User login
Preventing Gout Flares and Hospitalizations Means Targeting These Serum Urate Levels
Clinical efforts to get patients with a history of gout to reach specific target serum urate (SU) levels less than either 5 or 6 mg/dL could prevent the great majority of gout flares and hospitalizations for them, according to a new study that tracked patients for a mean of 8.3 years.
The findings, which appeared February 6 in JAMA, “support the value of target serum urate levels in gout flare prevention in primary care, where most gout patients are treated,” rheumatologist and study coauthor Hyon K. Choi, MD, DrPH, of Harvard Medical School and Massachusetts General Hospital, Boston, told this news organization. However, Dr. Choi noted that “the value of relying on target urate levels is not accepted in primary care practice,” and the author of an accompanying commentary said that the jury is still out about the best strategy to prevent flares.

Gout is caused by monosodium urate crystallization within the joints, which occurs when SU levels exceed the saturation point for uric acid crystallization in the body: approximately 6.8 mg/dL. “Studies have found strongly graded associations between serum urate levels above the saturation point and the risk of developing new cases of gout among individuals without gout at baseline,” Dr. Choi said. “However, associations between serum urate levels and the risk of recurrent flares among preexisting gout patients, which is relevant to clinical gout care practice, has not been established.”
Dr. Choi added that “despite the emphasis in US and European rheumatology guidelines on the use of urate-lowering therapy to treat-to-target serum urate level — eg, under 6 or 5 mg/dL — the proportions of flares associated with such target urate levels remained unknown.”
Study Shows Relationship Between SU Levels and Recurrent Flares
For the study, researchers tracked 3613 patients aged 40-69 with gout in the UK Biobank database from 2006-2010 to 2017 or 2020. The patients, 86% of whom were men, had a mean age of 60 years and about 96% were White.
Among the patients, 1773 new episodes of acute gout occurred in 27% of the patients (16% had one episode, 6% had two episodes, and 5% had at least three episodes). These were treated in primary care or required hospitalizations. The other 73% of patients had no new acute gout episodes.
Overall, 95% of flares occurred in those with baseline SU levels ≥ 6 mg/dL, and 98% occurred in those with levels ≥ 5 mg/dL.
Patients with baseline SU levels < 6.0 mg/dL had an acute gout flare rate of 10.6 per 1000 person-years. In comparison, relative risks for acute gout flares per 1000 person-years were 3.16 at baseline SU levels of 6.0-6.9 mg/dL, 6.20 for 7.0-7.9 mg/dL, 7.70 for 8.0-8.9 mg/dL, 9.80 for 9.0-9.9 mg/dL, and 11.26 for > 10 mg/dL after adjustment for various possible confounders (P < .001).
The researchers identified 64 hospitalizations with gout as the main discharge diagnosis, and 97% occurred in patients with baseline SU levels ≥ 6 mg/dL. All were in patients with baseline SU levels ≥ 5 mg/dL.
“An important feature of this study was that serum urate measurements were obtained from all gout patients at the study baseline, irrespective of clinical needs or flare status,” Dr. Choi said. “Prior studies failed to reveal the truly compelling nature of relations between serum urate levels and recurrent flares among preexisting gout patients.”
As for the cost of SU tests, Dr. Choi said they can run as low as $2. “Portable tests similar to home glucose measurement for diabetes patients are also being adopted by certain gout care practices,” he said.
The findings matter, Dr. Choi said, because SU is not tracked in the “vast majority of gout patients” in primary care. Instead, primary care doctors — as per the guidelines of the American College of Physicians — often adopt an approach that treats symptoms as needed instead of tracking and lowering SU levels, he said. In fact, “95% and 98% of gout flares can be potentially preventable at the population level if serum urate levels < 6 and < 5 mg/dL can be met, respectively, and 100% of hospitalizations for gout could be preventable with serum urate < 5 mg/dL,” he said.
As for limitations, the authors noted that participants in the UK Biobank “typically have a better socioeconomic status and are healthier than the UK general population,” and they added that “these data may underestimate the number of acute gout flares in the cohort.” Also, 55% of the total 502,490 patients in the UK Biobank were excluded owing to lack of primary care data.
Study ‘Offers the Kind of Evidence That We Need’
In an accompanying commentary, University of Alabama at Birmingham rheumatologist Angelo L. Gaffo, MD, MSPH, also noted that the study population was overwhelmingly White, had a low mean SU level (6.9 mg/dL), and had a low level of comorbidities, making the sample “poorly representative of the most commonly described gout populations.”
However, he also noted that there is “growing evidence linking serum urate levels with clinical outcomes,” with a pair of studies — one from 2021 and the other from 2022 — linking reductions in SU to < 6 md/dL to lower flare rates.

Dr. Gaffo told this news organization that although rheumatology guidelines support a treat-to-target strategy, “we haven›t generated a whole lot of important evidence to support it.”
The new study “offers the kind of evidence that we need,” he said, “but this is not going to be the ultimate answer.” That will only come from randomized clinical trials in the works that will pit the treat-to-target approach vs the primary care–favored strategy of titrating treatment until flares are controlled, he said.
Even though evidence is sparse, Dr. Gaffo said he still believes in the treat-to-target strategy: “I believe it is the best way to treat gout.”
What’s next? Researchers hope to understand how to better reach target SU goals in clinical practice, Dr. Choi said. “Involving nurses, pharmacists, or interactive online or app systems — as in other chronic treat-to-target care such as anticoagulation care, blood pressure, or lipid care — is actively being researched.”
He added that “we are trying to find the effective and safe medications and nonpharmacologic measures to reduce the urate burden, which can also simultaneously take care of gout’s frequent cardiovascular-kidney comorbidities.”
The US National Institutes of Health supported the study. Dr. Choi reports receiving grants from Horizon and serving on a board or committee for LG Chem, Shanton, and ANI Pharmaceuticals. Some other authors report an employment and stockholder relationship with Regeneron and support from the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health, and Rheumatology Research Foundation. Dr. Gaffo reports personal fees from PK MED, SOBI/Selecta, Atom, and UpToDate.
A version of this article first appeared on Medscape.com.
Clinical efforts to get patients with a history of gout to reach specific target serum urate (SU) levels less than either 5 or 6 mg/dL could prevent the great majority of gout flares and hospitalizations for them, according to a new study that tracked patients for a mean of 8.3 years.
The findings, which appeared February 6 in JAMA, “support the value of target serum urate levels in gout flare prevention in primary care, where most gout patients are treated,” rheumatologist and study coauthor Hyon K. Choi, MD, DrPH, of Harvard Medical School and Massachusetts General Hospital, Boston, told this news organization. However, Dr. Choi noted that “the value of relying on target urate levels is not accepted in primary care practice,” and the author of an accompanying commentary said that the jury is still out about the best strategy to prevent flares.
Gout is caused by monosodium urate crystallization within the joints, which occurs when SU levels exceed the saturation point for uric acid crystallization in the body: approximately 6.8 mg/dL. “Studies have found strongly graded associations between serum urate levels above the saturation point and the risk of developing new cases of gout among individuals without gout at baseline,” Dr. Choi said. “However, associations between serum urate levels and the risk of recurrent flares among preexisting gout patients, which is relevant to clinical gout care practice, has not been established.”
Dr. Choi added that “despite the emphasis in US and European rheumatology guidelines on the use of urate-lowering therapy to treat-to-target serum urate level — eg, under 6 or 5 mg/dL — the proportions of flares associated with such target urate levels remained unknown.”
Study Shows Relationship Between SU Levels and Recurrent Flares
For the study, researchers tracked 3613 patients aged 40-69 with gout in the UK Biobank database from 2006-2010 to 2017 or 2020. The patients, 86% of whom were men, had a mean age of 60 years and about 96% were White.
Among the patients, 1773 new episodes of acute gout occurred in 27% of the patients (16% had one episode, 6% had two episodes, and 5% had at least three episodes). These were treated in primary care or required hospitalizations. The other 73% of patients had no new acute gout episodes.
Overall, 95% of flares occurred in those with baseline SU levels ≥ 6 mg/dL, and 98% occurred in those with levels ≥ 5 mg/dL.
Patients with baseline SU levels < 6.0 mg/dL had an acute gout flare rate of 10.6 per 1000 person-years. In comparison, relative risks for acute gout flares per 1000 person-years were 3.16 at baseline SU levels of 6.0-6.9 mg/dL, 6.20 for 7.0-7.9 mg/dL, 7.70 for 8.0-8.9 mg/dL, 9.80 for 9.0-9.9 mg/dL, and 11.26 for > 10 mg/dL after adjustment for various possible confounders (P < .001).
The researchers identified 64 hospitalizations with gout as the main discharge diagnosis, and 97% occurred in patients with baseline SU levels ≥ 6 mg/dL. All were in patients with baseline SU levels ≥ 5 mg/dL.
“An important feature of this study was that serum urate measurements were obtained from all gout patients at the study baseline, irrespective of clinical needs or flare status,” Dr. Choi said. “Prior studies failed to reveal the truly compelling nature of relations between serum urate levels and recurrent flares among preexisting gout patients.”
As for the cost of SU tests, Dr. Choi said they can run as low as $2. “Portable tests similar to home glucose measurement for diabetes patients are also being adopted by certain gout care practices,” he said.
The findings matter, Dr. Choi said, because SU is not tracked in the “vast majority of gout patients” in primary care. Instead, primary care doctors — as per the guidelines of the American College of Physicians — often adopt an approach that treats symptoms as needed instead of tracking and lowering SU levels, he said. In fact, “95% and 98% of gout flares can be potentially preventable at the population level if serum urate levels < 6 and < 5 mg/dL can be met, respectively, and 100% of hospitalizations for gout could be preventable with serum urate < 5 mg/dL,” he said.
As for limitations, the authors noted that participants in the UK Biobank “typically have a better socioeconomic status and are healthier than the UK general population,” and they added that “these data may underestimate the number of acute gout flares in the cohort.” Also, 55% of the total 502,490 patients in the UK Biobank were excluded owing to lack of primary care data.
Study ‘Offers the Kind of Evidence That We Need’
In an accompanying commentary, University of Alabama at Birmingham rheumatologist Angelo L. Gaffo, MD, MSPH, also noted that the study population was overwhelmingly White, had a low mean SU level (6.9 mg/dL), and had a low level of comorbidities, making the sample “poorly representative of the most commonly described gout populations.”
However, he also noted that there is “growing evidence linking serum urate levels with clinical outcomes,” with a pair of studies — one from 2021 and the other from 2022 — linking reductions in SU to < 6 md/dL to lower flare rates.
Dr. Gaffo told this news organization that although rheumatology guidelines support a treat-to-target strategy, “we haven›t generated a whole lot of important evidence to support it.”
The new study “offers the kind of evidence that we need,” he said, “but this is not going to be the ultimate answer.” That will only come from randomized clinical trials in the works that will pit the treat-to-target approach vs the primary care–favored strategy of titrating treatment until flares are controlled, he said.
Even though evidence is sparse, Dr. Gaffo said he still believes in the treat-to-target strategy: “I believe it is the best way to treat gout.”
What’s next? Researchers hope to understand how to better reach target SU goals in clinical practice, Dr. Choi said. “Involving nurses, pharmacists, or interactive online or app systems — as in other chronic treat-to-target care such as anticoagulation care, blood pressure, or lipid care — is actively being researched.”
He added that “we are trying to find the effective and safe medications and nonpharmacologic measures to reduce the urate burden, which can also simultaneously take care of gout’s frequent cardiovascular-kidney comorbidities.”
The US National Institutes of Health supported the study. Dr. Choi reports receiving grants from Horizon and serving on a board or committee for LG Chem, Shanton, and ANI Pharmaceuticals. Some other authors report an employment and stockholder relationship with Regeneron and support from the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health, and Rheumatology Research Foundation. Dr. Gaffo reports personal fees from PK MED, SOBI/Selecta, Atom, and UpToDate.
A version of this article first appeared on Medscape.com.
Clinical efforts to get patients with a history of gout to reach specific target serum urate (SU) levels less than either 5 or 6 mg/dL could prevent the great majority of gout flares and hospitalizations for them, according to a new study that tracked patients for a mean of 8.3 years.
The findings, which appeared February 6 in JAMA, “support the value of target serum urate levels in gout flare prevention in primary care, where most gout patients are treated,” rheumatologist and study coauthor Hyon K. Choi, MD, DrPH, of Harvard Medical School and Massachusetts General Hospital, Boston, told this news organization. However, Dr. Choi noted that “the value of relying on target urate levels is not accepted in primary care practice,” and the author of an accompanying commentary said that the jury is still out about the best strategy to prevent flares.
Gout is caused by monosodium urate crystallization within the joints, which occurs when SU levels exceed the saturation point for uric acid crystallization in the body: approximately 6.8 mg/dL. “Studies have found strongly graded associations between serum urate levels above the saturation point and the risk of developing new cases of gout among individuals without gout at baseline,” Dr. Choi said. “However, associations between serum urate levels and the risk of recurrent flares among preexisting gout patients, which is relevant to clinical gout care practice, has not been established.”
Dr. Choi added that “despite the emphasis in US and European rheumatology guidelines on the use of urate-lowering therapy to treat-to-target serum urate level — eg, under 6 or 5 mg/dL — the proportions of flares associated with such target urate levels remained unknown.”
Study Shows Relationship Between SU Levels and Recurrent Flares
For the study, researchers tracked 3613 patients aged 40-69 with gout in the UK Biobank database from 2006-2010 to 2017 or 2020. The patients, 86% of whom were men, had a mean age of 60 years and about 96% were White.
Among the patients, 1773 new episodes of acute gout occurred in 27% of the patients (16% had one episode, 6% had two episodes, and 5% had at least three episodes). These were treated in primary care or required hospitalizations. The other 73% of patients had no new acute gout episodes.
Overall, 95% of flares occurred in those with baseline SU levels ≥ 6 mg/dL, and 98% occurred in those with levels ≥ 5 mg/dL.
Patients with baseline SU levels < 6.0 mg/dL had an acute gout flare rate of 10.6 per 1000 person-years. In comparison, relative risks for acute gout flares per 1000 person-years were 3.16 at baseline SU levels of 6.0-6.9 mg/dL, 6.20 for 7.0-7.9 mg/dL, 7.70 for 8.0-8.9 mg/dL, 9.80 for 9.0-9.9 mg/dL, and 11.26 for > 10 mg/dL after adjustment for various possible confounders (P < .001).
The researchers identified 64 hospitalizations with gout as the main discharge diagnosis, and 97% occurred in patients with baseline SU levels ≥ 6 mg/dL. All were in patients with baseline SU levels ≥ 5 mg/dL.
“An important feature of this study was that serum urate measurements were obtained from all gout patients at the study baseline, irrespective of clinical needs or flare status,” Dr. Choi said. “Prior studies failed to reveal the truly compelling nature of relations between serum urate levels and recurrent flares among preexisting gout patients.”
As for the cost of SU tests, Dr. Choi said they can run as low as $2. “Portable tests similar to home glucose measurement for diabetes patients are also being adopted by certain gout care practices,” he said.
