User login
Surgery adds little after successful chemo in metastatic breast cancer
SAN ANTONIO – In patients with metastatic breast cancer who responded favorably to initial chemotherapy, radiotherapy and surgical removal of primary tumors failed to enhance overall survival, a new study has shown.
In an interview at the San Antonio Breast Cancer Symposium, study investigator Dr. Rajendra Badwe offers his perspectives on loco-regional treatment vs. chemotherapy alone, and he discusses why surgical removal of primary tumors might be linked to later spread of metastatic disease.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – In patients with metastatic breast cancer who responded favorably to initial chemotherapy, radiotherapy and surgical removal of primary tumors failed to enhance overall survival, a new study has shown.
In an interview at the San Antonio Breast Cancer Symposium, study investigator Dr. Rajendra Badwe offers his perspectives on loco-regional treatment vs. chemotherapy alone, and he discusses why surgical removal of primary tumors might be linked to later spread of metastatic disease.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – In patients with metastatic breast cancer who responded favorably to initial chemotherapy, radiotherapy and surgical removal of primary tumors failed to enhance overall survival, a new study has shown.
In an interview at the San Antonio Breast Cancer Symposium, study investigator Dr. Rajendra Badwe offers his perspectives on loco-regional treatment vs. chemotherapy alone, and he discusses why surgical removal of primary tumors might be linked to later spread of metastatic disease.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Psychoeducation, compliance contracts curb postsurgery alcohol abuse
ATLANTA – Pre–bariatric surgery psychoeducation and compliance contracts are two ways to help lower the risk of patient alcohol abuse after surgery.
"Surgery itself changes a patient’s susceptibility to alcohol," said Leslie Heinberg, Ph.D., director of behavioral services for the Bariatric and Metabolic Institute at Cleveland Clinic. "There’s going to be increased sensitivity to alcohol and decreased tolerance," Dr. Heinberg said at Obesity Week, presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
Programs that screen and triage bariatric surgery candidates, as well as inform them of how alcohol will affect them post surgery, can help manage their risk, according to Dr. Heinberg.
"I tell patients: ‘You’re going to get drunk very easily, very quickly, and it’s going to last a very long time.’ "
Dr. Heinberg cited a case cross-over trial that showed how at 6 months post gastric bypass surgery, patients had higher postoperative peak blood alcohol content levels after drinking one 5-ounce glass of red wine, and took longer to recover than they did before surgery.
"Patients that have one glass of red wine before surgery, they’re about at .02 [blood alcohol content], and they’re legally fine," she said. "Six months after surgery, they’re legally drunk." (J. Am. Coll. Surg. 2011;212:209-14).
The physical experience of drinking alcohol changes post surgery, too. "Postop, people are more likely to report that they feel dizzy and lightheaded and have double vision," said Dr. Heinberg, also professor of medicine in the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University.
‘Addiction transfer’
Reasons for the increased susceptibility in this patient population include the change in ratio between body weight and alcohol concentration, as well as the physiologic change inherent to gastric bypass where a pouch is placed in the jejunum. "There is a bolus of alcohol that hits and hits very quickly," said Dr. Heinberg.
Another reason is that in weight-loss surgery, one of the body’s primary sources of antialcohol dehydrogenase, the stomach, has been reduced in volume, she said.
Dr. Heinberg also said new data suggest "addiction transfer," thought to be the result of the body’s shared neural pathways for compulsive eating and substance abuse, might lead to either relapse in patients with histories of alcohol abuse or new-onset alcoholism in those who may not have abused alcohol, but who were compulsive eaters (Arch. Gen. Psychiatry. 2011;68:808-16).
Risk predictors
Dr. Heinberg cited a longitudinal study showing that predictors of risk included being male; presurgery use of tobacco, alcohol, and recreational drugs; having weak social support networks; and having gastric bypass surgery rather than other surgical weight loss procedures (JAMA 2012;307:2516-25).
The "good news," said Dr. Heinberg, is that contrary to her own hypothesis, a study of 400 patients with a history of substance abuse, controlled for presurgical body mass index, surgery type, gender, and race showed that people with a history of substance abuse had lost more weight 2 years after surgery (Surg. Obes. Relat. Dis. 2012 8:357-63).

"I think people who achieve abstinence have figured out how to completely change their lifestyle," said Dr. Heinberg. "Maybe those skills that helped them quit drinking are helping them post surgery."
Improved compliance
In an online questionnaire, 84% of 318 bariatric surgery patients surveyed admitted they continued to drink after their surgery, said Dr. Heinberg. "I think it’s important to screen each and every patient for all kinds of alcohol problems."
To help ensure compliance, she suggested clinics use free screening tools and guidelines available from the National Institute on Alcohol Abuse and Alcoholism. She described various levels of psychoeducation in use at her clinic, depending upon how severe the risk per the screening.
Participants deemed by her clinic to be at greater risk are given substance risk reduction education, which includes pre- and posttests. This helps avoid patients’ claims that they were unaware of the risks of alcohol after the surgery, said Dr. Heinberg. "We just pull out the test and say, ‘You got a 100%."
In some cases, she suggested that asking a patient who is a compliance risk concern to sign a contract agreeing not to drink after the surgery might help "get around risk management."
Dr. Heinberg concluded that this is a "vulnerable" patient population that may not be aware of the risks posed by alcohol post surgery. "Most programs need to think about putting this in their informed consent and providing more psychoeducation prior to surgery, sometimes even behavioral contracts," she said.
ATLANTA – Pre–bariatric surgery psychoeducation and compliance contracts are two ways to help lower the risk of patient alcohol abuse after surgery.
"Surgery itself changes a patient’s susceptibility to alcohol," said Leslie Heinberg, Ph.D., director of behavioral services for the Bariatric and Metabolic Institute at Cleveland Clinic. "There’s going to be increased sensitivity to alcohol and decreased tolerance," Dr. Heinberg said at Obesity Week, presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
Programs that screen and triage bariatric surgery candidates, as well as inform them of how alcohol will affect them post surgery, can help manage their risk, according to Dr. Heinberg.
"I tell patients: ‘You’re going to get drunk very easily, very quickly, and it’s going to last a very long time.’ "
Dr. Heinberg cited a case cross-over trial that showed how at 6 months post gastric bypass surgery, patients had higher postoperative peak blood alcohol content levels after drinking one 5-ounce glass of red wine, and took longer to recover than they did before surgery.
"Patients that have one glass of red wine before surgery, they’re about at .02 [blood alcohol content], and they’re legally fine," she said. "Six months after surgery, they’re legally drunk." (J. Am. Coll. Surg. 2011;212:209-14).
The physical experience of drinking alcohol changes post surgery, too. "Postop, people are more likely to report that they feel dizzy and lightheaded and have double vision," said Dr. Heinberg, also professor of medicine in the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University.
‘Addiction transfer’
Reasons for the increased susceptibility in this patient population include the change in ratio between body weight and alcohol concentration, as well as the physiologic change inherent to gastric bypass where a pouch is placed in the jejunum. "There is a bolus of alcohol that hits and hits very quickly," said Dr. Heinberg.
Another reason is that in weight-loss surgery, one of the body’s primary sources of antialcohol dehydrogenase, the stomach, has been reduced in volume, she said.
Dr. Heinberg also said new data suggest "addiction transfer," thought to be the result of the body’s shared neural pathways for compulsive eating and substance abuse, might lead to either relapse in patients with histories of alcohol abuse or new-onset alcoholism in those who may not have abused alcohol, but who were compulsive eaters (Arch. Gen. Psychiatry. 2011;68:808-16).
Risk predictors
Dr. Heinberg cited a longitudinal study showing that predictors of risk included being male; presurgery use of tobacco, alcohol, and recreational drugs; having weak social support networks; and having gastric bypass surgery rather than other surgical weight loss procedures (JAMA 2012;307:2516-25).
The "good news," said Dr. Heinberg, is that contrary to her own hypothesis, a study of 400 patients with a history of substance abuse, controlled for presurgical body mass index, surgery type, gender, and race showed that people with a history of substance abuse had lost more weight 2 years after surgery (Surg. Obes. Relat. Dis. 2012 8:357-63).
"I think people who achieve abstinence have figured out how to completely change their lifestyle," said Dr. Heinberg. "Maybe those skills that helped them quit drinking are helping them post surgery."
Improved compliance
In an online questionnaire, 84% of 318 bariatric surgery patients surveyed admitted they continued to drink after their surgery, said Dr. Heinberg. "I think it’s important to screen each and every patient for all kinds of alcohol problems."
To help ensure compliance, she suggested clinics use free screening tools and guidelines available from the National Institute on Alcohol Abuse and Alcoholism. She described various levels of psychoeducation in use at her clinic, depending upon how severe the risk per the screening.
Participants deemed by her clinic to be at greater risk are given substance risk reduction education, which includes pre- and posttests. This helps avoid patients’ claims that they were unaware of the risks of alcohol after the surgery, said Dr. Heinberg. "We just pull out the test and say, ‘You got a 100%."
In some cases, she suggested that asking a patient who is a compliance risk concern to sign a contract agreeing not to drink after the surgery might help "get around risk management."
Dr. Heinberg concluded that this is a "vulnerable" patient population that may not be aware of the risks posed by alcohol post surgery. "Most programs need to think about putting this in their informed consent and providing more psychoeducation prior to surgery, sometimes even behavioral contracts," she said.
ATLANTA – Pre–bariatric surgery psychoeducation and compliance contracts are two ways to help lower the risk of patient alcohol abuse after surgery.
"Surgery itself changes a patient’s susceptibility to alcohol," said Leslie Heinberg, Ph.D., director of behavioral services for the Bariatric and Metabolic Institute at Cleveland Clinic. "There’s going to be increased sensitivity to alcohol and decreased tolerance," Dr. Heinberg said at Obesity Week, presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
Programs that screen and triage bariatric surgery candidates, as well as inform them of how alcohol will affect them post surgery, can help manage their risk, according to Dr. Heinberg.
"I tell patients: ‘You’re going to get drunk very easily, very quickly, and it’s going to last a very long time.’ "
Dr. Heinberg cited a case cross-over trial that showed how at 6 months post gastric bypass surgery, patients had higher postoperative peak blood alcohol content levels after drinking one 5-ounce glass of red wine, and took longer to recover than they did before surgery.
"Patients that have one glass of red wine before surgery, they’re about at .02 [blood alcohol content], and they’re legally fine," she said. "Six months after surgery, they’re legally drunk." (J. Am. Coll. Surg. 2011;212:209-14).
The physical experience of drinking alcohol changes post surgery, too. "Postop, people are more likely to report that they feel dizzy and lightheaded and have double vision," said Dr. Heinberg, also professor of medicine in the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University.
‘Addiction transfer’
Reasons for the increased susceptibility in this patient population include the change in ratio between body weight and alcohol concentration, as well as the physiologic change inherent to gastric bypass where a pouch is placed in the jejunum. "There is a bolus of alcohol that hits and hits very quickly," said Dr. Heinberg.
Another reason is that in weight-loss surgery, one of the body’s primary sources of antialcohol dehydrogenase, the stomach, has been reduced in volume, she said.
Dr. Heinberg also said new data suggest "addiction transfer," thought to be the result of the body’s shared neural pathways for compulsive eating and substance abuse, might lead to either relapse in patients with histories of alcohol abuse or new-onset alcoholism in those who may not have abused alcohol, but who were compulsive eaters (Arch. Gen. Psychiatry. 2011;68:808-16).
Risk predictors
Dr. Heinberg cited a longitudinal study showing that predictors of risk included being male; presurgery use of tobacco, alcohol, and recreational drugs; having weak social support networks; and having gastric bypass surgery rather than other surgical weight loss procedures (JAMA 2012;307:2516-25).
The "good news," said Dr. Heinberg, is that contrary to her own hypothesis, a study of 400 patients with a history of substance abuse, controlled for presurgical body mass index, surgery type, gender, and race showed that people with a history of substance abuse had lost more weight 2 years after surgery (Surg. Obes. Relat. Dis. 2012 8:357-63).
"I think people who achieve abstinence have figured out how to completely change their lifestyle," said Dr. Heinberg. "Maybe those skills that helped them quit drinking are helping them post surgery."
Improved compliance
In an online questionnaire, 84% of 318 bariatric surgery patients surveyed admitted they continued to drink after their surgery, said Dr. Heinberg. "I think it’s important to screen each and every patient for all kinds of alcohol problems."
To help ensure compliance, she suggested clinics use free screening tools and guidelines available from the National Institute on Alcohol Abuse and Alcoholism. She described various levels of psychoeducation in use at her clinic, depending upon how severe the risk per the screening.
Participants deemed by her clinic to be at greater risk are given substance risk reduction education, which includes pre- and posttests. This helps avoid patients’ claims that they were unaware of the risks of alcohol after the surgery, said Dr. Heinberg. "We just pull out the test and say, ‘You got a 100%."
In some cases, she suggested that asking a patient who is a compliance risk concern to sign a contract agreeing not to drink after the surgery might help "get around risk management."
Dr. Heinberg concluded that this is a "vulnerable" patient population that may not be aware of the risks posed by alcohol post surgery. "Most programs need to think about putting this in their informed consent and providing more psychoeducation prior to surgery, sometimes even behavioral contracts," she said.
EXPERT ANALYSIS FROM OBESITY WEEK

Radiotherapy can be omitted for many older breast cancer patients
SAN ANTONIO – Avoiding whole-breast radiation therapy is a reasonable – and even attractive – option for many older women with early-stage breast cancer, according to the results of the Postoperative Radiotherapy in Minimum-Risk Elderly (PRIME II) trial.
The patient population identified in PRIME II as being suitable for omission of postoperative radiotherapy on the basis of a relatively benign natural history consists of women aged 65 or older who are on adjuvant hormone therapy after undergoing lumpectomy with clear margins for estrogen receptor–rich, axillary node–negative breast cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PRIME II was a six-country trial in which 1,326 patients 65 or older with hormone receptor–positive early breast cancer were randomized to radiotherapy or no radiotherapy following breast-conserving surgery and endocrine therapy. The 5-year actuarial rate of ipsilateral breast cancer recurrence – the primary study endpoint – was 1.3% in those who received radiotherapy and 4.1% in those who did not, Dr. Ian H. Kunkler reported at the San Antonio Breast Cancer Symposium.
The 5-year actuarial rate of overall survival was 94.2% in patients randomized to radiotherapy and closely similar at 93.8% in the no-radiotherapy group, added Dr. Kunkler, professor of clinical oncology at the University of Edinburgh.
The relative benefit of radiotherapy was even smaller in the 91% of subjects who had estrogen-rich tumors as defined by an ER score of at least 7. They had a local recurrence rate of 3.2% with radiotherapy and 0.8% without. While that absolute 2.4% difference was statistically significant, it is arguably not clinically meaningful. For every 100 women who fit the description carefully defined in PRIME II and who undergo radiotherapy, three will have a recurrence prevented, one will have a recurrence anyway, and 96 will have had treatment that was not beneficial, he said.

