User login
Uterus Transplants in Women With Uterine-Factor Infertility Show High Rate of Live Births
TOPLINE:
Uterus transplants in women with absolute uterine-factor infertility resulted in a 70% success rate of women later giving birth.
METHODOLOGY:
- The study included 20 women with uterine-factor infertility, a condition in which women do not have a uterus or have one that is not functional; each patient had at least one functioning ovary and uterine abnormalities.
- All patients underwent womb transplantation at a large US specialized care center between 2016 and 2019.
- The transplant was performed using grafts from 18 living donors and two deceased donors.
- Patients received anti-rejection medication until the transplanted uterus was removed following one or two live births or graft failure.
- Researchers measured uterus graft survival and subsequent live births.
TAKEAWAY:
- Out of the 20 participants, 14 (70%) had successful uterus transplants and all 14 gave birth to at least one healthy infant.
- Half of the successful pregnancies had complications, which included gestational hypertension (14%), cervical insufficiency (14%), and preterm labor (14%).
- None of the 16 live-born infants had congenital malformations, and no developmental delays were observed as of May 2024.
- Four of the 18 living donors experienced grade 3 complications, including ureteral obstruction and thermal injury to the ureters.
IN PRACTICE:
“Uterus transplant was technically feasible and was associated with a high live birth rate following successful graft survival,” wrote the authors of the study. “Adverse events were common, with medical and surgical risks affecting recipients as well as donors.”
SOURCE:
The study was led by Giuliano Testa, MD, MBA, of Baylor University Medical Center in Dallas, Texas, and was published online in JAMA Network.
LIMITATIONS:
The findings are based on data from a single center. The sample size was small. The high cost of uterus transplants limits generalizability.
DISCLOSURES:
No disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Uterus transplants in women with absolute uterine-factor infertility resulted in a 70% success rate of women later giving birth.
METHODOLOGY:
- The study included 20 women with uterine-factor infertility, a condition in which women do not have a uterus or have one that is not functional; each patient had at least one functioning ovary and uterine abnormalities.
- All patients underwent womb transplantation at a large US specialized care center between 2016 and 2019.
- The transplant was performed using grafts from 18 living donors and two deceased donors.
- Patients received anti-rejection medication until the transplanted uterus was removed following one or two live births or graft failure.
- Researchers measured uterus graft survival and subsequent live births.
TAKEAWAY:
- Out of the 20 participants, 14 (70%) had successful uterus transplants and all 14 gave birth to at least one healthy infant.
- Half of the successful pregnancies had complications, which included gestational hypertension (14%), cervical insufficiency (14%), and preterm labor (14%).
- None of the 16 live-born infants had congenital malformations, and no developmental delays were observed as of May 2024.
- Four of the 18 living donors experienced grade 3 complications, including ureteral obstruction and thermal injury to the ureters.
IN PRACTICE:
“Uterus transplant was technically feasible and was associated with a high live birth rate following successful graft survival,” wrote the authors of the study. “Adverse events were common, with medical and surgical risks affecting recipients as well as donors.”
SOURCE:
The study was led by Giuliano Testa, MD, MBA, of Baylor University Medical Center in Dallas, Texas, and was published online in JAMA Network.
LIMITATIONS:
The findings are based on data from a single center. The sample size was small. The high cost of uterus transplants limits generalizability.
DISCLOSURES:
No disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Uterus transplants in women with absolute uterine-factor infertility resulted in a 70% success rate of women later giving birth.
METHODOLOGY:
- The study included 20 women with uterine-factor infertility, a condition in which women do not have a uterus or have one that is not functional; each patient had at least one functioning ovary and uterine abnormalities.
- All patients underwent womb transplantation at a large US specialized care center between 2016 and 2019.
- The transplant was performed using grafts from 18 living donors and two deceased donors.
- Patients received anti-rejection medication until the transplanted uterus was removed following one or two live births or graft failure.
- Researchers measured uterus graft survival and subsequent live births.
TAKEAWAY:
- Out of the 20 participants, 14 (70%) had successful uterus transplants and all 14 gave birth to at least one healthy infant.
- Half of the successful pregnancies had complications, which included gestational hypertension (14%), cervical insufficiency (14%), and preterm labor (14%).
- None of the 16 live-born infants had congenital malformations, and no developmental delays were observed as of May 2024.
- Four of the 18 living donors experienced grade 3 complications, including ureteral obstruction and thermal injury to the ureters.
IN PRACTICE:
“Uterus transplant was technically feasible and was associated with a high live birth rate following successful graft survival,” wrote the authors of the study. “Adverse events were common, with medical and surgical risks affecting recipients as well as donors.”
SOURCE:
The study was led by Giuliano Testa, MD, MBA, of Baylor University Medical Center in Dallas, Texas, and was published online in JAMA Network.
LIMITATIONS:
The findings are based on data from a single center. The sample size was small. The high cost of uterus transplants limits generalizability.
DISCLOSURES:
No disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Rural Women Face Greater Challenges in Perimenopause
Women in the perimenopausal period who live in rural areas have a higher prevalence of symptoms typical of this period and a poorer health-related quality of life than women living in urban areas, according to a cross-sectional study that was conducted in Spain.
Cristina Llaneza Suárez, a specialist in family and community medicine and the lead author of the study, told this news organization that women living in rural areas face greater difficulties with access to healthcare services, employment, and transportation and a heavier burden of caregiving. She mentioned that these barriers “can represent an added challenge during the perimenopausal stage, when significant life changes generally occur for all women.” The challenges may lead to “poorer health-related quality of life during perimenopause, compared with women living in urban areas.”
The research group led by Dr. Llaneza aimed to test the hypothesis that sociodemographic characteristics influence symptoms and quality of life in women in perimenopause. They enrolled 270 women aged 45-55 years from eight autonomous communities in Spain who had variability in their menstrual cycles (lasting more than 7 days or amenorrhea greater than 60 days but less than a year).
This cross-sectional study was conducted from December 2019 to April 2023, using the short version of the Cervantes scale to assess health-related quality of life and the Beck Depression Inventory to evaluate associated depressive symptoms.
Among the main findings of the study was that sociocultural factors can influence the perception of perimenopausal symptoms. Living in rural areas has a negative effect on health-related quality of life scales, and this finding is consistent with those of previous studies conducted on women in India, Turkey, Poland, and Peru.
In addition, the selected sample of women experiencing changes in their menstrual cycles and residing in rural areas showed a high prevalence of hot flashes (70% overall and 80% in rural areas) and a poorer quality of life in women with obesity.
“It is striking that, although there is a worse perception of quality of life during perimenopause in women living in rural areas, the proportion of women experiencing some degree of depressive symptoms, according to the Beck inventory, was similar to that of women residing in urban areas,” said Dr. Llaneza. She noted that “no worse scores were observed in sexuality or in the couple relationship.”
Rural Physicians’ Role
Women in the perimenopausal period face significant challenges resulting from inadequate access to healthcare services and limited awareness about menopause. In many countries, this topic is still taboo, both in the family environment and in workplaces and health centers.
Dr. Llaneza mentioned that when she began her training as a primary care physician in a rural population, she witnessed firsthand some of the barriers that women in this age group face, such as limited access to healthcare due to a lack of public transportation. She added that, coupled with this challenge, “there are no regular public transport services that allow independent access for patients, and many [women] lack a driver’s license, making them dependent on others to receive healthcare.” Another important point that she identified was the lack of health education in rural populations, which leads to a minimization of perimenopausal symptoms and causes delays in prevention and early detection.
According to the World Health Organization, healthcare professionals often lack the necessary training to recognize and treat the symptoms of perimenopause and postmenopause. This situation, coupled with the limited attention given to the sexual well-being of menopausal women, contributes to gynecological problems and risks for sexually transmitted infections in this population. The absence of specific health policies and funding for menopause exacerbates the situation, particularly in regions where other health needs compete for limited resources.
Dr. Llaneza noted that primary care physicians in rural areas are responsible for leading primary prevention actions through community interventions that contribute to improving health. Community physicians in rural areas have a lower patient load than urban physicians do. Therefore, “this allows for a more thorough management and closer monitoring of these conditions, which highlights the importance of prevention of perimenopausal symptoms and community education,” she said.
An important goal in improving the quality of life of women in the perimenopausal period is reducing symptoms. Hormone replacement therapy is the cornerstone of treatment, along with nonhormonal therapies such as the use of isoflavones. However, the aforementioned barriers lead to a delay in initiating effective treatment.
Dr. Llaneza added that the main limitation that she encountered during her clinical practice in rural areas regarding the initiation of hormonal therapy was “the reluctance of certain professionals to start it, as they consider that these drugs should be prescribed by menopause specialists because of potential side effects and the increased risk for developing breast cancer.”
Call for Training
Dr. Llaneza and her research team emphasized the need for further research on new drugs for controlling vasomotor symptoms, expressing their interest in conducting additional studies. “We would like to conduct a study on the use of these therapies in perimenopausal and postmenopausal women residing in rural areas.
“We believe that our data may be of interest to healthcare authorities seeking to combat population exodus in rural areas,” they wrote. In addition, they recommended additional training for rural primary care physicians on perimenopause and menopause topics regarding prevention, management, and access, as well as further awareness about preventing depressive symptoms in this population.
Dr. Llaneza declared that she has no relevant financial relationships.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Women in the perimenopausal period who live in rural areas have a higher prevalence of symptoms typical of this period and a poorer health-related quality of life than women living in urban areas, according to a cross-sectional study that was conducted in Spain.
Cristina Llaneza Suárez, a specialist in family and community medicine and the lead author of the study, told this news organization that women living in rural areas face greater difficulties with access to healthcare services, employment, and transportation and a heavier burden of caregiving. She mentioned that these barriers “can represent an added challenge during the perimenopausal stage, when significant life changes generally occur for all women.” The challenges may lead to “poorer health-related quality of life during perimenopause, compared with women living in urban areas.”
The research group led by Dr. Llaneza aimed to test the hypothesis that sociodemographic characteristics influence symptoms and quality of life in women in perimenopause. They enrolled 270 women aged 45-55 years from eight autonomous communities in Spain who had variability in their menstrual cycles (lasting more than 7 days or amenorrhea greater than 60 days but less than a year).
This cross-sectional study was conducted from December 2019 to April 2023, using the short version of the Cervantes scale to assess health-related quality of life and the Beck Depression Inventory to evaluate associated depressive symptoms.
Among the main findings of the study was that sociocultural factors can influence the perception of perimenopausal symptoms. Living in rural areas has a negative effect on health-related quality of life scales, and this finding is consistent with those of previous studies conducted on women in India, Turkey, Poland, and Peru.
In addition, the selected sample of women experiencing changes in their menstrual cycles and residing in rural areas showed a high prevalence of hot flashes (70% overall and 80% in rural areas) and a poorer quality of life in women with obesity.
“It is striking that, although there is a worse perception of quality of life during perimenopause in women living in rural areas, the proportion of women experiencing some degree of depressive symptoms, according to the Beck inventory, was similar to that of women residing in urban areas,” said Dr. Llaneza. She noted that “no worse scores were observed in sexuality or in the couple relationship.”
Rural Physicians’ Role
Women in the perimenopausal period face significant challenges resulting from inadequate access to healthcare services and limited awareness about menopause. In many countries, this topic is still taboo, both in the family environment and in workplaces and health centers.
Dr. Llaneza mentioned that when she began her training as a primary care physician in a rural population, she witnessed firsthand some of the barriers that women in this age group face, such as limited access to healthcare due to a lack of public transportation. She added that, coupled with this challenge, “there are no regular public transport services that allow independent access for patients, and many [women] lack a driver’s license, making them dependent on others to receive healthcare.” Another important point that she identified was the lack of health education in rural populations, which leads to a minimization of perimenopausal symptoms and causes delays in prevention and early detection.
According to the World Health Organization, healthcare professionals often lack the necessary training to recognize and treat the symptoms of perimenopause and postmenopause. This situation, coupled with the limited attention given to the sexual well-being of menopausal women, contributes to gynecological problems and risks for sexually transmitted infections in this population. The absence of specific health policies and funding for menopause exacerbates the situation, particularly in regions where other health needs compete for limited resources.
Dr. Llaneza noted that primary care physicians in rural areas are responsible for leading primary prevention actions through community interventions that contribute to improving health. Community physicians in rural areas have a lower patient load than urban physicians do. Therefore, “this allows for a more thorough management and closer monitoring of these conditions, which highlights the importance of prevention of perimenopausal symptoms and community education,” she said.
An important goal in improving the quality of life of women in the perimenopausal period is reducing symptoms. Hormone replacement therapy is the cornerstone of treatment, along with nonhormonal therapies such as the use of isoflavones. However, the aforementioned barriers lead to a delay in initiating effective treatment.
Dr. Llaneza added that the main limitation that she encountered during her clinical practice in rural areas regarding the initiation of hormonal therapy was “the reluctance of certain professionals to start it, as they consider that these drugs should be prescribed by menopause specialists because of potential side effects and the increased risk for developing breast cancer.”
Call for Training
Dr. Llaneza and her research team emphasized the need for further research on new drugs for controlling vasomotor symptoms, expressing their interest in conducting additional studies. “We would like to conduct a study on the use of these therapies in perimenopausal and postmenopausal women residing in rural areas.
