User login
Herbal medicines and supplements carry risk of hepatoxicity
LONDON – Herbal medicines and other home remedies or supplements are a significant cause of hepatotoxicity experts warned recently during a symposium at the International Liver Congress, which unintentionally coincided with World Homeopathy Awareness Week.
Although they are not at the very top of the list when it comes to drug-induced liver injury (DILI) – that accolade being reserved for antimicrobial agents used to treat tuberculosis – the use of homeopathy-based approaches are potentially on the increase in the western world and the use of such substances are often not reported to physicians.

"Herbal medicines represent a significant cause of liver injury," Dr. Dominique Larrey (Central University Hospital, Montpellier, France), said at the meeting that was sponsored by the European Association for the Study of the Liver. "Herbs can cause almost the whole spectrum of hepatic and biliary lesions, acute hepatitis being the most frequent one," he added.
The rise of herbal medicine
Dr. Larrey, who works in the liver and transplantation department of Saint Eloi Hospital, also in Montpellier, noted that the use of herbs in traditional medicine was very important in many parts of the world, notably in Asia, Africa, and Central and South America. They are used for both traditional and cultural reasons, he added, are often easy to access and are low cost in comparison to regulated medicines.
Their use is probably on the increase in western countries for a variety of reasons, Dr. Larrey suggested, such as the migration of people from cultures in which the use of traditional medicines is high, to the thinking that "what is natural can only be good" and "herbal medicines are considered completely innocuous in contrast to classical drugs." Furthermore, the lack of satisfactory treatments for some severe diseases – cancer, multiple sclerosis, AIDS, and hepatitis C virus infection to name a few – mean that people often are willing to try out complementary or alternative medicines (CAM).
In the United States, the total sale of herbal remedies in 2010 was an estimated $5.2 billion per year, having increased around 3% a year over the past decade, Dr. Larrey pointed out.
The problem is that patients do not often tell their doctors about their use of CAM. A staggering 90% of patients taking the anticoagulant drug warfarin – which is renowned for having a very narrow therapeutic window and careful monitoring is required – were taking herbal medicines in one study, he said.
Prospective studies on the use of herbal medicines in western countries are scarce but those that have been conducted specifically in patients with liver disease suggest that as many as one-fifth (Hepatology 2008;47:605-12) to one-third (Gastroenterology 2001;120[Suppl 1]:A228) might be taking herbal remedies unbeknownst to their doctor.
The problem of assessment
There are limited data on how frequently herbal medicines cause liver damage, but estimates range from 2% to 16%, Dr. Larrey observed, adding that reported cases could be just the tip of the iceberg.
"Herbal medicine hepatoxicity is clearly underestimated for many reasons," he suggested. First, their intake is hard to analyze. Second, the mechanism of liver damage is often uncertain, and third, it is hard to confirm causality. Indeed, herbal medicines do not have to undergo the rigorous testing or regulation in the same way that prescribed medicines do, and sales via the Internet make them easily available to all.
There is then the uncertainty of what is really in the preparations, if they contain the right plant at all or the wrong part of it, and then whether or not they have been stored correctly, or if they have been contaminated with other liver-damaging agents or microorganisms.
Advice for physicians
DILI from prescription and nonprescription medicines is an important but rare event in the westernized world, Dr. Robert Fontana of the University of Michigan in Ann Arbor said in an interview. However, because it can bring about very bad and unpredictable liver injury, it is of great importance for hepatologists and general family physicians alike.

"In the United States and I think worldwide, the frequency in use of [herbal treatments] is increasing and as we start to see registry data I think we will start to see more and more cases [of hepatoxicity]," Dr. Fontana said.
Dr. Fontana is part of the National Institutes of Health–funded Drug-Induced Liver Injury Network (DILIN), a multicenter, prospective registry looking at the etiologies, risk factors, and outcomes of DILI in the United States (Drug Saf. 2009;32:55-68). Data from the registry show the prevalence of herbal and dietary supplements is around 9% (n = 300) in confirmed DILI cases.
"Patients need to tell their doctors what they are taking," he advised, adding that, as physicians, "we all need to be aware and maybe ask more questions of our patients."
The LiverTox website – produced by the National Institute of Diabetes and Digestive and Kidney Diseases and the National Library of Medicine – is a valuable online and freely available resource for determining if a medication, herbal, or other supplement is known to cause liver problems. This is going to have a new chapter on herbal medicines, Dr. Fontana said, and is worth using in daily practice to help advise patients on the prescription or CAM they might be taking.
Dr. Larrey and Dr. Fontana had no disclosures relevant to their comments.
New Chinese herbal medicine inhibits HCV activity
A compound named SBEL1 after the laboratory in which it was discovered has multiple effects on the hepatitis C virus (HCV) life cycle, according to data from a late-breaking poster presented at the meeting.
Researchers from the Systems Biology of Epithelia Laboratory at the National Taiwan University, Taipei, screened six herbal medicines and found that one of these – SBEL1 – inhibited HCV activity by about 90% in infected cells.
Cheng-Wei Lin and Ming-Jiun Yu pretreated liver cells with the herbal extract and then infected these cells with HCV. Compared with control cells, SBEL1-treated cells contained 23% less viral protein. This suggested that SBEL1 prevented HCV from entering the pretreated cells.
Their findings also suggested that SBEL1 reduced internal-ribosome entry site–mediated translation, a process vital for viral protein production, and might also have interfered with the RNA replication process.
"SBEL1 has demonstrated significant inhibition of HCV at multiple stages of the viral life cycle," Dr. Markus Peck-Radosavljevic, the secretary-general of the European Association for the Study of the Liver, said in a press release issued by the Society.
Dr. Peck-Radosavljevic (University of Vienna, Austria), who was not involved in the research, added that this "is an exciting discovery because it allows us to gain a deeper understanding of the virus and its interactions with other compounds. Ultimately, this adds to our library of knowledge that may bring us closer to improving future treatment options."
LONDON – Herbal medicines and other home remedies or supplements are a significant cause of hepatotoxicity experts warned recently during a symposium at the International Liver Congress, which unintentionally coincided with World Homeopathy Awareness Week.
Although they are not at the very top of the list when it comes to drug-induced liver injury (DILI) – that accolade being reserved for antimicrobial agents used to treat tuberculosis – the use of homeopathy-based approaches are potentially on the increase in the western world and the use of such substances are often not reported to physicians.
"Herbal medicines represent a significant cause of liver injury," Dr. Dominique Larrey (Central University Hospital, Montpellier, France), said at the meeting that was sponsored by the European Association for the Study of the Liver. "Herbs can cause almost the whole spectrum of hepatic and biliary lesions, acute hepatitis being the most frequent one," he added.
The rise of herbal medicine
Dr. Larrey, who works in the liver and transplantation department of Saint Eloi Hospital, also in Montpellier, noted that the use of herbs in traditional medicine was very important in many parts of the world, notably in Asia, Africa, and Central and South America. They are used for both traditional and cultural reasons, he added, are often easy to access and are low cost in comparison to regulated medicines.
Their use is probably on the increase in western countries for a variety of reasons, Dr. Larrey suggested, such as the migration of people from cultures in which the use of traditional medicines is high, to the thinking that "what is natural can only be good" and "herbal medicines are considered completely innocuous in contrast to classical drugs." Furthermore, the lack of satisfactory treatments for some severe diseases – cancer, multiple sclerosis, AIDS, and hepatitis C virus infection to name a few – mean that people often are willing to try out complementary or alternative medicines (CAM).
In the United States, the total sale of herbal remedies in 2010 was an estimated $5.2 billion per year, having increased around 3% a year over the past decade, Dr. Larrey pointed out.
The problem is that patients do not often tell their doctors about their use of CAM. A staggering 90% of patients taking the anticoagulant drug warfarin – which is renowned for having a very narrow therapeutic window and careful monitoring is required – were taking herbal medicines in one study, he said.
Prospective studies on the use of herbal medicines in western countries are scarce but those that have been conducted specifically in patients with liver disease suggest that as many as one-fifth (Hepatology 2008;47:605-12) to one-third (Gastroenterology 2001;120[Suppl 1]:A228) might be taking herbal remedies unbeknownst to their doctor.
The problem of assessment
There are limited data on how frequently herbal medicines cause liver damage, but estimates range from 2% to 16%, Dr. Larrey observed, adding that reported cases could be just the tip of the iceberg.
"Herbal medicine hepatoxicity is clearly underestimated for many reasons," he suggested. First, their intake is hard to analyze. Second, the mechanism of liver damage is often uncertain, and third, it is hard to confirm causality. Indeed, herbal medicines do not have to undergo the rigorous testing or regulation in the same way that prescribed medicines do, and sales via the Internet make them easily available to all.
There is then the uncertainty of what is really in the preparations, if they contain the right plant at all or the wrong part of it, and then whether or not they have been stored correctly, or if they have been contaminated with other liver-damaging agents or microorganisms.
Advice for physicians
DILI from prescription and nonprescription medicines is an important but rare event in the westernized world, Dr. Robert Fontana of the University of Michigan in Ann Arbor said in an interview. However, because it can bring about very bad and unpredictable liver injury, it is of great importance for hepatologists and general family physicians alike.
"In the United States and I think worldwide, the frequency in use of [herbal treatments] is increasing and as we start to see registry data I think we will start to see more and more cases [of hepatoxicity]," Dr. Fontana said.
Dr. Fontana is part of the National Institutes of Health–funded Drug-Induced Liver Injury Network (DILIN), a multicenter, prospective registry looking at the etiologies, risk factors, and outcomes of DILI in the United States (Drug Saf. 2009;32:55-68). Data from the registry show the prevalence of herbal and dietary supplements is around 9% (n = 300) in confirmed DILI cases.
"Patients need to tell their doctors what they are taking," he advised, adding that, as physicians, "we all need to be aware and maybe ask more questions of our patients."
The LiverTox website – produced by the National Institute of Diabetes and Digestive and Kidney Diseases and the National Library of Medicine – is a valuable online and freely available resource for determining if a medication, herbal, or other supplement is known to cause liver problems. This is going to have a new chapter on herbal medicines, Dr. Fontana said, and is worth using in daily practice to help advise patients on the prescription or CAM they might be taking.
Dr. Larrey and Dr. Fontana had no disclosures relevant to their comments.
New Chinese herbal medicine inhibits HCV activity
A compound named SBEL1 after the laboratory in which it was discovered has multiple effects on the hepatitis C virus (HCV) life cycle, according to data from a late-breaking poster presented at the meeting.
Researchers from the Systems Biology of Epithelia Laboratory at the National Taiwan University, Taipei, screened six herbal medicines and found that one of these – SBEL1 – inhibited HCV activity by about 90% in infected cells.
Cheng-Wei Lin and Ming-Jiun Yu pretreated liver cells with the herbal extract and then infected these cells with HCV. Compared with control cells, SBEL1-treated cells contained 23% less viral protein. This suggested that SBEL1 prevented HCV from entering the pretreated cells.
Their findings also suggested that SBEL1 reduced internal-ribosome entry site–mediated translation, a process vital for viral protein production, and might also have interfered with the RNA replication process.
"SBEL1 has demonstrated significant inhibition of HCV at multiple stages of the viral life cycle," Dr. Markus Peck-Radosavljevic, the secretary-general of the European Association for the Study of the Liver, said in a press release issued by the Society.
Dr. Peck-Radosavljevic (University of Vienna, Austria), who was not involved in the research, added that this "is an exciting discovery because it allows us to gain a deeper understanding of the virus and its interactions with other compounds. Ultimately, this adds to our library of knowledge that may bring us closer to improving future treatment options."
