User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Reducing hypersalivation
We would like to counter the suggestion to use benztropine or clonidine as a means to control clozapine-induced hypersalivation as suggested in “Reducing clozapine-induced hypersalivation” (Pearls, Current Psychiatry, October 2011, p. 77-78).
As stated in the article, clozapine is an antagonist for all known muscarinic receptors except M4—where it is an agonist—making it a potent anticholinergic medication with the potential to cause excessive saliva production.1,2 Another proposed mechanism for clozapine-induced hypersalivation is its antagonist activity at α-1 receptors, thus the suggestion to use clonidine to combat this side effect. The use of benztropine, another medication with known anticholinergic activity, or clonidine, a medication that may cause additional hypotension, to treat clozapine-induced hypersalivation may cause further unwanted complications and may not be the best option to treat this troubling side effect.
We have had great success locally using medications such as atropine or ipratropium as first-line treatments for clozapine-induced hypersalivation in an effort to minimize additional systemic side effects, such as those seen with benztropine and clonidine. Atropine eye drops administered orally, starting with 1 drop and titrated up to 2 drops twice daily to adequate response, has been shown to be successful according to patient opinion in several case reports.3 Alternatively, intranasal ipratropium orally administered 1 to 2 sprays, up to 3 times daily has shown improvement in clozapine-induced hypersalivation according to patient report.3 Although controlled trials to support the use of topical treatment for clozapine-induced hypersalivation are necessary, attempting to minimize additional adverse effects warrants a trial of atropine or ipratropium before using systemically acting medications such as benztropine or clonidine.
Sarah Hutfilz, PharmD
PGY1 Pharmacy Practice Resident
Department of Pharmacy
University of North Carolina Hospitals and Clinics
Clinical Instructor
University of North Carolina
Eshelman School of Pharmacy
Shauna Garris, PharmD, BCPP
Neurology/Psychiatry Clinical Specialist
Department of Pharmacy
University of North Carolina Hospitals and Clinics
Clinical Assistant Professor
University of North Carolina
Eshelman School of Pharmacy
M. Lindsey Kennedy, PharmD, BCPS, BCPP
Psychiatry Clinical Specialist
Department of Pharmacy
University of North Carolina Hospitals and Clinics
Clinical Assistant Professor
University of North Carolina School
of Medicine
University of North Carolina
Eshelman School of Pharmacy
Chapel Hill, NC
The authors respond
We thank Drs. Hutfilz, Garris, and Kennedy for their response and comments. We acknowledge that the medications we suggested have potentially harmful adverse effects; however, they are evidence-based. Atropine eye drops and ipratropium are interesting suggestions; if their use is based on evidence, they should have been included in the article.
We agree that further studies may show these topical approaches to be superior, but our recommendation, based on the best evidence available from the clinical studies, would be to use medications that have been studied while advocating for further study of medications with a theoretical superiority that is not yet proven.
Gurprit Lamba, MD
Geriatric Psychiatry Fellow
Partners HealthCare Geriatric Psychiatry Fellowship
Boston, MA
James M. Ellison, MD, MPH
Associate Professor of Psychiatry
Harvard Medical School
Boston, MA
We would like to counter the suggestion to use benztropine or clonidine as a means to control clozapine-induced hypersalivation as suggested in “Reducing clozapine-induced hypersalivation” (Pearls, Current Psychiatry, October 2011, p. 77-78).
As stated in the article, clozapine is an antagonist for all known muscarinic receptors except M4—where it is an agonist—making it a potent anticholinergic medication with the potential to cause excessive saliva production.1,2 Another proposed mechanism for clozapine-induced hypersalivation is its antagonist activity at α-1 receptors, thus the suggestion to use clonidine to combat this side effect. The use of benztropine, another medication with known anticholinergic activity, or clonidine, a medication that may cause additional hypotension, to treat clozapine-induced hypersalivation may cause further unwanted complications and may not be the best option to treat this troubling side effect.
We have had great success locally using medications such as atropine or ipratropium as first-line treatments for clozapine-induced hypersalivation in an effort to minimize additional systemic side effects, such as those seen with benztropine and clonidine. Atropine eye drops administered orally, starting with 1 drop and titrated up to 2 drops twice daily to adequate response, has been shown to be successful according to patient opinion in several case reports.3 Alternatively, intranasal ipratropium orally administered 1 to 2 sprays, up to 3 times daily has shown improvement in clozapine-induced hypersalivation according to patient report.3 Although controlled trials to support the use of topical treatment for clozapine-induced hypersalivation are necessary, attempting to minimize additional adverse effects warrants a trial of atropine or ipratropium before using systemically acting medications such as benztropine or clonidine.
Sarah Hutfilz, PharmD
PGY1 Pharmacy Practice Resident
Department of Pharmacy
University of North Carolina Hospitals and Clinics
Clinical Instructor
University of North Carolina
Eshelman School of Pharmacy
Shauna Garris, PharmD, BCPP
Neurology/Psychiatry Clinical Specialist
Department of Pharmacy
University of North Carolina Hospitals and Clinics
Clinical Assistant Professor
University of North Carolina
Eshelman School of Pharmacy
M. Lindsey Kennedy, PharmD, BCPS, BCPP
Psychiatry Clinical Specialist
Department of Pharmacy
University of North Carolina Hospitals and Clinics
Clinical Assistant Professor
University of North Carolina School
of Medicine
University of North Carolina
Eshelman School of Pharmacy
Chapel Hill, NC
The authors respond
We thank Drs. Hutfilz, Garris, and Kennedy for their response and comments. We acknowledge that the medications we suggested have potentially harmful adverse effects; however, they are evidence-based. Atropine eye drops and ipratropium are interesting suggestions; if their use is based on evidence, they should have been included in the article.
We agree that further studies may show these topical approaches to be superior, but our recommendation, based on the best evidence available from the clinical studies, would be to use medications that have been studied while advocating for further study of medications with a theoretical superiority that is not yet proven.
Gurprit Lamba, MD
Geriatric Psychiatry Fellow
Partners HealthCare Geriatric Psychiatry Fellowship
Boston, MA
James M. Ellison, MD, MPH
Associate Professor of Psychiatry
Harvard Medical School
Boston, MA
We would like to counter the suggestion to use benztropine or clonidine as a means to control clozapine-induced hypersalivation as suggested in “Reducing clozapine-induced hypersalivation” (Pearls, Current Psychiatry, October 2011, p. 77-78).
As stated in the article, clozapine is an antagonist for all known muscarinic receptors except M4—where it is an agonist—making it a potent anticholinergic medication with the potential to cause excessive saliva production.1,2 Another proposed mechanism for clozapine-induced hypersalivation is its antagonist activity at α-1 receptors, thus the suggestion to use clonidine to combat this side effect. The use of benztropine, another medication with known anticholinergic activity, or clonidine, a medication that may cause additional hypotension, to treat clozapine-induced hypersalivation may cause further unwanted complications and may not be the best option to treat this troubling side effect.
We have had great success locally using medications such as atropine or ipratropium as first-line treatments for clozapine-induced hypersalivation in an effort to minimize additional systemic side effects, such as those seen with benztropine and clonidine. Atropine eye drops administered orally, starting with 1 drop and titrated up to 2 drops twice daily to adequate response, has been shown to be successful according to patient opinion in several case reports.3 Alternatively, intranasal ipratropium orally administered 1 to 2 sprays, up to 3 times daily has shown improvement in clozapine-induced hypersalivation according to patient report.3 Although controlled trials to support the use of topical treatment for clozapine-induced hypersalivation are necessary, attempting to minimize additional adverse effects warrants a trial of atropine or ipratropium before using systemically acting medications such as benztropine or clonidine.
Sarah Hutfilz, PharmD
PGY1 Pharmacy Practice Resident
Department of Pharmacy
University of North Carolina Hospitals and Clinics
Clinical Instructor
University of North Carolina
Eshelman School of Pharmacy
Shauna Garris, PharmD, BCPP
Neurology/Psychiatry Clinical Specialist
Department of Pharmacy
University of North Carolina Hospitals and Clinics
Clinical Assistant Professor
University of North Carolina
Eshelman School of Pharmacy
M. Lindsey Kennedy, PharmD, BCPS, BCPP
Psychiatry Clinical Specialist
Department of Pharmacy
University of North Carolina Hospitals and Clinics
Clinical Assistant Professor
University of North Carolina School
of Medicine
University of North Carolina
Eshelman School of Pharmacy
Chapel Hill, NC
The authors respond
We thank Drs. Hutfilz, Garris, and Kennedy for their response and comments. We acknowledge that the medications we suggested have potentially harmful adverse effects; however, they are evidence-based. Atropine eye drops and ipratropium are interesting suggestions; if their use is based on evidence, they should have been included in the article.
We agree that further studies may show these topical approaches to be superior, but our recommendation, based on the best evidence available from the clinical studies, would be to use medications that have been studied while advocating for further study of medications with a theoretical superiority that is not yet proven.
Gurprit Lamba, MD
Geriatric Psychiatry Fellow
Partners HealthCare Geriatric Psychiatry Fellowship
Boston, MA
James M. Ellison, MD, MPH
Associate Professor of Psychiatry
Harvard Medical School
Boston, MA
Striving for greatness
As an advanced practice nurse in psychiatry who is passionate about my work, I was re-motivated by Dr. Nasrallah’s editorial on the model psychiatrist (“The model psychiatrist: 7 domains of excellence,” From the Editor, Current Psychiatry, November 2011, p. 5-6). It was great to see that these traits are being encouraged and practiced. I appreciated the piece, as well as the support that it gives to all types of mental health practitioners, telling us that there are still psychiatrists striving for “greatness.”
Gretchen Moeller, MSN-BC
Linden Oaks at Edward Hospital
St. Charles, IL
As an advanced practice nurse in psychiatry who is passionate about my work, I was re-motivated by Dr. Nasrallah’s editorial on the model psychiatrist (“The model psychiatrist: 7 domains of excellence,” From the Editor, Current Psychiatry, November 2011, p. 5-6). It was great to see that these traits are being encouraged and practiced. I appreciated the piece, as well as the support that it gives to all types of mental health practitioners, telling us that there are still psychiatrists striving for “greatness.”
Gretchen Moeller, MSN-BC
Linden Oaks at Edward Hospital
St. Charles, IL
As an advanced practice nurse in psychiatry who is passionate about my work, I was re-motivated by Dr. Nasrallah’s editorial on the model psychiatrist (“The model psychiatrist: 7 domains of excellence,” From the Editor, Current Psychiatry, November 2011, p. 5-6). It was great to see that these traits are being encouraged and practiced. I appreciated the piece, as well as the support that it gives to all types of mental health practitioners, telling us that there are still psychiatrists striving for “greatness.”
Gretchen Moeller, MSN-BC
Linden Oaks at Edward Hospital
St. Charles, IL
Clinical application of the SAFER and ATRQ
Nonsuicidal self-injury: How categorization guides treatment
Discuss this article at www.facebook.com/CurrentPsychiatry
Formerly called self-mutilation, self-injury, or self-harm, nonsuicidal self-injury (NSSI) is the deliberate and direct alteration or destruction of healthy body tissue without suicidal intent; these behaviors range from skin cutting or burning to eye enucleation or amputation of body parts. NSSI must be deliberate, as opposed to accidental or indirect behaviors—such as overdoses or ingesting harmful substances—that cause injury that is uncertain, ambiguous as to course, or invisible (the injuries do not disfigure observable body tissue).1 NSSI acts are done without an intent to die, although persons who self-harm may have suicidal ideation and passive thoughts of dying.2 Persons who repeatedly engage in NSSI and are demoralized over their inability to control it are at risk for suicide attempts.3
NSSI can be classified as nonpathological or pathological.4 Culturally sanctioned, nonpathological NSSI consists of body modification practices such as tattoos or piercing. Body modification practices may be a sublimation of pathological NSSI. For a description of nonpathological NSSI, see the Box.5 Pathological NSSI typically is a method of emotional regulation. Understanding why patients engage in pathological NSSI and how it is categorized can help guide assessment and treatment.
Body modification practices and rituals are culturally sanctioned forms of nonsuicidal self-injury (NSSI). Body modification practices include tattooing and piercing earlobes, nipples, and other body parts to accommodate jewelry. Most practices are harmless but when carried to extremes, they may point to underlying neuroses. For some patients, a tattoo or piercing may be psychologically beneficial—eg, to reclaim one’s body after an attack or rape.5
Body modification rituals, such as head gashing by Sufi healers, penis cutting during aboriginal coming-of-age ceremonies, and Hindu body piercing to attain spiritual goals, are meaningful activities that reflect the tradition, symbolism, and beliefs of a society. These rituals serve an elemental purpose by correcting or preventing destabilizing conditions that threaten people and communities, such as mental and physical diseases; angry gods, spirits, or ancestors; failure of children to accept adult responsibilities; conflicts (eg, male-female, intergenerational, interclass, intertribal); loosening of clear social role distinctions; loss of group identity; immoral or sinful behaviors; and ecological disasters.
These rituals are effective because participants believe they promote healing, spirituality, and social order. Knowledge about body modification practices and rituals in which NSSI is perceived to be therapeutic opens the door to an understanding of pathological NSSI as a form of self-help behavior and allows clinicians to have a more empathic interaction with patients who self-injure.
Why people engage in NSSI
NSSI is best regarded as a pathological approach to emotional regulation and distress tolerance that provides rapid but temporary relief from disturbing thoughts, feelings, and emotions. For approximately 90% of patients, NSSI decreases symptoms, most commonly untenable anxiety (“It’s like popping a balloon”), depressed mood, racing thoughts, swirling emotions, anger, hallucinations, and flashbacks.6,7 In some instances, NSSI generates desired feelings and self-stimulation during periods of dissociation, depersonalization, grief, insecurity, loneliness, extreme boredom, self-pity, and alienation.8,9 NSSI also may signal distress to elicit a caring response from others or provide a means of escape from intolerable social situations.10Table 1 lists factors associated with NSSI.
Table 1
Factors associated with NSSI
| High levels of negative and unpleasant thoughts and feelingsa |
| Poor communication skills and problem-solving abilitiesb |
| Abuse, maltreatment, hostility, and marked criticism during childhoodc,d |
| Under- or over-arousal responses to stressb |
| High valuation of NSSI to achieve a desired responsee |
| Need for self-punishmenta |
| Modeling behaviors based on exposure to NSSI among peers, on the Internet—ie, postings on YouTube—and in the mediaf |
| NSSI: nonsuicidal self-injury Source: References
|
The functional approach
One model of classifying NSSI focuses on the behavioral functions it serves.11,12 In this model, the most common function of NSSI is removal or escape from an aversive affective or cognitive state (automatic positive reinforcement). Automatic negative reinforcement explains using NSSI to generate feelings—eg, by patients with anhedonia or numbness. NSSI also may be used as a signal of distress to gain attention, access helpful environmental resources (social positive reinforcement), or remove distressing interpersonal demands (social negative reinforcement).
The functional model is key to providing thorough clinical evaluations that should include understanding the antecedent and consequent thoughts, feelings, situations, triggers, and vulnerabilities related to NSSI acts.
The medical approach
A descriptive, phenomenological model of NSSI classification uses concepts and terminology with which most psychiatrists are familiar, takes into account patients who have comorbid psychiatric disorders, is based on atheoretical, descriptive observations, and fits into what might be regarded as a “medical model.” In this classification, NSSI usually is regarded as a symptom or associated feature of a specific psychiatric disorder, although it may occur in persons who do not meet diagnostic criteria of a mental illness—eg, “copycat” cutting in high school students.13,14 NSSI may fall within 4 descriptive categories: major, stereotypic, compulsive, or impulsive. For psychiatric disorders associated with these types of pathological NSSI, see Table 2.
Major NSSI includes infrequent acts that destroy significant body tissue, such as eye enucleation and amputation of body parts. They are sudden, messy, and often bloody acts. Seventy-five percent occur during a psychotic state, mainly schizophrenia; of these, approximately one-half occur during a first psychotic episode.15 The reasons patients typically offer for such behavior often defy logical understanding—eg, to enhance general well-being—but most center on religion, such as a concrete interpretation of biblical texts about removing an offending eye or hand or becoming an eunuch,16,17 or on sexuality, such as controlling troubling hypersexuality or fear of giving in to homosexual urges.18
Stereotypic NSSI acts, most commonly associated with severe and profound mental retardation, include repetitive head banging; eye gouging; biting lips, the tongue, cheeks, or fingers; and face or head slapping. The behaviors may be monotonously repetitive, have a rhythmic pattern, and be performed without shame or guilt in the presence of onlookers.
Compulsive NSSI encompasses repetitive behaviors such as severe skin scratching and nail biting, hair pulling (trichotillomania), and skin digging (delusional parasitosis).
Impulsive NSSI consists of acts such as skin cutting, burning, and carving; sticking pins or other objects under the skin or into the chest or abdomen; interfering with wound healing; and smashing hand or foot bones. These behaviors usually are episodic and occur more frequently in females. The average age of onset in patients who engage in impulsive NSSI is 12 to 14, although it may occur throughout the life cycle.
One or 2 isolated instances of impulsive NSSI do not have much prognostic importance unless they are serious enough to warrant an emergency department visit. The real danger is when the behavior becomes repetitive and “addictive.” The crossover from episodic to repetitive usually varies from 5 to 10 episodes.
Persons who engage in repetitive NSSI may use multiple methods, but skin cutting predominates. Such persons often develop a self-identity as a “cutter,” are preoccupied with their NSSI, may carve words into their skin, and may perform acts of self-harm with other self-injurers. Some may cut themselves hundreds or even thousands of times, creating scars that result in social morbidity. They often seek professional help avidly, but may become so demoralized over their inability to stop their NSSI that they are at risk for suicide.3 In some repetitive self-injurers, other impulsive behaviors such as bulimia or substance abuse may alternate or coexist with NSSI. This pattern often runs its course in 5 to 15 years and may end abruptly, especially in patients with borderline personality disorder.
Table 2
Psychiatric disorders associated with pathological NSSI
| Type of NSSI | Related psychiatric disorders |
|---|---|
| Major | Alcohol/drug intoxication, body integrity identity disordera |
| Stereotypic | Autism,b Tourette’s syndrome,c Lesch-Nyhan syndrome,d hereditary neuropathies,e mental retardation |
| Compulsive | Trichotillomania, delusional parasitosis |
| Impulsive | Anxiety disorders (generalized, acute stress, posttraumatic stress, obsessive-compulsive, substance-inducedf-h); borderline, histrionic, and antisocial personality disordersi,j; somatoform and factitious disordersk,l; dissociative identity and depersonalization disordersm,n; anorexia and bulimia nervosao,p; depressive disordersq,r; bipolar disorders; schizophreniat,u; alcohol use disorderv; kleptomaniaw |
| NSSI: nonsuicidal self-injury Source: References
| |
First-line treatment: Psychotherapy
Many studies have demonstrated the efficacy of psychotherapy as the primary treatment for NSSI.19-21 Except for patients with Lesch-Nyhan syndrome or other rare neurologic syndromes, the biologic causes of NSSI, including the role of endogenous opioids, are unclear. No medications are FDA-approved for NSSI. Pharmacotherapy may help NSSI patients, but such treatment recommendations are based on clinical experience, and polypharmacy is common.22 Studies have not demonstrated specific benefits or consistent efficacy of pharmacotherapy for NSSI.23
Major NSSI. Prevention is key to addressing major NSSI. Consider atypical antipsychotics for psychotic patients who are preoccupied with religion, the Bible, or sexuality, as well as those who dramatically and suddenly change their appearance by cutting off their hair, engaging in extreme body modification practices, or wearing bizarre clothes.24 In my clinical experience, agitated patients who have committed major NSSI are at high risk for a second episode and should receive pharmacotherapy based on treatment guidelines and hospitalized until the agitation is controlled.
Stereotypic NSSI. Patients with this form of NSSI often cannot articulate what is bothering them. With input from caretakers, assess the likelihood that a patient is reacting to pain. Analgesics may be effective. Also check for infections such as otitis media. Selecting a medication can be challenging. Start with a moderate dose of a selective serotonin reuptake inhibitor (SSRI), then slowly add an atypical antipsychotic, followed by a mood stabilizer, then clonidine, and then a beta blocker; a trial of naltrexone also is an option.23 Behavior therapy is the primary treatment.
Compulsive NSSI. Compulsive NSSI patients typically seek help from dermatologists or family physicians. Literature on psychiatric treatment is limited, but SSRIs, lithium, benzodiazepines, and atypical antipsychotics (for delusional parasitosis) may be effective. N-acetylcysteine, 600 mg twice a day, may relieve trichotillomania.25 Treatment should include psychotherapy.
Impulsive NSSI. Patients who engage in episodic impulsive NSSI should receive pharmacotherapy for underlying psychiatric illnesses such as generalized anxiety disorder, posttraumatic stress disorder, or depression. Do not automatically diagnose borderline personality disorder. Patients whose NSSI behavior is uncontrollable initially should receive high doses of SSRIs that can be lowered when impulsivity decreases, atypical antipsychotics, and a mood stabilizer such as lamotrigine. Psychotherapy is vital, especially dialectical behavior therapy. Cognitive-behavioral and interpersonal therapies also are effective, as is psychodynamic therapy.19-21
NSSI patients and their families may benefit from Web sites that provide information, advice, monitored blogs, and support groups (see Related Resources).
- Favazza A. Bodies under siege: self-mutilation, nonsuicidal self-injury, and body modification in culture and psychiatry. 3rd ed. Baltimore, MD: Johns Hopkins University Press; 2011.
- Nock MK. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC: American Psychological Association; 2009.
- Cornell University Family Life Development Center. About self-injury. www.crpsib.com/whatissi.asp.
Drug Brand Names
- Clonidine • Catapres, Kapvay
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Naltrexone • ReVia
Disclosure
Dr. Favazza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Walsh BW, Rosen PM. Self-mutilation: theory research, and treatment. New York, NY: Guilford Press; 2008:32.
2. Nock MK, Favazza AR. Nonsuicidal self-injury: definition and classification. In: Nock MK ed. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC: American Psychological Association; 2009:9-18.
3. Favazza AR, Conterio K. Female habitual self-mutilators. Acta Psychiatr Scand. 1989;79(3):283-289.
4. Favazza A. Bodies under siege: self-mutilation nonsuicidal self-injury, and body modification in culture and psychiatry. 3rd ed. Baltimore, MD: Johns Hopkins University Press; 2011.
5. Gallina R. Tattoos and body piercing. In: Vale V Juno A, eds. Modern primitives. San Francisco, CA: Re/Search Publications; 1989:101-105.
6. Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: the experiential avoidance model. Behav Res Ther. 2006;44(3):371-394.
7. Nock MK, Prinstein MJ. Contextual features and behavioral functions of self-mutilation among adolescents. J Abnorm Psychol. 2005;114(1):140-146.
8. Miller F, Bashkin EA. Depersonalization and self-mutilation. Psychoanal Q. 1974;43(4):638-649.
9. Klonsky ED. The functions of deliberate self-injury: a review of the evidence. Clin Psychol Rev. 2007;27(2):226-239.
10. Nock MK. Actions speak louder than words: an elaborated theoretical model of the social functions of self-injury and other harmful behaviors. Appl Prev Psychol. 2008;12(4):159-168.
11. Nock MK, Prinstein MJ. A functional approach to the assessment of self-mutilative behavior. J Consult Clin Psychol. 2004;72(5):885-890.
12. Nock MK, Prinstein MJ. Contextual features and behavioral functions of self-mutilation among adolescents. J Abnorm Psychol. 2005;114(1):140-146.
13. Favazza AR, Rosenthal RJ. Diagnostic issues in self-mutilation. Hosp Community Psychiatry. 1993;44(2):134-140.
14. Rosen PM, Walsh BW. Patterns of contagion in self-mutilation epidemics. Am J Psychiatry. 1989;146(5):656-658.
15. Large M, Babidge N, Andrews D, et al. Major self-mutilation in the first episode of psychosis. Schizophr Bull. 2009;35(5):1012-1021.
