User login
Redo carotid endarterectomy is more risky than previously estimated
NEW YORK – It is well known that reoperative carotid endarterectomy can be technically challenging because of the scarring left from the initial procedure, but an analysis of a large database presented at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation also revealed that the risk of complications, particularly stroke, is greater.

When “redo” carotid endarterectomies were compared with the index primary procedure collected in the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database, the odds ratio for stroke was several times greater (odds ratio, 3.71; P = .002) on univariate analysis, reported Jeffrey J. Siracuse, MD, associate professor of surgery and radiology at Boston University.
Previous single-center reports of redo endarterectomies “showed terrific results, really no perioperative stroke or morbidity, but this is older data from a different era,” said Dr. Siracuse, who undertook this study to determine whether “real-world” data would tell a different story.
In this study, 75,943 primary carotid endarterectomies and 140 redo procedures were identified in the ACS NSQIP database and compared. The redo population had a significantly higher incidence of end-stage renal disease (3.6% vs. 1.1%; P = .004), but history of stroke, whether with deficit (20.8% vs. 15.4%) or without (11.5% vs. 9.1%), was numerically higher among those undergoing a primary procedure even though these differences did not reach statistical significance. Baseline demographics and comorbidities were otherwise similar.
Presumably because of the difficulty of recanalizing scarred tissue, the mean procedure time for redos was longer than that for the primary procedures (137 vs. 49 minutes; P less than .001), but there were no significant differences in the rate of surgical site infections (0.7% vs. 0.3%; P = .482), return to the operating room (3.6% vs. 4%; P = .853), or 30-day readmissions (2.1% vs. 6.9%; P = .810) for the redo and index procedures, respectively.
Although perioperative MI rates were higher in the redo group (2.1%) than in the primary endarterectomy group (0.9%), this difference did not reach statistical significance (P = .125). However, a multivariate analysis associated redo carotid endarterectomy procedures with a nearly threefold increase in risk of a composite of major adverse cardiovascular events when compared on a multivariate analysis (OR, 2.76; P = .007), Dr. Siracuse reported.
For the surgeons considering a redo carotid endarterectomy, these data “inform a risk-benefit analysis,” according to Dr. Siracuse, but he also said that redo procedures still should be considered a viable strategy when considered in the context of other options.
Presenting a case he performed just prior to the VEITHsymposium, Dr. Siracuse displayed CT images that showed internal and common carotids with more than 75% stenosis in an 80-year-old women 7 years after a primary carotid endarterectomy. The tight stenoses and the evidence of substantial intra-arterial debris were concerns, but a decision to perform a redo endarterectomy was reached after other options, including stenting, were considered.
“She did great. She went home and has had no more symptoms,” Dr. Siracuse reported. “The point is you still have to take these [potential redo endarterectomies] on a case-by case basis.”
Dr. Siracuse reported he had no financial relationships relevant to this study.
NEW YORK – It is well known that reoperative carotid endarterectomy can be technically challenging because of the scarring left from the initial procedure, but an analysis of a large database presented at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation also revealed that the risk of complications, particularly stroke, is greater.
When “redo” carotid endarterectomies were compared with the index primary procedure collected in the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database, the odds ratio for stroke was several times greater (odds ratio, 3.71; P = .002) on univariate analysis, reported Jeffrey J. Siracuse, MD, associate professor of surgery and radiology at Boston University.
Previous single-center reports of redo endarterectomies “showed terrific results, really no perioperative stroke or morbidity, but this is older data from a different era,” said Dr. Siracuse, who undertook this study to determine whether “real-world” data would tell a different story.
In this study, 75,943 primary carotid endarterectomies and 140 redo procedures were identified in the ACS NSQIP database and compared. The redo population had a significantly higher incidence of end-stage renal disease (3.6% vs. 1.1%; P = .004), but history of stroke, whether with deficit (20.8% vs. 15.4%) or without (11.5% vs. 9.1%), was numerically higher among those undergoing a primary procedure even though these differences did not reach statistical significance. Baseline demographics and comorbidities were otherwise similar.
Presumably because of the difficulty of recanalizing scarred tissue, the mean procedure time for redos was longer than that for the primary procedures (137 vs. 49 minutes; P less than .001), but there were no significant differences in the rate of surgical site infections (0.7% vs. 0.3%; P = .482), return to the operating room (3.6% vs. 4%; P = .853), or 30-day readmissions (2.1% vs. 6.9%; P = .810) for the redo and index procedures, respectively.
Although perioperative MI rates were higher in the redo group (2.1%) than in the primary endarterectomy group (0.9%), this difference did not reach statistical significance (P = .125). However, a multivariate analysis associated redo carotid endarterectomy procedures with a nearly threefold increase in risk of a composite of major adverse cardiovascular events when compared on a multivariate analysis (OR, 2.76; P = .007), Dr. Siracuse reported.
For the surgeons considering a redo carotid endarterectomy, these data “inform a risk-benefit analysis,” according to Dr. Siracuse, but he also said that redo procedures still should be considered a viable strategy when considered in the context of other options.
Presenting a case he performed just prior to the VEITHsymposium, Dr. Siracuse displayed CT images that showed internal and common carotids with more than 75% stenosis in an 80-year-old women 7 years after a primary carotid endarterectomy. The tight stenoses and the evidence of substantial intra-arterial debris were concerns, but a decision to perform a redo endarterectomy was reached after other options, including stenting, were considered.
“She did great. She went home and has had no more symptoms,” Dr. Siracuse reported. “The point is you still have to take these [potential redo endarterectomies] on a case-by case basis.”
Dr. Siracuse reported he had no financial relationships relevant to this study.
NEW YORK – It is well known that reoperative carotid endarterectomy can be technically challenging because of the scarring left from the initial procedure, but an analysis of a large database presented at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation also revealed that the risk of complications, particularly stroke, is greater.
When “redo” carotid endarterectomies were compared with the index primary procedure collected in the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database, the odds ratio for stroke was several times greater (odds ratio, 3.71; P = .002) on univariate analysis, reported Jeffrey J. Siracuse, MD, associate professor of surgery and radiology at Boston University.
Previous single-center reports of redo endarterectomies “showed terrific results, really no perioperative stroke or morbidity, but this is older data from a different era,” said Dr. Siracuse, who undertook this study to determine whether “real-world” data would tell a different story.
In this study, 75,943 primary carotid endarterectomies and 140 redo procedures were identified in the ACS NSQIP database and compared. The redo population had a significantly higher incidence of end-stage renal disease (3.6% vs. 1.1%; P = .004), but history of stroke, whether with deficit (20.8% vs. 15.4%) or without (11.5% vs. 9.1%), was numerically higher among those undergoing a primary procedure even though these differences did not reach statistical significance. Baseline demographics and comorbidities were otherwise similar.
Presumably because of the difficulty of recanalizing scarred tissue, the mean procedure time for redos was longer than that for the primary procedures (137 vs. 49 minutes; P less than .001), but there were no significant differences in the rate of surgical site infections (0.7% vs. 0.3%; P = .482), return to the operating room (3.6% vs. 4%; P = .853), or 30-day readmissions (2.1% vs. 6.9%; P = .810) for the redo and index procedures, respectively.
Although perioperative MI rates were higher in the redo group (2.1%) than in the primary endarterectomy group (0.9%), this difference did not reach statistical significance (P = .125). However, a multivariate analysis associated redo carotid endarterectomy procedures with a nearly threefold increase in risk of a composite of major adverse cardiovascular events when compared on a multivariate analysis (OR, 2.76; P = .007), Dr. Siracuse reported.
For the surgeons considering a redo carotid endarterectomy, these data “inform a risk-benefit analysis,” according to Dr. Siracuse, but he also said that redo procedures still should be considered a viable strategy when considered in the context of other options.
Presenting a case he performed just prior to the VEITHsymposium, Dr. Siracuse displayed CT images that showed internal and common carotids with more than 75% stenosis in an 80-year-old women 7 years after a primary carotid endarterectomy. The tight stenoses and the evidence of substantial intra-arterial debris were concerns, but a decision to perform a redo endarterectomy was reached after other options, including stenting, were considered.
“She did great. She went home and has had no more symptoms,” Dr. Siracuse reported. “The point is you still have to take these [potential redo endarterectomies] on a case-by case basis.”
Dr. Siracuse reported he had no financial relationships relevant to this study.
REPORTING FROM VEITHSYMPOSIUM
Key clinical point:
Major finding: The odds ratio for stroke is 3.71 times higher (P = .002) with redo than with primary carotid endarterectomy.
Study details: Multivariate retrospective database analysis.
Disclosures: Dr. Siracuse reported he had no financial relationships relevant to this study.
Healthier lifestyle in midlife women reduces subclinical carotid atherosclerosis
Women who have a healthier lifestyle during the menopausal transition could significantly reduce their risk of cardiovascular disease, new research suggests.

Because women experience a steeper increase in CVD risk during and after the menopausal transition, researchers analyzed data from the Study of Women’s Health Across the Nation (SWAN), a prospective longitudinal cohort study of 1,143 women aged 42-52 years. The report is in JAHA: Journal of the American Heart Association.
The analysis revealed that women with the highest average Healthy Lifestyle Score – a composite score of dietary quality, levels of physical activity, and smoking – over 10 years of follow-up had a 0.024-mm smaller common carotid artery intima-media thickness and 0.16-mm smaller adventitial diameter, compared to those with the lowest average score. This was after adjustment for confounders and physiological risk factors such as ethnicity, age, menopausal status, body mass index, and cholesterol levels.
“Smoking, unhealthy diet, and lack of physical activity are three well-known modifiable behavioral risk factors for CVD,” wrote Dongqing Wang of the University of Michigan, Ann Arbor, and his coauthors. “Even after adjusting for the lifestyle-related physiological risk factors, the adherence to a healthy lifestyle composed of abstinence from smoking, healthy diet, and regular engagement in physical activity is inversely associated with atherosclerosis in midlife women.”
Women with higher average health lifestyle score also had lower levels of carotid plaque after adjustment for confounding factors, but this was no longer significant after adjustment for physiological risk factors.
The authors analyzed the three components of the healthy lifestyle score separately, and found that not smoking was strongly and significantly associated with lower scores for all three measures of subclinical atherosclerosis. Women who never smoked across the duration of the study had a 49% lower odds of having a high carotid plaque index compared with women who smoked at some point during the follow-up period.
The analysis showed an inverse association between average Alternate Healthy Eating Index score – a measure of diet quality – and smaller common carotid artery adventitial diameter, although after adjustment for BMI this association was no longer statistically significant. Likewise, the association between dietary quality and intima-media thickness was only marginally significant and lost that significance after adjustment for BMI.
Long-term physical activity was only marginally significantly associated with common carotid artery intima-media thickness, but this was not significant after adjustment for physiological risk factors. No association was found between physical activity and common carotid artery adventitial diameter or carotid plaque.
The authors said that 1.7% of the study population managed to stay in the top category for all three components of healthy lifestyle at all three follow-up time points in the study.
“The low prevalence of a healthy lifestyle in midlife women highlights the potential for lifestyle interventions aimed at this vulnerable population,” they wrote.
In particular, they highlighted abstinence from smoking as having the strongest impact on all three measures of subclinical atherosclerosis, which is known to affect women more than men. However, the outcomes from diet and physical activity weren’t so strong: The authors suggested that BMI could partly mediate the effects of healthier diet and greater levels of physical activity.
One strength of the study was its ethnically diverse population, which included African American, Chinese, and Hispanic women in addition to non-Hispanic white women. However, the study was not powered to examine the impacts ethnicity may have had on outcomes, the researchers wrote.
The Study of Women’s Health Across the Nation is supported by the National Institutes of Health. No conflicts of interest were declared.
SOURCE: Wang D et al. JAHA 2018 Nov. 28.
Women who have a healthier lifestyle during the menopausal transition could significantly reduce their risk of cardiovascular disease, new research suggests.
Because women experience a steeper increase in CVD risk during and after the menopausal transition, researchers analyzed data from the Study of Women’s Health Across the Nation (SWAN), a prospective longitudinal cohort study of 1,143 women aged 42-52 years. The report is in JAHA: Journal of the American Heart Association.
The analysis revealed that women with the highest average Healthy Lifestyle Score – a composite score of dietary quality, levels of physical activity, and smoking – over 10 years of follow-up had a 0.024-mm smaller common carotid artery intima-media thickness and 0.16-mm smaller adventitial diameter, compared to those with the lowest average score. This was after adjustment for confounders and physiological risk factors such as ethnicity, age, menopausal status, body mass index, and cholesterol levels.
“Smoking, unhealthy diet, and lack of physical activity are three well-known modifiable behavioral risk factors for CVD,” wrote Dongqing Wang of the University of Michigan, Ann Arbor, and his coauthors. “Even after adjusting for the lifestyle-related physiological risk factors, the adherence to a healthy lifestyle composed of abstinence from smoking, healthy diet, and regular engagement in physical activity is inversely associated with atherosclerosis in midlife women.”
Women with higher average health lifestyle score also had lower levels of carotid plaque after adjustment for confounding factors, but this was no longer significant after adjustment for physiological risk factors.
The authors analyzed the three components of the healthy lifestyle score separately, and found that not smoking was strongly and significantly associated with lower scores for all three measures of subclinical atherosclerosis. Women who never smoked across the duration of the study had a 49% lower odds of having a high carotid plaque index compared with women who smoked at some point during the follow-up period.
The analysis showed an inverse association between average Alternate Healthy Eating Index score – a measure of diet quality – and smaller common carotid artery adventitial diameter, although after adjustment for BMI this association was no longer statistically significant. Likewise, the association between dietary quality and intima-media thickness was only marginally significant and lost that significance after adjustment for BMI.
Long-term physical activity was only marginally significantly associated with common carotid artery intima-media thickness, but this was not significant after adjustment for physiological risk factors. No association was found between physical activity and common carotid artery adventitial diameter or carotid plaque.
The authors said that 1.7% of the study population managed to stay in the top category for all three components of healthy lifestyle at all three follow-up time points in the study.
“The low prevalence of a healthy lifestyle in midlife women highlights the potential for lifestyle interventions aimed at this vulnerable population,” they wrote.
In particular, they highlighted abstinence from smoking as having the strongest impact on all three measures of subclinical atherosclerosis, which is known to affect women more than men. However, the outcomes from diet and physical activity weren’t so strong: The authors suggested that BMI could partly mediate the effects of healthier diet and greater levels of physical activity.
One strength of the study was its ethnically diverse population, which included African American, Chinese, and Hispanic women in addition to non-Hispanic white women. However, the study was not powered to examine the impacts ethnicity may have had on outcomes, the researchers wrote.
The Study of Women’s Health Across the Nation is supported by the National Institutes of Health. No conflicts of interest were declared.
SOURCE: Wang D et al. JAHA 2018 Nov. 28.
Women who have a healthier lifestyle during the menopausal transition could significantly reduce their risk of cardiovascular disease, new research suggests.
Because women experience a steeper increase in CVD risk during and after the menopausal transition, researchers analyzed data from the Study of Women’s Health Across the Nation (SWAN), a prospective longitudinal cohort study of 1,143 women aged 42-52 years. The report is in JAHA: Journal of the American Heart Association.
The analysis revealed that women with the highest average Healthy Lifestyle Score – a composite score of dietary quality, levels of physical activity, and smoking – over 10 years of follow-up had a 0.024-mm smaller common carotid artery intima-media thickness and 0.16-mm smaller adventitial diameter, compared to those with the lowest average score. This was after adjustment for confounders and physiological risk factors such as ethnicity, age, menopausal status, body mass index, and cholesterol levels.
“Smoking, unhealthy diet, and lack of physical activity are three well-known modifiable behavioral risk factors for CVD,” wrote Dongqing Wang of the University of Michigan, Ann Arbor, and his coauthors. “Even after adjusting for the lifestyle-related physiological risk factors, the adherence to a healthy lifestyle composed of abstinence from smoking, healthy diet, and regular engagement in physical activity is inversely associated with atherosclerosis in midlife women.”
Women with higher average health lifestyle score also had lower levels of carotid plaque after adjustment for confounding factors, but this was no longer significant after adjustment for physiological risk factors.
The authors analyzed the three components of the healthy lifestyle score separately, and found that not smoking was strongly and significantly associated with lower scores for all three measures of subclinical atherosclerosis. Women who never smoked across the duration of the study had a 49% lower odds of having a high carotid plaque index compared with women who smoked at some point during the follow-up period.
The analysis showed an inverse association between average Alternate Healthy Eating Index score – a measure of diet quality – and smaller common carotid artery adventitial diameter, although after adjustment for BMI this association was no longer statistically significant. Likewise, the association between dietary quality and intima-media thickness was only marginally significant and lost that significance after adjustment for BMI.
Long-term physical activity was only marginally significantly associated with common carotid artery intima-media thickness, but this was not significant after adjustment for physiological risk factors. No association was found between physical activity and common carotid artery adventitial diameter or carotid plaque.
The authors said that 1.7% of the study population managed to stay in the top category for all three components of healthy lifestyle at all three follow-up time points in the study.
“The low prevalence of a healthy lifestyle in midlife women highlights the potential for lifestyle interventions aimed at this vulnerable population,” they wrote.
In particular, they highlighted abstinence from smoking as having the strongest impact on all three measures of subclinical atherosclerosis, which is known to affect women more than men. However, the outcomes from diet and physical activity weren’t so strong: The authors suggested that BMI could partly mediate the effects of healthier diet and greater levels of physical activity.
One strength of the study was its ethnically diverse population, which included African American, Chinese, and Hispanic women in addition to non-Hispanic white women. However, the study was not powered to examine the impacts ethnicity may have had on outcomes, the researchers wrote.
The Study of Women’s Health Across the Nation is supported by the National Institutes of Health. No conflicts of interest were declared.
SOURCE: Wang D et al. JAHA 2018 Nov. 28.
FROM JAHA: JOURNAL OF THE AMERICAN HEART ASSOCIATION
Key clinical point: .
Major finding: Following a healthier diet and not smoking were significantly linked with lower subclinical carotid atherosclerosis in menopausal women.
Study details: A prospective, longitudinal cohort study of 1,143 women.
Disclosures: The Study of Women’s Health Across the Nation is supported by the National Institutes of Health. No conflicts of interest were declared.
Source: Wang D et al. JAHA 2018 Nov. 28.
Open AAA repair mortality rates doubled for very-low-volume surgeons
NEW YORK – If New York State is representative, the risk of bad outcomes in patients undergoing open abdominal aortic aneurysm repair (OAR) or carotid endarterectomy (CEA), including death in the case of OAR, is about double when performed by very low- versus higher-volume surgeons, according to data presented at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
“What should we do to fix the problem? We could require surgeons to track their outcomes in quality improvement registry,” suggested Jack L. Cronenwett, MD, professor of surgery, Geisel School of Medicine at Dartmouth, Hanover, N.H.
