User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Using a ‘MAP’ to navigate follow-up visits
Knowing each patient’s problems and life situation is critical to conducting an effective follow-up examination. But with limits on your time and patients often changing psychiatrists, keeping track can be challenging.
A multiaxial problem (MAP) list, which we devised based on clinical experience, can help you organize key symptoms and remember which issues to address during repeat visits. It can quickly get you up to speed with a patient who:
- has multiple disorders or symptoms
- is treatment-resistant
- has not been seen in months or years
- is a candidate for a change in treatment
- or was treated by another psychiatrist.
Table
Sample multiaxial problem (MAP) list
| Jane Doe. Age 49—white female. Continuous with exacerbations since age 19. | |
|---|---|
Axis A
| Axis C
|
Axis B
| Axis D
|
Creating the list
The MAP list can be compiled from information obtained by:
- asking the patient to list complaints
- reviewing the patient’s chart
- interviewing family members
- or talking with other care team members.
On a blank sheet of paper, write at the top the patient’s name, age, race/sex (for fast identification), and age at onset of symptoms (to differentiate between chronic, episodic, and recent onset).
Then draw four quadrants and organize the information as follows (Table):
- Axis A—symptoms and issues addressed by the psychiatrist
- Axis B—behavior patterns and attitudes that might affect treatment. Also include intellectual limitations. A behavior attributed to a personality disorder (such as selfmutilation) falls under Axis A because the psychiatrist would treat it directly.
- Axis C—physical symptoms or disorders to be addressed by another physician
- Axis D—psychosocial, physical, and other patient stressors. A physical illness may fall under both Axes C and D if the stress is significant.
Pertinent negatives such as “No suicide attempt” may be recorded on Axis A or C, psychological strengths/coping skills on Axis B, and supportive persons and factors (such as “Mother helps financially”) on Axis D.
Using the list
Keep the MAP list handy while seeing the patient. Start by going through the symptoms/problems listed under Axis A. Review the patterns noted under Axis B and look for ways to promote insight and coping by reflecting those patterns back to the patient. For the hypothetical patient illustrated in the Table, we would prescribe a medication, then tell her, “We’ve discussed your pattern of stopping medications because you’re afraid of becoming dependent on them. We need to discuss this further so that you can keep taking this medication regularly.”
Next, check the physical conditions under Axis C before choosing a medication to avoid possible drug-drug interactions or side effects. We find that Axis C also helps us ensure that the patient seeks appropriate medical care from another physician. Finally, Axis D reminds us to be empathic toward patients who report psychosocial stressors and to intervene where appropriate.
Remember that the MAP list is not a substitute for taking a full history and physical.
MAP maintenance
Revise the MAP list after each visit as the patient responds to treatment or as his or her life changes. For example, a psychosocial stressor that has been resolved should be struck, although some cases call for leaving the item in and noting “resolved” or “in remission” after it. For example, even if a patient was no longer being physically abused by her spouse, we would not delete the problem because we would want to keep monitoring it.
Include only relevant data on the list or it will become unwieldy. Add diagnoses only if they are certain.
Dr. Mago is assistant professor of psychiatry, Thomas Jefferson University, Philadelphia.
Dr. Joshi is a fellow in child and adolescent psychiatry at Massachusetts General Hospital, Boston.
Knowing each patient’s problems and life situation is critical to conducting an effective follow-up examination. But with limits on your time and patients often changing psychiatrists, keeping track can be challenging.
A multiaxial problem (MAP) list, which we devised based on clinical experience, can help you organize key symptoms and remember which issues to address during repeat visits. It can quickly get you up to speed with a patient who:
- has multiple disorders or symptoms
- is treatment-resistant
- has not been seen in months or years
- is a candidate for a change in treatment
- or was treated by another psychiatrist.
Table
Sample multiaxial problem (MAP) list
| Jane Doe. Age 49—white female. Continuous with exacerbations since age 19. | |
|---|---|
Axis A
| Axis C
|
Axis B
| Axis D
|
Creating the list
The MAP list can be compiled from information obtained by:
- asking the patient to list complaints
- reviewing the patient’s chart
- interviewing family members
- or talking with other care team members.
On a blank sheet of paper, write at the top the patient’s name, age, race/sex (for fast identification), and age at onset of symptoms (to differentiate between chronic, episodic, and recent onset).
Then draw four quadrants and organize the information as follows (Table):
- Axis A—symptoms and issues addressed by the psychiatrist
- Axis B—behavior patterns and attitudes that might affect treatment. Also include intellectual limitations. A behavior attributed to a personality disorder (such as selfmutilation) falls under Axis A because the psychiatrist would treat it directly.
- Axis C—physical symptoms or disorders to be addressed by another physician
- Axis D—psychosocial, physical, and other patient stressors. A physical illness may fall under both Axes C and D if the stress is significant.
Pertinent negatives such as “No suicide attempt” may be recorded on Axis A or C, psychological strengths/coping skills on Axis B, and supportive persons and factors (such as “Mother helps financially”) on Axis D.
Using the list
Keep the MAP list handy while seeing the patient. Start by going through the symptoms/problems listed under Axis A. Review the patterns noted under Axis B and look for ways to promote insight and coping by reflecting those patterns back to the patient. For the hypothetical patient illustrated in the Table, we would prescribe a medication, then tell her, “We’ve discussed your pattern of stopping medications because you’re afraid of becoming dependent on them. We need to discuss this further so that you can keep taking this medication regularly.”
Next, check the physical conditions under Axis C before choosing a medication to avoid possible drug-drug interactions or side effects. We find that Axis C also helps us ensure that the patient seeks appropriate medical care from another physician. Finally, Axis D reminds us to be empathic toward patients who report psychosocial stressors and to intervene where appropriate.
Remember that the MAP list is not a substitute for taking a full history and physical.
MAP maintenance
Revise the MAP list after each visit as the patient responds to treatment or as his or her life changes. For example, a psychosocial stressor that has been resolved should be struck, although some cases call for leaving the item in and noting “resolved” or “in remission” after it. For example, even if a patient was no longer being physically abused by her spouse, we would not delete the problem because we would want to keep monitoring it.
Include only relevant data on the list or it will become unwieldy. Add diagnoses only if they are certain.
Knowing each patient’s problems and life situation is critical to conducting an effective follow-up examination. But with limits on your time and patients often changing psychiatrists, keeping track can be challenging.
A multiaxial problem (MAP) list, which we devised based on clinical experience, can help you organize key symptoms and remember which issues to address during repeat visits. It can quickly get you up to speed with a patient who:
- has multiple disorders or symptoms
- is treatment-resistant
- has not been seen in months or years
- is a candidate for a change in treatment
- or was treated by another psychiatrist.
Table
Sample multiaxial problem (MAP) list
| Jane Doe. Age 49—white female. Continuous with exacerbations since age 19. | |
|---|---|
Axis A
| Axis C
|
Axis B
| Axis D
|
Creating the list
The MAP list can be compiled from information obtained by:
- asking the patient to list complaints
- reviewing the patient’s chart
- interviewing family members
- or talking with other care team members.
On a blank sheet of paper, write at the top the patient’s name, age, race/sex (for fast identification), and age at onset of symptoms (to differentiate between chronic, episodic, and recent onset).
Then draw four quadrants and organize the information as follows (Table):
- Axis A—symptoms and issues addressed by the psychiatrist
- Axis B—behavior patterns and attitudes that might affect treatment. Also include intellectual limitations. A behavior attributed to a personality disorder (such as selfmutilation) falls under Axis A because the psychiatrist would treat it directly.
- Axis C—physical symptoms or disorders to be addressed by another physician
- Axis D—psychosocial, physical, and other patient stressors. A physical illness may fall under both Axes C and D if the stress is significant.
Pertinent negatives such as “No suicide attempt” may be recorded on Axis A or C, psychological strengths/coping skills on Axis B, and supportive persons and factors (such as “Mother helps financially”) on Axis D.
Using the list
Keep the MAP list handy while seeing the patient. Start by going through the symptoms/problems listed under Axis A. Review the patterns noted under Axis B and look for ways to promote insight and coping by reflecting those patterns back to the patient. For the hypothetical patient illustrated in the Table, we would prescribe a medication, then tell her, “We’ve discussed your pattern of stopping medications because you’re afraid of becoming dependent on them. We need to discuss this further so that you can keep taking this medication regularly.”
Next, check the physical conditions under Axis C before choosing a medication to avoid possible drug-drug interactions or side effects. We find that Axis C also helps us ensure that the patient seeks appropriate medical care from another physician. Finally, Axis D reminds us to be empathic toward patients who report psychosocial stressors and to intervene where appropriate.
Remember that the MAP list is not a substitute for taking a full history and physical.
MAP maintenance
Revise the MAP list after each visit as the patient responds to treatment or as his or her life changes. For example, a psychosocial stressor that has been resolved should be struck, although some cases call for leaving the item in and noting “resolved” or “in remission” after it. For example, even if a patient was no longer being physically abused by her spouse, we would not delete the problem because we would want to keep monitoring it.
Include only relevant data on the list or it will become unwieldy. Add diagnoses only if they are certain.
Dr. Mago is assistant professor of psychiatry, Thomas Jefferson University, Philadelphia.
Dr. Joshi is a fellow in child and adolescent psychiatry at Massachusetts General Hospital, Boston.
Dr. Mago is assistant professor of psychiatry, Thomas Jefferson University, Philadelphia.
Dr. Joshi is a fellow in child and adolescent psychiatry at Massachusetts General Hospital, Boston.
Revised ‘SAD PERSONS’ helps assess suicide risk
The SAD PERSONS scale, an acronym based on 10 suicide risk factors,1 has found widespread acceptance in assessing the likelihood of a suicide attempt. It also has been adapted for use with children.2
However, a major risk factor omitted from the scale is the availability of a lethal means for suicide, such as a firearm, stockpiled medication, or other potentially lethal item. In particular, where firearm ownership levels are higher, a disproportionately higher number of people die from suicide.3
Include ‘Availability of lethal means’
SAD PERSONS can be modified to “SAD PERSONAS” to remedy this omission, with the second ‘A’ representing “Availability of lethal means” (Table). This modification reminds the clinician to ask about lethal means when assessing suicidality. If lethal means are available, the clinician can then take whatever action is reasonably indicated to reduce the likelihood of a suicide.
Eliminate scoring
Because the listed risk factors are not equivalent with regard to suicide potential, a second modification is to eliminate scoring.
In SAD PERSONS, one point is scored for each risk factor. Consider these two patients:
- a man who is depressed and has an organized plan to shoot himself with his handgun
- an elderly widower who has dementia and is physically ill.
Both men would score a 4, but the risk of suicide would be substantially greater in the first case. Suicide risk factors are qualitative—not quantitative—measures and should be considered within the overall context of the clinical presentation.
Table
Modified SAD PERSONAS scale
| Sex |
| Age |
| Depression |
| Previous attempt |
| Ethanol abuse |
| Rational thinking loss |
| Social supports lacking |
| Organized plan |
| No spouse |
| Availability of lethal means |
| Sickness |
| Eliminate scoring. Consider risk factors within the context of the clinical presentation |
1. Patterson WM, Dohn HH, Bird J, Patterson GA. Evaluation of suicidal patients: the SAD PERSONS scale. Psychosomatics 1983;24:343-9.
2. Juhnke GA. The adapted-SAD PERSONS: a suicide assessment scale designed for use with children. Elementary School Guidance & Counseling 1996;30:252-8.
3. Miller M, Azrael D, Hemenway D. Household firearm ownership and suicide rates in the United States. Epidemiology 2002;13:517-24.
Dr. Campbell is assistant professor, department of psychiatry, Case Western Reserve University School of Medicine, Cleveland, OH, and is clinical director, division of ambulatory care, department of psychiatry, University Hospitals of Cleveland.
The SAD PERSONS scale, an acronym based on 10 suicide risk factors,1 has found widespread acceptance in assessing the likelihood of a suicide attempt. It also has been adapted for use with children.2
However, a major risk factor omitted from the scale is the availability of a lethal means for suicide, such as a firearm, stockpiled medication, or other potentially lethal item. In particular, where firearm ownership levels are higher, a disproportionately higher number of people die from suicide.3
Include ‘Availability of lethal means’
SAD PERSONS can be modified to “SAD PERSONAS” to remedy this omission, with the second ‘A’ representing “Availability of lethal means” (Table). This modification reminds the clinician to ask about lethal means when assessing suicidality. If lethal means are available, the clinician can then take whatever action is reasonably indicated to reduce the likelihood of a suicide.
Eliminate scoring
Because the listed risk factors are not equivalent with regard to suicide potential, a second modification is to eliminate scoring.
In SAD PERSONS, one point is scored for each risk factor. Consider these two patients:
- a man who is depressed and has an organized plan to shoot himself with his handgun
- an elderly widower who has dementia and is physically ill.
Both men would score a 4, but the risk of suicide would be substantially greater in the first case. Suicide risk factors are qualitative—not quantitative—measures and should be considered within the overall context of the clinical presentation.
Table
Modified SAD PERSONAS scale
| Sex |
| Age |
| Depression |
| Previous attempt |
| Ethanol abuse |
| Rational thinking loss |
| Social supports lacking |
| Organized plan |
| No spouse |
| Availability of lethal means |
| Sickness |
| Eliminate scoring. Consider risk factors within the context of the clinical presentation |
The SAD PERSONS scale, an acronym based on 10 suicide risk factors,1 has found widespread acceptance in assessing the likelihood of a suicide attempt. It also has been adapted for use with children.2
However, a major risk factor omitted from the scale is the availability of a lethal means for suicide, such as a firearm, stockpiled medication, or other potentially lethal item. In particular, where firearm ownership levels are higher, a disproportionately higher number of people die from suicide.3
Include ‘Availability of lethal means’
SAD PERSONS can be modified to “SAD PERSONAS” to remedy this omission, with the second ‘A’ representing “Availability of lethal means” (Table). This modification reminds the clinician to ask about lethal means when assessing suicidality. If lethal means are available, the clinician can then take whatever action is reasonably indicated to reduce the likelihood of a suicide.
Eliminate scoring
Because the listed risk factors are not equivalent with regard to suicide potential, a second modification is to eliminate scoring.
In SAD PERSONS, one point is scored for each risk factor. Consider these two patients:
- a man who is depressed and has an organized plan to shoot himself with his handgun
- an elderly widower who has dementia and is physically ill.
Both men would score a 4, but the risk of suicide would be substantially greater in the first case. Suicide risk factors are qualitative—not quantitative—measures and should be considered within the overall context of the clinical presentation.
Table
Modified SAD PERSONAS scale
| Sex |
| Age |
| Depression |
| Previous attempt |
| Ethanol abuse |
| Rational thinking loss |
| Social supports lacking |
| Organized plan |
| No spouse |
| Availability of lethal means |
| Sickness |
| Eliminate scoring. Consider risk factors within the context of the clinical presentation |
1. Patterson WM, Dohn HH, Bird J, Patterson GA. Evaluation of suicidal patients: the SAD PERSONS scale. Psychosomatics 1983;24:343-9.
2. Juhnke GA. The adapted-SAD PERSONS: a suicide assessment scale designed for use with children. Elementary School Guidance & Counseling 1996;30:252-8.
3. Miller M, Azrael D, Hemenway D. Household firearm ownership and suicide rates in the United States. Epidemiology 2002;13:517-24.
Dr. Campbell is assistant professor, department of psychiatry, Case Western Reserve University School of Medicine, Cleveland, OH, and is clinical director, division of ambulatory care, department of psychiatry, University Hospitals of Cleveland.
1. Patterson WM, Dohn HH, Bird J, Patterson GA. Evaluation of suicidal patients: the SAD PERSONS scale. Psychosomatics 1983;24:343-9.
2. Juhnke GA. The adapted-SAD PERSONS: a suicide assessment scale designed for use with children. Elementary School Guidance & Counseling 1996;30:252-8.
3. Miller M, Azrael D, Hemenway D. Household firearm ownership and suicide rates in the United States. Epidemiology 2002;13:517-24.
Dr. Campbell is assistant professor, department of psychiatry, Case Western Reserve University School of Medicine, Cleveland, OH, and is clinical director, division of ambulatory care, department of psychiatry, University Hospitals of Cleveland.
Prescribing to preserve or restore sexual function
Many psychotropics can cause erectile dysfunction (ED) and other sexual problems (Tables 1 and 2). This side effect can discourage treatment compliance and jeopardize outcomes.
This article offers evidence-based strategies for preventing and treating psychotropic-induced ED. We also review information psychiatrists need to share with primary care physicians when treating a patient with ED.
Case report: A good relationship
Mr. A, age 52, has experienced diminishing erectile function for 6 months and now cannot achieve an erection. His relationship with his wife is good; he attributes loss of libido to his erection problem.
A pack-a-day smoker since age 18, Mr. A has type 2 diabetes and has been taking metformin, 850 mg bid, for 2 years. For about 2 months he has been taking sertraline, 50 mg, for depression and reports significantly improved mood, sleep, concentration, and appetite. He also has been taking lisinopril, 20 mg/d, for hypertension, and simvastatin, 40 mg nightly, for hyperlipidemia.
Table 1
Antidepressants associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Monoamine oxidase inhibitors | Unknown | ED (rare), retarded ejaculation(rare) |
| Selective serotonin reuptake inhibitors | Increased serum prolactin (possible) Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | Decreased libido ED Anorgasmia Delayed/retarded ejaculation |
| Tricyclic antidepressants | CNS depression Anticholinergic activity | Decreased libido ED |
| Venlafaxine | Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | ED Anorgasmia Delayed/retarded ejaculation |
| ED: Erectile dysfunction | ||
Mr. A’s hemoglobin A1C is 9.8%, indicating poor diabetes control. His blood pressure is 168/94 mm Hg, well above his goal of <135/80. He has no chest pain or history of myocardial infarction; a recent exercise stress test indicated no coronary disease.
Discussion. Several medical causes—diabetes, hypertension, hyperlipidemia, and 34 years of heavy smoking—could explain Mr. A’s ED. Vascular disease is suspected, although the stress test was negative.
Identifying a specific cause is crucial to treating ED but may be difficult. Up to 80% of cases can be traced to one or more organic causes.1 Mr. A’s depression could be a factor, although psychogenic ED is not common. Adding the selective serotonin reuptake inhibitor (SSRI) sertraline may also have worsened his ED.
Other possible causes of ED include:
- nonpsychotropic drugs (to view a list of agents, see this article at currentpsychiatry.com)
- decreased libido, delayed orgasm, and anorgasmia. Decreased libido and anorgasmia are often misdiagnosed as primary ED because the presenting symptoms are similar.
ED treatment begins with managing underlying medical problems, although optimal control alone may not alleviate ED. Encourage the patient to stop smoking and offer smoking cessation strategies.
Alert the primary care physician and patient when prescribing a psychotropic associated with sexual side effects, and explain the drug’s potential benefits. Assess baseline sexual function before starting the psychotropic so that changes in sexual function can be detected. Report your findings to the referring physician after each visit.
If ED is believed to be psychotropic-induced:
- maintain the psychotropic regimen for 6 to 8 weeksto see if the patient builds a tolerance to its sexual side effects.
- lower the psychotropic dosage. In one study,2 nearly 75% of patients whose SSRI dosages were reduced by one-half reported improved sexual function with sustained antidepressant effectiveness. This SSRIeffect has been replicated and has also been demonstrated with imipramine.3-5
- schedule 1- to 2-day drug “holidays” (on weekends, for example) for medications with a short halflife (such as sertraline or paroxetine) if the underlying condition permits.7
Table 2
Other psychotropics associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Amphetamines | Increased relative sympathetic nervous syndrome/parasympathetic nervous system activity | ED |
| Anticholinergics | Anticholinergic activity | ED |
| Antipsychotics (typical and atypical) | CNS depression, increased serum prolactin Anticholinergic activity Alpha1-receptor blockade Decreased internal urethral sphincter closure | Decreased libido ED Retarded ejaculation Retrograde ejaculation |
| Barbiturates, benzodiazepines, CNS depressants | CNS depression | Decreased libido |
| Carbamazepine, gabapentin | Decreased androgenic activity | Decreased libido, ED, retarded ejaculation |
| Disulfiram | Unknown | ED |
| Dopamine-receptor agonists | Unknown | ED |
| Dopamine-receptor antagonists | Increased serum prolactin | Decreased libido |
| ED: Erectile dysfunction | ||
If these measures do not work, individualized treatment of the sexual dysfunction becomes necessary. For some patients, switching psychotropics may be necessary to ensure compliance and preserve response. In cases such as Mr. A’s, however, the physician and patient may not want to stop a psychotropic that is working. For these patients, consider adding a drug to restore sexual function.
If ED persists after treatment, the primary care physician may refer the patient to a urologist.
Case report:Continued
Mr. A was advised to quit smoking and control his blood pressure and diabetes. His primary care doctor restarted lisinopril, 20 mg/d, increased his metformin to 1,000 mg bid, and added sildenafil, 50 mg before anticipated sexual activity. Mr. A says sildenafil has worked well.
Psychotropics and sexual dysfunction
Several physiologic processes contribute to psychotropics’ sexual side effects.
Libido is primarily a function of hormonal and CNS control. By contrast, erectile functions are mediated through local parasympathetic stimulation and ejaculation, which are controlled by norepinephrine. Orgasm is a cerebral cortical event distinct from ejaculation; either process can be disturbed independently. Elevated central serotonin levels inhibit orgasm and, to a lesser extent, ejaculation. Dopamine elevation over time leads to hyperprolactinemia and resultant hypotestosteronemia, decreasing libido.
SSRIs have been associated with ED and ejaculatory disturbances. A high serotonin-to-dopamine reuptake inhibition ratio associated with these agents may contribute to ED. Paroxetine has a higher serotonin-to-dopamine reuptake inhibition ratio—and is associated with a higher incidence of sexual dysfunction—than other SSRIs.7
Elevated central serotonin concentrations associated with SSRIs may also inhibit orgasm. SSRIs have been used to prolong orgasm in patients experiencing premature ejaculation.8
Venlafaxine, a serotonin/norepinephrine reuptake inhibitor, exhibits similar effects on sexual function as SSRIs, probably via the same serotonin/dopamine reuptake mechanisms. The lowest effective dosage can still cause sexual dysfunction but may reduce the likelihood.
TCAs. Tricyclic antidepressants may have fewer effects on sexual function than SSRIs. The mechanisms by which TCAs decrease libido and cause ED seem to be mediated through their CNS sedative and local anticholinergic effects.
MAOIs. Monoamine oxidase inhibitors have fewer effects on sexual function than SSRIs or TCAs, but these agents are rarely used to treat depression because of their adverse effects and drug-drug interactions.
Other antidepressants. Trazodone and nefazodone exhibit similar mechanisms of antidepressant action as SSRIs, but neither agent causes significant ED or ejaculatory disturbances. Priapism has been described with use of these agents, however.
Avoid using nefazodone in patients with hepatic dysfunction and in those who have taken an MAOI within 14 days.
Mirtazapine, a novel antidepressant with antiserotonergic actions, and bupropion, a dopamine and norepinephrine reuptake inhibitor, are not associated with significant sexual dysfunction compared with placebo. These agents are good alternatives to SSRIs9-11 and may alleviate sexual dysfunction when used to augment SSRIs.12,13
Lithium has been shown to decrease libido and cause ED. Lithium-mediated CNS sedation contributes to decreased libido; other mechanisms of lithium’s sexual side effects are not known. It is unclear whether lower dosages reduce the likelihood of sexual dysfunction.
Anticonvulsants. In two small studies, phenytoin increased sex hormone-binding globulin, resulting in lower free testosterone levels, which may lead to sexual dysfunction.18,19 Barbiturates have been shown to decrease libido, probably because of CNS sedation. Carbamazepine and gabapentin exhibit antiandrogenic effects, leading to various types of sexual dysfunction. These effects have not been observed with oxcarbazepine, however.
Lamotrigine may be an effective alternative in patients exhibiting sexual dysfunction with gabapentin.20
Typical antipsychotics can impair all aspects of sexual function:14
- CNS sedation and hyperprolactinemia account for decreased libido.
- Local anticholinergic effects may cause ED. Thus, the greater the anticholinergic effects, the presumably higher the incidence of ED.
- Alpha-receptor blockade and inhibition of inner urethral sphincter closure may cause retarded and retrograde ejaculation, respectively.
Of the conventional antipsychotics, thioridazine is associated with the highest incidence of sexual dysfunction.15
Table 3
Side effects, drug interactions associated with PDE-5 inhibitors
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Sildenafil | Dyspepsia, flushing, headache, hypotension, myocardial infarction (rare), nasal congestion, rash, visual disturbances | CYP-2C9 inducers and inhibitors (minor alterations in sildenafil plasma concentration) CYP-3A4 inducers and inhibitors (major alterations in sildenafil plasma concentration) Dihydrocodeine (rare priapism) Nitrates (severe hypotension) |
| Tadalafil* | Headache, dyspepsia, back pain, myalgia, nasal congestion, flushing, pain in limb, visual disturbances | CYP-3A4 inhibitors (increase tadalafil exposure) Alpha blockers other than tamsulosin (hypotension) Nitrates (severe hypotension) |
| Vardenafil* | Dizziness, dyspepsia, headache, hypotension | CYP-3A4 inducers and inhibitors (altered vardenafil plasma concentration) Nitrates (severe hypotension) |
| * Tadalafil and vardenafil are still undergoing post-marketing surveillance. This explains in part why fewer adverse effects and drug-drug interactions have been reported with these agents than with sildenafil. | ||
Atypical antipsychotics exhibit fewer adverse effects on sexual function than their typical counterparts, but the mechanisms that mediate these effects are the same.
Of these agents, risperidone causes the greatest prolactin elevation.16 Aripiprazole may also be associated with minimal sexual dysfunction.17 Other atypicals decrease prolactin levels or raise them transiently,16,17 so consider switching to one of these agents if a patient experiences ED.
Anxiolytics. Benzodiazepines, with their CNS sedative effects, are associated with decreased libido. Their potential for abuse may augment this effect. Buspirone, a novel anxiolytic that exhibits serotonergic and dopaminergic effects, is not associated with significant sexual dysfunction and may be a viable alternative.
Others. Amphetamines can increase the local sympathetic-to-parasympathetic activity ratio, resulting in ED. This effect is more pronounced with long-term use, though it is also seen with short-term use.
ED also has been reported in patients taking disulfiram, though it is unclear whether the drug or long-term alcohol use caused the dysfunction.
Drug treatment of ED
Because primary ED is a quality-of-life issue and not a health risk, few comparative trials have tested medications that improve erectile function. Thus, ED drug treatment may require trials of two or more agents.
Adverse effects and drug-drug interactions of selected agents used for ED treatment are listed in Tables 3 and 4.
Phosphodiesterase (PDE-5) inhibitors have become widely used as first-line oral medications for ED secondary to numerous causes. Sildenafil has demonstrated effectiveness in treating SSRI-induced ED compared with placebo. Tadalafil and vardenafil have not been studied in patients taking SSRIs.
Table 4
Side effects, drug interactions associated with other ED agents
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Amantadine | Aggression, altered mentation, anxiety, heart failure (rare), insomnia, leukopenia (rare), nausea Livedo reticularis (with extended use), neuroleptic malignant syndrome (upon discontinuation), orthostatic hypotension, psychoses | Bupropion (increased adverse events) Triamterene (may increase amantadine plasma concentration) |
| Bethanechol | Cholinergic effects (increased GI motility, lacrimation, miosis, urinary frequency) Diaphoresis, flushing, headache, hypotension, tachycardia | Anticholinergics (decreased effects of both agents) Cholinesterase inhibitors (increased cholinergic effects), Ganglionic blockers (severe hypotension) |
| Bupropion | Agitation, amblyopia, arrhythmias (rare), constipation, diaphoresis, dizziness, extrapyramidal symptoms (rare), headache, hypertension Hypoprolactinemia, insomnia, leukopenia (minor), nausea/vomiting Alcohol psychoses (rare), seizures, serum sickness (rare), taste perversion, tinnitus, tremor, urinary frequency Urticaria, weight gain (rare), weight loss, xerostomia | CYP-2D6 inducers and inhibitors (altered bupropion plasma concentration) Dopamine-receptor agonists (increased adverse effects) MAOIs (increased seizures and psychoses) QT-prolonging agents (increased QT-prolongation) Alcohol, systemic steroids, theophylline (increased seizures) |
| Mirtazapine | Somnolence, constipation, xerostomia, increased appetite, weight gain, dizziness, abnormal dreams, confusion Hyperlipidemia, flu-like symptoms, back pain | MAO inhibitors, linezolid, CNS depressants (increased sedative effects) Alcohol (may increase CNS depression) St John’s wort (may decrease mirtazapine levels) |
| Ropinirole | Abdominal pain, anxiety, arthralgias, confusion, constipation, diaphoresis, dyskinesias, dyspepsia, headache Hallucinations, insomnia, nausea/vomiting, orthostatic hypotension, peripheral edema Somnolence, tremor, upper respiratory infection, urinary tract infection, visual disturbances, xerostomia | CYP-1A2 inducers and inhibitors (altered ropinirole plasma concentration) Dopamine-receptor antagonists (decreased efficacy of both agents) |
In one 6-week study,21 54.4% of patients taking both an SSRI and sildenafil, up to 100 mg, showed significantly improved erectile function, arousal, ejaculation, orgasm, and overall satisfaction. In another study,22 SSRI-treated patients receiving sildenafil, 5 to 200 mg before sexual activity, reported noticeably improved ability to achieve and maintain erection, ejaculate, and achieve orgasm.
Sildenafil should not be taken concomitantly with agents or products containing nitrates. Use sildenafil with caution in patients with a blood pressure >170/110 mm Hg or <90/50 mm Hg, unstable angina, or retinitis pigmentosa. Also use sildenafil cautiously in patients who have suffered myocardial infarction, stroke, or life-threatening arrhythmia within the last 6 months.
Bupropion. In double-blind trials,11,12 the agent’s sustained-release form has shown effectiveness as an alternative or adjunct to SSRIs in treating SSRI-induced ED. Prescribe at 150 mg nightly when used as an adjunct.
Bupropion is contraindicated in patients with bulimia, anorexia nervosa, and seizure disorders, and in patients taking MAOIs. Use bupropion cautiously in patients with cranial trauma, renal or hepatic insufficiency, uncontrolled hypertension, myocardial infarction, unstable cardiovascular disease, psychosis, and bipolar disorder, and in patients abusing alcohol or taking warfarin.
Amantadine, an oral dopamine-receptor agonist with innate cholinergic effects, has shown effectiveness against SSRI-induced ED when given at 200 mg bid in a small trial.23
Avoid using amantadine in patients with closed-angle glaucoma, and use with caution in patients with heart failure and in persons age 65 and older.
Mirtazapine, 15 mg/d, has shown effectiveness as an SSRI alternative and as SSRI augmentation therapy to alleviate sexual dysfunction.12,13
Mirtazapine is contraindicated in patients with hypersensitivity or in patients who have used an MAOI within 14 days. Be careful when combining mirtazapine with an SSRI as the combination may increase the risk of serotonin syndrome.
Ropinirole, an oral dopamine 2-receptor agonist used to treat Parkinson’s disease, has shown effectiveness against antidepressant-induced ED when given at 0.25 mg/d and titrated across 4 weeks to 2 to 4 mg/d.24 Use ropinirole carefully in patients with bradycardia, dyskinesias, hallucinations, renal or hepatic insufficiency, and hypotension.
Bethanechol, an oral cholinergic agent used to treat urinary retention, has been described in case reports to alleviate TCA-induced ED when given at 20 mg 1 to 2 hours before sexual activity.25,26 Bethanechol is contraindicated in patients with hyperthyroidism, peptic ulcer disease, asthma, bradycardia, hypotension, coronary artery disease, epilepsy, Parkinson’s disease, urinary bladder neck obstruction, spastic GI disturbances, acute inflammatory GI lesions, peritonitis, and vagotonia.
Related resources
- Miller TA. Diagnostic evaluation of erectile dysfunction. Am Fam Physician 2000;61:95-110.
- Viera AJ, Clenney TL, Shenenberger DW, Green GF. Newer pharmacologic alternatives for erectile dysfunction. Am Fam Physician 1999;60:1159-72.
- British Medical Journal Web site search: erectile dysfunction. http://bmj.bmjjournals.com/cgi/collection/erectile_dysfunction
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Bethanechol • Urecholine
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Dihydrocodeine • Synalgos
- Disulfiram • Antabuse
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Linezolid • Zyvox
- Lisinopril • Prinivil, others
- Lithium • Eskalith, others
- Metformin • Glucophage
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Risperidone • Risperdal
- Ropinirole • Requip
- Sertraline • Zoloft
- Sildenafil • Viagra
- Simvastatin • Zocor
- Tadalafil • Cialis
- Triamterene • Dyazide, others
- Trazodone • Desyrel, others
- Vardenafil • Levitra
- Warfarin • Coumadin
Disclosure
Dr. Viera and Mr. Conrad report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Choksi is a regional scientific manager for cardiovascular medicine with Novartis Pharmaceuticals Corp. When he co-wrote this article he was clinical coordinator, pharmacy department, Naval Hospital, Jacksonville, FL.
1. National Institutes of Health consensus conference on impotence. JAMA 1993;270:83-90.
2. Montejo-Gonzalez AL, Llorca G, Izquierdo JA, et al. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther 1997;23:176-94.
3. Harrison WM, Rabkin JG, Ehrhardt AA, et al. Effects of antidepressant medication on sexual function: a controlled study. J Clin Psychopharmacol 1986;6:144-9.
4. Benazzi F, Mazzoli M. Fluoxetine-induced sexual dysfunction: a dose-dependent effect? Pharmacopsychiatry 1994;27:246.-
5. Clinical management of depression: bupropion—an update. Monograph series, vol.1, no. 1. Proceedings of a closed symposium: Antidepressant drug therapy: bupropion—an update meeting, Boca Raton, FL, October 30-31, 1992.
6. Rothschild AJ. Selective serotonin reuptake inhibitor-induced sexual dysfunction: efficacy of a drug holiday. Am J Psychiatry 1995;152:1514-16.
7. Rosen RC, Lane RM, Menza M. Effects of SSRIs on sexual function: a critical review. J Clin Psychopharmacol 1999;19:67-85.
8. Waldinger MD, Hengeveld MW, Zwinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 1998;18:274-81.
9. Koutouvidis N, Pratikakis M, Fotiadou A. The use of mirtazapine in a group of 11 patients following poor compliance to selective serotonin reuptake inhibitor treatment due to sexual dysfunction. Int Clin Psychopharmacol 1999;14:253-5.
10. Gelenberg AJ, McGahuey C, Laukes C, et al. Mirtazapine substitution in SSRI-induced sexual dysfunction. J Clin Psychiatry 2000;61:356-60.
11. Segraves RT, Kavoussi R, Hughes AR, et al. Evaluation of sexual functioning in depressed outpatients: a double-blind comparison of sustained-release bupropion and sertraline treatment. J Clin Psychopharmacol 2000;20:122-8.
12. Masand PS, Ashton AK, Gupta S, Frank B. Sustained-release bupropion for selective serotonin reuptake inhibitor-induced sexual dysfunction: a randomized, double-blind, placebo-controlled, parallel-group study. Am J Psychiatry 2001;158:805-7.
13. Farah A. Relief of SSRI-induced sexual dysfunction with mirtazapine treatment. J Clin Psychiatry 1999;60:260-1.
14. Smith SM, O’Keane V, Murray R. Sexual dysfunction in patients taking conventional antipsychotic medication. Br J Psychiatry 2002;181:49-55.
15. Kotin J, Wilbert DE, Verburg D, Soldinger SM. Thioridazine and sexual dysfunction. Am J Psychiatry 1976;133:82-5.
16. Guthrie SK. Clinical issues associated with maintenance treatment of patients with schizophrenia. Am J Health-Syst Pharm 2002;59(suppl 5):519-24.
17. Goodnick PJ, Rodriguez L, Santana O. Antipsychotics: impact on prolactin levels. Expert Opin Pharmacother 2002;3:1381-91.
18. Brunet M, Rodamilans M, Martinez-Osaba MJ, et al. Effects of long-term antiepileptic therapy on the catabolism of testosterone. Pharmacol Toxicol 1995;76:371-5.
19. Heroz AG, Levesque LA, Drislane FW, et al. Phenytoin-induced elevation of serum estradiol and reproductive dysfunction in men with epilepsy. Epilepsia 1991;32:550-3.
20. Husain AM, Carwile ST, Miller PP, Radtke RA. Improved sexual function in three men taking lamotrigine for epilepsy. South Med J 2000;93:335-6.
21. Nurnberg HG, Hensley PL, Gelenberg AJ, et al. Treatment of antidepressant-associated sexual dysfunction with sildenafil. A randomized controlled trial. JAMA 2003;289:56-64.
22. Nurnberg HG, Gelenberg A, Hargreave TB, et al. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001;158:1926-8.
23. Shrivastava RK, Shrivastava S, Overweg N, Schmitt M. Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. J Clin Psychopharmacol 1995;15:83-4.
24. Worthington JJ, 3rd, Simon NM, Korbly NB, et al. Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol 2002;17:307-10.
25. Gross MD. Reversal by bethanechol of sexual dysfunction caused by anticholinergic antidepressants. Am J Psychiatry 1982;139:1193-4.
26. Yager J. Bethanechol chloride can reverse erectile and ejaculatory dysfunction induced by tricyclic antidepressants and mazindol: case report. J Clin Psychiatry 1986;47:210-11.
Many psychotropics can cause erectile dysfunction (ED) and other sexual problems (Tables 1 and 2). This side effect can discourage treatment compliance and jeopardize outcomes.
This article offers evidence-based strategies for preventing and treating psychotropic-induced ED. We also review information psychiatrists need to share with primary care physicians when treating a patient with ED.
Case report: A good relationship
Mr. A, age 52, has experienced diminishing erectile function for 6 months and now cannot achieve an erection. His relationship with his wife is good; he attributes loss of libido to his erection problem.
A pack-a-day smoker since age 18, Mr. A has type 2 diabetes and has been taking metformin, 850 mg bid, for 2 years. For about 2 months he has been taking sertraline, 50 mg, for depression and reports significantly improved mood, sleep, concentration, and appetite. He also has been taking lisinopril, 20 mg/d, for hypertension, and simvastatin, 40 mg nightly, for hyperlipidemia.
Table 1
Antidepressants associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Monoamine oxidase inhibitors | Unknown | ED (rare), retarded ejaculation(rare) |
| Selective serotonin reuptake inhibitors | Increased serum prolactin (possible) Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | Decreased libido ED Anorgasmia Delayed/retarded ejaculation |
| Tricyclic antidepressants | CNS depression Anticholinergic activity | Decreased libido ED |
| Venlafaxine | Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | ED Anorgasmia Delayed/retarded ejaculation |
| ED: Erectile dysfunction | ||
Mr. A’s hemoglobin A1C is 9.8%, indicating poor diabetes control. His blood pressure is 168/94 mm Hg, well above his goal of <135/80. He has no chest pain or history of myocardial infarction; a recent exercise stress test indicated no coronary disease.
Discussion. Several medical causes—diabetes, hypertension, hyperlipidemia, and 34 years of heavy smoking—could explain Mr. A’s ED. Vascular disease is suspected, although the stress test was negative.
Identifying a specific cause is crucial to treating ED but may be difficult. Up to 80% of cases can be traced to one or more organic causes.1 Mr. A’s depression could be a factor, although psychogenic ED is not common. Adding the selective serotonin reuptake inhibitor (SSRI) sertraline may also have worsened his ED.
Other possible causes of ED include:
- nonpsychotropic drugs (to view a list of agents, see this article at currentpsychiatry.com)
- decreased libido, delayed orgasm, and anorgasmia. Decreased libido and anorgasmia are often misdiagnosed as primary ED because the presenting symptoms are similar.
ED treatment begins with managing underlying medical problems, although optimal control alone may not alleviate ED. Encourage the patient to stop smoking and offer smoking cessation strategies.
Alert the primary care physician and patient when prescribing a psychotropic associated with sexual side effects, and explain the drug’s potential benefits. Assess baseline sexual function before starting the psychotropic so that changes in sexual function can be detected. Report your findings to the referring physician after each visit.
If ED is believed to be psychotropic-induced:
- maintain the psychotropic regimen for 6 to 8 weeksto see if the patient builds a tolerance to its sexual side effects.
- lower the psychotropic dosage. In one study,2 nearly 75% of patients whose SSRI dosages were reduced by one-half reported improved sexual function with sustained antidepressant effectiveness. This SSRIeffect has been replicated and has also been demonstrated with imipramine.3-5
- schedule 1- to 2-day drug “holidays” (on weekends, for example) for medications with a short halflife (such as sertraline or paroxetine) if the underlying condition permits.7
Table 2
Other psychotropics associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Amphetamines | Increased relative sympathetic nervous syndrome/parasympathetic nervous system activity | ED |
| Anticholinergics | Anticholinergic activity | ED |
| Antipsychotics (typical and atypical) | CNS depression, increased serum prolactin Anticholinergic activity Alpha1-receptor blockade Decreased internal urethral sphincter closure | Decreased libido ED Retarded ejaculation Retrograde ejaculation |
| Barbiturates, benzodiazepines, CNS depressants | CNS depression | Decreased libido |
| Carbamazepine, gabapentin | Decreased androgenic activity | Decreased libido, ED, retarded ejaculation |
| Disulfiram | Unknown | ED |
| Dopamine-receptor agonists | Unknown | ED |
| Dopamine-receptor antagonists | Increased serum prolactin | Decreased libido |
| ED: Erectile dysfunction | ||
If these measures do not work, individualized treatment of the sexual dysfunction becomes necessary. For some patients, switching psychotropics may be necessary to ensure compliance and preserve response. In cases such as Mr. A’s, however, the physician and patient may not want to stop a psychotropic that is working. For these patients, consider adding a drug to restore sexual function.
If ED persists after treatment, the primary care physician may refer the patient to a urologist.
Case report:Continued
Mr. A was advised to quit smoking and control his blood pressure and diabetes. His primary care doctor restarted lisinopril, 20 mg/d, increased his metformin to 1,000 mg bid, and added sildenafil, 50 mg before anticipated sexual activity. Mr. A says sildenafil has worked well.
Psychotropics and sexual dysfunction
Several physiologic processes contribute to psychotropics’ sexual side effects.
Libido is primarily a function of hormonal and CNS control. By contrast, erectile functions are mediated through local parasympathetic stimulation and ejaculation, which are controlled by norepinephrine. Orgasm is a cerebral cortical event distinct from ejaculation; either process can be disturbed independently. Elevated central serotonin levels inhibit orgasm and, to a lesser extent, ejaculation. Dopamine elevation over time leads to hyperprolactinemia and resultant hypotestosteronemia, decreasing libido.
SSRIs have been associated with ED and ejaculatory disturbances. A high serotonin-to-dopamine reuptake inhibition ratio associated with these agents may contribute to ED. Paroxetine has a higher serotonin-to-dopamine reuptake inhibition ratio—and is associated with a higher incidence of sexual dysfunction—than other SSRIs.7
Elevated central serotonin concentrations associated with SSRIs may also inhibit orgasm. SSRIs have been used to prolong orgasm in patients experiencing premature ejaculation.8
Venlafaxine, a serotonin/norepinephrine reuptake inhibitor, exhibits similar effects on sexual function as SSRIs, probably via the same serotonin/dopamine reuptake mechanisms. The lowest effective dosage can still cause sexual dysfunction but may reduce the likelihood.
TCAs. Tricyclic antidepressants may have fewer effects on sexual function than SSRIs. The mechanisms by which TCAs decrease libido and cause ED seem to be mediated through their CNS sedative and local anticholinergic effects.
MAOIs. Monoamine oxidase inhibitors have fewer effects on sexual function than SSRIs or TCAs, but these agents are rarely used to treat depression because of their adverse effects and drug-drug interactions.
Other antidepressants. Trazodone and nefazodone exhibit similar mechanisms of antidepressant action as SSRIs, but neither agent causes significant ED or ejaculatory disturbances. Priapism has been described with use of these agents, however.