16. Kushner AW. Two cases of auto-castration due to religious delusions. Br J Med Psychol. 1967;40(3):293-298.
17. Moskovitz RA, Byrd T. Rescuing the angel within: PCP-related self-enucleation. Psychosomatics. 1983;24(4):402-403,406.
18. Cleveland SE. Three cases of self-castration. J Nerv Ment Dis. 1956;123(4):386-391.
19. Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. 2006;63(7):757-766.
20. Kahng S, Iwata BA, Lewin AB. Behavioral treatment of self-injury 1964 to 2000. Am J Ment Retard. 2002;107(3):212-221.
21. Levy KN, Yeomans FE, Diamond D. Psychodynamic treatments of self-injury. J Clin Psychol. 2007;63(11):1105-1120.
22. Lott IT, McGregor M, Engelman L, et al. Longitudinal prescribing patterns for psychoactive medications in community-based individuals with developmental disabilities: utilization of pharmacy records. J Intellect Disabil Res. 2004;48(Pt 6):563-571.
23. Sandman CA. Psychopharmacologic treatment of nonsuicidal self-injury. In: Nock MK ed. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC: American Psychological Association; 2009:291-322.
24. Sweeny S, Zamecnik K. Predictors of self-mutilation in patients with schizophrenia. Am J Psychiatry. 1981;138(8):1086-1089.
25. Grant JE, Odlaug BL, Kim SW. N-acetylcysteine a glutamate modulator, in the treatment of trichotillomania: a double-blind, placebo-controlled study. Arch Gen Psychiatry. 2009;66(7):756-763.
Discuss this article at www.facebook.com/CurrentPsychiatry
Formerly called self-mutilation, self-injury, or self-harm, nonsuicidal self-injury (NSSI) is the deliberate and direct alteration or destruction of healthy body tissue without suicidal intent; these behaviors range from skin cutting or burning to eye enucleation or amputation of body parts. NSSI must be deliberate, as opposed to accidental or indirect behaviors—such as overdoses or ingesting harmful substances—that cause injury that is uncertain, ambiguous as to course, or invisible (the injuries do not disfigure observable body tissue).1 NSSI acts are done without an intent to die, although persons who self-harm may have suicidal ideation and passive thoughts of dying.2 Persons who repeatedly engage in NSSI and are demoralized over their inability to control it are at risk for suicide attempts.3
NSSI can be classified as nonpathological or pathological.4 Culturally sanctioned, nonpathological NSSI consists of body modification practices such as tattoos or piercing. Body modification practices may be a sublimation of pathological NSSI. For a description of nonpathological NSSI, see the Box.5 Pathological NSSI typically is a method of emotional regulation. Understanding why patients engage in pathological NSSI and how it is categorized can help guide assessment and treatment.
Body modification practices and rituals are culturally sanctioned forms of nonsuicidal self-injury (NSSI). Body modification practices include tattooing and piercing earlobes, nipples, and other body parts to accommodate jewelry. Most practices are harmless but when carried to extremes, they may point to underlying neuroses. For some patients, a tattoo or piercing may be psychologically beneficial—eg, to reclaim one’s body after an attack or rape.5
Body modification rituals, such as head gashing by Sufi healers, penis cutting during aboriginal coming-of-age ceremonies, and Hindu body piercing to attain spiritual goals, are meaningful activities that reflect the tradition, symbolism, and beliefs of a society. These rituals serve an elemental purpose by correcting or preventing destabilizing conditions that threaten people and communities, such as mental and physical diseases; angry gods, spirits, or ancestors; failure of children to accept adult responsibilities; conflicts (eg, male-female, intergenerational, interclass, intertribal); loosening of clear social role distinctions; loss of group identity; immoral or sinful behaviors; and ecological disasters.
These rituals are effective because participants believe they promote healing, spirituality, and social order. Knowledge about body modification practices and rituals in which NSSI is perceived to be therapeutic opens the door to an understanding of pathological NSSI as a form of self-help behavior and allows clinicians to have a more empathic interaction with patients who self-injure.
Why people engage in NSSI
NSSI is best regarded as a pathological approach to emotional regulation and distress tolerance that provides rapid but temporary relief from disturbing thoughts, feelings, and emotions. For approximately 90% of patients, NSSI decreases symptoms, most commonly untenable anxiety (“It’s like popping a balloon”), depressed mood, racing thoughts, swirling emotions, anger, hallucinations, and flashbacks.6,7 In some instances, NSSI generates desired feelings and self-stimulation during periods of dissociation, depersonalization, grief, insecurity, loneliness, extreme boredom, self-pity, and alienation.8,9 NSSI also may signal distress to elicit a caring response from others or provide a means of escape from intolerable social situations.10Table 1 lists factors associated with NSSI.
Table 1
Factors associated with NSSI
| High levels of negative and unpleasant thoughts and feelingsa |
| Poor communication skills and problem-solving abilitiesb |
| Abuse, maltreatment, hostility, and marked criticism during childhoodc,d |
| Under- or over-arousal responses to stressb |
| High valuation of NSSI to achieve a desired responsee |
| Need for self-punishmenta |
| Modeling behaviors based on exposure to NSSI among peers, on the Internet—ie, postings on YouTube—and in the mediaf |
| NSSI: nonsuicidal self-injury Source: References
|
The functional approach
One model of classifying NSSI focuses on the behavioral functions it serves.11,12 In this model, the most common function of NSSI is removal or escape from an aversive affective or cognitive state (automatic positive reinforcement). Automatic negative reinforcement explains using NSSI to generate feelings—eg, by patients with anhedonia or numbness. NSSI also may be used as a signal of distress to gain attention, access helpful environmental resources (social positive reinforcement), or remove distressing interpersonal demands (social negative reinforcement).
The functional model is key to providing thorough clinical evaluations that should include understanding the antecedent and consequent thoughts, feelings, situations, triggers, and vulnerabilities related to NSSI acts.
The medical approach
A descriptive, phenomenological model of NSSI classification uses concepts and terminology with which most psychiatrists are familiar, takes into account patients who have comorbid psychiatric disorders, is based on atheoretical, descriptive observations, and fits into what might be regarded as a “medical model.” In this classification, NSSI usually is regarded as a symptom or associated feature of a specific psychiatric disorder, although it may occur in persons who do not meet diagnostic criteria of a mental illness—eg, “copycat” cutting in high school students.13,14 NSSI may fall within 4 descriptive categories: major, stereotypic, compulsive, or impulsive. For psychiatric disorders associated with these types of pathological NSSI, see Table 2.
Major NSSI includes infrequent acts that destroy significant body tissue, such as eye enucleation and amputation of body parts. They are sudden, messy, and often bloody acts. Seventy-five percent occur during a psychotic state, mainly schizophrenia; of these, approximately one-half occur during a first psychotic episode.15 The reasons patients typically offer for such behavior often defy logical understanding—eg, to enhance general well-being—but most center on religion, such as a concrete interpretation of biblical texts about removing an offending eye or hand or becoming an eunuch,16,17 or on sexuality, such as controlling troubling hypersexuality or fear of giving in to homosexual urges.18
Stereotypic NSSI acts, most commonly associated with severe and profound mental retardation, include repetitive head banging; eye gouging; biting lips, the tongue, cheeks, or fingers; and face or head slapping. The behaviors may be monotonously repetitive, have a rhythmic pattern, and be performed without shame or guilt in the presence of onlookers.
Compulsive NSSI encompasses repetitive behaviors such as severe skin scratching and nail biting, hair pulling (trichotillomania), and skin digging (delusional parasitosis).
Impulsive NSSI consists of acts such as skin cutting, burning, and carving; sticking pins or other objects under the skin or into the chest or abdomen; interfering with wound healing; and smashing hand or foot bones. These behaviors usually are episodic and occur more frequently in females. The average age of onset in patients who engage in impulsive NSSI is 12 to 14, although it may occur throughout the life cycle.
One or 2 isolated instances of impulsive NSSI do not have much prognostic importance unless they are serious enough to warrant an emergency department visit. The real danger is when the behavior becomes repetitive and “addictive.” The crossover from episodic to repetitive usually varies from 5 to 10 episodes.
Persons who engage in repetitive NSSI may use multiple methods, but skin cutting predominates. Such persons often develop a self-identity as a “cutter,” are preoccupied with their NSSI, may carve words into their skin, and may perform acts of self-harm with other self-injurers. Some may cut themselves hundreds or even thousands of times, creating scars that result in social morbidity. They often seek professional help avidly, but may become so demoralized over their inability to stop their NSSI that they are at risk for suicide.3 In some repetitive self-injurers, other impulsive behaviors such as bulimia or substance abuse may alternate or coexist with NSSI. This pattern often runs its course in 5 to 15 years and may end abruptly, especially in patients with borderline personality disorder.
Table 2
Psychiatric disorders associated with pathological NSSI
| Type of NSSI | Related psychiatric disorders |
|---|---|
| Major | Alcohol/drug intoxication, body integrity identity disordera |
| Stereotypic | Autism,b Tourette’s syndrome,c Lesch-Nyhan syndrome,d hereditary neuropathies,e mental retardation |
| Compulsive | Trichotillomania, delusional parasitosis |
| Impulsive | Anxiety disorders (generalized, acute stress, posttraumatic stress, obsessive-compulsive, substance-inducedf-h); borderline, histrionic, and antisocial personality disordersi,j; somatoform and factitious disordersk,l; dissociative identity and depersonalization disordersm,n; anorexia and bulimia nervosao,p; depressive disordersq,r; bipolar disorders; schizophreniat,u; alcohol use disorderv; kleptomaniaw |
| NSSI: nonsuicidal self-injury Source: References
| |
First-line treatment: Psychotherapy
Many studies have demonstrated the efficacy of psychotherapy as the primary treatment for NSSI.19-21 Except for patients with Lesch-Nyhan syndrome or other rare neurologic syndromes, the biologic causes of NSSI, including the role of endogenous opioids, are unclear. No medications are FDA-approved for NSSI. Pharmacotherapy may help NSSI patients, but such treatment recommendations are based on clinical experience, and polypharmacy is common.22 Studies have not demonstrated specific benefits or consistent efficacy of pharmacotherapy for NSSI.23
Major NSSI. Prevention is key to addressing major NSSI. Consider atypical antipsychotics for psychotic patients who are preoccupied with religion, the Bible, or sexuality, as well as those who dramatically and suddenly change their appearance by cutting off their hair, engaging in extreme body modification practices, or wearing bizarre clothes.24 In my clinical experience, agitated patients who have committed major NSSI are at high risk for a second episode and should receive pharmacotherapy based on treatment guidelines and hospitalized until the agitation is controlled.
Stereotypic NSSI. Patients with this form of NSSI often cannot articulate what is bothering them. With input from caretakers, assess the likelihood that a patient is reacting to pain. Analgesics may be effective. Also check for infections such as otitis media. Selecting a medication can be challenging. Start with a moderate dose of a selective serotonin reuptake inhibitor (SSRI), then slowly add an atypical antipsychotic, followed by a mood stabilizer, then clonidine, and then a beta blocker; a trial of naltrexone also is an option.23 Behavior therapy is the primary treatment.
Compulsive NSSI. Compulsive NSSI patients typically seek help from dermatologists or family physicians. Literature on psychiatric treatment is limited, but SSRIs, lithium, benzodiazepines, and atypical antipsychotics (for delusional parasitosis) may be effective. N-acetylcysteine, 600 mg twice a day, may relieve trichotillomania.25 Treatment should include psychotherapy.
Impulsive NSSI. Patients who engage in episodic impulsive NSSI should receive pharmacotherapy for underlying psychiatric illnesses such as generalized anxiety disorder, posttraumatic stress disorder, or depression. Do not automatically diagnose borderline personality disorder. Patients whose NSSI behavior is uncontrollable initially should receive high doses of SSRIs that can be lowered when impulsivity decreases, atypical antipsychotics, and a mood stabilizer such as lamotrigine. Psychotherapy is vital, especially dialectical behavior therapy. Cognitive-behavioral and interpersonal therapies also are effective, as is psychodynamic therapy.19-21
NSSI patients and their families may benefit from Web sites that provide information, advice, monitored blogs, and support groups (see Related Resources).
- Favazza A. Bodies under siege: self-mutilation, nonsuicidal self-injury, and body modification in culture and psychiatry. 3rd ed. Baltimore, MD: Johns Hopkins University Press; 2011.
- Nock MK. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC: American Psychological Association; 2009.
- Cornell University Family Life Development Center. About self-injury. www.crpsib.com/whatissi.asp.
Drug Brand Names
- Clonidine • Catapres, Kapvay
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Naltrexone • ReVia
Disclosure
Dr. Favazza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Formerly called self-mutilation, self-injury, or self-harm, nonsuicidal self-injury (NSSI) is the deliberate and direct alteration or destruction of healthy body tissue without suicidal intent; these behaviors range from skin cutting or burning to eye enucleation or amputation of body parts. NSSI must be deliberate, as opposed to accidental or indirect behaviors—such as overdoses or ingesting harmful substances—that cause injury that is uncertain, ambiguous as to course, or invisible (the injuries do not disfigure observable body tissue).1 NSSI acts are done without an intent to die, although persons who self-harm may have suicidal ideation and passive thoughts of dying.2 Persons who repeatedly engage in NSSI and are demoralized over their inability to control it are at risk for suicide attempts.3
NSSI can be classified as nonpathological or pathological.4 Culturally sanctioned, nonpathological NSSI consists of body modification practices such as tattoos or piercing. Body modification practices may be a sublimation of pathological NSSI. For a description of nonpathological NSSI, see the Box.5 Pathological NSSI typically is a method of emotional regulation. Understanding why patients engage in pathological NSSI and how it is categorized can help guide assessment and treatment.
Body modification practices and rituals are culturally sanctioned forms of nonsuicidal self-injury (NSSI). Body modification practices include tattooing and piercing earlobes, nipples, and other body parts to accommodate jewelry. Most practices are harmless but when carried to extremes, they may point to underlying neuroses. For some patients, a tattoo or piercing may be psychologically beneficial—eg, to reclaim one’s body after an attack or rape.5
Body modification rituals, such as head gashing by Sufi healers, penis cutting during aboriginal coming-of-age ceremonies, and Hindu body piercing to attain spiritual goals, are meaningful activities that reflect the tradition, symbolism, and beliefs of a society. These rituals serve an elemental purpose by correcting or preventing destabilizing conditions that threaten people and communities, such as mental and physical diseases; angry gods, spirits, or ancestors; failure of children to accept adult responsibilities; conflicts (eg, male-female, intergenerational, interclass, intertribal); loosening of clear social role distinctions; loss of group identity; immoral or sinful behaviors; and ecological disasters.
These rituals are effective because participants believe they promote healing, spirituality, and social order. Knowledge about body modification practices and rituals in which NSSI is perceived to be therapeutic opens the door to an understanding of pathological NSSI as a form of self-help behavior and allows clinicians to have a more empathic interaction with patients who self-injure.
Why people engage in NSSI
NSSI is best regarded as a pathological approach to emotional regulation and distress tolerance that provides rapid but temporary relief from disturbing thoughts, feelings, and emotions. For approximately 90% of patients, NSSI decreases symptoms, most commonly untenable anxiety (“It’s like popping a balloon”), depressed mood, racing thoughts, swirling emotions, anger, hallucinations, and flashbacks.6,7 In some instances, NSSI generates desired feelings and self-stimulation during periods of dissociation, depersonalization, grief, insecurity, loneliness, extreme boredom, self-pity, and alienation.8,9 NSSI also may signal distress to elicit a caring response from others or provide a means of escape from intolerable social situations.10Table 1 lists factors associated with NSSI.
Table 1
Factors associated with NSSI
| High levels of negative and unpleasant thoughts and feelingsa |
| Poor communication skills and problem-solving abilitiesb |
| Abuse, maltreatment, hostility, and marked criticism during childhoodc,d |
| Under- or over-arousal responses to stressb |
| High valuation of NSSI to achieve a desired responsee |
| Need for self-punishmenta |
| Modeling behaviors based on exposure to NSSI among peers, on the Internet—ie, postings on YouTube—and in the mediaf |
| NSSI: nonsuicidal self-injury Source: References
|
The functional approach
One model of classifying NSSI focuses on the behavioral functions it serves.11,12 In this model, the most common function of NSSI is removal or escape from an aversive affective or cognitive state (automatic positive reinforcement). Automatic negative reinforcement explains using NSSI to generate feelings—eg, by patients with anhedonia or numbness. NSSI also may be used as a signal of distress to gain attention, access helpful environmental resources (social positive reinforcement), or remove distressing interpersonal demands (social negative reinforcement).
The functional model is key to providing thorough clinical evaluations that should include understanding the antecedent and consequent thoughts, feelings, situations, triggers, and vulnerabilities related to NSSI acts.
The medical approach
A descriptive, phenomenological model of NSSI classification uses concepts and terminology with which most psychiatrists are familiar, takes into account patients who have comorbid psychiatric disorders, is based on atheoretical, descriptive observations, and fits into what might be regarded as a “medical model.” In this classification, NSSI usually is regarded as a symptom or associated feature of a specific psychiatric disorder, although it may occur in persons who do not meet diagnostic criteria of a mental illness—eg, “copycat” cutting in high school students.13,14 NSSI may fall within 4 descriptive categories: major, stereotypic, compulsive, or impulsive. For psychiatric disorders associated with these types of pathological NSSI, see Table 2.
Major NSSI includes infrequent acts that destroy significant body tissue, such as eye enucleation and amputation of body parts. They are sudden, messy, and often bloody acts. Seventy-five percent occur during a psychotic state, mainly schizophrenia; of these, approximately one-half occur during a first psychotic episode.15 The reasons patients typically offer for such behavior often defy logical understanding—eg, to enhance general well-being—but most center on religion, such as a concrete interpretation of biblical texts about removing an offending eye or hand or becoming an eunuch,16,17 or on sexuality, such as controlling troubling hypersexuality or fear of giving in to homosexual urges.18
Stereotypic NSSI acts, most commonly associated with severe and profound mental retardation, include repetitive head banging; eye gouging; biting lips, the tongue, cheeks, or fingers; and face or head slapping. The behaviors may be monotonously repetitive, have a rhythmic pattern, and be performed without shame or guilt in the presence of onlookers.
Compulsive NSSI encompasses repetitive behaviors such as severe skin scratching and nail biting, hair pulling (trichotillomania), and skin digging (delusional parasitosis).
Impulsive NSSI consists of acts such as skin cutting, burning, and carving; sticking pins or other objects under the skin or into the chest or abdomen; interfering with wound healing; and smashing hand or foot bones. These behaviors usually are episodic and occur more frequently in females. The average age of onset in patients who engage in impulsive NSSI is 12 to 14, although it may occur throughout the life cycle.
One or 2 isolated instances of impulsive NSSI do not have much prognostic importance unless they are serious enough to warrant an emergency department visit. The real danger is when the behavior becomes repetitive and “addictive.” The crossover from episodic to repetitive usually varies from 5 to 10 episodes.
Persons who engage in repetitive NSSI may use multiple methods, but skin cutting predominates. Such persons often develop a self-identity as a “cutter,” are preoccupied with their NSSI, may carve words into their skin, and may perform acts of self-harm with other self-injurers. Some may cut themselves hundreds or even thousands of times, creating scars that result in social morbidity. They often seek professional help avidly, but may become so demoralized over their inability to stop their NSSI that they are at risk for suicide.3 In some repetitive self-injurers, other impulsive behaviors such as bulimia or substance abuse may alternate or coexist with NSSI. This pattern often runs its course in 5 to 15 years and may end abruptly, especially in patients with borderline personality disorder.
Table 2
Psychiatric disorders associated with pathological NSSI
| Type of NSSI | Related psychiatric disorders |
|---|---|
| Major | Alcohol/drug intoxication, body integrity identity disordera |
| Stereotypic | Autism,b Tourette’s syndrome,c Lesch-Nyhan syndrome,d hereditary neuropathies,e mental retardation |
| Compulsive | Trichotillomania, delusional parasitosis |
| Impulsive | Anxiety disorders (generalized, acute stress, posttraumatic stress, obsessive-compulsive, substance-inducedf-h); borderline, histrionic, and antisocial personality disordersi,j; somatoform and factitious disordersk,l; dissociative identity and depersonalization disordersm,n; anorexia and bulimia nervosao,p; depressive disordersq,r; bipolar disorders; schizophreniat,u; alcohol use disorderv; kleptomaniaw |
| NSSI: nonsuicidal self-injury Source: References
| |
First-line treatment: Psychotherapy
Many studies have demonstrated the efficacy of psychotherapy as the primary treatment for NSSI.19-21 Except for patients with Lesch-Nyhan syndrome or other rare neurologic syndromes, the biologic causes of NSSI, including the role of endogenous opioids, are unclear. No medications are FDA-approved for NSSI. Pharmacotherapy may help NSSI patients, but such treatment recommendations are based on clinical experience, and polypharmacy is common.22 Studies have not demonstrated specific benefits or consistent efficacy of pharmacotherapy for NSSI.23
Major NSSI. Prevention is key to addressing major NSSI. Consider atypical antipsychotics for psychotic patients who are preoccupied with religion, the Bible, or sexuality, as well as those who dramatically and suddenly change their appearance by cutting off their hair, engaging in extreme body modification practices, or wearing bizarre clothes.24 In my clinical experience, agitated patients who have committed major NSSI are at high risk for a second episode and should receive pharmacotherapy based on treatment guidelines and hospitalized until the agitation is controlled.
Stereotypic NSSI. Patients with this form of NSSI often cannot articulate what is bothering them. With input from caretakers, assess the likelihood that a patient is reacting to pain. Analgesics may be effective. Also check for infections such as otitis media. Selecting a medication can be challenging. Start with a moderate dose of a selective serotonin reuptake inhibitor (SSRI), then slowly add an atypical antipsychotic, followed by a mood stabilizer, then clonidine, and then a beta blocker; a trial of naltrexone also is an option.23 Behavior therapy is the primary treatment.
Compulsive NSSI. Compulsive NSSI patients typically seek help from dermatologists or family physicians. Literature on psychiatric treatment is limited, but SSRIs, lithium, benzodiazepines, and atypical antipsychotics (for delusional parasitosis) may be effective. N-acetylcysteine, 600 mg twice a day, may relieve trichotillomania.25 Treatment should include psychotherapy.
Impulsive NSSI. Patients who engage in episodic impulsive NSSI should receive pharmacotherapy for underlying psychiatric illnesses such as generalized anxiety disorder, posttraumatic stress disorder, or depression. Do not automatically diagnose borderline personality disorder. Patients whose NSSI behavior is uncontrollable initially should receive high doses of SSRIs that can be lowered when impulsivity decreases, atypical antipsychotics, and a mood stabilizer such as lamotrigine. Psychotherapy is vital, especially dialectical behavior therapy. Cognitive-behavioral and interpersonal therapies also are effective, as is psychodynamic therapy.19-21
NSSI patients and their families may benefit from Web sites that provide information, advice, monitored blogs, and support groups (see Related Resources).
- Favazza A. Bodies under siege: self-mutilation, nonsuicidal self-injury, and body modification in culture and psychiatry. 3rd ed. Baltimore, MD: Johns Hopkins University Press; 2011.
- Nock MK. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC: American Psychological Association; 2009.
- Cornell University Family Life Development Center. About self-injury. www.crpsib.com/whatissi.asp.
Drug Brand Names
- Clonidine • Catapres, Kapvay
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Naltrexone • ReVia
Disclosure
Dr. Favazza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Walsh BW, Rosen PM. Self-mutilation: theory research, and treatment. New York, NY: Guilford Press; 2008:32.
2. Nock MK, Favazza AR. Nonsuicidal self-injury: definition and classification. In: Nock MK ed. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC: American Psychological Association; 2009:9-18.
