User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Alcohol withdrawal: When to choose an adjunctive anticonvulsant
Benzodiazepines are the mainstay of alcohol detoxification treatment, with extensive evidence supporting their efficacy and relative safety.1 The risk of benzodiazepine-alcohol interaction, however, and psychomotor and cognitive impairments associated with benzodiazepine use may limit early rehabilitation efforts in hospitalized patients.2 Cross-tolerance with alcohol also limits benzodiazepines’ potential benefit in outpatients with substance use disorders.
Adding anticonvulsants to acute benzodiazepine therapy has been shown to decrease alcohol withdrawal symptom severity, reduce seizure risk, and support recovery, particularly in patients with multiple alcohol withdrawal episodes. After detoxification, long-term anticonvulsant use may reduce relapse risk by decreasing post-cessation craving, without abuse liability.3
Although not all studies endorse adding anticonvulsants to benzodiazepines for managing alcohol withdrawal syndrome (AWS),4 we present 3 cases in which anticonvulsants were used successfully as adjuncts to lorazepam. Valproic acid, levetiracetam, and gabapentin offer advantages in acute and long-term therapy of alcohol dependence with efficacy in AWS, low abuse potential, benign safety profile, and mood-stabilizing properties.
Neurobiologic rationale
AWS manifests as a cluster of clinical symptoms including delirium tremens (DTs) and seizures (Table 1). Its pathophysiology can be explained by alcohol’s agonist effect on the gamma-aminobutyric acid (GABA) system and antagonist effect on the glutamatergic system (Table 2).5
Chronic alcohol intake leads to neuroadaptation in the brain in the form of down-regulation of GABAA receptors and upregulation of N-methyl-D-aspartate receptors. During alcohol withdrawal, this neuroadaptation leads to a decrease in central GABA activity and an increase in glutamate activity, resulting in hyperexcitation, anxiety, and seizures.6
Little data exist regarding time to relapse after detoxification in alcohol-dependent patients. One theory—called “protracted withdrawal syndrome” (Table 1)—suggests that abstinent alcoholics return to drinking because of the same, but attenuated, neuroadaptations that trigger acute AWS.7
Advantages of adjunct therapy. Ntais et al8 evaluated benzodiazepines’ effectiveness and safety in treating AWS in a clinical review of 57 randomized, controlled trials totaling 4,051 patients. Benzodiazepines showed similar success rates as other drugs (relative risk [RR] 1.00) or anticonvulsants in particular (RR 0.88), as measured by changes in Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) scores at the end of treatment. Benzodiazepines also offered significant benefit for seizure control compared with nonanticonvulsants (RR 0.23), but less when compared with anti convulsants (RR 1.99).
Although the literature does not support anticonvulsant use for monotherapy in AWS, anticonvulsants show potential as adjunctive therapy. Valproic acid, levetiracetam, and gabapentin offer unique mechanisms of action (Table 3) and demonstrate advantages over benzodiazepine monotherapy for AWS. Adjunctive use of valproic acid,8,9 levetiracetam,10 and gabapentin11,12 in detoxification also has demonstrated efficacy in reducing risk of relapse and delaying relapse.
The neurobiologic rationale for using anticonvulsants in acute AWS is speculative, but these agents appear to:
- inhibit “kindling” (neuronal changes that may be associated with repeated intoxications)
- facilitate GABAergic mechanisms.9
Table 1
Alcohol withdrawal: Acute vs long-term symptoms
| Alcohol withdrawal syndrome | Protracted withdrawal syndrome | |
|---|---|---|
| Description | Cluster of symptoms in alcohol-dependent persons after heavy or prolonged alcohol use has lessened or ceased | Constellation of symptoms lasting weeks to months after alcohol use ends |
| Presentation | Develops during acute detoxification period and lasts 5 to 7 days | Develops after 5- to 7-day acute detoxification period and may persist for 1 year |
| Symptoms | Mild: insomnia, tremor, anxiety, GI upset, headache, diaphoresis, palpitations, anorexia Severe: alcoholic hallucinosis Seizures (generalized tonic-clonic) occur in up to 25% of withdrawal episodes, usually within 24 hours after alcohol cessation Delirium tremens (characterized by hallucinations, disorientation, tachycardia, hypertension, low-grade fever, agitation, and diaphoresis) occurs in up to 5% of patients undergoing withdrawal, may be delayed 4 to 5 days, and has mortality rates reaching 15% | Sleep disruption; anxiety; depressive symptoms; irritability; increased breathing rate, body temperature, blood pressure, and pulse |
| GI: gastrointestinal | ||
| Source: Click here for a bibliography | ||
Table 2
How alcohol affects GABA and glutamate neurotransmitters
| GABA | Glutamate | |
|---|---|---|
| GABA, the brain’s primary inhibitory neurotransmitter, renders nerve cells less sensitive to further signaling | Glutamate, the brain’s major excitatory neurotransmitter, renders nerve cells more sensitive to further signaling | |
| Alcohol facilitates the inhibitory function of the GABAA receptor, allowing more GABA to traverse the receptor, and leading to alcohol’s intoxicating effects | Alcohol seems to inhibit the excitatory function of the NMDA glutamate receptor, believed to play a role in memory, learning, and generation of seizures | |
| During alcohol withdrawal, brain GABA concentrations fall below normal and GABAA receptor sensitivity may be reduced | Long-term alcohol exposure produces an adaptive increase in the function of NMDA receptors and results in development of glutamate-NMDA supersensitivity | |
| In the absence of alcohol, the resulting decrease in inhibitory function may contribute to symptoms of CNS hyperactivity associated with acute and protracted alcohol withdrawal | Acute alcohol withdrawal activates glutamate systems, leading to autonomic nervous system hyperactivity; alcohol withdrawal seizures are associated with increased NMDA receptor function | |
| GABA: gamma-aminobutyric acid; NMDA: N-methyl-D-aspartate | ||
| Source: Click here for a bibliography | ||
Table 3
Mechanisms of action of benzodiazepines vs 3 anticonvulsants
| Agent | Mechanism of action |
|---|---|
| Benzodiazepines | Activate GABAA chloride ionophore, increasing affinity of GABAA receptor for GABA and augmenting frequency of chloride channel openinga |
| Valproic acid | GABA modulation and possibly second messenger systems; may inhibit Na1+ and/or Ca2+ channel, thereby boosting GABA and glutamate actionb |
| Levetiracetam | Decreases high voltage activated Ca2+ channels; unique binding site (synaptic vesicle protein SV2A) is thought to be involved in calcium-dependent regulation of neurotransmitter vesicle exocytosisc |
| Gabapentin | GABA analog; unique binding site (Ca2+ channel subunit in brain) decreases calcium influx and inhibits release of excitatory amino acids and monoaminesd |
| GABA: gamma-aminobutyric acid | |
| Source: Click here for a bibliography | |
CASE REPORT 1: Valproic acid for alcohol overdose
After attempting suicide with an alcohol overdose, Ms. J, age 45, is transferred from the emergency room (ER) to our psychiatry consult service 10 hours after admission. Her symptoms include nausea, tremor, headaches, agitation, disorientation, and auditory hallucinations.
Medical history reveals 25 years of alcohol dependence, multiple hospitalizations for withdrawal, and many failed attempts to quit. Ms. J reports consuming an average of 16 drink equivalents (eg, 12 oz beers) daily but denies illicit drug use.
Lab values on admission include blood alcohol concentration (BAC) 290 mg/dL (0.29%), mean corpuscular volume (MCV) 96 fL, gamma-glutamyltransferase (GGT) 164 U/L, aspartate aminotransferase (AST) 43 U/L, alanine aminotransferase (ALT) 31 U/L, and alkaline phosphatase (ALP) 151 U/L. Urine drug screen, acetaminophen, salicylate, vitamin B1 (thiamine), B12 (cyanocobalamin), B9 (folate), and electrolytes (including magnesium) are normal.
We assess alcohol withdrawal severity using the CIWA-Ar (Click here to view/download a copy of this scale). Ms. J’s initial score is 17, indicating a risk of moderate alcohol withdrawal if untreated.
In the ER, Ms. J is placed on a symptom-triggered benzodiazepine detoxification protocol with lorazepam. We add IV valproic acid, 1,250 mg (based on 20 mg/kg body weight)13 divided into 2 doses over the first 24 hours, then maintain IV valproic acid at 500 mg twice daily (Table 4). Within 12 hours of starting combination therapy, Ms. J scores 7 on the CIWA-Ar—indicating mild withdrawal—with subsequent scores <5. She scores 0 with no residual withdrawal symptoms within 36 hours.
Ms. J requires lorazepam, 7 mg, during the 10 hours before valproic acid is added. She requires only 2 mg lorazepam over the next 3 days and reports no side effects related to IV valproic acid. At discharge, Ms. J begins extended-release oral valproic acid, 1,250 mg (based on 25 mg/kg body weight)13 once daily for 2 weeks, until she can obtain outpatient follow-up.
Table 4
Benzodiazepines and anticonvulsants for alcohol detoxification
| Benzodiazepines | Valproic acid | Levetiracetam | Gabapentin | |
|---|---|---|---|---|
| Loading dose | None | 20 mg/kg of body weight, divided into 2 doses for first 24 hours | 1,500 mg IV once daily | 400 mg PO qid |
| Maintenance dose | Day 1: 2 mg tid Day 2: 2 mg morning, 1 mg afternoon, 2 mg evening Day 3: 1 mg tid Day 4: 1 mg bid Day 5: 1 mg Day 6: none | 500 mg IV bid | Either 500 mg IV tid or 1,000 mg PO bid after 2 to 3 days of treatment | 1,200 mg PO tid |
| Side effects | Impaired consciousness, respiratory depression, hypotension | Dizziness, drowsiness, hair loss/thinning, nausea, tremor, weight gain | Somnolence, asthenia, dizziness, coordination difficulties | Somnolence, dizziness, ataxia, fatigue |
| Drug interactions | ↑ BZ: cimetidine, oral contraceptives, ethanol (acute), disulfiram, isoniazid, propranolol ↓ BZ: rifampin, ethanol (chronic) | ↑ VPA: aspirin, felbamate, fluoxetine, isoniazid ↓ VPA: carbamazepine, lamotrigine, phenobarbital, phenytoin, ritonavir | None | ↓ GBP 20%: antacids |
| BZ: benzodiazepine; GBP: gabapentin; PO: per os (by mouth); VPA: valproic acid | ||||
| Source: Click here for a bibliography | ||||
Less lorazepam needed
Adjunctive anticonvulsants can reduce the amount of lorazepam required during detoxification.14,15 Compared with benzodiazepine monotherapy, the advantages of combination therapy—particularly in outpatient alcohol withdrawal treatment and relapse prevention—include:
- minimal interaction with alcohol (avoiding increased psychomotor deficits, cognitive impairment, and intoxication)15
- lower abuse potential
- possible efficacy in mood stabilization before, during, and after withdrawal (Table 5).16
Given the risk of seizures during AWS, anticonvulsants seem to make empirical sense. One study reported a 1% incidence of withdrawal-related seizures in 545 alcohol-dependent inpatients treated with valproic acid.17 Another case series of 37 patients found no acute sequelae when valproic acid was used for AWS.18
Anticonvulsants such as valproic acid may reduce the frequency and severity of alcohol relapse, whereas benzodiazepines may increase relapse risk.19 During a 6-week trial, patients receiving valproic acid maintenance therapy had greater abstinence rates and improved drinking outcomes compared with detoxification-only groups.9
One disadvantage of valproic acid is potential hepatotoxicity, an important consideration in patients with liver damage. Fortunately, Ms. J’s AST and ALT values remained within normal limits during valproic acid treatment.
Table 5
Pharmacologic profiles of benzodiazepines vs 3 anticonvulsants
| Benzodiazepines | Valproic acid | Levetiracetam | Gabapentin | |
|---|---|---|---|---|
| Metabolism | CYP 2C19: diazepam CYP 3A3/4: alprazolam, clonazepam, diazepam, triazolam Phase II only: lorazepam, temazepam, oxazepam | >95% hepatic, of which <20% occurs via CYP isoenzymes | Not extensively metabolized; renal clearance; not involved with hepatic CYP isoenzymes | Not metabolized; secreted via kidneys as unchanged drug |
| Sedation | Mild to moderate | Mild to moderate | Mild to moderate | Moderate to severe |
| Synergistic effects with alcohol | Yes | No | No | No |
| Paradoxical disinhibition | Yes | No | No | No |
| Risk of addiction in outpatient therapy | Yes | No | No | No |
| CYP: cytochrome P450 | ||||
| Source: Click here for a bibliography | ||||
CASE REPORT 2: Levetiracetam for withdrawal seizures
Mr. H, age 42, presents to the ER after suffering a seizure. His medical history includes hypertension, alcohol dependence, and seizures during alcohol withdrawal. He denies a history of psychiatric illness, and his family history is unknown. He is noncompliant with hypertension treatment, which includes clonidine. Mr. H reports his usual alcohol consumption as a 6-pack of beer nightly during the week and a 12-pack nightly on weekends. He says his last drink was 4 days before admission.
Mr. H scores 19 on the CIWA-Ar, placing him at risk for moderate withdrawal. Head CT shows diffuse atrophy, without evidence of an acute intracranial process. BAC is zero on admission, and urine drug screen is negative. Amylase, lipase, and lactate dehydrogenase (LDH) levels suggest acute pancreatitis. AST is elevated to 131 U/L, ALT is elevated to 42 U/L, but MCV is within normal limits.
The psychiatric service is consulted on day 2 of admission, and we prescribe levetiracetam, 500 mg IV every 8 hours.20 IV lorazepam also is available as needed: 1 mg every 8 hours for the first 2 days, then 1 mg every 12 hours for 2 days, then 1 mg every 24 hours. The patient’s CIWA-Ar score is 9 on days 2 and 3 of admission, followed by scores consistently between 2 and 3 after scheduled levetiracetam administration. Mr. H requires 3 mg of lorazepam the remainder of his hospitalization. He is discharged on day 7 with a CIWA-Ar score of 2, and reports no adverse effects related to levetiracetam. He leaves the hospital with a 2-week prescription for oral levetiracetam, 500 mg tid.
Advantages of levetiracetam
Levetiracetam is FDA-approved for adjunctive treatment of adults with partial-onset seizures.21 Successful AWS treatment with adjunctive levetiracetam has been supported by few but promising studies.10,20 Potential advantages of levetiracetam in detoxification include:
- a lack of GABAergic properties, which limits the risk of intoxication or respiratory insufficiency when combined with alcohol21
- low drug-drug interaction risk because of nonhepatic metabolism and primary renal excretion.22,23
We selected levetiracetam for Mr. H because of his history of alcohol withdrawal seizures and acute pancreatitis. Anticonvulsants may be more effective than lorazepam in reducing the risk of alcohol withdrawal seizures,24 and we felt valproic acid might not be safe for him because of its low but real risk of pancreatitis.13 We based our levetiracetam dosing on a small open-label trial20 and product information for treating adults with partial-onset seizures.25
Studies also demonstrate levetiracetam’s potential for relapse prevention during outpatient therapy. In a 10-week trial, levetiracetam decreased the number of standard drinks in alcohol-dependent patients from 5.3 to 1.7 per day.10 This was a small open trial, however, and large controlled trials support the usefulness of other, FDA-approved medications—including disulfiram, naltrexone, and acamprosate—for alcohol relapse prevention.
CASE REPORT 3: Gabapentin for acute withdrawal
Mr. B, age 38, presents to the ER after a 13-day alcohol binge. He has been drinking increasing amounts of alcohol over 6 weeks. Three months earlier, Mr. B was admitted for alcohol withdrawal treatment and received 49 mg of lorazepam over 3 days. This resulted in his transfer from the step-down unit to the intensive care unit for increased agitation, possibly caused by paradoxical disinhibition from excessive lorazepam use.26
Mr. B’s medical history is significant for alcohol-induced seizures, DTs, traumatic brain injury related to craniotomy, and right arm amputation. Mr. B drinks approximately 24 beers per day. He denies tobacco use but admits to past use of cocaine, marijuana, and heroin.
On admission, Mr. B’s BAC is 360 mg/dL (0.36%), AST is elevated at 72 U/L, ALT at 42 U/L, and LDH significantly elevated at 384 U/L. Urine drug screen is negative, and his CIWA-Ar score is 23. His score of –1 on the Richmond Agitation and Sedation Scale (RASS)27 correlates with very mild sedation.
Guided by Bonnet et al28 and clinical experience, we start Mr. B on gabapentin, 1,200 mg tid, and IV lorazepam, 2 mg every 8 hours as needed for breakthrough withdrawal. We decrease lorazepam by 50% every other day until Mr. B is discharged. On days 2, 3, and 4, Mr. B’s CIWA-Ar scores are 6, 9, and 2, respectively. His RASS score drops from –1 on days 1 and 2 to 0 until discharge, indicating an alert and calm state.
Mr. B requires a total of 2 mg of lorazepam throughout hospitalization. He finishes alcohol detoxification on day 4 and is discharged with a prescription for gabapentin, 1,200 mg tid. Two weeks later, when he is admitted to a 28-day inpatient alcohol rehabilitation unit, Mr. B has not relapsed.
More abstinent days
Gabapentin is FDA-approved as adjunctive therapy for partial seizures. Off-label, it has been generally efficacious as an adjunct in alcohol detoxification.29-32 We chose adjunctive anticonvulsant therapy for Mr. B because of his history of alcohol-induced seizures. We chose gabapentin instead of valproic acid because of Mr. B’s liver damage and gabapentin’s lack of hepatic metabolism.
Gabapentin may reduce alcohol consumption and craving in alcohol-dependent patients. By increasing the number of abstinent days, gabapentin may help patients maintain abstinence.33 Gabapentin does not appear to interact clinically with alcohol, causing neither sedation nor synergistic effects.34 Its relative lack of abuse potential may be valuable in outpatient alcohol withdrawal treatment and in maintaining alcohol abstinence after detoxification.
Related resource
- Asplund CA, Aaronson JW, Aaronson HE. 3 regimens for alcohol withdrawal and detoxification. J Fam Pract. 2004;53(7):545-554. www.jfponline.com/Pages.asp?AID=1730.
Drug brand names
- Acamprosate • Campral
- Alprazolam • Xanax
- Carbamazepine • Carbatrol
- Cimetidine • Tagamet
- Clonazepam • Klonopin
- Clonidine • Catapres
- Diazepam • Valium
- Disulfiram • Antabuse
- Felbamate • Felbatol
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Isoniazid • Nydrazid
- Lamotrigine • Lamictal
- Levetiracetam • Keppra
- Lorazepam • Ativan
- Naltrexone • ReVia, Vivitrol
- Oxazepam • Serax
- Phenobarbital • Luminal
- Phenytoin • Dilantin
- Propranolol • Inderal
- Rifampin • Rifadin
- Ritonavir • Norvir
- Temazepam • Restoril
- Triazolam • Halcion
- Valproic acid • Depakote, Depakene
Disclosures
Dr. Spiegel is a speaker for Pfizer Inc. and GlaxoSmithKline.
Dr. Radac reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The authors thank Rishi Laroia, MD, Robert Swanson, MD, and Adam W. Coe, MD for their contributions to this article.
1. Mayo-Smith MF, Cushman P, Hill AJ, et al. Pharmacological management of alcohol withdrawal. JAMA. 1997;278:144-151.
2. Myrick H, Brady KT, Malcom R. Divalproex in the treatment of alcohol withdrawal—statistical data included. Am J Drug Alcohol Abuse. 2000;26(1):155-160.
3. Johnson BA, Swift RM, Addolorato G, et al. Safety and efficacy of GABAergic medications for treating alcoholism. Alcohol Clin Exp Res. 2005;29(2):248-254.
4. Lum E, Gorman SK, Slavik RS. Valproic acid management of acute alcohol withdrawal. Ann Pharmacother. 2006;40(3):441-448.
5. Trevisan LA, Boutros N, Petrakis IL, et al. Complications of alcohol withdrawal: pathophysiological insights. Alcohol Health Res World. 1998;22(1):61-66.
6. Esel E. Neurobiology of alcohol withdrawal inhibitory and excitatory neurotransmitters. Turk Psikiyatri Derg. 2006;7(2):129-138.
7. Myrick H, Brady KT. The use of divalproex in the treatment of addictive disorders. Psychopharmacol Bull. 2003;37(suppl 2):89-97.
8. Brady KT, Myrick H, Henderson S, et al. The use of divalproex in alcohol relapse prevention: a pilot study. Drug Alcohol Depend. 2002;67(3):323-330.
9. Longo L, Campbell T, Hubatch S. Divalproex sodium (Depakote) for alcohol withdrawal and relapse prevention. J Addict Dis. 2002;21(2):55-64.
10. Sarid-Segal O, Piechniczek-Buczek J, Knapp C, et al. The effects of levetiracetam on alcohol consumption in alcohol-dependent subjects: an open label study. Am J Drug Alcohol Abuse. 2008;34(4):441-447.
11. American Psychiatric Association. Treatments of psychiatric disorders: a task force report of the American Psychiatric Association. Washington, DC: American Psychiatric Association Press; 1989:187.
12. Mason BJ, Light JM, Williams LD, et al. Proof-of-concept human laboratory study for protracted abstinence in alcohol dependence: effects of gabapentin. Addict Biol. 2009;14(1):73-83.
13. Physicians’ Desk Reference 2009. 63rd ed. Montvale, NJ: Physicians’ Desk Reference; 2008:423-431.
14. Malcolm R, Ballenger JC, Sturgis ET, et al. Double-blind controlled trial comparing carbamazepine to oxazepam treatment of alcohol withdrawal. Am J Psychiatry. 1989;146:617-621.
15. Myrick H, Anton R, Voronin K, et al. A double-blind evaluation of gabapentin on alcohol effects and drinking in a clinical laboratory paradigm. Alcohol Clin Exp Res. 2007;31(2):221-227.
16. Malcolm R, Myrick H, Brady KT, et al. Update on anticonvulsants for the treatment of alcohol withdrawal. Am J Addict. 2001;10(suppl):16-23.
17. Davis LL, Ryan W, Adinoff B, et al. Comprehensive review of the psychiatric uses of valproate. J Clin Psychopharm. 2000;20(1 suppl 1):1S-17S.
18. Rosenthal RN, Perkel C, Singh P, et al. A pilot open randomized trial of valproate and phenobarbital in the treatment of acute alcohol withdrawal. Am J Addict. 1998;7:189-197.
19. Book SW, Myrick H. Novel anticonvulsants in the treatment of alcoholism. Expert Opin Investig Drugs. 2005;14(4):371-376.
20. Krebs M, Leopold K, Richter C, et al. Levetiracetam for the treatment of alcohol withdrawal syndrome: an open-label pilot trial. J Clin Psychopharmacol. 2006;26(3):347-349.
21. LaRoche SM, Helmers SL. The new antiepileptic drugs: scientific review. JAMA. 2004;291:605-614.
22. Chabolla DR, Harnois DM, Meschia JF. Levetiracetam monotherapy for liver transplant patients with seizures. Transplant Proc. 2003;35:1480-1481.
23. Paul F, Meencke HJ. Levetiracetam in focal epilepsy and hepatic porphyria: a case report. Epilepsia. 2004;45:559-560.
24. Ntais C, Pakos E, Kyzas P, et al. Benzodiazepines for alcohol withdrawal. Cochrane Database Syst Rev. 2005;(3):CD005063.-
25. Physicians’ Desk Reference 2009. 63rd ed. Montvale, NJ: Physicians’ Desk Reference; 2008:3131-3143.
26. Saias T, Gallarda T. Paradoxical aggressive reactions to benzodiazepine use: a review. Encephale. 2008;34(4):330-336.
27. Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation–Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166:1338-1344.
28. Bonnet U, Banger M, Leweke FM, et al. Treatment of acute alcohol withdrawal with gabapentin: results from a controlled two-center trial. J Clin Psychopharmacol. 2003;23(5):514-519.
29. Myrick H, Malcolm R, Brady KT. Gabapentin treatment of alcohol withdrawal. Am J Psychiatry. 1998;155:1626.-
30. Bonnet U, Banger M, Leweke FM, et al. Treatment of alcohol withdrawal syndrome with gabapentin. Pharmacopsychiatry. 1999;32:107-109.
31. Mariani JJ, Rosenthal RN, Tross S, et al. A randomized, open-label, controlled trial of gabapentin and phenobarbital in the treatment of alcohol withdrawal. Am J Addict. 2006;15(1):76-84.
32. Voris J, Smith NL, Rao SM, et al. Gabapentin for the treatment of ethanol withdrawal. Subst Abus. 2003;24(2):129-132.
33. Furieri FA, Nakamura-Palacios EM. Gabapentin reduces alcohol consumption and craving: a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. 2007;68(11):1691-1700.
34. Bisaga A, Evans SM. The acute effects of gabapentin in combination with alcohol in heavy drinkers. Drug Alcohol Depend. 2006;83(1):25-32.
Benzodiazepines are the mainstay of alcohol detoxification treatment, with extensive evidence supporting their efficacy and relative safety.1 The risk of benzodiazepine-alcohol interaction, however, and psychomotor and cognitive impairments associated with benzodiazepine use may limit early rehabilitation efforts in hospitalized patients.2 Cross-tolerance with alcohol also limits benzodiazepines’ potential benefit in outpatients with substance use disorders.
Adding anticonvulsants to acute benzodiazepine therapy has been shown to decrease alcohol withdrawal symptom severity, reduce seizure risk, and support recovery, particularly in patients with multiple alcohol withdrawal episodes. After detoxification, long-term anticonvulsant use may reduce relapse risk by decreasing post-cessation craving, without abuse liability.3
Although not all studies endorse adding anticonvulsants to benzodiazepines for managing alcohol withdrawal syndrome (AWS),4 we present 3 cases in which anticonvulsants were used successfully as adjuncts to lorazepam. Valproic acid, levetiracetam, and gabapentin offer advantages in acute and long-term therapy of alcohol dependence with efficacy in AWS, low abuse potential, benign safety profile, and mood-stabilizing properties.
Neurobiologic rationale
AWS manifests as a cluster of clinical symptoms including delirium tremens (DTs) and seizures (Table 1). Its pathophysiology can be explained by alcohol’s agonist effect on the gamma-aminobutyric acid (GABA) system and antagonist effect on the glutamatergic system (Table 2).5
Chronic alcohol intake leads to neuroadaptation in the brain in the form of down-regulation of GABAA receptors and upregulation of N-methyl-D-aspartate receptors. During alcohol withdrawal, this neuroadaptation leads to a decrease in central GABA activity and an increase in glutamate activity, resulting in hyperexcitation, anxiety, and seizures.6
Little data exist regarding time to relapse after detoxification in alcohol-dependent patients. One theory—called “protracted withdrawal syndrome” (Table 1)—suggests that abstinent alcoholics return to drinking because of the same, but attenuated, neuroadaptations that trigger acute AWS.7
Advantages of adjunct therapy. Ntais et al8 evaluated benzodiazepines’ effectiveness and safety in treating AWS in a clinical review of 57 randomized, controlled trials totaling 4,051 patients. Benzodiazepines showed similar success rates as other drugs (relative risk [RR] 1.00) or anticonvulsants in particular (RR 0.88), as measured by changes in Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) scores at the end of treatment. Benzodiazepines also offered significant benefit for seizure control compared with nonanticonvulsants (RR 0.23), but less when compared with anti convulsants (RR 1.99).
Although the literature does not support anticonvulsant use for monotherapy in AWS, anticonvulsants show potential as adjunctive therapy. Valproic acid, levetiracetam, and gabapentin offer unique mechanisms of action (Table 3) and demonstrate advantages over benzodiazepine monotherapy for AWS. Adjunctive use of valproic acid,8,9 levetiracetam,10 and gabapentin11,12 in detoxification also has demonstrated efficacy in reducing risk of relapse and delaying relapse.
The neurobiologic rationale for using anticonvulsants in acute AWS is speculative, but these agents appear to:
- inhibit “kindling” (neuronal changes that may be associated with repeated intoxications)
- facilitate GABAergic mechanisms.9
Table 1
Alcohol withdrawal: Acute vs long-term symptoms
| Alcohol withdrawal syndrome | Protracted withdrawal syndrome | |
|---|---|---|
| Description | Cluster of symptoms in alcohol-dependent persons after heavy or prolonged alcohol use has lessened or ceased | Constellation of symptoms lasting weeks to months after alcohol use ends |
| Presentation | Develops during acute detoxification period and lasts 5 to 7 days | Develops after 5- to 7-day acute detoxification period and may persist for 1 year |
| Symptoms | Mild: insomnia, tremor, anxiety, GI upset, headache, diaphoresis, palpitations, anorexia Severe: alcoholic hallucinosis Seizures (generalized tonic-clonic) occur in up to 25% of withdrawal episodes, usually within 24 hours after alcohol cessation Delirium tremens (characterized by hallucinations, disorientation, tachycardia, hypertension, low-grade fever, agitation, and diaphoresis) occurs in up to 5% of patients undergoing withdrawal, may be delayed 4 to 5 days, and has mortality rates reaching 15% | Sleep disruption; anxiety; depressive symptoms; irritability; increased breathing rate, body temperature, blood pressure, and pulse |
| GI: gastrointestinal | ||
| Source: Click here for a bibliography | ||
Table 2
How alcohol affects GABA and glutamate neurotransmitters
| GABA | Glutamate | |
|---|---|---|
| GABA, the brain’s primary inhibitory neurotransmitter, renders nerve cells less sensitive to further signaling | Glutamate, the brain’s major excitatory neurotransmitter, renders nerve cells more sensitive to further signaling | |
| Alcohol facilitates the inhibitory function of the GABAA receptor, allowing more GABA to traverse the receptor, and leading to alcohol’s intoxicating effects | Alcohol seems to inhibit the excitatory function of the NMDA glutamate receptor, believed to play a role in memory, learning, and generation of seizures | |
| During alcohol withdrawal, brain GABA concentrations fall below normal and GABAA receptor sensitivity may be reduced | Long-term alcohol exposure produces an adaptive increase in the function of NMDA receptors and results in development of glutamate-NMDA supersensitivity | |
| In the absence of alcohol, the resulting decrease in inhibitory function may contribute to symptoms of CNS hyperactivity associated with acute and protracted alcohol withdrawal | Acute alcohol withdrawal activates glutamate systems, leading to autonomic nervous system hyperactivity; alcohol withdrawal seizures are associated with increased NMDA receptor function | |
| GABA: gamma-aminobutyric acid; NMDA: N-methyl-D-aspartate | ||
| Source: Click here for a bibliography | ||
Table 3
Mechanisms of action of benzodiazepines vs 3 anticonvulsants
| Agent | Mechanism of action |
|---|---|
| Benzodiazepines | Activate GABAA chloride ionophore, increasing affinity of GABAA receptor for GABA and augmenting frequency of chloride channel openinga |
| Valproic acid | GABA modulation and possibly second messenger systems; may inhibit Na1+ and/or Ca2+ channel, thereby boosting GABA and glutamate actionb |
| Levetiracetam | Decreases high voltage activated Ca2+ channels; unique binding site (synaptic vesicle protein SV2A) is thought to be involved in calcium-dependent regulation of neurotransmitter vesicle exocytosisc |
| Gabapentin | GABA analog; unique binding site (Ca2+ channel subunit in brain) decreases calcium influx and inhibits release of excitatory amino acids and monoaminesd |
| GABA: gamma-aminobutyric acid | |
| Source: Click here for a bibliography | |
CASE REPORT 1: Valproic acid for alcohol overdose
After attempting suicide with an alcohol overdose, Ms. J, age 45, is transferred from the emergency room (ER) to our psychiatry consult service 10 hours after admission. Her symptoms include nausea, tremor, headaches, agitation, disorientation, and auditory hallucinations.
Medical history reveals 25 years of alcohol dependence, multiple hospitalizations for withdrawal, and many failed attempts to quit. Ms. J reports consuming an average of 16 drink equivalents (eg, 12 oz beers) daily but denies illicit drug use.
Lab values on admission include blood alcohol concentration (BAC) 290 mg/dL (0.29%), mean corpuscular volume (MCV) 96 fL, gamma-glutamyltransferase (GGT) 164 U/L, aspartate aminotransferase (AST) 43 U/L, alanine aminotransferase (ALT) 31 U/L, and alkaline phosphatase (ALP) 151 U/L. Urine drug screen, acetaminophen, salicylate, vitamin B1 (thiamine), B12 (cyanocobalamin), B9 (folate), and electrolytes (including magnesium) are normal.
We assess alcohol withdrawal severity using the CIWA-Ar (Click here to view/download a copy of this scale). Ms. J’s initial score is 17, indicating a risk of moderate alcohol withdrawal if untreated.
In the ER, Ms. J is placed on a symptom-triggered benzodiazepine detoxification protocol with lorazepam. We add IV valproic acid, 1,250 mg (based on 20 mg/kg body weight)13 divided into 2 doses over the first 24 hours, then maintain IV valproic acid at 500 mg twice daily (Table 4). Within 12 hours of starting combination therapy, Ms. J scores 7 on the CIWA-Ar—indicating mild withdrawal—with subsequent scores <5. She scores 0 with no residual withdrawal symptoms within 36 hours.
Ms. J requires lorazepam, 7 mg, during the 10 hours before valproic acid is added. She requires only 2 mg lorazepam over the next 3 days and reports no side effects related to IV valproic acid. At discharge, Ms. J begins extended-release oral valproic acid, 1,250 mg (based on 25 mg/kg body weight)13 once daily for 2 weeks, until she can obtain outpatient follow-up.
Table 4
Benzodiazepines and anticonvulsants for alcohol detoxification
| Benzodiazepines | Valproic acid | Levetiracetam | Gabapentin | |
|---|---|---|---|---|
| Loading dose | None | 20 mg/kg of body weight, divided into 2 doses for first 24 hours | 1,500 mg IV once daily | 400 mg PO qid |
| Maintenance dose | Day 1: 2 mg tid Day 2: 2 mg morning, 1 mg afternoon, 2 mg evening Day 3: 1 mg tid Day 4: 1 mg bid Day 5: 1 mg Day 6: none | 500 mg IV bid | Either 500 mg IV tid or 1,000 mg PO bid after 2 to 3 days of treatment | 1,200 mg PO tid |
| Side effects | Impaired consciousness, respiratory depression, hypotension | Dizziness, drowsiness, hair loss/thinning, nausea, tremor, weight gain | Somnolence, asthenia, dizziness, coordination difficulties | Somnolence, dizziness, ataxia, fatigue |
| Drug interactions | ↑ BZ: cimetidine, oral contraceptives, ethanol (acute), disulfiram, isoniazid, propranolol ↓ BZ: rifampin, ethanol (chronic) | ↑ VPA: aspirin, felbamate, fluoxetine, isoniazid ↓ VPA: carbamazepine, lamotrigine, phenobarbital, phenytoin, ritonavir | None | ↓ GBP 20%: antacids |
| BZ: benzodiazepine; GBP: gabapentin; PO: per os (by mouth); VPA: valproic acid | ||||
| Source: Click here for a bibliography | ||||
Less lorazepam needed
Adjunctive anticonvulsants can reduce the amount of lorazepam required during detoxification.14,15 Compared with benzodiazepine monotherapy, the advantages of combination therapy—particularly in outpatient alcohol withdrawal treatment and relapse prevention—include:
- minimal interaction with alcohol (avoiding increased psychomotor deficits, cognitive impairment, and intoxication)15
- lower abuse potential
- possible efficacy in mood stabilization before, during, and after withdrawal (Table 5).16
Given the risk of seizures during AWS, anticonvulsants seem to make empirical sense. One study reported a 1% incidence of withdrawal-related seizures in 545 alcohol-dependent inpatients treated with valproic acid.17 Another case series of 37 patients found no acute sequelae when valproic acid was used for AWS.18
Anticonvulsants such as valproic acid may reduce the frequency and severity of alcohol relapse, whereas benzodiazepines may increase relapse risk.19 During a 6-week trial, patients receiving valproic acid maintenance therapy had greater abstinence rates and improved drinking outcomes compared with detoxification-only groups.9
One disadvantage of valproic acid is potential hepatotoxicity, an important consideration in patients with liver damage. Fortunately, Ms. J’s AST and ALT values remained within normal limits during valproic acid treatment.
Table 5
Pharmacologic profiles of benzodiazepines vs 3 anticonvulsants
| Benzodiazepines | Valproic acid | Levetiracetam | Gabapentin | |
|---|---|---|---|---|
| Metabolism | CYP 2C19: diazepam CYP 3A3/4: alprazolam, clonazepam, diazepam, triazolam Phase II only: lorazepam, temazepam, oxazepam | >95% hepatic, of which <20% occurs via CYP isoenzymes | Not extensively metabolized; renal clearance; not involved with hepatic CYP isoenzymes | Not metabolized; secreted via kidneys as unchanged drug |
| Sedation | Mild to moderate | Mild to moderate | Mild to moderate | Moderate to severe |
| Synergistic effects with alcohol | Yes | No | No | No |
| Paradoxical disinhibition | Yes | No | No | No |
| Risk of addiction in outpatient therapy | Yes | No | No | No |
| CYP: cytochrome P450 | ||||
| Source: Click here for a bibliography | ||||
CASE REPORT 2: Levetiracetam for withdrawal seizures
Mr. H, age 42, presents to the ER after suffering a seizure. His medical history includes hypertension, alcohol dependence, and seizures during alcohol withdrawal. He denies a history of psychiatric illness, and his family history is unknown. He is noncompliant with hypertension treatment, which includes clonidine. Mr. H reports his usual alcohol consumption as a 6-pack of beer nightly during the week and a 12-pack nightly on weekends. He says his last drink was 4 days before admission.
Mr. H scores 19 on the CIWA-Ar, placing him at risk for moderate withdrawal. Head CT shows diffuse atrophy, without evidence of an acute intracranial process. BAC is zero on admission, and urine drug screen is negative. Amylase, lipase, and lactate dehydrogenase (LDH) levels suggest acute pancreatitis. AST is elevated to 131 U/L, ALT is elevated to 42 U/L, but MCV is within normal limits.