The outcomes were evaluated from inpatient data gathered from patients undergoing OAR or CEA in an all-payer database involving every hospital discharge in New York State. Surgeons were defined as very-low-volume for a given procedure if they averaged one or less per year, though the results held true if very-low-volume was defined as less than three cases per year, according to Dr. Cronenwett.
The database had outcomes on 8,781 OAR procedures and 68,896 CEA procedures performed from 2000 to 2014.
Of the 614 surgeons who performed one or more OARs over this period, 318 (51.8%) were defined as low-volume surgeons. Despite their substantial representation, they performed just 7.6% of the procedures.
When outcomes from procedures performed by very-low-volume surgeons were compared to those done by higher-volume surgeons, the mortality rates without adjustments were nearly double (6.7% vs. 3.5%; P less than .001). Procedures performed by low-volume surgeons were associated with far higher rates of sepsis or shock (5.7% vs. 3.7%; P = .008), and patients treated by low-volume surgeons were more likely to spend 9 or more days in the hospital (39.3% vs. 30.1%; P less than .001).
When fully adjusted for other variables, “low-volume surgeons had twofold higher odds [OR 2.09] of postoperative death,” Dr. Cronenwett reported.
Of the 1,071 surgeons who performed CEA over this period, 512 (47.8%) were low-volume. They performed 1.3% of the procedures.
Mortality and sepsis or shock following CEA were less than 1% in procedures performed by either low- or higher-volume surgeons without significant differences. However, procedures performed by low-volume surgeons were associated with a three-times higher rate of myocardial infarction (1.5% vs. 0.5%; P less than .001) and a 65% higher rate of stroke (3.5% vs. 2.1%; P = .003).
In addition, patients who underwent CEA performed by a low-volume surgeon had a significantly higher rate of 30-day readmission (11.5% vs. 8.5%; P = .002) and a significantly longer median length of stay (2 days vs. 1 day; P less than .001) than did those treated by a higher-volume surgeon.
Whether OAR or CEA, patients treated by a low-volume surgeon were more likely to have Medicaid coverage. The fact that procedures by low-volume surgeons were more likely to be performed in New York City than other areas of the state suggest that access to care was not a variable, according to Dr. Cronenwett.
Surgeon volume was calculated in this study by dividing the total number of OAR or CEA procedures performed by the number of years that the surgeon was in practice in New York State. Surgeons were classified as vascular surgeons if 75% or more of their surgical practice involved vascular procedures, cardiac surgeons if more than 20% of their surgical practice involved cardiac procedures, and general surgeons if they did not meet either of these criteria.
Of OAR procedures were done by a higher-volume surgeon, approximately 65% were by vascular specialists, 5% were by cardiac specialists, and the remaining were by general surgeons.
Of OAR procedures were done by a low-volume surgeon, approximately 25% were by vascular surgeons, 20% were by cardiac surgeons, and the remaining were by general surgeons. For CEA, there was a somewhat greater representation of general surgeons in both categories, but the patterns were similar.
Dr. Cronenwett argued that more rigorous steps should be taken to ensure that those with proven skills perform OAR and CEA and that open abdominal aortic aneurysm repair should be performed only by high-volume surgeons and hospitals. He suggested there are a variety of incentives or disincentives that could help, but he stressed the importance of tracking results and making them available to referring physicians and to patients.
“Some of the low-volume surgeons are probably not tracking their results so are not even aware of these bad outcomes,” he added.
Dr. Cronenwett reported that he had no relevant disclosures.
NEW YORK – If New York State is representative, the risk of bad outcomes in patients undergoing open abdominal aortic aneurysm repair (OAR) or carotid endarterectomy (CEA), including death in the case of OAR, is about double when performed by very low- versus higher-volume surgeons, according to data presented at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
“What should we do to fix the problem? We could require surgeons to track their outcomes in quality improvement registry,” suggested Jack L. Cronenwett, MD, professor of surgery, Geisel School of Medicine at Dartmouth, Hanover, N.H.
The outcomes were evaluated from inpatient data gathered from patients undergoing OAR or CEA in an all-payer database involving every hospital discharge in New York State. Surgeons were defined as very-low-volume for a given procedure if they averaged one or less per year, though the results held true if very-low-volume was defined as less than three cases per year, according to Dr. Cronenwett.
The database had outcomes on 8,781 OAR procedures and 68,896 CEA procedures performed from 2000 to 2014.
Of the 614 surgeons who performed one or more OARs over this period, 318 (51.8%) were defined as low-volume surgeons. Despite their substantial representation, they performed just 7.6% of the procedures.
When outcomes from procedures performed by very-low-volume surgeons were compared to those done by higher-volume surgeons, the mortality rates without adjustments were nearly double (6.7% vs. 3.5%; P less than .001). Procedures performed by low-volume surgeons were associated with far higher rates of sepsis or shock (5.7% vs. 3.7%; P = .008), and patients treated by low-volume surgeons were more likely to spend 9 or more days in the hospital (39.3% vs. 30.1%; P less than .001).
When fully adjusted for other variables, “low-volume surgeons had twofold higher odds [OR 2.09] of postoperative death,” Dr. Cronenwett reported.
Of the 1,071 surgeons who performed CEA over this period, 512 (47.8%) were low-volume. They performed 1.3% of the procedures.
Mortality and sepsis or shock following CEA were less than 1% in procedures performed by either low- or higher-volume surgeons without significant differences. However, procedures performed by low-volume surgeons were associated with a three-times higher rate of myocardial infarction (1.5% vs. 0.5%; P less than .001) and a 65% higher rate of stroke (3.5% vs. 2.1%; P = .003).
In addition, patients who underwent CEA performed by a low-volume surgeon had a significantly higher rate of 30-day readmission (11.5% vs. 8.5%; P = .002) and a significantly longer median length of stay (2 days vs. 1 day; P less than .001) than did those treated by a higher-volume surgeon.
Whether OAR or CEA, patients treated by a low-volume surgeon were more likely to have Medicaid coverage. The fact that procedures by low-volume surgeons were more likely to be performed in New York City than other areas of the state suggest that access to care was not a variable, according to Dr. Cronenwett.
Surgeon volume was calculated in this study by dividing the total number of OAR or CEA procedures performed by the number of years that the surgeon was in practice in New York State. Surgeons were classified as vascular surgeons if 75% or more of their surgical practice involved vascular procedures, cardiac surgeons if more than 20% of their surgical practice involved cardiac procedures, and general surgeons if they did not meet either of these criteria.
Of OAR procedures were done by a higher-volume surgeon, approximately 65% were by vascular specialists, 5% were by cardiac specialists, and the remaining were by general surgeons.
Of OAR procedures were done by a low-volume surgeon, approximately 25% were by vascular surgeons, 20% were by cardiac surgeons, and the remaining were by general surgeons. For CEA, there was a somewhat greater representation of general surgeons in both categories, but the patterns were similar.
Dr. Cronenwett argued that more rigorous steps should be taken to ensure that those with proven skills perform OAR and CEA and that open abdominal aortic aneurysm repair should be performed only by high-volume surgeons and hospitals. He suggested there are a variety of incentives or disincentives that could help, but he stressed the importance of tracking results and making them available to referring physicians and to patients.
“Some of the low-volume surgeons are probably not tracking their results so are not even aware of these bad outcomes,” he added.
Dr. Cronenwett reported that he had no relevant disclosures.
NEW YORK – If New York State is representative, the risk of bad outcomes in patients undergoing open abdominal aortic aneurysm repair (OAR) or carotid endarterectomy (CEA), including death in the case of OAR, is about double when performed by very low- versus higher-volume surgeons, according to data presented at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
“What should we do to fix the problem? We could require surgeons to track their outcomes in quality improvement registry,” suggested Jack L. Cronenwett, MD, professor of surgery, Geisel School of Medicine at Dartmouth, Hanover, N.H.
The outcomes were evaluated from inpatient data gathered from patients undergoing OAR or CEA in an all-payer database involving every hospital discharge in New York State. Surgeons were defined as very-low-volume for a given procedure if they averaged one or less per year, though the results held true if very-low-volume was defined as less than three cases per year, according to Dr. Cronenwett.
The database had outcomes on 8,781 OAR procedures and 68,896 CEA procedures performed from 2000 to 2014.
Of the 614 surgeons who performed one or more OARs over this period, 318 (51.8%) were defined as low-volume surgeons. Despite their substantial representation, they performed just 7.6% of the procedures.
When outcomes from procedures performed by very-low-volume surgeons were compared to those done by higher-volume surgeons, the mortality rates without adjustments were nearly double (6.7% vs. 3.5%; P less than .001). Procedures performed by low-volume surgeons were associated with far higher rates of sepsis or shock (5.7% vs. 3.7%; P = .008), and patients treated by low-volume surgeons were more likely to spend 9 or more days in the hospital (39.3% vs. 30.1%; P less than .001).
When fully adjusted for other variables, “low-volume surgeons had twofold higher odds [OR 2.09] of postoperative death,” Dr. Cronenwett reported.
Of the 1,071 surgeons who performed CEA over this period, 512 (47.8%) were low-volume. They performed 1.3% of the procedures.
Mortality and sepsis or shock following CEA were less than 1% in procedures performed by either low- or higher-volume surgeons without significant differences. However, procedures performed by low-volume surgeons were associated with a three-times higher rate of myocardial infarction (1.5% vs. 0.5%; P less than .001) and a 65% higher rate of stroke (3.5% vs. 2.1%; P = .003).
In addition, patients who underwent CEA performed by a low-volume surgeon had a significantly higher rate of 30-day readmission (11.5% vs. 8.5%; P = .002) and a significantly longer median length of stay (2 days vs. 1 day; P less than .001) than did those treated by a higher-volume surgeon.
Whether OAR or CEA, patients treated by a low-volume surgeon were more likely to have Medicaid coverage. The fact that procedures by low-volume surgeons were more likely to be performed in New York City than other areas of the state suggest that access to care was not a variable, according to Dr. Cronenwett.
Surgeon volume was calculated in this study by dividing the total number of OAR or CEA procedures performed by the number of years that the surgeon was in practice in New York State. Surgeons were classified as vascular surgeons if 75% or more of their surgical practice involved vascular procedures, cardiac surgeons if more than 20% of their surgical practice involved cardiac procedures, and general surgeons if they did not meet either of these criteria.
Of OAR procedures were done by a higher-volume surgeon, approximately 65% were by vascular specialists, 5% were by cardiac specialists, and the remaining were by general surgeons.
Of OAR procedures were done by a low-volume surgeon, approximately 25% were by vascular surgeons, 20% were by cardiac surgeons, and the remaining were by general surgeons. For CEA, there was a somewhat greater representation of general surgeons in both categories, but the patterns were similar.
Dr. Cronenwett argued that more rigorous steps should be taken to ensure that those with proven skills perform OAR and CEA and that open abdominal aortic aneurysm repair should be performed only by high-volume surgeons and hospitals. He suggested there are a variety of incentives or disincentives that could help, but he stressed the importance of tracking results and making them available to referring physicians and to patients.
“Some of the low-volume surgeons are probably not tracking their results so are not even aware of these bad outcomes,” he added.
Dr. Cronenwett reported that he had no relevant disclosures.
REPORTING FROM VEITHSYMPOSIUM
Key clinical point:
Major finding: In-hospital mortality is approximately double (OR 2.09; P less than .001) for very low-volume relative to high-volume surgeon.
Study details: Retrospective database review.
Disclosures: Dr. Cronenwett reports no conflicts of interest.
Source: Cronenwett JL et al. 2018; 45th VEITHsymposium.
Young adults with hypertension may be at higher CVD risk
a pair of recent studies published in JAMA suggest.

In one study, investigators applied the 2017 American College of Cardiology/American Heart Association blood pressure criteria to nearly 5,000 U.S. young adults followed for approximately 20 years and who had up to a 3.5-fold risk associated with hypertension versus normal blood pressure.
The second study of almost 2.5 million Korean young adults, followed for 10 years, similarly found increased risks of cardiovascular disease later in life for those who had stage 1 or 2 hypertension between the ages of 20 and 39 years.
“These findings from a second country on the opposite side of the globe are consistent with those of the U.S. study, providing further support for the ACC/AHA guideline definitions of hypertension,” Naomi D.L. Fisher, MD, deputy editor, JAMA, and Gregory Curfman, MD, Brigham and Women’s Hospital, Boston, said in an editorial also appearing in JAMA.
Disagreement over the ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults threatens to distract from their potential benefits, Dr. Fisher and Dr. Curfman wrote in that editorial.
By redefining stage 1 hypertension as 130/80 mm Hg or higher, down from 140/90 mm Hg or higher, the 2017 ACC/AHA increased the prevalence of hypertension in the United States from 31.9% to 45.6%, they noted.
“Given the magnitude and reach of the global problem of hypertension, it is imperative that dedicated control efforts at the population level intensify,” they said.
U.S. study
The U.S. study, described in JAMA by Yuichiro Yano, MD, PhD, department of community and family medicine, Duke University, Durham, N.C., and his colleagues, was based on analysis of a prospective cohort study, CARDIA (Coronary Artery Risk Development in Young Adults Study), which started in 1985 and enrolled 5,115 black and white adults aged 18-30 years.
They applied the ACC/AHA blood pressure criteria based on each participants’ highest measurement before the age of 40 years, and correlated that with incident cardiovascular disease events that occurred over a median follow-up of 18.8 years.
Patients with normal blood pressure had a cardiovascular disease incidence rate of 1.37/1,000 person-years, compared with 2.74/1,000 person-years for those with elevated blood pressure, 3.15 for stage 1 hypertension, and 8.04 for stage 2 hypertension, investigators found.
That translated into increased risks of cardiovascular disease for those with elevated blood pressure versus those with normal blood pressure. After multivariable adjustment, the hazard ratio for cardiovascular disease was 1.67 (95% confidence interval, 1.01-2.77) for elevated blood pressure, 1.75 (95% CI, 1.22-2.53) for stage 1 hypertension, and 3.49 (95% CI, 2.42-5.05) for stage 2, Dr. Yano and his colleagues reported.
“The ACC/AHA blood pressure classification system may help identify young adults at higher risk for CVD events,” they concluded.
South Korean study
Similar findings were shown in a population-based cohort study, also published in JAMA, that included 2,488,101 adults aged 20-39 years in Korean National Health Insurance Service records.
The investigators looked at mean blood pressure levels from an initial health examination that took place during 2002-2003 and a second examination during 2004-2005.
Follow-up was shorter than the U.S. study, with a median duration of 10 years, reported Joung Sik Son, MD, department of family medicine and biomedical sciences, Seoul (South Korea) National University, and coauthors.
Even so, investigators detected an elevated risk of cardiovascular events for individuals with stage 1 or 2 hypertension versus those with normal blood pressure.
For men with baseline stage 1 hypertension based on the mean values and using the latest ACC/AHA blood pressure criteria, the incidence of cardiovascular disease was 215/100,000 person-years, versus 164 for those with normal blood pressure, with an adjusted hazard ratio of 1.25 (95% CI, 1.21-1.28), the authors said. Likewise, women with stage 1 hypertension had an incidence of 131/100,000 person-years versus 40 for women with normal blood pressure, with a hazard ratio of 1.27 (95% CI, 1.21-1.34).
Men with stage 2 hypertension likewise had a higher cardiovascular disease incidence than did those with normal blood pressure (336 vs. 164 per 100,000 person-years; adjusted HR 1.76), with similar findings seen in women, the report shows.
“Despite the relatively low absolute risk, the difference in absolute risk and the fact that sustained hypertension during longer durations is associated with higher risk of CVD [cardiovascular disease] indicate that early blood pressure management among young adults may lead to significant public health benefits by reducing CVD risk later in life,” Dr. Son and colleagues wrote in a discussion of the results.
Authors of the U.S. study reported disclosures related to Amarin, Amgen, and Novartis outside of the submitted work, as well as grants from the National Heart, Lung, and Blood Institute and National Institutes of Health during the conduct of the study.
Authors of the South Korean study reported no conflict of interest disclosures. That study was supported by the Ministry of Health and Welfare and the Ministry of Education of Korea, along with grants from the National Research Foundation of Korea.
SOURCES: Yano Y et al. JAMA. 2018;302(17):1774-82; Son JS et al. JAMA. 2018;302(17):1783-92.
These two studies suggest that a higher blood pressure level in young adulthood is associated with a greater hazard of premature cardiovascular disease, according to Ramachandran S. Vasan, MD.
However, observing an elevated risk of premature cardiovascular disease does necessarily prove causality, or establish that intervening to lower blood pressure in this age group would lessen that risk, he said in an editorial.
The studies are notable for showing that half to nearly 60% of younger adults had levels of blood pressure considered not normal, he added in the editorial, which appears in JAMA.
It is not clear why so many young adults would manifest higher blood pressure levels in these studies, he said, noting that the umbrella of young adults with hypertension likely includes patients with a variety of subtypes. Those including white-coat hypertension, peripheral amplification with normal central blood pressure, hyperadrenergic state, isolated systolic hypertension, and a smaller subset with secondary hypertension.
“These distinct pathophenotypes may have varying natural histories and their management approaches may be distinctive, suggesting the importance and potential role of subphenotyping of elevated blood pressure in young adults to facilitate treatment decisions,” he wrote in his editorial.
The two studies raise key questions, such as whether there are modifiable social, behavioral, or cultural factors that could prevent elevated blood pressure in younger people, he said.
To date, a substantial body of evidence does suggest that blood pressure levels evolve over the course of life, driven by environmental factors superimposed on genetic risks, and modified by sex and race.
“Overall, these data emphasize that primary prevention of higher blood pressure levels must begin in childhood,” he said.
Ramachandran S. Vasan, MD, is with the section of preventive medicine and epidemiology at Boston University. He reported no conflict of interest disclosures related to his editorial, which was supported by the National Heart, Lung, and Blood Institute’s Framingham Heart Study and a grant from the National Institutes of Health. JAMA. 2018;320(17):1760-3. doi:10.1001/jama.2018.16068.
These two studies suggest that a higher blood pressure level in young adulthood is associated with a greater hazard of premature cardiovascular disease, according to Ramachandran S. Vasan, MD.
However, observing an elevated risk of premature cardiovascular disease does necessarily prove causality, or establish that intervening to lower blood pressure in this age group would lessen that risk, he said in an editorial.
The studies are notable for showing that half to nearly 60% of younger adults had levels of blood pressure considered not normal, he added in the editorial, which appears in JAMA.