3. Favazza AR, Conterio K. Female habitual self-mutilators. Acta Psychiatr Scand. 1989;79(3):283-289.
4. Favazza A. Bodies under siege: self-mutilation nonsuicidal self-injury, and body modification in culture and psychiatry. 3rd ed. Baltimore, MD: Johns Hopkins University Press; 2011.
5. Gallina R. Tattoos and body piercing. In: Vale V Juno A, eds. Modern primitives. San Francisco, CA: Re/Search Publications; 1989:101-105.
6. Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: the experiential avoidance model. Behav Res Ther. 2006;44(3):371-394.
7. Nock MK, Prinstein MJ. Contextual features and behavioral functions of self-mutilation among adolescents. J Abnorm Psychol. 2005;114(1):140-146.
8. Miller F, Bashkin EA. Depersonalization and self-mutilation. Psychoanal Q. 1974;43(4):638-649.
9. Klonsky ED. The functions of deliberate self-injury: a review of the evidence. Clin Psychol Rev. 2007;27(2):226-239.
10. Nock MK. Actions speak louder than words: an elaborated theoretical model of the social functions of self-injury and other harmful behaviors. Appl Prev Psychol. 2008;12(4):159-168.
11. Nock MK, Prinstein MJ. A functional approach to the assessment of self-mutilative behavior. J Consult Clin Psychol. 2004;72(5):885-890.
12. Nock MK, Prinstein MJ. Contextual features and behavioral functions of self-mutilation among adolescents. J Abnorm Psychol. 2005;114(1):140-146.
13. Favazza AR, Rosenthal RJ. Diagnostic issues in self-mutilation. Hosp Community Psychiatry. 1993;44(2):134-140.
14. Rosen PM, Walsh BW. Patterns of contagion in self-mutilation epidemics. Am J Psychiatry. 1989;146(5):656-658.
15. Large M, Babidge N, Andrews D, et al. Major self-mutilation in the first episode of psychosis. Schizophr Bull. 2009;35(5):1012-1021.
16. Kushner AW. Two cases of auto-castration due to religious delusions. Br J Med Psychol. 1967;40(3):293-298.
17. Moskovitz RA, Byrd T. Rescuing the angel within: PCP-related self-enucleation. Psychosomatics. 1983;24(4):402-403,406.
18. Cleveland SE. Three cases of self-castration. J Nerv Ment Dis. 1956;123(4):386-391.
19. Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. 2006;63(7):757-766.
20. Kahng S, Iwata BA, Lewin AB. Behavioral treatment of self-injury 1964 to 2000. Am J Ment Retard. 2002;107(3):212-221.
21. Levy KN, Yeomans FE, Diamond D. Psychodynamic treatments of self-injury. J Clin Psychol. 2007;63(11):1105-1120.
22. Lott IT, McGregor M, Engelman L, et al. Longitudinal prescribing patterns for psychoactive medications in community-based individuals with developmental disabilities: utilization of pharmacy records. J Intellect Disabil Res. 2004;48(Pt 6):563-571.
23. Sandman CA. Psychopharmacologic treatment of nonsuicidal self-injury. In: Nock MK ed. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC: American Psychological Association; 2009:291-322.
24. Sweeny S, Zamecnik K. Predictors of self-mutilation in patients with schizophrenia. Am J Psychiatry. 1981;138(8):1086-1089.
25. Grant JE, Odlaug BL, Kim SW. N-acetylcysteine a glutamate modulator, in the treatment of trichotillomania: a double-blind, placebo-controlled study. Arch Gen Psychiatry. 2009;66(7):756-763.
1. Walsh BW, Rosen PM. Self-mutilation: theory research, and treatment. New York, NY: Guilford Press; 2008:32.
2. Nock MK, Favazza AR. Nonsuicidal self-injury: definition and classification. In: Nock MK ed. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC: American Psychological Association; 2009:9-18.
3. Favazza AR, Conterio K. Female habitual self-mutilators. Acta Psychiatr Scand. 1989;79(3):283-289.
4. Favazza A. Bodies under siege: self-mutilation nonsuicidal self-injury, and body modification in culture and psychiatry. 3rd ed. Baltimore, MD: Johns Hopkins University Press; 2011.
5. Gallina R. Tattoos and body piercing. In: Vale V Juno A, eds. Modern primitives. San Francisco, CA: Re/Search Publications; 1989:101-105.
6. Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: the experiential avoidance model. Behav Res Ther. 2006;44(3):371-394.
7. Nock MK, Prinstein MJ. Contextual features and behavioral functions of self-mutilation among adolescents. J Abnorm Psychol. 2005;114(1):140-146.
8. Miller F, Bashkin EA. Depersonalization and self-mutilation. Psychoanal Q. 1974;43(4):638-649.
9. Klonsky ED. The functions of deliberate self-injury: a review of the evidence. Clin Psychol Rev. 2007;27(2):226-239.
10. Nock MK. Actions speak louder than words: an elaborated theoretical model of the social functions of self-injury and other harmful behaviors. Appl Prev Psychol. 2008;12(4):159-168.
11. Nock MK, Prinstein MJ. A functional approach to the assessment of self-mutilative behavior. J Consult Clin Psychol. 2004;72(5):885-890.
12. Nock MK, Prinstein MJ. Contextual features and behavioral functions of self-mutilation among adolescents. J Abnorm Psychol. 2005;114(1):140-146.
13. Favazza AR, Rosenthal RJ. Diagnostic issues in self-mutilation. Hosp Community Psychiatry. 1993;44(2):134-140.
14. Rosen PM, Walsh BW. Patterns of contagion in self-mutilation epidemics. Am J Psychiatry. 1989;146(5):656-658.
15. Large M, Babidge N, Andrews D, et al. Major self-mutilation in the first episode of psychosis. Schizophr Bull. 2009;35(5):1012-1021.
16. Kushner AW. Two cases of auto-castration due to religious delusions. Br J Med Psychol. 1967;40(3):293-298.
17. Moskovitz RA, Byrd T. Rescuing the angel within: PCP-related self-enucleation. Psychosomatics. 1983;24(4):402-403,406.
18. Cleveland SE. Three cases of self-castration. J Nerv Ment Dis. 1956;123(4):386-391.
19. Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. 2006;63(7):757-766.
20. Kahng S, Iwata BA, Lewin AB. Behavioral treatment of self-injury 1964 to 2000. Am J Ment Retard. 2002;107(3):212-221.
21. Levy KN, Yeomans FE, Diamond D. Psychodynamic treatments of self-injury. J Clin Psychol. 2007;63(11):1105-1120.
22. Lott IT, McGregor M, Engelman L, et al. Longitudinal prescribing patterns for psychoactive medications in community-based individuals with developmental disabilities: utilization of pharmacy records. J Intellect Disabil Res. 2004;48(Pt 6):563-571.
23. Sandman CA. Psychopharmacologic treatment of nonsuicidal self-injury. In: Nock MK ed. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC: American Psychological Association; 2009:291-322.
24. Sweeny S, Zamecnik K. Predictors of self-mutilation in patients with schizophrenia. Am J Psychiatry. 1981;138(8):1086-1089.
25. Grant JE, Odlaug BL, Kim SW. N-acetylcysteine a glutamate modulator, in the treatment of trichotillomania: a double-blind, placebo-controlled study. Arch Gen Psychiatry. 2009;66(7):756-763.
Obsessive and inattentive
CASE: Perfect breath
Mr. C, a 20-year-old college student, is diagnosed with obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and tic disorder (TD). His obsessions consist of a persistent sense that he is not breathing “correctly” or “perfectly.” He compulsively holds his breath to “rush blood to my head” until “the pressure feels just right.” Mr. C says that his OCD has had longstanding, significant negative impact on his academic performance and capacity to engage in other activities. Tics have been present for years and manifest as coughing and throat-clearing. After multiple syncopal epi-sodes from breath-holding with Valsalva maneuver—some of which caused falls and head injury—Mr. C is admitted to a residential psychiatric unit specializing in treating OCD. At the time of his admission, his Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores1,2 are 23 total, 12 on the obsessions subscale, and 11 on the compulsions subscale, indicating moderate to severe illness. Cognitive-behavioral therapy (CBT) is offered, along with a combination of escitalopram, 60 mg/d, and quetiapine, 50 mg/d. Quetiapine is over-sedating at subtherapeutic doses and Mr. C’s compulsions worsen. He reports that “[it] took longer and longer to get the ‘just right’ feeling.’” Quetiapine is discontinued and risperidone, 0.5 mg/d, is started, which decreases the frequency of his tics. When he is discharged after a 36-day stay, Mr. C’s Y-BOCS scores are greatly improved at 13 total, 7 on the obsessions subscale, and 3 on the compulsions subscale.
Mr. C’s psychologist refers him to our outpatient clinic for continued psychiatric evaluation and treatment of his OCD, ADHD, and TD. At this time, he is prescribed escitalopram, 60 mg/d, and risperidone, 0.5 mg/d, along with CBT with his psychologist. We do not readminister the Y-BOCS at this time, but Mr. C reports that his OCD is “60% improved.” However, he describes prominent obsessive thoughts regarding his breathing similar to those he experienced before residential treatment. These obsessive thoughts arise in the context of specific environmental “triggers,” such as other people coughing or his own tics. The obsessions lead to compulsive urges to engage in breath-holding rituals. Mr. C experiences the thoughts and compulsions as deeply troubling and they consume 5 to 6 hours each day. Mr. C reports impaired concentration in class and during studying: “I can focus for 5 minutes, then not for 2 minutes, then for 3 minutes… I can never stay focused for more than a couple minutes,” before becoming distracted “by my OCD” or other environmental stimuli. We note on exam prominent breath-holding occurring several times per minute. Mr. C says his OCD has not impaired his ability to socialize.
Mr. C notes that he has been exposed to an array of CBT techniques, but he has difficulty using these techniques because his “mind wanders” or he lacks “motivation.” He admits he occasionally has taken a classmate’s ADHD medication (mixed amphetamine salts [MAS], dose unspecified) and found it improved his ability to focus on his academic work.
The authors’ observations
Researchers have established a relationship among OCD, ADHD, and TD across all combinations of comorbidity (OCD and ADHD,3 ADHD and TD,4 OCD and TD,5,6 and all 3 entities7). Data suggests a poorer prognosis for OCD when comorbid with either or both of these conditions.8 Researchers have raised concerns that psychostimulants could exacerbate or potentiate tic behaviors in patients with ADHD,9,10 although safe and effective use of these medications has been documented in controlled trials of patients with comorbid ADHD and tics.11-13 Furthermore, tic suppression has been reported with psychostimulants,14 as well as a differential effect of stimulants on motor vs vocal tics.15 Despite these data (Table 1),9-15 the FDA regards using psychostimulants in patients with TD as a contraindication,16 although clinicians often recognize that this practice may be unavoidable in some circumstances because of high comorbidity rates. Psychostimulants could exacerbate obsessions or compulsions in some patients because of their dopaminergic properties or through mitigation of the purported anti-obsessional properties of dopamine antagonists.17
Although there is evidence that the prevalence of prescribed psychostimulant abuse is low among ADHD patients,18 diversion of prescribed medication is a risk inherent in the use of these agents, particularly among college-age patients.19,20
Table 1
Evidence of effect of psychostimulants on tics
| Study/disorder(s) | Medication and study design | Relevant findings |
|---|---|---|
| Lipkin et al, 19949; ADHD without TD | Chart review (N = 122) to determine the incidence of tics or dyskinesias in children treated with stimulants | Approximately 9% of children developed tics or dyskinesias, which predominantly were transient, with <1% developing chronic tics or Tourette’s syndrome. Personal or family tic history and medication selection or dosage were not related to onset of tics or dyskinesias |
| Gadow et al, 199515; ADHD with TD | Methylphenidate variable dose, placebo-controlled, 2-week trials (N = 24) | All children’s ADHD symptoms improved. At a 0.1 mg/kg dose, motor tics observed in the classroom increased, but there were fewer vocal tics observed in the lunchroom |
| Castellanos et al, 199710; ADHD with Tourette’s syndrome | Methylphenidate, dextroamphetamine, variable-dose, double-blind, placebo-controlled, 9-week crossover (N = 20) | 3 patients had consistent worsening of tics while taking stimulants. Stimulants reduced hyperactivity rates compared with placebo (P = .03). Stimulants improved ADHD symptoms and had acceptable effects on tics. Methylphenidate was better tolerated than dextroamphetamine |
| Gadow et al, 199911; ADHD with TD | 34 methylphenidate-treated children, followed at 6-month intervals for 2 years | No evidence that frequency or severity of motor or vocal tics changed during maintenance therapy |
| Tourette Syndrome Study Group, 200213; ADHD with TD | Clonidine alone, methylphenidate alone, clonidine plus methylphenidate, or placebo | Worsening of tics was not reported in any group at a rate significantly higher than placebo. Tic severity was more reduced in the 2 clonidine groups than in the methylphenidate group |
| Lyon et al, 201014; ADHD with Tourette’s syndrome | Dexmethylphenidate, single-dose challenge. Ten patients with or without TSP | Acute dexmethylphenidate administration resulted in tic suppression but did not augment TSP |
| Gadow et al, 200712; ADHD with TD | Double-blind, placebo-controlled, 2-week trials each of 3 doses of methylphenidate and placebo (N = 71) | MPH-IR did not alter the overall severity of TD or OCD behaviors. Teacher ratings indicated that MPH-IR therapy decreased tic frequency and severity |
| ADHD: attention-deficit/hyperactivity disorder; MPH-IR: methylphenidate immediate release; OCD: obsessive-compulsive disorder; TD: tic disorder; TSP: tic suppression protocol | ||
TREATMENT: Weighing options
To manage impaired attention and executive function difficulties secondary to ADHD, we offer Mr. C several options, including bupropion, modafinil, and memantine augmentation. Mr. C asks for a psychostimulant because exam week is approaching and he wants a treatment with quick therapeutic effect. We discuss with Mr. C the potential for dopaminergic agents, such as psychostimulants, to exacerbate tics or OCD symptoms. Ultimately, we prescribe immediate-release MAS, 20 mg/d.
Two days later, Mr. C says he has taken 3 MAS doses and describes a marked reduction in obsessions, significant decrease in frequency of “triggers,” and greater capacity to use CBT saying, “when I am [triggered], I am able to move past the urges without doing any compulsions.” Daily time spent “stuck on” obsessions or compulsions decreases from 5 to 6 hours per day to “about 2 and a half minutes.”
Mr. C reports a modest increase in the prevalence of tics, experienced as “little throat clears and quick stuttering of breath.” He notes that, although in the past such tics would be followed by urges for “perfecting the tic and making it feel just right,” he presently “had no desire to do so.”
OUTCOME: Sharper focus
Increasing MAS immediate release from 20 mg/d to 30 mg/d suppresses Mr. C’s obsessions and compulsions for 8 hours. On the 19th day of treatment, MAS immediate release was replaced with an extended release formulation, 30 mg/d, which preserves therapeutic effect and tolerability for 16 weeks. Repeat Y-BOCS yields 9 total, 3 on obsessions subscale, and 6 on compulsions subscale scores.
One month later, Mr. C reports that his symptoms have been “improving ever since” the previous appointment. He continues to be able to access skills for managing his OCD and is doing well in his 2 accelerated summer courses, saying “I focus really well” in 3-hour class sessions. On exam, tic behaviors are nearly absent. Mr. C describes occasional bouts of anxiety associated with urges to engage in tic behaviors, in turn arising from fear of symptomatic recurrence as he worked toward stopping smoking as advised by his primary care physician and psychiatrist.
The authors’ observations
The results of the repeat Y-BOCS are consistent with improvement in obsessions but possible worsening of compulsions since Mr. C was discharged from residential treatment. Alternatively, compulsions may have worsened immediately after discharge and declined again with introduction of MAS.
A substantial body of literature describes the challenges associated with treating ADHD with comorbid tics, including the relative degree of risk of tic exacerbation associated with treating ADHD with psychostimulants. The range of FDA-approved pharmacologic options for treatment of this comorbidity is limited (Table 2),21 particularly given the risk for tardive dyskinesia associated with the typical antipsychotics haloperidol and chlorpromazine. Data support using the α-2 agonist clonidine to treat hyperactivity associated with ADHD22 and TD23 and an extended-release preparation of this medication is FDA-approved for the former but not the latter indication (an α-2A receptor subtype agonist, guanfacine, also is FDA-approved for ADHD in pediatric patients). Mr. C’s experience of robust, sustained reduction in obsessions, if not compulsions, after treatment with MAS is consistent with the few studies of stimulant use in ADHD with comorbid OCD.24,25
Effective treatment of ADHD may help Mr. C better access CBT strategies and thereby potentiate treatment of comorbid OCD.
Table 2
FDA-approved medications for ADHD, OCD, and TD
| Disorder | Medications |
|---|---|
| ADHD | Amphetamine (racemic), atomoxetine, chlorpromazine (hyperactivity), clonidine extended release, dexmethylphenidate, dextroamphetamine, guanfacine extended release, haloperidol (hyperactivity, second-line), lisdexamfetamine, methylphenidate (racemic) |
| OCD | Clomipramine, fluoxetine, fluvoxamine, paroxetine, sertraline |
| TD/Tourette’s syndrome | Haloperidol (Tourette’s), pimozide (Tourette’s) |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder; TD: tic disorder Source: Reference 21 | |
Related Resources
- Pliszka SR. Treating ADHD and comorbid disorders: psychosocial and psychopharmacological interventions. New York, NY: The Guilford Press; 2011.
- Pollak Y, Benarroch F, Kanengisser L, et al. Tourette syndrome-associated psychopathology: roles of comorbid attention-deficit hyperactivity disorder and obsessive-compulsive disorder. J Dev Behav Pediatr. 2009;30(5):413-419.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Clonidine extended release • Kapvay
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guanfacine • Intuniv, Tenex
- Haloperidol • Haldol
- Lisdexamfetamine • Vyvanse
- Memantine • Namenda
- Methylphenidate • Methylin, Ritalin
- Modafinil • Provigil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use and reliability. Arch Gen Psych. 1989;46(11):1006-1011.
2. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: II. Validity. Arch Gen Psych. 1989;46(11):1012-1016.
3. Geller DA, Biederman J, Faraone S, et al. Re-examining comorbidity of obsessive compulsive and attention-deficit hyperactivity disorder using an empirically derived taxonomy. Eur Child Adolesc Psychiatry. 2004;13(2):83-91.
4. Freeman RD. Attention deficit hyperactivity disorder in the presence of Tourette syndrome. Neurol Clin. 1997;15(2):411-420.
5. Geller DA. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr Clin North Am. 2006;29(2):353-370.
6. Eapen V, Fox-Hiley P, Banerjee S, et al. Clinical features and associated psychopathology in a Tourette syndrome cohort. Acta Neurol Scand. 2004;109(4):255-260.
7. Kano Y, Ohta M, Nagai Y, et al. Association between Tourette syndrome and comorbidities in Japan. Brain Dev. 2010;32(3):201-207.
8. Grados M, Riddle M. Do all obsessive-compulsive disorder subtypes respond to medication? Int Rev Psychiatry. 2008;20(2):189-193.
9. Lipkin PH, Goldstein IH, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 1994;148(8):859-861.
10. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry. 1997;36(5):589-596.
11. Gadow K, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry. 1999;56(4):330-333.
12. Gadow KD, Sverd J, Nolan EE, et al. Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):840-848.
13. Tourette’s Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology. 2002;58(4):527-536.
14. Lyon GJ, Samar SM, Conelea C, et al. Testing tic suppression: comparing the effects of dexmethylphenidate to no mediation in children and adolescents with attention-deficit/hyperactivity disorder and Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):283-289.
15. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry. 1995;52(6):444-455.
16. Bloch MH, Panza KE, Landerso-Weisenberger A, et al. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry. 2009;48(9):884-893.
17. McDougle CJ, Goodman WK, Price LH. Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry. 1994;55(suppl):24-31.
18. Wilens TE, Morrison NR. The intersection of attention-deficit/hyperactivity disorder and substance abuse. Curr Opin Psychiatry. 2011;24(4):280-285.
19. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
20. Schubiner H. Substance abuse in patients with attention-deficit hyperactivity disorder: therapeutic implications. CNS Drugs. 2005;19(8):643-655.
21. Stahl SM. The prescriber’s guide. Stahl’s essential psychopharmacology. 3rd ed. New York NY: Cambridge University Press; 2009.
22. Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(2):171-179.
23. Hedderick EF, Morris CM, Singer HS. Double-blind crossover study of clonidine and levetiracetam in Tourette syndrome. Pediatr Neurol. 2009;40(6):420-425.
24. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11(4):237-241.
25. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80(3):231-235.
CASE: Perfect breath
Mr. C, a 20-year-old college student, is diagnosed with obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and tic disorder (TD). His obsessions consist of a persistent sense that he is not breathing “correctly” or “perfectly.” He compulsively holds his breath to “rush blood to my head” until “the pressure feels just right.” Mr. C says that his OCD has had longstanding, significant negative impact on his academic performance and capacity to engage in other activities. Tics have been present for years and manifest as coughing and throat-clearing. After multiple syncopal epi-sodes from breath-holding with Valsalva maneuver—some of which caused falls and head injury—Mr. C is admitted to a residential psychiatric unit specializing in treating OCD. At the time of his admission, his Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores1,2 are 23 total, 12 on the obsessions subscale, and 11 on the compulsions subscale, indicating moderate to severe illness. Cognitive-behavioral therapy (CBT) is offered, along with a combination of escitalopram, 60 mg/d, and quetiapine, 50 mg/d. Quetiapine is over-sedating at subtherapeutic doses and Mr. C’s compulsions worsen. He reports that “[it] took longer and longer to get the ‘just right’ feeling.’” Quetiapine is discontinued and risperidone, 0.5 mg/d, is started, which decreases the frequency of his tics. When he is discharged after a 36-day stay, Mr. C’s Y-BOCS scores are greatly improved at 13 total, 7 on the obsessions subscale, and 3 on the compulsions subscale.
Mr. C’s psychologist refers him to our outpatient clinic for continued psychiatric evaluation and treatment of his OCD, ADHD, and TD. At this time, he is prescribed escitalopram, 60 mg/d, and risperidone, 0.5 mg/d, along with CBT with his psychologist. We do not readminister the Y-BOCS at this time, but Mr. C reports that his OCD is “60% improved.” However, he describes prominent obsessive thoughts regarding his breathing similar to those he experienced before residential treatment. These obsessive thoughts arise in the context of specific environmental “triggers,” such as other people coughing or his own tics. The obsessions lead to compulsive urges to engage in breath-holding rituals. Mr. C experiences the thoughts and compulsions as deeply troubling and they consume 5 to 6 hours each day. Mr. C reports impaired concentration in class and during studying: “I can focus for 5 minutes, then not for 2 minutes, then for 3 minutes… I can never stay focused for more than a couple minutes,” before becoming distracted “by my OCD” or other environmental stimuli. We note on exam prominent breath-holding occurring several times per minute. Mr. C says his OCD has not impaired his ability to socialize.
Mr. C notes that he has been exposed to an array of CBT techniques, but he has difficulty using these techniques because his “mind wanders” or he lacks “motivation.” He admits he occasionally has taken a classmate’s ADHD medication (mixed amphetamine salts [MAS], dose unspecified) and found it improved his ability to focus on his academic work.