“We believe that our data may be of interest to healthcare authorities seeking to combat population exodus in rural areas,” they wrote. In addition, they recommended additional training for rural primary care physicians on perimenopause and menopause topics regarding prevention, management, and access, as well as further awareness about preventing depressive symptoms in this population.
Dr. Llaneza declared that she has no relevant financial relationships.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Women in the perimenopausal period who live in rural areas have a higher prevalence of symptoms typical of this period and a poorer health-related quality of life than women living in urban areas, according to a cross-sectional study that was conducted in Spain.
Cristina Llaneza Suárez, a specialist in family and community medicine and the lead author of the study, told this news organization that women living in rural areas face greater difficulties with access to healthcare services, employment, and transportation and a heavier burden of caregiving. She mentioned that these barriers “can represent an added challenge during the perimenopausal stage, when significant life changes generally occur for all women.” The challenges may lead to “poorer health-related quality of life during perimenopause, compared with women living in urban areas.”
The research group led by Dr. Llaneza aimed to test the hypothesis that sociodemographic characteristics influence symptoms and quality of life in women in perimenopause. They enrolled 270 women aged 45-55 years from eight autonomous communities in Spain who had variability in their menstrual cycles (lasting more than 7 days or amenorrhea greater than 60 days but less than a year).
This cross-sectional study was conducted from December 2019 to April 2023, using the short version of the Cervantes scale to assess health-related quality of life and the Beck Depression Inventory to evaluate associated depressive symptoms.
Among the main findings of the study was that sociocultural factors can influence the perception of perimenopausal symptoms. Living in rural areas has a negative effect on health-related quality of life scales, and this finding is consistent with those of previous studies conducted on women in India, Turkey, Poland, and Peru.
In addition, the selected sample of women experiencing changes in their menstrual cycles and residing in rural areas showed a high prevalence of hot flashes (70% overall and 80% in rural areas) and a poorer quality of life in women with obesity.
“It is striking that, although there is a worse perception of quality of life during perimenopause in women living in rural areas, the proportion of women experiencing some degree of depressive symptoms, according to the Beck inventory, was similar to that of women residing in urban areas,” said Dr. Llaneza. She noted that “no worse scores were observed in sexuality or in the couple relationship.”
Rural Physicians’ Role
Women in the perimenopausal period face significant challenges resulting from inadequate access to healthcare services and limited awareness about menopause. In many countries, this topic is still taboo, both in the family environment and in workplaces and health centers.
Dr. Llaneza mentioned that when she began her training as a primary care physician in a rural population, she witnessed firsthand some of the barriers that women in this age group face, such as limited access to healthcare due to a lack of public transportation. She added that, coupled with this challenge, “there are no regular public transport services that allow independent access for patients, and many [women] lack a driver’s license, making them dependent on others to receive healthcare.” Another important point that she identified was the lack of health education in rural populations, which leads to a minimization of perimenopausal symptoms and causes delays in prevention and early detection.
According to the World Health Organization, healthcare professionals often lack the necessary training to recognize and treat the symptoms of perimenopause and postmenopause. This situation, coupled with the limited attention given to the sexual well-being of menopausal women, contributes to gynecological problems and risks for sexually transmitted infections in this population. The absence of specific health policies and funding for menopause exacerbates the situation, particularly in regions where other health needs compete for limited resources.
Dr. Llaneza noted that primary care physicians in rural areas are responsible for leading primary prevention actions through community interventions that contribute to improving health. Community physicians in rural areas have a lower patient load than urban physicians do. Therefore, “this allows for a more thorough management and closer monitoring of these conditions, which highlights the importance of prevention of perimenopausal symptoms and community education,” she said.
An important goal in improving the quality of life of women in the perimenopausal period is reducing symptoms. Hormone replacement therapy is the cornerstone of treatment, along with nonhormonal therapies such as the use of isoflavones. However, the aforementioned barriers lead to a delay in initiating effective treatment.
Dr. Llaneza added that the main limitation that she encountered during her clinical practice in rural areas regarding the initiation of hormonal therapy was “the reluctance of certain professionals to start it, as they consider that these drugs should be prescribed by menopause specialists because of potential side effects and the increased risk for developing breast cancer.”
Call for Training
Dr. Llaneza and her research team emphasized the need for further research on new drugs for controlling vasomotor symptoms, expressing their interest in conducting additional studies. “We would like to conduct a study on the use of these therapies in perimenopausal and postmenopausal women residing in rural areas.
“We believe that our data may be of interest to healthcare authorities seeking to combat population exodus in rural areas,” they wrote. In addition, they recommended additional training for rural primary care physicians on perimenopause and menopause topics regarding prevention, management, and access, as well as further awareness about preventing depressive symptoms in this population.
Dr. Llaneza declared that she has no relevant financial relationships.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
CBD Use in Pregnant People Double That of Nonpregnant Counterparts
Pregnant women in a large North American sample reported nearly double the rate of cannabidiol (CBD) use compared with nonpregnant women, new data published in a research letter in Obstetrics & Gynecology indicates.
Healthcare providers should be aware of the high rate of CBD use in pregnancy, especially as legal use of cannabis is increasing faster than evidence on outcomes for exposed offspring, note the researchers, led by Devika Bhatia, MD, from the Department of Psychiatry, Colorado School of Medicine, University of Colorado Anschutz Medical Campus in Aurora.
In an accompanying editorial, Torri D. Metz, MD, MS, deputy editor for obstetrics for Obstetrics & Gynecology, writes that the study “is critically important.” She points out that pregnant individuals may perceive that CBD is a safe drug to use in pregnancy, despite there being essentially no data examining whether or not this is the case.
Large Dataset From United States and Canada
Researchers used data from the International Cannabis Policy Study (2019-2021), a repeated cross-sectional survey of people aged 16-65 years in the United States and Canada. There were 66,457 women in the sample, including 1096 pregnant women.
Particularly concerning, the authors write, is the prenatal use of CBD-only products. Those products are advertised to contain only CBD, rather than tetrahydrocannabinol (THC). They point out CBD-only products are often legal in North America and often marketed as supplements.
The prevalence of CBD-only use in pregnant women in the study was 20.4% compared with 11.3% among nonpregnant women, P < .001. The top reason for use by pregnant women was anxiety (58.4%). Other top reasons included depression (40.3%), posttraumatic stress disorder (32.1%), pain (52.3%), headache (35.6%), and nausea or vomiting (31.9%).
“Nonpregnant women were significantly more likely to report using CBD for pain, sleep, general well-being, and ‘other’ physical or mental health reasons, or to not use CBD for mental health,” the authors write, adding that the reasons for CBD use highlight drivers that may be important to address in treating pregnant patients.
Provider Endorsement in Some Cases
Dr. Metz, associate professor of obstetrics and gynecology with the University of Utah Health in Salt Lake City, says in some cases women may be getting endorsement of CBD use from their provider or at least implied support when CBD is prescribed. In the study, pregnant women had 2.33 times greater adjusted odds of having a CBD prescription than nonpregnant women (95% confidence interval, 1.27-2.88).
She points to another cross-sectional study of more than 10,000 participants using PRAMS (Pregnancy Risk Assessment Monitoring System) data that found that “from 2017 to 2019, 63% of pregnant women reported that they were not told to avoid cannabis use in pregnancy, and 8% noted that they were advised to use cannabis by their prenatal care practitioner.”
The American College of Obstetricians and Gynecologists recommends against prescribing cannabis products for pregnant or lactating women.
Studies that have explored THC and its metabolites have shown “a consistent association between cannabis use and decreased fetal growth,” Dr. Metz noted. “There also remain persistent concerns about the long-term neurodevelopmental effects of maternal cannabis use on the fetus and, subsequently, the newborn.”
Limitations of the study include the self-reported responses and participants’ ability to accurately distinguish between CBD-only and THC-containing products.
Because self-reports of CBD use in pregnancy may be drastically underestimated and nonreliable, Dr. Metz writes, development of blood and urine screens to help detect CBD product use “will be helpful in moving the field forward.”
Study senior author David Hammond, PhD, has been a paid expert witness on behalf of public health authorities in response to legal challenges from the cannabis, tobacco, vaping, and food industries. Other authors did not report any potential conflicts. Dr. Metz reports personal fees from Pfizer, and grants from Pfizer for her role as a site principal investigator for SARS-CoV-2 vaccination and for her role as a site PI for RSV vaccination in pregnancy study.
Pregnant women in a large North American sample reported nearly double the rate of cannabidiol (CBD) use compared with nonpregnant women, new data published in a research letter in Obstetrics & Gynecology indicates.
Healthcare providers should be aware of the high rate of CBD use in pregnancy, especially as legal use of cannabis is increasing faster than evidence on outcomes for exposed offspring, note the researchers, led by Devika Bhatia, MD, from the Department of Psychiatry, Colorado School of Medicine, University of Colorado Anschutz Medical Campus in Aurora.
In an accompanying editorial, Torri D. Metz, MD, MS, deputy editor for obstetrics for Obstetrics & Gynecology, writes that the study “is critically important.” She points out that pregnant individuals may perceive that CBD is a safe drug to use in pregnancy, despite there being essentially no data examining whether or not this is the case.
Large Dataset From United States and Canada
Researchers used data from the International Cannabis Policy Study (2019-2021), a repeated cross-sectional survey of people aged 16-65 years in the United States and Canada. There were 66,457 women in the sample, including 1096 pregnant women.
Particularly concerning, the authors write, is the prenatal use of CBD-only products. Those products are advertised to contain only CBD, rather than tetrahydrocannabinol (THC). They point out CBD-only products are often legal in North America and often marketed as supplements.
The prevalence of CBD-only use in pregnant women in the study was 20.4% compared with 11.3% among nonpregnant women, P < .001. The top reason for use by pregnant women was anxiety (58.4%). Other top reasons included depression (40.3%), posttraumatic stress disorder (32.1%), pain (52.3%), headache (35.6%), and nausea or vomiting (31.9%).
“Nonpregnant women were significantly more likely to report using CBD for pain, sleep, general well-being, and ‘other’ physical or mental health reasons, or to not use CBD for mental health,” the authors write, adding that the reasons for CBD use highlight drivers that may be important to address in treating pregnant patients.
Provider Endorsement in Some Cases
Dr. Metz, associate professor of obstetrics and gynecology with the University of Utah Health in Salt Lake City, says in some cases women may be getting endorsement of CBD use from their provider or at least implied support when CBD is prescribed. In the study, pregnant women had 2.33 times greater adjusted odds of having a CBD prescription than nonpregnant women (95% confidence interval, 1.27-2.88).
She points to another cross-sectional study of more than 10,000 participants using PRAMS (Pregnancy Risk Assessment Monitoring System) data that found that “from 2017 to 2019, 63% of pregnant women reported that they were not told to avoid cannabis use in pregnancy, and 8% noted that they were advised to use cannabis by their prenatal care practitioner.”
The American College of Obstetricians and Gynecologists recommends against prescribing cannabis products for pregnant or lactating women.
Studies that have explored THC and its metabolites have shown “a consistent association between cannabis use and decreased fetal growth,” Dr. Metz noted. “There also remain persistent concerns about the long-term neurodevelopmental effects of maternal cannabis use on the fetus and, subsequently, the newborn.”
Limitations of the study include the self-reported responses and participants’ ability to accurately distinguish between CBD-only and THC-containing products.
Because self-reports of CBD use in pregnancy may be drastically underestimated and nonreliable, Dr. Metz writes, development of blood and urine screens to help detect CBD product use “will be helpful in moving the field forward.”
Study senior author David Hammond, PhD, has been a paid expert witness on behalf of public health authorities in response to legal challenges from the cannabis, tobacco, vaping, and food industries. Other authors did not report any potential conflicts. Dr. Metz reports personal fees from Pfizer, and grants from Pfizer for her role as a site principal investigator for SARS-CoV-2 vaccination and for her role as a site PI for RSV vaccination in pregnancy study.
Pregnant women in a large North American sample reported nearly double the rate of cannabidiol (CBD) use compared with nonpregnant women, new data published in a research letter in Obstetrics & Gynecology indicates.
Healthcare providers should be aware of the high rate of CBD use in pregnancy, especially as legal use of cannabis is increasing faster than evidence on outcomes for exposed offspring, note the researchers, led by Devika Bhatia, MD, from the Department of Psychiatry, Colorado School of Medicine, University of Colorado Anschutz Medical Campus in Aurora.
In an accompanying editorial, Torri D. Metz, MD, MS, deputy editor for obstetrics for Obstetrics & Gynecology, writes that the study “is critically important.” She points out that pregnant individuals may perceive that CBD is a safe drug to use in pregnancy, despite there being essentially no data examining whether or not this is the case.
Large Dataset From United States and Canada
Researchers used data from the International Cannabis Policy Study (2019-2021), a repeated cross-sectional survey of people aged 16-65 years in the United States and Canada. There were 66,457 women in the sample, including 1096 pregnant women.
Particularly concerning, the authors write, is the prenatal use of CBD-only products. Those products are advertised to contain only CBD, rather than tetrahydrocannabinol (THC). They point out CBD-only products are often legal in North America and often marketed as supplements.