The findings matter, Dr. Choi said, because SU is not tracked in the “vast majority of gout patients” in primary care. Instead, primary care doctors — as per the guidelines of the American College of Physicians — often adopt an approach that treats symptoms as needed instead of tracking and lowering SU levels, he said. In fact, “95% and 98% of gout flares can be potentially preventable at the population level if serum urate levels < 6 and < 5 mg/dL can be met, respectively, and 100% of hospitalizations for gout could be preventable with serum urate < 5 mg/dL,” he said.
As for limitations, the authors noted that participants in the UK Biobank “typically have a better socioeconomic status and are healthier than the UK general population,” and they added that “these data may underestimate the number of acute gout flares in the cohort.” Also, 55% of the total 502,490 patients in the UK Biobank were excluded owing to lack of primary care data.
Study ‘Offers the Kind of Evidence That We Need’
In an accompanying commentary, University of Alabama at Birmingham rheumatologist Angelo L. Gaffo, MD, MSPH, also noted that the study population was overwhelmingly White, had a low mean SU level (6.9 mg/dL), and had a low level of comorbidities, making the sample “poorly representative of the most commonly described gout populations.”
However, he also noted that there is “growing evidence linking serum urate levels with clinical outcomes,” with a pair of studies — one from 2021 and the other from 2022 — linking reductions in SU to < 6 md/dL to lower flare rates.
Dr. Gaffo told this news organization that although rheumatology guidelines support a treat-to-target strategy, “we haven›t generated a whole lot of important evidence to support it.”
The new study “offers the kind of evidence that we need,” he said, “but this is not going to be the ultimate answer.” That will only come from randomized clinical trials in the works that will pit the treat-to-target approach vs the primary care–favored strategy of titrating treatment until flares are controlled, he said.
Even though evidence is sparse, Dr. Gaffo said he still believes in the treat-to-target strategy: “I believe it is the best way to treat gout.”
What’s next? Researchers hope to understand how to better reach target SU goals in clinical practice, Dr. Choi said. “Involving nurses, pharmacists, or interactive online or app systems — as in other chronic treat-to-target care such as anticoagulation care, blood pressure, or lipid care — is actively being researched.”
He added that “we are trying to find the effective and safe medications and nonpharmacologic measures to reduce the urate burden, which can also simultaneously take care of gout’s frequent cardiovascular-kidney comorbidities.”
The US National Institutes of Health supported the study. Dr. Choi reports receiving grants from Horizon and serving on a board or committee for LG Chem, Shanton, and ANI Pharmaceuticals. Some other authors report an employment and stockholder relationship with Regeneron and support from the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health, and Rheumatology Research Foundation. Dr. Gaffo reports personal fees from PK MED, SOBI/Selecta, Atom, and UpToDate.
A version of this article first appeared on Medscape.com.
FROM JAMA
Comorbidities and Disease Type Weigh Heavily in Pregnancy Outcomes of Immune-Mediated Inflammatory Diseases
Comorbidities may play a large role in driving poor pregnancy outcomes in pregnant people with certain immune-mediated inflammatory diseases (IMIDs).
In a new study of 12 individual IMIDs, people with rheumatoid arthritis (RA) or inflammatory bowel disease (IBD) did not have signficantly increased risk for preterm birth (PTB) or low birth weight (LBW), compared with people who did not have an IMID, after adjusting for additional chronic conditions and other confounding factors.

The study was published online on February 1 in eClinicalMedicine.
While many studies have explored the relationships between pregnancy outcomes and IMIDs, “the impact of comorbidities on the relation between IMIDs and pregnancy course is insufficiently examined,” the authors wrote. These previous studies also tended to have a small sample size.
Pregnancy Outcome Risks Varied Between IMIDs
To remedy this, researchers used electronic health record data from Providence St Joseph Health — a multistate integrated healthcare system — to identify more than 365,000 pregnant people with live births between January 1, 2013, and December 31, 2022. The cohort included more than 5700 people with at least one of 12 IMIDs: Psoriasis, IBD, RA, spondyloarthritis (SpA), multiple sclerosis, systemic lupus erythematosus (SLE), psoriatic arthritis (PsA), antiphospholipid syndrome (APS), Sjögren syndrome (SjS), vasculitis, sarcoidosis, and systemic sclerosis. The study included only live births with a gestational age of 20 weeks or greater.
Researchers compared maternal-fetal health outcomes between the two groups, controlling for comorbidities including diabetes, cardiovascular disease, chronic kidney disease, obesity, and depression. They also accounted for confounding variables including race, age, smoking status, and socioeconomic status.
In total, 83% of people in the IMID group had no immunomodulatory medication prescriptions during their pregnancy. Of the 17% taking medication, 48%-70% continued taking their medication until delivery. Most patients were White, comprising 62.9% of the non-IMID group and 73.1% of the IMID group.
After adjusting for comorbidities, patients with any of the 12 IMIDs had a 10%-20% higher risk for PTB, LBW, small for gestation age (SGA), and cesarean section than did comparators.
But these risks varied between IMIDs. Patients with RA and IBD did not have an increased risk for PTB or LBW. However, when researchers did not control for comorbidities, pregnancy risks were higher and showed statistical significance in these two groups.
“This suggests that for RA and IBD, comorbidities may be a more important factor for adverse outcomes than the underlying autoimmune disease,” senior author Jennifer Hadlock, MD, an associate professor and director of medical data science at the Institute for Systems Biology in Seattle, Washington, said in a video accompanying a press release.
Overall, the analysis found that women with IMIDs were approximately two to three times more likely to have chronic comorbidities than the control group.
Like previous studies, there was a strong association between SLE and APS and poor pregnancy outcomes, even after controlling for confounding factors. Patients with SpA had a 50% increased risk for PTB, while those with SLE and APS had more than a twofold higher risk. Patients with SLE were 90% more likely than comparators to deliver babies with an SGA condition, while RA patients had a 30% higher risk. SLE was the only condition with an increased risk for LBW (relative risk, 3.5). IBD, RA, PsA, SpA, SLE, APS, and SjS were all associated with a higher likelihood of delivery via cesarean section.
“The findings of this study reveal that the associations between IMIDs and adverse pregnancy outcomes are influenced by the specific type of IMIDs and the presence of comorbidities,” the authors wrote.
A Large Study, But How Representative Is It?
Asked to comment on the study, Catherine Sims, MD, a rheumatologist at Duke University Medical Center in Durham, North Carolina, noted that the analysis was much larger than many reproductive rheumatology studies, and “their statistics were phenomenal.”

She agreed that “not all autoimmune diseases are created equal when it comes to pregnancy-associated risks.” However, she added that this study’s patient population may not be totally representative of pregnant people with IMIDs or autoimmune diseases.
“We’re making generalizations about autoimmune diseases based on this demographic of White women who are not taking immunosuppression,” she said.
“We know that race and ethnicity play a huge role in pregnancy outcomes, and Black women have higher maternal and fetal morbidity and mortality, which is likely related to systemic racism and biases in the medical system,” she added. “While the study did control for sociodemographic factors, the population studied is not diverse.”
Only 17% of people with IMID in the cohort were on immunosuppressive medication, which could suggest low disease activity in the study population, Dr. Sims said. If the population generally had well-controlled disease, that could have positioned them for better pregnancy outcomes.
The authors noted that their analysis did not have information on IMID disease activity or severity — one of the limitations of the study.
However, the authors argued that the observed low prescription rate during the study may have increased poor pregnancy outcomes.
“Although this reflects real-world care in the population studied, results from this study may show higher risk than might be achieved with recommended care guidelines,” they wrote.
Ultimately, the authors argued that these findings show how co-occurring health conditions can affect pregnancy outcomes in autoimmune diseases, particularly for RA and IBD.
“There is a need to take comorbidities into consideration for guidelines for patients with inflammatory bowel disease and rheumatoid arthritis and when designing future research to investigate maternal health in patients with IMIDs,” they wrote.
The study was funded by the National Institutes of Health. Dr. Sims declared no relevant financial relationships. Dr. Hadlock has received research funding (paid to the institute) from Pfizer, Novartis, Janssen, Bristol-Myers Squibb, and Gilead.
A version of this article first appeared on Medscape.com.
Comorbidities may play a large role in driving poor pregnancy outcomes in pregnant people with certain immune-mediated inflammatory diseases (IMIDs).
In a new study of 12 individual IMIDs, people with rheumatoid arthritis (RA) or inflammatory bowel disease (IBD) did not have signficantly increased risk for preterm birth (PTB) or low birth weight (LBW), compared with people who did not have an IMID, after adjusting for additional chronic conditions and other confounding factors.
The study was published online on February 1 in eClinicalMedicine.
While many studies have explored the relationships between pregnancy outcomes and IMIDs, “the impact of comorbidities on the relation between IMIDs and pregnancy course is insufficiently examined,” the authors wrote. These previous studies also tended to have a small sample size.
Pregnancy Outcome Risks Varied Between IMIDs
To remedy this, researchers used electronic health record data from Providence St Joseph Health — a multistate integrated healthcare system — to identify more than 365,000 pregnant people with live births between January 1, 2013, and December 31, 2022. The cohort included more than 5700 people with at least one of 12 IMIDs: Psoriasis, IBD, RA, spondyloarthritis (SpA), multiple sclerosis, systemic lupus erythematosus (SLE), psoriatic arthritis (PsA), antiphospholipid syndrome (APS), Sjögren syndrome (SjS), vasculitis, sarcoidosis, and systemic sclerosis. The study included only live births with a gestational age of 20 weeks or greater.
Researchers compared maternal-fetal health outcomes between the two groups, controlling for comorbidities including diabetes, cardiovascular disease, chronic kidney disease, obesity, and depression. They also accounted for confounding variables including race, age, smoking status, and socioeconomic status.
In total, 83% of people in the IMID group had no immunomodulatory medication prescriptions during their pregnancy. Of the 17% taking medication, 48%-70% continued taking their medication until delivery. Most patients were White, comprising 62.9% of the non-IMID group and 73.1% of the IMID group.
After adjusting for comorbidities, patients with any of the 12 IMIDs had a 10%-20% higher risk for PTB, LBW, small for gestation age (SGA), and cesarean section than did comparators.
But these risks varied between IMIDs. Patients with RA and IBD did not have an increased risk for PTB or LBW. However, when researchers did not control for comorbidities, pregnancy risks were higher and showed statistical significance in these two groups.
“This suggests that for RA and IBD, comorbidities may be a more important factor for adverse outcomes than the underlying autoimmune disease,” senior author Jennifer Hadlock, MD, an associate professor and director of medical data science at the Institute for Systems Biology in Seattle, Washington, said in a video accompanying a press release.
Overall, the analysis found that women with IMIDs were approximately two to three times more likely to have chronic comorbidities than the control group.
Like previous studies, there was a strong association between SLE and APS and poor pregnancy outcomes, even after controlling for confounding factors. Patients with SpA had a 50% increased risk for PTB, while those with SLE and APS had more than a twofold higher risk. Patients with SLE were 90% more likely than comparators to deliver babies with an SGA condition, while RA patients had a 30% higher risk. SLE was the only condition with an increased risk for LBW (relative risk, 3.5). IBD, RA, PsA, SpA, SLE, APS, and SjS were all associated with a higher likelihood of delivery via cesarean section.
“The findings of this study reveal that the associations between IMIDs and adverse pregnancy outcomes are influenced by the specific type of IMIDs and the presence of comorbidities,” the authors wrote.
A Large Study, But How Representative Is It?
Asked to comment on the study, Catherine Sims, MD, a rheumatologist at Duke University Medical Center in Durham, North Carolina, noted that the analysis was much larger than many reproductive rheumatology studies, and “their statistics were phenomenal.”
She agreed that “not all autoimmune diseases are created equal when it comes to pregnancy-associated risks.” However, she added that this study’s patient population may not be totally representative of pregnant people with IMIDs or autoimmune diseases.
“We’re making generalizations about autoimmune diseases based on this demographic of White women who are not taking immunosuppression,” she said.
“We know that race and ethnicity play a huge role in pregnancy outcomes, and Black women have higher maternal and fetal morbidity and mortality, which is likely related to systemic racism and biases in the medical system,” she added. “While the study did control for sociodemographic factors, the population studied is not diverse.”
Only 17% of people with IMID in the cohort were on immunosuppressive medication, which could suggest low disease activity in the study population, Dr. Sims said. If the population generally had well-controlled disease, that could have positioned them for better pregnancy outcomes.
The authors noted that their analysis did not have information on IMID disease activity or severity — one of the limitations of the study.
However, the authors argued that the observed low prescription rate during the study may have increased poor pregnancy outcomes.
“Although this reflects real-world care in the population studied, results from this study may show higher risk than might be achieved with recommended care guidelines,” they wrote.
Ultimately, the authors argued that these findings show how co-occurring health conditions can affect pregnancy outcomes in autoimmune diseases, particularly for RA and IBD.
“There is a need to take comorbidities into consideration for guidelines for patients with inflammatory bowel disease and rheumatoid arthritis and when designing future research to investigate maternal health in patients with IMIDs,” they wrote.
The study was funded by the National Institutes of Health. Dr. Sims declared no relevant financial relationships. Dr. Hadlock has received research funding (paid to the institute) from Pfizer, Novartis, Janssen, Bristol-Myers Squibb, and Gilead.
A version of this article first appeared on Medscape.com.
Comorbidities may play a large role in driving poor pregnancy outcomes in pregnant people with certain immune-mediated inflammatory diseases (IMIDs).
In a new study of 12 individual IMIDs, people with rheumatoid arthritis (RA) or inflammatory bowel disease (IBD) did not have signficantly increased risk for preterm birth (PTB) or low birth weight (LBW), compared with people who did not have an IMID, after adjusting for additional chronic conditions and other confounding factors.
The study was published online on February 1 in eClinicalMedicine.
While many studies have explored the relationships between pregnancy outcomes and IMIDs, “the impact of comorbidities on the relation between IMIDs and pregnancy course is insufficiently examined,” the authors wrote. These previous studies also tended to have a small sample size.
Pregnancy Outcome Risks Varied Between IMIDs
To remedy this, researchers used electronic health record data from Providence St Joseph Health — a multistate integrated healthcare system — to identify more than 365,000 pregnant people with live births between January 1, 2013, and December 31, 2022. The cohort included more than 5700 people with at least one of 12 IMIDs: Psoriasis, IBD, RA, spondyloarthritis (SpA), multiple sclerosis, systemic lupus erythematosus (SLE), psoriatic arthritis (PsA), antiphospholipid syndrome (APS), Sjögren syndrome (SjS), vasculitis, sarcoidosis, and systemic sclerosis. The study included only live births with a gestational age of 20 weeks or greater.
Researchers compared maternal-fetal health outcomes between the two groups, controlling for comorbidities including diabetes, cardiovascular disease, chronic kidney disease, obesity, and depression. They also accounted for confounding variables including race, age, smoking status, and socioeconomic status.
In total, 83% of people in the IMID group had no immunomodulatory medication prescriptions during their pregnancy. Of the 17% taking medication, 48%-70% continued taking their medication until delivery. Most patients were White, comprising 62.9% of the non-IMID group and 73.1% of the IMID group.
After adjusting for comorbidities, patients with any of the 12 IMIDs had a 10%-20% higher risk for PTB, LBW, small for gestation age (SGA), and cesarean section than did comparators.