The psychiatric service is consulted on day 2 of admission, and we prescribe levetiracetam, 500 mg IV every 8 hours.20 IV lorazepam also is available as needed: 1 mg every 8 hours for the first 2 days, then 1 mg every 12 hours for 2 days, then 1 mg every 24 hours. The patient’s CIWA-Ar score is 9 on days 2 and 3 of admission, followed by scores consistently between 2 and 3 after scheduled levetiracetam administration. Mr. H requires 3 mg of lorazepam the remainder of his hospitalization. He is discharged on day 7 with a CIWA-Ar score of 2, and reports no adverse effects related to levetiracetam. He leaves the hospital with a 2-week prescription for oral levetiracetam, 500 mg tid.
Advantages of levetiracetam
Levetiracetam is FDA-approved for adjunctive treatment of adults with partial-onset seizures.21 Successful AWS treatment with adjunctive levetiracetam has been supported by few but promising studies.10,20 Potential advantages of levetiracetam in detoxification include:
- a lack of GABAergic properties, which limits the risk of intoxication or respiratory insufficiency when combined with alcohol21
- low drug-drug interaction risk because of nonhepatic metabolism and primary renal excretion.22,23
We selected levetiracetam for Mr. H because of his history of alcohol withdrawal seizures and acute pancreatitis. Anticonvulsants may be more effective than lorazepam in reducing the risk of alcohol withdrawal seizures,24 and we felt valproic acid might not be safe for him because of its low but real risk of pancreatitis.13 We based our levetiracetam dosing on a small open-label trial20 and product information for treating adults with partial-onset seizures.25
Studies also demonstrate levetiracetam’s potential for relapse prevention during outpatient therapy. In a 10-week trial, levetiracetam decreased the number of standard drinks in alcohol-dependent patients from 5.3 to 1.7 per day.10 This was a small open trial, however, and large controlled trials support the usefulness of other, FDA-approved medications—including disulfiram, naltrexone, and acamprosate—for alcohol relapse prevention.
CASE REPORT 3: Gabapentin for acute withdrawal
Mr. B, age 38, presents to the ER after a 13-day alcohol binge. He has been drinking increasing amounts of alcohol over 6 weeks. Three months earlier, Mr. B was admitted for alcohol withdrawal treatment and received 49 mg of lorazepam over 3 days. This resulted in his transfer from the step-down unit to the intensive care unit for increased agitation, possibly caused by paradoxical disinhibition from excessive lorazepam use.26
Mr. B’s medical history is significant for alcohol-induced seizures, DTs, traumatic brain injury related to craniotomy, and right arm amputation. Mr. B drinks approximately 24 beers per day. He denies tobacco use but admits to past use of cocaine, marijuana, and heroin.
On admission, Mr. B’s BAC is 360 mg/dL (0.36%), AST is elevated at 72 U/L, ALT at 42 U/L, and LDH significantly elevated at 384 U/L. Urine drug screen is negative, and his CIWA-Ar score is 23. His score of –1 on the Richmond Agitation and Sedation Scale (RASS)27 correlates with very mild sedation.
Guided by Bonnet et al28 and clinical experience, we start Mr. B on gabapentin, 1,200 mg tid, and IV lorazepam, 2 mg every 8 hours as needed for breakthrough withdrawal. We decrease lorazepam by 50% every other day until Mr. B is discharged. On days 2, 3, and 4, Mr. B’s CIWA-Ar scores are 6, 9, and 2, respectively. His RASS score drops from –1 on days 1 and 2 to 0 until discharge, indicating an alert and calm state.
Mr. B requires a total of 2 mg of lorazepam throughout hospitalization. He finishes alcohol detoxification on day 4 and is discharged with a prescription for gabapentin, 1,200 mg tid. Two weeks later, when he is admitted to a 28-day inpatient alcohol rehabilitation unit, Mr. B has not relapsed.
More abstinent days
Gabapentin is FDA-approved as adjunctive therapy for partial seizures. Off-label, it has been generally efficacious as an adjunct in alcohol detoxification.29-32 We chose adjunctive anticonvulsant therapy for Mr. B because of his history of alcohol-induced seizures. We chose gabapentin instead of valproic acid because of Mr. B’s liver damage and gabapentin’s lack of hepatic metabolism.
Gabapentin may reduce alcohol consumption and craving in alcohol-dependent patients. By increasing the number of abstinent days, gabapentin may help patients maintain abstinence.33 Gabapentin does not appear to interact clinically with alcohol, causing neither sedation nor synergistic effects.34 Its relative lack of abuse potential may be valuable in outpatient alcohol withdrawal treatment and in maintaining alcohol abstinence after detoxification.
Related resource
- Asplund CA, Aaronson JW, Aaronson HE. 3 regimens for alcohol withdrawal and detoxification. J Fam Pract. 2004;53(7):545-554. www.jfponline.com/Pages.asp?AID=1730.
Drug brand names
- Acamprosate • Campral
- Alprazolam • Xanax
- Carbamazepine • Carbatrol
- Cimetidine • Tagamet
- Clonazepam • Klonopin
- Clonidine • Catapres
- Diazepam • Valium
- Disulfiram • Antabuse
- Felbamate • Felbatol
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Isoniazid • Nydrazid
- Lamotrigine • Lamictal
- Levetiracetam • Keppra
- Lorazepam • Ativan
- Naltrexone • ReVia, Vivitrol
- Oxazepam • Serax
- Phenobarbital • Luminal
- Phenytoin • Dilantin
- Propranolol • Inderal
- Rifampin • Rifadin
- Ritonavir • Norvir
- Temazepam • Restoril
- Triazolam • Halcion
- Valproic acid • Depakote, Depakene
Disclosures
Dr. Spiegel is a speaker for Pfizer Inc. and GlaxoSmithKline.
Dr. Radac reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The authors thank Rishi Laroia, MD, Robert Swanson, MD, and Adam W. Coe, MD for their contributions to this article.
Benzodiazepines are the mainstay of alcohol detoxification treatment, with extensive evidence supporting their efficacy and relative safety.1 The risk of benzodiazepine-alcohol interaction, however, and psychomotor and cognitive impairments associated with benzodiazepine use may limit early rehabilitation efforts in hospitalized patients.2 Cross-tolerance with alcohol also limits benzodiazepines’ potential benefit in outpatients with substance use disorders.
Adding anticonvulsants to acute benzodiazepine therapy has been shown to decrease alcohol withdrawal symptom severity, reduce seizure risk, and support recovery, particularly in patients with multiple alcohol withdrawal episodes. After detoxification, long-term anticonvulsant use may reduce relapse risk by decreasing post-cessation craving, without abuse liability.3
Although not all studies endorse adding anticonvulsants to benzodiazepines for managing alcohol withdrawal syndrome (AWS),4 we present 3 cases in which anticonvulsants were used successfully as adjuncts to lorazepam. Valproic acid, levetiracetam, and gabapentin offer advantages in acute and long-term therapy of alcohol dependence with efficacy in AWS, low abuse potential, benign safety profile, and mood-stabilizing properties.
Neurobiologic rationale
AWS manifests as a cluster of clinical symptoms including delirium tremens (DTs) and seizures (Table 1). Its pathophysiology can be explained by alcohol’s agonist effect on the gamma-aminobutyric acid (GABA) system and antagonist effect on the glutamatergic system (Table 2).5
Chronic alcohol intake leads to neuroadaptation in the brain in the form of down-regulation of GABAA receptors and upregulation of N-methyl-D-aspartate receptors. During alcohol withdrawal, this neuroadaptation leads to a decrease in central GABA activity and an increase in glutamate activity, resulting in hyperexcitation, anxiety, and seizures.6
Little data exist regarding time to relapse after detoxification in alcohol-dependent patients. One theory—called “protracted withdrawal syndrome” (Table 1)—suggests that abstinent alcoholics return to drinking because of the same, but attenuated, neuroadaptations that trigger acute AWS.7
Advantages of adjunct therapy. Ntais et al8 evaluated benzodiazepines’ effectiveness and safety in treating AWS in a clinical review of 57 randomized, controlled trials totaling 4,051 patients. Benzodiazepines showed similar success rates as other drugs (relative risk [RR] 1.00) or anticonvulsants in particular (RR 0.88), as measured by changes in Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) scores at the end of treatment. Benzodiazepines also offered significant benefit for seizure control compared with nonanticonvulsants (RR 0.23), but less when compared with anti convulsants (RR 1.99).
Although the literature does not support anticonvulsant use for monotherapy in AWS, anticonvulsants show potential as adjunctive therapy. Valproic acid, levetiracetam, and gabapentin offer unique mechanisms of action (Table 3) and demonstrate advantages over benzodiazepine monotherapy for AWS. Adjunctive use of valproic acid,8,9 levetiracetam,10 and gabapentin11,12 in detoxification also has demonstrated efficacy in reducing risk of relapse and delaying relapse.
The neurobiologic rationale for using anticonvulsants in acute AWS is speculative, but these agents appear to:
- inhibit “kindling” (neuronal changes that may be associated with repeated intoxications)
- facilitate GABAergic mechanisms.9
Table 1
Alcohol withdrawal: Acute vs long-term symptoms
| Alcohol withdrawal syndrome | Protracted withdrawal syndrome | |
|---|---|---|
| Description | Cluster of symptoms in alcohol-dependent persons after heavy or prolonged alcohol use has lessened or ceased | Constellation of symptoms lasting weeks to months after alcohol use ends |
| Presentation | Develops during acute detoxification period and lasts 5 to 7 days | Develops after 5- to 7-day acute detoxification period and may persist for 1 year |
| Symptoms | Mild: insomnia, tremor, anxiety, GI upset, headache, diaphoresis, palpitations, anorexia Severe: alcoholic hallucinosis Seizures (generalized tonic-clonic) occur in up to 25% of withdrawal episodes, usually within 24 hours after alcohol cessation Delirium tremens (characterized by hallucinations, disorientation, tachycardia, hypertension, low-grade fever, agitation, and diaphoresis) occurs in up to 5% of patients undergoing withdrawal, may be delayed 4 to 5 days, and has mortality rates reaching 15% | Sleep disruption; anxiety; depressive symptoms; irritability; increased breathing rate, body temperature, blood pressure, and pulse |
| GI: gastrointestinal | ||
| Source: Click here for a bibliography | ||
Table 2
How alcohol affects GABA and glutamate neurotransmitters
| GABA | Glutamate | |
|---|---|---|
| GABA, the brain’s primary inhibitory neurotransmitter, renders nerve cells less sensitive to further signaling | Glutamate, the brain’s major excitatory neurotransmitter, renders nerve cells more sensitive to further signaling | |
| Alcohol facilitates the inhibitory function of the GABAA receptor, allowing more GABA to traverse the receptor, and leading to alcohol’s intoxicating effects | Alcohol seems to inhibit the excitatory function of the NMDA glutamate receptor, believed to play a role in memory, learning, and generation of seizures | |
| During alcohol withdrawal, brain GABA concentrations fall below normal and GABAA receptor sensitivity may be reduced | Long-term alcohol exposure produces an adaptive increase in the function of NMDA receptors and results in development of glutamate-NMDA supersensitivity | |
| In the absence of alcohol, the resulting decrease in inhibitory function may contribute to symptoms of CNS hyperactivity associated with acute and protracted alcohol withdrawal | Acute alcohol withdrawal activates glutamate systems, leading to autonomic nervous system hyperactivity; alcohol withdrawal seizures are associated with increased NMDA receptor function | |
| GABA: gamma-aminobutyric acid; NMDA: N-methyl-D-aspartate | ||
| Source: Click here for a bibliography | ||
Table 3
Mechanisms of action of benzodiazepines vs 3 anticonvulsants
| Agent | Mechanism of action |
|---|---|
| Benzodiazepines | Activate GABAA chloride ionophore, increasing affinity of GABAA receptor for GABA and augmenting frequency of chloride channel openinga |
| Valproic acid | GABA modulation and possibly second messenger systems; may inhibit Na1+ and/or Ca2+ channel, thereby boosting GABA and glutamate actionb |
| Levetiracetam | Decreases high voltage activated Ca2+ channels; unique binding site (synaptic vesicle protein SV2A) is thought to be involved in calcium-dependent regulation of neurotransmitter vesicle exocytosisc |
| Gabapentin | GABA analog; unique binding site (Ca2+ channel subunit in brain) decreases calcium influx and inhibits release of excitatory amino acids and monoaminesd |
| GABA: gamma-aminobutyric acid | |
| Source: Click here for a bibliography | |
CASE REPORT 1: Valproic acid for alcohol overdose
After attempting suicide with an alcohol overdose, Ms. J, age 45, is transferred from the emergency room (ER) to our psychiatry consult service 10 hours after admission. Her symptoms include nausea, tremor, headaches, agitation, disorientation, and auditory hallucinations.
Medical history reveals 25 years of alcohol dependence, multiple hospitalizations for withdrawal, and many failed attempts to quit. Ms. J reports consuming an average of 16 drink equivalents (eg, 12 oz beers) daily but denies illicit drug use.
Lab values on admission include blood alcohol concentration (BAC) 290 mg/dL (0.29%), mean corpuscular volume (MCV) 96 fL, gamma-glutamyltransferase (GGT) 164 U/L, aspartate aminotransferase (AST) 43 U/L, alanine aminotransferase (ALT) 31 U/L, and alkaline phosphatase (ALP) 151 U/L. Urine drug screen, acetaminophen, salicylate, vitamin B1 (thiamine), B12 (cyanocobalamin), B9 (folate), and electrolytes (including magnesium) are normal.
We assess alcohol withdrawal severity using the CIWA-Ar (Click here to view/download a copy of this scale). Ms. J’s initial score is 17, indicating a risk of moderate alcohol withdrawal if untreated.
In the ER, Ms. J is placed on a symptom-triggered benzodiazepine detoxification protocol with lorazepam. We add IV valproic acid, 1,250 mg (based on 20 mg/kg body weight)13 divided into 2 doses over the first 24 hours, then maintain IV valproic acid at 500 mg twice daily (Table 4). Within 12 hours of starting combination therapy, Ms. J scores 7 on the CIWA-Ar—indicating mild withdrawal—with subsequent scores <5. She scores 0 with no residual withdrawal symptoms within 36 hours.
Ms. J requires lorazepam, 7 mg, during the 10 hours before valproic acid is added. She requires only 2 mg lorazepam over the next 3 days and reports no side effects related to IV valproic acid. At discharge, Ms. J begins extended-release oral valproic acid, 1,250 mg (based on 25 mg/kg body weight)13 once daily for 2 weeks, until she can obtain outpatient follow-up.
Table 4
Benzodiazepines and anticonvulsants for alcohol detoxification
| Benzodiazepines | Valproic acid | Levetiracetam | Gabapentin | |
|---|---|---|---|---|
| Loading dose | None | 20 mg/kg of body weight, divided into 2 doses for first 24 hours | 1,500 mg IV once daily | 400 mg PO qid |
| Maintenance dose | Day 1: 2 mg tid Day 2: 2 mg morning, 1 mg afternoon, 2 mg evening Day 3: 1 mg tid Day 4: 1 mg bid Day 5: 1 mg Day 6: none | 500 mg IV bid | Either 500 mg IV tid or 1,000 mg PO bid after 2 to 3 days of treatment | 1,200 mg PO tid |
| Side effects | Impaired consciousness, respiratory depression, hypotension | Dizziness, drowsiness, hair loss/thinning, nausea, tremor, weight gain | Somnolence, asthenia, dizziness, coordination difficulties | Somnolence, dizziness, ataxia, fatigue |
| Drug interactions | ↑ BZ: cimetidine, oral contraceptives, ethanol (acute), disulfiram, isoniazid, propranolol ↓ BZ: rifampin, ethanol (chronic) | ↑ VPA: aspirin, felbamate, fluoxetine, isoniazid ↓ VPA: carbamazepine, lamotrigine, phenobarbital, phenytoin, ritonavir | None | ↓ GBP 20%: antacids |
| BZ: benzodiazepine; GBP: gabapentin; PO: per os (by mouth); VPA: valproic acid | ||||
| Source: Click here for a bibliography | ||||
Less lorazepam needed
Adjunctive anticonvulsants can reduce the amount of lorazepam required during detoxification.14,15 Compared with benzodiazepine monotherapy, the advantages of combination therapy—particularly in outpatient alcohol withdrawal treatment and relapse prevention—include:
- minimal interaction with alcohol (avoiding increased psychomotor deficits, cognitive impairment, and intoxication)15
- lower abuse potential
- possible efficacy in mood stabilization before, during, and after withdrawal (Table 5).16
Given the risk of seizures during AWS, anticonvulsants seem to make empirical sense. One study reported a 1% incidence of withdrawal-related seizures in 545 alcohol-dependent inpatients treated with valproic acid.17 Another case series of 37 patients found no acute sequelae when valproic acid was used for AWS.18
Anticonvulsants such as valproic acid may reduce the frequency and severity of alcohol relapse, whereas benzodiazepines may increase relapse risk.19 During a 6-week trial, patients receiving valproic acid maintenance therapy had greater abstinence rates and improved drinking outcomes compared with detoxification-only groups.9
One disadvantage of valproic acid is potential hepatotoxicity, an important consideration in patients with liver damage. Fortunately, Ms. J’s AST and ALT values remained within normal limits during valproic acid treatment.
Table 5
Pharmacologic profiles of benzodiazepines vs 3 anticonvulsants
| Benzodiazepines | Valproic acid | Levetiracetam | Gabapentin | |
|---|---|---|---|---|
| Metabolism | CYP 2C19: diazepam CYP 3A3/4: alprazolam, clonazepam, diazepam, triazolam Phase II only: lorazepam, temazepam, oxazepam | >95% hepatic, of which <20% occurs via CYP isoenzymes | Not extensively metabolized; renal clearance; not involved with hepatic CYP isoenzymes | Not metabolized; secreted via kidneys as unchanged drug |
| Sedation | Mild to moderate | Mild to moderate | Mild to moderate | Moderate to severe |
| Synergistic effects with alcohol | Yes | No | No | No |
| Paradoxical disinhibition | Yes | No | No | No |
| Risk of addiction in outpatient therapy | Yes | No | No | No |
| CYP: cytochrome P450 | ||||
| Source: Click here for a bibliography | ||||
CASE REPORT 2: Levetiracetam for withdrawal seizures
Mr. H, age 42, presents to the ER after suffering a seizure. His medical history includes hypertension, alcohol dependence, and seizures during alcohol withdrawal. He denies a history of psychiatric illness, and his family history is unknown. He is noncompliant with hypertension treatment, which includes clonidine. Mr. H reports his usual alcohol consumption as a 6-pack of beer nightly during the week and a 12-pack nightly on weekends. He says his last drink was 4 days before admission.
Mr. H scores 19 on the CIWA-Ar, placing him at risk for moderate withdrawal. Head CT shows diffuse atrophy, without evidence of an acute intracranial process. BAC is zero on admission, and urine drug screen is negative. Amylase, lipase, and lactate dehydrogenase (LDH) levels suggest acute pancreatitis. AST is elevated to 131 U/L, ALT is elevated to 42 U/L, but MCV is within normal limits.
The psychiatric service is consulted on day 2 of admission, and we prescribe levetiracetam, 500 mg IV every 8 hours.20 IV lorazepam also is available as needed: 1 mg every 8 hours for the first 2 days, then 1 mg every 12 hours for 2 days, then 1 mg every 24 hours. The patient’s CIWA-Ar score is 9 on days 2 and 3 of admission, followed by scores consistently between 2 and 3 after scheduled levetiracetam administration. Mr. H requires 3 mg of lorazepam the remainder of his hospitalization. He is discharged on day 7 with a CIWA-Ar score of 2, and reports no adverse effects related to levetiracetam. He leaves the hospital with a 2-week prescription for oral levetiracetam, 500 mg tid.
Advantages of levetiracetam
Levetiracetam is FDA-approved for adjunctive treatment of adults with partial-onset seizures.21 Successful AWS treatment with adjunctive levetiracetam has been supported by few but promising studies.10,20 Potential advantages of levetiracetam in detoxification include:
- a lack of GABAergic properties, which limits the risk of intoxication or respiratory insufficiency when combined with alcohol21
- low drug-drug interaction risk because of nonhepatic metabolism and primary renal excretion.22,23
We selected levetiracetam for Mr. H because of his history of alcohol withdrawal seizures and acute pancreatitis. Anticonvulsants may be more effective than lorazepam in reducing the risk of alcohol withdrawal seizures,24 and we felt valproic acid might not be safe for him because of its low but real risk of pancreatitis.13 We based our levetiracetam dosing on a small open-label trial20 and product information for treating adults with partial-onset seizures.25
Studies also demonstrate levetiracetam’s potential for relapse prevention during outpatient therapy. In a 10-week trial, levetiracetam decreased the number of standard drinks in alcohol-dependent patients from 5.3 to 1.7 per day.10 This was a small open trial, however, and large controlled trials support the usefulness of other, FDA-approved medications—including disulfiram, naltrexone, and acamprosate—for alcohol relapse prevention.
CASE REPORT 3: Gabapentin for acute withdrawal
Mr. B, age 38, presents to the ER after a 13-day alcohol binge. He has been drinking increasing amounts of alcohol over 6 weeks. Three months earlier, Mr. B was admitted for alcohol withdrawal treatment and received 49 mg of lorazepam over 3 days. This resulted in his transfer from the step-down unit to the intensive care unit for increased agitation, possibly caused by paradoxical disinhibition from excessive lorazepam use.26
Mr. B’s medical history is significant for alcohol-induced seizures, DTs, traumatic brain injury related to craniotomy, and right arm amputation. Mr. B drinks approximately 24 beers per day. He denies tobacco use but admits to past use of cocaine, marijuana, and heroin.
On admission, Mr. B’s BAC is 360 mg/dL (0.36%), AST is elevated at 72 U/L, ALT at 42 U/L, and LDH significantly elevated at 384 U/L. Urine drug screen is negative, and his CIWA-Ar score is 23. His score of –1 on the Richmond Agitation and Sedation Scale (RASS)27 correlates with very mild sedation.
Guided by Bonnet et al28 and clinical experience, we start Mr. B on gabapentin, 1,200 mg tid, and IV lorazepam, 2 mg every 8 hours as needed for breakthrough withdrawal. We decrease lorazepam by 50% every other day until Mr. B is discharged. On days 2, 3, and 4, Mr. B’s CIWA-Ar scores are 6, 9, and 2, respectively. His RASS score drops from –1 on days 1 and 2 to 0 until discharge, indicating an alert and calm state.
Mr. B requires a total of 2 mg of lorazepam throughout hospitalization. He finishes alcohol detoxification on day 4 and is discharged with a prescription for gabapentin, 1,200 mg tid. Two weeks later, when he is admitted to a 28-day inpatient alcohol rehabilitation unit, Mr. B has not relapsed.
More abstinent days
Gabapentin is FDA-approved as adjunctive therapy for partial seizures. Off-label, it has been generally efficacious as an adjunct in alcohol detoxification.29-32 We chose adjunctive anticonvulsant therapy for Mr. B because of his history of alcohol-induced seizures. We chose gabapentin instead of valproic acid because of Mr. B’s liver damage and gabapentin’s lack of hepatic metabolism.
Gabapentin may reduce alcohol consumption and craving in alcohol-dependent patients. By increasing the number of abstinent days, gabapentin may help patients maintain abstinence.33 Gabapentin does not appear to interact clinically with alcohol, causing neither sedation nor synergistic effects.34 Its relative lack of abuse potential may be valuable in outpatient alcohol withdrawal treatment and in maintaining alcohol abstinence after detoxification.
Related resource
- Asplund CA, Aaronson JW, Aaronson HE. 3 regimens for alcohol withdrawal and detoxification. J Fam Pract. 2004;53(7):545-554. www.jfponline.com/Pages.asp?AID=1730.
Drug brand names
- Acamprosate • Campral
- Alprazolam • Xanax
- Carbamazepine • Carbatrol
- Cimetidine • Tagamet
- Clonazepam • Klonopin
- Clonidine • Catapres
- Diazepam • Valium
- Disulfiram • Antabuse
- Felbamate • Felbatol
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Isoniazid • Nydrazid
- Lamotrigine • Lamictal
- Levetiracetam • Keppra
- Lorazepam • Ativan
- Naltrexone • ReVia, Vivitrol
- Oxazepam • Serax
- Phenobarbital • Luminal
- Phenytoin • Dilantin
- Propranolol • Inderal
- Rifampin • Rifadin
- Ritonavir • Norvir
- Temazepam • Restoril
- Triazolam • Halcion
- Valproic acid • Depakote, Depakene
Disclosures
Dr. Spiegel is a speaker for Pfizer Inc. and GlaxoSmithKline.
Dr. Radac reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The authors thank Rishi Laroia, MD, Robert Swanson, MD, and Adam W. Coe, MD for their contributions to this article.
1. Mayo-Smith MF, Cushman P, Hill AJ, et al. Pharmacological management of alcohol withdrawal. JAMA. 1997;278:144-151.
2. Myrick H, Brady KT, Malcom R. Divalproex in the treatment of alcohol withdrawal—statistical data included. Am J Drug Alcohol Abuse. 2000;26(1):155-160.
3. Johnson BA, Swift RM, Addolorato G, et al. Safety and efficacy of GABAergic medications for treating alcoholism. Alcohol Clin Exp Res. 2005;29(2):248-254.
4. Lum E, Gorman SK, Slavik RS. Valproic acid management of acute alcohol withdrawal. Ann Pharmacother. 2006;40(3):441-448.
5. Trevisan LA, Boutros N, Petrakis IL, et al. Complications of alcohol withdrawal: pathophysiological insights. Alcohol Health Res World. 1998;22(1):61-66.
6. Esel E. Neurobiology of alcohol withdrawal inhibitory and excitatory neurotransmitters. Turk Psikiyatri Derg. 2006;7(2):129-138.
7. Myrick H, Brady KT. The use of divalproex in the treatment of addictive disorders. Psychopharmacol Bull. 2003;37(suppl 2):89-97.
8. Brady KT, Myrick H, Henderson S, et al. The use of divalproex in alcohol relapse prevention: a pilot study. Drug Alcohol Depend. 2002;67(3):323-330.
9. Longo L, Campbell T, Hubatch S. Divalproex sodium (Depakote) for alcohol withdrawal and relapse prevention. J Addict Dis. 2002;21(2):55-64.
10. Sarid-Segal O, Piechniczek-Buczek J, Knapp C, et al. The effects of levetiracetam on alcohol consumption in alcohol-dependent subjects: an open label study. Am J Drug Alcohol Abuse. 2008;34(4):441-447.
11. American Psychiatric Association. Treatments of psychiatric disorders: a task force report of the American Psychiatric Association. Washington, DC: American Psychiatric Association Press; 1989:187.
12. Mason BJ, Light JM, Williams LD, et al. Proof-of-concept human laboratory study for protracted abstinence in alcohol dependence: effects of gabapentin. Addict Biol. 2009;14(1):73-83.
13. Physicians’ Desk Reference 2009. 63rd ed. Montvale, NJ: Physicians’ Desk Reference; 2008:423-431.
14. Malcolm R, Ballenger JC, Sturgis ET, et al. Double-blind controlled trial comparing carbamazepine to oxazepam treatment of alcohol withdrawal. Am J Psychiatry. 1989;146:617-621.
15. Myrick H, Anton R, Voronin K, et al. A double-blind evaluation of gabapentin on alcohol effects and drinking in a clinical laboratory paradigm. Alcohol Clin Exp Res. 2007;31(2):221-227.
16. Malcolm R, Myrick H, Brady KT, et al. Update on anticonvulsants for the treatment of alcohol withdrawal. Am J Addict. 2001;10(suppl):16-23.
17. Davis LL, Ryan W, Adinoff B, et al. Comprehensive review of the psychiatric uses of valproate. J Clin Psychopharm. 2000;20(1 suppl 1):1S-17S.
18. Rosenthal RN, Perkel C, Singh P, et al. A pilot open randomized trial of valproate and phenobarbital in the treatment of acute alcohol withdrawal. Am J Addict. 1998;7:189-197.
19. Book SW, Myrick H. Novel anticonvulsants in the treatment of alcoholism. Expert Opin Investig Drugs. 2005;14(4):371-376.
20. Krebs M, Leopold K, Richter C, et al. Levetiracetam for the treatment of alcohol withdrawal syndrome: an open-label pilot trial. J Clin Psychopharmacol. 2006;26(3):347-349.
21. LaRoche SM, Helmers SL. The new antiepileptic drugs: scientific review. JAMA. 2004;291:605-614.
22. Chabolla DR, Harnois DM, Meschia JF. Levetiracetam monotherapy for liver transplant patients with seizures. Transplant Proc. 2003;35:1480-1481.
23. Paul F, Meencke HJ. Levetiracetam in focal epilepsy and hepatic porphyria: a case report. Epilepsia. 2004;45:559-560.
24. Ntais C, Pakos E, Kyzas P, et al. Benzodiazepines for alcohol withdrawal. Cochrane Database Syst Rev. 2005;(3):CD005063.-
25. Physicians’ Desk Reference 2009. 63rd ed. Montvale, NJ: Physicians’ Desk Reference; 2008:3131-3143.
26. Saias T, Gallarda T. Paradoxical aggressive reactions to benzodiazepine use: a review. Encephale. 2008;34(4):330-336.
27. Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation–Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166:1338-1344.
28. Bonnet U, Banger M, Leweke FM, et al. Treatment of acute alcohol withdrawal with gabapentin: results from a controlled two-center trial. J Clin Psychopharmacol. 2003;23(5):514-519.
29. Myrick H, Malcolm R, Brady KT. Gabapentin treatment of alcohol withdrawal. Am J Psychiatry. 1998;155:1626.-
30. Bonnet U, Banger M, Leweke FM, et al. Treatment of alcohol withdrawal syndrome with gabapentin. Pharmacopsychiatry. 1999;32:107-109.
31. Mariani JJ, Rosenthal RN, Tross S, et al. A randomized, open-label, controlled trial of gabapentin and phenobarbital in the treatment of alcohol withdrawal. Am J Addict. 2006;15(1):76-84.
32. Voris J, Smith NL, Rao SM, et al. Gabapentin for the treatment of ethanol withdrawal. Subst Abus. 2003;24(2):129-132.
33. Furieri FA, Nakamura-Palacios EM. Gabapentin reduces alcohol consumption and craving: a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. 2007;68(11):1691-1700.
34. Bisaga A, Evans SM. The acute effects of gabapentin in combination with alcohol in heavy drinkers. Drug Alcohol Depend. 2006;83(1):25-32.
1. Mayo-Smith MF, Cushman P, Hill AJ, et al. Pharmacological management of alcohol withdrawal. JAMA. 1997;278:144-151.
2. Myrick H, Brady KT, Malcom R. Divalproex in the treatment of alcohol withdrawal—statistical data included. Am J Drug Alcohol Abuse. 2000;26(1):155-160.
3. Johnson BA, Swift RM, Addolorato G, et al. Safety and efficacy of GABAergic medications for treating alcoholism. Alcohol Clin Exp Res. 2005;29(2):248-254.
4. Lum E, Gorman SK, Slavik RS. Valproic acid management of acute alcohol withdrawal. Ann Pharmacother. 2006;40(3):441-448.
5. Trevisan LA, Boutros N, Petrakis IL, et al. Complications of alcohol withdrawal: pathophysiological insights. Alcohol Health Res World. 1998;22(1):61-66.
6. Esel E. Neurobiology of alcohol withdrawal inhibitory and excitatory neurotransmitters. Turk Psikiyatri Derg. 2006;7(2):129-138.
7. Myrick H, Brady KT. The use of divalproex in the treatment of addictive disorders. Psychopharmacol Bull. 2003;37(suppl 2):89-97.
8. Brady KT, Myrick H, Henderson S, et al. The use of divalproex in alcohol relapse prevention: a pilot study. Drug Alcohol Depend. 2002;67(3):323-330.
9. Longo L, Campbell T, Hubatch S. Divalproex sodium (Depakote) for alcohol withdrawal and relapse prevention. J Addict Dis. 2002;21(2):55-64.
10. Sarid-Segal O, Piechniczek-Buczek J, Knapp C, et al. The effects of levetiracetam on alcohol consumption in alcohol-dependent subjects: an open label study. Am J Drug Alcohol Abuse. 2008;34(4):441-447.
11. American Psychiatric Association. Treatments of psychiatric disorders: a task force report of the American Psychiatric Association. Washington, DC: American Psychiatric Association Press; 1989:187.
12. Mason BJ, Light JM, Williams LD, et al. Proof-of-concept human laboratory study for protracted abstinence in alcohol dependence: effects of gabapentin. Addict Biol. 2009;14(1):73-83.
13. Physicians’ Desk Reference 2009. 63rd ed. Montvale, NJ: Physicians’ Desk Reference; 2008:423-431.
14. Malcolm R, Ballenger JC, Sturgis ET, et al. Double-blind controlled trial comparing carbamazepine to oxazepam treatment of alcohol withdrawal. Am J Psychiatry. 1989;146:617-621.
15. Myrick H, Anton R, Voronin K, et al. A double-blind evaluation of gabapentin on alcohol effects and drinking in a clinical laboratory paradigm. Alcohol Clin Exp Res. 2007;31(2):221-227.
16. Malcolm R, Myrick H, Brady KT, et al. Update on anticonvulsants for the treatment of alcohol withdrawal. Am J Addict. 2001;10(suppl):16-23.
17. Davis LL, Ryan W, Adinoff B, et al. Comprehensive review of the psychiatric uses of valproate. J Clin Psychopharm. 2000;20(1 suppl 1):1S-17S.
18. Rosenthal RN, Perkel C, Singh P, et al. A pilot open randomized trial of valproate and phenobarbital in the treatment of acute alcohol withdrawal. Am J Addict. 1998;7:189-197.
19. Book SW, Myrick H. Novel anticonvulsants in the treatment of alcoholism. Expert Opin Investig Drugs. 2005;14(4):371-376.
20. Krebs M, Leopold K, Richter C, et al. Levetiracetam for the treatment of alcohol withdrawal syndrome: an open-label pilot trial. J Clin Psychopharmacol. 2006;26(3):347-349.
21. LaRoche SM, Helmers SL. The new antiepileptic drugs: scientific review. JAMA. 2004;291:605-614.
22. Chabolla DR, Harnois DM, Meschia JF. Levetiracetam monotherapy for liver transplant patients with seizures. Transplant Proc. 2003;35:1480-1481.
23. Paul F, Meencke HJ. Levetiracetam in focal epilepsy and hepatic porphyria: a case report. Epilepsia. 2004;45:559-560.
24. Ntais C, Pakos E, Kyzas P, et al. Benzodiazepines for alcohol withdrawal. Cochrane Database Syst Rev. 2005;(3):CD005063.-
25. Physicians’ Desk Reference 2009. 63rd ed. Montvale, NJ: Physicians’ Desk Reference; 2008:3131-3143.
26. Saias T, Gallarda T. Paradoxical aggressive reactions to benzodiazepine use: a review. Encephale. 2008;34(4):330-336.
27. Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation–Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166:1338-1344.
28. Bonnet U, Banger M, Leweke FM, et al. Treatment of acute alcohol withdrawal with gabapentin: results from a controlled two-center trial. J Clin Psychopharmacol. 2003;23(5):514-519.
29. Myrick H, Malcolm R, Brady KT. Gabapentin treatment of alcohol withdrawal. Am J Psychiatry. 1998;155:1626.-
30. Bonnet U, Banger M, Leweke FM, et al. Treatment of alcohol withdrawal syndrome with gabapentin. Pharmacopsychiatry. 1999;32:107-109.
31. Mariani JJ, Rosenthal RN, Tross S, et al. A randomized, open-label, controlled trial of gabapentin and phenobarbital in the treatment of alcohol withdrawal. Am J Addict. 2006;15(1):76-84.
32. Voris J, Smith NL, Rao SM, et al. Gabapentin for the treatment of ethanol withdrawal. Subst Abus. 2003;24(2):129-132.
33. Furieri FA, Nakamura-Palacios EM. Gabapentin reduces alcohol consumption and craving: a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. 2007;68(11):1691-1700.
34. Bisaga A, Evans SM. The acute effects of gabapentin in combination with alcohol in heavy drinkers. Drug Alcohol Depend. 2006;83(1):25-32.
Reducing polypharmacy: When less is more
Up to one-third of psychiatric out-patients in 2006 received ≥3 medications, compared with 17% a decade earlier.1 Polypharmacy is expensive, increases the risk of adverse effects, and may contribute to nonadherence. Although we recognize that at times long medication lists are justified, we offer 4 principles to help you limit unnecessary polypharmacy.
Do not treat patients’ symptoms indefinitely
William Osler stressed the importance of treating diseases, not symptoms.2 Symptoms without a diagnosis are experiences. Whether physicians should treat experiences is an ethical question; however, even if your answer is “yes,” such treatment should be transient. Symptoms occurring within a diagnosis should be treated conservatively, but humanely, only while waiting for syndromal relief.3
Do not use syndrome-oriented drugs to treat symptoms
Mood disorders are not just unpleasant emotions, and anxiety disorders are more than simply nervousness. Medications that are effective for psychopathologic syndromes might not help isolated patient complaints. For example, antidepressants do not simply lift sadness, nor do they usually relieve the nonsyndromal “anxiety” many patients report. Some clinicians might disagree with this recommendation based on flaws in DSM-IV-TR taxonomy; however, these shortcomings do not translate into pharmacologic efficacy.
Do not accumulate medications when faced with nonresponse
If the first 3 medications you prescribed were working, you wouldn’t need to add a fourth. Consider discontinuing one medication for every new one you start. This principle can help you set limits with patients who demand more medications to try to eradicate nonsyndromal distress or clinically significant symptoms that psychopharmacology cannot address. Nonresponse to aggressive treatment should trigger a reassessment of the original diagnosis.
Do not match ‘soft’ diagnoses with ‘soft’ treatments
“Soft” diagnoses come in 2 types:
- an equivocal or mild psychopathologic picture that may be called, for example, “soft bipolar illness”
- using imprecise terms as diagnostic proxies, such as “depression and anxiety.”
Patients with soft diagnoses often receive combinations of lower-than-standard dosages or drugs with milder side effects but substandard efficacy. For these patients, we recommend postponing pharmacotherapy or “firming up” the diagnosis and then initiating the standard of care.
1. Mojtabai R, Olfson M. National trends in psychotropic medication polypharmacy in office-based psychiatry. Arch Gen Psychiatry. 2010;67:26-36.
