User login
Optimal management of patients with chronic kidney disease
SCOTTSDALE, ARIZ. – Optimal management of patients with chronic kidney disease involves knowing what can be modified, understanding that much is uncertain, and having the wisdom to know the difference, suggested an anesthesiologist at a meeting on perioperative medicine sponsored by the University of Miami.
"There is a lot to be done in terms of evaluation of chronic kidney disease and also defining interventions," said Dr. Claus U. Niemann, professor of anesthesia and surgery at the University of California, San Francisco.
Kidney disease is identified either by markers of function such as glomerular filtration rate (GFR), markers of damage such as proteinuria, and markers of volume sense, such as edema, ascites, and urinary sodium excretion.
None of these measures is particularly accurate at measuring disease, however. For example, GFR is not observed directly but estimated from creatinine clearance, which is produced by the body in varying amounts daily and which depends on muscle mass, so that values for a young, muscular man will be higher than those of a small, older woman, Dr. Niemann noted.
In addition, even in people without kidney disease, GFR declines gradually with age, from about 116 mL/min per 1.73 m2 for people in their 20s, to about 75 mL/min per 1.73 m2 in those aged 70 years and older.
In 2002, the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (K/DOQI) developed a five-stage classification for chronic kidney disease (CKD), based on GFR, with CKD defined as either a GFR of less than 60 mL/min per 1.73 m2 for more than 3 months or evidence of kidney damage for more than 3 months, based on the presence of abnormalities such as proteinuria. The classification notes that a combination of GFR less than 60 mL/min per 1.73 m2 and proteinuria is prognostic.
The classification includes moderately and severely reduced GFR, with respective rates of 30-59 and 15-29 mL/min per 1.73 m2, respectively, and end-stage renal disease, with a GFR less than 15 mL/min per 1.73 m2 or a need for dialysis,
The most common cause of CKD is diabetic nephropathy or hypertensive nephrosclerosis, which account for 67% of all cases. About 1 in 5 or 1 in 6 Americans has some form of CKD, and the problem can be lifelong, Dr. Niemann said.
Risk stratification
The goal of perioperative management of patients with CKD is to prevent further renal impairment from acute kidney injury, a rapid reduction in kidney function as measured by a significant rise in serum creatinine levels or reduction in urine output within 48 hours of exposure.
Approximately 5%-7% of all hospitalized patients experience some degree of acute kidney injury and changes in serum creatinine of only 0.3 mg/dL have been associated with greater length of stay and increased morbidity and mortality, Dr. Niemann said.
"What is really necessary is that we do perioperative risk stratification. We want to identify the subset of patients who are at risk, we can do tests potentially, and we want to understand what the procedure is, put it in the context of the patient and his renal disease, and then hopefully define a plan and get him to surgery," Dr. Niemann said.
Defining perioperative renal risk involves determining as best as possible the extent of renal insufficiency or CKD, the etiology of the kidney disease (including severity and complications), and the risk of loss of kidney function from the planned or urgent/emergent surgery. The preop clinical team should also know where the patient will be discharged after surgery (home, ICU, floor).
Risk factors for in-hospital acute renal failure include baseline risks, such as age, diabetes, heart or liver failure, and male sex; acute clinical conditions, such as sepsis, hypotension, shock, volume depletion, or rhabdomyolysis; and use of nephrotoxic agents, such as contrast media, aminoglycosides, chemotherapy drugs, or NSAIDs.
Mixed results
Dr. Niemann noted that in a systematic review of possible interventions for protecting renal function in the perioperative period found little in the way of solid evidence to support the use of various interventions, including dopamine agonists or analogs, loop diuretics, mannitol, calcium inhibitors, angiotensin-converting enzyme (ACE) inhibitors, N-acetylcysteine in contrast studies or surgery, or sodium bicarbonate (Cochrane Database of Syst. Rev. 2013;9:CD003590 [doi:10.1002/14651858.CD003590.pub]).
"The long and the short of it is that no interventions have definitely been shown to make a big difference in randomized trials," he said.
Nonetheless, to prevent further loss of renal function in at-risk patients, clinicians should optimize modifiable variables, such as blood pressure, and discontinue nephrotoxic medications, such as NSAIDs.
In addition, the perioperative team should strive to better control acidosis, anemia, and hyperphosphatemia.
"I think what is really important is that you counsel the patient in the preop clinic," Dr. Niemann said.
Preoperative clinic staff should review the procedure and risks based on the presence and severity of the patient’s CKD and outline possible outcomes based on the best available evidence.
"We do it for the heart, but we don’t do it for the kidney," he commented.
During surgery, the team should be aware of the risks of a potential "second hit" – that is, an acute injury on top of chronic disease, and after surgery, clinicians should monitor for the known risk factors, such as sepsis and infection, he said.
Dr. Niemann reported no relevant conflicts.
SCOTTSDALE, ARIZ. – Optimal management of patients with chronic kidney disease involves knowing what can be modified, understanding that much is uncertain, and having the wisdom to know the difference, suggested an anesthesiologist at a meeting on perioperative medicine sponsored by the University of Miami.
"There is a lot to be done in terms of evaluation of chronic kidney disease and also defining interventions," said Dr. Claus U. Niemann, professor of anesthesia and surgery at the University of California, San Francisco.
Kidney disease is identified either by markers of function such as glomerular filtration rate (GFR), markers of damage such as proteinuria, and markers of volume sense, such as edema, ascites, and urinary sodium excretion.
None of these measures is particularly accurate at measuring disease, however. For example, GFR is not observed directly but estimated from creatinine clearance, which is produced by the body in varying amounts daily and which depends on muscle mass, so that values for a young, muscular man will be higher than those of a small, older woman, Dr. Niemann noted.
In addition, even in people without kidney disease, GFR declines gradually with age, from about 116 mL/min per 1.73 m2 for people in their 20s, to about 75 mL/min per 1.73 m2 in those aged 70 years and older.
In 2002, the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (K/DOQI) developed a five-stage classification for chronic kidney disease (CKD), based on GFR, with CKD defined as either a GFR of less than 60 mL/min per 1.73 m2 for more than 3 months or evidence of kidney damage for more than 3 months, based on the presence of abnormalities such as proteinuria. The classification notes that a combination of GFR less than 60 mL/min per 1.73 m2 and proteinuria is prognostic.
The classification includes moderately and severely reduced GFR, with respective rates of 30-59 and 15-29 mL/min per 1.73 m2, respectively, and end-stage renal disease, with a GFR less than 15 mL/min per 1.73 m2 or a need for dialysis,
The most common cause of CKD is diabetic nephropathy or hypertensive nephrosclerosis, which account for 67% of all cases. About 1 in 5 or 1 in 6 Americans has some form of CKD, and the problem can be lifelong, Dr. Niemann said.
Risk stratification
The goal of perioperative management of patients with CKD is to prevent further renal impairment from acute kidney injury, a rapid reduction in kidney function as measured by a significant rise in serum creatinine levels or reduction in urine output within 48 hours of exposure.
Approximately 5%-7% of all hospitalized patients experience some degree of acute kidney injury and changes in serum creatinine of only 0.3 mg/dL have been associated with greater length of stay and increased morbidity and mortality, Dr. Niemann said.
"What is really necessary is that we do perioperative risk stratification. We want to identify the subset of patients who are at risk, we can do tests potentially, and we want to understand what the procedure is, put it in the context of the patient and his renal disease, and then hopefully define a plan and get him to surgery," Dr. Niemann said.
Defining perioperative renal risk involves determining as best as possible the extent of renal insufficiency or CKD, the etiology of the kidney disease (including severity and complications), and the risk of loss of kidney function from the planned or urgent/emergent surgery. The preop clinical team should also know where the patient will be discharged after surgery (home, ICU, floor).
Risk factors for in-hospital acute renal failure include baseline risks, such as age, diabetes, heart or liver failure, and male sex; acute clinical conditions, such as sepsis, hypotension, shock, volume depletion, or rhabdomyolysis; and use of nephrotoxic agents, such as contrast media, aminoglycosides, chemotherapy drugs, or NSAIDs.
Mixed results
Dr. Niemann noted that in a systematic review of possible interventions for protecting renal function in the perioperative period found little in the way of solid evidence to support the use of various interventions, including dopamine agonists or analogs, loop diuretics, mannitol, calcium inhibitors, angiotensin-converting enzyme (ACE) inhibitors, N-acetylcysteine in contrast studies or surgery, or sodium bicarbonate (Cochrane Database of Syst. Rev. 2013;9:CD003590 [doi:10.1002/14651858.CD003590.pub]).
"The long and the short of it is that no interventions have definitely been shown to make a big difference in randomized trials," he said.
Nonetheless, to prevent further loss of renal function in at-risk patients, clinicians should optimize modifiable variables, such as blood pressure, and discontinue nephrotoxic medications, such as NSAIDs.
In addition, the perioperative team should strive to better control acidosis, anemia, and hyperphosphatemia.
"I think what is really important is that you counsel the patient in the preop clinic," Dr. Niemann said.
Preoperative clinic staff should review the procedure and risks based on the presence and severity of the patient’s CKD and outline possible outcomes based on the best available evidence.
"We do it for the heart, but we don’t do it for the kidney," he commented.
During surgery, the team should be aware of the risks of a potential "second hit" – that is, an acute injury on top of chronic disease, and after surgery, clinicians should monitor for the known risk factors, such as sepsis and infection, he said.
Dr. Niemann reported no relevant conflicts.
SCOTTSDALE, ARIZ. – Optimal management of patients with chronic kidney disease involves knowing what can be modified, understanding that much is uncertain, and having the wisdom to know the difference, suggested an anesthesiologist at a meeting on perioperative medicine sponsored by the University of Miami.
"There is a lot to be done in terms of evaluation of chronic kidney disease and also defining interventions," said Dr. Claus U. Niemann, professor of anesthesia and surgery at the University of California, San Francisco.
Kidney disease is identified either by markers of function such as glomerular filtration rate (GFR), markers of damage such as proteinuria, and markers of volume sense, such as edema, ascites, and urinary sodium excretion.
None of these measures is particularly accurate at measuring disease, however. For example, GFR is not observed directly but estimated from creatinine clearance, which is produced by the body in varying amounts daily and which depends on muscle mass, so that values for a young, muscular man will be higher than those of a small, older woman, Dr. Niemann noted.
In addition, even in people without kidney disease, GFR declines gradually with age, from about 116 mL/min per 1.73 m2 for people in their 20s, to about 75 mL/min per 1.73 m2 in those aged 70 years and older.
In 2002, the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (K/DOQI) developed a five-stage classification for chronic kidney disease (CKD), based on GFR, with CKD defined as either a GFR of less than 60 mL/min per 1.73 m2 for more than 3 months or evidence of kidney damage for more than 3 months, based on the presence of abnormalities such as proteinuria. The classification notes that a combination of GFR less than 60 mL/min per 1.73 m2 and proteinuria is prognostic.
The classification includes moderately and severely reduced GFR, with respective rates of 30-59 and 15-29 mL/min per 1.73 m2, respectively, and end-stage renal disease, with a GFR less than 15 mL/min per 1.73 m2 or a need for dialysis,
The most common cause of CKD is diabetic nephropathy or hypertensive nephrosclerosis, which account for 67% of all cases. About 1 in 5 or 1 in 6 Americans has some form of CKD, and the problem can be lifelong, Dr. Niemann said.
Risk stratification
The goal of perioperative management of patients with CKD is to prevent further renal impairment from acute kidney injury, a rapid reduction in kidney function as measured by a significant rise in serum creatinine levels or reduction in urine output within 48 hours of exposure.