"I think we’re really at the cusp of overtreatment here. I think it’s a matter for discussion between the physician and patient as to whether that very modest benefit is worth the potential complications of radiotherapy and the burdens of ongoing treatment, as well as the costs to the health service. Older patients find radiotherapy very burdensome, the relative benefits are very small, and there is no compromise in terms of overall survival with its omission," Dr. Kunkler said.
An important caveat: Among the 9% of patients with low estrogen receptor status, the local recurrence rate was 11.1% with no radiotherapy compared to zero with radiation.
"This is a group for whom radiotherapy should not be omitted," Dr. Kunkler declared.
More than one-half of all early breast cancers present in women aged 65 or older. While postoperative radiotherapy after lumpectomy has been the standard of care regardless of age and other risk factors, there has been only sparse high-quality supporting evidence for this practice in older patients.
Dr. Kunkler estimated that the PRIME II findings are generalizable to 60%-70% of all breast cancer patients over age 65. He predicted that the PRIME II study will "very likely" alter practice in the United Kingdom, and symposium codirector Dr. C. Kent Osborne predicted that the study will be practice changing in the United States as well.

"When I was in training, everybody thought that more was better: more drug treatment, more radiation, more surgery, high-dose chemotherapy, and bone marrow transplant. As we’ve evolved over the last 3 decades, that’s turning out not to be the case. I think we’re gradually doing less and less treatment, either with radiotherapy or with surgery, to control the local disease in appropriate patients. And I think more and more people will begin to accept it," said Dr. Osborne, director of the Dan L. Duncan Cancer Center and the Lester and Sue Smith Breast Center at Baylor College of Medicine, Houston.
PRIME II was funded by the Chief Scientist Office for Scotland. Dr. Kunkler declared having no conflicts of interest.
SAN ANTONIO – Avoiding whole-breast radiation therapy is a reasonable – and even attractive – option for many older women with early-stage breast cancer, according to the results of the Postoperative Radiotherapy in Minimum-Risk Elderly (PRIME II) trial.
The patient population identified in PRIME II as being suitable for omission of postoperative radiotherapy on the basis of a relatively benign natural history consists of women aged 65 or older who are on adjuvant hormone therapy after undergoing lumpectomy with clear margins for estrogen receptor–rich, axillary node–negative breast cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PRIME II was a six-country trial in which 1,326 patients 65 or older with hormone receptor–positive early breast cancer were randomized to radiotherapy or no radiotherapy following breast-conserving surgery and endocrine therapy. The 5-year actuarial rate of ipsilateral breast cancer recurrence – the primary study endpoint – was 1.3% in those who received radiotherapy and 4.1% in those who did not, Dr. Ian H. Kunkler reported at the San Antonio Breast Cancer Symposium.
The 5-year actuarial rate of overall survival was 94.2% in patients randomized to radiotherapy and closely similar at 93.8% in the no-radiotherapy group, added Dr. Kunkler, professor of clinical oncology at the University of Edinburgh.
The relative benefit of radiotherapy was even smaller in the 91% of subjects who had estrogen-rich tumors as defined by an ER score of at least 7. They had a local recurrence rate of 3.2% with radiotherapy and 0.8% without. While that absolute 2.4% difference was statistically significant, it is arguably not clinically meaningful. For every 100 women who fit the description carefully defined in PRIME II and who undergo radiotherapy, three will have a recurrence prevented, one will have a recurrence anyway, and 96 will have had treatment that was not beneficial, he said.
"I think we’re really at the cusp of overtreatment here. I think it’s a matter for discussion between the physician and patient as to whether that very modest benefit is worth the potential complications of radiotherapy and the burdens of ongoing treatment, as well as the costs to the health service. Older patients find radiotherapy very burdensome, the relative benefits are very small, and there is no compromise in terms of overall survival with its omission," Dr. Kunkler said.
An important caveat: Among the 9% of patients with low estrogen receptor status, the local recurrence rate was 11.1% with no radiotherapy compared to zero with radiation.
"This is a group for whom radiotherapy should not be omitted," Dr. Kunkler declared.
More than one-half of all early breast cancers present in women aged 65 or older. While postoperative radiotherapy after lumpectomy has been the standard of care regardless of age and other risk factors, there has been only sparse high-quality supporting evidence for this practice in older patients.
Dr. Kunkler estimated that the PRIME II findings are generalizable to 60%-70% of all breast cancer patients over age 65. He predicted that the PRIME II study will "very likely" alter practice in the United Kingdom, and symposium codirector Dr. C. Kent Osborne predicted that the study will be practice changing in the United States as well.
"When I was in training, everybody thought that more was better: more drug treatment, more radiation, more surgery, high-dose chemotherapy, and bone marrow transplant. As we’ve evolved over the last 3 decades, that’s turning out not to be the case. I think we’re gradually doing less and less treatment, either with radiotherapy or with surgery, to control the local disease in appropriate patients. And I think more and more people will begin to accept it," said Dr. Osborne, director of the Dan L. Duncan Cancer Center and the Lester and Sue Smith Breast Center at Baylor College of Medicine, Houston.
PRIME II was funded by the Chief Scientist Office for Scotland. Dr. Kunkler declared having no conflicts of interest.
SAN ANTONIO – Avoiding whole-breast radiation therapy is a reasonable – and even attractive – option for many older women with early-stage breast cancer, according to the results of the Postoperative Radiotherapy in Minimum-Risk Elderly (PRIME II) trial.
The patient population identified in PRIME II as being suitable for omission of postoperative radiotherapy on the basis of a relatively benign natural history consists of women aged 65 or older who are on adjuvant hormone therapy after undergoing lumpectomy with clear margins for estrogen receptor–rich, axillary node–negative breast cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PRIME II was a six-country trial in which 1,326 patients 65 or older with hormone receptor–positive early breast cancer were randomized to radiotherapy or no radiotherapy following breast-conserving surgery and endocrine therapy. The 5-year actuarial rate of ipsilateral breast cancer recurrence – the primary study endpoint – was 1.3% in those who received radiotherapy and 4.1% in those who did not, Dr. Ian H. Kunkler reported at the San Antonio Breast Cancer Symposium.
The 5-year actuarial rate of overall survival was 94.2% in patients randomized to radiotherapy and closely similar at 93.8% in the no-radiotherapy group, added Dr. Kunkler, professor of clinical oncology at the University of Edinburgh.
The relative benefit of radiotherapy was even smaller in the 91% of subjects who had estrogen-rich tumors as defined by an ER score of at least 7. They had a local recurrence rate of 3.2% with radiotherapy and 0.8% without. While that absolute 2.4% difference was statistically significant, it is arguably not clinically meaningful. For every 100 women who fit the description carefully defined in PRIME II and who undergo radiotherapy, three will have a recurrence prevented, one will have a recurrence anyway, and 96 will have had treatment that was not beneficial, he said.
"I think we’re really at the cusp of overtreatment here. I think it’s a matter for discussion between the physician and patient as to whether that very modest benefit is worth the potential complications of radiotherapy and the burdens of ongoing treatment, as well as the costs to the health service. Older patients find radiotherapy very burdensome, the relative benefits are very small, and there is no compromise in terms of overall survival with its omission," Dr. Kunkler said.
An important caveat: Among the 9% of patients with low estrogen receptor status, the local recurrence rate was 11.1% with no radiotherapy compared to zero with radiation.
"This is a group for whom radiotherapy should not be omitted," Dr. Kunkler declared.
More than one-half of all early breast cancers present in women aged 65 or older. While postoperative radiotherapy after lumpectomy has been the standard of care regardless of age and other risk factors, there has been only sparse high-quality supporting evidence for this practice in older patients.
Dr. Kunkler estimated that the PRIME II findings are generalizable to 60%-70% of all breast cancer patients over age 65. He predicted that the PRIME II study will "very likely" alter practice in the United Kingdom, and symposium codirector Dr. C. Kent Osborne predicted that the study will be practice changing in the United States as well.
"When I was in training, everybody thought that more was better: more drug treatment, more radiation, more surgery, high-dose chemotherapy, and bone marrow transplant. As we’ve evolved over the last 3 decades, that’s turning out not to be the case. I think we’re gradually doing less and less treatment, either with radiotherapy or with surgery, to control the local disease in appropriate patients. And I think more and more people will begin to accept it," said Dr. Osborne, director of the Dan L. Duncan Cancer Center and the Lester and Sue Smith Breast Center at Baylor College of Medicine, Houston.
PRIME II was funded by the Chief Scientist Office for Scotland. Dr. Kunkler declared having no conflicts of interest.
AT SABCS 2013
Major finding: The 5-year ipsilateral breast cancer recurrence rate in a selected population of older women undergoing breast-conserving surgery and adjuvant hormone therapy was 1.3% with postoperative radiotherapy and 4.1% without it, a modest difference that did not impact overall survival.
Data source: A prospective randomized trial in six countries, involving 1,326 patients aged 65 or older who underwent lumpectomy with clear margins for hormone receptor–positive, axillary node–negative breast cancer and were on adjuvant endocrine therapy. They were randomized to postoperative radiotherapy or no radiotherapy.
Disclosures: The PRIME II study was funded by the Chief Scientist Office for Scotland. The presenter reported having no financial conflicts.

Complication gap narrows between low- and high-volume bariatric centers
WASHINGTON – Annual case volume appears to be falling out as a safety factor in bariatric surgery, Dr. Oliver Varban said at the annual clinical congress of the American College of Surgeons.
In the early days of the procedure, facilities that performed more than 125 operations each year had significantly better safety outcomes than did those performing fewer operations. But that difference is fading, particularly as laparoscopy continues to supplant open surgery, said Dr. Varban of the University of Michigan Health Systems, Ann Arbor.
"Over time, safety is improving in both high- and low-volume centers, with lower rates of complications, morbidity, and mortality. The inverse relationship does still persist, but that effect is attenuating."
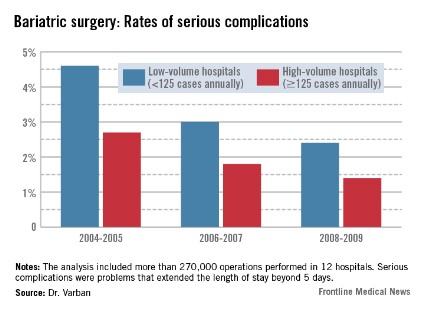
Dr. Varban conducted a review of more than 270,000 bariatric surgery procedures performed in 12 hospitals from 2004 to 2009. He separated the hospitals by annual case volume: 125 or more and less than 125 per year.
In each year, about two-thirds of the procedures were completed in high-volume hospitals. The type of surgery also varied over the study period. During 2004-2005, laparoscopic and open procedures were about equally common. By 2006-2007, laparoscopic operations made up 65% of all bariatric procedures, and that held steady through 2008-2009.
The type of procedure evolved as well, Dr. Varban noted. In 2004-2005, gastric banding comprised about 5% of the operations. By 2006-2007, that had risen to 20%, and by 2008-2009, the number was close to 30%.
In the first era, low-volume hospitals had significantly higher rates of any complication than did high-volume centers (9.3% vs. 6%). By 2006-2007, the difference had narrowed but was still statistically significant (7% vs. 4.8%). By 2008-2009, the difference was no longer significant (5.6% vs. 4.5%).
A multivariate analysis that controlled for type of surgery and patient demographics found a similar trend. The risk of any complication remained significantly elevated at low-volume centers during all three periods (odds ratio, 1.33 in 2004-2005; 1.35 in 2006-2007; and 1.21 in 2008-2009).

