User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Greater travel distance reduces rates of abortion
Travel distance is an important determinant of access to abortion care in the United States, new findings show.
Increases in median travel distance to the nearest abortion care facility were associated with significant reductions in median abortion rate.
The abortion rate was 21.1 per 1,000 female residents of reproductive age among those who lived less than 5 miles from a facility, but that number dropped to 3.9/1,000 for those living 120 miles or further away.
Overall, in a model of 3,107 U.S. counties that included 62.5 million women of reproductive age, there were an estimated 696,760 abortions (at a mean rate of 11.1/1,000). The authors estimate that if abortion services were integrated into primary care, an additional 18,190 abortions would be performed (mean rate, 11.4/1,000).
Similarly, if telemedicine became widely available in this setting, this would allow approximately 70,920 abortions (mean rate 12.3/1,000). The study was published online in JAMA Open Network.
Reducing travel distances to abortion facilities would increase access, but additional clinics and providers would be needed to meet the demand. But as the population density of many counties with poor access is low, innovative strategies are also needed.
Integrating abortion into primary care or making medication abortion care available by telemedicine may decrease this unmet need, and lead author Kirsten Thompson, MPH, noted that there is growing evidence that both solutions are quite feasible to implement.
“A study published in 2018 has led primary care providers to adopt the same regimen for miscarriage care, showing that they are interested and capable, despite the barriers posed by the mifepristone [Risk Evaluation and Mitigation Strategy] program for these patients,” said Ms. Thompson, who is program and communications director, Bixby Center for Global Reproductive Health, University of California, San Francisco. “Medical education programs designed specifically for primary care providers have trained family medicine and other clinicians in abortion care for over a decade.”
As for telemedicine, Ms. Thompson explained that, during the pandemic, a preliminary injunction in a federal court case and then the Food and Drug Administration suspended enforcement of the in-person requirements of the mifepristone REMS. “In states that allow medical abortion care by telemedicine, providers have been able to offer remote care when medically appropriate, including mailing medical abortion pills to patients at home,” she said. “Researchers have already published evidence on the safety of and patient satisfaction with this approach.”
However, there are two main barriers to the widespread adoption of medical abortion by telemedicine in the United States. “One is the potentially temporary nature of the FDA’s enforcement discretion and second, are the 19 states with laws that ban it, singling out medical abortion as somehow different from other forms of care by telemedicine,” she said.
Study details
About one in four women in the United States will terminate a pregnancy during their lifetime, but the issue is highly contentious and many states have implemented policies that restrict access to abortion care. The authors pointed out that studies have documented clinic closures and women being unable to obtain abortion care, with low-income women and non-White women being disproportionately affected. Increased travel to a provider has also been associated with delays in care as well as increased costs and stress.
Prior research has shown that the further a woman lives from a facility, the less likely she is to obtain abortion care. In this study, Ms. Thompson and colleagues examined the association between travel distance to the nearest abortion care facility and the abortion rate, and then modeled the effect of reduced travel distance on rates.
They first conducted a cross-sectional geographic analysis using the American Community Survey and the U.S. Census to calculate county-level abortion rates per 1,000 women aged between 15 and 44 years. The 2015 data covered 1,948 counties in 27 states.
Abortion rates were then estimated for 3,107 counties in 48 states and the effect of different travel distance scenarios on the abortion rate was also estimated by multivariable model. Data were collected from April 2018 to October 2019.
There were 37.3 million women of reproductive age residing in the 27 states, and a total of 428,720 reported abortions (mean rate, 11.5/1,000; median rate, 9.9/1,000 women).
When looking at all 48 states, the population-weighted mean travel distance to the nearest facility was 25.6 miles, with a median travel distance of 8.2 miles.
A multivariable model showed that a greater travel distance was associated with lower abortion rates. When compared with traveling less than 5 miles, the abortion rate declined by 0.05/1,000 for women traveling between 5 to less than 15 miles for care, 0.22 for those traveling 15 to less than 30 miles, 0.34 for 30 to less than 60 miles, 0.43 for 60 to less than 120 miles, and 0.73 for those traveling 120 miles or more.
They estimated that, if all travel was under 30 miles, there would be a 2.6% increase or 18,190 additional abortions. A simulation also showed that there would be a 10.2% increase (70,920 additional abortions) using medication via telemedicine.
Solutions are feasible
Approached for an independent comment, Sarah W. Prager, MD, MAS, professor of obstetrics and gynecology and division chief, complex family planning, at the University of Washington, Seattle, agreed that the solutions proposed by the authors were feasible.
“More than a third of abortions that are eligible are now done with medication,” she said, “And 89% of abortions are done in the first trimester.”
What this means is that early first-trimester abortions can conceivably be performed in the primary care setting. “Any primary care clinician – whether it’s a family practice or internal medicine physician, or nurse practitioner or nurse midwife – can all be trained to do aspiration or prescribe medication in the first trimester,” said Dr. Prager. “So it could easily be integrated into primary care settings if there was motivation for that to happen.”
However, she emphasized that more is involved than just training the provider. “The whole clinic has to buy into it,” Dr. Prager explained. “The nurses have to be willing to assist, you need the medical assistants, the scheduler or person who works the front desk – the whole clinic system has to buy into it and that’s where it becomes more challenging.”
The individual provider may be willing, but the system may still not be allowing that to happen. “This is also where telemedicine can come in, where the medication can be mailed so it can circumvent the problem to a certain extent,” Dr. Prager added. “You don’t have to have the infrastructure in the same way.”
But many states already have laws in place to make that illegal, especially for abortion care even if they allow it for similar types of care.
Another expert also weighed in and agreed that these two solutions can potentially be implemented.
“The concept of decreased rates of abortion associated with greater distances traveled is not new, but what is unique to this manuscript is the estimations that the authors conducted in understanding the impact of expanding access to abortion among primary care and telehealth providers,” said Catherine Cansino, MD, MPH, associate clinical professor in the department of obstetrics and gynecology, University of California, Davis.
“The study provides convincing evidence regarding the need to strengthen infrastructures that support expansion of these services in primary care settings, among physicians and advanced care practitioners,” she said. “Training to provide medical abortion and first-trimester surgical abortion is simple. Many primary care providers are already doing gynecologic procedures – IUD insertions, colposcopies, endometrial biopsies.”
Thus, she noted, adding abortion care “to their toolkit isn’t too far of a stretch.”
As for telemedicine, Dr. Cansino pointed out how the COVID-19 pandemic has also expanded what both patients and providers think are safe options for providing and receiving good care. “Consultations through telemedicine coupled with access to medications for medical abortion through local pharmacies or express mail is definitely safe and feasible.”
The study was supported by the William and Flora Hewlett Foundation and by an anonymous foundation for general operating support (Ms Thompson). Ms. Thompson reported receiving personal fees from GenBioPro outside the submitted work. Dr. Cansino and Dr. Prager have no disclosures.
Travel distance is an important determinant of access to abortion care in the United States, new findings show.
Increases in median travel distance to the nearest abortion care facility were associated with significant reductions in median abortion rate.
The abortion rate was 21.1 per 1,000 female residents of reproductive age among those who lived less than 5 miles from a facility, but that number dropped to 3.9/1,000 for those living 120 miles or further away.
Overall, in a model of 3,107 U.S. counties that included 62.5 million women of reproductive age, there were an estimated 696,760 abortions (at a mean rate of 11.1/1,000). The authors estimate that if abortion services were integrated into primary care, an additional 18,190 abortions would be performed (mean rate, 11.4/1,000).
Similarly, if telemedicine became widely available in this setting, this would allow approximately 70,920 abortions (mean rate 12.3/1,000). The study was published online in JAMA Open Network.
Reducing travel distances to abortion facilities would increase access, but additional clinics and providers would be needed to meet the demand. But as the population density of many counties with poor access is low, innovative strategies are also needed.
Integrating abortion into primary care or making medication abortion care available by telemedicine may decrease this unmet need, and lead author Kirsten Thompson, MPH, noted that there is growing evidence that both solutions are quite feasible to implement.
“A study published in 2018 has led primary care providers to adopt the same regimen for miscarriage care, showing that they are interested and capable, despite the barriers posed by the mifepristone [Risk Evaluation and Mitigation Strategy] program for these patients,” said Ms. Thompson, who is program and communications director, Bixby Center for Global Reproductive Health, University of California, San Francisco. “Medical education programs designed specifically for primary care providers have trained family medicine and other clinicians in abortion care for over a decade.”
As for telemedicine, Ms. Thompson explained that, during the pandemic, a preliminary injunction in a federal court case and then the Food and Drug Administration suspended enforcement of the in-person requirements of the mifepristone REMS. “In states that allow medical abortion care by telemedicine, providers have been able to offer remote care when medically appropriate, including mailing medical abortion pills to patients at home,” she said. “Researchers have already published evidence on the safety of and patient satisfaction with this approach.”
However, there are two main barriers to the widespread adoption of medical abortion by telemedicine in the United States. “One is the potentially temporary nature of the FDA’s enforcement discretion and second, are the 19 states with laws that ban it, singling out medical abortion as somehow different from other forms of care by telemedicine,” she said.
Study details
About one in four women in the United States will terminate a pregnancy during their lifetime, but the issue is highly contentious and many states have implemented policies that restrict access to abortion care. The authors pointed out that studies have documented clinic closures and women being unable to obtain abortion care, with low-income women and non-White women being disproportionately affected. Increased travel to a provider has also been associated with delays in care as well as increased costs and stress.
Prior research has shown that the further a woman lives from a facility, the less likely she is to obtain abortion care. In this study, Ms. Thompson and colleagues examined the association between travel distance to the nearest abortion care facility and the abortion rate, and then modeled the effect of reduced travel distance on rates.
They first conducted a cross-sectional geographic analysis using the American Community Survey and the U.S. Census to calculate county-level abortion rates per 1,000 women aged between 15 and 44 years. The 2015 data covered 1,948 counties in 27 states.
Abortion rates were then estimated for 3,107 counties in 48 states and the effect of different travel distance scenarios on the abortion rate was also estimated by multivariable model. Data were collected from April 2018 to October 2019.
There were 37.3 million women of reproductive age residing in the 27 states, and a total of 428,720 reported abortions (mean rate, 11.5/1,000; median rate, 9.9/1,000 women).
When looking at all 48 states, the population-weighted mean travel distance to the nearest facility was 25.6 miles, with a median travel distance of 8.2 miles.
A multivariable model showed that a greater travel distance was associated with lower abortion rates. When compared with traveling less than 5 miles, the abortion rate declined by 0.05/1,000 for women traveling between 5 to less than 15 miles for care, 0.22 for those traveling 15 to less than 30 miles, 0.34 for 30 to less than 60 miles, 0.43 for 60 to less than 120 miles, and 0.73 for those traveling 120 miles or more.
They estimated that, if all travel was under 30 miles, there would be a 2.6% increase or 18,190 additional abortions. A simulation also showed that there would be a 10.2% increase (70,920 additional abortions) using medication via telemedicine.
Solutions are feasible
Approached for an independent comment, Sarah W. Prager, MD, MAS, professor of obstetrics and gynecology and division chief, complex family planning, at the University of Washington, Seattle, agreed that the solutions proposed by the authors were feasible.
“More than a third of abortions that are eligible are now done with medication,” she said, “And 89% of abortions are done in the first trimester.”
What this means is that early first-trimester abortions can conceivably be performed in the primary care setting. “Any primary care clinician – whether it’s a family practice or internal medicine physician, or nurse practitioner or nurse midwife – can all be trained to do aspiration or prescribe medication in the first trimester,” said Dr. Prager. “So it could easily be integrated into primary care settings if there was motivation for that to happen.”
However, she emphasized that more is involved than just training the provider. “The whole clinic has to buy into it,” Dr. Prager explained. “The nurses have to be willing to assist, you need the medical assistants, the scheduler or person who works the front desk – the whole clinic system has to buy into it and that’s where it becomes more challenging.”
The individual provider may be willing, but the system may still not be allowing that to happen. “This is also where telemedicine can come in, where the medication can be mailed so it can circumvent the problem to a certain extent,” Dr. Prager added. “You don’t have to have the infrastructure in the same way.”
But many states already have laws in place to make that illegal, especially for abortion care even if they allow it for similar types of care.
Another expert also weighed in and agreed that these two solutions can potentially be implemented.
“The concept of decreased rates of abortion associated with greater distances traveled is not new, but what is unique to this manuscript is the estimations that the authors conducted in understanding the impact of expanding access to abortion among primary care and telehealth providers,” said Catherine Cansino, MD, MPH, associate clinical professor in the department of obstetrics and gynecology, University of California, Davis.
“The study provides convincing evidence regarding the need to strengthen infrastructures that support expansion of these services in primary care settings, among physicians and advanced care practitioners,” she said. “Training to provide medical abortion and first-trimester surgical abortion is simple. Many primary care providers are already doing gynecologic procedures – IUD insertions, colposcopies, endometrial biopsies.”
Thus, she noted, adding abortion care “to their toolkit isn’t too far of a stretch.”
As for telemedicine, Dr. Cansino pointed out how the COVID-19 pandemic has also expanded what both patients and providers think are safe options for providing and receiving good care. “Consultations through telemedicine coupled with access to medications for medical abortion through local pharmacies or express mail is definitely safe and feasible.”
The study was supported by the William and Flora Hewlett Foundation and by an anonymous foundation for general operating support (Ms Thompson). Ms. Thompson reported receiving personal fees from GenBioPro outside the submitted work. Dr. Cansino and Dr. Prager have no disclosures.
Travel distance is an important determinant of access to abortion care in the United States, new findings show.
Increases in median travel distance to the nearest abortion care facility were associated with significant reductions in median abortion rate.
The abortion rate was 21.1 per 1,000 female residents of reproductive age among those who lived less than 5 miles from a facility, but that number dropped to 3.9/1,000 for those living 120 miles or further away.
Overall, in a model of 3,107 U.S. counties that included 62.5 million women of reproductive age, there were an estimated 696,760 abortions (at a mean rate of 11.1/1,000). The authors estimate that if abortion services were integrated into primary care, an additional 18,190 abortions would be performed (mean rate, 11.4/1,000).
Similarly, if telemedicine became widely available in this setting, this would allow approximately 70,920 abortions (mean rate 12.3/1,000). The study was published online in JAMA Open Network.
Reducing travel distances to abortion facilities would increase access, but additional clinics and providers would be needed to meet the demand. But as the population density of many counties with poor access is low, innovative strategies are also needed.
Integrating abortion into primary care or making medication abortion care available by telemedicine may decrease this unmet need, and lead author Kirsten Thompson, MPH, noted that there is growing evidence that both solutions are quite feasible to implement.
“A study published in 2018 has led primary care providers to adopt the same regimen for miscarriage care, showing that they are interested and capable, despite the barriers posed by the mifepristone [Risk Evaluation and Mitigation Strategy] program for these patients,” said Ms. Thompson, who is program and communications director, Bixby Center for Global Reproductive Health, University of California, San Francisco. “Medical education programs designed specifically for primary care providers have trained family medicine and other clinicians in abortion care for over a decade.”
As for telemedicine, Ms. Thompson explained that, during the pandemic, a preliminary injunction in a federal court case and then the Food and Drug Administration suspended enforcement of the in-person requirements of the mifepristone REMS. “In states that allow medical abortion care by telemedicine, providers have been able to offer remote care when medically appropriate, including mailing medical abortion pills to patients at home,” she said. “Researchers have already published evidence on the safety of and patient satisfaction with this approach.”
However, there are two main barriers to the widespread adoption of medical abortion by telemedicine in the United States. “One is the potentially temporary nature of the FDA’s enforcement discretion and second, are the 19 states with laws that ban it, singling out medical abortion as somehow different from other forms of care by telemedicine,” she said.
Study details
About one in four women in the United States will terminate a pregnancy during their lifetime, but the issue is highly contentious and many states have implemented policies that restrict access to abortion care. The authors pointed out that studies have documented clinic closures and women being unable to obtain abortion care, with low-income women and non-White women being disproportionately affected. Increased travel to a provider has also been associated with delays in care as well as increased costs and stress.
Prior research has shown that the further a woman lives from a facility, the less likely she is to obtain abortion care. In this study, Ms. Thompson and colleagues examined the association between travel distance to the nearest abortion care facility and the abortion rate, and then modeled the effect of reduced travel distance on rates.
They first conducted a cross-sectional geographic analysis using the American Community Survey and the U.S. Census to calculate county-level abortion rates per 1,000 women aged between 15 and 44 years. The 2015 data covered 1,948 counties in 27 states.
Abortion rates were then estimated for 3,107 counties in 48 states and the effect of different travel distance scenarios on the abortion rate was also estimated by multivariable model. Data were collected from April 2018 to October 2019.
There were 37.3 million women of reproductive age residing in the 27 states, and a total of 428,720 reported abortions (mean rate, 11.5/1,000; median rate, 9.9/1,000 women).
When looking at all 48 states, the population-weighted mean travel distance to the nearest facility was 25.6 miles, with a median travel distance of 8.2 miles.
A multivariable model showed that a greater travel distance was associated with lower abortion rates. When compared with traveling less than 5 miles, the abortion rate declined by 0.05/1,000 for women traveling between 5 to less than 15 miles for care, 0.22 for those traveling 15 to less than 30 miles, 0.34 for 30 to less than 60 miles, 0.43 for 60 to less than 120 miles, and 0.73 for those traveling 120 miles or more.
They estimated that, if all travel was under 30 miles, there would be a 2.6% increase or 18,190 additional abortions. A simulation also showed that there would be a 10.2% increase (70,920 additional abortions) using medication via telemedicine.
Solutions are feasible
Approached for an independent comment, Sarah W. Prager, MD, MAS, professor of obstetrics and gynecology and division chief, complex family planning, at the University of Washington, Seattle, agreed that the solutions proposed by the authors were feasible.
“More than a third of abortions that are eligible are now done with medication,” she said, “And 89% of abortions are done in the first trimester.”
What this means is that early first-trimester abortions can conceivably be performed in the primary care setting. “Any primary care clinician – whether it’s a family practice or internal medicine physician, or nurse practitioner or nurse midwife – can all be trained to do aspiration or prescribe medication in the first trimester,” said Dr. Prager. “So it could easily be integrated into primary care settings if there was motivation for that to happen.”
However, she emphasized that more is involved than just training the provider. “The whole clinic has to buy into it,” Dr. Prager explained. “The nurses have to be willing to assist, you need the medical assistants, the scheduler or person who works the front desk – the whole clinic system has to buy into it and that’s where it becomes more challenging.”