Approximately 5%-7% of all hospitalized patients experience some degree of acute kidney injury and changes in serum creatinine of only 0.3 mg/dL have been associated with greater length of stay and increased morbidity and mortality, Dr. Niemann said.
"What is really necessary is that we do perioperative risk stratification. We want to identify the subset of patients who are at risk, we can do tests potentially, and we want to understand what the procedure is, put it in the context of the patient and his renal disease, and then hopefully define a plan and get him to surgery," Dr. Niemann said.
Defining perioperative renal risk involves determining as best as possible the extent of renal insufficiency or CKD, the etiology of the kidney disease (including severity and complications), and the risk of loss of kidney function from the planned or urgent/emergent surgery. The preop clinical team should also know where the patient will be discharged after surgery (home, ICU, floor).
Risk factors for in-hospital acute renal failure include baseline risks, such as age, diabetes, heart or liver failure, and male sex; acute clinical conditions, such as sepsis, hypotension, shock, volume depletion, or rhabdomyolysis; and use of nephrotoxic agents, such as contrast media, aminoglycosides, chemotherapy drugs, or NSAIDs.
Mixed results
Dr. Niemann noted that in a systematic review of possible interventions for protecting renal function in the perioperative period found little in the way of solid evidence to support the use of various interventions, including dopamine agonists or analogs, loop diuretics, mannitol, calcium inhibitors, angiotensin-converting enzyme (ACE) inhibitors, N-acetylcysteine in contrast studies or surgery, or sodium bicarbonate (Cochrane Database of Syst. Rev. 2013;9:CD003590 [doi:10.1002/14651858.CD003590.pub]).
"The long and the short of it is that no interventions have definitely been shown to make a big difference in randomized trials," he said.
Nonetheless, to prevent further loss of renal function in at-risk patients, clinicians should optimize modifiable variables, such as blood pressure, and discontinue nephrotoxic medications, such as NSAIDs.
In addition, the perioperative team should strive to better control acidosis, anemia, and hyperphosphatemia.
"I think what is really important is that you counsel the patient in the preop clinic," Dr. Niemann said.
Preoperative clinic staff should review the procedure and risks based on the presence and severity of the patient’s CKD and outline possible outcomes based on the best available evidence.
"We do it for the heart, but we don’t do it for the kidney," he commented.
During surgery, the team should be aware of the risks of a potential "second hit" – that is, an acute injury on top of chronic disease, and after surgery, clinicians should monitor for the known risk factors, such as sepsis and infection, he said.
Dr. Niemann reported no relevant conflicts.
AT THE PERIOPERATIVE MEDICINE SUMMIT
Childhood glomerular disease associated with adult hypertension
Men who had glomerular disease as children were at increased risk for developing hypertension as adults, according to a study published in JAMA.
Dr. Asaf Vivante and his colleagues studied 38,144 healthy men in the Staff Periodic Examination Center (SPEC) of the Israeli Defense Forces Medical Corps, 264 of whom had a medical history of resolved childhood glomerular disease.
All participants had a baseline evaluation at age 17, during which the diagnosis of resolved childhood glomerular disease (including childhood acute glomerulonephritis and nephrotic syndrome) was determined. Men with unresolved childhood glomerular disease, hypertension, diabetes, active rheumatic diseases, or any other kidney or urinary tract disorders were excluded. SPEC follow-up visits occurred until hypertension diagnosis, retirement from service, or Dec. 31, 2010, whichever came first.
At a mean follow-up of 18 years, 2,856 men developed hypertension. Of men with a history of resolved childhood glomerular disease, 13.6% had hypertension as adults, compared with 7.4% who had no childhood kidney disease (hazard ratio, 1.67; 95% confidence interval, 1.20-2.31; P = .002 when adjusted for age and body mass index) (JAMA 2014;311:1155-7).
The researchers cited a few limitations of the study, including a lack of information on the exact glomerular histopathologic injury during childhood and the young age of the study population at the end of follow-up.
Database access was provided by the Israeli Defense Forces Medical Corps. One coauthor reported receiving travel reimbursement from the European Cooperation in Science and Technology. No other disclosures were reported.
Men who had glomerular disease as children were at increased risk for developing hypertension as adults, according to a study published in JAMA.
Dr. Asaf Vivante and his colleagues studied 38,144 healthy men in the Staff Periodic Examination Center (SPEC) of the Israeli Defense Forces Medical Corps, 264 of whom had a medical history of resolved childhood glomerular disease.
All participants had a baseline evaluation at age 17, during which the diagnosis of resolved childhood glomerular disease (including childhood acute glomerulonephritis and nephrotic syndrome) was determined. Men with unresolved childhood glomerular disease, hypertension, diabetes, active rheumatic diseases, or any other kidney or urinary tract disorders were excluded. SPEC follow-up visits occurred until hypertension diagnosis, retirement from service, or Dec. 31, 2010, whichever came first.
At a mean follow-up of 18 years, 2,856 men developed hypertension. Of men with a history of resolved childhood glomerular disease, 13.6% had hypertension as adults, compared with 7.4% who had no childhood kidney disease (hazard ratio, 1.67; 95% confidence interval, 1.20-2.31; P = .002 when adjusted for age and body mass index) (JAMA 2014;311:1155-7).
The researchers cited a few limitations of the study, including a lack of information on the exact glomerular histopathologic injury during childhood and the young age of the study population at the end of follow-up.
Database access was provided by the Israeli Defense Forces Medical Corps. One coauthor reported receiving travel reimbursement from the European Cooperation in Science and Technology. No other disclosures were reported.
Men who had glomerular disease as children were at increased risk for developing hypertension as adults, according to a study published in JAMA.
Dr. Asaf Vivante and his colleagues studied 38,144 healthy men in the Staff Periodic Examination Center (SPEC) of the Israeli Defense Forces Medical Corps, 264 of whom had a medical history of resolved childhood glomerular disease.
All participants had a baseline evaluation at age 17, during which the diagnosis of resolved childhood glomerular disease (including childhood acute glomerulonephritis and nephrotic syndrome) was determined. Men with unresolved childhood glomerular disease, hypertension, diabetes, active rheumatic diseases, or any other kidney or urinary tract disorders were excluded. SPEC follow-up visits occurred until hypertension diagnosis, retirement from service, or Dec. 31, 2010, whichever came first.
At a mean follow-up of 18 years, 2,856 men developed hypertension. Of men with a history of resolved childhood glomerular disease, 13.6% had hypertension as adults, compared with 7.4% who had no childhood kidney disease (hazard ratio, 1.67; 95% confidence interval, 1.20-2.31; P = .002 when adjusted for age and body mass index) (JAMA 2014;311:1155-7).
The researchers cited a few limitations of the study, including a lack of information on the exact glomerular histopathologic injury during childhood and the young age of the study population at the end of follow-up.
Database access was provided by the Israeli Defense Forces Medical Corps. One coauthor reported receiving travel reimbursement from the European Cooperation in Science and Technology. No other disclosures were reported.
FROM JAMA
Major finding: Of men with a history of resolved childhood glomerular disease, 13.6% developed hypertension as adults, compared with 7.4% of men who had no childhood kidney disease (hazard ratio, 1.67; 95% confidence interval, 1.20-2.31; P = .002 when adjusted for age and body mass index).
Data source: An analysis using Cox proportional hazards models of 38,144 healthy men in the Staff Periodic Examination Center (SPEC) of the Israeli Defense Forces Medical Corps, 264 of whom had a history of resolved childhood glomerular disease.
Disclosures: Database access was provided by the Israeli Defense Forces Medical Corps. One coauthor reported receiving travel reimbursement from the European Cooperation in Science and Technology. No other disclosures were reported.
TNFR1 shown as marker for mortality risk in type 2 diabetes with kidney disease
Tumor necrosis factor receptor 1 is an effective marker for all-cause mortality in type 2 diabetes with kidney disease, according to results of a French study.
Additionally, TNFR1 was found to add clinical utility to the U.K. Prospective Diabetes Study (UKPDS) outcome equation for mortality.
"Our data showed a clear and graded relationship between concentrations of serum TNFR1 and risk of all-cause mortality," Pierre Jean Saulnier, Ph.D., of the University of Poitiers (France) and his colleagues wrote.
In a follow-up analysis of the SURDIAGENE study, designed to identify genetic and environmental causes of micro- and macrovascular complications in type 2 diabetes, investigators followed 522 patients with baseline urinary albumin to creatinine ratios (uACR) greater than 30 mg/mmol, an estimated glomerular filtration rate (eGFR) greater than 60 mL/min per 1.73 m2, or both. Patients with a history of myocardial infarction and/or stroke were considered to have cardiovascular disease at baseline (Diabetes Care 2014 March 12 [doi:10.2337/dc13-2580]).
The primary endpoint was all-cause mortality. The secondary endpoint was the occurrence of a composite renal outcome in patients who did not have end-stage renal disease at baseline. The median duration of the study was 48 months. In that time, 196 deaths occurred.
The increased rate of death correlated with increased levels of TNFR1 across quartiles: 4.7% patient years in the first quartile, 7.7% in the second, 9.3% in the third, and 15.9% in the fourth.
Of note, when the investigators ran a multivariate analysis using age, diabetes duration, hemoglobin A1c, uACR, and eGFR, they found that the risk of death tripled in patients in the fourth quartile (adjusted hazard ratio, 2.98), compared with patients in the first quartile.
When TNFR1 was combined with the UKDPS equation, which uses age, diabetes duration, sex, ethnicity, current smoking status, systolic blood pressure, HbA1c, body mass index, eGFR, heart rate, atrial fibrillation, albuminuria, and peripheral vascular disease, the predictive value for mortality improved significantly (P = .03).
TNFR1 is a proinflammatory marker that a growing body of literature indicates has prognostic value for cardiovascular disease in patients with diabetes. "Our current findings add to this literature," the researchers wrote, adding that while it was not the focus of their study, the data may contribute to understanding the role of TNFR1 in vasculopathy and diabetes-related events such as amputation.
None of the authors of this study reported any relevant disclosures. Funding was provided by the French Ministry of Health, among others.
Tumor necrosis factor receptor 1 is an effective marker for all-cause mortality in type 2 diabetes with kidney disease, according to results of a French study.
Additionally, TNFR1 was found to add clinical utility to the U.K. Prospective Diabetes Study (UKPDS) outcome equation for mortality.
"Our data showed a clear and graded relationship between concentrations of serum TNFR1 and risk of all-cause mortality," Pierre Jean Saulnier, Ph.D., of the University of Poitiers (France) and his colleagues wrote.
In a follow-up analysis of the SURDIAGENE study, designed to identify genetic and environmental causes of micro- and macrovascular complications in type 2 diabetes, investigators followed 522 patients with baseline urinary albumin to creatinine ratios (uACR) greater than 30 mg/mmol, an estimated glomerular filtration rate (eGFR) greater than 60 mL/min per 1.73 m2, or both. Patients with a history of myocardial infarction and/or stroke were considered to have cardiovascular disease at baseline (Diabetes Care 2014 March 12 [doi:10.2337/dc13-2580]).
The primary endpoint was all-cause mortality. The secondary endpoint was the occurrence of a composite renal outcome in patients who did not have end-stage renal disease at baseline. The median duration of the study was 48 months. In that time, 196 deaths occurred.
The increased rate of death correlated with increased levels of TNFR1 across quartiles: 4.7% patient years in the first quartile, 7.7% in the second, 9.3% in the third, and 15.9% in the fourth.
Of note, when the investigators ran a multivariate analysis using age, diabetes duration, hemoglobin A1c, uACR, and eGFR, they found that the risk of death tripled in patients in the fourth quartile (adjusted hazard ratio, 2.98), compared with patients in the first quartile.
