User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Update on eating disorders Eating disorders: Which treatments are most effective
Compared with other psychiatric diagnoses, eating disorders are relatively new. Bulimia nervosa was first described as a distinct syndrome in 1979, Update on Eating Disorders.” In part 1 Harrison G. Pope, Jr., MD, and James I. Hudson, MD, ScD, of Harvard Medical School describe how to avoid undertreating bulimia nervosa. Future issues will feature insights on:
- anorexia nervosa by Katherine A. Halmi, MD, Weill Medical College of Cornell University
- binge eating by Susan L. McElroy, MD, Renu Kotwal, MD, and Rakesh M. Kaneria, MD, University of Cincinnati College of Medicine.
Rigorous clinical research by these experts and others has helped weed out unsubstantiated theories while providing empiric evidence of eating disorders’ biological and psychological roots. This series updates the evidence for choosing medications and psychotherapies that have shown the greatest therapeutic promise.

Paul E. Keck, Jr, MD
Deputy Editor, Current Psychiatry
Paul E. Keck, Jr, MD
Deputy Editor, Current Psychiatry
Paul E. Keck, Jr, MD
Deputy Editor, Current Psychiatry
Compared with other psychiatric diagnoses, eating disorders are relatively new. Bulimia nervosa was first described as a distinct syndrome in 1979, Update on Eating Disorders.” In part 1 Harrison G. Pope, Jr., MD, and James I. Hudson, MD, ScD, of Harvard Medical School describe how to avoid undertreating bulimia nervosa. Future issues will feature insights on:
- anorexia nervosa by Katherine A. Halmi, MD, Weill Medical College of Cornell University
- binge eating by Susan L. McElroy, MD, Renu Kotwal, MD, and Rakesh M. Kaneria, MD, University of Cincinnati College of Medicine.
Rigorous clinical research by these experts and others has helped weed out unsubstantiated theories while providing empiric evidence of eating disorders’ biological and psychological roots. This series updates the evidence for choosing medications and psychotherapies that have shown the greatest therapeutic promise.
Compared with other psychiatric diagnoses, eating disorders are relatively new. Bulimia nervosa was first described as a distinct syndrome in 1979, Update on Eating Disorders.” In part 1 Harrison G. Pope, Jr., MD, and James I. Hudson, MD, ScD, of Harvard Medical School describe how to avoid undertreating bulimia nervosa. Future issues will feature insights on:
- anorexia nervosa by Katherine A. Halmi, MD, Weill Medical College of Cornell University
- binge eating by Susan L. McElroy, MD, Renu Kotwal, MD, and Rakesh M. Kaneria, MD, University of Cincinnati College of Medicine.
Rigorous clinical research by these experts and others has helped weed out unsubstantiated theories while providing empiric evidence of eating disorders’ biological and psychological roots. This series updates the evidence for choosing medications and psychotherapies that have shown the greatest therapeutic promise.
When a patient threatens terrorism
Mr. Z, age 38, came to the United States from a predominantly Islamic country to study science and engineering. While in graduate school, he was seen by a primary care physician for complaints of hypersomnia; reduced appetite with an approximate 15-lb weight loss; impaired concentration and memory, which hurt his academic performance; low energy; and occasional thoughts about dying.
Mr. Z’s physical examination and lab results were unremarkable, and he reported no psychiatric history. He was diagnosed with depression and was prescribed sertraline, 50 mg/d, but he refused to take it. He declined referral to a psychiatrist but agreed to weekly psychotherapy with a psychology intern at the student mental health center.
During therapy, Mr. Z said he constantly felt lonely. He feared being ostracized because of his Islamic beliefs and lifestyle, yet reported tremendous guilt over violating Islamic codes forbidding premarital sex. He told his therapist that his longing for a romantic relationship was “contaminating” his soul, and fantasized that death would free him of impure, sexual thoughts.
The severity of Mr. Z’s depression and his preoccupation with death alarmed the therapist. She referred him to a clinic psychiatrist, but Mr. Z refused to see him, saying that his depression was a punishment from God for his sexual sins. He vowed to repent by undergoing psychotherapy.
Continued therapy: A ‘religious awakening’
During the first 4 months of therapy, Mr. Z’s Beck Depression Inventory score fell from 32 to 17, indicating mild depression.
Mr. Z then reported that he experienced a “religious awakening” and began describing his mood and experiences in religious terms. He thanked his therapist for “saving his soul.”
The therapist was stunned by Mr. Z’s sudden transformation in mood and affect. He slept 7 to 8 hours a night, and his academic performance improved dramatically. He exhibited stable (though bright) affect and no thought disorder. His therapist viewed his use of religious terminology, though significant, as a cultural artifact because there were no signs of psychosis. Although no objective signs of mania or hypomania were apparent, the therapist suspected he might have bipolar disorder. She again tried unsuccessfully to refer him to a psychiatrist.
Then came Sept. 11, 2001.
Mr. Z was traumatized by the terrorist attacks on the World Trade Center and the Pentagon. He feared a backlash against Muslims in the United States but showed no signs of paranoia.
A few months later, however, Mr. Z became preoccupied with the attacks and harbored conspiracy theories alleging that the United States government had committed them. His speech was rapid and pressured, and he slept only 2 to 3 hours nightly. We later learned that he had not attended class for months and only sporadically showed up for lab work.
Mr. Z then began to fear he was under surveillance and that his visa would be revoked. His affect became increasingly intense during psychotherapy, and he frequently used religious metaphors and concepts. His therapist realized he was suffering a worsening manic episode, although suicidal or homicidal thoughts were not present.
Down with ‘nonbelievers’
During a subsequent session, Mr. Z reported that he had become engaged to marry a well-known supermodel. He also announced a plan to “rid the world of nonbelievers”—people who were not devout Christians, Jews, or Muslims. His three-stage plan called for:
- gently persuading nonbelievers to change their beliefs and lifestyles
- threatening nonbelievers who did not repent after polite persuasion
- “eliminating all the nonbelievers” who did not respond to intimidation.
Mr. Z viewed his therapist as “commander of the believers” and considered the three-phased plan to be her will. She questioned Mr. Z extensively about how, when, and against whom he intended to carry out this plan. He identified no specific targets, but did say, “I’ll know what do to when the time comes. I am an engineer, and I know a lot about explosives.”
The therapist then recommended an emergency psychiatric evaluation, which Mr. Z declined. She immediately notified the mental health clinic’s attending psychiatrist.
What are the therapist’s options? Can Mr. Z be involuntarily committed based on his threats of violence against “nonbelievers?”
Dr. Kennedy’s and Dr. Klafter’s observations
Two legal principles justify involuntary commitment of a patient who poses a threat to himself or the public:
Police power refers to the government’s role in maintaining public safety. State commitment statutes usually require that a mentally ill person pose a significant and imminent threat to the public. The psychiatrist who files an affidavit alleging danger does not need absolute certainty or perfect information but must act in good faith.1
Parens patriae, or paternalism, refers to government intervention on behalf of persons incapable of managing their lives.1
Psychiatric treatment of unwilling patients is possible in some states. Family members and/or mental health professionals can petition the court to compel outpatient psychiatric treatment.
Because an emergency evaluation produces a thorough and controlled psychiatric assessment (and minimal deprivation of personal liberty), a psychiatrist with any doubt about the patient’s condition should move toward commitment.
Psychiatric patients can be involuntarily committed through a two-step process: emergency hospitalization and judicial commitment.
Laws vary from state to state but they usually allow mental health professionals and law enforcement officials to complete a written statement documenting their belief that an individual suffers from a mental illness and poses substantial danger to self or others.
This form allows police to civilly arrest and transport the individual to a hospital for an emergency evaluation. The hospital then must complete the evaluation within a specified period, usually 24 hours.
If the evaluator finds that the individual is mentally ill and dangerous, he or she must then file an affidavit with the probate court, again within a specified period.
A court hearing is then scheduled. The individual is usually granted due-process rights, including the right to an attorney and an independent psychiatric evaluation. The judge then must decide whether the individual is mentally ill and dangerous, usually based on a “clear and convincing” evidence standard.
Before resorting to legal coercion, try scheduling more-frequent appointments to monitor symptom progression. This would allow faster response when civil commitment criteria are met.
A psychiatrist or other mental health professional can request an emergency evaluation based on information from a knowledgeable intermediary or family member—even if the clinician did not recently or directly interview the patient.2 For example, a psychologist could receive information from a case manager who encountered the patient decompensating. It would be impractical to require a psychiatrist to see a decompensating patient before an evaluation can be ordered.
Hospitalization: A ‘blood-drinking monster’
With no security staff immediately available, the attending psychiatrist and therapist sent Mr. Z home.
The psychiatrist then submitted an application for involuntary hospitalization—in which the doctor summarized the case—and faxed it to the local psychiatric emergency service. The police were notified and—after verifying that the appropriate paperwork had been completed—arrested Mr. Z at his home and brought him to the emergency service for an assessment. Mr. Z was then hospitalized. (Box 1).
Mr. Z was found to be harboring bizarre, grandiose, persecutory, and religious delusions. He claimed that a blood-drinking monster was lurking inside the hospital, and that his hospitalization was part of a conspiracy to persecute Muslims. He considered the Sept. 11 attacks fictitious and claimed that widely broadcast television news footage of the attacks was a computer-animated video. The patient refused all medications while hospitalized.
After 3 days, the court ordered Mr. Z’s discharge, citing lack of evidence that he posed any danger to self or others. At his mental health probate hearing, he managed to conceal his psychotic symptoms while testifying. The court expressed concern over his technical training in explosives but ruled that he was not dangerous because he had never used this knowledge to commit violence.
Upon discharge, Mr. Z declined outpatient psychiatric treatment. The therapist then told Mr. Z that she would terminate psychotherapy after two sessions unless he visited a psychiatrist. Mr. Z again refused, and psychotherapy was terminated.
Although 30 days’ notice is generally appropriate for terminating a provider-patient relationship, a longer or shorter period may be needed depending on:
- Reason for termination. Immediate termination can be justified if the patient has assaulted or threatened the clinician.
- Provider-patient relationship duration. In general, the shorter the relationship, the more leeway there is toward shortening the required notice.
- Type of care being provided. Psychiatric care involving medications or highly intensive interventions calls for longer notice to effect a smooth transition to the next caregiver.
- Availability of alternatives. The general wait time to obtain a new-intake appointment with another psychiatrist needs to be factored into the length of notice.
Letters and notes regarding termination can be used as evidence in court proceedings. When judging a patient abandonment case, the courts will rely on documentation of the reasons for termination and the process used to end treatment.
Source: Slovenko R. Law in psychiatry. New York: Brunner-Routledge, 2002:770-1.
Would you terminate psychotherapy at this point? Could the therapist’s actions be viewed as patient abandonment?
Dr. Kennedy’s and Dr. Klafter’s observations
The formation of a professional relationship establishes a duty of care and requires the clinician to provide reasonable notice of termination and alternative sources of care. Although 30 days’ notice is generally appropriate, several factors may dictate the need for more or less notice (Box 2).
In Mr. Z’s case, we view the psychologist’s behavior as appropriate because:
- Without psychotropics, Mr. Z’s psychosis would likely persist. To continue treating him with psychotherapy alone would fall below the standard of care.
- By threatening to terminate psychotherapy, the therapist tried to use the patient’s transference and desire to maintain the therapeutic relationship as an incentive to accept medication.
Continued observation: A clue from the past
Mr. Z’s brother, who was contacted by the treatment team, reported that the patient had never been violent. He did note, however, that as an adolescent Mr. Z talked about joining a terrorist organization, though he had never followed through. The brother tried to persuade Mr. Z to leave school and live with him on the West Coast, but he instead chose to continue his studies.
Mr. Z’s hospital treatment team realized that his continued work in engineering—where he had access to explosive materials—posed a significant risk given his impaired judgment. Acting on a forensic expert’s advice, the team warned university officials about Mr. Z’s mental state and preoccupation with violence. The FBI was also contacted.
Was the treatment team justified in reporting Mr. Z’s behavior to authorities, even though he never identified any potential victims?
Dr. Kennedy’s and Dr. Klafter’s observations
Various legislative and judicial remedies—some more restrictive than others—address the psychiatrist’s duty to third parties:3
- Some states require psychiatrists to notify or protect third parties when any danger is foreseeable, regardless of threat or victim.
- Other states require specific threats but charge the psychiatrist with foreseeing all potential victims regardless of whether they were named.
- Still other states limit protection to identifiable victims, even if no threat is issued.
- In some states the psychiatrist is responsible only if the patient makes specific threats to identifiable victims.
Again, psychiatrists need to make their best professional judgments in good faith about risk of violence. Hospitalizing a threatening patient provides the most protection to third parties, but this option is intrusive, coercive, and is not always appropriate or feasible. If the threat is directed toward the public rather than specific individuals or groups, law enforcement agencies can reduce the risk somewhat through monitoring and surveillance.
Although it is a judgment call, clinicians should notify:
- all persons or organizations against whom a patient might commit violence
- and those who might be targeted as instruments for violence towards others, such as family members who have guns the patient could obtain.
A terrorist would not likely seek psychiatric help relative to his goals of terrorism because such behavior is not rooted in major mental illness. However, the heightened sense of paranoia and anxiety created by events involving terrorism, religious animosity, and hatred provide patients who struggle with psychosis an outlet for their paranoia. As such, we should take a patient’s terroristic threats seriously.
Conclusion: Going home
The university granted Mr. Z medical leave and placed him on academic probation for 2 months, during which he returned to his native country to stay with his parents.
The faculty later dismissed Mr. Z from the program, citing poor academic and laboratory performance. His visa expired, with renewal contingent upon enrollment in a full-time academic program.
Related resources
- American Academy of Psychiatry and the Law. www.aapl.org.
Drug brand names
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Mr. Z, age 38, came to the United States from a predominantly Islamic country to study science and engineering. While in graduate school, he was seen by a primary care physician for complaints of hypersomnia; reduced appetite with an approximate 15-lb weight loss; impaired concentration and memory, which hurt his academic performance; low energy; and occasional thoughts about dying.
Mr. Z’s physical examination and lab results were unremarkable, and he reported no psychiatric history. He was diagnosed with depression and was prescribed sertraline, 50 mg/d, but he refused to take it. He declined referral to a psychiatrist but agreed to weekly psychotherapy with a psychology intern at the student mental health center.
During therapy, Mr. Z said he constantly felt lonely. He feared being ostracized because of his Islamic beliefs and lifestyle, yet reported tremendous guilt over violating Islamic codes forbidding premarital sex. He told his therapist that his longing for a romantic relationship was “contaminating” his soul, and fantasized that death would free him of impure, sexual thoughts.
The severity of Mr. Z’s depression and his preoccupation with death alarmed the therapist. She referred him to a clinic psychiatrist, but Mr. Z refused to see him, saying that his depression was a punishment from God for his sexual sins. He vowed to repent by undergoing psychotherapy.
Continued therapy: A ‘religious awakening’
During the first 4 months of therapy, Mr. Z’s Beck Depression Inventory score fell from 32 to 17, indicating mild depression.
Mr. Z then reported that he experienced a “religious awakening” and began describing his mood and experiences in religious terms. He thanked his therapist for “saving his soul.”
The therapist was stunned by Mr. Z’s sudden transformation in mood and affect. He slept 7 to 8 hours a night, and his academic performance improved dramatically. He exhibited stable (though bright) affect and no thought disorder. His therapist viewed his use of religious terminology, though significant, as a cultural artifact because there were no signs of psychosis. Although no objective signs of mania or hypomania were apparent, the therapist suspected he might have bipolar disorder. She again tried unsuccessfully to refer him to a psychiatrist.
Then came Sept. 11, 2001.
Mr. Z was traumatized by the terrorist attacks on the World Trade Center and the Pentagon. He feared a backlash against Muslims in the United States but showed no signs of paranoia.
A few months later, however, Mr. Z became preoccupied with the attacks and harbored conspiracy theories alleging that the United States government had committed them. His speech was rapid and pressured, and he slept only 2 to 3 hours nightly. We later learned that he had not attended class for months and only sporadically showed up for lab work.
Mr. Z then began to fear he was under surveillance and that his visa would be revoked. His affect became increasingly intense during psychotherapy, and he frequently used religious metaphors and concepts. His therapist realized he was suffering a worsening manic episode, although suicidal or homicidal thoughts were not present.
Down with ‘nonbelievers’
During a subsequent session, Mr. Z reported that he had become engaged to marry a well-known supermodel. He also announced a plan to “rid the world of nonbelievers”—people who were not devout Christians, Jews, or Muslims. His three-stage plan called for:
- gently persuading nonbelievers to change their beliefs and lifestyles
- threatening nonbelievers who did not repent after polite persuasion
- “eliminating all the nonbelievers” who did not respond to intimidation.
Mr. Z viewed his therapist as “commander of the believers” and considered the three-phased plan to be her will. She questioned Mr. Z extensively about how, when, and against whom he intended to carry out this plan. He identified no specific targets, but did say, “I’ll know what do to when the time comes. I am an engineer, and I know a lot about explosives.”
The therapist then recommended an emergency psychiatric evaluation, which Mr. Z declined. She immediately notified the mental health clinic’s attending psychiatrist.
What are the therapist’s options? Can Mr. Z be involuntarily committed based on his threats of violence against “nonbelievers?”
Dr. Kennedy’s and Dr. Klafter’s observations
Two legal principles justify involuntary commitment of a patient who poses a threat to himself or the public:
Police power refers to the government’s role in maintaining public safety. State commitment statutes usually require that a mentally ill person pose a significant and imminent threat to the public. The psychiatrist who files an affidavit alleging danger does not need absolute certainty or perfect information but must act in good faith.1
Parens patriae, or paternalism, refers to government intervention on behalf of persons incapable of managing their lives.1
Psychiatric treatment of unwilling patients is possible in some states. Family members and/or mental health professionals can petition the court to compel outpatient psychiatric treatment.
Because an emergency evaluation produces a thorough and controlled psychiatric assessment (and minimal deprivation of personal liberty), a psychiatrist with any doubt about the patient’s condition should move toward commitment.
Psychiatric patients can be involuntarily committed through a two-step process: emergency hospitalization and judicial commitment.
Laws vary from state to state but they usually allow mental health professionals and law enforcement officials to complete a written statement documenting their belief that an individual suffers from a mental illness and poses substantial danger to self or others.
This form allows police to civilly arrest and transport the individual to a hospital for an emergency evaluation. The hospital then must complete the evaluation within a specified period, usually 24 hours.
If the evaluator finds that the individual is mentally ill and dangerous, he or she must then file an affidavit with the probate court, again within a specified period.
A court hearing is then scheduled. The individual is usually granted due-process rights, including the right to an attorney and an independent psychiatric evaluation. The judge then must decide whether the individual is mentally ill and dangerous, usually based on a “clear and convincing” evidence standard.
Before resorting to legal coercion, try scheduling more-frequent appointments to monitor symptom progression. This would allow faster response when civil commitment criteria are met.
A psychiatrist or other mental health professional can request an emergency evaluation based on information from a knowledgeable intermediary or family member—even if the clinician did not recently or directly interview the patient.2 For example, a psychologist could receive information from a case manager who encountered the patient decompensating. It would be impractical to require a psychiatrist to see a decompensating patient before an evaluation can be ordered.
Hospitalization: A ‘blood-drinking monster’
With no security staff immediately available, the attending psychiatrist and therapist sent Mr. Z home.
The psychiatrist then submitted an application for involuntary hospitalization—in which the doctor summarized the case—and faxed it to the local psychiatric emergency service. The police were notified and—after verifying that the appropriate paperwork had been completed—arrested Mr. Z at his home and brought him to the emergency service for an assessment. Mr. Z was then hospitalized. (Box 1).
Mr. Z was found to be harboring bizarre, grandiose, persecutory, and religious delusions. He claimed that a blood-drinking monster was lurking inside the hospital, and that his hospitalization was part of a conspiracy to persecute Muslims. He considered the Sept. 11 attacks fictitious and claimed that widely broadcast television news footage of the attacks was a computer-animated video. The patient refused all medications while hospitalized.
After 3 days, the court ordered Mr. Z’s discharge, citing lack of evidence that he posed any danger to self or others. At his mental health probate hearing, he managed to conceal his psychotic symptoms while testifying. The court expressed concern over his technical training in explosives but ruled that he was not dangerous because he had never used this knowledge to commit violence.
Upon discharge, Mr. Z declined outpatient psychiatric treatment. The therapist then told Mr. Z that she would terminate psychotherapy after two sessions unless he visited a psychiatrist. Mr. Z again refused, and psychotherapy was terminated.
Although 30 days’ notice is generally appropriate for terminating a provider-patient relationship, a longer or shorter period may be needed depending on:
- Reason for termination. Immediate termination can be justified if the patient has assaulted or threatened the clinician.
- Provider-patient relationship duration. In general, the shorter the relationship, the more leeway there is toward shortening the required notice.
- Type of care being provided. Psychiatric care involving medications or highly intensive interventions calls for longer notice to effect a smooth transition to the next caregiver.
- Availability of alternatives. The general wait time to obtain a new-intake appointment with another psychiatrist needs to be factored into the length of notice.
Letters and notes regarding termination can be used as evidence in court proceedings. When judging a patient abandonment case, the courts will rely on documentation of the reasons for termination and the process used to end treatment.
Source: Slovenko R. Law in psychiatry. New York: Brunner-Routledge, 2002:770-1.
Would you terminate psychotherapy at this point? Could the therapist’s actions be viewed as patient abandonment?
Dr. Kennedy’s and Dr. Klafter’s observations
The formation of a professional relationship establishes a duty of care and requires the clinician to provide reasonable notice of termination and alternative sources of care. Although 30 days’ notice is generally appropriate, several factors may dictate the need for more or less notice (Box 2).
In Mr. Z’s case, we view the psychologist’s behavior as appropriate because:
- Without psychotropics, Mr. Z’s psychosis would likely persist. To continue treating him with psychotherapy alone would fall below the standard of care.
- By threatening to terminate psychotherapy, the therapist tried to use the patient’s transference and desire to maintain the therapeutic relationship as an incentive to accept medication.
Continued observation: A clue from the past
Mr. Z’s brother, who was contacted by the treatment team, reported that the patient had never been violent. He did note, however, that as an adolescent Mr. Z talked about joining a terrorist organization, though he had never followed through. The brother tried to persuade Mr. Z to leave school and live with him on the West Coast, but he instead chose to continue his studies.
Mr. Z’s hospital treatment team realized that his continued work in engineering—where he had access to explosive materials—posed a significant risk given his impaired judgment. Acting on a forensic expert’s advice, the team warned university officials about Mr. Z’s mental state and preoccupation with violence. The FBI was also contacted.
Was the treatment team justified in reporting Mr. Z’s behavior to authorities, even though he never identified any potential victims?
Dr. Kennedy’s and Dr. Klafter’s observations
Various legislative and judicial remedies—some more restrictive than others—address the psychiatrist’s duty to third parties:3
- Some states require psychiatrists to notify or protect third parties when any danger is foreseeable, regardless of threat or victim.
- Other states require specific threats but charge the psychiatrist with foreseeing all potential victims regardless of whether they were named.
- Still other states limit protection to identifiable victims, even if no threat is issued.
- In some states the psychiatrist is responsible only if the patient makes specific threats to identifiable victims.
Again, psychiatrists need to make their best professional judgments in good faith about risk of violence. Hospitalizing a threatening patient provides the most protection to third parties, but this option is intrusive, coercive, and is not always appropriate or feasible. If the threat is directed toward the public rather than specific individuals or groups, law enforcement agencies can reduce the risk somewhat through monitoring and surveillance.
Although it is a judgment call, clinicians should notify:
- all persons or organizations against whom a patient might commit violence
- and those who might be targeted as instruments for violence towards others, such as family members who have guns the patient could obtain.
A terrorist would not likely seek psychiatric help relative to his goals of terrorism because such behavior is not rooted in major mental illness. However, the heightened sense of paranoia and anxiety created by events involving terrorism, religious animosity, and hatred provide patients who struggle with psychosis an outlet for their paranoia. As such, we should take a patient’s terroristic threats seriously.
Conclusion: Going home
The university granted Mr. Z medical leave and placed him on academic probation for 2 months, during which he returned to his native country to stay with his parents.
The faculty later dismissed Mr. Z from the program, citing poor academic and laboratory performance. His visa expired, with renewal contingent upon enrollment in a full-time academic program.
Related resources
- American Academy of Psychiatry and the Law. www.aapl.org.
Drug brand names
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Mr. Z, age 38, came to the United States from a predominantly Islamic country to study science and engineering. While in graduate school, he was seen by a primary care physician for complaints of hypersomnia; reduced appetite with an approximate 15-lb weight loss; impaired concentration and memory, which hurt his academic performance; low energy; and occasional thoughts about dying.
Mr. Z’s physical examination and lab results were unremarkable, and he reported no psychiatric history. He was diagnosed with depression and was prescribed sertraline, 50 mg/d, but he refused to take it. He declined referral to a psychiatrist but agreed to weekly psychotherapy with a psychology intern at the student mental health center.
During therapy, Mr. Z said he constantly felt lonely. He feared being ostracized because of his Islamic beliefs and lifestyle, yet reported tremendous guilt over violating Islamic codes forbidding premarital sex. He told his therapist that his longing for a romantic relationship was “contaminating” his soul, and fantasized that death would free him of impure, sexual thoughts.
The severity of Mr. Z’s depression and his preoccupation with death alarmed the therapist. She referred him to a clinic psychiatrist, but Mr. Z refused to see him, saying that his depression was a punishment from God for his sexual sins. He vowed to repent by undergoing psychotherapy.
Continued therapy: A ‘religious awakening’
During the first 4 months of therapy, Mr. Z’s Beck Depression Inventory score fell from 32 to 17, indicating mild depression.
Mr. Z then reported that he experienced a “religious awakening” and began describing his mood and experiences in religious terms. He thanked his therapist for “saving his soul.”
The therapist was stunned by Mr. Z’s sudden transformation in mood and affect. He slept 7 to 8 hours a night, and his academic performance improved dramatically. He exhibited stable (though bright) affect and no thought disorder. His therapist viewed his use of religious terminology, though significant, as a cultural artifact because there were no signs of psychosis. Although no objective signs of mania or hypomania were apparent, the therapist suspected he might have bipolar disorder. She again tried unsuccessfully to refer him to a psychiatrist.
Then came Sept. 11, 2001.
Mr. Z was traumatized by the terrorist attacks on the World Trade Center and the Pentagon. He feared a backlash against Muslims in the United States but showed no signs of paranoia.
A few months later, however, Mr. Z became preoccupied with the attacks and harbored conspiracy theories alleging that the United States government had committed them. His speech was rapid and pressured, and he slept only 2 to 3 hours nightly. We later learned that he had not attended class for months and only sporadically showed up for lab work.
Mr. Z then began to fear he was under surveillance and that his visa would be revoked. His affect became increasingly intense during psychotherapy, and he frequently used religious metaphors and concepts. His therapist realized he was suffering a worsening manic episode, although suicidal or homicidal thoughts were not present.
Down with ‘nonbelievers’
During a subsequent session, Mr. Z reported that he had become engaged to marry a well-known supermodel. He also announced a plan to “rid the world of nonbelievers”—people who were not devout Christians, Jews, or Muslims. His three-stage plan called for:
- gently persuading nonbelievers to change their beliefs and lifestyles
- threatening nonbelievers who did not repent after polite persuasion
- “eliminating all the nonbelievers” who did not respond to intimidation.
Mr. Z viewed his therapist as “commander of the believers” and considered the three-phased plan to be her will. She questioned Mr. Z extensively about how, when, and against whom he intended to carry out this plan. He identified no specific targets, but did say, “I’ll know what do to when the time comes. I am an engineer, and I know a lot about explosives.”
The therapist then recommended an emergency psychiatric evaluation, which Mr. Z declined. She immediately notified the mental health clinic’s attending psychiatrist.
What are the therapist’s options? Can Mr. Z be involuntarily committed based on his threats of violence against “nonbelievers?”
Dr. Kennedy’s and Dr. Klafter’s observations
Two legal principles justify involuntary commitment of a patient who poses a threat to himself or the public:
Police power refers to the government’s role in maintaining public safety. State commitment statutes usually require that a mentally ill person pose a significant and imminent threat to the public. The psychiatrist who files an affidavit alleging danger does not need absolute certainty or perfect information but must act in good faith.1
Parens patriae, or paternalism, refers to government intervention on behalf of persons incapable of managing their lives.1
Psychiatric treatment of unwilling patients is possible in some states. Family members and/or mental health professionals can petition the court to compel outpatient psychiatric treatment.
Because an emergency evaluation produces a thorough and controlled psychiatric assessment (and minimal deprivation of personal liberty), a psychiatrist with any doubt about the patient’s condition should move toward commitment.
Psychiatric patients can be involuntarily committed through a two-step process: emergency hospitalization and judicial commitment.
Laws vary from state to state but they usually allow mental health professionals and law enforcement officials to complete a written statement documenting their belief that an individual suffers from a mental illness and poses substantial danger to self or others.
This form allows police to civilly arrest and transport the individual to a hospital for an emergency evaluation. The hospital then must complete the evaluation within a specified period, usually 24 hours.
If the evaluator finds that the individual is mentally ill and dangerous, he or she must then file an affidavit with the probate court, again within a specified period.
A court hearing is then scheduled. The individual is usually granted due-process rights, including the right to an attorney and an independent psychiatric evaluation. The judge then must decide whether the individual is mentally ill and dangerous, usually based on a “clear and convincing” evidence standard.
Before resorting to legal coercion, try scheduling more-frequent appointments to monitor symptom progression. This would allow faster response when civil commitment criteria are met.
A psychiatrist or other mental health professional can request an emergency evaluation based on information from a knowledgeable intermediary or family member—even if the clinician did not recently or directly interview the patient.2 For example, a psychologist could receive information from a case manager who encountered the patient decompensating. It would be impractical to require a psychiatrist to see a decompensating patient before an evaluation can be ordered.
Hospitalization: A ‘blood-drinking monster’
With no security staff immediately available, the attending psychiatrist and therapist sent Mr. Z home.
The psychiatrist then submitted an application for involuntary hospitalization—in which the doctor summarized the case—and faxed it to the local psychiatric emergency service. The police were notified and—after verifying that the appropriate paperwork had been completed—arrested Mr. Z at his home and brought him to the emergency service for an assessment. Mr. Z was then hospitalized. (Box 1).
Mr. Z was found to be harboring bizarre, grandiose, persecutory, and religious delusions. He claimed that a blood-drinking monster was lurking inside the hospital, and that his hospitalization was part of a conspiracy to persecute Muslims. He considered the Sept. 11 attacks fictitious and claimed that widely broadcast television news footage of the attacks was a computer-animated video. The patient refused all medications while hospitalized.
After 3 days, the court ordered Mr. Z’s discharge, citing lack of evidence that he posed any danger to self or others. At his mental health probate hearing, he managed to conceal his psychotic symptoms while testifying. The court expressed concern over his technical training in explosives but ruled that he was not dangerous because he had never used this knowledge to commit violence.
Upon discharge, Mr. Z declined outpatient psychiatric treatment. The therapist then told Mr. Z that she would terminate psychotherapy after two sessions unless he visited a psychiatrist. Mr. Z again refused, and psychotherapy was terminated.
Although 30 days’ notice is generally appropriate for terminating a provider-patient relationship, a longer or shorter period may be needed depending on:
- Reason for termination. Immediate termination can be justified if the patient has assaulted or threatened the clinician.
- Provider-patient relationship duration. In general, the shorter the relationship, the more leeway there is toward shortening the required notice.
- Type of care being provided. Psychiatric care involving medications or highly intensive interventions calls for longer notice to effect a smooth transition to the next caregiver.
- Availability of alternatives. The general wait time to obtain a new-intake appointment with another psychiatrist needs to be factored into the length of notice.
Letters and notes regarding termination can be used as evidence in court proceedings. When judging a patient abandonment case, the courts will rely on documentation of the reasons for termination and the process used to end treatment.
Source: Slovenko R. Law in psychiatry. New York: Brunner-Routledge, 2002:770-1.
Would you terminate psychotherapy at this point? Could the therapist’s actions be viewed as patient abandonment?
Dr. Kennedy’s and Dr. Klafter’s observations
The formation of a professional relationship establishes a duty of care and requires the clinician to provide reasonable notice of termination and alternative sources of care. Although 30 days’ notice is generally appropriate, several factors may dictate the need for more or less notice (Box 2).
In Mr. Z’s case, we view the psychologist’s behavior as appropriate because:
- Without psychotropics, Mr. Z’s psychosis would likely persist. To continue treating him with psychotherapy alone would fall below the standard of care.
- By threatening to terminate psychotherapy, the therapist tried to use the patient’s transference and desire to maintain the therapeutic relationship as an incentive to accept medication.
Continued observation: A clue from the past
Mr. Z’s brother, who was contacted by the treatment team, reported that the patient had never been violent. He did note, however, that as an adolescent Mr. Z talked about joining a terrorist organization, though he had never followed through. The brother tried to persuade Mr. Z to leave school and live with him on the West Coast, but he instead chose to continue his studies.
Mr. Z’s hospital treatment team realized that his continued work in engineering—where he had access to explosive materials—posed a significant risk given his impaired judgment. Acting on a forensic expert’s advice, the team warned university officials about Mr. Z’s mental state and preoccupation with violence. The FBI was also contacted.
Was the treatment team justified in reporting Mr. Z’s behavior to authorities, even though he never identified any potential victims?
Dr. Kennedy’s and Dr. Klafter’s observations
Various legislative and judicial remedies—some more restrictive than others—address the psychiatrist’s duty to third parties:3
- Some states require psychiatrists to notify or protect third parties when any danger is foreseeable, regardless of threat or victim.
- Other states require specific threats but charge the psychiatrist with foreseeing all potential victims regardless of whether they were named.
- Still other states limit protection to identifiable victims, even if no threat is issued.
- In some states the psychiatrist is responsible only if the patient makes specific threats to identifiable victims.
Again, psychiatrists need to make their best professional judgments in good faith about risk of violence. Hospitalizing a threatening patient provides the most protection to third parties, but this option is intrusive, coercive, and is not always appropriate or feasible. If the threat is directed toward the public rather than specific individuals or groups, law enforcement agencies can reduce the risk somewhat through monitoring and surveillance.
Although it is a judgment call, clinicians should notify:
- all persons or organizations against whom a patient might commit violence
- and those who might be targeted as instruments for violence towards others, such as family members who have guns the patient could obtain.
A terrorist would not likely seek psychiatric help relative to his goals of terrorism because such behavior is not rooted in major mental illness. However, the heightened sense of paranoia and anxiety created by events involving terrorism, religious animosity, and hatred provide patients who struggle with psychosis an outlet for their paranoia. As such, we should take a patient’s terroristic threats seriously.
Conclusion: Going home
The university granted Mr. Z medical leave and placed him on academic probation for 2 months, during which he returned to his native country to stay with his parents.
The faculty later dismissed Mr. Z from the program, citing poor academic and laboratory performance. His visa expired, with renewal contingent upon enrollment in a full-time academic program.
Related resources
- American Academy of Psychiatry and the Law. www.aapl.org.
Drug brand names
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Update on eating disorders Bulimia nervosa: Persistent disorder requires equally persistent treatment
Thousands of scientific papers have been written about bulimia, but not all patients receive effective treatments that produce remission.
To set the record straight and help psychiatrists avoid undertreating bulimia, this article discusses:
- evidence for using antidepressants, even when patients are not “depressed”
- merits of psychotherapies, including those shown to work and those that can harm
- augmentation therapies that can help increase response from partial to full remission.
Initial evaluation
Diagnosis. Bulimia nervosa is characterized by eating binges, followed by purging behaviors such as self-induced vomiting or laxative abuse1,2 (Table 1). It affects 1% to 3% of adolescent girls and young women and occurs in women 5 to 10 times more often than in men.
Bulimia is often persistent. About one-half of bulimic patients—including those who have been treated—continue to show eating disorder features on long-term follow-up.3,4
Psychiatric comorbidity. Most bulimic patients report a history of other psychiatric disorders, especially major depressive and bipolar disorders and anxiety disorders such as panic disorder, social phobia, and obsessive-compulsive disorder (OCD).5 Because these psychiatric comorbidities may occur before, during, or after bulimia nervosa, one cannot assume that mood or anxiety disorders are a cause or consequence of bulimia. Instead, bulimia nervosa, mood disorders, and anxiety disorders may be different expressions of a shared etiologic abnormality.
Table 1
DSM-IV-TR diagnostic criteria for bulimia nervosa
|
| Specify type: |
| Purging type: during the current episode of bulimia nervosa, the person has regularly engaged in self-induced vomiting or the misuse of laxatives, diuretics, or enemas |
| Non-purging type: during the current episode of bulimia nervosa, the person has used other inappropriate compensatory behaviors, such as fasting or excessive exercise but has not regularly engaged in self-induced vomiting or the misuse of laxatives, diuretics, or enemas |
| Source: Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, 4th ed, text rev. Copyright 2000 American Psychiatric Association. |
Evidence supporting this hypothesis comes from studies showing that these disorders:
- respond to several chemically unrelated families of antidepressants6,7
- frequently co-occur in individual patients5,7
- frequently co-aggregate in families.7-9
We have published this evidence6,7 and proposed that bulimia nervosa may be one form of a larger underlying disorder, which we termed “affective spectrum disorder.”
Antidepressants are often rapidly effective in treating bulimic symptoms,10 regardless of whether patients exhibit depressive symptoms. Thus, there is no reason to withhold antidepressant therapy simply because a bulimic patient is not depressed. The term “antidepressant” may be a misnomer; these drugs are effective for numerous conditions, of which depression is only one.
Anorexic symptoms. Co-occurring depressive or anxiety disorders in a bulimic patient will not greatly alter treatment. The antidepressants and psychotherapies typically used to treat bulimia are often equally effective for affective disorders. Co-occurring anorexia nervosa, however, is a more serious concern.
Bulimic patients often display a history of anorexia nervosa; in many cases, the patient develops anorexia nervosa as a teenager and then progresses to bulimia nervosa across several years. Her prognosis is much better if her weight normalizes with the shift to bulimia nervosa, than if her weight remains well below normal for her height. It is unclear why medications and psychotherapy are much less effective in bulimic patients with anorexic symptoms than in those with bulimia alone. Watch for further details on anorexia nervosa as this series continues in future issues of.
Medical considerations. Potential medical complications—mostly consequences of vomiting or laxative use—are important to consider when you assess a bulimic patient:1
- The acid in vomitus may gradually erode tooth enamel, requiring dental consultation.
- Vomitus may inflame salivary gland ducts, though the swelling is usually benign.
- Frequent vomiting may result in hypokalemia and alkalosis, although aggressive medical treatment usually is not needed.
Ask about ipecac use. To induce vomiting, some patients may abuse ipecac syrup, which can cause cardiomyopathy.11
Inpatient or outpatient? Unless the bulimic patient displays severe and medically dangerous anorexic symptoms, she can usually be treated as an outpatient. However, evaluate her carefully for suicidal ideation—which is not uncommon in bulimia nervosa—and consider inpatient treatment if necessary.
Medication vs. psychotherapy
The relative merits of medication versus psychotherapy in treating bulimia nervosa continue to be debated. The Cochrane Database of Systematic Reviews includes meta-analyses of both drug therapy12 and psychotherapy13 for bulimia nervosa. The 2001 drug therapy review found that “the use of a single antidepressant agent was clinically effective,” with no one drug clearly superior to another. Notably, this review was published before recent findings on topiramate.
The corresponding 2002 review of psychotherapy concludes—somewhat more cautiously—that “there is a small body of evidence for the efficacy of cognitive-behavior therapy in bulimia nervosa and similar syndromes, but the quality of trials is very variable and sample sizes are often small.”
In bulimia nervosa and other psychiatric disorders, comparing psychotherapy with drug therapy is hazardous because several factors bias the comparison in favor of psychotherapy. These factors include an expectational effect, a responsibility effect, and differential generalizability of study results.
Expectational effect. Patients in clinical trials are aware that they are receiving psychotherapy and, presumably, that study investigators hope to demonstrate its efficacy. This might account for much of psychotherapy’s apparent effect, as even placebos can produce 30% to 50% improvement in bulimia.14
Responsibility effect. If a patient fails to improve in a drug study, she will conclude that the drug has failed. But if she fails to improve in a psychotherapy study, she may conclude that she has failed. Because psychological treatments generally require patients to work in therapy, the patient may feel partially responsible for the outcome. Thus, to avoid cognitive dissonance, she may consciously or unconsciously exaggerate her improvement, both in her own mind and when reporting to treaters.
Differential generalizability. Psychological study protocols, such as administering several months of a behavioral treatment, usually mimic clinical practice fairly well. This is not the case with drug study protocols.
No responsible clinician would inflexibly administer a single dosage of a single drug for a fixed period to every bulimic patient and then declare failure for all nonresponders, as is done in study protocols. In practice, the clinician can offer nonresponders augmentation strategies and additional drug trials. Thus, calculations of bulimia response rates in drug studies substantially understate response to drug therapy in clinical practice.
Table 2
How effective are medications in treating bulimia nervosa?
| Medication | Evidence for efficacy | Remarks |
|---|---|---|
| Antidepressants | ||
| Selective serotonin reuptake inhibitors | +++ | Fluoxetine is only SSRI studied in controlled trials |
| Tricyclics | +++ | Generally more side effects than SSRIs |
| Monoamine oxidase inhibitors | ++ | High rates of remission, but dietary restrictions |
| Trazodone | ++ | Only one controlled trial |
| Venlafaxine, mirtazapine, nefazodone | ? | No controlled trials, but probably effective |
| Bupropion | (++) | Not recommended; caused seizures in bulimic patients |
| Anticonvulsants | ||
| Topiramate | ++ | Only one controlled trial, but substantial effect size |
| Phenytoin | + | Little efficacy in only controlled study |
| Carbamazepine | + | May be useful in bulimia with comorbid bipolar disorder |
| Valproate | + | May be useful in bulimia with comorbid bipolar disorder |
| Other agents | ||
| Liothyronine | + | Augmentation agent in patients with incomplete antidepressant response |
| Lithium | + | Ineffective in only controlled trial; possible augmentation strategy |
| Naltrexone | 0 | Ineffective in two controlled trials |
| Ondansetron | + | One controlled trial |
| 0 No apparent efficacy | ||
| + Occasional effect; limited evidence | ||
| ++ Clear effect; good evidence from controlled trial(s) | ||
| +++ Strongly documented effect; evidence from multiple controlled trials. | ||
| ( ) Negative effect | ||
One also might note that psychological study findings have not “sold” well in the clinical practice marketplace. For example, in a recent survey of more than 220 bulimic women treated with psychotherapy, only 6.9% said they received a full course of cognitive behavioral therapy (CBT)14 —despite two decades of evidence of its efficacy. By contrast, untested, inefficacious, and possibly harmful psychotherapies for bulimia—including recovered-memory therapy—appear to be thriving.
