User login
VIDEO: How to improve cancer survivorship planning
BRUSSELS – National Cancer Institute Director Catherine Alfano, Ph.D., summarizes the institute’s work on improving cancer survivor planning, better coordinating survivor care, and gathering new data on long-term outcomes. She made her remarks during the Cancer Survivorship Summit in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
BRUSSELS – National Cancer Institute Director Catherine Alfano, Ph.D., summarizes the institute’s work on improving cancer survivor planning, better coordinating survivor care, and gathering new data on long-term outcomes. She made her remarks during the Cancer Survivorship Summit in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
BRUSSELS – National Cancer Institute Director Catherine Alfano, Ph.D., summarizes the institute’s work on improving cancer survivor planning, better coordinating survivor care, and gathering new data on long-term outcomes. She made her remarks during the Cancer Survivorship Summit in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE CANCER SURVIVORSHIP SUMMIT
Palliative care is not just for the dying
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.

Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
On Twitter @sherryboschert
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
|
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
|
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.
Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.
Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
On Twitter @sherryboschert
EXPERT ANALYSIS FROM THE CRITICAL CARE CONGRESS

Palliative care is not just for the dying
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.

Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
If you’re interested in more about these topics, you can join a discussion on this topic within the Critical Care e-Community. Simply log in to ecommunity.chestnet.org and find the Critical Care group. If you’re not part of the Critical Care NetWork, log in to chestnet.org and add the Critical Care NetWork to your profile.
Questions? Contact [email protected].
On Twitter @sherryboschert
|
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
|
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
|
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.
Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
If you’re interested in more about these topics, you can join a discussion on this topic within the Critical Care e-Community. Simply log in to ecommunity.chestnet.org and find the Critical Care group. If you’re not part of the Critical Care NetWork, log in to chestnet.org and add the Critical Care NetWork to your profile.
Questions? Contact [email protected].
On Twitter @sherryboschert
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.
Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
If you’re interested in more about these topics, you can join a discussion on this topic within the Critical Care e-Community. Simply log in to ecommunity.chestnet.org and find the Critical Care group. If you’re not part of the Critical Care NetWork, log in to chestnet.org and add the Critical Care NetWork to your profile.
Questions? Contact [email protected].
On Twitter @sherryboschert
EXPERT ANALYSIS FROM THE CRITICAL CARE CONGRESS

Relatively few in ICUs get end-of-life communication training
SAN FRANCISCO – Despite training recommendations, half of physicians and less than a third of nurses surveyed in adult intensive care units at 56 California hospitals reported receiving formal training in talking with patients and families about end-of-life.
A 2008 consensus statement by the American College of Critical Care Medicine included a recommendation for end-of-life communication skills training for clinicians to improve the care of patients dying in ICUs (Crit. Care Med. 2008;36:953-63).
Dr. Matthew H.R. Anstey and his associates approached 149 California hospitals to gauge the extent of implementation of this recommendation. At 56 hospitals, doctors and nurses who work in adult ICUs voluntarily completed an anonymous web-based survey. Eighty-four percent of the 1,363 respondents were nurses, he reported in a poster presentation at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.

Overall, 32% of the respondents said they had received formal training in communication skills. A significantly higher percentage of doctors had undergone training (50%) compared with nurses (29%), said Dr. Anstey, who is currently a lecturer in anesthesia at Harvard Medical School, Boston.
Sixty-six percent of all respondents agreed that "nurses are present during the communication of end-of-life information to the family" at their institution. Nurses were significantly more likely to agree with this statement (69%) than were doctors (52%).
Both doctors and nurses were very supportive of the idea of formal communication training for ICU providers. When asked about possible strategies to reduce inappropriate care for ICU patients, 91% of respondents said communication training would have a positive effect, Dr. Anstey reported.
This could be accomplished by requiring ICU physicians to complete a communication training module for ongoing credentialing, he said in an interview. Either individual hospitals could require this as part of credentialing for privileges to work in the ICU, or state medical boards could require it, similar to the California Medical Board’s requirement that physicians obtain some continuing medical education in pain management, he suggested.
The characteristics of participating hospitals were similar to those of nonparticipating hospitals in the sizes of the hospitals and ICUs, their regional location in California, and the proportions of hospitals that are teaching facilities. The 93 nonparticipating hospitals were significantly more likely to be for-profit hospitals (59%) compared with participating hospitals (7%), and significantly less likely to be part of a hospital system containing more than three hospitals (54%) compared with participating hospitals (75%).
Dr. Anstey reported having no financial disclosures. His research was in conjunction with a Commonwealth Fund Harkness Fellowship in Health Care Policy and Practice for which he was placed at Kaiser Permanente in California.
On Twitter @sherryboschert
I am not at all surprised, nor am I disappointed by these findings. As a nation we are headed in the right direction with improving communication around end-of-life (EOL) issues.

|
|
One of the recommendations coming from 2008 guidelines by the American College of Physicians has to do with communicating advance directives and addressing the EOL topic with our patients. I am thrilled that we are beginning to have guidelines and recommendations like these to use as stimulation and leverage, improving the patient experience. If we reflect on some relatively depressing data from the last few years looking at internal medicine physicians at the University of California, San Francisco, admitting acutely ill patients and having advance directive discussions with them (J. Gen. Intern. Med. 2011;26:359-66), then I am encouraged by the findings in this ICU study. While the patient population (medical floor vs. ICU) is somewhat different, both populations benefit from advance care planning.
Barriers to end-of-life communications in ICUs include deficits in communication skills and a lack of time. The average amount of time, conservatively, is 45 minutes for these discussions. Care providers may avoid these discussions because of difficulty with their own emotions, perceiving the family as "difficult," a lack of understanding between the health care provider and the patient or family, and poor compliance. There’s little – if any – reimbursement, space is an issue as there are very few family conference rooms in hospitals, and there is mixed messaging by the numerous teams or specialties involved. The list goes on!
The Gundersen Health System in La Crosse, Wisc., is a good example of how to create a successful system of advance care planning. No one does it better. Also, the "premier programs" listed on the website of the Improving Palliative Care in the ICU (IPAL-ICU) Project are examples of leaders in the field.
Training in advance care planning is part of the education of students and residents at our institution. The University of Texas and Seton Healthcare jointly are creating a medical school in Austin. We plan to have all medical students spend time with our palliative care team and learn these communication skills. We began work on the IPAL-ICU program at two of our large hospitals. We also have put in a proposal to teach these skills to our providers and other providers within our community.
Finally, our program is collaborating with elderly advocacy groups in town to train their nurses and social workers in having upstream discussions with the population they serve so that decisions are addressed before hospitalization.
Dr. Stephen J. Bekanich, codirector of the palliative care program at Seton Healthcare, Austin, Tex., coauthors the Palliatively Speaking blog for Hospitalist News. He reported having no financial disclosures.
I am not at all surprised, nor am I disappointed by these findings. As a nation we are headed in the right direction with improving communication around end-of-life (EOL) issues.
|
|
|
One of the recommendations coming from 2008 guidelines by the American College of Physicians has to do with communicating advance directives and addressing the EOL topic with our patients. I am thrilled that we are beginning to have guidelines and recommendations like these to use as stimulation and leverage, improving the patient experience. If we reflect on some relatively depressing data from the last few years looking at internal medicine physicians at the University of California, San Francisco, admitting acutely ill patients and having advance directive discussions with them (J. Gen. Intern. Med. 2011;26:359-66), then I am encouraged by the findings in this ICU study. While the patient population (medical floor vs. ICU) is somewhat different, both populations benefit from advance care planning.
Barriers to end-of-life communications in ICUs include deficits in communication skills and a lack of time. The average amount of time, conservatively, is 45 minutes for these discussions. Care providers may avoid these discussions because of difficulty with their own emotions, perceiving the family as "difficult," a lack of understanding between the health care provider and the patient or family, and poor compliance. There’s little – if any – reimbursement, space is an issue as there are very few family conference rooms in hospitals, and there is mixed messaging by the numerous teams or specialties involved. The list goes on!
The Gundersen Health System in La Crosse, Wisc., is a good example of how to create a successful system of advance care planning. No one does it better. Also, the "premier programs" listed on the website of the Improving Palliative Care in the ICU (IPAL-ICU) Project are examples of leaders in the field.
