User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Bedside psychotherapy
Dr. Sermsak Lolak’s well-written article on bedside psychotherapy (August 2004) stresses the importance of psychiatrists’ psychotherapeutic skills in medical settings. As our roles have shrunk to that of medication management in this era of managed care, this article is timely.
Regularly practicing psychotherapy in consultation and liaison psychiatry, however, is difficult because of several logistical issues:
- Length of stay. The 21-day hospital stay in Dr. Lolak’s example is an exception. On consult service, psychiatrists see up to 40% of patients for three follow-up visits or fewer.1
- Inability to plan therapy. Often a patient is discharged without the psychiatric consultant’s knowledge or input.
- Reimbursement for follow-up psychotherapeutic visits. Most consultation and liaison psychiatrists generate income through billing; follow-up visits are not routinely reimbursed.
To address these issues, the psychiatrist needs to consider every visit as final and make every session complete in itself.
Although we clinically and intuitively recognize the benefits of ultra-brief psychotherapeutic interventions, clinical trials are needed to show their efficacy. These data would also provide rationale for payers to reimburse follow-up therapeutic visits.
Narsimha R. Pinninti MD, MBBS
Assistant professor of psychiatry
University of Medicine and Dentistry of New Jersey
Cherry Hill, NJ
- Strain JJ, Ginsburg J, Fulop G, Strain JJ. Follow-up of psychiatric comorbidity in the general hospital. Int J Psychiatry Med 1990;20:227–34.
Dr. Lolak responds
Dr. Pinninti raises two commonly recognized major problems in consultation psychiatry:
- Visiting a hospitalized patient in a timely manner is often inconvenient.
- Reimbursement is limited.
These are among the many reasons that the American Board of Psychiatry and Neurology now recognizes psychosomatic medicine as a subspecialty. Hospital-based consultation psychiatrists who can see patients in a timely manner are needed. Often hospitals must subsidize a consultation psychiatrist’s position, but this expense offsets the risks of not seeing these patients.
Evidence for brief psychosocial treatment is another issue. Much of what we do is not supported by randomized controlled trials, but we cannot ignore our patients’ needs until more evidence is gathered. We hope a sufficient cadre of consultation psychiatrists do the research Dr. Pinninti suggests.
Sermsak Lolak, MD
Consultation-liaison psychiatry fellow
Thomas Wise, MD
Professor and vice chairman
Department of psychiatry Georgetown University,
Washington, DC
Dr. Sermsak Lolak’s well-written article on bedside psychotherapy (August 2004) stresses the importance of psychiatrists’ psychotherapeutic skills in medical settings. As our roles have shrunk to that of medication management in this era of managed care, this article is timely.
Regularly practicing psychotherapy in consultation and liaison psychiatry, however, is difficult because of several logistical issues:
- Length of stay. The 21-day hospital stay in Dr. Lolak’s example is an exception. On consult service, psychiatrists see up to 40% of patients for three follow-up visits or fewer.1
- Inability to plan therapy. Often a patient is discharged without the psychiatric consultant’s knowledge or input.
- Reimbursement for follow-up psychotherapeutic visits. Most consultation and liaison psychiatrists generate income through billing; follow-up visits are not routinely reimbursed.
To address these issues, the psychiatrist needs to consider every visit as final and make every session complete in itself.
Although we clinically and intuitively recognize the benefits of ultra-brief psychotherapeutic interventions, clinical trials are needed to show their efficacy. These data would also provide rationale for payers to reimburse follow-up therapeutic visits.
Narsimha R. Pinninti MD, MBBS
Assistant professor of psychiatry
University of Medicine and Dentistry of New Jersey
Cherry Hill, NJ
- Strain JJ, Ginsburg J, Fulop G, Strain JJ. Follow-up of psychiatric comorbidity in the general hospital. Int J Psychiatry Med 1990;20:227–34.
Dr. Lolak responds
Dr. Pinninti raises two commonly recognized major problems in consultation psychiatry:
- Visiting a hospitalized patient in a timely manner is often inconvenient.
- Reimbursement is limited.
These are among the many reasons that the American Board of Psychiatry and Neurology now recognizes psychosomatic medicine as a subspecialty. Hospital-based consultation psychiatrists who can see patients in a timely manner are needed. Often hospitals must subsidize a consultation psychiatrist’s position, but this expense offsets the risks of not seeing these patients.
Evidence for brief psychosocial treatment is another issue. Much of what we do is not supported by randomized controlled trials, but we cannot ignore our patients’ needs until more evidence is gathered. We hope a sufficient cadre of consultation psychiatrists do the research Dr. Pinninti suggests.
Sermsak Lolak, MD
Consultation-liaison psychiatry fellow
Thomas Wise, MD
Professor and vice chairman
Department of psychiatry Georgetown University,
Washington, DC
Dr. Sermsak Lolak’s well-written article on bedside psychotherapy (August 2004) stresses the importance of psychiatrists’ psychotherapeutic skills in medical settings. As our roles have shrunk to that of medication management in this era of managed care, this article is timely.
Regularly practicing psychotherapy in consultation and liaison psychiatry, however, is difficult because of several logistical issues:
- Length of stay. The 21-day hospital stay in Dr. Lolak’s example is an exception. On consult service, psychiatrists see up to 40% of patients for three follow-up visits or fewer.1
- Inability to plan therapy. Often a patient is discharged without the psychiatric consultant’s knowledge or input.
- Reimbursement for follow-up psychotherapeutic visits. Most consultation and liaison psychiatrists generate income through billing; follow-up visits are not routinely reimbursed.
To address these issues, the psychiatrist needs to consider every visit as final and make every session complete in itself.
Although we clinically and intuitively recognize the benefits of ultra-brief psychotherapeutic interventions, clinical trials are needed to show their efficacy. These data would also provide rationale for payers to reimburse follow-up therapeutic visits.
Narsimha R. Pinninti MD, MBBS
Assistant professor of psychiatry
University of Medicine and Dentistry of New Jersey
Cherry Hill, NJ
- Strain JJ, Ginsburg J, Fulop G, Strain JJ. Follow-up of psychiatric comorbidity in the general hospital. Int J Psychiatry Med 1990;20:227–34.
Dr. Lolak responds
Dr. Pinninti raises two commonly recognized major problems in consultation psychiatry:
- Visiting a hospitalized patient in a timely manner is often inconvenient.
- Reimbursement is limited.
These are among the many reasons that the American Board of Psychiatry and Neurology now recognizes psychosomatic medicine as a subspecialty. Hospital-based consultation psychiatrists who can see patients in a timely manner are needed. Often hospitals must subsidize a consultation psychiatrist’s position, but this expense offsets the risks of not seeing these patients.
Evidence for brief psychosocial treatment is another issue. Much of what we do is not supported by randomized controlled trials, but we cannot ignore our patients’ needs until more evidence is gathered. We hope a sufficient cadre of consultation psychiatrists do the research Dr. Pinninti suggests.
Sermsak Lolak, MD
Consultation-liaison psychiatry fellow
Thomas Wise, MD
Professor and vice chairman
Department of psychiatry Georgetown University,
Washington, DC
Aggressive antipsychotic dosing
Reading “High-dose antipsychotics: Desperation or data-driven?” (Current Psychiatry, August 2004) brings back memories.
In 1980, I worked in a rural hospital. Our psychiatrist gave patients with acute mania a loading dosage of lithium, 900 mg tid to qid on day one, and drew a level in the morning. He reduced the dosage daily until target symptoms improved and/or serum concentration reached the high therapeutic range, or until side effects occurred.
During acute mania, the psychiatrist controlled unsafe agitation with short-acting barbiturates. Some extremely hostile, aggressive patients got IM sodium amobarbital. We observed the patient one-on-one until he or she awoke and could take fluids, food, and lithium. When manic symptoms began escalating, the patient again was medicated and the cycle continued. This cycle might continue for 1 to 3 days with decreasing frequency and sedation based on behavior.
Although I’m not advocating this regimen, it worked well from an empirical perspective. Our patients never acted out or had breathing problems.
Thomas Dowling, RN, MSN
St. Peter’s Hospital, Albany, NY
Reading “High-dose antipsychotics: Desperation or data-driven?” (Current Psychiatry, August 2004) brings back memories.
In 1980, I worked in a rural hospital. Our psychiatrist gave patients with acute mania a loading dosage of lithium, 900 mg tid to qid on day one, and drew a level in the morning. He reduced the dosage daily until target symptoms improved and/or serum concentration reached the high therapeutic range, or until side effects occurred.
During acute mania, the psychiatrist controlled unsafe agitation with short-acting barbiturates. Some extremely hostile, aggressive patients got IM sodium amobarbital. We observed the patient one-on-one until he or she awoke and could take fluids, food, and lithium. When manic symptoms began escalating, the patient again was medicated and the cycle continued. This cycle might continue for 1 to 3 days with decreasing frequency and sedation based on behavior.
Although I’m not advocating this regimen, it worked well from an empirical perspective. Our patients never acted out or had breathing problems.
Thomas Dowling, RN, MSN
St. Peter’s Hospital, Albany, NY
Reading “High-dose antipsychotics: Desperation or data-driven?” (Current Psychiatry, August 2004) brings back memories.
In 1980, I worked in a rural hospital. Our psychiatrist gave patients with acute mania a loading dosage of lithium, 900 mg tid to qid on day one, and drew a level in the morning. He reduced the dosage daily until target symptoms improved and/or serum concentration reached the high therapeutic range, or until side effects occurred.
During acute mania, the psychiatrist controlled unsafe agitation with short-acting barbiturates. Some extremely hostile, aggressive patients got IM sodium amobarbital. We observed the patient one-on-one until he or she awoke and could take fluids, food, and lithium. When manic symptoms began escalating, the patient again was medicated and the cycle continued. This cycle might continue for 1 to 3 days with decreasing frequency and sedation based on behavior.
Although I’m not advocating this regimen, it worked well from an empirical perspective. Our patients never acted out or had breathing problems.
Thomas Dowling, RN, MSN
St. Peter’s Hospital, Albany, NY
A ‘FRESH’ way to manage trauma
Ameliorating emotional trauma is key to avoiding long-term functional impairment. Consider a FRESH approach that involves families/friends, reassurance/retelling, education, addressing substance abuse, sleeplessness, and suicide risk, and taking a careful history.
Family and friends can be valuable to treatment but clinicians often overlook their importance. Overwhelmed or traumatized family members who are not counseled about the patient’s symptoms can undermine treatment by dismissing symptoms and withdrawing support. Involve them by emphasizing their supportive role. Alert them to normal and problematic trauma responses and stress disorder symptoms.
Reassurance/retelling. Explain that emotional pain is normal but usually fades with time. Consider effects of survivor guilt: Encourage the patient to retell the experience, but do not demand this. Help patients identify and correct thought distortions that foster avoidance. Though controversial,1 critical incident debriefing and cognitive-behavioral therapy can help the patient recount the trauma and ultimately restore a sense of self, enjoyment of life, and expectations of safety, control, and trust.2
Educate patients about normal variable stress responses. Warn traumatized patients against engaging in high-risk behaviors, through which they may try to deny their vulnerability, fear, and loss of control. Explain symptoms and risk factors for depression, posttraumatic stress disorder (PTSD), and other anxiety disorders.
Substance abuse, sleeplessness, and suicide are possible outcomes of trauma. Prescribe a non-narcotic sleep-promoting medication if insomnia is problematic. Alternately, consider a selective serotonin or serotonin-norepinephrine reuptake inhibitor3,4 at normal or low starting dosages if presenting symptoms suggest an emerging anxiety or mood disorder or PTSD. Watch for signs of survivor guilt—such as an unrealistic sense of responsibility for the trauma—that can lead to depression with suicide risk after a significant loss.
History. Watch for factors that predict PTSD and comorbid disorders (trauma severity and chronicity, involvement of interpersonal violence, fear of death). Previous trauma, PTSD, depression, anxiety, personality disorder, childhood victimization, substance abuse, and poor social support increase the risk. Avoidance, numbing, dissociation, high guilt, and low acknowledged anger correlate with increased PTSD risk. Follow up with patients who exhibit these risk factors every 1 to 2 weeks with medication and/or psychotherapy.
1. Cloak NL, Edwards P. Psychological first aid: Emergency care for terrorism and disaster survivors. Current Psychiatry 2004;3(5):12-23.
2. Bisson JI. Early interventions following traumatic events. Psychiatr Ann 2003;1:37-44.
3. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58:485-92.
4. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8.
Dr. Sobel is a clinical instructor, University of California-San Diego School of Medicine, and consulting psychiatrist, University of San Diego Counseling Center.
Ameliorating emotional trauma is key to avoiding long-term functional impairment. Consider a FRESH approach that involves families/friends, reassurance/retelling, education, addressing substance abuse, sleeplessness, and suicide risk, and taking a careful history.
Family and friends can be valuable to treatment but clinicians often overlook their importance. Overwhelmed or traumatized family members who are not counseled about the patient’s symptoms can undermine treatment by dismissing symptoms and withdrawing support. Involve them by emphasizing their supportive role. Alert them to normal and problematic trauma responses and stress disorder symptoms.
Reassurance/retelling. Explain that emotional pain is normal but usually fades with time. Consider effects of survivor guilt: Encourage the patient to retell the experience, but do not demand this. Help patients identify and correct thought distortions that foster avoidance. Though controversial,1 critical incident debriefing and cognitive-behavioral therapy can help the patient recount the trauma and ultimately restore a sense of self, enjoyment of life, and expectations of safety, control, and trust.2
Educate patients about normal variable stress responses. Warn traumatized patients against engaging in high-risk behaviors, through which they may try to deny their vulnerability, fear, and loss of control. Explain symptoms and risk factors for depression, posttraumatic stress disorder (PTSD), and other anxiety disorders.
Substance abuse, sleeplessness, and suicide are possible outcomes of trauma. Prescribe a non-narcotic sleep-promoting medication if insomnia is problematic. Alternately, consider a selective serotonin or serotonin-norepinephrine reuptake inhibitor3,4 at normal or low starting dosages if presenting symptoms suggest an emerging anxiety or mood disorder or PTSD. Watch for signs of survivor guilt—such as an unrealistic sense of responsibility for the trauma—that can lead to depression with suicide risk after a significant loss.
History. Watch for factors that predict PTSD and comorbid disorders (trauma severity and chronicity, involvement of interpersonal violence, fear of death). Previous trauma, PTSD, depression, anxiety, personality disorder, childhood victimization, substance abuse, and poor social support increase the risk. Avoidance, numbing, dissociation, high guilt, and low acknowledged anger correlate with increased PTSD risk. Follow up with patients who exhibit these risk factors every 1 to 2 weeks with medication and/or psychotherapy.
Ameliorating emotional trauma is key to avoiding long-term functional impairment. Consider a FRESH approach that involves families/friends, reassurance/retelling, education, addressing substance abuse, sleeplessness, and suicide risk, and taking a careful history.
Family and friends can be valuable to treatment but clinicians often overlook their importance. Overwhelmed or traumatized family members who are not counseled about the patient’s symptoms can undermine treatment by dismissing symptoms and withdrawing support. Involve them by emphasizing their supportive role. Alert them to normal and problematic trauma responses and stress disorder symptoms.
Reassurance/retelling. Explain that emotional pain is normal but usually fades with time. Consider effects of survivor guilt: Encourage the patient to retell the experience, but do not demand this. Help patients identify and correct thought distortions that foster avoidance. Though controversial,1 critical incident debriefing and cognitive-behavioral therapy can help the patient recount the trauma and ultimately restore a sense of self, enjoyment of life, and expectations of safety, control, and trust.2
Educate patients about normal variable stress responses. Warn traumatized patients against engaging in high-risk behaviors, through which they may try to deny their vulnerability, fear, and loss of control. Explain symptoms and risk factors for depression, posttraumatic stress disorder (PTSD), and other anxiety disorders.
Substance abuse, sleeplessness, and suicide are possible outcomes of trauma. Prescribe a non-narcotic sleep-promoting medication if insomnia is problematic. Alternately, consider a selective serotonin or serotonin-norepinephrine reuptake inhibitor3,4 at normal or low starting dosages if presenting symptoms suggest an emerging anxiety or mood disorder or PTSD. Watch for signs of survivor guilt—such as an unrealistic sense of responsibility for the trauma—that can lead to depression with suicide risk after a significant loss.
History. Watch for factors that predict PTSD and comorbid disorders (trauma severity and chronicity, involvement of interpersonal violence, fear of death). Previous trauma, PTSD, depression, anxiety, personality disorder, childhood victimization, substance abuse, and poor social support increase the risk. Avoidance, numbing, dissociation, high guilt, and low acknowledged anger correlate with increased PTSD risk. Follow up with patients who exhibit these risk factors every 1 to 2 weeks with medication and/or psychotherapy.
1. Cloak NL, Edwards P. Psychological first aid: Emergency care for terrorism and disaster survivors. Current Psychiatry 2004;3(5):12-23.
2. Bisson JI. Early interventions following traumatic events. Psychiatr Ann 2003;1:37-44.
3. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58:485-92.
4. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8.
Dr. Sobel is a clinical instructor, University of California-San Diego School of Medicine, and consulting psychiatrist, University of San Diego Counseling Center.
1. Cloak NL, Edwards P. Psychological first aid: Emergency care for terrorism and disaster survivors. Current Psychiatry 2004;3(5):12-23.
2. Bisson JI. Early interventions following traumatic events. Psychiatr Ann 2003;1:37-44.
3. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58:485-92.
4. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8.
Dr. Sobel is a clinical instructor, University of California-San Diego School of Medicine, and consulting psychiatrist, University of San Diego Counseling Center.
Liability in patient suicide
Clinical psychiatrists often find it hard to evaluate suicide risk and understand their potential legal liability. Prevalence of suicidality compounds this challenge: Up to one-third of the general population in the United States have suicidal thoughts at some point.1 Although most people who consider suicide do not act on those thoughts, 51% of psychiatrists report having had a patient who committed suicide.2
Because patient suicide risk is real, psychiatrists often worry about malpractice claims. Although post-suicide lawsuits account for the largest number of malpractice suits against psychiatrists,3,4 a psychiatrist’s risk of being sued for malpractice is still quite low.3 Even when sued, clinicians win up to 80% of cases.3
Still, with malpractice claims increasing overall, clinicians should understand their potential liability in preventing suicide and the basic principles behind a malpractice claim.
Patient jumps from window after suicide watch is called off
Los Angeles County (CA) superior court
A 24-year-old man was hospitalized after attempting suicide by ingesting prescription pills and alcohol. He was admitted to the general medical floor with a 24-hour sitter to guard against additional suicide attempts. When the psychiatrist tried to evaluate him, he found the patient unresponsive because of the pills’ effects.
The next day, the psychiatrist evaluated the patient and recommended that the patient be transferred to the psychiatric unit and that the sitter be continued. Four hours later, without a further evaluation, the psychiatrist recommended moving the patient to another room and canceling the sitter.
The next day, the patient jumped from his sixth-floor hospital room window. He sustained traumatic brain injury.
The patient’s guardian ad litem argued that discontinuing the sitter was negligent. The defendant argued that discontinuation was within the parameters of proper care.
- The jury found for the defense.
Patient commits suicide hours after ER discharge
Lake County (IL) circuit court
A 36-year-old man was being treated by a psychiatrist for major depressive disorder. The patient owned several guns for hunting and target shooting and had a state-issued firearm owner’s identification card.
In October 2003, the patient presented to the emergency room and was examined by a mental health assessment staff. The psychiatrist recommended voluntary admission to the psychiatric unit for 23 hours.
The patient’s father discouraged the admission and stated that the patient could lose his gun owner’s card as a result. The patient was subsequently discharged. Within 24 hours after discharge, the patient shot himself in the chest and died.
The deceased’s estate argued that the psychiatrist should have admitted the patient involuntarily. The psychiatrist claimed no obligation to involuntary admission and argued that the patient did not meet criteria typically used for such admission.
- The jury found for the defense.
Doctor’s hanging attempt in hospital causes permanent brain damage
Morris County (NJ) district court
A cardiologist was admitted to the hospital’s psychiatric unit after decompensating. While hospitalized, he attempted suicide by hanging in a clinic bathroom. He suffered permanent brain injury as a result of the hanging. Because the injury left him in a childlike state, he required constant care.
The patient’s attorney argued that hospital personnel knew he was suicidal yet did not adequately supervise him. The attorney also argued that the injury cost his client $5 million in lost income.
The defense reported that the hospital had placed the patient on suicide watch and that staff checked him every 5 minutes. The defense also argued that the bathroom where the suicide was attempted was impossible to monitor.
- The jury found for the defense.
Dr. Grant’s observations
To win a malpractice claim, the injured party must show four things:
Duty to care for the patient existed based on the provider’s relationship with the patient. Whether on a hospital floor or in the emergency room, once a doctor-patient relationship has been established, the provider agrees to provide non-negligent care.
Negligence. The physician or hospital personnel acted negligently and violated the duty of care. This concept is based upon a “standard of care” —ie, what other psychiatrists would do in this situation.
Harm. Even if someone has acted negligently, a malpractice case cannot go forward if no harm has been suffered.
Causation. The negligent act caused the harm.
The defendants most likely won the cases cited above because the injured parties could not establish negligence. Clinicians are not negligent for merely failing to predict suicide, as the inability to predict suicide has been demonstrated.5,6 Clinicians, however, must follow the profession’s standard of care, assess the relative degree of risk, and form a treatment and safety plan consistent with that risk.4
Based on relevant case law, the following actions can decrease the risk of patient suicide—and a resultant malpractice claim:
- Conduct a comprehensive evaluation of the patient and his or her suicide risk. Ask about:
- Consider hospitalizing at-risk patients. If you decide against hospitalization, provide a comprehensive safety plan. In the gun owner’s case, such a plan would include arranging with the family to remove firearms. Implement additional anti-suicide precautions, such as more-intensive outpatient therapy or involving family members in treatment.
- Document suicide risk assessment and the reasons for your treatment decisions. Juries may interpret lack of documented information in the patient’s favor.
- Design a treatment plan for hospitalized patients to reduce suicide risk. Consider the patient’s reaction to constant surveillance. For example, checking a paranoid patient every 5 minutes may be more therapeutic than a constant watch while providing adequate safety. Thoroughly document your reasons behind the plan.
1. Hirschfeld RMA, Russell JM. Assessment and treatment of suicidal patients. N Engl J Med 1997;337:910-5.
2. Chemtob CM, Hamada RS, Bauer GB, et al. Patient suicide: frequency and impact on psychiatrists. Am J Psychiatry 1988;145:224-8.
3. Baerger DR. Risk management with the suicidal patient: lessons from case law. Prof Psychol Res Pract 2001;32:359-66.
4. Packman WL, O’Connor Pennuto T, Bongar B, Orthwein J. Legal issues of professional negligence in suicide cases. Behav Sci Law 2004;22:697-713.
5. Pokorny AD. Prediction of suicide in psychiatric patients. Arch Gen Psychiatry 1983;40:249-57.
6. Pokorny AD. Suicide prediction revisited. Suicide Life Threat Behav 1993;23:1-10.
7. Bell v. New York City Health and Hospitals Corp., 456 NYS 2d 787 (App. Div. 1982).
8. Simon RI. The suicidal patient. In: Lifson LE, Simon SI (eds). The mental health practitioner and the law: A comprehensive handbook. Cambridge, MA: Harvard University Press, 1998;166-86.
Clinical psychiatrists often find it hard to evaluate suicide risk and understand their potential legal liability. Prevalence of suicidality compounds this challenge: Up to one-third of the general population in the United States have suicidal thoughts at some point.1 Although most people who consider suicide do not act on those thoughts, 51% of psychiatrists report having had a patient who committed suicide.2
Because patient suicide risk is real, psychiatrists often worry about malpractice claims. Although post-suicide lawsuits account for the largest number of malpractice suits against psychiatrists,3,4 a psychiatrist’s risk of being sued for malpractice is still quite low.3 Even when sued, clinicians win up to 80% of cases.3
Still, with malpractice claims increasing overall, clinicians should understand their potential liability in preventing suicide and the basic principles behind a malpractice claim.
Patient jumps from window after suicide watch is called off
Los Angeles County (CA) superior court
A 24-year-old man was hospitalized after attempting suicide by ingesting prescription pills and alcohol. He was admitted to the general medical floor with a 24-hour sitter to guard against additional suicide attempts. When the psychiatrist tried to evaluate him, he found the patient unresponsive because of the pills’ effects.
The next day, the psychiatrist evaluated the patient and recommended that the patient be transferred to the psychiatric unit and that the sitter be continued. Four hours later, without a further evaluation, the psychiatrist recommended moving the patient to another room and canceling the sitter.
The next day, the patient jumped from his sixth-floor hospital room window. He sustained traumatic brain injury.
The patient’s guardian ad litem argued that discontinuing the sitter was negligent. The defendant argued that discontinuation was within the parameters of proper care.
- The jury found for the defense.
Patient commits suicide hours after ER discharge
Lake County (IL) circuit court
A 36-year-old man was being treated by a psychiatrist for major depressive disorder. The patient owned several guns for hunting and target shooting and had a state-issued firearm owner’s identification card.
In October 2003, the patient presented to the emergency room and was examined by a mental health assessment staff. The psychiatrist recommended voluntary admission to the psychiatric unit for 23 hours.
The patient’s father discouraged the admission and stated that the patient could lose his gun owner’s card as a result. The patient was subsequently discharged. Within 24 hours after discharge, the patient shot himself in the chest and died.
The deceased’s estate argued that the psychiatrist should have admitted the patient involuntarily. The psychiatrist claimed no obligation to involuntary admission and argued that the patient did not meet criteria typically used for such admission.
- The jury found for the defense.
Doctor’s hanging attempt in hospital causes permanent brain damage
Morris County (NJ) district court
A cardiologist was admitted to the hospital’s psychiatric unit after decompensating. While hospitalized, he attempted suicide by hanging in a clinic bathroom. He suffered permanent brain injury as a result of the hanging. Because the injury left him in a childlike state, he required constant care.
The patient’s attorney argued that hospital personnel knew he was suicidal yet did not adequately supervise him. The attorney also argued that the injury cost his client $5 million in lost income.
The defense reported that the hospital had placed the patient on suicide watch and that staff checked him every 5 minutes. The defense also argued that the bathroom where the suicide was attempted was impossible to monitor.
- The jury found for the defense.
Dr. Grant’s observations
To win a malpractice claim, the injured party must show four things:
Duty to care for the patient existed based on the provider’s relationship with the patient. Whether on a hospital floor or in the emergency room, once a doctor-patient relationship has been established, the provider agrees to provide non-negligent care.
Negligence. The physician or hospital personnel acted negligently and violated the duty of care. This concept is based upon a “standard of care” —ie, what other psychiatrists would do in this situation.
Harm. Even if someone has acted negligently, a malpractice case cannot go forward if no harm has been suffered.
Causation. The negligent act caused the harm.
The defendants most likely won the cases cited above because the injured parties could not establish negligence. Clinicians are not negligent for merely failing to predict suicide, as the inability to predict suicide has been demonstrated.5,6 Clinicians, however, must follow the profession’s standard of care, assess the relative degree of risk, and form a treatment and safety plan consistent with that risk.4
Based on relevant case law, the following actions can decrease the risk of patient suicide—and a resultant malpractice claim:
- Conduct a comprehensive evaluation of the patient and his or her suicide risk. Ask about:
- Consider hospitalizing at-risk patients. If you decide against hospitalization, provide a comprehensive safety plan. In the gun owner’s case, such a plan would include arranging with the family to remove firearms. Implement additional anti-suicide precautions, such as more-intensive outpatient therapy or involving family members in treatment.
- Document suicide risk assessment and the reasons for your treatment decisions. Juries may interpret lack of documented information in the patient’s favor.
- Design a treatment plan for hospitalized patients to reduce suicide risk. Consider the patient’s reaction to constant surveillance. For example, checking a paranoid patient every 5 minutes may be more therapeutic than a constant watch while providing adequate safety. Thoroughly document your reasons behind the plan.
Clinical psychiatrists often find it hard to evaluate suicide risk and understand their potential legal liability. Prevalence of suicidality compounds this challenge: Up to one-third of the general population in the United States have suicidal thoughts at some point.1 Although most people who consider suicide do not act on those thoughts, 51% of psychiatrists report having had a patient who committed suicide.2
Because patient suicide risk is real, psychiatrists often worry about malpractice claims. Although post-suicide lawsuits account for the largest number of malpractice suits against psychiatrists,3,4 a psychiatrist’s risk of being sued for malpractice is still quite low.3 Even when sued, clinicians win up to 80% of cases.3
Still, with malpractice claims increasing overall, clinicians should understand their potential liability in preventing suicide and the basic principles behind a malpractice claim.
Patient jumps from window after suicide watch is called off
Los Angeles County (CA) superior court
A 24-year-old man was hospitalized after attempting suicide by ingesting prescription pills and alcohol. He was admitted to the general medical floor with a 24-hour sitter to guard against additional suicide attempts. When the psychiatrist tried to evaluate him, he found the patient unresponsive because of the pills’ effects.
The next day, the psychiatrist evaluated the patient and recommended that the patient be transferred to the psychiatric unit and that the sitter be continued. Four hours later, without a further evaluation, the psychiatrist recommended moving the patient to another room and canceling the sitter.
The next day, the patient jumped from his sixth-floor hospital room window. He sustained traumatic brain injury.
The patient’s guardian ad litem argued that discontinuing the sitter was negligent. The defendant argued that discontinuation was within the parameters of proper care.
- The jury found for the defense.
Patient commits suicide hours after ER discharge
Lake County (IL) circuit court
A 36-year-old man was being treated by a psychiatrist for major depressive disorder. The patient owned several guns for hunting and target shooting and had a state-issued firearm owner’s identification card.
In October 2003, the patient presented to the emergency room and was examined by a mental health assessment staff. The psychiatrist recommended voluntary admission to the psychiatric unit for 23 hours.
The patient’s father discouraged the admission and stated that the patient could lose his gun owner’s card as a result. The patient was subsequently discharged. Within 24 hours after discharge, the patient shot himself in the chest and died.
The deceased’s estate argued that the psychiatrist should have admitted the patient involuntarily. The psychiatrist claimed no obligation to involuntary admission and argued that the patient did not meet criteria typically used for such admission.
- The jury found for the defense.
Doctor’s hanging attempt in hospital causes permanent brain damage
Morris County (NJ) district court
A cardiologist was admitted to the hospital’s psychiatric unit after decompensating. While hospitalized, he attempted suicide by hanging in a clinic bathroom. He suffered permanent brain injury as a result of the hanging. Because the injury left him in a childlike state, he required constant care.
The patient’s attorney argued that hospital personnel knew he was suicidal yet did not adequately supervise him. The attorney also argued that the injury cost his client $5 million in lost income.
The defense reported that the hospital had placed the patient on suicide watch and that staff checked him every 5 minutes. The defense also argued that the bathroom where the suicide was attempted was impossible to monitor.
- The jury found for the defense.
Dr. Grant’s observations
To win a malpractice claim, the injured party must show four things:
Duty to care for the patient existed based on the provider’s relationship with the patient. Whether on a hospital floor or in the emergency room, once a doctor-patient relationship has been established, the provider agrees to provide non-negligent care.
Negligence. The physician or hospital personnel acted negligently and violated the duty of care. This concept is based upon a “standard of care” —ie, what other psychiatrists would do in this situation.
Harm. Even if someone has acted negligently, a malpractice case cannot go forward if no harm has been suffered.
Causation. The negligent act caused the harm.
The defendants most likely won the cases cited above because the injured parties could not establish negligence. Clinicians are not negligent for merely failing to predict suicide, as the inability to predict suicide has been demonstrated.5,6 Clinicians, however, must follow the profession’s standard of care, assess the relative degree of risk, and form a treatment and safety plan consistent with that risk.4
Based on relevant case law, the following actions can decrease the risk of patient suicide—and a resultant malpractice claim:
- Conduct a comprehensive evaluation of the patient and his or her suicide risk. Ask about:
- Consider hospitalizing at-risk patients. If you decide against hospitalization, provide a comprehensive safety plan. In the gun owner’s case, such a plan would include arranging with the family to remove firearms. Implement additional anti-suicide precautions, such as more-intensive outpatient therapy or involving family members in treatment.
- Document suicide risk assessment and the reasons for your treatment decisions. Juries may interpret lack of documented information in the patient’s favor.
- Design a treatment plan for hospitalized patients to reduce suicide risk. Consider the patient’s reaction to constant surveillance. For example, checking a paranoid patient every 5 minutes may be more therapeutic than a constant watch while providing adequate safety. Thoroughly document your reasons behind the plan.
1. Hirschfeld RMA, Russell JM. Assessment and treatment of suicidal patients. N Engl J Med 1997;337:910-5.
2. Chemtob CM, Hamada RS, Bauer GB, et al. Patient suicide: frequency and impact on psychiatrists. Am J Psychiatry 1988;145:224-8.
3. Baerger DR. Risk management with the suicidal patient: lessons from case law. Prof Psychol Res Pract 2001;32:359-66.
4. Packman WL, O’Connor Pennuto T, Bongar B, Orthwein J. Legal issues of professional negligence in suicide cases. Behav Sci Law 2004;22:697-713.
5. Pokorny AD. Prediction of suicide in psychiatric patients. Arch Gen Psychiatry 1983;40:249-57.
6. Pokorny AD. Suicide prediction revisited. Suicide Life Threat Behav 1993;23:1-10.
7. Bell v. New York City Health and Hospitals Corp., 456 NYS 2d 787 (App. Div. 1982).
8. Simon RI. The suicidal patient. In: Lifson LE, Simon SI (eds). The mental health practitioner and the law: A comprehensive handbook. Cambridge, MA: Harvard University Press, 1998;166-86.