The prevalence of CBD-only use in pregnant women in the study was 20.4% compared with 11.3% among nonpregnant women, P < .001. The top reason for use by pregnant women was anxiety (58.4%). Other top reasons included depression (40.3%), posttraumatic stress disorder (32.1%), pain (52.3%), headache (35.6%), and nausea or vomiting (31.9%).
“Nonpregnant women were significantly more likely to report using CBD for pain, sleep, general well-being, and ‘other’ physical or mental health reasons, or to not use CBD for mental health,” the authors write, adding that the reasons for CBD use highlight drivers that may be important to address in treating pregnant patients.
Provider Endorsement in Some Cases
Dr. Metz, associate professor of obstetrics and gynecology with the University of Utah Health in Salt Lake City, says in some cases women may be getting endorsement of CBD use from their provider or at least implied support when CBD is prescribed. In the study, pregnant women had 2.33 times greater adjusted odds of having a CBD prescription than nonpregnant women (95% confidence interval, 1.27-2.88).
She points to another cross-sectional study of more than 10,000 participants using PRAMS (Pregnancy Risk Assessment Monitoring System) data that found that “from 2017 to 2019, 63% of pregnant women reported that they were not told to avoid cannabis use in pregnancy, and 8% noted that they were advised to use cannabis by their prenatal care practitioner.”
The American College of Obstetricians and Gynecologists recommends against prescribing cannabis products for pregnant or lactating women.
Studies that have explored THC and its metabolites have shown “a consistent association between cannabis use and decreased fetal growth,” Dr. Metz noted. “There also remain persistent concerns about the long-term neurodevelopmental effects of maternal cannabis use on the fetus and, subsequently, the newborn.”
Limitations of the study include the self-reported responses and participants’ ability to accurately distinguish between CBD-only and THC-containing products.
Because self-reports of CBD use in pregnancy may be drastically underestimated and nonreliable, Dr. Metz writes, development of blood and urine screens to help detect CBD product use “will be helpful in moving the field forward.”
Study senior author David Hammond, PhD, has been a paid expert witness on behalf of public health authorities in response to legal challenges from the cannabis, tobacco, vaping, and food industries. Other authors did not report any potential conflicts. Dr. Metz reports personal fees from Pfizer, and grants from Pfizer for her role as a site principal investigator for SARS-CoV-2 vaccination and for her role as a site PI for RSV vaccination in pregnancy study.
FROM OBSTETRICS & GYNECOLOGY
Data Trends 2024: Women's Health
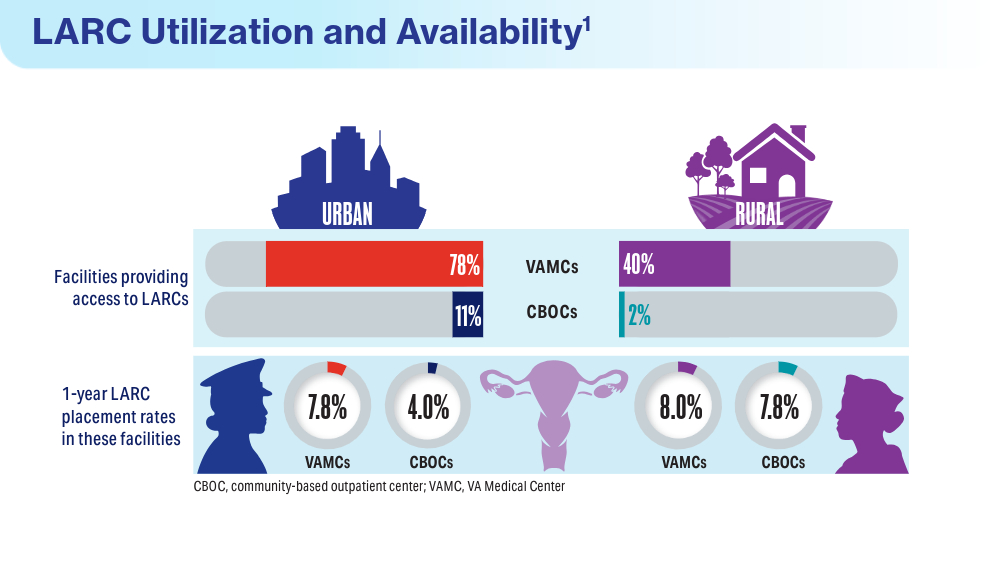
Mahorter S, Vinekar K, Shaw JG, et al. Variations in provision of long-acting reversible contraception across Veterans Health Administration facilities. J Gen Intern Med. 2023;38(suppl 3):865-867. doi:10.1007/s11606-023-08123-5
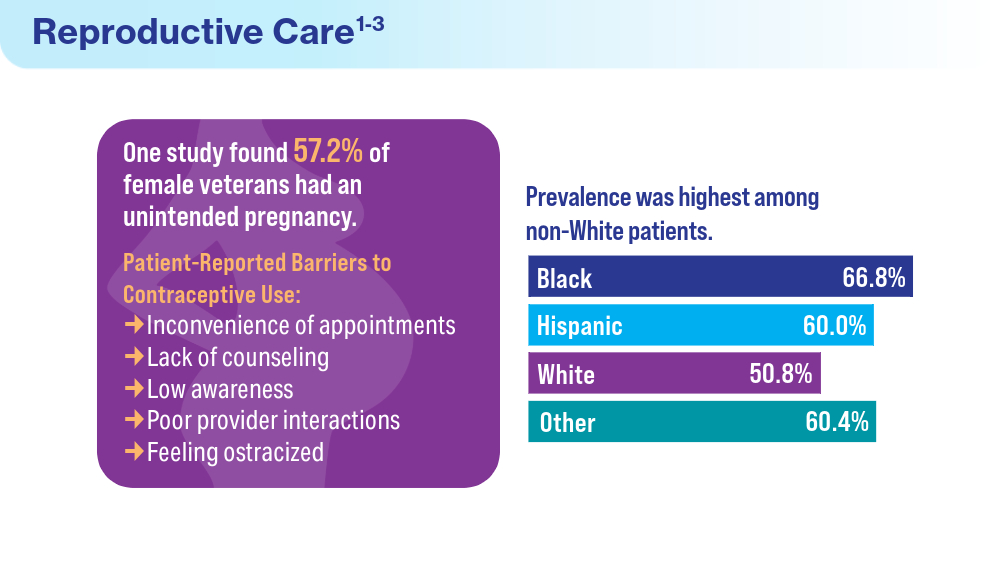
Quinn DA, Sileanu FE, Zhao X, Mor MK, Judge-Golden C, Callegari LS, Borrero S. History of unintended pregnancy and patterns of contraceptive use among racial and ethnic minority women veterans. Am J Obstet Gynecol. 2020;223(4):564.e1-564.e13. doi:10.1016/j.ajog.2020.02.042
Wolgemuth TE, Cuddeback M, Callegari LS, Rodriguez KL, Zhao X, Borrero S. Perceived Barriers and Facilitators to Contraceptive Use Among Women Veterans Accessing the Veterans Affairs Healthcare System. Womens Health Issues. 2020;30(1):57-63. doi:10.1016/j.whi.2019.08.005
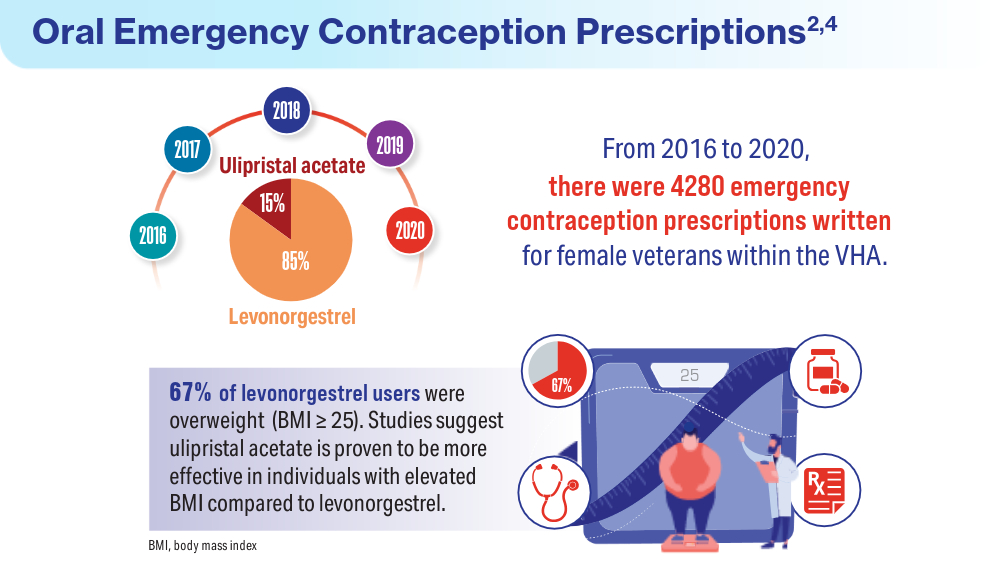
Gawron LM, He T, Lewis L, Fudin H, Callegari LS, Turok DK, Stevens V. Oral emergency contraception provision in the Veterans Health Administration: a retrospective cohort study. J Gen Intern Med. 2022;37(suppl 3):685-689. doi:10.1007/s11606-022-07596-0
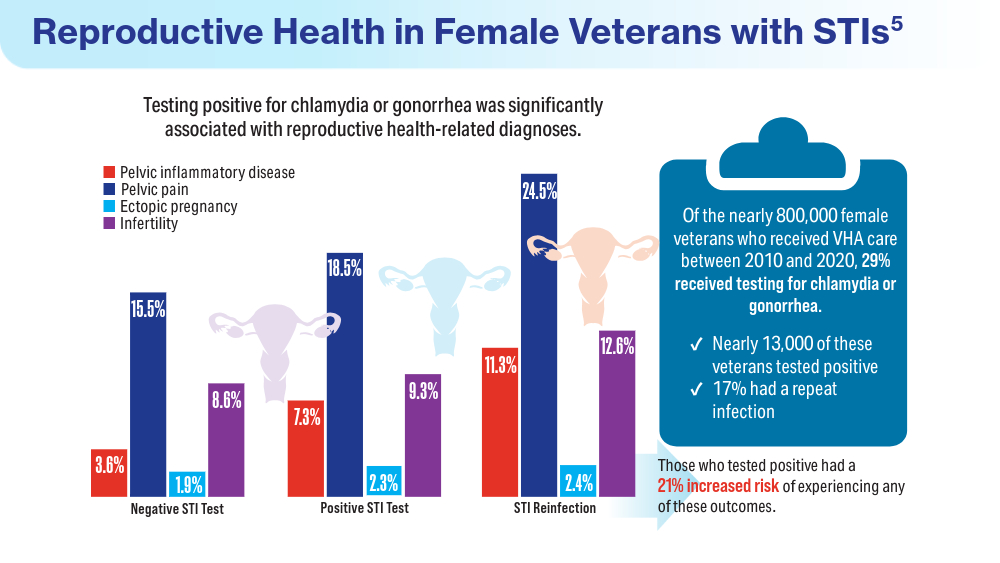
Gardella CM, Borgerding J, Maier MM, Beste LA. Chlamydial and gonococcal infections and adverse reproductive health conditions among patients assigned female at birth in the Veterans Health Administration. Sex Transm Dis. 2024;51(5):p 320-324. doi:10.1097/OLQ.0000000000001932
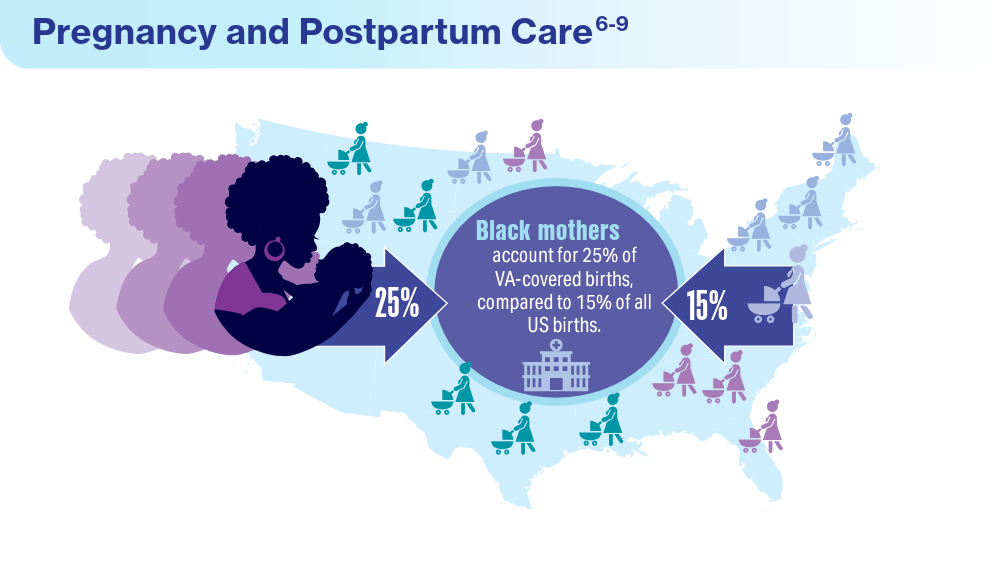
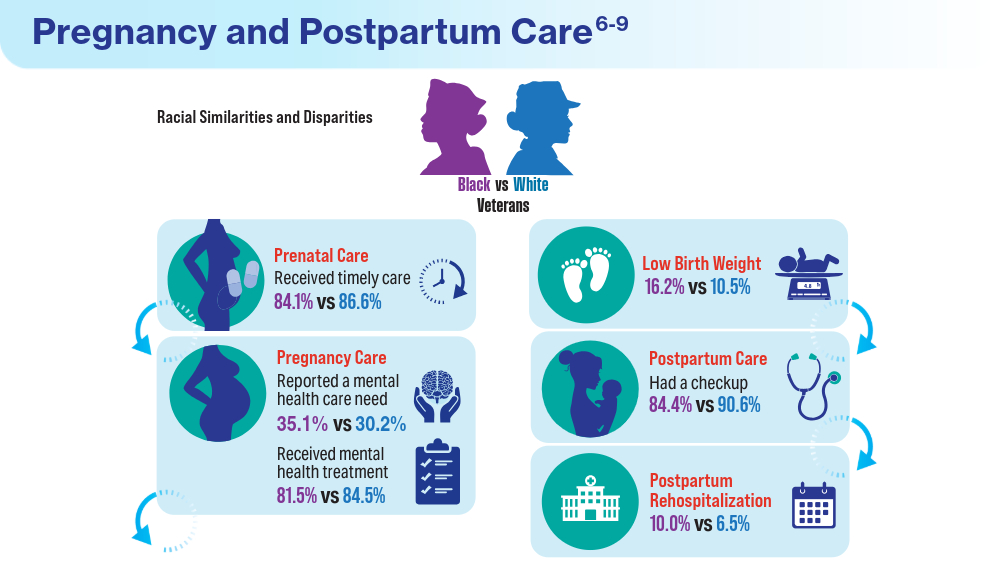
Katon JG, Bossick AS, Tartaglione EV, et al. Assessing racial disparities in access, use, and outcomes for pregnant and postpartum veterans and their infants in Veterans Health Administration. J Womens Health (Larchmt). 2023;32(7):757-766. doi:10.1089/jwh.2022.0507
Katon J, Bossick A, Tartaglione E, et al. Survey of Veterans Receiving VA Maternity Care Benefits: A Report Sponsored by the VHA Office of Women's Health Department of Veterans Affairs. VA Office of Women's Health: Washington, DC; 2021.
