User login
Blood Eosinophil-Directed Prednisolone Proves Noninferior to Standard Care for COPD Exacerbations
TOPLINE:
Both blood eosinophil-directed treatment (BET) and standard care treatment (ST) similarly reduced treatment failure following acute exacerbations in chronic obstructive pulmonary disease (COPD).
METHODOLOGY:
- The researchers randomized 152 adults with a mean age of 70 years to BET or a placebo (if eosinophil counts were less than 2%) or to standard care treatment regardless of baseline eosinophil counts; the final population available for analysis included 47 patients in the blood eosinophil group and 46 in the primary care group, with 73 and 71 exacerbations, respectively.
- Participants were assessed at baseline and at day 14, day 30, and day 90 after exacerbation; the primary outcome was the rate of treatment failure at 30 days post exacerbation, defined as any need for retreatment with antibiotics or steroids, hospitalization, or death; secondary outcomes included health-related quality of life, forced expiratory volume in 1 second, and visual analogue score respiratory symptoms.
- Participants were recruited from 14 general practices between November 6, 2017, and April 30, 2020; the study was terminated on April 30, 2023, because of the COVID-19 pandemic.
TAKEAWAY:
- BET was noninferior to ST in a noninferiority analysis.
- At 30 days post exacerbation, 14 treatment failures had occurred in the BET group and 23 in the ST group; the relative risk was 0.60 (P = .070).
- The frequency of adverse events was similar between the groups; the most common adverse events were glycosuria and hospital admission for COPD exacerbation (2% in the BET group and 1% in the ST group for both event types), and no deaths occurred during the study period.
- Subgroup analysis showed the greatest benefit in both groups was to patients with higher eosinophil counts who received prednisolone.
IN PRACTICE:
“There was improvement of lung function, quality of life, and symptoms in exacerbations with low eosinophil count independent of whether placebo or prednisolone was prescribed,” the authors wrote in their discussion.
SOURCE:
The lead author on the study was Sanjay Ramakrishnan, MBBS, University of Oxford, United Kingdom. The study was published online in Lancet Respiratory Medicine .
LIMITATIONS:
A key limitation was an error in the randomization code that prevented the trial’s completion as a superiority study; other limitations included the relatively low number of exacerbations associated with low eosinophil counts and reduction in the recommended length of treatment with prednisolone during the study period.
DISCLOSURES:
The study was supported by the National Institute for Health and Care Research. Dr. Ramakrishnan disclosed personal salary support from the National Institute for Health and Care Research, an unrestricted research grant from AstraZeneca to his institution, and speaker fees and conference travel support from AstraZeneca, all unrelated to the current study.
A version of this article first appeared on Medscape.com.
TOPLINE:
Both blood eosinophil-directed treatment (BET) and standard care treatment (ST) similarly reduced treatment failure following acute exacerbations in chronic obstructive pulmonary disease (COPD).
METHODOLOGY:
- The researchers randomized 152 adults with a mean age of 70 years to BET or a placebo (if eosinophil counts were less than 2%) or to standard care treatment regardless of baseline eosinophil counts; the final population available for analysis included 47 patients in the blood eosinophil group and 46 in the primary care group, with 73 and 71 exacerbations, respectively.
- Participants were assessed at baseline and at day 14, day 30, and day 90 after exacerbation; the primary outcome was the rate of treatment failure at 30 days post exacerbation, defined as any need for retreatment with antibiotics or steroids, hospitalization, or death; secondary outcomes included health-related quality of life, forced expiratory volume in 1 second, and visual analogue score respiratory symptoms.
- Participants were recruited from 14 general practices between November 6, 2017, and April 30, 2020; the study was terminated on April 30, 2023, because of the COVID-19 pandemic.
TAKEAWAY:
- BET was noninferior to ST in a noninferiority analysis.
- At 30 days post exacerbation, 14 treatment failures had occurred in the BET group and 23 in the ST group; the relative risk was 0.60 (P = .070).
- The frequency of adverse events was similar between the groups; the most common adverse events were glycosuria and hospital admission for COPD exacerbation (2% in the BET group and 1% in the ST group for both event types), and no deaths occurred during the study period.
- Subgroup analysis showed the greatest benefit in both groups was to patients with higher eosinophil counts who received prednisolone.
IN PRACTICE:
“There was improvement of lung function, quality of life, and symptoms in exacerbations with low eosinophil count independent of whether placebo or prednisolone was prescribed,” the authors wrote in their discussion.
SOURCE:
The lead author on the study was Sanjay Ramakrishnan, MBBS, University of Oxford, United Kingdom. The study was published online in Lancet Respiratory Medicine .
LIMITATIONS:
A key limitation was an error in the randomization code that prevented the trial’s completion as a superiority study; other limitations included the relatively low number of exacerbations associated with low eosinophil counts and reduction in the recommended length of treatment with prednisolone during the study period.
DISCLOSURES:
The study was supported by the National Institute for Health and Care Research. Dr. Ramakrishnan disclosed personal salary support from the National Institute for Health and Care Research, an unrestricted research grant from AstraZeneca to his institution, and speaker fees and conference travel support from AstraZeneca, all unrelated to the current study.
A version of this article first appeared on Medscape.com.
TOPLINE:
Both blood eosinophil-directed treatment (BET) and standard care treatment (ST) similarly reduced treatment failure following acute exacerbations in chronic obstructive pulmonary disease (COPD).
METHODOLOGY:
- The researchers randomized 152 adults with a mean age of 70 years to BET or a placebo (if eosinophil counts were less than 2%) or to standard care treatment regardless of baseline eosinophil counts; the final population available for analysis included 47 patients in the blood eosinophil group and 46 in the primary care group, with 73 and 71 exacerbations, respectively.
- Participants were assessed at baseline and at day 14, day 30, and day 90 after exacerbation; the primary outcome was the rate of treatment failure at 30 days post exacerbation, defined as any need for retreatment with antibiotics or steroids, hospitalization, or death; secondary outcomes included health-related quality of life, forced expiratory volume in 1 second, and visual analogue score respiratory symptoms.
- Participants were recruited from 14 general practices between November 6, 2017, and April 30, 2020; the study was terminated on April 30, 2023, because of the COVID-19 pandemic.
TAKEAWAY:
- BET was noninferior to ST in a noninferiority analysis.
- At 30 days post exacerbation, 14 treatment failures had occurred in the BET group and 23 in the ST group; the relative risk was 0.60 (P = .070).
- The frequency of adverse events was similar between the groups; the most common adverse events were glycosuria and hospital admission for COPD exacerbation (2% in the BET group and 1% in the ST group for both event types), and no deaths occurred during the study period.
- Subgroup analysis showed the greatest benefit in both groups was to patients with higher eosinophil counts who received prednisolone.
IN PRACTICE:
“There was improvement of lung function, quality of life, and symptoms in exacerbations with low eosinophil count independent of whether placebo or prednisolone was prescribed,” the authors wrote in their discussion.
SOURCE:
The lead author on the study was Sanjay Ramakrishnan, MBBS, University of Oxford, United Kingdom. The study was published online in Lancet Respiratory Medicine .
LIMITATIONS:
A key limitation was an error in the randomization code that prevented the trial’s completion as a superiority study; other limitations included the relatively low number of exacerbations associated with low eosinophil counts and reduction in the recommended length of treatment with prednisolone during the study period.
DISCLOSURES:
The study was supported by the National Institute for Health and Care Research. Dr. Ramakrishnan disclosed personal salary support from the National Institute for Health and Care Research, an unrestricted research grant from AstraZeneca to his institution, and speaker fees and conference travel support from AstraZeneca, all unrelated to the current study.
A version of this article first appeared on Medscape.com.
Roflumilast foam gets nod as new option for seborrheic dermatitis
The in a press release.
The 0.3% foam, marketed as Zoryve, applied once-daily, is indicated for patients aged 9 years and older with seborrheic dermatitis, and can be used anywhere on the body, including areas with hair, with no limits on duration of use, according to the company, Arcutis. A 0.3% cream formulation of roflumilast was previously approved by the FDA for the topical treatment of plaque psoriasis in patients aged 6 years and older.
Approval was based on data from the phase 3 STRATUM trial and an accompanying phase 2 study known as Trial 203. These studies included a total of 683 adults and youth aged 9 years and older with seborrheic dermatitis. Participants were randomized to roflumilast or a placebo.
At 8 weeks, 79.5 % of patients on roflumilast met the primary efficacy endpoint of Investigator Global Assessment (IGA) scores of 0 or 1 (clear or almost clear) compared with 58.0% of patients on placebo (P < .001); the results were similar in the phase 2 Trial 203 (73.1% vs. 40.8%, respectively; P < .001). Overall, more than 50% of the patients on roflumilast achieved a clear score.
Patients in the roflumilast group also showed significant improvement in all secondary endpoints, including itching, scaling, and erythema, according to the company.
In the STRATUM study, 62.8% of roflumilast-treated patients and 40.6% of placebo patients achieved a 4-point or more reduction in itch based on the Worst Itch Numerical Rating Score (P =.0001), and 28% of roflumilast-treated patients reported significant itch improvement within the first 48 hours of use, compared with 13% of placebo patients (P = .0024).
Over a treatment period of up to 1 year, no treatment-related severe adverse events were reported in the phase 2 and 3 studies. The incidence of treatment emergent adverse events was similar between the treatment and placebo groups, and the most common adverse events (occurring in 1% of more of patients) across both studies were nasopharyngitis (1.5%), nausea (1.3%), and headache (1.1%).
Roflumilast foam is scheduled to be available by the end of January 2024, according to the company. The product is for topical use only, and contraindicated for individuals with severe liver impairment.
The in a press release.
The 0.3% foam, marketed as Zoryve, applied once-daily, is indicated for patients aged 9 years and older with seborrheic dermatitis, and can be used anywhere on the body, including areas with hair, with no limits on duration of use, according to the company, Arcutis. A 0.3% cream formulation of roflumilast was previously approved by the FDA for the topical treatment of plaque psoriasis in patients aged 6 years and older.
Approval was based on data from the phase 3 STRATUM trial and an accompanying phase 2 study known as Trial 203. These studies included a total of 683 adults and youth aged 9 years and older with seborrheic dermatitis. Participants were randomized to roflumilast or a placebo.
At 8 weeks, 79.5 % of patients on roflumilast met the primary efficacy endpoint of Investigator Global Assessment (IGA) scores of 0 or 1 (clear or almost clear) compared with 58.0% of patients on placebo (P < .001); the results were similar in the phase 2 Trial 203 (73.1% vs. 40.8%, respectively; P < .001). Overall, more than 50% of the patients on roflumilast achieved a clear score.
Patients in the roflumilast group also showed significant improvement in all secondary endpoints, including itching, scaling, and erythema, according to the company.
In the STRATUM study, 62.8% of roflumilast-treated patients and 40.6% of placebo patients achieved a 4-point or more reduction in itch based on the Worst Itch Numerical Rating Score (P =.0001), and 28% of roflumilast-treated patients reported significant itch improvement within the first 48 hours of use, compared with 13% of placebo patients (P = .0024).
Over a treatment period of up to 1 year, no treatment-related severe adverse events were reported in the phase 2 and 3 studies. The incidence of treatment emergent adverse events was similar between the treatment and placebo groups, and the most common adverse events (occurring in 1% of more of patients) across both studies were nasopharyngitis (1.5%), nausea (1.3%), and headache (1.1%).
Roflumilast foam is scheduled to be available by the end of January 2024, according to the company. The product is for topical use only, and contraindicated for individuals with severe liver impairment.
The in a press release.
The 0.3% foam, marketed as Zoryve, applied once-daily, is indicated for patients aged 9 years and older with seborrheic dermatitis, and can be used anywhere on the body, including areas with hair, with no limits on duration of use, according to the company, Arcutis. A 0.3% cream formulation of roflumilast was previously approved by the FDA for the topical treatment of plaque psoriasis in patients aged 6 years and older.
Approval was based on data from the phase 3 STRATUM trial and an accompanying phase 2 study known as Trial 203. These studies included a total of 683 adults and youth aged 9 years and older with seborrheic dermatitis. Participants were randomized to roflumilast or a placebo.
At 8 weeks, 79.5 % of patients on roflumilast met the primary efficacy endpoint of Investigator Global Assessment (IGA) scores of 0 or 1 (clear or almost clear) compared with 58.0% of patients on placebo (P < .001); the results were similar in the phase 2 Trial 203 (73.1% vs. 40.8%, respectively; P < .001). Overall, more than 50% of the patients on roflumilast achieved a clear score.
Patients in the roflumilast group also showed significant improvement in all secondary endpoints, including itching, scaling, and erythema, according to the company.