Recommendation. Interpret with caution any head-to-head comparisons of psychological versus drug therapies—especially when clinical practice recommendations are made. Certain psychological therapies provided by specifically-trained individuals likely do help patients with bulimia nervosa. However, biases inherent to the studies may inflate psychological therapies’ efficacy when compared with that of drug therapy.
Therefore, for a psychiatrist who does not specialize in eating disorders to offer exclusively psychological therapy to a bulimic patient—while withholding or postponing drug therapy—may now be a questionable practice.
Choosing drug therapies
Although consensus is lacking on an optimal treatment trial sequence for bulimia nervosa, we suggest a rational approach based on the evidence and our experience (Algorithm).
First-line antidepressants. A selective serotonin reuptake inhibitor (SSRI) trial is usually the first choice (Table 2), and some data suggest that higher-than-usual dosages may be required. For example, in a large multicenter trial of fluoxetine in bulimia nervosa, 60 mg/d was considerably more effective than 20 mg/d for reducing binge eating behavior and vomiting frequency.15
Based on our observations, however, we believe that noncompliance or irregular compliance may account for this difference in response. Bulimic patients’ impulsive and obsessional behavior may keep them from taking their medications as prescribed. The higher fluoxetine dosage may therefore have been more effective simply because it ensured adequate plasma levels, even when patients missed or forgot multiple doses.
Augmenting agents. A first antidepressant trial rarely leads to complete remission of bulimic symptoms. This is not a serious concern, however, because many other options are available.
Liothyronine. Partial responders to SSRIs often become complete responders when we add a 10-day trial of liothyronine (T3), 25 μg/d. If this fails, we may try augmenting with lithium carbonate, although bulimic patients are often afraid of weight gain or lithium’s other side effects.
Topiramate. A newer augmentation strategy is to add the anticonvulsant topiramate. Used alone, topiramate demonstrated effectiveness for bulimia nervosa in one placebo-controlled, double-blind trial.16
Adding topiramate to an antidepressant regimen will likely reduce any remaining bulimic symptoms. In addition, topiramate often produces weight loss—a side effect that bulimic patients usually welcome. It remains unclear whether topiramate’s weight-loss effects might pose a hazard in patients with simultaneous bulimic and anorexic symptoms.
Other antidepressants. If the above strategies fail, other antidepressant options include venlafaxine, tricyclics, and monoamine oxidase inhibitors. Bupropion is not recommended in bulimia nervosa; one trial17 of this agent resulted in a much higher rate of grand mal seizures in bulimic patients than in patients taking bupropion for depression.
In bulimic patients with concomitant bipolar disorder, the anticonvulsants carbamazepine and valproate often reduce affective and bulimic symptoms. By contrast, the anticonvulsant phenytoin—once thought to be useful in bulimia nervosa10 —offers little benefit for either bulimic or affective symptoms.
Persistence is important when initial medication trials fail. One unblinded study followed 36 bulimic patients 9 to 19 months after they completed a controlled study with trazodone.18 Of the 26 patients who tried a second or third antidepressant, 17 (65%) achieved remission of bulimia on follow-up. Of the 10 patients who declined a second or third trial, only 1 (10%) attained remission.
Notably, these study results were obtained before the SSRIs and other newer antidepressants or topiramate became available. Cooperative patients using present-day medications might be able to achieve remission rates that exceed 65%.
Algorithm Proposed treatment approach to bulimia nervosa

Table 3
How effective are psychotherapies in treating bulimia nervosa?
| Psychotherapy | Evidence for efficacy | Remarks |
|---|---|---|
| Cognitive behavioral therapy (CBT) | +++ | Controlled evidence for efficacy in individual and group treatment |
| Interpersonal psychotherapy (IPT) | ++ | Effective, but slower than CBT |
| Exposure with response prevention | + | May be added to other behavioral techniques, though additive benefit questionable |
| Dialectical behavior therapy | + | Highly structured behavioral technique originally developed for borderline personality disorder |
| Self-help groups | + | Frequently considered very helpful by patients |
| Psychodynamic psychotherapy | 0 | “Recovered memory” approaches are frankly harmful |
| Eye movement desensitization and reprocessing (EMDR) | 0 | Dubious theoretical basis; no methodologically acceptable evidence for efficacy |
| 0 No apparent efficacy | ||
| + Occasional effect; limited evidence | ||
| ++ Clear effect; good evidence from controlled trial(s) | ||
| +++ Strongly documented effect; evidence from multiple controlled trials. | ||
Psychotherapy
Cognitive-behavioral therapy. CBT—given either individually or in groups—is the most effective psychotherapy for bulimia (Table 3).19 CBT typically involves 3 to 6 months of helping the patient focus on her bulimic behaviors and on specific attitudes—such as unrealistic preoccupations with being “too fat”—that perpetuate the behaviors.
In practice, unfortunately, few bulimic patients are offered CBT, perhaps because few clinicians are trained in the specific approach used for bulimia nervosa.19 If you are not trained in using CBT for bulimia and do not have access to colleagues who offer this treatment, you may begin with medication plus simple behavioral treatments, such as:
- offering supportive therapy in the office
- referring patients to self-help groups for persons with eating disorders.
If this strategy fails, encourage patients to consider CBT—even if they must travel some distance to obtain it.
Other specialized psychotherapies. Dialectical behavior therapy and interpersonal psychotherapy appear to be effective in bulimia. Again, however, clinicians who lack training in these techniques or access to local experts may be unable to offer them. Psychodynamic therapy does not appear to offer greater benefit in bulimia nervosa than ordinary supportive counseling.
Dubious therapies. One psychodynamic approach—regrettably still practiced—is “recovered memory therapy.” Therapists who use it claim that childhood sexual abuse or other trauma can cause bulimic symptoms but patients have repressed the memory of these events.20
No methodologically sound evidence has shown that childhood sexual abuse can cause bulimia nervosa years or decades later.21 Nor is there acceptable evidence that people can repress the memory of a traumatic experience.22 Therapists administering recovered memory therapy have been subjected to malpractice judgments totaling tens of millions of dollars from suits filed by patients who eventually realized that so-called “recovered” memories were false.23
Another dubious therapy—eye movement desensitization and reprocessing (EMDR)—also may involve attempts to “recover” memories of putative traumatic events.24 No methodologically sound evidence has shown that EMDR is effective in bulimic patients, and the technique’s theoretical basis is questionable.24,25
Related resources
- Mental Health Net/Eating disorders. http://eatingdisorders.mentalhelp.net
- National Association of Anorexia Nervosa and Associated Disorders (ANAD). www.altrue.net/site/anadweb/
- Association for Advancement of Behavior Therapy. www.aabt.org
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Lithium • Lithobid, Eskalith
- Nortriptyline • Pamelor, Aventyl
- Sertraline • Zoloft
- Topiramate • Topamax
- Trazodone • Desyrel
- Liothyronine • Cytomel
- Venlafaxine • Effexor
Disclosure
Dr. Pope receives research support from Ortho-McNeil Pharmaceuticals and is a consultant to Solvay Pharmaceuticals and Auxilium Pharmaceuticals.
Dr. Hudson receives research support from and is a consultant to Eli Lilly & Co. and Ortho-McNeil Pharmaceuticals.
1. Mehler PS. Clinical practice. Bulimia nervosa. N Engl J Med 2003;349(9):875-81.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association,2000.
3. Fisher M. The course and outcome of eating disorders in adults and in adolescents: a review. Adolesc Med 2003;14(1):149-58.
4. Fairburn CG, Norman PA, Welch SL, et al. A prospective study of outcome in bulimia nervosa and the long-term effects of three psychological treatments. Arch Gen Psychiatry 1995;52(4):304-12.
5. Hudson JI, Pope HG, Jr, Yurgelun-Todd D, et al. A controlled study of lifetime prevalence of affective and other psychiatric disorders in bulimic outpatients. Am J Psychiatry 1987;144(10):1283-7.
6. Hudson JI, Pope HG, Jr. Affective spectrum disorder: does antidepressant response identify a family of disorders with a common pathophysiology? Am J Psychiatry 1990;147(5):552-64.
7. Hudson JI, Mangweth B, Pope HG, Jr, et al. Family study of affective spectrum disorder. Arch Gen Psychiatry 2003;60:170-7.
8. Hudson JI, Laird NM, Betensky RA, et al. Multivariate logistic regression for familial aggregation of two disorders: II. Analysis of studies of eating and mood disorders. Am J Epidemiology 2001;153(5):506-14.
9. Mangweth B, Hudson JI, Pope HG, Jr, et al. Family study of the aggregation of eating disorders and mood disorders. Psychol Med (in press).
10. Hudson JI, Pope HG, Jr, Carter WP. Pharmacologic therapy of bulimia nervosa. In: Goldstein D (ed). The management of eating disorders and obesity (2nd ed) Totowa, NJ: Humana Press, Inc.(in press).
11. Pope HG, Jr, Hudson JI, Nixon RA, Herridge PL. The epidemiology of ipecac abuse. N Engl J Med 1986;14(4):245-6.
12. Hay PJ, Bacaltchuk J. Psychotherapy for bulimia nervosa and binging. Cochrane Database Syst Rev 2003;(1):CD000562.-
13. Bacaltchuk J, Hay P. Antidepressants versus placebo for people with bulimia nervosa. Cochrane Database Syst Rev 2001;(4):CD003391.-
14. Crow S, Mussell MP, Peterson C, et al. Prior treatment received by patients with bulimia nervosa. Int J Eating Disord 1999;25(1):39-44.
15. Fluoxetine Bulimia Collaborative Study Group Fluoxetine in the treatment of bulimia nervosa: a multicenter placebo-controlled, double-blind trial. Arch Gen Psychiatry 1992;49:139-47.
16. Hoopes S, Reimherr F, Hedges D, et al. Part 1:Topiramate in the treatment of bulimia nervosa: a randomized, double-blind, placebocontrolled trial. J Clin Psychiatry (in press).
17. Horne RL, Ferguson JM, Pope HG, Jr, et al. Treatment of bulimia with bupropion: a controlled multi-center trial. J Clin Psychiatry 1988;49(7):262-6.
18. Pope HG, Jr, McElroy SL, Keck PE, Jr, Hudson JI. Long-term pharmacotherapy of bulimia nervosa. J Clin Psychopharmacol 1989;9(5):385-6.
19. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361(9355):407-16.
20. Pope HG, Jr, Hudson JI. “Recovered memory” therapy for eating disorders: implications of the Ramona verdict. Int J Eat Disord 1996;19(2):139-45.
21. Pope HG, Jr, Hudson JI. Does childhood sexual abuse cause adult psychiatric disorders? Essentials of methodology. J Psychiatry Law 1995;Fall:363-81.
22. Pope HG, Jr, Oliva PS, Hudson JI. Repressed memories. The scientific status of research on repressed memories. In: Faigman DL, Kaye DH, Saks MJ, Sanders J (eds). Science in the law: social and behavioral science issues St. Paul, MN: West Group, 2002;487-526.
23. Cannell J, Hudson JI, Pope HG, Jr. Standards for informed consent in recovered memory therapy. J Am Acad Psychiatry Law 2001;29(2):138-47.
24. Hudson JI, Chase EA, Pope HG, Jr. Eye movement desensitization and reprocessing in eating disorders: caution against premature acceptance. Int J Eat Disord 1998;23:1-5.
25. McNally RJ. EMDR and mesmerism: a comparative historical analysis. J Anxiety Disord 1999;13(1-2):225-36.
Thousands of scientific papers have been written about bulimia, but not all patients receive effective treatments that produce remission.
To set the record straight and help psychiatrists avoid undertreating bulimia, this article discusses:
- evidence for using antidepressants, even when patients are not “depressed”
- merits of psychotherapies, including those shown to work and those that can harm
- augmentation therapies that can help increase response from partial to full remission.
Initial evaluation
Diagnosis. Bulimia nervosa is characterized by eating binges, followed by purging behaviors such as self-induced vomiting or laxative abuse1,2 (Table 1). It affects 1% to 3% of adolescent girls and young women and occurs in women 5 to 10 times more often than in men.
Bulimia is often persistent. About one-half of bulimic patients—including those who have been treated—continue to show eating disorder features on long-term follow-up.3,4
Psychiatric comorbidity. Most bulimic patients report a history of other psychiatric disorders, especially major depressive and bipolar disorders and anxiety disorders such as panic disorder, social phobia, and obsessive-compulsive disorder (OCD).5 Because these psychiatric comorbidities may occur before, during, or after bulimia nervosa, one cannot assume that mood or anxiety disorders are a cause or consequence of bulimia. Instead, bulimia nervosa, mood disorders, and anxiety disorders may be different expressions of a shared etiologic abnormality.
Table 1
DSM-IV-TR diagnostic criteria for bulimia nervosa
|
| Specify type: |
| Purging type: during the current episode of bulimia nervosa, the person has regularly engaged in self-induced vomiting or the misuse of laxatives, diuretics, or enemas |
| Non-purging type: during the current episode of bulimia nervosa, the person has used other inappropriate compensatory behaviors, such as fasting or excessive exercise but has not regularly engaged in self-induced vomiting or the misuse of laxatives, diuretics, or enemas |
| Source: Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, 4th ed, text rev. Copyright 2000 American Psychiatric Association. |
Evidence supporting this hypothesis comes from studies showing that these disorders:
- respond to several chemically unrelated families of antidepressants6,7
- frequently co-occur in individual patients5,7
- frequently co-aggregate in families.7-9
We have published this evidence6,7 and proposed that bulimia nervosa may be one form of a larger underlying disorder, which we termed “affective spectrum disorder.”
Antidepressants are often rapidly effective in treating bulimic symptoms,10 regardless of whether patients exhibit depressive symptoms. Thus, there is no reason to withhold antidepressant therapy simply because a bulimic patient is not depressed. The term “antidepressant” may be a misnomer; these drugs are effective for numerous conditions, of which depression is only one.
Anorexic symptoms. Co-occurring depressive or anxiety disorders in a bulimic patient will not greatly alter treatment. The antidepressants and psychotherapies typically used to treat bulimia are often equally effective for affective disorders. Co-occurring anorexia nervosa, however, is a more serious concern.
Bulimic patients often display a history of anorexia nervosa; in many cases, the patient develops anorexia nervosa as a teenager and then progresses to bulimia nervosa across several years. Her prognosis is much better if her weight normalizes with the shift to bulimia nervosa, than if her weight remains well below normal for her height. It is unclear why medications and psychotherapy are much less effective in bulimic patients with anorexic symptoms than in those with bulimia alone. Watch for further details on anorexia nervosa as this series continues in future issues of.
Medical considerations. Potential medical complications—mostly consequences of vomiting or laxative use—are important to consider when you assess a bulimic patient:1
- The acid in vomitus may gradually erode tooth enamel, requiring dental consultation.
- Vomitus may inflame salivary gland ducts, though the swelling is usually benign.
- Frequent vomiting may result in hypokalemia and alkalosis, although aggressive medical treatment usually is not needed.
Ask about ipecac use. To induce vomiting, some patients may abuse ipecac syrup, which can cause cardiomyopathy.11
Inpatient or outpatient? Unless the bulimic patient displays severe and medically dangerous anorexic symptoms, she can usually be treated as an outpatient. However, evaluate her carefully for suicidal ideation—which is not uncommon in bulimia nervosa—and consider inpatient treatment if necessary.
Medication vs. psychotherapy
The relative merits of medication versus psychotherapy in treating bulimia nervosa continue to be debated. The Cochrane Database of Systematic Reviews includes meta-analyses of both drug therapy12 and psychotherapy13 for bulimia nervosa. The 2001 drug therapy review found that “the use of a single antidepressant agent was clinically effective,” with no one drug clearly superior to another. Notably, this review was published before recent findings on topiramate.
The corresponding 2002 review of psychotherapy concludes—somewhat more cautiously—that “there is a small body of evidence for the efficacy of cognitive-behavior therapy in bulimia nervosa and similar syndromes, but the quality of trials is very variable and sample sizes are often small.”
In bulimia nervosa and other psychiatric disorders, comparing psychotherapy with drug therapy is hazardous because several factors bias the comparison in favor of psychotherapy. These factors include an expectational effect, a responsibility effect, and differential generalizability of study results.
Expectational effect. Patients in clinical trials are aware that they are receiving psychotherapy and, presumably, that study investigators hope to demonstrate its efficacy. This might account for much of psychotherapy’s apparent effect, as even placebos can produce 30% to 50% improvement in bulimia.14
Responsibility effect. If a patient fails to improve in a drug study, she will conclude that the drug has failed. But if she fails to improve in a psychotherapy study, she may conclude that she has failed. Because psychological treatments generally require patients to work in therapy, the patient may feel partially responsible for the outcome. Thus, to avoid cognitive dissonance, she may consciously or unconsciously exaggerate her improvement, both in her own mind and when reporting to treaters.
Differential generalizability. Psychological study protocols, such as administering several months of a behavioral treatment, usually mimic clinical practice fairly well. This is not the case with drug study protocols.
No responsible clinician would inflexibly administer a single dosage of a single drug for a fixed period to every bulimic patient and then declare failure for all nonresponders, as is done in study protocols. In practice, the clinician can offer nonresponders augmentation strategies and additional drug trials. Thus, calculations of bulimia response rates in drug studies substantially understate response to drug therapy in clinical practice.
Table 2
How effective are medications in treating bulimia nervosa?
| Medication | Evidence for efficacy | Remarks |
|---|---|---|
| Antidepressants | ||
| Selective serotonin reuptake inhibitors | +++ | Fluoxetine is only SSRI studied in controlled trials |
| Tricyclics | +++ | Generally more side effects than SSRIs |
| Monoamine oxidase inhibitors | ++ | High rates of remission, but dietary restrictions |
| Trazodone | ++ | Only one controlled trial |
| Venlafaxine, mirtazapine, nefazodone | ? | No controlled trials, but probably effective |
| Bupropion | (++) | Not recommended; caused seizures in bulimic patients |
| Anticonvulsants | ||
| Topiramate | ++ | Only one controlled trial, but substantial effect size |
| Phenytoin | + | Little efficacy in only controlled study |
| Carbamazepine | + | May be useful in bulimia with comorbid bipolar disorder |
| Valproate | + | May be useful in bulimia with comorbid bipolar disorder |
| Other agents | ||
| Liothyronine | + | Augmentation agent in patients with incomplete antidepressant response |
| Lithium | + | Ineffective in only controlled trial; possible augmentation strategy |
| Naltrexone | 0 | Ineffective in two controlled trials |
| Ondansetron | + | One controlled trial |
| 0 No apparent efficacy | ||
| + Occasional effect; limited evidence | ||
| ++ Clear effect; good evidence from controlled trial(s) | ||
| +++ Strongly documented effect; evidence from multiple controlled trials. | ||
| ( ) Negative effect | ||
One also might note that psychological study findings have not “sold” well in the clinical practice marketplace. For example, in a recent survey of more than 220 bulimic women treated with psychotherapy, only 6.9% said they received a full course of cognitive behavioral therapy (CBT)14 —despite two decades of evidence of its efficacy. By contrast, untested, inefficacious, and possibly harmful psychotherapies for bulimia—including recovered-memory therapy—appear to be thriving.
Recommendation. Interpret with caution any head-to-head comparisons of psychological versus drug therapies—especially when clinical practice recommendations are made. Certain psychological therapies provided by specifically-trained individuals likely do help patients with bulimia nervosa. However, biases inherent to the studies may inflate psychological therapies’ efficacy when compared with that of drug therapy.
Therefore, for a psychiatrist who does not specialize in eating disorders to offer exclusively psychological therapy to a bulimic patient—while withholding or postponing drug therapy—may now be a questionable practice.
Choosing drug therapies
Although consensus is lacking on an optimal treatment trial sequence for bulimia nervosa, we suggest a rational approach based on the evidence and our experience (Algorithm).
First-line antidepressants. A selective serotonin reuptake inhibitor (SSRI) trial is usually the first choice (Table 2), and some data suggest that higher-than-usual dosages may be required. For example, in a large multicenter trial of fluoxetine in bulimia nervosa, 60 mg/d was considerably more effective than 20 mg/d for reducing binge eating behavior and vomiting frequency.15
Based on our observations, however, we believe that noncompliance or irregular compliance may account for this difference in response. Bulimic patients’ impulsive and obsessional behavior may keep them from taking their medications as prescribed. The higher fluoxetine dosage may therefore have been more effective simply because it ensured adequate plasma levels, even when patients missed or forgot multiple doses.
Augmenting agents. A first antidepressant trial rarely leads to complete remission of bulimic symptoms. This is not a serious concern, however, because many other options are available.
Liothyronine. Partial responders to SSRIs often become complete responders when we add a 10-day trial of liothyronine (T3), 25 μg/d. If this fails, we may try augmenting with lithium carbonate, although bulimic patients are often afraid of weight gain or lithium’s other side effects.
Topiramate. A newer augmentation strategy is to add the anticonvulsant topiramate. Used alone, topiramate demonstrated effectiveness for bulimia nervosa in one placebo-controlled, double-blind trial.16
Adding topiramate to an antidepressant regimen will likely reduce any remaining bulimic symptoms. In addition, topiramate often produces weight loss—a side effect that bulimic patients usually welcome. It remains unclear whether topiramate’s weight-loss effects might pose a hazard in patients with simultaneous bulimic and anorexic symptoms.
Other antidepressants. If the above strategies fail, other antidepressant options include venlafaxine, tricyclics, and monoamine oxidase inhibitors. Bupropion is not recommended in bulimia nervosa; one trial17 of this agent resulted in a much higher rate of grand mal seizures in bulimic patients than in patients taking bupropion for depression.
In bulimic patients with concomitant bipolar disorder, the anticonvulsants carbamazepine and valproate often reduce affective and bulimic symptoms. By contrast, the anticonvulsant phenytoin—once thought to be useful in bulimia nervosa10 —offers little benefit for either bulimic or affective symptoms.
Persistence is important when initial medication trials fail. One unblinded study followed 36 bulimic patients 9 to 19 months after they completed a controlled study with trazodone.18 Of the 26 patients who tried a second or third antidepressant, 17 (65%) achieved remission of bulimia on follow-up. Of the 10 patients who declined a second or third trial, only 1 (10%) attained remission.
Notably, these study results were obtained before the SSRIs and other newer antidepressants or topiramate became available. Cooperative patients using present-day medications might be able to achieve remission rates that exceed 65%.
Algorithm Proposed treatment approach to bulimia nervosa
Table 3
How effective are psychotherapies in treating bulimia nervosa?
| Psychotherapy | Evidence for efficacy | Remarks |
|---|---|---|
| Cognitive behavioral therapy (CBT) | +++ | Controlled evidence for efficacy in individual and group treatment |
| Interpersonal psychotherapy (IPT) | ++ | Effective, but slower than CBT |
| Exposure with response prevention | + | May be added to other behavioral techniques, though additive benefit questionable |
| Dialectical behavior therapy | + | Highly structured behavioral technique originally developed for borderline personality disorder |
| Self-help groups | + | Frequently considered very helpful by patients |
| Psychodynamic psychotherapy | 0 | “Recovered memory” approaches are frankly harmful |
| Eye movement desensitization and reprocessing (EMDR) | 0 | Dubious theoretical basis; no methodologically acceptable evidence for efficacy |
| 0 No apparent efficacy | ||
| + Occasional effect; limited evidence | ||
| ++ Clear effect; good evidence from controlled trial(s) | ||
| +++ Strongly documented effect; evidence from multiple controlled trials. | ||
Psychotherapy
Cognitive-behavioral therapy. CBT—given either individually or in groups—is the most effective psychotherapy for bulimia (Table 3).19 CBT typically involves 3 to 6 months of helping the patient focus on her bulimic behaviors and on specific attitudes—such as unrealistic preoccupations with being “too fat”—that perpetuate the behaviors.
In practice, unfortunately, few bulimic patients are offered CBT, perhaps because few clinicians are trained in the specific approach used for bulimia nervosa.19 If you are not trained in using CBT for bulimia and do not have access to colleagues who offer this treatment, you may begin with medication plus simple behavioral treatments, such as:
- offering supportive therapy in the office
- referring patients to self-help groups for persons with eating disorders.
If this strategy fails, encourage patients to consider CBT—even if they must travel some distance to obtain it.
Other specialized psychotherapies. Dialectical behavior therapy and interpersonal psychotherapy appear to be effective in bulimia. Again, however, clinicians who lack training in these techniques or access to local experts may be unable to offer them. Psychodynamic therapy does not appear to offer greater benefit in bulimia nervosa than ordinary supportive counseling.
Dubious therapies. One psychodynamic approach—regrettably still practiced—is “recovered memory therapy.” Therapists who use it claim that childhood sexual abuse or other trauma can cause bulimic symptoms but patients have repressed the memory of these events.20
No methodologically sound evidence has shown that childhood sexual abuse can cause bulimia nervosa years or decades later.21 Nor is there acceptable evidence that people can repress the memory of a traumatic experience.22 Therapists administering recovered memory therapy have been subjected to malpractice judgments totaling tens of millions of dollars from suits filed by patients who eventually realized that so-called “recovered” memories were false.23
Another dubious therapy—eye movement desensitization and reprocessing (EMDR)—also may involve attempts to “recover” memories of putative traumatic events.24 No methodologically sound evidence has shown that EMDR is effective in bulimic patients, and the technique’s theoretical basis is questionable.24,25
Related resources
- Mental Health Net/Eating disorders. http://eatingdisorders.mentalhelp.net
- National Association of Anorexia Nervosa and Associated Disorders (ANAD). www.altrue.net/site/anadweb/
- Association for Advancement of Behavior Therapy. www.aabt.org
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Lithium • Lithobid, Eskalith
- Nortriptyline • Pamelor, Aventyl
- Sertraline • Zoloft
- Topiramate • Topamax
- Trazodone • Desyrel
- Liothyronine • Cytomel
- Venlafaxine • Effexor
Disclosure
Dr. Pope receives research support from Ortho-McNeil Pharmaceuticals and is a consultant to Solvay Pharmaceuticals and Auxilium Pharmaceuticals.
Dr. Hudson receives research support from and is a consultant to Eli Lilly & Co. and Ortho-McNeil Pharmaceuticals.
Thousands of scientific papers have been written about bulimia, but not all patients receive effective treatments that produce remission.
To set the record straight and help psychiatrists avoid undertreating bulimia, this article discusses:
- evidence for using antidepressants, even when patients are not “depressed”
- merits of psychotherapies, including those shown to work and those that can harm
- augmentation therapies that can help increase response from partial to full remission.
Initial evaluation
Diagnosis. Bulimia nervosa is characterized by eating binges, followed by purging behaviors such as self-induced vomiting or laxative abuse1,2 (Table 1). It affects 1% to 3% of adolescent girls and young women and occurs in women 5 to 10 times more often than in men.
Bulimia is often persistent. About one-half of bulimic patients—including those who have been treated—continue to show eating disorder features on long-term follow-up.3,4
Psychiatric comorbidity. Most bulimic patients report a history of other psychiatric disorders, especially major depressive and bipolar disorders and anxiety disorders such as panic disorder, social phobia, and obsessive-compulsive disorder (OCD).5 Because these psychiatric comorbidities may occur before, during, or after bulimia nervosa, one cannot assume that mood or anxiety disorders are a cause or consequence of bulimia. Instead, bulimia nervosa, mood disorders, and anxiety disorders may be different expressions of a shared etiologic abnormality.
Table 1
DSM-IV-TR diagnostic criteria for bulimia nervosa
|
| Specify type: |
| Purging type: during the current episode of bulimia nervosa, the person has regularly engaged in self-induced vomiting or the misuse of laxatives, diuretics, or enemas |
| Non-purging type: during the current episode of bulimia nervosa, the person has used other inappropriate compensatory behaviors, such as fasting or excessive exercise but has not regularly engaged in self-induced vomiting or the misuse of laxatives, diuretics, or enemas |
| Source: Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, 4th ed, text rev. Copyright 2000 American Psychiatric Association. |
Evidence supporting this hypothesis comes from studies showing that these disorders:
- respond to several chemically unrelated families of antidepressants6,7
- frequently co-occur in individual patients5,7
- frequently co-aggregate in families.7-9
We have published this evidence6,7 and proposed that bulimia nervosa may be one form of a larger underlying disorder, which we termed “affective spectrum disorder.”
Antidepressants are often rapidly effective in treating bulimic symptoms,10 regardless of whether patients exhibit depressive symptoms. Thus, there is no reason to withhold antidepressant therapy simply because a bulimic patient is not depressed. The term “antidepressant” may be a misnomer; these drugs are effective for numerous conditions, of which depression is only one.
Anorexic symptoms. Co-occurring depressive or anxiety disorders in a bulimic patient will not greatly alter treatment. The antidepressants and psychotherapies typically used to treat bulimia are often equally effective for affective disorders. Co-occurring anorexia nervosa, however, is a more serious concern.
Bulimic patients often display a history of anorexia nervosa; in many cases, the patient develops anorexia nervosa as a teenager and then progresses to bulimia nervosa across several years. Her prognosis is much better if her weight normalizes with the shift to bulimia nervosa, than if her weight remains well below normal for her height. It is unclear why medications and psychotherapy are much less effective in bulimic patients with anorexic symptoms than in those with bulimia alone. Watch for further details on anorexia nervosa as this series continues in future issues of.
Medical considerations. Potential medical complications—mostly consequences of vomiting or laxative use—are important to consider when you assess a bulimic patient:1
- The acid in vomitus may gradually erode tooth enamel, requiring dental consultation.
- Vomitus may inflame salivary gland ducts, though the swelling is usually benign.
- Frequent vomiting may result in hypokalemia and alkalosis, although aggressive medical treatment usually is not needed.
Ask about ipecac use. To induce vomiting, some patients may abuse ipecac syrup, which can cause cardiomyopathy.11
Inpatient or outpatient? Unless the bulimic patient displays severe and medically dangerous anorexic symptoms, she can usually be treated as an outpatient. However, evaluate her carefully for suicidal ideation—which is not uncommon in bulimia nervosa—and consider inpatient treatment if necessary.
Medication vs. psychotherapy
The relative merits of medication versus psychotherapy in treating bulimia nervosa continue to be debated. The Cochrane Database of Systematic Reviews includes meta-analyses of both drug therapy12 and psychotherapy13 for bulimia nervosa. The 2001 drug therapy review found that “the use of a single antidepressant agent was clinically effective,” with no one drug clearly superior to another. Notably, this review was published before recent findings on topiramate.
The corresponding 2002 review of psychotherapy concludes—somewhat more cautiously—that “there is a small body of evidence for the efficacy of cognitive-behavior therapy in bulimia nervosa and similar syndromes, but the quality of trials is very variable and sample sizes are often small.”
In bulimia nervosa and other psychiatric disorders, comparing psychotherapy with drug therapy is hazardous because several factors bias the comparison in favor of psychotherapy. These factors include an expectational effect, a responsibility effect, and differential generalizability of study results.
Expectational effect. Patients in clinical trials are aware that they are receiving psychotherapy and, presumably, that study investigators hope to demonstrate its efficacy. This might account for much of psychotherapy’s apparent effect, as even placebos can produce 30% to 50% improvement in bulimia.14
Responsibility effect. If a patient fails to improve in a drug study, she will conclude that the drug has failed. But if she fails to improve in a psychotherapy study, she may conclude that she has failed. Because psychological treatments generally require patients to work in therapy, the patient may feel partially responsible for the outcome. Thus, to avoid cognitive dissonance, she may consciously or unconsciously exaggerate her improvement, both in her own mind and when reporting to treaters.
Differential generalizability. Psychological study protocols, such as administering several months of a behavioral treatment, usually mimic clinical practice fairly well. This is not the case with drug study protocols.
No responsible clinician would inflexibly administer a single dosage of a single drug for a fixed period to every bulimic patient and then declare failure for all nonresponders, as is done in study protocols. In practice, the clinician can offer nonresponders augmentation strategies and additional drug trials. Thus, calculations of bulimia response rates in drug studies substantially understate response to drug therapy in clinical practice.
Table 2
How effective are medications in treating bulimia nervosa?
| Medication | Evidence for efficacy | Remarks |
|---|---|---|
| Antidepressants | ||
| Selective serotonin reuptake inhibitors | +++ | Fluoxetine is only SSRI studied in controlled trials |
| Tricyclics | +++ | Generally more side effects than SSRIs |
| Monoamine oxidase inhibitors | ++ | High rates of remission, but dietary restrictions |
| Trazodone | ++ | Only one controlled trial |
| Venlafaxine, mirtazapine, nefazodone | ? | No controlled trials, but probably effective |
| Bupropion | (++) | Not recommended; caused seizures in bulimic patients |
| Anticonvulsants | ||
| Topiramate | ++ | Only one controlled trial, but substantial effect size |
| Phenytoin | + | Little efficacy in only controlled study |
| Carbamazepine | + | May be useful in bulimia with comorbid bipolar disorder |
| Valproate | + | May be useful in bulimia with comorbid bipolar disorder |
| Other agents | ||
| Liothyronine | + | Augmentation agent in patients with incomplete antidepressant response |
| Lithium | + | Ineffective in only controlled trial; possible augmentation strategy |
| Naltrexone | 0 | Ineffective in two controlled trials |
| Ondansetron | + | One controlled trial |
| 0 No apparent efficacy | ||
| + Occasional effect; limited evidence | ||
| ++ Clear effect; good evidence from controlled trial(s) | ||
| +++ Strongly documented effect; evidence from multiple controlled trials. | ||
| ( ) Negative effect | ||
One also might note that psychological study findings have not “sold” well in the clinical practice marketplace. For example, in a recent survey of more than 220 bulimic women treated with psychotherapy, only 6.9% said they received a full course of cognitive behavioral therapy (CBT)14 —despite two decades of evidence of its efficacy. By contrast, untested, inefficacious, and possibly harmful psychotherapies for bulimia—including recovered-memory therapy—appear to be thriving.
Recommendation. Interpret with caution any head-to-head comparisons of psychological versus drug therapies—especially when clinical practice recommendations are made. Certain psychological therapies provided by specifically-trained individuals likely do help patients with bulimia nervosa. However, biases inherent to the studies may inflate psychological therapies’ efficacy when compared with that of drug therapy.
Therefore, for a psychiatrist who does not specialize in eating disorders to offer exclusively psychological therapy to a bulimic patient—while withholding or postponing drug therapy—may now be a questionable practice.
Choosing drug therapies
Although consensus is lacking on an optimal treatment trial sequence for bulimia nervosa, we suggest a rational approach based on the evidence and our experience (Algorithm).
First-line antidepressants. A selective serotonin reuptake inhibitor (SSRI) trial is usually the first choice (Table 2), and some data suggest that higher-than-usual dosages may be required. For example, in a large multicenter trial of fluoxetine in bulimia nervosa, 60 mg/d was considerably more effective than 20 mg/d for reducing binge eating behavior and vomiting frequency.15
Based on our observations, however, we believe that noncompliance or irregular compliance may account for this difference in response. Bulimic patients’ impulsive and obsessional behavior may keep them from taking their medications as prescribed. The higher fluoxetine dosage may therefore have been more effective simply because it ensured adequate plasma levels, even when patients missed or forgot multiple doses.
Augmenting agents. A first antidepressant trial rarely leads to complete remission of bulimic symptoms. This is not a serious concern, however, because many other options are available.
Liothyronine. Partial responders to SSRIs often become complete responders when we add a 10-day trial of liothyronine (T3), 25 μg/d. If this fails, we may try augmenting with lithium carbonate, although bulimic patients are often afraid of weight gain or lithium’s other side effects.
Topiramate. A newer augmentation strategy is to add the anticonvulsant topiramate. Used alone, topiramate demonstrated effectiveness for bulimia nervosa in one placebo-controlled, double-blind trial.16
Adding topiramate to an antidepressant regimen will likely reduce any remaining bulimic symptoms. In addition, topiramate often produces weight loss—a side effect that bulimic patients usually welcome. It remains unclear whether topiramate’s weight-loss effects might pose a hazard in patients with simultaneous bulimic and anorexic symptoms.
Other antidepressants. If the above strategies fail, other antidepressant options include venlafaxine, tricyclics, and monoamine oxidase inhibitors. Bupropion is not recommended in bulimia nervosa; one trial17 of this agent resulted in a much higher rate of grand mal seizures in bulimic patients than in patients taking bupropion for depression.
In bulimic patients with concomitant bipolar disorder, the anticonvulsants carbamazepine and valproate often reduce affective and bulimic symptoms. By contrast, the anticonvulsant phenytoin—once thought to be useful in bulimia nervosa10 —offers little benefit for either bulimic or affective symptoms.
Persistence is important when initial medication trials fail. One unblinded study followed 36 bulimic patients 9 to 19 months after they completed a controlled study with trazodone.18 Of the 26 patients who tried a second or third antidepressant, 17 (65%) achieved remission of bulimia on follow-up. Of the 10 patients who declined a second or third trial, only 1 (10%) attained remission.
Notably, these study results were obtained before the SSRIs and other newer antidepressants or topiramate became available. Cooperative patients using present-day medications might be able to achieve remission rates that exceed 65%.
Algorithm Proposed treatment approach to bulimia nervosa
Table 3
How effective are psychotherapies in treating bulimia nervosa?
| Psychotherapy | Evidence for efficacy | Remarks |
|---|---|---|
| Cognitive behavioral therapy (CBT) | +++ | Controlled evidence for efficacy in individual and group treatment |
| Interpersonal psychotherapy (IPT) | ++ | Effective, but slower than CBT |
| Exposure with response prevention | + | May be added to other behavioral techniques, though additive benefit questionable |
| Dialectical behavior therapy | + | Highly structured behavioral technique originally developed for borderline personality disorder |
| Self-help groups | + | Frequently considered very helpful by patients |
| Psychodynamic psychotherapy | 0 | “Recovered memory” approaches are frankly harmful |
| Eye movement desensitization and reprocessing (EMDR) | 0 | Dubious theoretical basis; no methodologically acceptable evidence for efficacy |
| 0 No apparent efficacy | ||
| + Occasional effect; limited evidence | ||
| ++ Clear effect; good evidence from controlled trial(s) | ||
| +++ Strongly documented effect; evidence from multiple controlled trials. | ||
Psychotherapy
Cognitive-behavioral therapy. CBT—given either individually or in groups—is the most effective psychotherapy for bulimia (Table 3).19 CBT typically involves 3 to 6 months of helping the patient focus on her bulimic behaviors and on specific attitudes—such as unrealistic preoccupations with being “too fat”—that perpetuate the behaviors.
In practice, unfortunately, few bulimic patients are offered CBT, perhaps because few clinicians are trained in the specific approach used for bulimia nervosa.19 If you are not trained in using CBT for bulimia and do not have access to colleagues who offer this treatment, you may begin with medication plus simple behavioral treatments, such as:
- offering supportive therapy in the office
- referring patients to self-help groups for persons with eating disorders.
If this strategy fails, encourage patients to consider CBT—even if they must travel some distance to obtain it.
Other specialized psychotherapies. Dialectical behavior therapy and interpersonal psychotherapy appear to be effective in bulimia. Again, however, clinicians who lack training in these techniques or access to local experts may be unable to offer them. Psychodynamic therapy does not appear to offer greater benefit in bulimia nervosa than ordinary supportive counseling.
Dubious therapies. One psychodynamic approach—regrettably still practiced—is “recovered memory therapy.” Therapists who use it claim that childhood sexual abuse or other trauma can cause bulimic symptoms but patients have repressed the memory of these events.20
No methodologically sound evidence has shown that childhood sexual abuse can cause bulimia nervosa years or decades later.21 Nor is there acceptable evidence that people can repress the memory of a traumatic experience.22 Therapists administering recovered memory therapy have been subjected to malpractice judgments totaling tens of millions of dollars from suits filed by patients who eventually realized that so-called “recovered” memories were false.23
Another dubious therapy—eye movement desensitization and reprocessing (EMDR)—also may involve attempts to “recover” memories of putative traumatic events.24 No methodologically sound evidence has shown that EMDR is effective in bulimic patients, and the technique’s theoretical basis is questionable.24,25
Related resources
- Mental Health Net/Eating disorders. http://eatingdisorders.mentalhelp.net
- National Association of Anorexia Nervosa and Associated Disorders (ANAD). www.altrue.net/site/anadweb/
- Association for Advancement of Behavior Therapy. www.aabt.org
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Lithium • Lithobid, Eskalith
- Nortriptyline • Pamelor, Aventyl
- Sertraline • Zoloft
- Topiramate • Topamax
- Trazodone • Desyrel
- Liothyronine • Cytomel
- Venlafaxine • Effexor
Disclosure
Dr. Pope receives research support from Ortho-McNeil Pharmaceuticals and is a consultant to Solvay Pharmaceuticals and Auxilium Pharmaceuticals.
Dr. Hudson receives research support from and is a consultant to Eli Lilly & Co. and Ortho-McNeil Pharmaceuticals.
1. Mehler PS. Clinical practice. Bulimia nervosa. N Engl J Med 2003;349(9):875-81.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association,2000.
3. Fisher M. The course and outcome of eating disorders in adults and in adolescents: a review. Adolesc Med 2003;14(1):149-58.
4. Fairburn CG, Norman PA, Welch SL, et al. A prospective study of outcome in bulimia nervosa and the long-term effects of three psychological treatments. Arch Gen Psychiatry 1995;52(4):304-12.
5. Hudson JI, Pope HG, Jr, Yurgelun-Todd D, et al. A controlled study of lifetime prevalence of affective and other psychiatric disorders in bulimic outpatients. Am J Psychiatry 1987;144(10):1283-7.
6. Hudson JI, Pope HG, Jr. Affective spectrum disorder: does antidepressant response identify a family of disorders with a common pathophysiology? Am J Psychiatry 1990;147(5):552-64.
7. Hudson JI, Mangweth B, Pope HG, Jr, et al. Family study of affective spectrum disorder. Arch Gen Psychiatry 2003;60:170-7.
8. Hudson JI, Laird NM, Betensky RA, et al. Multivariate logistic regression for familial aggregation of two disorders: II. Analysis of studies of eating and mood disorders. Am J Epidemiology 2001;153(5):506-14.
9. Mangweth B, Hudson JI, Pope HG, Jr, et al. Family study of the aggregation of eating disorders and mood disorders. Psychol Med (in press).
10. Hudson JI, Pope HG, Jr, Carter WP. Pharmacologic therapy of bulimia nervosa. In: Goldstein D (ed). The management of eating disorders and obesity (2nd ed) Totowa, NJ: Humana Press, Inc.(in press).
11. Pope HG, Jr, Hudson JI, Nixon RA, Herridge PL. The epidemiology of ipecac abuse. N Engl J Med 1986;14(4):245-6.
12. Hay PJ, Bacaltchuk J. Psychotherapy for bulimia nervosa and binging. Cochrane Database Syst Rev 2003;(1):CD000562.-
13. Bacaltchuk J, Hay P. Antidepressants versus placebo for people with bulimia nervosa. Cochrane Database Syst Rev 2001;(4):CD003391.-
14. Crow S, Mussell MP, Peterson C, et al. Prior treatment received by patients with bulimia nervosa. Int J Eating Disord 1999;25(1):39-44.