Frayne SM, Phibbs SC, Saechao F, et al. Sourcebook: Women Veterans in the Veterans Health Administration. Vol 4. Longitudinal Trends in Sociodemographics, Utilization, Health Profile, and Geographic Distribution. Veterans Health Administration, Department of Veterans Affairs: Washington, DC; 2018.
March of Dimes Peristats: Birth. 2022. Updated January 2024. Accessed May 15, 2024. https://www.marchofdimes.org/peristats/
Katon JG, Hoggatt KJ, Balasubramanian V, et al. Reproductive health diagnoses of women veterans using Department of Veterans Affairs health care. Med Care. 2015;53(4 Suppl 1):S63–S67. doi:10.1097/MLR.0000000000000295
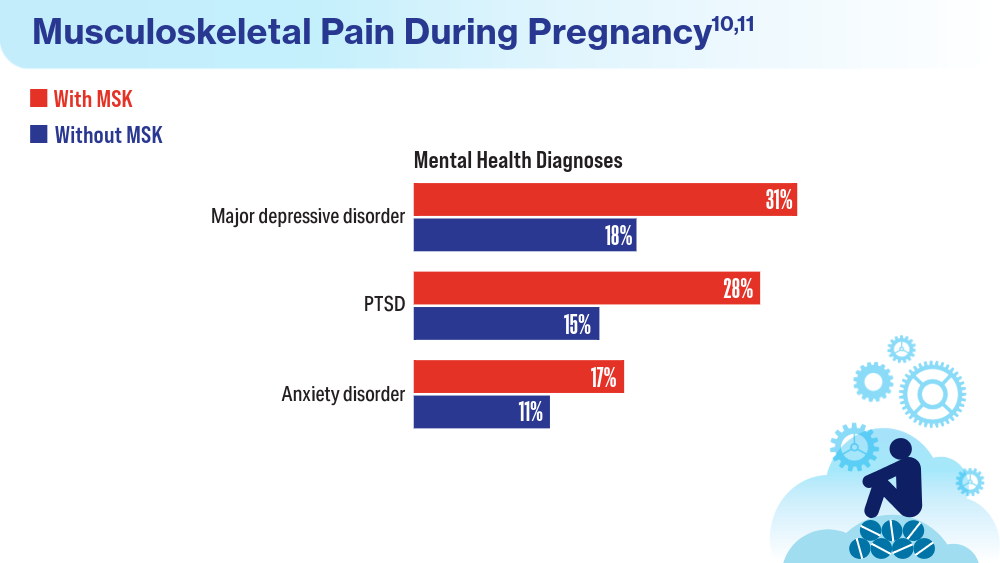
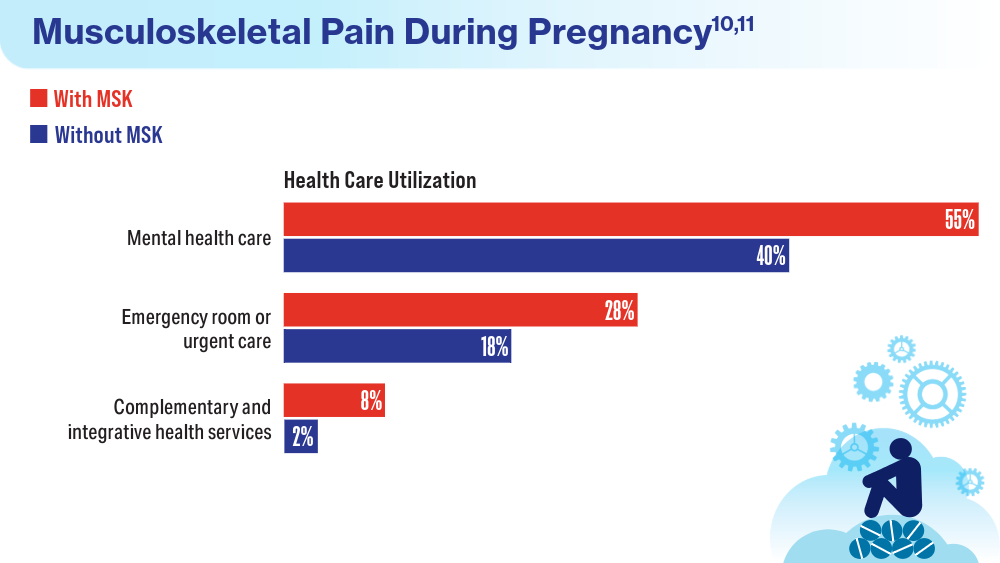
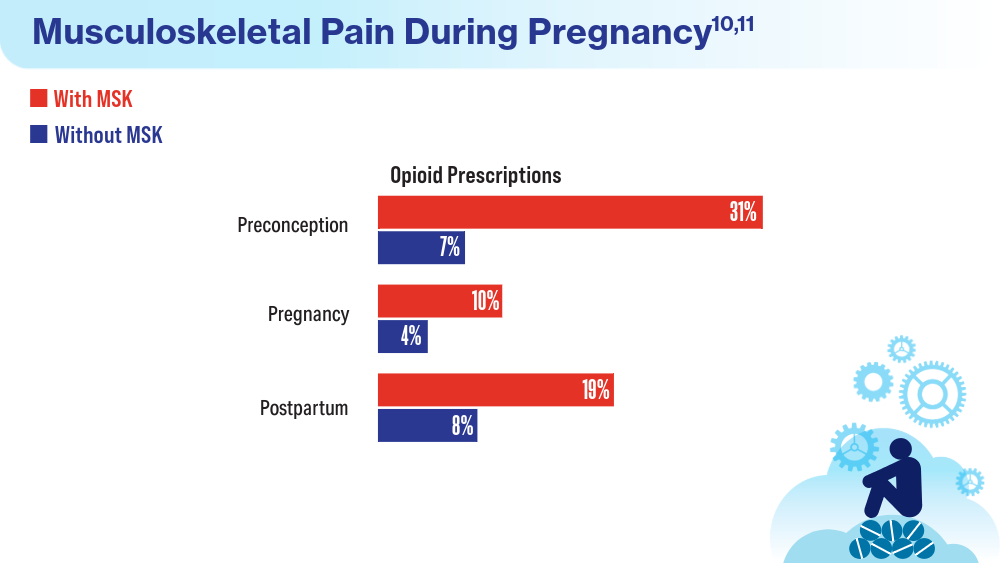
Kroll-Desrosiers A, Wallace KF, Higgins DM, Martino S, Mattocks KM. Musculoskeletal pain during pregnancy among veterans: associations with health and health care utilization. Womens Health Issues. 2024;34(1):90-97. doi:10.1016/j.whi.2023.07.004
Mahorter S, Vinekar K, Shaw JG, et al. Variations in provision of long-acting reversible contraception across Veterans Health Administration facilities. J Gen Intern Med. 2023;38(suppl 3):865-867. doi:10.1007/s11606-023-08123-5
Quinn DA, Sileanu FE, Zhao X, Mor MK, Judge-Golden C, Callegari LS, Borrero S. History of unintended pregnancy and patterns of contraceptive use among racial and ethnic minority women veterans. Am J Obstet Gynecol. 2020;223(4):564.e1-564.e13. doi:10.1016/j.ajog.2020.02.042
Wolgemuth TE, Cuddeback M, Callegari LS, Rodriguez KL, Zhao X, Borrero S. Perceived Barriers and Facilitators to Contraceptive Use Among Women Veterans Accessing the Veterans Affairs Healthcare System. Womens Health Issues. 2020;30(1):57-63. doi:10.1016/j.whi.2019.08.005
Gawron LM, He T, Lewis L, Fudin H, Callegari LS, Turok DK, Stevens V. Oral emergency contraception provision in the Veterans Health Administration: a retrospective cohort study. J Gen Intern Med. 2022;37(suppl 3):685-689. doi:10.1007/s11606-022-07596-0
Gardella CM, Borgerding J, Maier MM, Beste LA. Chlamydial and gonococcal infections and adverse reproductive health conditions among patients assigned female at birth in the Veterans Health Administration. Sex Transm Dis. 2024;51(5):p 320-324. doi:10.1097/OLQ.0000000000001932
Katon JG, Bossick AS, Tartaglione EV, et al. Assessing racial disparities in access, use, and outcomes for pregnant and postpartum veterans and their infants in Veterans Health Administration. J Womens Health (Larchmt). 2023;32(7):757-766. doi:10.1089/jwh.2022.0507
Katon J, Bossick A, Tartaglione E, et al. Survey of Veterans Receiving VA Maternity Care Benefits: A Report Sponsored by the VHA Office of Women's Health Department of Veterans Affairs. VA Office of Women's Health: Washington, DC; 2021.
Frayne SM, Phibbs SC, Saechao F, et al. Sourcebook: Women Veterans in the Veterans Health Administration. Vol 4. Longitudinal Trends in Sociodemographics, Utilization, Health Profile, and Geographic Distribution. Veterans Health Administration, Department of Veterans Affairs: Washington, DC; 2018.
March of Dimes Peristats: Birth. 2022. Updated January 2024. Accessed May 15, 2024. https://www.marchofdimes.org/peristats/
Katon JG, Hoggatt KJ, Balasubramanian V, et al. Reproductive health diagnoses of women veterans using Department of Veterans Affairs health care. Med Care. 2015;53(4 Suppl 1):S63–S67. doi:10.1097/MLR.0000000000000295
Kroll-Desrosiers A, Wallace KF, Higgins DM, Martino S, Mattocks KM. Musculoskeletal pain during pregnancy among veterans: associations with health and health care utilization. Womens Health Issues. 2024;34(1):90-97. doi:10.1016/j.whi.2023.07.004
Mahorter S, Vinekar K, Shaw JG, et al. Variations in provision of long-acting reversible contraception across Veterans Health Administration facilities. J Gen Intern Med. 2023;38(suppl 3):865-867. doi:10.1007/s11606-023-08123-5
Quinn DA, Sileanu FE, Zhao X, Mor MK, Judge-Golden C, Callegari LS, Borrero S. History of unintended pregnancy and patterns of contraceptive use among racial and ethnic minority women veterans. Am J Obstet Gynecol. 2020;223(4):564.e1-564.e13. doi:10.1016/j.ajog.2020.02.042
Wolgemuth TE, Cuddeback M, Callegari LS, Rodriguez KL, Zhao X, Borrero S. Perceived Barriers and Facilitators to Contraceptive Use Among Women Veterans Accessing the Veterans Affairs Healthcare System. Womens Health Issues. 2020;30(1):57-63. doi:10.1016/j.whi.2019.08.005
Gawron LM, He T, Lewis L, Fudin H, Callegari LS, Turok DK, Stevens V. Oral emergency contraception provision in the Veterans Health Administration: a retrospective cohort study. J Gen Intern Med. 2022;37(suppl 3):685-689. doi:10.1007/s11606-022-07596-0
Gardella CM, Borgerding J, Maier MM, Beste LA. Chlamydial and gonococcal infections and adverse reproductive health conditions among patients assigned female at birth in the Veterans Health Administration. Sex Transm Dis. 2024;51(5):p 320-324. doi:10.1097/OLQ.0000000000001932
Katon JG, Bossick AS, Tartaglione EV, et al. Assessing racial disparities in access, use, and outcomes for pregnant and postpartum veterans and their infants in Veterans Health Administration. J Womens Health (Larchmt). 2023;32(7):757-766. doi:10.1089/jwh.2022.0507
Katon J, Bossick A, Tartaglione E, et al. Survey of Veterans Receiving VA Maternity Care Benefits: A Report Sponsored by the VHA Office of Women's Health Department of Veterans Affairs. VA Office of Women's Health: Washington, DC; 2021.