In the STRATUM study, 62.8% of roflumilast-treated patients and 40.6% of placebo patients achieved a 4-point or more reduction in itch based on the Worst Itch Numerical Rating Score (P =.0001), and 28% of roflumilast-treated patients reported significant itch improvement within the first 48 hours of use, compared with 13% of placebo patients (P = .0024).
Over a treatment period of up to 1 year, no treatment-related severe adverse events were reported in the phase 2 and 3 studies. The incidence of treatment emergent adverse events was similar between the treatment and placebo groups, and the most common adverse events (occurring in 1% of more of patients) across both studies were nasopharyngitis (1.5%), nausea (1.3%), and headache (1.1%).
Roflumilast foam is scheduled to be available by the end of January 2024, according to the company. The product is for topical use only, and contraindicated for individuals with severe liver impairment.
Catheter-directed strategy improves pulmonary artery occlusion
Use of pharmacomechanical catheter-directory thrombolysis significantly reduced the number of pulmonary artery branches with total or subtotal occlusions in patients with acute pulmonary embolism, based on data from more than 100 individuals.
Reduced distal vascular volume is a significant predictor of 30-day and 90-day mortality in acute pulmonary embolism (PE) patients, and pulmonary obstruction is often the cause, wrote Riyaz Bashir, MD, of Temple University, Philadelphia, Pennsylvania, and colleagues.
, the researchers said.
“The recently published RESCUE (Recombinant tPA by Endovascular Administration for the Treatment of Submassive PE Using CDT for the Reduction of Thrombus Burden) trial showed a 35.9% reduction in PA obstruction using the Refined Modified Miller Index (RMMI), the largest reduction of all published catheter studies with core lab measurement, with similar doses of tissue plasminogen activator (tPA),” the researchers wrote.
The Bashir endovascular catheter was designed to maximize thrombus reduction via a pharmacomechanical infusion. The catheter features an expandable basket of 6 nitinol-reinforced infusion limbs.
“There are three crucial goals that we want to accomplish in patients who have a severe pulmonary embolism,” Dr. Bashir said in an interview. “Those include, in the order of importance, survival, recovery of right ventricular function, and resolution of blocked pulmonary arteries; both segmental and proximal pulmonary arteries,” he said.
Most previous studies have focused on the first two goals, but they still need to evaluate the resolution of PA blockages carefully, said Dr. Bashir. “In our clinical practice, we have seen a large number of patients who develop debilitating shortness of breath from these blockages. We decided to carefully evaluate these blockages before and after pharmacomechanical catheter-directed thrombolysis with the Bashir endovascular catheter using the core lab data from the RESCUE study,” he said.
In the current study published in JACC: Advances), the researchers used baseline and 48-hour posttreatment contrast-enhanced chest computed tomography angiography of adult PE patients with right ventricular dilatation.
The study population included 107 adults with acute intermediate-risk PE who were treated with pharmacomechanical catheter-directory thrombolysis (PM-CDT) at 18 sites in the United States. Of these, 98 had intermediate high-risk PE with elevated troponin and/or brain-type natriuretic peptide (BNP) levels and 102 had bilateral PE.
The primary endpoint was the change in the number of segmental and proximal PA branches with total or subtotal occlusions (defined as > 65%) after 48 hours compared to baseline. Occlusions were assessed using McNemar’s test.
Patients with bilateral PE received two Bashir catheters; those with unilateral PE received one catheter each.
Each patient received a pulse spray of 2 mg of recombinant tPA (r-tPA) into each lung, followed by 5 mg of r-tPA over 5 hours; the total dose was 7 mg of r-tPA for patients with unilateral PEs and 14 mg for those with bilateral PEs, the researchers said. The median times for catheter placement and total procedure were 15 minutes and 54 minutes, respectively.
The number of segmental PA branches with total or subtotal occlusions decreased significantly, from 40.5% at baseline to 11.7% at 48 hours, and proximal PA branch total or subtotal occlusions decreased significantly, from 28.7% at baseline to 11.0% at 48 hours (P < 0.0001 for both).
The magnitude of the reductions in both total and subtotal occlusions of segmental arteries was significantly correlated with the extent of right ventricle recovery (measured by the reduction in right ventricular/left ventricular ratio) with a correlation coefficient of 0.287 (P = .0026); however, this correlation was not observed in the proximal PA arteries (correlation coefficient 0.132, P = .173).
One major bleeding event occurred within 72 hours in a patient who also experienced a device-related left common iliac vein thrombosis while not taking anticoagulation medication, and one death unrelated to PE occurred within 30 days.
“The two findings that surprised me include, first, a more than 70% reduction in total and subtotal occlusions in the segmental arteries with such a low dose of r-tPA and, second, the resolution of the blockages was seen not only in the arteries where the device was placed but also at remote sites away from the location of the catheter,” Dr. Bashir told this news organization.
The findings were limited by several factors including the lack of long-term clinical follow-up outcomes data and lack of comparison groups who underwent other treatments.
However, “This study implies that we now have a safe therapy for these patients that improves survival and right ventricular recovery in addition to dramatically improving blocked pulmonary arteries,” Dr. Bashir said.
As for additional research, “we need all the current and future prospective pulmonary embolism studies to include an assessment of pulmonary artery blockage resolution as an essential endpoint,” he said.
Catheter Expands Treatment Options
The current study, a subgroup analysis of the RESCUE trial, was one of the first to examine the impact of catheter-directed lysis on distal occlusions, study coauthor Parth M. Rali, MD, said in an interview.
To this point, literature has been limited to evaluation for proximal disease, said Dr. Rali, director of thoracic surgery and medicine and part of the Pulmonary Embolism Response Team at Temple University Hospital, Philadelphia.
Dr. Rali said he was encouraged to see confirmation that the BEC catheter, because of its design, works in patients with proximal or distal occlusive disease.
In clinical practice, “the catheter provides an additional option for care in patients with multiple distal occlusive disease when a systemic tissue plasminogen activator (tPA), may put patient at high bleeding risk,” Dr. Rali said.
Looking ahead, a prospective, observational multicenter study would be useful to validate the findings from the post hoc analysis of the current study, he noted.
The study was sponsored by the National Heart, Lung, and Blood Institute, Commonwealth of Pennsylvania, and Thrombolex Inc., a medical device company developing interventional catheter-based therapies for the rapid and effective treatment of acute venous thromboembolic disorders. Dr. Bashir is a cofounder and has an equity interest in Thrombolex Inc. Dr. Rali disclosed serving as a consultant for Thrombolex, Inari Medical, Viz AI, and ThinkSono.
Use of pharmacomechanical catheter-directory thrombolysis significantly reduced the number of pulmonary artery branches with total or subtotal occlusions in patients with acute pulmonary embolism, based on data from more than 100 individuals.
Reduced distal vascular volume is a significant predictor of 30-day and 90-day mortality in acute pulmonary embolism (PE) patients, and pulmonary obstruction is often the cause, wrote Riyaz Bashir, MD, of Temple University, Philadelphia, Pennsylvania, and colleagues.
, the researchers said.
“The recently published RESCUE (Recombinant tPA by Endovascular Administration for the Treatment of Submassive PE Using CDT for the Reduction of Thrombus Burden) trial showed a 35.9% reduction in PA obstruction using the Refined Modified Miller Index (RMMI), the largest reduction of all published catheter studies with core lab measurement, with similar doses of tissue plasminogen activator (tPA),” the researchers wrote.
The Bashir endovascular catheter was designed to maximize thrombus reduction via a pharmacomechanical infusion. The catheter features an expandable basket of 6 nitinol-reinforced infusion limbs.
“There are three crucial goals that we want to accomplish in patients who have a severe pulmonary embolism,” Dr. Bashir said in an interview. “Those include, in the order of importance, survival, recovery of right ventricular function, and resolution of blocked pulmonary arteries; both segmental and proximal pulmonary arteries,” he said.
Most previous studies have focused on the first two goals, but they still need to evaluate the resolution of PA blockages carefully, said Dr. Bashir. “In our clinical practice, we have seen a large number of patients who develop debilitating shortness of breath from these blockages. We decided to carefully evaluate these blockages before and after pharmacomechanical catheter-directed thrombolysis with the Bashir endovascular catheter using the core lab data from the RESCUE study,” he said.
In the current study published in JACC: Advances), the researchers used baseline and 48-hour posttreatment contrast-enhanced chest computed tomography angiography of adult PE patients with right ventricular dilatation.
The study population included 107 adults with acute intermediate-risk PE who were treated with pharmacomechanical catheter-directory thrombolysis (PM-CDT) at 18 sites in the United States. Of these, 98 had intermediate high-risk PE with elevated troponin and/or brain-type natriuretic peptide (BNP) levels and 102 had bilateral PE.
The primary endpoint was the change in the number of segmental and proximal PA branches with total or subtotal occlusions (defined as > 65%) after 48 hours compared to baseline. Occlusions were assessed using McNemar’s test.
Patients with bilateral PE received two Bashir catheters; those with unilateral PE received one catheter each.
Each patient received a pulse spray of 2 mg of recombinant tPA (r-tPA) into each lung, followed by 5 mg of r-tPA over 5 hours; the total dose was 7 mg of r-tPA for patients with unilateral PEs and 14 mg for those with bilateral PEs, the researchers said. The median times for catheter placement and total procedure were 15 minutes and 54 minutes, respectively.
The number of segmental PA branches with total or subtotal occlusions decreased significantly, from 40.5% at baseline to 11.7% at 48 hours, and proximal PA branch total or subtotal occlusions decreased significantly, from 28.7% at baseline to 11.0% at 48 hours (P < 0.0001 for both).
The magnitude of the reductions in both total and subtotal occlusions of segmental arteries was significantly correlated with the extent of right ventricle recovery (measured by the reduction in right ventricular/left ventricular ratio) with a correlation coefficient of 0.287 (P = .0026); however, this correlation was not observed in the proximal PA arteries (correlation coefficient 0.132, P = .173).
One major bleeding event occurred within 72 hours in a patient who also experienced a device-related left common iliac vein thrombosis while not taking anticoagulation medication, and one death unrelated to PE occurred within 30 days.
“The two findings that surprised me include, first, a more than 70% reduction in total and subtotal occlusions in the segmental arteries with such a low dose of r-tPA and, second, the resolution of the blockages was seen not only in the arteries where the device was placed but also at remote sites away from the location of the catheter,” Dr. Bashir told this news organization.
The findings were limited by several factors including the lack of long-term clinical follow-up outcomes data and lack of comparison groups who underwent other treatments.
However, “This study implies that we now have a safe therapy for these patients that improves survival and right ventricular recovery in addition to dramatically improving blocked pulmonary arteries,” Dr. Bashir said.
As for additional research, “we need all the current and future prospective pulmonary embolism studies to include an assessment of pulmonary artery blockage resolution as an essential endpoint,” he said.
Catheter Expands Treatment Options
The current study, a subgroup analysis of the RESCUE trial, was one of the first to examine the impact of catheter-directed lysis on distal occlusions, study coauthor Parth M. Rali, MD, said in an interview.
To this point, literature has been limited to evaluation for proximal disease, said Dr. Rali, director of thoracic surgery and medicine and part of the Pulmonary Embolism Response Team at Temple University Hospital, Philadelphia.
Dr. Rali said he was encouraged to see confirmation that the BEC catheter, because of its design, works in patients with proximal or distal occlusive disease.
In clinical practice, “the catheter provides an additional option for care in patients with multiple distal occlusive disease when a systemic tissue plasminogen activator (tPA), may put patient at high bleeding risk,” Dr. Rali said.
Looking ahead, a prospective, observational multicenter study would be useful to validate the findings from the post hoc analysis of the current study, he noted.
The study was sponsored by the National Heart, Lung, and Blood Institute, Commonwealth of Pennsylvania, and Thrombolex Inc., a medical device company developing interventional catheter-based therapies for the rapid and effective treatment of acute venous thromboembolic disorders. Dr. Bashir is a cofounder and has an equity interest in Thrombolex Inc. Dr. Rali disclosed serving as a consultant for Thrombolex, Inari Medical, Viz AI, and ThinkSono.
Use of pharmacomechanical catheter-directory thrombolysis significantly reduced the number of pulmonary artery branches with total or subtotal occlusions in patients with acute pulmonary embolism, based on data from more than 100 individuals.
Reduced distal vascular volume is a significant predictor of 30-day and 90-day mortality in acute pulmonary embolism (PE) patients, and pulmonary obstruction is often the cause, wrote Riyaz Bashir, MD, of Temple University, Philadelphia, Pennsylvania, and colleagues.
, the researchers said.
“The recently published RESCUE (Recombinant tPA by Endovascular Administration for the Treatment of Submassive PE Using CDT for the Reduction of Thrombus Burden) trial showed a 35.9% reduction in PA obstruction using the Refined Modified Miller Index (RMMI), the largest reduction of all published catheter studies with core lab measurement, with similar doses of tissue plasminogen activator (tPA),” the researchers wrote.
