User login
Medical Research Highlights Palliative Care Contributions
Palliative care increasingly is the subject of clinical and administrative research in medical literature, with investigators examining its impact on costs and utilization of hospital care and other health services, as well as on such outcomes as pain and symptom management and patient and family satisfaction with health services.
An influential study of cost savings associated with hospital palliative care consultation services, conducted by R. Sean Morrison, MD, and colleagues at the National Palliative Care Research Center at Mount Sinai School of Medicine in New York City, matched 2,630 palliative care patients to 18,472 “usual care patients” and concluded that the cost savings averaged $4,988 per patient in direct costs per day for those dying in the hospital.3 A follow-up study in 2010 confirmed these results, and Dr. Morrison and colleagues have documented improved quality from palliative care based on a survey of bereaved family members of patients who received palliative care.4,5
A 2010 study by a group at Massachusetts General Hospital, led by Jennifer Temel, MD, reached the surprising conclusion that early palliative care for patients with metastatic non-small-cell lung cancer led not only to significant improvements in quality of life and mood and less provision of aggressive care at the end of life—but also to longer survival.6 The researchers have studied possible mechanisms for this result, as well as the integration of palliative care with oncology and the importance of palliative care support provided outside of the hospital, in community-based and outpatient settings. 7,8,9
Community-based palliative care is a significant new direction for palliative care in America, and the availability of palliative care outside of the hospital’s four walls is viewed as important to improving care transitions and preventing readmissions in the seriously ill patients typically targeted for palliative care. The effects of palliative care on 30-day readmissions rates was studied by Susan Enguidanos, PhD, MPH, and colleagues at the University of Southern California School of Gerontology; they found that receipt of palliative care following hospital discharge were a significant factor in reducing 30-day rehospitalizations.10
A study from Albert Einstein College of Medicine in New York explored outcomes from a dedicated acute palliative care unit in an academic medical center, while others have looked at the diverse landscape of palliative care in outpatient clinics and its potential for rapid growth.11,12
—Larry Beresford
References
- Lupu D. American Academy of Hospice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician workforce shortage. J Pain Symptom Manage. 2010;40(6):899-911.
- Quill TE, Abernethy AP. Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med. 2013;368(13):1173-1175.
- Morrison RS, Penrod JD, Cassel JB, et al. Palliative Care Leadership Centers' Outcomes Group. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
- Penrod JD, Deb P, Dellenbaugh C, et al. Hospital-based palliative care consultation: effects on hospital cost. J Palliat Med. 2010;13(8):973-979.
- Gelfman LP, Meier DE, Morrison RS. Does palliative care improve quality? A survey of bereaved family members. J Pain Symptom Manage. 2008;36(1):22-28.
- Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
- Irwin KE, Greer JA, Khatib J, Temel JS, Pirl WF. Early palliative care and metastatic non-small cell lung cancer: potential mechanisms of prolonged survival. Chron Respir Dis. 2013;10(1):35-47.
- Von Roenn JN, Temel J. The integration of palliative care and oncology: the evidence. Oncology. 2011;25(13):1258-1260,1262,1264-1265.
- Yoong J, Park ER, Greer JA, etc. Early palliative care in advanced lung cancer: a qualitative study. JAMA Intern Med. 2013;173(4):283-290.
- Enguidanos S, Vesper E, Lorenz K. 30-day readmissions among seriously ill older adults. J Palliat Med. 2012;15(12):1356-1361.
- Eti S, O’Mahony S, McHugh M, Guilbe R, Blank A, Selwyn P. Outcomes of the acute palliative care unit in an academic medical center [published online ahead of print May 10, 2013]. Am J Hosp Palliat Care. PMID: 23666616.
- Smith AK, Thai JN, Bakitas MA, et al. The diverse landscape of palliative care clinics. J Palliat Med. 2013;16(6):661-668.
Palliative care increasingly is the subject of clinical and administrative research in medical literature, with investigators examining its impact on costs and utilization of hospital care and other health services, as well as on such outcomes as pain and symptom management and patient and family satisfaction with health services.
An influential study of cost savings associated with hospital palliative care consultation services, conducted by R. Sean Morrison, MD, and colleagues at the National Palliative Care Research Center at Mount Sinai School of Medicine in New York City, matched 2,630 palliative care patients to 18,472 “usual care patients” and concluded that the cost savings averaged $4,988 per patient in direct costs per day for those dying in the hospital.3 A follow-up study in 2010 confirmed these results, and Dr. Morrison and colleagues have documented improved quality from palliative care based on a survey of bereaved family members of patients who received palliative care.4,5
A 2010 study by a group at Massachusetts General Hospital, led by Jennifer Temel, MD, reached the surprising conclusion that early palliative care for patients with metastatic non-small-cell lung cancer led not only to significant improvements in quality of life and mood and less provision of aggressive care at the end of life—but also to longer survival.6 The researchers have studied possible mechanisms for this result, as well as the integration of palliative care with oncology and the importance of palliative care support provided outside of the hospital, in community-based and outpatient settings. 7,8,9
Community-based palliative care is a significant new direction for palliative care in America, and the availability of palliative care outside of the hospital’s four walls is viewed as important to improving care transitions and preventing readmissions in the seriously ill patients typically targeted for palliative care. The effects of palliative care on 30-day readmissions rates was studied by Susan Enguidanos, PhD, MPH, and colleagues at the University of Southern California School of Gerontology; they found that receipt of palliative care following hospital discharge were a significant factor in reducing 30-day rehospitalizations.10
A study from Albert Einstein College of Medicine in New York explored outcomes from a dedicated acute palliative care unit in an academic medical center, while others have looked at the diverse landscape of palliative care in outpatient clinics and its potential for rapid growth.11,12
—Larry Beresford
References
- Lupu D. American Academy of Hospice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician workforce shortage. J Pain Symptom Manage. 2010;40(6):899-911.
- Quill TE, Abernethy AP. Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med. 2013;368(13):1173-1175.
- Morrison RS, Penrod JD, Cassel JB, et al. Palliative Care Leadership Centers' Outcomes Group. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
- Penrod JD, Deb P, Dellenbaugh C, et al. Hospital-based palliative care consultation: effects on hospital cost. J Palliat Med. 2010;13(8):973-979.
- Gelfman LP, Meier DE, Morrison RS. Does palliative care improve quality? A survey of bereaved family members. J Pain Symptom Manage. 2008;36(1):22-28.
- Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
- Irwin KE, Greer JA, Khatib J, Temel JS, Pirl WF. Early palliative care and metastatic non-small cell lung cancer: potential mechanisms of prolonged survival. Chron Respir Dis. 2013;10(1):35-47.
- Von Roenn JN, Temel J. The integration of palliative care and oncology: the evidence. Oncology. 2011;25(13):1258-1260,1262,1264-1265.
- Yoong J, Park ER, Greer JA, etc. Early palliative care in advanced lung cancer: a qualitative study. JAMA Intern Med. 2013;173(4):283-290.
- Enguidanos S, Vesper E, Lorenz K. 30-day readmissions among seriously ill older adults. J Palliat Med. 2012;15(12):1356-1361.
- Eti S, O’Mahony S, McHugh M, Guilbe R, Blank A, Selwyn P. Outcomes of the acute palliative care unit in an academic medical center [published online ahead of print May 10, 2013]. Am J Hosp Palliat Care. PMID: 23666616.
- Smith AK, Thai JN, Bakitas MA, et al. The diverse landscape of palliative care clinics. J Palliat Med. 2013;16(6):661-668.
Palliative care increasingly is the subject of clinical and administrative research in medical literature, with investigators examining its impact on costs and utilization of hospital care and other health services, as well as on such outcomes as pain and symptom management and patient and family satisfaction with health services.
An influential study of cost savings associated with hospital palliative care consultation services, conducted by R. Sean Morrison, MD, and colleagues at the National Palliative Care Research Center at Mount Sinai School of Medicine in New York City, matched 2,630 palliative care patients to 18,472 “usual care patients” and concluded that the cost savings averaged $4,988 per patient in direct costs per day for those dying in the hospital.3 A follow-up study in 2010 confirmed these results, and Dr. Morrison and colleagues have documented improved quality from palliative care based on a survey of bereaved family members of patients who received palliative care.4,5
A 2010 study by a group at Massachusetts General Hospital, led by Jennifer Temel, MD, reached the surprising conclusion that early palliative care for patients with metastatic non-small-cell lung cancer led not only to significant improvements in quality of life and mood and less provision of aggressive care at the end of life—but also to longer survival.6 The researchers have studied possible mechanisms for this result, as well as the integration of palliative care with oncology and the importance of palliative care support provided outside of the hospital, in community-based and outpatient settings. 7,8,9
Community-based palliative care is a significant new direction for palliative care in America, and the availability of palliative care outside of the hospital’s four walls is viewed as important to improving care transitions and preventing readmissions in the seriously ill patients typically targeted for palliative care. The effects of palliative care on 30-day readmissions rates was studied by Susan Enguidanos, PhD, MPH, and colleagues at the University of Southern California School of Gerontology; they found that receipt of palliative care following hospital discharge were a significant factor in reducing 30-day rehospitalizations.10
A study from Albert Einstein College of Medicine in New York explored outcomes from a dedicated acute palliative care unit in an academic medical center, while others have looked at the diverse landscape of palliative care in outpatient clinics and its potential for rapid growth.11,12
—Larry Beresford
References
- Lupu D. American Academy of Hospice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician workforce shortage. J Pain Symptom Manage. 2010;40(6):899-911.
- Quill TE, Abernethy AP. Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med. 2013;368(13):1173-1175.
- Morrison RS, Penrod JD, Cassel JB, et al. Palliative Care Leadership Centers' Outcomes Group. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
- Penrod JD, Deb P, Dellenbaugh C, et al. Hospital-based palliative care consultation: effects on hospital cost. J Palliat Med. 2010;13(8):973-979.
- Gelfman LP, Meier DE, Morrison RS. Does palliative care improve quality? A survey of bereaved family members. J Pain Symptom Manage. 2008;36(1):22-28.
- Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
- Irwin KE, Greer JA, Khatib J, Temel JS, Pirl WF. Early palliative care and metastatic non-small cell lung cancer: potential mechanisms of prolonged survival. Chron Respir Dis. 2013;10(1):35-47.
- Von Roenn JN, Temel J. The integration of palliative care and oncology: the evidence. Oncology. 2011;25(13):1258-1260,1262,1264-1265.
- Yoong J, Park ER, Greer JA, etc. Early palliative care in advanced lung cancer: a qualitative study. JAMA Intern Med. 2013;173(4):283-290.
- Enguidanos S, Vesper E, Lorenz K. 30-day readmissions among seriously ill older adults. J Palliat Med. 2012;15(12):1356-1361.
- Eti S, O’Mahony S, McHugh M, Guilbe R, Blank A, Selwyn P. Outcomes of the acute palliative care unit in an academic medical center [published online ahead of print May 10, 2013]. Am J Hosp Palliat Care. PMID: 23666616.
- Smith AK, Thai JN, Bakitas MA, et al. The diverse landscape of palliative care clinics. J Palliat Med. 2013;16(6):661-668.
Benefits of a Palliative Care Consultation
Valerie Phillips was diagnosed with stage IV breast cancer in 2010 and is a shining example of the difference a palliative care consultation can make. After she was diagnosed, the Austin, Texas, native continued to work and enjoy a relatively normal life. But when the disease metastasized to her hip, she began to take opioid analgesics for the pain.
Phillips says she felt foolish when she ended up in the ED, profoundly uncomfortable from a four-day impaction due to the analgesic and oral cancer drugs. “But nobody told me about all that,” she says.
She thinks her oncologist was giving good care, “but her area was treating the disease.”
Upon admission, a hospitalist referred Phillips for an inpatient palliative care consultation with Stephen Bekanich, MD, a former hospitalist who now co-directs Seton Palliative Care for the Seton Health System in Austin.
“I learned there’s a big difference between fighting the disease and treating the needs of the patient as a person,” Phillips explains. “A palliative care doctor like Stephen changes everything. He found a way for me to better navigate the healthcare system, carrying all of that information in his head. He said to me, ‘OK, we’re going to make sure this doesn’t happen again.’
I trusted him—and it worked.” Phillips says she understands that her long-term prospects aren’t great, and she expects to enroll in hospice soon. She hasn’t been back to the hospital, but has continued to see Dr. Bekanich as an outpatient.
“For me, there was an informational and educational gap, and I have a master’s degree and a career in management,” she says. “Stephen was able to tie everything together for me.”
Phillips says hospitalists should focus on the connection between disease treatment and the quality of life palliative care affords. “They should go hand in hand. Patients should be able to count on somebody who can take us by the hand and make the whole process as painless—and worry-free—as possible.”
—Larry Beresford
Valerie Phillips was diagnosed with stage IV breast cancer in 2010 and is a shining example of the difference a palliative care consultation can make. After she was diagnosed, the Austin, Texas, native continued to work and enjoy a relatively normal life. But when the disease metastasized to her hip, she began to take opioid analgesics for the pain.
Phillips says she felt foolish when she ended up in the ED, profoundly uncomfortable from a four-day impaction due to the analgesic and oral cancer drugs. “But nobody told me about all that,” she says.
She thinks her oncologist was giving good care, “but her area was treating the disease.”
Upon admission, a hospitalist referred Phillips for an inpatient palliative care consultation with Stephen Bekanich, MD, a former hospitalist who now co-directs Seton Palliative Care for the Seton Health System in Austin.