2. Osler W. Aequanimitas. 3rd edy. New York, NY: McGraw-Hill Professional; 1932.
3. Ghaemi SN. Toward a Hippocratic psychopharmacology. Can J Psychiatry. 2008;53(3):189-196.
Up to one-third of psychiatric out-patients in 2006 received ≥3 medications, compared with 17% a decade earlier.1 Polypharmacy is expensive, increases the risk of adverse effects, and may contribute to nonadherence. Although we recognize that at times long medication lists are justified, we offer 4 principles to help you limit unnecessary polypharmacy.
Do not treat patients’ symptoms indefinitely
William Osler stressed the importance of treating diseases, not symptoms.2 Symptoms without a diagnosis are experiences. Whether physicians should treat experiences is an ethical question; however, even if your answer is “yes,” such treatment should be transient. Symptoms occurring within a diagnosis should be treated conservatively, but humanely, only while waiting for syndromal relief.3
Do not use syndrome-oriented drugs to treat symptoms
Mood disorders are not just unpleasant emotions, and anxiety disorders are more than simply nervousness. Medications that are effective for psychopathologic syndromes might not help isolated patient complaints. For example, antidepressants do not simply lift sadness, nor do they usually relieve the nonsyndromal “anxiety” many patients report. Some clinicians might disagree with this recommendation based on flaws in DSM-IV-TR taxonomy; however, these shortcomings do not translate into pharmacologic efficacy.
Do not accumulate medications when faced with nonresponse
If the first 3 medications you prescribed were working, you wouldn’t need to add a fourth. Consider discontinuing one medication for every new one you start. This principle can help you set limits with patients who demand more medications to try to eradicate nonsyndromal distress or clinically significant symptoms that psychopharmacology cannot address. Nonresponse to aggressive treatment should trigger a reassessment of the original diagnosis.
Do not match ‘soft’ diagnoses with ‘soft’ treatments
“Soft” diagnoses come in 2 types:
- an equivocal or mild psychopathologic picture that may be called, for example, “soft bipolar illness”
- using imprecise terms as diagnostic proxies, such as “depression and anxiety.”
Patients with soft diagnoses often receive combinations of lower-than-standard dosages or drugs with milder side effects but substandard efficacy. For these patients, we recommend postponing pharmacotherapy or “firming up” the diagnosis and then initiating the standard of care.
Up to one-third of psychiatric out-patients in 2006 received ≥3 medications, compared with 17% a decade earlier.1 Polypharmacy is expensive, increases the risk of adverse effects, and may contribute to nonadherence. Although we recognize that at times long medication lists are justified, we offer 4 principles to help you limit unnecessary polypharmacy.
Do not treat patients’ symptoms indefinitely
William Osler stressed the importance of treating diseases, not symptoms.2 Symptoms without a diagnosis are experiences. Whether physicians should treat experiences is an ethical question; however, even if your answer is “yes,” such treatment should be transient. Symptoms occurring within a diagnosis should be treated conservatively, but humanely, only while waiting for syndromal relief.3
Do not use syndrome-oriented drugs to treat symptoms
Mood disorders are not just unpleasant emotions, and anxiety disorders are more than simply nervousness. Medications that are effective for psychopathologic syndromes might not help isolated patient complaints. For example, antidepressants do not simply lift sadness, nor do they usually relieve the nonsyndromal “anxiety” many patients report. Some clinicians might disagree with this recommendation based on flaws in DSM-IV-TR taxonomy; however, these shortcomings do not translate into pharmacologic efficacy.
Do not accumulate medications when faced with nonresponse
If the first 3 medications you prescribed were working, you wouldn’t need to add a fourth. Consider discontinuing one medication for every new one you start. This principle can help you set limits with patients who demand more medications to try to eradicate nonsyndromal distress or clinically significant symptoms that psychopharmacology cannot address. Nonresponse to aggressive treatment should trigger a reassessment of the original diagnosis.
Do not match ‘soft’ diagnoses with ‘soft’ treatments
“Soft” diagnoses come in 2 types:
- an equivocal or mild psychopathologic picture that may be called, for example, “soft bipolar illness”
- using imprecise terms as diagnostic proxies, such as “depression and anxiety.”
Patients with soft diagnoses often receive combinations of lower-than-standard dosages or drugs with milder side effects but substandard efficacy. For these patients, we recommend postponing pharmacotherapy or “firming up” the diagnosis and then initiating the standard of care.
1. Mojtabai R, Olfson M. National trends in psychotropic medication polypharmacy in office-based psychiatry. Arch Gen Psychiatry. 2010;67:26-36.
2. Osler W. Aequanimitas. 3rd edy. New York, NY: McGraw-Hill Professional; 1932.
3. Ghaemi SN. Toward a Hippocratic psychopharmacology. Can J Psychiatry. 2008;53(3):189-196.
1. Mojtabai R, Olfson M. National trends in psychotropic medication polypharmacy in office-based psychiatry. Arch Gen Psychiatry. 2010;67:26-36.
2. Osler W. Aequanimitas. 3rd edy. New York, NY: McGraw-Hill Professional; 1932.
3. Ghaemi SN. Toward a Hippocratic psychopharmacology. Can J Psychiatry. 2008;53(3):189-196.
Did brain trauma lead to crime?
CASE: Self-reported TBI
When charged with raping a 19-year-old woman, Mr. P, age 32, pleads not guilty by reason of insanity (NGRI). He has a self-reported history of traumatic brain injury (TBI) and claims that since suffering a blow to the head 8 years before the rape, he has experienced episodes of personality changes, psychosis, and violent behavior. Mr. P is adamant that any wrongdoing on his part was beyond his control, and he argues that consequences of the brain injury, such as hallucinations and aggressive behavior, had recently emerged. The court asks that a forensic psychiatrist evaluate Mr. P.
An only child, Mr. P was raised by his mother in an inner city area. His father was dependent on alcohol and cocaine and abandoned the family shortly after Mr. P’s birth. Mr. P abuses alcohol, as evidenced by previous driving under the influence charges, but denies illicit drug use. He graduated from high school with average grades and denies a history of disciplinary action at school or home. Although Mr. P was charged with misdemeanors in his late teens, the sexual assault is his first felony charge. Mr. P describes himself as a “charmer.”
After high school, Mr. P worked full-time in construction, where he claims he suffered a traumatic blow to the head. Despite this injury, he continued to work and socialize and never sought treatment at a mental health clinic.
The authors’ observations
Although defendants may legitimately suffer from TBI and resultant complications, many individuals capitalize on a history of minor head injury to support their NGRI defense.1 Forensic psychiatrists must retain a healthy degree of clinical suspicion for malingering in defendants who claim NGRI as a result of complications from brain injury, especially when the injury and complications are not documented and simply patient-reported.
TBI is a CNS injury that occurs when an outside force traumatically injures the brain and can cause a variety of physical, cognitive, emotional, and behavioral effects ( Table 1 ).2 Cognitive deficits include:
- impaired attention
- disrupted insight
- poor judgment
- thought disorders.
Reduced processing speed, distractibility, and deficits in executive functions such as abstract reasoning, planning, problem solving, and multitasking have been documented. Memory loss—the most common cognitive impairment among head-injured people—occurs in 20% to 79% of people with closed head trauma, depending on injury severity.3 People who have suffered TBI may have difficulty understanding or producing spoken or written language, or with more subtle aspects of communication, such as body language.
TBI may cause emotional or behavioral problems and personality changes. Mood and affect changes are common. TBI predisposes patients to obsessive-compulsive disorder, substance abuse, dysthymia, clinical depression, bipolar disorder, phobias, panic disorder, and schizophrenia.4 Frontal lobe injuries have been correlated with disinhibition and inappropriate or childish behavior, and temporal lobe injuries with irritability and aggression.5
Table 1
TBI symptoms correspond to area of injury
| Area of injury | Motor/sensory | Psychiatric/behavioral | Cognitive |
|---|---|---|---|
| Brain stem | Decreased vital capacity in breathing, dysphagia | Sleep difficulties | Inability to categorize objects, difficulty with organization |
| Frontal lobe | Aphasia, praxis | Disinhibition, personality changes | Impaired executive function |
| Cerebellum | Nystagmus, tremor | Labile emotions | Inability to process information |
| Parietal lobe | Apraxia | Personality changes | Neglect |
| Occipital lobe | Visual field cuts; diminished proprioception | Visual hallucinations | Color agnosia; inability to recognize words; difficulty reading, writing, and recognizing drawn objects |
| Temporal lobe | Seizure | Libido changes, humorless verbosity, aggression, olfactory perceptual changes | Prosopagnosia, aphasia, agnosia, memory loss, inattention |
| TBI: traumatic brain injury | |||
| Source: Reference 2 | |||
TBI and the insanity defense
The M’Naghten Rule of 1843 requires that for an insanity defense, the defendant must have a mental disease or defect that causes him not to know the nature and quality or the wrongfulness of his act.6 TBI is an abnormal condition of the mind leading to a mental disease that can substantially affect control of emotions and behaviors.
Nevertheless, TBI-induced criminality remains controversial.7 Theories on the etiology of impulse dyscontrol resulting from TBI have suggested structural damage to the brain and altered neurotransmitters. In TBI, the amygdala—which is located within the anterior temporal lobe and adjoins emotions to thoughts—often is injured. Damage to this structure leads to poor impulse control and violent behavior. Damage to specific neurotransmitter systems that causes elevated norepinephrine and dopamine levels and reduced serotonin levels have also been implicated as a cause of impulse dyscontrol in TBI patients.8
In theory, TBI patients potentially could have enough cognitive impairment to have a substantial lack of appreciation of the criminality or wrongfulness of an act. TBI-related impulsivity and cognitive impairment can lead to recklessness and negligence.9 The U.S. Supreme Court has acknowledged that CNS dysfunction affects judgment, reality testing, and self-control.10
EVALUATION: Vague answers
To determine whether Mr. P’s defense is plausible, the forensic psychiatrist must pay attention to the details of the patient’s presentation and history. During the interview, Mr. P quickly shifts from cooperative to obstinate and restricted. He ruminates on the head injury causing him to suffer auditory hallucinations, which he claims he always obeys. Mr. P refuses to provide details of the hallucinations, however, and answers most questions about the head injury or his defense with vague answers, including “I don’t know.”
Because of Mr. P’s reluctance to share information, his lack of psychiatric symptoms other than those he self-reports, and the presence of potential secondary gain from an NGRI defense, the psychiatrist begins to suspect malingering.
The authors’ observations
Malingering is a condition—not a diagnosis—characterized by intentional production of false or grossly exaggerated physical or psychological symptoms motivated by external incentives.11 The presence of external incentives distinguishes malingering from psychiatric illnesses such as factitious and somatoform disorders, in which there is no apparent external incentive. Malingering of psychiatric symptoms occurs in up to 20% of forensic patients, 5% of military recruits, and 1% of mental health patients.5 Stimuli for malingering range from seeking food and shelter to avoiding criminal responsibility ( Table 2 ). Malingering is more common in individuals being evaluated for criminal responsibility than for competence to stand trial. The 3 categories of malingering are:
Table 2
Common external incentives for malingering
| Evading criminal responsibility |
| Disability claims/financial gain |
| Avoiding military duty |
| Evading work |
| Obtaining drugs |
| Seeking food/shelter |
- pure malingering—feigning a nonexistent disorder
- partial malingering—consciously exaggerating real symptoms
- false imputation—ascribing real symptoms to a cause the individual knows is unrelated to the symptoms.12
Determining if a defendant with a history of TBI is malingering requires a multi-step approach that encompasses the clinical interview, a thorough review of collateral data, and focused psychological testing. In interviews, psychiatrists detect approximately 50% of lies, which is no better than would be discovered by chance.13 If you suspect a patient is malingering, combine a structured clinical interview with collateral sources such as old hospital records, treatment history, insurance records, police reports, and interviews with close family and friends.
TBI patients’ poor cognition, memory deficits, and inattention will prove challenging. Malingering patients who attempt to capitalize on a pre-existing TBI to evade responsibility for a current criminal charge may grossly exaggerate or even fake intellectual deficits. Be patient with such defendants and remain aware that such people will give vague or hedging answers to straightforward questions, often accompanied by “I don’t know.” Prolonging the interview may be helpful because it may fatigue a defendant who is faking.12
Some patients who malinger after sustaining a TBI will attempt to feign psychotic symptoms. Table 3 14 illustrates criteria for assessing a patient suspected of malingering psychosis and Table 4 14 highlights atypical psychotic symptoms that suggest feigning illness. Malingering of psychosis can be both assessed in the interview and through testing.
Table 3
Criteria for malingered psychosis
| A. Understandable motive to malinger |
| B. Marked variability of presentation as evidenced by ≥1 of the following: 1. Marked discrepancies in interview and non-interview behaviors 2. Gross inconsistencies in reported psychotic symptoms 3. Blatant contradictions between reported prior episodes and documented psychiatric history |
| C. Improbable psychiatric symptoms as evidenced by ≥1 of the following: 1. Reporting elaborate psychotic symptoms that lack common paranoid, grandiose, or religious themes 2. Sudden emergence of purported symptoms to explain antisocial behavior 3. Atypical hallucinations and delusions |
| D. Confirmation of malingering by either: 1. Admission of malingering following confrontation, or 2. Presence of strong corroborative information, such as psychometric data or history of malingering |
| Source: Reference 14 |
Table 4
Atypical psychotic symptoms that suggest malingering
| Hallucinations |
| Continuous rather than intermittent |
| Vague or inaudible auditory hallucinations |
| Stilted language reported in hallucinations |
| Inability to state strategies to diminish voices |
| Self-report that all command hallucinations were obeyed |
| Visual hallucinations in black and white |
| Delusions |
| Abrupt onset or termination |
| Eagerness to call attention to delusions |
| Conduct markedly inconsistent with delusions |
| Bizarre content without disordered thinking |
| Source: Reference 14 |
Psychological testing
Several standardized diagnostic instruments can be used to help determine whether a patient is feigning or exaggerating psychotic symptoms or cognitive impairments ( Table 5 ). Testing for a patient such as Mr. P—who attributes any criminal wrongdoing to psychosis and also cites limited cognition as a reason for trouble in the interview—would include personality tests, tests to assess exaggerations of psychosis, and cognitive tests.
In the forensic setting, the preferred personality test is the MMPI-2.15 It consists of 567 items, with 10 clinical scales and several validity scales. The F scale, “faking good” or “faking bad,” detects people who are answering questions with the goal of appearing better or worse than they actually are. The Personal Assessment Inventory (PAI)16 is a 344-item test with a 4-point response format. The 22 scales cover a range of important axis I and II psychopathology.
SIRS17 is the gold standard in detecting malingered psychiatric illness; it includes questions about rare symptoms and uncommon symptom pairing. M-FAST18 was developed to provide a brief, reliable screen for malingered mental illness. It has shown good validity and high correlation with the SIRS and MMPI-2.
Tests of exaggerated cognitive impairment are extremely important in evaluating patients who claim to suffer from complications following TBI. TOMM19 —a 50-item recognition test designed to discriminate between true memory-impaired patients and malingerers—is the most studied and valid of such tests. Defendants’ scores that meet the recommended criteria for detecting malingering—≥5 errors on the retention trial—were found to also report a history of head injury.1
Although not as well validated, the Portland Digit Recognition Test (PDRT)20 is an alternative to the TOMM. This test is a forced-choice measure of recognition designed for assessing the possibility of malingering in individuals claiming mental illness because of head injury. The Victoria Symptoms Validity Test (VSVT)21 is used in outpatient and inpatient settings and also uses a forced-choice model to assess possible exaggeration or feigning of cognitive impairments. Finally, the Word Memory Test (WMT)22 is a neuropsychological assessment that evaluates the effort participants put forth.
Table 5
Standardized diagnostic instruments for detecting malingering
| Test | Clinical use |
|---|---|
| Personality | |
| MMPI-2 | F scale detects lying. Several validity scales |
| PAI | Covers a range of axis I and II psychopathology |
| Psychotic symptoms | |
| SIRS | Gold standard in detecting exaggerated psychotic symptoms |
| M-FAST | Screening tool to assess exaggerated psychosis; brief and reliable |
| Cognitive impairment | |
| TOMM | Highest validity of all tools to test memory malingering |
| PDRT | Assesses the possibility of malingering. Not widely studied and validity/reliability are suspect |
| VSVT | Useful for inpatient and outpatient settings |
| WMT | Evaluates effort put forth by the participant |
| M-FAST: Miller Forensic Assessment of Symptoms Test; MMPI-2: Minnesota Multiphasic Personality Inventory; PAI: Personal Assessment Inventory; PDRT: Portland Digit Recognition Test; SIRS: Structured Interview of Reported Symptoms; TOMM: Test of Memory Malingering; VSVT: Victoria Symptoms Validity Test; WMT: Word Memory Test | |
OUTCOME: Unsupported claims
Mr. P’s hospital records reveal a very minor head trauma that resulted in no structural brain abnormalities on imaging tests. Collateral interviews with Mr. P’s family and close friends fail to support the defendant’s claim that after the accident he began to experience behavioral changes and periods of psychosis. Mr. P’s SIRS and TOMM scores indicate malingering, and the psychiatrist did not support his NGRI defense.
Related resource
- Williamson DJ. Neurocognitive impairment: feigned, exaggerated, or real? Current Psychiatry. 2007;6(8):19-37.
Disclosure
Dr. Nasrallah receives research grant/research support from Forest Pharmaceuticals, GlaxoSmithKline, Janssen, Otsuka America Pharmaceuticals, Pfizer Inc., Roche, sanofi-aventis, and Shire, is on the advisory board of Abbott Laboratories, AstraZeneca, Janssen, Novartis, Pfizer Inc., and Merck, and is on the speakers’ bureau for Abbott Laboratories, AstraZeneca, Janssen, Novartis, Pfizer Inc., and Merck.
Dr. Farrell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Delain SL, Stafford KP, Yosef SB. Use of the TOMM in a criminal court forensic assessment setting. Assessment. 2003;10(4):370-381.
2. Rao V, Lyketsos C. Neuropsychiatric sequelae of traumatic brain injury Psychosomatics. 2000;41:95-103.
3. Hall RC, Hall RC, Chapman MJ. Definition, diagnosis, and forensic implications of postconcussional syndrome. Psychosomatics. 2005;46(3):195-202.
4. Arlinghaus KA, Shoaib AM, Price TRP. Neuropsychiatric assessment. In: Silver JM, McAllister TW, Yudofsky SC. Textbook of traumatic brain injury. Arlington, VA: American Psychiatric Publishing, Inc.; 2005:63-65.
5. West S, Noffsinger S. Is this patient not guilty by reason of insanity? Current Psychiatry. 2005;5(8):54-62.
6. Barzman D, Kennedy J, Fozdar M. Does traumatic brain injury cause violence? Current Psychiatry. 2002;1(4):49-55.
7. Silver JM, Yudofsky SC, Hales RE. Neuropsychiatry of traumatic brain injury. Washington, DC: American Psychiatric Press, Inc.; 1994.
8. Melton GB, Petrila J, Poythress NG, et al. Psychological evaluations for the courts. New York, NY: The Guilford Press; 1997.
9. Lewis DO, Pincus JH, Feldman M, et al. Psychiatric, neurological, and psychoeducational characteristics of 15 death row inmates in the United States. Am J Psychiatry. 1986;143:838-845.
10. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
11. Sadock VA. Kaplan and Sadock’s synopsis of psychiatry. Philadelphia, PA: Lippincott, Williams, and Wilkins; 2007:887.
12. Resnick PJ. Faking it: how to determine malingered psychosis. Current Psychiatry. 2005;4(11):12-25.
13. Samuel RZ, Mittenberg W. Determination of malingering in disability claims. Primary Psychiatry. 2005;12(12):60-68.
14. Resnick PJ. Malingered psychosis. In: Rogers R, ed. Clinical assessment of malingering. 2nd ed. New York, NY: The Guilford Press; 1997:47-67.
15. Hathaway SR, McKinley JC. The Minnesota Multiphasic Personality Inventory-2. Minneapolis, MN: University of Minnesota Press; 1989.
16. Rogers R, Sewell KW, Morey LC, et al. Detection of feigned mental disorder on the personality assessment inventory: a discriminate analysis. J Pers Assess. 1996;67:629-640.
17. Rogers R, Bagby RM, Dickens SE. Structured Interview of Reported Symptoms (SIRS). Lutz, FL: Psychological Assessment Resources; 1992.
18. Miller H. Miller Forensic Assessment of Symptoms Test (M-FAST). Professional Manual. Lutz, FL: Psychological Assessment Resources; 2001.
19. Tombaugh TN. The Test of Memory Malingering. Toronto, ON, Canada: Multi-Health Systems; 1996.
20. Binder LM. Malingering following minor head trauma. Clin Neuropsychol. 1990;4:25-36.
21. Slick D, Hopp G, Strauss E, et al. Victoria Symptom Validity Test professional manual. Lutz, FL: Psychological Assessment Resources; 1997.
22. Green P. Word Memory Test. Edmonton, Alberta, Canada: Green’s Publishing; 2003.
CASE: Self-reported TBI
When charged with raping a 19-year-old woman, Mr. P, age 32, pleads not guilty by reason of insanity (NGRI). He has a self-reported history of traumatic brain injury (TBI) and claims that since suffering a blow to the head 8 years before the rape, he has experienced episodes of personality changes, psychosis, and violent behavior. Mr. P is adamant that any wrongdoing on his part was beyond his control, and he argues that consequences of the brain injury, such as hallucinations and aggressive behavior, had recently emerged. The court asks that a forensic psychiatrist evaluate Mr. P.
An only child, Mr. P was raised by his mother in an inner city area. His father was dependent on alcohol and cocaine and abandoned the family shortly after Mr. P’s birth. Mr. P abuses alcohol, as evidenced by previous driving under the influence charges, but denies illicit drug use. He graduated from high school with average grades and denies a history of disciplinary action at school or home. Although Mr. P was charged with misdemeanors in his late teens, the sexual assault is his first felony charge. Mr. P describes himself as a “charmer.”
After high school, Mr. P worked full-time in construction, where he claims he suffered a traumatic blow to the head. Despite this injury, he continued to work and socialize and never sought treatment at a mental health clinic.
The authors’ observations
Although defendants may legitimately suffer from TBI and resultant complications, many individuals capitalize on a history of minor head injury to support their NGRI defense.1 Forensic psychiatrists must retain a healthy degree of clinical suspicion for malingering in defendants who claim NGRI as a result of complications from brain injury, especially when the injury and complications are not documented and simply patient-reported.
TBI is a CNS injury that occurs when an outside force traumatically injures the brain and can cause a variety of physical, cognitive, emotional, and behavioral effects ( Table 1 ).2 Cognitive deficits include:
- impaired attention
- disrupted insight
- poor judgment
- thought disorders.
Reduced processing speed, distractibility, and deficits in executive functions such as abstract reasoning, planning, problem solving, and multitasking have been documented. Memory loss—the most common cognitive impairment among head-injured people—occurs in 20% to 79% of people with closed head trauma, depending on injury severity.3 People who have suffered TBI may have difficulty understanding or producing spoken or written language, or with more subtle aspects of communication, such as body language.
TBI may cause emotional or behavioral problems and personality changes. Mood and affect changes are common. TBI predisposes patients to obsessive-compulsive disorder, substance abuse, dysthymia, clinical depression, bipolar disorder, phobias, panic disorder, and schizophrenia.4 Frontal lobe injuries have been correlated with disinhibition and inappropriate or childish behavior, and temporal lobe injuries with irritability and aggression.5
Table 1
TBI symptoms correspond to area of injury
| Area of injury | Motor/sensory | Psychiatric/behavioral | Cognitive |
|---|---|---|---|
| Brain stem | Decreased vital capacity in breathing, dysphagia | Sleep difficulties | Inability to categorize objects, difficulty with organization |
| Frontal lobe | Aphasia, praxis | Disinhibition, personality changes | Impaired executive function |
| Cerebellum | Nystagmus, tremor | Labile emotions | Inability to process information |
| Parietal lobe | Apraxia | Personality changes | Neglect |
| Occipital lobe | Visual field cuts; diminished proprioception | Visual hallucinations | Color agnosia; inability to recognize words; difficulty reading, writing, and recognizing drawn objects |
| Temporal lobe | Seizure | Libido changes, humorless verbosity, aggression, olfactory perceptual changes | Prosopagnosia, aphasia, agnosia, memory loss, inattention |
| TBI: traumatic brain injury | |||
| Source: Reference 2 | |||
TBI and the insanity defense
The M’Naghten Rule of 1843 requires that for an insanity defense, the defendant must have a mental disease or defect that causes him not to know the nature and quality or the wrongfulness of his act.6 TBI is an abnormal condition of the mind leading to a mental disease that can substantially affect control of emotions and behaviors.
Nevertheless, TBI-induced criminality remains controversial.7 Theories on the etiology of impulse dyscontrol resulting from TBI have suggested structural damage to the brain and altered neurotransmitters. In TBI, the amygdala—which is located within the anterior temporal lobe and adjoins emotions to thoughts—often is injured. Damage to this structure leads to poor impulse control and violent behavior. Damage to specific neurotransmitter systems that causes elevated norepinephrine and dopamine levels and reduced serotonin levels have also been implicated as a cause of impulse dyscontrol in TBI patients.8
In theory, TBI patients potentially could have enough cognitive impairment to have a substantial lack of appreciation of the criminality or wrongfulness of an act. TBI-related impulsivity and cognitive impairment can lead to recklessness and negligence.9 The U.S. Supreme Court has acknowledged that CNS dysfunction affects judgment, reality testing, and self-control.10
EVALUATION: Vague answers
To determine whether Mr. P’s defense is plausible, the forensic psychiatrist must pay attention to the details of the patient’s presentation and history. During the interview, Mr. P quickly shifts from cooperative to obstinate and restricted. He ruminates on the head injury causing him to suffer auditory hallucinations, which he claims he always obeys. Mr. P refuses to provide details of the hallucinations, however, and answers most questions about the head injury or his defense with vague answers, including “I don’t know.”
Because of Mr. P’s reluctance to share information, his lack of psychiatric symptoms other than those he self-reports, and the presence of potential secondary gain from an NGRI defense, the psychiatrist begins to suspect malingering.
The authors’ observations
Malingering is a condition—not a diagnosis—characterized by intentional production of false or grossly exaggerated physical or psychological symptoms motivated by external incentives.11 The presence of external incentives distinguishes malingering from psychiatric illnesses such as factitious and somatoform disorders, in which there is no apparent external incentive. Malingering of psychiatric symptoms occurs in up to 20% of forensic patients, 5% of military recruits, and 1% of mental health patients.5 Stimuli for malingering range from seeking food and shelter to avoiding criminal responsibility ( Table 2 ). Malingering is more common in individuals being evaluated for criminal responsibility than for competence to stand trial. The 3 categories of malingering are:
Table 2
Common external incentives for malingering
| Evading criminal responsibility |
| Disability claims/financial gain |
| Avoiding military duty |
| Evading work |
| Obtaining drugs |
| Seeking food/shelter |
- pure malingering—feigning a nonexistent disorder
- partial malingering—consciously exaggerating real symptoms
- false imputation—ascribing real symptoms to a cause the individual knows is unrelated to the symptoms.12
Determining if a defendant with a history of TBI is malingering requires a multi-step approach that encompasses the clinical interview, a thorough review of collateral data, and focused psychological testing. In interviews, psychiatrists detect approximately 50% of lies, which is no better than would be discovered by chance.13 If you suspect a patient is malingering, combine a structured clinical interview with collateral sources such as old hospital records, treatment history, insurance records, police reports, and interviews with close family and friends.
TBI patients’ poor cognition, memory deficits, and inattention will prove challenging. Malingering patients who attempt to capitalize on a pre-existing TBI to evade responsibility for a current criminal charge may grossly exaggerate or even fake intellectual deficits. Be patient with such defendants and remain aware that such people will give vague or hedging answers to straightforward questions, often accompanied by “I don’t know.” Prolonging the interview may be helpful because it may fatigue a defendant who is faking.12
Some patients who malinger after sustaining a TBI will attempt to feign psychotic symptoms. Table 3 14 illustrates criteria for assessing a patient suspected of malingering psychosis and Table 4 14 highlights atypical psychotic symptoms that suggest feigning illness. Malingering of psychosis can be both assessed in the interview and through testing.
Table 3
Criteria for malingered psychosis
| A. Understandable motive to malinger |
| B. Marked variability of presentation as evidenced by ≥1 of the following: 1. Marked discrepancies in interview and non-interview behaviors 2. Gross inconsistencies in reported psychotic symptoms 3. Blatant contradictions between reported prior episodes and documented psychiatric history |
| C. Improbable psychiatric symptoms as evidenced by ≥1 of the following: 1. Reporting elaborate psychotic symptoms that lack common paranoid, grandiose, or religious themes 2. Sudden emergence of purported symptoms to explain antisocial behavior 3. Atypical hallucinations and delusions |
| D. Confirmation of malingering by either: 1. Admission of malingering following confrontation, or 2. Presence of strong corroborative information, such as psychometric data or history of malingering |
| Source: Reference 14 |
Table 4
Atypical psychotic symptoms that suggest malingering
| Hallucinations |
| Continuous rather than intermittent |
| Vague or inaudible auditory hallucinations |
| Stilted language reported in hallucinations |
| Inability to state strategies to diminish voices |
| Self-report that all command hallucinations were obeyed |
| Visual hallucinations in black and white |
| Delusions |
| Abrupt onset or termination |
| Eagerness to call attention to delusions |
| Conduct markedly inconsistent with delusions |
| Bizarre content without disordered thinking |
| Source: Reference 14 |
Psychological testing
Several standardized diagnostic instruments can be used to help determine whether a patient is feigning or exaggerating psychotic symptoms or cognitive impairments ( Table 5 ). Testing for a patient such as Mr. P—who attributes any criminal wrongdoing to psychosis and also cites limited cognition as a reason for trouble in the interview—would include personality tests, tests to assess exaggerations of psychosis, and cognitive tests.
In the forensic setting, the preferred personality test is the MMPI-2.15 It consists of 567 items, with 10 clinical scales and several validity scales. The F scale, “faking good” or “faking bad,” detects people who are answering questions with the goal of appearing better or worse than they actually are. The Personal Assessment Inventory (PAI)16 is a 344-item test with a 4-point response format. The 22 scales cover a range of important axis I and II psychopathology.
SIRS17 is the gold standard in detecting malingered psychiatric illness; it includes questions about rare symptoms and uncommon symptom pairing. M-FAST18 was developed to provide a brief, reliable screen for malingered mental illness. It has shown good validity and high correlation with the SIRS and MMPI-2.
Tests of exaggerated cognitive impairment are extremely important in evaluating patients who claim to suffer from complications following TBI. TOMM19 —a 50-item recognition test designed to discriminate between true memory-impaired patients and malingerers—is the most studied and valid of such tests. Defendants’ scores that meet the recommended criteria for detecting malingering—≥5 errors on the retention trial—were found to also report a history of head injury.1
Although not as well validated, the Portland Digit Recognition Test (PDRT)20 is an alternative to the TOMM. This test is a forced-choice measure of recognition designed for assessing the possibility of malingering in individuals claiming mental illness because of head injury. The Victoria Symptoms Validity Test (VSVT)21 is used in outpatient and inpatient settings and also uses a forced-choice model to assess possible exaggeration or feigning of cognitive impairments. Finally, the Word Memory Test (WMT)22 is a neuropsychological assessment that evaluates the effort participants put forth.
Table 5
Standardized diagnostic instruments for detecting malingering
| Test | Clinical use |
|---|---|
| Personality | |
| MMPI-2 | F scale detects lying. Several validity scales |
| PAI | Covers a range of axis I and II psychopathology |
| Psychotic symptoms | |
| SIRS | Gold standard in detecting exaggerated psychotic symptoms |
| M-FAST | Screening tool to assess exaggerated psychosis; brief and reliable |
| Cognitive impairment | |
| TOMM | Highest validity of all tools to test memory malingering |
| PDRT | Assesses the possibility of malingering. Not widely studied and validity/reliability are suspect |
| VSVT | Useful for inpatient and outpatient settings |
| WMT | Evaluates effort put forth by the participant |
| M-FAST: Miller Forensic Assessment of Symptoms Test; MMPI-2: Minnesota Multiphasic Personality Inventory; PAI: Personal Assessment Inventory; PDRT: Portland Digit Recognition Test; SIRS: Structured Interview of Reported Symptoms; TOMM: Test of Memory Malingering; VSVT: Victoria Symptoms Validity Test; WMT: Word Memory Test | |
OUTCOME: Unsupported claims
Mr. P’s hospital records reveal a very minor head trauma that resulted in no structural brain abnormalities on imaging tests. Collateral interviews with Mr. P’s family and close friends fail to support the defendant’s claim that after the accident he began to experience behavioral changes and periods of psychosis. Mr. P’s SIRS and TOMM scores indicate malingering, and the psychiatrist did not support his NGRI defense.
Related resource
- Williamson DJ. Neurocognitive impairment: feigned, exaggerated, or real? Current Psychiatry. 2007;6(8):19-37.
Disclosure
Dr. Nasrallah receives research grant/research support from Forest Pharmaceuticals, GlaxoSmithKline, Janssen, Otsuka America Pharmaceuticals, Pfizer Inc., Roche, sanofi-aventis, and Shire, is on the advisory board of Abbott Laboratories, AstraZeneca, Janssen, Novartis, Pfizer Inc., and Merck, and is on the speakers’ bureau for Abbott Laboratories, AstraZeneca, Janssen, Novartis, Pfizer Inc., and Merck.
Dr. Farrell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Self-reported TBI
When charged with raping a 19-year-old woman, Mr. P, age 32, pleads not guilty by reason of insanity (NGRI). He has a self-reported history of traumatic brain injury (TBI) and claims that since suffering a blow to the head 8 years before the rape, he has experienced episodes of personality changes, psychosis, and violent behavior. Mr. P is adamant that any wrongdoing on his part was beyond his control, and he argues that consequences of the brain injury, such as hallucinations and aggressive behavior, had recently emerged. The court asks that a forensic psychiatrist evaluate Mr. P.
An only child, Mr. P was raised by his mother in an inner city area. His father was dependent on alcohol and cocaine and abandoned the family shortly after Mr. P’s birth. Mr. P abuses alcohol, as evidenced by previous driving under the influence charges, but denies illicit drug use. He graduated from high school with average grades and denies a history of disciplinary action at school or home. Although Mr. P was charged with misdemeanors in his late teens, the sexual assault is his first felony charge. Mr. P describes himself as a “charmer.”
After high school, Mr. P worked full-time in construction, where he claims he suffered a traumatic blow to the head. Despite this injury, he continued to work and socialize and never sought treatment at a mental health clinic.
The authors’ observations
Although defendants may legitimately suffer from TBI and resultant complications, many individuals capitalize on a history of minor head injury to support their NGRI defense.1 Forensic psychiatrists must retain a healthy degree of clinical suspicion for malingering in defendants who claim NGRI as a result of complications from brain injury, especially when the injury and complications are not documented and simply patient-reported.
TBI is a CNS injury that occurs when an outside force traumatically injures the brain and can cause a variety of physical, cognitive, emotional, and behavioral effects ( Table 1 ).2 Cognitive deficits include:
- impaired attention
- disrupted insight
- poor judgment
- thought disorders.
Reduced processing speed, distractibility, and deficits in executive functions such as abstract reasoning, planning, problem solving, and multitasking have been documented. Memory loss—the most common cognitive impairment among head-injured people—occurs in 20% to 79% of people with closed head trauma, depending on injury severity.3 People who have suffered TBI may have difficulty understanding or producing spoken or written language, or with more subtle aspects of communication, such as body language.
TBI may cause emotional or behavioral problems and personality changes. Mood and affect changes are common. TBI predisposes patients to obsessive-compulsive disorder, substance abuse, dysthymia, clinical depression, bipolar disorder, phobias, panic disorder, and schizophrenia.4 Frontal lobe injuries have been correlated with disinhibition and inappropriate or childish behavior, and temporal lobe injuries with irritability and aggression.5
Table 1
TBI symptoms correspond to area of injury
| Area of injury | Motor/sensory | Psychiatric/behavioral | Cognitive |
|---|---|---|---|
| Brain stem | Decreased vital capacity in breathing, dysphagia | Sleep difficulties | Inability to categorize objects, difficulty with organization |
| Frontal lobe | Aphasia, praxis | Disinhibition, personality changes | Impaired executive function |
| Cerebellum | Nystagmus, tremor | Labile emotions | Inability to process information |
| Parietal lobe | Apraxia | Personality changes | Neglect |
| Occipital lobe | Visual field cuts; diminished proprioception | Visual hallucinations | Color agnosia; inability to recognize words; difficulty reading, writing, and recognizing drawn objects |
| Temporal lobe | Seizure | Libido changes, humorless verbosity, aggression, olfactory perceptual changes | Prosopagnosia, aphasia, agnosia, memory loss, inattention |
| TBI: traumatic brain injury | |||
| Source: Reference 2 | |||
TBI and the insanity defense
The M’Naghten Rule of 1843 requires that for an insanity defense, the defendant must have a mental disease or defect that causes him not to know the nature and quality or the wrongfulness of his act.6 TBI is an abnormal condition of the mind leading to a mental disease that can substantially affect control of emotions and behaviors.
Nevertheless, TBI-induced criminality remains controversial.7 Theories on the etiology of impulse dyscontrol resulting from TBI have suggested structural damage to the brain and altered neurotransmitters. In TBI, the amygdala—which is located within the anterior temporal lobe and adjoins emotions to thoughts—often is injured. Damage to this structure leads to poor impulse control and violent behavior. Damage to specific neurotransmitter systems that causes elevated norepinephrine and dopamine levels and reduced serotonin levels have also been implicated as a cause of impulse dyscontrol in TBI patients.8
In theory, TBI patients potentially could have enough cognitive impairment to have a substantial lack of appreciation of the criminality or wrongfulness of an act. TBI-related impulsivity and cognitive impairment can lead to recklessness and negligence.9 The U.S. Supreme Court has acknowledged that CNS dysfunction affects judgment, reality testing, and self-control.10
EVALUATION: Vague answers
To determine whether Mr. P’s defense is plausible, the forensic psychiatrist must pay attention to the details of the patient’s presentation and history. During the interview, Mr. P quickly shifts from cooperative to obstinate and restricted. He ruminates on the head injury causing him to suffer auditory hallucinations, which he claims he always obeys. Mr. P refuses to provide details of the hallucinations, however, and answers most questions about the head injury or his defense with vague answers, including “I don’t know.”
