User login
A New ADC for Lung Cancer: Datopotamab Deruxtecan Now Approved by FDA
This transcript has been edited for clarity.
Hello. It’s Mark Kris, from Memorial Sloan Kettering, talking about a birthday gift I received on June 23 when the FDA approved the indication of datopotamab deruxtecan for people with lung cancers. We have another drug, our third ADC (antibody-drug conjugate) to fight lung cancer, so that’s a gift.
Let’s talk a little bit about that agent. It’s an interesting twist in our practice patterns. What can the drug do? It had a response rate of 45%, which is really important in patients that had EGFR mutations with progression on osimertinib. We really need drugs in that space. The duration of response was about 7 months, which is significant.
One interesting thing in the approval, [was] that the response rate of the blinded folks was greater than that in the investigator-assessed response by about 10%. It’s very interesting. Clearly, we have another drug, and we have it in a space where we need it.
Let’s talk a bit about the toxicity. I’m going to focus more on the paper by Bardia et al that compared datopotamab deruxtecan to various chemo drugs in breast cancer, not in lung cancer. You can take this a little bit with a grain of salt.
First, they saw a whole different array of side effects with datopotamab deruxtecan, things that we don’t normally deal with here. Nausea, stomatitis, alopecia, dry eye, and vomiting. All of those were more than 10% more common in patients that received datopotamab deruxtecan compared to the control. The only things that were more common with the control were neutropenia, leukopenia, and hand-foot syndrome in patients that had capecitabine.
One thing, though, is while you say, “Oh, these weren’t dangerous side effects,” they surely were lifestyle altering. Nobody wants to have these side effects on a daily basis. Again, there’s an increasing awareness about these kinds of lower-grade but still lifestyle-disrupting side effects. When it goes on day after day, you really have to balance that into the benefit you’re going to receive.
I think the second important point is how, when we use this drug, we’re going to have to go to another level to deal with the adverse effects that we are going to see. The first would be nausea and emesis. It is a highly emetogenic regimen based on the NCCN (National Comprehensive Cancer Network) guidelines, so you would need either 3 or 4 antiemetic drugs. That’s number one.
Number two, because of the potential eye problems, you need an eye exam before treatment — and the label says at least annually — with any symptoms. I think it’s very important that you give the patients eyedrops, and in general, the preservative-free eyedrops are the ones that are most effective.
Stomatitis is a very common side effect with that agent. It’s really not seen with the other drugs that even contain the same warhead. There, dexamethasone rinses are important. Now, this is a compounded medicine so you need to be very careful in making sure that you identify pharmacies that will prepare this and will have it available for the patients that need it.
Last, there is the risk of hypersensitivity reactions and there’s a recommendation for premedication for that. As you think about using datopotamab deruxtecan, you need to have all your ducks in a row to treat side effects. You need prophylaxis for hypersensitivity reactions, nausea, and emesis.
The patient will need an eye exam. You need to prepare the patient for possible dry eye and teach them which eyedrops are the best. You also need to ensure the availability of dexamethasone rinses and mouth washes. All that needs to be in place to make sure that the patient can safely use the drug.
I think it’s going to be a useful drug. We don’t yet have a uniformly available way to select patients for its use other than EGFR. I should note that the approval is for EGFR-mutated lung cancers. It doesn’t say which type of mutation, so that would give you some latitude in giving it for exon 20 atypicals as well as for the common sensitizing mutation.
We have another drug. It’s clearly going to be a useful one. It clearly comes with many adverse effects that we don’t normally treat on an everyday basis, we’re used to the diarrhea and skin changes that come on with the EGFR TKIs.
This pattern of side effects is different and requires some additional attention, but with it, the drug can be useful. I’m glad that we have yet another way to fight this disease.
Mark G. Kris, MD, Professor of Medicine, Weill Cornell Medical College; Attending Physician, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York , has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo; Received research grant from: National Institute of Health; Received income in an amount equal to or greater than $250 from: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo Others: Editorial support from Genentech
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. It’s Mark Kris, from Memorial Sloan Kettering, talking about a birthday gift I received on June 23 when the FDA approved the indication of datopotamab deruxtecan for people with lung cancers. We have another drug, our third ADC (antibody-drug conjugate) to fight lung cancer, so that’s a gift.
Let’s talk a little bit about that agent. It’s an interesting twist in our practice patterns. What can the drug do? It had a response rate of 45%, which is really important in patients that had EGFR mutations with progression on osimertinib. We really need drugs in that space. The duration of response was about 7 months, which is significant.
One interesting thing in the approval, [was] that the response rate of the blinded folks was greater than that in the investigator-assessed response by about 10%. It’s very interesting. Clearly, we have another drug, and we have it in a space where we need it.
Let’s talk a bit about the toxicity. I’m going to focus more on the paper by Bardia et al that compared datopotamab deruxtecan to various chemo drugs in breast cancer, not in lung cancer. You can take this a little bit with a grain of salt.
First, they saw a whole different array of side effects with datopotamab deruxtecan, things that we don’t normally deal with here. Nausea, stomatitis, alopecia, dry eye, and vomiting. All of those were more than 10% more common in patients that received datopotamab deruxtecan compared to the control. The only things that were more common with the control were neutropenia, leukopenia, and hand-foot syndrome in patients that had capecitabine.
One thing, though, is while you say, “Oh, these weren’t dangerous side effects,” they surely were lifestyle altering. Nobody wants to have these side effects on a daily basis. Again, there’s an increasing awareness about these kinds of lower-grade but still lifestyle-disrupting side effects. When it goes on day after day, you really have to balance that into the benefit you’re going to receive.
I think the second important point is how, when we use this drug, we’re going to have to go to another level to deal with the adverse effects that we are going to see. The first would be nausea and emesis. It is a highly emetogenic regimen based on the NCCN (National Comprehensive Cancer Network) guidelines, so you would need either 3 or 4 antiemetic drugs. That’s number one.
Number two, because of the potential eye problems, you need an eye exam before treatment — and the label says at least annually — with any symptoms. I think it’s very important that you give the patients eyedrops, and in general, the preservative-free eyedrops are the ones that are most effective.
Stomatitis is a very common side effect with that agent. It’s really not seen with the other drugs that even contain the same warhead. There, dexamethasone rinses are important. Now, this is a compounded medicine so you need to be very careful in making sure that you identify pharmacies that will prepare this and will have it available for the patients that need it.
Last, there is the risk of hypersensitivity reactions and there’s a recommendation for premedication for that. As you think about using datopotamab deruxtecan, you need to have all your ducks in a row to treat side effects. You need prophylaxis for hypersensitivity reactions, nausea, and emesis.
The patient will need an eye exam. You need to prepare the patient for possible dry eye and teach them which eyedrops are the best. You also need to ensure the availability of dexamethasone rinses and mouth washes. All that needs to be in place to make sure that the patient can safely use the drug.
I think it’s going to be a useful drug. We don’t yet have a uniformly available way to select patients for its use other than EGFR. I should note that the approval is for EGFR-mutated lung cancers. It doesn’t say which type of mutation, so that would give you some latitude in giving it for exon 20 atypicals as well as for the common sensitizing mutation.
We have another drug. It’s clearly going to be a useful one. It clearly comes with many adverse effects that we don’t normally treat on an everyday basis, we’re used to the diarrhea and skin changes that come on with the EGFR TKIs.
This pattern of side effects is different and requires some additional attention, but with it, the drug can be useful. I’m glad that we have yet another way to fight this disease.
Mark G. Kris, MD, Professor of Medicine, Weill Cornell Medical College; Attending Physician, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York , has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo; Received research grant from: National Institute of Health; Received income in an amount equal to or greater than $250 from: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo Others: Editorial support from Genentech
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. It’s Mark Kris, from Memorial Sloan Kettering, talking about a birthday gift I received on June 23 when the FDA approved the indication of datopotamab deruxtecan for people with lung cancers. We have another drug, our third ADC (antibody-drug conjugate) to fight lung cancer, so that’s a gift.
Let’s talk a little bit about that agent. It’s an interesting twist in our practice patterns. What can the drug do? It had a response rate of 45%, which is really important in patients that had EGFR mutations with progression on osimertinib. We really need drugs in that space. The duration of response was about 7 months, which is significant.
One interesting thing in the approval, [was] that the response rate of the blinded folks was greater than that in the investigator-assessed response by about 10%. It’s very interesting. Clearly, we have another drug, and we have it in a space where we need it.
Let’s talk a bit about the toxicity. I’m going to focus more on the paper by Bardia et al that compared datopotamab deruxtecan to various chemo drugs in breast cancer, not in lung cancer. You can take this a little bit with a grain of salt.
First, they saw a whole different array of side effects with datopotamab deruxtecan, things that we don’t normally deal with here. Nausea, stomatitis, alopecia, dry eye, and vomiting. All of those were more than 10% more common in patients that received datopotamab deruxtecan compared to the control. The only things that were more common with the control were neutropenia, leukopenia, and hand-foot syndrome in patients that had capecitabine.
One thing, though, is while you say, “Oh, these weren’t dangerous side effects,” they surely were lifestyle altering. Nobody wants to have these side effects on a daily basis. Again, there’s an increasing awareness about these kinds of lower-grade but still lifestyle-disrupting side effects. When it goes on day after day, you really have to balance that into the benefit you’re going to receive.
I think the second important point is how, when we use this drug, we’re going to have to go to another level to deal with the adverse effects that we are going to see. The first would be nausea and emesis. It is a highly emetogenic regimen based on the NCCN (National Comprehensive Cancer Network) guidelines, so you would need either 3 or 4 antiemetic drugs. That’s number one.
Number two, because of the potential eye problems, you need an eye exam before treatment — and the label says at least annually — with any symptoms. I think it’s very important that you give the patients eyedrops, and in general, the preservative-free eyedrops are the ones that are most effective.
Stomatitis is a very common side effect with that agent. It’s really not seen with the other drugs that even contain the same warhead. There, dexamethasone rinses are important. Now, this is a compounded medicine so you need to be very careful in making sure that you identify pharmacies that will prepare this and will have it available for the patients that need it.
Last, there is the risk of hypersensitivity reactions and there’s a recommendation for premedication for that. As you think about using datopotamab deruxtecan, you need to have all your ducks in a row to treat side effects. You need prophylaxis for hypersensitivity reactions, nausea, and emesis.
The patient will need an eye exam. You need to prepare the patient for possible dry eye and teach them which eyedrops are the best. You also need to ensure the availability of dexamethasone rinses and mouth washes. All that needs to be in place to make sure that the patient can safely use the drug.
I think it’s going to be a useful drug. We don’t yet have a uniformly available way to select patients for its use other than EGFR. I should note that the approval is for EGFR-mutated lung cancers. It doesn’t say which type of mutation, so that would give you some latitude in giving it for exon 20 atypicals as well as for the common sensitizing mutation.
We have another drug. It’s clearly going to be a useful one. It clearly comes with many adverse effects that we don’t normally treat on an everyday basis, we’re used to the diarrhea and skin changes that come on with the EGFR TKIs.
This pattern of side effects is different and requires some additional attention, but with it, the drug can be useful. I’m glad that we have yet another way to fight this disease.
Mark G. Kris, MD, Professor of Medicine, Weill Cornell Medical College; Attending Physician, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York , has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo; Received research grant from: National Institute of Health; Received income in an amount equal to or greater than $250 from: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo Others: Editorial support from Genentech
A version of this article first appeared on Medscape.com.
New Treatment Guidance Issued for Challenging Overlap of Hypermobility Syndromes and GI Symptoms
to help clinicians comprehend such cases.
“Recognizing and treating GI symptoms in patients with hEDS or hypermobility spectrum disorders and comorbid POTS or MCAS present major challenges for clinicians, who often feel under equipped to address their needs,” AGA reported in the update, published in Clinical Gastroenterology and Hepatology.
Importantly, “the poor understanding of these overlapping syndromes can lead to nonstandardized approaches to diagnostic evaluation and management,” the authors noted.
“Gastroenterology providers should be aware of the features of [these syndromes] to recognize the full complexity of patients presenting with multisystemic symptoms.”
Hypermobility spectrum disorders, which include hEDS, are typically genetic, and patients experience pain along with joint hypermobility, or extreme flexibility of joints beyond the normal range of motion.
With research showing that most of those patients — up to 98% — also experience GI symptoms, gastroenterologists may be encountering them more commonly than realized, Lucinda A. Harris, MD, AGAF, of the Mayo Clinic School of Medicine, in Scottsdale, Arizona, explained to GI & Hepatology News.

“As our knowledge in gastroenterology has progressed, we realize that hypermobility itself predisposes individuals to disorders of brain-gut interaction,” she said. “We may only be seeing the tip of the iceberg when it comes to diagnosing patients with hypermobility.”
Additionally, “many of these patients have POTS, which has also been increasingly diagnosed,” Harris added. “The strong overlap of these conditions prompted us to present this data.”
With a lack of evidence-based understanding of the overlapping syndromes, AGA’s guidance does not carry formal ratings but is drawn from a review of the published literature and expert opinion.
In addition to the key recommendation of being aware of the observed combination of syndromes, their recommendations include:
- Regarding testing: Testing for POTS/MCAS should be targeted to patients presenting with clinical manifestations of the disorders, but universal testing for POTS/MCAS in all patients with hEDS or hypermobility spectrum disorders is not currently supported by the evidence, the guidance advises.
- Gastroenterologists seeing patients with disorders of gut-brain interaction should inquire about joint hypermobility and strongly consider incorporating the Beighton score for assessing joint hypermobility into their practice as a screening tool; if the screen is positive, gastroenterologists may consider applying 2017 diagnostic criteria to diagnose hEDS or offer appropriate referral to a specialist where resources are available, the AGA recommends.
- Medical management: Management of GI symptoms in hEDS or hypermobility spectrum disorders and POTS/MCAS should focus on treating the most prominent GI symptoms and abnormal GI function test results.
- In addition to general disorders of gut-brain interactions and GI motility disorder treatment, management should also include treating any symptoms attributable to POTS and/or MCAS.
Treatment of POTS may include increasing fluid and salt intake, exercise training, and use of compression garments. Special pharmacological treatments for volume expansion, heart rate control, and vasoconstriction with integrated care from multiple specialties (eg, cardiology, neurology) should be considered in patients who do not respond to conservative lifestyle measures.
In patients presenting to gastroenterology providers, testing for mast cell disorders including MCAS should be considered in patients with hEDS or hypermobility spectrum disorders and disorders of gut-brain interaction with episodic symptoms that suggest a more generalized mast cell disorder involving two or more physiological systems. However, current data does not support the use of these tests for routine evaluation of GI symptoms in all patients with hEDS or hypermobility spectrum disorders without clinical or laboratory evidence of a primary or secondary mast cell disorder, the authors noted.
Harris explained that patients presenting with gut-brain disorders are often mistakenly classified as having irritable bowel syndrome or dyspepsia, whereas these conditions may be affecting the GI disorders they have.
“For example, a patient with Ehlers-Danlos syndrome might have problems with constipation, which is impacted by pelvic floor dysfunction,” she said. “Due to their hypermobility, they may experience more pelvic floor descent than usual.”