The Bashir endovascular catheter was designed to maximize thrombus reduction via a pharmacomechanical infusion. The catheter features an expandable basket of 6 nitinol-reinforced infusion limbs.
“There are three crucial goals that we want to accomplish in patients who have a severe pulmonary embolism,” Dr. Bashir said in an interview. “Those include, in the order of importance, survival, recovery of right ventricular function, and resolution of blocked pulmonary arteries; both segmental and proximal pulmonary arteries,” he said.
Most previous studies have focused on the first two goals, but they still need to evaluate the resolution of PA blockages carefully, said Dr. Bashir. “In our clinical practice, we have seen a large number of patients who develop debilitating shortness of breath from these blockages. We decided to carefully evaluate these blockages before and after pharmacomechanical catheter-directed thrombolysis with the Bashir endovascular catheter using the core lab data from the RESCUE study,” he said.
In the current study published in JACC: Advances), the researchers used baseline and 48-hour posttreatment contrast-enhanced chest computed tomography angiography of adult PE patients with right ventricular dilatation.
The study population included 107 adults with acute intermediate-risk PE who were treated with pharmacomechanical catheter-directory thrombolysis (PM-CDT) at 18 sites in the United States. Of these, 98 had intermediate high-risk PE with elevated troponin and/or brain-type natriuretic peptide (BNP) levels and 102 had bilateral PE.
The primary endpoint was the change in the number of segmental and proximal PA branches with total or subtotal occlusions (defined as > 65%) after 48 hours compared to baseline. Occlusions were assessed using McNemar’s test.
Patients with bilateral PE received two Bashir catheters; those with unilateral PE received one catheter each.
Each patient received a pulse spray of 2 mg of recombinant tPA (r-tPA) into each lung, followed by 5 mg of r-tPA over 5 hours; the total dose was 7 mg of r-tPA for patients with unilateral PEs and 14 mg for those with bilateral PEs, the researchers said. The median times for catheter placement and total procedure were 15 minutes and 54 minutes, respectively.
The number of segmental PA branches with total or subtotal occlusions decreased significantly, from 40.5% at baseline to 11.7% at 48 hours, and proximal PA branch total or subtotal occlusions decreased significantly, from 28.7% at baseline to 11.0% at 48 hours (P < 0.0001 for both).
The magnitude of the reductions in both total and subtotal occlusions of segmental arteries was significantly correlated with the extent of right ventricle recovery (measured by the reduction in right ventricular/left ventricular ratio) with a correlation coefficient of 0.287 (P = .0026); however, this correlation was not observed in the proximal PA arteries (correlation coefficient 0.132, P = .173).
One major bleeding event occurred within 72 hours in a patient who also experienced a device-related left common iliac vein thrombosis while not taking anticoagulation medication, and one death unrelated to PE occurred within 30 days.
“The two findings that surprised me include, first, a more than 70% reduction in total and subtotal occlusions in the segmental arteries with such a low dose of r-tPA and, second, the resolution of the blockages was seen not only in the arteries where the device was placed but also at remote sites away from the location of the catheter,” Dr. Bashir told this news organization.
The findings were limited by several factors including the lack of long-term clinical follow-up outcomes data and lack of comparison groups who underwent other treatments.
However, “This study implies that we now have a safe therapy for these patients that improves survival and right ventricular recovery in addition to dramatically improving blocked pulmonary arteries,” Dr. Bashir said.
As for additional research, “we need all the current and future prospective pulmonary embolism studies to include an assessment of pulmonary artery blockage resolution as an essential endpoint,” he said.
Catheter Expands Treatment Options
The current study, a subgroup analysis of the RESCUE trial, was one of the first to examine the impact of catheter-directed lysis on distal occlusions, study coauthor Parth M. Rali, MD, said in an interview.
To this point, literature has been limited to evaluation for proximal disease, said Dr. Rali, director of thoracic surgery and medicine and part of the Pulmonary Embolism Response Team at Temple University Hospital, Philadelphia.
Dr. Rali said he was encouraged to see confirmation that the BEC catheter, because of its design, works in patients with proximal or distal occlusive disease.
In clinical practice, “the catheter provides an additional option for care in patients with multiple distal occlusive disease when a systemic tissue plasminogen activator (tPA), may put patient at high bleeding risk,” Dr. Rali said.
Looking ahead, a prospective, observational multicenter study would be useful to validate the findings from the post hoc analysis of the current study, he noted.
The study was sponsored by the National Heart, Lung, and Blood Institute, Commonwealth of Pennsylvania, and Thrombolex Inc., a medical device company developing interventional catheter-based therapies for the rapid and effective treatment of acute venous thromboembolic disorders. Dr. Bashir is a cofounder and has an equity interest in Thrombolex Inc. Dr. Rali disclosed serving as a consultant for Thrombolex, Inari Medical, Viz AI, and ThinkSono.
FROM JACC: ADVANCES
Slow-to-moderate weight loss better than rapid with antiobesity drugs in OA
TOPLINE:
Individuals with overweight or obesity and knee or hip osteoarthritis (OA) who used antiobesity medications and achieved slow-to-moderate weight loss had a lower risk for all-cause mortality than did those with weight gain or stable weight in a population-based cohort study emulating a randomized controlled trial. Patients who rapidly lost weight had mortality similar to those with weight gain or stable weight.
METHODOLOGY:
- The researchers used the IQVIA Medical Research Database to identify overweight or obese individuals with knee or hip OA; they conducted a hypothetical trial comparing the effects of slow-to-moderate weight loss (defined as 2%-10% of body weight) and rapid weight loss (defined as 5% or more of body weight) within 1 year of starting antiobesity medications.
- The final analysis included patients with a mean age of 60.9 years who met the criteria for treatment adherence to orlistat (n = 3028), sibutramine (n = 2919), or rimonabant (n = 797).
- The primary outcome was all-cause mortality over a 5-year follow-up period; secondary outcomes included hypertension, type 2 diabetes, and venous thromboembolism.
TAKEAWAY:
- All-cause mortality at 5 years was 5.3% with weight gain or stable weight, 4.0% with slow to moderate weight loss, and 5.4% with rapid weight loss.
- Hazard ratios for all-cause mortality were 0.72 (95% CI, 0.56-0.92) for slow to moderate weight loss and 0.99 (95% CI, 0.67-1.44) for the rapid weight loss group.
- Weight loss was associated with the secondary outcomes of reduced hypertension, type 2 diabetes, and venous thromboembolism in a dose-dependent manner.
- A slightly increased risk for cardiovascular disease occurred in the rapid weight loss group, compared with the weight gain or stable group, but this difference was not significant.
IN PRACTICE:
“Our finding that gradual weight loss by antiobesity medications lowers all-cause mortality, if confirmed by future studies, could guide policy-making and improve the well-being of patients with overweight or obesity and knee or hip OA,” the researchers wrote.
SOURCE:
The lead author on the study was Jie Wei, MD, of Central South University, Changsha, China. The study was published online in Arthritis & Rheumatology.
LIMITATIONS:
Study limitations included the inability to control for factors such as exercise, diet, and disease severity; the inability to assess the risk for cause-specific mortality; and the inability to account for the impact of pain reduction and improved function as a result of weight loss.
DISCLOSURES:
The study was supported by the National Key Research and Development Plan, the National Natural Science Foundation of China, the Project Program of National Clinical Research Center for Geriatric Disorders, the Natural Science Foundation of Hunan Province, the Central South University Innovation-Driven Research Programme, and the Science and Technology Innovation Program of Hunan Province. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Individuals with overweight or obesity and knee or hip osteoarthritis (OA) who used antiobesity medications and achieved slow-to-moderate weight loss had a lower risk for all-cause mortality than did those with weight gain or stable weight in a population-based cohort study emulating a randomized controlled trial. Patients who rapidly lost weight had mortality similar to those with weight gain or stable weight.
METHODOLOGY:
- The researchers used the IQVIA Medical Research Database to identify overweight or obese individuals with knee or hip OA; they conducted a hypothetical trial comparing the effects of slow-to-moderate weight loss (defined as 2%-10% of body weight) and rapid weight loss (defined as 5% or more of body weight) within 1 year of starting antiobesity medications.
- The final analysis included patients with a mean age of 60.9 years who met the criteria for treatment adherence to orlistat (n = 3028), sibutramine (n = 2919), or rimonabant (n = 797).
- The primary outcome was all-cause mortality over a 5-year follow-up period; secondary outcomes included hypertension, type 2 diabetes, and venous thromboembolism.
TAKEAWAY:
- All-cause mortality at 5 years was 5.3% with weight gain or stable weight, 4.0% with slow to moderate weight loss, and 5.4% with rapid weight loss.
- Hazard ratios for all-cause mortality were 0.72 (95% CI, 0.56-0.92) for slow to moderate weight loss and 0.99 (95% CI, 0.67-1.44) for the rapid weight loss group.
- Weight loss was associated with the secondary outcomes of reduced hypertension, type 2 diabetes, and venous thromboembolism in a dose-dependent manner.
- A slightly increased risk for cardiovascular disease occurred in the rapid weight loss group, compared with the weight gain or stable group, but this difference was not significant.
IN PRACTICE:
“Our finding that gradual weight loss by antiobesity medications lowers all-cause mortality, if confirmed by future studies, could guide policy-making and improve the well-being of patients with overweight or obesity and knee or hip OA,” the researchers wrote.
SOURCE:
The lead author on the study was Jie Wei, MD, of Central South University, Changsha, China. The study was published online in Arthritis & Rheumatology.
LIMITATIONS:
Study limitations included the inability to control for factors such as exercise, diet, and disease severity; the inability to assess the risk for cause-specific mortality; and the inability to account for the impact of pain reduction and improved function as a result of weight loss.
DISCLOSURES:
The study was supported by the National Key Research and Development Plan, the National Natural Science Foundation of China, the Project Program of National Clinical Research Center for Geriatric Disorders, the Natural Science Foundation of Hunan Province, the Central South University Innovation-Driven Research Programme, and the Science and Technology Innovation Program of Hunan Province. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Individuals with overweight or obesity and knee or hip osteoarthritis (OA) who used antiobesity medications and achieved slow-to-moderate weight loss had a lower risk for all-cause mortality than did those with weight gain or stable weight in a population-based cohort study emulating a randomized controlled trial. Patients who rapidly lost weight had mortality similar to those with weight gain or stable weight.
METHODOLOGY:
- The researchers used the IQVIA Medical Research Database to identify overweight or obese individuals with knee or hip OA; they conducted a hypothetical trial comparing the effects of slow-to-moderate weight loss (defined as 2%-10% of body weight) and rapid weight loss (defined as 5% or more of body weight) within 1 year of starting antiobesity medications.
- The final analysis included patients with a mean age of 60.9 years who met the criteria for treatment adherence to orlistat (n = 3028), sibutramine (n = 2919), or rimonabant (n = 797).
- The primary outcome was all-cause mortality over a 5-year follow-up period; secondary outcomes included hypertension, type 2 diabetes, and venous thromboembolism.
TAKEAWAY:
- All-cause mortality at 5 years was 5.3% with weight gain or stable weight, 4.0% with slow to moderate weight loss, and 5.4% with rapid weight loss.
- Hazard ratios for all-cause mortality were 0.72 (95% CI, 0.56-0.92) for slow to moderate weight loss and 0.99 (95% CI, 0.67-1.44) for the rapid weight loss group.
- Weight loss was associated with the secondary outcomes of reduced hypertension, type 2 diabetes, and venous thromboembolism in a dose-dependent manner.
- A slightly increased risk for cardiovascular disease occurred in the rapid weight loss group, compared with the weight gain or stable group, but this difference was not significant.
IN PRACTICE:
“Our finding that gradual weight loss by antiobesity medications lowers all-cause mortality, if confirmed by future studies, could guide policy-making and improve the well-being of patients with overweight or obesity and knee or hip OA,” the researchers wrote.
SOURCE:
The lead author on the study was Jie Wei, MD, of Central South University, Changsha, China. The study was published online in Arthritis & Rheumatology.
LIMITATIONS:
Study limitations included the inability to control for factors such as exercise, diet, and disease severity; the inability to assess the risk for cause-specific mortality; and the inability to account for the impact of pain reduction and improved function as a result of weight loss.
DISCLOSURES:
The study was supported by the National Key Research and Development Plan, the National Natural Science Foundation of China, the Project Program of National Clinical Research Center for Geriatric Disorders, the Natural Science Foundation of Hunan Province, the Central South University Innovation-Driven Research Programme, and the Science and Technology Innovation Program of Hunan Province. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Acne stigma persists across social and professional settings
from more than 1300 individuals.