LONDON – Herbal medicines and other home remedies or supplements are a significant cause of hepatotoxicity experts warned recently during a symposium at the International Liver Congress, which unintentionally coincided with World Homeopathy Awareness Week.
Although they are not at the very top of the list when it comes to drug-induced liver injury (DILI) – that accolade being reserved for antimicrobial agents used to treat tuberculosis – the use of homeopathy-based approaches are potentially on the increase in the western world and the use of such substances are often not reported to physicians.
"Herbal medicines represent a significant cause of liver injury," Dr. Dominique Larrey (Central University Hospital, Montpellier, France), said at the meeting that was sponsored by the European Association for the Study of the Liver. "Herbs can cause almost the whole spectrum of hepatic and biliary lesions, acute hepatitis being the most frequent one," he added.
The rise of herbal medicine
Dr. Larrey, who works in the liver and transplantation department of Saint Eloi Hospital, also in Montpellier, noted that the use of herbs in traditional medicine was very important in many parts of the world, notably in Asia, Africa, and Central and South America. They are used for both traditional and cultural reasons, he added, are often easy to access and are low cost in comparison to regulated medicines.
Their use is probably on the increase in western countries for a variety of reasons, Dr. Larrey suggested, such as the migration of people from cultures in which the use of traditional medicines is high, to the thinking that "what is natural can only be good" and "herbal medicines are considered completely innocuous in contrast to classical drugs." Furthermore, the lack of satisfactory treatments for some severe diseases – cancer, multiple sclerosis, AIDS, and hepatitis C virus infection to name a few – mean that people often are willing to try out complementary or alternative medicines (CAM).
In the United States, the total sale of herbal remedies in 2010 was an estimated $5.2 billion per year, having increased around 3% a year over the past decade, Dr. Larrey pointed out.
The problem is that patients do not often tell their doctors about their use of CAM. A staggering 90% of patients taking the anticoagulant drug warfarin – which is renowned for having a very narrow therapeutic window and careful monitoring is required – were taking herbal medicines in one study, he said.
Prospective studies on the use of herbal medicines in western countries are scarce but those that have been conducted specifically in patients with liver disease suggest that as many as one-fifth (Hepatology 2008;47:605-12) to one-third (Gastroenterology 2001;120[Suppl 1]:A228) might be taking herbal remedies unbeknownst to their doctor.
The problem of assessment
There are limited data on how frequently herbal medicines cause liver damage, but estimates range from 2% to 16%, Dr. Larrey observed, adding that reported cases could be just the tip of the iceberg.
"Herbal medicine hepatoxicity is clearly underestimated for many reasons," he suggested. First, their intake is hard to analyze. Second, the mechanism of liver damage is often uncertain, and third, it is hard to confirm causality. Indeed, herbal medicines do not have to undergo the rigorous testing or regulation in the same way that prescribed medicines do, and sales via the Internet make them easily available to all.
There is then the uncertainty of what is really in the preparations, if they contain the right plant at all or the wrong part of it, and then whether or not they have been stored correctly, or if they have been contaminated with other liver-damaging agents or microorganisms.
Advice for physicians
DILI from prescription and nonprescription medicines is an important but rare event in the westernized world, Dr. Robert Fontana of the University of Michigan in Ann Arbor said in an interview. However, because it can bring about very bad and unpredictable liver injury, it is of great importance for hepatologists and general family physicians alike.
"In the United States and I think worldwide, the frequency in use of [herbal treatments] is increasing and as we start to see registry data I think we will start to see more and more cases [of hepatoxicity]," Dr. Fontana said.
Dr. Fontana is part of the National Institutes of Health–funded Drug-Induced Liver Injury Network (DILIN), a multicenter, prospective registry looking at the etiologies, risk factors, and outcomes of DILI in the United States (Drug Saf. 2009;32:55-68). Data from the registry show the prevalence of herbal and dietary supplements is around 9% (n = 300) in confirmed DILI cases.
"Patients need to tell their doctors what they are taking," he advised, adding that, as physicians, "we all need to be aware and maybe ask more questions of our patients."
The LiverTox website – produced by the National Institute of Diabetes and Digestive and Kidney Diseases and the National Library of Medicine – is a valuable online and freely available resource for determining if a medication, herbal, or other supplement is known to cause liver problems. This is going to have a new chapter on herbal medicines, Dr. Fontana said, and is worth using in daily practice to help advise patients on the prescription or CAM they might be taking.
Dr. Larrey and Dr. Fontana had no disclosures relevant to their comments.
New Chinese herbal medicine inhibits HCV activity
A compound named SBEL1 after the laboratory in which it was discovered has multiple effects on the hepatitis C virus (HCV) life cycle, according to data from a late-breaking poster presented at the meeting.
Researchers from the Systems Biology of Epithelia Laboratory at the National Taiwan University, Taipei, screened six herbal medicines and found that one of these – SBEL1 – inhibited HCV activity by about 90% in infected cells.
Cheng-Wei Lin and Ming-Jiun Yu pretreated liver cells with the herbal extract and then infected these cells with HCV. Compared with control cells, SBEL1-treated cells contained 23% less viral protein. This suggested that SBEL1 prevented HCV from entering the pretreated cells.
Their findings also suggested that SBEL1 reduced internal-ribosome entry site–mediated translation, a process vital for viral protein production, and might also have interfered with the RNA replication process.
"SBEL1 has demonstrated significant inhibition of HCV at multiple stages of the viral life cycle," Dr. Markus Peck-Radosavljevic, the secretary-general of the European Association for the Study of the Liver, said in a press release issued by the Society.
Dr. Peck-Radosavljevic (University of Vienna, Austria), who was not involved in the research, added that this "is an exciting discovery because it allows us to gain a deeper understanding of the virus and its interactions with other compounds. Ultimately, this adds to our library of knowledge that may bring us closer to improving future treatment options."
AT THE INTERNATIONAL LIVER CONGRESS 2014

Lorazepam not superior to diazepam in pediatric status epilepticus
The efficacy and safety of lorazepam were not superior to diazepam in a clinical trial of pediatric status epilepticus, investigators reported online April 22 in JAMA.
Both drugs effectively halted status epilepticus in more than 70% of children and adolescents and caused severe respiratory depression in less than 20%, said Dr. James Chamberlain of the Children’s National Medical Center, Washington, and his associates in the Pediatric Emergency Care Applied Research Network (PECARN).
"Taken together with the results of the RAMPART trial, it would appear that either diazepam, lorazepam, or midazolam could be chosen as a reasonable first-line therapy" for pediatric status epilepticus, the researchers said. Many prehospital systems prefer diazepam because it does not require refrigeration, they noted (JAMA 2014;311:1652-60 [doi:10.1001/jama.2014.2625]).
The multicenter, randomized, double-blind trial included 272 patients aged 3 months to less than 18 years who presented to one of 11 academic pediatric emergency departments with generalized tonic-clonic convulsive status epilepticus. Patients received intravenous diazepam (0.2 mg/kg) or lorazepam (0.1 mg/kg), with half the dose repeated at 5 minutes if needed. If status epilepticus continued at 12 minutes, patients received fosphenytoin or phenytoin.
Status epilepticus ceased by 10 minutes and did not recur for at least 30 minutes in 97 (72.9%) patients given lorazepam and in 101 (72.1%) patients treated with diazepam. The absolute efficacy difference was 0.8% (95% confidence interval, –11.4% to 9.8%). Severe respiratory depression – the primary safety outcome – occurred in 17.6% of lorazepam patients and 16.0% of diazepam patients, for an absolute risk difference of just 1.6% (95% CI, –9.9% to 6.8%), Dr. James Chamberlain and his associates reported.
Rates of secondary outcomes also were similar, except that sedation was more common in the lorazepam group (66.9% vs. 50% for diazepam; absolute risk difference, 16.9%; 95% CI, 6.1% to 27.7%).
The study was a superiority trial, not a noninferiority trial, so the two drugs could not be assumed to be statistically equivalent, the researchers said. "Although the point estimates for both efficacy and safety outcomes are similar in the two groups, the confidence intervals suggest that one medication could be superior in efficacy by as much as approximately 10% to 11% and in safety by approximately 7% to 10%," they wrote. They concluded that new treatment options for pediatric status epilepticus are needed, given the extent of medication failure and respiratory depression observed in both study groups.
The Eunice Kennedy Shriver National Institute of Child Health and Human Development funded the study. Dr. Pamela Okada reported receiving a grant from NICHD during the study. Dr. Prashant Mahajan, Dr. Richard Lichenstein, and Dr. Joseph Grubenhoff reported having received grants from the National Institutes of Health during the study. The remaining authors reported no relevant financial disclosures.
The efficacy and safety of lorazepam were not superior to diazepam in a clinical trial of pediatric status epilepticus, investigators reported online April 22 in JAMA.
Both drugs effectively halted status epilepticus in more than 70% of children and adolescents and caused severe respiratory depression in less than 20%, said Dr. James Chamberlain of the Children’s National Medical Center, Washington, and his associates in the Pediatric Emergency Care Applied Research Network (PECARN).
"Taken together with the results of the RAMPART trial, it would appear that either diazepam, lorazepam, or midazolam could be chosen as a reasonable first-line therapy" for pediatric status epilepticus, the researchers said. Many prehospital systems prefer diazepam because it does not require refrigeration, they noted (JAMA 2014;311:1652-60 [doi:10.1001/jama.2014.2625]).
The multicenter, randomized, double-blind trial included 272 patients aged 3 months to less than 18 years who presented to one of 11 academic pediatric emergency departments with generalized tonic-clonic convulsive status epilepticus. Patients received intravenous diazepam (0.2 mg/kg) or lorazepam (0.1 mg/kg), with half the dose repeated at 5 minutes if needed. If status epilepticus continued at 12 minutes, patients received fosphenytoin or phenytoin.
Status epilepticus ceased by 10 minutes and did not recur for at least 30 minutes in 97 (72.9%) patients given lorazepam and in 101 (72.1%) patients treated with diazepam. The absolute efficacy difference was 0.8% (95% confidence interval, –11.4% to 9.8%). Severe respiratory depression – the primary safety outcome – occurred in 17.6% of lorazepam patients and 16.0% of diazepam patients, for an absolute risk difference of just 1.6% (95% CI, –9.9% to 6.8%), Dr. James Chamberlain and his associates reported.
Rates of secondary outcomes also were similar, except that sedation was more common in the lorazepam group (66.9% vs. 50% for diazepam; absolute risk difference, 16.9%; 95% CI, 6.1% to 27.7%).
The study was a superiority trial, not a noninferiority trial, so the two drugs could not be assumed to be statistically equivalent, the researchers said. "Although the point estimates for both efficacy and safety outcomes are similar in the two groups, the confidence intervals suggest that one medication could be superior in efficacy by as much as approximately 10% to 11% and in safety by approximately 7% to 10%," they wrote. They concluded that new treatment options for pediatric status epilepticus are needed, given the extent of medication failure and respiratory depression observed in both study groups.
The Eunice Kennedy Shriver National Institute of Child Health and Human Development funded the study. Dr. Pamela Okada reported receiving a grant from NICHD during the study. Dr. Prashant Mahajan, Dr. Richard Lichenstein, and Dr. Joseph Grubenhoff reported having received grants from the National Institutes of Health during the study. The remaining authors reported no relevant financial disclosures.
The efficacy and safety of lorazepam were not superior to diazepam in a clinical trial of pediatric status epilepticus, investigators reported online April 22 in JAMA.
Both drugs effectively halted status epilepticus in more than 70% of children and adolescents and caused severe respiratory depression in less than 20%, said Dr. James Chamberlain of the Children’s National Medical Center, Washington, and his associates in the Pediatric Emergency Care Applied Research Network (PECARN).
