User login
Supplement Captures Snapshot of Melanoma Epidemiology
While the recently published supplement on melanoma in the Journal of the American Academy of Dermatology doesn’t offer evidence of many new trends, it does provide an important estimate of the burden of the disease and suggests new targets for education and surveillance.
"The best way to characterize this nice ensemble of studies is that it literally takes a pulse on the epidemic," Dr. Hensin Tsao said of the collection of studies (J. Am. Acad. Dermatol 2011;65[suppl. 1]:S1-143) in an interview. Dr. Tsao is the clinical director of the Melanoma Center and Pigmented Lesion Center at Massachusetts General Hospital in Boston.

Dr. Randall K. Roenigk, a professor of dermatology at the Mayo Clinic in Rochester, Minn., agreed. "It summarizes some facts that are pretty well known but it solidifies some [others]," he said in an interview.
The supplements were published as a joint effort by the American Academy of Dermatology and the Centers for Disease Control and Prevention. The included studies were largely based on data from the Surveillance, Epidemiology, and End Results (SEER) registry that is maintained by the National Cancer Institute.
"The incidence of melanoma is still increasing, and the mortality has not decreased," said Dr. Tsao. "So the biggest take-home message is that this burden is still growing."
Dr. Roenigk noted that "people interpret that one of two ways. They either say that it’s increasing because we’re doing a better job of surveillance or that people are just getting more cancers. However, he added, "some people say that the death rate should also increase if the incidence rate is increasing; but because it’s flat, some people say that maybe our criteria for diagnosis have changed a little bit ... I don’t know if [the supplement] answers that. It’s a little bit of a controversy. But the positive spin on it would be that while the incidence rate is increasing, we’re able to catch it in time that the death rate is staying about the same."
The take home messages from the supplement include: cancer incidence is increasing in younger individuals, particularly younger women; the greatest melanoma mortality is seen among elderly men; and dermatologists have an important chance to improve surveillance of melanoma by reporting their data to registries, such as the SEER database.
Young Women
The study of melanoma in adolescents and young adults aged 15-39 years (J. Am. Acad. Dermatol 2011;65[suppl. 1]:S38-49) found the incidence of melanoma to be rising in that age group. "There have been a number of studies in this younger age group showing the incidence shooting up, especially among women," said Dr. Tsao. "This study substantiates previously published data."
According to Dr. Roenigk, it has been suggested that "the increased incidence in melanoma could just be due to people living longer ... but obviously with people under the age of 40 it’s not so much living longer, it’s probably behavioral or it’s environmental ... but not necessarily longevity."
Dr. Tsao noted that the increasing melanoma incidence in this age group "has implications for what we can do now on some regulatory level ... and for what we expect to happen in 20 years. Are we going to get a whole cohort of advanced-disease women because there is a lag time in the formation of [melanomas] ... It’s a cautionary tale for the future but it’s certainly a point of intervention now."
Tanning beds continue to be a source of controversy at all levels of government nationwide. The AAD, states, local organizations, and others are working to tackle the issue of access to tanning beds.
Education may prove even harder. "We have a lot of room to improve ... despite pretty heavy messaging ... people are either fatigued with the message or they have competing interests," said Dr. Tsao. "There are even more and more studies out there suggesting that even the long-wave ‘safer tans’ like UVA can cause the same types of genetic damage ... I’m not sure that the words ‘safe tan’ makes any sense. A lot of exposure even to long-wave UVA may lead to the chronic skin cancer environment in the skin."
Older Men
The other newer information asks who is dying from melanoma. "Overall, yes, young women are getting melanoma," but if you’re asking who is dying from melanoma, it is old men. You’ll see this theme throughout many of the articles," said Dr. Tsao. "Elderly men are getting to be the most susceptible group – it appears – for melanoma if you look at the death rates." In this age group the rates of melanoma mortality are much greater in men than in women (J. Am. Acad. Dermatol 2011;65[suppl. 1]:S78-86).
"This is going to have clinical impact down the line," Dr. Tsao noted. "Many of these [older] people have melanomas on the head and neck, which appear to have a worse prognosis." These tumors are thick, often nodular in subtype and with a lot of negative features in the pathology report. "We don’t really understand this phenotype – it may be the tumor, it may be the host, it may be the chronically sun-damaged skin surface."
However, "the question is how you get that group to be potentially screened – and how screening within this group is going to impact mortality," he noted. "We’re still optimistic that with proper screening, we can make a difference in mortality."
Dr. Tsao uses the mnemonic MENN (male, elderly, neck/scalp/trunk, nodular type melanoma) to thoroughly check for melanomas in this patient population, regardless of the reason for presentation.
Melanoma Registries
"One of the ways that we can study the burden of a skin disease is by having nationalized records. It doesn’t exist for most other skin diseases," said Dr. Tsao. "Still, most dermatologists in practice don’t think about registering their melanomas, even though this is one of the most codified disorders in all of dermatology ... maybe this is something that we need to work on ... the only way that we can make progress toward documenting the burden of skin disease is that we document the burden of skin disease."
There are likely a large number of melanomas that are diagnosed in the community and the question is whether those are getting recorded in a registry. "In most large hospitals or tertiary care centers, cancers undergo registration. But this may not be the case in private practice," Dr. Tsao said. "If we’re underestimating the burden of melanoma, then in some ways we’re shortchanging ourselves. Given the long-range surveillance, dermatologists are becoming the primary caretakers of melanoma patients in this country in terms of sheer volume ... dermatologists have an opportunity to detect at an early stage and to deflect these patients away from advanced disease."
While the recently published supplement on melanoma in the Journal of the American Academy of Dermatology doesn’t offer evidence of many new trends, it does provide an important estimate of the burden of the disease and suggests new targets for education and surveillance.
"The best way to characterize this nice ensemble of studies is that it literally takes a pulse on the epidemic," Dr. Hensin Tsao said of the collection of studies (J. Am. Acad. Dermatol 2011;65[suppl. 1]:S1-143) in an interview. Dr. Tsao is the clinical director of the Melanoma Center and Pigmented Lesion Center at Massachusetts General Hospital in Boston.
Dr. Randall K. Roenigk, a professor of dermatology at the Mayo Clinic in Rochester, Minn., agreed. "It summarizes some facts that are pretty well known but it solidifies some [others]," he said in an interview.
The supplements were published as a joint effort by the American Academy of Dermatology and the Centers for Disease Control and Prevention. The included studies were largely based on data from the Surveillance, Epidemiology, and End Results (SEER) registry that is maintained by the National Cancer Institute.
"The incidence of melanoma is still increasing, and the mortality has not decreased," said Dr. Tsao. "So the biggest take-home message is that this burden is still growing."
Dr. Roenigk noted that "people interpret that one of two ways. They either say that it’s increasing because we’re doing a better job of surveillance or that people are just getting more cancers. However, he added, "some people say that the death rate should also increase if the incidence rate is increasing; but because it’s flat, some people say that maybe our criteria for diagnosis have changed a little bit ... I don’t know if [the supplement] answers that. It’s a little bit of a controversy. But the positive spin on it would be that while the incidence rate is increasing, we’re able to catch it in time that the death rate is staying about the same."
The take home messages from the supplement include: cancer incidence is increasing in younger individuals, particularly younger women; the greatest melanoma mortality is seen among elderly men; and dermatologists have an important chance to improve surveillance of melanoma by reporting their data to registries, such as the SEER database.
Young Women
The study of melanoma in adolescents and young adults aged 15-39 years (J. Am. Acad. Dermatol 2011;65[suppl. 1]:S38-49) found the incidence of melanoma to be rising in that age group. "There have been a number of studies in this younger age group showing the incidence shooting up, especially among women," said Dr. Tsao. "This study substantiates previously published data."
According to Dr. Roenigk, it has been suggested that "the increased incidence in melanoma could just be due to people living longer ... but obviously with people under the age of 40 it’s not so much living longer, it’s probably behavioral or it’s environmental ... but not necessarily longevity."
Dr. Tsao noted that the increasing melanoma incidence in this age group "has implications for what we can do now on some regulatory level ... and for what we expect to happen in 20 years. Are we going to get a whole cohort of advanced-disease women because there is a lag time in the formation of [melanomas] ... It’s a cautionary tale for the future but it’s certainly a point of intervention now."
Tanning beds continue to be a source of controversy at all levels of government nationwide. The AAD, states, local organizations, and others are working to tackle the issue of access to tanning beds.
Education may prove even harder. "We have a lot of room to improve ... despite pretty heavy messaging ... people are either fatigued with the message or they have competing interests," said Dr. Tsao. "There are even more and more studies out there suggesting that even the long-wave ‘safer tans’ like UVA can cause the same types of genetic damage ... I’m not sure that the words ‘safe tan’ makes any sense. A lot of exposure even to long-wave UVA may lead to the chronic skin cancer environment in the skin."
Older Men
The other newer information asks who is dying from melanoma. "Overall, yes, young women are getting melanoma," but if you’re asking who is dying from melanoma, it is old men. You’ll see this theme throughout many of the articles," said Dr. Tsao. "Elderly men are getting to be the most susceptible group – it appears – for melanoma if you look at the death rates." In this age group the rates of melanoma mortality are much greater in men than in women (J. Am. Acad. Dermatol 2011;65[suppl. 1]:S78-86).
"This is going to have clinical impact down the line," Dr. Tsao noted. "Many of these [older] people have melanomas on the head and neck, which appear to have a worse prognosis." These tumors are thick, often nodular in subtype and with a lot of negative features in the pathology report. "We don’t really understand this phenotype – it may be the tumor, it may be the host, it may be the chronically sun-damaged skin surface."
However, "the question is how you get that group to be potentially screened – and how screening within this group is going to impact mortality," he noted. "We’re still optimistic that with proper screening, we can make a difference in mortality."
Dr. Tsao uses the mnemonic MENN (male, elderly, neck/scalp/trunk, nodular type melanoma) to thoroughly check for melanomas in this patient population, regardless of the reason for presentation.
Melanoma Registries
"One of the ways that we can study the burden of a skin disease is by having nationalized records. It doesn’t exist for most other skin diseases," said Dr. Tsao. "Still, most dermatologists in practice don’t think about registering their melanomas, even though this is one of the most codified disorders in all of dermatology ... maybe this is something that we need to work on ... the only way that we can make progress toward documenting the burden of skin disease is that we document the burden of skin disease."
There are likely a large number of melanomas that are diagnosed in the community and the question is whether those are getting recorded in a registry. "In most large hospitals or tertiary care centers, cancers undergo registration. But this may not be the case in private practice," Dr. Tsao said. "If we’re underestimating the burden of melanoma, then in some ways we’re shortchanging ourselves. Given the long-range surveillance, dermatologists are becoming the primary caretakers of melanoma patients in this country in terms of sheer volume ... dermatologists have an opportunity to detect at an early stage and to deflect these patients away from advanced disease."
While the recently published supplement on melanoma in the Journal of the American Academy of Dermatology doesn’t offer evidence of many new trends, it does provide an important estimate of the burden of the disease and suggests new targets for education and surveillance.
"The best way to characterize this nice ensemble of studies is that it literally takes a pulse on the epidemic," Dr. Hensin Tsao said of the collection of studies (J. Am. Acad. Dermatol 2011;65[suppl. 1]:S1-143) in an interview. Dr. Tsao is the clinical director of the Melanoma Center and Pigmented Lesion Center at Massachusetts General Hospital in Boston.
Dr. Randall K. Roenigk, a professor of dermatology at the Mayo Clinic in Rochester, Minn., agreed. "It summarizes some facts that are pretty well known but it solidifies some [others]," he said in an interview.
The supplements were published as a joint effort by the American Academy of Dermatology and the Centers for Disease Control and Prevention. The included studies were largely based on data from the Surveillance, Epidemiology, and End Results (SEER) registry that is maintained by the National Cancer Institute.
"The incidence of melanoma is still increasing, and the mortality has not decreased," said Dr. Tsao. "So the biggest take-home message is that this burden is still growing."
Dr. Roenigk noted that "people interpret that one of two ways. They either say that it’s increasing because we’re doing a better job of surveillance or that people are just getting more cancers. However, he added, "some people say that the death rate should also increase if the incidence rate is increasing; but because it’s flat, some people say that maybe our criteria for diagnosis have changed a little bit ... I don’t know if [the supplement] answers that. It’s a little bit of a controversy. But the positive spin on it would be that while the incidence rate is increasing, we’re able to catch it in time that the death rate is staying about the same."
The take home messages from the supplement include: cancer incidence is increasing in younger individuals, particularly younger women; the greatest melanoma mortality is seen among elderly men; and dermatologists have an important chance to improve surveillance of melanoma by reporting their data to registries, such as the SEER database.
Young Women
The study of melanoma in adolescents and young adults aged 15-39 years (J. Am. Acad. Dermatol 2011;65[suppl. 1]:S38-49) found the incidence of melanoma to be rising in that age group. "There have been a number of studies in this younger age group showing the incidence shooting up, especially among women," said Dr. Tsao. "This study substantiates previously published data."
According to Dr. Roenigk, it has been suggested that "the increased incidence in melanoma could just be due to people living longer ... but obviously with people under the age of 40 it’s not so much living longer, it’s probably behavioral or it’s environmental ... but not necessarily longevity."
Dr. Tsao noted that the increasing melanoma incidence in this age group "has implications for what we can do now on some regulatory level ... and for what we expect to happen in 20 years. Are we going to get a whole cohort of advanced-disease women because there is a lag time in the formation of [melanomas] ... It’s a cautionary tale for the future but it’s certainly a point of intervention now."
Tanning beds continue to be a source of controversy at all levels of government nationwide. The AAD, states, local organizations, and others are working to tackle the issue of access to tanning beds.
Education may prove even harder. "We have a lot of room to improve ... despite pretty heavy messaging ... people are either fatigued with the message or they have competing interests," said Dr. Tsao. "There are even more and more studies out there suggesting that even the long-wave ‘safer tans’ like UVA can cause the same types of genetic damage ... I’m not sure that the words ‘safe tan’ makes any sense. A lot of exposure even to long-wave UVA may lead to the chronic skin cancer environment in the skin."
Older Men
The other newer information asks who is dying from melanoma. "Overall, yes, young women are getting melanoma," but if you’re asking who is dying from melanoma, it is old men. You’ll see this theme throughout many of the articles," said Dr. Tsao. "Elderly men are getting to be the most susceptible group – it appears – for melanoma if you look at the death rates." In this age group the rates of melanoma mortality are much greater in men than in women (J. Am. Acad. Dermatol 2011;65[suppl. 1]:S78-86).
"This is going to have clinical impact down the line," Dr. Tsao noted. "Many of these [older] people have melanomas on the head and neck, which appear to have a worse prognosis." These tumors are thick, often nodular in subtype and with a lot of negative features in the pathology report. "We don’t really understand this phenotype – it may be the tumor, it may be the host, it may be the chronically sun-damaged skin surface."
However, "the question is how you get that group to be potentially screened – and how screening within this group is going to impact mortality," he noted. "We’re still optimistic that with proper screening, we can make a difference in mortality."
Dr. Tsao uses the mnemonic MENN (male, elderly, neck/scalp/trunk, nodular type melanoma) to thoroughly check for melanomas in this patient population, regardless of the reason for presentation.
Melanoma Registries
"One of the ways that we can study the burden of a skin disease is by having nationalized records. It doesn’t exist for most other skin diseases," said Dr. Tsao. "Still, most dermatologists in practice don’t think about registering their melanomas, even though this is one of the most codified disorders in all of dermatology ... maybe this is something that we need to work on ... the only way that we can make progress toward documenting the burden of skin disease is that we document the burden of skin disease."
There are likely a large number of melanomas that are diagnosed in the community and the question is whether those are getting recorded in a registry. "In most large hospitals or tertiary care centers, cancers undergo registration. But this may not be the case in private practice," Dr. Tsao said. "If we’re underestimating the burden of melanoma, then in some ways we’re shortchanging ourselves. Given the long-range surveillance, dermatologists are becoming the primary caretakers of melanoma patients in this country in terms of sheer volume ... dermatologists have an opportunity to detect at an early stage and to deflect these patients away from advanced disease."
Rheumatoid Arthritis Doubled Fracture Risk in Younger Women
CHICAGO – Rheumatoid arthritis more than doubles the risk of fracture in women younger than age 50, according to the results of a large population-based study.
While it’s well known that the disease drives up fracture risk in older men and women, independent of glucocorticoid use, these findings suggest that "we need to make our [younger female] patients aware" that they, too, are at increased risk so they can take precautions by not smoking, and by maintaining adequate calcium, vitamin D, and activity levels, Dr. Shreyasee Amin said at the annual meeting of the American College of Rheumatology.
Dr. Amin and colleagues at the Mayo Clinic in Rochester, Minn., analyzed data from the Rochester Epidemiologic Project, which includes inpatient and outpatient medical records for residents of Olmstead County, Minn.
The population-based cohort included 1,171 women (70%) and men (30%) diagnosed with RA during 1955-2007. Those individuals were compared with age- and sex-matched controls without RA. The researchers followed subjects until death or their last available follow-up.*
Among women with RA, 308 were younger than 50 years; among men with RA, 110 were younger than 50 years.