When TNFR1 was combined with the UKDPS equation, which uses age, diabetes duration, sex, ethnicity, current smoking status, systolic blood pressure, HbA1c, body mass index, eGFR, heart rate, atrial fibrillation, albuminuria, and peripheral vascular disease, the predictive value for mortality improved significantly (P = .03).
TNFR1 is a proinflammatory marker that a growing body of literature indicates has prognostic value for cardiovascular disease in patients with diabetes. "Our current findings add to this literature," the researchers wrote, adding that while it was not the focus of their study, the data may contribute to understanding the role of TNFR1 in vasculopathy and diabetes-related events such as amputation.
None of the authors of this study reported any relevant disclosures. Funding was provided by the French Ministry of Health, among others.
Tumor necrosis factor receptor 1 is an effective marker for all-cause mortality in type 2 diabetes with kidney disease, according to results of a French study.
Additionally, TNFR1 was found to add clinical utility to the U.K. Prospective Diabetes Study (UKPDS) outcome equation for mortality.
"Our data showed a clear and graded relationship between concentrations of serum TNFR1 and risk of all-cause mortality," Pierre Jean Saulnier, Ph.D., of the University of Poitiers (France) and his colleagues wrote.
In a follow-up analysis of the SURDIAGENE study, designed to identify genetic and environmental causes of micro- and macrovascular complications in type 2 diabetes, investigators followed 522 patients with baseline urinary albumin to creatinine ratios (uACR) greater than 30 mg/mmol, an estimated glomerular filtration rate (eGFR) greater than 60 mL/min per 1.73 m2, or both. Patients with a history of myocardial infarction and/or stroke were considered to have cardiovascular disease at baseline (Diabetes Care 2014 March 12 [doi:10.2337/dc13-2580]).
The primary endpoint was all-cause mortality. The secondary endpoint was the occurrence of a composite renal outcome in patients who did not have end-stage renal disease at baseline. The median duration of the study was 48 months. In that time, 196 deaths occurred.
The increased rate of death correlated with increased levels of TNFR1 across quartiles: 4.7% patient years in the first quartile, 7.7% in the second, 9.3% in the third, and 15.9% in the fourth.
Of note, when the investigators ran a multivariate analysis using age, diabetes duration, hemoglobin A1c, uACR, and eGFR, they found that the risk of death tripled in patients in the fourth quartile (adjusted hazard ratio, 2.98), compared with patients in the first quartile.
When TNFR1 was combined with the UKDPS equation, which uses age, diabetes duration, sex, ethnicity, current smoking status, systolic blood pressure, HbA1c, body mass index, eGFR, heart rate, atrial fibrillation, albuminuria, and peripheral vascular disease, the predictive value for mortality improved significantly (P = .03).
TNFR1 is a proinflammatory marker that a growing body of literature indicates has prognostic value for cardiovascular disease in patients with diabetes. "Our current findings add to this literature," the researchers wrote, adding that while it was not the focus of their study, the data may contribute to understanding the role of TNFR1 in vasculopathy and diabetes-related events such as amputation.
None of the authors of this study reported any relevant disclosures. Funding was provided by the French Ministry of Health, among others.
FROM DIABETES CARE
Major finding: Increased rate of death correlated with increased rates of TNFR1 across quartiles: 4.7% patient years; 7.7%; 9.3%; 15.9%.
Data source: A prospective, single-center study of 522 patients.
Disclosures: None of the authors of this study reported any relevant disclosures. Funding was provided by the French Ministry of Health, among others.
Managing acute pyelonephritis during pregnancy
Acute pyelonephritis is a serious and common medical complication of pregnancy. It is estimated to occur in up to 1%-2% of pregnancies and is a common nonobstetrical indication for antepartum hospital admissions. Its prevalence is probably even higher in obstetrical clinics serving underserved inner-city populations such as ours in Newark, N.J.
The diagnosis of acute pyelonephritis is based on clinical signs and symptoms. Patients usually feel ill and have fever, chills, flank pain (usually right-sided), dysuria, and urgency and frequency. Nausea and vomiting also may be present. Laboratory abnormalities may include pyuria and bacteriuria, with white blood cell counts often predictive of pyelonephritis. A urine culture and sensitivity will often reveal Escherichia coli, but other less commonly found causative organisms may be detected as well.

It is the prevailing view that most pregnant women with acute pyelonephritis should be hospitalized for careful monitoring, evaluated for possible sepsis, and treated with parenteral antibiotics. Recently published retrospective cohort studies, as well as our own experience, have emphasized that the risks of preterm labor and delivery in these patients can be significant, as can the risks of septic shock and other complications. Treatment, therefore, should be aggressive, with careful monitoring and charting of vital signs, including urinary output; and fetal monitoring and monitoring of uterine contractions. That way one can identify patients who are not responding to treatment or who may be developing septic shock or preterm labor.
Studies have shown that 10%-12% of all pregnant women have asymptomatic bacteriuria. Because physiologic changes associated with pregnancy encourage urinary stasis, there is an increased risk of progression to acute pyelonephritis with the potential for serious infectious complications, even in pregnant women who are otherwise healthy. By and large, however, pyelonephritis is usually a preventable problem given access to prenatal care. Screening for asymptomatic bacteriuria during the first prenatal visit is important, and repeat screening in each trimester in women who are at high risk for recurrent infection is critical for preventing symptomatic and possibly severe infection.
Our screening preference is to perform a urine culture and sensitivity test at the first prenatal visit. Other providers may utilize a urinalysis and leukocyte esterase test initially, but as this approach is not as sensitive or specific, it must be followed by a urine culture and sensitivity testing if the urinalysis results are positive. Obstetricians and others providing prenatal care should utilize whatever approach works best for their patients and environment. Most importantly, screening for asymptomatic bacteriuria must occur early in the pregnancy.
Additional urine culture and sensitivity testing are advisable for patients who are at high risk for urinary tract infections, such as those who have had frequent UTIs before pregnancy and those who have anemia, sickle cell trait, a history of renal stones, diabetes mellitus, obesity, or neurologic disorders (such as neurogenic bladder and multiple sclerosis). Considering the increase in prevalence of obesity and diabetes, these high-risk patients represent a growing proportion of the obstetric population and appear to be at increased risk of UTIs as well. Women of increasing age and increasing parity also may be at higher risk of developing UTIs during pregnancy.
Cranberry juice has been touted for years as an effective remedy for the prevention and treatment of UTIs in women, and I advise my patients who have a UTI during pregnancy, who have diabetes, or who have other risk factors, to drink a glass of unsweetened cranberry juice each day. No definitive mechanism of action has been established, but it appears that cranberry juice prevents or interferes with the adherence of bacteria (particularly E. coli) to uroepithelial cells. It is important to emphasize to patients to consume unsweetened cranberry juice and not cranberry juice cocktail because of the high sugar content in the latter.
Recent research has emphasized that pregnancies of women who develop pyelonephritis are more likely to be complicated by spontaneous preterm birth, septicemia, and other adverse outcomes. In a retrospective cohort study of more than 546,000 singleton pregnancies delivered in all Kaiser Permanente of Southern California hospitals from 1993 to 2010, women with pyelonephritis were almost 57 times more likely than those without pyelonephritis to develop septicemia and 1.3 times more likely to have spontaneous preterm birth.
In addition, pregnancies of women with pyelonephritis were 2.6 times more likely than those of the baseline obstetric population to be complicated by anemia and 16.5 times more likely to be complicated by acute renal failure (Am. J. Obstet. Gynecol. 2014;210:219.e1-6). The overall incidence of acute antepartum pyelonephritis in this cohort study was relatively low compared with the incidence in other populations – 0.5% – which is not surprising given that patients in Kaiser’s integrated health care system routinely receive prenatal screening for asymptomatic bacteriuria.
Another retrospective population-based study comparing almost 220,000 singleton pregnancies of patients with and without acute pyelonephritis concluded that the infection is an independent risk factor for preterm delivery (Eur. J. Obstet. Gynecol. Reprod. Biol 2012;162:24-7).
After admission to the hospital, patients must be carefully monitored for uterine contractions and changes in vital signs and fetal heart rate. Several years ago, in an effort to empirically and synergistically target E. coli, the most common cause of UTIs and pyelonephritis, we began administering both an extended-spectrum cephalosporin (intravenous ceftriaxone) and an antimicrobial that will target gram-negative organisms, such as an aminoglycoside (gentamicin) or aztreonam.
We established this protocol because reviews of the outcomes at our institution indicated that intravenous ceftriaxone alone had not prevented some of our patients from developing septic shock in the first 8-20 hours post admission, despite the fact that culture and sensitivity results later indicated that the organism was E. coli and sensitive to the antimicrobial.
While we have not yet done any formal data analysis since changing our protocol, the combination parenteral antimicrobial regimen prescribed on admission appears to be effective in preventing the development of septic shock. We prescribe ceftriaxone 2 g intravenously once a day and gentamicin 5 mg/kg per day. Both drugs are continued until the patient improves clinically and has been afebrile for 48 hours.
At discharge, patients are prescribed a 10- to 14-day oral antimicrobial regimen dependent upon the culture and sensitivity report. Because at least 50% of E. coli are resistant to penicillin-like antimicrobials, the initial treatment no longer involves the use of ampicillin or amoxicillin. A repeat urine culture test at the end of treatment to confirm clearance of the infection is essential.
The possibility of anatomical obstructions in the urinary system should be investigated in pregnant patients who have multiple UTIs or who are unresponsive to appropriate antibiotic therapy for pyelonephritis. In this group we have performed ultrasound of the urinary tract system and have diagnosed renal stones as the risk factor for recurrent UTI. These patients are prescribed antimicrobial prophylaxis for the duration of the pregnancy. After delivery, they are referred to a urologist for follow-up care and treatment.
Dr. Apuzzio reported that he has no disclosures relevant to this Master Class.
Dr. Apuzzio is a professor in the department of obstetrics, gynecology, and women’s health, director of prenatal diagnosis and infectious diseases, professor of radiology, and director of maternal-fetal medicine at Rutgers New Jersey Medical School, Newark.
Acute pyelonephritis is a serious and common medical complication of pregnancy. It is estimated to occur in up to 1%-2% of pregnancies and is a common nonobstetrical indication for antepartum hospital admissions. Its prevalence is probably even higher in obstetrical clinics serving underserved inner-city populations such as ours in Newark, N.J.
The diagnosis of acute pyelonephritis is based on clinical signs and symptoms. Patients usually feel ill and have fever, chills, flank pain (usually right-sided), dysuria, and urgency and frequency. Nausea and vomiting also may be present. Laboratory abnormalities may include pyuria and bacteriuria, with white blood cell counts often predictive of pyelonephritis. A urine culture and sensitivity will often reveal Escherichia coli, but other less commonly found causative organisms may be detected as well.
It is the prevailing view that most pregnant women with acute pyelonephritis should be hospitalized for careful monitoring, evaluated for possible sepsis, and treated with parenteral antibiotics. Recently published retrospective cohort studies, as well as our own experience, have emphasized that the risks of preterm labor and delivery in these patients can be significant, as can the risks of septic shock and other complications. Treatment, therefore, should be aggressive, with careful monitoring and charting of vital signs, including urinary output; and fetal monitoring and monitoring of uterine contractions. That way one can identify patients who are not responding to treatment or who may be developing septic shock or preterm labor.
Studies have shown that 10%-12% of all pregnant women have asymptomatic bacteriuria. Because physiologic changes associated with pregnancy encourage urinary stasis, there is an increased risk of progression to acute pyelonephritis with the potential for serious infectious complications, even in pregnant women who are otherwise healthy. By and large, however, pyelonephritis is usually a preventable problem given access to prenatal care. Screening for asymptomatic bacteriuria during the first prenatal visit is important, and repeat screening in each trimester in women who are at high risk for recurrent infection is critical for preventing symptomatic and possibly severe infection.