Training in advance care planning is part of the education of students and residents at our institution. The University of Texas and Seton Healthcare jointly are creating a medical school in Austin. We plan to have all medical students spend time with our palliative care team and learn these communication skills. We began work on the IPAL-ICU program at two of our large hospitals. We also have put in a proposal to teach these skills to our providers and other providers within our community.
Finally, our program is collaborating with elderly advocacy groups in town to train their nurses and social workers in having upstream discussions with the population they serve so that decisions are addressed before hospitalization.
Dr. Stephen J. Bekanich, codirector of the palliative care program at Seton Healthcare, Austin, Tex., coauthors the Palliatively Speaking blog for Hospitalist News. He reported having no financial disclosures.
I am not at all surprised, nor am I disappointed by these findings. As a nation we are headed in the right direction with improving communication around end-of-life (EOL) issues.
|
|
|
One of the recommendations coming from 2008 guidelines by the American College of Physicians has to do with communicating advance directives and addressing the EOL topic with our patients. I am thrilled that we are beginning to have guidelines and recommendations like these to use as stimulation and leverage, improving the patient experience. If we reflect on some relatively depressing data from the last few years looking at internal medicine physicians at the University of California, San Francisco, admitting acutely ill patients and having advance directive discussions with them (J. Gen. Intern. Med. 2011;26:359-66), then I am encouraged by the findings in this ICU study. While the patient population (medical floor vs. ICU) is somewhat different, both populations benefit from advance care planning.
Barriers to end-of-life communications in ICUs include deficits in communication skills and a lack of time. The average amount of time, conservatively, is 45 minutes for these discussions. Care providers may avoid these discussions because of difficulty with their own emotions, perceiving the family as "difficult," a lack of understanding between the health care provider and the patient or family, and poor compliance. There’s little – if any – reimbursement, space is an issue as there are very few family conference rooms in hospitals, and there is mixed messaging by the numerous teams or specialties involved. The list goes on!
The Gundersen Health System in La Crosse, Wisc., is a good example of how to create a successful system of advance care planning. No one does it better. Also, the "premier programs" listed on the website of the Improving Palliative Care in the ICU (IPAL-ICU) Project are examples of leaders in the field.
Training in advance care planning is part of the education of students and residents at our institution. The University of Texas and Seton Healthcare jointly are creating a medical school in Austin. We plan to have all medical students spend time with our palliative care team and learn these communication skills. We began work on the IPAL-ICU program at two of our large hospitals. We also have put in a proposal to teach these skills to our providers and other providers within our community.
Finally, our program is collaborating with elderly advocacy groups in town to train their nurses and social workers in having upstream discussions with the population they serve so that decisions are addressed before hospitalization.
Dr. Stephen J. Bekanich, codirector of the palliative care program at Seton Healthcare, Austin, Tex., coauthors the Palliatively Speaking blog for Hospitalist News. He reported having no financial disclosures.
SAN FRANCISCO – Despite training recommendations, half of physicians and less than a third of nurses surveyed in adult intensive care units at 56 California hospitals reported receiving formal training in talking with patients and families about end-of-life.
A 2008 consensus statement by the American College of Critical Care Medicine included a recommendation for end-of-life communication skills training for clinicians to improve the care of patients dying in ICUs (Crit. Care Med. 2008;36:953-63).
Dr. Matthew H.R. Anstey and his associates approached 149 California hospitals to gauge the extent of implementation of this recommendation. At 56 hospitals, doctors and nurses who work in adult ICUs voluntarily completed an anonymous web-based survey. Eighty-four percent of the 1,363 respondents were nurses, he reported in a poster presentation at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Overall, 32% of the respondents said they had received formal training in communication skills. A significantly higher percentage of doctors had undergone training (50%) compared with nurses (29%), said Dr. Anstey, who is currently a lecturer in anesthesia at Harvard Medical School, Boston.
Sixty-six percent of all respondents agreed that "nurses are present during the communication of end-of-life information to the family" at their institution. Nurses were significantly more likely to agree with this statement (69%) than were doctors (52%).
Both doctors and nurses were very supportive of the idea of formal communication training for ICU providers. When asked about possible strategies to reduce inappropriate care for ICU patients, 91% of respondents said communication training would have a positive effect, Dr. Anstey reported.
This could be accomplished by requiring ICU physicians to complete a communication training module for ongoing credentialing, he said in an interview. Either individual hospitals could require this as part of credentialing for privileges to work in the ICU, or state medical boards could require it, similar to the California Medical Board’s requirement that physicians obtain some continuing medical education in pain management, he suggested.
The characteristics of participating hospitals were similar to those of nonparticipating hospitals in the sizes of the hospitals and ICUs, their regional location in California, and the proportions of hospitals that are teaching facilities. The 93 nonparticipating hospitals were significantly more likely to be for-profit hospitals (59%) compared with participating hospitals (7%), and significantly less likely to be part of a hospital system containing more than three hospitals (54%) compared with participating hospitals (75%).
Dr. Anstey reported having no financial disclosures. His research was in conjunction with a Commonwealth Fund Harkness Fellowship in Health Care Policy and Practice for which he was placed at Kaiser Permanente in California.
On Twitter @sherryboschert
SAN FRANCISCO – Despite training recommendations, half of physicians and less than a third of nurses surveyed in adult intensive care units at 56 California hospitals reported receiving formal training in talking with patients and families about end-of-life.
A 2008 consensus statement by the American College of Critical Care Medicine included a recommendation for end-of-life communication skills training for clinicians to improve the care of patients dying in ICUs (Crit. Care Med. 2008;36:953-63).
Dr. Matthew H.R. Anstey and his associates approached 149 California hospitals to gauge the extent of implementation of this recommendation. At 56 hospitals, doctors and nurses who work in adult ICUs voluntarily completed an anonymous web-based survey. Eighty-four percent of the 1,363 respondents were nurses, he reported in a poster presentation at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Overall, 32% of the respondents said they had received formal training in communication skills. A significantly higher percentage of doctors had undergone training (50%) compared with nurses (29%), said Dr. Anstey, who is currently a lecturer in anesthesia at Harvard Medical School, Boston.
Sixty-six percent of all respondents agreed that "nurses are present during the communication of end-of-life information to the family" at their institution. Nurses were significantly more likely to agree with this statement (69%) than were doctors (52%).
Both doctors and nurses were very supportive of the idea of formal communication training for ICU providers. When asked about possible strategies to reduce inappropriate care for ICU patients, 91% of respondents said communication training would have a positive effect, Dr. Anstey reported.
This could be accomplished by requiring ICU physicians to complete a communication training module for ongoing credentialing, he said in an interview. Either individual hospitals could require this as part of credentialing for privileges to work in the ICU, or state medical boards could require it, similar to the California Medical Board’s requirement that physicians obtain some continuing medical education in pain management, he suggested.
The characteristics of participating hospitals were similar to those of nonparticipating hospitals in the sizes of the hospitals and ICUs, their regional location in California, and the proportions of hospitals that are teaching facilities. The 93 nonparticipating hospitals were significantly more likely to be for-profit hospitals (59%) compared with participating hospitals (7%), and significantly less likely to be part of a hospital system containing more than three hospitals (54%) compared with participating hospitals (75%).
Dr. Anstey reported having no financial disclosures. His research was in conjunction with a Commonwealth Fund Harkness Fellowship in Health Care Policy and Practice for which he was placed at Kaiser Permanente in California.
On Twitter @sherryboschert
AT THE CRITICAL CARE CONGRESS

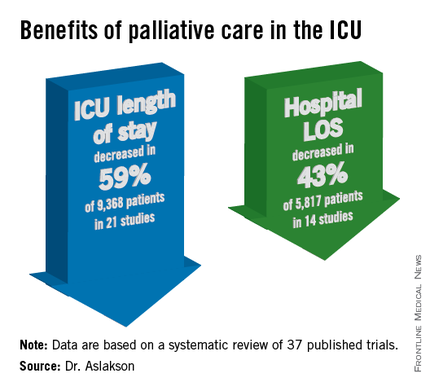
Palliative care shortens ICU, hospital stays, review data show
SAN FRANCISCO – Palliative care in the intensive care unit reduces the length of stay in the ICU and the hospital without changing mortality rates or family satisfaction, according to a review of the literature.
Although measurements of family satisfaction overall didn’t change much from palliative care of a loved one in the ICU, some measures of components of satisfaction increased with palliative care, such as improved communication with the physician, better consensus around the goals of care, and decreased anxiety and depression in family members, reported Dr. Rebecca A. Aslakson of Johns Hopkins University, Baltimore.
