User login
PRAGMA-CF shows disease progression of cystic fibrosis in children
reported Nynke R. Bouma, BSc, and colleagues.
“Even though bronchiectasis is present in 60% to 80% of children with CF in school age, the extent and severity of bronchiectasis in preschool children are generally lower ... however, diffuse airway abnormalities such as airway wall thickening and mucus plugging are observed in many preschool children. It is hypothesized that these preschool airway changes reflect diffuse airway disease that eventually will result in bronchiectasis in school age,” they noted.
The PRAGMA-CF image scoring system can measure airway disease and can also be used to monitor disease progression, noted Ms. Bouma of Sophia Children’s Hospital, Rotterdam, and colleagues. The study was published in Pediatric Pulmonology. PRAGMA-CF is a composite score of airway wall thickening, mucus plugging, and bronchiectasis as percent disease (%disease). “In preschool children, %disease measured by PRAGMA-CF on chest CT allows quantification of early clinically relevant morphological features of CF airway disease and it is associated with later school-age bronchiectasis,” the team wrote. “These findings support the use of %disease as a clinically relevant outcome measure in early CF lung disease.”
The team conducted a prospective cohort study of 61 children (mean age 4 years) with cystic fibrosis, following them for a mean of 5 years. A total of 122 CT scans were available from this group, in addition to spirometry data and cystic fibrosis quality of life scores.
From preschool age to school age, the %disease on PRAGMA-CF increased significantly, from a mean of 0.7% to 1.73%. Scores on another composite measuring tool (%MUPAT, a composite score of airway wall thickening and mucus plugging) went from 0.46 to 0.58 – not a significant difference.
A multivariate analysis corrected for age in each school group and the type of scanner used to acquire the images. That analysis determined that each 1% increase in %disease at preschool age resulted in an increase of 1.18% of bronchiectasis at school age.
A cross-sectional analysis of the group at school age found significant associations between the %disease and percent of forced expiratory volume and the cystic fibrosis quality of life score.
At least one pulmonary exacerbation requiring intravenous antibiotics occurred in 19 of the patients. However, the investigators didn’t find any significant interactions between the %disease in preschool and these exacerbations..
“These findings are in line with previous studies in school‐aged children that showed that mucus plugging is associated with inflammation and airway wall thickening, and that these are thought to be risk factors for later bronchiectasis,” they concluded. “On the basis of our findings, we suggest that %disease and %MUPAT could be used as a clinically relevant outcome measure in clinical studies in preschool patients with cystic fibrosis, as these measures predict later bronchiectasis. Percent disease may be preferred as it captures all the principal features of CF airways disease including bronchiectasis.”
Ms. Bouma had no financial disclosures.
SOURCE: Bouma NR et al. Pediatr Pulmonol. 2019 Sep 9 doi: 10.1002/ppul.24498; Rosenow et al. Am J Respir Crit Care Med. 2015 May 15. doi: 10.1164/rccm.201501-0061OC.
reported Nynke R. Bouma, BSc, and colleagues.
“Even though bronchiectasis is present in 60% to 80% of children with CF in school age, the extent and severity of bronchiectasis in preschool children are generally lower ... however, diffuse airway abnormalities such as airway wall thickening and mucus plugging are observed in many preschool children. It is hypothesized that these preschool airway changes reflect diffuse airway disease that eventually will result in bronchiectasis in school age,” they noted.
The PRAGMA-CF image scoring system can measure airway disease and can also be used to monitor disease progression, noted Ms. Bouma of Sophia Children’s Hospital, Rotterdam, and colleagues. The study was published in Pediatric Pulmonology. PRAGMA-CF is a composite score of airway wall thickening, mucus plugging, and bronchiectasis as percent disease (%disease). “In preschool children, %disease measured by PRAGMA-CF on chest CT allows quantification of early clinically relevant morphological features of CF airway disease and it is associated with later school-age bronchiectasis,” the team wrote. “These findings support the use of %disease as a clinically relevant outcome measure in early CF lung disease.”
The team conducted a prospective cohort study of 61 children (mean age 4 years) with cystic fibrosis, following them for a mean of 5 years. A total of 122 CT scans were available from this group, in addition to spirometry data and cystic fibrosis quality of life scores.
From preschool age to school age, the %disease on PRAGMA-CF increased significantly, from a mean of 0.7% to 1.73%. Scores on another composite measuring tool (%MUPAT, a composite score of airway wall thickening and mucus plugging) went from 0.46 to 0.58 – not a significant difference.
A multivariate analysis corrected for age in each school group and the type of scanner used to acquire the images. That analysis determined that each 1% increase in %disease at preschool age resulted in an increase of 1.18% of bronchiectasis at school age.
A cross-sectional analysis of the group at school age found significant associations between the %disease and percent of forced expiratory volume and the cystic fibrosis quality of life score.
At least one pulmonary exacerbation requiring intravenous antibiotics occurred in 19 of the patients. However, the investigators didn’t find any significant interactions between the %disease in preschool and these exacerbations..
“These findings are in line with previous studies in school‐aged children that showed that mucus plugging is associated with inflammation and airway wall thickening, and that these are thought to be risk factors for later bronchiectasis,” they concluded. “On the basis of our findings, we suggest that %disease and %MUPAT could be used as a clinically relevant outcome measure in clinical studies in preschool patients with cystic fibrosis, as these measures predict later bronchiectasis. Percent disease may be preferred as it captures all the principal features of CF airways disease including bronchiectasis.”
Ms. Bouma had no financial disclosures.
SOURCE: Bouma NR et al. Pediatr Pulmonol. 2019 Sep 9 doi: 10.1002/ppul.24498; Rosenow et al. Am J Respir Crit Care Med. 2015 May 15. doi: 10.1164/rccm.201501-0061OC.
reported Nynke R. Bouma, BSc, and colleagues.
“Even though bronchiectasis is present in 60% to 80% of children with CF in school age, the extent and severity of bronchiectasis in preschool children are generally lower ... however, diffuse airway abnormalities such as airway wall thickening and mucus plugging are observed in many preschool children. It is hypothesized that these preschool airway changes reflect diffuse airway disease that eventually will result in bronchiectasis in school age,” they noted.
The PRAGMA-CF image scoring system can measure airway disease and can also be used to monitor disease progression, noted Ms. Bouma of Sophia Children’s Hospital, Rotterdam, and colleagues. The study was published in Pediatric Pulmonology. PRAGMA-CF is a composite score of airway wall thickening, mucus plugging, and bronchiectasis as percent disease (%disease). “In preschool children, %disease measured by PRAGMA-CF on chest CT allows quantification of early clinically relevant morphological features of CF airway disease and it is associated with later school-age bronchiectasis,” the team wrote. “These findings support the use of %disease as a clinically relevant outcome measure in early CF lung disease.”
The team conducted a prospective cohort study of 61 children (mean age 4 years) with cystic fibrosis, following them for a mean of 5 years. A total of 122 CT scans were available from this group, in addition to spirometry data and cystic fibrosis quality of life scores.
From preschool age to school age, the %disease on PRAGMA-CF increased significantly, from a mean of 0.7% to 1.73%. Scores on another composite measuring tool (%MUPAT, a composite score of airway wall thickening and mucus plugging) went from 0.46 to 0.58 – not a significant difference.
A multivariate analysis corrected for age in each school group and the type of scanner used to acquire the images. That analysis determined that each 1% increase in %disease at preschool age resulted in an increase of 1.18% of bronchiectasis at school age.
A cross-sectional analysis of the group at school age found significant associations between the %disease and percent of forced expiratory volume and the cystic fibrosis quality of life score.
At least one pulmonary exacerbation requiring intravenous antibiotics occurred in 19 of the patients. However, the investigators didn’t find any significant interactions between the %disease in preschool and these exacerbations..
“These findings are in line with previous studies in school‐aged children that showed that mucus plugging is associated with inflammation and airway wall thickening, and that these are thought to be risk factors for later bronchiectasis,” they concluded. “On the basis of our findings, we suggest that %disease and %MUPAT could be used as a clinically relevant outcome measure in clinical studies in preschool patients with cystic fibrosis, as these measures predict later bronchiectasis. Percent disease may be preferred as it captures all the principal features of CF airways disease including bronchiectasis.”
Ms. Bouma had no financial disclosures.
SOURCE: Bouma NR et al. Pediatr Pulmonol. 2019 Sep 9 doi: 10.1002/ppul.24498; Rosenow et al. Am J Respir Crit Care Med. 2015 May 15. doi: 10.1164/rccm.201501-0061OC.
FROM PEDIATRIC PULMONOLOGY
Indwelling endoscopic biliary stents reduced risk of recurrent strictures in chronic pancreatitis
Sundeep Lakhtakia, MD, and colleagues reported in Gastrointestinal Endoscopy.
Patients with severe disease at baseline were more than twice as likely to develop a postprocedural stricture (odds ratio, 2.4). Longer baseline stricture length was less predictive, but it was still significantly associated with increased risk (OR, 1.2), according to Dr. Lakhtakia of the Asian Institute of Gastroenterology, Hyderabad, India, and coauthors.
The results indicate that indwelling biliary stenting is a reasonable and beneficial procedure for many of these patients, wrote Dr. Lakhtakia and coauthors.
“The major message to be taken from this study is that in patients with chronic [symptomatic] pancreatitis ... associated with benign biliary strictures, the single placement of a fully covered self-expanding metal stent for an intended indwell of 10-12 months allows more than 60% to remain free of symptoms up to 5 years later without additional intervention.”
The prospective nonrandomized study comprised 118 patients with chronic symptomatic pancreatitis and benign biliary strictures. All received a stent with removal scheduled for 10-12 months later. Patients were followed for 5 years. The primary endpoints were stricture resolution and freedom from recurrence at the end of follow-up.
Patients were a mean of 52 years old; most (83%) were male. At baseline, the mean total bilirubin was 1.4 mg/dL, and the mean alkaline phosphate level was 338.7 IU/L. Mean stricture length was 23.7 mm, but varied from 7.2 to 40 mm. Severe disease was present in 70%.
Among the cohort, five cases (4.2%) were considered treatment failures, with four lost to follow-up and one treated surgically for chronic pancreatitis progression. Another five experienced a spontaneous complete distal stent migration. The rest of the cohort (108) had their scheduled stent removal. At that time, 95 of the 118 experienced successful stent removal, without serious adverse events or the need for immediate replacement.
At 5 years, patients were reassessed, with the primary follow-up endpoint of stricture resolution. Secondary endpoints were time to stricture recurrence and/or changes in liver function tests. Overall, 79.7% (94) of the overall cohort showed stricture resolution at 5 years.
Among the 108 who had a successful removal, a longer time of stent indwell was associated with a decreased chance of recurrent placement. Among those with the longer indwell (median, 344 days), the risk reduction was 34% (OR, 0.66). Of the 94 patients with stricture resolution at stent removal, 77.4% remained stent free at 5 years.
At the end of follow-up, 56 patients had symptomatic data available. Most (53) had not experienced symptoms of biliary obstruction and/or cholestasis. The other three had been symptom free at 48 months but had incomplete or missing 5-year data.
By 5 years, 19 patients needed a new stent. Of these, 13 had symptoms of biliary obstruction.
About 23% of stented patients had a stent-related serious adverse event. These included cholangitis (9.3%), abdominal pain (5%), pancreatitis (3.4%), cholecystitis (2%), and cholestasis (1.7%).
About 80% of the 19 patients who had a stricture recurrence experienced a serious adverse event in the month before recurrent stent placement. The most common were cholangitis, cholestasis, abdominal pain, and cholelithiasis.
In a univariate analysis, recurrence risk was significantly associated with severe baseline disease and longer stricture length. The associations remained significant in the multivariate model.
“Strikingly, patients with initial stricture resolution at [stent] removal ... were very likely to have long-term stricture resolution” the authors noted.
Dr. Lakhtakia had no financial disclosures.
SOURCE: Lakhtakia S et al. Gastrointest Endosc. 2019. doi: 10.1016/j.gie.2019.08.037.
Sundeep Lakhtakia, MD, and colleagues reported in Gastrointestinal Endoscopy.
Patients with severe disease at baseline were more than twice as likely to develop a postprocedural stricture (odds ratio, 2.4). Longer baseline stricture length was less predictive, but it was still significantly associated with increased risk (OR, 1.2), according to Dr. Lakhtakia of the Asian Institute of Gastroenterology, Hyderabad, India, and coauthors.
The results indicate that indwelling biliary stenting is a reasonable and beneficial procedure for many of these patients, wrote Dr. Lakhtakia and coauthors.
“The major message to be taken from this study is that in patients with chronic [symptomatic] pancreatitis ... associated with benign biliary strictures, the single placement of a fully covered self-expanding metal stent for an intended indwell of 10-12 months allows more than 60% to remain free of symptoms up to 5 years later without additional intervention.”
The prospective nonrandomized study comprised 118 patients with chronic symptomatic pancreatitis and benign biliary strictures. All received a stent with removal scheduled for 10-12 months later. Patients were followed for 5 years. The primary endpoints were stricture resolution and freedom from recurrence at the end of follow-up.
Patients were a mean of 52 years old; most (83%) were male. At baseline, the mean total bilirubin was 1.4 mg/dL, and the mean alkaline phosphate level was 338.7 IU/L. Mean stricture length was 23.7 mm, but varied from 7.2 to 40 mm. Severe disease was present in 70%.
Among the cohort, five cases (4.2%) were considered treatment failures, with four lost to follow-up and one treated surgically for chronic pancreatitis progression. Another five experienced a spontaneous complete distal stent migration. The rest of the cohort (108) had their scheduled stent removal. At that time, 95 of the 118 experienced successful stent removal, without serious adverse events or the need for immediate replacement.
At 5 years, patients were reassessed, with the primary follow-up endpoint of stricture resolution. Secondary endpoints were time to stricture recurrence and/or changes in liver function tests. Overall, 79.7% (94) of the overall cohort showed stricture resolution at 5 years.
Among the 108 who had a successful removal, a longer time of stent indwell was associated with a decreased chance of recurrent placement. Among those with the longer indwell (median, 344 days), the risk reduction was 34% (OR, 0.66). Of the 94 patients with stricture resolution at stent removal, 77.4% remained stent free at 5 years.
At the end of follow-up, 56 patients had symptomatic data available. Most (53) had not experienced symptoms of biliary obstruction and/or cholestasis. The other three had been symptom free at 48 months but had incomplete or missing 5-year data.
By 5 years, 19 patients needed a new stent. Of these, 13 had symptoms of biliary obstruction.
About 23% of stented patients had a stent-related serious adverse event. These included cholangitis (9.3%), abdominal pain (5%), pancreatitis (3.4%), cholecystitis (2%), and cholestasis (1.7%).
About 80% of the 19 patients who had a stricture recurrence experienced a serious adverse event in the month before recurrent stent placement. The most common were cholangitis, cholestasis, abdominal pain, and cholelithiasis.
In a univariate analysis, recurrence risk was significantly associated with severe baseline disease and longer stricture length. The associations remained significant in the multivariate model.
“Strikingly, patients with initial stricture resolution at [stent] removal ... were very likely to have long-term stricture resolution” the authors noted.
Dr. Lakhtakia had no financial disclosures.
SOURCE: Lakhtakia S et al. Gastrointest Endosc. 2019. doi: 10.1016/j.gie.2019.08.037.
Sundeep Lakhtakia, MD, and colleagues reported in Gastrointestinal Endoscopy.
Patients with severe disease at baseline were more than twice as likely to develop a postprocedural stricture (odds ratio, 2.4). Longer baseline stricture length was less predictive, but it was still significantly associated with increased risk (OR, 1.2), according to Dr. Lakhtakia of the Asian Institute of Gastroenterology, Hyderabad, India, and coauthors.