Self-stigma among people with acne has been examined in previous studies; however, “little is known about the prevalence and magnitude of stigmatizing attitudes of the general public toward individuals with acne,” wrote Ali Shields of Drexel University, Philadelphia, Pennsylvania, and her coauthors.
In the study, recently published in JAMA Dermatology, they reviewed survey data from 1357 adults aged 18 years and older who were identified through an online national research registry (ResearchMatch). The mean age of the participants was 42.4 years range). 67.7% were female.
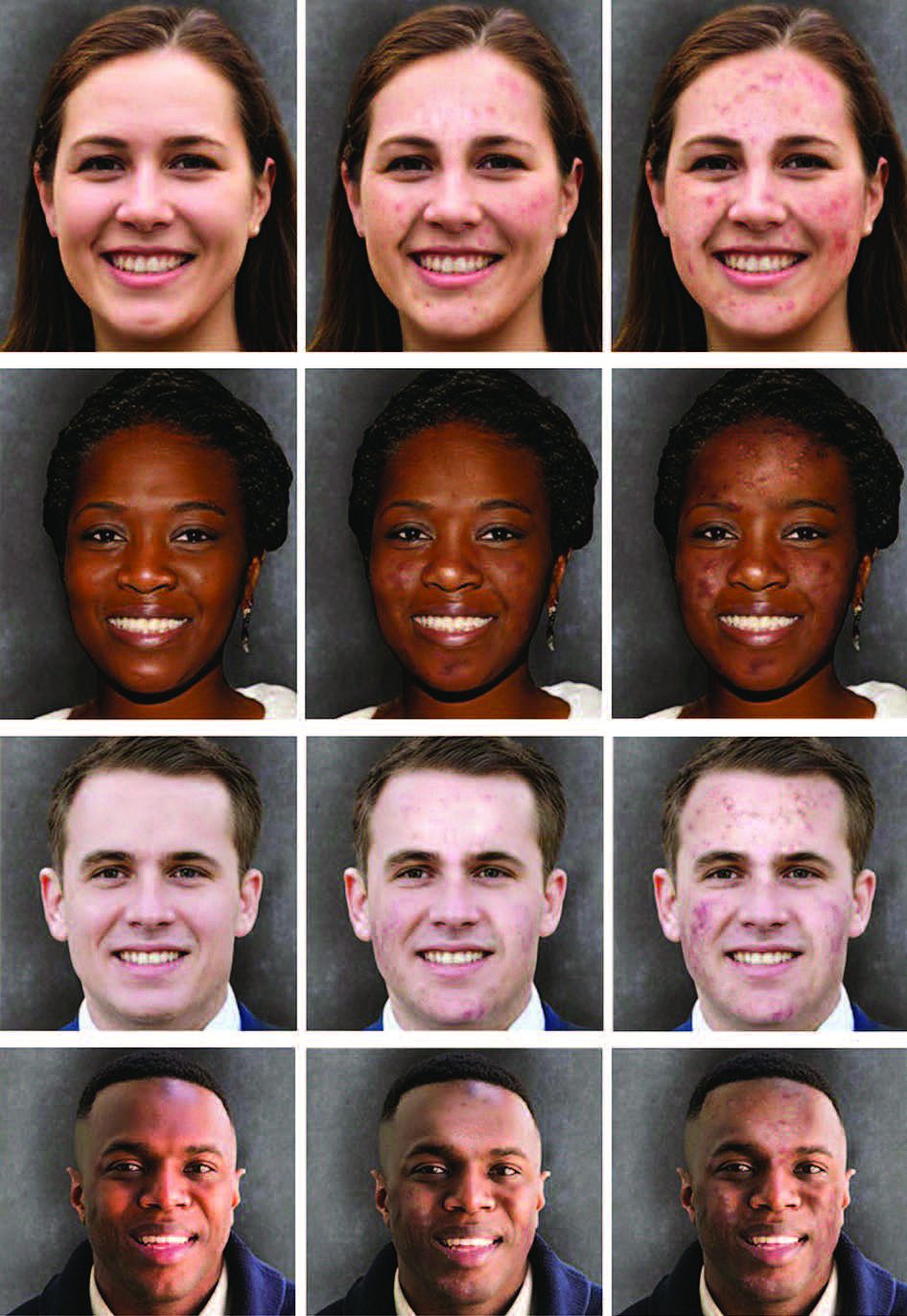
Participants were randomly shown 1 of 12 standardized portraits of individuals that varied in skin tone, sex, and acne severity. They responded to questions about stigmatizing attitudes with respect to the portrait, including stereotype endorsement and desire for social distance.
With regard to social distance, survey participants were significantly less comfortable being friends with people with severe acne, compared with those who did not have acne (adjusted coefficient [aC], -0.28, P = .003). Compared with people without acne, participants also reported significantly less comfort in hiring someone with severe acne (aC, -0.33; P < .001), having physical contact (aC, -0.26; P = .006), dating (aC, -0.44; P = .004), and posting photos with that person on social media (aC, -0.50; P < .001).
With regard to common acne stereotypes, survey participants also rated individuals with severe acne as significantly more likely than those without acne to have poor hygiene and to be unattractive, unintelligent, unlikeable, immature, and untrustworthy (aCs, -1.04, -0.89, -0.42, -0.36, -0.52, and -0.40, respectively; P < .001 for all).
In a linear regression analysis, the researchers found no evidence of association modification by sex of the portraits presented, but found evidence that “the effect size of association of acne with stereotype endorsement was greater for individuals with dark skin.”
The findings were limited by several factors including the potential differences in degree of severity between images after the addition of acne because the baseline images were not exact controls for each other: Therefore comparisons between image sets based on skin tone or sex should be interpreted cautiously, the researchers noted. Other limitations included the homogeneous population of survey respondents and the inability to account for all aspects of stigma, they said.
However, the results illustrate the persistent stigma associated with acne and “highlight the need to identify approaches to reduce stigmatizing attitudes in the community and for adequate access to care, which might prevent negative downstream effects related to these stigmatizing attitudes,” the authors concluded.
The study was supported by a grant from the National Institute of Arthritis and Musculoskeletal Diseases to corresponding author John S. Barbieri, MD. Coauthor Arash Mostaghimi, MD, disclosed personal fees from hims & hers, AbbVie, Sun Pharmaceutical Industries, Pfizer, Digital Diagnostics, Lilly, Equillium, ASLAN Pharmaceuticals, Boehringer Ingelheim, Fig.1 Beauty, Acom Healthcare, and Olaplex outside the current study. Dr. Barbieri disclosed personal fees from Dexcel Pharma for consulting outside the current study.
from more than 1300 individuals.
Self-stigma among people with acne has been examined in previous studies; however, “little is known about the prevalence and magnitude of stigmatizing attitudes of the general public toward individuals with acne,” wrote Ali Shields of Drexel University, Philadelphia, Pennsylvania, and her coauthors.
In the study, recently published in JAMA Dermatology, they reviewed survey data from 1357 adults aged 18 years and older who were identified through an online national research registry (ResearchMatch). The mean age of the participants was 42.4 years range). 67.7% were female.
Participants were randomly shown 1 of 12 standardized portraits of individuals that varied in skin tone, sex, and acne severity. They responded to questions about stigmatizing attitudes with respect to the portrait, including stereotype endorsement and desire for social distance.
With regard to social distance, survey participants were significantly less comfortable being friends with people with severe acne, compared with those who did not have acne (adjusted coefficient [aC], -0.28, P = .003). Compared with people without acne, participants also reported significantly less comfort in hiring someone with severe acne (aC, -0.33; P < .001), having physical contact (aC, -0.26; P = .006), dating (aC, -0.44; P = .004), and posting photos with that person on social media (aC, -0.50; P < .001).
With regard to common acne stereotypes, survey participants also rated individuals with severe acne as significantly more likely than those without acne to have poor hygiene and to be unattractive, unintelligent, unlikeable, immature, and untrustworthy (aCs, -1.04, -0.89, -0.42, -0.36, -0.52, and -0.40, respectively; P < .001 for all).
In a linear regression analysis, the researchers found no evidence of association modification by sex of the portraits presented, but found evidence that “the effect size of association of acne with stereotype endorsement was greater for individuals with dark skin.”
The findings were limited by several factors including the potential differences in degree of severity between images after the addition of acne because the baseline images were not exact controls for each other: Therefore comparisons between image sets based on skin tone or sex should be interpreted cautiously, the researchers noted. Other limitations included the homogeneous population of survey respondents and the inability to account for all aspects of stigma, they said.
However, the results illustrate the persistent stigma associated with acne and “highlight the need to identify approaches to reduce stigmatizing attitudes in the community and for adequate access to care, which might prevent negative downstream effects related to these stigmatizing attitudes,” the authors concluded.
The study was supported by a grant from the National Institute of Arthritis and Musculoskeletal Diseases to corresponding author John S. Barbieri, MD. Coauthor Arash Mostaghimi, MD, disclosed personal fees from hims & hers, AbbVie, Sun Pharmaceutical Industries, Pfizer, Digital Diagnostics, Lilly, Equillium, ASLAN Pharmaceuticals, Boehringer Ingelheim, Fig.1 Beauty, Acom Healthcare, and Olaplex outside the current study. Dr. Barbieri disclosed personal fees from Dexcel Pharma for consulting outside the current study.
from more than 1300 individuals.
Self-stigma among people with acne has been examined in previous studies; however, “little is known about the prevalence and magnitude of stigmatizing attitudes of the general public toward individuals with acne,” wrote Ali Shields of Drexel University, Philadelphia, Pennsylvania, and her coauthors.
In the study, recently published in JAMA Dermatology, they reviewed survey data from 1357 adults aged 18 years and older who were identified through an online national research registry (ResearchMatch). The mean age of the participants was 42.4 years range). 67.7% were female.
Participants were randomly shown 1 of 12 standardized portraits of individuals that varied in skin tone, sex, and acne severity. They responded to questions about stigmatizing attitudes with respect to the portrait, including stereotype endorsement and desire for social distance.
With regard to social distance, survey participants were significantly less comfortable being friends with people with severe acne, compared with those who did not have acne (adjusted coefficient [aC], -0.28, P = .003). Compared with people without acne, participants also reported significantly less comfort in hiring someone with severe acne (aC, -0.33; P < .001), having physical contact (aC, -0.26; P = .006), dating (aC, -0.44; P = .004), and posting photos with that person on social media (aC, -0.50; P < .001).
With regard to common acne stereotypes, survey participants also rated individuals with severe acne as significantly more likely than those without acne to have poor hygiene and to be unattractive, unintelligent, unlikeable, immature, and untrustworthy (aCs, -1.04, -0.89, -0.42, -0.36, -0.52, and -0.40, respectively; P < .001 for all).
In a linear regression analysis, the researchers found no evidence of association modification by sex of the portraits presented, but found evidence that “the effect size of association of acne with stereotype endorsement was greater for individuals with dark skin.”
The findings were limited by several factors including the potential differences in degree of severity between images after the addition of acne because the baseline images were not exact controls for each other: Therefore comparisons between image sets based on skin tone or sex should be interpreted cautiously, the researchers noted. Other limitations included the homogeneous population of survey respondents and the inability to account for all aspects of stigma, they said.
However, the results illustrate the persistent stigma associated with acne and “highlight the need to identify approaches to reduce stigmatizing attitudes in the community and for adequate access to care, which might prevent negative downstream effects related to these stigmatizing attitudes,” the authors concluded.
The study was supported by a grant from the National Institute of Arthritis and Musculoskeletal Diseases to corresponding author John S. Barbieri, MD. Coauthor Arash Mostaghimi, MD, disclosed personal fees from hims & hers, AbbVie, Sun Pharmaceutical Industries, Pfizer, Digital Diagnostics, Lilly, Equillium, ASLAN Pharmaceuticals, Boehringer Ingelheim, Fig.1 Beauty, Acom Healthcare, and Olaplex outside the current study. Dr. Barbieri disclosed personal fees from Dexcel Pharma for consulting outside the current study.
FROM JAMA DERMATOLOGY
Low-dose naltrexone falls short for fibromyalgia
TOPLINE:
Women with fibromyalgia who received low-dose naltrexone showed no significant improvement in pain at 12 weeks, compared with those who received placebo in a randomized trial.
METHODOLOGY:
- The researchers randomly assigned 99 women with fibromyalgia at a single center in Denmark to a daily dose of 6 mg of naltrexone or a placebo for 12 weeks.
- The primary outcome was within-group change in pain intensity from baseline to 12 weeks, measured using an 11-point numeric rating scale (NRS) and the Fibromyalgia Impact Questionnaire-Revised (FIQR); outcomes were measured at 4, 8, and 12 weeks.