The findings have been submitted for publication, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Dr. Aslakson and her associates were unable to perform a formal meta-analysis of the 37 published trials of palliative care in the ICU because of the heterogeneity of the studies, which looked at more than 40 different outcomes. Instead, their systematic review grouped results under four outcomes that commonly were measured, and assessed those either by the number of studies or by the number of patients studied.
ICU length of stay decreased with palliative care in 13 of 21 studies (62%) that used this outcome and in 59% of 9,368 patients in those studies. Hospital length of stay decreased with palliative care in 8 of 14 studies (57%) and in 43% of 5,817 patients. Family satisfaction did not decrease in any studies or families and increased in only 1 of 14 studies (7%) and in 2% of families of 4,927 patients, Dr. Aslakson reported.
Mortality rates did not change with palliative care in 14 of 16 studies (88%) that assessed mortality and in 57% of 5,969 patients in those studies. Mortality increased in one small study (6%) and decreased in one larger study (6%).
"Talking about big-picture issues and goals of care doesn’t lead to people dying," Dr. Aslakson said. "No harm came in any of these studies." Some separate studies of palliative care outside of ICUs reported that this increases hope, "because people feel that they have more control over their choices and what’s happening to their loved ones," she added.
Integrative vs. consultative model
Dr. Aslakson and her associates also reviewed studies based on whether the interventions used integrative or consultative models of palliative care.
Generally, consultative models bring outsiders into the ICU to help provide palliative care, and integrative models train the ICU team to be the palliative care providers. In reality, the two models may overlap. For this review, the investigators applied mutually exclusive definitions to 36 of the studies. In 18 studies of integrative interventions, members of the ICU team were the only caregivers in face-to-face interactions with the patient and families. In 18 studies of consultative interventions, palliative care providers included others besides the ICU team.
In the studies of integrative palliative care, ICU length of stay decreased with palliative care in four of nine studies (44%) that measured this outcome and in 52% of 6,963 patients in those studies, she reported. Hospital length of stay decreased in two of five studies (40%) and in 24% of 3,812 patients. Family satisfaction changed in none of 15 studies, and mortality decreased in 1 of 5 studies (20%) and in 34% of 3,807 patients.
In the studies of consultative care, ICU length of stay decreased with palliative care in 9 of 12 studies (75%) that measured this outcome and in 79% of 2,405 patients in those studies. Hospital length of stay decreased in six of nine studies (67%) and in 79% of 2,005 patients. Family satisfaction increased in one of four studies (25%) and in 21% of 429 patients. Mortality increased in 1 of 11 studies (9%) and in 5% of 2,162 patients.
One model isn’t necessarily better than the other, Dr. Aslakson said. Integrative palliative care may work best in a closed ICU with perhaps four or five intensivists in a relatively small unit. An integrative approach can be much more difficult in open or semiopen ICUs that have "40 different doctors floating around," she said. "We tried that in my unit, and it didn’t work that well."

Different ICUs need palliative care models that fit them. "Look at your unit, the way it works, and who the providers are, then look at the literature and see what matches that and what might work for your unit," she said.
Outcomes of improved communication
A previous, separate review of the medical literature identified 21 controlled trials of 16 interventions to improve communication in ICUs between families and care providers. Overall, the interventions improved emotional outcomes for families and reduced ICU length of stay and treatment intensity (Chest 2011;139:543-54), she noted.
Yet another prior review of the literature reported that interventions to promote family meetings, use empathetic communication skills, and employ palliative care consultations improved family satisfaction and reduced ICU length of stay and the adverse effects of family bereavement (Curr. Opin. Crit. Care 2009;15:569-77).
Dr. Aslakson reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
SAN FRANCISCO – Palliative care in the intensive care unit reduces the length of stay in the ICU and the hospital without changing mortality rates or family satisfaction, according to a review of the literature.
Although measurements of family satisfaction overall didn’t change much from palliative care of a loved one in the ICU, some measures of components of satisfaction increased with palliative care, such as improved communication with the physician, better consensus around the goals of care, and decreased anxiety and depression in family members, reported Dr. Rebecca A. Aslakson of Johns Hopkins University, Baltimore.
The findings have been submitted for publication, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Dr. Aslakson and her associates were unable to perform a formal meta-analysis of the 37 published trials of palliative care in the ICU because of the heterogeneity of the studies, which looked at more than 40 different outcomes. Instead, their systematic review grouped results under four outcomes that commonly were measured, and assessed those either by the number of studies or by the number of patients studied.
ICU length of stay decreased with palliative care in 13 of 21 studies (62%) that used this outcome and in 59% of 9,368 patients in those studies. Hospital length of stay decreased with palliative care in 8 of 14 studies (57%) and in 43% of 5,817 patients. Family satisfaction did not decrease in any studies or families and increased in only 1 of 14 studies (7%) and in 2% of families of 4,927 patients, Dr. Aslakson reported.
Mortality rates did not change with palliative care in 14 of 16 studies (88%) that assessed mortality and in 57% of 5,969 patients in those studies. Mortality increased in one small study (6%) and decreased in one larger study (6%).
"Talking about big-picture issues and goals of care doesn’t lead to people dying," Dr. Aslakson said. "No harm came in any of these studies." Some separate studies of palliative care outside of ICUs reported that this increases hope, "because people feel that they have more control over their choices and what’s happening to their loved ones," she added.
Integrative vs. consultative model
Dr. Aslakson and her associates also reviewed studies based on whether the interventions used integrative or consultative models of palliative care.
Generally, consultative models bring outsiders into the ICU to help provide palliative care, and integrative models train the ICU team to be the palliative care providers. In reality, the two models may overlap. For this review, the investigators applied mutually exclusive definitions to 36 of the studies. In 18 studies of integrative interventions, members of the ICU team were the only caregivers in face-to-face interactions with the patient and families. In 18 studies of consultative interventions, palliative care providers included others besides the ICU team.
In the studies of integrative palliative care, ICU length of stay decreased with palliative care in four of nine studies (44%) that measured this outcome and in 52% of 6,963 patients in those studies, she reported. Hospital length of stay decreased in two of five studies (40%) and in 24% of 3,812 patients. Family satisfaction changed in none of 15 studies, and mortality decreased in 1 of 5 studies (20%) and in 34% of 3,807 patients.
In the studies of consultative care, ICU length of stay decreased with palliative care in 9 of 12 studies (75%) that measured this outcome and in 79% of 2,405 patients in those studies. Hospital length of stay decreased in six of nine studies (67%) and in 79% of 2,005 patients. Family satisfaction increased in one of four studies (25%) and in 21% of 429 patients. Mortality increased in 1 of 11 studies (9%) and in 5% of 2,162 patients.
One model isn’t necessarily better than the other, Dr. Aslakson said. Integrative palliative care may work best in a closed ICU with perhaps four or five intensivists in a relatively small unit. An integrative approach can be much more difficult in open or semiopen ICUs that have "40 different doctors floating around," she said. "We tried that in my unit, and it didn’t work that well."
Different ICUs need palliative care models that fit them. "Look at your unit, the way it works, and who the providers are, then look at the literature and see what matches that and what might work for your unit," she said.
Outcomes of improved communication
A previous, separate review of the medical literature identified 21 controlled trials of 16 interventions to improve communication in ICUs between families and care providers. Overall, the interventions improved emotional outcomes for families and reduced ICU length of stay and treatment intensity (Chest 2011;139:543-54), she noted.
Yet another prior review of the literature reported that interventions to promote family meetings, use empathetic communication skills, and employ palliative care consultations improved family satisfaction and reduced ICU length of stay and the adverse effects of family bereavement (Curr. Opin. Crit. Care 2009;15:569-77).
Dr. Aslakson reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
SAN FRANCISCO – Palliative care in the intensive care unit reduces the length of stay in the ICU and the hospital without changing mortality rates or family satisfaction, according to a review of the literature.
Although measurements of family satisfaction overall didn’t change much from palliative care of a loved one in the ICU, some measures of components of satisfaction increased with palliative care, such as improved communication with the physician, better consensus around the goals of care, and decreased anxiety and depression in family members, reported Dr. Rebecca A. Aslakson of Johns Hopkins University, Baltimore.