Causes of fractures were categorized by whether they were incidental or not and by trauma severity: severe (for example, motor vehicle accident), moderate (fall from standing height or less), spontaneous, and pathologic (malignancy). Severe or pathologic fractures were not included in the analysis.
Overall, women with RA had a 63% greater risk of fracture than women without RA. Women with RA aged 50 years or older had a 43% greater risk of fracture, and women younger than 50 years had more than twice the risk of a fracture (Hazard Ratio, 2.34).
Overall, men with RA had a 40% greater risk of a fracture, compared with those without the disease. Among men aged 50 years and older, those with RA tended to have a greater risk of fracture. In men with RA who were younger than age 50, "we didn’t see enough fractures to determine whether they were at high risk for fracture before the age of 50," said the rheumatologist.
Steroids, which are commonly used to treat the disease, can put individuals at greater risk of fracture. But RA patients also tend to have a greater risk of fracture, independent of their steroid use. "The disease itself may play a role in the loss of bone because the inflammation that drives the joint disease also affects the cells of the bone that increase bone loss," she said.
The study primarily involved a white population, so the results can’t be extrapolated to other races or ethic groups with RA.
Dr. Amin reported that she is on the scientific advisory board for Merck.
* Correction, 11/10/2011: The original version of this story misstated how patients in this study were followed. Patients were followed until death or their last available follow-up, not their first fracture.
CHICAGO – Rheumatoid arthritis more than doubles the risk of fracture in women younger than age 50, according to the results of a large population-based study.
While it’s well known that the disease drives up fracture risk in older men and women, independent of glucocorticoid use, these findings suggest that "we need to make our [younger female] patients aware" that they, too, are at increased risk so they can take precautions by not smoking, and by maintaining adequate calcium, vitamin D, and activity levels, Dr. Shreyasee Amin said at the annual meeting of the American College of Rheumatology.
Dr. Amin and colleagues at the Mayo Clinic in Rochester, Minn., analyzed data from the Rochester Epidemiologic Project, which includes inpatient and outpatient medical records for residents of Olmstead County, Minn.
The population-based cohort included 1,171 women (70%) and men (30%) diagnosed with RA during 1955-2007. Those individuals were compared with age- and sex-matched controls without RA. The researchers followed subjects until death or their last available follow-up.*
Among women with RA, 308 were younger than 50 years; among men with RA, 110 were younger than 50 years.
Causes of fractures were categorized by whether they were incidental or not and by trauma severity: severe (for example, motor vehicle accident), moderate (fall from standing height or less), spontaneous, and pathologic (malignancy). Severe or pathologic fractures were not included in the analysis.
Overall, women with RA had a 63% greater risk of fracture than women without RA. Women with RA aged 50 years or older had a 43% greater risk of fracture, and women younger than 50 years had more than twice the risk of a fracture (Hazard Ratio, 2.34).
Overall, men with RA had a 40% greater risk of a fracture, compared with those without the disease. Among men aged 50 years and older, those with RA tended to have a greater risk of fracture. In men with RA who were younger than age 50, "we didn’t see enough fractures to determine whether they were at high risk for fracture before the age of 50," said the rheumatologist.
Steroids, which are commonly used to treat the disease, can put individuals at greater risk of fracture. But RA patients also tend to have a greater risk of fracture, independent of their steroid use. "The disease itself may play a role in the loss of bone because the inflammation that drives the joint disease also affects the cells of the bone that increase bone loss," she said.
The study primarily involved a white population, so the results can’t be extrapolated to other races or ethic groups with RA.
Dr. Amin reported that she is on the scientific advisory board for Merck.
* Correction, 11/10/2011: The original version of this story misstated how patients in this study were followed. Patients were followed until death or their last available follow-up, not their first fracture.
CHICAGO – Rheumatoid arthritis more than doubles the risk of fracture in women younger than age 50, according to the results of a large population-based study.
While it’s well known that the disease drives up fracture risk in older men and women, independent of glucocorticoid use, these findings suggest that "we need to make our [younger female] patients aware" that they, too, are at increased risk so they can take precautions by not smoking, and by maintaining adequate calcium, vitamin D, and activity levels, Dr. Shreyasee Amin said at the annual meeting of the American College of Rheumatology.
Dr. Amin and colleagues at the Mayo Clinic in Rochester, Minn., analyzed data from the Rochester Epidemiologic Project, which includes inpatient and outpatient medical records for residents of Olmstead County, Minn.
The population-based cohort included 1,171 women (70%) and men (30%) diagnosed with RA during 1955-2007. Those individuals were compared with age- and sex-matched controls without RA. The researchers followed subjects until death or their last available follow-up.*
Among women with RA, 308 were younger than 50 years; among men with RA, 110 were younger than 50 years.
Causes of fractures were categorized by whether they were incidental or not and by trauma severity: severe (for example, motor vehicle accident), moderate (fall from standing height or less), spontaneous, and pathologic (malignancy). Severe or pathologic fractures were not included in the analysis.
Overall, women with RA had a 63% greater risk of fracture than women without RA. Women with RA aged 50 years or older had a 43% greater risk of fracture, and women younger than 50 years had more than twice the risk of a fracture (Hazard Ratio, 2.34).
Overall, men with RA had a 40% greater risk of a fracture, compared with those without the disease. Among men aged 50 years and older, those with RA tended to have a greater risk of fracture. In men with RA who were younger than age 50, "we didn’t see enough fractures to determine whether they were at high risk for fracture before the age of 50," said the rheumatologist.
Steroids, which are commonly used to treat the disease, can put individuals at greater risk of fracture. But RA patients also tend to have a greater risk of fracture, independent of their steroid use. "The disease itself may play a role in the loss of bone because the inflammation that drives the joint disease also affects the cells of the bone that increase bone loss," she said.
The study primarily involved a white population, so the results can’t be extrapolated to other races or ethic groups with RA.
Dr. Amin reported that she is on the scientific advisory board for Merck.
* Correction, 11/10/2011: The original version of this story misstated how patients in this study were followed. Patients were followed until death or their last available follow-up, not their first fracture.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: Overall, women with RA had a 63% greater risk of fracture than women without RA. Women with RA aged 50 years or older had a 43% greater risk of fracture and women younger than 50 years had more than twice the risk of a fracture (Hazard Ratio, 2.34).
Data Source: A large population-based study.
Disclosures: Dr. Amin reported that she is on the scientific advisory board for Merck.
Mild Lupus Means Healthy Pregnancies for Most Women
CHICAGO – Women with low-activity systemic lupus erythematosus can have healthy pregnancies with few complications, even those with a history of renal disease.
"The good news was that the overall pregnancy adverse outcome was 19%, so 81% of the women [with low-activity disease] had a very favorable outcome," lead author Dr. Jill Buyon said when she announced the results of the largest such study to date at the annual meeting of the American College of Rheumatology.
The findings are very good news for women with systemic lupus erythematosus (SLE) who want to become pregnant. "Previous data suggested that women with lupus would have difficulty with regard to their own health and the health of their fetus and subsequent baby, [so] many rheumatologists have discouraged these women from childbearing," said Dr. Buyon, a professor of medicine and associate director of the division of rheumatology at New York University.
The findings suggest that rheumatologists should advise patients with very active disease to hold off on pregnancy until the disease is under better control, she said.
This study is part of a larger project, the PROMISSE (Predictors of Pregnancy Outcome: Biomarkers in Antiphospholipid Antibody Syndrome and Systemic Lupus Erythematosus) study. "We also felt that this would be a huge opportunity to evaluate patients, whom we [rheumatologists] would normally advise to get pregnant," she said.
This study comprises four groups: women who only have antiphospholipid antibodies (group 1); women with lupus and antiphospholipid antibodies (group 2); women with lupus but no antiphospholipid antibodies (group 3); and a very selective group of healthy women, who already had a previously healthy child and no major pregnancy losses (group 4).
A total of 10 sites participated in the study, which included both rheumatologists and obstetricians. The study was initiated in 2003. At the time that the abstract was written, 700 women had been recruited to this study; at the time of abstract submission, 599 pregnancies had been completed.
Patients were all enrolled prior to 12 weeks’ gestation and were seen by a rheumatologist every trimester. Women were excluded from the study if they had a multifetal pregnancy; were on more than 20 mg/day of prednisone; had a proteinuria level greater than 1 g/day; and/or had a creatinine level greater than 1.2 mg/dL.
An adverse pregnancy outcome was strictly defined as at least one of the following: fetal/neonatal death; birth indicated at less than 36 weeks due to placental insufficiency, hypertension, or preeclampsia; and small for gestational age (less than fifth percentile).
In addition, mild/moderate and severe flares were defined by the SLEPDAI (SLE Pregnancy Disease Activity Index) score, which excludes physiologic changes of pregnancy but incorporates the components of the SELENA (Safety of Estrogen in Lupus Erythematosus National Assessment), as well as changes in clinical parameters and medications, and physician’s global assessment.
The researchers evaluated 333 women from their first trimester until 3 months post partum. Nearly half of the women were ethnicities other than white, an important characteristic given that women from minority groups can have an increased risk of SLE.
Also importantly, 31% had a history of previous lupus affecting their kidneys. "This is really important because when we see a young woman who develops lupus nephritis – and that’s a fairly serious manifestation of the disease – they always ask, ‘Even if I get better from this, does that mean that I can never have a child?’ " said Dr. Buyon.
Half of the women with a prior history of lupus nephritis had anti-DNA antibodies, "which many of us worry quite a bit about and suggests perhaps a more serious disease." However, their baseline characteristics were good in terms of low disease activity and disease stability.
When enrolled in the study, 60% of the women were taking hydroxychloroquine, 41% were taking prednisone, and 18% were taking azathioprine. On average, the participants’ lupus was relatively inactive
Fetal death occurred in 4.5%. "But if you look at the national population, this is about 2%," Dr. Buyon said.
Neonatal death in this cohort was very similar to that for neonatal death nationally: 1.2%, compared with 1% nationally.
Indicated preterm delivery or small for gestational age occurred in 9.1% of SLE pregnancies. In addition, 10% of the mothers developed preeclampsia; the national level is closer to 4%.
Greater levels of lupus activity and greater levels of antiphospholipid antibodies – particularly the lupus anticoagulant – were associated with poorer outcomes.
The researchers also performed a multivariate analysis to identify independent predictors of these poor outcomes. They found that a history of renal disease predicted a poor pregnancy outcome.
The researchers then looked at maternal outcomes. "I think this is where the news is extraordinary. ... Our mild-moderate flair rate was 18%, which we were obviously very excited about," Dr. Buyon said. Only 15 patients had a severe flare-up, and most flares did not require medication.
The study was funded by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Buyon reported that she has no relevant financial disclosures.
CHICAGO – Women with low-activity systemic lupus erythematosus can have healthy pregnancies with few complications, even those with a history of renal disease.
"The good news was that the overall pregnancy adverse outcome was 19%, so 81% of the women [with low-activity disease] had a very favorable outcome," lead author Dr. Jill Buyon said when she announced the results of the largest such study to date at the annual meeting of the American College of Rheumatology.
The findings are very good news for women with systemic lupus erythematosus (SLE) who want to become pregnant. "Previous data suggested that women with lupus would have difficulty with regard to their own health and the health of their fetus and subsequent baby, [so] many rheumatologists have discouraged these women from childbearing," said Dr. Buyon, a professor of medicine and associate director of the division of rheumatology at New York University.
The findings suggest that rheumatologists should advise patients with very active disease to hold off on pregnancy until the disease is under better control, she said.
This study is part of a larger project, the PROMISSE (Predictors of Pregnancy Outcome: Biomarkers in Antiphospholipid Antibody Syndrome and Systemic Lupus Erythematosus) study. "We also felt that this would be a huge opportunity to evaluate patients, whom we [rheumatologists] would normally advise to get pregnant," she said.
This study comprises four groups: women who only have antiphospholipid antibodies (group 1); women with lupus and antiphospholipid antibodies (group 2); women with lupus but no antiphospholipid antibodies (group 3); and a very selective group of healthy women, who already had a previously healthy child and no major pregnancy losses (group 4).
A total of 10 sites participated in the study, which included both rheumatologists and obstetricians. The study was initiated in 2003. At the time that the abstract was written, 700 women had been recruited to this study; at the time of abstract submission, 599 pregnancies had been completed.
Patients were all enrolled prior to 12 weeks’ gestation and were seen by a rheumatologist every trimester. Women were excluded from the study if they had a multifetal pregnancy; were on more than 20 mg/day of prednisone; had a proteinuria level greater than 1 g/day; and/or had a creatinine level greater than 1.2 mg/dL.
An adverse pregnancy outcome was strictly defined as at least one of the following: fetal/neonatal death; birth indicated at less than 36 weeks due to placental insufficiency, hypertension, or preeclampsia; and small for gestational age (less than fifth percentile).
In addition, mild/moderate and severe flares were defined by the SLEPDAI (SLE Pregnancy Disease Activity Index) score, which excludes physiologic changes of pregnancy but incorporates the components of the SELENA (Safety of Estrogen in Lupus Erythematosus National Assessment), as well as changes in clinical parameters and medications, and physician’s global assessment.
The researchers evaluated 333 women from their first trimester until 3 months post partum. Nearly half of the women were ethnicities other than white, an important characteristic given that women from minority groups can have an increased risk of SLE.
Also importantly, 31% had a history of previous lupus affecting their kidneys. "This is really important because when we see a young woman who develops lupus nephritis – and that’s a fairly serious manifestation of the disease – they always ask, ‘Even if I get better from this, does that mean that I can never have a child?’ " said Dr. Buyon.
Half of the women with a prior history of lupus nephritis had anti-DNA antibodies, "which many of us worry quite a bit about and suggests perhaps a more serious disease." However, their baseline characteristics were good in terms of low disease activity and disease stability.
When enrolled in the study, 60% of the women were taking hydroxychloroquine, 41% were taking prednisone, and 18% were taking azathioprine. On average, the participants’ lupus was relatively inactive
Fetal death occurred in 4.5%. "But if you look at the national population, this is about 2%," Dr. Buyon said.
Neonatal death in this cohort was very similar to that for neonatal death nationally: 1.2%, compared with 1% nationally.
Indicated preterm delivery or small for gestational age occurred in 9.1% of SLE pregnancies. In addition, 10% of the mothers developed preeclampsia; the national level is closer to 4%.
Greater levels of lupus activity and greater levels of antiphospholipid antibodies – particularly the lupus anticoagulant – were associated with poorer outcomes.
The researchers also performed a multivariate analysis to identify independent predictors of these poor outcomes. They found that a history of renal disease predicted a poor pregnancy outcome.
The researchers then looked at maternal outcomes. "I think this is where the news is extraordinary. ... Our mild-moderate flair rate was 18%, which we were obviously very excited about," Dr. Buyon said. Only 15 patients had a severe flare-up, and most flares did not require medication.
The study was funded by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Buyon reported that she has no relevant financial disclosures.
CHICAGO – Women with low-activity systemic lupus erythematosus can have healthy pregnancies with few complications, even those with a history of renal disease.
"The good news was that the overall pregnancy adverse outcome was 19%, so 81% of the women [with low-activity disease] had a very favorable outcome," lead author Dr. Jill Buyon said when she announced the results of the largest such study to date at the annual meeting of the American College of Rheumatology.
The findings are very good news for women with systemic lupus erythematosus (SLE) who want to become pregnant. "Previous data suggested that women with lupus would have difficulty with regard to their own health and the health of their fetus and subsequent baby, [so] many rheumatologists have discouraged these women from childbearing," said Dr. Buyon, a professor of medicine and associate director of the division of rheumatology at New York University.
The findings suggest that rheumatologists should advise patients with very active disease to hold off on pregnancy until the disease is under better control, she said.
This study is part of a larger project, the PROMISSE (Predictors of Pregnancy Outcome: Biomarkers in Antiphospholipid Antibody Syndrome and Systemic Lupus Erythematosus) study. "We also felt that this would be a huge opportunity to evaluate patients, whom we [rheumatologists] would normally advise to get pregnant," she said.
This study comprises four groups: women who only have antiphospholipid antibodies (group 1); women with lupus and antiphospholipid antibodies (group 2); women with lupus but no antiphospholipid antibodies (group 3); and a very selective group of healthy women, who already had a previously healthy child and no major pregnancy losses (group 4).
A total of 10 sites participated in the study, which included both rheumatologists and obstetricians. The study was initiated in 2003. At the time that the abstract was written, 700 women had been recruited to this study; at the time of abstract submission, 599 pregnancies had been completed.
Patients were all enrolled prior to 12 weeks’ gestation and were seen by a rheumatologist every trimester. Women were excluded from the study if they had a multifetal pregnancy; were on more than 20 mg/day of prednisone; had a proteinuria level greater than 1 g/day; and/or had a creatinine level greater than 1.2 mg/dL.
An adverse pregnancy outcome was strictly defined as at least one of the following: fetal/neonatal death; birth indicated at less than 36 weeks due to placental insufficiency, hypertension, or preeclampsia; and small for gestational age (less than fifth percentile).
In addition, mild/moderate and severe flares were defined by the SLEPDAI (SLE Pregnancy Disease Activity Index) score, which excludes physiologic changes of pregnancy but incorporates the components of the SELENA (Safety of Estrogen in Lupus Erythematosus National Assessment), as well as changes in clinical parameters and medications, and physician’s global assessment.