“I learned there’s a big difference between fighting the disease and treating the needs of the patient as a person,” Phillips explains. “A palliative care doctor like Stephen changes everything. He found a way for me to better navigate the healthcare system, carrying all of that information in his head. He said to me, ‘OK, we’re going to make sure this doesn’t happen again.’
I trusted him—and it worked.” Phillips says she understands that her long-term prospects aren’t great, and she expects to enroll in hospice soon. She hasn’t been back to the hospital, but has continued to see Dr. Bekanich as an outpatient.
“For me, there was an informational and educational gap, and I have a master’s degree and a career in management,” she says. “Stephen was able to tie everything together for me.”
Phillips says hospitalists should focus on the connection between disease treatment and the quality of life palliative care affords. “They should go hand in hand. Patients should be able to count on somebody who can take us by the hand and make the whole process as painless—and worry-free—as possible.”
—Larry Beresford
Valerie Phillips was diagnosed with stage IV breast cancer in 2010 and is a shining example of the difference a palliative care consultation can make. After she was diagnosed, the Austin, Texas, native continued to work and enjoy a relatively normal life. But when the disease metastasized to her hip, she began to take opioid analgesics for the pain.
Phillips says she felt foolish when she ended up in the ED, profoundly uncomfortable from a four-day impaction due to the analgesic and oral cancer drugs. “But nobody told me about all that,” she says.
She thinks her oncologist was giving good care, “but her area was treating the disease.”
Upon admission, a hospitalist referred Phillips for an inpatient palliative care consultation with Stephen Bekanich, MD, a former hospitalist who now co-directs Seton Palliative Care for the Seton Health System in Austin.
“I learned there’s a big difference between fighting the disease and treating the needs of the patient as a person,” Phillips explains. “A palliative care doctor like Stephen changes everything. He found a way for me to better navigate the healthcare system, carrying all of that information in his head. He said to me, ‘OK, we’re going to make sure this doesn’t happen again.’
I trusted him—and it worked.” Phillips says she understands that her long-term prospects aren’t great, and she expects to enroll in hospice soon. She hasn’t been back to the hospital, but has continued to see Dr. Bekanich as an outpatient.
“For me, there was an informational and educational gap, and I have a master’s degree and a career in management,” she says. “Stephen was able to tie everything together for me.”
Phillips says hospitalists should focus on the connection between disease treatment and the quality of life palliative care affords. “They should go hand in hand. Patients should be able to count on somebody who can take us by the hand and make the whole process as painless—and worry-free—as possible.”
—Larry Beresford
Palliative Care Can Be Incredibly Intense, Richly Rewarding for Hospitalists


After nine years in practice as a hospitalist in community and academic settings, Leonard Noronha, MD, applied for and in July 2012 became the inaugural, full-year, full-time fellow in hospice and palliative medicine (HPM) at the University of New Mexico in Albuquerque, one of approximately 200 such positions nationwide. The fellowship training qualifies him to sit for HPM subspecialty medical board certification.
Dr. Noronha says he was casually acquainted with the concept of palliative care from residency but didn’t know “when to ask for a palliative care consultation or what they offered.”
“I also had a sense that discussions about feeding tubes, for example, could happen better and easier than they typically did,” he says.
His interest piqued as he learned more about palliative care at hospitalist meetings.
“I grew more excited about it and came to realize that it is something I’d find rewarding and enjoyable, if I could get good at it,” Dr. Noronha says. “Over time, I found more satisfaction in palliative care encounters with patients—and became less comfortable with what I perceived as occasionally inappropriate and excessive testing and treatment [for some hospitalized patients who weren’t offered palliative care].”
Palliative care is a medical specialty that focuses on comfort, relief of symptoms, and clarifying patients’ treatment goals. It is commonly provided as an interdisciplinary consultation service in hospitals. Advocates say it can be offered concurrently with other medical therapies for any seriously ill patient, particularly when there are physical, psychosocial, or spiritual complications, and it is not limited to patients approaching death.
Experienced clinicians say palliative care maximizes quality of life and empowers patients and their families to make treatment decisions more in line with their hopes and values. They also say palliative care gives an emotional lift to providers, while reducing hospital expenditures. Some also suggest that palliative care is an additional tool for enhancing care transitions, potentially affecting readmission rates.
For Dr. Noronha, the one-year fellowship required a significant cut in pay, but he was prepared for the financial hardship.
“It was a great decision for me,” he says. “Some of my colleagues had encouraged me to think about using the experiential pathway to HPM board certification, but I knew I’d do better in the structured environment of a fellowship.
“There have been times when I’ve been outside of my comfort zone, sometimes feeling like the least experienced person in the room. But I knew the fellowship would help—and it did.”
He says the training gives him a better appreciation for things like illness trajectories, the nuances of goal clarification, and the benefit of an extra set of eyes and ears to assess the patient.
After completing his fellowship, Dr. Noronha became UNM’s second full-time palliative medicine faculty. He encourages hospitalists to talk to the palliative care service at their institutions and request consultations for complex, seriously ill patients who might benefit.
As for his new career path, he says that often he is asked if palliative care is depressing. “Some of these situations can be tragic, but I find the work very rewarding,” he says.
Service Models
In some settings, palliative care is incorporated into the hospitalist service. Hospitalists are scheduled for palliative care shifts or have palliative care visits incorporated into daily rounds. Such blended positions could be a recruiting incentive for some physicians who want to do both.
In other settings, palliative care is a separate service. Consultations are ordered as needed by hospitalists and other physicians.
Advocates like Marianne Novelli, MD, FHM, FACP, say hospitalists play a pivotal role in providing the basics of palliative care for seriously ill, hospitalized patients.
“Palliative care is part and parcel of what we do as hospitalists with the people we serve—who by definition are very sick, even to get into the hospital,” says Dr. Novelli, formerly the chief of the division of hospital medicine at Kaiser Permanente in Denver, Colo. She rotated off that leadership position in 2011 and has since divided her time between hospital medicine and palliative care shifts in the hospital, although she now does palliative care exclusively.
Initially, she watched palliative care consults and asked for mentorship from the palliative care team. Although it took time to get used to the advisory role of the consultant, and to working with a team, she eventually became board certified in HPM.
“Palliative care is incredibly intense but richly rewarding work,” she says. “The patients you see are never simple. It allows us to practice the type of medicine we originally set out to do, with people at the most vulnerable times in their lives.”
Workforce, Fellowship, Board Certification
In October 2012, 3,356 physicians passed the hospice and palliative medicine subspecialty board exams offered by the American Board of Medical Specialties and 10 of its constituent specialty boards, with the lion’s share of them certified by the American Board of Internal Medicine. That more than doubled the number of physicians earning the HPM credential since its inception in 2008.
Even with the surge in palliative care training, workforce studies suggest the U.S. is woefully short of credentialed palliative care physicians. And many think hospitalists can help fill that void.
The Center to Advance Palliative Care (CAPC, www.capc.org) counts 1,400 hospital-based palliative care programs in the U.S., while the Centers for Medicare & Medicaid Services (CMS) recognizes about 3,500 Medicare-certified hospice programs. A 2010 estimate by Dale Lupu and the American Academy of Hospice and Palliative Medicine (AAHPM), however, suggested a need for between 4,487 and 10,810 palliative care physician FTEs just to staff existing programs at appropriate levels—without considering growth for the field or its spread into outpatient settings.1
In the past, mid-career physicians had an experiential pathway to the HPM board exam, based on hours worked with a hospice or palliative care team, but physicians now must complete an HPM fellowship of at least one year in order to sit for the boards. And, according to AAHPM, only 234 HPM fellowship positions are offered nationwide by 85 approved fellowship programs.

A one-year fellowship is a big commitment for an established hospitalist, according to Stephen Bekanich, MD, co-director of Seton Palliative Care at Seton Healthcare, an 11-hospital system in Austin, Texas. A former hospitalist, Dr. Bekanich says that in his region a fellow stipend is about $70,000, whereas typical hospitalist compensation is in the mid- to upper-$200,000s.
AAHPM is exploring other approaches to expanding the workforce with mid-career physicians. One approach, authored by Timothy Quill, MD, and Amy Abernethy, MD, the past and current AAHPM board presidents, is to develop a two-tiered system in which palliative medicine specialists teach basic palliative care techniques and approaches to primary care physicians, hospitalists, and such specialists as oncologists.2 The article also suggested equipping clinicians with the tools to recognize when more specialized help is needed.
“As in any medical discipline, some core elements of palliative care, such as aligning treatment with a patient’s goals and basic symptom management, should be routine aspects of care delivered by any practitioner,” Drs. Quill and Abernethy wrote. “Other skills are more complex and take years of training to learn and apply, such as negotiating a difficult family meeting, addressing veiled existential distress, and managing refractory symptoms.”
Dr. Bekanich is trying the two-tiered approach at Seton Healthcare. At facilities with no palliative care service, he is transplanting palliative-trained nurse practitioners in hospital medicine groups.
“This model is locked into our budget for fiscal year 2014,” Dr. Bekanich says. “We’ll train folks, starting with hospitalists and primary care physicians.”
The training will start with a pair of three-hour sessions on palliative care techniques for hospitalists and PCPs, followed by homework assignments. “Then we’ll meet again in three months to do some role plays,” he says.
Two final rounds of training will focus on skills, philosophy, values, and practice.

—Marianne Novelli, MD, FHM, FACP, former chief of the division of hospital medicine, Kaiser Permanente, Denver, Colo.
On-the-Job Training
David Weissman, MD, FACP, a palliative care specialist in Milwaukee, Wis., and consultant to the CAPC, recommends hospitalists do what they can to improve their knowledge and skills. “There are a lot of opportunities for palliative care training out there,” he says.
HM conferences often include palliative care content. AAHPM and CAPC offer annual conferences that immerse participants in content, with opportunities to mingle with palliative care colleagues. AAHPM also offers specific content through its “Unipac” series of nine self-study training modules (www.aahpm.org/resources/default/unipac-4th-edition.html.)

On the job, Dr. Weissman says hospitalists should ask for consults for patients with complex needs. Also pay attention to how the service works and what it recommends. Taking a couple of days to round with the palliative care service could be very educational. It may be possible to take a part-time position with the team, providing weekend or vacation coverage. Hospitalists can participate on planning or advisory committees for palliative care in their hospitals or on quality improvement projects.
“If there isn’t a palliative care service, advocate for developing one,” he says.
Local hospice programs, especially those with inpatient hospice facilities that need daily physician coverage, might have part-time staff positions, which could be a great moonlighting opportunity for hospitalists and a way to learn a lot very quickly.
“I can tell the difference between physicians who have spent time working in a hospice, where you can learn about caring for people at the end of life because most of the patients are so sick, and those who have not,” says Porter Storey, MD, FACP, AAHPM’s executive vice president and a practicing palliative care physician in Colorado. “You can learn how to use the medications to get someone comfortable quickly and how to talk to families in crisis. It can be some of the most rewarding work you can possibly do—especially when you have the time and training to do it well for some of the most challenging of patients and families.”
Dr. Storey recommends that hospitalists join AAHPM, use its professional materials, attend its annual meetings, and, if they feel a calling, consider fellowship training as the next big step.
“Palliative care programs are growing in number and size but are chronically understaffed,” says Steven Pantilat, MD, SFHM, hospitalist and director of the Palliative Care Program at the University of California at San Francisco. “This creates a great opportunity for hospitalists. I have heard of places that were having trouble recruiting palliative care physicians but were willing to sponsor a hospitalist to go and do a fellowship, supplementing their salary as an incentive—and a reasonable one—for a hospitalist interested in making a career move.”
He says that palliative care, like hospital medicine, has been a significant value-add in many hospitals and health systems. More importantly, it correlates to positive patient outcomes (see “Research Highlights Palliative Care Contributions,”).

“What’s new is how it connects to current issues like improved care transitions and readmissions reduction,” Dr. Pantilat says.
Advocates say palliative care helps to match medical services to patient preferences, thereby improving patient satisfaction scores, especially for those who aren’t likely to achieve good outcomes. Dr. Pantilat says it puts plans in place for patients to get the right services for the post-discharge period and for responding to anticipated problems like chest pain.
“It’s not just how to get patients out of the hospital as quickly as possible,” he says, “but to do that with a plan that sets them up to succeed at home.”
Larry Beresford is a freelance writer in San Francisco.
References
- Lupu D. American Academy of Hospice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician workforce shortage. J Pain Symptom Manage. 2010;40(6):899-911.
- Quill TE, Abernethy AP. Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med. 2013;368(13):1173-1175.
- Morrison RS, Penrod JD, Cassel JB, et al. Palliative Care Leadership Centers' Outcomes Group. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
- Penrod JD, Deb P, Dellenbaugh C, et al. Hospital-based palliative care consultation: effects on hospital cost. J Palliat Med. 2010;13(8):973-979.
- Gelfman LP, Meier DE, Morrison RS. Does palliative care improve quality? A survey of bereaved family members. J Pain Symptom Manage. 2008;36(1):22-28.
- Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
- Irwin KE, Greer JA, Khatib J, Temel JS, Pirl WF. Early palliative care and metastatic non-small cell lung cancer: potential mechanisms of prolonged survival. Chron Respir Dis. 2013;10(1):35-47.
- Von Roenn JN, Temel J. The integration of palliative care and oncology: the evidence. Oncology. 2011;25(13):1258-1260,1262,1264-1265.
- Yoong J, Park ER, Greer JA, etc. Early palliative care in advanced lung cancer: a qualitative study. JAMA Intern Med. 2013;173(4):283-290.
- Enguidanos S, Vesper E, Lorenz K. 30-day readmissions among seriously ill older adults. J Palliat Med. 2012;15(12):1356-1361.