The findings have been submitted for publication, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Dr. Aslakson and her associates were unable to perform a formal meta-analysis of the 37 published trials of palliative care in the ICU because of the heterogeneity of the studies, which looked at more than 40 different outcomes. Instead, their systematic review grouped results under four outcomes that commonly were measured, and assessed those either by the number of studies or by the number of patients studied.
ICU length of stay decreased with palliative care in 13 of 21 studies (62%) that used this outcome and in 59% of 9,368 patients in those studies. Hospital length of stay decreased with palliative care in 8 of 14 studies (57%) and in 43% of 5,817 patients. Family satisfaction did not decrease in any studies or families and increased in only 1 of 14 studies (7%) and in 2% of families of 4,927 patients, Dr. Aslakson reported.
Mortality rates did not change with palliative care in 14 of 16 studies (88%) that assessed mortality and in 57% of 5,969 patients in those studies. Mortality increased in one small study (6%) and decreased in one larger study (6%).
"Talking about big-picture issues and goals of care doesn’t lead to people dying," Dr. Aslakson said. "No harm came in any of these studies." Some separate studies of palliative care outside of ICUs reported that this increases hope, "because people feel that they have more control over their choices and what’s happening to their loved ones," she added.
Integrative vs. consultative model
Dr. Aslakson and her associates also reviewed studies based on whether the interventions used integrative or consultative models of palliative care.
Generally, consultative models bring outsiders into the ICU to help provide palliative care, and integrative models train the ICU team to be the palliative care providers. In reality, the two models may overlap. For this review, the investigators applied mutually exclusive definitions to 36 of the studies. In 18 studies of integrative interventions, members of the ICU team were the only caregivers in face-to-face interactions with the patient and families. In 18 studies of consultative interventions, palliative care providers included others besides the ICU team.
In the studies of integrative palliative care, ICU length of stay decreased with palliative care in four of nine studies (44%) that measured this outcome and in 52% of 6,963 patients in those studies, she reported. Hospital length of stay decreased in two of five studies (40%) and in 24% of 3,812 patients. Family satisfaction changed in none of 15 studies, and mortality decreased in 1 of 5 studies (20%) and in 34% of 3,807 patients.
In the studies of consultative care, ICU length of stay decreased with palliative care in 9 of 12 studies (75%) that measured this outcome and in 79% of 2,405 patients in those studies. Hospital length of stay decreased in six of nine studies (67%) and in 79% of 2,005 patients. Family satisfaction increased in one of four studies (25%) and in 21% of 429 patients. Mortality increased in 1 of 11 studies (9%) and in 5% of 2,162 patients.
One model isn’t necessarily better than the other, Dr. Aslakson said. Integrative palliative care may work best in a closed ICU with perhaps four or five intensivists in a relatively small unit. An integrative approach can be much more difficult in open or semiopen ICUs that have "40 different doctors floating around," she said. "We tried that in my unit, and it didn’t work that well."
Different ICUs need palliative care models that fit them. "Look at your unit, the way it works, and who the providers are, then look at the literature and see what matches that and what might work for your unit," she said.
Outcomes of improved communication
A previous, separate review of the medical literature identified 21 controlled trials of 16 interventions to improve communication in ICUs between families and care providers. Overall, the interventions improved emotional outcomes for families and reduced ICU length of stay and treatment intensity (Chest 2011;139:543-54), she noted.
Yet another prior review of the literature reported that interventions to promote family meetings, use empathetic communication skills, and employ palliative care consultations improved family satisfaction and reduced ICU length of stay and the adverse effects of family bereavement (Curr. Opin. Crit. Care 2009;15:569-77).
Dr. Aslakson reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
AT THE CRITICAL CARE CONGRESS
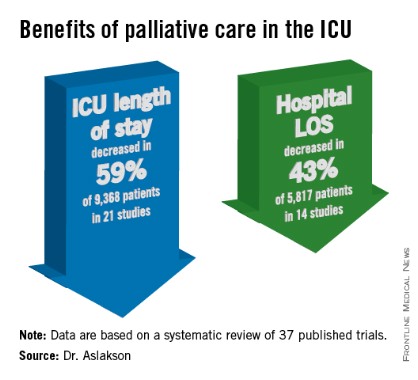
Comfort care informs critical care societies’ Choosing Wisely list
SAN FRANCISCO – Four critical care societies released a list of the top five things that intensivists should avoid doing, part of the larger Choosing Wisely campaign to reduce unnecessary and costly medical practices. The list includes a potentially difficult issue: offering patients' families the option of comfort care in lieu of continuing life support.
Fifth on the list, the life-support item may be the most controversial and is also the one that the representatives felt the most strongly about including, whether or not it saves many resources, according to Dr. Hannah Wunsch, who served on the collaborative task force. "Many ... patients receive aggressive life-sustaining therapies, in part due to clinicians’ failures to elicit patients’ values and goals, and to provide patient-centered recommendations," the task force wrote.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Discussion of the list, which was announced at the Critical Care Congress, quickly turned to how to implement the recommendations, including how to empower families to challenge physicians or nurses when they see these steps being taken in the care of a loved one.
The Society for Critical Care Medicine, which sponsored the Congress, collaborated with the American College of Chest Physicians, the American Thoracic Society, and the American Association of Critical Care Nurses to create the list. It’s the first Choosing Wisely list to include collaboration with a nursing organization and only the second that’s a product of collaboration instead of being issued by a sole medical society, said Dr. Scott D. Halpern of the University of Pennsylvania, Philadelphia, chair of the collaborative group.
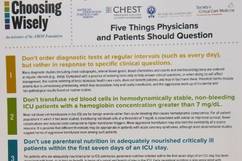
The four groups – the Critical Care Societies Collaborative – started with a list of 58 medical practices that they found objectionable, which they trimmed to 9 items based on the strength of evidence and their prevalence, relevance, and cost, explained Dr. Wunsch of the department of anesthesiology at Columbia University Medical Center, N.Y. Discussion winnowed that to the Top 5, an arbitrary number selected by the Choosing Wisely campaign that everyone should recognize as "a starting point," she said.
A two-page document of the critical care list can be downloaded from the Choosing Wisely website. It includes some of the sources for the recommendations and these top five "don’ts" displayed on the front:
1. Don’t order diagnostic tests at regular intervals (such as every day), but rather in response to specific clinical questions. Ordering diagnostic studies such as x-rays, arterial blood gases, blood counts, blood chemistries, or ECGs daily or at routine intervals drives up costs, doesn’t benefit patients, and may harm them through radiation exposure, inducing anemia, or triggering aggressive follow-up of incidental results. "I think this has become more prevalent with electronic medical records," where one click can order x-rays for the next 5 days, she said.

2. Don’t transfuse red blood cells in hemodynamically stable, non-bleeding ICU patients with a hemoglobin concentration greater than 7 mg/dL. Blood is a scarce resource, and studies show that limiting red blood cell transfusions to thresholds of 7 mg/dL or higher does not worsen survival, complications, or costs, and causes fewer complications. Different thresholds may be appropriate for patients with acute coronary syndrome, but even in this subgroup aggressive transfusion is harmful, most observational studies suggest.
3. Don’t use parenteral nutrition in adequately nourished critically ill patients within the first 7 days of an ICU stay. Early parenteral nutrition is harmful, even in patients who cannot tolerate enteral nutrition, if they were adequately nourished prior to ICU admission. The evidence is less clear for patients with nosocomial infections, and early parenteral nutrition may benefit patients who were severely malnourished right before ICU admission.
A study to be published soon shows that 90% of parenteral nutrition in the United States starts within 7 days of admission, usually within the first 2 days, Dr. Wunsch said. "It’s definitely more prevalent than I think many of us realize," she said.

4. Don’t deeply sedate mechanically ventilated patients without a specific indication and without daily attempts to lighten sedation. Deep sedation of patients on mechanical ventilation prolongs the duration of ventilation and hospitalization. Several protocols for limiting sedation have been shown to improve patient outcomes.
5. Don’t continue life support for patients at high risk of death or severely impaired functional recovery without offering patients and their families the alternative of care focused entirely on comfort. When an audience member expressed concern about discontinuation of life support possibly increasing premature deaths, Dr. Wunsch stressed that the second part of the statement is key – giving the family the choice of comfort care or continuing life support.
The simplicity of the Choosing Wisely list and its focus on overuse and costs make it possible to pursue unconventional ways of making it widely adopted, such as empowering families to question care, said Dr. Jeremy M. Kahn of the University of Pittsburgh. The 5 recommendations are far fewer than the 85 recommendations in the 2002 Surviving Sepsis campaign, for example, and the Choosing Wisely campaign has partnered with Consumer Reports and engaged the lay press to help spread the word, he said.
