User login
FDA approves alogliptin, alone and in combinations
After several years of reviews and rejections, the dipeptidyl peptidase IV inhibitor alogliptin has finally been approved by the Food and Drug Administration.
The FDA approved three versions of the product: as a single agent (Nesina); in combination with metformin (Kazano); and, in combination with pioglitazone (Oseni). All are indicated for treatment of type 2 diabetes in combination with diet and exercise.

Alogliptin is designed to slow the inactivation of incretin hormones GLP-1 (glucagonlike peptide–1) and GIP (glucose-dependent insulinotropic peptide), according to the drug’s maker, Takeda Pharmaceutical Company Ltd. Oseni is the first product approved in the United States that includes a DPP-4 inhibitor and a thiazolidinedione in a single tablet, the company said.
That unique combination may be of interest to clinicians, said Dr. Paul Jellinger, professor of clinical medicine at the University of Miami, Division of Endocrinology. First, a one-pill combination offers convenience for patients. And, the combination of a DPP-4 inhibitor and a TZD robustly drops hemoglobin A1C and also makes physiologic sense since they work by two different mechanisms, added Dr. Jellinger.
He notes that in carefully selected patients, pioglitazone is useful to reverse or diminish insulin resistance and also to treat and minimize the appearance of fatty liver. “The same patient that you would think of using pioglitazone for is probably an ideal candidate for a combination of pioglitazone and a DPP-4 inhibitor like alogliptin,” said Dr. Jellinger, who practices at The Center for Diabetes & Endocrine Care in Hollywood, Florida.
Patients should be monitored for pioglitazone side effects such as heart failure, weight gain, edema, and more rarely, small bone fractures, he said. They should also be screened for bladder cancer several times yearly.Alogliptin is the fourth DPP-4 inhibitor to win FDA approval. Merck’s sitagliptin (Januvia) is the market leader; the others in the class are saxagliptin (Onglyza, marketed by AstraZeneca and Bristol-Myers Squibb) and linagliptin (Tradjenta, marketed by Boehringer Ingelheim and Lilly).
These approvals are 5 years in the making. Takeda submitted an application for the drug in 2008, but was tripped up by several developments. First, shortly after concerns were raised in 2007 about a link between rosiglitazone (Avandia) and an increased risk of myocardial infarction, the FDA in 2008 began requiring all diabetes therapies to demonstrate cardiovascular safety. Takeda had to restart its clinical development to incorporate trials with cardiovascular endpoints. The company subsequently received two requests – one for alogliptin as a single agent and another for the combination with pioglitazone – for more information, because of safety concerns.
As a result, the agency’s approval for each product is a mixed bag, with each carrying different warnings and requirements.
The single agent, Nesina, showed in more than 14 trials that it reduced hemoglobin A1c by 0.4-0.6 percentage points compared with placebo over 26 weeks. It will be available in 6.25-mg, 12.5-mg, and 25-mg tablets. But the agency is requiring five postmarketing studies for alogliptin as a single agent: an enhanced pharmacovigilance program to monitor for liver abnormalities, serious cases of pancreatitis, and severe hypersensitivity reactions; and three pediatric studies under the Pediatric Research Equity Act (PREA), including a dose-finding study and two safety and efficacy studies, one with Nesina as a monotherapy and one with Nesina and metformin.
The metformin combination, Kazano, reduced HbA1c by 1.1 percentage points more than Nesina, and 0.5 percentage points more than metformin alone in four clinical trials. The two dosages are 12.5 mg alogliptin/500 mg metformin and 12.5 mg/1,000 mg. The FDA is requiring two postmarketing studies for Kazano: a program to monitor for liver abnormalities, serious pancreatitis, and severe hypersensitivity reactions; and a pediatric safety and efficacy study. Kazano will carry a boxed warning for lactic acidosis.
Oseni, the alogliptin/pioglitazone combination, in six fixed-dose formulations (5 mg/15 mg, 25 mg/30 mg, 25 mg/45 mg, 12.5 mg/15 mg, 12.5 mg/30 mg, and 12.5 mg/45 mg), reduced HbA1c by 0.4-0.9 percentage points more than alogliptin alone, and 0.4-0.6 percentage points better than pioglitazone alone in studies. Takeda will have to conduct a postmarketing study on liver abnormalities, pancreatitis, and hypersensitivity reactions for Oseni, as well. The drug will have a boxed warning for heart failure.
Both Oseni and Nesina are approved in Japan, but those are the only other global approvals for the products.
Although there has been some concern with all diabetes therapeutics and cardiovascular safety, a recent meta-analysis showed that DPP-4 inhibitors may substantially reduce the risk of major cardiovascular events. The study, funded by Bristol-Myers Squibb and AstraZeneca, was reported at the annual scientific sessions of the American Heart Association in late November.
Twitter @aliciaault
After several years of reviews and rejections, the dipeptidyl peptidase IV inhibitor alogliptin has finally been approved by the Food and Drug Administration.
The FDA approved three versions of the product: as a single agent (Nesina); in combination with metformin (Kazano); and, in combination with pioglitazone (Oseni). All are indicated for treatment of type 2 diabetes in combination with diet and exercise.
Alogliptin is designed to slow the inactivation of incretin hormones GLP-1 (glucagonlike peptide–1) and GIP (glucose-dependent insulinotropic peptide), according to the drug’s maker, Takeda Pharmaceutical Company Ltd. Oseni is the first product approved in the United States that includes a DPP-4 inhibitor and a thiazolidinedione in a single tablet, the company said.
That unique combination may be of interest to clinicians, said Dr. Paul Jellinger, professor of clinical medicine at the University of Miami, Division of Endocrinology. First, a one-pill combination offers convenience for patients. And, the combination of a DPP-4 inhibitor and a TZD robustly drops hemoglobin A1C and also makes physiologic sense since they work by two different mechanisms, added Dr. Jellinger.
He notes that in carefully selected patients, pioglitazone is useful to reverse or diminish insulin resistance and also to treat and minimize the appearance of fatty liver. “The same patient that you would think of using pioglitazone for is probably an ideal candidate for a combination of pioglitazone and a DPP-4 inhibitor like alogliptin,” said Dr. Jellinger, who practices at The Center for Diabetes & Endocrine Care in Hollywood, Florida.
Patients should be monitored for pioglitazone side effects such as heart failure, weight gain, edema, and more rarely, small bone fractures, he said. They should also be screened for bladder cancer several times yearly.Alogliptin is the fourth DPP-4 inhibitor to win FDA approval. Merck’s sitagliptin (Januvia) is the market leader; the others in the class are saxagliptin (Onglyza, marketed by AstraZeneca and Bristol-Myers Squibb) and linagliptin (Tradjenta, marketed by Boehringer Ingelheim and Lilly).
These approvals are 5 years in the making. Takeda submitted an application for the drug in 2008, but was tripped up by several developments. First, shortly after concerns were raised in 2007 about a link between rosiglitazone (Avandia) and an increased risk of myocardial infarction, the FDA in 2008 began requiring all diabetes therapies to demonstrate cardiovascular safety. Takeda had to restart its clinical development to incorporate trials with cardiovascular endpoints. The company subsequently received two requests – one for alogliptin as a single agent and another for the combination with pioglitazone – for more information, because of safety concerns.
As a result, the agency’s approval for each product is a mixed bag, with each carrying different warnings and requirements.
The single agent, Nesina, showed in more than 14 trials that it reduced hemoglobin A1c by 0.4-0.6 percentage points compared with placebo over 26 weeks. It will be available in 6.25-mg, 12.5-mg, and 25-mg tablets. But the agency is requiring five postmarketing studies for alogliptin as a single agent: an enhanced pharmacovigilance program to monitor for liver abnormalities, serious cases of pancreatitis, and severe hypersensitivity reactions; and three pediatric studies under the Pediatric Research Equity Act (PREA), including a dose-finding study and two safety and efficacy studies, one with Nesina as a monotherapy and one with Nesina and metformin.
The metformin combination, Kazano, reduced HbA1c by 1.1 percentage points more than Nesina, and 0.5 percentage points more than metformin alone in four clinical trials. The two dosages are 12.5 mg alogliptin/500 mg metformin and 12.5 mg/1,000 mg. The FDA is requiring two postmarketing studies for Kazano: a program to monitor for liver abnormalities, serious pancreatitis, and severe hypersensitivity reactions; and a pediatric safety and efficacy study. Kazano will carry a boxed warning for lactic acidosis.
Oseni, the alogliptin/pioglitazone combination, in six fixed-dose formulations (5 mg/15 mg, 25 mg/30 mg, 25 mg/45 mg, 12.5 mg/15 mg, 12.5 mg/30 mg, and 12.5 mg/45 mg), reduced HbA1c by 0.4-0.9 percentage points more than alogliptin alone, and 0.4-0.6 percentage points better than pioglitazone alone in studies. Takeda will have to conduct a postmarketing study on liver abnormalities, pancreatitis, and hypersensitivity reactions for Oseni, as well. The drug will have a boxed warning for heart failure.
Both Oseni and Nesina are approved in Japan, but those are the only other global approvals for the products.
Although there has been some concern with all diabetes therapeutics and cardiovascular safety, a recent meta-analysis showed that DPP-4 inhibitors may substantially reduce the risk of major cardiovascular events. The study, funded by Bristol-Myers Squibb and AstraZeneca, was reported at the annual scientific sessions of the American Heart Association in late November.
Twitter @aliciaault
After several years of reviews and rejections, the dipeptidyl peptidase IV inhibitor alogliptin has finally been approved by the Food and Drug Administration.
The FDA approved three versions of the product: as a single agent (Nesina); in combination with metformin (Kazano); and, in combination with pioglitazone (Oseni). All are indicated for treatment of type 2 diabetes in combination with diet and exercise.
Alogliptin is designed to slow the inactivation of incretin hormones GLP-1 (glucagonlike peptide–1) and GIP (glucose-dependent insulinotropic peptide), according to the drug’s maker, Takeda Pharmaceutical Company Ltd. Oseni is the first product approved in the United States that includes a DPP-4 inhibitor and a thiazolidinedione in a single tablet, the company said.
That unique combination may be of interest to clinicians, said Dr. Paul Jellinger, professor of clinical medicine at the University of Miami, Division of Endocrinology. First, a one-pill combination offers convenience for patients. And, the combination of a DPP-4 inhibitor and a TZD robustly drops hemoglobin A1C and also makes physiologic sense since they work by two different mechanisms, added Dr. Jellinger.
He notes that in carefully selected patients, pioglitazone is useful to reverse or diminish insulin resistance and also to treat and minimize the appearance of fatty liver. “The same patient that you would think of using pioglitazone for is probably an ideal candidate for a combination of pioglitazone and a DPP-4 inhibitor like alogliptin,” said Dr. Jellinger, who practices at The Center for Diabetes & Endocrine Care in Hollywood, Florida.
Patients should be monitored for pioglitazone side effects such as heart failure, weight gain, edema, and more rarely, small bone fractures, he said. They should also be screened for bladder cancer several times yearly.Alogliptin is the fourth DPP-4 inhibitor to win FDA approval. Merck’s sitagliptin (Januvia) is the market leader; the others in the class are saxagliptin (Onglyza, marketed by AstraZeneca and Bristol-Myers Squibb) and linagliptin (Tradjenta, marketed by Boehringer Ingelheim and Lilly).
These approvals are 5 years in the making. Takeda submitted an application for the drug in 2008, but was tripped up by several developments. First, shortly after concerns were raised in 2007 about a link between rosiglitazone (Avandia) and an increased risk of myocardial infarction, the FDA in 2008 began requiring all diabetes therapies to demonstrate cardiovascular safety. Takeda had to restart its clinical development to incorporate trials with cardiovascular endpoints. The company subsequently received two requests – one for alogliptin as a single agent and another for the combination with pioglitazone – for more information, because of safety concerns.
As a result, the agency’s approval for each product is a mixed bag, with each carrying different warnings and requirements.
The single agent, Nesina, showed in more than 14 trials that it reduced hemoglobin A1c by 0.4-0.6 percentage points compared with placebo over 26 weeks. It will be available in 6.25-mg, 12.5-mg, and 25-mg tablets. But the agency is requiring five postmarketing studies for alogliptin as a single agent: an enhanced pharmacovigilance program to monitor for liver abnormalities, serious cases of pancreatitis, and severe hypersensitivity reactions; and three pediatric studies under the Pediatric Research Equity Act (PREA), including a dose-finding study and two safety and efficacy studies, one with Nesina as a monotherapy and one with Nesina and metformin.