- Eti S, O’Mahony S, McHugh M, Guilbe R, Blank A, Selwyn P. Outcomes of the acute palliative care unit in an academic medical center [published online ahead of print May 10, 2013]. Am J Hosp Palliat Care. PMID: 23666616.
- Smith AK, Thai JN, Bakitas MA, et al. The diverse landscape of palliative care clinics. J Palliat Med. 2013;16(6):661-668.
After nine years in practice as a hospitalist in community and academic settings, Leonard Noronha, MD, applied for and in July 2012 became the inaugural, full-year, full-time fellow in hospice and palliative medicine (HPM) at the University of New Mexico in Albuquerque, one of approximately 200 such positions nationwide. The fellowship training qualifies him to sit for HPM subspecialty medical board certification.
Dr. Noronha says he was casually acquainted with the concept of palliative care from residency but didn’t know “when to ask for a palliative care consultation or what they offered.”
“I also had a sense that discussions about feeding tubes, for example, could happen better and easier than they typically did,” he says.
His interest piqued as he learned more about palliative care at hospitalist meetings.
“I grew more excited about it and came to realize that it is something I’d find rewarding and enjoyable, if I could get good at it,” Dr. Noronha says. “Over time, I found more satisfaction in palliative care encounters with patients—and became less comfortable with what I perceived as occasionally inappropriate and excessive testing and treatment [for some hospitalized patients who weren’t offered palliative care].”
Palliative care is a medical specialty that focuses on comfort, relief of symptoms, and clarifying patients’ treatment goals. It is commonly provided as an interdisciplinary consultation service in hospitals. Advocates say it can be offered concurrently with other medical therapies for any seriously ill patient, particularly when there are physical, psychosocial, or spiritual complications, and it is not limited to patients approaching death.
Experienced clinicians say palliative care maximizes quality of life and empowers patients and their families to make treatment decisions more in line with their hopes and values. They also say palliative care gives an emotional lift to providers, while reducing hospital expenditures. Some also suggest that palliative care is an additional tool for enhancing care transitions, potentially affecting readmission rates.
For Dr. Noronha, the one-year fellowship required a significant cut in pay, but he was prepared for the financial hardship.
“It was a great decision for me,” he says. “Some of my colleagues had encouraged me to think about using the experiential pathway to HPM board certification, but I knew I’d do better in the structured environment of a fellowship.
“There have been times when I’ve been outside of my comfort zone, sometimes feeling like the least experienced person in the room. But I knew the fellowship would help—and it did.”
He says the training gives him a better appreciation for things like illness trajectories, the nuances of goal clarification, and the benefit of an extra set of eyes and ears to assess the patient.
After completing his fellowship, Dr. Noronha became UNM’s second full-time palliative medicine faculty. He encourages hospitalists to talk to the palliative care service at their institutions and request consultations for complex, seriously ill patients who might benefit.
As for his new career path, he says that often he is asked if palliative care is depressing. “Some of these situations can be tragic, but I find the work very rewarding,” he says.
Service Models
In some settings, palliative care is incorporated into the hospitalist service. Hospitalists are scheduled for palliative care shifts or have palliative care visits incorporated into daily rounds. Such blended positions could be a recruiting incentive for some physicians who want to do both.
In other settings, palliative care is a separate service. Consultations are ordered as needed by hospitalists and other physicians.
Advocates like Marianne Novelli, MD, FHM, FACP, say hospitalists play a pivotal role in providing the basics of palliative care for seriously ill, hospitalized patients.
“Palliative care is part and parcel of what we do as hospitalists with the people we serve—who by definition are very sick, even to get into the hospital,” says Dr. Novelli, formerly the chief of the division of hospital medicine at Kaiser Permanente in Denver, Colo. She rotated off that leadership position in 2011 and has since divided her time between hospital medicine and palliative care shifts in the hospital, although she now does palliative care exclusively.
Initially, she watched palliative care consults and asked for mentorship from the palliative care team. Although it took time to get used to the advisory role of the consultant, and to working with a team, she eventually became board certified in HPM.
“Palliative care is incredibly intense but richly rewarding work,” she says. “The patients you see are never simple. It allows us to practice the type of medicine we originally set out to do, with people at the most vulnerable times in their lives.”
Workforce, Fellowship, Board Certification
In October 2012, 3,356 physicians passed the hospice and palliative medicine subspecialty board exams offered by the American Board of Medical Specialties and 10 of its constituent specialty boards, with the lion’s share of them certified by the American Board of Internal Medicine. That more than doubled the number of physicians earning the HPM credential since its inception in 2008.
Even with the surge in palliative care training, workforce studies suggest the U.S. is woefully short of credentialed palliative care physicians. And many think hospitalists can help fill that void.
The Center to Advance Palliative Care (CAPC, www.capc.org) counts 1,400 hospital-based palliative care programs in the U.S., while the Centers for Medicare & Medicaid Services (CMS) recognizes about 3,500 Medicare-certified hospice programs. A 2010 estimate by Dale Lupu and the American Academy of Hospice and Palliative Medicine (AAHPM), however, suggested a need for between 4,487 and 10,810 palliative care physician FTEs just to staff existing programs at appropriate levels—without considering growth for the field or its spread into outpatient settings.1
In the past, mid-career physicians had an experiential pathway to the HPM board exam, based on hours worked with a hospice or palliative care team, but physicians now must complete an HPM fellowship of at least one year in order to sit for the boards. And, according to AAHPM, only 234 HPM fellowship positions are offered nationwide by 85 approved fellowship programs.
A one-year fellowship is a big commitment for an established hospitalist, according to Stephen Bekanich, MD, co-director of Seton Palliative Care at Seton Healthcare, an 11-hospital system in Austin, Texas. A former hospitalist, Dr. Bekanich says that in his region a fellow stipend is about $70,000, whereas typical hospitalist compensation is in the mid- to upper-$200,000s.
AAHPM is exploring other approaches to expanding the workforce with mid-career physicians. One approach, authored by Timothy Quill, MD, and Amy Abernethy, MD, the past and current AAHPM board presidents, is to develop a two-tiered system in which palliative medicine specialists teach basic palliative care techniques and approaches to primary care physicians, hospitalists, and such specialists as oncologists.2 The article also suggested equipping clinicians with the tools to recognize when more specialized help is needed.
“As in any medical discipline, some core elements of palliative care, such as aligning treatment with a patient’s goals and basic symptom management, should be routine aspects of care delivered by any practitioner,” Drs. Quill and Abernethy wrote. “Other skills are more complex and take years of training to learn and apply, such as negotiating a difficult family meeting, addressing veiled existential distress, and managing refractory symptoms.”
Dr. Bekanich is trying the two-tiered approach at Seton Healthcare. At facilities with no palliative care service, he is transplanting palliative-trained nurse practitioners in hospital medicine groups.
“This model is locked into our budget for fiscal year 2014,” Dr. Bekanich says. “We’ll train folks, starting with hospitalists and primary care physicians.”
The training will start with a pair of three-hour sessions on palliative care techniques for hospitalists and PCPs, followed by homework assignments. “Then we’ll meet again in three months to do some role plays,” he says.
Two final rounds of training will focus on skills, philosophy, values, and practice.
—Marianne Novelli, MD, FHM, FACP, former chief of the division of hospital medicine, Kaiser Permanente, Denver, Colo.
On-the-Job Training
David Weissman, MD, FACP, a palliative care specialist in Milwaukee, Wis., and consultant to the CAPC, recommends hospitalists do what they can to improve their knowledge and skills. “There are a lot of opportunities for palliative care training out there,” he says.
HM conferences often include palliative care content. AAHPM and CAPC offer annual conferences that immerse participants in content, with opportunities to mingle with palliative care colleagues. AAHPM also offers specific content through its “Unipac” series of nine self-study training modules (www.aahpm.org/resources/default/unipac-4th-edition.html.)
On the job, Dr. Weissman says hospitalists should ask for consults for patients with complex needs. Also pay attention to how the service works and what it recommends. Taking a couple of days to round with the palliative care service could be very educational. It may be possible to take a part-time position with the team, providing weekend or vacation coverage. Hospitalists can participate on planning or advisory committees for palliative care in their hospitals or on quality improvement projects.
“If there isn’t a palliative care service, advocate for developing one,” he says.
Local hospice programs, especially those with inpatient hospice facilities that need daily physician coverage, might have part-time staff positions, which could be a great moonlighting opportunity for hospitalists and a way to learn a lot very quickly.
“I can tell the difference between physicians who have spent time working in a hospice, where you can learn about caring for people at the end of life because most of the patients are so sick, and those who have not,” says Porter Storey, MD, FACP, AAHPM’s executive vice president and a practicing palliative care physician in Colorado. “You can learn how to use the medications to get someone comfortable quickly and how to talk to families in crisis. It can be some of the most rewarding work you can possibly do—especially when you have the time and training to do it well for some of the most challenging of patients and families.”
Dr. Storey recommends that hospitalists join AAHPM, use its professional materials, attend its annual meetings, and, if they feel a calling, consider fellowship training as the next big step.
“Palliative care programs are growing in number and size but are chronically understaffed,” says Steven Pantilat, MD, SFHM, hospitalist and director of the Palliative Care Program at the University of California at San Francisco. “This creates a great opportunity for hospitalists. I have heard of places that were having trouble recruiting palliative care physicians but were willing to sponsor a hospitalist to go and do a fellowship, supplementing their salary as an incentive—and a reasonable one—for a hospitalist interested in making a career move.”
He says that palliative care, like hospital medicine, has been a significant value-add in many hospitals and health systems. More importantly, it correlates to positive patient outcomes (see “Research Highlights Palliative Care Contributions,”).
“What’s new is how it connects to current issues like improved care transitions and readmissions reduction,” Dr. Pantilat says.
Advocates say palliative care helps to match medical services to patient preferences, thereby improving patient satisfaction scores, especially for those who aren’t likely to achieve good outcomes. Dr. Pantilat says it puts plans in place for patients to get the right services for the post-discharge period and for responding to anticipated problems like chest pain.
“It’s not just how to get patients out of the hospital as quickly as possible,” he says, “but to do that with a plan that sets them up to succeed at home.”
Larry Beresford is a freelance writer in San Francisco.
References
- Lupu D. American Academy of Hospice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician workforce shortage. J Pain Symptom Manage. 2010;40(6):899-911.
- Quill TE, Abernethy AP. Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med. 2013;368(13):1173-1175.
- Morrison RS, Penrod JD, Cassel JB, et al. Palliative Care Leadership Centers' Outcomes Group. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
- Penrod JD, Deb P, Dellenbaugh C, et al. Hospital-based palliative care consultation: effects on hospital cost. J Palliat Med. 2010;13(8):973-979.
- Gelfman LP, Meier DE, Morrison RS. Does palliative care improve quality? A survey of bereaved family members. J Pain Symptom Manage. 2008;36(1):22-28.
- Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
- Irwin KE, Greer JA, Khatib J, Temel JS, Pirl WF. Early palliative care and metastatic non-small cell lung cancer: potential mechanisms of prolonged survival. Chron Respir Dis. 2013;10(1):35-47.
- Von Roenn JN, Temel J. The integration of palliative care and oncology: the evidence. Oncology. 2011;25(13):1258-1260,1262,1264-1265.
- Yoong J, Park ER, Greer JA, etc. Early palliative care in advanced lung cancer: a qualitative study. JAMA Intern Med. 2013;173(4):283-290.
- Enguidanos S, Vesper E, Lorenz K. 30-day readmissions among seriously ill older adults. J Palliat Med. 2012;15(12):1356-1361.
- Eti S, O’Mahony S, McHugh M, Guilbe R, Blank A, Selwyn P. Outcomes of the acute palliative care unit in an academic medical center [published online ahead of print May 10, 2013]. Am J Hosp Palliat Care. PMID: 23666616.
- Smith AK, Thai JN, Bakitas MA, et al. The diverse landscape of palliative care clinics. J Palliat Med. 2013;16(6):661-668.
After nine years in practice as a hospitalist in community and academic settings, Leonard Noronha, MD, applied for and in July 2012 became the inaugural, full-year, full-time fellow in hospice and palliative medicine (HPM) at the University of New Mexico in Albuquerque, one of approximately 200 such positions nationwide. The fellowship training qualifies him to sit for HPM subspecialty medical board certification.
Dr. Noronha says he was casually acquainted with the concept of palliative care from residency but didn’t know “when to ask for a palliative care consultation or what they offered.”
“I also had a sense that discussions about feeding tubes, for example, could happen better and easier than they typically did,” he says.
His interest piqued as he learned more about palliative care at hospitalist meetings.
“I grew more excited about it and came to realize that it is something I’d find rewarding and enjoyable, if I could get good at it,” Dr. Noronha says. “Over time, I found more satisfaction in palliative care encounters with patients—and became less comfortable with what I perceived as occasionally inappropriate and excessive testing and treatment [for some hospitalized patients who weren’t offered palliative care].”
Palliative care is a medical specialty that focuses on comfort, relief of symptoms, and clarifying patients’ treatment goals. It is commonly provided as an interdisciplinary consultation service in hospitals. Advocates say it can be offered concurrently with other medical therapies for any seriously ill patient, particularly when there are physical, psychosocial, or spiritual complications, and it is not limited to patients approaching death.
Experienced clinicians say palliative care maximizes quality of life and empowers patients and their families to make treatment decisions more in line with their hopes and values. They also say palliative care gives an emotional lift to providers, while reducing hospital expenditures. Some also suggest that palliative care is an additional tool for enhancing care transitions, potentially affecting readmission rates.