It is not clear why so many young adults would manifest higher blood pressure levels in these studies, he said, noting that the umbrella of young adults with hypertension likely includes patients with a variety of subtypes. Those including white-coat hypertension, peripheral amplification with normal central blood pressure, hyperadrenergic state, isolated systolic hypertension, and a smaller subset with secondary hypertension.
“These distinct pathophenotypes may have varying natural histories and their management approaches may be distinctive, suggesting the importance and potential role of subphenotyping of elevated blood pressure in young adults to facilitate treatment decisions,” he wrote in his editorial.
The two studies raise key questions, such as whether there are modifiable social, behavioral, or cultural factors that could prevent elevated blood pressure in younger people, he said.
To date, a substantial body of evidence does suggest that blood pressure levels evolve over the course of life, driven by environmental factors superimposed on genetic risks, and modified by sex and race.
“Overall, these data emphasize that primary prevention of higher blood pressure levels must begin in childhood,” he said.
Ramachandran S. Vasan, MD, is with the section of preventive medicine and epidemiology at Boston University. He reported no conflict of interest disclosures related to his editorial, which was supported by the National Heart, Lung, and Blood Institute’s Framingham Heart Study and a grant from the National Institutes of Health. JAMA. 2018;320(17):1760-3. doi:10.1001/jama.2018.16068.
These two studies suggest that a higher blood pressure level in young adulthood is associated with a greater hazard of premature cardiovascular disease, according to Ramachandran S. Vasan, MD.
However, observing an elevated risk of premature cardiovascular disease does necessarily prove causality, or establish that intervening to lower blood pressure in this age group would lessen that risk, he said in an editorial.
The studies are notable for showing that half to nearly 60% of younger adults had levels of blood pressure considered not normal, he added in the editorial, which appears in JAMA.
It is not clear why so many young adults would manifest higher blood pressure levels in these studies, he said, noting that the umbrella of young adults with hypertension likely includes patients with a variety of subtypes. Those including white-coat hypertension, peripheral amplification with normal central blood pressure, hyperadrenergic state, isolated systolic hypertension, and a smaller subset with secondary hypertension.
“These distinct pathophenotypes may have varying natural histories and their management approaches may be distinctive, suggesting the importance and potential role of subphenotyping of elevated blood pressure in young adults to facilitate treatment decisions,” he wrote in his editorial.
The two studies raise key questions, such as whether there are modifiable social, behavioral, or cultural factors that could prevent elevated blood pressure in younger people, he said.
To date, a substantial body of evidence does suggest that blood pressure levels evolve over the course of life, driven by environmental factors superimposed on genetic risks, and modified by sex and race.
“Overall, these data emphasize that primary prevention of higher blood pressure levels must begin in childhood,” he said.
Ramachandran S. Vasan, MD, is with the section of preventive medicine and epidemiology at Boston University. He reported no conflict of interest disclosures related to his editorial, which was supported by the National Heart, Lung, and Blood Institute’s Framingham Heart Study and a grant from the National Institutes of Health. JAMA. 2018;320(17):1760-3. doi:10.1001/jama.2018.16068.
a pair of recent studies published in JAMA suggest.
In one study, investigators applied the 2017 American College of Cardiology/American Heart Association blood pressure criteria to nearly 5,000 U.S. young adults followed for approximately 20 years and who had up to a 3.5-fold risk associated with hypertension versus normal blood pressure.
The second study of almost 2.5 million Korean young adults, followed for 10 years, similarly found increased risks of cardiovascular disease later in life for those who had stage 1 or 2 hypertension between the ages of 20 and 39 years.
“These findings from a second country on the opposite side of the globe are consistent with those of the U.S. study, providing further support for the ACC/AHA guideline definitions of hypertension,” Naomi D.L. Fisher, MD, deputy editor, JAMA, and Gregory Curfman, MD, Brigham and Women’s Hospital, Boston, said in an editorial also appearing in JAMA.
Disagreement over the ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults threatens to distract from their potential benefits, Dr. Fisher and Dr. Curfman wrote in that editorial.
By redefining stage 1 hypertension as 130/80 mm Hg or higher, down from 140/90 mm Hg or higher, the 2017 ACC/AHA increased the prevalence of hypertension in the United States from 31.9% to 45.6%, they noted.
“Given the magnitude and reach of the global problem of hypertension, it is imperative that dedicated control efforts at the population level intensify,” they said.
U.S. study
The U.S. study, described in JAMA by Yuichiro Yano, MD, PhD, department of community and family medicine, Duke University, Durham, N.C., and his colleagues, was based on analysis of a prospective cohort study, CARDIA (Coronary Artery Risk Development in Young Adults Study), which started in 1985 and enrolled 5,115 black and white adults aged 18-30 years.
They applied the ACC/AHA blood pressure criteria based on each participants’ highest measurement before the age of 40 years, and correlated that with incident cardiovascular disease events that occurred over a median follow-up of 18.8 years.
Patients with normal blood pressure had a cardiovascular disease incidence rate of 1.37/1,000 person-years, compared with 2.74/1,000 person-years for those with elevated blood pressure, 3.15 for stage 1 hypertension, and 8.04 for stage 2 hypertension, investigators found.
That translated into increased risks of cardiovascular disease for those with elevated blood pressure versus those with normal blood pressure. After multivariable adjustment, the hazard ratio for cardiovascular disease was 1.67 (95% confidence interval, 1.01-2.77) for elevated blood pressure, 1.75 (95% CI, 1.22-2.53) for stage 1 hypertension, and 3.49 (95% CI, 2.42-5.05) for stage 2, Dr. Yano and his colleagues reported.
“The ACC/AHA blood pressure classification system may help identify young adults at higher risk for CVD events,” they concluded.
South Korean study
Similar findings were shown in a population-based cohort study, also published in JAMA, that included 2,488,101 adults aged 20-39 years in Korean National Health Insurance Service records.
The investigators looked at mean blood pressure levels from an initial health examination that took place during 2002-2003 and a second examination during 2004-2005.
Follow-up was shorter than the U.S. study, with a median duration of 10 years, reported Joung Sik Son, MD, department of family medicine and biomedical sciences, Seoul (South Korea) National University, and coauthors.
Even so, investigators detected an elevated risk of cardiovascular events for individuals with stage 1 or 2 hypertension versus those with normal blood pressure.
For men with baseline stage 1 hypertension based on the mean values and using the latest ACC/AHA blood pressure criteria, the incidence of cardiovascular disease was 215/100,000 person-years, versus 164 for those with normal blood pressure, with an adjusted hazard ratio of 1.25 (95% CI, 1.21-1.28), the authors said. Likewise, women with stage 1 hypertension had an incidence of 131/100,000 person-years versus 40 for women with normal blood pressure, with a hazard ratio of 1.27 (95% CI, 1.21-1.34).
Men with stage 2 hypertension likewise had a higher cardiovascular disease incidence than did those with normal blood pressure (336 vs. 164 per 100,000 person-years; adjusted HR 1.76), with similar findings seen in women, the report shows.
“Despite the relatively low absolute risk, the difference in absolute risk and the fact that sustained hypertension during longer durations is associated with higher risk of CVD [cardiovascular disease] indicate that early blood pressure management among young adults may lead to significant public health benefits by reducing CVD risk later in life,” Dr. Son and colleagues wrote in a discussion of the results.
Authors of the U.S. study reported disclosures related to Amarin, Amgen, and Novartis outside of the submitted work, as well as grants from the National Heart, Lung, and Blood Institute and National Institutes of Health during the conduct of the study.
Authors of the South Korean study reported no conflict of interest disclosures. That study was supported by the Ministry of Health and Welfare and the Ministry of Education of Korea, along with grants from the National Research Foundation of Korea.
SOURCES: Yano Y et al. JAMA. 2018;302(17):1774-82; Son JS et al. JAMA. 2018;302(17):1783-92.
a pair of recent studies published in JAMA suggest.
In one study, investigators applied the 2017 American College of Cardiology/American Heart Association blood pressure criteria to nearly 5,000 U.S. young adults followed for approximately 20 years and who had up to a 3.5-fold risk associated with hypertension versus normal blood pressure.
The second study of almost 2.5 million Korean young adults, followed for 10 years, similarly found increased risks of cardiovascular disease later in life for those who had stage 1 or 2 hypertension between the ages of 20 and 39 years.
“These findings from a second country on the opposite side of the globe are consistent with those of the U.S. study, providing further support for the ACC/AHA guideline definitions of hypertension,” Naomi D.L. Fisher, MD, deputy editor, JAMA, and Gregory Curfman, MD, Brigham and Women’s Hospital, Boston, said in an editorial also appearing in JAMA.
Disagreement over the ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults threatens to distract from their potential benefits, Dr. Fisher and Dr. Curfman wrote in that editorial.
By redefining stage 1 hypertension as 130/80 mm Hg or higher, down from 140/90 mm Hg or higher, the 2017 ACC/AHA increased the prevalence of hypertension in the United States from 31.9% to 45.6%, they noted.
“Given the magnitude and reach of the global problem of hypertension, it is imperative that dedicated control efforts at the population level intensify,” they said.
U.S. study
The U.S. study, described in JAMA by Yuichiro Yano, MD, PhD, department of community and family medicine, Duke University, Durham, N.C., and his colleagues, was based on analysis of a prospective cohort study, CARDIA (Coronary Artery Risk Development in Young Adults Study), which started in 1985 and enrolled 5,115 black and white adults aged 18-30 years.
They applied the ACC/AHA blood pressure criteria based on each participants’ highest measurement before the age of 40 years, and correlated that with incident cardiovascular disease events that occurred over a median follow-up of 18.8 years.
Patients with normal blood pressure had a cardiovascular disease incidence rate of 1.37/1,000 person-years, compared with 2.74/1,000 person-years for those with elevated blood pressure, 3.15 for stage 1 hypertension, and 8.04 for stage 2 hypertension, investigators found.
That translated into increased risks of cardiovascular disease for those with elevated blood pressure versus those with normal blood pressure. After multivariable adjustment, the hazard ratio for cardiovascular disease was 1.67 (95% confidence interval, 1.01-2.77) for elevated blood pressure, 1.75 (95% CI, 1.22-2.53) for stage 1 hypertension, and 3.49 (95% CI, 2.42-5.05) for stage 2, Dr. Yano and his colleagues reported.
“The ACC/AHA blood pressure classification system may help identify young adults at higher risk for CVD events,” they concluded.
South Korean study
Similar findings were shown in a population-based cohort study, also published in JAMA, that included 2,488,101 adults aged 20-39 years in Korean National Health Insurance Service records.
The investigators looked at mean blood pressure levels from an initial health examination that took place during 2002-2003 and a second examination during 2004-2005.
Follow-up was shorter than the U.S. study, with a median duration of 10 years, reported Joung Sik Son, MD, department of family medicine and biomedical sciences, Seoul (South Korea) National University, and coauthors.
Even so, investigators detected an elevated risk of cardiovascular events for individuals with stage 1 or 2 hypertension versus those with normal blood pressure.
For men with baseline stage 1 hypertension based on the mean values and using the latest ACC/AHA blood pressure criteria, the incidence of cardiovascular disease was 215/100,000 person-years, versus 164 for those with normal blood pressure, with an adjusted hazard ratio of 1.25 (95% CI, 1.21-1.28), the authors said. Likewise, women with stage 1 hypertension had an incidence of 131/100,000 person-years versus 40 for women with normal blood pressure, with a hazard ratio of 1.27 (95% CI, 1.21-1.34).
Men with stage 2 hypertension likewise had a higher cardiovascular disease incidence than did those with normal blood pressure (336 vs. 164 per 100,000 person-years; adjusted HR 1.76), with similar findings seen in women, the report shows.
“Despite the relatively low absolute risk, the difference in absolute risk and the fact that sustained hypertension during longer durations is associated with higher risk of CVD [cardiovascular disease] indicate that early blood pressure management among young adults may lead to significant public health benefits by reducing CVD risk later in life,” Dr. Son and colleagues wrote in a discussion of the results.
Authors of the U.S. study reported disclosures related to Amarin, Amgen, and Novartis outside of the submitted work, as well as grants from the National Heart, Lung, and Blood Institute and National Institutes of Health during the conduct of the study.
Authors of the South Korean study reported no conflict of interest disclosures. That study was supported by the Ministry of Health and Welfare and the Ministry of Education of Korea, along with grants from the National Research Foundation of Korea.
SOURCES: Yano Y et al. JAMA. 2018;302(17):1774-82; Son JS et al. JAMA. 2018;302(17):1783-92.
FROM JAMA
Vascular ultrasound reasonable for first-line imaging of large-vessel GCA
CHICAGO – Vascular ultrasound showed high sensitivity and specificity for diagnosing large-vessel giant-cell arteritis (LV-GCA) in a prospective study of patients with suspected new-onset disease.
The findings highlight the value of vascular ultrasound – in the hands of experienced sonographers – as a first-line imaging test in this setting, Berit Dalsgaard Nielsen, MD, reported at the annual meeting of the American College of Rheumatology.
Of 41 control subjects without LV-GCA, none had a positive ultrasound, whereas 36 of 45 LV-GCA patients had a positive ultrasound, which gives the test a specificity of 100% and sensitivity of 80%, Dr. Nielsen of Aarhus (Denmark) University Hospital said during a press briefing at the meeting.
Ultrasound was performed on the carotid artery in the neck and axillary arteries under the arm, which are easily accessible by ultrasound.
“These patients also had temporal arteries evaluated, and if we included this evaluation in the diagnostic performance, it showed a sensitivity of 91%,” she noted, explaining that temporal artery ultrasound alone conferred 71% sensitivity. “So it actually helped us identify more GCA patients.”
The study subjects were adults with suspected GCA. Inclusion criteria included age of at least 50 years, C-reactive protein of more than 15 mg/L or erythrocyte sedimentation rate of more than 40 mm, and either cranial symptoms, new-onset limb claudication, protracted constitutional symptoms, or polymyalgia rheumatica (PMR) symptoms. Patients were excluded if they had recent or ongoing glucocorticoid or disease-modifying antirheumatic drug treatment, a previous GCA or PMR diagnosis, or a large vessel inflammation that mimicked LV-GCA.
Clinical evaluations and imaging tests were performed prior to treatment initiation. The reference diagnosis was a clinical diagnosis of GCA and a positive 18F-FDG PET/CT scan, Dr Nielsen said, adding that ultrasound examinations were performed by experienced sonographers who were blinded to the PET/CT results.
Of the 86 patients included, 45 had LV-GCA with or without concomitant cranial GCA, 10 had isolated cranial GCA, 21 had PMR, and 10 were diagnosed with other diseases. The patients found to not have LV-GCA were considered control subjects.
The findings are notable because, while PET is considered the gold standard, it is very expensive and not always readily available, Dr. Nielsen said.
Additionally, while cranial-GCA patients generally present with symptoms such as headache, jaw claudication, and visual disturbances that are considered typical for GCA, LV-GCA patients rarely present with these symptoms.
Rather, these LV-GCA patients tend to present with constitutional symptoms mimicking infection or cancer, and they undergo extensive examination programs before the diagnosis is established. For this reason, diagnosis is often delayed for several months in LV-GCA patients until late in the disease course.
“During this time they often experience a decline in physical ability,” she said. “So in this disease subset of patients with GCA, there’s an unmet need for earlier recognition and earlier diagnosis.”
New recommendations from the European League Against Rheumatism call for early diagnostic imaging in all cases of suspected GCA, she added, noting that, for cranial-GCA symptoms, temporal artery ultrasound is recommended first line, but for those who present without cranial symptoms, no particular imaging modality is recommended because of a lack of comparative and diagnostic accuracy data in LV-GCA.
Biopsy has traditionally been used in these cases, but now imaging can be substituted – and vascular ultrasound is an attractive first-line option given its affordability and availability.
Indeed, the current findings support its use in this setting, she said.
“We think that these results indicate that ultrasound should not only be the first-line imaging test in patients presenting with cranial symptoms, but also in patients suspected of GCA presenting with constitutional symptoms, and if this examination is included in the standard examinations in fast-track clinics, it may overcome the delay in diagnosis and the patients can be treated earlier. It may also spare the unneeded examinations performed in these patients,” she concluded.
Dr. Nielsen disclosed a relationship with Roche.
SOURCE: Nielsen B et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 2905.
CHICAGO – Vascular ultrasound showed high sensitivity and specificity for diagnosing large-vessel giant-cell arteritis (LV-GCA) in a prospective study of patients with suspected new-onset disease.
The findings highlight the value of vascular ultrasound – in the hands of experienced sonographers – as a first-line imaging test in this setting, Berit Dalsgaard Nielsen, MD, reported at the annual meeting of the American College of Rheumatology.
Of 41 control subjects without LV-GCA, none had a positive ultrasound, whereas 36 of 45 LV-GCA patients had a positive ultrasound, which gives the test a specificity of 100% and sensitivity of 80%, Dr. Nielsen of Aarhus (Denmark) University Hospital said during a press briefing at the meeting.
Ultrasound was performed on the carotid artery in the neck and axillary arteries under the arm, which are easily accessible by ultrasound.
“These patients also had temporal arteries evaluated, and if we included this evaluation in the diagnostic performance, it showed a sensitivity of 91%,” she noted, explaining that temporal artery ultrasound alone conferred 71% sensitivity. “So it actually helped us identify more GCA patients.”
The study subjects were adults with suspected GCA. Inclusion criteria included age of at least 50 years, C-reactive protein of more than 15 mg/L or erythrocyte sedimentation rate of more than 40 mm, and either cranial symptoms, new-onset limb claudication, protracted constitutional symptoms, or polymyalgia rheumatica (PMR) symptoms. Patients were excluded if they had recent or ongoing glucocorticoid or disease-modifying antirheumatic drug treatment, a previous GCA or PMR diagnosis, or a large vessel inflammation that mimicked LV-GCA.
Clinical evaluations and imaging tests were performed prior to treatment initiation. The reference diagnosis was a clinical diagnosis of GCA and a positive 18F-FDG PET/CT scan, Dr Nielsen said, adding that ultrasound examinations were performed by experienced sonographers who were blinded to the PET/CT results.
Of the 86 patients included, 45 had LV-GCA with or without concomitant cranial GCA, 10 had isolated cranial GCA, 21 had PMR, and 10 were diagnosed with other diseases. The patients found to not have LV-GCA were considered control subjects.
The findings are notable because, while PET is considered the gold standard, it is very expensive and not always readily available, Dr. Nielsen said.
Additionally, while cranial-GCA patients generally present with symptoms such as headache, jaw claudication, and visual disturbances that are considered typical for GCA, LV-GCA patients rarely present with these symptoms.
