User login
European Academy of Dermatology & Venereology (EADV): Annual Congress
Open Wide: New Insights Into Burning Mouth Syndrome
AMSTERDAM – The incidence of burning mouth syndrome is considerably lower than previously reported, according to findings from the first population-based study of the disorder.
The age- and gender-adjusted incidence of burning mouth syndrome during 2000-2010 in Olmsted County, Minn., was 11.4 cases per 100,000 person-years, John J. Kohorst reported at the annual congress of the European Academy of Dermatology and Venereology.
Prior epidemiologic studies have reported prevalence rates all over the map, from 1% to 40%, probably in large part because they used a variety of definitions for burning mouth syndrome. The new population-based study focused on disease incidence rather than prevalence utilized a standardized definition for the diagnosis: subjective burning pain of the oral mucosa in the absence of physical findings or an identifiable extraneous cause. All cases had to be diagnosed by a physician participating in the Rochester (Minn.) Epidemiology Project, explained Mr. Kohorst, a medical student at the Mayo Medical School in Rochester.
Because burning mouth syndrome is a diagnosis of exclusion, typically a year or more goes by and three different physicians are consulted before the correct diagnosis is made.
The pathogenesis of burning mouth syndrome remains poorly understood. It is predominantly a disorder affecting postmenopausal women. In the Minnesota study, for example, women accounted for 84% of the 169 individuals diagnosed with new-onset burning mouth syndrome during the study period. The incidence among women was 18.8 cases per 100,000 person-years, compared with 3.7 per 100,000 person-years in men. The incidence climbed sharply after age 50 in both men and women, achieving a peak rate of 70.3 cases per 100,000 person-years among women age 70-79.
Some prior studies have reported a strong association between burning mouth syndrome and smoking that wasn’t evident in the Olmsted County population-based study. Only 11% of the Minnesota patients with new-onset burning mouth syndrome were current smokers and 63% were never-smokers, rates mirroring those of the county’s general population, according to Mr. Kohorst.
Eighty-eight percent of patients reported bilateral as opposed to unilateral mouth pain. The tongue was the sole involved site in 53% of cases. Forty-two percent of patients rated the pain as mild, while 13% characterized it as severe based upon a score of 8 or more on a 10-point scale. Most affected patients described the burning pain as a continuous feature throughout their day.
The next step in this research project will be to investigate the potential role of concurrent disease states and medication use in the incidence and prevalence of burning mouth syndrome in the county’s population, Mr. Kohorst said.
He reported having no financial conflicts regarding this study.
AMSTERDAM – The incidence of burning mouth syndrome is considerably lower than previously reported, according to findings from the first population-based study of the disorder.
The age- and gender-adjusted incidence of burning mouth syndrome during 2000-2010 in Olmsted County, Minn., was 11.4 cases per 100,000 person-years, John J. Kohorst reported at the annual congress of the European Academy of Dermatology and Venereology.
Prior epidemiologic studies have reported prevalence rates all over the map, from 1% to 40%, probably in large part because they used a variety of definitions for burning mouth syndrome. The new population-based study focused on disease incidence rather than prevalence utilized a standardized definition for the diagnosis: subjective burning pain of the oral mucosa in the absence of physical findings or an identifiable extraneous cause. All cases had to be diagnosed by a physician participating in the Rochester (Minn.) Epidemiology Project, explained Mr. Kohorst, a medical student at the Mayo Medical School in Rochester.
Because burning mouth syndrome is a diagnosis of exclusion, typically a year or more goes by and three different physicians are consulted before the correct diagnosis is made.
The pathogenesis of burning mouth syndrome remains poorly understood. It is predominantly a disorder affecting postmenopausal women. In the Minnesota study, for example, women accounted for 84% of the 169 individuals diagnosed with new-onset burning mouth syndrome during the study period. The incidence among women was 18.8 cases per 100,000 person-years, compared with 3.7 per 100,000 person-years in men. The incidence climbed sharply after age 50 in both men and women, achieving a peak rate of 70.3 cases per 100,000 person-years among women age 70-79.
Some prior studies have reported a strong association between burning mouth syndrome and smoking that wasn’t evident in the Olmsted County population-based study. Only 11% of the Minnesota patients with new-onset burning mouth syndrome were current smokers and 63% were never-smokers, rates mirroring those of the county’s general population, according to Mr. Kohorst.
Eighty-eight percent of patients reported bilateral as opposed to unilateral mouth pain. The tongue was the sole involved site in 53% of cases. Forty-two percent of patients rated the pain as mild, while 13% characterized it as severe based upon a score of 8 or more on a 10-point scale. Most affected patients described the burning pain as a continuous feature throughout their day.
The next step in this research project will be to investigate the potential role of concurrent disease states and medication use in the incidence and prevalence of burning mouth syndrome in the county’s population, Mr. Kohorst said.
He reported having no financial conflicts regarding this study.
AMSTERDAM – The incidence of burning mouth syndrome is considerably lower than previously reported, according to findings from the first population-based study of the disorder.
The age- and gender-adjusted incidence of burning mouth syndrome during 2000-2010 in Olmsted County, Minn., was 11.4 cases per 100,000 person-years, John J. Kohorst reported at the annual congress of the European Academy of Dermatology and Venereology.
Prior epidemiologic studies have reported prevalence rates all over the map, from 1% to 40%, probably in large part because they used a variety of definitions for burning mouth syndrome. The new population-based study focused on disease incidence rather than prevalence utilized a standardized definition for the diagnosis: subjective burning pain of the oral mucosa in the absence of physical findings or an identifiable extraneous cause. All cases had to be diagnosed by a physician participating in the Rochester (Minn.) Epidemiology Project, explained Mr. Kohorst, a medical student at the Mayo Medical School in Rochester.
Because burning mouth syndrome is a diagnosis of exclusion, typically a year or more goes by and three different physicians are consulted before the correct diagnosis is made.
The pathogenesis of burning mouth syndrome remains poorly understood. It is predominantly a disorder affecting postmenopausal women. In the Minnesota study, for example, women accounted for 84% of the 169 individuals diagnosed with new-onset burning mouth syndrome during the study period. The incidence among women was 18.8 cases per 100,000 person-years, compared with 3.7 per 100,000 person-years in men. The incidence climbed sharply after age 50 in both men and women, achieving a peak rate of 70.3 cases per 100,000 person-years among women age 70-79.
Some prior studies have reported a strong association between burning mouth syndrome and smoking that wasn’t evident in the Olmsted County population-based study. Only 11% of the Minnesota patients with new-onset burning mouth syndrome were current smokers and 63% were never-smokers, rates mirroring those of the county’s general population, according to Mr. Kohorst.
Eighty-eight percent of patients reported bilateral as opposed to unilateral mouth pain. The tongue was the sole involved site in 53% of cases. Forty-two percent of patients rated the pain as mild, while 13% characterized it as severe based upon a score of 8 or more on a 10-point scale. Most affected patients described the burning pain as a continuous feature throughout their day.
The next step in this research project will be to investigate the potential role of concurrent disease states and medication use in the incidence and prevalence of burning mouth syndrome in the county’s population, Mr. Kohorst said.
He reported having no financial conflicts regarding this study.
AT THE EADV CONGRESS

Open wide: new insights into burning mouth syndrome
AMSTERDAM – The incidence of burning mouth syndrome is considerably lower than previously reported, according to findings from the first population-based study of the disorder.
The age- and gender-adjusted incidence of burning mouth syndrome during 2000-2010 in Olmsted County, Minn., was 11.4 cases per 100,000 person-years, John J. Kohorst reported at the annual congress of the European Academy of Dermatology and Venereology.

Prior epidemiologic studies have reported prevalence rates all over the map, from 1% to 40%, probably in large part because they used a variety of definitions for burning mouth syndrome. The new population-based study focused on disease incidence rather than prevalence utilized a standardized definition for the diagnosis: subjective burning pain of the oral mucosa in the absence of physical findings or an identifiable extraneous cause. All cases had to be diagnosed by a physician participating in the Rochester (Minn.) Epidemiology Project, explained Mr. Kohorst, a medical student at the Mayo Medical School in Rochester.
Because burning mouth syndrome is a diagnosis of exclusion, typically a year or more goes by and three different physicians are consulted before the correct diagnosis is made.