Because of Mr. P’s reluctance to share information, his lack of psychiatric symptoms other than those he self-reports, and the presence of potential secondary gain from an NGRI defense, the psychiatrist begins to suspect malingering.
The authors’ observations
Malingering is a condition—not a diagnosis—characterized by intentional production of false or grossly exaggerated physical or psychological symptoms motivated by external incentives.11 The presence of external incentives distinguishes malingering from psychiatric illnesses such as factitious and somatoform disorders, in which there is no apparent external incentive. Malingering of psychiatric symptoms occurs in up to 20% of forensic patients, 5% of military recruits, and 1% of mental health patients.5 Stimuli for malingering range from seeking food and shelter to avoiding criminal responsibility ( Table 2 ). Malingering is more common in individuals being evaluated for criminal responsibility than for competence to stand trial. The 3 categories of malingering are:
Table 2
Common external incentives for malingering
| Evading criminal responsibility |
| Disability claims/financial gain |
| Avoiding military duty |
| Evading work |
| Obtaining drugs |
| Seeking food/shelter |
- pure malingering—feigning a nonexistent disorder
- partial malingering—consciously exaggerating real symptoms
- false imputation—ascribing real symptoms to a cause the individual knows is unrelated to the symptoms.12
Determining if a defendant with a history of TBI is malingering requires a multi-step approach that encompasses the clinical interview, a thorough review of collateral data, and focused psychological testing. In interviews, psychiatrists detect approximately 50% of lies, which is no better than would be discovered by chance.13 If you suspect a patient is malingering, combine a structured clinical interview with collateral sources such as old hospital records, treatment history, insurance records, police reports, and interviews with close family and friends.
TBI patients’ poor cognition, memory deficits, and inattention will prove challenging. Malingering patients who attempt to capitalize on a pre-existing TBI to evade responsibility for a current criminal charge may grossly exaggerate or even fake intellectual deficits. Be patient with such defendants and remain aware that such people will give vague or hedging answers to straightforward questions, often accompanied by “I don’t know.” Prolonging the interview may be helpful because it may fatigue a defendant who is faking.12
Some patients who malinger after sustaining a TBI will attempt to feign psychotic symptoms. Table 3 14 illustrates criteria for assessing a patient suspected of malingering psychosis and Table 4 14 highlights atypical psychotic symptoms that suggest feigning illness. Malingering of psychosis can be both assessed in the interview and through testing.
Table 3
Criteria for malingered psychosis
| A. Understandable motive to malinger |
| B. Marked variability of presentation as evidenced by ≥1 of the following: 1. Marked discrepancies in interview and non-interview behaviors 2. Gross inconsistencies in reported psychotic symptoms 3. Blatant contradictions between reported prior episodes and documented psychiatric history |
| C. Improbable psychiatric symptoms as evidenced by ≥1 of the following: 1. Reporting elaborate psychotic symptoms that lack common paranoid, grandiose, or religious themes 2. Sudden emergence of purported symptoms to explain antisocial behavior 3. Atypical hallucinations and delusions |
| D. Confirmation of malingering by either: 1. Admission of malingering following confrontation, or 2. Presence of strong corroborative information, such as psychometric data or history of malingering |
| Source: Reference 14 |
Table 4
Atypical psychotic symptoms that suggest malingering
| Hallucinations |
| Continuous rather than intermittent |
| Vague or inaudible auditory hallucinations |
| Stilted language reported in hallucinations |
| Inability to state strategies to diminish voices |
| Self-report that all command hallucinations were obeyed |
| Visual hallucinations in black and white |
| Delusions |
| Abrupt onset or termination |
| Eagerness to call attention to delusions |
| Conduct markedly inconsistent with delusions |
| Bizarre content without disordered thinking |
| Source: Reference 14 |
Psychological testing
Several standardized diagnostic instruments can be used to help determine whether a patient is feigning or exaggerating psychotic symptoms or cognitive impairments ( Table 5 ). Testing for a patient such as Mr. P—who attributes any criminal wrongdoing to psychosis and also cites limited cognition as a reason for trouble in the interview—would include personality tests, tests to assess exaggerations of psychosis, and cognitive tests.
In the forensic setting, the preferred personality test is the MMPI-2.15 It consists of 567 items, with 10 clinical scales and several validity scales. The F scale, “faking good” or “faking bad,” detects people who are answering questions with the goal of appearing better or worse than they actually are. The Personal Assessment Inventory (PAI)16 is a 344-item test with a 4-point response format. The 22 scales cover a range of important axis I and II psychopathology.
SIRS17 is the gold standard in detecting malingered psychiatric illness; it includes questions about rare symptoms and uncommon symptom pairing. M-FAST18 was developed to provide a brief, reliable screen for malingered mental illness. It has shown good validity and high correlation with the SIRS and MMPI-2.
Tests of exaggerated cognitive impairment are extremely important in evaluating patients who claim to suffer from complications following TBI. TOMM19 —a 50-item recognition test designed to discriminate between true memory-impaired patients and malingerers—is the most studied and valid of such tests. Defendants’ scores that meet the recommended criteria for detecting malingering—≥5 errors on the retention trial—were found to also report a history of head injury.1
Although not as well validated, the Portland Digit Recognition Test (PDRT)20 is an alternative to the TOMM. This test is a forced-choice measure of recognition designed for assessing the possibility of malingering in individuals claiming mental illness because of head injury. The Victoria Symptoms Validity Test (VSVT)21 is used in outpatient and inpatient settings and also uses a forced-choice model to assess possible exaggeration or feigning of cognitive impairments. Finally, the Word Memory Test (WMT)22 is a neuropsychological assessment that evaluates the effort participants put forth.
Table 5
Standardized diagnostic instruments for detecting malingering
| Test | Clinical use |
|---|---|
| Personality | |
| MMPI-2 | F scale detects lying. Several validity scales |
| PAI | Covers a range of axis I and II psychopathology |
| Psychotic symptoms | |
| SIRS | Gold standard in detecting exaggerated psychotic symptoms |
| M-FAST | Screening tool to assess exaggerated psychosis; brief and reliable |
| Cognitive impairment | |
| TOMM | Highest validity of all tools to test memory malingering |
| PDRT | Assesses the possibility of malingering. Not widely studied and validity/reliability are suspect |
| VSVT | Useful for inpatient and outpatient settings |
| WMT | Evaluates effort put forth by the participant |
| M-FAST: Miller Forensic Assessment of Symptoms Test; MMPI-2: Minnesota Multiphasic Personality Inventory; PAI: Personal Assessment Inventory; PDRT: Portland Digit Recognition Test; SIRS: Structured Interview of Reported Symptoms; TOMM: Test of Memory Malingering; VSVT: Victoria Symptoms Validity Test; WMT: Word Memory Test | |
OUTCOME: Unsupported claims
Mr. P’s hospital records reveal a very minor head trauma that resulted in no structural brain abnormalities on imaging tests. Collateral interviews with Mr. P’s family and close friends fail to support the defendant’s claim that after the accident he began to experience behavioral changes and periods of psychosis. Mr. P’s SIRS and TOMM scores indicate malingering, and the psychiatrist did not support his NGRI defense.
Related resource
- Williamson DJ. Neurocognitive impairment: feigned, exaggerated, or real? Current Psychiatry. 2007;6(8):19-37.
Disclosure
Dr. Nasrallah receives research grant/research support from Forest Pharmaceuticals, GlaxoSmithKline, Janssen, Otsuka America Pharmaceuticals, Pfizer Inc., Roche, sanofi-aventis, and Shire, is on the advisory board of Abbott Laboratories, AstraZeneca, Janssen, Novartis, Pfizer Inc., and Merck, and is on the speakers’ bureau for Abbott Laboratories, AstraZeneca, Janssen, Novartis, Pfizer Inc., and Merck.
Dr. Farrell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Delain SL, Stafford KP, Yosef SB. Use of the TOMM in a criminal court forensic assessment setting. Assessment. 2003;10(4):370-381.
2. Rao V, Lyketsos C. Neuropsychiatric sequelae of traumatic brain injury Psychosomatics. 2000;41:95-103.
3. Hall RC, Hall RC, Chapman MJ. Definition, diagnosis, and forensic implications of postconcussional syndrome. Psychosomatics. 2005;46(3):195-202.
4. Arlinghaus KA, Shoaib AM, Price TRP. Neuropsychiatric assessment. In: Silver JM, McAllister TW, Yudofsky SC. Textbook of traumatic brain injury. Arlington, VA: American Psychiatric Publishing, Inc.; 2005:63-65.
5. West S, Noffsinger S. Is this patient not guilty by reason of insanity? Current Psychiatry. 2005;5(8):54-62.
6. Barzman D, Kennedy J, Fozdar M. Does traumatic brain injury cause violence? Current Psychiatry. 2002;1(4):49-55.
7. Silver JM, Yudofsky SC, Hales RE. Neuropsychiatry of traumatic brain injury. Washington, DC: American Psychiatric Press, Inc.; 1994.
8. Melton GB, Petrila J, Poythress NG, et al. Psychological evaluations for the courts. New York, NY: The Guilford Press; 1997.
9. Lewis DO, Pincus JH, Feldman M, et al. Psychiatric, neurological, and psychoeducational characteristics of 15 death row inmates in the United States. Am J Psychiatry. 1986;143:838-845.
10. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
11. Sadock VA. Kaplan and Sadock’s synopsis of psychiatry. Philadelphia, PA: Lippincott, Williams, and Wilkins; 2007:887.
12. Resnick PJ. Faking it: how to determine malingered psychosis. Current Psychiatry. 2005;4(11):12-25.
13. Samuel RZ, Mittenberg W. Determination of malingering in disability claims. Primary Psychiatry. 2005;12(12):60-68.
14. Resnick PJ. Malingered psychosis. In: Rogers R, ed. Clinical assessment of malingering. 2nd ed. New York, NY: The Guilford Press; 1997:47-67.
15. Hathaway SR, McKinley JC. The Minnesota Multiphasic Personality Inventory-2. Minneapolis, MN: University of Minnesota Press; 1989.
16. Rogers R, Sewell KW, Morey LC, et al. Detection of feigned mental disorder on the personality assessment inventory: a discriminate analysis. J Pers Assess. 1996;67:629-640.
17. Rogers R, Bagby RM, Dickens SE. Structured Interview of Reported Symptoms (SIRS). Lutz, FL: Psychological Assessment Resources; 1992.
18. Miller H. Miller Forensic Assessment of Symptoms Test (M-FAST). Professional Manual. Lutz, FL: Psychological Assessment Resources; 2001.
19. Tombaugh TN. The Test of Memory Malingering. Toronto, ON, Canada: Multi-Health Systems; 1996.
20. Binder LM. Malingering following minor head trauma. Clin Neuropsychol. 1990;4:25-36.
21. Slick D, Hopp G, Strauss E, et al. Victoria Symptom Validity Test professional manual. Lutz, FL: Psychological Assessment Resources; 1997.
22. Green P. Word Memory Test. Edmonton, Alberta, Canada: Green’s Publishing; 2003.
1. Delain SL, Stafford KP, Yosef SB. Use of the TOMM in a criminal court forensic assessment setting. Assessment. 2003;10(4):370-381.
2. Rao V, Lyketsos C. Neuropsychiatric sequelae of traumatic brain injury Psychosomatics. 2000;41:95-103.
3. Hall RC, Hall RC, Chapman MJ. Definition, diagnosis, and forensic implications of postconcussional syndrome. Psychosomatics. 2005;46(3):195-202.
4. Arlinghaus KA, Shoaib AM, Price TRP. Neuropsychiatric assessment. In: Silver JM, McAllister TW, Yudofsky SC. Textbook of traumatic brain injury. Arlington, VA: American Psychiatric Publishing, Inc.; 2005:63-65.
5. West S, Noffsinger S. Is this patient not guilty by reason of insanity? Current Psychiatry. 2005;5(8):54-62.
6. Barzman D, Kennedy J, Fozdar M. Does traumatic brain injury cause violence? Current Psychiatry. 2002;1(4):49-55.
7. Silver JM, Yudofsky SC, Hales RE. Neuropsychiatry of traumatic brain injury. Washington, DC: American Psychiatric Press, Inc.; 1994.
8. Melton GB, Petrila J, Poythress NG, et al. Psychological evaluations for the courts. New York, NY: The Guilford Press; 1997.
9. Lewis DO, Pincus JH, Feldman M, et al. Psychiatric, neurological, and psychoeducational characteristics of 15 death row inmates in the United States. Am J Psychiatry. 1986;143:838-845.
10. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
11. Sadock VA. Kaplan and Sadock’s synopsis of psychiatry. Philadelphia, PA: Lippincott, Williams, and Wilkins; 2007:887.
12. Resnick PJ. Faking it: how to determine malingered psychosis. Current Psychiatry. 2005;4(11):12-25.
13. Samuel RZ, Mittenberg W. Determination of malingering in disability claims. Primary Psychiatry. 2005;12(12):60-68.
14. Resnick PJ. Malingered psychosis. In: Rogers R, ed. Clinical assessment of malingering. 2nd ed. New York, NY: The Guilford Press; 1997:47-67.
15. Hathaway SR, McKinley JC. The Minnesota Multiphasic Personality Inventory-2. Minneapolis, MN: University of Minnesota Press; 1989.
16. Rogers R, Sewell KW, Morey LC, et al. Detection of feigned mental disorder on the personality assessment inventory: a discriminate analysis. J Pers Assess. 1996;67:629-640.
17. Rogers R, Bagby RM, Dickens SE. Structured Interview of Reported Symptoms (SIRS). Lutz, FL: Psychological Assessment Resources; 1992.
18. Miller H. Miller Forensic Assessment of Symptoms Test (M-FAST). Professional Manual. Lutz, FL: Psychological Assessment Resources; 2001.
19. Tombaugh TN. The Test of Memory Malingering. Toronto, ON, Canada: Multi-Health Systems; 1996.
20. Binder LM. Malingering following minor head trauma. Clin Neuropsychol. 1990;4:25-36.
21. Slick D, Hopp G, Strauss E, et al. Victoria Symptom Validity Test professional manual. Lutz, FL: Psychological Assessment Resources; 1997.
22. Green P. Word Memory Test. Edmonton, Alberta, Canada: Green’s Publishing; 2003.
Children with tic disorders: How to match treatment with symptoms
Sammy, age 7, is referred to you by his pediatrician because of a 4-week history of frequent eye blinking. His parents say he blinks a lot when bored but very little when playing baseball. They recall that he also has intermittently sniffed and nodded his head over the last 12 months. Neither Sammy nor his friends seem to be bothered by the blinking. Except for the tics, Sammy’s physical and mental status exams are normal.
Since preschool, Sammy’s teachers have complained that his backpack and desk are always a mess. Sammy is well-meaning but forgetful in his chores at home. A paternal uncle has head-turning movements, counts his steps, and becomes distressed if books on his shelf are not in alphabetical order.
Tics, such as strong eye blinks or repetitive shoulder shrugs, can distress a child or his/her parents, but the conditions associated with tic disorders often are more problematic than the tic disorder itself. High rates of comorbid conditions are recognized in persons with Tourette syndrome, including:
- obsessive-compulsive disorder (OCD) in >80%1
- attention-deficit/hyperactivity disorder (ADHD) in ≤70%2
- anxiety disorders in 30%3
- rage, aggression, learning disabilities, and autism less commonly.
The strategy we recommend for managing tic disorders includes assessing tic severity, educating the family about the illness, determining whether a comorbid condition is present, and managing these conditions appropriately. Above all, we emphasize a risk-benefit analysis guided by the Hippocratic principle of “do no harm.”
Characteristics of tic disorders
You diagnose Sammy with Tourette syndrome because he meets DSM-IV-TR criteria of at least 2 motor tics and 1 vocal tic that have persisted for 1 year without more than a 3-month hiatus, with tic onset before age 18. Because tics may resemble other movement disorders, you rule out stereotypies, dystonia, chorea, ballism, and myoclonus (Table 1). You explain to his parents that Sammy’s condition is a heritable, neurobehavioral disorder that typically begins in childhood and is associated in families with OCD, ADHD, and autism spectrum disorders.
His parents ask about the difference between tics and other movements. You explain that eye-blinking tics—like other motor tics—appear as sudden, repetitive, stereotyped, nonrhythmic movements that involve discrete muscle groups. (View a video of a patient with tics.) Simple motor tics are focal movements involving 1 group of muscles, whereas complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements (Table 2).
Table 1
Features of 5 movement disorders that may resemble tics
| Tics | Stereotypies | Dystonia | Chorea | Ballism | Myoclonus |
|---|---|---|---|---|---|
| Sudden, repetitive, stereotyped, nonrhythmic movements or sounds | Patterned, nonpurposeful movement | Cocontraction of agonist and antagonist muscles, causing an abnormal twisting posture | Continuous, flowing, nonrhythmic, nonpurposeful movement | Forceful, flinging, large amplitude choreic movement | Sudden, quick, shock-like movement |
| Usually start after age 3 | Usually start before age 3 and resolve by adolescence | More common in adults | — | — | — |
| Decrease when focused; increase when stressed, anxious, fatigued, or bored | Occur when the child is excited | Worsens during motor tasks | Worsens during motor tasks | Worsens during motor tasks | — |
| Comorbid conditions include OCD and ADHD | Common in children with mental retardation or autism | — | Can occur after streptococcal infection | Can occur after streptococcal infection | — |
| Preceded by a premonitory urge or sensation | Possibly preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge |
| Temporarily suppressible | Suppressible | Not suppressible | Partially suppressible; can incorporate into semi-purposeful movements | Partially suppressible | Not suppressible |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder | |||||
Table 2
Characteristics of simple and complex motor and vocal tics*
| Simple tics | Complex tics |
|---|---|
| Eye blinking or eye rolling Nose, mouth, tongue, or facial grimaces (nose twitch, nasal flaring, chewing lip, teeth grinding, sticking out tongue, mouth stretching, lip licking) Head jerks or movements (neck stretching, touching chin to shoulder) Shoulder jerks/movements (shoulder shrugging, jerking a shoulder) Arm or hand movements (flexing or extending arms or fingers) Coughing Throat clearing, grunting Sniffing, snorting, shouting Humming | Jumping Spinning Touching objects or people Throwing objects Repeating others’ action (echopraxia) Obscene gestures (copropraxia) Repeating one’s own words (palilalia) Repeating what someone else said (echolalia) Obscene, inappropriate words (coprolalia) |
| *Simple tics are focal movements involving 1 group of muscles; complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements | |
Older children frequently describe a premonitory urge prior to the tic. Patients typically can suppress tics for a transient period of time, although during tic suppression they usually feel restless and anticipate performing their tic. The ultimate performance of the tic brings relief. Tic suppression also occurs during focused activity. Emotional stress, fatigue, illness, or boredom can exacerbate tics.
To begin monitoring Sammy’s clinical course, you administer 3 assessment tools described inTable 3. You explain to Sammy’s parents that these tests will be repeated yearly or when tics worsen. However, you tell his parents that these scores alone will not determine present or future clinical decisions, including treatments. You also recommend that they connect with support groups on the Tourette Syndrome Association (TSA) Web site.
CASE CONTINUED: Changes over time
Sammy’s parents appreciate your explanation and say they will share information from the TSA Web site with Sammy’s principal, teachers, and classmates. The family agrees to return in 6 months or sooner if the tics worsen.
By age 8, Sammy develops multiple tics: facial grimacing, looking upwards, punching movements, whistling, and throat clearing. He is slightly bothered by these tics, and his friends have asked him about them. He tells them he has Tourette syndrome, and that usually ends the questioning. He returns for a follow-up visit because his parents notice a dramatic increase in his tics after Sammy’s father loses his job.
Treatment options
When deciding to treat a child’s tics, the first step is to determine whether to pursue a nonpharmacologic or pharmacologic approach (Algorithm). To tailor an approach most suited for an individual child, discuss with the family their feelings about therapy and medications. This information—along with tic severity—will help determine a treatment plan.
Behavior therapy and medication are management strategies; neither can cure a tic disorder. The most conservative approach to tic treatment is to:
- provide the child and family with basic guidelines for managing tics
- help alleviate environmental stress and other potential triggers.
Algorithm: Recommended treatment of tics in children and adolescents
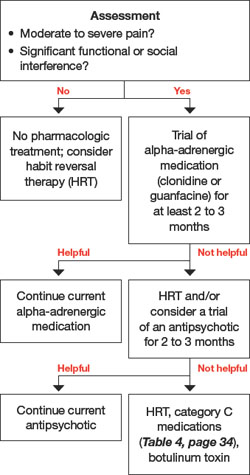
CASE CONTINUED: A first intervention
You discuss treatment options with Sammy’s family, and they view medication as a last resort. Sammy does not seem to be bothered by his tics, and his parents do not wish to start him on daily medications. Given this situation, habit reversal therapy (HRT) is appropriate for Sammy because he is old enough to participate in HRT to reduce his tics.
HRT is an effective nonpharmacologic approach to help children with tics.4 Its 3 components are:
- awareness training
- competing response training
- social support.5
This simplified version of the original HRT can be completed in eight 1-hour sessions. Good candidates are patients who are cognitively mature enough to understand the therapy’s goals and compliant with frequent clinic visits. They also must practice the strategies at home.
It should not be difficult for psychiatrists to learn HRT—or refer to therapists who are willing to learn it—with the available instructional manual.
CASE CONTINUED: Practicing alternatives
You ask Sammy to imitate his tics. After helping him become more aware of his tics, you encourage him to develop a more socially appropriate movement to engage in whenever he feels the urge to punch. Sammy chooses to clench his fist in his pocket. He also learns to breathe in whenever he has an urge to whistle. you advise Sammy’s parents to reward his efforts to suppress the tics. He practices the strategies daily.
At age 12, Sammy returns to your office. He has begun to have frequent neck-jerking tics, which cause neck pain and daily headaches. He also is slapping his thigh and having frequent vocal tics characterized by loud shrieking. The vocal tics are disruptive in class, even though Sammy sits toward the back of the room. Sammy’s classmates tease him, and he is very frustrated.
Medication approach
The decision to start a medication for tics is complex. Scores from the YGTSS, PUTS, and GTS-QOL scales (Table 3) provide only a partial clinical picture. This decision should be reached after a detailed discussion with the family about benefits and risks of medications and ensuring that everyone’s expectations are reasonable.
A variety of medications are available to treat patients with tics (Table 4). No medication can completely eliminate tics, however, and many have substantial side effects. Before initiating medical treatment, consider 3 questions:
- Is moderate or severe pain involved?
- Is there significant functional interference?
- Is there significant social disruption despite efforts to optimize the social environment for the child?
Sammy’s frequent neck-jerking tics now cause chronic daily headaches, and his shrieking vocal tics are interfering with classroom activities, so we recommended a 3-month trial of guanfacine following the dosing schedule in Table 4.
Table 3
3 scales for assessing tic severity and impact on functioning
| Instrument | Purpose | Description | Design | Administration frequency |
|---|---|---|---|---|
| Yale Global Tic Severity Scale (YGTSS) | Assess tic severity | Review of motor and vocal tics. Rate number, frequency, intensity, complexity, and interference on a 5-point scale | Clinician-rated | Annual and as needed for increased tics |
| Premonitory Urge for Tics Scale (PUTS) | Detect the presence of unpleasant sensations that precedes tics | 10 questions | Self-report | Annual and as needed for increased tics |
| Gilles de la Tourette Syndrome Quality of Life Scale (GTS-QOL) | Measure quality of life | 27 questions, 4 subscales: psychological, physical, obsessional, and cognitive | Self-report | Annual and as needed for increased tics |
Table 4
Medications with evidence of tic-suppressing effects*
| Category A evidence | ||
|---|---|---|
| Medication | Starting dose | Target dose |
| Haloperidol | 0.25 to 0.5 mg/d | 1 to 4 mg/d |
| Pimozide | 0.5 to 1 mg/d | 2 to 8 mg/d |
| Risperidone | 0.25 to 0.5 mg/d | 1 to 3 mg/d |
| Category B evidence | ||
| Medication | Starting dose | Target dose |
| Fluphenazine | 0.5 to 1 mg/d | 1.5 to 10 mg/d |
| Ziprasidone | 5 to 10 mg/d | 10 to 80 mg/d |
| Clonidine | 0.025 to 0.05 mg/d | 0.1 to 0.3 mg/d |
| Guanfacine | 0.5 to 1 mg/d | 1 to 3 mg/d |
| Botulinum toxin | 30 to 300 units | |
| Category C evidence | ||
| Medication | Starting dose | Target dose |
| Olanzapine | 2.5 to 5 mg/d | 2.5 to 12.5 mg/d |
| Tetrabenazine | 25 mg/d | 37.5 to 150 mg/d |
| Baclofen | 10 mg/d | 40 to 60 mg/d |
| Nicotine patch | 7 mg/d | 7 to 21 mg/d |
| Mecamylamine | 2.5 mg/d | 2.5 to 7.5 mg/d |
| Flutamide | 250 mg/d | 750 mg/d |
| *Category A: supported by ≥2 placebo-controlled trials; category B: supported by 1 placebo-controlled trial; category C: supported by open-label study | ||
| Source: Reference 6 | ||
The first-line pharmacologic agent for tic suppression generally is an alpha-adrenergic medication, unless the tics are severe.6
Clonidine and guanfacine usually are started at low doses and increased gradually. Although not as effective as neuroleptics, alpha-adrenergics have a lower potential for side effects and are easier to use because no laboratory tests need to be monitored. Adverse effects associated with alpha-adrenergic medications include sedation, dry mouth, dizziness, headache, and rebound hypertension if discontinued abruptly.
If tics are causing pain, some clinicians prefer conservative measures such as heat or ice, massage, analgesics, relaxation therapy, and reassurance.
Second-line agents include typical and atypical antipsychotics. Haloperidol and pimozide have shown efficacy in reducing tics in placebo- controlled studies,7,8 as have risperidone (in 4 randomized controlled trials [RCTs]) and ziprasidone (in 1 RCT).9,10 The emergence of serious side effects is a risk for both typical and atypical antipsychotics (Table 5).
Table 5
Potential adverse effects of antipsychotic treatment in children*
| Adverse effect | Examples |
|---|---|
| Sedation | — |
| Acute dystonic reactions | Oculogyric crisis, torticollis |
| Appetite changes | Weight gain |
| Endocrine abnormalities | Amenorrhea, diabetes, galactorrhea, gynecomastia, hyperprolactinemia |
| Cognitive effects | Impaired concentration |
| Akathisia | Difficulty sitting still |
| ECG changes | Prolonged QT interval |
| Parkinsonism | Tremor, bradykinesia, rigidity, postural instability |
| Tardive syndrome | Orofacial dyskinesia, chorea, dystonia, myoclonus, tics |
| Neuroleptic malignant syndrome | Potentially fatal; consists of muscular rigidity, fever, autonomic dysfunction, labile blood pressure, sweating, urinary incontinence, fluctuating level of consciousness, leukocytosis, elevated serum creatine kinase |
| *Potential adverse effects are listed from most to least likely to occur | |
As part of your informed consent discussion, weigh the risk of side effects against the benefits of treatment. Point out to patients and their families that they can expect to see a decrease in tic frequency, but symptoms will not necessarily disappear with any medication. We tell our patients that with antipsychotics the best we can hope for is to reduce tic frequency by approximately one-half.6
When treating tics, start with 1 medication. However, if the tics are severe enough to require more than 1 medication, check for drug interactions.
Third-line agents. Agents that have not been tested in placebo-controlled trials can be considered third line; these are listed as category C (supported by open-label studies) in Table 4. Botulinum toxin injection has been found to be effective for motor and vocal tics.11,12 Botulinum toxin and implantation of deep brain stimulators13 are invasive options and generally are reserved for severe, treatment-resistant tics.
CASE CONTINUED: Managing antipsychotics
After trying guanfacine for 12 weeks, Sammy notices no tic reduction. His parents consent to a low dose of risperidone. you review with them the American Psychiatric Association (APA)/American Diabetes Association (ADA) guidelines14 for managing metabolic problems in patients treated with atypical antipsychotics.
As instructed in the APA/ADA guidelines, obtain baseline measurements and monitor for metabolic effects of antipsychotic therapy over time (Table 6). Sammy starts risperidone at 0.5 mg once daily. After 2 weeks, he notices a decrease in his tics. At the 3-month visit after starting risperidone, he is happy with his risperidone dose and does not want to increase it. He has gained 3 pounds, and you instruct him to eat a well-balanced diet and exercise routinely. At the 6-month visit, his tics are minimal and his weight has stabilized.
Table 6
Children receiving antipsychotics: monitoring recommendations
| Clinical information | Frequency |
|---|---|
| Family history | Initial visit |
| Weight | Baseline, monthly |
| Height | Baseline, monthly |
| BMI | Baseline, monthly |
| Waist circumference | Baseline, annually |
| Blood pressure | Baseline, 3 months after treatment starts, and annually thereafter |
| Fasting lipid profile | Baseline, every 3 months initially, then every 6 months thereafter |
| Fasting serum glucose | Baseline, every 3 months, then every 6 months thereafter |
| BMI: body mass index | |
| Source: References 14,16 | |
You recommend that Sammy remain on risperidone for another 3 months of stability and then begin to taper this medication. You review the risks and benefits of long-term treatment with risperidone, pointing out that it may lead to abnormal movements upon withdrawal, and explain that you typically do not treat children with antipsychotics for more than one year continuously.
CASE CONTINUED: Comorbid symptoms
Since starting 7th grade, Sammy has worried excessively about making mistakes. He spends 6 hours each night on homework, which he often does not turn in because of anxiety about not getting answers perfectly right. Classmates notice that Sammy taps the door 3 times when he comes into the classroom and that he steps over the black tiles in the hallway.
Consider the presence and impact of comorbid OCD or ADHD, which can impair children’s quality of life more than tics themselves.15 Assessment scales can help you make a diagnosis and monitor treatment.
If you suspect OCD, the clinician-rated Children’s Yale Brown Obsessive Compulsive Scale is the gold standard for describing the phenomenology and measuring symptom severity. Additional scales to measure symptoms’ impact on family life include the Leyton Obsessional Inventory—child version, Family Accommodation Scale for OCD, and Child OCD Impact Scale.
ADHD scales include the Conners Parent Rating Scale—Revised, Conners Teacher Rating Scale—Revised, Swanson, Nolan, and Pelham, or the Vanderbilt ADHD Diagnostic Parent and Teacher Rating Scales. Because ADHD symptoms must be present in more than 1 environment to meet diagnostic criteria, ask parents and teachers to complete the Conners or Vanderbilt scales.
In children who present with a tic disorder plus a comorbid condition, prioritize treatment by determining which symptoms interfere with the child’s ability to function at school, at home, and in the social arena. Children who require treatment for >1 disorder often are referred initially for cognitive-behavioral therapy for OCD symptoms while receiving pharmacologic treatment for ADHD and/or Tourette syndrome. When necessary, it is usually safe to combine antipsychotics, stimulants, and selective serotonin reuptake inhibitors, although medication interactions should be reviewed in each specific case.
Related resources
- Woods DW. Managing Tourette syndrome: a behavioral intervention for children and adults. Therapist guide. New York, NY: Oxford University Press; 2008.
- Tourette Syndrome Association. www.tsa-usa.org.
- International OCD Foundation. www.ocfoundation.org.
Drug brand names
- Baclofen • Lioresal
- Botulinum toxin • Botox, Myobloc
- Clomipramine • Anafranil
- Clonidine • Catapres
- Guanfacine • Tenex
- Fluphenazine • Prolixin
- Flutamide • Eulexin
- Haloperidol • Haldol
- Mecamylamine • Inversine
- Nicotine patch • NicoDerm
- Olanzapine • Zyprexa
- Pimozide • Orap
- Risperidone • Risperdal
- Tetrabenazine • Xenazine
- Ziprasidone • Geodon
Disclosures
Dr. Harris has received research support from the Translational Research Initiative at Cincinnati Children’s Hospital Medical Center.
Dr. Wu reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Robertson M. Tourette syndrome, associated conditions and the complexities of treatment. Brain. 2000;123(3):425-462.
2. Freeman R. For the Tourette Syndrome International Database Consortium. Tic disorders and ADHD: answers from a worldwide clinical dataset on Tourette syndrome. Eur Child Adolesc Psychiatry. 2007;16(suppl 1):15-23.
3. Stefl M. Mental health needs associated with Tourette syndrome. Am J Public Health. 1984;74:1310-1313.
4. Deckersbach T, Rauch S, Buhlmann U, et al. Habit reversal versus supportive psychotherapy in Tourette’s disorder: a randomized controlled trial and predictors of treatment response. Behav Res Ther. 2006;44:1079-1090.
5. Woods DW, Miltenberger RG. Habit reversal: a review of applications and variations. J Behav Ther Exp Psychiatry. 1995;26:123-131.
6. Scahill L, Erenberg G, Berlin C, et al. Contemporary assessment and pharmacotherapy of Tourette syndrome. NeuroRx. 2006;3(2):192-206.
7. Shapiro E, Shapiro A, Fulop G, et al. Controlled study of haloperidol, pimozide, and placebo for the treatment of Gilles de la Tourette’s syndrome. 1989;46:722-730.
8. Sallee F, Nesbitt L, Jackson C, et al. Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette’s disorder. Am J Psychiatry. 1997;154:1057-1062.
9. Scahill L, Leckman J, Schultz R, et al. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology. 2003;60:1130-1135.
10. Sallee F, Kurlan R, Goetz C, et al. Ziprasidone treatment of children and adolescents with Tourette’s syndrome: a pilot study. J Am Acad Child Adolesc Psychiatry. 2000;39(3):292-299.
11. Marras C, Andrews D, Sime E, et al. Botulinum toxin for simple motor tics: a randomized, double-blind, controlled clinical trial. Neurology. 2001;56(5):605-610.
12. Porta M, Maggioni G, Ottaviani F, et al. Treatment of phonic tics in patients with Tourette’s syndrome using botulinum toxin type A. Neurol Sci. 2004;24(6):420-423.
13. Porta M, Sevello D, Sassi M, et al. Issues related to deep brain stimulation for treatment-refractory Tourette’s syndrome. Eur Neurol. 2009;62(5):264-273.
14. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65:1335-1342.
15. Bernard BA, Stebbins GT, Siegel S, et al. Determinants of quality of life in children with Gilles de la Tourette syndrome. Mov Disord. 2009;24(7):1070-1073.
16. Understanding the risks of antipsychotic treatment in young people. Advice for managing side effects in children and teenagers. Harv Ment Health Lett. 2009;25(9):1-3.
Sammy, age 7, is referred to you by his pediatrician because of a 4-week history of frequent eye blinking. His parents say he blinks a lot when bored but very little when playing baseball. They recall that he also has intermittently sniffed and nodded his head over the last 12 months. Neither Sammy nor his friends seem to be bothered by the blinking. Except for the tics, Sammy’s physical and mental status exams are normal.
Since preschool, Sammy’s teachers have complained that his backpack and desk are always a mess. Sammy is well-meaning but forgetful in his chores at home. A paternal uncle has head-turning movements, counts his steps, and becomes distressed if books on his shelf are not in alphabetical order.
Tics, such as strong eye blinks or repetitive shoulder shrugs, can distress a child or his/her parents, but the conditions associated with tic disorders often are more problematic than the tic disorder itself. High rates of comorbid conditions are recognized in persons with Tourette syndrome, including:
- obsessive-compulsive disorder (OCD) in >80%1
- attention-deficit/hyperactivity disorder (ADHD) in ≤70%2
- anxiety disorders in 30%3
- rage, aggression, learning disabilities, and autism less commonly.
The strategy we recommend for managing tic disorders includes assessing tic severity, educating the family about the illness, determining whether a comorbid condition is present, and managing these conditions appropriately. Above all, we emphasize a risk-benefit analysis guided by the Hippocratic principle of “do no harm.”
Characteristics of tic disorders
You diagnose Sammy with Tourette syndrome because he meets DSM-IV-TR criteria of at least 2 motor tics and 1 vocal tic that have persisted for 1 year without more than a 3-month hiatus, with tic onset before age 18. Because tics may resemble other movement disorders, you rule out stereotypies, dystonia, chorea, ballism, and myoclonus (Table 1). You explain to his parents that Sammy’s condition is a heritable, neurobehavioral disorder that typically begins in childhood and is associated in families with OCD, ADHD, and autism spectrum disorders.
His parents ask about the difference between tics and other movements. You explain that eye-blinking tics—like other motor tics—appear as sudden, repetitive, stereotyped, nonrhythmic movements that involve discrete muscle groups. (View a video of a patient with tics.) Simple motor tics are focal movements involving 1 group of muscles, whereas complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements (Table 2).
Table 1
Features of 5 movement disorders that may resemble tics
| Tics | Stereotypies | Dystonia | Chorea | Ballism | Myoclonus |
|---|---|---|---|---|---|
| Sudden, repetitive, stereotyped, nonrhythmic movements or sounds | Patterned, nonpurposeful movement | Cocontraction of agonist and antagonist muscles, causing an abnormal twisting posture | Continuous, flowing, nonrhythmic, nonpurposeful movement | Forceful, flinging, large amplitude choreic movement | Sudden, quick, shock-like movement |
| Usually start after age 3 | Usually start before age 3 and resolve by adolescence | More common in adults | — | — | — |
| Decrease when focused; increase when stressed, anxious, fatigued, or bored | Occur when the child is excited | Worsens during motor tasks | Worsens during motor tasks | Worsens during motor tasks | — |
| Comorbid conditions include OCD and ADHD | Common in children with mental retardation or autism | — | Can occur after streptococcal infection | Can occur after streptococcal infection | — |
| Preceded by a premonitory urge or sensation | Possibly preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge |
| Temporarily suppressible | Suppressible | Not suppressible | Partially suppressible; can incorporate into semi-purposeful movements | Partially suppressible | Not suppressible |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder | |||||
Table 2
Characteristics of simple and complex motor and vocal tics*
| Simple tics | Complex tics |
|---|---|
| Eye blinking or eye rolling Nose, mouth, tongue, or facial grimaces (nose twitch, nasal flaring, chewing lip, teeth grinding, sticking out tongue, mouth stretching, lip licking) Head jerks or movements (neck stretching, touching chin to shoulder) Shoulder jerks/movements (shoulder shrugging, jerking a shoulder) Arm or hand movements (flexing or extending arms or fingers) Coughing Throat clearing, grunting Sniffing, snorting, shouting Humming | Jumping Spinning Touching objects or people Throwing objects Repeating others’ action (echopraxia) Obscene gestures (copropraxia) Repeating one’s own words (palilalia) Repeating what someone else said (echolalia) Obscene, inappropriate words (coprolalia) |
| *Simple tics are focal movements involving 1 group of muscles; complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements | |
Older children frequently describe a premonitory urge prior to the tic. Patients typically can suppress tics for a transient period of time, although during tic suppression they usually feel restless and anticipate performing their tic. The ultimate performance of the tic brings relief. Tic suppression also occurs during focused activity. Emotional stress, fatigue, illness, or boredom can exacerbate tics.