But these risks varied between IMIDs. Patients with RA and IBD did not have an increased risk for PTB or LBW. However, when researchers did not control for comorbidities, pregnancy risks were higher and showed statistical significance in these two groups.
“This suggests that for RA and IBD, comorbidities may be a more important factor for adverse outcomes than the underlying autoimmune disease,” senior author Jennifer Hadlock, MD, an associate professor and director of medical data science at the Institute for Systems Biology in Seattle, Washington, said in a video accompanying a press release.
Overall, the analysis found that women with IMIDs were approximately two to three times more likely to have chronic comorbidities than the control group.
Like previous studies, there was a strong association between SLE and APS and poor pregnancy outcomes, even after controlling for confounding factors. Patients with SpA had a 50% increased risk for PTB, while those with SLE and APS had more than a twofold higher risk. Patients with SLE were 90% more likely than comparators to deliver babies with an SGA condition, while RA patients had a 30% higher risk. SLE was the only condition with an increased risk for LBW (relative risk, 3.5). IBD, RA, PsA, SpA, SLE, APS, and SjS were all associated with a higher likelihood of delivery via cesarean section.
“The findings of this study reveal that the associations between IMIDs and adverse pregnancy outcomes are influenced by the specific type of IMIDs and the presence of comorbidities,” the authors wrote.
A Large Study, But How Representative Is It?
Asked to comment on the study, Catherine Sims, MD, a rheumatologist at Duke University Medical Center in Durham, North Carolina, noted that the analysis was much larger than many reproductive rheumatology studies, and “their statistics were phenomenal.”
She agreed that “not all autoimmune diseases are created equal when it comes to pregnancy-associated risks.” However, she added that this study’s patient population may not be totally representative of pregnant people with IMIDs or autoimmune diseases.
“We’re making generalizations about autoimmune diseases based on this demographic of White women who are not taking immunosuppression,” she said.
“We know that race and ethnicity play a huge role in pregnancy outcomes, and Black women have higher maternal and fetal morbidity and mortality, which is likely related to systemic racism and biases in the medical system,” she added. “While the study did control for sociodemographic factors, the population studied is not diverse.”
Only 17% of people with IMID in the cohort were on immunosuppressive medication, which could suggest low disease activity in the study population, Dr. Sims said. If the population generally had well-controlled disease, that could have positioned them for better pregnancy outcomes.
The authors noted that their analysis did not have information on IMID disease activity or severity — one of the limitations of the study.
However, the authors argued that the observed low prescription rate during the study may have increased poor pregnancy outcomes.
“Although this reflects real-world care in the population studied, results from this study may show higher risk than might be achieved with recommended care guidelines,” they wrote.
Ultimately, the authors argued that these findings show how co-occurring health conditions can affect pregnancy outcomes in autoimmune diseases, particularly for RA and IBD.
“There is a need to take comorbidities into consideration for guidelines for patients with inflammatory bowel disease and rheumatoid arthritis and when designing future research to investigate maternal health in patients with IMIDs,” they wrote.
The study was funded by the National Institutes of Health. Dr. Sims declared no relevant financial relationships. Dr. Hadlock has received research funding (paid to the institute) from Pfizer, Novartis, Janssen, Bristol-Myers Squibb, and Gilead.
A version of this article first appeared on Medscape.com.
FROM ECLINICALMEDICINE
New Findings on Vitamin D, Omega-3 Supplements for Preventing Autoimmune Diseases
Two years after the end of a randomized trial that showed a benefit of daily vitamin D and omega-3 fatty acid (n-3 FA) supplementation for reducing risk for autoimmune diseases, the salubrious effects of daily vitamin D appear to have waned after the supplement was discontinued, while the protection from n-3 lived on for at least 2 additional years.
As previously reported, the randomized VITAL, which was designed primarily to study the effects of vitamin D and n-3 supplementation on incident cancer and cardiovascular disease, also showed that 5 years of vitamin D supplementation was associated with a 22% reduction in risk for confirmed autoimmune diseases, and 5 years of n-3 FA supplementation was associated with an 18% reduction in confirmed and probable incident autoimmune diseases.
Now, investigators Karen H. Costenbader, MD, MPH, of Brigham & Women’s Hospital in Boston, Massachusetts, and colleagues reported that among 21,592 participants in VITAL who agreed to be followed for an additional 2 years after discontinuation, the protection against autoimmune diseases from daily vitamin D (cholecalciferol; 2000 IU/d) was no longer statistically significant, but the benefits of daily marine n-3 FAs (1 g/d as a fish-oil capsule containing 460 mg of eicosapentaenoic acid and 380 mg of docosahexaenoic acid) remained significant.
“VITAL observational extension results suggest that vitamin D supplementation should be given on a continuous basis for long-term prevention of [autoimmune diseases]. The beneficial effects of n-3 fatty acids, however, may be prolonged for at least 2 years after discontinuation,” they wrote in an article published in Arthritis & Rheumatology.
Dr. Costenbader told this news organization that the results of the observational extension study suggest that the benefits of vitamin D “wear off more quickly, and it should be continued for a longer period of time or indefinitely, rather than only for 5 years.”
In addition to the disparity in the duration of the protective effect, the investigators also saw differences in the effects across different autoimmune diseases.
“The protective effect of vitamin D seemed strongest for psoriasis, while for omega-3 fatty acids, the protective effects were strongest for rheumatoid arthritis and inflammatory bowel disease,” she said.
Mixed Effects
In an interview with this news organization, Janet Funk, MD, MS, vice chair of research in the Department of Medicine and professor in the School of Nutritional Science and Wellness at the University of Arizona, Tucson, Arizona, who was not involved in the study, saidthat the results suggest that while each supplement may offer protection against autoimmune diseases, the effects are inconsistent and may not apply to all patients.
“I think the VITAL extension results suggest that either supplement (or both together) may have benefits in reducing risk of autoimmune diseases, including possible persistent effects posttreatment, but that these effects are nuanced (ie, only in normal weight post-vitamin D treatment) and possibly not uniform across all autoimmune diseases (including possible adverse effects for some — eg, inverse association between prior omega-3 and psoriasis and tendency for increased autoimmune thyroid disease for vitamin D), although the study was not powered sufficiently to draw disease-specific conclusions,” she said.
In an editorial accompanying the study, rheumatologist Joel M. Kremer, MD, of Albany Medical College and the Corrona Research Foundation in Delray Beach, Florida, wrote that “[T]he studies by Dr. Costenbader, et al. have shed new light on the possibility that dietary supplements of n-3 FA [fatty acid] may prevent the onset of [autoimmune disease]. The sustained benefits they describe for as long as 2 years after the supplements are discontinued are consistent with the chronicity of FA species in cellular plasma membranes where they serve as substrates for a diverse array of salient metabolic and inflammatory pathways.”
VITAL Then
To test whether vitamin D or marine-derived long-chain n-3 FA supplementation could protect against autoimmune disease over time, Dr. Costenbader and colleagues piggybacked an ancillary study onto the VITAL trial, which had primary outcomes of cancer and cardiovascular disease incidence.
A total of 25,871 participants were enrolled, including 12,786 men aged 50 and older and 13,085 women aged 55 and older. The study had a 2 × 2 factorial design, with patients randomly assigned to vitamin D 2000 IU/d or placebo and then further randomized to either 1 g/d n-3 FAs or placebo in both the vitamin D and placebo primary randomization arms.
In multivariate analysis adjusted for age, sex, race, and other supplement arm, vitamin D alone was associated with a hazard ratio (HR) of 0.68 (P = .02) for incident autoimmune disease, n-3 alone was associated with a nonsignificant HR of 0.74, and the combination was associated with an HR of 0.69 (P = .03). However, when probable incident autoimmune disease cases were included, the effect of n-3 became significant, with an HR of 0.82.
VITAL Now
In the current analysis, Dr. Costenbader and colleagues reported observational data on 21,592 VITAL participants, a sample representing 83.5% of those who were initially randomized, and 87.9% of those who were alive and could be contacted at the end of the study.
As in the initial trial, the investigators used annual questionnaires to assess incident autoimmune diseases during the randomized follow-up. Participants were asked about new-onset, doctor-diagnosed rheumatoid arthritis, polymyalgia rheumatica, psoriasis, autoimmune thyroid disease, and inflammatory bowel disease. Participants could also write in any other new autoimmune disease diagnoses.
There were 236 new cases of confirmed autoimmune disease that occurred since the initial publication of the trial results, as well as 65 probable cases identified during the median 5.3 years of the randomized portion, and 42 probable cases diagnosed during the 2-year observational phase.
The investigators found that after the 2-year observation period, 255 participants initially randomized to receive vitamin D had a newly developed confirmed autoimmune disease, compared with 259 of those initially randomized to a vitamin D placebo. This translated into a nonsignificant HR of 0.98.
Adding probable autoimmune cases to the confirmed cases made little difference, resulting in a nonsignificant adjusted HR of 0.95.
In contrast, there were 234 confirmed autoimmune disease cases among patients initially assigned to n-3, compared with 280 among patients randomized to the n-3 placebo, translating into a statistically significant HR of 0.83 for new-onset autoimmune disease with n-3.
Dr. Costenbader and colleagues acknowledged that the study was limited by the use of doses intended to prevent cancer or cardiovascular disease and that higher doses intended for high-risk or nutritionally deficient populations might reveal larger effects of supplementation. In addition, they noted the difficulty of identifying the timing and onset of incident disease, and that the small number of cases that occurred during the 2-year observational period precluded detailed analyses of individual autoimmune diseases.
The study was funded by grants from the National Institutes of Health. Dr. Costenbader, Dr. Funk, and Dr. Kremer reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Two years after the end of a randomized trial that showed a benefit of daily vitamin D and omega-3 fatty acid (n-3 FA) supplementation for reducing risk for autoimmune diseases, the salubrious effects of daily vitamin D appear to have waned after the supplement was discontinued, while the protection from n-3 lived on for at least 2 additional years.
As previously reported, the randomized VITAL, which was designed primarily to study the effects of vitamin D and n-3 supplementation on incident cancer and cardiovascular disease, also showed that 5 years of vitamin D supplementation was associated with a 22% reduction in risk for confirmed autoimmune diseases, and 5 years of n-3 FA supplementation was associated with an 18% reduction in confirmed and probable incident autoimmune diseases.
Now, investigators Karen H. Costenbader, MD, MPH, of Brigham & Women’s Hospital in Boston, Massachusetts, and colleagues reported that among 21,592 participants in VITAL who agreed to be followed for an additional 2 years after discontinuation, the protection against autoimmune diseases from daily vitamin D (cholecalciferol; 2000 IU/d) was no longer statistically significant, but the benefits of daily marine n-3 FAs (1 g/d as a fish-oil capsule containing 460 mg of eicosapentaenoic acid and 380 mg of docosahexaenoic acid) remained significant.
“VITAL observational extension results suggest that vitamin D supplementation should be given on a continuous basis for long-term prevention of [autoimmune diseases]. The beneficial effects of n-3 fatty acids, however, may be prolonged for at least 2 years after discontinuation,” they wrote in an article published in Arthritis & Rheumatology.
Dr. Costenbader told this news organization that the results of the observational extension study suggest that the benefits of vitamin D “wear off more quickly, and it should be continued for a longer period of time or indefinitely, rather than only for 5 years.”
In addition to the disparity in the duration of the protective effect, the investigators also saw differences in the effects across different autoimmune diseases.
“The protective effect of vitamin D seemed strongest for psoriasis, while for omega-3 fatty acids, the protective effects were strongest for rheumatoid arthritis and inflammatory bowel disease,” she said.
Mixed Effects
In an interview with this news organization, Janet Funk, MD, MS, vice chair of research in the Department of Medicine and professor in the School of Nutritional Science and Wellness at the University of Arizona, Tucson, Arizona, who was not involved in the study, saidthat the results suggest that while each supplement may offer protection against autoimmune diseases, the effects are inconsistent and may not apply to all patients.
“I think the VITAL extension results suggest that either supplement (or both together) may have benefits in reducing risk of autoimmune diseases, including possible persistent effects posttreatment, but that these effects are nuanced (ie, only in normal weight post-vitamin D treatment) and possibly not uniform across all autoimmune diseases (including possible adverse effects for some — eg, inverse association between prior omega-3 and psoriasis and tendency for increased autoimmune thyroid disease for vitamin D), although the study was not powered sufficiently to draw disease-specific conclusions,” she said.
In an editorial accompanying the study, rheumatologist Joel M. Kremer, MD, of Albany Medical College and the Corrona Research Foundation in Delray Beach, Florida, wrote that “[T]he studies by Dr. Costenbader, et al. have shed new light on the possibility that dietary supplements of n-3 FA [fatty acid] may prevent the onset of [autoimmune disease]. The sustained benefits they describe for as long as 2 years after the supplements are discontinued are consistent with the chronicity of FA species in cellular plasma membranes where they serve as substrates for a diverse array of salient metabolic and inflammatory pathways.”
VITAL Then
To test whether vitamin D or marine-derived long-chain n-3 FA supplementation could protect against autoimmune disease over time, Dr. Costenbader and colleagues piggybacked an ancillary study onto the VITAL trial, which had primary outcomes of cancer and cardiovascular disease incidence.
A total of 25,871 participants were enrolled, including 12,786 men aged 50 and older and 13,085 women aged 55 and older. The study had a 2 × 2 factorial design, with patients randomly assigned to vitamin D 2000 IU/d or placebo and then further randomized to either 1 g/d n-3 FAs or placebo in both the vitamin D and placebo primary randomization arms.
In multivariate analysis adjusted for age, sex, race, and other supplement arm, vitamin D alone was associated with a hazard ratio (HR) of 0.68 (P = .02) for incident autoimmune disease, n-3 alone was associated with a nonsignificant HR of 0.74, and the combination was associated with an HR of 0.69 (P = .03). However, when probable incident autoimmune disease cases were included, the effect of n-3 became significant, with an HR of 0.82.
VITAL Now
In the current analysis, Dr. Costenbader and colleagues reported observational data on 21,592 VITAL participants, a sample representing 83.5% of those who were initially randomized, and 87.9% of those who were alive and could be contacted at the end of the study.
As in the initial trial, the investigators used annual questionnaires to assess incident autoimmune diseases during the randomized follow-up. Participants were asked about new-onset, doctor-diagnosed rheumatoid arthritis, polymyalgia rheumatica, psoriasis, autoimmune thyroid disease, and inflammatory bowel disease. Participants could also write in any other new autoimmune disease diagnoses.
There were 236 new cases of confirmed autoimmune disease that occurred since the initial publication of the trial results, as well as 65 probable cases identified during the median 5.3 years of the randomized portion, and 42 probable cases diagnosed during the 2-year observational phase.
The investigators found that after the 2-year observation period, 255 participants initially randomized to receive vitamin D had a newly developed confirmed autoimmune disease, compared with 259 of those initially randomized to a vitamin D placebo. This translated into a nonsignificant HR of 0.98.
Adding probable autoimmune cases to the confirmed cases made little difference, resulting in a nonsignificant adjusted HR of 0.95.