1. Hirschfeld RMA, Russell JM. Assessment and treatment of suicidal patients. N Engl J Med 1997;337:910-5.
2. Chemtob CM, Hamada RS, Bauer GB, et al. Patient suicide: frequency and impact on psychiatrists. Am J Psychiatry 1988;145:224-8.
3. Baerger DR. Risk management with the suicidal patient: lessons from case law. Prof Psychol Res Pract 2001;32:359-66.
4. Packman WL, O’Connor Pennuto T, Bongar B, Orthwein J. Legal issues of professional negligence in suicide cases. Behav Sci Law 2004;22:697-713.
5. Pokorny AD. Prediction of suicide in psychiatric patients. Arch Gen Psychiatry 1983;40:249-57.
6. Pokorny AD. Suicide prediction revisited. Suicide Life Threat Behav 1993;23:1-10.
7. Bell v. New York City Health and Hospitals Corp., 456 NYS 2d 787 (App. Div. 1982).
8. Simon RI. The suicidal patient. In: Lifson LE, Simon SI (eds). The mental health practitioner and the law: A comprehensive handbook. Cambridge, MA: Harvard University Press, 1998;166-86.
Somatoform disorders: food for thought
HISTORY: UNHAPPY NEW YEAR
On New Year’s Day Ms. M, age 43, begins experiencing persistent left-leg numbness, fatigue, and what she calls a “superallergic sensitivity to anything I put in my mouth.”
A few days later she sees her internist, who finds no medical cause and suspects that her symptoms are psychological. The internist prescribes fluoxetine, 10 mg/d. Fifteen minutes after taking the first dose, the patient reports “an anaphylactic episode,” which she describes as “screaming and shaking.”
Acting on the internist’s suggestion, Ms. M presents to me on Jan. 10. Her parents bring her to the appointment, as she feels too weak to drive.
A chemical engineer with a six-figure income, Ms. M has lived on her own most of her adult life but has stayed the past week with her elderly parents. With her vacation leave about to end, she says she is too weak and tired to return to work. She complains of extreme fatigue after eating most foods; after some meals, she says, welts surface throughout her body. Now living on bananas and homemade apple-sauce, she has lost 5 lbs in less than 2 weeks.
An only child, Ms. M is an award-winning athlete. She has enjoyed her career, which has taken her around the world. She has no significant psychiatric or medical history or family history of allergy or autoimmune disease. She says she is not depressed and is sleeping normally. Her Mini-Mental State Examination score of 30 indicates no cognitive impairment.
Ms. M denies feeling depressed. She mentions that her boyfriend broke off their relationship days before New Year’s Eve—the day on which she had expected they would become engaged. She sees no relationship between disappointment over this breakup and the symptoms that followed almost immediately. She has never had another intimate relationship and describes people she knows as “acquaintances” or “work buddies” rather than as friends.
Table 1
Diagnostic criteria for hypochondriasis
|
| Specify if: With poor insight: if, for most of the time during the current episode, the person does not recognize that the concern about having a serious illness is excessive or unreasonable. |
| Source: Tables 1 through 3 reprinted with permission from the Diagnostic and statistical manual of mental disorders (4th ed, text revision). |
| Copyright 2000.American Psychiatric Association. |
Ms. M refuses to try another psychotropic, fearing another “anaphylactic” episode like the one she described after the fluoxetine dose. She is willing to start psychotherapy, however.
Dr. Bernstein’s observations
Ms. M. complains of an array of food allergies and fatigue with no subjective feelings of depression. She has an athletic physique, is attractive without cosmetics, and is casually but neatly dressed, indicating good organization.
At this point, no physical or medical cause has been found for Ms. M’s symptoms, nor does she meet DSM-IV-TR criteria for hypochondriasis (Table 1). Her symptoms have persisted for 10 days—far short of the 6 months the diagnosis requires. Ms. M also believes that her medical problem is inconvenient but not serious.
Even though Ms. M denies feeling depressed, her symptoms most closely suggest depression with somatic complaints. She is not substantially distressed, but her symptoms are impairing her social and occupational functioning.
Antidepressants—particularly selective serotonin reuptake inhibitors—can help depressed patients with somatic symptoms, and low-dose atypical antipsychotics alternately are used to treat major depressive disorder with somatic delusions. Ms. M, however, will not try another medication, making psychotherapy my only treatment option.
TREATMENT: ‘SURFING’ FOR CLUES
For 6 months, Ms. M attends weekly psychodynamic psychotherapy sessions regularly and on time. She is courteous and pleasant, but her fatigue persists.
Early in treatment, Ms. M spends hours searching the Internet for doctors who specialize in malabsorption syndrome, allergy, and rare infectious diseases. Numerous internists, allergists, and immunologists perform blood work and other laboratory tests on her. She has the results—reams of clinical data—sent to me. I also order tests for HIV, syphilis, and gonorrhea. None of the results indicates a physical disorder. She refuses patch or intradermal testing for allergy, fearing anaphylaxis.
Ms. M also spends much of her day preparing her own meals. She introduces “new foods” one at a time, but reports that these trials often lead to fatigue and cause her to break out in welts. During psychotherapy, she points to bumps and rashes throughout her body that I cannot see.
Six months into psychotherapy, Ms. M is still staying with her parents and has not returned to work, citing disabling fatigue. Her parents, frustrated with her apparent unwillingness to get better, set a deadline for her to move out of their home. She finds an apartment nearby but about 2 miles from the train line she would use to commute to work. She refuses to take a taxi to the train station because of the expense, will not drive to the station because she cannot get up early, and will not drive directly to work for fear of tiring while driving. She refuses her company’s offer to let her work part time from home.
Ms. M’s company keeps her job open for her, but she is still not returning to work. After 1 year, the company finally fires her, then calls her a few months later asking if she’ll come back; she again says no. She collects disability benefits and taps into her savings and investment dividends to make ends meet. In discussing her lack of income during psychotherapy, Ms. M does not appear distressed.
Table 2
Undifferentiated somatoform disorder: diagnostic criteria
|
Dr. Bernstein’s observations
Although Ms. M meets criteria for undifferentiated somatoform disorder ( Table 2), her belief that she has a medical problem is tenacious and her disability persists despite lack of a medical diagnosis. To me, this suggests a delusional disorder (Table 3 ).
Table 3
Diagnostic criteria for delusional disorder
|
| Somatic type: delusions that the person has some physical defect or general medical condition. |
For 6 months, although she has cooperated with psychotherapy, Ms. M’s complaints have been unyielding. Despite our good relationship, she will not trust my recommendations to try a psychotropic. Nor does psychotherapy or the cooperation of her former employer enable her to resume her once-rewarding career, even part-time.
Ms. M is reclusive but not suspicious. She has no grandiose or paranoid delusions or hallucinations. She has had no depersonalization or derealization episodes, and no affective component exists. She is profoundly convinced that she suddenly developed severe, incapacitating food allergies. Her lifestyle has deteriorated—she feels unable to work and even her parents have virtually abandoned her—yet she seems oddly content.
How does Ms. M compare with other patients with:
- undifferentiated somatic disorder
- delusional disorder?
Dr. Bernstein’s observations
Somatoform disorder. Patients with undifferentiated somatoform disorder usually exhibit fluctuating symptoms, which often can be mitigated with psychodynamic therapy. In time, most accept that their problem is psychological rather than physical or that anxiety or depression are contributing to symptom fluctuation. Patients usually continue or resume social and vocational functioning.
By contrast, Ms. M believes immutably that her symptoms have an undiscovered physical cause. This belief has dramatically changed her life: She has sacrificed her career, social life, health insurance, even her financial security.
The depth and seeming permanence of Ms. M’s state does not distress her. She is not regressed nor affectively or cognitively impaired. She reports seeing and feeling welts and rashes that were not visible to me or to other medical/alternative medical specialists, suggesting reality testing impairment. I perceived no other break in reality testing during psychotherapy.
Delusional disorder can be treated with medication or cognitive-behavioral therapy. I once treated a young man who believed that his head was coming to a point, causing him tremendous emotional distress. An antipsychotic resulted in prompt remission.
By contrast, Ms. M has a delusional belief that food and medicine make her sick and could lead to anaphylaxis. She will not take medication, even in a hospital.
Perhaps someday we will find a neurobiological or biochemical cause for Ms. M’s behavior. Positron-emission tomography or augmented MRI could uncover such clues, but both tests require ingesting a foreign substance—something Ms. M will not do.
FOLLOW-UP: MS. M’S NEW LIFE
Having exhausted her savings and work disability benefits, Ms. M receives Social Security disability benefits. With her health insurance coverage having expired, she stops psychotherapy after 2 years and pursues no further medical workup.
Two years after presenting to me, she does not seem depressed but her presenting picture is unchanged. She sounds happy and cognitively intact. Her life revolves around her perceived disability.
Ms. M has spent much of the last 2 years alone in her apartment, content in her solitude. She has resumed playing tennis but only occasionally and has not resumed the sport for which she has won many awards. She says she feels slightly better but remains too tired to return to work. She has gradually expanded her menu to about a dozen foods. Despite her problems Ms. M, who is 5 feet 2 inches, has maintained her weight (114 lbs) and attractiveness.
All the while, Ms. M has refused medication. I repeatedly suggest hospitalization so that she can take psychotropics in a safe, supervised setting, but she declines.
Related resources
- Pilowsky I. Abnormal Illness Behaviour. New York: John Wiley & Sons, 1997.
- Isaac A, Wise T. A low-frustration strategy for treating somatization. Current Psychiatry 2003;2(8):32-50.
Drug brand names
- Fluoxetine • Prozac
Disclosure
Dr. Bernstein reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
HISTORY: UNHAPPY NEW YEAR
On New Year’s Day Ms. M, age 43, begins experiencing persistent left-leg numbness, fatigue, and what she calls a “superallergic sensitivity to anything I put in my mouth.”
A few days later she sees her internist, who finds no medical cause and suspects that her symptoms are psychological. The internist prescribes fluoxetine, 10 mg/d. Fifteen minutes after taking the first dose, the patient reports “an anaphylactic episode,” which she describes as “screaming and shaking.”
Acting on the internist’s suggestion, Ms. M presents to me on Jan. 10. Her parents bring her to the appointment, as she feels too weak to drive.
A chemical engineer with a six-figure income, Ms. M has lived on her own most of her adult life but has stayed the past week with her elderly parents. With her vacation leave about to end, she says she is too weak and tired to return to work. She complains of extreme fatigue after eating most foods; after some meals, she says, welts surface throughout her body. Now living on bananas and homemade apple-sauce, she has lost 5 lbs in less than 2 weeks.
An only child, Ms. M is an award-winning athlete. She has enjoyed her career, which has taken her around the world. She has no significant psychiatric or medical history or family history of allergy or autoimmune disease. She says she is not depressed and is sleeping normally. Her Mini-Mental State Examination score of 30 indicates no cognitive impairment.
Ms. M denies feeling depressed. She mentions that her boyfriend broke off their relationship days before New Year’s Eve—the day on which she had expected they would become engaged. She sees no relationship between disappointment over this breakup and the symptoms that followed almost immediately. She has never had another intimate relationship and describes people she knows as “acquaintances” or “work buddies” rather than as friends.
Table 1
Diagnostic criteria for hypochondriasis
|
| Specify if: With poor insight: if, for most of the time during the current episode, the person does not recognize that the concern about having a serious illness is excessive or unreasonable. |
| Source: Tables 1 through 3 reprinted with permission from the Diagnostic and statistical manual of mental disorders (4th ed, text revision). |
| Copyright 2000.American Psychiatric Association. |
Ms. M refuses to try another psychotropic, fearing another “anaphylactic” episode like the one she described after the fluoxetine dose. She is willing to start psychotherapy, however.
Dr. Bernstein’s observations
Ms. M. complains of an array of food allergies and fatigue with no subjective feelings of depression. She has an athletic physique, is attractive without cosmetics, and is casually but neatly dressed, indicating good organization.
At this point, no physical or medical cause has been found for Ms. M’s symptoms, nor does she meet DSM-IV-TR criteria for hypochondriasis (Table 1). Her symptoms have persisted for 10 days—far short of the 6 months the diagnosis requires. Ms. M also believes that her medical problem is inconvenient but not serious.
Even though Ms. M denies feeling depressed, her symptoms most closely suggest depression with somatic complaints. She is not substantially distressed, but her symptoms are impairing her social and occupational functioning.
Antidepressants—particularly selective serotonin reuptake inhibitors—can help depressed patients with somatic symptoms, and low-dose atypical antipsychotics alternately are used to treat major depressive disorder with somatic delusions. Ms. M, however, will not try another medication, making psychotherapy my only treatment option.
TREATMENT: ‘SURFING’ FOR CLUES
For 6 months, Ms. M attends weekly psychodynamic psychotherapy sessions regularly and on time. She is courteous and pleasant, but her fatigue persists.
Early in treatment, Ms. M spends hours searching the Internet for doctors who specialize in malabsorption syndrome, allergy, and rare infectious diseases. Numerous internists, allergists, and immunologists perform blood work and other laboratory tests on her. She has the results—reams of clinical data—sent to me. I also order tests for HIV, syphilis, and gonorrhea. None of the results indicates a physical disorder. She refuses patch or intradermal testing for allergy, fearing anaphylaxis.
Ms. M also spends much of her day preparing her own meals. She introduces “new foods” one at a time, but reports that these trials often lead to fatigue and cause her to break out in welts. During psychotherapy, she points to bumps and rashes throughout her body that I cannot see.
Six months into psychotherapy, Ms. M is still staying with her parents and has not returned to work, citing disabling fatigue. Her parents, frustrated with her apparent unwillingness to get better, set a deadline for her to move out of their home. She finds an apartment nearby but about 2 miles from the train line she would use to commute to work. She refuses to take a taxi to the train station because of the expense, will not drive to the station because she cannot get up early, and will not drive directly to work for fear of tiring while driving. She refuses her company’s offer to let her work part time from home.
Ms. M’s company keeps her job open for her, but she is still not returning to work. After 1 year, the company finally fires her, then calls her a few months later asking if she’ll come back; she again says no. She collects disability benefits and taps into her savings and investment dividends to make ends meet. In discussing her lack of income during psychotherapy, Ms. M does not appear distressed.
Table 2
Undifferentiated somatoform disorder: diagnostic criteria
|
Dr. Bernstein’s observations
Although Ms. M meets criteria for undifferentiated somatoform disorder ( Table 2), her belief that she has a medical problem is tenacious and her disability persists despite lack of a medical diagnosis. To me, this suggests a delusional disorder (Table 3 ).
Table 3
Diagnostic criteria for delusional disorder
|
| Somatic type: delusions that the person has some physical defect or general medical condition. |
For 6 months, although she has cooperated with psychotherapy, Ms. M’s complaints have been unyielding. Despite our good relationship, she will not trust my recommendations to try a psychotropic. Nor does psychotherapy or the cooperation of her former employer enable her to resume her once-rewarding career, even part-time.
Ms. M is reclusive but not suspicious. She has no grandiose or paranoid delusions or hallucinations. She has had no depersonalization or derealization episodes, and no affective component exists. She is profoundly convinced that she suddenly developed severe, incapacitating food allergies. Her lifestyle has deteriorated—she feels unable to work and even her parents have virtually abandoned her—yet she seems oddly content.
How does Ms. M compare with other patients with:
- undifferentiated somatic disorder
- delusional disorder?
Dr. Bernstein’s observations
Somatoform disorder. Patients with undifferentiated somatoform disorder usually exhibit fluctuating symptoms, which often can be mitigated with psychodynamic therapy. In time, most accept that their problem is psychological rather than physical or that anxiety or depression are contributing to symptom fluctuation. Patients usually continue or resume social and vocational functioning.
By contrast, Ms. M believes immutably that her symptoms have an undiscovered physical cause. This belief has dramatically changed her life: She has sacrificed her career, social life, health insurance, even her financial security.
The depth and seeming permanence of Ms. M’s state does not distress her. She is not regressed nor affectively or cognitively impaired. She reports seeing and feeling welts and rashes that were not visible to me or to other medical/alternative medical specialists, suggesting reality testing impairment. I perceived no other break in reality testing during psychotherapy.
Delusional disorder can be treated with medication or cognitive-behavioral therapy. I once treated a young man who believed that his head was coming to a point, causing him tremendous emotional distress. An antipsychotic resulted in prompt remission.
By contrast, Ms. M has a delusional belief that food and medicine make her sick and could lead to anaphylaxis. She will not take medication, even in a hospital.
Perhaps someday we will find a neurobiological or biochemical cause for Ms. M’s behavior. Positron-emission tomography or augmented MRI could uncover such clues, but both tests require ingesting a foreign substance—something Ms. M will not do.
FOLLOW-UP: MS. M’S NEW LIFE
Having exhausted her savings and work disability benefits, Ms. M receives Social Security disability benefits. With her health insurance coverage having expired, she stops psychotherapy after 2 years and pursues no further medical workup.
Two years after presenting to me, she does not seem depressed but her presenting picture is unchanged. She sounds happy and cognitively intact. Her life revolves around her perceived disability.
Ms. M has spent much of the last 2 years alone in her apartment, content in her solitude. She has resumed playing tennis but only occasionally and has not resumed the sport for which she has won many awards. She says she feels slightly better but remains too tired to return to work. She has gradually expanded her menu to about a dozen foods. Despite her problems Ms. M, who is 5 feet 2 inches, has maintained her weight (114 lbs) and attractiveness.
All the while, Ms. M has refused medication. I repeatedly suggest hospitalization so that she can take psychotropics in a safe, supervised setting, but she declines.
Related resources
- Pilowsky I. Abnormal Illness Behaviour. New York: John Wiley & Sons, 1997.
- Isaac A, Wise T. A low-frustration strategy for treating somatization. Current Psychiatry 2003;2(8):32-50.
Drug brand names
- Fluoxetine • Prozac
Disclosure
Dr. Bernstein reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
HISTORY: UNHAPPY NEW YEAR
On New Year’s Day Ms. M, age 43, begins experiencing persistent left-leg numbness, fatigue, and what she calls a “superallergic sensitivity to anything I put in my mouth.”
A few days later she sees her internist, who finds no medical cause and suspects that her symptoms are psychological. The internist prescribes fluoxetine, 10 mg/d. Fifteen minutes after taking the first dose, the patient reports “an anaphylactic episode,” which she describes as “screaming and shaking.”
Acting on the internist’s suggestion, Ms. M presents to me on Jan. 10. Her parents bring her to the appointment, as she feels too weak to drive.
A chemical engineer with a six-figure income, Ms. M has lived on her own most of her adult life but has stayed the past week with her elderly parents. With her vacation leave about to end, she says she is too weak and tired to return to work. She complains of extreme fatigue after eating most foods; after some meals, she says, welts surface throughout her body. Now living on bananas and homemade apple-sauce, she has lost 5 lbs in less than 2 weeks.
An only child, Ms. M is an award-winning athlete. She has enjoyed her career, which has taken her around the world. She has no significant psychiatric or medical history or family history of allergy or autoimmune disease. She says she is not depressed and is sleeping normally. Her Mini-Mental State Examination score of 30 indicates no cognitive impairment.
Ms. M denies feeling depressed. She mentions that her boyfriend broke off their relationship days before New Year’s Eve—the day on which she had expected they would become engaged. She sees no relationship between disappointment over this breakup and the symptoms that followed almost immediately. She has never had another intimate relationship and describes people she knows as “acquaintances” or “work buddies” rather than as friends.
Table 1
Diagnostic criteria for hypochondriasis
|
| Specify if: With poor insight: if, for most of the time during the current episode, the person does not recognize that the concern about having a serious illness is excessive or unreasonable. |
| Source: Tables 1 through 3 reprinted with permission from the Diagnostic and statistical manual of mental disorders (4th ed, text revision). |
| Copyright 2000.American Psychiatric Association. |
Ms. M refuses to try another psychotropic, fearing another “anaphylactic” episode like the one she described after the fluoxetine dose. She is willing to start psychotherapy, however.
Dr. Bernstein’s observations
Ms. M. complains of an array of food allergies and fatigue with no subjective feelings of depression. She has an athletic physique, is attractive without cosmetics, and is casually but neatly dressed, indicating good organization.
At this point, no physical or medical cause has been found for Ms. M’s symptoms, nor does she meet DSM-IV-TR criteria for hypochondriasis (Table 1). Her symptoms have persisted for 10 days—far short of the 6 months the diagnosis requires. Ms. M also believes that her medical problem is inconvenient but not serious.
Even though Ms. M denies feeling depressed, her symptoms most closely suggest depression with somatic complaints. She is not substantially distressed, but her symptoms are impairing her social and occupational functioning.
Antidepressants—particularly selective serotonin reuptake inhibitors—can help depressed patients with somatic symptoms, and low-dose atypical antipsychotics alternately are used to treat major depressive disorder with somatic delusions. Ms. M, however, will not try another medication, making psychotherapy my only treatment option.
TREATMENT: ‘SURFING’ FOR CLUES
For 6 months, Ms. M attends weekly psychodynamic psychotherapy sessions regularly and on time. She is courteous and pleasant, but her fatigue persists.
Early in treatment, Ms. M spends hours searching the Internet for doctors who specialize in malabsorption syndrome, allergy, and rare infectious diseases. Numerous internists, allergists, and immunologists perform blood work and other laboratory tests on her. She has the results—reams of clinical data—sent to me. I also order tests for HIV, syphilis, and gonorrhea. None of the results indicates a physical disorder. She refuses patch or intradermal testing for allergy, fearing anaphylaxis.
Ms. M also spends much of her day preparing her own meals. She introduces “new foods” one at a time, but reports that these trials often lead to fatigue and cause her to break out in welts. During psychotherapy, she points to bumps and rashes throughout her body that I cannot see.
Six months into psychotherapy, Ms. M is still staying with her parents and has not returned to work, citing disabling fatigue. Her parents, frustrated with her apparent unwillingness to get better, set a deadline for her to move out of their home. She finds an apartment nearby but about 2 miles from the train line she would use to commute to work. She refuses to take a taxi to the train station because of the expense, will not drive to the station because she cannot get up early, and will not drive directly to work for fear of tiring while driving. She refuses her company’s offer to let her work part time from home.
Ms. M’s company keeps her job open for her, but she is still not returning to work. After 1 year, the company finally fires her, then calls her a few months later asking if she’ll come back; she again says no. She collects disability benefits and taps into her savings and investment dividends to make ends meet. In discussing her lack of income during psychotherapy, Ms. M does not appear distressed.
Table 2
Undifferentiated somatoform disorder: diagnostic criteria
|
Dr. Bernstein’s observations
Although Ms. M meets criteria for undifferentiated somatoform disorder ( Table 2), her belief that she has a medical problem is tenacious and her disability persists despite lack of a medical diagnosis. To me, this suggests a delusional disorder (Table 3 ).
Table 3
Diagnostic criteria for delusional disorder
|
| Somatic type: delusions that the person has some physical defect or general medical condition. |
For 6 months, although she has cooperated with psychotherapy, Ms. M’s complaints have been unyielding. Despite our good relationship, she will not trust my recommendations to try a psychotropic. Nor does psychotherapy or the cooperation of her former employer enable her to resume her once-rewarding career, even part-time.
Ms. M is reclusive but not suspicious. She has no grandiose or paranoid delusions or hallucinations. She has had no depersonalization or derealization episodes, and no affective component exists. She is profoundly convinced that she suddenly developed severe, incapacitating food allergies. Her lifestyle has deteriorated—she feels unable to work and even her parents have virtually abandoned her—yet she seems oddly content.
How does Ms. M compare with other patients with:
- undifferentiated somatic disorder
- delusional disorder?
Dr. Bernstein’s observations
Somatoform disorder. Patients with undifferentiated somatoform disorder usually exhibit fluctuating symptoms, which often can be mitigated with psychodynamic therapy. In time, most accept that their problem is psychological rather than physical or that anxiety or depression are contributing to symptom fluctuation. Patients usually continue or resume social and vocational functioning.
By contrast, Ms. M believes immutably that her symptoms have an undiscovered physical cause. This belief has dramatically changed her life: She has sacrificed her career, social life, health insurance, even her financial security.
The depth and seeming permanence of Ms. M’s state does not distress her. She is not regressed nor affectively or cognitively impaired. She reports seeing and feeling welts and rashes that were not visible to me or to other medical/alternative medical specialists, suggesting reality testing impairment. I perceived no other break in reality testing during psychotherapy.
Delusional disorder can be treated with medication or cognitive-behavioral therapy. I once treated a young man who believed that his head was coming to a point, causing him tremendous emotional distress. An antipsychotic resulted in prompt remission.
By contrast, Ms. M has a delusional belief that food and medicine make her sick and could lead to anaphylaxis. She will not take medication, even in a hospital.
Perhaps someday we will find a neurobiological or biochemical cause for Ms. M’s behavior. Positron-emission tomography or augmented MRI could uncover such clues, but both tests require ingesting a foreign substance—something Ms. M will not do.
FOLLOW-UP: MS. M’S NEW LIFE
Having exhausted her savings and work disability benefits, Ms. M receives Social Security disability benefits. With her health insurance coverage having expired, she stops psychotherapy after 2 years and pursues no further medical workup.
Two years after presenting to me, she does not seem depressed but her presenting picture is unchanged. She sounds happy and cognitively intact. Her life revolves around her perceived disability.
Ms. M has spent much of the last 2 years alone in her apartment, content in her solitude. She has resumed playing tennis but only occasionally and has not resumed the sport for which she has won many awards. She says she feels slightly better but remains too tired to return to work. She has gradually expanded her menu to about a dozen foods. Despite her problems Ms. M, who is 5 feet 2 inches, has maintained her weight (114 lbs) and attractiveness.
All the while, Ms. M has refused medication. I repeatedly suggest hospitalization so that she can take psychotropics in a safe, supervised setting, but she declines.
Related resources
- Pilowsky I. Abnormal Illness Behaviour. New York: John Wiley & Sons, 1997.
- Isaac A, Wise T. A low-frustration strategy for treating somatization. Current Psychiatry 2003;2(8):32-50.
Drug brand names
- Fluoxetine • Prozac
Disclosure
Dr. Bernstein reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Stumped? 5 steps to find the latest evidence
When grappling with difficult cases, clinicians often wonder, “What does the evidence say, and how can I find it?” Thanks to evidence-based medicine (EBM), study results are easier to track down and apply to patient care.
From our experience, we tell how to use EBM’s 5 steps and offer tips and shortcuts to help you quickly find the evidence you need.
SPEEDING RESEARCH TO PRACTICE
Health care is rich in evidence-based innovations, but successful innovations are often disseminated slowly—if at all—to practitioners.1 Studies that demonstrate effective treatments for mental disorders may take considerable time to find their way into clinical practice.2 Similar delays have been noted in other specialties, depriving patients of the most up-to-date medical treatments. Academic medical center surveys show that up to 40% of clinical decisions are not supported by the literature.3,4
Faculty at McMaster University in Canada developed evidence-based medicine as a medical education model by which physicians would rely on the literature—rather than textbooks or tradition—to solve patient problems.7 EBM’s influence on psychiatry has been greatest in the United Kingdom through efforts of its National Health Service, the Centre for Evidence-Based Mental Health at the University of Oxford, and the journal, Evidence-Based Mental Health.5
The U.S. experience. Given managed care’s influence on American medicine, one might expect EBM to have had a similar effect in the United States. This has not been the case, however, perhaps because for-profit HMOs have focused more on controlling costs rather than improving quality.
The U.S. Agency for Healthcare Research and Quality has funded evidence-based practice centers that produce systematic reviews but has done relatively little to promote EBM teaching and practice. Instead, professional organizations such as the American College of Physicians and journals such as JAMA have taken the lead in teaching physicians about EBM.
Residents learning EBM. Most EBM instruction occurs in medical school primary care departments. This is changing, however, now that the Accreditation Council for Graduate Medical Education (ACGME) requires all residents to show competence in EBM methods.8 ACGME requires residency programs in all specialties—including psychiatry—to ensure that graduates achieve EBM core competencies, including being able to use the process described in this article.
Two problems that daunt psychiatrists and other physicians—information overload and uncritical acceptance of information—contribute to less-than-optimal care.5
Information overload. With thousands of medical journals and millions of articles being published, no clinician can keep up with all developments in his or her field. Furthermore, study results often appear contradictory.
Review articles summarize the literature, but most are “journalistic” or “narrative”—not systematic reviews—and thus are subject to author bias in the studies cited and methods used to summarize conflicting results.4 Textbook chapters have the added problem of being almost immediately out-of-date.6
Uncritical acceptance of information occurs when clinicians rely too heavily on personal experiences, noncritiqued study results, expert opinion, and pharmaceutical industry influence.4,6
Two approaches could narrow the gap between research and practice:
- clinical practice guidelines and pathways, a “top-down” approach favored by administrators
- evidence-based medicine, a “bottom-up” approach favored—and developed by—medical educators (Box 1).5,7,8
EBM and patient care. EBM has been described as “partly a philosophy, partly a skill, and partly…a set of tools.”9 David Sackett—often considered the father of EBM—has defined it as “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.”10
Although some critics disagree, clinical expertise plays an important role in EBM, as the clinician must integrate research evidence, patient preferences, and the patient’s clinical condition when making decisions.11
EBM’S 5 ACTION STEPS
With EBM, evidence from the medical literature is applied to patient care through 5 action steps:
- Formulate the question.
- Search for answers.
- Appraise the evidence.
- Apply the evidence to the patient.
- Assess the outcome.5,6,12
Step 1: Formulate the question. EBM begins with a clinical question related to the diagnosis, treatment, prognosis, or cause of a patient’s illness. The question is formatted to include the patient’s problem or diagnosis, the intervention of interest and any comparison intervention, and the outcome of interest.
Take, for example, this question: “In patients with bipolar disorder, is lamotrigine as effective as lithium in preventing relapse?” In this format:
- bipolar disorder is the diagnosis
- lamotrigine is the intervention of interest
- lithium is the comparison intervention
- relapse is the outcome of interest.
Step 2: Search for answers. Because answering different types of questions requires different types of evidence, this step involves determining the most appropriate type of evidence and searching for it.13
Evidence hierarchies (Table 1) 5,6,12,14 indicate that certain types of evidence are considered more credible than others. The higher the level of evidence, the more likely it is to provide valid, unbiased estimates of an intervention’s effect.
Table 1
Hierarchy for studies of therapy or harm
| Quality* | Type of evidence |
|---|---|
| 1a | Systematic review of randomized controlled trials (RCTs) |
| 1b | Individual RCT with narrow confidence interval |
| 2a | Systematic review of cohort studies |
| 2b | Individual cohort study RCT with <80% follow-up |
| 2c | Outcomes research Ecological study |
| 3a | Systematic review of case-control studies |
| 3b | Individual case-control study |
| 4 | Case series |
| 5 | Expert opinion |
| * Highest- to lowest-quality evidence | |
| Source: Adapted from references 5,6,12, and 14 | |
For example, observational studies may give misleading results, compared with randomized, controlled, clinical trials.15 Expert opinion—which does not necessarily reflect the best evidence in the literature—is considered the lowest evidence level.16
Beginning the literature search with Medline—as many clinicians do—is relatively inefficient. Searching the massive National Library of Medicine database often identifies a large number of articles, which you then must appraise for validity.
More efficient is Haynes’ “4S” strategy of:
It gives priority to sources of high-quality, pre-appraised information ( Table 2), so that you may omit Step 3—appraisal—in the EBM process.
Table 2
“4S” approach to answering clinical questions
| Category | Examples | Web site |
|---|---|---|
| Systems (comprehensive sources) | Clinical Evidence | http://www.clinicalevidence.com |
| National electronic Library for Mental Health | http://www.nelmh.org | |
| APA Practice Guidelines | http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm | |
| National Guideline Clearinghouse | http://www.guideline.gov | |
| Synopses (structured abstracts) | Evidence-Based Mental Health | http://ebmh.bmjjournals.com |
| ACP Journal Club | http://www.acpjc.org/ | |
| Syntheses (systematic reviews) | Cochrane Database of Systematic Reviews | http://www.update-software.com/abstracts/mainindex.htm |
| Database of Abstracts of Reviews of Effectiveness (DARE) | http://www.york.ac.uk/inst/crd/darehp.htm | |
| Health Technology Assessment (HTA) database | http://www.york.ac.uk/inst/crd/htahp.htm | |
| Studies (original articles) | Medline (PubMed) | http://www.ncbi.nlm.nih.gov/entrez/query/static/clinical.html |
| Source: Adapted from references 12 and 17. | ||
Systems. A system is an information source that covers a variety of diagnoses, summarizes the results of high-quality systematic reviews, is frequently updated, and is linked to the original studies. Three examples are:
- Clinical Evidence, a journal published semi-annually in the United Kingdom that is also available online (www.clinicalevidence.com). Its ease of use, frequent updates, and clear links to the best evidence make it a good starting point.
- National electronic Library for Mental Health (NeLMH) (www.nelmh.org), created by the U.K.’s Centre for Evidence-Based Mental Health.18 It provides information only about depression, schizophrenia, and suicide but may become the model for evidence-based psychiatry.
- Evidence-based clinical practice guidelines developed by the American Psychiatric Association9 and other organizations. Many of these are included in the National Guideline Clearinghouse (www.guideline.gov), produced by the U.S. Department of Health and Human Service’s Agency for Healthcare Research and Quality.