For Dr. Noronha, the one-year fellowship required a significant cut in pay, but he was prepared for the financial hardship.
“It was a great decision for me,” he says. “Some of my colleagues had encouraged me to think about using the experiential pathway to HPM board certification, but I knew I’d do better in the structured environment of a fellowship.
“There have been times when I’ve been outside of my comfort zone, sometimes feeling like the least experienced person in the room. But I knew the fellowship would help—and it did.”
He says the training gives him a better appreciation for things like illness trajectories, the nuances of goal clarification, and the benefit of an extra set of eyes and ears to assess the patient.
After completing his fellowship, Dr. Noronha became UNM’s second full-time palliative medicine faculty. He encourages hospitalists to talk to the palliative care service at their institutions and request consultations for complex, seriously ill patients who might benefit.
As for his new career path, he says that often he is asked if palliative care is depressing. “Some of these situations can be tragic, but I find the work very rewarding,” he says.
Service Models
In some settings, palliative care is incorporated into the hospitalist service. Hospitalists are scheduled for palliative care shifts or have palliative care visits incorporated into daily rounds. Such blended positions could be a recruiting incentive for some physicians who want to do both.
In other settings, palliative care is a separate service. Consultations are ordered as needed by hospitalists and other physicians.
Advocates like Marianne Novelli, MD, FHM, FACP, say hospitalists play a pivotal role in providing the basics of palliative care for seriously ill, hospitalized patients.
“Palliative care is part and parcel of what we do as hospitalists with the people we serve—who by definition are very sick, even to get into the hospital,” says Dr. Novelli, formerly the chief of the division of hospital medicine at Kaiser Permanente in Denver, Colo. She rotated off that leadership position in 2011 and has since divided her time between hospital medicine and palliative care shifts in the hospital, although she now does palliative care exclusively.
Initially, she watched palliative care consults and asked for mentorship from the palliative care team. Although it took time to get used to the advisory role of the consultant, and to working with a team, she eventually became board certified in HPM.
“Palliative care is incredibly intense but richly rewarding work,” she says. “The patients you see are never simple. It allows us to practice the type of medicine we originally set out to do, with people at the most vulnerable times in their lives.”
Workforce, Fellowship, Board Certification
In October 2012, 3,356 physicians passed the hospice and palliative medicine subspecialty board exams offered by the American Board of Medical Specialties and 10 of its constituent specialty boards, with the lion’s share of them certified by the American Board of Internal Medicine. That more than doubled the number of physicians earning the HPM credential since its inception in 2008.
Even with the surge in palliative care training, workforce studies suggest the U.S. is woefully short of credentialed palliative care physicians. And many think hospitalists can help fill that void.
The Center to Advance Palliative Care (CAPC, www.capc.org) counts 1,400 hospital-based palliative care programs in the U.S., while the Centers for Medicare & Medicaid Services (CMS) recognizes about 3,500 Medicare-certified hospice programs. A 2010 estimate by Dale Lupu and the American Academy of Hospice and Palliative Medicine (AAHPM), however, suggested a need for between 4,487 and 10,810 palliative care physician FTEs just to staff existing programs at appropriate levels—without considering growth for the field or its spread into outpatient settings.1
In the past, mid-career physicians had an experiential pathway to the HPM board exam, based on hours worked with a hospice or palliative care team, but physicians now must complete an HPM fellowship of at least one year in order to sit for the boards. And, according to AAHPM, only 234 HPM fellowship positions are offered nationwide by 85 approved fellowship programs.
A one-year fellowship is a big commitment for an established hospitalist, according to Stephen Bekanich, MD, co-director of Seton Palliative Care at Seton Healthcare, an 11-hospital system in Austin, Texas. A former hospitalist, Dr. Bekanich says that in his region a fellow stipend is about $70,000, whereas typical hospitalist compensation is in the mid- to upper-$200,000s.
AAHPM is exploring other approaches to expanding the workforce with mid-career physicians. One approach, authored by Timothy Quill, MD, and Amy Abernethy, MD, the past and current AAHPM board presidents, is to develop a two-tiered system in which palliative medicine specialists teach basic palliative care techniques and approaches to primary care physicians, hospitalists, and such specialists as oncologists.2 The article also suggested equipping clinicians with the tools to recognize when more specialized help is needed.
“As in any medical discipline, some core elements of palliative care, such as aligning treatment with a patient’s goals and basic symptom management, should be routine aspects of care delivered by any practitioner,” Drs. Quill and Abernethy wrote. “Other skills are more complex and take years of training to learn and apply, such as negotiating a difficult family meeting, addressing veiled existential distress, and managing refractory symptoms.”
Dr. Bekanich is trying the two-tiered approach at Seton Healthcare. At facilities with no palliative care service, he is transplanting palliative-trained nurse practitioners in hospital medicine groups.
“This model is locked into our budget for fiscal year 2014,” Dr. Bekanich says. “We’ll train folks, starting with hospitalists and primary care physicians.”
The training will start with a pair of three-hour sessions on palliative care techniques for hospitalists and PCPs, followed by homework assignments. “Then we’ll meet again in three months to do some role plays,” he says.
Two final rounds of training will focus on skills, philosophy, values, and practice.
—Marianne Novelli, MD, FHM, FACP, former chief of the division of hospital medicine, Kaiser Permanente, Denver, Colo.
On-the-Job Training
David Weissman, MD, FACP, a palliative care specialist in Milwaukee, Wis., and consultant to the CAPC, recommends hospitalists do what they can to improve their knowledge and skills. “There are a lot of opportunities for palliative care training out there,” he says.
HM conferences often include palliative care content. AAHPM and CAPC offer annual conferences that immerse participants in content, with opportunities to mingle with palliative care colleagues. AAHPM also offers specific content through its “Unipac” series of nine self-study training modules (www.aahpm.org/resources/default/unipac-4th-edition.html.)
On the job, Dr. Weissman says hospitalists should ask for consults for patients with complex needs. Also pay attention to how the service works and what it recommends. Taking a couple of days to round with the palliative care service could be very educational. It may be possible to take a part-time position with the team, providing weekend or vacation coverage. Hospitalists can participate on planning or advisory committees for palliative care in their hospitals or on quality improvement projects.
“If there isn’t a palliative care service, advocate for developing one,” he says.
Local hospice programs, especially those with inpatient hospice facilities that need daily physician coverage, might have part-time staff positions, which could be a great moonlighting opportunity for hospitalists and a way to learn a lot very quickly.
“I can tell the difference between physicians who have spent time working in a hospice, where you can learn about caring for people at the end of life because most of the patients are so sick, and those who have not,” says Porter Storey, MD, FACP, AAHPM’s executive vice president and a practicing palliative care physician in Colorado. “You can learn how to use the medications to get someone comfortable quickly and how to talk to families in crisis. It can be some of the most rewarding work you can possibly do—especially when you have the time and training to do it well for some of the most challenging of patients and families.”
Dr. Storey recommends that hospitalists join AAHPM, use its professional materials, attend its annual meetings, and, if they feel a calling, consider fellowship training as the next big step.
“Palliative care programs are growing in number and size but are chronically understaffed,” says Steven Pantilat, MD, SFHM, hospitalist and director of the Palliative Care Program at the University of California at San Francisco. “This creates a great opportunity for hospitalists. I have heard of places that were having trouble recruiting palliative care physicians but were willing to sponsor a hospitalist to go and do a fellowship, supplementing their salary as an incentive—and a reasonable one—for a hospitalist interested in making a career move.”
He says that palliative care, like hospital medicine, has been a significant value-add in many hospitals and health systems. More importantly, it correlates to positive patient outcomes (see “Research Highlights Palliative Care Contributions,”).
“What’s new is how it connects to current issues like improved care transitions and readmissions reduction,” Dr. Pantilat says.
Advocates say palliative care helps to match medical services to patient preferences, thereby improving patient satisfaction scores, especially for those who aren’t likely to achieve good outcomes. Dr. Pantilat says it puts plans in place for patients to get the right services for the post-discharge period and for responding to anticipated problems like chest pain.
“It’s not just how to get patients out of the hospital as quickly as possible,” he says, “but to do that with a plan that sets them up to succeed at home.”
Larry Beresford is a freelance writer in San Francisco.
References
- Lupu D. American Academy of Hospice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician workforce shortage. J Pain Symptom Manage. 2010;40(6):899-911.
- Quill TE, Abernethy AP. Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med. 2013;368(13):1173-1175.
- Morrison RS, Penrod JD, Cassel JB, et al. Palliative Care Leadership Centers' Outcomes Group. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
- Penrod JD, Deb P, Dellenbaugh C, et al. Hospital-based palliative care consultation: effects on hospital cost. J Palliat Med. 2010;13(8):973-979.
- Gelfman LP, Meier DE, Morrison RS. Does palliative care improve quality? A survey of bereaved family members. J Pain Symptom Manage. 2008;36(1):22-28.
- Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
- Irwin KE, Greer JA, Khatib J, Temel JS, Pirl WF. Early palliative care and metastatic non-small cell lung cancer: potential mechanisms of prolonged survival. Chron Respir Dis. 2013;10(1):35-47.
- Von Roenn JN, Temel J. The integration of palliative care and oncology: the evidence. Oncology. 2011;25(13):1258-1260,1262,1264-1265.
- Yoong J, Park ER, Greer JA, etc. Early palliative care in advanced lung cancer: a qualitative study. JAMA Intern Med. 2013;173(4):283-290.
- Enguidanos S, Vesper E, Lorenz K. 30-day readmissions among seriously ill older adults. J Palliat Med. 2012;15(12):1356-1361.
- Eti S, O’Mahony S, McHugh M, Guilbe R, Blank A, Selwyn P. Outcomes of the acute palliative care unit in an academic medical center [published online ahead of print May 10, 2013]. Am J Hosp Palliat Care. PMID: 23666616.
- Smith AK, Thai JN, Bakitas MA, et al. The diverse landscape of palliative care clinics. J Palliat Med. 2013;16(6):661-668.
Five criteria doubled palliative care, cut hospital readmissions
Using five characteristics doubled palliative care consults for patients with solid tumors in a small study at one facility. As a result, hospice utilization rates increased by more than 10% and 30-day readmission rates decreased from 36% to 17%, Dr. Kerin Adelson reported during a press briefing held in advance of the symposium on quality care sponsored by the American Society of Clinical Oncology, where the results of the pilot program will be presented in full.
The criteria used to prompt palliative care consults in patients with sold tumors are as follows:
• Stage IV disease.
• Stage III lung or pancreatic cancer.
• Prior hospitalization within 30-days, excluding routine chemotherapy.
• Hospitalization lasting longer than 7 days.
• Uncontrolled symptoms including pain, nausea/vomiting, dyspnea, delirium, and psychological distress.
"Too many patients receive palliative care too late or go without it altogether. This results in inadequate pain control, emotional distress for patients and caregivers, and overuse of aggressive medical interventions. By increasing access to palliative care services, we hoped to help patients clarify their own treatment goals and, in turn, align our clinical goals with those of our patients," said Dr. Adelson of Mount Sinai Hospital, N.Y.
Over 3 months, 68 patients at the center with solid tumors qualified for the palliative care consultations. The investigators compared outcomes for these patients with rates of palliative care for 51 patients during a 6-week period before the program was implemented.
Before the routine use of the criteria, 41% of the patients received a palliative care consultation. After the program was implemented, this rate doubled to 82% – a significant increase (P less than .0001). Thirty-day readmission rates fell from 36% before use of the criteria to 17% after use of the criteria – also a significant improvement (P = .022). Hospice utilization increased from 14% before to 25% after – a difference that was not statistically significant (P = .146).
The investigators also assessed data from the entire Mount Sinai University Health System Consortium, comparing outcomes during the pilot study to the averages seen within the system during the previous year.
Projecting results from the pilot study onto that data, about 60% of patients admitted with a solid tumor would have been eligible for a consult under the investigational criteria. The intervention would have reduced 30-day readmission rates from 22% to 13% and would have significantly lowered the mortality index – an inpatient death rate that controls for the severity of illness – from 1.39 to 0.59, according to Dr. Adelson.
"This means that fewer patients were dying in acute hospital settings than would be expected for the severity of illness," she said.
Before the five criteria were established, the facility had no guidelines and relied on the treating oncologist’s discretion for identifying patients who needed palliative care consults, said Dr. Adelson, who determined the criteria in collaboration with her Mount Sinai colleagues. Now, patients who meet any of the criteria are offered a palliative care consultation, which could lead to new symptomatic treatments or to hospice care at home or in the hospital.
The facility has now decided to create a palliative care team that will provide consultation for every patient who meets the new criteria, she added.
Dr. Adelson had no financial disclosures related to her presentation.
Using five characteristics doubled palliative care consults for patients with solid tumors in a small study at one facility. As a result, hospice utilization rates increased by more than 10% and 30-day readmission rates decreased from 36% to 17%, Dr. Kerin Adelson reported during a press briefing held in advance of the symposium on quality care sponsored by the American Society of Clinical Oncology, where the results of the pilot program will be presented in full.
The criteria used to prompt palliative care consults in patients with sold tumors are as follows:
• Stage IV disease.
• Stage III lung or pancreatic cancer.
• Prior hospitalization within 30-days, excluding routine chemotherapy.
• Hospitalization lasting longer than 7 days.
• Uncontrolled symptoms including pain, nausea/vomiting, dyspnea, delirium, and psychological distress.
"Too many patients receive palliative care too late or go without it altogether. This results in inadequate pain control, emotional distress for patients and caregivers, and overuse of aggressive medical interventions. By increasing access to palliative care services, we hoped to help patients clarify their own treatment goals and, in turn, align our clinical goals with those of our patients," said Dr. Adelson of Mount Sinai Hospital, N.Y.