Rather, these LV-GCA patients tend to present with constitutional symptoms mimicking infection or cancer, and they undergo extensive examination programs before the diagnosis is established. For this reason, diagnosis is often delayed for several months in LV-GCA patients until late in the disease course.
“During this time they often experience a decline in physical ability,” she said. “So in this disease subset of patients with GCA, there’s an unmet need for earlier recognition and earlier diagnosis.”
New recommendations from the European League Against Rheumatism call for early diagnostic imaging in all cases of suspected GCA, she added, noting that, for cranial-GCA symptoms, temporal artery ultrasound is recommended first line, but for those who present without cranial symptoms, no particular imaging modality is recommended because of a lack of comparative and diagnostic accuracy data in LV-GCA.
Biopsy has traditionally been used in these cases, but now imaging can be substituted – and vascular ultrasound is an attractive first-line option given its affordability and availability.
Indeed, the current findings support its use in this setting, she said.
“We think that these results indicate that ultrasound should not only be the first-line imaging test in patients presenting with cranial symptoms, but also in patients suspected of GCA presenting with constitutional symptoms, and if this examination is included in the standard examinations in fast-track clinics, it may overcome the delay in diagnosis and the patients can be treated earlier. It may also spare the unneeded examinations performed in these patients,” she concluded.
Dr. Nielsen disclosed a relationship with Roche.
SOURCE: Nielsen B et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 2905.
CHICAGO – Vascular ultrasound showed high sensitivity and specificity for diagnosing large-vessel giant-cell arteritis (LV-GCA) in a prospective study of patients with suspected new-onset disease.
The findings highlight the value of vascular ultrasound – in the hands of experienced sonographers – as a first-line imaging test in this setting, Berit Dalsgaard Nielsen, MD, reported at the annual meeting of the American College of Rheumatology.
Of 41 control subjects without LV-GCA, none had a positive ultrasound, whereas 36 of 45 LV-GCA patients had a positive ultrasound, which gives the test a specificity of 100% and sensitivity of 80%, Dr. Nielsen of Aarhus (Denmark) University Hospital said during a press briefing at the meeting.
Ultrasound was performed on the carotid artery in the neck and axillary arteries under the arm, which are easily accessible by ultrasound.
“These patients also had temporal arteries evaluated, and if we included this evaluation in the diagnostic performance, it showed a sensitivity of 91%,” she noted, explaining that temporal artery ultrasound alone conferred 71% sensitivity. “So it actually helped us identify more GCA patients.”
The study subjects were adults with suspected GCA. Inclusion criteria included age of at least 50 years, C-reactive protein of more than 15 mg/L or erythrocyte sedimentation rate of more than 40 mm, and either cranial symptoms, new-onset limb claudication, protracted constitutional symptoms, or polymyalgia rheumatica (PMR) symptoms. Patients were excluded if they had recent or ongoing glucocorticoid or disease-modifying antirheumatic drug treatment, a previous GCA or PMR diagnosis, or a large vessel inflammation that mimicked LV-GCA.
Clinical evaluations and imaging tests were performed prior to treatment initiation. The reference diagnosis was a clinical diagnosis of GCA and a positive 18F-FDG PET/CT scan, Dr Nielsen said, adding that ultrasound examinations were performed by experienced sonographers who were blinded to the PET/CT results.
Of the 86 patients included, 45 had LV-GCA with or without concomitant cranial GCA, 10 had isolated cranial GCA, 21 had PMR, and 10 were diagnosed with other diseases. The patients found to not have LV-GCA were considered control subjects.
The findings are notable because, while PET is considered the gold standard, it is very expensive and not always readily available, Dr. Nielsen said.
Additionally, while cranial-GCA patients generally present with symptoms such as headache, jaw claudication, and visual disturbances that are considered typical for GCA, LV-GCA patients rarely present with these symptoms.
Rather, these LV-GCA patients tend to present with constitutional symptoms mimicking infection or cancer, and they undergo extensive examination programs before the diagnosis is established. For this reason, diagnosis is often delayed for several months in LV-GCA patients until late in the disease course.
“During this time they often experience a decline in physical ability,” she said. “So in this disease subset of patients with GCA, there’s an unmet need for earlier recognition and earlier diagnosis.”
New recommendations from the European League Against Rheumatism call for early diagnostic imaging in all cases of suspected GCA, she added, noting that, for cranial-GCA symptoms, temporal artery ultrasound is recommended first line, but for those who present without cranial symptoms, no particular imaging modality is recommended because of a lack of comparative and diagnostic accuracy data in LV-GCA.
Biopsy has traditionally been used in these cases, but now imaging can be substituted – and vascular ultrasound is an attractive first-line option given its affordability and availability.
Indeed, the current findings support its use in this setting, she said.
“We think that these results indicate that ultrasound should not only be the first-line imaging test in patients presenting with cranial symptoms, but also in patients suspected of GCA presenting with constitutional symptoms, and if this examination is included in the standard examinations in fast-track clinics, it may overcome the delay in diagnosis and the patients can be treated earlier. It may also spare the unneeded examinations performed in these patients,” she concluded.
Dr. Nielsen disclosed a relationship with Roche.
SOURCE: Nielsen B et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 2905.
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point: Vascular ultrasound is reasonable for first-line maging of suspected LV-GCA.
Major finding: Vascular ultrasound had 100% specificity and 80% sensitivity.
Study details: A prospective study of 86 patients.
Disclosures: Dr. Nielsen disclosed a relationship with Roche.
Source: Nielsen BD et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 2905.
Ultrasound denervation tops RF ablation for resistant hypertension
SAN DIEGO – Denervation of the main renal arteries with ultrasound is more effective than radiofrequency (RF) ablation at lowering blood pressure in patients with resistant hypertension, according to a single-center, randomized trial from Germany.

Dubbed RADIOSOUND–HTN, it was the first time the two emerging technologies have been pitted against each other. At 3-month follow-up, the 42 patients randomized to ultrasound ablation with the Paradise catheter (ReCor Medical) had a mean systolic daytime blood pressure reduction of 13.2 mm Hg on ambulatory monitoring, vs. 6.5 mm Hg among 39 patients randomized to RF ablation with Medtronic’s Symplicity Spyral catheter (P = .043).
Meanwhile, 39 patients randomized to both main artery and side branch ablation with the Spyral had a mean reduction of 8.3 mm Hg, slightly better than RF ablation of the main renal arteries alone, but the difference was not statistically significant, and “no definite conclusion on the value of an additional side branch ablation can be drawn,” said senior investigator Philipp Lurz , MD, PhD, a cardiologist at the University of Leipzig, Germany, and his colleagues (Circulation. 2018 Sep 25. doi: 10.1161/circulationaha.118.037654).
Denervation was probably more complete with the Paradise catheter, which might explain the results. Ultrasound energy penetrates about 6-7 mm from the lumen, reaching up to 90% of sympathetic nerve fibers, while RF energy penetrates 3-4 mm; indeed, the idea of going into the branches with RF ablation is because nerve fibers are closer to the lumen surface, Dr. Lurz said at the Transcatheter Cardiovascular Therapeutics (TCT) annual meeting, where he presented the study, which was simultaneously published in Circulation.
Also, the Paradise catheter – an endovascular balloon device inflated to fit the lumen – delivers fully circumferential, ringlike ablations with each application, while the Spyral catheter delivers four ablations simultaneously in a spiral pattern, and requires more ablations to create a similar effect, according to Dr. Lurz.
About two-thirds of patients in all three arms responded to treatment, meaning at least a 5 mm Hg drop in systolic blood pressure. Among the nonresponders, it’s possible that their hypertension wasn’t caused by sympathetic overdrive. “Future trials should focus on identifying these patients to avoid futile” procedures, and define “specific anatomic predictors associated with a more effective” renal denervation, Dr. Lurz and his team said in their study report.
The researchers noted that “the present study included patients with larger renal arteries” – at least one renal artery 5.5 mm or greater in diameter – “based on the assumption that sympathetic fibers are in greater distance from the lumen than in smaller arteries, and therefore ... higher penetration depth would be more relevant ... Results might have differed in a cohort of patients with smaller renal artery diameters.”
Both Paradise and Spyral are in pivotal trials for Food and Drug Administration approval.
The subjects were an average of 64 years. The majority were men, and there were no significant differences in baseline characteristics between the arms. The mean baseline daytime blood pressure was 153/86 mm Hg despite treatment with three or more classes of antihypertensives dosed to at least 50% of their maximum. There was no drug testing to confirm patients were taking their medications, but their general practitioners vouched for their adherence.
One patient in the ultrasound arm group developed a pseudoaneurysm treated successfully by compression. One of the RF subjects developed a postprocedural intracapsular and retroperitoneal hematoma that resolved spontaneously. No renal vascular complications or stenoses were detected at follow-up.
There was no industry funding for the work. Dr. Lurz is a speaker and consultant for both ReCor Medical and Medtronic.
SOURCE: Fengler K et al. TCT 2018, Abstract.
SAN DIEGO – Denervation of the main renal arteries with ultrasound is more effective than radiofrequency (RF) ablation at lowering blood pressure in patients with resistant hypertension, according to a single-center, randomized trial from Germany.
Dubbed RADIOSOUND–HTN, it was the first time the two emerging technologies have been pitted against each other. At 3-month follow-up, the 42 patients randomized to ultrasound ablation with the Paradise catheter (ReCor Medical) had a mean systolic daytime blood pressure reduction of 13.2 mm Hg on ambulatory monitoring, vs. 6.5 mm Hg among 39 patients randomized to RF ablation with Medtronic’s Symplicity Spyral catheter (P = .043).
Meanwhile, 39 patients randomized to both main artery and side branch ablation with the Spyral had a mean reduction of 8.3 mm Hg, slightly better than RF ablation of the main renal arteries alone, but the difference was not statistically significant, and “no definite conclusion on the value of an additional side branch ablation can be drawn,” said senior investigator Philipp Lurz , MD, PhD, a cardiologist at the University of Leipzig, Germany, and his colleagues (Circulation. 2018 Sep 25. doi: 10.1161/circulationaha.118.037654).
Denervation was probably more complete with the Paradise catheter, which might explain the results. Ultrasound energy penetrates about 6-7 mm from the lumen, reaching up to 90% of sympathetic nerve fibers, while RF energy penetrates 3-4 mm; indeed, the idea of going into the branches with RF ablation is because nerve fibers are closer to the lumen surface, Dr. Lurz said at the Transcatheter Cardiovascular Therapeutics (TCT) annual meeting, where he presented the study, which was simultaneously published in Circulation.
Also, the Paradise catheter – an endovascular balloon device inflated to fit the lumen – delivers fully circumferential, ringlike ablations with each application, while the Spyral catheter delivers four ablations simultaneously in a spiral pattern, and requires more ablations to create a similar effect, according to Dr. Lurz.
About two-thirds of patients in all three arms responded to treatment, meaning at least a 5 mm Hg drop in systolic blood pressure. Among the nonresponders, it’s possible that their hypertension wasn’t caused by sympathetic overdrive. “Future trials should focus on identifying these patients to avoid futile” procedures, and define “specific anatomic predictors associated with a more effective” renal denervation, Dr. Lurz and his team said in their study report.
The researchers noted that “the present study included patients with larger renal arteries” – at least one renal artery 5.5 mm or greater in diameter – “based on the assumption that sympathetic fibers are in greater distance from the lumen than in smaller arteries, and therefore ... higher penetration depth would be more relevant ... Results might have differed in a cohort of patients with smaller renal artery diameters.”
Both Paradise and Spyral are in pivotal trials for Food and Drug Administration approval.
The subjects were an average of 64 years. The majority were men, and there were no significant differences in baseline characteristics between the arms. The mean baseline daytime blood pressure was 153/86 mm Hg despite treatment with three or more classes of antihypertensives dosed to at least 50% of their maximum. There was no drug testing to confirm patients were taking their medications, but their general practitioners vouched for their adherence.
One patient in the ultrasound arm group developed a pseudoaneurysm treated successfully by compression. One of the RF subjects developed a postprocedural intracapsular and retroperitoneal hematoma that resolved spontaneously. No renal vascular complications or stenoses were detected at follow-up.
There was no industry funding for the work. Dr. Lurz is a speaker and consultant for both ReCor Medical and Medtronic.
SOURCE: Fengler K et al. TCT 2018, Abstract.
SAN DIEGO – Denervation of the main renal arteries with ultrasound is more effective than radiofrequency (RF) ablation at lowering blood pressure in patients with resistant hypertension, according to a single-center, randomized trial from Germany.
Dubbed RADIOSOUND–HTN, it was the first time the two emerging technologies have been pitted against each other. At 3-month follow-up, the 42 patients randomized to ultrasound ablation with the Paradise catheter (ReCor Medical) had a mean systolic daytime blood pressure reduction of 13.2 mm Hg on ambulatory monitoring, vs. 6.5 mm Hg among 39 patients randomized to RF ablation with Medtronic’s Symplicity Spyral catheter (P = .043).
Meanwhile, 39 patients randomized to both main artery and side branch ablation with the Spyral had a mean reduction of 8.3 mm Hg, slightly better than RF ablation of the main renal arteries alone, but the difference was not statistically significant, and “no definite conclusion on the value of an additional side branch ablation can be drawn,” said senior investigator Philipp Lurz , MD, PhD, a cardiologist at the University of Leipzig, Germany, and his colleagues (Circulation. 2018 Sep 25. doi: 10.1161/circulationaha.118.037654).
Denervation was probably more complete with the Paradise catheter, which might explain the results. Ultrasound energy penetrates about 6-7 mm from the lumen, reaching up to 90% of sympathetic nerve fibers, while RF energy penetrates 3-4 mm; indeed, the idea of going into the branches with RF ablation is because nerve fibers are closer to the lumen surface, Dr. Lurz said at the Transcatheter Cardiovascular Therapeutics (TCT) annual meeting, where he presented the study, which was simultaneously published in Circulation.
Also, the Paradise catheter – an endovascular balloon device inflated to fit the lumen – delivers fully circumferential, ringlike ablations with each application, while the Spyral catheter delivers four ablations simultaneously in a spiral pattern, and requires more ablations to create a similar effect, according to Dr. Lurz.
About two-thirds of patients in all three arms responded to treatment, meaning at least a 5 mm Hg drop in systolic blood pressure. Among the nonresponders, it’s possible that their hypertension wasn’t caused by sympathetic overdrive. “Future trials should focus on identifying these patients to avoid futile” procedures, and define “specific anatomic predictors associated with a more effective” renal denervation, Dr. Lurz and his team said in their study report.
The researchers noted that “the present study included patients with larger renal arteries” – at least one renal artery 5.5 mm or greater in diameter – “based on the assumption that sympathetic fibers are in greater distance from the lumen than in smaller arteries, and therefore ... higher penetration depth would be more relevant ... Results might have differed in a cohort of patients with smaller renal artery diameters.”
Both Paradise and Spyral are in pivotal trials for Food and Drug Administration approval.
The subjects were an average of 64 years. The majority were men, and there were no significant differences in baseline characteristics between the arms. The mean baseline daytime blood pressure was 153/86 mm Hg despite treatment with three or more classes of antihypertensives dosed to at least 50% of their maximum. There was no drug testing to confirm patients were taking their medications, but their general practitioners vouched for their adherence.
One patient in the ultrasound arm group developed a pseudoaneurysm treated successfully by compression. One of the RF subjects developed a postprocedural intracapsular and retroperitoneal hematoma that resolved spontaneously. No renal vascular complications or stenoses were detected at follow-up.
There was no industry funding for the work. Dr. Lurz is a speaker and consultant for both ReCor Medical and Medtronic.
SOURCE: Fengler K et al. TCT 2018, Abstract.
REPORTING FROM TCT 2018
Key clinical point: Denervation might be more complete with ultrasound.
Major finding: Patients randomized to ultrasound ablation had a mean systolic blood pressure reduction of 13.2 mm Hg, vs. 6.5 mm Hg among patients randomized to RF ablation (P = .043).
Study details: Randomized trial with 120 subjects
Disclosures: There was no industry funding for the work. The senior investigator is a speaker and consultant for both ReCor Medical and Medtronic.
Source: Fengler K et al. TCT 2018, Abstract.
Comparison of Cardiovascular Outcomes Between Statin Monotherapy and Fish Oil and Statin Combination Therapy in a Veteran Population
The Centers for Disease Control and Prevention lists cardiovascular-related diseases as a leading cause of mortality.1 The medication class of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors, more commonly known as statins, is first-line therapy to prevent negative cardiovascular outcomes and reduce premature death.2 Additional hyperlipidemia medications, such as fish oil, can be added for potential cardiovascular benefit.
Yokoyama and colleagues demonstrated that fish oil is a promising treatment for the prevention of major coronary events in patients with hypercholesterolemia.3 Furthermore, Macchia and colleagues found reductions in cardiovascular outcomes and all-cause mortality in postmyocardial infarction patients treated with fish oil and statin combination therapy.4 In contrast, the Outcomes Reduction with an Initial Glargine Intervention (ORIGIN) trial found glucose intolerant and patients with diabetes mellitus did not have improved cardiovascular outcomes with fish oil therapy.5 Likewise The Risk and Prevention Study Collaborative Group found fish oil supplementation provided no benefit for primary prevention in patients with multiple cardiovascular risk factors.6 These studies demonstrate fish oil therapy can cause diverse cardiovascular outcomes in different patient populations.
Currently, there are no studies examining the impact of fish oil and statin combination therapy on the US veteran population. The research of Yokoyama, Macchia, and The Risk and Prevention Study Collaborative Group took place in Japanese and Italian populations, which impacts their external validity.
This study aims to help the US Department of Veterans Affairs (VA) primary care providers and clinical pharmacists address the role of fish oil and statin combination therapy in the prevention of cardiovascular disease and all-cause mortality in the veteran population. The addition of fish oil to statin therapy was compared with an established standard of care, statin monotherapy, in veterans at the Fargo Veterans Affairs Health Care System (FVAHCS).