To begin monitoring Sammy’s clinical course, you administer 3 assessment tools described inTable 3. You explain to Sammy’s parents that these tests will be repeated yearly or when tics worsen. However, you tell his parents that these scores alone will not determine present or future clinical decisions, including treatments. You also recommend that they connect with support groups on the Tourette Syndrome Association (TSA) Web site.
CASE CONTINUED: Changes over time
Sammy’s parents appreciate your explanation and say they will share information from the TSA Web site with Sammy’s principal, teachers, and classmates. The family agrees to return in 6 months or sooner if the tics worsen.
By age 8, Sammy develops multiple tics: facial grimacing, looking upwards, punching movements, whistling, and throat clearing. He is slightly bothered by these tics, and his friends have asked him about them. He tells them he has Tourette syndrome, and that usually ends the questioning. He returns for a follow-up visit because his parents notice a dramatic increase in his tics after Sammy’s father loses his job.
Treatment options
When deciding to treat a child’s tics, the first step is to determine whether to pursue a nonpharmacologic or pharmacologic approach (Algorithm). To tailor an approach most suited for an individual child, discuss with the family their feelings about therapy and medications. This information—along with tic severity—will help determine a treatment plan.
Behavior therapy and medication are management strategies; neither can cure a tic disorder. The most conservative approach to tic treatment is to:
- provide the child and family with basic guidelines for managing tics
- help alleviate environmental stress and other potential triggers.
Algorithm: Recommended treatment of tics in children and adolescents
CASE CONTINUED: A first intervention
You discuss treatment options with Sammy’s family, and they view medication as a last resort. Sammy does not seem to be bothered by his tics, and his parents do not wish to start him on daily medications. Given this situation, habit reversal therapy (HRT) is appropriate for Sammy because he is old enough to participate in HRT to reduce his tics.
HRT is an effective nonpharmacologic approach to help children with tics.4 Its 3 components are:
- awareness training
- competing response training
- social support.5
This simplified version of the original HRT can be completed in eight 1-hour sessions. Good candidates are patients who are cognitively mature enough to understand the therapy’s goals and compliant with frequent clinic visits. They also must practice the strategies at home.
It should not be difficult for psychiatrists to learn HRT—or refer to therapists who are willing to learn it—with the available instructional manual.
CASE CONTINUED: Practicing alternatives
You ask Sammy to imitate his tics. After helping him become more aware of his tics, you encourage him to develop a more socially appropriate movement to engage in whenever he feels the urge to punch. Sammy chooses to clench his fist in his pocket. He also learns to breathe in whenever he has an urge to whistle. you advise Sammy’s parents to reward his efforts to suppress the tics. He practices the strategies daily.
At age 12, Sammy returns to your office. He has begun to have frequent neck-jerking tics, which cause neck pain and daily headaches. He also is slapping his thigh and having frequent vocal tics characterized by loud shrieking. The vocal tics are disruptive in class, even though Sammy sits toward the back of the room. Sammy’s classmates tease him, and he is very frustrated.
Medication approach
The decision to start a medication for tics is complex. Scores from the YGTSS, PUTS, and GTS-QOL scales (Table 3) provide only a partial clinical picture. This decision should be reached after a detailed discussion with the family about benefits and risks of medications and ensuring that everyone’s expectations are reasonable.
A variety of medications are available to treat patients with tics (Table 4). No medication can completely eliminate tics, however, and many have substantial side effects. Before initiating medical treatment, consider 3 questions:
- Is moderate or severe pain involved?
- Is there significant functional interference?
- Is there significant social disruption despite efforts to optimize the social environment for the child?
Sammy’s frequent neck-jerking tics now cause chronic daily headaches, and his shrieking vocal tics are interfering with classroom activities, so we recommended a 3-month trial of guanfacine following the dosing schedule in Table 4.
Table 3
3 scales for assessing tic severity and impact on functioning
| Instrument | Purpose | Description | Design | Administration frequency |
|---|---|---|---|---|
| Yale Global Tic Severity Scale (YGTSS) | Assess tic severity | Review of motor and vocal tics. Rate number, frequency, intensity, complexity, and interference on a 5-point scale | Clinician-rated | Annual and as needed for increased tics |
| Premonitory Urge for Tics Scale (PUTS) | Detect the presence of unpleasant sensations that precedes tics | 10 questions | Self-report | Annual and as needed for increased tics |
| Gilles de la Tourette Syndrome Quality of Life Scale (GTS-QOL) | Measure quality of life | 27 questions, 4 subscales: psychological, physical, obsessional, and cognitive | Self-report | Annual and as needed for increased tics |
Table 4
Medications with evidence of tic-suppressing effects*
| Category A evidence | ||
|---|---|---|
| Medication | Starting dose | Target dose |
| Haloperidol | 0.25 to 0.5 mg/d | 1 to 4 mg/d |
| Pimozide | 0.5 to 1 mg/d | 2 to 8 mg/d |
| Risperidone | 0.25 to 0.5 mg/d | 1 to 3 mg/d |
| Category B evidence | ||
| Medication | Starting dose | Target dose |
| Fluphenazine | 0.5 to 1 mg/d | 1.5 to 10 mg/d |
| Ziprasidone | 5 to 10 mg/d | 10 to 80 mg/d |
| Clonidine | 0.025 to 0.05 mg/d | 0.1 to 0.3 mg/d |
| Guanfacine | 0.5 to 1 mg/d | 1 to 3 mg/d |
| Botulinum toxin | 30 to 300 units | |
| Category C evidence | ||
| Medication | Starting dose | Target dose |
| Olanzapine | 2.5 to 5 mg/d | 2.5 to 12.5 mg/d |
| Tetrabenazine | 25 mg/d | 37.5 to 150 mg/d |
| Baclofen | 10 mg/d | 40 to 60 mg/d |
| Nicotine patch | 7 mg/d | 7 to 21 mg/d |
| Mecamylamine | 2.5 mg/d | 2.5 to 7.5 mg/d |
| Flutamide | 250 mg/d | 750 mg/d |
| *Category A: supported by ≥2 placebo-controlled trials; category B: supported by 1 placebo-controlled trial; category C: supported by open-label study | ||
| Source: Reference 6 | ||
The first-line pharmacologic agent for tic suppression generally is an alpha-adrenergic medication, unless the tics are severe.6
Clonidine and guanfacine usually are started at low doses and increased gradually. Although not as effective as neuroleptics, alpha-adrenergics have a lower potential for side effects and are easier to use because no laboratory tests need to be monitored. Adverse effects associated with alpha-adrenergic medications include sedation, dry mouth, dizziness, headache, and rebound hypertension if discontinued abruptly.
If tics are causing pain, some clinicians prefer conservative measures such as heat or ice, massage, analgesics, relaxation therapy, and reassurance.
Second-line agents include typical and atypical antipsychotics. Haloperidol and pimozide have shown efficacy in reducing tics in placebo- controlled studies,7,8 as have risperidone (in 4 randomized controlled trials [RCTs]) and ziprasidone (in 1 RCT).9,10 The emergence of serious side effects is a risk for both typical and atypical antipsychotics (Table 5).
Table 5
Potential adverse effects of antipsychotic treatment in children*
| Adverse effect | Examples |
|---|---|
| Sedation | — |
| Acute dystonic reactions | Oculogyric crisis, torticollis |
| Appetite changes | Weight gain |
| Endocrine abnormalities | Amenorrhea, diabetes, galactorrhea, gynecomastia, hyperprolactinemia |
| Cognitive effects | Impaired concentration |
| Akathisia | Difficulty sitting still |
| ECG changes | Prolonged QT interval |
| Parkinsonism | Tremor, bradykinesia, rigidity, postural instability |
| Tardive syndrome | Orofacial dyskinesia, chorea, dystonia, myoclonus, tics |
| Neuroleptic malignant syndrome | Potentially fatal; consists of muscular rigidity, fever, autonomic dysfunction, labile blood pressure, sweating, urinary incontinence, fluctuating level of consciousness, leukocytosis, elevated serum creatine kinase |
| *Potential adverse effects are listed from most to least likely to occur | |
As part of your informed consent discussion, weigh the risk of side effects against the benefits of treatment. Point out to patients and their families that they can expect to see a decrease in tic frequency, but symptoms will not necessarily disappear with any medication. We tell our patients that with antipsychotics the best we can hope for is to reduce tic frequency by approximately one-half.6
When treating tics, start with 1 medication. However, if the tics are severe enough to require more than 1 medication, check for drug interactions.
Third-line agents. Agents that have not been tested in placebo-controlled trials can be considered third line; these are listed as category C (supported by open-label studies) in Table 4. Botulinum toxin injection has been found to be effective for motor and vocal tics.11,12 Botulinum toxin and implantation of deep brain stimulators13 are invasive options and generally are reserved for severe, treatment-resistant tics.
CASE CONTINUED: Managing antipsychotics
After trying guanfacine for 12 weeks, Sammy notices no tic reduction. His parents consent to a low dose of risperidone. you review with them the American Psychiatric Association (APA)/American Diabetes Association (ADA) guidelines14 for managing metabolic problems in patients treated with atypical antipsychotics.
As instructed in the APA/ADA guidelines, obtain baseline measurements and monitor for metabolic effects of antipsychotic therapy over time (Table 6). Sammy starts risperidone at 0.5 mg once daily. After 2 weeks, he notices a decrease in his tics. At the 3-month visit after starting risperidone, he is happy with his risperidone dose and does not want to increase it. He has gained 3 pounds, and you instruct him to eat a well-balanced diet and exercise routinely. At the 6-month visit, his tics are minimal and his weight has stabilized.
Table 6
Children receiving antipsychotics: monitoring recommendations
| Clinical information | Frequency |
|---|---|
| Family history | Initial visit |
| Weight | Baseline, monthly |
| Height | Baseline, monthly |
| BMI | Baseline, monthly |
| Waist circumference | Baseline, annually |
| Blood pressure | Baseline, 3 months after treatment starts, and annually thereafter |
| Fasting lipid profile | Baseline, every 3 months initially, then every 6 months thereafter |
| Fasting serum glucose | Baseline, every 3 months, then every 6 months thereafter |
| BMI: body mass index | |
| Source: References 14,16 | |
You recommend that Sammy remain on risperidone for another 3 months of stability and then begin to taper this medication. You review the risks and benefits of long-term treatment with risperidone, pointing out that it may lead to abnormal movements upon withdrawal, and explain that you typically do not treat children with antipsychotics for more than one year continuously.
CASE CONTINUED: Comorbid symptoms
Since starting 7th grade, Sammy has worried excessively about making mistakes. He spends 6 hours each night on homework, which he often does not turn in because of anxiety about not getting answers perfectly right. Classmates notice that Sammy taps the door 3 times when he comes into the classroom and that he steps over the black tiles in the hallway.
Consider the presence and impact of comorbid OCD or ADHD, which can impair children’s quality of life more than tics themselves.15 Assessment scales can help you make a diagnosis and monitor treatment.
If you suspect OCD, the clinician-rated Children’s Yale Brown Obsessive Compulsive Scale is the gold standard for describing the phenomenology and measuring symptom severity. Additional scales to measure symptoms’ impact on family life include the Leyton Obsessional Inventory—child version, Family Accommodation Scale for OCD, and Child OCD Impact Scale.
ADHD scales include the Conners Parent Rating Scale—Revised, Conners Teacher Rating Scale—Revised, Swanson, Nolan, and Pelham, or the Vanderbilt ADHD Diagnostic Parent and Teacher Rating Scales. Because ADHD symptoms must be present in more than 1 environment to meet diagnostic criteria, ask parents and teachers to complete the Conners or Vanderbilt scales.
In children who present with a tic disorder plus a comorbid condition, prioritize treatment by determining which symptoms interfere with the child’s ability to function at school, at home, and in the social arena. Children who require treatment for >1 disorder often are referred initially for cognitive-behavioral therapy for OCD symptoms while receiving pharmacologic treatment for ADHD and/or Tourette syndrome. When necessary, it is usually safe to combine antipsychotics, stimulants, and selective serotonin reuptake inhibitors, although medication interactions should be reviewed in each specific case.
Related resources
- Woods DW. Managing Tourette syndrome: a behavioral intervention for children and adults. Therapist guide. New York, NY: Oxford University Press; 2008.
- Tourette Syndrome Association. www.tsa-usa.org.
- International OCD Foundation. www.ocfoundation.org.
Drug brand names
- Baclofen • Lioresal
- Botulinum toxin • Botox, Myobloc
- Clomipramine • Anafranil
- Clonidine • Catapres
- Guanfacine • Tenex
- Fluphenazine • Prolixin
- Flutamide • Eulexin
- Haloperidol • Haldol
- Mecamylamine • Inversine
- Nicotine patch • NicoDerm
- Olanzapine • Zyprexa
- Pimozide • Orap
- Risperidone • Risperdal
- Tetrabenazine • Xenazine
- Ziprasidone • Geodon
Disclosures
Dr. Harris has received research support from the Translational Research Initiative at Cincinnati Children’s Hospital Medical Center.
Dr. Wu reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Sammy, age 7, is referred to you by his pediatrician because of a 4-week history of frequent eye blinking. His parents say he blinks a lot when bored but very little when playing baseball. They recall that he also has intermittently sniffed and nodded his head over the last 12 months. Neither Sammy nor his friends seem to be bothered by the blinking. Except for the tics, Sammy’s physical and mental status exams are normal.
Since preschool, Sammy’s teachers have complained that his backpack and desk are always a mess. Sammy is well-meaning but forgetful in his chores at home. A paternal uncle has head-turning movements, counts his steps, and becomes distressed if books on his shelf are not in alphabetical order.
Tics, such as strong eye blinks or repetitive shoulder shrugs, can distress a child or his/her parents, but the conditions associated with tic disorders often are more problematic than the tic disorder itself. High rates of comorbid conditions are recognized in persons with Tourette syndrome, including:
- obsessive-compulsive disorder (OCD) in >80%1
- attention-deficit/hyperactivity disorder (ADHD) in ≤70%2
- anxiety disorders in 30%3
- rage, aggression, learning disabilities, and autism less commonly.
The strategy we recommend for managing tic disorders includes assessing tic severity, educating the family about the illness, determining whether a comorbid condition is present, and managing these conditions appropriately. Above all, we emphasize a risk-benefit analysis guided by the Hippocratic principle of “do no harm.”
Characteristics of tic disorders
You diagnose Sammy with Tourette syndrome because he meets DSM-IV-TR criteria of at least 2 motor tics and 1 vocal tic that have persisted for 1 year without more than a 3-month hiatus, with tic onset before age 18. Because tics may resemble other movement disorders, you rule out stereotypies, dystonia, chorea, ballism, and myoclonus (Table 1). You explain to his parents that Sammy’s condition is a heritable, neurobehavioral disorder that typically begins in childhood and is associated in families with OCD, ADHD, and autism spectrum disorders.
His parents ask about the difference between tics and other movements. You explain that eye-blinking tics—like other motor tics—appear as sudden, repetitive, stereotyped, nonrhythmic movements that involve discrete muscle groups. (View a video of a patient with tics.) Simple motor tics are focal movements involving 1 group of muscles, whereas complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements (Table 2).
Table 1
Features of 5 movement disorders that may resemble tics
| Tics | Stereotypies | Dystonia | Chorea | Ballism | Myoclonus |
|---|---|---|---|---|---|
| Sudden, repetitive, stereotyped, nonrhythmic movements or sounds | Patterned, nonpurposeful movement | Cocontraction of agonist and antagonist muscles, causing an abnormal twisting posture | Continuous, flowing, nonrhythmic, nonpurposeful movement | Forceful, flinging, large amplitude choreic movement | Sudden, quick, shock-like movement |
| Usually start after age 3 | Usually start before age 3 and resolve by adolescence | More common in adults | — | — | — |
| Decrease when focused; increase when stressed, anxious, fatigued, or bored | Occur when the child is excited | Worsens during motor tasks | Worsens during motor tasks | Worsens during motor tasks | — |
| Comorbid conditions include OCD and ADHD | Common in children with mental retardation or autism | — | Can occur after streptococcal infection | Can occur after streptococcal infection | — |
| Preceded by a premonitory urge or sensation | Possibly preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge |
| Temporarily suppressible | Suppressible | Not suppressible | Partially suppressible; can incorporate into semi-purposeful movements | Partially suppressible | Not suppressible |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder | |||||
Table 2
Characteristics of simple and complex motor and vocal tics*
| Simple tics | Complex tics |
|---|---|
| Eye blinking or eye rolling Nose, mouth, tongue, or facial grimaces (nose twitch, nasal flaring, chewing lip, teeth grinding, sticking out tongue, mouth stretching, lip licking) Head jerks or movements (neck stretching, touching chin to shoulder) Shoulder jerks/movements (shoulder shrugging, jerking a shoulder) Arm or hand movements (flexing or extending arms or fingers) Coughing Throat clearing, grunting Sniffing, snorting, shouting Humming | Jumping Spinning Touching objects or people Throwing objects Repeating others’ action (echopraxia) Obscene gestures (copropraxia) Repeating one’s own words (palilalia) Repeating what someone else said (echolalia) Obscene, inappropriate words (coprolalia) |
| *Simple tics are focal movements involving 1 group of muscles; complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements | |
Older children frequently describe a premonitory urge prior to the tic. Patients typically can suppress tics for a transient period of time, although during tic suppression they usually feel restless and anticipate performing their tic. The ultimate performance of the tic brings relief. Tic suppression also occurs during focused activity. Emotional stress, fatigue, illness, or boredom can exacerbate tics.
To begin monitoring Sammy’s clinical course, you administer 3 assessment tools described inTable 3. You explain to Sammy’s parents that these tests will be repeated yearly or when tics worsen. However, you tell his parents that these scores alone will not determine present or future clinical decisions, including treatments. You also recommend that they connect with support groups on the Tourette Syndrome Association (TSA) Web site.
CASE CONTINUED: Changes over time
Sammy’s parents appreciate your explanation and say they will share information from the TSA Web site with Sammy’s principal, teachers, and classmates. The family agrees to return in 6 months or sooner if the tics worsen.
By age 8, Sammy develops multiple tics: facial grimacing, looking upwards, punching movements, whistling, and throat clearing. He is slightly bothered by these tics, and his friends have asked him about them. He tells them he has Tourette syndrome, and that usually ends the questioning. He returns for a follow-up visit because his parents notice a dramatic increase in his tics after Sammy’s father loses his job.
Treatment options
When deciding to treat a child’s tics, the first step is to determine whether to pursue a nonpharmacologic or pharmacologic approach (Algorithm). To tailor an approach most suited for an individual child, discuss with the family their feelings about therapy and medications. This information—along with tic severity—will help determine a treatment plan.
Behavior therapy and medication are management strategies; neither can cure a tic disorder. The most conservative approach to tic treatment is to:
- provide the child and family with basic guidelines for managing tics
- help alleviate environmental stress and other potential triggers.
Algorithm: Recommended treatment of tics in children and adolescents
CASE CONTINUED: A first intervention
You discuss treatment options with Sammy’s family, and they view medication as a last resort. Sammy does not seem to be bothered by his tics, and his parents do not wish to start him on daily medications. Given this situation, habit reversal therapy (HRT) is appropriate for Sammy because he is old enough to participate in HRT to reduce his tics.
HRT is an effective nonpharmacologic approach to help children with tics.4 Its 3 components are:
- awareness training
- competing response training
- social support.5
This simplified version of the original HRT can be completed in eight 1-hour sessions. Good candidates are patients who are cognitively mature enough to understand the therapy’s goals and compliant with frequent clinic visits. They also must practice the strategies at home.
It should not be difficult for psychiatrists to learn HRT—or refer to therapists who are willing to learn it—with the available instructional manual.
CASE CONTINUED: Practicing alternatives
You ask Sammy to imitate his tics. After helping him become more aware of his tics, you encourage him to develop a more socially appropriate movement to engage in whenever he feels the urge to punch. Sammy chooses to clench his fist in his pocket. He also learns to breathe in whenever he has an urge to whistle. you advise Sammy’s parents to reward his efforts to suppress the tics. He practices the strategies daily.
At age 12, Sammy returns to your office. He has begun to have frequent neck-jerking tics, which cause neck pain and daily headaches. He also is slapping his thigh and having frequent vocal tics characterized by loud shrieking. The vocal tics are disruptive in class, even though Sammy sits toward the back of the room. Sammy’s classmates tease him, and he is very frustrated.
Medication approach
The decision to start a medication for tics is complex. Scores from the YGTSS, PUTS, and GTS-QOL scales (Table 3) provide only a partial clinical picture. This decision should be reached after a detailed discussion with the family about benefits and risks of medications and ensuring that everyone’s expectations are reasonable.
A variety of medications are available to treat patients with tics (Table 4). No medication can completely eliminate tics, however, and many have substantial side effects. Before initiating medical treatment, consider 3 questions:
- Is moderate or severe pain involved?
- Is there significant functional interference?
- Is there significant social disruption despite efforts to optimize the social environment for the child?
Sammy’s frequent neck-jerking tics now cause chronic daily headaches, and his shrieking vocal tics are interfering with classroom activities, so we recommended a 3-month trial of guanfacine following the dosing schedule in Table 4.
Table 3
3 scales for assessing tic severity and impact on functioning
| Instrument | Purpose | Description | Design | Administration frequency |
|---|---|---|---|---|
| Yale Global Tic Severity Scale (YGTSS) | Assess tic severity | Review of motor and vocal tics. Rate number, frequency, intensity, complexity, and interference on a 5-point scale | Clinician-rated | Annual and as needed for increased tics |
| Premonitory Urge for Tics Scale (PUTS) | Detect the presence of unpleasant sensations that precedes tics | 10 questions | Self-report | Annual and as needed for increased tics |
| Gilles de la Tourette Syndrome Quality of Life Scale (GTS-QOL) | Measure quality of life | 27 questions, 4 subscales: psychological, physical, obsessional, and cognitive | Self-report | Annual and as needed for increased tics |
Table 4
Medications with evidence of tic-suppressing effects*
| Category A evidence | ||
|---|---|---|
| Medication | Starting dose | Target dose |
| Haloperidol | 0.25 to 0.5 mg/d | 1 to 4 mg/d |
| Pimozide | 0.5 to 1 mg/d | 2 to 8 mg/d |
| Risperidone | 0.25 to 0.5 mg/d | 1 to 3 mg/d |
| Category B evidence | ||
| Medication | Starting dose | Target dose |
| Fluphenazine | 0.5 to 1 mg/d | 1.5 to 10 mg/d |
| Ziprasidone | 5 to 10 mg/d | 10 to 80 mg/d |
| Clonidine | 0.025 to 0.05 mg/d | 0.1 to 0.3 mg/d |
| Guanfacine | 0.5 to 1 mg/d | 1 to 3 mg/d |
| Botulinum toxin | 30 to 300 units | |
| Category C evidence | ||
| Medication | Starting dose | Target dose |
| Olanzapine | 2.5 to 5 mg/d | 2.5 to 12.5 mg/d |
| Tetrabenazine | 25 mg/d | 37.5 to 150 mg/d |
| Baclofen | 10 mg/d | 40 to 60 mg/d |
| Nicotine patch | 7 mg/d | 7 to 21 mg/d |
| Mecamylamine | 2.5 mg/d | 2.5 to 7.5 mg/d |
| Flutamide | 250 mg/d | 750 mg/d |
| *Category A: supported by ≥2 placebo-controlled trials; category B: supported by 1 placebo-controlled trial; category C: supported by open-label study | ||
| Source: Reference 6 | ||
The first-line pharmacologic agent for tic suppression generally is an alpha-adrenergic medication, unless the tics are severe.6
Clonidine and guanfacine usually are started at low doses and increased gradually. Although not as effective as neuroleptics, alpha-adrenergics have a lower potential for side effects and are easier to use because no laboratory tests need to be monitored. Adverse effects associated with alpha-adrenergic medications include sedation, dry mouth, dizziness, headache, and rebound hypertension if discontinued abruptly.
If tics are causing pain, some clinicians prefer conservative measures such as heat or ice, massage, analgesics, relaxation therapy, and reassurance.
Second-line agents include typical and atypical antipsychotics. Haloperidol and pimozide have shown efficacy in reducing tics in placebo- controlled studies,7,8 as have risperidone (in 4 randomized controlled trials [RCTs]) and ziprasidone (in 1 RCT).9,10 The emergence of serious side effects is a risk for both typical and atypical antipsychotics (Table 5).
Table 5
Potential adverse effects of antipsychotic treatment in children*
| Adverse effect | Examples |
|---|---|
| Sedation | — |
| Acute dystonic reactions | Oculogyric crisis, torticollis |
| Appetite changes | Weight gain |
| Endocrine abnormalities | Amenorrhea, diabetes, galactorrhea, gynecomastia, hyperprolactinemia |
| Cognitive effects | Impaired concentration |
| Akathisia | Difficulty sitting still |
| ECG changes | Prolonged QT interval |
| Parkinsonism | Tremor, bradykinesia, rigidity, postural instability |
| Tardive syndrome | Orofacial dyskinesia, chorea, dystonia, myoclonus, tics |
| Neuroleptic malignant syndrome | Potentially fatal; consists of muscular rigidity, fever, autonomic dysfunction, labile blood pressure, sweating, urinary incontinence, fluctuating level of consciousness, leukocytosis, elevated serum creatine kinase |
| *Potential adverse effects are listed from most to least likely to occur | |
As part of your informed consent discussion, weigh the risk of side effects against the benefits of treatment. Point out to patients and their families that they can expect to see a decrease in tic frequency, but symptoms will not necessarily disappear with any medication. We tell our patients that with antipsychotics the best we can hope for is to reduce tic frequency by approximately one-half.6
When treating tics, start with 1 medication. However, if the tics are severe enough to require more than 1 medication, check for drug interactions.
Third-line agents. Agents that have not been tested in placebo-controlled trials can be considered third line; these are listed as category C (supported by open-label studies) in Table 4. Botulinum toxin injection has been found to be effective for motor and vocal tics.11,12 Botulinum toxin and implantation of deep brain stimulators13 are invasive options and generally are reserved for severe, treatment-resistant tics.
CASE CONTINUED: Managing antipsychotics
After trying guanfacine for 12 weeks, Sammy notices no tic reduction. His parents consent to a low dose of risperidone. you review with them the American Psychiatric Association (APA)/American Diabetes Association (ADA) guidelines14 for managing metabolic problems in patients treated with atypical antipsychotics.
As instructed in the APA/ADA guidelines, obtain baseline measurements and monitor for metabolic effects of antipsychotic therapy over time (Table 6). Sammy starts risperidone at 0.5 mg once daily. After 2 weeks, he notices a decrease in his tics. At the 3-month visit after starting risperidone, he is happy with his risperidone dose and does not want to increase it. He has gained 3 pounds, and you instruct him to eat a well-balanced diet and exercise routinely. At the 6-month visit, his tics are minimal and his weight has stabilized.
Table 6
Children receiving antipsychotics: monitoring recommendations
| Clinical information | Frequency |
|---|---|
| Family history | Initial visit |
| Weight | Baseline, monthly |
| Height | Baseline, monthly |
| BMI | Baseline, monthly |
| Waist circumference | Baseline, annually |
| Blood pressure | Baseline, 3 months after treatment starts, and annually thereafter |
| Fasting lipid profile | Baseline, every 3 months initially, then every 6 months thereafter |
| Fasting serum glucose | Baseline, every 3 months, then every 6 months thereafter |
| BMI: body mass index | |
| Source: References 14,16 | |
You recommend that Sammy remain on risperidone for another 3 months of stability and then begin to taper this medication. You review the risks and benefits of long-term treatment with risperidone, pointing out that it may lead to abnormal movements upon withdrawal, and explain that you typically do not treat children with antipsychotics for more than one year continuously.
CASE CONTINUED: Comorbid symptoms
Since starting 7th grade, Sammy has worried excessively about making mistakes. He spends 6 hours each night on homework, which he often does not turn in because of anxiety about not getting answers perfectly right. Classmates notice that Sammy taps the door 3 times when he comes into the classroom and that he steps over the black tiles in the hallway.
Consider the presence and impact of comorbid OCD or ADHD, which can impair children’s quality of life more than tics themselves.15 Assessment scales can help you make a diagnosis and monitor treatment.
If you suspect OCD, the clinician-rated Children’s Yale Brown Obsessive Compulsive Scale is the gold standard for describing the phenomenology and measuring symptom severity. Additional scales to measure symptoms’ impact on family life include the Leyton Obsessional Inventory—child version, Family Accommodation Scale for OCD, and Child OCD Impact Scale.
ADHD scales include the Conners Parent Rating Scale—Revised, Conners Teacher Rating Scale—Revised, Swanson, Nolan, and Pelham, or the Vanderbilt ADHD Diagnostic Parent and Teacher Rating Scales. Because ADHD symptoms must be present in more than 1 environment to meet diagnostic criteria, ask parents and teachers to complete the Conners or Vanderbilt scales.
In children who present with a tic disorder plus a comorbid condition, prioritize treatment by determining which symptoms interfere with the child’s ability to function at school, at home, and in the social arena. Children who require treatment for >1 disorder often are referred initially for cognitive-behavioral therapy for OCD symptoms while receiving pharmacologic treatment for ADHD and/or Tourette syndrome. When necessary, it is usually safe to combine antipsychotics, stimulants, and selective serotonin reuptake inhibitors, although medication interactions should be reviewed in each specific case.
Related resources
- Woods DW. Managing Tourette syndrome: a behavioral intervention for children and adults. Therapist guide. New York, NY: Oxford University Press; 2008.
- Tourette Syndrome Association. www.tsa-usa.org.
- International OCD Foundation. www.ocfoundation.org.
Drug brand names
- Baclofen • Lioresal
- Botulinum toxin • Botox, Myobloc
- Clomipramine • Anafranil
- Clonidine • Catapres
- Guanfacine • Tenex
- Fluphenazine • Prolixin
- Flutamide • Eulexin
- Haloperidol • Haldol
- Mecamylamine • Inversine
- Nicotine patch • NicoDerm
- Olanzapine • Zyprexa
- Pimozide • Orap
- Risperidone • Risperdal
- Tetrabenazine • Xenazine
- Ziprasidone • Geodon
Disclosures
Dr. Harris has received research support from the Translational Research Initiative at Cincinnati Children’s Hospital Medical Center.
Dr. Wu reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Robertson M. Tourette syndrome, associated conditions and the complexities of treatment. Brain. 2000;123(3):425-462.
2. Freeman R. For the Tourette Syndrome International Database Consortium. Tic disorders and ADHD: answers from a worldwide clinical dataset on Tourette syndrome. Eur Child Adolesc Psychiatry. 2007;16(suppl 1):15-23.
3. Stefl M. Mental health needs associated with Tourette syndrome. Am J Public Health. 1984;74:1310-1313.
4. Deckersbach T, Rauch S, Buhlmann U, et al. Habit reversal versus supportive psychotherapy in Tourette’s disorder: a randomized controlled trial and predictors of treatment response. Behav Res Ther. 2006;44:1079-1090.
5. Woods DW, Miltenberger RG. Habit reversal: a review of applications and variations. J Behav Ther Exp Psychiatry. 1995;26:123-131.
6. Scahill L, Erenberg G, Berlin C, et al. Contemporary assessment and pharmacotherapy of Tourette syndrome. NeuroRx. 2006;3(2):192-206.
7. Shapiro E, Shapiro A, Fulop G, et al. Controlled study of haloperidol, pimozide, and placebo for the treatment of Gilles de la Tourette’s syndrome. 1989;46:722-730.
8. Sallee F, Nesbitt L, Jackson C, et al. Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette’s disorder. Am J Psychiatry. 1997;154:1057-1062.
9. Scahill L, Leckman J, Schultz R, et al. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology. 2003;60:1130-1135.
10. Sallee F, Kurlan R, Goetz C, et al. Ziprasidone treatment of children and adolescents with Tourette’s syndrome: a pilot study. J Am Acad Child Adolesc Psychiatry. 2000;39(3):292-299.
11. Marras C, Andrews D, Sime E, et al. Botulinum toxin for simple motor tics: a randomized, double-blind, controlled clinical trial. Neurology. 2001;56(5):605-610.
12. Porta M, Maggioni G, Ottaviani F, et al. Treatment of phonic tics in patients with Tourette’s syndrome using botulinum toxin type A. Neurol Sci. 2004;24(6):420-423.
13. Porta M, Sevello D, Sassi M, et al. Issues related to deep brain stimulation for treatment-refractory Tourette’s syndrome. Eur Neurol. 2009;62(5):264-273.
14. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65:1335-1342.
15. Bernard BA, Stebbins GT, Siegel S, et al. Determinants of quality of life in children with Gilles de la Tourette syndrome. Mov Disord. 2009;24(7):1070-1073.
16. Understanding the risks of antipsychotic treatment in young people. Advice for managing side effects in children and teenagers. Harv Ment Health Lett. 2009;25(9):1-3.
1. Robertson M. Tourette syndrome, associated conditions and the complexities of treatment. Brain. 2000;123(3):425-462.
2. Freeman R. For the Tourette Syndrome International Database Consortium. Tic disorders and ADHD: answers from a worldwide clinical dataset on Tourette syndrome. Eur Child Adolesc Psychiatry. 2007;16(suppl 1):15-23.
3. Stefl M. Mental health needs associated with Tourette syndrome. Am J Public Health. 1984;74:1310-1313.
4. Deckersbach T, Rauch S, Buhlmann U, et al. Habit reversal versus supportive psychotherapy in Tourette’s disorder: a randomized controlled trial and predictors of treatment response. Behav Res Ther. 2006;44:1079-1090.
5. Woods DW, Miltenberger RG. Habit reversal: a review of applications and variations. J Behav Ther Exp Psychiatry. 1995;26:123-131.
6. Scahill L, Erenberg G, Berlin C, et al. Contemporary assessment and pharmacotherapy of Tourette syndrome. NeuroRx. 2006;3(2):192-206.
7. Shapiro E, Shapiro A, Fulop G, et al. Controlled study of haloperidol, pimozide, and placebo for the treatment of Gilles de la Tourette’s syndrome. 1989;46:722-730.
8. Sallee F, Nesbitt L, Jackson C, et al. Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette’s disorder. Am J Psychiatry. 1997;154:1057-1062.
9. Scahill L, Leckman J, Schultz R, et al. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology. 2003;60:1130-1135.
10. Sallee F, Kurlan R, Goetz C, et al. Ziprasidone treatment of children and adolescents with Tourette’s syndrome: a pilot study. J Am Acad Child Adolesc Psychiatry. 2000;39(3):292-299.
11. Marras C, Andrews D, Sime E, et al. Botulinum toxin for simple motor tics: a randomized, double-blind, controlled clinical trial. Neurology. 2001;56(5):605-610.
12. Porta M, Maggioni G, Ottaviani F, et al. Treatment of phonic tics in patients with Tourette’s syndrome using botulinum toxin type A. Neurol Sci. 2004;24(6):420-423.
13. Porta M, Sevello D, Sassi M, et al. Issues related to deep brain stimulation for treatment-refractory Tourette’s syndrome. Eur Neurol. 2009;62(5):264-273.
14. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65:1335-1342.
15. Bernard BA, Stebbins GT, Siegel S, et al. Determinants of quality of life in children with Gilles de la Tourette syndrome. Mov Disord. 2009;24(7):1070-1073.
16. Understanding the risks of antipsychotic treatment in young people. Advice for managing side effects in children and teenagers. Harv Ment Health Lett. 2009;25(9):1-3.
Discontinuing an antidepressant?
Most psychiatrists have encountered patients who report distressing symptoms when they have forgotten to take their antidepressant for a few days or during changes in the medication regimen. A discontinuation syndrome can occur with almost any antidepressant, highlighting the need to slowly taper these medications when discontinuation is part of a treatment plan.
This article discusses antidepressant discontinuation syndrome (ADS) in a patient who experienced substantial distress after a rapid antidepressant taper in preparation for electroconvulsive therapy (ECT). My goal is to raise awareness of ADS, promote early detection of the syndrome, and address proper prevention and management strategies.
CASE REPORT: Feeling ‘worse than ever’
Mr. J, a 32-year-old tax accountant, is hospitalized for a major depressive episode (MDE) associated with deteriorating function and suicidal ideation. This second lifetime MDE started 8 months before his admission to an inpatient mood disorders unit.
Mr. J initially was treated with fluoxetine, up to 40 mg/d across 14 weeks, with good tolerability but no significant benefit. His psychiatrist switched Mr. J to bupropion but stopped it after 4 weeks because of side effects—including headaches, insomnia, and tremor—and limited antidepressant benefit. Venlafaxine XR was initiated next, at 150 mg/d within the first 2 weeks, increased to 225 mg/d at week 6, then titrated to 300 mg/d at week 10. After 10 weeks, aripiprazole, 5 mg/d, was added because Mr. J showed only partial, limited response to venlafaxine XR and this antipsychotic is indicated for adjunctive treatment of major depressive disorder.
Mr. J reported mild, transient restlessness but otherwise he tolerated the medications well, and he claimed excellent adherence. After 6 additional weeks of treatment, however, Mr. J was hospitalized because of persistent severely depressed mood, increasing suicidal ideation, and inability to function at work.