The pattern of serious complications (problems that extended the length of stay beyond 5 days) was similar, with a rate of 4.6% vs. 2.7% in the early era; 3% vs. 1.8% in the middle era; and 2.4% vs. 1.4% in the final era. The risk of serious complications was significantly higher in the low-volume group in every era (OR 1.35, 1.43, and 1.44, respectively).
The rates of reoperation were higher in low-volume centers in every era, and declined as time went on. However, the difference between low- and high-volume centers in terms of reoperation rates was nonsignificant at every time point (1.5% vs. 1.06%; 1% vs. 0.75%; 0.78% vs. 0.67%). Similarly, the adjusted odds ratios were nonsignificant (OR 1.22, 1.28, and 1.20).
Although overall the mortality rates were low and remained low, they declined significantly in both groups over the study period (from 0.22% vs. 0.1% and 0.09% vs. 0.04%). Only in the first era was the difference statistically significant, with an adjusted OR of 1.71.
Dr. Varban had no financial disclosures.
WASHINGTON – Annual case volume appears to be falling out as a safety factor in bariatric surgery, Dr. Oliver Varban said at the annual clinical congress of the American College of Surgeons.
In the early days of the procedure, facilities that performed more than 125 operations each year had significantly better safety outcomes than did those performing fewer operations. But that difference is fading, particularly as laparoscopy continues to supplant open surgery, said Dr. Varban of the University of Michigan Health Systems, Ann Arbor.
"Over time, safety is improving in both high- and low-volume centers, with lower rates of complications, morbidity, and mortality. The inverse relationship does still persist, but that effect is attenuating."
Dr. Varban conducted a review of more than 270,000 bariatric surgery procedures performed in 12 hospitals from 2004 to 2009. He separated the hospitals by annual case volume: 125 or more and less than 125 per year.
In each year, about two-thirds of the procedures were completed in high-volume hospitals. The type of surgery also varied over the study period. During 2004-2005, laparoscopic and open procedures were about equally common. By 2006-2007, laparoscopic operations made up 65% of all bariatric procedures, and that held steady through 2008-2009.
The type of procedure evolved as well, Dr. Varban noted. In 2004-2005, gastric banding comprised about 5% of the operations. By 2006-2007, that had risen to 20%, and by 2008-2009, the number was close to 30%.
In the first era, low-volume hospitals had significantly higher rates of any complication than did high-volume centers (9.3% vs. 6%). By 2006-2007, the difference had narrowed but was still statistically significant (7% vs. 4.8%). By 2008-2009, the difference was no longer significant (5.6% vs. 4.5%).
A multivariate analysis that controlled for type of surgery and patient demographics found a similar trend. The risk of any complication remained significantly elevated at low-volume centers during all three periods (odds ratio, 1.33 in 2004-2005; 1.35 in 2006-2007; and 1.21 in 2008-2009).
The pattern of serious complications (problems that extended the length of stay beyond 5 days) was similar, with a rate of 4.6% vs. 2.7% in the early era; 3% vs. 1.8% in the middle era; and 2.4% vs. 1.4% in the final era. The risk of serious complications was significantly higher in the low-volume group in every era (OR 1.35, 1.43, and 1.44, respectively).
The rates of reoperation were higher in low-volume centers in every era, and declined as time went on. However, the difference between low- and high-volume centers in terms of reoperation rates was nonsignificant at every time point (1.5% vs. 1.06%; 1% vs. 0.75%; 0.78% vs. 0.67%). Similarly, the adjusted odds ratios were nonsignificant (OR 1.22, 1.28, and 1.20).
Although overall the mortality rates were low and remained low, they declined significantly in both groups over the study period (from 0.22% vs. 0.1% and 0.09% vs. 0.04%). Only in the first era was the difference statistically significant, with an adjusted OR of 1.71.
Dr. Varban had no financial disclosures.
WASHINGTON – Annual case volume appears to be falling out as a safety factor in bariatric surgery, Dr. Oliver Varban said at the annual clinical congress of the American College of Surgeons.
In the early days of the procedure, facilities that performed more than 125 operations each year had significantly better safety outcomes than did those performing fewer operations. But that difference is fading, particularly as laparoscopy continues to supplant open surgery, said Dr. Varban of the University of Michigan Health Systems, Ann Arbor.
"Over time, safety is improving in both high- and low-volume centers, with lower rates of complications, morbidity, and mortality. The inverse relationship does still persist, but that effect is attenuating."
Dr. Varban conducted a review of more than 270,000 bariatric surgery procedures performed in 12 hospitals from 2004 to 2009. He separated the hospitals by annual case volume: 125 or more and less than 125 per year.
In each year, about two-thirds of the procedures were completed in high-volume hospitals. The type of surgery also varied over the study period. During 2004-2005, laparoscopic and open procedures were about equally common. By 2006-2007, laparoscopic operations made up 65% of all bariatric procedures, and that held steady through 2008-2009.
The type of procedure evolved as well, Dr. Varban noted. In 2004-2005, gastric banding comprised about 5% of the operations. By 2006-2007, that had risen to 20%, and by 2008-2009, the number was close to 30%.
In the first era, low-volume hospitals had significantly higher rates of any complication than did high-volume centers (9.3% vs. 6%). By 2006-2007, the difference had narrowed but was still statistically significant (7% vs. 4.8%). By 2008-2009, the difference was no longer significant (5.6% vs. 4.5%).
A multivariate analysis that controlled for type of surgery and patient demographics found a similar trend. The risk of any complication remained significantly elevated at low-volume centers during all three periods (odds ratio, 1.33 in 2004-2005; 1.35 in 2006-2007; and 1.21 in 2008-2009).
The pattern of serious complications (problems that extended the length of stay beyond 5 days) was similar, with a rate of 4.6% vs. 2.7% in the early era; 3% vs. 1.8% in the middle era; and 2.4% vs. 1.4% in the final era. The risk of serious complications was significantly higher in the low-volume group in every era (OR 1.35, 1.43, and 1.44, respectively).
The rates of reoperation were higher in low-volume centers in every era, and declined as time went on. However, the difference between low- and high-volume centers in terms of reoperation rates was nonsignificant at every time point (1.5% vs. 1.06%; 1% vs. 0.75%; 0.78% vs. 0.67%). Similarly, the adjusted odds ratios were nonsignificant (OR 1.22, 1.28, and 1.20).
Although overall the mortality rates were low and remained low, they declined significantly in both groups over the study period (from 0.22% vs. 0.1% and 0.09% vs. 0.04%). Only in the first era was the difference statistically significant, with an adjusted OR of 1.71.
Dr. Varban had no financial disclosures.
AT THE ACS CLINICAL CONGRESS
Major finding: From 2004 to 2009, the rates of serious complications, reoperation, and mortality improved in low-volume hospitals, bringing their results closer to those seen in high-volume centers.
Data source: The study included data on more than 270,000 bariatric surgical procedures.
Disclosures: Dr. Varban had no financial disclosures.
Fistula risk quadrupled with hyperthermia during pancreaticoduodenectomy
SAN FRANCISCO – A patient body temperature higher than 99.5° F (37.5° C) at the end of elective pancreaticoduodenectomy predicted a fourfold increased risk of postoperative pancreatic fistula in a retrospective study of 123 patients.
Two factors independently predicted a significantly increased risk for postoperative pancreatic fistula in a multivariate logistic regression analysis – body temperature at the end of surgery and a soft pancreatic texture (which conferred a 34-fold increase in risk), Dr. Tadashi Tanioku and his associates.
It wasn’t clear whether pancreatic fistula caused the intraoperative elevated body temperature or the hyperthermia contributed to postoperative development of fistula, but the findings suggest that body temperature at the conclusion of surgery may provide a clue to a patient’s risk of postoperative pancreatic fistula, said Dr. Tanioku of Wakayama (Japan) Medical University.
The study included all patients who underwent pancreaticoduodenectomy for benign or malignant diseases in the pancreatic head and the periampullary region during a 2-year period at his hospital. Thirty-six percent developed postoperative pancreatic fistulas, the investigators reported in a poster presentation at the annual meeting of the American Society of Anesthesiologists.
In a univariate logistic regression analysis, significant predictors for postoperative pancreatic fistula included a body temperature higher than 99.5 degrees Fahrenheit in 45% of patients, soft pancreatic texture in 52%, and a pancreatic duct diameter less than 3 mm in 43% of patients. Having a body mass index greater than 25 kg/m2 (in 17% of patients) was not a significant predictor).
Previous studies have reported an association between hyperthermia on postoperative day 3 after pancreaticoduodenectomy and the development of postoperative pancreatic fistula. Other data have shown an association between intraoperative hyperthermia during colorectal surgery and increased risk of postoperative anastomotic leakage.
In general, operative mortality after pancreaticoduodenectomy had declined to less than 5% but postoperative morality rates are still 40%-50%, mainly from postoperative pancreatic fistula, Dr. Tanioku said.
Patients who developed pancreatic fistula were significantly younger than those who didn’t (a mean of 68 vs. 72 years, respectively) and were significantly more likely to have a main pancreatic duct diameter less than 3 mm (59% vs. 30%, respectively). Fifty-nine percent of patients who developed postoperative fistulas and 37% of those who didn’t had a body temperature higher than 99.5° F at the end of surgery. Eighty-six percent of patients who went on to develop fistulas and 29% of those who didn’t had a soft pancreatic texture.
Dr. Tanioku reported having no financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – A patient body temperature higher than 99.5° F (37.5° C) at the end of elective pancreaticoduodenectomy predicted a fourfold increased risk of postoperative pancreatic fistula in a retrospective study of 123 patients.
Two factors independently predicted a significantly increased risk for postoperative pancreatic fistula in a multivariate logistic regression analysis – body temperature at the end of surgery and a soft pancreatic texture (which conferred a 34-fold increase in risk), Dr. Tadashi Tanioku and his associates.
It wasn’t clear whether pancreatic fistula caused the intraoperative elevated body temperature or the hyperthermia contributed to postoperative development of fistula, but the findings suggest that body temperature at the conclusion of surgery may provide a clue to a patient’s risk of postoperative pancreatic fistula, said Dr. Tanioku of Wakayama (Japan) Medical University.
The study included all patients who underwent pancreaticoduodenectomy for benign or malignant diseases in the pancreatic head and the periampullary region during a 2-year period at his hospital. Thirty-six percent developed postoperative pancreatic fistulas, the investigators reported in a poster presentation at the annual meeting of the American Society of Anesthesiologists.
In a univariate logistic regression analysis, significant predictors for postoperative pancreatic fistula included a body temperature higher than 99.5 degrees Fahrenheit in 45% of patients, soft pancreatic texture in 52%, and a pancreatic duct diameter less than 3 mm in 43% of patients. Having a body mass index greater than 25 kg/m2 (in 17% of patients) was not a significant predictor).
Previous studies have reported an association between hyperthermia on postoperative day 3 after pancreaticoduodenectomy and the development of postoperative pancreatic fistula. Other data have shown an association between intraoperative hyperthermia during colorectal surgery and increased risk of postoperative anastomotic leakage.
In general, operative mortality after pancreaticoduodenectomy had declined to less than 5% but postoperative morality rates are still 40%-50%, mainly from postoperative pancreatic fistula, Dr. Tanioku said.
Patients who developed pancreatic fistula were significantly younger than those who didn’t (a mean of 68 vs. 72 years, respectively) and were significantly more likely to have a main pancreatic duct diameter less than 3 mm (59% vs. 30%, respectively). Fifty-nine percent of patients who developed postoperative fistulas and 37% of those who didn’t had a body temperature higher than 99.5° F at the end of surgery. Eighty-six percent of patients who went on to develop fistulas and 29% of those who didn’t had a soft pancreatic texture.
Dr. Tanioku reported having no financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – A patient body temperature higher than 99.5° F (37.5° C) at the end of elective pancreaticoduodenectomy predicted a fourfold increased risk of postoperative pancreatic fistula in a retrospective study of 123 patients.
Two factors independently predicted a significantly increased risk for postoperative pancreatic fistula in a multivariate logistic regression analysis – body temperature at the end of surgery and a soft pancreatic texture (which conferred a 34-fold increase in risk), Dr. Tadashi Tanioku and his associates.
It wasn’t clear whether pancreatic fistula caused the intraoperative elevated body temperature or the hyperthermia contributed to postoperative development of fistula, but the findings suggest that body temperature at the conclusion of surgery may provide a clue to a patient’s risk of postoperative pancreatic fistula, said Dr. Tanioku of Wakayama (Japan) Medical University.
The study included all patients who underwent pancreaticoduodenectomy for benign or malignant diseases in the pancreatic head and the periampullary region during a 2-year period at his hospital. Thirty-six percent developed postoperative pancreatic fistulas, the investigators reported in a poster presentation at the annual meeting of the American Society of Anesthesiologists.
In a univariate logistic regression analysis, significant predictors for postoperative pancreatic fistula included a body temperature higher than 99.5 degrees Fahrenheit in 45% of patients, soft pancreatic texture in 52%, and a pancreatic duct diameter less than 3 mm in 43% of patients. Having a body mass index greater than 25 kg/m2 (in 17% of patients) was not a significant predictor).
Previous studies have reported an association between hyperthermia on postoperative day 3 after pancreaticoduodenectomy and the development of postoperative pancreatic fistula. Other data have shown an association between intraoperative hyperthermia during colorectal surgery and increased risk of postoperative anastomotic leakage.
In general, operative mortality after pancreaticoduodenectomy had declined to less than 5% but postoperative morality rates are still 40%-50%, mainly from postoperative pancreatic fistula, Dr. Tanioku said.
Patients who developed pancreatic fistula were significantly younger than those who didn’t (a mean of 68 vs. 72 years, respectively) and were significantly more likely to have a main pancreatic duct diameter less than 3 mm (59% vs. 30%, respectively). Fifty-nine percent of patients who developed postoperative fistulas and 37% of those who didn’t had a body temperature higher than 99.5° F at the end of surgery. Eighty-six percent of patients who went on to develop fistulas and 29% of those who didn’t had a soft pancreatic texture.
Dr. Tanioku reported having no financial disclosures.
On Twitter @sherryboschert
AT THE ASA ANNUAL MEETING
Major finding: The likelihood of postoperative pancreatic fistula quadrupled in patients with a body temperature higher than 99.5 degrees F at the end of pancreaticoduodenectomy.
Data source: Retrospective study of 123 patients undergoing elective pancreaticoduodenectomy at one hospital.
Disclosures: Dr. Tanioku reported having no financial disclosures.
Bariatric surgery benefits in type 2 diabetes linked to disease duration
MELBOURNE – The benefits of bariatric surgery in people with type 2 diabetes are significantly reduced with longer disease duration at the time of surgery and with time since surgery, a long-running, prospective, controlled study has found.
The Swedish Obese Subjects study showed that 72% of surgery patients achieved remission at 2 years after treatment, compared with 16% of control patients.
Furthermore, 15 years after surgery, 31% of the surgery patients remained in remission, compared to 7% of control patients, according to data presented at the International Diabetes Federation world congress.
When stratified by disease duration at baseline, newly diagnosed patients maintained significantly higher remission rates at 2, 10 and 15 years’ follow-up (roughly 94%, 60%, and 47%, respectively) than did those who had had diabetes for more than 3 years at baseline (about 39%, 12%, and 9%).