Our screening preference is to perform a urine culture and sensitivity test at the first prenatal visit. Other providers may utilize a urinalysis and leukocyte esterase test initially, but as this approach is not as sensitive or specific, it must be followed by a urine culture and sensitivity testing if the urinalysis results are positive. Obstetricians and others providing prenatal care should utilize whatever approach works best for their patients and environment. Most importantly, screening for asymptomatic bacteriuria must occur early in the pregnancy.
Additional urine culture and sensitivity testing are advisable for patients who are at high risk for urinary tract infections, such as those who have had frequent UTIs before pregnancy and those who have anemia, sickle cell trait, a history of renal stones, diabetes mellitus, obesity, or neurologic disorders (such as neurogenic bladder and multiple sclerosis). Considering the increase in prevalence of obesity and diabetes, these high-risk patients represent a growing proportion of the obstetric population and appear to be at increased risk of UTIs as well. Women of increasing age and increasing parity also may be at higher risk of developing UTIs during pregnancy.
Cranberry juice has been touted for years as an effective remedy for the prevention and treatment of UTIs in women, and I advise my patients who have a UTI during pregnancy, who have diabetes, or who have other risk factors, to drink a glass of unsweetened cranberry juice each day. No definitive mechanism of action has been established, but it appears that cranberry juice prevents or interferes with the adherence of bacteria (particularly E. coli) to uroepithelial cells. It is important to emphasize to patients to consume unsweetened cranberry juice and not cranberry juice cocktail because of the high sugar content in the latter.
Recent research has emphasized that pregnancies of women who develop pyelonephritis are more likely to be complicated by spontaneous preterm birth, septicemia, and other adverse outcomes. In a retrospective cohort study of more than 546,000 singleton pregnancies delivered in all Kaiser Permanente of Southern California hospitals from 1993 to 2010, women with pyelonephritis were almost 57 times more likely than those without pyelonephritis to develop septicemia and 1.3 times more likely to have spontaneous preterm birth.
In addition, pregnancies of women with pyelonephritis were 2.6 times more likely than those of the baseline obstetric population to be complicated by anemia and 16.5 times more likely to be complicated by acute renal failure (Am. J. Obstet. Gynecol. 2014;210:219.e1-6). The overall incidence of acute antepartum pyelonephritis in this cohort study was relatively low compared with the incidence in other populations – 0.5% – which is not surprising given that patients in Kaiser’s integrated health care system routinely receive prenatal screening for asymptomatic bacteriuria.
Another retrospective population-based study comparing almost 220,000 singleton pregnancies of patients with and without acute pyelonephritis concluded that the infection is an independent risk factor for preterm delivery (Eur. J. Obstet. Gynecol. Reprod. Biol 2012;162:24-7).
After admission to the hospital, patients must be carefully monitored for uterine contractions and changes in vital signs and fetal heart rate. Several years ago, in an effort to empirically and synergistically target E. coli, the most common cause of UTIs and pyelonephritis, we began administering both an extended-spectrum cephalosporin (intravenous ceftriaxone) and an antimicrobial that will target gram-negative organisms, such as an aminoglycoside (gentamicin) or aztreonam.
We established this protocol because reviews of the outcomes at our institution indicated that intravenous ceftriaxone alone had not prevented some of our patients from developing septic shock in the first 8-20 hours post admission, despite the fact that culture and sensitivity results later indicated that the organism was E. coli and sensitive to the antimicrobial.
While we have not yet done any formal data analysis since changing our protocol, the combination parenteral antimicrobial regimen prescribed on admission appears to be effective in preventing the development of septic shock. We prescribe ceftriaxone 2 g intravenously once a day and gentamicin 5 mg/kg per day. Both drugs are continued until the patient improves clinically and has been afebrile for 48 hours.
At discharge, patients are prescribed a 10- to 14-day oral antimicrobial regimen dependent upon the culture and sensitivity report. Because at least 50% of E. coli are resistant to penicillin-like antimicrobials, the initial treatment no longer involves the use of ampicillin or amoxicillin. A repeat urine culture test at the end of treatment to confirm clearance of the infection is essential.
The possibility of anatomical obstructions in the urinary system should be investigated in pregnant patients who have multiple UTIs or who are unresponsive to appropriate antibiotic therapy for pyelonephritis. In this group we have performed ultrasound of the urinary tract system and have diagnosed renal stones as the risk factor for recurrent UTI. These patients are prescribed antimicrobial prophylaxis for the duration of the pregnancy. After delivery, they are referred to a urologist for follow-up care and treatment.
Dr. Apuzzio reported that he has no disclosures relevant to this Master Class.
Dr. Apuzzio is a professor in the department of obstetrics, gynecology, and women’s health, director of prenatal diagnosis and infectious diseases, professor of radiology, and director of maternal-fetal medicine at Rutgers New Jersey Medical School, Newark.
Acute pyelonephritis is a serious and common medical complication of pregnancy. It is estimated to occur in up to 1%-2% of pregnancies and is a common nonobstetrical indication for antepartum hospital admissions. Its prevalence is probably even higher in obstetrical clinics serving underserved inner-city populations such as ours in Newark, N.J.
The diagnosis of acute pyelonephritis is based on clinical signs and symptoms. Patients usually feel ill and have fever, chills, flank pain (usually right-sided), dysuria, and urgency and frequency. Nausea and vomiting also may be present. Laboratory abnormalities may include pyuria and bacteriuria, with white blood cell counts often predictive of pyelonephritis. A urine culture and sensitivity will often reveal Escherichia coli, but other less commonly found causative organisms may be detected as well.
It is the prevailing view that most pregnant women with acute pyelonephritis should be hospitalized for careful monitoring, evaluated for possible sepsis, and treated with parenteral antibiotics. Recently published retrospective cohort studies, as well as our own experience, have emphasized that the risks of preterm labor and delivery in these patients can be significant, as can the risks of septic shock and other complications. Treatment, therefore, should be aggressive, with careful monitoring and charting of vital signs, including urinary output; and fetal monitoring and monitoring of uterine contractions. That way one can identify patients who are not responding to treatment or who may be developing septic shock or preterm labor.
Studies have shown that 10%-12% of all pregnant women have asymptomatic bacteriuria. Because physiologic changes associated with pregnancy encourage urinary stasis, there is an increased risk of progression to acute pyelonephritis with the potential for serious infectious complications, even in pregnant women who are otherwise healthy. By and large, however, pyelonephritis is usually a preventable problem given access to prenatal care. Screening for asymptomatic bacteriuria during the first prenatal visit is important, and repeat screening in each trimester in women who are at high risk for recurrent infection is critical for preventing symptomatic and possibly severe infection.
Our screening preference is to perform a urine culture and sensitivity test at the first prenatal visit. Other providers may utilize a urinalysis and leukocyte esterase test initially, but as this approach is not as sensitive or specific, it must be followed by a urine culture and sensitivity testing if the urinalysis results are positive. Obstetricians and others providing prenatal care should utilize whatever approach works best for their patients and environment. Most importantly, screening for asymptomatic bacteriuria must occur early in the pregnancy.
Additional urine culture and sensitivity testing are advisable for patients who are at high risk for urinary tract infections, such as those who have had frequent UTIs before pregnancy and those who have anemia, sickle cell trait, a history of renal stones, diabetes mellitus, obesity, or neurologic disorders (such as neurogenic bladder and multiple sclerosis). Considering the increase in prevalence of obesity and diabetes, these high-risk patients represent a growing proportion of the obstetric population and appear to be at increased risk of UTIs as well. Women of increasing age and increasing parity also may be at higher risk of developing UTIs during pregnancy.
Cranberry juice has been touted for years as an effective remedy for the prevention and treatment of UTIs in women, and I advise my patients who have a UTI during pregnancy, who have diabetes, or who have other risk factors, to drink a glass of unsweetened cranberry juice each day. No definitive mechanism of action has been established, but it appears that cranberry juice prevents or interferes with the adherence of bacteria (particularly E. coli) to uroepithelial cells. It is important to emphasize to patients to consume unsweetened cranberry juice and not cranberry juice cocktail because of the high sugar content in the latter.
Recent research has emphasized that pregnancies of women who develop pyelonephritis are more likely to be complicated by spontaneous preterm birth, septicemia, and other adverse outcomes. In a retrospective cohort study of more than 546,000 singleton pregnancies delivered in all Kaiser Permanente of Southern California hospitals from 1993 to 2010, women with pyelonephritis were almost 57 times more likely than those without pyelonephritis to develop septicemia and 1.3 times more likely to have spontaneous preterm birth.
In addition, pregnancies of women with pyelonephritis were 2.6 times more likely than those of the baseline obstetric population to be complicated by anemia and 16.5 times more likely to be complicated by acute renal failure (Am. J. Obstet. Gynecol. 2014;210:219.e1-6). The overall incidence of acute antepartum pyelonephritis in this cohort study was relatively low compared with the incidence in other populations – 0.5% – which is not surprising given that patients in Kaiser’s integrated health care system routinely receive prenatal screening for asymptomatic bacteriuria.
Another retrospective population-based study comparing almost 220,000 singleton pregnancies of patients with and without acute pyelonephritis concluded that the infection is an independent risk factor for preterm delivery (Eur. J. Obstet. Gynecol. Reprod. Biol 2012;162:24-7).
After admission to the hospital, patients must be carefully monitored for uterine contractions and changes in vital signs and fetal heart rate. Several years ago, in an effort to empirically and synergistically target E. coli, the most common cause of UTIs and pyelonephritis, we began administering both an extended-spectrum cephalosporin (intravenous ceftriaxone) and an antimicrobial that will target gram-negative organisms, such as an aminoglycoside (gentamicin) or aztreonam.
We established this protocol because reviews of the outcomes at our institution indicated that intravenous ceftriaxone alone had not prevented some of our patients from developing septic shock in the first 8-20 hours post admission, despite the fact that culture and sensitivity results later indicated that the organism was E. coli and sensitive to the antimicrobial.
While we have not yet done any formal data analysis since changing our protocol, the combination parenteral antimicrobial regimen prescribed on admission appears to be effective in preventing the development of septic shock. We prescribe ceftriaxone 2 g intravenously once a day and gentamicin 5 mg/kg per day. Both drugs are continued until the patient improves clinically and has been afebrile for 48 hours.
At discharge, patients are prescribed a 10- to 14-day oral antimicrobial regimen dependent upon the culture and sensitivity report. Because at least 50% of E. coli are resistant to penicillin-like antimicrobials, the initial treatment no longer involves the use of ampicillin or amoxicillin. A repeat urine culture test at the end of treatment to confirm clearance of the infection is essential.
The possibility of anatomical obstructions in the urinary system should be investigated in pregnant patients who have multiple UTIs or who are unresponsive to appropriate antibiotic therapy for pyelonephritis. In this group we have performed ultrasound of the urinary tract system and have diagnosed renal stones as the risk factor for recurrent UTI. These patients are prescribed antimicrobial prophylaxis for the duration of the pregnancy. After delivery, they are referred to a urologist for follow-up care and treatment.
Dr. Apuzzio reported that he has no disclosures relevant to this Master Class.
Dr. Apuzzio is a professor in the department of obstetrics, gynecology, and women’s health, director of prenatal diagnosis and infectious diseases, professor of radiology, and director of maternal-fetal medicine at Rutgers New Jersey Medical School, Newark.
Positive surgical margins do not independently predict prostate cancer mortality
Positive surgical margins alone do not predict death from prostate cancer in men who undergo radical prostatectomy, investigators reported in the April issue of European Urology.