15. Fluoxetine Bulimia Collaborative Study Group Fluoxetine in the treatment of bulimia nervosa: a multicenter placebo-controlled, double-blind trial. Arch Gen Psychiatry 1992;49:139-47.
16. Hoopes S, Reimherr F, Hedges D, et al. Part 1:Topiramate in the treatment of bulimia nervosa: a randomized, double-blind, placebocontrolled trial. J Clin Psychiatry (in press).
17. Horne RL, Ferguson JM, Pope HG, Jr, et al. Treatment of bulimia with bupropion: a controlled multi-center trial. J Clin Psychiatry 1988;49(7):262-6.
18. Pope HG, Jr, McElroy SL, Keck PE, Jr, Hudson JI. Long-term pharmacotherapy of bulimia nervosa. J Clin Psychopharmacol 1989;9(5):385-6.
19. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361(9355):407-16.
20. Pope HG, Jr, Hudson JI. “Recovered memory” therapy for eating disorders: implications of the Ramona verdict. Int J Eat Disord 1996;19(2):139-45.
21. Pope HG, Jr, Hudson JI. Does childhood sexual abuse cause adult psychiatric disorders? Essentials of methodology. J Psychiatry Law 1995;Fall:363-81.
22. Pope HG, Jr, Oliva PS, Hudson JI. Repressed memories. The scientific status of research on repressed memories. In: Faigman DL, Kaye DH, Saks MJ, Sanders J (eds). Science in the law: social and behavioral science issues St. Paul, MN: West Group, 2002;487-526.
23. Cannell J, Hudson JI, Pope HG, Jr. Standards for informed consent in recovered memory therapy. J Am Acad Psychiatry Law 2001;29(2):138-47.
24. Hudson JI, Chase EA, Pope HG, Jr. Eye movement desensitization and reprocessing in eating disorders: caution against premature acceptance. Int J Eat Disord 1998;23:1-5.
25. McNally RJ. EMDR and mesmerism: a comparative historical analysis. J Anxiety Disord 1999;13(1-2):225-36.
1. Mehler PS. Clinical practice. Bulimia nervosa. N Engl J Med 2003;349(9):875-81.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association,2000.
3. Fisher M. The course and outcome of eating disorders in adults and in adolescents: a review. Adolesc Med 2003;14(1):149-58.
4. Fairburn CG, Norman PA, Welch SL, et al. A prospective study of outcome in bulimia nervosa and the long-term effects of three psychological treatments. Arch Gen Psychiatry 1995;52(4):304-12.
5. Hudson JI, Pope HG, Jr, Yurgelun-Todd D, et al. A controlled study of lifetime prevalence of affective and other psychiatric disorders in bulimic outpatients. Am J Psychiatry 1987;144(10):1283-7.
6. Hudson JI, Pope HG, Jr. Affective spectrum disorder: does antidepressant response identify a family of disorders with a common pathophysiology? Am J Psychiatry 1990;147(5):552-64.
7. Hudson JI, Mangweth B, Pope HG, Jr, et al. Family study of affective spectrum disorder. Arch Gen Psychiatry 2003;60:170-7.
8. Hudson JI, Laird NM, Betensky RA, et al. Multivariate logistic regression for familial aggregation of two disorders: II. Analysis of studies of eating and mood disorders. Am J Epidemiology 2001;153(5):506-14.
9. Mangweth B, Hudson JI, Pope HG, Jr, et al. Family study of the aggregation of eating disorders and mood disorders. Psychol Med (in press).
10. Hudson JI, Pope HG, Jr, Carter WP. Pharmacologic therapy of bulimia nervosa. In: Goldstein D (ed). The management of eating disorders and obesity (2nd ed) Totowa, NJ: Humana Press, Inc.(in press).
11. Pope HG, Jr, Hudson JI, Nixon RA, Herridge PL. The epidemiology of ipecac abuse. N Engl J Med 1986;14(4):245-6.
12. Hay PJ, Bacaltchuk J. Psychotherapy for bulimia nervosa and binging. Cochrane Database Syst Rev 2003;(1):CD000562.-
13. Bacaltchuk J, Hay P. Antidepressants versus placebo for people with bulimia nervosa. Cochrane Database Syst Rev 2001;(4):CD003391.-
14. Crow S, Mussell MP, Peterson C, et al. Prior treatment received by patients with bulimia nervosa. Int J Eating Disord 1999;25(1):39-44.
15. Fluoxetine Bulimia Collaborative Study Group Fluoxetine in the treatment of bulimia nervosa: a multicenter placebo-controlled, double-blind trial. Arch Gen Psychiatry 1992;49:139-47.
16. Hoopes S, Reimherr F, Hedges D, et al. Part 1:Topiramate in the treatment of bulimia nervosa: a randomized, double-blind, placebocontrolled trial. J Clin Psychiatry (in press).
17. Horne RL, Ferguson JM, Pope HG, Jr, et al. Treatment of bulimia with bupropion: a controlled multi-center trial. J Clin Psychiatry 1988;49(7):262-6.
18. Pope HG, Jr, McElroy SL, Keck PE, Jr, Hudson JI. Long-term pharmacotherapy of bulimia nervosa. J Clin Psychopharmacol 1989;9(5):385-6.
19. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361(9355):407-16.
20. Pope HG, Jr, Hudson JI. “Recovered memory” therapy for eating disorders: implications of the Ramona verdict. Int J Eat Disord 1996;19(2):139-45.
21. Pope HG, Jr, Hudson JI. Does childhood sexual abuse cause adult psychiatric disorders? Essentials of methodology. J Psychiatry Law 1995;Fall:363-81.
22. Pope HG, Jr, Oliva PS, Hudson JI. Repressed memories. The scientific status of research on repressed memories. In: Faigman DL, Kaye DH, Saks MJ, Sanders J (eds). Science in the law: social and behavioral science issues St. Paul, MN: West Group, 2002;487-526.
23. Cannell J, Hudson JI, Pope HG, Jr. Standards for informed consent in recovered memory therapy. J Am Acad Psychiatry Law 2001;29(2):138-47.
24. Hudson JI, Chase EA, Pope HG, Jr. Eye movement desensitization and reprocessing in eating disorders: caution against premature acceptance. Int J Eat Disord 1998;23:1-5.
25. McNally RJ. EMDR and mesmerism: a comparative historical analysis. J Anxiety Disord 1999;13(1-2):225-36.
Captive of the mirror: ‘I pick at my face all day, every day’
Lying in the hospital bed, her face covered in bandages, Ms. S talked of suicide while awaiting reconstructive surgery on her nose: “If the only way to stop is by killing myself, I will.” When asked what she wanted to stop, she replied, “The picking. I pick at my face all day, every day.”
Ms. S, age 22, had picked a hole through the bridge of her nose, and her face was scarred and covered with scabs. Every morning for 5 years, she had gotten up, dressed, and then—after washing her face—felt intense, uncontrollable urges to pick at her face. Hours would go by and she was still picking, even as her face started to bleed: “I try to resist, but I can’t.”
Ms. S started picking her face when she was 17. She missed so much of high school because of time spent picking that she did not graduate. She now lives alone on medical disability. Conscious of her facial scarring, she rarely goes out in public. “People stare at me as if I’m a zoo animal; it’s so painful,” she says.
After her plastic surgery, she told the staff psychiatrist she had never sought help because she thought no one would understand her behavior. “It doesn’t make sense to me, and I’ve lived with it for years.”
Patients such as Ms. S often suffer in isolation for years, unaware that skin picking is a psychiatric disorder that can be treated successfully. Some are referred to psychiatrists through hospital emergency rooms or by dermatologists; others commit suicide, as Ms. S threatened to do.
In our practice, we recognize skin picking in patients with comorbid mood and anxiety disorders, body dysmorphic disorder (BDD), substance use disorders, impulse control disorders such as trichotillomania or kleptomania, and personality disorders.
Based on recent evidence and our experience, we discuss three steps to help you diagnose pathologic skin picking. We then examine treatment options that have shown benefit for skinpicking patients, including habit reversal psychotherapy and medications.
WHAT IS SKIN PICKING?
Pathologic skin picking is repetitive, ritualistic, or impulsive picking of normal skin, leading to tissue damage, personal distress, and impaired functioning.1 The behavior has been described for more than 100 years but remains poorly understood, under-diagnosed, and under-treated.2,3
Most people pick at their hands or face to a limited extent,4 and picking does not by itself suggest a psychiatric disorder. Pathology exists in the focus, duration, and extent of the behavior, as well as reasons for picking, associated emotions, and resulting problems. Persons with pathologic skin picking report irresistible, intrusive, and/or senseless thoughts of picking or impulses to pick, accompanied by marked distress.1 Pathologic skin picking is recurrent and usually results in noticeable skin damage, although many patients try to camouflage the lesions or scarring with makeup.
Pathologic skin picking’s prevalence is unknown. One early study estimated that 2% of dermatology patients suffer from skin picking.1 Two clinical studies found that 3.8% of college students4 and 28% of patients with BDD meet diagnostic criteria.5,6
TWEEZERS, RAZOR BLADES, KNIVES…
Persons who engage in pathologic skin picking typically spend substantial time picking. Most often they pick the face, but any body part—lips, arms, hands, or legs—may be the focus. They may pick at blemishes, pimples, scars, or healthy skin. Some use their hands and fingernails to pick, and others use pins, tweezers, razor blades, or knives. Picking may worsen in the evening.2,7
Although picking episodes may last only a few minutes, many patients have multiple episodes each day. Some pick for as long as 12 hours every day,2,5 which often leads to scarring and disfigurement. In one study, 90% of patients had at least minor tissue damage, 61% suffered infections, and 45% had “deep craters” because of picking.2
Reasons for picking. Many patients pick to relieve discomfort or tension.1 Others pick to improve their appearance, as in BDD, or to remove perceived dirt or contaminants, as in obsessive-compulsive disorder (OCD).1,5 Still others say they pick as a habit, with minimal awareness.1 Itching or uneven skin may also cause the behavior.1,3 We have found that a patient may pick for several of these reasons. Most report:
- tension before picking
- satisfaction during picking
- guilt, shame, and dysphoria after picking.1
Social impairment. Shame after picking episodes often leads patients to cover lesions with clothing or makeup and to avoid social contact.7 Substantial social and occupational impairment have been reported3,5,7 because of the hours spent picking and from avoiding people because of disfigurement.
Physical injury. Skin picking may cause serious injuries. Some of our patients have required emergency medical intervention and sutures after picking through a major blood vessel (such as the facial artery). One woman—who picked at a pimple on her neck with tweezers—lacerated her carotid artery, causing a near-fatal hemorrhage that required emergency surgery.8
Suicide risk. In a series of 123 patients with BDD, 33 (27%) excessively picked their skin and 10 of those who picked their skin (33%) had attempted suicide.5 In a case series of 31 patients with skin picking, 10% had attempted suicide.2 We know of several young women whose chief complaint was skin picking and who committed suicide.5
Gender. The gender ratio of patients with skin picking remains unclear. In two case series that totaled 65 patients, 87% to 92% of those with pathologic skin picking were female.2,7 In the series of patients with BDD, 58% of the 33 who compulsively picked their skin were female.5 On the other hand, most of 28 patients seen in a dermatology clinic for neurotic excoriations were male.9
Onset and chronicity. Pathologic skin picking may develop at any age, but it usually manifests in late adolescence or early adulthood, often after onset of a dermatologic illness such as acne2 or in response to itching.3 Although long-term studies have not been done, the disorder appears to often be chronic, with waxing and waning of picking intensity and frequency.1,2
Table 1
Skin picking: 3 steps to diagnosis and treatment
| Step 1: Assess reasons for skin picking Dermatologic or medical disorder?
Psychiatric disorder?
Impulse control disorder, not otherwise specified? |
| Step 2: Assess picking severity Treat comorbid mood or anxiety disorders Treat skin picking if:
|
| Step 3: Provide recommended treatment For adults Habit reversal therapy plus medication is usually necessary For children and adolescents Habit reversal therapy alone for mild to moderate symptoms Habit reversal therapy plus medication for severe symptoms |
Comorbid psychopathology. In clinical settings, common comorbid psychopathologies include mood disorders (in 48% to 68% of patients with skin picking), anxiety disorders (41% to 64%), and alcohol use disorders (39%).2
In one patient sample, 71% of skin pickers met criteria for at least one personality disorder (48% had obsessive-compulsive personality disorder, and 26% met criteria for borderline personality disorder).2
Table 2
Medications with evidence of benefit for skin picking*
| Medication | Dosage | Type of evidence |
|---|---|---|
| SSRIs | ||
| Citalopram | 40 mg/d | Case report (effective only with inositol augmentation)16 |
| Fluoxetine | 20 to 80 mg/d | Case reports5,14-15 and two double-blind studies23-24 |
| Fluvoxamine | 100 to 300 mg/d | Case report,8 open-label study,21 and double-blind trial22 |
| Sertraline | 50 to 200 mg/d | Open-label study9 |
| Other agents | ||
| Clomipramine | 50 mg/d | Case report3 |
| Doxepin | 30 mg/d | Case report1 |
| Naltrexone | 50 mg/d | Case report20 |
| Olanzapine | 2.5 to 7.5 mg/d | Case report17 |
| Pimozide | 4 mg/d | Case report18 |
| * Off-label uses; little scientific evidence supports using medications other than SSRIs for treating skin picking. Inform patients of the evidence for using any medication, risk of side effects including change in cardiac conduction (pimozide, clomipramine), seizure risk (pimozide, clomipramine), and tardive dyskinesia (pimozide), and potential interactions with other medications (all of the above). | ||
PRIMARY VS. SECONDARY DISORDER
Is skin picking an independent disorder or a symptom of other psychiatric disorders? Although skin picking is not included in DSM-IV and has no formal diagnostic criteria, some forms of this behavior may belong among the impulse control disorders.
Patients often report an urge to pick their skin in response to increasing tension,1,3 and picking results in transient relief or pleasure.1,2 This description mirrors that of other impulse control disorders, such as trichotillomania and kleptomania. In fact, one study found that trichotillomania and kleptomania were common comorbidities among patients with skin picking (23% and 16%, respectively).2 In 34 patients with psychogenic excoriation, only 7 (21%) appeared to have skin picking as a primary complaint, unaccounted for by another psychiatric disorder.7
Skin picking may also be a symptom of other psychiatric disorders. To determine whether another disorder is present, we ask patients why they pick their skin. Patients may be reluctant to reveal either the picking or the underlying disorder because of embarrassment and shame. The diagnosis can often be clarified by asking about the following conditions:
Body dysmorphic disorder. Nearly 30% of patients with BDD pick their skin to a pathologic extent.5,6 The purpose of picking in BDD is to remove or minimize a nonexistent or slight imperfection in appearance (such as scars, pimples, bumps).5,6
Obsessive-compulsive disorder. Patients with OCD may pick their skin in response to contamination obsessions.1 Picking is often repetitive and ritualistic, and—as with compulsions—the behavior may reduce tension.10
Genetic disorders. Skin picking may be a symptom of Prader-Willi syndrome, a genetic disorder characterized by muscular hypotonia, short stature, characteristic facial features, intellectual disabilities, hypogonadism, hyperphagia, and an increased obesity risk. In one study, 97% of patients with Prader-Willi syndrome engaged in skin picking.11
Delusional disorder. Delusions of parasitosis may result in skin picking, as patients attempt to remove imagined parasites or other vermin from on or under their skin.12
Dermatitis artefacta. Patients may consciously create skin lesions to assume the sick role. Onethird of patients presenting to dermatologists with a disease that is primarily psychiatric may be suffering from dermatitis artefacta.13
TREATMENT RECOMMENDATIONS
Successful clinical care of pathologic skin picking requires perseverance and patience from both patient and clinician.
Treatment begins with a thorough dermatologic examination for medical causes of skin picking (such as atopic dermatitis or scabies) and to treat excoriations (such as with antibiotics for infection). After the dermatologist has ruled out a medical cause, carefully assess the patient’s picking behavior and related psychiatric problems (Table 1).
- If picking is secondary to a psychiatric disorder, begin by providing appropriate treatment for that disorder.
- If picking results from BDD or OCD, we recommend habit reversal therapy combined with medication.
- If picking appears to be an independent impulse control disorder, simultaneous habit reversal therapy and medication is usually necessary to reduce symptoms.
SSRIs are a reasonable first medication because of evidence for their efficacy in reducing skin picking. Higher dosages—comparable to those used in treating OCD—are usually required to improve skin-picking behavior. You may need to try another SSRI if the first trial results in partial or no response.
In our experience, augmenting an SSRI with naltrexone, 50 mg/d, helps reduce intrusive urges to pick and is worth considering if SSRI therapy results in only partial response.
Children or adolescents. Depending upon symptom severity, a trial of habit reversal therapy may be appropriate before you recommend using medication.
EVIDENCE FOR DRUG THERAPY
Although few treatment studies have been done, skin picking does appear to respond to medication (Table 2).
Because no medications are approved to treat skin-picking behavior, inform patients of any “off-label” uses and the scientific or clinical evidence for considering medication treatment.
Case reports and case series. Selective serotonin reuptake inhibitors (SSRIs) appear most effective in patients with picking behavior, including:
- fluvoxamine, 300 mg/d, in one case report8
- fluoxetine, 20 to 80 mg/d, in several case reports.5,14-15
In a series of 33 patients with BDD and compulsive skin picking, one-half (49%) of a variety of SSRI treatment trials improved BDD symptoms and skin picking behavior. The percentage of patients who improved was not examined. Dermatologic treatment alone was effective for only 15% of patients.5
Medications other than SSRIs have also been studied. One patient improved within 3 weeks of taking the tricyclic antidepressant clomipramine, 50 mg/d.3 Another patient picked her skin less often 4 weeks after inositol, 18 grams/d, was added to citalopram, 40 mg/d. Inositol, a nonprescription isomer of glucose, is a precursor in the phosphatidylinositol second-messenger cycle, which may play a role at certain serotonin receptors.16 The patient was given 6 grams dissolved in water three times daily.
Case reports have also suggested that olanzapine, pimozide, doxepin, and naltrexone may be beneficial in reducing skin excoriations. These reports often involved patients with psychiatric and medical comorbidities.17-20
Table 3
Habit reversal: 5 components in patient learning
| Awareness about picking behavior |
| Relaxation to reduce anxiety |
| Competing responses to learn behaviors incompatible with picking (such as fist clenching) |
| Rewarding oneself for successfully resisting picking |
| Generalizing the behavioral control |
Open-label studies. In an open-label study of 28 patients with neurotic excoriation treated in a dermatology clinic, 68% improved within 1 month with sertraline, mean dosage 95 mg/d.9 Similarly, open-label fluvoxamine, mean dosage 112.5 mg/d, was effective in reducing skin excoriation in 7 of 14 patients treated for 12 weeks in a psychiatric setting.21
Double-blind studies. In a double-blind study using fluvoxamine with supportive psychotherapy in patients with psychocutaneous disorders, all five patients with acne excoriee improved after 4 weeks of medication treatment (none was randomized to placebo).22
In a 10-week, double-blind study, 10 patients were assigned to fluoxetine, mean dosage 53.0 ± 16.4 mg/d, and 11 to placebo. A patient self-report visual analog scale showed that fluoxetine was significantly more effective than placebo in reducing picking behavior. Two other measures did not show significant improvement, however, perhaps because of the small sample size.23
In a third study, 8 of 15 patients responded to open-label fluoxetine, 20 to 60 mg/d after 6 weeks. The responders were then randomized to 6 additional weeks of fluoxetine or placebo. All four patients assigned to continue active medication maintained their improvement. Symptoms returned to baseline by week 12 in the four assigned to placebo.24
EVIDENCE FOR HABIT REVERSAL THERAPY
No controlled trials have examined psychosocial treatments for skin picking, but several psychotherapeutic interventions appear promising. Habit reversal has shown promise in three case reports totaling seven patients and appears to reduce picking behavior within a few weeks.25-27
In a case series, three patients were successfully treated with habit reversal (Table 3) and cognitive-behavioral techniques, consisting of:
- awareness training (using a skin-picking diary)
- competing response techniques (such as making a fist or squeezing a ball)
- emotion regulation skills
- psychoeducation
- cognitive restructuring (such as using Socratic questioning to produce rational alternatives) in situations that elicit the urge to pick.28
In another case series, 22 dermatology patients with skin picking received psychotherapy with insight-oriented and behavioral components. Therapy included attention to developmental issues and active conflicts, cognitive restructuring, and tools to manage aggression and social relations. Although treatment duration varied— the mean was weekly for 14 months—skin lesions healed in 17 patients (77%).29
Related resources
- Obsessive-Compulsive Foundation http://www.ocfoundation.org
- Koran LM. Obsessive-compulsive and related disorders in adults: A comprehensive clinical guide. Cambridge, UK: Cambridge University Press, 1999.
- Phillips KA. The broken mirror: Recognizing and treating body dysmorphic disorder. New York: Oxford University Press, 1996.
Drug brand names
- Citalopram • Celexa
- Clomipramine • Anafranil
- Doxepin • Sinequan
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Pimozide • Orap
- Sertraline • Zoloft
Disclosure
Dr. Grant reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Phillips receives research support from Eli Lilly and Co., Forest Pharmaceuticals, and Gate Pharmaceuticals; she is a speaker for or consultant to Eli Lilly and Co., Forest Pharmaceuticals, and UCB Pharma.
1. Arnold LM, Auchenbach MB, McElroy SL. Psychogenic excoriation: clinical features, proposed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs 2001;15:351-9.
2. Wilhelm S, Keuthen NJ, Deckersbach T, et al. Self-injurious skin picking: clinical characteristics and comorbidity. J Clin Psychiatry 1999;60:454-9.
3. Gupta MA, Gupta AK, Haberman HF. Neurotic excoriations: a review and some new perspectives. Compr Psychiatry 1986;27:381-6.
4. Keuthen NJ, Deckersbach T, Wilhelm S, et al. Repetitive skinpicking in a student population and comparison with a sample of self-injurious skin-pickers. Psychosomatics 2000;41:210-15.
5. Phillips KA, Taub SL. Skin picking as a symptom of body dysmorphic disorder. Psychopharmacol Bull 1995;31:279-88.
6. Phillips KA, Diaz S. Gender differences in body dysmorphic disorder. J Nerv Ment Dis 1997;185:570-7
7. Arnold LM, McElroy SL, Mutasim DF, et al. Characteristics of 34 adults with psychogenic excoriation. J Clin Psychiatry 1998;59:509-14.
8. O’Sullivan RL, Phillips KA, Keuthen NJ, Wilhelm S. Near fatal skin picking from delusional body dysmorphic disorder responsive to fluvoxamine. Psychosomatics 1999;40:79-81.
9. Kalivas J, Kalivas L, Gilman D, Hayden CT. Sertraline in the treatment of neurotic excoriations and related disorders [letter]. Arch Dermatol 1996;132:589-90.
10. Stein DJ, Hollander E. Dermatology and conditions related to obsessive-compulsive disorder. J Am Acad Dermatol 1992;26:237-42.
11. Dykens E, Shah B. Psychiatric disorders in Prader-Willi syndrome: epidemiology and management. CNS Drugs 2003;17:167-78.
12. Bishop ER. Monosymptomatic hypochondriacal syndromes in dermatology. J Am Acad Dermatol 1983;9:152-8.
13. Koblenzer CS. Dermatitis artefacta: clinical features and approaches to treatment. Am J Clin Dermatol 2000;1:47-55.
14. Stein DJ, Hutt CS, Spitz JL, Hollander E. Compulsive picking and obsessive-compulsive disorder. Psychosomatics 1993;34:177-80.
15. Stout RJ. Fluoxetine for the treatment of compulsive facial picking [letter]. Am J Psychiatry 1990;147:370.-
16. Seedat S, Stein DJ, Harvey BH. Inositol in the treatment of trichotillomania and compulsive skin picking [letter]. J Clin Psychiatry 2001;62:60-1.
17. Gupta MA, Gupta AK. Olanzapine is effective in the management of some self-induced dermatoses: three case reports. Cutis 2000;66:143-6.
18. Duke EE. Clinical experience with pimozide: emphasis on its use in postherpetic neuralgia. J Am Acad Dermatol 1983;8:845-50.
19. Harris BA, Sherertz EF, Flowers FP. Improvement of chronic neurotic excoriations with oral doxepin therapy. Int J Dermatol 1987;26:541-3.
20. Lienemann J, Walker FD. Reversal of self-abusive behavior with naltrexone [letter]. J Clin Psychopharmacol 1989;9:448-9.
21. Arnold LM, Mutasim DF, Dwight MM, et al. An open clinical trial of fluvoxamine treatment of psychogenic excoriation. J Clin Psychopharmacol 1999;19:15-18.
22. Hendrickx B, Van Moffaert M, Spiers R, Von Frenckell R. The treatment of psychocutaneous disorders: a new approach. Curr Ther Res Clin Exp 1991;49:111-19.
23. Simeon D, Stein DJ, Gross S, et al. A double-blind trial of fluoxetine in pathologic skin picking. J Clin Psychiatry 1997;58:341-7.
24. Bloch MR, Elliott M, Thompson H, Koran LM. Fluoxetine in pathologic skin-picking: open-label and double-blind results. Psychosomatics 2001;42:314-19.
25. Kent A, Drummond LM. Acne excoriee—a case report of treatment using habit-reversal. Clin Exp Dermatol 1989;14:163-4.
26. Rosenbaum MS, Ayllon T. The behavioral treatment of neurodermatitis through habit-reversal. Behav Res Ther 1981;19:313-18.
27. Twohig MP, Woods DW. Habit reversal as a treatment for chronic skin picking in typically developing adult male siblings. J App Behav Analysis 2001;34:217-20.
28. Deckersbach T, Wilhelm S, Keuthen NJ, et al. Cognitive-behavior therapy for self-injurious skin picking. Behav Modif 2002;26:361-77.
29. Fruensgaard K. Psychotherapy and neurotic excoriations. Int J Dermatol 1991;30:262-5.
Lying in the hospital bed, her face covered in bandages, Ms. S talked of suicide while awaiting reconstructive surgery on her nose: “If the only way to stop is by killing myself, I will.” When asked what she wanted to stop, she replied, “The picking. I pick at my face all day, every day.”
Ms. S, age 22, had picked a hole through the bridge of her nose, and her face was scarred and covered with scabs. Every morning for 5 years, she had gotten up, dressed, and then—after washing her face—felt intense, uncontrollable urges to pick at her face. Hours would go by and she was still picking, even as her face started to bleed: “I try to resist, but I can’t.”
Ms. S started picking her face when she was 17. She missed so much of high school because of time spent picking that she did not graduate. She now lives alone on medical disability. Conscious of her facial scarring, she rarely goes out in public. “People stare at me as if I’m a zoo animal; it’s so painful,” she says.
After her plastic surgery, she told the staff psychiatrist she had never sought help because she thought no one would understand her behavior. “It doesn’t make sense to me, and I’ve lived with it for years.”
Patients such as Ms. S often suffer in isolation for years, unaware that skin picking is a psychiatric disorder that can be treated successfully. Some are referred to psychiatrists through hospital emergency rooms or by dermatologists; others commit suicide, as Ms. S threatened to do.
In our practice, we recognize skin picking in patients with comorbid mood and anxiety disorders, body dysmorphic disorder (BDD), substance use disorders, impulse control disorders such as trichotillomania or kleptomania, and personality disorders.
Based on recent evidence and our experience, we discuss three steps to help you diagnose pathologic skin picking. We then examine treatment options that have shown benefit for skinpicking patients, including habit reversal psychotherapy and medications.
WHAT IS SKIN PICKING?
Pathologic skin picking is repetitive, ritualistic, or impulsive picking of normal skin, leading to tissue damage, personal distress, and impaired functioning.1 The behavior has been described for more than 100 years but remains poorly understood, under-diagnosed, and under-treated.2,3
Most people pick at their hands or face to a limited extent,4 and picking does not by itself suggest a psychiatric disorder. Pathology exists in the focus, duration, and extent of the behavior, as well as reasons for picking, associated emotions, and resulting problems. Persons with pathologic skin picking report irresistible, intrusive, and/or senseless thoughts of picking or impulses to pick, accompanied by marked distress.1 Pathologic skin picking is recurrent and usually results in noticeable skin damage, although many patients try to camouflage the lesions or scarring with makeup.
Pathologic skin picking’s prevalence is unknown. One early study estimated that 2% of dermatology patients suffer from skin picking.1 Two clinical studies found that 3.8% of college students4 and 28% of patients with BDD meet diagnostic criteria.5,6
TWEEZERS, RAZOR BLADES, KNIVES…
Persons who engage in pathologic skin picking typically spend substantial time picking. Most often they pick the face, but any body part—lips, arms, hands, or legs—may be the focus. They may pick at blemishes, pimples, scars, or healthy skin. Some use their hands and fingernails to pick, and others use pins, tweezers, razor blades, or knives. Picking may worsen in the evening.2,7
Although picking episodes may last only a few minutes, many patients have multiple episodes each day. Some pick for as long as 12 hours every day,2,5 which often leads to scarring and disfigurement. In one study, 90% of patients had at least minor tissue damage, 61% suffered infections, and 45% had “deep craters” because of picking.2
Reasons for picking. Many patients pick to relieve discomfort or tension.1 Others pick to improve their appearance, as in BDD, or to remove perceived dirt or contaminants, as in obsessive-compulsive disorder (OCD).1,5 Still others say they pick as a habit, with minimal awareness.1 Itching or uneven skin may also cause the behavior.1,3 We have found that a patient may pick for several of these reasons. Most report:
- tension before picking
- satisfaction during picking
- guilt, shame, and dysphoria after picking.1
Social impairment. Shame after picking episodes often leads patients to cover lesions with clothing or makeup and to avoid social contact.7 Substantial social and occupational impairment have been reported3,5,7 because of the hours spent picking and from avoiding people because of disfigurement.
Physical injury. Skin picking may cause serious injuries. Some of our patients have required emergency medical intervention and sutures after picking through a major blood vessel (such as the facial artery). One woman—who picked at a pimple on her neck with tweezers—lacerated her carotid artery, causing a near-fatal hemorrhage that required emergency surgery.8
Suicide risk. In a series of 123 patients with BDD, 33 (27%) excessively picked their skin and 10 of those who picked their skin (33%) had attempted suicide.5 In a case series of 31 patients with skin picking, 10% had attempted suicide.2 We know of several young women whose chief complaint was skin picking and who committed suicide.5
Gender. The gender ratio of patients with skin picking remains unclear. In two case series that totaled 65 patients, 87% to 92% of those with pathologic skin picking were female.2,7 In the series of patients with BDD, 58% of the 33 who compulsively picked their skin were female.5 On the other hand, most of 28 patients seen in a dermatology clinic for neurotic excoriations were male.9
Onset and chronicity. Pathologic skin picking may develop at any age, but it usually manifests in late adolescence or early adulthood, often after onset of a dermatologic illness such as acne2 or in response to itching.3 Although long-term studies have not been done, the disorder appears to often be chronic, with waxing and waning of picking intensity and frequency.1,2
Table 1
Skin picking: 3 steps to diagnosis and treatment
| Step 1: Assess reasons for skin picking Dermatologic or medical disorder?
Psychiatric disorder?
Impulse control disorder, not otherwise specified? |
| Step 2: Assess picking severity Treat comorbid mood or anxiety disorders Treat skin picking if:
|
| Step 3: Provide recommended treatment For adults Habit reversal therapy plus medication is usually necessary For children and adolescents Habit reversal therapy alone for mild to moderate symptoms Habit reversal therapy plus medication for severe symptoms |
Comorbid psychopathology. In clinical settings, common comorbid psychopathologies include mood disorders (in 48% to 68% of patients with skin picking), anxiety disorders (41% to 64%), and alcohol use disorders (39%).2
In one patient sample, 71% of skin pickers met criteria for at least one personality disorder (48% had obsessive-compulsive personality disorder, and 26% met criteria for borderline personality disorder).2
Table 2
Medications with evidence of benefit for skin picking*
| Medication | Dosage | Type of evidence |
|---|---|---|
| SSRIs | ||
| Citalopram | 40 mg/d | Case report (effective only with inositol augmentation)16 |
| Fluoxetine | 20 to 80 mg/d | Case reports5,14-15 and two double-blind studies23-24 |
| Fluvoxamine | 100 to 300 mg/d | Case report,8 open-label study,21 and double-blind trial22 |
| Sertraline | 50 to 200 mg/d | Open-label study9 |
| Other agents | ||
| Clomipramine | 50 mg/d | Case report3 |
| Doxepin | 30 mg/d | Case report1 |
| Naltrexone | 50 mg/d | Case report20 |
| Olanzapine | 2.5 to 7.5 mg/d | Case report17 |
| Pimozide | 4 mg/d | Case report18 |
| * Off-label uses; little scientific evidence supports using medications other than SSRIs for treating skin picking. Inform patients of the evidence for using any medication, risk of side effects including change in cardiac conduction (pimozide, clomipramine), seizure risk (pimozide, clomipramine), and tardive dyskinesia (pimozide), and potential interactions with other medications (all of the above). | ||
PRIMARY VS. SECONDARY DISORDER
Is skin picking an independent disorder or a symptom of other psychiatric disorders? Although skin picking is not included in DSM-IV and has no formal diagnostic criteria, some forms of this behavior may belong among the impulse control disorders.
Patients often report an urge to pick their skin in response to increasing tension,1,3 and picking results in transient relief or pleasure.1,2 This description mirrors that of other impulse control disorders, such as trichotillomania and kleptomania. In fact, one study found that trichotillomania and kleptomania were common comorbidities among patients with skin picking (23% and 16%, respectively).2 In 34 patients with psychogenic excoriation, only 7 (21%) appeared to have skin picking as a primary complaint, unaccounted for by another psychiatric disorder.7
Skin picking may also be a symptom of other psychiatric disorders. To determine whether another disorder is present, we ask patients why they pick their skin. Patients may be reluctant to reveal either the picking or the underlying disorder because of embarrassment and shame. The diagnosis can often be clarified by asking about the following conditions:
Body dysmorphic disorder. Nearly 30% of patients with BDD pick their skin to a pathologic extent.5,6 The purpose of picking in BDD is to remove or minimize a nonexistent or slight imperfection in appearance (such as scars, pimples, bumps).5,6
Obsessive-compulsive disorder. Patients with OCD may pick their skin in response to contamination obsessions.1 Picking is often repetitive and ritualistic, and—as with compulsions—the behavior may reduce tension.10
Genetic disorders. Skin picking may be a symptom of Prader-Willi syndrome, a genetic disorder characterized by muscular hypotonia, short stature, characteristic facial features, intellectual disabilities, hypogonadism, hyperphagia, and an increased obesity risk. In one study, 97% of patients with Prader-Willi syndrome engaged in skin picking.11
Delusional disorder. Delusions of parasitosis may result in skin picking, as patients attempt to remove imagined parasites or other vermin from on or under their skin.12
Dermatitis artefacta. Patients may consciously create skin lesions to assume the sick role. Onethird of patients presenting to dermatologists with a disease that is primarily psychiatric may be suffering from dermatitis artefacta.13
TREATMENT RECOMMENDATIONS
Successful clinical care of pathologic skin picking requires perseverance and patience from both patient and clinician.
Treatment begins with a thorough dermatologic examination for medical causes of skin picking (such as atopic dermatitis or scabies) and to treat excoriations (such as with antibiotics for infection). After the dermatologist has ruled out a medical cause, carefully assess the patient’s picking behavior and related psychiatric problems (Table 1).
- If picking is secondary to a psychiatric disorder, begin by providing appropriate treatment for that disorder.
- If picking results from BDD or OCD, we recommend habit reversal therapy combined with medication.
- If picking appears to be an independent impulse control disorder, simultaneous habit reversal therapy and medication is usually necessary to reduce symptoms.
SSRIs are a reasonable first medication because of evidence for their efficacy in reducing skin picking. Higher dosages—comparable to those used in treating OCD—are usually required to improve skin-picking behavior. You may need to try another SSRI if the first trial results in partial or no response.
In our experience, augmenting an SSRI with naltrexone, 50 mg/d, helps reduce intrusive urges to pick and is worth considering if SSRI therapy results in only partial response.
Children or adolescents. Depending upon symptom severity, a trial of habit reversal therapy may be appropriate before you recommend using medication.
EVIDENCE FOR DRUG THERAPY
Although few treatment studies have been done, skin picking does appear to respond to medication (Table 2).
Because no medications are approved to treat skin-picking behavior, inform patients of any “off-label” uses and the scientific or clinical evidence for considering medication treatment.
Case reports and case series. Selective serotonin reuptake inhibitors (SSRIs) appear most effective in patients with picking behavior, including:
- fluvoxamine, 300 mg/d, in one case report8
- fluoxetine, 20 to 80 mg/d, in several case reports.5,14-15
In a series of 33 patients with BDD and compulsive skin picking, one-half (49%) of a variety of SSRI treatment trials improved BDD symptoms and skin picking behavior. The percentage of patients who improved was not examined. Dermatologic treatment alone was effective for only 15% of patients.5
Medications other than SSRIs have also been studied. One patient improved within 3 weeks of taking the tricyclic antidepressant clomipramine, 50 mg/d.3 Another patient picked her skin less often 4 weeks after inositol, 18 grams/d, was added to citalopram, 40 mg/d. Inositol, a nonprescription isomer of glucose, is a precursor in the phosphatidylinositol second-messenger cycle, which may play a role at certain serotonin receptors.16 The patient was given 6 grams dissolved in water three times daily.
Case reports have also suggested that olanzapine, pimozide, doxepin, and naltrexone may be beneficial in reducing skin excoriations. These reports often involved patients with psychiatric and medical comorbidities.17-20
Table 3
Habit reversal: 5 components in patient learning
| Awareness about picking behavior |
| Relaxation to reduce anxiety |
| Competing responses to learn behaviors incompatible with picking (such as fist clenching) |
| Rewarding oneself for successfully resisting picking |
| Generalizing the behavioral control |
Open-label studies. In an open-label study of 28 patients with neurotic excoriation treated in a dermatology clinic, 68% improved within 1 month with sertraline, mean dosage 95 mg/d.9 Similarly, open-label fluvoxamine, mean dosage 112.5 mg/d, was effective in reducing skin excoriation in 7 of 14 patients treated for 12 weeks in a psychiatric setting.21
Double-blind studies. In a double-blind study using fluvoxamine with supportive psychotherapy in patients with psychocutaneous disorders, all five patients with acne excoriee improved after 4 weeks of medication treatment (none was randomized to placebo).22
In a 10-week, double-blind study, 10 patients were assigned to fluoxetine, mean dosage 53.0 ± 16.4 mg/d, and 11 to placebo. A patient self-report visual analog scale showed that fluoxetine was significantly more effective than placebo in reducing picking behavior. Two other measures did not show significant improvement, however, perhaps because of the small sample size.23
In a third study, 8 of 15 patients responded to open-label fluoxetine, 20 to 60 mg/d after 6 weeks. The responders were then randomized to 6 additional weeks of fluoxetine or placebo. All four patients assigned to continue active medication maintained their improvement. Symptoms returned to baseline by week 12 in the four assigned to placebo.24
EVIDENCE FOR HABIT REVERSAL THERAPY
No controlled trials have examined psychosocial treatments for skin picking, but several psychotherapeutic interventions appear promising. Habit reversal has shown promise in three case reports totaling seven patients and appears to reduce picking behavior within a few weeks.25-27
In a case series, three patients were successfully treated with habit reversal (Table 3) and cognitive-behavioral techniques, consisting of:
- awareness training (using a skin-picking diary)
- competing response techniques (such as making a fist or squeezing a ball)
- emotion regulation skills
- psychoeducation
- cognitive restructuring (such as using Socratic questioning to produce rational alternatives) in situations that elicit the urge to pick.28
In another case series, 22 dermatology patients with skin picking received psychotherapy with insight-oriented and behavioral components. Therapy included attention to developmental issues and active conflicts, cognitive restructuring, and tools to manage aggression and social relations. Although treatment duration varied— the mean was weekly for 14 months—skin lesions healed in 17 patients (77%).29
Related resources
- Obsessive-Compulsive Foundation http://www.ocfoundation.org
- Koran LM. Obsessive-compulsive and related disorders in adults: A comprehensive clinical guide. Cambridge, UK: Cambridge University Press, 1999.
- Phillips KA. The broken mirror: Recognizing and treating body dysmorphic disorder. New York: Oxford University Press, 1996.
Drug brand names
- Citalopram • Celexa
- Clomipramine • Anafranil
- Doxepin • Sinequan
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Pimozide • Orap
- Sertraline • Zoloft
Disclosure
Dr. Grant reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Phillips receives research support from Eli Lilly and Co., Forest Pharmaceuticals, and Gate Pharmaceuticals; she is a speaker for or consultant to Eli Lilly and Co., Forest Pharmaceuticals, and UCB Pharma.
Lying in the hospital bed, her face covered in bandages, Ms. S talked of suicide while awaiting reconstructive surgery on her nose: “If the only way to stop is by killing myself, I will.” When asked what she wanted to stop, she replied, “The picking. I pick at my face all day, every day.”
Ms. S, age 22, had picked a hole through the bridge of her nose, and her face was scarred and covered with scabs. Every morning for 5 years, she had gotten up, dressed, and then—after washing her face—felt intense, uncontrollable urges to pick at her face. Hours would go by and she was still picking, even as her face started to bleed: “I try to resist, but I can’t.”
Ms. S started picking her face when she was 17. She missed so much of high school because of time spent picking that she did not graduate. She now lives alone on medical disability. Conscious of her facial scarring, she rarely goes out in public. “People stare at me as if I’m a zoo animal; it’s so painful,” she says.
After her plastic surgery, she told the staff psychiatrist she had never sought help because she thought no one would understand her behavior. “It doesn’t make sense to me, and I’ve lived with it for years.”
Patients such as Ms. S often suffer in isolation for years, unaware that skin picking is a psychiatric disorder that can be treated successfully. Some are referred to psychiatrists through hospital emergency rooms or by dermatologists; others commit suicide, as Ms. S threatened to do.
In our practice, we recognize skin picking in patients with comorbid mood and anxiety disorders, body dysmorphic disorder (BDD), substance use disorders, impulse control disorders such as trichotillomania or kleptomania, and personality disorders.
Based on recent evidence and our experience, we discuss three steps to help you diagnose pathologic skin picking. We then examine treatment options that have shown benefit for skinpicking patients, including habit reversal psychotherapy and medications.
WHAT IS SKIN PICKING?