“If we do not recognize this, the patient risks developing rectal prolapse or not effectively addressing their constipation.”
Regarding patient characteristics, Harris said that those with hEDS and POTS appear to more likely be women and tend to present in younger patients, aged 18-50 years. Of note, there is no genetic test for hEDS.
“The take-home point for clinicians should be to consider POTS and Ehlers-Danlos syndrome when encountering young female patients with symptoms of palpitations, hypermobility, and orthostatic intolerance,” she said.
“Recognizing hypermobility is crucial, not only for GI symptoms but also to prevent joint dislocations, tendon ruptures, and other connective tissue issues.”
Clinicians are further urged to “offer informed counseling, and guide patients away from unreliable sources or fragmented care to foster therapeutic relationships and evidence-based care,” the authors added.
Deciphering Gut-Brain Disorder Challenges
Commenting to GI & Hepatology News, Clair Francomano, MD, a professor of medical and molecular genetics at the Indiana University School of Medicine, in Indianapolis, said the new guidance sheds important light on the syndromes.

“I’m delighted to see this guidance offered through the AGA as it will encourage gastroenterologists to think of EDS, POTS and MCAS when they are evaluating patients with disorders of gut-brain interaction,” Francomano said.
“This should allow patients to receive more accurate and timely diagnoses and appropriate management.”
Francomano noted that the Ehlers-Danlos Society, which provides information for clinicians and patients alike on the syndromes, and where she serves on the medical scientific board, has also been active in raising awareness.
“While co-occurrence of POTS and MCAS with EDS has in fact been recognized for many years, I do think awareness is increasing, in large part due to the advocacy and educational efforts of the Ehlers-Danlos Society,” she said.
The take-home message? “When clinicians see disorders of the gut-brain axis, POTS or MCAS, they should be thinking, ‘Could this be related to joint hypermobility or Ehlers-Danlos syndrome?’” Francomano said.
Harris reported serving as a consultant for AbbVie, Ardelyx, Salix, and Gemelli Biotech and reported receiving research support from Takeda and Anyx. Francomano did not report any relevant disclosures.
A version of this article appeared on Medscape.com.
to help clinicians comprehend such cases.
“Recognizing and treating GI symptoms in patients with hEDS or hypermobility spectrum disorders and comorbid POTS or MCAS present major challenges for clinicians, who often feel under equipped to address their needs,” AGA reported in the update, published in Clinical Gastroenterology and Hepatology.
Importantly, “the poor understanding of these overlapping syndromes can lead to nonstandardized approaches to diagnostic evaluation and management,” the authors noted.
“Gastroenterology providers should be aware of the features of [these syndromes] to recognize the full complexity of patients presenting with multisystemic symptoms.”
Hypermobility spectrum disorders, which include hEDS, are typically genetic, and patients experience pain along with joint hypermobility, or extreme flexibility of joints beyond the normal range of motion.
With research showing that most of those patients — up to 98% — also experience GI symptoms, gastroenterologists may be encountering them more commonly than realized, Lucinda A. Harris, MD, AGAF, of the Mayo Clinic School of Medicine, in Scottsdale, Arizona, explained to GI & Hepatology News.
“As our knowledge in gastroenterology has progressed, we realize that hypermobility itself predisposes individuals to disorders of brain-gut interaction,” she said. “We may only be seeing the tip of the iceberg when it comes to diagnosing patients with hypermobility.”
Additionally, “many of these patients have POTS, which has also been increasingly diagnosed,” Harris added. “The strong overlap of these conditions prompted us to present this data.”
With a lack of evidence-based understanding of the overlapping syndromes, AGA’s guidance does not carry formal ratings but is drawn from a review of the published literature and expert opinion.
In addition to the key recommendation of being aware of the observed combination of syndromes, their recommendations include:
- Regarding testing: Testing for POTS/MCAS should be targeted to patients presenting with clinical manifestations of the disorders, but universal testing for POTS/MCAS in all patients with hEDS or hypermobility spectrum disorders is not currently supported by the evidence, the guidance advises.
- Gastroenterologists seeing patients with disorders of gut-brain interaction should inquire about joint hypermobility and strongly consider incorporating the Beighton score for assessing joint hypermobility into their practice as a screening tool; if the screen is positive, gastroenterologists may consider applying 2017 diagnostic criteria to diagnose hEDS or offer appropriate referral to a specialist where resources are available, the AGA recommends.
- Medical management: Management of GI symptoms in hEDS or hypermobility spectrum disorders and POTS/MCAS should focus on treating the most prominent GI symptoms and abnormal GI function test results.
- In addition to general disorders of gut-brain interactions and GI motility disorder treatment, management should also include treating any symptoms attributable to POTS and/or MCAS.
Treatment of POTS may include increasing fluid and salt intake, exercise training, and use of compression garments. Special pharmacological treatments for volume expansion, heart rate control, and vasoconstriction with integrated care from multiple specialties (eg, cardiology, neurology) should be considered in patients who do not respond to conservative lifestyle measures.
In patients presenting to gastroenterology providers, testing for mast cell disorders including MCAS should be considered in patients with hEDS or hypermobility spectrum disorders and disorders of gut-brain interaction with episodic symptoms that suggest a more generalized mast cell disorder involving two or more physiological systems. However, current data does not support the use of these tests for routine evaluation of GI symptoms in all patients with hEDS or hypermobility spectrum disorders without clinical or laboratory evidence of a primary or secondary mast cell disorder, the authors noted.
Harris explained that patients presenting with gut-brain disorders are often mistakenly classified as having irritable bowel syndrome or dyspepsia, whereas these conditions may be affecting the GI disorders they have.
“For example, a patient with Ehlers-Danlos syndrome might have problems with constipation, which is impacted by pelvic floor dysfunction,” she said. “Due to their hypermobility, they may experience more pelvic floor descent than usual.”
“If we do not recognize this, the patient risks developing rectal prolapse or not effectively addressing their constipation.”
Regarding patient characteristics, Harris said that those with hEDS and POTS appear to more likely be women and tend to present in younger patients, aged 18-50 years. Of note, there is no genetic test for hEDS.
“The take-home point for clinicians should be to consider POTS and Ehlers-Danlos syndrome when encountering young female patients with symptoms of palpitations, hypermobility, and orthostatic intolerance,” she said.
“Recognizing hypermobility is crucial, not only for GI symptoms but also to prevent joint dislocations, tendon ruptures, and other connective tissue issues.”
Clinicians are further urged to “offer informed counseling, and guide patients away from unreliable sources or fragmented care to foster therapeutic relationships and evidence-based care,” the authors added.
Deciphering Gut-Brain Disorder Challenges
Commenting to GI & Hepatology News, Clair Francomano, MD, a professor of medical and molecular genetics at the Indiana University School of Medicine, in Indianapolis, said the new guidance sheds important light on the syndromes.
“I’m delighted to see this guidance offered through the AGA as it will encourage gastroenterologists to think of EDS, POTS and MCAS when they are evaluating patients with disorders of gut-brain interaction,” Francomano said.
“This should allow patients to receive more accurate and timely diagnoses and appropriate management.”
Francomano noted that the Ehlers-Danlos Society, which provides information for clinicians and patients alike on the syndromes, and where she serves on the medical scientific board, has also been active in raising awareness.
“While co-occurrence of POTS and MCAS with EDS has in fact been recognized for many years, I do think awareness is increasing, in large part due to the advocacy and educational efforts of the Ehlers-Danlos Society,” she said.
The take-home message? “When clinicians see disorders of the gut-brain axis, POTS or MCAS, they should be thinking, ‘Could this be related to joint hypermobility or Ehlers-Danlos syndrome?’” Francomano said.
Harris reported serving as a consultant for AbbVie, Ardelyx, Salix, and Gemelli Biotech and reported receiving research support from Takeda and Anyx. Francomano did not report any relevant disclosures.
A version of this article appeared on Medscape.com.
to help clinicians comprehend such cases.
“Recognizing and treating GI symptoms in patients with hEDS or hypermobility spectrum disorders and comorbid POTS or MCAS present major challenges for clinicians, who often feel under equipped to address their needs,” AGA reported in the update, published in Clinical Gastroenterology and Hepatology.
Importantly, “the poor understanding of these overlapping syndromes can lead to nonstandardized approaches to diagnostic evaluation and management,” the authors noted.
“Gastroenterology providers should be aware of the features of [these syndromes] to recognize the full complexity of patients presenting with multisystemic symptoms.”
Hypermobility spectrum disorders, which include hEDS, are typically genetic, and patients experience pain along with joint hypermobility, or extreme flexibility of joints beyond the normal range of motion.
With research showing that most of those patients — up to 98% — also experience GI symptoms, gastroenterologists may be encountering them more commonly than realized, Lucinda A. Harris, MD, AGAF, of the Mayo Clinic School of Medicine, in Scottsdale, Arizona, explained to GI & Hepatology News.
“As our knowledge in gastroenterology has progressed, we realize that hypermobility itself predisposes individuals to disorders of brain-gut interaction,” she said. “We may only be seeing the tip of the iceberg when it comes to diagnosing patients with hypermobility.”
Additionally, “many of these patients have POTS, which has also been increasingly diagnosed,” Harris added. “The strong overlap of these conditions prompted us to present this data.”
With a lack of evidence-based understanding of the overlapping syndromes, AGA’s guidance does not carry formal ratings but is drawn from a review of the published literature and expert opinion.
In addition to the key recommendation of being aware of the observed combination of syndromes, their recommendations include:
- Regarding testing: Testing for POTS/MCAS should be targeted to patients presenting with clinical manifestations of the disorders, but universal testing for POTS/MCAS in all patients with hEDS or hypermobility spectrum disorders is not currently supported by the evidence, the guidance advises.
- Gastroenterologists seeing patients with disorders of gut-brain interaction should inquire about joint hypermobility and strongly consider incorporating the Beighton score for assessing joint hypermobility into their practice as a screening tool; if the screen is positive, gastroenterologists may consider applying 2017 diagnostic criteria to diagnose hEDS or offer appropriate referral to a specialist where resources are available, the AGA recommends.
- Medical management: Management of GI symptoms in hEDS or hypermobility spectrum disorders and POTS/MCAS should focus on treating the most prominent GI symptoms and abnormal GI function test results.
- In addition to general disorders of gut-brain interactions and GI motility disorder treatment, management should also include treating any symptoms attributable to POTS and/or MCAS.
Treatment of POTS may include increasing fluid and salt intake, exercise training, and use of compression garments. Special pharmacological treatments for volume expansion, heart rate control, and vasoconstriction with integrated care from multiple specialties (eg, cardiology, neurology) should be considered in patients who do not respond to conservative lifestyle measures.
In patients presenting to gastroenterology providers, testing for mast cell disorders including MCAS should be considered in patients with hEDS or hypermobility spectrum disorders and disorders of gut-brain interaction with episodic symptoms that suggest a more generalized mast cell disorder involving two or more physiological systems. However, current data does not support the use of these tests for routine evaluation of GI symptoms in all patients with hEDS or hypermobility spectrum disorders without clinical or laboratory evidence of a primary or secondary mast cell disorder, the authors noted.
Harris explained that patients presenting with gut-brain disorders are often mistakenly classified as having irritable bowel syndrome or dyspepsia, whereas these conditions may be affecting the GI disorders they have.
“For example, a patient with Ehlers-Danlos syndrome might have problems with constipation, which is impacted by pelvic floor dysfunction,” she said. “Due to their hypermobility, they may experience more pelvic floor descent than usual.”
“If we do not recognize this, the patient risks developing rectal prolapse or not effectively addressing their constipation.”
Regarding patient characteristics, Harris said that those with hEDS and POTS appear to more likely be women and tend to present in younger patients, aged 18-50 years. Of note, there is no genetic test for hEDS.
“The take-home point for clinicians should be to consider POTS and Ehlers-Danlos syndrome when encountering young female patients with symptoms of palpitations, hypermobility, and orthostatic intolerance,” she said.
“Recognizing hypermobility is crucial, not only for GI symptoms but also to prevent joint dislocations, tendon ruptures, and other connective tissue issues.”
Clinicians are further urged to “offer informed counseling, and guide patients away from unreliable sources or fragmented care to foster therapeutic relationships and evidence-based care,” the authors added.
Deciphering Gut-Brain Disorder Challenges
Commenting to GI & Hepatology News, Clair Francomano, MD, a professor of medical and molecular genetics at the Indiana University School of Medicine, in Indianapolis, said the new guidance sheds important light on the syndromes.
“I’m delighted to see this guidance offered through the AGA as it will encourage gastroenterologists to think of EDS, POTS and MCAS when they are evaluating patients with disorders of gut-brain interaction,” Francomano said.
“This should allow patients to receive more accurate and timely diagnoses and appropriate management.”
Francomano noted that the Ehlers-Danlos Society, which provides information for clinicians and patients alike on the syndromes, and where she serves on the medical scientific board, has also been active in raising awareness.
“While co-occurrence of POTS and MCAS with EDS has in fact been recognized for many years, I do think awareness is increasing, in large part due to the advocacy and educational efforts of the Ehlers-Danlos Society,” she said.
The take-home message? “When clinicians see disorders of the gut-brain axis, POTS or MCAS, they should be thinking, ‘Could this be related to joint hypermobility or Ehlers-Danlos syndrome?’” Francomano said.
Harris reported serving as a consultant for AbbVie, Ardelyx, Salix, and Gemelli Biotech and reported receiving research support from Takeda and Anyx. Francomano did not report any relevant disclosures.
A version of this article appeared on Medscape.com.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Out-of-Pocket Prep Costs Reduce Screening Colonoscopy Uptake, Especially in Vulnerable Populations
, a large insurance-claims analysis in Gastroenterology reported.
Moreover, this cost-sharing contravenes the preventive-care provisions for bowel preparation mandated by the Affordable Care Act (ACA).
Led by Gastroenterologist Eric D. Shah, MD, MBA, a clinical associate professor at the University of Michigan in Ann Arbor, Michigan, the study found a significant proportion of prescribed bowel preparation claims — 53% for commercial plans and 83% for Medicare — still involve patient cost-sharing, indicating noncompliance with ACA guidelines. Although expense-sharing was less prevalent among Medicaid claims (just 27%), it was not eliminated, suggesting room for improvement in coverage enforcement across the board.

“Colon cancer is unique in that it can be prevented with colonoscopy, but where are the patients? Bowel prep is a major reason that patients defer screening,” Shah told GI & Hepatology News. He said his group was quite surprised that the majority in the study cohort were paying something out of pocket when these costs should have been covered. “Primary care doctors may not think to ask about bowel prep costs when they order screening colonoscopies.”
The findings emerged from an analysis of 2,593,079 prescription drug claims: 52.9% from commercial plans, 35% from Medicare Part D plans, and 8.3% from Medicaid plans.
“These patient costs of $30 or $50 are a real not a theoretical deterrent,” said Whitney Jones, MD, a gastroenterologist, adjunct clinical professor at the University of Louisville in Louisville, Kentucky, and founder of the nonprofit Colon Cancer Prevention Project. Jones was not involved in the analysis. “Some insurers require prior patient authorization for the low-dose preps, but gastroenterologists are doing so many colonoscopies they don’t always have time to get a PA [prior authorization] on everyone.”