The results indicate that indwelling biliary stenting is a reasonable and beneficial procedure for many of these patients, wrote Dr. Lakhtakia and coauthors.
“The major message to be taken from this study is that in patients with chronic [symptomatic] pancreatitis ... associated with benign biliary strictures, the single placement of a fully covered self-expanding metal stent for an intended indwell of 10-12 months allows more than 60% to remain free of symptoms up to 5 years later without additional intervention.”
The prospective nonrandomized study comprised 118 patients with chronic symptomatic pancreatitis and benign biliary strictures. All received a stent with removal scheduled for 10-12 months later. Patients were followed for 5 years. The primary endpoints were stricture resolution and freedom from recurrence at the end of follow-up.
Patients were a mean of 52 years old; most (83%) were male. At baseline, the mean total bilirubin was 1.4 mg/dL, and the mean alkaline phosphate level was 338.7 IU/L. Mean stricture length was 23.7 mm, but varied from 7.2 to 40 mm. Severe disease was present in 70%.
Among the cohort, five cases (4.2%) were considered treatment failures, with four lost to follow-up and one treated surgically for chronic pancreatitis progression. Another five experienced a spontaneous complete distal stent migration. The rest of the cohort (108) had their scheduled stent removal. At that time, 95 of the 118 experienced successful stent removal, without serious adverse events or the need for immediate replacement.
At 5 years, patients were reassessed, with the primary follow-up endpoint of stricture resolution. Secondary endpoints were time to stricture recurrence and/or changes in liver function tests. Overall, 79.7% (94) of the overall cohort showed stricture resolution at 5 years.
Among the 108 who had a successful removal, a longer time of stent indwell was associated with a decreased chance of recurrent placement. Among those with the longer indwell (median, 344 days), the risk reduction was 34% (OR, 0.66). Of the 94 patients with stricture resolution at stent removal, 77.4% remained stent free at 5 years.
At the end of follow-up, 56 patients had symptomatic data available. Most (53) had not experienced symptoms of biliary obstruction and/or cholestasis. The other three had been symptom free at 48 months but had incomplete or missing 5-year data.
By 5 years, 19 patients needed a new stent. Of these, 13 had symptoms of biliary obstruction.
About 23% of stented patients had a stent-related serious adverse event. These included cholangitis (9.3%), abdominal pain (5%), pancreatitis (3.4%), cholecystitis (2%), and cholestasis (1.7%).
About 80% of the 19 patients who had a stricture recurrence experienced a serious adverse event in the month before recurrent stent placement. The most common were cholangitis, cholestasis, abdominal pain, and cholelithiasis.
In a univariate analysis, recurrence risk was significantly associated with severe baseline disease and longer stricture length. The associations remained significant in the multivariate model.
“Strikingly, patients with initial stricture resolution at [stent] removal ... were very likely to have long-term stricture resolution” the authors noted.
Dr. Lakhtakia had no financial disclosures.
SOURCE: Lakhtakia S et al. Gastrointest Endosc. 2019. doi: 10.1016/j.gie.2019.08.037.
FROM GASTROINTESTINAL ENDOSCOPY
Peanut allergy pill gets thumbs-up from FDA advisory panel
A pill designed to desensitize peanut-allergic children and teenagers may be on the way.
aged 4-17 years old with a confirmed peanut allergy. Conditions for approval include stipulations that a black-box warning and medication use guide are included in the packaging, the panel said. The FDA usually follows the recommendations of its advisory panels.

The committee members voted 7-2 that the drug was effective and 8-1 that it was safe.
John Kelso, MD, the sole dissenter on safety, voiced concerns about the dearth of long-term follow-up in Aimmune Therapeutic’s body of research and the finding that children who received the treatment during the dose-escalation and maintenance periods had twice the number of allergic reactions requiring epinephrine, compared with those who received placebo. There are no long-term safety data to rely on yet, he added.
“Efficacy has not been demonstrated, except on the day the peanut challenge is administered,” said Dr. Kelso, an allergist at the Scripps Clinic, San Diego, adding that only long-term follow-up data would fully convince him that the drug’s benefits outweigh the risks.
In the discussion, however, other committee members pointed out that new drugs are often approved without long-term efficacy and safety data. Those data are extrapolated from clinical trials, and only real-world experience will confirm the data, they noted.
Company representatives did not explicitly address the potential cost of the therapy, but a recent review by the Institute for Clinical and Economic Review estimated the cost to be $4,200 a year. Palforzia would have to be taken every day, for an unknown amount of time, to maintain peanut tolerance.
“Using prices from analysts for AR101 ($4,200 a year), we estimated that only 41% of eligible patients could be treated in a given year without exceeding ICER’s budget impact threshold,” the institute concluded in a publicly released analysis.
Palforzia comes in individual packs of capsules filled with peanut protein, not flour. The capsules come in doses of 0.5, 1, 10, 20, and 100, and 300 mg. A single-dose sachet contains 300 mg. Treatment begins with 0.5-6 mg over 1 day and escalates every 2 weeks until 300 mg is reached or there is a reaction requiring epinephrine. Passing at least a 300-mg dose was the requirement for exiting the escalation phase and moving on to the daily, year-long maintenance phase.
The four efficacy studies presented showed that 96% of patients tolerated 300 mg, 84% tolerated 600 mg, and 63% 1,000 mg – about 10 times the reactive dose observed in the placebo controls.
“Only 125 mg of peanut protein – the amount in about half a peanut kernel – can be enough to provoke a reaction,” said Daniel Adelman, MD, chief medical officer of Aimmune. If patients can tolerate 600 mg of protein – the equivalent of two kernels, accidental ingestion will result in a “predictable, manageable” reaction.
“This is truly a clinically significant result for patients and families who report lives dictated by the allergy,” Dr. Adelman said.
Consistent manufacturing processes and positive safety data should reassure clinicians and patients that they are receiving a safe, effective, and well-regulated treatment, he added.
The capsule, however, is not a panacea. The company advises that families continue with the peanut avoidance diet. “It’s important to remember that reactive episodes can occur with dosing, and accidental exposures can occur at unpredictable times, away from home, and despite the best efforts at avoidance,” Dr. Adelman said. “This is not a drug for everyone, but it is an effective desensitization tool and would clearly be the first therapy to treat a food allergy, providing statistically significant and clinically important improvement. Outcomes align with patients’ goals.”
Safety was assessed in 709 treated patients who received the medication and 292 who received placebo. Treatment-related adverse events were most common in initial dosing: 89% of the treatment group and 58% of the placebo group experienced at least one adverse event during that time. Adverse events were mostly mild to moderate and decreased in severity over the study period. They included abdominal pain (45% active vs. 18% placebo), throat irritation (40% vs. 17%), pruritus (33% vs. 20%), vomiting (37% vs. 16%), cough (32% vs. 24%), nausea (32% vs. 14%), urticaria (28% vs. 19%), and upper abdominal pain (30% vs. 14%).
Discontinuations caused by these adverse events were infrequent, with only 1.8% of participants who were taking the active capsule and 1% of those taking placebo discontinuing the study product during initial dose escalation. Only the severe systemic allergic reactions were considered to be anaphylaxis, and they had to affect at least two body systems.
Respiratory events were more common in those in the active group, especially in children with asthma. These events included cough, wheezing, dyspnea, dysphonia, throat irritation and tightness, and exercise-induced asthma. There was, however, no “concerning change” in asthma control.
Systemic allergic reactions and anaphylaxis were more common in the active-dose group. Systemic reactions during dose escalation occurred in 9.4% of active patients and 3.8% those taking placebo. During the maintenance phase, they occurred in 8.7% and 1.7% of patients, respectively. Three patients in the active group had a serious systemic reaction – two during up-dosing and one during maintenance.
During initial dose escalation and up-dosing combined, 6.1% of patients in the active group and 3.1% in the placebo group had a systemic reaction requiring epinephrine. This was most often administered outside of the clinic.
There were 12 cases of eosinophilic esophagitis, all of which resolved after withdrawal from the study medication.
Aimmune submitted a risk-management proposal that includes the following:
- The first dose of each progressive dose must be administered in a facility that is equipped to treat systemic allergic reactions.
- Families must have a valid prescription for injectable epinephrine before treatment starts and must demonstrate that they know how to use it.
- There must be distribution controls in every pharmacy that dispenses the product.
- Packaging will be dose specific to ensure proper at-home administration.
- Pharmacologic questionnaires will be used as data collection instruments.
- Professional and patient-focused labeling will include a medication guide and educational material.
Palforzia is not the only peanut desensitization product in the works. DBC Technology has resubmitted its biologics license application to the FDA in the hope of getting approval for its peanut allergy treatment, the Viaskin Peanut patch.
The patch is designed to desensitize allergic children aged 4-11 years through a skin-patch method known as epicutaneous immunotherapy. Results from two controlled clinical trials were included in the submission. The company is also investigating the potential of this form of skin-patch therapy for milk and egg allergies.
Correction, 9/15/19: An earlier version of this article did not clearly state that the panel recommended approval rather than granted approval for the drug.
A pill designed to desensitize peanut-allergic children and teenagers may be on the way.
aged 4-17 years old with a confirmed peanut allergy. Conditions for approval include stipulations that a black-box warning and medication use guide are included in the packaging, the panel said. The FDA usually follows the recommendations of its advisory panels.
The committee members voted 7-2 that the drug was effective and 8-1 that it was safe.
John Kelso, MD, the sole dissenter on safety, voiced concerns about the dearth of long-term follow-up in Aimmune Therapeutic’s body of research and the finding that children who received the treatment during the dose-escalation and maintenance periods had twice the number of allergic reactions requiring epinephrine, compared with those who received placebo. There are no long-term safety data to rely on yet, he added.
“Efficacy has not been demonstrated, except on the day the peanut challenge is administered,” said Dr. Kelso, an allergist at the Scripps Clinic, San Diego, adding that only long-term follow-up data would fully convince him that the drug’s benefits outweigh the risks.
In the discussion, however, other committee members pointed out that new drugs are often approved without long-term efficacy and safety data. Those data are extrapolated from clinical trials, and only real-world experience will confirm the data, they noted.
Company representatives did not explicitly address the potential cost of the therapy, but a recent review by the Institute for Clinical and Economic Review estimated the cost to be $4,200 a year. Palforzia would have to be taken every day, for an unknown amount of time, to maintain peanut tolerance.
“Using prices from analysts for AR101 ($4,200 a year), we estimated that only 41% of eligible patients could be treated in a given year without exceeding ICER’s budget impact threshold,” the institute concluded in a publicly released analysis.
Palforzia comes in individual packs of capsules filled with peanut protein, not flour. The capsules come in doses of 0.5, 1, 10, 20, and 100, and 300 mg. A single-dose sachet contains 300 mg. Treatment begins with 0.5-6 mg over 1 day and escalates every 2 weeks until 300 mg is reached or there is a reaction requiring epinephrine. Passing at least a 300-mg dose was the requirement for exiting the escalation phase and moving on to the daily, year-long maintenance phase.
The four efficacy studies presented showed that 96% of patients tolerated 300 mg, 84% tolerated 600 mg, and 63% 1,000 mg – about 10 times the reactive dose observed in the placebo controls.
“Only 125 mg of peanut protein – the amount in about half a peanut kernel – can be enough to provoke a reaction,” said Daniel Adelman, MD, chief medical officer of Aimmune. If patients can tolerate 600 mg of protein – the equivalent of two kernels, accidental ingestion will result in a “predictable, manageable” reaction.
“This is truly a clinically significant result for patients and families who report lives dictated by the allergy,” Dr. Adelman said.
Consistent manufacturing processes and positive safety data should reassure clinicians and patients that they are receiving a safe, effective, and well-regulated treatment, he added.
The capsule, however, is not a panacea. The company advises that families continue with the peanut avoidance diet. “It’s important to remember that reactive episodes can occur with dosing, and accidental exposures can occur at unpredictable times, away from home, and despite the best efforts at avoidance,” Dr. Adelman said. “This is not a drug for everyone, but it is an effective desensitization tool and would clearly be the first therapy to treat a food allergy, providing statistically significant and clinically important improvement. Outcomes align with patients’ goals.”
Safety was assessed in 709 treated patients who received the medication and 292 who received placebo. Treatment-related adverse events were most common in initial dosing: 89% of the treatment group and 58% of the placebo group experienced at least one adverse event during that time. Adverse events were mostly mild to moderate and decreased in severity over the study period. They included abdominal pain (45% active vs. 18% placebo), throat irritation (40% vs. 17%), pruritus (33% vs. 20%), vomiting (37% vs. 16%), cough (32% vs. 24%), nausea (32% vs. 14%), urticaria (28% vs. 19%), and upper abdominal pain (30% vs. 14%).
Discontinuations caused by these adverse events were infrequent, with only 1.8% of participants who were taking the active capsule and 1% of those taking placebo discontinuing the study product during initial dose escalation. Only the severe systemic allergic reactions were considered to be anaphylaxis, and they had to affect at least two body systems.
Respiratory events were more common in those in the active group, especially in children with asthma. These events included cough, wheezing, dyspnea, dysphonia, throat irritation and tightness, and exercise-induced asthma. There was, however, no “concerning change” in asthma control.
Systemic allergic reactions and anaphylaxis were more common in the active-dose group. Systemic reactions during dose escalation occurred in 9.4% of active patients and 3.8% those taking placebo. During the maintenance phase, they occurred in 8.7% and 1.7% of patients, respectively. Three patients in the active group had a serious systemic reaction – two during up-dosing and one during maintenance.
During initial dose escalation and up-dosing combined, 6.1% of patients in the active group and 3.1% in the placebo group had a systemic reaction requiring epinephrine. This was most often administered outside of the clinic.
There were 12 cases of eosinophilic esophagitis, all of which resolved after withdrawal from the study medication.
Aimmune submitted a risk-management proposal that includes the following:
- The first dose of each progressive dose must be administered in a facility that is equipped to treat systemic allergic reactions.
- Families must have a valid prescription for injectable epinephrine before treatment starts and must demonstrate that they know how to use it.
- There must be distribution controls in every pharmacy that dispenses the product.
- Packaging will be dose specific to ensure proper at-home administration.
- Pharmacologic questionnaires will be used as data collection instruments.
- Professional and patient-focused labeling will include a medication guide and educational material.
Palforzia is not the only peanut desensitization product in the works. DBC Technology has resubmitted its biologics license application to the FDA in the hope of getting approval for its peanut allergy treatment, the Viaskin Peanut patch.
The patch is designed to desensitize allergic children aged 4-11 years through a skin-patch method known as epicutaneous immunotherapy. Results from two controlled clinical trials were included in the submission. The company is also investigating the potential of this form of skin-patch therapy for milk and egg allergies.
Correction, 9/15/19: An earlier version of this article did not clearly state that the panel recommended approval rather than granted approval for the drug.
A pill designed to desensitize peanut-allergic children and teenagers may be on the way.
aged 4-17 years old with a confirmed peanut allergy. Conditions for approval include stipulations that a black-box warning and medication use guide are included in the packaging, the panel said. The FDA usually follows the recommendations of its advisory panels.
The committee members voted 7-2 that the drug was effective and 8-1 that it was safe.
John Kelso, MD, the sole dissenter on safety, voiced concerns about the dearth of long-term follow-up in Aimmune Therapeutic’s body of research and the finding that children who received the treatment during the dose-escalation and maintenance periods had twice the number of allergic reactions requiring epinephrine, compared with those who received placebo. There are no long-term safety data to rely on yet, he added.