The authors’ observations
Researchers have established a relationship among OCD, ADHD, and TD across all combinations of comorbidity (OCD and ADHD,3 ADHD and TD,4 OCD and TD,5,6 and all 3 entities7). Data suggests a poorer prognosis for OCD when comorbid with either or both of these conditions.8 Researchers have raised concerns that psychostimulants could exacerbate or potentiate tic behaviors in patients with ADHD,9,10 although safe and effective use of these medications has been documented in controlled trials of patients with comorbid ADHD and tics.11-13 Furthermore, tic suppression has been reported with psychostimulants,14 as well as a differential effect of stimulants on motor vs vocal tics.15 Despite these data (Table 1),9-15 the FDA regards using psychostimulants in patients with TD as a contraindication,16 although clinicians often recognize that this practice may be unavoidable in some circumstances because of high comorbidity rates. Psychostimulants could exacerbate obsessions or compulsions in some patients because of their dopaminergic properties or through mitigation of the purported anti-obsessional properties of dopamine antagonists.17
Although there is evidence that the prevalence of prescribed psychostimulant abuse is low among ADHD patients,18 diversion of prescribed medication is a risk inherent in the use of these agents, particularly among college-age patients.19,20
Table 1
Evidence of effect of psychostimulants on tics
| Study/disorder(s) | Medication and study design | Relevant findings |
|---|---|---|
| Lipkin et al, 19949; ADHD without TD | Chart review (N = 122) to determine the incidence of tics or dyskinesias in children treated with stimulants | Approximately 9% of children developed tics or dyskinesias, which predominantly were transient, with <1% developing chronic tics or Tourette’s syndrome. Personal or family tic history and medication selection or dosage were not related to onset of tics or dyskinesias |
| Gadow et al, 199515; ADHD with TD | Methylphenidate variable dose, placebo-controlled, 2-week trials (N = 24) | All children’s ADHD symptoms improved. At a 0.1 mg/kg dose, motor tics observed in the classroom increased, but there were fewer vocal tics observed in the lunchroom |
| Castellanos et al, 199710; ADHD with Tourette’s syndrome | Methylphenidate, dextroamphetamine, variable-dose, double-blind, placebo-controlled, 9-week crossover (N = 20) | 3 patients had consistent worsening of tics while taking stimulants. Stimulants reduced hyperactivity rates compared with placebo (P = .03). Stimulants improved ADHD symptoms and had acceptable effects on tics. Methylphenidate was better tolerated than dextroamphetamine |
| Gadow et al, 199911; ADHD with TD | 34 methylphenidate-treated children, followed at 6-month intervals for 2 years | No evidence that frequency or severity of motor or vocal tics changed during maintenance therapy |
| Tourette Syndrome Study Group, 200213; ADHD with TD | Clonidine alone, methylphenidate alone, clonidine plus methylphenidate, or placebo | Worsening of tics was not reported in any group at a rate significantly higher than placebo. Tic severity was more reduced in the 2 clonidine groups than in the methylphenidate group |
| Lyon et al, 201014; ADHD with Tourette’s syndrome | Dexmethylphenidate, single-dose challenge. Ten patients with or without TSP | Acute dexmethylphenidate administration resulted in tic suppression but did not augment TSP |
| Gadow et al, 200712; ADHD with TD | Double-blind, placebo-controlled, 2-week trials each of 3 doses of methylphenidate and placebo (N = 71) | MPH-IR did not alter the overall severity of TD or OCD behaviors. Teacher ratings indicated that MPH-IR therapy decreased tic frequency and severity |
| ADHD: attention-deficit/hyperactivity disorder; MPH-IR: methylphenidate immediate release; OCD: obsessive-compulsive disorder; TD: tic disorder; TSP: tic suppression protocol | ||
TREATMENT: Weighing options
To manage impaired attention and executive function difficulties secondary to ADHD, we offer Mr. C several options, including bupropion, modafinil, and memantine augmentation. Mr. C asks for a psychostimulant because exam week is approaching and he wants a treatment with quick therapeutic effect. We discuss with Mr. C the potential for dopaminergic agents, such as psychostimulants, to exacerbate tics or OCD symptoms. Ultimately, we prescribe immediate-release MAS, 20 mg/d.
Two days later, Mr. C says he has taken 3 MAS doses and describes a marked reduction in obsessions, significant decrease in frequency of “triggers,” and greater capacity to use CBT saying, “when I am [triggered], I am able to move past the urges without doing any compulsions.” Daily time spent “stuck on” obsessions or compulsions decreases from 5 to 6 hours per day to “about 2 and a half minutes.”
Mr. C reports a modest increase in the prevalence of tics, experienced as “little throat clears and quick stuttering of breath.” He notes that, although in the past such tics would be followed by urges for “perfecting the tic and making it feel just right,” he presently “had no desire to do so.”
OUTCOME: Sharper focus
Increasing MAS immediate release from 20 mg/d to 30 mg/d suppresses Mr. C’s obsessions and compulsions for 8 hours. On the 19th day of treatment, MAS immediate release was replaced with an extended release formulation, 30 mg/d, which preserves therapeutic effect and tolerability for 16 weeks. Repeat Y-BOCS yields 9 total, 3 on obsessions subscale, and 6 on compulsions subscale scores.
One month later, Mr. C reports that his symptoms have been “improving ever since” the previous appointment. He continues to be able to access skills for managing his OCD and is doing well in his 2 accelerated summer courses, saying “I focus really well” in 3-hour class sessions. On exam, tic behaviors are nearly absent. Mr. C describes occasional bouts of anxiety associated with urges to engage in tic behaviors, in turn arising from fear of symptomatic recurrence as he worked toward stopping smoking as advised by his primary care physician and psychiatrist.
The authors’ observations
The results of the repeat Y-BOCS are consistent with improvement in obsessions but possible worsening of compulsions since Mr. C was discharged from residential treatment. Alternatively, compulsions may have worsened immediately after discharge and declined again with introduction of MAS.
A substantial body of literature describes the challenges associated with treating ADHD with comorbid tics, including the relative degree of risk of tic exacerbation associated with treating ADHD with psychostimulants. The range of FDA-approved pharmacologic options for treatment of this comorbidity is limited (Table 2),21 particularly given the risk for tardive dyskinesia associated with the typical antipsychotics haloperidol and chlorpromazine. Data support using the α-2 agonist clonidine to treat hyperactivity associated with ADHD22 and TD23 and an extended-release preparation of this medication is FDA-approved for the former but not the latter indication (an α-2A receptor subtype agonist, guanfacine, also is FDA-approved for ADHD in pediatric patients). Mr. C’s experience of robust, sustained reduction in obsessions, if not compulsions, after treatment with MAS is consistent with the few studies of stimulant use in ADHD with comorbid OCD.24,25
Effective treatment of ADHD may help Mr. C better access CBT strategies and thereby potentiate treatment of comorbid OCD.
Table 2
FDA-approved medications for ADHD, OCD, and TD
| Disorder | Medications |
|---|---|
| ADHD | Amphetamine (racemic), atomoxetine, chlorpromazine (hyperactivity), clonidine extended release, dexmethylphenidate, dextroamphetamine, guanfacine extended release, haloperidol (hyperactivity, second-line), lisdexamfetamine, methylphenidate (racemic) |
| OCD | Clomipramine, fluoxetine, fluvoxamine, paroxetine, sertraline |
| TD/Tourette’s syndrome | Haloperidol (Tourette’s), pimozide (Tourette’s) |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder; TD: tic disorder Source: Reference 21 | |
Related Resources
- Pliszka SR. Treating ADHD and comorbid disorders: psychosocial and psychopharmacological interventions. New York, NY: The Guilford Press; 2011.
- Pollak Y, Benarroch F, Kanengisser L, et al. Tourette syndrome-associated psychopathology: roles of comorbid attention-deficit hyperactivity disorder and obsessive-compulsive disorder. J Dev Behav Pediatr. 2009;30(5):413-419.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Clonidine extended release • Kapvay
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guanfacine • Intuniv, Tenex
- Haloperidol • Haldol
- Lisdexamfetamine • Vyvanse
- Memantine • Namenda
- Methylphenidate • Methylin, Ritalin
- Modafinil • Provigil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Perfect breath
Mr. C, a 20-year-old college student, is diagnosed with obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and tic disorder (TD). His obsessions consist of a persistent sense that he is not breathing “correctly” or “perfectly.” He compulsively holds his breath to “rush blood to my head” until “the pressure feels just right.” Mr. C says that his OCD has had longstanding, significant negative impact on his academic performance and capacity to engage in other activities. Tics have been present for years and manifest as coughing and throat-clearing. After multiple syncopal epi-sodes from breath-holding with Valsalva maneuver—some of which caused falls and head injury—Mr. C is admitted to a residential psychiatric unit specializing in treating OCD. At the time of his admission, his Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores1,2 are 23 total, 12 on the obsessions subscale, and 11 on the compulsions subscale, indicating moderate to severe illness. Cognitive-behavioral therapy (CBT) is offered, along with a combination of escitalopram, 60 mg/d, and quetiapine, 50 mg/d. Quetiapine is over-sedating at subtherapeutic doses and Mr. C’s compulsions worsen. He reports that “[it] took longer and longer to get the ‘just right’ feeling.’” Quetiapine is discontinued and risperidone, 0.5 mg/d, is started, which decreases the frequency of his tics. When he is discharged after a 36-day stay, Mr. C’s Y-BOCS scores are greatly improved at 13 total, 7 on the obsessions subscale, and 3 on the compulsions subscale.
Mr. C’s psychologist refers him to our outpatient clinic for continued psychiatric evaluation and treatment of his OCD, ADHD, and TD. At this time, he is prescribed escitalopram, 60 mg/d, and risperidone, 0.5 mg/d, along with CBT with his psychologist. We do not readminister the Y-BOCS at this time, but Mr. C reports that his OCD is “60% improved.” However, he describes prominent obsessive thoughts regarding his breathing similar to those he experienced before residential treatment. These obsessive thoughts arise in the context of specific environmental “triggers,” such as other people coughing or his own tics. The obsessions lead to compulsive urges to engage in breath-holding rituals. Mr. C experiences the thoughts and compulsions as deeply troubling and they consume 5 to 6 hours each day. Mr. C reports impaired concentration in class and during studying: “I can focus for 5 minutes, then not for 2 minutes, then for 3 minutes… I can never stay focused for more than a couple minutes,” before becoming distracted “by my OCD” or other environmental stimuli. We note on exam prominent breath-holding occurring several times per minute. Mr. C says his OCD has not impaired his ability to socialize.
Mr. C notes that he has been exposed to an array of CBT techniques, but he has difficulty using these techniques because his “mind wanders” or he lacks “motivation.” He admits he occasionally has taken a classmate’s ADHD medication (mixed amphetamine salts [MAS], dose unspecified) and found it improved his ability to focus on his academic work.
The authors’ observations
Researchers have established a relationship among OCD, ADHD, and TD across all combinations of comorbidity (OCD and ADHD,3 ADHD and TD,4 OCD and TD,5,6 and all 3 entities7). Data suggests a poorer prognosis for OCD when comorbid with either or both of these conditions.8 Researchers have raised concerns that psychostimulants could exacerbate or potentiate tic behaviors in patients with ADHD,9,10 although safe and effective use of these medications has been documented in controlled trials of patients with comorbid ADHD and tics.11-13 Furthermore, tic suppression has been reported with psychostimulants,14 as well as a differential effect of stimulants on motor vs vocal tics.15 Despite these data (Table 1),9-15 the FDA regards using psychostimulants in patients with TD as a contraindication,16 although clinicians often recognize that this practice may be unavoidable in some circumstances because of high comorbidity rates. Psychostimulants could exacerbate obsessions or compulsions in some patients because of their dopaminergic properties or through mitigation of the purported anti-obsessional properties of dopamine antagonists.17
Although there is evidence that the prevalence of prescribed psychostimulant abuse is low among ADHD patients,18 diversion of prescribed medication is a risk inherent in the use of these agents, particularly among college-age patients.19,20
Table 1
Evidence of effect of psychostimulants on tics
| Study/disorder(s) | Medication and study design | Relevant findings |
|---|---|---|
| Lipkin et al, 19949; ADHD without TD | Chart review (N = 122) to determine the incidence of tics or dyskinesias in children treated with stimulants | Approximately 9% of children developed tics or dyskinesias, which predominantly were transient, with <1% developing chronic tics or Tourette’s syndrome. Personal or family tic history and medication selection or dosage were not related to onset of tics or dyskinesias |
| Gadow et al, 199515; ADHD with TD | Methylphenidate variable dose, placebo-controlled, 2-week trials (N = 24) | All children’s ADHD symptoms improved. At a 0.1 mg/kg dose, motor tics observed in the classroom increased, but there were fewer vocal tics observed in the lunchroom |
| Castellanos et al, 199710; ADHD with Tourette’s syndrome | Methylphenidate, dextroamphetamine, variable-dose, double-blind, placebo-controlled, 9-week crossover (N = 20) | 3 patients had consistent worsening of tics while taking stimulants. Stimulants reduced hyperactivity rates compared with placebo (P = .03). Stimulants improved ADHD symptoms and had acceptable effects on tics. Methylphenidate was better tolerated than dextroamphetamine |
| Gadow et al, 199911; ADHD with TD | 34 methylphenidate-treated children, followed at 6-month intervals for 2 years | No evidence that frequency or severity of motor or vocal tics changed during maintenance therapy |
| Tourette Syndrome Study Group, 200213; ADHD with TD | Clonidine alone, methylphenidate alone, clonidine plus methylphenidate, or placebo | Worsening of tics was not reported in any group at a rate significantly higher than placebo. Tic severity was more reduced in the 2 clonidine groups than in the methylphenidate group |
| Lyon et al, 201014; ADHD with Tourette’s syndrome | Dexmethylphenidate, single-dose challenge. Ten patients with or without TSP | Acute dexmethylphenidate administration resulted in tic suppression but did not augment TSP |
| Gadow et al, 200712; ADHD with TD | Double-blind, placebo-controlled, 2-week trials each of 3 doses of methylphenidate and placebo (N = 71) | MPH-IR did not alter the overall severity of TD or OCD behaviors. Teacher ratings indicated that MPH-IR therapy decreased tic frequency and severity |
| ADHD: attention-deficit/hyperactivity disorder; MPH-IR: methylphenidate immediate release; OCD: obsessive-compulsive disorder; TD: tic disorder; TSP: tic suppression protocol | ||
TREATMENT: Weighing options
To manage impaired attention and executive function difficulties secondary to ADHD, we offer Mr. C several options, including bupropion, modafinil, and memantine augmentation. Mr. C asks for a psychostimulant because exam week is approaching and he wants a treatment with quick therapeutic effect. We discuss with Mr. C the potential for dopaminergic agents, such as psychostimulants, to exacerbate tics or OCD symptoms. Ultimately, we prescribe immediate-release MAS, 20 mg/d.
Two days later, Mr. C says he has taken 3 MAS doses and describes a marked reduction in obsessions, significant decrease in frequency of “triggers,” and greater capacity to use CBT saying, “when I am [triggered], I am able to move past the urges without doing any compulsions.” Daily time spent “stuck on” obsessions or compulsions decreases from 5 to 6 hours per day to “about 2 and a half minutes.”
Mr. C reports a modest increase in the prevalence of tics, experienced as “little throat clears and quick stuttering of breath.” He notes that, although in the past such tics would be followed by urges for “perfecting the tic and making it feel just right,” he presently “had no desire to do so.”
OUTCOME: Sharper focus
Increasing MAS immediate release from 20 mg/d to 30 mg/d suppresses Mr. C’s obsessions and compulsions for 8 hours. On the 19th day of treatment, MAS immediate release was replaced with an extended release formulation, 30 mg/d, which preserves therapeutic effect and tolerability for 16 weeks. Repeat Y-BOCS yields 9 total, 3 on obsessions subscale, and 6 on compulsions subscale scores.
One month later, Mr. C reports that his symptoms have been “improving ever since” the previous appointment. He continues to be able to access skills for managing his OCD and is doing well in his 2 accelerated summer courses, saying “I focus really well” in 3-hour class sessions. On exam, tic behaviors are nearly absent. Mr. C describes occasional bouts of anxiety associated with urges to engage in tic behaviors, in turn arising from fear of symptomatic recurrence as he worked toward stopping smoking as advised by his primary care physician and psychiatrist.
The authors’ observations
The results of the repeat Y-BOCS are consistent with improvement in obsessions but possible worsening of compulsions since Mr. C was discharged from residential treatment. Alternatively, compulsions may have worsened immediately after discharge and declined again with introduction of MAS.
A substantial body of literature describes the challenges associated with treating ADHD with comorbid tics, including the relative degree of risk of tic exacerbation associated with treating ADHD with psychostimulants. The range of FDA-approved pharmacologic options for treatment of this comorbidity is limited (Table 2),21 particularly given the risk for tardive dyskinesia associated with the typical antipsychotics haloperidol and chlorpromazine. Data support using the α-2 agonist clonidine to treat hyperactivity associated with ADHD22 and TD23 and an extended-release preparation of this medication is FDA-approved for the former but not the latter indication (an α-2A receptor subtype agonist, guanfacine, also is FDA-approved for ADHD in pediatric patients). Mr. C’s experience of robust, sustained reduction in obsessions, if not compulsions, after treatment with MAS is consistent with the few studies of stimulant use in ADHD with comorbid OCD.24,25
Effective treatment of ADHD may help Mr. C better access CBT strategies and thereby potentiate treatment of comorbid OCD.
Table 2
FDA-approved medications for ADHD, OCD, and TD
| Disorder | Medications |
|---|---|
| ADHD | Amphetamine (racemic), atomoxetine, chlorpromazine (hyperactivity), clonidine extended release, dexmethylphenidate, dextroamphetamine, guanfacine extended release, haloperidol (hyperactivity, second-line), lisdexamfetamine, methylphenidate (racemic) |
| OCD | Clomipramine, fluoxetine, fluvoxamine, paroxetine, sertraline |
| TD/Tourette’s syndrome | Haloperidol (Tourette’s), pimozide (Tourette’s) |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder; TD: tic disorder Source: Reference 21 | |
Related Resources
- Pliszka SR. Treating ADHD and comorbid disorders: psychosocial and psychopharmacological interventions. New York, NY: The Guilford Press; 2011.
- Pollak Y, Benarroch F, Kanengisser L, et al. Tourette syndrome-associated psychopathology: roles of comorbid attention-deficit hyperactivity disorder and obsessive-compulsive disorder. J Dev Behav Pediatr. 2009;30(5):413-419.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Clonidine extended release • Kapvay
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guanfacine • Intuniv, Tenex
- Haloperidol • Haldol
- Lisdexamfetamine • Vyvanse
- Memantine • Namenda
- Methylphenidate • Methylin, Ritalin
- Modafinil • Provigil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use and reliability. Arch Gen Psych. 1989;46(11):1006-1011.
2. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: II. Validity. Arch Gen Psych. 1989;46(11):1012-1016.
3. Geller DA, Biederman J, Faraone S, et al. Re-examining comorbidity of obsessive compulsive and attention-deficit hyperactivity disorder using an empirically derived taxonomy. Eur Child Adolesc Psychiatry. 2004;13(2):83-91.
4. Freeman RD. Attention deficit hyperactivity disorder in the presence of Tourette syndrome. Neurol Clin. 1997;15(2):411-420.
5. Geller DA. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr Clin North Am. 2006;29(2):353-370.
6. Eapen V, Fox-Hiley P, Banerjee S, et al. Clinical features and associated psychopathology in a Tourette syndrome cohort. Acta Neurol Scand. 2004;109(4):255-260.
7. Kano Y, Ohta M, Nagai Y, et al. Association between Tourette syndrome and comorbidities in Japan. Brain Dev. 2010;32(3):201-207.
8. Grados M, Riddle M. Do all obsessive-compulsive disorder subtypes respond to medication? Int Rev Psychiatry. 2008;20(2):189-193.
9. Lipkin PH, Goldstein IH, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 1994;148(8):859-861.
10. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry. 1997;36(5):589-596.
11. Gadow K, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry. 1999;56(4):330-333.
12. Gadow KD, Sverd J, Nolan EE, et al. Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):840-848.
13. Tourette’s Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology. 2002;58(4):527-536.
14. Lyon GJ, Samar SM, Conelea C, et al. Testing tic suppression: comparing the effects of dexmethylphenidate to no mediation in children and adolescents with attention-deficit/hyperactivity disorder and Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):283-289.
15. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry. 1995;52(6):444-455.
16. Bloch MH, Panza KE, Landerso-Weisenberger A, et al. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry. 2009;48(9):884-893.
17. McDougle CJ, Goodman WK, Price LH. Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry. 1994;55(suppl):24-31.
18. Wilens TE, Morrison NR. The intersection of attention-deficit/hyperactivity disorder and substance abuse. Curr Opin Psychiatry. 2011;24(4):280-285.
19. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
20. Schubiner H. Substance abuse in patients with attention-deficit hyperactivity disorder: therapeutic implications. CNS Drugs. 2005;19(8):643-655.
21. Stahl SM. The prescriber’s guide. Stahl’s essential psychopharmacology. 3rd ed. New York NY: Cambridge University Press; 2009.
22. Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(2):171-179.
23. Hedderick EF, Morris CM, Singer HS. Double-blind crossover study of clonidine and levetiracetam in Tourette syndrome. Pediatr Neurol. 2009;40(6):420-425.
24. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11(4):237-241.
25. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80(3):231-235.
1. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use and reliability. Arch Gen Psych. 1989;46(11):1006-1011.
2. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: II. Validity. Arch Gen Psych. 1989;46(11):1012-1016.
3. Geller DA, Biederman J, Faraone S, et al. Re-examining comorbidity of obsessive compulsive and attention-deficit hyperactivity disorder using an empirically derived taxonomy. Eur Child Adolesc Psychiatry. 2004;13(2):83-91.
4. Freeman RD. Attention deficit hyperactivity disorder in the presence of Tourette syndrome. Neurol Clin. 1997;15(2):411-420.
5. Geller DA. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr Clin North Am. 2006;29(2):353-370.
6. Eapen V, Fox-Hiley P, Banerjee S, et al. Clinical features and associated psychopathology in a Tourette syndrome cohort. Acta Neurol Scand. 2004;109(4):255-260.
7. Kano Y, Ohta M, Nagai Y, et al. Association between Tourette syndrome and comorbidities in Japan. Brain Dev. 2010;32(3):201-207.
8. Grados M, Riddle M. Do all obsessive-compulsive disorder subtypes respond to medication? Int Rev Psychiatry. 2008;20(2):189-193.
9. Lipkin PH, Goldstein IH, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 1994;148(8):859-861.
10. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry. 1997;36(5):589-596.
11. Gadow K, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry. 1999;56(4):330-333.
12. Gadow KD, Sverd J, Nolan EE, et al. Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):840-848.
13. Tourette’s Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology. 2002;58(4):527-536.
14. Lyon GJ, Samar SM, Conelea C, et al. Testing tic suppression: comparing the effects of dexmethylphenidate to no mediation in children and adolescents with attention-deficit/hyperactivity disorder and Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):283-289.
15. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry. 1995;52(6):444-455.
16. Bloch MH, Panza KE, Landerso-Weisenberger A, et al. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry. 2009;48(9):884-893.
17. McDougle CJ, Goodman WK, Price LH. Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry. 1994;55(suppl):24-31.
18. Wilens TE, Morrison NR. The intersection of attention-deficit/hyperactivity disorder and substance abuse. Curr Opin Psychiatry. 2011;24(4):280-285.
19. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
20. Schubiner H. Substance abuse in patients with attention-deficit hyperactivity disorder: therapeutic implications. CNS Drugs. 2005;19(8):643-655.
21. Stahl SM. The prescriber’s guide. Stahl’s essential psychopharmacology. 3rd ed. New York NY: Cambridge University Press; 2009.
22. Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(2):171-179.
23. Hedderick EF, Morris CM, Singer HS. Double-blind crossover study of clonidine and levetiracetam in Tourette syndrome. Pediatr Neurol. 2009;40(6):420-425.
24. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11(4):237-241.
25. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80(3):231-235.
Not ’antipsychiatry’; Defending Dr. Szasz; Perpetrators of abuse
Not ’antipsychiatry’
Dr. Nasrallah misrepresents Drs. Jacques Lacan, Erich Fromm, Theodore Lidz, and others in his December 2011 editorial (“The antipsychiatry movement: Who and why,” From the Editor, Current Psychiatry, December 2011, p. 4-6, 53). They were not antipsychiatry, nor am I.