These data came from the SOS (Swedish Obese Subjects) study, a nonrandomized, prospective, observational study involving 2,010 obese subjects who underwent bariatric surgery in 1987-2001, when they were 37-60 years old. A total of 68% of the bariatric surgery recipients had vertical band gastroplasty, 19% underwent gastric banding, and 13% had a Roux en-Y gastric bypass. They were extensively matched by 18 variables to 2,037 obese controls. The SOS study is being conducted at 25 surgical departments and 480 primary care clinics across Sweden. Follow-up is ongoing.
There were 343 individuals with type 2 diabetes in the surgical group and 260 in the control group, enabling a secondary analysis of the impact of bariatric surgery in type 2 diabetes.
Presenter Markku Peltonen said that although bariatric surgery achieves impressive results in the short-term, there is considerable relapse in the longer term.
"It’s typical of bariatric surgery that you achieve the greatest weight loss initially, after 2 years, then there is a slow regain again and this was observed in this study," said Dr. Peltonen, director of the department of chronic disease prevention at the National Institute for Health and Welfare, Helsinki.
"Even in the long term, they are doing much better than the controls who were treated with traditional weight management means," he said in an interview.
This also extended to the microvascular and macrovascular complications of diabetes, with the study showing a significant 47% lower incidence of complications in the surgery group, compared with the control group.
However, these benefits were also attenuated by disease duration. Patients who had had diabetes for more than 3 years and were treated with surgery showed no significant differences in diabetes complication rates, compared with the patients given medical care only.
Dr. Peltonen said he was surprised by the degree of impact that disease duration had on the outcomes of surgery.
"Somehow the expectation would be that we would see an effect even in those people with long diabetes duration, because they have a serious, advanced disease but it looks like, based on our results, that maybe it’s so that the disease has advanced for so long that bariatric surgery cannot reverse that development."
Session chair John Dixon said the SOS study represented the pinnacle of long-term data for bariatric surgery, and offered impressive insights.
"The fact that 31% of these patients are still in remission from diabetes some 15 years down the track is extraordinary, because we know the deterioration of beta cells is significant and this group has held it off for a long time," said Dr. Dixon, head of clinical obesity research at the Baker IDI Heart and Diabetes Institute in Melbourne.
Dr. Dixon said the finding that patients treated early fared better and had a reduction in long-term complications was also a very important clinical finding, suggesting that bariatric surgery should be considered earlier in obese patients not getting good control with conventional therapy.
SOS was supported by the Swedish Research Council, the Swedish Foundation for Strategic Research, and the Swedish government. Some study investigators authors had received paid lectureships, held stock in, or were on the advisory boards for pharmaceutical companies.
MELBOURNE – The benefits of bariatric surgery in people with type 2 diabetes are significantly reduced with longer disease duration at the time of surgery and with time since surgery, a long-running, prospective, controlled study has found.
The Swedish Obese Subjects study showed that 72% of surgery patients achieved remission at 2 years after treatment, compared with 16% of control patients.
Furthermore, 15 years after surgery, 31% of the surgery patients remained in remission, compared to 7% of control patients, according to data presented at the International Diabetes Federation world congress.
When stratified by disease duration at baseline, newly diagnosed patients maintained significantly higher remission rates at 2, 10 and 15 years’ follow-up (roughly 94%, 60%, and 47%, respectively) than did those who had had diabetes for more than 3 years at baseline (about 39%, 12%, and 9%).
These data came from the SOS (Swedish Obese Subjects) study, a nonrandomized, prospective, observational study involving 2,010 obese subjects who underwent bariatric surgery in 1987-2001, when they were 37-60 years old. A total of 68% of the bariatric surgery recipients had vertical band gastroplasty, 19% underwent gastric banding, and 13% had a Roux en-Y gastric bypass. They were extensively matched by 18 variables to 2,037 obese controls. The SOS study is being conducted at 25 surgical departments and 480 primary care clinics across Sweden. Follow-up is ongoing.
There were 343 individuals with type 2 diabetes in the surgical group and 260 in the control group, enabling a secondary analysis of the impact of bariatric surgery in type 2 diabetes.
Presenter Markku Peltonen said that although bariatric surgery achieves impressive results in the short-term, there is considerable relapse in the longer term.
"It’s typical of bariatric surgery that you achieve the greatest weight loss initially, after 2 years, then there is a slow regain again and this was observed in this study," said Dr. Peltonen, director of the department of chronic disease prevention at the National Institute for Health and Welfare, Helsinki.
"Even in the long term, they are doing much better than the controls who were treated with traditional weight management means," he said in an interview.
This also extended to the microvascular and macrovascular complications of diabetes, with the study showing a significant 47% lower incidence of complications in the surgery group, compared with the control group.
However, these benefits were also attenuated by disease duration. Patients who had had diabetes for more than 3 years and were treated with surgery showed no significant differences in diabetes complication rates, compared with the patients given medical care only.
Dr. Peltonen said he was surprised by the degree of impact that disease duration had on the outcomes of surgery.
"Somehow the expectation would be that we would see an effect even in those people with long diabetes duration, because they have a serious, advanced disease but it looks like, based on our results, that maybe it’s so that the disease has advanced for so long that bariatric surgery cannot reverse that development."
Session chair John Dixon said the SOS study represented the pinnacle of long-term data for bariatric surgery, and offered impressive insights.
"The fact that 31% of these patients are still in remission from diabetes some 15 years down the track is extraordinary, because we know the deterioration of beta cells is significant and this group has held it off for a long time," said Dr. Dixon, head of clinical obesity research at the Baker IDI Heart and Diabetes Institute in Melbourne.
Dr. Dixon said the finding that patients treated early fared better and had a reduction in long-term complications was also a very important clinical finding, suggesting that bariatric surgery should be considered earlier in obese patients not getting good control with conventional therapy.
SOS was supported by the Swedish Research Council, the Swedish Foundation for Strategic Research, and the Swedish government. Some study investigators authors had received paid lectureships, held stock in, or were on the advisory boards for pharmaceutical companies.
MELBOURNE – The benefits of bariatric surgery in people with type 2 diabetes are significantly reduced with longer disease duration at the time of surgery and with time since surgery, a long-running, prospective, controlled study has found.
The Swedish Obese Subjects study showed that 72% of surgery patients achieved remission at 2 years after treatment, compared with 16% of control patients.
Furthermore, 15 years after surgery, 31% of the surgery patients remained in remission, compared to 7% of control patients, according to data presented at the International Diabetes Federation world congress.
When stratified by disease duration at baseline, newly diagnosed patients maintained significantly higher remission rates at 2, 10 and 15 years’ follow-up (roughly 94%, 60%, and 47%, respectively) than did those who had had diabetes for more than 3 years at baseline (about 39%, 12%, and 9%).
These data came from the SOS (Swedish Obese Subjects) study, a nonrandomized, prospective, observational study involving 2,010 obese subjects who underwent bariatric surgery in 1987-2001, when they were 37-60 years old. A total of 68% of the bariatric surgery recipients had vertical band gastroplasty, 19% underwent gastric banding, and 13% had a Roux en-Y gastric bypass. They were extensively matched by 18 variables to 2,037 obese controls. The SOS study is being conducted at 25 surgical departments and 480 primary care clinics across Sweden. Follow-up is ongoing.
There were 343 individuals with type 2 diabetes in the surgical group and 260 in the control group, enabling a secondary analysis of the impact of bariatric surgery in type 2 diabetes.
Presenter Markku Peltonen said that although bariatric surgery achieves impressive results in the short-term, there is considerable relapse in the longer term.
"It’s typical of bariatric surgery that you achieve the greatest weight loss initially, after 2 years, then there is a slow regain again and this was observed in this study," said Dr. Peltonen, director of the department of chronic disease prevention at the National Institute for Health and Welfare, Helsinki.
"Even in the long term, they are doing much better than the controls who were treated with traditional weight management means," he said in an interview.
This also extended to the microvascular and macrovascular complications of diabetes, with the study showing a significant 47% lower incidence of complications in the surgery group, compared with the control group.
However, these benefits were also attenuated by disease duration. Patients who had had diabetes for more than 3 years and were treated with surgery showed no significant differences in diabetes complication rates, compared with the patients given medical care only.
Dr. Peltonen said he was surprised by the degree of impact that disease duration had on the outcomes of surgery.
"Somehow the expectation would be that we would see an effect even in those people with long diabetes duration, because they have a serious, advanced disease but it looks like, based on our results, that maybe it’s so that the disease has advanced for so long that bariatric surgery cannot reverse that development."
Session chair John Dixon said the SOS study represented the pinnacle of long-term data for bariatric surgery, and offered impressive insights.
"The fact that 31% of these patients are still in remission from diabetes some 15 years down the track is extraordinary, because we know the deterioration of beta cells is significant and this group has held it off for a long time," said Dr. Dixon, head of clinical obesity research at the Baker IDI Heart and Diabetes Institute in Melbourne.
Dr. Dixon said the finding that patients treated early fared better and had a reduction in long-term complications was also a very important clinical finding, suggesting that bariatric surgery should be considered earlier in obese patients not getting good control with conventional therapy.
SOS was supported by the Swedish Research Council, the Swedish Foundation for Strategic Research, and the Swedish government. Some study investigators authors had received paid lectureships, held stock in, or were on the advisory boards for pharmaceutical companies.
FROM THE WORLD DIABETES CONGRESS
Major finding: Type 2 diabetes remission persisted after 2 and 15 years in 72% and 31% of bariatric surgery patients, vs. 16% and 7% of matched control patients. Those with newly diagnosed disease at baseline maintained significantly higher remission rates at 2 and 15 years’ follow-up (94% and 47%) than did those who had had diabetes for more than 3 years (39% and 9%).
Data source: A subanalysis of the Swedish Obese Subjects study, which included 343 type 2 diabetes patients who underwent bariatric surgery in 1987-2001 and 260 matched control patients.
Disclosures: SOS was supported by the Swedish Research Council, the Swedish Foundation for Strategic Research, and the Swedish government. Some of the investigators declared paid lectureships, stock ownership, and board membership in pharmaceutical companies.

Point/Counterpoint – Are SCIP measures efficacious?
POINT: SCIP is both efficacious and effective.
The Surgical Care Improvement Project (SCIP) was a national campaign that set out to reduce surgical mortality and morbidity by 25% by 2010 through recommendations in targeted areas: wound infections, perioperative MIs, and venous thromboembolism. The recommendations have become pay-for-performance measures. There are seven in the area of infectious disease to reduce surgical site infections. There is one measure for reducing perioperative MI: Continue beta-blockers (for patients who are on them) in the perioperative period. For venous thromboembolism prevention, give prophylaxis within 24 hours before to 24 hours after surgery.
It’s key to understand the difference between efficacy and effectiveness. I think we would all agree that the SCIP measures have efficacy. Efficacy trials determine whether an intervention produces the expected result under ideal circumstances. Effectiveness trials measure the degree of beneficial effect under "real world" clinical conditions. The problem with effectiveness trials is that those real-world conditions may change the effect, or they might just change the ability to measure the effect.