Pathologic skin picking is repetitive, ritualistic, or impulsive picking of normal skin, leading to tissue damage, personal distress, and impaired functioning.1 The behavior has been described for more than 100 years but remains poorly understood, under-diagnosed, and under-treated.2,3
Most people pick at their hands or face to a limited extent,4 and picking does not by itself suggest a psychiatric disorder. Pathology exists in the focus, duration, and extent of the behavior, as well as reasons for picking, associated emotions, and resulting problems. Persons with pathologic skin picking report irresistible, intrusive, and/or senseless thoughts of picking or impulses to pick, accompanied by marked distress.1 Pathologic skin picking is recurrent and usually results in noticeable skin damage, although many patients try to camouflage the lesions or scarring with makeup.
Pathologic skin picking’s prevalence is unknown. One early study estimated that 2% of dermatology patients suffer from skin picking.1 Two clinical studies found that 3.8% of college students4 and 28% of patients with BDD meet diagnostic criteria.5,6
TWEEZERS, RAZOR BLADES, KNIVES…
Persons who engage in pathologic skin picking typically spend substantial time picking. Most often they pick the face, but any body part—lips, arms, hands, or legs—may be the focus. They may pick at blemishes, pimples, scars, or healthy skin. Some use their hands and fingernails to pick, and others use pins, tweezers, razor blades, or knives. Picking may worsen in the evening.2,7
Although picking episodes may last only a few minutes, many patients have multiple episodes each day. Some pick for as long as 12 hours every day,2,5 which often leads to scarring and disfigurement. In one study, 90% of patients had at least minor tissue damage, 61% suffered infections, and 45% had “deep craters” because of picking.2
Reasons for picking. Many patients pick to relieve discomfort or tension.1 Others pick to improve their appearance, as in BDD, or to remove perceived dirt or contaminants, as in obsessive-compulsive disorder (OCD).1,5 Still others say they pick as a habit, with minimal awareness.1 Itching or uneven skin may also cause the behavior.1,3 We have found that a patient may pick for several of these reasons. Most report:
- tension before picking
- satisfaction during picking
- guilt, shame, and dysphoria after picking.1
Social impairment. Shame after picking episodes often leads patients to cover lesions with clothing or makeup and to avoid social contact.7 Substantial social and occupational impairment have been reported3,5,7 because of the hours spent picking and from avoiding people because of disfigurement.
Physical injury. Skin picking may cause serious injuries. Some of our patients have required emergency medical intervention and sutures after picking through a major blood vessel (such as the facial artery). One woman—who picked at a pimple on her neck with tweezers—lacerated her carotid artery, causing a near-fatal hemorrhage that required emergency surgery.8
Suicide risk. In a series of 123 patients with BDD, 33 (27%) excessively picked their skin and 10 of those who picked their skin (33%) had attempted suicide.5 In a case series of 31 patients with skin picking, 10% had attempted suicide.2 We know of several young women whose chief complaint was skin picking and who committed suicide.5
Gender. The gender ratio of patients with skin picking remains unclear. In two case series that totaled 65 patients, 87% to 92% of those with pathologic skin picking were female.2,7 In the series of patients with BDD, 58% of the 33 who compulsively picked their skin were female.5 On the other hand, most of 28 patients seen in a dermatology clinic for neurotic excoriations were male.9
Onset and chronicity. Pathologic skin picking may develop at any age, but it usually manifests in late adolescence or early adulthood, often after onset of a dermatologic illness such as acne2 or in response to itching.3 Although long-term studies have not been done, the disorder appears to often be chronic, with waxing and waning of picking intensity and frequency.1,2
Table 1
Skin picking: 3 steps to diagnosis and treatment
| Step 1: Assess reasons for skin picking Dermatologic or medical disorder?
Psychiatric disorder?
Impulse control disorder, not otherwise specified? |
| Step 2: Assess picking severity Treat comorbid mood or anxiety disorders Treat skin picking if:
|
| Step 3: Provide recommended treatment For adults Habit reversal therapy plus medication is usually necessary For children and adolescents Habit reversal therapy alone for mild to moderate symptoms Habit reversal therapy plus medication for severe symptoms |
Comorbid psychopathology. In clinical settings, common comorbid psychopathologies include mood disorders (in 48% to 68% of patients with skin picking), anxiety disorders (41% to 64%), and alcohol use disorders (39%).2
In one patient sample, 71% of skin pickers met criteria for at least one personality disorder (48% had obsessive-compulsive personality disorder, and 26% met criteria for borderline personality disorder).2
Table 2
Medications with evidence of benefit for skin picking*
| Medication | Dosage | Type of evidence |
|---|---|---|
| SSRIs | ||
| Citalopram | 40 mg/d | Case report (effective only with inositol augmentation)16 |
| Fluoxetine | 20 to 80 mg/d | Case reports5,14-15 and two double-blind studies23-24 |
| Fluvoxamine | 100 to 300 mg/d | Case report,8 open-label study,21 and double-blind trial22 |
| Sertraline | 50 to 200 mg/d | Open-label study9 |
| Other agents | ||
| Clomipramine | 50 mg/d | Case report3 |
| Doxepin | 30 mg/d | Case report1 |
| Naltrexone | 50 mg/d | Case report20 |
| Olanzapine | 2.5 to 7.5 mg/d | Case report17 |
| Pimozide | 4 mg/d | Case report18 |
| * Off-label uses; little scientific evidence supports using medications other than SSRIs for treating skin picking. Inform patients of the evidence for using any medication, risk of side effects including change in cardiac conduction (pimozide, clomipramine), seizure risk (pimozide, clomipramine), and tardive dyskinesia (pimozide), and potential interactions with other medications (all of the above). | ||
PRIMARY VS. SECONDARY DISORDER
Is skin picking an independent disorder or a symptom of other psychiatric disorders? Although skin picking is not included in DSM-IV and has no formal diagnostic criteria, some forms of this behavior may belong among the impulse control disorders.
Patients often report an urge to pick their skin in response to increasing tension,1,3 and picking results in transient relief or pleasure.1,2 This description mirrors that of other impulse control disorders, such as trichotillomania and kleptomania. In fact, one study found that trichotillomania and kleptomania were common comorbidities among patients with skin picking (23% and 16%, respectively).2 In 34 patients with psychogenic excoriation, only 7 (21%) appeared to have skin picking as a primary complaint, unaccounted for by another psychiatric disorder.7
Skin picking may also be a symptom of other psychiatric disorders. To determine whether another disorder is present, we ask patients why they pick their skin. Patients may be reluctant to reveal either the picking or the underlying disorder because of embarrassment and shame. The diagnosis can often be clarified by asking about the following conditions:
Body dysmorphic disorder. Nearly 30% of patients with BDD pick their skin to a pathologic extent.5,6 The purpose of picking in BDD is to remove or minimize a nonexistent or slight imperfection in appearance (such as scars, pimples, bumps).5,6
Obsessive-compulsive disorder. Patients with OCD may pick their skin in response to contamination obsessions.1 Picking is often repetitive and ritualistic, and—as with compulsions—the behavior may reduce tension.10
Genetic disorders. Skin picking may be a symptom of Prader-Willi syndrome, a genetic disorder characterized by muscular hypotonia, short stature, characteristic facial features, intellectual disabilities, hypogonadism, hyperphagia, and an increased obesity risk. In one study, 97% of patients with Prader-Willi syndrome engaged in skin picking.11
Delusional disorder. Delusions of parasitosis may result in skin picking, as patients attempt to remove imagined parasites or other vermin from on or under their skin.12
Dermatitis artefacta. Patients may consciously create skin lesions to assume the sick role. Onethird of patients presenting to dermatologists with a disease that is primarily psychiatric may be suffering from dermatitis artefacta.13
TREATMENT RECOMMENDATIONS
Successful clinical care of pathologic skin picking requires perseverance and patience from both patient and clinician.
Treatment begins with a thorough dermatologic examination for medical causes of skin picking (such as atopic dermatitis or scabies) and to treat excoriations (such as with antibiotics for infection). After the dermatologist has ruled out a medical cause, carefully assess the patient’s picking behavior and related psychiatric problems (Table 1).
- If picking is secondary to a psychiatric disorder, begin by providing appropriate treatment for that disorder.
- If picking results from BDD or OCD, we recommend habit reversal therapy combined with medication.
- If picking appears to be an independent impulse control disorder, simultaneous habit reversal therapy and medication is usually necessary to reduce symptoms.
SSRIs are a reasonable first medication because of evidence for their efficacy in reducing skin picking. Higher dosages—comparable to those used in treating OCD—are usually required to improve skin-picking behavior. You may need to try another SSRI if the first trial results in partial or no response.
In our experience, augmenting an SSRI with naltrexone, 50 mg/d, helps reduce intrusive urges to pick and is worth considering if SSRI therapy results in only partial response.
Children or adolescents. Depending upon symptom severity, a trial of habit reversal therapy may be appropriate before you recommend using medication.
EVIDENCE FOR DRUG THERAPY
Although few treatment studies have been done, skin picking does appear to respond to medication (Table 2).
Because no medications are approved to treat skin-picking behavior, inform patients of any “off-label” uses and the scientific or clinical evidence for considering medication treatment.
Case reports and case series. Selective serotonin reuptake inhibitors (SSRIs) appear most effective in patients with picking behavior, including:
- fluvoxamine, 300 mg/d, in one case report8
- fluoxetine, 20 to 80 mg/d, in several case reports.5,14-15
In a series of 33 patients with BDD and compulsive skin picking, one-half (49%) of a variety of SSRI treatment trials improved BDD symptoms and skin picking behavior. The percentage of patients who improved was not examined. Dermatologic treatment alone was effective for only 15% of patients.5
Medications other than SSRIs have also been studied. One patient improved within 3 weeks of taking the tricyclic antidepressant clomipramine, 50 mg/d.3 Another patient picked her skin less often 4 weeks after inositol, 18 grams/d, was added to citalopram, 40 mg/d. Inositol, a nonprescription isomer of glucose, is a precursor in the phosphatidylinositol second-messenger cycle, which may play a role at certain serotonin receptors.16 The patient was given 6 grams dissolved in water three times daily.
Case reports have also suggested that olanzapine, pimozide, doxepin, and naltrexone may be beneficial in reducing skin excoriations. These reports often involved patients with psychiatric and medical comorbidities.17-20
Table 3
Habit reversal: 5 components in patient learning
| Awareness about picking behavior |
| Relaxation to reduce anxiety |
| Competing responses to learn behaviors incompatible with picking (such as fist clenching) |
| Rewarding oneself for successfully resisting picking |
| Generalizing the behavioral control |
Open-label studies. In an open-label study of 28 patients with neurotic excoriation treated in a dermatology clinic, 68% improved within 1 month with sertraline, mean dosage 95 mg/d.9 Similarly, open-label fluvoxamine, mean dosage 112.5 mg/d, was effective in reducing skin excoriation in 7 of 14 patients treated for 12 weeks in a psychiatric setting.21
Double-blind studies. In a double-blind study using fluvoxamine with supportive psychotherapy in patients with psychocutaneous disorders, all five patients with acne excoriee improved after 4 weeks of medication treatment (none was randomized to placebo).22
In a 10-week, double-blind study, 10 patients were assigned to fluoxetine, mean dosage 53.0 ± 16.4 mg/d, and 11 to placebo. A patient self-report visual analog scale showed that fluoxetine was significantly more effective than placebo in reducing picking behavior. Two other measures did not show significant improvement, however, perhaps because of the small sample size.23
In a third study, 8 of 15 patients responded to open-label fluoxetine, 20 to 60 mg/d after 6 weeks. The responders were then randomized to 6 additional weeks of fluoxetine or placebo. All four patients assigned to continue active medication maintained their improvement. Symptoms returned to baseline by week 12 in the four assigned to placebo.24
EVIDENCE FOR HABIT REVERSAL THERAPY
No controlled trials have examined psychosocial treatments for skin picking, but several psychotherapeutic interventions appear promising. Habit reversal has shown promise in three case reports totaling seven patients and appears to reduce picking behavior within a few weeks.25-27
In a case series, three patients were successfully treated with habit reversal (Table 3) and cognitive-behavioral techniques, consisting of:
- awareness training (using a skin-picking diary)
- competing response techniques (such as making a fist or squeezing a ball)
- emotion regulation skills
- psychoeducation
- cognitive restructuring (such as using Socratic questioning to produce rational alternatives) in situations that elicit the urge to pick.28
In another case series, 22 dermatology patients with skin picking received psychotherapy with insight-oriented and behavioral components. Therapy included attention to developmental issues and active conflicts, cognitive restructuring, and tools to manage aggression and social relations. Although treatment duration varied— the mean was weekly for 14 months—skin lesions healed in 17 patients (77%).29
Related resources
- Obsessive-Compulsive Foundation http://www.ocfoundation.org
- Koran LM. Obsessive-compulsive and related disorders in adults: A comprehensive clinical guide. Cambridge, UK: Cambridge University Press, 1999.
- Phillips KA. The broken mirror: Recognizing and treating body dysmorphic disorder. New York: Oxford University Press, 1996.
Drug brand names
- Citalopram • Celexa
- Clomipramine • Anafranil
- Doxepin • Sinequan
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Pimozide • Orap
- Sertraline • Zoloft
Disclosure
Dr. Grant reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Phillips receives research support from Eli Lilly and Co., Forest Pharmaceuticals, and Gate Pharmaceuticals; she is a speaker for or consultant to Eli Lilly and Co., Forest Pharmaceuticals, and UCB Pharma.
1. Arnold LM, Auchenbach MB, McElroy SL. Psychogenic excoriation: clinical features, proposed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs 2001;15:351-9.
2. Wilhelm S, Keuthen NJ, Deckersbach T, et al. Self-injurious skin picking: clinical characteristics and comorbidity. J Clin Psychiatry 1999;60:454-9.
3. Gupta MA, Gupta AK, Haberman HF. Neurotic excoriations: a review and some new perspectives. Compr Psychiatry 1986;27:381-6.
4. Keuthen NJ, Deckersbach T, Wilhelm S, et al. Repetitive skinpicking in a student population and comparison with a sample of self-injurious skin-pickers. Psychosomatics 2000;41:210-15.
5. Phillips KA, Taub SL. Skin picking as a symptom of body dysmorphic disorder. Psychopharmacol Bull 1995;31:279-88.
6. Phillips KA, Diaz S. Gender differences in body dysmorphic disorder. J Nerv Ment Dis 1997;185:570-7
7. Arnold LM, McElroy SL, Mutasim DF, et al. Characteristics of 34 adults with psychogenic excoriation. J Clin Psychiatry 1998;59:509-14.
8. O’Sullivan RL, Phillips KA, Keuthen NJ, Wilhelm S. Near fatal skin picking from delusional body dysmorphic disorder responsive to fluvoxamine. Psychosomatics 1999;40:79-81.
9. Kalivas J, Kalivas L, Gilman D, Hayden CT. Sertraline in the treatment of neurotic excoriations and related disorders [letter]. Arch Dermatol 1996;132:589-90.
10. Stein DJ, Hollander E. Dermatology and conditions related to obsessive-compulsive disorder. J Am Acad Dermatol 1992;26:237-42.
11. Dykens E, Shah B. Psychiatric disorders in Prader-Willi syndrome: epidemiology and management. CNS Drugs 2003;17:167-78.
12. Bishop ER. Monosymptomatic hypochondriacal syndromes in dermatology. J Am Acad Dermatol 1983;9:152-8.
13. Koblenzer CS. Dermatitis artefacta: clinical features and approaches to treatment. Am J Clin Dermatol 2000;1:47-55.
14. Stein DJ, Hutt CS, Spitz JL, Hollander E. Compulsive picking and obsessive-compulsive disorder. Psychosomatics 1993;34:177-80.
15. Stout RJ. Fluoxetine for the treatment of compulsive facial picking [letter]. Am J Psychiatry 1990;147:370.-
16. Seedat S, Stein DJ, Harvey BH. Inositol in the treatment of trichotillomania and compulsive skin picking [letter]. J Clin Psychiatry 2001;62:60-1.
17. Gupta MA, Gupta AK. Olanzapine is effective in the management of some self-induced dermatoses: three case reports. Cutis 2000;66:143-6.
18. Duke EE. Clinical experience with pimozide: emphasis on its use in postherpetic neuralgia. J Am Acad Dermatol 1983;8:845-50.
19. Harris BA, Sherertz EF, Flowers FP. Improvement of chronic neurotic excoriations with oral doxepin therapy. Int J Dermatol 1987;26:541-3.
20. Lienemann J, Walker FD. Reversal of self-abusive behavior with naltrexone [letter]. J Clin Psychopharmacol 1989;9:448-9.
21. Arnold LM, Mutasim DF, Dwight MM, et al. An open clinical trial of fluvoxamine treatment of psychogenic excoriation. J Clin Psychopharmacol 1999;19:15-18.
22. Hendrickx B, Van Moffaert M, Spiers R, Von Frenckell R. The treatment of psychocutaneous disorders: a new approach. Curr Ther Res Clin Exp 1991;49:111-19.
23. Simeon D, Stein DJ, Gross S, et al. A double-blind trial of fluoxetine in pathologic skin picking. J Clin Psychiatry 1997;58:341-7.
24. Bloch MR, Elliott M, Thompson H, Koran LM. Fluoxetine in pathologic skin-picking: open-label and double-blind results. Psychosomatics 2001;42:314-19.
25. Kent A, Drummond LM. Acne excoriee—a case report of treatment using habit-reversal. Clin Exp Dermatol 1989;14:163-4.
26. Rosenbaum MS, Ayllon T. The behavioral treatment of neurodermatitis through habit-reversal. Behav Res Ther 1981;19:313-18.
27. Twohig MP, Woods DW. Habit reversal as a treatment for chronic skin picking in typically developing adult male siblings. J App Behav Analysis 2001;34:217-20.
28. Deckersbach T, Wilhelm S, Keuthen NJ, et al. Cognitive-behavior therapy for self-injurious skin picking. Behav Modif 2002;26:361-77.
29. Fruensgaard K. Psychotherapy and neurotic excoriations. Int J Dermatol 1991;30:262-5.
1. Arnold LM, Auchenbach MB, McElroy SL. Psychogenic excoriation: clinical features, proposed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs 2001;15:351-9.
2. Wilhelm S, Keuthen NJ, Deckersbach T, et al. Self-injurious skin picking: clinical characteristics and comorbidity. J Clin Psychiatry 1999;60:454-9.
3. Gupta MA, Gupta AK, Haberman HF. Neurotic excoriations: a review and some new perspectives. Compr Psychiatry 1986;27:381-6.
4. Keuthen NJ, Deckersbach T, Wilhelm S, et al. Repetitive skinpicking in a student population and comparison with a sample of self-injurious skin-pickers. Psychosomatics 2000;41:210-15.
5. Phillips KA, Taub SL. Skin picking as a symptom of body dysmorphic disorder. Psychopharmacol Bull 1995;31:279-88.
6. Phillips KA, Diaz S. Gender differences in body dysmorphic disorder. J Nerv Ment Dis 1997;185:570-7
7. Arnold LM, McElroy SL, Mutasim DF, et al. Characteristics of 34 adults with psychogenic excoriation. J Clin Psychiatry 1998;59:509-14.
8. O’Sullivan RL, Phillips KA, Keuthen NJ, Wilhelm S. Near fatal skin picking from delusional body dysmorphic disorder responsive to fluvoxamine. Psychosomatics 1999;40:79-81.
9. Kalivas J, Kalivas L, Gilman D, Hayden CT. Sertraline in the treatment of neurotic excoriations and related disorders [letter]. Arch Dermatol 1996;132:589-90.
10. Stein DJ, Hollander E. Dermatology and conditions related to obsessive-compulsive disorder. J Am Acad Dermatol 1992;26:237-42.
11. Dykens E, Shah B. Psychiatric disorders in Prader-Willi syndrome: epidemiology and management. CNS Drugs 2003;17:167-78.
12. Bishop ER. Monosymptomatic hypochondriacal syndromes in dermatology. J Am Acad Dermatol 1983;9:152-8.
13. Koblenzer CS. Dermatitis artefacta: clinical features and approaches to treatment. Am J Clin Dermatol 2000;1:47-55.
14. Stein DJ, Hutt CS, Spitz JL, Hollander E. Compulsive picking and obsessive-compulsive disorder. Psychosomatics 1993;34:177-80.
15. Stout RJ. Fluoxetine for the treatment of compulsive facial picking [letter]. Am J Psychiatry 1990;147:370.-
16. Seedat S, Stein DJ, Harvey BH. Inositol in the treatment of trichotillomania and compulsive skin picking [letter]. J Clin Psychiatry 2001;62:60-1.
17. Gupta MA, Gupta AK. Olanzapine is effective in the management of some self-induced dermatoses: three case reports. Cutis 2000;66:143-6.
18. Duke EE. Clinical experience with pimozide: emphasis on its use in postherpetic neuralgia. J Am Acad Dermatol 1983;8:845-50.
19. Harris BA, Sherertz EF, Flowers FP. Improvement of chronic neurotic excoriations with oral doxepin therapy. Int J Dermatol 1987;26:541-3.
20. Lienemann J, Walker FD. Reversal of self-abusive behavior with naltrexone [letter]. J Clin Psychopharmacol 1989;9:448-9.
21. Arnold LM, Mutasim DF, Dwight MM, et al. An open clinical trial of fluvoxamine treatment of psychogenic excoriation. J Clin Psychopharmacol 1999;19:15-18.
22. Hendrickx B, Van Moffaert M, Spiers R, Von Frenckell R. The treatment of psychocutaneous disorders: a new approach. Curr Ther Res Clin Exp 1991;49:111-19.
23. Simeon D, Stein DJ, Gross S, et al. A double-blind trial of fluoxetine in pathologic skin picking. J Clin Psychiatry 1997;58:341-7.
24. Bloch MR, Elliott M, Thompson H, Koran LM. Fluoxetine in pathologic skin-picking: open-label and double-blind results. Psychosomatics 2001;42:314-19.
25. Kent A, Drummond LM. Acne excoriee—a case report of treatment using habit-reversal. Clin Exp Dermatol 1989;14:163-4.
26. Rosenbaum MS, Ayllon T. The behavioral treatment of neurodermatitis through habit-reversal. Behav Res Ther 1981;19:313-18.
27. Twohig MP, Woods DW. Habit reversal as a treatment for chronic skin picking in typically developing adult male siblings. J App Behav Analysis 2001;34:217-20.
28. Deckersbach T, Wilhelm S, Keuthen NJ, et al. Cognitive-behavior therapy for self-injurious skin picking. Behav Modif 2002;26:361-77.
29. Fruensgaard K. Psychotherapy and neurotic excoriations. Int J Dermatol 1991;30:262-5.
IM risperidone: Long-acting atypical antipsychotic
Patients with chronic schizophrenia are notoriously inconsistent in adhering to medications.1 Partial compliance is a serious problem because the resulting psychotic relapses often lead to progressive neurologic and clinical deterioration as well as social and vocational impairment.
Long-acting, “depot” formulations of first-generation antipsychotics (haloperidol decanoate and fluphenazine decanoate) have been used over the past 25 years to ensure adherence in the least-compliant patients. These formulations, however, are not widely used because of the risks of tardive dyskinesia (TD) and other movement disorders.
Atypical antipsychotics—with their reduced risk of TD—have become the standard of care in managing schizophrenia and related psychosis over the long term.2 All are administered orally, however, and—until now—none has been available in a long-acting formulation.
The FDA recently approved a long-acting, injectable form of risperidone (Table 1), based on results of a 12-week, placebo-controlled trial and a 1-year open-label trial. The clinical and functional improvements seen in chronic schizophrenia patients who received long-acting risperidone for 1 to 3 years may change prevailing notions of the potential to stabilize and restore function in this severe brain disorder.
Table 1
Injectable, long-acting risperidone: Fast facts
| Drug brand name: Risperdal Consta |
| Class: Long-acting injectable atypical antipsychotic |
| FDA-approved indications: Schizophrenia |
| Approval date: Oct. 29, 2003 |
| Manufacturer: Janssen Pharmaceutica |
| Dosing forms: 25 mg, 37.5 mg, 50 mg |
| Recommended dosage: Most adult patients will be started at 25 mg every 2 weeks, with dosages titrated upward as needed |
| Estimated date of availability: By January 2004 |
| Dosing equivalencies (approximate): 25 mg IM biweekly = 3 mg/d oral 37.5 mg IM biweekly = 4.5 mg/d oral 50 mg IM biweekly = 5 to 6 mg/d oral |
HOW LONG-ACTING RISPERIDONE WORKS
Long-acting injectable risperidone has the same mechanism of action as oral risperidone. The injectable form is delivered into muscle tissue by microspheres that encapsulate the drug into a biodegradable polymer. The microspheres undergo gradual hydrolysis, resulting in a gradual release of risperidone into the blood stream. The drug then crosses the blood-brain barrier to block dopamine D2 and serotonin 5HT2A receptors in brain tissue, which is accepted as the pharmacodynamic basis for the efficacy of atypical antipsychotics. Risperidone’s receptor-binding profile is shown in Table 2.
CLINICAL PHARMACOKINETICS
Full release of long-acting risperidone from the gradually hydrolyzing microspheres starts about 3 weeks after an intramuscular (IM) injection. Thus, supplemental oral risperidone is recommended during the first 3 weeks of IM injections. Release is then maintained for 4 to 6 weeks. Steady-state plasma levels are reached after four biweekly injections. Risperidone is absorbed completely from the microspheres, which are biodegradable to carbon dioxide and water.
In plasma, risperidone is oxidized by the cytochrome P-450 isoenzyme CYP 2D6 to 9-hydroxy risperidone, an active metabolite similar to risperidone in its pharmacologic characteristics and efficacy. Risperidone is also metabolized via N-dealkylation. The plasma protein binding of risperidone is 90% and that of 9-hydroxy risperidone is 77%. After several biweekly IM injections of 25 or 50 mg during clinical trials, median trough and peak plasma concentrations of active moiety fluctuated between 9.9 and 19.2 ng/ml and 17.9 and 45.5 ng/ml, respectively.
Table 2
Receptor-binding profile of risperidone long-acting formulation
| Receptor type | Effects |
|---|---|
| Dopamine D2 | Antagonism (< haloperidol) |
| Serotonin 5HT2A | Antagonism (170 times > haloperidol) |
| Alpha 1 | Low affinity |
| Alpha 2 | Low affinity |
| Histaminic | Low affinity |
| Muscarinic | No affinity |
Risperidone plasma concentrations may be affected by interactions with other psychotropics that inhibit or induce the oxidative enzyme CYP 2D6 (Table 3).
Clearance of risperidone and 9-hydroxy risperidone is decreased by 60% in patients with severe kidney disease, as compared with healthy subjects. Plasma levels and maximum drug concentrations are 25 to 32% lower with long-acting risperidone than with oral risperidone. This difference may account for the injectable formulation’s more favorable side-effect profile because lower peaks means a lower likelihood of side effects.
Table 3
Potential drug-drug interactions with risperidone long-acting microspheres
| Drug | CYP enzyme affected | Effect on plasma concentration of risperidone |
|---|---|---|
| Fluphenazine | 2D6 | Increase |
| Paroxetine | 2D6 | Increase |
| Carbamazepine | 2D6 | Decrease |
RESULTS FROM CLINICAL TRIALS
Long-acting risperidone was tested at doses of 25, 50, and 75 mg in a 12-week, double-blind trial of 400 patients with acute relapse of schizophrenia.4 During the 3-week initial titration, patients also received the usual dosage of oral risperidone (3 to 5 mg/d) for schizophrenia. Oral risperidone can be discontinued 3 weeks after the first injection (ie, 1 week after the second injection). Measurement of serum concentrations is not needed because the microspheres encapsulating risperidone have been shown in bioavailability studies to begin disintegrating and releasing risperidone 3 weeks after being deposited into muscle tissue.
All three doses were more effective than placebo in reducing total, positive, and negative symptom scores, as measured by the Positive and Negative Syndrome Scale (PANSS). The 75-mg dose showed no greater efficacy than the 50-mg dose.
In a second, open-label study, 775 stable outpatients with schizophrenia or schizoaffective disorder received biweekly injections of 25, 50, or 75 mg of long-acting risperidone for 1 year. All three doses improved the baseline PANSS scores significantly, above and beyond the patients’ stable clinical status. These results indicate that injectable long-acting risperidone can further stabilize schizophrenia beyond the usual response to oral antipsychotics.5
Notably, patients’ quality-of-life scores—as measured by the 36-item Short-Form Health Survey (SF-36)—were significantly lower than U.S. norms at baseline. At the end of the study, patients’ scores had increased to within the norm range.6 The completion rate in this 1-year study was 65%; patients dropped out because of insufficient response (7%) or adverse events (5%), or they withdrew consent (15%) or were lost to follow-up (3%).
SAFETY AND TOLERABILITY
Few side effects were seen in the 12-week and 1-year trials. Extrapyramidal symptoms as measured by the Extrapyramidal Symptom Rating Scale declined from baseline by 67% with the 25-mg dose, by 50% with the 50-mg dose, and by 33% with the 75-mg dose in the 12-week study. Patients who had TD at baseline also improved by the end of the 1-year study, suggesting that long-acting risperidone has a low risk of TD.7 Also:
- Although prolactin levels were elevated compared with baseline, they were 18% lower with long-acting risperidone than with oral risperidone, possibly because of lower plasma peaks of the drug in the long-acting formulation.
- Injection site pain or redness was minimal, as measured by patient ratings.
- Mean weight gain after 12 weeks was 0.5 kg with the 25-mg dose, 1.2 kg with the 50-mg dose, and 1.9 kg with the 75-mg dose. After 52 weeks, weight gain was 1.8 kg, 2.1 kg, and 2.7 kg, respectively.
- QTc prolongation—as measured with random ECGs—was negligible with all doses.
REPARATIVE EFFECTS?
Based on clinical trial results, long-acting risperidone appears to be highly effective in treating and preventing relapse of acute psychotic episodes in schizophrenia. Its injectable formulation ensures that compliance is far more consistent than with oral atypical antipsychotics.
Patients who had been disabled with chronic schizophrenia improved dramatically after about 1 year of biweekly injections of long-acting risperidone. Many were able to return to school to finish a degree, go back to holding full-time jobs, or develop close personal relationships such as dating. Total PANSS scores after 1 year of treatment approached the low 40s in some patients, which is similar to what a healthy person might score on the PANSS on certain days. This pattern, which justifies the term “recovery,” suggests that uninterrupted, long-term atypical antipsychotic treatment may have reparative and/or neuroprotective effects on the brain in schizophrenia.8
Candidates for long-acting injectable risperidone include:
- first-episode patients
- patients with a history of partial or complete noncompliance
- patients who become violent or assaultive when they relapse
- and those receiving depot injections of haloperidol decanoate or fluphenazine decanoate.
Long-acting injectable atypical antipsychotics may become the standard of care for treating newonset schizophrenia.9 The goal would be to return patients to baseline functioning as soon as possible, rather than resorting to a long-acting antipsychotic only after repetitive relapses, adverse neuroplastic changes, and psychosocial decline.
Related resources
- Lasser R, Bossie C, Zhu Y, Gharahawi G. Does constant therapy infer optimal efficacy in schizophrenia? Moving to an advanced pharmacotherapeutic option. Schizophr Res 2003;60:291.
- Risperdal Consta Web site. www.risperdalconsta.com
Drug brand names
- Carbamazepine • Tegretol
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Paroxetine • Paxil
Disclosure
The author participated in the 12-week controlled clinical trial of long-acting, injectable risperidone and in an open-label extension for more than 3 additional years.
Dr. Nasrallah reports that he also receives research/grant support from and is a consultant to and speaker for AstraZeneca Pharmaceuticals, Janssen Pharmaceutica, and Pfizer Inc., and is a consultant to and speaker for Bristol-Myers Squibb Co. and Abbott Laboratories.
Acknowledgment
The author thanks Peggy Grause for her assistance in preparing this manuscript for publication.
1. Barnes TR, Curson DA. Long-acting depot antipsychotics: a riskbenefit assessment. Drug Safety 1994;10:464-79.
2. Nasrallah HA, Smeltzer DJ. Contemporary diagnosis and management of the patient with schizophrenia. Philadelphia: Handbooks in Health Care, 2002.
3. Kane JM, Eerdekens M, Lindenmayer JP, et al. Long-acting injectable risperidone: efficacy and safety of the first long-acting atypical antipsychotic. Am J Psychiatry 2003;160:1125-32.
4. Remington G, Light M, Lasser R, et al. Can stable patients with schizophrenia improve? The impact of partial compliance versus constant therapy. Schizophr Res 2003;60:300.-
5. Nasrallah HA, Duchesne J, Mehnert A, Janagap C. Improved quality of life in schizophrenia with long-acting intramuscular risperidone. J Neuropsychopharmacol 2002;5(suppl):390.-
6. Chouinard G, Lasser R, Bossie C, et al. Does a long-acting atypical antipsychotic offer a low risk of tardive dyskinesia in patients with schizophrenia? Schizophr Res 2003;60:277.-
7. Nasrallah HA, Mahadik S, Evans D, Keshavan M. Are atypical antipsychotics neuroprotective? Evidence from animal and human studies. Biol Psychiatry 2002;51(suppl 8S):25.-
8. Thompson PM, Vidal C, Giedd JN, et al. Mapping adolescent brain change reveals dynamic wave of accelerated gray matter loss in very early-onset schizophrenia. PNAS 2001;98:11,650-5.
Patients with chronic schizophrenia are notoriously inconsistent in adhering to medications.1 Partial compliance is a serious problem because the resulting psychotic relapses often lead to progressive neurologic and clinical deterioration as well as social and vocational impairment.
Long-acting, “depot” formulations of first-generation antipsychotics (haloperidol decanoate and fluphenazine decanoate) have been used over the past 25 years to ensure adherence in the least-compliant patients. These formulations, however, are not widely used because of the risks of tardive dyskinesia (TD) and other movement disorders.
Atypical antipsychotics—with their reduced risk of TD—have become the standard of care in managing schizophrenia and related psychosis over the long term.2 All are administered orally, however, and—until now—none has been available in a long-acting formulation.
The FDA recently approved a long-acting, injectable form of risperidone (Table 1), based on results of a 12-week, placebo-controlled trial and a 1-year open-label trial. The clinical and functional improvements seen in chronic schizophrenia patients who received long-acting risperidone for 1 to 3 years may change prevailing notions of the potential to stabilize and restore function in this severe brain disorder.
Table 1
Injectable, long-acting risperidone: Fast facts
| Drug brand name: Risperdal Consta |
| Class: Long-acting injectable atypical antipsychotic |
| FDA-approved indications: Schizophrenia |
| Approval date: Oct. 29, 2003 |
| Manufacturer: Janssen Pharmaceutica |
| Dosing forms: 25 mg, 37.5 mg, 50 mg |
| Recommended dosage: Most adult patients will be started at 25 mg every 2 weeks, with dosages titrated upward as needed |
| Estimated date of availability: By January 2004 |
| Dosing equivalencies (approximate): 25 mg IM biweekly = 3 mg/d oral 37.5 mg IM biweekly = 4.5 mg/d oral 50 mg IM biweekly = 5 to 6 mg/d oral |
HOW LONG-ACTING RISPERIDONE WORKS
Long-acting injectable risperidone has the same mechanism of action as oral risperidone. The injectable form is delivered into muscle tissue by microspheres that encapsulate the drug into a biodegradable polymer. The microspheres undergo gradual hydrolysis, resulting in a gradual release of risperidone into the blood stream. The drug then crosses the blood-brain barrier to block dopamine D2 and serotonin 5HT2A receptors in brain tissue, which is accepted as the pharmacodynamic basis for the efficacy of atypical antipsychotics. Risperidone’s receptor-binding profile is shown in Table 2.
CLINICAL PHARMACOKINETICS
Full release of long-acting risperidone from the gradually hydrolyzing microspheres starts about 3 weeks after an intramuscular (IM) injection. Thus, supplemental oral risperidone is recommended during the first 3 weeks of IM injections. Release is then maintained for 4 to 6 weeks. Steady-state plasma levels are reached after four biweekly injections. Risperidone is absorbed completely from the microspheres, which are biodegradable to carbon dioxide and water.
In plasma, risperidone is oxidized by the cytochrome P-450 isoenzyme CYP 2D6 to 9-hydroxy risperidone, an active metabolite similar to risperidone in its pharmacologic characteristics and efficacy. Risperidone is also metabolized via N-dealkylation. The plasma protein binding of risperidone is 90% and that of 9-hydroxy risperidone is 77%. After several biweekly IM injections of 25 or 50 mg during clinical trials, median trough and peak plasma concentrations of active moiety fluctuated between 9.9 and 19.2 ng/ml and 17.9 and 45.5 ng/ml, respectively.
Table 2
Receptor-binding profile of risperidone long-acting formulation
| Receptor type | Effects |
|---|---|
| Dopamine D2 | Antagonism (< haloperidol) |
| Serotonin 5HT2A | Antagonism (170 times > haloperidol) |
| Alpha 1 | Low affinity |
| Alpha 2 | Low affinity |
| Histaminic | Low affinity |
| Muscarinic | No affinity |
Risperidone plasma concentrations may be affected by interactions with other psychotropics that inhibit or induce the oxidative enzyme CYP 2D6 (Table 3).
Clearance of risperidone and 9-hydroxy risperidone is decreased by 60% in patients with severe kidney disease, as compared with healthy subjects. Plasma levels and maximum drug concentrations are 25 to 32% lower with long-acting risperidone than with oral risperidone. This difference may account for the injectable formulation’s more favorable side-effect profile because lower peaks means a lower likelihood of side effects.
Table 3
Potential drug-drug interactions with risperidone long-acting microspheres
| Drug | CYP enzyme affected | Effect on plasma concentration of risperidone |
|---|---|---|
| Fluphenazine | 2D6 | Increase |
| Paroxetine | 2D6 | Increase |
| Carbamazepine | 2D6 | Decrease |
RESULTS FROM CLINICAL TRIALS
Long-acting risperidone was tested at doses of 25, 50, and 75 mg in a 12-week, double-blind trial of 400 patients with acute relapse of schizophrenia.4 During the 3-week initial titration, patients also received the usual dosage of oral risperidone (3 to 5 mg/d) for schizophrenia. Oral risperidone can be discontinued 3 weeks after the first injection (ie, 1 week after the second injection). Measurement of serum concentrations is not needed because the microspheres encapsulating risperidone have been shown in bioavailability studies to begin disintegrating and releasing risperidone 3 weeks after being deposited into muscle tissue.
All three doses were more effective than placebo in reducing total, positive, and negative symptom scores, as measured by the Positive and Negative Syndrome Scale (PANSS). The 75-mg dose showed no greater efficacy than the 50-mg dose.
In a second, open-label study, 775 stable outpatients with schizophrenia or schizoaffective disorder received biweekly injections of 25, 50, or 75 mg of long-acting risperidone for 1 year. All three doses improved the baseline PANSS scores significantly, above and beyond the patients’ stable clinical status. These results indicate that injectable long-acting risperidone can further stabilize schizophrenia beyond the usual response to oral antipsychotics.5
Notably, patients’ quality-of-life scores—as measured by the 36-item Short-Form Health Survey (SF-36)—were significantly lower than U.S. norms at baseline. At the end of the study, patients’ scores had increased to within the norm range.6 The completion rate in this 1-year study was 65%; patients dropped out because of insufficient response (7%) or adverse events (5%), or they withdrew consent (15%) or were lost to follow-up (3%).
SAFETY AND TOLERABILITY
Few side effects were seen in the 12-week and 1-year trials. Extrapyramidal symptoms as measured by the Extrapyramidal Symptom Rating Scale declined from baseline by 67% with the 25-mg dose, by 50% with the 50-mg dose, and by 33% with the 75-mg dose in the 12-week study. Patients who had TD at baseline also improved by the end of the 1-year study, suggesting that long-acting risperidone has a low risk of TD.7 Also:
- Although prolactin levels were elevated compared with baseline, they were 18% lower with long-acting risperidone than with oral risperidone, possibly because of lower plasma peaks of the drug in the long-acting formulation.
- Injection site pain or redness was minimal, as measured by patient ratings.
- Mean weight gain after 12 weeks was 0.5 kg with the 25-mg dose, 1.2 kg with the 50-mg dose, and 1.9 kg with the 75-mg dose. After 52 weeks, weight gain was 1.8 kg, 2.1 kg, and 2.7 kg, respectively.
- QTc prolongation—as measured with random ECGs—was negligible with all doses.
REPARATIVE EFFECTS?
Based on clinical trial results, long-acting risperidone appears to be highly effective in treating and preventing relapse of acute psychotic episodes in schizophrenia. Its injectable formulation ensures that compliance is far more consistent than with oral atypical antipsychotics.
Patients who had been disabled with chronic schizophrenia improved dramatically after about 1 year of biweekly injections of long-acting risperidone. Many were able to return to school to finish a degree, go back to holding full-time jobs, or develop close personal relationships such as dating. Total PANSS scores after 1 year of treatment approached the low 40s in some patients, which is similar to what a healthy person might score on the PANSS on certain days. This pattern, which justifies the term “recovery,” suggests that uninterrupted, long-term atypical antipsychotic treatment may have reparative and/or neuroprotective effects on the brain in schizophrenia.8
Candidates for long-acting injectable risperidone include:
- first-episode patients
- patients with a history of partial or complete noncompliance
- patients who become violent or assaultive when they relapse
- and those receiving depot injections of haloperidol decanoate or fluphenazine decanoate.
Long-acting injectable atypical antipsychotics may become the standard of care for treating newonset schizophrenia.9 The goal would be to return patients to baseline functioning as soon as possible, rather than resorting to a long-acting antipsychotic only after repetitive relapses, adverse neuroplastic changes, and psychosocial decline.
Related resources
- Lasser R, Bossie C, Zhu Y, Gharahawi G. Does constant therapy infer optimal efficacy in schizophrenia? Moving to an advanced pharmacotherapeutic option. Schizophr Res 2003;60:291.
- Risperdal Consta Web site. www.risperdalconsta.com
Drug brand names
- Carbamazepine • Tegretol
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Paroxetine • Paxil
Disclosure
The author participated in the 12-week controlled clinical trial of long-acting, injectable risperidone and in an open-label extension for more than 3 additional years.
Dr. Nasrallah reports that he also receives research/grant support from and is a consultant to and speaker for AstraZeneca Pharmaceuticals, Janssen Pharmaceutica, and Pfizer Inc., and is a consultant to and speaker for Bristol-Myers Squibb Co. and Abbott Laboratories.
Acknowledgment
The author thanks Peggy Grause for her assistance in preparing this manuscript for publication.
Patients with chronic schizophrenia are notoriously inconsistent in adhering to medications.1 Partial compliance is a serious problem because the resulting psychotic relapses often lead to progressive neurologic and clinical deterioration as well as social and vocational impairment.