Avoid using nefazodone in patients with hepatic dysfunction and in those who have taken an MAOI within 14 days.
Mirtazapine, a novel antidepressant with antiserotonergic actions, and bupropion, a dopamine and norepinephrine reuptake inhibitor, are not associated with significant sexual dysfunction compared with placebo. These agents are good alternatives to SSRIs9-11 and may alleviate sexual dysfunction when used to augment SSRIs.12,13
Lithium has been shown to decrease libido and cause ED. Lithium-mediated CNS sedation contributes to decreased libido; other mechanisms of lithium’s sexual side effects are not known. It is unclear whether lower dosages reduce the likelihood of sexual dysfunction.
Anticonvulsants. In two small studies, phenytoin increased sex hormone-binding globulin, resulting in lower free testosterone levels, which may lead to sexual dysfunction.18,19 Barbiturates have been shown to decrease libido, probably because of CNS sedation. Carbamazepine and gabapentin exhibit antiandrogenic effects, leading to various types of sexual dysfunction. These effects have not been observed with oxcarbazepine, however.
Lamotrigine may be an effective alternative in patients exhibiting sexual dysfunction with gabapentin.20
Typical antipsychotics can impair all aspects of sexual function:14
- CNS sedation and hyperprolactinemia account for decreased libido.
- Local anticholinergic effects may cause ED. Thus, the greater the anticholinergic effects, the presumably higher the incidence of ED.
- Alpha-receptor blockade and inhibition of inner urethral sphincter closure may cause retarded and retrograde ejaculation, respectively.
Of the conventional antipsychotics, thioridazine is associated with the highest incidence of sexual dysfunction.15
Table 3
Side effects, drug interactions associated with PDE-5 inhibitors
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Sildenafil | Dyspepsia, flushing, headache, hypotension, myocardial infarction (rare), nasal congestion, rash, visual disturbances | CYP-2C9 inducers and inhibitors (minor alterations in sildenafil plasma concentration) CYP-3A4 inducers and inhibitors (major alterations in sildenafil plasma concentration) Dihydrocodeine (rare priapism) Nitrates (severe hypotension) |
| Tadalafil* | Headache, dyspepsia, back pain, myalgia, nasal congestion, flushing, pain in limb, visual disturbances | CYP-3A4 inhibitors (increase tadalafil exposure) Alpha blockers other than tamsulosin (hypotension) Nitrates (severe hypotension) |
| Vardenafil* | Dizziness, dyspepsia, headache, hypotension | CYP-3A4 inducers and inhibitors (altered vardenafil plasma concentration) Nitrates (severe hypotension) |
| * Tadalafil and vardenafil are still undergoing post-marketing surveillance. This explains in part why fewer adverse effects and drug-drug interactions have been reported with these agents than with sildenafil. | ||
Atypical antipsychotics exhibit fewer adverse effects on sexual function than their typical counterparts, but the mechanisms that mediate these effects are the same.
Of these agents, risperidone causes the greatest prolactin elevation.16 Aripiprazole may also be associated with minimal sexual dysfunction.17 Other atypicals decrease prolactin levels or raise them transiently,16,17 so consider switching to one of these agents if a patient experiences ED.
Anxiolytics. Benzodiazepines, with their CNS sedative effects, are associated with decreased libido. Their potential for abuse may augment this effect. Buspirone, a novel anxiolytic that exhibits serotonergic and dopaminergic effects, is not associated with significant sexual dysfunction and may be a viable alternative.
Others. Amphetamines can increase the local sympathetic-to-parasympathetic activity ratio, resulting in ED. This effect is more pronounced with long-term use, though it is also seen with short-term use.
ED also has been reported in patients taking disulfiram, though it is unclear whether the drug or long-term alcohol use caused the dysfunction.
Drug treatment of ED
Because primary ED is a quality-of-life issue and not a health risk, few comparative trials have tested medications that improve erectile function. Thus, ED drug treatment may require trials of two or more agents.
Adverse effects and drug-drug interactions of selected agents used for ED treatment are listed in Tables 3 and 4.
Phosphodiesterase (PDE-5) inhibitors have become widely used as first-line oral medications for ED secondary to numerous causes. Sildenafil has demonstrated effectiveness in treating SSRI-induced ED compared with placebo. Tadalafil and vardenafil have not been studied in patients taking SSRIs.
Table 4
Side effects, drug interactions associated with other ED agents
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Amantadine | Aggression, altered mentation, anxiety, heart failure (rare), insomnia, leukopenia (rare), nausea Livedo reticularis (with extended use), neuroleptic malignant syndrome (upon discontinuation), orthostatic hypotension, psychoses | Bupropion (increased adverse events) Triamterene (may increase amantadine plasma concentration) |
| Bethanechol | Cholinergic effects (increased GI motility, lacrimation, miosis, urinary frequency) Diaphoresis, flushing, headache, hypotension, tachycardia | Anticholinergics (decreased effects of both agents) Cholinesterase inhibitors (increased cholinergic effects), Ganglionic blockers (severe hypotension) |
| Bupropion | Agitation, amblyopia, arrhythmias (rare), constipation, diaphoresis, dizziness, extrapyramidal symptoms (rare), headache, hypertension Hypoprolactinemia, insomnia, leukopenia (minor), nausea/vomiting Alcohol psychoses (rare), seizures, serum sickness (rare), taste perversion, tinnitus, tremor, urinary frequency Urticaria, weight gain (rare), weight loss, xerostomia | CYP-2D6 inducers and inhibitors (altered bupropion plasma concentration) Dopamine-receptor agonists (increased adverse effects) MAOIs (increased seizures and psychoses) QT-prolonging agents (increased QT-prolongation) Alcohol, systemic steroids, theophylline (increased seizures) |
| Mirtazapine | Somnolence, constipation, xerostomia, increased appetite, weight gain, dizziness, abnormal dreams, confusion Hyperlipidemia, flu-like symptoms, back pain | MAO inhibitors, linezolid, CNS depressants (increased sedative effects) Alcohol (may increase CNS depression) St John’s wort (may decrease mirtazapine levels) |
| Ropinirole | Abdominal pain, anxiety, arthralgias, confusion, constipation, diaphoresis, dyskinesias, dyspepsia, headache Hallucinations, insomnia, nausea/vomiting, orthostatic hypotension, peripheral edema Somnolence, tremor, upper respiratory infection, urinary tract infection, visual disturbances, xerostomia | CYP-1A2 inducers and inhibitors (altered ropinirole plasma concentration) Dopamine-receptor antagonists (decreased efficacy of both agents) |
In one 6-week study,21 54.4% of patients taking both an SSRI and sildenafil, up to 100 mg, showed significantly improved erectile function, arousal, ejaculation, orgasm, and overall satisfaction. In another study,22 SSRI-treated patients receiving sildenafil, 5 to 200 mg before sexual activity, reported noticeably improved ability to achieve and maintain erection, ejaculate, and achieve orgasm.
Sildenafil should not be taken concomitantly with agents or products containing nitrates. Use sildenafil with caution in patients with a blood pressure >170/110 mm Hg or <90/50 mm Hg, unstable angina, or retinitis pigmentosa. Also use sildenafil cautiously in patients who have suffered myocardial infarction, stroke, or life-threatening arrhythmia within the last 6 months.
Bupropion. In double-blind trials,11,12 the agent’s sustained-release form has shown effectiveness as an alternative or adjunct to SSRIs in treating SSRI-induced ED. Prescribe at 150 mg nightly when used as an adjunct.
Bupropion is contraindicated in patients with bulimia, anorexia nervosa, and seizure disorders, and in patients taking MAOIs. Use bupropion cautiously in patients with cranial trauma, renal or hepatic insufficiency, uncontrolled hypertension, myocardial infarction, unstable cardiovascular disease, psychosis, and bipolar disorder, and in patients abusing alcohol or taking warfarin.
Amantadine, an oral dopamine-receptor agonist with innate cholinergic effects, has shown effectiveness against SSRI-induced ED when given at 200 mg bid in a small trial.23
Avoid using amantadine in patients with closed-angle glaucoma, and use with caution in patients with heart failure and in persons age 65 and older.
Mirtazapine, 15 mg/d, has shown effectiveness as an SSRI alternative and as SSRI augmentation therapy to alleviate sexual dysfunction.12,13
Mirtazapine is contraindicated in patients with hypersensitivity or in patients who have used an MAOI within 14 days. Be careful when combining mirtazapine with an SSRI as the combination may increase the risk of serotonin syndrome.
Ropinirole, an oral dopamine 2-receptor agonist used to treat Parkinson’s disease, has shown effectiveness against antidepressant-induced ED when given at 0.25 mg/d and titrated across 4 weeks to 2 to 4 mg/d.24 Use ropinirole carefully in patients with bradycardia, dyskinesias, hallucinations, renal or hepatic insufficiency, and hypotension.
Bethanechol, an oral cholinergic agent used to treat urinary retention, has been described in case reports to alleviate TCA-induced ED when given at 20 mg 1 to 2 hours before sexual activity.25,26 Bethanechol is contraindicated in patients with hyperthyroidism, peptic ulcer disease, asthma, bradycardia, hypotension, coronary artery disease, epilepsy, Parkinson’s disease, urinary bladder neck obstruction, spastic GI disturbances, acute inflammatory GI lesions, peritonitis, and vagotonia.
Related resources
- Miller TA. Diagnostic evaluation of erectile dysfunction. Am Fam Physician 2000;61:95-110.
- Viera AJ, Clenney TL, Shenenberger DW, Green GF. Newer pharmacologic alternatives for erectile dysfunction. Am Fam Physician 1999;60:1159-72.
- British Medical Journal Web site search: erectile dysfunction. http://bmj.bmjjournals.com/cgi/collection/erectile_dysfunction
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Bethanechol • Urecholine
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Dihydrocodeine • Synalgos
- Disulfiram • Antabuse
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Linezolid • Zyvox
- Lisinopril • Prinivil, others
- Lithium • Eskalith, others
- Metformin • Glucophage
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Risperidone • Risperdal
- Ropinirole • Requip
- Sertraline • Zoloft
- Sildenafil • Viagra
- Simvastatin • Zocor
- Tadalafil • Cialis
- Triamterene • Dyazide, others
- Trazodone • Desyrel, others
- Vardenafil • Levitra
- Warfarin • Coumadin
Disclosure
Dr. Viera and Mr. Conrad report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Choksi is a regional scientific manager for cardiovascular medicine with Novartis Pharmaceuticals Corp. When he co-wrote this article he was clinical coordinator, pharmacy department, Naval Hospital, Jacksonville, FL.
Many psychotropics can cause erectile dysfunction (ED) and other sexual problems (Tables 1 and 2). This side effect can discourage treatment compliance and jeopardize outcomes.
This article offers evidence-based strategies for preventing and treating psychotropic-induced ED. We also review information psychiatrists need to share with primary care physicians when treating a patient with ED.
Case report: A good relationship
Mr. A, age 52, has experienced diminishing erectile function for 6 months and now cannot achieve an erection. His relationship with his wife is good; he attributes loss of libido to his erection problem.
A pack-a-day smoker since age 18, Mr. A has type 2 diabetes and has been taking metformin, 850 mg bid, for 2 years. For about 2 months he has been taking sertraline, 50 mg, for depression and reports significantly improved mood, sleep, concentration, and appetite. He also has been taking lisinopril, 20 mg/d, for hypertension, and simvastatin, 40 mg nightly, for hyperlipidemia.
Table 1
Antidepressants associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Monoamine oxidase inhibitors | Unknown | ED (rare), retarded ejaculation(rare) |
| Selective serotonin reuptake inhibitors | Increased serum prolactin (possible) Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | Decreased libido ED Anorgasmia Delayed/retarded ejaculation |
| Tricyclic antidepressants | CNS depression Anticholinergic activity | Decreased libido ED |
| Venlafaxine | Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | ED Anorgasmia Delayed/retarded ejaculation |
| ED: Erectile dysfunction | ||
Mr. A’s hemoglobin A1C is 9.8%, indicating poor diabetes control. His blood pressure is 168/94 mm Hg, well above his goal of <135/80. He has no chest pain or history of myocardial infarction; a recent exercise stress test indicated no coronary disease.
Discussion. Several medical causes—diabetes, hypertension, hyperlipidemia, and 34 years of heavy smoking—could explain Mr. A’s ED. Vascular disease is suspected, although the stress test was negative.
Identifying a specific cause is crucial to treating ED but may be difficult. Up to 80% of cases can be traced to one or more organic causes.1 Mr. A’s depression could be a factor, although psychogenic ED is not common. Adding the selective serotonin reuptake inhibitor (SSRI) sertraline may also have worsened his ED.
Other possible causes of ED include:
- nonpsychotropic drugs (to view a list of agents, see this article at currentpsychiatry.com)
- decreased libido, delayed orgasm, and anorgasmia. Decreased libido and anorgasmia are often misdiagnosed as primary ED because the presenting symptoms are similar.
ED treatment begins with managing underlying medical problems, although optimal control alone may not alleviate ED. Encourage the patient to stop smoking and offer smoking cessation strategies.
Alert the primary care physician and patient when prescribing a psychotropic associated with sexual side effects, and explain the drug’s potential benefits. Assess baseline sexual function before starting the psychotropic so that changes in sexual function can be detected. Report your findings to the referring physician after each visit.
If ED is believed to be psychotropic-induced:
- maintain the psychotropic regimen for 6 to 8 weeksto see if the patient builds a tolerance to its sexual side effects.
- lower the psychotropic dosage. In one study,2 nearly 75% of patients whose SSRI dosages were reduced by one-half reported improved sexual function with sustained antidepressant effectiveness. This SSRIeffect has been replicated and has also been demonstrated with imipramine.3-5
- schedule 1- to 2-day drug “holidays” (on weekends, for example) for medications with a short halflife (such as sertraline or paroxetine) if the underlying condition permits.7
Table 2
Other psychotropics associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Amphetamines | Increased relative sympathetic nervous syndrome/parasympathetic nervous system activity | ED |
| Anticholinergics | Anticholinergic activity | ED |
| Antipsychotics (typical and atypical) | CNS depression, increased serum prolactin Anticholinergic activity Alpha1-receptor blockade Decreased internal urethral sphincter closure | Decreased libido ED Retarded ejaculation Retrograde ejaculation |
| Barbiturates, benzodiazepines, CNS depressants | CNS depression | Decreased libido |
| Carbamazepine, gabapentin | Decreased androgenic activity | Decreased libido, ED, retarded ejaculation |
| Disulfiram | Unknown | ED |
| Dopamine-receptor agonists | Unknown | ED |
| Dopamine-receptor antagonists | Increased serum prolactin | Decreased libido |
| ED: Erectile dysfunction | ||
If these measures do not work, individualized treatment of the sexual dysfunction becomes necessary. For some patients, switching psychotropics may be necessary to ensure compliance and preserve response. In cases such as Mr. A’s, however, the physician and patient may not want to stop a psychotropic that is working. For these patients, consider adding a drug to restore sexual function.
If ED persists after treatment, the primary care physician may refer the patient to a urologist.
Case report:Continued
Mr. A was advised to quit smoking and control his blood pressure and diabetes. His primary care doctor restarted lisinopril, 20 mg/d, increased his metformin to 1,000 mg bid, and added sildenafil, 50 mg before anticipated sexual activity. Mr. A says sildenafil has worked well.
Psychotropics and sexual dysfunction
Several physiologic processes contribute to psychotropics’ sexual side effects.
Libido is primarily a function of hormonal and CNS control. By contrast, erectile functions are mediated through local parasympathetic stimulation and ejaculation, which are controlled by norepinephrine. Orgasm is a cerebral cortical event distinct from ejaculation; either process can be disturbed independently. Elevated central serotonin levels inhibit orgasm and, to a lesser extent, ejaculation. Dopamine elevation over time leads to hyperprolactinemia and resultant hypotestosteronemia, decreasing libido.
SSRIs have been associated with ED and ejaculatory disturbances. A high serotonin-to-dopamine reuptake inhibition ratio associated with these agents may contribute to ED. Paroxetine has a higher serotonin-to-dopamine reuptake inhibition ratio—and is associated with a higher incidence of sexual dysfunction—than other SSRIs.7
Elevated central serotonin concentrations associated with SSRIs may also inhibit orgasm. SSRIs have been used to prolong orgasm in patients experiencing premature ejaculation.8
Venlafaxine, a serotonin/norepinephrine reuptake inhibitor, exhibits similar effects on sexual function as SSRIs, probably via the same serotonin/dopamine reuptake mechanisms. The lowest effective dosage can still cause sexual dysfunction but may reduce the likelihood.
TCAs. Tricyclic antidepressants may have fewer effects on sexual function than SSRIs. The mechanisms by which TCAs decrease libido and cause ED seem to be mediated through their CNS sedative and local anticholinergic effects.
MAOIs. Monoamine oxidase inhibitors have fewer effects on sexual function than SSRIs or TCAs, but these agents are rarely used to treat depression because of their adverse effects and drug-drug interactions.
Other antidepressants. Trazodone and nefazodone exhibit similar mechanisms of antidepressant action as SSRIs, but neither agent causes significant ED or ejaculatory disturbances. Priapism has been described with use of these agents, however.
Avoid using nefazodone in patients with hepatic dysfunction and in those who have taken an MAOI within 14 days.
Mirtazapine, a novel antidepressant with antiserotonergic actions, and bupropion, a dopamine and norepinephrine reuptake inhibitor, are not associated with significant sexual dysfunction compared with placebo. These agents are good alternatives to SSRIs9-11 and may alleviate sexual dysfunction when used to augment SSRIs.12,13
Lithium has been shown to decrease libido and cause ED. Lithium-mediated CNS sedation contributes to decreased libido; other mechanisms of lithium’s sexual side effects are not known. It is unclear whether lower dosages reduce the likelihood of sexual dysfunction.
Anticonvulsants. In two small studies, phenytoin increased sex hormone-binding globulin, resulting in lower free testosterone levels, which may lead to sexual dysfunction.18,19 Barbiturates have been shown to decrease libido, probably because of CNS sedation. Carbamazepine and gabapentin exhibit antiandrogenic effects, leading to various types of sexual dysfunction. These effects have not been observed with oxcarbazepine, however.
Lamotrigine may be an effective alternative in patients exhibiting sexual dysfunction with gabapentin.20
Typical antipsychotics can impair all aspects of sexual function:14
- CNS sedation and hyperprolactinemia account for decreased libido.
- Local anticholinergic effects may cause ED. Thus, the greater the anticholinergic effects, the presumably higher the incidence of ED.
- Alpha-receptor blockade and inhibition of inner urethral sphincter closure may cause retarded and retrograde ejaculation, respectively.
Of the conventional antipsychotics, thioridazine is associated with the highest incidence of sexual dysfunction.15
Table 3
Side effects, drug interactions associated with PDE-5 inhibitors
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Sildenafil | Dyspepsia, flushing, headache, hypotension, myocardial infarction (rare), nasal congestion, rash, visual disturbances | CYP-2C9 inducers and inhibitors (minor alterations in sildenafil plasma concentration) CYP-3A4 inducers and inhibitors (major alterations in sildenafil plasma concentration) Dihydrocodeine (rare priapism) Nitrates (severe hypotension) |
| Tadalafil* | Headache, dyspepsia, back pain, myalgia, nasal congestion, flushing, pain in limb, visual disturbances | CYP-3A4 inhibitors (increase tadalafil exposure) Alpha blockers other than tamsulosin (hypotension) Nitrates (severe hypotension) |
| Vardenafil* | Dizziness, dyspepsia, headache, hypotension | CYP-3A4 inducers and inhibitors (altered vardenafil plasma concentration) Nitrates (severe hypotension) |
| * Tadalafil and vardenafil are still undergoing post-marketing surveillance. This explains in part why fewer adverse effects and drug-drug interactions have been reported with these agents than with sildenafil. | ||
Atypical antipsychotics exhibit fewer adverse effects on sexual function than their typical counterparts, but the mechanisms that mediate these effects are the same.
Of these agents, risperidone causes the greatest prolactin elevation.16 Aripiprazole may also be associated with minimal sexual dysfunction.17 Other atypicals decrease prolactin levels or raise them transiently,16,17 so consider switching to one of these agents if a patient experiences ED.
Anxiolytics. Benzodiazepines, with their CNS sedative effects, are associated with decreased libido. Their potential for abuse may augment this effect. Buspirone, a novel anxiolytic that exhibits serotonergic and dopaminergic effects, is not associated with significant sexual dysfunction and may be a viable alternative.
Others. Amphetamines can increase the local sympathetic-to-parasympathetic activity ratio, resulting in ED. This effect is more pronounced with long-term use, though it is also seen with short-term use.
ED also has been reported in patients taking disulfiram, though it is unclear whether the drug or long-term alcohol use caused the dysfunction.
Drug treatment of ED
Because primary ED is a quality-of-life issue and not a health risk, few comparative trials have tested medications that improve erectile function. Thus, ED drug treatment may require trials of two or more agents.
Adverse effects and drug-drug interactions of selected agents used for ED treatment are listed in Tables 3 and 4.
Phosphodiesterase (PDE-5) inhibitors have become widely used as first-line oral medications for ED secondary to numerous causes. Sildenafil has demonstrated effectiveness in treating SSRI-induced ED compared with placebo. Tadalafil and vardenafil have not been studied in patients taking SSRIs.
Table 4
Side effects, drug interactions associated with other ED agents
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Amantadine | Aggression, altered mentation, anxiety, heart failure (rare), insomnia, leukopenia (rare), nausea Livedo reticularis (with extended use), neuroleptic malignant syndrome (upon discontinuation), orthostatic hypotension, psychoses | Bupropion (increased adverse events) Triamterene (may increase amantadine plasma concentration) |
| Bethanechol | Cholinergic effects (increased GI motility, lacrimation, miosis, urinary frequency) Diaphoresis, flushing, headache, hypotension, tachycardia | Anticholinergics (decreased effects of both agents) Cholinesterase inhibitors (increased cholinergic effects), Ganglionic blockers (severe hypotension) |
| Bupropion | Agitation, amblyopia, arrhythmias (rare), constipation, diaphoresis, dizziness, extrapyramidal symptoms (rare), headache, hypertension Hypoprolactinemia, insomnia, leukopenia (minor), nausea/vomiting Alcohol psychoses (rare), seizures, serum sickness (rare), taste perversion, tinnitus, tremor, urinary frequency Urticaria, weight gain (rare), weight loss, xerostomia | CYP-2D6 inducers and inhibitors (altered bupropion plasma concentration) Dopamine-receptor agonists (increased adverse effects) MAOIs (increased seizures and psychoses) QT-prolonging agents (increased QT-prolongation) Alcohol, systemic steroids, theophylline (increased seizures) |
| Mirtazapine | Somnolence, constipation, xerostomia, increased appetite, weight gain, dizziness, abnormal dreams, confusion Hyperlipidemia, flu-like symptoms, back pain | MAO inhibitors, linezolid, CNS depressants (increased sedative effects) Alcohol (may increase CNS depression) St John’s wort (may decrease mirtazapine levels) |
| Ropinirole | Abdominal pain, anxiety, arthralgias, confusion, constipation, diaphoresis, dyskinesias, dyspepsia, headache Hallucinations, insomnia, nausea/vomiting, orthostatic hypotension, peripheral edema Somnolence, tremor, upper respiratory infection, urinary tract infection, visual disturbances, xerostomia | CYP-1A2 inducers and inhibitors (altered ropinirole plasma concentration) Dopamine-receptor antagonists (decreased efficacy of both agents) |
In one 6-week study,21 54.4% of patients taking both an SSRI and sildenafil, up to 100 mg, showed significantly improved erectile function, arousal, ejaculation, orgasm, and overall satisfaction. In another study,22 SSRI-treated patients receiving sildenafil, 5 to 200 mg before sexual activity, reported noticeably improved ability to achieve and maintain erection, ejaculate, and achieve orgasm.
Sildenafil should not be taken concomitantly with agents or products containing nitrates. Use sildenafil with caution in patients with a blood pressure >170/110 mm Hg or <90/50 mm Hg, unstable angina, or retinitis pigmentosa. Also use sildenafil cautiously in patients who have suffered myocardial infarction, stroke, or life-threatening arrhythmia within the last 6 months.
Bupropion. In double-blind trials,11,12 the agent’s sustained-release form has shown effectiveness as an alternative or adjunct to SSRIs in treating SSRI-induced ED. Prescribe at 150 mg nightly when used as an adjunct.
Bupropion is contraindicated in patients with bulimia, anorexia nervosa, and seizure disorders, and in patients taking MAOIs. Use bupropion cautiously in patients with cranial trauma, renal or hepatic insufficiency, uncontrolled hypertension, myocardial infarction, unstable cardiovascular disease, psychosis, and bipolar disorder, and in patients abusing alcohol or taking warfarin.
Amantadine, an oral dopamine-receptor agonist with innate cholinergic effects, has shown effectiveness against SSRI-induced ED when given at 200 mg bid in a small trial.23
Avoid using amantadine in patients with closed-angle glaucoma, and use with caution in patients with heart failure and in persons age 65 and older.
Mirtazapine, 15 mg/d, has shown effectiveness as an SSRI alternative and as SSRI augmentation therapy to alleviate sexual dysfunction.12,13
Mirtazapine is contraindicated in patients with hypersensitivity or in patients who have used an MAOI within 14 days. Be careful when combining mirtazapine with an SSRI as the combination may increase the risk of serotonin syndrome.
Ropinirole, an oral dopamine 2-receptor agonist used to treat Parkinson’s disease, has shown effectiveness against antidepressant-induced ED when given at 0.25 mg/d and titrated across 4 weeks to 2 to 4 mg/d.24 Use ropinirole carefully in patients with bradycardia, dyskinesias, hallucinations, renal or hepatic insufficiency, and hypotension.
Bethanechol, an oral cholinergic agent used to treat urinary retention, has been described in case reports to alleviate TCA-induced ED when given at 20 mg 1 to 2 hours before sexual activity.25,26 Bethanechol is contraindicated in patients with hyperthyroidism, peptic ulcer disease, asthma, bradycardia, hypotension, coronary artery disease, epilepsy, Parkinson’s disease, urinary bladder neck obstruction, spastic GI disturbances, acute inflammatory GI lesions, peritonitis, and vagotonia.
Related resources
- Miller TA. Diagnostic evaluation of erectile dysfunction. Am Fam Physician 2000;61:95-110.
- Viera AJ, Clenney TL, Shenenberger DW, Green GF. Newer pharmacologic alternatives for erectile dysfunction. Am Fam Physician 1999;60:1159-72.
- British Medical Journal Web site search: erectile dysfunction. http://bmj.bmjjournals.com/cgi/collection/erectile_dysfunction
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Bethanechol • Urecholine
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Dihydrocodeine • Synalgos
- Disulfiram • Antabuse
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Linezolid • Zyvox
- Lisinopril • Prinivil, others
- Lithium • Eskalith, others
- Metformin • Glucophage
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Risperidone • Risperdal
- Ropinirole • Requip
- Sertraline • Zoloft
- Sildenafil • Viagra
- Simvastatin • Zocor
- Tadalafil • Cialis
- Triamterene • Dyazide, others
- Trazodone • Desyrel, others
- Vardenafil • Levitra
- Warfarin • Coumadin
Disclosure
Dr. Viera and Mr. Conrad report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Choksi is a regional scientific manager for cardiovascular medicine with Novartis Pharmaceuticals Corp. When he co-wrote this article he was clinical coordinator, pharmacy department, Naval Hospital, Jacksonville, FL.
1. National Institutes of Health consensus conference on impotence. JAMA 1993;270:83-90.
2. Montejo-Gonzalez AL, Llorca G, Izquierdo JA, et al. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther 1997;23:176-94.
3. Harrison WM, Rabkin JG, Ehrhardt AA, et al. Effects of antidepressant medication on sexual function: a controlled study. J Clin Psychopharmacol 1986;6:144-9.
4. Benazzi F, Mazzoli M. Fluoxetine-induced sexual dysfunction: a dose-dependent effect? Pharmacopsychiatry 1994;27:246.-
5. Clinical management of depression: bupropion—an update. Monograph series, vol.1, no. 1. Proceedings of a closed symposium: Antidepressant drug therapy: bupropion—an update meeting, Boca Raton, FL, October 30-31, 1992.
6. Rothschild AJ. Selective serotonin reuptake inhibitor-induced sexual dysfunction: efficacy of a drug holiday. Am J Psychiatry 1995;152:1514-16.
7. Rosen RC, Lane RM, Menza M. Effects of SSRIs on sexual function: a critical review. J Clin Psychopharmacol 1999;19:67-85.
8. Waldinger MD, Hengeveld MW, Zwinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 1998;18:274-81.
9. Koutouvidis N, Pratikakis M, Fotiadou A. The use of mirtazapine in a group of 11 patients following poor compliance to selective serotonin reuptake inhibitor treatment due to sexual dysfunction. Int Clin Psychopharmacol 1999;14:253-5.
10. Gelenberg AJ, McGahuey C, Laukes C, et al. Mirtazapine substitution in SSRI-induced sexual dysfunction. J Clin Psychiatry 2000;61:356-60.
11. Segraves RT, Kavoussi R, Hughes AR, et al. Evaluation of sexual functioning in depressed outpatients: a double-blind comparison of sustained-release bupropion and sertraline treatment. J Clin Psychopharmacol 2000;20:122-8.
12. Masand PS, Ashton AK, Gupta S, Frank B. Sustained-release bupropion for selective serotonin reuptake inhibitor-induced sexual dysfunction: a randomized, double-blind, placebo-controlled, parallel-group study. Am J Psychiatry 2001;158:805-7.
13. Farah A. Relief of SSRI-induced sexual dysfunction with mirtazapine treatment. J Clin Psychiatry 1999;60:260-1.
14. Smith SM, O’Keane V, Murray R. Sexual dysfunction in patients taking conventional antipsychotic medication. Br J Psychiatry 2002;181:49-55.
15. Kotin J, Wilbert DE, Verburg D, Soldinger SM. Thioridazine and sexual dysfunction. Am J Psychiatry 1976;133:82-5.
16. Guthrie SK. Clinical issues associated with maintenance treatment of patients with schizophrenia. Am J Health-Syst Pharm 2002;59(suppl 5):519-24.
17. Goodnick PJ, Rodriguez L, Santana O. Antipsychotics: impact on prolactin levels. Expert Opin Pharmacother 2002;3:1381-91.
18. Brunet M, Rodamilans M, Martinez-Osaba MJ, et al. Effects of long-term antiepileptic therapy on the catabolism of testosterone. Pharmacol Toxicol 1995;76:371-5.
19. Heroz AG, Levesque LA, Drislane FW, et al. Phenytoin-induced elevation of serum estradiol and reproductive dysfunction in men with epilepsy. Epilepsia 1991;32:550-3.
20. Husain AM, Carwile ST, Miller PP, Radtke RA. Improved sexual function in three men taking lamotrigine for epilepsy. South Med J 2000;93:335-6.
21. Nurnberg HG, Hensley PL, Gelenberg AJ, et al. Treatment of antidepressant-associated sexual dysfunction with sildenafil. A randomized controlled trial. JAMA 2003;289:56-64.
22. Nurnberg HG, Gelenberg A, Hargreave TB, et al. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001;158:1926-8.
23. Shrivastava RK, Shrivastava S, Overweg N, Schmitt M. Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. J Clin Psychopharmacol 1995;15:83-4.
24. Worthington JJ, 3rd, Simon NM, Korbly NB, et al. Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol 2002;17:307-10.
25. Gross MD. Reversal by bethanechol of sexual dysfunction caused by anticholinergic antidepressants. Am J Psychiatry 1982;139:1193-4.
26. Yager J. Bethanechol chloride can reverse erectile and ejaculatory dysfunction induced by tricyclic antidepressants and mazindol: case report. J Clin Psychiatry 1986;47:210-11.
1. National Institutes of Health consensus conference on impotence. JAMA 1993;270:83-90.
2. Montejo-Gonzalez AL, Llorca G, Izquierdo JA, et al. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther 1997;23:176-94.
3. Harrison WM, Rabkin JG, Ehrhardt AA, et al. Effects of antidepressant medication on sexual function: a controlled study. J Clin Psychopharmacol 1986;6:144-9.
4. Benazzi F, Mazzoli M. Fluoxetine-induced sexual dysfunction: a dose-dependent effect? Pharmacopsychiatry 1994;27:246.-
5. Clinical management of depression: bupropion—an update. Monograph series, vol.1, no. 1. Proceedings of a closed symposium: Antidepressant drug therapy: bupropion—an update meeting, Boca Raton, FL, October 30-31, 1992.
6. Rothschild AJ. Selective serotonin reuptake inhibitor-induced sexual dysfunction: efficacy of a drug holiday. Am J Psychiatry 1995;152:1514-16.
7. Rosen RC, Lane RM, Menza M. Effects of SSRIs on sexual function: a critical review. J Clin Psychopharmacol 1999;19:67-85.
8. Waldinger MD, Hengeveld MW, Zwinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 1998;18:274-81.
9. Koutouvidis N, Pratikakis M, Fotiadou A. The use of mirtazapine in a group of 11 patients following poor compliance to selective serotonin reuptake inhibitor treatment due to sexual dysfunction. Int Clin Psychopharmacol 1999;14:253-5.
10. Gelenberg AJ, McGahuey C, Laukes C, et al. Mirtazapine substitution in SSRI-induced sexual dysfunction. J Clin Psychiatry 2000;61:356-60.
11. Segraves RT, Kavoussi R, Hughes AR, et al. Evaluation of sexual functioning in depressed outpatients: a double-blind comparison of sustained-release bupropion and sertraline treatment. J Clin Psychopharmacol 2000;20:122-8.
12. Masand PS, Ashton AK, Gupta S, Frank B. Sustained-release bupropion for selective serotonin reuptake inhibitor-induced sexual dysfunction: a randomized, double-blind, placebo-controlled, parallel-group study. Am J Psychiatry 2001;158:805-7.
13. Farah A. Relief of SSRI-induced sexual dysfunction with mirtazapine treatment. J Clin Psychiatry 1999;60:260-1.
14. Smith SM, O’Keane V, Murray R. Sexual dysfunction in patients taking conventional antipsychotic medication. Br J Psychiatry 2002;181:49-55.
15. Kotin J, Wilbert DE, Verburg D, Soldinger SM. Thioridazine and sexual dysfunction. Am J Psychiatry 1976;133:82-5.
16. Guthrie SK. Clinical issues associated with maintenance treatment of patients with schizophrenia. Am J Health-Syst Pharm 2002;59(suppl 5):519-24.
17. Goodnick PJ, Rodriguez L, Santana O. Antipsychotics: impact on prolactin levels. Expert Opin Pharmacother 2002;3:1381-91.
18. Brunet M, Rodamilans M, Martinez-Osaba MJ, et al. Effects of long-term antiepileptic therapy on the catabolism of testosterone. Pharmacol Toxicol 1995;76:371-5.
19. Heroz AG, Levesque LA, Drislane FW, et al. Phenytoin-induced elevation of serum estradiol and reproductive dysfunction in men with epilepsy. Epilepsia 1991;32:550-3.
20. Husain AM, Carwile ST, Miller PP, Radtke RA. Improved sexual function in three men taking lamotrigine for epilepsy. South Med J 2000;93:335-6.
21. Nurnberg HG, Hensley PL, Gelenberg AJ, et al. Treatment of antidepressant-associated sexual dysfunction with sildenafil. A randomized controlled trial. JAMA 2003;289:56-64.
22. Nurnberg HG, Gelenberg A, Hargreave TB, et al. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001;158:1926-8.
23. Shrivastava RK, Shrivastava S, Overweg N, Schmitt M. Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. J Clin Psychopharmacol 1995;15:83-4.
24. Worthington JJ, 3rd, Simon NM, Korbly NB, et al. Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol 2002;17:307-10.
25. Gross MD. Reversal by bethanechol of sexual dysfunction caused by anticholinergic antidepressants. Am J Psychiatry 1982;139:1193-4.
26. Yager J. Bethanechol chloride can reverse erectile and ejaculatory dysfunction induced by tricyclic antidepressants and mazindol: case report. J Clin Psychiatry 1986;47:210-11.
Chemical ‘warfare’ in Philadelphia
Emergency presentation: A rough commute
Mr. R, age 25, presented to the emergency room confused and severely agitated. That morning, his parents found him in his Philadelphia apartment covering his mouth and nose with a T-shirt to guard against imminent chemical warfare.
The day before, Mr. R had developed auditory and visual hallucinations and paranoid and persecutory delusions. That day, on his way to work, he said he had seen “terrorists releasing toxic chemicals into the air” and heard “whispers of terrorists plotting an attack on the East Coast.”
Mr. R showed no suicidal or homicidal ideations. He denied significant medical or surgical history but reported that he had recently been diagnosed with depression after a “bad Ecstasy experience.” For 6 months he had been taking paroxetine, 20 mg once daily, and bupropion, 150 mg once daily, for his depression.
At age 18, Mr. R was diagnosed with attention-deficit/hyperactivity disorder (ADHD) after years of struggling through school with impaired concentration. At that time, he began taking methylphenidate, 10 mg each morning, and completed 3 years of college in North Carolina. He then dropped out of college and attempted suicide twice.
After the second suicide attempt, a psychiatrist diagnosed Mr. R as having major depression. The psychiatrist discontinued methylphenidate and started bupropion, dosage unknown. After 1 year, he stopped taking the antidepressant, thinking he no longer needed it.
Last year, Mr. R moved back to Philadelphia to be closer to his parents. Shortly afterward, he began obtaining methylphenidate illegally and later starting using cocaine, marijuana, amphetamines, and 3,4-methylenedioxymethamphetamine (“Ecstasy”).
At presentation, Mr. R’s mood was dysphoric with bizarre affect. Eye contact was poor with easy distractibility. Speech was pressured, with full range. His thought process was grossly disorganized with tangential thinking and flight of ideas. His short- and long-term memory were intact; insight and judgment were limited. A Mini-Mental State Examination could not be completed because of his disorganization and distractibility.
Does Mr. R. have schizophrenia or schizoaffective disorder? Or are his symptoms related to ADHD or substance abuse?
The authors’ observations
Mr. R’s paranoid delusions and hallucinations may suggest schizophrenia. With his history of suicide attempts, a depressive or schizoaffective disorder may also be considered.
However, Mr. R is close with his family and has several friends. His parents say he has not been withdrawn or paranoid, and there is no known family history of mood disorder, substance abuse, or other psychiatric illness. Mr. R also has been working steadily and had worked the night before presenting to us, so schizophrenia and schizoaffective disorder are ruled out. ADHD and abuse of multiple substances could explain his behavior because overdose of stimulants and illicit drugs may produce a psychotic event.
Further history: The power of addiction
After more questioning, Mr. R said that he had recently started using gamma butyrolactone (GBL) in a failed attempt to build muscle. For 4 months he had been taking 3.5 oz of GBL daily—0.25 oz every 2 to 3 hours and 0.75 oz at night to help him sleep.
Within 6 hours of his most recent GBL dose (reportedly 1 oz), Mr. R developed intractable nausea, vomiting, and flatus, followed quickly by anxiety, palpitations, and generalized hand/body tremors that disturbed his sleep. Hallucinations and delusions started the next day.
At presentation, Mr. R’s blood pressure was 188/92 mm Hg, his heart rate was 110 bpm, and his respiratory rate was 22 breaths per minute. Pupils were 5 mm and reactive with intact extraocular movement. A urine drug screen indicated amphetamine use.
Mr. R was tentatively diagnosed as having GBL withdrawal syndrome and was admitted for observation and treatment. The psychiatry service followed him for change in mental status and drug dependence.
Can a withdrawal syndrome reasonably account for Mr. R’s symptoms?
The authors’ observations
GBL is a precursor of gamma-hydroxybutyrate (GHB), a highly addictive agent that is used illicitly, typically at parties and nightclubs (Box). GBL is among the clinical analogues of GHB that have become popular street drugs.
GHB withdrawal syndrome has only recently been described in the literature and is virtually indistinguishable from withdrawal after cessation of GBL and other precursors. To date, 71 deaths have been attributed to GHB withdrawal.2
A constellation of symptoms exhibited by Mr. R point to GHB withdrawal, which should be included in the differential diagnosis of any sedative/hypnotic withdrawal (Table 1).
How GHB works. GHB easily crosses the blood-brain barrier. Like other sedative/hypnotics, its depressant effects on the brain in low doses (2 to 4 grams) produce a euphoric feeling as inhibitions are depressed. Profound coma or death result from higher doses (>4 grams).3 Heart rate may also be slowed and CNS effects may result in myoclonus, producing seizure-like movements. Combining GHB with other drugs can increase the other agents’ depressant effects, leading to confusion, amnesia, vomiting, irregular breathing, or death.2
Introduced in 1960 as an anesthetic, gamma-hydroxybutyrate (GHB) has become a notorious recreational drug. It is often called the “date rape drug” because of its intoxicating sedative effects.
Users have viewed GHB as a dietary supplement that can also enhance athletic and sexual performance, relieve depression, and induce sleep. Weightlifters have used GHB to quickly build muscle while avoiding side effects associated with anabolic steroids.
As more products containing GHB were introduced, many serious adverse events—including seizure, respiratory depression, and profound decreases in consciousness—were identified with its use and misuse. Although the Food and Drug Administration banned over-the-counter sales of GHB in 1990,1 the agent is still widely available on the black market and over the Internet.
GHB also is marketed through its chemical precursors, specifically GBL and 1,4-butanediol. These precursors are rapidly and systemically converted to the active GHB product. GBL is hydrolyzed by a peripheral lactonase, and 1,4-butanediol is processed by alcohol dehydrogenase and aldehyde dehydrogenase—the enzymes involved in ethanol degradation.1
A tiny increase in GHB dose can dramatically increase the symptoms and risk of overdose.4 GHB’s effects are also variable: A 1-teaspoon dose can produce the desired “high” one time and an overdose the next.
GHB and ethanol share a common mechanism of action.5 At pharmacologic doses, GHB appears to act in part through effects on the structurally related GABA neurotransmitter or its receptors.
Not surprisingly, a withdrawal syndrome characterized by delirium and autonomic instability ensues after GHB use is abruptly stopped. By functioning as indirect GABA agonists and ultimately evoking inhibitory neurotransmission, benzodiazepines and most barbiturates may alleviate GHB withdrawal symptoms.4 Thiamine is added to prevent Wernicke-Korsakoff syndrome, as is seen in alcohol withdrawal.5
GHB withdrawal. Symptoms are divided into three phases:
• Phase 1 (acute, first 24 hours). Presenting symptoms include anxiety, restlessness, insomnia, tremor, diaphoresis, tachycardia, and hypertension. Nausea and vomiting are variable but can be unrelenting.
While symptoms vary in severity, most prominent are agitation, restlessness, and insomnia. Some patients do not sleep for days after their last dose, and diffuse body tremors prevent them from sitting or lying still. Tachycardia and hypertension are hard to evaluate at this phase because patients present at different stages of withdrawal. Initial blood pressure readings as high as 240/130 mm Hg and heart rates of 120 bpm have been reported, however.
• Phase 2 (days 2 through 6). Worsening autonomic symptoms, progressive GI symptoms, and overall worsening of the withdrawal mark this tumultuous period. Patients usually present at this point—in acute distress and no longer able to self-treat.
Confusion, delirium, and florid psychosis characterize this phase. Mr. R’s paranoid delusions and hallucinations are the most common form of psychosis seen in GHB withdrawal.5 In some cases, the psychosis impairs social, occupational, and other functioning.