On admission, Mr. J is evaluated and agrees to ECT. To meet the ECT service’s protocol, venlafaxine XR is reduced to 150 mg/d for 2 days and then stopped when ECT is started. Aripiprazole is continued at 5 mg/d.
Mr. J tolerates the first ECT treatment well, but the morning before his second treatment he complains of feeling “worse than ever.” An agitated Mr. J reports dramatically intensified suicidal ideation—much more intrusive than before he was hospitalized. He also complains of diffuse muscle aches and cramps, runny nose, nausea, headache, and burning sensations in both arms and hands. He withdraws consent for ECT and returns to the mood disorders unit for ongoing treatment.
Could this be ADS?
Yes, it could. In this case, the inpatient psychiatrist and treatment team were lulled into a false sense of security by Mr. J’s history of few side effects with various treatments and medication changes. The ECT service wanted the patient off venlafaxine XR before beginning ECT, and the treatment team believed a quick taper would not cause discontinuation symptoms because Mr. J was taking an “extended-release” medication.
Within 72 hours, Mr. J went from taking 300 mg/d of venlafaxine XR to none. Within 2 days of cessation, he complained of symptoms that could characterize a discontinuation syndrome. A potential red herring in this case is that the patient complained of feeling worse after his first ECT treatment, and one might erroneously think the myalgias, headache, and other somatic symptoms were side effects of ECT and/or anesthesia.
Typical ADS symptoms
Nearly all antidepressant classes are associated with ADS. Symptoms vary from patient to patient but typically include the “FINISH” syndrome: flu-like symptoms, ###bold/bold###nsomnia, nausea, ###bold/bold###mbalance, sensory disturbances, and hyperarousal (anxiety/agitation) (Table 1).1
Adverse effects after stopping tricyclic antidepressants have been well documented. They may include FINISH syndrome features as well as cholinergic overdrive or “rebound” such as abdominal cramping and diarrhea.2-4 Reports of ADS after patients stopped selective serotonin reuptake inhibitors (SSRIs) emerged soon after these agents were introduced.5-7 Similarly, ADS has been reported with serotonin-norepinephrine reuptake inhibitors (SNRIs), including venlafaxine,8-10 venlafaxine XR,11 and duloxetine.12 ADS symptoms are similar with SSRIs and SNRIs, generally without the anticholinergic effects associated with tricyclic antidepressant discontinuation.
Fewer reports of discontinuation syndrome exist for bupropion, mirtazapine, monoamine oxidase inhibitors (MAOIs), and nefazodone.13-17 Discontinuation-emergent syndromes with these non-SSRI/non-SNRI antidepressants tend to present differently. With MAOIs, for example, neuropsychiatric symptoms such as severe anxiety, agitation, pressured speech, sleeplessness or drowsiness, hallucinations, delirium, and paranoid psychosis can be prominent.17
The prevalence of ADS is unclear, and published estimates vary widely because of the lack of large controlled studies. ADS rates with SSRIs/SNRIs have been reported from as low as 0% for fluoxetine to higher rates for shorter half-life antidepressants:
- 2.2% with sertraline
- 14% with fluvoxamine
- 20% with paroxetine
- 30.8% with clomipramine.
These rates come from a retrospective case note review of patients who discontinued antidepressants under supervision.18 In a small cohort of outpatients being treated for major depressive disorder, stopping venlafaxine XR was associated with discontinuation symptoms for the next 3 days in 7 of 9 patients (78%), compared with 2 of 9 patients (22%) stopping placebo.11
Diagnostic criteria have been proposed for ADS associated with serotonin (5-HT) reuptake inhibitors.19-22 Proposed ADS definitions differ somewhat, but essentially 3 features guide the diagnosis:
- appearance of characteristic symptoms (Table 2)21,23
- timing of those symptoms, which usually emerge within 1 week of abrupt cessation or marked reduction of the antidepressant
- symptoms generally are mild, short-lived, self-limiting, and/or rapidly reversed by restarting the original antidepressant.
Evidence suggests shorter half-life antidepressants may be associated with the highest risk for ADS, but other risk factors remain presumptive (Table 3).
Table 1
FINISH: Symptoms of antidepressant discontinuation syndrome
| Flu-like symptoms |
| Insomnia |
| Nausea |
| Imbalance |
| Sensory disturbances |
| Hyperarousal (anxiety/agitation) |
| Source: Reference 1 |
Table 2
ADS symptoms can range across a variety of system clusters
| System cluster | Symptoms |
|---|---|
| Neurosensory | Vertigo, paresthesias, shock-like reactions, myalgias, numbness, sensitivity to sound, unusual visual sensations, ringing in the ears |
| Neuromotor | Tremor, myoclonus, ataxia/gait instability, visual changes, restless legs, problems with speech, tongue movements |
| Gastrointestinal | Nausea, vomiting, cramps/bloating, diarrhea, anorexia |
| Neuropsychiatric | Anxiety/panic, depression, mood swings, suicidal ideation, irritability, impulsivity, confusion, psychosis |
| Vasomotor | Diaphoresis, flushing, temperature intolerance |
| Other | Headache, insomnia, vivid dreams, nightmares, lethargy/fatigue, flu-like symptoms |
| ADS: antidepressant discontinuation syndrome | |
| Source: Construct suggested by Shelton,21 with additional symptoms added from other sources, including the discontinuation symptom checklist of Rosenbaum et al23 | |
Table 3
Possible patient risk factors for developing ADS*
| Abrupt antidepressant discontinuation |
| Shorter half-life antidepressants |
| Intermittent nonadherence/noncompliance |
| Interrupted treatment or use of ‘drug holiday’ |
| Specific antidepressant properties (such as potent [5-HT] receptor antagonism, cholinergic effects) |
| Younger patient age (including children and adolescents) |
| Female gender |
| Pregnancy |
| Neonate/breast-fed infant (mother on antidepressant therapy) |
| History of ADS |
| Vulnerability to depressive relapse |
| Duration of treatment (possible increased risk with more than 4 to 6 weeks of antidepressant exposure) |
| Switches to or between generic antidepressant formulations (related to variations in bioequivalence) |
| History of early adverse reactions when the antidepressant was initiated |
| ADS: antidepressant discontinuation syndrome |
| *Risk factors for ADS have not been rigorously studied in randomized controlled trials. Possible risk factors in this table were found in case reports |
What causes ADS?
Although the exact cause of ADS is unknown, the literature proposes several theories.
Because of the central serotonin system’s complex connections, acute reduction in synaptic serotonin when an SSRI or SNRI is abruptly or too quickly stopped may be the first in a cascade of steps affecting transmission of multiple monoamines. Parallels have been drawn between the phenomenon observed with rapid depletion of tryptophan—the essential amino acid precursor for the synthesis of 5-HT—and ADS seen with abrupt discontinuation of serotonergic antidepressants. This suggests that acute drops in neurotransmitter levels can precipitate neuropsychiatric and somatic manifestations of ADS.24
Patients’ uncomfortable symptoms likely are caused by the serotonin, norepinephrine, and cholinergic systems and their complex interactions.25 Individual genetic factors may influence patients’ vulnerability for ADS.
Managing ADS
Awareness and prevention. ADS can be misinterpreted as side effects of newly started treatment after an antidepressant is stopped. In Mr. J’s case, the appearance of muscle aches, headaches, and other ADS symptoms after ECT was started easily could have been perceived as adverse effects of ECT. Mr. J’s agitation and increased suicidal ideation could lead a clinician to mistakenly think that MDE was worsening because the antidepressant was stopped before ECT became effective. Being aware of ADS can prevent misdiagnosis and allow you to quickly identify the condition, manage the reversible syndrome, and continue with new treatment plan—in this case, ECT.
You can help prevent ADS by educating patients about the need to adhere to antidepressant regimens and to avoid missing doses. Consider ADS risk factors—particularly medications’ half-lives—before you start, change, or stop antidepressant therapy. Gradually taper all antidepressants being discontinued, with the possible exception of fluoxetine (which, including its active metabolite, has an elimination half-life of approximately 1 to 2 weeks).
Tapering antidepressants is more art than science because we have no controlled data to support any particular tapering regimen. Tailor the taper duration based on each patient’s response to sequential dosage reductions. Antidepressants with shorter half-lives—such as venlafaxine or paroxetine—may need to be tapered more slowly, perhaps by reducing the dosage by 25% every 4 to 6 weeks. If you plan to switch medications, this process may be expedited during a cross-taper to another antidepressant. You still may see discontinuation symptoms, however, depending on which new agent is chosen and which is being stopped.
Treating ADS. Appropriately recognizing ADS risk and slowly tapering antidepressants as needed usually prevents clinically significant distress associated with discontinuation. For some patients, however, ADS may be particularly severe or prolonged, or may emerge at the end of a slow taper.
Challenging cases may be more likely with paroxetine or venlafaxine—even the extended-release or controlled-release preparations. The elimination half-life of paroxetine is 15 to 20 hours, and the half-lives of venlafaxine and venlafaxine XR are 5 to 11 hours. Desvenlafaxine’s half-life is 11 hours, and product labeling of this enantiomer of racemic venlafaxine notes that discontinuation symptoms have occurred.26 ADS treatment depends on the severity of the reaction and whether or not further antidepressant therapy is necessary.
For mild ADS, reassurance and treatment focused on specific symptoms—such as sedative-hypnotics for insomnia or benzodiazepines for anxiety—may be all that is needed, because ADS tends to gradually resolve over an average of 10 days.27
For more severe ADS, or when ongoing antidepressant therapy is indicated, restarting the recently withdrawn antidepressant at the pre-ADS dosage typically resolves the syndrome within 24 hours. Then employ a slower, more cautious taper when next attempting to discontinue that antidepressant.
Another option. An alternate management strategy is to substitute fluoxetine to suppress ADS associated with shorter half-life SSRIs or SNRIs. Case reports18,20,28 suggest that fluoxetine, 5 to 20 mg/d, can be used to ameliorate venlafaxine-induced ADS. Fluoxetine can be tried as monotherapy for 1 to 2 weeks and then rapidly tapered or stopped. Others have suggested combination therapy, such as:
- restarting venlafaxine at the pre-ADS dose plus fluoxetine, 20 mg/d
- tapering venlafaxine by 50% every 5 days until stopped
- reducing fluoxetine 1 week later to 10 mg/d for 5 days
- then stopping fluoxetine.28
In general, SSRIs should not be co-administered with SNRIs long-term because of potential additive adverse effects such as serotonin syndrome. Combining fluoxetine with an SNRI such as venlafaxine for the purpose of tapering off venlafaxine and reducing ADS risk probably is safe, however, as long as the fluoxetine dose is low (5 to 20 mg) and SNRI reduction begins immediately, with a plan for complete tapering.
CASE CONTINUED: ECT treatment proceeds
Venlafaxine XR is not restarted to address Mr. J’s suspected ADS because of concerns about potential increased risk for cardiac events (asystole, prolonged bradycardia) during ECT with concomitant venlafaxine use.29,30 Fluoxetine, which rarely may prolong ECT-induced seizures, is deemed a safer choice and is started immediately at 20 mg/d.
Because of Mr. J’s other symptoms, we prescribe lorazepam, 0.5 mg bid, for anxiety for 2 days; increase aripiprazole to 5 mg bid for agitation; and add zolpidem, 10 mg at bedtime, for insomnia. The following day, Mr. J reports substantial relief from ADS symptoms, including myalgias, paresthesias, and suicidal ideation.21,23
His second ECT treatment is administered the next day, followed by a successful course of 9 treatments and partial remission of the MDE within 3 weeks. Fluoxetine is reduced to 10 mg/d one week into the ECT series, then discontinued one week later. No signs of emergent ADS are seen at discharge or 2-week outpatient follow-up. Mr. J achieves full remission with maintenance ECT plus bedtime doses of mirtazapine, 30 mg, and aripiprazole, 7.5 mg, across 6 months of follow-up care.
Related resources
- Schatzberg AF, Blier P, Delgado PL, et al. Antidepressant discontinuation syndrome: consensus panel recommendations for clinical management and additional research. J Clin Psychiatry. 2006;67(suppl 4):27-30.
- American Family Physician. Patient handout on antidepressant discontinuation. www.aafp.org/afp/2006/0801/p457.html.
- Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry. 1998;44(2):77-87. See appendix for discontinuation-emergent signs and symptoms checklist.
Drug brand names
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Clomipramine • Anafranil
- Desvenlafaxine • Pristiq
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
- Venlafaxine extended-release • Effexor XR
- Zolpidem • Ambien
Disclosure
Dr. Muzina reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
When Dr. Muzina submitted this article to Current Psychiatry, he was director, Center for Mood Disorders Treatment and Research, Cleveland Clinic Neurological Institute, Cleveland, OH.
1. Berber MJ. FINISH: remembering the discontinuation syndrome. Flu-like symptoms, insomnia, nausea, imbalance, sensory disturbances, and hyperarousal (anxiety/agitation). J Clin Psychiatry. 1998;59(5):255.-
2. Ceccherini-Nelli A, Bardellini L, Cur A, et al. Antidepressant withdrawal: prospective findings. Am J Psychiatry. 1993;150(1):165.-
3. Dilsaver SC, Kronfol Z, Sackellares JC, et al. Antidepressant withdrawal syndromes: evidence supporting the cholinergic overdrive hypothesis. J Clin Psychopharmacol. 1983;3(3):157-164.
4. Garner EM, Kelly MW, Thompson DF. Tricyclic antidepressant withdrawal syndrome. Ann Pharmacother. 1993;27(9):1068-1072.
5. Barr LC, Goodman WK, Price LH. Physical symptoms associated with paroxetine discontinuation. Am J Psychiatry. 1994;151(2):289.-
6. Frost L, Lal S. Shock-like sensations after discontinuation of selective serotonin reuptake inhibitors. Am J Psychiatry. 1995;152(5):810.-
7. Louie AK, Lannon RA, Ajari LJ. Withdrawal reaction after sertraline discontinuation. Am J Psychiatry. 1994;151(3):450-451.
8. Benazzi F. Venlafaxine withdrawal symptoms. Can J Psychiatry. 1996;41(7):487.-
9. Farah A, Lauer TE. Possible venlafaxine withdrawal syndrome. Am J Psychiatry. 1996;153(4):576.-
10. Louie AK, Lannon RA, Kirsch MA, et al. Venlafaxine withdrawal reactions. Am J Psychiatry. 1996;153(12):1652.-
11. Fava M, Mulroy R, Alpert J, et al. Emergence of adverse events following discontinuation of treatment with extended-release venlafaxine. Am J Psychiatry. 1997;154(12):1760-1762.
12. Perahia DG, Kajdasz DK, Desaiah D, et al. Symptoms following abrupt discontinuation of duloxetine treatment in patients with major depressive disorder. J Affect Disord. 2005;89(1-3):207-212.
13. Benazzi F. Mirtazapine withdrawal symptoms. Can J Psychiatry. 1998;43(5):525.-
14. Benazzi F. Nefazodone withdrawal symptoms. Can J Psychiatry. 1998;43(2):194-195.
15. Berigan TR. Bupropion-associated withdrawal symptoms revisited: a case report. Prim Care Companion J Clin Psychiatry. 2002;4(2):78.-
16. Berigan TR, Harazin JS. Bupropion-associated withdrawal symptoms: a case report. Prim Care Companion J Clin Psychiatry. 1999;1(2):50-51.
17. Dilsaver SC. Monoamine oxidase inhibitor withdrawal phenomena: symptoms and pathophysiology. Acta Psychiatr Scand. 1988;78(1):1-7.
18. Coupland NJ, Bell CJ, Potokar JP. Serotonin reuptake inhibitor withdrawal. J Clin Psychopharmacol. 1996;16(5):356-362.
19. Black K, Shea C, Dursun S, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: proposed diagnostic criteria. J Psychiatry Neurosci. 2000;25(3):255-261.
20. Haddad PM. Antidepressant discontinuation syndromes. Drug Saf. 2001;24(3):183-197.
21. Shelton RC. The nature of the discontinuation syndrome associated with antidepressant drugs. J Clin Psychiatry. 2006;67(suppl 4):3-7.
22. Schatzberg AF, Haddad P, Kaplan EM, et al. Serotonin reuptake inhibitor discontinuation syndrome: a hypothetical definition. Discontinuation consensus panel. J Clin Psychiatry. 1997;58(suppl 7):5-10.
23. Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry. 1998;44(2):77-87.
24. Delgado PL. Monoamine depletion studies: implications for antidepressant discontinuation syndrome. J Clin Psychiatry. 2006;67(suppl 4):22-26.
25. Blier P, Tremblay P. Physiologic mechanisms underlying the antidepressant discontinuation syndrome. J Clin Psychiatry. 2006;67(suppl 4):8-13.
26. Wyeth. Desvenlafaxine (Pristiq) prescribing information. Available at: http://www.wyeth.com/content/showlabeling.asp?id=497. Accessed January 27, 2010.
27. Price JS, Waller PC, Wood SM, et al. A comparison of the post-marketing safety of four selective serotonin re-uptake inhibitors including the investigation of symptoms occurring on withdrawal. Br J Clin Pharmacol. 1996;42(6):757-763.
28. Benazzi F. SSRI discontinuation syndrome treated with fluoxetine. Int J Geriatr Psychiatry. 1998;13(6):421-422.
29. Agelink MM, Zeit T, Klieser E. Prolonged bradycardia complicates antidepressive treatment with venlafaxine and ECT. Br J Psychiatry. 1998;173:441.-
30. Gonzalez-Pinto A, Gutierrez M, Gonzalez N, et al. Efficacy and safety of venlafaxine-ECT combination in treatment-resistant depression. J Neuropsychiatry Clin Neurosci. 2002;14(2):206-209.
Most psychiatrists have encountered patients who report distressing symptoms when they have forgotten to take their antidepressant for a few days or during changes in the medication regimen. A discontinuation syndrome can occur with almost any antidepressant, highlighting the need to slowly taper these medications when discontinuation is part of a treatment plan.
This article discusses antidepressant discontinuation syndrome (ADS) in a patient who experienced substantial distress after a rapid antidepressant taper in preparation for electroconvulsive therapy (ECT). My goal is to raise awareness of ADS, promote early detection of the syndrome, and address proper prevention and management strategies.
CASE REPORT: Feeling ‘worse than ever’
Mr. J, a 32-year-old tax accountant, is hospitalized for a major depressive episode (MDE) associated with deteriorating function and suicidal ideation. This second lifetime MDE started 8 months before his admission to an inpatient mood disorders unit.
Mr. J initially was treated with fluoxetine, up to 40 mg/d across 14 weeks, with good tolerability but no significant benefit. His psychiatrist switched Mr. J to bupropion but stopped it after 4 weeks because of side effects—including headaches, insomnia, and tremor—and limited antidepressant benefit. Venlafaxine XR was initiated next, at 150 mg/d within the first 2 weeks, increased to 225 mg/d at week 6, then titrated to 300 mg/d at week 10. After 10 weeks, aripiprazole, 5 mg/d, was added because Mr. J showed only partial, limited response to venlafaxine XR and this antipsychotic is indicated for adjunctive treatment of major depressive disorder.
Mr. J reported mild, transient restlessness but otherwise he tolerated the medications well, and he claimed excellent adherence. After 6 additional weeks of treatment, however, Mr. J was hospitalized because of persistent severely depressed mood, increasing suicidal ideation, and inability to function at work.
On admission, Mr. J is evaluated and agrees to ECT. To meet the ECT service’s protocol, venlafaxine XR is reduced to 150 mg/d for 2 days and then stopped when ECT is started. Aripiprazole is continued at 5 mg/d.
Mr. J tolerates the first ECT treatment well, but the morning before his second treatment he complains of feeling “worse than ever.” An agitated Mr. J reports dramatically intensified suicidal ideation—much more intrusive than before he was hospitalized. He also complains of diffuse muscle aches and cramps, runny nose, nausea, headache, and burning sensations in both arms and hands. He withdraws consent for ECT and returns to the mood disorders unit for ongoing treatment.
Could this be ADS?
Yes, it could. In this case, the inpatient psychiatrist and treatment team were lulled into a false sense of security by Mr. J’s history of few side effects with various treatments and medication changes. The ECT service wanted the patient off venlafaxine XR before beginning ECT, and the treatment team believed a quick taper would not cause discontinuation symptoms because Mr. J was taking an “extended-release” medication.
Within 72 hours, Mr. J went from taking 300 mg/d of venlafaxine XR to none. Within 2 days of cessation, he complained of symptoms that could characterize a discontinuation syndrome. A potential red herring in this case is that the patient complained of feeling worse after his first ECT treatment, and one might erroneously think the myalgias, headache, and other somatic symptoms were side effects of ECT and/or anesthesia.
Typical ADS symptoms
Nearly all antidepressant classes are associated with ADS. Symptoms vary from patient to patient but typically include the “FINISH” syndrome: flu-like symptoms, ###bold/bold###nsomnia, nausea, ###bold/bold###mbalance, sensory disturbances, and hyperarousal (anxiety/agitation) (Table 1).1
Adverse effects after stopping tricyclic antidepressants have been well documented. They may include FINISH syndrome features as well as cholinergic overdrive or “rebound” such as abdominal cramping and diarrhea.2-4 Reports of ADS after patients stopped selective serotonin reuptake inhibitors (SSRIs) emerged soon after these agents were introduced.5-7 Similarly, ADS has been reported with serotonin-norepinephrine reuptake inhibitors (SNRIs), including venlafaxine,8-10 venlafaxine XR,11 and duloxetine.12 ADS symptoms are similar with SSRIs and SNRIs, generally without the anticholinergic effects associated with tricyclic antidepressant discontinuation.
Fewer reports of discontinuation syndrome exist for bupropion, mirtazapine, monoamine oxidase inhibitors (MAOIs), and nefazodone.13-17 Discontinuation-emergent syndromes with these non-SSRI/non-SNRI antidepressants tend to present differently. With MAOIs, for example, neuropsychiatric symptoms such as severe anxiety, agitation, pressured speech, sleeplessness or drowsiness, hallucinations, delirium, and paranoid psychosis can be prominent.17
The prevalence of ADS is unclear, and published estimates vary widely because of the lack of large controlled studies. ADS rates with SSRIs/SNRIs have been reported from as low as 0% for fluoxetine to higher rates for shorter half-life antidepressants:
- 2.2% with sertraline
- 14% with fluvoxamine
- 20% with paroxetine
- 30.8% with clomipramine.
These rates come from a retrospective case note review of patients who discontinued antidepressants under supervision.18 In a small cohort of outpatients being treated for major depressive disorder, stopping venlafaxine XR was associated with discontinuation symptoms for the next 3 days in 7 of 9 patients (78%), compared with 2 of 9 patients (22%) stopping placebo.11
Diagnostic criteria have been proposed for ADS associated with serotonin (5-HT) reuptake inhibitors.19-22 Proposed ADS definitions differ somewhat, but essentially 3 features guide the diagnosis:
- appearance of characteristic symptoms (Table 2)21,23
- timing of those symptoms, which usually emerge within 1 week of abrupt cessation or marked reduction of the antidepressant
- symptoms generally are mild, short-lived, self-limiting, and/or rapidly reversed by restarting the original antidepressant.
Evidence suggests shorter half-life antidepressants may be associated with the highest risk for ADS, but other risk factors remain presumptive (Table 3).
Table 1
FINISH: Symptoms of antidepressant discontinuation syndrome
| Flu-like symptoms |
| Insomnia |
| Nausea |
| Imbalance |
| Sensory disturbances |
| Hyperarousal (anxiety/agitation) |
| Source: Reference 1 |
Table 2
ADS symptoms can range across a variety of system clusters
| System cluster | Symptoms |
|---|---|
| Neurosensory | Vertigo, paresthesias, shock-like reactions, myalgias, numbness, sensitivity to sound, unusual visual sensations, ringing in the ears |
| Neuromotor | Tremor, myoclonus, ataxia/gait instability, visual changes, restless legs, problems with speech, tongue movements |
| Gastrointestinal | Nausea, vomiting, cramps/bloating, diarrhea, anorexia |
| Neuropsychiatric | Anxiety/panic, depression, mood swings, suicidal ideation, irritability, impulsivity, confusion, psychosis |
| Vasomotor | Diaphoresis, flushing, temperature intolerance |
| Other | Headache, insomnia, vivid dreams, nightmares, lethargy/fatigue, flu-like symptoms |
| ADS: antidepressant discontinuation syndrome | |
| Source: Construct suggested by Shelton,21 with additional symptoms added from other sources, including the discontinuation symptom checklist of Rosenbaum et al23 | |
Table 3
Possible patient risk factors for developing ADS*
| Abrupt antidepressant discontinuation |
| Shorter half-life antidepressants |
| Intermittent nonadherence/noncompliance |
| Interrupted treatment or use of ‘drug holiday’ |
| Specific antidepressant properties (such as potent [5-HT] receptor antagonism, cholinergic effects) |
| Younger patient age (including children and adolescents) |
| Female gender |
| Pregnancy |
| Neonate/breast-fed infant (mother on antidepressant therapy) |
| History of ADS |
| Vulnerability to depressive relapse |
| Duration of treatment (possible increased risk with more than 4 to 6 weeks of antidepressant exposure) |
| Switches to or between generic antidepressant formulations (related to variations in bioequivalence) |
| History of early adverse reactions when the antidepressant was initiated |
| ADS: antidepressant discontinuation syndrome |
| *Risk factors for ADS have not been rigorously studied in randomized controlled trials. Possible risk factors in this table were found in case reports |
What causes ADS?
Although the exact cause of ADS is unknown, the literature proposes several theories.
Because of the central serotonin system’s complex connections, acute reduction in synaptic serotonin when an SSRI or SNRI is abruptly or too quickly stopped may be the first in a cascade of steps affecting transmission of multiple monoamines. Parallels have been drawn between the phenomenon observed with rapid depletion of tryptophan—the essential amino acid precursor for the synthesis of 5-HT—and ADS seen with abrupt discontinuation of serotonergic antidepressants. This suggests that acute drops in neurotransmitter levels can precipitate neuropsychiatric and somatic manifestations of ADS.24
Patients’ uncomfortable symptoms likely are caused by the serotonin, norepinephrine, and cholinergic systems and their complex interactions.25 Individual genetic factors may influence patients’ vulnerability for ADS.
Managing ADS
Awareness and prevention. ADS can be misinterpreted as side effects of newly started treatment after an antidepressant is stopped. In Mr. J’s case, the appearance of muscle aches, headaches, and other ADS symptoms after ECT was started easily could have been perceived as adverse effects of ECT. Mr. J’s agitation and increased suicidal ideation could lead a clinician to mistakenly think that MDE was worsening because the antidepressant was stopped before ECT became effective. Being aware of ADS can prevent misdiagnosis and allow you to quickly identify the condition, manage the reversible syndrome, and continue with new treatment plan—in this case, ECT.
You can help prevent ADS by educating patients about the need to adhere to antidepressant regimens and to avoid missing doses. Consider ADS risk factors—particularly medications’ half-lives—before you start, change, or stop antidepressant therapy. Gradually taper all antidepressants being discontinued, with the possible exception of fluoxetine (which, including its active metabolite, has an elimination half-life of approximately 1 to 2 weeks).
Tapering antidepressants is more art than science because we have no controlled data to support any particular tapering regimen. Tailor the taper duration based on each patient’s response to sequential dosage reductions. Antidepressants with shorter half-lives—such as venlafaxine or paroxetine—may need to be tapered more slowly, perhaps by reducing the dosage by 25% every 4 to 6 weeks. If you plan to switch medications, this process may be expedited during a cross-taper to another antidepressant. You still may see discontinuation symptoms, however, depending on which new agent is chosen and which is being stopped.
Treating ADS. Appropriately recognizing ADS risk and slowly tapering antidepressants as needed usually prevents clinically significant distress associated with discontinuation. For some patients, however, ADS may be particularly severe or prolonged, or may emerge at the end of a slow taper.
Challenging cases may be more likely with paroxetine or venlafaxine—even the extended-release or controlled-release preparations. The elimination half-life of paroxetine is 15 to 20 hours, and the half-lives of venlafaxine and venlafaxine XR are 5 to 11 hours. Desvenlafaxine’s half-life is 11 hours, and product labeling of this enantiomer of racemic venlafaxine notes that discontinuation symptoms have occurred.26 ADS treatment depends on the severity of the reaction and whether or not further antidepressant therapy is necessary.
For mild ADS, reassurance and treatment focused on specific symptoms—such as sedative-hypnotics for insomnia or benzodiazepines for anxiety—may be all that is needed, because ADS tends to gradually resolve over an average of 10 days.27
For more severe ADS, or when ongoing antidepressant therapy is indicated, restarting the recently withdrawn antidepressant at the pre-ADS dosage typically resolves the syndrome within 24 hours. Then employ a slower, more cautious taper when next attempting to discontinue that antidepressant.
Another option. An alternate management strategy is to substitute fluoxetine to suppress ADS associated with shorter half-life SSRIs or SNRIs. Case reports18,20,28 suggest that fluoxetine, 5 to 20 mg/d, can be used to ameliorate venlafaxine-induced ADS. Fluoxetine can be tried as monotherapy for 1 to 2 weeks and then rapidly tapered or stopped. Others have suggested combination therapy, such as:
- restarting venlafaxine at the pre-ADS dose plus fluoxetine, 20 mg/d
- tapering venlafaxine by 50% every 5 days until stopped
- reducing fluoxetine 1 week later to 10 mg/d for 5 days
- then stopping fluoxetine.28
In general, SSRIs should not be co-administered with SNRIs long-term because of potential additive adverse effects such as serotonin syndrome. Combining fluoxetine with an SNRI such as venlafaxine for the purpose of tapering off venlafaxine and reducing ADS risk probably is safe, however, as long as the fluoxetine dose is low (5 to 20 mg) and SNRI reduction begins immediately, with a plan for complete tapering.
CASE CONTINUED: ECT treatment proceeds
Venlafaxine XR is not restarted to address Mr. J’s suspected ADS because of concerns about potential increased risk for cardiac events (asystole, prolonged bradycardia) during ECT with concomitant venlafaxine use.29,30 Fluoxetine, which rarely may prolong ECT-induced seizures, is deemed a safer choice and is started immediately at 20 mg/d.
Because of Mr. J’s other symptoms, we prescribe lorazepam, 0.5 mg bid, for anxiety for 2 days; increase aripiprazole to 5 mg bid for agitation; and add zolpidem, 10 mg at bedtime, for insomnia. The following day, Mr. J reports substantial relief from ADS symptoms, including myalgias, paresthesias, and suicidal ideation.21,23
His second ECT treatment is administered the next day, followed by a successful course of 9 treatments and partial remission of the MDE within 3 weeks. Fluoxetine is reduced to 10 mg/d one week into the ECT series, then discontinued one week later. No signs of emergent ADS are seen at discharge or 2-week outpatient follow-up. Mr. J achieves full remission with maintenance ECT plus bedtime doses of mirtazapine, 30 mg, and aripiprazole, 7.5 mg, across 6 months of follow-up care.
Related resources
- Schatzberg AF, Blier P, Delgado PL, et al. Antidepressant discontinuation syndrome: consensus panel recommendations for clinical management and additional research. J Clin Psychiatry. 2006;67(suppl 4):27-30.
- American Family Physician. Patient handout on antidepressant discontinuation. www.aafp.org/afp/2006/0801/p457.html.
- Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry. 1998;44(2):77-87. See appendix for discontinuation-emergent signs and symptoms checklist.
Drug brand names
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Clomipramine • Anafranil
- Desvenlafaxine • Pristiq
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
- Venlafaxine extended-release • Effexor XR
- Zolpidem • Ambien
Disclosure
Dr. Muzina reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
When Dr. Muzina submitted this article to Current Psychiatry, he was director, Center for Mood Disorders Treatment and Research, Cleveland Clinic Neurological Institute, Cleveland, OH.
Most psychiatrists have encountered patients who report distressing symptoms when they have forgotten to take their antidepressant for a few days or during changes in the medication regimen. A discontinuation syndrome can occur with almost any antidepressant, highlighting the need to slowly taper these medications when discontinuation is part of a treatment plan.
This article discusses antidepressant discontinuation syndrome (ADS) in a patient who experienced substantial distress after a rapid antidepressant taper in preparation for electroconvulsive therapy (ECT). My goal is to raise awareness of ADS, promote early detection of the syndrome, and address proper prevention and management strategies.
CASE REPORT: Feeling ‘worse than ever’
Mr. J, a 32-year-old tax accountant, is hospitalized for a major depressive episode (MDE) associated with deteriorating function and suicidal ideation. This second lifetime MDE started 8 months before his admission to an inpatient mood disorders unit.
Mr. J initially was treated with fluoxetine, up to 40 mg/d across 14 weeks, with good tolerability but no significant benefit. His psychiatrist switched Mr. J to bupropion but stopped it after 4 weeks because of side effects—including headaches, insomnia, and tremor—and limited antidepressant benefit. Venlafaxine XR was initiated next, at 150 mg/d within the first 2 weeks, increased to 225 mg/d at week 6, then titrated to 300 mg/d at week 10. After 10 weeks, aripiprazole, 5 mg/d, was added because Mr. J showed only partial, limited response to venlafaxine XR and this antipsychotic is indicated for adjunctive treatment of major depressive disorder.
Mr. J reported mild, transient restlessness but otherwise he tolerated the medications well, and he claimed excellent adherence. After 6 additional weeks of treatment, however, Mr. J was hospitalized because of persistent severely depressed mood, increasing suicidal ideation, and inability to function at work.
On admission, Mr. J is evaluated and agrees to ECT. To meet the ECT service’s protocol, venlafaxine XR is reduced to 150 mg/d for 2 days and then stopped when ECT is started. Aripiprazole is continued at 5 mg/d.
Mr. J tolerates the first ECT treatment well, but the morning before his second treatment he complains of feeling “worse than ever.” An agitated Mr. J reports dramatically intensified suicidal ideation—much more intrusive than before he was hospitalized. He also complains of diffuse muscle aches and cramps, runny nose, nausea, headache, and burning sensations in both arms and hands. He withdraws consent for ECT and returns to the mood disorders unit for ongoing treatment.
Could this be ADS?
Yes, it could. In this case, the inpatient psychiatrist and treatment team were lulled into a false sense of security by Mr. J’s history of few side effects with various treatments and medication changes. The ECT service wanted the patient off venlafaxine XR before beginning ECT, and the treatment team believed a quick taper would not cause discontinuation symptoms because Mr. J was taking an “extended-release” medication.
Within 72 hours, Mr. J went from taking 300 mg/d of venlafaxine XR to none. Within 2 days of cessation, he complained of symptoms that could characterize a discontinuation syndrome. A potential red herring in this case is that the patient complained of feeling worse after his first ECT treatment, and one might erroneously think the myalgias, headache, and other somatic symptoms were side effects of ECT and/or anesthesia.
Typical ADS symptoms
Nearly all antidepressant classes are associated with ADS. Symptoms vary from patient to patient but typically include the “FINISH” syndrome: flu-like symptoms, ###bold/bold###nsomnia, nausea, ###bold/bold###mbalance, sensory disturbances, and hyperarousal (anxiety/agitation) (Table 1).1
Adverse effects after stopping tricyclic antidepressants have been well documented. They may include FINISH syndrome features as well as cholinergic overdrive or “rebound” such as abdominal cramping and diarrhea.2-4 Reports of ADS after patients stopped selective serotonin reuptake inhibitors (SSRIs) emerged soon after these agents were introduced.5-7 Similarly, ADS has been reported with serotonin-norepinephrine reuptake inhibitors (SNRIs), including venlafaxine,8-10 venlafaxine XR,11 and duloxetine.12 ADS symptoms are similar with SSRIs and SNRIs, generally without the anticholinergic effects associated with tricyclic antidepressant discontinuation.
Fewer reports of discontinuation syndrome exist for bupropion, mirtazapine, monoamine oxidase inhibitors (MAOIs), and nefazodone.13-17 Discontinuation-emergent syndromes with these non-SSRI/non-SNRI antidepressants tend to present differently. With MAOIs, for example, neuropsychiatric symptoms such as severe anxiety, agitation, pressured speech, sleeplessness or drowsiness, hallucinations, delirium, and paranoid psychosis can be prominent.17
The prevalence of ADS is unclear, and published estimates vary widely because of the lack of large controlled studies. ADS rates with SSRIs/SNRIs have been reported from as low as 0% for fluoxetine to higher rates for shorter half-life antidepressants:
- 2.2% with sertraline
- 14% with fluvoxamine
- 20% with paroxetine
- 30.8% with clomipramine.
These rates come from a retrospective case note review of patients who discontinued antidepressants under supervision.18 In a small cohort of outpatients being treated for major depressive disorder, stopping venlafaxine XR was associated with discontinuation symptoms for the next 3 days in 7 of 9 patients (78%), compared with 2 of 9 patients (22%) stopping placebo.11
Diagnostic criteria have been proposed for ADS associated with serotonin (5-HT) reuptake inhibitors.19-22 Proposed ADS definitions differ somewhat, but essentially 3 features guide the diagnosis:
- appearance of characteristic symptoms (Table 2)21,23
- timing of those symptoms, which usually emerge within 1 week of abrupt cessation or marked reduction of the antidepressant
- symptoms generally are mild, short-lived, self-limiting, and/or rapidly reversed by restarting the original antidepressant.
Evidence suggests shorter half-life antidepressants may be associated with the highest risk for ADS, but other risk factors remain presumptive (Table 3).