“Efficacy has not been demonstrated, except on the day the peanut challenge is administered,” said Dr. Kelso, an allergist at the Scripps Clinic, San Diego, adding that only long-term follow-up data would fully convince him that the drug’s benefits outweigh the risks.
In the discussion, however, other committee members pointed out that new drugs are often approved without long-term efficacy and safety data. Those data are extrapolated from clinical trials, and only real-world experience will confirm the data, they noted.
Company representatives did not explicitly address the potential cost of the therapy, but a recent review by the Institute for Clinical and Economic Review estimated the cost to be $4,200 a year. Palforzia would have to be taken every day, for an unknown amount of time, to maintain peanut tolerance.
“Using prices from analysts for AR101 ($4,200 a year), we estimated that only 41% of eligible patients could be treated in a given year without exceeding ICER’s budget impact threshold,” the institute concluded in a publicly released analysis.
Palforzia comes in individual packs of capsules filled with peanut protein, not flour. The capsules come in doses of 0.5, 1, 10, 20, and 100, and 300 mg. A single-dose sachet contains 300 mg. Treatment begins with 0.5-6 mg over 1 day and escalates every 2 weeks until 300 mg is reached or there is a reaction requiring epinephrine. Passing at least a 300-mg dose was the requirement for exiting the escalation phase and moving on to the daily, year-long maintenance phase.
The four efficacy studies presented showed that 96% of patients tolerated 300 mg, 84% tolerated 600 mg, and 63% 1,000 mg – about 10 times the reactive dose observed in the placebo controls.
“Only 125 mg of peanut protein – the amount in about half a peanut kernel – can be enough to provoke a reaction,” said Daniel Adelman, MD, chief medical officer of Aimmune. If patients can tolerate 600 mg of protein – the equivalent of two kernels, accidental ingestion will result in a “predictable, manageable” reaction.
“This is truly a clinically significant result for patients and families who report lives dictated by the allergy,” Dr. Adelman said.
Consistent manufacturing processes and positive safety data should reassure clinicians and patients that they are receiving a safe, effective, and well-regulated treatment, he added.
The capsule, however, is not a panacea. The company advises that families continue with the peanut avoidance diet. “It’s important to remember that reactive episodes can occur with dosing, and accidental exposures can occur at unpredictable times, away from home, and despite the best efforts at avoidance,” Dr. Adelman said. “This is not a drug for everyone, but it is an effective desensitization tool and would clearly be the first therapy to treat a food allergy, providing statistically significant and clinically important improvement. Outcomes align with patients’ goals.”
Safety was assessed in 709 treated patients who received the medication and 292 who received placebo. Treatment-related adverse events were most common in initial dosing: 89% of the treatment group and 58% of the placebo group experienced at least one adverse event during that time. Adverse events were mostly mild to moderate and decreased in severity over the study period. They included abdominal pain (45% active vs. 18% placebo), throat irritation (40% vs. 17%), pruritus (33% vs. 20%), vomiting (37% vs. 16%), cough (32% vs. 24%), nausea (32% vs. 14%), urticaria (28% vs. 19%), and upper abdominal pain (30% vs. 14%).
Discontinuations caused by these adverse events were infrequent, with only 1.8% of participants who were taking the active capsule and 1% of those taking placebo discontinuing the study product during initial dose escalation. Only the severe systemic allergic reactions were considered to be anaphylaxis, and they had to affect at least two body systems.
Respiratory events were more common in those in the active group, especially in children with asthma. These events included cough, wheezing, dyspnea, dysphonia, throat irritation and tightness, and exercise-induced asthma. There was, however, no “concerning change” in asthma control.
Systemic allergic reactions and anaphylaxis were more common in the active-dose group. Systemic reactions during dose escalation occurred in 9.4% of active patients and 3.8% those taking placebo. During the maintenance phase, they occurred in 8.7% and 1.7% of patients, respectively. Three patients in the active group had a serious systemic reaction – two during up-dosing and one during maintenance.
During initial dose escalation and up-dosing combined, 6.1% of patients in the active group and 3.1% in the placebo group had a systemic reaction requiring epinephrine. This was most often administered outside of the clinic.
There were 12 cases of eosinophilic esophagitis, all of which resolved after withdrawal from the study medication.
Aimmune submitted a risk-management proposal that includes the following:
- The first dose of each progressive dose must be administered in a facility that is equipped to treat systemic allergic reactions.
- Families must have a valid prescription for injectable epinephrine before treatment starts and must demonstrate that they know how to use it.
- There must be distribution controls in every pharmacy that dispenses the product.
- Packaging will be dose specific to ensure proper at-home administration.
- Pharmacologic questionnaires will be used as data collection instruments.
- Professional and patient-focused labeling will include a medication guide and educational material.
Palforzia is not the only peanut desensitization product in the works. DBC Technology has resubmitted its biologics license application to the FDA in the hope of getting approval for its peanut allergy treatment, the Viaskin Peanut patch.
The patch is designed to desensitize allergic children aged 4-11 years through a skin-patch method known as epicutaneous immunotherapy. Results from two controlled clinical trials were included in the submission. The company is also investigating the potential of this form of skin-patch therapy for milk and egg allergies.
Correction, 9/15/19: An earlier version of this article did not clearly state that the panel recommended approval rather than granted approval for the drug.
FROM THE FDA ALLERGENIC PRODUCTS ADVISORY COMMITTEE MEETING
Nivolumab may be beneficial for recurrent or metastatic cervical cancer
The checkpoint inhibitor nivolumab may hold some promise for treating women with metastatic gynecologic cancers, especially cervical disease, according to cohort results from the phase 1/2 CheckMate 358 trial.
Of twenty-four patients enrolled in the recurrent/metastatic cervical and vaginal/vulvar carcinoma cohorts, 26.3% of patients with cervical cancer and 20% with vaginal/vulvar cancers experienced an objective response, R. Wendel Naumann, MD, and colleagues reported in the Journal of Clinical Oncology.
Median overall survival was 21.9 months (95% confidence interval, 15.1 months to not reached) among patients with cervical cancer. Because of the small size of the vaginal/vulvar cohort, median overall survival was not calculated.
“Given the lack of effective therapy and low survival rates for patients with metastatic disease in these gynecologic cancers, the results reported here are of strong clinical interest and underscore the growing role of immune checkpoint inhibitors in this patient population,” the investigators wrote.
Checkmate 358 is investigating nivolumab in patients with virus-associated cancers. Patients receive nivolumab monotherapy (240 mg intravenously every 2 weeks for 2 years) until disease progression, unacceptable side effects, or withdrawal of consent.
The median age was 51 years in the cervical cohort (n = 19) and 59 in the vaginal/vulvar cohort (n = 5). HPV status was positive in 83.3% of those with cervical disease and 40% of those with vaginal/vulvar disease. Ten cervical tumors and four vaginal/vulvar tumors expressed PD-L1.
The median duration of nivolumab treatment was 5.6 months in the cervical cohort and 6.7 months in the vaginal/vulvar cohort. Median follow-up was 19 months and 10 months, respectively.
At 12 months and 18 months, 40.0% of the cervical cohort and 20% of the vaginal/vulvar cohort were still alive.
The most common treatment-related adverse effects were diarrhea and decreased appetite. One patient in the cervical cohort discontinued treatment because of pneumonitis, which was considered treatment related.
Bristol-Myers Squibb funded the study. Several of Dr. Naumann’s associates reported relationships with the company and four others are employed by Bristol-Myers Squibb.
SOURCE: Naumann RW et al. J Clin Oncol. 2019 Sep 5. doi: 10.1200JCP.19.00739.
The checkpoint inhibitor nivolumab may hold some promise for treating women with metastatic gynecologic cancers, especially cervical disease, according to cohort results from the phase 1/2 CheckMate 358 trial.
Of twenty-four patients enrolled in the recurrent/metastatic cervical and vaginal/vulvar carcinoma cohorts, 26.3% of patients with cervical cancer and 20% with vaginal/vulvar cancers experienced an objective response, R. Wendel Naumann, MD, and colleagues reported in the Journal of Clinical Oncology.
Median overall survival was 21.9 months (95% confidence interval, 15.1 months to not reached) among patients with cervical cancer. Because of the small size of the vaginal/vulvar cohort, median overall survival was not calculated.
“Given the lack of effective therapy and low survival rates for patients with metastatic disease in these gynecologic cancers, the results reported here are of strong clinical interest and underscore the growing role of immune checkpoint inhibitors in this patient population,” the investigators wrote.
Checkmate 358 is investigating nivolumab in patients with virus-associated cancers. Patients receive nivolumab monotherapy (240 mg intravenously every 2 weeks for 2 years) until disease progression, unacceptable side effects, or withdrawal of consent.
The median age was 51 years in the cervical cohort (n = 19) and 59 in the vaginal/vulvar cohort (n = 5). HPV status was positive in 83.3% of those with cervical disease and 40% of those with vaginal/vulvar disease. Ten cervical tumors and four vaginal/vulvar tumors expressed PD-L1.
The median duration of nivolumab treatment was 5.6 months in the cervical cohort and 6.7 months in the vaginal/vulvar cohort. Median follow-up was 19 months and 10 months, respectively.
At 12 months and 18 months, 40.0% of the cervical cohort and 20% of the vaginal/vulvar cohort were still alive.
The most common treatment-related adverse effects were diarrhea and decreased appetite. One patient in the cervical cohort discontinued treatment because of pneumonitis, which was considered treatment related.
Bristol-Myers Squibb funded the study. Several of Dr. Naumann’s associates reported relationships with the company and four others are employed by Bristol-Myers Squibb.
SOURCE: Naumann RW et al. J Clin Oncol. 2019 Sep 5. doi: 10.1200JCP.19.00739.
The checkpoint inhibitor nivolumab may hold some promise for treating women with metastatic gynecologic cancers, especially cervical disease, according to cohort results from the phase 1/2 CheckMate 358 trial.
Of twenty-four patients enrolled in the recurrent/metastatic cervical and vaginal/vulvar carcinoma cohorts, 26.3% of patients with cervical cancer and 20% with vaginal/vulvar cancers experienced an objective response, R. Wendel Naumann, MD, and colleagues reported in the Journal of Clinical Oncology.
Median overall survival was 21.9 months (95% confidence interval, 15.1 months to not reached) among patients with cervical cancer. Because of the small size of the vaginal/vulvar cohort, median overall survival was not calculated.
“Given the lack of effective therapy and low survival rates for patients with metastatic disease in these gynecologic cancers, the results reported here are of strong clinical interest and underscore the growing role of immune checkpoint inhibitors in this patient population,” the investigators wrote.
Checkmate 358 is investigating nivolumab in patients with virus-associated cancers. Patients receive nivolumab monotherapy (240 mg intravenously every 2 weeks for 2 years) until disease progression, unacceptable side effects, or withdrawal of consent.
The median age was 51 years in the cervical cohort (n = 19) and 59 in the vaginal/vulvar cohort (n = 5). HPV status was positive in 83.3% of those with cervical disease and 40% of those with vaginal/vulvar disease. Ten cervical tumors and four vaginal/vulvar tumors expressed PD-L1.
The median duration of nivolumab treatment was 5.6 months in the cervical cohort and 6.7 months in the vaginal/vulvar cohort. Median follow-up was 19 months and 10 months, respectively.
At 12 months and 18 months, 40.0% of the cervical cohort and 20% of the vaginal/vulvar cohort were still alive.
The most common treatment-related adverse effects were diarrhea and decreased appetite. One patient in the cervical cohort discontinued treatment because of pneumonitis, which was considered treatment related.
Bristol-Myers Squibb funded the study. Several of Dr. Naumann’s associates reported relationships with the company and four others are employed by Bristol-Myers Squibb.
SOURCE: Naumann RW et al. J Clin Oncol. 2019 Sep 5. doi: 10.1200JCP.19.00739.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Ankylosing spondylitis severity, comorbidities higher in blacks than in whites
While ankylosing spondylitis may be more common among whites, black patients have more comorbidities and express higher disease activity, Dilpreet Kaur Singh, MD, and Marina Magrey, MBBS, reported in The Journal of Rheumatology.
A retrospective review of a large U.S. medical database conducted by Dr. Singh and Dr. Magrey of MetroHealth Medical Center, Cleveland, found that black patients had higher erythrocyte sedimentation rates and C-reactive protein, and a higher prevalence of anterior uveitis, hypertension, diabetes, and depression, compared with white patients. (Dr. Singh, who was a rheumatology fellow at MetroHealth at the time of the study, is now a practicing rheumatologist in Springfield, Mass.)
Disease severity in AS is “thought to be genetically mediated but cultural, social, or economic factors may also be contributing to this racial disparity,” the investigators wrote. “Further research is needed to determine the role of factors other than genetic factors like HLA-B27 positivity that contribute to worsening disease severity.”
The authors extracted data recorded during 1999-2017 from the Explorys platform, a clinical research informatics tool with data from more than 50 million patients in 26 major integrated health care systems in the United States.
The current study comprised 10,990 AS patients with at least two visits to a rheumatologist. Most (84%) were white; 8% were black. Sex was equally distributed in both groups. Positivity for HLA-B27 was similar among whites (26%) and blacks (20%). A majority of patients smoked (65%), and smoking was more common among whites than among blacks (67% vs. 59%).
Disease characteristics suggested that AS was more severe among blacks. Significantly greater proportions of black patients had elevated erythrocyte sedimentation rate (62% vs. 48% of whites) and C-reactive protein (68% vs. 54%). Blacks also experienced significantly greater rates of anterior uveitis (8% vs. 4%), hypertension (29% vs. 22%), diabetes (27% vs. 17%), and depression (36% vs. 32%).
Blacks experienced higher rates of peripheral arthritis, enthesopathy, dactylitis, and inflammatory bowel disease, although these differences were not statistically significant when compared with whites.
Whites, however, had significantly higher rates of psoriasis (10% vs. 6.5%).
Most of the cohort (87%) received NSAIDs; 39% used tumor necrosis factor inhibitors. There were no significant between-group treatment differences.
The authors reported no potential conflicts of interest and no source of financial support.
SOURCE: Singh DK et al. J Rheumatol. 2019 Sep 1. doi: 10.3899/jrheum.181019.
While ankylosing spondylitis may be more common among whites, black patients have more comorbidities and express higher disease activity, Dilpreet Kaur Singh, MD, and Marina Magrey, MBBS, reported in The Journal of Rheumatology.
A retrospective review of a large U.S. medical database conducted by Dr. Singh and Dr. Magrey of MetroHealth Medical Center, Cleveland, found that black patients had higher erythrocyte sedimentation rates and C-reactive protein, and a higher prevalence of anterior uveitis, hypertension, diabetes, and depression, compared with white patients. (Dr. Singh, who was a rheumatology fellow at MetroHealth at the time of the study, is now a practicing rheumatologist in Springfield, Mass.)
Disease severity in AS is “thought to be genetically mediated but cultural, social, or economic factors may also be contributing to this racial disparity,” the investigators wrote. “Further research is needed to determine the role of factors other than genetic factors like HLA-B27 positivity that contribute to worsening disease severity.”
The authors extracted data recorded during 1999-2017 from the Explorys platform, a clinical research informatics tool with data from more than 50 million patients in 26 major integrated health care systems in the United States.
The current study comprised 10,990 AS patients with at least two visits to a rheumatologist. Most (84%) were white; 8% were black. Sex was equally distributed in both groups. Positivity for HLA-B27 was similar among whites (26%) and blacks (20%). A majority of patients smoked (65%), and smoking was more common among whites than among blacks (67% vs. 59%).
Disease characteristics suggested that AS was more severe among blacks. Significantly greater proportions of black patients had elevated erythrocyte sedimentation rate (62% vs. 48% of whites) and C-reactive protein (68% vs. 54%). Blacks also experienced significantly greater rates of anterior uveitis (8% vs. 4%), hypertension (29% vs. 22%), diabetes (27% vs. 17%), and depression (36% vs. 32%).