Over 3 months, 68 patients at the center with solid tumors qualified for the palliative care consultations. The investigators compared outcomes for these patients with rates of palliative care for 51 patients during a 6-week period before the program was implemented.
Before the routine use of the criteria, 41% of the patients received a palliative care consultation. After the program was implemented, this rate doubled to 82% – a significant increase (P less than .0001). Thirty-day readmission rates fell from 36% before use of the criteria to 17% after use of the criteria – also a significant improvement (P = .022). Hospice utilization increased from 14% before to 25% after – a difference that was not statistically significant (P = .146).
The investigators also assessed data from the entire Mount Sinai University Health System Consortium, comparing outcomes during the pilot study to the averages seen within the system during the previous year.
Projecting results from the pilot study onto that data, about 60% of patients admitted with a solid tumor would have been eligible for a consult under the investigational criteria. The intervention would have reduced 30-day readmission rates from 22% to 13% and would have significantly lowered the mortality index – an inpatient death rate that controls for the severity of illness – from 1.39 to 0.59, according to Dr. Adelson.
"This means that fewer patients were dying in acute hospital settings than would be expected for the severity of illness," she said.
Before the five criteria were established, the facility had no guidelines and relied on the treating oncologist’s discretion for identifying patients who needed palliative care consults, said Dr. Adelson, who determined the criteria in collaboration with her Mount Sinai colleagues. Now, patients who meet any of the criteria are offered a palliative care consultation, which could lead to new symptomatic treatments or to hospice care at home or in the hospital.
The facility has now decided to create a palliative care team that will provide consultation for every patient who meets the new criteria, she added.
Dr. Adelson had no financial disclosures related to her presentation.
Using five characteristics doubled palliative care consults for patients with solid tumors in a small study at one facility. As a result, hospice utilization rates increased by more than 10% and 30-day readmission rates decreased from 36% to 17%, Dr. Kerin Adelson reported during a press briefing held in advance of the symposium on quality care sponsored by the American Society of Clinical Oncology, where the results of the pilot program will be presented in full.
The criteria used to prompt palliative care consults in patients with sold tumors are as follows:
• Stage IV disease.
• Stage III lung or pancreatic cancer.
• Prior hospitalization within 30-days, excluding routine chemotherapy.
• Hospitalization lasting longer than 7 days.
• Uncontrolled symptoms including pain, nausea/vomiting, dyspnea, delirium, and psychological distress.
"Too many patients receive palliative care too late or go without it altogether. This results in inadequate pain control, emotional distress for patients and caregivers, and overuse of aggressive medical interventions. By increasing access to palliative care services, we hoped to help patients clarify their own treatment goals and, in turn, align our clinical goals with those of our patients," said Dr. Adelson of Mount Sinai Hospital, N.Y.
Over 3 months, 68 patients at the center with solid tumors qualified for the palliative care consultations. The investigators compared outcomes for these patients with rates of palliative care for 51 patients during a 6-week period before the program was implemented.
Before the routine use of the criteria, 41% of the patients received a palliative care consultation. After the program was implemented, this rate doubled to 82% – a significant increase (P less than .0001). Thirty-day readmission rates fell from 36% before use of the criteria to 17% after use of the criteria – also a significant improvement (P = .022). Hospice utilization increased from 14% before to 25% after – a difference that was not statistically significant (P = .146).
The investigators also assessed data from the entire Mount Sinai University Health System Consortium, comparing outcomes during the pilot study to the averages seen within the system during the previous year.
Projecting results from the pilot study onto that data, about 60% of patients admitted with a solid tumor would have been eligible for a consult under the investigational criteria. The intervention would have reduced 30-day readmission rates from 22% to 13% and would have significantly lowered the mortality index – an inpatient death rate that controls for the severity of illness – from 1.39 to 0.59, according to Dr. Adelson.
"This means that fewer patients were dying in acute hospital settings than would be expected for the severity of illness," she said.
Before the five criteria were established, the facility had no guidelines and relied on the treating oncologist’s discretion for identifying patients who needed palliative care consults, said Dr. Adelson, who determined the criteria in collaboration with her Mount Sinai colleagues. Now, patients who meet any of the criteria are offered a palliative care consultation, which could lead to new symptomatic treatments or to hospice care at home or in the hospital.
The facility has now decided to create a palliative care team that will provide consultation for every patient who meets the new criteria, she added.
Dr. Adelson had no financial disclosures related to her presentation.
FROM THE ASCO QUALITY CARE SYMPOSIUM
Major finding: Thirty-day readmission rates fell from 36% before use of the criteria to 17% after use of the criteria – a significant improvement (P = .022).
Data source: A comparison of outcomes in 68 patients treated over 3 months with the criteria in place and in 51 patients treated during a 6-week period before the program was implemented.
Disclosures: The researchers had no relevant financial disclosures.
Hospital-Based Palliative Care Reduces Length of Stay, Charges, Invasive Procedures, ICU Deaths

Clinical question: What are the characteristics of children who died in children’s hospitals while receiving palliative care (PC) compared to those who did not?
Background: Approximately 44,000 children die annually in hospitals in the U.S. Since the American Academy of Pediatrics (AAP) released a statement in August 2000 that presented an integrated model for providing PC to children with life-threatening conditions, pediatric PC programs have increased steadily in number. Children who receive PC services are commonly afflicted by genetic/congenital disorders, neuromuscular disorders, and cancer diagnoses. Although it is estimated that 6,320 people under the age of 24 received PC services in 2010, little data exist comparing pediatric inpatients receiving PC and those who do not.
Study design: Multicenter retrospective cohort study.
Setting: More than 40 freestanding children’s hospitals.
Synopsis: Using the Pediatric Health Information System (PHIS) database, which collects administrative and clinical data from more than 40 freestanding children’s hospitals belonging to the Children’s Hospital Association, researchers analyzed the characteristics of children under the age of 18 who died in the hospital more than five days after admission from 2001 to 2011. They extracted demographic data and categorized patients using major diagnostic categories (MDC) based on major organ system or etiology of disease. Identification of patients receiving PC services was by ICD-9 codes, and utilization of medications and procedures was identified by clinical transaction codes (CTC) and ICD-9 codes. The unit billing the last hospital day determined location of death.
Of the 24,342 children studied, only 3.8% received PC services based on coding. Patients less likely to receive PC services included black children (2.3%), those with circulatory diseases (2.8%), and those with neonatal diseases (1.9%). Children who did receive PC services had a significantly lower median length of stay (17 vs. 21 days), average daily charges ($9,348 vs. $11,806), received significantly fewer interventions (mechanical ventilation, invasive monitoring, surgical procedures), and died less frequently in an ICU setting (60% vs. 88%). PC services disproportionately altered the care of children with lymphatic/hematopoietic diseases, significantly decreasing use of mechanical ventilation (75% to 22%) and death in an ICU setting (66% to 21%).
Bottom line: Provision of PC services to children dying in children’s hospitals remains low. It is even lower for children with certain racial backgrounds and disease processes. When provided, PC services reduce length of stay, average daily charges, invasive procedures, and death in an ICU setting.
Citation: Keele L, Keenan HT, Sheetz J. Differences in characteristics of dying children who receive and do not receive palliative care. Pediatrics. 2013;132(1):72-78.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FAAP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: What are the characteristics of children who died in children’s hospitals while receiving palliative care (PC) compared to those who did not?
Background: Approximately 44,000 children die annually in hospitals in the U.S. Since the American Academy of Pediatrics (AAP) released a statement in August 2000 that presented an integrated model for providing PC to children with life-threatening conditions, pediatric PC programs have increased steadily in number. Children who receive PC services are commonly afflicted by genetic/congenital disorders, neuromuscular disorders, and cancer diagnoses. Although it is estimated that 6,320 people under the age of 24 received PC services in 2010, little data exist comparing pediatric inpatients receiving PC and those who do not.
Study design: Multicenter retrospective cohort study.
Setting: More than 40 freestanding children’s hospitals.
Synopsis: Using the Pediatric Health Information System (PHIS) database, which collects administrative and clinical data from more than 40 freestanding children’s hospitals belonging to the Children’s Hospital Association, researchers analyzed the characteristics of children under the age of 18 who died in the hospital more than five days after admission from 2001 to 2011. They extracted demographic data and categorized patients using major diagnostic categories (MDC) based on major organ system or etiology of disease. Identification of patients receiving PC services was by ICD-9 codes, and utilization of medications and procedures was identified by clinical transaction codes (CTC) and ICD-9 codes. The unit billing the last hospital day determined location of death.
Of the 24,342 children studied, only 3.8% received PC services based on coding. Patients less likely to receive PC services included black children (2.3%), those with circulatory diseases (2.8%), and those with neonatal diseases (1.9%). Children who did receive PC services had a significantly lower median length of stay (17 vs. 21 days), average daily charges ($9,348 vs. $11,806), received significantly fewer interventions (mechanical ventilation, invasive monitoring, surgical procedures), and died less frequently in an ICU setting (60% vs. 88%). PC services disproportionately altered the care of children with lymphatic/hematopoietic diseases, significantly decreasing use of mechanical ventilation (75% to 22%) and death in an ICU setting (66% to 21%).
Bottom line: Provision of PC services to children dying in children’s hospitals remains low. It is even lower for children with certain racial backgrounds and disease processes. When provided, PC services reduce length of stay, average daily charges, invasive procedures, and death in an ICU setting.
Citation: Keele L, Keenan HT, Sheetz J. Differences in characteristics of dying children who receive and do not receive palliative care. Pediatrics. 2013;132(1):72-78.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FAAP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: What are the characteristics of children who died in children’s hospitals while receiving palliative care (PC) compared to those who did not?
Background: Approximately 44,000 children die annually in hospitals in the U.S. Since the American Academy of Pediatrics (AAP) released a statement in August 2000 that presented an integrated model for providing PC to children with life-threatening conditions, pediatric PC programs have increased steadily in number. Children who receive PC services are commonly afflicted by genetic/congenital disorders, neuromuscular disorders, and cancer diagnoses. Although it is estimated that 6,320 people under the age of 24 received PC services in 2010, little data exist comparing pediatric inpatients receiving PC and those who do not.
Study design: Multicenter retrospective cohort study.
Setting: More than 40 freestanding children’s hospitals.
Synopsis: Using the Pediatric Health Information System (PHIS) database, which collects administrative and clinical data from more than 40 freestanding children’s hospitals belonging to the Children’s Hospital Association, researchers analyzed the characteristics of children under the age of 18 who died in the hospital more than five days after admission from 2001 to 2011. They extracted demographic data and categorized patients using major diagnostic categories (MDC) based on major organ system or etiology of disease. Identification of patients receiving PC services was by ICD-9 codes, and utilization of medications and procedures was identified by clinical transaction codes (CTC) and ICD-9 codes. The unit billing the last hospital day determined location of death.
Of the 24,342 children studied, only 3.8% received PC services based on coding. Patients less likely to receive PC services included black children (2.3%), those with circulatory diseases (2.8%), and those with neonatal diseases (1.9%). Children who did receive PC services had a significantly lower median length of stay (17 vs. 21 days), average daily charges ($9,348 vs. $11,806), received significantly fewer interventions (mechanical ventilation, invasive monitoring, surgical procedures), and died less frequently in an ICU setting (60% vs. 88%). PC services disproportionately altered the care of children with lymphatic/hematopoietic diseases, significantly decreasing use of mechanical ventilation (75% to 22%) and death in an ICU setting (66% to 21%).
Bottom line: Provision of PC services to children dying in children’s hospitals remains low. It is even lower for children with certain racial backgrounds and disease processes. When provided, PC services reduce length of stay, average daily charges, invasive procedures, and death in an ICU setting.
Citation: Keele L, Keenan HT, Sheetz J. Differences in characteristics of dying children who receive and do not receive palliative care. Pediatrics. 2013;132(1):72-78.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FAAP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Hospice usage up but not delivered soon enough, study finds
LEBANON, N.H. – Medicare patients with advanced cancer are more likely to receive hospice care than in previous years, although it is still too late in their treatment to deliver the full benefits of palliative care, according to a report issued by the Dartmouth Institute for Health Policy and Clinical Practice.
The report also states that geography and the treatment styles favored by individual health systems, rather than patient preferences, drive the level of intensive, end-of-life treatments used.
The findings are part of the Dartmouth Atlas Project, which uses Medicare data to examine how health care resources are allocated nationally. The report is the institute’s first longitudinal analysis of trends in end-of-life care for advanced cancer patients across regions, academic medical centers, and National Cancer Institute–designated cancer centers.
Controlling for patient age, sex, race, tumor type, and non–cancer-related comorbidities, the investigators found that, when compared with similar data collected from 2003 to 2007 and published by the institute in 2010, the number of advanced cancer patients on Medicare dying in the hospital decreased by an average of 28.8% during 2003-2007 to 24.7% in 2010. An increase from 54.6% to 61.3% in the number of patients who were enrolled in hospice in the last month of life was also found. The number of patients for whom hospice was initiated during the last 3 days of life increased from 8.3% during 2003-2007 to 10.9% in 2010.
When asked in an interview about the importance of starting hospice sooner in terminal care, Dr. Lorenzo Norris, director of psycho-oncology services at George Washington University Medical Center in Washington, said, "The biggest misconception is that hospice is strictly for end of life. Palliative care is just good medicine. If you limit the hospice care to the last 3 days, you’ve already limited the options a patient has. If you offer palliative care 5 or 6 months out, you can start reducing symptom burdens and increase a patient’s quality of life, which is very important because during that last year to 6 months is when patients are finishing unresolved financial and relationship issues. Palliative care allows them to more fully engage in their life."