With the increasing use of blood and stool-based CRC testing, he added, “when you get a positive result, it’s really important to have the procedure quickly.” And appropriate bowel preparation is a small, cost-effective portion of the total costs of colonoscopy, a procedure that ultimately saves insurers significant money in treatment costs.
The authors noted that while CRC is the second-leading cause of cancer-related deaths in the US, screening rates remain low, with only 59% of adults aged 45 years or older up to date with screening. Screening rates are particularly low among racial and ethnic minority groups as compared with White individuals, a disparity that highlights the need to address existing barriers and enhance screening efforts.
In the current study, shared costs by bowel preparation volume also varied. Low-volume formulations had consistently higher out-of-pocket costs: a median of $60 for low-volume vs $10 for high-volume in commercial plans. In Medicare, 75% of high-volume claims had shared costs compared with 90% for their low-volume counterparts. The cost-sharing difference was slightly narrower with Medicaid: 27% of high-volume claims vs 30% of low-volume claims.
This is concerning, as low-volume options, which are preferred by patients for their better tolerability, can enhance uptake and adherence and improve colonoscopy outcomes. Shah advises physicians to consider prescribing low-volume preparations. “Let patients know about the potential out-of-pocket cost and about copay cards and assistance programs and use high-volume preps as an alternative rather than a go-to,” he said.
As to costs across insurance types, among commercial plans, the median nonzero out-of-pocket cost was $10 for high-volume and $60 for low-volume product claims. For Medicare, the median nonzero out-of-pocket cost was $8 for high-volume and $55.99 for low-volume products.

Under the ACA, CRC screening is classified as a recommended preventive service, requiring health plans to cover it without cost-sharing. Although the Centers for Medicare & Medicaid Services previously tried to enforce this mandate in 2015 and 2016, stating that colonoscopy preparation medications should be covered at no cost, many health plans are still not compliant.
At the nonfederal level, Jones noted, Kentucky, which has a significant high-risk population, recently became the first state to pass legislation requiring health benefit plans to cover all guideline-recommended CRC exams and lab tests.
For its part, AGA has also called on payers to eliminate all cost-sharing barriers across the CRC screening continuum.
Of note, the study authors said, the higher compliance with the ACA mandate in commercial and Medicaid plans than in Medicare highlights disparities that may disproportionately affect vulnerable older adults. While nearly half of commercial patients and nearly three quarters of Medicaid patients incurred zero out-of-pocket costs, fewer than 17% of Medicare beneficiaries, or 1 in 6, did so.
Although these costs may be low relative to the colonoscopy, they nevertheless can deter uptake of preventive screenings, potentially leading to higher CRC incidence and mortality. “While some patients may be willing to pay modest out-of-pocket costs, any required payment, however small, can serve as a barrier to preventative care, particularly in underserved populations,” they wrote. “These financial barriers will continue to contribute to widening disparities and hinder progress toward equitable screening outcomes.”
In the meantime, said Shah, “Physicians should advocate now to their representatives in Congress that bowel prep costs should already be covered as part of the ACA.”
This study was funded by Sebela Pharmaceuticals, maker of SUFLAVE preparation. The authors had no conflicts of interest to declare. Jones is a speaker and consultant for Grail LLC.
A version of this article appeared on Medscape.com.
, a large insurance-claims analysis in Gastroenterology reported.
Moreover, this cost-sharing contravenes the preventive-care provisions for bowel preparation mandated by the Affordable Care Act (ACA).
Led by Gastroenterologist Eric D. Shah, MD, MBA, a clinical associate professor at the University of Michigan in Ann Arbor, Michigan, the study found a significant proportion of prescribed bowel preparation claims — 53% for commercial plans and 83% for Medicare — still involve patient cost-sharing, indicating noncompliance with ACA guidelines. Although expense-sharing was less prevalent among Medicaid claims (just 27%), it was not eliminated, suggesting room for improvement in coverage enforcement across the board.
“Colon cancer is unique in that it can be prevented with colonoscopy, but where are the patients? Bowel prep is a major reason that patients defer screening,” Shah told GI & Hepatology News. He said his group was quite surprised that the majority in the study cohort were paying something out of pocket when these costs should have been covered. “Primary care doctors may not think to ask about bowel prep costs when they order screening colonoscopies.”
The findings emerged from an analysis of 2,593,079 prescription drug claims: 52.9% from commercial plans, 35% from Medicare Part D plans, and 8.3% from Medicaid plans.
“These patient costs of $30 or $50 are a real not a theoretical deterrent,” said Whitney Jones, MD, a gastroenterologist, adjunct clinical professor at the University of Louisville in Louisville, Kentucky, and founder of the nonprofit Colon Cancer Prevention Project. Jones was not involved in the analysis. “Some insurers require prior patient authorization for the low-dose preps, but gastroenterologists are doing so many colonoscopies they don’t always have time to get a PA [prior authorization] on everyone.”
With the increasing use of blood and stool-based CRC testing, he added, “when you get a positive result, it’s really important to have the procedure quickly.” And appropriate bowel preparation is a small, cost-effective portion of the total costs of colonoscopy, a procedure that ultimately saves insurers significant money in treatment costs.
The authors noted that while CRC is the second-leading cause of cancer-related deaths in the US, screening rates remain low, with only 59% of adults aged 45 years or older up to date with screening. Screening rates are particularly low among racial and ethnic minority groups as compared with White individuals, a disparity that highlights the need to address existing barriers and enhance screening efforts.
In the current study, shared costs by bowel preparation volume also varied. Low-volume formulations had consistently higher out-of-pocket costs: a median of $60 for low-volume vs $10 for high-volume in commercial plans. In Medicare, 75% of high-volume claims had shared costs compared with 90% for their low-volume counterparts. The cost-sharing difference was slightly narrower with Medicaid: 27% of high-volume claims vs 30% of low-volume claims.
This is concerning, as low-volume options, which are preferred by patients for their better tolerability, can enhance uptake and adherence and improve colonoscopy outcomes. Shah advises physicians to consider prescribing low-volume preparations. “Let patients know about the potential out-of-pocket cost and about copay cards and assistance programs and use high-volume preps as an alternative rather than a go-to,” he said.
As to costs across insurance types, among commercial plans, the median nonzero out-of-pocket cost was $10 for high-volume and $60 for low-volume product claims. For Medicare, the median nonzero out-of-pocket cost was $8 for high-volume and $55.99 for low-volume products.
Under the ACA, CRC screening is classified as a recommended preventive service, requiring health plans to cover it without cost-sharing. Although the Centers for Medicare & Medicaid Services previously tried to enforce this mandate in 2015 and 2016, stating that colonoscopy preparation medications should be covered at no cost, many health plans are still not compliant.
At the nonfederal level, Jones noted, Kentucky, which has a significant high-risk population, recently became the first state to pass legislation requiring health benefit plans to cover all guideline-recommended CRC exams and lab tests.
For its part, AGA has also called on payers to eliminate all cost-sharing barriers across the CRC screening continuum.
Of note, the study authors said, the higher compliance with the ACA mandate in commercial and Medicaid plans than in Medicare highlights disparities that may disproportionately affect vulnerable older adults. While nearly half of commercial patients and nearly three quarters of Medicaid patients incurred zero out-of-pocket costs, fewer than 17% of Medicare beneficiaries, or 1 in 6, did so.
Although these costs may be low relative to the colonoscopy, they nevertheless can deter uptake of preventive screenings, potentially leading to higher CRC incidence and mortality. “While some patients may be willing to pay modest out-of-pocket costs, any required payment, however small, can serve as a barrier to preventative care, particularly in underserved populations,” they wrote. “These financial barriers will continue to contribute to widening disparities and hinder progress toward equitable screening outcomes.”
In the meantime, said Shah, “Physicians should advocate now to their representatives in Congress that bowel prep costs should already be covered as part of the ACA.”
This study was funded by Sebela Pharmaceuticals, maker of SUFLAVE preparation. The authors had no conflicts of interest to declare. Jones is a speaker and consultant for Grail LLC.
A version of this article appeared on Medscape.com.
, a large insurance-claims analysis in Gastroenterology reported.
Moreover, this cost-sharing contravenes the preventive-care provisions for bowel preparation mandated by the Affordable Care Act (ACA).
Led by Gastroenterologist Eric D. Shah, MD, MBA, a clinical associate professor at the University of Michigan in Ann Arbor, Michigan, the study found a significant proportion of prescribed bowel preparation claims — 53% for commercial plans and 83% for Medicare — still involve patient cost-sharing, indicating noncompliance with ACA guidelines. Although expense-sharing was less prevalent among Medicaid claims (just 27%), it was not eliminated, suggesting room for improvement in coverage enforcement across the board.
“Colon cancer is unique in that it can be prevented with colonoscopy, but where are the patients? Bowel prep is a major reason that patients defer screening,” Shah told GI & Hepatology News. He said his group was quite surprised that the majority in the study cohort were paying something out of pocket when these costs should have been covered. “Primary care doctors may not think to ask about bowel prep costs when they order screening colonoscopies.”
The findings emerged from an analysis of 2,593,079 prescription drug claims: 52.9% from commercial plans, 35% from Medicare Part D plans, and 8.3% from Medicaid plans.
“These patient costs of $30 or $50 are a real not a theoretical deterrent,” said Whitney Jones, MD, a gastroenterologist, adjunct clinical professor at the University of Louisville in Louisville, Kentucky, and founder of the nonprofit Colon Cancer Prevention Project. Jones was not involved in the analysis. “Some insurers require prior patient authorization for the low-dose preps, but gastroenterologists are doing so many colonoscopies they don’t always have time to get a PA [prior authorization] on everyone.”
With the increasing use of blood and stool-based CRC testing, he added, “when you get a positive result, it’s really important to have the procedure quickly.” And appropriate bowel preparation is a small, cost-effective portion of the total costs of colonoscopy, a procedure that ultimately saves insurers significant money in treatment costs.
The authors noted that while CRC is the second-leading cause of cancer-related deaths in the US, screening rates remain low, with only 59% of adults aged 45 years or older up to date with screening. Screening rates are particularly low among racial and ethnic minority groups as compared with White individuals, a disparity that highlights the need to address existing barriers and enhance screening efforts.
In the current study, shared costs by bowel preparation volume also varied. Low-volume formulations had consistently higher out-of-pocket costs: a median of $60 for low-volume vs $10 for high-volume in commercial plans. In Medicare, 75% of high-volume claims had shared costs compared with 90% for their low-volume counterparts. The cost-sharing difference was slightly narrower with Medicaid: 27% of high-volume claims vs 30% of low-volume claims.
This is concerning, as low-volume options, which are preferred by patients for their better tolerability, can enhance uptake and adherence and improve colonoscopy outcomes. Shah advises physicians to consider prescribing low-volume preparations. “Let patients know about the potential out-of-pocket cost and about copay cards and assistance programs and use high-volume preps as an alternative rather than a go-to,” he said.
As to costs across insurance types, among commercial plans, the median nonzero out-of-pocket cost was $10 for high-volume and $60 for low-volume product claims. For Medicare, the median nonzero out-of-pocket cost was $8 for high-volume and $55.99 for low-volume products.
Under the ACA, CRC screening is classified as a recommended preventive service, requiring health plans to cover it without cost-sharing. Although the Centers for Medicare & Medicaid Services previously tried to enforce this mandate in 2015 and 2016, stating that colonoscopy preparation medications should be covered at no cost, many health plans are still not compliant.
At the nonfederal level, Jones noted, Kentucky, which has a significant high-risk population, recently became the first state to pass legislation requiring health benefit plans to cover all guideline-recommended CRC exams and lab tests.
For its part, AGA has also called on payers to eliminate all cost-sharing barriers across the CRC screening continuum.
Of note, the study authors said, the higher compliance with the ACA mandate in commercial and Medicaid plans than in Medicare highlights disparities that may disproportionately affect vulnerable older adults. While nearly half of commercial patients and nearly three quarters of Medicaid patients incurred zero out-of-pocket costs, fewer than 17% of Medicare beneficiaries, or 1 in 6, did so.
Although these costs may be low relative to the colonoscopy, they nevertheless can deter uptake of preventive screenings, potentially leading to higher CRC incidence and mortality. “While some patients may be willing to pay modest out-of-pocket costs, any required payment, however small, can serve as a barrier to preventative care, particularly in underserved populations,” they wrote. “These financial barriers will continue to contribute to widening disparities and hinder progress toward equitable screening outcomes.”
In the meantime, said Shah, “Physicians should advocate now to their representatives in Congress that bowel prep costs should already be covered as part of the ACA.”
This study was funded by Sebela Pharmaceuticals, maker of SUFLAVE preparation. The authors had no conflicts of interest to declare. Jones is a speaker and consultant for Grail LLC.
A version of this article appeared on Medscape.com.
FROM GASTROENTEROLOGY
Diet Rich in Ultraprocessed Grains Increases Risk for IBD
, a large study has found.
The sweeping analysis of 124,590 adults from 21 countries found that those eating at least 19 g of ultraprocessed grains a day were about twice as likely to be diagnosed with IBD as peers eating less than 9 g daily.
“Our study adds robust evidence from a large, diverse global cohort that frequent consumption of ultraprocessed grains is associated with an increased risk of developing inflammatory bowel disease,” Neeraj Narula, MD, MPH, gastroenterologist and associate professor of medicine, McMaster University, Hamilton, Ontario, Canada, told GI & Hepatology News.

The study also “further clarifies that not all grains carry risk — minimally processed grains like fresh bread and rice were associated with lower risk even. These results build on and specify previous findings linking ultraprocessed foods more broadly to IBD,” Narula said.
The study was published in The American Journal of Gastroenterology.
Diet Matters to IBD Risk
According to the latest US data (2021-2023), ultraprocessed foods made up 62% of daily calories for young people and 53% for adults in 2021-2023.
The Prospective Urban Rural Epidemiology (PURE) study has followed participants aged 35-70 years for a median of nearly 13 years. At enrollment, volunteers completed country-specific food-frequency questionnaires, enabling researchers to quantify usual intake of more than 130 food items and track new cases of IBD reported at biennial follow-ups.
The researchers classified packaged breads, sweet breakfast cereals, crackers, pastries and ready-to-heat pizza or pasta as ultraprocessed grains because they are refined and typically contain additives such as emulsifiers and preservatives. Fresh bakery bread and plain rice were analyzed separately as minimally processed grain references.
During a median of 12.9 years, 605 participants developed IBD; 497 developed ulcerative colitis (UC) and 108 developed Crohn’s disease.
Increased intake of ultraprocessed grains was associated with a higher risk for IBD, with hazard ratios (HR) of 2.08 for intake of ≥ 50 g/d and 1.37 for 19-50 g/d compared to intake of < 19 g/d. The increased risk was largely driven by a significantly increased risk for UC (HR, 2.46) and not Crohn’s disease (HR, 0.98).
Among the different ultraprocessed grain products, packaged bread stood out: Consuming ≥ 30 g/d of packaged bread (a little more than one slice) was associated with a greater than twofold increased risk for IBD (HR, 2.11) compared to no intake of packaged bread.