In contrast, there were 234 confirmed autoimmune disease cases among patients initially assigned to n-3, compared with 280 among patients randomized to the n-3 placebo, translating into a statistically significant HR of 0.83 for new-onset autoimmune disease with n-3.
Dr. Costenbader and colleagues acknowledged that the study was limited by the use of doses intended to prevent cancer or cardiovascular disease and that higher doses intended for high-risk or nutritionally deficient populations might reveal larger effects of supplementation. In addition, they noted the difficulty of identifying the timing and onset of incident disease, and that the small number of cases that occurred during the 2-year observational period precluded detailed analyses of individual autoimmune diseases.
The study was funded by grants from the National Institutes of Health. Dr. Costenbader, Dr. Funk, and Dr. Kremer reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Two years after the end of a randomized trial that showed a benefit of daily vitamin D and omega-3 fatty acid (n-3 FA) supplementation for reducing risk for autoimmune diseases, the salubrious effects of daily vitamin D appear to have waned after the supplement was discontinued, while the protection from n-3 lived on for at least 2 additional years.
As previously reported, the randomized VITAL, which was designed primarily to study the effects of vitamin D and n-3 supplementation on incident cancer and cardiovascular disease, also showed that 5 years of vitamin D supplementation was associated with a 22% reduction in risk for confirmed autoimmune diseases, and 5 years of n-3 FA supplementation was associated with an 18% reduction in confirmed and probable incident autoimmune diseases.
Now, investigators Karen H. Costenbader, MD, MPH, of Brigham & Women’s Hospital in Boston, Massachusetts, and colleagues reported that among 21,592 participants in VITAL who agreed to be followed for an additional 2 years after discontinuation, the protection against autoimmune diseases from daily vitamin D (cholecalciferol; 2000 IU/d) was no longer statistically significant, but the benefits of daily marine n-3 FAs (1 g/d as a fish-oil capsule containing 460 mg of eicosapentaenoic acid and 380 mg of docosahexaenoic acid) remained significant.
“VITAL observational extension results suggest that vitamin D supplementation should be given on a continuous basis for long-term prevention of [autoimmune diseases]. The beneficial effects of n-3 fatty acids, however, may be prolonged for at least 2 years after discontinuation,” they wrote in an article published in Arthritis & Rheumatology.
Dr. Costenbader told this news organization that the results of the observational extension study suggest that the benefits of vitamin D “wear off more quickly, and it should be continued for a longer period of time or indefinitely, rather than only for 5 years.”
In addition to the disparity in the duration of the protective effect, the investigators also saw differences in the effects across different autoimmune diseases.
“The protective effect of vitamin D seemed strongest for psoriasis, while for omega-3 fatty acids, the protective effects were strongest for rheumatoid arthritis and inflammatory bowel disease,” she said.
Mixed Effects
In an interview with this news organization, Janet Funk, MD, MS, vice chair of research in the Department of Medicine and professor in the School of Nutritional Science and Wellness at the University of Arizona, Tucson, Arizona, who was not involved in the study, saidthat the results suggest that while each supplement may offer protection against autoimmune diseases, the effects are inconsistent and may not apply to all patients.
“I think the VITAL extension results suggest that either supplement (or both together) may have benefits in reducing risk of autoimmune diseases, including possible persistent effects posttreatment, but that these effects are nuanced (ie, only in normal weight post-vitamin D treatment) and possibly not uniform across all autoimmune diseases (including possible adverse effects for some — eg, inverse association between prior omega-3 and psoriasis and tendency for increased autoimmune thyroid disease for vitamin D), although the study was not powered sufficiently to draw disease-specific conclusions,” she said.
In an editorial accompanying the study, rheumatologist Joel M. Kremer, MD, of Albany Medical College and the Corrona Research Foundation in Delray Beach, Florida, wrote that “[T]he studies by Dr. Costenbader, et al. have shed new light on the possibility that dietary supplements of n-3 FA [fatty acid] may prevent the onset of [autoimmune disease]. The sustained benefits they describe for as long as 2 years after the supplements are discontinued are consistent with the chronicity of FA species in cellular plasma membranes where they serve as substrates for a diverse array of salient metabolic and inflammatory pathways.”
VITAL Then
To test whether vitamin D or marine-derived long-chain n-3 FA supplementation could protect against autoimmune disease over time, Dr. Costenbader and colleagues piggybacked an ancillary study onto the VITAL trial, which had primary outcomes of cancer and cardiovascular disease incidence.
A total of 25,871 participants were enrolled, including 12,786 men aged 50 and older and 13,085 women aged 55 and older. The study had a 2 × 2 factorial design, with patients randomly assigned to vitamin D 2000 IU/d or placebo and then further randomized to either 1 g/d n-3 FAs or placebo in both the vitamin D and placebo primary randomization arms.
In multivariate analysis adjusted for age, sex, race, and other supplement arm, vitamin D alone was associated with a hazard ratio (HR) of 0.68 (P = .02) for incident autoimmune disease, n-3 alone was associated with a nonsignificant HR of 0.74, and the combination was associated with an HR of 0.69 (P = .03). However, when probable incident autoimmune disease cases were included, the effect of n-3 became significant, with an HR of 0.82.
VITAL Now
In the current analysis, Dr. Costenbader and colleagues reported observational data on 21,592 VITAL participants, a sample representing 83.5% of those who were initially randomized, and 87.9% of those who were alive and could be contacted at the end of the study.
As in the initial trial, the investigators used annual questionnaires to assess incident autoimmune diseases during the randomized follow-up. Participants were asked about new-onset, doctor-diagnosed rheumatoid arthritis, polymyalgia rheumatica, psoriasis, autoimmune thyroid disease, and inflammatory bowel disease. Participants could also write in any other new autoimmune disease diagnoses.
There were 236 new cases of confirmed autoimmune disease that occurred since the initial publication of the trial results, as well as 65 probable cases identified during the median 5.3 years of the randomized portion, and 42 probable cases diagnosed during the 2-year observational phase.
The investigators found that after the 2-year observation period, 255 participants initially randomized to receive vitamin D had a newly developed confirmed autoimmune disease, compared with 259 of those initially randomized to a vitamin D placebo. This translated into a nonsignificant HR of 0.98.
Adding probable autoimmune cases to the confirmed cases made little difference, resulting in a nonsignificant adjusted HR of 0.95.
In contrast, there were 234 confirmed autoimmune disease cases among patients initially assigned to n-3, compared with 280 among patients randomized to the n-3 placebo, translating into a statistically significant HR of 0.83 for new-onset autoimmune disease with n-3.
Dr. Costenbader and colleagues acknowledged that the study was limited by the use of doses intended to prevent cancer or cardiovascular disease and that higher doses intended for high-risk or nutritionally deficient populations might reveal larger effects of supplementation. In addition, they noted the difficulty of identifying the timing and onset of incident disease, and that the small number of cases that occurred during the 2-year observational period precluded detailed analyses of individual autoimmune diseases.
The study was funded by grants from the National Institutes of Health. Dr. Costenbader, Dr. Funk, and Dr. Kremer reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM ARTHRITIS & RHEUMATOLOGY
Calcium Pyrophosphate Deposition Disease Nearly Doubles Fracture Risk
Patients with calcium pyrophosphate deposition (CPPD) disease, also known as pseudogout, have an 80% higher risk for fracture than individuals who do not have the disease, according to a new analysis.
This trend was driven by wrist fractures, where there was a more than threefold increased risk.
Previous studies identified an association between CPPD and low bone mineral density, and there is growing evidence suggesting that the dysregulation of osteoprotegerin — a molecule that is important in the regulation of osteoclasts — may be associated with early-onset CPPD, noted Sara K. Tedeschi, MD, MPH, the lead author of the study and head of crystal-induced arthritic diseases at Brigham and Women’s Hospital, Boston, Massachusetts.

However, CPPD’s association with fracture risk has yet to be explored.
In the study, Dr. Tedeschi and colleagues used Mass General Brigham electronic health record (EHR) data from 1991 to 2023 to identify 1148 individuals with acute calcium pyrophosphate (CPP) crystal arthritis. The index date was defined as the first documentation of pseudogout or synovial fluid CPP crystals. These patients were matched to 3730 comparators based on healthcare encounters within 30 days of the index date of a patient with CPPD. Patients were also matched based on the year of their first EHR encounter. Patients with a fracture documented prior to the index date were excluded from the analysis.
The primary outcome was the first fracture of the humerus, knee, wrist, hip, or pelvis, detected via published algorithms using diagnostic and procedural codes.
The research was published on January 14 in Arthritis & Rheumatology.
Although participants were not matched on age or sex, the average age was 73, and most participants were female. In total, 83.1% of participants in the CPPD group and 80.0% of those in the control group were White.
After adjustment for confounding factors including age, sex, comorbidities, and glucocorticoid use, CPPD was associated with an 80% higher risk for any fracture (hazard risk [HR], 1.8). Fracture risk was highest for the wrist (HR, 3.6).
Patients with CPPD had a 40% higher risk to experience a humerus or pelvis fracture and a 30% higher risk for hip fractures, but the results were not statistically significant.
The results were similar for sensitivity analyses that excluded patients who were prescribed glucocorticoids, treatment for osteoporosis, or had a diagnosis of rheumatoid arthritis.

Asked to comment, John D. FitzGerald, MD, PhD, clinical chief of rheumatology at the University of California, Los Angeles, noted that these associations were “convincing and strong. I thought it was a very good study and important work. CPPD is common and osteoporosis is common, so better understanding the connection is important.”
It’s still not clear why the risk for wrist fractures was highest, but Dr. Tedeschi had two hypotheses. The researchers were unable to assess for falls in this dataset, but it’s possible that patients with CPPD experiencing joint pain could fall and try to brace themselves with an outstretched arm, leading to a wrist fracture.
CPPD also commonly affects the wrist, “so it’s possible that if CPPD is affecting the wrist and if there is an association between CPPD and low bone density, maybe there’s particularly low bone density at the wrist,” she said.
Dr. FitzGerald agreed that both hypotheses were plausible, but “with the retrospective study, there could be a lot of things that are unobserved or unexplained,” he added.
Dr. Tedeschi is interested in exploring what could be causing the association with an increased fracture risk in future research.
“I hope this draws attention to the fact that people with CPPD can have related medical problems that are outside of their joints,” added Dr. Tedeschi. “Thinking about routine screening for osteopenia and osteoporosis could be a good first step in patients with CPPD.”
The study was funded by grants from the US National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Tedeschi has worked as a consultant for Novartis. Dr. FitzGerald reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Patients with calcium pyrophosphate deposition (CPPD) disease, also known as pseudogout, have an 80% higher risk for fracture than individuals who do not have the disease, according to a new analysis.
This trend was driven by wrist fractures, where there was a more than threefold increased risk.
Previous studies identified an association between CPPD and low bone mineral density, and there is growing evidence suggesting that the dysregulation of osteoprotegerin — a molecule that is important in the regulation of osteoclasts — may be associated with early-onset CPPD, noted Sara K. Tedeschi, MD, MPH, the lead author of the study and head of crystal-induced arthritic diseases at Brigham and Women’s Hospital, Boston, Massachusetts.
However, CPPD’s association with fracture risk has yet to be explored.
In the study, Dr. Tedeschi and colleagues used Mass General Brigham electronic health record (EHR) data from 1991 to 2023 to identify 1148 individuals with acute calcium pyrophosphate (CPP) crystal arthritis. The index date was defined as the first documentation of pseudogout or synovial fluid CPP crystals. These patients were matched to 3730 comparators based on healthcare encounters within 30 days of the index date of a patient with CPPD. Patients were also matched based on the year of their first EHR encounter. Patients with a fracture documented prior to the index date were excluded from the analysis.
The primary outcome was the first fracture of the humerus, knee, wrist, hip, or pelvis, detected via published algorithms using diagnostic and procedural codes.
The research was published on January 14 in Arthritis & Rheumatology.
Although participants were not matched on age or sex, the average age was 73, and most participants were female. In total, 83.1% of participants in the CPPD group and 80.0% of those in the control group were White.
After adjustment for confounding factors including age, sex, comorbidities, and glucocorticoid use, CPPD was associated with an 80% higher risk for any fracture (hazard risk [HR], 1.8). Fracture risk was highest for the wrist (HR, 3.6).
Patients with CPPD had a 40% higher risk to experience a humerus or pelvis fracture and a 30% higher risk for hip fractures, but the results were not statistically significant.
The results were similar for sensitivity analyses that excluded patients who were prescribed glucocorticoids, treatment for osteoporosis, or had a diagnosis of rheumatoid arthritis.
Asked to comment, John D. FitzGerald, MD, PhD, clinical chief of rheumatology at the University of California, Los Angeles, noted that these associations were “convincing and strong. I thought it was a very good study and important work. CPPD is common and osteoporosis is common, so better understanding the connection is important.”
It’s still not clear why the risk for wrist fractures was highest, but Dr. Tedeschi had two hypotheses. The researchers were unable to assess for falls in this dataset, but it’s possible that patients with CPPD experiencing joint pain could fall and try to brace themselves with an outstretched arm, leading to a wrist fracture.
CPPD also commonly affects the wrist, “so it’s possible that if CPPD is affecting the wrist and if there is an association between CPPD and low bone density, maybe there’s particularly low bone density at the wrist,” she said.
Dr. FitzGerald agreed that both hypotheses were plausible, but “with the retrospective study, there could be a lot of things that are unobserved or unexplained,” he added.
Dr. Tedeschi is interested in exploring what could be causing the association with an increased fracture risk in future research.
“I hope this draws attention to the fact that people with CPPD can have related medical problems that are outside of their joints,” added Dr. Tedeschi. “Thinking about routine screening for osteopenia and osteoporosis could be a good first step in patients with CPPD.”
The study was funded by grants from the US National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Tedeschi has worked as a consultant for Novartis. Dr. FitzGerald reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Patients with calcium pyrophosphate deposition (CPPD) disease, also known as pseudogout, have an 80% higher risk for fracture than individuals who do not have the disease, according to a new analysis.
This trend was driven by wrist fractures, where there was a more than threefold increased risk.
Previous studies identified an association between CPPD and low bone mineral density, and there is growing evidence suggesting that the dysregulation of osteoprotegerin — a molecule that is important in the regulation of osteoclasts — may be associated with early-onset CPPD, noted Sara K. Tedeschi, MD, MPH, the lead author of the study and head of crystal-induced arthritic diseases at Brigham and Women’s Hospital, Boston, Massachusetts.
However, CPPD’s association with fracture risk has yet to be explored.
In the study, Dr. Tedeschi and colleagues used Mass General Brigham electronic health record (EHR) data from 1991 to 2023 to identify 1148 individuals with acute calcium pyrophosphate (CPP) crystal arthritis. The index date was defined as the first documentation of pseudogout or synovial fluid CPP crystals. These patients were matched to 3730 comparators based on healthcare encounters within 30 days of the index date of a patient with CPPD. Patients were also matched based on the year of their first EHR encounter. Patients with a fracture documented prior to the index date were excluded from the analysis.
The primary outcome was the first fracture of the humerus, knee, wrist, hip, or pelvis, detected via published algorithms using diagnostic and procedural codes.