Long-acting, “depot” formulations of first-generation antipsychotics (haloperidol decanoate and fluphenazine decanoate) have been used over the past 25 years to ensure adherence in the least-compliant patients. These formulations, however, are not widely used because of the risks of tardive dyskinesia (TD) and other movement disorders.
Atypical antipsychotics—with their reduced risk of TD—have become the standard of care in managing schizophrenia and related psychosis over the long term.2 All are administered orally, however, and—until now—none has been available in a long-acting formulation.
The FDA recently approved a long-acting, injectable form of risperidone (Table 1), based on results of a 12-week, placebo-controlled trial and a 1-year open-label trial. The clinical and functional improvements seen in chronic schizophrenia patients who received long-acting risperidone for 1 to 3 years may change prevailing notions of the potential to stabilize and restore function in this severe brain disorder.
Table 1
Injectable, long-acting risperidone: Fast facts
| Drug brand name: Risperdal Consta |
| Class: Long-acting injectable atypical antipsychotic |
| FDA-approved indications: Schizophrenia |
| Approval date: Oct. 29, 2003 |
| Manufacturer: Janssen Pharmaceutica |
| Dosing forms: 25 mg, 37.5 mg, 50 mg |
| Recommended dosage: Most adult patients will be started at 25 mg every 2 weeks, with dosages titrated upward as needed |
| Estimated date of availability: By January 2004 |
| Dosing equivalencies (approximate): 25 mg IM biweekly = 3 mg/d oral 37.5 mg IM biweekly = 4.5 mg/d oral 50 mg IM biweekly = 5 to 6 mg/d oral |
HOW LONG-ACTING RISPERIDONE WORKS
Long-acting injectable risperidone has the same mechanism of action as oral risperidone. The injectable form is delivered into muscle tissue by microspheres that encapsulate the drug into a biodegradable polymer. The microspheres undergo gradual hydrolysis, resulting in a gradual release of risperidone into the blood stream. The drug then crosses the blood-brain barrier to block dopamine D2 and serotonin 5HT2A receptors in brain tissue, which is accepted as the pharmacodynamic basis for the efficacy of atypical antipsychotics. Risperidone’s receptor-binding profile is shown in Table 2.
CLINICAL PHARMACOKINETICS
Full release of long-acting risperidone from the gradually hydrolyzing microspheres starts about 3 weeks after an intramuscular (IM) injection. Thus, supplemental oral risperidone is recommended during the first 3 weeks of IM injections. Release is then maintained for 4 to 6 weeks. Steady-state plasma levels are reached after four biweekly injections. Risperidone is absorbed completely from the microspheres, which are biodegradable to carbon dioxide and water.
In plasma, risperidone is oxidized by the cytochrome P-450 isoenzyme CYP 2D6 to 9-hydroxy risperidone, an active metabolite similar to risperidone in its pharmacologic characteristics and efficacy. Risperidone is also metabolized via N-dealkylation. The plasma protein binding of risperidone is 90% and that of 9-hydroxy risperidone is 77%. After several biweekly IM injections of 25 or 50 mg during clinical trials, median trough and peak plasma concentrations of active moiety fluctuated between 9.9 and 19.2 ng/ml and 17.9 and 45.5 ng/ml, respectively.
Table 2
Receptor-binding profile of risperidone long-acting formulation
| Receptor type | Effects |
|---|---|
| Dopamine D2 | Antagonism (< haloperidol) |
| Serotonin 5HT2A | Antagonism (170 times > haloperidol) |
| Alpha 1 | Low affinity |
| Alpha 2 | Low affinity |
| Histaminic | Low affinity |
| Muscarinic | No affinity |
Risperidone plasma concentrations may be affected by interactions with other psychotropics that inhibit or induce the oxidative enzyme CYP 2D6 (Table 3).
Clearance of risperidone and 9-hydroxy risperidone is decreased by 60% in patients with severe kidney disease, as compared with healthy subjects. Plasma levels and maximum drug concentrations are 25 to 32% lower with long-acting risperidone than with oral risperidone. This difference may account for the injectable formulation’s more favorable side-effect profile because lower peaks means a lower likelihood of side effects.
Table 3
Potential drug-drug interactions with risperidone long-acting microspheres
| Drug | CYP enzyme affected | Effect on plasma concentration of risperidone |
|---|---|---|
| Fluphenazine | 2D6 | Increase |
| Paroxetine | 2D6 | Increase |
| Carbamazepine | 2D6 | Decrease |
RESULTS FROM CLINICAL TRIALS
Long-acting risperidone was tested at doses of 25, 50, and 75 mg in a 12-week, double-blind trial of 400 patients with acute relapse of schizophrenia.4 During the 3-week initial titration, patients also received the usual dosage of oral risperidone (3 to 5 mg/d) for schizophrenia. Oral risperidone can be discontinued 3 weeks after the first injection (ie, 1 week after the second injection). Measurement of serum concentrations is not needed because the microspheres encapsulating risperidone have been shown in bioavailability studies to begin disintegrating and releasing risperidone 3 weeks after being deposited into muscle tissue.
All three doses were more effective than placebo in reducing total, positive, and negative symptom scores, as measured by the Positive and Negative Syndrome Scale (PANSS). The 75-mg dose showed no greater efficacy than the 50-mg dose.
In a second, open-label study, 775 stable outpatients with schizophrenia or schizoaffective disorder received biweekly injections of 25, 50, or 75 mg of long-acting risperidone for 1 year. All three doses improved the baseline PANSS scores significantly, above and beyond the patients’ stable clinical status. These results indicate that injectable long-acting risperidone can further stabilize schizophrenia beyond the usual response to oral antipsychotics.5
Notably, patients’ quality-of-life scores—as measured by the 36-item Short-Form Health Survey (SF-36)—were significantly lower than U.S. norms at baseline. At the end of the study, patients’ scores had increased to within the norm range.6 The completion rate in this 1-year study was 65%; patients dropped out because of insufficient response (7%) or adverse events (5%), or they withdrew consent (15%) or were lost to follow-up (3%).
SAFETY AND TOLERABILITY
Few side effects were seen in the 12-week and 1-year trials. Extrapyramidal symptoms as measured by the Extrapyramidal Symptom Rating Scale declined from baseline by 67% with the 25-mg dose, by 50% with the 50-mg dose, and by 33% with the 75-mg dose in the 12-week study. Patients who had TD at baseline also improved by the end of the 1-year study, suggesting that long-acting risperidone has a low risk of TD.7 Also:
- Although prolactin levels were elevated compared with baseline, they were 18% lower with long-acting risperidone than with oral risperidone, possibly because of lower plasma peaks of the drug in the long-acting formulation.
- Injection site pain or redness was minimal, as measured by patient ratings.
- Mean weight gain after 12 weeks was 0.5 kg with the 25-mg dose, 1.2 kg with the 50-mg dose, and 1.9 kg with the 75-mg dose. After 52 weeks, weight gain was 1.8 kg, 2.1 kg, and 2.7 kg, respectively.
- QTc prolongation—as measured with random ECGs—was negligible with all doses.
REPARATIVE EFFECTS?
Based on clinical trial results, long-acting risperidone appears to be highly effective in treating and preventing relapse of acute psychotic episodes in schizophrenia. Its injectable formulation ensures that compliance is far more consistent than with oral atypical antipsychotics.
Patients who had been disabled with chronic schizophrenia improved dramatically after about 1 year of biweekly injections of long-acting risperidone. Many were able to return to school to finish a degree, go back to holding full-time jobs, or develop close personal relationships such as dating. Total PANSS scores after 1 year of treatment approached the low 40s in some patients, which is similar to what a healthy person might score on the PANSS on certain days. This pattern, which justifies the term “recovery,” suggests that uninterrupted, long-term atypical antipsychotic treatment may have reparative and/or neuroprotective effects on the brain in schizophrenia.8
Candidates for long-acting injectable risperidone include:
- first-episode patients
- patients with a history of partial or complete noncompliance
- patients who become violent or assaultive when they relapse
- and those receiving depot injections of haloperidol decanoate or fluphenazine decanoate.
Long-acting injectable atypical antipsychotics may become the standard of care for treating newonset schizophrenia.9 The goal would be to return patients to baseline functioning as soon as possible, rather than resorting to a long-acting antipsychotic only after repetitive relapses, adverse neuroplastic changes, and psychosocial decline.
Related resources
- Lasser R, Bossie C, Zhu Y, Gharahawi G. Does constant therapy infer optimal efficacy in schizophrenia? Moving to an advanced pharmacotherapeutic option. Schizophr Res 2003;60:291.
- Risperdal Consta Web site. www.risperdalconsta.com
Drug brand names
- Carbamazepine • Tegretol
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Paroxetine • Paxil
Disclosure
The author participated in the 12-week controlled clinical trial of long-acting, injectable risperidone and in an open-label extension for more than 3 additional years.
Dr. Nasrallah reports that he also receives research/grant support from and is a consultant to and speaker for AstraZeneca Pharmaceuticals, Janssen Pharmaceutica, and Pfizer Inc., and is a consultant to and speaker for Bristol-Myers Squibb Co. and Abbott Laboratories.
Acknowledgment
The author thanks Peggy Grause for her assistance in preparing this manuscript for publication.
1. Barnes TR, Curson DA. Long-acting depot antipsychotics: a riskbenefit assessment. Drug Safety 1994;10:464-79.
2. Nasrallah HA, Smeltzer DJ. Contemporary diagnosis and management of the patient with schizophrenia. Philadelphia: Handbooks in Health Care, 2002.
3. Kane JM, Eerdekens M, Lindenmayer JP, et al. Long-acting injectable risperidone: efficacy and safety of the first long-acting atypical antipsychotic. Am J Psychiatry 2003;160:1125-32.
4. Remington G, Light M, Lasser R, et al. Can stable patients with schizophrenia improve? The impact of partial compliance versus constant therapy. Schizophr Res 2003;60:300.-
5. Nasrallah HA, Duchesne J, Mehnert A, Janagap C. Improved quality of life in schizophrenia with long-acting intramuscular risperidone. J Neuropsychopharmacol 2002;5(suppl):390.-
6. Chouinard G, Lasser R, Bossie C, et al. Does a long-acting atypical antipsychotic offer a low risk of tardive dyskinesia in patients with schizophrenia? Schizophr Res 2003;60:277.-
7. Nasrallah HA, Mahadik S, Evans D, Keshavan M. Are atypical antipsychotics neuroprotective? Evidence from animal and human studies. Biol Psychiatry 2002;51(suppl 8S):25.-
8. Thompson PM, Vidal C, Giedd JN, et al. Mapping adolescent brain change reveals dynamic wave of accelerated gray matter loss in very early-onset schizophrenia. PNAS 2001;98:11,650-5.
1. Barnes TR, Curson DA. Long-acting depot antipsychotics: a riskbenefit assessment. Drug Safety 1994;10:464-79.
2. Nasrallah HA, Smeltzer DJ. Contemporary diagnosis and management of the patient with schizophrenia. Philadelphia: Handbooks in Health Care, 2002.
3. Kane JM, Eerdekens M, Lindenmayer JP, et al. Long-acting injectable risperidone: efficacy and safety of the first long-acting atypical antipsychotic. Am J Psychiatry 2003;160:1125-32.
4. Remington G, Light M, Lasser R, et al. Can stable patients with schizophrenia improve? The impact of partial compliance versus constant therapy. Schizophr Res 2003;60:300.-
5. Nasrallah HA, Duchesne J, Mehnert A, Janagap C. Improved quality of life in schizophrenia with long-acting intramuscular risperidone. J Neuropsychopharmacol 2002;5(suppl):390.-
6. Chouinard G, Lasser R, Bossie C, et al. Does a long-acting atypical antipsychotic offer a low risk of tardive dyskinesia in patients with schizophrenia? Schizophr Res 2003;60:277.-
7. Nasrallah HA, Mahadik S, Evans D, Keshavan M. Are atypical antipsychotics neuroprotective? Evidence from animal and human studies. Biol Psychiatry 2002;51(suppl 8S):25.-
8. Thompson PM, Vidal C, Giedd JN, et al. Mapping adolescent brain change reveals dynamic wave of accelerated gray matter loss in very early-onset schizophrenia. PNAS 2001;98:11,650-5.
Neuroleptic malignant syndrome: Still a risk, but which patients may be in danger?
Potentially fatal neuroleptic malignant syndrome (NMS)—though less common than in the past—can happen with either conventional or atypical antipsychotics.1,2 To help you protect patients when prescribing antipsychotics or consulting with other clinicians about these drugs, this article discusses:
- risk factors and clinical features that warn of NMS onset
- differential diagnosis of disease states most often confused with NMS
- management recommendations, including supportive measures and specific interventions such as benzodiazepines, dopamine agonists, dantrolene, and electroconvulsive therapy (ECT).
WHY NMS REMAINS RELEVANT
NMS remains a risk in susceptible patients receiving atypical antipsychotics, according to clinical reports and drug adverse event surveys (Figure).2
Moreover, NMS continues to be reported with conventional antipsychotics, which remain in widespread use. Patients who receive long-acting depot conventional antipsychotics are at risk for prolonged NMS episodes.
Figure 55 NMS cases reported with use of antipsychotics, 1998-2002
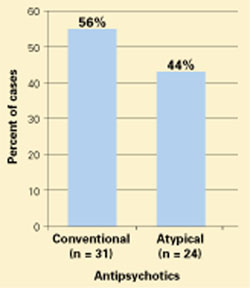
Probable or definite neuroleptic malignant syndrome cases associated with antipsychotic monotherapy reported to the Neuroleptic Malignant Syndrome Information Service.NMS in medical settings. Psychiatrists may be consulted when patients develop NMS while receiving conventional antipsychotics or other dopaminereceptor antagonists used in medical settings.3,4 Haloperidol remains the recommended drug of choice for treating agitation and delirium and continues to be the single most common trigger of NMS. Although often overlooked, antiemetics and sedatives with neuroleptic properties—such as prochlorperazine, metoclopramide, and promethazine—also have triggered NMS.
Other hyperthermic conditions. NMS is often considered in the differential diagnosis of patients who develop fever or encephalopathy while being treated with psychotropics. In these acute, complex, and often grave situations, psychiatrists may be consulted to recommend treatment for behavioral control or to distinguish NMS from other conditions.
NEWER VS. OLDER ANTIPSYCHOTICS
Has NMS incidence declined with the atypical agents? Probably, but providing proof is difficult:
- NMS is uncommon; its incidence in psychiatric patients treated with conventional antipsychotics is approximately 0.2%.5 To demonstrate reduced NMS incidence with atypicals, a very large sample of patients would be required to reach statistical significance.
- As doctors have used lower doses of conventional agents—which reduces the risk of NMS—any beneficial impact from atypicals has become more difficult to detect.5,6
- Reports of NMS frequency with atypicals may be inflated by bias in publishing adverse events with newer versus older agents.
- Patients switched to atypicals may represent a high-risk group that is intolerant or resistant to conventional antipsychotics.
So far, few unequivocal cases of NMS have been attributed to the use of quetiapine, ziprasidone, or aripiprazole, the most recently introduced atypicals. Moreover, case reports of NMS associated with clozapine, risperidone, or olanzapine2 are often difficult to interpret because of incomplete clinical details, varying diagnostic criteria, and concomitant use of more than one antipsychotic.
Milder NMS? Do the newer antipsychotics produce an “atypical” or milder form of NMS? Case reports indicate that extreme temperature elevations and extrapyramidal dysfunction are less frequent in NMS associated with atypical compared with conventional antipsychotics.2 However, case descriptions of NMS were heterogeneous even with conventional agents, and clinicians’ growing awareness of NMS even before atypicals were introduced allowed for earlier diagnosis of mild and partial NMS cases.7
CLINICAL FEATURES OF NMS
Regardless of drug selection, it is important to recognize early and mild signs of NMS. Any case can progress to a fulminant form that is more difficult to treat.
Patients at risk. NMS may be more likely to develop in patients with:5,6,8
- dehydration
- agitation
- low serum iron
- underlying brain damage
- catatonia.
Some patients may have genetic abnormalities in central dopamine systems that increase their susceptibility to NMS.6,9
Fifteen to 20% of patients who develop NMS have experienced a previous episode while taking antipsychotics, which is why taking a careful drug history is important.5,6 Although most often reported with therapeutic antipsychotic doses, NMS has been associated with rapid dose titration, especially when given parenterally.8
On the other hand, the practical value of these risk factors is often limited in individual cases and may lead one to overestimate NMS risk. NMS is rare and idiosyncratic. Risk factors may not outweigh antipsychotics’ benefits when these drugs are indicated for a patient with psychosis.
Incipient NMS. Identifying early signs of NMS may be impossible in fulminant cases, but patients with incipient NMS may show:
- unexpected mental status changes
- new-onset catatonia
- refractory extrapyramidal and bulbar signs such as rigidity, dysphagia, or dysarthria.5,7,10
Other clues to NMS onset include tachycardia, tachypnea, and elevated temperature or serum creatine phosphokinase (CPK). These signs, however, do not precede or progress to NMS in all cases. A high index of suspicion for NMS, tempered by sound clinical judgment, is called for when assessing all patients receiving antipsychotics.
Diagnostic criteria. Clinical signs of NMS as a fullblown hypermetabolic syndrome are distinctive and well described (Table 1).5,6,11,12 Elevated temperature is accompanied by profuse sweating. Extreme temperatures (>104° F), especially if prolonged or associated with hypoxia or hypotension, pose a high risk for brain damage, rhabdomyolysis, disseminated intravascular coagulation, multisystem organ failure, and death.
Muscle rigidity is a characteristic finding and may be accompanied by tremors, cogwheeling, myoclonus, or rhabdomyolysis. Changes in vital signs—such as tachycardia and tachypnea—are typical.
Mental status examination usually reveals catatonic signs of mutism and stupor, but delirium and coma also have been described. No laboratory findings are specific for NMS, but elevated white blood cell counts, low serum iron, metabolic acidosis, hypoxia, and elevated serum CPK and catecholamines have been reported.
Table 1
Common clinical features of NMS
| Signs and symptoms | Altered level of consciousness, catatonia, dysarthria, dysphagia, elevated temperature, labile blood pressure, muscle rigidity, mutism, myoclonus, tachycardia, tachypnea, tremor |
| Laboratory findings | Elevated catecholamines and serum creatine phosphokinase, hypoxia, leukocytosis, low serum iron, metabolic acidosis |
Resolution. If recognized promptly, NMS resolves within 1 to 2 weeks in two-thirds of patients after antipsychotics are discontinued. The average recovery time of 7 to 10 days may be prolonged in patients who were taking long-acting depot antipsychotics or in those with persistent residual catatonic symptoms.13
Risk of death. NMS remains potentially fatal, especially if high temperatures develop or episodes are prolonged. Causes of death include cardiorespiratory arrest, renal failure, pulmonary emboli, pneumonia, sepsis, disseminated intravascular coagulation, and multisystem organ failure.
DIFFERENTIAL DIAGNOSIS
Differential diagnosis of NMS encompasses disorders that present with fever and encephalopathy.5,6,12 Primary brain disorders that resemble NMS include:9,14-16
- infections
- acute psychotic disorders that progress to malignant catatonia or delirious mania
- midbrain structural lesions
- seizures.
Also exclude hormonal and autoimmune disorders and environmental heatstroke (Table 2).17,18 Similar hyperthermic syndromes have been reported with other toxins and drugs, including malignant hyperthermia of anesthesia, serotonin syndrome, and dopamine agonist withdrawal in patients with Parkinson’s disease (Table 3).5,6,19
Table 2
7 disease states most often confused with NMS
| Infections |
| Malignant catatonia secondary to psychotic disorders |
| Benign extrapyramidal side effects |
| Agitated delirium from diverse causes |
| Environmental heatstroke |
| Serotonin syndrome |
| Withdrawal from dopamine agonists, other drugs, or alcohol |
| Source: Neuroleptic Malignant Syndrome Information Service hotline |
Table 3
Drugs that can cause NMS-like hyperthermic syndromes
| Anticholinergics Dopamine antagonists Hallucinogens Inhalational anesthetics Monoamine oxidase inhibitors Psychostimulants Salicylates | Serotonergic drugs Succinylcholine Withdrawal from: • Dopamine agonists • Alcohol • Sedative/hypnotics • Baclofen |
MANAGING NMS
The standard approach to managing patients with NMS includes four steps:
- recognize the diagnosis early
- exclude alternate causes of symptoms
- discontinue suspected triggering drugs
- provide supportive care to reduce temperatures, ensure fluid balance, and detect complications.5,6,20
Beyond supportive care, several specific therapies have been proposed based on theoretical mechanisms of NMS and meta-analyses of offlabel use in anecdotal clinical reports (Table 4). If benzodiazepines, dopamine agonists, or dantrolene are effective, taper slowly after recovery to prevent rebound symptoms.
Benzodiazepines. Given the concept of NMS as a form of catatonia, benzodiazepines have been used effectively in some cases.20,21 A trial of lorazepam, 1 to 2 mg parenterally, is a reasonable first step. Higher doses may be required, with adequate monitoring of respiratory status. Oral lorazepam can maintain the therapeutic effect.
Dopamine agonists. To reverse the parkinsonism and dopamine antagonist properties of antipsychotics, dopamine agonists such as bromocriptine or amantadine have been tried and have reduced NMS duration and mortality.20,22,23 Newer drugs such as ropinorole and pramipexole may also be useful. Dopaminergic drugs, however, can worsen psychosis and cause hypotension and emesis.
Dantrolene may reduce hyperthermia related to skeletal muscle hypermetabolism of any cause and has been effective in rapidly reducing extreme temperatures in some NMS cases.20,22-26 Dantrolene is given IV, 1 to 2.5 mg/kg every 6 hours. An oral form can be substituted if a response is obtained. Dantrolene can impair respiratory and hepatic function and should not be combined with calcium channel blockers.
ECT is increasingly recognized as an effective NMS treatment and should not be overlooked for patients:
Standard ECT is given, although nondepolarizing muscle relaxants instead of succinylcholine are used in patients with serious rhabdomyolysis to avoid the risk of hyperkalemia.20
Recommendation. Although these modalities offer a spectrum of therapeutic options, it is premature to recommend any single remedy over others or over supportive care alone because:
- randomized, controlled trials have not been conducted
- NMS episodes are heterogeneous in presentation and outcome
- the syndrome is often self-limited after antipsychotics are discontinued.
I recommend that you choose therapies empirically, based on the character, severity, and duration of symptoms in a given case.5,6,20
Table 4
How to treat neuroleptic malignant syndrome
| General measures | Diagnose early, discontinue antipsychotic, provide supportive care |
| Specific interventions under investigation | |
| Benzodiazepines | Parenteral lorazepam, 1 to 2 mg or higher; monitor respiratory status |
| Dopamine agonists | Bromocriptine, 2.5 mg every 8 hours or amantadine, 100 mg every 8 hours; monitor psychosis, blood pressure, nausea |
| Dantrolene | 1 to 2.5 mg/kg IV every 6 hours; monitor respiratory and hepatic function; avoid calcium channel blockers |
| ECT | Standard administration; avoid succinylcholine in patients with rhabdomyolysis |
REDUCING RISK OF RECURRENCE
Patients vary in susceptibility to recurrence after they recover from NMS, but the risk approaches 30% with future exposure to antipsychotics.5,6 You may be able to minimize recurrence risk by:
- reducing risk factors, such as dehydration
- considering alternatives to antipsychotics, such as treating bipolar disorder with lithium or ECT
- using atypical instead of conventional antipsychotics, starting with low dosages and titrating slowly.
Before you reintroduce antipsychotics, carefully document informed consent and your rationale for treatment decisions in the patient’s chart.
Related resources
- Neuroleptic Malignant Syndrome Information Service. Hotline for health professionals. (888) 667-8367. www.nmsis.org
- Mann SC, Caroff SN, Keck PE Jr, Lazarus A. Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003.
- Caroff SN, Mann SC, Francis A, Fricchione GL. Catatonia: from psychopathology to neurobiology. Washington, DC: American Psychiatric Publishing (in press).
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Bromocriptine • Parlodel
- Clozapine • Clozaril
- Dantrolene • Dantrium
- Haloperidol • Haldol
- Lorazepam • Ativan
- Metoclopramide • Reglan
- Olanzapine • Zyprexa
- Pramipexole • Mirapex
- Prochlorperazine • Compazine
- Promethazine • Phenergan
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ropinirole • Requip
- Ziprasidone • Geodon
Disclosure
Dr. Caroff receives research support from Janssen Pharmaceutica and Pfizer Inc., and is a consultant to Eli Lilly and Co. and Bristol-Myers Squibb Co.
1. Caroff SN, Mann SC, Campbell EC, Sullivan KA. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry 2002;63(suppl 4):12-19.
2. Caroff SN, Mann SC, Campbell EC. Atypical antipsychotics and neuroleptic malignant syndrome. Psychiatric Annals 2000;30(5):314-21.
3. Caroff SN, Rosenberg H, Mann SC, et al. Neuroleptic malignant syndrome in the perioperative setting. Am J Anesthesiology 2001;28(8):387-93.
4. Caroff SN, Rosenberg H, Mann SC, et al. Neuroleptic malignant syndrome in the critical care unit. Crit Care Med 2002;30(11):2609.-
5. Caroff SN, Mann SC. Neuroleptic malignant syndrome. Med Clin North Am 1993;77(1):185-202.
6. Caroff SN. Neuroleptic malignant syndrome. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing Inc., 2003;1-44.
7. Velamoor VR, Swamy GN, Parmar RS, et al. Management of suspected neuroleptic malignant syndrome. Can J Psychiatry 1995;40(9):545-50.
8. Keck PE, Jr, Pope HG, Jr, Cohen BM, et al. Risk factors for neuroleptic malignant syndrome. Arch Gen Psychiatry 1989;46:914-18.
9. Mann SC. Malignant catatonia. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003;121-43.
10. Velamoor VR, Norman RMG, Caroff SN, et al. Progression of symptoms in neuroleptic malignant syndrome. J Nerv Ment Dis 1994;182(3):168-73.
11. Delay J, Pichot P, Lemperiere T, et al. Un neuroleptique majeur non-phenothiazine et non reserpinique, l’haloperidol, dans le traitement des psychoses. Annales Medico-Psychologique 1960;118(1):145-52.
12. Caroff SN. The neuroleptic malignant syndrome. J Clin Psychiatry 1980;41(3):79-83.
13. Caroff SN, Mann SC, Keck PE, Jr, Francis A. Residual catatonic state following neuroleptic malignant syndrome. J Clin Psychopharmacol 2000;20(2):257-9.
14. Caroff SN, Mann SC, McCarthy M, et al. Acute infectious encephalitis complicated by neuroleptic malignant syndrome. J Clin Psychopharmacol 1998;18(4):349-51.
15. Caroff SN, Mann SC, Gliatto MF, et al. Psychiatric manifestations of acute viral encephalitis. Psychiatric Annals 2001;31(3):193-204.
16. Caroff SN, Mann SC, Francis A, Fricchione GL (eds). Catatonia: from psychopathology to neurobiology. Washington, DC: American Psychiatric Publishing (in press).
17. Mann SC. Thermoregulatory mechanisms and antipsychotic drugrelated heatstroke. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003;45-74.
18. Caroff SN, Mann SC, Campbell EC. Risk of fatal heatstroke after hospitalization. Psychiatric Serv 2000;51(7):938.-
19. Keck PE, Jr. Serotonin syndrome. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003;75-92.
20. Davis JM, Caroff SN, Mann SC. Treatment of neuroleptic malignant syndrome. Psychiatric Annals 2000;30(5):325-31.
21. Francis A, Chandragiri S, Rizvi S, et al. Lorazepam a treatment for neuroleptic malignant syndrome? CNS Spectrums 2000;5(7):54-7.
22. Sakkas P, Davis JM, Hua J, Wang Z. Pharmacotherapy of neuroleptic malignant syndrome. Psychiatr Ann 1991;21:157-64.
23. Rosenberg MR, Green M. Neuroleptic malignant syndrome: review of response to therapy. Arch Intern Med 1989;149:1927-31.
24. Henderson A, Longdon P. Fulminant metoclopramide-induced neuroleptic malignant syndrome rapidly responsive to intravenous dantrolene. Aust N Z J Med 1991;21:742-3.
25. Yamawaki S, Morio M, Kazamatsuri G, et al. Clinical evaluation and effective usage of dantrolene sodium in neuroleptic malignant syndrome. Kiso to Rinsyou (Clinical Reports) 1993;27(3):1045-66.
26. Tsutsumi Y, Yamamoto K, Matsuura S, et al. The treatment of neuroleptic malignant syndrome using dantrolene sodium. Psychiatry Clin Neurosci 1998;52:433-8.
27. Nisijima K, Ishiguro T. Electroconvulsive therapy for the treatment of neuroleptic malignant syndrome: a report of five cases. J ECT 1999;15:158-63.
28. Troller JN, Sachdev PS. Electroconvulsive treatment of neuroleptic malignant syndrome: a review and report of cases. Aust N Z J Psychiatry 1999;33:650-9.
Potentially fatal neuroleptic malignant syndrome (NMS)—though less common than in the past—can happen with either conventional or atypical antipsychotics.1,2 To help you protect patients when prescribing antipsychotics or consulting with other clinicians about these drugs, this article discusses:
- risk factors and clinical features that warn of NMS onset
- differential diagnosis of disease states most often confused with NMS
- management recommendations, including supportive measures and specific interventions such as benzodiazepines, dopamine agonists, dantrolene, and electroconvulsive therapy (ECT).
WHY NMS REMAINS RELEVANT
NMS remains a risk in susceptible patients receiving atypical antipsychotics, according to clinical reports and drug adverse event surveys (Figure).2
Moreover, NMS continues to be reported with conventional antipsychotics, which remain in widespread use. Patients who receive long-acting depot conventional antipsychotics are at risk for prolonged NMS episodes.
Figure 55 NMS cases reported with use of antipsychotics, 1998-2002
Probable or definite neuroleptic malignant syndrome cases associated with antipsychotic monotherapy reported to the Neuroleptic Malignant Syndrome Information Service.NMS in medical settings. Psychiatrists may be consulted when patients develop NMS while receiving conventional antipsychotics or other dopaminereceptor antagonists used in medical settings.3,4 Haloperidol remains the recommended drug of choice for treating agitation and delirium and continues to be the single most common trigger of NMS. Although often overlooked, antiemetics and sedatives with neuroleptic properties—such as prochlorperazine, metoclopramide, and promethazine—also have triggered NMS.
Other hyperthermic conditions. NMS is often considered in the differential diagnosis of patients who develop fever or encephalopathy while being treated with psychotropics. In these acute, complex, and often grave situations, psychiatrists may be consulted to recommend treatment for behavioral control or to distinguish NMS from other conditions.
NEWER VS. OLDER ANTIPSYCHOTICS
Has NMS incidence declined with the atypical agents? Probably, but providing proof is difficult:
- NMS is uncommon; its incidence in psychiatric patients treated with conventional antipsychotics is approximately 0.2%.5 To demonstrate reduced NMS incidence with atypicals, a very large sample of patients would be required to reach statistical significance.
- As doctors have used lower doses of conventional agents—which reduces the risk of NMS—any beneficial impact from atypicals has become more difficult to detect.5,6
- Reports of NMS frequency with atypicals may be inflated by bias in publishing adverse events with newer versus older agents.
- Patients switched to atypicals may represent a high-risk group that is intolerant or resistant to conventional antipsychotics.
So far, few unequivocal cases of NMS have been attributed to the use of quetiapine, ziprasidone, or aripiprazole, the most recently introduced atypicals. Moreover, case reports of NMS associated with clozapine, risperidone, or olanzapine2 are often difficult to interpret because of incomplete clinical details, varying diagnostic criteria, and concomitant use of more than one antipsychotic.
Milder NMS? Do the newer antipsychotics produce an “atypical” or milder form of NMS? Case reports indicate that extreme temperature elevations and extrapyramidal dysfunction are less frequent in NMS associated with atypical compared with conventional antipsychotics.2 However, case descriptions of NMS were heterogeneous even with conventional agents, and clinicians’ growing awareness of NMS even before atypicals were introduced allowed for earlier diagnosis of mild and partial NMS cases.7
CLINICAL FEATURES OF NMS
Regardless of drug selection, it is important to recognize early and mild signs of NMS. Any case can progress to a fulminant form that is more difficult to treat.
Patients at risk. NMS may be more likely to develop in patients with:5,6,8
- dehydration
- agitation
- low serum iron
- underlying brain damage
- catatonia.
Some patients may have genetic abnormalities in central dopamine systems that increase their susceptibility to NMS.6,9
Fifteen to 20% of patients who develop NMS have experienced a previous episode while taking antipsychotics, which is why taking a careful drug history is important.5,6 Although most often reported with therapeutic antipsychotic doses, NMS has been associated with rapid dose titration, especially when given parenterally.8
On the other hand, the practical value of these risk factors is often limited in individual cases and may lead one to overestimate NMS risk. NMS is rare and idiosyncratic. Risk factors may not outweigh antipsychotics’ benefits when these drugs are indicated for a patient with psychosis.
Incipient NMS. Identifying early signs of NMS may be impossible in fulminant cases, but patients with incipient NMS may show:
- unexpected mental status changes
- new-onset catatonia
- refractory extrapyramidal and bulbar signs such as rigidity, dysphagia, or dysarthria.5,7,10
Other clues to NMS onset include tachycardia, tachypnea, and elevated temperature or serum creatine phosphokinase (CPK). These signs, however, do not precede or progress to NMS in all cases. A high index of suspicion for NMS, tempered by sound clinical judgment, is called for when assessing all patients receiving antipsychotics.
Diagnostic criteria. Clinical signs of NMS as a fullblown hypermetabolic syndrome are distinctive and well described (Table 1).5,6,11,12 Elevated temperature is accompanied by profuse sweating. Extreme temperatures (>104° F), especially if prolonged or associated with hypoxia or hypotension, pose a high risk for brain damage, rhabdomyolysis, disseminated intravascular coagulation, multisystem organ failure, and death.
Muscle rigidity is a characteristic finding and may be accompanied by tremors, cogwheeling, myoclonus, or rhabdomyolysis. Changes in vital signs—such as tachycardia and tachypnea—are typical.
Mental status examination usually reveals catatonic signs of mutism and stupor, but delirium and coma also have been described. No laboratory findings are specific for NMS, but elevated white blood cell counts, low serum iron, metabolic acidosis, hypoxia, and elevated serum CPK and catecholamines have been reported.
Table 1
Common clinical features of NMS
| Signs and symptoms | Altered level of consciousness, catatonia, dysarthria, dysphagia, elevated temperature, labile blood pressure, muscle rigidity, mutism, myoclonus, tachycardia, tachypnea, tremor |
| Laboratory findings | Elevated catecholamines and serum creatine phosphokinase, hypoxia, leukocytosis, low serum iron, metabolic acidosis |
Resolution. If recognized promptly, NMS resolves within 1 to 2 weeks in two-thirds of patients after antipsychotics are discontinued. The average recovery time of 7 to 10 days may be prolonged in patients who were taking long-acting depot antipsychotics or in those with persistent residual catatonic symptoms.13
Risk of death. NMS remains potentially fatal, especially if high temperatures develop or episodes are prolonged. Causes of death include cardiorespiratory arrest, renal failure, pulmonary emboli, pneumonia, sepsis, disseminated intravascular coagulation, and multisystem organ failure.
DIFFERENTIAL DIAGNOSIS
Differential diagnosis of NMS encompasses disorders that present with fever and encephalopathy.5,6,12 Primary brain disorders that resemble NMS include:9,14-16
- infections
- acute psychotic disorders that progress to malignant catatonia or delirious mania
- midbrain structural lesions
- seizures.
Also exclude hormonal and autoimmune disorders and environmental heatstroke (Table 2).17,18 Similar hyperthermic syndromes have been reported with other toxins and drugs, including malignant hyperthermia of anesthesia, serotonin syndrome, and dopamine agonist withdrawal in patients with Parkinson’s disease (Table 3).5,6,19
Table 2
7 disease states most often confused with NMS
| Infections |
| Malignant catatonia secondary to psychotic disorders |
| Benign extrapyramidal side effects |
| Agitated delirium from diverse causes |
| Environmental heatstroke |
| Serotonin syndrome |
| Withdrawal from dopamine agonists, other drugs, or alcohol |
| Source: Neuroleptic Malignant Syndrome Information Service hotline |
Table 3
Drugs that can cause NMS-like hyperthermic syndromes
| Anticholinergics Dopamine antagonists Hallucinogens Inhalational anesthetics Monoamine oxidase inhibitors Psychostimulants Salicylates | Serotonergic drugs Succinylcholine Withdrawal from: • Dopamine agonists • Alcohol • Sedative/hypnotics • Baclofen |
MANAGING NMS
The standard approach to managing patients with NMS includes four steps:
- recognize the diagnosis early
- exclude alternate causes of symptoms
- discontinue suspected triggering drugs
- provide supportive care to reduce temperatures, ensure fluid balance, and detect complications.5,6,20
Beyond supportive care, several specific therapies have been proposed based on theoretical mechanisms of NMS and meta-analyses of offlabel use in anecdotal clinical reports (Table 4). If benzodiazepines, dopamine agonists, or dantrolene are effective, taper slowly after recovery to prevent rebound symptoms.
Benzodiazepines. Given the concept of NMS as a form of catatonia, benzodiazepines have been used effectively in some cases.20,21 A trial of lorazepam, 1 to 2 mg parenterally, is a reasonable first step. Higher doses may be required, with adequate monitoring of respiratory status. Oral lorazepam can maintain the therapeutic effect.
Dopamine agonists. To reverse the parkinsonism and dopamine antagonist properties of antipsychotics, dopamine agonists such as bromocriptine or amantadine have been tried and have reduced NMS duration and mortality.20,22,23 Newer drugs such as ropinorole and pramipexole may also be useful. Dopaminergic drugs, however, can worsen psychosis and cause hypotension and emesis.
Dantrolene may reduce hyperthermia related to skeletal muscle hypermetabolism of any cause and has been effective in rapidly reducing extreme temperatures in some NMS cases.20,22-26 Dantrolene is given IV, 1 to 2.5 mg/kg every 6 hours. An oral form can be substituted if a response is obtained. Dantrolene can impair respiratory and hepatic function and should not be combined with calcium channel blockers.
ECT is increasingly recognized as an effective NMS treatment and should not be overlooked for patients:
Standard ECT is given, although nondepolarizing muscle relaxants instead of succinylcholine are used in patients with serious rhabdomyolysis to avoid the risk of hyperkalemia.20
Recommendation. Although these modalities offer a spectrum of therapeutic options, it is premature to recommend any single remedy over others or over supportive care alone because:
- randomized, controlled trials have not been conducted
- NMS episodes are heterogeneous in presentation and outcome
- the syndrome is often self-limited after antipsychotics are discontinued.
I recommend that you choose therapies empirically, based on the character, severity, and duration of symptoms in a given case.5,6,20
Table 4
How to treat neuroleptic malignant syndrome
| General measures | Diagnose early, discontinue antipsychotic, provide supportive care |
| Specific interventions under investigation | |
| Benzodiazepines | Parenteral lorazepam, 1 to 2 mg or higher; monitor respiratory status |
| Dopamine agonists | Bromocriptine, 2.5 mg every 8 hours or amantadine, 100 mg every 8 hours; monitor psychosis, blood pressure, nausea |
| Dantrolene | 1 to 2.5 mg/kg IV every 6 hours; monitor respiratory and hepatic function; avoid calcium channel blockers |
| ECT | Standard administration; avoid succinylcholine in patients with rhabdomyolysis |
REDUCING RISK OF RECURRENCE
Patients vary in susceptibility to recurrence after they recover from NMS, but the risk approaches 30% with future exposure to antipsychotics.5,6 You may be able to minimize recurrence risk by:
- reducing risk factors, such as dehydration
- considering alternatives to antipsychotics, such as treating bipolar disorder with lithium or ECT
- using atypical instead of conventional antipsychotics, starting with low dosages and titrating slowly.
Before you reintroduce antipsychotics, carefully document informed consent and your rationale for treatment decisions in the patient’s chart.
Related resources
- Neuroleptic Malignant Syndrome Information Service. Hotline for health professionals. (888) 667-8367. www.nmsis.org
- Mann SC, Caroff SN, Keck PE Jr, Lazarus A. Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003.
- Caroff SN, Mann SC, Francis A, Fricchione GL. Catatonia: from psychopathology to neurobiology. Washington, DC: American Psychiatric Publishing (in press).
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Bromocriptine • Parlodel
- Clozapine • Clozaril
- Dantrolene • Dantrium
- Haloperidol • Haldol
- Lorazepam • Ativan
- Metoclopramide • Reglan
- Olanzapine • Zyprexa
- Pramipexole • Mirapex
- Prochlorperazine • Compazine
- Promethazine • Phenergan
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ropinirole • Requip
- Ziprasidone • Geodon
Disclosure
Dr. Caroff receives research support from Janssen Pharmaceutica and Pfizer Inc., and is a consultant to Eli Lilly and Co. and Bristol-Myers Squibb Co.
Potentially fatal neuroleptic malignant syndrome (NMS)—though less common than in the past—can happen with either conventional or atypical antipsychotics.1,2 To help you protect patients when prescribing antipsychotics or consulting with other clinicians about these drugs, this article discusses:
- risk factors and clinical features that warn of NMS onset
- differential diagnosis of disease states most often confused with NMS
- management recommendations, including supportive measures and specific interventions such as benzodiazepines, dopamine agonists, dantrolene, and electroconvulsive therapy (ECT).
WHY NMS REMAINS RELEVANT
NMS remains a risk in susceptible patients receiving atypical antipsychotics, according to clinical reports and drug adverse event surveys (Figure).2
Moreover, NMS continues to be reported with conventional antipsychotics, which remain in widespread use. Patients who receive long-acting depot conventional antipsychotics are at risk for prolonged NMS episodes.
Figure 55 NMS cases reported with use of antipsychotics, 1998-2002
Probable or definite neuroleptic malignant syndrome cases associated with antipsychotic monotherapy reported to the Neuroleptic Malignant Syndrome Information Service.NMS in medical settings. Psychiatrists may be consulted when patients develop NMS while receiving conventional antipsychotics or other dopaminereceptor antagonists used in medical settings.3,4 Haloperidol remains the recommended drug of choice for treating agitation and delirium and continues to be the single most common trigger of NMS. Although often overlooked, antiemetics and sedatives with neuroleptic properties—such as prochlorperazine, metoclopramide, and promethazine—also have triggered NMS.
Other hyperthermic conditions. NMS is often considered in the differential diagnosis of patients who develop fever or encephalopathy while being treated with psychotropics. In these acute, complex, and often grave situations, psychiatrists may be consulted to recommend treatment for behavioral control or to distinguish NMS from other conditions.
NEWER VS. OLDER ANTIPSYCHOTICS
Has NMS incidence declined with the atypical agents? Probably, but providing proof is difficult:
- NMS is uncommon; its incidence in psychiatric patients treated with conventional antipsychotics is approximately 0.2%.5 To demonstrate reduced NMS incidence with atypicals, a very large sample of patients would be required to reach statistical significance.