The researchers evaluated 333 women from their first trimester until 3 months post partum. Nearly half of the women were ethnicities other than white, an important characteristic given that women from minority groups can have an increased risk of SLE.
Also importantly, 31% had a history of previous lupus affecting their kidneys. "This is really important because when we see a young woman who develops lupus nephritis – and that’s a fairly serious manifestation of the disease – they always ask, ‘Even if I get better from this, does that mean that I can never have a child?’ " said Dr. Buyon.
Half of the women with a prior history of lupus nephritis had anti-DNA antibodies, "which many of us worry quite a bit about and suggests perhaps a more serious disease." However, their baseline characteristics were good in terms of low disease activity and disease stability.
When enrolled in the study, 60% of the women were taking hydroxychloroquine, 41% were taking prednisone, and 18% were taking azathioprine. On average, the participants’ lupus was relatively inactive
Fetal death occurred in 4.5%. "But if you look at the national population, this is about 2%," Dr. Buyon said.
Neonatal death in this cohort was very similar to that for neonatal death nationally: 1.2%, compared with 1% nationally.
Indicated preterm delivery or small for gestational age occurred in 9.1% of SLE pregnancies. In addition, 10% of the mothers developed preeclampsia; the national level is closer to 4%.
Greater levels of lupus activity and greater levels of antiphospholipid antibodies – particularly the lupus anticoagulant – were associated with poorer outcomes.
The researchers also performed a multivariate analysis to identify independent predictors of these poor outcomes. They found that a history of renal disease predicted a poor pregnancy outcome.
The researchers then looked at maternal outcomes. "I think this is where the news is extraordinary. ... Our mild-moderate flair rate was 18%, which we were obviously very excited about," Dr. Buyon said. Only 15 patients had a severe flare-up, and most flares did not require medication.
The study was funded by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Buyon reported that she has no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: In all, 81% of the women with low-activity disease had a favorable outcome. Indicated preterm delivery or small for gestational age occurred in 9.1% of SLE pregnancies. In addition, 10% of the mothers developed preeclampsia; the national level is closer to 4%.
Data Source: A study of 333 pregnancies in women with low-activity systemic lupus erythematosus as part of the PROMISSE (Predictors of Pregnancy Outcome: Biomarkers in Antiphospholipid Antibody Syndrome and Systemic Lupus Erythematosus) study.
Disclosures: The study was funded by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Buyon reported that she has no relevant financial disclosures.
Cancer Risk From Biologics in RA Shown Negligible
CHICAGO – Patients with rheumatoid arthritis on antitumor necrosis factor drugs have no greater risk of developing solid cancers than RA patients on disease-modifying antirheumatic drugs, according to an analysis of registry data on more than 15,000 patients tracked for up to 5 years.
Among the 15,262 patients in the RA registry, 91 of the 3,543 participants taking DMARDs (2.6%) and 295 among 11,719 participants taking anti-TNF drugs (2.5%) developed solid cancers.
"I think these results are very reassuring and follow on nicely from results of early clinical trials. Overall, the risk of solid cancer with anti-TNF therapy does not appear to be increased," lead author Dr. Kimme Hyrich said at the annual meeting of the American College of Rheumatology.
"Of course this represents therapy only up to 5 years, and we know that cancer in general can take many, many years to develop or become clinically apparent. Therefore we need to continue to follow these patients," Dr. Hyrich noted.
The study corroborates previous studies showing a minimal cancer risk associated with the use of anti-TNF agents, many of which have been used in the treatment of RA for more than 10 years. "When they were first available for widespread use, I think there was a continuing anxiety about whether or not an agent, which blocks occult tumor necrosis factor, would actually increase the risk of cancer in patients with rheumatoid arthritis," said Dr. Hyrich, who is senior lecturer and consultant in rheumatology at the University of Manchester (England).
Studies since have been limited primarily to meta-analyses of randomized controlled trials of anti-TNF drugs. These trials tend to be of limited duration, and the participating patients tend to be highly screened. The participants may not represent patients in typical practice, Dr. Hyrich said.
In 2001, the British Society for Rheumatology Biologics Register was established to track the progress of patients with severe rheumatoid arthritis and other rheumatic diseases who are taking anti-TNF therapy. The registry also tracks patients with moderate to severe RA who are being treated with nonbiologic DMARDs; these patients served as a control group in this analysis.
Cancer cases were also identified by reviewing patient records. The study data were linked with the U.K. National Health Service Information Center’s national cancer register. "This is a mandatory reporting cancer register where every confirmed cancer in the United Kingdom is recorded," she explained.
The analysis was limited to solid cancers, specifically excluding lymphoma, leukemia, and skin cancers. The researchers compared the risk out to 5 years’ follow-up for those receiving anti-TNF therapies with the risk for those receiving nonbiologic DMARD therapies.
Dr. Hyrich noted that there were differences between the two patient groups. In particular, more men were on DMARDs, and those on DMARDs were slightly older. "Both of these are recognized risk factors for cancer in general," he said. The results, however, were statistically adjusted to balance the risk between the two groups. The investigators found no significant differences between the groups after adjustment.
Dr. Hyrich reported having no relevant financial disclosures.
CHICAGO – Patients with rheumatoid arthritis on antitumor necrosis factor drugs have no greater risk of developing solid cancers than RA patients on disease-modifying antirheumatic drugs, according to an analysis of registry data on more than 15,000 patients tracked for up to 5 years.
Among the 15,262 patients in the RA registry, 91 of the 3,543 participants taking DMARDs (2.6%) and 295 among 11,719 participants taking anti-TNF drugs (2.5%) developed solid cancers.
"I think these results are very reassuring and follow on nicely from results of early clinical trials. Overall, the risk of solid cancer with anti-TNF therapy does not appear to be increased," lead author Dr. Kimme Hyrich said at the annual meeting of the American College of Rheumatology.
"Of course this represents therapy only up to 5 years, and we know that cancer in general can take many, many years to develop or become clinically apparent. Therefore we need to continue to follow these patients," Dr. Hyrich noted.
The study corroborates previous studies showing a minimal cancer risk associated with the use of anti-TNF agents, many of which have been used in the treatment of RA for more than 10 years. "When they were first available for widespread use, I think there was a continuing anxiety about whether or not an agent, which blocks occult tumor necrosis factor, would actually increase the risk of cancer in patients with rheumatoid arthritis," said Dr. Hyrich, who is senior lecturer and consultant in rheumatology at the University of Manchester (England).
Studies since have been limited primarily to meta-analyses of randomized controlled trials of anti-TNF drugs. These trials tend to be of limited duration, and the participating patients tend to be highly screened. The participants may not represent patients in typical practice, Dr. Hyrich said.
In 2001, the British Society for Rheumatology Biologics Register was established to track the progress of patients with severe rheumatoid arthritis and other rheumatic diseases who are taking anti-TNF therapy. The registry also tracks patients with moderate to severe RA who are being treated with nonbiologic DMARDs; these patients served as a control group in this analysis.
Cancer cases were also identified by reviewing patient records. The study data were linked with the U.K. National Health Service Information Center’s national cancer register. "This is a mandatory reporting cancer register where every confirmed cancer in the United Kingdom is recorded," she explained.
The analysis was limited to solid cancers, specifically excluding lymphoma, leukemia, and skin cancers. The researchers compared the risk out to 5 years’ follow-up for those receiving anti-TNF therapies with the risk for those receiving nonbiologic DMARD therapies.
Dr. Hyrich noted that there were differences between the two patient groups. In particular, more men were on DMARDs, and those on DMARDs were slightly older. "Both of these are recognized risk factors for cancer in general," he said. The results, however, were statistically adjusted to balance the risk between the two groups. The investigators found no significant differences between the groups after adjustment.
Dr. Hyrich reported having no relevant financial disclosures.
CHICAGO – Patients with rheumatoid arthritis on antitumor necrosis factor drugs have no greater risk of developing solid cancers than RA patients on disease-modifying antirheumatic drugs, according to an analysis of registry data on more than 15,000 patients tracked for up to 5 years.
Among the 15,262 patients in the RA registry, 91 of the 3,543 participants taking DMARDs (2.6%) and 295 among 11,719 participants taking anti-TNF drugs (2.5%) developed solid cancers.
"I think these results are very reassuring and follow on nicely from results of early clinical trials. Overall, the risk of solid cancer with anti-TNF therapy does not appear to be increased," lead author Dr. Kimme Hyrich said at the annual meeting of the American College of Rheumatology.
"Of course this represents therapy only up to 5 years, and we know that cancer in general can take many, many years to develop or become clinically apparent. Therefore we need to continue to follow these patients," Dr. Hyrich noted.
The study corroborates previous studies showing a minimal cancer risk associated with the use of anti-TNF agents, many of which have been used in the treatment of RA for more than 10 years. "When they were first available for widespread use, I think there was a continuing anxiety about whether or not an agent, which blocks occult tumor necrosis factor, would actually increase the risk of cancer in patients with rheumatoid arthritis," said Dr. Hyrich, who is senior lecturer and consultant in rheumatology at the University of Manchester (England).
Studies since have been limited primarily to meta-analyses of randomized controlled trials of anti-TNF drugs. These trials tend to be of limited duration, and the participating patients tend to be highly screened. The participants may not represent patients in typical practice, Dr. Hyrich said.
In 2001, the British Society for Rheumatology Biologics Register was established to track the progress of patients with severe rheumatoid arthritis and other rheumatic diseases who are taking anti-TNF therapy. The registry also tracks patients with moderate to severe RA who are being treated with nonbiologic DMARDs; these patients served as a control group in this analysis.
Cancer cases were also identified by reviewing patient records. The study data were linked with the U.K. National Health Service Information Center’s national cancer register. "This is a mandatory reporting cancer register where every confirmed cancer in the United Kingdom is recorded," she explained.
The analysis was limited to solid cancers, specifically excluding lymphoma, leukemia, and skin cancers. The researchers compared the risk out to 5 years’ follow-up for those receiving anti-TNF therapies with the risk for those receiving nonbiologic DMARD therapies.
Dr. Hyrich noted that there were differences between the two patient groups. In particular, more men were on DMARDs, and those on DMARDs were slightly older. "Both of these are recognized risk factors for cancer in general," he said. The results, however, were statistically adjusted to balance the risk between the two groups. The investigators found no significant differences between the groups after adjustment.
Dr. Hyrich reported having no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: During 5 years of follow-up, 91 of the 3,543 participants taking DMARDs (2.6%) and 295 among 11,719 participants taking anti-TNF drugs (2.5%)developed solid cancers.
Data Source: An analysis of data from the British Society for Rheumatology Biologics Register.
Disclosures: Dr. Hyrich reported having no relevant financial disclosures.
Osteoarthritis May Drive Up Risk of Falling, Fracture
CHICAGO – Despite their bigger bones, postmenopausal women with osteoarthritis appear to be at a greater risk of falls and subsequent fractures, compared to their counterparts without the joint disease, according to an analysis of data from a longitudinal study of more than 50,000 women.
Among the 51,386 women in GLOW (Global Longitudinal Study of Osteoporosis in Women), 40% had osteoarthritis (OA). Women with OA experienced almost 30% more falls and had a 20% greater risk of fracture than those without OA, lead author Dr. Daniel Prieto-Alhambra said at the annual meeting of the American College of Rheumatology.
"We know that patients with osteoarthritis have bigger bones, and some have actually suggested that these bones are more resistant." However, recent papers have suggested that patients with osteoarthritis experience more falls than the general population, said Dr. Prieto-Alhambra, who is a postdoctoral research fellow at the Hospital del Mar and Municipal Institute of Medical Research in Barcelona.
Coauthor Dr. Nigel Arden noted that "we’ve seen this in other cohorts before. What was new here was that the falls would actually explain the increased risk of fracture, whereas in other cohorts, it hasn’t explained it."
Part of the disconnect between bigger bones and fractures in OA is that bone mineral density (BMD) measurements do not provide an accurate picture of BMD. "The bone density measurement is a two-dimensional measurement of a three-dimensional bone," said Dr. Arden in an interview. Individuals with OA have up to an 8% greater BMD when viewed two dimensionally. However, "when you look at volumetric density, as we’ve done in another cohort, their density is the same [as those without OA] – they just have bigger bones."
All of this can lead to a potential overestimate of BMD. "In osteoporosis, we use bone density as a predictor of fracture. People with osteoarthritis have an increased bone density and therefore should have a low risk of fracture but they have an increased risk of fracture. Therefore, we were concerned that people were being falsely reassured by their increased bone density measurements," Dr. Arden added.
In addition, "when they get osteoarthritis, they have increased rates of bone loss, which again is an independent risk factor for fracture," said Dr. Arden, who is a professor of rheumatology at the University of Oxford (England).
The study included 60,393 women aged 55 years or older. For 3 years, participants from several countries, including the United States, Canada, Australia, United Kingdom, Spain, and others, were surveyed annually. Women who were at least 55 years old and who visited a practice within the previous 2 years were eligible. The women were mailed a self-administered questionnaire at baseline; follow-up questionnaires were sent at 12-month intervals for 3 years. Participants were asked if a doctor or other health care provider had told them that they had osteoarthritis or degenerative joint disease. Information on incident falls and fractures and potential confounders were self-reported. For this analysis, women with missing baseline OA or fracture information, as well as those with celiac disease or rheumatoid arthritis, were excluded.
The unadjusted hazard ratio for fracture among OA patients was 1.40 and this remained significant after multivariable adjustment (HR, 1.21). Falls were also more likely in women with OA (adjusted HR, 1.27). The association between OA and fracture remained significant even after adjusting for baseline falls (HR, 1.16).
"If falls explain the increased risk of fracture, we need to work out why these people are falling and have public health interventions to reduce those risks of falls – through physiotherapy, nutrition, and help around the home," said Dr. Arden. "We also need to worry that when we do an osteoporosis estimation that we [consider] osteoarthritis as an extra risk factor."
"We need to pay more attention to pain relief, exercise, and support around the home ... and when we assess their osteoporosis risk we need to think that their bone density may be falsely reassuring," Dr. Arden said.
Dr. Prieto-Alhambra and Dr. Arden reported that they have no relevant disclosures.
CHICAGO – Despite their bigger bones, postmenopausal women with osteoarthritis appear to be at a greater risk of falls and subsequent fractures, compared to their counterparts without the joint disease, according to an analysis of data from a longitudinal study of more than 50,000 women.
Among the 51,386 women in GLOW (Global Longitudinal Study of Osteoporosis in Women), 40% had osteoarthritis (OA). Women with OA experienced almost 30% more falls and had a 20% greater risk of fracture than those without OA, lead author Dr. Daniel Prieto-Alhambra said at the annual meeting of the American College of Rheumatology.
"We know that patients with osteoarthritis have bigger bones, and some have actually suggested that these bones are more resistant." However, recent papers have suggested that patients with osteoarthritis experience more falls than the general population, said Dr. Prieto-Alhambra, who is a postdoctoral research fellow at the Hospital del Mar and Municipal Institute of Medical Research in Barcelona.
Coauthor Dr. Nigel Arden noted that "we’ve seen this in other cohorts before. What was new here was that the falls would actually explain the increased risk of fracture, whereas in other cohorts, it hasn’t explained it."
Part of the disconnect between bigger bones and fractures in OA is that bone mineral density (BMD) measurements do not provide an accurate picture of BMD. "The bone density measurement is a two-dimensional measurement of a three-dimensional bone," said Dr. Arden in an interview. Individuals with OA have up to an 8% greater BMD when viewed two dimensionally. However, "when you look at volumetric density, as we’ve done in another cohort, their density is the same [as those without OA] – they just have bigger bones."
All of this can lead to a potential overestimate of BMD. "In osteoporosis, we use bone density as a predictor of fracture. People with osteoarthritis have an increased bone density and therefore should have a low risk of fracture but they have an increased risk of fracture. Therefore, we were concerned that people were being falsely reassured by their increased bone density measurements," Dr. Arden added.
In addition, "when they get osteoarthritis, they have increased rates of bone loss, which again is an independent risk factor for fracture," said Dr. Arden, who is a professor of rheumatology at the University of Oxford (England).
The study included 60,393 women aged 55 years or older. For 3 years, participants from several countries, including the United States, Canada, Australia, United Kingdom, Spain, and others, were surveyed annually. Women who were at least 55 years old and who visited a practice within the previous 2 years were eligible. The women were mailed a self-administered questionnaire at baseline; follow-up questionnaires were sent at 12-month intervals for 3 years. Participants were asked if a doctor or other health care provider had told them that they had osteoarthritis or degenerative joint disease. Information on incident falls and fractures and potential confounders were self-reported. For this analysis, women with missing baseline OA or fracture information, as well as those with celiac disease or rheumatoid arthritis, were excluded.
The unadjusted hazard ratio for fracture among OA patients was 1.40 and this remained significant after multivariable adjustment (HR, 1.21). Falls were also more likely in women with OA (adjusted HR, 1.27). The association between OA and fracture remained significant even after adjusting for baseline falls (HR, 1.16).
"If falls explain the increased risk of fracture, we need to work out why these people are falling and have public health interventions to reduce those risks of falls – through physiotherapy, nutrition, and help around the home," said Dr. Arden. "We also need to worry that when we do an osteoporosis estimation that we [consider] osteoarthritis as an extra risk factor."