The individual provider may be willing, but the system may still not be allowing that to happen. “This is also where telemedicine can come in, where the medication can be mailed so it can circumvent the problem to a certain extent,” Dr. Prager added. “You don’t have to have the infrastructure in the same way.”
But many states already have laws in place to make that illegal, especially for abortion care even if they allow it for similar types of care.
Another expert also weighed in and agreed that these two solutions can potentially be implemented.
“The concept of decreased rates of abortion associated with greater distances traveled is not new, but what is unique to this manuscript is the estimations that the authors conducted in understanding the impact of expanding access to abortion among primary care and telehealth providers,” said Catherine Cansino, MD, MPH, associate clinical professor in the department of obstetrics and gynecology, University of California, Davis.
“The study provides convincing evidence regarding the need to strengthen infrastructures that support expansion of these services in primary care settings, among physicians and advanced care practitioners,” she said. “Training to provide medical abortion and first-trimester surgical abortion is simple. Many primary care providers are already doing gynecologic procedures – IUD insertions, colposcopies, endometrial biopsies.”
Thus, she noted, adding abortion care “to their toolkit isn’t too far of a stretch.”
As for telemedicine, Dr. Cansino pointed out how the COVID-19 pandemic has also expanded what both patients and providers think are safe options for providing and receiving good care. “Consultations through telemedicine coupled with access to medications for medical abortion through local pharmacies or express mail is definitely safe and feasible.”
The study was supported by the William and Flora Hewlett Foundation and by an anonymous foundation for general operating support (Ms Thompson). Ms. Thompson reported receiving personal fees from GenBioPro outside the submitted work. Dr. Cansino and Dr. Prager have no disclosures.
FROM JAMA NETWORK OPEN
Antimicrobial resistance threat continues during COVID-19
The stark realities of antimicrobial resistance – including rising rates of difficult-to-treat infections, lack of a robust pipeline of future antimicrobials, and COVID-19 treatments that leave people more vulnerable to infections – remain urgent priorities, experts say.
For some patients, the pandemic and antimicrobial resistance (AMR) are intertwined.
“One patient I’m seeing now in service really underscores how the two interact,” Vance Fowler, MD, said during a June 30 media briefing sponsored by the Infectious Diseases Society of America (IDSA). A man in his mid-40s, married with a small child, developed COVID-19 in early January 2021. He was intubated, spent about 1 month in the ICU, and managed to survive.
“But since then he has been struck with a series of progressively more drug resistant bacteria,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C., and chair of the IDSA Antimicrobial Resistance Committee.
The patient acquired Pseudomonas ventilator-associated pneumonia. Although the infection initially responded to standard antibiotics, he has experienced relapses over the past few months. Through these multiple infections the Pseudomonas grew increasingly pan-resistant to treatment.
The only remaining antimicrobial agent for this patient, Dr. Fowler said, is “a case study in what we are describing ... a drug that is used relatively infrequently, that is fairly expensive, but for that particular patient is absolutely vital.”
A ‘terrifying’ personal experience
Tori Kinamon, a Duke University medical student and Food and Drug Administration antibacterial drug resistance fellow, joined Dr. Fowler at the IDSA briefing. She shared her personal journey of surviving a methicillin-resistant Staphylococcus aureus (MRSA) infection, one that sparked her interest in becoming a physician.
“I had a very frightening and unexpected confrontation with antimicrobial resistance when I was a freshman in college,” Ms. Kinamon said.
A few days after competing in a Division One gymnastics championship, she felt a gradual onset of pain in her left hamstring. The pain grew acutely worse and, within days, her leg become red, swollen, and painful to the touch.
Ms. Kinamon was admitted to the hospital for suspected cellulitis and put on intravenous antibiotics.
“However, my clinical condition continued to decline,” she recalled. “Imaging studies revealed a 15-cm abscess deep in my hamstring.”
The limb- and life-threatening infection left her wondering if she would come out of surgery with both legs.
“Ultimately, I had eight surgeries in 2 weeks,” she said.
“As a 19-year-old collegiate athlete, that’s terrifying. And I never imagined that something like that would happen to me – until it did,” said Ms. Kinamon, who is an NCAA infection prevention advocate.
When Ms. Kinamon’s kidneys could no longer tolerate vancomycin, she was switched to daptomycin.
“I reflect quite frequently on how having that one extra drug in the stockpile had a significant impact on my outcome,” she said.
Incentivizing new antimicrobial agents
A lack of new antimicrobials in development is not a new story.
“There’s been a chill that’s been sustained on the antibiotic development field. Most large pharmaceutical companies have left the area of anti-infectants and the bulk of research and development is now in small pharmaceutical companies,” Dr. Fowler said. “And they’re struggling.”
One potential solution is the Pasteur Act, a bipartisan bill reintroduced in Congress and supported by IDSA. The bill encourages pharmaceutical companies to develop new antimicrobial agents with funding not linked to sales or use of the drugs.
Furthermore, the bill emphasizes appropriate use of these agents through effective stewardship programs.
Although some institutions shifted resources away from AMR out of necessity when COVID-19 struck, “I can say certainly from our experience at Duke that at least stewardship was alive and well. It was not relegated to the side,” Dr. Fowler said.
“In fact,” he added, “if anything, COVID really emphasized the importance of stewardship” by helping clinicians with guidance on the use of remdesivir and other antivirals during the pandemic.
Also, in some instances, treatments used to keep people with COVID-19 alive can paradoxically place them at higher risk for other infections, Dr. Fowler said, citing corticosteroids as an example.
Everyone’s concern
AMR isn’t just an issue in hospital settings, either. Ms. Kinamon reiterated that she picked up the infection in an athletic environment.
“Antimicrobial resistance is not just a problem for ICU patients in the hospital. I was the healthiest I had ever been and just very nearly escaped death due to one of these infections,” she said. ”As rates of resistance rise as these pathogens become more virulent, AMR is becoming more and more of a community threat,” she added.
Furthermore, consumers are partially to blame as well, Dr. Fowler noted.
“It’s interesting when you look at the surveys of the numbers of patients that have used someone else’s antibiotics” or leftover antimicrobial agents from a prior infection.
“It’s really startling ... that’s the sort of antibiotic overuse that directly contributes to antibacterial resistance,” he said.
Reasons for optimism
Promising advances in diagnostics, treatment, and prevention of AMRs are underway, Dr. Fowler said.
“It always gets me really excited to talk about it. It’s amazing what technology and scientific discovery can bring to this discussion and to this threat,” he said.
For example, there is a “silent revolution” in diagnostics with the aim to rapidly provide life-saving actionable data on a real patient in nearly real time.
Traditionally, “you start off by treating what should be there” while awaiting results of tests to narrow down therapy, Dr. Fowler said. However, a whole host of new platforms are in development to reduce the time to susceptibility results. This kind of technology has “the potential to transform our ability to take care of patients, giving them the right drug at the right time and no more,” he said.
Another promising avenue of research involves bacteriophages. Dr. Fowler is principal investigator on a clinical trial underway to evaluate bacteriophages as adjunct therapy for MRSA bacteremia.
When it comes to prevention on AMR infections in the future, “I continue to be optimistic about the possibility of vaccines to prevent many of these infections,” Dr. Fowler said, adding that companies are working on vaccines against these kinds of infections caused by MRSA or Escherichia coli, for example.
Patient outcomes
The man in his 40s with the multidrug resistant Pseudomonas infections “is now to the point where he’s walking in the halls and I think he’ll get out of the hospital eventually,” Dr. Fowler said.
“But his life is forever changed,” he added.
Ms. Kinamon’s recovery from MRSA included time in the ICU, 1 month in a regular hospital setting, and 5 months at home.
“It sparked my interest in antibiotic research and development because I see myself as a direct beneficiary of the stockpile of antibiotics that were available to treat my infection,” Ms. Kinamon said. “Now as a medical student working with patients who have similar infections, I feel a deep empathy and connectedness to them because they ask the same questions that I did.”
A version of this article first appeared on WebMD.com.
The stark realities of antimicrobial resistance – including rising rates of difficult-to-treat infections, lack of a robust pipeline of future antimicrobials, and COVID-19 treatments that leave people more vulnerable to infections – remain urgent priorities, experts say.
For some patients, the pandemic and antimicrobial resistance (AMR) are intertwined.
“One patient I’m seeing now in service really underscores how the two interact,” Vance Fowler, MD, said during a June 30 media briefing sponsored by the Infectious Diseases Society of America (IDSA). A man in his mid-40s, married with a small child, developed COVID-19 in early January 2021. He was intubated, spent about 1 month in the ICU, and managed to survive.
“But since then he has been struck with a series of progressively more drug resistant bacteria,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C., and chair of the IDSA Antimicrobial Resistance Committee.
The patient acquired Pseudomonas ventilator-associated pneumonia. Although the infection initially responded to standard antibiotics, he has experienced relapses over the past few months. Through these multiple infections the Pseudomonas grew increasingly pan-resistant to treatment.
The only remaining antimicrobial agent for this patient, Dr. Fowler said, is “a case study in what we are describing ... a drug that is used relatively infrequently, that is fairly expensive, but for that particular patient is absolutely vital.”
A ‘terrifying’ personal experience
Tori Kinamon, a Duke University medical student and Food and Drug Administration antibacterial drug resistance fellow, joined Dr. Fowler at the IDSA briefing. She shared her personal journey of surviving a methicillin-resistant Staphylococcus aureus (MRSA) infection, one that sparked her interest in becoming a physician.
“I had a very frightening and unexpected confrontation with antimicrobial resistance when I was a freshman in college,” Ms. Kinamon said.
A few days after competing in a Division One gymnastics championship, she felt a gradual onset of pain in her left hamstring. The pain grew acutely worse and, within days, her leg become red, swollen, and painful to the touch.
Ms. Kinamon was admitted to the hospital for suspected cellulitis and put on intravenous antibiotics.
“However, my clinical condition continued to decline,” she recalled. “Imaging studies revealed a 15-cm abscess deep in my hamstring.”
The limb- and life-threatening infection left her wondering if she would come out of surgery with both legs.
“Ultimately, I had eight surgeries in 2 weeks,” she said.
“As a 19-year-old collegiate athlete, that’s terrifying. And I never imagined that something like that would happen to me – until it did,” said Ms. Kinamon, who is an NCAA infection prevention advocate.
When Ms. Kinamon’s kidneys could no longer tolerate vancomycin, she was switched to daptomycin.
“I reflect quite frequently on how having that one extra drug in the stockpile had a significant impact on my outcome,” she said.
Incentivizing new antimicrobial agents
A lack of new antimicrobials in development is not a new story.
“There’s been a chill that’s been sustained on the antibiotic development field. Most large pharmaceutical companies have left the area of anti-infectants and the bulk of research and development is now in small pharmaceutical companies,” Dr. Fowler said. “And they’re struggling.”
One potential solution is the Pasteur Act, a bipartisan bill reintroduced in Congress and supported by IDSA. The bill encourages pharmaceutical companies to develop new antimicrobial agents with funding not linked to sales or use of the drugs.
Furthermore, the bill emphasizes appropriate use of these agents through effective stewardship programs.
Although some institutions shifted resources away from AMR out of necessity when COVID-19 struck, “I can say certainly from our experience at Duke that at least stewardship was alive and well. It was not relegated to the side,” Dr. Fowler said.
“In fact,” he added, “if anything, COVID really emphasized the importance of stewardship” by helping clinicians with guidance on the use of remdesivir and other antivirals during the pandemic.
Also, in some instances, treatments used to keep people with COVID-19 alive can paradoxically place them at higher risk for other infections, Dr. Fowler said, citing corticosteroids as an example.
Everyone’s concern
AMR isn’t just an issue in hospital settings, either. Ms. Kinamon reiterated that she picked up the infection in an athletic environment.
“Antimicrobial resistance is not just a problem for ICU patients in the hospital. I was the healthiest I had ever been and just very nearly escaped death due to one of these infections,” she said. ”As rates of resistance rise as these pathogens become more virulent, AMR is becoming more and more of a community threat,” she added.
Furthermore, consumers are partially to blame as well, Dr. Fowler noted.
“It’s interesting when you look at the surveys of the numbers of patients that have used someone else’s antibiotics” or leftover antimicrobial agents from a prior infection.
“It’s really startling ... that’s the sort of antibiotic overuse that directly contributes to antibacterial resistance,” he said.
Reasons for optimism
Promising advances in diagnostics, treatment, and prevention of AMRs are underway, Dr. Fowler said.
“It always gets me really excited to talk about it. It’s amazing what technology and scientific discovery can bring to this discussion and to this threat,” he said.
For example, there is a “silent revolution” in diagnostics with the aim to rapidly provide life-saving actionable data on a real patient in nearly real time.
Traditionally, “you start off by treating what should be there” while awaiting results of tests to narrow down therapy, Dr. Fowler said. However, a whole host of new platforms are in development to reduce the time to susceptibility results. This kind of technology has “the potential to transform our ability to take care of patients, giving them the right drug at the right time and no more,” he said.
Another promising avenue of research involves bacteriophages. Dr. Fowler is principal investigator on a clinical trial underway to evaluate bacteriophages as adjunct therapy for MRSA bacteremia.
When it comes to prevention on AMR infections in the future, “I continue to be optimistic about the possibility of vaccines to prevent many of these infections,” Dr. Fowler said, adding that companies are working on vaccines against these kinds of infections caused by MRSA or Escherichia coli, for example.
Patient outcomes
The man in his 40s with the multidrug resistant Pseudomonas infections “is now to the point where he’s walking in the halls and I think he’ll get out of the hospital eventually,” Dr. Fowler said.
“But his life is forever changed,” he added.
Ms. Kinamon’s recovery from MRSA included time in the ICU, 1 month in a regular hospital setting, and 5 months at home.
“It sparked my interest in antibiotic research and development because I see myself as a direct beneficiary of the stockpile of antibiotics that were available to treat my infection,” Ms. Kinamon said. “Now as a medical student working with patients who have similar infections, I feel a deep empathy and connectedness to them because they ask the same questions that I did.”
A version of this article first appeared on WebMD.com.
The stark realities of antimicrobial resistance – including rising rates of difficult-to-treat infections, lack of a robust pipeline of future antimicrobials, and COVID-19 treatments that leave people more vulnerable to infections – remain urgent priorities, experts say.
For some patients, the pandemic and antimicrobial resistance (AMR) are intertwined.
“One patient I’m seeing now in service really underscores how the two interact,” Vance Fowler, MD, said during a June 30 media briefing sponsored by the Infectious Diseases Society of America (IDSA). A man in his mid-40s, married with a small child, developed COVID-19 in early January 2021. He was intubated, spent about 1 month in the ICU, and managed to survive.
“But since then he has been struck with a series of progressively more drug resistant bacteria,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C., and chair of the IDSA Antimicrobial Resistance Committee.
The patient acquired Pseudomonas ventilator-associated pneumonia. Although the infection initially responded to standard antibiotics, he has experienced relapses over the past few months. Through these multiple infections the Pseudomonas grew increasingly pan-resistant to treatment.
The only remaining antimicrobial agent for this patient, Dr. Fowler said, is “a case study in what we are describing ... a drug that is used relatively infrequently, that is fairly expensive, but for that particular patient is absolutely vital.”
A ‘terrifying’ personal experience
Tori Kinamon, a Duke University medical student and Food and Drug Administration antibacterial drug resistance fellow, joined Dr. Fowler at the IDSA briefing. She shared her personal journey of surviving a methicillin-resistant Staphylococcus aureus (MRSA) infection, one that sparked her interest in becoming a physician.
“I had a very frightening and unexpected confrontation with antimicrobial resistance when I was a freshman in college,” Ms. Kinamon said.
A few days after competing in a Division One gymnastics championship, she felt a gradual onset of pain in her left hamstring. The pain grew acutely worse and, within days, her leg become red, swollen, and painful to the touch.
Ms. Kinamon was admitted to the hospital for suspected cellulitis and put on intravenous antibiotics.
“However, my clinical condition continued to decline,” she recalled. “Imaging studies revealed a 15-cm abscess deep in my hamstring.”
The limb- and life-threatening infection left her wondering if she would come out of surgery with both legs.
“Ultimately, I had eight surgeries in 2 weeks,” she said.
“As a 19-year-old collegiate athlete, that’s terrifying. And I never imagined that something like that would happen to me – until it did,” said Ms. Kinamon, who is an NCAA infection prevention advocate.
When Ms. Kinamon’s kidneys could no longer tolerate vancomycin, she was switched to daptomycin.
“I reflect quite frequently on how having that one extra drug in the stockpile had a significant impact on my outcome,” she said.
Incentivizing new antimicrobial agents
A lack of new antimicrobials in development is not a new story.
“There’s been a chill that’s been sustained on the antibiotic development field. Most large pharmaceutical companies have left the area of anti-infectants and the bulk of research and development is now in small pharmaceutical companies,” Dr. Fowler said. “And they’re struggling.”
One potential solution is the Pasteur Act, a bipartisan bill reintroduced in Congress and supported by IDSA. The bill encourages pharmaceutical companies to develop new antimicrobial agents with funding not linked to sales or use of the drugs.
Furthermore, the bill emphasizes appropriate use of these agents through effective stewardship programs.
Although some institutions shifted resources away from AMR out of necessity when COVID-19 struck, “I can say certainly from our experience at Duke that at least stewardship was alive and well. It was not relegated to the side,” Dr. Fowler said.
“In fact,” he added, “if anything, COVID really emphasized the importance of stewardship” by helping clinicians with guidance on the use of remdesivir and other antivirals during the pandemic.
Also, in some instances, treatments used to keep people with COVID-19 alive can paradoxically place them at higher risk for other infections, Dr. Fowler said, citing corticosteroids as an example.
Everyone’s concern
AMR isn’t just an issue in hospital settings, either. Ms. Kinamon reiterated that she picked up the infection in an athletic environment.
“Antimicrobial resistance is not just a problem for ICU patients in the hospital. I was the healthiest I had ever been and just very nearly escaped death due to one of these infections,” she said. ”As rates of resistance rise as these pathogens become more virulent, AMR is becoming more and more of a community threat,” she added.
Furthermore, consumers are partially to blame as well, Dr. Fowler noted.
“It’s interesting when you look at the surveys of the numbers of patients that have used someone else’s antibiotics” or leftover antimicrobial agents from a prior infection.
“It’s really startling ... that’s the sort of antibiotic overuse that directly contributes to antibacterial resistance,” he said.
Reasons for optimism
Promising advances in diagnostics, treatment, and prevention of AMRs are underway, Dr. Fowler said.