The metformin combination, Kazano, reduced HbA1c by 1.1 percentage points more than Nesina, and 0.5 percentage points more than metformin alone in four clinical trials. The two dosages are 12.5 mg alogliptin/500 mg metformin and 12.5 mg/1,000 mg. The FDA is requiring two postmarketing studies for Kazano: a program to monitor for liver abnormalities, serious pancreatitis, and severe hypersensitivity reactions; and a pediatric safety and efficacy study. Kazano will carry a boxed warning for lactic acidosis.
Oseni, the alogliptin/pioglitazone combination, in six fixed-dose formulations (5 mg/15 mg, 25 mg/30 mg, 25 mg/45 mg, 12.5 mg/15 mg, 12.5 mg/30 mg, and 12.5 mg/45 mg), reduced HbA1c by 0.4-0.9 percentage points more than alogliptin alone, and 0.4-0.6 percentage points better than pioglitazone alone in studies. Takeda will have to conduct a postmarketing study on liver abnormalities, pancreatitis, and hypersensitivity reactions for Oseni, as well. The drug will have a boxed warning for heart failure.
Both Oseni and Nesina are approved in Japan, but those are the only other global approvals for the products.
Although there has been some concern with all diabetes therapeutics and cardiovascular safety, a recent meta-analysis showed that DPP-4 inhibitors may substantially reduce the risk of major cardiovascular events. The study, funded by Bristol-Myers Squibb and AstraZeneca, was reported at the annual scientific sessions of the American Heart Association in late November.
Twitter @aliciaault

FDA approves bevacizumab for second-line combinations
Bevacizumab is now approved by the Food and Drug Administration for use in combination with fluoropyrimidine-irinotecan–based or fluoropyrimidine-oxaliplatin–based chemotherapy for metastatic colorectal cancer in patients whose disease has progressed on a first-line bevacizumab-containing regimen.
The agency based its approval on results from the 820-patient ML18147 study, funded by Genentech, which markets bevacizumab as Avastin. In that trial, median overall survival for those who received the bevacizumab combination in the first and second line was 11.2 months, compared with 9.8 months for those who had combinations that did not contain bevacizumab. The median progression-free survival was 5.7 months for those receiving the combination with bevacizumab, compared with 4.1 months for the others.
The results of ML18147 were presented at the 2012 American Society of Clinical Oncology annual meeting.
"The majority of people diagnosed with metastatic colorectal cancer receive Avastin plus chemotherapy as their initial treatment," said Dr. Hal Barron, chief medical officer and head of Global Product Development for Genentech, in a statement. "These people now have the option to continue with Avastin plus a new chemotherapy after their cancer worsens, which may help them live longer than changing to the new chemotherapy alone."
The Food and Drug Administration (FDA) said that the safety data from the ML18147 study were similar to bevacizumab’s known safety profile, especially in previous trials of metastatic colorectal cancer.
Genentech noted that this is the third approval for bevacizumab in that disease that is based on improved overall survival. The drug is approved in Europe in combination with fluoropyrimidine-based chemotherapy in metastatic carcinoma of the colon or rectum.
According to the FDA, patients receiving bevacizumab in combination with fluoropyrimidine-irinotecan–based or fluoropyrimidine-oxaliplatin–based chemotherapy after progression on a first-line bevacizumab-containing regimen should receive 5 mg/kg administered every 2 weeks or 7.5 mg/kg administered every 3 weeks as a 60-minute intravenous infusion.
Full prescribing information is available here.
On Twitter @aliciaault
Bevacizumab is now approved by the Food and Drug Administration for use in combination with fluoropyrimidine-irinotecan–based or fluoropyrimidine-oxaliplatin–based chemotherapy for metastatic colorectal cancer in patients whose disease has progressed on a first-line bevacizumab-containing regimen.
The agency based its approval on results from the 820-patient ML18147 study, funded by Genentech, which markets bevacizumab as Avastin. In that trial, median overall survival for those who received the bevacizumab combination in the first and second line was 11.2 months, compared with 9.8 months for those who had combinations that did not contain bevacizumab. The median progression-free survival was 5.7 months for those receiving the combination with bevacizumab, compared with 4.1 months for the others.
The results of ML18147 were presented at the 2012 American Society of Clinical Oncology annual meeting.
"The majority of people diagnosed with metastatic colorectal cancer receive Avastin plus chemotherapy as their initial treatment," said Dr. Hal Barron, chief medical officer and head of Global Product Development for Genentech, in a statement. "These people now have the option to continue with Avastin plus a new chemotherapy after their cancer worsens, which may help them live longer than changing to the new chemotherapy alone."
The Food and Drug Administration (FDA) said that the safety data from the ML18147 study were similar to bevacizumab’s known safety profile, especially in previous trials of metastatic colorectal cancer.
Genentech noted that this is the third approval for bevacizumab in that disease that is based on improved overall survival. The drug is approved in Europe in combination with fluoropyrimidine-based chemotherapy in metastatic carcinoma of the colon or rectum.
According to the FDA, patients receiving bevacizumab in combination with fluoropyrimidine-irinotecan–based or fluoropyrimidine-oxaliplatin–based chemotherapy after progression on a first-line bevacizumab-containing regimen should receive 5 mg/kg administered every 2 weeks or 7.5 mg/kg administered every 3 weeks as a 60-minute intravenous infusion.
Full prescribing information is available here.
On Twitter @aliciaault
Bevacizumab is now approved by the Food and Drug Administration for use in combination with fluoropyrimidine-irinotecan–based or fluoropyrimidine-oxaliplatin–based chemotherapy for metastatic colorectal cancer in patients whose disease has progressed on a first-line bevacizumab-containing regimen.
The agency based its approval on results from the 820-patient ML18147 study, funded by Genentech, which markets bevacizumab as Avastin. In that trial, median overall survival for those who received the bevacizumab combination in the first and second line was 11.2 months, compared with 9.8 months for those who had combinations that did not contain bevacizumab. The median progression-free survival was 5.7 months for those receiving the combination with bevacizumab, compared with 4.1 months for the others.
The results of ML18147 were presented at the 2012 American Society of Clinical Oncology annual meeting.
"The majority of people diagnosed with metastatic colorectal cancer receive Avastin plus chemotherapy as their initial treatment," said Dr. Hal Barron, chief medical officer and head of Global Product Development for Genentech, in a statement. "These people now have the option to continue with Avastin plus a new chemotherapy after their cancer worsens, which may help them live longer than changing to the new chemotherapy alone."
The Food and Drug Administration (FDA) said that the safety data from the ML18147 study were similar to bevacizumab’s known safety profile, especially in previous trials of metastatic colorectal cancer.
Genentech noted that this is the third approval for bevacizumab in that disease that is based on improved overall survival. The drug is approved in Europe in combination with fluoropyrimidine-based chemotherapy in metastatic carcinoma of the colon or rectum.
According to the FDA, patients receiving bevacizumab in combination with fluoropyrimidine-irinotecan–based or fluoropyrimidine-oxaliplatin–based chemotherapy after progression on a first-line bevacizumab-containing regimen should receive 5 mg/kg administered every 2 weeks or 7.5 mg/kg administered every 3 weeks as a 60-minute intravenous infusion.
Full prescribing information is available here.
On Twitter @aliciaault
Cancer deaths declined 20% since 1991
Cancer deaths have declined 20% since 1991, which means there were 1.2 million fewer deaths from cancer in 2009, according to the American Cancer Society.
The overall cancer death rate decreased from 215 per 100,000 in 1991 to 173 per 100,000 in 2009. Death rates declined more sharply for cancers of the lung and prostate in men, for breast cancers in women, and for colon and rectal cancers for men and women. The ACS attributes the drops to decreases in smoking and improvements in early detection and treatment.

The most common causes of cancer death in Americans, accounting for 50% of cancer deaths, are cancers of the lung and bronchus, prostate, and colorectum in men; and cancers of the lung and bronchus, breast, and colorectum in women. This year, there will be 1.6 million cancer cases and 580,350 cancer deaths; lung cancers will account for 25% of cancer deaths in men and women this year, according to estimates from the ACS.
The mortality figures and incidence data are contained in two reports: Cancer Facts & Figures 2013 and Cancer Statistics 2013, both published in CA: A Cancer Journal for Clinicians. (doi:10.3322/caac.21166). The reports were published online on Jan. 18.
Incidence rates are on the decline for most cancers with the exception of melanoma, and liver, thyroid and pancreatic cancer.
Dr. Daniel M. Siegel, president of the American Academy of Dermatology, said in a statement that a rising incidence of melanoma "is particularly concerning because skin cancer can often be easily prevented and detected." Dr. Siegel said that the AAD and its members "are actively working to reduce the incidence of skin cancer and change society’s attitudes and behaviors toward sun exposure and tanning."
Death rates from pancreatic cancer have increased over the last decade, due to what the ACS called "a lack progress in primary prevention, early diagnosis, and treatment of this cancer." The ACS report included a special section devoted to updated information on the occurrence and treatment of pancreatic cancer. Most patients with pancreatic cancer die within a year of diagnosis; the 5-year survival rate is 6%.
The ACS also noted that the disparity in cancer outcomes based on ethnicity and income, "particularly [among] those diagnosed with colorectal or breast cancer where earlier detection and better treatments are credited for the improving trends," said John R. Seffrin, Ph.D., chief executive officer of the ACS, in a statement. "We can and must close this gap so that people are not punished for having the misfortune of being born poor and disadvantaged."
The 5-year survival rate in 2002-2008 for white women with breast cancer, for instance, was 92%, whereas for black women, it was 78%. For colon cancer, the 5-year survival rate was 66% for whites, but 55% for blacks.
On Twitter @aliciaault
Cancer deaths have declined 20% since 1991, which means there were 1.2 million fewer deaths from cancer in 2009, according to the American Cancer Society.
The overall cancer death rate decreased from 215 per 100,000 in 1991 to 173 per 100,000 in 2009. Death rates declined more sharply for cancers of the lung and prostate in men, for breast cancers in women, and for colon and rectal cancers for men and women. The ACS attributes the drops to decreases in smoking and improvements in early detection and treatment.
The most common causes of cancer death in Americans, accounting for 50% of cancer deaths, are cancers of the lung and bronchus, prostate, and colorectum in men; and cancers of the lung and bronchus, breast, and colorectum in women. This year, there will be 1.6 million cancer cases and 580,350 cancer deaths; lung cancers will account for 25% of cancer deaths in men and women this year, according to estimates from the ACS.
The mortality figures and incidence data are contained in two reports: Cancer Facts & Figures 2013 and Cancer Statistics 2013, both published in CA: A Cancer Journal for Clinicians. (doi:10.3322/caac.21166). The reports were published online on Jan. 18.
Incidence rates are on the decline for most cancers with the exception of melanoma, and liver, thyroid and pancreatic cancer.
Dr. Daniel M. Siegel, president of the American Academy of Dermatology, said in a statement that a rising incidence of melanoma "is particularly concerning because skin cancer can often be easily prevented and detected." Dr. Siegel said that the AAD and its members "are actively working to reduce the incidence of skin cancer and change society’s attitudes and behaviors toward sun exposure and tanning."
Death rates from pancreatic cancer have increased over the last decade, due to what the ACS called "a lack progress in primary prevention, early diagnosis, and treatment of this cancer." The ACS report included a special section devoted to updated information on the occurrence and treatment of pancreatic cancer. Most patients with pancreatic cancer die within a year of diagnosis; the 5-year survival rate is 6%.
The ACS also noted that the disparity in cancer outcomes based on ethnicity and income, "particularly [among] those diagnosed with colorectal or breast cancer where earlier detection and better treatments are credited for the improving trends," said John R. Seffrin, Ph.D., chief executive officer of the ACS, in a statement. "We can and must close this gap so that people are not punished for having the misfortune of being born poor and disadvantaged."
The 5-year survival rate in 2002-2008 for white women with breast cancer, for instance, was 92%, whereas for black women, it was 78%. For colon cancer, the 5-year survival rate was 66% for whites, but 55% for blacks.