- Secondary outcomes included the global impact of FIQR total scores, as well as FIQR scores for tenderness, fatigue, , , anxiety, memory, stiffness, and physical function.
TAKEAWAY:
- The patients ranged in age from 18 to 64 years, with a mean age of 50.6 years, and all but one was White.
- At 12 weeks, the mean change in pain intensity was greater in the naltrexone group compared with the placebo group (−1.3 points vs −0.9 points, respectively), but the difference was not statistically significant.
- Of the secondary outcomes, only memory problems related to fibromyalgia showed significant improvement with naltrexone compared with placebo (−0.93 vs −0.30; P = .004), although the significance was lost after adjusting for multiplicity.
- Adverse events were infrequent and similar between the groups; four of 49 patients in the naltrexone group and three of 50 in the placebo group discontinued their assigned treatments because of side effects, and no safety concerns appeared related to the 6-mg dose.
IN PRACTICE:
“At this time we recommend that off-label treatment of patients who have responded to low-dose naltrexone should not be terminated, but we recommend against initiating low-dose naltrexone for low-dose naltrexone-naive patients with fibromyalgia pending the results of additional adequately powered studies with distinctive inflammatory and autoantibody patient profiles,” Winfried Häuser, MD, of the Center for Pain Medicine and Mental Health, Saarbrücken, Germany, and Mary-Ann Fitzcharles, MD, of McGill University Health Centre, Montreal, Canada, wrote in an accompanying editorial.
SOURCE:
The lead author of the study was Karin Due Bruun, MD, of Odense University Hospital, Denmark. The full study and accompanying editorial were published online in The Lancet Rheumatology.
LIMITATIONS:
The study was only powered to detect a difference of 1.0 NRS points for pain intensity; other limitations include the homogenous population that prevents generalizability to other groups and the relatively short follow-up period.
DISCLOSURES:
The study was supported by the Danish Rheumatism Association, Odense University Hospital, Danielsen’s Foundation, and the Oak Foundation. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Women with fibromyalgia who received low-dose naltrexone showed no significant improvement in pain at 12 weeks, compared with those who received placebo in a randomized trial.
METHODOLOGY:
- The researchers randomly assigned 99 women with fibromyalgia at a single center in Denmark to a daily dose of 6 mg of naltrexone or a placebo for 12 weeks.
- The primary outcome was within-group change in pain intensity from baseline to 12 weeks, measured using an 11-point numeric rating scale (NRS) and the Fibromyalgia Impact Questionnaire-Revised (FIQR); outcomes were measured at 4, 8, and 12 weeks.
- Secondary outcomes included the global impact of FIQR total scores, as well as FIQR scores for tenderness, fatigue, , , anxiety, memory, stiffness, and physical function.
TAKEAWAY:
- The patients ranged in age from 18 to 64 years, with a mean age of 50.6 years, and all but one was White.
- At 12 weeks, the mean change in pain intensity was greater in the naltrexone group compared with the placebo group (−1.3 points vs −0.9 points, respectively), but the difference was not statistically significant.
- Of the secondary outcomes, only memory problems related to fibromyalgia showed significant improvement with naltrexone compared with placebo (−0.93 vs −0.30; P = .004), although the significance was lost after adjusting for multiplicity.
- Adverse events were infrequent and similar between the groups; four of 49 patients in the naltrexone group and three of 50 in the placebo group discontinued their assigned treatments because of side effects, and no safety concerns appeared related to the 6-mg dose.
IN PRACTICE:
“At this time we recommend that off-label treatment of patients who have responded to low-dose naltrexone should not be terminated, but we recommend against initiating low-dose naltrexone for low-dose naltrexone-naive patients with fibromyalgia pending the results of additional adequately powered studies with distinctive inflammatory and autoantibody patient profiles,” Winfried Häuser, MD, of the Center for Pain Medicine and Mental Health, Saarbrücken, Germany, and Mary-Ann Fitzcharles, MD, of McGill University Health Centre, Montreal, Canada, wrote in an accompanying editorial.
SOURCE:
The lead author of the study was Karin Due Bruun, MD, of Odense University Hospital, Denmark. The full study and accompanying editorial were published online in The Lancet Rheumatology.
LIMITATIONS:
The study was only powered to detect a difference of 1.0 NRS points for pain intensity; other limitations include the homogenous population that prevents generalizability to other groups and the relatively short follow-up period.
DISCLOSURES:
The study was supported by the Danish Rheumatism Association, Odense University Hospital, Danielsen’s Foundation, and the Oak Foundation. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Women with fibromyalgia who received low-dose naltrexone showed no significant improvement in pain at 12 weeks, compared with those who received placebo in a randomized trial.
METHODOLOGY:
- The researchers randomly assigned 99 women with fibromyalgia at a single center in Denmark to a daily dose of 6 mg of naltrexone or a placebo for 12 weeks.
- The primary outcome was within-group change in pain intensity from baseline to 12 weeks, measured using an 11-point numeric rating scale (NRS) and the Fibromyalgia Impact Questionnaire-Revised (FIQR); outcomes were measured at 4, 8, and 12 weeks.
- Secondary outcomes included the global impact of FIQR total scores, as well as FIQR scores for tenderness, fatigue, , , anxiety, memory, stiffness, and physical function.
TAKEAWAY:
- The patients ranged in age from 18 to 64 years, with a mean age of 50.6 years, and all but one was White.
- At 12 weeks, the mean change in pain intensity was greater in the naltrexone group compared with the placebo group (−1.3 points vs −0.9 points, respectively), but the difference was not statistically significant.
- Of the secondary outcomes, only memory problems related to fibromyalgia showed significant improvement with naltrexone compared with placebo (−0.93 vs −0.30; P = .004), although the significance was lost after adjusting for multiplicity.
- Adverse events were infrequent and similar between the groups; four of 49 patients in the naltrexone group and three of 50 in the placebo group discontinued their assigned treatments because of side effects, and no safety concerns appeared related to the 6-mg dose.
IN PRACTICE:
“At this time we recommend that off-label treatment of patients who have responded to low-dose naltrexone should not be terminated, but we recommend against initiating low-dose naltrexone for low-dose naltrexone-naive patients with fibromyalgia pending the results of additional adequately powered studies with distinctive inflammatory and autoantibody patient profiles,” Winfried Häuser, MD, of the Center for Pain Medicine and Mental Health, Saarbrücken, Germany, and Mary-Ann Fitzcharles, MD, of McGill University Health Centre, Montreal, Canada, wrote in an accompanying editorial.
SOURCE:
The lead author of the study was Karin Due Bruun, MD, of Odense University Hospital, Denmark. The full study and accompanying editorial were published online in The Lancet Rheumatology.
LIMITATIONS:
The study was only powered to detect a difference of 1.0 NRS points for pain intensity; other limitations include the homogenous population that prevents generalizability to other groups and the relatively short follow-up period.
DISCLOSURES:
The study was supported by the Danish Rheumatism Association, Odense University Hospital, Danielsen’s Foundation, and the Oak Foundation. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Bimekizumab shows promise for palmoplantar pustular psoriasis
.
PPP is a type of pustular psoriasis that remains a treatment challenge, and available treatments for palmoplantar plaque psoriasis with pustules also “remain unsatisfactory,” according to Thierry Passeron, MD, PhD, of the dermatology service at Centre Hospitalier Universitaire de Nice (France), and colleagues. Bimekizumab, an anti-interleukin (IL)-17A and anti-IL-17F antibody therapy, has been used for psoriasis and psoriatic arthritis (PsA), but its effectiveness for PPP has not been studied, they said. In the United States, bimekizumab (Bimzelx), administered subcutaneously, was recently approved for treating moderate to severe plaque psoriasis in adults; in the European Union, it is approved for treating psoriasis, in addition to psoriatic arthritis, axial spondyloarthritis and ankylosing spondylitis.
In the case series published in JAMA Dermatology, Dr. Passeron and coinvestigators identified 11 adults with PPP and 10 with palmoplantar plaque psoriasis with pustules who were treated at one of seven tertiary dermatology centers in France from September 2022 through June 2023. PPP also has been associated with bone and joint inflammation in SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome.
All patients received bimekizumab for at least 3 months. The patients — 19 women and 2 men — ranged in age from 24 to 68 years (mean age, 46 years). The primary outcome was complete clearance, defined as an Investigator Global Assessment (IGA) score of 0.
A total of 17 patients achieved an IGA score of zero in 1-4 months. Over 3-6 months, three patients achieved an IGA score of 1 (almost clear), and one patient achieved an IGA score of 2 (mild).
Three patients with PPP also had acrodermatitis continua of Hallopeau; in these patients, nail involvement improved by 50%-70% after 4-6 months of bimekizumab use. Two patients with SAPHO experienced complete clearance of skin lesions associated with improvement in joint pain.
Four patients developed oral and genital candidiasis during treatment, but all were treated successfully with antifungals. None of the patients discontinued bimekizumab because of adverse events. “All patients are still receiving treatment, and their psoriatic lesions remain controlled,” the authors wrote.
“The rapid and consistent improvement observed in the present case series supports the effectiveness of bimekizumab therapy in managing PPP, palmoplantar plaque psoriasis with pustules, and SAPHO syndrome,” they said in their discussion.
The study findings were limited by several factors including the small sample size and short follow-up period, and by the inclusion of only patients with severe disease; and prospective, placebo-controlled studies are needed to confirm the results, the researchers noted.
However, the results suggest that bimekizumab could be a treatment approach for PPP, palmoplantar plaque psoriasis with pustules, and SAPHO syndrome, and warrant a prospective, randomized, placebo-controlled, randomized clinical trial to confirm the findings, they concluded.
Dr. Passeron disclosed fees from AbbVie, ACM Pharma, Almirall, Boehringer Ingelheim, Bristol Myers Squibb, Calypso, Celgene, Galderma, Genzyme/Sanofi, GlaxoSmithKline, Incyte, Janssen, LEO Pharma, Eli Lilly, Novartis, Roivant Sciences, Sun Pharmaceuticals, and VYNE Therapeutics outside the current study; he is a cofounder of Yukin Therapeutics. Three authors disclosed receiving personal fees from UCB, manufacturer of bimekizumab, outside of the submitted work, another author disclosed receiving personal fees from UCB during the conduct of the study, and another reported receiving grants from UCB and several other companies, outside the submitted work.
The study findings were also presented at a meeting, Les Journées Dermatologiques de Paris 2023, on December 6, in Paris.
.
PPP is a type of pustular psoriasis that remains a treatment challenge, and available treatments for palmoplantar plaque psoriasis with pustules also “remain unsatisfactory,” according to Thierry Passeron, MD, PhD, of the dermatology service at Centre Hospitalier Universitaire de Nice (France), and colleagues. Bimekizumab, an anti-interleukin (IL)-17A and anti-IL-17F antibody therapy, has been used for psoriasis and psoriatic arthritis (PsA), but its effectiveness for PPP has not been studied, they said. In the United States, bimekizumab (Bimzelx), administered subcutaneously, was recently approved for treating moderate to severe plaque psoriasis in adults; in the European Union, it is approved for treating psoriasis, in addition to psoriatic arthritis, axial spondyloarthritis and ankylosing spondylitis.
In the case series published in JAMA Dermatology, Dr. Passeron and coinvestigators identified 11 adults with PPP and 10 with palmoplantar plaque psoriasis with pustules who were treated at one of seven tertiary dermatology centers in France from September 2022 through June 2023. PPP also has been associated with bone and joint inflammation in SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome.
All patients received bimekizumab for at least 3 months. The patients — 19 women and 2 men — ranged in age from 24 to 68 years (mean age, 46 years). The primary outcome was complete clearance, defined as an Investigator Global Assessment (IGA) score of 0.
A total of 17 patients achieved an IGA score of zero in 1-4 months. Over 3-6 months, three patients achieved an IGA score of 1 (almost clear), and one patient achieved an IGA score of 2 (mild).
Three patients with PPP also had acrodermatitis continua of Hallopeau; in these patients, nail involvement improved by 50%-70% after 4-6 months of bimekizumab use. Two patients with SAPHO experienced complete clearance of skin lesions associated with improvement in joint pain.
Four patients developed oral and genital candidiasis during treatment, but all were treated successfully with antifungals. None of the patients discontinued bimekizumab because of adverse events. “All patients are still receiving treatment, and their psoriatic lesions remain controlled,” the authors wrote.
“The rapid and consistent improvement observed in the present case series supports the effectiveness of bimekizumab therapy in managing PPP, palmoplantar plaque psoriasis with pustules, and SAPHO syndrome,” they said in their discussion.
The study findings were limited by several factors including the small sample size and short follow-up period, and by the inclusion of only patients with severe disease; and prospective, placebo-controlled studies are needed to confirm the results, the researchers noted.