I believe that the SCIP measures have proven efficacy because they all are based upon randomized controlled trials that were identified by systematic reviews amenable to meta-analysis. All of these measures are Level 1 recommendations, based on the highest forms of evidence. The studies that Dr. Barash uses to criticize SCIP measures are cohort studies. They do not randomize. There may be unknown confounding variables.
There have been effectiveness trials that show that the SCIP measures do work. One showed a 27% decrease in surgical site infections, another showed a 62% decrease in surgical site infections, and a third showed a 39% decrease in surgical site infections.
Perhaps the strongest endorsement of efficacy of the SCIP measures comes from Dr. Kaveh G. Shojania, who has written several reviews of the efficacy of medical interventions. This guy is like Mikey from the old Life cereal commercials ... he hates everything. He said there were 11 patient safety practices rated most highly in terms of strength of the evidence, and 3 are SCIP measures: appropriate use of prophylaxis to prevent venous thromboembolism in patients at risk, use of perioperative beta-blockers in appropriate patients, and appropriate use of antibiotic prophylaxis in surgical patients (AHRQ Publication No. 01-E058).
Several trials published by pretty good researchers in reputable journals show a lack of effectiveness of SCIP measures. Even those researchers admit to the efficacy of SCIP measures. The lead investigator of the best effectiveness trial, a retrospective cohort study, wrote, "There are several explanations as to why we did not observe an association between timely antibiotic administration and surgical site infection (SSI). The first is that timely antibiotic administration does not diminish SSI risk. This is an unlikely interpretation. There are numerous randomized controlled trials and observational studies that demonstrate the efficacy of prophylactic antibiotics in reducing SSI for various surgical procedures" (Ann. Surg. 2011;254:494-9).
A separate retrospective cohort study showed a decrease in surgical site infection only if two or more SCIP recommendations were followed (JAMA 2010;303:2479-85). Shocking – if you give the wrong antibiotic at the right time, it might not work.
Another retrospective cohort study found no association with adjusted complications and SCIP compliance. Hospitals in the lowest compliance group had patients in lower-income ZIP codes and lower unadjusted complication rates. So, poor people go home and don’t come back, perhaps because of payment considerations. The study didn’t have enough patients; it also used measures that don’t apply to SCIP (Arch. Surg. 2010;145:999-1004).
SCIP did not design these measures for pay-for-performance programs. The intent was to decrease perioperative complications by 25% by 2010. When you start changing the baseline with pay-for-performance, it doesn’t work. In a study by Hawkins et al., the authors tested the hypothesis that documented compliance with antibiotic prophylaxis guidelines on a pediatric surgery service does not reflect adherence to guidelines as intended. In a 7-week observational study of elective pediatric surgical cases, adherence was evaluated for appropriate administration, type, timing, weight-based dosing, and redosing of antibiotics. Prophylactic antibiotics were administered appropriately in 141 of 143 cases (99%). Of 100 cases in which antibiotic prophylaxis was indicated, compliance was documented in 100% of cases in the electronic medical record; but only 48% of cases adhered to all five guidelines. Lack of adherence was due primarily to dosing or timing errors.
The SCIP measures, however, are based on best evidence. They are tightly linked with the desired outcomes. They are measurable and effectible, as demonstrated in multiple randomized controlled trials. Studies of effectiveness have had variable results due to methodological flaws.
Dr. Lagasse is a professor of anesthesiology and director of quality management at the Yale School of Medicine, New Haven, Conn. He is on the steering committee for the Surgical Care Improvement Project. He reported having no financial disclosures.
COUNTERPOINT: Studies have not shown effectiveness.
When it was created, SCIP did not reflect reality. SCIP started at the U.S. Department of Veterans Affairs, which conducted a 10-year study. They found a 25% relative risk reduction, but that was only a 0.8% absolute risk reduction for the incidence of complications, a drop from about 3.1% to about 2.3% (Arch. Surg. 2002;137:20-27).
It would be great to have randomized controlled trials on the effectiveness of SCIP, but it’s not happening. We’re going to have to go by high-fidelity observational trials, which according to a number of researchers in the field have the same impact as randomized controlled trials.
One study of 35,543 patients in 44 hospitals found a whopping 27% reduction in surgical site infections, but that was only a 0.6% absolute reduction, from about 2.5% to about 1.9% (Am. J. Surg. 2005;190:9-15). There was no significant difference between groups.
Another study showed improved compliance with SCIP measures, but no change in surgical site infection rate (Dis. Colon Rectum 2010;53:24-30). This is the theme in study after study after study.