Dr. Kahn described a recent uncomfortable experience in which he had to question some of the medical care being offered to a hospitalized family member. It wasn’t easy to speak up, even though he’s a physician, and it must be even harder for lay people, he said. Hanging a sign in every ICU with the Choosing Wisely list might help empower families to speak up, one physician suggested during the discussion.
Incorporating decision-support prompts in electronic health records also could help physicians adhere to the Choosing Wisely recommendations, Dr. Kahn said.
Beyond the five items that made the Choosing Wisely list, the four runners-up were issues of antimicrobial duration; CT or MRI scanning for altered level of consciousness; vascular catheter indications; and ICU admission criteria for patients with poor prognosis, Dr. Wunsch said.
The Critical Care Societies Collaborative represents approximately 150,000 critical care providers, according to Dr. Curtis Sessler, president-designate of the American College of Chest Physicians.
The Choosing Wisely campaign, a project of the ABIM Foundation, released lists of "Five Things Physicians and Patients Should Question" by 9 medical societies in April 2012 and 17 more in February 2013, with the development of more lists ongoing.
The speakers reported having no financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – Four critical care societies released a list of the top five things that intensivists should avoid doing, part of the larger Choosing Wisely campaign to reduce unnecessary and costly medical practices. The list includes a potentially difficult issue: offering patients' families the option of comfort care in lieu of continuing life support.
Fifth on the list, the life-support item may be the most controversial and is also the one that the representatives felt the most strongly about including, whether or not it saves many resources, according to Dr. Hannah Wunsch, who served on the collaborative task force. "Many ... patients receive aggressive life-sustaining therapies, in part due to clinicians’ failures to elicit patients’ values and goals, and to provide patient-centered recommendations," the task force wrote.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Discussion of the list, which was announced at the Critical Care Congress, quickly turned to how to implement the recommendations, including how to empower families to challenge physicians or nurses when they see these steps being taken in the care of a loved one.
The Society for Critical Care Medicine, which sponsored the Congress, collaborated with the American College of Chest Physicians, the American Thoracic Society, and the American Association of Critical Care Nurses to create the list. It’s the first Choosing Wisely list to include collaboration with a nursing organization and only the second that’s a product of collaboration instead of being issued by a sole medical society, said Dr. Scott D. Halpern of the University of Pennsylvania, Philadelphia, chair of the collaborative group.
The four groups – the Critical Care Societies Collaborative – started with a list of 58 medical practices that they found objectionable, which they trimmed to 9 items based on the strength of evidence and their prevalence, relevance, and cost, explained Dr. Wunsch of the department of anesthesiology at Columbia University Medical Center, N.Y. Discussion winnowed that to the Top 5, an arbitrary number selected by the Choosing Wisely campaign that everyone should recognize as "a starting point," she said.
A two-page document of the critical care list can be downloaded from the Choosing Wisely website. It includes some of the sources for the recommendations and these top five "don’ts" displayed on the front:
1. Don’t order diagnostic tests at regular intervals (such as every day), but rather in response to specific clinical questions. Ordering diagnostic studies such as x-rays, arterial blood gases, blood counts, blood chemistries, or ECGs daily or at routine intervals drives up costs, doesn’t benefit patients, and may harm them through radiation exposure, inducing anemia, or triggering aggressive follow-up of incidental results. "I think this has become more prevalent with electronic medical records," where one click can order x-rays for the next 5 days, she said.
2. Don’t transfuse red blood cells in hemodynamically stable, non-bleeding ICU patients with a hemoglobin concentration greater than 7 mg/dL. Blood is a scarce resource, and studies show that limiting red blood cell transfusions to thresholds of 7 mg/dL or higher does not worsen survival, complications, or costs, and causes fewer complications. Different thresholds may be appropriate for patients with acute coronary syndrome, but even in this subgroup aggressive transfusion is harmful, most observational studies suggest.
3. Don’t use parenteral nutrition in adequately nourished critically ill patients within the first 7 days of an ICU stay. Early parenteral nutrition is harmful, even in patients who cannot tolerate enteral nutrition, if they were adequately nourished prior to ICU admission. The evidence is less clear for patients with nosocomial infections, and early parenteral nutrition may benefit patients who were severely malnourished right before ICU admission.
A study to be published soon shows that 90% of parenteral nutrition in the United States starts within 7 days of admission, usually within the first 2 days, Dr. Wunsch said. "It’s definitely more prevalent than I think many of us realize," she said.
4. Don’t deeply sedate mechanically ventilated patients without a specific indication and without daily attempts to lighten sedation. Deep sedation of patients on mechanical ventilation prolongs the duration of ventilation and hospitalization. Several protocols for limiting sedation have been shown to improve patient outcomes.
5. Don’t continue life support for patients at high risk of death or severely impaired functional recovery without offering patients and their families the alternative of care focused entirely on comfort. When an audience member expressed concern about discontinuation of life support possibly increasing premature deaths, Dr. Wunsch stressed that the second part of the statement is key – giving the family the choice of comfort care or continuing life support.
The simplicity of the Choosing Wisely list and its focus on overuse and costs make it possible to pursue unconventional ways of making it widely adopted, such as empowering families to question care, said Dr. Jeremy M. Kahn of the University of Pittsburgh. The 5 recommendations are far fewer than the 85 recommendations in the 2002 Surviving Sepsis campaign, for example, and the Choosing Wisely campaign has partnered with Consumer Reports and engaged the lay press to help spread the word, he said.
Dr. Kahn described a recent uncomfortable experience in which he had to question some of the medical care being offered to a hospitalized family member. It wasn’t easy to speak up, even though he’s a physician, and it must be even harder for lay people, he said. Hanging a sign in every ICU with the Choosing Wisely list might help empower families to speak up, one physician suggested during the discussion.
Incorporating decision-support prompts in electronic health records also could help physicians adhere to the Choosing Wisely recommendations, Dr. Kahn said.
Beyond the five items that made the Choosing Wisely list, the four runners-up were issues of antimicrobial duration; CT or MRI scanning for altered level of consciousness; vascular catheter indications; and ICU admission criteria for patients with poor prognosis, Dr. Wunsch said.
The Critical Care Societies Collaborative represents approximately 150,000 critical care providers, according to Dr. Curtis Sessler, president-designate of the American College of Chest Physicians.
The Choosing Wisely campaign, a project of the ABIM Foundation, released lists of "Five Things Physicians and Patients Should Question" by 9 medical societies in April 2012 and 17 more in February 2013, with the development of more lists ongoing.
The speakers reported having no financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – Four critical care societies released a list of the top five things that intensivists should avoid doing, part of the larger Choosing Wisely campaign to reduce unnecessary and costly medical practices. The list includes a potentially difficult issue: offering patients' families the option of comfort care in lieu of continuing life support.
Fifth on the list, the life-support item may be the most controversial and is also the one that the representatives felt the most strongly about including, whether or not it saves many resources, according to Dr. Hannah Wunsch, who served on the collaborative task force. "Many ... patients receive aggressive life-sustaining therapies, in part due to clinicians’ failures to elicit patients’ values and goals, and to provide patient-centered recommendations," the task force wrote.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Discussion of the list, which was announced at the Critical Care Congress, quickly turned to how to implement the recommendations, including how to empower families to challenge physicians or nurses when they see these steps being taken in the care of a loved one.
The Society for Critical Care Medicine, which sponsored the Congress, collaborated with the American College of Chest Physicians, the American Thoracic Society, and the American Association of Critical Care Nurses to create the list. It’s the first Choosing Wisely list to include collaboration with a nursing organization and only the second that’s a product of collaboration instead of being issued by a sole medical society, said Dr. Scott D. Halpern of the University of Pennsylvania, Philadelphia, chair of the collaborative group.
The four groups – the Critical Care Societies Collaborative – started with a list of 58 medical practices that they found objectionable, which they trimmed to 9 items based on the strength of evidence and their prevalence, relevance, and cost, explained Dr. Wunsch of the department of anesthesiology at Columbia University Medical Center, N.Y. Discussion winnowed that to the Top 5, an arbitrary number selected by the Choosing Wisely campaign that everyone should recognize as "a starting point," she said.