Table 1
Comparison of sedative-hypnotic withdrawal syndromes
| Substance | Onset | Duration of severe symptoms | Autonomic instability* | Neurologic/psychiatric symptoms | Mortality | Major mechanism inducing withdrawal state‡ |
|---|---|---|---|---|---|---|
| GHB | <6 hours | 5 to 12 days | Mild | Severe | <1% | Loss of GHB, GABAA, and GABAB-mediated inhibition |
| Benzodiazepines | 1 to 3 days | 5 to 9 days | Moderate | Moderate | 1% | Loss of GABAA-mediated inhibition |
| Baclofen | 12 to 96 hours | 8 days | Moderate | Severe | None reported | Loss of GABAB-mediated inhibition |
| Ethanol | <6 hours | 10 to 14 days | Severe | Moderate to severe | 5% to 15% | Loss of GABAA-mediated inhibition; disinhibition of NMDA receptors |
| NMDA: N-methyl D-aspartate. | ||||||
| GHB: Gamma-hydroxybutyrate | ||||||
| *Marked by tachycardia, fever, hypertension, and/or diaphoresis. | ||||||
| ‡All withdrawal states involve multifactorial processes. | ||||||
| Source: Reference 5 | ||||||
Underlying or concurrent causes of delirium must be ruled out. Patients at this stage often require physical restraint or immediate sedation to prevent injury and dangerous complications, including hyperthermia and rhabdomyolysis. Benzodiazepines are often used in high doses1 for sedation. IV hydration and antiemetics are also treatment mainstays. Atypical antipsychotics are added ASAP to control the paranoia.
• Phase 3 (days 7 through 13). Symptoms usually resolve at this stage. The delirium most often clears first, followed by restored autonomic stability and GI rest. While decreased sleep and periods of psychosis persist, agitation is less severe. The patient is discharged on average after 11 days.
Intense outpatient follow-up should include individual psychotherapy, substance abuse counseling, and drug therapy. Highly addictive medications should be avoided because of the patient’s substance abuse history.
Did Mr. R accurately report the amount of GBL he had taken? How should GBL and GHB blood levels be measured, given the agents’ rapid absorption rates?
The authors’ observations
As with most drugs of abuse, high doses over time contribute to severe GHB withdrawal syndrome. GHB doses taken before withdrawal are up to 10 times greater than those taken in typical recreational use.5
However, quantifying GHB levels with standard urine drug screens is nearly impossible because:
- the agent is absorbed within 20 to 60 minutes
- only 2% to 5% of the agent is eliminated in the urine.
GHB—which comes in powder, tablet, and liquid form and is usually dissolved in water before use—often is mixed with other drugs or alcohol. Varying preparations and use with multiple substances can produce inconsistent GHB levels and decrease sensitivity and specificity in routine drug screening. GHB abusers also report the amount ingested in “capfuls,” ounces, and teaspoons, making accurate quantification harder still.2
Though infrequently used because of feasibility and cost, gas chromatography and infrared spectroscopy of a urine specimen are the only known methods for determining GHB levels. Chronic GHB use, negative polypharmacy history, and negative urine and blood analysis for alcohol, benzodiazepines, sedative-hypnotics, or other substances usually confirm GHB withdrawal diagnosis.1
Treatment: ‘Bad’ medicine
In the ER, Mr. R was given two 1-mg doses of lorazepam IV 1 hour apart. After 1 hour, his vital signs improved slightly (heart rate: 100/min; blood pressure: 165/99 mm Hg). Thiamine and folate were also started. Mr. R’s severe agitation and paranoia persisted, so three more 2-mg doses of lorazepam IV were given at 4-hour intervals.
Within 2 days, Mr. R was transferred to the voluntary inpatient psychiatric unit. His nausea, vomiting, and autonomic instability resolved, but his delirium and psychosis persisted. Quetiapine, 100 mg bid, was started to address his psychosis, and bupropion, 150 mg once daily, was restarted to manage his previously diagnosed depression. Three days after starting bupropion, Mr. R’s mood improved based on patient reports and Clinical Global Impression scores (6 at baseline, 2 at discharge), but his persecutory delusions persisted, causing mild anxiety.
The next day, Mr. R’s auditory and visual hallucinations had ceased, his preoccupation with terrorists began to subside, and his concentration, sleep, and appetite were improving. By day 6 of hospitalization, he still complained of mild tremors and anxiety, but his persecutory delusions resolved.
After 9 days, Mr. R was discharged. Autonomic stability was achieved and his delirium had mostly resolved. Outpatient drug rehabilitation and psychiatric services were arranged.
As of this writing, Mr. R had not sought outpatient treatment. His current medical status is unknown.
Related resources
- Miglani J, Kim K, Chahil R. Gamma-hydroxybutyrate withdrawal delirium: a case report. Gen Hosp Psychiatry. 2000;22:213-6.
- Columbo G, Agabio R, Lobina C, et al. Cross tolerance to ethanol and gamma-hydroxybutyric acid. Eur J Pharmacol. 1995;273:235-8.
- Project GHB. www.projectghb.org
Drug brand names
- Bupropion • Wellbutrin
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta
- Paroxetine • Paxil
- Quetiapine • Seroquel
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Craig K, Gomez H, McManus J, et al. Severe gamma-hydroxybutyrate withdrawal: a case report and literature review. J Emerg Med. 2000;18:65-70.
2. Project GHB: Death list. Available at: http://www.projectghb.org/deathlist.html. Accessed Jan. 30, 2004.
3. Li J, Stokes SA, Woeckener A. A tale of novel intoxication: a review of the effects of gamma-hydroxybutyric acid with recommendations for management. Ann Emerg Med. 1998;31:729-36.
4. Sivilotti ML, Burns MJ, Aaron CK, Greenberg MJ. Pentobarbital for severe gamma-butyrolactone withdrawal. Ann Emerg Med. 2001;38:660-5.
5. Dyer JE, Roth B, Hyma B. Gamma hydroxybutyrate withdrawal syndrome. Ann Emerg Med. 2001;37:147-53.
Emergency presentation: A rough commute
Mr. R, age 25, presented to the emergency room confused and severely agitated. That morning, his parents found him in his Philadelphia apartment covering his mouth and nose with a T-shirt to guard against imminent chemical warfare.
The day before, Mr. R had developed auditory and visual hallucinations and paranoid and persecutory delusions. That day, on his way to work, he said he had seen “terrorists releasing toxic chemicals into the air” and heard “whispers of terrorists plotting an attack on the East Coast.”
Mr. R showed no suicidal or homicidal ideations. He denied significant medical or surgical history but reported that he had recently been diagnosed with depression after a “bad Ecstasy experience.” For 6 months he had been taking paroxetine, 20 mg once daily, and bupropion, 150 mg once daily, for his depression.
At age 18, Mr. R was diagnosed with attention-deficit/hyperactivity disorder (ADHD) after years of struggling through school with impaired concentration. At that time, he began taking methylphenidate, 10 mg each morning, and completed 3 years of college in North Carolina. He then dropped out of college and attempted suicide twice.
After the second suicide attempt, a psychiatrist diagnosed Mr. R as having major depression. The psychiatrist discontinued methylphenidate and started bupropion, dosage unknown. After 1 year, he stopped taking the antidepressant, thinking he no longer needed it.
Last year, Mr. R moved back to Philadelphia to be closer to his parents. Shortly afterward, he began obtaining methylphenidate illegally and later starting using cocaine, marijuana, amphetamines, and 3,4-methylenedioxymethamphetamine (“Ecstasy”).
At presentation, Mr. R’s mood was dysphoric with bizarre affect. Eye contact was poor with easy distractibility. Speech was pressured, with full range. His thought process was grossly disorganized with tangential thinking and flight of ideas. His short- and long-term memory were intact; insight and judgment were limited. A Mini-Mental State Examination could not be completed because of his disorganization and distractibility.
Does Mr. R. have schizophrenia or schizoaffective disorder? Or are his symptoms related to ADHD or substance abuse?
The authors’ observations
Mr. R’s paranoid delusions and hallucinations may suggest schizophrenia. With his history of suicide attempts, a depressive or schizoaffective disorder may also be considered.
However, Mr. R is close with his family and has several friends. His parents say he has not been withdrawn or paranoid, and there is no known family history of mood disorder, substance abuse, or other psychiatric illness. Mr. R also has been working steadily and had worked the night before presenting to us, so schizophrenia and schizoaffective disorder are ruled out. ADHD and abuse of multiple substances could explain his behavior because overdose of stimulants and illicit drugs may produce a psychotic event.
Further history: The power of addiction
After more questioning, Mr. R said that he had recently started using gamma butyrolactone (GBL) in a failed attempt to build muscle. For 4 months he had been taking 3.5 oz of GBL daily—0.25 oz every 2 to 3 hours and 0.75 oz at night to help him sleep.
Within 6 hours of his most recent GBL dose (reportedly 1 oz), Mr. R developed intractable nausea, vomiting, and flatus, followed quickly by anxiety, palpitations, and generalized hand/body tremors that disturbed his sleep. Hallucinations and delusions started the next day.
At presentation, Mr. R’s blood pressure was 188/92 mm Hg, his heart rate was 110 bpm, and his respiratory rate was 22 breaths per minute. Pupils were 5 mm and reactive with intact extraocular movement. A urine drug screen indicated amphetamine use.
Mr. R was tentatively diagnosed as having GBL withdrawal syndrome and was admitted for observation and treatment. The psychiatry service followed him for change in mental status and drug dependence.
Can a withdrawal syndrome reasonably account for Mr. R’s symptoms?
The authors’ observations
GBL is a precursor of gamma-hydroxybutyrate (GHB), a highly addictive agent that is used illicitly, typically at parties and nightclubs (Box). GBL is among the clinical analogues of GHB that have become popular street drugs.
GHB withdrawal syndrome has only recently been described in the literature and is virtually indistinguishable from withdrawal after cessation of GBL and other precursors. To date, 71 deaths have been attributed to GHB withdrawal.2
A constellation of symptoms exhibited by Mr. R point to GHB withdrawal, which should be included in the differential diagnosis of any sedative/hypnotic withdrawal (Table 1).
How GHB works. GHB easily crosses the blood-brain barrier. Like other sedative/hypnotics, its depressant effects on the brain in low doses (2 to 4 grams) produce a euphoric feeling as inhibitions are depressed. Profound coma or death result from higher doses (>4 grams).3 Heart rate may also be slowed and CNS effects may result in myoclonus, producing seizure-like movements. Combining GHB with other drugs can increase the other agents’ depressant effects, leading to confusion, amnesia, vomiting, irregular breathing, or death.2
Introduced in 1960 as an anesthetic, gamma-hydroxybutyrate (GHB) has become a notorious recreational drug. It is often called the “date rape drug” because of its intoxicating sedative effects.
Users have viewed GHB as a dietary supplement that can also enhance athletic and sexual performance, relieve depression, and induce sleep. Weightlifters have used GHB to quickly build muscle while avoiding side effects associated with anabolic steroids.
As more products containing GHB were introduced, many serious adverse events—including seizure, respiratory depression, and profound decreases in consciousness—were identified with its use and misuse. Although the Food and Drug Administration banned over-the-counter sales of GHB in 1990,1 the agent is still widely available on the black market and over the Internet.
GHB also is marketed through its chemical precursors, specifically GBL and 1,4-butanediol. These precursors are rapidly and systemically converted to the active GHB product. GBL is hydrolyzed by a peripheral lactonase, and 1,4-butanediol is processed by alcohol dehydrogenase and aldehyde dehydrogenase—the enzymes involved in ethanol degradation.1
A tiny increase in GHB dose can dramatically increase the symptoms and risk of overdose.4 GHB’s effects are also variable: A 1-teaspoon dose can produce the desired “high” one time and an overdose the next.
GHB and ethanol share a common mechanism of action.5 At pharmacologic doses, GHB appears to act in part through effects on the structurally related GABA neurotransmitter or its receptors.
Not surprisingly, a withdrawal syndrome characterized by delirium and autonomic instability ensues after GHB use is abruptly stopped. By functioning as indirect GABA agonists and ultimately evoking inhibitory neurotransmission, benzodiazepines and most barbiturates may alleviate GHB withdrawal symptoms.4 Thiamine is added to prevent Wernicke-Korsakoff syndrome, as is seen in alcohol withdrawal.5
GHB withdrawal. Symptoms are divided into three phases:
• Phase 1 (acute, first 24 hours). Presenting symptoms include anxiety, restlessness, insomnia, tremor, diaphoresis, tachycardia, and hypertension. Nausea and vomiting are variable but can be unrelenting.
While symptoms vary in severity, most prominent are agitation, restlessness, and insomnia. Some patients do not sleep for days after their last dose, and diffuse body tremors prevent them from sitting or lying still. Tachycardia and hypertension are hard to evaluate at this phase because patients present at different stages of withdrawal. Initial blood pressure readings as high as 240/130 mm Hg and heart rates of 120 bpm have been reported, however.
• Phase 2 (days 2 through 6). Worsening autonomic symptoms, progressive GI symptoms, and overall worsening of the withdrawal mark this tumultuous period. Patients usually present at this point—in acute distress and no longer able to self-treat.
Confusion, delirium, and florid psychosis characterize this phase. Mr. R’s paranoid delusions and hallucinations are the most common form of psychosis seen in GHB withdrawal.5 In some cases, the psychosis impairs social, occupational, and other functioning.
Table 1
Comparison of sedative-hypnotic withdrawal syndromes
| Substance | Onset | Duration of severe symptoms | Autonomic instability* | Neurologic/psychiatric symptoms | Mortality | Major mechanism inducing withdrawal state‡ |
|---|---|---|---|---|---|---|
| GHB | <6 hours | 5 to 12 days | Mild | Severe | <1% | Loss of GHB, GABAA, and GABAB-mediated inhibition |
| Benzodiazepines | 1 to 3 days | 5 to 9 days | Moderate | Moderate | 1% | Loss of GABAA-mediated inhibition |
| Baclofen | 12 to 96 hours | 8 days | Moderate | Severe | None reported | Loss of GABAB-mediated inhibition |
| Ethanol | <6 hours | 10 to 14 days | Severe | Moderate to severe | 5% to 15% | Loss of GABAA-mediated inhibition; disinhibition of NMDA receptors |
| NMDA: N-methyl D-aspartate. | ||||||
| GHB: Gamma-hydroxybutyrate | ||||||
| *Marked by tachycardia, fever, hypertension, and/or diaphoresis. | ||||||
| ‡All withdrawal states involve multifactorial processes. | ||||||
| Source: Reference 5 | ||||||
Underlying or concurrent causes of delirium must be ruled out. Patients at this stage often require physical restraint or immediate sedation to prevent injury and dangerous complications, including hyperthermia and rhabdomyolysis. Benzodiazepines are often used in high doses1 for sedation. IV hydration and antiemetics are also treatment mainstays. Atypical antipsychotics are added ASAP to control the paranoia.
• Phase 3 (days 7 through 13). Symptoms usually resolve at this stage. The delirium most often clears first, followed by restored autonomic stability and GI rest. While decreased sleep and periods of psychosis persist, agitation is less severe. The patient is discharged on average after 11 days.
Intense outpatient follow-up should include individual psychotherapy, substance abuse counseling, and drug therapy. Highly addictive medications should be avoided because of the patient’s substance abuse history.
Did Mr. R accurately report the amount of GBL he had taken? How should GBL and GHB blood levels be measured, given the agents’ rapid absorption rates?
The authors’ observations
As with most drugs of abuse, high doses over time contribute to severe GHB withdrawal syndrome. GHB doses taken before withdrawal are up to 10 times greater than those taken in typical recreational use.5
However, quantifying GHB levels with standard urine drug screens is nearly impossible because:
- the agent is absorbed within 20 to 60 minutes
- only 2% to 5% of the agent is eliminated in the urine.
GHB—which comes in powder, tablet, and liquid form and is usually dissolved in water before use—often is mixed with other drugs or alcohol. Varying preparations and use with multiple substances can produce inconsistent GHB levels and decrease sensitivity and specificity in routine drug screening. GHB abusers also report the amount ingested in “capfuls,” ounces, and teaspoons, making accurate quantification harder still.2
Though infrequently used because of feasibility and cost, gas chromatography and infrared spectroscopy of a urine specimen are the only known methods for determining GHB levels. Chronic GHB use, negative polypharmacy history, and negative urine and blood analysis for alcohol, benzodiazepines, sedative-hypnotics, or other substances usually confirm GHB withdrawal diagnosis.1
Treatment: ‘Bad’ medicine
In the ER, Mr. R was given two 1-mg doses of lorazepam IV 1 hour apart. After 1 hour, his vital signs improved slightly (heart rate: 100/min; blood pressure: 165/99 mm Hg). Thiamine and folate were also started. Mr. R’s severe agitation and paranoia persisted, so three more 2-mg doses of lorazepam IV were given at 4-hour intervals.
Within 2 days, Mr. R was transferred to the voluntary inpatient psychiatric unit. His nausea, vomiting, and autonomic instability resolved, but his delirium and psychosis persisted. Quetiapine, 100 mg bid, was started to address his psychosis, and bupropion, 150 mg once daily, was restarted to manage his previously diagnosed depression. Three days after starting bupropion, Mr. R’s mood improved based on patient reports and Clinical Global Impression scores (6 at baseline, 2 at discharge), but his persecutory delusions persisted, causing mild anxiety.
The next day, Mr. R’s auditory and visual hallucinations had ceased, his preoccupation with terrorists began to subside, and his concentration, sleep, and appetite were improving. By day 6 of hospitalization, he still complained of mild tremors and anxiety, but his persecutory delusions resolved.
After 9 days, Mr. R was discharged. Autonomic stability was achieved and his delirium had mostly resolved. Outpatient drug rehabilitation and psychiatric services were arranged.
As of this writing, Mr. R had not sought outpatient treatment. His current medical status is unknown.
Related resources
- Miglani J, Kim K, Chahil R. Gamma-hydroxybutyrate withdrawal delirium: a case report. Gen Hosp Psychiatry. 2000;22:213-6.
- Columbo G, Agabio R, Lobina C, et al. Cross tolerance to ethanol and gamma-hydroxybutyric acid. Eur J Pharmacol. 1995;273:235-8.
- Project GHB. www.projectghb.org
Drug brand names
- Bupropion • Wellbutrin
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta
- Paroxetine • Paxil
- Quetiapine • Seroquel
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Emergency presentation: A rough commute
Mr. R, age 25, presented to the emergency room confused and severely agitated. That morning, his parents found him in his Philadelphia apartment covering his mouth and nose with a T-shirt to guard against imminent chemical warfare.
The day before, Mr. R had developed auditory and visual hallucinations and paranoid and persecutory delusions. That day, on his way to work, he said he had seen “terrorists releasing toxic chemicals into the air” and heard “whispers of terrorists plotting an attack on the East Coast.”
Mr. R showed no suicidal or homicidal ideations. He denied significant medical or surgical history but reported that he had recently been diagnosed with depression after a “bad Ecstasy experience.” For 6 months he had been taking paroxetine, 20 mg once daily, and bupropion, 150 mg once daily, for his depression.
At age 18, Mr. R was diagnosed with attention-deficit/hyperactivity disorder (ADHD) after years of struggling through school with impaired concentration. At that time, he began taking methylphenidate, 10 mg each morning, and completed 3 years of college in North Carolina. He then dropped out of college and attempted suicide twice.
After the second suicide attempt, a psychiatrist diagnosed Mr. R as having major depression. The psychiatrist discontinued methylphenidate and started bupropion, dosage unknown. After 1 year, he stopped taking the antidepressant, thinking he no longer needed it.
Last year, Mr. R moved back to Philadelphia to be closer to his parents. Shortly afterward, he began obtaining methylphenidate illegally and later starting using cocaine, marijuana, amphetamines, and 3,4-methylenedioxymethamphetamine (“Ecstasy”).
At presentation, Mr. R’s mood was dysphoric with bizarre affect. Eye contact was poor with easy distractibility. Speech was pressured, with full range. His thought process was grossly disorganized with tangential thinking and flight of ideas. His short- and long-term memory were intact; insight and judgment were limited. A Mini-Mental State Examination could not be completed because of his disorganization and distractibility.
Does Mr. R. have schizophrenia or schizoaffective disorder? Or are his symptoms related to ADHD or substance abuse?
The authors’ observations
Mr. R’s paranoid delusions and hallucinations may suggest schizophrenia. With his history of suicide attempts, a depressive or schizoaffective disorder may also be considered.
However, Mr. R is close with his family and has several friends. His parents say he has not been withdrawn or paranoid, and there is no known family history of mood disorder, substance abuse, or other psychiatric illness. Mr. R also has been working steadily and had worked the night before presenting to us, so schizophrenia and schizoaffective disorder are ruled out. ADHD and abuse of multiple substances could explain his behavior because overdose of stimulants and illicit drugs may produce a psychotic event.
Further history: The power of addiction
After more questioning, Mr. R said that he had recently started using gamma butyrolactone (GBL) in a failed attempt to build muscle. For 4 months he had been taking 3.5 oz of GBL daily—0.25 oz every 2 to 3 hours and 0.75 oz at night to help him sleep.
Within 6 hours of his most recent GBL dose (reportedly 1 oz), Mr. R developed intractable nausea, vomiting, and flatus, followed quickly by anxiety, palpitations, and generalized hand/body tremors that disturbed his sleep. Hallucinations and delusions started the next day.
At presentation, Mr. R’s blood pressure was 188/92 mm Hg, his heart rate was 110 bpm, and his respiratory rate was 22 breaths per minute. Pupils were 5 mm and reactive with intact extraocular movement. A urine drug screen indicated amphetamine use.
Mr. R was tentatively diagnosed as having GBL withdrawal syndrome and was admitted for observation and treatment. The psychiatry service followed him for change in mental status and drug dependence.
Can a withdrawal syndrome reasonably account for Mr. R’s symptoms?
The authors’ observations
GBL is a precursor of gamma-hydroxybutyrate (GHB), a highly addictive agent that is used illicitly, typically at parties and nightclubs (Box). GBL is among the clinical analogues of GHB that have become popular street drugs.
GHB withdrawal syndrome has only recently been described in the literature and is virtually indistinguishable from withdrawal after cessation of GBL and other precursors. To date, 71 deaths have been attributed to GHB withdrawal.2
A constellation of symptoms exhibited by Mr. R point to GHB withdrawal, which should be included in the differential diagnosis of any sedative/hypnotic withdrawal (Table 1).
How GHB works. GHB easily crosses the blood-brain barrier. Like other sedative/hypnotics, its depressant effects on the brain in low doses (2 to 4 grams) produce a euphoric feeling as inhibitions are depressed. Profound coma or death result from higher doses (>4 grams).3 Heart rate may also be slowed and CNS effects may result in myoclonus, producing seizure-like movements. Combining GHB with other drugs can increase the other agents’ depressant effects, leading to confusion, amnesia, vomiting, irregular breathing, or death.2
Introduced in 1960 as an anesthetic, gamma-hydroxybutyrate (GHB) has become a notorious recreational drug. It is often called the “date rape drug” because of its intoxicating sedative effects.
Users have viewed GHB as a dietary supplement that can also enhance athletic and sexual performance, relieve depression, and induce sleep. Weightlifters have used GHB to quickly build muscle while avoiding side effects associated with anabolic steroids.
As more products containing GHB were introduced, many serious adverse events—including seizure, respiratory depression, and profound decreases in consciousness—were identified with its use and misuse. Although the Food and Drug Administration banned over-the-counter sales of GHB in 1990,1 the agent is still widely available on the black market and over the Internet.
GHB also is marketed through its chemical precursors, specifically GBL and 1,4-butanediol. These precursors are rapidly and systemically converted to the active GHB product. GBL is hydrolyzed by a peripheral lactonase, and 1,4-butanediol is processed by alcohol dehydrogenase and aldehyde dehydrogenase—the enzymes involved in ethanol degradation.1
A tiny increase in GHB dose can dramatically increase the symptoms and risk of overdose.4 GHB’s effects are also variable: A 1-teaspoon dose can produce the desired “high” one time and an overdose the next.
GHB and ethanol share a common mechanism of action.5 At pharmacologic doses, GHB appears to act in part through effects on the structurally related GABA neurotransmitter or its receptors.
Not surprisingly, a withdrawal syndrome characterized by delirium and autonomic instability ensues after GHB use is abruptly stopped. By functioning as indirect GABA agonists and ultimately evoking inhibitory neurotransmission, benzodiazepines and most barbiturates may alleviate GHB withdrawal symptoms.4 Thiamine is added to prevent Wernicke-Korsakoff syndrome, as is seen in alcohol withdrawal.5
GHB withdrawal. Symptoms are divided into three phases:
• Phase 1 (acute, first 24 hours). Presenting symptoms include anxiety, restlessness, insomnia, tremor, diaphoresis, tachycardia, and hypertension. Nausea and vomiting are variable but can be unrelenting.
While symptoms vary in severity, most prominent are agitation, restlessness, and insomnia. Some patients do not sleep for days after their last dose, and diffuse body tremors prevent them from sitting or lying still. Tachycardia and hypertension are hard to evaluate at this phase because patients present at different stages of withdrawal. Initial blood pressure readings as high as 240/130 mm Hg and heart rates of 120 bpm have been reported, however.
• Phase 2 (days 2 through 6). Worsening autonomic symptoms, progressive GI symptoms, and overall worsening of the withdrawal mark this tumultuous period. Patients usually present at this point—in acute distress and no longer able to self-treat.
Confusion, delirium, and florid psychosis characterize this phase. Mr. R’s paranoid delusions and hallucinations are the most common form of psychosis seen in GHB withdrawal.5 In some cases, the psychosis impairs social, occupational, and other functioning.
Table 1
Comparison of sedative-hypnotic withdrawal syndromes
| Substance | Onset | Duration of severe symptoms | Autonomic instability* | Neurologic/psychiatric symptoms | Mortality | Major mechanism inducing withdrawal state‡ |
|---|---|---|---|---|---|---|
| GHB | <6 hours | 5 to 12 days | Mild | Severe | <1% | Loss of GHB, GABAA, and GABAB-mediated inhibition |
| Benzodiazepines | 1 to 3 days | 5 to 9 days | Moderate | Moderate | 1% | Loss of GABAA-mediated inhibition |
| Baclofen | 12 to 96 hours | 8 days | Moderate | Severe | None reported | Loss of GABAB-mediated inhibition |
| Ethanol | <6 hours | 10 to 14 days | Severe | Moderate to severe | 5% to 15% | Loss of GABAA-mediated inhibition; disinhibition of NMDA receptors |
| NMDA: N-methyl D-aspartate. | ||||||
| GHB: Gamma-hydroxybutyrate | ||||||
| *Marked by tachycardia, fever, hypertension, and/or diaphoresis. | ||||||
| ‡All withdrawal states involve multifactorial processes. | ||||||
| Source: Reference 5 | ||||||
Underlying or concurrent causes of delirium must be ruled out. Patients at this stage often require physical restraint or immediate sedation to prevent injury and dangerous complications, including hyperthermia and rhabdomyolysis. Benzodiazepines are often used in high doses1 for sedation. IV hydration and antiemetics are also treatment mainstays. Atypical antipsychotics are added ASAP to control the paranoia.
• Phase 3 (days 7 through 13). Symptoms usually resolve at this stage. The delirium most often clears first, followed by restored autonomic stability and GI rest. While decreased sleep and periods of psychosis persist, agitation is less severe. The patient is discharged on average after 11 days.
Intense outpatient follow-up should include individual psychotherapy, substance abuse counseling, and drug therapy. Highly addictive medications should be avoided because of the patient’s substance abuse history.
Did Mr. R accurately report the amount of GBL he had taken? How should GBL and GHB blood levels be measured, given the agents’ rapid absorption rates?
The authors’ observations
As with most drugs of abuse, high doses over time contribute to severe GHB withdrawal syndrome. GHB doses taken before withdrawal are up to 10 times greater than those taken in typical recreational use.5
However, quantifying GHB levels with standard urine drug screens is nearly impossible because:
- the agent is absorbed within 20 to 60 minutes
- only 2% to 5% of the agent is eliminated in the urine.
GHB—which comes in powder, tablet, and liquid form and is usually dissolved in water before use—often is mixed with other drugs or alcohol. Varying preparations and use with multiple substances can produce inconsistent GHB levels and decrease sensitivity and specificity in routine drug screening. GHB abusers also report the amount ingested in “capfuls,” ounces, and teaspoons, making accurate quantification harder still.2
Though infrequently used because of feasibility and cost, gas chromatography and infrared spectroscopy of a urine specimen are the only known methods for determining GHB levels. Chronic GHB use, negative polypharmacy history, and negative urine and blood analysis for alcohol, benzodiazepines, sedative-hypnotics, or other substances usually confirm GHB withdrawal diagnosis.1
Treatment: ‘Bad’ medicine
In the ER, Mr. R was given two 1-mg doses of lorazepam IV 1 hour apart. After 1 hour, his vital signs improved slightly (heart rate: 100/min; blood pressure: 165/99 mm Hg). Thiamine and folate were also started. Mr. R’s severe agitation and paranoia persisted, so three more 2-mg doses of lorazepam IV were given at 4-hour intervals.
Within 2 days, Mr. R was transferred to the voluntary inpatient psychiatric unit. His nausea, vomiting, and autonomic instability resolved, but his delirium and psychosis persisted. Quetiapine, 100 mg bid, was started to address his psychosis, and bupropion, 150 mg once daily, was restarted to manage his previously diagnosed depression. Three days after starting bupropion, Mr. R’s mood improved based on patient reports and Clinical Global Impression scores (6 at baseline, 2 at discharge), but his persecutory delusions persisted, causing mild anxiety.
The next day, Mr. R’s auditory and visual hallucinations had ceased, his preoccupation with terrorists began to subside, and his concentration, sleep, and appetite were improving. By day 6 of hospitalization, he still complained of mild tremors and anxiety, but his persecutory delusions resolved.
After 9 days, Mr. R was discharged. Autonomic stability was achieved and his delirium had mostly resolved. Outpatient drug rehabilitation and psychiatric services were arranged.
As of this writing, Mr. R had not sought outpatient treatment. His current medical status is unknown.
Related resources
- Miglani J, Kim K, Chahil R. Gamma-hydroxybutyrate withdrawal delirium: a case report. Gen Hosp Psychiatry. 2000;22:213-6.
- Columbo G, Agabio R, Lobina C, et al. Cross tolerance to ethanol and gamma-hydroxybutyric acid. Eur J Pharmacol. 1995;273:235-8.
- Project GHB. www.projectghb.org
Drug brand names
- Bupropion • Wellbutrin
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta
- Paroxetine • Paxil
- Quetiapine • Seroquel
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Craig K, Gomez H, McManus J, et al. Severe gamma-hydroxybutyrate withdrawal: a case report and literature review. J Emerg Med. 2000;18:65-70.
2. Project GHB: Death list. Available at: http://www.projectghb.org/deathlist.html. Accessed Jan. 30, 2004.
3. Li J, Stokes SA, Woeckener A. A tale of novel intoxication: a review of the effects of gamma-hydroxybutyric acid with recommendations for management. Ann Emerg Med. 1998;31:729-36.
4. Sivilotti ML, Burns MJ, Aaron CK, Greenberg MJ. Pentobarbital for severe gamma-butyrolactone withdrawal. Ann Emerg Med. 2001;38:660-5.
5. Dyer JE, Roth B, Hyma B. Gamma hydroxybutyrate withdrawal syndrome. Ann Emerg Med. 2001;37:147-53.
1. Craig K, Gomez H, McManus J, et al. Severe gamma-hydroxybutyrate withdrawal: a case report and literature review. J Emerg Med. 2000;18:65-70.
2. Project GHB: Death list. Available at: http://www.projectghb.org/deathlist.html. Accessed Jan. 30, 2004.
3. Li J, Stokes SA, Woeckener A. A tale of novel intoxication: a review of the effects of gamma-hydroxybutyric acid with recommendations for management. Ann Emerg Med. 1998;31:729-36.
4. Sivilotti ML, Burns MJ, Aaron CK, Greenberg MJ. Pentobarbital for severe gamma-butyrolactone withdrawal. Ann Emerg Med. 2001;38:660-5.
5. Dyer JE, Roth B, Hyma B. Gamma hydroxybutyrate withdrawal syndrome. Ann Emerg Med. 2001;37:147-53.
Update on eating disorders Anorexia nervosa: Dual therapy can bring patients back from the brink
Ms. J started losing weight deliberately at age 14 while attending boarding school. She lost 25 lbs by jogging 6 miles per day, exercising another 2 hours, avoiding meat, abusing laxatives, and drinking large quantities of coffee.
She was referred to a school counselor because of her weight loss and returned home. She was happier at a local high school and recovered to normal weight. In college, however, she reverted to compulsive exercising and preoccupation with her weight after the break-up of her first intimate relationship.
Now at age 22, Ms. J has persistently failed to gain weight during outpatient therapy for anorexia nervosa. At 5′7″ she weighs 98 lbs. On the day she was to be hospitalized involuntarily, she took 25 diphenhydramine tablets, which her psychiatrist viewed as a suicide threat. The overdose was treated in the emergency room with ipecac syrup, and she was admitted for inpatient eating disorder treatment.
Like Ms. J, patients with anorexia nervosa resist treatment and deny having most diagnostic signs and symptoms. Based on the evidence and my 30 years of treating anorectic patients,1 this article offers suggestions to help you:
- gather accurate histories from patients and their families
- identify common psychiatric comorbidities
- gain the patient’s trust during treatment
- provide effective dual therapy, with cognitive-behavioral and pharmacologic components.
Table 1
Diagnostic criteria for anorexia nervosa
| Underweight (<85% of normal for age and height) |
| Fear of gaining weight or becoming fat, even though underweight |
| Disturbed conceptualization of body shape and weight, denial of seriousness of low body weight, or overemphasis on body shape and weight in self-evaluation |
Amenorrhea. Subtypes:
|
| Source: Adapted with permission from Diagnostic and statistical manual of mental disorders (4th ed. text revision). |
| Copyright 2000 American Psychiatric Association. |
Making the diagnosis
Anorexia nervosa is characterized by underweight, fear of gaining weight, disturbed body concept, and amenorrhea (Table 1). Its core psychological symptoms have been described as:
- relentless pursuit of thinness
- denial of cachexia
- and feelings of general ineffectiveness.2
The patient may say she feels fat even though emaciated or that parts of her body are too large. This disturbed experience of body weight or shape may represent sublimation and displacement for feelings of inadequacy. Because anorectic patients stay thin so effectively, they may feel a sense of accomplishment by evaluating themselves in terms of their thinness. Cognitive therapy focuses on correcting patients’ pervasive sense of inadequacy, as manifest in maturity fears and lack of confidence in coping with life’s problems.3
Subtypes. Anorexia nervosa has two subtypes—restricting and binge eating/purging—that differ in behavioral and medical symptoms.4 Patients with binge eating/purging show:
- higher rates of impulsivity (suicide attempts, self-mutilation, stealing, and alcohol and other substance abuse)
- more-prevalent impulsive personality disorders (borderline personality disorder, hysterical personality disorder)
- medical problems caused by purging.
Restricting-type patients are often dependent and submissive, with difficulty separating from parents. These patients may be preoccupied with orderliness, perfectionism, and control.
Recommendation. A structured interview to diagnose anorexia nervosa is summarized in Table 2. Because the patient will likely deny her symptoms, it is usually necessary to also interview family members or close friends.
Psychiatric comorbidity
Case report continued: A ‘perfectionist.’
School for Ms. J required great effort, and she spent many hours studying. Her upper-middle-class parents described her as “a perfectionist.” The family placed considerable emphasis on doing the “correct” thing.
During adolescence, Ms. J developed a major depressive episode that lasted 4 months. She also developed obsessions and compulsions unrelated to her eating disorder. She obsessively ruminated about the correct things to say in social circumstances and devoted 4 hours per day to cleaning and checking compulsions. She felt she had to wash her car every time before going out; if she could not, she would cancel her social plans.
Table 2
Diagnosis of anorexia nervosa: Questions to ask*
| Weight history | -What was her highest weight and lowest weight (after weight loss) -At what ages did these weights occur? -Ask about her present weight before you weigh her |
| Eating behavior | -What does she eat and when from morning awakening to bedtime? -Does she eat with the family less often than in the past? -Is she binging? |
| Purging behavior | -Is she inducing vomiting? -Is she using laxatives, diuretics, ipecac, or enemas? |
| Preoccupations and rituals concerning food and weight | -Does she constantly count calories and express concern about fat content in foods? -Does she often gaze in the mirror and comment about being fat? -How often does she weigh herself? -Does she express fear of being unable to stop eating? |
| Activity | -Is she jogging, bike riding, or doing aerobics? -How often, and for how long? -Is she overactive at home, such as pacing? |
| Menstrual history | -At what age did menses begin? -What was the date of her last period? -How regular is her cycle? |
| Psychiatric comorbidity | -Does she have symptoms of depression? -Impulsive behavior (suicide attempts or self-mutilation)? -Drug or alcohol abuse? -Anxiety (obsessive-compulsive behaviors, social phobia, generalized anxiety, fearfulness)? -Personality disorders? |
| * Because patients with anorexia nervosa often deny their symptoms and conceal their food intake, it is usually necessary to interview family members or close friends as well as the patient. | |
In college, she began abusing alcohol and was arrested once for driving while intoxicated.
Depression is the most common comorbidity in anorexia nervosa. Two-thirds of anorectic patients in a 10-year follow-up study reported a history of major depressive disorder.5 Suicide, starvation, and electrolyte imbalance are the three major causes of death. Among severely ill patients who require hospitalization, 10% to 20% die, though the suicide rate is undocumented.
Compulsions. Anorectics’ preoccupations about food and eating rituals have been compared with compulsions, though less than 20% of patients meet diagnostic criteria for obsessive-compulsive disorder.6
Substance abuse. Bulimic anorectics report more alcohol and substance use and abuse than restricting anorectics.7 The most common substances of abuse are cannabis, cocaine, stimulants, and over-the-counter pills such as diet aids.
Personality disorders. Up to 50% of patients with anorexia nervosa—particularly the binge/purge subtype—have personality disorders. Borderline personality disorder is especially common among binge/purge types,8 and avoidant personality disorder is more common among restricting types.
Table 3
Diagnostic signs of emaciation and purging in patients with anorexia nervosa
Emaciation
|
Purging
|
Personality disorders usually reflect instability in interpersonal relationships, poor self-image, or fluctuating affect. Patients may show a pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Sexuality. Psychosocial and sexual development is often delayed in adolescent anorectics. In adults, interest in sex often plummets with anorexia onset, although binge/purge-type patients occasionally become promiscuous.
Medical signs
Case report continued: Abnormal ECG.
Ms. J was hospitalized after her weight dropped below 75% of normal for her age, height, and body build. She showed signs of electrolyte disturbance, including severe bradycardia (pulse rate 40) and ST-segment abnormalities on ECG.
Clinical signs of emaciation and purging can assist with diagnosis and in making decisions about medical treatment, including hospitalization (Table 3). Patients who purge are often weak and have puffy cheeks or parotid gland enlargement. They may have fainting spells and scars on their hands from stimulating vomiting. Laxative abuse may decrease colon motility and worsen constipation.
Neuroendocrine changes secondary to dieting and weight loss include:
- increased corticotropin-releasing hormone secretion
- blunted diurnal cortisol fluctuation
- decreased follicle-stimulating hormone (FSH) secretion
- impaired growth hormone regulation
- decreased luteinizing hormone (LH) secretion
- mildly decreased triiodothyronine
- erratic vasopressin secretion.
Measuring these changes is unnecessary, as general nutritional rehabilitation with weight gain will correct them.
Neurotransmitter function. Emaciated anorectics have a blunted response to pharmacologic probes for dopamine, reduced CSF norepinephrine turnover, and decreased CSF serotonin. Neuroimaging studies suggest that serotonin dysfunction may persist after weight is restored, although these findings require replication.
Treatment priorities
Effective therapies. Open studies indicate that multidimensional treatment—medical management, psychoeducation, and individual cognitive-behavioral therapy (CBT)—is most effective for anorexia nervosa. The fewer than 10 controlled trials that address anorexia nervosa treatment show:
- the more severe the illness, the more intense the treatment required
- outpatient therapy is most successful in patients who have had the illness <6 months, are not binging and vomiting, and have parents who participate in family therapy.
Hospitalization. An emaciated patient who is irritable, depressed, preoccupied with food, and sleep-deprived is unlikely to make progress toward behavioral change. The first goal, therefore, is to restore her nutritional state to normal.
Severely ill anorectic patients require hospitalization for daily monitoring of weight, calorie intake, urine output, and serum electrolytes and amylase (to assess purging behavior). Hospitalization is indicated for:
- loss of >20% of normal weight for age, height, and bone structure
- >6 months of repeated hospitalizations and underweight
- psychotic depression or serious suicide attempt
- incapacitating obsessions and compulsions, related or not to the eating disorder
- serious comorbid medical conditions, such as edema, hypoproteinemia, severe anemia, cardiac arrhythmia, or hypokalemic alkalosis (serum K+ < 2.5 mEq/L).
Keeping a patient in the hospital long enough to provide effective medical and psychological therapy has become difficult, however, because of medical insurance restrictions (Box). The result: poorer outcomes and increased relapse rates compared with 10 years ago.9-12
Hospital treatment of eating disorders has shifted from long-term care of a chronic disorder to stabilization of acute episodes. For some patients, this change has been deleterious and not cost-effective.
A decade ago, eating disorder hospitalizations were covered primarily by private insurance. Today, health maintenance organizations, managed care oversight of private insurance, and public funding are the primary sources of payment. These insurers often limit payment for eating disorder hospitalization, the most costly aspect of psychiatric care.
Poor outcomes and a high relapse rate have been documented in anorexia nervosa patients who left the hospital while underweight.9-11 From 1984 to 1998:
- average hospital stays for anorexia nervosa decreased from 150 days to 23.7 days
- readmissions increased from 0% to 27% of total admissions
- anorectic patients’ average body mass index at discharge dropped from 19.3 to 17.7, a statistically significant difference.12
For psychiatrists, this trend means many outpatients with anorexia nervosa will require repeated hospitalizations that will not substantially improve their anorectic behaviors.
Nutritional rehabilitation and behavior changes can often correct the medical complications of emaciation and purging. Lost bone density is seldom restored, but nutritional rehabilitation can prevent further bone loss.13 Women who remain amenorrheic for several years after weight restoration tend to be more psychologically disturbed than those who resume menses rapidly.14
Cognitive-behavioral therapy
Other authors have discussed CBT for anorexia nervosa.3,15 In general, the key tasks—operationalizing beliefs, evaluating autonomic thoughts, testing prospective hypotheses, and examining underlying assumptions—are accomplished by assessing anorexia’s distorted cognitions. No satisfactory controlled studies have examined any other type of individual psychotherapy for treating anorexia nervosa.
Alliance building. Patients with anorexia find it difficult to participate in therapeutic relationships. They are terrified of gaining weight and readily drop out of treatment. To build a therapeutic alliance:
- begin by helping the patient develop a history of her significant life events
- proceed slowly, praising her for every small attempt at changing her behavior
- set realistic therapy goals, considering her degree of resistance.
Monitoring. Behavior therapy consists primarily of positive reinforcements for weight gain. For this, we weigh outpatients weekly and inpatients daily. Outpatients are taught to keep diaries of daily food intake, stressful events, and emotional responses to them. The therapist begins each session by examining the patient’s diary with her and discussing how life events affect her eating behavior.
Cognitive restructuring helps patients identify their disturbed cognitions and challenge core beliefs about self-image. In this process, they become aware of their negative thoughts and develop arguments and evidence to support and refute the thoughts’ validity. They then form a reasoned conclusion based on the evidence.
Even if patients do not accept this logical conclusion, we encourage them to behave as if they believe it to be true. By doing this repeatedly, they eventually obtain some symptom relief.
Response-prevention techniques can help stop binging and purging. For example, we may require inpatients to sit together for 1 hour after eating. Because most patients will not vomit in front of each other, they learn how to resist vomiting and eventually experience reduced anxiety without vomiting after a meal.
Problem solving helps patients to reason through difficult food-related or interpersonal situations. The patient states the problem, then generates as many solutions as possible with the therapist’s assistance. She chooses one solution and puts it into effect, usually for 1 week. She then discusses the results with her therapist and decides whether to try another solution.
Family therapy. A family analysis—including a brief psychiatric history and evaluation of interactions—is recommended for all patients who live at home. This analysis can help you decide what type of family therapy or counseling to recommend.
Some families respond well with the parents and patient together in therapy sessions, whereas others are more comfortable with separate counseling. In a recent controlled study, anorectic patients younger than age 18 did equally well whether they were counseled with the family or separately.16
Brief therapy sessions are sometimes the most effective method to address family issues. When this is not possible, you and the patient can discuss family relationships in individual therapy.