"Taken together with the results of the RAMPART trial, it would appear that either diazepam, lorazepam, or midazolam could be chosen as a reasonable first-line therapy" for pediatric status epilepticus, the researchers said. Many prehospital systems prefer diazepam because it does not require refrigeration, they noted (JAMA 2014;311:1652-60 [doi:10.1001/jama.2014.2625]).
The multicenter, randomized, double-blind trial included 272 patients aged 3 months to less than 18 years who presented to one of 11 academic pediatric emergency departments with generalized tonic-clonic convulsive status epilepticus. Patients received intravenous diazepam (0.2 mg/kg) or lorazepam (0.1 mg/kg), with half the dose repeated at 5 minutes if needed. If status epilepticus continued at 12 minutes, patients received fosphenytoin or phenytoin.
Status epilepticus ceased by 10 minutes and did not recur for at least 30 minutes in 97 (72.9%) patients given lorazepam and in 101 (72.1%) patients treated with diazepam. The absolute efficacy difference was 0.8% (95% confidence interval, –11.4% to 9.8%). Severe respiratory depression – the primary safety outcome – occurred in 17.6% of lorazepam patients and 16.0% of diazepam patients, for an absolute risk difference of just 1.6% (95% CI, –9.9% to 6.8%), Dr. James Chamberlain and his associates reported.
Rates of secondary outcomes also were similar, except that sedation was more common in the lorazepam group (66.9% vs. 50% for diazepam; absolute risk difference, 16.9%; 95% CI, 6.1% to 27.7%).
The study was a superiority trial, not a noninferiority trial, so the two drugs could not be assumed to be statistically equivalent, the researchers said. "Although the point estimates for both efficacy and safety outcomes are similar in the two groups, the confidence intervals suggest that one medication could be superior in efficacy by as much as approximately 10% to 11% and in safety by approximately 7% to 10%," they wrote. They concluded that new treatment options for pediatric status epilepticus are needed, given the extent of medication failure and respiratory depression observed in both study groups.
The Eunice Kennedy Shriver National Institute of Child Health and Human Development funded the study. Dr. Pamela Okada reported receiving a grant from NICHD during the study. Dr. Prashant Mahajan, Dr. Richard Lichenstein, and Dr. Joseph Grubenhoff reported having received grants from the National Institutes of Health during the study. The remaining authors reported no relevant financial disclosures.
FROM JAMA
Major finding: Status epilepticus ceased by 10 minutes and did not recur for at least 30 minutes in 101 (72.1%) patients treated with diazepam and 97 (72.9%) patients given lorazepam, for an absolute efficacy difference of 0.8% (95% confidence interval, –11.4% to 9.8%).
Data source: A randomized, double-blind, multicenter superiority trial of 273 pediatric patients with convulsive status epilepticus.
Disclosures: The Eunice Kennedy Shriver National Institute of Child Health and Human Development funded the study. Dr. Pamela Okada reported receiving a grant from NICHD during the study. Dr. Prashant Mahajan, Dr. Richard Lichenstein, and Dr. Joseph Grubenhoff reported having received grants from the National Institutes of Health during the study. The remaining authors reported no relevant financial disclosures.
Pulsatile tinnitus looms large in fibromuscular dysplasia
WASHINGTON – Think cerebrovascular fibromuscular dysplasia in a middle-aged woman who presents with a complaint of pulsatile tinnitus.
That’s the take-home message from a new analysis of the United States Registry for Fibromuscular Dysplasia. The data highlight pulsatile tinnitus as an important clinical manifestation of fibromuscular dysplasia (FMD). Indeed, it was a presenting symptom in one-third of 720 patients included in the national registry, Dr. Redah Z. Mahmood reported at the annual meeting of the American College of Cardiology.
FMD is a nonatherosclerotic, noninflammatory form of vascular disease. It is predominantly a disease of middle-aged women: 91% of patients in the registry were women, as were 98% of patients who presented with pulsatile tinnitus. The mean age at symptom onset for registry participants was 48.8 years, although on average another 4.2 years passed before FMD was diagnosed on the basis of angiography or noninvasive imaging, noted Dr. Mahmood of the Cleveland Clinic.
FMD presents a formidable diagnostic challenge because of its potential to appear in virtually any arterial vascular bed and its lack of specific symptoms. The FMD registry was formed in 2008 in an effort to shed new light on the disorder. The association with pulsatile tinnitus is particularly helpful in raising the index of suspicion, he continued.
Patients with pulsatile tinnitus as a presenting symptom of FMD were more likely than those without that complaint to have frequent headaches, by a margin of 71%-47%. Nearly half of FMD patients with pulsatile tinnitus reported neck pain, compared with 19% without pulsatile tinnitus. Dizziness, transient ischemic attacks, cervical bruit, and Horner syndrome also were significantly more common in the pulsatile tinnitus group. This cluster of symptoms reflects the pulsatile tinnitus group’s increased prevalence of FMD of the medial fibroplasia type involving the extracranial carotid and vertebral artery beds. Patients with pulsatile tinnitus were not more likely, however, to present with stroke, which was a presenting symptom in only about 8% of patients.
Patients with pulsatile tinnitus had a reduced likelihood of renal and mesenteric involvement. Fifty-three percent of them had hypertension, compared with 67% of FMD patients without pulsatile tinnitus.
Thirty-two percent of FMD patients with pulsatile tinnitus had a history of an anxiety disorder, a rate twice that of patients without pulsatile tinnitus. Intriguingly, 84% of patients with pulsatile tinnitus had a history of use of oral contraceptives or hormone replacement therapy, compared with 56% of those without pulsatile tinnitus.
This study was sponsored by the Fibromuscular Dysplasia Study of America, a nonprofit organization. Dr. Mahmood reported having no financial conflicts.
WASHINGTON – Think cerebrovascular fibromuscular dysplasia in a middle-aged woman who presents with a complaint of pulsatile tinnitus.
That’s the take-home message from a new analysis of the United States Registry for Fibromuscular Dysplasia. The data highlight pulsatile tinnitus as an important clinical manifestation of fibromuscular dysplasia (FMD). Indeed, it was a presenting symptom in one-third of 720 patients included in the national registry, Dr. Redah Z. Mahmood reported at the annual meeting of the American College of Cardiology.
FMD is a nonatherosclerotic, noninflammatory form of vascular disease. It is predominantly a disease of middle-aged women: 91% of patients in the registry were women, as were 98% of patients who presented with pulsatile tinnitus. The mean age at symptom onset for registry participants was 48.8 years, although on average another 4.2 years passed before FMD was diagnosed on the basis of angiography or noninvasive imaging, noted Dr. Mahmood of the Cleveland Clinic.
FMD presents a formidable diagnostic challenge because of its potential to appear in virtually any arterial vascular bed and its lack of specific symptoms. The FMD registry was formed in 2008 in an effort to shed new light on the disorder. The association with pulsatile tinnitus is particularly helpful in raising the index of suspicion, he continued.
Patients with pulsatile tinnitus as a presenting symptom of FMD were more likely than those without that complaint to have frequent headaches, by a margin of 71%-47%. Nearly half of FMD patients with pulsatile tinnitus reported neck pain, compared with 19% without pulsatile tinnitus. Dizziness, transient ischemic attacks, cervical bruit, and Horner syndrome also were significantly more common in the pulsatile tinnitus group. This cluster of symptoms reflects the pulsatile tinnitus group’s increased prevalence of FMD of the medial fibroplasia type involving the extracranial carotid and vertebral artery beds. Patients with pulsatile tinnitus were not more likely, however, to present with stroke, which was a presenting symptom in only about 8% of patients.
Patients with pulsatile tinnitus had a reduced likelihood of renal and mesenteric involvement. Fifty-three percent of them had hypertension, compared with 67% of FMD patients without pulsatile tinnitus.
Thirty-two percent of FMD patients with pulsatile tinnitus had a history of an anxiety disorder, a rate twice that of patients without pulsatile tinnitus. Intriguingly, 84% of patients with pulsatile tinnitus had a history of use of oral contraceptives or hormone replacement therapy, compared with 56% of those without pulsatile tinnitus.
This study was sponsored by the Fibromuscular Dysplasia Study of America, a nonprofit organization. Dr. Mahmood reported having no financial conflicts.
WASHINGTON – Think cerebrovascular fibromuscular dysplasia in a middle-aged woman who presents with a complaint of pulsatile tinnitus.
That’s the take-home message from a new analysis of the United States Registry for Fibromuscular Dysplasia. The data highlight pulsatile tinnitus as an important clinical manifestation of fibromuscular dysplasia (FMD). Indeed, it was a presenting symptom in one-third of 720 patients included in the national registry, Dr. Redah Z. Mahmood reported at the annual meeting of the American College of Cardiology.
FMD is a nonatherosclerotic, noninflammatory form of vascular disease. It is predominantly a disease of middle-aged women: 91% of patients in the registry were women, as were 98% of patients who presented with pulsatile tinnitus. The mean age at symptom onset for registry participants was 48.8 years, although on average another 4.2 years passed before FMD was diagnosed on the basis of angiography or noninvasive imaging, noted Dr. Mahmood of the Cleveland Clinic.
FMD presents a formidable diagnostic challenge because of its potential to appear in virtually any arterial vascular bed and its lack of specific symptoms. The FMD registry was formed in 2008 in an effort to shed new light on the disorder. The association with pulsatile tinnitus is particularly helpful in raising the index of suspicion, he continued.
Patients with pulsatile tinnitus as a presenting symptom of FMD were more likely than those without that complaint to have frequent headaches, by a margin of 71%-47%. Nearly half of FMD patients with pulsatile tinnitus reported neck pain, compared with 19% without pulsatile tinnitus. Dizziness, transient ischemic attacks, cervical bruit, and Horner syndrome also were significantly more common in the pulsatile tinnitus group. This cluster of symptoms reflects the pulsatile tinnitus group’s increased prevalence of FMD of the medial fibroplasia type involving the extracranial carotid and vertebral artery beds. Patients with pulsatile tinnitus were not more likely, however, to present with stroke, which was a presenting symptom in only about 8% of patients.
Patients with pulsatile tinnitus had a reduced likelihood of renal and mesenteric involvement. Fifty-three percent of them had hypertension, compared with 67% of FMD patients without pulsatile tinnitus.
Thirty-two percent of FMD patients with pulsatile tinnitus had a history of an anxiety disorder, a rate twice that of patients without pulsatile tinnitus. Intriguingly, 84% of patients with pulsatile tinnitus had a history of use of oral contraceptives or hormone replacement therapy, compared with 56% of those without pulsatile tinnitus.
This study was sponsored by the Fibromuscular Dysplasia Study of America, a nonprofit organization. Dr. Mahmood reported having no financial conflicts.
AT ACC 14
Major finding: Pulsatile tinnitus was a presenting symptom in one-third of a large group of patients with fibromuscular dysplasia.
Data source: This was a study of 720 patients with confirmed fibromuscular dysplasia at 11 centers participating in the United States Registry for Fibromuscular Dysplasia.
Disclosures: The study was sponsored by the Fibromuscular Dysplasia Study of America. The presenter reported having no financial conflicts.
Chronic inflammation linked to high-grade prostate cancer
Men whose benign prostate biopsy cores showed signs of chronic inflammation had more than twice the odds of high-grade prostate cancer, investigators reported online April 18 in Cancer Epidemiology, Biomarkers & Prevention.
The association existed even when prostate-specific antigen was low (less than 2 ng/mL at biopsy), suggesting that the results were not due to detection bias, said Dr. Bora Gurel of Johns Hopkins University, Baltimore, and his associates.