Table 1
FINISH: Symptoms of antidepressant discontinuation syndrome
| Flu-like symptoms |
| Insomnia |
| Nausea |
| Imbalance |
| Sensory disturbances |
| Hyperarousal (anxiety/agitation) |
| Source: Reference 1 |
Table 2
ADS symptoms can range across a variety of system clusters
| System cluster | Symptoms |
|---|---|
| Neurosensory | Vertigo, paresthesias, shock-like reactions, myalgias, numbness, sensitivity to sound, unusual visual sensations, ringing in the ears |
| Neuromotor | Tremor, myoclonus, ataxia/gait instability, visual changes, restless legs, problems with speech, tongue movements |
| Gastrointestinal | Nausea, vomiting, cramps/bloating, diarrhea, anorexia |
| Neuropsychiatric | Anxiety/panic, depression, mood swings, suicidal ideation, irritability, impulsivity, confusion, psychosis |
| Vasomotor | Diaphoresis, flushing, temperature intolerance |
| Other | Headache, insomnia, vivid dreams, nightmares, lethargy/fatigue, flu-like symptoms |
| ADS: antidepressant discontinuation syndrome | |
| Source: Construct suggested by Shelton,21 with additional symptoms added from other sources, including the discontinuation symptom checklist of Rosenbaum et al23 | |
Table 3
Possible patient risk factors for developing ADS*
| Abrupt antidepressant discontinuation |
| Shorter half-life antidepressants |
| Intermittent nonadherence/noncompliance |
| Interrupted treatment or use of ‘drug holiday’ |
| Specific antidepressant properties (such as potent [5-HT] receptor antagonism, cholinergic effects) |
| Younger patient age (including children and adolescents) |
| Female gender |
| Pregnancy |
| Neonate/breast-fed infant (mother on antidepressant therapy) |
| History of ADS |
| Vulnerability to depressive relapse |
| Duration of treatment (possible increased risk with more than 4 to 6 weeks of antidepressant exposure) |
| Switches to or between generic antidepressant formulations (related to variations in bioequivalence) |
| History of early adverse reactions when the antidepressant was initiated |
| ADS: antidepressant discontinuation syndrome |
| *Risk factors for ADS have not been rigorously studied in randomized controlled trials. Possible risk factors in this table were found in case reports |
What causes ADS?
Although the exact cause of ADS is unknown, the literature proposes several theories.
Because of the central serotonin system’s complex connections, acute reduction in synaptic serotonin when an SSRI or SNRI is abruptly or too quickly stopped may be the first in a cascade of steps affecting transmission of multiple monoamines. Parallels have been drawn between the phenomenon observed with rapid depletion of tryptophan—the essential amino acid precursor for the synthesis of 5-HT—and ADS seen with abrupt discontinuation of serotonergic antidepressants. This suggests that acute drops in neurotransmitter levels can precipitate neuropsychiatric and somatic manifestations of ADS.24
Patients’ uncomfortable symptoms likely are caused by the serotonin, norepinephrine, and cholinergic systems and their complex interactions.25 Individual genetic factors may influence patients’ vulnerability for ADS.
Managing ADS
Awareness and prevention. ADS can be misinterpreted as side effects of newly started treatment after an antidepressant is stopped. In Mr. J’s case, the appearance of muscle aches, headaches, and other ADS symptoms after ECT was started easily could have been perceived as adverse effects of ECT. Mr. J’s agitation and increased suicidal ideation could lead a clinician to mistakenly think that MDE was worsening because the antidepressant was stopped before ECT became effective. Being aware of ADS can prevent misdiagnosis and allow you to quickly identify the condition, manage the reversible syndrome, and continue with new treatment plan—in this case, ECT.
You can help prevent ADS by educating patients about the need to adhere to antidepressant regimens and to avoid missing doses. Consider ADS risk factors—particularly medications’ half-lives—before you start, change, or stop antidepressant therapy. Gradually taper all antidepressants being discontinued, with the possible exception of fluoxetine (which, including its active metabolite, has an elimination half-life of approximately 1 to 2 weeks).
Tapering antidepressants is more art than science because we have no controlled data to support any particular tapering regimen. Tailor the taper duration based on each patient’s response to sequential dosage reductions. Antidepressants with shorter half-lives—such as venlafaxine or paroxetine—may need to be tapered more slowly, perhaps by reducing the dosage by 25% every 4 to 6 weeks. If you plan to switch medications, this process may be expedited during a cross-taper to another antidepressant. You still may see discontinuation symptoms, however, depending on which new agent is chosen and which is being stopped.
Treating ADS. Appropriately recognizing ADS risk and slowly tapering antidepressants as needed usually prevents clinically significant distress associated with discontinuation. For some patients, however, ADS may be particularly severe or prolonged, or may emerge at the end of a slow taper.
Challenging cases may be more likely with paroxetine or venlafaxine—even the extended-release or controlled-release preparations. The elimination half-life of paroxetine is 15 to 20 hours, and the half-lives of venlafaxine and venlafaxine XR are 5 to 11 hours. Desvenlafaxine’s half-life is 11 hours, and product labeling of this enantiomer of racemic venlafaxine notes that discontinuation symptoms have occurred.26 ADS treatment depends on the severity of the reaction and whether or not further antidepressant therapy is necessary.
For mild ADS, reassurance and treatment focused on specific symptoms—such as sedative-hypnotics for insomnia or benzodiazepines for anxiety—may be all that is needed, because ADS tends to gradually resolve over an average of 10 days.27
For more severe ADS, or when ongoing antidepressant therapy is indicated, restarting the recently withdrawn antidepressant at the pre-ADS dosage typically resolves the syndrome within 24 hours. Then employ a slower, more cautious taper when next attempting to discontinue that antidepressant.
Another option. An alternate management strategy is to substitute fluoxetine to suppress ADS associated with shorter half-life SSRIs or SNRIs. Case reports18,20,28 suggest that fluoxetine, 5 to 20 mg/d, can be used to ameliorate venlafaxine-induced ADS. Fluoxetine can be tried as monotherapy for 1 to 2 weeks and then rapidly tapered or stopped. Others have suggested combination therapy, such as:
- restarting venlafaxine at the pre-ADS dose plus fluoxetine, 20 mg/d
- tapering venlafaxine by 50% every 5 days until stopped
- reducing fluoxetine 1 week later to 10 mg/d for 5 days
- then stopping fluoxetine.28
In general, SSRIs should not be co-administered with SNRIs long-term because of potential additive adverse effects such as serotonin syndrome. Combining fluoxetine with an SNRI such as venlafaxine for the purpose of tapering off venlafaxine and reducing ADS risk probably is safe, however, as long as the fluoxetine dose is low (5 to 20 mg) and SNRI reduction begins immediately, with a plan for complete tapering.
CASE CONTINUED: ECT treatment proceeds
Venlafaxine XR is not restarted to address Mr. J’s suspected ADS because of concerns about potential increased risk for cardiac events (asystole, prolonged bradycardia) during ECT with concomitant venlafaxine use.29,30 Fluoxetine, which rarely may prolong ECT-induced seizures, is deemed a safer choice and is started immediately at 20 mg/d.
Because of Mr. J’s other symptoms, we prescribe lorazepam, 0.5 mg bid, for anxiety for 2 days; increase aripiprazole to 5 mg bid for agitation; and add zolpidem, 10 mg at bedtime, for insomnia. The following day, Mr. J reports substantial relief from ADS symptoms, including myalgias, paresthesias, and suicidal ideation.21,23
His second ECT treatment is administered the next day, followed by a successful course of 9 treatments and partial remission of the MDE within 3 weeks. Fluoxetine is reduced to 10 mg/d one week into the ECT series, then discontinued one week later. No signs of emergent ADS are seen at discharge or 2-week outpatient follow-up. Mr. J achieves full remission with maintenance ECT plus bedtime doses of mirtazapine, 30 mg, and aripiprazole, 7.5 mg, across 6 months of follow-up care.
Related resources
- Schatzberg AF, Blier P, Delgado PL, et al. Antidepressant discontinuation syndrome: consensus panel recommendations for clinical management and additional research. J Clin Psychiatry. 2006;67(suppl 4):27-30.
- American Family Physician. Patient handout on antidepressant discontinuation. www.aafp.org/afp/2006/0801/p457.html.
- Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry. 1998;44(2):77-87. See appendix for discontinuation-emergent signs and symptoms checklist.
Drug brand names
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Clomipramine • Anafranil
- Desvenlafaxine • Pristiq
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
- Venlafaxine extended-release • Effexor XR
- Zolpidem • Ambien
Disclosure
Dr. Muzina reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
When Dr. Muzina submitted this article to Current Psychiatry, he was director, Center for Mood Disorders Treatment and Research, Cleveland Clinic Neurological Institute, Cleveland, OH.
1. Berber MJ. FINISH: remembering the discontinuation syndrome. Flu-like symptoms, insomnia, nausea, imbalance, sensory disturbances, and hyperarousal (anxiety/agitation). J Clin Psychiatry. 1998;59(5):255.-
2. Ceccherini-Nelli A, Bardellini L, Cur A, et al. Antidepressant withdrawal: prospective findings. Am J Psychiatry. 1993;150(1):165.-
3. Dilsaver SC, Kronfol Z, Sackellares JC, et al. Antidepressant withdrawal syndromes: evidence supporting the cholinergic overdrive hypothesis. J Clin Psychopharmacol. 1983;3(3):157-164.
4. Garner EM, Kelly MW, Thompson DF. Tricyclic antidepressant withdrawal syndrome. Ann Pharmacother. 1993;27(9):1068-1072.
5. Barr LC, Goodman WK, Price LH. Physical symptoms associated with paroxetine discontinuation. Am J Psychiatry. 1994;151(2):289.-
6. Frost L, Lal S. Shock-like sensations after discontinuation of selective serotonin reuptake inhibitors. Am J Psychiatry. 1995;152(5):810.-
7. Louie AK, Lannon RA, Ajari LJ. Withdrawal reaction after sertraline discontinuation. Am J Psychiatry. 1994;151(3):450-451.
8. Benazzi F. Venlafaxine withdrawal symptoms. Can J Psychiatry. 1996;41(7):487.-
9. Farah A, Lauer TE. Possible venlafaxine withdrawal syndrome. Am J Psychiatry. 1996;153(4):576.-
10. Louie AK, Lannon RA, Kirsch MA, et al. Venlafaxine withdrawal reactions. Am J Psychiatry. 1996;153(12):1652.-
11. Fava M, Mulroy R, Alpert J, et al. Emergence of adverse events following discontinuation of treatment with extended-release venlafaxine. Am J Psychiatry. 1997;154(12):1760-1762.
12. Perahia DG, Kajdasz DK, Desaiah D, et al. Symptoms following abrupt discontinuation of duloxetine treatment in patients with major depressive disorder. J Affect Disord. 2005;89(1-3):207-212.
13. Benazzi F. Mirtazapine withdrawal symptoms. Can J Psychiatry. 1998;43(5):525.-
14. Benazzi F. Nefazodone withdrawal symptoms. Can J Psychiatry. 1998;43(2):194-195.
15. Berigan TR. Bupropion-associated withdrawal symptoms revisited: a case report. Prim Care Companion J Clin Psychiatry. 2002;4(2):78.-
16. Berigan TR, Harazin JS. Bupropion-associated withdrawal symptoms: a case report. Prim Care Companion J Clin Psychiatry. 1999;1(2):50-51.
17. Dilsaver SC. Monoamine oxidase inhibitor withdrawal phenomena: symptoms and pathophysiology. Acta Psychiatr Scand. 1988;78(1):1-7.
18. Coupland NJ, Bell CJ, Potokar JP. Serotonin reuptake inhibitor withdrawal. J Clin Psychopharmacol. 1996;16(5):356-362.
19. Black K, Shea C, Dursun S, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: proposed diagnostic criteria. J Psychiatry Neurosci. 2000;25(3):255-261.
20. Haddad PM. Antidepressant discontinuation syndromes. Drug Saf. 2001;24(3):183-197.
21. Shelton RC. The nature of the discontinuation syndrome associated with antidepressant drugs. J Clin Psychiatry. 2006;67(suppl 4):3-7.
22. Schatzberg AF, Haddad P, Kaplan EM, et al. Serotonin reuptake inhibitor discontinuation syndrome: a hypothetical definition. Discontinuation consensus panel. J Clin Psychiatry. 1997;58(suppl 7):5-10.
23. Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry. 1998;44(2):77-87.
24. Delgado PL. Monoamine depletion studies: implications for antidepressant discontinuation syndrome. J Clin Psychiatry. 2006;67(suppl 4):22-26.
25. Blier P, Tremblay P. Physiologic mechanisms underlying the antidepressant discontinuation syndrome. J Clin Psychiatry. 2006;67(suppl 4):8-13.
26. Wyeth. Desvenlafaxine (Pristiq) prescribing information. Available at: http://www.wyeth.com/content/showlabeling.asp?id=497. Accessed January 27, 2010.
27. Price JS, Waller PC, Wood SM, et al. A comparison of the post-marketing safety of four selective serotonin re-uptake inhibitors including the investigation of symptoms occurring on withdrawal. Br J Clin Pharmacol. 1996;42(6):757-763.
28. Benazzi F. SSRI discontinuation syndrome treated with fluoxetine. Int J Geriatr Psychiatry. 1998;13(6):421-422.
29. Agelink MM, Zeit T, Klieser E. Prolonged bradycardia complicates antidepressive treatment with venlafaxine and ECT. Br J Psychiatry. 1998;173:441.-
30. Gonzalez-Pinto A, Gutierrez M, Gonzalez N, et al. Efficacy and safety of venlafaxine-ECT combination in treatment-resistant depression. J Neuropsychiatry Clin Neurosci. 2002;14(2):206-209.
1. Berber MJ. FINISH: remembering the discontinuation syndrome. Flu-like symptoms, insomnia, nausea, imbalance, sensory disturbances, and hyperarousal (anxiety/agitation). J Clin Psychiatry. 1998;59(5):255.-
2. Ceccherini-Nelli A, Bardellini L, Cur A, et al. Antidepressant withdrawal: prospective findings. Am J Psychiatry. 1993;150(1):165.-
3. Dilsaver SC, Kronfol Z, Sackellares JC, et al. Antidepressant withdrawal syndromes: evidence supporting the cholinergic overdrive hypothesis. J Clin Psychopharmacol. 1983;3(3):157-164.
4. Garner EM, Kelly MW, Thompson DF. Tricyclic antidepressant withdrawal syndrome. Ann Pharmacother. 1993;27(9):1068-1072.
5. Barr LC, Goodman WK, Price LH. Physical symptoms associated with paroxetine discontinuation. Am J Psychiatry. 1994;151(2):289.-
6. Frost L, Lal S. Shock-like sensations after discontinuation of selective serotonin reuptake inhibitors. Am J Psychiatry. 1995;152(5):810.-
7. Louie AK, Lannon RA, Ajari LJ. Withdrawal reaction after sertraline discontinuation. Am J Psychiatry. 1994;151(3):450-451.
8. Benazzi F. Venlafaxine withdrawal symptoms. Can J Psychiatry. 1996;41(7):487.-
9. Farah A, Lauer TE. Possible venlafaxine withdrawal syndrome. Am J Psychiatry. 1996;153(4):576.-
10. Louie AK, Lannon RA, Kirsch MA, et al. Venlafaxine withdrawal reactions. Am J Psychiatry. 1996;153(12):1652.-
11. Fava M, Mulroy R, Alpert J, et al. Emergence of adverse events following discontinuation of treatment with extended-release venlafaxine. Am J Psychiatry. 1997;154(12):1760-1762.
12. Perahia DG, Kajdasz DK, Desaiah D, et al. Symptoms following abrupt discontinuation of duloxetine treatment in patients with major depressive disorder. J Affect Disord. 2005;89(1-3):207-212.
13. Benazzi F. Mirtazapine withdrawal symptoms. Can J Psychiatry. 1998;43(5):525.-
14. Benazzi F. Nefazodone withdrawal symptoms. Can J Psychiatry. 1998;43(2):194-195.
15. Berigan TR. Bupropion-associated withdrawal symptoms revisited: a case report. Prim Care Companion J Clin Psychiatry. 2002;4(2):78.-
16. Berigan TR, Harazin JS. Bupropion-associated withdrawal symptoms: a case report. Prim Care Companion J Clin Psychiatry. 1999;1(2):50-51.
17. Dilsaver SC. Monoamine oxidase inhibitor withdrawal phenomena: symptoms and pathophysiology. Acta Psychiatr Scand. 1988;78(1):1-7.
18. Coupland NJ, Bell CJ, Potokar JP. Serotonin reuptake inhibitor withdrawal. J Clin Psychopharmacol. 1996;16(5):356-362.
19. Black K, Shea C, Dursun S, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: proposed diagnostic criteria. J Psychiatry Neurosci. 2000;25(3):255-261.
20. Haddad PM. Antidepressant discontinuation syndromes. Drug Saf. 2001;24(3):183-197.
21. Shelton RC. The nature of the discontinuation syndrome associated with antidepressant drugs. J Clin Psychiatry. 2006;67(suppl 4):3-7.
22. Schatzberg AF, Haddad P, Kaplan EM, et al. Serotonin reuptake inhibitor discontinuation syndrome: a hypothetical definition. Discontinuation consensus panel. J Clin Psychiatry. 1997;58(suppl 7):5-10.
23. Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry. 1998;44(2):77-87.
24. Delgado PL. Monoamine depletion studies: implications for antidepressant discontinuation syndrome. J Clin Psychiatry. 2006;67(suppl 4):22-26.
25. Blier P, Tremblay P. Physiologic mechanisms underlying the antidepressant discontinuation syndrome. J Clin Psychiatry. 2006;67(suppl 4):8-13.
26. Wyeth. Desvenlafaxine (Pristiq) prescribing information. Available at: http://www.wyeth.com/content/showlabeling.asp?id=497. Accessed January 27, 2010.
27. Price JS, Waller PC, Wood SM, et al. A comparison of the post-marketing safety of four selective serotonin re-uptake inhibitors including the investigation of symptoms occurring on withdrawal. Br J Clin Pharmacol. 1996;42(6):757-763.
28. Benazzi F. SSRI discontinuation syndrome treated with fluoxetine. Int J Geriatr Psychiatry. 1998;13(6):421-422.
29. Agelink MM, Zeit T, Klieser E. Prolonged bradycardia complicates antidepressive treatment with venlafaxine and ECT. Br J Psychiatry. 1998;173:441.-
30. Gonzalez-Pinto A, Gutierrez M, Gonzalez N, et al. Efficacy and safety of venlafaxine-ECT combination in treatment-resistant depression. J Neuropsychiatry Clin Neurosci. 2002;14(2):206-209.
Paliperidone palmitate: Once-monthly treatment option for schizophrenia
Paliperidone palmitate (9-hydroxyrisperidone) is an injectable, once-monthly atypical antipsychotic medication, FDA-approved in July 2009 for acute and/or maintenance treatment of schizophrenia. This aqueous-based, extremely slowly dissolving depot medication is well tolerated and causes few drug-drug interactions.1 Clinically, paliperidone palmitate and its parent drug, intramuscular (IM) risperidone, have similarities and differences.
Clinical information
Paliperidone palmitate is available in 39-mg, 78-mg, 117-mg, 156-mg, and 234-mg formulations. Once administered, it hydrolyzes and diffuses slowly and provides paliperidone doses equivalent to 25 mg, 50 mg, 75 mg, 100 mg, and 150 mg, respectively. The 234-mg dose of paliperidone palmitate is equivalent to 12 mg oral paliperidone, 117 mg to 6 mg, and 39 to 78 mg to 3 mg, respectively (visit this article at CurrentPsychiatry.com to learn more about paliperidone palmitate).
Pharmacokinetics. This palmitate ester of paliperidone is an aqueous suspension utilizing nanocrystal molecules. The increased surface area leads to rapid medication release and a short time to steady state. Active paliperidone plasma levels were detected at day 1, meaning co-administration with the oral formulation is not necessary. Paliperidone palmitate’s slow dissolution rate results in a half-life of 25 to 49 days. The fast onset of action and long half-life simplifies administration.
Co-administration with carbamazepine decreases paliperidone levels, whereas divalproex causes an increase. Up to 60% of paliperidone is excreted unchanged through the kidneys, which means patients with impaired renal function require a lower dosage. Because the liver has only a minimal role in paliperidone palmitate’s metabolism, dose adjustment is needed only for patients with severe hepatic dysfunction.1
Administration. Before starting this medication, test for allergy with a dose of oral paliperidone. Then administer 2 consecutive loading doses of paliperidone palmitate by deltoid IM injection; first 234 mg, and then a 156-mg dose after 7 to 10 days. Monthly injections of 117 mg are recommended, although higher or lower dosages can be used depending on the clinical situation. The first 2 injections should be in the deltoid muscle because plasma concentrations are 28% higher with deltoid vs gluteal administration. Subsequent injections can alternate between gluteal and deltoid sites.
If a dose is missed within 6 weeks of the last injection, administer the most recently used dosage. For discontinuation of 6 weeks to 6 months, administer 2 injections of the previously stabilized dose separated by 1 week, followed by the regular monthly dosage. After >6 months, begin the initial loading dose regimen.1
Paliperidone palmitate is available in prefilled syringes that do not require refrigeration or reconstitution. Use a 22-gauge needle for deltoid injections and for patients weighing >200 lbs. Use a 23-gauge needle for gluteal injections in non-obese individuals. Do not inject into a blood vessel, and alternate injection sites between sides of the body each month.1
Table
Paliperidone palmitate: Fast facts
| Brand name: Invega Sustenna |
| Indication: Acute and/or maintenance treatment of patients with schizophrenia |
| Approval date: July 31, 2009 |
| Manufacturer: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc. |
| Dosing forms: 39-, 78-, 117-, 156-, and 234-mg doses of injectable solutions |
| Cost: Is not covered by private insurance and requires prior authorization for Medicare or Medicaid coverage. According to Internet pharmacies, monthly paliperidone costs: •$255 for 39 mg •$509 for 78 mg •$763 for 117 mg •$1,017 for 156 mg •$1,525 for 234 mg. Monthly costs for IM risperidone are: •$302 for 12.5 mg •$642 for 25 mg •$934 for 37.5 mg •$1,280 for 50 mg. |
Efficacy
In a 9-week, phase II, double-blind study, mean Positive and Negative Syndrome Scale (PANSS) scores improved in patients receiving paliperidone, 78 mg or 156 mg (mean change -5.2 and -7.8, respectively) compared with placebo (6.2). Two percent of the paliperidone group discontinued the agent, compared with 10% of placebo. Although extrapyramidal symptoms were comparable in all groups (1%), 5% of patients receiving 78 mg and 8% of patients receiving 156 mg reported parkinsonian adverse events, compared with 1% with placebo.2
In other double-blind, placebo-controlled trials, paliperidone dosages from 25 mg to 150 mg were associated with a decrease in positive and negative symptoms in 1,540 subjects.1 During a 1-year study, 18% of patients taking paliperidone palmitate relapsed, compared with 48% for placebo.1
In a 53-week study, both paliperidone palmitate and IM risperidone were effective in decreasing positive and negative symptoms; however, risperidone-treated patients showed greater therapeutic response.3 Mean PANSS score changes in patients receiving paliperidone were -11.6, compared with -14.4 with risperidone. Psychotic relapse occurred in 14% of IM risperidone patients and 18% of paliperidone palmitate patients.3
In an unpublished 13-week, randomized, double-blind study conducted by the drug’s manufacturer, paliperidone palmitate, 78 mg to 234 mg once monthly, and long-acting risperidone, 25 mg to 50 mg every other week with supplemental oral risperidone for 2 to 3 weeks, were reported as equivalent.1 Both groups showed similar decrease in PANSS scores (-18.6 vs -17.9); however, reported adverse events were slightly higher in patients receiving paliperidone (57.9% vs 52.8%).1
Adverse events
Common side effects include insomnia (15%), anxiety (10%), and headaches (9%). Dizziness, agitation, gastrointestinal upset, hypotension, and urinary tract infection have been reported. Rarely, tachycardia, clinically nonsignificant QTc prolongation, and tardive dyskinesia occur. Increased prolactin levels have been observed, particularly in females. This drug should not be prescribed to pregnant or lactating women or elderly patients with dementia-related psychosis. In the 13-week trial, patients gained up to 3.3 lbs. Other adverse effects include allergic reactions, blood dyscrasias, elevated liver enzymes, lower seizure thresholds, body temperature dysregulation, neuroleptic malignant syndrome, dysphagia, and motor impairments.1
Clinically significant adverse effects were reported in 25% of paliperidone-treated subjects compared with 20% in the risperidone IM group. The discontinuation rate was 5% for paliperidone palmitate, compared with 3% for IM risperidone. Hyperkinesia with paliperidone (6%) was less prominent than with risperidone (10%).3
Drug brand names
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Paliperidone • Invega
- Paliperidone palmitate • Invega Sustenna
- Risperidone IM • Risperdal Consta
Disclosure
Dr. Lindenmayer has received grant support from AstraZeneca, Otsuka, Pfizer Inc., Dainippon Sumitomo, Azur, Janssen, Eli Lilly and Company, and National Institute of Mental Health. He is a consultant to Eli Lilly and Company and Janssen. Drs. Sedky, Nazir, and Lippmann report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgments
The authors thank Dr. Roop Parlapalli, an observer physician at University of Louisville School of Medicine, for his editorial revision.
1. Invega Sustenna [package insert]. Titusville, NJ: Janssen; 2009.
2. Kramer M, Litman R, Hough D, et al. Paliperidone palmitate, a potential long-acting treatment for patients with schizophrenia. Results of a randomized, double-blind, placebo-controlled efficacy and safety study. Int J Neuropsychopharmacol. 2009;27:1-13.
3. Fleischhacker W. A randomized, double blind, parallel-group comparative study of flexibly dosed paliperidone palmitate (25, 50, 75, or 100 mg eq.) administered every 4 weeks and flexibly dosed Risperdal® Consta® (25, 37.5, or 50 mg) administered every 2 weeks in subjects with schizophrenia. Available at: http://download.veritasmedicine.com/PDF/CR004195_CSR.pdf. Accessed November 23, 2009.
Paliperidone palmitate (9-hydroxyrisperidone) is an injectable, once-monthly atypical antipsychotic medication, FDA-approved in July 2009 for acute and/or maintenance treatment of schizophrenia. This aqueous-based, extremely slowly dissolving depot medication is well tolerated and causes few drug-drug interactions.1 Clinically, paliperidone palmitate and its parent drug, intramuscular (IM) risperidone, have similarities and differences.
Clinical information
Paliperidone palmitate is available in 39-mg, 78-mg, 117-mg, 156-mg, and 234-mg formulations. Once administered, it hydrolyzes and diffuses slowly and provides paliperidone doses equivalent to 25 mg, 50 mg, 75 mg, 100 mg, and 150 mg, respectively. The 234-mg dose of paliperidone palmitate is equivalent to 12 mg oral paliperidone, 117 mg to 6 mg, and 39 to 78 mg to 3 mg, respectively (visit this article at CurrentPsychiatry.com to learn more about paliperidone palmitate).
Pharmacokinetics. This palmitate ester of paliperidone is an aqueous suspension utilizing nanocrystal molecules. The increased surface area leads to rapid medication release and a short time to steady state. Active paliperidone plasma levels were detected at day 1, meaning co-administration with the oral formulation is not necessary. Paliperidone palmitate’s slow dissolution rate results in a half-life of 25 to 49 days. The fast onset of action and long half-life simplifies administration.
Co-administration with carbamazepine decreases paliperidone levels, whereas divalproex causes an increase. Up to 60% of paliperidone is excreted unchanged through the kidneys, which means patients with impaired renal function require a lower dosage. Because the liver has only a minimal role in paliperidone palmitate’s metabolism, dose adjustment is needed only for patients with severe hepatic dysfunction.1
Administration. Before starting this medication, test for allergy with a dose of oral paliperidone. Then administer 2 consecutive loading doses of paliperidone palmitate by deltoid IM injection; first 234 mg, and then a 156-mg dose after 7 to 10 days. Monthly injections of 117 mg are recommended, although higher or lower dosages can be used depending on the clinical situation. The first 2 injections should be in the deltoid muscle because plasma concentrations are 28% higher with deltoid vs gluteal administration. Subsequent injections can alternate between gluteal and deltoid sites.
If a dose is missed within 6 weeks of the last injection, administer the most recently used dosage. For discontinuation of 6 weeks to 6 months, administer 2 injections of the previously stabilized dose separated by 1 week, followed by the regular monthly dosage. After >6 months, begin the initial loading dose regimen.1
Paliperidone palmitate is available in prefilled syringes that do not require refrigeration or reconstitution. Use a 22-gauge needle for deltoid injections and for patients weighing >200 lbs. Use a 23-gauge needle for gluteal injections in non-obese individuals. Do not inject into a blood vessel, and alternate injection sites between sides of the body each month.1
Table
Paliperidone palmitate: Fast facts
| Brand name: Invega Sustenna |
| Indication: Acute and/or maintenance treatment of patients with schizophrenia |
| Approval date: July 31, 2009 |
| Manufacturer: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc. |
| Dosing forms: 39-, 78-, 117-, 156-, and 234-mg doses of injectable solutions |
| Cost: Is not covered by private insurance and requires prior authorization for Medicare or Medicaid coverage. According to Internet pharmacies, monthly paliperidone costs: •$255 for 39 mg •$509 for 78 mg •$763 for 117 mg •$1,017 for 156 mg •$1,525 for 234 mg. Monthly costs for IM risperidone are: •$302 for 12.5 mg •$642 for 25 mg •$934 for 37.5 mg •$1,280 for 50 mg. |
Efficacy
In a 9-week, phase II, double-blind study, mean Positive and Negative Syndrome Scale (PANSS) scores improved in patients receiving paliperidone, 78 mg or 156 mg (mean change -5.2 and -7.8, respectively) compared with placebo (6.2). Two percent of the paliperidone group discontinued the agent, compared with 10% of placebo. Although extrapyramidal symptoms were comparable in all groups (1%), 5% of patients receiving 78 mg and 8% of patients receiving 156 mg reported parkinsonian adverse events, compared with 1% with placebo.2
In other double-blind, placebo-controlled trials, paliperidone dosages from 25 mg to 150 mg were associated with a decrease in positive and negative symptoms in 1,540 subjects.1 During a 1-year study, 18% of patients taking paliperidone palmitate relapsed, compared with 48% for placebo.1
In a 53-week study, both paliperidone palmitate and IM risperidone were effective in decreasing positive and negative symptoms; however, risperidone-treated patients showed greater therapeutic response.3 Mean PANSS score changes in patients receiving paliperidone were -11.6, compared with -14.4 with risperidone. Psychotic relapse occurred in 14% of IM risperidone patients and 18% of paliperidone palmitate patients.3
In an unpublished 13-week, randomized, double-blind study conducted by the drug’s manufacturer, paliperidone palmitate, 78 mg to 234 mg once monthly, and long-acting risperidone, 25 mg to 50 mg every other week with supplemental oral risperidone for 2 to 3 weeks, were reported as equivalent.1 Both groups showed similar decrease in PANSS scores (-18.6 vs -17.9); however, reported adverse events were slightly higher in patients receiving paliperidone (57.9% vs 52.8%).1
Adverse events
Common side effects include insomnia (15%), anxiety (10%), and headaches (9%). Dizziness, agitation, gastrointestinal upset, hypotension, and urinary tract infection have been reported. Rarely, tachycardia, clinically nonsignificant QTc prolongation, and tardive dyskinesia occur. Increased prolactin levels have been observed, particularly in females. This drug should not be prescribed to pregnant or lactating women or elderly patients with dementia-related psychosis. In the 13-week trial, patients gained up to 3.3 lbs. Other adverse effects include allergic reactions, blood dyscrasias, elevated liver enzymes, lower seizure thresholds, body temperature dysregulation, neuroleptic malignant syndrome, dysphagia, and motor impairments.1
Clinically significant adverse effects were reported in 25% of paliperidone-treated subjects compared with 20% in the risperidone IM group. The discontinuation rate was 5% for paliperidone palmitate, compared with 3% for IM risperidone. Hyperkinesia with paliperidone (6%) was less prominent than with risperidone (10%).3
Drug brand names
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Paliperidone • Invega
- Paliperidone palmitate • Invega Sustenna
- Risperidone IM • Risperdal Consta
Disclosure
Dr. Lindenmayer has received grant support from AstraZeneca, Otsuka, Pfizer Inc., Dainippon Sumitomo, Azur, Janssen, Eli Lilly and Company, and National Institute of Mental Health. He is a consultant to Eli Lilly and Company and Janssen. Drs. Sedky, Nazir, and Lippmann report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgments
The authors thank Dr. Roop Parlapalli, an observer physician at University of Louisville School of Medicine, for his editorial revision.
Paliperidone palmitate (9-hydroxyrisperidone) is an injectable, once-monthly atypical antipsychotic medication, FDA-approved in July 2009 for acute and/or maintenance treatment of schizophrenia. This aqueous-based, extremely slowly dissolving depot medication is well tolerated and causes few drug-drug interactions.1 Clinically, paliperidone palmitate and its parent drug, intramuscular (IM) risperidone, have similarities and differences.
Clinical information
Paliperidone palmitate is available in 39-mg, 78-mg, 117-mg, 156-mg, and 234-mg formulations. Once administered, it hydrolyzes and diffuses slowly and provides paliperidone doses equivalent to 25 mg, 50 mg, 75 mg, 100 mg, and 150 mg, respectively. The 234-mg dose of paliperidone palmitate is equivalent to 12 mg oral paliperidone, 117 mg to 6 mg, and 39 to 78 mg to 3 mg, respectively (visit this article at CurrentPsychiatry.com to learn more about paliperidone palmitate).
Pharmacokinetics. This palmitate ester of paliperidone is an aqueous suspension utilizing nanocrystal molecules. The increased surface area leads to rapid medication release and a short time to steady state. Active paliperidone plasma levels were detected at day 1, meaning co-administration with the oral formulation is not necessary. Paliperidone palmitate’s slow dissolution rate results in a half-life of 25 to 49 days. The fast onset of action and long half-life simplifies administration.
Co-administration with carbamazepine decreases paliperidone levels, whereas divalproex causes an increase. Up to 60% of paliperidone is excreted unchanged through the kidneys, which means patients with impaired renal function require a lower dosage. Because the liver has only a minimal role in paliperidone palmitate’s metabolism, dose adjustment is needed only for patients with severe hepatic dysfunction.1
Administration. Before starting this medication, test for allergy with a dose of oral paliperidone. Then administer 2 consecutive loading doses of paliperidone palmitate by deltoid IM injection; first 234 mg, and then a 156-mg dose after 7 to 10 days. Monthly injections of 117 mg are recommended, although higher or lower dosages can be used depending on the clinical situation. The first 2 injections should be in the deltoid muscle because plasma concentrations are 28% higher with deltoid vs gluteal administration. Subsequent injections can alternate between gluteal and deltoid sites.
If a dose is missed within 6 weeks of the last injection, administer the most recently used dosage. For discontinuation of 6 weeks to 6 months, administer 2 injections of the previously stabilized dose separated by 1 week, followed by the regular monthly dosage. After >6 months, begin the initial loading dose regimen.1
Paliperidone palmitate is available in prefilled syringes that do not require refrigeration or reconstitution. Use a 22-gauge needle for deltoid injections and for patients weighing >200 lbs. Use a 23-gauge needle for gluteal injections in non-obese individuals. Do not inject into a blood vessel, and alternate injection sites between sides of the body each month.1
Table
Paliperidone palmitate: Fast facts
| Brand name: Invega Sustenna |
| Indication: Acute and/or maintenance treatment of patients with schizophrenia |
| Approval date: July 31, 2009 |
| Manufacturer: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc. |
| Dosing forms: 39-, 78-, 117-, 156-, and 234-mg doses of injectable solutions |
| Cost: Is not covered by private insurance and requires prior authorization for Medicare or Medicaid coverage. According to Internet pharmacies, monthly paliperidone costs: •$255 for 39 mg •$509 for 78 mg •$763 for 117 mg •$1,017 for 156 mg •$1,525 for 234 mg. Monthly costs for IM risperidone are: •$302 for 12.5 mg •$642 for 25 mg •$934 for 37.5 mg •$1,280 for 50 mg. |
Efficacy
In a 9-week, phase II, double-blind study, mean Positive and Negative Syndrome Scale (PANSS) scores improved in patients receiving paliperidone, 78 mg or 156 mg (mean change -5.2 and -7.8, respectively) compared with placebo (6.2). Two percent of the paliperidone group discontinued the agent, compared with 10% of placebo. Although extrapyramidal symptoms were comparable in all groups (1%), 5% of patients receiving 78 mg and 8% of patients receiving 156 mg reported parkinsonian adverse events, compared with 1% with placebo.2
In other double-blind, placebo-controlled trials, paliperidone dosages from 25 mg to 150 mg were associated with a decrease in positive and negative symptoms in 1,540 subjects.1 During a 1-year study, 18% of patients taking paliperidone palmitate relapsed, compared with 48% for placebo.1
In a 53-week study, both paliperidone palmitate and IM risperidone were effective in decreasing positive and negative symptoms; however, risperidone-treated patients showed greater therapeutic response.3 Mean PANSS score changes in patients receiving paliperidone were -11.6, compared with -14.4 with risperidone. Psychotic relapse occurred in 14% of IM risperidone patients and 18% of paliperidone palmitate patients.3
In an unpublished 13-week, randomized, double-blind study conducted by the drug’s manufacturer, paliperidone palmitate, 78 mg to 234 mg once monthly, and long-acting risperidone, 25 mg to 50 mg every other week with supplemental oral risperidone for 2 to 3 weeks, were reported as equivalent.1 Both groups showed similar decrease in PANSS scores (-18.6 vs -17.9); however, reported adverse events were slightly higher in patients receiving paliperidone (57.9% vs 52.8%).1
Adverse events
Common side effects include insomnia (15%), anxiety (10%), and headaches (9%). Dizziness, agitation, gastrointestinal upset, hypotension, and urinary tract infection have been reported. Rarely, tachycardia, clinically nonsignificant QTc prolongation, and tardive dyskinesia occur. Increased prolactin levels have been observed, particularly in females. This drug should not be prescribed to pregnant or lactating women or elderly patients with dementia-related psychosis. In the 13-week trial, patients gained up to 3.3 lbs. Other adverse effects include allergic reactions, blood dyscrasias, elevated liver enzymes, lower seizure thresholds, body temperature dysregulation, neuroleptic malignant syndrome, dysphagia, and motor impairments.1
Clinically significant adverse effects were reported in 25% of paliperidone-treated subjects compared with 20% in the risperidone IM group. The discontinuation rate was 5% for paliperidone palmitate, compared with 3% for IM risperidone. Hyperkinesia with paliperidone (6%) was less prominent than with risperidone (10%).3
Drug brand names
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Paliperidone • Invega
- Paliperidone palmitate • Invega Sustenna
- Risperidone IM • Risperdal Consta
Disclosure
Dr. Lindenmayer has received grant support from AstraZeneca, Otsuka, Pfizer Inc., Dainippon Sumitomo, Azur, Janssen, Eli Lilly and Company, and National Institute of Mental Health. He is a consultant to Eli Lilly and Company and Janssen. Drs. Sedky, Nazir, and Lippmann report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgments
The authors thank Dr. Roop Parlapalli, an observer physician at University of Louisville School of Medicine, for his editorial revision.