Synopses. If a system does not answer a clinical question, look for synopses—structured abstracts of high-quality systematic reviews or original articles. Synopses are brief and pre-appraised for quality, allowing you to quickly get the point without reading a lengthy article. For psychiatry, Evidence-Based Mental Health and ACP Journal Club are the best synopses sources.
Syntheses. If you don’t find a synopsis to answer your question, then search for a synthesis—a high-quality systematic review. The best source is the Cochrane Database of Systematic Reviews;20 others include:
- Database of Abstracts of Reviews of Effectiveness (DARE)
- Health Technology Assessment (HTA) database.
Table 3
Web sites for learning more about EBM
| Organization | Web site |
|---|---|
| Centre for Evidence-Based Medicine (Oxford) | http://www.cebm.net |
| Centre for Evidence-Based Medicine (Toronto) | http://www.cebm.utoronto.ca |
| Centre for Evidence-Based Mental Health | http://www.cebmh.com |
| EBM Education Center of Excellence | http://www.hsl.unc.edu/ahec/ebmcoe/pages/teaching.htm |
| Evidence-based Medicine Resource Center | http://www.ebmny.org |
| Netting the Evidence | http://www.nettingtheevidence.org.uk |
| University of Sheffield Health Informatics | http://www.shef.ac.uk/~scharr/ir/mschi/ |
| Users’ Guides to the Medical Literature | http://ugi.usersguides.org |
Studies. Only if the first three “S’s” fail to yield an answer would you then search Medline or similar databases for applicable studies.
The PubMed Clinical Queries interface lets you specify the type of question (therapy, diagnosis, etiology, or prognosis) and whether the search is to be sensitive or specific. You can also use filters built into this interface when searching for systematic reviews.
Step 3: Appraise the evidence. After you find an article, appraise its validity and importance. Checklists for appraising studies may be found in EBM texts4,6,12 or downloaded from Web sites (Table 3). Specific appraisal questions to ask depend on the study design and your clinical question.
Step 4: Apply the results to your patient. Assuming the evidence is valid, important, and feasible in your setting, consider your patient’s preferences21 and apply the results.
Step 5: Assess the outcome. Evaluate your performance in searching the literature, and assess the patient’s response.
STREAMLINING THE EBM PROCESS
Studies in academic settings have shown that the full 5-step model can be incorporated into daily practice.6,12 In nonacademic settings, however, practitioners complain about lack of time and information resources, as well as inadequate EBM skills.11,12 Two shortcuts can streamline the process:
Use the 5-step process selectively; it is not required for every patient encounter.6,12 After you research a question for one patient with a particular diagnosis, you can apply the answer to similar patients. Because most psychiatrists’ patients fall into relatively few diagnostic categories, only the exceptional patient would trigger the full 5-step process.
Use pre-appraised information sources. With online databases such as Clinical Evidence and Evidence-Based Mental Health, you can find information quickly, often in the time it takes to use textbooks.5,12,17
Excellent EBM texts4,6,12 and online resources may be useful (Table 3). Courses are listed on the EBM Education Center of Excellence Web site, and the Centre for Evidence-Based Mental Health at Oxford University offers an outstanding course for psychiatrists.
Related resources
- Gray GE. Concise guide to evidence-based psychiatry. Washington, DC: American Psychiatric Publishing, 2004.
- Greenhalgh T. How to read a paper: the basics of evidence-based medicine (2nd ed). London, BMJ Books, 2001.
- Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
- Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: how to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
Acknowledgment
Supported in part by a grant from the National Institute of Mental Health (5-R24-MH61456-03).
1. Berwick DM. Disseminating innovations in health care. JAMA 2003;289:1969-75
2. Drake RE, Goldman HH, Leff HS, et al. Implementing evidence-based practices in routine mental health settings. Psychiatr Serv 2001;52:179-82
3. Geddes JR, Game D, Jenkins NE, et al. What proportion of primary psychiatric interventions are based on evidence from randomised controlled trials? Qual Health Care 1996;5:215-17.
4. Greenhalgh T. How to read a paper: the basics of evidence based medicine (2nd ed). London: BMJ Books, 2001.
5. Gray GE. Evidence-based medicine: an introduction for psychiatrists. J Psychiatr Pract 2002;8:5-13.
6. Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: How to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
7. Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to the teaching of medicine. JAMA 1992;268:2420-5.
8. Accreditation Council for Graduate Medical Education General competencies [ACGME Outcome Project Web site], 2001. Available at: http://www.acgme.org/outcome/. Accessed May 5, 2004.
9. Dawes M. Preface. In: Dawes M, Davies P, Gray A, et al (eds). Evidence-based practice: a primer for health professionals New York: Churchill Livingstone, 1999.
10. Sackett DL, Rosenberg WMC, Gray JAM, et al. Evidence-based medicine: what it is and what it isn’t. BMJ 1996;312:71-2.
11. Straus SE, McAlister FA. Evidence-based medicine: a commentary on common criticisms. Can Med Assoc J 2000;163:837-41.
12. Gray GE. Concise guide to evidence-based psychiatry Washington, DC: American Psychiatric Publishing, 2004.
13. Glasziou P, Vandenbroucke J, Chalmers I. Assessing the quality of research. BMJ 2004;328:39-41.
14. Phillips B, Ball C, Sackett D, et al. Centre for Evidence-Based Medicine: Levels of evidence and grades of recommendations, May 2001. Available at: http://www.cebm.net/levels_of_evidence.asp. Accessed Sept. 18, 2004.
15. Lacchetti C, Guyatt G. Therapy and validity: surprising results of randomized controlled trials. In: Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
16. Antman EM, Lau J, Kupelnick B, et al. A comparison of results of meta-analyses of randomized control trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA 1992;268:240-8.
17. Haynes RB. Of studies, summaries, synopses, and systems: the “4S” evolution of services for finding current best evidence. Evid Based Ment Health 2001;4:37-9.
18. Dearness KL, Tomlin A. Development of the National Electronic Library for Mental Health: providing evidence-based information for all. Health Info Libr J 2001;18:167-74.
19. American Psychiatric Association. Practice guidelines for the treatment of psychiatric disorders: compendium 2002. Washington, DC: American Psychiatric Publishing, 2002.
20. Antes G. Oxman AD for the Cochrane Collaboration. The Cochrane Collaboration in the 20th Century. In: Egger M, Smith GD, Altman DG (eds). Systematic reviews in health care: meta-analysis in context London: BMJBooks, 2001.
21. Say RE, Thomson R. The importance of patient p in treatment decisions—challenges for doctors. BMJ 2003;327:542-5.
When grappling with difficult cases, clinicians often wonder, “What does the evidence say, and how can I find it?” Thanks to evidence-based medicine (EBM), study results are easier to track down and apply to patient care.
From our experience, we tell how to use EBM’s 5 steps and offer tips and shortcuts to help you quickly find the evidence you need.
SPEEDING RESEARCH TO PRACTICE
Health care is rich in evidence-based innovations, but successful innovations are often disseminated slowly—if at all—to practitioners.1 Studies that demonstrate effective treatments for mental disorders may take considerable time to find their way into clinical practice.2 Similar delays have been noted in other specialties, depriving patients of the most up-to-date medical treatments. Academic medical center surveys show that up to 40% of clinical decisions are not supported by the literature.3,4
Faculty at McMaster University in Canada developed evidence-based medicine as a medical education model by which physicians would rely on the literature—rather than textbooks or tradition—to solve patient problems.7 EBM’s influence on psychiatry has been greatest in the United Kingdom through efforts of its National Health Service, the Centre for Evidence-Based Mental Health at the University of Oxford, and the journal, Evidence-Based Mental Health.5
The U.S. experience. Given managed care’s influence on American medicine, one might expect EBM to have had a similar effect in the United States. This has not been the case, however, perhaps because for-profit HMOs have focused more on controlling costs rather than improving quality.
The U.S. Agency for Healthcare Research and Quality has funded evidence-based practice centers that produce systematic reviews but has done relatively little to promote EBM teaching and practice. Instead, professional organizations such as the American College of Physicians and journals such as JAMA have taken the lead in teaching physicians about EBM.
Residents learning EBM. Most EBM instruction occurs in medical school primary care departments. This is changing, however, now that the Accreditation Council for Graduate Medical Education (ACGME) requires all residents to show competence in EBM methods.8 ACGME requires residency programs in all specialties—including psychiatry—to ensure that graduates achieve EBM core competencies, including being able to use the process described in this article.
Two problems that daunt psychiatrists and other physicians—information overload and uncritical acceptance of information—contribute to less-than-optimal care.5
Information overload. With thousands of medical journals and millions of articles being published, no clinician can keep up with all developments in his or her field. Furthermore, study results often appear contradictory.
Review articles summarize the literature, but most are “journalistic” or “narrative”—not systematic reviews—and thus are subject to author bias in the studies cited and methods used to summarize conflicting results.4 Textbook chapters have the added problem of being almost immediately out-of-date.6
Uncritical acceptance of information occurs when clinicians rely too heavily on personal experiences, noncritiqued study results, expert opinion, and pharmaceutical industry influence.4,6
Two approaches could narrow the gap between research and practice:
- clinical practice guidelines and pathways, a “top-down” approach favored by administrators
- evidence-based medicine, a “bottom-up” approach favored—and developed by—medical educators (Box 1).5,7,8
EBM and patient care. EBM has been described as “partly a philosophy, partly a skill, and partly…a set of tools.”9 David Sackett—often considered the father of EBM—has defined it as “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.”10
Although some critics disagree, clinical expertise plays an important role in EBM, as the clinician must integrate research evidence, patient preferences, and the patient’s clinical condition when making decisions.11
EBM’S 5 ACTION STEPS
With EBM, evidence from the medical literature is applied to patient care through 5 action steps:
- Formulate the question.
- Search for answers.
- Appraise the evidence.
- Apply the evidence to the patient.
- Assess the outcome.5,6,12
Step 1: Formulate the question. EBM begins with a clinical question related to the diagnosis, treatment, prognosis, or cause of a patient’s illness. The question is formatted to include the patient’s problem or diagnosis, the intervention of interest and any comparison intervention, and the outcome of interest.
Take, for example, this question: “In patients with bipolar disorder, is lamotrigine as effective as lithium in preventing relapse?” In this format:
- bipolar disorder is the diagnosis
- lamotrigine is the intervention of interest
- lithium is the comparison intervention
- relapse is the outcome of interest.
Step 2: Search for answers. Because answering different types of questions requires different types of evidence, this step involves determining the most appropriate type of evidence and searching for it.13
Evidence hierarchies (Table 1) 5,6,12,14 indicate that certain types of evidence are considered more credible than others. The higher the level of evidence, the more likely it is to provide valid, unbiased estimates of an intervention’s effect.
Table 1
Hierarchy for studies of therapy or harm
| Quality* | Type of evidence |
|---|---|
| 1a | Systematic review of randomized controlled trials (RCTs) |
| 1b | Individual RCT with narrow confidence interval |
| 2a | Systematic review of cohort studies |
| 2b | Individual cohort study RCT with <80% follow-up |
| 2c | Outcomes research Ecological study |
| 3a | Systematic review of case-control studies |
| 3b | Individual case-control study |
| 4 | Case series |
| 5 | Expert opinion |
| * Highest- to lowest-quality evidence | |
| Source: Adapted from references 5,6,12, and 14 | |
For example, observational studies may give misleading results, compared with randomized, controlled, clinical trials.15 Expert opinion—which does not necessarily reflect the best evidence in the literature—is considered the lowest evidence level.16
Beginning the literature search with Medline—as many clinicians do—is relatively inefficient. Searching the massive National Library of Medicine database often identifies a large number of articles, which you then must appraise for validity.
More efficient is Haynes’ “4S” strategy of:
It gives priority to sources of high-quality, pre-appraised information ( Table 2), so that you may omit Step 3—appraisal—in the EBM process.
Table 2
“4S” approach to answering clinical questions
| Category | Examples | Web site |
|---|---|---|
| Systems (comprehensive sources) | Clinical Evidence | http://www.clinicalevidence.com |
| National electronic Library for Mental Health | http://www.nelmh.org | |
| APA Practice Guidelines | http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm | |
| National Guideline Clearinghouse | http://www.guideline.gov | |
| Synopses (structured abstracts) | Evidence-Based Mental Health | http://ebmh.bmjjournals.com |
| ACP Journal Club | http://www.acpjc.org/ | |
| Syntheses (systematic reviews) | Cochrane Database of Systematic Reviews | http://www.update-software.com/abstracts/mainindex.htm |
| Database of Abstracts of Reviews of Effectiveness (DARE) | http://www.york.ac.uk/inst/crd/darehp.htm | |
| Health Technology Assessment (HTA) database | http://www.york.ac.uk/inst/crd/htahp.htm | |
| Studies (original articles) | Medline (PubMed) | http://www.ncbi.nlm.nih.gov/entrez/query/static/clinical.html |
| Source: Adapted from references 12 and 17. | ||
Systems. A system is an information source that covers a variety of diagnoses, summarizes the results of high-quality systematic reviews, is frequently updated, and is linked to the original studies. Three examples are:
- Clinical Evidence, a journal published semi-annually in the United Kingdom that is also available online (www.clinicalevidence.com). Its ease of use, frequent updates, and clear links to the best evidence make it a good starting point.
- National electronic Library for Mental Health (NeLMH) (www.nelmh.org), created by the U.K.’s Centre for Evidence-Based Mental Health.18 It provides information only about depression, schizophrenia, and suicide but may become the model for evidence-based psychiatry.
- Evidence-based clinical practice guidelines developed by the American Psychiatric Association9 and other organizations. Many of these are included in the National Guideline Clearinghouse (www.guideline.gov), produced by the U.S. Department of Health and Human Service’s Agency for Healthcare Research and Quality.
Synopses. If a system does not answer a clinical question, look for synopses—structured abstracts of high-quality systematic reviews or original articles. Synopses are brief and pre-appraised for quality, allowing you to quickly get the point without reading a lengthy article. For psychiatry, Evidence-Based Mental Health and ACP Journal Club are the best synopses sources.
Syntheses. If you don’t find a synopsis to answer your question, then search for a synthesis—a high-quality systematic review. The best source is the Cochrane Database of Systematic Reviews;20 others include:
- Database of Abstracts of Reviews of Effectiveness (DARE)
- Health Technology Assessment (HTA) database.
Table 3
Web sites for learning more about EBM
| Organization | Web site |
|---|---|
| Centre for Evidence-Based Medicine (Oxford) | http://www.cebm.net |
| Centre for Evidence-Based Medicine (Toronto) | http://www.cebm.utoronto.ca |
| Centre for Evidence-Based Mental Health | http://www.cebmh.com |
| EBM Education Center of Excellence | http://www.hsl.unc.edu/ahec/ebmcoe/pages/teaching.htm |
| Evidence-based Medicine Resource Center | http://www.ebmny.org |
| Netting the Evidence | http://www.nettingtheevidence.org.uk |
| University of Sheffield Health Informatics | http://www.shef.ac.uk/~scharr/ir/mschi/ |
| Users’ Guides to the Medical Literature | http://ugi.usersguides.org |
Studies. Only if the first three “S’s” fail to yield an answer would you then search Medline or similar databases for applicable studies.
The PubMed Clinical Queries interface lets you specify the type of question (therapy, diagnosis, etiology, or prognosis) and whether the search is to be sensitive or specific. You can also use filters built into this interface when searching for systematic reviews.
Step 3: Appraise the evidence. After you find an article, appraise its validity and importance. Checklists for appraising studies may be found in EBM texts4,6,12 or downloaded from Web sites (Table 3). Specific appraisal questions to ask depend on the study design and your clinical question.
Step 4: Apply the results to your patient. Assuming the evidence is valid, important, and feasible in your setting, consider your patient’s preferences21 and apply the results.
Step 5: Assess the outcome. Evaluate your performance in searching the literature, and assess the patient’s response.
STREAMLINING THE EBM PROCESS
Studies in academic settings have shown that the full 5-step model can be incorporated into daily practice.6,12 In nonacademic settings, however, practitioners complain about lack of time and information resources, as well as inadequate EBM skills.11,12 Two shortcuts can streamline the process:
Use the 5-step process selectively; it is not required for every patient encounter.6,12 After you research a question for one patient with a particular diagnosis, you can apply the answer to similar patients. Because most psychiatrists’ patients fall into relatively few diagnostic categories, only the exceptional patient would trigger the full 5-step process.
Use pre-appraised information sources. With online databases such as Clinical Evidence and Evidence-Based Mental Health, you can find information quickly, often in the time it takes to use textbooks.5,12,17
Excellent EBM texts4,6,12 and online resources may be useful (Table 3). Courses are listed on the EBM Education Center of Excellence Web site, and the Centre for Evidence-Based Mental Health at Oxford University offers an outstanding course for psychiatrists.
Related resources
- Gray GE. Concise guide to evidence-based psychiatry. Washington, DC: American Psychiatric Publishing, 2004.
- Greenhalgh T. How to read a paper: the basics of evidence-based medicine (2nd ed). London, BMJ Books, 2001.
- Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
- Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: how to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
Acknowledgment
Supported in part by a grant from the National Institute of Mental Health (5-R24-MH61456-03).
When grappling with difficult cases, clinicians often wonder, “What does the evidence say, and how can I find it?” Thanks to evidence-based medicine (EBM), study results are easier to track down and apply to patient care.
From our experience, we tell how to use EBM’s 5 steps and offer tips and shortcuts to help you quickly find the evidence you need.
SPEEDING RESEARCH TO PRACTICE
Health care is rich in evidence-based innovations, but successful innovations are often disseminated slowly—if at all—to practitioners.1 Studies that demonstrate effective treatments for mental disorders may take considerable time to find their way into clinical practice.2 Similar delays have been noted in other specialties, depriving patients of the most up-to-date medical treatments. Academic medical center surveys show that up to 40% of clinical decisions are not supported by the literature.3,4
Faculty at McMaster University in Canada developed evidence-based medicine as a medical education model by which physicians would rely on the literature—rather than textbooks or tradition—to solve patient problems.7 EBM’s influence on psychiatry has been greatest in the United Kingdom through efforts of its National Health Service, the Centre for Evidence-Based Mental Health at the University of Oxford, and the journal, Evidence-Based Mental Health.5
The U.S. experience. Given managed care’s influence on American medicine, one might expect EBM to have had a similar effect in the United States. This has not been the case, however, perhaps because for-profit HMOs have focused more on controlling costs rather than improving quality.
The U.S. Agency for Healthcare Research and Quality has funded evidence-based practice centers that produce systematic reviews but has done relatively little to promote EBM teaching and practice. Instead, professional organizations such as the American College of Physicians and journals such as JAMA have taken the lead in teaching physicians about EBM.
Residents learning EBM. Most EBM instruction occurs in medical school primary care departments. This is changing, however, now that the Accreditation Council for Graduate Medical Education (ACGME) requires all residents to show competence in EBM methods.8 ACGME requires residency programs in all specialties—including psychiatry—to ensure that graduates achieve EBM core competencies, including being able to use the process described in this article.
Two problems that daunt psychiatrists and other physicians—information overload and uncritical acceptance of information—contribute to less-than-optimal care.5
Information overload. With thousands of medical journals and millions of articles being published, no clinician can keep up with all developments in his or her field. Furthermore, study results often appear contradictory.
Review articles summarize the literature, but most are “journalistic” or “narrative”—not systematic reviews—and thus are subject to author bias in the studies cited and methods used to summarize conflicting results.4 Textbook chapters have the added problem of being almost immediately out-of-date.6
Uncritical acceptance of information occurs when clinicians rely too heavily on personal experiences, noncritiqued study results, expert opinion, and pharmaceutical industry influence.4,6
Two approaches could narrow the gap between research and practice:
- clinical practice guidelines and pathways, a “top-down” approach favored by administrators
- evidence-based medicine, a “bottom-up” approach favored—and developed by—medical educators (Box 1).5,7,8
EBM and patient care. EBM has been described as “partly a philosophy, partly a skill, and partly…a set of tools.”9 David Sackett—often considered the father of EBM—has defined it as “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.”10
Although some critics disagree, clinical expertise plays an important role in EBM, as the clinician must integrate research evidence, patient preferences, and the patient’s clinical condition when making decisions.11
EBM’S 5 ACTION STEPS
With EBM, evidence from the medical literature is applied to patient care through 5 action steps:
- Formulate the question.
- Search for answers.
- Appraise the evidence.
- Apply the evidence to the patient.
- Assess the outcome.5,6,12
Step 1: Formulate the question. EBM begins with a clinical question related to the diagnosis, treatment, prognosis, or cause of a patient’s illness. The question is formatted to include the patient’s problem or diagnosis, the intervention of interest and any comparison intervention, and the outcome of interest.
Take, for example, this question: “In patients with bipolar disorder, is lamotrigine as effective as lithium in preventing relapse?” In this format:
- bipolar disorder is the diagnosis
- lamotrigine is the intervention of interest
- lithium is the comparison intervention
- relapse is the outcome of interest.
Step 2: Search for answers. Because answering different types of questions requires different types of evidence, this step involves determining the most appropriate type of evidence and searching for it.13
Evidence hierarchies (Table 1) 5,6,12,14 indicate that certain types of evidence are considered more credible than others. The higher the level of evidence, the more likely it is to provide valid, unbiased estimates of an intervention’s effect.
Table 1
Hierarchy for studies of therapy or harm
| Quality* | Type of evidence |
|---|---|
| 1a | Systematic review of randomized controlled trials (RCTs) |
| 1b | Individual RCT with narrow confidence interval |
| 2a | Systematic review of cohort studies |
| 2b | Individual cohort study RCT with <80% follow-up |
| 2c | Outcomes research Ecological study |
| 3a | Systematic review of case-control studies |
| 3b | Individual case-control study |
| 4 | Case series |
| 5 | Expert opinion |
| * Highest- to lowest-quality evidence | |
| Source: Adapted from references 5,6,12, and 14 | |
For example, observational studies may give misleading results, compared with randomized, controlled, clinical trials.15 Expert opinion—which does not necessarily reflect the best evidence in the literature—is considered the lowest evidence level.16
Beginning the literature search with Medline—as many clinicians do—is relatively inefficient. Searching the massive National Library of Medicine database often identifies a large number of articles, which you then must appraise for validity.
More efficient is Haynes’ “4S” strategy of:
It gives priority to sources of high-quality, pre-appraised information ( Table 2), so that you may omit Step 3—appraisal—in the EBM process.
Table 2
“4S” approach to answering clinical questions
| Category | Examples | Web site |
|---|---|---|
| Systems (comprehensive sources) | Clinical Evidence | http://www.clinicalevidence.com |
| National electronic Library for Mental Health | http://www.nelmh.org | |
| APA Practice Guidelines | http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm | |
| National Guideline Clearinghouse | http://www.guideline.gov | |
| Synopses (structured abstracts) | Evidence-Based Mental Health | http://ebmh.bmjjournals.com |
| ACP Journal Club | http://www.acpjc.org/ | |
| Syntheses (systematic reviews) | Cochrane Database of Systematic Reviews | http://www.update-software.com/abstracts/mainindex.htm |
| Database of Abstracts of Reviews of Effectiveness (DARE) | http://www.york.ac.uk/inst/crd/darehp.htm | |
| Health Technology Assessment (HTA) database | http://www.york.ac.uk/inst/crd/htahp.htm | |
| Studies (original articles) | Medline (PubMed) | http://www.ncbi.nlm.nih.gov/entrez/query/static/clinical.html |
| Source: Adapted from references 12 and 17. | ||
Systems. A system is an information source that covers a variety of diagnoses, summarizes the results of high-quality systematic reviews, is frequently updated, and is linked to the original studies. Three examples are:
- Clinical Evidence, a journal published semi-annually in the United Kingdom that is also available online (www.clinicalevidence.com). Its ease of use, frequent updates, and clear links to the best evidence make it a good starting point.
- National electronic Library for Mental Health (NeLMH) (www.nelmh.org), created by the U.K.’s Centre for Evidence-Based Mental Health.18 It provides information only about depression, schizophrenia, and suicide but may become the model for evidence-based psychiatry.
- Evidence-based clinical practice guidelines developed by the American Psychiatric Association9 and other organizations. Many of these are included in the National Guideline Clearinghouse (www.guideline.gov), produced by the U.S. Department of Health and Human Service’s Agency for Healthcare Research and Quality.
Synopses. If a system does not answer a clinical question, look for synopses—structured abstracts of high-quality systematic reviews or original articles. Synopses are brief and pre-appraised for quality, allowing you to quickly get the point without reading a lengthy article. For psychiatry, Evidence-Based Mental Health and ACP Journal Club are the best synopses sources.
Syntheses. If you don’t find a synopsis to answer your question, then search for a synthesis—a high-quality systematic review. The best source is the Cochrane Database of Systematic Reviews;20 others include:
- Database of Abstracts of Reviews of Effectiveness (DARE)
- Health Technology Assessment (HTA) database.
Table 3
Web sites for learning more about EBM
| Organization | Web site |
|---|---|
| Centre for Evidence-Based Medicine (Oxford) | http://www.cebm.net |
| Centre for Evidence-Based Medicine (Toronto) | http://www.cebm.utoronto.ca |
| Centre for Evidence-Based Mental Health | http://www.cebmh.com |
| EBM Education Center of Excellence | http://www.hsl.unc.edu/ahec/ebmcoe/pages/teaching.htm |
| Evidence-based Medicine Resource Center | http://www.ebmny.org |
| Netting the Evidence | http://www.nettingtheevidence.org.uk |
| University of Sheffield Health Informatics | http://www.shef.ac.uk/~scharr/ir/mschi/ |
| Users’ Guides to the Medical Literature | http://ugi.usersguides.org |
Studies. Only if the first three “S’s” fail to yield an answer would you then search Medline or similar databases for applicable studies.
The PubMed Clinical Queries interface lets you specify the type of question (therapy, diagnosis, etiology, or prognosis) and whether the search is to be sensitive or specific. You can also use filters built into this interface when searching for systematic reviews.
Step 3: Appraise the evidence. After you find an article, appraise its validity and importance. Checklists for appraising studies may be found in EBM texts4,6,12 or downloaded from Web sites (Table 3). Specific appraisal questions to ask depend on the study design and your clinical question.
Step 4: Apply the results to your patient. Assuming the evidence is valid, important, and feasible in your setting, consider your patient’s preferences21 and apply the results.
Step 5: Assess the outcome. Evaluate your performance in searching the literature, and assess the patient’s response.
STREAMLINING THE EBM PROCESS
Studies in academic settings have shown that the full 5-step model can be incorporated into daily practice.6,12 In nonacademic settings, however, practitioners complain about lack of time and information resources, as well as inadequate EBM skills.11,12 Two shortcuts can streamline the process:
Use the 5-step process selectively; it is not required for every patient encounter.6,12 After you research a question for one patient with a particular diagnosis, you can apply the answer to similar patients. Because most psychiatrists’ patients fall into relatively few diagnostic categories, only the exceptional patient would trigger the full 5-step process.
Use pre-appraised information sources. With online databases such as Clinical Evidence and Evidence-Based Mental Health, you can find information quickly, often in the time it takes to use textbooks.5,12,17
Excellent EBM texts4,6,12 and online resources may be useful (Table 3). Courses are listed on the EBM Education Center of Excellence Web site, and the Centre for Evidence-Based Mental Health at Oxford University offers an outstanding course for psychiatrists.
Related resources
- Gray GE. Concise guide to evidence-based psychiatry. Washington, DC: American Psychiatric Publishing, 2004.
- Greenhalgh T. How to read a paper: the basics of evidence-based medicine (2nd ed). London, BMJ Books, 2001.
- Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
- Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: how to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
Acknowledgment
Supported in part by a grant from the National Institute of Mental Health (5-R24-MH61456-03).
1. Berwick DM. Disseminating innovations in health care. JAMA 2003;289:1969-75
2. Drake RE, Goldman HH, Leff HS, et al. Implementing evidence-based practices in routine mental health settings. Psychiatr Serv 2001;52:179-82
3. Geddes JR, Game D, Jenkins NE, et al. What proportion of primary psychiatric interventions are based on evidence from randomised controlled trials? Qual Health Care 1996;5:215-17.
4. Greenhalgh T. How to read a paper: the basics of evidence based medicine (2nd ed). London: BMJ Books, 2001.
5. Gray GE. Evidence-based medicine: an introduction for psychiatrists. J Psychiatr Pract 2002;8:5-13.
6. Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: How to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
7. Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to the teaching of medicine. JAMA 1992;268:2420-5.
8. Accreditation Council for Graduate Medical Education General competencies [ACGME Outcome Project Web site], 2001. Available at: http://www.acgme.org/outcome/. Accessed May 5, 2004.
9. Dawes M. Preface. In: Dawes M, Davies P, Gray A, et al (eds). Evidence-based practice: a primer for health professionals New York: Churchill Livingstone, 1999.
10. Sackett DL, Rosenberg WMC, Gray JAM, et al. Evidence-based medicine: what it is and what it isn’t. BMJ 1996;312:71-2.
11. Straus SE, McAlister FA. Evidence-based medicine: a commentary on common criticisms. Can Med Assoc J 2000;163:837-41.
12. Gray GE. Concise guide to evidence-based psychiatry Washington, DC: American Psychiatric Publishing, 2004.
13. Glasziou P, Vandenbroucke J, Chalmers I. Assessing the quality of research. BMJ 2004;328:39-41.
14. Phillips B, Ball C, Sackett D, et al. Centre for Evidence-Based Medicine: Levels of evidence and grades of recommendations, May 2001. Available at: http://www.cebm.net/levels_of_evidence.asp. Accessed Sept. 18, 2004.
15. Lacchetti C, Guyatt G. Therapy and validity: surprising results of randomized controlled trials. In: Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
16. Antman EM, Lau J, Kupelnick B, et al. A comparison of results of meta-analyses of randomized control trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA 1992;268:240-8.
17. Haynes RB. Of studies, summaries, synopses, and systems: the “4S” evolution of services for finding current best evidence. Evid Based Ment Health 2001;4:37-9.
18. Dearness KL, Tomlin A. Development of the National Electronic Library for Mental Health: providing evidence-based information for all. Health Info Libr J 2001;18:167-74.
19. American Psychiatric Association. Practice guidelines for the treatment of psychiatric disorders: compendium 2002. Washington, DC: American Psychiatric Publishing, 2002.
20. Antes G. Oxman AD for the Cochrane Collaboration. The Cochrane Collaboration in the 20th Century. In: Egger M, Smith GD, Altman DG (eds). Systematic reviews in health care: meta-analysis in context London: BMJBooks, 2001.
21. Say RE, Thomson R. The importance of patient p in treatment decisions—challenges for doctors. BMJ 2003;327:542-5.
1. Berwick DM. Disseminating innovations in health care. JAMA 2003;289:1969-75
2. Drake RE, Goldman HH, Leff HS, et al. Implementing evidence-based practices in routine mental health settings. Psychiatr Serv 2001;52:179-82
3. Geddes JR, Game D, Jenkins NE, et al. What proportion of primary psychiatric interventions are based on evidence from randomised controlled trials? Qual Health Care 1996;5:215-17.
4. Greenhalgh T. How to read a paper: the basics of evidence based medicine (2nd ed). London: BMJ Books, 2001.
5. Gray GE. Evidence-based medicine: an introduction for psychiatrists. J Psychiatr Pract 2002;8:5-13.
6. Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: How to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
7. Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to the teaching of medicine. JAMA 1992;268:2420-5.
8. Accreditation Council for Graduate Medical Education General competencies [ACGME Outcome Project Web site], 2001. Available at: http://www.acgme.org/outcome/. Accessed May 5, 2004.
9. Dawes M. Preface. In: Dawes M, Davies P, Gray A, et al (eds). Evidence-based practice: a primer for health professionals New York: Churchill Livingstone, 1999.
10. Sackett DL, Rosenberg WMC, Gray JAM, et al. Evidence-based medicine: what it is and what it isn’t. BMJ 1996;312:71-2.
11. Straus SE, McAlister FA. Evidence-based medicine: a commentary on common criticisms. Can Med Assoc J 2000;163:837-41.
12. Gray GE. Concise guide to evidence-based psychiatry Washington, DC: American Psychiatric Publishing, 2004.
13. Glasziou P, Vandenbroucke J, Chalmers I. Assessing the quality of research. BMJ 2004;328:39-41.
14. Phillips B, Ball C, Sackett D, et al. Centre for Evidence-Based Medicine: Levels of evidence and grades of recommendations, May 2001. Available at: http://www.cebm.net/levels_of_evidence.asp. Accessed Sept. 18, 2004.
15. Lacchetti C, Guyatt G. Therapy and validity: surprising results of randomized controlled trials. In: Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
16. Antman EM, Lau J, Kupelnick B, et al. A comparison of results of meta-analyses of randomized control trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA 1992;268:240-8.
17. Haynes RB. Of studies, summaries, synopses, and systems: the “4S” evolution of services for finding current best evidence. Evid Based Ment Health 2001;4:37-9.
18. Dearness KL, Tomlin A. Development of the National Electronic Library for Mental Health: providing evidence-based information for all. Health Info Libr J 2001;18:167-74.
19. American Psychiatric Association. Practice guidelines for the treatment of psychiatric disorders: compendium 2002. Washington, DC: American Psychiatric Publishing, 2002.
20. Antes G. Oxman AD for the Cochrane Collaboration. The Cochrane Collaboration in the 20th Century. In: Egger M, Smith GD, Altman DG (eds). Systematic reviews in health care: meta-analysis in context London: BMJBooks, 2001.