However, the results suggest that bimekizumab could be a treatment approach for PPP, palmoplantar plaque psoriasis with pustules, and SAPHO syndrome, and warrant a prospective, randomized, placebo-controlled, randomized clinical trial to confirm the findings, they concluded.
Dr. Passeron disclosed fees from AbbVie, ACM Pharma, Almirall, Boehringer Ingelheim, Bristol Myers Squibb, Calypso, Celgene, Galderma, Genzyme/Sanofi, GlaxoSmithKline, Incyte, Janssen, LEO Pharma, Eli Lilly, Novartis, Roivant Sciences, Sun Pharmaceuticals, and VYNE Therapeutics outside the current study; he is a cofounder of Yukin Therapeutics. Three authors disclosed receiving personal fees from UCB, manufacturer of bimekizumab, outside of the submitted work, another author disclosed receiving personal fees from UCB during the conduct of the study, and another reported receiving grants from UCB and several other companies, outside the submitted work.
The study findings were also presented at a meeting, Les Journées Dermatologiques de Paris 2023, on December 6, in Paris.
.
PPP is a type of pustular psoriasis that remains a treatment challenge, and available treatments for palmoplantar plaque psoriasis with pustules also “remain unsatisfactory,” according to Thierry Passeron, MD, PhD, of the dermatology service at Centre Hospitalier Universitaire de Nice (France), and colleagues. Bimekizumab, an anti-interleukin (IL)-17A and anti-IL-17F antibody therapy, has been used for psoriasis and psoriatic arthritis (PsA), but its effectiveness for PPP has not been studied, they said. In the United States, bimekizumab (Bimzelx), administered subcutaneously, was recently approved for treating moderate to severe plaque psoriasis in adults; in the European Union, it is approved for treating psoriasis, in addition to psoriatic arthritis, axial spondyloarthritis and ankylosing spondylitis.
In the case series published in JAMA Dermatology, Dr. Passeron and coinvestigators identified 11 adults with PPP and 10 with palmoplantar plaque psoriasis with pustules who were treated at one of seven tertiary dermatology centers in France from September 2022 through June 2023. PPP also has been associated with bone and joint inflammation in SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome.
All patients received bimekizumab for at least 3 months. The patients — 19 women and 2 men — ranged in age from 24 to 68 years (mean age, 46 years). The primary outcome was complete clearance, defined as an Investigator Global Assessment (IGA) score of 0.
A total of 17 patients achieved an IGA score of zero in 1-4 months. Over 3-6 months, three patients achieved an IGA score of 1 (almost clear), and one patient achieved an IGA score of 2 (mild).
Three patients with PPP also had acrodermatitis continua of Hallopeau; in these patients, nail involvement improved by 50%-70% after 4-6 months of bimekizumab use. Two patients with SAPHO experienced complete clearance of skin lesions associated with improvement in joint pain.
Four patients developed oral and genital candidiasis during treatment, but all were treated successfully with antifungals. None of the patients discontinued bimekizumab because of adverse events. “All patients are still receiving treatment, and their psoriatic lesions remain controlled,” the authors wrote.
“The rapid and consistent improvement observed in the present case series supports the effectiveness of bimekizumab therapy in managing PPP, palmoplantar plaque psoriasis with pustules, and SAPHO syndrome,” they said in their discussion.
The study findings were limited by several factors including the small sample size and short follow-up period, and by the inclusion of only patients with severe disease; and prospective, placebo-controlled studies are needed to confirm the results, the researchers noted.
However, the results suggest that bimekizumab could be a treatment approach for PPP, palmoplantar plaque psoriasis with pustules, and SAPHO syndrome, and warrant a prospective, randomized, placebo-controlled, randomized clinical trial to confirm the findings, they concluded.
Dr. Passeron disclosed fees from AbbVie, ACM Pharma, Almirall, Boehringer Ingelheim, Bristol Myers Squibb, Calypso, Celgene, Galderma, Genzyme/Sanofi, GlaxoSmithKline, Incyte, Janssen, LEO Pharma, Eli Lilly, Novartis, Roivant Sciences, Sun Pharmaceuticals, and VYNE Therapeutics outside the current study; he is a cofounder of Yukin Therapeutics. Three authors disclosed receiving personal fees from UCB, manufacturer of bimekizumab, outside of the submitted work, another author disclosed receiving personal fees from UCB during the conduct of the study, and another reported receiving grants from UCB and several other companies, outside the submitted work.
The study findings were also presented at a meeting, Les Journées Dermatologiques de Paris 2023, on December 6, in Paris.
FROM JAMA DERMATOLOGY
Elagolix curbs heavy bleeding linked to uterine leiomyomas
Uterine leiomyomas are common in premenopausal women, and 60% experience heavy menstrual bleeding, but nonsurgical options as an alternative to hysterectomy are limited, wrote Eric Brown, MD, of Gyn-Care, Atlanta, Georgia, and colleagues.
Elagolix sodium, an oral, short-acting nonpeptide, gonadotropin-releasing hormone antagonist, has been approved by the Food and Drug Administration at a dose of 300 mg twice daily with add-back therapy for up to 24 months of use. However, this treatment protocol is contraindicated or not preferable for some patients, the researchers said.
In a study published in Obstetrics & Gynecology , the researchers randomized 54 women to 150 mg of oral elagolix once daily, and 28 to a placebo for 6 months to investigate the safety and efficacy of the lower dose. The study population included women aged 18-51 years with a history of heavy menstrual bleeding association with uterine leiomyomas. Approximately two-thirds (65.9%) were Black.
The primary endpoint was the proportion of patients who met the criteria of menstrual blood loss volume less than 80 mL during the final month of treatment and menstrual blood loss volume reduction of 50% or more from baseline to the final month of treatment.
After 6 months, nearly half (49.4%) of the elagolix group met the study endpoint compared with 23.3% of the placebo group (P = .035).
Elagolix patients showed significantly greater reductions in both mean and median menstrual blood loss volumes compared with the placebo patients over the study period, and significant differences between the groups in the mean reduction of menstrual blood loss were evident after 1 month of treatment (P < .05 for months 1, 2, 3, and 5).
Results were similar in a further sensitivity analysis in which patients with incomplete final month data were considered nonresponders; 44.4% of elagolix patients and 21.4% of patients met the primary endpoint.
Overall, 51.9% of elagolix patients and 39.3% of placebo patients reported adverse events; the most common were headache and hot flush. Three patients (5.6%) in the elagolix group discontinued the drug because of adverse events. No serious or severe adverse events were reported in the elagolix group; both cases of reported serious adverse events (COVID-19 and an enlarged uvula) occurred in placebo patients.
Patient-reported outcomes were significantly greater in the elagolix patients, based on symptom severity score, 5 of 6 Uterine Fibroid Symptom and Quality of Life (UFS-QOL) health-related quality of life subscales, and the HRQOL total score at the end of the study.
The findings were limited by several factors including the small study population and lenient eligibility criteria that may have led to a higher placebo response rate, and the study did not monitor bone mineral density, the researchers noted.
However, the results suggest that elagolix at a 150-mg dose was well tolerated, with a safety profile similar to that seen in women who took the drug for endometriosis pain, and may be an option for women with contraindications to other therapy or for those who prefer once-daily dosing, they concluded.
The study was funded by AbbVie. Lead author Dr. Brown had no additional financial conflicts to disclose, but several coauthors disclosed relationships with AbbVie and other companies.
Uterine leiomyomas are common in premenopausal women, and 60% experience heavy menstrual bleeding, but nonsurgical options as an alternative to hysterectomy are limited, wrote Eric Brown, MD, of Gyn-Care, Atlanta, Georgia, and colleagues.
Elagolix sodium, an oral, short-acting nonpeptide, gonadotropin-releasing hormone antagonist, has been approved by the Food and Drug Administration at a dose of 300 mg twice daily with add-back therapy for up to 24 months of use. However, this treatment protocol is contraindicated or not preferable for some patients, the researchers said.
In a study published in Obstetrics & Gynecology , the researchers randomized 54 women to 150 mg of oral elagolix once daily, and 28 to a placebo for 6 months to investigate the safety and efficacy of the lower dose. The study population included women aged 18-51 years with a history of heavy menstrual bleeding association with uterine leiomyomas. Approximately two-thirds (65.9%) were Black.
The primary endpoint was the proportion of patients who met the criteria of menstrual blood loss volume less than 80 mL during the final month of treatment and menstrual blood loss volume reduction of 50% or more from baseline to the final month of treatment.
After 6 months, nearly half (49.4%) of the elagolix group met the study endpoint compared with 23.3% of the placebo group (P = .035).
Elagolix patients showed significantly greater reductions in both mean and median menstrual blood loss volumes compared with the placebo patients over the study period, and significant differences between the groups in the mean reduction of menstrual blood loss were evident after 1 month of treatment (P < .05 for months 1, 2, 3, and 5).
Results were similar in a further sensitivity analysis in which patients with incomplete final month data were considered nonresponders; 44.4% of elagolix patients and 21.4% of patients met the primary endpoint.
Overall, 51.9% of elagolix patients and 39.3% of placebo patients reported adverse events; the most common were headache and hot flush. Three patients (5.6%) in the elagolix group discontinued the drug because of adverse events. No serious or severe adverse events were reported in the elagolix group; both cases of reported serious adverse events (COVID-19 and an enlarged uvula) occurred in placebo patients.
Patient-reported outcomes were significantly greater in the elagolix patients, based on symptom severity score, 5 of 6 Uterine Fibroid Symptom and Quality of Life (UFS-QOL) health-related quality of life subscales, and the HRQOL total score at the end of the study.
The findings were limited by several factors including the small study population and lenient eligibility criteria that may have led to a higher placebo response rate, and the study did not monitor bone mineral density, the researchers noted.
However, the results suggest that elagolix at a 150-mg dose was well tolerated, with a safety profile similar to that seen in women who took the drug for endometriosis pain, and may be an option for women with contraindications to other therapy or for those who prefer once-daily dosing, they concluded.
The study was funded by AbbVie. Lead author Dr. Brown had no additional financial conflicts to disclose, but several coauthors disclosed relationships with AbbVie and other companies.
Uterine leiomyomas are common in premenopausal women, and 60% experience heavy menstrual bleeding, but nonsurgical options as an alternative to hysterectomy are limited, wrote Eric Brown, MD, of Gyn-Care, Atlanta, Georgia, and colleagues.
Elagolix sodium, an oral, short-acting nonpeptide, gonadotropin-releasing hormone antagonist, has been approved by the Food and Drug Administration at a dose of 300 mg twice daily with add-back therapy for up to 24 months of use. However, this treatment protocol is contraindicated or not preferable for some patients, the researchers said.
In a study published in Obstetrics & Gynecology , the researchers randomized 54 women to 150 mg of oral elagolix once daily, and 28 to a placebo for 6 months to investigate the safety and efficacy of the lower dose. The study population included women aged 18-51 years with a history of heavy menstrual bleeding association with uterine leiomyomas. Approximately two-thirds (65.9%) were Black.
The primary endpoint was the proportion of patients who met the criteria of menstrual blood loss volume less than 80 mL during the final month of treatment and menstrual blood loss volume reduction of 50% or more from baseline to the final month of treatment.
After 6 months, nearly half (49.4%) of the elagolix group met the study endpoint compared with 23.3% of the placebo group (P = .035).
Elagolix patients showed significantly greater reductions in both mean and median menstrual blood loss volumes compared with the placebo patients over the study period, and significant differences between the groups in the mean reduction of menstrual blood loss were evident after 1 month of treatment (P < .05 for months 1, 2, 3, and 5).
Results were similar in a further sensitivity analysis in which patients with incomplete final month data were considered nonresponders; 44.4% of elagolix patients and 21.4% of patients met the primary endpoint.
Overall, 51.9% of elagolix patients and 39.3% of placebo patients reported adverse events; the most common were headache and hot flush. Three patients (5.6%) in the elagolix group discontinued the drug because of adverse events. No serious or severe adverse events were reported in the elagolix group; both cases of reported serious adverse events (COVID-19 and an enlarged uvula) occurred in placebo patients.
Patient-reported outcomes were significantly greater in the elagolix patients, based on symptom severity score, 5 of 6 Uterine Fibroid Symptom and Quality of Life (UFS-QOL) health-related quality of life subscales, and the HRQOL total score at the end of the study.
The findings were limited by several factors including the small study population and lenient eligibility criteria that may have led to a higher placebo response rate, and the study did not monitor bone mineral density, the researchers noted.
However, the results suggest that elagolix at a 150-mg dose was well tolerated, with a safety profile similar to that seen in women who took the drug for endometriosis pain, and may be an option for women with contraindications to other therapy or for those who prefer once-daily dosing, they concluded.
The study was funded by AbbVie. Lead author Dr. Brown had no additional financial conflicts to disclose, but several coauthors disclosed relationships with AbbVie and other companies.