The research was published on January 14 in Arthritis & Rheumatology.
Although participants were not matched on age or sex, the average age was 73, and most participants were female. In total, 83.1% of participants in the CPPD group and 80.0% of those in the control group were White.
After adjustment for confounding factors including age, sex, comorbidities, and glucocorticoid use, CPPD was associated with an 80% higher risk for any fracture (hazard risk [HR], 1.8). Fracture risk was highest for the wrist (HR, 3.6).
Patients with CPPD had a 40% higher risk to experience a humerus or pelvis fracture and a 30% higher risk for hip fractures, but the results were not statistically significant.
The results were similar for sensitivity analyses that excluded patients who were prescribed glucocorticoids, treatment for osteoporosis, or had a diagnosis of rheumatoid arthritis.
Asked to comment, John D. FitzGerald, MD, PhD, clinical chief of rheumatology at the University of California, Los Angeles, noted that these associations were “convincing and strong. I thought it was a very good study and important work. CPPD is common and osteoporosis is common, so better understanding the connection is important.”
It’s still not clear why the risk for wrist fractures was highest, but Dr. Tedeschi had two hypotheses. The researchers were unable to assess for falls in this dataset, but it’s possible that patients with CPPD experiencing joint pain could fall and try to brace themselves with an outstretched arm, leading to a wrist fracture.
CPPD also commonly affects the wrist, “so it’s possible that if CPPD is affecting the wrist and if there is an association between CPPD and low bone density, maybe there’s particularly low bone density at the wrist,” she said.
Dr. FitzGerald agreed that both hypotheses were plausible, but “with the retrospective study, there could be a lot of things that are unobserved or unexplained,” he added.
Dr. Tedeschi is interested in exploring what could be causing the association with an increased fracture risk in future research.
“I hope this draws attention to the fact that people with CPPD can have related medical problems that are outside of their joints,” added Dr. Tedeschi. “Thinking about routine screening for osteopenia and osteoporosis could be a good first step in patients with CPPD.”
The study was funded by grants from the US National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Tedeschi has worked as a consultant for Novartis. Dr. FitzGerald reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM ARTHRITIS & RHEUMATOLOGY
Proinflammatory Diet May Prompt Worse Pain Course in Knee OA
TOPLINE:
Higher scores on the dietary inflammatory index in patients with knee osteoarthritis (KOA) were associated with an increased risk of experiencing greater pain over 10 years of follow-up.
METHODOLOGY:
- The researchers recruited 944 adults aged 50-80 years from the community; the mean age at baseline was 62.9 years, 51% were female, the mean body mass index was 27.9 kg/m2, and 60% had radiographic KOA at baseline.
- Magnetic resonance imaging was used to identify structural changes in the knee based on cartilage volume and bone marrow lesions at baseline and follow-up; knee pain was assessed using the Western Ontario and McMaster Universities Osteoarthritis Index pain questionnaire.
- Dietary inflammation was measured using energy-adjusted dietary inflammatory index (E-DII) scores based on nutritional information from the Food-Frequency Questionnaire (FFQ).
TAKEAWAY:
- Over a follow-up period of 10.7 years, higher E-DII scores were positively associated with increased pain scores (beta = 0.21) after adjustment for age, sex, body mass index, steps per day, education, emotional problems, employment status, comorbidities, and radiographic KOA.
- E-DII scores were not associated with tibial cartilage volume loss or overall bone marrow loss.
- Patients with higher E-DII scores had a significantly higher risk of being on a moderate pain trajectory (relative risk ratio, 1.19), compared with those who followed a minimal pain trajectory over the follow-up period.
IN PRACTICE:
“An anti-inflammatory diet may reduce pain among KOA patients. Future trials investigating the potential of an anti-inflammatory diet for pain relief in KOA are warranted,” the researchers wrote.
SOURCE:
The lead author on the study was Canchen Ma, PhD, of the University of Tasmania, Hobart, Australia. The study was published online in Arthritis Care & Research.
LIMITATIONS:
The study used a relatively small number of nutrients from the FFQ to calculate the E-DII scores; participants also exhibited a narrower range of E-DII scores than previous studies. The researchers were unable to account for pharmacologic or preventive treatments.
DISCLOSURES:
The study was supported by the National Health and Medical Research Council of Australia (NHMRC) and Arthritis Australia. Several authors received support from the National Heart Foundation Fellowship, the NHMRC Leadership Fellowship, the NHMRC Practitioner Fellowship, and the NHMRC Early Career Fellowship. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Higher scores on the dietary inflammatory index in patients with knee osteoarthritis (KOA) were associated with an increased risk of experiencing greater pain over 10 years of follow-up.
METHODOLOGY:
- The researchers recruited 944 adults aged 50-80 years from the community; the mean age at baseline was 62.9 years, 51% were female, the mean body mass index was 27.9 kg/m2, and 60% had radiographic KOA at baseline.
- Magnetic resonance imaging was used to identify structural changes in the knee based on cartilage volume and bone marrow lesions at baseline and follow-up; knee pain was assessed using the Western Ontario and McMaster Universities Osteoarthritis Index pain questionnaire.
- Dietary inflammation was measured using energy-adjusted dietary inflammatory index (E-DII) scores based on nutritional information from the Food-Frequency Questionnaire (FFQ).
TAKEAWAY:
- Over a follow-up period of 10.7 years, higher E-DII scores were positively associated with increased pain scores (beta = 0.21) after adjustment for age, sex, body mass index, steps per day, education, emotional problems, employment status, comorbidities, and radiographic KOA.
- E-DII scores were not associated with tibial cartilage volume loss or overall bone marrow loss.
- Patients with higher E-DII scores had a significantly higher risk of being on a moderate pain trajectory (relative risk ratio, 1.19), compared with those who followed a minimal pain trajectory over the follow-up period.
IN PRACTICE:
“An anti-inflammatory diet may reduce pain among KOA patients. Future trials investigating the potential of an anti-inflammatory diet for pain relief in KOA are warranted,” the researchers wrote.
SOURCE:
The lead author on the study was Canchen Ma, PhD, of the University of Tasmania, Hobart, Australia. The study was published online in Arthritis Care & Research.
LIMITATIONS:
The study used a relatively small number of nutrients from the FFQ to calculate the E-DII scores; participants also exhibited a narrower range of E-DII scores than previous studies. The researchers were unable to account for pharmacologic or preventive treatments.
DISCLOSURES:
The study was supported by the National Health and Medical Research Council of Australia (NHMRC) and Arthritis Australia. Several authors received support from the National Heart Foundation Fellowship, the NHMRC Leadership Fellowship, the NHMRC Practitioner Fellowship, and the NHMRC Early Career Fellowship. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Higher scores on the dietary inflammatory index in patients with knee osteoarthritis (KOA) were associated with an increased risk of experiencing greater pain over 10 years of follow-up.
METHODOLOGY:
- The researchers recruited 944 adults aged 50-80 years from the community; the mean age at baseline was 62.9 years, 51% were female, the mean body mass index was 27.9 kg/m2, and 60% had radiographic KOA at baseline.
- Magnetic resonance imaging was used to identify structural changes in the knee based on cartilage volume and bone marrow lesions at baseline and follow-up; knee pain was assessed using the Western Ontario and McMaster Universities Osteoarthritis Index pain questionnaire.
- Dietary inflammation was measured using energy-adjusted dietary inflammatory index (E-DII) scores based on nutritional information from the Food-Frequency Questionnaire (FFQ).
TAKEAWAY:
- Over a follow-up period of 10.7 years, higher E-DII scores were positively associated with increased pain scores (beta = 0.21) after adjustment for age, sex, body mass index, steps per day, education, emotional problems, employment status, comorbidities, and radiographic KOA.
- E-DII scores were not associated with tibial cartilage volume loss or overall bone marrow loss.
- Patients with higher E-DII scores had a significantly higher risk of being on a moderate pain trajectory (relative risk ratio, 1.19), compared with those who followed a minimal pain trajectory over the follow-up period.
IN PRACTICE:
“An anti-inflammatory diet may reduce pain among KOA patients. Future trials investigating the potential of an anti-inflammatory diet for pain relief in KOA are warranted,” the researchers wrote.
SOURCE:
The lead author on the study was Canchen Ma, PhD, of the University of Tasmania, Hobart, Australia. The study was published online in Arthritis Care & Research.
LIMITATIONS:
The study used a relatively small number of nutrients from the FFQ to calculate the E-DII scores; participants also exhibited a narrower range of E-DII scores than previous studies. The researchers were unable to account for pharmacologic or preventive treatments.
DISCLOSURES:
The study was supported by the National Health and Medical Research Council of Australia (NHMRC) and Arthritis Australia. Several authors received support from the National Heart Foundation Fellowship, the NHMRC Leadership Fellowship, the NHMRC Practitioner Fellowship, and the NHMRC Early Career Fellowship. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Breaking the Diagnostic Bottleneck in RA
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).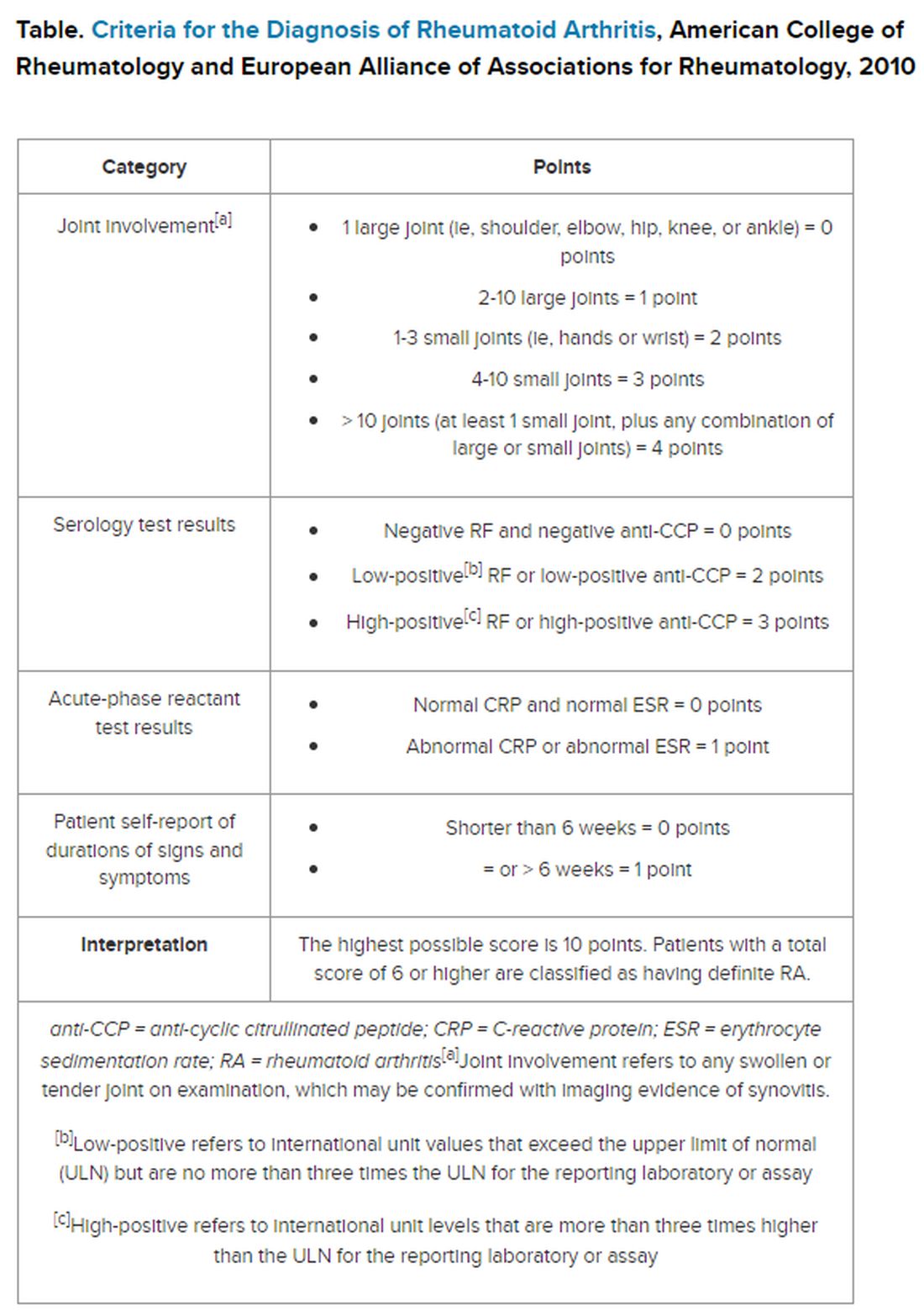
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
A Paradox? Higher Male Fertility Seen With Inflammatory Arthritis
TOPLINE:
Men with an inflammatory arthritis (IA) diagnosis are less likely to be childless than healthy comparators, according to an epidemiological study.
METHODS:
- 10,865 men in the Norwegian Arthritis Registry were compared with 54,325 men without IA, matched by age and location.
- In the arthritis group, 37% had rheumatoid arthritis, 33% had psoriatic arthritis, and 30% had spondyloarthritis.
- Researchers used childlessness and number of children as proxies for male fertility.
TAKEAWAY:
- 21% of men with IA were childless compared with 27% in the healthy cohort (P < .001).
- On an average, a man with IA had 1.80 children whereas a man in the control group had 1.69 children (P < .001).
- These findings were consistent over time, but the most pronounced difference between groups was seen in men diagnosed after the year 2000.
IN PRACTICE:
The finding “is novel and generates new hypotheses regarding associations between fertility, inflammatory rheumatic diseases, and immune-modulating drugs,” the authors wrote.
SOURCE:
First author Gudrun David Sigmo, of the department of rheumatology at Stavanger (Norway) University Hospital, and colleagues had their work published online on January 23, 2024, in Annals of the Rheumatic Diseases.
LIMITATIONS:
The analysis relied on administrative data, and researchers did not have data on confounding factors.
DISCLOSURES:
The study was funded by the nonprofit organizations Aslaug Anders fond, Astri og Edvard Riisøens legat, Det alminnelige medisinske forskningsfond, Pahles legat, and Fagsenter for medisins-ke kvalitetsregistre i Helse Vest. The authors declared no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
Men with an inflammatory arthritis (IA) diagnosis are less likely to be childless than healthy comparators, according to an epidemiological study.
METHODS:
- 10,865 men in the Norwegian Arthritis Registry were compared with 54,325 men without IA, matched by age and location.
- In the arthritis group, 37% had rheumatoid arthritis, 33% had psoriatic arthritis, and 30% had spondyloarthritis.
- Researchers used childlessness and number of children as proxies for male fertility.
TAKEAWAY:
- 21% of men with IA were childless compared with 27% in the healthy cohort (P < .001).
- On an average, a man with IA had 1.80 children whereas a man in the control group had 1.69 children (P < .001).
- These findings were consistent over time, but the most pronounced difference between groups was seen in men diagnosed after the year 2000.
IN PRACTICE:
The finding “is novel and generates new hypotheses regarding associations between fertility, inflammatory rheumatic diseases, and immune-modulating drugs,” the authors wrote.