Positive surgical margins (PSMs) were not significantly associated with prostate cancer–specific mortality after adjustment for fixed covariates and postoperative radiotherapy, reported Dr. Andrew J. Stephenson, of the Cleveland Clinic’s Glickman Urological & Kidney Institute, and his associates.
Investigators analyzed data from 11,521 men with localized prostate cancer. Patients had undergone radical prostatectomy at four universities and cancer centers between 1987 and 2005.
At 15 years of follow-up, the prostate cancer–specific mortality for men with negative surgical margins was 6%, compared with 10% for men with PSMs (P less than .001).
But PSMs did not independently predict prostate cancer–specific mortality in regression models, the investigators reported (Eur. Urol. 2004;65:675-80).
That finding was true when researchers modeled only fixed covariates, such as age, Gleason score, seminal vesicle invasion, lymph node involvement, prostate-specific antigen (PSA), and extraprostatic extension (hazard ratio, 1.04; 95% confidence interval, 0.7-1.5), and also when they adjusted for postoperative radiotherapy, either as a single parameter (HR, 0.96; 95% CI, 0.7-1.4) or as early versus late treatment (HR, 1.01; 95% CI, 0.7-1.4).
The lack of an association called into question "the rationale for postoperative radiotherapy for PSMs in the absence of other adverse features," as well as "the relevance of PSM rates as a measure of surgical proficiency," the investigators said.
Even expert pathologists may not agree on PSMs and whether PSMs could be artifacts from surgery or pathologic processing, they noted. In addition, residual cancer from PSMs could lack biological characteristics needed for progression.
However, PSMs "should be avoided" because they worry patients and significantly increase the risks of biochemical recurrence and need for secondary treatment, Dr. Stephenson and associates said.
All patients in the study were treated at high-volume hospitals, and PSMs at low-volume hospitals could have a different prognosis. The study also lacked data on length and number of PSMs, the investigators noted.
Dr. Stephenson was partially supported by the Robert Wood Johnson Foundation Physician Faculty Scholars Program and the Astellas/American Urological Association Rising Stars in Urology Program. He reported no relevant financial conflicts of interest.
The "important and new aspect of this study," said Dr. Markus Graefen and Dr. Hartwig Huland, is that it accounted for postoperative radiotherapy. Previous studies modeled only fixed pathologic variables.
The data show that a positive surgical margin "is the product of a large cancer with a bad prognosis rather than an independent risk factor" for cancer-specific mortality, they said.
However, the study could not address whether or not to withhold early radiotherapy and wait for a PSA relapse to deliver early salvage radiotherapy. That answer requires results from the RADICALS (Radiotherapy and Androgen Deprivation in Combination after Local Surgery) study, which randomized patients to adjuvant radiotherapy or early salvage radiotherapy with and without additional hormonal therapy.
In the meantime, clinicians can help ease patients’ fears by explaining that positive surgical margins indicate the need for further treatment, but do not independently increase their risk of dying from prostate cancer.
Dr. Markus Graefen and Dr. Hartwig Huland are with the Martini-Klinik Prostate Cancer Center, University-Hospital Hamburg-Eppendorf, Germany. These remarks were taken from their editorial accompanying Dr. Stephenson’s report (Eur. Urol. 2014;65:681-2).
The "important and new aspect of this study," said Dr. Markus Graefen and Dr. Hartwig Huland, is that it accounted for postoperative radiotherapy. Previous studies modeled only fixed pathologic variables.
The data show that a positive surgical margin "is the product of a large cancer with a bad prognosis rather than an independent risk factor" for cancer-specific mortality, they said.
However, the study could not address whether or not to withhold early radiotherapy and wait for a PSA relapse to deliver early salvage radiotherapy. That answer requires results from the RADICALS (Radiotherapy and Androgen Deprivation in Combination after Local Surgery) study, which randomized patients to adjuvant radiotherapy or early salvage radiotherapy with and without additional hormonal therapy.
In the meantime, clinicians can help ease patients’ fears by explaining that positive surgical margins indicate the need for further treatment, but do not independently increase their risk of dying from prostate cancer.
Dr. Markus Graefen and Dr. Hartwig Huland are with the Martini-Klinik Prostate Cancer Center, University-Hospital Hamburg-Eppendorf, Germany. These remarks were taken from their editorial accompanying Dr. Stephenson’s report (Eur. Urol. 2014;65:681-2).
The "important and new aspect of this study," said Dr. Markus Graefen and Dr. Hartwig Huland, is that it accounted for postoperative radiotherapy. Previous studies modeled only fixed pathologic variables.
The data show that a positive surgical margin "is the product of a large cancer with a bad prognosis rather than an independent risk factor" for cancer-specific mortality, they said.
However, the study could not address whether or not to withhold early radiotherapy and wait for a PSA relapse to deliver early salvage radiotherapy. That answer requires results from the RADICALS (Radiotherapy and Androgen Deprivation in Combination after Local Surgery) study, which randomized patients to adjuvant radiotherapy or early salvage radiotherapy with and without additional hormonal therapy.
In the meantime, clinicians can help ease patients’ fears by explaining that positive surgical margins indicate the need for further treatment, but do not independently increase their risk of dying from prostate cancer.
Dr. Markus Graefen and Dr. Hartwig Huland are with the Martini-Klinik Prostate Cancer Center, University-Hospital Hamburg-Eppendorf, Germany. These remarks were taken from their editorial accompanying Dr. Stephenson’s report (Eur. Urol. 2014;65:681-2).
Positive surgical margins alone do not predict death from prostate cancer in men who undergo radical prostatectomy, investigators reported in the April issue of European Urology.
Positive surgical margins (PSMs) were not significantly associated with prostate cancer–specific mortality after adjustment for fixed covariates and postoperative radiotherapy, reported Dr. Andrew J. Stephenson, of the Cleveland Clinic’s Glickman Urological & Kidney Institute, and his associates.
Investigators analyzed data from 11,521 men with localized prostate cancer. Patients had undergone radical prostatectomy at four universities and cancer centers between 1987 and 2005.
At 15 years of follow-up, the prostate cancer–specific mortality for men with negative surgical margins was 6%, compared with 10% for men with PSMs (P less than .001).
But PSMs did not independently predict prostate cancer–specific mortality in regression models, the investigators reported (Eur. Urol. 2004;65:675-80).
That finding was true when researchers modeled only fixed covariates, such as age, Gleason score, seminal vesicle invasion, lymph node involvement, prostate-specific antigen (PSA), and extraprostatic extension (hazard ratio, 1.04; 95% confidence interval, 0.7-1.5), and also when they adjusted for postoperative radiotherapy, either as a single parameter (HR, 0.96; 95% CI, 0.7-1.4) or as early versus late treatment (HR, 1.01; 95% CI, 0.7-1.4).
The lack of an association called into question "the rationale for postoperative radiotherapy for PSMs in the absence of other adverse features," as well as "the relevance of PSM rates as a measure of surgical proficiency," the investigators said.
Even expert pathologists may not agree on PSMs and whether PSMs could be artifacts from surgery or pathologic processing, they noted. In addition, residual cancer from PSMs could lack biological characteristics needed for progression.
However, PSMs "should be avoided" because they worry patients and significantly increase the risks of biochemical recurrence and need for secondary treatment, Dr. Stephenson and associates said.
All patients in the study were treated at high-volume hospitals, and PSMs at low-volume hospitals could have a different prognosis. The study also lacked data on length and number of PSMs, the investigators noted.
Dr. Stephenson was partially supported by the Robert Wood Johnson Foundation Physician Faculty Scholars Program and the Astellas/American Urological Association Rising Stars in Urology Program. He reported no relevant financial conflicts of interest.
Positive surgical margins alone do not predict death from prostate cancer in men who undergo radical prostatectomy, investigators reported in the April issue of European Urology.
Positive surgical margins (PSMs) were not significantly associated with prostate cancer–specific mortality after adjustment for fixed covariates and postoperative radiotherapy, reported Dr. Andrew J. Stephenson, of the Cleveland Clinic’s Glickman Urological & Kidney Institute, and his associates.
Investigators analyzed data from 11,521 men with localized prostate cancer. Patients had undergone radical prostatectomy at four universities and cancer centers between 1987 and 2005.
At 15 years of follow-up, the prostate cancer–specific mortality for men with negative surgical margins was 6%, compared with 10% for men with PSMs (P less than .001).
But PSMs did not independently predict prostate cancer–specific mortality in regression models, the investigators reported (Eur. Urol. 2004;65:675-80).
That finding was true when researchers modeled only fixed covariates, such as age, Gleason score, seminal vesicle invasion, lymph node involvement, prostate-specific antigen (PSA), and extraprostatic extension (hazard ratio, 1.04; 95% confidence interval, 0.7-1.5), and also when they adjusted for postoperative radiotherapy, either as a single parameter (HR, 0.96; 95% CI, 0.7-1.4) or as early versus late treatment (HR, 1.01; 95% CI, 0.7-1.4).
The lack of an association called into question "the rationale for postoperative radiotherapy for PSMs in the absence of other adverse features," as well as "the relevance of PSM rates as a measure of surgical proficiency," the investigators said.
Even expert pathologists may not agree on PSMs and whether PSMs could be artifacts from surgery or pathologic processing, they noted. In addition, residual cancer from PSMs could lack biological characteristics needed for progression.
However, PSMs "should be avoided" because they worry patients and significantly increase the risks of biochemical recurrence and need for secondary treatment, Dr. Stephenson and associates said.
All patients in the study were treated at high-volume hospitals, and PSMs at low-volume hospitals could have a different prognosis. The study also lacked data on length and number of PSMs, the investigators noted.
Dr. Stephenson was partially supported by the Robert Wood Johnson Foundation Physician Faculty Scholars Program and the Astellas/American Urological Association Rising Stars in Urology Program. He reported no relevant financial conflicts of interest.
FROM EUROPEAN UROLOGY
Major finding: Positive surgical margins were not significantly associated with prostate cancer–specific mortality within 15 years of radical prostatectomy after adjustment for fixed covariates and postoperative radiotherapy.
Data source: Multicenter cohort study of 11,521 men with localized prostate cancer who underwent radical prostatectomy between 1987 and 2005.
Disclosures: Dr. Stephenson was partially supported by the Robert Wood Johnson Foundation Physician Faculty Scholars Program and the Astellas/American Urological Association Rising Stars in Urology Program. Dr. Stephenson, Dr. Graefen, and Dr. Huland reported no relevant financial conflicts of interest.
Adherence Issues With Overactive Bladder Treatment
More than 50% of patients taking an anticholinergic drug for symptoms of overactive bladder (OAB) stop taking their medicine—and at least half of those stop within the first 6 months. Two-thirds of patients never start again. That’s according to a study by researchers from Beaumont Hospital in Royal Oak, Michigan; Xcenda, LLC in Palm Harbor, Florida; and Allergan, Inc. in Irvine, California, who analyzed medical, pharmacy, and other data from the IMS LifeLink Health Plan Claims Database of 103,250 patients with OAB.
Anticholinergic drugs included oxybutynin, tolterodine, trospium, fesoterodine, and solifenacin, but 42% of patients received tolterodine extended release (ER) as their index prescription. To be considered a discontinuation, the patient had to have a gap of at least 45 days in therapy, based on fill dates and days’ supply. The corresponding time to treatment failure (TTF) was estimated as the number of days between the index date and the date of the first medication switch or estimated discontinuation date. Treatment reinitiation was defined as the documentation of a filled prescription for any anticholinergic agent after a discontinuation period of at least 45 days. The researchers in this study used claims data to avoid the problem of self-reported adherence, since patients often overstate their adherence to medications.