Frayne SM, Phibbs SC, Saechao F, et al. Sourcebook: Women Veterans in the Veterans Health Administration. Vol 4. Longitudinal Trends in Sociodemographics, Utilization, Health Profile, and Geographic Distribution. Veterans Health Administration, Department of Veterans Affairs: Washington, DC; 2018.
March of Dimes Peristats: Birth. 2022. Updated January 2024. Accessed May 15, 2024. https://www.marchofdimes.org/peristats/
Katon JG, Hoggatt KJ, Balasubramanian V, et al. Reproductive health diagnoses of women veterans using Department of Veterans Affairs health care. Med Care. 2015;53(4 Suppl 1):S63–S67. doi:10.1097/MLR.0000000000000295
Kroll-Desrosiers A, Wallace KF, Higgins DM, Martino S, Mattocks KM. Musculoskeletal pain during pregnancy among veterans: associations with health and health care utilization. Womens Health Issues. 2024;34(1):90-97. doi:10.1016/j.whi.2023.07.004


Type 2 Diabetes Fracture Risk Likely Due to Impaired Physical Function
, according to a Swedish prospective observational study in JAMA Network Open.
The study was conducted in more than 3000 Swedish women by Mattias Lorentzon, MD, a professor of geriatric medicine at Gothenburg University, and chief physician at the Osteoporosis Clinic at Sahlgrenska University Hospital in Mölndal, and colleagues.
Older women with T2D had higher BMD, better bone microarchitecture, and a similar bone material strength index (BMSi) but poorer physical performance and higher fracture risk than women without diabetes.
Women with T2D had 9.1% higher body weight, a 9.5% higher body mass index (BMI), and 6.3% higher appendicular lean mass index (lean mass divided by height squared) than controls.
The T2D group also had a lower prevalence of reported osteoporosis medication use vs controls: 3.4% vs 7.5%, respectively.
Prolonged diabetes treatment and insulin use were associated with higher fracture risk and poorer physical performance despite better bone characteristics.
“Our results demonstrate that checking and monitoring physical function is important to identify diabetes patients with a high risk of fractures and suggest that improving physical function may be important to reduce the risk of fractures in these patients,” Dr. Lorentzon told this news organization.
He speculated that the better bone microarchitecture in women with T2D could be due to both higher body weight and adiposity as well as to hormonal differences such as higher estradiol levels.
Study Details
A fractures study was performed in the Gothenburg area from March 2013 to May 2016 with follow-up of incident fracture data completed in March 2023. Data were collected from questionnaires and through examination of anthropometrics, physical function, and bone measurements using dual-energy x-ray absorptiometry and high-resolution peripheral computed tomography. A subsample underwent bone microindentation to assess BMSi.
Among the cohort’s 3008 women, ages 75-80 (mean, 77.8), 294 patients with T2D were compared with 2714 same-age unaffected women.
During a median follow-up of 7.3 years, 1071 incident fractures, 853 major osteoporotic fractures, and 232 hip fractures occurred. In models adjusted for age, BMI, clinical risk factors, and femoral neck BMD, T2D was associated with an increased risk of any fracture: hazard ratio (HR), 1.26; (95% CI, 1.04-1.54), and major osteoporotic fracture (HR, 1.25; 95% CI, 1.00-1.56).
Most fractures were due to falls, with the most common affected sites being the forearm, upper arm, spine, and hip, Dr. Lorentzon said.
Among the findings:
- In bone microarchitecture, women with T2D had higher BMD at all sites: total hip, 4.4% higher; femoral neck, 4.9% higher; and lumbar spine, 5.2% higher.
- At the tibia, the T2D group had 7.4% greater cortical area and 1.3% greater density, as well as 8.7% higher trabecular bone volume fraction.
“Our findings regarding BMD are consistent with previous publications showing higher BMD in individuals with T2D compared with those without diabetes,” Dr. Lorentzon said. A 2012 meta-analysis, for example, showed higher BMD levels in T2D patients. “Some smaller studies, however, have found worse bone microstructure and lower bone material strength in contrast to the results from our study,” Dr. Lorentzon said.
- There was no difference in BMSi, with a mean of 78 in both groups.
- The T2D group had lower performance on all physical function tests: a 9.7% lower grip strength, 9.9% slower gait speed, and 13.9% slower timed up-and-go time than women without diabetes.
“We found all parameters regarding physical function, such as muscle strength, balance, and performance, were much worse in women with diabetes than in those without,” Dr. Lorentzon said. “Dizziness could also be a contributor to the increased risk of falls, but this factor was not investigated in our study.”
Commenting on the study but not involved in it, Anthony J. Pick, MD, an endocrinologist at Northwestern Medicine Lake Forest Hospital in Lake Forest, Illinois, said sarcopenia is a common and often under-recognized problem in older adults and is especially prevalent in T2D, obesity, and heart failure. “I believe that ‘exercise is medicine’ is a key concept for metabolic and osteoporosis patients — and wellness and longevity in general — and I certainly hope studies like this drive awareness of the importance of engaging in strengthening exercises.”
Dr. Pick noted some nuances in this study suggesting there may be some impairments in bone quality beyond the strength and fall risk issue, “so this is likely a complex area.”
This study was supported by the Swedish Research Council, the Inga-Britt and Arne Lundberg Foundation, and Sahlgrenska University Hospital. Dr. Lorentzon reported personal fees from UCB Pharma, Amgen, Parexel International, Astellas, and Gedeon Richter outside the submitted work. Coauthor Dr. Johansson reported lecture fees from Union Chimique Belge (UCB) Pharma outside the submitted work. Dr. Axelsson reported personal fees from Amgen, Meda/Mylan, and Lilly outside the submitted work. Dr. Pick had no relevant conflicts of interest.
, according to a Swedish prospective observational study in JAMA Network Open.
The study was conducted in more than 3000 Swedish women by Mattias Lorentzon, MD, a professor of geriatric medicine at Gothenburg University, and chief physician at the Osteoporosis Clinic at Sahlgrenska University Hospital in Mölndal, and colleagues.
Older women with T2D had higher BMD, better bone microarchitecture, and a similar bone material strength index (BMSi) but poorer physical performance and higher fracture risk than women without diabetes.
Women with T2D had 9.1% higher body weight, a 9.5% higher body mass index (BMI), and 6.3% higher appendicular lean mass index (lean mass divided by height squared) than controls.
The T2D group also had a lower prevalence of reported osteoporosis medication use vs controls: 3.4% vs 7.5%, respectively.
Prolonged diabetes treatment and insulin use were associated with higher fracture risk and poorer physical performance despite better bone characteristics.
“Our results demonstrate that checking and monitoring physical function is important to identify diabetes patients with a high risk of fractures and suggest that improving physical function may be important to reduce the risk of fractures in these patients,” Dr. Lorentzon told this news organization.
He speculated that the better bone microarchitecture in women with T2D could be due to both higher body weight and adiposity as well as to hormonal differences such as higher estradiol levels.
Study Details
A fractures study was performed in the Gothenburg area from March 2013 to May 2016 with follow-up of incident fracture data completed in March 2023. Data were collected from questionnaires and through examination of anthropometrics, physical function, and bone measurements using dual-energy x-ray absorptiometry and high-resolution peripheral computed tomography. A subsample underwent bone microindentation to assess BMSi.
Among the cohort’s 3008 women, ages 75-80 (mean, 77.8), 294 patients with T2D were compared with 2714 same-age unaffected women.
During a median follow-up of 7.3 years, 1071 incident fractures, 853 major osteoporotic fractures, and 232 hip fractures occurred. In models adjusted for age, BMI, clinical risk factors, and femoral neck BMD, T2D was associated with an increased risk of any fracture: hazard ratio (HR), 1.26; (95% CI, 1.04-1.54), and major osteoporotic fracture (HR, 1.25; 95% CI, 1.00-1.56).
Most fractures were due to falls, with the most common affected sites being the forearm, upper arm, spine, and hip, Dr. Lorentzon said.
Among the findings:
- In bone microarchitecture, women with T2D had higher BMD at all sites: total hip, 4.4% higher; femoral neck, 4.9% higher; and lumbar spine, 5.2% higher.
- At the tibia, the T2D group had 7.4% greater cortical area and 1.3% greater density, as well as 8.7% higher trabecular bone volume fraction.
“Our findings regarding BMD are consistent with previous publications showing higher BMD in individuals with T2D compared with those without diabetes,” Dr. Lorentzon said. A 2012 meta-analysis, for example, showed higher BMD levels in T2D patients. “Some smaller studies, however, have found worse bone microstructure and lower bone material strength in contrast to the results from our study,” Dr. Lorentzon said.
- There was no difference in BMSi, with a mean of 78 in both groups.
- The T2D group had lower performance on all physical function tests: a 9.7% lower grip strength, 9.9% slower gait speed, and 13.9% slower timed up-and-go time than women without diabetes.
“We found all parameters regarding physical function, such as muscle strength, balance, and performance, were much worse in women with diabetes than in those without,” Dr. Lorentzon said. “Dizziness could also be a contributor to the increased risk of falls, but this factor was not investigated in our study.”
Commenting on the study but not involved in it, Anthony J. Pick, MD, an endocrinologist at Northwestern Medicine Lake Forest Hospital in Lake Forest, Illinois, said sarcopenia is a common and often under-recognized problem in older adults and is especially prevalent in T2D, obesity, and heart failure. “I believe that ‘exercise is medicine’ is a key concept for metabolic and osteoporosis patients — and wellness and longevity in general — and I certainly hope studies like this drive awareness of the importance of engaging in strengthening exercises.”
Dr. Pick noted some nuances in this study suggesting there may be some impairments in bone quality beyond the strength and fall risk issue, “so this is likely a complex area.”
This study was supported by the Swedish Research Council, the Inga-Britt and Arne Lundberg Foundation, and Sahlgrenska University Hospital. Dr. Lorentzon reported personal fees from UCB Pharma, Amgen, Parexel International, Astellas, and Gedeon Richter outside the submitted work. Coauthor Dr. Johansson reported lecture fees from Union Chimique Belge (UCB) Pharma outside the submitted work. Dr. Axelsson reported personal fees from Amgen, Meda/Mylan, and Lilly outside the submitted work. Dr. Pick had no relevant conflicts of interest.
, according to a Swedish prospective observational study in JAMA Network Open.
The study was conducted in more than 3000 Swedish women by Mattias Lorentzon, MD, a professor of geriatric medicine at Gothenburg University, and chief physician at the Osteoporosis Clinic at Sahlgrenska University Hospital in Mölndal, and colleagues.
Older women with T2D had higher BMD, better bone microarchitecture, and a similar bone material strength index (BMSi) but poorer physical performance and higher fracture risk than women without diabetes.
Women with T2D had 9.1% higher body weight, a 9.5% higher body mass index (BMI), and 6.3% higher appendicular lean mass index (lean mass divided by height squared) than controls.
The T2D group also had a lower prevalence of reported osteoporosis medication use vs controls: 3.4% vs 7.5%, respectively.
Prolonged diabetes treatment and insulin use were associated with higher fracture risk and poorer physical performance despite better bone characteristics.
“Our results demonstrate that checking and monitoring physical function is important to identify diabetes patients with a high risk of fractures and suggest that improving physical function may be important to reduce the risk of fractures in these patients,” Dr. Lorentzon told this news organization.
He speculated that the better bone microarchitecture in women with T2D could be due to both higher body weight and adiposity as well as to hormonal differences such as higher estradiol levels.
Study Details
A fractures study was performed in the Gothenburg area from March 2013 to May 2016 with follow-up of incident fracture data completed in March 2023. Data were collected from questionnaires and through examination of anthropometrics, physical function, and bone measurements using dual-energy x-ray absorptiometry and high-resolution peripheral computed tomography. A subsample underwent bone microindentation to assess BMSi.
Among the cohort’s 3008 women, ages 75-80 (mean, 77.8), 294 patients with T2D were compared with 2714 same-age unaffected women.
During a median follow-up of 7.3 years, 1071 incident fractures, 853 major osteoporotic fractures, and 232 hip fractures occurred. In models adjusted for age, BMI, clinical risk factors, and femoral neck BMD, T2D was associated with an increased risk of any fracture: hazard ratio (HR), 1.26; (95% CI, 1.04-1.54), and major osteoporotic fracture (HR, 1.25; 95% CI, 1.00-1.56).
Most fractures were due to falls, with the most common affected sites being the forearm, upper arm, spine, and hip, Dr. Lorentzon said.
Among the findings:
- In bone microarchitecture, women with T2D had higher BMD at all sites: total hip, 4.4% higher; femoral neck, 4.9% higher; and lumbar spine, 5.2% higher.