21. Say RE, Thomson R. The importance of patient p in treatment decisions—challenges for doctors. BMJ 2003;327:542-5.
Psychogenic or epileptic seizures? How to clinch the diagnosis
When you evaluate patients whose seizures could be epileptic or psychogenic, the evidence points to three useful diagnostic steps:
- Step 1: Characterize the seizure by its triggers and presentation.
- Step 2: Identify psychiatric comorbidity that might be precipitating psychogenic nonepileptic seizures (PNES).1
- Step 3: Obtain video EEG and blood tests for physiologic confirmation of epilepsy.
Using a case illustration, this article describes how to accomplish these steps by seeking clues in the patient’s seizure and psychiatric histories and choosing high-yield laboratory tests. When a PNES diagnosis becomes clear, we suggest an empathic approach that can help patients develop healthier responses to stress.
Patients with psychogenic nonepileptic seizure (PNES)have high rates of repressed anger and life stressors. Psychodynamic interpretations postulate PNES as an unconscious conversion of emotional distress into physical symptoms, unlike factitious disorder’s intentionality. Repressed traumatic childhood sexual experience may be significant.2
Family dynamics. PNES may be a maladaptive communication method by which an individual uses behavior to manipulate the environment to meet emotional needs or to compensate for an environment intolerant of direct verbal expression.3
Characteristics. PNES patients are a heterogeneous group. They average a full-scale IQ of 92 in the lower quartile of intellectual capacity and neuropsychological functioning. PNES usually presents in the 20s but may occur at any age. PNES is more common in women than men (ratio 4:1).4,5
Comorbidities. Up to 40% of patients treated at epilepsy centers are reported to have both epilepsy and PNES.4,5 In a 1-year study at an EEG-video monitoring unit, however, only 9.4% of PNES patients had interictal epileptiform discharges to support a coexisting diagnosis of epilepsy.4
PNES may be highly associated with somatoform disorder, mood disorder, anxiety disorder, brief reactive psychosis, or schizophreniform disorder.6
CASE: A DIFFERENT KIND OF SEIZURE
Ms. X’s husband brought her to the emergency room after her third tonic-clonic convulsion within 1 week. He reported that her eyes suddenly rolled up and she became limp and fell down after they argued about money. She suffered a minor temple laceration, but this seizure—unlike past episodes—was not associated with mouth foaming or fecal or urinary incontinence.
Ms. X, age 35, has a history of seizure disorder and 5 years of unemployment when seizures were uncontrolled. Her seizures have been stabilized for 18 months with phenytoin, 300 mg bid. She has been hospitalized twice for major depressive disorder, most recently 2 years ago. Since then, her depression has been in remission with paroxetine, 20 mg once daily. She does not abuse drugs or alcohol. She has been married 8 years, has no children, and receives disability income.
Ms. X was stabilized and admitted for neurologic evaluation. CT and MRI were normal, EEG recordings were unremarkable, and blood workup revealed slightly elevated creatine kinase but normal prolactin. Her phenytoin serum level was 12 mcg/mL (therapeutic range, 5 to 20 mcg/mL). When video-EEG recording during one seizure revealed no abnormality, the neurologist requested psychiatric consultation.
PNES: NOT A ‘PSEUDO’ SEIZURE
Patients with PNES are a heterogeneous population (Box)2-6 that appears repeatedly at emergency rooms, resulting in multiple investigations and treatment with antiepileptic medications. Those with both PNES and epileptic seizure disorders, such as Ms. X, present a particularly difficult clinical dilemma as:
- discontinuing anticonvulsants may exacerbate epileptic seizures
- increasing the medication in the mistaken belief that a seizure breakthrough has occurred could result in toxic serum levels.
Psychological stressors may precipitate PNES in a person who has never had a seizure or in someone with co-existing epilepsy. Patients with PNES frequently deny a correlation between emotional stress and their seizures, whereas the opposite usually holds for patients who have experienced an epileptic seizure.7,8
PNES has been called “pseudoseizure” a term we believe is unfair to patients because the etiologic determinants are mostly subconscious.9 Although one author has defended the term,10 we agree with others that “pseudoseizure” can give a misleading impression that patients feign their symptoms.9
Psychiatric comorbidity. When PNES is suspected, a careful history is essential to identify precipitating psychiatric comorbidity, such as somatoform, somatization, conversion, or dissociative disorder. PNES may also be precipitated by or coexist with mood and anxiety disorders, schizophrenia, malingering and factitious disorders, diffuse organic brain disease, and developmental disorders (Table 1).11,12
CASE CONTINUED: AN IMPORTANT CLUE
Ms. X was admitted to the psychiatric unit. Her psychiatric history showed recurrent depressive disorder and excluded head injury. She was mildly depressed but expressed minimal cognitive and biological depressive symptoms in the mental status examination. She denied suicidal or homicidal thoughts. Perception, thought process, and cognition were normal.
With her consent, the psychiatrist obtained collateral information from her brother. He reported that his sister had received a diagnosis of “pseudoseizures” about 5 years before this presentation. The brother was unsure of any emotional precipitants.
Table 1
Psychiatric disorders that may precipitate or coexist with PNES
| Psychopathology | Differentiation |
|---|---|
| Somatoform disorders | Physical symptoms suggest a medical condition but are not the result of a medical condition, substance, or another mental disorder such as panic disorder or schizophrenia |
| Conversion disorder | Psychological symptoms expressed as neurologic symptoms—such as paralysis, blindness, or paresthesia—in the absence of a known medical or neurologic disorder |
| Dissociative disorder | Disruption in consciousness, memory, identity, or perception that may be sudden or gradual, transient or chronic |
| Depressive disorders | Mood or anxiety symptoms related to depressive, bipolar, panic, posttraumatic stress, or acute stress disorders may coexist with PNES |
| Psychotic disorders | Schizophrenia may be associated with seizure-like events in some patients12 |
| Factitious disorder | Seizure-like symptoms may be produced intentionally for secondary gain (as in malingering) or feigned to assume a sick role (as in factitious disorder) |
| Developmental disorders | In a patient with mental retardation, PNES may result from reinforced operant behavior patterns |
| Source: Diagnostic and statistical manual of mental disorders (4th ed., text rev).11 | |
PNES OR EPILEPSY?
Initial assessment of suspected PNES includes a medical, psychiatric, social, psychological, and substance abuse history, as well as a thorough physical examination.
In patients with suspected PNES, obtain collateral histories of seizure precipitants, abortants, childhood events, and family history. Ms. X, for example, has a history of depression and at least one past episode of probable PNES, as described by her brother. An argument with her husband apparently precipitated the most recent seizure episode.
Table 2
Psychogenic seizures PNES vs. epileptic seizures: Differences in presentation*
| Clinical features | Psychogenic nonepileptic seizures (PNES) | Epileptic seizures |
|---|---|---|
| Duration | Variable | Short (20 to 70 seconds) |
| Pattern | Variable | Stereotyped |
| Frequency | Variable | Paroxysmal, cluster |
| Cause | Emotional | Organic |
| Occurs in presence of others | Yes | Variable |
| Occurs during sleep | Rare | Yes |
| Incontinence | Rare | Frequent |
| Biting pattern | Tip of tongue, lips | Side of tongue, cheek |
| Convulsion | Bizarre, trashing, sexual movements | Tonic-clonic |
| Injury | Infrequent, mild | Infrequent, severe |
| Pupillary reflex | Normal | Slow, nonreactive |
| Babinski’s reflex | No | Yes, if convulsion |
| Orientation afterwards | Clear | Confused |
| Postictal stupor | Rare | Frequent |
| Serum prolactin | Normal | Elevated (>18 ng/mL in men; >30 ng/mL in nonpregnant women) |
| EEG | Normal | Abnormal or variable |
| * Apply loosely, as the spectrum of seizure types within epilepsy is very large. | ||
| Source: Adapted from reference 13. | ||
PNES features. Clinical features (Table 2)13—although not definitive—can help differentiate PNES from epileptic seizure.1 PNES features to look for include:
- prolonged and bizarre prodrome
- prominent out-of-phase ictal or postictal activity
- clear-cut precipitants, especially in an emotionally charged atmosphere
- lack of falls or injuries
- fluctuating consciousness or vivid recall of details during ictal moments.
PNES’ physical symptoms are not voluntary. Patients often have out-of-phase upper- and lower-extremity movements and vocalization as the event starts, as opposed to about 20 seconds into the event when true tonic-clonic seizure makes the tonic-clonic transformation. Other common features are high-amplitude, forward pelvic thrusting, and lack of rigidity. Weeping during an apparent seizure strongly suggests a nonepileptic event.14
Ictal duration can be useful in assessment. Events that resemble tonic-clonic seizure but continue for >70 seconds or <20 seconds raise suspicion of nonepileptic seizures, although status epilepticus is possible.
Prolactin elevation. Epileptic tonic-clonic and partial complex seizures increase serum prolactin and are most reliable approximately 20 minutes after event onset. Nipple manipulation can spuriously increase serum prolactin, so observe female patients for this behavior if a seizure occurs in your presence. Psychotropics such as chlorpromazine and haloperidol may also elevate serum prolactin.
INVESTIGATIONS
Video EEG recording is available in most neurologic centers and is the investigation of choice. Epileptic seizure is characterized by recruitment of seizure activity in a physiologic distribution and postictal slowing, which would be difficult for a patient to imitate.
Unlike traditional EEG, video EEG shows evidence of electrographic paroxysmal changes immediately before, during, or after an epileptic seizure.15 Seizure presentations without paroxysmal electrographic changes would be considered PNES.
Traditional EEG is not recommended for a PNES workup because seizure activity is not recorded and myogenic infarcts may obscure readings. Moreover, because interictal EEG changes may occur even in patients with PNES, these changes in isolation cannot be interpreted as evidence of epilepsy.16
Laboratory testing includes full blood count, electrolytes, urea and creatinine, urine drug screen, and thyroid and liver function tests, as well as serum levels in patients taking anticonvulsants. These tests may exclude some seizure causes (such as hypokalemia or hypocalcemia with electrolyte disturbances) and provide baseline values for monitoring drug toxicity. Thyroid function testing will rule out hypo- or hyperthyroidism in patients with comorbid depressive or anxiety disorders. Urine drug screen reveals evidence of drug abuse—a possible organic seizure disorder precipitant.
Normal serum prolactin (men: 2 to 18 ng/mL; nonpregnant women: 3 to 30 ng/mL), cortisol (5 to 22 mcg/dL, morning blood specimen), and creatine kinase (50 to 200 U/L) rise substantially after an epileptic—but not psychogenic—seizure.17 Note, however, that creatine kinase and prolactin may be as elevated in PNES as in an epileptic seizure if PNES presents with vigorous muscular activity.18
Psychological testing may help distinguish PNES from epileptic seizure:
- Minnesota Multiphasic Personality Inventory (MMPI) is fairly sensitive and shows statistically significant differences between PNES and epileptic seizures in hypochondriasis, depression, hysteria, and schizophrenia.19
- Washington Psychosocial Seizure Inventory helps identify etiologic subgroups among PNES patients.9
Others. As in Ms. X’s case, CT and MRI for cerebral pathology may not help.20 Provocative techniques21 based on suggestibility also may have little value because PNES can be provoked in patients with documented epileptic seizures. Hypnosis has been used in attempts to demonstrate the psychogenic component of nonepileptic seizures by reversing ictal and postictal amnesia. Patients with PNES seem to be more responsive to hypnosis than those with epileptic seizures.22
CASE CONTINUED: EXPLAINING THE DIAGNOSIS
The psychiatric team concluded that even though Ms. X has a seizure disorder, this particular episode was psychogenic. This conclusion was based on the emotional precipitant, her brother’s collateral history, video EEG recordings, and her history of depression.
The psychiatrist explained to Ms. X that PNES and seizure disorders can coexist and that a PNES diagnosis does not imply that a patient is lying. It simply means that some seizures are precipitated by psychoemotional events.
Unlike some patients with PNES, Ms. X accepted the diagnosis without anger. Because her epilepsy and depression were stable, the psychiatrist did not change her phenytoin or paroxetine dosages. She was discharged, with follow-up care by a psychiatrist and neurologist.
TELLING AND TREATING THE PATIENT
It is important to present a PNES diagnosis with care because some patients react with aggressive denial and suicidal behavior. A patient who believes he or she has been perceived as a liar or “fake” may feel humiliated,9 which is why we prefer the term “PNES” rather than “pseudoseizure.”
PNES treatment calls for collaboration among the neurologist, psychiatrist, psychologist, therapists, support workers, and family. When PNES is clearly the only cause of seizures, avoid treating with anticonvulsants. If PNES coexists with a treated seizure disorder, no change in anticonvulsant dosage is necessary, especially if blood levels are normal.
Target the underlying psychiatric disorder, using medication and cognitive-behavioral therapy as appropriate. Advise patients and families that the seizure-like events may continue for some time but will disappear as the patient develops more-effective and appropriate coping strategies.
Prognosis. Favorable prognostic factors include being female, effective early intervention, normal premorbid psychological make-up, and good family support. Studies have shown that:
- up to 40% of treated PNES patients remained event-free for a median of 5 years.23
- prognosis may depend on spell type (catatonic is more favorable than “thrashing”) and illness duration (<1 year is more favorable than >1 year).24
Related resources
- Riley LT, Roy A. Pseudoseizures. Baltimore: Lippincott, Williams and Wilkins, 1982.
- Epilepsy.com. Psychogenic seizures. Resource for patients. www.epilepsy.com/epilepsy/seizure_psychogenic.html Accessed Oct. 14, 2004.
- Epilepsy Foundation. Information for patients and families. www.epilepsyfoundation.org. Search for nonepileptic seizures. Accessed Oct. 14, 2004.
Drug brand names
- Chlorpromazine • Thorazine
- Haloperidol • Haldol
- Phenytoin • Dilantin
- Paroxetine • Paxil
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Riley TL, Brannon WL, Jr. Recognition of pseudoseizures. Acta Neurol Scand 1991;83(2):129-32.
2. Goodwin J, Simms M, Bergman R. Hysterical seizures: a sequel to incest. Am J Orthopsychiatry 1979;49:698-703.
3. Krawetz P, Fleisher W, Pillay N, et al. Family functioning in subjects with pseudoseizures and epilepsy. J Nerv Ment Dis 2001;189(1):38-43.
4. Gates JR, Luciano D, Devinsky O. The classification and treatment of nonepileptic events. In: Devinsky O, Theodore WH (eds). Epilepsy and behavior. New York: Wiley-Liss, 1991;251-63.
5. Vossler DG. Nonepileptic seizures of physiologic origin. J Epilepsy 1995;8:1-10.
6. Wyllie E, Glazer JP, Benbadis S, et al. Psychiatric features of children and adolescents with pseudoseizures. Arch Pediatr Adolesc Med 1999;153(3):244-8.
7. Luciano D, Perrine K, Clayton B, Devinsky O. Stress as a seizure precipitant and its relationship to ictal focus [abstract]. Epilepsia 1992;33(suppl 3):130.-
8. Betts T. Epilepsy and stress [editorial]. BMJ 1992;305:378-9.
9. Chabolla DR, Krahn LE, So EL, Rummans TA. Psychogenic nonepileptic seizures. Mayo Foundation for Medical Education and Research (symposium, part Ii, vol. 71[5]). May 1996;493-500.
10. Slavney PR. In defense of pseudoseizure (comment). Gen Hosp Psychiatry 1994;16(4):243-5.
11. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association, 2000.
12. Matsuura M, Oana Y, Kato M, et al. A multicenter study on the prevalence of psychiatric disorders among new referrals for epilepsy in Japan. Epilepsia 2003;44(1):107-14.
13. Oommen KJ. Pseudoseizures: Diagnostic guidelines. Comprehensive Oklahoma Program for Epilepsy (COPE), 2000. Available at w3.ouhsc.edu/neuro/division/cope/pseudosz.htm. Accessed Oct. 14, 2004.
14. Walczak TS, Bogolioubov A. Weeping during psychogenic non-epileptic seizures. Epilepsia 1996;37(2):208-10.
15. Mohan KK, Markand ON, Salanova V. Diagnostic utility of video EEG monitoring in paroxysmal events. Acta Neurol Scand 1996;94(5):320-5.
16. Reuber M, Fernandez G, Bauer J, et al. Interictal EEG abnormalities in patients with psychogenic nonepileptic seizures. Epilepsia 2002;43(9):1013-20.
17. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985;35:31-5.
18. Alving J. Serum prolactin levels are elevated also after pseudoepileptic seizures. Seizure 1998;7(2):85-9.
19. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184-7.
20. Lelliott PT, Fenwick P. Cerebral pathology in pseudoseizures. Acta Neurol Scand 1992;85(3):177-80.
21. Guberman A. Psychogenic pseudoseizures in non-epileptic patients. Can J Psychiatry 1982;27:401-4.
22. Kuyk J, Jacobs LD, Aldenkamp AP, et al. Pseudoepileptic seizures: hypnosis as a diagnostic tool. Seizure 1995;4(2):123-8.
23. Holmes GL, Sackellares JC, McKiernan J, et al. Evaluation of childhood pseudoseizures using EEG telemetry and video tape monitoring. J Pediatr 1980;97(4):554-8.
24. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41(10):1330-4.
When you evaluate patients whose seizures could be epileptic or psychogenic, the evidence points to three useful diagnostic steps:
- Step 1: Characterize the seizure by its triggers and presentation.
- Step 2: Identify psychiatric comorbidity that might be precipitating psychogenic nonepileptic seizures (PNES).1
- Step 3: Obtain video EEG and blood tests for physiologic confirmation of epilepsy.
Using a case illustration, this article describes how to accomplish these steps by seeking clues in the patient’s seizure and psychiatric histories and choosing high-yield laboratory tests. When a PNES diagnosis becomes clear, we suggest an empathic approach that can help patients develop healthier responses to stress.
Patients with psychogenic nonepileptic seizure (PNES)have high rates of repressed anger and life stressors. Psychodynamic interpretations postulate PNES as an unconscious conversion of emotional distress into physical symptoms, unlike factitious disorder’s intentionality. Repressed traumatic childhood sexual experience may be significant.2
Family dynamics. PNES may be a maladaptive communication method by which an individual uses behavior to manipulate the environment to meet emotional needs or to compensate for an environment intolerant of direct verbal expression.3
Characteristics. PNES patients are a heterogeneous group. They average a full-scale IQ of 92 in the lower quartile of intellectual capacity and neuropsychological functioning. PNES usually presents in the 20s but may occur at any age. PNES is more common in women than men (ratio 4:1).4,5
Comorbidities. Up to 40% of patients treated at epilepsy centers are reported to have both epilepsy and PNES.4,5 In a 1-year study at an EEG-video monitoring unit, however, only 9.4% of PNES patients had interictal epileptiform discharges to support a coexisting diagnosis of epilepsy.4
PNES may be highly associated with somatoform disorder, mood disorder, anxiety disorder, brief reactive psychosis, or schizophreniform disorder.6
CASE: A DIFFERENT KIND OF SEIZURE
Ms. X’s husband brought her to the emergency room after her third tonic-clonic convulsion within 1 week. He reported that her eyes suddenly rolled up and she became limp and fell down after they argued about money. She suffered a minor temple laceration, but this seizure—unlike past episodes—was not associated with mouth foaming or fecal or urinary incontinence.
Ms. X, age 35, has a history of seizure disorder and 5 years of unemployment when seizures were uncontrolled. Her seizures have been stabilized for 18 months with phenytoin, 300 mg bid. She has been hospitalized twice for major depressive disorder, most recently 2 years ago. Since then, her depression has been in remission with paroxetine, 20 mg once daily. She does not abuse drugs or alcohol. She has been married 8 years, has no children, and receives disability income.
Ms. X was stabilized and admitted for neurologic evaluation. CT and MRI were normal, EEG recordings were unremarkable, and blood workup revealed slightly elevated creatine kinase but normal prolactin. Her phenytoin serum level was 12 mcg/mL (therapeutic range, 5 to 20 mcg/mL). When video-EEG recording during one seizure revealed no abnormality, the neurologist requested psychiatric consultation.
PNES: NOT A ‘PSEUDO’ SEIZURE
Patients with PNES are a heterogeneous population (Box)2-6 that appears repeatedly at emergency rooms, resulting in multiple investigations and treatment with antiepileptic medications. Those with both PNES and epileptic seizure disorders, such as Ms. X, present a particularly difficult clinical dilemma as:
- discontinuing anticonvulsants may exacerbate epileptic seizures
- increasing the medication in the mistaken belief that a seizure breakthrough has occurred could result in toxic serum levels.
Psychological stressors may precipitate PNES in a person who has never had a seizure or in someone with co-existing epilepsy. Patients with PNES frequently deny a correlation between emotional stress and their seizures, whereas the opposite usually holds for patients who have experienced an epileptic seizure.7,8
PNES has been called “pseudoseizure” a term we believe is unfair to patients because the etiologic determinants are mostly subconscious.9 Although one author has defended the term,10 we agree with others that “pseudoseizure” can give a misleading impression that patients feign their symptoms.9
Psychiatric comorbidity. When PNES is suspected, a careful history is essential to identify precipitating psychiatric comorbidity, such as somatoform, somatization, conversion, or dissociative disorder. PNES may also be precipitated by or coexist with mood and anxiety disorders, schizophrenia, malingering and factitious disorders, diffuse organic brain disease, and developmental disorders (Table 1).11,12
CASE CONTINUED: AN IMPORTANT CLUE
Ms. X was admitted to the psychiatric unit. Her psychiatric history showed recurrent depressive disorder and excluded head injury. She was mildly depressed but expressed minimal cognitive and biological depressive symptoms in the mental status examination. She denied suicidal or homicidal thoughts. Perception, thought process, and cognition were normal.
With her consent, the psychiatrist obtained collateral information from her brother. He reported that his sister had received a diagnosis of “pseudoseizures” about 5 years before this presentation. The brother was unsure of any emotional precipitants.
Table 1
Psychiatric disorders that may precipitate or coexist with PNES
| Psychopathology | Differentiation |
|---|---|
| Somatoform disorders | Physical symptoms suggest a medical condition but are not the result of a medical condition, substance, or another mental disorder such as panic disorder or schizophrenia |
| Conversion disorder | Psychological symptoms expressed as neurologic symptoms—such as paralysis, blindness, or paresthesia—in the absence of a known medical or neurologic disorder |
| Dissociative disorder | Disruption in consciousness, memory, identity, or perception that may be sudden or gradual, transient or chronic |
| Depressive disorders | Mood or anxiety symptoms related to depressive, bipolar, panic, posttraumatic stress, or acute stress disorders may coexist with PNES |
| Psychotic disorders | Schizophrenia may be associated with seizure-like events in some patients12 |
| Factitious disorder | Seizure-like symptoms may be produced intentionally for secondary gain (as in malingering) or feigned to assume a sick role (as in factitious disorder) |
| Developmental disorders | In a patient with mental retardation, PNES may result from reinforced operant behavior patterns |
| Source: Diagnostic and statistical manual of mental disorders (4th ed., text rev).11 | |
PNES OR EPILEPSY?
Initial assessment of suspected PNES includes a medical, psychiatric, social, psychological, and substance abuse history, as well as a thorough physical examination.
In patients with suspected PNES, obtain collateral histories of seizure precipitants, abortants, childhood events, and family history. Ms. X, for example, has a history of depression and at least one past episode of probable PNES, as described by her brother. An argument with her husband apparently precipitated the most recent seizure episode.
Table 2
Psychogenic seizures PNES vs. epileptic seizures: Differences in presentation*
| Clinical features | Psychogenic nonepileptic seizures (PNES) | Epileptic seizures |
|---|---|---|
| Duration | Variable | Short (20 to 70 seconds) |
| Pattern | Variable | Stereotyped |
| Frequency | Variable | Paroxysmal, cluster |
| Cause | Emotional | Organic |
| Occurs in presence of others | Yes | Variable |
| Occurs during sleep | Rare | Yes |
| Incontinence | Rare | Frequent |
| Biting pattern | Tip of tongue, lips | Side of tongue, cheek |
| Convulsion | Bizarre, trashing, sexual movements | Tonic-clonic |
| Injury | Infrequent, mild | Infrequent, severe |
| Pupillary reflex | Normal | Slow, nonreactive |
| Babinski’s reflex | No | Yes, if convulsion |
| Orientation afterwards | Clear | Confused |
| Postictal stupor | Rare | Frequent |
| Serum prolactin | Normal | Elevated (>18 ng/mL in men; >30 ng/mL in nonpregnant women) |
| EEG | Normal | Abnormal or variable |
| * Apply loosely, as the spectrum of seizure types within epilepsy is very large. | ||
| Source: Adapted from reference 13. | ||
PNES features. Clinical features (Table 2)13—although not definitive—can help differentiate PNES from epileptic seizure.1 PNES features to look for include:
- prolonged and bizarre prodrome
- prominent out-of-phase ictal or postictal activity
- clear-cut precipitants, especially in an emotionally charged atmosphere
- lack of falls or injuries
- fluctuating consciousness or vivid recall of details during ictal moments.
PNES’ physical symptoms are not voluntary. Patients often have out-of-phase upper- and lower-extremity movements and vocalization as the event starts, as opposed to about 20 seconds into the event when true tonic-clonic seizure makes the tonic-clonic transformation. Other common features are high-amplitude, forward pelvic thrusting, and lack of rigidity. Weeping during an apparent seizure strongly suggests a nonepileptic event.14
Ictal duration can be useful in assessment. Events that resemble tonic-clonic seizure but continue for >70 seconds or <20 seconds raise suspicion of nonepileptic seizures, although status epilepticus is possible.
Prolactin elevation. Epileptic tonic-clonic and partial complex seizures increase serum prolactin and are most reliable approximately 20 minutes after event onset. Nipple manipulation can spuriously increase serum prolactin, so observe female patients for this behavior if a seizure occurs in your presence. Psychotropics such as chlorpromazine and haloperidol may also elevate serum prolactin.
INVESTIGATIONS
Video EEG recording is available in most neurologic centers and is the investigation of choice. Epileptic seizure is characterized by recruitment of seizure activity in a physiologic distribution and postictal slowing, which would be difficult for a patient to imitate.
Unlike traditional EEG, video EEG shows evidence of electrographic paroxysmal changes immediately before, during, or after an epileptic seizure.15 Seizure presentations without paroxysmal electrographic changes would be considered PNES.
Traditional EEG is not recommended for a PNES workup because seizure activity is not recorded and myogenic infarcts may obscure readings. Moreover, because interictal EEG changes may occur even in patients with PNES, these changes in isolation cannot be interpreted as evidence of epilepsy.16
Laboratory testing includes full blood count, electrolytes, urea and creatinine, urine drug screen, and thyroid and liver function tests, as well as serum levels in patients taking anticonvulsants. These tests may exclude some seizure causes (such as hypokalemia or hypocalcemia with electrolyte disturbances) and provide baseline values for monitoring drug toxicity. Thyroid function testing will rule out hypo- or hyperthyroidism in patients with comorbid depressive or anxiety disorders. Urine drug screen reveals evidence of drug abuse—a possible organic seizure disorder precipitant.
Normal serum prolactin (men: 2 to 18 ng/mL; nonpregnant women: 3 to 30 ng/mL), cortisol (5 to 22 mcg/dL, morning blood specimen), and creatine kinase (50 to 200 U/L) rise substantially after an epileptic—but not psychogenic—seizure.17 Note, however, that creatine kinase and prolactin may be as elevated in PNES as in an epileptic seizure if PNES presents with vigorous muscular activity.18
Psychological testing may help distinguish PNES from epileptic seizure:
- Minnesota Multiphasic Personality Inventory (MMPI) is fairly sensitive and shows statistically significant differences between PNES and epileptic seizures in hypochondriasis, depression, hysteria, and schizophrenia.19
- Washington Psychosocial Seizure Inventory helps identify etiologic subgroups among PNES patients.9
Others. As in Ms. X’s case, CT and MRI for cerebral pathology may not help.20 Provocative techniques21 based on suggestibility also may have little value because PNES can be provoked in patients with documented epileptic seizures. Hypnosis has been used in attempts to demonstrate the psychogenic component of nonepileptic seizures by reversing ictal and postictal amnesia. Patients with PNES seem to be more responsive to hypnosis than those with epileptic seizures.22
CASE CONTINUED: EXPLAINING THE DIAGNOSIS
The psychiatric team concluded that even though Ms. X has a seizure disorder, this particular episode was psychogenic. This conclusion was based on the emotional precipitant, her brother’s collateral history, video EEG recordings, and her history of depression.
The psychiatrist explained to Ms. X that PNES and seizure disorders can coexist and that a PNES diagnosis does not imply that a patient is lying. It simply means that some seizures are precipitated by psychoemotional events.
Unlike some patients with PNES, Ms. X accepted the diagnosis without anger. Because her epilepsy and depression were stable, the psychiatrist did not change her phenytoin or paroxetine dosages. She was discharged, with follow-up care by a psychiatrist and neurologist.
TELLING AND TREATING THE PATIENT
It is important to present a PNES diagnosis with care because some patients react with aggressive denial and suicidal behavior. A patient who believes he or she has been perceived as a liar or “fake” may feel humiliated,9 which is why we prefer the term “PNES” rather than “pseudoseizure.”
PNES treatment calls for collaboration among the neurologist, psychiatrist, psychologist, therapists, support workers, and family. When PNES is clearly the only cause of seizures, avoid treating with anticonvulsants. If PNES coexists with a treated seizure disorder, no change in anticonvulsant dosage is necessary, especially if blood levels are normal.
Target the underlying psychiatric disorder, using medication and cognitive-behavioral therapy as appropriate. Advise patients and families that the seizure-like events may continue for some time but will disappear as the patient develops more-effective and appropriate coping strategies.
Prognosis. Favorable prognostic factors include being female, effective early intervention, normal premorbid psychological make-up, and good family support. Studies have shown that:
- up to 40% of treated PNES patients remained event-free for a median of 5 years.23
- prognosis may depend on spell type (catatonic is more favorable than “thrashing”) and illness duration (<1 year is more favorable than >1 year).24
Related resources
- Riley LT, Roy A. Pseudoseizures. Baltimore: Lippincott, Williams and Wilkins, 1982.
- Epilepsy.com. Psychogenic seizures. Resource for patients. www.epilepsy.com/epilepsy/seizure_psychogenic.html Accessed Oct. 14, 2004.
- Epilepsy Foundation. Information for patients and families. www.epilepsyfoundation.org. Search for nonepileptic seizures. Accessed Oct. 14, 2004.
Drug brand names
- Chlorpromazine • Thorazine
- Haloperidol • Haldol
- Phenytoin • Dilantin
- Paroxetine • Paxil
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
When you evaluate patients whose seizures could be epileptic or psychogenic, the evidence points to three useful diagnostic steps:
- Step 1: Characterize the seizure by its triggers and presentation.
- Step 2: Identify psychiatric comorbidity that might be precipitating psychogenic nonepileptic seizures (PNES).1
- Step 3: Obtain video EEG and blood tests for physiologic confirmation of epilepsy.
Using a case illustration, this article describes how to accomplish these steps by seeking clues in the patient’s seizure and psychiatric histories and choosing high-yield laboratory tests. When a PNES diagnosis becomes clear, we suggest an empathic approach that can help patients develop healthier responses to stress.
Patients with psychogenic nonepileptic seizure (PNES)have high rates of repressed anger and life stressors. Psychodynamic interpretations postulate PNES as an unconscious conversion of emotional distress into physical symptoms, unlike factitious disorder’s intentionality. Repressed traumatic childhood sexual experience may be significant.2
Family dynamics. PNES may be a maladaptive communication method by which an individual uses behavior to manipulate the environment to meet emotional needs or to compensate for an environment intolerant of direct verbal expression.3
Characteristics. PNES patients are a heterogeneous group. They average a full-scale IQ of 92 in the lower quartile of intellectual capacity and neuropsychological functioning. PNES usually presents in the 20s but may occur at any age. PNES is more common in women than men (ratio 4:1).4,5
Comorbidities. Up to 40% of patients treated at epilepsy centers are reported to have both epilepsy and PNES.4,5 In a 1-year study at an EEG-video monitoring unit, however, only 9.4% of PNES patients had interictal epileptiform discharges to support a coexisting diagnosis of epilepsy.4
PNES may be highly associated with somatoform disorder, mood disorder, anxiety disorder, brief reactive psychosis, or schizophreniform disorder.6
CASE: A DIFFERENT KIND OF SEIZURE
Ms. X’s husband brought her to the emergency room after her third tonic-clonic convulsion within 1 week. He reported that her eyes suddenly rolled up and she became limp and fell down after they argued about money. She suffered a minor temple laceration, but this seizure—unlike past episodes—was not associated with mouth foaming or fecal or urinary incontinence.
Ms. X, age 35, has a history of seizure disorder and 5 years of unemployment when seizures were uncontrolled. Her seizures have been stabilized for 18 months with phenytoin, 300 mg bid. She has been hospitalized twice for major depressive disorder, most recently 2 years ago. Since then, her depression has been in remission with paroxetine, 20 mg once daily. She does not abuse drugs or alcohol. She has been married 8 years, has no children, and receives disability income.
Ms. X was stabilized and admitted for neurologic evaluation. CT and MRI were normal, EEG recordings were unremarkable, and blood workup revealed slightly elevated creatine kinase but normal prolactin. Her phenytoin serum level was 12 mcg/mL (therapeutic range, 5 to 20 mcg/mL). When video-EEG recording during one seizure revealed no abnormality, the neurologist requested psychiatric consultation.