Blacks experienced higher rates of peripheral arthritis, enthesopathy, dactylitis, and inflammatory bowel disease, although these differences were not statistically significant when compared with whites.
Whites, however, had significantly higher rates of psoriasis (10% vs. 6.5%).
Most of the cohort (87%) received NSAIDs; 39% used tumor necrosis factor inhibitors. There were no significant between-group treatment differences.
The authors reported no potential conflicts of interest and no source of financial support.
SOURCE: Singh DK et al. J Rheumatol. 2019 Sep 1. doi: 10.3899/jrheum.181019.
While ankylosing spondylitis may be more common among whites, black patients have more comorbidities and express higher disease activity, Dilpreet Kaur Singh, MD, and Marina Magrey, MBBS, reported in The Journal of Rheumatology.
A retrospective review of a large U.S. medical database conducted by Dr. Singh and Dr. Magrey of MetroHealth Medical Center, Cleveland, found that black patients had higher erythrocyte sedimentation rates and C-reactive protein, and a higher prevalence of anterior uveitis, hypertension, diabetes, and depression, compared with white patients. (Dr. Singh, who was a rheumatology fellow at MetroHealth at the time of the study, is now a practicing rheumatologist in Springfield, Mass.)
Disease severity in AS is “thought to be genetically mediated but cultural, social, or economic factors may also be contributing to this racial disparity,” the investigators wrote. “Further research is needed to determine the role of factors other than genetic factors like HLA-B27 positivity that contribute to worsening disease severity.”
The authors extracted data recorded during 1999-2017 from the Explorys platform, a clinical research informatics tool with data from more than 50 million patients in 26 major integrated health care systems in the United States.
The current study comprised 10,990 AS patients with at least two visits to a rheumatologist. Most (84%) were white; 8% were black. Sex was equally distributed in both groups. Positivity for HLA-B27 was similar among whites (26%) and blacks (20%). A majority of patients smoked (65%), and smoking was more common among whites than among blacks (67% vs. 59%).
Disease characteristics suggested that AS was more severe among blacks. Significantly greater proportions of black patients had elevated erythrocyte sedimentation rate (62% vs. 48% of whites) and C-reactive protein (68% vs. 54%). Blacks also experienced significantly greater rates of anterior uveitis (8% vs. 4%), hypertension (29% vs. 22%), diabetes (27% vs. 17%), and depression (36% vs. 32%).
Blacks experienced higher rates of peripheral arthritis, enthesopathy, dactylitis, and inflammatory bowel disease, although these differences were not statistically significant when compared with whites.
Whites, however, had significantly higher rates of psoriasis (10% vs. 6.5%).
Most of the cohort (87%) received NSAIDs; 39% used tumor necrosis factor inhibitors. There were no significant between-group treatment differences.
The authors reported no potential conflicts of interest and no source of financial support.
SOURCE: Singh DK et al. J Rheumatol. 2019 Sep 1. doi: 10.3899/jrheum.181019.
FROM THE JOURNAL OF RHEUMATOLOGY
For trans children, early gender ID conversion efforts damage lifelong mental health
Gender identity conversion efforts during early childhood quadruple lifetime risk of suicidal behavior for transgender people, a study of almost 28,000 adults has determined.
The findings prompted the authors to issue a blanket warning against the controversial treatment, which already has been decried by several medical associations.
“Our results support policy positions … which state that gender identity–conversion therapy should not be conducted for transgender patients at any age, Jack L. Turban, MD, and colleagues wrote in JAMA Psychiatry.
The American Academy of Child and Adolescent Psychiatry, the American Psychiatric Association, the American Academy of Pediatrics, and the American Medical Association all strongly warn against any kind of gender conversion efforts.
The significantly increased risk of suicidal behavior was similar whether the gender identity–conversion effort (GICE) was administered by a clinician or a cleric. “This suggests that any process of intervening to alter gender identity is associated with poorer mental health regardless of whether the intervention occurred within a secular or religious framework,” wrote Dr. Turban of Massachusetts General Hospital, Boston, and coauthors.
The study – the largest of its kind thus far – comprised 27,715 transgender adults included in the 2015 U.S. Transgender Survey, conducted by the National Center for Transgender Equality.
In the current study, investigators focused on the question: “Did any professional (such as a psychologist, counselor, or religious advisor) try to make you identify only with your sex assigned at birth (in other words, try to stop you being trans)?”
They compared responses among subjects who reported exposure to GICE before age 10 years with those who did not.
Subjects were aged a mean of 31 years when they participated in the survey. Slightly less than half (42.8%) were assigned male sex at birth. Most (19,751) had discussed their gender identity with a professional. Nearly 20% (3,869) reported some exposure to GICE; 35% said a religious adviser had conducted the effort.
In this group, exposure had significant negative lifetime effects on mental health. These subjects were at a 56% increased risk of psychological distress within the month before taking the survey (odds ratio, 1.56), and more than twice as likely to have tried at least once to end their lives by suicide (OR, 2.27).
But the negative effects were even more pronounced among the small group of 206 who reported exposure to GICE before they were 10 years old. In a multivariate analysis adjusted for demographics, GICE before age 10 more than quadrupled the risk of lifetime suicide attempts (OR, 4.15). Again, it didn’t matter whether a medical or religious professional administered GICE.
“A plausible association of these practices with poor mental health outcomes can be conceptualized through the minority stress framework; that is, elevated stigma-related stress from exposure to GICE may increase general emotion dysregulation, interpersonal dysfunction, and maladaptive cognitions,” the investigators wrote. “Although this study suggests that exposure to GICE is associated with increased odds of suicide attempts, GICE are not the only way in which minority group stress manifests, and thus, other factors are also likely to be associated with suicidality among gender-diverse people.”
“One potential explanation for this is that, compared with persons in the sexual-minority group, many persons in the gender-minority group must interact with clinical professionals to be medically and surgically affirmed in their identities. This higher prevalence of interactions with clinical professionals among people in the gender minority group may lead to greater risk of experiencing conversion effort.”
The authors cited the sample size of the study as one of its many strengths. One limitation includes the study’s cross-sectional design.
Dr. Turban reported collecting royalties from Springer for an upcoming textbook about pediatric gender identity. The other coauthors reported no disclosures.
SOURCE: Turban JL et al. JAMA Psychiatry. 2019 Sep 11. doi: 10.1001/jamapsychiatry.2019.2285.
Gender identity conversion efforts during early childhood quadruple lifetime risk of suicidal behavior for transgender people, a study of almost 28,000 adults has determined.
The findings prompted the authors to issue a blanket warning against the controversial treatment, which already has been decried by several medical associations.
“Our results support policy positions … which state that gender identity–conversion therapy should not be conducted for transgender patients at any age, Jack L. Turban, MD, and colleagues wrote in JAMA Psychiatry.
The American Academy of Child and Adolescent Psychiatry, the American Psychiatric Association, the American Academy of Pediatrics, and the American Medical Association all strongly warn against any kind of gender conversion efforts.
The significantly increased risk of suicidal behavior was similar whether the gender identity–conversion effort (GICE) was administered by a clinician or a cleric. “This suggests that any process of intervening to alter gender identity is associated with poorer mental health regardless of whether the intervention occurred within a secular or religious framework,” wrote Dr. Turban of Massachusetts General Hospital, Boston, and coauthors.
The study – the largest of its kind thus far – comprised 27,715 transgender adults included in the 2015 U.S. Transgender Survey, conducted by the National Center for Transgender Equality.
In the current study, investigators focused on the question: “Did any professional (such as a psychologist, counselor, or religious advisor) try to make you identify only with your sex assigned at birth (in other words, try to stop you being trans)?”
They compared responses among subjects who reported exposure to GICE before age 10 years with those who did not.
Subjects were aged a mean of 31 years when they participated in the survey. Slightly less than half (42.8%) were assigned male sex at birth. Most (19,751) had discussed their gender identity with a professional. Nearly 20% (3,869) reported some exposure to GICE; 35% said a religious adviser had conducted the effort.
In this group, exposure had significant negative lifetime effects on mental health. These subjects were at a 56% increased risk of psychological distress within the month before taking the survey (odds ratio, 1.56), and more than twice as likely to have tried at least once to end their lives by suicide (OR, 2.27).
But the negative effects were even more pronounced among the small group of 206 who reported exposure to GICE before they were 10 years old. In a multivariate analysis adjusted for demographics, GICE before age 10 more than quadrupled the risk of lifetime suicide attempts (OR, 4.15). Again, it didn’t matter whether a medical or religious professional administered GICE.
“A plausible association of these practices with poor mental health outcomes can be conceptualized through the minority stress framework; that is, elevated stigma-related stress from exposure to GICE may increase general emotion dysregulation, interpersonal dysfunction, and maladaptive cognitions,” the investigators wrote. “Although this study suggests that exposure to GICE is associated with increased odds of suicide attempts, GICE are not the only way in which minority group stress manifests, and thus, other factors are also likely to be associated with suicidality among gender-diverse people.”
“One potential explanation for this is that, compared with persons in the sexual-minority group, many persons in the gender-minority group must interact with clinical professionals to be medically and surgically affirmed in their identities. This higher prevalence of interactions with clinical professionals among people in the gender minority group may lead to greater risk of experiencing conversion effort.”
The authors cited the sample size of the study as one of its many strengths. One limitation includes the study’s cross-sectional design.
Dr. Turban reported collecting royalties from Springer for an upcoming textbook about pediatric gender identity. The other coauthors reported no disclosures.
SOURCE: Turban JL et al. JAMA Psychiatry. 2019 Sep 11. doi: 10.1001/jamapsychiatry.2019.2285.
Gender identity conversion efforts during early childhood quadruple lifetime risk of suicidal behavior for transgender people, a study of almost 28,000 adults has determined.
The findings prompted the authors to issue a blanket warning against the controversial treatment, which already has been decried by several medical associations.
“Our results support policy positions … which state that gender identity–conversion therapy should not be conducted for transgender patients at any age, Jack L. Turban, MD, and colleagues wrote in JAMA Psychiatry.
The American Academy of Child and Adolescent Psychiatry, the American Psychiatric Association, the American Academy of Pediatrics, and the American Medical Association all strongly warn against any kind of gender conversion efforts.
The significantly increased risk of suicidal behavior was similar whether the gender identity–conversion effort (GICE) was administered by a clinician or a cleric. “This suggests that any process of intervening to alter gender identity is associated with poorer mental health regardless of whether the intervention occurred within a secular or religious framework,” wrote Dr. Turban of Massachusetts General Hospital, Boston, and coauthors.
The study – the largest of its kind thus far – comprised 27,715 transgender adults included in the 2015 U.S. Transgender Survey, conducted by the National Center for Transgender Equality.
In the current study, investigators focused on the question: “Did any professional (such as a psychologist, counselor, or religious advisor) try to make you identify only with your sex assigned at birth (in other words, try to stop you being trans)?”
They compared responses among subjects who reported exposure to GICE before age 10 years with those who did not.
Subjects were aged a mean of 31 years when they participated in the survey. Slightly less than half (42.8%) were assigned male sex at birth. Most (19,751) had discussed their gender identity with a professional. Nearly 20% (3,869) reported some exposure to GICE; 35% said a religious adviser had conducted the effort.
In this group, exposure had significant negative lifetime effects on mental health. These subjects were at a 56% increased risk of psychological distress within the month before taking the survey (odds ratio, 1.56), and more than twice as likely to have tried at least once to end their lives by suicide (OR, 2.27).
But the negative effects were even more pronounced among the small group of 206 who reported exposure to GICE before they were 10 years old. In a multivariate analysis adjusted for demographics, GICE before age 10 more than quadrupled the risk of lifetime suicide attempts (OR, 4.15). Again, it didn’t matter whether a medical or religious professional administered GICE.
“A plausible association of these practices with poor mental health outcomes can be conceptualized through the minority stress framework; that is, elevated stigma-related stress from exposure to GICE may increase general emotion dysregulation, interpersonal dysfunction, and maladaptive cognitions,” the investigators wrote. “Although this study suggests that exposure to GICE is associated with increased odds of suicide attempts, GICE are not the only way in which minority group stress manifests, and thus, other factors are also likely to be associated with suicidality among gender-diverse people.”
“One potential explanation for this is that, compared with persons in the sexual-minority group, many persons in the gender-minority group must interact with clinical professionals to be medically and surgically affirmed in their identities. This higher prevalence of interactions with clinical professionals among people in the gender minority group may lead to greater risk of experiencing conversion effort.”
The authors cited the sample size of the study as one of its many strengths. One limitation includes the study’s cross-sectional design.
Dr. Turban reported collecting royalties from Springer for an upcoming textbook about pediatric gender identity. The other coauthors reported no disclosures.
SOURCE: Turban JL et al. JAMA Psychiatry. 2019 Sep 11. doi: 10.1001/jamapsychiatry.2019.2285.
FROM JAMA PSYCHIATRY
Key clinical point: Gender identity–conversion efforts exert lifelong negative mental health impacts on transgender children.
Major finding: Exposure before age 10 years more than quadrupled the risk of lifetime suicidal behavior.
Study details: The cohort comprised 27,715 transgender adults.
Disclosures: Dr. Turban reported collecting royalties from Springer for an upcoming textbook about pediatric gender identity. No other financial disclosures were reported.
Source: Turban JL et al. JAMA Psychiatry. 2019 Sep 11. doi: 10.1001/jamapsychiatry.2019.2285.
Vape lung disease cases exceed 400, 3 dead
Vitamin E acetate is one possible culprit in the mysterious vaping-associated lung disease that has killed three patients, sickened 450, and baffled clinicians and investigators all summer.

Another death may be linked to the disorder, officials said during a joint press briefing held by the Centers for Disease Control and Prevention and the Food and Drug Administration. In all, 450 potential cases have been reported and e-cigarette use confirmed in 215. Cases have occurred in 33 states and one territory. A total of 84% of the patients reported having used tetrahydrocannabinol (THC) products in e-cigarette devices.
A preliminary report on the situation by Jennifer Layden, MD, of the department of public health in Illinois and colleagues – including a preliminary case definition – was simultaneously released in the New England Journal of Medicine (2019 Sep 6. doi: 10.1056/NEJMoa1911614).
No single device or substance was common to all the cases, leading officials to issue a blanket warning against e-cigarettes, especially those containing THC.
“We believe a chemical exposure is likely related, but more information is needed to determine what substances. Some labs have identified vitamin E acetate in some samples,” said Dana Meaney-Delman, MD, MPH, incident manager, CDC 2019 Lung Injury Response. “Continued investigation is needed to identify the risk associated with a specific product or substance.”
Besides vitamin E acetate, federal labs are looking at other cannabinoids, cutting agents, diluting agents, pesticides, opioids, and toxins.
Officials also issued a general warning about the products. Youths, young people, and pregnant women should never use e-cigarettes, they cautioned, and no one should buy them from a noncertified source, a street vendor, or a social contact. Even cartridges originally obtained from a certified source should never have been altered in any way.
Dr. Layden and colleagues reported that bilateral lung infiltrates was characterized in 98% of the 53 patients hospitalized with the recently reported e-cigarette–induced lung injury. Nonspecific constitutional symptoms, including fever, chills, weight loss, and fatigue, were present in all of the patients.
Patients may show some symptoms days or even weeks before acute respiratory failure develops, and many had sought medical help before that. All presented with bilateral lung infiltrates, part of an evolving case definition. Many complained of nonspecific constitutional symptoms, including fever, chills, gastrointestinal symptoms, and weight loss. Of the patients who underwent bronchoscopy, many were diagnosed as having lipoid pneumonia, a rare condition characterized by lipid-laden macrophages.