On Twitter @aliciaault
Cancer deaths have declined 20% since 1991, which means there were 1.2 million fewer deaths from cancer in 2009, according to the American Cancer Society.
The overall cancer death rate decreased from 215 per 100,000 in 1991 to 173 per 100,000 in 2009. Death rates declined more sharply for cancers of the lung and prostate in men, for breast cancers in women, and for colon and rectal cancers for men and women. The ACS attributes the drops to decreases in smoking and improvements in early detection and treatment.
The most common causes of cancer death in Americans, accounting for 50% of cancer deaths, are cancers of the lung and bronchus, prostate, and colorectum in men; and cancers of the lung and bronchus, breast, and colorectum in women. This year, there will be 1.6 million cancer cases and 580,350 cancer deaths; lung cancers will account for 25% of cancer deaths in men and women this year, according to estimates from the ACS.
The mortality figures and incidence data are contained in two reports: Cancer Facts & Figures 2013 and Cancer Statistics 2013, both published in CA: A Cancer Journal for Clinicians. (doi:10.3322/caac.21166). The reports were published online on Jan. 18.
Incidence rates are on the decline for most cancers with the exception of melanoma, and liver, thyroid and pancreatic cancer.
Dr. Daniel M. Siegel, president of the American Academy of Dermatology, said in a statement that a rising incidence of melanoma "is particularly concerning because skin cancer can often be easily prevented and detected." Dr. Siegel said that the AAD and its members "are actively working to reduce the incidence of skin cancer and change society’s attitudes and behaviors toward sun exposure and tanning."
Death rates from pancreatic cancer have increased over the last decade, due to what the ACS called "a lack progress in primary prevention, early diagnosis, and treatment of this cancer." The ACS report included a special section devoted to updated information on the occurrence and treatment of pancreatic cancer. Most patients with pancreatic cancer die within a year of diagnosis; the 5-year survival rate is 6%.
The ACS also noted that the disparity in cancer outcomes based on ethnicity and income, "particularly [among] those diagnosed with colorectal or breast cancer where earlier detection and better treatments are credited for the improving trends," said John R. Seffrin, Ph.D., chief executive officer of the ACS, in a statement. "We can and must close this gap so that people are not punished for having the misfortune of being born poor and disadvantaged."
The 5-year survival rate in 2002-2008 for white women with breast cancer, for instance, was 92%, whereas for black women, it was 78%. For colon cancer, the 5-year survival rate was 66% for whites, but 55% for blacks.
On Twitter @aliciaault
FROM CA: A CANCER JOURNAL FOR CLINICIANS

FDA approves Botox for overactive bladder
The Food and Drug Administration on Jan. 18 approved Botox for patients with overactive bladder who have contraindications to or don’t respond to anticholinergics.
"Clinical studies have demonstrated Botox’s ability to significantly reduce the frequency of urinary incontinence," Dr. Hylton V. Joffe, director of the Division of Reproductive and Urologic Products in the Food and Drug Administration’s Center for Drug Evaluation and Research, said in a statement.
"With the approval of Botox [onabotulinumtoxinA], we have a new treatment option to offer these patients that has demonstrated efficacy in reducing urinary leakage and other symptoms of OAB with the effect lasting up to 6 months," Dr. Victor Nitti, vice chairman in the department of urology at NYU Langone Medical Center, said in a statement released by Botox maker Allergan.
Overactive bladder (OAB) results in an uncontrolled urge to urinate, frequent urination, and uncontrollable leakage of urine, according to the Allergan statement. About 14.7 million American adults have overactive bladder, and 3.3 million use anticholinergics; however, at least half of them stop taking the drugs within a year because of intolerance.
Botox injected into the bladder muscle relaxes the organ and increases its storage capacity, thus reducing incontinence, according to the FDA. The Botox is injected via cystoscopy.
The FDA evaluated the drug’s safety and efficacy for overactive bladder through two studies in which 1,105 patients were randomly assigned to receive injections of 100 units of Botox (20 injections of 5 units each) or placebo. At 12 weeks, patients who received Botox had 1.6 to 1.9 fewer incidents of incontinence per day, and also needed to urinate less frequently.
The treatment needs to be repeated to maintain effectiveness; the FDA recommends at least 12 weeks between injections. Side effects during trials included urinary tract infections, painful urination, and urinary retention.
Patients must take antibiotics before, during, and a few days after Botox treatment to reduce infection risk.
On Twitter @aliciaault
The Food and Drug Administration on Jan. 18 approved Botox for patients with overactive bladder who have contraindications to or don’t respond to anticholinergics.
"Clinical studies have demonstrated Botox’s ability to significantly reduce the frequency of urinary incontinence," Dr. Hylton V. Joffe, director of the Division of Reproductive and Urologic Products in the Food and Drug Administration’s Center for Drug Evaluation and Research, said in a statement.
"With the approval of Botox [onabotulinumtoxinA], we have a new treatment option to offer these patients that has demonstrated efficacy in reducing urinary leakage and other symptoms of OAB with the effect lasting up to 6 months," Dr. Victor Nitti, vice chairman in the department of urology at NYU Langone Medical Center, said in a statement released by Botox maker Allergan.
Overactive bladder (OAB) results in an uncontrolled urge to urinate, frequent urination, and uncontrollable leakage of urine, according to the Allergan statement. About 14.7 million American adults have overactive bladder, and 3.3 million use anticholinergics; however, at least half of them stop taking the drugs within a year because of intolerance.
Botox injected into the bladder muscle relaxes the organ and increases its storage capacity, thus reducing incontinence, according to the FDA. The Botox is injected via cystoscopy.
The FDA evaluated the drug’s safety and efficacy for overactive bladder through two studies in which 1,105 patients were randomly assigned to receive injections of 100 units of Botox (20 injections of 5 units each) or placebo. At 12 weeks, patients who received Botox had 1.6 to 1.9 fewer incidents of incontinence per day, and also needed to urinate less frequently.
The treatment needs to be repeated to maintain effectiveness; the FDA recommends at least 12 weeks between injections. Side effects during trials included urinary tract infections, painful urination, and urinary retention.
Patients must take antibiotics before, during, and a few days after Botox treatment to reduce infection risk.
On Twitter @aliciaault
The Food and Drug Administration on Jan. 18 approved Botox for patients with overactive bladder who have contraindications to or don’t respond to anticholinergics.
"Clinical studies have demonstrated Botox’s ability to significantly reduce the frequency of urinary incontinence," Dr. Hylton V. Joffe, director of the Division of Reproductive and Urologic Products in the Food and Drug Administration’s Center for Drug Evaluation and Research, said in a statement.
"With the approval of Botox [onabotulinumtoxinA], we have a new treatment option to offer these patients that has demonstrated efficacy in reducing urinary leakage and other symptoms of OAB with the effect lasting up to 6 months," Dr. Victor Nitti, vice chairman in the department of urology at NYU Langone Medical Center, said in a statement released by Botox maker Allergan.
Overactive bladder (OAB) results in an uncontrolled urge to urinate, frequent urination, and uncontrollable leakage of urine, according to the Allergan statement. About 14.7 million American adults have overactive bladder, and 3.3 million use anticholinergics; however, at least half of them stop taking the drugs within a year because of intolerance.
Botox injected into the bladder muscle relaxes the organ and increases its storage capacity, thus reducing incontinence, according to the FDA. The Botox is injected via cystoscopy.
The FDA evaluated the drug’s safety and efficacy for overactive bladder through two studies in which 1,105 patients were randomly assigned to receive injections of 100 units of Botox (20 injections of 5 units each) or placebo. At 12 weeks, patients who received Botox had 1.6 to 1.9 fewer incidents of incontinence per day, and also needed to urinate less frequently.
The treatment needs to be repeated to maintain effectiveness; the FDA recommends at least 12 weeks between injections. Side effects during trials included urinary tract infections, painful urination, and urinary retention.
Patients must take antibiotics before, during, and a few days after Botox treatment to reduce infection risk.
On Twitter @aliciaault
Obama gun control proposal addresses doctors' concerns
President Obama’s wide range of proposals to address gun violence in the United States included a clarification that physicians should be allowed to discuss firearm safety with their patients.
The plan states, "Doctors and other health care providers also need to be able to ask about firearms in their patients’ homes and safe storage of those firearms, especially if their patients show signs of certain mental illnesses or if they have a young child or mentally ill family member at home."
The clarification was issued in response to recent concerns that the Affordable Care Act prohibited physicians from asking about firearms in the home. That is not true, according to the White House, which also added that "the administration will issue guidance clarifying that the Affordable Care Act does not prohibit or otherwise regulate communication between doctors and patients, including about firearms."

Several groups representing physicians, including the American Psychiatric Association, the American Academy of Family Physicians, the American Academy of Pediatrics, and the American College of Physicians, praised the administration’s initiatives.
"We are glad that the president has clarified that doctors are not prohibited from asking their patients about guns in their homes," Dr. Dilip V. Jeste, president of the APA, said in a statement. "The APA has consistently advocated for such a position."
In a statement, the ACP said that "state governments must also do their part, by not imposing restrictions on engaging in such discussions with their patients, as some state legislatures have attempted to do."
"Family physicians need to be able to have appropriate medical conversations with our patients about gun safety, and researchers need the ability to study gun safety," said Dr. Jeffrey Cain, president of the American Academy of Family Physicians (AAFP), in a recent blog post, calling for a broader recognition of gun violence as a public health issue.
Physician organizations also said they supported the President’s executive order directing the Centers for Disease Control and Prevention to study gun violence. In his remarks, the president said, "While year after year, those who oppose even modest gun safety measures have threatened to defund scientific or medical research into the causes of gun violence, I will direct the Centers for Disease Control to go ahead and study the best ways to reduce it."
In addition, the proposal seeks $10 million from Congress for CDC to research the relationship between video games, media images, and violence, and $20 million from Congress to expand the National Violent Death Reporting System to all 50 states.
As part of the gun control package, the president also issued executive orders seeking reviews of gun locks and other safety technologies. He is asking Congress to reinstate the assault weapons ban and to limit large-capacity ammunition magazines.
Congress also will have to approve several other proposals, including $55 million for a new initiative (Project AWARE), which covers teacher training and coordination of referrals to make sure students get mental health treatment, $25 million for state-based strategies to support young adults with mental health or substance abuse issues, and $25 million for student mental health services. The president also wants Congress to provide $50 million to train 5,000 mental health professionals who can target children and young adults.

The proposal also emphasized the need for parity of mental health coverage with medical and surgical health benefits, and noted that the administration intends to issue soon the final regulations for the Mental Health Parity and Addiction Equity Act of 2008. Parity will be further fleshed out under the essential benefits requirements called for by the Affordable Care Act, according to the proposal. A final rule on the essential health benefits package is expected in February.
"We are heartened that the administration plans to finalize rules governing mental health parity under the 2008 Mental Health Parity and Addiction Equity Act, the Affordable Care Act, and Medicaid," said Dr. Jeste of the APA. "We strongly urge the administration to close loopholes involving so-called ‘nonquantitative treatment limits’ and to ensure that health plans deliver a full scope of mental health services in order to comply with the law."
The ACP said that it also has long supported parity and increased access to mental health services, especially for young adults. The organization said in its statement that it "agrees on the urgency of adoption of policies that include these and other measures and is committed to being part of the change outlined by the president."
The AAP said that it was pleased that the proposals reflected recommendations the group made during a Jan. 3 meeting with the White House Task Force on Gun Violence Prevention.
In a statement, Dr. Thomas K. McInerny, AAP president said, "The AAP agrees with the President that we must improve the identification of mental illnesses through increased screening, address inadequate insurance coverage and high out-of-pocket costs that create barriers to access, strengthen the overall quality of mental health access, and improve and expand the Medicaid reimbursement policy to include mental health and developmental services."
On Twitter @aliciaault
President Obama’s wide range of proposals to address gun violence in the United States included a clarification that physicians should be allowed to discuss firearm safety with their patients.
The plan states, "Doctors and other health care providers also need to be able to ask about firearms in their patients’ homes and safe storage of those firearms, especially if their patients show signs of certain mental illnesses or if they have a young child or mentally ill family member at home."