SOURCE:
First author Gudrun David Sigmo, of the department of rheumatology at Stavanger (Norway) University Hospital, and colleagues had their work published online on January 23, 2024, in Annals of the Rheumatic Diseases.
LIMITATIONS:
The analysis relied on administrative data, and researchers did not have data on confounding factors.
DISCLOSURES:
The study was funded by the nonprofit organizations Aslaug Anders fond, Astri og Edvard Riisøens legat, Det alminnelige medisinske forskningsfond, Pahles legat, and Fagsenter for medisins-ke kvalitetsregistre i Helse Vest. The authors declared no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
Men with an inflammatory arthritis (IA) diagnosis are less likely to be childless than healthy comparators, according to an epidemiological study.
METHODS:
- 10,865 men in the Norwegian Arthritis Registry were compared with 54,325 men without IA, matched by age and location.
- In the arthritis group, 37% had rheumatoid arthritis, 33% had psoriatic arthritis, and 30% had spondyloarthritis.
- Researchers used childlessness and number of children as proxies for male fertility.
TAKEAWAY:
- 21% of men with IA were childless compared with 27% in the healthy cohort (P < .001).
- On an average, a man with IA had 1.80 children whereas a man in the control group had 1.69 children (P < .001).
- These findings were consistent over time, but the most pronounced difference between groups was seen in men diagnosed after the year 2000.
IN PRACTICE:
The finding “is novel and generates new hypotheses regarding associations between fertility, inflammatory rheumatic diseases, and immune-modulating drugs,” the authors wrote.
SOURCE:
First author Gudrun David Sigmo, of the department of rheumatology at Stavanger (Norway) University Hospital, and colleagues had their work published online on January 23, 2024, in Annals of the Rheumatic Diseases.
LIMITATIONS:
The analysis relied on administrative data, and researchers did not have data on confounding factors.
DISCLOSURES:
The study was funded by the nonprofit organizations Aslaug Anders fond, Astri og Edvard Riisøens legat, Det alminnelige medisinske forskningsfond, Pahles legat, and Fagsenter for medisins-ke kvalitetsregistre i Helse Vest. The authors declared no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Vibrating Belt Receives Approval to Help Women With Osteopenia Keep Bone Strength
The US Food and Drug Administration (FDA) has approved a wearable belt device for postmenopausal women with osteopenia, the precursor to osteoporosis, according to the company’s manufacturer, Bone Health Technologies.
According to the company, the device (Osteoboost) is the first nonpharmacologic device-based, prescription-only treatment for postmenopausal women with low bone density. It has not been tested for ability to reduce fracture risk.

The device is worn around the hips and delivers calibrated mild vibrations to the hips and lumbar spine to help preserve bone strength and density. A vibration pack is mounted to the back of the belt.
FDA approval, announced on January 18, was based on the findings of a National Institutes of Health–funded double-blinded, sham-controlled study of 126 women with low bone density conducted at the University of Nebraska Medical Center in Omaha. The data were shared at the 2023 Endocrine Society and American Society for Bone and Mineral Research annual meetings and published in the Journal of the Endocrine Society.
Lead investigator Laura D. Bilek, PT, PhD, associate dean for research and associate professor at the University of Nebraska, and colleagues wrote that the primary outcome measurement was the change in vertebral strength measured by CT scans for women who used the device a minimum of three times per week compared with a sham group who wore a belt that emitted sound but had no vibrations.
Compressive strength and volumetric density of the first lumbar vertebra were analyzed.
In the active-belt group, women lost, on average, 0.48% bone strength, while those in the sham group lost nearly 2.84% (P = .014), about five times as much. Results also showed that participants in the active treatment group who used the device three times per week lost 0.29% bone mineral density (BMD) compared with the 1.97% BMD lost in the control group. No adverse events were reported in the study.
Sonali Khandelwal, MD, a rheumatologist at Rush University in Chicago, told this news organization there’s considerable fear among some patients about long-term use of available medications for bone health, “so any modality that is nontherapeutic — not a pill — is always exciting.”
The endpoints of the study are one good measure, she said, but she emphasized that it will be important to show that the improved bone density from the belt that is described in this study “is a true marker of decreased fracture risk.”
Because there are no apparent side effects, she said it may be effective in combination with weight-bearing exercise, vitamin D and calcium, and/or medication, depending on severity of bone loss.
Current medications on the market for osteoporosis have been shown to improve bone strength and reduce fracture risk, she noted.
“It could help; I just don’t think we have enough evidence that it will completely treat the bone loss,” Dr. Khandelwal said.
She said she sees the potential population most interested in the belt as premenopausal women with a family history of bone loss who may not meet the level of bone loss for medical management but are interested in prevention.
“I also think of individuals who might already meet medication needs but are completely averse to being on medication,” she said. The bulk of her practice is treating bone loss, she said, estimating that 20% of her patients do not want to be on medication.
Bone Health Technologies CEO Laura Yecies, MBA, told this news organization the company has not yet set the price for the device and noted that because it will be available by prescription only, out-of-pocket costs and copays will differ. She said the company expects to begin shipping later this year. Requests for update notifications can be made at the company’s website.
Dr. Bilek told this news organization the device was tested for a year, so it’s unclear how long people with osteopenia would need to wear the belt for maximum benefit.
The theory behind the mechanism of action, she said, “is that the vibration actually inhibits the cells [osteoclasts] that take away bone mass.”
The researchers included only postmenopausal women with osteopenia in the study, but Dr. Bilek said she would like to test the device on other groups, such as men with prostate cancer getting testosterone-blocking therapy, which can result in loss of bone density. An estimated 34 million people in the United States have osteopenia.
Dr. Bilek said a next step for the study is to enroll a more diverse cohort at an additional center to test the device because most of the women in this one were White.
She noted that women’s bone mass peaks at age 30 and then starts to decline.
“When women hit menopause, there’s a really rapid decline [in bone strength] for the next 5-7 years and then the decline levels off. If we can slow that decline, hopefully that woman’s bone density is maintained at a higher level throughout their life,” Dr. Bilek said.
Dr. Bilek is a scientific adviser to Bone Health Technologies. She and many coauthors of the study received grants or fees from the company and own stock in or are employees of the company. Ms. Yecies is the founder and CEO of Bone Health Technologies. Dr. Khandelwal had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved a wearable belt device for postmenopausal women with osteopenia, the precursor to osteoporosis, according to the company’s manufacturer, Bone Health Technologies.
According to the company, the device (Osteoboost) is the first nonpharmacologic device-based, prescription-only treatment for postmenopausal women with low bone density. It has not been tested for ability to reduce fracture risk.
The device is worn around the hips and delivers calibrated mild vibrations to the hips and lumbar spine to help preserve bone strength and density. A vibration pack is mounted to the back of the belt.
FDA approval, announced on January 18, was based on the findings of a National Institutes of Health–funded double-blinded, sham-controlled study of 126 women with low bone density conducted at the University of Nebraska Medical Center in Omaha. The data were shared at the 2023 Endocrine Society and American Society for Bone and Mineral Research annual meetings and published in the Journal of the Endocrine Society.
Lead investigator Laura D. Bilek, PT, PhD, associate dean for research and associate professor at the University of Nebraska, and colleagues wrote that the primary outcome measurement was the change in vertebral strength measured by CT scans for women who used the device a minimum of three times per week compared with a sham group who wore a belt that emitted sound but had no vibrations.
Compressive strength and volumetric density of the first lumbar vertebra were analyzed.
In the active-belt group, women lost, on average, 0.48% bone strength, while those in the sham group lost nearly 2.84% (P = .014), about five times as much. Results also showed that participants in the active treatment group who used the device three times per week lost 0.29% bone mineral density (BMD) compared with the 1.97% BMD lost in the control group. No adverse events were reported in the study.
Sonali Khandelwal, MD, a rheumatologist at Rush University in Chicago, told this news organization there’s considerable fear among some patients about long-term use of available medications for bone health, “so any modality that is nontherapeutic — not a pill — is always exciting.”
The endpoints of the study are one good measure, she said, but she emphasized that it will be important to show that the improved bone density from the belt that is described in this study “is a true marker of decreased fracture risk.”
Because there are no apparent side effects, she said it may be effective in combination with weight-bearing exercise, vitamin D and calcium, and/or medication, depending on severity of bone loss.
Current medications on the market for osteoporosis have been shown to improve bone strength and reduce fracture risk, she noted.
“It could help; I just don’t think we have enough evidence that it will completely treat the bone loss,” Dr. Khandelwal said.
She said she sees the potential population most interested in the belt as premenopausal women with a family history of bone loss who may not meet the level of bone loss for medical management but are interested in prevention.
“I also think of individuals who might already meet medication needs but are completely averse to being on medication,” she said. The bulk of her practice is treating bone loss, she said, estimating that 20% of her patients do not want to be on medication.
Bone Health Technologies CEO Laura Yecies, MBA, told this news organization the company has not yet set the price for the device and noted that because it will be available by prescription only, out-of-pocket costs and copays will differ. She said the company expects to begin shipping later this year. Requests for update notifications can be made at the company’s website.
Dr. Bilek told this news organization the device was tested for a year, so it’s unclear how long people with osteopenia would need to wear the belt for maximum benefit.
The theory behind the mechanism of action, she said, “is that the vibration actually inhibits the cells [osteoclasts] that take away bone mass.”
The researchers included only postmenopausal women with osteopenia in the study, but Dr. Bilek said she would like to test the device on other groups, such as men with prostate cancer getting testosterone-blocking therapy, which can result in loss of bone density. An estimated 34 million people in the United States have osteopenia.
Dr. Bilek said a next step for the study is to enroll a more diverse cohort at an additional center to test the device because most of the women in this one were White.
She noted that women’s bone mass peaks at age 30 and then starts to decline.
“When women hit menopause, there’s a really rapid decline [in bone strength] for the next 5-7 years and then the decline levels off. If we can slow that decline, hopefully that woman’s bone density is maintained at a higher level throughout their life,” Dr. Bilek said.
Dr. Bilek is a scientific adviser to Bone Health Technologies. She and many coauthors of the study received grants or fees from the company and own stock in or are employees of the company. Ms. Yecies is the founder and CEO of Bone Health Technologies. Dr. Khandelwal had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved a wearable belt device for postmenopausal women with osteopenia, the precursor to osteoporosis, according to the company’s manufacturer, Bone Health Technologies.
According to the company, the device (Osteoboost) is the first nonpharmacologic device-based, prescription-only treatment for postmenopausal women with low bone density. It has not been tested for ability to reduce fracture risk.
The device is worn around the hips and delivers calibrated mild vibrations to the hips and lumbar spine to help preserve bone strength and density. A vibration pack is mounted to the back of the belt.
FDA approval, announced on January 18, was based on the findings of a National Institutes of Health–funded double-blinded, sham-controlled study of 126 women with low bone density conducted at the University of Nebraska Medical Center in Omaha. The data were shared at the 2023 Endocrine Society and American Society for Bone and Mineral Research annual meetings and published in the Journal of the Endocrine Society.
Lead investigator Laura D. Bilek, PT, PhD, associate dean for research and associate professor at the University of Nebraska, and colleagues wrote that the primary outcome measurement was the change in vertebral strength measured by CT scans for women who used the device a minimum of three times per week compared with a sham group who wore a belt that emitted sound but had no vibrations.
Compressive strength and volumetric density of the first lumbar vertebra were analyzed.
In the active-belt group, women lost, on average, 0.48% bone strength, while those in the sham group lost nearly 2.84% (P = .014), about five times as much. Results also showed that participants in the active treatment group who used the device three times per week lost 0.29% bone mineral density (BMD) compared with the 1.97% BMD lost in the control group. No adverse events were reported in the study.
Sonali Khandelwal, MD, a rheumatologist at Rush University in Chicago, told this news organization there’s considerable fear among some patients about long-term use of available medications for bone health, “so any modality that is nontherapeutic — not a pill — is always exciting.”
The endpoints of the study are one good measure, she said, but she emphasized that it will be important to show that the improved bone density from the belt that is described in this study “is a true marker of decreased fracture risk.”
Because there are no apparent side effects, she said it may be effective in combination with weight-bearing exercise, vitamin D and calcium, and/or medication, depending on severity of bone loss.
Current medications on the market for osteoporosis have been shown to improve bone strength and reduce fracture risk, she noted.
“It could help; I just don’t think we have enough evidence that it will completely treat the bone loss,” Dr. Khandelwal said.
She said she sees the potential population most interested in the belt as premenopausal women with a family history of bone loss who may not meet the level of bone loss for medical management but are interested in prevention.
“I also think of individuals who might already meet medication needs but are completely averse to being on medication,” she said. The bulk of her practice is treating bone loss, she said, estimating that 20% of her patients do not want to be on medication.
Bone Health Technologies CEO Laura Yecies, MBA, told this news organization the company has not yet set the price for the device and noted that because it will be available by prescription only, out-of-pocket costs and copays will differ. She said the company expects to begin shipping later this year. Requests for update notifications can be made at the company’s website.
Dr. Bilek told this news organization the device was tested for a year, so it’s unclear how long people with osteopenia would need to wear the belt for maximum benefit.
The theory behind the mechanism of action, she said, “is that the vibration actually inhibits the cells [osteoclasts] that take away bone mass.”
The researchers included only postmenopausal women with osteopenia in the study, but Dr. Bilek said she would like to test the device on other groups, such as men with prostate cancer getting testosterone-blocking therapy, which can result in loss of bone density. An estimated 34 million people in the United States have osteopenia.
Dr. Bilek said a next step for the study is to enroll a more diverse cohort at an additional center to test the device because most of the women in this one were White.
She noted that women’s bone mass peaks at age 30 and then starts to decline.
“When women hit menopause, there’s a really rapid decline [in bone strength] for the next 5-7 years and then the decline levels off. If we can slow that decline, hopefully that woman’s bone density is maintained at a higher level throughout their life,” Dr. Bilek said.
Dr. Bilek is a scientific adviser to Bone Health Technologies. She and many coauthors of the study received grants or fees from the company and own stock in or are employees of the company. Ms. Yecies is the founder and CEO of Bone Health Technologies. Dr. Khandelwal had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Is RA Disease Activity Assessed Too Little After Starting TNFi?
TOPLINE:
Less than half of patients with rheumatoid arthritis (RA) initiating a first-line tumor necrosis factor inhibitor (TNFi) in clinical practice had a recorded composite disease activity assessment at the start of the treatment, and many remained on that treatment for years without evidence recorded in their electronic medical record of achieving low-disease activity or remission.
METHODOLOGY:
- Researchers reviewed data from 1651 adults aged 18 years and older with moderate to severe RA at baseline or follow-up in the electronic medical record database of the American Rheumatology Network, a large community network of independent practices with > 200 rheumatologists across the United States.
- Patients received a TNFi as their first advanced therapy between January 2014 and August 2021 and were assessed for measurement of disease activity with the Clinical Disease Activity Index (CDAI) or Routine Assessment of Patient Index Data 3 (RAPID3) at baseline and follow-up visits.
TAKEAWAY:
- Among the patients with moderate to severe RA, 47.2% of patients remained on first-line TNFi therapy 1 year after initiation despite no evidence of achieving treatment targets of low disease activity or remission (defined as CDAI ≤ 10 and/or RAPID3 ≤ 2).