- As doctors have used lower doses of conventional agents—which reduces the risk of NMS—any beneficial impact from atypicals has become more difficult to detect.5,6
- Reports of NMS frequency with atypicals may be inflated by bias in publishing adverse events with newer versus older agents.
- Patients switched to atypicals may represent a high-risk group that is intolerant or resistant to conventional antipsychotics.
So far, few unequivocal cases of NMS have been attributed to the use of quetiapine, ziprasidone, or aripiprazole, the most recently introduced atypicals. Moreover, case reports of NMS associated with clozapine, risperidone, or olanzapine2 are often difficult to interpret because of incomplete clinical details, varying diagnostic criteria, and concomitant use of more than one antipsychotic.
Milder NMS? Do the newer antipsychotics produce an “atypical” or milder form of NMS? Case reports indicate that extreme temperature elevations and extrapyramidal dysfunction are less frequent in NMS associated with atypical compared with conventional antipsychotics.2 However, case descriptions of NMS were heterogeneous even with conventional agents, and clinicians’ growing awareness of NMS even before atypicals were introduced allowed for earlier diagnosis of mild and partial NMS cases.7
CLINICAL FEATURES OF NMS
Regardless of drug selection, it is important to recognize early and mild signs of NMS. Any case can progress to a fulminant form that is more difficult to treat.
Patients at risk. NMS may be more likely to develop in patients with:5,6,8
- dehydration
- agitation
- low serum iron
- underlying brain damage
- catatonia.
Some patients may have genetic abnormalities in central dopamine systems that increase their susceptibility to NMS.6,9
Fifteen to 20% of patients who develop NMS have experienced a previous episode while taking antipsychotics, which is why taking a careful drug history is important.5,6 Although most often reported with therapeutic antipsychotic doses, NMS has been associated with rapid dose titration, especially when given parenterally.8
On the other hand, the practical value of these risk factors is often limited in individual cases and may lead one to overestimate NMS risk. NMS is rare and idiosyncratic. Risk factors may not outweigh antipsychotics’ benefits when these drugs are indicated for a patient with psychosis.
Incipient NMS. Identifying early signs of NMS may be impossible in fulminant cases, but patients with incipient NMS may show:
- unexpected mental status changes
- new-onset catatonia
- refractory extrapyramidal and bulbar signs such as rigidity, dysphagia, or dysarthria.5,7,10
Other clues to NMS onset include tachycardia, tachypnea, and elevated temperature or serum creatine phosphokinase (CPK). These signs, however, do not precede or progress to NMS in all cases. A high index of suspicion for NMS, tempered by sound clinical judgment, is called for when assessing all patients receiving antipsychotics.
Diagnostic criteria. Clinical signs of NMS as a fullblown hypermetabolic syndrome are distinctive and well described (Table 1).5,6,11,12 Elevated temperature is accompanied by profuse sweating. Extreme temperatures (>104° F), especially if prolonged or associated with hypoxia or hypotension, pose a high risk for brain damage, rhabdomyolysis, disseminated intravascular coagulation, multisystem organ failure, and death.
Muscle rigidity is a characteristic finding and may be accompanied by tremors, cogwheeling, myoclonus, or rhabdomyolysis. Changes in vital signs—such as tachycardia and tachypnea—are typical.
Mental status examination usually reveals catatonic signs of mutism and stupor, but delirium and coma also have been described. No laboratory findings are specific for NMS, but elevated white blood cell counts, low serum iron, metabolic acidosis, hypoxia, and elevated serum CPK and catecholamines have been reported.
Table 1
Common clinical features of NMS
| Signs and symptoms | Altered level of consciousness, catatonia, dysarthria, dysphagia, elevated temperature, labile blood pressure, muscle rigidity, mutism, myoclonus, tachycardia, tachypnea, tremor |
| Laboratory findings | Elevated catecholamines and serum creatine phosphokinase, hypoxia, leukocytosis, low serum iron, metabolic acidosis |
Resolution. If recognized promptly, NMS resolves within 1 to 2 weeks in two-thirds of patients after antipsychotics are discontinued. The average recovery time of 7 to 10 days may be prolonged in patients who were taking long-acting depot antipsychotics or in those with persistent residual catatonic symptoms.13
Risk of death. NMS remains potentially fatal, especially if high temperatures develop or episodes are prolonged. Causes of death include cardiorespiratory arrest, renal failure, pulmonary emboli, pneumonia, sepsis, disseminated intravascular coagulation, and multisystem organ failure.
DIFFERENTIAL DIAGNOSIS
Differential diagnosis of NMS encompasses disorders that present with fever and encephalopathy.5,6,12 Primary brain disorders that resemble NMS include:9,14-16
- infections
- acute psychotic disorders that progress to malignant catatonia or delirious mania
- midbrain structural lesions
- seizures.
Also exclude hormonal and autoimmune disorders and environmental heatstroke (Table 2).17,18 Similar hyperthermic syndromes have been reported with other toxins and drugs, including malignant hyperthermia of anesthesia, serotonin syndrome, and dopamine agonist withdrawal in patients with Parkinson’s disease (Table 3).5,6,19
Table 2
7 disease states most often confused with NMS
| Infections |
| Malignant catatonia secondary to psychotic disorders |
| Benign extrapyramidal side effects |
| Agitated delirium from diverse causes |
| Environmental heatstroke |
| Serotonin syndrome |
| Withdrawal from dopamine agonists, other drugs, or alcohol |
| Source: Neuroleptic Malignant Syndrome Information Service hotline |
Table 3
Drugs that can cause NMS-like hyperthermic syndromes
| Anticholinergics Dopamine antagonists Hallucinogens Inhalational anesthetics Monoamine oxidase inhibitors Psychostimulants Salicylates | Serotonergic drugs Succinylcholine Withdrawal from: • Dopamine agonists • Alcohol • Sedative/hypnotics • Baclofen |
MANAGING NMS
The standard approach to managing patients with NMS includes four steps:
- recognize the diagnosis early
- exclude alternate causes of symptoms
- discontinue suspected triggering drugs
- provide supportive care to reduce temperatures, ensure fluid balance, and detect complications.5,6,20
Beyond supportive care, several specific therapies have been proposed based on theoretical mechanisms of NMS and meta-analyses of offlabel use in anecdotal clinical reports (Table 4). If benzodiazepines, dopamine agonists, or dantrolene are effective, taper slowly after recovery to prevent rebound symptoms.
Benzodiazepines. Given the concept of NMS as a form of catatonia, benzodiazepines have been used effectively in some cases.20,21 A trial of lorazepam, 1 to 2 mg parenterally, is a reasonable first step. Higher doses may be required, with adequate monitoring of respiratory status. Oral lorazepam can maintain the therapeutic effect.
Dopamine agonists. To reverse the parkinsonism and dopamine antagonist properties of antipsychotics, dopamine agonists such as bromocriptine or amantadine have been tried and have reduced NMS duration and mortality.20,22,23 Newer drugs such as ropinorole and pramipexole may also be useful. Dopaminergic drugs, however, can worsen psychosis and cause hypotension and emesis.
Dantrolene may reduce hyperthermia related to skeletal muscle hypermetabolism of any cause and has been effective in rapidly reducing extreme temperatures in some NMS cases.20,22-26 Dantrolene is given IV, 1 to 2.5 mg/kg every 6 hours. An oral form can be substituted if a response is obtained. Dantrolene can impair respiratory and hepatic function and should not be combined with calcium channel blockers.
ECT is increasingly recognized as an effective NMS treatment and should not be overlooked for patients:
Standard ECT is given, although nondepolarizing muscle relaxants instead of succinylcholine are used in patients with serious rhabdomyolysis to avoid the risk of hyperkalemia.20
Recommendation. Although these modalities offer a spectrum of therapeutic options, it is premature to recommend any single remedy over others or over supportive care alone because:
- randomized, controlled trials have not been conducted
- NMS episodes are heterogeneous in presentation and outcome
- the syndrome is often self-limited after antipsychotics are discontinued.
I recommend that you choose therapies empirically, based on the character, severity, and duration of symptoms in a given case.5,6,20
Table 4
How to treat neuroleptic malignant syndrome
| General measures | Diagnose early, discontinue antipsychotic, provide supportive care |
| Specific interventions under investigation | |
| Benzodiazepines | Parenteral lorazepam, 1 to 2 mg or higher; monitor respiratory status |
| Dopamine agonists | Bromocriptine, 2.5 mg every 8 hours or amantadine, 100 mg every 8 hours; monitor psychosis, blood pressure, nausea |
| Dantrolene | 1 to 2.5 mg/kg IV every 6 hours; monitor respiratory and hepatic function; avoid calcium channel blockers |
| ECT | Standard administration; avoid succinylcholine in patients with rhabdomyolysis |
REDUCING RISK OF RECURRENCE
Patients vary in susceptibility to recurrence after they recover from NMS, but the risk approaches 30% with future exposure to antipsychotics.5,6 You may be able to minimize recurrence risk by:
- reducing risk factors, such as dehydration
- considering alternatives to antipsychotics, such as treating bipolar disorder with lithium or ECT
- using atypical instead of conventional antipsychotics, starting with low dosages and titrating slowly.
Before you reintroduce antipsychotics, carefully document informed consent and your rationale for treatment decisions in the patient’s chart.
Related resources
- Neuroleptic Malignant Syndrome Information Service. Hotline for health professionals. (888) 667-8367. www.nmsis.org
- Mann SC, Caroff SN, Keck PE Jr, Lazarus A. Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003.
- Caroff SN, Mann SC, Francis A, Fricchione GL. Catatonia: from psychopathology to neurobiology. Washington, DC: American Psychiatric Publishing (in press).
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Bromocriptine • Parlodel
- Clozapine • Clozaril
- Dantrolene • Dantrium
- Haloperidol • Haldol
- Lorazepam • Ativan
- Metoclopramide • Reglan
- Olanzapine • Zyprexa
- Pramipexole • Mirapex
- Prochlorperazine • Compazine
- Promethazine • Phenergan
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ropinirole • Requip
- Ziprasidone • Geodon
Disclosure
Dr. Caroff receives research support from Janssen Pharmaceutica and Pfizer Inc., and is a consultant to Eli Lilly and Co. and Bristol-Myers Squibb Co.
1. Caroff SN, Mann SC, Campbell EC, Sullivan KA. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry 2002;63(suppl 4):12-19.
2. Caroff SN, Mann SC, Campbell EC. Atypical antipsychotics and neuroleptic malignant syndrome. Psychiatric Annals 2000;30(5):314-21.
3. Caroff SN, Rosenberg H, Mann SC, et al. Neuroleptic malignant syndrome in the perioperative setting. Am J Anesthesiology 2001;28(8):387-93.
4. Caroff SN, Rosenberg H, Mann SC, et al. Neuroleptic malignant syndrome in the critical care unit. Crit Care Med 2002;30(11):2609.-
5. Caroff SN, Mann SC. Neuroleptic malignant syndrome. Med Clin North Am 1993;77(1):185-202.
6. Caroff SN. Neuroleptic malignant syndrome. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing Inc., 2003;1-44.
7. Velamoor VR, Swamy GN, Parmar RS, et al. Management of suspected neuroleptic malignant syndrome. Can J Psychiatry 1995;40(9):545-50.
8. Keck PE, Jr, Pope HG, Jr, Cohen BM, et al. Risk factors for neuroleptic malignant syndrome. Arch Gen Psychiatry 1989;46:914-18.
9. Mann SC. Malignant catatonia. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003;121-43.
10. Velamoor VR, Norman RMG, Caroff SN, et al. Progression of symptoms in neuroleptic malignant syndrome. J Nerv Ment Dis 1994;182(3):168-73.
11. Delay J, Pichot P, Lemperiere T, et al. Un neuroleptique majeur non-phenothiazine et non reserpinique, l’haloperidol, dans le traitement des psychoses. Annales Medico-Psychologique 1960;118(1):145-52.
12. Caroff SN. The neuroleptic malignant syndrome. J Clin Psychiatry 1980;41(3):79-83.
13. Caroff SN, Mann SC, Keck PE, Jr, Francis A. Residual catatonic state following neuroleptic malignant syndrome. J Clin Psychopharmacol 2000;20(2):257-9.
14. Caroff SN, Mann SC, McCarthy M, et al. Acute infectious encephalitis complicated by neuroleptic malignant syndrome. J Clin Psychopharmacol 1998;18(4):349-51.
15. Caroff SN, Mann SC, Gliatto MF, et al. Psychiatric manifestations of acute viral encephalitis. Psychiatric Annals 2001;31(3):193-204.
16. Caroff SN, Mann SC, Francis A, Fricchione GL (eds). Catatonia: from psychopathology to neurobiology. Washington, DC: American Psychiatric Publishing (in press).
17. Mann SC. Thermoregulatory mechanisms and antipsychotic drugrelated heatstroke. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003;45-74.
18. Caroff SN, Mann SC, Campbell EC. Risk of fatal heatstroke after hospitalization. Psychiatric Serv 2000;51(7):938.-
19. Keck PE, Jr. Serotonin syndrome. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003;75-92.
20. Davis JM, Caroff SN, Mann SC. Treatment of neuroleptic malignant syndrome. Psychiatric Annals 2000;30(5):325-31.
21. Francis A, Chandragiri S, Rizvi S, et al. Lorazepam a treatment for neuroleptic malignant syndrome? CNS Spectrums 2000;5(7):54-7.
22. Sakkas P, Davis JM, Hua J, Wang Z. Pharmacotherapy of neuroleptic malignant syndrome. Psychiatr Ann 1991;21:157-64.
23. Rosenberg MR, Green M. Neuroleptic malignant syndrome: review of response to therapy. Arch Intern Med 1989;149:1927-31.
24. Henderson A, Longdon P. Fulminant metoclopramide-induced neuroleptic malignant syndrome rapidly responsive to intravenous dantrolene. Aust N Z J Med 1991;21:742-3.
25. Yamawaki S, Morio M, Kazamatsuri G, et al. Clinical evaluation and effective usage of dantrolene sodium in neuroleptic malignant syndrome. Kiso to Rinsyou (Clinical Reports) 1993;27(3):1045-66.
26. Tsutsumi Y, Yamamoto K, Matsuura S, et al. The treatment of neuroleptic malignant syndrome using dantrolene sodium. Psychiatry Clin Neurosci 1998;52:433-8.
27. Nisijima K, Ishiguro T. Electroconvulsive therapy for the treatment of neuroleptic malignant syndrome: a report of five cases. J ECT 1999;15:158-63.
28. Troller JN, Sachdev PS. Electroconvulsive treatment of neuroleptic malignant syndrome: a review and report of cases. Aust N Z J Psychiatry 1999;33:650-9.
1. Caroff SN, Mann SC, Campbell EC, Sullivan KA. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry 2002;63(suppl 4):12-19.
2. Caroff SN, Mann SC, Campbell EC. Atypical antipsychotics and neuroleptic malignant syndrome. Psychiatric Annals 2000;30(5):314-21.
3. Caroff SN, Rosenberg H, Mann SC, et al. Neuroleptic malignant syndrome in the perioperative setting. Am J Anesthesiology 2001;28(8):387-93.
4. Caroff SN, Rosenberg H, Mann SC, et al. Neuroleptic malignant syndrome in the critical care unit. Crit Care Med 2002;30(11):2609.-
5. Caroff SN, Mann SC. Neuroleptic malignant syndrome. Med Clin North Am 1993;77(1):185-202.
6. Caroff SN. Neuroleptic malignant syndrome. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing Inc., 2003;1-44.
7. Velamoor VR, Swamy GN, Parmar RS, et al. Management of suspected neuroleptic malignant syndrome. Can J Psychiatry 1995;40(9):545-50.
8. Keck PE, Jr, Pope HG, Jr, Cohen BM, et al. Risk factors for neuroleptic malignant syndrome. Arch Gen Psychiatry 1989;46:914-18.
9. Mann SC. Malignant catatonia. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003;121-43.
10. Velamoor VR, Norman RMG, Caroff SN, et al. Progression of symptoms in neuroleptic malignant syndrome. J Nerv Ment Dis 1994;182(3):168-73.
11. Delay J, Pichot P, Lemperiere T, et al. Un neuroleptique majeur non-phenothiazine et non reserpinique, l’haloperidol, dans le traitement des psychoses. Annales Medico-Psychologique 1960;118(1):145-52.
12. Caroff SN. The neuroleptic malignant syndrome. J Clin Psychiatry 1980;41(3):79-83.
13. Caroff SN, Mann SC, Keck PE, Jr, Francis A. Residual catatonic state following neuroleptic malignant syndrome. J Clin Psychopharmacol 2000;20(2):257-9.
14. Caroff SN, Mann SC, McCarthy M, et al. Acute infectious encephalitis complicated by neuroleptic malignant syndrome. J Clin Psychopharmacol 1998;18(4):349-51.
15. Caroff SN, Mann SC, Gliatto MF, et al. Psychiatric manifestations of acute viral encephalitis. Psychiatric Annals 2001;31(3):193-204.
16. Caroff SN, Mann SC, Francis A, Fricchione GL (eds). Catatonia: from psychopathology to neurobiology. Washington, DC: American Psychiatric Publishing (in press).
17. Mann SC. Thermoregulatory mechanisms and antipsychotic drugrelated heatstroke. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003;45-74.
18. Caroff SN, Mann SC, Campbell EC. Risk of fatal heatstroke after hospitalization. Psychiatric Serv 2000;51(7):938.-
19. Keck PE, Jr. Serotonin syndrome. In: Mann SC, Caroff SN, Keck PE Jr, Lazarus A (eds). Neuroleptic malignant syndrome and related conditions (2nd ed). Washington, DC: American Psychiatric Publishing, 2003;75-92.
20. Davis JM, Caroff SN, Mann SC. Treatment of neuroleptic malignant syndrome. Psychiatric Annals 2000;30(5):325-31.
21. Francis A, Chandragiri S, Rizvi S, et al. Lorazepam a treatment for neuroleptic malignant syndrome? CNS Spectrums 2000;5(7):54-7.
22. Sakkas P, Davis JM, Hua J, Wang Z. Pharmacotherapy of neuroleptic malignant syndrome. Psychiatr Ann 1991;21:157-64.
23. Rosenberg MR, Green M. Neuroleptic malignant syndrome: review of response to therapy. Arch Intern Med 1989;149:1927-31.
24. Henderson A, Longdon P. Fulminant metoclopramide-induced neuroleptic malignant syndrome rapidly responsive to intravenous dantrolene. Aust N Z J Med 1991;21:742-3.
25. Yamawaki S, Morio M, Kazamatsuri G, et al. Clinical evaluation and effective usage of dantrolene sodium in neuroleptic malignant syndrome. Kiso to Rinsyou (Clinical Reports) 1993;27(3):1045-66.
26. Tsutsumi Y, Yamamoto K, Matsuura S, et al. The treatment of neuroleptic malignant syndrome using dantrolene sodium. Psychiatry Clin Neurosci 1998;52:433-8.
27. Nisijima K, Ishiguro T. Electroconvulsive therapy for the treatment of neuroleptic malignant syndrome: a report of five cases. J ECT 1999;15:158-63.
28. Troller JN, Sachdev PS. Electroconvulsive treatment of neuroleptic malignant syndrome: a review and report of cases. Aust N Z J Psychiatry 1999;33:650-9.
Practice, not malpractice: 3 clinical habits to reduce liability risk
Psychiatrists’ risk of malpractice liability1 is broadening as courts consider the uncertainties of off-label prescribing, telemedicine, and confidentiality. Juries are holding mental health practitioners responsible for harm done both to and by psychiatric patients.
How you keep medical records, communicate with patients and colleagues, and arrange consultations can reduce your malpractice risk (Box 1).4-9 We offer recommendations based on court decisions and other evidence for managing:
- traditional risks—such as patient violence and suicide, adverse drug reactions, sex with patients, faulty termination of treatment, and supervisory and consultative relationships4
- newer risks—such as recovered memory, off-label prescribing, practice guidelines, and e-mail and confidentiality.
1. Keep thorough medical records
The most powerful defense against a malpractice suit is a well-documented chart. It can often prevent a malpractice suit by providing evidence that the physician adequately evaluated the available information and made good-faith efforts with his or her best judgment. Juries are typically forgiving of mistakes made in this context.4,5
Write legibly, and sign and date all entries. Try to think out loud in the chart. By outlining your thoughts about differential diagnosis, risks and benefits, and treatment options, you can help a jury understand your decision-making process and show that you carefully evaluated the situation. When documenting difficult cases, for example, imagine a plaintiff’s attorney reading your notes to a jury.6
2. Communicate freely with patients
Careful interaction with patients and their families can also prevent lawsuits. Communicating includes preparing patients for what to expect during treatment sessions, encouraging feedback, and even using humor.7 Freely sharing treatment information with patients can build a sense of mutual decision-making and responsibility.8 Acknowledging treatment limitations and deflating unrealistic expectations can also protect you.
Patients who file malpractice suits are often seeking an apology or expression of regret from their physicians. It is appropriate and prudent to admit and apologize for minor errors. It is also appropriate to express condolence over what both sides agree is a severe, negative outcome.9 Expressing sympathy is not equivalent to admitting wrongdoing.
3. Seek consultation as needed
Discussing difficult or ambiguous cases with peers, supervisors, or legal staff can help shield you from liability. For example:
- Second opinions may help you make difficult clinical decisions.
- Peers and supervisors may provide useful suggestions to improve patient care.
- Legal staff can give advice regarding liability.
The fact that you sought consultation can be used in court as evidence against negligence, as it shows you tried to ensure appropriate care for your patient.9
This article describes general guidelines and is not intended to constitute legal advice. All practitioners have a responsibility to know the laws of the jurisdictions in which they practice.
PREVENTING PATIENT VIOLENCE
The case that opened Pandora’s box. Prosenjit Poddar, a student at the University of California at Berkeley, was infatuated with coed Tanya Tarasoff and told his psychologist he intended to kill her. The psychologist notified his psychiatric supervisor and called campus police.
The psychologist told police Poddar was dangerous to himself and others. He stated that he would sign an emergency hold if they would bring Poddar to the hospital.
The police apprehended Poddar but released him. Poddar dropped out of therapy and 2 months later fatally stabbed Ms. Tarasoff.
Ms. Tarasoff’s parents sued those who treated Poddar and the University of California.2 After a complicated legal course, the California Supreme Court ruled that once a therapist determines—or should have determined—that a patient poses a serious danger of violence to others, “he bears a duty to exercise reasonable care to protect the foreseeable victim of that danger.”3
The 1976 Tarasoff ruling has become a national standard of practice, leading to numerous other patient violence lawsuits. In these cases, psychiatrists are most likely to be found liable when recently released inpatients commit violent acts, particularly if the physician had reason to know the patient was dangerous and failed to take adequate precautions or appropriately assess the patient.4
Wider interpretations. Cases in several states have extended the Tarasoff ruling. In at least two cases, this standard has been applied when the patient threatened no specific victim before committing violence:
- A New Jersey court (McIntosh v. Milano, 1979) found a psychiatrist liable for malpractice on grounds that a therapist has a duty to protect society, just as a doctor must protect society by reporting carriers of dangerous diseases.
- A Nebraska court (Lipari v. Sears, Roebuck, and Co., 1980) held that physicians have a duty to protect—even if the specific identity of victims is unknown—so long as the physician should know that the patient presents an unreasonable risk of harm to others.2
Auto accidents. Tarasoff liability also has been extended to auto accidents. In Washington state (Petersen v. Washington, 1983), a psychiatrist was held liable for injuries to victims of an accident caused by a psychiatric patient. The court ruled that the psychiatrist had a duty to take reasonable precautions to protect any foreseeable persons from being endangered by the patient.
In a similar case in Wisconsin (Schuster and Schuster v. Altenberg, et al., 1988), the court ruled that damages could be awarded to anyone whose harm could have been prevented had the physician practiced according to professional standards.2
Other extensions include cases such as Naidu v. Laird, 1988, in which patient violence occurred more than 5 months after hospitalization.2 Vermont has extended the Tarasoff precedent to property destruction by psychiatric patients.10
Recommendation. Most states require a psychiatrist to protect against only specific threats to identifiable victims.10 To defend yourself against a Tarasoff-type suit, you must show that you:
- carefully assessed the patient’s risk for violence
- provided appropriate care
- and took appropriate precautions.
The most protective evidence is a medical record documenting that you thoroughly assessed a patient for risk of violence (Table).4,11
If you are unsure about how to manage a patient you believe may be dangerous to himself or others, consult with supervisors, peers, and legal advisors. Many states have Tarasoff-like statutes that specify the conditions that require action and the appropriate actions.
In states without specific statutes, options that generally satisfy Tarasoff requirements include hospitalizing the patient, notifying authorities, and/or warning the potential victim.10 As the Tarasoff case demonstrated, notifying authorities may not substitute for warning or hospitalizing.2
SUICIDE RISK? DOCUMENT CAREFULLY
Patient suicide accounts for one-fifth of claims covered by the American Psychiatric Association (APA) insurance plan.
In court, key points of challenge to a physician’s judgment in a suicide case include the admission evaluation and any status changes. Thorough risk assessment includes carefully reviewing existing records, evaluating risk factors for suicide, and seeking advice from colleagues or supervisors when appropriate.4
Recommendation. Document for every inpatient admission, discharge, or status change that the patient’s risk for suicide was assessed. List risk factors, protective factors, and risk for self-harm.
Explicitly address in the patient’s chart any comments about suicidality (such as heard by nursing staff).9 Document your rationale for medical decisions and orders, consistently follow unit policies, and explain risks and benefits of hospitalization to patients and their families.
Before discharge, schedule appropriate follow-up and make reasonable efforts to ensure medication adherence.4
SEX WITH PATIENTS IS UNPROTECTED
Sexual involvement with patients is indefensible and uncontestable in malpractice cases. Even so, up to 9% of male therapists and 3% of female therapists report in surveys that they have had sexual interaction with their patients.4
In 1985 the APA excluded sex with patients from its malpractice insurance coverage. Courts generally consider a treatment to be within the standard of care if a respectable minority of physicians consider it to be appropriate. Sex with patients is considered an absolute deviation from the standard of care, and no respectable minority of practitioners supports this practice. Because patients are substantially harmed, sex with patients is considered prima facie malpractice.12
Table
Is this patient dangerous? Risk factors for violence
| Psychiatric |
|
| Demographic |
|
| Socioeconomic |
|
WHEN MEDICATIONS CAUSE HARM
Adverse drug reactions—particularly tardive dyskinesia (TD)—are a source of significant losses in malpractice cases. Multimillion-dollar awards have been granted, especially when neuroleptic antipsychotics have been given in excessive dosages without proper monitoring.13
Informed consent has been a particularly difficult issue with the use of neuroleptic medications. Many doctors worry that patients who fear developing TD will not take prescribed neuroleptics. A study of North Carolina psychiatrists in the 1980s revealed that only 30% mentioned TD when telling their patients about neuroleptics’ possible side effects.13
The fact that a patient develops TD while taking an antipsychotic does not establish grounds for malpractice; a valid malpractice suit must also establish negligence. Negligence could include failing to obtain appropriate informed consent or continuing to prescribe an antipsychotic without adequately examining the patient.4
Informed consent does not require a patient to fully understand everything about a medication. The patient must understand the information a reasonable patient would want to know. Obvious misunderstandings must be corrected.
Recommendation. Consider informed consent a process, rather than one event—especially when you give neuroleptics for acute psychotic episodes. You can establish, review, and refresh consent in follow-up visits as medications help patients become more coherent and organized.
If you doubt a patient’s capacity to provide informed consent, a court determination may be necessary. In emergencies, however, treatment becomes a priority, even if the patient’s capacity to make rational decisions has not been established.13
TERMINATE TREATMENT WITH CAUTION
Terminating treatment can lead to malpractice, particularly if a patient becomes suicidal or violent. Psychiatrists have the right to choose their patients but cannot terminate care if a patient is acutely ill or requires emergency care.
Ensuring appropriate follow-up for patients at risk for decompensation often requires more than providing a referral or phone number. With the patient’s permission, for example, you could contact his subsequent psychiatrist or work with his support network to ensure that he receives follow-up care.14
Recommendation. With stable patients, send a written notice of termination and specify a reasonable period, usually 30 days. Send the letter by certified mail, and request a return receipt. Offer to help the patient find a new doctor, and say that you will forward the patient’s records to the new doctor when you receive appropriate release-of-information paperwork.15
LET THE SUPERVISOR BEWARE
Under the legal concept of respondeat superior (“let the master reply”), liability for the actions of subordinates may be transferred upward to the supervisor.4 For psychiatrists, supervisory liability obviously applies to teaching residents but may also apply in joint care, as with psychologists or social workers.
Recommendation. As a co-treating psychiatrist, you may be liable for other therapists’ actions unless you formally distinguish your role as a prescriber and not as a supervisor.9
When you prescribe medications for patients of nonphysician therapists, be sure you, the therapist, and patient understand the nature of your collaboration. Document the type of relationship and your discussion with the patient in the patient’s chart.
WATCH OUT FOR ‘CURBSIDE’ CONSULTS
Consult-liaison psychiatrists typically face a lower malpractice risk than do those who provide primary treatment. Duty to care for the patient is usually established by a formal consult request, after which the psychiatrist examines the patient and recommends treatment to the primary team.
You can, however, establish duty without meeting a patient. If sufficiently detailed, an informal “curbside” consult may establish a duty and corresponding liability16 (Box 2).4,5,9,17.18
Liability is usually shared with the primary team but may be related to how much responsibility you assume in the patient’s care. Any direct treatment—electroconvulsive therapy, psychotherapy, prescribing, writing orders in the chart—can elevate your risk to the primary level. Similarly, if the patient is harmed because the primary treater followed a consulting psychiatrist’s negligent advice, the psychiatrist can be found solely liable.
When you recommend a treatment, you share a portion of liability for informed consent. If neither you nor the provider obtains appropriate informed consent, you may both share liability for adverse outcomes. Both teams also share the duty to report child and elder abuse.16
Recommendation. Establish an explicit division of responsibilities with the primary team, including who writes orders and manages medications and who provides follow-up and discharge planning.
For curbside consults, inform the primary physician that you are providing general information and not a specific treatment recommendation. If the case is too complicated for general information to be useful, a formal consultation would serve the patient better. In written consultations, specify:
- the reason for the consult
- the issues addressed
- and the parties responsible for follow-up.16
RECOVERED MEMORY? FORGET PROSECUTION
In 1994, a father successfully sued his daughter’s therapists for implanting false memories of incest. A California court awarded him $500,000 on grounds that the therapists owed a duty of care to the patient’s parents as well as to the patient. Since then, multimillion-dollar cases have been litigated on grounds of false recovered memories, and some insurers exclude coverage for “revival of memory.”12
Most therapists who have been found liable have strongly supported the accuracy of their patients’ memories. These memories have usually contained bizarre features, including satanic abuse, baby breeding, human sacrifice, and cannibalism. Therapists in these cases have often recommended that their patients press charges or file lawsuits against their alleged abusers.
Lawsuits against therapists have been won on grounds that they used unorthodox procedures without informed consent, negligently or recklessly implanted memories of abuse, negligently reinforced such memories, and failed to sufficiently investigate the memories’ accuracy.19
Malpractice requires four conditions:
- A doctor-patient relationship was established.
- The physician practiced below the standard of care.
- The patient was harmed.
- The patient’s harm was a direct result of the physician’s failure to practice at the standard of care.4
Standard of care. A treatment may be considered within the standard of care so long as a “respectable minority” of practitioners considers it appropriate.17 Standard of care may be established by expert testimony, published texts, or practice guidelines18 and tends to be flexible in medical specialties—such as mental health—that allow for multiple treatment options.
Preponderance of evidence. In court proceedings, the plaintiff must establish malpractice by a reponderance of the evidence, which means “more likely than not.” This is a much less-stringent level of proof than beyond a reasonable doubt, as is required in criminal cases.9
Although a preponderance of the evidence may seem disturbingly easy to establish, courts are often forgiving of adverse outcomes caused by judgment errors if the physician acted in good faith and followed professional standards.4,5
Recommendation. Patients in therapy sometimes report newly found memories. To reduce your risk:
- obtain informed consent from patients before you begin any psychotherapy
- carefully document therapy session details when patients divulge new memories—particularly of abuse
- avoid encouraging patients to act on recovered memories.19
OFF-LABEL DRUG USE: KNOW THE LITERATURE
Off-label prescribing is both common and legal but may increase a physician’s liability risk if adverse events occur. Cases in Minnesota, Texas, and Louisiana have established precedents for using the Physician’s Desk Reference or package inserts to establish a standard of care.
In 1970 the Minnesota Supreme Court held that deviating from the package insert constituted prima facie evidence of negligence. This interpretation shifts the burden of proof from the plaintiff to the physician, who must then prove that he or she was not negligent when prescribing the drug.20
Recommendation. Off-label prescribing is an important component of modern psychiatric care. Research supports most accepted off-label prescribing, at least to the point of establishing a respectable minority for a standard of care (Box 2).
When prescribing, know which indications are FDA-approved and which are off-label. For off-label prescribing, know the literature supporting that use and notify patients of off-label status as you document informed consent.20
PROS AND CONS OF PRACTICE GUIDELINES
Clinical practice guidelines developed by professional organizations to assist physicians have also acquired legal ramifications. Difficult questions about guidelines include:
- Do they set the standard of care, or are they merely suggestions?
- Do they provide a defense against liability?
- How does a practitioner select between conflicting guidelines?
On the other hand, following clinical guidelines can protect you in cases with adverse outcomes. In a study of insurance company claims, approximately one-fourth of plaintiff’s attorneys who were surveyed said they had refused cases because the physician had followed practice guidelines. Conversely, one-fourth of defense attorneys said they had been influenced to settle cases because the physicians they represented had not followed practice guidelines.21
Liability cases involving practice guidelines have produced varying decisions. As a rule of thumb, courts tend to find that more-specific guidelines constitute a standard of care, whereas more-general guidelines are flexible suggestions.
Recommendation. If the court finds that existing guidelines establish the standard of care and your care has deviated from the guidelines with adverse consequences, the burden of proof shifts to you to prove that you were not negligent.18 When guidelines exist, know them and be prepared to defend decisions that deviate from them.
TELEMEDICINE: DANGERS IN CYBERSPACE
Unauthorized use or disclosure of patients’ electronic information can leave physicians liable for invasion of privacy and breach of confidentiality.22
E-mail communication with a patient may also be sufficient to establish a duty of care, especially if the patient presents diagnostic information and the physician provides medical advice. Once duty to care is established, the physician is responsible for ongoing care or may face charges of abandonment.
Establishing duty to patients through e-mail is particularly troublesome, as patients may be writing from another state where you are not licensed to practice. Several states have explicitly forbidden unlicensed telemedicine; others have offered limited licenses for telemedicine practice.22
Using e-mail to communicate with established patients introduces other liabilities. E-mail is legally considered part of the medical record and is subject to discovery in legal proceedings. Failure to preserve important patient e-mail may be evidence of negligence, especially in cases involving the medical record.
On the other hand, e-mail can be surprisingly permanent; it is virtually impossible to definitively delete e-mail that contains sensitive or embarrassing information. Deleted e-mail frequently can be recovered, and every e-mail exists in multiple copies, including the sender’s, the receiver’s, and at least one in a centralized server.23
Recommendation. Reduce liability risks with informed consent if you use e-mail to communicate with existing patients. Minimize e-mail contact with nonestablished patients, and make sure the confidentiality of patients’ communications is secure.22
Related resources
- Gutheil TG, Appelbaum PS. Clinical handbook of psychiatry and the law (3rd ed). Philadelphia: Lippincott Williams & Wilkins, 2000.
- American Psychiatric Association. Practice guidelines. http://www.psych.org/clin_res/prac_guide.cfm
1. Slawson PF, Guggenheim FG. Psychiatric malpractice: a review of the national loss experience. Am J Psychiatry 1984;141:979-81.
2. Buckner F, Firestone M. Where the public peril begins: 25 years after Tarasoff. J Legal Med 2000;21(2):187-222.
3. Tarasoff v. Regents of the University of California, 551 P.2d 334 (California 1976).
4. Menninger WW. The impact of litigation and court decisions on clinical practice. Bull Menninger Clin 1989;53:203-14.
5. Davenport J. Documenting high-risk cases to avoid malpractice liability. Fam Pract Manag 2000;7(9):33-6.
6. Rice B. How plaintiffs’ lawyers pick their targets. Medical Economics 2000;8:94-110.
7. Levinson W, Roter DL, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA 1997;277(7):553-9.
8. Condon JT. Medical litigation the aetiological role of psychological and interpersonal factors. Med J Aust 1992;157:768-70.
9. Gutheil TG, Appelbaum PS. Clinical handbook of psychiatry and the law (3rd ed). Philadelphia: Lippincott Williams & Wilkins; 2000.
10. Resnick PJ, Scott CL. Legal issues in treating perpetrators and victims of violence. Psychiatr Clin North Am 1997;20(2):473-87.
11. Resnick PJ. Risk assessment for violence (lecture). Cleveland, OH: Case Western Reserve University, June 26, 2003.
12. Slovenko R. Malpractice in psychotherapy. Psychiatr Clin North Am 1999;22(1):1-15.
13. Mills MJ, Eth S. Legal liability with psychotropic drug use: extrapyramidal syndromes and tardive dyskinesia. J Clin Psychiatry 1987;48(9S):28-33.
14. Appelbaum PS. Can a psychiatrist be held responsible when a patient commits murder? Law Psychiatry 2002;53(1):27-9.
15. Tan MW, McDonough WJ. Risk management in psychiatry. Psychiatr Clin North Am 1990;13(1):135-47.
16. Garrick TR, Weinstock R. Liability of psychiatric consultants. Psychosomatics 1994;35:474-84.
17. Bradford GE. The “respectable minority” doctrine in Missouri medical negligence law. J Missouri Bar 2000;56(6):326-34.
18. Jacobson PD. Legal and policy considerations in using clinical practice guidelines. Am J Cardiol 1997;30(8B):74H-79H.
19. Scheflin AW, Spiegel D. From courtroom to couch: working with repressed memory and avoiding lawsuits. Psychiatr Clin North Am 1998;21(4):847-67.
20. Bradford GE, Elben CC. The drug package insert and the PDR as establishing the standard of care in prescription drug liability cases. J Missouri Bar 2001;57(5):233-42.
21. Hyams AL, Brandenburg JA, Lipsitz SR, et al. Practice guidelines and malpractice litigation: a two-way street. Ann Intern Med 1995;122(6):450-5.
22. Jones J. MD liability for electronic medical communications. Physician’s News Digest [serial online] 2000;(5).
23. Spielberg AR. Online without a net: physician-patient communication by electronic mail. Am J Law Med 1999;25:267-95.
Psychiatrists’ risk of malpractice liability1 is broadening as courts consider the uncertainties of off-label prescribing, telemedicine, and confidentiality. Juries are holding mental health practitioners responsible for harm done both to and by psychiatric patients.
How you keep medical records, communicate with patients and colleagues, and arrange consultations can reduce your malpractice risk (Box 1).4-9 We offer recommendations based on court decisions and other evidence for managing:
- traditional risks—such as patient violence and suicide, adverse drug reactions, sex with patients, faulty termination of treatment, and supervisory and consultative relationships4
- newer risks—such as recovered memory, off-label prescribing, practice guidelines, and e-mail and confidentiality.
1. Keep thorough medical records
The most powerful defense against a malpractice suit is a well-documented chart. It can often prevent a malpractice suit by providing evidence that the physician adequately evaluated the available information and made good-faith efforts with his or her best judgment. Juries are typically forgiving of mistakes made in this context.4,5
Write legibly, and sign and date all entries. Try to think out loud in the chart. By outlining your thoughts about differential diagnosis, risks and benefits, and treatment options, you can help a jury understand your decision-making process and show that you carefully evaluated the situation. When documenting difficult cases, for example, imagine a plaintiff’s attorney reading your notes to a jury.6
2. Communicate freely with patients
Careful interaction with patients and their families can also prevent lawsuits. Communicating includes preparing patients for what to expect during treatment sessions, encouraging feedback, and even using humor.7 Freely sharing treatment information with patients can build a sense of mutual decision-making and responsibility.8 Acknowledging treatment limitations and deflating unrealistic expectations can also protect you.
Patients who file malpractice suits are often seeking an apology or expression of regret from their physicians. It is appropriate and prudent to admit and apologize for minor errors. It is also appropriate to express condolence over what both sides agree is a severe, negative outcome.9 Expressing sympathy is not equivalent to admitting wrongdoing.
3. Seek consultation as needed
Discussing difficult or ambiguous cases with peers, supervisors, or legal staff can help shield you from liability. For example:
- Second opinions may help you make difficult clinical decisions.
- Peers and supervisors may provide useful suggestions to improve patient care.
- Legal staff can give advice regarding liability.
The fact that you sought consultation can be used in court as evidence against negligence, as it shows you tried to ensure appropriate care for your patient.9
This article describes general guidelines and is not intended to constitute legal advice. All practitioners have a responsibility to know the laws of the jurisdictions in which they practice.
PREVENTING PATIENT VIOLENCE
The case that opened Pandora’s box. Prosenjit Poddar, a student at the University of California at Berkeley, was infatuated with coed Tanya Tarasoff and told his psychologist he intended to kill her. The psychologist notified his psychiatric supervisor and called campus police.
The psychologist told police Poddar was dangerous to himself and others. He stated that he would sign an emergency hold if they would bring Poddar to the hospital.
The police apprehended Poddar but released him. Poddar dropped out of therapy and 2 months later fatally stabbed Ms. Tarasoff.
Ms. Tarasoff’s parents sued those who treated Poddar and the University of California.2 After a complicated legal course, the California Supreme Court ruled that once a therapist determines—or should have determined—that a patient poses a serious danger of violence to others, “he bears a duty to exercise reasonable care to protect the foreseeable victim of that danger.”3
The 1976 Tarasoff ruling has become a national standard of practice, leading to numerous other patient violence lawsuits. In these cases, psychiatrists are most likely to be found liable when recently released inpatients commit violent acts, particularly if the physician had reason to know the patient was dangerous and failed to take adequate precautions or appropriately assess the patient.4
Wider interpretations. Cases in several states have extended the Tarasoff ruling. In at least two cases, this standard has been applied when the patient threatened no specific victim before committing violence:
- A New Jersey court (McIntosh v. Milano, 1979) found a psychiatrist liable for malpractice on grounds that a therapist has a duty to protect society, just as a doctor must protect society by reporting carriers of dangerous diseases.