I am “anti” the sort of concrete biological reductionism espoused by Dr. Nasrallah. The psychiatrist nattily dressed in a white jacket and a neat suit and tie looks like a real doctor, but the so-called rigorous objective medical practice he does ignores a huge domain that psychiatry used to be concerned about. In effect, under the leadership of those such as Dr. Nasrallah, psychiatry has “lost its mind.” The disorders we treat are real disorders, but getting rid of the mental dimension and reducing all to “brain disorders” reduces our effectiveness in helping patients, is not humane, and flees from the truth. Psychiatry needs to re-find its mind.
Ronald Abramson, MD, DLFAPA
Associate Clinical Professor of Psychiatry
Tufts University School of Medicine
Boston, MA
Defending Dr. Szasz
Dr. Nasrallah’s editorial (“The antipsychiatry movement: Who and why,” From the Editor, Current Psychiatry, December 2011, p. 4-6, 53) on the antipsychiatry movement was an excellent historical overview. It also was right on target in its conclusion, namely, that antipsychiatry can help keep psychiatry honest and rigorous.
However, the portrayal of Dr. Thomas Szasz as an antipsychiatrist is not wholly correct. For decades, Dr. Szasz has severely criticized both psychiatry and the antipsychiatry movement. Like antipsychiatrists, he is critical of psychiatry, but unlike antipsychiatrists, Dr. Szasz steadfastly has defended the right of consenting individuals to engage in treatment, as long as their participation is voluntary. It is this libertarian streak, the idea that people are free to choose any treatment arrangement they desire—including psychiatry—that distinguishes Dr. Szasz from antipsychiatrists such as Drs. Theodore Lidz, R.D. Laing, and others.
Thomas Rosko, MD
Private Practice
Los Angeles, CA
Perpetrators of abuse
Dr. Nasrallah appears to be deliberately avoiding some of the real abuses perpetrated by modern-day psychiatry (“The antipsychiatry movement: Who and why,” From the Editor, Current Psychiatry, December 2011, p. 4-6, 53), including deliberately misdiagnosing alcoholics and drug abusers as bipolar in order to give them mood stabilizers, often while they are actively abusing substances.
It seems unfathomable for a physician to document a history of depressive episodes, let alone manic episodes, in someone who has been either intoxicated or in early withdrawal constantly over the years, yet this is done routinely. The abuser is happy to play along, as long as the psychiatrist prescribes benzodiazepines along with valproic acid, lithium, or lamotrigine for the patient’s persistent panic attacks and chronic insomnia.
This psychiatric version of “when you have a hammer, everything is a nail” extends to the treatment of uncomplicated grief with antidepressants, additionally labeling oppositional defiant adolescents as bipolar to give them mood stabilizers, and, of course, treating large-portion junk food eaters for “bulimia,” placing them into eating disorder programs, and prescribing psychotropics.
Dr. Nasrallah’s examples of old abuses are a “straw man” argument and unfortunately divert attention from the legitimate concerns about “scientific” modern psychiatry.
Ronald Cann, MD
Private Practice
San Diego, CA
Dr. Nasrallah responds
I appreciate the letters from Drs. Abramson, Rosko, and Cann. I particularly liked their “healthy skepticism” about parts of my editorial about antipsychiatry.
My clinical training was heavily “mind-oriented” with intensive psychodynamic as well as behavioral psychotherapy (not cognitive-behavioral therapy), and my National Institute of Mental Health research training was heavily “brain oriented” with a neuroscience focus. I integrated both brain (hardware) and mind (software) in my work with each patient and it worked spectacularly well for both of us! George Engel, the father of the biopsychosocial model, was one of my residency supervisors at the University of Rochester, so I was “inoculated” by his mentorship against the hazards of biological reductionism, to which Dr. Abramson assumes I subscribe.
Dr. Thomas Szasz certainly was more of a libertarian than an antipsychiatrist and did a great injustice to patients with severe brain disorders, such as schizophrenia, by asserting that they are competent enough to choose or deny treatment, possibly because of the early state of neurobiology research 50 years ago when the neurotoxic effects of psychosis were still undiscovered. Unlike persons with healthy brains and prefrontal executive functions that enable sound decision-making, schizophrenia patients have anosognosia—the neurologic term for lack of insight and self-monitoring—severe cognitive deficits in processing information and decision-making, and reality distortion, and they lack the capacity to determine that they urgently need treatment. Witness the death of thousands of schizophrenia patients who were abruptly released from Italy’s asylums in the 1980s because they lacked the basic brain functions needed to survive. It was a tragic mistake to leave them to their own devices in the name of freedom, conceptualized by lay legislators who had no idea how impaired the brain is in many schizophrenia patients.
Finally, Dr. Szasz practiced long before research demonstrated that the longer psychosis went untreated, the worse the deterioration and functional outcome. Thus, his stance to let patients with psychosis refuse medications significantly harmed those patients, worsened their symptoms, and reduced their chance for remission.
Dr. Cann’s allegations of the “real abuses” of modern day psychiatry are to the best of my knowledge just that–allegations. I have never seen valid documentation of the large-scale abuses he cites, although an occasional deviation occurs in any profession. The practice guidelines for various psychiatric disorders never recommend what Dr. Cann claims is happening with diagnostic distortions and ulterior motives.
Psychiatry still is evolving as a medical discipline and there are comorbidities that confound the primary diagnosis—such as anxiety or heavy drinking in bipolar disorder—but research is actively seeking a biopsychosocial explanation. The Epidemiological Catchment Area study,1 published 20 years ago before any of the current medications were introduced, is upheld as the best estimate of the prevalence of psychiatric disorders in the United States—approximately 25% lifetime risk, which means approximately 75 million children, adolescents, and adults have a diagnosable psychiatric disorder. Some of them receive good evidence-based treatments and some do not, but many more never receive any treatment and suffer in quiet desperation.
Henry A. Nasrallah, MD
Editor-in-Chief
Not ’antipsychiatry’
Dr. Nasrallah misrepresents Drs. Jacques Lacan, Erich Fromm, Theodore Lidz, and others in his December 2011 editorial (“The antipsychiatry movement: Who and why,” From the Editor, Current Psychiatry, December 2011, p. 4-6, 53). They were not antipsychiatry, nor am I.
I am “anti” the sort of concrete biological reductionism espoused by Dr. Nasrallah. The psychiatrist nattily dressed in a white jacket and a neat suit and tie looks like a real doctor, but the so-called rigorous objective medical practice he does ignores a huge domain that psychiatry used to be concerned about. In effect, under the leadership of those such as Dr. Nasrallah, psychiatry has “lost its mind.” The disorders we treat are real disorders, but getting rid of the mental dimension and reducing all to “brain disorders” reduces our effectiveness in helping patients, is not humane, and flees from the truth. Psychiatry needs to re-find its mind.
Ronald Abramson, MD, DLFAPA
Associate Clinical Professor of Psychiatry
Tufts University School of Medicine
Boston, MA
Defending Dr. Szasz
Dr. Nasrallah’s editorial (“The antipsychiatry movement: Who and why,” From the Editor, Current Psychiatry, December 2011, p. 4-6, 53) on the antipsychiatry movement was an excellent historical overview. It also was right on target in its conclusion, namely, that antipsychiatry can help keep psychiatry honest and rigorous.
However, the portrayal of Dr. Thomas Szasz as an antipsychiatrist is not wholly correct. For decades, Dr. Szasz has severely criticized both psychiatry and the antipsychiatry movement. Like antipsychiatrists, he is critical of psychiatry, but unlike antipsychiatrists, Dr. Szasz steadfastly has defended the right of consenting individuals to engage in treatment, as long as their participation is voluntary. It is this libertarian streak, the idea that people are free to choose any treatment arrangement they desire—including psychiatry—that distinguishes Dr. Szasz from antipsychiatrists such as Drs. Theodore Lidz, R.D. Laing, and others.
Thomas Rosko, MD
Private Practice
Los Angeles, CA
Perpetrators of abuse
Dr. Nasrallah appears to be deliberately avoiding some of the real abuses perpetrated by modern-day psychiatry (“The antipsychiatry movement: Who and why,” From the Editor, Current Psychiatry, December 2011, p. 4-6, 53), including deliberately misdiagnosing alcoholics and drug abusers as bipolar in order to give them mood stabilizers, often while they are actively abusing substances.
It seems unfathomable for a physician to document a history of depressive episodes, let alone manic episodes, in someone who has been either intoxicated or in early withdrawal constantly over the years, yet this is done routinely. The abuser is happy to play along, as long as the psychiatrist prescribes benzodiazepines along with valproic acid, lithium, or lamotrigine for the patient’s persistent panic attacks and chronic insomnia.
This psychiatric version of “when you have a hammer, everything is a nail” extends to the treatment of uncomplicated grief with antidepressants, additionally labeling oppositional defiant adolescents as bipolar to give them mood stabilizers, and, of course, treating large-portion junk food eaters for “bulimia,” placing them into eating disorder programs, and prescribing psychotropics.
Dr. Nasrallah’s examples of old abuses are a “straw man” argument and unfortunately divert attention from the legitimate concerns about “scientific” modern psychiatry.
Ronald Cann, MD
Private Practice
San Diego, CA
Dr. Nasrallah responds
I appreciate the letters from Drs. Abramson, Rosko, and Cann. I particularly liked their “healthy skepticism” about parts of my editorial about antipsychiatry.
My clinical training was heavily “mind-oriented” with intensive psychodynamic as well as behavioral psychotherapy (not cognitive-behavioral therapy), and my National Institute of Mental Health research training was heavily “brain oriented” with a neuroscience focus. I integrated both brain (hardware) and mind (software) in my work with each patient and it worked spectacularly well for both of us! George Engel, the father of the biopsychosocial model, was one of my residency supervisors at the University of Rochester, so I was “inoculated” by his mentorship against the hazards of biological reductionism, to which Dr. Abramson assumes I subscribe.
Dr. Thomas Szasz certainly was more of a libertarian than an antipsychiatrist and did a great injustice to patients with severe brain disorders, such as schizophrenia, by asserting that they are competent enough to choose or deny treatment, possibly because of the early state of neurobiology research 50 years ago when the neurotoxic effects of psychosis were still undiscovered. Unlike persons with healthy brains and prefrontal executive functions that enable sound decision-making, schizophrenia patients have anosognosia—the neurologic term for lack of insight and self-monitoring—severe cognitive deficits in processing information and decision-making, and reality distortion, and they lack the capacity to determine that they urgently need treatment. Witness the death of thousands of schizophrenia patients who were abruptly released from Italy’s asylums in the 1980s because they lacked the basic brain functions needed to survive. It was a tragic mistake to leave them to their own devices in the name of freedom, conceptualized by lay legislators who had no idea how impaired the brain is in many schizophrenia patients.
Finally, Dr. Szasz practiced long before research demonstrated that the longer psychosis went untreated, the worse the deterioration and functional outcome. Thus, his stance to let patients with psychosis refuse medications significantly harmed those patients, worsened their symptoms, and reduced their chance for remission.
Dr. Cann’s allegations of the “real abuses” of modern day psychiatry are to the best of my knowledge just that–allegations. I have never seen valid documentation of the large-scale abuses he cites, although an occasional deviation occurs in any profession. The practice guidelines for various psychiatric disorders never recommend what Dr. Cann claims is happening with diagnostic distortions and ulterior motives.
Psychiatry still is evolving as a medical discipline and there are comorbidities that confound the primary diagnosis—such as anxiety or heavy drinking in bipolar disorder—but research is actively seeking a biopsychosocial explanation. The Epidemiological Catchment Area study,1 published 20 years ago before any of the current medications were introduced, is upheld as the best estimate of the prevalence of psychiatric disorders in the United States—approximately 25% lifetime risk, which means approximately 75 million children, adolescents, and adults have a diagnosable psychiatric disorder. Some of them receive good evidence-based treatments and some do not, but many more never receive any treatment and suffer in quiet desperation.
Henry A. Nasrallah, MD
Editor-in-Chief
Not ’antipsychiatry’
Dr. Nasrallah misrepresents Drs. Jacques Lacan, Erich Fromm, Theodore Lidz, and others in his December 2011 editorial (“The antipsychiatry movement: Who and why,” From the Editor, Current Psychiatry, December 2011, p. 4-6, 53). They were not antipsychiatry, nor am I.
I am “anti” the sort of concrete biological reductionism espoused by Dr. Nasrallah. The psychiatrist nattily dressed in a white jacket and a neat suit and tie looks like a real doctor, but the so-called rigorous objective medical practice he does ignores a huge domain that psychiatry used to be concerned about. In effect, under the leadership of those such as Dr. Nasrallah, psychiatry has “lost its mind.” The disorders we treat are real disorders, but getting rid of the mental dimension and reducing all to “brain disorders” reduces our effectiveness in helping patients, is not humane, and flees from the truth. Psychiatry needs to re-find its mind.
Ronald Abramson, MD, DLFAPA
Associate Clinical Professor of Psychiatry
Tufts University School of Medicine
Boston, MA
Defending Dr. Szasz
Dr. Nasrallah’s editorial (“The antipsychiatry movement: Who and why,” From the Editor, Current Psychiatry, December 2011, p. 4-6, 53) on the antipsychiatry movement was an excellent historical overview. It also was right on target in its conclusion, namely, that antipsychiatry can help keep psychiatry honest and rigorous.
However, the portrayal of Dr. Thomas Szasz as an antipsychiatrist is not wholly correct. For decades, Dr. Szasz has severely criticized both psychiatry and the antipsychiatry movement. Like antipsychiatrists, he is critical of psychiatry, but unlike antipsychiatrists, Dr. Szasz steadfastly has defended the right of consenting individuals to engage in treatment, as long as their participation is voluntary. It is this libertarian streak, the idea that people are free to choose any treatment arrangement they desire—including psychiatry—that distinguishes Dr. Szasz from antipsychiatrists such as Drs. Theodore Lidz, R.D. Laing, and others.
Thomas Rosko, MD
Private Practice
Los Angeles, CA
Perpetrators of abuse
Dr. Nasrallah appears to be deliberately avoiding some of the real abuses perpetrated by modern-day psychiatry (“The antipsychiatry movement: Who and why,” From the Editor, Current Psychiatry, December 2011, p. 4-6, 53), including deliberately misdiagnosing alcoholics and drug abusers as bipolar in order to give them mood stabilizers, often while they are actively abusing substances.
It seems unfathomable for a physician to document a history of depressive episodes, let alone manic episodes, in someone who has been either intoxicated or in early withdrawal constantly over the years, yet this is done routinely. The abuser is happy to play along, as long as the psychiatrist prescribes benzodiazepines along with valproic acid, lithium, or lamotrigine for the patient’s persistent panic attacks and chronic insomnia.
This psychiatric version of “when you have a hammer, everything is a nail” extends to the treatment of uncomplicated grief with antidepressants, additionally labeling oppositional defiant adolescents as bipolar to give them mood stabilizers, and, of course, treating large-portion junk food eaters for “bulimia,” placing them into eating disorder programs, and prescribing psychotropics.
Dr. Nasrallah’s examples of old abuses are a “straw man” argument and unfortunately divert attention from the legitimate concerns about “scientific” modern psychiatry.
Ronald Cann, MD
Private Practice
San Diego, CA
Dr. Nasrallah responds
I appreciate the letters from Drs. Abramson, Rosko, and Cann. I particularly liked their “healthy skepticism” about parts of my editorial about antipsychiatry.
My clinical training was heavily “mind-oriented” with intensive psychodynamic as well as behavioral psychotherapy (not cognitive-behavioral therapy), and my National Institute of Mental Health research training was heavily “brain oriented” with a neuroscience focus. I integrated both brain (hardware) and mind (software) in my work with each patient and it worked spectacularly well for both of us! George Engel, the father of the biopsychosocial model, was one of my residency supervisors at the University of Rochester, so I was “inoculated” by his mentorship against the hazards of biological reductionism, to which Dr. Abramson assumes I subscribe.
Dr. Thomas Szasz certainly was more of a libertarian than an antipsychiatrist and did a great injustice to patients with severe brain disorders, such as schizophrenia, by asserting that they are competent enough to choose or deny treatment, possibly because of the early state of neurobiology research 50 years ago when the neurotoxic effects of psychosis were still undiscovered. Unlike persons with healthy brains and prefrontal executive functions that enable sound decision-making, schizophrenia patients have anosognosia—the neurologic term for lack of insight and self-monitoring—severe cognitive deficits in processing information and decision-making, and reality distortion, and they lack the capacity to determine that they urgently need treatment. Witness the death of thousands of schizophrenia patients who were abruptly released from Italy’s asylums in the 1980s because they lacked the basic brain functions needed to survive. It was a tragic mistake to leave them to their own devices in the name of freedom, conceptualized by lay legislators who had no idea how impaired the brain is in many schizophrenia patients.
Finally, Dr. Szasz practiced long before research demonstrated that the longer psychosis went untreated, the worse the deterioration and functional outcome. Thus, his stance to let patients with psychosis refuse medications significantly harmed those patients, worsened their symptoms, and reduced their chance for remission.
Dr. Cann’s allegations of the “real abuses” of modern day psychiatry are to the best of my knowledge just that–allegations. I have never seen valid documentation of the large-scale abuses he cites, although an occasional deviation occurs in any profession. The practice guidelines for various psychiatric disorders never recommend what Dr. Cann claims is happening with diagnostic distortions and ulterior motives.
Psychiatry still is evolving as a medical discipline and there are comorbidities that confound the primary diagnosis—such as anxiety or heavy drinking in bipolar disorder—but research is actively seeking a biopsychosocial explanation. The Epidemiological Catchment Area study,1 published 20 years ago before any of the current medications were introduced, is upheld as the best estimate of the prevalence of psychiatric disorders in the United States—approximately 25% lifetime risk, which means approximately 75 million children, adolescents, and adults have a diagnosable psychiatric disorder. Some of them receive good evidence-based treatments and some do not, but many more never receive any treatment and suffer in quiet desperation.
Henry A. Nasrallah, MD
Editor-in-Chief
P-glycoprotein: Why this drug transporter may be clinically important
Discuss this article at www.facebook.com/CurrentPsychiatry
• Venlafaxine has been shown to decrease indinavir concentrations in cellular models and healthy individuals in a controlled trial.
• It is not known if this effect would occur with other protease inhibitors; however, most protease inhibitors are P-glycoprotein substrates.
• In preliminary cellular models, desvenlafaxine did not have the same effect.
• It is not known if other psychotropics have the same effect on P-glycoprotein or other efflux proteins.
Mr. B, age 32, was diagnosed with human immunodeficiency virus (HIV) approximately 10 years ago. His current HIV regimen is highly active antiretroviral therapy, which includes the protease inhibitor (PI) indinavir and the combination product lamivudine and zidovudine, 2 nucleoside reverse transcriptase inhibitors. He shows no symptoms and his viral load has been undetectable for 9 years.
Several months ago, Mr. B reported to his primary care physician feelings of depressed mood, anhedonia, significant weight loss, fatigue, and feelings of worthlessness. He was diagnosed with major depressive disorder and started venlafaxine, 150 mg/d. The depressive episode is now in remission and the only major side effect he experiences is lethargy. His physician decides to check Mr. B’s viral load, which is 1,100 copies/mL. This viral load value indicates a significant elevation from the baseline (<48 copies/mL), which although still low, is considered virologic failure.1 To rule out a lab error the viral load test is replicated, but the result is the same.
Mr. B’s case may represent an interaction between his antidepressant and one of his antiviral drugs that is a P-glycoprotein substrate. This protein transports a variety of drug substrates across cell membranes and affects the distribution and elimination of many prescription and nonprescription medications. Whether a drug induces or inhibits P-glycoprotein can affect plasma and cellular concentrations of drugs and can lead to unexpected increases or decreases in plasma concentrations of the affected drug. Understanding P-glycoprotein’s role can help you choose effective psychotropics for patients such as Mr. B.
Change in drug effect
Because depression is common among patients with HIV, my colleagues and I evaluated the pharmacokinetic effects of indinavir on venlafaxine and venlafaxine on indinavir to determine if venlafaxine would be safe to use in a patient taking a PI because of potential cytochrome P450 (CYP450) drug interactions in both classes of medications.2 Adding venlafaxine resulted in a 36% decrease in maximum concentrations for indinavir and a 28% decrease in area under the curve Figure.2 Study participants were healthy individuals; however, we concluded that had we studied patients with HIV, indinavir efficacy could decrease, resulting in an increased viral load. After this study, the manufacturer of venlafaxine included a caution about this combination in the product labeling.3 Because the extended-release formulation includes the same compound, the same effect could be expected and was included in the most recent version of the extended-release venlafaxine prescribing information.4
What is interesting about the venlafaxine-indinavir interaction is that there was no change in either agent’s half-life and therefore no reason to assume this effect was a traditional CYP450 drug interaction. The investigators considered other types of drug interactions and focused on mechanisms that could be presystemic, ie, affecting the absorption and bioavailability of indinavir. This led investigators to believe that the mechanism involved a drug transport protein such as P-glycoprotein, which is present in gut lumen. Subsequent studies have shown in a cellular model that venlafaxine—but not desvenlafaxine—is an inducer of P-glycoprotein and breast cancer resistant protein (BCRP).5,6 Researchers are conducting animal studies to attempt to duplicate the cellular models. However, it could be presumed that the study of venlafaxine and indinavir in healthy individuals already had demonstrated this effect.2
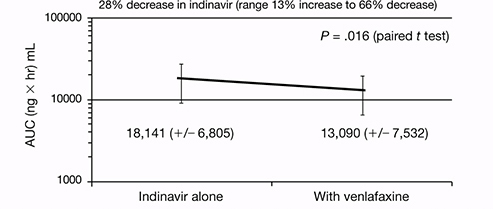
Figure: Indinavir area under the curve before and after steady state venlafaxine
Decrease in area under the curve (AUC) for indinavir when healthy individuals achieved steady state dosing of venlafaxine
Source: Reference 2
Cause and effect
P-glycoprotein transports drugs or other foreign compounds out of the cells (efflux) of the target tissue so they can be further metabolized by metabolic enzymes for elimination. These proteins are called efflux proteins. There are many efflux proteins in addition to P-glycoprotein; a common one is BCRP, which confers resistance to some anticancer drugs. In addition to the gut lumen and breast tissue, efflux proteins are present in most tissues throughout the body, including the blood-brain barrier.
If drug A inhibits an efflux protein, then drug B would be able to enter the target tissue with greater ease and not be “kicked out” because the efflux system would be disabled. This could result in higher-than-expected tissue concentrations of drug B. Pharmaceutical companies often perform P-glycoprotein inhibition studies before a drug is marketed and include this data in the prescribing information.
If, on the other hand, drug A induces an efflux protein, then drug B would be “kicked out” at a greater rate than normal because the efflux system would be working in overdrive. In this case, tissue concentrations of drug B would be lower than expected and could lead to therapeutic failure. Typically, pharmaceutical companies either do not conduct these induction studies, or if they are performed, they often are not described in prescribing information. This lack of efficacy has been well documented with chemotherapeutic failure caused by drug efflux by BCRP.7 It is likely that Mr. B’s viral load increased when venlafaxine was added to his regimen—the antidepressant induced P-glycoprotein, which reduced indinavir concentrations and subsequent therapeutic effect.
Clinicians should review specific medications they are considering using if the drugs have a narrow therapeutic index or if therapeutic failure from subtherapeutic or supratherapeutic doses would be considered problematic Table.8 Kim9 provides a comprehensive list of P-glycoprotein substrates, inhibitors, and inducers. However, keep in mind that the list of substrates, inhibitors, and inducers changes regularly as new research becomes available.
Table
Selected psychotropics that affect P-glycoprotein
| Substrates | |
| Amitriptyline | Paroxetine |
| Carbamazepine | Quetiapine |
| Chlorpromazine | Risperidone |
| Citalopram | Sertraline |
| Doxepin | Topiramate |
| Nortriptyline | Venlafaxine |
| Olanzapine | |
| Inhibitors | |
| Amitriptyline | Imipramine |
| Carbamazepine | Nefazodone |
| Chlorpromazine | Paroxetine |
| Desipramine | Sertraline |
| Disulfiram | Thioridazine |
| Fluoxetine | Trifluoperazine |
| Fluvoxamine | Trimipramine |
| Haloperidol | |
| Inducersa | |
| Amitriptyline | Phenothiazines |
| Nefazodone | Trazodone |
| aData supporting induction is limited Source: Reference 8 | |
- Linnet K, Ejsing TB. A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol. 2008;18(3):157-169.