PNES: NOT A ‘PSEUDO’ SEIZURE
Patients with PNES are a heterogeneous population (Box)2-6 that appears repeatedly at emergency rooms, resulting in multiple investigations and treatment with antiepileptic medications. Those with both PNES and epileptic seizure disorders, such as Ms. X, present a particularly difficult clinical dilemma as:
- discontinuing anticonvulsants may exacerbate epileptic seizures
- increasing the medication in the mistaken belief that a seizure breakthrough has occurred could result in toxic serum levels.
Psychological stressors may precipitate PNES in a person who has never had a seizure or in someone with co-existing epilepsy. Patients with PNES frequently deny a correlation between emotional stress and their seizures, whereas the opposite usually holds for patients who have experienced an epileptic seizure.7,8
PNES has been called “pseudoseizure” a term we believe is unfair to patients because the etiologic determinants are mostly subconscious.9 Although one author has defended the term,10 we agree with others that “pseudoseizure” can give a misleading impression that patients feign their symptoms.9
Psychiatric comorbidity. When PNES is suspected, a careful history is essential to identify precipitating psychiatric comorbidity, such as somatoform, somatization, conversion, or dissociative disorder. PNES may also be precipitated by or coexist with mood and anxiety disorders, schizophrenia, malingering and factitious disorders, diffuse organic brain disease, and developmental disorders (Table 1).11,12
CASE CONTINUED: AN IMPORTANT CLUE
Ms. X was admitted to the psychiatric unit. Her psychiatric history showed recurrent depressive disorder and excluded head injury. She was mildly depressed but expressed minimal cognitive and biological depressive symptoms in the mental status examination. She denied suicidal or homicidal thoughts. Perception, thought process, and cognition were normal.
With her consent, the psychiatrist obtained collateral information from her brother. He reported that his sister had received a diagnosis of “pseudoseizures” about 5 years before this presentation. The brother was unsure of any emotional precipitants.
Table 1
Psychiatric disorders that may precipitate or coexist with PNES
| Psychopathology | Differentiation |
|---|---|
| Somatoform disorders | Physical symptoms suggest a medical condition but are not the result of a medical condition, substance, or another mental disorder such as panic disorder or schizophrenia |
| Conversion disorder | Psychological symptoms expressed as neurologic symptoms—such as paralysis, blindness, or paresthesia—in the absence of a known medical or neurologic disorder |
| Dissociative disorder | Disruption in consciousness, memory, identity, or perception that may be sudden or gradual, transient or chronic |
| Depressive disorders | Mood or anxiety symptoms related to depressive, bipolar, panic, posttraumatic stress, or acute stress disorders may coexist with PNES |
| Psychotic disorders | Schizophrenia may be associated with seizure-like events in some patients12 |
| Factitious disorder | Seizure-like symptoms may be produced intentionally for secondary gain (as in malingering) or feigned to assume a sick role (as in factitious disorder) |
| Developmental disorders | In a patient with mental retardation, PNES may result from reinforced operant behavior patterns |
| Source: Diagnostic and statistical manual of mental disorders (4th ed., text rev).11 | |
PNES OR EPILEPSY?
Initial assessment of suspected PNES includes a medical, psychiatric, social, psychological, and substance abuse history, as well as a thorough physical examination.
In patients with suspected PNES, obtain collateral histories of seizure precipitants, abortants, childhood events, and family history. Ms. X, for example, has a history of depression and at least one past episode of probable PNES, as described by her brother. An argument with her husband apparently precipitated the most recent seizure episode.
Table 2
Psychogenic seizures PNES vs. epileptic seizures: Differences in presentation*
| Clinical features | Psychogenic nonepileptic seizures (PNES) | Epileptic seizures |
|---|---|---|
| Duration | Variable | Short (20 to 70 seconds) |
| Pattern | Variable | Stereotyped |
| Frequency | Variable | Paroxysmal, cluster |
| Cause | Emotional | Organic |
| Occurs in presence of others | Yes | Variable |
| Occurs during sleep | Rare | Yes |
| Incontinence | Rare | Frequent |
| Biting pattern | Tip of tongue, lips | Side of tongue, cheek |
| Convulsion | Bizarre, trashing, sexual movements | Tonic-clonic |
| Injury | Infrequent, mild | Infrequent, severe |
| Pupillary reflex | Normal | Slow, nonreactive |
| Babinski’s reflex | No | Yes, if convulsion |
| Orientation afterwards | Clear | Confused |
| Postictal stupor | Rare | Frequent |
| Serum prolactin | Normal | Elevated (>18 ng/mL in men; >30 ng/mL in nonpregnant women) |
| EEG | Normal | Abnormal or variable |
| * Apply loosely, as the spectrum of seizure types within epilepsy is very large. | ||
| Source: Adapted from reference 13. | ||
PNES features. Clinical features (Table 2)13—although not definitive—can help differentiate PNES from epileptic seizure.1 PNES features to look for include:
- prolonged and bizarre prodrome
- prominent out-of-phase ictal or postictal activity
- clear-cut precipitants, especially in an emotionally charged atmosphere
- lack of falls or injuries
- fluctuating consciousness or vivid recall of details during ictal moments.
PNES’ physical symptoms are not voluntary. Patients often have out-of-phase upper- and lower-extremity movements and vocalization as the event starts, as opposed to about 20 seconds into the event when true tonic-clonic seizure makes the tonic-clonic transformation. Other common features are high-amplitude, forward pelvic thrusting, and lack of rigidity. Weeping during an apparent seizure strongly suggests a nonepileptic event.14
Ictal duration can be useful in assessment. Events that resemble tonic-clonic seizure but continue for >70 seconds or <20 seconds raise suspicion of nonepileptic seizures, although status epilepticus is possible.
Prolactin elevation. Epileptic tonic-clonic and partial complex seizures increase serum prolactin and are most reliable approximately 20 minutes after event onset. Nipple manipulation can spuriously increase serum prolactin, so observe female patients for this behavior if a seizure occurs in your presence. Psychotropics such as chlorpromazine and haloperidol may also elevate serum prolactin.
INVESTIGATIONS
Video EEG recording is available in most neurologic centers and is the investigation of choice. Epileptic seizure is characterized by recruitment of seizure activity in a physiologic distribution and postictal slowing, which would be difficult for a patient to imitate.
Unlike traditional EEG, video EEG shows evidence of electrographic paroxysmal changes immediately before, during, or after an epileptic seizure.15 Seizure presentations without paroxysmal electrographic changes would be considered PNES.
Traditional EEG is not recommended for a PNES workup because seizure activity is not recorded and myogenic infarcts may obscure readings. Moreover, because interictal EEG changes may occur even in patients with PNES, these changes in isolation cannot be interpreted as evidence of epilepsy.16
Laboratory testing includes full blood count, electrolytes, urea and creatinine, urine drug screen, and thyroid and liver function tests, as well as serum levels in patients taking anticonvulsants. These tests may exclude some seizure causes (such as hypokalemia or hypocalcemia with electrolyte disturbances) and provide baseline values for monitoring drug toxicity. Thyroid function testing will rule out hypo- or hyperthyroidism in patients with comorbid depressive or anxiety disorders. Urine drug screen reveals evidence of drug abuse—a possible organic seizure disorder precipitant.
Normal serum prolactin (men: 2 to 18 ng/mL; nonpregnant women: 3 to 30 ng/mL), cortisol (5 to 22 mcg/dL, morning blood specimen), and creatine kinase (50 to 200 U/L) rise substantially after an epileptic—but not psychogenic—seizure.17 Note, however, that creatine kinase and prolactin may be as elevated in PNES as in an epileptic seizure if PNES presents with vigorous muscular activity.18
Psychological testing may help distinguish PNES from epileptic seizure:
- Minnesota Multiphasic Personality Inventory (MMPI) is fairly sensitive and shows statistically significant differences between PNES and epileptic seizures in hypochondriasis, depression, hysteria, and schizophrenia.19
- Washington Psychosocial Seizure Inventory helps identify etiologic subgroups among PNES patients.9
Others. As in Ms. X’s case, CT and MRI for cerebral pathology may not help.20 Provocative techniques21 based on suggestibility also may have little value because PNES can be provoked in patients with documented epileptic seizures. Hypnosis has been used in attempts to demonstrate the psychogenic component of nonepileptic seizures by reversing ictal and postictal amnesia. Patients with PNES seem to be more responsive to hypnosis than those with epileptic seizures.22
CASE CONTINUED: EXPLAINING THE DIAGNOSIS
The psychiatric team concluded that even though Ms. X has a seizure disorder, this particular episode was psychogenic. This conclusion was based on the emotional precipitant, her brother’s collateral history, video EEG recordings, and her history of depression.
The psychiatrist explained to Ms. X that PNES and seizure disorders can coexist and that a PNES diagnosis does not imply that a patient is lying. It simply means that some seizures are precipitated by psychoemotional events.
Unlike some patients with PNES, Ms. X accepted the diagnosis without anger. Because her epilepsy and depression were stable, the psychiatrist did not change her phenytoin or paroxetine dosages. She was discharged, with follow-up care by a psychiatrist and neurologist.
TELLING AND TREATING THE PATIENT
It is important to present a PNES diagnosis with care because some patients react with aggressive denial and suicidal behavior. A patient who believes he or she has been perceived as a liar or “fake” may feel humiliated,9 which is why we prefer the term “PNES” rather than “pseudoseizure.”
PNES treatment calls for collaboration among the neurologist, psychiatrist, psychologist, therapists, support workers, and family. When PNES is clearly the only cause of seizures, avoid treating with anticonvulsants. If PNES coexists with a treated seizure disorder, no change in anticonvulsant dosage is necessary, especially if blood levels are normal.
Target the underlying psychiatric disorder, using medication and cognitive-behavioral therapy as appropriate. Advise patients and families that the seizure-like events may continue for some time but will disappear as the patient develops more-effective and appropriate coping strategies.
Prognosis. Favorable prognostic factors include being female, effective early intervention, normal premorbid psychological make-up, and good family support. Studies have shown that:
- up to 40% of treated PNES patients remained event-free for a median of 5 years.23
- prognosis may depend on spell type (catatonic is more favorable than “thrashing”) and illness duration (<1 year is more favorable than >1 year).24
Related resources
- Riley LT, Roy A. Pseudoseizures. Baltimore: Lippincott, Williams and Wilkins, 1982.
- Epilepsy.com. Psychogenic seizures. Resource for patients. www.epilepsy.com/epilepsy/seizure_psychogenic.html Accessed Oct. 14, 2004.
- Epilepsy Foundation. Information for patients and families. www.epilepsyfoundation.org. Search for nonepileptic seizures. Accessed Oct. 14, 2004.
Drug brand names
- Chlorpromazine • Thorazine
- Haloperidol • Haldol
- Phenytoin • Dilantin
- Paroxetine • Paxil
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Riley TL, Brannon WL, Jr. Recognition of pseudoseizures. Acta Neurol Scand 1991;83(2):129-32.
2. Goodwin J, Simms M, Bergman R. Hysterical seizures: a sequel to incest. Am J Orthopsychiatry 1979;49:698-703.
3. Krawetz P, Fleisher W, Pillay N, et al. Family functioning in subjects with pseudoseizures and epilepsy. J Nerv Ment Dis 2001;189(1):38-43.
4. Gates JR, Luciano D, Devinsky O. The classification and treatment of nonepileptic events. In: Devinsky O, Theodore WH (eds). Epilepsy and behavior. New York: Wiley-Liss, 1991;251-63.
5. Vossler DG. Nonepileptic seizures of physiologic origin. J Epilepsy 1995;8:1-10.
6. Wyllie E, Glazer JP, Benbadis S, et al. Psychiatric features of children and adolescents with pseudoseizures. Arch Pediatr Adolesc Med 1999;153(3):244-8.
7. Luciano D, Perrine K, Clayton B, Devinsky O. Stress as a seizure precipitant and its relationship to ictal focus [abstract]. Epilepsia 1992;33(suppl 3):130.-
8. Betts T. Epilepsy and stress [editorial]. BMJ 1992;305:378-9.
9. Chabolla DR, Krahn LE, So EL, Rummans TA. Psychogenic nonepileptic seizures. Mayo Foundation for Medical Education and Research (symposium, part Ii, vol. 71[5]). May 1996;493-500.
10. Slavney PR. In defense of pseudoseizure (comment). Gen Hosp Psychiatry 1994;16(4):243-5.
11. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association, 2000.
12. Matsuura M, Oana Y, Kato M, et al. A multicenter study on the prevalence of psychiatric disorders among new referrals for epilepsy in Japan. Epilepsia 2003;44(1):107-14.
13. Oommen KJ. Pseudoseizures: Diagnostic guidelines. Comprehensive Oklahoma Program for Epilepsy (COPE), 2000. Available at w3.ouhsc.edu/neuro/division/cope/pseudosz.htm. Accessed Oct. 14, 2004.
14. Walczak TS, Bogolioubov A. Weeping during psychogenic non-epileptic seizures. Epilepsia 1996;37(2):208-10.
15. Mohan KK, Markand ON, Salanova V. Diagnostic utility of video EEG monitoring in paroxysmal events. Acta Neurol Scand 1996;94(5):320-5.
16. Reuber M, Fernandez G, Bauer J, et al. Interictal EEG abnormalities in patients with psychogenic nonepileptic seizures. Epilepsia 2002;43(9):1013-20.
17. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985;35:31-5.
18. Alving J. Serum prolactin levels are elevated also after pseudoepileptic seizures. Seizure 1998;7(2):85-9.
19. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184-7.
20. Lelliott PT, Fenwick P. Cerebral pathology in pseudoseizures. Acta Neurol Scand 1992;85(3):177-80.
21. Guberman A. Psychogenic pseudoseizures in non-epileptic patients. Can J Psychiatry 1982;27:401-4.
22. Kuyk J, Jacobs LD, Aldenkamp AP, et al. Pseudoepileptic seizures: hypnosis as a diagnostic tool. Seizure 1995;4(2):123-8.
23. Holmes GL, Sackellares JC, McKiernan J, et al. Evaluation of childhood pseudoseizures using EEG telemetry and video tape monitoring. J Pediatr 1980;97(4):554-8.
24. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41(10):1330-4.
1. Riley TL, Brannon WL, Jr. Recognition of pseudoseizures. Acta Neurol Scand 1991;83(2):129-32.
2. Goodwin J, Simms M, Bergman R. Hysterical seizures: a sequel to incest. Am J Orthopsychiatry 1979;49:698-703.
3. Krawetz P, Fleisher W, Pillay N, et al. Family functioning in subjects with pseudoseizures and epilepsy. J Nerv Ment Dis 2001;189(1):38-43.
4. Gates JR, Luciano D, Devinsky O. The classification and treatment of nonepileptic events. In: Devinsky O, Theodore WH (eds). Epilepsy and behavior. New York: Wiley-Liss, 1991;251-63.
5. Vossler DG. Nonepileptic seizures of physiologic origin. J Epilepsy 1995;8:1-10.
6. Wyllie E, Glazer JP, Benbadis S, et al. Psychiatric features of children and adolescents with pseudoseizures. Arch Pediatr Adolesc Med 1999;153(3):244-8.
7. Luciano D, Perrine K, Clayton B, Devinsky O. Stress as a seizure precipitant and its relationship to ictal focus [abstract]. Epilepsia 1992;33(suppl 3):130.-
8. Betts T. Epilepsy and stress [editorial]. BMJ 1992;305:378-9.
9. Chabolla DR, Krahn LE, So EL, Rummans TA. Psychogenic nonepileptic seizures. Mayo Foundation for Medical Education and Research (symposium, part Ii, vol. 71[5]). May 1996;493-500.
10. Slavney PR. In defense of pseudoseizure (comment). Gen Hosp Psychiatry 1994;16(4):243-5.
11. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association, 2000.
12. Matsuura M, Oana Y, Kato M, et al. A multicenter study on the prevalence of psychiatric disorders among new referrals for epilepsy in Japan. Epilepsia 2003;44(1):107-14.
13. Oommen KJ. Pseudoseizures: Diagnostic guidelines. Comprehensive Oklahoma Program for Epilepsy (COPE), 2000. Available at w3.ouhsc.edu/neuro/division/cope/pseudosz.htm. Accessed Oct. 14, 2004.
14. Walczak TS, Bogolioubov A. Weeping during psychogenic non-epileptic seizures. Epilepsia 1996;37(2):208-10.
15. Mohan KK, Markand ON, Salanova V. Diagnostic utility of video EEG monitoring in paroxysmal events. Acta Neurol Scand 1996;94(5):320-5.
16. Reuber M, Fernandez G, Bauer J, et al. Interictal EEG abnormalities in patients with psychogenic nonepileptic seizures. Epilepsia 2002;43(9):1013-20.
17. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985;35:31-5.
18. Alving J. Serum prolactin levels are elevated also after pseudoepileptic seizures. Seizure 1998;7(2):85-9.
19. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184-7.
20. Lelliott PT, Fenwick P. Cerebral pathology in pseudoseizures. Acta Neurol Scand 1992;85(3):177-80.
21. Guberman A. Psychogenic pseudoseizures in non-epileptic patients. Can J Psychiatry 1982;27:401-4.
22. Kuyk J, Jacobs LD, Aldenkamp AP, et al. Pseudoepileptic seizures: hypnosis as a diagnostic tool. Seizure 1995;4(2):123-8.
23. Holmes GL, Sackellares JC, McKiernan J, et al. Evaluation of childhood pseudoseizures using EEG telemetry and video tape monitoring. J Pediatr 1980;97(4):554-8.
24. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41(10):1330-4.
Bipolar moving target: Draw a bead on rapid cycling with type-specific therapies
Rapid-cycling bipolar disorder is a moving target, with treatment-resistant depression recurring frequently and alternating with hypomanic/manic episodes (Box).1,2 Can one medication adequately treat these complicated patients, or is combination therapy necessary? If more than one medication is needed, are some combinations more effective than others?
This article attempts to answer these questions by:
- discussing recent treatment trial results
- suggesting an algorithm for managing hypomanic/manic and depressive episodes in rapid-cycling patients with bipolar disorder types I or II.
CLINICAL CHARACTERISTICS
Rapid cycling is associated most consistently with female gender and bipolar II disorder2 (Table); why these two groups are primarily affected is unknown. Results of studies linking rapid cycling with hypothyroidism, gonadal steroid effects, family history, and substance use have been inconsistent and contradictory.2
Age of onset. Recent studies examining bipolar disorder’s age of onset have contradicted earlier rapid-cycling literature. In two large studies, Schneck et al3 and Coryell et al4 found rapid cycling associated with early onset of bipolar illness. The authors note that high rates of rapid cycling in children and adolescents resemble adult rapid cycling and speculate that early-onset bipolar illness might lead to rapid cycling vulnerability.5
Rapid cycling—defined in DSM-IV-TR as four or more depressive, manic, hypomanic, or mixed episodes in the previous 12 months—is considered a longitudinal course specifier for bipolar I or II disorder.1 Episodes must be demarcated by:
- full or partial remission lasting at least 2 months
- or a switch to a mood state of opposite polarity.
Cycling variations include ultra-rapid (1 day to 1 week), ultra-ultra rapid or ultradian (<24 hours), and continuous (no euthymic periods between mood episodes). Rapid cycling occurs in an estimated 15% to 25% of patients with bipolar disorder,2 though psychiatrists in specialty and tertiary referral centers see higher percentages because of the illness’ refractory nature.
Transient vs persistent state. Rapid cycling is thought to be either a transient state in long-term bipolar illness or a more chronic expression of the illness. Several studies6,7 have described rapid cycling as a transient phenomenon, whereas others8-11 have found a more persistent rapid cycling course during follow-up. Interestingly, a recent study11 suggested the mood-cycle pattern may be the most important predictor of rapid cycling. Patients with a depression–hypomania/mania-euthymia course demonstrated more-persistent rapid cycling than did those with a hypomania/mania-depression-euthymia course.
Antidepressants. Antidepressants’ role in initiating or exacerbating rapid cycling also remains unclear. Wehr et al8 found that discontinuing antidepressants contributed to cycling cessation or slowing. However, two prospective studies by Coryell et al4 that controlled for major depression found no association between antidepressant use and rapid cycling.
More recently, Yildiz and Sachs12 found a possible gender-specific relationship between antidepressants and rapid cycling. Women exposed to antidepressants before their first hypomanic/manic episode were more likely to develop rapid cycling than women who were not so exposed. This association was not evident in men.
NO DEFINITIVE CHOICES
Any discussion of treating rapid-cycling bipolar disorder is based on limited data, as few prospective studies of this exclusive cohort exist. Many studies report on mixed cohorts of refractory bipolar patients that include rapid cyclers, but separate analyses of rapid-cycling subgroups are not usually reported. Notable exceptions are recent studies by Calabrese et al, which are discussed below.
Lithium. Dunner and Fieve13 were the first to suggest that rapid-cycling bipolar patients respond poorly to lithium maintenance monotherapy. Later studies, however, suggested that lithium could benefit rapid cyclers, primarily in reducing hypomanic or manic episodes.
Baldessarini et al10 found that lithium was less effective for rapid than nonrapid cyclers only in reducing recurrence of depressive episodes. Kukopulos et al14 reported that lithium response in rapid cyclers increased from 16% to 78% after antidepressants were stopped, suggesting that a positive response to lithium may require more limited antidepressant use (or patients not having been exposed to antidepressants at all).
Thus, lithium prophylaxis has at least partial efficacy in many rapid cyclers, especially when antidepressants are avoided.
Divalproex. As with lithium, divalproex sodium appears more effective in treating and preventing hypomanic/manic episodes than depressive episodes in bipolar patients with rapid-cycling illness. Six open studies showed that patients who had not responded to lithium tended to do better with divalproex.15
Calabrese et al then tested the hypothesis that rapid cycling predicts nonresponse to lithium and positive response to divalproex.16 In a randomized controlled trial, they enrolled 254 recently hypomanic/manic rapid-cycling outpatients in an open-label stabilization phase involving combination lithium and divalproex therapy. Stabilized patients were then randomized to monotherapy with lithium, serum level ≥ 0.8 mEq/L, or divalproex, serum level ≥ 50 mcg/mL. Only 60 patients (24%) met stability criteria for randomization, achieving a persistent bimodal response as measured by continuous weeks of:
- Hamilton depression scale (24-item) score ≤ 20
- Young Mania Rating Scale score ≤ 12.5
- Global Assessment Scale score ≥ 51.
Most nonresponse was attributed to refractory depression.
After 20 months of maintenance therapy, about one-half of patients relapsed on either monotherapy. In the survival analysis, the median time to any mood episode was 45 weeks with divalproex monotherapy and 18 weeks with lithium monotherapy, although this difference was not statistically significant. The small sample size and high dropout rate may have created a false-negative error in this study.
Thus, these data did not show divalproex monotherapy to be more effective than lithium monotherapy in managing rapid-cycling bipolar disorder. The combination proved more effective in treating mania than depression and superior to monotherapy. This finding underscores combination therapy’s importance and the need to use mood stabilizers that also treat the depressed phase of bipolar disorder in rapid cyclers.
Table
Clinical characteristics of rapid cycling
| Prevalence approximately 15% to 25% in patients with bipolar disorder |
| More common in women than men |
| More common with type II than type I bipolar disorder |
| Primarily a depressive disease |
| Low treatment response rates and high recurrence risk |
| Associated with antidepressant use in some cases |
Carbamazepine. Recent data refute earlier reports suggesting that rapid cycling predicted positive response to carbamazepine. Multiple open studies and four controlled studies suggest that carbamazepine—like lithium and divalproex—possesses moderate to marked efficacy in the hypomanic/manic phase but poor to moderate efficacy in the depressed phase of rapid-cycling bipolar disorder.17
Lamotrigine. Lamotrigine is the first mood-stabilizing agent that has shown efficacy in maintenance treatment of bipolar depression and rapid cycling. In a double-blind, prospective, placebo-controlled trial, Calabrese et al18 enrolled 324 rapid-cycling patients with bipolar disorder type I or II in an open-label stabilization phase with lamotrigine. The 182 stabilized patients were then randomly assigned to receive either lamotrigine (mean 288 +/- 94 mg/d) or placebo.
For 6 months, 41% of patients receiving lamotrigine and 26% of those receiving placebo remained stable without relapse (P = 0.03), although the difference was statistically significant only for the bipolar II subtype. Lamotrigine appeared most effective in patients with the biphasic pattern of depression-hypomania/mania-euthymia.
Topiramate. Most studies of topiramate in rapid cycling have been retrospective and/or small add-on studies to existing mood stabilizers, with topiramate use associated with moderately or markedly improved manic symptoms.19 Evidence supports further controlled investigations, particularly because topiramate’s weight-loss effects may help overweight or obese patients.
Gabapentin. Gabapentin’s efficacy in rapid cycling has not been established. Although open-label studies showed a 67% response rate when gabapentin was used as adjunctive therapy, two double-blind, placebocontrolled studies of bipolar patients failed to show efficacy.20,21
Atypical antipsychotics. Five atypical antipsychotics—aripiprazole, olanzapine, quetiapine, risperidone, and ziprasidone—are FDA-approved for treating acute mania. Olanzapine is also indicated for bipolar maintenance treatment and has the most data showing efficacy in rapid cycling:
- In a 3-week, placebo-controlled study of 139 patients with bipolar I acute mania, olanzapine (median modal 15 mg/d) reduced manic symptoms to a statistically significantly extent in the 45 rapid cyclers.22
- A long-term prospective study followed 23 patients—30% of whom were rapid cyclers—who used olanzapine (mean 8.2 mg/d) as an adjunct to mood stabilizers. Manic and depressive symptoms were reduced significantly in the cohort, which was followed for a mean of 303 days.23
- An 8-week, double-blind, placebo-controlled study24 compared olanzapine monotherapy with the olanzapine/fluoxetine combination (OFC) in 833 depressed bipolar I patients, of whom 315 (37%) had rapid cycling. Mean olanzapine dosage was 9.7 mg in monotherapy and 7.4 mg in combination therapy; mean fluoxetine dosage was 39.3 mg.
A follow-up analysis25 showed that rapid cyclers’ depressive symptoms improved rapidly, and this improvement was sustained with OFC but not olanzapine monotherapy. Nonrapid-cycling patients responded to both treatments.
Other atypicals have shown partial efficacy in rapid-cycling bipolar disorder, although the studies have had methodologic limitations. Suppes et al26 conducted the first controlled trial using clozapine as add-on therapy in a 1-year, randomized evaluation of 38 patients with treatment-refractory bipolar disorder. The 21 rapid cyclers received a mean peak of 234 mg/d. Brief Psychiatric Rating Scale and Clinical Global Improvement scores improved significantly overall, but data specific to the rapid-cycling patients were not reported.
Small, open-label studies using risperidone and quetiapine as adjuncts to mood stabilizers have shown modest efficacy in rapid cycling, usually in treating manic symptoms. A recent 8-week, double-blind, placebo-controlled trial of quetiapine in bipolar depression showed promising results, though its efficacy in rapid cycling was not reported.27
RECOMMENDED TREATMENT
Because coincidental cycling may give the false appearance of efficacy in the short term, we recommend that you treat rapid cyclers methodically and judge outcomes over several months or cycle-lengths. A general approach includes:
- identify and treat underlying medical illnesses, such as hypothyroidism
- identify and treat comorbid alcohol/drug abuse
- taper or discontinue cycle-inducing agents such as antidepressants or sympathomimetics
- use standard mood stabilizers and/or atypical antipsychotics alone or in combination (Algorithm).
Algorithm Managing manic and depressive phases of rapid-cycling bipolar disorder
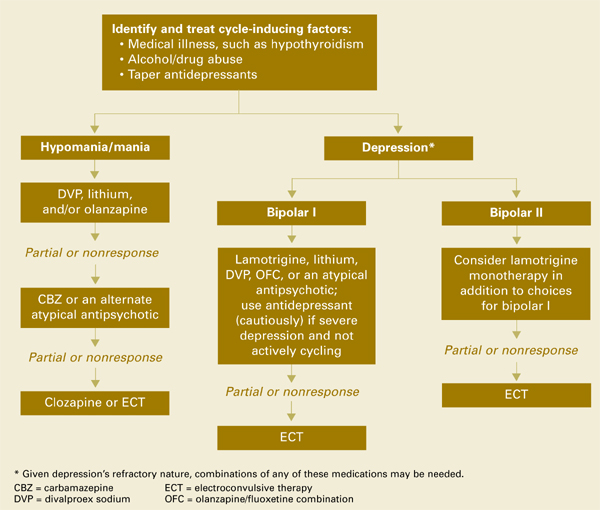
Treating acute mania in rapid-cycling patients is similar to managing this phase in nonrapid cyclers. First-tier therapy includes established mood stabilizers such as lithium, divalproex, or atypical antipsychotics. Carbamazepine is usually considered second-tier because of its effects on other medications via cytochrome P-450 system induction, and limited data exist on oxcarbazepine’s efficacy. Lamotrigine has not been proven effective in acute mania. If monotherapy is ineffective, try combinations of mood stabilizers and/or atypical antipsychotics.
Treating the depressed phase in rapid cyclers is far more difficult than treating acute mania and may depend on bipolar subtype:
- Bipolar I patients likely will require one or more mood stabilizers (such as lithium, divalproex, olanzapine) plus add-on lamotrigine.
- Bipolar II patients may benefit from lamotrigine alone.
- Atypical antipsychotics that have putative antidepressant effects without apparent cycle-accelerating effects may also be considered. At this time, olanzapine has the most data.
Given depression’s refractory nature in rapid-cycling bipolar illness, you may need to combine any of the above medications, try electroconvulsive therapy, or use more-experimental strategies such as:
- omega-3 fatty acids
- donepezil
- pramipexole
- high-dose levothyroxine/T4.
Antidepressants. Before using antidepressants to treat bipolar depression, consider carefully the risk of initiating or exacerbating rapid cycling. No definitive evidence is available to guide your decision.
Likewise, the optimal duration of antidepressant treatment is unclear, although tapering the antidepressant as tolerated may be prudent after depressive symptoms are in remission.
Psychosocial interventions. Finally, don’t overlook psychosocial interventions. Bipolar-specific psychotherapies can enhance compliance, lessen depression, and improve treatment response.28
CONCLUSION
Standard mood stabilizers appear to show partial efficacy in rapid cycling’s hypomanic/manic phase but only modest efficacy in the depressed phase. Lamotrigine appears more-promising in treating depressive than acute manic episodes and may be particularly effective for bipolar II patients. Evidence is growing that atypical antipsychotics also have partial efficacy in treating rapid cyclers, though whether this effect is phase-specific is unclear. As no single agent provides ideal bimodal treatment, combination therapy is recommended.
Related resources
- Bipolar Clinic and Research Program. Massachusetts General Hospital. Includes tools for clinicians and the clinical site for the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). www.manicdepressive.org. Accessed Oct. 14, 2004.
- Goodwin FK, Jamison KR. Manic-depressive illness. New York: Oxford University Press, 1990.
- Marneros A, Goodwin FK (eds). Bipolar disorders: Mixed states, rapid cycling and atypical bipolar disorder. Cambridge, UK: Cambridge University Press (in press).
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Carbatrol, others
- Clozapine • Clozaril
- Donepezil • Aricept
- Divalproex sodium • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid, others
- Lithium • Lithobid, others
- Olanzapine • Zyprexa
- Olanzapine/fluoxetine • Symbyax
- Oxcarbazepine • Trileptal
- Pramipexole • Mirapex
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Topiramate • Topamax
- Ziprasidone • Geodon
Disclosures
Dr. Altman is a speaker for Forest Pharmaceuticals, Janssen Pharmaceutica, AstraZeneca Pharmaceuticals, and Abbott Laboratories.
Dr. Schneck is a consultant to AstraZeneca Pharmaceuticals, UCB Pharma, and Bristol-Myers Squibb Co. and a speaker for AstraZeneca Pharmaceuticals.
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association, 2000.
2. Kupka RW, Luckenbaugh DA, Post RM, et al. Rapid and non-rapid cycling bipolar disorder: a meta-analysis of clinical studies. J Clin Psychiatry 2003;64(12):1483-94.
3. Schneck CD, Miklowitz DJ, Calabrese JR, et al. Phenomenology of rapid cycling bipolar disorder: data from the first 500 participants in the Systematic Treatment Enhancement Program. Am J Psychiatry 2004;161(10):1902-8.
4. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry 2003;60(9):914-20.
5. Findling RL, Gracious BL, McNamara NK, et al. Rapid, continuous cycling and psychiatric comorbidity in pediatric bipolar I disorder. Bipolar Disord 2001;3:202-10.
6. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry 1992;49:126-31.
7. Maj M, Magliano L, Pirozzi R, et al. Validity of rapid cycling as a course specifier for bipolar disorder. Am J Psychiatry 1994;151:1015-19.
8. Wehr TA, Sack DA, Rosenthal NE, Cowdry RW. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry 1988;145:179-84.
9. Bauer MS, Calabrese J, Dunner DL, et al. Multisite data reanalysis of the validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry 1994;151:506-15.
10. Baldessarini RJ, Tondo L, Floris G, Hennen J. Effects of rapid cycling on response to lithium maintenance treatment in 360 bipolar I and II disorder patients. J Affect Disord 2000;61:13-22.
11. Koukopoulos A, Sani G, Koukopoulos AE, et al. Duration and stability of the rapid-cycling course: a long-term personal follow-up of 109 patients. J Affect Disord 2003;73:75-85.