Medications
Many medications have been used to treat anorexia nervosa, though few randomized, placebo-controlled studies exist. Because evidence does not support using psychotropics as monotherapy for anorexia nervosa, medication is considered adjunctive to CBT.
Chlorpromazine can help the hospitalized, severely ill patient who is overwhelmed with uncontrollable behavioral rituals and thoughts of losing weight. This antipsychotic helps reduce anorectic preoccupations and anxiety and helps make patients more amenable to therapy.
Start chlorpromazine at 10 mg tid and increase gradually until the patient can eat without extreme anxiety. Usual maximum dosage is 50 mg tid. Monitor blood pressure, tardive dyskinesia, and decreased white blood cell count.
Olanzapine may help induce weight gain and reduce anxiety in anorectic patients.17 Controlled and open-label studies are under way.
We start olanzapine at 2.5 mg/d and increase gradually to 10 or 15 mg/d. At this dosage, patients’ anxiety about eating is usually substantially reduced. Sedation is the most common side effect.
Anorexia patients often refuse to take olanzapine for fear of weight gain. If a patient’s emaciation is life-threatening, we may seek court permission to medicate her involuntarily. We reassure her that we will discontinue olanzapine when she reaches her target weight.
Serotonin in anorexia. Central serotonin pathways modulate feeding behavior. Serotonin antagonists—such as cyproheptadine—increase food intake and weight gain, whereas serotonin agonists—such as selective serotonin reuptake inhibitors (SSRIs)—decrease food intake.
Serotonin pathways also may modulate obsessive-compulsive and impulsive behaviors. Both serotonin agonists and antagonists can be useful adjuncts in treating anorexia nervosa.
In a double-blind, placebo-controlled trial, cyproheptadine, 4 to 8 mg tid, was associated with weight gain and reduced depressive symptoms in anorexia nervosa patients.18 Unlike tricyclic antidepressants, cyproheptadine does not reduce blood pressure or increase heart rate, which makes it attractive for emaciated anorectic patients. Dosages up to 28 mg/d can be used safely.
The SSRI fluoxetine may help prevent weight loss relapse in anorexia nervosa and reduce obsessive-compulsive behaviors.19 In open studies of low-weight anorectics, however, fluoxetine had little impact on weight or other clinically meaningful variables.20 Thus, this agent is recommended for preventing weight-loss relapse only in patients who are within 10% to 15% of ideal body weight.
Outpatient care
Case report continued: Ongoing therapy
During hospitalization, Ms. J participated in all therapeutic modalities but had difficulty eating enough to gain weight. She reached her target weight of 127 lbs in about 7 weeks but gained no sense of purpose in life.
She is starting an intensive outpatient program using CBT to maintain her weight and further address the core psychopathology of her illness. Her maintenance therapy includes attending Alcoholics Anonymous meetings, ongoing fluoxetine (20 mg/d) to prevent weight-loss relapse, and CBT for obsessions and compulsions not related to her eating disorder.
Related resources
- Halmi KA. Eating disorders: Anorexia, bulimia nervosa and obesity. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry, 4th ed. Washington, DC: American Psychiatric Publishing, 2003:1001-21.
- Academy of Eating Disorders. www.aedweb.org
- Anorexia Nervosa & Associated Disorders (ANAD). www.anad.org
Drug brand names
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Olanzapine • Zyprexa
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Halmi KA. Anorexia nervosa: demographic and clinical features in 94 cases. Psychosom Med 1974;36:18-24.
2. Bruch AH. Eating disorders: obesity, anorexia nervosa, and the person within. New York, Basic books, 1973.
3. Kleifield E, Wagner S, Halmi KA. Cognitive behavioral treatment of anorexia nervosa. Psychiatr Clin North Am 1996;19:715-34.
4. Halmi KA. Eating disorders. In: Martin A, Scahill L, Charney DS Leckman JF (eds). Pediatric pharmacology. New York: Oxford University Press, 2002;592-602.
5. Halmi KA, Eckert E, Marci P, Cohen J. Comorbidity of psychiatric diagnoses in anorexia nervosa. Arch Gen Psychiatry 1991;48:712-18.
6. Braun DL, Sunday SR, Halmi KA. Psychiatric comorbidity in patients with eating disorders. Psychol Med 1994;24:859-67.
7. Holderness CC, Brooks-Gunn J, Warren MP. Comorbidity of eating disorders and substance abuse review of the literature. Int J Eat Disord 1994;16:1-34.
8. Herzog DB, Keller M, Lavori P. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry 1992;53:147-52.
9. Baran S, Weltzin T, Kaye W. Low discharge weight and outcome in anorexia nervosa. Am J Psychiatry 1995;150:1070-2.
10. Commerford MC, Licinio J, Halmi KA. Guidelines for discharging eating disorder patients. Eat Disord 1997;5:69-74.
11. Howard W, Evans K, Quinter-Howard C, et al. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am J Psychiatry 1999;156:1697-1702.
12. Wiseman C, Sunday SR, Klapper F, et al. Changing patterns of hospitalization in eating disorder patients. Int J Eat Disord 2001;30:69-74.
13. Newman M, Halmi KA. The relationship of bone density to estradiol and cortisol in anorexia nervosa and bulimia nervosa. Psychiatr Res 1989;29:105-12.
14. Falk JR, Halmi KA. Amenorrhea in anorexia nervosa: examination of the critical body hypothesis. Biol Psychiatr 1982;17:799-806.
15. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res 1982;6:1223-50.
16. Dare C. Eisler. Family therapy and eating disorders. In: Fairburn CR, Brownell KD (eds). Eating disorders and obesity. New York: Guilford Press, 2002;314-19.
17. Powers P, Santana CA, Bannon YS. Olanzapine in the treatment of anorexia nervosa: an open label trial. Int J Eat Disord 2002;32:146-54.
18. Halmi KA, Eckert ED, Ladu T, Cohen J. Anorexia nervosa: treatment efficacy of cyproheptadine and amitriptyline. Arch Gen Psychiatry 1986;43:177-81.
19. Kaye W. The use of fluoxetine to prevent relapse in anorexia nervosa (presentation). Pittsburgh, PA: Eating Disorder Research Society annual meeting, 1996.
20. Ferguson C, Lavia M, Crossan P. Are serotonin selective reuptake inhibitors effective in underweight anorexia nervosa? Int J Eat Disord 1999;25:11-17.
Ms. J started losing weight deliberately at age 14 while attending boarding school. She lost 25 lbs by jogging 6 miles per day, exercising another 2 hours, avoiding meat, abusing laxatives, and drinking large quantities of coffee.
She was referred to a school counselor because of her weight loss and returned home. She was happier at a local high school and recovered to normal weight. In college, however, she reverted to compulsive exercising and preoccupation with her weight after the break-up of her first intimate relationship.
Now at age 22, Ms. J has persistently failed to gain weight during outpatient therapy for anorexia nervosa. At 5′7″ she weighs 98 lbs. On the day she was to be hospitalized involuntarily, she took 25 diphenhydramine tablets, which her psychiatrist viewed as a suicide threat. The overdose was treated in the emergency room with ipecac syrup, and she was admitted for inpatient eating disorder treatment.
Like Ms. J, patients with anorexia nervosa resist treatment and deny having most diagnostic signs and symptoms. Based on the evidence and my 30 years of treating anorectic patients,1 this article offers suggestions to help you:
- gather accurate histories from patients and their families
- identify common psychiatric comorbidities
- gain the patient’s trust during treatment
- provide effective dual therapy, with cognitive-behavioral and pharmacologic components.
Table 1
Diagnostic criteria for anorexia nervosa
| Underweight (<85% of normal for age and height) |
| Fear of gaining weight or becoming fat, even though underweight |
| Disturbed conceptualization of body shape and weight, denial of seriousness of low body weight, or overemphasis on body shape and weight in self-evaluation |
Amenorrhea. Subtypes:
|
| Source: Adapted with permission from Diagnostic and statistical manual of mental disorders (4th ed. text revision). |
| Copyright 2000 American Psychiatric Association. |
Making the diagnosis
Anorexia nervosa is characterized by underweight, fear of gaining weight, disturbed body concept, and amenorrhea (Table 1). Its core psychological symptoms have been described as:
- relentless pursuit of thinness
- denial of cachexia
- and feelings of general ineffectiveness.2
The patient may say she feels fat even though emaciated or that parts of her body are too large. This disturbed experience of body weight or shape may represent sublimation and displacement for feelings of inadequacy. Because anorectic patients stay thin so effectively, they may feel a sense of accomplishment by evaluating themselves in terms of their thinness. Cognitive therapy focuses on correcting patients’ pervasive sense of inadequacy, as manifest in maturity fears and lack of confidence in coping with life’s problems.3
Subtypes. Anorexia nervosa has two subtypes—restricting and binge eating/purging—that differ in behavioral and medical symptoms.4 Patients with binge eating/purging show:
- higher rates of impulsivity (suicide attempts, self-mutilation, stealing, and alcohol and other substance abuse)
- more-prevalent impulsive personality disorders (borderline personality disorder, hysterical personality disorder)
- medical problems caused by purging.
Restricting-type patients are often dependent and submissive, with difficulty separating from parents. These patients may be preoccupied with orderliness, perfectionism, and control.
Recommendation. A structured interview to diagnose anorexia nervosa is summarized in Table 2. Because the patient will likely deny her symptoms, it is usually necessary to also interview family members or close friends.
Psychiatric comorbidity
Case report continued: A ‘perfectionist.’
School for Ms. J required great effort, and she spent many hours studying. Her upper-middle-class parents described her as “a perfectionist.” The family placed considerable emphasis on doing the “correct” thing.
During adolescence, Ms. J developed a major depressive episode that lasted 4 months. She also developed obsessions and compulsions unrelated to her eating disorder. She obsessively ruminated about the correct things to say in social circumstances and devoted 4 hours per day to cleaning and checking compulsions. She felt she had to wash her car every time before going out; if she could not, she would cancel her social plans.
Table 2
Diagnosis of anorexia nervosa: Questions to ask*
| Weight history | -What was her highest weight and lowest weight (after weight loss) -At what ages did these weights occur? -Ask about her present weight before you weigh her |
| Eating behavior | -What does she eat and when from morning awakening to bedtime? -Does she eat with the family less often than in the past? -Is she binging? |
| Purging behavior | -Is she inducing vomiting? -Is she using laxatives, diuretics, ipecac, or enemas? |
| Preoccupations and rituals concerning food and weight | -Does she constantly count calories and express concern about fat content in foods? -Does she often gaze in the mirror and comment about being fat? -How often does she weigh herself? -Does she express fear of being unable to stop eating? |
| Activity | -Is she jogging, bike riding, or doing aerobics? -How often, and for how long? -Is she overactive at home, such as pacing? |
| Menstrual history | -At what age did menses begin? -What was the date of her last period? -How regular is her cycle? |
| Psychiatric comorbidity | -Does she have symptoms of depression? -Impulsive behavior (suicide attempts or self-mutilation)? -Drug or alcohol abuse? -Anxiety (obsessive-compulsive behaviors, social phobia, generalized anxiety, fearfulness)? -Personality disorders? |
| * Because patients with anorexia nervosa often deny their symptoms and conceal their food intake, it is usually necessary to interview family members or close friends as well as the patient. | |
In college, she began abusing alcohol and was arrested once for driving while intoxicated.
Depression is the most common comorbidity in anorexia nervosa. Two-thirds of anorectic patients in a 10-year follow-up study reported a history of major depressive disorder.5 Suicide, starvation, and electrolyte imbalance are the three major causes of death. Among severely ill patients who require hospitalization, 10% to 20% die, though the suicide rate is undocumented.
Compulsions. Anorectics’ preoccupations about food and eating rituals have been compared with compulsions, though less than 20% of patients meet diagnostic criteria for obsessive-compulsive disorder.6
Substance abuse. Bulimic anorectics report more alcohol and substance use and abuse than restricting anorectics.7 The most common substances of abuse are cannabis, cocaine, stimulants, and over-the-counter pills such as diet aids.
Personality disorders. Up to 50% of patients with anorexia nervosa—particularly the binge/purge subtype—have personality disorders. Borderline personality disorder is especially common among binge/purge types,8 and avoidant personality disorder is more common among restricting types.
Table 3
Diagnostic signs of emaciation and purging in patients with anorexia nervosa
Emaciation
|
Purging
|
Personality disorders usually reflect instability in interpersonal relationships, poor self-image, or fluctuating affect. Patients may show a pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Sexuality. Psychosocial and sexual development is often delayed in adolescent anorectics. In adults, interest in sex often plummets with anorexia onset, although binge/purge-type patients occasionally become promiscuous.
Medical signs
Case report continued: Abnormal ECG.
Ms. J was hospitalized after her weight dropped below 75% of normal for her age, height, and body build. She showed signs of electrolyte disturbance, including severe bradycardia (pulse rate 40) and ST-segment abnormalities on ECG.
Clinical signs of emaciation and purging can assist with diagnosis and in making decisions about medical treatment, including hospitalization (Table 3). Patients who purge are often weak and have puffy cheeks or parotid gland enlargement. They may have fainting spells and scars on their hands from stimulating vomiting. Laxative abuse may decrease colon motility and worsen constipation.
Neuroendocrine changes secondary to dieting and weight loss include:
- increased corticotropin-releasing hormone secretion
- blunted diurnal cortisol fluctuation
- decreased follicle-stimulating hormone (FSH) secretion
- impaired growth hormone regulation
- decreased luteinizing hormone (LH) secretion
- mildly decreased triiodothyronine
- erratic vasopressin secretion.
Measuring these changes is unnecessary, as general nutritional rehabilitation with weight gain will correct them.
Neurotransmitter function. Emaciated anorectics have a blunted response to pharmacologic probes for dopamine, reduced CSF norepinephrine turnover, and decreased CSF serotonin. Neuroimaging studies suggest that serotonin dysfunction may persist after weight is restored, although these findings require replication.
Treatment priorities
Effective therapies. Open studies indicate that multidimensional treatment—medical management, psychoeducation, and individual cognitive-behavioral therapy (CBT)—is most effective for anorexia nervosa. The fewer than 10 controlled trials that address anorexia nervosa treatment show:
- the more severe the illness, the more intense the treatment required
- outpatient therapy is most successful in patients who have had the illness <6 months, are not binging and vomiting, and have parents who participate in family therapy.
Hospitalization. An emaciated patient who is irritable, depressed, preoccupied with food, and sleep-deprived is unlikely to make progress toward behavioral change. The first goal, therefore, is to restore her nutritional state to normal.
Severely ill anorectic patients require hospitalization for daily monitoring of weight, calorie intake, urine output, and serum electrolytes and amylase (to assess purging behavior). Hospitalization is indicated for:
- loss of >20% of normal weight for age, height, and bone structure
- >6 months of repeated hospitalizations and underweight
- psychotic depression or serious suicide attempt
- incapacitating obsessions and compulsions, related or not to the eating disorder
- serious comorbid medical conditions, such as edema, hypoproteinemia, severe anemia, cardiac arrhythmia, or hypokalemic alkalosis (serum K+ < 2.5 mEq/L).
Keeping a patient in the hospital long enough to provide effective medical and psychological therapy has become difficult, however, because of medical insurance restrictions (Box). The result: poorer outcomes and increased relapse rates compared with 10 years ago.9-12
Hospital treatment of eating disorders has shifted from long-term care of a chronic disorder to stabilization of acute episodes. For some patients, this change has been deleterious and not cost-effective.
A decade ago, eating disorder hospitalizations were covered primarily by private insurance. Today, health maintenance organizations, managed care oversight of private insurance, and public funding are the primary sources of payment. These insurers often limit payment for eating disorder hospitalization, the most costly aspect of psychiatric care.
Poor outcomes and a high relapse rate have been documented in anorexia nervosa patients who left the hospital while underweight.9-11 From 1984 to 1998:
- average hospital stays for anorexia nervosa decreased from 150 days to 23.7 days
- readmissions increased from 0% to 27% of total admissions
- anorectic patients’ average body mass index at discharge dropped from 19.3 to 17.7, a statistically significant difference.12
For psychiatrists, this trend means many outpatients with anorexia nervosa will require repeated hospitalizations that will not substantially improve their anorectic behaviors.
Nutritional rehabilitation and behavior changes can often correct the medical complications of emaciation and purging. Lost bone density is seldom restored, but nutritional rehabilitation can prevent further bone loss.13 Women who remain amenorrheic for several years after weight restoration tend to be more psychologically disturbed than those who resume menses rapidly.14
Cognitive-behavioral therapy
Other authors have discussed CBT for anorexia nervosa.3,15 In general, the key tasks—operationalizing beliefs, evaluating autonomic thoughts, testing prospective hypotheses, and examining underlying assumptions—are accomplished by assessing anorexia’s distorted cognitions. No satisfactory controlled studies have examined any other type of individual psychotherapy for treating anorexia nervosa.
Alliance building. Patients with anorexia find it difficult to participate in therapeutic relationships. They are terrified of gaining weight and readily drop out of treatment. To build a therapeutic alliance:
- begin by helping the patient develop a history of her significant life events
- proceed slowly, praising her for every small attempt at changing her behavior
- set realistic therapy goals, considering her degree of resistance.
Monitoring. Behavior therapy consists primarily of positive reinforcements for weight gain. For this, we weigh outpatients weekly and inpatients daily. Outpatients are taught to keep diaries of daily food intake, stressful events, and emotional responses to them. The therapist begins each session by examining the patient’s diary with her and discussing how life events affect her eating behavior.
Cognitive restructuring helps patients identify their disturbed cognitions and challenge core beliefs about self-image. In this process, they become aware of their negative thoughts and develop arguments and evidence to support and refute the thoughts’ validity. They then form a reasoned conclusion based on the evidence.
Even if patients do not accept this logical conclusion, we encourage them to behave as if they believe it to be true. By doing this repeatedly, they eventually obtain some symptom relief.
Response-prevention techniques can help stop binging and purging. For example, we may require inpatients to sit together for 1 hour after eating. Because most patients will not vomit in front of each other, they learn how to resist vomiting and eventually experience reduced anxiety without vomiting after a meal.
Problem solving helps patients to reason through difficult food-related or interpersonal situations. The patient states the problem, then generates as many solutions as possible with the therapist’s assistance. She chooses one solution and puts it into effect, usually for 1 week. She then discusses the results with her therapist and decides whether to try another solution.
Family therapy. A family analysis—including a brief psychiatric history and evaluation of interactions—is recommended for all patients who live at home. This analysis can help you decide what type of family therapy or counseling to recommend.
Some families respond well with the parents and patient together in therapy sessions, whereas others are more comfortable with separate counseling. In a recent controlled study, anorectic patients younger than age 18 did equally well whether they were counseled with the family or separately.16
Brief therapy sessions are sometimes the most effective method to address family issues. When this is not possible, you and the patient can discuss family relationships in individual therapy.
Medications
Many medications have been used to treat anorexia nervosa, though few randomized, placebo-controlled studies exist. Because evidence does not support using psychotropics as monotherapy for anorexia nervosa, medication is considered adjunctive to CBT.
Chlorpromazine can help the hospitalized, severely ill patient who is overwhelmed with uncontrollable behavioral rituals and thoughts of losing weight. This antipsychotic helps reduce anorectic preoccupations and anxiety and helps make patients more amenable to therapy.
Start chlorpromazine at 10 mg tid and increase gradually until the patient can eat without extreme anxiety. Usual maximum dosage is 50 mg tid. Monitor blood pressure, tardive dyskinesia, and decreased white blood cell count.
Olanzapine may help induce weight gain and reduce anxiety in anorectic patients.17 Controlled and open-label studies are under way.
We start olanzapine at 2.5 mg/d and increase gradually to 10 or 15 mg/d. At this dosage, patients’ anxiety about eating is usually substantially reduced. Sedation is the most common side effect.
Anorexia patients often refuse to take olanzapine for fear of weight gain. If a patient’s emaciation is life-threatening, we may seek court permission to medicate her involuntarily. We reassure her that we will discontinue olanzapine when she reaches her target weight.
Serotonin in anorexia. Central serotonin pathways modulate feeding behavior. Serotonin antagonists—such as cyproheptadine—increase food intake and weight gain, whereas serotonin agonists—such as selective serotonin reuptake inhibitors (SSRIs)—decrease food intake.
Serotonin pathways also may modulate obsessive-compulsive and impulsive behaviors. Both serotonin agonists and antagonists can be useful adjuncts in treating anorexia nervosa.
In a double-blind, placebo-controlled trial, cyproheptadine, 4 to 8 mg tid, was associated with weight gain and reduced depressive symptoms in anorexia nervosa patients.18 Unlike tricyclic antidepressants, cyproheptadine does not reduce blood pressure or increase heart rate, which makes it attractive for emaciated anorectic patients. Dosages up to 28 mg/d can be used safely.
The SSRI fluoxetine may help prevent weight loss relapse in anorexia nervosa and reduce obsessive-compulsive behaviors.19 In open studies of low-weight anorectics, however, fluoxetine had little impact on weight or other clinically meaningful variables.20 Thus, this agent is recommended for preventing weight-loss relapse only in patients who are within 10% to 15% of ideal body weight.
Outpatient care
Case report continued: Ongoing therapy
During hospitalization, Ms. J participated in all therapeutic modalities but had difficulty eating enough to gain weight. She reached her target weight of 127 lbs in about 7 weeks but gained no sense of purpose in life.
She is starting an intensive outpatient program using CBT to maintain her weight and further address the core psychopathology of her illness. Her maintenance therapy includes attending Alcoholics Anonymous meetings, ongoing fluoxetine (20 mg/d) to prevent weight-loss relapse, and CBT for obsessions and compulsions not related to her eating disorder.
Related resources
- Halmi KA. Eating disorders: Anorexia, bulimia nervosa and obesity. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry, 4th ed. Washington, DC: American Psychiatric Publishing, 2003:1001-21.
- Academy of Eating Disorders. www.aedweb.org
- Anorexia Nervosa & Associated Disorders (ANAD). www.anad.org
Drug brand names
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Olanzapine • Zyprexa
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Ms. J started losing weight deliberately at age 14 while attending boarding school. She lost 25 lbs by jogging 6 miles per day, exercising another 2 hours, avoiding meat, abusing laxatives, and drinking large quantities of coffee.
She was referred to a school counselor because of her weight loss and returned home. She was happier at a local high school and recovered to normal weight. In college, however, she reverted to compulsive exercising and preoccupation with her weight after the break-up of her first intimate relationship.
Now at age 22, Ms. J has persistently failed to gain weight during outpatient therapy for anorexia nervosa. At 5′7″ she weighs 98 lbs. On the day she was to be hospitalized involuntarily, she took 25 diphenhydramine tablets, which her psychiatrist viewed as a suicide threat. The overdose was treated in the emergency room with ipecac syrup, and she was admitted for inpatient eating disorder treatment.
Like Ms. J, patients with anorexia nervosa resist treatment and deny having most diagnostic signs and symptoms. Based on the evidence and my 30 years of treating anorectic patients,1 this article offers suggestions to help you:
- gather accurate histories from patients and their families
- identify common psychiatric comorbidities
- gain the patient’s trust during treatment
- provide effective dual therapy, with cognitive-behavioral and pharmacologic components.
Table 1
Diagnostic criteria for anorexia nervosa
| Underweight (<85% of normal for age and height) |
| Fear of gaining weight or becoming fat, even though underweight |
| Disturbed conceptualization of body shape and weight, denial of seriousness of low body weight, or overemphasis on body shape and weight in self-evaluation |
Amenorrhea. Subtypes:
|
| Source: Adapted with permission from Diagnostic and statistical manual of mental disorders (4th ed. text revision). |
| Copyright 2000 American Psychiatric Association. |
Making the diagnosis
Anorexia nervosa is characterized by underweight, fear of gaining weight, disturbed body concept, and amenorrhea (Table 1). Its core psychological symptoms have been described as:
- relentless pursuit of thinness
- denial of cachexia
- and feelings of general ineffectiveness.2
The patient may say she feels fat even though emaciated or that parts of her body are too large. This disturbed experience of body weight or shape may represent sublimation and displacement for feelings of inadequacy. Because anorectic patients stay thin so effectively, they may feel a sense of accomplishment by evaluating themselves in terms of their thinness. Cognitive therapy focuses on correcting patients’ pervasive sense of inadequacy, as manifest in maturity fears and lack of confidence in coping with life’s problems.3
Subtypes. Anorexia nervosa has two subtypes—restricting and binge eating/purging—that differ in behavioral and medical symptoms.4 Patients with binge eating/purging show:
- higher rates of impulsivity (suicide attempts, self-mutilation, stealing, and alcohol and other substance abuse)
- more-prevalent impulsive personality disorders (borderline personality disorder, hysterical personality disorder)
- medical problems caused by purging.
Restricting-type patients are often dependent and submissive, with difficulty separating from parents. These patients may be preoccupied with orderliness, perfectionism, and control.
Recommendation. A structured interview to diagnose anorexia nervosa is summarized in Table 2. Because the patient will likely deny her symptoms, it is usually necessary to also interview family members or close friends.
Psychiatric comorbidity
Case report continued: A ‘perfectionist.’
School for Ms. J required great effort, and she spent many hours studying. Her upper-middle-class parents described her as “a perfectionist.” The family placed considerable emphasis on doing the “correct” thing.
During adolescence, Ms. J developed a major depressive episode that lasted 4 months. She also developed obsessions and compulsions unrelated to her eating disorder. She obsessively ruminated about the correct things to say in social circumstances and devoted 4 hours per day to cleaning and checking compulsions. She felt she had to wash her car every time before going out; if she could not, she would cancel her social plans.
Table 2
Diagnosis of anorexia nervosa: Questions to ask*
| Weight history | -What was her highest weight and lowest weight (after weight loss) -At what ages did these weights occur? -Ask about her present weight before you weigh her |
| Eating behavior | -What does she eat and when from morning awakening to bedtime? -Does she eat with the family less often than in the past? -Is she binging? |
| Purging behavior | -Is she inducing vomiting? -Is she using laxatives, diuretics, ipecac, or enemas? |
| Preoccupations and rituals concerning food and weight | -Does she constantly count calories and express concern about fat content in foods? -Does she often gaze in the mirror and comment about being fat? -How often does she weigh herself? -Does she express fear of being unable to stop eating? |
| Activity | -Is she jogging, bike riding, or doing aerobics? -How often, and for how long? -Is she overactive at home, such as pacing? |
| Menstrual history | -At what age did menses begin? -What was the date of her last period? -How regular is her cycle? |
| Psychiatric comorbidity | -Does she have symptoms of depression? -Impulsive behavior (suicide attempts or self-mutilation)? -Drug or alcohol abuse? -Anxiety (obsessive-compulsive behaviors, social phobia, generalized anxiety, fearfulness)? -Personality disorders? |
| * Because patients with anorexia nervosa often deny their symptoms and conceal their food intake, it is usually necessary to interview family members or close friends as well as the patient. | |
In college, she began abusing alcohol and was arrested once for driving while intoxicated.
Depression is the most common comorbidity in anorexia nervosa. Two-thirds of anorectic patients in a 10-year follow-up study reported a history of major depressive disorder.5 Suicide, starvation, and electrolyte imbalance are the three major causes of death. Among severely ill patients who require hospitalization, 10% to 20% die, though the suicide rate is undocumented.
Compulsions. Anorectics’ preoccupations about food and eating rituals have been compared with compulsions, though less than 20% of patients meet diagnostic criteria for obsessive-compulsive disorder.6
Substance abuse. Bulimic anorectics report more alcohol and substance use and abuse than restricting anorectics.7 The most common substances of abuse are cannabis, cocaine, stimulants, and over-the-counter pills such as diet aids.
Personality disorders. Up to 50% of patients with anorexia nervosa—particularly the binge/purge subtype—have personality disorders. Borderline personality disorder is especially common among binge/purge types,8 and avoidant personality disorder is more common among restricting types.
Table 3
Diagnostic signs of emaciation and purging in patients with anorexia nervosa
Emaciation
|
Purging
|
Personality disorders usually reflect instability in interpersonal relationships, poor self-image, or fluctuating affect. Patients may show a pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Sexuality. Psychosocial and sexual development is often delayed in adolescent anorectics. In adults, interest in sex often plummets with anorexia onset, although binge/purge-type patients occasionally become promiscuous.
Medical signs
Case report continued: Abnormal ECG.
Ms. J was hospitalized after her weight dropped below 75% of normal for her age, height, and body build. She showed signs of electrolyte disturbance, including severe bradycardia (pulse rate 40) and ST-segment abnormalities on ECG.
Clinical signs of emaciation and purging can assist with diagnosis and in making decisions about medical treatment, including hospitalization (Table 3). Patients who purge are often weak and have puffy cheeks or parotid gland enlargement. They may have fainting spells and scars on their hands from stimulating vomiting. Laxative abuse may decrease colon motility and worsen constipation.
Neuroendocrine changes secondary to dieting and weight loss include:
- increased corticotropin-releasing hormone secretion
- blunted diurnal cortisol fluctuation
- decreased follicle-stimulating hormone (FSH) secretion
- impaired growth hormone regulation
- decreased luteinizing hormone (LH) secretion
- mildly decreased triiodothyronine
- erratic vasopressin secretion.
Measuring these changes is unnecessary, as general nutritional rehabilitation with weight gain will correct them.
Neurotransmitter function. Emaciated anorectics have a blunted response to pharmacologic probes for dopamine, reduced CSF norepinephrine turnover, and decreased CSF serotonin. Neuroimaging studies suggest that serotonin dysfunction may persist after weight is restored, although these findings require replication.
Treatment priorities
Effective therapies. Open studies indicate that multidimensional treatment—medical management, psychoeducation, and individual cognitive-behavioral therapy (CBT)—is most effective for anorexia nervosa. The fewer than 10 controlled trials that address anorexia nervosa treatment show:
- the more severe the illness, the more intense the treatment required
- outpatient therapy is most successful in patients who have had the illness <6 months, are not binging and vomiting, and have parents who participate in family therapy.
Hospitalization. An emaciated patient who is irritable, depressed, preoccupied with food, and sleep-deprived is unlikely to make progress toward behavioral change. The first goal, therefore, is to restore her nutritional state to normal.
Severely ill anorectic patients require hospitalization for daily monitoring of weight, calorie intake, urine output, and serum electrolytes and amylase (to assess purging behavior). Hospitalization is indicated for:
- loss of >20% of normal weight for age, height, and bone structure
- >6 months of repeated hospitalizations and underweight
- psychotic depression or serious suicide attempt
- incapacitating obsessions and compulsions, related or not to the eating disorder
- serious comorbid medical conditions, such as edema, hypoproteinemia, severe anemia, cardiac arrhythmia, or hypokalemic alkalosis (serum K+ < 2.5 mEq/L).
Keeping a patient in the hospital long enough to provide effective medical and psychological therapy has become difficult, however, because of medical insurance restrictions (Box). The result: poorer outcomes and increased relapse rates compared with 10 years ago.9-12
Hospital treatment of eating disorders has shifted from long-term care of a chronic disorder to stabilization of acute episodes. For some patients, this change has been deleterious and not cost-effective.
A decade ago, eating disorder hospitalizations were covered primarily by private insurance. Today, health maintenance organizations, managed care oversight of private insurance, and public funding are the primary sources of payment. These insurers often limit payment for eating disorder hospitalization, the most costly aspect of psychiatric care.
Poor outcomes and a high relapse rate have been documented in anorexia nervosa patients who left the hospital while underweight.9-11 From 1984 to 1998:
- average hospital stays for anorexia nervosa decreased from 150 days to 23.7 days
- readmissions increased from 0% to 27% of total admissions
- anorectic patients’ average body mass index at discharge dropped from 19.3 to 17.7, a statistically significant difference.12
For psychiatrists, this trend means many outpatients with anorexia nervosa will require repeated hospitalizations that will not substantially improve their anorectic behaviors.
Nutritional rehabilitation and behavior changes can often correct the medical complications of emaciation and purging. Lost bone density is seldom restored, but nutritional rehabilitation can prevent further bone loss.13 Women who remain amenorrheic for several years after weight restoration tend to be more psychologically disturbed than those who resume menses rapidly.14
Cognitive-behavioral therapy
Other authors have discussed CBT for anorexia nervosa.3,15 In general, the key tasks—operationalizing beliefs, evaluating autonomic thoughts, testing prospective hypotheses, and examining underlying assumptions—are accomplished by assessing anorexia’s distorted cognitions. No satisfactory controlled studies have examined any other type of individual psychotherapy for treating anorexia nervosa.
Alliance building. Patients with anorexia find it difficult to participate in therapeutic relationships. They are terrified of gaining weight and readily drop out of treatment. To build a therapeutic alliance:
- begin by helping the patient develop a history of her significant life events
- proceed slowly, praising her for every small attempt at changing her behavior
- set realistic therapy goals, considering her degree of resistance.
Monitoring. Behavior therapy consists primarily of positive reinforcements for weight gain. For this, we weigh outpatients weekly and inpatients daily. Outpatients are taught to keep diaries of daily food intake, stressful events, and emotional responses to them. The therapist begins each session by examining the patient’s diary with her and discussing how life events affect her eating behavior.
Cognitive restructuring helps patients identify their disturbed cognitions and challenge core beliefs about self-image. In this process, they become aware of their negative thoughts and develop arguments and evidence to support and refute the thoughts’ validity. They then form a reasoned conclusion based on the evidence.
Even if patients do not accept this logical conclusion, we encourage them to behave as if they believe it to be true. By doing this repeatedly, they eventually obtain some symptom relief.
Response-prevention techniques can help stop binging and purging. For example, we may require inpatients to sit together for 1 hour after eating. Because most patients will not vomit in front of each other, they learn how to resist vomiting and eventually experience reduced anxiety without vomiting after a meal.
Problem solving helps patients to reason through difficult food-related or interpersonal situations. The patient states the problem, then generates as many solutions as possible with the therapist’s assistance. She chooses one solution and puts it into effect, usually for 1 week. She then discusses the results with her therapist and decides whether to try another solution.
Family therapy. A family analysis—including a brief psychiatric history and evaluation of interactions—is recommended for all patients who live at home. This analysis can help you decide what type of family therapy or counseling to recommend.
Some families respond well with the parents and patient together in therapy sessions, whereas others are more comfortable with separate counseling. In a recent controlled study, anorectic patients younger than age 18 did equally well whether they were counseled with the family or separately.16
Brief therapy sessions are sometimes the most effective method to address family issues. When this is not possible, you and the patient can discuss family relationships in individual therapy.
Medications
Many medications have been used to treat anorexia nervosa, though few randomized, placebo-controlled studies exist. Because evidence does not support using psychotropics as monotherapy for anorexia nervosa, medication is considered adjunctive to CBT.
Chlorpromazine can help the hospitalized, severely ill patient who is overwhelmed with uncontrollable behavioral rituals and thoughts of losing weight. This antipsychotic helps reduce anorectic preoccupations and anxiety and helps make patients more amenable to therapy.
Start chlorpromazine at 10 mg tid and increase gradually until the patient can eat without extreme anxiety. Usual maximum dosage is 50 mg tid. Monitor blood pressure, tardive dyskinesia, and decreased white blood cell count.
Olanzapine may help induce weight gain and reduce anxiety in anorectic patients.17 Controlled and open-label studies are under way.
We start olanzapine at 2.5 mg/d and increase gradually to 10 or 15 mg/d. At this dosage, patients’ anxiety about eating is usually substantially reduced. Sedation is the most common side effect.
Anorexia patients often refuse to take olanzapine for fear of weight gain. If a patient’s emaciation is life-threatening, we may seek court permission to medicate her involuntarily. We reassure her that we will discontinue olanzapine when she reaches her target weight.
Serotonin in anorexia. Central serotonin pathways modulate feeding behavior. Serotonin antagonists—such as cyproheptadine—increase food intake and weight gain, whereas serotonin agonists—such as selective serotonin reuptake inhibitors (SSRIs)—decrease food intake.
Serotonin pathways also may modulate obsessive-compulsive and impulsive behaviors. Both serotonin agonists and antagonists can be useful adjuncts in treating anorexia nervosa.
In a double-blind, placebo-controlled trial, cyproheptadine, 4 to 8 mg tid, was associated with weight gain and reduced depressive symptoms in anorexia nervosa patients.18 Unlike tricyclic antidepressants, cyproheptadine does not reduce blood pressure or increase heart rate, which makes it attractive for emaciated anorectic patients. Dosages up to 28 mg/d can be used safely.
The SSRI fluoxetine may help prevent weight loss relapse in anorexia nervosa and reduce obsessive-compulsive behaviors.19 In open studies of low-weight anorectics, however, fluoxetine had little impact on weight or other clinically meaningful variables.20 Thus, this agent is recommended for preventing weight-loss relapse only in patients who are within 10% to 15% of ideal body weight.
Outpatient care
Case report continued: Ongoing therapy
During hospitalization, Ms. J participated in all therapeutic modalities but had difficulty eating enough to gain weight. She reached her target weight of 127 lbs in about 7 weeks but gained no sense of purpose in life.
She is starting an intensive outpatient program using CBT to maintain her weight and further address the core psychopathology of her illness. Her maintenance therapy includes attending Alcoholics Anonymous meetings, ongoing fluoxetine (20 mg/d) to prevent weight-loss relapse, and CBT for obsessions and compulsions not related to her eating disorder.
Related resources
- Halmi KA. Eating disorders: Anorexia, bulimia nervosa and obesity. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry, 4th ed. Washington, DC: American Psychiatric Publishing, 2003:1001-21.
- Academy of Eating Disorders. www.aedweb.org
- Anorexia Nervosa & Associated Disorders (ANAD). www.anad.org
Drug brand names
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Olanzapine • Zyprexa
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Halmi KA. Anorexia nervosa: demographic and clinical features in 94 cases. Psychosom Med 1974;36:18-24.
2. Bruch AH. Eating disorders: obesity, anorexia nervosa, and the person within. New York, Basic books, 1973.
3. Kleifield E, Wagner S, Halmi KA. Cognitive behavioral treatment of anorexia nervosa. Psychiatr Clin North Am 1996;19:715-34.
4. Halmi KA. Eating disorders. In: Martin A, Scahill L, Charney DS Leckman JF (eds). Pediatric pharmacology. New York: Oxford University Press, 2002;592-602.
5. Halmi KA, Eckert E, Marci P, Cohen J. Comorbidity of psychiatric diagnoses in anorexia nervosa. Arch Gen Psychiatry 1991;48:712-18.
6. Braun DL, Sunday SR, Halmi KA. Psychiatric comorbidity in patients with eating disorders. Psychol Med 1994;24:859-67.
7. Holderness CC, Brooks-Gunn J, Warren MP. Comorbidity of eating disorders and substance abuse review of the literature. Int J Eat Disord 1994;16:1-34.
8. Herzog DB, Keller M, Lavori P. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry 1992;53:147-52.
9. Baran S, Weltzin T, Kaye W. Low discharge weight and outcome in anorexia nervosa. Am J Psychiatry 1995;150:1070-2.
10. Commerford MC, Licinio J, Halmi KA. Guidelines for discharging eating disorder patients. Eat Disord 1997;5:69-74.
11. Howard W, Evans K, Quinter-Howard C, et al. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am J Psychiatry 1999;156:1697-1702.
12. Wiseman C, Sunday SR, Klapper F, et al. Changing patterns of hospitalization in eating disorder patients. Int J Eat Disord 2001;30:69-74.
13. Newman M, Halmi KA. The relationship of bone density to estradiol and cortisol in anorexia nervosa and bulimia nervosa. Psychiatr Res 1989;29:105-12.
14. Falk JR, Halmi KA. Amenorrhea in anorexia nervosa: examination of the critical body hypothesis. Biol Psychiatr 1982;17:799-806.
15. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res 1982;6:1223-50.
16. Dare C. Eisler. Family therapy and eating disorders. In: Fairburn CR, Brownell KD (eds). Eating disorders and obesity. New York: Guilford Press, 2002;314-19.
17. Powers P, Santana CA, Bannon YS. Olanzapine in the treatment of anorexia nervosa: an open label trial. Int J Eat Disord 2002;32:146-54.
18. Halmi KA, Eckert ED, Ladu T, Cohen J. Anorexia nervosa: treatment efficacy of cyproheptadine and amitriptyline. Arch Gen Psychiatry 1986;43:177-81.
19. Kaye W. The use of fluoxetine to prevent relapse in anorexia nervosa (presentation). Pittsburgh, PA: Eating Disorder Research Society annual meeting, 1996.
20. Ferguson C, Lavia M, Crossan P. Are serotonin selective reuptake inhibitors effective in underweight anorexia nervosa? Int J Eat Disord 1999;25:11-17.
1. Halmi KA. Anorexia nervosa: demographic and clinical features in 94 cases. Psychosom Med 1974;36:18-24.
2. Bruch AH. Eating disorders: obesity, anorexia nervosa, and the person within. New York, Basic books, 1973.
3. Kleifield E, Wagner S, Halmi KA. Cognitive behavioral treatment of anorexia nervosa. Psychiatr Clin North Am 1996;19:715-34.
4. Halmi KA. Eating disorders. In: Martin A, Scahill L, Charney DS Leckman JF (eds). Pediatric pharmacology. New York: Oxford University Press, 2002;592-602.
5. Halmi KA, Eckert E, Marci P, Cohen J. Comorbidity of psychiatric diagnoses in anorexia nervosa. Arch Gen Psychiatry 1991;48:712-18.
6. Braun DL, Sunday SR, Halmi KA. Psychiatric comorbidity in patients with eating disorders. Psychol Med 1994;24:859-67.
7. Holderness CC, Brooks-Gunn J, Warren MP. Comorbidity of eating disorders and substance abuse review of the literature. Int J Eat Disord 1994;16:1-34.
8. Herzog DB, Keller M, Lavori P. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry 1992;53:147-52.
9. Baran S, Weltzin T, Kaye W. Low discharge weight and outcome in anorexia nervosa. Am J Psychiatry 1995;150:1070-2.
10. Commerford MC, Licinio J, Halmi KA. Guidelines for discharging eating disorder patients. Eat Disord 1997;5:69-74.
11. Howard W, Evans K, Quinter-Howard C, et al. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am J Psychiatry 1999;156:1697-1702.
12. Wiseman C, Sunday SR, Klapper F, et al. Changing patterns of hospitalization in eating disorder patients. Int J Eat Disord 2001;30:69-74.
13. Newman M, Halmi KA. The relationship of bone density to estradiol and cortisol in anorexia nervosa and bulimia nervosa. Psychiatr Res 1989;29:105-12.
14. Falk JR, Halmi KA. Amenorrhea in anorexia nervosa: examination of the critical body hypothesis. Biol Psychiatr 1982;17:799-806.
15. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res 1982;6:1223-50.
16. Dare C. Eisler. Family therapy and eating disorders. In: Fairburn CR, Brownell KD (eds). Eating disorders and obesity. New York: Guilford Press, 2002;314-19.
17. Powers P, Santana CA, Bannon YS. Olanzapine in the treatment of anorexia nervosa: an open label trial. Int J Eat Disord 2002;32:146-54.
18. Halmi KA, Eckert ED, Ladu T, Cohen J. Anorexia nervosa: treatment efficacy of cyproheptadine and amitriptyline. Arch Gen Psychiatry 1986;43:177-81.
19. Kaye W. The use of fluoxetine to prevent relapse in anorexia nervosa (presentation). Pittsburgh, PA: Eating Disorder Research Society annual meeting, 1996.
20. Ferguson C, Lavia M, Crossan P. Are serotonin selective reuptake inhibitors effective in underweight anorexia nervosa? Int J Eat Disord 1999;25:11-17.
Treatment-resistant depression: Is there any other kind?
f
Before I see them, most of my depressed patients have failed an SSRI trial prescribed by their primary care physicians. Some have already tried two or more antidepressants. I bet your practice is the same.
Unfortunately, few medications have been tested on patients with treatment-resistant depression. To gain FDA approval, an investigational drug needs to show a treatment effect greater than placebo, and testing a drug on a treatment-resistant population is risky for pharmaceutical companies. Compared with monotherapy, even fewer large-scale studies have combined two or more medications for major depressive disorder.