In contrast, greater consumption of fresh bread was associated with a reduced risk of developing IBD (HR, 0.61 for ≥ 65 g/d and 0.45 for 16-65 g/d compared to < 16 g/d).
Increased intake of rice was also associated with a lower risk of developing IBD (HR, 0.63 for ≥ 1 serving/d and 0.99 for < 1 serving/d).
When the researchers widened the lens to all ultraprocessed foods — from sodas to salty snacks — the risk for IBD climbed further.
Participants eating at least five servings a day had nearly a fourfold greater odds of IBD than those eating fewer than one serving (HR, 3.95) — a finding consistent with other data from the PURE study cohort.
What to Tell Patients?
The authors acknowledged in their paper that it’s difficult — if not impossible — to completely avoid ultraprocessed food in the Western diet.
They said their findings support “public health strategies to promote consumption of whole and minimally processed foods while reducing the consumption of highly processed alternatives.”
“I tell my patients that emerging literature shows an association between ultraprocessed food intake and IBD risk, but it’s not yet clear whether simply cutting out those foods will improve disease activity once IBD is established,” Narula told GI & Hepatology News.
“However, I still encourage patients to reduce ultraprocessed foods and to follow a Mediterranean-style diet — focusing on minimally processed grains, fruits, vegetables, healthy fats, and lean proteins — to support overall gut and general health,” Narula said.
Reached for comment, Ashwin Ananthakrishnan, MD, MPH, AGAF, associate professor of medicine, Massachusetts General Hospital, Boston, who wasn’t part of the study, said it “adds incrementally to the growing data on how ultraprocessed foods may affect the risk of IBD.”

“They (and others) have previously shown a link between general ultraprocessed food consumption and risk of IBD. Others have shown that some of this is mediated through refined grains. This study more specifically studies that question and demonstrates an association,” said Ananthkrishnan.
“This should not be used, however, to counsel patients. It does not study the impact of grain intake on patients with IBD. It may help inform population level preventive strategies (or in high-risk individuals) but requires more confirmation since there is significant heterogeneity between the various countries in this cohort. Countries that have high refined grain intake are also enriched in several other IBD risk factors (including genetics),” Ananthkrishnan told GI & Hepatology News.
The PURE study is an investigator-initiated study funded by the Population Health Research Institute, Hamilton Health Sciences Research Institute, Canadian Institutes of Health Research, and Heart and Stroke Foundation of Ontario. It received support from Canadian Institutes of Health Research’s Strategy for Patient Oriented Research, Ontario SPOR Support Unit, and Ontario Ministry of Health and Long-Term Care and unrestricted grants from several pharmaceutical companies. Narula declared receiving honoraria from Janssen, Abbvie, Takeda, Pfizer, Sandoz, Novartis, Iterative Health, Innomar Strategies, Fresinius Kabi, Amgen, Organon, Eli Lilly, and Ferring. Ananthkrishnan declared having no relevant disclosures.
A version of this article appeared on Medscape.com.
, a large study has found.
The sweeping analysis of 124,590 adults from 21 countries found that those eating at least 19 g of ultraprocessed grains a day were about twice as likely to be diagnosed with IBD as peers eating less than 9 g daily.
“Our study adds robust evidence from a large, diverse global cohort that frequent consumption of ultraprocessed grains is associated with an increased risk of developing inflammatory bowel disease,” Neeraj Narula, MD, MPH, gastroenterologist and associate professor of medicine, McMaster University, Hamilton, Ontario, Canada, told GI & Hepatology News.
The study also “further clarifies that not all grains carry risk — minimally processed grains like fresh bread and rice were associated with lower risk even. These results build on and specify previous findings linking ultraprocessed foods more broadly to IBD,” Narula said.
The study was published in The American Journal of Gastroenterology.
Diet Matters to IBD Risk
According to the latest US data (2021-2023), ultraprocessed foods made up 62% of daily calories for young people and 53% for adults in 2021-2023.
The Prospective Urban Rural Epidemiology (PURE) study has followed participants aged 35-70 years for a median of nearly 13 years. At enrollment, volunteers completed country-specific food-frequency questionnaires, enabling researchers to quantify usual intake of more than 130 food items and track new cases of IBD reported at biennial follow-ups.
The researchers classified packaged breads, sweet breakfast cereals, crackers, pastries and ready-to-heat pizza or pasta as ultraprocessed grains because they are refined and typically contain additives such as emulsifiers and preservatives. Fresh bakery bread and plain rice were analyzed separately as minimally processed grain references.
During a median of 12.9 years, 605 participants developed IBD; 497 developed ulcerative colitis (UC) and 108 developed Crohn’s disease.
Increased intake of ultraprocessed grains was associated with a higher risk for IBD, with hazard ratios (HR) of 2.08 for intake of ≥ 50 g/d and 1.37 for 19-50 g/d compared to intake of < 19 g/d. The increased risk was largely driven by a significantly increased risk for UC (HR, 2.46) and not Crohn’s disease (HR, 0.98).
Among the different ultraprocessed grain products, packaged bread stood out: Consuming ≥ 30 g/d of packaged bread (a little more than one slice) was associated with a greater than twofold increased risk for IBD (HR, 2.11) compared to no intake of packaged bread.
In contrast, greater consumption of fresh bread was associated with a reduced risk of developing IBD (HR, 0.61 for ≥ 65 g/d and 0.45 for 16-65 g/d compared to < 16 g/d).
Increased intake of rice was also associated with a lower risk of developing IBD (HR, 0.63 for ≥ 1 serving/d and 0.99 for < 1 serving/d).
When the researchers widened the lens to all ultraprocessed foods — from sodas to salty snacks — the risk for IBD climbed further.
Participants eating at least five servings a day had nearly a fourfold greater odds of IBD than those eating fewer than one serving (HR, 3.95) — a finding consistent with other data from the PURE study cohort.
What to Tell Patients?
The authors acknowledged in their paper that it’s difficult — if not impossible — to completely avoid ultraprocessed food in the Western diet.
They said their findings support “public health strategies to promote consumption of whole and minimally processed foods while reducing the consumption of highly processed alternatives.”
“I tell my patients that emerging literature shows an association between ultraprocessed food intake and IBD risk, but it’s not yet clear whether simply cutting out those foods will improve disease activity once IBD is established,” Narula told GI & Hepatology News.
“However, I still encourage patients to reduce ultraprocessed foods and to follow a Mediterranean-style diet — focusing on minimally processed grains, fruits, vegetables, healthy fats, and lean proteins — to support overall gut and general health,” Narula said.
Reached for comment, Ashwin Ananthakrishnan, MD, MPH, AGAF, associate professor of medicine, Massachusetts General Hospital, Boston, who wasn’t part of the study, said it “adds incrementally to the growing data on how ultraprocessed foods may affect the risk of IBD.”
“They (and others) have previously shown a link between general ultraprocessed food consumption and risk of IBD. Others have shown that some of this is mediated through refined grains. This study more specifically studies that question and demonstrates an association,” said Ananthkrishnan.
“This should not be used, however, to counsel patients. It does not study the impact of grain intake on patients with IBD. It may help inform population level preventive strategies (or in high-risk individuals) but requires more confirmation since there is significant heterogeneity between the various countries in this cohort. Countries that have high refined grain intake are also enriched in several other IBD risk factors (including genetics),” Ananthkrishnan told GI & Hepatology News.
The PURE study is an investigator-initiated study funded by the Population Health Research Institute, Hamilton Health Sciences Research Institute, Canadian Institutes of Health Research, and Heart and Stroke Foundation of Ontario. It received support from Canadian Institutes of Health Research’s Strategy for Patient Oriented Research, Ontario SPOR Support Unit, and Ontario Ministry of Health and Long-Term Care and unrestricted grants from several pharmaceutical companies. Narula declared receiving honoraria from Janssen, Abbvie, Takeda, Pfizer, Sandoz, Novartis, Iterative Health, Innomar Strategies, Fresinius Kabi, Amgen, Organon, Eli Lilly, and Ferring. Ananthkrishnan declared having no relevant disclosures.
A version of this article appeared on Medscape.com.
, a large study has found.
The sweeping analysis of 124,590 adults from 21 countries found that those eating at least 19 g of ultraprocessed grains a day were about twice as likely to be diagnosed with IBD as peers eating less than 9 g daily.
“Our study adds robust evidence from a large, diverse global cohort that frequent consumption of ultraprocessed grains is associated with an increased risk of developing inflammatory bowel disease,” Neeraj Narula, MD, MPH, gastroenterologist and associate professor of medicine, McMaster University, Hamilton, Ontario, Canada, told GI & Hepatology News.
The study also “further clarifies that not all grains carry risk — minimally processed grains like fresh bread and rice were associated with lower risk even. These results build on and specify previous findings linking ultraprocessed foods more broadly to IBD,” Narula said.
The study was published in The American Journal of Gastroenterology.
Diet Matters to IBD Risk
According to the latest US data (2021-2023), ultraprocessed foods made up 62% of daily calories for young people and 53% for adults in 2021-2023.
The Prospective Urban Rural Epidemiology (PURE) study has followed participants aged 35-70 years for a median of nearly 13 years. At enrollment, volunteers completed country-specific food-frequency questionnaires, enabling researchers to quantify usual intake of more than 130 food items and track new cases of IBD reported at biennial follow-ups.
The researchers classified packaged breads, sweet breakfast cereals, crackers, pastries and ready-to-heat pizza or pasta as ultraprocessed grains because they are refined and typically contain additives such as emulsifiers and preservatives. Fresh bakery bread and plain rice were analyzed separately as minimally processed grain references.
During a median of 12.9 years, 605 participants developed IBD; 497 developed ulcerative colitis (UC) and 108 developed Crohn’s disease.
Increased intake of ultraprocessed grains was associated with a higher risk for IBD, with hazard ratios (HR) of 2.08 for intake of ≥ 50 g/d and 1.37 for 19-50 g/d compared to intake of < 19 g/d. The increased risk was largely driven by a significantly increased risk for UC (HR, 2.46) and not Crohn’s disease (HR, 0.98).
Among the different ultraprocessed grain products, packaged bread stood out: Consuming ≥ 30 g/d of packaged bread (a little more than one slice) was associated with a greater than twofold increased risk for IBD (HR, 2.11) compared to no intake of packaged bread.
In contrast, greater consumption of fresh bread was associated with a reduced risk of developing IBD (HR, 0.61 for ≥ 65 g/d and 0.45 for 16-65 g/d compared to < 16 g/d).
Increased intake of rice was also associated with a lower risk of developing IBD (HR, 0.63 for ≥ 1 serving/d and 0.99 for < 1 serving/d).
When the researchers widened the lens to all ultraprocessed foods — from sodas to salty snacks — the risk for IBD climbed further.
Participants eating at least five servings a day had nearly a fourfold greater odds of IBD than those eating fewer than one serving (HR, 3.95) — a finding consistent with other data from the PURE study cohort.
What to Tell Patients?
The authors acknowledged in their paper that it’s difficult — if not impossible — to completely avoid ultraprocessed food in the Western diet.
They said their findings support “public health strategies to promote consumption of whole and minimally processed foods while reducing the consumption of highly processed alternatives.”
“I tell my patients that emerging literature shows an association between ultraprocessed food intake and IBD risk, but it’s not yet clear whether simply cutting out those foods will improve disease activity once IBD is established,” Narula told GI & Hepatology News.
“However, I still encourage patients to reduce ultraprocessed foods and to follow a Mediterranean-style diet — focusing on minimally processed grains, fruits, vegetables, healthy fats, and lean proteins — to support overall gut and general health,” Narula said.
Reached for comment, Ashwin Ananthakrishnan, MD, MPH, AGAF, associate professor of medicine, Massachusetts General Hospital, Boston, who wasn’t part of the study, said it “adds incrementally to the growing data on how ultraprocessed foods may affect the risk of IBD.”
“They (and others) have previously shown a link between general ultraprocessed food consumption and risk of IBD. Others have shown that some of this is mediated through refined grains. This study more specifically studies that question and demonstrates an association,” said Ananthkrishnan.
“This should not be used, however, to counsel patients. It does not study the impact of grain intake on patients with IBD. It may help inform population level preventive strategies (or in high-risk individuals) but requires more confirmation since there is significant heterogeneity between the various countries in this cohort. Countries that have high refined grain intake are also enriched in several other IBD risk factors (including genetics),” Ananthkrishnan told GI & Hepatology News.
The PURE study is an investigator-initiated study funded by the Population Health Research Institute, Hamilton Health Sciences Research Institute, Canadian Institutes of Health Research, and Heart and Stroke Foundation of Ontario. It received support from Canadian Institutes of Health Research’s Strategy for Patient Oriented Research, Ontario SPOR Support Unit, and Ontario Ministry of Health and Long-Term Care and unrestricted grants from several pharmaceutical companies. Narula declared receiving honoraria from Janssen, Abbvie, Takeda, Pfizer, Sandoz, Novartis, Iterative Health, Innomar Strategies, Fresinius Kabi, Amgen, Organon, Eli Lilly, and Ferring. Ananthkrishnan declared having no relevant disclosures.
A version of this article appeared on Medscape.com.
Journal Highlights: May-July 2025
Esophagus/Motility
Nguyen AD, et al. AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.05.011.
Hartnett DA, et al. Distribution of Esophageal Eosinophilia as a Predictor of Proton Pump Inhibitor Response in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.06.032.
Gyawali CP, et al. pH Impedance Monitoring on Proton Pump Inhibitor Therapy Impacts Management Decisions in Proven GERD but not in Unproven GERD. Clin Gastroenterol Hepatol. 2025 May. doi: 10.1016/j.cgh.2025.02.032.
Stomach
Wiklund AK, et al. Risk of Gastric Adenocarcinoma After Eradication of Helicobacter pylori. Gastroenterology. 2025 Feb. doi: 10.1053/j.gastro.2025.01.239.
Sonaiya S, et al. Over-the-Scope Clip versus Standard Endoscopic Therapy as First-Line Intervention for Nonvariceal Upper Gastrointestinal Bleeding: A Cost-Effectiveness Analysis. Tech Innov Gastrointest. 2025 Jun. doi: 10.1016/j.tige.2025.250935.
Colon
Hassan C, et al. Colon Cancer Screening, Surveillance, and Treatment: Novel Artificial Intelligence Driving Strategies in the Management of Colon Lesions. Gastroenterology. 2025 Mar. doi: 10.1053/j.gastro.2025.02.021.

Pancreas
Wilcox CM, et al; US Pancreatic Disease Study Group. Management of the Disconnected Pancreatic Duct in Pancreatic Necrosis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.05.024.
Ghimire C, et al. The effect of advances in pancreatic cancer treatment in population mortality: A SEER-based study. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100739.
Hepatology
Canivet CM, et al. Validation of the AASLD/EASL Multi-Step Screening Strategies for MASLD. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100747.
Miscellaneous
Chang L, et al. Gut Feelings: The Critical Role of Interoception in Obesity and Disorders of Gut-Brain Interaction. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.04.002.