A two-page document of the critical care list can be downloaded from the Choosing Wisely website. It includes some of the sources for the recommendations and these top five "don’ts" displayed on the front:
1. Don’t order diagnostic tests at regular intervals (such as every day), but rather in response to specific clinical questions. Ordering diagnostic studies such as x-rays, arterial blood gases, blood counts, blood chemistries, or ECGs daily or at routine intervals drives up costs, doesn’t benefit patients, and may harm them through radiation exposure, inducing anemia, or triggering aggressive follow-up of incidental results. "I think this has become more prevalent with electronic medical records," where one click can order x-rays for the next 5 days, she said.
2. Don’t transfuse red blood cells in hemodynamically stable, non-bleeding ICU patients with a hemoglobin concentration greater than 7 mg/dL. Blood is a scarce resource, and studies show that limiting red blood cell transfusions to thresholds of 7 mg/dL or higher does not worsen survival, complications, or costs, and causes fewer complications. Different thresholds may be appropriate for patients with acute coronary syndrome, but even in this subgroup aggressive transfusion is harmful, most observational studies suggest.
3. Don’t use parenteral nutrition in adequately nourished critically ill patients within the first 7 days of an ICU stay. Early parenteral nutrition is harmful, even in patients who cannot tolerate enteral nutrition, if they were adequately nourished prior to ICU admission. The evidence is less clear for patients with nosocomial infections, and early parenteral nutrition may benefit patients who were severely malnourished right before ICU admission.
A study to be published soon shows that 90% of parenteral nutrition in the United States starts within 7 days of admission, usually within the first 2 days, Dr. Wunsch said. "It’s definitely more prevalent than I think many of us realize," she said.
4. Don’t deeply sedate mechanically ventilated patients without a specific indication and without daily attempts to lighten sedation. Deep sedation of patients on mechanical ventilation prolongs the duration of ventilation and hospitalization. Several protocols for limiting sedation have been shown to improve patient outcomes.
5. Don’t continue life support for patients at high risk of death or severely impaired functional recovery without offering patients and their families the alternative of care focused entirely on comfort. When an audience member expressed concern about discontinuation of life support possibly increasing premature deaths, Dr. Wunsch stressed that the second part of the statement is key – giving the family the choice of comfort care or continuing life support.
The simplicity of the Choosing Wisely list and its focus on overuse and costs make it possible to pursue unconventional ways of making it widely adopted, such as empowering families to question care, said Dr. Jeremy M. Kahn of the University of Pittsburgh. The 5 recommendations are far fewer than the 85 recommendations in the 2002 Surviving Sepsis campaign, for example, and the Choosing Wisely campaign has partnered with Consumer Reports and engaged the lay press to help spread the word, he said.
Dr. Kahn described a recent uncomfortable experience in which he had to question some of the medical care being offered to a hospitalized family member. It wasn’t easy to speak up, even though he’s a physician, and it must be even harder for lay people, he said. Hanging a sign in every ICU with the Choosing Wisely list might help empower families to speak up, one physician suggested during the discussion.
Incorporating decision-support prompts in electronic health records also could help physicians adhere to the Choosing Wisely recommendations, Dr. Kahn said.
Beyond the five items that made the Choosing Wisely list, the four runners-up were issues of antimicrobial duration; CT or MRI scanning for altered level of consciousness; vascular catheter indications; and ICU admission criteria for patients with poor prognosis, Dr. Wunsch said.
The Critical Care Societies Collaborative represents approximately 150,000 critical care providers, according to Dr. Curtis Sessler, president-designate of the American College of Chest Physicians.
The Choosing Wisely campaign, a project of the ABIM Foundation, released lists of "Five Things Physicians and Patients Should Question" by 9 medical societies in April 2012 and 17 more in February 2013, with the development of more lists ongoing.
The speakers reported having no financial disclosures.
On Twitter @sherryboschert
AT THE CRITICAL CARE CONGRESS
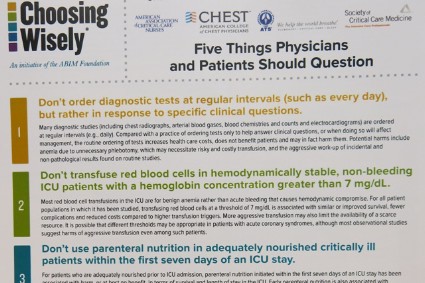
Never ‘do nothing’ at end of life
Providing end-of-life care – is one of the toughest, most painful things we are called upon to do. Who among us has not had the gut-wrenching experience of informing a spouse of 50+ years that within a few short days, their life together will come to an abrupt end? No more anniversaries. No more anything.
I don’t think physicians can truly appreciate what patients’ loved ones go through when they are dying, until we become that loved one. I got my revelation when I was the caregiver and hospice physician for a very close relative who ultimately died from cancer in my home. I had asked an oncologist friend of mine to take on her case when she relocated to live with me. To my surprise, my relative found my colleague to be rather cold and unfeeling, just when she needed a compassionate physician the most.
I deeply understand the field of medicine, had care provided by a clinician/friend, and my relative still had a subpar experience, so what must it like for those without a medical background?
I recently spoke with a friend whose elderly aunt had just passed away. In addition to the grief she felt, she had to deal with frustration and anguish about how her aunt was treated in her final days. Her aunt’s DNI (do not intubate) status was mistakenly assumed by some on her health care team to mean "DNT" (do not treat). Basic care, such as intravenous fluids in the face of inadequate oral intake, was even neglected. To add insult to injury, the family – those who actually knew her belief system, feelings, and wishes – was not allowed to partner with the health care team to create the plan for her end-of-life care.
While we often wrestle with how to talk to family, including what we should and should not say, perhaps we should begin by learning a little about the background of the family members so we can tailor our conversations to a level appropriate to their level of understanding – great or small– of health care.
We can learn a lot by talking to friends about the experiences they have when a loved one dies. How were they and their family member treated by physicians and how did they respond to that treatment? What do they wish had happened differently? What made the transition from this life more difficult and what made it easier?
My friend’s words of wisdom for hospitalists center on communication and respect: "Each patient and family should be treated as if they are Kennedys or Annenbergs from the start."
Dr. Hester is a hospitalist with Baltimore-Washington Medical Center who has a passion for empowering patients to partner in their health care. She is the creator of the Patient Whiz, a patient-engagement app for iOS.
Providing end-of-life care – is one of the toughest, most painful things we are called upon to do. Who among us has not had the gut-wrenching experience of informing a spouse of 50+ years that within a few short days, their life together will come to an abrupt end? No more anniversaries. No more anything.
I don’t think physicians can truly appreciate what patients’ loved ones go through when they are dying, until we become that loved one. I got my revelation when I was the caregiver and hospice physician for a very close relative who ultimately died from cancer in my home. I had asked an oncologist friend of mine to take on her case when she relocated to live with me. To my surprise, my relative found my colleague to be rather cold and unfeeling, just when she needed a compassionate physician the most.
I deeply understand the field of medicine, had care provided by a clinician/friend, and my relative still had a subpar experience, so what must it like for those without a medical background?
I recently spoke with a friend whose elderly aunt had just passed away. In addition to the grief she felt, she had to deal with frustration and anguish about how her aunt was treated in her final days. Her aunt’s DNI (do not intubate) status was mistakenly assumed by some on her health care team to mean "DNT" (do not treat). Basic care, such as intravenous fluids in the face of inadequate oral intake, was even neglected. To add insult to injury, the family – those who actually knew her belief system, feelings, and wishes – was not allowed to partner with the health care team to create the plan for her end-of-life care.
While we often wrestle with how to talk to family, including what we should and should not say, perhaps we should begin by learning a little about the background of the family members so we can tailor our conversations to a level appropriate to their level of understanding – great or small– of health care.
We can learn a lot by talking to friends about the experiences they have when a loved one dies. How were they and their family member treated by physicians and how did they respond to that treatment? What do they wish had happened differently? What made the transition from this life more difficult and what made it easier?
My friend’s words of wisdom for hospitalists center on communication and respect: "Each patient and family should be treated as if they are Kennedys or Annenbergs from the start."
Dr. Hester is a hospitalist with Baltimore-Washington Medical Center who has a passion for empowering patients to partner in their health care. She is the creator of the Patient Whiz, a patient-engagement app for iOS.
Providing end-of-life care – is one of the toughest, most painful things we are called upon to do. Who among us has not had the gut-wrenching experience of informing a spouse of 50+ years that within a few short days, their life together will come to an abrupt end? No more anniversaries. No more anything.