- At the tibia, the T2D group had 7.4% greater cortical area and 1.3% greater density, as well as 8.7% higher trabecular bone volume fraction.
“Our findings regarding BMD are consistent with previous publications showing higher BMD in individuals with T2D compared with those without diabetes,” Dr. Lorentzon said. A 2012 meta-analysis, for example, showed higher BMD levels in T2D patients. “Some smaller studies, however, have found worse bone microstructure and lower bone material strength in contrast to the results from our study,” Dr. Lorentzon said.
- There was no difference in BMSi, with a mean of 78 in both groups.
- The T2D group had lower performance on all physical function tests: a 9.7% lower grip strength, 9.9% slower gait speed, and 13.9% slower timed up-and-go time than women without diabetes.
“We found all parameters regarding physical function, such as muscle strength, balance, and performance, were much worse in women with diabetes than in those without,” Dr. Lorentzon said. “Dizziness could also be a contributor to the increased risk of falls, but this factor was not investigated in our study.”
Commenting on the study but not involved in it, Anthony J. Pick, MD, an endocrinologist at Northwestern Medicine Lake Forest Hospital in Lake Forest, Illinois, said sarcopenia is a common and often under-recognized problem in older adults and is especially prevalent in T2D, obesity, and heart failure. “I believe that ‘exercise is medicine’ is a key concept for metabolic and osteoporosis patients — and wellness and longevity in general — and I certainly hope studies like this drive awareness of the importance of engaging in strengthening exercises.”
Dr. Pick noted some nuances in this study suggesting there may be some impairments in bone quality beyond the strength and fall risk issue, “so this is likely a complex area.”
This study was supported by the Swedish Research Council, the Inga-Britt and Arne Lundberg Foundation, and Sahlgrenska University Hospital. Dr. Lorentzon reported personal fees from UCB Pharma, Amgen, Parexel International, Astellas, and Gedeon Richter outside the submitted work. Coauthor Dr. Johansson reported lecture fees from Union Chimique Belge (UCB) Pharma outside the submitted work. Dr. Axelsson reported personal fees from Amgen, Meda/Mylan, and Lilly outside the submitted work. Dr. Pick had no relevant conflicts of interest.
FROM JAMA NETWORK OPEN
Federal Health Care Data Trends 2024

Federal Health Care Data Trends is a special supplement to Federal Practitioner, showcasing the latest research in health care for veterans and active-duty military members via compelling infographics. Click below to view highlights from the issue:
Federal Health Care Data Trends is a special supplement to Federal Practitioner, showcasing the latest research in health care for veterans and active-duty military members via compelling infographics. Click below to view highlights from the issue:
Federal Health Care Data Trends is a special supplement to Federal Practitioner, showcasing the latest research in health care for veterans and active-duty military members via compelling infographics. Click below to view highlights from the issue:
Is Buprenorphine/Naloxone Safer Than Buprenorphine Alone During Pregnancy?
TOPLINE:
Buprenorphine combined with naloxone during pregnancy is associated with lower risks for neonatal abstinence syndrome and neonatal intensive care unit admission than buprenorphine alone. The study also found no significant differences in major congenital malformations between the two treatments.
METHODOLOGY:
- Researchers conducted a population-based cohort study using healthcare utilization data of people who were insured by Medicaid between 2000 and 2018.
- A total of 8695 pregnant individuals were included, with 3369 exposed to buprenorphine/naloxone and 5326 exposed to buprenorphine alone during the first trimester.
- Outcome measures included major congenital malformations, low birth weight, neonatal abstinence syndrome, neonatal intensive care unit admission, preterm birth, respiratory symptoms, small for gestational age, cesarean delivery, and maternal morbidity.
- The study excluded pregnancies with chromosomal anomalies, first-trimester exposure to known teratogens, or methadone use during baseline or the first trimester.
TAKEAWAY:
- According to the authors, buprenorphine/naloxone exposure during pregnancy was associated with a lower risk for neonatal abstinence syndrome (weighted risk ratio [RR], 0.77; 95% CI, 0.70-0.84) than buprenorphine alone.
- The researchers found a modestly lower risk for neonatal intensive care unit admission (weighted RR, 0.91; 95% CI, 0.85-0.98) and small risk for gestational age (weighted RR, 0.86; 95% CI, 0.75-0.98) in the buprenorphine/naloxone group.
- No significant differences were observed between the two groups in major congenital malformations, low birth weight, preterm birth, respiratory symptoms, or cesarean delivery.
IN PRACTICE:
“For the outcomes assessed, compared with buprenorphine alone, buprenorphine combined with naloxone during pregnancy appears to be a safe treatment option. This supports the view that both formulations are reasonable options for treatment of OUD in pregnancy, affirming flexibility in collaborative treatment decision-making,” the study authors wrote.
SOURCE:
The study was led by Loreen Straub, MD, MS, of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital and Harvard Medical School in Boston. It was published online in JAMA.
LIMITATIONS:
Some potential confounders, such as alcohol use and cigarette smoking, may not have been recorded in claims data. The findings for many of the neonatal and maternal outcomes suggest that confounding by unmeasured factors is an unlikely explanation for the associations observed. Individuals identified as exposed based on filled prescriptions might not have used the medication. The study used outcome algorithms with relatively high positive predictive values to minimize outcome misclassification. The cohort was restricted to live births to enable linkage to infants and to assess neonatal outcomes.
DISCLOSURES:
Various authors reported receiving grants and personal fees from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Drug Abuse, Roche, Moderna, Takeda, and Janssen Global, among others.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Buprenorphine combined with naloxone during pregnancy is associated with lower risks for neonatal abstinence syndrome and neonatal intensive care unit admission than buprenorphine alone. The study also found no significant differences in major congenital malformations between the two treatments.
METHODOLOGY:
- Researchers conducted a population-based cohort study using healthcare utilization data of people who were insured by Medicaid between 2000 and 2018.
- A total of 8695 pregnant individuals were included, with 3369 exposed to buprenorphine/naloxone and 5326 exposed to buprenorphine alone during the first trimester.
- Outcome measures included major congenital malformations, low birth weight, neonatal abstinence syndrome, neonatal intensive care unit admission, preterm birth, respiratory symptoms, small for gestational age, cesarean delivery, and maternal morbidity.
- The study excluded pregnancies with chromosomal anomalies, first-trimester exposure to known teratogens, or methadone use during baseline or the first trimester.
TAKEAWAY:
- According to the authors, buprenorphine/naloxone exposure during pregnancy was associated with a lower risk for neonatal abstinence syndrome (weighted risk ratio [RR], 0.77; 95% CI, 0.70-0.84) than buprenorphine alone.
- The researchers found a modestly lower risk for neonatal intensive care unit admission (weighted RR, 0.91; 95% CI, 0.85-0.98) and small risk for gestational age (weighted RR, 0.86; 95% CI, 0.75-0.98) in the buprenorphine/naloxone group.
- No significant differences were observed between the two groups in major congenital malformations, low birth weight, preterm birth, respiratory symptoms, or cesarean delivery.
IN PRACTICE:
“For the outcomes assessed, compared with buprenorphine alone, buprenorphine combined with naloxone during pregnancy appears to be a safe treatment option. This supports the view that both formulations are reasonable options for treatment of OUD in pregnancy, affirming flexibility in collaborative treatment decision-making,” the study authors wrote.
SOURCE:
The study was led by Loreen Straub, MD, MS, of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital and Harvard Medical School in Boston. It was published online in JAMA.
LIMITATIONS:
Some potential confounders, such as alcohol use and cigarette smoking, may not have been recorded in claims data. The findings for many of the neonatal and maternal outcomes suggest that confounding by unmeasured factors is an unlikely explanation for the associations observed. Individuals identified as exposed based on filled prescriptions might not have used the medication. The study used outcome algorithms with relatively high positive predictive values to minimize outcome misclassification. The cohort was restricted to live births to enable linkage to infants and to assess neonatal outcomes.
DISCLOSURES:
Various authors reported receiving grants and personal fees from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Drug Abuse, Roche, Moderna, Takeda, and Janssen Global, among others.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Buprenorphine combined with naloxone during pregnancy is associated with lower risks for neonatal abstinence syndrome and neonatal intensive care unit admission than buprenorphine alone. The study also found no significant differences in major congenital malformations between the two treatments.
METHODOLOGY:
- Researchers conducted a population-based cohort study using healthcare utilization data of people who were insured by Medicaid between 2000 and 2018.
- A total of 8695 pregnant individuals were included, with 3369 exposed to buprenorphine/naloxone and 5326 exposed to buprenorphine alone during the first trimester.
- Outcome measures included major congenital malformations, low birth weight, neonatal abstinence syndrome, neonatal intensive care unit admission, preterm birth, respiratory symptoms, small for gestational age, cesarean delivery, and maternal morbidity.
- The study excluded pregnancies with chromosomal anomalies, first-trimester exposure to known teratogens, or methadone use during baseline or the first trimester.
TAKEAWAY:
- According to the authors, buprenorphine/naloxone exposure during pregnancy was associated with a lower risk for neonatal abstinence syndrome (weighted risk ratio [RR], 0.77; 95% CI, 0.70-0.84) than buprenorphine alone.
- The researchers found a modestly lower risk for neonatal intensive care unit admission (weighted RR, 0.91; 95% CI, 0.85-0.98) and small risk for gestational age (weighted RR, 0.86; 95% CI, 0.75-0.98) in the buprenorphine/naloxone group.
- No significant differences were observed between the two groups in major congenital malformations, low birth weight, preterm birth, respiratory symptoms, or cesarean delivery.
IN PRACTICE:
“For the outcomes assessed, compared with buprenorphine alone, buprenorphine combined with naloxone during pregnancy appears to be a safe treatment option. This supports the view that both formulations are reasonable options for treatment of OUD in pregnancy, affirming flexibility in collaborative treatment decision-making,” the study authors wrote.
SOURCE:
The study was led by Loreen Straub, MD, MS, of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital and Harvard Medical School in Boston. It was published online in JAMA.
LIMITATIONS:
Some potential confounders, such as alcohol use and cigarette smoking, may not have been recorded in claims data. The findings for many of the neonatal and maternal outcomes suggest that confounding by unmeasured factors is an unlikely explanation for the associations observed. Individuals identified as exposed based on filled prescriptions might not have used the medication. The study used outcome algorithms with relatively high positive predictive values to minimize outcome misclassification. The cohort was restricted to live births to enable linkage to infants and to assess neonatal outcomes.
DISCLOSURES:
Various authors reported receiving grants and personal fees from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Drug Abuse, Roche, Moderna, Takeda, and Janssen Global, among others.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
PCOS Increases Eating Disorder Risk
TOPLINE:
Women with polycystic ovary syndrome (PCOS) have higher odds of some eating disorders, including bulimia nervosa, binge eating disorder, and disordered eating, regardless of weight.
METHODOLOGY:
- A small systematic review and meta-analysis showed increased odds of any eating disorders and disordered eating scores in adult women with PCOS compared with women without PCOS.
- As part of the 2023 update of the International Evidence-based Guideline for the Assessment of and Management of PCOS, the same researchers updated and expanded their analysis to include adolescents and specific eating disorders and to evaluate the effect of body mass index (BMI) on these risks.
- They included 20 cross-sectional studies involving 28,922 women with PCOS and 258,619 women without PCOS; PCOS was diagnosed by either National Institutes of Health or Rotterdam criteria, as well as by patient self-report or hospital records.
- Eating disorders were screened using a validated disordered eating screening tool or diagnostic criteria from the Diagnostic and Statistical Manual of Mental Disorders.
- The outcomes of interest included the prevalence of any eating disorder, individual eating disorders, disordered eating, and mean disordered eating scores.
TAKEAWAY:
- Women with PCOS had 53% higher odds (odds ratio [OR], 1.53; 95% CI, 1.29-1.82; eight studies) of any eating disorder than control individuals without PCOS.
- The likelihood of bulimia nervosa (OR, 1.34; 95% CI, 1.17-1.54; five studies) and binge eating disorder (OR, 2.09; 95% CI, 1.18-3.72; four studies) was higher in women with PCOS, but no significant association was found for anorexia nervosa.
- The mean disordered eating scores and odds of disordered eating were higher in women with PCOS (standardized mean difference [SMD], 0.52; 95% CI, 0.28-0.77; 13 studies; and OR, 2.84; 95% CI, 1.0-8.04; eight studies; respectively).
- Disordered eating scores were higher in both the normal and higher weight categories (BMI < 25; SMD, 0.36; 95% CI, 0.15-0.58; five studies; and BMI ≥ 25; SMD, 0.68; 95% CI, 0.22-1.13; four studies; respectively).
IN PRACTICE:
“Our findings emphasize the importance of screening women with PCOS for eating disorders before clinicians share any lifestyle advice,” the lead author said in a press release. “The lifestyle modifications we often recommend for women with PCOS — including physical activity, healthy diet, and behavior modifications — could hinder the recovery process for eating disorders.”
SOURCE:
The study was led by Laura G. Cooney, MD, MSCE, University of Wisconsin, Madison, and published online in the Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The included studies were observational in nature, limiting the ability to adjust for potential confounders. The cross-sectional design of the included studies precluded determining whether the diagnosis of PCOS or the symptoms of disordered eating occurred first. Studies from 10 countries were included, but limited data from developing or Asian countries restrict the generalizability of the results.