In this issue, A. John Rush, MD, of the University of Texas Southwestern Medical Center, provides the best synthesis I have seen of the literature on treatment-resistant depression. I am already incorporating his insights into my clinical practice.
Not to minimize the suffering of patients with treatment-resistant depression, but I believe this disorder saved psychiatry. Ten years ago, doomsayers predicted psychiatry’s demise, assuming anyone could do psychotherapy and any physician could prescribe 20 mg of Prozac. Those predictions have proven wrong, and demand for psychiatrists has grown.
We do not compete with primary care physicians. The more depressed patients our medical colleagues treat, the more treatment-resistant cases they refer for psychiatric care. We may not be seeing as many patients with nontreatment depression, but fewer with major depressive disorder are suffering without receiving effective treatment.

James Randolph Hillard, MD
Editor-in-Chief
James Randolph Hillard, MD
Editor-in-Chief
James Randolph Hillard, MD
Editor-in-Chief
f
Before I see them, most of my depressed patients have failed an SSRI trial prescribed by their primary care physicians. Some have already tried two or more antidepressants. I bet your practice is the same.
Unfortunately, few medications have been tested on patients with treatment-resistant depression. To gain FDA approval, an investigational drug needs to show a treatment effect greater than placebo, and testing a drug on a treatment-resistant population is risky for pharmaceutical companies. Compared with monotherapy, even fewer large-scale studies have combined two or more medications for major depressive disorder.
In this issue, A. John Rush, MD, of the University of Texas Southwestern Medical Center, provides the best synthesis I have seen of the literature on treatment-resistant depression. I am already incorporating his insights into my clinical practice.
Not to minimize the suffering of patients with treatment-resistant depression, but I believe this disorder saved psychiatry. Ten years ago, doomsayers predicted psychiatry’s demise, assuming anyone could do psychotherapy and any physician could prescribe 20 mg of Prozac. Those predictions have proven wrong, and demand for psychiatrists has grown.
We do not compete with primary care physicians. The more depressed patients our medical colleagues treat, the more treatment-resistant cases they refer for psychiatric care. We may not be seeing as many patients with nontreatment depression, but fewer with major depressive disorder are suffering without receiving effective treatment.
f
Before I see them, most of my depressed patients have failed an SSRI trial prescribed by their primary care physicians. Some have already tried two or more antidepressants. I bet your practice is the same.
Unfortunately, few medications have been tested on patients with treatment-resistant depression. To gain FDA approval, an investigational drug needs to show a treatment effect greater than placebo, and testing a drug on a treatment-resistant population is risky for pharmaceutical companies. Compared with monotherapy, even fewer large-scale studies have combined two or more medications for major depressive disorder.
In this issue, A. John Rush, MD, of the University of Texas Southwestern Medical Center, provides the best synthesis I have seen of the literature on treatment-resistant depression. I am already incorporating his insights into my clinical practice.
Not to minimize the suffering of patients with treatment-resistant depression, but I believe this disorder saved psychiatry. Ten years ago, doomsayers predicted psychiatry’s demise, assuming anyone could do psychotherapy and any physician could prescribe 20 mg of Prozac. Those predictions have proven wrong, and demand for psychiatrists has grown.
We do not compete with primary care physicians. The more depressed patients our medical colleagues treat, the more treatment-resistant cases they refer for psychiatric care. We may not be seeing as many patients with nontreatment depression, but fewer with major depressive disorder are suffering without receiving effective treatment.
Bipolar treatment update: Evidence is driving change in mania, depression algorithms
Many well-controlled trials in the past 4 years have evaluated new medications for treating bipolar disorder. It’s time to build a consensus on how this data may apply to clinical practice.
This year, our group will re-examine the Texas Medication Algorithm Project (TMAP) treatment algorithms for bipolar I disorder.
What makes TMAP unique? It is the first project to evaluate treatment algorithm use in community mental health settings for patients with a history of mania (see Box).1-5 Severely, persistently ill outpatients such as these are seldom included in research but are frequently seen in clinical practice.
To preview for psychiatrists the changes expected in 2004, this article describes the goals of TMAP and the controlled study on which the medication algorithms are based. We review the medication algorithms of 2000 as a starting point and present the evidence that is changing clinical practice.
Guiding principles of TMAP
A treatment algorithm is no substitute for clinical judgment; rather, medication guidelines and algorithms are guideposts to help the clinician and patient collaboratively develop the most effective medication strategy with the fewest side effects.
The Texas Medication Algorithm Project (TMAP)1-3 is a public and academic collaboration started in 1996 to develop evidence- and consensus-based medication treatment algorithms for schizophrenia, major depressive disorder, and bipolar disorder.
TMAP’s goal is to establish “best practices” to encourage uniformity of care, achieve the best possible patient outcomes, and use mental health care dollars most efficiently. The project includes four phases, in which the treatment algorithms were developed, compared with treatment-as-usual, put into practice, and will undergo periodic updates.4 The next update begins this year.
The comparison of algorithms for treating bipolar mania/hypomania and depression included 409 patients (mean age 38 to 40) with bipolar I disorder or schizoaffective disorder, bipolar type. These patients were severely and persistently mentally ill, from a diverse ethnic population, and significantly impaired in functioning.
During 12 months of treatment, psychiatric symptoms diminished more rapidly in patients in the algorithm group—as measured by the Brief Psychiatric Rating Scale (BPRS-24)—compared with those receiving usual treatment. After the first 3 months, the usual-treatment patients also showed diminished symptoms. At study’s end, symptom severity between the groups was not significantly different; both groups showed improvement.
Manic and psychotic symptoms—measured by Clinician-Administered Rating Scale subscales (CARS-M)5—improved significantly more in the algorithm group in the first 3 months, and this gap between the two groups was sustained for 12 months. Depressive symptoms declined, but no overall differences were noted between the two groups. Side effect rates and functioning were also similar.
TMAP’s treatment manual (see Related resources) describes clinicians’ preferred tactics and decision points, which we summarize here. The guidelines are an ongoing effort to apply evidence-based medicine to everyday practice and are meant to be adapted to patient needs.
Treatment goals that guided TMAP algorithm development are:
- symptomatic remission
- full return of psychosocial functioning
- prevention of relapse and recurrence.
Suggestions came from controlled clinical trials, open trials, retrospective data analyses, expert clinical consensus, and input from consumers.
Treatment selection. Initial algorithm stages recommend simple treatments (in terms of safety, tolerability, and side effects), whereas later stages recommend more-complicated regimens. A patient’s symptoms, comorbid conditions, and treatment history guide treatment selection. Patients may enter an algorithm at any stage, depending on their clinical presentation and medication history.
The clinician may consider patient preference when deciding among equivalent medications. The algorithm strongly encourages patients and families to participate, such as by keeping daily mood charts and completing symptom and side-effect checklists. When clinicians face a choice among medication brands, generics, or forms (such as immediate- versus slow-release), agents with greater tolerability are preferred.
Patient management. When patients enter the algorithm, clinic visits are frequent (such as every 2 weeks). Follow-up appointments address medication adherence, dosage adjustments, and side effects or adverse reactions.
If a patient’s symptoms show no change after two treatment stages, re-evaluate the diagnosis and consider mitigating factors such as substance abuse. Patients who complete acute treatment should receive continuation treatment.
Documentation. Clinicians are advised to document decision points and the rationale for treatment choices made outside the algorithm package.
Treating mania or hypomania
After clinical evaluation confirms the diagnosis of bipolar illness,4 the TMAP mania/hypomania algorithm (Algorithm 1) splits into three treatment pathways:
- euphoric mania/hypomania
- mixed or dysphoric mania/hypomania
- psychotic mania.
These pathways recognize the need for differing approaches to initial monotherapy and later two-drug combinations. If a patient develops persistent or severe depressive symptoms, the bipolar algorithm for a major depressive episode (Algorithm 2) is used during depressive periods with the primary mania algorithm.
Treatment recommendations. The key to using mood stabilizers is to achieve the optimum response—assuming good tolerability—before switching to another agent. Adjust medication dosages one at a time to allow adequate response and assessment.
When switching medications, use an overlap-and-taper strategy, assuming there is no medical necessity to stop a drug abruptly. Add the new medication, then gradually taper the one that is being discontinued. Monitor serum levels.
Discontinue antidepressants when appropriate in patients with hypomania/mania or rapid cycling, and continually evaluate suicide and homicide potential of patients in mixed or depressive states.
Stage 1: Monotherapy. First medication choices are lithium, divalproex, or olanzapine. For mixed or dysphoric mania, the algorithm recommends divalproex (preferred over valproic acid because of tolerability and side effects) or olanzapine.6 Data suggest dysphoric manic patients are less likely to respond to lithium.7 A Consensus Panel minority expressed concern about using olanzapine as first-line monotherapy for acute mania because of limited data on the drug’s long-term safety. Patients with partial response or residual symptoms may move to stage 2 or switch to other medication options within stage 1.
Patients with psychotic mania move directly to stage 4 for a broader range of combination therapy.
Stage 2: Combination therapy. Combination therapy has become the standard of care in treating most patients with bipolar disorder. The algorithm recommends using two agents:
- lithium or an anticonvulsant plus another anticonvulsant ([Li or AC]+AC)
- or lithium or an anticonvulsant plus an atypical antipsychotic ([Li or AC]+AAP).8
Recommended agents include lithium, divalproex, oxcarbazepine, olanzapine, or risperidone. The experts recommended oxcarbazepine as first choice because it is better tolerated and interacts with fewer drugs than carbamazepine and does not require serum level monitoring.9
A Consensus Panel minority expressed concern that few studies had examined using oxcarbazepine in bipolar disorder. Carbamazepine was also considered an option.
Stages 3 and 4: Other two-drug combinations. Other two-drug combinations are tried at these stages, drawing from the same pool of medication classes described in stage 2.
Stage 4 broadens the choice of atypical antipsychotic by adding quetiapine10 and ziprasidone11 to the recommended stage-2 agents olanzapine and risperidone. When the 2000 algorithm was developed, limited data were available on using some newer atypicals in patients with bipolar mania. Based on recent, high-quality studies of mono- and combination therapy—including quetiapine,10 ziprasidone,11 risperidone,12,13 and aripiprazole14 —the 2004 algorithm update panel will likely recommend using atypicals earlier, including at stage 1.
Algorithm 1 Treating mania/hypomania in patients with bipolar I disorder
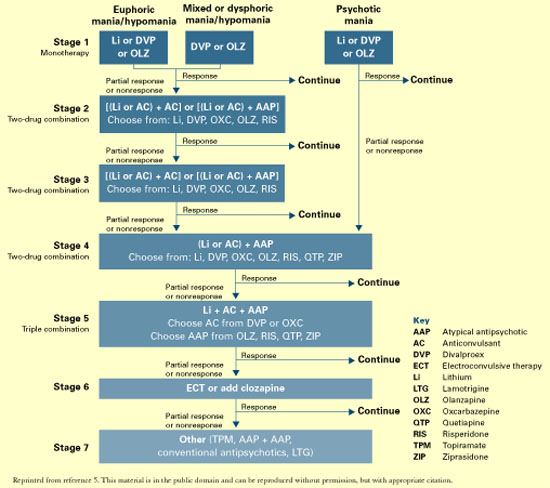
Stage 5: Triple-drug combination. Lithium, an anticonvulsant (divalproex or oxcarbazepine), and an atypical antipsychotic (olanzapine, risperidone, quetiapine, or ziprasidone) is a recommended triple-drug combination. In the 2004 update, the choices will likely expand to include all the newer atypicals and will list carbamazepine as an option.
Stage 6: ECT or clozapine. For patients with inadequate response to triple-drug combinations, the algorithm recommends adding electroconvulsive therapy (ECT) or clozapine.
ECT15 is recommended three times a week until the patient achieves remission of manic symptoms or fails to achieve a sustained response over three to six treatment cycles. Treatment resistance is declared if no response is seen after 6 to 10 treatment cycles.
Clozapine’s16 recommendation at this stage is consistent with its use in patients who fail to respond to other atypical antipsychotics. Blood monitoring for agranulocytosis is required; other adverse effects include an increased risk of seizures, myocarditis, and orthostatic hypotension.
Stage 7: Other. Treatment options such as topiramate17,18 and lamotrigine19 are recommended at this stage. These recommendations also will be reviewed and likely revised.
Treating bipolar depression
The TMAP algorithm for treating depression in bipolar disorder (Algorithm 2) assumes that anti-depressants will be used only with optimum mood-stabilizer levels because of the risk of inducing manic symptoms. The bipolar depression algorithm is always used with the primary algorithm for mania/hypomania.
The patient’s clinical presentation guides medication selection. For the “pure” bipolar I patient with a major depressive episode but little mood lability or hypomania, starting an antide-pressant is a clear decision. On the other hand, patients with predominant depressive symptoms plus dysphoric hypomania, mood lability, and irritability need a balance of mood-stabilizing drugs and antidepressants.
Stage 1: Mood stabilizer. Initiate a mood stabilizer and optimize the dosage. Choices are the same mood stabilizers listed in the hypomania/mania treatment algorithm.
Stage 2: Antidepressant. Adding an antidepressant implies that depressive symptoms are severe enough to change treatment. Antidepressant options include a selective serotonin reuptake inhibitor (SSRI), sustained-release bupropion, or lamotrigine.20
Using SSRIs is supported by widespread clinical experience and offers the convenience of once-daily dosing. Recommended SSRIs include fluoxetine, paroxetine, fluvoxamine, sertraline, and citalopram. The SSRI escitalopram was introduced after the 2000 algorithms were published; evidence for using it and other newer medications will be reviewed for the 2004 update.
The recommendation for sustained-release bupropion is consistent with the algorithm principle to use medications in the most well-tolerated form when accessible and available.
With lamotrigine, review with patients the risk of serious rash. To minimize rash risk, start lamotrigine slowly and follow the recommended titration schedule.
Stage 3: Multiple choices. At this stage, no definitive studies, safety data, or tolerability issues are available to rank the medication choices. The algorithm suggests:
- adding lithium21 or a second antidepressant
- or switching to an alternate antidepressant such as venlafaxine or nefazodone.
If a patient moves to stage 3 because of side effects with one antidepressant class, a different class—preferably with a contrasting side-effect profile—is recommended.
Algorithm 2 Treating depression in bipolar I disorder*
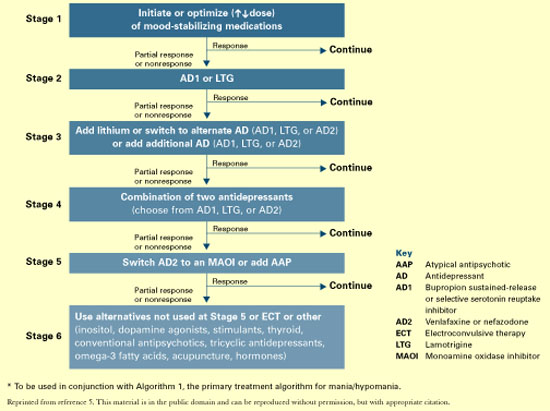
Stage 4: Two antidepressants. To enhance clinical response, the algorithm recommends combining two antidepressants, preferably from different classes. Monitor patients closely for side effects.
Stage 5. Antipsychotic or MAOI. At this stage, the algorithm recommends adding an atypical antipsychotic22 or switching to a monoamine oxidase inhibitor (MAOI).
Early evidence supported the efficacy of MAOIs in bipolar depression. However, the panel ranked MAOIs lower in the algorithm because they are associated with more bothersome side effects than SSRIs and other antidepressants. When using MAOIs, provide patients with dietary restriction guidelines.
Stage 6. Other therapies. Therapies such as ECT or “other” interventions are recommended at this stage. ECT has proven efficacy in bipolar depression and is appropriate for patients with limited medication response. The panel gave ECT a low ranking because of limited availability, lack of patient acceptance, and newer options.
Medication options include experimental treatments with limited evidence, such as inositol, dopamine agonists, stimulants, thyroid supplementation, conventional antipsychotics, and tri-cyclic antidepressants.
Acute to maintenance treatment
Adjunctive treatments for agitation, insomnia, GI upset, sedation, headache, and tremor are recommended in the physician manual supporting the TMAP guidelines (see Related resources). The manual also suggests ways to manage medication side effects and modify the algorithms for inpatients.
Patient and family psychoeducation plays an important role in helping the patient:
- identify prodromal bipolar symptoms
- understand the need to take medications as prescribed.
Continuation treatment. After mania or hypomania remits, continue medication(s) at the effective acute-phase dosages for at least 3 months. Use follow-up visits to enhance patient adherence, detect early symptoms of relapse, and monitor for side effects.
During the late continuation phase, after a period of sustained stability, clinicians can try to simplify the medications. When discontinuing a medication, taper the dosage by no more than 25% per week. If symptoms recur, promptly return to acute-phase treatment. Consider restarting medications and titrating up to the dosage(s) that resulted in remission.
In a depressive episode, continue the antidepressant(s) for 1 to 3 months at the effective acutephase dosage(s). Follow up frequently, and educate patients to watch for symptom recurrence and to communicate with you to assess when medication changes are needed.
Maintenance treatment. Relatively few well-controlled studies on long-term management of bipolar patients were available for the 2000 algorithm update.23 In general, all patients need mood stabilizer(s) to prevent relapse, using the lowest dosage that maintains therapeutic efficacy. Based on new evidence for lamotrigine and atypical antipsychotics—including FDAapproval of olanzapine for bipolar maintenace therapy—we anticipate recommendations will be expanded and more delineated in the 2004 update.
Discontinuing antidepressants after 3 to 6 months of initial treatment is now recommended. However, a recent retrospective case series suggests that continuing antidepressants at least 1 year after initial successful therapy may protect against depressive relapse. During this study, continuing antidepressants more than 3 to 6 months did not appear to increase the risk of switching to mania.24
Should antidepressants be continued or discontinued after successful acute treatment of a bipolar I depressive episode? This is an active area of research and debate as to the most appropriate strategy. The 2004 algorithm update panel will consider recent evidence that supports continuing antidepressants after symptom remission.24
- Texas Medication Algorithm Project algorithms and physician manual. Texas Department of Mental Health and Mental Retardation. http://www.mhmr.state.tx.us/centraloffice/medicaldirector/TIMA.html
- American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. Am J Psychiatry 2002; 159(4):suppl 2.
- Depression and Bipolar Support Alliance. www.dbsalliance.org
Drug brand names
- Bupropion • Wellbutrin SR
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Inositol • Various
- Lamotrigine • Lamictal
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Valproic acid • Depakene
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
Dr. Shivakumar reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Suppes receives research support from or is a consultant to Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, National Institutes of Mental Health, Novartis Pharmaceuticals Corp., Pfizer Inc., Pharmaceutical Research Institute, Ortho-McNeil Pharmaceutical, Robert Wood Johnson Pharmaceutical Research Institute, The Stanley Medical Research Institute, and UCB Pharma.
1. Gilbert DA, Altshuler KZ, Rago WV, et al. Texas Medication Algorithm Project: definitions, rationale, and methods to develop medication algorithms. J Clin Psychiatry 1998;59:345-51.
2. Altshuler KZ, Rush AJ. Computerized Texas Medication Algorithm Project undergoes testing. Outcomes Accountability Alert 1999;4(1):10-11.
3. Rush AJ, Crismon ML, Kashner TM, et al. Texas Medication Algorithm Project, Phase 3 (TMAP-3): rationale and study design. J Clin Psychiatry 2003;64(4):357-69.
4. Altman E, Hedeker D, Janicak P, et al. The Clinician-Administered Rating Scale For Mania (CARS-M): development, reliability, and validity. Biol Psychiatry 1994;36:124-34.
5. Suppes T, Dennehy EB, Swann AC, et al. Report of the Texas consensus conference panel on medication treatment of bipolar disorder 2000. J Clin Psychiatry 2002;63:288-99.
6. Dennehy EB, Doyle K, Suppes T. The efficacy of olanzapine monotherapy for acute hypomania or mania in an outpatient setting. Int Clin Psychopharmacol 2003;18(3):143-5.
7. Dilsaver SC, Swann AC, Shoaib AM, et al. The manic syndrome: factors which may predict a patient’s response to lithium, carbamazepine and valproate. J Psych Neurosci 1993;18:61-6.
8. Tohen M, Chengappa KNR, Suppes T, et al. Efficacy of olanzapine in combination with valproate or lithium in the treatment of mania in patients partially nonresponsive to valproate or lithium monotherapy. Arch Gen Psychiatry 2002;59(1):62-9.
9. Emrich HM. Studies with oxcarbazepine (Trileptal) in acute mania. Int Clin Psychopharmacol 1990;190(5,suppl):83-8.
10. Vieta E, Parramon G, Padrell E, et al. Quetiapine in the treatment of rapid cycling bipolar disorder. Bipolar Disord 2002;4(5):335-40.
11. Keck PE, Versiani M, Potkin S, et al. Ziprasidone in the treatment of acute bipolar mania: a three week placebo-controlled, double-blinded randomized trial. Am J Psychiatry 2003;160(4):741-8.
12. Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus risperidone or placebo in the treatment of acute mania. International, double-blinded, randomised controlled trial. Br J Psychiatry 2003;182:141-7.
13. Sachs GS, Grossman F, Ghaemi SN, et al. Combination of a mood stabilizer with risperidone or haloperidol for treatment of acute mania: a double-blind, placebo-controlled comparison of efficacy and safety. Am J Psychiatry 2002;159(7):1146-54.
14. Keck PE, Jr, Marcus R, Tourkodimitris S, et al. Aripiprazole study group. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. Am J Psychiatry 2003;160(9):1651-8.
15. Mukherjee S, Sackeim HA, Schnur DB. Electroconvulsive therapy of acute manic episode: a review of 50 years’ experience. Am J Psychiatry 1988;45:727-32.
16. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trail of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156(8):1164-9.
17. Guille C, Sachs G. Clinical outcome of adjunctive topiramate treatment in a sample of refractory bipolar patients with comorbid conditions. Prog Neuropsychopharmacol Biol Psychiatry 2002;26(6):1035-9.
18. Vieta E, Torrent C, Garcia-Ribas G, et al. Use of topiramate in treatment-resistant bipolar spectrum disorders. J Clin Psychopharmacol 2002;22(4):431-5.
19. Calabrese JR, Suppes T, Bowden CL, et al. A double blinded, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61:841-50.
20. Calabrese JR, Bowden CL, Sachs GS, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder. J Clin Psychiatry 2003;64(9):1013-24.
21. Bauer M, Dopfmer S. Lithium augmentation in treatment-resistant depression: meta-analysis of placebo-controlled studies. J Clin Psychopharmacology 1999;19:427-34.
22. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
23. Baldessarini RJ, Tohen M, Tondo L. Maintenance treatment in bipolar disorder (comment). Arch Gen Psychiatry 2000;57:490-2.
24. Altshuler L, Suppes T, Black D, et al. Impact of antidepressant discontinuation after acute bipolar depression remission on rates of depressive relapse at 1-year follow-up. Am J Psychiatry 2003;160:1252-62.
Many well-controlled trials in the past 4 years have evaluated new medications for treating bipolar disorder. It’s time to build a consensus on how this data may apply to clinical practice.
This year, our group will re-examine the Texas Medication Algorithm Project (TMAP) treatment algorithms for bipolar I disorder.
What makes TMAP unique? It is the first project to evaluate treatment algorithm use in community mental health settings for patients with a history of mania (see Box).1-5 Severely, persistently ill outpatients such as these are seldom included in research but are frequently seen in clinical practice.
To preview for psychiatrists the changes expected in 2004, this article describes the goals of TMAP and the controlled study on which the medication algorithms are based. We review the medication algorithms of 2000 as a starting point and present the evidence that is changing clinical practice.
Guiding principles of TMAP
A treatment algorithm is no substitute for clinical judgment; rather, medication guidelines and algorithms are guideposts to help the clinician and patient collaboratively develop the most effective medication strategy with the fewest side effects.
The Texas Medication Algorithm Project (TMAP)1-3 is a public and academic collaboration started in 1996 to develop evidence- and consensus-based medication treatment algorithms for schizophrenia, major depressive disorder, and bipolar disorder.
TMAP’s goal is to establish “best practices” to encourage uniformity of care, achieve the best possible patient outcomes, and use mental health care dollars most efficiently. The project includes four phases, in which the treatment algorithms were developed, compared with treatment-as-usual, put into practice, and will undergo periodic updates.4 The next update begins this year.
The comparison of algorithms for treating bipolar mania/hypomania and depression included 409 patients (mean age 38 to 40) with bipolar I disorder or schizoaffective disorder, bipolar type. These patients were severely and persistently mentally ill, from a diverse ethnic population, and significantly impaired in functioning.
During 12 months of treatment, psychiatric symptoms diminished more rapidly in patients in the algorithm group—as measured by the Brief Psychiatric Rating Scale (BPRS-24)—compared with those receiving usual treatment. After the first 3 months, the usual-treatment patients also showed diminished symptoms. At study’s end, symptom severity between the groups was not significantly different; both groups showed improvement.
Manic and psychotic symptoms—measured by Clinician-Administered Rating Scale subscales (CARS-M)5—improved significantly more in the algorithm group in the first 3 months, and this gap between the two groups was sustained for 12 months. Depressive symptoms declined, but no overall differences were noted between the two groups. Side effect rates and functioning were also similar.
TMAP’s treatment manual (see Related resources) describes clinicians’ preferred tactics and decision points, which we summarize here. The guidelines are an ongoing effort to apply evidence-based medicine to everyday practice and are meant to be adapted to patient needs.
Treatment goals that guided TMAP algorithm development are:
- symptomatic remission
- full return of psychosocial functioning
- prevention of relapse and recurrence.
Suggestions came from controlled clinical trials, open trials, retrospective data analyses, expert clinical consensus, and input from consumers.
Treatment selection. Initial algorithm stages recommend simple treatments (in terms of safety, tolerability, and side effects), whereas later stages recommend more-complicated regimens. A patient’s symptoms, comorbid conditions, and treatment history guide treatment selection. Patients may enter an algorithm at any stage, depending on their clinical presentation and medication history.
The clinician may consider patient preference when deciding among equivalent medications. The algorithm strongly encourages patients and families to participate, such as by keeping daily mood charts and completing symptom and side-effect checklists. When clinicians face a choice among medication brands, generics, or forms (such as immediate- versus slow-release), agents with greater tolerability are preferred.
Patient management. When patients enter the algorithm, clinic visits are frequent (such as every 2 weeks). Follow-up appointments address medication adherence, dosage adjustments, and side effects or adverse reactions.
If a patient’s symptoms show no change after two treatment stages, re-evaluate the diagnosis and consider mitigating factors such as substance abuse. Patients who complete acute treatment should receive continuation treatment.
Documentation. Clinicians are advised to document decision points and the rationale for treatment choices made outside the algorithm package.
Treating mania or hypomania
After clinical evaluation confirms the diagnosis of bipolar illness,4 the TMAP mania/hypomania algorithm (Algorithm 1) splits into three treatment pathways:
- euphoric mania/hypomania
- mixed or dysphoric mania/hypomania
- psychotic mania.
These pathways recognize the need for differing approaches to initial monotherapy and later two-drug combinations. If a patient develops persistent or severe depressive symptoms, the bipolar algorithm for a major depressive episode (Algorithm 2) is used during depressive periods with the primary mania algorithm.
Treatment recommendations. The key to using mood stabilizers is to achieve the optimum response—assuming good tolerability—before switching to another agent. Adjust medication dosages one at a time to allow adequate response and assessment.
When switching medications, use an overlap-and-taper strategy, assuming there is no medical necessity to stop a drug abruptly. Add the new medication, then gradually taper the one that is being discontinued. Monitor serum levels.
Discontinue antidepressants when appropriate in patients with hypomania/mania or rapid cycling, and continually evaluate suicide and homicide potential of patients in mixed or depressive states.
Stage 1: Monotherapy. First medication choices are lithium, divalproex, or olanzapine. For mixed or dysphoric mania, the algorithm recommends divalproex (preferred over valproic acid because of tolerability and side effects) or olanzapine.6 Data suggest dysphoric manic patients are less likely to respond to lithium.7 A Consensus Panel minority expressed concern about using olanzapine as first-line monotherapy for acute mania because of limited data on the drug’s long-term safety. Patients with partial response or residual symptoms may move to stage 2 or switch to other medication options within stage 1.
Patients with psychotic mania move directly to stage 4 for a broader range of combination therapy.
Stage 2: Combination therapy. Combination therapy has become the standard of care in treating most patients with bipolar disorder. The algorithm recommends using two agents:
- lithium or an anticonvulsant plus another anticonvulsant ([Li or AC]+AC)
- or lithium or an anticonvulsant plus an atypical antipsychotic ([Li or AC]+AAP).8
Recommended agents include lithium, divalproex, oxcarbazepine, olanzapine, or risperidone. The experts recommended oxcarbazepine as first choice because it is better tolerated and interacts with fewer drugs than carbamazepine and does not require serum level monitoring.9
A Consensus Panel minority expressed concern that few studies had examined using oxcarbazepine in bipolar disorder. Carbamazepine was also considered an option.
Stages 3 and 4: Other two-drug combinations. Other two-drug combinations are tried at these stages, drawing from the same pool of medication classes described in stage 2.
Stage 4 broadens the choice of atypical antipsychotic by adding quetiapine10 and ziprasidone11 to the recommended stage-2 agents olanzapine and risperidone. When the 2000 algorithm was developed, limited data were available on using some newer atypicals in patients with bipolar mania. Based on recent, high-quality studies of mono- and combination therapy—including quetiapine,10 ziprasidone,11 risperidone,12,13 and aripiprazole14 —the 2004 algorithm update panel will likely recommend using atypicals earlier, including at stage 1.
Algorithm 1 Treating mania/hypomania in patients with bipolar I disorder
Stage 5: Triple-drug combination. Lithium, an anticonvulsant (divalproex or oxcarbazepine), and an atypical antipsychotic (olanzapine, risperidone, quetiapine, or ziprasidone) is a recommended triple-drug combination. In the 2004 update, the choices will likely expand to include all the newer atypicals and will list carbamazepine as an option.
Stage 6: ECT or clozapine. For patients with inadequate response to triple-drug combinations, the algorithm recommends adding electroconvulsive therapy (ECT) or clozapine.
ECT15 is recommended three times a week until the patient achieves remission of manic symptoms or fails to achieve a sustained response over three to six treatment cycles. Treatment resistance is declared if no response is seen after 6 to 10 treatment cycles.
Clozapine’s16 recommendation at this stage is consistent with its use in patients who fail to respond to other atypical antipsychotics. Blood monitoring for agranulocytosis is required; other adverse effects include an increased risk of seizures, myocarditis, and orthostatic hypotension.
Stage 7: Other. Treatment options such as topiramate17,18 and lamotrigine19 are recommended at this stage. These recommendations also will be reviewed and likely revised.
Treating bipolar depression
The TMAP algorithm for treating depression in bipolar disorder (Algorithm 2) assumes that anti-depressants will be used only with optimum mood-stabilizer levels because of the risk of inducing manic symptoms. The bipolar depression algorithm is always used with the primary algorithm for mania/hypomania.
The patient’s clinical presentation guides medication selection. For the “pure” bipolar I patient with a major depressive episode but little mood lability or hypomania, starting an antide-pressant is a clear decision. On the other hand, patients with predominant depressive symptoms plus dysphoric hypomania, mood lability, and irritability need a balance of mood-stabilizing drugs and antidepressants.
Stage 1: Mood stabilizer. Initiate a mood stabilizer and optimize the dosage. Choices are the same mood stabilizers listed in the hypomania/mania treatment algorithm.
Stage 2: Antidepressant. Adding an antidepressant implies that depressive symptoms are severe enough to change treatment. Antidepressant options include a selective serotonin reuptake inhibitor (SSRI), sustained-release bupropion, or lamotrigine.20
Using SSRIs is supported by widespread clinical experience and offers the convenience of once-daily dosing. Recommended SSRIs include fluoxetine, paroxetine, fluvoxamine, sertraline, and citalopram. The SSRI escitalopram was introduced after the 2000 algorithms were published; evidence for using it and other newer medications will be reviewed for the 2004 update.
The recommendation for sustained-release bupropion is consistent with the algorithm principle to use medications in the most well-tolerated form when accessible and available.
With lamotrigine, review with patients the risk of serious rash. To minimize rash risk, start lamotrigine slowly and follow the recommended titration schedule.
Stage 3: Multiple choices. At this stage, no definitive studies, safety data, or tolerability issues are available to rank the medication choices. The algorithm suggests:
- adding lithium21 or a second antidepressant
- or switching to an alternate antidepressant such as venlafaxine or nefazodone.
If a patient moves to stage 3 because of side effects with one antidepressant class, a different class—preferably with a contrasting side-effect profile—is recommended.
Algorithm 2 Treating depression in bipolar I disorder*
Stage 4: Two antidepressants. To enhance clinical response, the algorithm recommends combining two antidepressants, preferably from different classes. Monitor patients closely for side effects.
Stage 5. Antipsychotic or MAOI. At this stage, the algorithm recommends adding an atypical antipsychotic22 or switching to a monoamine oxidase inhibitor (MAOI).
Early evidence supported the efficacy of MAOIs in bipolar depression. However, the panel ranked MAOIs lower in the algorithm because they are associated with more bothersome side effects than SSRIs and other antidepressants. When using MAOIs, provide patients with dietary restriction guidelines.
Stage 6. Other therapies. Therapies such as ECT or “other” interventions are recommended at this stage. ECT has proven efficacy in bipolar depression and is appropriate for patients with limited medication response. The panel gave ECT a low ranking because of limited availability, lack of patient acceptance, and newer options.
Medication options include experimental treatments with limited evidence, such as inositol, dopamine agonists, stimulants, thyroid supplementation, conventional antipsychotics, and tri-cyclic antidepressants.
Acute to maintenance treatment
Adjunctive treatments for agitation, insomnia, GI upset, sedation, headache, and tremor are recommended in the physician manual supporting the TMAP guidelines (see Related resources). The manual also suggests ways to manage medication side effects and modify the algorithms for inpatients.
Patient and family psychoeducation plays an important role in helping the patient:
- identify prodromal bipolar symptoms
- understand the need to take medications as prescribed.
Continuation treatment. After mania or hypomania remits, continue medication(s) at the effective acute-phase dosages for at least 3 months. Use follow-up visits to enhance patient adherence, detect early symptoms of relapse, and monitor for side effects.
During the late continuation phase, after a period of sustained stability, clinicians can try to simplify the medications. When discontinuing a medication, taper the dosage by no more than 25% per week. If symptoms recur, promptly return to acute-phase treatment. Consider restarting medications and titrating up to the dosage(s) that resulted in remission.
In a depressive episode, continue the antidepressant(s) for 1 to 3 months at the effective acutephase dosage(s). Follow up frequently, and educate patients to watch for symptom recurrence and to communicate with you to assess when medication changes are needed.
Maintenance treatment. Relatively few well-controlled studies on long-term management of bipolar patients were available for the 2000 algorithm update.23 In general, all patients need mood stabilizer(s) to prevent relapse, using the lowest dosage that maintains therapeutic efficacy. Based on new evidence for lamotrigine and atypical antipsychotics—including FDAapproval of olanzapine for bipolar maintenace therapy—we anticipate recommendations will be expanded and more delineated in the 2004 update.
Discontinuing antidepressants after 3 to 6 months of initial treatment is now recommended. However, a recent retrospective case series suggests that continuing antidepressants at least 1 year after initial successful therapy may protect against depressive relapse. During this study, continuing antidepressants more than 3 to 6 months did not appear to increase the risk of switching to mania.24
Should antidepressants be continued or discontinued after successful acute treatment of a bipolar I depressive episode? This is an active area of research and debate as to the most appropriate strategy. The 2004 algorithm update panel will consider recent evidence that supports continuing antidepressants after symptom remission.24
- Texas Medication Algorithm Project algorithms and physician manual. Texas Department of Mental Health and Mental Retardation. http://www.mhmr.state.tx.us/centraloffice/medicaldirector/TIMA.html
- American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. Am J Psychiatry 2002; 159(4):suppl 2.
- Depression and Bipolar Support Alliance. www.dbsalliance.org
Drug brand names
- Bupropion • Wellbutrin SR
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Inositol • Various
- Lamotrigine • Lamictal
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Valproic acid • Depakene
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
Dr. Shivakumar reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Suppes receives research support from or is a consultant to Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, National Institutes of Mental Health, Novartis Pharmaceuticals Corp., Pfizer Inc., Pharmaceutical Research Institute, Ortho-McNeil Pharmaceutical, Robert Wood Johnson Pharmaceutical Research Institute, The Stanley Medical Research Institute, and UCB Pharma.
Many well-controlled trials in the past 4 years have evaluated new medications for treating bipolar disorder. It’s time to build a consensus on how this data may apply to clinical practice.
This year, our group will re-examine the Texas Medication Algorithm Project (TMAP) treatment algorithms for bipolar I disorder.
What makes TMAP unique? It is the first project to evaluate treatment algorithm use in community mental health settings for patients with a history of mania (see Box).1-5 Severely, persistently ill outpatients such as these are seldom included in research but are frequently seen in clinical practice.
To preview for psychiatrists the changes expected in 2004, this article describes the goals of TMAP and the controlled study on which the medication algorithms are based. We review the medication algorithms of 2000 as a starting point and present the evidence that is changing clinical practice.
Guiding principles of TMAP
A treatment algorithm is no substitute for clinical judgment; rather, medication guidelines and algorithms are guideposts to help the clinician and patient collaboratively develop the most effective medication strategy with the fewest side effects.
The Texas Medication Algorithm Project (TMAP)1-3 is a public and academic collaboration started in 1996 to develop evidence- and consensus-based medication treatment algorithms for schizophrenia, major depressive disorder, and bipolar disorder.
TMAP’s goal is to establish “best practices” to encourage uniformity of care, achieve the best possible patient outcomes, and use mental health care dollars most efficiently. The project includes four phases, in which the treatment algorithms were developed, compared with treatment-as-usual, put into practice, and will undergo periodic updates.4 The next update begins this year.
The comparison of algorithms for treating bipolar mania/hypomania and depression included 409 patients (mean age 38 to 40) with bipolar I disorder or schizoaffective disorder, bipolar type. These patients were severely and persistently mentally ill, from a diverse ethnic population, and significantly impaired in functioning.
During 12 months of treatment, psychiatric symptoms diminished more rapidly in patients in the algorithm group—as measured by the Brief Psychiatric Rating Scale (BPRS-24)—compared with those receiving usual treatment. After the first 3 months, the usual-treatment patients also showed diminished symptoms. At study’s end, symptom severity between the groups was not significantly different; both groups showed improvement.
Manic and psychotic symptoms—measured by Clinician-Administered Rating Scale subscales (CARS-M)5—improved significantly more in the algorithm group in the first 3 months, and this gap between the two groups was sustained for 12 months. Depressive symptoms declined, but no overall differences were noted between the two groups. Side effect rates and functioning were also similar.
TMAP’s treatment manual (see Related resources) describes clinicians’ preferred tactics and decision points, which we summarize here. The guidelines are an ongoing effort to apply evidence-based medicine to everyday practice and are meant to be adapted to patient needs.
Treatment goals that guided TMAP algorithm development are:
- symptomatic remission
- full return of psychosocial functioning
- prevention of relapse and recurrence.
Suggestions came from controlled clinical trials, open trials, retrospective data analyses, expert clinical consensus, and input from consumers.
Treatment selection. Initial algorithm stages recommend simple treatments (in terms of safety, tolerability, and side effects), whereas later stages recommend more-complicated regimens. A patient’s symptoms, comorbid conditions, and treatment history guide treatment selection. Patients may enter an algorithm at any stage, depending on their clinical presentation and medication history.
The clinician may consider patient preference when deciding among equivalent medications. The algorithm strongly encourages patients and families to participate, such as by keeping daily mood charts and completing symptom and side-effect checklists. When clinicians face a choice among medication brands, generics, or forms (such as immediate- versus slow-release), agents with greater tolerability are preferred.
Patient management. When patients enter the algorithm, clinic visits are frequent (such as every 2 weeks). Follow-up appointments address medication adherence, dosage adjustments, and side effects or adverse reactions.
If a patient’s symptoms show no change after two treatment stages, re-evaluate the diagnosis and consider mitigating factors such as substance abuse. Patients who complete acute treatment should receive continuation treatment.
Documentation. Clinicians are advised to document decision points and the rationale for treatment choices made outside the algorithm package.
Treating mania or hypomania
After clinical evaluation confirms the diagnosis of bipolar illness,4 the TMAP mania/hypomania algorithm (Algorithm 1) splits into three treatment pathways:
- euphoric mania/hypomania
- mixed or dysphoric mania/hypomania
- psychotic mania.
These pathways recognize the need for differing approaches to initial monotherapy and later two-drug combinations. If a patient develops persistent or severe depressive symptoms, the bipolar algorithm for a major depressive episode (Algorithm 2) is used during depressive periods with the primary mania algorithm.
Treatment recommendations. The key to using mood stabilizers is to achieve the optimum response—assuming good tolerability—before switching to another agent. Adjust medication dosages one at a time to allow adequate response and assessment.
When switching medications, use an overlap-and-taper strategy, assuming there is no medical necessity to stop a drug abruptly. Add the new medication, then gradually taper the one that is being discontinued. Monitor serum levels.
Discontinue antidepressants when appropriate in patients with hypomania/mania or rapid cycling, and continually evaluate suicide and homicide potential of patients in mixed or depressive states.
Stage 1: Monotherapy. First medication choices are lithium, divalproex, or olanzapine. For mixed or dysphoric mania, the algorithm recommends divalproex (preferred over valproic acid because of tolerability and side effects) or olanzapine.6 Data suggest dysphoric manic patients are less likely to respond to lithium.7 A Consensus Panel minority expressed concern about using olanzapine as first-line monotherapy for acute mania because of limited data on the drug’s long-term safety. Patients with partial response or residual symptoms may move to stage 2 or switch to other medication options within stage 1.
Patients with psychotic mania move directly to stage 4 for a broader range of combination therapy.
Stage 2: Combination therapy. Combination therapy has become the standard of care in treating most patients with bipolar disorder. The algorithm recommends using two agents:
- lithium or an anticonvulsant plus another anticonvulsant ([Li or AC]+AC)
- or lithium or an anticonvulsant plus an atypical antipsychotic ([Li or AC]+AAP).8
Recommended agents include lithium, divalproex, oxcarbazepine, olanzapine, or risperidone. The experts recommended oxcarbazepine as first choice because it is better tolerated and interacts with fewer drugs than carbamazepine and does not require serum level monitoring.9
A Consensus Panel minority expressed concern that few studies had examined using oxcarbazepine in bipolar disorder. Carbamazepine was also considered an option.
Stages 3 and 4: Other two-drug combinations. Other two-drug combinations are tried at these stages, drawing from the same pool of medication classes described in stage 2.
Stage 4 broadens the choice of atypical antipsychotic by adding quetiapine10 and ziprasidone11 to the recommended stage-2 agents olanzapine and risperidone. When the 2000 algorithm was developed, limited data were available on using some newer atypicals in patients with bipolar mania. Based on recent, high-quality studies of mono- and combination therapy—including quetiapine,10 ziprasidone,11 risperidone,12,13 and aripiprazole14 —the 2004 algorithm update panel will likely recommend using atypicals earlier, including at stage 1.
Algorithm 1 Treating mania/hypomania in patients with bipolar I disorder
Stage 5: Triple-drug combination. Lithium, an anticonvulsant (divalproex or oxcarbazepine), and an atypical antipsychotic (olanzapine, risperidone, quetiapine, or ziprasidone) is a recommended triple-drug combination. In the 2004 update, the choices will likely expand to include all the newer atypicals and will list carbamazepine as an option.
Stage 6: ECT or clozapine. For patients with inadequate response to triple-drug combinations, the algorithm recommends adding electroconvulsive therapy (ECT) or clozapine.
ECT15 is recommended three times a week until the patient achieves remission of manic symptoms or fails to achieve a sustained response over three to six treatment cycles. Treatment resistance is declared if no response is seen after 6 to 10 treatment cycles.