The clarification was issued in response to recent concerns that the Affordable Care Act prohibited physicians from asking about firearms in the home. That is not true, according to the White House, which also added that "the administration will issue guidance clarifying that the Affordable Care Act does not prohibit or otherwise regulate communication between doctors and patients, including about firearms."
Several groups representing physicians, including the American Psychiatric Association, the American Academy of Family Physicians, the American Academy of Pediatrics, and the American College of Physicians, praised the administration’s initiatives.
"We are glad that the president has clarified that doctors are not prohibited from asking their patients about guns in their homes," Dr. Dilip V. Jeste, president of the APA, said in a statement. "The APA has consistently advocated for such a position."
In a statement, the ACP said that "state governments must also do their part, by not imposing restrictions on engaging in such discussions with their patients, as some state legislatures have attempted to do."
"Family physicians need to be able to have appropriate medical conversations with our patients about gun safety, and researchers need the ability to study gun safety," said Dr. Jeffrey Cain, president of the American Academy of Family Physicians (AAFP), in a recent blog post, calling for a broader recognition of gun violence as a public health issue.
Physician organizations also said they supported the President’s executive order directing the Centers for Disease Control and Prevention to study gun violence. In his remarks, the president said, "While year after year, those who oppose even modest gun safety measures have threatened to defund scientific or medical research into the causes of gun violence, I will direct the Centers for Disease Control to go ahead and study the best ways to reduce it."
In addition, the proposal seeks $10 million from Congress for CDC to research the relationship between video games, media images, and violence, and $20 million from Congress to expand the National Violent Death Reporting System to all 50 states.
As part of the gun control package, the president also issued executive orders seeking reviews of gun locks and other safety technologies. He is asking Congress to reinstate the assault weapons ban and to limit large-capacity ammunition magazines.
Congress also will have to approve several other proposals, including $55 million for a new initiative (Project AWARE), which covers teacher training and coordination of referrals to make sure students get mental health treatment, $25 million for state-based strategies to support young adults with mental health or substance abuse issues, and $25 million for student mental health services. The president also wants Congress to provide $50 million to train 5,000 mental health professionals who can target children and young adults.
The proposal also emphasized the need for parity of mental health coverage with medical and surgical health benefits, and noted that the administration intends to issue soon the final regulations for the Mental Health Parity and Addiction Equity Act of 2008. Parity will be further fleshed out under the essential benefits requirements called for by the Affordable Care Act, according to the proposal. A final rule on the essential health benefits package is expected in February.
"We are heartened that the administration plans to finalize rules governing mental health parity under the 2008 Mental Health Parity and Addiction Equity Act, the Affordable Care Act, and Medicaid," said Dr. Jeste of the APA. "We strongly urge the administration to close loopholes involving so-called ‘nonquantitative treatment limits’ and to ensure that health plans deliver a full scope of mental health services in order to comply with the law."
The ACP said that it also has long supported parity and increased access to mental health services, especially for young adults. The organization said in its statement that it "agrees on the urgency of adoption of policies that include these and other measures and is committed to being part of the change outlined by the president."
The AAP said that it was pleased that the proposals reflected recommendations the group made during a Jan. 3 meeting with the White House Task Force on Gun Violence Prevention.
In a statement, Dr. Thomas K. McInerny, AAP president said, "The AAP agrees with the President that we must improve the identification of mental illnesses through increased screening, address inadequate insurance coverage and high out-of-pocket costs that create barriers to access, strengthen the overall quality of mental health access, and improve and expand the Medicaid reimbursement policy to include mental health and developmental services."
On Twitter @aliciaault
President Obama’s wide range of proposals to address gun violence in the United States included a clarification that physicians should be allowed to discuss firearm safety with their patients.
The plan states, "Doctors and other health care providers also need to be able to ask about firearms in their patients’ homes and safe storage of those firearms, especially if their patients show signs of certain mental illnesses or if they have a young child or mentally ill family member at home."
The clarification was issued in response to recent concerns that the Affordable Care Act prohibited physicians from asking about firearms in the home. That is not true, according to the White House, which also added that "the administration will issue guidance clarifying that the Affordable Care Act does not prohibit or otherwise regulate communication between doctors and patients, including about firearms."
Several groups representing physicians, including the American Psychiatric Association, the American Academy of Family Physicians, the American Academy of Pediatrics, and the American College of Physicians, praised the administration’s initiatives.
"We are glad that the president has clarified that doctors are not prohibited from asking their patients about guns in their homes," Dr. Dilip V. Jeste, president of the APA, said in a statement. "The APA has consistently advocated for such a position."
In a statement, the ACP said that "state governments must also do their part, by not imposing restrictions on engaging in such discussions with their patients, as some state legislatures have attempted to do."
"Family physicians need to be able to have appropriate medical conversations with our patients about gun safety, and researchers need the ability to study gun safety," said Dr. Jeffrey Cain, president of the American Academy of Family Physicians (AAFP), in a recent blog post, calling for a broader recognition of gun violence as a public health issue.
Physician organizations also said they supported the President’s executive order directing the Centers for Disease Control and Prevention to study gun violence. In his remarks, the president said, "While year after year, those who oppose even modest gun safety measures have threatened to defund scientific or medical research into the causes of gun violence, I will direct the Centers for Disease Control to go ahead and study the best ways to reduce it."
In addition, the proposal seeks $10 million from Congress for CDC to research the relationship between video games, media images, and violence, and $20 million from Congress to expand the National Violent Death Reporting System to all 50 states.
As part of the gun control package, the president also issued executive orders seeking reviews of gun locks and other safety technologies. He is asking Congress to reinstate the assault weapons ban and to limit large-capacity ammunition magazines.
Congress also will have to approve several other proposals, including $55 million for a new initiative (Project AWARE), which covers teacher training and coordination of referrals to make sure students get mental health treatment, $25 million for state-based strategies to support young adults with mental health or substance abuse issues, and $25 million for student mental health services. The president also wants Congress to provide $50 million to train 5,000 mental health professionals who can target children and young adults.
The proposal also emphasized the need for parity of mental health coverage with medical and surgical health benefits, and noted that the administration intends to issue soon the final regulations for the Mental Health Parity and Addiction Equity Act of 2008. Parity will be further fleshed out under the essential benefits requirements called for by the Affordable Care Act, according to the proposal. A final rule on the essential health benefits package is expected in February.
"We are heartened that the administration plans to finalize rules governing mental health parity under the 2008 Mental Health Parity and Addiction Equity Act, the Affordable Care Act, and Medicaid," said Dr. Jeste of the APA. "We strongly urge the administration to close loopholes involving so-called ‘nonquantitative treatment limits’ and to ensure that health plans deliver a full scope of mental health services in order to comply with the law."
The ACP said that it also has long supported parity and increased access to mental health services, especially for young adults. The organization said in its statement that it "agrees on the urgency of adoption of policies that include these and other measures and is committed to being part of the change outlined by the president."
The AAP said that it was pleased that the proposals reflected recommendations the group made during a Jan. 3 meeting with the White House Task Force on Gun Violence Prevention.
In a statement, Dr. Thomas K. McInerny, AAP president said, "The AAP agrees with the President that we must improve the identification of mental illnesses through increased screening, address inadequate insurance coverage and high out-of-pocket costs that create barriers to access, strengthen the overall quality of mental health access, and improve and expand the Medicaid reimbursement policy to include mental health and developmental services."
On Twitter @aliciaault

Primary care inaccurately estimates cancer risk
Primary care physicians’ assessments of the risks and benefits of cancer screening didn’t match with reality, based on the results of a survey of beliefs and behaviors around cancer risk.
"We were really surprised at the high percentage of physicians who were inaccurately estimating risk," said Dr. Laura-Mae Baldwin, professor of family medicine at the University of Washington, Seattle, who presented on behalf of her colleagues a slice of data from the survey of 3,200 physicians. "This has the potential for average-risk patients to receive unnecessary testing, and for high-risk patients to miss opportunities for prevention or early detection."

The cross-sectional national survey used the 2008 American Medical Association master file to randomly sample family physicians, general internists, and obstetrician-gynecologists. The physicians were all under age 65 and practiced in either a hospital or an office. They were contacted by mail, and given encouragement in the form of a $20 bill. In a second mailing, nonresponders received a written note from Dr. Baldwin. Overall, there was a 62% response rate: 591 family physicians, 414 general internists, and 569 ob.gyns. took part.
Survey participants were given a 12-page booklet with a particular patient vignette and a photo of the patient. The example included a medical and family history, along with age, race, sex, insurance status, and some other characteristics.
The researchers focused on ovarian cancer in particular because the Centers for Disease Control and Prevention, which funded the study, had a special interest in that cancer.
For instance, one vignette presented a 51-year-old white woman who came in because she wanted to be sure she was up to date on various tests. She had no medical problems, but had not seen a physician in 3 years. Her father had hypertension and her mother died of ovarian cancer at age 65. The other family history was negative, and there was an unremarkable physical exam.
The researchers had 258 variations for the different vignettes, varying age, race, insurance status, whether the patient asked for ovarian cancer screening, and family history. Physicians were asked to give their best estimate for this patient, and for other example patients, of risk for breast, ovarian, and colon cancer. They were asked to state whether the patient had a risk that was the same as that of the general population, somewhat higher, or much higher.
For a woman who was at the same risk as the general population for ovarian cancer, 72% of physicians were in agreement. However, 26% estimated the women were at somewhat higher risk and 1%, at much higher risk. For women at somewhat higher risk for ovarian cancer, however, 7% of physicians correctly assessed risk. Risk was assessed as somewhat higher or much higher by 90%, Dr. Baldwin reported at the annual meeting of the North American Primary Care Research Group.
For a woman at high risk for ovarian cancer, 35% of physicians correctly estimated that risk. Most physicians estimated risk as somewhat higher, but 11% thought her risk was the same as that for the general population.
The assessments of risk for colon cancer were similarly inaccurate. For the vignette of the woman at the same risk as the general population, 62% of physicians were on target, and 39% overestimated the risk.
There were no significant differences among the specialties, but ob.gyns. tended to be more accurate in their screening decisions, said Dr. Baldwin. An analysis showed that providers’ personal history with cancer influenced their recommended screening behaviors, said Dr. Baldwin. She did not present specific data on that issue.
The study did have some limitations in that physicians were given somewhat limited information about the patient’s risk. Dr. Baldwin said it’s important to study physician behaviors further, especially since so many in the survey underestimated risk in a woman who clearly was at high risk for ovarian cancer.
Primary care physicians’ assessments of the risks and benefits of cancer screening didn’t match with reality, based on the results of a survey of beliefs and behaviors around cancer risk.
"We were really surprised at the high percentage of physicians who were inaccurately estimating risk," said Dr. Laura-Mae Baldwin, professor of family medicine at the University of Washington, Seattle, who presented on behalf of her colleagues a slice of data from the survey of 3,200 physicians. "This has the potential for average-risk patients to receive unnecessary testing, and for high-risk patients to miss opportunities for prevention or early detection."
The cross-sectional national survey used the 2008 American Medical Association master file to randomly sample family physicians, general internists, and obstetrician-gynecologists. The physicians were all under age 65 and practiced in either a hospital or an office. They were contacted by mail, and given encouragement in the form of a $20 bill. In a second mailing, nonresponders received a written note from Dr. Baldwin. Overall, there was a 62% response rate: 591 family physicians, 414 general internists, and 569 ob.gyns. took part.
Survey participants were given a 12-page booklet with a particular patient vignette and a photo of the patient. The example included a medical and family history, along with age, race, sex, insurance status, and some other characteristics.
The researchers focused on ovarian cancer in particular because the Centers for Disease Control and Prevention, which funded the study, had a special interest in that cancer.
For instance, one vignette presented a 51-year-old white woman who came in because she wanted to be sure she was up to date on various tests. She had no medical problems, but had not seen a physician in 3 years. Her father had hypertension and her mother died of ovarian cancer at age 65. The other family history was negative, and there was an unremarkable physical exam.
The researchers had 258 variations for the different vignettes, varying age, race, insurance status, whether the patient asked for ovarian cancer screening, and family history. Physicians were asked to give their best estimate for this patient, and for other example patients, of risk for breast, ovarian, and colon cancer. They were asked to state whether the patient had a risk that was the same as that of the general population, somewhat higher, or much higher.