The nested case-control study included 191 patients with biopsy-proven prostate cancer and 209 cancer-free patients from the placebo arm of the Prostate Cancer Prevention Trial. To measure the presence and extent of inflammation, a pathologist who was blinded to case-control status examined stained tissue sections from benign areas of prostate biopsy cores. The presence of any inflammatory cells, both acute inflammatory cells and chronic inflammatory cells (cells with an appearance consistent with that of lymphocytes and macrophages) in the benign tissue for each biopsy core on each slide, were noted.
Signs of inflammation were found in at least one biopsy core in 78.2% of controls, 86.2% of cases overall, and 88.4% of high-grade cases. Most of the signs of inflammation in both controls and cases reflected chronic inflammation.
Men who had at least one biopsy core with inflammation had greater odds of a prostate cancer diagnosis (odds ratio, 1.78; 95% confidence interval, 1.04–3.06) than men who had zero cores with inflammation, and even greater odds of a high-grade diagnosis (OR, 2.24; 95% CI, 1.06-4.71), the researchers reported (Cancer Epidemiol. Biomarkers Prev. 2014 April 18 [doi: 10.1158/1055-9965.EPI-13-1126]).
But it was unclear if inflammation preceded cancer onset, because the biopsy cores were obtained to evaluate patients for prostate cancer, the investigators said.
The finding that inflammation, primarily chronic, in benign prostate tissue is associated with an increased odds of prostate cancer, and high-grade prostate cancer in particular, will inform the etiology of this disease, the investigators concluded.
"Identifying those men at highest risk of developing aggressive disease is the first step in being able to prevent lethal prostate cancer," they said. "Rather than targeting interventions to all healthy men, which may result in unintended harms, if causal, the findings from our work may allow preventive interventions to be targeted to those men who would benefit the most," they wrote.
The National Cancer Institute funded the study. The authors disclosed no relevant financial conflicts of interest.
Men whose benign prostate biopsy cores showed signs of chronic inflammation had more than twice the odds of high-grade prostate cancer, investigators reported online April 18 in Cancer Epidemiology, Biomarkers & Prevention.
The association existed even when prostate-specific antigen was low (less than 2 ng/mL at biopsy), suggesting that the results were not due to detection bias, said Dr. Bora Gurel of Johns Hopkins University, Baltimore, and his associates.
The nested case-control study included 191 patients with biopsy-proven prostate cancer and 209 cancer-free patients from the placebo arm of the Prostate Cancer Prevention Trial. To measure the presence and extent of inflammation, a pathologist who was blinded to case-control status examined stained tissue sections from benign areas of prostate biopsy cores. The presence of any inflammatory cells, both acute inflammatory cells and chronic inflammatory cells (cells with an appearance consistent with that of lymphocytes and macrophages) in the benign tissue for each biopsy core on each slide, were noted.
Signs of inflammation were found in at least one biopsy core in 78.2% of controls, 86.2% of cases overall, and 88.4% of high-grade cases. Most of the signs of inflammation in both controls and cases reflected chronic inflammation.
Men who had at least one biopsy core with inflammation had greater odds of a prostate cancer diagnosis (odds ratio, 1.78; 95% confidence interval, 1.04–3.06) than men who had zero cores with inflammation, and even greater odds of a high-grade diagnosis (OR, 2.24; 95% CI, 1.06-4.71), the researchers reported (Cancer Epidemiol. Biomarkers Prev. 2014 April 18 [doi: 10.1158/1055-9965.EPI-13-1126]).
But it was unclear if inflammation preceded cancer onset, because the biopsy cores were obtained to evaluate patients for prostate cancer, the investigators said.
The finding that inflammation, primarily chronic, in benign prostate tissue is associated with an increased odds of prostate cancer, and high-grade prostate cancer in particular, will inform the etiology of this disease, the investigators concluded.
"Identifying those men at highest risk of developing aggressive disease is the first step in being able to prevent lethal prostate cancer," they said. "Rather than targeting interventions to all healthy men, which may result in unintended harms, if causal, the findings from our work may allow preventive interventions to be targeted to those men who would benefit the most," they wrote.
The National Cancer Institute funded the study. The authors disclosed no relevant financial conflicts of interest.
Men whose benign prostate biopsy cores showed signs of chronic inflammation had more than twice the odds of high-grade prostate cancer, investigators reported online April 18 in Cancer Epidemiology, Biomarkers & Prevention.
The association existed even when prostate-specific antigen was low (less than 2 ng/mL at biopsy), suggesting that the results were not due to detection bias, said Dr. Bora Gurel of Johns Hopkins University, Baltimore, and his associates.
The nested case-control study included 191 patients with biopsy-proven prostate cancer and 209 cancer-free patients from the placebo arm of the Prostate Cancer Prevention Trial. To measure the presence and extent of inflammation, a pathologist who was blinded to case-control status examined stained tissue sections from benign areas of prostate biopsy cores. The presence of any inflammatory cells, both acute inflammatory cells and chronic inflammatory cells (cells with an appearance consistent with that of lymphocytes and macrophages) in the benign tissue for each biopsy core on each slide, were noted.
Signs of inflammation were found in at least one biopsy core in 78.2% of controls, 86.2% of cases overall, and 88.4% of high-grade cases. Most of the signs of inflammation in both controls and cases reflected chronic inflammation.
Men who had at least one biopsy core with inflammation had greater odds of a prostate cancer diagnosis (odds ratio, 1.78; 95% confidence interval, 1.04–3.06) than men who had zero cores with inflammation, and even greater odds of a high-grade diagnosis (OR, 2.24; 95% CI, 1.06-4.71), the researchers reported (Cancer Epidemiol. Biomarkers Prev. 2014 April 18 [doi: 10.1158/1055-9965.EPI-13-1126]).
But it was unclear if inflammation preceded cancer onset, because the biopsy cores were obtained to evaluate patients for prostate cancer, the investigators said.
The finding that inflammation, primarily chronic, in benign prostate tissue is associated with an increased odds of prostate cancer, and high-grade prostate cancer in particular, will inform the etiology of this disease, the investigators concluded.
"Identifying those men at highest risk of developing aggressive disease is the first step in being able to prevent lethal prostate cancer," they said. "Rather than targeting interventions to all healthy men, which may result in unintended harms, if causal, the findings from our work may allow preventive interventions to be targeted to those men who would benefit the most," they wrote.
The National Cancer Institute funded the study. The authors disclosed no relevant financial conflicts of interest.
FROM CANCER EPIDEMIOLOGY, BIOMARKERS & PREVENTION
Major finding: Men with at least one prostate biopsy core with inflammation had 2.24 times the odds of high-grade prostate cancer as men who had no cores with inflammation (95% confidence interval, 1.06-4.71).
Data source: Nested case-control study of 191 biopsy-proven prostate cancer cases and 209 cancer-free controls. Researchers analyzed stained prostate tissue sections from benign areas of biopsy cores.
Disclosures: The National Cancer Institute funded the study. The authors disclosed no relevant financial conflicts of interest.
Urine culture essential for UTI diagnosis in febrile neonates
All febrile infants under 1 month old should receive a urine culture because of the prevalence of urinary tract infections and the inadequacy of other clinical parameters in identifying urinary tract infection risk, according to results of a recent study.
Approximately one in six infants aged 30 days or younger experienced urinary tract infections (UTIs), and males were more than twice as likely as females to have one, reported Dr. William Bonadio and Dr. Gary Maida of Maimonides Medical Center in New York.
Infants with a UTI should receive renal ultrasound imaging because nearly half of those with UTIs had radiographic anatomic abnormalities, the authors reported (Pediatr. Infect. Dis. J. 2014;33:342-4).
Of 670 febrile infants evaluated for sepsis in the emergency department at Maimonides Medical Center between 2004 and 2013, a total of 15.4% of the 651 receiving a urine culture had a UTI. Of these, 73% were male, and 47% had anatomic abnormalities appearing on renal ultrasound imaging.
The patients with abnormalities included 19 with pelviectasis and 26 with hydronephrosis. In the 21 patients with hydronephrosis who received a voiding cystourethrogram, 5 had vesicoureteral reflux. None of the infants had bacterial meningitis, and four had urosepsis.
Meanwhile the sensitivity of clinical symptoms, including fever height, CBC total white blood cell count, and urine dipstick test, was insufficient to determine risk of UTI in infants. Among those with UTIs, only 40% had a CBC total white blood cell count of at least 15,000/mm3, and 39% had a fever of 102° F or greater; 79% tested positive for leukocyte esterase or nitrite with a urine dipstick test.
"Reliance on urine dipstick test results to determine whether to perform a urine culture would have resulted in missed diagnosis of 21% of UTI cases in our cohort," the authors wrote. "Similarly, microscopic urinalysis was relatively insensitive at identifying those with underlying UTI."
Escherichia coli was the most common uropathogen, identified in 71% of the patients with UTI, followed by Enterococcus (10%), and Klebsiella species (10%).
The researchers did not report external funding. The authors reported no disclosures.
Dr. Bonadio and Dr. Maida provide a consecutive study that is illuminating for a number of reasons. It’s been well known that a high percentage of febrile neonates have UTI. As many studies have either lumped together patients aged up to 90 days or evaluated those exclusively with the comorbidity of respiratory syncytial virus plus bronchiolitis, this paper dedicating attention to the neonatal period is useful. As the study notes, recent American Academy of Pediatrics guidelines intentionally excluded the 0- to 2-month period because of a paucity of data.
A frequent question is whether a febrile neonate needs a lumbar puncture after diagnosis of UTI. While the standard of care for infants aged less than 30 days is a complete febrile sepsis work-up, including lumbar puncture, this study adds to the body of literature suggesting that an infant older than 30 days, and certainly older than 60 days, does not always need an lumbar puncture once UTI is identified as the source of fever. Two other findings of note are the relatively low frequency of neonates with a WBC greater than 15,000/mm3 (39%) and the much higher than previously described incidence of renal system anomalies. Digging deeper, almost half of the 47% of renal anomalies were transient. Nonetheless, this may change management or make the recommendation for evaluation that much stronger after a single UTI.

|
|
Dr. Bonadio has made numerous varied contributions to the field of pediatrics, with a keen eye to clinical utility. Both for the contribution of more cases of UTI without meningitis and the incidence of anomalies in males with UTIs, this study again helps practitioners practice good medicine.
Dr. Amy Baxter is director of emergency research for Pediatric Emergency Medicine Associates, Children’s Healthcare of Atlanta at Scottish Rite; CEO of MMJ Labs; and a clinical associate professor of emergency medicine at the Medical College of Georgia, Augusta. Dr. Baxter invented Buzzy Personal Pain Solution and is the owner and CEO of Buzzy4shots.com. She has no other disclosures.
Dr. Bonadio and Dr. Maida provide a consecutive study that is illuminating for a number of reasons. It’s been well known that a high percentage of febrile neonates have UTI. As many studies have either lumped together patients aged up to 90 days or evaluated those exclusively with the comorbidity of respiratory syncytial virus plus bronchiolitis, this paper dedicating attention to the neonatal period is useful. As the study notes, recent American Academy of Pediatrics guidelines intentionally excluded the 0- to 2-month period because of a paucity of data.