DISCLOSURES:
This study was conducted to inform recommendations of the 2023 International Evidence-based Guideline in PCOS, which was funded by the Australian National Health and Medical Research Council, Centre for Research Excellence in Polycystic Ovary Syndrome, and other sources. The authors declared no conflicts of interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Women with polycystic ovary syndrome (PCOS) have higher odds of some eating disorders, including bulimia nervosa, binge eating disorder, and disordered eating, regardless of weight.
METHODOLOGY:
- A small systematic review and meta-analysis showed increased odds of any eating disorders and disordered eating scores in adult women with PCOS compared with women without PCOS.
- As part of the 2023 update of the International Evidence-based Guideline for the Assessment of and Management of PCOS, the same researchers updated and expanded their analysis to include adolescents and specific eating disorders and to evaluate the effect of body mass index (BMI) on these risks.
- They included 20 cross-sectional studies involving 28,922 women with PCOS and 258,619 women without PCOS; PCOS was diagnosed by either National Institutes of Health or Rotterdam criteria, as well as by patient self-report or hospital records.
- Eating disorders were screened using a validated disordered eating screening tool or diagnostic criteria from the Diagnostic and Statistical Manual of Mental Disorders.
- The outcomes of interest included the prevalence of any eating disorder, individual eating disorders, disordered eating, and mean disordered eating scores.
TAKEAWAY:
- Women with PCOS had 53% higher odds (odds ratio [OR], 1.53; 95% CI, 1.29-1.82; eight studies) of any eating disorder than control individuals without PCOS.
- The likelihood of bulimia nervosa (OR, 1.34; 95% CI, 1.17-1.54; five studies) and binge eating disorder (OR, 2.09; 95% CI, 1.18-3.72; four studies) was higher in women with PCOS, but no significant association was found for anorexia nervosa.
- The mean disordered eating scores and odds of disordered eating were higher in women with PCOS (standardized mean difference [SMD], 0.52; 95% CI, 0.28-0.77; 13 studies; and OR, 2.84; 95% CI, 1.0-8.04; eight studies; respectively).
- Disordered eating scores were higher in both the normal and higher weight categories (BMI < 25; SMD, 0.36; 95% CI, 0.15-0.58; five studies; and BMI ≥ 25; SMD, 0.68; 95% CI, 0.22-1.13; four studies; respectively).
IN PRACTICE:
“Our findings emphasize the importance of screening women with PCOS for eating disorders before clinicians share any lifestyle advice,” the lead author said in a press release. “The lifestyle modifications we often recommend for women with PCOS — including physical activity, healthy diet, and behavior modifications — could hinder the recovery process for eating disorders.”
SOURCE:
The study was led by Laura G. Cooney, MD, MSCE, University of Wisconsin, Madison, and published online in the Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The included studies were observational in nature, limiting the ability to adjust for potential confounders. The cross-sectional design of the included studies precluded determining whether the diagnosis of PCOS or the symptoms of disordered eating occurred first. Studies from 10 countries were included, but limited data from developing or Asian countries restrict the generalizability of the results.
DISCLOSURES:
This study was conducted to inform recommendations of the 2023 International Evidence-based Guideline in PCOS, which was funded by the Australian National Health and Medical Research Council, Centre for Research Excellence in Polycystic Ovary Syndrome, and other sources. The authors declared no conflicts of interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Women with polycystic ovary syndrome (PCOS) have higher odds of some eating disorders, including bulimia nervosa, binge eating disorder, and disordered eating, regardless of weight.
METHODOLOGY:
- A small systematic review and meta-analysis showed increased odds of any eating disorders and disordered eating scores in adult women with PCOS compared with women without PCOS.
- As part of the 2023 update of the International Evidence-based Guideline for the Assessment of and Management of PCOS, the same researchers updated and expanded their analysis to include adolescents and specific eating disorders and to evaluate the effect of body mass index (BMI) on these risks.
- They included 20 cross-sectional studies involving 28,922 women with PCOS and 258,619 women without PCOS; PCOS was diagnosed by either National Institutes of Health or Rotterdam criteria, as well as by patient self-report or hospital records.
- Eating disorders were screened using a validated disordered eating screening tool or diagnostic criteria from the Diagnostic and Statistical Manual of Mental Disorders.
- The outcomes of interest included the prevalence of any eating disorder, individual eating disorders, disordered eating, and mean disordered eating scores.
TAKEAWAY:
- Women with PCOS had 53% higher odds (odds ratio [OR], 1.53; 95% CI, 1.29-1.82; eight studies) of any eating disorder than control individuals without PCOS.
- The likelihood of bulimia nervosa (OR, 1.34; 95% CI, 1.17-1.54; five studies) and binge eating disorder (OR, 2.09; 95% CI, 1.18-3.72; four studies) was higher in women with PCOS, but no significant association was found for anorexia nervosa.
- The mean disordered eating scores and odds of disordered eating were higher in women with PCOS (standardized mean difference [SMD], 0.52; 95% CI, 0.28-0.77; 13 studies; and OR, 2.84; 95% CI, 1.0-8.04; eight studies; respectively).
- Disordered eating scores were higher in both the normal and higher weight categories (BMI < 25; SMD, 0.36; 95% CI, 0.15-0.58; five studies; and BMI ≥ 25; SMD, 0.68; 95% CI, 0.22-1.13; four studies; respectively).
IN PRACTICE:
“Our findings emphasize the importance of screening women with PCOS for eating disorders before clinicians share any lifestyle advice,” the lead author said in a press release. “The lifestyle modifications we often recommend for women with PCOS — including physical activity, healthy diet, and behavior modifications — could hinder the recovery process for eating disorders.”
SOURCE:
The study was led by Laura G. Cooney, MD, MSCE, University of Wisconsin, Madison, and published online in the Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The included studies were observational in nature, limiting the ability to adjust for potential confounders. The cross-sectional design of the included studies precluded determining whether the diagnosis of PCOS or the symptoms of disordered eating occurred first. Studies from 10 countries were included, but limited data from developing or Asian countries restrict the generalizability of the results.
DISCLOSURES:
This study was conducted to inform recommendations of the 2023 International Evidence-based Guideline in PCOS, which was funded by the Australian National Health and Medical Research Council, Centre for Research Excellence in Polycystic Ovary Syndrome, and other sources. The authors declared no conflicts of interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Sexual Arousal Cream Promising in Some Subsets of Women
Topical sildenafil (citrate) cream 3.6% used by healthy premenopausal women with a primary symptom of female sexual arousal disorder did not show statistically significant improvement over placebo in the coprimary or secondary endpoints over a 3-month period in new preliminary study data published in Obstetrics & Gynecology.
Topical sildenafil cream is currently used for erectile dysfunction in men. There are no US Food and Drug Administration–approved treatments for female sexual arousal disorder, which affects up to 26% of women in the United States by some estimates.
Isabella Johnson, senior manager of product development at Daré Bioscience, San Diego, California, led a phase 2b, exploratory, randomized, placebo-controlled, double-blind study of sildenafil cream’s potential to help women improve their sexual experiences.
The study included 200 women with female sexual arousal disorder randomized to sildenafil cream (n = 101) or placebo cream (n = 99); 177 completed the trial and made up the intention-to-treat group. Healthy premenopausal women at least 18 years old and their sexual partners were screened for the study.
The authors report that the primary endpoints were scores on Sexual Function Questionnaire (SFQ28) arousal sensation domain and question 14 on the Female Sexual Distress Scale — Desire/Arousal/Orgasm (FSD-DAO), which asks “How often in the past 30 days did you feel concerned by difficulties with sexual arousal?” The secondary endpoint was the average number and average proportion of satisfactory sexual events. Topical sildenafil was not more effective than placebo with these primary or secondary endpoints.
Some Subgroups Benefited
However, a post hoc analysis told a different story. “[A]mong a subset of women with female sexual arousal disorder only or female sexual arousal disorder with concomitant decreased desire, we found either trends or significant improvements in sexual functioning with sildenafil cream compared with placebo cream across multiple aspects of sexual function,” the authors write.
The researchers also noted that several FSDS-DAO questions, other than question 14, asked about generalized feelings related to sexual distress and interpersonal difficulties and scores on those questions showed significant improvement with sildenafil cream compared with placebo in the exploratory subset.
“The total FSDS-DAO score decreased by about 7 points for sildenafil cream users in the subset population (a clinically meaningful decrease in sexual distress) compared with a two-point decrease for placebo cream users (P = .10),” they write.
Post Hoc Analysis Is Exploratory
JoAnn V. Pinkerton, MD, with the Department of Obstetrics and Gynecology, University of Virginia Health in Charlottesville, writes in an editorial that because the authors did not adjust for multiple hypothesis testing, the post hoc subset analyses should be considered only exploratory.
She notes that the trial was underpowered partly because it was halted after recruitment challenges during the COVID-19 pandemic. The small sample size and the varied reasons for arousal disorder among the women “may have limited the ability to find a positive outcome.”
, Dr. Pinkerton writes.
“Because improvement in genital arousal is thought to be due to the increased genital blood flow from sildenafil citrate, the subset of participants found least likely to benefit from sildenafil citrate cream were those with concomitant orgasmic dysfunction with or without genital pain,” she writes.
Data May Inform Phase 3 Trial
This phase 2b trial sets the stage for a phase 3 trial, she writes, to evaluate sildenafil topical cream in women with female sexual arousal disorder in the subsets where there were positive findings (those with or without a secondary diagnosis of decreased desire) but not among women having difficulty reaching orgasm.
“If positive, it could lead to a new therapeutic area for the unmet treatment needs of premenopausal and postmenopausal women with female sexual arousal disorder,” Dr. Pinkerton writes.
A study coauthor, Clint Dart, reports money was paid to his institution from Daré Bioscience, he provided independent data verification, and he is an employee of Premier Research. Isabella Johnson, Andrea Ries Thurman, MD, Jessica Hatheway, MBA, David R. Friend, PhD, and Andrew Goldstein, MD, are employees of Daré Bioscience. Katherine A. Cornell is an employee of Strategic Science & Technologies, LLC. C. Paige Brainard, MD, was financially compensated by Del Sol Research Management and her practice received funding from Daré Bioscience for study-specific activities. Dr. Goldstein also reported receiving payments from Nuvig, Ipsen, and AbbVie. Dr. Pinkerton’s institution received funds from Bayer Pharmaceuticals as she served as PI for a multinational clinical trial.
Topical sildenafil (citrate) cream 3.6% used by healthy premenopausal women with a primary symptom of female sexual arousal disorder did not show statistically significant improvement over placebo in the coprimary or secondary endpoints over a 3-month period in new preliminary study data published in Obstetrics & Gynecology.
Topical sildenafil cream is currently used for erectile dysfunction in men. There are no US Food and Drug Administration–approved treatments for female sexual arousal disorder, which affects up to 26% of women in the United States by some estimates.
Isabella Johnson, senior manager of product development at Daré Bioscience, San Diego, California, led a phase 2b, exploratory, randomized, placebo-controlled, double-blind study of sildenafil cream’s potential to help women improve their sexual experiences.
The study included 200 women with female sexual arousal disorder randomized to sildenafil cream (n = 101) or placebo cream (n = 99); 177 completed the trial and made up the intention-to-treat group. Healthy premenopausal women at least 18 years old and their sexual partners were screened for the study.
The authors report that the primary endpoints were scores on Sexual Function Questionnaire (SFQ28) arousal sensation domain and question 14 on the Female Sexual Distress Scale — Desire/Arousal/Orgasm (FSD-DAO), which asks “How often in the past 30 days did you feel concerned by difficulties with sexual arousal?” The secondary endpoint was the average number and average proportion of satisfactory sexual events. Topical sildenafil was not more effective than placebo with these primary or secondary endpoints.
Some Subgroups Benefited
However, a post hoc analysis told a different story. “[A]mong a subset of women with female sexual arousal disorder only or female sexual arousal disorder with concomitant decreased desire, we found either trends or significant improvements in sexual functioning with sildenafil cream compared with placebo cream across multiple aspects of sexual function,” the authors write.
The researchers also noted that several FSDS-DAO questions, other than question 14, asked about generalized feelings related to sexual distress and interpersonal difficulties and scores on those questions showed significant improvement with sildenafil cream compared with placebo in the exploratory subset.
“The total FSDS-DAO score decreased by about 7 points for sildenafil cream users in the subset population (a clinically meaningful decrease in sexual distress) compared with a two-point decrease for placebo cream users (P = .10),” they write.
Post Hoc Analysis Is Exploratory
JoAnn V. Pinkerton, MD, with the Department of Obstetrics and Gynecology, University of Virginia Health in Charlottesville, writes in an editorial that because the authors did not adjust for multiple hypothesis testing, the post hoc subset analyses should be considered only exploratory.
She notes that the trial was underpowered partly because it was halted after recruitment challenges during the COVID-19 pandemic. The small sample size and the varied reasons for arousal disorder among the women “may have limited the ability to find a positive outcome.”
, Dr. Pinkerton writes.
“Because improvement in genital arousal is thought to be due to the increased genital blood flow from sildenafil citrate, the subset of participants found least likely to benefit from sildenafil citrate cream were those with concomitant orgasmic dysfunction with or without genital pain,” she writes.