For a woman who was at the same risk as the general population for ovarian cancer, 72% of physicians were in agreement. However, 26% estimated the women were at somewhat higher risk and 1%, at much higher risk. For women at somewhat higher risk for ovarian cancer, however, 7% of physicians correctly assessed risk. Risk was assessed as somewhat higher or much higher by 90%, Dr. Baldwin reported at the annual meeting of the North American Primary Care Research Group.
For a woman at high risk for ovarian cancer, 35% of physicians correctly estimated that risk. Most physicians estimated risk as somewhat higher, but 11% thought her risk was the same as that for the general population.
The assessments of risk for colon cancer were similarly inaccurate. For the vignette of the woman at the same risk as the general population, 62% of physicians were on target, and 39% overestimated the risk.
There were no significant differences among the specialties, but ob.gyns. tended to be more accurate in their screening decisions, said Dr. Baldwin. An analysis showed that providers’ personal history with cancer influenced their recommended screening behaviors, said Dr. Baldwin. She did not present specific data on that issue.
The study did have some limitations in that physicians were given somewhat limited information about the patient’s risk. Dr. Baldwin said it’s important to study physician behaviors further, especially since so many in the survey underestimated risk in a woman who clearly was at high risk for ovarian cancer.
Primary care physicians’ assessments of the risks and benefits of cancer screening didn’t match with reality, based on the results of a survey of beliefs and behaviors around cancer risk.
"We were really surprised at the high percentage of physicians who were inaccurately estimating risk," said Dr. Laura-Mae Baldwin, professor of family medicine at the University of Washington, Seattle, who presented on behalf of her colleagues a slice of data from the survey of 3,200 physicians. "This has the potential for average-risk patients to receive unnecessary testing, and for high-risk patients to miss opportunities for prevention or early detection."
The cross-sectional national survey used the 2008 American Medical Association master file to randomly sample family physicians, general internists, and obstetrician-gynecologists. The physicians were all under age 65 and practiced in either a hospital or an office. They were contacted by mail, and given encouragement in the form of a $20 bill. In a second mailing, nonresponders received a written note from Dr. Baldwin. Overall, there was a 62% response rate: 591 family physicians, 414 general internists, and 569 ob.gyns. took part.
Survey participants were given a 12-page booklet with a particular patient vignette and a photo of the patient. The example included a medical and family history, along with age, race, sex, insurance status, and some other characteristics.
The researchers focused on ovarian cancer in particular because the Centers for Disease Control and Prevention, which funded the study, had a special interest in that cancer.
For instance, one vignette presented a 51-year-old white woman who came in because she wanted to be sure she was up to date on various tests. She had no medical problems, but had not seen a physician in 3 years. Her father had hypertension and her mother died of ovarian cancer at age 65. The other family history was negative, and there was an unremarkable physical exam.
The researchers had 258 variations for the different vignettes, varying age, race, insurance status, whether the patient asked for ovarian cancer screening, and family history. Physicians were asked to give their best estimate for this patient, and for other example patients, of risk for breast, ovarian, and colon cancer. They were asked to state whether the patient had a risk that was the same as that of the general population, somewhat higher, or much higher.
For a woman who was at the same risk as the general population for ovarian cancer, 72% of physicians were in agreement. However, 26% estimated the women were at somewhat higher risk and 1%, at much higher risk. For women at somewhat higher risk for ovarian cancer, however, 7% of physicians correctly assessed risk. Risk was assessed as somewhat higher or much higher by 90%, Dr. Baldwin reported at the annual meeting of the North American Primary Care Research Group.
For a woman at high risk for ovarian cancer, 35% of physicians correctly estimated that risk. Most physicians estimated risk as somewhat higher, but 11% thought her risk was the same as that for the general population.
The assessments of risk for colon cancer were similarly inaccurate. For the vignette of the woman at the same risk as the general population, 62% of physicians were on target, and 39% overestimated the risk.
There were no significant differences among the specialties, but ob.gyns. tended to be more accurate in their screening decisions, said Dr. Baldwin. An analysis showed that providers’ personal history with cancer influenced their recommended screening behaviors, said Dr. Baldwin. She did not present specific data on that issue.
The study did have some limitations in that physicians were given somewhat limited information about the patient’s risk. Dr. Baldwin said it’s important to study physician behaviors further, especially since so many in the survey underestimated risk in a woman who clearly was at high risk for ovarian cancer.
AT THE ANNUAL MEETING OF THE NORTH AMERICAN PRIMARY CARE RESEARCH GROUP
Major Finding: For a woman at high risk for ovarian cancer, 35% of surveyed physicians correctly estimated that risk, and 11% thought her risk was the same as that for the general population.
Data Source: Data from a national, cross-sectional survey of 3,200 physicians.
Disclosures: The study was funded by the Centers for Disease Control and Prevention.

Newly labeled sunscreens surface on shelves
Sunscreens that have proven their protective ability and feature updated, more-consumer-friendly labeling are hitting store shelves, but they currently share space with older products that may not have passed muster with the Food and Drug Administration.
This mix of old and new packaging coincides with an FDA announcement that, later this year, it will review sunscreen ingredient safety and the potential approval of additional UVA-blocking agents.
In January, the agency issued its semiannual agenda for the coming year. That list included two sunscreen-related items.
The FDA said it would issue an "advance notice of proposed rulemaking" in July on how it will address sunscreen ingredient safety, which is the first step in a three-step process that culminates in a final rule.
The agency also said it would take a similar early step in the regulatory process for new ingredients manufacturers would like to add to their products.
At least six additional UVA filters are awaiting FDA approval, said Dr. Steven Q. Wang, director of dermatologic surgery and dermatology at the Memorial Sloan-Kettering Cancer Center, Basking Ridge, N.J. Currently, only two UVA-blocking agents – avobenzone and zinc oxide – are approved in the United States, but many others are available in Europe and elsewhere around the world.
Dr. Wang said he is looking forward to progress on UVA blockers; he noted that although both UVA and UVB contribute to skin cancer development, UVA penetrates deeper into the skin, contributes to more DNA damage, and plays a larger role in skin aging. A study of sunscreens from 1997 to 2009 by Dr. Wang showed that increasing numbers of products contained either avobenzone or zinc oxide, matching their claims of UVA protection.
In the late 1990s, 81% of the products surveyed claimed to protect against UVA, but only 5% actually contained a UVA blocker. By 2009, 80% of the products still made the claim, and 70% contained UVA-blocking agents. The study was published in the January issue of the journal Photochemical & Photobiological Sciences (Photochem. Photobiol. Sci. 2013;12:197-202).

Based on these findings, many of the products on the market in the past decade already met the FDA’s new criteria – announced in June 2011 – to claim protection against skin cancer, Dr. Wang said. And, clinicians and consumers should be reassured that products that meet the FDA labeling rules are effective and safe, he added.
Because they have already met the FDA’s effectiveness criteria, most products have not needed to be reformulated, said Farah Ahmed, chair of the sunscreen task force at the Personal Care Products Council.
But manufacturers have relabeled products to conform to the FDA’s rules, she said. The Council estimates that at least 4,500 products marketed in the United States claim an SPF, which subjects them to the FDA sunscreen rules. The product list includes not only sunscreens but lip balms, daily moisturizers, makeup, and any other product that contains a sunscreen component.
Products that have proved through testing that they protect against UVA and UVB radiation can claim that they are "broad spectrum" and will be labeled as SPF 15 or higher. The label also will be able to claim that the product can protect against sunburn, and, if used as directed with other sun protection measures, can reduce the risk of skin cancer and early skin aging.
Any product not labeled as "broad spectrum" or that has an SPF value between 2 and 14 will carry a warning: "Skin Cancer/Skin Aging Alert: Spending time in the sun increases your risk of skin cancer and early skin aging. This product has been shown only to help prevent sunburn, not skin cancer or early skin aging."
Under the revised labeling, no product can claim to be waterproof or sweatproof. If a product claims to be water resistant, the product’s label must state how long a user "can expect to get the declared SPF level of protection while swimming or sweating, based on standard testing," according to the FDA.
For more information, visit the agency’s website.
There may still be products on store shelves that have the old labeling, said Ms. Ahmed. That’s because the FDA has allowed a phase-in. Retailers also can choose to sell remaining stocks of the old products or remove them. "I think we’ll continue to see a mix of both products on the shelves," said Ms. Ahmed.
The situation creates the potential for confusion among consumers, although the FDA rules were meant to create a uniform label to help increase sun protection knowledge and the use of sun protection products.
Dr. Wang says he is telling patients to look for products that are labeled "broad spectrum" on the front, which is the best indicator that they are newly labeled and in compliance with FDA rules.
The FDA has been criticized for years for not finalizing the "monograph" – the accepted criteria or recipe – for sunscreen products. Although a final monograph is nowhere in sight, Dr. Wang said that he thought the agency had "done a reasonable job" in setting the cutoff point for products that could claim UVA protection against cancer at the accepted wavelength of 370 nm.
The FDA also plans to examine whether products labeled with an SPF greater than 50 provide any better protection than an SPF 50 sunscreen. The agency proposed in June 2011 that sunscreens with an SPF greater than 50 be labeled "SPF 50-plus," but nothing further has been issued. For now, consumers will continue to see sunscreens labeled as SPF 70, 80, or even 100.
There has been some difference of opinion on whether higher-SPF products are more beneficial. Dr. Wang said he recommends an SPF 30 product for daily use, but suggests higher SPFs for recreational activities that put users in the sun for longer periods.
The FDA also asked for more data on sunscreen-containing wipes, powders, body washes, and shampoos.
Finally, there may be some controversy down the road when the agency takes a closer look at the safety of ingredients in sun protection products. The Washington-based Environmental Working Group has criticized the safety of some of those ingredients – in particular oxybenzone and retinyl palmitate – and did so again last year in its annual review of sunscreens.
The American Academy of Dermatology refuted the group, saying that there is no evidence that these ingredients are dangerous. The AAD backs the use of a water-resistant, broad-spectrum sunscreen that protects against UVA and UVB radiation, with an SPF 30 or higher, in conjunction with limiting sun exposure and wearing sun-protective clothing.
Dr. Wang agrees that oxybenzone and retinyl palmitate appear to be safe, but he says that some manufacturers have been removing the vitamin A derivative because of the bad publicity. Oxybenzone also may be removed as newer UVA blockers are approved, he said. "But right now, we don’t have any other alternatives," he noted.
For help selecting and using sunscreens effectively, click here.
Dr. Wang disclosed that he is a consultant for L’Oreal, and that he has collaborated with researchers at Procter & Gamble, but has not received any compensation from that company.
On Twitter @aliciaault
Sunscreens that have proven their protective ability and feature updated, more-consumer-friendly labeling are hitting store shelves, but they currently share space with older products that may not have passed muster with the Food and Drug Administration.
This mix of old and new packaging coincides with an FDA announcement that, later this year, it will review sunscreen ingredient safety and the potential approval of additional UVA-blocking agents.
In January, the agency issued its semiannual agenda for the coming year. That list included two sunscreen-related items.
The FDA said it would issue an "advance notice of proposed rulemaking" in July on how it will address sunscreen ingredient safety, which is the first step in a three-step process that culminates in a final rule.
The agency also said it would take a similar early step in the regulatory process for new ingredients manufacturers would like to add to their products.
At least six additional UVA filters are awaiting FDA approval, said Dr. Steven Q. Wang, director of dermatologic surgery and dermatology at the Memorial Sloan-Kettering Cancer Center, Basking Ridge, N.J. Currently, only two UVA-blocking agents – avobenzone and zinc oxide – are approved in the United States, but many others are available in Europe and elsewhere around the world.
Dr. Wang said he is looking forward to progress on UVA blockers; he noted that although both UVA and UVB contribute to skin cancer development, UVA penetrates deeper into the skin, contributes to more DNA damage, and plays a larger role in skin aging. A study of sunscreens from 1997 to 2009 by Dr. Wang showed that increasing numbers of products contained either avobenzone or zinc oxide, matching their claims of UVA protection.
In the late 1990s, 81% of the products surveyed claimed to protect against UVA, but only 5% actually contained a UVA blocker. By 2009, 80% of the products still made the claim, and 70% contained UVA-blocking agents. The study was published in the January issue of the journal Photochemical & Photobiological Sciences (Photochem. Photobiol. Sci. 2013;12:197-202).
Based on these findings, many of the products on the market in the past decade already met the FDA’s new criteria – announced in June 2011 – to claim protection against skin cancer, Dr. Wang said. And, clinicians and consumers should be reassured that products that meet the FDA labeling rules are effective and safe, he added.
Because they have already met the FDA’s effectiveness criteria, most products have not needed to be reformulated, said Farah Ahmed, chair of the sunscreen task force at the Personal Care Products Council.
But manufacturers have relabeled products to conform to the FDA’s rules, she said. The Council estimates that at least 4,500 products marketed in the United States claim an SPF, which subjects them to the FDA sunscreen rules. The product list includes not only sunscreens but lip balms, daily moisturizers, makeup, and any other product that contains a sunscreen component.
Products that have proved through testing that they protect against UVA and UVB radiation can claim that they are "broad spectrum" and will be labeled as SPF 15 or higher. The label also will be able to claim that the product can protect against sunburn, and, if used as directed with other sun protection measures, can reduce the risk of skin cancer and early skin aging.
Any product not labeled as "broad spectrum" or that has an SPF value between 2 and 14 will carry a warning: "Skin Cancer/Skin Aging Alert: Spending time in the sun increases your risk of skin cancer and early skin aging. This product has been shown only to help prevent sunburn, not skin cancer or early skin aging."
Under the revised labeling, no product can claim to be waterproof or sweatproof. If a product claims to be water resistant, the product’s label must state how long a user "can expect to get the declared SPF level of protection while swimming or sweating, based on standard testing," according to the FDA.
For more information, visit the agency’s website.
There may still be products on store shelves that have the old labeling, said Ms. Ahmed. That’s because the FDA has allowed a phase-in. Retailers also can choose to sell remaining stocks of the old products or remove them. "I think we’ll continue to see a mix of both products on the shelves," said Ms. Ahmed.
The situation creates the potential for confusion among consumers, although the FDA rules were meant to create a uniform label to help increase sun protection knowledge and the use of sun protection products.
Dr. Wang says he is telling patients to look for products that are labeled "broad spectrum" on the front, which is the best indicator that they are newly labeled and in compliance with FDA rules.
The FDA has been criticized for years for not finalizing the "monograph" – the accepted criteria or recipe – for sunscreen products. Although a final monograph is nowhere in sight, Dr. Wang said that he thought the agency had "done a reasonable job" in setting the cutoff point for products that could claim UVA protection against cancer at the accepted wavelength of 370 nm.
The FDA also plans to examine whether products labeled with an SPF greater than 50 provide any better protection than an SPF 50 sunscreen. The agency proposed in June 2011 that sunscreens with an SPF greater than 50 be labeled "SPF 50-plus," but nothing further has been issued. For now, consumers will continue to see sunscreens labeled as SPF 70, 80, or even 100.
There has been some difference of opinion on whether higher-SPF products are more beneficial. Dr. Wang said he recommends an SPF 30 product for daily use, but suggests higher SPFs for recreational activities that put users in the sun for longer periods.
The FDA also asked for more data on sunscreen-containing wipes, powders, body washes, and shampoos.
Finally, there may be some controversy down the road when the agency takes a closer look at the safety of ingredients in sun protection products. The Washington-based Environmental Working Group has criticized the safety of some of those ingredients – in particular oxybenzone and retinyl palmitate – and did so again last year in its annual review of sunscreens.
The American Academy of Dermatology refuted the group, saying that there is no evidence that these ingredients are dangerous. The AAD backs the use of a water-resistant, broad-spectrum sunscreen that protects against UVA and UVB radiation, with an SPF 30 or higher, in conjunction with limiting sun exposure and wearing sun-protective clothing.
Dr. Wang agrees that oxybenzone and retinyl palmitate appear to be safe, but he says that some manufacturers have been removing the vitamin A derivative because of the bad publicity. Oxybenzone also may be removed as newer UVA blockers are approved, he said. "But right now, we don’t have any other alternatives," he noted.
For help selecting and using sunscreens effectively, click here.
Dr. Wang disclosed that he is a consultant for L’Oreal, and that he has collaborated with researchers at Procter & Gamble, but has not received any compensation from that company.
On Twitter @aliciaault
Sunscreens that have proven their protective ability and feature updated, more-consumer-friendly labeling are hitting store shelves, but they currently share space with older products that may not have passed muster with the Food and Drug Administration.
This mix of old and new packaging coincides with an FDA announcement that, later this year, it will review sunscreen ingredient safety and the potential approval of additional UVA-blocking agents.
In January, the agency issued its semiannual agenda for the coming year. That list included two sunscreen-related items.
The FDA said it would issue an "advance notice of proposed rulemaking" in July on how it will address sunscreen ingredient safety, which is the first step in a three-step process that culminates in a final rule.
The agency also said it would take a similar early step in the regulatory process for new ingredients manufacturers would like to add to their products.
At least six additional UVA filters are awaiting FDA approval, said Dr. Steven Q. Wang, director of dermatologic surgery and dermatology at the Memorial Sloan-Kettering Cancer Center, Basking Ridge, N.J. Currently, only two UVA-blocking agents – avobenzone and zinc oxide – are approved in the United States, but many others are available in Europe and elsewhere around the world.
Dr. Wang said he is looking forward to progress on UVA blockers; he noted that although both UVA and UVB contribute to skin cancer development, UVA penetrates deeper into the skin, contributes to more DNA damage, and plays a larger role in skin aging. A study of sunscreens from 1997 to 2009 by Dr. Wang showed that increasing numbers of products contained either avobenzone or zinc oxide, matching their claims of UVA protection.
In the late 1990s, 81% of the products surveyed claimed to protect against UVA, but only 5% actually contained a UVA blocker. By 2009, 80% of the products still made the claim, and 70% contained UVA-blocking agents. The study was published in the January issue of the journal Photochemical & Photobiological Sciences (Photochem. Photobiol. Sci. 2013;12:197-202).
Based on these findings, many of the products on the market in the past decade already met the FDA’s new criteria – announced in June 2011 – to claim protection against skin cancer, Dr. Wang said. And, clinicians and consumers should be reassured that products that meet the FDA labeling rules are effective and safe, he added.
Because they have already met the FDA’s effectiveness criteria, most products have not needed to be reformulated, said Farah Ahmed, chair of the sunscreen task force at the Personal Care Products Council.
But manufacturers have relabeled products to conform to the FDA’s rules, she said. The Council estimates that at least 4,500 products marketed in the United States claim an SPF, which subjects them to the FDA sunscreen rules. The product list includes not only sunscreens but lip balms, daily moisturizers, makeup, and any other product that contains a sunscreen component.
Products that have proved through testing that they protect against UVA and UVB radiation can claim that they are "broad spectrum" and will be labeled as SPF 15 or higher. The label also will be able to claim that the product can protect against sunburn, and, if used as directed with other sun protection measures, can reduce the risk of skin cancer and early skin aging.
Any product not labeled as "broad spectrum" or that has an SPF value between 2 and 14 will carry a warning: "Skin Cancer/Skin Aging Alert: Spending time in the sun increases your risk of skin cancer and early skin aging. This product has been shown only to help prevent sunburn, not skin cancer or early skin aging."
Under the revised labeling, no product can claim to be waterproof or sweatproof. If a product claims to be water resistant, the product’s label must state how long a user "can expect to get the declared SPF level of protection while swimming or sweating, based on standard testing," according to the FDA.
For more information, visit the agency’s website.
There may still be products on store shelves that have the old labeling, said Ms. Ahmed. That’s because the FDA has allowed a phase-in. Retailers also can choose to sell remaining stocks of the old products or remove them. "I think we’ll continue to see a mix of both products on the shelves," said Ms. Ahmed.
The situation creates the potential for confusion among consumers, although the FDA rules were meant to create a uniform label to help increase sun protection knowledge and the use of sun protection products.
Dr. Wang says he is telling patients to look for products that are labeled "broad spectrum" on the front, which is the best indicator that they are newly labeled and in compliance with FDA rules.
The FDA has been criticized for years for not finalizing the "monograph" – the accepted criteria or recipe – for sunscreen products. Although a final monograph is nowhere in sight, Dr. Wang said that he thought the agency had "done a reasonable job" in setting the cutoff point for products that could claim UVA protection against cancer at the accepted wavelength of 370 nm.
The FDA also plans to examine whether products labeled with an SPF greater than 50 provide any better protection than an SPF 50 sunscreen. The agency proposed in June 2011 that sunscreens with an SPF greater than 50 be labeled "SPF 50-plus," but nothing further has been issued. For now, consumers will continue to see sunscreens labeled as SPF 70, 80, or even 100.
There has been some difference of opinion on whether higher-SPF products are more beneficial. Dr. Wang said he recommends an SPF 30 product for daily use, but suggests higher SPFs for recreational activities that put users in the sun for longer periods.
The FDA also asked for more data on sunscreen-containing wipes, powders, body washes, and shampoos.
Finally, there may be some controversy down the road when the agency takes a closer look at the safety of ingredients in sun protection products. The Washington-based Environmental Working Group has criticized the safety of some of those ingredients – in particular oxybenzone and retinyl palmitate – and did so again last year in its annual review of sunscreens.
The American Academy of Dermatology refuted the group, saying that there is no evidence that these ingredients are dangerous. The AAD backs the use of a water-resistant, broad-spectrum sunscreen that protects against UVA and UVB radiation, with an SPF 30 or higher, in conjunction with limiting sun exposure and wearing sun-protective clothing.
Dr. Wang agrees that oxybenzone and retinyl palmitate appear to be safe, but he says that some manufacturers have been removing the vitamin A derivative because of the bad publicity. Oxybenzone also may be removed as newer UVA blockers are approved, he said. "But right now, we don’t have any other alternatives," he noted.
For help selecting and using sunscreens effectively, click here.
Dr. Wang disclosed that he is a consultant for L’Oreal, and that he has collaborated with researchers at Procter & Gamble, but has not received any compensation from that company.
On Twitter @aliciaault
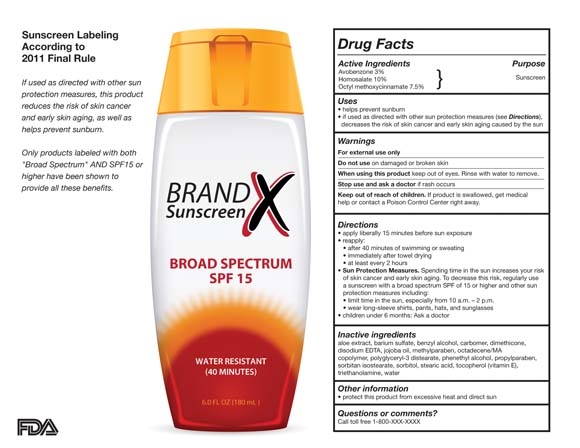
Physician spending a top driver of health costs in 2011
WASHINGTON – Spending on physician and clinical services was the second biggest driver of the increase in health costs in 2011, according to the Centers for Medicare and Medicaid Services.
The nation spent $2.7 trillion on health care in 2011, or about $8,600 per person, according to an annual tally by CMS economists published Jan. 7 in the journal Health Affairs (2013;32:87-99).

The Affordable Care Act (ACA) had only a minimal impact on health spending in 2011, mainly because most of the provisions do not go into effect until 2014, according to the CMS officials.
Slightly more than 70% of the nation’s health bill is paid for by some form of insurance – 33% by private insurance, 21% by Medicare, and 15% by Medicaid, with the remainder paid by other programs.
Health spending has stayed relatively stable over the last 3 years, rising 3.9% in each of the years 2009, 2010, and 2011, which are historically low numbers. Health care also has consumed a similar share of the nation’s gross domestic product (18%) each year for the past few years.
Despite the stability, spending grew in certain areas, indicating that the nation could be poised for a rebound in spending growth. In particular, spending on prescription drugs and physician and clinical services grew faster than in previous years. But it’s not all bad news, according to Rick Foster, chief actuary for the CMS.
"There’s a growing amount of evidence that health care providers are getting it – getting that the future can’t be the same as the past – that the future will have to involve greater efforts for efficiency," Mr. Foster said at a briefing called by the CMS to discuss the analysis. He added that eventually, these efficiencies could offset other factors contributing to the growth in health spending.
Physician and clinical services are considered a single spending category by the CMS. Clinical services include outpatient care centers, freestanding ambulatory surgical centers, and medical and diagnostic labs.