- A Nebraska court (Lipari v. Sears, Roebuck, and Co., 1980) held that physicians have a duty to protect—even if the specific identity of victims is unknown—so long as the physician should know that the patient presents an unreasonable risk of harm to others.2
Auto accidents. Tarasoff liability also has been extended to auto accidents. In Washington state (Petersen v. Washington, 1983), a psychiatrist was held liable for injuries to victims of an accident caused by a psychiatric patient. The court ruled that the psychiatrist had a duty to take reasonable precautions to protect any foreseeable persons from being endangered by the patient.
In a similar case in Wisconsin (Schuster and Schuster v. Altenberg, et al., 1988), the court ruled that damages could be awarded to anyone whose harm could have been prevented had the physician practiced according to professional standards.2
Other extensions include cases such as Naidu v. Laird, 1988, in which patient violence occurred more than 5 months after hospitalization.2 Vermont has extended the Tarasoff precedent to property destruction by psychiatric patients.10
Recommendation. Most states require a psychiatrist to protect against only specific threats to identifiable victims.10 To defend yourself against a Tarasoff-type suit, you must show that you:
- carefully assessed the patient’s risk for violence
- provided appropriate care
- and took appropriate precautions.
The most protective evidence is a medical record documenting that you thoroughly assessed a patient for risk of violence (Table).4,11
If you are unsure about how to manage a patient you believe may be dangerous to himself or others, consult with supervisors, peers, and legal advisors. Many states have Tarasoff-like statutes that specify the conditions that require action and the appropriate actions.
In states without specific statutes, options that generally satisfy Tarasoff requirements include hospitalizing the patient, notifying authorities, and/or warning the potential victim.10 As the Tarasoff case demonstrated, notifying authorities may not substitute for warning or hospitalizing.2
SUICIDE RISK? DOCUMENT CAREFULLY
Patient suicide accounts for one-fifth of claims covered by the American Psychiatric Association (APA) insurance plan.
In court, key points of challenge to a physician’s judgment in a suicide case include the admission evaluation and any status changes. Thorough risk assessment includes carefully reviewing existing records, evaluating risk factors for suicide, and seeking advice from colleagues or supervisors when appropriate.4
Recommendation. Document for every inpatient admission, discharge, or status change that the patient’s risk for suicide was assessed. List risk factors, protective factors, and risk for self-harm.
Explicitly address in the patient’s chart any comments about suicidality (such as heard by nursing staff).9 Document your rationale for medical decisions and orders, consistently follow unit policies, and explain risks and benefits of hospitalization to patients and their families.
Before discharge, schedule appropriate follow-up and make reasonable efforts to ensure medication adherence.4
SEX WITH PATIENTS IS UNPROTECTED
Sexual involvement with patients is indefensible and uncontestable in malpractice cases. Even so, up to 9% of male therapists and 3% of female therapists report in surveys that they have had sexual interaction with their patients.4
In 1985 the APA excluded sex with patients from its malpractice insurance coverage. Courts generally consider a treatment to be within the standard of care if a respectable minority of physicians consider it to be appropriate. Sex with patients is considered an absolute deviation from the standard of care, and no respectable minority of practitioners supports this practice. Because patients are substantially harmed, sex with patients is considered prima facie malpractice.12
Table
Is this patient dangerous? Risk factors for violence
| Psychiatric |
|
| Demographic |
|
| Socioeconomic |
|
WHEN MEDICATIONS CAUSE HARM
Adverse drug reactions—particularly tardive dyskinesia (TD)—are a source of significant losses in malpractice cases. Multimillion-dollar awards have been granted, especially when neuroleptic antipsychotics have been given in excessive dosages without proper monitoring.13
Informed consent has been a particularly difficult issue with the use of neuroleptic medications. Many doctors worry that patients who fear developing TD will not take prescribed neuroleptics. A study of North Carolina psychiatrists in the 1980s revealed that only 30% mentioned TD when telling their patients about neuroleptics’ possible side effects.13
The fact that a patient develops TD while taking an antipsychotic does not establish grounds for malpractice; a valid malpractice suit must also establish negligence. Negligence could include failing to obtain appropriate informed consent or continuing to prescribe an antipsychotic without adequately examining the patient.4
Informed consent does not require a patient to fully understand everything about a medication. The patient must understand the information a reasonable patient would want to know. Obvious misunderstandings must be corrected.
Recommendation. Consider informed consent a process, rather than one event—especially when you give neuroleptics for acute psychotic episodes. You can establish, review, and refresh consent in follow-up visits as medications help patients become more coherent and organized.
If you doubt a patient’s capacity to provide informed consent, a court determination may be necessary. In emergencies, however, treatment becomes a priority, even if the patient’s capacity to make rational decisions has not been established.13
TERMINATE TREATMENT WITH CAUTION
Terminating treatment can lead to malpractice, particularly if a patient becomes suicidal or violent. Psychiatrists have the right to choose their patients but cannot terminate care if a patient is acutely ill or requires emergency care.
Ensuring appropriate follow-up for patients at risk for decompensation often requires more than providing a referral or phone number. With the patient’s permission, for example, you could contact his subsequent psychiatrist or work with his support network to ensure that he receives follow-up care.14
Recommendation. With stable patients, send a written notice of termination and specify a reasonable period, usually 30 days. Send the letter by certified mail, and request a return receipt. Offer to help the patient find a new doctor, and say that you will forward the patient’s records to the new doctor when you receive appropriate release-of-information paperwork.15
LET THE SUPERVISOR BEWARE
Under the legal concept of respondeat superior (“let the master reply”), liability for the actions of subordinates may be transferred upward to the supervisor.4 For psychiatrists, supervisory liability obviously applies to teaching residents but may also apply in joint care, as with psychologists or social workers.
Recommendation. As a co-treating psychiatrist, you may be liable for other therapists’ actions unless you formally distinguish your role as a prescriber and not as a supervisor.9
When you prescribe medications for patients of nonphysician therapists, be sure you, the therapist, and patient understand the nature of your collaboration. Document the type of relationship and your discussion with the patient in the patient’s chart.
WATCH OUT FOR ‘CURBSIDE’ CONSULTS
Consult-liaison psychiatrists typically face a lower malpractice risk than do those who provide primary treatment. Duty to care for the patient is usually established by a formal consult request, after which the psychiatrist examines the patient and recommends treatment to the primary team.
You can, however, establish duty without meeting a patient. If sufficiently detailed, an informal “curbside” consult may establish a duty and corresponding liability16 (Box 2).4,5,9,17.18
Liability is usually shared with the primary team but may be related to how much responsibility you assume in the patient’s care. Any direct treatment—electroconvulsive therapy, psychotherapy, prescribing, writing orders in the chart—can elevate your risk to the primary level. Similarly, if the patient is harmed because the primary treater followed a consulting psychiatrist’s negligent advice, the psychiatrist can be found solely liable.
When you recommend a treatment, you share a portion of liability for informed consent. If neither you nor the provider obtains appropriate informed consent, you may both share liability for adverse outcomes. Both teams also share the duty to report child and elder abuse.16
Recommendation. Establish an explicit division of responsibilities with the primary team, including who writes orders and manages medications and who provides follow-up and discharge planning.
For curbside consults, inform the primary physician that you are providing general information and not a specific treatment recommendation. If the case is too complicated for general information to be useful, a formal consultation would serve the patient better. In written consultations, specify:
- the reason for the consult
- the issues addressed
- and the parties responsible for follow-up.16
RECOVERED MEMORY? FORGET PROSECUTION
In 1994, a father successfully sued his daughter’s therapists for implanting false memories of incest. A California court awarded him $500,000 on grounds that the therapists owed a duty of care to the patient’s parents as well as to the patient. Since then, multimillion-dollar cases have been litigated on grounds of false recovered memories, and some insurers exclude coverage for “revival of memory.”12
Most therapists who have been found liable have strongly supported the accuracy of their patients’ memories. These memories have usually contained bizarre features, including satanic abuse, baby breeding, human sacrifice, and cannibalism. Therapists in these cases have often recommended that their patients press charges or file lawsuits against their alleged abusers.
Lawsuits against therapists have been won on grounds that they used unorthodox procedures without informed consent, negligently or recklessly implanted memories of abuse, negligently reinforced such memories, and failed to sufficiently investigate the memories’ accuracy.19
Malpractice requires four conditions:
- A doctor-patient relationship was established.
- The physician practiced below the standard of care.
- The patient was harmed.
- The patient’s harm was a direct result of the physician’s failure to practice at the standard of care.4
Standard of care. A treatment may be considered within the standard of care so long as a “respectable minority” of practitioners considers it appropriate.17 Standard of care may be established by expert testimony, published texts, or practice guidelines18 and tends to be flexible in medical specialties—such as mental health—that allow for multiple treatment options.
Preponderance of evidence. In court proceedings, the plaintiff must establish malpractice by a reponderance of the evidence, which means “more likely than not.” This is a much less-stringent level of proof than beyond a reasonable doubt, as is required in criminal cases.9
Although a preponderance of the evidence may seem disturbingly easy to establish, courts are often forgiving of adverse outcomes caused by judgment errors if the physician acted in good faith and followed professional standards.4,5
Recommendation. Patients in therapy sometimes report newly found memories. To reduce your risk:
- obtain informed consent from patients before you begin any psychotherapy
- carefully document therapy session details when patients divulge new memories—particularly of abuse
- avoid encouraging patients to act on recovered memories.19
OFF-LABEL DRUG USE: KNOW THE LITERATURE
Off-label prescribing is both common and legal but may increase a physician’s liability risk if adverse events occur. Cases in Minnesota, Texas, and Louisiana have established precedents for using the Physician’s Desk Reference or package inserts to establish a standard of care.
In 1970 the Minnesota Supreme Court held that deviating from the package insert constituted prima facie evidence of negligence. This interpretation shifts the burden of proof from the plaintiff to the physician, who must then prove that he or she was not negligent when prescribing the drug.20
Recommendation. Off-label prescribing is an important component of modern psychiatric care. Research supports most accepted off-label prescribing, at least to the point of establishing a respectable minority for a standard of care (Box 2).
When prescribing, know which indications are FDA-approved and which are off-label. For off-label prescribing, know the literature supporting that use and notify patients of off-label status as you document informed consent.20
PROS AND CONS OF PRACTICE GUIDELINES
Clinical practice guidelines developed by professional organizations to assist physicians have also acquired legal ramifications. Difficult questions about guidelines include:
- Do they set the standard of care, or are they merely suggestions?
- Do they provide a defense against liability?
- How does a practitioner select between conflicting guidelines?
On the other hand, following clinical guidelines can protect you in cases with adverse outcomes. In a study of insurance company claims, approximately one-fourth of plaintiff’s attorneys who were surveyed said they had refused cases because the physician had followed practice guidelines. Conversely, one-fourth of defense attorneys said they had been influenced to settle cases because the physicians they represented had not followed practice guidelines.21
Liability cases involving practice guidelines have produced varying decisions. As a rule of thumb, courts tend to find that more-specific guidelines constitute a standard of care, whereas more-general guidelines are flexible suggestions.
Recommendation. If the court finds that existing guidelines establish the standard of care and your care has deviated from the guidelines with adverse consequences, the burden of proof shifts to you to prove that you were not negligent.18 When guidelines exist, know them and be prepared to defend decisions that deviate from them.
TELEMEDICINE: DANGERS IN CYBERSPACE
Unauthorized use or disclosure of patients’ electronic information can leave physicians liable for invasion of privacy and breach of confidentiality.22
E-mail communication with a patient may also be sufficient to establish a duty of care, especially if the patient presents diagnostic information and the physician provides medical advice. Once duty to care is established, the physician is responsible for ongoing care or may face charges of abandonment.
Establishing duty to patients through e-mail is particularly troublesome, as patients may be writing from another state where you are not licensed to practice. Several states have explicitly forbidden unlicensed telemedicine; others have offered limited licenses for telemedicine practice.22
Using e-mail to communicate with established patients introduces other liabilities. E-mail is legally considered part of the medical record and is subject to discovery in legal proceedings. Failure to preserve important patient e-mail may be evidence of negligence, especially in cases involving the medical record.
On the other hand, e-mail can be surprisingly permanent; it is virtually impossible to definitively delete e-mail that contains sensitive or embarrassing information. Deleted e-mail frequently can be recovered, and every e-mail exists in multiple copies, including the sender’s, the receiver’s, and at least one in a centralized server.23
Recommendation. Reduce liability risks with informed consent if you use e-mail to communicate with existing patients. Minimize e-mail contact with nonestablished patients, and make sure the confidentiality of patients’ communications is secure.22
Related resources
- Gutheil TG, Appelbaum PS. Clinical handbook of psychiatry and the law (3rd ed). Philadelphia: Lippincott Williams & Wilkins, 2000.
- American Psychiatric Association. Practice guidelines. http://www.psych.org/clin_res/prac_guide.cfm
Psychiatrists’ risk of malpractice liability1 is broadening as courts consider the uncertainties of off-label prescribing, telemedicine, and confidentiality. Juries are holding mental health practitioners responsible for harm done both to and by psychiatric patients.
How you keep medical records, communicate with patients and colleagues, and arrange consultations can reduce your malpractice risk (Box 1).4-9 We offer recommendations based on court decisions and other evidence for managing:
- traditional risks—such as patient violence and suicide, adverse drug reactions, sex with patients, faulty termination of treatment, and supervisory and consultative relationships4
- newer risks—such as recovered memory, off-label prescribing, practice guidelines, and e-mail and confidentiality.
1. Keep thorough medical records
The most powerful defense against a malpractice suit is a well-documented chart. It can often prevent a malpractice suit by providing evidence that the physician adequately evaluated the available information and made good-faith efforts with his or her best judgment. Juries are typically forgiving of mistakes made in this context.4,5
Write legibly, and sign and date all entries. Try to think out loud in the chart. By outlining your thoughts about differential diagnosis, risks and benefits, and treatment options, you can help a jury understand your decision-making process and show that you carefully evaluated the situation. When documenting difficult cases, for example, imagine a plaintiff’s attorney reading your notes to a jury.6
2. Communicate freely with patients
Careful interaction with patients and their families can also prevent lawsuits. Communicating includes preparing patients for what to expect during treatment sessions, encouraging feedback, and even using humor.7 Freely sharing treatment information with patients can build a sense of mutual decision-making and responsibility.8 Acknowledging treatment limitations and deflating unrealistic expectations can also protect you.
Patients who file malpractice suits are often seeking an apology or expression of regret from their physicians. It is appropriate and prudent to admit and apologize for minor errors. It is also appropriate to express condolence over what both sides agree is a severe, negative outcome.9 Expressing sympathy is not equivalent to admitting wrongdoing.
3. Seek consultation as needed
Discussing difficult or ambiguous cases with peers, supervisors, or legal staff can help shield you from liability. For example:
- Second opinions may help you make difficult clinical decisions.
- Peers and supervisors may provide useful suggestions to improve patient care.
- Legal staff can give advice regarding liability.
The fact that you sought consultation can be used in court as evidence against negligence, as it shows you tried to ensure appropriate care for your patient.9
This article describes general guidelines and is not intended to constitute legal advice. All practitioners have a responsibility to know the laws of the jurisdictions in which they practice.
PREVENTING PATIENT VIOLENCE
The case that opened Pandora’s box. Prosenjit Poddar, a student at the University of California at Berkeley, was infatuated with coed Tanya Tarasoff and told his psychologist he intended to kill her. The psychologist notified his psychiatric supervisor and called campus police.
The psychologist told police Poddar was dangerous to himself and others. He stated that he would sign an emergency hold if they would bring Poddar to the hospital.
The police apprehended Poddar but released him. Poddar dropped out of therapy and 2 months later fatally stabbed Ms. Tarasoff.
Ms. Tarasoff’s parents sued those who treated Poddar and the University of California.2 After a complicated legal course, the California Supreme Court ruled that once a therapist determines—or should have determined—that a patient poses a serious danger of violence to others, “he bears a duty to exercise reasonable care to protect the foreseeable victim of that danger.”3
The 1976 Tarasoff ruling has become a national standard of practice, leading to numerous other patient violence lawsuits. In these cases, psychiatrists are most likely to be found liable when recently released inpatients commit violent acts, particularly if the physician had reason to know the patient was dangerous and failed to take adequate precautions or appropriately assess the patient.4
Wider interpretations. Cases in several states have extended the Tarasoff ruling. In at least two cases, this standard has been applied when the patient threatened no specific victim before committing violence:
- A New Jersey court (McIntosh v. Milano, 1979) found a psychiatrist liable for malpractice on grounds that a therapist has a duty to protect society, just as a doctor must protect society by reporting carriers of dangerous diseases.
- A Nebraska court (Lipari v. Sears, Roebuck, and Co., 1980) held that physicians have a duty to protect—even if the specific identity of victims is unknown—so long as the physician should know that the patient presents an unreasonable risk of harm to others.2
Auto accidents. Tarasoff liability also has been extended to auto accidents. In Washington state (Petersen v. Washington, 1983), a psychiatrist was held liable for injuries to victims of an accident caused by a psychiatric patient. The court ruled that the psychiatrist had a duty to take reasonable precautions to protect any foreseeable persons from being endangered by the patient.
In a similar case in Wisconsin (Schuster and Schuster v. Altenberg, et al., 1988), the court ruled that damages could be awarded to anyone whose harm could have been prevented had the physician practiced according to professional standards.2
Other extensions include cases such as Naidu v. Laird, 1988, in which patient violence occurred more than 5 months after hospitalization.2 Vermont has extended the Tarasoff precedent to property destruction by psychiatric patients.10
Recommendation. Most states require a psychiatrist to protect against only specific threats to identifiable victims.10 To defend yourself against a Tarasoff-type suit, you must show that you:
- carefully assessed the patient’s risk for violence
- provided appropriate care
- and took appropriate precautions.
The most protective evidence is a medical record documenting that you thoroughly assessed a patient for risk of violence (Table).4,11
If you are unsure about how to manage a patient you believe may be dangerous to himself or others, consult with supervisors, peers, and legal advisors. Many states have Tarasoff-like statutes that specify the conditions that require action and the appropriate actions.
In states without specific statutes, options that generally satisfy Tarasoff requirements include hospitalizing the patient, notifying authorities, and/or warning the potential victim.10 As the Tarasoff case demonstrated, notifying authorities may not substitute for warning or hospitalizing.2
SUICIDE RISK? DOCUMENT CAREFULLY
Patient suicide accounts for one-fifth of claims covered by the American Psychiatric Association (APA) insurance plan.
In court, key points of challenge to a physician’s judgment in a suicide case include the admission evaluation and any status changes. Thorough risk assessment includes carefully reviewing existing records, evaluating risk factors for suicide, and seeking advice from colleagues or supervisors when appropriate.4
Recommendation. Document for every inpatient admission, discharge, or status change that the patient’s risk for suicide was assessed. List risk factors, protective factors, and risk for self-harm.
Explicitly address in the patient’s chart any comments about suicidality (such as heard by nursing staff).9 Document your rationale for medical decisions and orders, consistently follow unit policies, and explain risks and benefits of hospitalization to patients and their families.
Before discharge, schedule appropriate follow-up and make reasonable efforts to ensure medication adherence.4
SEX WITH PATIENTS IS UNPROTECTED
Sexual involvement with patients is indefensible and uncontestable in malpractice cases. Even so, up to 9% of male therapists and 3% of female therapists report in surveys that they have had sexual interaction with their patients.4
In 1985 the APA excluded sex with patients from its malpractice insurance coverage. Courts generally consider a treatment to be within the standard of care if a respectable minority of physicians consider it to be appropriate. Sex with patients is considered an absolute deviation from the standard of care, and no respectable minority of practitioners supports this practice. Because patients are substantially harmed, sex with patients is considered prima facie malpractice.12
Table
Is this patient dangerous? Risk factors for violence
| Psychiatric |
|
| Demographic |
|
| Socioeconomic |
|
WHEN MEDICATIONS CAUSE HARM
Adverse drug reactions—particularly tardive dyskinesia (TD)—are a source of significant losses in malpractice cases. Multimillion-dollar awards have been granted, especially when neuroleptic antipsychotics have been given in excessive dosages without proper monitoring.13
Informed consent has been a particularly difficult issue with the use of neuroleptic medications. Many doctors worry that patients who fear developing TD will not take prescribed neuroleptics. A study of North Carolina psychiatrists in the 1980s revealed that only 30% mentioned TD when telling their patients about neuroleptics’ possible side effects.13
The fact that a patient develops TD while taking an antipsychotic does not establish grounds for malpractice; a valid malpractice suit must also establish negligence. Negligence could include failing to obtain appropriate informed consent or continuing to prescribe an antipsychotic without adequately examining the patient.4
Informed consent does not require a patient to fully understand everything about a medication. The patient must understand the information a reasonable patient would want to know. Obvious misunderstandings must be corrected.
Recommendation. Consider informed consent a process, rather than one event—especially when you give neuroleptics for acute psychotic episodes. You can establish, review, and refresh consent in follow-up visits as medications help patients become more coherent and organized.
If you doubt a patient’s capacity to provide informed consent, a court determination may be necessary. In emergencies, however, treatment becomes a priority, even if the patient’s capacity to make rational decisions has not been established.13
TERMINATE TREATMENT WITH CAUTION
Terminating treatment can lead to malpractice, particularly if a patient becomes suicidal or violent. Psychiatrists have the right to choose their patients but cannot terminate care if a patient is acutely ill or requires emergency care.
Ensuring appropriate follow-up for patients at risk for decompensation often requires more than providing a referral or phone number. With the patient’s permission, for example, you could contact his subsequent psychiatrist or work with his support network to ensure that he receives follow-up care.14
Recommendation. With stable patients, send a written notice of termination and specify a reasonable period, usually 30 days. Send the letter by certified mail, and request a return receipt. Offer to help the patient find a new doctor, and say that you will forward the patient’s records to the new doctor when you receive appropriate release-of-information paperwork.15
LET THE SUPERVISOR BEWARE
Under the legal concept of respondeat superior (“let the master reply”), liability for the actions of subordinates may be transferred upward to the supervisor.4 For psychiatrists, supervisory liability obviously applies to teaching residents but may also apply in joint care, as with psychologists or social workers.
Recommendation. As a co-treating psychiatrist, you may be liable for other therapists’ actions unless you formally distinguish your role as a prescriber and not as a supervisor.9
When you prescribe medications for patients of nonphysician therapists, be sure you, the therapist, and patient understand the nature of your collaboration. Document the type of relationship and your discussion with the patient in the patient’s chart.
WATCH OUT FOR ‘CURBSIDE’ CONSULTS
Consult-liaison psychiatrists typically face a lower malpractice risk than do those who provide primary treatment. Duty to care for the patient is usually established by a formal consult request, after which the psychiatrist examines the patient and recommends treatment to the primary team.
You can, however, establish duty without meeting a patient. If sufficiently detailed, an informal “curbside” consult may establish a duty and corresponding liability16 (Box 2).4,5,9,17.18
Liability is usually shared with the primary team but may be related to how much responsibility you assume in the patient’s care. Any direct treatment—electroconvulsive therapy, psychotherapy, prescribing, writing orders in the chart—can elevate your risk to the primary level. Similarly, if the patient is harmed because the primary treater followed a consulting psychiatrist’s negligent advice, the psychiatrist can be found solely liable.
When you recommend a treatment, you share a portion of liability for informed consent. If neither you nor the provider obtains appropriate informed consent, you may both share liability for adverse outcomes. Both teams also share the duty to report child and elder abuse.16
Recommendation. Establish an explicit division of responsibilities with the primary team, including who writes orders and manages medications and who provides follow-up and discharge planning.
For curbside consults, inform the primary physician that you are providing general information and not a specific treatment recommendation. If the case is too complicated for general information to be useful, a formal consultation would serve the patient better. In written consultations, specify:
- the reason for the consult
- the issues addressed
- and the parties responsible for follow-up.16
RECOVERED MEMORY? FORGET PROSECUTION
In 1994, a father successfully sued his daughter’s therapists for implanting false memories of incest. A California court awarded him $500,000 on grounds that the therapists owed a duty of care to the patient’s parents as well as to the patient. Since then, multimillion-dollar cases have been litigated on grounds of false recovered memories, and some insurers exclude coverage for “revival of memory.”12
Most therapists who have been found liable have strongly supported the accuracy of their patients’ memories. These memories have usually contained bizarre features, including satanic abuse, baby breeding, human sacrifice, and cannibalism. Therapists in these cases have often recommended that their patients press charges or file lawsuits against their alleged abusers.
Lawsuits against therapists have been won on grounds that they used unorthodox procedures without informed consent, negligently or recklessly implanted memories of abuse, negligently reinforced such memories, and failed to sufficiently investigate the memories’ accuracy.19
Malpractice requires four conditions:
- A doctor-patient relationship was established.
- The physician practiced below the standard of care.
- The patient was harmed.
- The patient’s harm was a direct result of the physician’s failure to practice at the standard of care.4
Standard of care. A treatment may be considered within the standard of care so long as a “respectable minority” of practitioners considers it appropriate.17 Standard of care may be established by expert testimony, published texts, or practice guidelines18 and tends to be flexible in medical specialties—such as mental health—that allow for multiple treatment options.
Preponderance of evidence. In court proceedings, the plaintiff must establish malpractice by a reponderance of the evidence, which means “more likely than not.” This is a much less-stringent level of proof than beyond a reasonable doubt, as is required in criminal cases.9
Although a preponderance of the evidence may seem disturbingly easy to establish, courts are often forgiving of adverse outcomes caused by judgment errors if the physician acted in good faith and followed professional standards.4,5
Recommendation. Patients in therapy sometimes report newly found memories. To reduce your risk:
- obtain informed consent from patients before you begin any psychotherapy
- carefully document therapy session details when patients divulge new memories—particularly of abuse
- avoid encouraging patients to act on recovered memories.19
OFF-LABEL DRUG USE: KNOW THE LITERATURE
Off-label prescribing is both common and legal but may increase a physician’s liability risk if adverse events occur. Cases in Minnesota, Texas, and Louisiana have established precedents for using the Physician’s Desk Reference or package inserts to establish a standard of care.
In 1970 the Minnesota Supreme Court held that deviating from the package insert constituted prima facie evidence of negligence. This interpretation shifts the burden of proof from the plaintiff to the physician, who must then prove that he or she was not negligent when prescribing the drug.20
Recommendation. Off-label prescribing is an important component of modern psychiatric care. Research supports most accepted off-label prescribing, at least to the point of establishing a respectable minority for a standard of care (Box 2).
When prescribing, know which indications are FDA-approved and which are off-label. For off-label prescribing, know the literature supporting that use and notify patients of off-label status as you document informed consent.20
PROS AND CONS OF PRACTICE GUIDELINES
Clinical practice guidelines developed by professional organizations to assist physicians have also acquired legal ramifications. Difficult questions about guidelines include:
- Do they set the standard of care, or are they merely suggestions?
- Do they provide a defense against liability?
- How does a practitioner select between conflicting guidelines?
On the other hand, following clinical guidelines can protect you in cases with adverse outcomes. In a study of insurance company claims, approximately one-fourth of plaintiff’s attorneys who were surveyed said they had refused cases because the physician had followed practice guidelines. Conversely, one-fourth of defense attorneys said they had been influenced to settle cases because the physicians they represented had not followed practice guidelines.21
Liability cases involving practice guidelines have produced varying decisions. As a rule of thumb, courts tend to find that more-specific guidelines constitute a standard of care, whereas more-general guidelines are flexible suggestions.
Recommendation. If the court finds that existing guidelines establish the standard of care and your care has deviated from the guidelines with adverse consequences, the burden of proof shifts to you to prove that you were not negligent.18 When guidelines exist, know them and be prepared to defend decisions that deviate from them.
TELEMEDICINE: DANGERS IN CYBERSPACE
Unauthorized use or disclosure of patients’ electronic information can leave physicians liable for invasion of privacy and breach of confidentiality.22
E-mail communication with a patient may also be sufficient to establish a duty of care, especially if the patient presents diagnostic information and the physician provides medical advice. Once duty to care is established, the physician is responsible for ongoing care or may face charges of abandonment.
Establishing duty to patients through e-mail is particularly troublesome, as patients may be writing from another state where you are not licensed to practice. Several states have explicitly forbidden unlicensed telemedicine; others have offered limited licenses for telemedicine practice.22
Using e-mail to communicate with established patients introduces other liabilities. E-mail is legally considered part of the medical record and is subject to discovery in legal proceedings. Failure to preserve important patient e-mail may be evidence of negligence, especially in cases involving the medical record.
On the other hand, e-mail can be surprisingly permanent; it is virtually impossible to definitively delete e-mail that contains sensitive or embarrassing information. Deleted e-mail frequently can be recovered, and every e-mail exists in multiple copies, including the sender’s, the receiver’s, and at least one in a centralized server.23
Recommendation. Reduce liability risks with informed consent if you use e-mail to communicate with existing patients. Minimize e-mail contact with nonestablished patients, and make sure the confidentiality of patients’ communications is secure.22
Related resources
- Gutheil TG, Appelbaum PS. Clinical handbook of psychiatry and the law (3rd ed). Philadelphia: Lippincott Williams & Wilkins, 2000.
- American Psychiatric Association. Practice guidelines. http://www.psych.org/clin_res/prac_guide.cfm
1. Slawson PF, Guggenheim FG. Psychiatric malpractice: a review of the national loss experience. Am J Psychiatry 1984;141:979-81.
2. Buckner F, Firestone M. Where the public peril begins: 25 years after Tarasoff. J Legal Med 2000;21(2):187-222.
3. Tarasoff v. Regents of the University of California, 551 P.2d 334 (California 1976).
4. Menninger WW. The impact of litigation and court decisions on clinical practice. Bull Menninger Clin 1989;53:203-14.
5. Davenport J. Documenting high-risk cases to avoid malpractice liability. Fam Pract Manag 2000;7(9):33-6.
6. Rice B. How plaintiffs’ lawyers pick their targets. Medical Economics 2000;8:94-110.
7. Levinson W, Roter DL, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA 1997;277(7):553-9.
8. Condon JT. Medical litigation the aetiological role of psychological and interpersonal factors. Med J Aust 1992;157:768-70.
9. Gutheil TG, Appelbaum PS. Clinical handbook of psychiatry and the law (3rd ed). Philadelphia: Lippincott Williams & Wilkins; 2000.
10. Resnick PJ, Scott CL. Legal issues in treating perpetrators and victims of violence. Psychiatr Clin North Am 1997;20(2):473-87.
11. Resnick PJ. Risk assessment for violence (lecture). Cleveland, OH: Case Western Reserve University, June 26, 2003.
12. Slovenko R. Malpractice in psychotherapy. Psychiatr Clin North Am 1999;22(1):1-15.
13. Mills MJ, Eth S. Legal liability with psychotropic drug use: extrapyramidal syndromes and tardive dyskinesia. J Clin Psychiatry 1987;48(9S):28-33.
14. Appelbaum PS. Can a psychiatrist be held responsible when a patient commits murder? Law Psychiatry 2002;53(1):27-9.
15. Tan MW, McDonough WJ. Risk management in psychiatry. Psychiatr Clin North Am 1990;13(1):135-47.
16. Garrick TR, Weinstock R. Liability of psychiatric consultants. Psychosomatics 1994;35:474-84.
17. Bradford GE. The “respectable minority” doctrine in Missouri medical negligence law. J Missouri Bar 2000;56(6):326-34.
18. Jacobson PD. Legal and policy considerations in using clinical practice guidelines. Am J Cardiol 1997;30(8B):74H-79H.
19. Scheflin AW, Spiegel D. From courtroom to couch: working with repressed memory and avoiding lawsuits. Psychiatr Clin North Am 1998;21(4):847-67.
20. Bradford GE, Elben CC. The drug package insert and the PDR as establishing the standard of care in prescription drug liability cases. J Missouri Bar 2001;57(5):233-42.
21. Hyams AL, Brandenburg JA, Lipsitz SR, et al. Practice guidelines and malpractice litigation: a two-way street. Ann Intern Med 1995;122(6):450-5.
22. Jones J. MD liability for electronic medical communications. Physician’s News Digest [serial online] 2000;(5).
23. Spielberg AR. Online without a net: physician-patient communication by electronic mail. Am J Law Med 1999;25:267-95.
1. Slawson PF, Guggenheim FG. Psychiatric malpractice: a review of the national loss experience. Am J Psychiatry 1984;141:979-81.
2. Buckner F, Firestone M. Where the public peril begins: 25 years after Tarasoff. J Legal Med 2000;21(2):187-222.
3. Tarasoff v. Regents of the University of California, 551 P.2d 334 (California 1976).
4. Menninger WW. The impact of litigation and court decisions on clinical practice. Bull Menninger Clin 1989;53:203-14.
5. Davenport J. Documenting high-risk cases to avoid malpractice liability. Fam Pract Manag 2000;7(9):33-6.
6. Rice B. How plaintiffs’ lawyers pick their targets. Medical Economics 2000;8:94-110.
7. Levinson W, Roter DL, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA 1997;277(7):553-9.
8. Condon JT. Medical litigation the aetiological role of psychological and interpersonal factors. Med J Aust 1992;157:768-70.
9. Gutheil TG, Appelbaum PS. Clinical handbook of psychiatry and the law (3rd ed). Philadelphia: Lippincott Williams & Wilkins; 2000.
10. Resnick PJ, Scott CL. Legal issues in treating perpetrators and victims of violence. Psychiatr Clin North Am 1997;20(2):473-87.
11. Resnick PJ. Risk assessment for violence (lecture). Cleveland, OH: Case Western Reserve University, June 26, 2003.
12. Slovenko R. Malpractice in psychotherapy. Psychiatr Clin North Am 1999;22(1):1-15.
13. Mills MJ, Eth S. Legal liability with psychotropic drug use: extrapyramidal syndromes and tardive dyskinesia. J Clin Psychiatry 1987;48(9S):28-33.
14. Appelbaum PS. Can a psychiatrist be held responsible when a patient commits murder? Law Psychiatry 2002;53(1):27-9.
15. Tan MW, McDonough WJ. Risk management in psychiatry. Psychiatr Clin North Am 1990;13(1):135-47.
16. Garrick TR, Weinstock R. Liability of psychiatric consultants. Psychosomatics 1994;35:474-84.
17. Bradford GE. The “respectable minority” doctrine in Missouri medical negligence law. J Missouri Bar 2000;56(6):326-34.
18. Jacobson PD. Legal and policy considerations in using clinical practice guidelines. Am J Cardiol 1997;30(8B):74H-79H.
19. Scheflin AW, Spiegel D. From courtroom to couch: working with repressed memory and avoiding lawsuits. Psychiatr Clin North Am 1998;21(4):847-67.
20. Bradford GE, Elben CC. The drug package insert and the PDR as establishing the standard of care in prescription drug liability cases. J Missouri Bar 2001;57(5):233-42.
21. Hyams AL, Brandenburg JA, Lipsitz SR, et al. Practice guidelines and malpractice litigation: a two-way street. Ann Intern Med 1995;122(6):450-5.
22. Jones J. MD liability for electronic medical communications. Physician’s News Digest [serial online] 2000;(5).
23. Spielberg AR. Online without a net: physician-patient communication by electronic mail. Am J Law Med 1999;25:267-95.
Regression, depression, and the facts of life
HISTORY: New school, old problems
Mr. E, age 13, was diagnosed with Down syndrome at birth and has mild mental retardation and bilateral sensorineural hearing loss. His pediatrician referred him to our child and adolescent psychiatry clinic for regressed behavior, depression, and apparent psychotic symptoms. He was also having problems sleeping and had begun puberty 8 months earlier.
Five months before referral, Mr. E had graduated from a small elementary school, where he was fully mainstreamed, to a large junior high school, where he spent most of the school day in a functional skills class. About that time, Mr. E began exhibiting nocturnal and daytime enuresis, loss of previously mastered skills, intolerance of novelty and change, and separation difficulty. Although toilet trained at age 7, he started having “accidents” at home, school, and elsewhere. He was reluctant to dress himself, and he resisted going to school.
The youth also talked to himself often and appeared to respond to internal stimuli. He “relived” conversations aloud, described imaginary friends to family and teachers, and spoke to a stuffed dog called Goofy. He would sit and stare into space for up to a half-hour, appearing preoccupied. Family members said he had exhibited these behaviors in grade school but until now appeared to have “outgrown” them.
Once sociable, Mr. E had become increasingly moody, negativistic, and isolative. He spent hours alone in his room. His mother, with whom he was close, reported that he was often angry with her for no apparent reason.
With puberty, his mother noted, Mr. E had begun kissing other developmentally disabled children. He also masturbated, but at his parents’ urging he restricted this activity to his room.
On evaluation, Mr. E was pleasant and outgoing. He had the facial dysmorphia and stature typical of Down syndrome. He smiled often and interacted well, and he attended and adapted to transitions in conversation and activities. His speech was dysarthric (with hyperglossia) and telegraphic; he could speak only four- to five-word sentences.
Was Mr. E exhibiting an adjustment reaction, depression, or a normal developmental response to puberty? Do his psychotic symptoms signal onset of schizophrenia?
Dr. Krassner’s and Kraus’ observations
Because Down syndrome is the most common genetic cause of mental retardation—seen in approximately 1 in 1,000 live births1—pediatricians and child psychiatrists see this disorder fairly frequently.
Regression, a form of coping exhibited by many children, is extremely common in youths with Down syndrome2 and often has a definite—though sometimes unclear—precipitant. We felt Mr. E’s move from a highly responsive, familiar school environment to a far less responsive one that accentuated his differences contributed to many of his symptoms.
Psychosis is less common in Down syndrome than in other developmental disabilities.2 Schizophrenia may occur, but diagnosis is complicated by cognition impairments, test-taking skills, and—in Mr. E’s case—inability to describe disordered thoughts or hallucinations due to poor language skills.3
Self-talk is common in Down syndrome and might be mistaken for psychosis. Note that despite his chronologic age, Mr. E is developmentally a 6-year-old, and self-talk and imaginary friends are considered normal behaviors for a child that age. What’s more, the stress of changing schools may have further compromised his developmental skills.
The FDA’s recent advisory about reports of increased suicidality in youths taking selective serotonin reuptake inhibitors (SSRIs) and other antidepressants for major depressive disorder during clinical trials has raised questions about using these agents in children and adolescents. Until more data become available, however, SSRIs remain the preferred drug therapy for pediatric depression.
- Based on our experience, we recommend citalopram, escitalopram, fluoxetine, and sertraline as first-line medications for pediatric depression because their side effects are relatively benign. The reported link between increased risk of suicidal ideation and behavior and use of paroxetine in pediatric patients has not been clearly established, so we cannot extrapolate that possible risk to other SSRIs.
- Newer antidepressants should be considered with caution in pediatric patients. Bupropion is contraindicated in patients with a history of seizures, bulimia, or anorexia. Mirtazapine is extremely sedating, with side effects such as weight gain and, in rare cases, agranulocytosis. Nefazodone comes with a “black box” warning for risk of liver toxicity. Trazodone is also sedating and carries a risk of priapism in boys.
- Older antidepressants, such as tricyclics, require extreme caution before prescribing to children and adolescents. Tricyclics, with their cardiac side effects, are not recommended for patients with Down syndrome, many of whom have cardiac pathology.
By contrast, depression is fairly common in Down syndrome, although it is much less prevalent in children than in adults with the developmental disorder.2
Finally, children with Down syndrome often enter puberty early, but without the cognitive or emotional maturity or knowledge to deal with the physiologic changes of adolescence.3 Parents often are reluctant to recognize their developmentally disabled child’s sexuality or are uncomfortable providing sexuality education.4 Mr. E’s parents clearly were unconvinced that his sexual behavior was normal for an adolescent.
TREATMENT Antidepressants lead to improvement
We felt Mr. E regressed secondary to emotional stress caused by switching schools. We viewed his psychotic symptoms as part of an adjustment disorder and attributed most of his other symptoms to depression. We anticipated Mr. E’s psychotic symptoms would remit spontaneously and focused on treating his mood and sleep disturbances.
We prescribed sertraline liquid suspension, 10 mg/d titrated across 3 weeks to 40 mg/d. We based our medication choice on clinical experience, mindful of a recent FDA advisory about the use of antidepressants in pediatric patients (Box 1). Also, the liquid suspension is easier to titrate than the tablet form, and we feared Mr. E might have trouble swallowing a tablet.
Mr. E’s mood and sociability improved after 3 to 4 weeks. Within 6 weeks, he regained some of his previously mastered daily activities. We added zolpidem, 10 mg nightly, to address his sleeping difficulties but discontinued the agent after 2 weeks, when his sleep patterns normalized.
At 2, 4, and 6 weeks, Mr. E was pleasant and cooperative, his thinking less concrete, and his speech more intelligible. His parents reported he was happier and more involved with family activities. At his mother’s request, sertraline was changed to 37.5 mg/d in tablet form. The patient remained stable for another month, during which his self-talk, though decreased, continued.
Two weeks later, Mr. E’s mother reported that, during a routine dermatologic examination for a chronic, presacral rash, the dermatologist noticed strategic shaving on the boy’s thighs, calves, and scrotum. Strategic shaving has been reported among sexually active youths as a means of purportedly increasing their sexual pleasure.
The dermatologist then told Mr. E’s mother that her son likely was sexually molested. Based on the boy’s differential rates of pubic hair growth, the doctor suspected that the molestation was chronic, dating back at least 3 months and probably continuing until the week before the examination. Upon hearing this, Mr. E’s parents were stunned and angry.
What behavioral signs might have suggested sexual abuse? How do the dermatologist’s findings alter diagnosis and treatment?
Dr. Krassner’s and Kraus’ observations
Given the dermatologist’s findings, Mr. E’s parents asked us whether their son’s presenting psychiatric symptoms were manifestations of posttraumatic stress disorder (PTSD).
Until now, explaining Mr. E’s symptoms as a reaction to changing schools seemed plausible. His symptoms were improving with treatment, and his sexual behaviors and interest in sexual topics were physiologically normal for his chronologic age. Despite his earlier pubertal experimentations, nothing in his psychosocial history indicated risk for sexual abuse or exploitation.
Still, children with Down syndrome are at higher risk for sexual exploitation than other children,4 so the possibility should have been explored with the parents. Psychiatrists should watch for physical signs of sexual abuse in these patients during the first examination (Box 2).4
But how is sexual abuse defined in this case? Deficient language skills prevented Mr. E from describing what happened to him, so determining whether he initiated sexual relations and with whom is nearly impossible. The act clearly could be considered abuse if Mr. E had been with an adult or older child—even if Mr. E consented. However, if Mr. E had initiated contact with another mentally retarded child, then cause, blame, and semantics become unclear. Either way, the incident could have caused PTSD.5
Diagnosing PTSD in non- or semi-verbal or retarded children is extremely difficult.6,7 Unlike adults with PTSD, pre-verbal children might not have recurrent, distressing recollections of the trauma, but symbolic displacement may characterize repetitive play, during which themes are expressed.8
Scheeringa et al have recommended PTSD criteria for preschool children, including:
- social withdrawal
- extreme temper tantrums
- loss of developmental skills
- new separation anxiety
- new onset of aggression
- new fears without obvious links to the trauma.5,6
Treating PTSD in children with developmental disabilities is also difficult. Modalities applicable to adults or mainstream children—such as psychodynamic psychotherapy, cognitive-behavioral therapy (CBT), exposure therapy, and medications—often do not help developmentally disabled children. For example, Mr. E lacks the cognitive apparatus to respond to CBT.