“It always gets me really excited to talk about it. It’s amazing what technology and scientific discovery can bring to this discussion and to this threat,” he said.
For example, there is a “silent revolution” in diagnostics with the aim to rapidly provide life-saving actionable data on a real patient in nearly real time.
Traditionally, “you start off by treating what should be there” while awaiting results of tests to narrow down therapy, Dr. Fowler said. However, a whole host of new platforms are in development to reduce the time to susceptibility results. This kind of technology has “the potential to transform our ability to take care of patients, giving them the right drug at the right time and no more,” he said.
Another promising avenue of research involves bacteriophages. Dr. Fowler is principal investigator on a clinical trial underway to evaluate bacteriophages as adjunct therapy for MRSA bacteremia.
When it comes to prevention on AMR infections in the future, “I continue to be optimistic about the possibility of vaccines to prevent many of these infections,” Dr. Fowler said, adding that companies are working on vaccines against these kinds of infections caused by MRSA or Escherichia coli, for example.
Patient outcomes
The man in his 40s with the multidrug resistant Pseudomonas infections “is now to the point where he’s walking in the halls and I think he’ll get out of the hospital eventually,” Dr. Fowler said.
“But his life is forever changed,” he added.
Ms. Kinamon’s recovery from MRSA included time in the ICU, 1 month in a regular hospital setting, and 5 months at home.
“It sparked my interest in antibiotic research and development because I see myself as a direct beneficiary of the stockpile of antibiotics that were available to treat my infection,” Ms. Kinamon said. “Now as a medical student working with patients who have similar infections, I feel a deep empathy and connectedness to them because they ask the same questions that I did.”
A version of this article first appeared on WebMD.com.
CDC notes sharp declines in breast and cervical cancer screening
The new data come from the National Breast and Cervical Cancer Early Detection Program (NBCCEDP), a program that provides cancer screening services to women with low income and inadequate health insurance.
The data show that the total number of screenings funded by the NBCCEDP declined by 87% for breast cancer screening and by 84% for cervical cancer screening in April 2020 in comparison with the previous 5-year averages for that month.
The declines in breast cancer screening varied from 84% among Hispanic women to 98% among American Indian/Alaskan Native women. The declines in cervical cancer screening varied from 82% among Black women to 92% among Asian Pacific Islander women.
In April 2020, breast cancer screening declined by 86% in metro areas, 88% in urban areas, and 89% in rural areas in comparison with respective 5-year averages. For cervical cancer screenings, the corresponding declines were 85%, 77%, and 82%.
The findings are consistent with those from studies conducted in insured populations, note the authors, led by the Amy DeGroff, PhD, MPH, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion.
“Prolonged delays in screening related to the COVID-19 pandemic may lead to delayed diagnoses, poor health consequences, and an increase in cancer disparities among women already experiencing health inequities,” the CDC states in a press release.
Women from racial and ethnic minority groups already face a disproportionate burden of cervical and breast cancers in the United States: Black women and Hispanic women have the highest rates of cervical cancer incidence (8.3 and 8.9 per 100,000 women, respectively, vs. 7.3 per 100,000 among White women) and the highest rates of cervical cancer deaths. Black women have the highest rate of breast cancer death (26.9 per 100,000 women, vs. 19.4 per 100,000 among White women), the study authors explain.
Although the volume of screening began to recover in May 2020 – test volumes for breast and cervical cancer were 39% and 40% below the 5-year average by June 2020 – breast cancer screening in rural areas remained 52% below the 5-year average, they report.
The findings were published online June 30 in Preventive Medicine.
“This study highlights a decline in cancer screening among women of racial and ethnic minority groups with low incomes when their access to medical services decreased at the beginning of the pandemic,” Dr. DeGroff comments in the CDC press release.
The findings “reinforce the need to safely maintain routine health care services during the pandemic, especially when the health care environment meets COVID-19 safety guidelines,” she adds.
The investigators used NBCCEDP administrative and program data reported to the CDC by awardees – organizations that receive funding to implement the NBCCEDP – to assess the impact of COVID-19 on the number of breast and cervical cancer screening tests administered through the program and the effects of COVID-19 on the availability of screening services and NBCCEDP awardees’ capacity to support partner clinics.
A total of 630,264 breast and 594,566 cervical cancer screening tests were conducted during the review period of January-June 2015-2020.
Despite COVID-related challenges, “a large number of awardees reported flexibility and creative efforts to reach women and support clinics’ resumption of clinical care, including screening, during the COVID-19 pandemic,” the authors write.
“[The] CDC encourages health care professionals to help minimize delays in testing by continuing routine cancer screening for women having symptoms or at high risk for breast or cervical cancer,” Dr. DeGroff commented. “The Early Detection Program can help women overcome barriers to health equity by educating them about the importance of routine screening, addressing their concerns about COVID-19 transmission, and helping them to safely access screening through interventions like patient navigation.”
Future studies will examine the effect of the pandemic on screening during the second half of 2020, when surges of COVID-19 and their timing varied geographically, they note.
A version of this article first appeared on Medscape.com.
The new data come from the National Breast and Cervical Cancer Early Detection Program (NBCCEDP), a program that provides cancer screening services to women with low income and inadequate health insurance.
The data show that the total number of screenings funded by the NBCCEDP declined by 87% for breast cancer screening and by 84% for cervical cancer screening in April 2020 in comparison with the previous 5-year averages for that month.
The declines in breast cancer screening varied from 84% among Hispanic women to 98% among American Indian/Alaskan Native women. The declines in cervical cancer screening varied from 82% among Black women to 92% among Asian Pacific Islander women.
In April 2020, breast cancer screening declined by 86% in metro areas, 88% in urban areas, and 89% in rural areas in comparison with respective 5-year averages. For cervical cancer screenings, the corresponding declines were 85%, 77%, and 82%.
The findings are consistent with those from studies conducted in insured populations, note the authors, led by the Amy DeGroff, PhD, MPH, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion.
“Prolonged delays in screening related to the COVID-19 pandemic may lead to delayed diagnoses, poor health consequences, and an increase in cancer disparities among women already experiencing health inequities,” the CDC states in a press release.
Women from racial and ethnic minority groups already face a disproportionate burden of cervical and breast cancers in the United States: Black women and Hispanic women have the highest rates of cervical cancer incidence (8.3 and 8.9 per 100,000 women, respectively, vs. 7.3 per 100,000 among White women) and the highest rates of cervical cancer deaths. Black women have the highest rate of breast cancer death (26.9 per 100,000 women, vs. 19.4 per 100,000 among White women), the study authors explain.
Although the volume of screening began to recover in May 2020 – test volumes for breast and cervical cancer were 39% and 40% below the 5-year average by June 2020 – breast cancer screening in rural areas remained 52% below the 5-year average, they report.
The findings were published online June 30 in Preventive Medicine.
“This study highlights a decline in cancer screening among women of racial and ethnic minority groups with low incomes when their access to medical services decreased at the beginning of the pandemic,” Dr. DeGroff comments in the CDC press release.
The findings “reinforce the need to safely maintain routine health care services during the pandemic, especially when the health care environment meets COVID-19 safety guidelines,” she adds.
The investigators used NBCCEDP administrative and program data reported to the CDC by awardees – organizations that receive funding to implement the NBCCEDP – to assess the impact of COVID-19 on the number of breast and cervical cancer screening tests administered through the program and the effects of COVID-19 on the availability of screening services and NBCCEDP awardees’ capacity to support partner clinics.
A total of 630,264 breast and 594,566 cervical cancer screening tests were conducted during the review period of January-June 2015-2020.
Despite COVID-related challenges, “a large number of awardees reported flexibility and creative efforts to reach women and support clinics’ resumption of clinical care, including screening, during the COVID-19 pandemic,” the authors write.
“[The] CDC encourages health care professionals to help minimize delays in testing by continuing routine cancer screening for women having symptoms or at high risk for breast or cervical cancer,” Dr. DeGroff commented. “The Early Detection Program can help women overcome barriers to health equity by educating them about the importance of routine screening, addressing their concerns about COVID-19 transmission, and helping them to safely access screening through interventions like patient navigation.”
Future studies will examine the effect of the pandemic on screening during the second half of 2020, when surges of COVID-19 and their timing varied geographically, they note.
A version of this article first appeared on Medscape.com.
The new data come from the National Breast and Cervical Cancer Early Detection Program (NBCCEDP), a program that provides cancer screening services to women with low income and inadequate health insurance.
The data show that the total number of screenings funded by the NBCCEDP declined by 87% for breast cancer screening and by 84% for cervical cancer screening in April 2020 in comparison with the previous 5-year averages for that month.
The declines in breast cancer screening varied from 84% among Hispanic women to 98% among American Indian/Alaskan Native women. The declines in cervical cancer screening varied from 82% among Black women to 92% among Asian Pacific Islander women.
In April 2020, breast cancer screening declined by 86% in metro areas, 88% in urban areas, and 89% in rural areas in comparison with respective 5-year averages. For cervical cancer screenings, the corresponding declines were 85%, 77%, and 82%.
The findings are consistent with those from studies conducted in insured populations, note the authors, led by the Amy DeGroff, PhD, MPH, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion.
“Prolonged delays in screening related to the COVID-19 pandemic may lead to delayed diagnoses, poor health consequences, and an increase in cancer disparities among women already experiencing health inequities,” the CDC states in a press release.
Women from racial and ethnic minority groups already face a disproportionate burden of cervical and breast cancers in the United States: Black women and Hispanic women have the highest rates of cervical cancer incidence (8.3 and 8.9 per 100,000 women, respectively, vs. 7.3 per 100,000 among White women) and the highest rates of cervical cancer deaths. Black women have the highest rate of breast cancer death (26.9 per 100,000 women, vs. 19.4 per 100,000 among White women), the study authors explain.
Although the volume of screening began to recover in May 2020 – test volumes for breast and cervical cancer were 39% and 40% below the 5-year average by June 2020 – breast cancer screening in rural areas remained 52% below the 5-year average, they report.
The findings were published online June 30 in Preventive Medicine.
“This study highlights a decline in cancer screening among women of racial and ethnic minority groups with low incomes when their access to medical services decreased at the beginning of the pandemic,” Dr. DeGroff comments in the CDC press release.
The findings “reinforce the need to safely maintain routine health care services during the pandemic, especially when the health care environment meets COVID-19 safety guidelines,” she adds.
The investigators used NBCCEDP administrative and program data reported to the CDC by awardees – organizations that receive funding to implement the NBCCEDP – to assess the impact of COVID-19 on the number of breast and cervical cancer screening tests administered through the program and the effects of COVID-19 on the availability of screening services and NBCCEDP awardees’ capacity to support partner clinics.
A total of 630,264 breast and 594,566 cervical cancer screening tests were conducted during the review period of January-June 2015-2020.
Despite COVID-related challenges, “a large number of awardees reported flexibility and creative efforts to reach women and support clinics’ resumption of clinical care, including screening, during the COVID-19 pandemic,” the authors write.
“[The] CDC encourages health care professionals to help minimize delays in testing by continuing routine cancer screening for women having symptoms or at high risk for breast or cervical cancer,” Dr. DeGroff commented. “The Early Detection Program can help women overcome barriers to health equity by educating them about the importance of routine screening, addressing their concerns about COVID-19 transmission, and helping them to safely access screening through interventions like patient navigation.”
Future studies will examine the effect of the pandemic on screening during the second half of 2020, when surges of COVID-19 and their timing varied geographically, they note.
A version of this article first appeared on Medscape.com.
New analysis puts U.S. psoriasis prevalence at 3%
, according to an analysis of national survey data from 2011 to 2014.
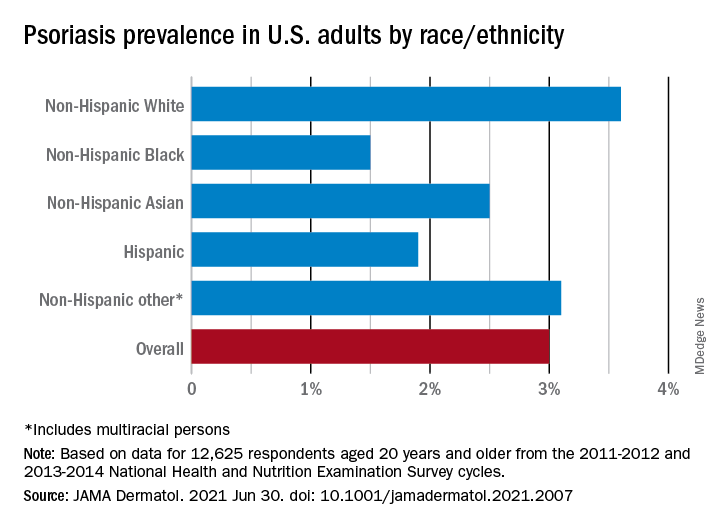
“The adult prevalence rate of 3.0% continues to place psoriasis as one of the most common immune-mediated diseases affecting adults” in the United States, April W. Armstrong, MD, MPH, and associates said in a report published in JAMA Dermatology. At that rate, approximately 7,560,000 Americans aged 20 years or older have psoriasis.
That overall rate among adults aged 20 years and older, based on data from the 2011-2012 and 2013-2014 cycles of the National Health and Nutrition Examination Survey (NHANES), did not change significantly when compared with the 2003-2004 NHANES, when it was 3.15% among those aged 20-59, said Dr. Armstrong, professor of dermatology, University of Southern California, Los Angeles, and associates.
For the 2011-2014 period, psoriasis prevalence was similar between women (3.2%) and men (2.8%) but was significantly associated with older age and White/non-White status. Those aged 50-59 years had the highest prevalence of any age group at 4.3% and those aged 70 and older had a rate of 3.9%, while those aged 20-29 were the lowest at 1.6%, the investigators reported.
The prevalence in non-Hispanic Whites in the United States was 3.6% over the study period, and their odds ratio for having psoriasis was 1.92, compared with non-White individuals. Asian respondents had a prevalence of 2.5%, with the Hispanic population at 1.9%, non-Hispanic Black respondents at 1.5%, and those identifying as other (including multiracial persons) at 3.1%, they said.
The NHANES sample consisted of 12,638 people who had participated in the question that asked if they had ever been diagnosed with psoriasis by a physician or other health care professional, of whom 12,625 gave a definitive yes or no answer, the investigators noted.
A much smaller number, 329, also answered a question about the severity of their disease: Fifty-six percent had little or no psoriasis, almost 22% reported 1-2 palms of involvement, 16% had 3-10 palms of involvement, and 5.5% said the coverage was more than 10 palms. Since the survey did not distinguish between treated and untreated patients, however, some “of those reporting low body surface area involvement may be receiving treatments that are controlling their otherwise more extensive disease,” they wrote.
Dr. Armstrong and another investigator said that they have received grants, personal fees, and honoraria from a number of pharmaceutical companies; two other investigators are employees of the National Psoriasis Foundation.
, according to an analysis of national survey data from 2011 to 2014.
“The adult prevalence rate of 3.0% continues to place psoriasis as one of the most common immune-mediated diseases affecting adults” in the United States, April W. Armstrong, MD, MPH, and associates said in a report published in JAMA Dermatology. At that rate, approximately 7,560,000 Americans aged 20 years or older have psoriasis.
That overall rate among adults aged 20 years and older, based on data from the 2011-2012 and 2013-2014 cycles of the National Health and Nutrition Examination Survey (NHANES), did not change significantly when compared with the 2003-2004 NHANES, when it was 3.15% among those aged 20-59, said Dr. Armstrong, professor of dermatology, University of Southern California, Los Angeles, and associates.
For the 2011-2014 period, psoriasis prevalence was similar between women (3.2%) and men (2.8%) but was significantly associated with older age and White/non-White status. Those aged 50-59 years had the highest prevalence of any age group at 4.3% and those aged 70 and older had a rate of 3.9%, while those aged 20-29 were the lowest at 1.6%, the investigators reported.
The prevalence in non-Hispanic Whites in the United States was 3.6% over the study period, and their odds ratio for having psoriasis was 1.92, compared with non-White individuals. Asian respondents had a prevalence of 2.5%, with the Hispanic population at 1.9%, non-Hispanic Black respondents at 1.5%, and those identifying as other (including multiracial persons) at 3.1%, they said.
The NHANES sample consisted of 12,638 people who had participated in the question that asked if they had ever been diagnosed with psoriasis by a physician or other health care professional, of whom 12,625 gave a definitive yes or no answer, the investigators noted.
A much smaller number, 329, also answered a question about the severity of their disease: Fifty-six percent had little or no psoriasis, almost 22% reported 1-2 palms of involvement, 16% had 3-10 palms of involvement, and 5.5% said the coverage was more than 10 palms. Since the survey did not distinguish between treated and untreated patients, however, some “of those reporting low body surface area involvement may be receiving treatments that are controlling their otherwise more extensive disease,” they wrote.
Dr. Armstrong and another investigator said that they have received grants, personal fees, and honoraria from a number of pharmaceutical companies; two other investigators are employees of the National Psoriasis Foundation.
, according to an analysis of national survey data from 2011 to 2014.
“The adult prevalence rate of 3.0% continues to place psoriasis as one of the most common immune-mediated diseases affecting adults” in the United States, April W. Armstrong, MD, MPH, and associates said in a report published in JAMA Dermatology. At that rate, approximately 7,560,000 Americans aged 20 years or older have psoriasis.
That overall rate among adults aged 20 years and older, based on data from the 2011-2012 and 2013-2014 cycles of the National Health and Nutrition Examination Survey (NHANES), did not change significantly when compared with the 2003-2004 NHANES, when it was 3.15% among those aged 20-59, said Dr. Armstrong, professor of dermatology, University of Southern California, Los Angeles, and associates.
For the 2011-2014 period, psoriasis prevalence was similar between women (3.2%) and men (2.8%) but was significantly associated with older age and White/non-White status. Those aged 50-59 years had the highest prevalence of any age group at 4.3% and those aged 70 and older had a rate of 3.9%, while those aged 20-29 were the lowest at 1.6%, the investigators reported.
The prevalence in non-Hispanic Whites in the United States was 3.6% over the study period, and their odds ratio for having psoriasis was 1.92, compared with non-White individuals. Asian respondents had a prevalence of 2.5%, with the Hispanic population at 1.9%, non-Hispanic Black respondents at 1.5%, and those identifying as other (including multiracial persons) at 3.1%, they said.
The NHANES sample consisted of 12,638 people who had participated in the question that asked if they had ever been diagnosed with psoriasis by a physician or other health care professional, of whom 12,625 gave a definitive yes or no answer, the investigators noted.