Data May Inform Phase 3 Trial
This phase 2b trial sets the stage for a phase 3 trial, she writes, to evaluate sildenafil topical cream in women with female sexual arousal disorder in the subsets where there were positive findings (those with or without a secondary diagnosis of decreased desire) but not among women having difficulty reaching orgasm.
“If positive, it could lead to a new therapeutic area for the unmet treatment needs of premenopausal and postmenopausal women with female sexual arousal disorder,” Dr. Pinkerton writes.
A study coauthor, Clint Dart, reports money was paid to his institution from Daré Bioscience, he provided independent data verification, and he is an employee of Premier Research. Isabella Johnson, Andrea Ries Thurman, MD, Jessica Hatheway, MBA, David R. Friend, PhD, and Andrew Goldstein, MD, are employees of Daré Bioscience. Katherine A. Cornell is an employee of Strategic Science & Technologies, LLC. C. Paige Brainard, MD, was financially compensated by Del Sol Research Management and her practice received funding from Daré Bioscience for study-specific activities. Dr. Goldstein also reported receiving payments from Nuvig, Ipsen, and AbbVie. Dr. Pinkerton’s institution received funds from Bayer Pharmaceuticals as she served as PI for a multinational clinical trial.
Topical sildenafil (citrate) cream 3.6% used by healthy premenopausal women with a primary symptom of female sexual arousal disorder did not show statistically significant improvement over placebo in the coprimary or secondary endpoints over a 3-month period in new preliminary study data published in Obstetrics & Gynecology.
Topical sildenafil cream is currently used for erectile dysfunction in men. There are no US Food and Drug Administration–approved treatments for female sexual arousal disorder, which affects up to 26% of women in the United States by some estimates.
Isabella Johnson, senior manager of product development at Daré Bioscience, San Diego, California, led a phase 2b, exploratory, randomized, placebo-controlled, double-blind study of sildenafil cream’s potential to help women improve their sexual experiences.
The study included 200 women with female sexual arousal disorder randomized to sildenafil cream (n = 101) or placebo cream (n = 99); 177 completed the trial and made up the intention-to-treat group. Healthy premenopausal women at least 18 years old and their sexual partners were screened for the study.
The authors report that the primary endpoints were scores on Sexual Function Questionnaire (SFQ28) arousal sensation domain and question 14 on the Female Sexual Distress Scale — Desire/Arousal/Orgasm (FSD-DAO), which asks “How often in the past 30 days did you feel concerned by difficulties with sexual arousal?” The secondary endpoint was the average number and average proportion of satisfactory sexual events. Topical sildenafil was not more effective than placebo with these primary or secondary endpoints.
Some Subgroups Benefited
However, a post hoc analysis told a different story. “[A]mong a subset of women with female sexual arousal disorder only or female sexual arousal disorder with concomitant decreased desire, we found either trends or significant improvements in sexual functioning with sildenafil cream compared with placebo cream across multiple aspects of sexual function,” the authors write.
The researchers also noted that several FSDS-DAO questions, other than question 14, asked about generalized feelings related to sexual distress and interpersonal difficulties and scores on those questions showed significant improvement with sildenafil cream compared with placebo in the exploratory subset.
“The total FSDS-DAO score decreased by about 7 points for sildenafil cream users in the subset population (a clinically meaningful decrease in sexual distress) compared with a two-point decrease for placebo cream users (P = .10),” they write.
Post Hoc Analysis Is Exploratory
JoAnn V. Pinkerton, MD, with the Department of Obstetrics and Gynecology, University of Virginia Health in Charlottesville, writes in an editorial that because the authors did not adjust for multiple hypothesis testing, the post hoc subset analyses should be considered only exploratory.
She notes that the trial was underpowered partly because it was halted after recruitment challenges during the COVID-19 pandemic. The small sample size and the varied reasons for arousal disorder among the women “may have limited the ability to find a positive outcome.”
, Dr. Pinkerton writes.
“Because improvement in genital arousal is thought to be due to the increased genital blood flow from sildenafil citrate, the subset of participants found least likely to benefit from sildenafil citrate cream were those with concomitant orgasmic dysfunction with or without genital pain,” she writes.
Data May Inform Phase 3 Trial
This phase 2b trial sets the stage for a phase 3 trial, she writes, to evaluate sildenafil topical cream in women with female sexual arousal disorder in the subsets where there were positive findings (those with or without a secondary diagnosis of decreased desire) but not among women having difficulty reaching orgasm.
“If positive, it could lead to a new therapeutic area for the unmet treatment needs of premenopausal and postmenopausal women with female sexual arousal disorder,” Dr. Pinkerton writes.
A study coauthor, Clint Dart, reports money was paid to his institution from Daré Bioscience, he provided independent data verification, and he is an employee of Premier Research. Isabella Johnson, Andrea Ries Thurman, MD, Jessica Hatheway, MBA, David R. Friend, PhD, and Andrew Goldstein, MD, are employees of Daré Bioscience. Katherine A. Cornell is an employee of Strategic Science & Technologies, LLC. C. Paige Brainard, MD, was financially compensated by Del Sol Research Management and her practice received funding from Daré Bioscience for study-specific activities. Dr. Goldstein also reported receiving payments from Nuvig, Ipsen, and AbbVie. Dr. Pinkerton’s institution received funds from Bayer Pharmaceuticals as she served as PI for a multinational clinical trial.
FROM OBSTETRICS & GYNECOLOGY
How Safe is Anti–IL-6 Therapy During Pregnancy?
TOPLINE:
The maternal and neonatal outcomes in pregnant women treated with anti–interleukin (IL)-6 therapy for COVID-19 are largely favorable, with transient neonatal cytopenia observed in around one third of the babies being the only possible adverse outcome that could be related to anti–IL-6 therapy.
METHODOLOGY:
- Despite guidance, very few pregnant women with COVID-19 are offered evidence-based therapies such as anti–IL-6 due to concerns regarding fetal safety in later pregnancy.
- In this retrospective study, researchers evaluated maternal and neonatal outcomes in 25 pregnant women with COVID-19 (mean age at admission, 33 years) treated with anti–IL-6 (tocilizumab or sarilumab) at two tertiary hospitals in London.
- Most women (n = 16) received anti–IL-6 in the third trimester of pregnancy, whereas nine received it during the second trimester.
- Maternal and neonatal outcomes were assessed through medical record reviews and maternal medicine networks, with follow-up for 12 months.
- The women included in the study constituted a high-risk population with severe COVID-19; 24 required level two or three critical care. All women were receiving at least three concomitant medications due to their critical illness.
TAKEAWAY:
- Overall, 24 of 25 women treated with IL-6 receptor antibodies survived until hospital discharge.
- The sole death occurred in a woman with severe COVID-19 pneumonitis who later developed myocarditis and cardiac arrest. The physicians believed that these complications were more likely due to severe COVID-19 rather than anti–IL-6 therapy.
- All pregnancies resulted in live births; however, 16 babies had to be delivered preterm due to COVID-19 complications.
- Transient cytopenia was observed in 6 of 19 babies in whom a full blood count was performed. All the six babies were premature, with cytopenia resolving within 7 days in four babies; one baby died from complications associated with extreme prematurity.
IN PRACTICE:
“Although the authors found mild, transitory cytopenia in some (6 of 19) exposed infants, most had been delivered prematurely due to progressive COVID-19–related morbidity, and distinguishing drug effects from similar prematurity-related effects is difficult,” wrote Steven L. Clark, MD, from the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, in an accompanying editorial.
SOURCE:
The study was led by Melanie Nana, MRCP, from the Department of Obstetric Medicine, St Thomas’ Hospital, London, England. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study was retrospective in design, which may have introduced bias. The small sample size of 25 women may have limited the generalizability of the findings. Additionally, the study did not include a control group, which made it difficult to attribute outcomes solely to anti–IL-6 therapy. The lack of long-term follow-up data on the neonates also limited the understanding of potential long-term effects.
DISCLOSURES:
This study did not receive any funding. Some authors, including the lead author, received speaker fees, grants, or consultancy fees from academic institutions or pharmaceutical companies or had other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The maternal and neonatal outcomes in pregnant women treated with anti–interleukin (IL)-6 therapy for COVID-19 are largely favorable, with transient neonatal cytopenia observed in around one third of the babies being the only possible adverse outcome that could be related to anti–IL-6 therapy.
METHODOLOGY:
- Despite guidance, very few pregnant women with COVID-19 are offered evidence-based therapies such as anti–IL-6 due to concerns regarding fetal safety in later pregnancy.
- In this retrospective study, researchers evaluated maternal and neonatal outcomes in 25 pregnant women with COVID-19 (mean age at admission, 33 years) treated with anti–IL-6 (tocilizumab or sarilumab) at two tertiary hospitals in London.
- Most women (n = 16) received anti–IL-6 in the third trimester of pregnancy, whereas nine received it during the second trimester.
- Maternal and neonatal outcomes were assessed through medical record reviews and maternal medicine networks, with follow-up for 12 months.
- The women included in the study constituted a high-risk population with severe COVID-19; 24 required level two or three critical care. All women were receiving at least three concomitant medications due to their critical illness.
TAKEAWAY:
- Overall, 24 of 25 women treated with IL-6 receptor antibodies survived until hospital discharge.
- The sole death occurred in a woman with severe COVID-19 pneumonitis who later developed myocarditis and cardiac arrest. The physicians believed that these complications were more likely due to severe COVID-19 rather than anti–IL-6 therapy.
- All pregnancies resulted in live births; however, 16 babies had to be delivered preterm due to COVID-19 complications.
- Transient cytopenia was observed in 6 of 19 babies in whom a full blood count was performed. All the six babies were premature, with cytopenia resolving within 7 days in four babies; one baby died from complications associated with extreme prematurity.
IN PRACTICE:
“Although the authors found mild, transitory cytopenia in some (6 of 19) exposed infants, most had been delivered prematurely due to progressive COVID-19–related morbidity, and distinguishing drug effects from similar prematurity-related effects is difficult,” wrote Steven L. Clark, MD, from the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, in an accompanying editorial.
SOURCE:
The study was led by Melanie Nana, MRCP, from the Department of Obstetric Medicine, St Thomas’ Hospital, London, England. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study was retrospective in design, which may have introduced bias. The small sample size of 25 women may have limited the generalizability of the findings. Additionally, the study did not include a control group, which made it difficult to attribute outcomes solely to anti–IL-6 therapy. The lack of long-term follow-up data on the neonates also limited the understanding of potential long-term effects.
DISCLOSURES:
This study did not receive any funding. Some authors, including the lead author, received speaker fees, grants, or consultancy fees from academic institutions or pharmaceutical companies or had other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The maternal and neonatal outcomes in pregnant women treated with anti–interleukin (IL)-6 therapy for COVID-19 are largely favorable, with transient neonatal cytopenia observed in around one third of the babies being the only possible adverse outcome that could be related to anti–IL-6 therapy.
METHODOLOGY:
- Despite guidance, very few pregnant women with COVID-19 are offered evidence-based therapies such as anti–IL-6 due to concerns regarding fetal safety in later pregnancy.
- In this retrospective study, researchers evaluated maternal and neonatal outcomes in 25 pregnant women with COVID-19 (mean age at admission, 33 years) treated with anti–IL-6 (tocilizumab or sarilumab) at two tertiary hospitals in London.
- Most women (n = 16) received anti–IL-6 in the third trimester of pregnancy, whereas nine received it during the second trimester.
- Maternal and neonatal outcomes were assessed through medical record reviews and maternal medicine networks, with follow-up for 12 months.
- The women included in the study constituted a high-risk population with severe COVID-19; 24 required level two or three critical care. All women were receiving at least three concomitant medications due to their critical illness.
TAKEAWAY:
- Overall, 24 of 25 women treated with IL-6 receptor antibodies survived until hospital discharge.
- The sole death occurred in a woman with severe COVID-19 pneumonitis who later developed myocarditis and cardiac arrest. The physicians believed that these complications were more likely due to severe COVID-19 rather than anti–IL-6 therapy.
- All pregnancies resulted in live births; however, 16 babies had to be delivered preterm due to COVID-19 complications.
- Transient cytopenia was observed in 6 of 19 babies in whom a full blood count was performed. All the six babies were premature, with cytopenia resolving within 7 days in four babies; one baby died from complications associated with extreme prematurity.
IN PRACTICE:
“Although the authors found mild, transitory cytopenia in some (6 of 19) exposed infants, most had been delivered prematurely due to progressive COVID-19–related morbidity, and distinguishing drug effects from similar prematurity-related effects is difficult,” wrote Steven L. Clark, MD, from the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, in an accompanying editorial.
SOURCE:
The study was led by Melanie Nana, MRCP, from the Department of Obstetric Medicine, St Thomas’ Hospital, London, England. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study was retrospective in design, which may have introduced bias. The small sample size of 25 women may have limited the generalizability of the findings. Additionally, the study did not include a control group, which made it difficult to attribute outcomes solely to anti–IL-6 therapy. The lack of long-term follow-up data on the neonates also limited the understanding of potential long-term effects.
DISCLOSURES:
This study did not receive any funding. Some authors, including the lead author, received speaker fees, grants, or consultancy fees from academic institutions or pharmaceutical companies or had other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.