Bashiri K, et al. Advancing Hemostatic Powder Technologies for Management of Gastrointestinal Bleeding: Challenges and Solutions. Tech Innov Gastrointest. 2025 Jul. doi: 10.1016/j.tige.2025.250940.
Dr. Trieu is assistant professor of medicine, interventional endoscopy, in the Division of Gastroenterology at Washington University in St. Louis School of Medicine, Missouri.
Esophagus/Motility
Nguyen AD, et al. AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.05.011.
Hartnett DA, et al. Distribution of Esophageal Eosinophilia as a Predictor of Proton Pump Inhibitor Response in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.06.032.
Gyawali CP, et al. pH Impedance Monitoring on Proton Pump Inhibitor Therapy Impacts Management Decisions in Proven GERD but not in Unproven GERD. Clin Gastroenterol Hepatol. 2025 May. doi: 10.1016/j.cgh.2025.02.032.
Stomach
Wiklund AK, et al. Risk of Gastric Adenocarcinoma After Eradication of Helicobacter pylori. Gastroenterology. 2025 Feb. doi: 10.1053/j.gastro.2025.01.239.
Sonaiya S, et al. Over-the-Scope Clip versus Standard Endoscopic Therapy as First-Line Intervention for Nonvariceal Upper Gastrointestinal Bleeding: A Cost-Effectiveness Analysis. Tech Innov Gastrointest. 2025 Jun. doi: 10.1016/j.tige.2025.250935.
Colon
Hassan C, et al. Colon Cancer Screening, Surveillance, and Treatment: Novel Artificial Intelligence Driving Strategies in the Management of Colon Lesions. Gastroenterology. 2025 Mar. doi: 10.1053/j.gastro.2025.02.021.
Pancreas
Wilcox CM, et al; US Pancreatic Disease Study Group. Management of the Disconnected Pancreatic Duct in Pancreatic Necrosis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.05.024.
Ghimire C, et al. The effect of advances in pancreatic cancer treatment in population mortality: A SEER-based study. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100739.
Hepatology
Canivet CM, et al. Validation of the AASLD/EASL Multi-Step Screening Strategies for MASLD. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100747.
Miscellaneous
Chang L, et al. Gut Feelings: The Critical Role of Interoception in Obesity and Disorders of Gut-Brain Interaction. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.04.002.
Bashiri K, et al. Advancing Hemostatic Powder Technologies for Management of Gastrointestinal Bleeding: Challenges and Solutions. Tech Innov Gastrointest. 2025 Jul. doi: 10.1016/j.tige.2025.250940.
Dr. Trieu is assistant professor of medicine, interventional endoscopy, in the Division of Gastroenterology at Washington University in St. Louis School of Medicine, Missouri.
Esophagus/Motility
Nguyen AD, et al. AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.05.011.
Hartnett DA, et al. Distribution of Esophageal Eosinophilia as a Predictor of Proton Pump Inhibitor Response in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.06.032.
Gyawali CP, et al. pH Impedance Monitoring on Proton Pump Inhibitor Therapy Impacts Management Decisions in Proven GERD but not in Unproven GERD. Clin Gastroenterol Hepatol. 2025 May. doi: 10.1016/j.cgh.2025.02.032.
Stomach
Wiklund AK, et al. Risk of Gastric Adenocarcinoma After Eradication of Helicobacter pylori. Gastroenterology. 2025 Feb. doi: 10.1053/j.gastro.2025.01.239.
Sonaiya S, et al. Over-the-Scope Clip versus Standard Endoscopic Therapy as First-Line Intervention for Nonvariceal Upper Gastrointestinal Bleeding: A Cost-Effectiveness Analysis. Tech Innov Gastrointest. 2025 Jun. doi: 10.1016/j.tige.2025.250935.
Colon
Hassan C, et al. Colon Cancer Screening, Surveillance, and Treatment: Novel Artificial Intelligence Driving Strategies in the Management of Colon Lesions. Gastroenterology. 2025 Mar. doi: 10.1053/j.gastro.2025.02.021.
Pancreas
Wilcox CM, et al; US Pancreatic Disease Study Group. Management of the Disconnected Pancreatic Duct in Pancreatic Necrosis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.05.024.
Ghimire C, et al. The effect of advances in pancreatic cancer treatment in population mortality: A SEER-based study. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100739.
Hepatology
Canivet CM, et al. Validation of the AASLD/EASL Multi-Step Screening Strategies for MASLD. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100747.
Miscellaneous
Chang L, et al. Gut Feelings: The Critical Role of Interoception in Obesity and Disorders of Gut-Brain Interaction. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.04.002.
Bashiri K, et al. Advancing Hemostatic Powder Technologies for Management of Gastrointestinal Bleeding: Challenges and Solutions. Tech Innov Gastrointest. 2025 Jul. doi: 10.1016/j.tige.2025.250940.
Dr. Trieu is assistant professor of medicine, interventional endoscopy, in the Division of Gastroenterology at Washington University in St. Louis School of Medicine, Missouri.
Federal Government Funds Program for Hepatitis C Care and Cure
, according to an HHS press release.
The program, known as the Hepatitis C Elimination Initiative Pilot, will be administered by the Substance and Mental Health Administration. “This program is designed to support communities severely affected by homelessness and to gain insights on effective ways to identify patients, complete treatment, cure infections, and reduce reinfection by hepatitis C,” according to the press release.
The upfront investment in hepatitis C management is projected to not only save lives, but also to save community health care costs in the long-term, according to the press release.
“This is a vigorous pilot program that provides the first steps toward the large goal of eliminating hepatitis C in the United States population,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University Medical Center, Nashville, Tennessee, in an interview.
Hepatitis C affects more than two million individuals in the US, and is often complicated by social and medical issues such as homelessness, substance abuse, and mental health issues, said Schaffner. Fortunately, hepatitis C can be treated with oral medications that cure the chronic viral infection, thereby ending ongoing liver injury and interrupting person-to-person transmission of the virus by sharing needles, he said.
Given that the population most affected with hepatitis C also is often homeless, with possible mental health issues and sharing of needles for illicit drug use, challenges in reaching this population include assuring them that the care they receive though this and other programs is nonjudgemental and helpful, Schaffner told GI & Hepatology News.
The oral medications that now can cure the chronic hepatitis C viral infections must be taken over a period of weeks, and patients who lead socially disorganized lives often need assistance to assure that the medicine is taken as intended, so trained and sensitive personnel who are committed to helping this population are needed to make treatment programs succeed, he said.
Looking ahead, “the purpose of the pilot studies that will be funded by this program is to explore various approaches to determine which are more successful in bringing patients in to be evaluated and then to complete treatment,” Schaffner added.
State and community-based organizations are among the entities eligible to apply for the program. Potential applicants can find information about the program and application materials on the SAMSHA website.
Schaffner had no financial conflicts to disclose.
A version of this article appeared on Medscape.com .
, according to an HHS press release.
The program, known as the Hepatitis C Elimination Initiative Pilot, will be administered by the Substance and Mental Health Administration. “This program is designed to support communities severely affected by homelessness and to gain insights on effective ways to identify patients, complete treatment, cure infections, and reduce reinfection by hepatitis C,” according to the press release.
The upfront investment in hepatitis C management is projected to not only save lives, but also to save community health care costs in the long-term, according to the press release.
“This is a vigorous pilot program that provides the first steps toward the large goal of eliminating hepatitis C in the United States population,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University Medical Center, Nashville, Tennessee, in an interview.
Hepatitis C affects more than two million individuals in the US, and is often complicated by social and medical issues such as homelessness, substance abuse, and mental health issues, said Schaffner. Fortunately, hepatitis C can be treated with oral medications that cure the chronic viral infection, thereby ending ongoing liver injury and interrupting person-to-person transmission of the virus by sharing needles, he said.
Given that the population most affected with hepatitis C also is often homeless, with possible mental health issues and sharing of needles for illicit drug use, challenges in reaching this population include assuring them that the care they receive though this and other programs is nonjudgemental and helpful, Schaffner told GI & Hepatology News.
The oral medications that now can cure the chronic hepatitis C viral infections must be taken over a period of weeks, and patients who lead socially disorganized lives often need assistance to assure that the medicine is taken as intended, so trained and sensitive personnel who are committed to helping this population are needed to make treatment programs succeed, he said.
Looking ahead, “the purpose of the pilot studies that will be funded by this program is to explore various approaches to determine which are more successful in bringing patients in to be evaluated and then to complete treatment,” Schaffner added.
State and community-based organizations are among the entities eligible to apply for the program. Potential applicants can find information about the program and application materials on the SAMSHA website.
Schaffner had no financial conflicts to disclose.
A version of this article appeared on Medscape.com .
, according to an HHS press release.
The program, known as the Hepatitis C Elimination Initiative Pilot, will be administered by the Substance and Mental Health Administration. “This program is designed to support communities severely affected by homelessness and to gain insights on effective ways to identify patients, complete treatment, cure infections, and reduce reinfection by hepatitis C,” according to the press release.
The upfront investment in hepatitis C management is projected to not only save lives, but also to save community health care costs in the long-term, according to the press release.
“This is a vigorous pilot program that provides the first steps toward the large goal of eliminating hepatitis C in the United States population,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University Medical Center, Nashville, Tennessee, in an interview.
Hepatitis C affects more than two million individuals in the US, and is often complicated by social and medical issues such as homelessness, substance abuse, and mental health issues, said Schaffner. Fortunately, hepatitis C can be treated with oral medications that cure the chronic viral infection, thereby ending ongoing liver injury and interrupting person-to-person transmission of the virus by sharing needles, he said.
Given that the population most affected with hepatitis C also is often homeless, with possible mental health issues and sharing of needles for illicit drug use, challenges in reaching this population include assuring them that the care they receive though this and other programs is nonjudgemental and helpful, Schaffner told GI & Hepatology News.
The oral medications that now can cure the chronic hepatitis C viral infections must be taken over a period of weeks, and patients who lead socially disorganized lives often need assistance to assure that the medicine is taken as intended, so trained and sensitive personnel who are committed to helping this population are needed to make treatment programs succeed, he said.
Looking ahead, “the purpose of the pilot studies that will be funded by this program is to explore various approaches to determine which are more successful in bringing patients in to be evaluated and then to complete treatment,” Schaffner added.
State and community-based organizations are among the entities eligible to apply for the program. Potential applicants can find information about the program and application materials on the SAMSHA website.
Schaffner had no financial conflicts to disclose.
A version of this article appeared on Medscape.com .
Follow-Up Colonoscopies Low After Blood-Based Screening
Most GI Service Chiefs Support POCUS Training, But Uptake Is Slow
, according to a national survey.
Low POCUS uptake may be explained by substantial barriers to implementation, including lack of trained instructors, necessary equipment, and support staff, lead author Keerthi Thallapureddy, MD, of the University of Texas Health San Antonio, and colleagues, reported.
“POCUS is being increasingly used by gastroenterologists due to its portability and real-time diagnostic ability,” the investigators wrote in Gastro Hep Advances, but “there is limited understanding of how gastroenterologists use POCUS.”
To learn more, the investigators conducted a nationwide survey of the VA healthcare system. Separate questionnaires were sent to chiefs of staff (n = 130) and GI service chiefs (n = 117), yielding response rates of 100% and 79%, respectively.
Respondents represented a wide distribution of geographic regions and institutional complexity levels, with 80% of GI groups based at high-complexity centers and 92% in urban locations. A minority (8%) reported the presence of a liver transplant program.
Data collection focused on the prevalence of POCUS use, types of clinical applications, institutional policies and training processes, and perceived or actual barriers to wider adoption. Barriers were sorted into three categories: training, equipment, and infrastructure.
Of the 93 GI service chiefs who participated in the survey, 44% reported that at least 1 gastroenterologist at their facility currently uses POCUS. Most common procedural uses were paracentesis (23%) and liver biopsy (13%), while ascites assessment (19%) and biliary visualization (7%) were the most common diagnostic uses.
Among the same respondents, 69% said they would support sending clinicians to a POCUS training course, and 37% said their teams had expressed an active interest in pursuing such training. Only 17% of facilities had a formal process in place to obtain POCUS training, and an equal proportion had implemented a facility-wide policy to guide its use.
Barriers to implementation were widespread and often multifactorial.
Most challenges related to training: 48% of sites reported a lack of trained providers, 28% cited insufficient funding for training, 24% noted a lack of training opportunities, and 14% reported difficulty securing travel funds.
Equipment limitations were also common, with 41% of sites lacking ultrasound machines and 27% lacking funding to purchase them.
Institutional infrastructure posed further hurdles. Nearly a quarter of GI chiefs (23%) reported lacking a clinician champion to lead implementation, while others cited a lack of support staff, simulation space, privileging criteria, image archiving capabilities, or standardized reporting forms.
“Our findings on current POCUS use, training, barriers, and infrastructure can guide expansion of POCUS use and training among GI groups,” Dr. Thallapureddy and colleagues wrote, noting that early efforts to expand access to GI-specific POCUS training are already underway.
They cited growing interest from national organizations such as the American Gastroenterological Association and the American Association for the Study of Liver Diseases, the latter of which piloted training workshops at the 2024 Liver Meeting. Similarly, the International Bowel Ultrasound Group now offers a 3-part certification program in intestinal ultrasound and is developing additional online and interactive modules to improve training accessibility.
The study was supported by the US Department of Veterans Affairs, Quality Enhancement Research Initiative Partnered Evaluation Initiative Grant, and the VA National Center for Patient Safety. The investigators reported no conflicts of interest.
, according to a national survey.
Low POCUS uptake may be explained by substantial barriers to implementation, including lack of trained instructors, necessary equipment, and support staff, lead author Keerthi Thallapureddy, MD, of the University of Texas Health San Antonio, and colleagues, reported.
“POCUS is being increasingly used by gastroenterologists due to its portability and real-time diagnostic ability,” the investigators wrote in Gastro Hep Advances, but “there is limited understanding of how gastroenterologists use POCUS.”
To learn more, the investigators conducted a nationwide survey of the VA healthcare system. Separate questionnaires were sent to chiefs of staff (n = 130) and GI service chiefs (n = 117), yielding response rates of 100% and 79%, respectively.
Respondents represented a wide distribution of geographic regions and institutional complexity levels, with 80% of GI groups based at high-complexity centers and 92% in urban locations. A minority (8%) reported the presence of a liver transplant program.
Data collection focused on the prevalence of POCUS use, types of clinical applications, institutional policies and training processes, and perceived or actual barriers to wider adoption. Barriers were sorted into three categories: training, equipment, and infrastructure.
Of the 93 GI service chiefs who participated in the survey, 44% reported that at least 1 gastroenterologist at their facility currently uses POCUS. Most common procedural uses were paracentesis (23%) and liver biopsy (13%), while ascites assessment (19%) and biliary visualization (7%) were the most common diagnostic uses.
Among the same respondents, 69% said they would support sending clinicians to a POCUS training course, and 37% said their teams had expressed an active interest in pursuing such training. Only 17% of facilities had a formal process in place to obtain POCUS training, and an equal proportion had implemented a facility-wide policy to guide its use.
Barriers to implementation were widespread and often multifactorial.