A frequent question is whether a febrile neonate needs a lumbar puncture after diagnosis of UTI. While the standard of care for infants aged less than 30 days is a complete febrile sepsis work-up, including lumbar puncture, this study adds to the body of literature suggesting that an infant older than 30 days, and certainly older than 60 days, does not always need an lumbar puncture once UTI is identified as the source of fever. Two other findings of note are the relatively low frequency of neonates with a WBC greater than 15,000/mm3 (39%) and the much higher than previously described incidence of renal system anomalies. Digging deeper, almost half of the 47% of renal anomalies were transient. Nonetheless, this may change management or make the recommendation for evaluation that much stronger after a single UTI.
|
|
|
Dr. Bonadio has made numerous varied contributions to the field of pediatrics, with a keen eye to clinical utility. Both for the contribution of more cases of UTI without meningitis and the incidence of anomalies in males with UTIs, this study again helps practitioners practice good medicine.
Dr. Amy Baxter is director of emergency research for Pediatric Emergency Medicine Associates, Children’s Healthcare of Atlanta at Scottish Rite; CEO of MMJ Labs; and a clinical associate professor of emergency medicine at the Medical College of Georgia, Augusta. Dr. Baxter invented Buzzy Personal Pain Solution and is the owner and CEO of Buzzy4shots.com. She has no other disclosures.
Dr. Bonadio and Dr. Maida provide a consecutive study that is illuminating for a number of reasons. It’s been well known that a high percentage of febrile neonates have UTI. As many studies have either lumped together patients aged up to 90 days or evaluated those exclusively with the comorbidity of respiratory syncytial virus plus bronchiolitis, this paper dedicating attention to the neonatal period is useful. As the study notes, recent American Academy of Pediatrics guidelines intentionally excluded the 0- to 2-month period because of a paucity of data.
A frequent question is whether a febrile neonate needs a lumbar puncture after diagnosis of UTI. While the standard of care for infants aged less than 30 days is a complete febrile sepsis work-up, including lumbar puncture, this study adds to the body of literature suggesting that an infant older than 30 days, and certainly older than 60 days, does not always need an lumbar puncture once UTI is identified as the source of fever. Two other findings of note are the relatively low frequency of neonates with a WBC greater than 15,000/mm3 (39%) and the much higher than previously described incidence of renal system anomalies. Digging deeper, almost half of the 47% of renal anomalies were transient. Nonetheless, this may change management or make the recommendation for evaluation that much stronger after a single UTI.
|
|
|
Dr. Bonadio has made numerous varied contributions to the field of pediatrics, with a keen eye to clinical utility. Both for the contribution of more cases of UTI without meningitis and the incidence of anomalies in males with UTIs, this study again helps practitioners practice good medicine.
Dr. Amy Baxter is director of emergency research for Pediatric Emergency Medicine Associates, Children’s Healthcare of Atlanta at Scottish Rite; CEO of MMJ Labs; and a clinical associate professor of emergency medicine at the Medical College of Georgia, Augusta. Dr. Baxter invented Buzzy Personal Pain Solution and is the owner and CEO of Buzzy4shots.com. She has no other disclosures.
All febrile infants under 1 month old should receive a urine culture because of the prevalence of urinary tract infections and the inadequacy of other clinical parameters in identifying urinary tract infection risk, according to results of a recent study.
Approximately one in six infants aged 30 days or younger experienced urinary tract infections (UTIs), and males were more than twice as likely as females to have one, reported Dr. William Bonadio and Dr. Gary Maida of Maimonides Medical Center in New York.
Infants with a UTI should receive renal ultrasound imaging because nearly half of those with UTIs had radiographic anatomic abnormalities, the authors reported (Pediatr. Infect. Dis. J. 2014;33:342-4).
Of 670 febrile infants evaluated for sepsis in the emergency department at Maimonides Medical Center between 2004 and 2013, a total of 15.4% of the 651 receiving a urine culture had a UTI. Of these, 73% were male, and 47% had anatomic abnormalities appearing on renal ultrasound imaging.
The patients with abnormalities included 19 with pelviectasis and 26 with hydronephrosis. In the 21 patients with hydronephrosis who received a voiding cystourethrogram, 5 had vesicoureteral reflux. None of the infants had bacterial meningitis, and four had urosepsis.
Meanwhile the sensitivity of clinical symptoms, including fever height, CBC total white blood cell count, and urine dipstick test, was insufficient to determine risk of UTI in infants. Among those with UTIs, only 40% had a CBC total white blood cell count of at least 15,000/mm3, and 39% had a fever of 102° F or greater; 79% tested positive for leukocyte esterase or nitrite with a urine dipstick test.
"Reliance on urine dipstick test results to determine whether to perform a urine culture would have resulted in missed diagnosis of 21% of UTI cases in our cohort," the authors wrote. "Similarly, microscopic urinalysis was relatively insensitive at identifying those with underlying UTI."
Escherichia coli was the most common uropathogen, identified in 71% of the patients with UTI, followed by Enterococcus (10%), and Klebsiella species (10%).
The researchers did not report external funding. The authors reported no disclosures.
All febrile infants under 1 month old should receive a urine culture because of the prevalence of urinary tract infections and the inadequacy of other clinical parameters in identifying urinary tract infection risk, according to results of a recent study.
Approximately one in six infants aged 30 days or younger experienced urinary tract infections (UTIs), and males were more than twice as likely as females to have one, reported Dr. William Bonadio and Dr. Gary Maida of Maimonides Medical Center in New York.
Infants with a UTI should receive renal ultrasound imaging because nearly half of those with UTIs had radiographic anatomic abnormalities, the authors reported (Pediatr. Infect. Dis. J. 2014;33:342-4).
Of 670 febrile infants evaluated for sepsis in the emergency department at Maimonides Medical Center between 2004 and 2013, a total of 15.4% of the 651 receiving a urine culture had a UTI. Of these, 73% were male, and 47% had anatomic abnormalities appearing on renal ultrasound imaging.
The patients with abnormalities included 19 with pelviectasis and 26 with hydronephrosis. In the 21 patients with hydronephrosis who received a voiding cystourethrogram, 5 had vesicoureteral reflux. None of the infants had bacterial meningitis, and four had urosepsis.
Meanwhile the sensitivity of clinical symptoms, including fever height, CBC total white blood cell count, and urine dipstick test, was insufficient to determine risk of UTI in infants. Among those with UTIs, only 40% had a CBC total white blood cell count of at least 15,000/mm3, and 39% had a fever of 102° F or greater; 79% tested positive for leukocyte esterase or nitrite with a urine dipstick test.
"Reliance on urine dipstick test results to determine whether to perform a urine culture would have resulted in missed diagnosis of 21% of UTI cases in our cohort," the authors wrote. "Similarly, microscopic urinalysis was relatively insensitive at identifying those with underlying UTI."
Escherichia coli was the most common uropathogen, identified in 71% of the patients with UTI, followed by Enterococcus (10%), and Klebsiella species (10%).
The researchers did not report external funding. The authors reported no disclosures.
FROM THE PEDIATRIC INFECTIOUS DISEASE JOURNAL
Key clinical point: A urine culture is needed to diagnose a UTI in neonates with a fever.
Major finding: When a urine culture was taken in 651 febrile infants evaluated for sepsis, 15.4% had a UTI.
Data source: 670 febrile infants were evaluated for sepsis in the emergency department at Maimonides Medical Center between 2004 and 2013.
Disclosures: The researchers did not report external funding. The authors reported no disclosures.

Walking doesn’t hurt, may help in CKD
Neither acute bouts of moderate walking nor regular moderate walking are unsafe in patients who have predialysis chronic kidney disease, and both types of exercise may actually reduce systemic inflammation and improve immune function in these patients, according to a report published in the Journal of the American Society of Nephrology.
CKD is associated with "a complex state of immune dysfunction in which signs of immune depression and immune activation paradoxically coexist." Moderate exercise may therefore enhance certain aspects of immune function while simultaneously exerting detrimental effects on other aspects, said Dr. João Viana of the school of sport, exercise, and health sciences, Loughborough (England) University, and his associates.

The investigators studied blood biomarkers of immune function and inflammation in 15 adults with predialysis CKD who participated in a single bout of "somewhat hard" walking on a motorized treadmill for 30 minutes. This induced "a systemic anti-inflammatory environment," as evidenced by a marked increase in plasma IL-10 levels. It also improved neutrophil responsiveness to an in vitro bacterial challenge during the hour following the exercise. It had no effect on T-lymphocyte or monocyte activation, the researchers said (J. Am. Soc. Nephrol. 2014; April 3; doi:10.1681/ASN.2013070702]).
In a separate analysis, Dr. Viana and his colleagues assessed the same blood biomarkers in 24 participants in a previous study, who had been assigned to either 6 months of regular home-based walking (13 predialysis CKD patients) or to their usual sedentary activity level (11 control subjects). The "exercisers" walked at a "somewhat hard" rate for 30 minutes per day, 5 times per week.
This regular walking also exerted systemic anti-inflammatory effects, as evidenced by a reduction in the IL-6 to IL-10 ratio and downregulation of T-lymphocyte and monocyte activation. It had no effect on circulating numbers of immune cells or on neutrophil degranulation response. Neither acute nor regular walking affected body weight, renal function, proteinuria, or blood pressure.
These findings suggest that walking "is safe from an immune and inflammatory perspective, and exerts anti-inflammatory effects at both systemic and cellular levels" in this patient population. Regular walking "has the potential to be an effective anti-inflammatory therapy in predialysis CKD patients and may in this way reduce the high risk of cardiovascular disease in these very vulnerable patients," the investigators noted.
The authors reported no financial disclosures.
Neither acute bouts of moderate walking nor regular moderate walking are unsafe in patients who have predialysis chronic kidney disease, and both types of exercise may actually reduce systemic inflammation and improve immune function in these patients, according to a report published in the Journal of the American Society of Nephrology.
CKD is associated with "a complex state of immune dysfunction in which signs of immune depression and immune activation paradoxically coexist." Moderate exercise may therefore enhance certain aspects of immune function while simultaneously exerting detrimental effects on other aspects, said Dr. João Viana of the school of sport, exercise, and health sciences, Loughborough (England) University, and his associates.
The investigators studied blood biomarkers of immune function and inflammation in 15 adults with predialysis CKD who participated in a single bout of "somewhat hard" walking on a motorized treadmill for 30 minutes. This induced "a systemic anti-inflammatory environment," as evidenced by a marked increase in plasma IL-10 levels. It also improved neutrophil responsiveness to an in vitro bacterial challenge during the hour following the exercise. It had no effect on T-lymphocyte or monocyte activation, the researchers said (J. Am. Soc. Nephrol. 2014; April 3; doi:10.1681/ASN.2013070702]).
In a separate analysis, Dr. Viana and his colleagues assessed the same blood biomarkers in 24 participants in a previous study, who had been assigned to either 6 months of regular home-based walking (13 predialysis CKD patients) or to their usual sedentary activity level (11 control subjects). The "exercisers" walked at a "somewhat hard" rate for 30 minutes per day, 5 times per week.
This regular walking also exerted systemic anti-inflammatory effects, as evidenced by a reduction in the IL-6 to IL-10 ratio and downregulation of T-lymphocyte and monocyte activation. It had no effect on circulating numbers of immune cells or on neutrophil degranulation response. Neither acute nor regular walking affected body weight, renal function, proteinuria, or blood pressure.
These findings suggest that walking "is safe from an immune and inflammatory perspective, and exerts anti-inflammatory effects at both systemic and cellular levels" in this patient population. Regular walking "has the potential to be an effective anti-inflammatory therapy in predialysis CKD patients and may in this way reduce the high risk of cardiovascular disease in these very vulnerable patients," the investigators noted.
The authors reported no financial disclosures.
Neither acute bouts of moderate walking nor regular moderate walking are unsafe in patients who have predialysis chronic kidney disease, and both types of exercise may actually reduce systemic inflammation and improve immune function in these patients, according to a report published in the Journal of the American Society of Nephrology.