A much smaller number, 329, also answered a question about the severity of their disease: Fifty-six percent had little or no psoriasis, almost 22% reported 1-2 palms of involvement, 16% had 3-10 palms of involvement, and 5.5% said the coverage was more than 10 palms. Since the survey did not distinguish between treated and untreated patients, however, some “of those reporting low body surface area involvement may be receiving treatments that are controlling their otherwise more extensive disease,” they wrote.
Dr. Armstrong and another investigator said that they have received grants, personal fees, and honoraria from a number of pharmaceutical companies; two other investigators are employees of the National Psoriasis Foundation.
FROM JAMA DERMATOLOGY
Women not told about need for contraception after IVF births
The contraceptive needs of women who have had in vitro fertilization (IVF) pregnancies are real but are being overlooked, according to study data presented at the Royal College of Obstetricians & Gynaecologists (RCOG) Virtual World Congress 2021.
The interview-based study found that women report not being routinely informed about the chance of spontaneous pregnancy after IVF. “There is scope to follow-up with women after IVF … but information about the chances of spontaneous births and need for contraception isn’t given,” said lead researcher Annette Thwaites, MD, an academic clinical fellow and a senior registrar in Community Sexual and Reproductive Health at Kings College Hospital, London.
“Fertility services, maternity services, and community services could all do more to give women information on contraception postnatally,” Dr. Thwaites said.
“Even if a woman has had IVF previously, a woman shouldn’t lose the right to plan the rest of her family,” she added. “We need to stop shielding these women from the information they really do need.”
Dr. Thwaites first came across the issue around contraception after IVF pregnancy while talking to new mothers in a postnatal ward for another study. Ward staff told her not to enter the rooms with women who had had IVF births, with the implication that these women would not need or want contraception.
With this in mind, Dr. Thwaites and colleagues aimed to better understand the contraceptive needs of women after successful IVF pregnancy to improve service delivery and prevent unplanned and rapid-repeat pregnancies after IVF.
The researchers interviewed 21 women who had spontaneous pregnancies after successful IVF. Participants were aged 35-50 years, the majority were White, British, professional, married for at least 10 years, and living in nuclear families.
Of the spontaneous post-IVF pregnancies in these women, outcomes included single (11) and multiple live births (1 twin), miscarriage (1), ectopic (1) termination of pregnancy (1), and three ongoing pregnancies.
After IVF pregnancy, most women said that they used no contraception or ineffective contraception and had never had a conversation around contraception after IVF.
The women also reported that spontaneous pregnancy was shocking and not universally welcomed, and interpregnancy intervals were often short.
In addition, comments by these women suggested certain aspects of the IVF experience reinforced their perceptions of subfertility. One is quoted as saying, “It seemed to be this big failure if you were having IVF.” Another said, “It’s bad enough that I’m having to conceive my baby like this.”
An unmet need
In her 30 years of practice, Melanie Davies, MD, has seen many women who experience natural pregnancy after IVF. She agrees it is important to address these women’s contraceptive needs but stresses that it needs to be approached carefully.
“It can stir up sensitivities to discuss this issue after having an IVF pregnancy,” said Dr. Davies, a consultant obstetrician and gynecologist at University College London Hospitals, London. “I think many women genuinely think that contraception after IVF just doesn’t apply, but lots of women do have natural pregnancies after IVF. I think women do need this information, but we need to be aware of the sensitivities around this issue, so the way we deliver it is crucial.”
Gwenda Burns, chief executive of the National Patient Charity Fertility Network UK, which supports people before, during, and after fertility treatment, agrees that the process leading up to a successful IVF birth can have lasting effects.
“Fertility struggles and going through fertility treatment can put an enormous strain on both physical and mental health and can have a long-lasting impact,” Ms. Burns said when asked to comment on the new study.
“It is vital that patients receive the right support, guidance, and advice following treatment, including when natural conception may still be possible,” Ms. Burns continued.
Growing population
Given the increasing use of IVF in recent years, Dr. Thwaites said the importance of understanding and meeting the contraceptive needs of women post-IVF is increasingly important. Also, people are turning to it earlier and for other reasons, such as women in same sex relationships, single women, pre-implantation genetic testing, and surrogates.
“During the recruitment process for the current study, I came across women who said since their IVF pregnancies they had no idea what they should do about contraception,” Dr. Thwaites said.
But she empathizes with health care professionals too. “I genuinely feel that health care professionals just don’t know how to advise women in this setting, so they avoid the topic of contraception altogether with these women. They are concerned about making women feel awkward or upsetting them. In my experience, there is very little said about IVF and contraception in the same breath.”
Women believe subfertility always persists after IVF
Among participants in the study, the causes of the women’s subfertility were wide-ranging and included tubal, anovulatory, male factor, joint, and unexplained, the latter of which affects 25% of couples with fertility issues. In the cohort, women had taken up to 9 years to conceive their first child and one had a donor egg conception.
After IVF, the chance of pregnancy will depend on the reason for the couple’s subfertility. “Given that a huge number of patients these days have unexplained subfertility. This is when there is no absolute cause of infertility identified, and it might not prevent a pregnancy but slows it down,” Dr. Davies said in an interview. “Such couples still have a chance of natural pregnancy.”
Polycystic ovary syndrome as a cause of subfertility is often associated with improvement in fertility after IVF, Dr. Davies noted. “This can improve after a spontaneous pregnancy or after IVF, even if the IVF is not a success, and this is possibly due to needling the ovary.”
Dr. Thwaites added that challenging women’s perceptions of their subfertility is critical if headway is to be made on this topic. Many women have persistent views concerning their subfertility after successful IVF, which may be rooted in previous failed treatment; need for repeat cycles or intracytoplasmic sperm injection (ICSI); low numbers of eggs collected; poor quality embryos; and pregnancy complications, to note some of the most common reasons.
“So many [women] feel that they are very lucky to have had a pregnancy because their journey has been difficult. They might have had a successful pregnancy, but they still hold a sense of personal failure,” said Dr. Thwaites. “Even after spontaneous pregnancy some women said it was a miracle or freak event. [Yet two of these] women had two spontaneous pregnancies.”
Remarkably, even after subsequent spontaneous pregnancy, use of contraception and the most effective methods remained low among participants.
As well as fixed beliefs concerning their subfertility, other barriers to contraception use included a lack of knowledge of likelihood of spontaneous pregnancy; lack of contraceptive experience; and inherent incentives towards shorter interpregnancy intervals (e.g., the convenience and privacy of undergoing further IVF while still on maternity leave and availability of frozen embryos).
Looking ahead, Dr. Thwaites says there is a clear need to link and/or expand the maternity services dataset to uncover the true rates of post-IVF spontaneous pregnancy.
Dr. Thwaites and Dr. Davies have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The contraceptive needs of women who have had in vitro fertilization (IVF) pregnancies are real but are being overlooked, according to study data presented at the Royal College of Obstetricians & Gynaecologists (RCOG) Virtual World Congress 2021.
The interview-based study found that women report not being routinely informed about the chance of spontaneous pregnancy after IVF. “There is scope to follow-up with women after IVF … but information about the chances of spontaneous births and need for contraception isn’t given,” said lead researcher Annette Thwaites, MD, an academic clinical fellow and a senior registrar in Community Sexual and Reproductive Health at Kings College Hospital, London.
“Fertility services, maternity services, and community services could all do more to give women information on contraception postnatally,” Dr. Thwaites said.
“Even if a woman has had IVF previously, a woman shouldn’t lose the right to plan the rest of her family,” she added. “We need to stop shielding these women from the information they really do need.”
Dr. Thwaites first came across the issue around contraception after IVF pregnancy while talking to new mothers in a postnatal ward for another study. Ward staff told her not to enter the rooms with women who had had IVF births, with the implication that these women would not need or want contraception.
With this in mind, Dr. Thwaites and colleagues aimed to better understand the contraceptive needs of women after successful IVF pregnancy to improve service delivery and prevent unplanned and rapid-repeat pregnancies after IVF.
The researchers interviewed 21 women who had spontaneous pregnancies after successful IVF. Participants were aged 35-50 years, the majority were White, British, professional, married for at least 10 years, and living in nuclear families.
Of the spontaneous post-IVF pregnancies in these women, outcomes included single (11) and multiple live births (1 twin), miscarriage (1), ectopic (1) termination of pregnancy (1), and three ongoing pregnancies.
After IVF pregnancy, most women said that they used no contraception or ineffective contraception and had never had a conversation around contraception after IVF.
The women also reported that spontaneous pregnancy was shocking and not universally welcomed, and interpregnancy intervals were often short.
In addition, comments by these women suggested certain aspects of the IVF experience reinforced their perceptions of subfertility. One is quoted as saying, “It seemed to be this big failure if you were having IVF.” Another said, “It’s bad enough that I’m having to conceive my baby like this.”
An unmet need
In her 30 years of practice, Melanie Davies, MD, has seen many women who experience natural pregnancy after IVF. She agrees it is important to address these women’s contraceptive needs but stresses that it needs to be approached carefully.
“It can stir up sensitivities to discuss this issue after having an IVF pregnancy,” said Dr. Davies, a consultant obstetrician and gynecologist at University College London Hospitals, London. “I think many women genuinely think that contraception after IVF just doesn’t apply, but lots of women do have natural pregnancies after IVF. I think women do need this information, but we need to be aware of the sensitivities around this issue, so the way we deliver it is crucial.”
Gwenda Burns, chief executive of the National Patient Charity Fertility Network UK, which supports people before, during, and after fertility treatment, agrees that the process leading up to a successful IVF birth can have lasting effects.
“Fertility struggles and going through fertility treatment can put an enormous strain on both physical and mental health and can have a long-lasting impact,” Ms. Burns said when asked to comment on the new study.
“It is vital that patients receive the right support, guidance, and advice following treatment, including when natural conception may still be possible,” Ms. Burns continued.
Growing population
Given the increasing use of IVF in recent years, Dr. Thwaites said the importance of understanding and meeting the contraceptive needs of women post-IVF is increasingly important. Also, people are turning to it earlier and for other reasons, such as women in same sex relationships, single women, pre-implantation genetic testing, and surrogates.
“During the recruitment process for the current study, I came across women who said since their IVF pregnancies they had no idea what they should do about contraception,” Dr. Thwaites said.
But she empathizes with health care professionals too. “I genuinely feel that health care professionals just don’t know how to advise women in this setting, so they avoid the topic of contraception altogether with these women. They are concerned about making women feel awkward or upsetting them. In my experience, there is very little said about IVF and contraception in the same breath.”
Women believe subfertility always persists after IVF
Among participants in the study, the causes of the women’s subfertility were wide-ranging and included tubal, anovulatory, male factor, joint, and unexplained, the latter of which affects 25% of couples with fertility issues. In the cohort, women had taken up to 9 years to conceive their first child and one had a donor egg conception.
After IVF, the chance of pregnancy will depend on the reason for the couple’s subfertility. “Given that a huge number of patients these days have unexplained subfertility. This is when there is no absolute cause of infertility identified, and it might not prevent a pregnancy but slows it down,” Dr. Davies said in an interview. “Such couples still have a chance of natural pregnancy.”
Polycystic ovary syndrome as a cause of subfertility is often associated with improvement in fertility after IVF, Dr. Davies noted. “This can improve after a spontaneous pregnancy or after IVF, even if the IVF is not a success, and this is possibly due to needling the ovary.”
Dr. Thwaites added that challenging women’s perceptions of their subfertility is critical if headway is to be made on this topic. Many women have persistent views concerning their subfertility after successful IVF, which may be rooted in previous failed treatment; need for repeat cycles or intracytoplasmic sperm injection (ICSI); low numbers of eggs collected; poor quality embryos; and pregnancy complications, to note some of the most common reasons.
“So many [women] feel that they are very lucky to have had a pregnancy because their journey has been difficult. They might have had a successful pregnancy, but they still hold a sense of personal failure,” said Dr. Thwaites. “Even after spontaneous pregnancy some women said it was a miracle or freak event. [Yet two of these] women had two spontaneous pregnancies.”
Remarkably, even after subsequent spontaneous pregnancy, use of contraception and the most effective methods remained low among participants.
As well as fixed beliefs concerning their subfertility, other barriers to contraception use included a lack of knowledge of likelihood of spontaneous pregnancy; lack of contraceptive experience; and inherent incentives towards shorter interpregnancy intervals (e.g., the convenience and privacy of undergoing further IVF while still on maternity leave and availability of frozen embryos).
Looking ahead, Dr. Thwaites says there is a clear need to link and/or expand the maternity services dataset to uncover the true rates of post-IVF spontaneous pregnancy.
Dr. Thwaites and Dr. Davies have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The contraceptive needs of women who have had in vitro fertilization (IVF) pregnancies are real but are being overlooked, according to study data presented at the Royal College of Obstetricians & Gynaecologists (RCOG) Virtual World Congress 2021.
The interview-based study found that women report not being routinely informed about the chance of spontaneous pregnancy after IVF. “There is scope to follow-up with women after IVF … but information about the chances of spontaneous births and need for contraception isn’t given,” said lead researcher Annette Thwaites, MD, an academic clinical fellow and a senior registrar in Community Sexual and Reproductive Health at Kings College Hospital, London.
“Fertility services, maternity services, and community services could all do more to give women information on contraception postnatally,” Dr. Thwaites said.
“Even if a woman has had IVF previously, a woman shouldn’t lose the right to plan the rest of her family,” she added. “We need to stop shielding these women from the information they really do need.”
Dr. Thwaites first came across the issue around contraception after IVF pregnancy while talking to new mothers in a postnatal ward for another study. Ward staff told her not to enter the rooms with women who had had IVF births, with the implication that these women would not need or want contraception.
With this in mind, Dr. Thwaites and colleagues aimed to better understand the contraceptive needs of women after successful IVF pregnancy to improve service delivery and prevent unplanned and rapid-repeat pregnancies after IVF.
The researchers interviewed 21 women who had spontaneous pregnancies after successful IVF. Participants were aged 35-50 years, the majority were White, British, professional, married for at least 10 years, and living in nuclear families.
Of the spontaneous post-IVF pregnancies in these women, outcomes included single (11) and multiple live births (1 twin), miscarriage (1), ectopic (1) termination of pregnancy (1), and three ongoing pregnancies.
After IVF pregnancy, most women said that they used no contraception or ineffective contraception and had never had a conversation around contraception after IVF.
The women also reported that spontaneous pregnancy was shocking and not universally welcomed, and interpregnancy intervals were often short.
In addition, comments by these women suggested certain aspects of the IVF experience reinforced their perceptions of subfertility. One is quoted as saying, “It seemed to be this big failure if you were having IVF.” Another said, “It’s bad enough that I’m having to conceive my baby like this.”
An unmet need
In her 30 years of practice, Melanie Davies, MD, has seen many women who experience natural pregnancy after IVF. She agrees it is important to address these women’s contraceptive needs but stresses that it needs to be approached carefully.
“It can stir up sensitivities to discuss this issue after having an IVF pregnancy,” said Dr. Davies, a consultant obstetrician and gynecologist at University College London Hospitals, London. “I think many women genuinely think that contraception after IVF just doesn’t apply, but lots of women do have natural pregnancies after IVF. I think women do need this information, but we need to be aware of the sensitivities around this issue, so the way we deliver it is crucial.”
Gwenda Burns, chief executive of the National Patient Charity Fertility Network UK, which supports people before, during, and after fertility treatment, agrees that the process leading up to a successful IVF birth can have lasting effects.
“Fertility struggles and going through fertility treatment can put an enormous strain on both physical and mental health and can have a long-lasting impact,” Ms. Burns said when asked to comment on the new study.
“It is vital that patients receive the right support, guidance, and advice following treatment, including when natural conception may still be possible,” Ms. Burns continued.
Growing population
Given the increasing use of IVF in recent years, Dr. Thwaites said the importance of understanding and meeting the contraceptive needs of women post-IVF is increasingly important. Also, people are turning to it earlier and for other reasons, such as women in same sex relationships, single women, pre-implantation genetic testing, and surrogates.
“During the recruitment process for the current study, I came across women who said since their IVF pregnancies they had no idea what they should do about contraception,” Dr. Thwaites said.
But she empathizes with health care professionals too. “I genuinely feel that health care professionals just don’t know how to advise women in this setting, so they avoid the topic of contraception altogether with these women. They are concerned about making women feel awkward or upsetting them. In my experience, there is very little said about IVF and contraception in the same breath.”
Women believe subfertility always persists after IVF
Among participants in the study, the causes of the women’s subfertility were wide-ranging and included tubal, anovulatory, male factor, joint, and unexplained, the latter of which affects 25% of couples with fertility issues. In the cohort, women had taken up to 9 years to conceive their first child and one had a donor egg conception.
After IVF, the chance of pregnancy will depend on the reason for the couple’s subfertility. “Given that a huge number of patients these days have unexplained subfertility. This is when there is no absolute cause of infertility identified, and it might not prevent a pregnancy but slows it down,” Dr. Davies said in an interview. “Such couples still have a chance of natural pregnancy.”
Polycystic ovary syndrome as a cause of subfertility is often associated with improvement in fertility after IVF, Dr. Davies noted. “This can improve after a spontaneous pregnancy or after IVF, even if the IVF is not a success, and this is possibly due to needling the ovary.”
Dr. Thwaites added that challenging women’s perceptions of their subfertility is critical if headway is to be made on this topic. Many women have persistent views concerning their subfertility after successful IVF, which may be rooted in previous failed treatment; need for repeat cycles or intracytoplasmic sperm injection (ICSI); low numbers of eggs collected; poor quality embryos; and pregnancy complications, to note some of the most common reasons.
“So many [women] feel that they are very lucky to have had a pregnancy because their journey has been difficult. They might have had a successful pregnancy, but they still hold a sense of personal failure,” said Dr. Thwaites. “Even after spontaneous pregnancy some women said it was a miracle or freak event. [Yet two of these] women had two spontaneous pregnancies.”
Remarkably, even after subsequent spontaneous pregnancy, use of contraception and the most effective methods remained low among participants.
As well as fixed beliefs concerning their subfertility, other barriers to contraception use included a lack of knowledge of likelihood of spontaneous pregnancy; lack of contraceptive experience; and inherent incentives towards shorter interpregnancy intervals (e.g., the convenience and privacy of undergoing further IVF while still on maternity leave and availability of frozen embryos).
Looking ahead, Dr. Thwaites says there is a clear need to link and/or expand the maternity services dataset to uncover the true rates of post-IVF spontaneous pregnancy.