“We don’t know the significance of the lipid-containing macrophages, and we don’t know if the lipids are endogenous or exogenous,” Dr. Meaney-Delman said.
The incidence of such cases appears to be rising rapidly, Dr. Layden noted. An epidemiologic review of cases in Illinois found that the mean monthly rate of visits related to severe respiratory illness in June-August was twice that observed during the same months last year.
SOURCE: Layden JE et al. N Engl J Med. 2019 Sep 6. doi: 1 0.1056/NEJMoa1911614.
Vitamin E acetate is one possible culprit in the mysterious vaping-associated lung disease that has killed three patients, sickened 450, and baffled clinicians and investigators all summer.
Another death may be linked to the disorder, officials said during a joint press briefing held by the Centers for Disease Control and Prevention and the Food and Drug Administration. In all, 450 potential cases have been reported and e-cigarette use confirmed in 215. Cases have occurred in 33 states and one territory. A total of 84% of the patients reported having used tetrahydrocannabinol (THC) products in e-cigarette devices.
A preliminary report on the situation by Jennifer Layden, MD, of the department of public health in Illinois and colleagues – including a preliminary case definition – was simultaneously released in the New England Journal of Medicine (2019 Sep 6. doi: 10.1056/NEJMoa1911614).
No single device or substance was common to all the cases, leading officials to issue a blanket warning against e-cigarettes, especially those containing THC.
“We believe a chemical exposure is likely related, but more information is needed to determine what substances. Some labs have identified vitamin E acetate in some samples,” said Dana Meaney-Delman, MD, MPH, incident manager, CDC 2019 Lung Injury Response. “Continued investigation is needed to identify the risk associated with a specific product or substance.”
Besides vitamin E acetate, federal labs are looking at other cannabinoids, cutting agents, diluting agents, pesticides, opioids, and toxins.
Officials also issued a general warning about the products. Youths, young people, and pregnant women should never use e-cigarettes, they cautioned, and no one should buy them from a noncertified source, a street vendor, or a social contact. Even cartridges originally obtained from a certified source should never have been altered in any way.
Dr. Layden and colleagues reported that bilateral lung infiltrates was characterized in 98% of the 53 patients hospitalized with the recently reported e-cigarette–induced lung injury. Nonspecific constitutional symptoms, including fever, chills, weight loss, and fatigue, were present in all of the patients.
Patients may show some symptoms days or even weeks before acute respiratory failure develops, and many had sought medical help before that. All presented with bilateral lung infiltrates, part of an evolving case definition. Many complained of nonspecific constitutional symptoms, including fever, chills, gastrointestinal symptoms, and weight loss. Of the patients who underwent bronchoscopy, many were diagnosed as having lipoid pneumonia, a rare condition characterized by lipid-laden macrophages.
“We don’t know the significance of the lipid-containing macrophages, and we don’t know if the lipids are endogenous or exogenous,” Dr. Meaney-Delman said.
The incidence of such cases appears to be rising rapidly, Dr. Layden noted. An epidemiologic review of cases in Illinois found that the mean monthly rate of visits related to severe respiratory illness in June-August was twice that observed during the same months last year.
SOURCE: Layden JE et al. N Engl J Med. 2019 Sep 6. doi: 1 0.1056/NEJMoa1911614.
Vitamin E acetate is one possible culprit in the mysterious vaping-associated lung disease that has killed three patients, sickened 450, and baffled clinicians and investigators all summer.
Another death may be linked to the disorder, officials said during a joint press briefing held by the Centers for Disease Control and Prevention and the Food and Drug Administration. In all, 450 potential cases have been reported and e-cigarette use confirmed in 215. Cases have occurred in 33 states and one territory. A total of 84% of the patients reported having used tetrahydrocannabinol (THC) products in e-cigarette devices.
A preliminary report on the situation by Jennifer Layden, MD, of the department of public health in Illinois and colleagues – including a preliminary case definition – was simultaneously released in the New England Journal of Medicine (2019 Sep 6. doi: 10.1056/NEJMoa1911614).
No single device or substance was common to all the cases, leading officials to issue a blanket warning against e-cigarettes, especially those containing THC.
“We believe a chemical exposure is likely related, but more information is needed to determine what substances. Some labs have identified vitamin E acetate in some samples,” said Dana Meaney-Delman, MD, MPH, incident manager, CDC 2019 Lung Injury Response. “Continued investigation is needed to identify the risk associated with a specific product or substance.”
Besides vitamin E acetate, federal labs are looking at other cannabinoids, cutting agents, diluting agents, pesticides, opioids, and toxins.
Officials also issued a general warning about the products. Youths, young people, and pregnant women should never use e-cigarettes, they cautioned, and no one should buy them from a noncertified source, a street vendor, or a social contact. Even cartridges originally obtained from a certified source should never have been altered in any way.
Dr. Layden and colleagues reported that bilateral lung infiltrates was characterized in 98% of the 53 patients hospitalized with the recently reported e-cigarette–induced lung injury. Nonspecific constitutional symptoms, including fever, chills, weight loss, and fatigue, were present in all of the patients.
Patients may show some symptoms days or even weeks before acute respiratory failure develops, and many had sought medical help before that. All presented with bilateral lung infiltrates, part of an evolving case definition. Many complained of nonspecific constitutional symptoms, including fever, chills, gastrointestinal symptoms, and weight loss. Of the patients who underwent bronchoscopy, many were diagnosed as having lipoid pneumonia, a rare condition characterized by lipid-laden macrophages.
“We don’t know the significance of the lipid-containing macrophages, and we don’t know if the lipids are endogenous or exogenous,” Dr. Meaney-Delman said.
The incidence of such cases appears to be rising rapidly, Dr. Layden noted. An epidemiologic review of cases in Illinois found that the mean monthly rate of visits related to severe respiratory illness in June-August was twice that observed during the same months last year.
SOURCE: Layden JE et al. N Engl J Med. 2019 Sep 6. doi: 1 0.1056/NEJMoa1911614.
FROM A CDC TELECONFERENCE AND NEJM
Hyperphosphorylated tau visible in TBI survivors decades after brain injury
Brain deposits of hyperphosphorylated tau are detectable in traumatic brain injury (TBI) patients 18-51 years after a single moderate to severe incident occurred, researchers reported Sept. 4 in Science Translational Medicine.
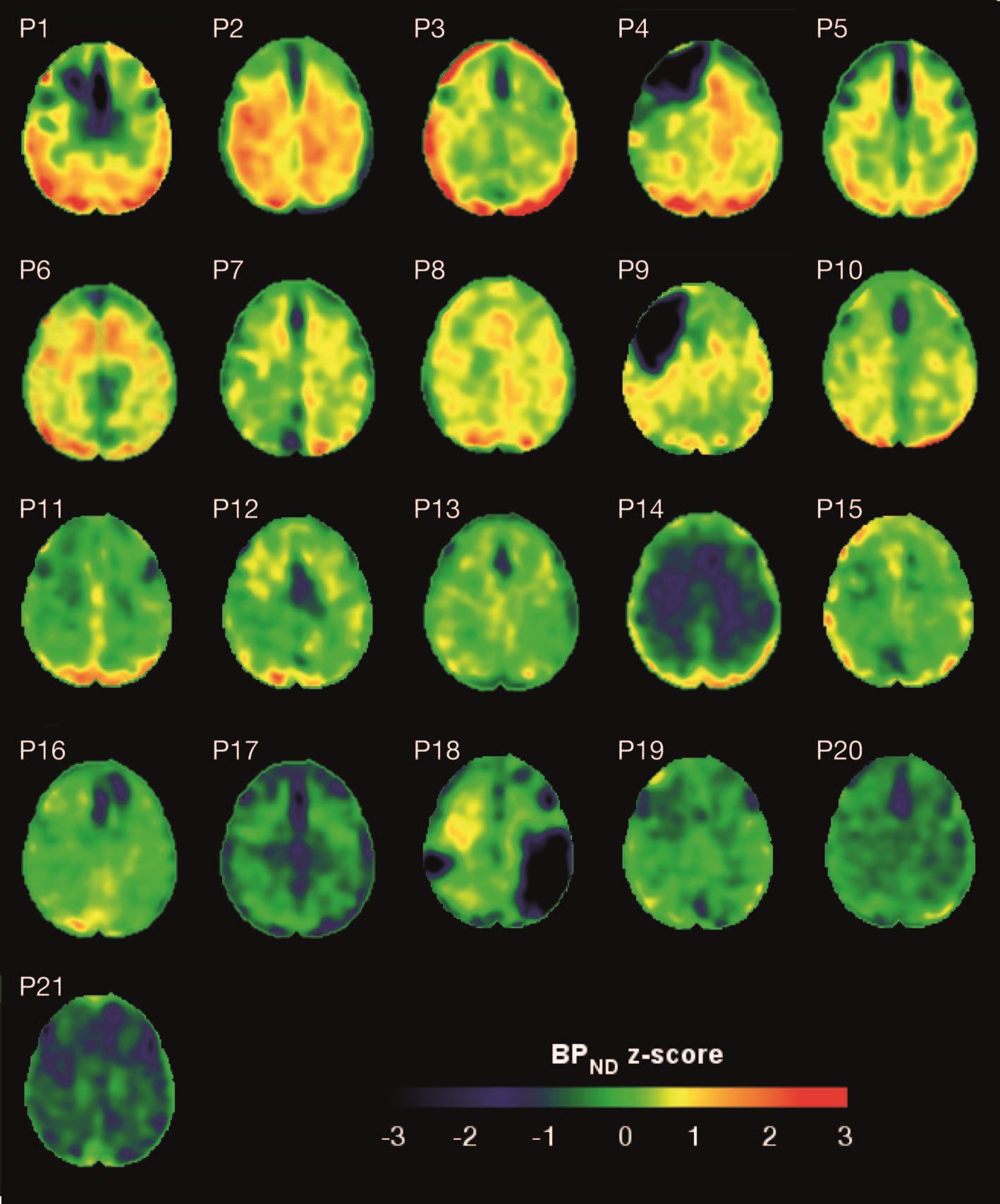
Imaging with the tau-specific PET radioligand flortaucipir showed that the protein was most apparent in the right occipital cortex, and was associated with changes in cognitive scores, tau and beta amyloid in cerebrospinal fluid (CSF), and white matter density, Nikos Gorgoraptis, PhD, of Imperial College London and his colleagues wrote.
“The ability to detect tau pathology in vivo after TBI has major potential implications for diagnosis and prognostication of clinical outcomes after TBI,” the researchers explained. “It is also likely to assist in patient selection and stratification for future treatment trials targeting tau.”
The cohort study comprised 21 subjects (median age, 49 years) who had experienced a single moderate to severe TBI a median of 32 years (range, 18-51 years) before enrollment. A control group comprised 11 noninjured adults who were matched for age and other demographic factors. Everyone underwent a PET scan with flortaucipir, brain MRI, CSF sampling, apolipoprotein E genotyping, and neuropsychological testing.
TBI subjects were grouped according to recovery status: good and disabled. Overall, they showed impairments on multiple cognitive domains (processing speed, executive function, motivation, inhibition, and verbal and visual memory), compared with controls. These findings were largely driven by the disabled group.
Eight TBI subjects had elevated tau binding greater than 2,000 voxels above the threshold of detection (equivalent to 16 cm3 of brain volume), and seven had an increase of 249-1,999 voxels above threshold. Tau binding in the remainder was similar to that in controls. Recovery status didn’t correlate with the tau-binding strength.
Overall, the tau-binding signal appeared most strongly in the right lateral occipital cortex, regardless of functional recovery status.
In TBI subjects, CSF total tau correlated significantly with flortaucipir uptake in cortical gray matter, but not white matter. CSF phosphorylated tau correlated with uptake in white matter, but not gray matter.
The investigators also examined fractional anisotropy, a measure of fiber density, axonal diameter, and myelination in white matter. In TBI subjects, there was more flortaucipir uptake in areas of decreased fractional anisotropy, including association, commissural, and projection tracts.
“Correlations were observed in the genu and body of the corpus callosum, as well as in several association tracts within the ipsilateral (right) hemisphere, including the cingulum bundle, inferior longitudinal fasciculus, uncinate fasciculus, and anterior thalamic radiation, but not in the contralateral hemisphere. Higher cortical flortaucipir [signal] was associated with reduced tissue density in remote white matter regions including the corpus callosum and right prefrontal white matter. The same analysis for gray matter density did not show an association.”
The increased tau signal in TBI subjects “is in keeping with a causative role for traumatic axonal injury in the pathophysiology of posttraumatic tau pathology,” the authors said. “Mechanical forces exerted at the time of head injury are thought to disrupt axonal organization, producing damage to microtubule structure and associated axonal tau. This damage may lead to hyperphosphorylation of tau, misfolding, and neurofibrillary tangle formation, which eventually causes neurodegeneration. Mechanical forces are maximal in points of geometric inflection such as the base of cortical sulci, where tau pathology is seen in chronic traumatic encephalopathy.”
These patterns suggest that tau imaging could provide valuable diagnostic information about the type of posttraumatic neurodegeneration, they said.
The work was supported by the Medical Research Council and UK Dementia Research Institute. None of the authors declared having any competing interests related to the current study. Some authors reported financial ties to pharmaceutical companies.
SOURCE: Gorgoraptis N et al. Sci Transl Med. 2019;11:eaaw1993. doi: 10.1126/scitranslmed.aaw1993.
Brain deposits of hyperphosphorylated tau are detectable in traumatic brain injury (TBI) patients 18-51 years after a single moderate to severe incident occurred, researchers reported Sept. 4 in Science Translational Medicine.
Imaging with the tau-specific PET radioligand flortaucipir showed that the protein was most apparent in the right occipital cortex, and was associated with changes in cognitive scores, tau and beta amyloid in cerebrospinal fluid (CSF), and white matter density, Nikos Gorgoraptis, PhD, of Imperial College London and his colleagues wrote.
“The ability to detect tau pathology in vivo after TBI has major potential implications for diagnosis and prognostication of clinical outcomes after TBI,” the researchers explained. “It is also likely to assist in patient selection and stratification for future treatment trials targeting tau.”
The cohort study comprised 21 subjects (median age, 49 years) who had experienced a single moderate to severe TBI a median of 32 years (range, 18-51 years) before enrollment. A control group comprised 11 noninjured adults who were matched for age and other demographic factors. Everyone underwent a PET scan with flortaucipir, brain MRI, CSF sampling, apolipoprotein E genotyping, and neuropsychological testing.
TBI subjects were grouped according to recovery status: good and disabled. Overall, they showed impairments on multiple cognitive domains (processing speed, executive function, motivation, inhibition, and verbal and visual memory), compared with controls. These findings were largely driven by the disabled group.
Eight TBI subjects had elevated tau binding greater than 2,000 voxels above the threshold of detection (equivalent to 16 cm3 of brain volume), and seven had an increase of 249-1,999 voxels above threshold. Tau binding in the remainder was similar to that in controls. Recovery status didn’t correlate with the tau-binding strength.
Overall, the tau-binding signal appeared most strongly in the right lateral occipital cortex, regardless of functional recovery status.
In TBI subjects, CSF total tau correlated significantly with flortaucipir uptake in cortical gray matter, but not white matter. CSF phosphorylated tau correlated with uptake in white matter, but not gray matter.
The investigators also examined fractional anisotropy, a measure of fiber density, axonal diameter, and myelination in white matter. In TBI subjects, there was more flortaucipir uptake in areas of decreased fractional anisotropy, including association, commissural, and projection tracts.