"We need to pay more attention to pain relief, exercise, and support around the home ... and when we assess their osteoporosis risk we need to think that their bone density may be falsely reassuring," Dr. Arden said.
Dr. Prieto-Alhambra and Dr. Arden reported that they have no relevant disclosures.
CHICAGO – Despite their bigger bones, postmenopausal women with osteoarthritis appear to be at a greater risk of falls and subsequent fractures, compared to their counterparts without the joint disease, according to an analysis of data from a longitudinal study of more than 50,000 women.
Among the 51,386 women in GLOW (Global Longitudinal Study of Osteoporosis in Women), 40% had osteoarthritis (OA). Women with OA experienced almost 30% more falls and had a 20% greater risk of fracture than those without OA, lead author Dr. Daniel Prieto-Alhambra said at the annual meeting of the American College of Rheumatology.
"We know that patients with osteoarthritis have bigger bones, and some have actually suggested that these bones are more resistant." However, recent papers have suggested that patients with osteoarthritis experience more falls than the general population, said Dr. Prieto-Alhambra, who is a postdoctoral research fellow at the Hospital del Mar and Municipal Institute of Medical Research in Barcelona.
Coauthor Dr. Nigel Arden noted that "we’ve seen this in other cohorts before. What was new here was that the falls would actually explain the increased risk of fracture, whereas in other cohorts, it hasn’t explained it."
Part of the disconnect between bigger bones and fractures in OA is that bone mineral density (BMD) measurements do not provide an accurate picture of BMD. "The bone density measurement is a two-dimensional measurement of a three-dimensional bone," said Dr. Arden in an interview. Individuals with OA have up to an 8% greater BMD when viewed two dimensionally. However, "when you look at volumetric density, as we’ve done in another cohort, their density is the same [as those without OA] – they just have bigger bones."
All of this can lead to a potential overestimate of BMD. "In osteoporosis, we use bone density as a predictor of fracture. People with osteoarthritis have an increased bone density and therefore should have a low risk of fracture but they have an increased risk of fracture. Therefore, we were concerned that people were being falsely reassured by their increased bone density measurements," Dr. Arden added.
In addition, "when they get osteoarthritis, they have increased rates of bone loss, which again is an independent risk factor for fracture," said Dr. Arden, who is a professor of rheumatology at the University of Oxford (England).
The study included 60,393 women aged 55 years or older. For 3 years, participants from several countries, including the United States, Canada, Australia, United Kingdom, Spain, and others, were surveyed annually. Women who were at least 55 years old and who visited a practice within the previous 2 years were eligible. The women were mailed a self-administered questionnaire at baseline; follow-up questionnaires were sent at 12-month intervals for 3 years. Participants were asked if a doctor or other health care provider had told them that they had osteoarthritis or degenerative joint disease. Information on incident falls and fractures and potential confounders were self-reported. For this analysis, women with missing baseline OA or fracture information, as well as those with celiac disease or rheumatoid arthritis, were excluded.
The unadjusted hazard ratio for fracture among OA patients was 1.40 and this remained significant after multivariable adjustment (HR, 1.21). Falls were also more likely in women with OA (adjusted HR, 1.27). The association between OA and fracture remained significant even after adjusting for baseline falls (HR, 1.16).
"If falls explain the increased risk of fracture, we need to work out why these people are falling and have public health interventions to reduce those risks of falls – through physiotherapy, nutrition, and help around the home," said Dr. Arden. "We also need to worry that when we do an osteoporosis estimation that we [consider] osteoarthritis as an extra risk factor."
"We need to pay more attention to pain relief, exercise, and support around the home ... and when we assess their osteoporosis risk we need to think that their bone density may be falsely reassuring," Dr. Arden said.
Dr. Prieto-Alhambra and Dr. Arden reported that they have no relevant disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: Women with osteoarthritis experienced almost 30% more falls and had a 20% greater risk of fracture than those without OA.
Data Source: An analysis of 51,386 women participating in GLOW (Global Longitudinal Study of Osteoporosis in Women).
Disclosures: Dr. Prieto-Alhambra and Dr. Arden reported that they have no relevant disclosures.
Prebiopsy Ciprofloxacin Still Best Choice to Prevent Infection
The use of prophylactic ciprofloxacin-containing regimens for prostate biopsies resulted in significantly fewer infective complications than did regimens containing co-amoxiclav and gentamicin, according to an audit of hospital records of 709 patients at one institution.
Researchers in the United Kingdom found that regimens containing ciprofloxacin resulted in an infective complications rate of 2.4%, compared with 12.9% for co-amoxiclav/gentamicin regimens.
The results of this 20-month audit supports the use of ciprofloxacin as part of a prophylactic regimen for transrectal ultrasound-guided prostate biopsy (TRUSP Bx), wrote Mr. Thomas Madden and his coinvestigators in the British Journal of Urology International (BJU International 2011;108:1597-602 [doi:10.1111/j.1464-410X.2011.10160.x]).
Prior to April 2008, patients undergoing TRUSP biopsy were treated with ciprofloxacin 500 mg orally prior to the procedure; followed by 500 mg ciprofloxacin twice daily for 5 days (regimen 1). After April 2008, patients were treated with ciprofloxacin 500 mg orally prior to procedure; followed by 500 mg ciprofloxacin twice daily for 3 days (regimen 2).
Subsequently various recommendations were made to help the hospital to reduce its incidence of Clostridium difficile infection and remain within national guidelines. This included restricting the use of fluoroquinolones and cephalosporins with substitution of co-amoxiclav. The standard antibiotic prophylaxis regimen for all surgeries, including urologic procedures, was changed in July 2008 to 120 mg intravenous gentamicin given 10 minutes preprocedure; followed by 375 mg co-amoxiclav given orally three times daily for 3 days (regimen 3).
In November 2008, the regimen was changed to 120 mg intravenous gentamicin given 10 minutes preprocedure; followed by 625 mg co-amoxiclav given orally three times daily for 3 days (regimen 4). In March 2009, the regimen was changed back to ciprofloxacin 500 mg given orally preprocedure; followed by ciprofloxacin 500 mg given twice daily for 3 days (regimen 5).
"Ciprofloxacin is well documented to achieve excellent prostatic tissue concentration."
"In view of the limited data supporting the change, it was agreed that postoperative infection rates should be monitored to confirm efficacy. This audit looks at the rates of infective complications before and after the change of antibiotic regimen," they wrote.
The investigators identified all patients undergoing TRUSP biopsy from January 2008 through March 2009 from clinic records. Because the electronic patient records at the Cambridge University Hospitals Trust stores all letters from clinics and any admissions, a search starting with the TRUSP Bx clinic letter was able to confirm the antibiotics chosen for prophylaxis. The audit continued for a further 6 months to assess the effect of returning to the use of quinolones as prophylaxis. Patients were divided into five groups based on the antibiotic regimen used.
The two (ciprofloxacin-based) regimens used before the intensive-support team visit were associated with infective complication rates of 0.8% and 2% with 5-day and 3-day courses of ciprofloxacin, respectively. After regimen 3 with gentamicin and co-amoxiclav 375 mg three times daily was introduced, the complication rate rose to 14.4%, and substituting a higher dosage of co-amoxiclav brought only a marginal drop to 11.4%. The incidence of infective complications fell to 3.8%, only after the protocol was changed back to ciprofloxacin.
Overall only 4 patients out of 454 (0.9%) who received ciprofloxacin were admitted for infective complications. In the combined groups given gentamicin/co-amoxiclav, 12 patients out of 255 (4.7%) were admitted with sepsis – which was a highly significant difference.
"Further analysis between the groups shows no significant difference between the 5-day and 3-day regimens of ciprofloxacin in terms of infective complications and no difference between the low-dose and high-dose regimens of co-amoxiclav and gentamicin," wrote Mr. Madden, a clinical fellow in the urology department of Addenbrooke’s Hospital in Cambridge, and his coinvestigators.
Analysis of patients with infective complications showed that only 47% of mid-stream urine specimens and 36% of blood culture samples grew any organisms. Notably, of those that did, 89% grew organisms that were sensitive to co-amoxiclav. "Ciprofloxacin is well documented to achieve excellent prostatic tissue concentrations and it is likely that this is the reason for its effectiveness as a prophylactic agent," the authors wrote.
"However, there should be some caution exercised when using ciprofloxacin as there is evidence that resistant microorganisms exist in the community. The four ciprofloxacin-resistant isolates in this study were evenly distributed between the groups of patients. This would seem to indicate a small but significant prevalence of resistance rather than increasing rates, although the numbers involved are too small in this study to draw firm conclusions."
Mr. Madden had no significant financial relationships to disclose.
The use of prophylactic ciprofloxacin-containing regimens for prostate biopsies resulted in significantly fewer infective complications than did regimens containing co-amoxiclav and gentamicin, according to an audit of hospital records of 709 patients at one institution.
Researchers in the United Kingdom found that regimens containing ciprofloxacin resulted in an infective complications rate of 2.4%, compared with 12.9% for co-amoxiclav/gentamicin regimens.
The results of this 20-month audit supports the use of ciprofloxacin as part of a prophylactic regimen for transrectal ultrasound-guided prostate biopsy (TRUSP Bx), wrote Mr. Thomas Madden and his coinvestigators in the British Journal of Urology International (BJU International 2011;108:1597-602 [doi:10.1111/j.1464-410X.2011.10160.x]).
Prior to April 2008, patients undergoing TRUSP biopsy were treated with ciprofloxacin 500 mg orally prior to the procedure; followed by 500 mg ciprofloxacin twice daily for 5 days (regimen 1). After April 2008, patients were treated with ciprofloxacin 500 mg orally prior to procedure; followed by 500 mg ciprofloxacin twice daily for 3 days (regimen 2).
Subsequently various recommendations were made to help the hospital to reduce its incidence of Clostridium difficile infection and remain within national guidelines. This included restricting the use of fluoroquinolones and cephalosporins with substitution of co-amoxiclav. The standard antibiotic prophylaxis regimen for all surgeries, including urologic procedures, was changed in July 2008 to 120 mg intravenous gentamicin given 10 minutes preprocedure; followed by 375 mg co-amoxiclav given orally three times daily for 3 days (regimen 3).
In November 2008, the regimen was changed to 120 mg intravenous gentamicin given 10 minutes preprocedure; followed by 625 mg co-amoxiclav given orally three times daily for 3 days (regimen 4). In March 2009, the regimen was changed back to ciprofloxacin 500 mg given orally preprocedure; followed by ciprofloxacin 500 mg given twice daily for 3 days (regimen 5).
"Ciprofloxacin is well documented to achieve excellent prostatic tissue concentration."
"In view of the limited data supporting the change, it was agreed that postoperative infection rates should be monitored to confirm efficacy. This audit looks at the rates of infective complications before and after the change of antibiotic regimen," they wrote.
The investigators identified all patients undergoing TRUSP biopsy from January 2008 through March 2009 from clinic records. Because the electronic patient records at the Cambridge University Hospitals Trust stores all letters from clinics and any admissions, a search starting with the TRUSP Bx clinic letter was able to confirm the antibiotics chosen for prophylaxis. The audit continued for a further 6 months to assess the effect of returning to the use of quinolones as prophylaxis. Patients were divided into five groups based on the antibiotic regimen used.
The two (ciprofloxacin-based) regimens used before the intensive-support team visit were associated with infective complication rates of 0.8% and 2% with 5-day and 3-day courses of ciprofloxacin, respectively. After regimen 3 with gentamicin and co-amoxiclav 375 mg three times daily was introduced, the complication rate rose to 14.4%, and substituting a higher dosage of co-amoxiclav brought only a marginal drop to 11.4%. The incidence of infective complications fell to 3.8%, only after the protocol was changed back to ciprofloxacin.
Overall only 4 patients out of 454 (0.9%) who received ciprofloxacin were admitted for infective complications. In the combined groups given gentamicin/co-amoxiclav, 12 patients out of 255 (4.7%) were admitted with sepsis – which was a highly significant difference.
"Further analysis between the groups shows no significant difference between the 5-day and 3-day regimens of ciprofloxacin in terms of infective complications and no difference between the low-dose and high-dose regimens of co-amoxiclav and gentamicin," wrote Mr. Madden, a clinical fellow in the urology department of Addenbrooke’s Hospital in Cambridge, and his coinvestigators.
Analysis of patients with infective complications showed that only 47% of mid-stream urine specimens and 36% of blood culture samples grew any organisms. Notably, of those that did, 89% grew organisms that were sensitive to co-amoxiclav. "Ciprofloxacin is well documented to achieve excellent prostatic tissue concentrations and it is likely that this is the reason for its effectiveness as a prophylactic agent," the authors wrote.
"However, there should be some caution exercised when using ciprofloxacin as there is evidence that resistant microorganisms exist in the community. The four ciprofloxacin-resistant isolates in this study were evenly distributed between the groups of patients. This would seem to indicate a small but significant prevalence of resistance rather than increasing rates, although the numbers involved are too small in this study to draw firm conclusions."
Mr. Madden had no significant financial relationships to disclose.
The use of prophylactic ciprofloxacin-containing regimens for prostate biopsies resulted in significantly fewer infective complications than did regimens containing co-amoxiclav and gentamicin, according to an audit of hospital records of 709 patients at one institution.
Researchers in the United Kingdom found that regimens containing ciprofloxacin resulted in an infective complications rate of 2.4%, compared with 12.9% for co-amoxiclav/gentamicin regimens.
The results of this 20-month audit supports the use of ciprofloxacin as part of a prophylactic regimen for transrectal ultrasound-guided prostate biopsy (TRUSP Bx), wrote Mr. Thomas Madden and his coinvestigators in the British Journal of Urology International (BJU International 2011;108:1597-602 [doi:10.1111/j.1464-410X.2011.10160.x]).
Prior to April 2008, patients undergoing TRUSP biopsy were treated with ciprofloxacin 500 mg orally prior to the procedure; followed by 500 mg ciprofloxacin twice daily for 5 days (regimen 1). After April 2008, patients were treated with ciprofloxacin 500 mg orally prior to procedure; followed by 500 mg ciprofloxacin twice daily for 3 days (regimen 2).
Subsequently various recommendations were made to help the hospital to reduce its incidence of Clostridium difficile infection and remain within national guidelines. This included restricting the use of fluoroquinolones and cephalosporins with substitution of co-amoxiclav. The standard antibiotic prophylaxis regimen for all surgeries, including urologic procedures, was changed in July 2008 to 120 mg intravenous gentamicin given 10 minutes preprocedure; followed by 375 mg co-amoxiclav given orally three times daily for 3 days (regimen 3).
In November 2008, the regimen was changed to 120 mg intravenous gentamicin given 10 minutes preprocedure; followed by 625 mg co-amoxiclav given orally three times daily for 3 days (regimen 4). In March 2009, the regimen was changed back to ciprofloxacin 500 mg given orally preprocedure; followed by ciprofloxacin 500 mg given twice daily for 3 days (regimen 5).
"Ciprofloxacin is well documented to achieve excellent prostatic tissue concentration."
"In view of the limited data supporting the change, it was agreed that postoperative infection rates should be monitored to confirm efficacy. This audit looks at the rates of infective complications before and after the change of antibiotic regimen," they wrote.
The investigators identified all patients undergoing TRUSP biopsy from January 2008 through March 2009 from clinic records. Because the electronic patient records at the Cambridge University Hospitals Trust stores all letters from clinics and any admissions, a search starting with the TRUSP Bx clinic letter was able to confirm the antibiotics chosen for prophylaxis. The audit continued for a further 6 months to assess the effect of returning to the use of quinolones as prophylaxis. Patients were divided into five groups based on the antibiotic regimen used.
The two (ciprofloxacin-based) regimens used before the intensive-support team visit were associated with infective complication rates of 0.8% and 2% with 5-day and 3-day courses of ciprofloxacin, respectively. After regimen 3 with gentamicin and co-amoxiclav 375 mg three times daily was introduced, the complication rate rose to 14.4%, and substituting a higher dosage of co-amoxiclav brought only a marginal drop to 11.4%. The incidence of infective complications fell to 3.8%, only after the protocol was changed back to ciprofloxacin.
Overall only 4 patients out of 454 (0.9%) who received ciprofloxacin were admitted for infective complications. In the combined groups given gentamicin/co-amoxiclav, 12 patients out of 255 (4.7%) were admitted with sepsis – which was a highly significant difference.
"Further analysis between the groups shows no significant difference between the 5-day and 3-day regimens of ciprofloxacin in terms of infective complications and no difference between the low-dose and high-dose regimens of co-amoxiclav and gentamicin," wrote Mr. Madden, a clinical fellow in the urology department of Addenbrooke’s Hospital in Cambridge, and his coinvestigators.
Analysis of patients with infective complications showed that only 47% of mid-stream urine specimens and 36% of blood culture samples grew any organisms. Notably, of those that did, 89% grew organisms that were sensitive to co-amoxiclav. "Ciprofloxacin is well documented to achieve excellent prostatic tissue concentrations and it is likely that this is the reason for its effectiveness as a prophylactic agent," the authors wrote.