FROM OBSTETRICS & GYNECOLOGY
Antihypertensives show similar long-term mortality rates
Long-term data showed negligible differences in mortality among hypertensive adults treated with thiazide-type diuretics, calcium channel blockers, or angiotensin-converting enzyme inhibitors in a review of nearly 33,000 individuals published in JAMA Network Open.
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) study was designed to compare initial antihypertensive treatments with a calcium channel blocker (CCB; amlodipine), an angiotensin-converting enzyme (ACE) inhibitor (lisinopril) or an alpha-blocker (doxazosin), and a thiazide-type diuretic (chlorthalidone).
The composite primary outcome was fatal coronary heart disease (CHD) or nonfatal myocardial infarction (MI), but long-term data were lacking, wrote Jose-Miguel Yamal, PhD, of University of Texas Health Science Center at Houston, and colleagues. A previous study with 8-13 years of follow-up showed no significant differences in mortality between the treatment groups, the researchers noted.
In the current study, a prespecified secondary analysis of ALLHAT, the researchers added 11 more years of data for a total of 19-24 years of follow-up after randomization.
In the original ALLHAT, 32,804 adults aged 55 years and older with a diagnosis of hypertension and at least one additional coronary heart disease risk factor were followed for 4-8 years for all-cause mortality. A subgroup of 22,754 were followed for fatal or nonfatal cardiovascular disease (CVD) for a mean of 13.7 years, with a maximum of 23.9 years.
The study occurred from Feb. 23, 1994, to Dec. 31, 2017. The participants were randomized to receive a thiazide-type diuretic (15,002 patients), a CCB (8,898 patients), or an ACE inhibitor (8,904 patients).
The primary outcome was CVD mortality; secondary outcomes included all-cause mortality, combined fatal and nonfatal CVD (CVD morbidity), and both morbidity and mortality for coronary heart disease, stroke, heart failure, end-stage renal disease, and cancer.
At 23 years, CVD mortality rates per 100 persons were 23.7, 21.6, and 23.8 in the diuretic, CCB, and ACE inhibitor groups, respectively. The adjusted hazard ratios were 0.97 for CCB vs. diuretics and 1.06 for ACE inhibitors vs. diuretics.
Although the risk of stroke mortality and of combined fatal and nonfatal hospitalized stroke was higher in the ACE inhibitor group compared with the diuretic group (adjusted hazard ratios 1.19 and 1.11, respectively), this increase was no longer significant after adjustment for multiple comparisons. “In contrast to the in-trial and 8-year to 13-year analyses, we now observed that the lisinopril group had an increased risk of kidney disease mortality that emerged after approximately 13 years after randomization, but this effect was attenuated after adjustment for baseline variables,” the researchers wrote in their discussion.
The findings were limited by several factors including the potential effect of unblinding if participants stopped the randomized drug, and by the lack of morbidity and mortality data on Canadian participants, Veterans Affairs participants, and those with no Medicare number, the researchers noted. Other limitations included the lack of data on posttrial medication use, blood pressure, and laboratory findings, they said.
However, the results over the follow-up period of up to 23 years supported those of the larger ALLHAT study, with similar outcomes among the drugs, and with 11 years of passive follow-up, “the results for lisinopril vs. chlorthalidone for stroke and stroke mortality are almost the same,” they concluded.
Findings support current practice, but new drug data are needed
The current study was important to determine whether there was a significant difference in long-term morbidity and mortality between patients treated with thiazide diuretics, calcium channel blockers and ACE inhibitors, Noel Deep, MD, said in an interview.
“Previously reported data had indicated no significant differences between patients randomized to one of these three classes of antihypertensive medications during the trial period or at 8-13 years post trial,” said Dr. Deep, a general internist in private practice in Antigo, Wisc., who was not involved in the study. Dr. Deep is chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
“This study reinforces the previously noted benefits of the three classes of antihypertensive medications, as well as the higher rates of cardiovascular disease and stroke in the ACE inhibitor arm,” he said.
In clinical practice, the results suggest that thiazide diuretics should be considered first-line agents for management of hypertension based on their noninferiority compared with ACE inhibitors and CCBs, and lower risk of stroke compared with ACE inhibitors, Dr. Deep said in an interview. “All three classes of antihypertensive medications are equally efficacious in blood pressure control and preventing all-cause mortality,” he said.
More research is needed in the wake of the introduction of other classes of antihypertensives since the original ALLHAT trial, Dr. Deep said. “It would be beneficial to assess the relative benefit/risks of those medications compared to the thiazide diuretics, and I would also look at studies comparing beta blockers to the thiazide diuretics,” he said. The question remains as to whether outcomes were affected by patients’ use of other classes of antihypertensives after the trial period, he said.
The study was supported by the National Institute on Aging of the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose and serves on the editorial advisory board of Internal Medicine News.
Long-term data showed negligible differences in mortality among hypertensive adults treated with thiazide-type diuretics, calcium channel blockers, or angiotensin-converting enzyme inhibitors in a review of nearly 33,000 individuals published in JAMA Network Open.
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) study was designed to compare initial antihypertensive treatments with a calcium channel blocker (CCB; amlodipine), an angiotensin-converting enzyme (ACE) inhibitor (lisinopril) or an alpha-blocker (doxazosin), and a thiazide-type diuretic (chlorthalidone).
The composite primary outcome was fatal coronary heart disease (CHD) or nonfatal myocardial infarction (MI), but long-term data were lacking, wrote Jose-Miguel Yamal, PhD, of University of Texas Health Science Center at Houston, and colleagues. A previous study with 8-13 years of follow-up showed no significant differences in mortality between the treatment groups, the researchers noted.
In the current study, a prespecified secondary analysis of ALLHAT, the researchers added 11 more years of data for a total of 19-24 years of follow-up after randomization.
In the original ALLHAT, 32,804 adults aged 55 years and older with a diagnosis of hypertension and at least one additional coronary heart disease risk factor were followed for 4-8 years for all-cause mortality. A subgroup of 22,754 were followed for fatal or nonfatal cardiovascular disease (CVD) for a mean of 13.7 years, with a maximum of 23.9 years.
The study occurred from Feb. 23, 1994, to Dec. 31, 2017. The participants were randomized to receive a thiazide-type diuretic (15,002 patients), a CCB (8,898 patients), or an ACE inhibitor (8,904 patients).
The primary outcome was CVD mortality; secondary outcomes included all-cause mortality, combined fatal and nonfatal CVD (CVD morbidity), and both morbidity and mortality for coronary heart disease, stroke, heart failure, end-stage renal disease, and cancer.
At 23 years, CVD mortality rates per 100 persons were 23.7, 21.6, and 23.8 in the diuretic, CCB, and ACE inhibitor groups, respectively. The adjusted hazard ratios were 0.97 for CCB vs. diuretics and 1.06 for ACE inhibitors vs. diuretics.
Although the risk of stroke mortality and of combined fatal and nonfatal hospitalized stroke was higher in the ACE inhibitor group compared with the diuretic group (adjusted hazard ratios 1.19 and 1.11, respectively), this increase was no longer significant after adjustment for multiple comparisons. “In contrast to the in-trial and 8-year to 13-year analyses, we now observed that the lisinopril group had an increased risk of kidney disease mortality that emerged after approximately 13 years after randomization, but this effect was attenuated after adjustment for baseline variables,” the researchers wrote in their discussion.
The findings were limited by several factors including the potential effect of unblinding if participants stopped the randomized drug, and by the lack of morbidity and mortality data on Canadian participants, Veterans Affairs participants, and those with no Medicare number, the researchers noted. Other limitations included the lack of data on posttrial medication use, blood pressure, and laboratory findings, they said.
However, the results over the follow-up period of up to 23 years supported those of the larger ALLHAT study, with similar outcomes among the drugs, and with 11 years of passive follow-up, “the results for lisinopril vs. chlorthalidone for stroke and stroke mortality are almost the same,” they concluded.
Findings support current practice, but new drug data are needed
The current study was important to determine whether there was a significant difference in long-term morbidity and mortality between patients treated with thiazide diuretics, calcium channel blockers and ACE inhibitors, Noel Deep, MD, said in an interview.
“Previously reported data had indicated no significant differences between patients randomized to one of these three classes of antihypertensive medications during the trial period or at 8-13 years post trial,” said Dr. Deep, a general internist in private practice in Antigo, Wisc., who was not involved in the study. Dr. Deep is chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
“This study reinforces the previously noted benefits of the three classes of antihypertensive medications, as well as the higher rates of cardiovascular disease and stroke in the ACE inhibitor arm,” he said.
In clinical practice, the results suggest that thiazide diuretics should be considered first-line agents for management of hypertension based on their noninferiority compared with ACE inhibitors and CCBs, and lower risk of stroke compared with ACE inhibitors, Dr. Deep said in an interview. “All three classes of antihypertensive medications are equally efficacious in blood pressure control and preventing all-cause mortality,” he said.
More research is needed in the wake of the introduction of other classes of antihypertensives since the original ALLHAT trial, Dr. Deep said. “It would be beneficial to assess the relative benefit/risks of those medications compared to the thiazide diuretics, and I would also look at studies comparing beta blockers to the thiazide diuretics,” he said. The question remains as to whether outcomes were affected by patients’ use of other classes of antihypertensives after the trial period, he said.
The study was supported by the National Institute on Aging of the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose and serves on the editorial advisory board of Internal Medicine News.
Long-term data showed negligible differences in mortality among hypertensive adults treated with thiazide-type diuretics, calcium channel blockers, or angiotensin-converting enzyme inhibitors in a review of nearly 33,000 individuals published in JAMA Network Open.
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) study was designed to compare initial antihypertensive treatments with a calcium channel blocker (CCB; amlodipine), an angiotensin-converting enzyme (ACE) inhibitor (lisinopril) or an alpha-blocker (doxazosin), and a thiazide-type diuretic (chlorthalidone).
The composite primary outcome was fatal coronary heart disease (CHD) or nonfatal myocardial infarction (MI), but long-term data were lacking, wrote Jose-Miguel Yamal, PhD, of University of Texas Health Science Center at Houston, and colleagues. A previous study with 8-13 years of follow-up showed no significant differences in mortality between the treatment groups, the researchers noted.
In the current study, a prespecified secondary analysis of ALLHAT, the researchers added 11 more years of data for a total of 19-24 years of follow-up after randomization.
In the original ALLHAT, 32,804 adults aged 55 years and older with a diagnosis of hypertension and at least one additional coronary heart disease risk factor were followed for 4-8 years for all-cause mortality. A subgroup of 22,754 were followed for fatal or nonfatal cardiovascular disease (CVD) for a mean of 13.7 years, with a maximum of 23.9 years.
The study occurred from Feb. 23, 1994, to Dec. 31, 2017. The participants were randomized to receive a thiazide-type diuretic (15,002 patients), a CCB (8,898 patients), or an ACE inhibitor (8,904 patients).
The primary outcome was CVD mortality; secondary outcomes included all-cause mortality, combined fatal and nonfatal CVD (CVD morbidity), and both morbidity and mortality for coronary heart disease, stroke, heart failure, end-stage renal disease, and cancer.
At 23 years, CVD mortality rates per 100 persons were 23.7, 21.6, and 23.8 in the diuretic, CCB, and ACE inhibitor groups, respectively. The adjusted hazard ratios were 0.97 for CCB vs. diuretics and 1.06 for ACE inhibitors vs. diuretics.
Although the risk of stroke mortality and of combined fatal and nonfatal hospitalized stroke was higher in the ACE inhibitor group compared with the diuretic group (adjusted hazard ratios 1.19 and 1.11, respectively), this increase was no longer significant after adjustment for multiple comparisons. “In contrast to the in-trial and 8-year to 13-year analyses, we now observed that the lisinopril group had an increased risk of kidney disease mortality that emerged after approximately 13 years after randomization, but this effect was attenuated after adjustment for baseline variables,” the researchers wrote in their discussion.
The findings were limited by several factors including the potential effect of unblinding if participants stopped the randomized drug, and by the lack of morbidity and mortality data on Canadian participants, Veterans Affairs participants, and those with no Medicare number, the researchers noted. Other limitations included the lack of data on posttrial medication use, blood pressure, and laboratory findings, they said.
However, the results over the follow-up period of up to 23 years supported those of the larger ALLHAT study, with similar outcomes among the drugs, and with 11 years of passive follow-up, “the results for lisinopril vs. chlorthalidone for stroke and stroke mortality are almost the same,” they concluded.
Findings support current practice, but new drug data are needed
The current study was important to determine whether there was a significant difference in long-term morbidity and mortality between patients treated with thiazide diuretics, calcium channel blockers and ACE inhibitors, Noel Deep, MD, said in an interview.