CKD is associated with "a complex state of immune dysfunction in which signs of immune depression and immune activation paradoxically coexist." Moderate exercise may therefore enhance certain aspects of immune function while simultaneously exerting detrimental effects on other aspects, said Dr. João Viana of the school of sport, exercise, and health sciences, Loughborough (England) University, and his associates.
The investigators studied blood biomarkers of immune function and inflammation in 15 adults with predialysis CKD who participated in a single bout of "somewhat hard" walking on a motorized treadmill for 30 minutes. This induced "a systemic anti-inflammatory environment," as evidenced by a marked increase in plasma IL-10 levels. It also improved neutrophil responsiveness to an in vitro bacterial challenge during the hour following the exercise. It had no effect on T-lymphocyte or monocyte activation, the researchers said (J. Am. Soc. Nephrol. 2014; April 3; doi:10.1681/ASN.2013070702]).
In a separate analysis, Dr. Viana and his colleagues assessed the same blood biomarkers in 24 participants in a previous study, who had been assigned to either 6 months of regular home-based walking (13 predialysis CKD patients) or to their usual sedentary activity level (11 control subjects). The "exercisers" walked at a "somewhat hard" rate for 30 minutes per day, 5 times per week.
This regular walking also exerted systemic anti-inflammatory effects, as evidenced by a reduction in the IL-6 to IL-10 ratio and downregulation of T-lymphocyte and monocyte activation. It had no effect on circulating numbers of immune cells or on neutrophil degranulation response. Neither acute nor regular walking affected body weight, renal function, proteinuria, or blood pressure.
These findings suggest that walking "is safe from an immune and inflammatory perspective, and exerts anti-inflammatory effects at both systemic and cellular levels" in this patient population. Regular walking "has the potential to be an effective anti-inflammatory therapy in predialysis CKD patients and may in this way reduce the high risk of cardiovascular disease in these very vulnerable patients," the investigators noted.
The authors reported no financial disclosures.
FROM THE JOURNAL OF THE AMERICAN SOCIETY OF NEPHROLOGY
Major finding: Both a single, "acute" bout of walking and a regular walking program improved several blood markers of systemic inflammation and several markers of immune function in patients with CKD.
Data source: An observational cohort study of 15 adults with predialysis CKD who participated in a single bout of walking exercise, and an analysis of blood biomarkers in 24 participants in a previous study of a 6-month program of regular walking exercise.
Disclosures: The authors reported no financial disclosures.

VIDEO: Exploring SYMPLICITY’s failure, Part 2
WASHINGTON – Far from being doomed after the failure SYMPLICITY HTN-3, renal denervation for refractory hypertension will continue to be explored. But it can’t go very far without finding a way to measure its effectiveness.
In Part 2 of our interview, Dr. Prakash Deedwania and Dr. George Bakris explore the options, and don’t miss the chance to talk about the controversial new hypertension guidelines.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
WASHINGTON – Far from being doomed after the failure SYMPLICITY HTN-3, renal denervation for refractory hypertension will continue to be explored. But it can’t go very far without finding a way to measure its effectiveness.
In Part 2 of our interview, Dr. Prakash Deedwania and Dr. George Bakris explore the options, and don’t miss the chance to talk about the controversial new hypertension guidelines.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
WASHINGTON – Far from being doomed after the failure SYMPLICITY HTN-3, renal denervation for refractory hypertension will continue to be explored. But it can’t go very far without finding a way to measure its effectiveness.
In Part 2 of our interview, Dr. Prakash Deedwania and Dr. George Bakris explore the options, and don’t miss the chance to talk about the controversial new hypertension guidelines.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
AT ACC 14

Angiography timing shown not a risk for AKI in most cardiac surgery
Acute kidney injury is a serious adverse effect of cardiac surgery, and contrast-induced nephropathy due to coronary angiography has been suggested as a potentially important component. However, the results of a retrospective study of more than 2,500 patients showed that acute kidney injury is significantly higher only in those patients who have combined cardiac surgery within 24 hours of catheterization.
The study by Dr. Giovanni Mariscalco of the Varese (Italy) University Hospital, and his colleagues assessed all consecutive patients undergoing cardiac surgery at the hospital between Jan. 1, 2005, and Dec. 31, 2011. The operations performed were isolated coronary artery bypass grafting (CABG), valve surgery with or without concomitant CABG, and proximal aortic procedures. After exclusion of patients who did not undergo cardiopulmonary bypass, a known major cause of acute kidney injury (AKI), and those who died during the procedure, a total of 2,504 patients remained. These patients had a mean age of 68.4 years and consisted mostly of men (67.3%), according to the report in the April issue of the International Journal of Cardiology.
The primary endpoint of the study was the effect of timing between cardiac catheterization and surgery on the development of AKI. Postoperative AKI was defined by the consensus RIFLE criteria (risk, injury, failure, loss of function, and end-stage renal disease), using the maximal change in serum creatinine and the estimated glomerular filtration rate during the first 7 days after surgery, compared with baseline values collected the day before surgery or immediately before surgery when cardiac catheterization was performed on the same day as the operation.
The researchers defined AKI as a 50% increase in the postoperative serum creatinine over baseline. Propensity analysis was used to match patients, who were then assessed both pre- and postmatch.
The overall incidence of AKI after surgery was 9.2% (230/2,504 patients). A breakdown by procedure showed that AKI occurred in 7.7% of isolated CABG patients, 12.2% of isolated valve patients, 9.5% of combined-procedure patients, and 9.5% of the proximal aorta surgery patients (Int. J. Cardiol. 2014;173:46-54).
As has been seen in previous studies, AKI was associated with patient-specific pre- and perioperative variables, including increased patient age, added comorbidities, longer cardiopulmonary bypass (CPB) times, higher rates of combined procedures, and the use of intra-aortic balloon pumps.
Unadjusted analysis of the total cohort showed AKI was significantly associated with contrast exposure within 1 day of surgery. However, in multivariable analysis, the time interval between catheterization and surgery as both a categorical and continuous variable was not an independent predictor of postoperative AKI for the total cohort. In subgroup analysis, only the combined valve and CABG group of patients showed an independent association of contrast exposure within 1 day before surgery and AKI in both the prematched (odds ratio, 2.69; P = .004) and the postmatched (OR, 3.68; P = .014) groups.
"Avoiding surgery within 1 day after contrast exposure should be recommended for patients undergoing valve surgery with concomitant CABG only. For other types of cardiac operations, delaying cardiac surgery after contrast exposure seems not to be justified," the researchers concluded.
Study limitations cited include its retrospective and single-institution nature and the statistical effect of different numbers of observations among the surgery groups. Patients affected with AKI also had higher rates of other postoperative complications, and AKI in some cases may have been the result of these rather than an independent event.
he study was supported by the Fondazione Cesare Bartorelli. The authors reported having no financial disclosures.
Acute kidney injury is a serious adverse effect of cardiac surgery, and contrast-induced nephropathy due to coronary angiography has been suggested as a potentially important component. However, the results of a retrospective study of more than 2,500 patients showed that acute kidney injury is significantly higher only in those patients who have combined cardiac surgery within 24 hours of catheterization.
The study by Dr. Giovanni Mariscalco of the Varese (Italy) University Hospital, and his colleagues assessed all consecutive patients undergoing cardiac surgery at the hospital between Jan. 1, 2005, and Dec. 31, 2011. The operations performed were isolated coronary artery bypass grafting (CABG), valve surgery with or without concomitant CABG, and proximal aortic procedures. After exclusion of patients who did not undergo cardiopulmonary bypass, a known major cause of acute kidney injury (AKI), and those who died during the procedure, a total of 2,504 patients remained. These patients had a mean age of 68.4 years and consisted mostly of men (67.3%), according to the report in the April issue of the International Journal of Cardiology.
The primary endpoint of the study was the effect of timing between cardiac catheterization and surgery on the development of AKI. Postoperative AKI was defined by the consensus RIFLE criteria (risk, injury, failure, loss of function, and end-stage renal disease), using the maximal change in serum creatinine and the estimated glomerular filtration rate during the first 7 days after surgery, compared with baseline values collected the day before surgery or immediately before surgery when cardiac catheterization was performed on the same day as the operation.
The researchers defined AKI as a 50% increase in the postoperative serum creatinine over baseline. Propensity analysis was used to match patients, who were then assessed both pre- and postmatch.
The overall incidence of AKI after surgery was 9.2% (230/2,504 patients). A breakdown by procedure showed that AKI occurred in 7.7% of isolated CABG patients, 12.2% of isolated valve patients, 9.5% of combined-procedure patients, and 9.5% of the proximal aorta surgery patients (Int. J. Cardiol. 2014;173:46-54).
As has been seen in previous studies, AKI was associated with patient-specific pre- and perioperative variables, including increased patient age, added comorbidities, longer cardiopulmonary bypass (CPB) times, higher rates of combined procedures, and the use of intra-aortic balloon pumps.
Unadjusted analysis of the total cohort showed AKI was significantly associated with contrast exposure within 1 day of surgery. However, in multivariable analysis, the time interval between catheterization and surgery as both a categorical and continuous variable was not an independent predictor of postoperative AKI for the total cohort. In subgroup analysis, only the combined valve and CABG group of patients showed an independent association of contrast exposure within 1 day before surgery and AKI in both the prematched (odds ratio, 2.69; P = .004) and the postmatched (OR, 3.68; P = .014) groups.
"Avoiding surgery within 1 day after contrast exposure should be recommended for patients undergoing valve surgery with concomitant CABG only. For other types of cardiac operations, delaying cardiac surgery after contrast exposure seems not to be justified," the researchers concluded.
Study limitations cited include its retrospective and single-institution nature and the statistical effect of different numbers of observations among the surgery groups. Patients affected with AKI also had higher rates of other postoperative complications, and AKI in some cases may have been the result of these rather than an independent event.
he study was supported by the Fondazione Cesare Bartorelli. The authors reported having no financial disclosures.
Acute kidney injury is a serious adverse effect of cardiac surgery, and contrast-induced nephropathy due to coronary angiography has been suggested as a potentially important component. However, the results of a retrospective study of more than 2,500 patients showed that acute kidney injury is significantly higher only in those patients who have combined cardiac surgery within 24 hours of catheterization.
The study by Dr. Giovanni Mariscalco of the Varese (Italy) University Hospital, and his colleagues assessed all consecutive patients undergoing cardiac surgery at the hospital between Jan. 1, 2005, and Dec. 31, 2011. The operations performed were isolated coronary artery bypass grafting (CABG), valve surgery with or without concomitant CABG, and proximal aortic procedures. After exclusion of patients who did not undergo cardiopulmonary bypass, a known major cause of acute kidney injury (AKI), and those who died during the procedure, a total of 2,504 patients remained. These patients had a mean age of 68.4 years and consisted mostly of men (67.3%), according to the report in the April issue of the International Journal of Cardiology.
The primary endpoint of the study was the effect of timing between cardiac catheterization and surgery on the development of AKI. Postoperative AKI was defined by the consensus RIFLE criteria (risk, injury, failure, loss of function, and end-stage renal disease), using the maximal change in serum creatinine and the estimated glomerular filtration rate during the first 7 days after surgery, compared with baseline values collected the day before surgery or immediately before surgery when cardiac catheterization was performed on the same day as the operation.
The researchers defined AKI as a 50% increase in the postoperative serum creatinine over baseline. Propensity analysis was used to match patients, who were then assessed both pre- and postmatch.