"However, there should be some caution exercised when using ciprofloxacin as there is evidence that resistant microorganisms exist in the community. The four ciprofloxacin-resistant isolates in this study were evenly distributed between the groups of patients. This would seem to indicate a small but significant prevalence of resistance rather than increasing rates, although the numbers involved are too small in this study to draw firm conclusions."
Mr. Madden had no significant financial relationships to disclose.
FROM THE BRITISH JOURNAL OF UROLOGY INTERNATIONAL
Major Finding: Ciprofloxacin-based regimens resulted in 2.4% infective complications, compared with 12.9% for co-amoxiclav/gentamicin regimens, when used prophylactically for transrectal ultrasound-guided prostate biopsy.
Data Source: A retrospective 20-month audit prophylactic regimens for transrectal ultrasound-guided prostate biopsy procedures in 709 patients.
Disclosures: Mr. Madden had no significant financial relationships to disclose.
Eyelid Plaque May Signal Severe Atherosclerosis
Major Finding: The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study.
Data Source: Patients were part of the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978; a total of 19,329 white women and men of Danish descent were included at baseline.
Disclosures: This study was funded by the Research Fund at Rigshospitalet, the Lundbeck Foundation, the Danish Medical Research Council, and the Danish Heart Foundation. The authors reported that they had no other financial disclosures.
Plaque occurring around the eyelids may offer clinicians a new way of identifying patients at an increased risk for myocardial infarction and severe atherosclerosis, a study has shown.
“The results from this study suggest that xanthelasmata are a cutaneous marker of atherosclerosis independent of lipid concentrations and thus should be considered in clinical practice as an independent and additional risk factor for myocardial infarction and ischemic heart disease,” Mette Christoffersen and her coinvestigators wrote in a study published online (BMJ 2011;343:d5497).
The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study of 12,745 patients. However, on multifactorial adjustment for arcus corneae, no hazard ratios remained significant. The presence of both xanthelasmata and arcus corneae significantly increased the risk of ischemic heart disease (HR, 1.56) but not any other outcomes after multifactorial adjustment.
Xanthelasmata palpebrarum are sharply demarcated, yellowish flat plaques that appear on the upper or lower eyelids, most often near the inner canthus. Xanthelasmata represent areas of macrophages containing lipids. Arcus corneae (or arcus senilis) is a gray-white-yellowish opacity that is located near the periphery of the cornea, though separated from the limbic margin by a clear corneal zone. Arcus corneae represents deposits of cholesteryl ester–rich lipid particles. It has been suggested that xanthelasmata and arcus corneae may be markers of proatherogenic changes in the vessels and thus markers of atherosclerosis.
“The findings from our study could be of particular value in societies where access to laboratory facilities, and thus lipid profile measurement, is difficult. In this setting, presence of xanthelasmata may be a useful predictor of underlying atherosclerotic disease. An easy registration of presence of xanthelasmata along with age and sex makes it possible to assess the risk of myocardial infarction and ischemic heart disease and thus to make sure that people at increased risk are managed accordingly with lifestyle changes and treatment to reduce low-density lipoprotein cholesterol,” wrote Ms. Christoffersen, a clinical biochemistry PhD student at Rigshospitalet in Copenhagen, and her colleagues.
They used data from the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978 with follow-up examinations. A total of 19,329 white women and men of Danish descent were drawn randomly from the Copenhagen Central Person Registry and invited to participate. Data came from a self-administered questionnaire, a physical examination, and blood samples.
For this analysis, the researchers included 12,745 people, for whom complete information on all relevant variables, including xanthelasmata and arcus corneae, were available at baseline. The patients were followed from baseline at the 1976-1978 examination to the end of May 2009 through the use of their unique Central Person Register number. No participants were lost to follow-up.
Trained nurses or medical laboratory technicians determined the presence of xanthelasmata and arcus corneae by careful visual inspection of the eyelids and the cornea during the physical examination. The investigators collected and verified diagnoses of MI and ischemic heart disease using ICD-8 and ICD-10 codes by reviewing all hospital admissions, diagnoses entered in the national Danish Patient Registry, all causes of death entered in the national Danish Causes of Death Registry, and medical records from hospitals and general practitioners.
The prevalence of xanthelasmata was 4.4% and similar in women and men. The prevalence of arcus corneae was 24.8% overall, but was lower in women than in men (20.1% vs. 30.2%), Ms. Christoffersen and her associates said.
Potential patients with ischemic cerebrovascular disease, including ischemic stroke, were collected from the national Danish Patient Registry and the national Danish Causes of Death Registry. Hospital records were reviewed by experienced neurologists. Ankle brachial index, a drop in blood pressure in the legs that predicts severe atherosclerosis, was determined in the 2001-2003 examination of the Copenhagen City Heart Study in 2,773 participants, who had also participated in the baseline examination and had complete information on all relevant variables, including xanthelasmata and arcus corneae.
Enzymatic methods were used on fresh plasma samples to measure plasma concentrations of total cholesterol, triglycerides, and high-density lipoprotein cholesterol, the last after precipitation of lipoproteins that contained apolipoprotein B.
The median follow-up was 22 years. In all, 1,872 participants developed MI, 3,699 developed ischemic heart disease, 1,498 developed ischemic strokes, 1,815 developed ischemic cerebrovascular disease, and 8,507 died.
The models were adjusted for age, sex, total cholesterol, triglycerides, body mass index, hypertension, diabetes, pack-years of smoking, alcohol consumption, physical activity, postmenopausal status, hormone therapy, education, income, and family history of ischemic vascular disease.
In this population, the “presence of xanthelasmata in itself predicts risk of myocardial infarction, ischemic heart disease, severe atherosclerosis, and death in the general population independent of well-known cardiovascular risk factors, including plasma cholesterol and triglyceride concentrations. In contrast, arcus corneae is not an important independent predictor of risk,” the authors concluded.
{kind=link}
Patients who have xanthelasmata palpebrarum (shown above) may require more aggressive management of their cardiovascular risk factors.
Source Courtesy Wikipedia/Klaus D. Peter, Gummersbach, Germany/Creative Commons License
View on the News
Findings Are Boon to Clinicians
In an accompanying editorial, Dr. Antonio B. Fernandez and Dr. Paul D. Thompson discussed the clinical relevance of the findings.
“In the linked prospective cohort study, Christoffersen and colleagues assess whether xanthelasmata and arcus corneae, individually and combined, predict risk of ischemic vascular disease and death in the general population,” Dr. Fernandez and Dr. Thompson wrote, noting that there are some good reasons for suspecting such a link (BMJ 2011;343:d5304).
“Both xanthelasmata and arcus corneae are composed of cholesteryl esters similar to those found in serum low-density lipoprotein cholesterol and very low-density lipoprotein cholesterol. They share similar risk factors and have pathophysiological similarities with atherosclerosis,” they noted.
Importantly, the results of this study confirm “that xanthelasmata are an important predictor of cardiovascular disease events and death beyond [their] known association with hyperlipidemia.”
However, “what do these results mean in practice?” they asked. “Overall, the evidence highlights the importance of a comprehensive physical examination and suggests that xanthelasmata could be used by general clinicians to help identify people at higher risk of cardiovascular disease. These people may have an enhanced biological propensity to deposition of cholesterol in vascular and soft tissue, which is not fully represented by their fasting lipid profiles. … Patients with xanthelasmata may therefore require more aggressive management of risk factors,” they concluded.
DR. FERNANDEZ is a clinical cardiology fellow at Brown University in Providence, R.I. DR. THOMPSON is the director of cardiology at Hartford (Conn.) Hospital. Dr. Thompson reported significant financial relationships with several pharmaceutical companies.
Major Finding: The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study.
Data Source: Patients were part of the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978; a total of 19,329 white women and men of Danish descent were included at baseline.
Disclosures: This study was funded by the Research Fund at Rigshospitalet, the Lundbeck Foundation, the Danish Medical Research Council, and the Danish Heart Foundation. The authors reported that they had no other financial disclosures.
Plaque occurring around the eyelids may offer clinicians a new way of identifying patients at an increased risk for myocardial infarction and severe atherosclerosis, a study has shown.
“The results from this study suggest that xanthelasmata are a cutaneous marker of atherosclerosis independent of lipid concentrations and thus should be considered in clinical practice as an independent and additional risk factor for myocardial infarction and ischemic heart disease,” Mette Christoffersen and her coinvestigators wrote in a study published online (BMJ 2011;343:d5497).
The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study of 12,745 patients. However, on multifactorial adjustment for arcus corneae, no hazard ratios remained significant. The presence of both xanthelasmata and arcus corneae significantly increased the risk of ischemic heart disease (HR, 1.56) but not any other outcomes after multifactorial adjustment.
Xanthelasmata palpebrarum are sharply demarcated, yellowish flat plaques that appear on the upper or lower eyelids, most often near the inner canthus. Xanthelasmata represent areas of macrophages containing lipids. Arcus corneae (or arcus senilis) is a gray-white-yellowish opacity that is located near the periphery of the cornea, though separated from the limbic margin by a clear corneal zone. Arcus corneae represents deposits of cholesteryl ester–rich lipid particles. It has been suggested that xanthelasmata and arcus corneae may be markers of proatherogenic changes in the vessels and thus markers of atherosclerosis.
“The findings from our study could be of particular value in societies where access to laboratory facilities, and thus lipid profile measurement, is difficult. In this setting, presence of xanthelasmata may be a useful predictor of underlying atherosclerotic disease. An easy registration of presence of xanthelasmata along with age and sex makes it possible to assess the risk of myocardial infarction and ischemic heart disease and thus to make sure that people at increased risk are managed accordingly with lifestyle changes and treatment to reduce low-density lipoprotein cholesterol,” wrote Ms. Christoffersen, a clinical biochemistry PhD student at Rigshospitalet in Copenhagen, and her colleagues.
They used data from the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978 with follow-up examinations. A total of 19,329 white women and men of Danish descent were drawn randomly from the Copenhagen Central Person Registry and invited to participate. Data came from a self-administered questionnaire, a physical examination, and blood samples.
For this analysis, the researchers included 12,745 people, for whom complete information on all relevant variables, including xanthelasmata and arcus corneae, were available at baseline. The patients were followed from baseline at the 1976-1978 examination to the end of May 2009 through the use of their unique Central Person Register number. No participants were lost to follow-up.
Trained nurses or medical laboratory technicians determined the presence of xanthelasmata and arcus corneae by careful visual inspection of the eyelids and the cornea during the physical examination. The investigators collected and verified diagnoses of MI and ischemic heart disease using ICD-8 and ICD-10 codes by reviewing all hospital admissions, diagnoses entered in the national Danish Patient Registry, all causes of death entered in the national Danish Causes of Death Registry, and medical records from hospitals and general practitioners.
The prevalence of xanthelasmata was 4.4% and similar in women and men. The prevalence of arcus corneae was 24.8% overall, but was lower in women than in men (20.1% vs. 30.2%), Ms. Christoffersen and her associates said.
Potential patients with ischemic cerebrovascular disease, including ischemic stroke, were collected from the national Danish Patient Registry and the national Danish Causes of Death Registry. Hospital records were reviewed by experienced neurologists. Ankle brachial index, a drop in blood pressure in the legs that predicts severe atherosclerosis, was determined in the 2001-2003 examination of the Copenhagen City Heart Study in 2,773 participants, who had also participated in the baseline examination and had complete information on all relevant variables, including xanthelasmata and arcus corneae.
Enzymatic methods were used on fresh plasma samples to measure plasma concentrations of total cholesterol, triglycerides, and high-density lipoprotein cholesterol, the last after precipitation of lipoproteins that contained apolipoprotein B.
The median follow-up was 22 years. In all, 1,872 participants developed MI, 3,699 developed ischemic heart disease, 1,498 developed ischemic strokes, 1,815 developed ischemic cerebrovascular disease, and 8,507 died.
The models were adjusted for age, sex, total cholesterol, triglycerides, body mass index, hypertension, diabetes, pack-years of smoking, alcohol consumption, physical activity, postmenopausal status, hormone therapy, education, income, and family history of ischemic vascular disease.
In this population, the “presence of xanthelasmata in itself predicts risk of myocardial infarction, ischemic heart disease, severe atherosclerosis, and death in the general population independent of well-known cardiovascular risk factors, including plasma cholesterol and triglyceride concentrations. In contrast, arcus corneae is not an important independent predictor of risk,” the authors concluded.
Patients who have xanthelasmata palpebrarum (shown above) may require more aggressive management of their cardiovascular risk factors.
Source Courtesy Wikipedia/Klaus D. Peter, Gummersbach, Germany/Creative Commons License
View on the News
Findings Are Boon to Clinicians
In an accompanying editorial, Dr. Antonio B. Fernandez and Dr. Paul D. Thompson discussed the clinical relevance of the findings.
“In the linked prospective cohort study, Christoffersen and colleagues assess whether xanthelasmata and arcus corneae, individually and combined, predict risk of ischemic vascular disease and death in the general population,” Dr. Fernandez and Dr. Thompson wrote, noting that there are some good reasons for suspecting such a link (BMJ 2011;343:d5304).
“Both xanthelasmata and arcus corneae are composed of cholesteryl esters similar to those found in serum low-density lipoprotein cholesterol and very low-density lipoprotein cholesterol. They share similar risk factors and have pathophysiological similarities with atherosclerosis,” they noted.
Importantly, the results of this study confirm “that xanthelasmata are an important predictor of cardiovascular disease events and death beyond [their] known association with hyperlipidemia.”
However, “what do these results mean in practice?” they asked. “Overall, the evidence highlights the importance of a comprehensive physical examination and suggests that xanthelasmata could be used by general clinicians to help identify people at higher risk of cardiovascular disease. These people may have an enhanced biological propensity to deposition of cholesterol in vascular and soft tissue, which is not fully represented by their fasting lipid profiles. … Patients with xanthelasmata may therefore require more aggressive management of risk factors,” they concluded.
DR. FERNANDEZ is a clinical cardiology fellow at Brown University in Providence, R.I. DR. THOMPSON is the director of cardiology at Hartford (Conn.) Hospital. Dr. Thompson reported significant financial relationships with several pharmaceutical companies.
Major Finding: The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study.
Data Source: Patients were part of the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978; a total of 19,329 white women and men of Danish descent were included at baseline.
Disclosures: This study was funded by the Research Fund at Rigshospitalet, the Lundbeck Foundation, the Danish Medical Research Council, and the Danish Heart Foundation. The authors reported that they had no other financial disclosures.
Plaque occurring around the eyelids may offer clinicians a new way of identifying patients at an increased risk for myocardial infarction and severe atherosclerosis, a study has shown.
“The results from this study suggest that xanthelasmata are a cutaneous marker of atherosclerosis independent of lipid concentrations and thus should be considered in clinical practice as an independent and additional risk factor for myocardial infarction and ischemic heart disease,” Mette Christoffersen and her coinvestigators wrote in a study published online (BMJ 2011;343:d5497).
The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study of 12,745 patients. However, on multifactorial adjustment for arcus corneae, no hazard ratios remained significant. The presence of both xanthelasmata and arcus corneae significantly increased the risk of ischemic heart disease (HR, 1.56) but not any other outcomes after multifactorial adjustment.
Xanthelasmata palpebrarum are sharply demarcated, yellowish flat plaques that appear on the upper or lower eyelids, most often near the inner canthus. Xanthelasmata represent areas of macrophages containing lipids. Arcus corneae (or arcus senilis) is a gray-white-yellowish opacity that is located near the periphery of the cornea, though separated from the limbic margin by a clear corneal zone. Arcus corneae represents deposits of cholesteryl ester–rich lipid particles. It has been suggested that xanthelasmata and arcus corneae may be markers of proatherogenic changes in the vessels and thus markers of atherosclerosis.
“The findings from our study could be of particular value in societies where access to laboratory facilities, and thus lipid profile measurement, is difficult. In this setting, presence of xanthelasmata may be a useful predictor of underlying atherosclerotic disease. An easy registration of presence of xanthelasmata along with age and sex makes it possible to assess the risk of myocardial infarction and ischemic heart disease and thus to make sure that people at increased risk are managed accordingly with lifestyle changes and treatment to reduce low-density lipoprotein cholesterol,” wrote Ms. Christoffersen, a clinical biochemistry PhD student at Rigshospitalet in Copenhagen, and her colleagues.
They used data from the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978 with follow-up examinations. A total of 19,329 white women and men of Danish descent were drawn randomly from the Copenhagen Central Person Registry and invited to participate. Data came from a self-administered questionnaire, a physical examination, and blood samples.
For this analysis, the researchers included 12,745 people, for whom complete information on all relevant variables, including xanthelasmata and arcus corneae, were available at baseline. The patients were followed from baseline at the 1976-1978 examination to the end of May 2009 through the use of their unique Central Person Register number. No participants were lost to follow-up.
Trained nurses or medical laboratory technicians determined the presence of xanthelasmata and arcus corneae by careful visual inspection of the eyelids and the cornea during the physical examination. The investigators collected and verified diagnoses of MI and ischemic heart disease using ICD-8 and ICD-10 codes by reviewing all hospital admissions, diagnoses entered in the national Danish Patient Registry, all causes of death entered in the national Danish Causes of Death Registry, and medical records from hospitals and general practitioners.