“Previously reported data had indicated no significant differences between patients randomized to one of these three classes of antihypertensive medications during the trial period or at 8-13 years post trial,” said Dr. Deep, a general internist in private practice in Antigo, Wisc., who was not involved in the study. Dr. Deep is chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
“This study reinforces the previously noted benefits of the three classes of antihypertensive medications, as well as the higher rates of cardiovascular disease and stroke in the ACE inhibitor arm,” he said.
In clinical practice, the results suggest that thiazide diuretics should be considered first-line agents for management of hypertension based on their noninferiority compared with ACE inhibitors and CCBs, and lower risk of stroke compared with ACE inhibitors, Dr. Deep said in an interview. “All three classes of antihypertensive medications are equally efficacious in blood pressure control and preventing all-cause mortality,” he said.
More research is needed in the wake of the introduction of other classes of antihypertensives since the original ALLHAT trial, Dr. Deep said. “It would be beneficial to assess the relative benefit/risks of those medications compared to the thiazide diuretics, and I would also look at studies comparing beta blockers to the thiazide diuretics,” he said. The question remains as to whether outcomes were affected by patients’ use of other classes of antihypertensives after the trial period, he said.
The study was supported by the National Institute on Aging of the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose and serves on the editorial advisory board of Internal Medicine News.
FROM JAMA NETWORK OPEN
Patients with hypermobile Ehlers-Danlos syndrome report skin laxity, scarring
.
The genetic cause of hEDS, a common inherited connective tissue disorder, remains unknown, wrote Alan Snyder, MD, of the department of dermatology and dermatologic surgery at Medical University of South Carolina, Charleston, and colleagues.
Previous research suggests that changes in dermal mechanics predispose these patients to a range of skin conditions including mast cell activation disorder (MCAD) spectrum and chronic spontaneous urticaria, abnormal scars or wound healing, piezogenic papules, dyshidrosis, skin laxity or softness, easy bruising, local anesthesia resistance, keratosis pilaris, striae, and hidradenitis suppurativa, the researchers wrote.
However, data on these and other dermatologic manifestations of hEDS are limited, they said.
The diagnosis of hEDS will continue to be made more frequently and carefully, as the condition becomes more recognized and understood in the medical community, especially with anticipated capabilities of genetic testing, Dr. Snyder said in an interview.
“Being able to be aware of disease-specific comorbidities, such as those discovered in this study, allows providers to better stratify phenotypes and improve patient disease co-management,” he said.
In the study, published in the Journal of the American Academy of Dermatology, the researchers reviewed data on 1,364 patients with ICD-10 or ICD-9 codes for hEDS or EDS unspecified who were seen at a single institution between June 2005 and May 2022. Most of the patients were White (95.4%) and female (86.7%); the average age was 29.2 years.
Of the 1,364 patients included in the chart review, 497 (36.4%) had documented skin manifestations. Of these, 118 (24.2%) had disorders of follicular occlusion (12 had hidradenitis suppurativa, 32 had folliculitis, and 74 had acne); 112 (23%) had eczema or atopic dermatitis, 98 (19.7%) had mast cell disorder, 32 (6.4%) had psoriasis, and 32 (6.4%) had wound healing issues (16 had hypertrophic keloids/scarring, 5 had abscesses, 3 had abnormal bruising, and 8 had other would healing issues).
The study also included results of a multiple-choice patient survey from 1,354 individuals. In the survey, approximately two-thirds of patients reported abnormal scarring, abnormal wound healing, and cutaneous laxity (61.7%, 69.0%, and 71.0%, respectively).
The findings were limited by several factors including the retrospective study design, lack of testing to confirm hEDS diagnosis, and the potential interdisciplinary selection bias for diagnoses, the authors noted.
However, the results support previous studies showing increased rates of occlusive conditions in hEDS and higher rates of acne, folliculitis, and psoriasis, and highlight the need for clinician education to manage patients and promote better outcomes, the researchers concluded.
Data Enhance Clinical Awareness
“Given the increasingly understood relation between TH2-directed and mast-cell mediated diseases and hEDS, it was not necessarily a surprise to find the increased prevalence of atopy and mast cell disease, but rather an interesting confirmation, within the limitations that exist with retrospective chart review,” Dr. Snyder told this news organization. “While it may make some intuitive sense that certain cohorts with higher risk of HS may have a higher risk of acne, this had not been reported in the literature to date,” he noted. “Given the high levels of patient reported issues with scarring and wound healing, I was surprised that so few analogous diagnoses were physician-reported in the medical records.”
In clinical practice, “health care professionals and patients need to be aware hEDS is associated with high rates of eczematous, mast-cell mediated and follicular occlusive cutaneous disorders,” Dr. Snyder said in an interview. “There seems to be a discrepancy between patients and physician awareness of scarring or wound healing issues in this patient population,” he added.
Looking ahead, “we need to better research and characterize the various hEDS phenotypes to understand who is at highest risk for various TH2-mediated or follicular occlusive disorders,” said Dr. Snyder. “Moreover, a greater understanding is needed of the wound healing inadequacies that predispose these patients to poor outcomes during dermatologic surgery,” he said.
The study was supported by the Ehlers-Danlos Society and the Milton and Tamar Maltz Family Foundation. The researchers had no financial conflicts to disclose.
.
The genetic cause of hEDS, a common inherited connective tissue disorder, remains unknown, wrote Alan Snyder, MD, of the department of dermatology and dermatologic surgery at Medical University of South Carolina, Charleston, and colleagues.
Previous research suggests that changes in dermal mechanics predispose these patients to a range of skin conditions including mast cell activation disorder (MCAD) spectrum and chronic spontaneous urticaria, abnormal scars or wound healing, piezogenic papules, dyshidrosis, skin laxity or softness, easy bruising, local anesthesia resistance, keratosis pilaris, striae, and hidradenitis suppurativa, the researchers wrote.
However, data on these and other dermatologic manifestations of hEDS are limited, they said.
The diagnosis of hEDS will continue to be made more frequently and carefully, as the condition becomes more recognized and understood in the medical community, especially with anticipated capabilities of genetic testing, Dr. Snyder said in an interview.
“Being able to be aware of disease-specific comorbidities, such as those discovered in this study, allows providers to better stratify phenotypes and improve patient disease co-management,” he said.
In the study, published in the Journal of the American Academy of Dermatology, the researchers reviewed data on 1,364 patients with ICD-10 or ICD-9 codes for hEDS or EDS unspecified who were seen at a single institution between June 2005 and May 2022. Most of the patients were White (95.4%) and female (86.7%); the average age was 29.2 years.
Of the 1,364 patients included in the chart review, 497 (36.4%) had documented skin manifestations. Of these, 118 (24.2%) had disorders of follicular occlusion (12 had hidradenitis suppurativa, 32 had folliculitis, and 74 had acne); 112 (23%) had eczema or atopic dermatitis, 98 (19.7%) had mast cell disorder, 32 (6.4%) had psoriasis, and 32 (6.4%) had wound healing issues (16 had hypertrophic keloids/scarring, 5 had abscesses, 3 had abnormal bruising, and 8 had other would healing issues).
The study also included results of a multiple-choice patient survey from 1,354 individuals. In the survey, approximately two-thirds of patients reported abnormal scarring, abnormal wound healing, and cutaneous laxity (61.7%, 69.0%, and 71.0%, respectively).
The findings were limited by several factors including the retrospective study design, lack of testing to confirm hEDS diagnosis, and the potential interdisciplinary selection bias for diagnoses, the authors noted.
However, the results support previous studies showing increased rates of occlusive conditions in hEDS and higher rates of acne, folliculitis, and psoriasis, and highlight the need for clinician education to manage patients and promote better outcomes, the researchers concluded.
Data Enhance Clinical Awareness
“Given the increasingly understood relation between TH2-directed and mast-cell mediated diseases and hEDS, it was not necessarily a surprise to find the increased prevalence of atopy and mast cell disease, but rather an interesting confirmation, within the limitations that exist with retrospective chart review,” Dr. Snyder told this news organization. “While it may make some intuitive sense that certain cohorts with higher risk of HS may have a higher risk of acne, this had not been reported in the literature to date,” he noted. “Given the high levels of patient reported issues with scarring and wound healing, I was surprised that so few analogous diagnoses were physician-reported in the medical records.”
In clinical practice, “health care professionals and patients need to be aware hEDS is associated with high rates of eczematous, mast-cell mediated and follicular occlusive cutaneous disorders,” Dr. Snyder said in an interview. “There seems to be a discrepancy between patients and physician awareness of scarring or wound healing issues in this patient population,” he added.
Looking ahead, “we need to better research and characterize the various hEDS phenotypes to understand who is at highest risk for various TH2-mediated or follicular occlusive disorders,” said Dr. Snyder. “Moreover, a greater understanding is needed of the wound healing inadequacies that predispose these patients to poor outcomes during dermatologic surgery,” he said.
The study was supported by the Ehlers-Danlos Society and the Milton and Tamar Maltz Family Foundation. The researchers had no financial conflicts to disclose.
.
The genetic cause of hEDS, a common inherited connective tissue disorder, remains unknown, wrote Alan Snyder, MD, of the department of dermatology and dermatologic surgery at Medical University of South Carolina, Charleston, and colleagues.
Previous research suggests that changes in dermal mechanics predispose these patients to a range of skin conditions including mast cell activation disorder (MCAD) spectrum and chronic spontaneous urticaria, abnormal scars or wound healing, piezogenic papules, dyshidrosis, skin laxity or softness, easy bruising, local anesthesia resistance, keratosis pilaris, striae, and hidradenitis suppurativa, the researchers wrote.
However, data on these and other dermatologic manifestations of hEDS are limited, they said.
The diagnosis of hEDS will continue to be made more frequently and carefully, as the condition becomes more recognized and understood in the medical community, especially with anticipated capabilities of genetic testing, Dr. Snyder said in an interview.
“Being able to be aware of disease-specific comorbidities, such as those discovered in this study, allows providers to better stratify phenotypes and improve patient disease co-management,” he said.
In the study, published in the Journal of the American Academy of Dermatology, the researchers reviewed data on 1,364 patients with ICD-10 or ICD-9 codes for hEDS or EDS unspecified who were seen at a single institution between June 2005 and May 2022. Most of the patients were White (95.4%) and female (86.7%); the average age was 29.2 years.
Of the 1,364 patients included in the chart review, 497 (36.4%) had documented skin manifestations. Of these, 118 (24.2%) had disorders of follicular occlusion (12 had hidradenitis suppurativa, 32 had folliculitis, and 74 had acne); 112 (23%) had eczema or atopic dermatitis, 98 (19.7%) had mast cell disorder, 32 (6.4%) had psoriasis, and 32 (6.4%) had wound healing issues (16 had hypertrophic keloids/scarring, 5 had abscesses, 3 had abnormal bruising, and 8 had other would healing issues).
The study also included results of a multiple-choice patient survey from 1,354 individuals. In the survey, approximately two-thirds of patients reported abnormal scarring, abnormal wound healing, and cutaneous laxity (61.7%, 69.0%, and 71.0%, respectively).
The findings were limited by several factors including the retrospective study design, lack of testing to confirm hEDS diagnosis, and the potential interdisciplinary selection bias for diagnoses, the authors noted.
However, the results support previous studies showing increased rates of occlusive conditions in hEDS and higher rates of acne, folliculitis, and psoriasis, and highlight the need for clinician education to manage patients and promote better outcomes, the researchers concluded.
Data Enhance Clinical Awareness
“Given the increasingly understood relation between TH2-directed and mast-cell mediated diseases and hEDS, it was not necessarily a surprise to find the increased prevalence of atopy and mast cell disease, but rather an interesting confirmation, within the limitations that exist with retrospective chart review,” Dr. Snyder told this news organization. “While it may make some intuitive sense that certain cohorts with higher risk of HS may have a higher risk of acne, this had not been reported in the literature to date,” he noted. “Given the high levels of patient reported issues with scarring and wound healing, I was surprised that so few analogous diagnoses were physician-reported in the medical records.”
In clinical practice, “health care professionals and patients need to be aware hEDS is associated with high rates of eczematous, mast-cell mediated and follicular occlusive cutaneous disorders,” Dr. Snyder said in an interview. “There seems to be a discrepancy between patients and physician awareness of scarring or wound healing issues in this patient population,” he added.
Looking ahead, “we need to better research and characterize the various hEDS phenotypes to understand who is at highest risk for various TH2-mediated or follicular occlusive disorders,” said Dr. Snyder. “Moreover, a greater understanding is needed of the wound healing inadequacies that predispose these patients to poor outcomes during dermatologic surgery,” he said.
The study was supported by the Ehlers-Danlos Society and the Milton and Tamar Maltz Family Foundation. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY