User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

Quick Byte: Take a seat
A survey of 305 inpatients showed that patients who reported that at least one provider sat down while caring for them were more likely to feel that their provider spent appropriate time with them and that their provider kept them well informed. The authors concluded that sitting down at a patient’s bedside improves some aspects of patients’ and families’ experience of their hospital care, and should be included in hospital efforts to improve the patient experience.
Reference
1. Adebusuyi OA et al. Does sitting enhance patient satisfaction in the hospital? [abstract]. J Hosp Med. 2017; 12 (suppl 2). Accessed Aug. 7, 2017.
A survey of 305 inpatients showed that patients who reported that at least one provider sat down while caring for them were more likely to feel that their provider spent appropriate time with them and that their provider kept them well informed. The authors concluded that sitting down at a patient’s bedside improves some aspects of patients’ and families’ experience of their hospital care, and should be included in hospital efforts to improve the patient experience.
Reference
1. Adebusuyi OA et al. Does sitting enhance patient satisfaction in the hospital? [abstract]. J Hosp Med. 2017; 12 (suppl 2). Accessed Aug. 7, 2017.
A survey of 305 inpatients showed that patients who reported that at least one provider sat down while caring for them were more likely to feel that their provider spent appropriate time with them and that their provider kept them well informed. The authors concluded that sitting down at a patient’s bedside improves some aspects of patients’ and families’ experience of their hospital care, and should be included in hospital efforts to improve the patient experience.
Reference
1. Adebusuyi OA et al. Does sitting enhance patient satisfaction in the hospital? [abstract]. J Hosp Med. 2017; 12 (suppl 2). Accessed Aug. 7, 2017.
Using “design thinking” to improve health care
Health care workers creating innovations by applying “design thinking” – “a human-centered approach to innovation” that comes from the business world – is a growing trend, according to a recent New York Times article.
“With design thinking, the innovations come from those who actually work there, providing feedback to designers to improve the final product,” wrote author Amitha Kalaichandran, MD, MHS.
“Health providers ... are uniquely positioned to come up with fresh solutions to health care problems,” Dr. Kalaichandran wrote. An example at her own hospital: The leader of the trauma team now wears an orange vest, clearly identifying who’s in charge in a potentially chaotic situation. It was an idea created by a hospital nurse.
“A 2016 report that looked at ways in which a health system can implement design thinking identified three principles behind the approach: empathy for the user, in this case a patient, doctor or other health care provider; the involvement of an interdisciplinary team; and rapid prototyping of the idea,” she wrote. “To develop a truly useful product, a comprehensive understanding of the problem the innovation aims to solve is paramount.”
In design thinking, described as creative, multidisciplinary thinking around a problem, groups naturally coalesce to find such solutions. The article cites examples such as Clinicians for Design, an international group of providers focused on improving hospital layouts, and Health Design by Us, a collaborative group that supports health care innovations such as a mobile system for diabetes management, designed by a patient.
Reference
Kalaichandran A. Design thinking for doctors and nurses. The New York Times. Aug. 3, 2017. Accessed Aug. 7, 2017.
Health care workers creating innovations by applying “design thinking” – “a human-centered approach to innovation” that comes from the business world – is a growing trend, according to a recent New York Times article.
“With design thinking, the innovations come from those who actually work there, providing feedback to designers to improve the final product,” wrote author Amitha Kalaichandran, MD, MHS.
“Health providers ... are uniquely positioned to come up with fresh solutions to health care problems,” Dr. Kalaichandran wrote. An example at her own hospital: The leader of the trauma team now wears an orange vest, clearly identifying who’s in charge in a potentially chaotic situation. It was an idea created by a hospital nurse.
“A 2016 report that looked at ways in which a health system can implement design thinking identified three principles behind the approach: empathy for the user, in this case a patient, doctor or other health care provider; the involvement of an interdisciplinary team; and rapid prototyping of the idea,” she wrote. “To develop a truly useful product, a comprehensive understanding of the problem the innovation aims to solve is paramount.”
In design thinking, described as creative, multidisciplinary thinking around a problem, groups naturally coalesce to find such solutions. The article cites examples such as Clinicians for Design, an international group of providers focused on improving hospital layouts, and Health Design by Us, a collaborative group that supports health care innovations such as a mobile system for diabetes management, designed by a patient.
Reference
Kalaichandran A. Design thinking for doctors and nurses. The New York Times. Aug. 3, 2017. Accessed Aug. 7, 2017.
Health care workers creating innovations by applying “design thinking” – “a human-centered approach to innovation” that comes from the business world – is a growing trend, according to a recent New York Times article.
“With design thinking, the innovations come from those who actually work there, providing feedback to designers to improve the final product,” wrote author Amitha Kalaichandran, MD, MHS.
“Health providers ... are uniquely positioned to come up with fresh solutions to health care problems,” Dr. Kalaichandran wrote. An example at her own hospital: The leader of the trauma team now wears an orange vest, clearly identifying who’s in charge in a potentially chaotic situation. It was an idea created by a hospital nurse.
“A 2016 report that looked at ways in which a health system can implement design thinking identified three principles behind the approach: empathy for the user, in this case a patient, doctor or other health care provider; the involvement of an interdisciplinary team; and rapid prototyping of the idea,” she wrote. “To develop a truly useful product, a comprehensive understanding of the problem the innovation aims to solve is paramount.”
In design thinking, described as creative, multidisciplinary thinking around a problem, groups naturally coalesce to find such solutions. The article cites examples such as Clinicians for Design, an international group of providers focused on improving hospital layouts, and Health Design by Us, a collaborative group that supports health care innovations such as a mobile system for diabetes management, designed by a patient.
Reference
Kalaichandran A. Design thinking for doctors and nurses. The New York Times. Aug. 3, 2017. Accessed Aug. 7, 2017.
Consider ‘impactibility’ to prevent hospital readmissions
With the goal of reducing 28-day or 30-day readmissions, some health care teams are turning to predictive models to identify patients at high risk for readmission and to efficiently focus resource-intensive prevention strategies. Recently, there’s been a rapid multiplying of these models.
Many of these models do accurately predict readmission risk, according to a recent BMJ editorial. “Among the 14 published models that target all unplanned readmissions (rather than readmissions for specific patient groups), the ‘C statistic’ ranges from 0.55 to 0.80, meaning that, when presented with two patients, these models correctly identify the higher risk individual between 55% and 80% of the time,” the authors wrote.
But, the authors suggested, the real value is not in simply making predictions but in using predictive models in ways that improve outcomes for patients.
“This will require linking predictive models to actionable opportunities for improving care,” they wrote. “Such linkages will most likely be identified through close collaboration between analytical teams, health care practitioners, and patients.” Being at high risk of readmission is not the only consideration; the patient must also be able to benefit from interventions being considered – they must be “impactible.”
“The distinction between predictive risk and impactibility might explain why practitioners tend to identify quite different patients for intervention than predictive risk models,” the authors wrote.
But together, predictive models and clinicians might produce more effective decisions than either does alone. “One of the strengths of predictive models is that they produce objective and consistent judgments regarding readmission risk, whereas clinical judgment can be affected by personal attitudes or attentiveness. Predictive risk models can also be operationalised across whole populations, and might therefore identify needs that would otherwise be missed by clinical teams (e.g., among more socioeconomically deprived neighbourhoods or groups with inadequate primary care). On the other hand, clinicians have access to a much wider range of information regarding patients than predictive risk models, which is essential to judge impactibility.”
The authors conclude, “The predictive modelling enterprise would benefit enormously from such collaboration because the real goal of this activity lies not in predicting the risk of readmission but in identifying patients at risk for preventable readmissions and ‘impactible’ by available interventions.”
Reference
Steventon A et al. Preventing hospital readmissions: The importance of considering ‘impactibility,’ not just predicted risk. BMJ Qual Saf. 2017 Oct;26(10):782-5. Accessed Oct. 9, 2017.
With the goal of reducing 28-day or 30-day readmissions, some health care teams are turning to predictive models to identify patients at high risk for readmission and to efficiently focus resource-intensive prevention strategies. Recently, there’s been a rapid multiplying of these models.
Many of these models do accurately predict readmission risk, according to a recent BMJ editorial. “Among the 14 published models that target all unplanned readmissions (rather than readmissions for specific patient groups), the ‘C statistic’ ranges from 0.55 to 0.80, meaning that, when presented with two patients, these models correctly identify the higher risk individual between 55% and 80% of the time,” the authors wrote.
But, the authors suggested, the real value is not in simply making predictions but in using predictive models in ways that improve outcomes for patients.
“This will require linking predictive models to actionable opportunities for improving care,” they wrote. “Such linkages will most likely be identified through close collaboration between analytical teams, health care practitioners, and patients.” Being at high risk of readmission is not the only consideration; the patient must also be able to benefit from interventions being considered – they must be “impactible.”
“The distinction between predictive risk and impactibility might explain why practitioners tend to identify quite different patients for intervention than predictive risk models,” the authors wrote.
But together, predictive models and clinicians might produce more effective decisions than either does alone. “One of the strengths of predictive models is that they produce objective and consistent judgments regarding readmission risk, whereas clinical judgment can be affected by personal attitudes or attentiveness. Predictive risk models can also be operationalised across whole populations, and might therefore identify needs that would otherwise be missed by clinical teams (e.g., among more socioeconomically deprived neighbourhoods or groups with inadequate primary care). On the other hand, clinicians have access to a much wider range of information regarding patients than predictive risk models, which is essential to judge impactibility.”
The authors conclude, “The predictive modelling enterprise would benefit enormously from such collaboration because the real goal of this activity lies not in predicting the risk of readmission but in identifying patients at risk for preventable readmissions and ‘impactible’ by available interventions.”
Reference
Steventon A et al. Preventing hospital readmissions: The importance of considering ‘impactibility,’ not just predicted risk. BMJ Qual Saf. 2017 Oct;26(10):782-5. Accessed Oct. 9, 2017.
With the goal of reducing 28-day or 30-day readmissions, some health care teams are turning to predictive models to identify patients at high risk for readmission and to efficiently focus resource-intensive prevention strategies. Recently, there’s been a rapid multiplying of these models.
Many of these models do accurately predict readmission risk, according to a recent BMJ editorial. “Among the 14 published models that target all unplanned readmissions (rather than readmissions for specific patient groups), the ‘C statistic’ ranges from 0.55 to 0.80, meaning that, when presented with two patients, these models correctly identify the higher risk individual between 55% and 80% of the time,” the authors wrote.
But, the authors suggested, the real value is not in simply making predictions but in using predictive models in ways that improve outcomes for patients.
“This will require linking predictive models to actionable opportunities for improving care,” they wrote. “Such linkages will most likely be identified through close collaboration between analytical teams, health care practitioners, and patients.” Being at high risk of readmission is not the only consideration; the patient must also be able to benefit from interventions being considered – they must be “impactible.”
“The distinction between predictive risk and impactibility might explain why practitioners tend to identify quite different patients for intervention than predictive risk models,” the authors wrote.
But together, predictive models and clinicians might produce more effective decisions than either does alone. “One of the strengths of predictive models is that they produce objective and consistent judgments regarding readmission risk, whereas clinical judgment can be affected by personal attitudes or attentiveness. Predictive risk models can also be operationalised across whole populations, and might therefore identify needs that would otherwise be missed by clinical teams (e.g., among more socioeconomically deprived neighbourhoods or groups with inadequate primary care). On the other hand, clinicians have access to a much wider range of information regarding patients than predictive risk models, which is essential to judge impactibility.”
The authors conclude, “The predictive modelling enterprise would benefit enormously from such collaboration because the real goal of this activity lies not in predicting the risk of readmission but in identifying patients at risk for preventable readmissions and ‘impactible’ by available interventions.”
Reference
Steventon A et al. Preventing hospital readmissions: The importance of considering ‘impactibility,’ not just predicted risk. BMJ Qual Saf. 2017 Oct;26(10):782-5. Accessed Oct. 9, 2017.
Guideline preview: ASH to recommend against VTE prophylaxis for lower-risk cancer patients
ATLANTA – An expert panel convened by the American Society of Hematology will recommend against routine venous thromboembolism (VTE) prophylaxis with low-molecular-weight heparin, except in patients deemed high risk, the panel chair told attendees at the group’s annual meeting.
The recommendations will be posted for public comment in early 2018 and are expected to be finalized and published later in the year.
The panel found strong evidence to recommend against prophylaxis in cancer patients at low risk of VTE, said Gary H. Lyman, MD, of the Fred Hutchinson Cancer Research Center and the University of Washington, both in Seattle.
For cancer patients at high risk of VTE, the panel will make a conditional recommendation – based on weaker evidence – in favor of low-molecular-weight thromboprophylaxis (LMWH) “with a caveat that patients should have no major bleeding risk or other contraindication to anticoagulation,” Dr. Lyman said.
The panel also found weaker evidence to support a conditional recommendation against routine prophylaxis in patients at intermediate risk of VTE, based on results from a systematic review.
These recommendations, which were described during a special education session at the annual meeting of the American Society of Hematology, are just one piece of a larger effort by ASH to develop evidence-based guidelines on VTE management. More than 100 thrombosis experts have reviewed evidence and drafted more than 200 recommendations on diagnosis, prevention, and treatment of VTE, according to ASH.
The cancer-specific recommendations described by Dr. Lyman are based in part on a meta-analysis of 17 randomized controlled trials of cancer patients receiving LMWH thromboprophylaxis that were published between 2008 and 2017. Across cancer types and settings, LMWH prophylaxis in these trials was associated with a reduced risk of VTE and an increased risk of bleeding, Dr. Lyman said.
For all cancer types, relative risk (RR) of VTE was 0.55 (95% confidence interval, 0.46-0.65), with an absolute risk reduction of just 2.7% “because of the low baseline risk of VTE in this setting,” Dr. Lyman said.
However, the baseline risk increased for certain cancer types, including lung cancer, which had a similar relative risk of 0.53 (95% CI, 0.41-0.69) but an absolute risk reduction of 4.3%, according to data Dr. Lyman presented. Likewise, pancreatic cancer was associated with a relative risk of 0.43 (95% CI, 0.25-0.73) but an absolute risk reduction of 10.1%.
Major bleeding across all trials was significantly increased (RR 1.40; 95% CI, 1.01-1.92), but the presented data show that, in absolute terms, the increase was just 0.7% overall and similarly, 0.7% and 0.9% for lung and pancreatic cancer, respectively.
However, VTE risk depends on more than the site of the cancer, Dr. Lyman noted. In their deliberations, the panel considered the validated Khorana Risk Score, which incorporates factors such as body mass index, platelet count, leukocyte count, and hemoglobin level.
Specific analysis of high-risk patients suggested a pronounced risk reduction associated with LMWH prophylaxis, according to Dr. Lyman, who noted that a patient-level analysis including nearly 8,000 patients from 13 randomized, controlled trials showed a relative risk of 0.58, with VTE events seen in 4.0% patients in the LMWH group versus 7.0% of controls.
The forthcoming ASH guidelines also will address other aspects of cancer-associated VTE, according to Dr. Lyman, including initial treatment, secondary prophylaxis, perioperative prophylaxis, and prophylaxis or treatment in patients with a central venous catheter.
“The risk of venous thromboembolism in patients with cancer is well recognized, and that risk is especially notable in patients receiving cancer treatment,” Dr. Lyman said.
Dr. Lyman reported having no relevant financial disclosures.
ATLANTA – An expert panel convened by the American Society of Hematology will recommend against routine venous thromboembolism (VTE) prophylaxis with low-molecular-weight heparin, except in patients deemed high risk, the panel chair told attendees at the group’s annual meeting.
The recommendations will be posted for public comment in early 2018 and are expected to be finalized and published later in the year.
The panel found strong evidence to recommend against prophylaxis in cancer patients at low risk of VTE, said Gary H. Lyman, MD, of the Fred Hutchinson Cancer Research Center and the University of Washington, both in Seattle.
For cancer patients at high risk of VTE, the panel will make a conditional recommendation – based on weaker evidence – in favor of low-molecular-weight thromboprophylaxis (LMWH) “with a caveat that patients should have no major bleeding risk or other contraindication to anticoagulation,” Dr. Lyman said.
The panel also found weaker evidence to support a conditional recommendation against routine prophylaxis in patients at intermediate risk of VTE, based on results from a systematic review.
These recommendations, which were described during a special education session at the annual meeting of the American Society of Hematology, are just one piece of a larger effort by ASH to develop evidence-based guidelines on VTE management. More than 100 thrombosis experts have reviewed evidence and drafted more than 200 recommendations on diagnosis, prevention, and treatment of VTE, according to ASH.
The cancer-specific recommendations described by Dr. Lyman are based in part on a meta-analysis of 17 randomized controlled trials of cancer patients receiving LMWH thromboprophylaxis that were published between 2008 and 2017. Across cancer types and settings, LMWH prophylaxis in these trials was associated with a reduced risk of VTE and an increased risk of bleeding, Dr. Lyman said.
For all cancer types, relative risk (RR) of VTE was 0.55 (95% confidence interval, 0.46-0.65), with an absolute risk reduction of just 2.7% “because of the low baseline risk of VTE in this setting,” Dr. Lyman said.
However, the baseline risk increased for certain cancer types, including lung cancer, which had a similar relative risk of 0.53 (95% CI, 0.41-0.69) but an absolute risk reduction of 4.3%, according to data Dr. Lyman presented. Likewise, pancreatic cancer was associated with a relative risk of 0.43 (95% CI, 0.25-0.73) but an absolute risk reduction of 10.1%.
Major bleeding across all trials was significantly increased (RR 1.40; 95% CI, 1.01-1.92), but the presented data show that, in absolute terms, the increase was just 0.7% overall and similarly, 0.7% and 0.9% for lung and pancreatic cancer, respectively.
However, VTE risk depends on more than the site of the cancer, Dr. Lyman noted. In their deliberations, the panel considered the validated Khorana Risk Score, which incorporates factors such as body mass index, platelet count, leukocyte count, and hemoglobin level.
Specific analysis of high-risk patients suggested a pronounced risk reduction associated with LMWH prophylaxis, according to Dr. Lyman, who noted that a patient-level analysis including nearly 8,000 patients from 13 randomized, controlled trials showed a relative risk of 0.58, with VTE events seen in 4.0% patients in the LMWH group versus 7.0% of controls.
The forthcoming ASH guidelines also will address other aspects of cancer-associated VTE, according to Dr. Lyman, including initial treatment, secondary prophylaxis, perioperative prophylaxis, and prophylaxis or treatment in patients with a central venous catheter.
“The risk of venous thromboembolism in patients with cancer is well recognized, and that risk is especially notable in patients receiving cancer treatment,” Dr. Lyman said.
Dr. Lyman reported having no relevant financial disclosures.
ATLANTA – An expert panel convened by the American Society of Hematology will recommend against routine venous thromboembolism (VTE) prophylaxis with low-molecular-weight heparin, except in patients deemed high risk, the panel chair told attendees at the group’s annual meeting.
The recommendations will be posted for public comment in early 2018 and are expected to be finalized and published later in the year.
The panel found strong evidence to recommend against prophylaxis in cancer patients at low risk of VTE, said Gary H. Lyman, MD, of the Fred Hutchinson Cancer Research Center and the University of Washington, both in Seattle.
For cancer patients at high risk of VTE, the panel will make a conditional recommendation – based on weaker evidence – in favor of low-molecular-weight thromboprophylaxis (LMWH) “with a caveat that patients should have no major bleeding risk or other contraindication to anticoagulation,” Dr. Lyman said.
The panel also found weaker evidence to support a conditional recommendation against routine prophylaxis in patients at intermediate risk of VTE, based on results from a systematic review.
These recommendations, which were described during a special education session at the annual meeting of the American Society of Hematology, are just one piece of a larger effort by ASH to develop evidence-based guidelines on VTE management. More than 100 thrombosis experts have reviewed evidence and drafted more than 200 recommendations on diagnosis, prevention, and treatment of VTE, according to ASH.
The cancer-specific recommendations described by Dr. Lyman are based in part on a meta-analysis of 17 randomized controlled trials of cancer patients receiving LMWH thromboprophylaxis that were published between 2008 and 2017. Across cancer types and settings, LMWH prophylaxis in these trials was associated with a reduced risk of VTE and an increased risk of bleeding, Dr. Lyman said.
For all cancer types, relative risk (RR) of VTE was 0.55 (95% confidence interval, 0.46-0.65), with an absolute risk reduction of just 2.7% “because of the low baseline risk of VTE in this setting,” Dr. Lyman said.
However, the baseline risk increased for certain cancer types, including lung cancer, which had a similar relative risk of 0.53 (95% CI, 0.41-0.69) but an absolute risk reduction of 4.3%, according to data Dr. Lyman presented. Likewise, pancreatic cancer was associated with a relative risk of 0.43 (95% CI, 0.25-0.73) but an absolute risk reduction of 10.1%.
Major bleeding across all trials was significantly increased (RR 1.40; 95% CI, 1.01-1.92), but the presented data show that, in absolute terms, the increase was just 0.7% overall and similarly, 0.7% and 0.9% for lung and pancreatic cancer, respectively.
However, VTE risk depends on more than the site of the cancer, Dr. Lyman noted. In their deliberations, the panel considered the validated Khorana Risk Score, which incorporates factors such as body mass index, platelet count, leukocyte count, and hemoglobin level.
Specific analysis of high-risk patients suggested a pronounced risk reduction associated with LMWH prophylaxis, according to Dr. Lyman, who noted that a patient-level analysis including nearly 8,000 patients from 13 randomized, controlled trials showed a relative risk of 0.58, with VTE events seen in 4.0% patients in the LMWH group versus 7.0% of controls.
The forthcoming ASH guidelines also will address other aspects of cancer-associated VTE, according to Dr. Lyman, including initial treatment, secondary prophylaxis, perioperative prophylaxis, and prophylaxis or treatment in patients with a central venous catheter.
“The risk of venous thromboembolism in patients with cancer is well recognized, and that risk is especially notable in patients receiving cancer treatment,” Dr. Lyman said.
Dr. Lyman reported having no relevant financial disclosures.
REPORTING FROM ASH 2017
Acute kidney injury linked with doubled inpatient VTEs
TORONTO – Hospitalized patients with acute kidney injury had more than double the inpatient rate of venous thromboembolism as had patients without acute kidney injury in a prospective, observational study of more than 6,000 hospitalized U.S. soldiers.

He offered four possible mechanisms to explain a link between AKI and VTE:
- Patients with AKI are in a hypercoagulable state.
- AKI alters the pharmacodynamics or pharmacokinetics of VTE prophylactic treatments.
- AKI is a marker of an illness that causes VTE.
- VTE leads to an increased rate of AKI rather than the other way around.
Dr. McMahon’s analysis also revealed that two other clinical conditions that are generally believed to raise VTE risk – obesity and impaired overall renal function identified with stagnant measures – did not correspond with a significantly elevated VTE rate in this study.
The data came from 6,552 adults hospitalized for at least 2 days at Walter Reed between September 2009 and March 2011. The study excluded patients with VTE at the time of admission and also those who had been treated with an anticoagulant at the time of admission. The patients averaged 55 years of age and were hospitalized for a median of 4 days. About 22% of patients received VTE prophylaxis with unfractionated heparin, about 41% received prophylaxis with low-molecular-weight heparin, and about 39% received no VTE prophylaxis (percentages total 102% because of rounding).
About 16% of the patients had been diagnosed with AKI at the time of admission, and an additional 8% developed AKI while hospitalized, defined as an increase in serum creatinine during hospitalization of at least 50% above baseline levels or an increase of more than 0.3 mg/dL above the level at time of admission. During hospitalization, 160 patients (2%) developed a new onset VTE.
In an analysis that adjusted for baseline differences in type of surgery, body mass index, sex, age, and prior hospitalizations during the prior 90 days, the results showed that patients with preexisting or new onset AKI had a 2.2-fold higher rate of VTE, compared with patients without AKI, and this difference was statistically significant, Dr. McMahon reported.
The analysis also showed a significant 62% relatively higher rate of VTE among soldiers hospitalized for a deployment-related event, as well as a significant 63% relatively lower VTE rate among patients not receiving medical prophylaxis, compared with patients receiving an anticoagulant. Dr. McMahon suggested that this lower rate of VTEs among patients not on prophylaxis reflected success in identifying which patients had an increased risk for VTE and hence received prophylaxis.
[email protected]
On Twitter @mitchelzoler
TORONTO – Hospitalized patients with acute kidney injury had more than double the inpatient rate of venous thromboembolism as had patients without acute kidney injury in a prospective, observational study of more than 6,000 hospitalized U.S. soldiers.
He offered four possible mechanisms to explain a link between AKI and VTE:
- Patients with AKI are in a hypercoagulable state.
- AKI alters the pharmacodynamics or pharmacokinetics of VTE prophylactic treatments.
- AKI is a marker of an illness that causes VTE.
- VTE leads to an increased rate of AKI rather than the other way around.
Dr. McMahon’s analysis also revealed that two other clinical conditions that are generally believed to raise VTE risk – obesity and impaired overall renal function identified with stagnant measures – did not correspond with a significantly elevated VTE rate in this study.
The data came from 6,552 adults hospitalized for at least 2 days at Walter Reed between September 2009 and March 2011. The study excluded patients with VTE at the time of admission and also those who had been treated with an anticoagulant at the time of admission. The patients averaged 55 years of age and were hospitalized for a median of 4 days. About 22% of patients received VTE prophylaxis with unfractionated heparin, about 41% received prophylaxis with low-molecular-weight heparin, and about 39% received no VTE prophylaxis (percentages total 102% because of rounding).
About 16% of the patients had been diagnosed with AKI at the time of admission, and an additional 8% developed AKI while hospitalized, defined as an increase in serum creatinine during hospitalization of at least 50% above baseline levels or an increase of more than 0.3 mg/dL above the level at time of admission. During hospitalization, 160 patients (2%) developed a new onset VTE.
In an analysis that adjusted for baseline differences in type of surgery, body mass index, sex, age, and prior hospitalizations during the prior 90 days, the results showed that patients with preexisting or new onset AKI had a 2.2-fold higher rate of VTE, compared with patients without AKI, and this difference was statistically significant, Dr. McMahon reported.
The analysis also showed a significant 62% relatively higher rate of VTE among soldiers hospitalized for a deployment-related event, as well as a significant 63% relatively lower VTE rate among patients not receiving medical prophylaxis, compared with patients receiving an anticoagulant. Dr. McMahon suggested that this lower rate of VTEs among patients not on prophylaxis reflected success in identifying which patients had an increased risk for VTE and hence received prophylaxis.
[email protected]
On Twitter @mitchelzoler
TORONTO – Hospitalized patients with acute kidney injury had more than double the inpatient rate of venous thromboembolism as had patients without acute kidney injury in a prospective, observational study of more than 6,000 hospitalized U.S. soldiers.
He offered four possible mechanisms to explain a link between AKI and VTE:
- Patients with AKI are in a hypercoagulable state.
- AKI alters the pharmacodynamics or pharmacokinetics of VTE prophylactic treatments.
- AKI is a marker of an illness that causes VTE.
- VTE leads to an increased rate of AKI rather than the other way around.
Dr. McMahon’s analysis also revealed that two other clinical conditions that are generally believed to raise VTE risk – obesity and impaired overall renal function identified with stagnant measures – did not correspond with a significantly elevated VTE rate in this study.
The data came from 6,552 adults hospitalized for at least 2 days at Walter Reed between September 2009 and March 2011. The study excluded patients with VTE at the time of admission and also those who had been treated with an anticoagulant at the time of admission. The patients averaged 55 years of age and were hospitalized for a median of 4 days. About 22% of patients received VTE prophylaxis with unfractionated heparin, about 41% received prophylaxis with low-molecular-weight heparin, and about 39% received no VTE prophylaxis (percentages total 102% because of rounding).
About 16% of the patients had been diagnosed with AKI at the time of admission, and an additional 8% developed AKI while hospitalized, defined as an increase in serum creatinine during hospitalization of at least 50% above baseline levels or an increase of more than 0.3 mg/dL above the level at time of admission. During hospitalization, 160 patients (2%) developed a new onset VTE.
In an analysis that adjusted for baseline differences in type of surgery, body mass index, sex, age, and prior hospitalizations during the prior 90 days, the results showed that patients with preexisting or new onset AKI had a 2.2-fold higher rate of VTE, compared with patients without AKI, and this difference was statistically significant, Dr. McMahon reported.
The analysis also showed a significant 62% relatively higher rate of VTE among soldiers hospitalized for a deployment-related event, as well as a significant 63% relatively lower VTE rate among patients not receiving medical prophylaxis, compared with patients receiving an anticoagulant. Dr. McMahon suggested that this lower rate of VTEs among patients not on prophylaxis reflected success in identifying which patients had an increased risk for VTE and hence received prophylaxis.
[email protected]
On Twitter @mitchelzoler
AT CHEST 2017
Key clinical point:
Major finding: Inpatients with AKI had an adjusted 2.2-fold higher rate of VTE, compared with other inpatients.
Data source: Prospective, observational data from 6,552 inpatients at a single U.S. military hospital.
Disclosures: Dr. McMahon had no disclosures.
Expanded hospital testing improves respiratory pathogen detection
SAN DIEGO – Systematic testing of acute respiratory illness patients can increase the likelihood of finding relevant pathogens, according to a study presented at an annual scientific meeting on infectious diseases.
Currently, hospitals conduct either nonroutine assessments or rely heavily on clinical laboratory testing among severe acute respiratory illness patients, which can lead to missing clinically key viruses.
Systematic testing expands on tests ordered and carried out at hospitals, expanding on them by testing for influenza, respiratory syncytial virus (RSV), human metapneumovirus, rhinovirus and enterovirus, adenovirus, coronavirus, and parainfluenza viruses 1-4. To test the efficacy of systematic testing, investigators studied 2,216 severe acute respiratory illness patients hospitalized in one of three hospitals in Minnesota during September 2015-August 2016. Patients were predominantly younger than 5 years old (57%) and had one or more chronic medical condition (63%).
Detection of at least one virus increased from 1,062 patients (48%) to 1,600 patients (72%) when comparing clinically ordered tests against expanded, systematic RT-PCR testing conducted through the Minnesota Health Department (MDH).
By patient age, viral detection increased by 27%, 24%, 18%, and 21% for patients aged younger than 5 years, 5-17 years, 18-64 years, and 65 years and older, respectively. Except for influenza viruses and RSV, the proportions of viruses identified, regardless of age, were all lower in hospital testing, compared with MDH testing.
“RSV targeting was almost systematic among children less than 5 years, but [accounted for] only 28% of RSV detection,” said Dr. Steffen in her presentation. “A smaller proportion of other respiratory viruses, including the human metapneumovirus, were detected at the hospital, and this was especially true for adults.”
Patients with rhinovirus and enterovirus saw a difference between hospital and expanded testing, increasing from a little over 300 patients detected, to nearly 800 patients.
“Patients admitted to the ICU were less likely to have a pathogen detection than those not admitted to the ICU, and those with one or more chronic medical condition had lower viral detection than those without,” Dr. Steffens said. “While testing at MDH did increase the percent of patients in each category, trends remained consistent and significant.”
Since testing information was only collected for patients with positive test results at the hospital, investigators were not able to compare testing practices between patients with and without viruses. This study may also have underrepresented pathogens detected through means other than the hospital laboratory, like rapid tests in emergency departments. The study was also limited by the short time frame of only 1 year.
The presenters reported no relevant financial disclosures.
SOURCE: Steffens A et al. Abstract 885.
SAN DIEGO – Systematic testing of acute respiratory illness patients can increase the likelihood of finding relevant pathogens, according to a study presented at an annual scientific meeting on infectious diseases.
Currently, hospitals conduct either nonroutine assessments or rely heavily on clinical laboratory testing among severe acute respiratory illness patients, which can lead to missing clinically key viruses.
Systematic testing expands on tests ordered and carried out at hospitals, expanding on them by testing for influenza, respiratory syncytial virus (RSV), human metapneumovirus, rhinovirus and enterovirus, adenovirus, coronavirus, and parainfluenza viruses 1-4. To test the efficacy of systematic testing, investigators studied 2,216 severe acute respiratory illness patients hospitalized in one of three hospitals in Minnesota during September 2015-August 2016. Patients were predominantly younger than 5 years old (57%) and had one or more chronic medical condition (63%).
Detection of at least one virus increased from 1,062 patients (48%) to 1,600 patients (72%) when comparing clinically ordered tests against expanded, systematic RT-PCR testing conducted through the Minnesota Health Department (MDH).
By patient age, viral detection increased by 27%, 24%, 18%, and 21% for patients aged younger than 5 years, 5-17 years, 18-64 years, and 65 years and older, respectively. Except for influenza viruses and RSV, the proportions of viruses identified, regardless of age, were all lower in hospital testing, compared with MDH testing.
“RSV targeting was almost systematic among children less than 5 years, but [accounted for] only 28% of RSV detection,” said Dr. Steffen in her presentation. “A smaller proportion of other respiratory viruses, including the human metapneumovirus, were detected at the hospital, and this was especially true for adults.”
Patients with rhinovirus and enterovirus saw a difference between hospital and expanded testing, increasing from a little over 300 patients detected, to nearly 800 patients.
“Patients admitted to the ICU were less likely to have a pathogen detection than those not admitted to the ICU, and those with one or more chronic medical condition had lower viral detection than those without,” Dr. Steffens said. “While testing at MDH did increase the percent of patients in each category, trends remained consistent and significant.”
Since testing information was only collected for patients with positive test results at the hospital, investigators were not able to compare testing practices between patients with and without viruses. This study may also have underrepresented pathogens detected through means other than the hospital laboratory, like rapid tests in emergency departments. The study was also limited by the short time frame of only 1 year.
The presenters reported no relevant financial disclosures.
SOURCE: Steffens A et al. Abstract 885.
SAN DIEGO – Systematic testing of acute respiratory illness patients can increase the likelihood of finding relevant pathogens, according to a study presented at an annual scientific meeting on infectious diseases.
Currently, hospitals conduct either nonroutine assessments or rely heavily on clinical laboratory testing among severe acute respiratory illness patients, which can lead to missing clinically key viruses.
Systematic testing expands on tests ordered and carried out at hospitals, expanding on them by testing for influenza, respiratory syncytial virus (RSV), human metapneumovirus, rhinovirus and enterovirus, adenovirus, coronavirus, and parainfluenza viruses 1-4. To test the efficacy of systematic testing, investigators studied 2,216 severe acute respiratory illness patients hospitalized in one of three hospitals in Minnesota during September 2015-August 2016. Patients were predominantly younger than 5 years old (57%) and had one or more chronic medical condition (63%).
Detection of at least one virus increased from 1,062 patients (48%) to 1,600 patients (72%) when comparing clinically ordered tests against expanded, systematic RT-PCR testing conducted through the Minnesota Health Department (MDH).
By patient age, viral detection increased by 27%, 24%, 18%, and 21% for patients aged younger than 5 years, 5-17 years, 18-64 years, and 65 years and older, respectively. Except for influenza viruses and RSV, the proportions of viruses identified, regardless of age, were all lower in hospital testing, compared with MDH testing.
“RSV targeting was almost systematic among children less than 5 years, but [accounted for] only 28% of RSV detection,” said Dr. Steffen in her presentation. “A smaller proportion of other respiratory viruses, including the human metapneumovirus, were detected at the hospital, and this was especially true for adults.”
Patients with rhinovirus and enterovirus saw a difference between hospital and expanded testing, increasing from a little over 300 patients detected, to nearly 800 patients.
“Patients admitted to the ICU were less likely to have a pathogen detection than those not admitted to the ICU, and those with one or more chronic medical condition had lower viral detection than those without,” Dr. Steffens said. “While testing at MDH did increase the percent of patients in each category, trends remained consistent and significant.”
Since testing information was only collected for patients with positive test results at the hospital, investigators were not able to compare testing practices between patients with and without viruses. This study may also have underrepresented pathogens detected through means other than the hospital laboratory, like rapid tests in emergency departments. The study was also limited by the short time frame of only 1 year.
The presenters reported no relevant financial disclosures.
SOURCE: Steffens A et al. Abstract 885.
REPORTING FROM ID WEEK 2017
Key clinical point:
Major finding: Among 2,216 patients studied, 1,600 (72%) were found to have at least one respiratory virus through expanded testing, compared with 1,062 (48%) patients tested through clincian-directed testing.
Study details: 2,351 severe acute respiratory illness patients hospitalized in one of three hospitals in Minnesota.
Disclosures: The presenter reported no relevant financial disclosures.
Source: Steffens A et al. Abstract 885.
New curriculum teaches value-based health care
While value has become an imperative in both training and health care delivery, few tools exist to teach hospitalists and other providers the basic concepts of value.
“Hospitalists are on the front lines of health care value delivery, and it is critical that we understand and embrace the concepts of value; however, we also need to be able to deliver upon these ideals,” said Christopher Moriates, MD, assistant dean for health care value at the University of Texas at Austin.

“As a hospitalist, I ensured that the content would be specifically applicable to our day-to-day world and experience,” Dr. Moriates said. “Using the modules, hospitalists can better understand how emerging tools, such as the University of Utah’s Value-Drive Outcome tool, can be used by hospitalists to improve value. The modules also dig into thorny subjects like understanding health care costs – for example, what really is the difference between costs and charges?”
The course is adaptive and interactive, using the latest in instructional technology, he said. Hospitalists can take the course independently and earn free CME credits; those who complete all three modules in this first collection will receive a certificate of completion and CME credit.
The goal is to release 10 modules over the course of this academic year, Dr. Moriates said. Future collections will cover “value-based health care delivery,” “how to deliver high-value care at the bedside,” and “how to deliver high-value care in systems.”
“As value-based health care is increasingly taught in medical schools and residency training, it is important for hospitalists – especially any of us that work with trainees – to be able to speak the same language and understand what our trainees now will know,” he said.
While value has become an imperative in both training and health care delivery, few tools exist to teach hospitalists and other providers the basic concepts of value.
“Hospitalists are on the front lines of health care value delivery, and it is critical that we understand and embrace the concepts of value; however, we also need to be able to deliver upon these ideals,” said Christopher Moriates, MD, assistant dean for health care value at the University of Texas at Austin.
“As a hospitalist, I ensured that the content would be specifically applicable to our day-to-day world and experience,” Dr. Moriates said. “Using the modules, hospitalists can better understand how emerging tools, such as the University of Utah’s Value-Drive Outcome tool, can be used by hospitalists to improve value. The modules also dig into thorny subjects like understanding health care costs – for example, what really is the difference between costs and charges?”
The course is adaptive and interactive, using the latest in instructional technology, he said. Hospitalists can take the course independently and earn free CME credits; those who complete all three modules in this first collection will receive a certificate of completion and CME credit.
The goal is to release 10 modules over the course of this academic year, Dr. Moriates said. Future collections will cover “value-based health care delivery,” “how to deliver high-value care at the bedside,” and “how to deliver high-value care in systems.”
“As value-based health care is increasingly taught in medical schools and residency training, it is important for hospitalists – especially any of us that work with trainees – to be able to speak the same language and understand what our trainees now will know,” he said.
While value has become an imperative in both training and health care delivery, few tools exist to teach hospitalists and other providers the basic concepts of value.
“Hospitalists are on the front lines of health care value delivery, and it is critical that we understand and embrace the concepts of value; however, we also need to be able to deliver upon these ideals,” said Christopher Moriates, MD, assistant dean for health care value at the University of Texas at Austin.
“As a hospitalist, I ensured that the content would be specifically applicable to our day-to-day world and experience,” Dr. Moriates said. “Using the modules, hospitalists can better understand how emerging tools, such as the University of Utah’s Value-Drive Outcome tool, can be used by hospitalists to improve value. The modules also dig into thorny subjects like understanding health care costs – for example, what really is the difference between costs and charges?”
The course is adaptive and interactive, using the latest in instructional technology, he said. Hospitalists can take the course independently and earn free CME credits; those who complete all three modules in this first collection will receive a certificate of completion and CME credit.
The goal is to release 10 modules over the course of this academic year, Dr. Moriates said. Future collections will cover “value-based health care delivery,” “how to deliver high-value care at the bedside,” and “how to deliver high-value care in systems.”
“As value-based health care is increasingly taught in medical schools and residency training, it is important for hospitalists – especially any of us that work with trainees – to be able to speak the same language and understand what our trainees now will know,” he said.
Managing mental health care at the hospital
The numbers tell a grim story. Nationwide, 43.7 million adult Americans experienced a mental health condition during 2016 – an increase of 1.2 million over the previous year. Mental health issues send almost 5.5 million people to emergency departments each year; nearly 60% of adults with a mental illness received no treatment at all.
If that massive – and growing – need is one side of the story, shrinking resources are the other. Mental health resources had already been diminishing for decades before the recession hit – and hit them especially hard. Between 2009 and 2012, states cut $5 billion in mental health services; during that time, at least 4,500 public psychiatric hospital beds nationwide disappeared – nearly 10% of the total supply. The bulk of those resources have never been restored.
Provider numbers also are falling. “Psychiatry is probably the top manpower shortage among all specialties,” said Joe Parks, MD, medical director of the National Council for Behavioral Health. “We have about a third the number of psychiatrists that most estimates say we need, and the number per capita is decreasing.” A significant percentage of psychiatrists – more than 50% – only accept cash, bypassing the low reimbursement rates even private insurance typically offers.

Hospitals, of course, feel those financial disincentives too, which discourage them from investments of their own. “It’s a difficult population to manage, and it’s difficult to manage the financial realities of mental health as well,” said John McHugh, PhD, assistant professor of health policy at Columbia University, New York. “If you were a hospital administrator looking to invest your last dollar and you have the option of investing it in a new heart institute or in behavioral health service, more likely than not, you’re going to invest it in the more profitable cardiovascular service line.”

Providers of last resort
But much of the burden of caring for this population ends up falling on hospitals by default. At Denver Health, Melanie Rylander, MD, medical director of the inpatient psychiatric unit, reports seeing this manifest in three categories of patients. First, there is an influx of people coming into the emergency department with primary mental health issues.
“We’re also seeing an influx of people coming in with physical problems, and upon assessment it becomes very clear very quickly that the real issue is an underlying mental health issue,” she said. Then there are the people coming in for the same physical problems over and over – maybe decompensated heart failure or COPD exacerbations – because mental health issues are impeding their ability to take care of themselves.
Some hospitalists say they feel ill equipped to care for these patients. “We don’t have the facility or the resources many times to properly care for their psychiatric needs when they’re in the hospital. It’s not really part of an internist’s training to be familiar with a lot of the medications,” said Atashi Mandal, MD, a hospitalist and pediatrician in Los Angeles. “Sometimes they get improperly medicated because we don’t know what else to do and the patient’s behavioral issues are escalating, so it’s really a difficult position.”
It’s a dispiriting experience for a hospitalist. “It really bothers me when I am trying to care for a patient who has psychiatric needs, and I feel I’m not able to do it, and I can’t find resources, and I feel that this patient’s needs are being neglected – not because we don’t care, and not because of a lack of effort by the staff. It’s just set up to fail,” Dr. Mandal said.
Ending the silo mentality
Encouraging a more holistic view of health across health care would be an important step to begin to address the problem – after all, the mind and the body are not separate.
“We work in silos, and we really have to stop doing that because these are intertwined,” said Corey Karlin-Zysman, MD, FHM, FACP, chief of the division of hospital medicine at Northwell Health. “A schizophrenic will become worse when they’re medically ill. That illness will be harder to treat if their psychiatric illness is active.” This is starting to happen in the outpatient setting, evidenced by the expansion of the integrated care model, where a primary care doctor is the lead physician working in combination with psychologists, psychiatrists, and social workers. Communication among providers becomes simpler, and patients don’t fall through the cracks as often while trying to navigate the system.

That idea of integration is also making its way into the hospital setting in various ways. In their efforts to bring the care to the patient, rather than the other way around, Dr. Karlin-Zysman’s hospital embedded two hospitalists in the neighboring inpatient psychiatric hospital; when patients need medical treatment, they can receive it without interrupting their behavioral health treatment. As a result, patients who used to end up in their emergency department don’t anymore, and their 30-day readmission rate has fallen by 50%.
But at its foundation, care integration is more of an attitude than a system; it begins with a mindset.
“We talk so much today about system reform, integrated systems, blah, blah,” said Lisa Rosenbaum, MD, a cardiologist at Brigham and Women’s Hospital, Boston. “I don’t want to make it seem like it’s not going to work, but what does it mean for the patient who is psychotic and has 10 problems, with whom you have 15 minutes? Taking good care of these patients means you have to take a deep breath and put in a lot of time and deal with all these things that have nothing to do with the health system under which you practice. There’s this ‘only so much you can do’ feeling that is a problem in itself, because there’s actually a lot we can do.”
Hospitals and communities
It’s axiomatic to say that a better approach to mental health would be based around prevention and early intervention, rather than the less crisis-oriented system we have now. Some efforts are being made in that direction, and they involve, and require, outreach outside the hospital.
“The best hospitals doing work in mental health are going beyond the hospital walls; they’re really looking at their community,” Dr. Nguyen said. “You have hospitals, like Accountable Care Organizations, who are trying to move earlier and think about mental health from a pediatric standpoint: How can we support parents and children during critical phases of brain growth? How can we provide prevention services?” Ultimately, those efforts should help lower future admission rates to EDs and hospitals.
That forward-looking approach may be necessary, but it’s also a challenge. “As a hospital administrator, I would think that you look out at the community and see this problem is not going away – in fact, it is likely going to get worse,” Dr. McHugh said. “A health system may look at themselves and say we have to take the lead on this.” The difficulty is that thinking of it in a sense of value to the community, and making the requisite investments, will have a very long period of payout; a health system that’s struggling may not be able to do it. “It’s the large [health systems] that tend to be more integrated … that are thinking about this much differently,” he said.
Still, the reality is that’s where the root of the problem lies, Dr. Rylander said – not in the hospital, but in the larger community. “In the absence of very basic needs – stable housing, food, heating – it’s really not reasonable to expect that people are going to take care of their physical needs,” she said. “It’s a much larger social issue: how to get resources so that these people can have stable places to live, they can get to and from appointments, that type of thing.”
Those needs are ongoing, of course. Many of these patients suffer from chronic conditions, meaning people will continue to need services and support, said Ron Honberg, JD, senior policy adviser for the National Alliance on Mental Illness. Often, people need services from different systems. “There are complexities in terms of navigating those systems and getting those systems to work well together. Until we make inroads in solving those things, or at least improving those things, the burdens are going to fall on the providers of last resort, and that includes hospitals,” he said.

A collaborative effort may be needed, but hospitals can still be active participants and even leaders.
“If hospitals really want to address these problems, they need to be part of the discussions taking place in communities among the various systems and providers and advocates,” Mr. Honberg said. “Ultimately, we need to develop a better community-based system of care, and a better way of handing people off from inpatient to community-based treatment, and some accountability in terms of requiring that people get services, so they don’t get rehospitalized quickly. You’re increasingly seeing accountability now with other health conditions; we’re measuring things in Medicare like rehospitalization rates and the like. We need to be doing that with mental health treatment as well.”
What a hospitalist can do
One thing hospitalists might consider is starting that practice at their own hospitals, measuring, recording, and sharing that kind of information.
“Hospitalists should measure systematically, and in a very neutral manner, the total burden and frequency of the problem and report it consistently to management, along with their assessment that this impairs the quality of care and creates patient risk,” Dr. Parks said. That information can help hospitalists lobby for access to psychiatric personnel, be that in person or through telemedicine. “We don’t have to lay hands on you. There’s no excuse for any hospital not having a contract in place for on-demand consultation in the ER and on the floors.”
Track outcomes, too, Dr. Mandal suggests. With access to the right personnel, are you getting patients out of the ED faster? Are you having fewer negative outcomes while these patients are in the hospital, such as having to use restraints or get security involved? “Hopefully you can get some data in terms of how much money you’ve saved by decreasing the length of stays and decreasing inadvertent adverse effects because the patients weren’t receiving the proper care,” he said.
As this challenge seems likely to continue to grow, hospitalists might consider finding more training in mental health issues themselves so they are more comfortable handling these issues, Dr. Parks said. “The average mini-psych rotation from medical school is only 4 weeks,” he noted. “The ob.gyn. is at least 8 weeks and often 12 weeks, and if you don’t go into ob.gyn., you’re going to see a lot more mentally ill people through the rest of your practice, no matter what you do, than you are going to see pregnant women.”
Just starting these conversations – with patients, with colleagues, with family and friends – might be the most important change of all. “Even though nobody is above these issues afflicting them, this is still something that is not part of an open dialogue, and this is something that affects our own colleagues,” Dr. Mandal said. “I don’t know how many more trainees jumping out of windows it will take, or colleagues going through depression and feeling that it’s a sign of weakness to even talk about it.
“We need to create safe harbors within our own medical communities and acknowledge that we ourselves can be prone to this,” he said. “Perhaps by doing that, we will develop more empathy and become more comfortable, not just with ourselves and our colleagues but also helping these patients. People get overwhelmed and throw their hands up because it is just such a difficult issue. I don’t want people to give up, both from the medical community and our society as a whole – we can’t give up.”
A med-psych unit pilot project
Med-psych units can be a good model to take on these challenges. At Long Island Jewish Medical Center, they launched a pilot project to see how one would work in their community and summarized the results in an SHM abstract.
The hospital shares a campus with a 200-bed inpatient psych hospital, and doctors were seeing a lot of back and forth between the two institutions, said Corey Karlin-Zysman, MD, FHM, FACP, chief of the division of hospital medicine at Northwell Health. “Patients would come into the hospital because they had an active medical issue, but because of their behavioral issues, they’d have to have continuous observation. It would not be uncommon for us to have sometimes close to 30 patients who needed 24-hour continuous observation to make sure they were not hurting themselves.” These PCAs or nurse’s assistants were doing 8-hour shifts, so each patient needed three. “The math is staggering – and with not any better outcomes.”
So the hospital created a 15-bed closed med-psych unit for medically ill patients with behavioral health disorders. They staffed it with a dedicated hospitalist, a nurse practitioner, a psychologist, and a nurse manager.
The number of patients requiring continuous observation fell to single digits. Once in their own unit, these patients caused less disruption and stress on the medical units. They had a lower length of stay compared to their previous admissions in other units, and this became one of the hospital’s highest performing units in terms of patient experience.
The biggest secret of their success, Dr. Karlin-Zysman said, is cohorting. “Instead of them going to the next open bed, wherever it may be, you get the patients all in one place geographically, with a team trained to manage those patients.” Another factor: it’s a hospitalist-run unit. “You can’t have 20 different doctors taking care of the patients; it’s one or two hospitalists running this unit.”
Care models like this can be a true win-win, and her hospital is using them more and more.
“I have a care model that’s a stroke unit; I have a care model that’s an onc unit and one that’s a pulmonary unit,” she said. “We’re creating these true teams, which I think hospitalists really like being part of. What’s that thing that makes them want to come to work every day? Things like this: running a care model, becoming specialized in something.” There are research and abstract opportunities for hospitalists on these units too, which also helps keep them engaged, she said. “I’ve used this care model and things like that to reduce burnout and keep people excited.”
The persistent mortality gap
Patients with mental illness tend to receive worse medical care than people without, studies have shown; they die an average of 25 years earlier, largely from preventable or treatable conditions such as cardiovascular disease and diabetes. The World Health Organization has called the problem “a hidden human rights emergency.”
In one in a series of articles on mental health, Lisa Rosenbaum, MD, a cardiologist at Brigham and Women’s Hospital, Boston, raises the question: Might physician attitudes toward mentally ill people contribute to this mortality gap, and if so, can we change them?
She recognizes the many obstacles physicians face in treating these patients. “The medicines we have are good but not great and can cause obesity and diabetes, which contributes to cardiovascular morbidity and mortality,” Dr. Rosenbaum said. “We have the adherence challenge for the psychiatric medications and for medications for chronic disease. It’s hard enough for anyone to take a medicine every day, and to do that if you’re homeless or you don’t have insight into the need for it, it’s really hard.”
Also, certain behaviors that are more common among people with serious mental illness – smoking, substance abuse, physical inactivity – increase their risk for chronic diseases.
These hurdles may foster a sense of helplessness among hospitalists who have just a small amount of time to spend with a patient, and attitudes may be hard to change.
“Negotiating more effectively about care refusals, more adeptly assessing capacity, and recognizing when our efforts to orchestrate care have been inadequate seem feasible,” Dr. Rosenbaum writes. “Far harder is overcoming any collective belief that what mentally ill people truly need is not something we can offer.” That’s why a truly honest examination of attitudes and biases is a necessary place to start.
She tells the story of one mentally ill patient she learned of in her research, who, after decades as the quintessential frequent flier in the ER, was living stably in the community. “No one could have known how many tries it would take to help him get there,” she writes. His doctor told her, “Let’s say 10 attempts are necessary. Someone needs to be number 2, 3 and 7. You just never know which number you are.”
Education for physicians
A course created by the National Alliance on Mental Illness addresses mental illness issues from a provider perspective.
“Although the description states that the course is intended for mental health professionals, it can be and has been used to educate and inform other healthcare professionals as well,” said Ron Honberg, JD, senior policy advisor for the National Alliance on Mental Illness. The standard course takes 15 hours; there is an abbreviated 4-hour alternative as well. More information can be found at http://www.nami.org/Find-Support/NAMI-Programs/NAMI-Provider-Education.
Sources
1. Szabo L. Cost of Not Caring: Nowhere to Go. USA Today. https://www.usatoday.com/story/news/nation/2014/05/12/mental-health-system-crisis/7746535/. Accessed March 10, 2017.
2. Mental Health America. The State of Mental Health in America. http://www.mentalhealthamerica.net/issues/state-mental-health-america. Accessed March 30, 2017.
3. Karlin-Zysman C, Lerner K, Warner-Cohen J. Creating a Hybrid Medicine and Psychiatric Unit to Manage Medically Ill Patients with Behavioral Health Disorders [abstract]. Journal of Hospital Medicine. 2015; 10 (suppl 2). http://www.shmabstracts.com/abstract/creating-a-hybrid-medicine-and-psychiatric-unit-to-manage-medically-ill-patients-with-behavioral-health-disorders/. Accessed March 19, 2017.
4. Garey J. When Doctors Discriminate. New York Times. http://www.nytimes.com/2013/08/11/opinion/sunday/when-doctors-discriminate.html. August 10, 2013. Accessed March 15, 2017.
5. Rosenbaum L. Closing the Mortality Gap – Mental Illness and Medical Care. N Engl J Med. 2016; 375:1585-1589. doi: 10.1056/NEJMms1610125.
6. Rosenbaum L. Unlearning Our Helplessness – Coexisting Serious Mental and Medical Illness. N Engl J Med. 2016;375:1690-4. doi: 10.1056/NEJMms1610127.
The numbers tell a grim story. Nationwide, 43.7 million adult Americans experienced a mental health condition during 2016 – an increase of 1.2 million over the previous year. Mental health issues send almost 5.5 million people to emergency departments each year; nearly 60% of adults with a mental illness received no treatment at all.
If that massive – and growing – need is one side of the story, shrinking resources are the other. Mental health resources had already been diminishing for decades before the recession hit – and hit them especially hard. Between 2009 and 2012, states cut $5 billion in mental health services; during that time, at least 4,500 public psychiatric hospital beds nationwide disappeared – nearly 10% of the total supply. The bulk of those resources have never been restored.
Provider numbers also are falling. “Psychiatry is probably the top manpower shortage among all specialties,” said Joe Parks, MD, medical director of the National Council for Behavioral Health. “We have about a third the number of psychiatrists that most estimates say we need, and the number per capita is decreasing.” A significant percentage of psychiatrists – more than 50% – only accept cash, bypassing the low reimbursement rates even private insurance typically offers.
Hospitals, of course, feel those financial disincentives too, which discourage them from investments of their own. “It’s a difficult population to manage, and it’s difficult to manage the financial realities of mental health as well,” said John McHugh, PhD, assistant professor of health policy at Columbia University, New York. “If you were a hospital administrator looking to invest your last dollar and you have the option of investing it in a new heart institute or in behavioral health service, more likely than not, you’re going to invest it in the more profitable cardiovascular service line.”
Providers of last resort
But much of the burden of caring for this population ends up falling on hospitals by default. At Denver Health, Melanie Rylander, MD, medical director of the inpatient psychiatric unit, reports seeing this manifest in three categories of patients. First, there is an influx of people coming into the emergency department with primary mental health issues.
“We’re also seeing an influx of people coming in with physical problems, and upon assessment it becomes very clear very quickly that the real issue is an underlying mental health issue,” she said. Then there are the people coming in for the same physical problems over and over – maybe decompensated heart failure or COPD exacerbations – because mental health issues are impeding their ability to take care of themselves.
Some hospitalists say they feel ill equipped to care for these patients. “We don’t have the facility or the resources many times to properly care for their psychiatric needs when they’re in the hospital. It’s not really part of an internist’s training to be familiar with a lot of the medications,” said Atashi Mandal, MD, a hospitalist and pediatrician in Los Angeles. “Sometimes they get improperly medicated because we don’t know what else to do and the patient’s behavioral issues are escalating, so it’s really a difficult position.”
It’s a dispiriting experience for a hospitalist. “It really bothers me when I am trying to care for a patient who has psychiatric needs, and I feel I’m not able to do it, and I can’t find resources, and I feel that this patient’s needs are being neglected – not because we don’t care, and not because of a lack of effort by the staff. It’s just set up to fail,” Dr. Mandal said.
Ending the silo mentality
Encouraging a more holistic view of health across health care would be an important step to begin to address the problem – after all, the mind and the body are not separate.
“We work in silos, and we really have to stop doing that because these are intertwined,” said Corey Karlin-Zysman, MD, FHM, FACP, chief of the division of hospital medicine at Northwell Health. “A schizophrenic will become worse when they’re medically ill. That illness will be harder to treat if their psychiatric illness is active.” This is starting to happen in the outpatient setting, evidenced by the expansion of the integrated care model, where a primary care doctor is the lead physician working in combination with psychologists, psychiatrists, and social workers. Communication among providers becomes simpler, and patients don’t fall through the cracks as often while trying to navigate the system.
That idea of integration is also making its way into the hospital setting in various ways. In their efforts to bring the care to the patient, rather than the other way around, Dr. Karlin-Zysman’s hospital embedded two hospitalists in the neighboring inpatient psychiatric hospital; when patients need medical treatment, they can receive it without interrupting their behavioral health treatment. As a result, patients who used to end up in their emergency department don’t anymore, and their 30-day readmission rate has fallen by 50%.
But at its foundation, care integration is more of an attitude than a system; it begins with a mindset.
“We talk so much today about system reform, integrated systems, blah, blah,” said Lisa Rosenbaum, MD, a cardiologist at Brigham and Women’s Hospital, Boston. “I don’t want to make it seem like it’s not going to work, but what does it mean for the patient who is psychotic and has 10 problems, with whom you have 15 minutes? Taking good care of these patients means you have to take a deep breath and put in a lot of time and deal with all these things that have nothing to do with the health system under which you practice. There’s this ‘only so much you can do’ feeling that is a problem in itself, because there’s actually a lot we can do.”
Hospitals and communities
It’s axiomatic to say that a better approach to mental health would be based around prevention and early intervention, rather than the less crisis-oriented system we have now. Some efforts are being made in that direction, and they involve, and require, outreach outside the hospital.
“The best hospitals doing work in mental health are going beyond the hospital walls; they’re really looking at their community,” Dr. Nguyen said. “You have hospitals, like Accountable Care Organizations, who are trying to move earlier and think about mental health from a pediatric standpoint: How can we support parents and children during critical phases of brain growth? How can we provide prevention services?” Ultimately, those efforts should help lower future admission rates to EDs and hospitals.
That forward-looking approach may be necessary, but it’s also a challenge. “As a hospital administrator, I would think that you look out at the community and see this problem is not going away – in fact, it is likely going to get worse,” Dr. McHugh said. “A health system may look at themselves and say we have to take the lead on this.” The difficulty is that thinking of it in a sense of value to the community, and making the requisite investments, will have a very long period of payout; a health system that’s struggling may not be able to do it. “It’s the large [health systems] that tend to be more integrated … that are thinking about this much differently,” he said.
Still, the reality is that’s where the root of the problem lies, Dr. Rylander said – not in the hospital, but in the larger community. “In the absence of very basic needs – stable housing, food, heating – it’s really not reasonable to expect that people are going to take care of their physical needs,” she said. “It’s a much larger social issue: how to get resources so that these people can have stable places to live, they can get to and from appointments, that type of thing.”
Those needs are ongoing, of course. Many of these patients suffer from chronic conditions, meaning people will continue to need services and support, said Ron Honberg, JD, senior policy adviser for the National Alliance on Mental Illness. Often, people need services from different systems. “There are complexities in terms of navigating those systems and getting those systems to work well together. Until we make inroads in solving those things, or at least improving those things, the burdens are going to fall on the providers of last resort, and that includes hospitals,” he said.
A collaborative effort may be needed, but hospitals can still be active participants and even leaders.
“If hospitals really want to address these problems, they need to be part of the discussions taking place in communities among the various systems and providers and advocates,” Mr. Honberg said. “Ultimately, we need to develop a better community-based system of care, and a better way of handing people off from inpatient to community-based treatment, and some accountability in terms of requiring that people get services, so they don’t get rehospitalized quickly. You’re increasingly seeing accountability now with other health conditions; we’re measuring things in Medicare like rehospitalization rates and the like. We need to be doing that with mental health treatment as well.”
What a hospitalist can do
One thing hospitalists might consider is starting that practice at their own hospitals, measuring, recording, and sharing that kind of information.
“Hospitalists should measure systematically, and in a very neutral manner, the total burden and frequency of the problem and report it consistently to management, along with their assessment that this impairs the quality of care and creates patient risk,” Dr. Parks said. That information can help hospitalists lobby for access to psychiatric personnel, be that in person or through telemedicine. “We don’t have to lay hands on you. There’s no excuse for any hospital not having a contract in place for on-demand consultation in the ER and on the floors.”
Track outcomes, too, Dr. Mandal suggests. With access to the right personnel, are you getting patients out of the ED faster? Are you having fewer negative outcomes while these patients are in the hospital, such as having to use restraints or get security involved? “Hopefully you can get some data in terms of how much money you’ve saved by decreasing the length of stays and decreasing inadvertent adverse effects because the patients weren’t receiving the proper care,” he said.
As this challenge seems likely to continue to grow, hospitalists might consider finding more training in mental health issues themselves so they are more comfortable handling these issues, Dr. Parks said. “The average mini-psych rotation from medical school is only 4 weeks,” he noted. “The ob.gyn. is at least 8 weeks and often 12 weeks, and if you don’t go into ob.gyn., you’re going to see a lot more mentally ill people through the rest of your practice, no matter what you do, than you are going to see pregnant women.”
Just starting these conversations – with patients, with colleagues, with family and friends – might be the most important change of all. “Even though nobody is above these issues afflicting them, this is still something that is not part of an open dialogue, and this is something that affects our own colleagues,” Dr. Mandal said. “I don’t know how many more trainees jumping out of windows it will take, or colleagues going through depression and feeling that it’s a sign of weakness to even talk about it.
“We need to create safe harbors within our own medical communities and acknowledge that we ourselves can be prone to this,” he said. “Perhaps by doing that, we will develop more empathy and become more comfortable, not just with ourselves and our colleagues but also helping these patients. People get overwhelmed and throw their hands up because it is just such a difficult issue. I don’t want people to give up, both from the medical community and our society as a whole – we can’t give up.”
A med-psych unit pilot project
Med-psych units can be a good model to take on these challenges. At Long Island Jewish Medical Center, they launched a pilot project to see how one would work in their community and summarized the results in an SHM abstract.
The hospital shares a campus with a 200-bed inpatient psych hospital, and doctors were seeing a lot of back and forth between the two institutions, said Corey Karlin-Zysman, MD, FHM, FACP, chief of the division of hospital medicine at Northwell Health. “Patients would come into the hospital because they had an active medical issue, but because of their behavioral issues, they’d have to have continuous observation. It would not be uncommon for us to have sometimes close to 30 patients who needed 24-hour continuous observation to make sure they were not hurting themselves.” These PCAs or nurse’s assistants were doing 8-hour shifts, so each patient needed three. “The math is staggering – and with not any better outcomes.”
So the hospital created a 15-bed closed med-psych unit for medically ill patients with behavioral health disorders. They staffed it with a dedicated hospitalist, a nurse practitioner, a psychologist, and a nurse manager.
The number of patients requiring continuous observation fell to single digits. Once in their own unit, these patients caused less disruption and stress on the medical units. They had a lower length of stay compared to their previous admissions in other units, and this became one of the hospital’s highest performing units in terms of patient experience.
The biggest secret of their success, Dr. Karlin-Zysman said, is cohorting. “Instead of them going to the next open bed, wherever it may be, you get the patients all in one place geographically, with a team trained to manage those patients.” Another factor: it’s a hospitalist-run unit. “You can’t have 20 different doctors taking care of the patients; it’s one or two hospitalists running this unit.”
Care models like this can be a true win-win, and her hospital is using them more and more.
“I have a care model that’s a stroke unit; I have a care model that’s an onc unit and one that’s a pulmonary unit,” she said. “We’re creating these true teams, which I think hospitalists really like being part of. What’s that thing that makes them want to come to work every day? Things like this: running a care model, becoming specialized in something.” There are research and abstract opportunities for hospitalists on these units too, which also helps keep them engaged, she said. “I’ve used this care model and things like that to reduce burnout and keep people excited.”
The persistent mortality gap
Patients with mental illness tend to receive worse medical care than people without, studies have shown; they die an average of 25 years earlier, largely from preventable or treatable conditions such as cardiovascular disease and diabetes. The World Health Organization has called the problem “a hidden human rights emergency.”
In one in a series of articles on mental health, Lisa Rosenbaum, MD, a cardiologist at Brigham and Women’s Hospital, Boston, raises the question: Might physician attitudes toward mentally ill people contribute to this mortality gap, and if so, can we change them?
She recognizes the many obstacles physicians face in treating these patients. “The medicines we have are good but not great and can cause obesity and diabetes, which contributes to cardiovascular morbidity and mortality,” Dr. Rosenbaum said. “We have the adherence challenge for the psychiatric medications and for medications for chronic disease. It’s hard enough for anyone to take a medicine every day, and to do that if you’re homeless or you don’t have insight into the need for it, it’s really hard.”
Also, certain behaviors that are more common among people with serious mental illness – smoking, substance abuse, physical inactivity – increase their risk for chronic diseases.
These hurdles may foster a sense of helplessness among hospitalists who have just a small amount of time to spend with a patient, and attitudes may be hard to change.
“Negotiating more effectively about care refusals, more adeptly assessing capacity, and recognizing when our efforts to orchestrate care have been inadequate seem feasible,” Dr. Rosenbaum writes. “Far harder is overcoming any collective belief that what mentally ill people truly need is not something we can offer.” That’s why a truly honest examination of attitudes and biases is a necessary place to start.
She tells the story of one mentally ill patient she learned of in her research, who, after decades as the quintessential frequent flier in the ER, was living stably in the community. “No one could have known how many tries it would take to help him get there,” she writes. His doctor told her, “Let’s say 10 attempts are necessary. Someone needs to be number 2, 3 and 7. You just never know which number you are.”
Education for physicians
A course created by the National Alliance on Mental Illness addresses mental illness issues from a provider perspective.
“Although the description states that the course is intended for mental health professionals, it can be and has been used to educate and inform other healthcare professionals as well,” said Ron Honberg, JD, senior policy advisor for the National Alliance on Mental Illness. The standard course takes 15 hours; there is an abbreviated 4-hour alternative as well. More information can be found at http://www.nami.org/Find-Support/NAMI-Programs/NAMI-Provider-Education.
Sources
1. Szabo L. Cost of Not Caring: Nowhere to Go. USA Today. https://www.usatoday.com/story/news/nation/2014/05/12/mental-health-system-crisis/7746535/. Accessed March 10, 2017.
2. Mental Health America. The State of Mental Health in America. http://www.mentalhealthamerica.net/issues/state-mental-health-america. Accessed March 30, 2017.
3. Karlin-Zysman C, Lerner K, Warner-Cohen J. Creating a Hybrid Medicine and Psychiatric Unit to Manage Medically Ill Patients with Behavioral Health Disorders [abstract]. Journal of Hospital Medicine. 2015; 10 (suppl 2). http://www.shmabstracts.com/abstract/creating-a-hybrid-medicine-and-psychiatric-unit-to-manage-medically-ill-patients-with-behavioral-health-disorders/. Accessed March 19, 2017.
4. Garey J. When Doctors Discriminate. New York Times. http://www.nytimes.com/2013/08/11/opinion/sunday/when-doctors-discriminate.html. August 10, 2013. Accessed March 15, 2017.
5. Rosenbaum L. Closing the Mortality Gap – Mental Illness and Medical Care. N Engl J Med. 2016; 375:1585-1589. doi: 10.1056/NEJMms1610125.
6. Rosenbaum L. Unlearning Our Helplessness – Coexisting Serious Mental and Medical Illness. N Engl J Med. 2016;375:1690-4. doi: 10.1056/NEJMms1610127.
The numbers tell a grim story. Nationwide, 43.7 million adult Americans experienced a mental health condition during 2016 – an increase of 1.2 million over the previous year. Mental health issues send almost 5.5 million people to emergency departments each year; nearly 60% of adults with a mental illness received no treatment at all.
If that massive – and growing – need is one side of the story, shrinking resources are the other. Mental health resources had already been diminishing for decades before the recession hit – and hit them especially hard. Between 2009 and 2012, states cut $5 billion in mental health services; during that time, at least 4,500 public psychiatric hospital beds nationwide disappeared – nearly 10% of the total supply. The bulk of those resources have never been restored.
Provider numbers also are falling. “Psychiatry is probably the top manpower shortage among all specialties,” said Joe Parks, MD, medical director of the National Council for Behavioral Health. “We have about a third the number of psychiatrists that most estimates say we need, and the number per capita is decreasing.” A significant percentage of psychiatrists – more than 50% – only accept cash, bypassing the low reimbursement rates even private insurance typically offers.
Hospitals, of course, feel those financial disincentives too, which discourage them from investments of their own. “It’s a difficult population to manage, and it’s difficult to manage the financial realities of mental health as well,” said John McHugh, PhD, assistant professor of health policy at Columbia University, New York. “If you were a hospital administrator looking to invest your last dollar and you have the option of investing it in a new heart institute or in behavioral health service, more likely than not, you’re going to invest it in the more profitable cardiovascular service line.”
Providers of last resort
But much of the burden of caring for this population ends up falling on hospitals by default. At Denver Health, Melanie Rylander, MD, medical director of the inpatient psychiatric unit, reports seeing this manifest in three categories of patients. First, there is an influx of people coming into the emergency department with primary mental health issues.
“We’re also seeing an influx of people coming in with physical problems, and upon assessment it becomes very clear very quickly that the real issue is an underlying mental health issue,” she said. Then there are the people coming in for the same physical problems over and over – maybe decompensated heart failure or COPD exacerbations – because mental health issues are impeding their ability to take care of themselves.
Some hospitalists say they feel ill equipped to care for these patients. “We don’t have the facility or the resources many times to properly care for their psychiatric needs when they’re in the hospital. It’s not really part of an internist’s training to be familiar with a lot of the medications,” said Atashi Mandal, MD, a hospitalist and pediatrician in Los Angeles. “Sometimes they get improperly medicated because we don’t know what else to do and the patient’s behavioral issues are escalating, so it’s really a difficult position.”
It’s a dispiriting experience for a hospitalist. “It really bothers me when I am trying to care for a patient who has psychiatric needs, and I feel I’m not able to do it, and I can’t find resources, and I feel that this patient’s needs are being neglected – not because we don’t care, and not because of a lack of effort by the staff. It’s just set up to fail,” Dr. Mandal said.
Ending the silo mentality
Encouraging a more holistic view of health across health care would be an important step to begin to address the problem – after all, the mind and the body are not separate.
“We work in silos, and we really have to stop doing that because these are intertwined,” said Corey Karlin-Zysman, MD, FHM, FACP, chief of the division of hospital medicine at Northwell Health. “A schizophrenic will become worse when they’re medically ill. That illness will be harder to treat if their psychiatric illness is active.” This is starting to happen in the outpatient setting, evidenced by the expansion of the integrated care model, where a primary care doctor is the lead physician working in combination with psychologists, psychiatrists, and social workers. Communication among providers becomes simpler, and patients don’t fall through the cracks as often while trying to navigate the system.
That idea of integration is also making its way into the hospital setting in various ways. In their efforts to bring the care to the patient, rather than the other way around, Dr. Karlin-Zysman’s hospital embedded two hospitalists in the neighboring inpatient psychiatric hospital; when patients need medical treatment, they can receive it without interrupting their behavioral health treatment. As a result, patients who used to end up in their emergency department don’t anymore, and their 30-day readmission rate has fallen by 50%.
But at its foundation, care integration is more of an attitude than a system; it begins with a mindset.
“We talk so much today about system reform, integrated systems, blah, blah,” said Lisa Rosenbaum, MD, a cardiologist at Brigham and Women’s Hospital, Boston. “I don’t want to make it seem like it’s not going to work, but what does it mean for the patient who is psychotic and has 10 problems, with whom you have 15 minutes? Taking good care of these patients means you have to take a deep breath and put in a lot of time and deal with all these things that have nothing to do with the health system under which you practice. There’s this ‘only so much you can do’ feeling that is a problem in itself, because there’s actually a lot we can do.”
Hospitals and communities
It’s axiomatic to say that a better approach to mental health would be based around prevention and early intervention, rather than the less crisis-oriented system we have now. Some efforts are being made in that direction, and they involve, and require, outreach outside the hospital.
“The best hospitals doing work in mental health are going beyond the hospital walls; they’re really looking at their community,” Dr. Nguyen said. “You have hospitals, like Accountable Care Organizations, who are trying to move earlier and think about mental health from a pediatric standpoint: How can we support parents and children during critical phases of brain growth? How can we provide prevention services?” Ultimately, those efforts should help lower future admission rates to EDs and hospitals.
That forward-looking approach may be necessary, but it’s also a challenge. “As a hospital administrator, I would think that you look out at the community and see this problem is not going away – in fact, it is likely going to get worse,” Dr. McHugh said. “A health system may look at themselves and say we have to take the lead on this.” The difficulty is that thinking of it in a sense of value to the community, and making the requisite investments, will have a very long period of payout; a health system that’s struggling may not be able to do it. “It’s the large [health systems] that tend to be more integrated … that are thinking about this much differently,” he said.
Still, the reality is that’s where the root of the problem lies, Dr. Rylander said – not in the hospital, but in the larger community. “In the absence of very basic needs – stable housing, food, heating – it’s really not reasonable to expect that people are going to take care of their physical needs,” she said. “It’s a much larger social issue: how to get resources so that these people can have stable places to live, they can get to and from appointments, that type of thing.”
Those needs are ongoing, of course. Many of these patients suffer from chronic conditions, meaning people will continue to need services and support, said Ron Honberg, JD, senior policy adviser for the National Alliance on Mental Illness. Often, people need services from different systems. “There are complexities in terms of navigating those systems and getting those systems to work well together. Until we make inroads in solving those things, or at least improving those things, the burdens are going to fall on the providers of last resort, and that includes hospitals,” he said.
A collaborative effort may be needed, but hospitals can still be active participants and even leaders.
“If hospitals really want to address these problems, they need to be part of the discussions taking place in communities among the various systems and providers and advocates,” Mr. Honberg said. “Ultimately, we need to develop a better community-based system of care, and a better way of handing people off from inpatient to community-based treatment, and some accountability in terms of requiring that people get services, so they don’t get rehospitalized quickly. You’re increasingly seeing accountability now with other health conditions; we’re measuring things in Medicare like rehospitalization rates and the like. We need to be doing that with mental health treatment as well.”
What a hospitalist can do
One thing hospitalists might consider is starting that practice at their own hospitals, measuring, recording, and sharing that kind of information.
“Hospitalists should measure systematically, and in a very neutral manner, the total burden and frequency of the problem and report it consistently to management, along with their assessment that this impairs the quality of care and creates patient risk,” Dr. Parks said. That information can help hospitalists lobby for access to psychiatric personnel, be that in person or through telemedicine. “We don’t have to lay hands on you. There’s no excuse for any hospital not having a contract in place for on-demand consultation in the ER and on the floors.”
Track outcomes, too, Dr. Mandal suggests. With access to the right personnel, are you getting patients out of the ED faster? Are you having fewer negative outcomes while these patients are in the hospital, such as having to use restraints or get security involved? “Hopefully you can get some data in terms of how much money you’ve saved by decreasing the length of stays and decreasing inadvertent adverse effects because the patients weren’t receiving the proper care,” he said.
As this challenge seems likely to continue to grow, hospitalists might consider finding more training in mental health issues themselves so they are more comfortable handling these issues, Dr. Parks said. “The average mini-psych rotation from medical school is only 4 weeks,” he noted. “The ob.gyn. is at least 8 weeks and often 12 weeks, and if you don’t go into ob.gyn., you’re going to see a lot more mentally ill people through the rest of your practice, no matter what you do, than you are going to see pregnant women.”
Just starting these conversations – with patients, with colleagues, with family and friends – might be the most important change of all. “Even though nobody is above these issues afflicting them, this is still something that is not part of an open dialogue, and this is something that affects our own colleagues,” Dr. Mandal said. “I don’t know how many more trainees jumping out of windows it will take, or colleagues going through depression and feeling that it’s a sign of weakness to even talk about it.
“We need to create safe harbors within our own medical communities and acknowledge that we ourselves can be prone to this,” he said. “Perhaps by doing that, we will develop more empathy and become more comfortable, not just with ourselves and our colleagues but also helping these patients. People get overwhelmed and throw their hands up because it is just such a difficult issue. I don’t want people to give up, both from the medical community and our society as a whole – we can’t give up.”
A med-psych unit pilot project
Med-psych units can be a good model to take on these challenges. At Long Island Jewish Medical Center, they launched a pilot project to see how one would work in their community and summarized the results in an SHM abstract.
The hospital shares a campus with a 200-bed inpatient psych hospital, and doctors were seeing a lot of back and forth between the two institutions, said Corey Karlin-Zysman, MD, FHM, FACP, chief of the division of hospital medicine at Northwell Health. “Patients would come into the hospital because they had an active medical issue, but because of their behavioral issues, they’d have to have continuous observation. It would not be uncommon for us to have sometimes close to 30 patients who needed 24-hour continuous observation to make sure they were not hurting themselves.” These PCAs or nurse’s assistants were doing 8-hour shifts, so each patient needed three. “The math is staggering – and with not any better outcomes.”
So the hospital created a 15-bed closed med-psych unit for medically ill patients with behavioral health disorders. They staffed it with a dedicated hospitalist, a nurse practitioner, a psychologist, and a nurse manager.
The number of patients requiring continuous observation fell to single digits. Once in their own unit, these patients caused less disruption and stress on the medical units. They had a lower length of stay compared to their previous admissions in other units, and this became one of the hospital’s highest performing units in terms of patient experience.
The biggest secret of their success, Dr. Karlin-Zysman said, is cohorting. “Instead of them going to the next open bed, wherever it may be, you get the patients all in one place geographically, with a team trained to manage those patients.” Another factor: it’s a hospitalist-run unit. “You can’t have 20 different doctors taking care of the patients; it’s one or two hospitalists running this unit.”
Care models like this can be a true win-win, and her hospital is using them more and more.
“I have a care model that’s a stroke unit; I have a care model that’s an onc unit and one that’s a pulmonary unit,” she said. “We’re creating these true teams, which I think hospitalists really like being part of. What’s that thing that makes them want to come to work every day? Things like this: running a care model, becoming specialized in something.” There are research and abstract opportunities for hospitalists on these units too, which also helps keep them engaged, she said. “I’ve used this care model and things like that to reduce burnout and keep people excited.”
The persistent mortality gap
Patients with mental illness tend to receive worse medical care than people without, studies have shown; they die an average of 25 years earlier, largely from preventable or treatable conditions such as cardiovascular disease and diabetes. The World Health Organization has called the problem “a hidden human rights emergency.”
In one in a series of articles on mental health, Lisa Rosenbaum, MD, a cardiologist at Brigham and Women’s Hospital, Boston, raises the question: Might physician attitudes toward mentally ill people contribute to this mortality gap, and if so, can we change them?
She recognizes the many obstacles physicians face in treating these patients. “The medicines we have are good but not great and can cause obesity and diabetes, which contributes to cardiovascular morbidity and mortality,” Dr. Rosenbaum said. “We have the adherence challenge for the psychiatric medications and for medications for chronic disease. It’s hard enough for anyone to take a medicine every day, and to do that if you’re homeless or you don’t have insight into the need for it, it’s really hard.”
Also, certain behaviors that are more common among people with serious mental illness – smoking, substance abuse, physical inactivity – increase their risk for chronic diseases.
These hurdles may foster a sense of helplessness among hospitalists who have just a small amount of time to spend with a patient, and attitudes may be hard to change.
“Negotiating more effectively about care refusals, more adeptly assessing capacity, and recognizing when our efforts to orchestrate care have been inadequate seem feasible,” Dr. Rosenbaum writes. “Far harder is overcoming any collective belief that what mentally ill people truly need is not something we can offer.” That’s why a truly honest examination of attitudes and biases is a necessary place to start.
She tells the story of one mentally ill patient she learned of in her research, who, after decades as the quintessential frequent flier in the ER, was living stably in the community. “No one could have known how many tries it would take to help him get there,” she writes. His doctor told her, “Let’s say 10 attempts are necessary. Someone needs to be number 2, 3 and 7. You just never know which number you are.”
Education for physicians
A course created by the National Alliance on Mental Illness addresses mental illness issues from a provider perspective.
“Although the description states that the course is intended for mental health professionals, it can be and has been used to educate and inform other healthcare professionals as well,” said Ron Honberg, JD, senior policy advisor for the National Alliance on Mental Illness. The standard course takes 15 hours; there is an abbreviated 4-hour alternative as well. More information can be found at http://www.nami.org/Find-Support/NAMI-Programs/NAMI-Provider-Education.
Sources
1. Szabo L. Cost of Not Caring: Nowhere to Go. USA Today. https://www.usatoday.com/story/news/nation/2014/05/12/mental-health-system-crisis/7746535/. Accessed March 10, 2017.
2. Mental Health America. The State of Mental Health in America. http://www.mentalhealthamerica.net/issues/state-mental-health-america. Accessed March 30, 2017.
3. Karlin-Zysman C, Lerner K, Warner-Cohen J. Creating a Hybrid Medicine and Psychiatric Unit to Manage Medically Ill Patients with Behavioral Health Disorders [abstract]. Journal of Hospital Medicine. 2015; 10 (suppl 2). http://www.shmabstracts.com/abstract/creating-a-hybrid-medicine-and-psychiatric-unit-to-manage-medically-ill-patients-with-behavioral-health-disorders/. Accessed March 19, 2017.