Most challenges related to training: 48% of sites reported a lack of trained providers, 28% cited insufficient funding for training, 24% noted a lack of training opportunities, and 14% reported difficulty securing travel funds.
Equipment limitations were also common, with 41% of sites lacking ultrasound machines and 27% lacking funding to purchase them.
Institutional infrastructure posed further hurdles. Nearly a quarter of GI chiefs (23%) reported lacking a clinician champion to lead implementation, while others cited a lack of support staff, simulation space, privileging criteria, image archiving capabilities, or standardized reporting forms.
“Our findings on current POCUS use, training, barriers, and infrastructure can guide expansion of POCUS use and training among GI groups,” Dr. Thallapureddy and colleagues wrote, noting that early efforts to expand access to GI-specific POCUS training are already underway.
They cited growing interest from national organizations such as the American Gastroenterological Association and the American Association for the Study of Liver Diseases, the latter of which piloted training workshops at the 2024 Liver Meeting. Similarly, the International Bowel Ultrasound Group now offers a 3-part certification program in intestinal ultrasound and is developing additional online and interactive modules to improve training accessibility.
The study was supported by the US Department of Veterans Affairs, Quality Enhancement Research Initiative Partnered Evaluation Initiative Grant, and the VA National Center for Patient Safety. The investigators reported no conflicts of interest.
, according to a national survey.
Low POCUS uptake may be explained by substantial barriers to implementation, including lack of trained instructors, necessary equipment, and support staff, lead author Keerthi Thallapureddy, MD, of the University of Texas Health San Antonio, and colleagues, reported.
“POCUS is being increasingly used by gastroenterologists due to its portability and real-time diagnostic ability,” the investigators wrote in Gastro Hep Advances, but “there is limited understanding of how gastroenterologists use POCUS.”
To learn more, the investigators conducted a nationwide survey of the VA healthcare system. Separate questionnaires were sent to chiefs of staff (n = 130) and GI service chiefs (n = 117), yielding response rates of 100% and 79%, respectively.
Respondents represented a wide distribution of geographic regions and institutional complexity levels, with 80% of GI groups based at high-complexity centers and 92% in urban locations. A minority (8%) reported the presence of a liver transplant program.
Data collection focused on the prevalence of POCUS use, types of clinical applications, institutional policies and training processes, and perceived or actual barriers to wider adoption. Barriers were sorted into three categories: training, equipment, and infrastructure.
Of the 93 GI service chiefs who participated in the survey, 44% reported that at least 1 gastroenterologist at their facility currently uses POCUS. Most common procedural uses were paracentesis (23%) and liver biopsy (13%), while ascites assessment (19%) and biliary visualization (7%) were the most common diagnostic uses.
Among the same respondents, 69% said they would support sending clinicians to a POCUS training course, and 37% said their teams had expressed an active interest in pursuing such training. Only 17% of facilities had a formal process in place to obtain POCUS training, and an equal proportion had implemented a facility-wide policy to guide its use.
Barriers to implementation were widespread and often multifactorial.
Most challenges related to training: 48% of sites reported a lack of trained providers, 28% cited insufficient funding for training, 24% noted a lack of training opportunities, and 14% reported difficulty securing travel funds.
Equipment limitations were also common, with 41% of sites lacking ultrasound machines and 27% lacking funding to purchase them.
Institutional infrastructure posed further hurdles. Nearly a quarter of GI chiefs (23%) reported lacking a clinician champion to lead implementation, while others cited a lack of support staff, simulation space, privileging criteria, image archiving capabilities, or standardized reporting forms.
“Our findings on current POCUS use, training, barriers, and infrastructure can guide expansion of POCUS use and training among GI groups,” Dr. Thallapureddy and colleagues wrote, noting that early efforts to expand access to GI-specific POCUS training are already underway.
They cited growing interest from national organizations such as the American Gastroenterological Association and the American Association for the Study of Liver Diseases, the latter of which piloted training workshops at the 2024 Liver Meeting. Similarly, the International Bowel Ultrasound Group now offers a 3-part certification program in intestinal ultrasound and is developing additional online and interactive modules to improve training accessibility.
The study was supported by the US Department of Veterans Affairs, Quality Enhancement Research Initiative Partnered Evaluation Initiative Grant, and the VA National Center for Patient Safety. The investigators reported no conflicts of interest.
FROM GASTRO HEP ADVANCES
AGA Women’s Committee Outlines Roadmap Towards Gender Equity
Despite the increasing number of women joining the field, GI remains one of the most male-dominated medical subspecialties. and has highlighted future directions to achieve gender equality in GI.
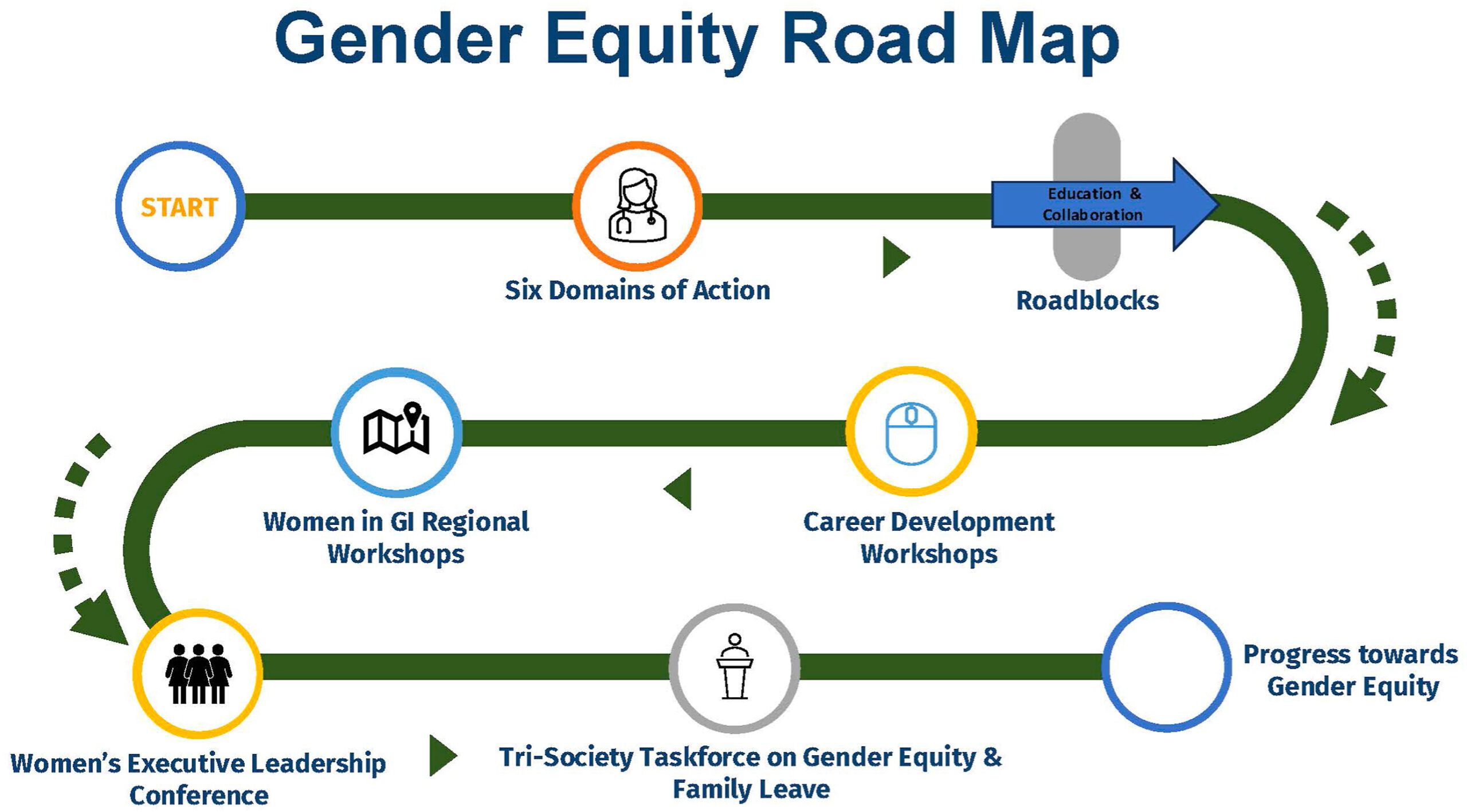
The AGA Gender Equity Framework outlines six domains of action, the current state and desired future state: bias & gender disparities, leadership & career advancement, wellness & balance, retention & recruitment, mentorship & sponsorship, and recognition.
Based on the desired future state, the group created a roadmap towards gender equity with measurable tactics. Career development workshops, including the Women in GI regional workshops and Women’s Executive Leadership Conference, are both crucial tactics.
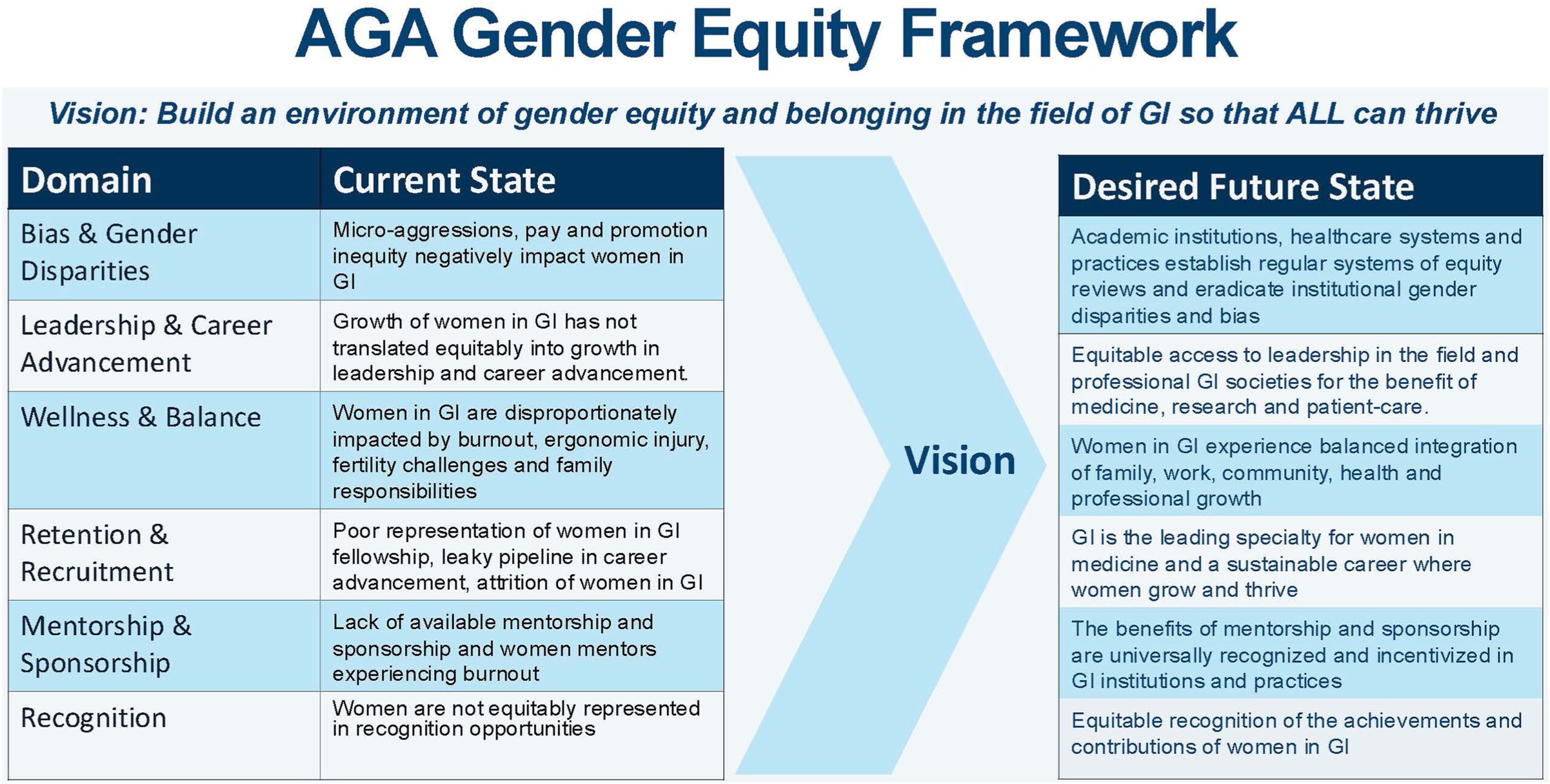
AGA outlined a few key areas for future gender equity efforts to focus on:
- Clearer GI-specific transparency guidelines regarding recruitment, salary, promotions, funding, and leadership.
- Pathway and research programs that help students from underrepresented backgrounds get involved and stay engaged in GI.
- Support networks (through GI societies, institutions, or other organizations) that help women connect, collaborate, and grow their careers.
The AGA Women’s Committee, along with other AGA committees, will continue to work to achieve the vision laid out in the AGA Gender Equity Framework and Gender Equity Road Map.
Despite the increasing number of women joining the field, GI remains one of the most male-dominated medical subspecialties. and has highlighted future directions to achieve gender equality in GI.
The AGA Gender Equity Framework outlines six domains of action, the current state and desired future state: bias & gender disparities, leadership & career advancement, wellness & balance, retention & recruitment, mentorship & sponsorship, and recognition.
Based on the desired future state, the group created a roadmap towards gender equity with measurable tactics. Career development workshops, including the Women in GI regional workshops and Women’s Executive Leadership Conference, are both crucial tactics.
AGA outlined a few key areas for future gender equity efforts to focus on:
- Clearer GI-specific transparency guidelines regarding recruitment, salary, promotions, funding, and leadership.
- Pathway and research programs that help students from underrepresented backgrounds get involved and stay engaged in GI.
- Support networks (through GI societies, institutions, or other organizations) that help women connect, collaborate, and grow their careers.
The AGA Women’s Committee, along with other AGA committees, will continue to work to achieve the vision laid out in the AGA Gender Equity Framework and Gender Equity Road Map.
Despite the increasing number of women joining the field, GI remains one of the most male-dominated medical subspecialties. and has highlighted future directions to achieve gender equality in GI.
The AGA Gender Equity Framework outlines six domains of action, the current state and desired future state: bias & gender disparities, leadership & career advancement, wellness & balance, retention & recruitment, mentorship & sponsorship, and recognition.
Based on the desired future state, the group created a roadmap towards gender equity with measurable tactics. Career development workshops, including the Women in GI regional workshops and Women’s Executive Leadership Conference, are both crucial tactics.
AGA outlined a few key areas for future gender equity efforts to focus on:
- Clearer GI-specific transparency guidelines regarding recruitment, salary, promotions, funding, and leadership.
- Pathway and research programs that help students from underrepresented backgrounds get involved and stay engaged in GI.
- Support networks (through GI societies, institutions, or other organizations) that help women connect, collaborate, and grow their careers.
The AGA Women’s Committee, along with other AGA committees, will continue to work to achieve the vision laid out in the AGA Gender Equity Framework and Gender Equity Road Map.