Dr. Thwaites and Dr. Davies have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pregnancy risk is low with negative test at IUD placement
Frequency or timing of unprotected intercourse within 14 days before IUD placement had no impact on pregnancy if a preplacement pregnancy test was negative, based on data from 655 women who received IUDs.
Many women present for emergency contraception with a history of unprotected intercourse, often beyond the 5-day guidelines for emergency contraception recommended by the World Health Organization, wrote Abena BakenRa, MD, of the University of California, Berkeley, and colleagues. “As such, we lack data on situations in which multiple episodes of unprotected intercourse occurred in the same menstrual cycle of use, especially episodes occurring more than 5 days before emergency contraception use,” the researchers said.
To determine pregnancy risk during a longer period before IUD placement, the researchers reviewed secondary data from a randomized trial of 655 women who received the copper T380A IUD or levonorgestrel 52-mg intrauterine system for emergency contraception. The women were aged 18-35 years and were enrolled at one of six family planning clinics in Utah between August 2016 and December 2019.
In a study published in Obstetrics & Gynecology, the researchers assessed pregnancies at 1 month after IUD placement. All of the women had a confirmed negative urine pregnancy test result immediately before IUD placement.
Overall, 286 women (43.7%) reported multiple episodes of unprotected intercourse, with a median of three episodes. A total of 95 women (14.4%) reported at least one unprotected intercourse episode at 6 days or more prior to IUD placement. No pregnancies were reported among women in either of these categories (0.0% for both). Pregnancy risk was 0.2% among those who reported unprotected intercourse within 5 days of IUD placement.
No pregnancies occurred in those who reported additional episodes of unprotected intercourse at 6-7 days, 6-10 days, or 6-14 days before IUD placement (0% for all).
In both the copper IUD and levonorgestrel groups, 68% and 74%, respectively, of the women reported that all fertile-window unprotected intercourse events occurred in the 5 days prior to IUD placement.
The study findings were limited by several factors including the lack of power for analysis of certain categories of assessment, such as pregnancy rates by timing or frequency, the inclusion of patients only from the state of Utah, and the potential underreporting of unprotected intercourse, the researchers noted. However, the findings were strengthened by the relatively large sample size, and by data on unprotected intercourse before IUD placement in a randomized, controlled trial that included two types of IUDs, they said.
“For these situations with multiple unprotected intercourse episodes and extended time between unprotected intercourse and emergency contraception request, potential users should be informed of the evidence of IUD emergency contraception efficacy, compared with the current state of uncertain data for oral emergency contraception methods,” the researchers said.
“Given the multitude of barriers that may impede timely presentation to care (insurance and cost concerns, difficulty finding a capable health care professional, or sexual assault trauma), these data are critical to patient-centered family planning care,” they concluded.
Data support IUD placement in practice
“Understanding potential barriers to placement of long-acting reversible contraception such as IUDs is essential to expanding access to contraception,” Iris Krishna, MD, of Emory University, Atlanta, said in an interview.
“This study is a secondary analysis of a randomized trial that compared copper versus levonorgestrel IUD placement for emergency contraception. Investigators were able to evaluate frequency and timing of unprotected intercourse up to 14 days prior to IUD placement and prospectively collect data assessing pregnancy risk 1 month after IUD placement,” she said.
The study findings suggest that the risk of pregnancy with unprotected intercourse within 14 days of IUD placement is low overall, and that this risk does not appear to increase with multiple episodes of unprotected intercourse during this time period, Dr. Krishna said. “In general, insertion of an IUD may occur at any time during the menstrual cycle as long as pregnancy may be reasonably excluded and clinicians are encouraged to initiate and place long-acting reversible contraceptives in a single visit, if possible,” she noted. However, “there is a paucity of data on risk of pregnancy when assessing efficacy of IUDs as emergency contraception with episodes of unprotected intercourse more than 5 days prior to IUD placement,” she added.
The study results also suggest that pregnancy risk is similar between women who reported unprotected intercourse within 5 days prior to IUD placement and those who reported unprotected intercourse up to 14 days prior to IUD placement, said Dr. Krishna. “These findings are clinically significant, as they add to our understanding of risk of pregnancy with unprotected intercourse up to 14 days prior to placement of an IUD,” she emphasized.
In practice, the study results “will help clinicians counsel patients on risk of pregnancy after IUD placement for emergency contraception,” said Dr. Krishna. “More studies evaluating risk of pregnancy after IUD placement for emergency contraception with episodes of unprotected intercourse more than 5 days prior to placement are needed to further assess the potential to expand the time frame for IUD use as emergency contraception,” she said. “Reducing barriers to IUD access, especially in setting of emergency contraception, is essential to lowering unintended pregnancy rates in the United States.”
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, as well as the University of Utah Population Health Research Foundation, the National Center for Research Resources, and the National Center for Advancing Translational Sciences at the National Institutes of Health. Several coauthors disclosed grant support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the Office of Research on Women’s Health of the National Institutes of Health. The researchers, as well as Dr. Krishna, had no financial conflicts to disclose.
Frequency or timing of unprotected intercourse within 14 days before IUD placement had no impact on pregnancy if a preplacement pregnancy test was negative, based on data from 655 women who received IUDs.
Many women present for emergency contraception with a history of unprotected intercourse, often beyond the 5-day guidelines for emergency contraception recommended by the World Health Organization, wrote Abena BakenRa, MD, of the University of California, Berkeley, and colleagues. “As such, we lack data on situations in which multiple episodes of unprotected intercourse occurred in the same menstrual cycle of use, especially episodes occurring more than 5 days before emergency contraception use,” the researchers said.
To determine pregnancy risk during a longer period before IUD placement, the researchers reviewed secondary data from a randomized trial of 655 women who received the copper T380A IUD or levonorgestrel 52-mg intrauterine system for emergency contraception. The women were aged 18-35 years and were enrolled at one of six family planning clinics in Utah between August 2016 and December 2019.
In a study published in Obstetrics & Gynecology, the researchers assessed pregnancies at 1 month after IUD placement. All of the women had a confirmed negative urine pregnancy test result immediately before IUD placement.
Overall, 286 women (43.7%) reported multiple episodes of unprotected intercourse, with a median of three episodes. A total of 95 women (14.4%) reported at least one unprotected intercourse episode at 6 days or more prior to IUD placement. No pregnancies were reported among women in either of these categories (0.0% for both). Pregnancy risk was 0.2% among those who reported unprotected intercourse within 5 days of IUD placement.
No pregnancies occurred in those who reported additional episodes of unprotected intercourse at 6-7 days, 6-10 days, or 6-14 days before IUD placement (0% for all).
In both the copper IUD and levonorgestrel groups, 68% and 74%, respectively, of the women reported that all fertile-window unprotected intercourse events occurred in the 5 days prior to IUD placement.
The study findings were limited by several factors including the lack of power for analysis of certain categories of assessment, such as pregnancy rates by timing or frequency, the inclusion of patients only from the state of Utah, and the potential underreporting of unprotected intercourse, the researchers noted. However, the findings were strengthened by the relatively large sample size, and by data on unprotected intercourse before IUD placement in a randomized, controlled trial that included two types of IUDs, they said.
“For these situations with multiple unprotected intercourse episodes and extended time between unprotected intercourse and emergency contraception request, potential users should be informed of the evidence of IUD emergency contraception efficacy, compared with the current state of uncertain data for oral emergency contraception methods,” the researchers said.
“Given the multitude of barriers that may impede timely presentation to care (insurance and cost concerns, difficulty finding a capable health care professional, or sexual assault trauma), these data are critical to patient-centered family planning care,” they concluded.
Data support IUD placement in practice
“Understanding potential barriers to placement of long-acting reversible contraception such as IUDs is essential to expanding access to contraception,” Iris Krishna, MD, of Emory University, Atlanta, said in an interview.
“This study is a secondary analysis of a randomized trial that compared copper versus levonorgestrel IUD placement for emergency contraception. Investigators were able to evaluate frequency and timing of unprotected intercourse up to 14 days prior to IUD placement and prospectively collect data assessing pregnancy risk 1 month after IUD placement,” she said.
The study findings suggest that the risk of pregnancy with unprotected intercourse within 14 days of IUD placement is low overall, and that this risk does not appear to increase with multiple episodes of unprotected intercourse during this time period, Dr. Krishna said. “In general, insertion of an IUD may occur at any time during the menstrual cycle as long as pregnancy may be reasonably excluded and clinicians are encouraged to initiate and place long-acting reversible contraceptives in a single visit, if possible,” she noted. However, “there is a paucity of data on risk of pregnancy when assessing efficacy of IUDs as emergency contraception with episodes of unprotected intercourse more than 5 days prior to IUD placement,” she added.
The study results also suggest that pregnancy risk is similar between women who reported unprotected intercourse within 5 days prior to IUD placement and those who reported unprotected intercourse up to 14 days prior to IUD placement, said Dr. Krishna. “These findings are clinically significant, as they add to our understanding of risk of pregnancy with unprotected intercourse up to 14 days prior to placement of an IUD,” she emphasized.
In practice, the study results “will help clinicians counsel patients on risk of pregnancy after IUD placement for emergency contraception,” said Dr. Krishna. “More studies evaluating risk of pregnancy after IUD placement for emergency contraception with episodes of unprotected intercourse more than 5 days prior to placement are needed to further assess the potential to expand the time frame for IUD use as emergency contraception,” she said. “Reducing barriers to IUD access, especially in setting of emergency contraception, is essential to lowering unintended pregnancy rates in the United States.”
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, as well as the University of Utah Population Health Research Foundation, the National Center for Research Resources, and the National Center for Advancing Translational Sciences at the National Institutes of Health. Several coauthors disclosed grant support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the Office of Research on Women’s Health of the National Institutes of Health. The researchers, as well as Dr. Krishna, had no financial conflicts to disclose.
Frequency or timing of unprotected intercourse within 14 days before IUD placement had no impact on pregnancy if a preplacement pregnancy test was negative, based on data from 655 women who received IUDs.
Many women present for emergency contraception with a history of unprotected intercourse, often beyond the 5-day guidelines for emergency contraception recommended by the World Health Organization, wrote Abena BakenRa, MD, of the University of California, Berkeley, and colleagues. “As such, we lack data on situations in which multiple episodes of unprotected intercourse occurred in the same menstrual cycle of use, especially episodes occurring more than 5 days before emergency contraception use,” the researchers said.
To determine pregnancy risk during a longer period before IUD placement, the researchers reviewed secondary data from a randomized trial of 655 women who received the copper T380A IUD or levonorgestrel 52-mg intrauterine system for emergency contraception. The women were aged 18-35 years and were enrolled at one of six family planning clinics in Utah between August 2016 and December 2019.
In a study published in Obstetrics & Gynecology, the researchers assessed pregnancies at 1 month after IUD placement. All of the women had a confirmed negative urine pregnancy test result immediately before IUD placement.
Overall, 286 women (43.7%) reported multiple episodes of unprotected intercourse, with a median of three episodes. A total of 95 women (14.4%) reported at least one unprotected intercourse episode at 6 days or more prior to IUD placement. No pregnancies were reported among women in either of these categories (0.0% for both). Pregnancy risk was 0.2% among those who reported unprotected intercourse within 5 days of IUD placement.
No pregnancies occurred in those who reported additional episodes of unprotected intercourse at 6-7 days, 6-10 days, or 6-14 days before IUD placement (0% for all).
In both the copper IUD and levonorgestrel groups, 68% and 74%, respectively, of the women reported that all fertile-window unprotected intercourse events occurred in the 5 days prior to IUD placement.
The study findings were limited by several factors including the lack of power for analysis of certain categories of assessment, such as pregnancy rates by timing or frequency, the inclusion of patients only from the state of Utah, and the potential underreporting of unprotected intercourse, the researchers noted. However, the findings were strengthened by the relatively large sample size, and by data on unprotected intercourse before IUD placement in a randomized, controlled trial that included two types of IUDs, they said.
“For these situations with multiple unprotected intercourse episodes and extended time between unprotected intercourse and emergency contraception request, potential users should be informed of the evidence of IUD emergency contraception efficacy, compared with the current state of uncertain data for oral emergency contraception methods,” the researchers said.
“Given the multitude of barriers that may impede timely presentation to care (insurance and cost concerns, difficulty finding a capable health care professional, or sexual assault trauma), these data are critical to patient-centered family planning care,” they concluded.
Data support IUD placement in practice
“Understanding potential barriers to placement of long-acting reversible contraception such as IUDs is essential to expanding access to contraception,” Iris Krishna, MD, of Emory University, Atlanta, said in an interview.
“This study is a secondary analysis of a randomized trial that compared copper versus levonorgestrel IUD placement for emergency contraception. Investigators were able to evaluate frequency and timing of unprotected intercourse up to 14 days prior to IUD placement and prospectively collect data assessing pregnancy risk 1 month after IUD placement,” she said.
The study findings suggest that the risk of pregnancy with unprotected intercourse within 14 days of IUD placement is low overall, and that this risk does not appear to increase with multiple episodes of unprotected intercourse during this time period, Dr. Krishna said. “In general, insertion of an IUD may occur at any time during the menstrual cycle as long as pregnancy may be reasonably excluded and clinicians are encouraged to initiate and place long-acting reversible contraceptives in a single visit, if possible,” she noted. However, “there is a paucity of data on risk of pregnancy when assessing efficacy of IUDs as emergency contraception with episodes of unprotected intercourse more than 5 days prior to IUD placement,” she added.
The study results also suggest that pregnancy risk is similar between women who reported unprotected intercourse within 5 days prior to IUD placement and those who reported unprotected intercourse up to 14 days prior to IUD placement, said Dr. Krishna. “These findings are clinically significant, as they add to our understanding of risk of pregnancy with unprotected intercourse up to 14 days prior to placement of an IUD,” she emphasized.
In practice, the study results “will help clinicians counsel patients on risk of pregnancy after IUD placement for emergency contraception,” said Dr. Krishna. “More studies evaluating risk of pregnancy after IUD placement for emergency contraception with episodes of unprotected intercourse more than 5 days prior to placement are needed to further assess the potential to expand the time frame for IUD use as emergency contraception,” she said. “Reducing barriers to IUD access, especially in setting of emergency contraception, is essential to lowering unintended pregnancy rates in the United States.”
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, as well as the University of Utah Population Health Research Foundation, the National Center for Research Resources, and the National Center for Advancing Translational Sciences at the National Institutes of Health. Several coauthors disclosed grant support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the Office of Research on Women’s Health of the National Institutes of Health. The researchers, as well as Dr. Krishna, had no financial conflicts to disclose.
FROM OBSTETRICS & GYNECOLOGY
Post–COVID-19 lung injury: What we know so far
With vaccination rates increasing and new infections declining, we all hope the worst of the COVID-19 pandemic is over (fingers crossed really tight). Regardless, the post–COVID-19 syndrome pandemic has already begun. What is post–COVID-19 syndrome (or long-haulers or long-COVID)? Is it standard postviral fatigue? Prolonged deconditioning following debilitating illness? Permanent lung or vascular injury? Common sense and past experience say it’s all of these.
In theory, the burden of actual lung injury post COVID-19 should be the easiest to quantify, so let’s discuss what we think we know. I’ve heard experts break post–COVID-19 lung injury into three broad categories:
- Preexisting lung disease that is exacerbated by acute COVID-19 infection.
- Acute COVID-19 infection that causes acute respiratory distress syndrome (ARDS) or other acute lung injury (ALI).
- Non–critically ill acute COVID-19 with residual lung damage and abnormal repair.
These categories are necessarily imprecise, making it challenging to fit some patients neatly into a single definition.
For patients in the first category, management will be dictated largely by the nature of the preexisting lung disease. For those in category two, we already know a lot about what their recovery from ARDS will look like. There’s no longer reason to believe that COVID-19–related ARDS is particularly unique, and all things being equal, lung recovery should mimic that seen with non–COVID-19 ARDS.
It’s going to take patience and time, and beyond targeted rehabilitation it’s not clear that we have anything available to expedite the process.
The third category of patients is the most intriguing. Is there a group of patients who have residual lung injury but didn’t have evident ARDS/ALI during their acute COVID-19 infection? Anecdotally we think so, but we know little about prevalence and less about management. A recent study published in Annals of the American Thoracic Society addresses both issues. In an observational report on patients recovering after being hospitalized with COVID-19 infection, the authors found that 3.6% of patients had residual lung injury that improved with 3 weeks of corticosteroid treatment.
The report is timely and helpful but hardly definitive. It’s observational, and patients required extensive screening and identification by a multidisciplinary committee of experts in interstitial lung disease. Patients were diagnosed as having organizing pneumonia (OP) as their “lung injury” if certain radiographic criteria were met. There were no biopsies. Last, there was no control group. Still, this report is critically important. It tells us that at 6 weeks post discharge, about 3.6% of patients who were hospitalized for COVID-19 will have persistent symptoms, radiographic abnormalities, and a plateau in their recovery.
Beyond that, it tells us little. Did these patients really have OP? It’s impossible to know. The CT findings used to establish the diagnosis are nonspecific. Response to steroids is consistent with OP, but the treatment course was quite short. If truly OP, one would expect a high relapse rate after steroid withdrawal. Patients weren’t followed long enough to monitor recurrence rates. Also, as appropriately discussed in the accompanying editorial, there’s no control group so we can’t know whether the patients treated with steroids would have recovered without treatment. There was objective improvement in lung function for the two to three patients they followed who did not receive steroids. However, it was of lesser magnitude than in the steroid group.
Post–COVID-19 symptoms will remain a challenge for the foreseeable future. More than 30 million patients have been diagnosed with COVID-19 in the United States and close to half will experience persistent dyspnea. Putting the numbers together, I conclude that the vast majority will not have identifiable lung injury that will benefit from steroids. I wish I could prescribe patience to both physicians and patients.
Dr. Holley is associate professor of medicine at Uniformed Services University and program director of pulmonary and critical care medicine at Walter Reed National Military Medical Center. He covers a wide range of topics in pulmonary, critical care, and sleep medicine.
A version of this article first appeared on Medscape.com.
With vaccination rates increasing and new infections declining, we all hope the worst of the COVID-19 pandemic is over (fingers crossed really tight). Regardless, the post–COVID-19 syndrome pandemic has already begun. What is post–COVID-19 syndrome (or long-haulers or long-COVID)? Is it standard postviral fatigue? Prolonged deconditioning following debilitating illness? Permanent lung or vascular injury? Common sense and past experience say it’s all of these.