4. Garey J. When Doctors Discriminate. New York Times. http://www.nytimes.com/2013/08/11/opinion/sunday/when-doctors-discriminate.html. August 10, 2013. Accessed March 15, 2017.
5. Rosenbaum L. Closing the Mortality Gap – Mental Illness and Medical Care. N Engl J Med. 2016; 375:1585-1589. doi: 10.1056/NEJMms1610125.
6. Rosenbaum L. Unlearning Our Helplessness – Coexisting Serious Mental and Medical Illness. N Engl J Med. 2016;375:1690-4. doi: 10.1056/NEJMms1610127.
Using post-acute and long-term care quality report cards
The challenges of hospital discharge planning are well known and yet have not been adequately addressed by hospitalists and discharge teams. As the complexity of patient care needs has grown, so has the difficulty in developing appropriate discharge goals for post-acute and long term care (LTC), choosing the appropriate setting(s), and selecting appropriate providers. Post-acute and LTC needs may include rehabilitation, nursing care, home health, supportive services, and/or palliative care1 in an institutional setting or at home from a wide array of providers with varying levels of quality.
Even though 52% of U.S. hospitals received penalties for having higher-than-expected readmissions between 2013 and 2017,2 inadequate discharge planning for post-acute and LTC continues to contribute to high rates of all-cause 30-day rehospitalization. The discharge process sometimes is deficient in: discussion of goals; assessment of discharge needs; appropriate choice of discharge locations; and the provision of additional or different home services.3 Discharge decisions are complicated by the stressful circumstances of hospitalization and discharge deadlines.

Hospital discharge planning decisions fall heavily on patients, families, and caregivers, often with inadequate information about choices and options. More than 30 states have passed the Caregiver Advise, Record, and Enable (CARE) Act into law to require hospitals to provide resources for family caregiver education and instruction,7 but hospitals do not have to provide information on all LTC options and provider quality ratings.
Quality report cards about LTC providers – a major innovation for consumer education and choice – are often not used in the discharge process for a number of reasons. A significant concern is that using report cards will extend the length of stay. Rather than extending the decision-making time and the length of stay, the use of report cards can reduce length of stay.9 A focus on identifying the first available nursing home bed or LTC provider often ignores the need to identify the most appropriate high-quality providers.

Hospitals and health plans often have established networks of post-acute and LTC providers and these networks must be taken into account in the discharge process. Most hospital and health plan networks have providers with a wide range of ratings, allowing for choices within networks.
The Centers for Medicare and Medicaid Services (CMS) established a web-based nursing home report card called Nursing Home Compare in 1998 that includes information on facility characteristics, deficiencies, staffing information (since 2000), and resident quality indicators (since 2002). In 2008, the website added a “five-star” rating system for all U.S. nursing homes and all-cause 30-day readmission rates and successful discharge rates from nursing homes were incorporated into the ratings in 2016.
CMS also established a web-based home health website, which provides quality ratings. This website has general information, quality measures, and patient surveys with information on readmission rates from home health agency services.

After establishment of the CMS Nursing Home Compare rating system in 2008, nursing homes improved their scores on certain quality measures and consumer demand significantly increased for the best (5-star) facilities and decreased for 1-star facilities.10 More recently, a clinical trial of the use of a personalized version of Nursing Home Compare in the hospital discharge planning process found greater patient satisfaction, patients being more likely to go to higher ranked nursing homes, patients traveling further to nursing homes, and patients having shorter hospital stays, compared with the control group.9
Quality report cards show wide variations within and across states ranging from one star (poorest quality) to five stars (highest quality). More than one-third of nursing homes had relatively low overall star ratings (1 or 2 stars) serving 39 percent of residents in 2015.11 Federal nursing home regulatory violations range from zero to more than 40 deficiencies (average of 7) with a scope and severity ranging from minor to widespread harm or jeopardy (including deaths).12 Total nurse staffing hours (average, 4.1 hours per resident day) range from less than 3 hours to more than 5.5 hours per resident day and RN hours are 3.5 times higher in some nursing homes than in the lowest staffed homes.13 Hospital readmission rates for short-stay residents from nursing homes also vary widely (4%-52%; average, 21%).12,14
Hospitalists and discharge planners should inform patients, families, and caregivers about the federal and state LTC quality report cards, provide education and choices, and engage and assist them in the decision making process. Hospitals, health plans, and accountable care organizations also need to be more informed about the availability of and benefits of using quality report cards for developing post-acute and LTC provider networks. The use of high quality LTC network providers should be able to reduce hospital length of stay and hospital readmission rates, and improve patient and caregiver satisfaction.
Charlene Harrington, PhD, RN, is professor of sociology and nursing; Leslie Ross, PhD, is a research specialist and principal investigator of the Calqualitycare.org website project; and Jeffrey Newman, MD, MPH, is a professor at the Institute for Health and Aging, all at the University of California, San Francisco.
References
1. Mor V et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff (Millwood). 2010;29(1):57-64.
2. Thompson, MP, Waters, TM, Kaplan et al. Most hospitals received annual penalties for excess readmissions, but some fared better than others. Health Aff (Millwood). 36(5):893-901.
3. Auerbach AD et al. Preventability and causes of readmissions in a national cohort of general medicine patients. JAMA Intern Med. 2016;176(4):484-93.
4. Jack B et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-87.
5. Hansen LO et al. Project BOOST: effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8)421-7.
6. Naylor MD et al. The care span: The importance of transitional care in achieving health reform. Health Aff (Millwood). 2011;30(4):746-54.
7. Coleman EA. Family caregivers as partners in care transitions: The caregiver advise record and enable act. J Hosp Med. 2016 Dec;11(12):883-5.
8. Leppin AL et al. Preventing 30-day hospital readmissions: a systematic review and meta-analysis of randomized trials. JAMA Internal Med. 2014;174(7):1095-107.
9. Mukamel DB et al. Personalizing nursing home compare and the discharge from hospitals to nursing homes. Health Serv Res. 2016;1(6):2076-2094.
10. Werner RM et al. Changes in consumer demand following public reporting of summary quality ratings: An evaluation in nursing homes. Health Serv Res. 2016;51 Suppl 2:1291-309.
11. Boccuti C et al. Reading the stars: nursing home quality star ratings, nationally and by state. Kaiser Family Foundation Issue Brief. May 2015.
12. Centers for Medicare and Medicaid Services. Nursing home compare data archives. May 2017 monthly files. Quality MSR Claims data. https://data.medicare.gov/data/archives/nursing-home-compare. Accessed July 15, 2017.
13. Harrington C et al. The need for higher minimum staffing standards in U.S. nursing homes. Health Serv Insights. 2016;9:13-9.
14. Mor V et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff (Millwood). 2010;29(1):57-64.
The challenges of hospital discharge planning are well known and yet have not been adequately addressed by hospitalists and discharge teams. As the complexity of patient care needs has grown, so has the difficulty in developing appropriate discharge goals for post-acute and long term care (LTC), choosing the appropriate setting(s), and selecting appropriate providers. Post-acute and LTC needs may include rehabilitation, nursing care, home health, supportive services, and/or palliative care1 in an institutional setting or at home from a wide array of providers with varying levels of quality.
Even though 52% of U.S. hospitals received penalties for having higher-than-expected readmissions between 2013 and 2017,2 inadequate discharge planning for post-acute and LTC continues to contribute to high rates of all-cause 30-day rehospitalization. The discharge process sometimes is deficient in: discussion of goals; assessment of discharge needs; appropriate choice of discharge locations; and the provision of additional or different home services.3 Discharge decisions are complicated by the stressful circumstances of hospitalization and discharge deadlines.
Hospital discharge planning decisions fall heavily on patients, families, and caregivers, often with inadequate information about choices and options. More than 30 states have passed the Caregiver Advise, Record, and Enable (CARE) Act into law to require hospitals to provide resources for family caregiver education and instruction,7 but hospitals do not have to provide information on all LTC options and provider quality ratings.
Quality report cards about LTC providers – a major innovation for consumer education and choice – are often not used in the discharge process for a number of reasons. A significant concern is that using report cards will extend the length of stay. Rather than extending the decision-making time and the length of stay, the use of report cards can reduce length of stay.9 A focus on identifying the first available nursing home bed or LTC provider often ignores the need to identify the most appropriate high-quality providers.
Hospitals and health plans often have established networks of post-acute and LTC providers and these networks must be taken into account in the discharge process. Most hospital and health plan networks have providers with a wide range of ratings, allowing for choices within networks.
The Centers for Medicare and Medicaid Services (CMS) established a web-based nursing home report card called Nursing Home Compare in 1998 that includes information on facility characteristics, deficiencies, staffing information (since 2000), and resident quality indicators (since 2002). In 2008, the website added a “five-star” rating system for all U.S. nursing homes and all-cause 30-day readmission rates and successful discharge rates from nursing homes were incorporated into the ratings in 2016.
CMS also established a web-based home health website, which provides quality ratings. This website has general information, quality measures, and patient surveys with information on readmission rates from home health agency services.
After establishment of the CMS Nursing Home Compare rating system in 2008, nursing homes improved their scores on certain quality measures and consumer demand significantly increased for the best (5-star) facilities and decreased for 1-star facilities.10 More recently, a clinical trial of the use of a personalized version of Nursing Home Compare in the hospital discharge planning process found greater patient satisfaction, patients being more likely to go to higher ranked nursing homes, patients traveling further to nursing homes, and patients having shorter hospital stays, compared with the control group.9
Quality report cards show wide variations within and across states ranging from one star (poorest quality) to five stars (highest quality). More than one-third of nursing homes had relatively low overall star ratings (1 or 2 stars) serving 39 percent of residents in 2015.11 Federal nursing home regulatory violations range from zero to more than 40 deficiencies (average of 7) with a scope and severity ranging from minor to widespread harm or jeopardy (including deaths).12 Total nurse staffing hours (average, 4.1 hours per resident day) range from less than 3 hours to more than 5.5 hours per resident day and RN hours are 3.5 times higher in some nursing homes than in the lowest staffed homes.13 Hospital readmission rates for short-stay residents from nursing homes also vary widely (4%-52%; average, 21%).12,14
Hospitalists and discharge planners should inform patients, families, and caregivers about the federal and state LTC quality report cards, provide education and choices, and engage and assist them in the decision making process. Hospitals, health plans, and accountable care organizations also need to be more informed about the availability of and benefits of using quality report cards for developing post-acute and LTC provider networks. The use of high quality LTC network providers should be able to reduce hospital length of stay and hospital readmission rates, and improve patient and caregiver satisfaction.
Charlene Harrington, PhD, RN, is professor of sociology and nursing; Leslie Ross, PhD, is a research specialist and principal investigator of the Calqualitycare.org website project; and Jeffrey Newman, MD, MPH, is a professor at the Institute for Health and Aging, all at the University of California, San Francisco.
References
1. Mor V et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff (Millwood). 2010;29(1):57-64.
2. Thompson, MP, Waters, TM, Kaplan et al. Most hospitals received annual penalties for excess readmissions, but some fared better than others. Health Aff (Millwood). 36(5):893-901.
3. Auerbach AD et al. Preventability and causes of readmissions in a national cohort of general medicine patients. JAMA Intern Med. 2016;176(4):484-93.
4. Jack B et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-87.
5. Hansen LO et al. Project BOOST: effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8)421-7.
6. Naylor MD et al. The care span: The importance of transitional care in achieving health reform. Health Aff (Millwood). 2011;30(4):746-54.
7. Coleman EA. Family caregivers as partners in care transitions: The caregiver advise record and enable act. J Hosp Med. 2016 Dec;11(12):883-5.
8. Leppin AL et al. Preventing 30-day hospital readmissions: a systematic review and meta-analysis of randomized trials. JAMA Internal Med. 2014;174(7):1095-107.
9. Mukamel DB et al. Personalizing nursing home compare and the discharge from hospitals to nursing homes. Health Serv Res. 2016;1(6):2076-2094.
10. Werner RM et al. Changes in consumer demand following public reporting of summary quality ratings: An evaluation in nursing homes. Health Serv Res. 2016;51 Suppl 2:1291-309.
11. Boccuti C et al. Reading the stars: nursing home quality star ratings, nationally and by state. Kaiser Family Foundation Issue Brief. May 2015.
12. Centers for Medicare and Medicaid Services. Nursing home compare data archives. May 2017 monthly files. Quality MSR Claims data. https://data.medicare.gov/data/archives/nursing-home-compare. Accessed July 15, 2017.
13. Harrington C et al. The need for higher minimum staffing standards in U.S. nursing homes. Health Serv Insights. 2016;9:13-9.
14. Mor V et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff (Millwood). 2010;29(1):57-64.
The challenges of hospital discharge planning are well known and yet have not been adequately addressed by hospitalists and discharge teams. As the complexity of patient care needs has grown, so has the difficulty in developing appropriate discharge goals for post-acute and long term care (LTC), choosing the appropriate setting(s), and selecting appropriate providers. Post-acute and LTC needs may include rehabilitation, nursing care, home health, supportive services, and/or palliative care1 in an institutional setting or at home from a wide array of providers with varying levels of quality.
Even though 52% of U.S. hospitals received penalties for having higher-than-expected readmissions between 2013 and 2017,2 inadequate discharge planning for post-acute and LTC continues to contribute to high rates of all-cause 30-day rehospitalization. The discharge process sometimes is deficient in: discussion of goals; assessment of discharge needs; appropriate choice of discharge locations; and the provision of additional or different home services.3 Discharge decisions are complicated by the stressful circumstances of hospitalization and discharge deadlines.
Hospital discharge planning decisions fall heavily on patients, families, and caregivers, often with inadequate information about choices and options. More than 30 states have passed the Caregiver Advise, Record, and Enable (CARE) Act into law to require hospitals to provide resources for family caregiver education and instruction,7 but hospitals do not have to provide information on all LTC options and provider quality ratings.