Initial treatment with the index drug failed in nearly all (92%) patients. Of those, only 6% were associated with switching drugs. More than half had permanently stopped all anticholinergic drugs at 24 months. Moreover, 33% of patients filled only 1 prescription, suggesting early failure (within the first 30 days).
The proportion of treatment failures was high across all primary diagnoses, ranging from 89% to 97%. Failure was also high regardless of the therapy. For instance, 90% of 43,902 patients on tolterodine ER and 96% of 2,246 patients on oxybutynin transdermal did not meet treatment goals. The researchers then took those numbers and pooled outcomes across all drugs to estimate the overall impact of anticholinergic treatment for patients with OAB and found that the mean TTF was 159 days.
Many patients (81%) who switched treatment during the 24-month study period also had no luck with the second drug. Treatment also failed for 29% who tried a third drug. Treatment failure didn’t always stop them from trying, though: About one-third started treatment again after a gap of at least 45 days, and about one-fifth restarted after 1 year.
Empirical studies of medications to treat chronic conditions have found persistence to OAB medications to be very low, the researchers say. When compared with oral antidiabetic drugs, angiotensin receptor blockers, statins, bisphosphonates, and prostaglandins, OAB medications had the lowest persistence rates at 6 months: 32% compared with 72% for oral antidiabetes drugs.
In research of patients with OAB, achievement of treatment goals is a strong predictor of treatment satisfaction, and dissatisfaction with treatment outcomes is the most common reason for patients stopping their treatment. Poor adherence to OAB drugs can have a negative impact on quality of life and increase the risk of medical sequelae, such as urinary tract infections. Thus, when anticholinergics fail, the researchers say, it’s important to give patients options, such as botulinum toxin A, sacral neuromodulation, and percutaneous tibial nerve stimulation.
Despite the “potential for better adherence” with some anticholinergic drugs, their findings suggest that the benefits of anticholinergic use in OAB are not being realized, and many patients may end up without any drug therapy at all.
Source
Chancellor MB, Migliaccio-Walle K, Bramley TJ, Chaudhari SL, Corbell C, Globe D. Clin Ther. 2013;35(11):1744-1751.
doi: 10.1016/j.clinthera.2013.08.017.
More than 50% of patients taking an anticholinergic drug for symptoms of overactive bladder (OAB) stop taking their medicine—and at least half of those stop within the first 6 months. Two-thirds of patients never start again. That’s according to a study by researchers from Beaumont Hospital in Royal Oak, Michigan; Xcenda, LLC in Palm Harbor, Florida; and Allergan, Inc. in Irvine, California, who analyzed medical, pharmacy, and other data from the IMS LifeLink Health Plan Claims Database of 103,250 patients with OAB.
Anticholinergic drugs included oxybutynin, tolterodine, trospium, fesoterodine, and solifenacin, but 42% of patients received tolterodine extended release (ER) as their index prescription. To be considered a discontinuation, the patient had to have a gap of at least 45 days in therapy, based on fill dates and days’ supply. The corresponding time to treatment failure (TTF) was estimated as the number of days between the index date and the date of the first medication switch or estimated discontinuation date. Treatment reinitiation was defined as the documentation of a filled prescription for any anticholinergic agent after a discontinuation period of at least 45 days. The researchers in this study used claims data to avoid the problem of self-reported adherence, since patients often overstate their adherence to medications.
Initial treatment with the index drug failed in nearly all (92%) patients. Of those, only 6% were associated with switching drugs. More than half had permanently stopped all anticholinergic drugs at 24 months. Moreover, 33% of patients filled only 1 prescription, suggesting early failure (within the first 30 days).
The proportion of treatment failures was high across all primary diagnoses, ranging from 89% to 97%. Failure was also high regardless of the therapy. For instance, 90% of 43,902 patients on tolterodine ER and 96% of 2,246 patients on oxybutynin transdermal did not meet treatment goals. The researchers then took those numbers and pooled outcomes across all drugs to estimate the overall impact of anticholinergic treatment for patients with OAB and found that the mean TTF was 159 days.
Many patients (81%) who switched treatment during the 24-month study period also had no luck with the second drug. Treatment also failed for 29% who tried a third drug. Treatment failure didn’t always stop them from trying, though: About one-third started treatment again after a gap of at least 45 days, and about one-fifth restarted after 1 year.
Empirical studies of medications to treat chronic conditions have found persistence to OAB medications to be very low, the researchers say. When compared with oral antidiabetic drugs, angiotensin receptor blockers, statins, bisphosphonates, and prostaglandins, OAB medications had the lowest persistence rates at 6 months: 32% compared with 72% for oral antidiabetes drugs.
In research of patients with OAB, achievement of treatment goals is a strong predictor of treatment satisfaction, and dissatisfaction with treatment outcomes is the most common reason for patients stopping their treatment. Poor adherence to OAB drugs can have a negative impact on quality of life and increase the risk of medical sequelae, such as urinary tract infections. Thus, when anticholinergics fail, the researchers say, it’s important to give patients options, such as botulinum toxin A, sacral neuromodulation, and percutaneous tibial nerve stimulation.
Despite the “potential for better adherence” with some anticholinergic drugs, their findings suggest that the benefits of anticholinergic use in OAB are not being realized, and many patients may end up without any drug therapy at all.
Source
Chancellor MB, Migliaccio-Walle K, Bramley TJ, Chaudhari SL, Corbell C, Globe D. Clin Ther. 2013;35(11):1744-1751.
doi: 10.1016/j.clinthera.2013.08.017.
More than 50% of patients taking an anticholinergic drug for symptoms of overactive bladder (OAB) stop taking their medicine—and at least half of those stop within the first 6 months. Two-thirds of patients never start again. That’s according to a study by researchers from Beaumont Hospital in Royal Oak, Michigan; Xcenda, LLC in Palm Harbor, Florida; and Allergan, Inc. in Irvine, California, who analyzed medical, pharmacy, and other data from the IMS LifeLink Health Plan Claims Database of 103,250 patients with OAB.
Anticholinergic drugs included oxybutynin, tolterodine, trospium, fesoterodine, and solifenacin, but 42% of patients received tolterodine extended release (ER) as their index prescription. To be considered a discontinuation, the patient had to have a gap of at least 45 days in therapy, based on fill dates and days’ supply. The corresponding time to treatment failure (TTF) was estimated as the number of days between the index date and the date of the first medication switch or estimated discontinuation date. Treatment reinitiation was defined as the documentation of a filled prescription for any anticholinergic agent after a discontinuation period of at least 45 days. The researchers in this study used claims data to avoid the problem of self-reported adherence, since patients often overstate their adherence to medications.
Initial treatment with the index drug failed in nearly all (92%) patients. Of those, only 6% were associated with switching drugs. More than half had permanently stopped all anticholinergic drugs at 24 months. Moreover, 33% of patients filled only 1 prescription, suggesting early failure (within the first 30 days).
The proportion of treatment failures was high across all primary diagnoses, ranging from 89% to 97%. Failure was also high regardless of the therapy. For instance, 90% of 43,902 patients on tolterodine ER and 96% of 2,246 patients on oxybutynin transdermal did not meet treatment goals. The researchers then took those numbers and pooled outcomes across all drugs to estimate the overall impact of anticholinergic treatment for patients with OAB and found that the mean TTF was 159 days.
Many patients (81%) who switched treatment during the 24-month study period also had no luck with the second drug. Treatment also failed for 29% who tried a third drug. Treatment failure didn’t always stop them from trying, though: About one-third started treatment again after a gap of at least 45 days, and about one-fifth restarted after 1 year.
Empirical studies of medications to treat chronic conditions have found persistence to OAB medications to be very low, the researchers say. When compared with oral antidiabetic drugs, angiotensin receptor blockers, statins, bisphosphonates, and prostaglandins, OAB medications had the lowest persistence rates at 6 months: 32% compared with 72% for oral antidiabetes drugs.
In research of patients with OAB, achievement of treatment goals is a strong predictor of treatment satisfaction, and dissatisfaction with treatment outcomes is the most common reason for patients stopping their treatment. Poor adherence to OAB drugs can have a negative impact on quality of life and increase the risk of medical sequelae, such as urinary tract infections. Thus, when anticholinergics fail, the researchers say, it’s important to give patients options, such as botulinum toxin A, sacral neuromodulation, and percutaneous tibial nerve stimulation.
Despite the “potential for better adherence” with some anticholinergic drugs, their findings suggest that the benefits of anticholinergic use in OAB are not being realized, and many patients may end up without any drug therapy at all.
Source
Chancellor MB, Migliaccio-Walle K, Bramley TJ, Chaudhari SL, Corbell C, Globe D. Clin Ther. 2013;35(11):1744-1751.
doi: 10.1016/j.clinthera.2013.08.017.
Maintenance percutaneous tibial nerve stimulation improved bladder symptoms in MS
Maintenance percutaneous tibial nerve stimulation in patients with multiple sclerosis led to sustained improvements in medically refractory lower urinary tract symptoms in a prospective, multicenter open-label trial.
All initial responders continued to respond after an average of 2 years of maintenance therapy, reported Dr. Claudio Gobbi of the Neurocentre of Southern Switzerland, Lugano, and his associates.
The prospective, multicenter open-label study recruited patients with multiple sclerosis who had lower urinary tract symptoms that had not responded to medical therapy. Symptom criteria included overactive bladder, incomplete voiding, hesitancy, poor or slow flow, prolonged and interrupted flow, and straining to void (J. Urol. 2014;191:697-702).
A total of 83 patients (mean age, 49 years; 62 women) completed 12 initial weekly sessions of percutaneous tibial nerve stimulation (PTNS). In all, 74 (89%) reported at least 50% improvement in lower urinary tract symptoms on the Patient Perception of Bladder Condition questionnaire.
These responders then underwent 30-minute PTNS maintenance sessions every 2, 3, or 4 weeks as needed. Most patients (60%) required treatment every 2 weeks, the researchers said.
After the 12 weekly PTNS treatments, most responders reported their bladder symptoms as moderately improved (based on a global response assessment), and mean treatment satisfaction was 70% (based on a visual analog scale). At 24 months’ follow-up, most patients described their symptoms as markedly improved, and mean treatment satisfaction was 82% (P less than .05).
The investigators also reported significant improvements over a 24-month period in measures of voiding and bladder diary parameters (including frequency of daytime urination, nocturia, and voided volume). Patients reported no relevant adverse effects of treatment.
Dr. Gobbi and his associates noted several caveats to their findings. The study probably lacked sufficient power to detect differences between subgroups, they said. The investigators also did not collect data on drinking habits or lifestyle modifications, each of which could have independently affected treatment outcomes. And the study included only patients who responded to and completed the initial treatment, which created a selection bias for patients willing to adhere to maintenance PTNS.
"Although the efficacy of PTNS was sustained for 2 years, the progressive neurologic course of MS with deteriorating bladder function may affect longer positive treatment outcomes," they added.
One author disclosed having financial interests or other relationships with Medtronic, Allergan, and Astellas. Dr. Gobbi and his other coauthors reported no conflicts of interest.
The most encouraging findings of this study were the clear improvements in voiding and voiding efficiency as well as overactive bladder symptoms, according to Dr. Gary E. Lemack.
He called the minimally invasive approach based on a nonimplantable technique "a welcome tool in our armamentarium" because it could benefit patients with multiple medical problems who need a repeat MRI.
Neuromodulation approaches have naturally evolved during the past 2 decades, said Dr. Lemack, citing recent reports that pudendal nerve stimulation, perianal stimulation, and sacral neuromodulation all directly affect overactive bladder contractions.
As new peripheral transcutaneous treatments for lower urinary tract symptoms emerge, we can expect an expansion of less-invasive neuromodulatory treatments that can be applied or maintained at home, he said.