On the other hand, behavioral therapy, reducing risk factors, minimizing dissociative triggers, and educating patients, parents, friends, and teachers about PTSD can help patients such as Mr. E.5 Attempting to provide structure and maintain routines is a cornerstone of any intervention.
- Aggression
- Anxiety
- Behavior, learning problems at school
- Depression
- Heightened somatic concerns
- Sexualized behavior
- Sleep disturbance
- Withdrawal
FURTHER TREATMENT A family in turmoil
We addressed Mr. E’s symptoms as PTSD-related, though his poor language skills kept us from identifying a trauma. Based on data regarding pediatric PTSD treatment,9 we increased sertraline to 50 mg/d and then to 75 mg/d across 2 weeks.
However, an intense legal investigation brought on by the parents, combined with ensuing tumult within the family, worsened Mr. E’s symptoms. His self-talk became more pronounced and his isolative behavior reappeared, suggesting that the intrusive, repetitive questioning caused him to re-experience the trauma.
We again increased sertraline, to 100 mg/d, and offered supportive therapy to Mr. E. We tried to educate his parents about understanding his symptoms and managing his behavior and strongly recommended that they undergo crisis therapy to keep their reactions and emotions from hurting Mr. E. The parents declined, however, and alleged that we did not adequately support their pursuit of a diagnosis or legal action, which for them had become synonymous with treatment.
Mr. E’s mother brought her son to a psychologist, who engaged him in play therapy. She followed her son around, noting everything he said. All the while, she failed to resolve her guilt and anger. When we explained to her that these actions were hurting Mr. E’s progress, she terminated therapy.
How would you have tried to keep Mr. E’s family in therapy?
Dr. Krassner’s and Kraus’ observations
Treating psychopathology in children carries the risk of strained relations with the patient’s family. The risk increases exponentially for developmentally disabled children, as they have little or no input and their parents are exquisitely sensitive to their needs. Further, the revelation that the parents might have somehow failed to avert or anticipate danger to the child complicates their emotional response.
Although the child is the patient, the parent is the consumer. Failure to gain or keep the parents’ confidence will hinder or destroy therapy.
We might have protected our working relationship with Mr. E’s parents by recognizing how fragile they were and how intensely they would react to any constructive criticism. Paradoxically, for the short-term we could have tolerated their detrimental behaviors toward Mr. E (such as repeated questioning) in the hopes of protecting a long-term relationship. Spending more time exploring the guilt, anger, and confusion that tormented Mr. E’s parents—particularly his mother—also might have helped.
Related resources
- Ryan RM. Recognition of psychosis in persons who do not use spoken communication. In: Ancill RJ, Holliday S, Higenbottam J (eds). Schizophrenia: exploring the spectrum of psychosis. New York: John Wiley & Sons, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Zolpidem • Ambien
1. Pueschel S. Children with Down syndrome. In: Levine M, Carey W, Crocker A, Gross R (eds). Developmental-behavioral pediatrics. Philadelphia: WB Saunders, 1983.
2. Hodapp RM. Down syndrome: developmental, psychiatric, and management issues. Child Adolesc Psychiatr Clin North Am 1996;5:881-94.
3. Feinstein C, Reiss AL. Psychiatric disorder in mentally retarded children and adolescents. Child Adolesc Psychiatr Clin North Am 1996;5:827-52.
4. Wilgosh L. Sexual abuse of children with disabilities: intervention and treatment issues for parents. Developmental Disabil Bull. Available at: http://www.ualberta.ca/~jpdasddc/bulletin/articles/wilgosh1993.html. Accessed Nov. 10, 2003.
5. Ryan RM. Posttraumatic stress disorder in persons with developmental disabilities. Community Health J 1994;30:45-54.
6. Scheeringa MS, Seanah CH, Myers L, Putnam FW. New findings on alternative criteria for PTSD in preschool children. J Am Acad Child Adolesc Psychiatry 2003;42:561-70.
7. Diagnostic and Statistical Manual of Mental Disorders (4th ed-text revision). Washington, DC: American Psychiatric Association, 2000.
8. Lonigan CJ, Phillips BM, Richey JA. Posttraumatic stress disorder in children: diagnosis, assessment, and associated features. Child Adolesc Psychiatr Clin North Am 2003;12:171-94.
9. Donnelly CL. Pharmacological treatment approaches for children and adolescents with posttraumatic stress disorder. Child Adolesc Psychiatr Clin North Am 2003;12:251-69.
HISTORY: New school, old problems
Mr. E, age 13, was diagnosed with Down syndrome at birth and has mild mental retardation and bilateral sensorineural hearing loss. His pediatrician referred him to our child and adolescent psychiatry clinic for regressed behavior, depression, and apparent psychotic symptoms. He was also having problems sleeping and had begun puberty 8 months earlier.
Five months before referral, Mr. E had graduated from a small elementary school, where he was fully mainstreamed, to a large junior high school, where he spent most of the school day in a functional skills class. About that time, Mr. E began exhibiting nocturnal and daytime enuresis, loss of previously mastered skills, intolerance of novelty and change, and separation difficulty. Although toilet trained at age 7, he started having “accidents” at home, school, and elsewhere. He was reluctant to dress himself, and he resisted going to school.
The youth also talked to himself often and appeared to respond to internal stimuli. He “relived” conversations aloud, described imaginary friends to family and teachers, and spoke to a stuffed dog called Goofy. He would sit and stare into space for up to a half-hour, appearing preoccupied. Family members said he had exhibited these behaviors in grade school but until now appeared to have “outgrown” them.
Once sociable, Mr. E had become increasingly moody, negativistic, and isolative. He spent hours alone in his room. His mother, with whom he was close, reported that he was often angry with her for no apparent reason.
With puberty, his mother noted, Mr. E had begun kissing other developmentally disabled children. He also masturbated, but at his parents’ urging he restricted this activity to his room.
On evaluation, Mr. E was pleasant and outgoing. He had the facial dysmorphia and stature typical of Down syndrome. He smiled often and interacted well, and he attended and adapted to transitions in conversation and activities. His speech was dysarthric (with hyperglossia) and telegraphic; he could speak only four- to five-word sentences.
Was Mr. E exhibiting an adjustment reaction, depression, or a normal developmental response to puberty? Do his psychotic symptoms signal onset of schizophrenia?
Dr. Krassner’s and Kraus’ observations
Because Down syndrome is the most common genetic cause of mental retardation—seen in approximately 1 in 1,000 live births1—pediatricians and child psychiatrists see this disorder fairly frequently.
Regression, a form of coping exhibited by many children, is extremely common in youths with Down syndrome2 and often has a definite—though sometimes unclear—precipitant. We felt Mr. E’s move from a highly responsive, familiar school environment to a far less responsive one that accentuated his differences contributed to many of his symptoms.
Psychosis is less common in Down syndrome than in other developmental disabilities.2 Schizophrenia may occur, but diagnosis is complicated by cognition impairments, test-taking skills, and—in Mr. E’s case—inability to describe disordered thoughts or hallucinations due to poor language skills.3
Self-talk is common in Down syndrome and might be mistaken for psychosis. Note that despite his chronologic age, Mr. E is developmentally a 6-year-old, and self-talk and imaginary friends are considered normal behaviors for a child that age. What’s more, the stress of changing schools may have further compromised his developmental skills.
The FDA’s recent advisory about reports of increased suicidality in youths taking selective serotonin reuptake inhibitors (SSRIs) and other antidepressants for major depressive disorder during clinical trials has raised questions about using these agents in children and adolescents. Until more data become available, however, SSRIs remain the preferred drug therapy for pediatric depression.
- Based on our experience, we recommend citalopram, escitalopram, fluoxetine, and sertraline as first-line medications for pediatric depression because their side effects are relatively benign. The reported link between increased risk of suicidal ideation and behavior and use of paroxetine in pediatric patients has not been clearly established, so we cannot extrapolate that possible risk to other SSRIs.
- Newer antidepressants should be considered with caution in pediatric patients. Bupropion is contraindicated in patients with a history of seizures, bulimia, or anorexia. Mirtazapine is extremely sedating, with side effects such as weight gain and, in rare cases, agranulocytosis. Nefazodone comes with a “black box” warning for risk of liver toxicity. Trazodone is also sedating and carries a risk of priapism in boys.
- Older antidepressants, such as tricyclics, require extreme caution before prescribing to children and adolescents. Tricyclics, with their cardiac side effects, are not recommended for patients with Down syndrome, many of whom have cardiac pathology.
By contrast, depression is fairly common in Down syndrome, although it is much less prevalent in children than in adults with the developmental disorder.2
Finally, children with Down syndrome often enter puberty early, but without the cognitive or emotional maturity or knowledge to deal with the physiologic changes of adolescence.3 Parents often are reluctant to recognize their developmentally disabled child’s sexuality or are uncomfortable providing sexuality education.4 Mr. E’s parents clearly were unconvinced that his sexual behavior was normal for an adolescent.
TREATMENT Antidepressants lead to improvement
We felt Mr. E regressed secondary to emotional stress caused by switching schools. We viewed his psychotic symptoms as part of an adjustment disorder and attributed most of his other symptoms to depression. We anticipated Mr. E’s psychotic symptoms would remit spontaneously and focused on treating his mood and sleep disturbances.
We prescribed sertraline liquid suspension, 10 mg/d titrated across 3 weeks to 40 mg/d. We based our medication choice on clinical experience, mindful of a recent FDA advisory about the use of antidepressants in pediatric patients (Box 1). Also, the liquid suspension is easier to titrate than the tablet form, and we feared Mr. E might have trouble swallowing a tablet.
Mr. E’s mood and sociability improved after 3 to 4 weeks. Within 6 weeks, he regained some of his previously mastered daily activities. We added zolpidem, 10 mg nightly, to address his sleeping difficulties but discontinued the agent after 2 weeks, when his sleep patterns normalized.
At 2, 4, and 6 weeks, Mr. E was pleasant and cooperative, his thinking less concrete, and his speech more intelligible. His parents reported he was happier and more involved with family activities. At his mother’s request, sertraline was changed to 37.5 mg/d in tablet form. The patient remained stable for another month, during which his self-talk, though decreased, continued.
Two weeks later, Mr. E’s mother reported that, during a routine dermatologic examination for a chronic, presacral rash, the dermatologist noticed strategic shaving on the boy’s thighs, calves, and scrotum. Strategic shaving has been reported among sexually active youths as a means of purportedly increasing their sexual pleasure.
The dermatologist then told Mr. E’s mother that her son likely was sexually molested. Based on the boy’s differential rates of pubic hair growth, the doctor suspected that the molestation was chronic, dating back at least 3 months and probably continuing until the week before the examination. Upon hearing this, Mr. E’s parents were stunned and angry.
What behavioral signs might have suggested sexual abuse? How do the dermatologist’s findings alter diagnosis and treatment?
Dr. Krassner’s and Kraus’ observations
Given the dermatologist’s findings, Mr. E’s parents asked us whether their son’s presenting psychiatric symptoms were manifestations of posttraumatic stress disorder (PTSD).
Until now, explaining Mr. E’s symptoms as a reaction to changing schools seemed plausible. His symptoms were improving with treatment, and his sexual behaviors and interest in sexual topics were physiologically normal for his chronologic age. Despite his earlier pubertal experimentations, nothing in his psychosocial history indicated risk for sexual abuse or exploitation.
Still, children with Down syndrome are at higher risk for sexual exploitation than other children,4 so the possibility should have been explored with the parents. Psychiatrists should watch for physical signs of sexual abuse in these patients during the first examination (Box 2).4
But how is sexual abuse defined in this case? Deficient language skills prevented Mr. E from describing what happened to him, so determining whether he initiated sexual relations and with whom is nearly impossible. The act clearly could be considered abuse if Mr. E had been with an adult or older child—even if Mr. E consented. However, if Mr. E had initiated contact with another mentally retarded child, then cause, blame, and semantics become unclear. Either way, the incident could have caused PTSD.5
Diagnosing PTSD in non- or semi-verbal or retarded children is extremely difficult.6,7 Unlike adults with PTSD, pre-verbal children might not have recurrent, distressing recollections of the trauma, but symbolic displacement may characterize repetitive play, during which themes are expressed.8
Scheeringa et al have recommended PTSD criteria for preschool children, including:
- social withdrawal
- extreme temper tantrums
- loss of developmental skills
- new separation anxiety
- new onset of aggression
- new fears without obvious links to the trauma.5,6
Treating PTSD in children with developmental disabilities is also difficult. Modalities applicable to adults or mainstream children—such as psychodynamic psychotherapy, cognitive-behavioral therapy (CBT), exposure therapy, and medications—often do not help developmentally disabled children. For example, Mr. E lacks the cognitive apparatus to respond to CBT.
On the other hand, behavioral therapy, reducing risk factors, minimizing dissociative triggers, and educating patients, parents, friends, and teachers about PTSD can help patients such as Mr. E.5 Attempting to provide structure and maintain routines is a cornerstone of any intervention.
- Aggression
- Anxiety
- Behavior, learning problems at school
- Depression
- Heightened somatic concerns
- Sexualized behavior
- Sleep disturbance
- Withdrawal
FURTHER TREATMENT A family in turmoil
We addressed Mr. E’s symptoms as PTSD-related, though his poor language skills kept us from identifying a trauma. Based on data regarding pediatric PTSD treatment,9 we increased sertraline to 50 mg/d and then to 75 mg/d across 2 weeks.
However, an intense legal investigation brought on by the parents, combined with ensuing tumult within the family, worsened Mr. E’s symptoms. His self-talk became more pronounced and his isolative behavior reappeared, suggesting that the intrusive, repetitive questioning caused him to re-experience the trauma.
We again increased sertraline, to 100 mg/d, and offered supportive therapy to Mr. E. We tried to educate his parents about understanding his symptoms and managing his behavior and strongly recommended that they undergo crisis therapy to keep their reactions and emotions from hurting Mr. E. The parents declined, however, and alleged that we did not adequately support their pursuit of a diagnosis or legal action, which for them had become synonymous with treatment.
Mr. E’s mother brought her son to a psychologist, who engaged him in play therapy. She followed her son around, noting everything he said. All the while, she failed to resolve her guilt and anger. When we explained to her that these actions were hurting Mr. E’s progress, she terminated therapy.
How would you have tried to keep Mr. E’s family in therapy?
Dr. Krassner’s and Kraus’ observations
Treating psychopathology in children carries the risk of strained relations with the patient’s family. The risk increases exponentially for developmentally disabled children, as they have little or no input and their parents are exquisitely sensitive to their needs. Further, the revelation that the parents might have somehow failed to avert or anticipate danger to the child complicates their emotional response.
Although the child is the patient, the parent is the consumer. Failure to gain or keep the parents’ confidence will hinder or destroy therapy.
We might have protected our working relationship with Mr. E’s parents by recognizing how fragile they were and how intensely they would react to any constructive criticism. Paradoxically, for the short-term we could have tolerated their detrimental behaviors toward Mr. E (such as repeated questioning) in the hopes of protecting a long-term relationship. Spending more time exploring the guilt, anger, and confusion that tormented Mr. E’s parents—particularly his mother—also might have helped.
Related resources
- Ryan RM. Recognition of psychosis in persons who do not use spoken communication. In: Ancill RJ, Holliday S, Higenbottam J (eds). Schizophrenia: exploring the spectrum of psychosis. New York: John Wiley & Sons, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Zolpidem • Ambien
HISTORY: New school, old problems
Mr. E, age 13, was diagnosed with Down syndrome at birth and has mild mental retardation and bilateral sensorineural hearing loss. His pediatrician referred him to our child and adolescent psychiatry clinic for regressed behavior, depression, and apparent psychotic symptoms. He was also having problems sleeping and had begun puberty 8 months earlier.
Five months before referral, Mr. E had graduated from a small elementary school, where he was fully mainstreamed, to a large junior high school, where he spent most of the school day in a functional skills class. About that time, Mr. E began exhibiting nocturnal and daytime enuresis, loss of previously mastered skills, intolerance of novelty and change, and separation difficulty. Although toilet trained at age 7, he started having “accidents” at home, school, and elsewhere. He was reluctant to dress himself, and he resisted going to school.
The youth also talked to himself often and appeared to respond to internal stimuli. He “relived” conversations aloud, described imaginary friends to family and teachers, and spoke to a stuffed dog called Goofy. He would sit and stare into space for up to a half-hour, appearing preoccupied. Family members said he had exhibited these behaviors in grade school but until now appeared to have “outgrown” them.
Once sociable, Mr. E had become increasingly moody, negativistic, and isolative. He spent hours alone in his room. His mother, with whom he was close, reported that he was often angry with her for no apparent reason.
With puberty, his mother noted, Mr. E had begun kissing other developmentally disabled children. He also masturbated, but at his parents’ urging he restricted this activity to his room.
On evaluation, Mr. E was pleasant and outgoing. He had the facial dysmorphia and stature typical of Down syndrome. He smiled often and interacted well, and he attended and adapted to transitions in conversation and activities. His speech was dysarthric (with hyperglossia) and telegraphic; he could speak only four- to five-word sentences.
Was Mr. E exhibiting an adjustment reaction, depression, or a normal developmental response to puberty? Do his psychotic symptoms signal onset of schizophrenia?
Dr. Krassner’s and Kraus’ observations
Because Down syndrome is the most common genetic cause of mental retardation—seen in approximately 1 in 1,000 live births1—pediatricians and child psychiatrists see this disorder fairly frequently.
Regression, a form of coping exhibited by many children, is extremely common in youths with Down syndrome2 and often has a definite—though sometimes unclear—precipitant. We felt Mr. E’s move from a highly responsive, familiar school environment to a far less responsive one that accentuated his differences contributed to many of his symptoms.
Psychosis is less common in Down syndrome than in other developmental disabilities.2 Schizophrenia may occur, but diagnosis is complicated by cognition impairments, test-taking skills, and—in Mr. E’s case—inability to describe disordered thoughts or hallucinations due to poor language skills.3
Self-talk is common in Down syndrome and might be mistaken for psychosis. Note that despite his chronologic age, Mr. E is developmentally a 6-year-old, and self-talk and imaginary friends are considered normal behaviors for a child that age. What’s more, the stress of changing schools may have further compromised his developmental skills.
The FDA’s recent advisory about reports of increased suicidality in youths taking selective serotonin reuptake inhibitors (SSRIs) and other antidepressants for major depressive disorder during clinical trials has raised questions about using these agents in children and adolescents. Until more data become available, however, SSRIs remain the preferred drug therapy for pediatric depression.
- Based on our experience, we recommend citalopram, escitalopram, fluoxetine, and sertraline as first-line medications for pediatric depression because their side effects are relatively benign. The reported link between increased risk of suicidal ideation and behavior and use of paroxetine in pediatric patients has not been clearly established, so we cannot extrapolate that possible risk to other SSRIs.
- Newer antidepressants should be considered with caution in pediatric patients. Bupropion is contraindicated in patients with a history of seizures, bulimia, or anorexia. Mirtazapine is extremely sedating, with side effects such as weight gain and, in rare cases, agranulocytosis. Nefazodone comes with a “black box” warning for risk of liver toxicity. Trazodone is also sedating and carries a risk of priapism in boys.
- Older antidepressants, such as tricyclics, require extreme caution before prescribing to children and adolescents. Tricyclics, with their cardiac side effects, are not recommended for patients with Down syndrome, many of whom have cardiac pathology.
By contrast, depression is fairly common in Down syndrome, although it is much less prevalent in children than in adults with the developmental disorder.2
Finally, children with Down syndrome often enter puberty early, but without the cognitive or emotional maturity or knowledge to deal with the physiologic changes of adolescence.3 Parents often are reluctant to recognize their developmentally disabled child’s sexuality or are uncomfortable providing sexuality education.4 Mr. E’s parents clearly were unconvinced that his sexual behavior was normal for an adolescent.
TREATMENT Antidepressants lead to improvement
We felt Mr. E regressed secondary to emotional stress caused by switching schools. We viewed his psychotic symptoms as part of an adjustment disorder and attributed most of his other symptoms to depression. We anticipated Mr. E’s psychotic symptoms would remit spontaneously and focused on treating his mood and sleep disturbances.
We prescribed sertraline liquid suspension, 10 mg/d titrated across 3 weeks to 40 mg/d. We based our medication choice on clinical experience, mindful of a recent FDA advisory about the use of antidepressants in pediatric patients (Box 1). Also, the liquid suspension is easier to titrate than the tablet form, and we feared Mr. E might have trouble swallowing a tablet.
Mr. E’s mood and sociability improved after 3 to 4 weeks. Within 6 weeks, he regained some of his previously mastered daily activities. We added zolpidem, 10 mg nightly, to address his sleeping difficulties but discontinued the agent after 2 weeks, when his sleep patterns normalized.
At 2, 4, and 6 weeks, Mr. E was pleasant and cooperative, his thinking less concrete, and his speech more intelligible. His parents reported he was happier and more involved with family activities. At his mother’s request, sertraline was changed to 37.5 mg/d in tablet form. The patient remained stable for another month, during which his self-talk, though decreased, continued.
Two weeks later, Mr. E’s mother reported that, during a routine dermatologic examination for a chronic, presacral rash, the dermatologist noticed strategic shaving on the boy’s thighs, calves, and scrotum. Strategic shaving has been reported among sexually active youths as a means of purportedly increasing their sexual pleasure.
The dermatologist then told Mr. E’s mother that her son likely was sexually molested. Based on the boy’s differential rates of pubic hair growth, the doctor suspected that the molestation was chronic, dating back at least 3 months and probably continuing until the week before the examination. Upon hearing this, Mr. E’s parents were stunned and angry.
What behavioral signs might have suggested sexual abuse? How do the dermatologist’s findings alter diagnosis and treatment?
Dr. Krassner’s and Kraus’ observations
Given the dermatologist’s findings, Mr. E’s parents asked us whether their son’s presenting psychiatric symptoms were manifestations of posttraumatic stress disorder (PTSD).
Until now, explaining Mr. E’s symptoms as a reaction to changing schools seemed plausible. His symptoms were improving with treatment, and his sexual behaviors and interest in sexual topics were physiologically normal for his chronologic age. Despite his earlier pubertal experimentations, nothing in his psychosocial history indicated risk for sexual abuse or exploitation.
Still, children with Down syndrome are at higher risk for sexual exploitation than other children,4 so the possibility should have been explored with the parents. Psychiatrists should watch for physical signs of sexual abuse in these patients during the first examination (Box 2).4
But how is sexual abuse defined in this case? Deficient language skills prevented Mr. E from describing what happened to him, so determining whether he initiated sexual relations and with whom is nearly impossible. The act clearly could be considered abuse if Mr. E had been with an adult or older child—even if Mr. E consented. However, if Mr. E had initiated contact with another mentally retarded child, then cause, blame, and semantics become unclear. Either way, the incident could have caused PTSD.5
Diagnosing PTSD in non- or semi-verbal or retarded children is extremely difficult.6,7 Unlike adults with PTSD, pre-verbal children might not have recurrent, distressing recollections of the trauma, but symbolic displacement may characterize repetitive play, during which themes are expressed.8
Scheeringa et al have recommended PTSD criteria for preschool children, including:
- social withdrawal
- extreme temper tantrums
- loss of developmental skills
- new separation anxiety
- new onset of aggression
- new fears without obvious links to the trauma.5,6
Treating PTSD in children with developmental disabilities is also difficult. Modalities applicable to adults or mainstream children—such as psychodynamic psychotherapy, cognitive-behavioral therapy (CBT), exposure therapy, and medications—often do not help developmentally disabled children. For example, Mr. E lacks the cognitive apparatus to respond to CBT.
On the other hand, behavioral therapy, reducing risk factors, minimizing dissociative triggers, and educating patients, parents, friends, and teachers about PTSD can help patients such as Mr. E.5 Attempting to provide structure and maintain routines is a cornerstone of any intervention.
- Aggression
- Anxiety
- Behavior, learning problems at school
- Depression
- Heightened somatic concerns
- Sexualized behavior
- Sleep disturbance
- Withdrawal
FURTHER TREATMENT A family in turmoil
We addressed Mr. E’s symptoms as PTSD-related, though his poor language skills kept us from identifying a trauma. Based on data regarding pediatric PTSD treatment,9 we increased sertraline to 50 mg/d and then to 75 mg/d across 2 weeks.
However, an intense legal investigation brought on by the parents, combined with ensuing tumult within the family, worsened Mr. E’s symptoms. His self-talk became more pronounced and his isolative behavior reappeared, suggesting that the intrusive, repetitive questioning caused him to re-experience the trauma.
We again increased sertraline, to 100 mg/d, and offered supportive therapy to Mr. E. We tried to educate his parents about understanding his symptoms and managing his behavior and strongly recommended that they undergo crisis therapy to keep their reactions and emotions from hurting Mr. E. The parents declined, however, and alleged that we did not adequately support their pursuit of a diagnosis or legal action, which for them had become synonymous with treatment.
Mr. E’s mother brought her son to a psychologist, who engaged him in play therapy. She followed her son around, noting everything he said. All the while, she failed to resolve her guilt and anger. When we explained to her that these actions were hurting Mr. E’s progress, she terminated therapy.
How would you have tried to keep Mr. E’s family in therapy?
Dr. Krassner’s and Kraus’ observations
Treating psychopathology in children carries the risk of strained relations with the patient’s family. The risk increases exponentially for developmentally disabled children, as they have little or no input and their parents are exquisitely sensitive to their needs. Further, the revelation that the parents might have somehow failed to avert or anticipate danger to the child complicates their emotional response.
Although the child is the patient, the parent is the consumer. Failure to gain or keep the parents’ confidence will hinder or destroy therapy.
We might have protected our working relationship with Mr. E’s parents by recognizing how fragile they were and how intensely they would react to any constructive criticism. Paradoxically, for the short-term we could have tolerated their detrimental behaviors toward Mr. E (such as repeated questioning) in the hopes of protecting a long-term relationship. Spending more time exploring the guilt, anger, and confusion that tormented Mr. E’s parents—particularly his mother—also might have helped.
Related resources
- Ryan RM. Recognition of psychosis in persons who do not use spoken communication. In: Ancill RJ, Holliday S, Higenbottam J (eds). Schizophrenia: exploring the spectrum of psychosis. New York: John Wiley & Sons, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Zolpidem • Ambien
1. Pueschel S. Children with Down syndrome. In: Levine M, Carey W, Crocker A, Gross R (eds). Developmental-behavioral pediatrics. Philadelphia: WB Saunders, 1983.
2. Hodapp RM. Down syndrome: developmental, psychiatric, and management issues. Child Adolesc Psychiatr Clin North Am 1996;5:881-94.
3. Feinstein C, Reiss AL. Psychiatric disorder in mentally retarded children and adolescents. Child Adolesc Psychiatr Clin North Am 1996;5:827-52.
4. Wilgosh L. Sexual abuse of children with disabilities: intervention and treatment issues for parents. Developmental Disabil Bull. Available at: http://www.ualberta.ca/~jpdasddc/bulletin/articles/wilgosh1993.html. Accessed Nov. 10, 2003.
5. Ryan RM. Posttraumatic stress disorder in persons with developmental disabilities. Community Health J 1994;30:45-54.
6. Scheeringa MS, Seanah CH, Myers L, Putnam FW. New findings on alternative criteria for PTSD in preschool children. J Am Acad Child Adolesc Psychiatry 2003;42:561-70.
7. Diagnostic and Statistical Manual of Mental Disorders (4th ed-text revision). Washington, DC: American Psychiatric Association, 2000.
8. Lonigan CJ, Phillips BM, Richey JA. Posttraumatic stress disorder in children: diagnosis, assessment, and associated features. Child Adolesc Psychiatr Clin North Am 2003;12:171-94.
9. Donnelly CL. Pharmacological treatment approaches for children and adolescents with posttraumatic stress disorder. Child Adolesc Psychiatr Clin North Am 2003;12:251-69.
1. Pueschel S. Children with Down syndrome. In: Levine M, Carey W, Crocker A, Gross R (eds). Developmental-behavioral pediatrics. Philadelphia: WB Saunders, 1983.
2. Hodapp RM. Down syndrome: developmental, psychiatric, and management issues. Child Adolesc Psychiatr Clin North Am 1996;5:881-94.
3. Feinstein C, Reiss AL. Psychiatric disorder in mentally retarded children and adolescents. Child Adolesc Psychiatr Clin North Am 1996;5:827-52.
4. Wilgosh L. Sexual abuse of children with disabilities: intervention and treatment issues for parents. Developmental Disabil Bull. Available at: http://www.ualberta.ca/~jpdasddc/bulletin/articles/wilgosh1993.html. Accessed Nov. 10, 2003.
5. Ryan RM. Posttraumatic stress disorder in persons with developmental disabilities. Community Health J 1994;30:45-54.
6. Scheeringa MS, Seanah CH, Myers L, Putnam FW. New findings on alternative criteria for PTSD in preschool children. J Am Acad Child Adolesc Psychiatry 2003;42:561-70.
7. Diagnostic and Statistical Manual of Mental Disorders (4th ed-text revision). Washington, DC: American Psychiatric Association, 2000.
8. Lonigan CJ, Phillips BM, Richey JA. Posttraumatic stress disorder in children: diagnosis, assessment, and associated features. Child Adolesc Psychiatr Clin North Am 2003;12:171-94.
9. Donnelly CL. Pharmacological treatment approaches for children and adolescents with posttraumatic stress disorder. Child Adolesc Psychiatr Clin North Am 2003;12:251-69.
Lithium in bipolar disorder
“Tips for using lithium in bipolar disorder” by West Magnon, MD (Pearls, CURRENT PSYCHIATRY, September 2003) was right on track.
I, too, have found that repeatedly measuring lithium levels is rarely warranted. The exception is when a manic patient is leaving the office and feels compelled to tell a joke. To me, this is suspiciously indicative of a bipolar illness and uncovers the need for a new lithium level determination in a previously diagnosed bipolar individual.
Leonard R. Friedman MD Revere, MA
“Tips for using lithium in bipolar disorder” by West Magnon, MD (Pearls, CURRENT PSYCHIATRY, September 2003) was right on track.
I, too, have found that repeatedly measuring lithium levels is rarely warranted. The exception is when a manic patient is leaving the office and feels compelled to tell a joke. To me, this is suspiciously indicative of a bipolar illness and uncovers the need for a new lithium level determination in a previously diagnosed bipolar individual.
Leonard R. Friedman MD Revere, MA
“Tips for using lithium in bipolar disorder” by West Magnon, MD (Pearls, CURRENT PSYCHIATRY, September 2003) was right on track.
I, too, have found that repeatedly measuring lithium levels is rarely warranted. The exception is when a manic patient is leaving the office and feels compelled to tell a joke. To me, this is suspiciously indicative of a bipolar illness and uncovers the need for a new lithium level determination in a previously diagnosed bipolar individual.
Leonard R. Friedman MD Revere, MA
Estrogen, HRT, and mood disorders

“Minding menopause” (CURRENT PSYCHIATRY, October 2003) provided an interesting and useful look at how to diagnose and treat menopause-related psychiatric symptoms.
However, Dr. Brizendine’s statement that “…the Women’s Health Initiative (WHI) trial reported that estrogen’s health risks…exceeded potential benefit during 5 years of therapy” requires some clarification.
After a mean of 5.2 years of follow-up, the WHI reported an increased risk of major cardiovascular events, breast cancer, and pulmonary emboli in the trial arm evaluating estrogen plus progestin versus placebo.1 The reduced incidence of hip fractures and colorectal cancers did not outweigh the adverse events. The results of the trial’s estrogen-versus-placebo arm (in women without a uterus) have not yet been reported.
Hormone replacement therapy, or HRT (estrogen plus progestin), is clearly no longer indicated to prevent chronic diseases in healthy postmenopausal women.2 Given the increase in breast cancer and symptomatic gallstones in patients taking estrogen,3 and uncertainty over how estrogen affects cardiovascular status, most clinicians now avoid estrogen for primary prevention, at least until the WHI reports its estrogen-only trial results.
As long as the risks and benefits are carefully explained, HRT can still be used to treat hot flashes.4 Although HRT does not have a clinically meaningful effect on health-related quality of life, it does reduce moderate to severe vasomotor symptoms.5
For now, the risks of estrogen therapy (in women without a uterus) should be presumed to be at least as serious as those of combined estrogen/progestin therapy. Though challenging, psychiatrists who treat menopause-related hot flashes and mood symptoms need to clearly understand the risks and benefits of estrogen and estrogen/progestin therapy.
Michael Rack MD
Assistant professor of internal medicine and psychiatry
University of Mississippi School of Medicine
Jackson, MS
- Yusuf S, Anand S. Hormone replacement therapy: a time for pause. CMAJ 2002;167:357–9.
- Day A. Lessons from the Women’s Health Initiative: Primary prevention and gender health. CMAJ 2002;167:361–2.
- Gupta G, Aronow WS. Hormone replacement therapy. An analysis of efficacy based on evidence. Geriatrics 2002;57(8):18–20, 23–4.
- Sherman FT. Hormone replacement therapy. The sudden halt of a clinical trial shakes long held beliefs. Geriatrics 2002;57(8):7.
- Hays J, Ockene JK, Brunner RL, et al. Effects of estrogen plus progestin on health-related quality of life. N Engl J Med 2003;348:1839–54.
Dr. Brizendine responds
Dr. Rack is right that the WHI has so far documented dangers of estrogen-progestin but not estrogen alone.
The WHI results clearly indicate that the risks of more than 5 years of estrogen-progestin HRT outweigh the benefits for the average woman. While we still don’t know the risks of estrogen-only therapy, the WHI trial’s estrogen-only arm—scheduled for completion in 2005—will provide valuable information on the safety of estrogen alone for women without a uterus.
It is somewhat comforting that after 7 years, predetermined risk limits have not forced termination of the estrogen-only trial. More than 6,500 women will soon enter their eighth year in the estrogen-only trial. Most physicians now feel they can treat severe hot flashes for up to 5 years with:
- estrogen in women without a uterus
- estrogen-progestin in women with a uterus.
In either case, patients must have no other contraindications to taking estrogen, including breast cancer risk, history of blood clotting, and gallbladder disease.
Women who cannot or will not take estrogen but have severe hot flashes may wish to try a selective serotonin reuptake inhibitor (SSRI) for hot flashes. Based on clinical experience, women with mood symptoms and hot flashes are likely to respond best to an SSRI.
Many women ages 40 to 60 develop mood symptoms during their perimenopause and menopause transitions. Familiarity with use of estrogen and SSRIs in this patient population is critical. Psychiatrists should be able to knowledgeably discuss the risks and benefits of HRT with patients, but HRT prescription is best left up to the patient’s Ob/Gyn or primary practitioner.
Louann Brizendine, MD
Clinical professor of psychiatry
Director, Women’s Mood and Hormone Clinic
University of California-San Francisco Medical School
“Minding menopause” (CURRENT PSYCHIATRY, October 2003) provided an interesting and useful look at how to diagnose and treat menopause-related psychiatric symptoms.
However, Dr. Brizendine’s statement that “…the Women’s Health Initiative (WHI) trial reported that estrogen’s health risks…exceeded potential benefit during 5 years of therapy” requires some clarification.
After a mean of 5.2 years of follow-up, the WHI reported an increased risk of major cardiovascular events, breast cancer, and pulmonary emboli in the trial arm evaluating estrogen plus progestin versus placebo.1 The reduced incidence of hip fractures and colorectal cancers did not outweigh the adverse events. The results of the trial’s estrogen-versus-placebo arm (in women without a uterus) have not yet been reported.
Hormone replacement therapy, or HRT (estrogen plus progestin), is clearly no longer indicated to prevent chronic diseases in healthy postmenopausal women.2 Given the increase in breast cancer and symptomatic gallstones in patients taking estrogen,3 and uncertainty over how estrogen affects cardiovascular status, most clinicians now avoid estrogen for primary prevention, at least until the WHI reports its estrogen-only trial results.
As long as the risks and benefits are carefully explained, HRT can still be used to treat hot flashes.4 Although HRT does not have a clinically meaningful effect on health-related quality of life, it does reduce moderate to severe vasomotor symptoms.5
For now, the risks of estrogen therapy (in women without a uterus) should be presumed to be at least as serious as those of combined estrogen/progestin therapy. Though challenging, psychiatrists who treat menopause-related hot flashes and mood symptoms need to clearly understand the risks and benefits of estrogen and estrogen/progestin therapy.
Michael Rack MD
Assistant professor of internal medicine and psychiatry
University of Mississippi School of Medicine
Jackson, MS
- Yusuf S, Anand S. Hormone replacement therapy: a time for pause. CMAJ 2002;167:357–9.
- Day A. Lessons from the Women’s Health Initiative: Primary prevention and gender health. CMAJ 2002;167:361–2.
- Gupta G, Aronow WS. Hormone replacement therapy. An analysis of efficacy based on evidence. Geriatrics 2002;57(8):18–20, 23–4.
- Sherman FT. Hormone replacement therapy. The sudden halt of a clinical trial shakes long held beliefs. Geriatrics 2002;57(8):7.
- Hays J, Ockene JK, Brunner RL, et al. Effects of estrogen plus progestin on health-related quality of life. N Engl J Med 2003;348:1839–54.
Dr. Brizendine responds
Dr. Rack is right that the WHI has so far documented dangers of estrogen-progestin but not estrogen alone.
The WHI results clearly indicate that the risks of more than 5 years of estrogen-progestin HRT outweigh the benefits for the average woman. While we still don’t know the risks of estrogen-only therapy, the WHI trial’s estrogen-only arm—scheduled for completion in 2005—will provide valuable information on the safety of estrogen alone for women without a uterus.
It is somewhat comforting that after 7 years, predetermined risk limits have not forced termination of the estrogen-only trial. More than 6,500 women will soon enter their eighth year in the estrogen-only trial. Most physicians now feel they can treat severe hot flashes for up to 5 years with:
- estrogen in women without a uterus
- estrogen-progestin in women with a uterus.
In either case, patients must have no other contraindications to taking estrogen, including breast cancer risk, history of blood clotting, and gallbladder disease.
Women who cannot or will not take estrogen but have severe hot flashes may wish to try a selective serotonin reuptake inhibitor (SSRI) for hot flashes. Based on clinical experience, women with mood symptoms and hot flashes are likely to respond best to an SSRI.
Many women ages 40 to 60 develop mood symptoms during their perimenopause and menopause transitions. Familiarity with use of estrogen and SSRIs in this patient population is critical. Psychiatrists should be able to knowledgeably discuss the risks and benefits of HRT with patients, but HRT prescription is best left up to the patient’s Ob/Gyn or primary practitioner.
Louann Brizendine, MD
Clinical professor of psychiatry
Director, Women’s Mood and Hormone Clinic
University of California-San Francisco Medical School
“Minding menopause” (CURRENT PSYCHIATRY, October 2003) provided an interesting and useful look at how to diagnose and treat menopause-related psychiatric symptoms.
However, Dr. Brizendine’s statement that “…the Women’s Health Initiative (WHI) trial reported that estrogen’s health risks…exceeded potential benefit during 5 years of therapy” requires some clarification.
After a mean of 5.2 years of follow-up, the WHI reported an increased risk of major cardiovascular events, breast cancer, and pulmonary emboli in the trial arm evaluating estrogen plus progestin versus placebo.1 The reduced incidence of hip fractures and colorectal cancers did not outweigh the adverse events. The results of the trial’s estrogen-versus-placebo arm (in women without a uterus) have not yet been reported.
Hormone replacement therapy, or HRT (estrogen plus progestin), is clearly no longer indicated to prevent chronic diseases in healthy postmenopausal women.2 Given the increase in breast cancer and symptomatic gallstones in patients taking estrogen,3 and uncertainty over how estrogen affects cardiovascular status, most clinicians now avoid estrogen for primary prevention, at least until the WHI reports its estrogen-only trial results.
As long as the risks and benefits are carefully explained, HRT can still be used to treat hot flashes.4 Although HRT does not have a clinically meaningful effect on health-related quality of life, it does reduce moderate to severe vasomotor symptoms.5
For now, the risks of estrogen therapy (in women without a uterus) should be presumed to be at least as serious as those of combined estrogen/progestin therapy. Though challenging, psychiatrists who treat menopause-related hot flashes and mood symptoms need to clearly understand the risks and benefits of estrogen and estrogen/progestin therapy.
Michael Rack MD
Assistant professor of internal medicine and psychiatry
University of Mississippi School of Medicine
Jackson, MS
- Yusuf S, Anand S. Hormone replacement therapy: a time for pause. CMAJ 2002;167:357–9.
- Day A. Lessons from the Women’s Health Initiative: Primary prevention and gender health. CMAJ 2002;167:361–2.
- Gupta G, Aronow WS. Hormone replacement therapy. An analysis of efficacy based on evidence. Geriatrics 2002;57(8):18–20, 23–4.
- Sherman FT. Hormone replacement therapy. The sudden halt of a clinical trial shakes long held beliefs. Geriatrics 2002;57(8):7.
- Hays J, Ockene JK, Brunner RL, et al. Effects of estrogen plus progestin on health-related quality of life. N Engl J Med 2003;348:1839–54.
Dr. Brizendine responds
Dr. Rack is right that the WHI has so far documented dangers of estrogen-progestin but not estrogen alone.
The WHI results clearly indicate that the risks of more than 5 years of estrogen-progestin HRT outweigh the benefits for the average woman. While we still don’t know the risks of estrogen-only therapy, the WHI trial’s estrogen-only arm—scheduled for completion in 2005—will provide valuable information on the safety of estrogen alone for women without a uterus.
It is somewhat comforting that after 7 years, predetermined risk limits have not forced termination of the estrogen-only trial. More than 6,500 women will soon enter their eighth year in the estrogen-only trial. Most physicians now feel they can treat severe hot flashes for up to 5 years with:
- estrogen in women without a uterus
- estrogen-progestin in women with a uterus.
In either case, patients must have no other contraindications to taking estrogen, including breast cancer risk, history of blood clotting, and gallbladder disease.
Women who cannot or will not take estrogen but have severe hot flashes may wish to try a selective serotonin reuptake inhibitor (SSRI) for hot flashes. Based on clinical experience, women with mood symptoms and hot flashes are likely to respond best to an SSRI.
Many women ages 40 to 60 develop mood symptoms during their perimenopause and menopause transitions. Familiarity with use of estrogen and SSRIs in this patient population is critical. Psychiatrists should be able to knowledgeably discuss the risks and benefits of HRT with patients, but HRT prescription is best left up to the patient’s Ob/Gyn or primary practitioner.
Louann Brizendine, MD
Clinical professor of psychiatry
Director, Women’s Mood and Hormone Clinic
University of California-San Francisco Medical School