The overall incidence of AKI after surgery was 9.2% (230/2,504 patients). A breakdown by procedure showed that AKI occurred in 7.7% of isolated CABG patients, 12.2% of isolated valve patients, 9.5% of combined-procedure patients, and 9.5% of the proximal aorta surgery patients (Int. J. Cardiol. 2014;173:46-54).
As has been seen in previous studies, AKI was associated with patient-specific pre- and perioperative variables, including increased patient age, added comorbidities, longer cardiopulmonary bypass (CPB) times, higher rates of combined procedures, and the use of intra-aortic balloon pumps.
Unadjusted analysis of the total cohort showed AKI was significantly associated with contrast exposure within 1 day of surgery. However, in multivariable analysis, the time interval between catheterization and surgery as both a categorical and continuous variable was not an independent predictor of postoperative AKI for the total cohort. In subgroup analysis, only the combined valve and CABG group of patients showed an independent association of contrast exposure within 1 day before surgery and AKI in both the prematched (odds ratio, 2.69; P = .004) and the postmatched (OR, 3.68; P = .014) groups.
"Avoiding surgery within 1 day after contrast exposure should be recommended for patients undergoing valve surgery with concomitant CABG only. For other types of cardiac operations, delaying cardiac surgery after contrast exposure seems not to be justified," the researchers concluded.
Study limitations cited include its retrospective and single-institution nature and the statistical effect of different numbers of observations among the surgery groups. Patients affected with AKI also had higher rates of other postoperative complications, and AKI in some cases may have been the result of these rather than an independent event.
he study was supported by the Fondazione Cesare Bartorelli. The authors reported having no financial disclosures.
FROM THE INTERNATIONAL JOURNAL OF CARDIOLOGY
Major finding: Only combined surgery plus contrast within 1 day before surgery was significantly associated with AKI in the prematched (OR, 2.69) and postmatched (OR, 3.68) groups.
Data source: A single-institute, retrospective study of 2,504 cardiac surgery patients.
Disclosures: The study was supported by the Fondazione Cesare Bartorelli. The authors reported having no financial disclosures.
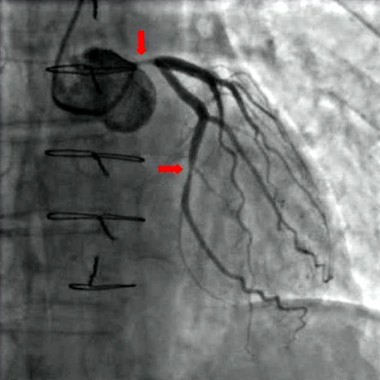
Ineffective renal denervation blamed for trial’s failure
WASHINGTON – Renal denervation’s not so simple after all.
Highly anticipated data from the large, sham-controlled renal-artery catheter denervation trial, SYMPLICITY HTN-3, gave its investigators reason to believe that inconsistent and inadequate delivery of nerve-ablating radiofrequency energy by inexperienced operators left too many patients undertreated, producing a neutral outcome for the primary endpoint, the study’s top-line result first reported in a company press release in January.
In the SYMPLICITY HTN-3 (Renal Denervation in Patients With Uncontrolled Hypertension) trial, the average systolic blood pressure reduction among the 364 patients randomized to renal denervation was 14 mm Hg, compared with an average 12 mm Hg reduction in 174 control patients who underwent a renal-artery angiogram masked to resemble a denervation procedure, a difference that was not statistically significant, falling substantially short of the prespecified 5 mm Hg between group difference necessary to fulfill superiority, Dr. Deepak L. Bhatt said at the annual meeting of the American College of Cardiology.

Although several factors likely led to the neutral outcome, including an unexpectedly robust blood pressure drop in the control arm, another major factor, many suspect, was inadequate delivery of the denervation treatment.
"It might be that the way we used the catheter wasn’t ideal," said Dr. Bhatt, coprincipal investigator of the study, professor of medicine at Harvard Medical School and executive director of interventional cardiology at Brigham and Women’s Hospital, both in Boston.
Concurrent with Dr. Bhatt’s report at the meeting a published version appeared online (N. Engl. J. Med. 2014 March 29 [doi:10.1056/NEJMoa1402670]).
"There is the concept that renal denervation is easy. As a catheter procedure it is easy, but to achieve denervation is far from easy," said Dr. Murray D. Esler, a professor of medicine at Monash University and senior director of the Baker IDI Heart and Diabetes Institute, both in Melbourne, and a pioneer of renal denervation who was involved in prior SYMPLICITY studies of the same renal-denervation device but was not a coinvestigator for the new trial.
"The SYMPLICITY 3 study made a mistake thinking it could get away with not giving the proceduralists any hands-on experience" before the trial. "There was none. The operators hadn’t done it before, and the trial’s designers would not have done that unless they thought that denervation was easy. Well, it’s not easy. There is a learning curve, and I think that’s the main explanation of what went wrong. "

Exacerbating the operators’ inexperience with denervation (they were all experienced interventional cardiologists) was a second flaw in the trial’s design: No method was used to monitor the efficacy of each denervation procedure, an easy decision because there is still no proven way to measure denervation efficacy during the procedure. Dr. Esler said he believes that he has a solution, one that involves testing for interrupted activity of the parallel, afferent nerves of the renal arteries using adenosine as a surrogate measure for denervation of the target efferent nerves. But while he is optimistic the adenosine approach will work, it is still at least several months from use in a trial.
In the first clinical study of renal denervation, a series of 50 patients treated at five centers in Australia and Europe reported just 5 years ago (Lancet 2009;373:1275-81), Dr. Esler, a lead investigator for that study, and his associates carefully tested the efficacy of denervation in 10 patients by measuring the direct effect of successful denervation, reduction of renal norepinephrine spillover. They reported that, in those 10 patients, renal denervation cut norepinephrine spillover by an average 47%, which correlated with an average reduction in systolic blood pressure of 22 mm Hg after 6 months.
But this effect from denervation was "far from uniform and ranged from zero to 85%," depending on who was doing the denervation. "It’s obviously operator dependent." Dr. Esler said in an interview. This observation of enormous variability in the physiologic impact of denervation "took on a new context with the failed trial. The denervation done by novices explains to some extent the spread [in results] and makes me think the same thing happened in SYMPLICITY 3."

"If you don’t do enough high-frequency burns or if the catheter doesn’t reach enough nerves" because of misplacement within the renal artery, the denervation won’t be very successful, noted Dr. George Bakris, professor of medicine and director of the comprehensive hypertension center at the University of Chicago and coprincipal investigator of SYMPLICITY HTN-3 along with Dr. Bhatt. "It certainly calls into question whether they denervated effectively. One could argue that if denervation were done appropriately" it would add to drug treatment, Dr. Bakris said in an interview. "This issue has come up about the quality of the denervation; the good news is that it can be done correctly," but that will require "a good understanding of what you are doing to the renal nerves and how much energy you need." SYMPLICITY HTN-3 "was a good but expensive learning experience," Dr. Bakris said.
The investigators "were performing a procedure, but they didn’t have the evidence that the procedure was accomplishing what it meant to accomplish," commented Dr. Anthony DeMaria, professor of medicine, the Judith and Jack White chair of cardiology, and director of the cardiovascular center at the University of California, San Diego, who was not involved in the trial. "Most of us feel there are tantalizing data to suggest that denervation can have a benefit, but they need to go back to the physiology to be sure they are denervating effectively."

Though Dr. Bakris and Dr. Esler cautioned that the study’s primary outcome was neutral, they see reason to hope that renal denervation will still prove to have an important and useful clinical effect.
"This report is the tip of the iceberg," Dr. Bakris noted. "When you look at the effect of denervation on blood pressure variability, heart rate variability, and total control over 24 hours using ambulatory blood pressure monitoring, you see a different picture," results that will be reported later this year, he said.
And Dr. Esler said that his experience using renal denervation on about 300 patients with treatment-resistant hypertension has convinced him that denervation can produce real benefits when done properly.
"I’m not changing my practice" using renal denervation on refractory patients, he said. "I accumulated a lot of patients with severe, resistant hypertension, patients whom I couldn’t control with seven or eight different drug classes. But when renal denervation came along, it was like chalk and cheese. Suddenly, I had a therapy that worked. My clinical experience in patients who didn’t budge with medications totally convinces me" that renal denervation works.
SYMPLICITY HTN-3 was sponsored by Medtronic, the company that markets the device tested in the study. Dr. Bhatt said that he has received research grants from Medtronic and five other companies. Dr. Esler said that he has received consulting fees, honoraria, and research grants from Medtronic. Dr. Bakris said that he has received personal fees from Medtronic and five other companies. Dr. DeMaria said that he has received research grants from Angioblast Systems, Cardiovascular Biotherapeutics, General Electric Medical, Gilead, and Lantheus.
On Twitter @mitchelzoler
WASHINGTON – Renal denervation’s not so simple after all.
Highly anticipated data from the large, sham-controlled renal-artery catheter denervation trial, SYMPLICITY HTN-3, gave its investigators reason to believe that inconsistent and inadequate delivery of nerve-ablating radiofrequency energy by inexperienced operators left too many patients undertreated, producing a neutral outcome for the primary endpoint, the study’s top-line result first reported in a company press release in January.
In the SYMPLICITY HTN-3 (Renal Denervation in Patients With Uncontrolled Hypertension) trial, the average systolic blood pressure reduction among the 364 patients randomized to renal denervation was 14 mm Hg, compared with an average 12 mm Hg reduction in 174 control patients who underwent a renal-artery angiogram masked to resemble a denervation procedure, a difference that was not statistically significant, falling substantially short of the prespecified 5 mm Hg between group difference necessary to fulfill superiority, Dr. Deepak L. Bhatt said at the annual meeting of the American College of Cardiology.
Although several factors likely led to the neutral outcome, including an unexpectedly robust blood pressure drop in the control arm, another major factor, many suspect, was inadequate delivery of the denervation treatment.
"It might be that the way we used the catheter wasn’t ideal," said Dr. Bhatt, coprincipal investigator of the study, professor of medicine at Harvard Medical School and executive director of interventional cardiology at Brigham and Women’s Hospital, both in Boston.
Concurrent with Dr. Bhatt’s report at the meeting a published version appeared online (N. Engl. J. Med. 2014 March 29 [doi:10.1056/NEJMoa1402670]).
"There is the concept that renal denervation is easy. As a catheter procedure it is easy, but to achieve denervation is far from easy," said Dr. Murray D. Esler, a professor of medicine at Monash University and senior director of the Baker IDI Heart and Diabetes Institute, both in Melbourne, and a pioneer of renal denervation who was involved in prior SYMPLICITY studies of the same renal-denervation device but was not a coinvestigator for the new trial.
"The SYMPLICITY 3 study made a mistake thinking it could get away with not giving the proceduralists any hands-on experience" before the trial. "There was none. The operators hadn’t done it before, and the trial’s designers would not have done that unless they thought that denervation was easy. Well, it’s not easy. There is a learning curve, and I think that’s the main explanation of what went wrong. "
Exacerbating the operators’ inexperience with denervation (they were all experienced interventional cardiologists) was a second flaw in the trial’s design: No method was used to monitor the efficacy of each denervation procedure, an easy decision because there is still no proven way to measure denervation efficacy during the procedure. Dr. Esler said he believes that he has a solution, one that involves testing for interrupted activity of the parallel, afferent nerves of the renal arteries using adenosine as a surrogate measure for denervation of the target efferent nerves. But while he is optimistic the adenosine approach will work, it is still at least several months from use in a trial.