A 2008 study enrolled 9,195 patients undergoing colorectal, orthopedic, or vascular surgery and looked at SCIP compliance vs. surgical site infection. The SCIP rate correlated with the hospital case mix. If you look at the SCIP rate in terms of antibiotic timing, SCIP is not significant. The study basically showed that variables other than timely antibiotic administration are affecting surgical site infection rates (J. Am. Coll. Surg. 2008;206:814-19).
Hospital performance on process measures may not be a good marker of surgical site infection or the outcome we’re looking at, according to another study, which reported that unmeasured effects may have a larger impact than the measured effects (Health Serv. Res. 2008;43:1464-84).
There is a randomized controlled trial that randomized patients to strict control with the SCIP measures or routine treatment at the hospital. The SCIP-treated patients had nearly twice the incidence of surgical site infections as the patients receiving standard treatment. The authors concluded that combining each of the SCIP factors into one big category doesn’t necessarily work (Arch. Surg. 2011;146:263-9).
Should we be evaluating outcome measures with performance measures (e.g., percent timely antibiotic administration) to determine whether they work or not? One editorial evaluated eight articles with data on 31,448 patients, looking just at antibiotic administration within 1 hour of surgery, a SCIP measure. It found a higher infection rate if antibiotics were administered within 30 minutes of incision (JAMA 2010;303:2527-2528).
There was no significant difference in another study between standard of care and SCIP for venous thromboembolism (Am. J. Surg. 2012;204:591-97). The authors wrote that there is no convincing evidence that improvements in compliance are associated with better outcomes. We see this time and time again.
When people find that SCIP is not working, they turn to other measures to reduce surgical site infection. The Comprehensive Unit-based Safety Program (CUSP) is targeted at a specific problem that a specific hospital is having in managing infections. It’s not coming from Washington; it’s based at the hospital. One study showed that following CUSP, there was a significant reduction in surgical site infections despite the fact that previous to that there was 95% compliance with SCIP standards (J. Am. Coll. Surg. 2012;215:193-200). SCIP was working, but it wasn’t affecting outcome.
Dr. Lagasse and I interpret one key study very differently. He abstracts a sentence from a Limitations section of the study and makes a sweeping generalization out of context. But the study showed no relationship between facility adherence to SCIP and the surgical site infection rate. The authors concluded, "Policies regarding continued SCIP measurement and reporting should be reassessed" (Ann. Surg. 2011;254:494-99).
The largest SCIP study to date from a single entity involved 32,459 patients in the Veterans Affairs medical system. Overall, antibiotics were administered within 28 minutes of surgical incision. Once they adjusted for confounders, they found no significant relationship between surgical site infection and the SCIP measures (JAMA 2013;148:649-57). No one has proven that giving antibiotics within 60 minutes of surgical incision gives you a lower infection rate.
SCIP measures divert resources and divert clinical care. They obscure the nuances of care. They may harm the hospital and the provider, and they raise unnecessary legal risk if an antibiotic is not given within 60 minutes of incision.
Dr. Barash is a professor of anesthesiology at Yale University, New Haven, Conn. He reported having no financial disclosures.
These are excerpts from a debate at the annual meeting of the American Society of Anesthesiologists.
POINT: SCIP is both efficacious and effective.
The Surgical Care Improvement Project (SCIP) was a national campaign that set out to reduce surgical mortality and morbidity by 25% by 2010 through recommendations in targeted areas: wound infections, perioperative MIs, and venous thromboembolism. The recommendations have become pay-for-performance measures. There are seven in the area of infectious disease to reduce surgical site infections. There is one measure for reducing perioperative MI: Continue beta-blockers (for patients who are on them) in the perioperative period. For venous thromboembolism prevention, give prophylaxis within 24 hours before to 24 hours after surgery.
It’s key to understand the difference between efficacy and effectiveness. I think we would all agree that the SCIP measures have efficacy. Efficacy trials determine whether an intervention produces the expected result under ideal circumstances. Effectiveness trials measure the degree of beneficial effect under "real world" clinical conditions. The problem with effectiveness trials is that those real-world conditions may change the effect, or they might just change the ability to measure the effect.
I believe that the SCIP measures have proven efficacy because they all are based upon randomized controlled trials that were identified by systematic reviews amenable to meta-analysis. All of these measures are Level 1 recommendations, based on the highest forms of evidence. The studies that Dr. Barash uses to criticize SCIP measures are cohort studies. They do not randomize. There may be unknown confounding variables.
There have been effectiveness trials that show that the SCIP measures do work. One showed a 27% decrease in surgical site infections, another showed a 62% decrease in surgical site infections, and a third showed a 39% decrease in surgical site infections.
Perhaps the strongest endorsement of efficacy of the SCIP measures comes from Dr. Kaveh G. Shojania, who has written several reviews of the efficacy of medical interventions. This guy is like Mikey from the old Life cereal commercials ... he hates everything. He said there were 11 patient safety practices rated most highly in terms of strength of the evidence, and 3 are SCIP measures: appropriate use of prophylaxis to prevent venous thromboembolism in patients at risk, use of perioperative beta-blockers in appropriate patients, and appropriate use of antibiotic prophylaxis in surgical patients (AHRQ Publication No. 01-E058).
Several trials published by pretty good researchers in reputable journals show a lack of effectiveness of SCIP measures. Even those researchers admit to the efficacy of SCIP measures. The lead investigator of the best effectiveness trial, a retrospective cohort study, wrote, "There are several explanations as to why we did not observe an association between timely antibiotic administration and surgical site infection (SSI). The first is that timely antibiotic administration does not diminish SSI risk. This is an unlikely interpretation. There are numerous randomized controlled trials and observational studies that demonstrate the efficacy of prophylactic antibiotics in reducing SSI for various surgical procedures" (Ann. Surg. 2011;254:494-9).
A separate retrospective cohort study showed a decrease in surgical site infection only if two or more SCIP recommendations were followed (JAMA 2010;303:2479-85). Shocking – if you give the wrong antibiotic at the right time, it might not work.
Another retrospective cohort study found no association with adjusted complications and SCIP compliance. Hospitals in the lowest compliance group had patients in lower-income ZIP codes and lower unadjusted complication rates. So, poor people go home and don’t come back, perhaps because of payment considerations. The study didn’t have enough patients; it also used measures that don’t apply to SCIP (Arch. Surg. 2010;145:999-1004).
SCIP did not design these measures for pay-for-performance programs. The intent was to decrease perioperative complications by 25% by 2010. When you start changing the baseline with pay-for-performance, it doesn’t work. In a study by Hawkins et al., the authors tested the hypothesis that documented compliance with antibiotic prophylaxis guidelines on a pediatric surgery service does not reflect adherence to guidelines as intended. In a 7-week observational study of elective pediatric surgical cases, adherence was evaluated for appropriate administration, type, timing, weight-based dosing, and redosing of antibiotics. Prophylactic antibiotics were administered appropriately in 141 of 143 cases (99%). Of 100 cases in which antibiotic prophylaxis was indicated, compliance was documented in 100% of cases in the electronic medical record; but only 48% of cases adhered to all five guidelines. Lack of adherence was due primarily to dosing or timing errors.
The SCIP measures, however, are based on best evidence. They are tightly linked with the desired outcomes. They are measurable and effectible, as demonstrated in multiple randomized controlled trials. Studies of effectiveness have had variable results due to methodological flaws.
Dr. Lagasse is a professor of anesthesiology and director of quality management at the Yale School of Medicine, New Haven, Conn. He is on the steering committee for the Surgical Care Improvement Project. He reported having no financial disclosures.
COUNTERPOINT: Studies have not shown effectiveness.
When it was created, SCIP did not reflect reality. SCIP started at the U.S. Department of Veterans Affairs, which conducted a 10-year study. They found a 25% relative risk reduction, but that was only a 0.8% absolute risk reduction for the incidence of complications, a drop from about 3.1% to about 2.3% (Arch. Surg. 2002;137:20-27).
It would be great to have randomized controlled trials on the effectiveness of SCIP, but it’s not happening. We’re going to have to go by high-fidelity observational trials, which according to a number of researchers in the field have the same impact as randomized controlled trials.
One study of 35,543 patients in 44 hospitals found a whopping 27% reduction in surgical site infections, but that was only a 0.6% absolute reduction, from about 2.5% to about 1.9% (Am. J. Surg. 2005;190:9-15). There was no significant difference between groups.
Another study showed improved compliance with SCIP measures, but no change in surgical site infection rate (Dis. Colon Rectum 2010;53:24-30). This is the theme in study after study after study.
A 2008 study enrolled 9,195 patients undergoing colorectal, orthopedic, or vascular surgery and looked at SCIP compliance vs. surgical site infection. The SCIP rate correlated with the hospital case mix. If you look at the SCIP rate in terms of antibiotic timing, SCIP is not significant. The study basically showed that variables other than timely antibiotic administration are affecting surgical site infection rates (J. Am. Coll. Surg. 2008;206:814-19).
Hospital performance on process measures may not be a good marker of surgical site infection or the outcome we’re looking at, according to another study, which reported that unmeasured effects may have a larger impact than the measured effects (Health Serv. Res. 2008;43:1464-84).
There is a randomized controlled trial that randomized patients to strict control with the SCIP measures or routine treatment at the hospital. The SCIP-treated patients had nearly twice the incidence of surgical site infections as the patients receiving standard treatment. The authors concluded that combining each of the SCIP factors into one big category doesn’t necessarily work (Arch. Surg. 2011;146:263-9).
Should we be evaluating outcome measures with performance measures (e.g., percent timely antibiotic administration) to determine whether they work or not? One editorial evaluated eight articles with data on 31,448 patients, looking just at antibiotic administration within 1 hour of surgery, a SCIP measure. It found a higher infection rate if antibiotics were administered within 30 minutes of incision (JAMA 2010;303:2527-2528).
There was no significant difference in another study between standard of care and SCIP for venous thromboembolism (Am. J. Surg. 2012;204:591-97). The authors wrote that there is no convincing evidence that improvements in compliance are associated with better outcomes. We see this time and time again.
When people find that SCIP is not working, they turn to other measures to reduce surgical site infection. The Comprehensive Unit-based Safety Program (CUSP) is targeted at a specific problem that a specific hospital is having in managing infections. It’s not coming from Washington; it’s based at the hospital. One study showed that following CUSP, there was a significant reduction in surgical site infections despite the fact that previous to that there was 95% compliance with SCIP standards (J. Am. Coll. Surg. 2012;215:193-200). SCIP was working, but it wasn’t affecting outcome.
Dr. Lagasse and I interpret one key study very differently. He abstracts a sentence from a Limitations section of the study and makes a sweeping generalization out of context. But the study showed no relationship between facility adherence to SCIP and the surgical site infection rate. The authors concluded, "Policies regarding continued SCIP measurement and reporting should be reassessed" (Ann. Surg. 2011;254:494-99).
The largest SCIP study to date from a single entity involved 32,459 patients in the Veterans Affairs medical system. Overall, antibiotics were administered within 28 minutes of surgical incision. Once they adjusted for confounders, they found no significant relationship between surgical site infection and the SCIP measures (JAMA 2013;148:649-57). No one has proven that giving antibiotics within 60 minutes of surgical incision gives you a lower infection rate.
SCIP measures divert resources and divert clinical care. They obscure the nuances of care. They may harm the hospital and the provider, and they raise unnecessary legal risk if an antibiotic is not given within 60 minutes of incision.
Dr. Barash is a professor of anesthesiology at Yale University, New Haven, Conn. He reported having no financial disclosures.
These are excerpts from a debate at the annual meeting of the American Society of Anesthesiologists.
POINT: SCIP is both efficacious and effective.
The Surgical Care Improvement Project (SCIP) was a national campaign that set out to reduce surgical mortality and morbidity by 25% by 2010 through recommendations in targeted areas: wound infections, perioperative MIs, and venous thromboembolism. The recommendations have become pay-for-performance measures. There are seven in the area of infectious disease to reduce surgical site infections. There is one measure for reducing perioperative MI: Continue beta-blockers (for patients who are on them) in the perioperative period. For venous thromboembolism prevention, give prophylaxis within 24 hours before to 24 hours after surgery.
It’s key to understand the difference between efficacy and effectiveness. I think we would all agree that the SCIP measures have efficacy. Efficacy trials determine whether an intervention produces the expected result under ideal circumstances. Effectiveness trials measure the degree of beneficial effect under "real world" clinical conditions. The problem with effectiveness trials is that those real-world conditions may change the effect, or they might just change the ability to measure the effect.
I believe that the SCIP measures have proven efficacy because they all are based upon randomized controlled trials that were identified by systematic reviews amenable to meta-analysis. All of these measures are Level 1 recommendations, based on the highest forms of evidence. The studies that Dr. Barash uses to criticize SCIP measures are cohort studies. They do not randomize. There may be unknown confounding variables.
There have been effectiveness trials that show that the SCIP measures do work. One showed a 27% decrease in surgical site infections, another showed a 62% decrease in surgical site infections, and a third showed a 39% decrease in surgical site infections.
Perhaps the strongest endorsement of efficacy of the SCIP measures comes from Dr. Kaveh G. Shojania, who has written several reviews of the efficacy of medical interventions. This guy is like Mikey from the old Life cereal commercials ... he hates everything. He said there were 11 patient safety practices rated most highly in terms of strength of the evidence, and 3 are SCIP measures: appropriate use of prophylaxis to prevent venous thromboembolism in patients at risk, use of perioperative beta-blockers in appropriate patients, and appropriate use of antibiotic prophylaxis in surgical patients (AHRQ Publication No. 01-E058).
Several trials published by pretty good researchers in reputable journals show a lack of effectiveness of SCIP measures. Even those researchers admit to the efficacy of SCIP measures. The lead investigator of the best effectiveness trial, a retrospective cohort study, wrote, "There are several explanations as to why we did not observe an association between timely antibiotic administration and surgical site infection (SSI). The first is that timely antibiotic administration does not diminish SSI risk. This is an unlikely interpretation. There are numerous randomized controlled trials and observational studies that demonstrate the efficacy of prophylactic antibiotics in reducing SSI for various surgical procedures" (Ann. Surg. 2011;254:494-9).
A separate retrospective cohort study showed a decrease in surgical site infection only if two or more SCIP recommendations were followed (JAMA 2010;303:2479-85). Shocking – if you give the wrong antibiotic at the right time, it might not work.
Another retrospective cohort study found no association with adjusted complications and SCIP compliance. Hospitals in the lowest compliance group had patients in lower-income ZIP codes and lower unadjusted complication rates. So, poor people go home and don’t come back, perhaps because of payment considerations. The study didn’t have enough patients; it also used measures that don’t apply to SCIP (Arch. Surg. 2010;145:999-1004).
SCIP did not design these measures for pay-for-performance programs. The intent was to decrease perioperative complications by 25% by 2010. When you start changing the baseline with pay-for-performance, it doesn’t work. In a study by Hawkins et al., the authors tested the hypothesis that documented compliance with antibiotic prophylaxis guidelines on a pediatric surgery service does not reflect adherence to guidelines as intended. In a 7-week observational study of elective pediatric surgical cases, adherence was evaluated for appropriate administration, type, timing, weight-based dosing, and redosing of antibiotics. Prophylactic antibiotics were administered appropriately in 141 of 143 cases (99%). Of 100 cases in which antibiotic prophylaxis was indicated, compliance was documented in 100% of cases in the electronic medical record; but only 48% of cases adhered to all five guidelines. Lack of adherence was due primarily to dosing or timing errors.
The SCIP measures, however, are based on best evidence. They are tightly linked with the desired outcomes. They are measurable and effectible, as demonstrated in multiple randomized controlled trials. Studies of effectiveness have had variable results due to methodological flaws.
Dr. Lagasse is a professor of anesthesiology and director of quality management at the Yale School of Medicine, New Haven, Conn. He is on the steering committee for the Surgical Care Improvement Project. He reported having no financial disclosures.
COUNTERPOINT: Studies have not shown effectiveness.
When it was created, SCIP did not reflect reality. SCIP started at the U.S. Department of Veterans Affairs, which conducted a 10-year study. They found a 25% relative risk reduction, but that was only a 0.8% absolute risk reduction for the incidence of complications, a drop from about 3.1% to about 2.3% (Arch. Surg. 2002;137:20-27).
It would be great to have randomized controlled trials on the effectiveness of SCIP, but it’s not happening. We’re going to have to go by high-fidelity observational trials, which according to a number of researchers in the field have the same impact as randomized controlled trials.
One study of 35,543 patients in 44 hospitals found a whopping 27% reduction in surgical site infections, but that was only a 0.6% absolute reduction, from about 2.5% to about 1.9% (Am. J. Surg. 2005;190:9-15). There was no significant difference between groups.
Another study showed improved compliance with SCIP measures, but no change in surgical site infection rate (Dis. Colon Rectum 2010;53:24-30). This is the theme in study after study after study.
A 2008 study enrolled 9,195 patients undergoing colorectal, orthopedic, or vascular surgery and looked at SCIP compliance vs. surgical site infection. The SCIP rate correlated with the hospital case mix. If you look at the SCIP rate in terms of antibiotic timing, SCIP is not significant. The study basically showed that variables other than timely antibiotic administration are affecting surgical site infection rates (J. Am. Coll. Surg. 2008;206:814-19).
Hospital performance on process measures may not be a good marker of surgical site infection or the outcome we’re looking at, according to another study, which reported that unmeasured effects may have a larger impact than the measured effects (Health Serv. Res. 2008;43:1464-84).
There is a randomized controlled trial that randomized patients to strict control with the SCIP measures or routine treatment at the hospital. The SCIP-treated patients had nearly twice the incidence of surgical site infections as the patients receiving standard treatment. The authors concluded that combining each of the SCIP factors into one big category doesn’t necessarily work (Arch. Surg. 2011;146:263-9).
Should we be evaluating outcome measures with performance measures (e.g., percent timely antibiotic administration) to determine whether they work or not? One editorial evaluated eight articles with data on 31,448 patients, looking just at antibiotic administration within 1 hour of surgery, a SCIP measure. It found a higher infection rate if antibiotics were administered within 30 minutes of incision (JAMA 2010;303:2527-2528).
There was no significant difference in another study between standard of care and SCIP for venous thromboembolism (Am. J. Surg. 2012;204:591-97). The authors wrote that there is no convincing evidence that improvements in compliance are associated with better outcomes. We see this time and time again.
When people find that SCIP is not working, they turn to other measures to reduce surgical site infection. The Comprehensive Unit-based Safety Program (CUSP) is targeted at a specific problem that a specific hospital is having in managing infections. It’s not coming from Washington; it’s based at the hospital. One study showed that following CUSP, there was a significant reduction in surgical site infections despite the fact that previous to that there was 95% compliance with SCIP standards (J. Am. Coll. Surg. 2012;215:193-200). SCIP was working, but it wasn’t affecting outcome.
Dr. Lagasse and I interpret one key study very differently. He abstracts a sentence from a Limitations section of the study and makes a sweeping generalization out of context. But the study showed no relationship between facility adherence to SCIP and the surgical site infection rate. The authors concluded, "Policies regarding continued SCIP measurement and reporting should be reassessed" (Ann. Surg. 2011;254:494-99).
The largest SCIP study to date from a single entity involved 32,459 patients in the Veterans Affairs medical system. Overall, antibiotics were administered within 28 minutes of surgical incision. Once they adjusted for confounders, they found no significant relationship between surgical site infection and the SCIP measures (JAMA 2013;148:649-57). No one has proven that giving antibiotics within 60 minutes of surgical incision gives you a lower infection rate.
SCIP measures divert resources and divert clinical care. They obscure the nuances of care. They may harm the hospital and the provider, and they raise unnecessary legal risk if an antibiotic is not given within 60 minutes of incision.
Dr. Barash is a professor of anesthesiology at Yale University, New Haven, Conn. He reported having no financial disclosures.
These are excerpts from a debate at the annual meeting of the American Society of Anesthesiologists.

Gastric banding benefited overweight, not just obese in type 2 diabetes
MELBOURNE – Gastric banding can achieve significant weight loss and remission of diabetes in patients with type 2 diabetes who are overweight but not obese, suggesting that a lower body mass index threshold could be considered for the procedure, according to results from a randomized controlled trial.
Type 2 diabetes patients with a BMI of 25-30 kg/m2 who received a laparoscopic gastric band achieved significantly greater weight loss (11 kg vs. 1 kg) and significantly higher rates of diabetes remission (52% vs. 8%) than did those who were treated with standard medical care.