- Approximately one third of patients remained on TNFi therapy for 2 (38.1%) or 3 (35.4%) years after initiation despite not achieving these targets. The median times to TNFi discontinuation was 30.4 months and to subsequent therapy initiation 68.3 months.
- A total of 52% discontinued their initial TNFi during the study period; among those who started a second therapy, 15% restarted the same TNFi, 45.6% started another TNFi, 27.6% started a non-TNFi biologic, and 11.5% started a Janus kinase inhibitor.
- The most common reported reasons for discontinuation were a combination of efficacy and intolerance, efficacy only, and intolerance only (26.9%, 25.3%, and 20.3%, respectively).
- Persistent pain was the most common reason for efficacy-related discontinuation (39.0%), followed by persistent inflammation/swelling and overall general discomfort (31.8% for both).
IN PRACTICE:
“Consistent monitoring of treatment response and timely switch to effective therapy as appropriate is needed in patients with RA initiating their first advanced therapies,” the researchers wrote.
SOURCE:
First author Colin Edgerton, MD, of Articularis Healthcare Group and American Rheumatology Network, Charleston, South Carolina, reported their work on January 14, 2024, in ACR Open Rheumatology.
LIMITATIONS:
The findings were limited by several factors including the retrospective design, incomplete data from electronic medical records, and reliance on physician documentation for drivers of discontinuation.
DISCLOSURES:
The study was supported by AbbVie. Lead author Edgerton also disclosed relationships with Novartis and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
TOPLINE:
Less than half of patients with rheumatoid arthritis (RA) initiating a first-line tumor necrosis factor inhibitor (TNFi) in clinical practice had a recorded composite disease activity assessment at the start of the treatment, and many remained on that treatment for years without evidence recorded in their electronic medical record of achieving low-disease activity or remission.
METHODOLOGY:
- Researchers reviewed data from 1651 adults aged 18 years and older with moderate to severe RA at baseline or follow-up in the electronic medical record database of the American Rheumatology Network, a large community network of independent practices with > 200 rheumatologists across the United States.
- Patients received a TNFi as their first advanced therapy between January 2014 and August 2021 and were assessed for measurement of disease activity with the Clinical Disease Activity Index (CDAI) or Routine Assessment of Patient Index Data 3 (RAPID3) at baseline and follow-up visits.
TAKEAWAY:
- Among the patients with moderate to severe RA, 47.2% of patients remained on first-line TNFi therapy 1 year after initiation despite no evidence of achieving treatment targets of low disease activity or remission (defined as CDAI ≤ 10 and/or RAPID3 ≤ 2).
- Approximately one third of patients remained on TNFi therapy for 2 (38.1%) or 3 (35.4%) years after initiation despite not achieving these targets. The median times to TNFi discontinuation was 30.4 months and to subsequent therapy initiation 68.3 months.
- A total of 52% discontinued their initial TNFi during the study period; among those who started a second therapy, 15% restarted the same TNFi, 45.6% started another TNFi, 27.6% started a non-TNFi biologic, and 11.5% started a Janus kinase inhibitor.
- The most common reported reasons for discontinuation were a combination of efficacy and intolerance, efficacy only, and intolerance only (26.9%, 25.3%, and 20.3%, respectively).
- Persistent pain was the most common reason for efficacy-related discontinuation (39.0%), followed by persistent inflammation/swelling and overall general discomfort (31.8% for both).
IN PRACTICE:
“Consistent monitoring of treatment response and timely switch to effective therapy as appropriate is needed in patients with RA initiating their first advanced therapies,” the researchers wrote.
SOURCE:
First author Colin Edgerton, MD, of Articularis Healthcare Group and American Rheumatology Network, Charleston, South Carolina, reported their work on January 14, 2024, in ACR Open Rheumatology.
LIMITATIONS:
The findings were limited by several factors including the retrospective design, incomplete data from electronic medical records, and reliance on physician documentation for drivers of discontinuation.
DISCLOSURES:
The study was supported by AbbVie. Lead author Edgerton also disclosed relationships with Novartis and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
TOPLINE:
Less than half of patients with rheumatoid arthritis (RA) initiating a first-line tumor necrosis factor inhibitor (TNFi) in clinical practice had a recorded composite disease activity assessment at the start of the treatment, and many remained on that treatment for years without evidence recorded in their electronic medical record of achieving low-disease activity or remission.
METHODOLOGY:
- Researchers reviewed data from 1651 adults aged 18 years and older with moderate to severe RA at baseline or follow-up in the electronic medical record database of the American Rheumatology Network, a large community network of independent practices with > 200 rheumatologists across the United States.
- Patients received a TNFi as their first advanced therapy between January 2014 and August 2021 and were assessed for measurement of disease activity with the Clinical Disease Activity Index (CDAI) or Routine Assessment of Patient Index Data 3 (RAPID3) at baseline and follow-up visits.
TAKEAWAY:
- Among the patients with moderate to severe RA, 47.2% of patients remained on first-line TNFi therapy 1 year after initiation despite no evidence of achieving treatment targets of low disease activity or remission (defined as CDAI ≤ 10 and/or RAPID3 ≤ 2).
- Approximately one third of patients remained on TNFi therapy for 2 (38.1%) or 3 (35.4%) years after initiation despite not achieving these targets. The median times to TNFi discontinuation was 30.4 months and to subsequent therapy initiation 68.3 months.
- A total of 52% discontinued their initial TNFi during the study period; among those who started a second therapy, 15% restarted the same TNFi, 45.6% started another TNFi, 27.6% started a non-TNFi biologic, and 11.5% started a Janus kinase inhibitor.
- The most common reported reasons for discontinuation were a combination of efficacy and intolerance, efficacy only, and intolerance only (26.9%, 25.3%, and 20.3%, respectively).
- Persistent pain was the most common reason for efficacy-related discontinuation (39.0%), followed by persistent inflammation/swelling and overall general discomfort (31.8% for both).
IN PRACTICE:
“Consistent monitoring of treatment response and timely switch to effective therapy as appropriate is needed in patients with RA initiating their first advanced therapies,” the researchers wrote.
SOURCE:
First author Colin Edgerton, MD, of Articularis Healthcare Group and American Rheumatology Network, Charleston, South Carolina, reported their work on January 14, 2024, in ACR Open Rheumatology.
LIMITATIONS:
The findings were limited by several factors including the retrospective design, incomplete data from electronic medical records, and reliance on physician documentation for drivers of discontinuation.
DISCLOSURES:
The study was supported by AbbVie. Lead author Edgerton also disclosed relationships with Novartis and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
Cutaneous lupus, dermatomyositis: Excitement growing around emerging therapies
ORLANDO, FLORIDA — Advances in treating medical conditions rarely emerge in a straight line. Oftentimes, progress comes in fits and starts, and therapies to treat cutaneous lupus erythematosus (CLE) and dermatomyositis are no exception.
Beyond approved treatments that deserve more attention, like belimumab, approved by the Food and Drug Administration (FDA) for systemic lupus erythematosus (SLE) in 2011, and Octagam 10%, an intravenous immune globulin (IVIG) preparation approved for dermatomyositis in 2021, anticipation is growing for emerging therapies and their potential to provide relief to patients, Anthony Fernandez, MD, PhD, said at the ODAC Dermatology, Aesthetic & Surgical Conference. The tyrosine kinase 2 (TYK2) inhibitor deucravacitinib, Janus kinase (JAK) inhibitors brepocitinib and baricitinib, and the monoclonal antibody anifrolumab, he noted, are prime examples.
“. In my opinion, this is the start of what will be the most exciting decade in the history of these two diseases,” said Dr. Fernandez, director of medical dermatology at the Cleveland Clinic.
Emerging Treatments for Cutaneous Lupus
Although SLE can involve many organ systems, the skin is one of the most affected. There are specific cutaneous lesions categorized as either acute cutaneous lupus, subacute cutaneous lupus, or chronic cutaneous lupus.
The oral TYK2 inhibitor deucravacitinib, for example, should be able to dampen interleukin responses in people with CLE, Dr. Fernandez said. Deucravacitinib was approved by the FDA to treat psoriasis in September 2022.

A phase 2 study published in 2023 focused on this agent for relief of systemic lupus. Improvements in cutaneous disease were a secondary endpoint. The trial demonstrated that the patients treated with deucravacitinib achieved a 56%-70% CLASI-50 response, depending on dosing, compared with a 17% response among those on placebo at week 48.
Based on the trial results, recruitment has begun for a phase 2 trial to evaluate deucravacitinib, compared with placebo, in patients with discoid and/or subacute cutaneous lupus. “This may be another medicine we have available to give to any of our patients with cutaneous lupus,” Dr. Fernandez said.
Anifrolumab Appears Promising
The FDA approval of anifrolumab, a type I interferon (IFN) receptor antagonist, for treating moderate to severe SLE in July 2021, for example, is good news for dermatologists and their patients, added Dr. Fernandez. “Almost immediately after approval, case studies showed marked improvement in patients with refractory cutaneous lupus.” While the therapy was approved for treating systemic lupus, it allows for off-label treatment of the cutaneous predominant form of the disease, he said.
Furthermore, the manufacturer of anifrolumab, AstraZeneca, is launching the LAVENDER clinical trial to assess the monoclonal antibody specifically for treating CLE. “This is a big deal because we may be able to prescribe anifrolumab for our cutaneous lupus patients who don’t have systemic lupus,” Dr. Fernandez said.
Phase 3 data supported use the of anifrolumab in systemic lupus, including the TULIP-2 trial, which demonstrated its superiority to placebo for reducing severity of systemic disease and lowering corticosteroid use. A study published in March 2023 of 11 patients showed that they had a “very fast response” to the agent, Dr. Fernandez said, with a 50% or greater improvement in the Cutaneous Lupus Erythematosus Disease Area and Severity Index activity score reached by all participants at week 16. Improvements of 50% or more in this scoring system are considered clinically meaningful, he added.
Upcoming Dermatomyositis Treatments
Why highlight emerging therapies for CLE and dermatomyositis in the same ODAC presentation? Although distinct conditions, these autoimmune conditions are both mediated by type 1 IFN inflammation.
Dermatomyositis is a relatively rare immune-mediated disease that most commonly affects the skin and muscle. Doctors score disease presentation, activity, and clinical improvements on a scale similar to CLASI for cutaneous lupus, the CDASI or Cutaneous Dermatomyositis Disease Area and Severity Index. Among people with CDASI activity scores of at least 14, which is the threshold for moderate to severe disease, a 20% improvement is clinically meaningful, Dr. Fernandez said. In addition, a 40% or greater improvement correlates with significant improvements in quality of life.
There is now more evidence for the use of IVIG to treat dermatomyositis. “Among those of us who treat dermatomyositis on a regular basis, we believe IVIG is the most potent treatment. We’ve known that for a long time,” Dr. Fernandez said.
Despite this tenet, for years, there was only one placebo-controlled trial, published in 1993, that evaluated IVIG treatment for dermatomyositis, and it included only 15 participants. That was until October 2022, he said, when the New England Journal of Medicine published a study comparing a specific brand of IVIG (Octagam) with placebo in 95 people with dermatomyositis.
In the study, 79% of participants treated with IVIG had a total improvement score of at least 20 (minimal improvement), the primary endpoint, at 16 weeks, compared with 44% of those receiving a placebo. Those treated with IVIG also had significant improvements in the CDASI score, a secondary endpoint, compared with those on placebo, he said.
Based on results of this trial, the FDA approved Octagam 10% for dermatomyositis in adults. Dr. Fernandez noted the approval is restricted to the brand of IVIG in the trial, not all IVIG products. However, “the FDA approval is most important to us because it gives us ammunition to fight for insurers to approve IVIG when we feel our patients with dermatomyositis need it,” regardless of the brand.
The Potential of JAK1 Inhibitors
An open-label study of the JAK inhibitor tofacitinib, published in December 2020, showed that mean changes in CDASI activity scores at 12 weeks were statistically significant compared with baseline in 10 people with dermatomyositis. “The importance of this study is that it is proof of concept that JAK inhibition can be effective for treating dermatomyositis, especially with active skin disease,” Dr. Fernandez said.
In addition, two large phase 3 trials are evaluating JAK inhibitor safety and efficacy for treating dermatomyositis. One is the VALOR trial, currently recruiting people with recalcitrant dermatomyositis to evaluate treatment with brepocitinib. Researchers in France are looking at another JAK inhibitor, baricitinib, for treating relapsing or treatment-naive dermatomyositis. Recruitment for the BIRD clinical trial is ongoing.
Monoclonal Antibody Showing Promise
“When it comes to looking specifically at dermatomyositis cutaneous disease, it’s been found that the levels of IFN beta correlate best with not only lesional skin type 1 IFN inflammatory signatures but also overall clinical disease activity,” Dr. Fernandez said. This correlation is stronger than for any other IFN-1-type cytokine active in the disorder.
“Perhaps blocking IFN beta might be best way to get control of dermatomyositis activity,” he added.
With that in mind, a phase 2 trial of dazukibart presented at the American Academy of Dermatology 2023 annual meeting highlighted the promise of this agent that targets type 1 IFN beta.
The primary endpoint was improvement in CDASI at 12 weeks. “This medication has remarkable efficacy,” Dr. Fernandez said. “We were one of the sites for this trial. Despite being blinded, there was no question about who was receiving drug and who was receiving placebo.”
“A minimal clinical improvement in disease activity was seen in more than 90%, so almost every patient who received this medication had meaningful improvement,” he added.
Based on the results, the manufacturer, Pfizer, is recruiting participants for a phase 3 trial to further assess dazukibart in dermatomyositis and polymyositis. Dr. Fernandez said, “This is a story you should pay attention to if you treat any dermatomyositis patients at all.”
Regarding these emerging therapies for CLE and dermatomyositis, “This looks very much like the early days of psoriasis, in the early 2000s, when there was a lot of activity developing treatments,” Dr. Fernandez said. “I will predict that within 10 years, we will have multiple novel agents available that will probably work better than anything we have today.”
Dr. Fernandez reported receiving grant and/or research support from Alexion, Incyte, Mallinckrodt Pharmaceuticals, Novartis, Pfizer, and Priovant Therapeutics; acting as a consultant or advisory board member for AbbVie, Biogen, Mallinckrodt Pharmaceuticals; and being a member of the speaker bureau or receiving honoraria for non-CME from AbbVie, Kyowa Kirin, and Mallinckrodt Pharmaceuticals.
A version of this article appeared on Medscape.com.
ORLANDO, FLORIDA — Advances in treating medical conditions rarely emerge in a straight line. Oftentimes, progress comes in fits and starts, and therapies to treat cutaneous lupus erythematosus (CLE) and dermatomyositis are no exception.
Beyond approved treatments that deserve more attention, like belimumab, approved by the Food and Drug Administration (FDA) for systemic lupus erythematosus (SLE) in 2011, and Octagam 10%, an intravenous immune globulin (IVIG) preparation approved for dermatomyositis in 2021, anticipation is growing for emerging therapies and their potential to provide relief to patients, Anthony Fernandez, MD, PhD, said at the ODAC Dermatology, Aesthetic & Surgical Conference. The tyrosine kinase 2 (TYK2) inhibitor deucravacitinib, Janus kinase (JAK) inhibitors brepocitinib and baricitinib, and the monoclonal antibody anifrolumab, he noted, are prime examples.