The prevalence of xanthelasmata was 4.4% and similar in women and men. The prevalence of arcus corneae was 24.8% overall, but was lower in women than in men (20.1% vs. 30.2%), Ms. Christoffersen and her associates said.
Potential patients with ischemic cerebrovascular disease, including ischemic stroke, were collected from the national Danish Patient Registry and the national Danish Causes of Death Registry. Hospital records were reviewed by experienced neurologists. Ankle brachial index, a drop in blood pressure in the legs that predicts severe atherosclerosis, was determined in the 2001-2003 examination of the Copenhagen City Heart Study in 2,773 participants, who had also participated in the baseline examination and had complete information on all relevant variables, including xanthelasmata and arcus corneae.
Enzymatic methods were used on fresh plasma samples to measure plasma concentrations of total cholesterol, triglycerides, and high-density lipoprotein cholesterol, the last after precipitation of lipoproteins that contained apolipoprotein B.
The median follow-up was 22 years. In all, 1,872 participants developed MI, 3,699 developed ischemic heart disease, 1,498 developed ischemic strokes, 1,815 developed ischemic cerebrovascular disease, and 8,507 died.
The models were adjusted for age, sex, total cholesterol, triglycerides, body mass index, hypertension, diabetes, pack-years of smoking, alcohol consumption, physical activity, postmenopausal status, hormone therapy, education, income, and family history of ischemic vascular disease.
In this population, the “presence of xanthelasmata in itself predicts risk of myocardial infarction, ischemic heart disease, severe atherosclerosis, and death in the general population independent of well-known cardiovascular risk factors, including plasma cholesterol and triglyceride concentrations. In contrast, arcus corneae is not an important independent predictor of risk,” the authors concluded.
Patients who have xanthelasmata palpebrarum (shown above) may require more aggressive management of their cardiovascular risk factors.
Source Courtesy Wikipedia/Klaus D. Peter, Gummersbach, Germany/Creative Commons License
View on the News
Findings Are Boon to Clinicians
In an accompanying editorial, Dr. Antonio B. Fernandez and Dr. Paul D. Thompson discussed the clinical relevance of the findings.
“In the linked prospective cohort study, Christoffersen and colleagues assess whether xanthelasmata and arcus corneae, individually and combined, predict risk of ischemic vascular disease and death in the general population,” Dr. Fernandez and Dr. Thompson wrote, noting that there are some good reasons for suspecting such a link (BMJ 2011;343:d5304).
“Both xanthelasmata and arcus corneae are composed of cholesteryl esters similar to those found in serum low-density lipoprotein cholesterol and very low-density lipoprotein cholesterol. They share similar risk factors and have pathophysiological similarities with atherosclerosis,” they noted.
Importantly, the results of this study confirm “that xanthelasmata are an important predictor of cardiovascular disease events and death beyond [their] known association with hyperlipidemia.”
However, “what do these results mean in practice?” they asked. “Overall, the evidence highlights the importance of a comprehensive physical examination and suggests that xanthelasmata could be used by general clinicians to help identify people at higher risk of cardiovascular disease. These people may have an enhanced biological propensity to deposition of cholesterol in vascular and soft tissue, which is not fully represented by their fasting lipid profiles. … Patients with xanthelasmata may therefore require more aggressive management of risk factors,” they concluded.
DR. FERNANDEZ is a clinical cardiology fellow at Brown University in Providence, R.I. DR. THOMPSON is the director of cardiology at Hartford (Conn.) Hospital. Dr. Thompson reported significant financial relationships with several pharmaceutical companies.
From BMJ
Inpatient Suicide Precaution Relies on Clinical Judgment
ANNAPOLIS, MD – Numerous suicide risk-assessment tools are available, but because none are perfect, the ability to prevent inpatient suicide hinges on a single factor, according to Dr. Robert P. Roca.
"It all comes down to clinical judgment. How do we guide clinical judgment?" Dr. Roca, vice president of medical affairs at Sheppard and Enoch Pratt Hospital, Towson, Md., asked at the annual meeting of the Southern Psychiatric Association. Basically, "it’s a synthetic clinical judgment that involves taking into account a whole lot of factors, and there’s really no test that tells us reliably what the answer is to this person’s risk."
About 5 years ago, Dr. Roca said, the Sheppard Pratt Health System looked retrospectively at its experience with inpatient suicide in its family and inpatient programs.
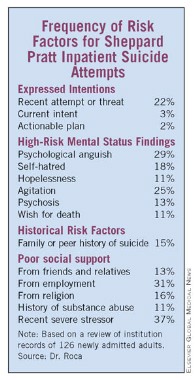
They found that men and women are equally likely to make serious attempts. Interestingly, the elderly were not disproportionately at risk. Nearly half of attempts occurred in the first 3 days; however, some attempts occurred when a patient appeared ready for discharge. Most patients who made serious attempts at suicide had unipolar or bipolar depression. Importantly, patients usually attempted hanging from a bedroom or bathroom door using bed linens or clothing.
Because attempts occur most often in bedrooms and bathrooms, careful design is needed to eliminate many hazards, such as using breakaway fixtures or down-sloping fixtures and avoiding breakable glass materials. "But a door is a potential gallows ... that was the vivid message that came across," he said. However, self-asphyxiation does not require hanging, and practically anything can become an instrument of self-harm.
"The most important message for me was that people who attempted suicide didn’t warn you in advance that they were going to do that," Dr. Roca said. "Certainly, a safety contract is no guarantee of safety."
Based on careful review of the records of patients who succeeded in committing suicide as an inpatient, the researchers identified several salient features of the mental status of these patients. These included intense psychological pain or anguish, intense self-loathing, delusions of guilt, agitation or perturbation, hopelessness, and a feeling that death would bring relief.
Universal precautions for these patients might include a physical environment that is safe yet therapeutically warm and a clinical milieu that inspires hope and rapidly relieves psychological distress, he said.
"You also need to be able to identify people who are at very, very high risk" and require special risk assessment. Early scales were simply inventories of demographic risk factors with limited evidence of reliability or validity. Subsequent scales were better researched, and included scales –such as the Beck Scale for Suicidal Ideation – with good reliability and validity but poor predictive value. Other scales were lengthy research tools that were impractical for clinical use and not designed to evaluate immediate risk.
More practical tools are available, but these are not perfect, either. The Nurses’ Global Assessment of Suicide Risk is a 15-item nurse-rated checklist. Scoring gives special weight to hopelessness, anhedonia, recent bereavement, and prior attempts. On this assessment, greater scores call for higher levels of engagement.
The Positive and Negative Suicidal Ideation Inventory (J. of Clin. Psychol. 2005;61:431-45) includes 14 items: eight "risk factors" and six "protective factors." Scoring uses a 5-point Likert scale. It has been validated in the adolescent and young adult populations in the Midwest, though it hasn’t been more broadly validated.
The clinicians at Sheppard Pratt have developed and are using their own assessment – the Sheppard Pratt Suicide Risk Assessment (SPSRA) – which includes 13 questions and three domains of risk: expressed intentions regarding suicide, mental status findings pertinent to risk, and aspects of history pertinent to risk. However, it is not a quantitative scale. The answers prompt clinicians to consider all three domains – not just expressed intentions – in their estimates of risk. The presence of any of these may increase suicide risk.
"The most important message for me was that people who attempted suicide didn’t warn you in advance that they were going to do that."
In terms of expressed intentions, these are important questions: Has there been a recent suicide attempt? Is there imminent suicide intent? Is there an actionable plan (a patient could realistically act upon this while in hospital)? If the answer to any of these three questions is yes, a high level of observation should be considered. If the patient’s answers demonstrate imminent intent and an actionable plan, an intensive level of observation should be ordered.
In terms of mental status findings, consider this question: Does the patient show extreme psychological pain or anguish, intense self-hatred, hopelessness, agitation or perturbation, psychosis (especially delusional guilt), or a wish for death? The presence of one or several of these might call for a high level of observation, even if the patient denies suicidal thoughts.
In terms of worrisome aspects of history, these are key questions: Has there been a recent severely distressing loss, disappointment, or threat? Does the patient lack social support from family, friends, church, and/or work? Is there an active substance abuse problem?
In bivariate analysis, imminent intent, an actionable plan, hopelessness, psychological pain, agitation, and wish for death were all significantly correlated with staff recommending suicidal observation or intense suicidal observation. On multivariate analysis, expressed intentions, wish for death, and hopelessness remained significant, Dr. Roca said.
Among hospitalized patients who attempted suicide, 17% had expressed imminent attempt or actionable plan; psychological anguish, hopelessness, and/or family history of suicide were each present in 58%; and 75% had three or more risk factors that were identified by the admitting clinician.
Lastly, it’s important to continuously perform risk assessment on vulnerable patients throughout the course of treatment.
Dr. Roca reported that he had no disclosures.
ANNAPOLIS, MD – Numerous suicide risk-assessment tools are available, but because none are perfect, the ability to prevent inpatient suicide hinges on a single factor, according to Dr. Robert P. Roca.
"It all comes down to clinical judgment. How do we guide clinical judgment?" Dr. Roca, vice president of medical affairs at Sheppard and Enoch Pratt Hospital, Towson, Md., asked at the annual meeting of the Southern Psychiatric Association. Basically, "it’s a synthetic clinical judgment that involves taking into account a whole lot of factors, and there’s really no test that tells us reliably what the answer is to this person’s risk."
About 5 years ago, Dr. Roca said, the Sheppard Pratt Health System looked retrospectively at its experience with inpatient suicide in its family and inpatient programs.
They found that men and women are equally likely to make serious attempts. Interestingly, the elderly were not disproportionately at risk. Nearly half of attempts occurred in the first 3 days; however, some attempts occurred when a patient appeared ready for discharge. Most patients who made serious attempts at suicide had unipolar or bipolar depression. Importantly, patients usually attempted hanging from a bedroom or bathroom door using bed linens or clothing.
Because attempts occur most often in bedrooms and bathrooms, careful design is needed to eliminate many hazards, such as using breakaway fixtures or down-sloping fixtures and avoiding breakable glass materials. "But a door is a potential gallows ... that was the vivid message that came across," he said. However, self-asphyxiation does not require hanging, and practically anything can become an instrument of self-harm.
"The most important message for me was that people who attempted suicide didn’t warn you in advance that they were going to do that," Dr. Roca said. "Certainly, a safety contract is no guarantee of safety."
Based on careful review of the records of patients who succeeded in committing suicide as an inpatient, the researchers identified several salient features of the mental status of these patients. These included intense psychological pain or anguish, intense self-loathing, delusions of guilt, agitation or perturbation, hopelessness, and a feeling that death would bring relief.
Universal precautions for these patients might include a physical environment that is safe yet therapeutically warm and a clinical milieu that inspires hope and rapidly relieves psychological distress, he said.
"You also need to be able to identify people who are at very, very high risk" and require special risk assessment. Early scales were simply inventories of demographic risk factors with limited evidence of reliability or validity. Subsequent scales were better researched, and included scales –such as the Beck Scale for Suicidal Ideation – with good reliability and validity but poor predictive value. Other scales were lengthy research tools that were impractical for clinical use and not designed to evaluate immediate risk.
More practical tools are available, but these are not perfect, either. The Nurses’ Global Assessment of Suicide Risk is a 15-item nurse-rated checklist. Scoring gives special weight to hopelessness, anhedonia, recent bereavement, and prior attempts. On this assessment, greater scores call for higher levels of engagement.
The Positive and Negative Suicidal Ideation Inventory (J. of Clin. Psychol. 2005;61:431-45) includes 14 items: eight "risk factors" and six "protective factors." Scoring uses a 5-point Likert scale. It has been validated in the adolescent and young adult populations in the Midwest, though it hasn’t been more broadly validated.
The clinicians at Sheppard Pratt have developed and are using their own assessment – the Sheppard Pratt Suicide Risk Assessment (SPSRA) – which includes 13 questions and three domains of risk: expressed intentions regarding suicide, mental status findings pertinent to risk, and aspects of history pertinent to risk. However, it is not a quantitative scale. The answers prompt clinicians to consider all three domains – not just expressed intentions – in their estimates of risk. The presence of any of these may increase suicide risk.
"The most important message for me was that people who attempted suicide didn’t warn you in advance that they were going to do that."
In terms of expressed intentions, these are important questions: Has there been a recent suicide attempt? Is there imminent suicide intent? Is there an actionable plan (a patient could realistically act upon this while in hospital)? If the answer to any of these three questions is yes, a high level of observation should be considered. If the patient’s answers demonstrate imminent intent and an actionable plan, an intensive level of observation should be ordered.
In terms of mental status findings, consider this question: Does the patient show extreme psychological pain or anguish, intense self-hatred, hopelessness, agitation or perturbation, psychosis (especially delusional guilt), or a wish for death? The presence of one or several of these might call for a high level of observation, even if the patient denies suicidal thoughts.
In terms of worrisome aspects of history, these are key questions: Has there been a recent severely distressing loss, disappointment, or threat? Does the patient lack social support from family, friends, church, and/or work? Is there an active substance abuse problem?
In bivariate analysis, imminent intent, an actionable plan, hopelessness, psychological pain, agitation, and wish for death were all significantly correlated with staff recommending suicidal observation or intense suicidal observation. On multivariate analysis, expressed intentions, wish for death, and hopelessness remained significant, Dr. Roca said.
Among hospitalized patients who attempted suicide, 17% had expressed imminent attempt or actionable plan; psychological anguish, hopelessness, and/or family history of suicide were each present in 58%; and 75% had three or more risk factors that were identified by the admitting clinician.
Lastly, it’s important to continuously perform risk assessment on vulnerable patients throughout the course of treatment.
Dr. Roca reported that he had no disclosures.
ANNAPOLIS, MD – Numerous suicide risk-assessment tools are available, but because none are perfect, the ability to prevent inpatient suicide hinges on a single factor, according to Dr. Robert P. Roca.
"It all comes down to clinical judgment. How do we guide clinical judgment?" Dr. Roca, vice president of medical affairs at Sheppard and Enoch Pratt Hospital, Towson, Md., asked at the annual meeting of the Southern Psychiatric Association. Basically, "it’s a synthetic clinical judgment that involves taking into account a whole lot of factors, and there’s really no test that tells us reliably what the answer is to this person’s risk."
About 5 years ago, Dr. Roca said, the Sheppard Pratt Health System looked retrospectively at its experience with inpatient suicide in its family and inpatient programs.
They found that men and women are equally likely to make serious attempts. Interestingly, the elderly were not disproportionately at risk. Nearly half of attempts occurred in the first 3 days; however, some attempts occurred when a patient appeared ready for discharge. Most patients who made serious attempts at suicide had unipolar or bipolar depression. Importantly, patients usually attempted hanging from a bedroom or bathroom door using bed linens or clothing.
Because attempts occur most often in bedrooms and bathrooms, careful design is needed to eliminate many hazards, such as using breakaway fixtures or down-sloping fixtures and avoiding breakable glass materials. "But a door is a potential gallows ... that was the vivid message that came across," he said. However, self-asphyxiation does not require hanging, and practically anything can become an instrument of self-harm.
"The most important message for me was that people who attempted suicide didn’t warn you in advance that they were going to do that," Dr. Roca said. "Certainly, a safety contract is no guarantee of safety."
Based on careful review of the records of patients who succeeded in committing suicide as an inpatient, the researchers identified several salient features of the mental status of these patients. These included intense psychological pain or anguish, intense self-loathing, delusions of guilt, agitation or perturbation, hopelessness, and a feeling that death would bring relief.
Universal precautions for these patients might include a physical environment that is safe yet therapeutically warm and a clinical milieu that inspires hope and rapidly relieves psychological distress, he said.
"You also need to be able to identify people who are at very, very high risk" and require special risk assessment. Early scales were simply inventories of demographic risk factors with limited evidence of reliability or validity. Subsequent scales were better researched, and included scales –such as the Beck Scale for Suicidal Ideation – with good reliability and validity but poor predictive value. Other scales were lengthy research tools that were impractical for clinical use and not designed to evaluate immediate risk.
More practical tools are available, but these are not perfect, either. The Nurses’ Global Assessment of Suicide Risk is a 15-item nurse-rated checklist. Scoring gives special weight to hopelessness, anhedonia, recent bereavement, and prior attempts. On this assessment, greater scores call for higher levels of engagement.
The Positive and Negative Suicidal Ideation Inventory (J. of Clin. Psychol. 2005;61:431-45) includes 14 items: eight "risk factors" and six "protective factors." Scoring uses a 5-point Likert scale. It has been validated in the adolescent and young adult populations in the Midwest, though it hasn’t been more broadly validated.
The clinicians at Sheppard Pratt have developed and are using their own assessment – the Sheppard Pratt Suicide Risk Assessment (SPSRA) – which includes 13 questions and three domains of risk: expressed intentions regarding suicide, mental status findings pertinent to risk, and aspects of history pertinent to risk. However, it is not a quantitative scale. The answers prompt clinicians to consider all three domains – not just expressed intentions – in their estimates of risk. The presence of any of these may increase suicide risk.
"The most important message for me was that people who attempted suicide didn’t warn you in advance that they were going to do that."
In terms of expressed intentions, these are important questions: Has there been a recent suicide attempt? Is there imminent suicide intent? Is there an actionable plan (a patient could realistically act upon this while in hospital)? If the answer to any of these three questions is yes, a high level of observation should be considered. If the patient’s answers demonstrate imminent intent and an actionable plan, an intensive level of observation should be ordered.