Methods
A retrospective chart review was conducted using the FVAHCS Computerized Patient Record System (CPRS). The institution’s review board and VA medical center approved the study. Eligible veterans with prescriptions for fish oil or statin therapy between January 1, 2000 and September 30, 2015 were randomly selected, reviewed, and sorted based on inclusion and exclusion criteria. 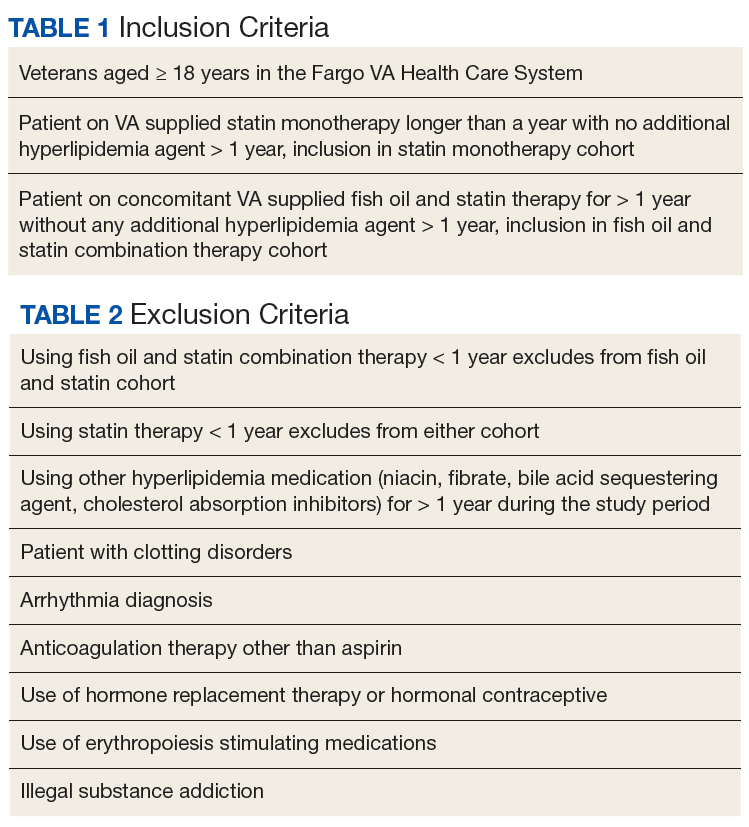
The primary outcome was time to aggregate cardiovascular events, specifically myocardial infarction (MI), stroke, transient ischemic attack, coronary artery bypass graft, and percutaneous intervention. Adverse cardiovascular event data were obtained from the veterans’ International Classification of Disease (ICD) 9 codes. Furthermore, the secondary outcome—time to all-cause mortality—was gathered by death records in CPRS. Time to these events was compared in veterans on fish oil and statin combination therapy or statin monotherapy. The date of the cardiovascular event or death was recorded for each outcome and was obtained by reviewing provider notes that documented the incidence. If a specific day or month of incidence was not documented, July 1 was selected as the default date for the adverse cardiovascular event.
Demographics, medication adherence, diagnoses, lab values within 90 days of initiation of therapy, and primary and secondary outcomes were collected. Demographics that included age, race, and sex all were obtained via chart review. Diagnoses were gathered using ICD 9 codes. Refill history was retrieved to assess adherence. Adherence was calculated by the total days of medication therapy divided by the total days within the study. Total days in the study was calculated by the duration of therapy days between therapy initiation date and a terminating factor. Terminating factors included an adverse cardiovascular event, death, or the study termination date.
Statistics
Demographic and other cohort characterization variables were compared either by a t test, rank sum test, or Fisher exact test given the character of the variable. Kaplan Meier analysis was used to evaluate time to aggregate cardiovascular events and all-cause mortality. VA Informatics and Computing Infrastructure (VINCI) R 3.4.3 was used for data analysis. One of the few combination studies by Macchia and colleagues gave an estimate of unadjusted incident rates for patients treated with statin monotherapy vs fish oil and statin combination therapy in patients having a recent MI.4 Based on this information, a power analysis determined that a 2% difference in incidence rate of adverse cardiovascular events could be detected between the 2 cohorts with 1,000 veterans in the statin cohort, and 500 veterans in the fish oil and statin cohort assuming a time to event interval of about 7.5 years. An α level of 0.05 was set to determine statistical significance.
Results
A total of 3,940 veterans with prescriptions for fish oil or statin therapy were randomly reviewed and sorted based on inclusion and exclusion criteria. This inclusion criteria resulted in 2,575 fish oil and statin combination patients and 1,365 statin monotherapy patients. Exclusion criteria produced a final total of 437 fish oil and statin combination patients and 559 statin monotherapy patients. Patient demographics are presented in Table 3. 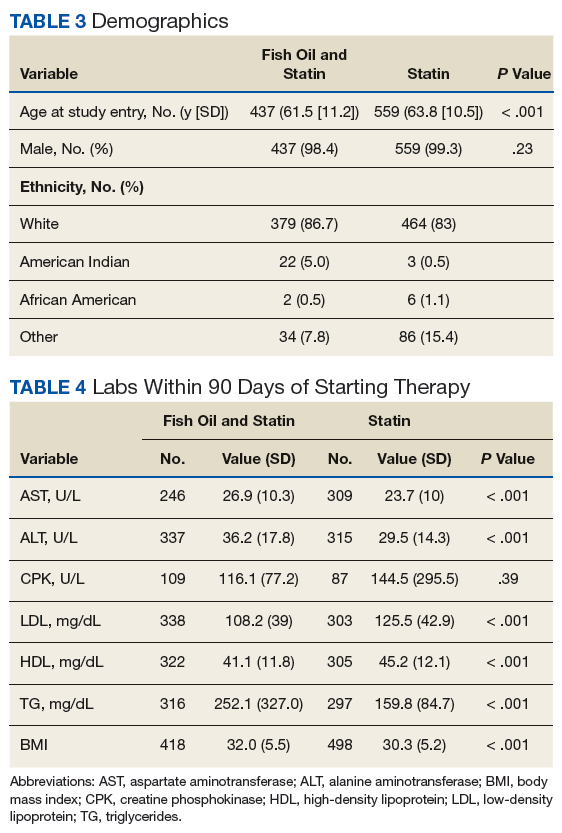
All baseline laboratory data were collected within 90 days of therapy initiation (Table 4). Statin monotherapy patients had lower triglyceride levels compared with those of the fish oil and statin combination patients. However, both high-density lipoprotein (HDL) and low-density lipoprotein (LDL) levels were higher in the statin monotherapy patients. As seen in Table 5, diagnosis of heart failure, hypertension, hypothyroidism, and dyslipidemia were higher in the statin monotherapy cohort, while tobacco use and pancreatitis were more prevalent in the fish oil and statin combination cohort. 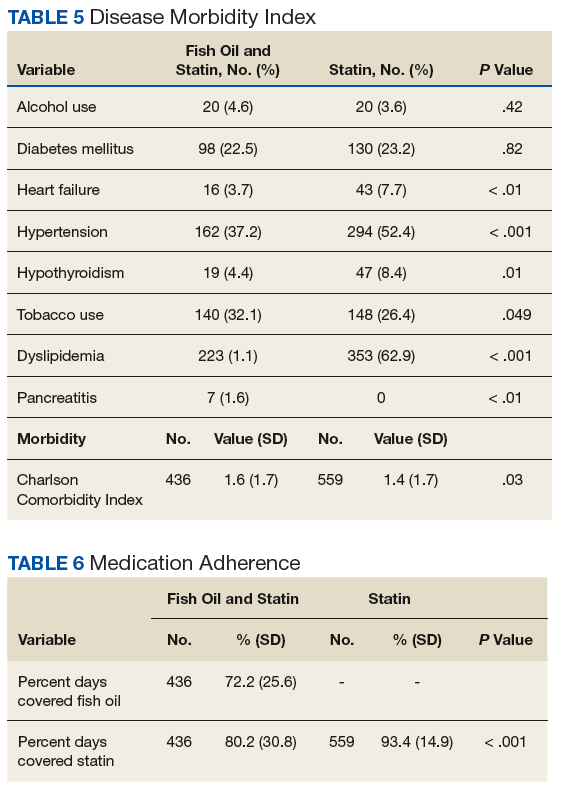
Kaplan Meier curves of the primary outcome, time to aggregate adverse cardiovascular event, and the secondary outcome, time to all-cause mortality are shown in Figure 1 and Figure 2, respectively. This shows adverse cardiovascular events and all-cause mortality for approximately 4,500 days for the fish oil and statin cohort and approximately 6,000 days for the statin monotherapy cohort.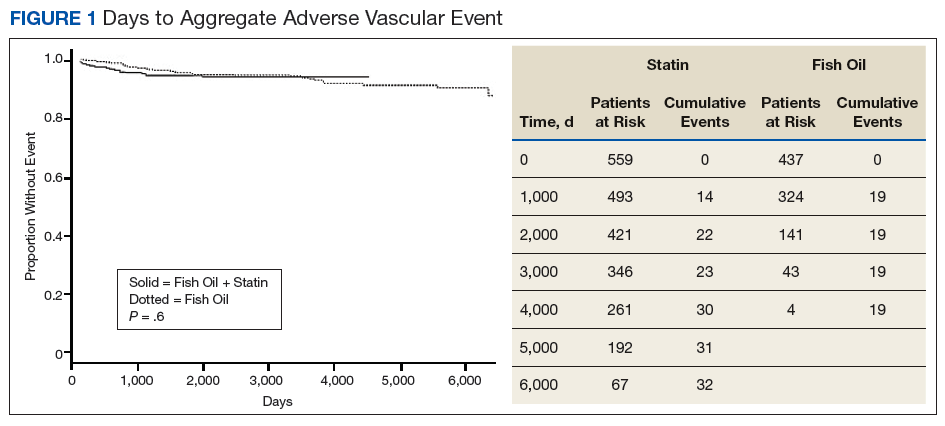
Discussion
Analysis of this study failed to detect a statistically significant difference for time to aggregate adverse cardiovascular events or all-cause mortality. This may be due to fewer adverse cardiovascular events and mortality in the 2 cohorts than was anticipated.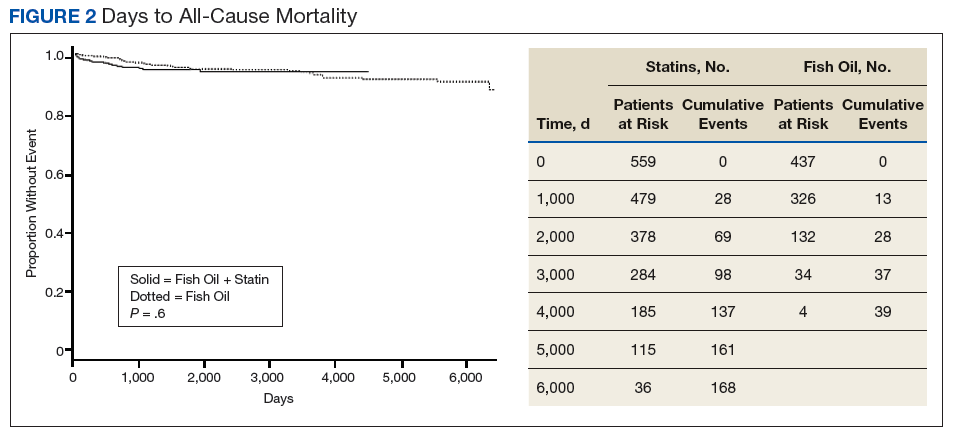
There are no studies examining fish oil and statin therapy in the veteran population and only limited studies comparing statin and fish oil combination therapy vs statin monotherapy for adverse cardiovascular outcomes and all-cause mortality. One of the few comparison studies was by Macchia and colleagues and consisted of 7,924 post MI patients in Italy. Over a 4-year period, researchers found a slight improvement in the adjusted paired-matched population for all-cause mortality in the fish oil and statin therapy cohort vs statin monotherapy (8.6% vs 13.6% P < .001).3 A benefit also was seen in the fish oil and statin cohort vs statin monotherapy in the adjusted paired-matched population for death or stroke (16.7% vs 11.5% P < .001).3
In contrast, this study did not address postmyocardial infarction patients exclusively. Rather, patients in this study had lower morbidity, which resulted in fewer adverse cardiovascular outcomes and a greater difficulty to detect a difference in this healthier population. These healthier patients may derive less benefit from primary or secondary prevention with statin and fish oil combination therapy.
In this study, there were extensive inclusion and exclusion criteria to assess the relationship between the cohorts for
Comparison of demographic data showed both cohorts were of similar age, sex, and race. Of note the Fargo veteran population was primarily white (> 80% in both cohorts). This is slightly higher than the percentage of whites for all US veterans. The slight difference most likely had a minimal clinical impact. Laboratory values recorded within 90 days of initiation of therapy were largely clinically similar except for triglycerides being significantly higher in the fish oil and statin combination cohort (Table 4). This may reflect selection bias, where providers may be more likely to add fish oil therapy for the potential to further control triglycerides.
Diagnoses of hypertension, heart failure, and dyslipidemia were higher in the statin monotherapy cohort. However, body mass index, tobacco use, and pancreatitis were statistically higher in fish oil and statin combination cohort. Even though there was a statistically significant difference in disease diagnoses, this likely created a minor clinical difference between the groups. This is further illustrated by the similarity of the Charlson Comorbidity Index of 1.6 for fish oil and statin cohort and 1.4 in statin monotherapy cohort.
Strengths
A strength of this study was its adherence rates. Adherence rates were high in both cohorts (Table 6). Fish oil and statin cohort did have slightly lower adherence compared with that of statin monotherapy. This may demonstrate extra pill burden influencing adherence. Overall demographics, laboratory values, disease, and adherence rates were clinically similar in both cohorts, thus reducing the potential for confounders.
Limitations
Limitations of this study include its retrospective chart review design. This design is susceptible to incorrect recording of events. The primary outcome, aggregate adverse cardiovascular events, may have been incorrectly recorded in the medical record as other diseases, such as coronary artery disease or heart disease, and therefore not captured by ICD 9 code retrieval. Also, important information, such as laboratory data, disease, and medication adherence, may not have been documented for all patients. Of note 1 patient in the fish oil and statin combination cohort did not have any recorded laboratory data, disease, or adherence data.
Another limitation is lack of access to medical notes from non-VA providers, which can result in missed data collection. To reduce this limitation, the study excluded veterans that received non-VA fish oil, statins, or other hyperlipidemia medications for > 1 year. Veterans were included only if they used VA-provided fish oil or statins. This inclusion and exclusion criteria reduced the chance of missing data from other facilities because it favored inclusion of only subjects that received care exclusively through the VA.
Last, on study initiation it was not realized that fish oil was not provided by the health care system until about the year 2004. This resulted in less risk days for the fish oil and statin cohort. However, Kaplan Meier analysis lessens this issue from being a confounder. Time to event rates for both the primary and secondary outcomes were similar and most likely would have continued to trend together with the same therapy duration.
Conclusion
Fish oil and statin combination therapy when compared with statin monotherapy failed to show that a statistically significant difference exists in the rates of MI, stroke, transient ischemic attack, coronary artery bypass graft, and percutaneous intervention. The clinical difference of fish oil and statin combination therapy vs statin monotherapy is most likely small or nonexistent. From our literature search, this is the only study concerning the use of fish oil and statin combination therapy in the veteran population. It is most likely that fish oil and statin combination therapy and statin monotherapy are similar for the reduction of time to aggregate adverse cardiovascular events and all-cause mortality in the veteran population.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Fargo VA Healthcare System.
1. Kochanek KD, Murphy SL, Xu J, Tejada-Vera B. Deaths: final data for 2014. https://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_04.pdf. Published June 30, 2016. Accessed July 26, 2018.
2. Stone NJ, Robinson JG, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.
3. Yokoyama M, Origasa H, Matsuzaki M, et al; Japan EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet. 2007;369(9567):1090-1098.
4. Macchia A, Romero M, D’Ettorre A, Tognoni G, Mariani J. Exploratory analysis on the use of statins with or without n-3 PUFA and major events in patients discharged for acute myocardial infarction: an observational retrospective study. PLoS One. 2013;8(5):e62772.
5. ORIGIN Trial Investigators, Bosch J, Gerstein HC, et al. n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N Engl J Med. 2012;367(4):309-318.
6. The Risk and Prevention Study Collaborative Group, Roncaglioni MC, Tombesi M, et al. n-3 fatty acids in patients with multiple cardiovascular risk factors. N Engl J Med. 2013;368(19):1800-1808.
7. Rizos EC, Ntzani EE, Bika E, Kostapanos MS, Elisaf MS. Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: a systematic review and meta-analysis. JAMA. 2012;308(10):1024-1033.
The Centers for Disease Control and Prevention lists cardiovascular-related diseases as a leading cause of mortality.1 The medication class of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors, more commonly known as statins, is first-line therapy to prevent negative cardiovascular outcomes and reduce premature death.2 Additional hyperlipidemia medications, such as fish oil, can be added for potential cardiovascular benefit.
Yokoyama and colleagues demonstrated that fish oil is a promising treatment for the prevention of major coronary events in patients with hypercholesterolemia.3 Furthermore, Macchia and colleagues found reductions in cardiovascular outcomes and all-cause mortality in postmyocardial infarction patients treated with fish oil and statin combination therapy.4 In contrast, the Outcomes Reduction with an Initial Glargine Intervention (ORIGIN) trial found glucose intolerant and patients with diabetes mellitus did not have improved cardiovascular outcomes with fish oil therapy.5 Likewise The Risk and Prevention Study Collaborative Group found fish oil supplementation provided no benefit for primary prevention in patients with multiple cardiovascular risk factors.6 These studies demonstrate fish oil therapy can cause diverse cardiovascular outcomes in different patient populations.
Currently, there are no studies examining the impact of fish oil and statin combination therapy on the US veteran population. The research of Yokoyama, Macchia, and The Risk and Prevention Study Collaborative Group took place in Japanese and Italian populations, which impacts their external validity.
This study aims to help the US Department of Veterans Affairs (VA) primary care providers and clinical pharmacists address the role of fish oil and statin combination therapy in the prevention of cardiovascular disease and all-cause mortality in the veteran population. The addition of fish oil to statin therapy was compared with an established standard of care, statin monotherapy, in veterans at the Fargo Veterans Affairs Health Care System (FVAHCS).
Methods
A retrospective chart review was conducted using the FVAHCS Computerized Patient Record System (CPRS). The institution’s review board and VA medical center approved the study. Eligible veterans with prescriptions for fish oil or statin therapy between January 1, 2000 and September 30, 2015 were randomly selected, reviewed, and sorted based on inclusion and exclusion criteria.
The primary outcome was time to aggregate cardiovascular events, specifically myocardial infarction (MI), stroke, transient ischemic attack, coronary artery bypass graft, and percutaneous intervention. Adverse cardiovascular event data were obtained from the veterans’ International Classification of Disease (ICD) 9 codes. Furthermore, the secondary outcome—time to all-cause mortality—was gathered by death records in CPRS. Time to these events was compared in veterans on fish oil and statin combination therapy or statin monotherapy. The date of the cardiovascular event or death was recorded for each outcome and was obtained by reviewing provider notes that documented the incidence. If a specific day or month of incidence was not documented, July 1 was selected as the default date for the adverse cardiovascular event.