In theory, the burden of actual lung injury post COVID-19 should be the easiest to quantify, so let’s discuss what we think we know. I’ve heard experts break post–COVID-19 lung injury into three broad categories:
- Preexisting lung disease that is exacerbated by acute COVID-19 infection.
- Acute COVID-19 infection that causes acute respiratory distress syndrome (ARDS) or other acute lung injury (ALI).
- Non–critically ill acute COVID-19 with residual lung damage and abnormal repair.
These categories are necessarily imprecise, making it challenging to fit some patients neatly into a single definition.
For patients in the first category, management will be dictated largely by the nature of the preexisting lung disease. For those in category two, we already know a lot about what their recovery from ARDS will look like. There’s no longer reason to believe that COVID-19–related ARDS is particularly unique, and all things being equal, lung recovery should mimic that seen with non–COVID-19 ARDS.
It’s going to take patience and time, and beyond targeted rehabilitation it’s not clear that we have anything available to expedite the process.
The third category of patients is the most intriguing. Is there a group of patients who have residual lung injury but didn’t have evident ARDS/ALI during their acute COVID-19 infection? Anecdotally we think so, but we know little about prevalence and less about management. A recent study published in Annals of the American Thoracic Society addresses both issues. In an observational report on patients recovering after being hospitalized with COVID-19 infection, the authors found that 3.6% of patients had residual lung injury that improved with 3 weeks of corticosteroid treatment.
The report is timely and helpful but hardly definitive. It’s observational, and patients required extensive screening and identification by a multidisciplinary committee of experts in interstitial lung disease. Patients were diagnosed as having organizing pneumonia (OP) as their “lung injury” if certain radiographic criteria were met. There were no biopsies. Last, there was no control group. Still, this report is critically important. It tells us that at 6 weeks post discharge, about 3.6% of patients who were hospitalized for COVID-19 will have persistent symptoms, radiographic abnormalities, and a plateau in their recovery.
Beyond that, it tells us little. Did these patients really have OP? It’s impossible to know. The CT findings used to establish the diagnosis are nonspecific. Response to steroids is consistent with OP, but the treatment course was quite short. If truly OP, one would expect a high relapse rate after steroid withdrawal. Patients weren’t followed long enough to monitor recurrence rates. Also, as appropriately discussed in the accompanying editorial, there’s no control group so we can’t know whether the patients treated with steroids would have recovered without treatment. There was objective improvement in lung function for the two to three patients they followed who did not receive steroids. However, it was of lesser magnitude than in the steroid group.
Post–COVID-19 symptoms will remain a challenge for the foreseeable future. More than 30 million patients have been diagnosed with COVID-19 in the United States and close to half will experience persistent dyspnea. Putting the numbers together, I conclude that the vast majority will not have identifiable lung injury that will benefit from steroids. I wish I could prescribe patience to both physicians and patients.
Dr. Holley is associate professor of medicine at Uniformed Services University and program director of pulmonary and critical care medicine at Walter Reed National Military Medical Center. He covers a wide range of topics in pulmonary, critical care, and sleep medicine.
A version of this article first appeared on Medscape.com.
With vaccination rates increasing and new infections declining, we all hope the worst of the COVID-19 pandemic is over (fingers crossed really tight). Regardless, the post–COVID-19 syndrome pandemic has already begun. What is post–COVID-19 syndrome (or long-haulers or long-COVID)? Is it standard postviral fatigue? Prolonged deconditioning following debilitating illness? Permanent lung or vascular injury? Common sense and past experience say it’s all of these.
In theory, the burden of actual lung injury post COVID-19 should be the easiest to quantify, so let’s discuss what we think we know. I’ve heard experts break post–COVID-19 lung injury into three broad categories:
- Preexisting lung disease that is exacerbated by acute COVID-19 infection.
- Acute COVID-19 infection that causes acute respiratory distress syndrome (ARDS) or other acute lung injury (ALI).
- Non–critically ill acute COVID-19 with residual lung damage and abnormal repair.
These categories are necessarily imprecise, making it challenging to fit some patients neatly into a single definition.
For patients in the first category, management will be dictated largely by the nature of the preexisting lung disease. For those in category two, we already know a lot about what their recovery from ARDS will look like. There’s no longer reason to believe that COVID-19–related ARDS is particularly unique, and all things being equal, lung recovery should mimic that seen with non–COVID-19 ARDS.
It’s going to take patience and time, and beyond targeted rehabilitation it’s not clear that we have anything available to expedite the process.
The third category of patients is the most intriguing. Is there a group of patients who have residual lung injury but didn’t have evident ARDS/ALI during their acute COVID-19 infection? Anecdotally we think so, but we know little about prevalence and less about management. A recent study published in Annals of the American Thoracic Society addresses both issues. In an observational report on patients recovering after being hospitalized with COVID-19 infection, the authors found that 3.6% of patients had residual lung injury that improved with 3 weeks of corticosteroid treatment.
The report is timely and helpful but hardly definitive. It’s observational, and patients required extensive screening and identification by a multidisciplinary committee of experts in interstitial lung disease. Patients were diagnosed as having organizing pneumonia (OP) as their “lung injury” if certain radiographic criteria were met. There were no biopsies. Last, there was no control group. Still, this report is critically important. It tells us that at 6 weeks post discharge, about 3.6% of patients who were hospitalized for COVID-19 will have persistent symptoms, radiographic abnormalities, and a plateau in their recovery.
Beyond that, it tells us little. Did these patients really have OP? It’s impossible to know. The CT findings used to establish the diagnosis are nonspecific. Response to steroids is consistent with OP, but the treatment course was quite short. If truly OP, one would expect a high relapse rate after steroid withdrawal. Patients weren’t followed long enough to monitor recurrence rates. Also, as appropriately discussed in the accompanying editorial, there’s no control group so we can’t know whether the patients treated with steroids would have recovered without treatment. There was objective improvement in lung function for the two to three patients they followed who did not receive steroids. However, it was of lesser magnitude than in the steroid group.
Post–COVID-19 symptoms will remain a challenge for the foreseeable future. More than 30 million patients have been diagnosed with COVID-19 in the United States and close to half will experience persistent dyspnea. Putting the numbers together, I conclude that the vast majority will not have identifiable lung injury that will benefit from steroids. I wish I could prescribe patience to both physicians and patients.
Dr. Holley is associate professor of medicine at Uniformed Services University and program director of pulmonary and critical care medicine at Walter Reed National Military Medical Center. He covers a wide range of topics in pulmonary, critical care, and sleep medicine.
A version of this article first appeared on Medscape.com.
‘Praise Diabetes’: Support programs in Black churches yield lasting A1c changes
A church-based diabetes self-management support intervention that incorporated parish nurses and peer leaders is feasible and may help improve diabetes-related outcomes in participants.

Sustained reductions in hemoglobin A1c and diabetes distress were seen in the Praise Diabetes Project, a 33-month study that piloted several different approaches to parish nurse and peer leader support at 21 urban churches in Michigan and Ohio, said Gretchen Piatt, MPH, PhD, associate professor in the department of learning health sciences at the University of Michigan, Ann Arbor, reported at the annual scientific sessions of the American Diabetes Association.
“Of the participants who achieved glycemic control following diabetes self-management education, a really large proportion – upward of 77% of participants across all the groups– achieved sustained glycemic control at 33 months,” Dr. Piatt said.
Findings from this study has helped diabetes educators better understand how to design effective support approaches that may have a long-term impact on glycemic control and diabetes distress, Dr. Piatt said.
The Praise Diabetes Project represents a “very smart strategy” of leveraging institutions that already exist in the African American community that are trusted and provide emotional support, said Tracey D. Brown, CEO of the ADA.
“This is about behavior change, really, at its crux,” Ms. Brown said in an interview. “To get there, you’ve got to have trust, and you have to have an emotional connection. If you don’t get either one of those things, then you really are not going to do anything in terms of changing behavior.”
Long-term solutions needed
Many studies show that diabetes self-management education can improve clinical and psychosocial outcomes, and reduce health care utilization and cost, at least in the short term, Dr. Piatt said. However, it’s less clear how those improvements can be sustained over longer periods of time.
“This then presents a critical need to develop and evaluate diabetes self-management support models that are ongoing, patient driven, and embedded within existing community infrastructures,” Dr. Piatt said in her presentation.
Working with churches is one approach to working within existing community infrastructures: “Churches are embedded in the community, they have the personnel oftentimes to facilitate these types of health programs, and most importantly, they have the established relationships with the community that brings about sustained changes,” Dr. Piatt said in her presentation.
Addressing diabetes education needs in urban, low-resource communities
The Praise Diabetes Project was a randomized, 33-month clinical trial conducted in 21 predominantly Black churches in Detroit; Flint, Mich.; and Toledo, Ohio, which are all urban, low-resource communities where diabetes is a significant public health problem, according to Dr. Piatt.
The study was designed to evaluate the relative effectiveness of three different approaches to diabetes self-management support at improving A1c and levels of diabetes distress, according to the investigators.
The churches were randomized to one of the support arms, including parish nurse plus peer leader support, parish nurse support by itself, or peer leader support by itself.
A total of 47 individuals were trained, including 31 peer leaders and 16 parish nurses.
All three interventions included an initial 6-month period of “enhanced usual care” during which biweekly newsletters that were distributed, according to Dr. Piatt. That was followed by 12 months of diabetes self-management support, and an additional 12 months of ongoing support facilitated by parish nurses and peer leaders on their own, without input from the research team or health care providers.
Participants in the program had to be at least 21 years old and under the care of a physician for their diabetes, according to Dr. Piatt. The parish nurses had to be registered nurses in Michigan or Ohio. Peer leaders had to be at least 21 years old, had at least an eighth-grade education, and had to commit to a 30-hour training program.
Peer leaders also had to be individuals living with diabetes: “Prior studies have found that, when peer leaders are actively working on their own self-management goals, they tend to be much more successful in helping others,” Dr. Piatt explained.
In addition to facilitating diabetes self-management education, the parish nurses and peer leaders in these interventions were responsible for recruitment, church announcements, room reservations, follow-up calls to participants, according to Dr. Piatt. Parish nurses also provided clinical content knowledge and supervised the peer leaders in the combined model.
Sustained reductions in A1c and diabetes distress
These diabetes self-management support approaches led to significant changes over time in A1c and diabetes distress, the primary outcomes of the study, Dr. Piatt said.
The peer leader support approach resulted in a statistically significant decline in A1c, from a mean of 8.0% at baseline to 7.7% at 33 months (P = .04), while nonsignificant declines were observed in the parish nurse and combined parish nurse–peer leader approach, according to the researcher.
Reductions in A1c persisted despite the COVID-19 pandemic, which began roughly 21 months into the study, she said.
Glycemic control remained steady over the course of the study, as illustrated by similar proportions of participants with A1c below 7% from baseline to 33 months, she added.
Sustained glycemic control was seen in all three groups, according to Dr. Piatt. For example, 42.7% of individuals in the parish nurse and peer leader support group achieved glycemic control following the intervention, and 88.5% of them sustained it at 33 months.
“I think this is one of the longest diabetes self-management education and diabetes self-management support interventions that’s out there right now, so we were so happy to see that sustained by glycemic control that far into the future,” she said.
Diabetes distress levels decreased steadily over time in all three groups, with declines that were statistically significant from baseline to 33 months in the parish nurse–only and peer leader–only groups, the investigator said.
The proportion of participants reporting moderate levels of diabetes distress dropped over time, especially in the peer leader support group, where there was a 50% reduction, she added.
Despite these findings, the study had limitations, according to Dr. Piatt, including some “burnout” that impacted participants, parish nurses, and peer leaders, especially after the pandemic started.
In addition, this type of intervention may have limited impact in the community at large: “We probably didn’t reach people who did not have good connection to the church,” Dr. Piatt said.
Dr. Piatt reported no conflicts of interest related to the research.
A church-based diabetes self-management support intervention that incorporated parish nurses and peer leaders is feasible and may help improve diabetes-related outcomes in participants.
Sustained reductions in hemoglobin A1c and diabetes distress were seen in the Praise Diabetes Project, a 33-month study that piloted several different approaches to parish nurse and peer leader support at 21 urban churches in Michigan and Ohio, said Gretchen Piatt, MPH, PhD, associate professor in the department of learning health sciences at the University of Michigan, Ann Arbor, reported at the annual scientific sessions of the American Diabetes Association.
“Of the participants who achieved glycemic control following diabetes self-management education, a really large proportion – upward of 77% of participants across all the groups– achieved sustained glycemic control at 33 months,” Dr. Piatt said.
Findings from this study has helped diabetes educators better understand how to design effective support approaches that may have a long-term impact on glycemic control and diabetes distress, Dr. Piatt said.
The Praise Diabetes Project represents a “very smart strategy” of leveraging institutions that already exist in the African American community that are trusted and provide emotional support, said Tracey D. Brown, CEO of the ADA.
“This is about behavior change, really, at its crux,” Ms. Brown said in an interview. “To get there, you’ve got to have trust, and you have to have an emotional connection. If you don’t get either one of those things, then you really are not going to do anything in terms of changing behavior.”
Long-term solutions needed
Many studies show that diabetes self-management education can improve clinical and psychosocial outcomes, and reduce health care utilization and cost, at least in the short term, Dr. Piatt said. However, it’s less clear how those improvements can be sustained over longer periods of time.
“This then presents a critical need to develop and evaluate diabetes self-management support models that are ongoing, patient driven, and embedded within existing community infrastructures,” Dr. Piatt said in her presentation.
Working with churches is one approach to working within existing community infrastructures: “Churches are embedded in the community, they have the personnel oftentimes to facilitate these types of health programs, and most importantly, they have the established relationships with the community that brings about sustained changes,” Dr. Piatt said in her presentation.
Addressing diabetes education needs in urban, low-resource communities
The Praise Diabetes Project was a randomized, 33-month clinical trial conducted in 21 predominantly Black churches in Detroit; Flint, Mich.; and Toledo, Ohio, which are all urban, low-resource communities where diabetes is a significant public health problem, according to Dr. Piatt.
The study was designed to evaluate the relative effectiveness of three different approaches to diabetes self-management support at improving A1c and levels of diabetes distress, according to the investigators.
The churches were randomized to one of the support arms, including parish nurse plus peer leader support, parish nurse support by itself, or peer leader support by itself.
A total of 47 individuals were trained, including 31 peer leaders and 16 parish nurses.
All three interventions included an initial 6-month period of “enhanced usual care” during which biweekly newsletters that were distributed, according to Dr. Piatt. That was followed by 12 months of diabetes self-management support, and an additional 12 months of ongoing support facilitated by parish nurses and peer leaders on their own, without input from the research team or health care providers.
Participants in the program had to be at least 21 years old and under the care of a physician for their diabetes, according to Dr. Piatt. The parish nurses had to be registered nurses in Michigan or Ohio. Peer leaders had to be at least 21 years old, had at least an eighth-grade education, and had to commit to a 30-hour training program.
Peer leaders also had to be individuals living with diabetes: “Prior studies have found that, when peer leaders are actively working on their own self-management goals, they tend to be much more successful in helping others,” Dr. Piatt explained.
In addition to facilitating diabetes self-management education, the parish nurses and peer leaders in these interventions were responsible for recruitment, church announcements, room reservations, follow-up calls to participants, according to Dr. Piatt. Parish nurses also provided clinical content knowledge and supervised the peer leaders in the combined model.
Sustained reductions in A1c and diabetes distress
These diabetes self-management support approaches led to significant changes over time in A1c and diabetes distress, the primary outcomes of the study, Dr. Piatt said.
The peer leader support approach resulted in a statistically significant decline in A1c, from a mean of 8.0% at baseline to 7.7% at 33 months (P = .04), while nonsignificant declines were observed in the parish nurse and combined parish nurse–peer leader approach, according to the researcher.
Reductions in A1c persisted despite the COVID-19 pandemic, which began roughly 21 months into the study, she said.
Glycemic control remained steady over the course of the study, as illustrated by similar proportions of participants with A1c below 7% from baseline to 33 months, she added.
Sustained glycemic control was seen in all three groups, according to Dr. Piatt. For example, 42.7% of individuals in the parish nurse and peer leader support group achieved glycemic control following the intervention, and 88.5% of them sustained it at 33 months.
“I think this is one of the longest diabetes self-management education and diabetes self-management support interventions that’s out there right now, so we were so happy to see that sustained by glycemic control that far into the future,” she said.
Diabetes distress levels decreased steadily over time in all three groups, with declines that were statistically significant from baseline to 33 months in the parish nurse–only and peer leader–only groups, the investigator said.
The proportion of participants reporting moderate levels of diabetes distress dropped over time, especially in the peer leader support group, where there was a 50% reduction, she added.
Despite these findings, the study had limitations, according to Dr. Piatt, including some “burnout” that impacted participants, parish nurses, and peer leaders, especially after the pandemic started.
In addition, this type of intervention may have limited impact in the community at large: “We probably didn’t reach people who did not have good connection to the church,” Dr. Piatt said.
Dr. Piatt reported no conflicts of interest related to the research.
A church-based diabetes self-management support intervention that incorporated parish nurses and peer leaders is feasible and may help improve diabetes-related outcomes in participants.
Sustained reductions in hemoglobin A1c and diabetes distress were seen in the Praise Diabetes Project, a 33-month study that piloted several different approaches to parish nurse and peer leader support at 21 urban churches in Michigan and Ohio, said Gretchen Piatt, MPH, PhD, associate professor in the department of learning health sciences at the University of Michigan, Ann Arbor, reported at the annual scientific sessions of the American Diabetes Association.
“Of the participants who achieved glycemic control following diabetes self-management education, a really large proportion – upward of 77% of participants across all the groups– achieved sustained glycemic control at 33 months,” Dr. Piatt said.
Findings from this study has helped diabetes educators better understand how to design effective support approaches that may have a long-term impact on glycemic control and diabetes distress, Dr. Piatt said.
The Praise Diabetes Project represents a “very smart strategy” of leveraging institutions that already exist in the African American community that are trusted and provide emotional support, said Tracey D. Brown, CEO of the ADA.
“This is about behavior change, really, at its crux,” Ms. Brown said in an interview. “To get there, you’ve got to have trust, and you have to have an emotional connection. If you don’t get either one of those things, then you really are not going to do anything in terms of changing behavior.”
Long-term solutions needed
Many studies show that diabetes self-management education can improve clinical and psychosocial outcomes, and reduce health care utilization and cost, at least in the short term, Dr. Piatt said. However, it’s less clear how those improvements can be sustained over longer periods of time.