Clozapine’s16 recommendation at this stage is consistent with its use in patients who fail to respond to other atypical antipsychotics. Blood monitoring for agranulocytosis is required; other adverse effects include an increased risk of seizures, myocarditis, and orthostatic hypotension.
Stage 7: Other. Treatment options such as topiramate17,18 and lamotrigine19 are recommended at this stage. These recommendations also will be reviewed and likely revised.
Treating bipolar depression
The TMAP algorithm for treating depression in bipolar disorder (Algorithm 2) assumes that anti-depressants will be used only with optimum mood-stabilizer levels because of the risk of inducing manic symptoms. The bipolar depression algorithm is always used with the primary algorithm for mania/hypomania.
The patient’s clinical presentation guides medication selection. For the “pure” bipolar I patient with a major depressive episode but little mood lability or hypomania, starting an antide-pressant is a clear decision. On the other hand, patients with predominant depressive symptoms plus dysphoric hypomania, mood lability, and irritability need a balance of mood-stabilizing drugs and antidepressants.
Stage 1: Mood stabilizer. Initiate a mood stabilizer and optimize the dosage. Choices are the same mood stabilizers listed in the hypomania/mania treatment algorithm.
Stage 2: Antidepressant. Adding an antidepressant implies that depressive symptoms are severe enough to change treatment. Antidepressant options include a selective serotonin reuptake inhibitor (SSRI), sustained-release bupropion, or lamotrigine.20
Using SSRIs is supported by widespread clinical experience and offers the convenience of once-daily dosing. Recommended SSRIs include fluoxetine, paroxetine, fluvoxamine, sertraline, and citalopram. The SSRI escitalopram was introduced after the 2000 algorithms were published; evidence for using it and other newer medications will be reviewed for the 2004 update.
The recommendation for sustained-release bupropion is consistent with the algorithm principle to use medications in the most well-tolerated form when accessible and available.
With lamotrigine, review with patients the risk of serious rash. To minimize rash risk, start lamotrigine slowly and follow the recommended titration schedule.
Stage 3: Multiple choices. At this stage, no definitive studies, safety data, or tolerability issues are available to rank the medication choices. The algorithm suggests:
- adding lithium21 or a second antidepressant
- or switching to an alternate antidepressant such as venlafaxine or nefazodone.
If a patient moves to stage 3 because of side effects with one antidepressant class, a different class—preferably with a contrasting side-effect profile—is recommended.
Algorithm 2 Treating depression in bipolar I disorder*
Stage 4: Two antidepressants. To enhance clinical response, the algorithm recommends combining two antidepressants, preferably from different classes. Monitor patients closely for side effects.
Stage 5. Antipsychotic or MAOI. At this stage, the algorithm recommends adding an atypical antipsychotic22 or switching to a monoamine oxidase inhibitor (MAOI).
Early evidence supported the efficacy of MAOIs in bipolar depression. However, the panel ranked MAOIs lower in the algorithm because they are associated with more bothersome side effects than SSRIs and other antidepressants. When using MAOIs, provide patients with dietary restriction guidelines.
Stage 6. Other therapies. Therapies such as ECT or “other” interventions are recommended at this stage. ECT has proven efficacy in bipolar depression and is appropriate for patients with limited medication response. The panel gave ECT a low ranking because of limited availability, lack of patient acceptance, and newer options.
Medication options include experimental treatments with limited evidence, such as inositol, dopamine agonists, stimulants, thyroid supplementation, conventional antipsychotics, and tri-cyclic antidepressants.
Acute to maintenance treatment
Adjunctive treatments for agitation, insomnia, GI upset, sedation, headache, and tremor are recommended in the physician manual supporting the TMAP guidelines (see Related resources). The manual also suggests ways to manage medication side effects and modify the algorithms for inpatients.
Patient and family psychoeducation plays an important role in helping the patient:
- identify prodromal bipolar symptoms
- understand the need to take medications as prescribed.
Continuation treatment. After mania or hypomania remits, continue medication(s) at the effective acute-phase dosages for at least 3 months. Use follow-up visits to enhance patient adherence, detect early symptoms of relapse, and monitor for side effects.
During the late continuation phase, after a period of sustained stability, clinicians can try to simplify the medications. When discontinuing a medication, taper the dosage by no more than 25% per week. If symptoms recur, promptly return to acute-phase treatment. Consider restarting medications and titrating up to the dosage(s) that resulted in remission.
In a depressive episode, continue the antidepressant(s) for 1 to 3 months at the effective acutephase dosage(s). Follow up frequently, and educate patients to watch for symptom recurrence and to communicate with you to assess when medication changes are needed.
Maintenance treatment. Relatively few well-controlled studies on long-term management of bipolar patients were available for the 2000 algorithm update.23 In general, all patients need mood stabilizer(s) to prevent relapse, using the lowest dosage that maintains therapeutic efficacy. Based on new evidence for lamotrigine and atypical antipsychotics—including FDAapproval of olanzapine for bipolar maintenace therapy—we anticipate recommendations will be expanded and more delineated in the 2004 update.
Discontinuing antidepressants after 3 to 6 months of initial treatment is now recommended. However, a recent retrospective case series suggests that continuing antidepressants at least 1 year after initial successful therapy may protect against depressive relapse. During this study, continuing antidepressants more than 3 to 6 months did not appear to increase the risk of switching to mania.24
Should antidepressants be continued or discontinued after successful acute treatment of a bipolar I depressive episode? This is an active area of research and debate as to the most appropriate strategy. The 2004 algorithm update panel will consider recent evidence that supports continuing antidepressants after symptom remission.24
- Texas Medication Algorithm Project algorithms and physician manual. Texas Department of Mental Health and Mental Retardation. http://www.mhmr.state.tx.us/centraloffice/medicaldirector/TIMA.html
- American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. Am J Psychiatry 2002; 159(4):suppl 2.
- Depression and Bipolar Support Alliance. www.dbsalliance.org
Drug brand names
- Bupropion • Wellbutrin SR
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Inositol • Various
- Lamotrigine • Lamictal
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Valproic acid • Depakene
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
Dr. Shivakumar reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Suppes receives research support from or is a consultant to Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, National Institutes of Mental Health, Novartis Pharmaceuticals Corp., Pfizer Inc., Pharmaceutical Research Institute, Ortho-McNeil Pharmaceutical, Robert Wood Johnson Pharmaceutical Research Institute, The Stanley Medical Research Institute, and UCB Pharma.
1. Gilbert DA, Altshuler KZ, Rago WV, et al. Texas Medication Algorithm Project: definitions, rationale, and methods to develop medication algorithms. J Clin Psychiatry 1998;59:345-51.
2. Altshuler KZ, Rush AJ. Computerized Texas Medication Algorithm Project undergoes testing. Outcomes Accountability Alert 1999;4(1):10-11.
3. Rush AJ, Crismon ML, Kashner TM, et al. Texas Medication Algorithm Project, Phase 3 (TMAP-3): rationale and study design. J Clin Psychiatry 2003;64(4):357-69.
4. Altman E, Hedeker D, Janicak P, et al. The Clinician-Administered Rating Scale For Mania (CARS-M): development, reliability, and validity. Biol Psychiatry 1994;36:124-34.
5. Suppes T, Dennehy EB, Swann AC, et al. Report of the Texas consensus conference panel on medication treatment of bipolar disorder 2000. J Clin Psychiatry 2002;63:288-99.
6. Dennehy EB, Doyle K, Suppes T. The efficacy of olanzapine monotherapy for acute hypomania or mania in an outpatient setting. Int Clin Psychopharmacol 2003;18(3):143-5.
7. Dilsaver SC, Swann AC, Shoaib AM, et al. The manic syndrome: factors which may predict a patient’s response to lithium, carbamazepine and valproate. J Psych Neurosci 1993;18:61-6.
8. Tohen M, Chengappa KNR, Suppes T, et al. Efficacy of olanzapine in combination with valproate or lithium in the treatment of mania in patients partially nonresponsive to valproate or lithium monotherapy. Arch Gen Psychiatry 2002;59(1):62-9.
9. Emrich HM. Studies with oxcarbazepine (Trileptal) in acute mania. Int Clin Psychopharmacol 1990;190(5,suppl):83-8.
10. Vieta E, Parramon G, Padrell E, et al. Quetiapine in the treatment of rapid cycling bipolar disorder. Bipolar Disord 2002;4(5):335-40.
11. Keck PE, Versiani M, Potkin S, et al. Ziprasidone in the treatment of acute bipolar mania: a three week placebo-controlled, double-blinded randomized trial. Am J Psychiatry 2003;160(4):741-8.
12. Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus risperidone or placebo in the treatment of acute mania. International, double-blinded, randomised controlled trial. Br J Psychiatry 2003;182:141-7.
13. Sachs GS, Grossman F, Ghaemi SN, et al. Combination of a mood stabilizer with risperidone or haloperidol for treatment of acute mania: a double-blind, placebo-controlled comparison of efficacy and safety. Am J Psychiatry 2002;159(7):1146-54.
14. Keck PE, Jr, Marcus R, Tourkodimitris S, et al. Aripiprazole study group. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. Am J Psychiatry 2003;160(9):1651-8.
15. Mukherjee S, Sackeim HA, Schnur DB. Electroconvulsive therapy of acute manic episode: a review of 50 years’ experience. Am J Psychiatry 1988;45:727-32.
16. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trail of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156(8):1164-9.
17. Guille C, Sachs G. Clinical outcome of adjunctive topiramate treatment in a sample of refractory bipolar patients with comorbid conditions. Prog Neuropsychopharmacol Biol Psychiatry 2002;26(6):1035-9.
18. Vieta E, Torrent C, Garcia-Ribas G, et al. Use of topiramate in treatment-resistant bipolar spectrum disorders. J Clin Psychopharmacol 2002;22(4):431-5.
19. Calabrese JR, Suppes T, Bowden CL, et al. A double blinded, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61:841-50.
20. Calabrese JR, Bowden CL, Sachs GS, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder. J Clin Psychiatry 2003;64(9):1013-24.
21. Bauer M, Dopfmer S. Lithium augmentation in treatment-resistant depression: meta-analysis of placebo-controlled studies. J Clin Psychopharmacology 1999;19:427-34.
22. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
23. Baldessarini RJ, Tohen M, Tondo L. Maintenance treatment in bipolar disorder (comment). Arch Gen Psychiatry 2000;57:490-2.
24. Altshuler L, Suppes T, Black D, et al. Impact of antidepressant discontinuation after acute bipolar depression remission on rates of depressive relapse at 1-year follow-up. Am J Psychiatry 2003;160:1252-62.
1. Gilbert DA, Altshuler KZ, Rago WV, et al. Texas Medication Algorithm Project: definitions, rationale, and methods to develop medication algorithms. J Clin Psychiatry 1998;59:345-51.
2. Altshuler KZ, Rush AJ. Computerized Texas Medication Algorithm Project undergoes testing. Outcomes Accountability Alert 1999;4(1):10-11.
3. Rush AJ, Crismon ML, Kashner TM, et al. Texas Medication Algorithm Project, Phase 3 (TMAP-3): rationale and study design. J Clin Psychiatry 2003;64(4):357-69.
4. Altman E, Hedeker D, Janicak P, et al. The Clinician-Administered Rating Scale For Mania (CARS-M): development, reliability, and validity. Biol Psychiatry 1994;36:124-34.
5. Suppes T, Dennehy EB, Swann AC, et al. Report of the Texas consensus conference panel on medication treatment of bipolar disorder 2000. J Clin Psychiatry 2002;63:288-99.
6. Dennehy EB, Doyle K, Suppes T. The efficacy of olanzapine monotherapy for acute hypomania or mania in an outpatient setting. Int Clin Psychopharmacol 2003;18(3):143-5.
7. Dilsaver SC, Swann AC, Shoaib AM, et al. The manic syndrome: factors which may predict a patient’s response to lithium, carbamazepine and valproate. J Psych Neurosci 1993;18:61-6.
8. Tohen M, Chengappa KNR, Suppes T, et al. Efficacy of olanzapine in combination with valproate or lithium in the treatment of mania in patients partially nonresponsive to valproate or lithium monotherapy. Arch Gen Psychiatry 2002;59(1):62-9.
9. Emrich HM. Studies with oxcarbazepine (Trileptal) in acute mania. Int Clin Psychopharmacol 1990;190(5,suppl):83-8.
10. Vieta E, Parramon G, Padrell E, et al. Quetiapine in the treatment of rapid cycling bipolar disorder. Bipolar Disord 2002;4(5):335-40.
11. Keck PE, Versiani M, Potkin S, et al. Ziprasidone in the treatment of acute bipolar mania: a three week placebo-controlled, double-blinded randomized trial. Am J Psychiatry 2003;160(4):741-8.
12. Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus risperidone or placebo in the treatment of acute mania. International, double-blinded, randomised controlled trial. Br J Psychiatry 2003;182:141-7.
13. Sachs GS, Grossman F, Ghaemi SN, et al. Combination of a mood stabilizer with risperidone or haloperidol for treatment of acute mania: a double-blind, placebo-controlled comparison of efficacy and safety. Am J Psychiatry 2002;159(7):1146-54.
14. Keck PE, Jr, Marcus R, Tourkodimitris S, et al. Aripiprazole study group. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. Am J Psychiatry 2003;160(9):1651-8.
15. Mukherjee S, Sackeim HA, Schnur DB. Electroconvulsive therapy of acute manic episode: a review of 50 years’ experience. Am J Psychiatry 1988;45:727-32.
16. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trail of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156(8):1164-9.
17. Guille C, Sachs G. Clinical outcome of adjunctive topiramate treatment in a sample of refractory bipolar patients with comorbid conditions. Prog Neuropsychopharmacol Biol Psychiatry 2002;26(6):1035-9.
18. Vieta E, Torrent C, Garcia-Ribas G, et al. Use of topiramate in treatment-resistant bipolar spectrum disorders. J Clin Psychopharmacol 2002;22(4):431-5.
19. Calabrese JR, Suppes T, Bowden CL, et al. A double blinded, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61:841-50.
20. Calabrese JR, Bowden CL, Sachs GS, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder. J Clin Psychiatry 2003;64(9):1013-24.
21. Bauer M, Dopfmer S. Lithium augmentation in treatment-resistant depression: meta-analysis of placebo-controlled studies. J Clin Psychopharmacology 1999;19:427-34.
22. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
23. Baldessarini RJ, Tohen M, Tondo L. Maintenance treatment in bipolar disorder (comment). Arch Gen Psychiatry 2000;57:490-2.
24. Altshuler L, Suppes T, Black D, et al. Impact of antidepressant discontinuation after acute bipolar depression remission on rates of depressive relapse at 1-year follow-up. Am J Psychiatry 2003;160:1252-62.
Vardenafil and tadalafil options for erectile dysfunction
Sildenafil has revolutionized management of erectile dysfunction (ED) over the past 5 years. The FDA recently approved two additional medications, vardenafil and tadalafil, for treating ED.
How vardenafil and tadalafil work
Like sildenafil, vardenafil and tadalafil are selective inhibitors of the phosphodiesterase (PDE) isoenzyme PDE-5, which is predominantly responsible for degrading cyclic guanosine monophosphate (cGMP) in the smooth muscle cells of the corpus cavernosum.
During sexual stimulation, nitric oxide is released from cavernous nerves and endothelial cells and activates the enzyme guanylate cyclase, resulting in increased cGMP synthesis. The cGMP triggers relaxation of smooth muscles, allowing increased blood flow into the penis and expansion of sinusoidal spaces; this prevents venous blood outflow and results in erection. The PDE-5 inhibitors can potentiate erections by enhancing and prolonging the smooth musclerelaxant effects of the nitric oxide-cGMP cascade in the corpus cavernosum.1 PDE-5 inhibitors have no effect without sexual stimulation.
Table 1
Pharmacokinetics of the PDE-5 inhibitors
| Sildenafil 100 mg | Vardenafil 20 mg | Tadalafil 20 mg | |
|---|---|---|---|
| Maximum concentration | 450 ng/mL | 20.9 ng/mL | 378 ng/mL |
| Time to maximum concentration | 1.0 hour | 0.7 hours | 2.0 hours |
| Half-life | 4 hours | 3.9 hours | 17.5 hours |
| Source: References 2 and 3 | |||
Although the three PDE-5 inhibitors have similar mechanisms of action, their selectivity differs for PDE-5 compared with the PDE-6 and PDE-11 isoenzymes. Sildenafil and vardenafil have lower selectivity than tadalafil for PDE-5 over PDE-6, which plays a role in phototransduction, the process by which light impulses are converted into nerve impulses in the retina. Thus, tadalafil is less likely than the other agents to cause visual disturbances such as abnormal color vision, increased brightness of light, or mild haziness.
Tadalafil shows lower selectivity than sildenafil or vardenafil for PDE-5 over PDE-11, meaning that tadalafil inhibits PDE-11 at clinical doses. PDE-11 is found in various tissues, but its physiologic significance and consequences of its inhibition are unknown.2
Pharmacokinetics
Vardenafil, tadalafil, and sildenafil have different pharmacokinetic characteristics (Table 1). A lower starting dosage is required with vardenafil than with sildenafil because of the former agent’s greater in vitro and in vivo potency, but whether this results in greater clinical efficacy or tolerability is unknown.3
Vardenafil and sildenafil reach maximum plasma concentration within 30 minutes to 2 hours (median 1 hour for sildenafil and 0.7 hour for vardenafil). By contrast, tadalafil reaches maximum concentration within 30 minutes to 6 hours (median 2 hours). However, studies of time to onset of erection indicate that about one-third of patients using the maximum recommended doses of any of these agents will experience onset within 14 to 16 minutes.4-6
Absorption rates for sildenafil and vardenafil are reduced when they are taken with a high-fat meal. High-fat foods do not affect tadalafil’s absorption rate.
Table 2
Vardenafil: Fast facts
| Drug brand name: Levitra |
| Class: Phosphodiesterase-5 inhibitor |
| FDA-approved indication: Erectile dysfunction |
| Approval date: August 19, 2003 |
| Manufacturer: Bayer Corp. (distributed by GlaxoSmithKline) |
| Dosing forms: 2.5 mg, 5 mg, 10 mg, 20 mg |
| Dosing recommendations: Start at 10 mg about 1 hour before sexual activity. Maximum recommended dose is 20 mg; maximum dosing frequency is once per day. Consider 5-mg starting dose for patients age 65 and older. |
Because of its 17.5-hour half-life, tadalafil has a longer period of activity than the other PDE-5 inhibitors. Most patients can complete sexual intercourse up to 36 hours after taking tadalafil, which potentially allows spontaneous sexual activity. Sildenafil and vardenafil each are effective for about 4 hours.
All three PDE-5 inhibitors are eliminated by hepatic metabolism, mainly by the CYP 3A4 hepatic enzyme. Therefore, concomitant use with CYP 3A4 inhibitors—such as ketoconazole, ritonavir, grapefruit juice, or erythromycin —results in increased plasma levels of these agents, and the use of CYP 3A4 inducers such as rifampin reduces plasma levels of the concomitant agent.
Table 3
Tadalafil: Fast facts
| Drug brand name: Cialis |
| Class: Phosphodiesterase-5 inhibitor |
| FDA-approved indication: Erectile dysfunction |
| Approval date: November 21, 2003 |
| Manufacturer: Eli Lilly and Co. |
| Dosing forms: 5 mg, 10 mg, 20 mg |
| Dosing recommendations: Start at 10 mg before anticipated sexual activity. Maximum recommended dose is 20 mg; maximum dosing frequency is once per day. |
Efficacy
Vardenafil (Table 2). In a placebo-controlled, 12-week trial,7 601 men with mildly to severely impaired erectile function received placebo or 5, 10, or 20 mg of vardenafil. Subjects receiving vardenafil at any dose saw significantly greater improvement in erectile function than did the placebo group. Percentage of successful intercourse ranged between 71% and 74% for the three vardenafil doses. For the 20-mg dose, 80% of patients experienced improved erections compared with 30% of those taking placebo.7
In another trial of 805 men with mild to severe ED,8 vardenafil in 5-mg, 10-mg, and 20-mg doses demonstrated efficacy versus placebo. Eighty-five percent of men using vardenafil, 20 mg, reported improved erections at 26 weeks compared with 28% in the placebo group.
Vardenafil, 10 mg and 20 mg, was also an effective ED treatment in men with type 1 or type 2 diabetes mellitus9 and in men who underwent radical prostatectomy.10
Tadalafil (Table 3). An integrated analysis11 of five randomized, placebo-controlled trials of tadalafil at 2.5, 5, 10, or 20 mg for at least 12 weeks found that the agent at all doses significantly enhanced erectile function in mild to severe ED compared with placebo. Successful intercourse was reported in 61% and 75% of sexual encounters among men treated with tadalafil, 10 and 20 mg respectively, compared with 32% in controls. Eighty-one percent of men taking tadalafil, 20 mg, reported improved erections compared with 35% of those taking placebo.
Tadalafil, 10 and 20 mg, also improved erectile function in men with type 1 or type 2 diabetes.12
Tolerability
All three PDE-5 inhibitors have been shown in clinical trials to be generally safe and well-tolerated. Apart from visual disturbances, all three agents have similar side effects.
- Patients taking vardenafil most commonly reported headaches, flushing, rhinitis, and dyspepsia. These effects were generally mild to moderate, dose-related, and transient.1
- Headache, back pain, myalgia, and dyspepsia were most commonly reported with tadalafil.13 Similarly, adverse events were mild or moderate, dose-related, and generally abated with treatment.
Treatment-related visual disturbances have been reported in 3% of patients taking sildenafil, >0.1% to <1% of men taking vardenafil, and <0.1% of those taking tadalafil.1 Laboratory parameters have been unaffected by treatment with the PDE-5 inhibitors, and treatment discontinuation due to adverse events has been consistently low.1
All three PDE-5 inhibitors cause vasodilatory effects and are contraindicated in patients using organic nitrates. Consensus guidelines have been developed for using PDE-5 inhibitors in patients with cardiovascular conditions.14
Related resources
- Rosen RC, Kostis JB. Overview of phosphodiesterase 5 inhibition in erectile dysfunction. Am J Cardiol 2003;92(suppl):9M-18M.
- The Process of Care Consensus Panel. Position paper: the process of care model for evaluation and treatment of erectile dysfunction. Int J Impot Res 1999;11:59-74.
- American Foundation for Urologic Disease. www.afud.org
Drug brand names
- Ketoconazole • Nizoral
- Rifampin • Rifadin
- Ritonavir • Kaletra, Norvir
- Sildenafil • Viagra
- Tadalafil • Cialis
- Vardenafil • Levitra
Disclosure
The author receives research/grant support and is a consultant to and speaker for Eli Lilly and Co. and Pfizer Inc.
1. Rosen RC, Kostis JB. Overview of phosphodiesterase 5 inhibition in erectile dysfunction. Am J Cardiol 2003;92(suppl):9M-18M.
2. Gresser U, Gleiter CH. Erectile dysfunction: comparison of efficacy and side effects of the PDE-5 inhibitors sildenafil, vardenafil and tadalafil—review of the literature. Eur J Med Res 2002;7:435-46.
3. Keating GM, Scott LJ. Vardenafil. A review of its use in erectile dysfunction. Drugs 2003;63:2673-2703.
4. Padma-Nathan H, Rosen RC, Shabsigh R, et al. Cialis (IC351) provides prompt response and extended period of responsiveness for the treatment of men with erectile dysfunction (ED). J Urol 2001;165(suppl):224.-
5. Padma-Nathan H, Kaufman J, Taylor T. Earliest time of onset of erections with vardenafil determined in an at-home setting. Chicago, IL: American Urological Association annual meeting, 2003.
6. Padma-Nathan H, Stecher VJ, Sweeney M, et al. Minimal time to successful intercourse after sildenafil citrate: results of a randomized, double-blind, placebo-controlled trial. Urology 2003;62:400-3.
7. Porst H, Rosen R, Padma-Nathan H, et al. The efficacy and tolerability of vardenafil, a new selective phosphodiesterase type 5 inhibitor, in patients with erectile dysfunction: the first at-home clinical trial. Int J Impot Res 2001;13:192-9.
8. Hellstrom WJ, Gittelman M, Karlin G, et al. Vardenafil for treatment of men with erectile dysfunction: efficacy and safety in a randomized, double-blind, placebo-controlled trial. J Androl 2002;23:763-71.
9. Goldstein I, Young JM, Fischer J, et al. Vardenafil, a highly selective PDE5 inhibitor, improves erectile function in patients with diabetes mellitus. Diabetes 2001;50(suppl 2):924.-
10. Brock G, Taylor T, Seger M. for the Vardenafil PROSPECT Group. Efficacy and tolerability of vardenafil in men with erectile dysfunction following radical prostatectomy. Eur Urol 2002;1:52.-
11. Brock GB, McMahon CG, Chen KK, et al. Efficacy and safety of tadalafil for the treatment of erectile dysfunction: results of integrated analyses. J Urol 2002;168:1332-6.
12. Sáenz de Tejada I, Anglin G, Knight JR, et al. Effects of tadalafil on erectile dysfunction in men with diabetes. Diabetes Care 2002;25:2159-64.
13. Padma-Nathan H. Efficacy and tolerability of tadalafil, a novel phosphodiesterase 5 inhibitor, in treatment of erectile dysfunction. Am J Cardiol 2003;92(suppl):19M-25M.
14. DeBusk R, Drory Y, Goldstein I, et al. Management of sexual dysfunction in patients with cardiovascular disease: recommendations of the Princeton Consensus Panel. Am J Cardiol 2000;86:175-81.
Sildenafil has revolutionized management of erectile dysfunction (ED) over the past 5 years. The FDA recently approved two additional medications, vardenafil and tadalafil, for treating ED.
How vardenafil and tadalafil work
Like sildenafil, vardenafil and tadalafil are selective inhibitors of the phosphodiesterase (PDE) isoenzyme PDE-5, which is predominantly responsible for degrading cyclic guanosine monophosphate (cGMP) in the smooth muscle cells of the corpus cavernosum.
During sexual stimulation, nitric oxide is released from cavernous nerves and endothelial cells and activates the enzyme guanylate cyclase, resulting in increased cGMP synthesis. The cGMP triggers relaxation of smooth muscles, allowing increased blood flow into the penis and expansion of sinusoidal spaces; this prevents venous blood outflow and results in erection. The PDE-5 inhibitors can potentiate erections by enhancing and prolonging the smooth musclerelaxant effects of the nitric oxide-cGMP cascade in the corpus cavernosum.1 PDE-5 inhibitors have no effect without sexual stimulation.
Table 1
Pharmacokinetics of the PDE-5 inhibitors
| Sildenafil 100 mg | Vardenafil 20 mg | Tadalafil 20 mg | |
|---|---|---|---|
| Maximum concentration | 450 ng/mL | 20.9 ng/mL | 378 ng/mL |
| Time to maximum concentration | 1.0 hour | 0.7 hours | 2.0 hours |
| Half-life | 4 hours | 3.9 hours | 17.5 hours |
| Source: References 2 and 3 | |||
Although the three PDE-5 inhibitors have similar mechanisms of action, their selectivity differs for PDE-5 compared with the PDE-6 and PDE-11 isoenzymes. Sildenafil and vardenafil have lower selectivity than tadalafil for PDE-5 over PDE-6, which plays a role in phototransduction, the process by which light impulses are converted into nerve impulses in the retina. Thus, tadalafil is less likely than the other agents to cause visual disturbances such as abnormal color vision, increased brightness of light, or mild haziness.
Tadalafil shows lower selectivity than sildenafil or vardenafil for PDE-5 over PDE-11, meaning that tadalafil inhibits PDE-11 at clinical doses. PDE-11 is found in various tissues, but its physiologic significance and consequences of its inhibition are unknown.2
Pharmacokinetics
Vardenafil, tadalafil, and sildenafil have different pharmacokinetic characteristics (Table 1). A lower starting dosage is required with vardenafil than with sildenafil because of the former agent’s greater in vitro and in vivo potency, but whether this results in greater clinical efficacy or tolerability is unknown.3
Vardenafil and sildenafil reach maximum plasma concentration within 30 minutes to 2 hours (median 1 hour for sildenafil and 0.7 hour for vardenafil). By contrast, tadalafil reaches maximum concentration within 30 minutes to 6 hours (median 2 hours). However, studies of time to onset of erection indicate that about one-third of patients using the maximum recommended doses of any of these agents will experience onset within 14 to 16 minutes.4-6
Absorption rates for sildenafil and vardenafil are reduced when they are taken with a high-fat meal. High-fat foods do not affect tadalafil’s absorption rate.
Table 2
Vardenafil: Fast facts
| Drug brand name: Levitra |
| Class: Phosphodiesterase-5 inhibitor |
| FDA-approved indication: Erectile dysfunction |
| Approval date: August 19, 2003 |
| Manufacturer: Bayer Corp. (distributed by GlaxoSmithKline) |
| Dosing forms: 2.5 mg, 5 mg, 10 mg, 20 mg |
| Dosing recommendations: Start at 10 mg about 1 hour before sexual activity. Maximum recommended dose is 20 mg; maximum dosing frequency is once per day. Consider 5-mg starting dose for patients age 65 and older. |
Because of its 17.5-hour half-life, tadalafil has a longer period of activity than the other PDE-5 inhibitors. Most patients can complete sexual intercourse up to 36 hours after taking tadalafil, which potentially allows spontaneous sexual activity. Sildenafil and vardenafil each are effective for about 4 hours.
All three PDE-5 inhibitors are eliminated by hepatic metabolism, mainly by the CYP 3A4 hepatic enzyme. Therefore, concomitant use with CYP 3A4 inhibitors—such as ketoconazole, ritonavir, grapefruit juice, or erythromycin —results in increased plasma levels of these agents, and the use of CYP 3A4 inducers such as rifampin reduces plasma levels of the concomitant agent.
Table 3
Tadalafil: Fast facts
| Drug brand name: Cialis |
| Class: Phosphodiesterase-5 inhibitor |
| FDA-approved indication: Erectile dysfunction |
| Approval date: November 21, 2003 |
| Manufacturer: Eli Lilly and Co. |
| Dosing forms: 5 mg, 10 mg, 20 mg |
| Dosing recommendations: Start at 10 mg before anticipated sexual activity. Maximum recommended dose is 20 mg; maximum dosing frequency is once per day. |
Efficacy
Vardenafil (Table 2). In a placebo-controlled, 12-week trial,7 601 men with mildly to severely impaired erectile function received placebo or 5, 10, or 20 mg of vardenafil. Subjects receiving vardenafil at any dose saw significantly greater improvement in erectile function than did the placebo group. Percentage of successful intercourse ranged between 71% and 74% for the three vardenafil doses. For the 20-mg dose, 80% of patients experienced improved erections compared with 30% of those taking placebo.7
In another trial of 805 men with mild to severe ED,8 vardenafil in 5-mg, 10-mg, and 20-mg doses demonstrated efficacy versus placebo. Eighty-five percent of men using vardenafil, 20 mg, reported improved erections at 26 weeks compared with 28% in the placebo group.
Vardenafil, 10 mg and 20 mg, was also an effective ED treatment in men with type 1 or type 2 diabetes mellitus9 and in men who underwent radical prostatectomy.10
Tadalafil (Table 3). An integrated analysis11 of five randomized, placebo-controlled trials of tadalafil at 2.5, 5, 10, or 20 mg for at least 12 weeks found that the agent at all doses significantly enhanced erectile function in mild to severe ED compared with placebo. Successful intercourse was reported in 61% and 75% of sexual encounters among men treated with tadalafil, 10 and 20 mg respectively, compared with 32% in controls. Eighty-one percent of men taking tadalafil, 20 mg, reported improved erections compared with 35% of those taking placebo.
Tadalafil, 10 and 20 mg, also improved erectile function in men with type 1 or type 2 diabetes.12
Tolerability
All three PDE-5 inhibitors have been shown in clinical trials to be generally safe and well-tolerated. Apart from visual disturbances, all three agents have similar side effects.
- Patients taking vardenafil most commonly reported headaches, flushing, rhinitis, and dyspepsia. These effects were generally mild to moderate, dose-related, and transient.1
- Headache, back pain, myalgia, and dyspepsia were most commonly reported with tadalafil.13 Similarly, adverse events were mild or moderate, dose-related, and generally abated with treatment.
Treatment-related visual disturbances have been reported in 3% of patients taking sildenafil, >0.1% to <1% of men taking vardenafil, and <0.1% of those taking tadalafil.1 Laboratory parameters have been unaffected by treatment with the PDE-5 inhibitors, and treatment discontinuation due to adverse events has been consistently low.1
All three PDE-5 inhibitors cause vasodilatory effects and are contraindicated in patients using organic nitrates. Consensus guidelines have been developed for using PDE-5 inhibitors in patients with cardiovascular conditions.14
Related resources
- Rosen RC, Kostis JB. Overview of phosphodiesterase 5 inhibition in erectile dysfunction. Am J Cardiol 2003;92(suppl):9M-18M.
- The Process of Care Consensus Panel. Position paper: the process of care model for evaluation and treatment of erectile dysfunction. Int J Impot Res 1999;11:59-74.
- American Foundation for Urologic Disease. www.afud.org
Drug brand names
- Ketoconazole • Nizoral
- Rifampin • Rifadin
- Ritonavir • Kaletra, Norvir
- Sildenafil • Viagra
- Tadalafil • Cialis
- Vardenafil • Levitra
Disclosure
The author receives research/grant support and is a consultant to and speaker for Eli Lilly and Co. and Pfizer Inc.
Sildenafil has revolutionized management of erectile dysfunction (ED) over the past 5 years. The FDA recently approved two additional medications, vardenafil and tadalafil, for treating ED.
How vardenafil and tadalafil work
Like sildenafil, vardenafil and tadalafil are selective inhibitors of the phosphodiesterase (PDE) isoenzyme PDE-5, which is predominantly responsible for degrading cyclic guanosine monophosphate (cGMP) in the smooth muscle cells of the corpus cavernosum.
During sexual stimulation, nitric oxide is released from cavernous nerves and endothelial cells and activates the enzyme guanylate cyclase, resulting in increased cGMP synthesis. The cGMP triggers relaxation of smooth muscles, allowing increased blood flow into the penis and expansion of sinusoidal spaces; this prevents venous blood outflow and results in erection. The PDE-5 inhibitors can potentiate erections by enhancing and prolonging the smooth musclerelaxant effects of the nitric oxide-cGMP cascade in the corpus cavernosum.1 PDE-5 inhibitors have no effect without sexual stimulation.
Table 1
Pharmacokinetics of the PDE-5 inhibitors
| Sildenafil 100 mg | Vardenafil 20 mg | Tadalafil 20 mg | |
|---|---|---|---|
| Maximum concentration | 450 ng/mL | 20.9 ng/mL | 378 ng/mL |
| Time to maximum concentration | 1.0 hour | 0.7 hours | 2.0 hours |
| Half-life | 4 hours | 3.9 hours | 17.5 hours |
| Source: References 2 and 3 | |||
Although the three PDE-5 inhibitors have similar mechanisms of action, their selectivity differs for PDE-5 compared with the PDE-6 and PDE-11 isoenzymes. Sildenafil and vardenafil have lower selectivity than tadalafil for PDE-5 over PDE-6, which plays a role in phototransduction, the process by which light impulses are converted into nerve impulses in the retina. Thus, tadalafil is less likely than the other agents to cause visual disturbances such as abnormal color vision, increased brightness of light, or mild haziness.
Tadalafil shows lower selectivity than sildenafil or vardenafil for PDE-5 over PDE-11, meaning that tadalafil inhibits PDE-11 at clinical doses. PDE-11 is found in various tissues, but its physiologic significance and consequences of its inhibition are unknown.2
Pharmacokinetics
Vardenafil, tadalafil, and sildenafil have different pharmacokinetic characteristics (Table 1). A lower starting dosage is required with vardenafil than with sildenafil because of the former agent’s greater in vitro and in vivo potency, but whether this results in greater clinical efficacy or tolerability is unknown.3
Vardenafil and sildenafil reach maximum plasma concentration within 30 minutes to 2 hours (median 1 hour for sildenafil and 0.7 hour for vardenafil). By contrast, tadalafil reaches maximum concentration within 30 minutes to 6 hours (median 2 hours). However, studies of time to onset of erection indicate that about one-third of patients using the maximum recommended doses of any of these agents will experience onset within 14 to 16 minutes.4-6
Absorption rates for sildenafil and vardenafil are reduced when they are taken with a high-fat meal. High-fat foods do not affect tadalafil’s absorption rate.
Table 2
Vardenafil: Fast facts
| Drug brand name: Levitra |
| Class: Phosphodiesterase-5 inhibitor |
| FDA-approved indication: Erectile dysfunction |
| Approval date: August 19, 2003 |
| Manufacturer: Bayer Corp. (distributed by GlaxoSmithKline) |
| Dosing forms: 2.5 mg, 5 mg, 10 mg, 20 mg |
| Dosing recommendations: Start at 10 mg about 1 hour before sexual activity. Maximum recommended dose is 20 mg; maximum dosing frequency is once per day. Consider 5-mg starting dose for patients age 65 and older. |
Because of its 17.5-hour half-life, tadalafil has a longer period of activity than the other PDE-5 inhibitors. Most patients can complete sexual intercourse up to 36 hours after taking tadalafil, which potentially allows spontaneous sexual activity. Sildenafil and vardenafil each are effective for about 4 hours.
All three PDE-5 inhibitors are eliminated by hepatic metabolism, mainly by the CYP 3A4 hepatic enzyme. Therefore, concomitant use with CYP 3A4 inhibitors—such as ketoconazole, ritonavir, grapefruit juice, or erythromycin —results in increased plasma levels of these agents, and the use of CYP 3A4 inducers such as rifampin reduces plasma levels of the concomitant agent.
Table 3
Tadalafil: Fast facts
| Drug brand name: Cialis |
| Class: Phosphodiesterase-5 inhibitor |
| FDA-approved indication: Erectile dysfunction |
| Approval date: November 21, 2003 |
| Manufacturer: Eli Lilly and Co. |
| Dosing forms: 5 mg, 10 mg, 20 mg |
| Dosing recommendations: Start at 10 mg before anticipated sexual activity. Maximum recommended dose is 20 mg; maximum dosing frequency is once per day. |
Efficacy
Vardenafil (Table 2). In a placebo-controlled, 12-week trial,7 601 men with mildly to severely impaired erectile function received placebo or 5, 10, or 20 mg of vardenafil. Subjects receiving vardenafil at any dose saw significantly greater improvement in erectile function than did the placebo group. Percentage of successful intercourse ranged between 71% and 74% for the three vardenafil doses. For the 20-mg dose, 80% of patients experienced improved erections compared with 30% of those taking placebo.7
In another trial of 805 men with mild to severe ED,8 vardenafil in 5-mg, 10-mg, and 20-mg doses demonstrated efficacy versus placebo. Eighty-five percent of men using vardenafil, 20 mg, reported improved erections at 26 weeks compared with 28% in the placebo group.
Vardenafil, 10 mg and 20 mg, was also an effective ED treatment in men with type 1 or type 2 diabetes mellitus9 and in men who underwent radical prostatectomy.10
Tadalafil (Table 3). An integrated analysis11 of five randomized, placebo-controlled trials of tadalafil at 2.5, 5, 10, or 20 mg for at least 12 weeks found that the agent at all doses significantly enhanced erectile function in mild to severe ED compared with placebo. Successful intercourse was reported in 61% and 75% of sexual encounters among men treated with tadalafil, 10 and 20 mg respectively, compared with 32% in controls. Eighty-one percent of men taking tadalafil, 20 mg, reported improved erections compared with 35% of those taking placebo.
Tadalafil, 10 and 20 mg, also improved erectile function in men with type 1 or type 2 diabetes.12
Tolerability
All three PDE-5 inhibitors have been shown in clinical trials to be generally safe and well-tolerated. Apart from visual disturbances, all three agents have similar side effects.
- Patients taking vardenafil most commonly reported headaches, flushing, rhinitis, and dyspepsia. These effects were generally mild to moderate, dose-related, and transient.1
- Headache, back pain, myalgia, and dyspepsia were most commonly reported with tadalafil.13 Similarly, adverse events were mild or moderate, dose-related, and generally abated with treatment.
Treatment-related visual disturbances have been reported in 3% of patients taking sildenafil, >0.1% to <1% of men taking vardenafil, and <0.1% of those taking tadalafil.1 Laboratory parameters have been unaffected by treatment with the PDE-5 inhibitors, and treatment discontinuation due to adverse events has been consistently low.1
All three PDE-5 inhibitors cause vasodilatory effects and are contraindicated in patients using organic nitrates. Consensus guidelines have been developed for using PDE-5 inhibitors in patients with cardiovascular conditions.14
Related resources
- Rosen RC, Kostis JB. Overview of phosphodiesterase 5 inhibition in erectile dysfunction. Am J Cardiol 2003;92(suppl):9M-18M.
- The Process of Care Consensus Panel. Position paper: the process of care model for evaluation and treatment of erectile dysfunction. Int J Impot Res 1999;11:59-74.
- American Foundation for Urologic Disease. www.afud.org
Drug brand names
- Ketoconazole • Nizoral
- Rifampin • Rifadin
- Ritonavir • Kaletra, Norvir
- Sildenafil • Viagra
- Tadalafil • Cialis
- Vardenafil • Levitra
Disclosure
The author receives research/grant support and is a consultant to and speaker for Eli Lilly and Co. and Pfizer Inc.
1. Rosen RC, Kostis JB. Overview of phosphodiesterase 5 inhibition in erectile dysfunction. Am J Cardiol 2003;92(suppl):9M-18M.
2. Gresser U, Gleiter CH. Erectile dysfunction: comparison of efficacy and side effects of the PDE-5 inhibitors sildenafil, vardenafil and tadalafil—review of the literature. Eur J Med Res 2002;7:435-46.
3. Keating GM, Scott LJ. Vardenafil. A review of its use in erectile dysfunction. Drugs 2003;63:2673-2703.
4. Padma-Nathan H, Rosen RC, Shabsigh R, et al. Cialis (IC351) provides prompt response and extended period of responsiveness for the treatment of men with erectile dysfunction (ED). J Urol 2001;165(suppl):224.-
5. Padma-Nathan H, Kaufman J, Taylor T. Earliest time of onset of erections with vardenafil determined in an at-home setting. Chicago, IL: American Urological Association annual meeting, 2003.
6. Padma-Nathan H, Stecher VJ, Sweeney M, et al. Minimal time to successful intercourse after sildenafil citrate: results of a randomized, double-blind, placebo-controlled trial. Urology 2003;62:400-3.
7. Porst H, Rosen R, Padma-Nathan H, et al. The efficacy and tolerability of vardenafil, a new selective phosphodiesterase type 5 inhibitor, in patients with erectile dysfunction: the first at-home clinical trial. Int J Impot Res 2001;13:192-9.
8. Hellstrom WJ, Gittelman M, Karlin G, et al. Vardenafil for treatment of men with erectile dysfunction: efficacy and safety in a randomized, double-blind, placebo-controlled trial. J Androl 2002;23:763-71.
9. Goldstein I, Young JM, Fischer J, et al. Vardenafil, a highly selective PDE5 inhibitor, improves erectile function in patients with diabetes mellitus. Diabetes 2001;50(suppl 2):924.-
10. Brock G, Taylor T, Seger M. for the Vardenafil PROSPECT Group. Efficacy and tolerability of vardenafil in men with erectile dysfunction following radical prostatectomy. Eur Urol 2002;1:52.-
11. Brock GB, McMahon CG, Chen KK, et al. Efficacy and safety of tadalafil for the treatment of erectile dysfunction: results of integrated analyses. J Urol 2002;168:1332-6.
12. Sáenz de Tejada I, Anglin G, Knight JR, et al. Effects of tadalafil on erectile dysfunction in men with diabetes. Diabetes Care 2002;25:2159-64.
13. Padma-Nathan H. Efficacy and tolerability of tadalafil, a novel phosphodiesterase 5 inhibitor, in treatment of erectile dysfunction. Am J Cardiol 2003;92(suppl):19M-25M.
14. DeBusk R, Drory Y, Goldstein I, et al. Management of sexual dysfunction in patients with cardiovascular disease: recommendations of the Princeton Consensus Panel. Am J Cardiol 2000;86:175-81.