- Weiss J, Dormann SM, Martin-Facklam M, et al. Inhibition of P-glycoprotein by newer antidepressants. J Pharmacol Exp Ther. 2003;305(1):197-204.
Drug Brand Names
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Desipramine • Norpramin
- Desvenlafaxine • Pristiq
- Disulfiram • Antabuse
- Doxepin • Adapin, Silenor
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Indinavir • Crixivan
- Lamivudine and zidovudine • Combivir
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Melleril
- Topiramate • Topamax
- Trazodone • Desyrel, Oleptro
- Trifluoperazine • Stelazine
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Disclosure
Dr. Levin receives grant/research support from Pfizer.
1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington DC: Department of Health and Human Services; January 10, 2011;1-166.
2. Levin GM, Nelson LA, DeVane CL, et al. A pharmacokinetic drug-drug interaction study of venlafaxine and indinavir. Psychopharmacol Bull. 2001;35(2):62-71.
3. Effexor [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2010.
4. Effexor XR [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2011.
5. Ehret MJ, Levin GM, Narasimhan M, et al. Venlafaxine induces P-glycoprotein in human Caco-2 cells. Hum Psychopharmacol. 2007;22(1):49-53.
6. Bachmeier CJ, Beaulieu-Abdelahad D, Ganey NJ, et al. Induction of drug efflux protein expression by venlafaxine but not desvenlafaxine. Biopharm Drug Dispos. 2011;32(4):233-244.
7. Rosenberg MF, Bikadi Z, Chan J, et al. The human breast cancer resistance protein (BCRP/ABCG2) shows conformational changes with mitoxantrone. Structure. 2010;18(4):482-493.
8. Oesterheld J. P-glycoprotein (PGP) table - the effect of drugs and foods. http://www.genemedrx.com/PGPtable.php. Accessed February 3 2012.
9. Kim RB. Drugs as P-glycoprotein substrates inhibitors, and inducers. Drug Metab Rev. 2002;34(1-2):47-54.
Gary M. Levin, PharmD, BCPP, FCCP
Dr. Levin is Associate Dean for Clinical Programs and Professor of Pharmacy Practice, College of Pharmacy, Roseman University of Health Sciences, Henderson, NV.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Gary M. Levin, PharmD, BCPP, FCCP
Dr. Levin is Associate Dean for Clinical Programs and Professor of Pharmacy Practice, College of Pharmacy, Roseman University of Health Sciences, Henderson, NV.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Gary M. Levin, PharmD, BCPP, FCCP
Dr. Levin is Associate Dean for Clinical Programs and Professor of Pharmacy Practice, College of Pharmacy, Roseman University of Health Sciences, Henderson, NV.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Discuss this article at www.facebook.com/CurrentPsychiatry
• Venlafaxine has been shown to decrease indinavir concentrations in cellular models and healthy individuals in a controlled trial.
• It is not known if this effect would occur with other protease inhibitors; however, most protease inhibitors are P-glycoprotein substrates.
• In preliminary cellular models, desvenlafaxine did not have the same effect.
• It is not known if other psychotropics have the same effect on P-glycoprotein or other efflux proteins.
Mr. B, age 32, was diagnosed with human immunodeficiency virus (HIV) approximately 10 years ago. His current HIV regimen is highly active antiretroviral therapy, which includes the protease inhibitor (PI) indinavir and the combination product lamivudine and zidovudine, 2 nucleoside reverse transcriptase inhibitors. He shows no symptoms and his viral load has been undetectable for 9 years.
Several months ago, Mr. B reported to his primary care physician feelings of depressed mood, anhedonia, significant weight loss, fatigue, and feelings of worthlessness. He was diagnosed with major depressive disorder and started venlafaxine, 150 mg/d. The depressive episode is now in remission and the only major side effect he experiences is lethargy. His physician decides to check Mr. B’s viral load, which is 1,100 copies/mL. This viral load value indicates a significant elevation from the baseline (<48 copies/mL), which although still low, is considered virologic failure.1 To rule out a lab error the viral load test is replicated, but the result is the same.
Mr. B’s case may represent an interaction between his antidepressant and one of his antiviral drugs that is a P-glycoprotein substrate. This protein transports a variety of drug substrates across cell membranes and affects the distribution and elimination of many prescription and nonprescription medications. Whether a drug induces or inhibits P-glycoprotein can affect plasma and cellular concentrations of drugs and can lead to unexpected increases or decreases in plasma concentrations of the affected drug. Understanding P-glycoprotein’s role can help you choose effective psychotropics for patients such as Mr. B.
Change in drug effect
Because depression is common among patients with HIV, my colleagues and I evaluated the pharmacokinetic effects of indinavir on venlafaxine and venlafaxine on indinavir to determine if venlafaxine would be safe to use in a patient taking a PI because of potential cytochrome P450 (CYP450) drug interactions in both classes of medications.2 Adding venlafaxine resulted in a 36% decrease in maximum concentrations for indinavir and a 28% decrease in area under the curve Figure.2 Study participants were healthy individuals; however, we concluded that had we studied patients with HIV, indinavir efficacy could decrease, resulting in an increased viral load. After this study, the manufacturer of venlafaxine included a caution about this combination in the product labeling.3 Because the extended-release formulation includes the same compound, the same effect could be expected and was included in the most recent version of the extended-release venlafaxine prescribing information.4
What is interesting about the venlafaxine-indinavir interaction is that there was no change in either agent’s half-life and therefore no reason to assume this effect was a traditional CYP450 drug interaction. The investigators considered other types of drug interactions and focused on mechanisms that could be presystemic, ie, affecting the absorption and bioavailability of indinavir. This led investigators to believe that the mechanism involved a drug transport protein such as P-glycoprotein, which is present in gut lumen. Subsequent studies have shown in a cellular model that venlafaxine—but not desvenlafaxine—is an inducer of P-glycoprotein and breast cancer resistant protein (BCRP).5,6 Researchers are conducting animal studies to attempt to duplicate the cellular models. However, it could be presumed that the study of venlafaxine and indinavir in healthy individuals already had demonstrated this effect.2
Figure: Indinavir area under the curve before and after steady state venlafaxine
Decrease in area under the curve (AUC) for indinavir when healthy individuals achieved steady state dosing of venlafaxine
Source: Reference 2
Cause and effect
P-glycoprotein transports drugs or other foreign compounds out of the cells (efflux) of the target tissue so they can be further metabolized by metabolic enzymes for elimination. These proteins are called efflux proteins. There are many efflux proteins in addition to P-glycoprotein; a common one is BCRP, which confers resistance to some anticancer drugs. In addition to the gut lumen and breast tissue, efflux proteins are present in most tissues throughout the body, including the blood-brain barrier.
If drug A inhibits an efflux protein, then drug B would be able to enter the target tissue with greater ease and not be “kicked out” because the efflux system would be disabled. This could result in higher-than-expected tissue concentrations of drug B. Pharmaceutical companies often perform P-glycoprotein inhibition studies before a drug is marketed and include this data in the prescribing information.
If, on the other hand, drug A induces an efflux protein, then drug B would be “kicked out” at a greater rate than normal because the efflux system would be working in overdrive. In this case, tissue concentrations of drug B would be lower than expected and could lead to therapeutic failure. Typically, pharmaceutical companies either do not conduct these induction studies, or if they are performed, they often are not described in prescribing information. This lack of efficacy has been well documented with chemotherapeutic failure caused by drug efflux by BCRP.7 It is likely that Mr. B’s viral load increased when venlafaxine was added to his regimen—the antidepressant induced P-glycoprotein, which reduced indinavir concentrations and subsequent therapeutic effect.
Clinicians should review specific medications they are considering using if the drugs have a narrow therapeutic index or if therapeutic failure from subtherapeutic or supratherapeutic doses would be considered problematic Table.8 Kim9 provides a comprehensive list of P-glycoprotein substrates, inhibitors, and inducers. However, keep in mind that the list of substrates, inhibitors, and inducers changes regularly as new research becomes available.
Table
Selected psychotropics that affect P-glycoprotein
| Substrates | |
| Amitriptyline | Paroxetine |
| Carbamazepine | Quetiapine |
| Chlorpromazine | Risperidone |
| Citalopram | Sertraline |
| Doxepin | Topiramate |
| Nortriptyline | Venlafaxine |
| Olanzapine | |
| Inhibitors | |
| Amitriptyline | Imipramine |
| Carbamazepine | Nefazodone |
| Chlorpromazine | Paroxetine |
| Desipramine | Sertraline |
| Disulfiram | Thioridazine |
| Fluoxetine | Trifluoperazine |
| Fluvoxamine | Trimipramine |
| Haloperidol | |
| Inducersa | |
| Amitriptyline | Phenothiazines |
| Nefazodone | Trazodone |
| aData supporting induction is limited Source: Reference 8 | |
- Linnet K, Ejsing TB. A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol. 2008;18(3):157-169.
- Weiss J, Dormann SM, Martin-Facklam M, et al. Inhibition of P-glycoprotein by newer antidepressants. J Pharmacol Exp Ther. 2003;305(1):197-204.
Drug Brand Names
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Desipramine • Norpramin
- Desvenlafaxine • Pristiq
- Disulfiram • Antabuse
- Doxepin • Adapin, Silenor
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Indinavir • Crixivan
- Lamivudine and zidovudine • Combivir
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Melleril
- Topiramate • Topamax
- Trazodone • Desyrel, Oleptro
- Trifluoperazine • Stelazine
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Disclosure
Dr. Levin receives grant/research support from Pfizer.
Discuss this article at www.facebook.com/CurrentPsychiatry
• Venlafaxine has been shown to decrease indinavir concentrations in cellular models and healthy individuals in a controlled trial.
• It is not known if this effect would occur with other protease inhibitors; however, most protease inhibitors are P-glycoprotein substrates.
• In preliminary cellular models, desvenlafaxine did not have the same effect.
• It is not known if other psychotropics have the same effect on P-glycoprotein or other efflux proteins.
Mr. B, age 32, was diagnosed with human immunodeficiency virus (HIV) approximately 10 years ago. His current HIV regimen is highly active antiretroviral therapy, which includes the protease inhibitor (PI) indinavir and the combination product lamivudine and zidovudine, 2 nucleoside reverse transcriptase inhibitors. He shows no symptoms and his viral load has been undetectable for 9 years.
Several months ago, Mr. B reported to his primary care physician feelings of depressed mood, anhedonia, significant weight loss, fatigue, and feelings of worthlessness. He was diagnosed with major depressive disorder and started venlafaxine, 150 mg/d. The depressive episode is now in remission and the only major side effect he experiences is lethargy. His physician decides to check Mr. B’s viral load, which is 1,100 copies/mL. This viral load value indicates a significant elevation from the baseline (<48 copies/mL), which although still low, is considered virologic failure.1 To rule out a lab error the viral load test is replicated, but the result is the same.
Mr. B’s case may represent an interaction between his antidepressant and one of his antiviral drugs that is a P-glycoprotein substrate. This protein transports a variety of drug substrates across cell membranes and affects the distribution and elimination of many prescription and nonprescription medications. Whether a drug induces or inhibits P-glycoprotein can affect plasma and cellular concentrations of drugs and can lead to unexpected increases or decreases in plasma concentrations of the affected drug. Understanding P-glycoprotein’s role can help you choose effective psychotropics for patients such as Mr. B.
Change in drug effect
Because depression is common among patients with HIV, my colleagues and I evaluated the pharmacokinetic effects of indinavir on venlafaxine and venlafaxine on indinavir to determine if venlafaxine would be safe to use in a patient taking a PI because of potential cytochrome P450 (CYP450) drug interactions in both classes of medications.2 Adding venlafaxine resulted in a 36% decrease in maximum concentrations for indinavir and a 28% decrease in area under the curve Figure.2 Study participants were healthy individuals; however, we concluded that had we studied patients with HIV, indinavir efficacy could decrease, resulting in an increased viral load. After this study, the manufacturer of venlafaxine included a caution about this combination in the product labeling.3 Because the extended-release formulation includes the same compound, the same effect could be expected and was included in the most recent version of the extended-release venlafaxine prescribing information.4
What is interesting about the venlafaxine-indinavir interaction is that there was no change in either agent’s half-life and therefore no reason to assume this effect was a traditional CYP450 drug interaction. The investigators considered other types of drug interactions and focused on mechanisms that could be presystemic, ie, affecting the absorption and bioavailability of indinavir. This led investigators to believe that the mechanism involved a drug transport protein such as P-glycoprotein, which is present in gut lumen. Subsequent studies have shown in a cellular model that venlafaxine—but not desvenlafaxine—is an inducer of P-glycoprotein and breast cancer resistant protein (BCRP).5,6 Researchers are conducting animal studies to attempt to duplicate the cellular models. However, it could be presumed that the study of venlafaxine and indinavir in healthy individuals already had demonstrated this effect.2
Figure: Indinavir area under the curve before and after steady state venlafaxine
Decrease in area under the curve (AUC) for indinavir when healthy individuals achieved steady state dosing of venlafaxine
Source: Reference 2
Cause and effect
P-glycoprotein transports drugs or other foreign compounds out of the cells (efflux) of the target tissue so they can be further metabolized by metabolic enzymes for elimination. These proteins are called efflux proteins. There are many efflux proteins in addition to P-glycoprotein; a common one is BCRP, which confers resistance to some anticancer drugs. In addition to the gut lumen and breast tissue, efflux proteins are present in most tissues throughout the body, including the blood-brain barrier.
If drug A inhibits an efflux protein, then drug B would be able to enter the target tissue with greater ease and not be “kicked out” because the efflux system would be disabled. This could result in higher-than-expected tissue concentrations of drug B. Pharmaceutical companies often perform P-glycoprotein inhibition studies before a drug is marketed and include this data in the prescribing information.
If, on the other hand, drug A induces an efflux protein, then drug B would be “kicked out” at a greater rate than normal because the efflux system would be working in overdrive. In this case, tissue concentrations of drug B would be lower than expected and could lead to therapeutic failure. Typically, pharmaceutical companies either do not conduct these induction studies, or if they are performed, they often are not described in prescribing information. This lack of efficacy has been well documented with chemotherapeutic failure caused by drug efflux by BCRP.7 It is likely that Mr. B’s viral load increased when venlafaxine was added to his regimen—the antidepressant induced P-glycoprotein, which reduced indinavir concentrations and subsequent therapeutic effect.
Clinicians should review specific medications they are considering using if the drugs have a narrow therapeutic index or if therapeutic failure from subtherapeutic or supratherapeutic doses would be considered problematic Table.8 Kim9 provides a comprehensive list of P-glycoprotein substrates, inhibitors, and inducers. However, keep in mind that the list of substrates, inhibitors, and inducers changes regularly as new research becomes available.
Table
Selected psychotropics that affect P-glycoprotein
| Substrates | |
| Amitriptyline | Paroxetine |
| Carbamazepine | Quetiapine |
| Chlorpromazine | Risperidone |
| Citalopram | Sertraline |
| Doxepin | Topiramate |
| Nortriptyline | Venlafaxine |
| Olanzapine | |
| Inhibitors | |
| Amitriptyline | Imipramine |
| Carbamazepine | Nefazodone |
| Chlorpromazine | Paroxetine |
| Desipramine | Sertraline |
| Disulfiram | Thioridazine |
| Fluoxetine | Trifluoperazine |
| Fluvoxamine | Trimipramine |
| Haloperidol | |
| Inducersa | |
| Amitriptyline | Phenothiazines |
| Nefazodone | Trazodone |
| aData supporting induction is limited Source: Reference 8 | |
- Linnet K, Ejsing TB. A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol. 2008;18(3):157-169.
- Weiss J, Dormann SM, Martin-Facklam M, et al. Inhibition of P-glycoprotein by newer antidepressants. J Pharmacol Exp Ther. 2003;305(1):197-204.
Drug Brand Names
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Desipramine • Norpramin
- Desvenlafaxine • Pristiq
- Disulfiram • Antabuse
- Doxepin • Adapin, Silenor
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Indinavir • Crixivan
- Lamivudine and zidovudine • Combivir
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Melleril
- Topiramate • Topamax
- Trazodone • Desyrel, Oleptro
- Trifluoperazine • Stelazine
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Disclosure
Dr. Levin receives grant/research support from Pfizer.
1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington DC: Department of Health and Human Services; January 10, 2011;1-166.
2. Levin GM, Nelson LA, DeVane CL, et al. A pharmacokinetic drug-drug interaction study of venlafaxine and indinavir. Psychopharmacol Bull. 2001;35(2):62-71.
3. Effexor [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2010.
4. Effexor XR [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2011.
5. Ehret MJ, Levin GM, Narasimhan M, et al. Venlafaxine induces P-glycoprotein in human Caco-2 cells. Hum Psychopharmacol. 2007;22(1):49-53.
6. Bachmeier CJ, Beaulieu-Abdelahad D, Ganey NJ, et al. Induction of drug efflux protein expression by venlafaxine but not desvenlafaxine. Biopharm Drug Dispos. 2011;32(4):233-244.
7. Rosenberg MF, Bikadi Z, Chan J, et al. The human breast cancer resistance protein (BCRP/ABCG2) shows conformational changes with mitoxantrone. Structure. 2010;18(4):482-493.
8. Oesterheld J. P-glycoprotein (PGP) table - the effect of drugs and foods. http://www.genemedrx.com/PGPtable.php. Accessed February 3 2012.
9. Kim RB. Drugs as P-glycoprotein substrates inhibitors, and inducers. Drug Metab Rev. 2002;34(1-2):47-54.
1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington DC: Department of Health and Human Services; January 10, 2011;1-166.
2. Levin GM, Nelson LA, DeVane CL, et al. A pharmacokinetic drug-drug interaction study of venlafaxine and indinavir. Psychopharmacol Bull. 2001;35(2):62-71.
3. Effexor [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2010.
4. Effexor XR [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2011.
5. Ehret MJ, Levin GM, Narasimhan M, et al. Venlafaxine induces P-glycoprotein in human Caco-2 cells. Hum Psychopharmacol. 2007;22(1):49-53.
6. Bachmeier CJ, Beaulieu-Abdelahad D, Ganey NJ, et al. Induction of drug efflux protein expression by venlafaxine but not desvenlafaxine. Biopharm Drug Dispos. 2011;32(4):233-244.
7. Rosenberg MF, Bikadi Z, Chan J, et al. The human breast cancer resistance protein (BCRP/ABCG2) shows conformational changes with mitoxantrone. Structure. 2010;18(4):482-493.
8. Oesterheld J. P-glycoprotein (PGP) table - the effect of drugs and foods. http://www.genemedrx.com/PGPtable.php. Accessed February 3 2012.
9. Kim RB. Drugs as P-glycoprotein substrates inhibitors, and inducers. Drug Metab Rev. 2002;34(1-2):47-54.
Psychostimulants and college students: 7 steps to prevent misuse
Discuss this article at www.facebook.com/CurrentPsychiatry
In a survey of 115 college students taking medication for attention-deficit/hyperactivity disorder (ADHD), 31% reported having taken their drugs more frequently or at a higher dose than prescribed, or used someone else’s medication since beginning college.1 Fifty-six percent reported being asked to give or sell their medication in the past 6 months; 26% of those solicited gave or sold their medication to a peer.1 The 3 most frequently reported reasons for misusing ADHD medications centered on studying: to improve concentration, to lengthen study time, and to feel less restless while studying.1
Although treating ADHD with first-line stimulants may reduce the incidence of substance use disorders,2,3 monitor patients closely to ensure therapeutic drugs are not being misused or abused.
- Use screening tools such as the CRAFFT test4 for adolescents and the 5-question RAFFT test for adults.5 Also, consider toxicology screenings.
- Consider extended-release formulations, which can reduce recreational stimulant use because subjective likeability is more strongly influenced by the drug delivery rate than by plasma concentration.
- Consider other medications/formulas such as a transdermal patch delivery of methylphenidate or prodrug formulations such as lisdexamfetamine, which is gut enzyme-dependent to hydrolyze into lysine and d-amphetamine. Also, consider nonstimulants such as atomoxetine, bupropion, or tricyclic antidepressants.
- Rule out mood disorders, especially depression, which may be driving the urge to get “high.”
- Involve family members or other forms of supervision, who may be able to better monitor medications.
- Improve physician/patient communication because active physician involvement and better patient communication about treatment-related issues is better for all involved.
- Provide triplicate prescriptions in person to avoid “prescriptions lost in the mail,” and keep a log of all prescriptions you dispense.
Disclosure
Dr. Jain reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rabiner DL, Anastopoulos AD, Costello EJ, et al. The misuse and diversion of prescribed ADHD medications by college students. J Atten Disord. 2009;13(2):144-153.
2. Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: a naturalistic controlled 10-year follow-up study. Am J Psychiatry. 2008;165(5):597-603.
3. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
4. The Center for Adolescent Substance Abuse Research. For teens. http://www.ceasar-boston.org/teens/test.php. Accessed January 19 2012.
5. Bastiaens L, Riccardi K, Sakhrani D. The RAFFT as a screening tool for adult substance use disorders. Am J Drug Alcohol Abuse. 2002;28(4):681-691.
Discuss this article at www.facebook.com/CurrentPsychiatry
In a survey of 115 college students taking medication for attention-deficit/hyperactivity disorder (ADHD), 31% reported having taken their drugs more frequently or at a higher dose than prescribed, or used someone else’s medication since beginning college.1 Fifty-six percent reported being asked to give or sell their medication in the past 6 months; 26% of those solicited gave or sold their medication to a peer.1 The 3 most frequently reported reasons for misusing ADHD medications centered on studying: to improve concentration, to lengthen study time, and to feel less restless while studying.1
Although treating ADHD with first-line stimulants may reduce the incidence of substance use disorders,2,3 monitor patients closely to ensure therapeutic drugs are not being misused or abused.
- Use screening tools such as the CRAFFT test4 for adolescents and the 5-question RAFFT test for adults.5 Also, consider toxicology screenings.
- Consider extended-release formulations, which can reduce recreational stimulant use because subjective likeability is more strongly influenced by the drug delivery rate than by plasma concentration.
- Consider other medications/formulas such as a transdermal patch delivery of methylphenidate or prodrug formulations such as lisdexamfetamine, which is gut enzyme-dependent to hydrolyze into lysine and d-amphetamine. Also, consider nonstimulants such as atomoxetine, bupropion, or tricyclic antidepressants.
- Rule out mood disorders, especially depression, which may be driving the urge to get “high.”
- Involve family members or other forms of supervision, who may be able to better monitor medications.
- Improve physician/patient communication because active physician involvement and better patient communication about treatment-related issues is better for all involved.
- Provide triplicate prescriptions in person to avoid “prescriptions lost in the mail,” and keep a log of all prescriptions you dispense.
Disclosure
Dr. Jain reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
In a survey of 115 college students taking medication for attention-deficit/hyperactivity disorder (ADHD), 31% reported having taken their drugs more frequently or at a higher dose than prescribed, or used someone else’s medication since beginning college.1 Fifty-six percent reported being asked to give or sell their medication in the past 6 months; 26% of those solicited gave or sold their medication to a peer.1 The 3 most frequently reported reasons for misusing ADHD medications centered on studying: to improve concentration, to lengthen study time, and to feel less restless while studying.1
Although treating ADHD with first-line stimulants may reduce the incidence of substance use disorders,2,3 monitor patients closely to ensure therapeutic drugs are not being misused or abused.
- Use screening tools such as the CRAFFT test4 for adolescents and the 5-question RAFFT test for adults.5 Also, consider toxicology screenings.