I don’t think physicians can truly appreciate what patients’ loved ones go through when they are dying, until we become that loved one. I got my revelation when I was the caregiver and hospice physician for a very close relative who ultimately died from cancer in my home. I had asked an oncologist friend of mine to take on her case when she relocated to live with me. To my surprise, my relative found my colleague to be rather cold and unfeeling, just when she needed a compassionate physician the most.
I deeply understand the field of medicine, had care provided by a clinician/friend, and my relative still had a subpar experience, so what must it like for those without a medical background?
I recently spoke with a friend whose elderly aunt had just passed away. In addition to the grief she felt, she had to deal with frustration and anguish about how her aunt was treated in her final days. Her aunt’s DNI (do not intubate) status was mistakenly assumed by some on her health care team to mean "DNT" (do not treat). Basic care, such as intravenous fluids in the face of inadequate oral intake, was even neglected. To add insult to injury, the family – those who actually knew her belief system, feelings, and wishes – was not allowed to partner with the health care team to create the plan for her end-of-life care.
While we often wrestle with how to talk to family, including what we should and should not say, perhaps we should begin by learning a little about the background of the family members so we can tailor our conversations to a level appropriate to their level of understanding – great or small– of health care.
We can learn a lot by talking to friends about the experiences they have when a loved one dies. How were they and their family member treated by physicians and how did they respond to that treatment? What do they wish had happened differently? What made the transition from this life more difficult and what made it easier?
My friend’s words of wisdom for hospitalists center on communication and respect: "Each patient and family should be treated as if they are Kennedys or Annenbergs from the start."
Dr. Hester is a hospitalist with Baltimore-Washington Medical Center who has a passion for empowering patients to partner in their health care. She is the creator of the Patient Whiz, a patient-engagement app for iOS.

Hospitalist Group Tackles Palliative Care; National Chain Explores Opportunities
At the Kaiser Permanente Medical Center in San Rafael, Calif., the 20 members of the hospitalist group were encouraged to study together in preparation for the October 2012 HPM boards. The group undertook weekly study sessions for the five months leading up to the exam. Sixteen hospitalists sat for the exam, along with oncologists, nephrologists, pulmonologists, and primary care physicians from the medical center.
All passed.
“For years, our hospitalist group has been doing actual rounding with the palliative care team on their own patients,” says Shideh Shadan, MD, the hospitalist group leader. “Everyone was on board with palliative care. It is now part of our daily care, and all we had to do was to sit down and study for the exam.”
Most of Kaiser’s HMO medical centers have designated interdisciplinary palliative care consultation teams. The one at San Rafael includes nurses, social workers, chaplains, and a part-time physician who is a hospitalist, Clay Angel, MD. Dr. Angel agrees that a cultural transformation has come about at Kaiser San Rafael through this collaboration. The two services are separate but closely connected.
“In hospital medicine, if you keep farming out what you do to specialists—if you’re not embracing palliative care as a hospitalist—you lose part of your practice,” he says.
Dr. Shadan says the study group “helped us to be more cohesive and more comfortable going to each other to ask for help. Palliative care is part of what we do—part of hospital medicine and of providing good care.”
Meanwhile, North Hollywood, Calif.-based IPC The Hospitalist Company, which is well-established in post-acute and long-term-care settings beyond the hospital walls, is now starting to explore palliative care approaches at the local level in a few of its 35 markets. Heather Zinzella-Cox, MD, who was part of a panel presentation on palliative care at HM13, is hospitalist practice group leader for IPC-Delaware. She also works part time as an associate medical director for a community hospice and helped to develop an inpatient palliative care team at a local community hospital.
“For me, as a post-acute hospitalist, every patient I see, I think about whether palliative care might benefit them,” says Dr. Zinzella-Cox, who is board certified in pain and in hospice and palliative medicine.
She says hospitalists need tools for identifying appropriate palliative care patients, along with training for how to communicate with them around goals of care, including simple language to help cue these conversations. She notes a “significant voltage drop” in information at the time of discharge, and the most careful discharge plans can fall apart in a hurry after the patient goes home.
IPC’s national practice group does not have a current policy or initiative for palliative care; however, there may be opportunities for further integrating palliative care with hospital medicine, says hospitalist Thomas Mathew, MD.
Larry Beresford is a freelance writer in San Francisco.
At the Kaiser Permanente Medical Center in San Rafael, Calif., the 20 members of the hospitalist group were encouraged to study together in preparation for the October 2012 HPM boards. The group undertook weekly study sessions for the five months leading up to the exam. Sixteen hospitalists sat for the exam, along with oncologists, nephrologists, pulmonologists, and primary care physicians from the medical center.
All passed.
“For years, our hospitalist group has been doing actual rounding with the palliative care team on their own patients,” says Shideh Shadan, MD, the hospitalist group leader. “Everyone was on board with palliative care. It is now part of our daily care, and all we had to do was to sit down and study for the exam.”
Most of Kaiser’s HMO medical centers have designated interdisciplinary palliative care consultation teams. The one at San Rafael includes nurses, social workers, chaplains, and a part-time physician who is a hospitalist, Clay Angel, MD. Dr. Angel agrees that a cultural transformation has come about at Kaiser San Rafael through this collaboration. The two services are separate but closely connected.
“In hospital medicine, if you keep farming out what you do to specialists—if you’re not embracing palliative care as a hospitalist—you lose part of your practice,” he says.
Dr. Shadan says the study group “helped us to be more cohesive and more comfortable going to each other to ask for help. Palliative care is part of what we do—part of hospital medicine and of providing good care.”
Meanwhile, North Hollywood, Calif.-based IPC The Hospitalist Company, which is well-established in post-acute and long-term-care settings beyond the hospital walls, is now starting to explore palliative care approaches at the local level in a few of its 35 markets. Heather Zinzella-Cox, MD, who was part of a panel presentation on palliative care at HM13, is hospitalist practice group leader for IPC-Delaware. She also works part time as an associate medical director for a community hospice and helped to develop an inpatient palliative care team at a local community hospital.
“For me, as a post-acute hospitalist, every patient I see, I think about whether palliative care might benefit them,” says Dr. Zinzella-Cox, who is board certified in pain and in hospice and palliative medicine.
She says hospitalists need tools for identifying appropriate palliative care patients, along with training for how to communicate with them around goals of care, including simple language to help cue these conversations. She notes a “significant voltage drop” in information at the time of discharge, and the most careful discharge plans can fall apart in a hurry after the patient goes home.
IPC’s national practice group does not have a current policy or initiative for palliative care; however, there may be opportunities for further integrating palliative care with hospital medicine, says hospitalist Thomas Mathew, MD.
Larry Beresford is a freelance writer in San Francisco.
At the Kaiser Permanente Medical Center in San Rafael, Calif., the 20 members of the hospitalist group were encouraged to study together in preparation for the October 2012 HPM boards. The group undertook weekly study sessions for the five months leading up to the exam. Sixteen hospitalists sat for the exam, along with oncologists, nephrologists, pulmonologists, and primary care physicians from the medical center.
All passed.
“For years, our hospitalist group has been doing actual rounding with the palliative care team on their own patients,” says Shideh Shadan, MD, the hospitalist group leader. “Everyone was on board with palliative care. It is now part of our daily care, and all we had to do was to sit down and study for the exam.”
Most of Kaiser’s HMO medical centers have designated interdisciplinary palliative care consultation teams. The one at San Rafael includes nurses, social workers, chaplains, and a part-time physician who is a hospitalist, Clay Angel, MD. Dr. Angel agrees that a cultural transformation has come about at Kaiser San Rafael through this collaboration. The two services are separate but closely connected.
“In hospital medicine, if you keep farming out what you do to specialists—if you’re not embracing palliative care as a hospitalist—you lose part of your practice,” he says.
Dr. Shadan says the study group “helped us to be more cohesive and more comfortable going to each other to ask for help. Palliative care is part of what we do—part of hospital medicine and of providing good care.”
Meanwhile, North Hollywood, Calif.-based IPC The Hospitalist Company, which is well-established in post-acute and long-term-care settings beyond the hospital walls, is now starting to explore palliative care approaches at the local level in a few of its 35 markets. Heather Zinzella-Cox, MD, who was part of a panel presentation on palliative care at HM13, is hospitalist practice group leader for IPC-Delaware. She also works part time as an associate medical director for a community hospice and helped to develop an inpatient palliative care team at a local community hospital.