1. Rosen RC, Kostis JB. Overview of phosphodiesterase 5 inhibition in erectile dysfunction. Am J Cardiol 2003;92(suppl):9M-18M.
2. Gresser U, Gleiter CH. Erectile dysfunction: comparison of efficacy and side effects of the PDE-5 inhibitors sildenafil, vardenafil and tadalafil—review of the literature. Eur J Med Res 2002;7:435-46.
3. Keating GM, Scott LJ. Vardenafil. A review of its use in erectile dysfunction. Drugs 2003;63:2673-2703.
4. Padma-Nathan H, Rosen RC, Shabsigh R, et al. Cialis (IC351) provides prompt response and extended period of responsiveness for the treatment of men with erectile dysfunction (ED). J Urol 2001;165(suppl):224.-
5. Padma-Nathan H, Kaufman J, Taylor T. Earliest time of onset of erections with vardenafil determined in an at-home setting. Chicago, IL: American Urological Association annual meeting, 2003.
6. Padma-Nathan H, Stecher VJ, Sweeney M, et al. Minimal time to successful intercourse after sildenafil citrate: results of a randomized, double-blind, placebo-controlled trial. Urology 2003;62:400-3.
7. Porst H, Rosen R, Padma-Nathan H, et al. The efficacy and tolerability of vardenafil, a new selective phosphodiesterase type 5 inhibitor, in patients with erectile dysfunction: the first at-home clinical trial. Int J Impot Res 2001;13:192-9.
8. Hellstrom WJ, Gittelman M, Karlin G, et al. Vardenafil for treatment of men with erectile dysfunction: efficacy and safety in a randomized, double-blind, placebo-controlled trial. J Androl 2002;23:763-71.
9. Goldstein I, Young JM, Fischer J, et al. Vardenafil, a highly selective PDE5 inhibitor, improves erectile function in patients with diabetes mellitus. Diabetes 2001;50(suppl 2):924.-
10. Brock G, Taylor T, Seger M. for the Vardenafil PROSPECT Group. Efficacy and tolerability of vardenafil in men with erectile dysfunction following radical prostatectomy. Eur Urol 2002;1:52.-
11. Brock GB, McMahon CG, Chen KK, et al. Efficacy and safety of tadalafil for the treatment of erectile dysfunction: results of integrated analyses. J Urol 2002;168:1332-6.
12. Sáenz de Tejada I, Anglin G, Knight JR, et al. Effects of tadalafil on erectile dysfunction in men with diabetes. Diabetes Care 2002;25:2159-64.
13. Padma-Nathan H. Efficacy and tolerability of tadalafil, a novel phosphodiesterase 5 inhibitor, in treatment of erectile dysfunction. Am J Cardiol 2003;92(suppl):19M-25M.
14. DeBusk R, Drory Y, Goldstein I, et al. Management of sexual dysfunction in patients with cardiovascular disease: recommendations of the Princeton Consensus Panel. Am J Cardiol 2000;86:175-81.
Using antipsychotics in patients with dementia
Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
Algorithm Treating behavioral symptoms in patients with dementia
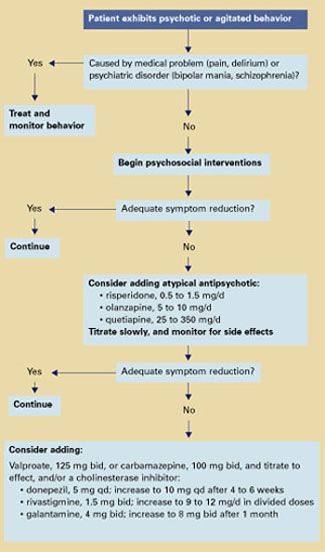
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|
Antipsychotic side effects
Atypical antipsychotics are more effective than conventional agents in treating negative symptoms and are associated with lower rates of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD).21
Tardive dyskinesia. All antipsychotics can cause TD, although the risk is about 10 times greater with conventionals than atypicals. With conventionals, the annual cumulative TD incidence for young adults is 4 to 5%,22 and rates are much higher for middle-aged and older adults receiving chronic therapy:
- 29% after 1 year
- 50% after 2 years
- 63% after 3 years.23
In older patients, use atypical rather than conventional antipsychotics to minimize TD risk. Observe carefully; if TD symptoms occur, cautiously withdraw the antipsychotic and consider trying another agent.
Other risks. Atypical antipsychotics may cause sedation, orthostatic hypotension (with an increased risk for falls), increased serum prolactin, and weight gain (Table 2).
Weight gain from atypical antipsychotics has been associated with adverse effects on glucose metabolism and increased risk for type 2 diabetes.24 Some might argue that weight gain associated with olanzapine and other atypicals might benefit low-weight older patients. The frail elderly need to increase muscle mass, however, and the atypicals are associated with increases in fat mass.
Increased serum prolactin with risperidone theoretically could lead to loss of bone density, but evidence of this effect in older patients does not exist.
Start low, go slow
Clozapine may help control treatment-resistant psychosis in patients with schizophrenia and manage patients with severe TD.25 However, clozapine’s increased risk of agranulocytosis, neurologic side effects (seizures, sedation, confusion), and anticholinergic effects limit its use in older patients, particularly those with neurodegenerative disorders (Table 2).
Dosing. In rare cases when using clozapine in older patients, start with 6.25 to 12.5 mg/d. Increase by 6.25 to 12.5 mg once or twice a week to 50 to 100 mg/d.
Risperidone has been used to treat agitation in older patients with dementia in two small studies:
In a 9-week, open-label trial, 15 patients (mean age 78) with dementia were given risperidone, 0.5 to 3 mg/d. Agitation improved significantly, as measured by the Cohen-Mansfield Agitation Inventory (CMAI)—a 29-item questionnaire completed by caregivers.26 CMAI scores at study’s end averaged 49.5, compared with 70.5 at baseline.27
A 12-week, placebo-controlled, doubleblind study examined risperidone—0.5, 1, or 2 mg/d—in 625 institutionalized patients (mean age 83) with dementia and agitation. Ninety-six patients had Functional Assessment Staging Rating Scale scores of 6A, indicating moderate to severe dementia. In patients receiving risperidone, these behavioral measures were significantly reduced:
- Behavior Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) total scores, which measure behavior severity
- BEHAVE-AD psychosis subscale scores
- BEHAVE-AD aggressiveness scores
- CMAI verbal and aggression scores.
Adverse effects were reported at 82% for all three risperidone dosages and 85% for placebo. Side effects including somnolence, EPS, and peripheral edema were dose-related.12
Another trial compared risperidone or haloperidol, 0.5 to 4 mg/d, with placebo in treating 344 patients with behavioral symptoms of dementia. After 12 weeks of risperidone, mean dosage 1.1 mg/d:
- mean total BEHAVE-AD score decreased by 53%, compared with 37% in the placebo group
- CMAI score decreased by 32%, compared with 18% in the placebo group.
EPS were more severe with haloperidol than with risperidone or placebo.28
Risk of stroke. A small but significantly increased incidence of stroke and stroke-like events was recently reported in older patients with dementia when treated with risperidone. These events occurred in double-blind, placebocontrolled trials in patients (mean age 82) with Alzheimer’s, vascular, and mixed dementias.
Pharmacokinetic changes can influence concentrations of drugs in tissue compartments over time. Drug absorption declines with normal aging, but a clinically significant decrease in total absorption of psychotropics appears not to occur.13
In the liver, lipid-soluble psychotropics are metabolized into pharmacologically active or inactive metabolites. Some metabolic pathways, such as demethylation, may be influenced by age, leading to increased plasma concentrations of drugs and their metabolites.14,15 However, hydroxylation tends not to be affected by age.16
The ratio of body fat to water increases with aging,13 increasing the volume of distribution for lipid-soluble psychotropics. An age-related decrease in glomerular filtration accounts in part for increased accumulation of hydrophilic metabolites in some older patients.17,18
Pharmacodynamic changes with aging occur in neurotransmitter systems within cellular processing, such as at receptor or reuptake levels.19 These changes may exaggerate drug-drug interactions or affect complex neurotransmitter interactions.
The number of neurons in nigrostriatal pathways declines with age. Decreases are also seen in tyrosine hydroxylase activity, presynaptic dopamine D2 receptors, and dopamine levels—which may be particularly relevant to a discussion of antipsychotic medications.20
The net effect of these changes is the need to prescribe lower-than-usual starting and target dosages of many medications, including antipsychotics.
Most patients who experienced cerebrovascular events had one or more stroke risk factors, including diabetes, hypertension, atrial fibrillation, heart arrhythmia, atherosclerosis, or heart failure. They did not show a pattern of reduced blood pressure or orthostatic changes.12,29
Table 2
Antipsychotic side effects and dosages in older patients with dementia*
| Side effect | Clozapine (6.25 to 100 mg/d) | Risperidone (0.5 to 1.5 mg/d) | Olanzapine (5 to 10 mg/d) | Quetiapine (25 to 350 mg/d) |
|---|---|---|---|---|
| Orthostasis | ++++ | ++++ | +++ | ++ |
| Sedation | +++++ | ++ | +++ | ++ |
| Prolactin increase | 0 | +++ | + | 0 |
| Weight gain | ++++ | + | +++ | + |
| EPS | 0/+ | ++ | + | 0/+ |
| Tardive dyskinesia | 0 | + | + | ? |
| Anticholinergic effects | ++++ | + | + | 0 |
| Seizure risk | +++ | + | + | + |
| Hematologic effects | +++ | + | + | + |
| Source: Adapted from references 15 and 16. | ||||
| * Side-effect profiles and recommended dosages of ziprasidone and aripiprazole in older patients are not yet established. | ||||
| EPS: Extrapyramidal symptoms | ||||
| Key: | ||||
| 0 = none | ||||
| + = slight | ||||
| +++ = mild | ||||
| +++++ = marked | ||||
| 0/+ = none to slight | ||||
| ++ = very mild | ||||
| ++++ = moderate | ||||
Dosing. For older patients with dementia and psychosis, start risperidone at 0.25 to 0.5 mg/d and increase by no more than 0.25 to 0.5 mg once or twice per week. Do not exceed 3 mg/d. For agitation, a 1998 Expert Consensus Guideline Series panel2 recommended starting risperidone at 0.25 to 0.5 mg/d and increasing to an average of 0.5 to 1.5 mg/d.
Olanzapine. Two double-blind, placebo-controlled studies have examined olanzapine in treating agitation associated with dementia.
Saterlee et al30 compared olanzapine, mean 2.4 mg/d, with placebo in outpatients (mean age 79) with Alzheimer’s disease and psychosis. No significant differences were noted in hepatic transaminase levels, leukopenia, EPS, or orthostatic changes.
In a later study,13 nursing home patients (mean age 83) with Alzheimer’s disease, psychosis, and agitation were randomly assigned to receive olanzapine—5, 10, or 15 mg/d—or placebo. After 6 weeks, patients receiving olanzapine, 5 or 10 mg/d, showed significant improvement in Neuropsychiatric Inventory (NPI) total core scores. Olanzapine, 15 mg/d, was not significantly more effective than placebo.
Adverse events such as somnolence and abnormal gait occurred more often with olanzapine than placebo. The somnolence rate with olanzapine was 14% for 5 mg/d and 13% for 10 mg/d, compared with 3% for placebo. For abnormal gait, the rate with olanzapine was 11% for 5 mg/d and 7% for 10 mg/d, compared with 1% for placebo.
Dosing. Start olanzapine at 2.5 mg/d, and increase after 1 to 3 days to 5 mg/d. If symptoms are not adequately controlled, titrate by 2.5-mg increments to 10 mg/d.
Quetiapine. One open-label study14 examined using quetiapine in older patients with psychotic disorders. The study enrolled 184 patients (mean age 76) with Alzheimer’s disease, Parkinson’s disease, schizophrenia, vascular dementia, schizoaffective disorder, bipolar disorder, or major depression. Before the trial, patients were taking various conventional and atypical antipsychotics.
Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impressions (CGI) scores improved significantly after 52 weeks of quetiapine, median 137.5 mg/d. BPRS scores improved 20% in 49% of patients who completed the study.
Less than one-half (48%) of enrolled patients completed the study. Reasons for withdrawal included lack of efficacy (19%), adverse events or illness (15%; adverse events alone, 11%), lost to follow-up (13%), protocol noncompliance (3%), or diminished need for treatment (2%).
EPS occurred in 13% of patients. Mean total scores on the Simpson-Angus Rating Scale for Extrapyramidal Side Effects decreased 1.8 points, indicating reduced parkinsonian symptoms.
Dosing. Start quetiapine at 25 mg once at bedtime or bid; increase in 25-mg increments until the lowest effective dosage is achieved.
Ziprasidone. Little data exist on using ziprasidone in long-term care. In one recent study,31 ziprasidone (mean 100 mg/d) was given to 62 patients ages 64 to 92 with medical illnesses plus major depression, bipolar disorder, schizoaffective disorder, Alzheimer’s disease, or multi-infarct dementia. A retrospective chart review of 10 patients showed decreased agitation, as mean NPI scores declined from 76 to 33.
Sedation was the most common side effect. QTc findings, postural hypotension, and syncope rates did not change. Despite its limitations, this study suggests that ziprasidone is safe and effective in treating psychosis associated with dementia or other disorders.
Aripiprazole. As with ziprasidone, little data exist to guide the use of aripiprazole in older patients. In a randomized preliminary trial,32 192 noninstitutionalized patients with Alzheimer’s disease and psychosis were treated for 10 weeks with aripiprazole, mean 10 mg/d, or placebo.
At 8 and 10 weeks, BPRS psychosis subscale scores improved significantly in patients taking aripiprazole, compared with placebo. EPS and akathisia improved, and somnolence was the most common side effect. Although this study enrolled noninstitutionalized patients with dementia, the results suggest that aripiprazole may help treat long-term care residents with neurodegenerative disorders and behavioral disturbances.
Related resources
- Zaraa AS. Dementia update: Pharmacologic management of agitation and psychosis in older demented patients. Geriatrics 2003;58(10):48-53.
- Mills EJ, Chow TW. Randomized controlled trials in long-term care of residents with dementia: a systematic review. J Am Med Dir Assoc 2003;4(6):302-7.
- Alzheimer’s Association. Treating agitation. www.alz.org/PhysCare/Treating/agitation.htm
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Donepezil • Aricept
- Galantamine • Reminyl
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Kasckow receives research support from, is a consultant to, or is a speaker for Eli Lilly & Co., Forest Laboratories, Solvay Pharmaceuticals, AstraZeneca Pharmaceuticals, Organon, Janssen Pharmaceutica, and Pfizer Inc.
Dr. Mulchahey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed receives research support form Forest Laboratories and is a speaker for Eli Lilly & Co.
1. Finkel S, Costa e Silva J, Cohen G, et al. Behavioral and psychological symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Am J Geriatr Psychiatry 1998;6:97-100.
2. The Expert Consensus Panel for Agitation in Dementia. Treatment of agitation in older persons with dementia. Postgrad Med 1998;4(suppl):1-88.
3. Cohen-Mansfield J. Nonpharmacologic interventions for inappropriate behaviors in dementia: a review, summary, and critique. Am J Geriatr Psychiatry 2001;9(4):361-81.
4. Davidson J. Pharmacologic treatment. In: Busse E, Blazer D (eds). Textbook of geriatric psychiatry (2nd ed). Washington DC: American Psychiatric Publishing, 1996:359-79.
5. Nies A, Robinson DS, Friedman MJ, et al. Relationship between age and tricyclic antidepressant plasma levels. Am J Psychiatry 1977;134(7):790-3.
6. Greenblatt DJ, Shader RJ. Benzodiazepine kinetics in the elderly. In: Usdin E (ed). Clinical pharmacology in psychiatry. New York: Elsevier, 1981;174-81.
7. Pollock BG, Perel JM, Altieri LP, et al. Debrisoquine hydroxylation phenotyping in geriatric psychopharmacology. Psychopharmacol Bull. 1992;28(2):163-8.
8. Nelson JC, Atillasoy E, Mazure C, Jatlow PI. Hydroxydesipramine in the elderly. J Clin Psychopharmacol 1988;8(6):428-33.
9. Young RC, Alexopoulos GS, Shamoian CA, et al. Plasma 10-hydroxynortriptyline in elderly depressed patients. Clin Pharmacol Ther 1984;35(4):540-4.
10. Cantillon M, Molchan SE, Little J. Pharmacological and neuroendocrine probes in neuropsychiatric illness. In: Coffey CE, Cummings JL (eds). Textbook of geriatric neuropsychiatry. Washington, DC: American Psychiatric Publishing, 1994.
11. Young RC, Meyers BS. Psychopharmacology. In: Sadovoy J, Lazarus LW, Jarvik LF, Grossberg GT (eds). Comprehensive review of geriatric psychiatry. Washington DC: American Psychiatric Publishing, 1996;755-817.
12. Katz IR, Jeste DV, Mintzer JE, et al. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. J Clin Psychiatry 1999;60(2):107-15.
13. Street JS, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer disease in nursing care facilities: a double-blind, randomized, placebo-controlled trial. The HGEU Study Group. Arch Gen Psychiatry 2000;57(10):968-76.
14. Tariot PN, Salzman C, Yeung PP, et al. Long-term use of quetiapine in elderly patients with psychotic disorders. Clin Ther 2000;22(9):1068-84.
15. Casey DE. The relationship of pharmacology to side effects. J Clin Psychiatry 1997;58(suppl):55-62.
16. Pickar D. Prospects for pharmacotherapy of schizophrenia. Lancet 1995;345:557-62.
17. Kasckow JW, McElroy SL, Cameron RL, et al. A pilot study on the use of divalproex sodium in the treatment of behavioral agitation in elderly patients with dementia: assessment with the BEHAVE-AD and CGI rating scales. Curr Ther Res 1997;58(12):981-9.
18. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155(1):54-61.
19. Kasckow JW. Cognitive enhancers for dementia: do they work? Current Psychiatry 2002;1(3):22-8.
20. Lacy C, Armstrong L, Goldman M, Lance L. (eds) Lexicomp drug information handbook. Hudson, OH: Lexicomp, 2003-2004:1225-27, 1189-90, 1026-27.
21. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47(6):716-19.
22. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
23. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995;52(9):756-65.
24. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
25. Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. JGeriatr Psychiatry Neurol 1995;8(1):12-15.
26. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in the nursing home. J Gerontol 1989;44(3):M77-84.
27. Lavretsky H, Sultzer D. A structured trial of risperidone for the treatment of agitation in dementia. Am J Geriatr Psychiatry 1998;6(2):127-35.
28. De Deyn PP, Rabheru K, Rasmussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53(5):946-55.
29. Brodaty H, Ames D, Snowdon J, et al. A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003;64(2):134-43.
30. Satterlee W, Reams SG, Burns PR, et al. A clinical update on olanzapine treatment in schizophrenia and in elderly Alzheimer’s disease patients (abstract). Psychopharmacol Bull 1995;31:534.-
31. Berkowitz A. Ziprasidone for elderly dementia: a case series (abstract). San Francisco, CA: American Psychiatric Association annual meeting, 2003.
32. De Deyn PP, Jeste D, Auby P, Carson W. Aripiprazole in dementia of the Alzheimer’s type (abstract). Honolulu, HI: American Association for Geriatric Psychiatry annual meeting, 2003.
Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
Algorithm Treating behavioral symptoms in patients with dementia
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|
Antipsychotic side effects
Atypical antipsychotics are more effective than conventional agents in treating negative symptoms and are associated with lower rates of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD).21
Tardive dyskinesia. All antipsychotics can cause TD, although the risk is about 10 times greater with conventionals than atypicals. With conventionals, the annual cumulative TD incidence for young adults is 4 to 5%,22 and rates are much higher for middle-aged and older adults receiving chronic therapy:
- 29% after 1 year
- 50% after 2 years
- 63% after 3 years.23
In older patients, use atypical rather than conventional antipsychotics to minimize TD risk. Observe carefully; if TD symptoms occur, cautiously withdraw the antipsychotic and consider trying another agent.
Other risks. Atypical antipsychotics may cause sedation, orthostatic hypotension (with an increased risk for falls), increased serum prolactin, and weight gain (Table 2).
Weight gain from atypical antipsychotics has been associated with adverse effects on glucose metabolism and increased risk for type 2 diabetes.24 Some might argue that weight gain associated with olanzapine and other atypicals might benefit low-weight older patients. The frail elderly need to increase muscle mass, however, and the atypicals are associated with increases in fat mass.
Increased serum prolactin with risperidone theoretically could lead to loss of bone density, but evidence of this effect in older patients does not exist.
Start low, go slow
Clozapine may help control treatment-resistant psychosis in patients with schizophrenia and manage patients with severe TD.25 However, clozapine’s increased risk of agranulocytosis, neurologic side effects (seizures, sedation, confusion), and anticholinergic effects limit its use in older patients, particularly those with neurodegenerative disorders (Table 2).
Dosing. In rare cases when using clozapine in older patients, start with 6.25 to 12.5 mg/d. Increase by 6.25 to 12.5 mg once or twice a week to 50 to 100 mg/d.
Risperidone has been used to treat agitation in older patients with dementia in two small studies:
In a 9-week, open-label trial, 15 patients (mean age 78) with dementia were given risperidone, 0.5 to 3 mg/d. Agitation improved significantly, as measured by the Cohen-Mansfield Agitation Inventory (CMAI)—a 29-item questionnaire completed by caregivers.26 CMAI scores at study’s end averaged 49.5, compared with 70.5 at baseline.27
A 12-week, placebo-controlled, doubleblind study examined risperidone—0.5, 1, or 2 mg/d—in 625 institutionalized patients (mean age 83) with dementia and agitation. Ninety-six patients had Functional Assessment Staging Rating Scale scores of 6A, indicating moderate to severe dementia. In patients receiving risperidone, these behavioral measures were significantly reduced:
- Behavior Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) total scores, which measure behavior severity
- BEHAVE-AD psychosis subscale scores
- BEHAVE-AD aggressiveness scores
- CMAI verbal and aggression scores.
Adverse effects were reported at 82% for all three risperidone dosages and 85% for placebo. Side effects including somnolence, EPS, and peripheral edema were dose-related.12
Another trial compared risperidone or haloperidol, 0.5 to 4 mg/d, with placebo in treating 344 patients with behavioral symptoms of dementia. After 12 weeks of risperidone, mean dosage 1.1 mg/d:
- mean total BEHAVE-AD score decreased by 53%, compared with 37% in the placebo group
- CMAI score decreased by 32%, compared with 18% in the placebo group.
EPS were more severe with haloperidol than with risperidone or placebo.28
Risk of stroke. A small but significantly increased incidence of stroke and stroke-like events was recently reported in older patients with dementia when treated with risperidone. These events occurred in double-blind, placebocontrolled trials in patients (mean age 82) with Alzheimer’s, vascular, and mixed dementias.
Pharmacokinetic changes can influence concentrations of drugs in tissue compartments over time. Drug absorption declines with normal aging, but a clinically significant decrease in total absorption of psychotropics appears not to occur.13
In the liver, lipid-soluble psychotropics are metabolized into pharmacologically active or inactive metabolites. Some metabolic pathways, such as demethylation, may be influenced by age, leading to increased plasma concentrations of drugs and their metabolites.14,15 However, hydroxylation tends not to be affected by age.16
The ratio of body fat to water increases with aging,13 increasing the volume of distribution for lipid-soluble psychotropics. An age-related decrease in glomerular filtration accounts in part for increased accumulation of hydrophilic metabolites in some older patients.17,18
Pharmacodynamic changes with aging occur in neurotransmitter systems within cellular processing, such as at receptor or reuptake levels.19 These changes may exaggerate drug-drug interactions or affect complex neurotransmitter interactions.
The number of neurons in nigrostriatal pathways declines with age. Decreases are also seen in tyrosine hydroxylase activity, presynaptic dopamine D2 receptors, and dopamine levels—which may be particularly relevant to a discussion of antipsychotic medications.20
The net effect of these changes is the need to prescribe lower-than-usual starting and target dosages of many medications, including antipsychotics.
Most patients who experienced cerebrovascular events had one or more stroke risk factors, including diabetes, hypertension, atrial fibrillation, heart arrhythmia, atherosclerosis, or heart failure. They did not show a pattern of reduced blood pressure or orthostatic changes.12,29
Table 2
Antipsychotic side effects and dosages in older patients with dementia*
| Side effect | Clozapine (6.25 to 100 mg/d) | Risperidone (0.5 to 1.5 mg/d) | Olanzapine (5 to 10 mg/d) | Quetiapine (25 to 350 mg/d) |
|---|---|---|---|---|
| Orthostasis | ++++ | ++++ | +++ | ++ |
| Sedation | +++++ | ++ | +++ | ++ |
| Prolactin increase | 0 | +++ | + | 0 |
| Weight gain | ++++ | + | +++ | + |
| EPS | 0/+ | ++ | + | 0/+ |
| Tardive dyskinesia | 0 | + | + | ? |
| Anticholinergic effects | ++++ | + | + | 0 |
| Seizure risk | +++ | + | + | + |
| Hematologic effects | +++ | + | + | + |
| Source: Adapted from references 15 and 16. | ||||
| * Side-effect profiles and recommended dosages of ziprasidone and aripiprazole in older patients are not yet established. | ||||
| EPS: Extrapyramidal symptoms | ||||
| Key: | ||||
| 0 = none | ||||
| + = slight | ||||
| +++ = mild | ||||
| +++++ = marked | ||||
| 0/+ = none to slight | ||||
| ++ = very mild | ||||
| ++++ = moderate | ||||
Dosing. For older patients with dementia and psychosis, start risperidone at 0.25 to 0.5 mg/d and increase by no more than 0.25 to 0.5 mg once or twice per week. Do not exceed 3 mg/d. For agitation, a 1998 Expert Consensus Guideline Series panel2 recommended starting risperidone at 0.25 to 0.5 mg/d and increasing to an average of 0.5 to 1.5 mg/d.
Olanzapine. Two double-blind, placebo-controlled studies have examined olanzapine in treating agitation associated with dementia.
Saterlee et al30 compared olanzapine, mean 2.4 mg/d, with placebo in outpatients (mean age 79) with Alzheimer’s disease and psychosis. No significant differences were noted in hepatic transaminase levels, leukopenia, EPS, or orthostatic changes.
In a later study,13 nursing home patients (mean age 83) with Alzheimer’s disease, psychosis, and agitation were randomly assigned to receive olanzapine—5, 10, or 15 mg/d—or placebo. After 6 weeks, patients receiving olanzapine, 5 or 10 mg/d, showed significant improvement in Neuropsychiatric Inventory (NPI) total core scores. Olanzapine, 15 mg/d, was not significantly more effective than placebo.
Adverse events such as somnolence and abnormal gait occurred more often with olanzapine than placebo. The somnolence rate with olanzapine was 14% for 5 mg/d and 13% for 10 mg/d, compared with 3% for placebo. For abnormal gait, the rate with olanzapine was 11% for 5 mg/d and 7% for 10 mg/d, compared with 1% for placebo.
Dosing. Start olanzapine at 2.5 mg/d, and increase after 1 to 3 days to 5 mg/d. If symptoms are not adequately controlled, titrate by 2.5-mg increments to 10 mg/d.
Quetiapine. One open-label study14 examined using quetiapine in older patients with psychotic disorders. The study enrolled 184 patients (mean age 76) with Alzheimer’s disease, Parkinson’s disease, schizophrenia, vascular dementia, schizoaffective disorder, bipolar disorder, or major depression. Before the trial, patients were taking various conventional and atypical antipsychotics.
Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impressions (CGI) scores improved significantly after 52 weeks of quetiapine, median 137.5 mg/d. BPRS scores improved 20% in 49% of patients who completed the study.
Less than one-half (48%) of enrolled patients completed the study. Reasons for withdrawal included lack of efficacy (19%), adverse events or illness (15%; adverse events alone, 11%), lost to follow-up (13%), protocol noncompliance (3%), or diminished need for treatment (2%).
EPS occurred in 13% of patients. Mean total scores on the Simpson-Angus Rating Scale for Extrapyramidal Side Effects decreased 1.8 points, indicating reduced parkinsonian symptoms.
Dosing. Start quetiapine at 25 mg once at bedtime or bid; increase in 25-mg increments until the lowest effective dosage is achieved.
Ziprasidone. Little data exist on using ziprasidone in long-term care. In one recent study,31 ziprasidone (mean 100 mg/d) was given to 62 patients ages 64 to 92 with medical illnesses plus major depression, bipolar disorder, schizoaffective disorder, Alzheimer’s disease, or multi-infarct dementia. A retrospective chart review of 10 patients showed decreased agitation, as mean NPI scores declined from 76 to 33.
Sedation was the most common side effect. QTc findings, postural hypotension, and syncope rates did not change. Despite its limitations, this study suggests that ziprasidone is safe and effective in treating psychosis associated with dementia or other disorders.
Aripiprazole. As with ziprasidone, little data exist to guide the use of aripiprazole in older patients. In a randomized preliminary trial,32 192 noninstitutionalized patients with Alzheimer’s disease and psychosis were treated for 10 weeks with aripiprazole, mean 10 mg/d, or placebo.
At 8 and 10 weeks, BPRS psychosis subscale scores improved significantly in patients taking aripiprazole, compared with placebo. EPS and akathisia improved, and somnolence was the most common side effect. Although this study enrolled noninstitutionalized patients with dementia, the results suggest that aripiprazole may help treat long-term care residents with neurodegenerative disorders and behavioral disturbances.
Related resources
- Zaraa AS. Dementia update: Pharmacologic management of agitation and psychosis in older demented patients. Geriatrics 2003;58(10):48-53.
- Mills EJ, Chow TW. Randomized controlled trials in long-term care of residents with dementia: a systematic review. J Am Med Dir Assoc 2003;4(6):302-7.
- Alzheimer’s Association. Treating agitation. www.alz.org/PhysCare/Treating/agitation.htm
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Donepezil • Aricept
- Galantamine • Reminyl
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Kasckow receives research support from, is a consultant to, or is a speaker for Eli Lilly & Co., Forest Laboratories, Solvay Pharmaceuticals, AstraZeneca Pharmaceuticals, Organon, Janssen Pharmaceutica, and Pfizer Inc.
Dr. Mulchahey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed receives research support form Forest Laboratories and is a speaker for Eli Lilly & Co.
Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
Algorithm Treating behavioral symptoms in patients with dementia
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|
Antipsychotic side effects
Atypical antipsychotics are more effective than conventional agents in treating negative symptoms and are associated with lower rates of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD).21
Tardive dyskinesia. All antipsychotics can cause TD, although the risk is about 10 times greater with conventionals than atypicals. With conventionals, the annual cumulative TD incidence for young adults is 4 to 5%,22 and rates are much higher for middle-aged and older adults receiving chronic therapy:
- 29% after 1 year
- 50% after 2 years
- 63% after 3 years.23
In older patients, use atypical rather than conventional antipsychotics to minimize TD risk. Observe carefully; if TD symptoms occur, cautiously withdraw the antipsychotic and consider trying another agent.
Other risks. Atypical antipsychotics may cause sedation, orthostatic hypotension (with an increased risk for falls), increased serum prolactin, and weight gain (Table 2).
Weight gain from atypical antipsychotics has been associated with adverse effects on glucose metabolism and increased risk for type 2 diabetes.24 Some might argue that weight gain associated with olanzapine and other atypicals might benefit low-weight older patients. The frail elderly need to increase muscle mass, however, and the atypicals are associated with increases in fat mass.
Increased serum prolactin with risperidone theoretically could lead to loss of bone density, but evidence of this effect in older patients does not exist.
Start low, go slow
Clozapine may help control treatment-resistant psychosis in patients with schizophrenia and manage patients with severe TD.25 However, clozapine’s increased risk of agranulocytosis, neurologic side effects (seizures, sedation, confusion), and anticholinergic effects limit its use in older patients, particularly those with neurodegenerative disorders (Table 2).
Dosing. In rare cases when using clozapine in older patients, start with 6.25 to 12.5 mg/d. Increase by 6.25 to 12.5 mg once or twice a week to 50 to 100 mg/d.
Risperidone has been used to treat agitation in older patients with dementia in two small studies:
In a 9-week, open-label trial, 15 patients (mean age 78) with dementia were given risperidone, 0.5 to 3 mg/d. Agitation improved significantly, as measured by the Cohen-Mansfield Agitation Inventory (CMAI)—a 29-item questionnaire completed by caregivers.26 CMAI scores at study’s end averaged 49.5, compared with 70.5 at baseline.27
A 12-week, placebo-controlled, doubleblind study examined risperidone—0.5, 1, or 2 mg/d—in 625 institutionalized patients (mean age 83) with dementia and agitation. Ninety-six patients had Functional Assessment Staging Rating Scale scores of 6A, indicating moderate to severe dementia. In patients receiving risperidone, these behavioral measures were significantly reduced:
- Behavior Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) total scores, which measure behavior severity
- BEHAVE-AD psychosis subscale scores
- BEHAVE-AD aggressiveness scores
- CMAI verbal and aggression scores.
Adverse effects were reported at 82% for all three risperidone dosages and 85% for placebo. Side effects including somnolence, EPS, and peripheral edema were dose-related.12
Another trial compared risperidone or haloperidol, 0.5 to 4 mg/d, with placebo in treating 344 patients with behavioral symptoms of dementia. After 12 weeks of risperidone, mean dosage 1.1 mg/d:
- mean total BEHAVE-AD score decreased by 53%, compared with 37% in the placebo group
- CMAI score decreased by 32%, compared with 18% in the placebo group.
EPS were more severe with haloperidol than with risperidone or placebo.28
Risk of stroke. A small but significantly increased incidence of stroke and stroke-like events was recently reported in older patients with dementia when treated with risperidone. These events occurred in double-blind, placebocontrolled trials in patients (mean age 82) with Alzheimer’s, vascular, and mixed dementias.
Pharmacokinetic changes can influence concentrations of drugs in tissue compartments over time. Drug absorption declines with normal aging, but a clinically significant decrease in total absorption of psychotropics appears not to occur.13
In the liver, lipid-soluble psychotropics are metabolized into pharmacologically active or inactive metabolites. Some metabolic pathways, such as demethylation, may be influenced by age, leading to increased plasma concentrations of drugs and their metabolites.14,15 However, hydroxylation tends not to be affected by age.16
The ratio of body fat to water increases with aging,13 increasing the volume of distribution for lipid-soluble psychotropics. An age-related decrease in glomerular filtration accounts in part for increased accumulation of hydrophilic metabolites in some older patients.17,18
Pharmacodynamic changes with aging occur in neurotransmitter systems within cellular processing, such as at receptor or reuptake levels.19 These changes may exaggerate drug-drug interactions or affect complex neurotransmitter interactions.
The number of neurons in nigrostriatal pathways declines with age. Decreases are also seen in tyrosine hydroxylase activity, presynaptic dopamine D2 receptors, and dopamine levels—which may be particularly relevant to a discussion of antipsychotic medications.20
The net effect of these changes is the need to prescribe lower-than-usual starting and target dosages of many medications, including antipsychotics.
Most patients who experienced cerebrovascular events had one or more stroke risk factors, including diabetes, hypertension, atrial fibrillation, heart arrhythmia, atherosclerosis, or heart failure. They did not show a pattern of reduced blood pressure or orthostatic changes.12,29
Table 2
Antipsychotic side effects and dosages in older patients with dementia*
| Side effect | Clozapine (6.25 to 100 mg/d) | Risperidone (0.5 to 1.5 mg/d) | Olanzapine (5 to 10 mg/d) | Quetiapine (25 to 350 mg/d) |
|---|---|---|---|---|
| Orthostasis | ++++ | ++++ | +++ | ++ |
| Sedation | +++++ | ++ | +++ | ++ |
| Prolactin increase | 0 | +++ | + | 0 |
| Weight gain | ++++ | + | +++ | + |
| EPS | 0/+ | ++ | + | 0/+ |
| Tardive dyskinesia | 0 | + | + | ? |
| Anticholinergic effects | ++++ | + | + | 0 |
| Seizure risk | +++ | + | + | + |
| Hematologic effects | +++ | + | + | + |
| Source: Adapted from references 15 and 16. | ||||
| * Side-effect profiles and recommended dosages of ziprasidone and aripiprazole in older patients are not yet established. | ||||
| EPS: Extrapyramidal symptoms | ||||
| Key: | ||||
| 0 = none | ||||
| + = slight | ||||
| +++ = mild | ||||
| +++++ = marked | ||||
| 0/+ = none to slight | ||||
| ++ = very mild | ||||
| ++++ = moderate | ||||
Dosing. For older patients with dementia and psychosis, start risperidone at 0.25 to 0.5 mg/d and increase by no more than 0.25 to 0.5 mg once or twice per week. Do not exceed 3 mg/d. For agitation, a 1998 Expert Consensus Guideline Series panel2 recommended starting risperidone at 0.25 to 0.5 mg/d and increasing to an average of 0.5 to 1.5 mg/d.
Olanzapine. Two double-blind, placebo-controlled studies have examined olanzapine in treating agitation associated with dementia.
Saterlee et al30 compared olanzapine, mean 2.4 mg/d, with placebo in outpatients (mean age 79) with Alzheimer’s disease and psychosis. No significant differences were noted in hepatic transaminase levels, leukopenia, EPS, or orthostatic changes.
In a later study,13 nursing home patients (mean age 83) with Alzheimer’s disease, psychosis, and agitation were randomly assigned to receive olanzapine—5, 10, or 15 mg/d—or placebo. After 6 weeks, patients receiving olanzapine, 5 or 10 mg/d, showed significant improvement in Neuropsychiatric Inventory (NPI) total core scores. Olanzapine, 15 mg/d, was not significantly more effective than placebo.
Adverse events such as somnolence and abnormal gait occurred more often with olanzapine than placebo. The somnolence rate with olanzapine was 14% for 5 mg/d and 13% for 10 mg/d, compared with 3% for placebo. For abnormal gait, the rate with olanzapine was 11% for 5 mg/d and 7% for 10 mg/d, compared with 1% for placebo.
Dosing. Start olanzapine at 2.5 mg/d, and increase after 1 to 3 days to 5 mg/d. If symptoms are not adequately controlled, titrate by 2.5-mg increments to 10 mg/d.
Quetiapine. One open-label study14 examined using quetiapine in older patients with psychotic disorders. The study enrolled 184 patients (mean age 76) with Alzheimer’s disease, Parkinson’s disease, schizophrenia, vascular dementia, schizoaffective disorder, bipolar disorder, or major depression. Before the trial, patients were taking various conventional and atypical antipsychotics.
Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impressions (CGI) scores improved significantly after 52 weeks of quetiapine, median 137.5 mg/d. BPRS scores improved 20% in 49% of patients who completed the study.
Less than one-half (48%) of enrolled patients completed the study. Reasons for withdrawal included lack of efficacy (19%), adverse events or illness (15%; adverse events alone, 11%), lost to follow-up (13%), protocol noncompliance (3%), or diminished need for treatment (2%).
EPS occurred in 13% of patients. Mean total scores on the Simpson-Angus Rating Scale for Extrapyramidal Side Effects decreased 1.8 points, indicating reduced parkinsonian symptoms.
Dosing. Start quetiapine at 25 mg once at bedtime or bid; increase in 25-mg increments until the lowest effective dosage is achieved.
Ziprasidone. Little data exist on using ziprasidone in long-term care. In one recent study,31 ziprasidone (mean 100 mg/d) was given to 62 patients ages 64 to 92 with medical illnesses plus major depression, bipolar disorder, schizoaffective disorder, Alzheimer’s disease, or multi-infarct dementia. A retrospective chart review of 10 patients showed decreased agitation, as mean NPI scores declined from 76 to 33.
Sedation was the most common side effect. QTc findings, postural hypotension, and syncope rates did not change. Despite its limitations, this study suggests that ziprasidone is safe and effective in treating psychosis associated with dementia or other disorders.
Aripiprazole. As with ziprasidone, little data exist to guide the use of aripiprazole in older patients. In a randomized preliminary trial,32 192 noninstitutionalized patients with Alzheimer’s disease and psychosis were treated for 10 weeks with aripiprazole, mean 10 mg/d, or placebo.
At 8 and 10 weeks, BPRS psychosis subscale scores improved significantly in patients taking aripiprazole, compared with placebo. EPS and akathisia improved, and somnolence was the most common side effect. Although this study enrolled noninstitutionalized patients with dementia, the results suggest that aripiprazole may help treat long-term care residents with neurodegenerative disorders and behavioral disturbances.
Related resources
- Zaraa AS. Dementia update: Pharmacologic management of agitation and psychosis in older demented patients. Geriatrics 2003;58(10):48-53.
- Mills EJ, Chow TW. Randomized controlled trials in long-term care of residents with dementia: a systematic review. J Am Med Dir Assoc 2003;4(6):302-7.
- Alzheimer’s Association. Treating agitation. www.alz.org/PhysCare/Treating/agitation.htm
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Donepezil • Aricept
- Galantamine • Reminyl
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Kasckow receives research support from, is a consultant to, or is a speaker for Eli Lilly & Co., Forest Laboratories, Solvay Pharmaceuticals, AstraZeneca Pharmaceuticals, Organon, Janssen Pharmaceutica, and Pfizer Inc.
Dr. Mulchahey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed receives research support form Forest Laboratories and is a speaker for Eli Lilly & Co.
1. Finkel S, Costa e Silva J, Cohen G, et al. Behavioral and psychological symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Am J Geriatr Psychiatry 1998;6:97-100.
2. The Expert Consensus Panel for Agitation in Dementia. Treatment of agitation in older persons with dementia. Postgrad Med 1998;4(suppl):1-88.
3. Cohen-Mansfield J. Nonpharmacologic interventions for inappropriate behaviors in dementia: a review, summary, and critique. Am J Geriatr Psychiatry 2001;9(4):361-81.
4. Davidson J. Pharmacologic treatment. In: Busse E, Blazer D (eds). Textbook of geriatric psychiatry (2nd ed). Washington DC: American Psychiatric Publishing, 1996:359-79.
5. Nies A, Robinson DS, Friedman MJ, et al. Relationship between age and tricyclic antidepressant plasma levels. Am J Psychiatry 1977;134(7):790-3.
6. Greenblatt DJ, Shader RJ. Benzodiazepine kinetics in the elderly. In: Usdin E (ed). Clinical pharmacology in psychiatry. New York: Elsevier, 1981;174-81.
7. Pollock BG, Perel JM, Altieri LP, et al. Debrisoquine hydroxylation phenotyping in geriatric psychopharmacology. Psychopharmacol Bull. 1992;28(2):163-8.
8. Nelson JC, Atillasoy E, Mazure C, Jatlow PI. Hydroxydesipramine in the elderly. J Clin Psychopharmacol 1988;8(6):428-33.
9. Young RC, Alexopoulos GS, Shamoian CA, et al. Plasma 10-hydroxynortriptyline in elderly depressed patients. Clin Pharmacol Ther 1984;35(4):540-4.
10. Cantillon M, Molchan SE, Little J. Pharmacological and neuroendocrine probes in neuropsychiatric illness. In: Coffey CE, Cummings JL (eds). Textbook of geriatric neuropsychiatry. Washington, DC: American Psychiatric Publishing, 1994.
11. Young RC, Meyers BS. Psychopharmacology. In: Sadovoy J, Lazarus LW, Jarvik LF, Grossberg GT (eds). Comprehensive review of geriatric psychiatry. Washington DC: American Psychiatric Publishing, 1996;755-817.
12. Katz IR, Jeste DV, Mintzer JE, et al. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. J Clin Psychiatry 1999;60(2):107-15.
13. Street JS, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer disease in nursing care facilities: a double-blind, randomized, placebo-controlled trial. The HGEU Study Group. Arch Gen Psychiatry 2000;57(10):968-76.
14. Tariot PN, Salzman C, Yeung PP, et al. Long-term use of quetiapine in elderly patients with psychotic disorders. Clin Ther 2000;22(9):1068-84.