“Correlations were observed in the genu and body of the corpus callosum, as well as in several association tracts within the ipsilateral (right) hemisphere, including the cingulum bundle, inferior longitudinal fasciculus, uncinate fasciculus, and anterior thalamic radiation, but not in the contralateral hemisphere. Higher cortical flortaucipir [signal] was associated with reduced tissue density in remote white matter regions including the corpus callosum and right prefrontal white matter. The same analysis for gray matter density did not show an association.”
The increased tau signal in TBI subjects “is in keeping with a causative role for traumatic axonal injury in the pathophysiology of posttraumatic tau pathology,” the authors said. “Mechanical forces exerted at the time of head injury are thought to disrupt axonal organization, producing damage to microtubule structure and associated axonal tau. This damage may lead to hyperphosphorylation of tau, misfolding, and neurofibrillary tangle formation, which eventually causes neurodegeneration. Mechanical forces are maximal in points of geometric inflection such as the base of cortical sulci, where tau pathology is seen in chronic traumatic encephalopathy.”
These patterns suggest that tau imaging could provide valuable diagnostic information about the type of posttraumatic neurodegeneration, they said.
The work was supported by the Medical Research Council and UK Dementia Research Institute. None of the authors declared having any competing interests related to the current study. Some authors reported financial ties to pharmaceutical companies.
SOURCE: Gorgoraptis N et al. Sci Transl Med. 2019;11:eaaw1993. doi: 10.1126/scitranslmed.aaw1993.
Brain deposits of hyperphosphorylated tau are detectable in traumatic brain injury (TBI) patients 18-51 years after a single moderate to severe incident occurred, researchers reported Sept. 4 in Science Translational Medicine.
Imaging with the tau-specific PET radioligand flortaucipir showed that the protein was most apparent in the right occipital cortex, and was associated with changes in cognitive scores, tau and beta amyloid in cerebrospinal fluid (CSF), and white matter density, Nikos Gorgoraptis, PhD, of Imperial College London and his colleagues wrote.
“The ability to detect tau pathology in vivo after TBI has major potential implications for diagnosis and prognostication of clinical outcomes after TBI,” the researchers explained. “It is also likely to assist in patient selection and stratification for future treatment trials targeting tau.”
The cohort study comprised 21 subjects (median age, 49 years) who had experienced a single moderate to severe TBI a median of 32 years (range, 18-51 years) before enrollment. A control group comprised 11 noninjured adults who were matched for age and other demographic factors. Everyone underwent a PET scan with flortaucipir, brain MRI, CSF sampling, apolipoprotein E genotyping, and neuropsychological testing.
TBI subjects were grouped according to recovery status: good and disabled. Overall, they showed impairments on multiple cognitive domains (processing speed, executive function, motivation, inhibition, and verbal and visual memory), compared with controls. These findings were largely driven by the disabled group.
Eight TBI subjects had elevated tau binding greater than 2,000 voxels above the threshold of detection (equivalent to 16 cm3 of brain volume), and seven had an increase of 249-1,999 voxels above threshold. Tau binding in the remainder was similar to that in controls. Recovery status didn’t correlate with the tau-binding strength.
Overall, the tau-binding signal appeared most strongly in the right lateral occipital cortex, regardless of functional recovery status.
In TBI subjects, CSF total tau correlated significantly with flortaucipir uptake in cortical gray matter, but not white matter. CSF phosphorylated tau correlated with uptake in white matter, but not gray matter.
The investigators also examined fractional anisotropy, a measure of fiber density, axonal diameter, and myelination in white matter. In TBI subjects, there was more flortaucipir uptake in areas of decreased fractional anisotropy, including association, commissural, and projection tracts.
“Correlations were observed in the genu and body of the corpus callosum, as well as in several association tracts within the ipsilateral (right) hemisphere, including the cingulum bundle, inferior longitudinal fasciculus, uncinate fasciculus, and anterior thalamic radiation, but not in the contralateral hemisphere. Higher cortical flortaucipir [signal] was associated with reduced tissue density in remote white matter regions including the corpus callosum and right prefrontal white matter. The same analysis for gray matter density did not show an association.”
The increased tau signal in TBI subjects “is in keeping with a causative role for traumatic axonal injury in the pathophysiology of posttraumatic tau pathology,” the authors said. “Mechanical forces exerted at the time of head injury are thought to disrupt axonal organization, producing damage to microtubule structure and associated axonal tau. This damage may lead to hyperphosphorylation of tau, misfolding, and neurofibrillary tangle formation, which eventually causes neurodegeneration. Mechanical forces are maximal in points of geometric inflection such as the base of cortical sulci, where tau pathology is seen in chronic traumatic encephalopathy.”
These patterns suggest that tau imaging could provide valuable diagnostic information about the type of posttraumatic neurodegeneration, they said.
The work was supported by the Medical Research Council and UK Dementia Research Institute. None of the authors declared having any competing interests related to the current study. Some authors reported financial ties to pharmaceutical companies.
SOURCE: Gorgoraptis N et al. Sci Transl Med. 2019;11:eaaw1993. doi: 10.1126/scitranslmed.aaw1993.
FROM SCIENCE TRANSLATIONAL MEDICINE
Five genetic variations associated with same-sex sexual behavior
There is no single “gay gene.”
There are, however, signals that nonheterosexual behavior has at least some genetic component, according to Andrea Ganna, PhD, and colleagues.
Five candidate genes found in a half-million subject genetic study each account for less than 1% of the variance in same-sex sexual behavior, the scientists found. Over the entire genome, genetic variants accounted for less than a quarter of such behavior.
None of the genetic signals can reliably predict sexual behavior, Benjamin Neale, PhD, director of genetics in the Stanley Center for Psychiatric Research at the Broad Institute of the Massachusetts Institute of Technology and Harvard Medical School, both in Boston, said in a telebriefing that included Dr. Ganna, a postdoctoral researcher in his lab. Instead, the variability of human sexuality is an entirely natural continuum of human behavior.
“Whether we are attracted exclusively to the opposite sex, the same sex, or both sexes falls along a spectrum that is an integral, and entirely normal, part of the human experience,” said Dr. Neale. “The choice of a sexual partner and the fraction of partners that are of the same sex are all consistent with this diversity being a key feature of our sexual behavior as a species and this diversity is a natural part of being human.”
The study, published in Science, clarifies findings of smaller, previous studies, which determined that sexual behavior is a combination of genetics and environment – although environment is a much more difficult association to assess.
“[Environment] can range from anything in utero, all the way all the way through who you happen to stand next to on the tube in the morning, right? That’s all potentially environmental factors that can have some influence on complex traits and so we don’t really understand,” Dr. Neale said.
However, he added, the concept of individual choice in sexual behaviors was beyond the scope of the study, which strictly centered on genetic associations with sexual behavior.
The study combined genetic information from three extant databases (the U.K. Biobank, National Longitudinal Study of Adolescent to Adult Health, the Molecular Genetic Study of Sexual Orientation, and the Child and Adolescent Twin Study in Sweden) with newly collected data from 23andMe, the technology company that provides at-home genetics tests largely used to determine ethnic origin.
The primary phenotype investigated was a binary measure: self-reported sexual behavior with someone of the same sex (nonheterosexuality) or someone of the opposite sex (heterosexuality).
“The binary variable also collapses rich and multifaceted diversity among nonheterosexuality individuals, wrote Dr. Ganna and his coauthors. Therefore, “we explored finer-scaled measurements and some of the complexities of the phenotype, although intricacies of the social and cultural influences on sexuality made it impossible to fully explore this complexity.”
The team also performed replication analyses on three smaller datasets: the Molecular Genetic Study of Sexual Orientation (2,308 U.S. adult males), Add Health (4,755 U.S. young adults), and the Child and Adolescent Twin Study in Sweden (8,093 Swedish adolescents). Data were available for 188,825 males and 220,170 females overall. When broken down by sexual behavior, data were available for 1,766 homosexual and 180,431 heterosexual males, and 693 homosexual and 214,062 heterosexual females.
The team identified two genes that significantly predicted same-sex sexual behavior (rs11114975-12q21.31 and rs10261857-7q31.2). Two more genes predicted same-sex sexual behavior in males only (rs28371400-15q21.3 and rs34730029-11q12.1), and one additional gene predicted the behavior in females only (rs13135637-4p14).
Three of the single nucleotide polymorphisms (SNPs) nominally replicated those in some of the other datasets, despite the much smaller sample sizes.
“The SNPs that reached genome-wide significance had very small effects (odds ratio, 1.1),” the authors wrote. “For example, in the U.K. Biobank, males with a GT genotype at the rs34730029 locus had 0.4% higher prevalence of same-sex sexual behavior than those with a TT genotype. Nevertheless, the contribution of all measured common SNPs in aggregate was estimated to [account for] 8%-25% of variation in female and male same-sex sexual behavior. … The discrepancy between the variance captured by the significant SNPs and all common SNPs suggests that same-sex sexual behavior, like most complex human traits, is influenced by the small, additive effects of very many genetic variants, most of which cannot be detected at the current sample size.”
The Child and Adolescent Twin Study in Sweden contained the youngest subjects. The polygenic scores in this dataset were significantly associated with sexual attraction at age 15 years, “suggesting that at least some of the genetic influences on same-sex sexual behavior manifest early in sexual development.”
The team also investigated the biological pathways associated with the SNPs. Among the male variants, rs34730029-11q12.1 contains numerous olfactory receptor genes.
“Second, rs28371400-15q21.3 had several indications of being involved in sex hormone regulation. The allele positively associated with same-sex sexual behavior is associated with higher rate of male pattern balding, in which sex-hormone sensitivity is implicated,” they wrote.
This is located near the TCF12 gene, related to a normal gonadal development in mice.
Among women, there were inverse associations with the level of sex hormone–binding globulin, which regulates the balance between testosterone and estrogen.
There were significant associations with some mental health traits, including loneliness, openness to experience, and risky behaviors such as smoking and using cannabis. There were also associations with depression and schizophrenia. The genetic correlations for bipolar disorder, cannabis use, and number of sexual partners were significantly higher in females than in males.
“We emphasize that the causal processes underlying these genetic correlations are unclear and could be generated by environmental factors relating to prejudice against individuals engaging in same-sex sexual behavior,” the authors wrote.
In an interview, Jack Drescher, MD, said he was not surprised by the findings and cited the results a twin study by J. Michael Bailey, PhD, and Richard C. Pillard, MD, as evidence of the complexities surrounding sexual orientation. The study examined the likelihood of one twin having a gay twin (Arch Gen Psychiatry. 1991 Dec;48[12]:1089-96).
“If you were a gay identical twin, you had a 52% chance of having a gay twin, he said. “If you were a gay fraternal twin, you only had a 22% chance of having a gay twin. The chance of an adoptive brother being gay was 11%. If homosexuality were simply a result of simple genetic transmission, then one would expect closer to 100% gay identical twins, since they both have the same genes.”
Dr. Drescher, clinical professor of psychiatry at the Center for Psychoanalytic Training and Research at Columbia University, New York, has written extensively about human sexuality, gender-conversion therapies, and gender.
The study by Dr. Ganna and associates as a whole invalidates several commonly used sexual behavior scales, including the Kinsey Scale, which is solely predicated upon self-reported attraction. The Klein Sexual Orientation Grid, which measures sexual behavior, fantasies, and sexual identification, is similarly problematic, the authors noted.
“Overall, our findings suggest that the most popular measures are based on a misconception of the underlying structure of sexual orientation and may need to be rethought. In particular, using separate measures of attraction to the opposite sex and attraction to the same sex, such as in the Sell Assessment of Sexual Orientation, would remove the assumption that these variables are perfectly inversely related and would enable more nuanced exploration of the full diversity of sexual orientation, including bisexuality and asexuality,” they wrote.
During the telebriefing discussion, Dr. Neale said the study supports the nuances in sexuality espoused by self-identified sexual orientation communities. “I think those things that we’ve learned include the idea that there is more diversity out there in the world. We see that diversity in the genetic analysis. And we reinforce that sort of message that the expanding acronyms in the LGBTQIA+ [lesbian, gay, bisexual, transgender, queer, intersex, asexual, and other] is justified.”
The study “underscores that there is an element of biology and it underscores that there’s an element of the environment,” he said. “And it underscores that this is a natural part of our species and so these are the things that both matter and there’s no way to get away from that idea.”
Several entities funded the study, including the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Ganna reported no financial conflicts. Two of the researchers and members of the 23andMe research team are 23andMe employees or hold stock options in the company. Another researcher is affiliated with Deep Genomics as a member of its scientific advisory board.
SOURCE: Ganna A et al. Science. 2019 Aug 30. doi: 10.1126/science.aat769.
A large study that reliably shows a genetic component to nonheterosexuality could have far-reaching societal and legal impact, Melinda C. Mills, PhD, wrote in an accompanying editorial (Science. 2019 Aug 30. doi: 10.1126/science.aay2726).
“Studies have indicated that same-sex orientation and behavior has a genetic basis and runs in families, yet specific genetic variants have not been isolated,” Dr. Mills wrote. “Evidence that sexual orientation has a biological component could shape acceptance and legal protection: 4%-10% of individuals report ever engaging in same-sex behavior in the United States, so this could affect a sizable proportion of the population.”
The half-million subject genome-wide association study by Ganna et al. could go a long way toward achieving that goal – much farther than prior studies, all of which were smaller and unreplicated.
“The genetic basis of same-sex orientation and sexual behavior has evaded discovery, largely because of the challenges of using small and nonrepresentative cohorts,” Dr. Mills wrote. “Initial evidence focused mostly on gay men, providing indirect and often speculative evidence of a relationship with fraternal birth order, prenatal exposure to sex hormones, neurodevelopmental traits, or maternal immunization to sex-specific proteins. Work in the 1990s isolated a relationship with the Xq28 region on the X chromosome. Subsequent studies found similarity in the sexual orientation of identical twins, with genetics explaining 18% (for women) and 37% (for men), with the remainder accounted for by directly shared environments (such as family or school) and nonshared environments (such as legalization or norms regarding same-sex behavior).”
Despite these findings, and others hinting at a heritable genetic cause, specific variants have not been identified – until now. The finding of five predictive genes, including two specific to males and one specific to females, is novel and exciting.
Attributing same-sex orientation to genetics could enhance civil rights or reduce stigma, she wrote. “Conversely, there are fears it provides a tool for intervention or ‘cure.’ Same-sex orientation has been classified as pathological and illegal, and remains criminalized in more than 70 countries, some with the death penalty.”
By calculating the overall potential genetic contribution of 8%-25% along with the identification of specific genetic loci, Ganna et al. showed “the potential magnitude of genetic effects that we may eventually measure and a sign that complex behaviors continue to have small, likely polygenic, influences.”
Dr. Mills is the Nuffield Professor of Sociology at the University of Oxford (England). She had no relevant financial disclosures.
A large study that reliably shows a genetic component to nonheterosexuality could have far-reaching societal and legal impact, Melinda C. Mills, PhD, wrote in an accompanying editorial (Science. 2019 Aug 30. doi: 10.1126/science.aay2726).
“Studies have indicated that same-sex orientation and behavior has a genetic basis and runs in families, yet specific genetic variants have not been isolated,” Dr. Mills wrote. “Evidence that sexual orientation has a biological component could shape acceptance and legal protection: 4%-10% of individuals report ever engaging in same-sex behavior in the United States, so this could affect a sizable proportion of the population.”
The half-million subject genome-wide association study by Ganna et al. could go a long way toward achieving that goal – much farther than prior studies, all of which were smaller and unreplicated.