These techniques will also be used in a wider range of patients, he added, including patients with neurogenic bladder symptoms who often suffer most from symptoms of overactive bladder.
Dr. Lemack is a urologist with the University of Texas Southwestern Medical Center at Dallas. He reported that he has financial interests or other relationships with Afferent Pharmaceuticals, Ferring, Merck, Pfizer, Astellas, and Allergan. These remarks were taken from his editorial accompanying Dr. Gobbi’s report (J. Urol. 2014;191:582-3).
The most encouraging findings of this study were the clear improvements in voiding and voiding efficiency as well as overactive bladder symptoms, according to Dr. Gary E. Lemack.
He called the minimally invasive approach based on a nonimplantable technique "a welcome tool in our armamentarium" because it could benefit patients with multiple medical problems who need a repeat MRI.
Neuromodulation approaches have naturally evolved during the past 2 decades, said Dr. Lemack, citing recent reports that pudendal nerve stimulation, perianal stimulation, and sacral neuromodulation all directly affect overactive bladder contractions.
As new peripheral transcutaneous treatments for lower urinary tract symptoms emerge, we can expect an expansion of less-invasive neuromodulatory treatments that can be applied or maintained at home, he said.
These techniques will also be used in a wider range of patients, he added, including patients with neurogenic bladder symptoms who often suffer most from symptoms of overactive bladder.
Dr. Lemack is a urologist with the University of Texas Southwestern Medical Center at Dallas. He reported that he has financial interests or other relationships with Afferent Pharmaceuticals, Ferring, Merck, Pfizer, Astellas, and Allergan. These remarks were taken from his editorial accompanying Dr. Gobbi’s report (J. Urol. 2014;191:582-3).
The most encouraging findings of this study were the clear improvements in voiding and voiding efficiency as well as overactive bladder symptoms, according to Dr. Gary E. Lemack.
He called the minimally invasive approach based on a nonimplantable technique "a welcome tool in our armamentarium" because it could benefit patients with multiple medical problems who need a repeat MRI.
Neuromodulation approaches have naturally evolved during the past 2 decades, said Dr. Lemack, citing recent reports that pudendal nerve stimulation, perianal stimulation, and sacral neuromodulation all directly affect overactive bladder contractions.
As new peripheral transcutaneous treatments for lower urinary tract symptoms emerge, we can expect an expansion of less-invasive neuromodulatory treatments that can be applied or maintained at home, he said.
These techniques will also be used in a wider range of patients, he added, including patients with neurogenic bladder symptoms who often suffer most from symptoms of overactive bladder.
Dr. Lemack is a urologist with the University of Texas Southwestern Medical Center at Dallas. He reported that he has financial interests or other relationships with Afferent Pharmaceuticals, Ferring, Merck, Pfizer, Astellas, and Allergan. These remarks were taken from his editorial accompanying Dr. Gobbi’s report (J. Urol. 2014;191:582-3).
Maintenance percutaneous tibial nerve stimulation in patients with multiple sclerosis led to sustained improvements in medically refractory lower urinary tract symptoms in a prospective, multicenter open-label trial.
All initial responders continued to respond after an average of 2 years of maintenance therapy, reported Dr. Claudio Gobbi of the Neurocentre of Southern Switzerland, Lugano, and his associates.
The prospective, multicenter open-label study recruited patients with multiple sclerosis who had lower urinary tract symptoms that had not responded to medical therapy. Symptom criteria included overactive bladder, incomplete voiding, hesitancy, poor or slow flow, prolonged and interrupted flow, and straining to void (J. Urol. 2014;191:697-702).
A total of 83 patients (mean age, 49 years; 62 women) completed 12 initial weekly sessions of percutaneous tibial nerve stimulation (PTNS). In all, 74 (89%) reported at least 50% improvement in lower urinary tract symptoms on the Patient Perception of Bladder Condition questionnaire.
These responders then underwent 30-minute PTNS maintenance sessions every 2, 3, or 4 weeks as needed. Most patients (60%) required treatment every 2 weeks, the researchers said.
After the 12 weekly PTNS treatments, most responders reported their bladder symptoms as moderately improved (based on a global response assessment), and mean treatment satisfaction was 70% (based on a visual analog scale). At 24 months’ follow-up, most patients described their symptoms as markedly improved, and mean treatment satisfaction was 82% (P less than .05).
The investigators also reported significant improvements over a 24-month period in measures of voiding and bladder diary parameters (including frequency of daytime urination, nocturia, and voided volume). Patients reported no relevant adverse effects of treatment.
Dr. Gobbi and his associates noted several caveats to their findings. The study probably lacked sufficient power to detect differences between subgroups, they said. The investigators also did not collect data on drinking habits or lifestyle modifications, each of which could have independently affected treatment outcomes. And the study included only patients who responded to and completed the initial treatment, which created a selection bias for patients willing to adhere to maintenance PTNS.
"Although the efficacy of PTNS was sustained for 2 years, the progressive neurologic course of MS with deteriorating bladder function may affect longer positive treatment outcomes," they added.
One author disclosed having financial interests or other relationships with Medtronic, Allergan, and Astellas. Dr. Gobbi and his other coauthors reported no conflicts of interest.
Maintenance percutaneous tibial nerve stimulation in patients with multiple sclerosis led to sustained improvements in medically refractory lower urinary tract symptoms in a prospective, multicenter open-label trial.
All initial responders continued to respond after an average of 2 years of maintenance therapy, reported Dr. Claudio Gobbi of the Neurocentre of Southern Switzerland, Lugano, and his associates.
The prospective, multicenter open-label study recruited patients with multiple sclerosis who had lower urinary tract symptoms that had not responded to medical therapy. Symptom criteria included overactive bladder, incomplete voiding, hesitancy, poor or slow flow, prolonged and interrupted flow, and straining to void (J. Urol. 2014;191:697-702).
A total of 83 patients (mean age, 49 years; 62 women) completed 12 initial weekly sessions of percutaneous tibial nerve stimulation (PTNS). In all, 74 (89%) reported at least 50% improvement in lower urinary tract symptoms on the Patient Perception of Bladder Condition questionnaire.
These responders then underwent 30-minute PTNS maintenance sessions every 2, 3, or 4 weeks as needed. Most patients (60%) required treatment every 2 weeks, the researchers said.
After the 12 weekly PTNS treatments, most responders reported their bladder symptoms as moderately improved (based on a global response assessment), and mean treatment satisfaction was 70% (based on a visual analog scale). At 24 months’ follow-up, most patients described their symptoms as markedly improved, and mean treatment satisfaction was 82% (P less than .05).
The investigators also reported significant improvements over a 24-month period in measures of voiding and bladder diary parameters (including frequency of daytime urination, nocturia, and voided volume). Patients reported no relevant adverse effects of treatment.
Dr. Gobbi and his associates noted several caveats to their findings. The study probably lacked sufficient power to detect differences between subgroups, they said. The investigators also did not collect data on drinking habits or lifestyle modifications, each of which could have independently affected treatment outcomes. And the study included only patients who responded to and completed the initial treatment, which created a selection bias for patients willing to adhere to maintenance PTNS.
"Although the efficacy of PTNS was sustained for 2 years, the progressive neurologic course of MS with deteriorating bladder function may affect longer positive treatment outcomes," they added.
One author disclosed having financial interests or other relationships with Medtronic, Allergan, and Astellas. Dr. Gobbi and his other coauthors reported no conflicts of interest.
FROM THE JOURNAL OF UROLOGY
Major finding: 74 of 83 patients (89%) reported at least 50% improvement after 12 weekly sessions of percutaneous tibial nerve stimulation. All initial responders had sustained benefits from maintenance therapy at 24 months’ follow-up.
Data source: A prospective, open-label multicenter trial of 83 patients with multiple sclerosis and medically refractory lower urinary tract symptoms.
Disclosures: One author disclosed having financial interests or other relationships with Medtronic, Allergan, and Astellas. Dr. Gobbi and his other coauthors reported no conflicts of interest.
Bladder incontinence up 43% in elderly since 1992
The prevalence of bladder incontinence rose from 21.1% in 1992 to 30.2% in 2010 for Medicare beneficiaries aged 65 years and older – an increase of 43%, according to data from the Medicare Current Beneficiary Survey.
Among white non-Hispanic patients, prevalence of bladder incontinence rose by 48% – going from 20.7% in 1992 to 30.6% in 2010. Prevalence in Hispanics rose from 22.7% in 1992 to 28.5% in 2010, for an increase of almost 26%. Black non-Hispanics saw their prevalence of bladder incontinence rise from 23.2% in 1992 to 27.7% in 2010 – an increase of more than 19%.
In the overall Medicare population for the same time period, bladder incontinence was reported almost twice as often among women – going from 25.8% in 1992 to 38.3% in 2010 – as in men – 13.4% in 1992 and 19.5% in 2010, according to MCBS data on the CDC Health Data Interactive.
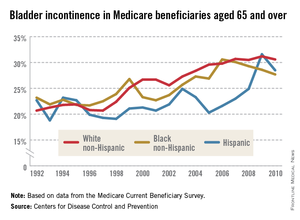
The prevalence of bladder incontinence rose from 21.1% in 1992 to 30.2% in 2010 for Medicare beneficiaries aged 65 years and older – an increase of 43%, according to data from the Medicare Current Beneficiary Survey.
Among white non-Hispanic patients, prevalence of bladder incontinence rose by 48% – going from 20.7% in 1992 to 30.6% in 2010. Prevalence in Hispanics rose from 22.7% in 1992 to 28.5% in 2010, for an increase of almost 26%. Black non-Hispanics saw their prevalence of bladder incontinence rise from 23.2% in 1992 to 27.7% in 2010 – an increase of more than 19%.
In the overall Medicare population for the same time period, bladder incontinence was reported almost twice as often among women – going from 25.8% in 1992 to 38.3% in 2010 – as in men – 13.4% in 1992 and 19.5% in 2010, according to MCBS data on the CDC Health Data Interactive.
The prevalence of bladder incontinence rose from 21.1% in 1992 to 30.2% in 2010 for Medicare beneficiaries aged 65 years and older – an increase of 43%, according to data from the Medicare Current Beneficiary Survey.
Among white non-Hispanic patients, prevalence of bladder incontinence rose by 48% – going from 20.7% in 1992 to 30.6% in 2010. Prevalence in Hispanics rose from 22.7% in 1992 to 28.5% in 2010, for an increase of almost 26%. Black non-Hispanics saw their prevalence of bladder incontinence rise from 23.2% in 1992 to 27.7% in 2010 – an increase of more than 19%.
In the overall Medicare population for the same time period, bladder incontinence was reported almost twice as often among women – going from 25.8% in 1992 to 38.3% in 2010 – as in men – 13.4% in 1992 and 19.5% in 2010, according to MCBS data on the CDC Health Data Interactive.
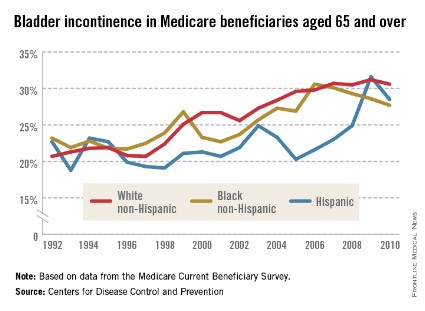
Acute kidney dysfunction related to nonviral comorbidities in chronic HCV
Among patients with chronic hepatitis C virus infection, viral factors such as viral load and HCV genotype "did not play any significant role in the causation of acute kidney dysfunction events" but known nonviral risk factors did, according to a report published online in the Journal of Clinical and Experimental Hepatology.
In a retrospective cohort study involving 468 patients with chronic HCV (mean age, 50 years) enrolled during a 1-year period at a single hepatology clinic and followed for 3 months to 6 years*, 124 episodes of acute kidney dysfunction developed in 63 patients.