Demographics, medication adherence, diagnoses, lab values within 90 days of initiation of therapy, and primary and secondary outcomes were collected. Demographics that included age, race, and sex all were obtained via chart review. Diagnoses were gathered using ICD 9 codes. Refill history was retrieved to assess adherence. Adherence was calculated by the total days of medication therapy divided by the total days within the study. Total days in the study was calculated by the duration of therapy days between therapy initiation date and a terminating factor. Terminating factors included an adverse cardiovascular event, death, or the study termination date.
Statistics
Demographic and other cohort characterization variables were compared either by a t test, rank sum test, or Fisher exact test given the character of the variable. Kaplan Meier analysis was used to evaluate time to aggregate cardiovascular events and all-cause mortality. VA Informatics and Computing Infrastructure (VINCI) R 3.4.3 was used for data analysis. One of the few combination studies by Macchia and colleagues gave an estimate of unadjusted incident rates for patients treated with statin monotherapy vs fish oil and statin combination therapy in patients having a recent MI.4 Based on this information, a power analysis determined that a 2% difference in incidence rate of adverse cardiovascular events could be detected between the 2 cohorts with 1,000 veterans in the statin cohort, and 500 veterans in the fish oil and statin cohort assuming a time to event interval of about 7.5 years. An α level of 0.05 was set to determine statistical significance.
Results
A total of 3,940 veterans with prescriptions for fish oil or statin therapy were randomly reviewed and sorted based on inclusion and exclusion criteria. This inclusion criteria resulted in 2,575 fish oil and statin combination patients and 1,365 statin monotherapy patients. Exclusion criteria produced a final total of 437 fish oil and statin combination patients and 559 statin monotherapy patients. Patient demographics are presented in Table 3.
All baseline laboratory data were collected within 90 days of therapy initiation (Table 4). Statin monotherapy patients had lower triglyceride levels compared with those of the fish oil and statin combination patients. However, both high-density lipoprotein (HDL) and low-density lipoprotein (LDL) levels were higher in the statin monotherapy patients. As seen in Table 5, diagnosis of heart failure, hypertension, hypothyroidism, and dyslipidemia were higher in the statin monotherapy cohort, while tobacco use and pancreatitis were more prevalent in the fish oil and statin combination cohort.
Kaplan Meier curves of the primary outcome, time to aggregate adverse cardiovascular event, and the secondary outcome, time to all-cause mortality are shown in Figure 1 and Figure 2, respectively. This shows adverse cardiovascular events and all-cause mortality for approximately 4,500 days for the fish oil and statin cohort and approximately 6,000 days for the statin monotherapy cohort.
Discussion
Analysis of this study failed to detect a statistically significant difference for time to aggregate adverse cardiovascular events or all-cause mortality. This may be due to fewer adverse cardiovascular events and mortality in the 2 cohorts than was anticipated.
There are no studies examining fish oil and statin therapy in the veteran population and only limited studies comparing statin and fish oil combination therapy vs statin monotherapy for adverse cardiovascular outcomes and all-cause mortality. One of the few comparison studies was by Macchia and colleagues and consisted of 7,924 post MI patients in Italy. Over a 4-year period, researchers found a slight improvement in the adjusted paired-matched population for all-cause mortality in the fish oil and statin therapy cohort vs statin monotherapy (8.6% vs 13.6% P < .001).3 A benefit also was seen in the fish oil and statin cohort vs statin monotherapy in the adjusted paired-matched population for death or stroke (16.7% vs 11.5% P < .001).3
In contrast, this study did not address postmyocardial infarction patients exclusively. Rather, patients in this study had lower morbidity, which resulted in fewer adverse cardiovascular outcomes and a greater difficulty to detect a difference in this healthier population. These healthier patients may derive less benefit from primary or secondary prevention with statin and fish oil combination therapy.
In this study, there were extensive inclusion and exclusion criteria to assess the relationship between the cohorts for
Comparison of demographic data showed both cohorts were of similar age, sex, and race. Of note the Fargo veteran population was primarily white (> 80% in both cohorts). This is slightly higher than the percentage of whites for all US veterans. The slight difference most likely had a minimal clinical impact. Laboratory values recorded within 90 days of initiation of therapy were largely clinically similar except for triglycerides being significantly higher in the fish oil and statin combination cohort (Table 4). This may reflect selection bias, where providers may be more likely to add fish oil therapy for the potential to further control triglycerides.
Diagnoses of hypertension, heart failure, and dyslipidemia were higher in the statin monotherapy cohort. However, body mass index, tobacco use, and pancreatitis were statistically higher in fish oil and statin combination cohort. Even though there was a statistically significant difference in disease diagnoses, this likely created a minor clinical difference between the groups. This is further illustrated by the similarity of the Charlson Comorbidity Index of 1.6 for fish oil and statin cohort and 1.4 in statin monotherapy cohort.
Strengths
A strength of this study was its adherence rates. Adherence rates were high in both cohorts (Table 6). Fish oil and statin cohort did have slightly lower adherence compared with that of statin monotherapy. This may demonstrate extra pill burden influencing adherence. Overall demographics, laboratory values, disease, and adherence rates were clinically similar in both cohorts, thus reducing the potential for confounders.
Limitations
Limitations of this study include its retrospective chart review design. This design is susceptible to incorrect recording of events. The primary outcome, aggregate adverse cardiovascular events, may have been incorrectly recorded in the medical record as other diseases, such as coronary artery disease or heart disease, and therefore not captured by ICD 9 code retrieval. Also, important information, such as laboratory data, disease, and medication adherence, may not have been documented for all patients. Of note 1 patient in the fish oil and statin combination cohort did not have any recorded laboratory data, disease, or adherence data.
Another limitation is lack of access to medical notes from non-VA providers, which can result in missed data collection. To reduce this limitation, the study excluded veterans that received non-VA fish oil, statins, or other hyperlipidemia medications for > 1 year. Veterans were included only if they used VA-provided fish oil or statins. This inclusion and exclusion criteria reduced the chance of missing data from other facilities because it favored inclusion of only subjects that received care exclusively through the VA.
Last, on study initiation it was not realized that fish oil was not provided by the health care system until about the year 2004. This resulted in less risk days for the fish oil and statin cohort. However, Kaplan Meier analysis lessens this issue from being a confounder. Time to event rates for both the primary and secondary outcomes were similar and most likely would have continued to trend together with the same therapy duration.
Conclusion
Fish oil and statin combination therapy when compared with statin monotherapy failed to show that a statistically significant difference exists in the rates of MI, stroke, transient ischemic attack, coronary artery bypass graft, and percutaneous intervention. The clinical difference of fish oil and statin combination therapy vs statin monotherapy is most likely small or nonexistent. From our literature search, this is the only study concerning the use of fish oil and statin combination therapy in the veteran population. It is most likely that fish oil and statin combination therapy and statin monotherapy are similar for the reduction of time to aggregate adverse cardiovascular events and all-cause mortality in the veteran population.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Fargo VA Healthcare System.
The Centers for Disease Control and Prevention lists cardiovascular-related diseases as a leading cause of mortality.1 The medication class of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors, more commonly known as statins, is first-line therapy to prevent negative cardiovascular outcomes and reduce premature death.2 Additional hyperlipidemia medications, such as fish oil, can be added for potential cardiovascular benefit.
Yokoyama and colleagues demonstrated that fish oil is a promising treatment for the prevention of major coronary events in patients with hypercholesterolemia.3 Furthermore, Macchia and colleagues found reductions in cardiovascular outcomes and all-cause mortality in postmyocardial infarction patients treated with fish oil and statin combination therapy.4 In contrast, the Outcomes Reduction with an Initial Glargine Intervention (ORIGIN) trial found glucose intolerant and patients with diabetes mellitus did not have improved cardiovascular outcomes with fish oil therapy.5 Likewise The Risk and Prevention Study Collaborative Group found fish oil supplementation provided no benefit for primary prevention in patients with multiple cardiovascular risk factors.6 These studies demonstrate fish oil therapy can cause diverse cardiovascular outcomes in different patient populations.
Currently, there are no studies examining the impact of fish oil and statin combination therapy on the US veteran population. The research of Yokoyama, Macchia, and The Risk and Prevention Study Collaborative Group took place in Japanese and Italian populations, which impacts their external validity.
This study aims to help the US Department of Veterans Affairs (VA) primary care providers and clinical pharmacists address the role of fish oil and statin combination therapy in the prevention of cardiovascular disease and all-cause mortality in the veteran population. The addition of fish oil to statin therapy was compared with an established standard of care, statin monotherapy, in veterans at the Fargo Veterans Affairs Health Care System (FVAHCS).
Methods
A retrospective chart review was conducted using the FVAHCS Computerized Patient Record System (CPRS). The institution’s review board and VA medical center approved the study. Eligible veterans with prescriptions for fish oil or statin therapy between January 1, 2000 and September 30, 2015 were randomly selected, reviewed, and sorted based on inclusion and exclusion criteria.
The primary outcome was time to aggregate cardiovascular events, specifically myocardial infarction (MI), stroke, transient ischemic attack, coronary artery bypass graft, and percutaneous intervention. Adverse cardiovascular event data were obtained from the veterans’ International Classification of Disease (ICD) 9 codes. Furthermore, the secondary outcome—time to all-cause mortality—was gathered by death records in CPRS. Time to these events was compared in veterans on fish oil and statin combination therapy or statin monotherapy. The date of the cardiovascular event or death was recorded for each outcome and was obtained by reviewing provider notes that documented the incidence. If a specific day or month of incidence was not documented, July 1 was selected as the default date for the adverse cardiovascular event.
Demographics, medication adherence, diagnoses, lab values within 90 days of initiation of therapy, and primary and secondary outcomes were collected. Demographics that included age, race, and sex all were obtained via chart review. Diagnoses were gathered using ICD 9 codes. Refill history was retrieved to assess adherence. Adherence was calculated by the total days of medication therapy divided by the total days within the study. Total days in the study was calculated by the duration of therapy days between therapy initiation date and a terminating factor. Terminating factors included an adverse cardiovascular event, death, or the study termination date.
Statistics
Demographic and other cohort characterization variables were compared either by a t test, rank sum test, or Fisher exact test given the character of the variable. Kaplan Meier analysis was used to evaluate time to aggregate cardiovascular events and all-cause mortality. VA Informatics and Computing Infrastructure (VINCI) R 3.4.3 was used for data analysis. One of the few combination studies by Macchia and colleagues gave an estimate of unadjusted incident rates for patients treated with statin monotherapy vs fish oil and statin combination therapy in patients having a recent MI.4 Based on this information, a power analysis determined that a 2% difference in incidence rate of adverse cardiovascular events could be detected between the 2 cohorts with 1,000 veterans in the statin cohort, and 500 veterans in the fish oil and statin cohort assuming a time to event interval of about 7.5 years. An α level of 0.05 was set to determine statistical significance.
Results
A total of 3,940 veterans with prescriptions for fish oil or statin therapy were randomly reviewed and sorted based on inclusion and exclusion criteria. This inclusion criteria resulted in 2,575 fish oil and statin combination patients and 1,365 statin monotherapy patients. Exclusion criteria produced a final total of 437 fish oil and statin combination patients and 559 statin monotherapy patients. Patient demographics are presented in Table 3.
All baseline laboratory data were collected within 90 days of therapy initiation (Table 4). Statin monotherapy patients had lower triglyceride levels compared with those of the fish oil and statin combination patients. However, both high-density lipoprotein (HDL) and low-density lipoprotein (LDL) levels were higher in the statin monotherapy patients. As seen in Table 5, diagnosis of heart failure, hypertension, hypothyroidism, and dyslipidemia were higher in the statin monotherapy cohort, while tobacco use and pancreatitis were more prevalent in the fish oil and statin combination cohort.
Kaplan Meier curves of the primary outcome, time to aggregate adverse cardiovascular event, and the secondary outcome, time to all-cause mortality are shown in Figure 1 and Figure 2, respectively. This shows adverse cardiovascular events and all-cause mortality for approximately 4,500 days for the fish oil and statin cohort and approximately 6,000 days for the statin monotherapy cohort.
Discussion
Analysis of this study failed to detect a statistically significant difference for time to aggregate adverse cardiovascular events or all-cause mortality. This may be due to fewer adverse cardiovascular events and mortality in the 2 cohorts than was anticipated.
There are no studies examining fish oil and statin therapy in the veteran population and only limited studies comparing statin and fish oil combination therapy vs statin monotherapy for adverse cardiovascular outcomes and all-cause mortality. One of the few comparison studies was by Macchia and colleagues and consisted of 7,924 post MI patients in Italy. Over a 4-year period, researchers found a slight improvement in the adjusted paired-matched population for all-cause mortality in the fish oil and statin therapy cohort vs statin monotherapy (8.6% vs 13.6% P < .001).3 A benefit also was seen in the fish oil and statin cohort vs statin monotherapy in the adjusted paired-matched population for death or stroke (16.7% vs 11.5% P < .001).3
In contrast, this study did not address postmyocardial infarction patients exclusively. Rather, patients in this study had lower morbidity, which resulted in fewer adverse cardiovascular outcomes and a greater difficulty to detect a difference in this healthier population. These healthier patients may derive less benefit from primary or secondary prevention with statin and fish oil combination therapy.
In this study, there were extensive inclusion and exclusion criteria to assess the relationship between the cohorts for
Comparison of demographic data showed both cohorts were of similar age, sex, and race. Of note the Fargo veteran population was primarily white (> 80% in both cohorts). This is slightly higher than the percentage of whites for all US veterans. The slight difference most likely had a minimal clinical impact. Laboratory values recorded within 90 days of initiation of therapy were largely clinically similar except for triglycerides being significantly higher in the fish oil and statin combination cohort (Table 4). This may reflect selection bias, where providers may be more likely to add fish oil therapy for the potential to further control triglycerides.
Diagnoses of hypertension, heart failure, and dyslipidemia were higher in the statin monotherapy cohort. However, body mass index, tobacco use, and pancreatitis were statistically higher in fish oil and statin combination cohort. Even though there was a statistically significant difference in disease diagnoses, this likely created a minor clinical difference between the groups. This is further illustrated by the similarity of the Charlson Comorbidity Index of 1.6 for fish oil and statin cohort and 1.4 in statin monotherapy cohort.
Strengths
A strength of this study was its adherence rates. Adherence rates were high in both cohorts (Table 6). Fish oil and statin cohort did have slightly lower adherence compared with that of statin monotherapy. This may demonstrate extra pill burden influencing adherence. Overall demographics, laboratory values, disease, and adherence rates were clinically similar in both cohorts, thus reducing the potential for confounders.
Limitations
Limitations of this study include its retrospective chart review design. This design is susceptible to incorrect recording of events. The primary outcome, aggregate adverse cardiovascular events, may have been incorrectly recorded in the medical record as other diseases, such as coronary artery disease or heart disease, and therefore not captured by ICD 9 code retrieval. Also, important information, such as laboratory data, disease, and medication adherence, may not have been documented for all patients. Of note 1 patient in the fish oil and statin combination cohort did not have any recorded laboratory data, disease, or adherence data.
Another limitation is lack of access to medical notes from non-VA providers, which can result in missed data collection. To reduce this limitation, the study excluded veterans that received non-VA fish oil, statins, or other hyperlipidemia medications for > 1 year. Veterans were included only if they used VA-provided fish oil or statins. This inclusion and exclusion criteria reduced the chance of missing data from other facilities because it favored inclusion of only subjects that received care exclusively through the VA.
Last, on study initiation it was not realized that fish oil was not provided by the health care system until about the year 2004. This resulted in less risk days for the fish oil and statin cohort. However, Kaplan Meier analysis lessens this issue from being a confounder. Time to event rates for both the primary and secondary outcomes were similar and most likely would have continued to trend together with the same therapy duration.
Conclusion
Fish oil and statin combination therapy when compared with statin monotherapy failed to show that a statistically significant difference exists in the rates of MI, stroke, transient ischemic attack, coronary artery bypass graft, and percutaneous intervention. The clinical difference of fish oil and statin combination therapy vs statin monotherapy is most likely small or nonexistent. From our literature search, this is the only study concerning the use of fish oil and statin combination therapy in the veteran population. It is most likely that fish oil and statin combination therapy and statin monotherapy are similar for the reduction of time to aggregate adverse cardiovascular events and all-cause mortality in the veteran population.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Fargo VA Healthcare System.
1. Kochanek KD, Murphy SL, Xu J, Tejada-Vera B. Deaths: final data for 2014. https://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_04.pdf. Published June 30, 2016. Accessed July 26, 2018.
2. Stone NJ, Robinson JG, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.
3. Yokoyama M, Origasa H, Matsuzaki M, et al; Japan EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet. 2007;369(9567):1090-1098.
4. Macchia A, Romero M, D’Ettorre A, Tognoni G, Mariani J. Exploratory analysis on the use of statins with or without n-3 PUFA and major events in patients discharged for acute myocardial infarction: an observational retrospective study. PLoS One. 2013;8(5):e62772.
5. ORIGIN Trial Investigators, Bosch J, Gerstein HC, et al. n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N Engl J Med. 2012;367(4):309-318.
6. The Risk and Prevention Study Collaborative Group, Roncaglioni MC, Tombesi M, et al. n-3 fatty acids in patients with multiple cardiovascular risk factors. N Engl J Med. 2013;368(19):1800-1808.
7. Rizos EC, Ntzani EE, Bika E, Kostapanos MS, Elisaf MS. Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: a systematic review and meta-analysis. JAMA. 2012;308(10):1024-1033.
1. Kochanek KD, Murphy SL, Xu J, Tejada-Vera B. Deaths: final data for 2014. https://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_04.pdf. Published June 30, 2016. Accessed July 26, 2018.
2. Stone NJ, Robinson JG, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.
3. Yokoyama M, Origasa H, Matsuzaki M, et al; Japan EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet. 2007;369(9567):1090-1098.
4. Macchia A, Romero M, D’Ettorre A, Tognoni G, Mariani J. Exploratory analysis on the use of statins with or without n-3 PUFA and major events in patients discharged for acute myocardial infarction: an observational retrospective study. PLoS One. 2013;8(5):e62772.
5. ORIGIN Trial Investigators, Bosch J, Gerstein HC, et al. n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N Engl J Med. 2012;367(4):309-318.
6. The Risk and Prevention Study Collaborative Group, Roncaglioni MC, Tombesi M, et al. n-3 fatty acids in patients with multiple cardiovascular risk factors. N Engl J Med. 2013;368(19):1800-1808.
7. Rizos EC, Ntzani EE, Bika E, Kostapanos MS, Elisaf MS. Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: a systematic review and meta-analysis. JAMA. 2012;308(10):1024-1033.