1. Invega Sustenna [package insert]. Titusville, NJ: Janssen; 2009.
2. Kramer M, Litman R, Hough D, et al. Paliperidone palmitate, a potential long-acting treatment for patients with schizophrenia. Results of a randomized, double-blind, placebo-controlled efficacy and safety study. Int J Neuropsychopharmacol. 2009;27:1-13.
3. Fleischhacker W. A randomized, double blind, parallel-group comparative study of flexibly dosed paliperidone palmitate (25, 50, 75, or 100 mg eq.) administered every 4 weeks and flexibly dosed Risperdal® Consta® (25, 37.5, or 50 mg) administered every 2 weeks in subjects with schizophrenia. Available at: http://download.veritasmedicine.com/PDF/CR004195_CSR.pdf. Accessed November 23, 2009.
1. Invega Sustenna [package insert]. Titusville, NJ: Janssen; 2009.
2. Kramer M, Litman R, Hough D, et al. Paliperidone palmitate, a potential long-acting treatment for patients with schizophrenia. Results of a randomized, double-blind, placebo-controlled efficacy and safety study. Int J Neuropsychopharmacol. 2009;27:1-13.
3. Fleischhacker W. A randomized, double blind, parallel-group comparative study of flexibly dosed paliperidone palmitate (25, 50, 75, or 100 mg eq.) administered every 4 weeks and flexibly dosed Risperdal® Consta® (25, 37.5, or 50 mg) administered every 2 weeks in subjects with schizophrenia. Available at: http://download.veritasmedicine.com/PDF/CR004195_CSR.pdf. Accessed November 23, 2009.
Splitting treatment: How to limit liability risk when you share a patient’s care
Dear Drs. Mossman and Weston:
In my psychiatric practice, I sometimes provide pharmacotherapy for patients treated by psychotherapists who practice independently. Am I liable for what these therapists do or don’t do—for example, not contacting me if a patient is suicidal or experiences a medication side effect? How much communication should occur between us? Sometimes—after a patient signs a release—I call the therapist and leave messages, but my calls are not returned. What should I do?—Submitted by “Dr. B”
Pharmacologic advances and altered reimbursement patterns have drastically changed how psychiatrists understand and manage mental problems. Not long ago, insight-oriented psychotherapy was the primary treatment—and often the only one—psychiatrists provided for outpatients. Nowadays, most visits to psychiatrists involve little or no in-depth psychotherapy,1 and many patients receive “joint treatment”—a psychiatrist performs the diagnostic and medical assessment and prescribes medications where appropriate, and a nonphysician provides other treatment services.
Psychiatrists need to be clear about their responsibilities for patients whom they “share” with other mental health professionals. In this article, we’ll discuss:
- forces that promote split treatment
- types of split-treatment relationships
- how to limit liability risk when you split treatment with an nonphysician mental health practitioner.
Dollars and cents reasons
Since the 1980s, psychiatrists have spent less time with their patients, provided less psychotherapy, and prescribed medications more frequently.2 An estimated 70% of outpatient visits to psychiatrists involve no psychotherapy.1
Market conditions are a major factor in these changes. Cost-containment policies and reduced private insurance payments for psychotherapy visits have incentivized psychiatrists to collaborate with less-well-paid psychotherapists. Combining medication and psychotherapy may be the best and most cost-effective treatment for mentally ill patients, but psychiatrists get paid more for three 15-minute “med checks” than for one 45-minute psychotherapy session.3-5
Although managed care payment patterns may be “perversely influencing” psychiatry (as one psychiatrist puts it)6 other factors contributing to the decline of psychotherapy include:
- new medications with fewer side effects
- aggressive pharmaceutical company promotions of psychotropics
- greater public acceptance of mental illness and its treatment
- an increasingly cohort of psychiatrists trained by teachers and mentors who emphasized biologic therapies.1
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
Forms of split treatment
Psychiatrists engage in several types of professional relationships that split the care provided to mentally ill patients (Table 1),7 and Dr. B has asked us to focus on one type of split-care relationship: a physician and psychotherapist treat the same patient, ideally collaborating to provide good clinical care.
Split, collaborative care is common throughout medicine. Most of us see medical specialists who treat different illnesses, but each doctor is responsible for the care he or she provides. An allergist knows what orthopedic surgery is, but we don’t expect our allergist to provide follow-up after arthroscopic surgery—and neither does our orthopedist.
The same considerations apply when a psychiatrist’s patient sees an independent nonphysician therapist. The psychiatrist provides the same care that a patient receiving only pharmacotherapy would need. The psychiatrist should not expect the collaborating therapist to monitor the patient’s pharmacotherapy—for example, by checking lab tests or asking about medication side effects—although the therapist is welcome to tell the psychiatrist about pharmacotherapy matters or encourage the patient to do so.
Table 1
Types of split-care relationships
| Type | Characteristics |
|---|---|
| Consultative | Develops when one licensed practitioner asks for the opinion of another |
| Informal (‘curbside’) | One practitioner describes clinical characteristics to another; patient’s identity is unknown to consultant |
| Formal | Consultant documents findings after reviewing record and/or examining patient; consultant knows patient’s identity |
| Supervisory | Mandated relationship between 2 professionals in which supervisee should follow supervisor’s recommendations |
| Collaborative | Credentialed professionals share ongoing responsibility for care and complementary aspects of a patient’s treatment |
| Same agency | Practitioners have distinct treatment roles (eg, therapist and prescriber) in several patients’ care and may have regular contact with each other; shared medical record |
| Independent | Practitioners lack regular contact; scope of treatment duties is established for the individual shared patient |
| Source: Reference 7 | |
Limiting liability
Psychiatrists who share patients with independent nonphysicians can take several steps to promote better care and limit potential liability.
Delegation. Do not delegate essential aspects of medical care. For example, tell young patients starting antidepressants (and minors’ legal guardians) about the risk of increased suicidal ideation, and provide close monitoring. Although it is acceptable for a patient to tell his or her therapist about worsening suicidal thoughts, instruct the patient to inform you as well.
Check them out. Before agreeing to split care, find out if the potential collaborator is credentialed, and respectfully inquire about his or her training and clinical approaches.8 Because unlicensed or uncredentialed therapists might not be held to the same practice standards as physicians and often have little or no malpractice insurance, psychiatrists who work with them may be assuming most of the clinical and legal liability.9 If a court is looking for a way to compensate an injured patient, it may hold the psychiatrist accountable for not knowing the therapist’s qualifications, failing to supervise the therapist, or failing to inform the patient of the therapist’s lack of qualifications.7,10
Establish the collaboration. Psychiatrists have a duty to ensure that their patients receive good care. Split treatment can help patients—who get 2 pairs of eyes monitoring them, plus 2 clinicians’ combined areas of skill—if the clinicians work together satisfactorily. Some psychiatrists recommend using initial consultation forms8 or contracts to spell out mutual expectations and establish important components of the relationship (Table 2).11,12 Other psychiatrists are comfortable with brief discussions with potential collaborators that cover:
- how the clinicians will divide treatment responsibilities
- circumstances when they will communicate
- patient coverage during each other’s vacations
- availability to patients during crises
- types of problems that would prompt the patient to contact the psychiatrist or therapist first.
Table 2
7 C’s of effective collaborative treatment
| Clarity about the relationship (collaborative, supervisory) and what each provider will do |
| Contract. A written agreement about duties and roles may help to dispel an assumption that the psychiatrist had supervisory responsibilities |
| Communication that occurs routinely between caregivers, even when treatment is going well |
| Consent by the patient, which requires that the patient knows, understands, and accepts each provider’s role |
| Comprehensive review of what’s happened in therapy, especially if the psychiatrist sees the patient infrequently |
| Credentialing. If the parties don’t know each other well, they should check out each other’s background |
| Consultation. Seek when problems arise in treatment or with the above arrangements |
| Source: References 11,12 |
Be sure to document these discussions as well as written consent for initial and ongoing communication in the patient’s medical record. Major treatment advances or setbacks, nonadherence, or termination of treatment by/with one clinician should prompt contact with the other clinician. Collaborating clinicians should communicate regularly even when treatment is going well, not only when big changes occur.8
Back to Dr. B
What should you do if a patient seeks pharmacotherapy and the therapist hasn’t contacted you? First, you probably should speak with your patient about the absence of interclinician communication, explain that it is important, and get the patient’s written permission to initiate contact. After contacting the therapist, you will be in a better position to determine how often you should see the patient and how often you need to share information with the therapist.
If you are uncomfortable sharing care with some or all nonphysician therapists, tell your patients. You might refer prospective patients to psychotherapists with whom you’re comfortable providing collaborative care or to other psychiatrists who accept split relationships.
Ideally, get patients’ written consent to share confidential information before you agree to participate in a shared treatment relationship. If patients refuse, you will not have access to all treatment information. This may adversely affect the quality of care and increase your liability risk.
In some cases, your discomfort with a split-treatment situation may make you decide to decline or terminate the treatment relationship. This is permissible if you give the patient proper notice, suggest other psychiatrists who might see the patient, and remain available for urgent matters for a reasonable time—usually 30 to 60 days—to allow the patient to contact another psychiatrist.10 When you discuss potential providers, explain that you don’t know these clinicians (if that’s the case) or whether they will agree to treat the patient.12
1. Mojtabai R, Olfson M. National trends in psychotherapy by office-based psychiatrists. Arch Gen Psychiatry. 2008;65:962-970.
2. Olfson M, Marcus SC, Pincus HA. Trends in office-based psychiatric practice. Am J Psychiatry. 1999;156:451-457.
3. Rosack J. Researchers learning why treatment combo is best. Psychiatr News. 2004;39(12):37.-
4. Thase ME, Greenhouse JB, Frank E, et al. Treatment of major depression with psychotherapy or psychotherapy-pharmacotherapy combinations. Arch Gen Psychiatry. 1997;54:1009-1015.
5. Dewan M. Are psychiatrists cost-effective? An analysis of integrated versus split treatment. Am J Psychiatry. 1999;156:324-326.
6. Clemens NA, MacKenzie KR, Griffith JL, et al. Psychotherapy by psychiatrists in a managed care environment: must it be an oxymoron? A forum from the APA commission on psychotherapy by psychiatrists. J Psychother Pract Res. 2001;10:53-62.
7. Sederer LI, Ellison J, Keyes C. Guidelines for prescribing psychiatrists in consultative, collaborative, and supervisory relationships. Psychiatr Serv. 1998;49:1197-1202.
8. Ellison JM. Teaching collaboration between pharmacotherapist and psychotherapist. Acad Psychiatry. 2005;29:195-202.
9. Sederer LI, Ellison J, Badaracco M, et al. Guidelines for prescribing psychiatrists in consultative, collaborative, or supervisory relationships. Cambridge, MA: Risk Management Foundation of the Harvard Medical Institutions; 1998. Available at: http://www.rmf.harvard.edu/files/documents/psychPr.pdf. Accessed January 4, 2010.
10. Melonas JM. Split treatment: does managed care change the risk to psychiatrists? Psychiatric Practice and Managed Care. 1999;5:5.-Available at: http://www.psychprogram.com/Risk_Management/news_splittreatment1.htm. Accessed January 4, 2010.
11. Gutheil TG, Simon RI. Abandonment of patients in split treatment. Harv Rev Psychiatry. 2003;11:175-179.
12. Reid WH. Organization liability: beyond respondeat superior. J Psychiatr Pract. 2004;4:258-262.

Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and adjunct professor of clinical psychiatry and training director, division of forensic psychiatry, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and adjunct professor of clinical psychiatry and training director, division of forensic psychiatry, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and adjunct professor of clinical psychiatry and training director, division of forensic psychiatry, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Dear Drs. Mossman and Weston:
In my psychiatric practice, I sometimes provide pharmacotherapy for patients treated by psychotherapists who practice independently. Am I liable for what these therapists do or don’t do—for example, not contacting me if a patient is suicidal or experiences a medication side effect? How much communication should occur between us? Sometimes—after a patient signs a release—I call the therapist and leave messages, but my calls are not returned. What should I do?—Submitted by “Dr. B”
Pharmacologic advances and altered reimbursement patterns have drastically changed how psychiatrists understand and manage mental problems. Not long ago, insight-oriented psychotherapy was the primary treatment—and often the only one—psychiatrists provided for outpatients. Nowadays, most visits to psychiatrists involve little or no in-depth psychotherapy,1 and many patients receive “joint treatment”—a psychiatrist performs the diagnostic and medical assessment and prescribes medications where appropriate, and a nonphysician provides other treatment services.
Psychiatrists need to be clear about their responsibilities for patients whom they “share” with other mental health professionals. In this article, we’ll discuss:
- forces that promote split treatment
- types of split-treatment relationships
- how to limit liability risk when you split treatment with an nonphysician mental health practitioner.
Dollars and cents reasons
Since the 1980s, psychiatrists have spent less time with their patients, provided less psychotherapy, and prescribed medications more frequently.2 An estimated 70% of outpatient visits to psychiatrists involve no psychotherapy.1
Market conditions are a major factor in these changes. Cost-containment policies and reduced private insurance payments for psychotherapy visits have incentivized psychiatrists to collaborate with less-well-paid psychotherapists. Combining medication and psychotherapy may be the best and most cost-effective treatment for mentally ill patients, but psychiatrists get paid more for three 15-minute “med checks” than for one 45-minute psychotherapy session.3-5
Although managed care payment patterns may be “perversely influencing” psychiatry (as one psychiatrist puts it)6 other factors contributing to the decline of psychotherapy include:
- new medications with fewer side effects
- aggressive pharmaceutical company promotions of psychotropics
- greater public acceptance of mental illness and its treatment
- an increasingly cohort of psychiatrists trained by teachers and mentors who emphasized biologic therapies.1
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
Forms of split treatment
Psychiatrists engage in several types of professional relationships that split the care provided to mentally ill patients (Table 1),7 and Dr. B has asked us to focus on one type of split-care relationship: a physician and psychotherapist treat the same patient, ideally collaborating to provide good clinical care.
Split, collaborative care is common throughout medicine. Most of us see medical specialists who treat different illnesses, but each doctor is responsible for the care he or she provides. An allergist knows what orthopedic surgery is, but we don’t expect our allergist to provide follow-up after arthroscopic surgery—and neither does our orthopedist.
The same considerations apply when a psychiatrist’s patient sees an independent nonphysician therapist. The psychiatrist provides the same care that a patient receiving only pharmacotherapy would need. The psychiatrist should not expect the collaborating therapist to monitor the patient’s pharmacotherapy—for example, by checking lab tests or asking about medication side effects—although the therapist is welcome to tell the psychiatrist about pharmacotherapy matters or encourage the patient to do so.
Table 1
Types of split-care relationships
| Type | Characteristics |
|---|---|
| Consultative | Develops when one licensed practitioner asks for the opinion of another |
| Informal (‘curbside’) | One practitioner describes clinical characteristics to another; patient’s identity is unknown to consultant |
| Formal | Consultant documents findings after reviewing record and/or examining patient; consultant knows patient’s identity |
| Supervisory | Mandated relationship between 2 professionals in which supervisee should follow supervisor’s recommendations |
| Collaborative | Credentialed professionals share ongoing responsibility for care and complementary aspects of a patient’s treatment |
| Same agency | Practitioners have distinct treatment roles (eg, therapist and prescriber) in several patients’ care and may have regular contact with each other; shared medical record |
| Independent | Practitioners lack regular contact; scope of treatment duties is established for the individual shared patient |
| Source: Reference 7 | |
Limiting liability
Psychiatrists who share patients with independent nonphysicians can take several steps to promote better care and limit potential liability.
Delegation. Do not delegate essential aspects of medical care. For example, tell young patients starting antidepressants (and minors’ legal guardians) about the risk of increased suicidal ideation, and provide close monitoring. Although it is acceptable for a patient to tell his or her therapist about worsening suicidal thoughts, instruct the patient to inform you as well.
Check them out. Before agreeing to split care, find out if the potential collaborator is credentialed, and respectfully inquire about his or her training and clinical approaches.8 Because unlicensed or uncredentialed therapists might not be held to the same practice standards as physicians and often have little or no malpractice insurance, psychiatrists who work with them may be assuming most of the clinical and legal liability.9 If a court is looking for a way to compensate an injured patient, it may hold the psychiatrist accountable for not knowing the therapist’s qualifications, failing to supervise the therapist, or failing to inform the patient of the therapist’s lack of qualifications.7,10
Establish the collaboration. Psychiatrists have a duty to ensure that their patients receive good care. Split treatment can help patients—who get 2 pairs of eyes monitoring them, plus 2 clinicians’ combined areas of skill—if the clinicians work together satisfactorily. Some psychiatrists recommend using initial consultation forms8 or contracts to spell out mutual expectations and establish important components of the relationship (Table 2).11,12 Other psychiatrists are comfortable with brief discussions with potential collaborators that cover:
- how the clinicians will divide treatment responsibilities
- circumstances when they will communicate
- patient coverage during each other’s vacations
- availability to patients during crises
- types of problems that would prompt the patient to contact the psychiatrist or therapist first.
Table 2
7 C’s of effective collaborative treatment
| Clarity about the relationship (collaborative, supervisory) and what each provider will do |
| Contract. A written agreement about duties and roles may help to dispel an assumption that the psychiatrist had supervisory responsibilities |
| Communication that occurs routinely between caregivers, even when treatment is going well |
| Consent by the patient, which requires that the patient knows, understands, and accepts each provider’s role |
| Comprehensive review of what’s happened in therapy, especially if the psychiatrist sees the patient infrequently |
| Credentialing. If the parties don’t know each other well, they should check out each other’s background |
| Consultation. Seek when problems arise in treatment or with the above arrangements |
| Source: References 11,12 |
Be sure to document these discussions as well as written consent for initial and ongoing communication in the patient’s medical record. Major treatment advances or setbacks, nonadherence, or termination of treatment by/with one clinician should prompt contact with the other clinician. Collaborating clinicians should communicate regularly even when treatment is going well, not only when big changes occur.8
Back to Dr. B
What should you do if a patient seeks pharmacotherapy and the therapist hasn’t contacted you? First, you probably should speak with your patient about the absence of interclinician communication, explain that it is important, and get the patient’s written permission to initiate contact. After contacting the therapist, you will be in a better position to determine how often you should see the patient and how often you need to share information with the therapist.
If you are uncomfortable sharing care with some or all nonphysician therapists, tell your patients. You might refer prospective patients to psychotherapists with whom you’re comfortable providing collaborative care or to other psychiatrists who accept split relationships.
Ideally, get patients’ written consent to share confidential information before you agree to participate in a shared treatment relationship. If patients refuse, you will not have access to all treatment information. This may adversely affect the quality of care and increase your liability risk.
In some cases, your discomfort with a split-treatment situation may make you decide to decline or terminate the treatment relationship. This is permissible if you give the patient proper notice, suggest other psychiatrists who might see the patient, and remain available for urgent matters for a reasonable time—usually 30 to 60 days—to allow the patient to contact another psychiatrist.10 When you discuss potential providers, explain that you don’t know these clinicians (if that’s the case) or whether they will agree to treat the patient.12
Dear Drs. Mossman and Weston:
In my psychiatric practice, I sometimes provide pharmacotherapy for patients treated by psychotherapists who practice independently. Am I liable for what these therapists do or don’t do—for example, not contacting me if a patient is suicidal or experiences a medication side effect? How much communication should occur between us? Sometimes—after a patient signs a release—I call the therapist and leave messages, but my calls are not returned. What should I do?—Submitted by “Dr. B”
Pharmacologic advances and altered reimbursement patterns have drastically changed how psychiatrists understand and manage mental problems. Not long ago, insight-oriented psychotherapy was the primary treatment—and often the only one—psychiatrists provided for outpatients. Nowadays, most visits to psychiatrists involve little or no in-depth psychotherapy,1 and many patients receive “joint treatment”—a psychiatrist performs the diagnostic and medical assessment and prescribes medications where appropriate, and a nonphysician provides other treatment services.
Psychiatrists need to be clear about their responsibilities for patients whom they “share” with other mental health professionals. In this article, we’ll discuss:
- forces that promote split treatment
- types of split-treatment relationships
- how to limit liability risk when you split treatment with an nonphysician mental health practitioner.
Dollars and cents reasons
Since the 1980s, psychiatrists have spent less time with their patients, provided less psychotherapy, and prescribed medications more frequently.2 An estimated 70% of outpatient visits to psychiatrists involve no psychotherapy.1
Market conditions are a major factor in these changes. Cost-containment policies and reduced private insurance payments for psychotherapy visits have incentivized psychiatrists to collaborate with less-well-paid psychotherapists. Combining medication and psychotherapy may be the best and most cost-effective treatment for mentally ill patients, but psychiatrists get paid more for three 15-minute “med checks” than for one 45-minute psychotherapy session.3-5
Although managed care payment patterns may be “perversely influencing” psychiatry (as one psychiatrist puts it)6 other factors contributing to the decline of psychotherapy include:
- new medications with fewer side effects
- aggressive pharmaceutical company promotions of psychotropics
- greater public acceptance of mental illness and its treatment
- an increasingly cohort of psychiatrists trained by teachers and mentors who emphasized biologic therapies.1
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
Forms of split treatment
Psychiatrists engage in several types of professional relationships that split the care provided to mentally ill patients (Table 1),7 and Dr. B has asked us to focus on one type of split-care relationship: a physician and psychotherapist treat the same patient, ideally collaborating to provide good clinical care.
Split, collaborative care is common throughout medicine. Most of us see medical specialists who treat different illnesses, but each doctor is responsible for the care he or she provides. An allergist knows what orthopedic surgery is, but we don’t expect our allergist to provide follow-up after arthroscopic surgery—and neither does our orthopedist.
The same considerations apply when a psychiatrist’s patient sees an independent nonphysician therapist. The psychiatrist provides the same care that a patient receiving only pharmacotherapy would need. The psychiatrist should not expect the collaborating therapist to monitor the patient’s pharmacotherapy—for example, by checking lab tests or asking about medication side effects—although the therapist is welcome to tell the psychiatrist about pharmacotherapy matters or encourage the patient to do so.
Table 1
Types of split-care relationships
| Type | Characteristics |
|---|---|
| Consultative | Develops when one licensed practitioner asks for the opinion of another |
| Informal (‘curbside’) | One practitioner describes clinical characteristics to another; patient’s identity is unknown to consultant |
| Formal | Consultant documents findings after reviewing record and/or examining patient; consultant knows patient’s identity |
| Supervisory | Mandated relationship between 2 professionals in which supervisee should follow supervisor’s recommendations |
| Collaborative | Credentialed professionals share ongoing responsibility for care and complementary aspects of a patient’s treatment |
| Same agency | Practitioners have distinct treatment roles (eg, therapist and prescriber) in several patients’ care and may have regular contact with each other; shared medical record |
| Independent | Practitioners lack regular contact; scope of treatment duties is established for the individual shared patient |
| Source: Reference 7 | |
Limiting liability
Psychiatrists who share patients with independent nonphysicians can take several steps to promote better care and limit potential liability.
Delegation. Do not delegate essential aspects of medical care. For example, tell young patients starting antidepressants (and minors’ legal guardians) about the risk of increased suicidal ideation, and provide close monitoring. Although it is acceptable for a patient to tell his or her therapist about worsening suicidal thoughts, instruct the patient to inform you as well.
Check them out. Before agreeing to split care, find out if the potential collaborator is credentialed, and respectfully inquire about his or her training and clinical approaches.8 Because unlicensed or uncredentialed therapists might not be held to the same practice standards as physicians and often have little or no malpractice insurance, psychiatrists who work with them may be assuming most of the clinical and legal liability.9 If a court is looking for a way to compensate an injured patient, it may hold the psychiatrist accountable for not knowing the therapist’s qualifications, failing to supervise the therapist, or failing to inform the patient of the therapist’s lack of qualifications.7,10
Establish the collaboration. Psychiatrists have a duty to ensure that their patients receive good care. Split treatment can help patients—who get 2 pairs of eyes monitoring them, plus 2 clinicians’ combined areas of skill—if the clinicians work together satisfactorily. Some psychiatrists recommend using initial consultation forms8 or contracts to spell out mutual expectations and establish important components of the relationship (Table 2).11,12 Other psychiatrists are comfortable with brief discussions with potential collaborators that cover:
- how the clinicians will divide treatment responsibilities
- circumstances when they will communicate
- patient coverage during each other’s vacations
- availability to patients during crises
- types of problems that would prompt the patient to contact the psychiatrist or therapist first.
Table 2
7 C’s of effective collaborative treatment
| Clarity about the relationship (collaborative, supervisory) and what each provider will do |
| Contract. A written agreement about duties and roles may help to dispel an assumption that the psychiatrist had supervisory responsibilities |
| Communication that occurs routinely between caregivers, even when treatment is going well |
| Consent by the patient, which requires that the patient knows, understands, and accepts each provider’s role |
| Comprehensive review of what’s happened in therapy, especially if the psychiatrist sees the patient infrequently |
| Credentialing. If the parties don’t know each other well, they should check out each other’s background |
| Consultation. Seek when problems arise in treatment or with the above arrangements |
| Source: References 11,12 |
Be sure to document these discussions as well as written consent for initial and ongoing communication in the patient’s medical record. Major treatment advances or setbacks, nonadherence, or termination of treatment by/with one clinician should prompt contact with the other clinician. Collaborating clinicians should communicate regularly even when treatment is going well, not only when big changes occur.8
Back to Dr. B
What should you do if a patient seeks pharmacotherapy and the therapist hasn’t contacted you? First, you probably should speak with your patient about the absence of interclinician communication, explain that it is important, and get the patient’s written permission to initiate contact. After contacting the therapist, you will be in a better position to determine how often you should see the patient and how often you need to share information with the therapist.
If you are uncomfortable sharing care with some or all nonphysician therapists, tell your patients. You might refer prospective patients to psychotherapists with whom you’re comfortable providing collaborative care or to other psychiatrists who accept split relationships.
Ideally, get patients’ written consent to share confidential information before you agree to participate in a shared treatment relationship. If patients refuse, you will not have access to all treatment information. This may adversely affect the quality of care and increase your liability risk.
In some cases, your discomfort with a split-treatment situation may make you decide to decline or terminate the treatment relationship. This is permissible if you give the patient proper notice, suggest other psychiatrists who might see the patient, and remain available for urgent matters for a reasonable time—usually 30 to 60 days—to allow the patient to contact another psychiatrist.10 When you discuss potential providers, explain that you don’t know these clinicians (if that’s the case) or whether they will agree to treat the patient.12
1. Mojtabai R, Olfson M. National trends in psychotherapy by office-based psychiatrists. Arch Gen Psychiatry. 2008;65:962-970.
2. Olfson M, Marcus SC, Pincus HA. Trends in office-based psychiatric practice. Am J Psychiatry. 1999;156:451-457.
3. Rosack J. Researchers learning why treatment combo is best. Psychiatr News. 2004;39(12):37.-
4. Thase ME, Greenhouse JB, Frank E, et al. Treatment of major depression with psychotherapy or psychotherapy-pharmacotherapy combinations. Arch Gen Psychiatry. 1997;54:1009-1015.
5. Dewan M. Are psychiatrists cost-effective? An analysis of integrated versus split treatment. Am J Psychiatry. 1999;156:324-326.
6. Clemens NA, MacKenzie KR, Griffith JL, et al. Psychotherapy by psychiatrists in a managed care environment: must it be an oxymoron? A forum from the APA commission on psychotherapy by psychiatrists. J Psychother Pract Res. 2001;10:53-62.
7. Sederer LI, Ellison J, Keyes C. Guidelines for prescribing psychiatrists in consultative, collaborative, and supervisory relationships. Psychiatr Serv. 1998;49:1197-1202.
8. Ellison JM. Teaching collaboration between pharmacotherapist and psychotherapist. Acad Psychiatry. 2005;29:195-202.
9. Sederer LI, Ellison J, Badaracco M, et al. Guidelines for prescribing psychiatrists in consultative, collaborative, or supervisory relationships. Cambridge, MA: Risk Management Foundation of the Harvard Medical Institutions; 1998. Available at: http://www.rmf.harvard.edu/files/documents/psychPr.pdf. Accessed January 4, 2010.
10. Melonas JM. Split treatment: does managed care change the risk to psychiatrists? Psychiatric Practice and Managed Care. 1999;5:5.-Available at: http://www.psychprogram.com/Risk_Management/news_splittreatment1.htm. Accessed January 4, 2010.
11. Gutheil TG, Simon RI. Abandonment of patients in split treatment. Harv Rev Psychiatry. 2003;11:175-179.
12. Reid WH. Organization liability: beyond respondeat superior. J Psychiatr Pract. 2004;4:258-262.
1. Mojtabai R, Olfson M. National trends in psychotherapy by office-based psychiatrists. Arch Gen Psychiatry. 2008;65:962-970.
2. Olfson M, Marcus SC, Pincus HA. Trends in office-based psychiatric practice. Am J Psychiatry. 1999;156:451-457.
3. Rosack J. Researchers learning why treatment combo is best. Psychiatr News. 2004;39(12):37.-
4. Thase ME, Greenhouse JB, Frank E, et al. Treatment of major depression with psychotherapy or psychotherapy-pharmacotherapy combinations. Arch Gen Psychiatry. 1997;54:1009-1015.
5. Dewan M. Are psychiatrists cost-effective? An analysis of integrated versus split treatment. Am J Psychiatry. 1999;156:324-326.
6. Clemens NA, MacKenzie KR, Griffith JL, et al. Psychotherapy by psychiatrists in a managed care environment: must it be an oxymoron? A forum from the APA commission on psychotherapy by psychiatrists. J Psychother Pract Res. 2001;10:53-62.
7. Sederer LI, Ellison J, Keyes C. Guidelines for prescribing psychiatrists in consultative, collaborative, and supervisory relationships. Psychiatr Serv. 1998;49:1197-1202.
8. Ellison JM. Teaching collaboration between pharmacotherapist and psychotherapist. Acad Psychiatry. 2005;29:195-202.
9. Sederer LI, Ellison J, Badaracco M, et al. Guidelines for prescribing psychiatrists in consultative, collaborative, or supervisory relationships. Cambridge, MA: Risk Management Foundation of the Harvard Medical Institutions; 1998. Available at: http://www.rmf.harvard.edu/files/documents/psychPr.pdf. Accessed January 4, 2010.
10. Melonas JM. Split treatment: does managed care change the risk to psychiatrists? Psychiatric Practice and Managed Care. 1999;5:5.-Available at: http://www.psychprogram.com/Risk_Management/news_splittreatment1.htm. Accessed January 4, 2010.
11. Gutheil TG, Simon RI. Abandonment of patients in split treatment. Harv Rev Psychiatry. 2003;11:175-179.
12. Reid WH. Organization liability: beyond respondeat superior. J Psychiatr Pract. 2004;4:258-262.
EBM can obscure realities
I appreciate Current Psychiatry’s practical approach, but psychiatry’s tidal wave of evidence-based medicine (EBM) guidelines can obscure obvious realities, in turn serving to dumb us down. The article “Clozapine for schizophrenia: Life-threatening or life-saving treatment?” (Current Psychiatry, December 2009) is an example of how so-called “objective” statistics hide fuzzy assumptions. The idea that those rare outpatients with support systems and egos consistently functional enough to adhere to lab testing and who accept their illness are representative of all schizophrenia patients is a whopper of an assumption. The author needs to consider the more mundane possibility that patient selection and not the drug itself may make the difference.
I feel that articles on “CBM” for common sense-based medicine or “WBM” for wisdom-based medicine would provide our profession with a fresh breath and a dose of reality. The drum-beat of the EBM march is promoted as a substitute for thinking, which it isn’t. It is just a tool.
Peggy Finston, MD
Prescott, AZ
I appreciate Current Psychiatry’s practical approach, but psychiatry’s tidal wave of evidence-based medicine (EBM) guidelines can obscure obvious realities, in turn serving to dumb us down. The article “Clozapine for schizophrenia: Life-threatening or life-saving treatment?” (Current Psychiatry, December 2009) is an example of how so-called “objective” statistics hide fuzzy assumptions. The idea that those rare outpatients with support systems and egos consistently functional enough to adhere to lab testing and who accept their illness are representative of all schizophrenia patients is a whopper of an assumption. The author needs to consider the more mundane possibility that patient selection and not the drug itself may make the difference.
I feel that articles on “CBM” for common sense-based medicine or “WBM” for wisdom-based medicine would provide our profession with a fresh breath and a dose of reality. The drum-beat of the EBM march is promoted as a substitute for thinking, which it isn’t. It is just a tool.
Peggy Finston, MD
Prescott, AZ
I appreciate Current Psychiatry’s practical approach, but psychiatry’s tidal wave of evidence-based medicine (EBM) guidelines can obscure obvious realities, in turn serving to dumb us down. The article “Clozapine for schizophrenia: Life-threatening or life-saving treatment?” (Current Psychiatry, December 2009) is an example of how so-called “objective” statistics hide fuzzy assumptions. The idea that those rare outpatients with support systems and egos consistently functional enough to adhere to lab testing and who accept their illness are representative of all schizophrenia patients is a whopper of an assumption. The author needs to consider the more mundane possibility that patient selection and not the drug itself may make the difference.
I feel that articles on “CBM” for common sense-based medicine or “WBM” for wisdom-based medicine would provide our profession with a fresh breath and a dose of reality. The drum-beat of the EBM march is promoted as a substitute for thinking, which it isn’t. It is just a tool.
Peggy Finston, MD
Prescott, AZ
Weighing clozapine’s risks
Thank you for publishing “Clozapine for schizophrenia: Life-threatening or life-saving treatment?” (Current Psychiatry, December 2009). In recent years, prescription rates for clozapine and long-acting injectables have been low, which is a disservice to our patients. We have seen the amazing impact clozapine can have on our patients’ lives compared with other antipsychotics, and it is a shame to not prescribe it because of red tape. I am amazed that patients will stay on a medication that has so many untoward side effects, as we saw in the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study. I think this is a testament to how effective the medication is.
Corey Yilmaz, MD
Southwest Behavioral Health Services
Tolleson, AZ
Thank you for publishing “Clozapine for schizophrenia: Life-threatening or life-saving treatment?” (Current Psychiatry, December 2009). In recent years, prescription rates for clozapine and long-acting injectables have been low, which is a disservice to our patients. We have seen the amazing impact clozapine can have on our patients’ lives compared with other antipsychotics, and it is a shame to not prescribe it because of red tape. I am amazed that patients will stay on a medication that has so many untoward side effects, as we saw in the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study. I think this is a testament to how effective the medication is.
Corey Yilmaz, MD
Southwest Behavioral Health Services
Tolleson, AZ
Thank you for publishing “Clozapine for schizophrenia: Life-threatening or life-saving treatment?” (Current Psychiatry, December 2009). In recent years, prescription rates for clozapine and long-acting injectables have been low, which is a disservice to our patients. We have seen the amazing impact clozapine can have on our patients’ lives compared with other antipsychotics, and it is a shame to not prescribe it because of red tape. I am amazed that patients will stay on a medication that has so many untoward side effects, as we saw in the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study. I think this is a testament to how effective the medication is.
Corey Yilmaz, MD
Southwest Behavioral Health Services
Tolleson, AZ
Could diet cause psychosis?
To add to Dr. Nasrallah’s New Year’s resolutions (“New Year’s resolutions to help our patients,” From the Editor, Current Psychiatry, January 2010), I suggest some fresh, out-of-the-box thinking about the basic causes of bipolar disorder and schizophrenia. It strikes me that 52 years ago, before I graduated from medical school, we knew that heart attacks, strokes, and many common cancers—breast, prostate, colon, etc.—were caused by our high-fat diet. We received no advice then or since about changing to a completely different diet. I wonder if it’s possible that our epidemic of psychoses also might be caused by the miserable diet we feed ourselves and our children. In the psychiatric literature, I have not seen a good comparison study of populations who follow a different diet. In Prevent and reverse heart disease, Caldwell Esselstyn Jr., MD, of the Cleveland Clinic states that in the genesis of heart disease “diet trumps genetics.” I wonder, is the brain any different?
James M. Donahue, MD
Indianapolis, IN
To add to Dr. Nasrallah’s New Year’s resolutions (“New Year’s resolutions to help our patients,” From the Editor, Current Psychiatry, January 2010), I suggest some fresh, out-of-the-box thinking about the basic causes of bipolar disorder and schizophrenia. It strikes me that 52 years ago, before I graduated from medical school, we knew that heart attacks, strokes, and many common cancers—breast, prostate, colon, etc.—were caused by our high-fat diet. We received no advice then or since about changing to a completely different diet. I wonder if it’s possible that our epidemic of psychoses also might be caused by the miserable diet we feed ourselves and our children. In the psychiatric literature, I have not seen a good comparison study of populations who follow a different diet. In Prevent and reverse heart disease, Caldwell Esselstyn Jr., MD, of the Cleveland Clinic states that in the genesis of heart disease “diet trumps genetics.” I wonder, is the brain any different?
James M. Donahue, MD
Indianapolis, IN
To add to Dr. Nasrallah’s New Year’s resolutions (“New Year’s resolutions to help our patients,” From the Editor, Current Psychiatry, January 2010), I suggest some fresh, out-of-the-box thinking about the basic causes of bipolar disorder and schizophrenia. It strikes me that 52 years ago, before I graduated from medical school, we knew that heart attacks, strokes, and many common cancers—breast, prostate, colon, etc.—were caused by our high-fat diet. We received no advice then or since about changing to a completely different diet. I wonder if it’s possible that our epidemic of psychoses also might be caused by the miserable diet we feed ourselves and our children. In the psychiatric literature, I have not seen a good comparison study of populations who follow a different diet. In Prevent and reverse heart disease, Caldwell Esselstyn Jr., MD, of the Cleveland Clinic states that in the genesis of heart disease “diet trumps genetics.” I wonder, is the brain any different?
James M. Donahue, MD
Indianapolis, IN