When viewed according to the medical center delivering the care, between 13% and 50% of Medicare patients with advanced cancer died in a hospital in 2010, rather than in a hospice setting – typically the patient’s home. These figures include data from NCI-designated cancer centers. Hospice treatment in the last month of life for patients treated in mid- and northwestern states such as Oregon and Iowa trended as much as nearly 50% higher than in places such as Alaska and New York City.
Addressing the reasons for regional variations in care, Dr. Ira Byock, director of palliative medicine at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., wrote in an accompanying editorial that, "Previous research has also shown that regional supply of health care resources, such as hospital and intensive care beds and imaging equipment, is one driver of the intensity of care, irrespective of the patient’s particular condition or illness level."
The analysts found the overall rate of ICU admissions for treatments such as intubation, a feeding tube, or cardiopulmonary resuscitation during the last month of life increased from 23.7% in the period between 2003 and 2007 to 28.8% in 2010. The number of days patients spent in the ICU in the last month of life varied more than fivefold across all centers, the analysts wrote.
"Our research continues to find that patients with advanced cancer are often receiving aggressive care until their final days, when we know that most patients would prefer care directed toward a better quality of life through hospice and palliative services. The increase in patients admitted to hospice care only days before death suggests that hospice services are often provided too late to provide much benefit," Dr. David C. Goodman, coprincipal investigator for the Dartmouth Atlas Project, said in a statement.
When asked why some oncologists are not referring their patients to hospice sooner, Dr. Clifford Hudis, president of the American Society of Clinical Oncology said, "There are many circumstances, based on culture, family dynamics, and patient’s wishes, where it is hard to communicate the value of hospice services. Some patients remain fearful of the very word and, in some situations, there is an unwillingness to acknowledge the severity of illnesses. These barriers can often be overcome through an increase in communication between doctors and patients about care goals and wishes."
When asked about the potential economic implications of the data, Dr. Goodman said, "The goal of better end-of-life care is to improve patient well-being. Often, it is less expensive to provide good care that patients want, [rather] than the usual care that patients receive."
The report also indicated that the number of patients who saw 10 or more different physicians during the last six months of their lives rose from 46.2% to 58.5%. The analysts interpreted this to mean "more patients may have experienced fragmented care."
In a statement Dr. Hudis encouraged the oncology community to "keep striving to deliver the right care at the right time." In an e-mail interview, Dr. Hudis wrote that, "The overall trend is a good one because it is concordant with the overall goals of ASCO: to make sure that every patient has access to the highest quality care throughout their disease experience."
Dr. Goodman and Dr. Byock report no relevant disclosures. The report was principally funded by the Robert Wood Johnson Foundation, with support from a consortium of funders including the WellPoint Foundation, the United Health Foundation, and the California HealthCare Foundation.
LEBANON, N.H. – Medicare patients with advanced cancer are more likely to receive hospice care than in previous years, although it is still too late in their treatment to deliver the full benefits of palliative care, according to a report issued by the Dartmouth Institute for Health Policy and Clinical Practice.
The report also states that geography and the treatment styles favored by individual health systems, rather than patient preferences, drive the level of intensive, end-of-life treatments used.
The findings are part of the Dartmouth Atlas Project, which uses Medicare data to examine how health care resources are allocated nationally. The report is the institute’s first longitudinal analysis of trends in end-of-life care for advanced cancer patients across regions, academic medical centers, and National Cancer Institute–designated cancer centers.
Controlling for patient age, sex, race, tumor type, and non–cancer-related comorbidities, the investigators found that, when compared with similar data collected from 2003 to 2007 and published by the institute in 2010, the number of advanced cancer patients on Medicare dying in the hospital decreased by an average of 28.8% during 2003-2007 to 24.7% in 2010. An increase from 54.6% to 61.3% in the number of patients who were enrolled in hospice in the last month of life was also found. The number of patients for whom hospice was initiated during the last 3 days of life increased from 8.3% during 2003-2007 to 10.9% in 2010.
When asked in an interview about the importance of starting hospice sooner in terminal care, Dr. Lorenzo Norris, director of psycho-oncology services at George Washington University Medical Center in Washington, said, "The biggest misconception is that hospice is strictly for end of life. Palliative care is just good medicine. If you limit the hospice care to the last 3 days, you’ve already limited the options a patient has. If you offer palliative care 5 or 6 months out, you can start reducing symptom burdens and increase a patient’s quality of life, which is very important because during that last year to 6 months is when patients are finishing unresolved financial and relationship issues. Palliative care allows them to more fully engage in their life."
When viewed according to the medical center delivering the care, between 13% and 50% of Medicare patients with advanced cancer died in a hospital in 2010, rather than in a hospice setting – typically the patient’s home. These figures include data from NCI-designated cancer centers. Hospice treatment in the last month of life for patients treated in mid- and northwestern states such as Oregon and Iowa trended as much as nearly 50% higher than in places such as Alaska and New York City.
Addressing the reasons for regional variations in care, Dr. Ira Byock, director of palliative medicine at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., wrote in an accompanying editorial that, "Previous research has also shown that regional supply of health care resources, such as hospital and intensive care beds and imaging equipment, is one driver of the intensity of care, irrespective of the patient’s particular condition or illness level."
The analysts found the overall rate of ICU admissions for treatments such as intubation, a feeding tube, or cardiopulmonary resuscitation during the last month of life increased from 23.7% in the period between 2003 and 2007 to 28.8% in 2010. The number of days patients spent in the ICU in the last month of life varied more than fivefold across all centers, the analysts wrote.
"Our research continues to find that patients with advanced cancer are often receiving aggressive care until their final days, when we know that most patients would prefer care directed toward a better quality of life through hospice and palliative services. The increase in patients admitted to hospice care only days before death suggests that hospice services are often provided too late to provide much benefit," Dr. David C. Goodman, coprincipal investigator for the Dartmouth Atlas Project, said in a statement.
When asked why some oncologists are not referring their patients to hospice sooner, Dr. Clifford Hudis, president of the American Society of Clinical Oncology said, "There are many circumstances, based on culture, family dynamics, and patient’s wishes, where it is hard to communicate the value of hospice services. Some patients remain fearful of the very word and, in some situations, there is an unwillingness to acknowledge the severity of illnesses. These barriers can often be overcome through an increase in communication between doctors and patients about care goals and wishes."
When asked about the potential economic implications of the data, Dr. Goodman said, "The goal of better end-of-life care is to improve patient well-being. Often, it is less expensive to provide good care that patients want, [rather] than the usual care that patients receive."
The report also indicated that the number of patients who saw 10 or more different physicians during the last six months of their lives rose from 46.2% to 58.5%. The analysts interpreted this to mean "more patients may have experienced fragmented care."
In a statement Dr. Hudis encouraged the oncology community to "keep striving to deliver the right care at the right time." In an e-mail interview, Dr. Hudis wrote that, "The overall trend is a good one because it is concordant with the overall goals of ASCO: to make sure that every patient has access to the highest quality care throughout their disease experience."
Dr. Goodman and Dr. Byock report no relevant disclosures. The report was principally funded by the Robert Wood Johnson Foundation, with support from a consortium of funders including the WellPoint Foundation, the United Health Foundation, and the California HealthCare Foundation.
LEBANON, N.H. – Medicare patients with advanced cancer are more likely to receive hospice care than in previous years, although it is still too late in their treatment to deliver the full benefits of palliative care, according to a report issued by the Dartmouth Institute for Health Policy and Clinical Practice.
The report also states that geography and the treatment styles favored by individual health systems, rather than patient preferences, drive the level of intensive, end-of-life treatments used.
The findings are part of the Dartmouth Atlas Project, which uses Medicare data to examine how health care resources are allocated nationally. The report is the institute’s first longitudinal analysis of trends in end-of-life care for advanced cancer patients across regions, academic medical centers, and National Cancer Institute–designated cancer centers.
Controlling for patient age, sex, race, tumor type, and non–cancer-related comorbidities, the investigators found that, when compared with similar data collected from 2003 to 2007 and published by the institute in 2010, the number of advanced cancer patients on Medicare dying in the hospital decreased by an average of 28.8% during 2003-2007 to 24.7% in 2010. An increase from 54.6% to 61.3% in the number of patients who were enrolled in hospice in the last month of life was also found. The number of patients for whom hospice was initiated during the last 3 days of life increased from 8.3% during 2003-2007 to 10.9% in 2010.
When asked in an interview about the importance of starting hospice sooner in terminal care, Dr. Lorenzo Norris, director of psycho-oncology services at George Washington University Medical Center in Washington, said, "The biggest misconception is that hospice is strictly for end of life. Palliative care is just good medicine. If you limit the hospice care to the last 3 days, you’ve already limited the options a patient has. If you offer palliative care 5 or 6 months out, you can start reducing symptom burdens and increase a patient’s quality of life, which is very important because during that last year to 6 months is when patients are finishing unresolved financial and relationship issues. Palliative care allows them to more fully engage in their life."
When viewed according to the medical center delivering the care, between 13% and 50% of Medicare patients with advanced cancer died in a hospital in 2010, rather than in a hospice setting – typically the patient’s home. These figures include data from NCI-designated cancer centers. Hospice treatment in the last month of life for patients treated in mid- and northwestern states such as Oregon and Iowa trended as much as nearly 50% higher than in places such as Alaska and New York City.
Addressing the reasons for regional variations in care, Dr. Ira Byock, director of palliative medicine at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., wrote in an accompanying editorial that, "Previous research has also shown that regional supply of health care resources, such as hospital and intensive care beds and imaging equipment, is one driver of the intensity of care, irrespective of the patient’s particular condition or illness level."
The analysts found the overall rate of ICU admissions for treatments such as intubation, a feeding tube, or cardiopulmonary resuscitation during the last month of life increased from 23.7% in the period between 2003 and 2007 to 28.8% in 2010. The number of days patients spent in the ICU in the last month of life varied more than fivefold across all centers, the analysts wrote.
"Our research continues to find that patients with advanced cancer are often receiving aggressive care until their final days, when we know that most patients would prefer care directed toward a better quality of life through hospice and palliative services. The increase in patients admitted to hospice care only days before death suggests that hospice services are often provided too late to provide much benefit," Dr. David C. Goodman, coprincipal investigator for the Dartmouth Atlas Project, said in a statement.
When asked why some oncologists are not referring their patients to hospice sooner, Dr. Clifford Hudis, president of the American Society of Clinical Oncology said, "There are many circumstances, based on culture, family dynamics, and patient’s wishes, where it is hard to communicate the value of hospice services. Some patients remain fearful of the very word and, in some situations, there is an unwillingness to acknowledge the severity of illnesses. These barriers can often be overcome through an increase in communication between doctors and patients about care goals and wishes."
When asked about the potential economic implications of the data, Dr. Goodman said, "The goal of better end-of-life care is to improve patient well-being. Often, it is less expensive to provide good care that patients want, [rather] than the usual care that patients receive."
The report also indicated that the number of patients who saw 10 or more different physicians during the last six months of their lives rose from 46.2% to 58.5%. The analysts interpreted this to mean "more patients may have experienced fragmented care."
In a statement Dr. Hudis encouraged the oncology community to "keep striving to deliver the right care at the right time." In an e-mail interview, Dr. Hudis wrote that, "The overall trend is a good one because it is concordant with the overall goals of ASCO: to make sure that every patient has access to the highest quality care throughout their disease experience."
Dr. Goodman and Dr. Byock report no relevant disclosures. The report was principally funded by the Robert Wood Johnson Foundation, with support from a consortium of funders including the WellPoint Foundation, the United Health Foundation, and the California HealthCare Foundation.
EXPERT ANALYSIS FROM THE DARTMOUTH ATLAS PROJECT

Networks: Telemedicine in Palliative Care, Sleep at CHEST 2013
Palliative and End-of-Life Care
Telemedicine as a tool for early family conferences in critically ill patients transferring to a tertiary care center
Evidence suggests that early palliative care consultations in critically ill patients may be associated with reduced health-care costs while improving family satisfaction. However, critically ill patients at smaller rural hospitals who are often transferred to tertiary care center (TCC) ICUs are often not able to participate in discussions regarding disease processes, prognosis, goals of care, and shared decision making until after they have been transferred. There is a gap in the standard of care related to early communication in this particular group of critically ill patients.
Telemedicine is a tool that we are using to provide family members and treatment teams the opportunity to participate in early family conferences and/or palliative care consultations prior to a patient transferring to a tertiary care center.
We conducted a small retrospective study of these telemedicine family conferences that showed 64% of patients did transfer to a TCC; however, ultimately 58% transferred back to the referring hospital for end of life care. We have also conducted a prospective qualitative study on the experience of participants of these conferences. Family members and clinicians have responded favorably to this form of communication, and we have created a structured intervention for use during these discussions.
We believe this telemedicine intervention will increase family satisfaction, decrease symptoms of posttraumatic stress disorder and anxiety among family members, and align care with patients’ wishes. In order to investigate this further, we are currently conducting a prospective comparative study of a structured telemedicine family conference intervention vs conference conducted after transfer.
Prema R., Menon, MD
Steering Committee Member
Sleep Medicine
AGuide guide to Sleep at CHEST 2013
I hope that you are all gearing up for our meeting this fall in Chicago; as always, the Program Committee has arranged a fantastic meeting with a diverse program, but I wanted to point out a couple of agenda items in the sleep curriculum that I thought would be worth highlighting.