In 2011, private and public payers spent $541 billion on physician and clinical services, accounting for 21% of the total $2.7 trillion health bill. Private health insurers covered 46% of the bill and Medicare paid 23%. Overall, there was a 4.3% increase in the growth of physician and clinical spending in 2011, which is still lower than the growth from 2002 to 2008. Physician spending, which accounts for 80% of the category, grew 3.6%, up from 2.8% the previous year.
The increase in growth was primarily driven by the complexity of services, said Micah Hartman, a statistician in the CMS Office of the Actuary, and the lead author of the report.
Physician and clinical spending also helped to drive an increase in Medicare spending, also due to increased complexity of care. But costs also went up as beneficiaries took advantage of free preventive services offered under the ACA, Mr. Hartman said.
Physician and clinical spending grew 7.6% in 2011, after 2 years of unusually slow growth. Overall, Medicare spent $554 billion in 2011. Seventy-five percent of that was spent on fee-for-service care; the remainder was spent for the Medicare Advantage program.
Medicaid spending shifted considerably in 2011.
Back in 2009, Medicaid saw a recession-related jump in enrollment. Federal legislation at the time increased the federal share of spending, cushioning the states from costs associated with the swell in enrollment. But by mid-2011, that increased federal match expired. As a result, the federal government’s Medicaid tab dropped by 7%, while the state share increased by 22%. Overall, states spent $29 billion more in 2011, even as they curbed benefits, restricted eligibility, and cut back on reimbursement rates, said Anne B. Martin, an economist in the CMS Office of the Actuary.
Another area where the health reform law may have had an impact was Medicare prescription drug spending. In 2011, Medicare beneficiaries spent less out of pocket because those who hit a spending level called the donut hole received a 50% discount on all additional brand name drugs.
That new benefit helped drive the growth of prescription drug spending to about 3%, compared to 0.4% in 2010.
Patients also shouldered a heavy load for those prescriptions and for other medical services. Out-of-pocket spending grew 3% in 2011, to $307 billion, accounting for 11% of total health spending. The increase was slightly more than in 2009-to-2010, but less than in the previous decade.
Patients spent more out-of-pocket in part because they are being asked to pay more by employer-sponsored plans and because increasingly, they are electing coverage through high-deductible health plans, also known as consumer-directed plans. Enrollment has grown by 20% a year the last few years; currently about 17% of insured Americans are in such plans, Mr. Hartman said.
In theory, the high-deductible plans make patients more cost-conscious. But their impact is not clear, Mr. Foster said. "The evidence is mixed to date as to how well these plans are working," he said, adding that costs are lower, but it’s unclear if that’s because the incentives are working or because healthier people are using the plans.
WASHINGTON – Spending on physician and clinical services was the second biggest driver of the increase in health costs in 2011, according to the Centers for Medicare and Medicaid Services.
The nation spent $2.7 trillion on health care in 2011, or about $8,600 per person, according to an annual tally by CMS economists published Jan. 7 in the journal Health Affairs (2013;32:87-99).
The Affordable Care Act (ACA) had only a minimal impact on health spending in 2011, mainly because most of the provisions do not go into effect until 2014, according to the CMS officials.
Slightly more than 70% of the nation’s health bill is paid for by some form of insurance – 33% by private insurance, 21% by Medicare, and 15% by Medicaid, with the remainder paid by other programs.
Health spending has stayed relatively stable over the last 3 years, rising 3.9% in each of the years 2009, 2010, and 2011, which are historically low numbers. Health care also has consumed a similar share of the nation’s gross domestic product (18%) each year for the past few years.
Despite the stability, spending grew in certain areas, indicating that the nation could be poised for a rebound in spending growth. In particular, spending on prescription drugs and physician and clinical services grew faster than in previous years. But it’s not all bad news, according to Rick Foster, chief actuary for the CMS.
"There’s a growing amount of evidence that health care providers are getting it – getting that the future can’t be the same as the past – that the future will have to involve greater efforts for efficiency," Mr. Foster said at a briefing called by the CMS to discuss the analysis. He added that eventually, these efficiencies could offset other factors contributing to the growth in health spending.
Physician and clinical services are considered a single spending category by the CMS. Clinical services include outpatient care centers, freestanding ambulatory surgical centers, and medical and diagnostic labs.
In 2011, private and public payers spent $541 billion on physician and clinical services, accounting for 21% of the total $2.7 trillion health bill. Private health insurers covered 46% of the bill and Medicare paid 23%. Overall, there was a 4.3% increase in the growth of physician and clinical spending in 2011, which is still lower than the growth from 2002 to 2008. Physician spending, which accounts for 80% of the category, grew 3.6%, up from 2.8% the previous year.
The increase in growth was primarily driven by the complexity of services, said Micah Hartman, a statistician in the CMS Office of the Actuary, and the lead author of the report.
Physician and clinical spending also helped to drive an increase in Medicare spending, also due to increased complexity of care. But costs also went up as beneficiaries took advantage of free preventive services offered under the ACA, Mr. Hartman said.
Physician and clinical spending grew 7.6% in 2011, after 2 years of unusually slow growth. Overall, Medicare spent $554 billion in 2011. Seventy-five percent of that was spent on fee-for-service care; the remainder was spent for the Medicare Advantage program.
Medicaid spending shifted considerably in 2011.
Back in 2009, Medicaid saw a recession-related jump in enrollment. Federal legislation at the time increased the federal share of spending, cushioning the states from costs associated with the swell in enrollment. But by mid-2011, that increased federal match expired. As a result, the federal government’s Medicaid tab dropped by 7%, while the state share increased by 22%. Overall, states spent $29 billion more in 2011, even as they curbed benefits, restricted eligibility, and cut back on reimbursement rates, said Anne B. Martin, an economist in the CMS Office of the Actuary.
Another area where the health reform law may have had an impact was Medicare prescription drug spending. In 2011, Medicare beneficiaries spent less out of pocket because those who hit a spending level called the donut hole received a 50% discount on all additional brand name drugs.
That new benefit helped drive the growth of prescription drug spending to about 3%, compared to 0.4% in 2010.
Patients also shouldered a heavy load for those prescriptions and for other medical services. Out-of-pocket spending grew 3% in 2011, to $307 billion, accounting for 11% of total health spending. The increase was slightly more than in 2009-to-2010, but less than in the previous decade.
Patients spent more out-of-pocket in part because they are being asked to pay more by employer-sponsored plans and because increasingly, they are electing coverage through high-deductible health plans, also known as consumer-directed plans. Enrollment has grown by 20% a year the last few years; currently about 17% of insured Americans are in such plans, Mr. Hartman said.
In theory, the high-deductible plans make patients more cost-conscious. But their impact is not clear, Mr. Foster said. "The evidence is mixed to date as to how well these plans are working," he said, adding that costs are lower, but it’s unclear if that’s because the incentives are working or because healthier people are using the plans.
WASHINGTON – Spending on physician and clinical services was the second biggest driver of the increase in health costs in 2011, according to the Centers for Medicare and Medicaid Services.
The nation spent $2.7 trillion on health care in 2011, or about $8,600 per person, according to an annual tally by CMS economists published Jan. 7 in the journal Health Affairs (2013;32:87-99).
The Affordable Care Act (ACA) had only a minimal impact on health spending in 2011, mainly because most of the provisions do not go into effect until 2014, according to the CMS officials.
Slightly more than 70% of the nation’s health bill is paid for by some form of insurance – 33% by private insurance, 21% by Medicare, and 15% by Medicaid, with the remainder paid by other programs.
Health spending has stayed relatively stable over the last 3 years, rising 3.9% in each of the years 2009, 2010, and 2011, which are historically low numbers. Health care also has consumed a similar share of the nation’s gross domestic product (18%) each year for the past few years.
Despite the stability, spending grew in certain areas, indicating that the nation could be poised for a rebound in spending growth. In particular, spending on prescription drugs and physician and clinical services grew faster than in previous years. But it’s not all bad news, according to Rick Foster, chief actuary for the CMS.
"There’s a growing amount of evidence that health care providers are getting it – getting that the future can’t be the same as the past – that the future will have to involve greater efforts for efficiency," Mr. Foster said at a briefing called by the CMS to discuss the analysis. He added that eventually, these efficiencies could offset other factors contributing to the growth in health spending.
Physician and clinical services are considered a single spending category by the CMS. Clinical services include outpatient care centers, freestanding ambulatory surgical centers, and medical and diagnostic labs.
In 2011, private and public payers spent $541 billion on physician and clinical services, accounting for 21% of the total $2.7 trillion health bill. Private health insurers covered 46% of the bill and Medicare paid 23%. Overall, there was a 4.3% increase in the growth of physician and clinical spending in 2011, which is still lower than the growth from 2002 to 2008. Physician spending, which accounts for 80% of the category, grew 3.6%, up from 2.8% the previous year.
The increase in growth was primarily driven by the complexity of services, said Micah Hartman, a statistician in the CMS Office of the Actuary, and the lead author of the report.
Physician and clinical spending also helped to drive an increase in Medicare spending, also due to increased complexity of care. But costs also went up as beneficiaries took advantage of free preventive services offered under the ACA, Mr. Hartman said.
Physician and clinical spending grew 7.6% in 2011, after 2 years of unusually slow growth. Overall, Medicare spent $554 billion in 2011. Seventy-five percent of that was spent on fee-for-service care; the remainder was spent for the Medicare Advantage program.
Medicaid spending shifted considerably in 2011.
Back in 2009, Medicaid saw a recession-related jump in enrollment. Federal legislation at the time increased the federal share of spending, cushioning the states from costs associated with the swell in enrollment. But by mid-2011, that increased federal match expired. As a result, the federal government’s Medicaid tab dropped by 7%, while the state share increased by 22%. Overall, states spent $29 billion more in 2011, even as they curbed benefits, restricted eligibility, and cut back on reimbursement rates, said Anne B. Martin, an economist in the CMS Office of the Actuary.
Another area where the health reform law may have had an impact was Medicare prescription drug spending. In 2011, Medicare beneficiaries spent less out of pocket because those who hit a spending level called the donut hole received a 50% discount on all additional brand name drugs.
That new benefit helped drive the growth of prescription drug spending to about 3%, compared to 0.4% in 2010.
Patients also shouldered a heavy load for those prescriptions and for other medical services. Out-of-pocket spending grew 3% in 2011, to $307 billion, accounting for 11% of total health spending. The increase was slightly more than in 2009-to-2010, but less than in the previous decade.
Patients spent more out-of-pocket in part because they are being asked to pay more by employer-sponsored plans and because increasingly, they are electing coverage through high-deductible health plans, also known as consumer-directed plans. Enrollment has grown by 20% a year the last few years; currently about 17% of insured Americans are in such plans, Mr. Hartman said.
In theory, the high-deductible plans make patients more cost-conscious. But their impact is not clear, Mr. Foster said. "The evidence is mixed to date as to how well these plans are working," he said, adding that costs are lower, but it’s unclear if that’s because the incentives are working or because healthier people are using the plans.
AT A BRIEFING CALLED BY THE CENTERS FOR MEDICARE AND MEDICAID SERVICES

Higher costs for internists, better preventive care?
NEW ORLEANS – The cost of care may be more expensive at an internist’s office, but it appears that internists may do a better job than family physicians in offering preventive care services such as flu shots and cancer screenings.
That’s according to an observational study of some 30,000 adults who had an internist, family physician, or specialist as their usual source of care.

Dr. Joshua J. Fenton of the department of family and community medicine at the University of California, Davis, and his colleagues analyzed data from the Medical Expenditures Panel Survey from 2000 to 2008 and selected adults who responded that they had one of those physicians as a usual source of care in the previous year. Surgeons and ob.gyns were excluded because the authors wanted to study prostate cancer screening, in addition to other outcomes.
Previous research has consistently shown that internists and specialists have higher costs than family physicians, but there have been few data showing whether those higher costs are justified through the delivery of better care – specifically, better preventive care. The authors hypothesized that preventive care delivery would be similar across the three physician groups, Dr. Fenton said at the annual meeting of the North American Primary Care Research Group.
Of the 29,503 adults who were selected, 73% had a family physician as their usual source of care, 23% had an internist, and 4% a specialist. Those who received their care from an internist or specialist were slightly older, had a greater illness burden, had a higher income, and were more likely to live in urban areas, he said.