In the first clinical study of renal denervation, a series of 50 patients treated at five centers in Australia and Europe reported just 5 years ago (Lancet 2009;373:1275-81), Dr. Esler, a lead investigator for that study, and his associates carefully tested the efficacy of denervation in 10 patients by measuring the direct effect of successful denervation, reduction of renal norepinephrine spillover. They reported that, in those 10 patients, renal denervation cut norepinephrine spillover by an average 47%, which correlated with an average reduction in systolic blood pressure of 22 mm Hg after 6 months.
But this effect from denervation was "far from uniform and ranged from zero to 85%," depending on who was doing the denervation. "It’s obviously operator dependent." Dr. Esler said in an interview. This observation of enormous variability in the physiologic impact of denervation "took on a new context with the failed trial. The denervation done by novices explains to some extent the spread [in results] and makes me think the same thing happened in SYMPLICITY 3."
"If you don’t do enough high-frequency burns or if the catheter doesn’t reach enough nerves" because of misplacement within the renal artery, the denervation won’t be very successful, noted Dr. George Bakris, professor of medicine and director of the comprehensive hypertension center at the University of Chicago and coprincipal investigator of SYMPLICITY HTN-3 along with Dr. Bhatt. "It certainly calls into question whether they denervated effectively. One could argue that if denervation were done appropriately" it would add to drug treatment, Dr. Bakris said in an interview. "This issue has come up about the quality of the denervation; the good news is that it can be done correctly," but that will require "a good understanding of what you are doing to the renal nerves and how much energy you need." SYMPLICITY HTN-3 "was a good but expensive learning experience," Dr. Bakris said.
The investigators "were performing a procedure, but they didn’t have the evidence that the procedure was accomplishing what it meant to accomplish," commented Dr. Anthony DeMaria, professor of medicine, the Judith and Jack White chair of cardiology, and director of the cardiovascular center at the University of California, San Diego, who was not involved in the trial. "Most of us feel there are tantalizing data to suggest that denervation can have a benefit, but they need to go back to the physiology to be sure they are denervating effectively."
Though Dr. Bakris and Dr. Esler cautioned that the study’s primary outcome was neutral, they see reason to hope that renal denervation will still prove to have an important and useful clinical effect.
"This report is the tip of the iceberg," Dr. Bakris noted. "When you look at the effect of denervation on blood pressure variability, heart rate variability, and total control over 24 hours using ambulatory blood pressure monitoring, you see a different picture," results that will be reported later this year, he said.
And Dr. Esler said that his experience using renal denervation on about 300 patients with treatment-resistant hypertension has convinced him that denervation can produce real benefits when done properly.
"I’m not changing my practice" using renal denervation on refractory patients, he said. "I accumulated a lot of patients with severe, resistant hypertension, patients whom I couldn’t control with seven or eight different drug classes. But when renal denervation came along, it was like chalk and cheese. Suddenly, I had a therapy that worked. My clinical experience in patients who didn’t budge with medications totally convinces me" that renal denervation works.
SYMPLICITY HTN-3 was sponsored by Medtronic, the company that markets the device tested in the study. Dr. Bhatt said that he has received research grants from Medtronic and five other companies. Dr. Esler said that he has received consulting fees, honoraria, and research grants from Medtronic. Dr. Bakris said that he has received personal fees from Medtronic and five other companies. Dr. DeMaria said that he has received research grants from Angioblast Systems, Cardiovascular Biotherapeutics, General Electric Medical, Gilead, and Lantheus.
On Twitter @mitchelzoler
WASHINGTON – Renal denervation’s not so simple after all.
Highly anticipated data from the large, sham-controlled renal-artery catheter denervation trial, SYMPLICITY HTN-3, gave its investigators reason to believe that inconsistent and inadequate delivery of nerve-ablating radiofrequency energy by inexperienced operators left too many patients undertreated, producing a neutral outcome for the primary endpoint, the study’s top-line result first reported in a company press release in January.
In the SYMPLICITY HTN-3 (Renal Denervation in Patients With Uncontrolled Hypertension) trial, the average systolic blood pressure reduction among the 364 patients randomized to renal denervation was 14 mm Hg, compared with an average 12 mm Hg reduction in 174 control patients who underwent a renal-artery angiogram masked to resemble a denervation procedure, a difference that was not statistically significant, falling substantially short of the prespecified 5 mm Hg between group difference necessary to fulfill superiority, Dr. Deepak L. Bhatt said at the annual meeting of the American College of Cardiology.
Although several factors likely led to the neutral outcome, including an unexpectedly robust blood pressure drop in the control arm, another major factor, many suspect, was inadequate delivery of the denervation treatment.
"It might be that the way we used the catheter wasn’t ideal," said Dr. Bhatt, coprincipal investigator of the study, professor of medicine at Harvard Medical School and executive director of interventional cardiology at Brigham and Women’s Hospital, both in Boston.
Concurrent with Dr. Bhatt’s report at the meeting a published version appeared online (N. Engl. J. Med. 2014 March 29 [doi:10.1056/NEJMoa1402670]).
"There is the concept that renal denervation is easy. As a catheter procedure it is easy, but to achieve denervation is far from easy," said Dr. Murray D. Esler, a professor of medicine at Monash University and senior director of the Baker IDI Heart and Diabetes Institute, both in Melbourne, and a pioneer of renal denervation who was involved in prior SYMPLICITY studies of the same renal-denervation device but was not a coinvestigator for the new trial.
"The SYMPLICITY 3 study made a mistake thinking it could get away with not giving the proceduralists any hands-on experience" before the trial. "There was none. The operators hadn’t done it before, and the trial’s designers would not have done that unless they thought that denervation was easy. Well, it’s not easy. There is a learning curve, and I think that’s the main explanation of what went wrong. "
Exacerbating the operators’ inexperience with denervation (they were all experienced interventional cardiologists) was a second flaw in the trial’s design: No method was used to monitor the efficacy of each denervation procedure, an easy decision because there is still no proven way to measure denervation efficacy during the procedure. Dr. Esler said he believes that he has a solution, one that involves testing for interrupted activity of the parallel, afferent nerves of the renal arteries using adenosine as a surrogate measure for denervation of the target efferent nerves. But while he is optimistic the adenosine approach will work, it is still at least several months from use in a trial.
In the first clinical study of renal denervation, a series of 50 patients treated at five centers in Australia and Europe reported just 5 years ago (Lancet 2009;373:1275-81), Dr. Esler, a lead investigator for that study, and his associates carefully tested the efficacy of denervation in 10 patients by measuring the direct effect of successful denervation, reduction of renal norepinephrine spillover. They reported that, in those 10 patients, renal denervation cut norepinephrine spillover by an average 47%, which correlated with an average reduction in systolic blood pressure of 22 mm Hg after 6 months.
But this effect from denervation was "far from uniform and ranged from zero to 85%," depending on who was doing the denervation. "It’s obviously operator dependent." Dr. Esler said in an interview. This observation of enormous variability in the physiologic impact of denervation "took on a new context with the failed trial. The denervation done by novices explains to some extent the spread [in results] and makes me think the same thing happened in SYMPLICITY 3."
"If you don’t do enough high-frequency burns or if the catheter doesn’t reach enough nerves" because of misplacement within the renal artery, the denervation won’t be very successful, noted Dr. George Bakris, professor of medicine and director of the comprehensive hypertension center at the University of Chicago and coprincipal investigator of SYMPLICITY HTN-3 along with Dr. Bhatt. "It certainly calls into question whether they denervated effectively. One could argue that if denervation were done appropriately" it would add to drug treatment, Dr. Bakris said in an interview. "This issue has come up about the quality of the denervation; the good news is that it can be done correctly," but that will require "a good understanding of what you are doing to the renal nerves and how much energy you need." SYMPLICITY HTN-3 "was a good but expensive learning experience," Dr. Bakris said.
The investigators "were performing a procedure, but they didn’t have the evidence that the procedure was accomplishing what it meant to accomplish," commented Dr. Anthony DeMaria, professor of medicine, the Judith and Jack White chair of cardiology, and director of the cardiovascular center at the University of California, San Diego, who was not involved in the trial. "Most of us feel there are tantalizing data to suggest that denervation can have a benefit, but they need to go back to the physiology to be sure they are denervating effectively."
Though Dr. Bakris and Dr. Esler cautioned that the study’s primary outcome was neutral, they see reason to hope that renal denervation will still prove to have an important and useful clinical effect.
"This report is the tip of the iceberg," Dr. Bakris noted. "When you look at the effect of denervation on blood pressure variability, heart rate variability, and total control over 24 hours using ambulatory blood pressure monitoring, you see a different picture," results that will be reported later this year, he said.
And Dr. Esler said that his experience using renal denervation on about 300 patients with treatment-resistant hypertension has convinced him that denervation can produce real benefits when done properly.
"I’m not changing my practice" using renal denervation on refractory patients, he said. "I accumulated a lot of patients with severe, resistant hypertension, patients whom I couldn’t control with seven or eight different drug classes. But when renal denervation came along, it was like chalk and cheese. Suddenly, I had a therapy that worked. My clinical experience in patients who didn’t budge with medications totally convinces me" that renal denervation works.
SYMPLICITY HTN-3 was sponsored by Medtronic, the company that markets the device tested in the study. Dr. Bhatt said that he has received research grants from Medtronic and five other companies. Dr. Esler said that he has received consulting fees, honoraria, and research grants from Medtronic. Dr. Bakris said that he has received personal fees from Medtronic and five other companies. Dr. DeMaria said that he has received research grants from Angioblast Systems, Cardiovascular Biotherapeutics, General Electric Medical, Gilead, and Lantheus.
On Twitter @mitchelzoler
AT ACC 14
Major finding: Renal denervation produced an average 14 mm Hg drop in systolic blood pressure, compared with an average 12 mm Hg decline in controls.
Data source: SYMPLICITY HTN-3, a randomized trial with 535 patients with uncontrolled hypertension who were treated at 88 U.S. sites.
Disclosures: SYMPLICITY HTN-3 was sponsored by Medtronic, the company that markets the device tested in the study. Dr. Bhatt said that he has received research grants from Medtronic and five other companies. Dr. Esler said that he has received consulting fees, honoraria, and research grants from Medtronic. Dr. Bakris said that he has received personal fees from Medtronic and five other companies. Dr. DeMaria said that he has received research grants from Angioblast Systems, Cardiovascular Biotherapeutics, General Electric Medical, Gilead, and Lantheus.

VIDEO: What explains SYMPLICITY HTN-3’s failure?
WASHINGTON – What can explain the failure of SYMPLICITY HTN-3? After clinical success in reducing blood pressure by 20-30 mm HG in patients with resistant hypertension, the renal denervation treatment showed no significant reduction in the first randomized trial in which control patients underwent sham operations.
According to two top hypertension experts, trial investigator Dr. George Bakris and Dr. Prakash Deedwania, physiology, behavior, and technology come to mind for starters, as explored in Part 1 of our interview.
WASHINGTON – What can explain the failure of SYMPLICITY HTN-3? After clinical success in reducing blood pressure by 20-30 mm HG in patients with resistant hypertension, the renal denervation treatment showed no significant reduction in the first randomized trial in which control patients underwent sham operations.
According to two top hypertension experts, trial investigator Dr. George Bakris and Dr. Prakash Deedwania, physiology, behavior, and technology come to mind for starters, as explored in Part 1 of our interview.
WASHINGTON – What can explain the failure of SYMPLICITY HTN-3? After clinical success in reducing blood pressure by 20-30 mm HG in patients with resistant hypertension, the renal denervation treatment showed no significant reduction in the first randomized trial in which control patients underwent sham operations.
According to two top hypertension experts, trial investigator Dr. George Bakris and Dr. Prakash Deedwania, physiology, behavior, and technology come to mind for starters, as explored in Part 1 of our interview.
At ACC 14