Evolving Standards of Practice: Esophageal Varices and Barrett’s Esophagus
Dear colleagues,
In the dynamic field of medicine, long-held practices are being reevaluated in light of new evidence and evolving standards of practice.

Dr. Anahita Rabiee discusses the importance of prioritizing non-selective beta blockers (NSBB) over endoscopic variceal ligation (EVL) in the primary prophylaxis of variceal bleeding in patients with compensated cirrhosis. Drawing on data from the PREDESCI trial and real-world experience, she argues that NSBB address the upstream driver—portal hypertension—more broadly and effectively than EVL. In a complementary piece, Dr. Tarek Sawas explores the nuanced landscape of screening and surveillance in Barrett’s esophagus. From how to manage irregular Z-lines, to rethinking the need for 1-year follow-up endoscopies and interpreting the implications of the BOSS trial, Dr. Sawas advocates for a more personalized, risk-based approach.
We hope these perspectives spark dialogue and reflection in your own practice. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
Choose NSBBs, Not EVL, in Patients with Compensated Cirrhosis
BY ANAHITA RABIEE, MD, MHS
I strongly favor the use of non selective beta blockers (NSBBs) in patients with compensated cirrhosis, rather than endoscopy and esophageal variceal ligation (EVL) for primary prophylaxis.
Since the results of PREDESCI trial (β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (CSPH)) were published in 2019, there has been much debate on the role of screening endoscopy and EVL for primary prophylaxis. While many argue that a single randomized trial should not overturn long standing practice, several compelling reasons convince me to choose NSBBs, when possible.
Recent guidance from major liver societies now recommends NSBBs as first line therapy for CSPH. Yet, adoption in clinical practice remains inconsistent.
Here is why I believe NSBB represent a better solution:

Treating Upstream, Not Just a Local Treatment
NSBBs such as propranolol and nadolol decrease portal pressure by decreasing portal venous inflow through β1 and β2 adrenergic blockade. Carvedilol is often preferred given its additional α1 adrenergic blocking activity making it the most effective one in decreasing the portal pressure. Therefore, NSBBs address the upstream driver of decompensation by decreasing portal pressures.
EVL, in contrast, is a local fix that only prevents variceal bleeding. Ascites, not variceal bleeding, is the most common initial decompensating event and is associated with high mortality. Preventing all forms of decompensation is clearly preferable to preventing just one.
Broader Eligibility, More Patients Benefit
CSPH is defined as hepatic venous pressure gradient (HVPG)>10 mmHg, the threshold where increased portal venous inflow secondary to splanchnic vasodilation and hyperdynamic circulation drives the increase in portal hypertension. This threshold has been shown to strongly predict decompensation in patients with compensated disease.
While all patients with varices have CSPH, not all patients with CSPH have varices. They can be identified by other non invasive criteria such as cross sectional imaging showing collaterals, or liver stiffness and platelet thresholds that have been previously validated. By restricting intervention to those with large varices and offering only EVL, we miss the opportunity to intervene earlier and to a broader group that would benefit from this treatment.
Comprehensive Protection Without Repeated Endoscopies
Once on an appropriate NSBB dose, patients are protected against variceal bleeding (at least as effectively as EVL). This eliminates the need for repeated surveillance endoscopies to identify and treat large varices in otherwise compensated patients.
Better Tolerated and – In Many Cases – Overlaps With Existing Medication List!
While overtreatment is a concern, regular endoscopies every two years are also burdensome. Many patients already need beta blockers for cardiac conditions such as atrial fibrillation, ischemic heart disease or hypertension. Carvedilol, in particular, offers dual benefit for both hepatologists and cardiologists.
It is important to emphasize that these arguments apply to compensated cirrhosis. In decompensated disease, the approach changes. After a variceal bleed, both NSBBs and EVL are required for secondary prophylaxis. In patients with prior ascites but no variceal bleed, the benefit of NSBBs is less pronounced since decompensation has already occurred. In this setting, NSBBs can still be used selectively, but only if systolic blood pressure remains above 90 mmHg.
The evidence supporting NSBBs over EVL in compensated cirrhosis is not perfect, but few things in medicine are. Given current data, NSBBs should be the first line therapy in compensated cirrhosis with CSPH. Once a patient is on an appropriate and tolerated NSBB dose, routine endoscopic surveillance is unnecessary. Endoscopy should be reserved for those who cannot tolerate NSBBs, in whom EVL is then indicated if large varices are present.
Dr. Rabiee is based at the Yale School of Medicine, New Haven, Connecticut, and the Veterans Affairs Connecticut Healthcare System, West Haven, Connecticut. She has no disclosures in regard to this article.
Rethinking Screening and Surveillance in Barrett’s Esophagus: Navigating Controversies and Nuances
BY TAREK SAWAS, MD, MPH
Barrett’s esophagus (BE) is a precursor to esophageal adenocarcinoma (EAC). Despite our comprehensive guidelines, many of the day-to-day decisions still rely on clinical judgment and honest conversations with patients. This article explores common scenarios in which management decisions are nuanced and the right answer remains debatable.
Irregular Z-Line/Ultrashort Segment BE: Leave Or Watch It?
Few findings provoke more confusion than irregular Z-line or intestinal metaplasia (IM) < 1 cm at the gastroesophageal junction (GEJ). For years, we have debated whether these subtle changes represent a precursor to EAC or simply a benign variant. We have wrestled with how to handle these cases from whether we should take biopsies to how to perform surveillance.
The American College of Gastroenterology (ACG) guideline suggests that irregular Z-lines should not be routinely biopsied or surveyed. Similarly, the upcoming American Gastroenterology Association (AGA) surveillance guideline suggests against surveillance of IM<1 cm citing the low individual annual risk of progression to high-grade dysplasia (HGD) and EAC of 0.23% per year which is lower than that of non-dysplastic Barrett’s esophagus (NDBE). However, this is not the entire picture.
Despite the low per-patient risk, IM<1cm is highly prevalent with columnar mucosa observed in approximately 15% of patients undergoing upper endoscopy. This paradox is unsettling. While any one patient with IM<1 cm is unlikely to progress to EAC, the group accounts for a meaningful share of the EAC burden. Some experts have argued that this justifies routine biopsy and surveillance in all patients with visible columnar mucosa regardless of length. However, this approach risks overwhelming our surveillance infrastructure.
A recent decision modeling analysis suggested that at the lowest progression rates, either no surveillance or one-time endoscopy can be considered. Based on these data, I do not regularly biopsy ultrashort segments unless the mucosa appears suspicious. In those with IM<1 cm detected during a high-quality endoscopic exam, no follow-up is needed. However, if the exam is suboptimal, I perform a 1-time high-quality repeat exam. If there is no evidence of dysplasia then I do not pursue any further surveillance.
The One-Year Follow-Up Endoscopy: Is It Necessary?
Another controversy is the one-year follow-up endoscopy after an initial diagnosis of NDBE. Proponents of this approach cite the high proportion of post endoscopy esophageal neoplasia and cancer (PEEN/PEEC) detected in the first year after diagnosis (missed HGD/EAC). In fact, PEEN account for about a quarter of all HGD/EAC cases diagnosed during surveillance.
While this approach might mitigate PEEN/PEEC risk, it may not be necessary if the index endoscopy is high quality. To ensure high quality exams, several best practices have been proposed including:
- Use of high-definition white light endoscopy (HD-WLE) with chromoendoscopy (virtual or dye based)
- Appropriate inspection time (1 minute per cm of circumferential BE)
- Accurate documentation using the Prague criteria
- Adherence to the Seattle protocol with additional targeted biopsies
If the index endoscopy meets these quality metrics, I typically do not bring the patient back at one year. However, if the exam quality is in question, then I repeat it at one year to establish a reliable baseline and rule out prevalent neoplasia.

Surveillance In NDBE: After BOSS, Do We Rethink Everything?
The recently published BOSS trial (Barrett’s Oesophagus Surveillance Study) has reignited the debate over the value of endoscopic surveillance in NDBE. In this study, 3,453 patients with NDBE across the UK were randomized to either surveillance endoscopy every two years or endoscopy only as clinically indicated. After a median follow-up of 12.8 years, the trial found no significant difference in all-cause mortality between the two groups.
While these findings are important, they should be interpreted with caution. First, the primary endpoint, all-cause mortality, is not optimal for evaluating surveillance for EAC. Surveillance is not intended to reduce all-cause mortality but rather to reduce EAC–related mortality. Second, a substantial number of patients in the no surveillance group still underwent endoscopy at intervals that were not meaningfully different from those in the surveillance group. If both groups receive similar exposure to endoscopy, the comparison loses power. Lastly, the trial was underpowered due to overestimation of progression risk during its initial design. As we have since learned, the risk of progression of NDBE is lower than originally assumed.
So where do we stand now? For me, the BOSS trial does not negate the value of surveillance. it reminds us that a one-size-fits-all approach is inefficient, and our strategy must be risk based. For low-risk individuals, particularly older adults with short-segment NDBE, surveillance may offer little benefit. But in healthier, younger patients with longer segments or additional risk factors, surveillance remains an essential tool for early neoplasia detection.
When to Stop Surveillance
Perhaps the most under-discussed point is when to stop surveillance. Existing guidelines do not account for competing mortality risks unrelated to EAC or provide specific recommendations regarding cessation of surveillance. The desired benefits of surveillance likely diminish with advanced age and greater comorbidity because of lower life expectancy and ineligibility for definitive therapy for EAC.
A recent modeling study found that the optimal ages for last surveillance were 81, 80, 77, and 73 years for men with no, mild, moderate, and severe comorbidity respectively and 75, 73, 73, and 69 years for women. In my practice, I discuss surveillance cessation in patients older than 75 based on their comorbidities. If the risk of progression is outweighed by the risk of the procedure or by the reality of limited life expectancy, we should not hesitate to consider surveillance cessation.
In summary, high-quality endoscopic exam in appropriately selected patients remains the cornerstone of BE surveillance. A more personalized, risk-based approach is needed taking into account competing comorbidities. Emerging technology through risk stratification tools such as biomarkers and artificial intelligence may refine our approach and help address the current limitations.
Dr. Sawas is based at the University of Texas Southwestern, Dallas, Texas. He has no disclosures in regard to this article.
Dear colleagues,
In the dynamic field of medicine, long-held practices are being reevaluated in light of new evidence and evolving standards of practice.
Dr. Anahita Rabiee discusses the importance of prioritizing non-selective beta blockers (NSBB) over endoscopic variceal ligation (EVL) in the primary prophylaxis of variceal bleeding in patients with compensated cirrhosis. Drawing on data from the PREDESCI trial and real-world experience, she argues that NSBB address the upstream driver—portal hypertension—more broadly and effectively than EVL. In a complementary piece, Dr. Tarek Sawas explores the nuanced landscape of screening and surveillance in Barrett’s esophagus. From how to manage irregular Z-lines, to rethinking the need for 1-year follow-up endoscopies and interpreting the implications of the BOSS trial, Dr. Sawas advocates for a more personalized, risk-based approach.
We hope these perspectives spark dialogue and reflection in your own practice. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
Choose NSBBs, Not EVL, in Patients with Compensated Cirrhosis
BY ANAHITA RABIEE, MD, MHS
I strongly favor the use of non selective beta blockers (NSBBs) in patients with compensated cirrhosis, rather than endoscopy and esophageal variceal ligation (EVL) for primary prophylaxis.
Since the results of PREDESCI trial (β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (CSPH)) were published in 2019, there has been much debate on the role of screening endoscopy and EVL for primary prophylaxis. While many argue that a single randomized trial should not overturn long standing practice, several compelling reasons convince me to choose NSBBs, when possible.
Recent guidance from major liver societies now recommends NSBBs as first line therapy for CSPH. Yet, adoption in clinical practice remains inconsistent.
Here is why I believe NSBB represent a better solution:
Treating Upstream, Not Just a Local Treatment
NSBBs such as propranolol and nadolol decrease portal pressure by decreasing portal venous inflow through β1 and β2 adrenergic blockade. Carvedilol is often preferred given its additional α1 adrenergic blocking activity making it the most effective one in decreasing the portal pressure. Therefore, NSBBs address the upstream driver of decompensation by decreasing portal pressures.
EVL, in contrast, is a local fix that only prevents variceal bleeding. Ascites, not variceal bleeding, is the most common initial decompensating event and is associated with high mortality. Preventing all forms of decompensation is clearly preferable to preventing just one.
Broader Eligibility, More Patients Benefit
CSPH is defined as hepatic venous pressure gradient (HVPG)>10 mmHg, the threshold where increased portal venous inflow secondary to splanchnic vasodilation and hyperdynamic circulation drives the increase in portal hypertension. This threshold has been shown to strongly predict decompensation in patients with compensated disease.
While all patients with varices have CSPH, not all patients with CSPH have varices. They can be identified by other non invasive criteria such as cross sectional imaging showing collaterals, or liver stiffness and platelet thresholds that have been previously validated. By restricting intervention to those with large varices and offering only EVL, we miss the opportunity to intervene earlier and to a broader group that would benefit from this treatment.
Comprehensive Protection Without Repeated Endoscopies
Once on an appropriate NSBB dose, patients are protected against variceal bleeding (at least as effectively as EVL). This eliminates the need for repeated surveillance endoscopies to identify and treat large varices in otherwise compensated patients.
Better Tolerated and – In Many Cases – Overlaps With Existing Medication List!
While overtreatment is a concern, regular endoscopies every two years are also burdensome. Many patients already need beta blockers for cardiac conditions such as atrial fibrillation, ischemic heart disease or hypertension. Carvedilol, in particular, offers dual benefit for both hepatologists and cardiologists.
It is important to emphasize that these arguments apply to compensated cirrhosis. In decompensated disease, the approach changes. After a variceal bleed, both NSBBs and EVL are required for secondary prophylaxis. In patients with prior ascites but no variceal bleed, the benefit of NSBBs is less pronounced since decompensation has already occurred. In this setting, NSBBs can still be used selectively, but only if systolic blood pressure remains above 90 mmHg.
The evidence supporting NSBBs over EVL in compensated cirrhosis is not perfect, but few things in medicine are. Given current data, NSBBs should be the first line therapy in compensated cirrhosis with CSPH. Once a patient is on an appropriate and tolerated NSBB dose, routine endoscopic surveillance is unnecessary. Endoscopy should be reserved for those who cannot tolerate NSBBs, in whom EVL is then indicated if large varices are present.
Dr. Rabiee is based at the Yale School of Medicine, New Haven, Connecticut, and the Veterans Affairs Connecticut Healthcare System, West Haven, Connecticut. She has no disclosures in regard to this article.
Rethinking Screening and Surveillance in Barrett’s Esophagus: Navigating Controversies and Nuances
BY TAREK SAWAS, MD, MPH
Barrett’s esophagus (BE) is a precursor to esophageal adenocarcinoma (EAC). Despite our comprehensive guidelines, many of the day-to-day decisions still rely on clinical judgment and honest conversations with patients. This article explores common scenarios in which management decisions are nuanced and the right answer remains debatable.
Irregular Z-Line/Ultrashort Segment BE: Leave Or Watch It?