- Consider extended-release formulations, which can reduce recreational stimulant use because subjective likeability is more strongly influenced by the drug delivery rate than by plasma concentration.
- Consider other medications/formulas such as a transdermal patch delivery of methylphenidate or prodrug formulations such as lisdexamfetamine, which is gut enzyme-dependent to hydrolyze into lysine and d-amphetamine. Also, consider nonstimulants such as atomoxetine, bupropion, or tricyclic antidepressants.
- Rule out mood disorders, especially depression, which may be driving the urge to get “high.”
- Involve family members or other forms of supervision, who may be able to better monitor medications.
- Improve physician/patient communication because active physician involvement and better patient communication about treatment-related issues is better for all involved.
- Provide triplicate prescriptions in person to avoid “prescriptions lost in the mail,” and keep a log of all prescriptions you dispense.
Disclosure
Dr. Jain reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rabiner DL, Anastopoulos AD, Costello EJ, et al. The misuse and diversion of prescribed ADHD medications by college students. J Atten Disord. 2009;13(2):144-153.
2. Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: a naturalistic controlled 10-year follow-up study. Am J Psychiatry. 2008;165(5):597-603.
3. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
4. The Center for Adolescent Substance Abuse Research. For teens. http://www.ceasar-boston.org/teens/test.php. Accessed January 19 2012.
5. Bastiaens L, Riccardi K, Sakhrani D. The RAFFT as a screening tool for adult substance use disorders. Am J Drug Alcohol Abuse. 2002;28(4):681-691.
1. Rabiner DL, Anastopoulos AD, Costello EJ, et al. The misuse and diversion of prescribed ADHD medications by college students. J Atten Disord. 2009;13(2):144-153.
2. Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: a naturalistic controlled 10-year follow-up study. Am J Psychiatry. 2008;165(5):597-603.
3. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
4. The Center for Adolescent Substance Abuse Research. For teens. http://www.ceasar-boston.org/teens/test.php. Accessed January 19 2012.
5. Bastiaens L, Riccardi K, Sakhrani D. The RAFFT as a screening tool for adult substance use disorders. Am J Drug Alcohol Abuse. 2002;28(4):681-691.
To best care for your patients, take care of yourself
Every psychiatrist has experienced professional highs and lows. Whether helping a schizophrenia patient return to college, collaborating effectively with nursing staff, or achieving board certification, doctors—like everyone else—thrive on success. These accomplishments motivate us to help others and advance our careers.
However, psychiatrists also are vulnerable to ego insults associated with unavoidable negative and sometimes disastrous outcomes of their work. Doctors fail to "cure" every patient, may be “fired” by a patient, or may lose a patient to suicide.
Physicians spend so much time caring for their patients that they often neglect their own health. Self-care is not a core competency for trainees and many residency programs ignore this important issue. Negative outcomes can have profound effects on physicians, including shock; crying/grief/sadness; changed relationships with colleagues; disassociation from the event; crises of faith in education, training, and competency; shame and embarrassment; fear of reprisal; grandiosity; or a belief that the physician should have been all-knowing. Even when a patient commits suicide, the impact of this difficult and painful event on the clinician often is ignored.1 Physician suicide rates have been reported to be higher than those of the general population.2 Barriers to self-preserving treatment include:
Time constraints. Many doctors work up to 80 hours per week. Self-preservation does not become a priority for professionals until a lack of self-care interferes with their personal or professional life.
Limited resources. Physicians, like the general public, find it difficult to get appointments with primary care physicians and psychiatrists. Some doctors feel guilty about taking a slot from another patient or failing to see one of their own patients during that time. Simply finding a provider who is comfortable treating another doctor may be a challenge.
Stigma. It can be embarrassing for doctors to admit they are human, are vulnerable, and have health care needs. Fear of scrutiny for having an illness such as depression is so severe that surveyed psychiatrists said they would rather treat themselves than seek professional help.3
Psychiatrists who face sensitive emotional material on an hourly basis are susceptible to internalizing their work. For those who work with the vulnerable and victimized, meeting our own needs is fundamental to our ability to thrive. Regular practices that promote reflection are crucial to a psychiatrist’s compassion and self-preservation. Suggestions for appropriate self-care are described in the Table.
Table
Psychiatrists’ health: Guidelines for self-preservation
| Practice | Examples |
|---|---|
| Define your professional role and know your level of competency | Work within the confines of your skill set Refer patients to more specialized physicians when you feel their illnesses are outside your scope of expertise Consult colleagues for help with difficult cases |
| Respect your own boundaries | Delineate professional and personal boundaries Reflect on "shades of gray" or ambiguity Seek reinforcement from a supervisor |
| Ask for help | Clearly articulate your needs to supervisors, colleagues, family, and friends Create a positive environment among colleagues |
| Be demanding of yourself and others | Expect yourself and others to live with honesty, integrity, and compassion Identify the source of any inability to maintain these standards Correct your behavior when your work is substandard |
| Treat depression | Find time to visit a mental health professional Seek out a physician skilled at and comfortable with treating physicians |
| Keep balance in life | Foster hobbies Exercise on a routine basis |
Discuss this article at www.facebook.com/CurrentPsychiatry
1. Hausman K. Psychiatrists often overwhelmed by a patient’s suicide. Psychiatric News. July 4 2003.
2. Schernhammer ES, Colditz GA. Suicide rates among physicians: a quantitative and gender assessment (meta-analysis). Am J Psychiatry. 2004;161(12):2295-2302.
3. Balon R. Psychiatrist attitudes toward self-treatment of their own depression. Psychother Psychosom. 2007;76(5):306-310.
Every psychiatrist has experienced professional highs and lows. Whether helping a schizophrenia patient return to college, collaborating effectively with nursing staff, or achieving board certification, doctors—like everyone else—thrive on success. These accomplishments motivate us to help others and advance our careers.
However, psychiatrists also are vulnerable to ego insults associated with unavoidable negative and sometimes disastrous outcomes of their work. Doctors fail to "cure" every patient, may be “fired” by a patient, or may lose a patient to suicide.
Physicians spend so much time caring for their patients that they often neglect their own health. Self-care is not a core competency for trainees and many residency programs ignore this important issue. Negative outcomes can have profound effects on physicians, including shock; crying/grief/sadness; changed relationships with colleagues; disassociation from the event; crises of faith in education, training, and competency; shame and embarrassment; fear of reprisal; grandiosity; or a belief that the physician should have been all-knowing. Even when a patient commits suicide, the impact of this difficult and painful event on the clinician often is ignored.1 Physician suicide rates have been reported to be higher than those of the general population.2 Barriers to self-preserving treatment include:
Time constraints. Many doctors work up to 80 hours per week. Self-preservation does not become a priority for professionals until a lack of self-care interferes with their personal or professional life.
Limited resources. Physicians, like the general public, find it difficult to get appointments with primary care physicians and psychiatrists. Some doctors feel guilty about taking a slot from another patient or failing to see one of their own patients during that time. Simply finding a provider who is comfortable treating another doctor may be a challenge.
Stigma. It can be embarrassing for doctors to admit they are human, are vulnerable, and have health care needs. Fear of scrutiny for having an illness such as depression is so severe that surveyed psychiatrists said they would rather treat themselves than seek professional help.3
Psychiatrists who face sensitive emotional material on an hourly basis are susceptible to internalizing their work. For those who work with the vulnerable and victimized, meeting our own needs is fundamental to our ability to thrive. Regular practices that promote reflection are crucial to a psychiatrist’s compassion and self-preservation. Suggestions for appropriate self-care are described in the Table.
Table
Psychiatrists’ health: Guidelines for self-preservation
| Practice | Examples |
|---|---|
| Define your professional role and know your level of competency | Work within the confines of your skill set Refer patients to more specialized physicians when you feel their illnesses are outside your scope of expertise Consult colleagues for help with difficult cases |
| Respect your own boundaries | Delineate professional and personal boundaries Reflect on "shades of gray" or ambiguity Seek reinforcement from a supervisor |
| Ask for help | Clearly articulate your needs to supervisors, colleagues, family, and friends Create a positive environment among colleagues |
| Be demanding of yourself and others | Expect yourself and others to live with honesty, integrity, and compassion Identify the source of any inability to maintain these standards Correct your behavior when your work is substandard |
| Treat depression | Find time to visit a mental health professional Seek out a physician skilled at and comfortable with treating physicians |
| Keep balance in life | Foster hobbies Exercise on a routine basis |
Discuss this article at www.facebook.com/CurrentPsychiatry
Every psychiatrist has experienced professional highs and lows. Whether helping a schizophrenia patient return to college, collaborating effectively with nursing staff, or achieving board certification, doctors—like everyone else—thrive on success. These accomplishments motivate us to help others and advance our careers.
However, psychiatrists also are vulnerable to ego insults associated with unavoidable negative and sometimes disastrous outcomes of their work. Doctors fail to "cure" every patient, may be “fired” by a patient, or may lose a patient to suicide.
Physicians spend so much time caring for their patients that they often neglect their own health. Self-care is not a core competency for trainees and many residency programs ignore this important issue. Negative outcomes can have profound effects on physicians, including shock; crying/grief/sadness; changed relationships with colleagues; disassociation from the event; crises of faith in education, training, and competency; shame and embarrassment; fear of reprisal; grandiosity; or a belief that the physician should have been all-knowing. Even when a patient commits suicide, the impact of this difficult and painful event on the clinician often is ignored.1 Physician suicide rates have been reported to be higher than those of the general population.2 Barriers to self-preserving treatment include:
Time constraints. Many doctors work up to 80 hours per week. Self-preservation does not become a priority for professionals until a lack of self-care interferes with their personal or professional life.
Limited resources. Physicians, like the general public, find it difficult to get appointments with primary care physicians and psychiatrists. Some doctors feel guilty about taking a slot from another patient or failing to see one of their own patients during that time. Simply finding a provider who is comfortable treating another doctor may be a challenge.
Stigma. It can be embarrassing for doctors to admit they are human, are vulnerable, and have health care needs. Fear of scrutiny for having an illness such as depression is so severe that surveyed psychiatrists said they would rather treat themselves than seek professional help.3
Psychiatrists who face sensitive emotional material on an hourly basis are susceptible to internalizing their work. For those who work with the vulnerable and victimized, meeting our own needs is fundamental to our ability to thrive. Regular practices that promote reflection are crucial to a psychiatrist’s compassion and self-preservation. Suggestions for appropriate self-care are described in the Table.
Table
Psychiatrists’ health: Guidelines for self-preservation
| Practice | Examples |
|---|---|
| Define your professional role and know your level of competency | Work within the confines of your skill set Refer patients to more specialized physicians when you feel their illnesses are outside your scope of expertise Consult colleagues for help with difficult cases |
| Respect your own boundaries | Delineate professional and personal boundaries Reflect on "shades of gray" or ambiguity Seek reinforcement from a supervisor |
| Ask for help | Clearly articulate your needs to supervisors, colleagues, family, and friends Create a positive environment among colleagues |
| Be demanding of yourself and others | Expect yourself and others to live with honesty, integrity, and compassion Identify the source of any inability to maintain these standards Correct your behavior when your work is substandard |
| Treat depression | Find time to visit a mental health professional Seek out a physician skilled at and comfortable with treating physicians |
| Keep balance in life | Foster hobbies Exercise on a routine basis |
Discuss this article at www.facebook.com/CurrentPsychiatry
1. Hausman K. Psychiatrists often overwhelmed by a patient’s suicide. Psychiatric News. July 4 2003.
2. Schernhammer ES, Colditz GA. Suicide rates among physicians: a quantitative and gender assessment (meta-analysis). Am J Psychiatry. 2004;161(12):2295-2302.
3. Balon R. Psychiatrist attitudes toward self-treatment of their own depression. Psychother Psychosom. 2007;76(5):306-310.
1. Hausman K. Psychiatrists often overwhelmed by a patient’s suicide. Psychiatric News. July 4 2003.
2. Schernhammer ES, Colditz GA. Suicide rates among physicians: a quantitative and gender assessment (meta-analysis). Am J Psychiatry. 2004;161(12):2295-2302.
3. Balon R. Psychiatrist attitudes toward self-treatment of their own depression. Psychother Psychosom. 2007;76(5):306-310.
Facebook: Social networking meets professional duty
Discuss this article at www.facebook.com/CurrentPsychiatry
Dear Dr. Mossman:
A patient has invited me to “friend” her on Facebook. I’m uncomfortable with this request, but I don’t want her to feel rejected. How should I respond?—Submitted by “Dr. V”
Among the many cultural developments that characterize the Internet era, few have had the impact of the social networking Web site Facebook. Because of Facebook, “friend” has become a transitive verb, and “like,” “wall,” “poke,” and “post” have acquired meanings that reflect new modes of communication and interpersonal connection. As of early 2012, Facebook had >800 million users.1 If you’re like most medical students, residents, and junior faculty members,2 you have a Facebook page.
The ubiquity of Facebook has added new dimensions to defining, teaching, and modeling professionalism in medicine.3,4 Facebook can be used to rapidly disseminate medical information through status updates and medical support groups.5 Professionals can create profiles, post their curricula vitae, and “like” professional journals—including Current Psychiatry.
But social media such as Facebook also present clinicians with new ethical and professional challenges.6 If you use Facebook personally or professionally, you need to decide how you will separate your personal and professional identities in a forum that rapidly distributes information across the Web for all to see. Sound, responsible decisions about your online profile can let you and your employing institutions prosper from the many benefits that accrue to savvy Facebook users—while avoiding potential embarrassments and liability.
Before you create a profile or “post” your next “status update” on your “wall,” you should:
- understand potential boundary violations
- know how to activate your security and privacy settings
- remember that you represent not only yourself but your profession.
Boundary crossings, violations
Feelings of online closeness and informality make receiving “friend” requests from patients far from uncommon.7 The Internet lets individuals quickly check out people and learn personal information (eg, where they live and what their homes cost) that was hard to discover 15 years ago. But the information on a person’s Facebook page usually is much more personal than what Internet searches reveal—and often much less dignified.
A quick Internet search of the phrase “professional boundaries” will show that concern about maintaining proper relationships between professionals and service recipients is not restricted to psychiatry. Yet the special, intensely personal nature of mental health care—especially psychotherapy—traditionally has made psychiatrists place special constraints on their relationships with patients.
Because psychiatrists recognize that even brief comments about ourselves can affect how patients feel, we refrain from forms of self-disclosure that non-psychiatric colleagues view as innocent.8 Psychiatrists also do not freely socialize with patients or provide care to persons we know well. We avoid blurring therapeutic and other types of relationships because such “boundary crossings” can cause problems and because “crossings” can be precursors to serious “boundary violations”—eg, sexual contact with patients.
Most doctors decline “friend” requests from patients because friending them could adversely affect the treatment relationship and could lead to new relationships that might interfere with patient care.9 The American Medical Association’s social media guidelines do not forbid friending patients, but physicians are advised to “consider separating personal and professional content online” and “maintain appropriate boundaries” with patients.10 The British Medical Association simply tells physicians to “politely refuse” patients’ friend requests.11
Privacy problems
Psychiatrists who friend patients need to be aware of potential privacy breeches among Facebook users. Individuals whose presence among a psychiatrist’s friends becomes known (eg, via a wall post) are revealing their connection to the psychiatrist, and other friends may surmise that an individual is a patient.
Also, Facebook’s “find friends” feature ostensibly lets Facebook locate individuals who are common to pairs of people and who can then be suggested as potential friends to others, but “find friends” imports members’ entire e-mail address books. If doctors who are on Facebook have patients in their webmail address books and have allowed “find friends,” then Facebook will import e-mail addresses, potentially disclosing associations between patients and their doctors.12
Facebook has tools that let users block their profiles from public view, but these privacy settings can be difficult to access and understand. Although social networking among medical trainees and new graduates is common in the culture of emerging professionals, most Facebook users allow anyone to view their profile—the default privacy setting.2,13 Even if you don’t friend patients, failing to privatize your account leaves your Facebook information readily available to the public, including your patients.
Professionalism in cyberspace
Under some circumstances, medical advice given in casual, outside-the-office contexts can establish a doctor-patient relationship, with all its accompanying obligations and liability risks. This is true of Facebook communications. If you communicate medical information or advice to someone in a form specific enough to be relied upon, you may be establishing a doctor-patient relationship. If harm comes to a person who relied upon your information, a negligence lawsuit could result—even though you never saw or spoke to the “patient.”14
Medical training programs have found that medical students and residents have posted work-related comments on Facebook that directly referenced specific patient situations or other patient care matters. Such actions can breach the Health Insurance Portability and Accountability Act of 1996 and can jeopardize careers.15 Medical professionals also have posted uncouth, inappropriate, and embarrassing content—profanity, frankly discriminatory language, tales of intoxication, and sexually explicit information. In a recent survey of 78 medical schools, 60% responded that their students had posted unprofessional online content.16 In 45 cases, schools reported such incidents and responded to follow-up questions about disciplinary actions; 30 schools gave informal warnings, and 2 schools reported student dismissals.
Using Facebook
Should psychiatrists stay off Facebook? Of course not. Many prominent American psychiatrists are on Facebook because, like everyone else, they enjoy keeping in contact with friends and family.17 Thousands of professional groups (eg, the American Psychiatric Association) and physician practices have Facebook pages. Institutions, schools, and agencies use social media to promote their curricula, notify students and staff of course changes, or organize meetings. Professionals join groups or “like” groups associated with their specialty to affiliate with each other, and they use Facebook to promote their practices, disseminate information, and network with colleagues.
Psychiatrists need not shy away from establishing an account on Facebook,18 but they should do so with greater circumspection than most persons, including physicians in other specialties. Table 1 lists several examples of Facebook behavior that all physicians should avoid.2,13,16,19,20
What about using Facebook to learn about your patients? Medical reports about checking Facebook to resolve emergencies have appeared,20 and forensic psychiatrists can use Facebook and other Internet resources to learn about evaluees.21 But if doctors search for information about a patient’s out-of-office behavior or statements, it may be like “driving down a patient’s street to see what he or she is up to,” which, although legal, seems inappropriate in a professional relationship.22
Recent experience suggests that medical schools and residencies should include “e-professionalism” in their curricula, emphasizing instruction and guidance on where personal and professional identities may intersect and where they should be kept separate. Table 2 lists several responses to the new challenges to medical professionalism posed by Facebook and other social media.5,6
Table 1
Facebook errors: What to avoid
| Category | Pitfalls |
|---|---|
| Information | Relationships, religious views, home address, and telephone number all may be readily viewable to the general public and patients if privacy settings are not properly configured |
| Photos | Intoxication, sexually explicit material, risk-taking behavior |
| “Wall posts” | Blatant comments about patients, disgruntlement with institution or supervisors |
| Security settings | Lack of privacy restrictions |
| “Friends” | Friending patients and supervisors |
| “Like” | “Liking” groups that contain pornographic material or other controversial topics |
| Source: References 2,13,16,19,20 | |
Table 2
Promoting e-professionalism
| Understand and activate all relevant privacy and security settings on social networking sites |
| Recognize the need to teach e-professionalism in the curricula of medical schools and residency training programs |
| Combine instruction on professional use of Facebook with teaching about relevant legal regulations in medicine (eg, HIPAA) |
| Guidance in online professionalism should come from faculty supervisors or program directors |
| Faculty should model appropriate Facebook behaviors for employees, medical students, and residents |
| Users of social media are well-advised to conduct Web searches on themselves and modify their pages to conform with professional standards |
| Politely decline patients’ “friend” requests |
| Discussions of medical professionalism, involving students, faculty, and employers, can help identify issues and define responses |
| Institutions should establish and enforce guidelines for Facebook professionalism |
| HIPAA: Health Insurance Portability and Accountability Act of 1996 Source: References 5,6 |
Responding to Dr. V
Psychiatrists should not “friend” patients. If you receive a “friend” request, you should proceed in 1 of the following ways:17
- Simply ignore the request. If your patient asks why you didn’t respond, explain that you use Facebook only for personal matters
- Ignore the request, and at the patient’s next appointment, mention the request and politely explain that you do not “friend” patients
- Ignore the request, but ask the patient about it at your next meeting. This is especially important for a patient whose treatment examines the doctor-patient relationship (eg, psychodynamic therapy), but may be valuable even in medication-focused care.
- Facebook. www.facebook.com.
- Foreman J. Think before you click. Boston Globe. April 12, 2010.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Facebook. Statistics. http://www.facebook.com/press/info.php?statistics. Accessed January 30, 2012.
2. MacDonald J, Sohn S, Ellis P. Privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2010;44(8):805-813.
3. Gorrindo T, Gorrindo PC, Groves JE. Intersection of online social networking with medical professionalism: can medicine police the Facebook boom? J Gen Intern Med. 2008;23(12):2155.-
4. Baer W, Schwartz AC. Teaching professionalism in the digital age on the psychiatric consultation-liaison service. Psychosomatics. 2011;52(4):303-309.
5. Landman MP, Shelton J, Kauffmann RM, et al. Guidelines for maintaining a professional compass in the era of social networking. J Surg Educ. 2010;67(6):381-386.
6. Guseh JS 2nd, Brendel RW, Brendel DH. Medical professionalism in the age of online social networking. J Med Ethics. 2009;35(9):584-586.
7. Devi S. Facebook friend request from a patient? Lancet. 2011;377(9772):1141-1142.
8. Gruenberg PB. Boundary violations. In: Wahl DS Polster DS, eds. Ethics primer. Arlington, VA: American Psychiatric Association; 2001. http://www.psych.org/Departments/EDU/residentmit/dl01.aspx. Accessed January 4, 2012.
9. Moubarak G, Guiot A, Benhamou Y, et al. Facebook activity of residents and fellows and its impact on the doctor-patient relationship. J Med Ethics. 2011;37(2):101-104.
10. American Medical Association. AMA policy: professionalism in the use of social media. http://www.ama-assn.org/ama/pub/meeting/professionalism-social-media.shtml. Accessed January 4 2012.
11. British Medical Association. Using social media: practical and ethical guidance for doctors and medical students. http://www.bma.org.uk/press_centre/video_social_media/socialmediaguidance2011.jsp. Accessed January 4 2012.
12. Wilson S. A bigger threat to patient privacy when doctors use Facebook. J Med Ethics. http://jme.bmj.com/content/37/2/101.abstract/reply#medethics_el_3625. Published December 20 2010. Accessed January 4, 2012.
13. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. J Gen Intern Med. 2008;23(7):954-957.
14. Reisman N. Avoid being too social when using social media. Plastic Surgery News. September 13 2011. http://www.psnextra.org/Columns/OLG-September-11.html. Accessed January 4, 2012.
15. Greysen SR, Kind T, Chretien KC. Online professionalism and the mirror of social media. J Gen Intern Med. 2010;25(11):1227-1229.
16. Chretien KC, Greysen SR, Chretien JP, et al. Online posting of unprofessional content by medical students. JAMA. 2009;302(12):1309-1315.
17. Arehart-Treichel J. Facebook can be useful–if you use common sense. Psychiatric News. 2011;46(22):5A.-
18. O’Hanlon S, Shannon B. Comments further to: privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2011;45(2):209.-
19. Metzger AH, Finley KN, Ulbrich TR, et al. Pharmacy faculty members’ perspectives on the student/faculty relationship in online social networks. Am J Pharm Educ. 2010;74(10):188.-
20. Ben-Yakov M, Snider C. How Facebook saved our day! Acad Emerg Med. 2011;18(11):1217-1219.
21. Metzner JL, Ash P. Commentary: the mental status examination in the age of the internet—challenges and opportunities. J Am Acad Psychiatry Law. 2010;38(1):27-31.