SPRINT: Pill burden affects ability to reach systolic BP control
CHICAGO –

“Five or more medications” meant total drug burden, both for hypertension and comorbidities. “When you are treating a patient for hypertension, you care about blood pressure, but you also need to care about” what else they are on, and their total drug burden, “because it affects their ability to get to their blood pressure goal, especially if you’re targeting intensive control,” said lead investigator Catherine Derington, PharmD, a postdoctoral fellow at the University of Colorado, Aurora.
Good old-fashioned exercise and weight loss remain potent non–pill options, she noted at the joint scientific sessions of AHA Council on Hypertension, AHA Council on Kidney in Cardiovascular Disease, and American Society of Hypertension.

The take-home message is to use more combination drugs for hypertension “to get patients on fewer pills.” Also, “eliminate drugs [patients] don’t need,” said SPRINT investigator William C. Cushman, MD, professor of medicine and physiology at the University of Tennessee, Memphis, when asked what he thought of the new findings.
SPRINT [Systolic Blood Pressure Intervention Trial] found that targeting systolic blood pressures below 120 mm Hg, as compared with less than 140 mm Hg, led to lower rates of MI, stroke, heart failure, and death from any cause.
Medication burden had no effect on patients in the 140 mm Hg group; they achieved a mean systolic blood pressure (SBP) of 136 mm Hg at 1 year, whether they were on fewer than five drugs a day or more. Hitting that target took an average of 1.8 hypertension medications.
Reaching 120 mm Hg generally took one extra drug (an average of 2.8), and the overall pill burden did matter; 2,463 patients in the intensive arm on fewer than five medications dropped their mean SBP 20 mm Hg at one year, while 1,698 taking more than five had a 15–mm Hg reduction. The group with the lower pill burden had a mean SBP of 120.6 mm Hg and those taking five or more had a mean SBP of 122.5 mm Hg. It’s a small difference but likely important.
Comorbidities in SPRINT included kidney and cardiovascular disease, among others, but the trial excluded patients with diabetes. Many patients were on statins and aspirin.
Pharmacy review is especially a good idea in the elderly.
Patients on five or more medications had higher rates of significant adverse events in the post hoc analysis (about 50% versus about 30%), including hypotension, syncope, electrolyte abnormalities, and acute kidney injury, regardless if they were in the 120–mm Hg or 140–mm Hg group.
About 45% in the intensive arm reported high adherence (Morisky Medication Adherence Scale-8 score greater than 8 at 12 months); medication burden made no difference. Oddly, in the standard-treatment arm, more patients on five or more drugs reported high adherence, 44.5% versus 38.1% among patients taking fewer,
The post hoc analysis was based on pill bottle review at baseline. Medication count did not affect hypertension treatment satisfaction, which was about 84% in the intensive and 77% in the standard arm.
There was no industry funding for the work. Dr. Derington didn’t have any disclosures.
CHICAGO –
“Five or more medications” meant total drug burden, both for hypertension and comorbidities. “When you are treating a patient for hypertension, you care about blood pressure, but you also need to care about” what else they are on, and their total drug burden, “because it affects their ability to get to their blood pressure goal, especially if you’re targeting intensive control,” said lead investigator Catherine Derington, PharmD, a postdoctoral fellow at the University of Colorado, Aurora.
Good old-fashioned exercise and weight loss remain potent non–pill options, she noted at the joint scientific sessions of AHA Council on Hypertension, AHA Council on Kidney in Cardiovascular Disease, and American Society of Hypertension.
The take-home message is to use more combination drugs for hypertension “to get patients on fewer pills.” Also, “eliminate drugs [patients] don’t need,” said SPRINT investigator William C. Cushman, MD, professor of medicine and physiology at the University of Tennessee, Memphis, when asked what he thought of the new findings.
SPRINT [Systolic Blood Pressure Intervention Trial] found that targeting systolic blood pressures below 120 mm Hg, as compared with less than 140 mm Hg, led to lower rates of MI, stroke, heart failure, and death from any cause.
Medication burden had no effect on patients in the 140 mm Hg group; they achieved a mean systolic blood pressure (SBP) of 136 mm Hg at 1 year, whether they were on fewer than five drugs a day or more. Hitting that target took an average of 1.8 hypertension medications.
Reaching 120 mm Hg generally took one extra drug (an average of 2.8), and the overall pill burden did matter; 2,463 patients in the intensive arm on fewer than five medications dropped their mean SBP 20 mm Hg at one year, while 1,698 taking more than five had a 15–mm Hg reduction. The group with the lower pill burden had a mean SBP of 120.6 mm Hg and those taking five or more had a mean SBP of 122.5 mm Hg. It’s a small difference but likely important.
Comorbidities in SPRINT included kidney and cardiovascular disease, among others, but the trial excluded patients with diabetes. Many patients were on statins and aspirin.
Pharmacy review is especially a good idea in the elderly.
Patients on five or more medications had higher rates of significant adverse events in the post hoc analysis (about 50% versus about 30%), including hypotension, syncope, electrolyte abnormalities, and acute kidney injury, regardless if they were in the 120–mm Hg or 140–mm Hg group.
About 45% in the intensive arm reported high adherence (Morisky Medication Adherence Scale-8 score greater than 8 at 12 months); medication burden made no difference. Oddly, in the standard-treatment arm, more patients on five or more drugs reported high adherence, 44.5% versus 38.1% among patients taking fewer,
The post hoc analysis was based on pill bottle review at baseline. Medication count did not affect hypertension treatment satisfaction, which was about 84% in the intensive and 77% in the standard arm.
There was no industry funding for the work. Dr. Derington didn’t have any disclosures.
CHICAGO –
“Five or more medications” meant total drug burden, both for hypertension and comorbidities. “When you are treating a patient for hypertension, you care about blood pressure, but you also need to care about” what else they are on, and their total drug burden, “because it affects their ability to get to their blood pressure goal, especially if you’re targeting intensive control,” said lead investigator Catherine Derington, PharmD, a postdoctoral fellow at the University of Colorado, Aurora.
Good old-fashioned exercise and weight loss remain potent non–pill options, she noted at the joint scientific sessions of AHA Council on Hypertension, AHA Council on Kidney in Cardiovascular Disease, and American Society of Hypertension.
The take-home message is to use more combination drugs for hypertension “to get patients on fewer pills.” Also, “eliminate drugs [patients] don’t need,” said SPRINT investigator William C. Cushman, MD, professor of medicine and physiology at the University of Tennessee, Memphis, when asked what he thought of the new findings.
SPRINT [Systolic Blood Pressure Intervention Trial] found that targeting systolic blood pressures below 120 mm Hg, as compared with less than 140 mm Hg, led to lower rates of MI, stroke, heart failure, and death from any cause.
Medication burden had no effect on patients in the 140 mm Hg group; they achieved a mean systolic blood pressure (SBP) of 136 mm Hg at 1 year, whether they were on fewer than five drugs a day or more. Hitting that target took an average of 1.8 hypertension medications.
Reaching 120 mm Hg generally took one extra drug (an average of 2.8), and the overall pill burden did matter; 2,463 patients in the intensive arm on fewer than five medications dropped their mean SBP 20 mm Hg at one year, while 1,698 taking more than five had a 15–mm Hg reduction. The group with the lower pill burden had a mean SBP of 120.6 mm Hg and those taking five or more had a mean SBP of 122.5 mm Hg. It’s a small difference but likely important.
Comorbidities in SPRINT included kidney and cardiovascular disease, among others, but the trial excluded patients with diabetes. Many patients were on statins and aspirin.
Pharmacy review is especially a good idea in the elderly.
Patients on five or more medications had higher rates of significant adverse events in the post hoc analysis (about 50% versus about 30%), including hypotension, syncope, electrolyte abnormalities, and acute kidney injury, regardless if they were in the 120–mm Hg or 140–mm Hg group.
About 45% in the intensive arm reported high adherence (Morisky Medication Adherence Scale-8 score greater than 8 at 12 months); medication burden made no difference. Oddly, in the standard-treatment arm, more patients on five or more drugs reported high adherence, 44.5% versus 38.1% among patients taking fewer,
The post hoc analysis was based on pill bottle review at baseline. Medication count did not affect hypertension treatment satisfaction, which was about 84% in the intensive and 77% in the standard arm.
There was no industry funding for the work. Dr. Derington didn’t have any disclosures.
REPORTING FROM JOINT HYPERTENSION 2018
Key clinical point: Consider overall pill burden when managing hypertension.
Major finding: Patients in the SPRINT trial were less likely to meet the intensive treatment goal – systolic blood pressure below 120 mm Hg – if they were taking five or more medications a day.
Study details: Post hoc analysis of the SPRINT trial
Disclosures: There was no industry funding, and the lead investigator didn’t have any disclosures.
Source: Derington C et al. Joint Hypertension 2018, Abstract P208.
ASPREE: What to do now about aspirin for healthy elderly people
Across-the-board use of aspirin for primary prevention is “not justified” based on the results of ASPREE as well as the equivocal results from other recent primary prevention trials, according to Prakash C. Deedwania, MD, clinical professor of medicine and chief of the cardiology division at the Veterans Affairs Medical Center/University of California San Francisco Program in Fresno.

The importance of interpreting these studies lies in the recognition that while low-risk people don’t benefit, patients who are at mid to high cardiovascular (CV) risk clearly might. Aspirin’s role in secondary prevention after an initial CV event is clearly established, Dr. Deedwania added.
In ASPREE, a randomized, double-blind, placebo-controlled trial including nearly 20,000 participants, daily aspirin increased rates of major hemorrhage and did not significantly decrease risks of cardiovascular events, death, or other outcomes in healthy elderly individuals.
Aspirin did not prolong disability-free survival, a composite endpoint that included death, dementia, and permanent physical disability, according to one of three separate reports on ASPREE that were published in the New England Journal of Medicine.
Cardiovascular disease rates were likewise not significantly different between aspirin and placebo, with a hazard ratio that ruled out the possibility of a major protective effect, lead author John J. McNeil, MBBS, PhD, of Monash University, Melbourne, said in a second report on ASPREE.
All-cause mortality was actually higher in the aspirin arm versus the placebo arm, attributable largely to an excess of cancer-related deaths, Dr. McNeil and colleagues said in their third full report in the journal. However, that mortality finding needs to be interpreted with caution, they noted, given that previous investigations have shown a protective effect of aspirin on cancer-related death.
Potential harms of “innocuous” drug
The ASPREE (Aspirin in Reducing Events in the Elderly) study evaluated the use of aspirin as primary prevention in 19,114 healthy subjects, with a median age of 74 years, enrolled at 34 centers in Australia and the United States between 2010 and 2014.
The patients, who did not have cardiovascular disease, dementia, or disability at baseline, were randomized to daily 100-mg enteric-coated aspirin or placebo.
The rate of death, dementia, or disability was 21.5 events per 1,000 person-years in the aspirin group, and 21.2 events per 1,000 person-years in the placebo group, with a hazard ratio of 1.01 (95% confidence interval, 0.92-1.11; P = .79), Dr. McNeil and colleagues reported.
The rate of major hemorrhage was 8.6 events per 1,000 person-years for aspirin versus 6.2 events per 1,000 person years for placebo (HR, 1.38; 95% CI, 1.18-1.62; P less than .001), investigators found.
Cardiovascular outcomes: expectations vs. reality
Investigators said they thought they might see a significant cardiovascular benefit of aspirin in ASPREE based on earlier studies and meta-analyses that suggested a benefit in other populations. However, the rate of cardiovascular disease at 4.7 years of follow-up was 10.7 events per 1,000 person-years for aspirin, and 11.3 per 1,000 person years for placebo (HR, 0.95; 95% CI, 0.83-1.08).
That hazard ratio “rules out the possibility of a major protective effect of aspirin but is compatible with a more modest lowering of risk of up to 17%,” Dr. McNeil and colleagues wrote.
The results are consistent with those of a recent meta-analysis including eight primary prevention trials, mainly in adults under 70 years of age. That analysis found a 17% reduction in nonfatal myocardial infarction risk, a 14% reduction in stroke risk, and a higher risk of serious bleeding for aspirin versus control groups.
Results of ASPREE have to be interpreted in light of event rates, which were much lower than the expected 22.4 events per 1,000 person-years, they added. The low event rate probably reflects both the relatively good health of the study subjects, and the declining rates of cardiovascular disease in recent years, they said.
“Because of these factors, the absolute benefit that results from any proportionally lower rate of cardiovascular disease may be less than the benefit observed in studies from previous decades and is less likely than it had been to outweigh the risk of adverse events from aspirin,” investigators said in their report.
Current guidelines state that the evidence is limited for use of aspirin as primary prevention of cardiovascular disease in the elderly. “Nevertheless, many millions of relatively healthy older persons in the United States and Australia take low-dose aspirin with the assumption that it will reduce the likelihood of future cardiovascular disease and stroke,” study authors said in a discussion of the results.
Excess deaths explored
There were also no significant differences between arms for the endpoints of death, dementia, or disability evaluated separately. However, the rate of death by any cause was numerically higher in the aspirin group versus the placebo group, at 12.7 and 11.1 events per 1,000 person-years, respectively (HR, 1.14; 95% CI, 1.01-1.29).
Cancer was the major contributor to the imbalance in deaths, ASPREE results show, at 1.6 excess deaths per 1,000 person-years. A total of 3.1% of patients in the aspirin group had cancer-related deaths, compared with 2.3% in the placebo arm of the trial (HR, 1.31; 95% CI, 1.10-1.56).
Mortality related to major hemorrhage contributed “only minimally” to the excess in deaths, investigators added in their report.
The finding of excess deaths in the aspirin arm of ASPREE contrasts with meta-analyses of previous prevention trials. According to investigators, those studies show a protective effect of aspirin on cancer-related death that is apparent after 4-5 years of continuous treatment.
Various cellular and molecular pathways relevant to cancer development, progression, and spread are influenced by aspirin, previous studies show.
“Questions may therefore arise about whether the biology of cancer differs among age groups with regard to the frequency of common molecular patterns, metastatic behavior, and treatment responses,” Dr. McNeil and coauthors wrote in their report.
Dr. McNeil reported nonfinancial support from Bayer received during the conduct of the study.
SOURCE: McNeil JJ et al. N Engl J Med. 2018 Sep 16.
Across-the-board use of aspirin for primary prevention is “not justified” based on the results of ASPREE as well as the equivocal results from other recent primary prevention trials, according to Prakash C. Deedwania, MD, clinical professor of medicine and chief of the cardiology division at the Veterans Affairs Medical Center/University of California San Francisco Program in Fresno.
The importance of interpreting these studies lies in the recognition that while low-risk people don’t benefit, patients who are at mid to high cardiovascular (CV) risk clearly might. Aspirin’s role in secondary prevention after an initial CV event is clearly established, Dr. Deedwania added.
In ASPREE, a randomized, double-blind, placebo-controlled trial including nearly 20,000 participants, daily aspirin increased rates of major hemorrhage and did not significantly decrease risks of cardiovascular events, death, or other outcomes in healthy elderly individuals.
Aspirin did not prolong disability-free survival, a composite endpoint that included death, dementia, and permanent physical disability, according to one of three separate reports on ASPREE that were published in the New England Journal of Medicine.
Cardiovascular disease rates were likewise not significantly different between aspirin and placebo, with a hazard ratio that ruled out the possibility of a major protective effect, lead author John J. McNeil, MBBS, PhD, of Monash University, Melbourne, said in a second report on ASPREE.
All-cause mortality was actually higher in the aspirin arm versus the placebo arm, attributable largely to an excess of cancer-related deaths, Dr. McNeil and colleagues said in their third full report in the journal. However, that mortality finding needs to be interpreted with caution, they noted, given that previous investigations have shown a protective effect of aspirin on cancer-related death.
Potential harms of “innocuous” drug
The ASPREE (Aspirin in Reducing Events in the Elderly) study evaluated the use of aspirin as primary prevention in 19,114 healthy subjects, with a median age of 74 years, enrolled at 34 centers in Australia and the United States between 2010 and 2014.
The patients, who did not have cardiovascular disease, dementia, or disability at baseline, were randomized to daily 100-mg enteric-coated aspirin or placebo.
The rate of death, dementia, or disability was 21.5 events per 1,000 person-years in the aspirin group, and 21.2 events per 1,000 person-years in the placebo group, with a hazard ratio of 1.01 (95% confidence interval, 0.92-1.11; P = .79), Dr. McNeil and colleagues reported.
The rate of major hemorrhage was 8.6 events per 1,000 person-years for aspirin versus 6.2 events per 1,000 person years for placebo (HR, 1.38; 95% CI, 1.18-1.62; P less than .001), investigators found.
Cardiovascular outcomes: expectations vs. reality
Investigators said they thought they might see a significant cardiovascular benefit of aspirin in ASPREE based on earlier studies and meta-analyses that suggested a benefit in other populations. However, the rate of cardiovascular disease at 4.7 years of follow-up was 10.7 events per 1,000 person-years for aspirin, and 11.3 per 1,000 person years for placebo (HR, 0.95; 95% CI, 0.83-1.08).
That hazard ratio “rules out the possibility of a major protective effect of aspirin but is compatible with a more modest lowering of risk of up to 17%,” Dr. McNeil and colleagues wrote.
The results are consistent with those of a recent meta-analysis including eight primary prevention trials, mainly in adults under 70 years of age. That analysis found a 17% reduction in nonfatal myocardial infarction risk, a 14% reduction in stroke risk, and a higher risk of serious bleeding for aspirin versus control groups.
Results of ASPREE have to be interpreted in light of event rates, which were much lower than the expected 22.4 events per 1,000 person-years, they added. The low event rate probably reflects both the relatively good health of the study subjects, and the declining rates of cardiovascular disease in recent years, they said.
“Because of these factors, the absolute benefit that results from any proportionally lower rate of cardiovascular disease may be less than the benefit observed in studies from previous decades and is less likely than it had been to outweigh the risk of adverse events from aspirin,” investigators said in their report.
Current guidelines state that the evidence is limited for use of aspirin as primary prevention of cardiovascular disease in the elderly. “Nevertheless, many millions of relatively healthy older persons in the United States and Australia take low-dose aspirin with the assumption that it will reduce the likelihood of future cardiovascular disease and stroke,” study authors said in a discussion of the results.
Excess deaths explored
There were also no significant differences between arms for the endpoints of death, dementia, or disability evaluated separately. However, the rate of death by any cause was numerically higher in the aspirin group versus the placebo group, at 12.7 and 11.1 events per 1,000 person-years, respectively (HR, 1.14; 95% CI, 1.01-1.29).
Cancer was the major contributor to the imbalance in deaths, ASPREE results show, at 1.6 excess deaths per 1,000 person-years. A total of 3.1% of patients in the aspirin group had cancer-related deaths, compared with 2.3% in the placebo arm of the trial (HR, 1.31; 95% CI, 1.10-1.56).