Quality report cards about LTC providers – a major innovation for consumer education and choice – are often not used in the discharge process for a number of reasons. A significant concern is that using report cards will extend the length of stay. Rather than extending the decision-making time and the length of stay, the use of report cards can reduce length of stay.9 A focus on identifying the first available nursing home bed or LTC provider often ignores the need to identify the most appropriate high-quality providers.
Hospitals and health plans often have established networks of post-acute and LTC providers and these networks must be taken into account in the discharge process. Most hospital and health plan networks have providers with a wide range of ratings, allowing for choices within networks.
The Centers for Medicare and Medicaid Services (CMS) established a web-based nursing home report card called Nursing Home Compare in 1998 that includes information on facility characteristics, deficiencies, staffing information (since 2000), and resident quality indicators (since 2002). In 2008, the website added a “five-star” rating system for all U.S. nursing homes and all-cause 30-day readmission rates and successful discharge rates from nursing homes were incorporated into the ratings in 2016.
CMS also established a web-based home health website, which provides quality ratings. This website has general information, quality measures, and patient surveys with information on readmission rates from home health agency services.
After establishment of the CMS Nursing Home Compare rating system in 2008, nursing homes improved their scores on certain quality measures and consumer demand significantly increased for the best (5-star) facilities and decreased for 1-star facilities.10 More recently, a clinical trial of the use of a personalized version of Nursing Home Compare in the hospital discharge planning process found greater patient satisfaction, patients being more likely to go to higher ranked nursing homes, patients traveling further to nursing homes, and patients having shorter hospital stays, compared with the control group.9
Quality report cards show wide variations within and across states ranging from one star (poorest quality) to five stars (highest quality). More than one-third of nursing homes had relatively low overall star ratings (1 or 2 stars) serving 39 percent of residents in 2015.11 Federal nursing home regulatory violations range from zero to more than 40 deficiencies (average of 7) with a scope and severity ranging from minor to widespread harm or jeopardy (including deaths).12 Total nurse staffing hours (average, 4.1 hours per resident day) range from less than 3 hours to more than 5.5 hours per resident day and RN hours are 3.5 times higher in some nursing homes than in the lowest staffed homes.13 Hospital readmission rates for short-stay residents from nursing homes also vary widely (4%-52%; average, 21%).12,14
Hospitalists and discharge planners should inform patients, families, and caregivers about the federal and state LTC quality report cards, provide education and choices, and engage and assist them in the decision making process. Hospitals, health plans, and accountable care organizations also need to be more informed about the availability of and benefits of using quality report cards for developing post-acute and LTC provider networks. The use of high quality LTC network providers should be able to reduce hospital length of stay and hospital readmission rates, and improve patient and caregiver satisfaction.
Charlene Harrington, PhD, RN, is professor of sociology and nursing; Leslie Ross, PhD, is a research specialist and principal investigator of the Calqualitycare.org website project; and Jeffrey Newman, MD, MPH, is a professor at the Institute for Health and Aging, all at the University of California, San Francisco.
References
1. Mor V et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff (Millwood). 2010;29(1):57-64.
2. Thompson, MP, Waters, TM, Kaplan et al. Most hospitals received annual penalties for excess readmissions, but some fared better than others. Health Aff (Millwood). 36(5):893-901.
3. Auerbach AD et al. Preventability and causes of readmissions in a national cohort of general medicine patients. JAMA Intern Med. 2016;176(4):484-93.
4. Jack B et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-87.
5. Hansen LO et al. Project BOOST: effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8)421-7.
6. Naylor MD et al. The care span: The importance of transitional care in achieving health reform. Health Aff (Millwood). 2011;30(4):746-54.
7. Coleman EA. Family caregivers as partners in care transitions: The caregiver advise record and enable act. J Hosp Med. 2016 Dec;11(12):883-5.
8. Leppin AL et al. Preventing 30-day hospital readmissions: a systematic review and meta-analysis of randomized trials. JAMA Internal Med. 2014;174(7):1095-107.
9. Mukamel DB et al. Personalizing nursing home compare and the discharge from hospitals to nursing homes. Health Serv Res. 2016;1(6):2076-2094.
10. Werner RM et al. Changes in consumer demand following public reporting of summary quality ratings: An evaluation in nursing homes. Health Serv Res. 2016;51 Suppl 2:1291-309.
11. Boccuti C et al. Reading the stars: nursing home quality star ratings, nationally and by state. Kaiser Family Foundation Issue Brief. May 2015.
12. Centers for Medicare and Medicaid Services. Nursing home compare data archives. May 2017 monthly files. Quality MSR Claims data. https://data.medicare.gov/data/archives/nursing-home-compare. Accessed July 15, 2017.
13. Harrington C et al. The need for higher minimum staffing standards in U.S. nursing homes. Health Serv Insights. 2016;9:13-9.
14. Mor V et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff (Millwood). 2010;29(1):57-64.
Pharmacomechanical thrombolysis does not reduce post-thrombotic syndrome risk
In patients with acute proximal deep vein thrombosis who were undergoing anticoagulation, adding pharmacomechanical catheter-directed thrombolysis did not reduce risk of the post-thrombotic syndrome, according to results of a phase 3, randomized, controlled trial.
Moreover, addition of pharmacomechanical thrombolysis increased risk of major bleeding risk, investigators wrote in a report published online Dec. 6 in the New England Journal of Medicine.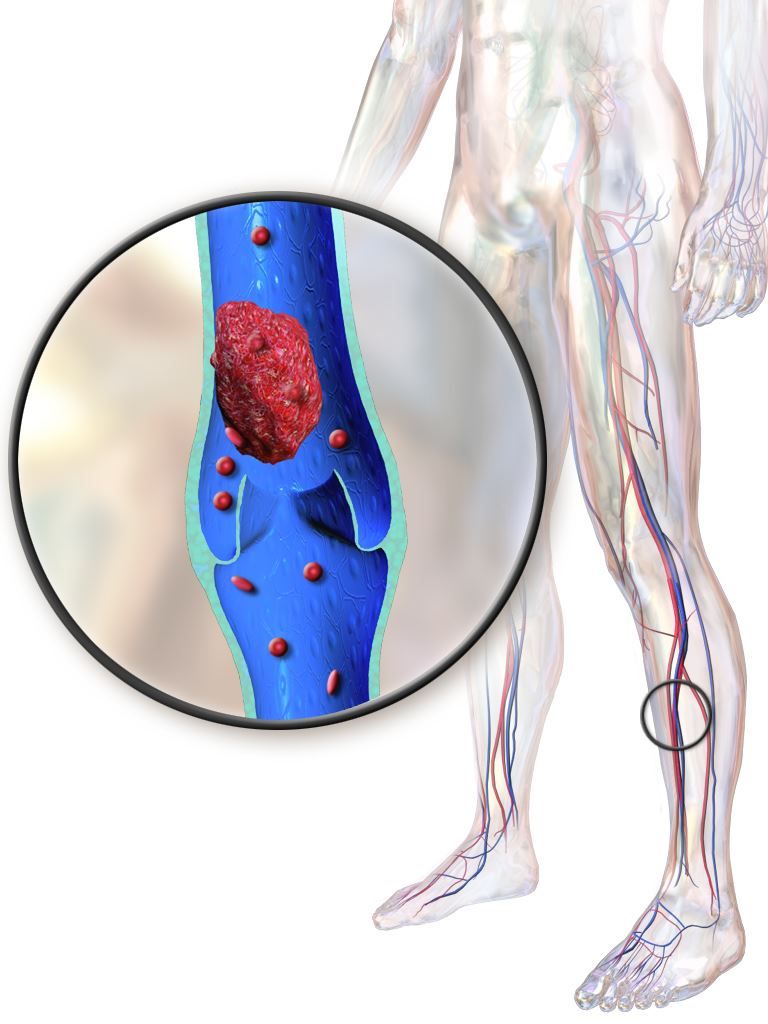
“Our trial, for uncertain reasons, did not confirm these findings,” wrote Suresh Vedantham, MD of Washington University, St. Louis, and his coauthors.
Post-thrombotic syndrome is associated with chronic limb swelling and pain, and can lead to leg ulcers, impaired quality of life, and major disability. About half of patients with proximal deep vein thrombosis (DVT) will develop the post-thrombotic syndrome within 2 years, despite use of anticoagulation therapy, Dr. Vedantham and his colleagues noted.
Pharmacomechanical thrombosis is the catheter-directed delivery of a fibrinolytic agent into the thrombus, along with aspiration or maceration of the thrombus. The goal of the treatment is to reduce the burden of thrombus, which in turn might reduce risk of the post-thrombotic syndrome.
However, in their randomized trial known as ATTRACT, which included 692 patients with an acute proximal DVT, rates of post-thrombotic syndrome between 6 to 24 months after intervention were 47% in the pharmacomechanical thrombolysis group and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56), according to the report (N Engl J Med. 2017;377:2240-52). Control group patients received no procedural intervention.
Major bleeds within 10 days of the intervention were 1.7% and 0.3% for the pharmacomechanical thrombolysis and control groups, respectively (P = .049).
By contrast, in the CAVENT trial, catheter-directed thrombolysis reduced the risk of the post-thrombotic syndrome over 5 years of follow-up (Lancet Haematol. 2016;3[2]:e64-71). Dr. Vedantham and his coauthors suggested that factors potentially explaining the difference in outcomes include the number of patients enrolled (692 in ATTRACT, versus 209 in CAVENT), or the greater use of mechanical therapies in ATTRACT versus longer recombinant tissue plasminogen activator infusions in CAVENT.
The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. Dr. Vedantham reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
In patients with acute proximal deep vein thrombosis who were undergoing anticoagulation, adding pharmacomechanical catheter-directed thrombolysis did not reduce risk of the post-thrombotic syndrome, according to results of a phase 3, randomized, controlled trial.
Moreover, addition of pharmacomechanical thrombolysis increased risk of major bleeding risk, investigators wrote in a report published online Dec. 6 in the New England Journal of Medicine.
“Our trial, for uncertain reasons, did not confirm these findings,” wrote Suresh Vedantham, MD of Washington University, St. Louis, and his coauthors.
Post-thrombotic syndrome is associated with chronic limb swelling and pain, and can lead to leg ulcers, impaired quality of life, and major disability. About half of patients with proximal deep vein thrombosis (DVT) will develop the post-thrombotic syndrome within 2 years, despite use of anticoagulation therapy, Dr. Vedantham and his colleagues noted.
Pharmacomechanical thrombosis is the catheter-directed delivery of a fibrinolytic agent into the thrombus, along with aspiration or maceration of the thrombus. The goal of the treatment is to reduce the burden of thrombus, which in turn might reduce risk of the post-thrombotic syndrome.
However, in their randomized trial known as ATTRACT, which included 692 patients with an acute proximal DVT, rates of post-thrombotic syndrome between 6 to 24 months after intervention were 47% in the pharmacomechanical thrombolysis group and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56), according to the report (N Engl J Med. 2017;377:2240-52). Control group patients received no procedural intervention.
Major bleeds within 10 days of the intervention were 1.7% and 0.3% for the pharmacomechanical thrombolysis and control groups, respectively (P = .049).
By contrast, in the CAVENT trial, catheter-directed thrombolysis reduced the risk of the post-thrombotic syndrome over 5 years of follow-up (Lancet Haematol. 2016;3[2]:e64-71). Dr. Vedantham and his coauthors suggested that factors potentially explaining the difference in outcomes include the number of patients enrolled (692 in ATTRACT, versus 209 in CAVENT), or the greater use of mechanical therapies in ATTRACT versus longer recombinant tissue plasminogen activator infusions in CAVENT.
The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. Dr. Vedantham reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
In patients with acute proximal deep vein thrombosis who were undergoing anticoagulation, adding pharmacomechanical catheter-directed thrombolysis did not reduce risk of the post-thrombotic syndrome, according to results of a phase 3, randomized, controlled trial.
Moreover, addition of pharmacomechanical thrombolysis increased risk of major bleeding risk, investigators wrote in a report published online Dec. 6 in the New England Journal of Medicine.
“Our trial, for uncertain reasons, did not confirm these findings,” wrote Suresh Vedantham, MD of Washington University, St. Louis, and his coauthors.
Post-thrombotic syndrome is associated with chronic limb swelling and pain, and can lead to leg ulcers, impaired quality of life, and major disability. About half of patients with proximal deep vein thrombosis (DVT) will develop the post-thrombotic syndrome within 2 years, despite use of anticoagulation therapy, Dr. Vedantham and his colleagues noted.
Pharmacomechanical thrombosis is the catheter-directed delivery of a fibrinolytic agent into the thrombus, along with aspiration or maceration of the thrombus. The goal of the treatment is to reduce the burden of thrombus, which in turn might reduce risk of the post-thrombotic syndrome.
However, in their randomized trial known as ATTRACT, which included 692 patients with an acute proximal DVT, rates of post-thrombotic syndrome between 6 to 24 months after intervention were 47% in the pharmacomechanical thrombolysis group and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56), according to the report (N Engl J Med. 2017;377:2240-52). Control group patients received no procedural intervention.
Major bleeds within 10 days of the intervention were 1.7% and 0.3% for the pharmacomechanical thrombolysis and control groups, respectively (P = .049).
By contrast, in the CAVENT trial, catheter-directed thrombolysis reduced the risk of the post-thrombotic syndrome over 5 years of follow-up (Lancet Haematol. 2016;3[2]:e64-71). Dr. Vedantham and his coauthors suggested that factors potentially explaining the difference in outcomes include the number of patients enrolled (692 in ATTRACT, versus 209 in CAVENT), or the greater use of mechanical therapies in ATTRACT versus longer recombinant tissue plasminogen activator infusions in CAVENT.
The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. Dr. Vedantham reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: Rates of post-thrombotic syndrome were 47% in the pharmacomechanical thrombolysis group, and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56).
Data source: A phase 3, multicenter, randomized, open-label, assessor-blinded, controlled clinical trial, including 692 patients with acute proximal deep vein thrombosis.
Disclosures: The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. First author Suresh Vedantham, MD, reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.