“For me, as a post-acute hospitalist, every patient I see, I think about whether palliative care might benefit them,” says Dr. Zinzella-Cox, who is board certified in pain and in hospice and palliative medicine.
She says hospitalists need tools for identifying appropriate palliative care patients, along with training for how to communicate with them around goals of care, including simple language to help cue these conversations. She notes a “significant voltage drop” in information at the time of discharge, and the most careful discharge plans can fall apart in a hurry after the patient goes home.
IPC’s national practice group does not have a current policy or initiative for palliative care; however, there may be opportunities for further integrating palliative care with hospital medicine, says hospitalist Thomas Mathew, MD.
Larry Beresford is a freelance writer in San Francisco.
American Academy of Hospice and Palliative Medicine EVP Explains Hospitalists' Important Role in End-of-Life Planning
Click here for excerpts of our interview with Porter Storey, MD, executive vice president of the American Academy of Hospice and Palliative Medicine.
Click here for excerpts of our interview with Porter Storey, MD, executive vice president of the American Academy of Hospice and Palliative Medicine.
Click here for excerpts of our interview with Porter Storey, MD, executive vice president of the American Academy of Hospice and Palliative Medicine.
SHM Backs Medicare Reimbursement for End-of-Life Care Counseling

Although inevitable, death is often difficult to conceptualize and even more sensitive to discuss. For hospitalists and other care providers, conversations about the end of life with families and caregivers can be fraught with emotion. The fact that something is uncomfortable does not mean it is not useful or valuable, however. Patients must be able to vocalize their end-of-life wishes and should feel confident that the healthcare system is able to respond.
To help with this effort, the Society of Hospital Medicine is supporting legislation that would encourage voluntary end-of-life conversations between patients and their healthcare providers. Sponsored by U.S. Rep. Earl Blumenauer (D-Ore.), the Personalize Your Care Act of 2013 (H.R. 1173) would make Medicare reimbursement available for advance-care planning consultations, establish grants for state-level physician orders for life-sustaining treatment (POLST) programs, and require that advance directives be honored across state lines.
Hospitalists are integral team leaders for coordinating care and, as such, are often highly involved in end-of-life care for patients. They are at the front lines of these conversations, often tasked to plan end-of-life care and then carry out those plans. Many of their patients are acutely ill and need to face these critical decisions, often in real time.
End-of-life planning, like many other cognitive medical services, is not adequately reimbursed under current Medicare payment policy. This legislation would authorize Medicare to provide coverage for voluntary advance care consultations every five years or following changes in health, health-related condition, or care setting of the patient.
SHM is strongly supportive of adequate reimbursement for the counseling these patients require in planning their end-of-life care. The bill would make these conversations a practicable addition to the care and counseling workflow for healthcare providers and would ensure that they could occur at reasonable intervals and at significant changes in health or life events. These conversations would help ensure that patient wishes are respected at the end of life and prevent the use of unwanted treatments or interventions.
As the healthcare system works toward being more coordinated and more patient-centered, voluntary advance care planning is essential. Patients often see multiple providers at the end of their lives and—particularly as questions arise—it is imperative that providers have access to the most up-to-date advance care plans. H.R. 1173 works to address this gap by moving toward electronic health record display of advance directives and POLST.
Hospitalists may be eligible for reimbursement for these consultations, particularly in cases where these discussions did not occur in the outpatient setting. SHM is actively working with Rep. Blumenauer to ensure that all providers in a position to have these important conversations would be appropriately reimbursed. Patients need to have an active mechanism to ensure that their wishes are appropriately followed; this legislation would give them better access to these important and difficult conversations.
Joshua Lapps is SHM’s government relations specialist.
Although inevitable, death is often difficult to conceptualize and even more sensitive to discuss. For hospitalists and other care providers, conversations about the end of life with families and caregivers can be fraught with emotion. The fact that something is uncomfortable does not mean it is not useful or valuable, however. Patients must be able to vocalize their end-of-life wishes and should feel confident that the healthcare system is able to respond.
To help with this effort, the Society of Hospital Medicine is supporting legislation that would encourage voluntary end-of-life conversations between patients and their healthcare providers. Sponsored by U.S. Rep. Earl Blumenauer (D-Ore.), the Personalize Your Care Act of 2013 (H.R. 1173) would make Medicare reimbursement available for advance-care planning consultations, establish grants for state-level physician orders for life-sustaining treatment (POLST) programs, and require that advance directives be honored across state lines.
Hospitalists are integral team leaders for coordinating care and, as such, are often highly involved in end-of-life care for patients. They are at the front lines of these conversations, often tasked to plan end-of-life care and then carry out those plans. Many of their patients are acutely ill and need to face these critical decisions, often in real time.
End-of-life planning, like many other cognitive medical services, is not adequately reimbursed under current Medicare payment policy. This legislation would authorize Medicare to provide coverage for voluntary advance care consultations every five years or following changes in health, health-related condition, or care setting of the patient.
SHM is strongly supportive of adequate reimbursement for the counseling these patients require in planning their end-of-life care. The bill would make these conversations a practicable addition to the care and counseling workflow for healthcare providers and would ensure that they could occur at reasonable intervals and at significant changes in health or life events. These conversations would help ensure that patient wishes are respected at the end of life and prevent the use of unwanted treatments or interventions.
As the healthcare system works toward being more coordinated and more patient-centered, voluntary advance care planning is essential. Patients often see multiple providers at the end of their lives and—particularly as questions arise—it is imperative that providers have access to the most up-to-date advance care plans. H.R. 1173 works to address this gap by moving toward electronic health record display of advance directives and POLST.
Hospitalists may be eligible for reimbursement for these consultations, particularly in cases where these discussions did not occur in the outpatient setting. SHM is actively working with Rep. Blumenauer to ensure that all providers in a position to have these important conversations would be appropriately reimbursed. Patients need to have an active mechanism to ensure that their wishes are appropriately followed; this legislation would give them better access to these important and difficult conversations.
Joshua Lapps is SHM’s government relations specialist.
Although inevitable, death is often difficult to conceptualize and even more sensitive to discuss. For hospitalists and other care providers, conversations about the end of life with families and caregivers can be fraught with emotion. The fact that something is uncomfortable does not mean it is not useful or valuable, however. Patients must be able to vocalize their end-of-life wishes and should feel confident that the healthcare system is able to respond.
To help with this effort, the Society of Hospital Medicine is supporting legislation that would encourage voluntary end-of-life conversations between patients and their healthcare providers. Sponsored by U.S. Rep. Earl Blumenauer (D-Ore.), the Personalize Your Care Act of 2013 (H.R. 1173) would make Medicare reimbursement available for advance-care planning consultations, establish grants for state-level physician orders for life-sustaining treatment (POLST) programs, and require that advance directives be honored across state lines.
Hospitalists are integral team leaders for coordinating care and, as such, are often highly involved in end-of-life care for patients. They are at the front lines of these conversations, often tasked to plan end-of-life care and then carry out those plans. Many of their patients are acutely ill and need to face these critical decisions, often in real time.
End-of-life planning, like many other cognitive medical services, is not adequately reimbursed under current Medicare payment policy. This legislation would authorize Medicare to provide coverage for voluntary advance care consultations every five years or following changes in health, health-related condition, or care setting of the patient.
SHM is strongly supportive of adequate reimbursement for the counseling these patients require in planning their end-of-life care. The bill would make these conversations a practicable addition to the care and counseling workflow for healthcare providers and would ensure that they could occur at reasonable intervals and at significant changes in health or life events. These conversations would help ensure that patient wishes are respected at the end of life and prevent the use of unwanted treatments or interventions.
As the healthcare system works toward being more coordinated and more patient-centered, voluntary advance care planning is essential. Patients often see multiple providers at the end of their lives and—particularly as questions arise—it is imperative that providers have access to the most up-to-date advance care plans. H.R. 1173 works to address this gap by moving toward electronic health record display of advance directives and POLST.
Hospitalists may be eligible for reimbursement for these consultations, particularly in cases where these discussions did not occur in the outpatient setting. SHM is actively working with Rep. Blumenauer to ensure that all providers in a position to have these important conversations would be appropriately reimbursed. Patients need to have an active mechanism to ensure that their wishes are appropriately followed; this legislation would give them better access to these important and difficult conversations.
Joshua Lapps is SHM’s government relations specialist.