12. Yildiz A, Sachs GS. Do antidepressants induce rapid cycling? A gender-specific association. J Clin Psychiatry 2003;64:814-18.
13. Dunner DL, Fieve RR. Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry 1974;30:229-33.
14. Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic-depressive cycle and changes caused by treatments. Pharmakopsychiatr Neuropsychopharmakol 1980;13:156-67.
15. Calabrese JR, Woyshville MJ, Kimmel SE, Rapport DJ. Predictors of valproate response in bipolar rapid cycling. J Clin Psychopharmacol 1993;13:280-3.
16. Calabrese JR, Shelton M, Rapport DJ, et al. A double-blind 20 month maintenance study of lithium vs. divalproex in rapid-cycling bipolar disorder [presentation]. Pittsburgh, PA: Fifth International Conference on Bipolar Disorder, June 12-14, 2003.
17. Calabrese JR, Bowden C, Woyshville MJ. Lithium and anticonvulsants in the treatment of bipolar disorders. In: Bloom E, Kupfer D (eds). Psychopharmacology: The third generation of progress. New York: Raven Press, 1995;1099-1112.
18. Calabrese JR, Suppes T, Bowden CL, et al. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61(11):841-50.
19. Marcotte D. Use of topiramate, a new anti-epileptic as a mood stabilizer. J Affect Disord 1998;50(2-3):245-51.
20. Pande AC, Crockatt JG, Janney CA, et al. Gabapentin in bipolar disorder: a placebo-controlled trial of adjunctive therapy. Gabapentin Bipolar Disorder Study Group. Bipolar Disord 2000;2(3 pt 2):249-55.
21. Frye MA, Ketter TA, Kimbrell TA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol 2000;20(6):607-14.
22. Sanger TM, Tohen M, Vieta E, et al. Olanzapine in the acute treatment of bipolar I disorder with a history of rapid cycling. J Affect Disord 2003;73:155-61.
23. Calabrese JR, Kasper S, Johnson G, et al. International consensus group on bipolar I depression treatment guidelines. J Clin Psychiatry 2004;65:569-79.
24. Tohen M, Vieta E, Calabrese J, et al. Efficacy of olanzapine and olanzapine-fluoxetine combination in the treatment of bipolar I depression. Arch Gen Psychiatry 2003;60:1079-88.
25. Keck P, Corya S, Andersen SW, et al. Analysis of olanzapine/fluoxetine combination in the treatment of rapid-cycling bipolar depression [presentation]. Boca Raton, FL: New Clinical Drug Evaluation Unit, 2003.
26. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156:1164-9.
27. Calabrese JR, Macfadden W, McCoy R, et al. Double-blind, placebo-controlled study of quetiapine in bipolar depression [presentation]. Phoenix, AZ: New Clinical Drug Evaluation Unit, 2004.
28. Craighead WE, Miklowitz DJ. Psychosocial interventions for bipolar disorder. J Clin Psychiatry 2000;61(suppl 13):58-64.
Rapid-cycling bipolar disorder is a moving target, with treatment-resistant depression recurring frequently and alternating with hypomanic/manic episodes (Box).1,2 Can one medication adequately treat these complicated patients, or is combination therapy necessary? If more than one medication is needed, are some combinations more effective than others?
This article attempts to answer these questions by:
- discussing recent treatment trial results
- suggesting an algorithm for managing hypomanic/manic and depressive episodes in rapid-cycling patients with bipolar disorder types I or II.
CLINICAL CHARACTERISTICS
Rapid cycling is associated most consistently with female gender and bipolar II disorder2 (Table); why these two groups are primarily affected is unknown. Results of studies linking rapid cycling with hypothyroidism, gonadal steroid effects, family history, and substance use have been inconsistent and contradictory.2
Age of onset. Recent studies examining bipolar disorder’s age of onset have contradicted earlier rapid-cycling literature. In two large studies, Schneck et al3 and Coryell et al4 found rapid cycling associated with early onset of bipolar illness. The authors note that high rates of rapid cycling in children and adolescents resemble adult rapid cycling and speculate that early-onset bipolar illness might lead to rapid cycling vulnerability.5
Rapid cycling—defined in DSM-IV-TR as four or more depressive, manic, hypomanic, or mixed episodes in the previous 12 months—is considered a longitudinal course specifier for bipolar I or II disorder.1 Episodes must be demarcated by:
- full or partial remission lasting at least 2 months
- or a switch to a mood state of opposite polarity.
Cycling variations include ultra-rapid (1 day to 1 week), ultra-ultra rapid or ultradian (<24 hours), and continuous (no euthymic periods between mood episodes). Rapid cycling occurs in an estimated 15% to 25% of patients with bipolar disorder,2 though psychiatrists in specialty and tertiary referral centers see higher percentages because of the illness’ refractory nature.
Transient vs persistent state. Rapid cycling is thought to be either a transient state in long-term bipolar illness or a more chronic expression of the illness. Several studies6,7 have described rapid cycling as a transient phenomenon, whereas others8-11 have found a more persistent rapid cycling course during follow-up. Interestingly, a recent study11 suggested the mood-cycle pattern may be the most important predictor of rapid cycling. Patients with a depression–hypomania/mania-euthymia course demonstrated more-persistent rapid cycling than did those with a hypomania/mania-depression-euthymia course.
Antidepressants. Antidepressants’ role in initiating or exacerbating rapid cycling also remains unclear. Wehr et al8 found that discontinuing antidepressants contributed to cycling cessation or slowing. However, two prospective studies by Coryell et al4 that controlled for major depression found no association between antidepressant use and rapid cycling.
More recently, Yildiz and Sachs12 found a possible gender-specific relationship between antidepressants and rapid cycling. Women exposed to antidepressants before their first hypomanic/manic episode were more likely to develop rapid cycling than women who were not so exposed. This association was not evident in men.
NO DEFINITIVE CHOICES
Any discussion of treating rapid-cycling bipolar disorder is based on limited data, as few prospective studies of this exclusive cohort exist. Many studies report on mixed cohorts of refractory bipolar patients that include rapid cyclers, but separate analyses of rapid-cycling subgroups are not usually reported. Notable exceptions are recent studies by Calabrese et al, which are discussed below.
Lithium. Dunner and Fieve13 were the first to suggest that rapid-cycling bipolar patients respond poorly to lithium maintenance monotherapy. Later studies, however, suggested that lithium could benefit rapid cyclers, primarily in reducing hypomanic or manic episodes.
Baldessarini et al10 found that lithium was less effective for rapid than nonrapid cyclers only in reducing recurrence of depressive episodes. Kukopulos et al14 reported that lithium response in rapid cyclers increased from 16% to 78% after antidepressants were stopped, suggesting that a positive response to lithium may require more limited antidepressant use (or patients not having been exposed to antidepressants at all).
Thus, lithium prophylaxis has at least partial efficacy in many rapid cyclers, especially when antidepressants are avoided.
Divalproex. As with lithium, divalproex sodium appears more effective in treating and preventing hypomanic/manic episodes than depressive episodes in bipolar patients with rapid-cycling illness. Six open studies showed that patients who had not responded to lithium tended to do better with divalproex.15
Calabrese et al then tested the hypothesis that rapid cycling predicts nonresponse to lithium and positive response to divalproex.16 In a randomized controlled trial, they enrolled 254 recently hypomanic/manic rapid-cycling outpatients in an open-label stabilization phase involving combination lithium and divalproex therapy. Stabilized patients were then randomized to monotherapy with lithium, serum level ≥ 0.8 mEq/L, or divalproex, serum level ≥ 50 mcg/mL. Only 60 patients (24%) met stability criteria for randomization, achieving a persistent bimodal response as measured by continuous weeks of:
- Hamilton depression scale (24-item) score ≤ 20
- Young Mania Rating Scale score ≤ 12.5
- Global Assessment Scale score ≥ 51.
Most nonresponse was attributed to refractory depression.
After 20 months of maintenance therapy, about one-half of patients relapsed on either monotherapy. In the survival analysis, the median time to any mood episode was 45 weeks with divalproex monotherapy and 18 weeks with lithium monotherapy, although this difference was not statistically significant. The small sample size and high dropout rate may have created a false-negative error in this study.
Thus, these data did not show divalproex monotherapy to be more effective than lithium monotherapy in managing rapid-cycling bipolar disorder. The combination proved more effective in treating mania than depression and superior to monotherapy. This finding underscores combination therapy’s importance and the need to use mood stabilizers that also treat the depressed phase of bipolar disorder in rapid cyclers.
Table
Clinical characteristics of rapid cycling
| Prevalence approximately 15% to 25% in patients with bipolar disorder |
| More common in women than men |
| More common with type II than type I bipolar disorder |
| Primarily a depressive disease |
| Low treatment response rates and high recurrence risk |
| Associated with antidepressant use in some cases |
Carbamazepine. Recent data refute earlier reports suggesting that rapid cycling predicted positive response to carbamazepine. Multiple open studies and four controlled studies suggest that carbamazepine—like lithium and divalproex—possesses moderate to marked efficacy in the hypomanic/manic phase but poor to moderate efficacy in the depressed phase of rapid-cycling bipolar disorder.17
Lamotrigine. Lamotrigine is the first mood-stabilizing agent that has shown efficacy in maintenance treatment of bipolar depression and rapid cycling. In a double-blind, prospective, placebo-controlled trial, Calabrese et al18 enrolled 324 rapid-cycling patients with bipolar disorder type I or II in an open-label stabilization phase with lamotrigine. The 182 stabilized patients were then randomly assigned to receive either lamotrigine (mean 288 +/- 94 mg/d) or placebo.
For 6 months, 41% of patients receiving lamotrigine and 26% of those receiving placebo remained stable without relapse (P = 0.03), although the difference was statistically significant only for the bipolar II subtype. Lamotrigine appeared most effective in patients with the biphasic pattern of depression-hypomania/mania-euthymia.
Topiramate. Most studies of topiramate in rapid cycling have been retrospective and/or small add-on studies to existing mood stabilizers, with topiramate use associated with moderately or markedly improved manic symptoms.19 Evidence supports further controlled investigations, particularly because topiramate’s weight-loss effects may help overweight or obese patients.
Gabapentin. Gabapentin’s efficacy in rapid cycling has not been established. Although open-label studies showed a 67% response rate when gabapentin was used as adjunctive therapy, two double-blind, placebocontrolled studies of bipolar patients failed to show efficacy.20,21
Atypical antipsychotics. Five atypical antipsychotics—aripiprazole, olanzapine, quetiapine, risperidone, and ziprasidone—are FDA-approved for treating acute mania. Olanzapine is also indicated for bipolar maintenance treatment and has the most data showing efficacy in rapid cycling:
- In a 3-week, placebo-controlled study of 139 patients with bipolar I acute mania, olanzapine (median modal 15 mg/d) reduced manic symptoms to a statistically significantly extent in the 45 rapid cyclers.22
- A long-term prospective study followed 23 patients—30% of whom were rapid cyclers—who used olanzapine (mean 8.2 mg/d) as an adjunct to mood stabilizers. Manic and depressive symptoms were reduced significantly in the cohort, which was followed for a mean of 303 days.23
- An 8-week, double-blind, placebo-controlled study24 compared olanzapine monotherapy with the olanzapine/fluoxetine combination (OFC) in 833 depressed bipolar I patients, of whom 315 (37%) had rapid cycling. Mean olanzapine dosage was 9.7 mg in monotherapy and 7.4 mg in combination therapy; mean fluoxetine dosage was 39.3 mg.
A follow-up analysis25 showed that rapid cyclers’ depressive symptoms improved rapidly, and this improvement was sustained with OFC but not olanzapine monotherapy. Nonrapid-cycling patients responded to both treatments.
Other atypicals have shown partial efficacy in rapid-cycling bipolar disorder, although the studies have had methodologic limitations. Suppes et al26 conducted the first controlled trial using clozapine as add-on therapy in a 1-year, randomized evaluation of 38 patients with treatment-refractory bipolar disorder. The 21 rapid cyclers received a mean peak of 234 mg/d. Brief Psychiatric Rating Scale and Clinical Global Improvement scores improved significantly overall, but data specific to the rapid-cycling patients were not reported.
Small, open-label studies using risperidone and quetiapine as adjuncts to mood stabilizers have shown modest efficacy in rapid cycling, usually in treating manic symptoms. A recent 8-week, double-blind, placebo-controlled trial of quetiapine in bipolar depression showed promising results, though its efficacy in rapid cycling was not reported.27
RECOMMENDED TREATMENT
Because coincidental cycling may give the false appearance of efficacy in the short term, we recommend that you treat rapid cyclers methodically and judge outcomes over several months or cycle-lengths. A general approach includes:
- identify and treat underlying medical illnesses, such as hypothyroidism
- identify and treat comorbid alcohol/drug abuse
- taper or discontinue cycle-inducing agents such as antidepressants or sympathomimetics
- use standard mood stabilizers and/or atypical antipsychotics alone or in combination (Algorithm).
Algorithm Managing manic and depressive phases of rapid-cycling bipolar disorder
Treating acute mania in rapid-cycling patients is similar to managing this phase in nonrapid cyclers. First-tier therapy includes established mood stabilizers such as lithium, divalproex, or atypical antipsychotics. Carbamazepine is usually considered second-tier because of its effects on other medications via cytochrome P-450 system induction, and limited data exist on oxcarbazepine’s efficacy. Lamotrigine has not been proven effective in acute mania. If monotherapy is ineffective, try combinations of mood stabilizers and/or atypical antipsychotics.
Treating the depressed phase in rapid cyclers is far more difficult than treating acute mania and may depend on bipolar subtype:
- Bipolar I patients likely will require one or more mood stabilizers (such as lithium, divalproex, olanzapine) plus add-on lamotrigine.
- Bipolar II patients may benefit from lamotrigine alone.
- Atypical antipsychotics that have putative antidepressant effects without apparent cycle-accelerating effects may also be considered. At this time, olanzapine has the most data.
Given depression’s refractory nature in rapid-cycling bipolar illness, you may need to combine any of the above medications, try electroconvulsive therapy, or use more-experimental strategies such as:
- omega-3 fatty acids
- donepezil
- pramipexole
- high-dose levothyroxine/T4.
Antidepressants. Before using antidepressants to treat bipolar depression, consider carefully the risk of initiating or exacerbating rapid cycling. No definitive evidence is available to guide your decision.
Likewise, the optimal duration of antidepressant treatment is unclear, although tapering the antidepressant as tolerated may be prudent after depressive symptoms are in remission.
Psychosocial interventions. Finally, don’t overlook psychosocial interventions. Bipolar-specific psychotherapies can enhance compliance, lessen depression, and improve treatment response.28
CONCLUSION
Standard mood stabilizers appear to show partial efficacy in rapid cycling’s hypomanic/manic phase but only modest efficacy in the depressed phase. Lamotrigine appears more-promising in treating depressive than acute manic episodes and may be particularly effective for bipolar II patients. Evidence is growing that atypical antipsychotics also have partial efficacy in treating rapid cyclers, though whether this effect is phase-specific is unclear. As no single agent provides ideal bimodal treatment, combination therapy is recommended.
Related resources
- Bipolar Clinic and Research Program. Massachusetts General Hospital. Includes tools for clinicians and the clinical site for the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). www.manicdepressive.org. Accessed Oct. 14, 2004.
- Goodwin FK, Jamison KR. Manic-depressive illness. New York: Oxford University Press, 1990.
- Marneros A, Goodwin FK (eds). Bipolar disorders: Mixed states, rapid cycling and atypical bipolar disorder. Cambridge, UK: Cambridge University Press (in press).
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Carbatrol, others
- Clozapine • Clozaril
- Donepezil • Aricept
- Divalproex sodium • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid, others
- Lithium • Lithobid, others
- Olanzapine • Zyprexa
- Olanzapine/fluoxetine • Symbyax
- Oxcarbazepine • Trileptal
- Pramipexole • Mirapex
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Topiramate • Topamax
- Ziprasidone • Geodon
Disclosures
Dr. Altman is a speaker for Forest Pharmaceuticals, Janssen Pharmaceutica, AstraZeneca Pharmaceuticals, and Abbott Laboratories.
Dr. Schneck is a consultant to AstraZeneca Pharmaceuticals, UCB Pharma, and Bristol-Myers Squibb Co. and a speaker for AstraZeneca Pharmaceuticals.
Rapid-cycling bipolar disorder is a moving target, with treatment-resistant depression recurring frequently and alternating with hypomanic/manic episodes (Box).1,2 Can one medication adequately treat these complicated patients, or is combination therapy necessary? If more than one medication is needed, are some combinations more effective than others?
This article attempts to answer these questions by:
- discussing recent treatment trial results
- suggesting an algorithm for managing hypomanic/manic and depressive episodes in rapid-cycling patients with bipolar disorder types I or II.
CLINICAL CHARACTERISTICS
Rapid cycling is associated most consistently with female gender and bipolar II disorder2 (Table); why these two groups are primarily affected is unknown. Results of studies linking rapid cycling with hypothyroidism, gonadal steroid effects, family history, and substance use have been inconsistent and contradictory.2
Age of onset. Recent studies examining bipolar disorder’s age of onset have contradicted earlier rapid-cycling literature. In two large studies, Schneck et al3 and Coryell et al4 found rapid cycling associated with early onset of bipolar illness. The authors note that high rates of rapid cycling in children and adolescents resemble adult rapid cycling and speculate that early-onset bipolar illness might lead to rapid cycling vulnerability.5
Rapid cycling—defined in DSM-IV-TR as four or more depressive, manic, hypomanic, or mixed episodes in the previous 12 months—is considered a longitudinal course specifier for bipolar I or II disorder.1 Episodes must be demarcated by:
- full or partial remission lasting at least 2 months
- or a switch to a mood state of opposite polarity.
Cycling variations include ultra-rapid (1 day to 1 week), ultra-ultra rapid or ultradian (<24 hours), and continuous (no euthymic periods between mood episodes). Rapid cycling occurs in an estimated 15% to 25% of patients with bipolar disorder,2 though psychiatrists in specialty and tertiary referral centers see higher percentages because of the illness’ refractory nature.
Transient vs persistent state. Rapid cycling is thought to be either a transient state in long-term bipolar illness or a more chronic expression of the illness. Several studies6,7 have described rapid cycling as a transient phenomenon, whereas others8-11 have found a more persistent rapid cycling course during follow-up. Interestingly, a recent study11 suggested the mood-cycle pattern may be the most important predictor of rapid cycling. Patients with a depression–hypomania/mania-euthymia course demonstrated more-persistent rapid cycling than did those with a hypomania/mania-depression-euthymia course.
Antidepressants. Antidepressants’ role in initiating or exacerbating rapid cycling also remains unclear. Wehr et al8 found that discontinuing antidepressants contributed to cycling cessation or slowing. However, two prospective studies by Coryell et al4 that controlled for major depression found no association between antidepressant use and rapid cycling.
More recently, Yildiz and Sachs12 found a possible gender-specific relationship between antidepressants and rapid cycling. Women exposed to antidepressants before their first hypomanic/manic episode were more likely to develop rapid cycling than women who were not so exposed. This association was not evident in men.
NO DEFINITIVE CHOICES
Any discussion of treating rapid-cycling bipolar disorder is based on limited data, as few prospective studies of this exclusive cohort exist. Many studies report on mixed cohorts of refractory bipolar patients that include rapid cyclers, but separate analyses of rapid-cycling subgroups are not usually reported. Notable exceptions are recent studies by Calabrese et al, which are discussed below.
Lithium. Dunner and Fieve13 were the first to suggest that rapid-cycling bipolar patients respond poorly to lithium maintenance monotherapy. Later studies, however, suggested that lithium could benefit rapid cyclers, primarily in reducing hypomanic or manic episodes.
Baldessarini et al10 found that lithium was less effective for rapid than nonrapid cyclers only in reducing recurrence of depressive episodes. Kukopulos et al14 reported that lithium response in rapid cyclers increased from 16% to 78% after antidepressants were stopped, suggesting that a positive response to lithium may require more limited antidepressant use (or patients not having been exposed to antidepressants at all).
Thus, lithium prophylaxis has at least partial efficacy in many rapid cyclers, especially when antidepressants are avoided.
Divalproex. As with lithium, divalproex sodium appears more effective in treating and preventing hypomanic/manic episodes than depressive episodes in bipolar patients with rapid-cycling illness. Six open studies showed that patients who had not responded to lithium tended to do better with divalproex.15
Calabrese et al then tested the hypothesis that rapid cycling predicts nonresponse to lithium and positive response to divalproex.16 In a randomized controlled trial, they enrolled 254 recently hypomanic/manic rapid-cycling outpatients in an open-label stabilization phase involving combination lithium and divalproex therapy. Stabilized patients were then randomized to monotherapy with lithium, serum level ≥ 0.8 mEq/L, or divalproex, serum level ≥ 50 mcg/mL. Only 60 patients (24%) met stability criteria for randomization, achieving a persistent bimodal response as measured by continuous weeks of:
- Hamilton depression scale (24-item) score ≤ 20
- Young Mania Rating Scale score ≤ 12.5
- Global Assessment Scale score ≥ 51.
Most nonresponse was attributed to refractory depression.
After 20 months of maintenance therapy, about one-half of patients relapsed on either monotherapy. In the survival analysis, the median time to any mood episode was 45 weeks with divalproex monotherapy and 18 weeks with lithium monotherapy, although this difference was not statistically significant. The small sample size and high dropout rate may have created a false-negative error in this study.
Thus, these data did not show divalproex monotherapy to be more effective than lithium monotherapy in managing rapid-cycling bipolar disorder. The combination proved more effective in treating mania than depression and superior to monotherapy. This finding underscores combination therapy’s importance and the need to use mood stabilizers that also treat the depressed phase of bipolar disorder in rapid cyclers.
Table
Clinical characteristics of rapid cycling
| Prevalence approximately 15% to 25% in patients with bipolar disorder |
| More common in women than men |
| More common with type II than type I bipolar disorder |
| Primarily a depressive disease |
| Low treatment response rates and high recurrence risk |
| Associated with antidepressant use in some cases |
Carbamazepine. Recent data refute earlier reports suggesting that rapid cycling predicted positive response to carbamazepine. Multiple open studies and four controlled studies suggest that carbamazepine—like lithium and divalproex—possesses moderate to marked efficacy in the hypomanic/manic phase but poor to moderate efficacy in the depressed phase of rapid-cycling bipolar disorder.17
Lamotrigine. Lamotrigine is the first mood-stabilizing agent that has shown efficacy in maintenance treatment of bipolar depression and rapid cycling. In a double-blind, prospective, placebo-controlled trial, Calabrese et al18 enrolled 324 rapid-cycling patients with bipolar disorder type I or II in an open-label stabilization phase with lamotrigine. The 182 stabilized patients were then randomly assigned to receive either lamotrigine (mean 288 +/- 94 mg/d) or placebo.
For 6 months, 41% of patients receiving lamotrigine and 26% of those receiving placebo remained stable without relapse (P = 0.03), although the difference was statistically significant only for the bipolar II subtype. Lamotrigine appeared most effective in patients with the biphasic pattern of depression-hypomania/mania-euthymia.
Topiramate. Most studies of topiramate in rapid cycling have been retrospective and/or small add-on studies to existing mood stabilizers, with topiramate use associated with moderately or markedly improved manic symptoms.19 Evidence supports further controlled investigations, particularly because topiramate’s weight-loss effects may help overweight or obese patients.
Gabapentin. Gabapentin’s efficacy in rapid cycling has not been established. Although open-label studies showed a 67% response rate when gabapentin was used as adjunctive therapy, two double-blind, placebocontrolled studies of bipolar patients failed to show efficacy.20,21
Atypical antipsychotics. Five atypical antipsychotics—aripiprazole, olanzapine, quetiapine, risperidone, and ziprasidone—are FDA-approved for treating acute mania. Olanzapine is also indicated for bipolar maintenance treatment and has the most data showing efficacy in rapid cycling:
- In a 3-week, placebo-controlled study of 139 patients with bipolar I acute mania, olanzapine (median modal 15 mg/d) reduced manic symptoms to a statistically significantly extent in the 45 rapid cyclers.22
- A long-term prospective study followed 23 patients—30% of whom were rapid cyclers—who used olanzapine (mean 8.2 mg/d) as an adjunct to mood stabilizers. Manic and depressive symptoms were reduced significantly in the cohort, which was followed for a mean of 303 days.23
- An 8-week, double-blind, placebo-controlled study24 compared olanzapine monotherapy with the olanzapine/fluoxetine combination (OFC) in 833 depressed bipolar I patients, of whom 315 (37%) had rapid cycling. Mean olanzapine dosage was 9.7 mg in monotherapy and 7.4 mg in combination therapy; mean fluoxetine dosage was 39.3 mg.
A follow-up analysis25 showed that rapid cyclers’ depressive symptoms improved rapidly, and this improvement was sustained with OFC but not olanzapine monotherapy. Nonrapid-cycling patients responded to both treatments.
Other atypicals have shown partial efficacy in rapid-cycling bipolar disorder, although the studies have had methodologic limitations. Suppes et al26 conducted the first controlled trial using clozapine as add-on therapy in a 1-year, randomized evaluation of 38 patients with treatment-refractory bipolar disorder. The 21 rapid cyclers received a mean peak of 234 mg/d. Brief Psychiatric Rating Scale and Clinical Global Improvement scores improved significantly overall, but data specific to the rapid-cycling patients were not reported.
Small, open-label studies using risperidone and quetiapine as adjuncts to mood stabilizers have shown modest efficacy in rapid cycling, usually in treating manic symptoms. A recent 8-week, double-blind, placebo-controlled trial of quetiapine in bipolar depression showed promising results, though its efficacy in rapid cycling was not reported.27
RECOMMENDED TREATMENT
Because coincidental cycling may give the false appearance of efficacy in the short term, we recommend that you treat rapid cyclers methodically and judge outcomes over several months or cycle-lengths. A general approach includes:
- identify and treat underlying medical illnesses, such as hypothyroidism
- identify and treat comorbid alcohol/drug abuse
- taper or discontinue cycle-inducing agents such as antidepressants or sympathomimetics
- use standard mood stabilizers and/or atypical antipsychotics alone or in combination (Algorithm).
Algorithm Managing manic and depressive phases of rapid-cycling bipolar disorder
Treating acute mania in rapid-cycling patients is similar to managing this phase in nonrapid cyclers. First-tier therapy includes established mood stabilizers such as lithium, divalproex, or atypical antipsychotics. Carbamazepine is usually considered second-tier because of its effects on other medications via cytochrome P-450 system induction, and limited data exist on oxcarbazepine’s efficacy. Lamotrigine has not been proven effective in acute mania. If monotherapy is ineffective, try combinations of mood stabilizers and/or atypical antipsychotics.
Treating the depressed phase in rapid cyclers is far more difficult than treating acute mania and may depend on bipolar subtype:
- Bipolar I patients likely will require one or more mood stabilizers (such as lithium, divalproex, olanzapine) plus add-on lamotrigine.
- Bipolar II patients may benefit from lamotrigine alone.
- Atypical antipsychotics that have putative antidepressant effects without apparent cycle-accelerating effects may also be considered. At this time, olanzapine has the most data.
Given depression’s refractory nature in rapid-cycling bipolar illness, you may need to combine any of the above medications, try electroconvulsive therapy, or use more-experimental strategies such as:
- omega-3 fatty acids
- donepezil
- pramipexole
- high-dose levothyroxine/T4.
Antidepressants. Before using antidepressants to treat bipolar depression, consider carefully the risk of initiating or exacerbating rapid cycling. No definitive evidence is available to guide your decision.
Likewise, the optimal duration of antidepressant treatment is unclear, although tapering the antidepressant as tolerated may be prudent after depressive symptoms are in remission.
Psychosocial interventions. Finally, don’t overlook psychosocial interventions. Bipolar-specific psychotherapies can enhance compliance, lessen depression, and improve treatment response.28
CONCLUSION
Standard mood stabilizers appear to show partial efficacy in rapid cycling’s hypomanic/manic phase but only modest efficacy in the depressed phase. Lamotrigine appears more-promising in treating depressive than acute manic episodes and may be particularly effective for bipolar II patients. Evidence is growing that atypical antipsychotics also have partial efficacy in treating rapid cyclers, though whether this effect is phase-specific is unclear. As no single agent provides ideal bimodal treatment, combination therapy is recommended.
Related resources
- Bipolar Clinic and Research Program. Massachusetts General Hospital. Includes tools for clinicians and the clinical site for the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). www.manicdepressive.org. Accessed Oct. 14, 2004.
- Goodwin FK, Jamison KR. Manic-depressive illness. New York: Oxford University Press, 1990.
- Marneros A, Goodwin FK (eds). Bipolar disorders: Mixed states, rapid cycling and atypical bipolar disorder. Cambridge, UK: Cambridge University Press (in press).
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Carbatrol, others
- Clozapine • Clozaril
- Donepezil • Aricept
- Divalproex sodium • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid, others
- Lithium • Lithobid, others
- Olanzapine • Zyprexa
- Olanzapine/fluoxetine • Symbyax
- Oxcarbazepine • Trileptal
- Pramipexole • Mirapex
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Topiramate • Topamax
- Ziprasidone • Geodon
Disclosures
Dr. Altman is a speaker for Forest Pharmaceuticals, Janssen Pharmaceutica, AstraZeneca Pharmaceuticals, and Abbott Laboratories.
Dr. Schneck is a consultant to AstraZeneca Pharmaceuticals, UCB Pharma, and Bristol-Myers Squibb Co. and a speaker for AstraZeneca Pharmaceuticals.
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association, 2000.
2. Kupka RW, Luckenbaugh DA, Post RM, et al. Rapid and non-rapid cycling bipolar disorder: a meta-analysis of clinical studies. J Clin Psychiatry 2003;64(12):1483-94.
3. Schneck CD, Miklowitz DJ, Calabrese JR, et al. Phenomenology of rapid cycling bipolar disorder: data from the first 500 participants in the Systematic Treatment Enhancement Program. Am J Psychiatry 2004;161(10):1902-8.
4. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry 2003;60(9):914-20.
5. Findling RL, Gracious BL, McNamara NK, et al. Rapid, continuous cycling and psychiatric comorbidity in pediatric bipolar I disorder. Bipolar Disord 2001;3:202-10.
6. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry 1992;49:126-31.
7. Maj M, Magliano L, Pirozzi R, et al. Validity of rapid cycling as a course specifier for bipolar disorder. Am J Psychiatry 1994;151:1015-19.
8. Wehr TA, Sack DA, Rosenthal NE, Cowdry RW. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry 1988;145:179-84.
9. Bauer MS, Calabrese J, Dunner DL, et al. Multisite data reanalysis of the validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry 1994;151:506-15.
10. Baldessarini RJ, Tondo L, Floris G, Hennen J. Effects of rapid cycling on response to lithium maintenance treatment in 360 bipolar I and II disorder patients. J Affect Disord 2000;61:13-22.
11. Koukopoulos A, Sani G, Koukopoulos AE, et al. Duration and stability of the rapid-cycling course: a long-term personal follow-up of 109 patients. J Affect Disord 2003;73:75-85.
12. Yildiz A, Sachs GS. Do antidepressants induce rapid cycling? A gender-specific association. J Clin Psychiatry 2003;64:814-18.
13. Dunner DL, Fieve RR. Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry 1974;30:229-33.
14. Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic-depressive cycle and changes caused by treatments. Pharmakopsychiatr Neuropsychopharmakol 1980;13:156-67.
15. Calabrese JR, Woyshville MJ, Kimmel SE, Rapport DJ. Predictors of valproate response in bipolar rapid cycling. J Clin Psychopharmacol 1993;13:280-3.
16. Calabrese JR, Shelton M, Rapport DJ, et al. A double-blind 20 month maintenance study of lithium vs. divalproex in rapid-cycling bipolar disorder [presentation]. Pittsburgh, PA: Fifth International Conference on Bipolar Disorder, June 12-14, 2003.
17. Calabrese JR, Bowden C, Woyshville MJ. Lithium and anticonvulsants in the treatment of bipolar disorders. In: Bloom E, Kupfer D (eds). Psychopharmacology: The third generation of progress. New York: Raven Press, 1995;1099-1112.
18. Calabrese JR, Suppes T, Bowden CL, et al. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61(11):841-50.
19. Marcotte D. Use of topiramate, a new anti-epileptic as a mood stabilizer. J Affect Disord 1998;50(2-3):245-51.
20. Pande AC, Crockatt JG, Janney CA, et al. Gabapentin in bipolar disorder: a placebo-controlled trial of adjunctive therapy. Gabapentin Bipolar Disorder Study Group. Bipolar Disord 2000;2(3 pt 2):249-55.
21. Frye MA, Ketter TA, Kimbrell TA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol 2000;20(6):607-14.
22. Sanger TM, Tohen M, Vieta E, et al. Olanzapine in the acute treatment of bipolar I disorder with a history of rapid cycling. J Affect Disord 2003;73:155-61.
23. Calabrese JR, Kasper S, Johnson G, et al. International consensus group on bipolar I depression treatment guidelines. J Clin Psychiatry 2004;65:569-79.
24. Tohen M, Vieta E, Calabrese J, et al. Efficacy of olanzapine and olanzapine-fluoxetine combination in the treatment of bipolar I depression. Arch Gen Psychiatry 2003;60:1079-88.
25. Keck P, Corya S, Andersen SW, et al. Analysis of olanzapine/fluoxetine combination in the treatment of rapid-cycling bipolar depression [presentation]. Boca Raton, FL: New Clinical Drug Evaluation Unit, 2003.
26. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156:1164-9.
27. Calabrese JR, Macfadden W, McCoy R, et al. Double-blind, placebo-controlled study of quetiapine in bipolar depression [presentation]. Phoenix, AZ: New Clinical Drug Evaluation Unit, 2004.
28. Craighead WE, Miklowitz DJ. Psychosocial interventions for bipolar disorder. J Clin Psychiatry 2000;61(suppl 13):58-64.
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association, 2000.
2. Kupka RW, Luckenbaugh DA, Post RM, et al. Rapid and non-rapid cycling bipolar disorder: a meta-analysis of clinical studies. J Clin Psychiatry 2003;64(12):1483-94.
3. Schneck CD, Miklowitz DJ, Calabrese JR, et al. Phenomenology of rapid cycling bipolar disorder: data from the first 500 participants in the Systematic Treatment Enhancement Program. Am J Psychiatry 2004;161(10):1902-8.
4. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry 2003;60(9):914-20.
5. Findling RL, Gracious BL, McNamara NK, et al. Rapid, continuous cycling and psychiatric comorbidity in pediatric bipolar I disorder. Bipolar Disord 2001;3:202-10.
6. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry 1992;49:126-31.
7. Maj M, Magliano L, Pirozzi R, et al. Validity of rapid cycling as a course specifier for bipolar disorder. Am J Psychiatry 1994;151:1015-19.
8. Wehr TA, Sack DA, Rosenthal NE, Cowdry RW. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry 1988;145:179-84.
9. Bauer MS, Calabrese J, Dunner DL, et al. Multisite data reanalysis of the validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry 1994;151:506-15.
10. Baldessarini RJ, Tondo L, Floris G, Hennen J. Effects of rapid cycling on response to lithium maintenance treatment in 360 bipolar I and II disorder patients. J Affect Disord 2000;61:13-22.
11. Koukopoulos A, Sani G, Koukopoulos AE, et al. Duration and stability of the rapid-cycling course: a long-term personal follow-up of 109 patients. J Affect Disord 2003;73:75-85.
12. Yildiz A, Sachs GS. Do antidepressants induce rapid cycling? A gender-specific association. J Clin Psychiatry 2003;64:814-18.
13. Dunner DL, Fieve RR. Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry 1974;30:229-33.
14. Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic-depressive cycle and changes caused by treatments. Pharmakopsychiatr Neuropsychopharmakol 1980;13:156-67.
15. Calabrese JR, Woyshville MJ, Kimmel SE, Rapport DJ. Predictors of valproate response in bipolar rapid cycling. J Clin Psychopharmacol 1993;13:280-3.
16. Calabrese JR, Shelton M, Rapport DJ, et al. A double-blind 20 month maintenance study of lithium vs. divalproex in rapid-cycling bipolar disorder [presentation]. Pittsburgh, PA: Fifth International Conference on Bipolar Disorder, June 12-14, 2003.
17. Calabrese JR, Bowden C, Woyshville MJ. Lithium and anticonvulsants in the treatment of bipolar disorders. In: Bloom E, Kupfer D (eds). Psychopharmacology: The third generation of progress. New York: Raven Press, 1995;1099-1112.
18. Calabrese JR, Suppes T, Bowden CL, et al. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61(11):841-50.
19. Marcotte D. Use of topiramate, a new anti-epileptic as a mood stabilizer. J Affect Disord 1998;50(2-3):245-51.
20. Pande AC, Crockatt JG, Janney CA, et al. Gabapentin in bipolar disorder: a placebo-controlled trial of adjunctive therapy. Gabapentin Bipolar Disorder Study Group. Bipolar Disord 2000;2(3 pt 2):249-55.
21. Frye MA, Ketter TA, Kimbrell TA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol 2000;20(6):607-14.
22. Sanger TM, Tohen M, Vieta E, et al. Olanzapine in the acute treatment of bipolar I disorder with a history of rapid cycling. J Affect Disord 2003;73:155-61.
23. Calabrese JR, Kasper S, Johnson G, et al. International consensus group on bipolar I depression treatment guidelines. J Clin Psychiatry 2004;65:569-79.
24. Tohen M, Vieta E, Calabrese J, et al. Efficacy of olanzapine and olanzapine-fluoxetine combination in the treatment of bipolar I depression. Arch Gen Psychiatry 2003;60:1079-88.
25. Keck P, Corya S, Andersen SW, et al. Analysis of olanzapine/fluoxetine combination in the treatment of rapid-cycling bipolar depression [presentation]. Boca Raton, FL: New Clinical Drug Evaluation Unit, 2003.
26. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156:1164-9.
27. Calabrese JR, Macfadden W, McCoy R, et al. Double-blind, placebo-controlled study of quetiapine in bipolar depression [presentation]. Phoenix, AZ: New Clinical Drug Evaluation Unit, 2004.
28. Craighead WE, Miklowitz DJ. Psychosocial interventions for bipolar disorder. J Clin Psychiatry 2000;61(suppl 13):58-64.
Risk taking adolescents: When and how to intervene
Boys will be boys” and other platitudes may condone adolescent reckless driving, substance use, or sexual promiscuity—but to write off dangerous behavior as normal would be a mistake. Because adolescent impulsivity and sensation-seeking may have physiologic as well as emotional causes,1,2 excessive risk taking may be treatable.
This article discusses the neurobiology of adolescent risk taking, suggests how to determine when such behavior may be pathologic, and offers a treatment approach for at-risk teens and their parents.
CASE: ‘WHAT’S WRONG WITH OUR SON?’
Josh, age 17, is brought to the adolescent psychiatry clinic by his distraught parents, who report their son has undergone a “personality change” over the past 2 years. They recall that he was respectful, studious, and soft-spoken until age 15. Since then, he has been skipping school, staying out late at night with his friends, and “obsessed” with TV poker games.
His parents recently discovered he has been gambling for money, which greatly upsets them. They also found a pack of cigarettes in their son’s car and are concerned that he might be using other substances. What finally prompted the psychiatric visit was Josh’s recent traffic citation for driving 25 miles over the speed limit.
CAUSES OF RISK TAKING
Normal development. In the absence of psychopathology, adolescent risk taking appears to be a normal development stage that is vital to successful transition to adulthood. This assumes that adolescents such as Josh learn to moderate their behavior and avoid long-term negative consequences.
Impulsivity and sensation seeking are recognized as key factors in adolescent risk taking Box 1.1-4 Apparently, these traits result primarily from incomplete neural circuit maturation. Adolescent brain regions involved in impulsivity and risk taking are also involved in reward, and these centers exhibit an exaggerated response to stimuli.5 This amplified response may help explain an adolescent’s propensity for risky behavior.
Despite potential hazards, adolescent risk taking may confer benefits. In taking risks, adolescents:
- explore adult behavior
- learn to accomplish increasingly difficult developmental tasks
- reinforce their self-esteem.
Adolescent risk-takers have been found to be more self-confident, to feel more accepted, and to be better liked than their more-cautious peers.6
Psychiatric comorbidity. Excessive risk taking can be associated with psychiatric illness, including bipolar mania, psychosis, substance abuse, and impulse control disorders. Individuals with borderline personality and other cluster B disorders have marked impulsivity and thus are prone to risky behavior.
Teens with attention-deficit/hyperactivity disorder (ADHD), conduct disorder, and oppositional-defiant disorder (ODD) also tend to exhibit high impulsivity.
Alcohol. 40% of adult alcoholics report having had their first alcoholism-related symptoms between ages 15 and 19.1
Gambling. 10% to 14% of adolescents engage in problem or pathologic gambling, and gambling typically begins at age 12.2
Automobile crashes are the leading cause of death among North American adolescents; both sexes ages 16 to 20 are at least twice as likely to be in a motor vehicle accident as are drivers ages 20 to 50.3
STDs. Each year, 3 million U.S. adolescents contract a sexually transmitted disease (STD). HIV infection is the seventh leading cause of death for Americans ages 13 to 24.4
Sexual activity. Adolescents are more likely than adults to engage in impulsive sexual behavior, to have multiple partners, and to fail to use contraceptives. Younger teens (ages 12 to 14) are more likely to engage in risky sexual practices than older teens (ages 16 to 19).4
CASE CONTINUED: JUST ‘HAVING FUN’
When interviewed alone, Josh admits to “occasional” truancy, which he attributes to being “bored” with school and wanting to spend time with his friends “doing fun stuff, like going to the beach.” He admits to gambling for money and smoking a half-pack of cigarettes daily, as well as drinking beer and smoking marijuana “a few times a week.”
Josh says he engages in these activities “because they’re fun,” and states he is annoyed by his parents’ concern. He blames the speeding ticket on “not paying attention.” He admits to drinking and driving but claims he always feels “in control.”
He also reports he has been sexually active since age 16 and often has had unprotected intercourse. When asked if he is concerned that he might contract a sexually transmitted disease or impregnate his partner, Josh appears ambivalent.
IMPULSIVITY IN ADOLESCENCE
Josh is engaging in numerous impulsive behaviors. Adolescents generally are more impulsive than adults, as demonstrated by their significantly higher impulsivity scores on standardized tests.7 Furthermore, as measured by improved response inhibition (go/no go tasks), the level of adolescent impulsivity is inversely related to age.8
Problem behavior syndrome. High impulsivity is predictive of problem gambling, drug use, and risky driving and sexual practices later in life.1,2,9-11 Adolescents with what some authors describe as a “problem behavior syndrome” engage in behaviors—such as substance use, risky sexual behavior,12 gambling,13 and reckless driving14—that share a common trend toward impulsivity.
Impaired data processing. Decision making has been proposed as a three-part cognitive process:
- accumulating sensory input
- processing this input and formulating a behavioral response appropriate to the situation
- planning and implementing the resultant motor output.2
Impulsivity is believed to result from impaired ability of the brain to process accumulated information or to formulate a response to it—or both. Impulsive individuals thus experience impaired data processing, in which they:
- misjudge the likely risk of a given action or overestimate their ability to accomplish a task
- show impaired response inhibition and thus find it difficult to resist an impulse to participate in a given activity.
Sensation seeking. Adolescents who exhibit risk-taking behavior may wish to experience the thrill of the behavior (sensation or novelty seeking). Alcoholic or drug-dependent individuals and those who engage in pathologic gambling or take chances while driving also demonstrate significantly impaired decision making.15-17 Adolescents who engage in these and other problem behaviors have similarly scored high on sensation-seeking scales.10,18
DECISION-MAKING BIOLOGY
At least four neural circuits process decisions, weighing the risks and benefits of a given situation and formulating a response. These circuits are:
- prefrontal cortices, including orbitofrontal, dorsolateral, and ventromedial
- ventral striatum, including the nucleus accumbens
- thalamus
- monoaminergic brainstem nuclei (ventral tegmental area [VTA] and raphe nuclei).19
Functional imaging studies—including MRI and PET, EEG, and electrophysiology—have confirmed that these four brain regions are integral to response inhibition and show abnormal activity in impulsive individuals.20,21 Indeed, prefrontal cortex damage has been extensively documented to cause marked impulsivity, poor decision making, and an increased propensity for substance abuse and dependency.1
Functional imaging studies also have shown that adolescents appear to use these neural regions inefficiently during decision making. Extensive areas of the involved brain regions are activated in individuals ages 8 to 20, whereas only focal activation occurs in adults.22
Dopamine. The nuclear accumbens (NA) plays an important role in processing afferent excitatory glutamatergic projections and then instigating the given response.23 Dopamine is released in the NA in response to a long list of stimuli, including:
- exposure to substances
- natural rewards such as food or sex
- stimulating situations, such as playing video games, gambling, or thrill seeking.2
Novel experiences and rewards that are delivered erratically cause an elevated dopamine release in the NA. This may explain, in part, the excitement one gains from activities with unpredictable outcomes, such as gambling, bungee jumping, parachuting, white-water rafting, or taking risks while driving.
As rewarding stimuli are re-experienced, dopamine response accelerates in magnitude, and the reward becomes progressively stronger as the experience is repeated. This repeated dopamine release in the NA changes the cellular proteins involved in signaling pathways thought to be associated with the transition from impulsive to compulsive behavior.2 Therefore, addiction may be caused by neurocircuitry changes induced by repeated dopamine release. Similarly, persons who engage in impulsive behavior may have hypersensitive dopamine-related reward circuitry, which may, in part, explain their predisposition to addictive behavior.
Serotonin. Serotonergic projections originate mainly in the midbrain’s raphe nuclei and are transmitted to the ventral tegmental area, NA, prefrontal cortex, amygdala, and hippocampus.1 Abnormal serotonin levels have been implicated in impaired impulse control2 and decreased CNS serotonin in impulsive behavior.24
Functional brain imaging studies have shown reduced serotonin neurotransmission in highly impulsive individuals, compared with normal controls.25 Administering serotonergic agents seems to markedly decrease impulsive behavior.26
Activity within this network is modulated by excitatory glutamatergic transmission and inhibitory GABAergic transmission within the cortices and by dopaminergic and serotonergic transmission within the VTA and raphe nuclei, respectively.2,20 Although all of these neurotransmitters have been implicated in impulsivity, dopamine and serotonin have been studied most extensively (box 2).1,2,23-26
CASE CONTINUED: PSYCHIATRIC WORKUP
Josh clearly is engaged in worrisome behavior with potential long-term consequences. To evaluate him for underlying psychopathology, the psychiatrist used a structured psychiatric exam, Minnesota Multi-phasic Personality Inventory (MMPI), and SNAP-IV Rating Scale for ADHD (see Related resources). Josh endorsed some depressive symptoms—which were also evident on the MMPI—but did not meet DSM-IVTR criteria for major depressive disorder. Neither were his symptoms diagnostic for any other Axis I or Axis II disorder.
Given the risk of harm and likelihood of worsening behavior over time, the psychiatrist schedules Josh for weekly psychotherapy and possible medication.
Psychosocial interventions are discussed with Josh’s parents, including monitoring his activities, restricting access to peers who have been a poor influence, reinforcing good behavior, and enlisting help from teachers and his friends’ parents. The effect of these interventions is to be explored in follow-up visits.
After months or years of conflict with their child, the parents of an adolescent with severe risk-taking behavior are often distraught and frustrated. You can comfort them by explaining:
- the biology of adolescent risk taking
- how you will treat such behavior in their adolescent
- and their role in the treatment plan.
Often the child’s behaviors have weakened their marriage, given adolescents’ tendency to divide and manipulate their parents. To help them set and maintain limits in the face of their child’s hostility:
Educate them to communicate with each other, to maintain a united front, and to set firm limits for their adolescent. For example, recommend that they:
- forbid cell phone use while the adolescent is driving
- limit the number of passengers allowed in the adolescent’s car to reduce distractions
- reduce the amount of money and free time available to the adolescent.
Counsel them that they are unlikely to receive the child’s respect or affection in the short term. Reassure them, however, that the child will thank them for their firm guidance after he or she matures to adulthood.
DEFINING DEGREES OF RISK
Although no criteria differentiate “normal” from “pathologic” risk taking, the definition of taking a risk implies potential adverse consequences. In evaluating the impulsive adolescent, it is important to determine which behaviors:
- can be instructive and promote maturation
- fall outside normal adolescent behavior and/or carry potentially severe outcomes.
Acceptable. Risk taking is acceptable if the potential adverse outcome is relatively benign and the adolescent is likely to learn from the experience. For example, driving 10 miles over the speed limit and receiving a ticket can lead to stricter observance of the speed limit.
Pathologic. Josh clearly exhibits risky behaviors that one would reasonably consider “pathologic,” as they carry potentially severe consequences that exceed any possible developmental gain. For example, drinking and driving can result in a DUI citation and/or a motor vehicle accident with physical injuries or death.
TREATMENT OPTIONS
Psychiatric comorbidity. When you evaluate an adolescent engaged in excessive risk taking, consider Axis I and II disorders characterized by marked impulsivity. If the patient meets diagnostic criteria for a psychopathology such as bipolar disorder or ADHD, treating the underlying condition will likely improve impulsivity.
Recommended approach. Even without an Axis I or Axis II disorder, adolescents who engage in pathologic risky behavior may benefit from psychosocial interventions (Box 3), psychotherapy, and perhaps medication.
Because very little evidence supports using psychotropics to treat pathologically impulsive adolescents, we recommend that you:
- first try psychosocial interventions and psychotherapy
- reserve medications for patients who do not respond adequately to nondrug approaches and engage in impulsive behaviors that pose a high risk for grave consequences.
Psychotherapy can be effective once the adolescent and clinician form a therapeutic alliance. Because Josh—like other such teens—will likely view his psychiatrist as “just another adult lecturing me on what to do,” focus first on establishing rapport by:
- getting to know him
- helping him feel at ease
- showing interest in his thoughts and empathy towards his concerns and complaints
- discussing anything but the reason his parents brought him to your office.
After you establish an alliance, focus therapy on helping the adolescent gain insight into his or her dangerous behaviors and their consequences. To illustrate to Josh the potential consequences of his behaviors, for example, you might introduce him to:
- someone disabled in a motor vehicle accident
- an HIV-positive activist
- a recovering alcoholic
- a long-time smoker with severe chronic obstructive pulmonary disease.
At-risk adolescents also could be encouraged to complete an educational program that teaches alternate activities for sensation seeking (such as skiing instead of high-speed driving).
Medication. Although the monoaminergic systems are known to modulate impulsive behavior, few studies have examined using medications to treat risk-taking adolescents, and no drugs are FDA-approved for this indication.
SSRIs. Selective serotonin reuptake inhibitors such as fluoxetine, sertraline, or escitalopram might be useful for treating excessive adolescent risk taking. A preliminary study with paroxetine—an SSRI not recommended for children and adolescents—suggests this class of antidepressants may help reduce impulsivity.26 In the absence of data specific to risk-taking behavior, we recommend using SSRI dosages similar to those used to treat mood disorders in adolescents.
Clomipramine acts mainly on the serotonin receptor, preventing serotonin reuptake in a manner similar to an SSRI. Because it has the greatest serotonergic effect in its drug class, clomipramine is the only tricyclic proven effective in obsessive-compulsive disorder.27 Although no data have shown that clomipramine affects impulsivity, it theoretically could be effective because of its effect on serotonin.
Divalproex sodium has been shown to effectively treat impulsivity, particularly in patients with autism spectrum disorders, intermittent explosive disorder, schizophrenia, borderline personality disorder, and bipolar disorder.27-30 As an off-label use, one could consider trying this agent in an adolescent with pathologic risk-taking behavior. Use the same dosages and obtain routine labs as indicated for adolescents with other disorders.
Adherence. Like Josh, adolescents who engage in high-risk behaviors often do not recognize their pathology and resist psychiatric intervention. Getting them to take medication or participate in psychotherapy can be quite difficult.
Adolescents are far more likely to adhere to treatment if you develop a rapport with them and they trust you. As psychotherapy and psychosocial interventions progress, patients become more likely to gain insight into their conditions and become more adherent.
Other options to encourage adherence include having the parent:
- administer the medication and ensure that the patient swallows it
- use rewards to reinforce the adolescent’s good behavior and adherence to treatment.
Follow up weekly with patients such as Josh who exhibit high-risk behaviors and require psychotherapy and medication. Follow less-acute patients 2 weeks after the initial evaluation, then monthly if they are responding to medication.
- Strauch B. The primal teen: what the new discoveries about the teenage brain tell us about our kids. New York: Doubleday, 2004.
- SNAP-IV Rating Scale to screen for attention-deficit/hyperactivity disorder. Is your child really ADD/ADHD? www.drbiofeedback.com. Accessed Sept. 8, 2004.
- Focus Adolescent Services. Resources and information for families with adolescent behavior problems, including high-risk behavior. http://www.focusas.com/BehavioralDisorders.html. Accessed Aug. 26, 2004.
Drug brand names
- Clomipramine • Anafranil
- Divalproex sodium • Depakote
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Sertraline • Zoloft
Disclosure
Dr. Husted reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr Shapira receives grant or research support from Abbott Laboratories, Janssen Pharmaceutica, Ortho-McNeil Pharmaceutical, Bristol-Myers Squibb Co., Eli Lilly and Co., and Pfizer Inc. He is a speaker for AstraZeneca Pharmaceuticals, Forest Laboratories, and Ortho-McNeil Pharmaceutical, Inc.
1. Chambers RA, Taylor JR, Potenza MN. Developmental neurocircuitry of motivation in adolescence: a critical period of addiction vulnerability. Am J Psychiatry 2003;160:1041-52.
2. Chambers RA, Potenza MN. Neurodevelopment, impulsivity, and adolescent gambling. J Gambl Stud 2003;19:53-84.
3. Turner C, McClure R. Age and gender differences in risk taking behavior as an explanation for high incidence of motor vehicle crashes as a driver in young males. Inj Control Saf Promot 2003;10:123-30.
4. Bachanas PJ, Morris MK, Lewis-Gess JK, et al. Psychological adjustment, substance use, HIV knowledge, and risky sexual behavior in at-risk minority females: developmental differences during adolescence. J Pediatr Psych 2002;27:373-84.
5. Goldstein RZ, Volkow ND. Drug addiction and its underlying neuro- biological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry 2002;159:1642-52.
6. Spear LP. The adolescent brain and age-related behavioral manifestations. Neurosci Biobehav Rev 2000;24:417-63.
7. Clayton R. Transitions in drug use: risk and protective factors. In: Glantz M, Pickens R (eds). Vulnerability to drug abuse. Washington, DC: American Psychological Association, 1992;15-52.
8. Tamm L, Menon V, Reiss AL. Maturation of brain function associated with response inhibition. J Am Acad Child Adolesc Psychiatry 2002;41:1231-8.
9. Jonah BA. Sensation seeking and risky driving: a review and synthesis of the literature. Accid Anal Prev 1997;29:651-6.
10. Vitaro F, Arseneault L, Tremblay RE. Dispositional predictors of problem gambling in male adolescents. Am J Psychiatry 1997;154:1769-70.
11. Malow RM, Devieux JG, Jennings T, et al. Substance-abusing adolescents at varying levels of HIV risk: psychosocial characteristics, drug use, and sexual behavior. J Subst Abuse 2001;13:103-17.
12. Donovan JE, Jessor R, Costa FM. Syndrome of problem behavior in adolescence: a replication. J Consult Clin Psychol 1988;56:762-5.
13. Vitaro F, Brendgen M, Ladouceur R, Tremblay RE. Gambling, delinquency, and drug use during adolescence: mutual influences and common risk factors. J Gambl Stud 2001;17:171-90.
14. Shope JT, Bingham CR. Drinking-driving as a component of problem driving and problem behavior in young adults. J Stud Alcohol 2002;63(1):24-33.
15. Potenza MN. The neurobiology of pathological gambling. Semin Clin Neuropsychiatry 2001;6:217-26.
16. Petry NM. Substance abuse, pathological gambling, and impulsiveness. Drug Alcohol Depend 2001;63:29-38.
17. Bechara A. Neurobiology of decision-making: risk and reward. Semin Clin Neuropsychiatry 2001;6:205-16.
18. Zuckerman M. Sensation seeking: the balance between risk and reward. In: Lipsitt LP, Mitnick LL (eds). Self-regulatory behavior and risk taking. Norwood, NJ: Ablex Publishing; 1992;143-52.
19. Masterman DL, Cummings JL. Frontal-subcortical circuits: the anatomical basis of executive, social and motivational behaviors. J Psychopharmacol 1997;11:107-14.
20. Horn NR, Dolan M, Elliot R, et al. Response inhibition and impulsivity: an fMRI study. Neuropsychologia 2003;41:1959-66.
21. Fallgatter AJ, Herrmann MJ. Electrophysiological assessment of impulsive behavior in healthy subjects. Neuropsychologia 2001;39:328-33.
22. Booth JR, Burman DD, Meyer JR, et al. Neural development of selective attention and response inhibition. Neuroimage 2003;20:737-51.
23. O’Donnell P, Greene J, Pabello N, et al. Modulation of cell firing in the nucleus accumbens. Ann NY Acad Sci 1999;877:157-75.
24. Nordin C, Eklundh T. Altered CSF 5-HIAA disposition in pathologic male gamblers. CNS Spectrums 1999;4:25-33.
25. Leyton M, Okazawa H, Diksic M, et al. Brain regional alpha-[11C] methyl-L-tryptophan trapping in impulsive subjects with borderline personality disorder. Am J Psychiatry 2001;158:775-82.
26. Cherek DR, Lane SD, Pietras CJ, Steinberg JL. Effects of chronic paroxetine administration on measures of aggressive and impulsive responses of adult males with a history of conduct disorder. Psychopharmacology (Berl) 2002;159:266-74.
27. Geller DA, Biederman J, Stewart SE, et al. Which SSRI? A meta-analysis of pharmacotherapy trials in pediatric obsessive-compulsive disorder. Am J Psychiatry 2003;160:1919-28.
28. Hollander E, Allen A, Lopez RP, et al. A preliminary double-blind, placebo-controlled trial of divalproex sodium in borderline personality disorder. J Clin Psychiatry 2001;62(3):199-203.
29. Swann AC. Treatment of aggression in patients with bipolar disorder. J Clin Psychiatry 1999;60(suppl 15):25-8.
30. Hollander E, Dolgoff-Kaspar R, Cartwright C, et al. An open trial of divalproex sodium in autism spectrum disorders. J Clin Psychiatry 2001;62:530-4.
Boys will be boys” and other platitudes may condone adolescent reckless driving, substance use, or sexual promiscuity—but to write off dangerous behavior as normal would be a mistake. Because adolescent impulsivity and sensation-seeking may have physiologic as well as emotional causes,1,2 excessive risk taking may be treatable.
This article discusses the neurobiology of adolescent risk taking, suggests how to determine when such behavior may be pathologic, and offers a treatment approach for at-risk teens and their parents.
CASE: ‘WHAT’S WRONG WITH OUR SON?’
Josh, age 17, is brought to the adolescent psychiatry clinic by his distraught parents, who report their son has undergone a “personality change” over the past 2 years. They recall that he was respectful, studious, and soft-spoken until age 15. Since then, he has been skipping school, staying out late at night with his friends, and “obsessed” with TV poker games.
His parents recently discovered he has been gambling for money, which greatly upsets them. They also found a pack of cigarettes in their son’s car and are concerned that he might be using other substances. What finally prompted the psychiatric visit was Josh’s recent traffic citation for driving 25 miles over the speed limit.
CAUSES OF RISK TAKING
Normal development. In the absence of psychopathology, adolescent risk taking appears to be a normal development stage that is vital to successful transition to adulthood. This assumes that adolescents such as Josh learn to moderate their behavior and avoid long-term negative consequences.
Impulsivity and sensation seeking are recognized as key factors in adolescent risk taking Box 1.1-4 Apparently, these traits result primarily from incomplete neural circuit maturation. Adolescent brain regions involved in impulsivity and risk taking are also involved in reward, and these centers exhibit an exaggerated response to stimuli.5 This amplified response may help explain an adolescent’s propensity for risky behavior.
Despite potential hazards, adolescent risk taking may confer benefits. In taking risks, adolescents:
- explore adult behavior
- learn to accomplish increasingly difficult developmental tasks
- reinforce their self-esteem.
Adolescent risk-takers have been found to be more self-confident, to feel more accepted, and to be better liked than their more-cautious peers.6
Psychiatric comorbidity. Excessive risk taking can be associated with psychiatric illness, including bipolar mania, psychosis, substance abuse, and impulse control disorders. Individuals with borderline personality and other cluster B disorders have marked impulsivity and thus are prone to risky behavior.
Teens with attention-deficit/hyperactivity disorder (ADHD), conduct disorder, and oppositional-defiant disorder (ODD) also tend to exhibit high impulsivity.
Alcohol. 40% of adult alcoholics report having had their first alcoholism-related symptoms between ages 15 and 19.1
Gambling. 10% to 14% of adolescents engage in problem or pathologic gambling, and gambling typically begins at age 12.2
Automobile crashes are the leading cause of death among North American adolescents; both sexes ages 16 to 20 are at least twice as likely to be in a motor vehicle accident as are drivers ages 20 to 50.3
STDs. Each year, 3 million U.S. adolescents contract a sexually transmitted disease (STD). HIV infection is the seventh leading cause of death for Americans ages 13 to 24.4
Sexual activity. Adolescents are more likely than adults to engage in impulsive sexual behavior, to have multiple partners, and to fail to use contraceptives. Younger teens (ages 12 to 14) are more likely to engage in risky sexual practices than older teens (ages 16 to 19).4
CASE CONTINUED: JUST ‘HAVING FUN’
When interviewed alone, Josh admits to “occasional” truancy, which he attributes to being “bored” with school and wanting to spend time with his friends “doing fun stuff, like going to the beach.” He admits to gambling for money and smoking a half-pack of cigarettes daily, as well as drinking beer and smoking marijuana “a few times a week.”
Josh says he engages in these activities “because they’re fun,” and states he is annoyed by his parents’ concern. He blames the speeding ticket on “not paying attention.” He admits to drinking and driving but claims he always feels “in control.”
He also reports he has been sexually active since age 16 and often has had unprotected intercourse. When asked if he is concerned that he might contract a sexually transmitted disease or impregnate his partner, Josh appears ambivalent.
IMPULSIVITY IN ADOLESCENCE
Josh is engaging in numerous impulsive behaviors. Adolescents generally are more impulsive than adults, as demonstrated by their significantly higher impulsivity scores on standardized tests.7 Furthermore, as measured by improved response inhibition (go/no go tasks), the level of adolescent impulsivity is inversely related to age.8
Problem behavior syndrome. High impulsivity is predictive of problem gambling, drug use, and risky driving and sexual practices later in life.1,2,9-11 Adolescents with what some authors describe as a “problem behavior syndrome” engage in behaviors—such as substance use, risky sexual behavior,12 gambling,13 and reckless driving14—that share a common trend toward impulsivity.
Impaired data processing. Decision making has been proposed as a three-part cognitive process:
- accumulating sensory input
- processing this input and formulating a behavioral response appropriate to the situation
- planning and implementing the resultant motor output.2
Impulsivity is believed to result from impaired ability of the brain to process accumulated information or to formulate a response to it—or both. Impulsive individuals thus experience impaired data processing, in which they:
- misjudge the likely risk of a given action or overestimate their ability to accomplish a task
- show impaired response inhibition and thus find it difficult to resist an impulse to participate in a given activity.
Sensation seeking. Adolescents who exhibit risk-taking behavior may wish to experience the thrill of the behavior (sensation or novelty seeking). Alcoholic or drug-dependent individuals and those who engage in pathologic gambling or take chances while driving also demonstrate significantly impaired decision making.15-17 Adolescents who engage in these and other problem behaviors have similarly scored high on sensation-seeking scales.10,18
DECISION-MAKING BIOLOGY
At least four neural circuits process decisions, weighing the risks and benefits of a given situation and formulating a response. These circuits are:
- prefrontal cortices, including orbitofrontal, dorsolateral, and ventromedial
- ventral striatum, including the nucleus accumbens
- thalamus
- monoaminergic brainstem nuclei (ventral tegmental area [VTA] and raphe nuclei).19
Functional imaging studies—including MRI and PET, EEG, and electrophysiology—have confirmed that these four brain regions are integral to response inhibition and show abnormal activity in impulsive individuals.20,21 Indeed, prefrontal cortex damage has been extensively documented to cause marked impulsivity, poor decision making, and an increased propensity for substance abuse and dependency.1
Functional imaging studies also have shown that adolescents appear to use these neural regions inefficiently during decision making. Extensive areas of the involved brain regions are activated in individuals ages 8 to 20, whereas only focal activation occurs in adults.22
Dopamine. The nuclear accumbens (NA) plays an important role in processing afferent excitatory glutamatergic projections and then instigating the given response.23 Dopamine is released in the NA in response to a long list of stimuli, including:
- exposure to substances
- natural rewards such as food or sex
- stimulating situations, such as playing video games, gambling, or thrill seeking.2
Novel experiences and rewards that are delivered erratically cause an elevated dopamine release in the NA. This may explain, in part, the excitement one gains from activities with unpredictable outcomes, such as gambling, bungee jumping, parachuting, white-water rafting, or taking risks while driving.
As rewarding stimuli are re-experienced, dopamine response accelerates in magnitude, and the reward becomes progressively stronger as the experience is repeated. This repeated dopamine release in the NA changes the cellular proteins involved in signaling pathways thought to be associated with the transition from impulsive to compulsive behavior.2 Therefore, addiction may be caused by neurocircuitry changes induced by repeated dopamine release. Similarly, persons who engage in impulsive behavior may have hypersensitive dopamine-related reward circuitry, which may, in part, explain their predisposition to addictive behavior.
Serotonin. Serotonergic projections originate mainly in the midbrain’s raphe nuclei and are transmitted to the ventral tegmental area, NA, prefrontal cortex, amygdala, and hippocampus.1 Abnormal serotonin levels have been implicated in impaired impulse control2 and decreased CNS serotonin in impulsive behavior.24
Functional brain imaging studies have shown reduced serotonin neurotransmission in highly impulsive individuals, compared with normal controls.25 Administering serotonergic agents seems to markedly decrease impulsive behavior.26
Activity within this network is modulated by excitatory glutamatergic transmission and inhibitory GABAergic transmission within the cortices and by dopaminergic and serotonergic transmission within the VTA and raphe nuclei, respectively.2,20 Although all of these neurotransmitters have been implicated in impulsivity, dopamine and serotonin have been studied most extensively (box 2).1,2,23-26
CASE CONTINUED: PSYCHIATRIC WORKUP
Josh clearly is engaged in worrisome behavior with potential long-term consequences. To evaluate him for underlying psychopathology, the psychiatrist used a structured psychiatric exam, Minnesota Multi-phasic Personality Inventory (MMPI), and SNAP-IV Rating Scale for ADHD (see Related resources). Josh endorsed some depressive symptoms—which were also evident on the MMPI—but did not meet DSM-IVTR criteria for major depressive disorder. Neither were his symptoms diagnostic for any other Axis I or Axis II disorder.