Mortality related to major hemorrhage contributed “only minimally” to the excess in deaths, investigators added in their report.
The finding of excess deaths in the aspirin arm of ASPREE contrasts with meta-analyses of previous prevention trials. According to investigators, those studies show a protective effect of aspirin on cancer-related death that is apparent after 4-5 years of continuous treatment.
Various cellular and molecular pathways relevant to cancer development, progression, and spread are influenced by aspirin, previous studies show.
“Questions may therefore arise about whether the biology of cancer differs among age groups with regard to the frequency of common molecular patterns, metastatic behavior, and treatment responses,” Dr. McNeil and coauthors wrote in their report.
Dr. McNeil reported nonfinancial support from Bayer received during the conduct of the study.
SOURCE: McNeil JJ et al. N Engl J Med. 2018 Sep 16.
Across-the-board use of aspirin for primary prevention is “not justified” based on the results of ASPREE as well as the equivocal results from other recent primary prevention trials, according to Prakash C. Deedwania, MD, clinical professor of medicine and chief of the cardiology division at the Veterans Affairs Medical Center/University of California San Francisco Program in Fresno.
The importance of interpreting these studies lies in the recognition that while low-risk people don’t benefit, patients who are at mid to high cardiovascular (CV) risk clearly might. Aspirin’s role in secondary prevention after an initial CV event is clearly established, Dr. Deedwania added.
In ASPREE, a randomized, double-blind, placebo-controlled trial including nearly 20,000 participants, daily aspirin increased rates of major hemorrhage and did not significantly decrease risks of cardiovascular events, death, or other outcomes in healthy elderly individuals.
Aspirin did not prolong disability-free survival, a composite endpoint that included death, dementia, and permanent physical disability, according to one of three separate reports on ASPREE that were published in the New England Journal of Medicine.
Cardiovascular disease rates were likewise not significantly different between aspirin and placebo, with a hazard ratio that ruled out the possibility of a major protective effect, lead author John J. McNeil, MBBS, PhD, of Monash University, Melbourne, said in a second report on ASPREE.
All-cause mortality was actually higher in the aspirin arm versus the placebo arm, attributable largely to an excess of cancer-related deaths, Dr. McNeil and colleagues said in their third full report in the journal. However, that mortality finding needs to be interpreted with caution, they noted, given that previous investigations have shown a protective effect of aspirin on cancer-related death.
Potential harms of “innocuous” drug
The ASPREE (Aspirin in Reducing Events in the Elderly) study evaluated the use of aspirin as primary prevention in 19,114 healthy subjects, with a median age of 74 years, enrolled at 34 centers in Australia and the United States between 2010 and 2014.
The patients, who did not have cardiovascular disease, dementia, or disability at baseline, were randomized to daily 100-mg enteric-coated aspirin or placebo.
The rate of death, dementia, or disability was 21.5 events per 1,000 person-years in the aspirin group, and 21.2 events per 1,000 person-years in the placebo group, with a hazard ratio of 1.01 (95% confidence interval, 0.92-1.11; P = .79), Dr. McNeil and colleagues reported.
The rate of major hemorrhage was 8.6 events per 1,000 person-years for aspirin versus 6.2 events per 1,000 person years for placebo (HR, 1.38; 95% CI, 1.18-1.62; P less than .001), investigators found.
Cardiovascular outcomes: expectations vs. reality
Investigators said they thought they might see a significant cardiovascular benefit of aspirin in ASPREE based on earlier studies and meta-analyses that suggested a benefit in other populations. However, the rate of cardiovascular disease at 4.7 years of follow-up was 10.7 events per 1,000 person-years for aspirin, and 11.3 per 1,000 person years for placebo (HR, 0.95; 95% CI, 0.83-1.08).
That hazard ratio “rules out the possibility of a major protective effect of aspirin but is compatible with a more modest lowering of risk of up to 17%,” Dr. McNeil and colleagues wrote.
The results are consistent with those of a recent meta-analysis including eight primary prevention trials, mainly in adults under 70 years of age. That analysis found a 17% reduction in nonfatal myocardial infarction risk, a 14% reduction in stroke risk, and a higher risk of serious bleeding for aspirin versus control groups.
Results of ASPREE have to be interpreted in light of event rates, which were much lower than the expected 22.4 events per 1,000 person-years, they added. The low event rate probably reflects both the relatively good health of the study subjects, and the declining rates of cardiovascular disease in recent years, they said.
“Because of these factors, the absolute benefit that results from any proportionally lower rate of cardiovascular disease may be less than the benefit observed in studies from previous decades and is less likely than it had been to outweigh the risk of adverse events from aspirin,” investigators said in their report.
Current guidelines state that the evidence is limited for use of aspirin as primary prevention of cardiovascular disease in the elderly. “Nevertheless, many millions of relatively healthy older persons in the United States and Australia take low-dose aspirin with the assumption that it will reduce the likelihood of future cardiovascular disease and stroke,” study authors said in a discussion of the results.
Excess deaths explored
There were also no significant differences between arms for the endpoints of death, dementia, or disability evaluated separately. However, the rate of death by any cause was numerically higher in the aspirin group versus the placebo group, at 12.7 and 11.1 events per 1,000 person-years, respectively (HR, 1.14; 95% CI, 1.01-1.29).
Cancer was the major contributor to the imbalance in deaths, ASPREE results show, at 1.6 excess deaths per 1,000 person-years. A total of 3.1% of patients in the aspirin group had cancer-related deaths, compared with 2.3% in the placebo arm of the trial (HR, 1.31; 95% CI, 1.10-1.56).
Mortality related to major hemorrhage contributed “only minimally” to the excess in deaths, investigators added in their report.
The finding of excess deaths in the aspirin arm of ASPREE contrasts with meta-analyses of previous prevention trials. According to investigators, those studies show a protective effect of aspirin on cancer-related death that is apparent after 4-5 years of continuous treatment.
Various cellular and molecular pathways relevant to cancer development, progression, and spread are influenced by aspirin, previous studies show.
“Questions may therefore arise about whether the biology of cancer differs among age groups with regard to the frequency of common molecular patterns, metastatic behavior, and treatment responses,” Dr. McNeil and coauthors wrote in their report.
Dr. McNeil reported nonfinancial support from Bayer received during the conduct of the study.
SOURCE: McNeil JJ et al. N Engl J Med. 2018 Sep 16.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
CVD-REAL 2: Lower mortality, CV risks with SGLT-2i vs. DPP-4i treatment in T2DM
ORLANDO – according to findings from the CVD-REAL 2 study.
CVD-REAL 2 is a real-world, observational cohort study involving the analysis of health records for two matched cohorts of patients with T2DM from 12 countries across the globe, including 181,620 SGLT-2 inhibitor recipients and 181,620 DPP-4 inhibitor recipients who were newly initiated on their respective treatments between December 2012 and November 2017. The respective rates of all-cause death were 0.83 and 1.33 per 100 patient-years (4,768 events; hazard ratio, 0.51), Shun Kohsaka, MD, of Keio University School of Medicine, Tokyo, and his colleagues reported in a late-breaking poster at the annual scientific sessions of the American Diabetes Association.
“HRs for all-cause death consistently favored SGLT-2 inhibitor vs. DPP-4 inhibitor in each country,” the investigators noted. “Directionally, the same results were observed in other cardiovascular outcomes, including [hospitalization for heart failure (HHF)], and the composite of all-cause death or HHF but modestly for [myocardial infarction] and stroke.”
The rates of hospitalization for heart failure per 100 patient-years were 0.80 and 1.08 in the SGLT-2 inhibitor and DPP-4 inhibitor groups (3,875 events; HR, 0.68), and for HHF plus all-cause death, they were 1.55 and 2.22 per 100 patient-years (7,807 events; HR, 0.67), respectively. The rates of myocardial infarction in the groups, respectively, were 0.53 and 0.58 per 100 patient-years (2,298 events; HR, 0.90), and for stroke, they were 0.82 and 0.99 per 100 patient-years (3,747 events; HR, 0.84), the investigators reported.
Study subjects in both cohorts had a mean age of 58 years, and 30% and 29% in the SGLT-2 inhibitor and DPP-4 inhibitor groups, respectively, had established cardiovascular disease. Only those newly initiated on either an SGLT-2 inhibitor or DPP-4 inhibitor were selected from each data source; fixed-dose combinations were allowed as long as there was no use of either drug during the year prior to enrollment.
In the SGLT-2 inhibitor cohort, most exposures (60.1%) were to dapagliflozin, followed by canagliflozin (23.8%) and empagliflozin (12.1%). The remaining exposures were to ipragliflozin, tofogliflozin, or luseogliflozin (0.3-2.8%). In the DPP-4 inhibitor group, most exposures (49.7%) were to sitagliptin, 18.9% were to linagliptin, 10.4% were to saxagliptin, and the remaining exposures were to alogliptin, gemigliptin, teneligliptin, anagliptin, evogliptin, and trelagliptin (0.1%-4.7%).
Those in the SGLT-2 inhibitor group were followed for a mean of 439 days, and those in the DPP-4 inhibitor group were followed for a mean of 446 days.
“The results were consistent across the subgroups of patients with and without established [cardiovascular disease], favoring SGLT-2 inhibitor vs. DPP-4 inhibitor for all outcomes,” they noted.
Both DPP-4 inhibitors and SGLT2 inhibitors are widely used in T2DM, and although clinical trials demonstrated lower risk of cardiovascular events with SGLT-2 inhibitors and a neutral effect on cardiovascular events with DPP-4 inhibitors, large comparative studies are lacking, the investigators explained.
Though limited by the possibility of residual, unmeasured confounding, as well as by a lack of mortality data in Japan and Singapore apart from the inpatient setting, the findings of this “large, contemporary analysis of real-world administrative data” are complementary to those from previous observational studies and clinical trials, they concluded, noting that “SGLT-2 inhibitor experience in real-world practice is still relatively short and longer-term follow-up is required to examine whether effects are sustained over time.”
The CVD-REAL studies are sponsored by AstraZeneca. Dr. Kohsaka reported receiving research support from Bayer Yakuhin and Daiichi Sankyo and serving on the speaker’s bureau for Bayer Yakuhin and Bristol-Myers Squibb.
SOURCE: Kohsaka S et al. ADA 2018, Abstract 124-LB.
ORLANDO – according to findings from the CVD-REAL 2 study.
CVD-REAL 2 is a real-world, observational cohort study involving the analysis of health records for two matched cohorts of patients with T2DM from 12 countries across the globe, including 181,620 SGLT-2 inhibitor recipients and 181,620 DPP-4 inhibitor recipients who were newly initiated on their respective treatments between December 2012 and November 2017. The respective rates of all-cause death were 0.83 and 1.33 per 100 patient-years (4,768 events; hazard ratio, 0.51), Shun Kohsaka, MD, of Keio University School of Medicine, Tokyo, and his colleagues reported in a late-breaking poster at the annual scientific sessions of the American Diabetes Association.
“HRs for all-cause death consistently favored SGLT-2 inhibitor vs. DPP-4 inhibitor in each country,” the investigators noted. “Directionally, the same results were observed in other cardiovascular outcomes, including [hospitalization for heart failure (HHF)], and the composite of all-cause death or HHF but modestly for [myocardial infarction] and stroke.”
The rates of hospitalization for heart failure per 100 patient-years were 0.80 and 1.08 in the SGLT-2 inhibitor and DPP-4 inhibitor groups (3,875 events; HR, 0.68), and for HHF plus all-cause death, they were 1.55 and 2.22 per 100 patient-years (7,807 events; HR, 0.67), respectively. The rates of myocardial infarction in the groups, respectively, were 0.53 and 0.58 per 100 patient-years (2,298 events; HR, 0.90), and for stroke, they were 0.82 and 0.99 per 100 patient-years (3,747 events; HR, 0.84), the investigators reported.
Study subjects in both cohorts had a mean age of 58 years, and 30% and 29% in the SGLT-2 inhibitor and DPP-4 inhibitor groups, respectively, had established cardiovascular disease. Only those newly initiated on either an SGLT-2 inhibitor or DPP-4 inhibitor were selected from each data source; fixed-dose combinations were allowed as long as there was no use of either drug during the year prior to enrollment.
In the SGLT-2 inhibitor cohort, most exposures (60.1%) were to dapagliflozin, followed by canagliflozin (23.8%) and empagliflozin (12.1%). The remaining exposures were to ipragliflozin, tofogliflozin, or luseogliflozin (0.3-2.8%). In the DPP-4 inhibitor group, most exposures (49.7%) were to sitagliptin, 18.9% were to linagliptin, 10.4% were to saxagliptin, and the remaining exposures were to alogliptin, gemigliptin, teneligliptin, anagliptin, evogliptin, and trelagliptin (0.1%-4.7%).
Those in the SGLT-2 inhibitor group were followed for a mean of 439 days, and those in the DPP-4 inhibitor group were followed for a mean of 446 days.
“The results were consistent across the subgroups of patients with and without established [cardiovascular disease], favoring SGLT-2 inhibitor vs. DPP-4 inhibitor for all outcomes,” they noted.
Both DPP-4 inhibitors and SGLT2 inhibitors are widely used in T2DM, and although clinical trials demonstrated lower risk of cardiovascular events with SGLT-2 inhibitors and a neutral effect on cardiovascular events with DPP-4 inhibitors, large comparative studies are lacking, the investigators explained.
Though limited by the possibility of residual, unmeasured confounding, as well as by a lack of mortality data in Japan and Singapore apart from the inpatient setting, the findings of this “large, contemporary analysis of real-world administrative data” are complementary to those from previous observational studies and clinical trials, they concluded, noting that “SGLT-2 inhibitor experience in real-world practice is still relatively short and longer-term follow-up is required to examine whether effects are sustained over time.”
The CVD-REAL studies are sponsored by AstraZeneca. Dr. Kohsaka reported receiving research support from Bayer Yakuhin and Daiichi Sankyo and serving on the speaker’s bureau for Bayer Yakuhin and Bristol-Myers Squibb.
SOURCE: Kohsaka S et al. ADA 2018, Abstract 124-LB.
ORLANDO – according to findings from the CVD-REAL 2 study.
CVD-REAL 2 is a real-world, observational cohort study involving the analysis of health records for two matched cohorts of patients with T2DM from 12 countries across the globe, including 181,620 SGLT-2 inhibitor recipients and 181,620 DPP-4 inhibitor recipients who were newly initiated on their respective treatments between December 2012 and November 2017. The respective rates of all-cause death were 0.83 and 1.33 per 100 patient-years (4,768 events; hazard ratio, 0.51), Shun Kohsaka, MD, of Keio University School of Medicine, Tokyo, and his colleagues reported in a late-breaking poster at the annual scientific sessions of the American Diabetes Association.
“HRs for all-cause death consistently favored SGLT-2 inhibitor vs. DPP-4 inhibitor in each country,” the investigators noted. “Directionally, the same results were observed in other cardiovascular outcomes, including [hospitalization for heart failure (HHF)], and the composite of all-cause death or HHF but modestly for [myocardial infarction] and stroke.”
The rates of hospitalization for heart failure per 100 patient-years were 0.80 and 1.08 in the SGLT-2 inhibitor and DPP-4 inhibitor groups (3,875 events; HR, 0.68), and for HHF plus all-cause death, they were 1.55 and 2.22 per 100 patient-years (7,807 events; HR, 0.67), respectively. The rates of myocardial infarction in the groups, respectively, were 0.53 and 0.58 per 100 patient-years (2,298 events; HR, 0.90), and for stroke, they were 0.82 and 0.99 per 100 patient-years (3,747 events; HR, 0.84), the investigators reported.
Study subjects in both cohorts had a mean age of 58 years, and 30% and 29% in the SGLT-2 inhibitor and DPP-4 inhibitor groups, respectively, had established cardiovascular disease. Only those newly initiated on either an SGLT-2 inhibitor or DPP-4 inhibitor were selected from each data source; fixed-dose combinations were allowed as long as there was no use of either drug during the year prior to enrollment.
In the SGLT-2 inhibitor cohort, most exposures (60.1%) were to dapagliflozin, followed by canagliflozin (23.8%) and empagliflozin (12.1%). The remaining exposures were to ipragliflozin, tofogliflozin, or luseogliflozin (0.3-2.8%). In the DPP-4 inhibitor group, most exposures (49.7%) were to sitagliptin, 18.9% were to linagliptin, 10.4% were to saxagliptin, and the remaining exposures were to alogliptin, gemigliptin, teneligliptin, anagliptin, evogliptin, and trelagliptin (0.1%-4.7%).
Those in the SGLT-2 inhibitor group were followed for a mean of 439 days, and those in the DPP-4 inhibitor group were followed for a mean of 446 days.
“The results were consistent across the subgroups of patients with and without established [cardiovascular disease], favoring SGLT-2 inhibitor vs. DPP-4 inhibitor for all outcomes,” they noted.
Both DPP-4 inhibitors and SGLT2 inhibitors are widely used in T2DM, and although clinical trials demonstrated lower risk of cardiovascular events with SGLT-2 inhibitors and a neutral effect on cardiovascular events with DPP-4 inhibitors, large comparative studies are lacking, the investigators explained.
Though limited by the possibility of residual, unmeasured confounding, as well as by a lack of mortality data in Japan and Singapore apart from the inpatient setting, the findings of this “large, contemporary analysis of real-world administrative data” are complementary to those from previous observational studies and clinical trials, they concluded, noting that “SGLT-2 inhibitor experience in real-world practice is still relatively short and longer-term follow-up is required to examine whether effects are sustained over time.”
The CVD-REAL studies are sponsored by AstraZeneca. Dr. Kohsaka reported receiving research support from Bayer Yakuhin and Daiichi Sankyo and serving on the speaker’s bureau for Bayer Yakuhin and Bristol-Myers Squibb.
SOURCE: Kohsaka S et al. ADA 2018, Abstract 124-LB.
REPORTING FROM ADA 2018
Key clinical point: SGLT-2 inhibitor treatment is associated with significantly lower risks of death, CV events, and stroke in T2DM, compared with DPP-4 inhibitor treatment.
Major finding: The rates of all-cause death in the SGLT-2 inhibitor and DPP-4 inhibitor groups, respectively, were 0.83 and 1.33 per 100 patient-years (4,768 events; hazard ratio, 0.51).
Study details: A multinational, observational cohort study of more than 360,000 subjects.
Disclosures: The CVD-REAL studies are sponsored by AstraZeneca. Dr. Kohsaka reported receiving research support from Bayer Yakuhin and Daiichi Sankyo and serving on the speaker’s bureau for Bayer Yakuhin and Bristol-Myers Squibb.
Source: Kohsaka S et al. ADA 2018, Abstract 124-LB.