22. Bosslet GT. Commentary: the good the bad, and the ugly of social media. Acad Emerg Med. 2011;18(11):1221-1222.

Douglas Mossman, MD
Dr. Mossman is administrative director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and Adjunct Professor of Clinical Psychiatry and Training Director for the University of Cincinnati Forensic Psychiatry Fellowship, Cincinnati, OH
Helen M. Farrell, MD
Dr. Farrell is an instructor at Harvard Medical School and a staff psychiatrist at Beth Israel Deaconess Medical Center, Boston, MA
Douglas Mossman, MD
Dr. Mossman is administrative director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and Adjunct Professor of Clinical Psychiatry and Training Director for the University of Cincinnati Forensic Psychiatry Fellowship, Cincinnati, OH
Helen M. Farrell, MD
Dr. Farrell is an instructor at Harvard Medical School and a staff psychiatrist at Beth Israel Deaconess Medical Center, Boston, MA
Douglas Mossman, MD
Dr. Mossman is administrative director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and Adjunct Professor of Clinical Psychiatry and Training Director for the University of Cincinnati Forensic Psychiatry Fellowship, Cincinnati, OH
Helen M. Farrell, MD
Dr. Farrell is an instructor at Harvard Medical School and a staff psychiatrist at Beth Israel Deaconess Medical Center, Boston, MA
Discuss this article at www.facebook.com/CurrentPsychiatry
Dear Dr. Mossman:
A patient has invited me to “friend” her on Facebook. I’m uncomfortable with this request, but I don’t want her to feel rejected. How should I respond?—Submitted by “Dr. V”
Among the many cultural developments that characterize the Internet era, few have had the impact of the social networking Web site Facebook. Because of Facebook, “friend” has become a transitive verb, and “like,” “wall,” “poke,” and “post” have acquired meanings that reflect new modes of communication and interpersonal connection. As of early 2012, Facebook had >800 million users.1 If you’re like most medical students, residents, and junior faculty members,2 you have a Facebook page.
The ubiquity of Facebook has added new dimensions to defining, teaching, and modeling professionalism in medicine.3,4 Facebook can be used to rapidly disseminate medical information through status updates and medical support groups.5 Professionals can create profiles, post their curricula vitae, and “like” professional journals—including Current Psychiatry.
But social media such as Facebook also present clinicians with new ethical and professional challenges.6 If you use Facebook personally or professionally, you need to decide how you will separate your personal and professional identities in a forum that rapidly distributes information across the Web for all to see. Sound, responsible decisions about your online profile can let you and your employing institutions prosper from the many benefits that accrue to savvy Facebook users—while avoiding potential embarrassments and liability.
Before you create a profile or “post” your next “status update” on your “wall,” you should:
- understand potential boundary violations
- know how to activate your security and privacy settings
- remember that you represent not only yourself but your profession.
Boundary crossings, violations
Feelings of online closeness and informality make receiving “friend” requests from patients far from uncommon.7 The Internet lets individuals quickly check out people and learn personal information (eg, where they live and what their homes cost) that was hard to discover 15 years ago. But the information on a person’s Facebook page usually is much more personal than what Internet searches reveal—and often much less dignified.
A quick Internet search of the phrase “professional boundaries” will show that concern about maintaining proper relationships between professionals and service recipients is not restricted to psychiatry. Yet the special, intensely personal nature of mental health care—especially psychotherapy—traditionally has made psychiatrists place special constraints on their relationships with patients.
Because psychiatrists recognize that even brief comments about ourselves can affect how patients feel, we refrain from forms of self-disclosure that non-psychiatric colleagues view as innocent.8 Psychiatrists also do not freely socialize with patients or provide care to persons we know well. We avoid blurring therapeutic and other types of relationships because such “boundary crossings” can cause problems and because “crossings” can be precursors to serious “boundary violations”—eg, sexual contact with patients.
Most doctors decline “friend” requests from patients because friending them could adversely affect the treatment relationship and could lead to new relationships that might interfere with patient care.9 The American Medical Association’s social media guidelines do not forbid friending patients, but physicians are advised to “consider separating personal and professional content online” and “maintain appropriate boundaries” with patients.10 The British Medical Association simply tells physicians to “politely refuse” patients’ friend requests.11
Privacy problems
Psychiatrists who friend patients need to be aware of potential privacy breeches among Facebook users. Individuals whose presence among a psychiatrist’s friends becomes known (eg, via a wall post) are revealing their connection to the psychiatrist, and other friends may surmise that an individual is a patient.
Also, Facebook’s “find friends” feature ostensibly lets Facebook locate individuals who are common to pairs of people and who can then be suggested as potential friends to others, but “find friends” imports members’ entire e-mail address books. If doctors who are on Facebook have patients in their webmail address books and have allowed “find friends,” then Facebook will import e-mail addresses, potentially disclosing associations between patients and their doctors.12
Facebook has tools that let users block their profiles from public view, but these privacy settings can be difficult to access and understand. Although social networking among medical trainees and new graduates is common in the culture of emerging professionals, most Facebook users allow anyone to view their profile—the default privacy setting.2,13 Even if you don’t friend patients, failing to privatize your account leaves your Facebook information readily available to the public, including your patients.
Professionalism in cyberspace
Under some circumstances, medical advice given in casual, outside-the-office contexts can establish a doctor-patient relationship, with all its accompanying obligations and liability risks. This is true of Facebook communications. If you communicate medical information or advice to someone in a form specific enough to be relied upon, you may be establishing a doctor-patient relationship. If harm comes to a person who relied upon your information, a negligence lawsuit could result—even though you never saw or spoke to the “patient.”14
Medical training programs have found that medical students and residents have posted work-related comments on Facebook that directly referenced specific patient situations or other patient care matters. Such actions can breach the Health Insurance Portability and Accountability Act of 1996 and can jeopardize careers.15 Medical professionals also have posted uncouth, inappropriate, and embarrassing content—profanity, frankly discriminatory language, tales of intoxication, and sexually explicit information. In a recent survey of 78 medical schools, 60% responded that their students had posted unprofessional online content.16 In 45 cases, schools reported such incidents and responded to follow-up questions about disciplinary actions; 30 schools gave informal warnings, and 2 schools reported student dismissals.
Using Facebook
Should psychiatrists stay off Facebook? Of course not. Many prominent American psychiatrists are on Facebook because, like everyone else, they enjoy keeping in contact with friends and family.17 Thousands of professional groups (eg, the American Psychiatric Association) and physician practices have Facebook pages. Institutions, schools, and agencies use social media to promote their curricula, notify students and staff of course changes, or organize meetings. Professionals join groups or “like” groups associated with their specialty to affiliate with each other, and they use Facebook to promote their practices, disseminate information, and network with colleagues.
Psychiatrists need not shy away from establishing an account on Facebook,18 but they should do so with greater circumspection than most persons, including physicians in other specialties. Table 1 lists several examples of Facebook behavior that all physicians should avoid.2,13,16,19,20
What about using Facebook to learn about your patients? Medical reports about checking Facebook to resolve emergencies have appeared,20 and forensic psychiatrists can use Facebook and other Internet resources to learn about evaluees.21 But if doctors search for information about a patient’s out-of-office behavior or statements, it may be like “driving down a patient’s street to see what he or she is up to,” which, although legal, seems inappropriate in a professional relationship.22
Recent experience suggests that medical schools and residencies should include “e-professionalism” in their curricula, emphasizing instruction and guidance on where personal and professional identities may intersect and where they should be kept separate. Table 2 lists several responses to the new challenges to medical professionalism posed by Facebook and other social media.5,6
Table 1
Facebook errors: What to avoid
| Category | Pitfalls |
|---|---|
| Information | Relationships, religious views, home address, and telephone number all may be readily viewable to the general public and patients if privacy settings are not properly configured |
| Photos | Intoxication, sexually explicit material, risk-taking behavior |
| “Wall posts” | Blatant comments about patients, disgruntlement with institution or supervisors |
| Security settings | Lack of privacy restrictions |
| “Friends” | Friending patients and supervisors |
| “Like” | “Liking” groups that contain pornographic material or other controversial topics |
| Source: References 2,13,16,19,20 | |
Table 2
Promoting e-professionalism
| Understand and activate all relevant privacy and security settings on social networking sites |
| Recognize the need to teach e-professionalism in the curricula of medical schools and residency training programs |
| Combine instruction on professional use of Facebook with teaching about relevant legal regulations in medicine (eg, HIPAA) |
| Guidance in online professionalism should come from faculty supervisors or program directors |
| Faculty should model appropriate Facebook behaviors for employees, medical students, and residents |
| Users of social media are well-advised to conduct Web searches on themselves and modify their pages to conform with professional standards |
| Politely decline patients’ “friend” requests |
| Discussions of medical professionalism, involving students, faculty, and employers, can help identify issues and define responses |
| Institutions should establish and enforce guidelines for Facebook professionalism |
| HIPAA: Health Insurance Portability and Accountability Act of 1996 Source: References 5,6 |
Responding to Dr. V
Psychiatrists should not “friend” patients. If you receive a “friend” request, you should proceed in 1 of the following ways:17
- Simply ignore the request. If your patient asks why you didn’t respond, explain that you use Facebook only for personal matters
- Ignore the request, and at the patient’s next appointment, mention the request and politely explain that you do not “friend” patients
- Ignore the request, but ask the patient about it at your next meeting. This is especially important for a patient whose treatment examines the doctor-patient relationship (eg, psychodynamic therapy), but may be valuable even in medication-focused care.
- Facebook. www.facebook.com.
- Foreman J. Think before you click. Boston Globe. April 12, 2010.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Dear Dr. Mossman:
A patient has invited me to “friend” her on Facebook. I’m uncomfortable with this request, but I don’t want her to feel rejected. How should I respond?—Submitted by “Dr. V”
Among the many cultural developments that characterize the Internet era, few have had the impact of the social networking Web site Facebook. Because of Facebook, “friend” has become a transitive verb, and “like,” “wall,” “poke,” and “post” have acquired meanings that reflect new modes of communication and interpersonal connection. As of early 2012, Facebook had >800 million users.1 If you’re like most medical students, residents, and junior faculty members,2 you have a Facebook page.
The ubiquity of Facebook has added new dimensions to defining, teaching, and modeling professionalism in medicine.3,4 Facebook can be used to rapidly disseminate medical information through status updates and medical support groups.5 Professionals can create profiles, post their curricula vitae, and “like” professional journals—including Current Psychiatry.
But social media such as Facebook also present clinicians with new ethical and professional challenges.6 If you use Facebook personally or professionally, you need to decide how you will separate your personal and professional identities in a forum that rapidly distributes information across the Web for all to see. Sound, responsible decisions about your online profile can let you and your employing institutions prosper from the many benefits that accrue to savvy Facebook users—while avoiding potential embarrassments and liability.
Before you create a profile or “post” your next “status update” on your “wall,” you should:
- understand potential boundary violations
- know how to activate your security and privacy settings
- remember that you represent not only yourself but your profession.
Boundary crossings, violations
Feelings of online closeness and informality make receiving “friend” requests from patients far from uncommon.7 The Internet lets individuals quickly check out people and learn personal information (eg, where they live and what their homes cost) that was hard to discover 15 years ago. But the information on a person’s Facebook page usually is much more personal than what Internet searches reveal—and often much less dignified.
A quick Internet search of the phrase “professional boundaries” will show that concern about maintaining proper relationships between professionals and service recipients is not restricted to psychiatry. Yet the special, intensely personal nature of mental health care—especially psychotherapy—traditionally has made psychiatrists place special constraints on their relationships with patients.
Because psychiatrists recognize that even brief comments about ourselves can affect how patients feel, we refrain from forms of self-disclosure that non-psychiatric colleagues view as innocent.8 Psychiatrists also do not freely socialize with patients or provide care to persons we know well. We avoid blurring therapeutic and other types of relationships because such “boundary crossings” can cause problems and because “crossings” can be precursors to serious “boundary violations”—eg, sexual contact with patients.
Most doctors decline “friend” requests from patients because friending them could adversely affect the treatment relationship and could lead to new relationships that might interfere with patient care.9 The American Medical Association’s social media guidelines do not forbid friending patients, but physicians are advised to “consider separating personal and professional content online” and “maintain appropriate boundaries” with patients.10 The British Medical Association simply tells physicians to “politely refuse” patients’ friend requests.11
Privacy problems
Psychiatrists who friend patients need to be aware of potential privacy breeches among Facebook users. Individuals whose presence among a psychiatrist’s friends becomes known (eg, via a wall post) are revealing their connection to the psychiatrist, and other friends may surmise that an individual is a patient.
Also, Facebook’s “find friends” feature ostensibly lets Facebook locate individuals who are common to pairs of people and who can then be suggested as potential friends to others, but “find friends” imports members’ entire e-mail address books. If doctors who are on Facebook have patients in their webmail address books and have allowed “find friends,” then Facebook will import e-mail addresses, potentially disclosing associations between patients and their doctors.12
Facebook has tools that let users block their profiles from public view, but these privacy settings can be difficult to access and understand. Although social networking among medical trainees and new graduates is common in the culture of emerging professionals, most Facebook users allow anyone to view their profile—the default privacy setting.2,13 Even if you don’t friend patients, failing to privatize your account leaves your Facebook information readily available to the public, including your patients.
Professionalism in cyberspace
Under some circumstances, medical advice given in casual, outside-the-office contexts can establish a doctor-patient relationship, with all its accompanying obligations and liability risks. This is true of Facebook communications. If you communicate medical information or advice to someone in a form specific enough to be relied upon, you may be establishing a doctor-patient relationship. If harm comes to a person who relied upon your information, a negligence lawsuit could result—even though you never saw or spoke to the “patient.”14
Medical training programs have found that medical students and residents have posted work-related comments on Facebook that directly referenced specific patient situations or other patient care matters. Such actions can breach the Health Insurance Portability and Accountability Act of 1996 and can jeopardize careers.15 Medical professionals also have posted uncouth, inappropriate, and embarrassing content—profanity, frankly discriminatory language, tales of intoxication, and sexually explicit information. In a recent survey of 78 medical schools, 60% responded that their students had posted unprofessional online content.16 In 45 cases, schools reported such incidents and responded to follow-up questions about disciplinary actions; 30 schools gave informal warnings, and 2 schools reported student dismissals.
Using Facebook
Should psychiatrists stay off Facebook? Of course not. Many prominent American psychiatrists are on Facebook because, like everyone else, they enjoy keeping in contact with friends and family.17 Thousands of professional groups (eg, the American Psychiatric Association) and physician practices have Facebook pages. Institutions, schools, and agencies use social media to promote their curricula, notify students and staff of course changes, or organize meetings. Professionals join groups or “like” groups associated with their specialty to affiliate with each other, and they use Facebook to promote their practices, disseminate information, and network with colleagues.
Psychiatrists need not shy away from establishing an account on Facebook,18 but they should do so with greater circumspection than most persons, including physicians in other specialties. Table 1 lists several examples of Facebook behavior that all physicians should avoid.2,13,16,19,20
What about using Facebook to learn about your patients? Medical reports about checking Facebook to resolve emergencies have appeared,20 and forensic psychiatrists can use Facebook and other Internet resources to learn about evaluees.21 But if doctors search for information about a patient’s out-of-office behavior or statements, it may be like “driving down a patient’s street to see what he or she is up to,” which, although legal, seems inappropriate in a professional relationship.22
Recent experience suggests that medical schools and residencies should include “e-professionalism” in their curricula, emphasizing instruction and guidance on where personal and professional identities may intersect and where they should be kept separate. Table 2 lists several responses to the new challenges to medical professionalism posed by Facebook and other social media.5,6
Table 1
Facebook errors: What to avoid
| Category | Pitfalls |
|---|---|
| Information | Relationships, religious views, home address, and telephone number all may be readily viewable to the general public and patients if privacy settings are not properly configured |
| Photos | Intoxication, sexually explicit material, risk-taking behavior |
| “Wall posts” | Blatant comments about patients, disgruntlement with institution or supervisors |
| Security settings | Lack of privacy restrictions |
| “Friends” | Friending patients and supervisors |
| “Like” | “Liking” groups that contain pornographic material or other controversial topics |
| Source: References 2,13,16,19,20 | |
Table 2
Promoting e-professionalism
| Understand and activate all relevant privacy and security settings on social networking sites |
| Recognize the need to teach e-professionalism in the curricula of medical schools and residency training programs |
| Combine instruction on professional use of Facebook with teaching about relevant legal regulations in medicine (eg, HIPAA) |
| Guidance in online professionalism should come from faculty supervisors or program directors |
| Faculty should model appropriate Facebook behaviors for employees, medical students, and residents |
| Users of social media are well-advised to conduct Web searches on themselves and modify their pages to conform with professional standards |
| Politely decline patients’ “friend” requests |
| Discussions of medical professionalism, involving students, faculty, and employers, can help identify issues and define responses |
| Institutions should establish and enforce guidelines for Facebook professionalism |
| HIPAA: Health Insurance Portability and Accountability Act of 1996 Source: References 5,6 |
Responding to Dr. V
Psychiatrists should not “friend” patients. If you receive a “friend” request, you should proceed in 1 of the following ways:17
- Simply ignore the request. If your patient asks why you didn’t respond, explain that you use Facebook only for personal matters
- Ignore the request, and at the patient’s next appointment, mention the request and politely explain that you do not “friend” patients
- Ignore the request, but ask the patient about it at your next meeting. This is especially important for a patient whose treatment examines the doctor-patient relationship (eg, psychodynamic therapy), but may be valuable even in medication-focused care.
- Facebook. www.facebook.com.
- Foreman J. Think before you click. Boston Globe. April 12, 2010.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Facebook. Statistics. http://www.facebook.com/press/info.php?statistics. Accessed January 30, 2012.
2. MacDonald J, Sohn S, Ellis P. Privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2010;44(8):805-813.
3. Gorrindo T, Gorrindo PC, Groves JE. Intersection of online social networking with medical professionalism: can medicine police the Facebook boom? J Gen Intern Med. 2008;23(12):2155.-
4. Baer W, Schwartz AC. Teaching professionalism in the digital age on the psychiatric consultation-liaison service. Psychosomatics. 2011;52(4):303-309.
5. Landman MP, Shelton J, Kauffmann RM, et al. Guidelines for maintaining a professional compass in the era of social networking. J Surg Educ. 2010;67(6):381-386.
6. Guseh JS 2nd, Brendel RW, Brendel DH. Medical professionalism in the age of online social networking. J Med Ethics. 2009;35(9):584-586.
7. Devi S. Facebook friend request from a patient? Lancet. 2011;377(9772):1141-1142.
8. Gruenberg PB. Boundary violations. In: Wahl DS Polster DS, eds. Ethics primer. Arlington, VA: American Psychiatric Association; 2001. http://www.psych.org/Departments/EDU/residentmit/dl01.aspx. Accessed January 4, 2012.
9. Moubarak G, Guiot A, Benhamou Y, et al. Facebook activity of residents and fellows and its impact on the doctor-patient relationship. J Med Ethics. 2011;37(2):101-104.
10. American Medical Association. AMA policy: professionalism in the use of social media. http://www.ama-assn.org/ama/pub/meeting/professionalism-social-media.shtml. Accessed January 4 2012.
11. British Medical Association. Using social media: practical and ethical guidance for doctors and medical students. http://www.bma.org.uk/press_centre/video_social_media/socialmediaguidance2011.jsp. Accessed January 4 2012.
12. Wilson S. A bigger threat to patient privacy when doctors use Facebook. J Med Ethics. http://jme.bmj.com/content/37/2/101.abstract/reply#medethics_el_3625. Published December 20 2010. Accessed January 4, 2012.
13. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. J Gen Intern Med. 2008;23(7):954-957.
14. Reisman N. Avoid being too social when using social media. Plastic Surgery News. September 13 2011. http://www.psnextra.org/Columns/OLG-September-11.html. Accessed January 4, 2012.
15. Greysen SR, Kind T, Chretien KC. Online professionalism and the mirror of social media. J Gen Intern Med. 2010;25(11):1227-1229.
16. Chretien KC, Greysen SR, Chretien JP, et al. Online posting of unprofessional content by medical students. JAMA. 2009;302(12):1309-1315.
17. Arehart-Treichel J. Facebook can be useful–if you use common sense. Psychiatric News. 2011;46(22):5A.-
18. O’Hanlon S, Shannon B. Comments further to: privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2011;45(2):209.-
19. Metzger AH, Finley KN, Ulbrich TR, et al. Pharmacy faculty members’ perspectives on the student/faculty relationship in online social networks. Am J Pharm Educ. 2010;74(10):188.-
20. Ben-Yakov M, Snider C. How Facebook saved our day! Acad Emerg Med. 2011;18(11):1217-1219.
21. Metzner JL, Ash P. Commentary: the mental status examination in the age of the internet—challenges and opportunities. J Am Acad Psychiatry Law. 2010;38(1):27-31.
22. Bosslet GT. Commentary: the good the bad, and the ugly of social media. Acad Emerg Med. 2011;18(11):1221-1222.
1. Facebook. Statistics. http://www.facebook.com/press/info.php?statistics. Accessed January 30, 2012.
2. MacDonald J, Sohn S, Ellis P. Privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2010;44(8):805-813.
3. Gorrindo T, Gorrindo PC, Groves JE. Intersection of online social networking with medical professionalism: can medicine police the Facebook boom? J Gen Intern Med. 2008;23(12):2155.-
4. Baer W, Schwartz AC. Teaching professionalism in the digital age on the psychiatric consultation-liaison service. Psychosomatics. 2011;52(4):303-309.
5. Landman MP, Shelton J, Kauffmann RM, et al. Guidelines for maintaining a professional compass in the era of social networking. J Surg Educ. 2010;67(6):381-386.
6. Guseh JS 2nd, Brendel RW, Brendel DH. Medical professionalism in the age of online social networking. J Med Ethics. 2009;35(9):584-586.
7. Devi S. Facebook friend request from a patient? Lancet. 2011;377(9772):1141-1142.
8. Gruenberg PB. Boundary violations. In: Wahl DS Polster DS, eds. Ethics primer. Arlington, VA: American Psychiatric Association; 2001. http://www.psych.org/Departments/EDU/residentmit/dl01.aspx. Accessed January 4, 2012.
9. Moubarak G, Guiot A, Benhamou Y, et al. Facebook activity of residents and fellows and its impact on the doctor-patient relationship. J Med Ethics. 2011;37(2):101-104.
10. American Medical Association. AMA policy: professionalism in the use of social media. http://www.ama-assn.org/ama/pub/meeting/professionalism-social-media.shtml. Accessed January 4 2012.
11. British Medical Association. Using social media: practical and ethical guidance for doctors and medical students. http://www.bma.org.uk/press_centre/video_social_media/socialmediaguidance2011.jsp. Accessed January 4 2012.
12. Wilson S. A bigger threat to patient privacy when doctors use Facebook. J Med Ethics. http://jme.bmj.com/content/37/2/101.abstract/reply#medethics_el_3625. Published December 20 2010. Accessed January 4, 2012.
13. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. J Gen Intern Med. 2008;23(7):954-957.
14. Reisman N. Avoid being too social when using social media. Plastic Surgery News. September 13 2011. http://www.psnextra.org/Columns/OLG-September-11.html. Accessed January 4, 2012.
15. Greysen SR, Kind T, Chretien KC. Online professionalism and the mirror of social media. J Gen Intern Med. 2010;25(11):1227-1229.
16. Chretien KC, Greysen SR, Chretien JP, et al. Online posting of unprofessional content by medical students. JAMA. 2009;302(12):1309-1315.
17. Arehart-Treichel J. Facebook can be useful–if you use common sense. Psychiatric News. 2011;46(22):5A.-
18. O’Hanlon S, Shannon B. Comments further to: privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2011;45(2):209.-
19. Metzger AH, Finley KN, Ulbrich TR, et al. Pharmacy faculty members’ perspectives on the student/faculty relationship in online social networks. Am J Pharm Educ. 2010;74(10):188.-
20. Ben-Yakov M, Snider C. How Facebook saved our day! Acad Emerg Med. 2011;18(11):1217-1219.
21. Metzner JL, Ash P. Commentary: the mental status examination in the age of the internet—challenges and opportunities. J Am Acad Psychiatry Law. 2010;38(1):27-31.
22. Bosslet GT. Commentary: the good the bad, and the ugly of social media. Acad Emerg Med. 2011;18(11):1221-1222.