“The genetic basis of same-sex orientation and sexual behavior has evaded discovery, largely because of the challenges of using small and nonrepresentative cohorts,” Dr. Mills wrote. “Initial evidence focused mostly on gay men, providing indirect and often speculative evidence of a relationship with fraternal birth order, prenatal exposure to sex hormones, neurodevelopmental traits, or maternal immunization to sex-specific proteins. Work in the 1990s isolated a relationship with the Xq28 region on the X chromosome. Subsequent studies found similarity in the sexual orientation of identical twins, with genetics explaining 18% (for women) and 37% (for men), with the remainder accounted for by directly shared environments (such as family or school) and nonshared environments (such as legalization or norms regarding same-sex behavior).”
Despite these findings, and others hinting at a heritable genetic cause, specific variants have not been identified – until now. The finding of five predictive genes, including two specific to males and one specific to females, is novel and exciting.
Attributing same-sex orientation to genetics could enhance civil rights or reduce stigma, she wrote. “Conversely, there are fears it provides a tool for intervention or ‘cure.’ Same-sex orientation has been classified as pathological and illegal, and remains criminalized in more than 70 countries, some with the death penalty.”
By calculating the overall potential genetic contribution of 8%-25% along with the identification of specific genetic loci, Ganna et al. showed “the potential magnitude of genetic effects that we may eventually measure and a sign that complex behaviors continue to have small, likely polygenic, influences.”
Dr. Mills is the Nuffield Professor of Sociology at the University of Oxford (England). She had no relevant financial disclosures.
A large study that reliably shows a genetic component to nonheterosexuality could have far-reaching societal and legal impact, Melinda C. Mills, PhD, wrote in an accompanying editorial (Science. 2019 Aug 30. doi: 10.1126/science.aay2726).
“Studies have indicated that same-sex orientation and behavior has a genetic basis and runs in families, yet specific genetic variants have not been isolated,” Dr. Mills wrote. “Evidence that sexual orientation has a biological component could shape acceptance and legal protection: 4%-10% of individuals report ever engaging in same-sex behavior in the United States, so this could affect a sizable proportion of the population.”
The half-million subject genome-wide association study by Ganna et al. could go a long way toward achieving that goal – much farther than prior studies, all of which were smaller and unreplicated.
“The genetic basis of same-sex orientation and sexual behavior has evaded discovery, largely because of the challenges of using small and nonrepresentative cohorts,” Dr. Mills wrote. “Initial evidence focused mostly on gay men, providing indirect and often speculative evidence of a relationship with fraternal birth order, prenatal exposure to sex hormones, neurodevelopmental traits, or maternal immunization to sex-specific proteins. Work in the 1990s isolated a relationship with the Xq28 region on the X chromosome. Subsequent studies found similarity in the sexual orientation of identical twins, with genetics explaining 18% (for women) and 37% (for men), with the remainder accounted for by directly shared environments (such as family or school) and nonshared environments (such as legalization or norms regarding same-sex behavior).”
Despite these findings, and others hinting at a heritable genetic cause, specific variants have not been identified – until now. The finding of five predictive genes, including two specific to males and one specific to females, is novel and exciting.
Attributing same-sex orientation to genetics could enhance civil rights or reduce stigma, she wrote. “Conversely, there are fears it provides a tool for intervention or ‘cure.’ Same-sex orientation has been classified as pathological and illegal, and remains criminalized in more than 70 countries, some with the death penalty.”
By calculating the overall potential genetic contribution of 8%-25% along with the identification of specific genetic loci, Ganna et al. showed “the potential magnitude of genetic effects that we may eventually measure and a sign that complex behaviors continue to have small, likely polygenic, influences.”
Dr. Mills is the Nuffield Professor of Sociology at the University of Oxford (England). She had no relevant financial disclosures.
There is no single “gay gene.”
There are, however, signals that nonheterosexual behavior has at least some genetic component, according to Andrea Ganna, PhD, and colleagues.
Five candidate genes found in a half-million subject genetic study each account for less than 1% of the variance in same-sex sexual behavior, the scientists found. Over the entire genome, genetic variants accounted for less than a quarter of such behavior.
None of the genetic signals can reliably predict sexual behavior, Benjamin Neale, PhD, director of genetics in the Stanley Center for Psychiatric Research at the Broad Institute of the Massachusetts Institute of Technology and Harvard Medical School, both in Boston, said in a telebriefing that included Dr. Ganna, a postdoctoral researcher in his lab. Instead, the variability of human sexuality is an entirely natural continuum of human behavior.
“Whether we are attracted exclusively to the opposite sex, the same sex, or both sexes falls along a spectrum that is an integral, and entirely normal, part of the human experience,” said Dr. Neale. “The choice of a sexual partner and the fraction of partners that are of the same sex are all consistent with this diversity being a key feature of our sexual behavior as a species and this diversity is a natural part of being human.”
The study, published in Science, clarifies findings of smaller, previous studies, which determined that sexual behavior is a combination of genetics and environment – although environment is a much more difficult association to assess.
“[Environment] can range from anything in utero, all the way all the way through who you happen to stand next to on the tube in the morning, right? That’s all potentially environmental factors that can have some influence on complex traits and so we don’t really understand,” Dr. Neale said.
However, he added, the concept of individual choice in sexual behaviors was beyond the scope of the study, which strictly centered on genetic associations with sexual behavior.
The study combined genetic information from three extant databases (the U.K. Biobank, National Longitudinal Study of Adolescent to Adult Health, the Molecular Genetic Study of Sexual Orientation, and the Child and Adolescent Twin Study in Sweden) with newly collected data from 23andMe, the technology company that provides at-home genetics tests largely used to determine ethnic origin.
The primary phenotype investigated was a binary measure: self-reported sexual behavior with someone of the same sex (nonheterosexuality) or someone of the opposite sex (heterosexuality).
“The binary variable also collapses rich and multifaceted diversity among nonheterosexuality individuals, wrote Dr. Ganna and his coauthors. Therefore, “we explored finer-scaled measurements and some of the complexities of the phenotype, although intricacies of the social and cultural influences on sexuality made it impossible to fully explore this complexity.”
The team also performed replication analyses on three smaller datasets: the Molecular Genetic Study of Sexual Orientation (2,308 U.S. adult males), Add Health (4,755 U.S. young adults), and the Child and Adolescent Twin Study in Sweden (8,093 Swedish adolescents). Data were available for 188,825 males and 220,170 females overall. When broken down by sexual behavior, data were available for 1,766 homosexual and 180,431 heterosexual males, and 693 homosexual and 214,062 heterosexual females.
The team identified two genes that significantly predicted same-sex sexual behavior (rs11114975-12q21.31 and rs10261857-7q31.2). Two more genes predicted same-sex sexual behavior in males only (rs28371400-15q21.3 and rs34730029-11q12.1), and one additional gene predicted the behavior in females only (rs13135637-4p14).
Three of the single nucleotide polymorphisms (SNPs) nominally replicated those in some of the other datasets, despite the much smaller sample sizes.
“The SNPs that reached genome-wide significance had very small effects (odds ratio, 1.1),” the authors wrote. “For example, in the U.K. Biobank, males with a GT genotype at the rs34730029 locus had 0.4% higher prevalence of same-sex sexual behavior than those with a TT genotype. Nevertheless, the contribution of all measured common SNPs in aggregate was estimated to [account for] 8%-25% of variation in female and male same-sex sexual behavior. … The discrepancy between the variance captured by the significant SNPs and all common SNPs suggests that same-sex sexual behavior, like most complex human traits, is influenced by the small, additive effects of very many genetic variants, most of which cannot be detected at the current sample size.”
The Child and Adolescent Twin Study in Sweden contained the youngest subjects. The polygenic scores in this dataset were significantly associated with sexual attraction at age 15 years, “suggesting that at least some of the genetic influences on same-sex sexual behavior manifest early in sexual development.”
The team also investigated the biological pathways associated with the SNPs. Among the male variants, rs34730029-11q12.1 contains numerous olfactory receptor genes.
“Second, rs28371400-15q21.3 had several indications of being involved in sex hormone regulation. The allele positively associated with same-sex sexual behavior is associated with higher rate of male pattern balding, in which sex-hormone sensitivity is implicated,” they wrote.
This is located near the TCF12 gene, related to a normal gonadal development in mice.
Among women, there were inverse associations with the level of sex hormone–binding globulin, which regulates the balance between testosterone and estrogen.
There were significant associations with some mental health traits, including loneliness, openness to experience, and risky behaviors such as smoking and using cannabis. There were also associations with depression and schizophrenia. The genetic correlations for bipolar disorder, cannabis use, and number of sexual partners were significantly higher in females than in males.
“We emphasize that the causal processes underlying these genetic correlations are unclear and could be generated by environmental factors relating to prejudice against individuals engaging in same-sex sexual behavior,” the authors wrote.
In an interview, Jack Drescher, MD, said he was not surprised by the findings and cited the results a twin study by J. Michael Bailey, PhD, and Richard C. Pillard, MD, as evidence of the complexities surrounding sexual orientation. The study examined the likelihood of one twin having a gay twin (Arch Gen Psychiatry. 1991 Dec;48[12]:1089-96).
“If you were a gay identical twin, you had a 52% chance of having a gay twin, he said. “If you were a gay fraternal twin, you only had a 22% chance of having a gay twin. The chance of an adoptive brother being gay was 11%. If homosexuality were simply a result of simple genetic transmission, then one would expect closer to 100% gay identical twins, since they both have the same genes.”
Dr. Drescher, clinical professor of psychiatry at the Center for Psychoanalytic Training and Research at Columbia University, New York, has written extensively about human sexuality, gender-conversion therapies, and gender.
The study by Dr. Ganna and associates as a whole invalidates several commonly used sexual behavior scales, including the Kinsey Scale, which is solely predicated upon self-reported attraction. The Klein Sexual Orientation Grid, which measures sexual behavior, fantasies, and sexual identification, is similarly problematic, the authors noted.
“Overall, our findings suggest that the most popular measures are based on a misconception of the underlying structure of sexual orientation and may need to be rethought. In particular, using separate measures of attraction to the opposite sex and attraction to the same sex, such as in the Sell Assessment of Sexual Orientation, would remove the assumption that these variables are perfectly inversely related and would enable more nuanced exploration of the full diversity of sexual orientation, including bisexuality and asexuality,” they wrote.
During the telebriefing discussion, Dr. Neale said the study supports the nuances in sexuality espoused by self-identified sexual orientation communities. “I think those things that we’ve learned include the idea that there is more diversity out there in the world. We see that diversity in the genetic analysis. And we reinforce that sort of message that the expanding acronyms in the LGBTQIA+ [lesbian, gay, bisexual, transgender, queer, intersex, asexual, and other] is justified.”
The study “underscores that there is an element of biology and it underscores that there’s an element of the environment,” he said. “And it underscores that this is a natural part of our species and so these are the things that both matter and there’s no way to get away from that idea.”
Several entities funded the study, including the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Ganna reported no financial conflicts. Two of the researchers and members of the 23andMe research team are 23andMe employees or hold stock options in the company. Another researcher is affiliated with Deep Genomics as a member of its scientific advisory board.
SOURCE: Ganna A et al. Science. 2019 Aug 30. doi: 10.1126/science.aat769.
There is no single “gay gene.”
There are, however, signals that nonheterosexual behavior has at least some genetic component, according to Andrea Ganna, PhD, and colleagues.
Five candidate genes found in a half-million subject genetic study each account for less than 1% of the variance in same-sex sexual behavior, the scientists found. Over the entire genome, genetic variants accounted for less than a quarter of such behavior.
None of the genetic signals can reliably predict sexual behavior, Benjamin Neale, PhD, director of genetics in the Stanley Center for Psychiatric Research at the Broad Institute of the Massachusetts Institute of Technology and Harvard Medical School, both in Boston, said in a telebriefing that included Dr. Ganna, a postdoctoral researcher in his lab. Instead, the variability of human sexuality is an entirely natural continuum of human behavior.
“Whether we are attracted exclusively to the opposite sex, the same sex, or both sexes falls along a spectrum that is an integral, and entirely normal, part of the human experience,” said Dr. Neale. “The choice of a sexual partner and the fraction of partners that are of the same sex are all consistent with this diversity being a key feature of our sexual behavior as a species and this diversity is a natural part of being human.”
The study, published in Science, clarifies findings of smaller, previous studies, which determined that sexual behavior is a combination of genetics and environment – although environment is a much more difficult association to assess.
“[Environment] can range from anything in utero, all the way all the way through who you happen to stand next to on the tube in the morning, right? That’s all potentially environmental factors that can have some influence on complex traits and so we don’t really understand,” Dr. Neale said.
However, he added, the concept of individual choice in sexual behaviors was beyond the scope of the study, which strictly centered on genetic associations with sexual behavior.
The study combined genetic information from three extant databases (the U.K. Biobank, National Longitudinal Study of Adolescent to Adult Health, the Molecular Genetic Study of Sexual Orientation, and the Child and Adolescent Twin Study in Sweden) with newly collected data from 23andMe, the technology company that provides at-home genetics tests largely used to determine ethnic origin.
The primary phenotype investigated was a binary measure: self-reported sexual behavior with someone of the same sex (nonheterosexuality) or someone of the opposite sex (heterosexuality).
“The binary variable also collapses rich and multifaceted diversity among nonheterosexuality individuals, wrote Dr. Ganna and his coauthors. Therefore, “we explored finer-scaled measurements and some of the complexities of the phenotype, although intricacies of the social and cultural influences on sexuality made it impossible to fully explore this complexity.”
The team also performed replication analyses on three smaller datasets: the Molecular Genetic Study of Sexual Orientation (2,308 U.S. adult males), Add Health (4,755 U.S. young adults), and the Child and Adolescent Twin Study in Sweden (8,093 Swedish adolescents). Data were available for 188,825 males and 220,170 females overall. When broken down by sexual behavior, data were available for 1,766 homosexual and 180,431 heterosexual males, and 693 homosexual and 214,062 heterosexual females.
The team identified two genes that significantly predicted same-sex sexual behavior (rs11114975-12q21.31 and rs10261857-7q31.2). Two more genes predicted same-sex sexual behavior in males only (rs28371400-15q21.3 and rs34730029-11q12.1), and one additional gene predicted the behavior in females only (rs13135637-4p14).
Three of the single nucleotide polymorphisms (SNPs) nominally replicated those in some of the other datasets, despite the much smaller sample sizes.
“The SNPs that reached genome-wide significance had very small effects (odds ratio, 1.1),” the authors wrote. “For example, in the U.K. Biobank, males with a GT genotype at the rs34730029 locus had 0.4% higher prevalence of same-sex sexual behavior than those with a TT genotype. Nevertheless, the contribution of all measured common SNPs in aggregate was estimated to [account for] 8%-25% of variation in female and male same-sex sexual behavior. … The discrepancy between the variance captured by the significant SNPs and all common SNPs suggests that same-sex sexual behavior, like most complex human traits, is influenced by the small, additive effects of very many genetic variants, most of which cannot be detected at the current sample size.”
The Child and Adolescent Twin Study in Sweden contained the youngest subjects. The polygenic scores in this dataset were significantly associated with sexual attraction at age 15 years, “suggesting that at least some of the genetic influences on same-sex sexual behavior manifest early in sexual development.”
The team also investigated the biological pathways associated with the SNPs. Among the male variants, rs34730029-11q12.1 contains numerous olfactory receptor genes.
“Second, rs28371400-15q21.3 had several indications of being involved in sex hormone regulation. The allele positively associated with same-sex sexual behavior is associated with higher rate of male pattern balding, in which sex-hormone sensitivity is implicated,” they wrote.
This is located near the TCF12 gene, related to a normal gonadal development in mice.
Among women, there were inverse associations with the level of sex hormone–binding globulin, which regulates the balance between testosterone and estrogen.