Few findings provoke more confusion than irregular Z-line or intestinal metaplasia (IM) < 1 cm at the gastroesophageal junction (GEJ). For years, we have debated whether these subtle changes represent a precursor to EAC or simply a benign variant. We have wrestled with how to handle these cases from whether we should take biopsies to how to perform surveillance.
The American College of Gastroenterology (ACG) guideline suggests that irregular Z-lines should not be routinely biopsied or surveyed. Similarly, the upcoming American Gastroenterology Association (AGA) surveillance guideline suggests against surveillance of IM<1 cm citing the low individual annual risk of progression to high-grade dysplasia (HGD) and EAC of 0.23% per year which is lower than that of non-dysplastic Barrett’s esophagus (NDBE). However, this is not the entire picture.
Despite the low per-patient risk, IM<1cm is highly prevalent with columnar mucosa observed in approximately 15% of patients undergoing upper endoscopy. This paradox is unsettling. While any one patient with IM<1 cm is unlikely to progress to EAC, the group accounts for a meaningful share of the EAC burden. Some experts have argued that this justifies routine biopsy and surveillance in all patients with visible columnar mucosa regardless of length. However, this approach risks overwhelming our surveillance infrastructure.
A recent decision modeling analysis suggested that at the lowest progression rates, either no surveillance or one-time endoscopy can be considered. Based on these data, I do not regularly biopsy ultrashort segments unless the mucosa appears suspicious. In those with IM<1 cm detected during a high-quality endoscopic exam, no follow-up is needed. However, if the exam is suboptimal, I perform a 1-time high-quality repeat exam. If there is no evidence of dysplasia then I do not pursue any further surveillance.
The One-Year Follow-Up Endoscopy: Is It Necessary?
Another controversy is the one-year follow-up endoscopy after an initial diagnosis of NDBE. Proponents of this approach cite the high proportion of post endoscopy esophageal neoplasia and cancer (PEEN/PEEC) detected in the first year after diagnosis (missed HGD/EAC). In fact, PEEN account for about a quarter of all HGD/EAC cases diagnosed during surveillance.
While this approach might mitigate PEEN/PEEC risk, it may not be necessary if the index endoscopy is high quality. To ensure high quality exams, several best practices have been proposed including:
- Use of high-definition white light endoscopy (HD-WLE) with chromoendoscopy (virtual or dye based)
- Appropriate inspection time (1 minute per cm of circumferential BE)
- Accurate documentation using the Prague criteria
- Adherence to the Seattle protocol with additional targeted biopsies
If the index endoscopy meets these quality metrics, I typically do not bring the patient back at one year. However, if the exam quality is in question, then I repeat it at one year to establish a reliable baseline and rule out prevalent neoplasia.
Surveillance In NDBE: After BOSS, Do We Rethink Everything?
The recently published BOSS trial (Barrett’s Oesophagus Surveillance Study) has reignited the debate over the value of endoscopic surveillance in NDBE. In this study, 3,453 patients with NDBE across the UK were randomized to either surveillance endoscopy every two years or endoscopy only as clinically indicated. After a median follow-up of 12.8 years, the trial found no significant difference in all-cause mortality between the two groups.
While these findings are important, they should be interpreted with caution. First, the primary endpoint, all-cause mortality, is not optimal for evaluating surveillance for EAC. Surveillance is not intended to reduce all-cause mortality but rather to reduce EAC–related mortality. Second, a substantial number of patients in the no surveillance group still underwent endoscopy at intervals that were not meaningfully different from those in the surveillance group. If both groups receive similar exposure to endoscopy, the comparison loses power. Lastly, the trial was underpowered due to overestimation of progression risk during its initial design. As we have since learned, the risk of progression of NDBE is lower than originally assumed.
So where do we stand now? For me, the BOSS trial does not negate the value of surveillance. it reminds us that a one-size-fits-all approach is inefficient, and our strategy must be risk based. For low-risk individuals, particularly older adults with short-segment NDBE, surveillance may offer little benefit. But in healthier, younger patients with longer segments or additional risk factors, surveillance remains an essential tool for early neoplasia detection.
When to Stop Surveillance
Perhaps the most under-discussed point is when to stop surveillance. Existing guidelines do not account for competing mortality risks unrelated to EAC or provide specific recommendations regarding cessation of surveillance. The desired benefits of surveillance likely diminish with advanced age and greater comorbidity because of lower life expectancy and ineligibility for definitive therapy for EAC.
A recent modeling study found that the optimal ages for last surveillance were 81, 80, 77, and 73 years for men with no, mild, moderate, and severe comorbidity respectively and 75, 73, 73, and 69 years for women. In my practice, I discuss surveillance cessation in patients older than 75 based on their comorbidities. If the risk of progression is outweighed by the risk of the procedure or by the reality of limited life expectancy, we should not hesitate to consider surveillance cessation.
In summary, high-quality endoscopic exam in appropriately selected patients remains the cornerstone of BE surveillance. A more personalized, risk-based approach is needed taking into account competing comorbidities. Emerging technology through risk stratification tools such as biomarkers and artificial intelligence may refine our approach and help address the current limitations.
Dr. Sawas is based at the University of Texas Southwestern, Dallas, Texas. He has no disclosures in regard to this article.
Dear colleagues,
In the dynamic field of medicine, long-held practices are being reevaluated in light of new evidence and evolving standards of practice.
Dr. Anahita Rabiee discusses the importance of prioritizing non-selective beta blockers (NSBB) over endoscopic variceal ligation (EVL) in the primary prophylaxis of variceal bleeding in patients with compensated cirrhosis. Drawing on data from the PREDESCI trial and real-world experience, she argues that NSBB address the upstream driver—portal hypertension—more broadly and effectively than EVL. In a complementary piece, Dr. Tarek Sawas explores the nuanced landscape of screening and surveillance in Barrett’s esophagus. From how to manage irregular Z-lines, to rethinking the need for 1-year follow-up endoscopies and interpreting the implications of the BOSS trial, Dr. Sawas advocates for a more personalized, risk-based approach.
We hope these perspectives spark dialogue and reflection in your own practice. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
Choose NSBBs, Not EVL, in Patients with Compensated Cirrhosis
BY ANAHITA RABIEE, MD, MHS
I strongly favor the use of non selective beta blockers (NSBBs) in patients with compensated cirrhosis, rather than endoscopy and esophageal variceal ligation (EVL) for primary prophylaxis.
Since the results of PREDESCI trial (β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (CSPH)) were published in 2019, there has been much debate on the role of screening endoscopy and EVL for primary prophylaxis. While many argue that a single randomized trial should not overturn long standing practice, several compelling reasons convince me to choose NSBBs, when possible.
Recent guidance from major liver societies now recommends NSBBs as first line therapy for CSPH. Yet, adoption in clinical practice remains inconsistent.
Here is why I believe NSBB represent a better solution:
Treating Upstream, Not Just a Local Treatment
NSBBs such as propranolol and nadolol decrease portal pressure by decreasing portal venous inflow through β1 and β2 adrenergic blockade. Carvedilol is often preferred given its additional α1 adrenergic blocking activity making it the most effective one in decreasing the portal pressure. Therefore, NSBBs address the upstream driver of decompensation by decreasing portal pressures.
EVL, in contrast, is a local fix that only prevents variceal bleeding. Ascites, not variceal bleeding, is the most common initial decompensating event and is associated with high mortality. Preventing all forms of decompensation is clearly preferable to preventing just one.
Broader Eligibility, More Patients Benefit
CSPH is defined as hepatic venous pressure gradient (HVPG)>10 mmHg, the threshold where increased portal venous inflow secondary to splanchnic vasodilation and hyperdynamic circulation drives the increase in portal hypertension. This threshold has been shown to strongly predict decompensation in patients with compensated disease.
While all patients with varices have CSPH, not all patients with CSPH have varices. They can be identified by other non invasive criteria such as cross sectional imaging showing collaterals, or liver stiffness and platelet thresholds that have been previously validated. By restricting intervention to those with large varices and offering only EVL, we miss the opportunity to intervene earlier and to a broader group that would benefit from this treatment.
Comprehensive Protection Without Repeated Endoscopies
Once on an appropriate NSBB dose, patients are protected against variceal bleeding (at least as effectively as EVL). This eliminates the need for repeated surveillance endoscopies to identify and treat large varices in otherwise compensated patients.
Better Tolerated and – In Many Cases – Overlaps With Existing Medication List!
While overtreatment is a concern, regular endoscopies every two years are also burdensome. Many patients already need beta blockers for cardiac conditions such as atrial fibrillation, ischemic heart disease or hypertension. Carvedilol, in particular, offers dual benefit for both hepatologists and cardiologists.
It is important to emphasize that these arguments apply to compensated cirrhosis. In decompensated disease, the approach changes. After a variceal bleed, both NSBBs and EVL are required for secondary prophylaxis. In patients with prior ascites but no variceal bleed, the benefit of NSBBs is less pronounced since decompensation has already occurred. In this setting, NSBBs can still be used selectively, but only if systolic blood pressure remains above 90 mmHg.
The evidence supporting NSBBs over EVL in compensated cirrhosis is not perfect, but few things in medicine are. Given current data, NSBBs should be the first line therapy in compensated cirrhosis with CSPH. Once a patient is on an appropriate and tolerated NSBB dose, routine endoscopic surveillance is unnecessary. Endoscopy should be reserved for those who cannot tolerate NSBBs, in whom EVL is then indicated if large varices are present.
Dr. Rabiee is based at the Yale School of Medicine, New Haven, Connecticut, and the Veterans Affairs Connecticut Healthcare System, West Haven, Connecticut. She has no disclosures in regard to this article.
Rethinking Screening and Surveillance in Barrett’s Esophagus: Navigating Controversies and Nuances
BY TAREK SAWAS, MD, MPH
Barrett’s esophagus (BE) is a precursor to esophageal adenocarcinoma (EAC). Despite our comprehensive guidelines, many of the day-to-day decisions still rely on clinical judgment and honest conversations with patients. This article explores common scenarios in which management decisions are nuanced and the right answer remains debatable.
Irregular Z-Line/Ultrashort Segment BE: Leave Or Watch It?
Few findings provoke more confusion than irregular Z-line or intestinal metaplasia (IM) < 1 cm at the gastroesophageal junction (GEJ). For years, we have debated whether these subtle changes represent a precursor to EAC or simply a benign variant. We have wrestled with how to handle these cases from whether we should take biopsies to how to perform surveillance.
The American College of Gastroenterology (ACG) guideline suggests that irregular Z-lines should not be routinely biopsied or surveyed. Similarly, the upcoming American Gastroenterology Association (AGA) surveillance guideline suggests against surveillance of IM<1 cm citing the low individual annual risk of progression to high-grade dysplasia (HGD) and EAC of 0.23% per year which is lower than that of non-dysplastic Barrett’s esophagus (NDBE). However, this is not the entire picture.
Despite the low per-patient risk, IM<1cm is highly prevalent with columnar mucosa observed in approximately 15% of patients undergoing upper endoscopy. This paradox is unsettling. While any one patient with IM<1 cm is unlikely to progress to EAC, the group accounts for a meaningful share of the EAC burden. Some experts have argued that this justifies routine biopsy and surveillance in all patients with visible columnar mucosa regardless of length. However, this approach risks overwhelming our surveillance infrastructure.
A recent decision modeling analysis suggested that at the lowest progression rates, either no surveillance or one-time endoscopy can be considered. Based on these data, I do not regularly biopsy ultrashort segments unless the mucosa appears suspicious. In those with IM<1 cm detected during a high-quality endoscopic exam, no follow-up is needed. However, if the exam is suboptimal, I perform a 1-time high-quality repeat exam. If there is no evidence of dysplasia then I do not pursue any further surveillance.
The One-Year Follow-Up Endoscopy: Is It Necessary?
Another controversy is the one-year follow-up endoscopy after an initial diagnosis of NDBE. Proponents of this approach cite the high proportion of post endoscopy esophageal neoplasia and cancer (PEEN/PEEC) detected in the first year after diagnosis (missed HGD/EAC). In fact, PEEN account for about a quarter of all HGD/EAC cases diagnosed during surveillance.
While this approach might mitigate PEEN/PEEC risk, it may not be necessary if the index endoscopy is high quality. To ensure high quality exams, several best practices have been proposed including:
- Use of high-definition white light endoscopy (HD-WLE) with chromoendoscopy (virtual or dye based)
- Appropriate inspection time (1 minute per cm of circumferential BE)
- Accurate documentation using the Prague criteria
- Adherence to the Seattle protocol with additional targeted biopsies
If the index endoscopy meets these quality metrics, I typically do not bring the patient back at one year. However, if the exam quality is in question, then I repeat it at one year to establish a reliable baseline and rule out prevalent neoplasia.
Surveillance In NDBE: After BOSS, Do We Rethink Everything?
The recently published BOSS trial (Barrett’s Oesophagus Surveillance Study) has reignited the debate over the value of endoscopic surveillance in NDBE. In this study, 3,453 patients with NDBE across the UK were randomized to either surveillance endoscopy every two years or endoscopy only as clinically indicated. After a median follow-up of 12.8 years, the trial found no significant difference in all-cause mortality between the two groups.
While these findings are important, they should be interpreted with caution. First, the primary endpoint, all-cause mortality, is not optimal for evaluating surveillance for EAC. Surveillance is not intended to reduce all-cause mortality but rather to reduce EAC–related mortality. Second, a substantial number of patients in the no surveillance group still underwent endoscopy at intervals that were not meaningfully different from those in the surveillance group. If both groups receive similar exposure to endoscopy, the comparison loses power. Lastly, the trial was underpowered due to overestimation of progression risk during its initial design. As we have since learned, the risk of progression of NDBE is lower than originally assumed.
So where do we stand now? For me, the BOSS trial does not negate the value of surveillance. it reminds us that a one-size-fits-all approach is inefficient, and our strategy must be risk based. For low-risk individuals, particularly older adults with short-segment NDBE, surveillance may offer little benefit. But in healthier, younger patients with longer segments or additional risk factors, surveillance remains an essential tool for early neoplasia detection.
When to Stop Surveillance
Perhaps the most under-discussed point is when to stop surveillance. Existing guidelines do not account for competing mortality risks unrelated to EAC or provide specific recommendations regarding cessation of surveillance. The desired benefits of surveillance likely diminish with advanced age and greater comorbidity because of lower life expectancy and ineligibility for definitive therapy for EAC.
A recent modeling study found that the optimal ages for last surveillance were 81, 80, 77, and 73 years for men with no, mild, moderate, and severe comorbidity respectively and 75, 73, 73, and 69 years for women. In my practice, I discuss surveillance cessation in patients older than 75 based on their comorbidities. If the risk of progression is outweighed by the risk of the procedure or by the reality of limited life expectancy, we should not hesitate to consider surveillance cessation.
In summary, high-quality endoscopic exam in appropriately selected patients remains the cornerstone of BE surveillance. A more personalized, risk-based approach is needed taking into account competing comorbidities. Emerging technology through risk stratification tools such as biomarkers and artificial intelligence may refine our approach and help address the current limitations.
Dr. Sawas is based at the University of Texas Southwestern, Dallas, Texas. He has no disclosures in regard to this article.