“This then presents a critical need to develop and evaluate diabetes self-management support models that are ongoing, patient driven, and embedded within existing community infrastructures,” Dr. Piatt said in her presentation.
Working with churches is one approach to working within existing community infrastructures: “Churches are embedded in the community, they have the personnel oftentimes to facilitate these types of health programs, and most importantly, they have the established relationships with the community that brings about sustained changes,” Dr. Piatt said in her presentation.
Addressing diabetes education needs in urban, low-resource communities
The Praise Diabetes Project was a randomized, 33-month clinical trial conducted in 21 predominantly Black churches in Detroit; Flint, Mich.; and Toledo, Ohio, which are all urban, low-resource communities where diabetes is a significant public health problem, according to Dr. Piatt.
The study was designed to evaluate the relative effectiveness of three different approaches to diabetes self-management support at improving A1c and levels of diabetes distress, according to the investigators.
The churches were randomized to one of the support arms, including parish nurse plus peer leader support, parish nurse support by itself, or peer leader support by itself.
A total of 47 individuals were trained, including 31 peer leaders and 16 parish nurses.
All three interventions included an initial 6-month period of “enhanced usual care” during which biweekly newsletters that were distributed, according to Dr. Piatt. That was followed by 12 months of diabetes self-management support, and an additional 12 months of ongoing support facilitated by parish nurses and peer leaders on their own, without input from the research team or health care providers.
Participants in the program had to be at least 21 years old and under the care of a physician for their diabetes, according to Dr. Piatt. The parish nurses had to be registered nurses in Michigan or Ohio. Peer leaders had to be at least 21 years old, had at least an eighth-grade education, and had to commit to a 30-hour training program.
Peer leaders also had to be individuals living with diabetes: “Prior studies have found that, when peer leaders are actively working on their own self-management goals, they tend to be much more successful in helping others,” Dr. Piatt explained.
In addition to facilitating diabetes self-management education, the parish nurses and peer leaders in these interventions were responsible for recruitment, church announcements, room reservations, follow-up calls to participants, according to Dr. Piatt. Parish nurses also provided clinical content knowledge and supervised the peer leaders in the combined model.
Sustained reductions in A1c and diabetes distress
These diabetes self-management support approaches led to significant changes over time in A1c and diabetes distress, the primary outcomes of the study, Dr. Piatt said.
The peer leader support approach resulted in a statistically significant decline in A1c, from a mean of 8.0% at baseline to 7.7% at 33 months (P = .04), while nonsignificant declines were observed in the parish nurse and combined parish nurse–peer leader approach, according to the researcher.
Reductions in A1c persisted despite the COVID-19 pandemic, which began roughly 21 months into the study, she said.
Glycemic control remained steady over the course of the study, as illustrated by similar proportions of participants with A1c below 7% from baseline to 33 months, she added.
Sustained glycemic control was seen in all three groups, according to Dr. Piatt. For example, 42.7% of individuals in the parish nurse and peer leader support group achieved glycemic control following the intervention, and 88.5% of them sustained it at 33 months.
“I think this is one of the longest diabetes self-management education and diabetes self-management support interventions that’s out there right now, so we were so happy to see that sustained by glycemic control that far into the future,” she said.
Diabetes distress levels decreased steadily over time in all three groups, with declines that were statistically significant from baseline to 33 months in the parish nurse–only and peer leader–only groups, the investigator said.
The proportion of participants reporting moderate levels of diabetes distress dropped over time, especially in the peer leader support group, where there was a 50% reduction, she added.
Despite these findings, the study had limitations, according to Dr. Piatt, including some “burnout” that impacted participants, parish nurses, and peer leaders, especially after the pandemic started.
In addition, this type of intervention may have limited impact in the community at large: “We probably didn’t reach people who did not have good connection to the church,” Dr. Piatt said.
Dr. Piatt reported no conflicts of interest related to the research.
FROM ADA 2020
Novel oral inhibitor may block intestinal damage in celiac disease
A novel oral inhibitor of transglutaminase 2 appears to block gluten-induced mucosal damage in patients with celiac disease at three different doses, based on proof-of-concept trial data from 132 patients.

“Currently, no drug therapy reliably prevents the effects of dietary gluten or has been approved by regulators to treat celiac disease,” which remains an unmet need in these patients, many of whom struggle with symptoms even when they adhere to a gluten-free diet, wrote Detlef Schuppan, MD, of Johannes Gutenberg University of Mainz (Germany) and colleagues.
Celiac disease is driven in part by the enzyme transglutaminase 2, and a transglutaminase 2 inhibitor known as ZED1227 has been tested safely in phase 1 trials, they reported.
“ZED1227 targets the intestinal mucosa predominantly and thereby mediates protection; thus, it is unaffected by the complexity of the food matrix and is less dependent on the timing of ingestion of gluten-containing food,” the researchers explained.
In a study published in the New England Journal of Medicine, the researchers assessed the safety and efficacy of three dose levels of ZED1227. Adults with controlled celiac disease were randomized to doses of 10 mg (41 patients), 50 mg (41 patients), and 100 mg (41 patients), and 40 patients received a placebo. Of these, 35, 39, 28, and 30 patients, respectively, had sufficient duodenal biopsy samples for analysis.
Patients underwent a daily gluten challenge of 3 g for 6 weeks. At the end of 6 weeks, the primary study endpoint of attenuation of gluten-induced mucosal damage was measured by the ratio of villus height to crypt depth.
Patients in all three treatment groups showed significant attenuation of mucosal damage. The change in the average ratio of villus height to crypt depth compared to placebo in the 10-mg, 50-mg, and 100-mg groups was 0.44, 0.49, and 0.48, respectively, with P values equal to .001 in the 10-mg group and less than .001 in the 50-mg and 100-mg groups.
Adverse events were similar across all treatment groups and the placebo group, with the exception of a rash in three patients in the 100-mg group. A total of 74 patients reported adverse events, and the most common were headache, nausea, diarrhea, vomiting, and abdominal pain. The investigators determined that from 34% to 55% of the adverse events across groups were related to the study drug or placebo.
Two patients developed serious adverse events that were deemed related to the study drug or placebo; one patient in the 50-mg group developed migraine with aura, and one placebo patient developed ventricular extrasystoles. The patients recovered after discontinuing the drug or placebo.
Secondary endpoints included intraepithelial lymphocyte density, the Celiac Symptom Index score, and the Celiac Disease Questionnaire score. Estimated changes in intraepithelial lymphocyte density, compared with placebo, were –2.7 cells per 100 epithelial cells in the 10-mg group, −4.2 cells per 100 epithelial cells in the 50-mg group, and −9.6 cells per 100 epithelial cells in the 100-mg group. Compared with those of patients taking placebo, the 6-week changes in Celiac Symptom Index scores and Celiac Disease Questionnaire scores suggested slight improvements in symptoms and quality of life for the 100-mg dose.
The study findings were limited by several factors including missing data and loss of several patients to follow-up, as well as the short trial duration and use of controlled gluten ingestion, the researchers noted. Larger studies involving real-world conditions of minor gluten ingestion are needed to support the preliminary signs of safety and efficacy, they said.
Study strengths include high levels of patient adherence to the treatment and the gluten challenge, they said. “Future studies of ZED1227 in more patients are needed to provide additional evidence of the safety and efficacy of the drug, potentially in real-life conditions with minor gluten ingestion,” they concluded.
Translating potential into practice
“An absence of mucosal damage is a critical criterion to ensure the long-term health of a patient, and this clinical trial in celiac disease meets this important endpoint,” Bana Jabri, MD, of the University of Chicago, wrote in an accompanying editorial.
The primary endpoint of no mucosal damage is “especially notable because it was achieved under a controlled gluten challenge, albeit with a relatively moderate amount of gluten (a regular diet contains 12 g of gluten daily, whereas the challenge involved 3 g daily) and for a short period of time,” Dr. Jabri said. The reduction of disease-associated symptoms and apparent improvement in quality of life with 100-mg dose added value to the findings, she said.
Future research areas include whether cross-reactive T cells, which were not analyzed in the current study, might “expand and become pathogenic after a long-term gluten challenge,” Dr. Jabri noted.
However, “ZED1227 is the first nondietary treatment that has preliminarily shown the capacity to prevent mucosal damage in persons with celiac disease,” she said.
“Although this trial is very encouraging, whether treatment with ZED1227, and more generally transglutaminase 2 inhibition, in patients with celiac disease will be efficient in real life and during long-term gluten exposure remains to be determined,” Dr. Jabri concluded.
Need for data on dosing consistency
“Celiac disease affects up to 2% of the population in many countries, and the main therapy of celiac disease is avoidance of gluten,” Kim Isaacs, MD, of the University of North Carolina, Chapel Hill, said in an interview. “This is challenging due to the ubiquitous nature of gluten in many food products,” she said. “Restrictive eating also affects social interaction which is often focused around food,” she added. “Availability of an oral therapy that is effective to treat celiac in the face of gluten exposure will have a profound impact on patients in terms of liberalization of dietary intake.”
Overall, “the changes in the villus height to crypt depth was similar between all the active treatment groups, whereas there was a dose-dependent reduction in transepithelial lymphocyte density,” Dr. Isaacs noted. “The symptom improvement was greatest in the 100-mg group, suggesting that symptoms may be related to a greater extent to the lymphocyte density than the minimal differences in villus height to crypt depth ratios seen in the active treatment groups,” she said.
Potential barriers to the use of the treatment include cost because “this will need to be a daily long-term therapy,” said Dr. Isaacs. “Compliance is a potential barrier as well,” she said. “This study looks at daily administration of the transglutaminase 2 inhibitor and shows a benefit, but it is not clear whether missing doses of the medication will have a prolonged impact on efficacy,” she emphasized. Consequently, long-term efficacy studies are needed, Dr. Isaacs said. Other research questions to answer include whether patients will become refractory to the beneficial effects over time, the effect of missing doses, and whether patients would lose all the benefits of the therapy if dosing is not consistent, she emphasized.
The study was funded by Dr. Falk Pharma. The researchers, as well as Dr. Jabri and Dr. Isaacs, had no financial conflicts to disclose. Dr. Isaacs is on the editorial advisory board of GI & Hepatology News.
A novel oral inhibitor of transglutaminase 2 appears to block gluten-induced mucosal damage in patients with celiac disease at three different doses, based on proof-of-concept trial data from 132 patients.
“Currently, no drug therapy reliably prevents the effects of dietary gluten or has been approved by regulators to treat celiac disease,” which remains an unmet need in these patients, many of whom struggle with symptoms even when they adhere to a gluten-free diet, wrote Detlef Schuppan, MD, of Johannes Gutenberg University of Mainz (Germany) and colleagues.
Celiac disease is driven in part by the enzyme transglutaminase 2, and a transglutaminase 2 inhibitor known as ZED1227 has been tested safely in phase 1 trials, they reported.
“ZED1227 targets the intestinal mucosa predominantly and thereby mediates protection; thus, it is unaffected by the complexity of the food matrix and is less dependent on the timing of ingestion of gluten-containing food,” the researchers explained.
In a study published in the New England Journal of Medicine, the researchers assessed the safety and efficacy of three dose levels of ZED1227. Adults with controlled celiac disease were randomized to doses of 10 mg (41 patients), 50 mg (41 patients), and 100 mg (41 patients), and 40 patients received a placebo. Of these, 35, 39, 28, and 30 patients, respectively, had sufficient duodenal biopsy samples for analysis.
Patients underwent a daily gluten challenge of 3 g for 6 weeks. At the end of 6 weeks, the primary study endpoint of attenuation of gluten-induced mucosal damage was measured by the ratio of villus height to crypt depth.
Patients in all three treatment groups showed significant attenuation of mucosal damage. The change in the average ratio of villus height to crypt depth compared to placebo in the 10-mg, 50-mg, and 100-mg groups was 0.44, 0.49, and 0.48, respectively, with P values equal to .001 in the 10-mg group and less than .001 in the 50-mg and 100-mg groups.
Adverse events were similar across all treatment groups and the placebo group, with the exception of a rash in three patients in the 100-mg group. A total of 74 patients reported adverse events, and the most common were headache, nausea, diarrhea, vomiting, and abdominal pain. The investigators determined that from 34% to 55% of the adverse events across groups were related to the study drug or placebo.
Two patients developed serious adverse events that were deemed related to the study drug or placebo; one patient in the 50-mg group developed migraine with aura, and one placebo patient developed ventricular extrasystoles. The patients recovered after discontinuing the drug or placebo.
Secondary endpoints included intraepithelial lymphocyte density, the Celiac Symptom Index score, and the Celiac Disease Questionnaire score. Estimated changes in intraepithelial lymphocyte density, compared with placebo, were –2.7 cells per 100 epithelial cells in the 10-mg group, −4.2 cells per 100 epithelial cells in the 50-mg group, and −9.6 cells per 100 epithelial cells in the 100-mg group. Compared with those of patients taking placebo, the 6-week changes in Celiac Symptom Index scores and Celiac Disease Questionnaire scores suggested slight improvements in symptoms and quality of life for the 100-mg dose.
The study findings were limited by several factors including missing data and loss of several patients to follow-up, as well as the short trial duration and use of controlled gluten ingestion, the researchers noted. Larger studies involving real-world conditions of minor gluten ingestion are needed to support the preliminary signs of safety and efficacy, they said.
Study strengths include high levels of patient adherence to the treatment and the gluten challenge, they said. “Future studies of ZED1227 in more patients are needed to provide additional evidence of the safety and efficacy of the drug, potentially in real-life conditions with minor gluten ingestion,” they concluded.
Translating potential into practice
“An absence of mucosal damage is a critical criterion to ensure the long-term health of a patient, and this clinical trial in celiac disease meets this important endpoint,” Bana Jabri, MD, of the University of Chicago, wrote in an accompanying editorial.
The primary endpoint of no mucosal damage is “especially notable because it was achieved under a controlled gluten challenge, albeit with a relatively moderate amount of gluten (a regular diet contains 12 g of gluten daily, whereas the challenge involved 3 g daily) and for a short period of time,” Dr. Jabri said. The reduction of disease-associated symptoms and apparent improvement in quality of life with 100-mg dose added value to the findings, she said.
Future research areas include whether cross-reactive T cells, which were not analyzed in the current study, might “expand and become pathogenic after a long-term gluten challenge,” Dr. Jabri noted.
However, “ZED1227 is the first nondietary treatment that has preliminarily shown the capacity to prevent mucosal damage in persons with celiac disease,” she said.
“Although this trial is very encouraging, whether treatment with ZED1227, and more generally transglutaminase 2 inhibition, in patients with celiac disease will be efficient in real life and during long-term gluten exposure remains to be determined,” Dr. Jabri concluded.
Need for data on dosing consistency
“Celiac disease affects up to 2% of the population in many countries, and the main therapy of celiac disease is avoidance of gluten,” Kim Isaacs, MD, of the University of North Carolina, Chapel Hill, said in an interview. “This is challenging due to the ubiquitous nature of gluten in many food products,” she said. “Restrictive eating also affects social interaction which is often focused around food,” she added. “Availability of an oral therapy that is effective to treat celiac in the face of gluten exposure will have a profound impact on patients in terms of liberalization of dietary intake.”
Overall, “the changes in the villus height to crypt depth was similar between all the active treatment groups, whereas there was a dose-dependent reduction in transepithelial lymphocyte density,” Dr. Isaacs noted. “The symptom improvement was greatest in the 100-mg group, suggesting that symptoms may be related to a greater extent to the lymphocyte density than the minimal differences in villus height to crypt depth ratios seen in the active treatment groups,” she said.
Potential barriers to the use of the treatment include cost because “this will need to be a daily long-term therapy,” said Dr. Isaacs. “Compliance is a potential barrier as well,” she said. “This study looks at daily administration of the transglutaminase 2 inhibitor and shows a benefit, but it is not clear whether missing doses of the medication will have a prolonged impact on efficacy,” she emphasized. Consequently, long-term efficacy studies are needed, Dr. Isaacs said. Other research questions to answer include whether patients will become refractory to the beneficial effects over time, the effect of missing doses, and whether patients would lose all the benefits of the therapy if dosing is not consistent, she emphasized.
The study was funded by Dr. Falk Pharma. The researchers, as well as Dr. Jabri and Dr. Isaacs, had no financial conflicts to disclose. Dr. Isaacs is on the editorial advisory board of GI & Hepatology News.
A novel oral inhibitor of transglutaminase 2 appears to block gluten-induced mucosal damage in patients with celiac disease at three different doses, based on proof-of-concept trial data from 132 patients.
“Currently, no drug therapy reliably prevents the effects of dietary gluten or has been approved by regulators to treat celiac disease,” which remains an unmet need in these patients, many of whom struggle with symptoms even when they adhere to a gluten-free diet, wrote Detlef Schuppan, MD, of Johannes Gutenberg University of Mainz (Germany) and colleagues.
Celiac disease is driven in part by the enzyme transglutaminase 2, and a transglutaminase 2 inhibitor known as ZED1227 has been tested safely in phase 1 trials, they reported.
“ZED1227 targets the intestinal mucosa predominantly and thereby mediates protection; thus, it is unaffected by the complexity of the food matrix and is less dependent on the timing of ingestion of gluten-containing food,” the researchers explained.
In a study published in the New England Journal of Medicine, the researchers assessed the safety and efficacy of three dose levels of ZED1227. Adults with controlled celiac disease were randomized to doses of 10 mg (41 patients), 50 mg (41 patients), and 100 mg (41 patients), and 40 patients received a placebo. Of these, 35, 39, 28, and 30 patients, respectively, had sufficient duodenal biopsy samples for analysis.
Patients underwent a daily gluten challenge of 3 g for 6 weeks. At the end of 6 weeks, the primary study endpoint of attenuation of gluten-induced mucosal damage was measured by the ratio of villus height to crypt depth.
Patients in all three treatment groups showed significant attenuation of mucosal damage. The change in the average ratio of villus height to crypt depth compared to placebo in the 10-mg, 50-mg, and 100-mg groups was 0.44, 0.49, and 0.48, respectively, with P values equal to .001 in the 10-mg group and less than .001 in the 50-mg and 100-mg groups.
Adverse events were similar across all treatment groups and the placebo group, with the exception of a rash in three patients in the 100-mg group. A total of 74 patients reported adverse events, and the most common were headache, nausea, diarrhea, vomiting, and abdominal pain. The investigators determined that from 34% to 55% of the adverse events across groups were related to the study drug or placebo.