There were significant associations with some mental health traits, including loneliness, openness to experience, and risky behaviors such as smoking and using cannabis. There were also associations with depression and schizophrenia. The genetic correlations for bipolar disorder, cannabis use, and number of sexual partners were significantly higher in females than in males.
“We emphasize that the causal processes underlying these genetic correlations are unclear and could be generated by environmental factors relating to prejudice against individuals engaging in same-sex sexual behavior,” the authors wrote.
In an interview, Jack Drescher, MD, said he was not surprised by the findings and cited the results a twin study by J. Michael Bailey, PhD, and Richard C. Pillard, MD, as evidence of the complexities surrounding sexual orientation. The study examined the likelihood of one twin having a gay twin (Arch Gen Psychiatry. 1991 Dec;48[12]:1089-96).
“If you were a gay identical twin, you had a 52% chance of having a gay twin, he said. “If you were a gay fraternal twin, you only had a 22% chance of having a gay twin. The chance of an adoptive brother being gay was 11%. If homosexuality were simply a result of simple genetic transmission, then one would expect closer to 100% gay identical twins, since they both have the same genes.”
Dr. Drescher, clinical professor of psychiatry at the Center for Psychoanalytic Training and Research at Columbia University, New York, has written extensively about human sexuality, gender-conversion therapies, and gender.
The study by Dr. Ganna and associates as a whole invalidates several commonly used sexual behavior scales, including the Kinsey Scale, which is solely predicated upon self-reported attraction. The Klein Sexual Orientation Grid, which measures sexual behavior, fantasies, and sexual identification, is similarly problematic, the authors noted.
“Overall, our findings suggest that the most popular measures are based on a misconception of the underlying structure of sexual orientation and may need to be rethought. In particular, using separate measures of attraction to the opposite sex and attraction to the same sex, such as in the Sell Assessment of Sexual Orientation, would remove the assumption that these variables are perfectly inversely related and would enable more nuanced exploration of the full diversity of sexual orientation, including bisexuality and asexuality,” they wrote.
During the telebriefing discussion, Dr. Neale said the study supports the nuances in sexuality espoused by self-identified sexual orientation communities. “I think those things that we’ve learned include the idea that there is more diversity out there in the world. We see that diversity in the genetic analysis. And we reinforce that sort of message that the expanding acronyms in the LGBTQIA+ [lesbian, gay, bisexual, transgender, queer, intersex, asexual, and other] is justified.”
The study “underscores that there is an element of biology and it underscores that there’s an element of the environment,” he said. “And it underscores that this is a natural part of our species and so these are the things that both matter and there’s no way to get away from that idea.”
Several entities funded the study, including the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Ganna reported no financial conflicts. Two of the researchers and members of the 23andMe research team are 23andMe employees or hold stock options in the company. Another researcher is affiliated with Deep Genomics as a member of its scientific advisory board.
SOURCE: Ganna A et al. Science. 2019 Aug 30. doi: 10.1126/science.aat769.
FROM SCIENCE
Key clinical point: Genetic variants do appear to contribute to same-sex sexual behaviors.
Major finding: Five single nucleotide polymorphisms each account for about 1% of the variability in sexual behavior, while across a large population, genetic variants account for 8%-25% of the variation.
Study details: The genome-wide association study was made up of about 500,000 subjects.
Disclosures: The study was funded by several entities, including the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Ganna reported no financial conflicts. Two of the researchers and members of the 23andMe research team are 23andMe employees or hold stock options in the company. Another researcher is affiliated with Deep Genomics as a member of its scientific advisory board.
Source: Ganna A et al. Science. 2019 Aug 30. doi: 10.1126/science.aat769.
Ambulatory BP monitoring slightly better than in-office measures for predicting cardiovascular outcomes
Continuous blood pressure monitoring is significantly better than in-office measurements at predicting the risk of cardiovascular events and death, although the additional prognostic benefit is quite small, wrote Wen-Yi Yang, MD, and colleagues. Their report is in JAMA.

In light of this finding, 24-hour monitoring is probably best reserved for select patients – especially those with white coat hypertension, and those who self-report hypertension but test within normal parameters in the office, said Philip Greenland, MD, Harry W. Dingman Professor of Cardiology at Northwestern University, Chicago, who wrote a perspective piece published along with the study.
“The good news is that, for the average patient, the office measurement is highly predictive and performs extremely well,” Dr. Greenland said in an interview. “Ambulatory monitoring will get you very little additional information. But if you are getting a 24-hour reading, the measures you probably want to focus on are the nighttime pressures and the overall 24-hour average.”
Dr. Yang of the University of Leuven, Belgium, and his team were “trying to make sense of this huge amount of data that’s available now that ambulatory blood pressure monitoring systems are much more common,” Dr. Greenland said. “The real clinical question is, ‘If I’m getting all this information, how do I interpret it?’ ”
To investigate this, the authors evaluated blood pressure and cardiovascular outcomes among more than 11,000 subjects enrolled in the International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcome (IDACO).
The median individual follow-up was about 14 years, although some patients were followed up to 22 years. All told, the study posted 153,140 person-years of follow-up. These patients were a mean of 55 years old at enrollment; almost 12% had a history of cardiovascular disease. Most (83%) had three automated in-office blood pressure measurements; 5% had two, and 2% had a single measurement. There were 55 24-hour ambulatory readings, 28 for daytime only, and 11 for nighttime.
The mean in-office automated BP was 135/82. The mean 24-hour BP was 123/74; the mean daytime pressure, 130/79; and the mean nighttime pressure, 113/65.
The authors recorded blood pressure–dipping status: 50% were normal, 18% had extreme dipping, 25% had no dipping, and 6% had reverse dipping. The mean dipping ratio was 0.87.
A regression analysis adjusted for sex, age, body mass index, smoking, and alcohol use, serum cholesterol, antihypertensive drugs, cardiovascular disease and diabetes.
Over the entire study period, there were 2,836 deaths and 2,049 cardiovascular events – a rate of 13.4 per 1,000 person-years. Both cardiovascular events and mortality were significantly associated with all ambulatory BP measurements, compared with in-office measurements. For nighttime systolic BP, the hazard ratio for mortality was 1.23 and 1.36 for cardiovascular events. For the 24-hour measure, the HR for mortality was 1.22, and for cardiovascular events, 1.45. Hazard ratios represented the risk associated with a 20–mm Hg higher systolic blood pressure or a 0.10 difference in dipping ratio.
However, the area under the curve for a single, in-office systolic BP was quite good, at 0.83 for mortality and 0.84 for cardiovascular events. Adding 24-hour measurements or nighttime systolic BP to the model resulted only in very, very small “incremental” improvements in AUC of 0.0013 and 0.0027, respectively
“The current population-based study confirmed previous research indicating that ambulatory BP monitoring over and beyond measures taken in clinicians’ offices improved risk stratification among patients with or suspected of having hypertension,” The authors wrote. “It strengthened the notion that nighttime BP measures carry valuable prognostic information.”
However, they admitted that the addition these measures offer to the AUC for BP measurements was “incremental.”
“This metric is not very sensitive in model comparisons if the basic model performs well, as was the case in the current study. … The prevailing perception among experts is that BP is the strongest modifiable risk factor. The small increments in change in the AUC challenge this concept. Thus an important issue in the evaluation of an additional risk prediction marker is how to interpret a small AUC increase, which many researchers believe is an imprecise metric because it increases only slightly with the introduction of an additional marker in multivariable-adjusted models, even if the marker under study carries great risk, as reflected by the odds ratio (or HR).”
One investigator, Krzysztof Narkiewicz, MD, reported receiving lecture fees from numerous pharmaceutical and device companies. No other disclosures were reported.
SOURCE: Yang W et al. JAMA. 2019;322(5):409-20.
Continuous blood pressure monitoring is significantly better than in-office measurements at predicting the risk of cardiovascular events and death, although the additional prognostic benefit is quite small, wrote Wen-Yi Yang, MD, and colleagues. Their report is in JAMA.
In light of this finding, 24-hour monitoring is probably best reserved for select patients – especially those with white coat hypertension, and those who self-report hypertension but test within normal parameters in the office, said Philip Greenland, MD, Harry W. Dingman Professor of Cardiology at Northwestern University, Chicago, who wrote a perspective piece published along with the study.
“The good news is that, for the average patient, the office measurement is highly predictive and performs extremely well,” Dr. Greenland said in an interview. “Ambulatory monitoring will get you very little additional information. But if you are getting a 24-hour reading, the measures you probably want to focus on are the nighttime pressures and the overall 24-hour average.”
Dr. Yang of the University of Leuven, Belgium, and his team were “trying to make sense of this huge amount of data that’s available now that ambulatory blood pressure monitoring systems are much more common,” Dr. Greenland said. “The real clinical question is, ‘If I’m getting all this information, how do I interpret it?’ ”
To investigate this, the authors evaluated blood pressure and cardiovascular outcomes among more than 11,000 subjects enrolled in the International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcome (IDACO).
The median individual follow-up was about 14 years, although some patients were followed up to 22 years. All told, the study posted 153,140 person-years of follow-up. These patients were a mean of 55 years old at enrollment; almost 12% had a history of cardiovascular disease. Most (83%) had three automated in-office blood pressure measurements; 5% had two, and 2% had a single measurement. There were 55 24-hour ambulatory readings, 28 for daytime only, and 11 for nighttime.
The mean in-office automated BP was 135/82. The mean 24-hour BP was 123/74; the mean daytime pressure, 130/79; and the mean nighttime pressure, 113/65.
The authors recorded blood pressure–dipping status: 50% were normal, 18% had extreme dipping, 25% had no dipping, and 6% had reverse dipping. The mean dipping ratio was 0.87.
A regression analysis adjusted for sex, age, body mass index, smoking, and alcohol use, serum cholesterol, antihypertensive drugs, cardiovascular disease and diabetes.
Over the entire study period, there were 2,836 deaths and 2,049 cardiovascular events – a rate of 13.4 per 1,000 person-years. Both cardiovascular events and mortality were significantly associated with all ambulatory BP measurements, compared with in-office measurements. For nighttime systolic BP, the hazard ratio for mortality was 1.23 and 1.36 for cardiovascular events. For the 24-hour measure, the HR for mortality was 1.22, and for cardiovascular events, 1.45. Hazard ratios represented the risk associated with a 20–mm Hg higher systolic blood pressure or a 0.10 difference in dipping ratio.
However, the area under the curve for a single, in-office systolic BP was quite good, at 0.83 for mortality and 0.84 for cardiovascular events. Adding 24-hour measurements or nighttime systolic BP to the model resulted only in very, very small “incremental” improvements in AUC of 0.0013 and 0.0027, respectively
“The current population-based study confirmed previous research indicating that ambulatory BP monitoring over and beyond measures taken in clinicians’ offices improved risk stratification among patients with or suspected of having hypertension,” The authors wrote. “It strengthened the notion that nighttime BP measures carry valuable prognostic information.”
However, they admitted that the addition these measures offer to the AUC for BP measurements was “incremental.”
“This metric is not very sensitive in model comparisons if the basic model performs well, as was the case in the current study. … The prevailing perception among experts is that BP is the strongest modifiable risk factor. The small increments in change in the AUC challenge this concept. Thus an important issue in the evaluation of an additional risk prediction marker is how to interpret a small AUC increase, which many researchers believe is an imprecise metric because it increases only slightly with the introduction of an additional marker in multivariable-adjusted models, even if the marker under study carries great risk, as reflected by the odds ratio (or HR).”
One investigator, Krzysztof Narkiewicz, MD, reported receiving lecture fees from numerous pharmaceutical and device companies. No other disclosures were reported.
SOURCE: Yang W et al. JAMA. 2019;322(5):409-20.
Continuous blood pressure monitoring is significantly better than in-office measurements at predicting the risk of cardiovascular events and death, although the additional prognostic benefit is quite small, wrote Wen-Yi Yang, MD, and colleagues. Their report is in JAMA.
In light of this finding, 24-hour monitoring is probably best reserved for select patients – especially those with white coat hypertension, and those who self-report hypertension but test within normal parameters in the office, said Philip Greenland, MD, Harry W. Dingman Professor of Cardiology at Northwestern University, Chicago, who wrote a perspective piece published along with the study.
“The good news is that, for the average patient, the office measurement is highly predictive and performs extremely well,” Dr. Greenland said in an interview. “Ambulatory monitoring will get you very little additional information. But if you are getting a 24-hour reading, the measures you probably want to focus on are the nighttime pressures and the overall 24-hour average.”
Dr. Yang of the University of Leuven, Belgium, and his team were “trying to make sense of this huge amount of data that’s available now that ambulatory blood pressure monitoring systems are much more common,” Dr. Greenland said. “The real clinical question is, ‘If I’m getting all this information, how do I interpret it?’ ”
To investigate this, the authors evaluated blood pressure and cardiovascular outcomes among more than 11,000 subjects enrolled in the International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcome (IDACO).
The median individual follow-up was about 14 years, although some patients were followed up to 22 years. All told, the study posted 153,140 person-years of follow-up. These patients were a mean of 55 years old at enrollment; almost 12% had a history of cardiovascular disease. Most (83%) had three automated in-office blood pressure measurements; 5% had two, and 2% had a single measurement. There were 55 24-hour ambulatory readings, 28 for daytime only, and 11 for nighttime.
The mean in-office automated BP was 135/82. The mean 24-hour BP was 123/74; the mean daytime pressure, 130/79; and the mean nighttime pressure, 113/65.
The authors recorded blood pressure–dipping status: 50% were normal, 18% had extreme dipping, 25% had no dipping, and 6% had reverse dipping. The mean dipping ratio was 0.87.
A regression analysis adjusted for sex, age, body mass index, smoking, and alcohol use, serum cholesterol, antihypertensive drugs, cardiovascular disease and diabetes.
Over the entire study period, there were 2,836 deaths and 2,049 cardiovascular events – a rate of 13.4 per 1,000 person-years. Both cardiovascular events and mortality were significantly associated with all ambulatory BP measurements, compared with in-office measurements. For nighttime systolic BP, the hazard ratio for mortality was 1.23 and 1.36 for cardiovascular events. For the 24-hour measure, the HR for mortality was 1.22, and for cardiovascular events, 1.45. Hazard ratios represented the risk associated with a 20–mm Hg higher systolic blood pressure or a 0.10 difference in dipping ratio.
However, the area under the curve for a single, in-office systolic BP was quite good, at 0.83 for mortality and 0.84 for cardiovascular events. Adding 24-hour measurements or nighttime systolic BP to the model resulted only in very, very small “incremental” improvements in AUC of 0.0013 and 0.0027, respectively
“The current population-based study confirmed previous research indicating that ambulatory BP monitoring over and beyond measures taken in clinicians’ offices improved risk stratification among patients with or suspected of having hypertension,” The authors wrote. “It strengthened the notion that nighttime BP measures carry valuable prognostic information.”
However, they admitted that the addition these measures offer to the AUC for BP measurements was “incremental.”
“This metric is not very sensitive in model comparisons if the basic model performs well, as was the case in the current study. … The prevailing perception among experts is that BP is the strongest modifiable risk factor. The small increments in change in the AUC challenge this concept. Thus an important issue in the evaluation of an additional risk prediction marker is how to interpret a small AUC increase, which many researchers believe is an imprecise metric because it increases only slightly with the introduction of an additional marker in multivariable-adjusted models, even if the marker under study carries great risk, as reflected by the odds ratio (or HR).”
One investigator, Krzysztof Narkiewicz, MD, reported receiving lecture fees from numerous pharmaceutical and device companies. No other disclosures were reported.
SOURCE: Yang W et al. JAMA. 2019;322(5):409-20.
FROM JAMA