According to an oral presentation at the International Diabetes Federation world congress, patients treated with gastric banding also required much less medication to achieve reductions in hemoglobin A1c.
"In the surgical group, we had a large number continuing metformin but basically very few taking other therapies, and the four people taking insulin all came off insulin by 2 years, whereas in the medical arm we had intensification of sulfonylurea, exenatide, insulin, and even gliptin therapy," said Dr. John Wentworth, an endocrinologist and research fellow at the Monash University Centre for Obesity Research and Education, Melbourne.
The study also found significant improvements in physical quality of life measures among the gastric banding group compared with the medical care group.
"Part of it was that people lost weight and they were pleased about it, but I think the other part was that they used less medication," Dr. Wentworth said in an interview.
Researchers also observed a small improvement in diastolic blood pressure, as well as significant improvements in insulin resistance and HDL levels, among patients treated with gastric banding.
The 2-year Australian study enrolled 51 overweight type 2 diabetes patients with relatively short disease duration (less than 5 years) and without underlying pancreatic pathology. Patients were randomized to either laparoscopic gastric banding or standard medical care involving regular consultations with a dietician, diabetes educator, and physician.
The study’s primary outcome was remission of diabetes at 2 years, which was defined as fasting and 2-hour glucose measurements of less than 7.0 mmol/L and less than 11.1 mmol/L, respectively, following an oral glucose challenge after at least 48 hours off medication.
Dr. Wentworth said gastric banding was a reasonable option in terms of achieving weight loss and improving glycemic outcomes with a much lower medication burden.
"Traditionally, bariatric surgery was a quite high risk procedure, looking back two or more decades, and you only targeted it to people who had very serious obesity and who had clear problems with it," Dr. Wentworth said.
"Things have become a lot safer in all types of bariatric surgery, so it becomes more of an option to offer people."
However, he stressed that the study population was carefully selected to include only people with shorter disease duration, and that gastric banding was not likely to achieve remission in patients with very long-standing and poorly controlled disease.
There were some complications in the surgical group, with one revision operation, and five episodes of esophageal obstruction in three patients, which required removal of fluid from the band.
A member of the audience pointed out that the medical care group might have achieved better results with greater use of glucagonlike peptide–1 (GLP-1) agonists, which can also have an effect on obesity. Dr. Wentworth said there was some use of the GLP-1 agonist exenatide, but it was not offered routinely to patients, and he acknowledged that this may have affected outcomes.
The Centre for Obesity Research and Education has received educational funding from Allergan, but there were no other financial conflicts of interest declared.
MELBOURNE – Gastric banding can achieve significant weight loss and remission of diabetes in patients with type 2 diabetes who are overweight but not obese, suggesting that a lower body mass index threshold could be considered for the procedure, according to results from a randomized controlled trial.
Type 2 diabetes patients with a BMI of 25-30 kg/m2 who received a laparoscopic gastric band achieved significantly greater weight loss (11 kg vs. 1 kg) and significantly higher rates of diabetes remission (52% vs. 8%) than did those who were treated with standard medical care.
According to an oral presentation at the International Diabetes Federation world congress, patients treated with gastric banding also required much less medication to achieve reductions in hemoglobin A1c.
"In the surgical group, we had a large number continuing metformin but basically very few taking other therapies, and the four people taking insulin all came off insulin by 2 years, whereas in the medical arm we had intensification of sulfonylurea, exenatide, insulin, and even gliptin therapy," said Dr. John Wentworth, an endocrinologist and research fellow at the Monash University Centre for Obesity Research and Education, Melbourne.
The study also found significant improvements in physical quality of life measures among the gastric banding group compared with the medical care group.
"Part of it was that people lost weight and they were pleased about it, but I think the other part was that they used less medication," Dr. Wentworth said in an interview.
Researchers also observed a small improvement in diastolic blood pressure, as well as significant improvements in insulin resistance and HDL levels, among patients treated with gastric banding.
The 2-year Australian study enrolled 51 overweight type 2 diabetes patients with relatively short disease duration (less than 5 years) and without underlying pancreatic pathology. Patients were randomized to either laparoscopic gastric banding or standard medical care involving regular consultations with a dietician, diabetes educator, and physician.
The study’s primary outcome was remission of diabetes at 2 years, which was defined as fasting and 2-hour glucose measurements of less than 7.0 mmol/L and less than 11.1 mmol/L, respectively, following an oral glucose challenge after at least 48 hours off medication.
Dr. Wentworth said gastric banding was a reasonable option in terms of achieving weight loss and improving glycemic outcomes with a much lower medication burden.
"Traditionally, bariatric surgery was a quite high risk procedure, looking back two or more decades, and you only targeted it to people who had very serious obesity and who had clear problems with it," Dr. Wentworth said.
"Things have become a lot safer in all types of bariatric surgery, so it becomes more of an option to offer people."
However, he stressed that the study population was carefully selected to include only people with shorter disease duration, and that gastric banding was not likely to achieve remission in patients with very long-standing and poorly controlled disease.
There were some complications in the surgical group, with one revision operation, and five episodes of esophageal obstruction in three patients, which required removal of fluid from the band.
A member of the audience pointed out that the medical care group might have achieved better results with greater use of glucagonlike peptide–1 (GLP-1) agonists, which can also have an effect on obesity. Dr. Wentworth said there was some use of the GLP-1 agonist exenatide, but it was not offered routinely to patients, and he acknowledged that this may have affected outcomes.
The Centre for Obesity Research and Education has received educational funding from Allergan, but there were no other financial conflicts of interest declared.
MELBOURNE – Gastric banding can achieve significant weight loss and remission of diabetes in patients with type 2 diabetes who are overweight but not obese, suggesting that a lower body mass index threshold could be considered for the procedure, according to results from a randomized controlled trial.
Type 2 diabetes patients with a BMI of 25-30 kg/m2 who received a laparoscopic gastric band achieved significantly greater weight loss (11 kg vs. 1 kg) and significantly higher rates of diabetes remission (52% vs. 8%) than did those who were treated with standard medical care.
According to an oral presentation at the International Diabetes Federation world congress, patients treated with gastric banding also required much less medication to achieve reductions in hemoglobin A1c.
"In the surgical group, we had a large number continuing metformin but basically very few taking other therapies, and the four people taking insulin all came off insulin by 2 years, whereas in the medical arm we had intensification of sulfonylurea, exenatide, insulin, and even gliptin therapy," said Dr. John Wentworth, an endocrinologist and research fellow at the Monash University Centre for Obesity Research and Education, Melbourne.
The study also found significant improvements in physical quality of life measures among the gastric banding group compared with the medical care group.
"Part of it was that people lost weight and they were pleased about it, but I think the other part was that they used less medication," Dr. Wentworth said in an interview.
Researchers also observed a small improvement in diastolic blood pressure, as well as significant improvements in insulin resistance and HDL levels, among patients treated with gastric banding.
The 2-year Australian study enrolled 51 overweight type 2 diabetes patients with relatively short disease duration (less than 5 years) and without underlying pancreatic pathology. Patients were randomized to either laparoscopic gastric banding or standard medical care involving regular consultations with a dietician, diabetes educator, and physician.
The study’s primary outcome was remission of diabetes at 2 years, which was defined as fasting and 2-hour glucose measurements of less than 7.0 mmol/L and less than 11.1 mmol/L, respectively, following an oral glucose challenge after at least 48 hours off medication.
Dr. Wentworth said gastric banding was a reasonable option in terms of achieving weight loss and improving glycemic outcomes with a much lower medication burden.
"Traditionally, bariatric surgery was a quite high risk procedure, looking back two or more decades, and you only targeted it to people who had very serious obesity and who had clear problems with it," Dr. Wentworth said.
"Things have become a lot safer in all types of bariatric surgery, so it becomes more of an option to offer people."
However, he stressed that the study population was carefully selected to include only people with shorter disease duration, and that gastric banding was not likely to achieve remission in patients with very long-standing and poorly controlled disease.
There were some complications in the surgical group, with one revision operation, and five episodes of esophageal obstruction in three patients, which required removal of fluid from the band.
A member of the audience pointed out that the medical care group might have achieved better results with greater use of glucagonlike peptide–1 (GLP-1) agonists, which can also have an effect on obesity. Dr. Wentworth said there was some use of the GLP-1 agonist exenatide, but it was not offered routinely to patients, and he acknowledged that this may have affected outcomes.
The Centre for Obesity Research and Education has received educational funding from Allergan, but there were no other financial conflicts of interest declared.
AT THE WORLD DIABETES CONGRESS
Major finding: Laparoscopic gastric banding resulted in significant weight loss (11 kg vs. 1 kg) and remission of diabetes (52% vs. 8%) at 2 years in overweight patients with type 2 diabetes, compared with those given standard medical care.
Data source: Randomized controlled trial of 51 patients with type 2 diabetes.
Disclosures: The Centre for Obesity Research and Education has received educational funding from Allergan, but there were no other financial conflicts of interest declared.

Cognitive impairment at baseline linked to poorer bariatric surgery outcomes
ATLANTA – Higher baseline levels of cognitive impairment are associated with poorer weight loss outcomes after bariatric surgery.
"People with problems of memory, problem solving, or attention prior to surgery show reduced ability to lose weight," said John Gunstad, Ph.D., at Obesity Week, presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
In a prospective study of 109 bariatric surgery patients enrolled in the LABS (Longitudinal Assessment of Bariatric Surgery) study and 41 obese matched controls who’d not had surgery, Dr. Gunstad, who is professor and chairman of neuroscience at Kent (Ohio) State University, and his colleagues assessed all participants’ cognitive function at baseline, at 12 weeks, and at 12, 24, and 36 months.

They found that 25% of all surgical patients had baseline cognitive impairment. "These were individuals who were at least 1.5 standard deviations below normal-weight persons in at least one cognitive domain," said Dr. Gunstad. "If these individuals came to my clinic, I would have to diagnose them with some kind of cognitive disorder."
Expanding the criteria to 1 standard deviation meant that 40% of participants had subtle impairment. "Patients who are coming in for bariatric surgery are between 5 and 8 times more likely to have cognitive impairment than their normal-weight counterparts. That’s a remarkable number," said Dr. Gunstad.
At 12 weeks, surgery patients who’d lost an average of 48 pounds showed gains in cognitive functioning. Overall, the study showed initial, rapid cognitive improvement, and then either continued or sustained improvement 3 years out.
"We went from a quarter of patients being clinically impaired prior to surgery," said Dr. Gunstad. "At 3 years after surgery, that number was down to 4%."
However, in a related study, Dr. Gunstad and his colleagues found that greater levels of cognitive impairment correlated to less weight loss at all follow-up points (Surg. Obes. Relat. Dis. 2013;9:765-70).
Dr. Gunstad said this was likely due to patient adherence issues after the tumult of bariatric surgery. "You have to eat in a different way. You have to think in a different way. You have to restructure every moment of your life," said Dr. Gunstad. "If you have problems with memory, problem solving, or organizing, it will be much more difficult to make and persist with those changes."
The clinical implication, said Dr. Gunstad, is that better screening of bariatric surgery candidates might be helpful. "If we know the cognitive status of our patients, it’s likely we will know what the outcomes will be," he said.
The drawback, he said, is that even though most third-party payers will cover the costs of evaluations, if a physician has a large practice of hundreds of patients, then the number of referrals might be overwhelming to the system, which might not have enough neuropsychologists to perform the tests.
Self-reporting might also be an issue because of the phenomenon of the "worried well" – the patients who overreport their problems – or because the patients with cognitive impairment won’t necessarily recognize the symptoms they need to report, said Dr. Gunstad.
By next year, said Dr. Gunstad, he hoped he and his colleagues will have finalized a better screening tool for clinicians who treat bariatric surgery patients.
Dr. Gunstad did not report any financial disclosures.
ATLANTA – Higher baseline levels of cognitive impairment are associated with poorer weight loss outcomes after bariatric surgery.
"People with problems of memory, problem solving, or attention prior to surgery show reduced ability to lose weight," said John Gunstad, Ph.D., at Obesity Week, presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
In a prospective study of 109 bariatric surgery patients enrolled in the LABS (Longitudinal Assessment of Bariatric Surgery) study and 41 obese matched controls who’d not had surgery, Dr. Gunstad, who is professor and chairman of neuroscience at Kent (Ohio) State University, and his colleagues assessed all participants’ cognitive function at baseline, at 12 weeks, and at 12, 24, and 36 months.
They found that 25% of all surgical patients had baseline cognitive impairment. "These were individuals who were at least 1.5 standard deviations below normal-weight persons in at least one cognitive domain," said Dr. Gunstad. "If these individuals came to my clinic, I would have to diagnose them with some kind of cognitive disorder."
Expanding the criteria to 1 standard deviation meant that 40% of participants had subtle impairment. "Patients who are coming in for bariatric surgery are between 5 and 8 times more likely to have cognitive impairment than their normal-weight counterparts. That’s a remarkable number," said Dr. Gunstad.
At 12 weeks, surgery patients who’d lost an average of 48 pounds showed gains in cognitive functioning. Overall, the study showed initial, rapid cognitive improvement, and then either continued or sustained improvement 3 years out.
"We went from a quarter of patients being clinically impaired prior to surgery," said Dr. Gunstad. "At 3 years after surgery, that number was down to 4%."
However, in a related study, Dr. Gunstad and his colleagues found that greater levels of cognitive impairment correlated to less weight loss at all follow-up points (Surg. Obes. Relat. Dis. 2013;9:765-70).
Dr. Gunstad said this was likely due to patient adherence issues after the tumult of bariatric surgery. "You have to eat in a different way. You have to think in a different way. You have to restructure every moment of your life," said Dr. Gunstad. "If you have problems with memory, problem solving, or organizing, it will be much more difficult to make and persist with those changes."
The clinical implication, said Dr. Gunstad, is that better screening of bariatric surgery candidates might be helpful. "If we know the cognitive status of our patients, it’s likely we will know what the outcomes will be," he said.
The drawback, he said, is that even though most third-party payers will cover the costs of evaluations, if a physician has a large practice of hundreds of patients, then the number of referrals might be overwhelming to the system, which might not have enough neuropsychologists to perform the tests.
Self-reporting might also be an issue because of the phenomenon of the "worried well" – the patients who overreport their problems – or because the patients with cognitive impairment won’t necessarily recognize the symptoms they need to report, said Dr. Gunstad.
By next year, said Dr. Gunstad, he hoped he and his colleagues will have finalized a better screening tool for clinicians who treat bariatric surgery patients.
Dr. Gunstad did not report any financial disclosures.
ATLANTA – Higher baseline levels of cognitive impairment are associated with poorer weight loss outcomes after bariatric surgery.
"People with problems of memory, problem solving, or attention prior to surgery show reduced ability to lose weight," said John Gunstad, Ph.D., at Obesity Week, presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
In a prospective study of 109 bariatric surgery patients enrolled in the LABS (Longitudinal Assessment of Bariatric Surgery) study and 41 obese matched controls who’d not had surgery, Dr. Gunstad, who is professor and chairman of neuroscience at Kent (Ohio) State University, and his colleagues assessed all participants’ cognitive function at baseline, at 12 weeks, and at 12, 24, and 36 months.
They found that 25% of all surgical patients had baseline cognitive impairment. "These were individuals who were at least 1.5 standard deviations below normal-weight persons in at least one cognitive domain," said Dr. Gunstad. "If these individuals came to my clinic, I would have to diagnose them with some kind of cognitive disorder."
Expanding the criteria to 1 standard deviation meant that 40% of participants had subtle impairment. "Patients who are coming in for bariatric surgery are between 5 and 8 times more likely to have cognitive impairment than their normal-weight counterparts. That’s a remarkable number," said Dr. Gunstad.
At 12 weeks, surgery patients who’d lost an average of 48 pounds showed gains in cognitive functioning. Overall, the study showed initial, rapid cognitive improvement, and then either continued or sustained improvement 3 years out.
"We went from a quarter of patients being clinically impaired prior to surgery," said Dr. Gunstad. "At 3 years after surgery, that number was down to 4%."
However, in a related study, Dr. Gunstad and his colleagues found that greater levels of cognitive impairment correlated to less weight loss at all follow-up points (Surg. Obes. Relat. Dis. 2013;9:765-70).
Dr. Gunstad said this was likely due to patient adherence issues after the tumult of bariatric surgery. "You have to eat in a different way. You have to think in a different way. You have to restructure every moment of your life," said Dr. Gunstad. "If you have problems with memory, problem solving, or organizing, it will be much more difficult to make and persist with those changes."
The clinical implication, said Dr. Gunstad, is that better screening of bariatric surgery candidates might be helpful. "If we know the cognitive status of our patients, it’s likely we will know what the outcomes will be," he said.
The drawback, he said, is that even though most third-party payers will cover the costs of evaluations, if a physician has a large practice of hundreds of patients, then the number of referrals might be overwhelming to the system, which might not have enough neuropsychologists to perform the tests.
Self-reporting might also be an issue because of the phenomenon of the "worried well" – the patients who overreport their problems – or because the patients with cognitive impairment won’t necessarily recognize the symptoms they need to report, said Dr. Gunstad.
By next year, said Dr. Gunstad, he hoped he and his colleagues will have finalized a better screening tool for clinicians who treat bariatric surgery patients.
Dr. Gunstad did not report any financial disclosures.
AT OBESITY WEEK