Two patients developed serious adverse events that were deemed related to the study drug or placebo; one patient in the 50-mg group developed migraine with aura, and one placebo patient developed ventricular extrasystoles. The patients recovered after discontinuing the drug or placebo.
Secondary endpoints included intraepithelial lymphocyte density, the Celiac Symptom Index score, and the Celiac Disease Questionnaire score. Estimated changes in intraepithelial lymphocyte density, compared with placebo, were –2.7 cells per 100 epithelial cells in the 10-mg group, −4.2 cells per 100 epithelial cells in the 50-mg group, and −9.6 cells per 100 epithelial cells in the 100-mg group. Compared with those of patients taking placebo, the 6-week changes in Celiac Symptom Index scores and Celiac Disease Questionnaire scores suggested slight improvements in symptoms and quality of life for the 100-mg dose.
The study findings were limited by several factors including missing data and loss of several patients to follow-up, as well as the short trial duration and use of controlled gluten ingestion, the researchers noted. Larger studies involving real-world conditions of minor gluten ingestion are needed to support the preliminary signs of safety and efficacy, they said.
Study strengths include high levels of patient adherence to the treatment and the gluten challenge, they said. “Future studies of ZED1227 in more patients are needed to provide additional evidence of the safety and efficacy of the drug, potentially in real-life conditions with minor gluten ingestion,” they concluded.
Translating potential into practice
“An absence of mucosal damage is a critical criterion to ensure the long-term health of a patient, and this clinical trial in celiac disease meets this important endpoint,” Bana Jabri, MD, of the University of Chicago, wrote in an accompanying editorial.
The primary endpoint of no mucosal damage is “especially notable because it was achieved under a controlled gluten challenge, albeit with a relatively moderate amount of gluten (a regular diet contains 12 g of gluten daily, whereas the challenge involved 3 g daily) and for a short period of time,” Dr. Jabri said. The reduction of disease-associated symptoms and apparent improvement in quality of life with 100-mg dose added value to the findings, she said.
Future research areas include whether cross-reactive T cells, which were not analyzed in the current study, might “expand and become pathogenic after a long-term gluten challenge,” Dr. Jabri noted.
However, “ZED1227 is the first nondietary treatment that has preliminarily shown the capacity to prevent mucosal damage in persons with celiac disease,” she said.
“Although this trial is very encouraging, whether treatment with ZED1227, and more generally transglutaminase 2 inhibition, in patients with celiac disease will be efficient in real life and during long-term gluten exposure remains to be determined,” Dr. Jabri concluded.
Need for data on dosing consistency
“Celiac disease affects up to 2% of the population in many countries, and the main therapy of celiac disease is avoidance of gluten,” Kim Isaacs, MD, of the University of North Carolina, Chapel Hill, said in an interview. “This is challenging due to the ubiquitous nature of gluten in many food products,” she said. “Restrictive eating also affects social interaction which is often focused around food,” she added. “Availability of an oral therapy that is effective to treat celiac in the face of gluten exposure will have a profound impact on patients in terms of liberalization of dietary intake.”
Overall, “the changes in the villus height to crypt depth was similar between all the active treatment groups, whereas there was a dose-dependent reduction in transepithelial lymphocyte density,” Dr. Isaacs noted. “The symptom improvement was greatest in the 100-mg group, suggesting that symptoms may be related to a greater extent to the lymphocyte density than the minimal differences in villus height to crypt depth ratios seen in the active treatment groups,” she said.
Potential barriers to the use of the treatment include cost because “this will need to be a daily long-term therapy,” said Dr. Isaacs. “Compliance is a potential barrier as well,” she said. “This study looks at daily administration of the transglutaminase 2 inhibitor and shows a benefit, but it is not clear whether missing doses of the medication will have a prolonged impact on efficacy,” she emphasized. Consequently, long-term efficacy studies are needed, Dr. Isaacs said. Other research questions to answer include whether patients will become refractory to the beneficial effects over time, the effect of missing doses, and whether patients would lose all the benefits of the therapy if dosing is not consistent, she emphasized.
The study was funded by Dr. Falk Pharma. The researchers, as well as Dr. Jabri and Dr. Isaacs, had no financial conflicts to disclose. Dr. Isaacs is on the editorial advisory board of GI & Hepatology News.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Rapid core antigen HCV tests could expand accessibility
A proposed rapid diagnostic test for hepatitis C viral infections that combines an inexpensive but lower-sensitivity core-antigen test with lab RNA confirmation of negative tests could expand testing and same-day initiation of antiviral therapy in places where resources are limited, investigators said.
Applying the proposed method to the Republic of Georgia, with a hepatitis C virus (HCV) prevalence of 5.4% as reported by the World Health Organization, would result in a 95.4% diagnosis rate, compared with 78.8% for lab-based RNA testing, which is the standard of care. Applied to Malaysia, the proposed method would boost diagnosis rates from 57.0% to 91.2%, reported Madeline Adee, MPH, from Massachusetts General Hospital’s Institute for Technology Assessment in Boston and colleagues.
“We found that a novel core antigen rapid diagnostic test for HCV could improve the diagnosis rate and result in cost savings. Although not yet developed, such a test could be a game changer and have a substantial impact on the feasibility and cost of HCV elimination, especially in low and middle-income countries,” they wrote in a poster presented at the meeting sponsored by the European Association for the Study of the Liver.
Although rapid diagnostic tests for HCV can improve diagnosis and treatment rates, currently available molecular tests are expensive and require a solid clinical laboratory infrastructure, which can put such tests out of the reach for clinicians in low- or middle-income countries. Rapid immunoassays based on HCV core antigens are comparative bargains, but their sensitivity ranges from 70% to 90%; in contrast, the third-generation HCV enzyme immunoassay has about a 98% sensitivity.
Could it work?
The proposed testing method would be likely to improve diagnosis, but whether that would translate into increased treatment is uncertain, commented Lesley Miller, MD, who specializes in HCV screening and treatment in underserved populations at Emory University, Atlanta.
“When we’re talking about hepatitis C, it’s all about the care cascade, the drop-off at each step from those who have the disease and aren’t diagnosed, to those who are tested and only partially diagnosed because they don’t have a confirmed infection, to those that get into care, get treated, and get cured,” she said in an interview.
“It’s all about closing the gaps in the care cascade in order to achieve elimination of the virus, which is what we’re all trying to do,” she added.
She pointed that there are certain at-risk populations in the United States, such as injectable-drug users, who might be able to benefit from such a system.
“These folks often have less access to traditional care, so bringing rapid testing and care to where those folks are is really important, so if we can deploy mobile units to areas where there is high prevalence and do it at the point of care, it simplifies the entire process,” she said.
Thomas J. Hoerger, PhD, a senior fellow in health economics and financing at the nonprofit research group RTI International in Research Triangle Park, N.C., said in an interview that the proposed model could eliminate the step in testing in which patients are required to return for confirmation.
“People don’t always come back for further testing, so if you can do it immediately and have the results of a screening test, you might be able to get people to come back more quickly. You still have the problem of the high cost of treatment, but this would at least make it a little more convenient,” he said.
He noted that the success of the strategy would be dependent on the sensitivity of the rapid core antigen test, it’s cost relative to HCV RNA testing, and whether the availability of the rapid test would translate into an improvement in follow-up.
Neither Dr. Miller nor Dr. Hoerger were involved in the study.
Evaluating the approach
To determine whether a lower-cost rapid test could be cost effective, the researchers created a microsimulation model of the natural history of HCV to compare potential outcomes from either core antigen rapid diagnostic testing with a base case sensitivity for HCV viremia of 80% with lab-based RNA confirmation for negative results or the current standard of care with lab-based RNA confirmation only.
The model incorporated METAVIR stage F0-F4, decompensated cirrhosis, hepatocellular carcinoma, and liver-related death. The investigators determined the baseline characteristics of HCV patients in each country based on different distributions of sex, HCV genotype, and METAVIR fibrosis stage.
They simulated outcomes for 10,000 adults in the Republic of Georgia, with an HCV prevalence of 5.4%, and Malaysia, with an HCV prevalence of 1.5%.
The model considers costs from a health care payer’s perspective, and the investigations performed deterministic and probabilistic sensitivity analyses to evaluate how the cost-effectiveness of testing pathways might change when various factors were plugged into the model.
As noted before, the investigators determined that the core antigen rapid test algorithm would improve diagnosis rates in Georgia from 78.8% to 95.4% and in Malaysia from 57.9% to 91.2%.
The use of the rapid test would also increase quality-adjusted life-years in Georgia by 207 per 10,000 and in Malaysia by 146 per 10,000.
Cost savings, primarily from averting the costs of care for patients with HCV, begin within the first year of the model. Over 50 years, the lifetime horizon cost savings in Georgia would be $232,000 per 10,000 people, and the corresponding savings in Malaysia would be $504,000 per 10,000 people.
Even when allowing for variations in parameters, the core antigen rapid diagnostic test approach remained the preferred model, the investigators reported.
The study was supported by the global health agency Unitaid. The researchers, Dr. Miller, and Dr. Hoerger reported no conflicts of interest relevant to the study.
A proposed rapid diagnostic test for hepatitis C viral infections that combines an inexpensive but lower-sensitivity core-antigen test with lab RNA confirmation of negative tests could expand testing and same-day initiation of antiviral therapy in places where resources are limited, investigators said.
Applying the proposed method to the Republic of Georgia, with a hepatitis C virus (HCV) prevalence of 5.4% as reported by the World Health Organization, would result in a 95.4% diagnosis rate, compared with 78.8% for lab-based RNA testing, which is the standard of care. Applied to Malaysia, the proposed method would boost diagnosis rates from 57.0% to 91.2%, reported Madeline Adee, MPH, from Massachusetts General Hospital’s Institute for Technology Assessment in Boston and colleagues.
“We found that a novel core antigen rapid diagnostic test for HCV could improve the diagnosis rate and result in cost savings. Although not yet developed, such a test could be a game changer and have a substantial impact on the feasibility and cost of HCV elimination, especially in low and middle-income countries,” they wrote in a poster presented at the meeting sponsored by the European Association for the Study of the Liver.
Although rapid diagnostic tests for HCV can improve diagnosis and treatment rates, currently available molecular tests are expensive and require a solid clinical laboratory infrastructure, which can put such tests out of the reach for clinicians in low- or middle-income countries. Rapid immunoassays based on HCV core antigens are comparative bargains, but their sensitivity ranges from 70% to 90%; in contrast, the third-generation HCV enzyme immunoassay has about a 98% sensitivity.
Could it work?
The proposed testing method would be likely to improve diagnosis, but whether that would translate into increased treatment is uncertain, commented Lesley Miller, MD, who specializes in HCV screening and treatment in underserved populations at Emory University, Atlanta.
“When we’re talking about hepatitis C, it’s all about the care cascade, the drop-off at each step from those who have the disease and aren’t diagnosed, to those who are tested and only partially diagnosed because they don’t have a confirmed infection, to those that get into care, get treated, and get cured,” she said in an interview.
“It’s all about closing the gaps in the care cascade in order to achieve elimination of the virus, which is what we’re all trying to do,” she added.
She pointed that there are certain at-risk populations in the United States, such as injectable-drug users, who might be able to benefit from such a system.
“These folks often have less access to traditional care, so bringing rapid testing and care to where those folks are is really important, so if we can deploy mobile units to areas where there is high prevalence and do it at the point of care, it simplifies the entire process,” she said.
Thomas J. Hoerger, PhD, a senior fellow in health economics and financing at the nonprofit research group RTI International in Research Triangle Park, N.C., said in an interview that the proposed model could eliminate the step in testing in which patients are required to return for confirmation.
“People don’t always come back for further testing, so if you can do it immediately and have the results of a screening test, you might be able to get people to come back more quickly. You still have the problem of the high cost of treatment, but this would at least make it a little more convenient,” he said.
He noted that the success of the strategy would be dependent on the sensitivity of the rapid core antigen test, it’s cost relative to HCV RNA testing, and whether the availability of the rapid test would translate into an improvement in follow-up.
Neither Dr. Miller nor Dr. Hoerger were involved in the study.
Evaluating the approach
To determine whether a lower-cost rapid test could be cost effective, the researchers created a microsimulation model of the natural history of HCV to compare potential outcomes from either core antigen rapid diagnostic testing with a base case sensitivity for HCV viremia of 80% with lab-based RNA confirmation for negative results or the current standard of care with lab-based RNA confirmation only.
The model incorporated METAVIR stage F0-F4, decompensated cirrhosis, hepatocellular carcinoma, and liver-related death. The investigators determined the baseline characteristics of HCV patients in each country based on different distributions of sex, HCV genotype, and METAVIR fibrosis stage.
They simulated outcomes for 10,000 adults in the Republic of Georgia, with an HCV prevalence of 5.4%, and Malaysia, with an HCV prevalence of 1.5%.
The model considers costs from a health care payer’s perspective, and the investigations performed deterministic and probabilistic sensitivity analyses to evaluate how the cost-effectiveness of testing pathways might change when various factors were plugged into the model.
As noted before, the investigators determined that the core antigen rapid test algorithm would improve diagnosis rates in Georgia from 78.8% to 95.4% and in Malaysia from 57.9% to 91.2%.
The use of the rapid test would also increase quality-adjusted life-years in Georgia by 207 per 10,000 and in Malaysia by 146 per 10,000.
Cost savings, primarily from averting the costs of care for patients with HCV, begin within the first year of the model. Over 50 years, the lifetime horizon cost savings in Georgia would be $232,000 per 10,000 people, and the corresponding savings in Malaysia would be $504,000 per 10,000 people.
Even when allowing for variations in parameters, the core antigen rapid diagnostic test approach remained the preferred model, the investigators reported.
The study was supported by the global health agency Unitaid. The researchers, Dr. Miller, and Dr. Hoerger reported no conflicts of interest relevant to the study.
A proposed rapid diagnostic test for hepatitis C viral infections that combines an inexpensive but lower-sensitivity core-antigen test with lab RNA confirmation of negative tests could expand testing and same-day initiation of antiviral therapy in places where resources are limited, investigators said.
Applying the proposed method to the Republic of Georgia, with a hepatitis C virus (HCV) prevalence of 5.4% as reported by the World Health Organization, would result in a 95.4% diagnosis rate, compared with 78.8% for lab-based RNA testing, which is the standard of care. Applied to Malaysia, the proposed method would boost diagnosis rates from 57.0% to 91.2%, reported Madeline Adee, MPH, from Massachusetts General Hospital’s Institute for Technology Assessment in Boston and colleagues.
“We found that a novel core antigen rapid diagnostic test for HCV could improve the diagnosis rate and result in cost savings. Although not yet developed, such a test could be a game changer and have a substantial impact on the feasibility and cost of HCV elimination, especially in low and middle-income countries,” they wrote in a poster presented at the meeting sponsored by the European Association for the Study of the Liver.
Although rapid diagnostic tests for HCV can improve diagnosis and treatment rates, currently available molecular tests are expensive and require a solid clinical laboratory infrastructure, which can put such tests out of the reach for clinicians in low- or middle-income countries. Rapid immunoassays based on HCV core antigens are comparative bargains, but their sensitivity ranges from 70% to 90%; in contrast, the third-generation HCV enzyme immunoassay has about a 98% sensitivity.
Could it work?
The proposed testing method would be likely to improve diagnosis, but whether that would translate into increased treatment is uncertain, commented Lesley Miller, MD, who specializes in HCV screening and treatment in underserved populations at Emory University, Atlanta.
“When we’re talking about hepatitis C, it’s all about the care cascade, the drop-off at each step from those who have the disease and aren’t diagnosed, to those who are tested and only partially diagnosed because they don’t have a confirmed infection, to those that get into care, get treated, and get cured,” she said in an interview.
“It’s all about closing the gaps in the care cascade in order to achieve elimination of the virus, which is what we’re all trying to do,” she added.
She pointed that there are certain at-risk populations in the United States, such as injectable-drug users, who might be able to benefit from such a system.
“These folks often have less access to traditional care, so bringing rapid testing and care to where those folks are is really important, so if we can deploy mobile units to areas where there is high prevalence and do it at the point of care, it simplifies the entire process,” she said.
Thomas J. Hoerger, PhD, a senior fellow in health economics and financing at the nonprofit research group RTI International in Research Triangle Park, N.C., said in an interview that the proposed model could eliminate the step in testing in which patients are required to return for confirmation.
“People don’t always come back for further testing, so if you can do it immediately and have the results of a screening test, you might be able to get people to come back more quickly. You still have the problem of the high cost of treatment, but this would at least make it a little more convenient,” he said.
He noted that the success of the strategy would be dependent on the sensitivity of the rapid core antigen test, it’s cost relative to HCV RNA testing, and whether the availability of the rapid test would translate into an improvement in follow-up.
Neither Dr. Miller nor Dr. Hoerger were involved in the study.
Evaluating the approach
To determine whether a lower-cost rapid test could be cost effective, the researchers created a microsimulation model of the natural history of HCV to compare potential outcomes from either core antigen rapid diagnostic testing with a base case sensitivity for HCV viremia of 80% with lab-based RNA confirmation for negative results or the current standard of care with lab-based RNA confirmation only.
The model incorporated METAVIR stage F0-F4, decompensated cirrhosis, hepatocellular carcinoma, and liver-related death. The investigators determined the baseline characteristics of HCV patients in each country based on different distributions of sex, HCV genotype, and METAVIR fibrosis stage.
They simulated outcomes for 10,000 adults in the Republic of Georgia, with an HCV prevalence of 5.4%, and Malaysia, with an HCV prevalence of 1.5%.
The model considers costs from a health care payer’s perspective, and the investigations performed deterministic and probabilistic sensitivity analyses to evaluate how the cost-effectiveness of testing pathways might change when various factors were plugged into the model.
As noted before, the investigators determined that the core antigen rapid test algorithm would improve diagnosis rates in Georgia from 78.8% to 95.4% and in Malaysia from 57.9% to 91.2%.
The use of the rapid test would also increase quality-adjusted life-years in Georgia by 207 per 10,000 and in Malaysia by 146 per 10,000.
Cost savings, primarily from averting the costs of care for patients with HCV, begin within the first year of the model. Over 50 years, the lifetime horizon cost savings in Georgia would be $232,000 per 10,000 people, and the corresponding savings in Malaysia would be $504,000 per 10,000 people.
Even when allowing for variations in parameters, the core antigen rapid diagnostic test approach remained the preferred model, the investigators reported.
The study was supported by the global health agency Unitaid. The researchers, Dr. Miller, and Dr. Hoerger reported no conflicts of interest relevant to the study.
FROM ILC 2021