Given the risk of harm and likelihood of worsening behavior over time, the psychiatrist schedules Josh for weekly psychotherapy and possible medication.
Psychosocial interventions are discussed with Josh’s parents, including monitoring his activities, restricting access to peers who have been a poor influence, reinforcing good behavior, and enlisting help from teachers and his friends’ parents. The effect of these interventions is to be explored in follow-up visits.
After months or years of conflict with their child, the parents of an adolescent with severe risk-taking behavior are often distraught and frustrated. You can comfort them by explaining:
- the biology of adolescent risk taking
- how you will treat such behavior in their adolescent
- and their role in the treatment plan.
Often the child’s behaviors have weakened their marriage, given adolescents’ tendency to divide and manipulate their parents. To help them set and maintain limits in the face of their child’s hostility:
Educate them to communicate with each other, to maintain a united front, and to set firm limits for their adolescent. For example, recommend that they:
- forbid cell phone use while the adolescent is driving
- limit the number of passengers allowed in the adolescent’s car to reduce distractions
- reduce the amount of money and free time available to the adolescent.
Counsel them that they are unlikely to receive the child’s respect or affection in the short term. Reassure them, however, that the child will thank them for their firm guidance after he or she matures to adulthood.
DEFINING DEGREES OF RISK
Although no criteria differentiate “normal” from “pathologic” risk taking, the definition of taking a risk implies potential adverse consequences. In evaluating the impulsive adolescent, it is important to determine which behaviors:
- can be instructive and promote maturation
- fall outside normal adolescent behavior and/or carry potentially severe outcomes.
Acceptable. Risk taking is acceptable if the potential adverse outcome is relatively benign and the adolescent is likely to learn from the experience. For example, driving 10 miles over the speed limit and receiving a ticket can lead to stricter observance of the speed limit.
Pathologic. Josh clearly exhibits risky behaviors that one would reasonably consider “pathologic,” as they carry potentially severe consequences that exceed any possible developmental gain. For example, drinking and driving can result in a DUI citation and/or a motor vehicle accident with physical injuries or death.
TREATMENT OPTIONS
Psychiatric comorbidity. When you evaluate an adolescent engaged in excessive risk taking, consider Axis I and II disorders characterized by marked impulsivity. If the patient meets diagnostic criteria for a psychopathology such as bipolar disorder or ADHD, treating the underlying condition will likely improve impulsivity.
Recommended approach. Even without an Axis I or Axis II disorder, adolescents who engage in pathologic risky behavior may benefit from psychosocial interventions (Box 3), psychotherapy, and perhaps medication.
Because very little evidence supports using psychotropics to treat pathologically impulsive adolescents, we recommend that you:
- first try psychosocial interventions and psychotherapy
- reserve medications for patients who do not respond adequately to nondrug approaches and engage in impulsive behaviors that pose a high risk for grave consequences.
Psychotherapy can be effective once the adolescent and clinician form a therapeutic alliance. Because Josh—like other such teens—will likely view his psychiatrist as “just another adult lecturing me on what to do,” focus first on establishing rapport by:
- getting to know him
- helping him feel at ease
- showing interest in his thoughts and empathy towards his concerns and complaints
- discussing anything but the reason his parents brought him to your office.
After you establish an alliance, focus therapy on helping the adolescent gain insight into his or her dangerous behaviors and their consequences. To illustrate to Josh the potential consequences of his behaviors, for example, you might introduce him to:
- someone disabled in a motor vehicle accident
- an HIV-positive activist
- a recovering alcoholic
- a long-time smoker with severe chronic obstructive pulmonary disease.
At-risk adolescents also could be encouraged to complete an educational program that teaches alternate activities for sensation seeking (such as skiing instead of high-speed driving).
Medication. Although the monoaminergic systems are known to modulate impulsive behavior, few studies have examined using medications to treat risk-taking adolescents, and no drugs are FDA-approved for this indication.
SSRIs. Selective serotonin reuptake inhibitors such as fluoxetine, sertraline, or escitalopram might be useful for treating excessive adolescent risk taking. A preliminary study with paroxetine—an SSRI not recommended for children and adolescents—suggests this class of antidepressants may help reduce impulsivity.26 In the absence of data specific to risk-taking behavior, we recommend using SSRI dosages similar to those used to treat mood disorders in adolescents.
Clomipramine acts mainly on the serotonin receptor, preventing serotonin reuptake in a manner similar to an SSRI. Because it has the greatest serotonergic effect in its drug class, clomipramine is the only tricyclic proven effective in obsessive-compulsive disorder.27 Although no data have shown that clomipramine affects impulsivity, it theoretically could be effective because of its effect on serotonin.
Divalproex sodium has been shown to effectively treat impulsivity, particularly in patients with autism spectrum disorders, intermittent explosive disorder, schizophrenia, borderline personality disorder, and bipolar disorder.27-30 As an off-label use, one could consider trying this agent in an adolescent with pathologic risk-taking behavior. Use the same dosages and obtain routine labs as indicated for adolescents with other disorders.
Adherence. Like Josh, adolescents who engage in high-risk behaviors often do not recognize their pathology and resist psychiatric intervention. Getting them to take medication or participate in psychotherapy can be quite difficult.
Adolescents are far more likely to adhere to treatment if you develop a rapport with them and they trust you. As psychotherapy and psychosocial interventions progress, patients become more likely to gain insight into their conditions and become more adherent.
Other options to encourage adherence include having the parent:
- administer the medication and ensure that the patient swallows it
- use rewards to reinforce the adolescent’s good behavior and adherence to treatment.
Follow up weekly with patients such as Josh who exhibit high-risk behaviors and require psychotherapy and medication. Follow less-acute patients 2 weeks after the initial evaluation, then monthly if they are responding to medication.
- Strauch B. The primal teen: what the new discoveries about the teenage brain tell us about our kids. New York: Doubleday, 2004.
- SNAP-IV Rating Scale to screen for attention-deficit/hyperactivity disorder. Is your child really ADD/ADHD? www.drbiofeedback.com. Accessed Sept. 8, 2004.
- Focus Adolescent Services. Resources and information for families with adolescent behavior problems, including high-risk behavior. http://www.focusas.com/BehavioralDisorders.html. Accessed Aug. 26, 2004.
Drug brand names
- Clomipramine • Anafranil
- Divalproex sodium • Depakote
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Sertraline • Zoloft
Disclosure
Dr. Husted reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr Shapira receives grant or research support from Abbott Laboratories, Janssen Pharmaceutica, Ortho-McNeil Pharmaceutical, Bristol-Myers Squibb Co., Eli Lilly and Co., and Pfizer Inc. He is a speaker for AstraZeneca Pharmaceuticals, Forest Laboratories, and Ortho-McNeil Pharmaceutical, Inc.
Boys will be boys” and other platitudes may condone adolescent reckless driving, substance use, or sexual promiscuity—but to write off dangerous behavior as normal would be a mistake. Because adolescent impulsivity and sensation-seeking may have physiologic as well as emotional causes,1,2 excessive risk taking may be treatable.
This article discusses the neurobiology of adolescent risk taking, suggests how to determine when such behavior may be pathologic, and offers a treatment approach for at-risk teens and their parents.
CASE: ‘WHAT’S WRONG WITH OUR SON?’
Josh, age 17, is brought to the adolescent psychiatry clinic by his distraught parents, who report their son has undergone a “personality change” over the past 2 years. They recall that he was respectful, studious, and soft-spoken until age 15. Since then, he has been skipping school, staying out late at night with his friends, and “obsessed” with TV poker games.
His parents recently discovered he has been gambling for money, which greatly upsets them. They also found a pack of cigarettes in their son’s car and are concerned that he might be using other substances. What finally prompted the psychiatric visit was Josh’s recent traffic citation for driving 25 miles over the speed limit.
CAUSES OF RISK TAKING
Normal development. In the absence of psychopathology, adolescent risk taking appears to be a normal development stage that is vital to successful transition to adulthood. This assumes that adolescents such as Josh learn to moderate their behavior and avoid long-term negative consequences.
Impulsivity and sensation seeking are recognized as key factors in adolescent risk taking Box 1.1-4 Apparently, these traits result primarily from incomplete neural circuit maturation. Adolescent brain regions involved in impulsivity and risk taking are also involved in reward, and these centers exhibit an exaggerated response to stimuli.5 This amplified response may help explain an adolescent’s propensity for risky behavior.
Despite potential hazards, adolescent risk taking may confer benefits. In taking risks, adolescents:
- explore adult behavior
- learn to accomplish increasingly difficult developmental tasks
- reinforce their self-esteem.
Adolescent risk-takers have been found to be more self-confident, to feel more accepted, and to be better liked than their more-cautious peers.6
Psychiatric comorbidity. Excessive risk taking can be associated with psychiatric illness, including bipolar mania, psychosis, substance abuse, and impulse control disorders. Individuals with borderline personality and other cluster B disorders have marked impulsivity and thus are prone to risky behavior.
Teens with attention-deficit/hyperactivity disorder (ADHD), conduct disorder, and oppositional-defiant disorder (ODD) also tend to exhibit high impulsivity.
Alcohol. 40% of adult alcoholics report having had their first alcoholism-related symptoms between ages 15 and 19.1
Gambling. 10% to 14% of adolescents engage in problem or pathologic gambling, and gambling typically begins at age 12.2
Automobile crashes are the leading cause of death among North American adolescents; both sexes ages 16 to 20 are at least twice as likely to be in a motor vehicle accident as are drivers ages 20 to 50.3
STDs. Each year, 3 million U.S. adolescents contract a sexually transmitted disease (STD). HIV infection is the seventh leading cause of death for Americans ages 13 to 24.4
Sexual activity. Adolescents are more likely than adults to engage in impulsive sexual behavior, to have multiple partners, and to fail to use contraceptives. Younger teens (ages 12 to 14) are more likely to engage in risky sexual practices than older teens (ages 16 to 19).4
CASE CONTINUED: JUST ‘HAVING FUN’
When interviewed alone, Josh admits to “occasional” truancy, which he attributes to being “bored” with school and wanting to spend time with his friends “doing fun stuff, like going to the beach.” He admits to gambling for money and smoking a half-pack of cigarettes daily, as well as drinking beer and smoking marijuana “a few times a week.”
Josh says he engages in these activities “because they’re fun,” and states he is annoyed by his parents’ concern. He blames the speeding ticket on “not paying attention.” He admits to drinking and driving but claims he always feels “in control.”
He also reports he has been sexually active since age 16 and often has had unprotected intercourse. When asked if he is concerned that he might contract a sexually transmitted disease or impregnate his partner, Josh appears ambivalent.
IMPULSIVITY IN ADOLESCENCE
Josh is engaging in numerous impulsive behaviors. Adolescents generally are more impulsive than adults, as demonstrated by their significantly higher impulsivity scores on standardized tests.7 Furthermore, as measured by improved response inhibition (go/no go tasks), the level of adolescent impulsivity is inversely related to age.8
Problem behavior syndrome. High impulsivity is predictive of problem gambling, drug use, and risky driving and sexual practices later in life.1,2,9-11 Adolescents with what some authors describe as a “problem behavior syndrome” engage in behaviors—such as substance use, risky sexual behavior,12 gambling,13 and reckless driving14—that share a common trend toward impulsivity.
Impaired data processing. Decision making has been proposed as a three-part cognitive process:
- accumulating sensory input
- processing this input and formulating a behavioral response appropriate to the situation
- planning and implementing the resultant motor output.2
Impulsivity is believed to result from impaired ability of the brain to process accumulated information or to formulate a response to it—or both. Impulsive individuals thus experience impaired data processing, in which they:
- misjudge the likely risk of a given action or overestimate their ability to accomplish a task
- show impaired response inhibition and thus find it difficult to resist an impulse to participate in a given activity.
Sensation seeking. Adolescents who exhibit risk-taking behavior may wish to experience the thrill of the behavior (sensation or novelty seeking). Alcoholic or drug-dependent individuals and those who engage in pathologic gambling or take chances while driving also demonstrate significantly impaired decision making.15-17 Adolescents who engage in these and other problem behaviors have similarly scored high on sensation-seeking scales.10,18
DECISION-MAKING BIOLOGY
At least four neural circuits process decisions, weighing the risks and benefits of a given situation and formulating a response. These circuits are:
- prefrontal cortices, including orbitofrontal, dorsolateral, and ventromedial
- ventral striatum, including the nucleus accumbens
- thalamus
- monoaminergic brainstem nuclei (ventral tegmental area [VTA] and raphe nuclei).19
Functional imaging studies—including MRI and PET, EEG, and electrophysiology—have confirmed that these four brain regions are integral to response inhibition and show abnormal activity in impulsive individuals.20,21 Indeed, prefrontal cortex damage has been extensively documented to cause marked impulsivity, poor decision making, and an increased propensity for substance abuse and dependency.1
Functional imaging studies also have shown that adolescents appear to use these neural regions inefficiently during decision making. Extensive areas of the involved brain regions are activated in individuals ages 8 to 20, whereas only focal activation occurs in adults.22
Dopamine. The nuclear accumbens (NA) plays an important role in processing afferent excitatory glutamatergic projections and then instigating the given response.23 Dopamine is released in the NA in response to a long list of stimuli, including:
- exposure to substances
- natural rewards such as food or sex
- stimulating situations, such as playing video games, gambling, or thrill seeking.2
Novel experiences and rewards that are delivered erratically cause an elevated dopamine release in the NA. This may explain, in part, the excitement one gains from activities with unpredictable outcomes, such as gambling, bungee jumping, parachuting, white-water rafting, or taking risks while driving.
As rewarding stimuli are re-experienced, dopamine response accelerates in magnitude, and the reward becomes progressively stronger as the experience is repeated. This repeated dopamine release in the NA changes the cellular proteins involved in signaling pathways thought to be associated with the transition from impulsive to compulsive behavior.2 Therefore, addiction may be caused by neurocircuitry changes induced by repeated dopamine release. Similarly, persons who engage in impulsive behavior may have hypersensitive dopamine-related reward circuitry, which may, in part, explain their predisposition to addictive behavior.
Serotonin. Serotonergic projections originate mainly in the midbrain’s raphe nuclei and are transmitted to the ventral tegmental area, NA, prefrontal cortex, amygdala, and hippocampus.1 Abnormal serotonin levels have been implicated in impaired impulse control2 and decreased CNS serotonin in impulsive behavior.24
Functional brain imaging studies have shown reduced serotonin neurotransmission in highly impulsive individuals, compared with normal controls.25 Administering serotonergic agents seems to markedly decrease impulsive behavior.26
Activity within this network is modulated by excitatory glutamatergic transmission and inhibitory GABAergic transmission within the cortices and by dopaminergic and serotonergic transmission within the VTA and raphe nuclei, respectively.2,20 Although all of these neurotransmitters have been implicated in impulsivity, dopamine and serotonin have been studied most extensively (box 2).1,2,23-26
CASE CONTINUED: PSYCHIATRIC WORKUP
Josh clearly is engaged in worrisome behavior with potential long-term consequences. To evaluate him for underlying psychopathology, the psychiatrist used a structured psychiatric exam, Minnesota Multi-phasic Personality Inventory (MMPI), and SNAP-IV Rating Scale for ADHD (see Related resources). Josh endorsed some depressive symptoms—which were also evident on the MMPI—but did not meet DSM-IVTR criteria for major depressive disorder. Neither were his symptoms diagnostic for any other Axis I or Axis II disorder.
Given the risk of harm and likelihood of worsening behavior over time, the psychiatrist schedules Josh for weekly psychotherapy and possible medication.
Psychosocial interventions are discussed with Josh’s parents, including monitoring his activities, restricting access to peers who have been a poor influence, reinforcing good behavior, and enlisting help from teachers and his friends’ parents. The effect of these interventions is to be explored in follow-up visits.
After months or years of conflict with their child, the parents of an adolescent with severe risk-taking behavior are often distraught and frustrated. You can comfort them by explaining:
- the biology of adolescent risk taking
- how you will treat such behavior in their adolescent
- and their role in the treatment plan.
Often the child’s behaviors have weakened their marriage, given adolescents’ tendency to divide and manipulate their parents. To help them set and maintain limits in the face of their child’s hostility:
Educate them to communicate with each other, to maintain a united front, and to set firm limits for their adolescent. For example, recommend that they:
- forbid cell phone use while the adolescent is driving
- limit the number of passengers allowed in the adolescent’s car to reduce distractions
- reduce the amount of money and free time available to the adolescent.
Counsel them that they are unlikely to receive the child’s respect or affection in the short term. Reassure them, however, that the child will thank them for their firm guidance after he or she matures to adulthood.
DEFINING DEGREES OF RISK
Although no criteria differentiate “normal” from “pathologic” risk taking, the definition of taking a risk implies potential adverse consequences. In evaluating the impulsive adolescent, it is important to determine which behaviors:
- can be instructive and promote maturation
- fall outside normal adolescent behavior and/or carry potentially severe outcomes.
Acceptable. Risk taking is acceptable if the potential adverse outcome is relatively benign and the adolescent is likely to learn from the experience. For example, driving 10 miles over the speed limit and receiving a ticket can lead to stricter observance of the speed limit.
Pathologic. Josh clearly exhibits risky behaviors that one would reasonably consider “pathologic,” as they carry potentially severe consequences that exceed any possible developmental gain. For example, drinking and driving can result in a DUI citation and/or a motor vehicle accident with physical injuries or death.
TREATMENT OPTIONS
Psychiatric comorbidity. When you evaluate an adolescent engaged in excessive risk taking, consider Axis I and II disorders characterized by marked impulsivity. If the patient meets diagnostic criteria for a psychopathology such as bipolar disorder or ADHD, treating the underlying condition will likely improve impulsivity.
Recommended approach. Even without an Axis I or Axis II disorder, adolescents who engage in pathologic risky behavior may benefit from psychosocial interventions (Box 3), psychotherapy, and perhaps medication.
Because very little evidence supports using psychotropics to treat pathologically impulsive adolescents, we recommend that you:
- first try psychosocial interventions and psychotherapy
- reserve medications for patients who do not respond adequately to nondrug approaches and engage in impulsive behaviors that pose a high risk for grave consequences.
Psychotherapy can be effective once the adolescent and clinician form a therapeutic alliance. Because Josh—like other such teens—will likely view his psychiatrist as “just another adult lecturing me on what to do,” focus first on establishing rapport by:
- getting to know him
- helping him feel at ease
- showing interest in his thoughts and empathy towards his concerns and complaints
- discussing anything but the reason his parents brought him to your office.
After you establish an alliance, focus therapy on helping the adolescent gain insight into his or her dangerous behaviors and their consequences. To illustrate to Josh the potential consequences of his behaviors, for example, you might introduce him to:
- someone disabled in a motor vehicle accident
- an HIV-positive activist
- a recovering alcoholic
- a long-time smoker with severe chronic obstructive pulmonary disease.
At-risk adolescents also could be encouraged to complete an educational program that teaches alternate activities for sensation seeking (such as skiing instead of high-speed driving).
Medication. Although the monoaminergic systems are known to modulate impulsive behavior, few studies have examined using medications to treat risk-taking adolescents, and no drugs are FDA-approved for this indication.
SSRIs. Selective serotonin reuptake inhibitors such as fluoxetine, sertraline, or escitalopram might be useful for treating excessive adolescent risk taking. A preliminary study with paroxetine—an SSRI not recommended for children and adolescents—suggests this class of antidepressants may help reduce impulsivity.26 In the absence of data specific to risk-taking behavior, we recommend using SSRI dosages similar to those used to treat mood disorders in adolescents.
Clomipramine acts mainly on the serotonin receptor, preventing serotonin reuptake in a manner similar to an SSRI. Because it has the greatest serotonergic effect in its drug class, clomipramine is the only tricyclic proven effective in obsessive-compulsive disorder.27 Although no data have shown that clomipramine affects impulsivity, it theoretically could be effective because of its effect on serotonin.
Divalproex sodium has been shown to effectively treat impulsivity, particularly in patients with autism spectrum disorders, intermittent explosive disorder, schizophrenia, borderline personality disorder, and bipolar disorder.27-30 As an off-label use, one could consider trying this agent in an adolescent with pathologic risk-taking behavior. Use the same dosages and obtain routine labs as indicated for adolescents with other disorders.
Adherence. Like Josh, adolescents who engage in high-risk behaviors often do not recognize their pathology and resist psychiatric intervention. Getting them to take medication or participate in psychotherapy can be quite difficult.
Adolescents are far more likely to adhere to treatment if you develop a rapport with them and they trust you. As psychotherapy and psychosocial interventions progress, patients become more likely to gain insight into their conditions and become more adherent.
Other options to encourage adherence include having the parent:
- administer the medication and ensure that the patient swallows it
- use rewards to reinforce the adolescent’s good behavior and adherence to treatment.
Follow up weekly with patients such as Josh who exhibit high-risk behaviors and require psychotherapy and medication. Follow less-acute patients 2 weeks after the initial evaluation, then monthly if they are responding to medication.
- Strauch B. The primal teen: what the new discoveries about the teenage brain tell us about our kids. New York: Doubleday, 2004.
- SNAP-IV Rating Scale to screen for attention-deficit/hyperactivity disorder. Is your child really ADD/ADHD? www.drbiofeedback.com. Accessed Sept. 8, 2004.
- Focus Adolescent Services. Resources and information for families with adolescent behavior problems, including high-risk behavior. http://www.focusas.com/BehavioralDisorders.html. Accessed Aug. 26, 2004.
Drug brand names
- Clomipramine • Anafranil
- Divalproex sodium • Depakote
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Sertraline • Zoloft
Disclosure
Dr. Husted reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr Shapira receives grant or research support from Abbott Laboratories, Janssen Pharmaceutica, Ortho-McNeil Pharmaceutical, Bristol-Myers Squibb Co., Eli Lilly and Co., and Pfizer Inc. He is a speaker for AstraZeneca Pharmaceuticals, Forest Laboratories, and Ortho-McNeil Pharmaceutical, Inc.
1. Chambers RA, Taylor JR, Potenza MN. Developmental neurocircuitry of motivation in adolescence: a critical period of addiction vulnerability. Am J Psychiatry 2003;160:1041-52.
2. Chambers RA, Potenza MN. Neurodevelopment, impulsivity, and adolescent gambling. J Gambl Stud 2003;19:53-84.
3. Turner C, McClure R. Age and gender differences in risk taking behavior as an explanation for high incidence of motor vehicle crashes as a driver in young males. Inj Control Saf Promot 2003;10:123-30.
4. Bachanas PJ, Morris MK, Lewis-Gess JK, et al. Psychological adjustment, substance use, HIV knowledge, and risky sexual behavior in at-risk minority females: developmental differences during adolescence. J Pediatr Psych 2002;27:373-84.
5. Goldstein RZ, Volkow ND. Drug addiction and its underlying neuro- biological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry 2002;159:1642-52.
6. Spear LP. The adolescent brain and age-related behavioral manifestations. Neurosci Biobehav Rev 2000;24:417-63.
7. Clayton R. Transitions in drug use: risk and protective factors. In: Glantz M, Pickens R (eds). Vulnerability to drug abuse. Washington, DC: American Psychological Association, 1992;15-52.
8. Tamm L, Menon V, Reiss AL. Maturation of brain function associated with response inhibition. J Am Acad Child Adolesc Psychiatry 2002;41:1231-8.
9. Jonah BA. Sensation seeking and risky driving: a review and synthesis of the literature. Accid Anal Prev 1997;29:651-6.
10. Vitaro F, Arseneault L, Tremblay RE. Dispositional predictors of problem gambling in male adolescents. Am J Psychiatry 1997;154:1769-70.
11. Malow RM, Devieux JG, Jennings T, et al. Substance-abusing adolescents at varying levels of HIV risk: psychosocial characteristics, drug use, and sexual behavior. J Subst Abuse 2001;13:103-17.
12. Donovan JE, Jessor R, Costa FM. Syndrome of problem behavior in adolescence: a replication. J Consult Clin Psychol 1988;56:762-5.
13. Vitaro F, Brendgen M, Ladouceur R, Tremblay RE. Gambling, delinquency, and drug use during adolescence: mutual influences and common risk factors. J Gambl Stud 2001;17:171-90.
14. Shope JT, Bingham CR. Drinking-driving as a component of problem driving and problem behavior in young adults. J Stud Alcohol 2002;63(1):24-33.
15. Potenza MN. The neurobiology of pathological gambling. Semin Clin Neuropsychiatry 2001;6:217-26.
16. Petry NM. Substance abuse, pathological gambling, and impulsiveness. Drug Alcohol Depend 2001;63:29-38.
17. Bechara A. Neurobiology of decision-making: risk and reward. Semin Clin Neuropsychiatry 2001;6:205-16.
18. Zuckerman M. Sensation seeking: the balance between risk and reward. In: Lipsitt LP, Mitnick LL (eds). Self-regulatory behavior and risk taking. Norwood, NJ: Ablex Publishing; 1992;143-52.
19. Masterman DL, Cummings JL. Frontal-subcortical circuits: the anatomical basis of executive, social and motivational behaviors. J Psychopharmacol 1997;11:107-14.
20. Horn NR, Dolan M, Elliot R, et al. Response inhibition and impulsivity: an fMRI study. Neuropsychologia 2003;41:1959-66.
21. Fallgatter AJ, Herrmann MJ. Electrophysiological assessment of impulsive behavior in healthy subjects. Neuropsychologia 2001;39:328-33.
22. Booth JR, Burman DD, Meyer JR, et al. Neural development of selective attention and response inhibition. Neuroimage 2003;20:737-51.
23. O’Donnell P, Greene J, Pabello N, et al. Modulation of cell firing in the nucleus accumbens. Ann NY Acad Sci 1999;877:157-75.
24. Nordin C, Eklundh T. Altered CSF 5-HIAA disposition in pathologic male gamblers. CNS Spectrums 1999;4:25-33.
25. Leyton M, Okazawa H, Diksic M, et al. Brain regional alpha-[11C] methyl-L-tryptophan trapping in impulsive subjects with borderline personality disorder. Am J Psychiatry 2001;158:775-82.
26. Cherek DR, Lane SD, Pietras CJ, Steinberg JL. Effects of chronic paroxetine administration on measures of aggressive and impulsive responses of adult males with a history of conduct disorder. Psychopharmacology (Berl) 2002;159:266-74.
27. Geller DA, Biederman J, Stewart SE, et al. Which SSRI? A meta-analysis of pharmacotherapy trials in pediatric obsessive-compulsive disorder. Am J Psychiatry 2003;160:1919-28.
28. Hollander E, Allen A, Lopez RP, et al. A preliminary double-blind, placebo-controlled trial of divalproex sodium in borderline personality disorder. J Clin Psychiatry 2001;62(3):199-203.
29. Swann AC. Treatment of aggression in patients with bipolar disorder. J Clin Psychiatry 1999;60(suppl 15):25-8.
30. Hollander E, Dolgoff-Kaspar R, Cartwright C, et al. An open trial of divalproex sodium in autism spectrum disorders. J Clin Psychiatry 2001;62:530-4.
1. Chambers RA, Taylor JR, Potenza MN. Developmental neurocircuitry of motivation in adolescence: a critical period of addiction vulnerability. Am J Psychiatry 2003;160:1041-52.
2. Chambers RA, Potenza MN. Neurodevelopment, impulsivity, and adolescent gambling. J Gambl Stud 2003;19:53-84.
3. Turner C, McClure R. Age and gender differences in risk taking behavior as an explanation for high incidence of motor vehicle crashes as a driver in young males. Inj Control Saf Promot 2003;10:123-30.
4. Bachanas PJ, Morris MK, Lewis-Gess JK, et al. Psychological adjustment, substance use, HIV knowledge, and risky sexual behavior in at-risk minority females: developmental differences during adolescence. J Pediatr Psych 2002;27:373-84.
5. Goldstein RZ, Volkow ND. Drug addiction and its underlying neuro- biological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry 2002;159:1642-52.
6. Spear LP. The adolescent brain and age-related behavioral manifestations. Neurosci Biobehav Rev 2000;24:417-63.
7. Clayton R. Transitions in drug use: risk and protective factors. In: Glantz M, Pickens R (eds). Vulnerability to drug abuse. Washington, DC: American Psychological Association, 1992;15-52.
8. Tamm L, Menon V, Reiss AL. Maturation of brain function associated with response inhibition. J Am Acad Child Adolesc Psychiatry 2002;41:1231-8.
9. Jonah BA. Sensation seeking and risky driving: a review and synthesis of the literature. Accid Anal Prev 1997;29:651-6.
10. Vitaro F, Arseneault L, Tremblay RE. Dispositional predictors of problem gambling in male adolescents. Am J Psychiatry 1997;154:1769-70.
11. Malow RM, Devieux JG, Jennings T, et al. Substance-abusing adolescents at varying levels of HIV risk: psychosocial characteristics, drug use, and sexual behavior. J Subst Abuse 2001;13:103-17.
12. Donovan JE, Jessor R, Costa FM. Syndrome of problem behavior in adolescence: a replication. J Consult Clin Psychol 1988;56:762-5.
13. Vitaro F, Brendgen M, Ladouceur R, Tremblay RE. Gambling, delinquency, and drug use during adolescence: mutual influences and common risk factors. J Gambl Stud 2001;17:171-90.
14. Shope JT, Bingham CR. Drinking-driving as a component of problem driving and problem behavior in young adults. J Stud Alcohol 2002;63(1):24-33.
15. Potenza MN. The neurobiology of pathological gambling. Semin Clin Neuropsychiatry 2001;6:217-26.
16. Petry NM. Substance abuse, pathological gambling, and impulsiveness. Drug Alcohol Depend 2001;63:29-38.
17. Bechara A. Neurobiology of decision-making: risk and reward. Semin Clin Neuropsychiatry 2001;6:205-16.
18. Zuckerman M. Sensation seeking: the balance between risk and reward. In: Lipsitt LP, Mitnick LL (eds). Self-regulatory behavior and risk taking. Norwood, NJ: Ablex Publishing; 1992;143-52.
19. Masterman DL, Cummings JL. Frontal-subcortical circuits: the anatomical basis of executive, social and motivational behaviors. J Psychopharmacol 1997;11:107-14.
20. Horn NR, Dolan M, Elliot R, et al. Response inhibition and impulsivity: an fMRI study. Neuropsychologia 2003;41:1959-66.
21. Fallgatter AJ, Herrmann MJ. Electrophysiological assessment of impulsive behavior in healthy subjects. Neuropsychologia 2001;39:328-33.
22. Booth JR, Burman DD, Meyer JR, et al. Neural development of selective attention and response inhibition. Neuroimage 2003;20:737-51.
23. O’Donnell P, Greene J, Pabello N, et al. Modulation of cell firing in the nucleus accumbens. Ann NY Acad Sci 1999;877:157-75.
24. Nordin C, Eklundh T. Altered CSF 5-HIAA disposition in pathologic male gamblers. CNS Spectrums 1999;4:25-33.
25. Leyton M, Okazawa H, Diksic M, et al. Brain regional alpha-[11C] methyl-L-tryptophan trapping in impulsive subjects with borderline personality disorder. Am J Psychiatry 2001;158:775-82.
26. Cherek DR, Lane SD, Pietras CJ, Steinberg JL. Effects of chronic paroxetine administration on measures of aggressive and impulsive responses of adult males with a history of conduct disorder. Psychopharmacology (Berl) 2002;159:266-74.
27. Geller DA, Biederman J, Stewart SE, et al. Which SSRI? A meta-analysis of pharmacotherapy trials in pediatric obsessive-compulsive disorder. Am J Psychiatry 2003;160:1919-28.
28. Hollander E, Allen A, Lopez RP, et al. A preliminary double-blind, placebo-controlled trial of divalproex sodium in borderline personality disorder. J Clin Psychiatry 2001;62(3):199-203.
29. Swann AC. Treatment of aggression in patients with bipolar disorder. J Clin Psychiatry 1999;60(suppl 15):25-8.
30. Hollander E, Dolgoff-Kaspar R, Cartwright C, et al. An open trial of divalproex sodium in autism spectrum disorders. J Clin Psychiatry 2001;62:530-4.
Correction
In last month’s Letters an editing error occurred in a letter by Dr. George Hilton and the reply by Dr. Edmund Higgins. The word “Oxytocin” was misread as “Oxycontin” and changed throughout to the incorrect “oxycodone” (Oxycontin’s generic name). Current Psychiatry regrets the error. See the corrected letter and reply at www.currentpsychiatry.com.
In last month’s Letters an editing error occurred in a letter by Dr. George Hilton and the reply by Dr. Edmund Higgins. The word “Oxytocin” was misread as “Oxycontin” and changed throughout to the incorrect “oxycodone” (Oxycontin’s generic name). Current Psychiatry regrets the error. See the corrected letter and reply at www.currentpsychiatry.com.
In last month’s Letters an editing error occurred in a letter by Dr. George Hilton and the reply by Dr. Edmund Higgins. The word “Oxytocin” was misread as “Oxycontin” and changed throughout to the incorrect “oxycodone” (Oxycontin’s generic name). Current Psychiatry regrets the error. See the corrected letter and reply at www.currentpsychiatry.com.