“. In my opinion, this is the start of what will be the most exciting decade in the history of these two diseases,” said Dr. Fernandez, director of medical dermatology at the Cleveland Clinic.
Emerging Treatments for Cutaneous Lupus
Although SLE can involve many organ systems, the skin is one of the most affected. There are specific cutaneous lesions categorized as either acute cutaneous lupus, subacute cutaneous lupus, or chronic cutaneous lupus.
The oral TYK2 inhibitor deucravacitinib, for example, should be able to dampen interleukin responses in people with CLE, Dr. Fernandez said. Deucravacitinib was approved by the FDA to treat psoriasis in September 2022.
A phase 2 study published in 2023 focused on this agent for relief of systemic lupus. Improvements in cutaneous disease were a secondary endpoint. The trial demonstrated that the patients treated with deucravacitinib achieved a 56%-70% CLASI-50 response, depending on dosing, compared with a 17% response among those on placebo at week 48.
Based on the trial results, recruitment has begun for a phase 2 trial to evaluate deucravacitinib, compared with placebo, in patients with discoid and/or subacute cutaneous lupus. “This may be another medicine we have available to give to any of our patients with cutaneous lupus,” Dr. Fernandez said.
Anifrolumab Appears Promising
The FDA approval of anifrolumab, a type I interferon (IFN) receptor antagonist, for treating moderate to severe SLE in July 2021, for example, is good news for dermatologists and their patients, added Dr. Fernandez. “Almost immediately after approval, case studies showed marked improvement in patients with refractory cutaneous lupus.” While the therapy was approved for treating systemic lupus, it allows for off-label treatment of the cutaneous predominant form of the disease, he said.
Furthermore, the manufacturer of anifrolumab, AstraZeneca, is launching the LAVENDER clinical trial to assess the monoclonal antibody specifically for treating CLE. “This is a big deal because we may be able to prescribe anifrolumab for our cutaneous lupus patients who don’t have systemic lupus,” Dr. Fernandez said.
Phase 3 data supported use the of anifrolumab in systemic lupus, including the TULIP-2 trial, which demonstrated its superiority to placebo for reducing severity of systemic disease and lowering corticosteroid use. A study published in March 2023 of 11 patients showed that they had a “very fast response” to the agent, Dr. Fernandez said, with a 50% or greater improvement in the Cutaneous Lupus Erythematosus Disease Area and Severity Index activity score reached by all participants at week 16. Improvements of 50% or more in this scoring system are considered clinically meaningful, he added.
Upcoming Dermatomyositis Treatments
Why highlight emerging therapies for CLE and dermatomyositis in the same ODAC presentation? Although distinct conditions, these autoimmune conditions are both mediated by type 1 IFN inflammation.
Dermatomyositis is a relatively rare immune-mediated disease that most commonly affects the skin and muscle. Doctors score disease presentation, activity, and clinical improvements on a scale similar to CLASI for cutaneous lupus, the CDASI or Cutaneous Dermatomyositis Disease Area and Severity Index. Among people with CDASI activity scores of at least 14, which is the threshold for moderate to severe disease, a 20% improvement is clinically meaningful, Dr. Fernandez said. In addition, a 40% or greater improvement correlates with significant improvements in quality of life.
There is now more evidence for the use of IVIG to treat dermatomyositis. “Among those of us who treat dermatomyositis on a regular basis, we believe IVIG is the most potent treatment. We’ve known that for a long time,” Dr. Fernandez said.
Despite this tenet, for years, there was only one placebo-controlled trial, published in 1993, that evaluated IVIG treatment for dermatomyositis, and it included only 15 participants. That was until October 2022, he said, when the New England Journal of Medicine published a study comparing a specific brand of IVIG (Octagam) with placebo in 95 people with dermatomyositis.
In the study, 79% of participants treated with IVIG had a total improvement score of at least 20 (minimal improvement), the primary endpoint, at 16 weeks, compared with 44% of those receiving a placebo. Those treated with IVIG also had significant improvements in the CDASI score, a secondary endpoint, compared with those on placebo, he said.
Based on results of this trial, the FDA approved Octagam 10% for dermatomyositis in adults. Dr. Fernandez noted the approval is restricted to the brand of IVIG in the trial, not all IVIG products. However, “the FDA approval is most important to us because it gives us ammunition to fight for insurers to approve IVIG when we feel our patients with dermatomyositis need it,” regardless of the brand.
The Potential of JAK1 Inhibitors
An open-label study of the JAK inhibitor tofacitinib, published in December 2020, showed that mean changes in CDASI activity scores at 12 weeks were statistically significant compared with baseline in 10 people with dermatomyositis. “The importance of this study is that it is proof of concept that JAK inhibition can be effective for treating dermatomyositis, especially with active skin disease,” Dr. Fernandez said.
In addition, two large phase 3 trials are evaluating JAK inhibitor safety and efficacy for treating dermatomyositis. One is the VALOR trial, currently recruiting people with recalcitrant dermatomyositis to evaluate treatment with brepocitinib. Researchers in France are looking at another JAK inhibitor, baricitinib, for treating relapsing or treatment-naive dermatomyositis. Recruitment for the BIRD clinical trial is ongoing.
Monoclonal Antibody Showing Promise
“When it comes to looking specifically at dermatomyositis cutaneous disease, it’s been found that the levels of IFN beta correlate best with not only lesional skin type 1 IFN inflammatory signatures but also overall clinical disease activity,” Dr. Fernandez said. This correlation is stronger than for any other IFN-1-type cytokine active in the disorder.
“Perhaps blocking IFN beta might be best way to get control of dermatomyositis activity,” he added.
With that in mind, a phase 2 trial of dazukibart presented at the American Academy of Dermatology 2023 annual meeting highlighted the promise of this agent that targets type 1 IFN beta.
The primary endpoint was improvement in CDASI at 12 weeks. “This medication has remarkable efficacy,” Dr. Fernandez said. “We were one of the sites for this trial. Despite being blinded, there was no question about who was receiving drug and who was receiving placebo.”
“A minimal clinical improvement in disease activity was seen in more than 90%, so almost every patient who received this medication had meaningful improvement,” he added.
Based on the results, the manufacturer, Pfizer, is recruiting participants for a phase 3 trial to further assess dazukibart in dermatomyositis and polymyositis. Dr. Fernandez said, “This is a story you should pay attention to if you treat any dermatomyositis patients at all.”
Regarding these emerging therapies for CLE and dermatomyositis, “This looks very much like the early days of psoriasis, in the early 2000s, when there was a lot of activity developing treatments,” Dr. Fernandez said. “I will predict that within 10 years, we will have multiple novel agents available that will probably work better than anything we have today.”
Dr. Fernandez reported receiving grant and/or research support from Alexion, Incyte, Mallinckrodt Pharmaceuticals, Novartis, Pfizer, and Priovant Therapeutics; acting as a consultant or advisory board member for AbbVie, Biogen, Mallinckrodt Pharmaceuticals; and being a member of the speaker bureau or receiving honoraria for non-CME from AbbVie, Kyowa Kirin, and Mallinckrodt Pharmaceuticals.
A version of this article appeared on Medscape.com.
ORLANDO, FLORIDA — Advances in treating medical conditions rarely emerge in a straight line. Oftentimes, progress comes in fits and starts, and therapies to treat cutaneous lupus erythematosus (CLE) and dermatomyositis are no exception.
Beyond approved treatments that deserve more attention, like belimumab, approved by the Food and Drug Administration (FDA) for systemic lupus erythematosus (SLE) in 2011, and Octagam 10%, an intravenous immune globulin (IVIG) preparation approved for dermatomyositis in 2021, anticipation is growing for emerging therapies and their potential to provide relief to patients, Anthony Fernandez, MD, PhD, said at the ODAC Dermatology, Aesthetic & Surgical Conference. The tyrosine kinase 2 (TYK2) inhibitor deucravacitinib, Janus kinase (JAK) inhibitors brepocitinib and baricitinib, and the monoclonal antibody anifrolumab, he noted, are prime examples.
“. In my opinion, this is the start of what will be the most exciting decade in the history of these two diseases,” said Dr. Fernandez, director of medical dermatology at the Cleveland Clinic.
Emerging Treatments for Cutaneous Lupus
Although SLE can involve many organ systems, the skin is one of the most affected. There are specific cutaneous lesions categorized as either acute cutaneous lupus, subacute cutaneous lupus, or chronic cutaneous lupus.
The oral TYK2 inhibitor deucravacitinib, for example, should be able to dampen interleukin responses in people with CLE, Dr. Fernandez said. Deucravacitinib was approved by the FDA to treat psoriasis in September 2022.
A phase 2 study published in 2023 focused on this agent for relief of systemic lupus. Improvements in cutaneous disease were a secondary endpoint. The trial demonstrated that the patients treated with deucravacitinib achieved a 56%-70% CLASI-50 response, depending on dosing, compared with a 17% response among those on placebo at week 48.
Based on the trial results, recruitment has begun for a phase 2 trial to evaluate deucravacitinib, compared with placebo, in patients with discoid and/or subacute cutaneous lupus. “This may be another medicine we have available to give to any of our patients with cutaneous lupus,” Dr. Fernandez said.
Anifrolumab Appears Promising
The FDA approval of anifrolumab, a type I interferon (IFN) receptor antagonist, for treating moderate to severe SLE in July 2021, for example, is good news for dermatologists and their patients, added Dr. Fernandez. “Almost immediately after approval, case studies showed marked improvement in patients with refractory cutaneous lupus.” While the therapy was approved for treating systemic lupus, it allows for off-label treatment of the cutaneous predominant form of the disease, he said.
Furthermore, the manufacturer of anifrolumab, AstraZeneca, is launching the LAVENDER clinical trial to assess the monoclonal antibody specifically for treating CLE. “This is a big deal because we may be able to prescribe anifrolumab for our cutaneous lupus patients who don’t have systemic lupus,” Dr. Fernandez said.
Phase 3 data supported use the of anifrolumab in systemic lupus, including the TULIP-2 trial, which demonstrated its superiority to placebo for reducing severity of systemic disease and lowering corticosteroid use. A study published in March 2023 of 11 patients showed that they had a “very fast response” to the agent, Dr. Fernandez said, with a 50% or greater improvement in the Cutaneous Lupus Erythematosus Disease Area and Severity Index activity score reached by all participants at week 16. Improvements of 50% or more in this scoring system are considered clinically meaningful, he added.
Upcoming Dermatomyositis Treatments
Why highlight emerging therapies for CLE and dermatomyositis in the same ODAC presentation? Although distinct conditions, these autoimmune conditions are both mediated by type 1 IFN inflammation.
Dermatomyositis is a relatively rare immune-mediated disease that most commonly affects the skin and muscle. Doctors score disease presentation, activity, and clinical improvements on a scale similar to CLASI for cutaneous lupus, the CDASI or Cutaneous Dermatomyositis Disease Area and Severity Index. Among people with CDASI activity scores of at least 14, which is the threshold for moderate to severe disease, a 20% improvement is clinically meaningful, Dr. Fernandez said. In addition, a 40% or greater improvement correlates with significant improvements in quality of life.
There is now more evidence for the use of IVIG to treat dermatomyositis. “Among those of us who treat dermatomyositis on a regular basis, we believe IVIG is the most potent treatment. We’ve known that for a long time,” Dr. Fernandez said.
Despite this tenet, for years, there was only one placebo-controlled trial, published in 1993, that evaluated IVIG treatment for dermatomyositis, and it included only 15 participants. That was until October 2022, he said, when the New England Journal of Medicine published a study comparing a specific brand of IVIG (Octagam) with placebo in 95 people with dermatomyositis.
In the study, 79% of participants treated with IVIG had a total improvement score of at least 20 (minimal improvement), the primary endpoint, at 16 weeks, compared with 44% of those receiving a placebo. Those treated with IVIG also had significant improvements in the CDASI score, a secondary endpoint, compared with those on placebo, he said.
Based on results of this trial, the FDA approved Octagam 10% for dermatomyositis in adults. Dr. Fernandez noted the approval is restricted to the brand of IVIG in the trial, not all IVIG products. However, “the FDA approval is most important to us because it gives us ammunition to fight for insurers to approve IVIG when we feel our patients with dermatomyositis need it,” regardless of the brand.
The Potential of JAK1 Inhibitors
An open-label study of the JAK inhibitor tofacitinib, published in December 2020, showed that mean changes in CDASI activity scores at 12 weeks were statistically significant compared with baseline in 10 people with dermatomyositis. “The importance of this study is that it is proof of concept that JAK inhibition can be effective for treating dermatomyositis, especially with active skin disease,” Dr. Fernandez said.
In addition, two large phase 3 trials are evaluating JAK inhibitor safety and efficacy for treating dermatomyositis. One is the VALOR trial, currently recruiting people with recalcitrant dermatomyositis to evaluate treatment with brepocitinib. Researchers in France are looking at another JAK inhibitor, baricitinib, for treating relapsing or treatment-naive dermatomyositis. Recruitment for the BIRD clinical trial is ongoing.
Monoclonal Antibody Showing Promise
“When it comes to looking specifically at dermatomyositis cutaneous disease, it’s been found that the levels of IFN beta correlate best with not only lesional skin type 1 IFN inflammatory signatures but also overall clinical disease activity,” Dr. Fernandez said. This correlation is stronger than for any other IFN-1-type cytokine active in the disorder.
“Perhaps blocking IFN beta might be best way to get control of dermatomyositis activity,” he added.
With that in mind, a phase 2 trial of dazukibart presented at the American Academy of Dermatology 2023 annual meeting highlighted the promise of this agent that targets type 1 IFN beta.
The primary endpoint was improvement in CDASI at 12 weeks. “This medication has remarkable efficacy,” Dr. Fernandez said. “We were one of the sites for this trial. Despite being blinded, there was no question about who was receiving drug and who was receiving placebo.”
“A minimal clinical improvement in disease activity was seen in more than 90%, so almost every patient who received this medication had meaningful improvement,” he added.
Based on the results, the manufacturer, Pfizer, is recruiting participants for a phase 3 trial to further assess dazukibart in dermatomyositis and polymyositis. Dr. Fernandez said, “This is a story you should pay attention to if you treat any dermatomyositis patients at all.”
Regarding these emerging therapies for CLE and dermatomyositis, “This looks very much like the early days of psoriasis, in the early 2000s, when there was a lot of activity developing treatments,” Dr. Fernandez said. “I will predict that within 10 years, we will have multiple novel agents available that will probably work better than anything we have today.”
Dr. Fernandez reported receiving grant and/or research support from Alexion, Incyte, Mallinckrodt Pharmaceuticals, Novartis, Pfizer, and Priovant Therapeutics; acting as a consultant or advisory board member for AbbVie, Biogen, Mallinckrodt Pharmaceuticals; and being a member of the speaker bureau or receiving honoraria for non-CME from AbbVie, Kyowa Kirin, and Mallinckrodt Pharmaceuticals.
A version of this article appeared on Medscape.com.
FROM ODAC 2024