On an unadjusted basis, the annual care expenditures were $4,682 for those seeing an FP, $6,356 for an internist, and $9,147 for specialist. After adjusting for a variety of factors, including use of care in the previous year, the cost for internists was 10% more and for specialists was 33% more than the cost for family physicians.
People seeing an internist had significantly increased odds of receiving a flu shot in the study year, when compared with a family physician. The odds of getting a shot with a specialist were similar to those with a family physician.
For mammograms – 11,806 women had one during the study year – those with an internist were slightly more likely to get the screen. About 82% of those seeing an internist had a mammogram, compared with 79% of those seeing a family physician and 78% of those seeing a specialist. Pap smear screening rates were similar across the three physician groups, with about 82% getting the test.
Some 15,000 patients had an up-to-date colorectal screen – defined as a fecal occult test within the prior year or lower endoscopy within the previous 5 years. Rates were highest for internists, at 53%, compared with 48% of those seeing a family physician and 44% of those using a specialist.
Patients seeing an internist also had significantly increased odds of having a prostate-specific antigen test.
The study was limited by its cross-sectional and observational design, said Dr. Fenton, who also noted that it’s possible that some preventive care may have been delivered by providers other than the usual source of care.
The finding that internists delivered more preventive services, however, "raises some questions about cost-effectiveness and value," he said.
Dr. Fenton reported no conflicts.
NEW ORLEANS – The cost of care may be more expensive at an internist’s office, but it appears that internists may do a better job than family physicians in offering preventive care services such as flu shots and cancer screenings.
That’s according to an observational study of some 30,000 adults who had an internist, family physician, or specialist as their usual source of care.
Dr. Joshua J. Fenton of the department of family and community medicine at the University of California, Davis, and his colleagues analyzed data from the Medical Expenditures Panel Survey from 2000 to 2008 and selected adults who responded that they had one of those physicians as a usual source of care in the previous year. Surgeons and ob.gyns were excluded because the authors wanted to study prostate cancer screening, in addition to other outcomes.
Previous research has consistently shown that internists and specialists have higher costs than family physicians, but there have been few data showing whether those higher costs are justified through the delivery of better care – specifically, better preventive care. The authors hypothesized that preventive care delivery would be similar across the three physician groups, Dr. Fenton said at the annual meeting of the North American Primary Care Research Group.
Of the 29,503 adults who were selected, 73% had a family physician as their usual source of care, 23% had an internist, and 4% a specialist. Those who received their care from an internist or specialist were slightly older, had a greater illness burden, had a higher income, and were more likely to live in urban areas, he said.
On an unadjusted basis, the annual care expenditures were $4,682 for those seeing an FP, $6,356 for an internist, and $9,147 for specialist. After adjusting for a variety of factors, including use of care in the previous year, the cost for internists was 10% more and for specialists was 33% more than the cost for family physicians.
People seeing an internist had significantly increased odds of receiving a flu shot in the study year, when compared with a family physician. The odds of getting a shot with a specialist were similar to those with a family physician.
For mammograms – 11,806 women had one during the study year – those with an internist were slightly more likely to get the screen. About 82% of those seeing an internist had a mammogram, compared with 79% of those seeing a family physician and 78% of those seeing a specialist. Pap smear screening rates were similar across the three physician groups, with about 82% getting the test.
Some 15,000 patients had an up-to-date colorectal screen – defined as a fecal occult test within the prior year or lower endoscopy within the previous 5 years. Rates were highest for internists, at 53%, compared with 48% of those seeing a family physician and 44% of those using a specialist.
Patients seeing an internist also had significantly increased odds of having a prostate-specific antigen test.
The study was limited by its cross-sectional and observational design, said Dr. Fenton, who also noted that it’s possible that some preventive care may have been delivered by providers other than the usual source of care.
The finding that internists delivered more preventive services, however, "raises some questions about cost-effectiveness and value," he said.
Dr. Fenton reported no conflicts.
NEW ORLEANS – The cost of care may be more expensive at an internist’s office, but it appears that internists may do a better job than family physicians in offering preventive care services such as flu shots and cancer screenings.
That’s according to an observational study of some 30,000 adults who had an internist, family physician, or specialist as their usual source of care.
Dr. Joshua J. Fenton of the department of family and community medicine at the University of California, Davis, and his colleagues analyzed data from the Medical Expenditures Panel Survey from 2000 to 2008 and selected adults who responded that they had one of those physicians as a usual source of care in the previous year. Surgeons and ob.gyns were excluded because the authors wanted to study prostate cancer screening, in addition to other outcomes.
Previous research has consistently shown that internists and specialists have higher costs than family physicians, but there have been few data showing whether those higher costs are justified through the delivery of better care – specifically, better preventive care. The authors hypothesized that preventive care delivery would be similar across the three physician groups, Dr. Fenton said at the annual meeting of the North American Primary Care Research Group.
Of the 29,503 adults who were selected, 73% had a family physician as their usual source of care, 23% had an internist, and 4% a specialist. Those who received their care from an internist or specialist were slightly older, had a greater illness burden, had a higher income, and were more likely to live in urban areas, he said.
On an unadjusted basis, the annual care expenditures were $4,682 for those seeing an FP, $6,356 for an internist, and $9,147 for specialist. After adjusting for a variety of factors, including use of care in the previous year, the cost for internists was 10% more and for specialists was 33% more than the cost for family physicians.
People seeing an internist had significantly increased odds of receiving a flu shot in the study year, when compared with a family physician. The odds of getting a shot with a specialist were similar to those with a family physician.
For mammograms – 11,806 women had one during the study year – those with an internist were slightly more likely to get the screen. About 82% of those seeing an internist had a mammogram, compared with 79% of those seeing a family physician and 78% of those seeing a specialist. Pap smear screening rates were similar across the three physician groups, with about 82% getting the test.
Some 15,000 patients had an up-to-date colorectal screen – defined as a fecal occult test within the prior year or lower endoscopy within the previous 5 years. Rates were highest for internists, at 53%, compared with 48% of those seeing a family physician and 44% of those using a specialist.
Patients seeing an internist also had significantly increased odds of having a prostate-specific antigen test.
The study was limited by its cross-sectional and observational design, said Dr. Fenton, who also noted that it’s possible that some preventive care may have been delivered by providers other than the usual source of care.
The finding that internists delivered more preventive services, however, "raises some questions about cost-effectiveness and value," he said.
Dr. Fenton reported no conflicts.
AT THE ANNUAL MEETING OF THE NORTH AMERICAN PRIMARY CARE RESEARCH GROUP
Major Finding: Internists delivered more preventive care than family physicians, but costs overall were 10% greater.
Data Source: A cross-sectional study of adults responding to the Medical Expenditures Panel Survey from 2000 to 2008 who had a family physician, internist, or specialist as a usual source of care.
Disclosures: Dr. Fenton reported no conflicts.

FDA approves teduglutide for short bowel syndrome
The Food and Drug Administration on Dec. 21 approved teduglutide, to be marketed under the trade name Gattex, to treat adults with short bowel syndrome (SBS) who need parenteral nutrition.
Teduglutide, a recombinant analogue of human glucagon-like peptide-2 (GLP-2), was unanimously recommended for approval by an FDA advisory panel in October. It is a once-daily subcutaneous injection that helps improve intestinal absorption of fluids and nutrients, reducing the frequency and volume of parenteral nutrition.
"Considering Gattex has been shown to significantly reduce or in some cases even eliminate the requirement for parenteral support, it may become a cornerstone therapy in the management of short bowel syndrome." Dr. Ken Fujioka of the Nutrition and Metabolic Research Center, Scripps Clinic, Del Mar, Calif., said in a statement issued by Gattex’s maker, NPA Pharmaceuticals.
It is the third drug to be approved by the FDA for SBS patients who are dependent on parenteral nutrition. Somatropin (Zorbtive) was approved in 2003 and glutamine (Nutrestore) in 2004.
"Today’s approval expands the available treatment options for patients with this life-threatening condition," Dr. Victoria Kusiak, deputy director of the Office of Drug Evaluation III in the FDA Center for Drug Evaluation and Research, said in a statement. "Because Gattex may cause other serious health conditions, it is critical that patients and health care professionals understand the drug’s potential and known safety risks."
Teduglutide therapy increases the risk of developing cancer and polyps in the intestine, obstructions in the intestine, gallbladder disease, biliary tract disease, and pancreatic disease. The drug will have a Risk Evaluation and Mitigation Strategy, consisting of a communication plan and training for prescribers, according to the FDA.
Pivotal data on the drug were published in September in Gastroenterology (Gastroenterology 2012 Sept. 13 [doi:10.1053/j.gastro.2012.09.007]).
The Food and Drug Administration on Dec. 21 approved teduglutide, to be marketed under the trade name Gattex, to treat adults with short bowel syndrome (SBS) who need parenteral nutrition.
Teduglutide, a recombinant analogue of human glucagon-like peptide-2 (GLP-2), was unanimously recommended for approval by an FDA advisory panel in October. It is a once-daily subcutaneous injection that helps improve intestinal absorption of fluids and nutrients, reducing the frequency and volume of parenteral nutrition.
"Considering Gattex has been shown to significantly reduce or in some cases even eliminate the requirement for parenteral support, it may become a cornerstone therapy in the management of short bowel syndrome." Dr. Ken Fujioka of the Nutrition and Metabolic Research Center, Scripps Clinic, Del Mar, Calif., said in a statement issued by Gattex’s maker, NPA Pharmaceuticals.
It is the third drug to be approved by the FDA for SBS patients who are dependent on parenteral nutrition. Somatropin (Zorbtive) was approved in 2003 and glutamine (Nutrestore) in 2004.
"Today’s approval expands the available treatment options for patients with this life-threatening condition," Dr. Victoria Kusiak, deputy director of the Office of Drug Evaluation III in the FDA Center for Drug Evaluation and Research, said in a statement. "Because Gattex may cause other serious health conditions, it is critical that patients and health care professionals understand the drug’s potential and known safety risks."
Teduglutide therapy increases the risk of developing cancer and polyps in the intestine, obstructions in the intestine, gallbladder disease, biliary tract disease, and pancreatic disease. The drug will have a Risk Evaluation and Mitigation Strategy, consisting of a communication plan and training for prescribers, according to the FDA.
Pivotal data on the drug were published in September in Gastroenterology (Gastroenterology 2012 Sept. 13 [doi:10.1053/j.gastro.2012.09.007]).
The Food and Drug Administration on Dec. 21 approved teduglutide, to be marketed under the trade name Gattex, to treat adults with short bowel syndrome (SBS) who need parenteral nutrition.
Teduglutide, a recombinant analogue of human glucagon-like peptide-2 (GLP-2), was unanimously recommended for approval by an FDA advisory panel in October. It is a once-daily subcutaneous injection that helps improve intestinal absorption of fluids and nutrients, reducing the frequency and volume of parenteral nutrition.
"Considering Gattex has been shown to significantly reduce or in some cases even eliminate the requirement for parenteral support, it may become a cornerstone therapy in the management of short bowel syndrome." Dr. Ken Fujioka of the Nutrition and Metabolic Research Center, Scripps Clinic, Del Mar, Calif., said in a statement issued by Gattex’s maker, NPA Pharmaceuticals.
It is the third drug to be approved by the FDA for SBS patients who are dependent on parenteral nutrition. Somatropin (Zorbtive) was approved in 2003 and glutamine (Nutrestore) in 2004.
"Today’s approval expands the available treatment options for patients with this life-threatening condition," Dr. Victoria Kusiak, deputy director of the Office of Drug Evaluation III in the FDA Center for Drug Evaluation and Research, said in a statement. "Because Gattex may cause other serious health conditions, it is critical that patients and health care professionals understand the drug’s potential and known safety risks."
Teduglutide therapy increases the risk of developing cancer and polyps in the intestine, obstructions in the intestine, gallbladder disease, biliary tract disease, and pancreatic disease. The drug will have a Risk Evaluation and Mitigation Strategy, consisting of a communication plan and training for prescribers, according to the FDA.
Pivotal data on the drug were published in September in Gastroenterology (Gastroenterology 2012 Sept. 13 [doi:10.1053/j.gastro.2012.09.007]).