In terms of mental status findings, consider this question: Does the patient show extreme psychological pain or anguish, intense self-hatred, hopelessness, agitation or perturbation, psychosis (especially delusional guilt), or a wish for death? The presence of one or several of these might call for a high level of observation, even if the patient denies suicidal thoughts.
In terms of worrisome aspects of history, these are key questions: Has there been a recent severely distressing loss, disappointment, or threat? Does the patient lack social support from family, friends, church, and/or work? Is there an active substance abuse problem?
In bivariate analysis, imminent intent, an actionable plan, hopelessness, psychological pain, agitation, and wish for death were all significantly correlated with staff recommending suicidal observation or intense suicidal observation. On multivariate analysis, expressed intentions, wish for death, and hopelessness remained significant, Dr. Roca said.
Among hospitalized patients who attempted suicide, 17% had expressed imminent attempt or actionable plan; psychological anguish, hopelessness, and/or family history of suicide were each present in 58%; and 75% had three or more risk factors that were identified by the admitting clinician.
Lastly, it’s important to continuously perform risk assessment on vulnerable patients throughout the course of treatment.
Dr. Roca reported that he had no disclosures.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOUTHERN PSYCHIATRY ASSOCIATION
Two Outpatient Interventions Help Beat Eating Disorders
ANNAPOLIS, MD. – Two treatment strategies appear to be effective in the management of and recovery from eating disorders, according to one eating disorder expert speaking at the annual meeting of the Southern Psychiatric Association.
Dr. Harry A. Brandt said the treatments – family-based treatment (FBT) and Cognitive Remediation Therapy (CRT) – are "really exciting and are ... helping patients a lot."
FBT has been shown to be very effective for adolescents with anorexia and is appropriate for children and adolescents who are medically stable. "The current focus leads to a shift from viewing the family as a cause of an eating disorder to, instead, evaluating family dynamics that might develop in the context of an eating disorder – perhaps functioning in a maintenance or perpetuating way," said Dr. Brandt, director of the Center for Eating Disorders at Sheppard Pratt, Baltimore.
In family-based treatment, no assumptions are made about the origin of the disorder. Instead, the focus is on what can be done. "The parents are engaged as a resource. No blame is directed at the parents or the kids with the eating disorder." Siblings also are involved, play a supportive role, and are protected for the job assigned to the parents.
FBT, an outpatient intervention designed to restore weight, requires a team approach that includes a primary therapist, a pediatrician, and a psychiatrist. Brief hospitalization might be necessary to resolve medical concerns.
Also, parents are viewed as the most useful resource in their child’s treatment under FBT. In fact, the parents play an active role in the recovery process and in restoring their child’s weight, Dr. Brandt said. Therapy is aimed at assisting/supporting the parents in their efforts to help their child recover from anorexia, so that adolescent development can get back on track.
At the start of treatment, the adolescent patient is viewed as incapacitated in terms of eating behaviors with an inability to maintain an optimal weight for age and height.
The therapist’s role is to be a coach or consultant to the parents and to empower them to develop strategies aimed at managing the anorexia and finding ways to help feed the child until weight restoration is achieved. The therapist also encourages sibling support and understanding.
Lastly, the therapist teaches the family to externalize the illness, modeling a no-blame approach with recognition that the eating disorder behaviors are mostly outside the control of the adolescent. "Instead of getting angry at the kid, the therapist helps the parents to get angry at the illness. A parent’s not going to get angry at a kid who develops pneumonia but might get angry at the bacteria that caused it," he said.
FBT works through three phases: weight restoration, returning control of eating to the adolescent, and establishing a healthy adolescent identity. "These are fluid. If we move into phase two and the child stops eating, we might have to go back to phase one for a span of time."
Parents are supported in their efforts to restore their child’s weight and are encouraged to present a united front. Parents monitor meals and snacks, while restricting physical activity.
The therapist reassures the parents that they will succeed. The therapist also conveys to the patient that while she has many fears about weight gain, these fears cannot deflect the parents’ efforts toward weight restoration.
Weight restoration takes precedence over almost any other issue until self-starvation has been reversed. Control can start to be returned to the adolescent when she has reached 90% of ideal body weight and is eating without too much resistance. The process is gradual and age dependent, however, Dr. Brandt said.
Establishing a healthy adolescent identity begins when the adolescent has achieved a healthy weight for age and height. Treatment focuses on general issues of adolescent development and ways in which the eating disorder affected this process. Goals include increased personal autonomy, relationships with peers, or getting ready to leave home for the first time.
The final stages of treatment focus on relapse prevention strategies; the identification and recognition of early warning signs for a developing relapse; and family responses to potential relapse. These responses should be outlined and an action plan should be developed.
Recently, a randomized, controlled trial for adolescents with bulimia compared FBT to supportive individual psychotherapy and showed promising results. Six months after treatment, almost 30% of participants who received family-based treatment were still abstinent from bingeing/purging, compared to only 10% of participants who received supportive psychotherapy, Dr. Brandt said in an interview. "FBT for young adults is still being developed and refined. A small number of trials have shown some positive results, but additional research using randomized controlled trials is necessary to determine if this is the best treatment for this older age group."
Cognitive-Remediation Therapy
"We know that cognitive process is very involved in anorexia," Dr. Brandt noted. This includes learning, reasoning, problem solving, perception, judgment, and concentration. Cognition provides the ability for people to analyze, discriminate, organize, categorize, memorize, and perform other functions that are influenced by emotions and social feelings.
A cognitive deficit is any impairment in the thought process. Cognitive remediation is working on "techniques to develop skills and strategies that maximize the cognitive abilities and compensate deficits with the idea of developing alternative strategies for impaired functioning," he said. The technique has been used successfully in schizophrenia, brain lesions, attention-deficit/hyperactivity disorder, and obsessive-compulsive disorder.
"Can the brain change? We know the brain is a plastic organ, so of course, it can change. ... Can we get our patients practicing skills that might help them with the kinds of distortions that we see in anorexia nervosa," he asked.
CRT has an objective of exercising connections in the brain that hopefully include functioning. "This seemed to have applicability to eating disorders," Dr. Brandt said. The technique also is used to encourage patients to reflect on the exercises, as a way of raising awareness of thinking styles. By using practice, reflection, and guided discovery, a patient’s thinking style can be improved.
CRT is attractive for several reasons. It’s relatively simple, and there’s a very clear specificity of the material. The therapist’s delivery of this treatment should be very motivational. "The therapist really gets involved in this, and our patients love it. The therapist basically plays games with the patient," Dr. Brandt said. "The therapist is open about what his or her thought processes are as he plays these games and the patients play along. "The patient hopefully learns something about their own cognitive style."
Dr. Brandt observed that CRT is different from cognitive-behavioral therapy, or CBT, because the latter focuses on symptoms of illness rather than on the structure of the thinking. CRT uses effectively neutral material targeting the thought processes with the goal of developing new types of thinking. There isn’t a focus on bingeing/purging or weight restoration."
However, "CRT is not meant to be a stand-alone treatment for eating disorders but as a supplement to more traditional therapies such as CBT and dialectical behavior therapy," he said in an interview. In CRT, cognitive processing skills are the target of treatment, while these skills are required for CBT. CBT requires being able to think, while CRT really focuses on improving the quality of the thinking.
"The application of CRT has little to do with a patient’s intelligence level and much to do with a patient’s thinking style. In fact, the goals of CRT are to help individuals learn about how their brains work so that they can develop new problem-solving skills and enhanced cognitive flexibility."
He added, "Patients with anorexia often struggle with rigid thought patterns and an over focus on details that serve to maintain the symptoms of the disorder. These patients are also commonly very resistant to treatment, and CRT’s nontraditional focus also helps provide opportunities to enhance the therapeutic alliance and increase the patient’s motivation to change."
It’s long been known that anorexia involves detail focus or weak central coherence. Patients with anorexia have an excessively detailed information processing style with a neglect of holistic thinking. "They can’t really see the big picture." They are very good at tasks that involve piecemeal information processing.
In addition, these patients tend to be inflexible and poor at set shifting. They are also very rule-bound. Set shifting is the ability to hold two different cognitive frameworks. Anorexia patients have rigid thinking, and applications of rules and habits. It’s important to talk with patients about their thought processes during exercises that attempt to improve flexible thinking.
Flexible thinking exercises are used to encourage switching between different stimuli. These exercises include illusions (seeing two different pictures in the same image), switching attention tasks, embedded word tasks, estimating tasks, and ecological tasks.
The aim of switching attention tasks is to practice switching between two difference pieces of information swiftly and accurately, while also holding in mind a rule that requires remembering the previous answer. Embedded word tasks are designed to practice identifying particular categories of information among irrelevant information. This requires seeing the bigger picture and the detail, increasing flexibility of thinking.
Exercises like these help patient recognize strengths and weaknesses of thinking styles, challenge anxieties related to those styles, build confidence, and acknowledge and appreciate their strengths.
Dr. Brandt reported that he has no relevant financial relationships.
ANNAPOLIS, MD. – Two treatment strategies appear to be effective in the management of and recovery from eating disorders, according to one eating disorder expert speaking at the annual meeting of the Southern Psychiatric Association.
Dr. Harry A. Brandt said the treatments – family-based treatment (FBT) and Cognitive Remediation Therapy (CRT) – are "really exciting and are ... helping patients a lot."
FBT has been shown to be very effective for adolescents with anorexia and is appropriate for children and adolescents who are medically stable. "The current focus leads to a shift from viewing the family as a cause of an eating disorder to, instead, evaluating family dynamics that might develop in the context of an eating disorder – perhaps functioning in a maintenance or perpetuating way," said Dr. Brandt, director of the Center for Eating Disorders at Sheppard Pratt, Baltimore.
In family-based treatment, no assumptions are made about the origin of the disorder. Instead, the focus is on what can be done. "The parents are engaged as a resource. No blame is directed at the parents or the kids with the eating disorder." Siblings also are involved, play a supportive role, and are protected for the job assigned to the parents.
FBT, an outpatient intervention designed to restore weight, requires a team approach that includes a primary therapist, a pediatrician, and a psychiatrist. Brief hospitalization might be necessary to resolve medical concerns.
Also, parents are viewed as the most useful resource in their child’s treatment under FBT. In fact, the parents play an active role in the recovery process and in restoring their child’s weight, Dr. Brandt said. Therapy is aimed at assisting/supporting the parents in their efforts to help their child recover from anorexia, so that adolescent development can get back on track.
At the start of treatment, the adolescent patient is viewed as incapacitated in terms of eating behaviors with an inability to maintain an optimal weight for age and height.
The therapist’s role is to be a coach or consultant to the parents and to empower them to develop strategies aimed at managing the anorexia and finding ways to help feed the child until weight restoration is achieved. The therapist also encourages sibling support and understanding.
Lastly, the therapist teaches the family to externalize the illness, modeling a no-blame approach with recognition that the eating disorder behaviors are mostly outside the control of the adolescent. "Instead of getting angry at the kid, the therapist helps the parents to get angry at the illness. A parent’s not going to get angry at a kid who develops pneumonia but might get angry at the bacteria that caused it," he said.
FBT works through three phases: weight restoration, returning control of eating to the adolescent, and establishing a healthy adolescent identity. "These are fluid. If we move into phase two and the child stops eating, we might have to go back to phase one for a span of time."
Parents are supported in their efforts to restore their child’s weight and are encouraged to present a united front. Parents monitor meals and snacks, while restricting physical activity.
The therapist reassures the parents that they will succeed. The therapist also conveys to the patient that while she has many fears about weight gain, these fears cannot deflect the parents’ efforts toward weight restoration.
Weight restoration takes precedence over almost any other issue until self-starvation has been reversed. Control can start to be returned to the adolescent when she has reached 90% of ideal body weight and is eating without too much resistance. The process is gradual and age dependent, however, Dr. Brandt said.
Establishing a healthy adolescent identity begins when the adolescent has achieved a healthy weight for age and height. Treatment focuses on general issues of adolescent development and ways in which the eating disorder affected this process. Goals include increased personal autonomy, relationships with peers, or getting ready to leave home for the first time.
The final stages of treatment focus on relapse prevention strategies; the identification and recognition of early warning signs for a developing relapse; and family responses to potential relapse. These responses should be outlined and an action plan should be developed.
Recently, a randomized, controlled trial for adolescents with bulimia compared FBT to supportive individual psychotherapy and showed promising results. Six months after treatment, almost 30% of participants who received family-based treatment were still abstinent from bingeing/purging, compared to only 10% of participants who received supportive psychotherapy, Dr. Brandt said in an interview. "FBT for young adults is still being developed and refined. A small number of trials have shown some positive results, but additional research using randomized controlled trials is necessary to determine if this is the best treatment for this older age group."
Cognitive-Remediation Therapy
"We know that cognitive process is very involved in anorexia," Dr. Brandt noted. This includes learning, reasoning, problem solving, perception, judgment, and concentration. Cognition provides the ability for people to analyze, discriminate, organize, categorize, memorize, and perform other functions that are influenced by emotions and social feelings.
A cognitive deficit is any impairment in the thought process. Cognitive remediation is working on "techniques to develop skills and strategies that maximize the cognitive abilities and compensate deficits with the idea of developing alternative strategies for impaired functioning," he said. The technique has been used successfully in schizophrenia, brain lesions, attention-deficit/hyperactivity disorder, and obsessive-compulsive disorder.
"Can the brain change? We know the brain is a plastic organ, so of course, it can change. ... Can we get our patients practicing skills that might help them with the kinds of distortions that we see in anorexia nervosa," he asked.
CRT has an objective of exercising connections in the brain that hopefully include functioning. "This seemed to have applicability to eating disorders," Dr. Brandt said. The technique also is used to encourage patients to reflect on the exercises, as a way of raising awareness of thinking styles. By using practice, reflection, and guided discovery, a patient’s thinking style can be improved.
CRT is attractive for several reasons. It’s relatively simple, and there’s a very clear specificity of the material. The therapist’s delivery of this treatment should be very motivational. "The therapist really gets involved in this, and our patients love it. The therapist basically plays games with the patient," Dr. Brandt said. "The therapist is open about what his or her thought processes are as he plays these games and the patients play along. "The patient hopefully learns something about their own cognitive style."
Dr. Brandt observed that CRT is different from cognitive-behavioral therapy, or CBT, because the latter focuses on symptoms of illness rather than on the structure of the thinking. CRT uses effectively neutral material targeting the thought processes with the goal of developing new types of thinking. There isn’t a focus on bingeing/purging or weight restoration."
However, "CRT is not meant to be a stand-alone treatment for eating disorders but as a supplement to more traditional therapies such as CBT and dialectical behavior therapy," he said in an interview. In CRT, cognitive processing skills are the target of treatment, while these skills are required for CBT. CBT requires being able to think, while CRT really focuses on improving the quality of the thinking.
"The application of CRT has little to do with a patient’s intelligence level and much to do with a patient’s thinking style. In fact, the goals of CRT are to help individuals learn about how their brains work so that they can develop new problem-solving skills and enhanced cognitive flexibility."
He added, "Patients with anorexia often struggle with rigid thought patterns and an over focus on details that serve to maintain the symptoms of the disorder. These patients are also commonly very resistant to treatment, and CRT’s nontraditional focus also helps provide opportunities to enhance the therapeutic alliance and increase the patient’s motivation to change."
It’s long been known that anorexia involves detail focus or weak central coherence. Patients with anorexia have an excessively detailed information processing style with a neglect of holistic thinking. "They can’t really see the big picture." They are very good at tasks that involve piecemeal information processing.
In addition, these patients tend to be inflexible and poor at set shifting. They are also very rule-bound. Set shifting is the ability to hold two different cognitive frameworks. Anorexia patients have rigid thinking, and applications of rules and habits. It’s important to talk with patients about their thought processes during exercises that attempt to improve flexible thinking.
Flexible thinking exercises are used to encourage switching between different stimuli. These exercises include illusions (seeing two different pictures in the same image), switching attention tasks, embedded word tasks, estimating tasks, and ecological tasks.
The aim of switching attention tasks is to practice switching between two difference pieces of information swiftly and accurately, while also holding in mind a rule that requires remembering the previous answer. Embedded word tasks are designed to practice identifying particular categories of information among irrelevant information. This requires seeing the bigger picture and the detail, increasing flexibility of thinking.
Exercises like these help patient recognize strengths and weaknesses of thinking styles, challenge anxieties related to those styles, build confidence, and acknowledge and appreciate their strengths.
Dr. Brandt reported that he has no relevant financial relationships.
ANNAPOLIS, MD. – Two treatment strategies appear to be effective in the management of and recovery from eating disorders, according to one eating disorder expert speaking at the annual meeting of the Southern Psychiatric Association.
Dr. Harry A. Brandt said the treatments – family-based treatment (FBT) and Cognitive Remediation Therapy (CRT) – are "really exciting and are ... helping patients a lot."
FBT has been shown to be very effective for adolescents with anorexia and is appropriate for children and adolescents who are medically stable. "The current focus leads to a shift from viewing the family as a cause of an eating disorder to, instead, evaluating family dynamics that might develop in the context of an eating disorder – perhaps functioning in a maintenance or perpetuating way," said Dr. Brandt, director of the Center for Eating Disorders at Sheppard Pratt, Baltimore.