Our postgraduate course on Saturday, October 26, was initially intended as a board review, before the ABIM saw fit to move up the examination date. As a result, this course will instead be a year-in-review, covering the best of the literature over the last 12 months; the session will also be supplemented by the use of an audience response system, allowing the audience to play along and show their knowledge of the newest developments in sleep medicine.
There is a ridiculous number of great sessions on Sunday, including "Management of Insomnia in 2013," developed based on results from our survey in the spring; this session will include a brief primer on cognitive behavioral therapy. Later that day will be one of our NetWork highlights, "Highly Controversial Topics in Sleep Medicine," with discussions on the growing use of sodium oxybate for insomnia and the role of modafinil for cognitive enhancement.
In the afternoon, Dr. Mark Rosekind, member of the National Transportation Safety Board, will be highlighting a session on sleep medicine and transportation safety. The day will be capped off by an evening session led by our NetWork Vice Chair, who will be orchestrating a panel discussion on the future of sleep medicine.
Attendance at Monday’s NetWork Open Forum is a must for anyone wanting to get more involved in the Sleep NetWork. The session will offer a chance to meet with NetWork leadership and to hear about the current activities and priorities of the Steering Committee. We are almost always looking for volunteers for one or more of our ongoing projects; attending the session ensures that you can both sign up and express your interest in person! In addition, you get to hear a great lecture, this year from Dr. Fred Turek.
The rest of the meeting is similarly packed; Tuesday will feature a panel discussion on sleep deprivation and the restriction of resident work hours. Wednesday houses our second NetWork highlight, "Intermittent Hypoxia and OSA Comorbidity," which may make many of us rethink our focus on the apnea-hypopnea index as the prime target for therapy of sleep-disordered breathing. Lastly, Thursday will feature a 4-hour symposium, "Sleep Medicine in 2013," highlighted by the debut of the College’s newest game show, "Who Wants to be a Somnologist?" with prizes for the winners.
For all of these reasons, 2013 is looking to be a spectacular year for sleep medicine education at CHEST, and there are many more sessions that I haven’t enough space to highlight. I sincerely hope that you will join us in Chicago and come by and say "hi" at the NetWork Forum!
Dr. David Schulman, FCCP
Chair
Body text starts here....
Second and subsequent grafs
Doctor’s Name and Bio
Body text starts here....
Second and subsequent grafs
Doctor’s Name and Bio
Body text starts here....
Second and subsequent grafs
Doctor’s Name and Bio
Palliative and End-of-Life Care
Telemedicine as a tool for early family conferences in critically ill patients transferring to a tertiary care center
Evidence suggests that early palliative care consultations in critically ill patients may be associated with reduced health-care costs while improving family satisfaction. However, critically ill patients at smaller rural hospitals who are often transferred to tertiary care center (TCC) ICUs are often not able to participate in discussions regarding disease processes, prognosis, goals of care, and shared decision making until after they have been transferred. There is a gap in the standard of care related to early communication in this particular group of critically ill patients.
Telemedicine is a tool that we are using to provide family members and treatment teams the opportunity to participate in early family conferences and/or palliative care consultations prior to a patient transferring to a tertiary care center.
We conducted a small retrospective study of these telemedicine family conferences that showed 64% of patients did transfer to a TCC; however, ultimately 58% transferred back to the referring hospital for end of life care. We have also conducted a prospective qualitative study on the experience of participants of these conferences. Family members and clinicians have responded favorably to this form of communication, and we have created a structured intervention for use during these discussions.
We believe this telemedicine intervention will increase family satisfaction, decrease symptoms of posttraumatic stress disorder and anxiety among family members, and align care with patients’ wishes. In order to investigate this further, we are currently conducting a prospective comparative study of a structured telemedicine family conference intervention vs conference conducted after transfer.
Prema R., Menon, MD
Steering Committee Member
Sleep Medicine
AGuide guide to Sleep at CHEST 2013
I hope that you are all gearing up for our meeting this fall in Chicago; as always, the Program Committee has arranged a fantastic meeting with a diverse program, but I wanted to point out a couple of agenda items in the sleep curriculum that I thought would be worth highlighting.
Our postgraduate course on Saturday, October 26, was initially intended as a board review, before the ABIM saw fit to move up the examination date. As a result, this course will instead be a year-in-review, covering the best of the literature over the last 12 months; the session will also be supplemented by the use of an audience response system, allowing the audience to play along and show their knowledge of the newest developments in sleep medicine.
There is a ridiculous number of great sessions on Sunday, including "Management of Insomnia in 2013," developed based on results from our survey in the spring; this session will include a brief primer on cognitive behavioral therapy. Later that day will be one of our NetWork highlights, "Highly Controversial Topics in Sleep Medicine," with discussions on the growing use of sodium oxybate for insomnia and the role of modafinil for cognitive enhancement.
In the afternoon, Dr. Mark Rosekind, member of the National Transportation Safety Board, will be highlighting a session on sleep medicine and transportation safety. The day will be capped off by an evening session led by our NetWork Vice Chair, who will be orchestrating a panel discussion on the future of sleep medicine.
Attendance at Monday’s NetWork Open Forum is a must for anyone wanting to get more involved in the Sleep NetWork. The session will offer a chance to meet with NetWork leadership and to hear about the current activities and priorities of the Steering Committee. We are almost always looking for volunteers for one or more of our ongoing projects; attending the session ensures that you can both sign up and express your interest in person! In addition, you get to hear a great lecture, this year from Dr. Fred Turek.
The rest of the meeting is similarly packed; Tuesday will feature a panel discussion on sleep deprivation and the restriction of resident work hours. Wednesday houses our second NetWork highlight, "Intermittent Hypoxia and OSA Comorbidity," which may make many of us rethink our focus on the apnea-hypopnea index as the prime target for therapy of sleep-disordered breathing. Lastly, Thursday will feature a 4-hour symposium, "Sleep Medicine in 2013," highlighted by the debut of the College’s newest game show, "Who Wants to be a Somnologist?" with prizes for the winners.
For all of these reasons, 2013 is looking to be a spectacular year for sleep medicine education at CHEST, and there are many more sessions that I haven’t enough space to highlight. I sincerely hope that you will join us in Chicago and come by and say "hi" at the NetWork Forum!
Dr. David Schulman, FCCP
Chair
Palliative and End-of-Life Care
Telemedicine as a tool for early family conferences in critically ill patients transferring to a tertiary care center
Evidence suggests that early palliative care consultations in critically ill patients may be associated with reduced health-care costs while improving family satisfaction. However, critically ill patients at smaller rural hospitals who are often transferred to tertiary care center (TCC) ICUs are often not able to participate in discussions regarding disease processes, prognosis, goals of care, and shared decision making until after they have been transferred. There is a gap in the standard of care related to early communication in this particular group of critically ill patients.
Telemedicine is a tool that we are using to provide family members and treatment teams the opportunity to participate in early family conferences and/or palliative care consultations prior to a patient transferring to a tertiary care center.
We conducted a small retrospective study of these telemedicine family conferences that showed 64% of patients did transfer to a TCC; however, ultimately 58% transferred back to the referring hospital for end of life care. We have also conducted a prospective qualitative study on the experience of participants of these conferences. Family members and clinicians have responded favorably to this form of communication, and we have created a structured intervention for use during these discussions.
We believe this telemedicine intervention will increase family satisfaction, decrease symptoms of posttraumatic stress disorder and anxiety among family members, and align care with patients’ wishes. In order to investigate this further, we are currently conducting a prospective comparative study of a structured telemedicine family conference intervention vs conference conducted after transfer.
Prema R., Menon, MD
Steering Committee Member
Sleep Medicine
AGuide guide to Sleep at CHEST 2013
I hope that you are all gearing up for our meeting this fall in Chicago; as always, the Program Committee has arranged a fantastic meeting with a diverse program, but I wanted to point out a couple of agenda items in the sleep curriculum that I thought would be worth highlighting.
Our postgraduate course on Saturday, October 26, was initially intended as a board review, before the ABIM saw fit to move up the examination date. As a result, this course will instead be a year-in-review, covering the best of the literature over the last 12 months; the session will also be supplemented by the use of an audience response system, allowing the audience to play along and show their knowledge of the newest developments in sleep medicine.
There is a ridiculous number of great sessions on Sunday, including "Management of Insomnia in 2013," developed based on results from our survey in the spring; this session will include a brief primer on cognitive behavioral therapy. Later that day will be one of our NetWork highlights, "Highly Controversial Topics in Sleep Medicine," with discussions on the growing use of sodium oxybate for insomnia and the role of modafinil for cognitive enhancement.
In the afternoon, Dr. Mark Rosekind, member of the National Transportation Safety Board, will be highlighting a session on sleep medicine and transportation safety. The day will be capped off by an evening session led by our NetWork Vice Chair, who will be orchestrating a panel discussion on the future of sleep medicine.
Attendance at Monday’s NetWork Open Forum is a must for anyone wanting to get more involved in the Sleep NetWork. The session will offer a chance to meet with NetWork leadership and to hear about the current activities and priorities of the Steering Committee. We are almost always looking for volunteers for one or more of our ongoing projects; attending the session ensures that you can both sign up and express your interest in person! In addition, you get to hear a great lecture, this year from Dr. Fred Turek.
The rest of the meeting is similarly packed; Tuesday will feature a panel discussion on sleep deprivation and the restriction of resident work hours. Wednesday houses our second NetWork highlight, "Intermittent Hypoxia and OSA Comorbidity," which may make many of us rethink our focus on the apnea-hypopnea index as the prime target for therapy of sleep-disordered breathing. Lastly, Thursday will feature a 4-hour symposium, "Sleep Medicine in 2013," highlighted by the debut of the College’s newest game show, "Who Wants to be a Somnologist?" with prizes for the winners.
For all of these reasons, 2013 is looking to be a spectacular year for sleep medicine education at CHEST, and there are many more sessions that I haven’t enough space to highlight. I sincerely hope that you will join us in Chicago and come by and say "hi" at the NetWork Forum!
Dr. David Schulman, FCCP
Chair
Few states meet palliative care benchmark
Only four states have effective strategies in place to improve access to and knowledge of palliative care services, the American Cancer Society Cancer Action Network reported.
The ACS CAN awarded top scores (5-6 points) to Connecticut, Maryland, Massachusetts, and Rhode Island using a scoring system that combines grades from the Center to Advance Palliative Care’s national palliative care report card with actions on model legislation.
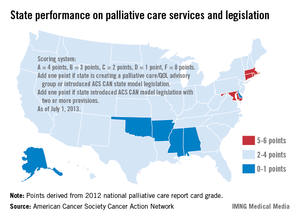
The four states passed laws "this session that focus on improving patient quality of life through palliative care," the ACS CAN noted, with Maryland finally crossing "the finish line with a palliative care bill after a 3-year effort."
The six states on the low end of the scoring range (0-1 points) were Alabama, Alaska, Arkansas, Delaware, Mississippi, and Oklahoma, the ACS CAN said in its report.
Palliative care is 1 of 10 legislative priority areas – including comprehensive smoke-free laws, tobacco taxes, restrictions on tanning bed use by minors, improved access to Medicaid, balanced pain policies, and time requirements for physical education in schools – measured by the ACS CAN. The network said that 38 states have reached benchmarks in three or fewer of the 10 areas, and that no states met the benchmarks in more than six areas.
"Many state legislatures are missing opportunities to enact laws and policies that could not only generate new revenue and long-term health savings, but also save lives," the ACS CAN said in a statement.
Only four states have effective strategies in place to improve access to and knowledge of palliative care services, the American Cancer Society Cancer Action Network reported.
The ACS CAN awarded top scores (5-6 points) to Connecticut, Maryland, Massachusetts, and Rhode Island using a scoring system that combines grades from the Center to Advance Palliative Care’s national palliative care report card with actions on model legislation.
The four states passed laws "this session that focus on improving patient quality of life through palliative care," the ACS CAN noted, with Maryland finally crossing "the finish line with a palliative care bill after a 3-year effort."
The six states on the low end of the scoring range (0-1 points) were Alabama, Alaska, Arkansas, Delaware, Mississippi, and Oklahoma, the ACS CAN said in its report.
Palliative care is 1 of 10 legislative priority areas – including comprehensive smoke-free laws, tobacco taxes, restrictions on tanning bed use by minors, improved access to Medicaid, balanced pain policies, and time requirements for physical education in schools – measured by the ACS CAN. The network said that 38 states have reached benchmarks in three or fewer of the 10 areas, and that no states met the benchmarks in more than six areas.
"Many state legislatures are missing opportunities to enact laws and policies that could not only generate new revenue and long-term health savings, but also save lives," the ACS CAN said in a statement.
Only four states have effective strategies in place to improve access to and knowledge of palliative care services, the American Cancer Society Cancer Action Network reported.
The ACS CAN awarded top scores (5-6 points) to Connecticut, Maryland, Massachusetts, and Rhode Island using a scoring system that combines grades from the Center to Advance Palliative Care’s national palliative care report card with actions on model legislation.
The four states passed laws "this session that focus on improving patient quality of life through palliative care," the ACS CAN noted, with Maryland finally crossing "the finish line with a palliative care bill after a 3-year effort."
The six states on the low end of the scoring range (0-1 points) were Alabama, Alaska, Arkansas, Delaware, Mississippi, and Oklahoma, the ACS CAN said in its report.
Palliative care is 1 of 10 legislative priority areas – including comprehensive smoke-free laws, tobacco taxes, restrictions on tanning bed use by minors, improved access to Medicaid, balanced pain policies, and time requirements for physical education in schools – measured by the ACS CAN. The network said that 38 states have reached benchmarks in three or fewer of the 10 areas, and that no states met the benchmarks in more than six areas.