Gastric bypass associated with reversal of aging process
ATLANTA – Gastric bypass was associated with the lengthening of telomeres, an indication that surgical weight loss may reverse aging in obese patients.
The most significant changes in telomere length occurred in patients with biomarkers indicative of higher levels of preoperative inflammation and cholesterol, according to findings presented by bariatric surgeon John Morton at this year’s Obesity Week.
"Telomeres are unique markers for aging and are linked to chronic diseases and things like smoking and depression," Dr. Morton said in an interview. "There are a lot of things that can potentially affect telomeres, but there aren’t a lot of things that can affect them in a positive sense."
Dr. Morton and his colleagues at Stanford (Calif.) University measured the baseline telomere length, weight, C-reactive protein (CRP) levels, cholesterol levels, and fasting insulin levels in 51 gastric bypass surgery patients (77% female, average age 49 years). The group’s mean body mass index was 44 kg/m2. The measurements were taken again at 3, 6, and 12 months. Telomere length was determined using quantitative polymerase chain reaction testing.

In all patients, excess body weight loss at 12 months averaged 71%; CRP levels, indicative of inflammation, dropped an average of more than 60%. Fasting insulin levels decreased from 24 uIU/mL at baseline to 6 uIU/mL when measured 1 year after surgery. These results were consistent with those of previous studies, but this study was the first to correlate such changes with the body’s biomarkers for aging, telomeres, Dr. Morton said.
Unexpected results
Telomere length did not change significantly across the cohort, but when analyzed according to CRP and LDL levels, significant changes in telomere length were found in patients whose levels of both were higher at baseline (P = .0387 and P = .005). In those whose baseline CRP was high, there also was a significant positive correlation between telomere lengthening and weight loss (P = .0498) and increases in HDL cholesterol level (P = .0176).
The results were somewhat unexpected. "The thing that surprised me the most was that if there were going to be changes, then they should be across the board," said Dr. Morton. "But where it really made a difference was in those who had [high levels of markers of] inflammation. It was a pretty specific result in a pretty specific population."
At least one other longitudinal study has shown the impact of nonsurgical intervention, namely a change in diet, on the length of telomeres (PLoS One 2013;8:e62781[doi:10.1371/journal.pone.0062781]), but Dr. Morton said the study, which emphasized eating less red meat and more fish, fresh vegetables, and olive oil did not demonstrate results that were notably different from his findings.
"One thing that study’s diet, the Mediterranean Diet, is known to do is to raise HDL," said Dr. Morton. "In our study we also saw a correlation between telomere lengthening and increases in HDL. That’s really hard to do. There aren’t a lot of medicines that can really affect the ‘good’ cholesterol."
‘Unique ability’ of gastric bypass
The study did not examine the relationship between telomeres and other kinds of surgical interventions for weight loss, but Dr. Morton said future studies on bariatric procedures such as the sleeve gastrectomy need to be conducted before they can be equated with bypass.
"Gastric bypass has a unique affect on inflammation that is independent of the other operations," said Dr. Morton, referring to data he presented earlier this year at the American College of Surgeons annual meeting, discussing the relationship between bypass and diabetes. "We have shown that C-reactive protein decreases more with gastric bypass than with other operations."
That of all the surgical interventions, gastric bypass has the greatest impact on diabetes, independent of weight loss, points to future research on inflammation, said Dr. Morton. "People are starting to think that type 2 diabetes is not just a burned-out pancreas, but that a lot of inflammation is involved."
Calling bariatric surgery a "platform for investigation" that can help [us] understand the connection between inflammation and the processes of disease in the general population, not just those with obesity, Dr. Morton said, "I think the future will elucidate some of those processes, and will come up with different interventions such as drugs."
Dr. Morton said he did not have any relevant financial disclosures.
ATLANTA – Gastric bypass was associated with the lengthening of telomeres, an indication that surgical weight loss may reverse aging in obese patients.
The most significant changes in telomere length occurred in patients with biomarkers indicative of higher levels of preoperative inflammation and cholesterol, according to findings presented by bariatric surgeon John Morton at this year’s Obesity Week.
"Telomeres are unique markers for aging and are linked to chronic diseases and things like smoking and depression," Dr. Morton said in an interview. "There are a lot of things that can potentially affect telomeres, but there aren’t a lot of things that can affect them in a positive sense."
Dr. Morton and his colleagues at Stanford (Calif.) University measured the baseline telomere length, weight, C-reactive protein (CRP) levels, cholesterol levels, and fasting insulin levels in 51 gastric bypass surgery patients (77% female, average age 49 years). The group’s mean body mass index was 44 kg/m2. The measurements were taken again at 3, 6, and 12 months. Telomere length was determined using quantitative polymerase chain reaction testing.
In all patients, excess body weight loss at 12 months averaged 71%; CRP levels, indicative of inflammation, dropped an average of more than 60%. Fasting insulin levels decreased from 24 uIU/mL at baseline to 6 uIU/mL when measured 1 year after surgery. These results were consistent with those of previous studies, but this study was the first to correlate such changes with the body’s biomarkers for aging, telomeres, Dr. Morton said.
Unexpected results
Telomere length did not change significantly across the cohort, but when analyzed according to CRP and LDL levels, significant changes in telomere length were found in patients whose levels of both were higher at baseline (P = .0387 and P = .005). In those whose baseline CRP was high, there also was a significant positive correlation between telomere lengthening and weight loss (P = .0498) and increases in HDL cholesterol level (P = .0176).
The results were somewhat unexpected. "The thing that surprised me the most was that if there were going to be changes, then they should be across the board," said Dr. Morton. "But where it really made a difference was in those who had [high levels of markers of] inflammation. It was a pretty specific result in a pretty specific population."
At least one other longitudinal study has shown the impact of nonsurgical intervention, namely a change in diet, on the length of telomeres (PLoS One 2013;8:e62781[doi:10.1371/journal.pone.0062781]), but Dr. Morton said the study, which emphasized eating less red meat and more fish, fresh vegetables, and olive oil did not demonstrate results that were notably different from his findings.
"One thing that study’s diet, the Mediterranean Diet, is known to do is to raise HDL," said Dr. Morton. "In our study we also saw a correlation between telomere lengthening and increases in HDL. That’s really hard to do. There aren’t a lot of medicines that can really affect the ‘good’ cholesterol."
‘Unique ability’ of gastric bypass
The study did not examine the relationship between telomeres and other kinds of surgical interventions for weight loss, but Dr. Morton said future studies on bariatric procedures such as the sleeve gastrectomy need to be conducted before they can be equated with bypass.
"Gastric bypass has a unique affect on inflammation that is independent of the other operations," said Dr. Morton, referring to data he presented earlier this year at the American College of Surgeons annual meeting, discussing the relationship between bypass and diabetes. "We have shown that C-reactive protein decreases more with gastric bypass than with other operations."
That of all the surgical interventions, gastric bypass has the greatest impact on diabetes, independent of weight loss, points to future research on inflammation, said Dr. Morton. "People are starting to think that type 2 diabetes is not just a burned-out pancreas, but that a lot of inflammation is involved."
Calling bariatric surgery a "platform for investigation" that can help [us] understand the connection between inflammation and the processes of disease in the general population, not just those with obesity, Dr. Morton said, "I think the future will elucidate some of those processes, and will come up with different interventions such as drugs."
Dr. Morton said he did not have any relevant financial disclosures.
ATLANTA – Gastric bypass was associated with the lengthening of telomeres, an indication that surgical weight loss may reverse aging in obese patients.
The most significant changes in telomere length occurred in patients with biomarkers indicative of higher levels of preoperative inflammation and cholesterol, according to findings presented by bariatric surgeon John Morton at this year’s Obesity Week.
"Telomeres are unique markers for aging and are linked to chronic diseases and things like smoking and depression," Dr. Morton said in an interview. "There are a lot of things that can potentially affect telomeres, but there aren’t a lot of things that can affect them in a positive sense."
Dr. Morton and his colleagues at Stanford (Calif.) University measured the baseline telomere length, weight, C-reactive protein (CRP) levels, cholesterol levels, and fasting insulin levels in 51 gastric bypass surgery patients (77% female, average age 49 years). The group’s mean body mass index was 44 kg/m2. The measurements were taken again at 3, 6, and 12 months. Telomere length was determined using quantitative polymerase chain reaction testing.
In all patients, excess body weight loss at 12 months averaged 71%; CRP levels, indicative of inflammation, dropped an average of more than 60%. Fasting insulin levels decreased from 24 uIU/mL at baseline to 6 uIU/mL when measured 1 year after surgery. These results were consistent with those of previous studies, but this study was the first to correlate such changes with the body’s biomarkers for aging, telomeres, Dr. Morton said.
Unexpected results
Telomere length did not change significantly across the cohort, but when analyzed according to CRP and LDL levels, significant changes in telomere length were found in patients whose levels of both were higher at baseline (P = .0387 and P = .005). In those whose baseline CRP was high, there also was a significant positive correlation between telomere lengthening and weight loss (P = .0498) and increases in HDL cholesterol level (P = .0176).
The results were somewhat unexpected. "The thing that surprised me the most was that if there were going to be changes, then they should be across the board," said Dr. Morton. "But where it really made a difference was in those who had [high levels of markers of] inflammation. It was a pretty specific result in a pretty specific population."
At least one other longitudinal study has shown the impact of nonsurgical intervention, namely a change in diet, on the length of telomeres (PLoS One 2013;8:e62781[doi:10.1371/journal.pone.0062781]), but Dr. Morton said the study, which emphasized eating less red meat and more fish, fresh vegetables, and olive oil did not demonstrate results that were notably different from his findings.
"One thing that study’s diet, the Mediterranean Diet, is known to do is to raise HDL," said Dr. Morton. "In our study we also saw a correlation between telomere lengthening and increases in HDL. That’s really hard to do. There aren’t a lot of medicines that can really affect the ‘good’ cholesterol."
‘Unique ability’ of gastric bypass
The study did not examine the relationship between telomeres and other kinds of surgical interventions for weight loss, but Dr. Morton said future studies on bariatric procedures such as the sleeve gastrectomy need to be conducted before they can be equated with bypass.
"Gastric bypass has a unique affect on inflammation that is independent of the other operations," said Dr. Morton, referring to data he presented earlier this year at the American College of Surgeons annual meeting, discussing the relationship between bypass and diabetes. "We have shown that C-reactive protein decreases more with gastric bypass than with other operations."
That of all the surgical interventions, gastric bypass has the greatest impact on diabetes, independent of weight loss, points to future research on inflammation, said Dr. Morton. "People are starting to think that type 2 diabetes is not just a burned-out pancreas, but that a lot of inflammation is involved."
Calling bariatric surgery a "platform for investigation" that can help [us] understand the connection between inflammation and the processes of disease in the general population, not just those with obesity, Dr. Morton said, "I think the future will elucidate some of those processes, and will come up with different interventions such as drugs."
Dr. Morton said he did not have any relevant financial disclosures.
AT OBESITY WEEK
Major finding: Significant increases in telomere length were observed after gastric bypass in individuals with high baseline CRP or LDL cholesterol levels (P = .0387 and P = .005, respectively); weight loss and increased levels of HDL cholesterol were positively correlated with telomere length in patients with high baseline CRP (P = .0498 and P = .0176).
Data source: A prospective study of 51 gastric bypass patients (77% female) whose telomere lengths, LDL, and CRP levels were measured at baseline and at 3,6, and 12 months.
Disclosures: Dr. Morton said he did not have any relevant financial disclosures.