In family-based treatment, no assumptions are made about the origin of the disorder. Instead, the focus is on what can be done. "The parents are engaged as a resource. No blame is directed at the parents or the kids with the eating disorder." Siblings also are involved, play a supportive role, and are protected for the job assigned to the parents.
FBT, an outpatient intervention designed to restore weight, requires a team approach that includes a primary therapist, a pediatrician, and a psychiatrist. Brief hospitalization might be necessary to resolve medical concerns.
Also, parents are viewed as the most useful resource in their child’s treatment under FBT. In fact, the parents play an active role in the recovery process and in restoring their child’s weight, Dr. Brandt said. Therapy is aimed at assisting/supporting the parents in their efforts to help their child recover from anorexia, so that adolescent development can get back on track.
At the start of treatment, the adolescent patient is viewed as incapacitated in terms of eating behaviors with an inability to maintain an optimal weight for age and height.
The therapist’s role is to be a coach or consultant to the parents and to empower them to develop strategies aimed at managing the anorexia and finding ways to help feed the child until weight restoration is achieved. The therapist also encourages sibling support and understanding.
Lastly, the therapist teaches the family to externalize the illness, modeling a no-blame approach with recognition that the eating disorder behaviors are mostly outside the control of the adolescent. "Instead of getting angry at the kid, the therapist helps the parents to get angry at the illness. A parent’s not going to get angry at a kid who develops pneumonia but might get angry at the bacteria that caused it," he said.
FBT works through three phases: weight restoration, returning control of eating to the adolescent, and establishing a healthy adolescent identity. "These are fluid. If we move into phase two and the child stops eating, we might have to go back to phase one for a span of time."
Parents are supported in their efforts to restore their child’s weight and are encouraged to present a united front. Parents monitor meals and snacks, while restricting physical activity.
The therapist reassures the parents that they will succeed. The therapist also conveys to the patient that while she has many fears about weight gain, these fears cannot deflect the parents’ efforts toward weight restoration.
Weight restoration takes precedence over almost any other issue until self-starvation has been reversed. Control can start to be returned to the adolescent when she has reached 90% of ideal body weight and is eating without too much resistance. The process is gradual and age dependent, however, Dr. Brandt said.
Establishing a healthy adolescent identity begins when the adolescent has achieved a healthy weight for age and height. Treatment focuses on general issues of adolescent development and ways in which the eating disorder affected this process. Goals include increased personal autonomy, relationships with peers, or getting ready to leave home for the first time.
The final stages of treatment focus on relapse prevention strategies; the identification and recognition of early warning signs for a developing relapse; and family responses to potential relapse. These responses should be outlined and an action plan should be developed.
Recently, a randomized, controlled trial for adolescents with bulimia compared FBT to supportive individual psychotherapy and showed promising results. Six months after treatment, almost 30% of participants who received family-based treatment were still abstinent from bingeing/purging, compared to only 10% of participants who received supportive psychotherapy, Dr. Brandt said in an interview. "FBT for young adults is still being developed and refined. A small number of trials have shown some positive results, but additional research using randomized controlled trials is necessary to determine if this is the best treatment for this older age group."
Cognitive-Remediation Therapy
"We know that cognitive process is very involved in anorexia," Dr. Brandt noted. This includes learning, reasoning, problem solving, perception, judgment, and concentration. Cognition provides the ability for people to analyze, discriminate, organize, categorize, memorize, and perform other functions that are influenced by emotions and social feelings.
A cognitive deficit is any impairment in the thought process. Cognitive remediation is working on "techniques to develop skills and strategies that maximize the cognitive abilities and compensate deficits with the idea of developing alternative strategies for impaired functioning," he said. The technique has been used successfully in schizophrenia, brain lesions, attention-deficit/hyperactivity disorder, and obsessive-compulsive disorder.
"Can the brain change? We know the brain is a plastic organ, so of course, it can change. ... Can we get our patients practicing skills that might help them with the kinds of distortions that we see in anorexia nervosa," he asked.
CRT has an objective of exercising connections in the brain that hopefully include functioning. "This seemed to have applicability to eating disorders," Dr. Brandt said. The technique also is used to encourage patients to reflect on the exercises, as a way of raising awareness of thinking styles. By using practice, reflection, and guided discovery, a patient’s thinking style can be improved.
CRT is attractive for several reasons. It’s relatively simple, and there’s a very clear specificity of the material. The therapist’s delivery of this treatment should be very motivational. "The therapist really gets involved in this, and our patients love it. The therapist basically plays games with the patient," Dr. Brandt said. "The therapist is open about what his or her thought processes are as he plays these games and the patients play along. "The patient hopefully learns something about their own cognitive style."
Dr. Brandt observed that CRT is different from cognitive-behavioral therapy, or CBT, because the latter focuses on symptoms of illness rather than on the structure of the thinking. CRT uses effectively neutral material targeting the thought processes with the goal of developing new types of thinking. There isn’t a focus on bingeing/purging or weight restoration."
However, "CRT is not meant to be a stand-alone treatment for eating disorders but as a supplement to more traditional therapies such as CBT and dialectical behavior therapy," he said in an interview. In CRT, cognitive processing skills are the target of treatment, while these skills are required for CBT. CBT requires being able to think, while CRT really focuses on improving the quality of the thinking.
"The application of CRT has little to do with a patient’s intelligence level and much to do with a patient’s thinking style. In fact, the goals of CRT are to help individuals learn about how their brains work so that they can develop new problem-solving skills and enhanced cognitive flexibility."
He added, "Patients with anorexia often struggle with rigid thought patterns and an over focus on details that serve to maintain the symptoms of the disorder. These patients are also commonly very resistant to treatment, and CRT’s nontraditional focus also helps provide opportunities to enhance the therapeutic alliance and increase the patient’s motivation to change."
It’s long been known that anorexia involves detail focus or weak central coherence. Patients with anorexia have an excessively detailed information processing style with a neglect of holistic thinking. "They can’t really see the big picture." They are very good at tasks that involve piecemeal information processing.
In addition, these patients tend to be inflexible and poor at set shifting. They are also very rule-bound. Set shifting is the ability to hold two different cognitive frameworks. Anorexia patients have rigid thinking, and applications of rules and habits. It’s important to talk with patients about their thought processes during exercises that attempt to improve flexible thinking.
Flexible thinking exercises are used to encourage switching between different stimuli. These exercises include illusions (seeing two different pictures in the same image), switching attention tasks, embedded word tasks, estimating tasks, and ecological tasks.
The aim of switching attention tasks is to practice switching between two difference pieces of information swiftly and accurately, while also holding in mind a rule that requires remembering the previous answer. Embedded word tasks are designed to practice identifying particular categories of information among irrelevant information. This requires seeing the bigger picture and the detail, increasing flexibility of thinking.
Exercises like these help patient recognize strengths and weaknesses of thinking styles, challenge anxieties related to those styles, build confidence, and acknowledge and appreciate their strengths.
Dr. Brandt reported that he has no relevant financial relationships.
EXPERT ANALYSIS FROM THE SOUTHERN PSYCHIATRIC ASSOCIATION
Chemoradiotherapy Boosts Survival in Elderly NSCLC Patients
STOCKHOLM – Patients aged 71 years and older with advanced non–small cell lung cancer showed significantly greater survival with carboplatin chemotherapy plus concurrent radiation than with radiotherapy alone in a Japan Clinical Oncology Group trial that included only elderly patients.
Median overall survival was significantly longer, at 22.4 months, for those who received chemoradiotherapy, compared with 16.9 months for those having radiation therapy alone (hazard ratio, 0.68; P = .0179). Median progression-free survival was also significantly longer (8.9 months) for those receiving chemoradiotherapy, compared with 6.8 months for those with radiation therapy alone (HR, 0.66; P = .0044).
"This is the first trial demonstrating the clinically significant benefits of concurrent chemoradiation therapy in elderly patients with stage III non–small-cell lung cancer," Dr. Shinji Atagi said at the European Multidisciplinary Cancer Congress.
"This combined modality is considered as the standard treatment for this population [in Japan]," added Dr. Atagi of the National Hospital Organization Kinki-Chuo Chest Medical Center in Osaka, Japan.
Invited discussant Dr. Johanna Kazmierska shared the enthusiasm about the trial and its results. "The study suggests that age is not the only determinant of management of the [older] patient. The overall patient status [usually] is not taken into consideration," said Dr. Kazmierska of the radiotherapy department at the Greater Poland Cancer Centre in Poznan, Poland.
"Assessment of potential differences in treatment results – for example, overall survival – [provides] a strong argument for us in the discussion of the treatment of elderly patients," she added.
Patients were included in the trial if they had cytologically and/or histologically confirmed stage IIA (except T3N1M0) or IIIB non–small cell lung cancer (NSCLC). They had to be at least 71 years of age and have had no previous chemotherapy or radiotherapy. They also could not be candidates for cisplatin-based combination chemotherapy.
Patients were randomly assigned to the radiotherapy (RT) arm or the chemoradiotherapy (CRT) arm. In all, 98 patients were randomized to receive RT alone and 99 patients received CRT. The median age for both groups was 77 years.
The RT consisted of 60 Gy in 30 fractions over 6 weeks. In the CRT arm, patients received the same radiotherapy dose as in the RT arm as well as concurrent intravenous administration of carboplatin (30 mg/m2 in a 30-minute infusion) 1 hour before every radiation treatment up to the first 20 fractions.
In March 2011 – after the second interim analysis was performed – the Data and SafetyMonitoring Board recommended early publication of this trial in accordance with a prespecified rule.
The overall objective response rate (complete plus partial response) was 52% in the CRT arm vs. 45% in the RT arm. The difference between the two groups was not significant, however.
Safety results showed 64% and 59% of patients in the CRT arm had grade 3/4 leukocytopenia and neutropenia, but there were no grade 3/4 cases of either side effect in the RT arm. The CRT group also had a greater incidence of grade 3/4 infection (15% vs. 4%). Four treatment-related deaths occurred in the RT arm, and three occurred in the CRT arm.
The joint congress was sponsored by the European Cancer Organization (ECCO), the European Society for Medical Oncology (ESMO), and the European Society for Radiation and Oncology (ESTRO).
The study was sponsored by the Japan Clinical Oncology Group, with support from Japanese Ministry of Health, Labour, and Welfare. No personal disclosures were presented.
STOCKHOLM – Patients aged 71 years and older with advanced non–small cell lung cancer showed significantly greater survival with carboplatin chemotherapy plus concurrent radiation than with radiotherapy alone in a Japan Clinical Oncology Group trial that included only elderly patients.
Median overall survival was significantly longer, at 22.4 months, for those who received chemoradiotherapy, compared with 16.9 months for those having radiation therapy alone (hazard ratio, 0.68; P = .0179). Median progression-free survival was also significantly longer (8.9 months) for those receiving chemoradiotherapy, compared with 6.8 months for those with radiation therapy alone (HR, 0.66; P = .0044).
"This is the first trial demonstrating the clinically significant benefits of concurrent chemoradiation therapy in elderly patients with stage III non–small-cell lung cancer," Dr. Shinji Atagi said at the European Multidisciplinary Cancer Congress.
"This combined modality is considered as the standard treatment for this population [in Japan]," added Dr. Atagi of the National Hospital Organization Kinki-Chuo Chest Medical Center in Osaka, Japan.
Invited discussant Dr. Johanna Kazmierska shared the enthusiasm about the trial and its results. "The study suggests that age is not the only determinant of management of the [older] patient. The overall patient status [usually] is not taken into consideration," said Dr. Kazmierska of the radiotherapy department at the Greater Poland Cancer Centre in Poznan, Poland.
"Assessment of potential differences in treatment results – for example, overall survival – [provides] a strong argument for us in the discussion of the treatment of elderly patients," she added.
Patients were included in the trial if they had cytologically and/or histologically confirmed stage IIA (except T3N1M0) or IIIB non–small cell lung cancer (NSCLC). They had to be at least 71 years of age and have had no previous chemotherapy or radiotherapy. They also could not be candidates for cisplatin-based combination chemotherapy.
Patients were randomly assigned to the radiotherapy (RT) arm or the chemoradiotherapy (CRT) arm. In all, 98 patients were randomized to receive RT alone and 99 patients received CRT. The median age for both groups was 77 years.
The RT consisted of 60 Gy in 30 fractions over 6 weeks. In the CRT arm, patients received the same radiotherapy dose as in the RT arm as well as concurrent intravenous administration of carboplatin (30 mg/m2 in a 30-minute infusion) 1 hour before every radiation treatment up to the first 20 fractions.
In March 2011 – after the second interim analysis was performed – the Data and SafetyMonitoring Board recommended early publication of this trial in accordance with a prespecified rule.
The overall objective response rate (complete plus partial response) was 52% in the CRT arm vs. 45% in the RT arm. The difference between the two groups was not significant, however.
Safety results showed 64% and 59% of patients in the CRT arm had grade 3/4 leukocytopenia and neutropenia, but there were no grade 3/4 cases of either side effect in the RT arm. The CRT group also had a greater incidence of grade 3/4 infection (15% vs. 4%). Four treatment-related deaths occurred in the RT arm, and three occurred in the CRT arm.
The joint congress was sponsored by the European Cancer Organization (ECCO), the European Society for Medical Oncology (ESMO), and the European Society for Radiation and Oncology (ESTRO).
The study was sponsored by the Japan Clinical Oncology Group, with support from Japanese Ministry of Health, Labour, and Welfare. No personal disclosures were presented.
STOCKHOLM – Patients aged 71 years and older with advanced non–small cell lung cancer showed significantly greater survival with carboplatin chemotherapy plus concurrent radiation than with radiotherapy alone in a Japan Clinical Oncology Group trial that included only elderly patients.
Median overall survival was significantly longer, at 22.4 months, for those who received chemoradiotherapy, compared with 16.9 months for those having radiation therapy alone (hazard ratio, 0.68; P = .0179). Median progression-free survival was also significantly longer (8.9 months) for those receiving chemoradiotherapy, compared with 6.8 months for those with radiation therapy alone (HR, 0.66; P = .0044).
"This is the first trial demonstrating the clinically significant benefits of concurrent chemoradiation therapy in elderly patients with stage III non–small-cell lung cancer," Dr. Shinji Atagi said at the European Multidisciplinary Cancer Congress.
"This combined modality is considered as the standard treatment for this population [in Japan]," added Dr. Atagi of the National Hospital Organization Kinki-Chuo Chest Medical Center in Osaka, Japan.
Invited discussant Dr. Johanna Kazmierska shared the enthusiasm about the trial and its results. "The study suggests that age is not the only determinant of management of the [older] patient. The overall patient status [usually] is not taken into consideration," said Dr. Kazmierska of the radiotherapy department at the Greater Poland Cancer Centre in Poznan, Poland.
"Assessment of potential differences in treatment results – for example, overall survival – [provides] a strong argument for us in the discussion of the treatment of elderly patients," she added.
Patients were included in the trial if they had cytologically and/or histologically confirmed stage IIA (except T3N1M0) or IIIB non–small cell lung cancer (NSCLC). They had to be at least 71 years of age and have had no previous chemotherapy or radiotherapy. They also could not be candidates for cisplatin-based combination chemotherapy.
Patients were randomly assigned to the radiotherapy (RT) arm or the chemoradiotherapy (CRT) arm. In all, 98 patients were randomized to receive RT alone and 99 patients received CRT. The median age for both groups was 77 years.
The RT consisted of 60 Gy in 30 fractions over 6 weeks. In the CRT arm, patients received the same radiotherapy dose as in the RT arm as well as concurrent intravenous administration of carboplatin (30 mg/m2 in a 30-minute infusion) 1 hour before every radiation treatment up to the first 20 fractions.
In March 2011 – after the second interim analysis was performed – the Data and SafetyMonitoring Board recommended early publication of this trial in accordance with a prespecified rule.
The overall objective response rate (complete plus partial response) was 52% in the CRT arm vs. 45% in the RT arm. The difference between the two groups was not significant, however.
Safety results showed 64% and 59% of patients in the CRT arm had grade 3/4 leukocytopenia and neutropenia, but there were no grade 3/4 cases of either side effect in the RT arm. The CRT group also had a greater incidence of grade 3/4 infection (15% vs. 4%). Four treatment-related deaths occurred in the RT arm, and three occurred in the CRT arm.
The joint congress was sponsored by the European Cancer Organization (ECCO), the European Society for Medical Oncology (ESMO), and the European Society for Radiation and Oncology (ESTRO).
The study was sponsored by the Japan Clinical Oncology Group, with support from Japanese Ministry of Health, Labour, and Welfare. No personal disclosures were presented.
FROM THE EUROPEAN MULTIDISCIPLINARY CANCER CONGRESS
Major Finding: Median overall survival was significantly longer at 22.4 months in patients who received chemotherapy and radiation vs. 16.9 months in those treated with radiation therapy alone (HR, 0.68; P = .0179).
Data Source: A trial of 197 elderly patients with advanced NSCLC.
Disclosures: The study was sponsored by the Japan Clinical Oncology Group, with support from the Japanese Ministry of Health, Labour, and Welfare. No personal disclosures were presented.