"Many state legislatures are missing opportunities to enact laws and policies that could not only generate new revenue and long-term health savings, but also save lives," the ACS CAN said in a statement.
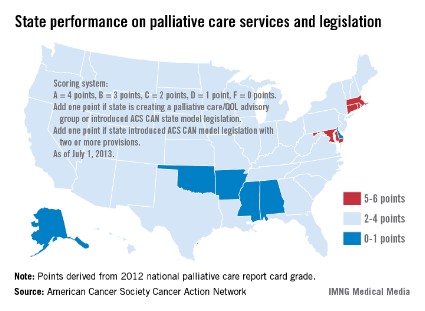
CHEST Foundation award project empowers patients and families through online palliative care resource
Designed to educate people about what palliative care is and what it offers, the website Palliative Care Services of Nebraska, www.palliativecarenebraska.com, states: "Palliative care is specialized medical care for people with serious life-limiting illnesses. Its focus lies in providing patients with relief from the symptoms, pain, and stress of illness, whatever the diagnosis. The goal is to improve quality of life for both the patient and the family."
That definition is one piece of a wealth of information available on the website, which was founded by Dr. Lisa Mansur, FCCP, recipient of The CHEST Foundation’s Roger C. Bone Advances in End-of-Life Care Award. In this instance, the term "end-of-life" care is slightly misleading because, as the website points out, "Palliative care is appropriate at any age and any stage in a serious illness and can be provided along with curative treatments." In this way it is different from its close cousin, hospice care, which is solely dedicated to comfort care when curative treatments are no longer appropriate or desired.
"The goal of the Palliative Care Services of Nebraska website is to empower people to learn and understand both the scientific and humanistic aspects of palliative care and to help them make informed decisions," she says. To that end, the site provides links to a wide array of articles, podcasts, and videos; a glossary of terms; and other resources for patients, families, caregivers, and medical professionals.
"Communication is a key tenet of palliative care," says Dr. Mansur. "Better communication equals better medicine." The emphasis on communication between patients, families, and doctors helps ensure that all needs – medical, emotional, spiritual, and practical – are fully met. In fact, Dr. Mansur calls what she and her colleagues practice "narrative medicine," with an emphasis on talking and listening rather than diagnosing and prescribing. That is not to say that patients do not receive treatment for their illness. If so desired, palliative care can work in concert with treatments meant to cure. But the focus is on the alleviation of symptoms, such as pain, fatigue, shortness of breath, loss of appetite, and anxiety or depression. Treatment might include medications along with things like massage and relaxation training. Palliative care focuses on the entire person, not just the illness. And it puts more choices in the patient’s hands.
A critical care specialist, Dr. Mansur recognized the need for palliative care in the critical care unit early in her career. She developed Palliative Care Services of Nebraska in 2010 in concert with Bryan Medical Center, where she is Director of Palliative Care, first as a hospital service with only one or two consultations a week. Since then the program has grown to accommodate up to 65 patients a week and includes an outpatient clinic, a staff of four advanced-practice nurses, and in-home visits for people who are too ill to come to the clinic. With her award from The CHEST Foundation, Dr. Mansur was able to greatly expand the website, which was launched in 2012.
The Roger C. Bone award supports leadership in end-of-life care that stresses the importance of communication, compassion, and effective listening. The award honors the late Roger C. Bone, MD, Master FCCP, who wrote about ethical and humanistic issues surrounding end-of-life decisions and stressed the importance of communication between physicians and patients. For more information about The CHEST Foundation grants and awards program, contact Lee Ann Fulton at [email protected].
Designed to educate people about what palliative care is and what it offers, the website Palliative Care Services of Nebraska, www.palliativecarenebraska.com, states: "Palliative care is specialized medical care for people with serious life-limiting illnesses. Its focus lies in providing patients with relief from the symptoms, pain, and stress of illness, whatever the diagnosis. The goal is to improve quality of life for both the patient and the family."
That definition is one piece of a wealth of information available on the website, which was founded by Dr. Lisa Mansur, FCCP, recipient of The CHEST Foundation’s Roger C. Bone Advances in End-of-Life Care Award. In this instance, the term "end-of-life" care is slightly misleading because, as the website points out, "Palliative care is appropriate at any age and any stage in a serious illness and can be provided along with curative treatments." In this way it is different from its close cousin, hospice care, which is solely dedicated to comfort care when curative treatments are no longer appropriate or desired.
"The goal of the Palliative Care Services of Nebraska website is to empower people to learn and understand both the scientific and humanistic aspects of palliative care and to help them make informed decisions," she says. To that end, the site provides links to a wide array of articles, podcasts, and videos; a glossary of terms; and other resources for patients, families, caregivers, and medical professionals.
"Communication is a key tenet of palliative care," says Dr. Mansur. "Better communication equals better medicine." The emphasis on communication between patients, families, and doctors helps ensure that all needs – medical, emotional, spiritual, and practical – are fully met. In fact, Dr. Mansur calls what she and her colleagues practice "narrative medicine," with an emphasis on talking and listening rather than diagnosing and prescribing. That is not to say that patients do not receive treatment for their illness. If so desired, palliative care can work in concert with treatments meant to cure. But the focus is on the alleviation of symptoms, such as pain, fatigue, shortness of breath, loss of appetite, and anxiety or depression. Treatment might include medications along with things like massage and relaxation training. Palliative care focuses on the entire person, not just the illness. And it puts more choices in the patient’s hands.
A critical care specialist, Dr. Mansur recognized the need for palliative care in the critical care unit early in her career. She developed Palliative Care Services of Nebraska in 2010 in concert with Bryan Medical Center, where she is Director of Palliative Care, first as a hospital service with only one or two consultations a week. Since then the program has grown to accommodate up to 65 patients a week and includes an outpatient clinic, a staff of four advanced-practice nurses, and in-home visits for people who are too ill to come to the clinic. With her award from The CHEST Foundation, Dr. Mansur was able to greatly expand the website, which was launched in 2012.
The Roger C. Bone award supports leadership in end-of-life care that stresses the importance of communication, compassion, and effective listening. The award honors the late Roger C. Bone, MD, Master FCCP, who wrote about ethical and humanistic issues surrounding end-of-life decisions and stressed the importance of communication between physicians and patients. For more information about The CHEST Foundation grants and awards program, contact Lee Ann Fulton at [email protected].
Designed to educate people about what palliative care is and what it offers, the website Palliative Care Services of Nebraska, www.palliativecarenebraska.com, states: "Palliative care is specialized medical care for people with serious life-limiting illnesses. Its focus lies in providing patients with relief from the symptoms, pain, and stress of illness, whatever the diagnosis. The goal is to improve quality of life for both the patient and the family."
That definition is one piece of a wealth of information available on the website, which was founded by Dr. Lisa Mansur, FCCP, recipient of The CHEST Foundation’s Roger C. Bone Advances in End-of-Life Care Award. In this instance, the term "end-of-life" care is slightly misleading because, as the website points out, "Palliative care is appropriate at any age and any stage in a serious illness and can be provided along with curative treatments." In this way it is different from its close cousin, hospice care, which is solely dedicated to comfort care when curative treatments are no longer appropriate or desired.
"The goal of the Palliative Care Services of Nebraska website is to empower people to learn and understand both the scientific and humanistic aspects of palliative care and to help them make informed decisions," she says. To that end, the site provides links to a wide array of articles, podcasts, and videos; a glossary of terms; and other resources for patients, families, caregivers, and medical professionals.
"Communication is a key tenet of palliative care," says Dr. Mansur. "Better communication equals better medicine." The emphasis on communication between patients, families, and doctors helps ensure that all needs – medical, emotional, spiritual, and practical – are fully met. In fact, Dr. Mansur calls what she and her colleagues practice "narrative medicine," with an emphasis on talking and listening rather than diagnosing and prescribing. That is not to say that patients do not receive treatment for their illness. If so desired, palliative care can work in concert with treatments meant to cure. But the focus is on the alleviation of symptoms, such as pain, fatigue, shortness of breath, loss of appetite, and anxiety or depression. Treatment might include medications along with things like massage and relaxation training. Palliative care focuses on the entire person, not just the illness. And it puts more choices in the patient’s hands.
A critical care specialist, Dr. Mansur recognized the need for palliative care in the critical care unit early in her career. She developed Palliative Care Services of Nebraska in 2010 in concert with Bryan Medical Center, where she is Director of Palliative Care, first as a hospital service with only one or two consultations a week. Since then the program has grown to accommodate up to 65 patients a week and includes an outpatient clinic, a staff of four advanced-practice nurses, and in-home visits for people who are too ill to come to the clinic. With her award from The CHEST Foundation, Dr. Mansur was able to greatly expand the website, which was launched in 2012.
The Roger C. Bone award supports leadership in end-of-life care that stresses the importance of communication, compassion, and effective listening. The award honors the late Roger C. Bone, MD, Master FCCP, who wrote about ethical and humanistic issues surrounding end-of-life decisions and stressed the importance of communication between physicians and patients. For more information about The CHEST Foundation grants and awards program, contact Lee Ann Fulton at [email protected].
Rising Medicare Spending for End-of-Life Care Brings Patients’ Wishes into Focus
A new report that shows ever-growing Medicare spending for chronically ill patients in the last two years of life can serve as a reminder for hospitalists to properly gauge patients’ wishes for end-of-life care, one of the authors says.
The brief from the Dartmouth Atlas Project [PDF] shows that from 2007 to 2010, average spending per patient in the last two years of life increased 15.2% to $69,947, and average spending in the last six months of life rose 13.4% to $36,392.
During the same three-year period, patients in their last six months of life were less likely to be hospitalized and logged more time in hospice care—21 days versus 18.3 days—reflecting the wishes of most patients to spend their last days in a homelike environment, the report notes. Accordingly, chronically ill Medicare patients were less likely to die in the hospital by the end of the study period.
David Goodman, MD, MS, co-principal investigator for Dartmouth Atlas of Health Care, says the growing use of hospice care and decreased hospitalization stays “aligns more closely with patients’ preferences.”
“The focus really needs to be on better diagnosis of patients’ preferences to reduce what has been well-documented as overutilization from the patient’s perspective,” Dr. Goodman says.
While costs and trends vary widely among regions and health-care systems, Dr. Goodman attributes the differences to local supplies of hospital beds and practice styles. For example, in regions with more beds, patients are more likely to spend time in the hospital near the end of life, he says. “There is definitely a national trend away from hospital care near the end of life,” he adds. “But that rate of change varies a lot from place to place. It’s helpful for hospitalists to understand where they fit on the spectrum.”
Visit our website for more information on end of life care.
A new report that shows ever-growing Medicare spending for chronically ill patients in the last two years of life can serve as a reminder for hospitalists to properly gauge patients’ wishes for end-of-life care, one of the authors says.
The brief from the Dartmouth Atlas Project [PDF] shows that from 2007 to 2010, average spending per patient in the last two years of life increased 15.2% to $69,947, and average spending in the last six months of life rose 13.4% to $36,392.
During the same three-year period, patients in their last six months of life were less likely to be hospitalized and logged more time in hospice care—21 days versus 18.3 days—reflecting the wishes of most patients to spend their last days in a homelike environment, the report notes. Accordingly, chronically ill Medicare patients were less likely to die in the hospital by the end of the study period.
David Goodman, MD, MS, co-principal investigator for Dartmouth Atlas of Health Care, says the growing use of hospice care and decreased hospitalization stays “aligns more closely with patients’ preferences.”
“The focus really needs to be on better diagnosis of patients’ preferences to reduce what has been well-documented as overutilization from the patient’s perspective,” Dr. Goodman says.
While costs and trends vary widely among regions and health-care systems, Dr. Goodman attributes the differences to local supplies of hospital beds and practice styles. For example, in regions with more beds, patients are more likely to spend time in the hospital near the end of life, he says. “There is definitely a national trend away from hospital care near the end of life,” he adds. “But that rate of change varies a lot from place to place. It’s helpful for hospitalists to understand where they fit on the spectrum.”
Visit our website for more information on end of life care.
A new report that shows ever-growing Medicare spending for chronically ill patients in the last two years of life can serve as a reminder for hospitalists to properly gauge patients’ wishes for end-of-life care, one of the authors says.
The brief from the Dartmouth Atlas Project [PDF] shows that from 2007 to 2010, average spending per patient in the last two years of life increased 15.2% to $69,947, and average spending in the last six months of life rose 13.4% to $36,392.
During the same three-year period, patients in their last six months of life were less likely to be hospitalized and logged more time in hospice care—21 days versus 18.3 days—reflecting the wishes of most patients to spend their last days in a homelike environment, the report notes. Accordingly, chronically ill Medicare patients were less likely to die in the hospital by the end of the study period.
David Goodman, MD, MS, co-principal investigator for Dartmouth Atlas of Health Care, says the growing use of hospice care and decreased hospitalization stays “aligns more closely with patients’ preferences.”
“The focus really needs to be on better diagnosis of patients’ preferences to reduce what has been well-documented as overutilization from the patient’s perspective,” Dr. Goodman says.
While costs and trends vary widely among regions and health-care systems, Dr. Goodman attributes the differences to local supplies of hospital beds and practice styles. For example, in regions with more beds, patients are more likely to spend time in the hospital near the end of life, he says. “There is definitely a national trend away from hospital care near the end of life,” he adds. “But that rate of change varies a lot from place to place. It’s helpful for hospitalists to understand where they fit on the spectrum.”
Visit our website for more information on end of life care.