15. Casey DE. The relationship of pharmacology to side effects. J Clin Psychiatry 1997;58(suppl):55-62.
16. Pickar D. Prospects for pharmacotherapy of schizophrenia. Lancet 1995;345:557-62.
17. Kasckow JW, McElroy SL, Cameron RL, et al. A pilot study on the use of divalproex sodium in the treatment of behavioral agitation in elderly patients with dementia: assessment with the BEHAVE-AD and CGI rating scales. Curr Ther Res 1997;58(12):981-9.
18. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155(1):54-61.
19. Kasckow JW. Cognitive enhancers for dementia: do they work? Current Psychiatry 2002;1(3):22-8.
20. Lacy C, Armstrong L, Goldman M, Lance L. (eds) Lexicomp drug information handbook. Hudson, OH: Lexicomp, 2003-2004:1225-27, 1189-90, 1026-27.
21. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47(6):716-19.
22. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
23. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995;52(9):756-65.
24. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
25. Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. JGeriatr Psychiatry Neurol 1995;8(1):12-15.
26. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in the nursing home. J Gerontol 1989;44(3):M77-84.
27. Lavretsky H, Sultzer D. A structured trial of risperidone for the treatment of agitation in dementia. Am J Geriatr Psychiatry 1998;6(2):127-35.
28. De Deyn PP, Rabheru K, Rasmussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53(5):946-55.
29. Brodaty H, Ames D, Snowdon J, et al. A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003;64(2):134-43.
30. Satterlee W, Reams SG, Burns PR, et al. A clinical update on olanzapine treatment in schizophrenia and in elderly Alzheimer’s disease patients (abstract). Psychopharmacol Bull 1995;31:534.-
31. Berkowitz A. Ziprasidone for elderly dementia: a case series (abstract). San Francisco, CA: American Psychiatric Association annual meeting, 2003.
32. De Deyn PP, Jeste D, Auby P, Carson W. Aripiprazole in dementia of the Alzheimer’s type (abstract). Honolulu, HI: American Association for Geriatric Psychiatry annual meeting, 2003.
1. Finkel S, Costa e Silva J, Cohen G, et al. Behavioral and psychological symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Am J Geriatr Psychiatry 1998;6:97-100.
2. The Expert Consensus Panel for Agitation in Dementia. Treatment of agitation in older persons with dementia. Postgrad Med 1998;4(suppl):1-88.
3. Cohen-Mansfield J. Nonpharmacologic interventions for inappropriate behaviors in dementia: a review, summary, and critique. Am J Geriatr Psychiatry 2001;9(4):361-81.
4. Davidson J. Pharmacologic treatment. In: Busse E, Blazer D (eds). Textbook of geriatric psychiatry (2nd ed). Washington DC: American Psychiatric Publishing, 1996:359-79.
5. Nies A, Robinson DS, Friedman MJ, et al. Relationship between age and tricyclic antidepressant plasma levels. Am J Psychiatry 1977;134(7):790-3.
6. Greenblatt DJ, Shader RJ. Benzodiazepine kinetics in the elderly. In: Usdin E (ed). Clinical pharmacology in psychiatry. New York: Elsevier, 1981;174-81.
7. Pollock BG, Perel JM, Altieri LP, et al. Debrisoquine hydroxylation phenotyping in geriatric psychopharmacology. Psychopharmacol Bull. 1992;28(2):163-8.
8. Nelson JC, Atillasoy E, Mazure C, Jatlow PI. Hydroxydesipramine in the elderly. J Clin Psychopharmacol 1988;8(6):428-33.
9. Young RC, Alexopoulos GS, Shamoian CA, et al. Plasma 10-hydroxynortriptyline in elderly depressed patients. Clin Pharmacol Ther 1984;35(4):540-4.
10. Cantillon M, Molchan SE, Little J. Pharmacological and neuroendocrine probes in neuropsychiatric illness. In: Coffey CE, Cummings JL (eds). Textbook of geriatric neuropsychiatry. Washington, DC: American Psychiatric Publishing, 1994.
11. Young RC, Meyers BS. Psychopharmacology. In: Sadovoy J, Lazarus LW, Jarvik LF, Grossberg GT (eds). Comprehensive review of geriatric psychiatry. Washington DC: American Psychiatric Publishing, 1996;755-817.
12. Katz IR, Jeste DV, Mintzer JE, et al. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. J Clin Psychiatry 1999;60(2):107-15.
13. Street JS, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer disease in nursing care facilities: a double-blind, randomized, placebo-controlled trial. The HGEU Study Group. Arch Gen Psychiatry 2000;57(10):968-76.
14. Tariot PN, Salzman C, Yeung PP, et al. Long-term use of quetiapine in elderly patients with psychotic disorders. Clin Ther 2000;22(9):1068-84.
15. Casey DE. The relationship of pharmacology to side effects. J Clin Psychiatry 1997;58(suppl):55-62.
16. Pickar D. Prospects for pharmacotherapy of schizophrenia. Lancet 1995;345:557-62.
17. Kasckow JW, McElroy SL, Cameron RL, et al. A pilot study on the use of divalproex sodium in the treatment of behavioral agitation in elderly patients with dementia: assessment with the BEHAVE-AD and CGI rating scales. Curr Ther Res 1997;58(12):981-9.
18. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155(1):54-61.
19. Kasckow JW. Cognitive enhancers for dementia: do they work? Current Psychiatry 2002;1(3):22-8.
20. Lacy C, Armstrong L, Goldman M, Lance L. (eds) Lexicomp drug information handbook. Hudson, OH: Lexicomp, 2003-2004:1225-27, 1189-90, 1026-27.
21. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47(6):716-19.
22. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
23. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995;52(9):756-65.
24. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
25. Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. JGeriatr Psychiatry Neurol 1995;8(1):12-15.
26. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in the nursing home. J Gerontol 1989;44(3):M77-84.
27. Lavretsky H, Sultzer D. A structured trial of risperidone for the treatment of agitation in dementia. Am J Geriatr Psychiatry 1998;6(2):127-35.
28. De Deyn PP, Rabheru K, Rasmussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53(5):946-55.
29. Brodaty H, Ames D, Snowdon J, et al. A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003;64(2):134-43.
30. Satterlee W, Reams SG, Burns PR, et al. A clinical update on olanzapine treatment in schizophrenia and in elderly Alzheimer’s disease patients (abstract). Psychopharmacol Bull 1995;31:534.-
31. Berkowitz A. Ziprasidone for elderly dementia: a case series (abstract). San Francisco, CA: American Psychiatric Association annual meeting, 2003.
32. De Deyn PP, Jeste D, Auby P, Carson W. Aripiprazole in dementia of the Alzheimer’s type (abstract). Honolulu, HI: American Association for Geriatric Psychiatry annual meeting, 2003.
Night terrors: a family affair
History: Terrors at age 8
Ms. J, age 35, began having sleepwalking episodes at age 8. At times they involved odd behaviors, such as carrying her brother’s shirt into the bathroom, placing it into the sink, and turning on the water.
As a child, Ms. J also began experiencing nocturnal awakenings characterized by panic and shouting. She sometimes saw a frightening image, usually of something falling on her. She would promptly return to sleep after each incident and had trouble remembering the event the next morning. The sleepwalking and awakening occurred monthly—more often when she was under stress or fatigued—until her early 20s.
At age 21, Ms. J. was under severe stress while preparing for a crucial graduate school examination and was losing much sleep. At this point, the episodes began to occur once or twice nightly.
She consulted a sleep specialist. EEG results were normal, but a sleep study was not helpful because she experienced no events that night. The specialist diagnosed Ms. J as having night terrors and prescribed clonazepam, 0.5 mg nightly. The agent did not prevent the events, but their frequency returned to baseline after Ms. J took her exam.
Were Ms. J’s clinical presentation and course consistent with night terrors? How would you treat her symptoms at this point?
The authors’ observations
Night terrors are an arousal disorder that usually begins in early childhood and affects 1% to 4% of the population.1 The disorder usually disappears before puberty.
Episodes of this parasomnia typically occur one to four times each month and can last several minutes. They are characterized by sudden awakenings with panic, disorientation, vocalization, and autonomic discharge. Patients sometimes see a frightening image. The events occur in stage 4 sleep, usually soon after falling asleep. Disorientation and a prompt return to sleep may follow.2 Sleeptalking and sleepwalking may also be present. The patient often cannot remember the event the next morning.
At this point, night terrors are a reasonable explanation for Ms. J’s nocturnal phenomena. Benzodiazepines, especially clonazepam, have been shown to decrease night terror frequency.3
Continued history: A new mother’s stress
At age 34, Ms. J gave birth to her first child. Weeks later, the nocturnal events began to occur at least three times nightly—every hour on some nights. Because their frequency disrupted her sleep, Ms. J constantly felt tired. Stress, emotional upset, and sleep deprivation exacerbated the events, which were stereotypical and included:
- sudden jerking of the right upper and/or lower extremities
- sudden sitting up and posing with the right arm flexed and internally rotated
- hallucinations of spiders or people
- sudden body flexion accompanied by an “electric shock” sensation in the head
- sitting up in bed, touching and picking at the sheets
- nonsensical speech after sitting up in bed
- sudden fear that Ms. J’s baby was hurt or dead, accompanied by searching the bed and under the pillow for the baby
- episodes of panic often accompanied by crying out, jumping out of bed and—in some cases—running.
Several times she ran down the stairs and out of the house while asleep. During one event, she jumped out of bed and fractured her foot. In another, she jumped from the bed and ran headfirst into a wall, causing bruising but no severe injury.
Each event was accompanied by confusion for 10 seconds to 3 minutes. Ms. J remembered about one-half the events; her husband described the remainder. She invariably returned to sleep immediately after each event.
A second sleep specialist diagnosed Ms. J as having night terrors. Unsatisfied with the diagnosis, she consulted a neurologist who specialized in epilepsy. The neurologist diagnosed her as having nocturnal frontal lobe epilepsy (NFLE) based on her history. A video EEG study—which showed spike and wave activity in the left frontal lobe during the nocturnal events—confirmed the diagnosis. The events all occurred during stage 2 sleep.
Is Ms. J’s latest diagnosis on target? Which clinical features in her case would differentiate sleep epilepsy from parasomnias?
The authors’ observations
Frontal lobe epilepsy can take many forms. Seizures can occur during sleep and/or while awake and consist of sudden, brief (<1 minute) motor attacks occurring in clusters. The prevalence of sleep epilepsy among persons with seizure disorders has been estimated at 7.5% to 45%, based on studies of small patient populations.4
Nocturnal frontal lobe seizures:
- occur only in non-REM (usually stage 2) sleep.
- can occur at any time of night
- usually begin in middle childhood to early adolescence, but onset in early childhood or adulthood has been reported.5 Seizures usually subside during adulthood (Table).6
Table
Characteristics of parasomnias and nocturnal epilepsy
| Nightmare (adult) | Night terror | Nocturnal epilepsy | |
|---|---|---|---|
| Incidence | 5 to 10% | 1 to 3% | Unknown |
| Sleep stage | During REM Anytime during the night the night | Stage 4 In first few hours of sleep | Often stage 2 Anytime during |
| Age of onset | Variable | Early childhood | Late childhood or adolescence Occasionally in adulthood |
| Change with age | Often diminishes with age May remit and recur | Diminishes with age Gone by young adulthood | Heterogeneous course May be less severe later in life |
| Symptoms | Frightening dreams Detailed story line No motor activity No injury | Inconsolable terror Not associated with dream Low-level motor activity Autonomic activation Injury rare | With or without fear and autonomic activation Hallucinations or illusions possible Stereotypical, paroxysmal motor activity Injury possible |
| Sleep resumption | Often delayed | Usually rapid | Usually rapid |
| Precipitating factors | PTSD Unusual stressors | PTSD Sleep deprivation | Sleep deprivation Physical and emotional stressors |
| Frequency | Irregular | 1 to 2 times per month or less | Extremely variable Can occur in clusters |
| Recollection | Variable | Often none | Variable |
| PTSD: Posttraumatic stress disorder | |||
These seizures are clinically polymorphous but stereotypical in each patient. Seizure type varies depending on which frontal lobe region is affected.
Nocturnal seizures universally have an explosive onset, with motor symptoms such as jerking, rocking, pelvic thrusting, tonic posturing, kicking, scrambling about, and touching the bed with one’s hand. Other possible occurrences include:
- sensory phenomena such as illusions and hallucinations, sensations of buzzing, vibration, and olfactory or gustatory sensations
- aphasia or other vocal events, such as laughing, screaming, or making odd noises
- fear and autonomic discharge simulating a night terror or panic attack.7
Confusion also is possible, although consciousness many times is preserved through the episode.
As with other seizures, sleep disruption exacerbates NFLE. Most patients have a normal interictal EEG.
Because NFLE is often misdiagnosed as a parasomnia, the psychiatrist needs to consider this disorder in the differential diagnosis. Any patient with a suspected parasomnia should be evaluated by a neurologist for NFLE if:
- the nocturnal events have not ceased by young adulthood
- events consist of prominent stereotypical motor symptoms that occur in clusters and/or have caused physical injury.
Extended history: Family stories
Ms. J’s neurologist asked whether any relatives have experienced similar nocturnal events.
Upon talking with family members, she learned that her aunt (her father’s sister) experienced nocturnal hallucinations and panic episodes well into her 50s. Her first cousin (her aunt’s daughter) also has nocturnal hallucinations and panic episodes and runs in her sleep. Two of her father’s cousins—twin brothers—were also affected. One of the brothers experienced explosive episodes, sometimes assaulting the other brother while asleep; he once had to be restrained from jumping out a window.
Other family members or surviving spouses described similar events that are clinically consistent with frontal lobe seizures. Interestingly, tic disorders run in the same branches of the family as the seizures.
Ms. J was diagnosed with autosomal dominant nocturnal frontal lobe epilepsy (ADNFLE) based on her diagnosis of NFLE and family history of similar events.
The authors’ observations
ADNFLE is an inherited disorder that displays 70% penetrance.8 Families in Australia, Canada, Spain, Japan, Korea, Germany, Great Britain, Italy, and Norway have been described with the disorder. No accurate prevalence data exist.9
Ms. J’s family traces its roots to Lithuania and White Russia (now Belarus) and is Ashkenazi Jewish. No literature describes the disorder in this population or these locations.
ADNFLE was the first genetic epilepsy to be associated with a defect in a single gene. It was recognized as a disorder in 1994, having previously been described with different names by multiple authors.
The disorderis a “channelopathy,” signifying a defective ion channel resulting in abnormal neuronal cell membrane conduction. The affected gene is the acetylcholine receptor, which is widely distributed in the brain. Missense mutations of the receptor gene lead to a change in an amino acid found in the center of the receptor pore. Ordinarily, the centers of ion channel pores are lined with hydrophobic amino acids to facilitate entrance of ions. The mutations in affected individuals result in a hydrophobic amino acid substitution. Different families display different mutations of the gene.10
In ADNFLE, there is mutation in the second transmembrane region of the alpha-4 subunit of the neuronal acetylcholine receptor. Defective receptors result in reduced channel permeability to calcium, causing fast desensitization and receptor hypoactivity. This has been postulated to cause an imbalance in excitatory/inhibitory synaptic transmission.11 Further study will elucidate the acetylcholine receptor’s relationship to brain functioning.
Treatment: Medication trial
Lamotrigine was started at 25 mg/d and titrated upward by 25 to 50 mg per week. When the dosage reached 500 mg/d, seizure frequency was reduced to once weekly.
Because Ms. J’s seizures were associated with stress and fatigue, she reduced her work hours and modified her job duties. Alcohol increased the frequency of the seizures, so she abstained from alcohol consumption. She also adhered to a consistent bedtime and slept at least 8 hours every night. After making these lifestyle modifications, Ms. J’s seizers decreased to once per month.
Why was lamotrigine chosen for Ms. J? What other drug options exist to treat sleep epilepsy?
The authors’ observations
Many clinicians consider carbamazepine the drug of choice for NFLE. Because NFLE is an epilepsy of partial onset, however, medications used to treat partial-onset epilepsy—including lamotrigine, topiramate, oxcarbazepine, gabapentin, and levetiracetam—are presumed to work as well. Because lamotrigine is considered the safest antiepileptic in pregnancy, the neurologist chose this agent for Ms. J.
Although comparative studies of antiepileptics for partial epilepsies have shown no difference in efficacy,12,13 no comparative studies of antiepileptics in NFLE have been published.
Related resources
- Hales RE, Yudofsky SC (eds). Textbook of neuropsychiatry (3rd ed). Washington, DC: American PsychiatricPublishing,1997. Specific chapters:
- Adams JM, Berkovic SF, Scheffer IE. Autosomal dominant nocturnal frontal lobe epilepsy. Gene Reviews. Available at: http://www.geneclinics.org/profiles/adnfle/. Accessed Dec. 22, 2003.
Drug brand names
- Carbamazepine • Tegretol
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levetiracetam • Keppra
- Oxcarbazepine • Trileptal
- Topiramate • Topamax
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Pagel JF. Nightmares and disorders of dreaming. Am Fam Phys 2000;61:2037-44.
2. Schenck CH. Parasomnias. Managing bizarre sleep-related behavior disorders. Postgrad Med 2000;107:145-56.
3. Schenck CH, Mahowald MW. Long-term, nightly benzodiazepine treatment of injurious parasomnias and other disorders of disrupted nocturnal sleep in 170 adults. Am J Med 1996;100:333-7.
4. Eisenman L, Attarian H. Sleep epilepsy. Neurology 2003;9:200-6.
5. Hirsch E, de Saint Martin A, Arzimanoglou A. New insights into the clinical management of partial epilepsies. Epilepsia 2000;41(suppl 5):S13-S17.
6. Zucconi M, Ferini-Strambi L. NREM parasomnias: arousal disorders and differentiation from nocturnal frontal lobe epilepsy. Clin Neurophysiol 2000;111(suppl 2):S129-S135.
7. Williamson PD, Jobst B. Frontal lobe epilepsy. Neocortical epilepsies. Adv Neurol 2000;84:215-42.
8. Leppert MF, Singh N. Susceptibility genes in human epilepsy. Semin Neurol 1999;19:397-405.
9. Itier V, Bertrand D. Mutations of the neuronal nicotinic acetylcholine receptors and their association with ADNFLE. Clin Neurophysiol 2002;32:99-107.
10. Motamedi GK, Lesser RP. Autosomal dominant nocturnal frontal lobe epilepsy. In: Fahn S, Frucht SJ, Halett M, Truong DD (eds). Myoclonus and paroxysmal dyskinesias. Advances in neurology, vol. 89. Philadelphia: Lippincott Williams & Wilkins, 2002;463-9.
11. Bertrand S, Weiland S, Berkovic SF, et al. Properties of neuronal nicotinic acetylcholine receptor mutants from humans suffering from autosomal dominant nocturnal frontal lobe epilepsy. Br. J Pharmacol 1998;125:751-60.
12. Brodie MJ, Chadwick DW, Anhut A, et al. Gabapentin versus lamotrigine monotherapy: a double-blind comparison in newly diagnosed epilepsy. Epilepsia 2002;43:993-1000.
13. Nieto-Barrera M, Brozmanova M, Capovilla G, et al. A comparison of monotherapy with lamotrigine or carbamazepine in patients with newly diagnosed partial epilepsy. Epilepsy Res 2001;46(2):145-55.
History: Terrors at age 8
Ms. J, age 35, began having sleepwalking episodes at age 8. At times they involved odd behaviors, such as carrying her brother’s shirt into the bathroom, placing it into the sink, and turning on the water.
As a child, Ms. J also began experiencing nocturnal awakenings characterized by panic and shouting. She sometimes saw a frightening image, usually of something falling on her. She would promptly return to sleep after each incident and had trouble remembering the event the next morning. The sleepwalking and awakening occurred monthly—more often when she was under stress or fatigued—until her early 20s.
At age 21, Ms. J. was under severe stress while preparing for a crucial graduate school examination and was losing much sleep. At this point, the episodes began to occur once or twice nightly.
She consulted a sleep specialist. EEG results were normal, but a sleep study was not helpful because she experienced no events that night. The specialist diagnosed Ms. J as having night terrors and prescribed clonazepam, 0.5 mg nightly. The agent did not prevent the events, but their frequency returned to baseline after Ms. J took her exam.
Were Ms. J’s clinical presentation and course consistent with night terrors? How would you treat her symptoms at this point?
The authors’ observations
Night terrors are an arousal disorder that usually begins in early childhood and affects 1% to 4% of the population.1 The disorder usually disappears before puberty.
Episodes of this parasomnia typically occur one to four times each month and can last several minutes. They are characterized by sudden awakenings with panic, disorientation, vocalization, and autonomic discharge. Patients sometimes see a frightening image. The events occur in stage 4 sleep, usually soon after falling asleep. Disorientation and a prompt return to sleep may follow.2 Sleeptalking and sleepwalking may also be present. The patient often cannot remember the event the next morning.
At this point, night terrors are a reasonable explanation for Ms. J’s nocturnal phenomena. Benzodiazepines, especially clonazepam, have been shown to decrease night terror frequency.3
Continued history: A new mother’s stress
At age 34, Ms. J gave birth to her first child. Weeks later, the nocturnal events began to occur at least three times nightly—every hour on some nights. Because their frequency disrupted her sleep, Ms. J constantly felt tired. Stress, emotional upset, and sleep deprivation exacerbated the events, which were stereotypical and included:
- sudden jerking of the right upper and/or lower extremities
- sudden sitting up and posing with the right arm flexed and internally rotated
- hallucinations of spiders or people
- sudden body flexion accompanied by an “electric shock” sensation in the head
- sitting up in bed, touching and picking at the sheets
- nonsensical speech after sitting up in bed
- sudden fear that Ms. J’s baby was hurt or dead, accompanied by searching the bed and under the pillow for the baby
- episodes of panic often accompanied by crying out, jumping out of bed and—in some cases—running.
Several times she ran down the stairs and out of the house while asleep. During one event, she jumped out of bed and fractured her foot. In another, she jumped from the bed and ran headfirst into a wall, causing bruising but no severe injury.
Each event was accompanied by confusion for 10 seconds to 3 minutes. Ms. J remembered about one-half the events; her husband described the remainder. She invariably returned to sleep immediately after each event.
A second sleep specialist diagnosed Ms. J as having night terrors. Unsatisfied with the diagnosis, she consulted a neurologist who specialized in epilepsy. The neurologist diagnosed her as having nocturnal frontal lobe epilepsy (NFLE) based on her history. A video EEG study—which showed spike and wave activity in the left frontal lobe during the nocturnal events—confirmed the diagnosis. The events all occurred during stage 2 sleep.
Is Ms. J’s latest diagnosis on target? Which clinical features in her case would differentiate sleep epilepsy from parasomnias?
The authors’ observations
Frontal lobe epilepsy can take many forms. Seizures can occur during sleep and/or while awake and consist of sudden, brief (<1 minute) motor attacks occurring in clusters. The prevalence of sleep epilepsy among persons with seizure disorders has been estimated at 7.5% to 45%, based on studies of small patient populations.4
Nocturnal frontal lobe seizures:
- occur only in non-REM (usually stage 2) sleep.
- can occur at any time of night
- usually begin in middle childhood to early adolescence, but onset in early childhood or adulthood has been reported.5 Seizures usually subside during adulthood (Table).6
Table
Characteristics of parasomnias and nocturnal epilepsy
| Nightmare (adult) | Night terror | Nocturnal epilepsy | |
|---|---|---|---|
| Incidence | 5 to 10% | 1 to 3% | Unknown |
| Sleep stage | During REM Anytime during the night the night | Stage 4 In first few hours of sleep | Often stage 2 Anytime during |
| Age of onset | Variable | Early childhood | Late childhood or adolescence Occasionally in adulthood |
| Change with age | Often diminishes with age May remit and recur | Diminishes with age Gone by young adulthood | Heterogeneous course May be less severe later in life |
| Symptoms | Frightening dreams Detailed story line No motor activity No injury | Inconsolable terror Not associated with dream Low-level motor activity Autonomic activation Injury rare | With or without fear and autonomic activation Hallucinations or illusions possible Stereotypical, paroxysmal motor activity Injury possible |
| Sleep resumption | Often delayed | Usually rapid | Usually rapid |
| Precipitating factors | PTSD Unusual stressors | PTSD Sleep deprivation | Sleep deprivation Physical and emotional stressors |
| Frequency | Irregular | 1 to 2 times per month or less | Extremely variable Can occur in clusters |
| Recollection | Variable | Often none | Variable |
| PTSD: Posttraumatic stress disorder | |||
These seizures are clinically polymorphous but stereotypical in each patient. Seizure type varies depending on which frontal lobe region is affected.
Nocturnal seizures universally have an explosive onset, with motor symptoms such as jerking, rocking, pelvic thrusting, tonic posturing, kicking, scrambling about, and touching the bed with one’s hand. Other possible occurrences include:
- sensory phenomena such as illusions and hallucinations, sensations of buzzing, vibration, and olfactory or gustatory sensations
- aphasia or other vocal events, such as laughing, screaming, or making odd noises
- fear and autonomic discharge simulating a night terror or panic attack.7
Confusion also is possible, although consciousness many times is preserved through the episode.
As with other seizures, sleep disruption exacerbates NFLE. Most patients have a normal interictal EEG.
Because NFLE is often misdiagnosed as a parasomnia, the psychiatrist needs to consider this disorder in the differential diagnosis. Any patient with a suspected parasomnia should be evaluated by a neurologist for NFLE if:
- the nocturnal events have not ceased by young adulthood
- events consist of prominent stereotypical motor symptoms that occur in clusters and/or have caused physical injury.
Extended history: Family stories
Ms. J’s neurologist asked whether any relatives have experienced similar nocturnal events.
Upon talking with family members, she learned that her aunt (her father’s sister) experienced nocturnal hallucinations and panic episodes well into her 50s. Her first cousin (her aunt’s daughter) also has nocturnal hallucinations and panic episodes and runs in her sleep. Two of her father’s cousins—twin brothers—were also affected. One of the brothers experienced explosive episodes, sometimes assaulting the other brother while asleep; he once had to be restrained from jumping out a window.
Other family members or surviving spouses described similar events that are clinically consistent with frontal lobe seizures. Interestingly, tic disorders run in the same branches of the family as the seizures.
Ms. J was diagnosed with autosomal dominant nocturnal frontal lobe epilepsy (ADNFLE) based on her diagnosis of NFLE and family history of similar events.
The authors’ observations
ADNFLE is an inherited disorder that displays 70% penetrance.8 Families in Australia, Canada, Spain, Japan, Korea, Germany, Great Britain, Italy, and Norway have been described with the disorder. No accurate prevalence data exist.9
Ms. J’s family traces its roots to Lithuania and White Russia (now Belarus) and is Ashkenazi Jewish. No literature describes the disorder in this population or these locations.
ADNFLE was the first genetic epilepsy to be associated with a defect in a single gene. It was recognized as a disorder in 1994, having previously been described with different names by multiple authors.
The disorderis a “channelopathy,” signifying a defective ion channel resulting in abnormal neuronal cell membrane conduction. The affected gene is the acetylcholine receptor, which is widely distributed in the brain. Missense mutations of the receptor gene lead to a change in an amino acid found in the center of the receptor pore. Ordinarily, the centers of ion channel pores are lined with hydrophobic amino acids to facilitate entrance of ions. The mutations in affected individuals result in a hydrophobic amino acid substitution. Different families display different mutations of the gene.10
In ADNFLE, there is mutation in the second transmembrane region of the alpha-4 subunit of the neuronal acetylcholine receptor. Defective receptors result in reduced channel permeability to calcium, causing fast desensitization and receptor hypoactivity. This has been postulated to cause an imbalance in excitatory/inhibitory synaptic transmission.11 Further study will elucidate the acetylcholine receptor’s relationship to brain functioning.
Treatment: Medication trial
Lamotrigine was started at 25 mg/d and titrated upward by 25 to 50 mg per week. When the dosage reached 500 mg/d, seizure frequency was reduced to once weekly.
Because Ms. J’s seizures were associated with stress and fatigue, she reduced her work hours and modified her job duties. Alcohol increased the frequency of the seizures, so she abstained from alcohol consumption. She also adhered to a consistent bedtime and slept at least 8 hours every night. After making these lifestyle modifications, Ms. J’s seizers decreased to once per month.
Why was lamotrigine chosen for Ms. J? What other drug options exist to treat sleep epilepsy?
The authors’ observations
Many clinicians consider carbamazepine the drug of choice for NFLE. Because NFLE is an epilepsy of partial onset, however, medications used to treat partial-onset epilepsy—including lamotrigine, topiramate, oxcarbazepine, gabapentin, and levetiracetam—are presumed to work as well. Because lamotrigine is considered the safest antiepileptic in pregnancy, the neurologist chose this agent for Ms. J.
Although comparative studies of antiepileptics for partial epilepsies have shown no difference in efficacy,12,13 no comparative studies of antiepileptics in NFLE have been published.
Related resources
- Hales RE, Yudofsky SC (eds). Textbook of neuropsychiatry (3rd ed). Washington, DC: American PsychiatricPublishing,1997. Specific chapters:
- Adams JM, Berkovic SF, Scheffer IE. Autosomal dominant nocturnal frontal lobe epilepsy. Gene Reviews. Available at: http://www.geneclinics.org/profiles/adnfle/. Accessed Dec. 22, 2003.
Drug brand names
- Carbamazepine • Tegretol
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levetiracetam • Keppra
- Oxcarbazepine • Trileptal
- Topiramate • Topamax
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
History: Terrors at age 8
Ms. J, age 35, began having sleepwalking episodes at age 8. At times they involved odd behaviors, such as carrying her brother’s shirt into the bathroom, placing it into the sink, and turning on the water.
As a child, Ms. J also began experiencing nocturnal awakenings characterized by panic and shouting. She sometimes saw a frightening image, usually of something falling on her. She would promptly return to sleep after each incident and had trouble remembering the event the next morning. The sleepwalking and awakening occurred monthly—more often when she was under stress or fatigued—until her early 20s.
At age 21, Ms. J. was under severe stress while preparing for a crucial graduate school examination and was losing much sleep. At this point, the episodes began to occur once or twice nightly.
She consulted a sleep specialist. EEG results were normal, but a sleep study was not helpful because she experienced no events that night. The specialist diagnosed Ms. J as having night terrors and prescribed clonazepam, 0.5 mg nightly. The agent did not prevent the events, but their frequency returned to baseline after Ms. J took her exam.
Were Ms. J’s clinical presentation and course consistent with night terrors? How would you treat her symptoms at this point?
The authors’ observations
Night terrors are an arousal disorder that usually begins in early childhood and affects 1% to 4% of the population.1 The disorder usually disappears before puberty.
Episodes of this parasomnia typically occur one to four times each month and can last several minutes. They are characterized by sudden awakenings with panic, disorientation, vocalization, and autonomic discharge. Patients sometimes see a frightening image. The events occur in stage 4 sleep, usually soon after falling asleep. Disorientation and a prompt return to sleep may follow.2 Sleeptalking and sleepwalking may also be present. The patient often cannot remember the event the next morning.
At this point, night terrors are a reasonable explanation for Ms. J’s nocturnal phenomena. Benzodiazepines, especially clonazepam, have been shown to decrease night terror frequency.3
Continued history: A new mother’s stress
At age 34, Ms. J gave birth to her first child. Weeks later, the nocturnal events began to occur at least three times nightly—every hour on some nights. Because their frequency disrupted her sleep, Ms. J constantly felt tired. Stress, emotional upset, and sleep deprivation exacerbated the events, which were stereotypical and included:
- sudden jerking of the right upper and/or lower extremities
- sudden sitting up and posing with the right arm flexed and internally rotated
- hallucinations of spiders or people
- sudden body flexion accompanied by an “electric shock” sensation in the head
- sitting up in bed, touching and picking at the sheets
- nonsensical speech after sitting up in bed
- sudden fear that Ms. J’s baby was hurt or dead, accompanied by searching the bed and under the pillow for the baby
- episodes of panic often accompanied by crying out, jumping out of bed and—in some cases—running.
Several times she ran down the stairs and out of the house while asleep. During one event, she jumped out of bed and fractured her foot. In another, she jumped from the bed and ran headfirst into a wall, causing bruising but no severe injury.
Each event was accompanied by confusion for 10 seconds to 3 minutes. Ms. J remembered about one-half the events; her husband described the remainder. She invariably returned to sleep immediately after each event.
A second sleep specialist diagnosed Ms. J as having night terrors. Unsatisfied with the diagnosis, she consulted a neurologist who specialized in epilepsy. The neurologist diagnosed her as having nocturnal frontal lobe epilepsy (NFLE) based on her history. A video EEG study—which showed spike and wave activity in the left frontal lobe during the nocturnal events—confirmed the diagnosis. The events all occurred during stage 2 sleep.
Is Ms. J’s latest diagnosis on target? Which clinical features in her case would differentiate sleep epilepsy from parasomnias?
The authors’ observations
Frontal lobe epilepsy can take many forms. Seizures can occur during sleep and/or while awake and consist of sudden, brief (<1 minute) motor attacks occurring in clusters. The prevalence of sleep epilepsy among persons with seizure disorders has been estimated at 7.5% to 45%, based on studies of small patient populations.4
Nocturnal frontal lobe seizures:
- occur only in non-REM (usually stage 2) sleep.
- can occur at any time of night
- usually begin in middle childhood to early adolescence, but onset in early childhood or adulthood has been reported.5 Seizures usually subside during adulthood (Table).6
Table
Characteristics of parasomnias and nocturnal epilepsy
| Nightmare (adult) | Night terror | Nocturnal epilepsy | |
|---|---|---|---|
| Incidence | 5 to 10% | 1 to 3% | Unknown |
| Sleep stage | During REM Anytime during the night the night | Stage 4 In first few hours of sleep | Often stage 2 Anytime during |
| Age of onset | Variable | Early childhood | Late childhood or adolescence Occasionally in adulthood |
| Change with age | Often diminishes with age May remit and recur | Diminishes with age Gone by young adulthood | Heterogeneous course May be less severe later in life |
| Symptoms | Frightening dreams Detailed story line No motor activity No injury | Inconsolable terror Not associated with dream Low-level motor activity Autonomic activation Injury rare | With or without fear and autonomic activation Hallucinations or illusions possible Stereotypical, paroxysmal motor activity Injury possible |
| Sleep resumption | Often delayed | Usually rapid | Usually rapid |
| Precipitating factors | PTSD Unusual stressors | PTSD Sleep deprivation | Sleep deprivation Physical and emotional stressors |
| Frequency | Irregular | 1 to 2 times per month or less | Extremely variable Can occur in clusters |
| Recollection | Variable | Often none | Variable |
| PTSD: Posttraumatic stress disorder | |||
These seizures are clinically polymorphous but stereotypical in each patient. Seizure type varies depending on which frontal lobe region is affected.
Nocturnal seizures universally have an explosive onset, with motor symptoms such as jerking, rocking, pelvic thrusting, tonic posturing, kicking, scrambling about, and touching the bed with one’s hand. Other possible occurrences include:
- sensory phenomena such as illusions and hallucinations, sensations of buzzing, vibration, and olfactory or gustatory sensations
- aphasia or other vocal events, such as laughing, screaming, or making odd noises
- fear and autonomic discharge simulating a night terror or panic attack.7
Confusion also is possible, although consciousness many times is preserved through the episode.
As with other seizures, sleep disruption exacerbates NFLE. Most patients have a normal interictal EEG.
Because NFLE is often misdiagnosed as a parasomnia, the psychiatrist needs to consider this disorder in the differential diagnosis. Any patient with a suspected parasomnia should be evaluated by a neurologist for NFLE if:
- the nocturnal events have not ceased by young adulthood
- events consist of prominent stereotypical motor symptoms that occur in clusters and/or have caused physical injury.
Extended history: Family stories
Ms. J’s neurologist asked whether any relatives have experienced similar nocturnal events.
Upon talking with family members, she learned that her aunt (her father’s sister) experienced nocturnal hallucinations and panic episodes well into her 50s. Her first cousin (her aunt’s daughter) also has nocturnal hallucinations and panic episodes and runs in her sleep. Two of her father’s cousins—twin brothers—were also affected. One of the brothers experienced explosive episodes, sometimes assaulting the other brother while asleep; he once had to be restrained from jumping out a window.
Other family members or surviving spouses described similar events that are clinically consistent with frontal lobe seizures. Interestingly, tic disorders run in the same branches of the family as the seizures.
Ms. J was diagnosed with autosomal dominant nocturnal frontal lobe epilepsy (ADNFLE) based on her diagnosis of NFLE and family history of similar events.
The authors’ observations
ADNFLE is an inherited disorder that displays 70% penetrance.8 Families in Australia, Canada, Spain, Japan, Korea, Germany, Great Britain, Italy, and Norway have been described with the disorder. No accurate prevalence data exist.9
Ms. J’s family traces its roots to Lithuania and White Russia (now Belarus) and is Ashkenazi Jewish. No literature describes the disorder in this population or these locations.
ADNFLE was the first genetic epilepsy to be associated with a defect in a single gene. It was recognized as a disorder in 1994, having previously been described with different names by multiple authors.
The disorderis a “channelopathy,” signifying a defective ion channel resulting in abnormal neuronal cell membrane conduction. The affected gene is the acetylcholine receptor, which is widely distributed in the brain. Missense mutations of the receptor gene lead to a change in an amino acid found in the center of the receptor pore. Ordinarily, the centers of ion channel pores are lined with hydrophobic amino acids to facilitate entrance of ions. The mutations in affected individuals result in a hydrophobic amino acid substitution. Different families display different mutations of the gene.10
In ADNFLE, there is mutation in the second transmembrane region of the alpha-4 subunit of the neuronal acetylcholine receptor. Defective receptors result in reduced channel permeability to calcium, causing fast desensitization and receptor hypoactivity. This has been postulated to cause an imbalance in excitatory/inhibitory synaptic transmission.11 Further study will elucidate the acetylcholine receptor’s relationship to brain functioning.
Treatment: Medication trial
Lamotrigine was started at 25 mg/d and titrated upward by 25 to 50 mg per week. When the dosage reached 500 mg/d, seizure frequency was reduced to once weekly.
Because Ms. J’s seizures were associated with stress and fatigue, she reduced her work hours and modified her job duties. Alcohol increased the frequency of the seizures, so she abstained from alcohol consumption. She also adhered to a consistent bedtime and slept at least 8 hours every night. After making these lifestyle modifications, Ms. J’s seizers decreased to once per month.
Why was lamotrigine chosen for Ms. J? What other drug options exist to treat sleep epilepsy?
The authors’ observations
Many clinicians consider carbamazepine the drug of choice for NFLE. Because NFLE is an epilepsy of partial onset, however, medications used to treat partial-onset epilepsy—including lamotrigine, topiramate, oxcarbazepine, gabapentin, and levetiracetam—are presumed to work as well. Because lamotrigine is considered the safest antiepileptic in pregnancy, the neurologist chose this agent for Ms. J.
Although comparative studies of antiepileptics for partial epilepsies have shown no difference in efficacy,12,13 no comparative studies of antiepileptics in NFLE have been published.
Related resources
- Hales RE, Yudofsky SC (eds). Textbook of neuropsychiatry (3rd ed). Washington, DC: American PsychiatricPublishing,1997. Specific chapters:
- Adams JM, Berkovic SF, Scheffer IE. Autosomal dominant nocturnal frontal lobe epilepsy. Gene Reviews. Available at: http://www.geneclinics.org/profiles/adnfle/. Accessed Dec. 22, 2003.
Drug brand names
- Carbamazepine • Tegretol
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levetiracetam • Keppra
- Oxcarbazepine • Trileptal
- Topiramate • Topamax
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Pagel JF. Nightmares and disorders of dreaming. Am Fam Phys 2000;61:2037-44.
2. Schenck CH. Parasomnias. Managing bizarre sleep-related behavior disorders. Postgrad Med 2000;107:145-56.
3. Schenck CH, Mahowald MW. Long-term, nightly benzodiazepine treatment of injurious parasomnias and other disorders of disrupted nocturnal sleep in 170 adults. Am J Med 1996;100:333-7.
4. Eisenman L, Attarian H. Sleep epilepsy. Neurology 2003;9:200-6.
5. Hirsch E, de Saint Martin A, Arzimanoglou A. New insights into the clinical management of partial epilepsies. Epilepsia 2000;41(suppl 5):S13-S17.
6. Zucconi M, Ferini-Strambi L. NREM parasomnias: arousal disorders and differentiation from nocturnal frontal lobe epilepsy. Clin Neurophysiol 2000;111(suppl 2):S129-S135.
7. Williamson PD, Jobst B. Frontal lobe epilepsy. Neocortical epilepsies. Adv Neurol 2000;84:215-42.
8. Leppert MF, Singh N. Susceptibility genes in human epilepsy. Semin Neurol 1999;19:397-405.
9. Itier V, Bertrand D. Mutations of the neuronal nicotinic acetylcholine receptors and their association with ADNFLE. Clin Neurophysiol 2002;32:99-107.
10. Motamedi GK, Lesser RP. Autosomal dominant nocturnal frontal lobe epilepsy. In: Fahn S, Frucht SJ, Halett M, Truong DD (eds). Myoclonus and paroxysmal dyskinesias. Advances in neurology, vol. 89. Philadelphia: Lippincott Williams & Wilkins, 2002;463-9.
11. Bertrand S, Weiland S, Berkovic SF, et al. Properties of neuronal nicotinic acetylcholine receptor mutants from humans suffering from autosomal dominant nocturnal frontal lobe epilepsy. Br. J Pharmacol 1998;125:751-60.
12. Brodie MJ, Chadwick DW, Anhut A, et al. Gabapentin versus lamotrigine monotherapy: a double-blind comparison in newly diagnosed epilepsy. Epilepsia 2002;43:993-1000.
13. Nieto-Barrera M, Brozmanova M, Capovilla G, et al. A comparison of monotherapy with lamotrigine or carbamazepine in patients with newly diagnosed partial epilepsy. Epilepsy Res 2001;46(2):145-55.
1. Pagel JF. Nightmares and disorders of dreaming. Am Fam Phys 2000;61:2037-44.
2. Schenck CH. Parasomnias. Managing bizarre sleep-related behavior disorders. Postgrad Med 2000;107:145-56.
3. Schenck CH, Mahowald MW. Long-term, nightly benzodiazepine treatment of injurious parasomnias and other disorders of disrupted nocturnal sleep in 170 adults. Am J Med 1996;100:333-7.
4. Eisenman L, Attarian H. Sleep epilepsy. Neurology 2003;9:200-6.
5. Hirsch E, de Saint Martin A, Arzimanoglou A. New insights into the clinical management of partial epilepsies. Epilepsia 2000;41(suppl 5):S13-S17.
6. Zucconi M, Ferini-Strambi L. NREM parasomnias: arousal disorders and differentiation from nocturnal frontal lobe epilepsy. Clin Neurophysiol 2000;111(suppl 2):S129-S135.
7. Williamson PD, Jobst B. Frontal lobe epilepsy. Neocortical epilepsies. Adv Neurol 2000;84:215-42.
8. Leppert MF, Singh N. Susceptibility genes in human epilepsy. Semin Neurol 1999;19:397-405.
9. Itier V, Bertrand D. Mutations of the neuronal nicotinic acetylcholine receptors and their association with ADNFLE. Clin Neurophysiol 2002;32:99-107.
10. Motamedi GK, Lesser RP. Autosomal dominant nocturnal frontal lobe epilepsy. In: Fahn S, Frucht SJ, Halett M, Truong DD (eds). Myoclonus and paroxysmal dyskinesias. Advances in neurology, vol. 89. Philadelphia: Lippincott Williams & Wilkins, 2002;463-9.
11. Bertrand S, Weiland S, Berkovic SF, et al. Properties of neuronal nicotinic acetylcholine receptor mutants from humans suffering from autosomal dominant nocturnal frontal lobe epilepsy. Br. J Pharmacol 1998;125:751-60.
12. Brodie MJ, Chadwick DW, Anhut A, et al. Gabapentin versus lamotrigine monotherapy: a double-blind comparison in newly diagnosed epilepsy. Epilepsia 2002;43:993-1000.
13. Nieto-Barrera M, Brozmanova M, Capovilla G, et al. A comparison of monotherapy with lamotrigine or carbamazepine in patients with newly diagnosed partial epilepsy. Epilepsy Res 2001;46(2):145-55.