Such dysfunction was significantly more likely to develop in those who had comorbid diabetes (47.6% prevalence, compared with 16.5% prevalence in nondiabetic participants), hypertension (69.8% prevalence, compared with 38.8% prevalence in nonhypertensive participants), or a history of IV drug use (44.4% prevalence, compared with 29.4% prevalence in nonusers), said Dr. Sanjaya Kumar Satapathy, who was with the division of gastroenterology at New York Medical College during the study, and his associates.
"Acute volume depletion secondary to nausea, vomiting, diarrhea, and large-volume paracentesis accounted for the major bulk of patients with acute kidney dysfunction. ... In addition, infections (n = 23) and GI bleeding (n = 9), the majority of which occurred in patients with advanced liver disease, appeared to play a significant role in developing acute kidney dysfunction," the investigators wrote (J. Clin. Exp. Hepatol. 2014 [doi:10.1016/j.jceh.2014.01.004]).
In contrast, the prevalence of acute kidney dysfunction showed no relation to baseline viral load; viral genotype; or the patient’s sex, race, body mass index, HIV status, or history regarding alcohol abuse. A total of 68 of the 124 acute kidney dysfunction events (54.8%) resolved completely, with serum creatinine returning to baseline levels; there was partial recovery in another 34.7% of the events, and the remaining 10.5% of cases progressed to either chronic kidney disease or end-stage renal disease.
Although acute kidney dysfunction is a well-known complication of cirrhosis and liver failure, most cases in this study (76%) developed in patients who did not have decompensated or advanced liver disease, noted Dr. Satapathy, who is now with the University of Tennessee, Memphis, and his associates.
No funding sources or potential conflicts of interest were disclosed.
*Correction, 4/1/2014: An earlier version of the article misstated the length of time patients were monitored.
Among patients with chronic hepatitis C virus infection, viral factors such as viral load and HCV genotype "did not play any significant role in the causation of acute kidney dysfunction events" but known nonviral risk factors did, according to a report published online in the Journal of Clinical and Experimental Hepatology.
In a retrospective cohort study involving 468 patients with chronic HCV (mean age, 50 years) enrolled during a 1-year period at a single hepatology clinic and followed for 3 months to 6 years*, 124 episodes of acute kidney dysfunction developed in 63 patients.
Such dysfunction was significantly more likely to develop in those who had comorbid diabetes (47.6% prevalence, compared with 16.5% prevalence in nondiabetic participants), hypertension (69.8% prevalence, compared with 38.8% prevalence in nonhypertensive participants), or a history of IV drug use (44.4% prevalence, compared with 29.4% prevalence in nonusers), said Dr. Sanjaya Kumar Satapathy, who was with the division of gastroenterology at New York Medical College during the study, and his associates.
"Acute volume depletion secondary to nausea, vomiting, diarrhea, and large-volume paracentesis accounted for the major bulk of patients with acute kidney dysfunction. ... In addition, infections (n = 23) and GI bleeding (n = 9), the majority of which occurred in patients with advanced liver disease, appeared to play a significant role in developing acute kidney dysfunction," the investigators wrote (J. Clin. Exp. Hepatol. 2014 [doi:10.1016/j.jceh.2014.01.004]).
In contrast, the prevalence of acute kidney dysfunction showed no relation to baseline viral load; viral genotype; or the patient’s sex, race, body mass index, HIV status, or history regarding alcohol abuse. A total of 68 of the 124 acute kidney dysfunction events (54.8%) resolved completely, with serum creatinine returning to baseline levels; there was partial recovery in another 34.7% of the events, and the remaining 10.5% of cases progressed to either chronic kidney disease or end-stage renal disease.
Although acute kidney dysfunction is a well-known complication of cirrhosis and liver failure, most cases in this study (76%) developed in patients who did not have decompensated or advanced liver disease, noted Dr. Satapathy, who is now with the University of Tennessee, Memphis, and his associates.
No funding sources or potential conflicts of interest were disclosed.
*Correction, 4/1/2014: An earlier version of the article misstated the length of time patients were monitored.
Among patients with chronic hepatitis C virus infection, viral factors such as viral load and HCV genotype "did not play any significant role in the causation of acute kidney dysfunction events" but known nonviral risk factors did, according to a report published online in the Journal of Clinical and Experimental Hepatology.
In a retrospective cohort study involving 468 patients with chronic HCV (mean age, 50 years) enrolled during a 1-year period at a single hepatology clinic and followed for 3 months to 6 years*, 124 episodes of acute kidney dysfunction developed in 63 patients.
Such dysfunction was significantly more likely to develop in those who had comorbid diabetes (47.6% prevalence, compared with 16.5% prevalence in nondiabetic participants), hypertension (69.8% prevalence, compared with 38.8% prevalence in nonhypertensive participants), or a history of IV drug use (44.4% prevalence, compared with 29.4% prevalence in nonusers), said Dr. Sanjaya Kumar Satapathy, who was with the division of gastroenterology at New York Medical College during the study, and his associates.
"Acute volume depletion secondary to nausea, vomiting, diarrhea, and large-volume paracentesis accounted for the major bulk of patients with acute kidney dysfunction. ... In addition, infections (n = 23) and GI bleeding (n = 9), the majority of which occurred in patients with advanced liver disease, appeared to play a significant role in developing acute kidney dysfunction," the investigators wrote (J. Clin. Exp. Hepatol. 2014 [doi:10.1016/j.jceh.2014.01.004]).
In contrast, the prevalence of acute kidney dysfunction showed no relation to baseline viral load; viral genotype; or the patient’s sex, race, body mass index, HIV status, or history regarding alcohol abuse. A total of 68 of the 124 acute kidney dysfunction events (54.8%) resolved completely, with serum creatinine returning to baseline levels; there was partial recovery in another 34.7% of the events, and the remaining 10.5% of cases progressed to either chronic kidney disease or end-stage renal disease.
Although acute kidney dysfunction is a well-known complication of cirrhosis and liver failure, most cases in this study (76%) developed in patients who did not have decompensated or advanced liver disease, noted Dr. Satapathy, who is now with the University of Tennessee, Memphis, and his associates.
No funding sources or potential conflicts of interest were disclosed.
*Correction, 4/1/2014: An earlier version of the article misstated the length of time patients were monitored.
FROM THE JOURNAL OF CLINICAL AND EXPERIMENTAL HEPATOLOGY
Major finding: Acute kidney dysfunction was significantly more likely to develop in HCV patients who had comorbid diabetes (47.6% prevalence, compared with 16.5% prevalence in nondiabetic participants), hypertension (69.8% prevalence, compared with 38.8% prevalence in nonhypertensive participants), or a history of IV drug use (44.4% prevalence, compared with 29.4% prevalence in nonusers).
Data source: A retrospective cohort study involving 468 patients with chronic HCV, of whom 63 developed 124 episodes of acute kidney dysfunction during follow-up of 3 months to 6 years.
Disclosures: No funding sources or potential conflicts of interest were disclosed.
FDA issues warning about using doripenem for ventilator-associated pneumonia
When used to treat ventilator-associated pneumonia, the antibacterial drug doripenem is linked to a greater risk of mortality and lower clinical cure rates compared with imipenem and cilastatin for injection, according to a drug safety communication issued by the Food and Drug Administration.
Doripenem, an intravenous penem antibacterial drug marketed as Doribax, is not approved to treat any type of pneumonia. A warning about increased mortality in patients with ventilator-associated pneumonia (VAP), for which the use of doripenem is unapproved, has been added to the drug’s label. In a statement posted on March 6, the FDA recommended that health care professionals "consider whether the benefits of Doribax treatment are likely to exceed its potential risks in patients who develop pneumonia while on ventilators."
The safety communication is based on an FDA analysis of a 3-year study comparing 7 days of treatment with doripenem to 10 days of treatment with imipenem and cilastatin in patients with VAP. All-cause mortality over 28 days was 23% among those treated with doripenem, compared with 16.7% among those treated with imipenem and cilastatin. Clinical cure rates also were lower in the doripenem-treated patients in the study, which was stopped prematurely in 2011.
The statement adds that doripenem, approved in 2007, "is still considered safe and effective" for treating adults with complicated intra-abdominal infections and complicated urinary tract infections, including pyelonephritis, which are FDA-approved indications.
In January 2012, the FDA issued a statement about the prematurely terminated study.
The revised doripenem label is available on the FDA website. The label change was made in January. Doripenem is manufactured by Shionogi.
Imipenem and cilastatin for injection is marketed as Primaxin in the United States.
Serious adverse events associated with doripenem should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch/.
When used to treat ventilator-associated pneumonia, the antibacterial drug doripenem is linked to a greater risk of mortality and lower clinical cure rates compared with imipenem and cilastatin for injection, according to a drug safety communication issued by the Food and Drug Administration.
Doripenem, an intravenous penem antibacterial drug marketed as Doribax, is not approved to treat any type of pneumonia. A warning about increased mortality in patients with ventilator-associated pneumonia (VAP), for which the use of doripenem is unapproved, has been added to the drug’s label. In a statement posted on March 6, the FDA recommended that health care professionals "consider whether the benefits of Doribax treatment are likely to exceed its potential risks in patients who develop pneumonia while on ventilators."
The safety communication is based on an FDA analysis of a 3-year study comparing 7 days of treatment with doripenem to 10 days of treatment with imipenem and cilastatin in patients with VAP. All-cause mortality over 28 days was 23% among those treated with doripenem, compared with 16.7% among those treated with imipenem and cilastatin. Clinical cure rates also were lower in the doripenem-treated patients in the study, which was stopped prematurely in 2011.
The statement adds that doripenem, approved in 2007, "is still considered safe and effective" for treating adults with complicated intra-abdominal infections and complicated urinary tract infections, including pyelonephritis, which are FDA-approved indications.
In January 2012, the FDA issued a statement about the prematurely terminated study.
The revised doripenem label is available on the FDA website. The label change was made in January. Doripenem is manufactured by Shionogi.
Imipenem and cilastatin for injection is marketed as Primaxin in the United States.
Serious adverse events associated with doripenem should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch/.
When used to treat ventilator-associated pneumonia, the antibacterial drug doripenem is linked to a greater risk of mortality and lower clinical cure rates compared with imipenem and cilastatin for injection, according to a drug safety communication issued by the Food and Drug Administration.
Doripenem, an intravenous penem antibacterial drug marketed as Doribax, is not approved to treat any type of pneumonia. A warning about increased mortality in patients with ventilator-associated pneumonia (VAP), for which the use of doripenem is unapproved, has been added to the drug’s label. In a statement posted on March 6, the FDA recommended that health care professionals "consider whether the benefits of Doribax treatment are likely to exceed its potential risks in patients who develop pneumonia while on ventilators."
The safety communication is based on an FDA analysis of a 3-year study comparing 7 days of treatment with doripenem to 10 days of treatment with imipenem and cilastatin in patients with VAP. All-cause mortality over 28 days was 23% among those treated with doripenem, compared with 16.7% among those treated with imipenem and cilastatin. Clinical cure rates also were lower in the doripenem-treated patients in the study, which was stopped prematurely in 2011.
The statement adds that doripenem, approved in 2007, "is still considered safe and effective" for treating adults with complicated intra-abdominal infections and complicated urinary tract infections, including pyelonephritis, which are FDA-approved indications.
In January 2012, the FDA issued a statement about the prematurely terminated study.
The revised doripenem label is available on the FDA website. The label change was made in January. Doripenem is manufactured by Shionogi.
Imipenem and cilastatin for injection is marketed as Primaxin in the United States.
Serious adverse events associated with doripenem should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch/.