The pathogenesis of burning mouth syndrome remains poorly understood. It is predominantly a disorder affecting postmenopausal women. In the Minnesota study, for example, women accounted for 84% of the 169 individuals diagnosed with new-onset burning mouth syndrome during the study period. The incidence among women was 18.8 cases per 100,000 person-years, compared with 3.7 per 100,000 person-years in men. The incidence climbed sharply after age 50 in both men and women, achieving a peak rate of 70.3 cases per 100,000 person-years among women age 70-79.
Some prior studies have reported a strong association between burning mouth syndrome and smoking that wasn’t evident in the Olmsted County population-based study. Only 11% of the Minnesota patients with new-onset burning mouth syndrome were current smokers and 63% were never-smokers, rates mirroring those of the county’s general population, according to Mr. Kohorst.
Eighty-eight percent of patients reported bilateral as opposed to unilateral mouth pain. The tongue was the sole involved site in 53% of cases. Forty-two percent of patients rated the pain as mild, while 13% characterized it as severe based upon a score of 8 or more on a 10-point scale. Most affected patients described the burning pain as a continuous feature throughout their day.
The next step in this research project will be to investigate the potential role of concurrent disease states and medication use in the incidence and prevalence of burning mouth syndrome in the county’s population, Mr. Kohorst said.
He reported having no financial conflicts regarding this study.
AMSTERDAM – The incidence of burning mouth syndrome is considerably lower than previously reported, according to findings from the first population-based study of the disorder.
The age- and gender-adjusted incidence of burning mouth syndrome during 2000-2010 in Olmsted County, Minn., was 11.4 cases per 100,000 person-years, John J. Kohorst reported at the annual congress of the European Academy of Dermatology and Venereology.
Prior epidemiologic studies have reported prevalence rates all over the map, from 1% to 40%, probably in large part because they used a variety of definitions for burning mouth syndrome. The new population-based study focused on disease incidence rather than prevalence utilized a standardized definition for the diagnosis: subjective burning pain of the oral mucosa in the absence of physical findings or an identifiable extraneous cause. All cases had to be diagnosed by a physician participating in the Rochester (Minn.) Epidemiology Project, explained Mr. Kohorst, a medical student at the Mayo Medical School in Rochester.
Because burning mouth syndrome is a diagnosis of exclusion, typically a year or more goes by and three different physicians are consulted before the correct diagnosis is made.
The pathogenesis of burning mouth syndrome remains poorly understood. It is predominantly a disorder affecting postmenopausal women. In the Minnesota study, for example, women accounted for 84% of the 169 individuals diagnosed with new-onset burning mouth syndrome during the study period. The incidence among women was 18.8 cases per 100,000 person-years, compared with 3.7 per 100,000 person-years in men. The incidence climbed sharply after age 50 in both men and women, achieving a peak rate of 70.3 cases per 100,000 person-years among women age 70-79.
Some prior studies have reported a strong association between burning mouth syndrome and smoking that wasn’t evident in the Olmsted County population-based study. Only 11% of the Minnesota patients with new-onset burning mouth syndrome were current smokers and 63% were never-smokers, rates mirroring those of the county’s general population, according to Mr. Kohorst.
Eighty-eight percent of patients reported bilateral as opposed to unilateral mouth pain. The tongue was the sole involved site in 53% of cases. Forty-two percent of patients rated the pain as mild, while 13% characterized it as severe based upon a score of 8 or more on a 10-point scale. Most affected patients described the burning pain as a continuous feature throughout their day.
The next step in this research project will be to investigate the potential role of concurrent disease states and medication use in the incidence and prevalence of burning mouth syndrome in the county’s population, Mr. Kohorst said.
He reported having no financial conflicts regarding this study.
AMSTERDAM – The incidence of burning mouth syndrome is considerably lower than previously reported, according to findings from the first population-based study of the disorder.
The age- and gender-adjusted incidence of burning mouth syndrome during 2000-2010 in Olmsted County, Minn., was 11.4 cases per 100,000 person-years, John J. Kohorst reported at the annual congress of the European Academy of Dermatology and Venereology.
Prior epidemiologic studies have reported prevalence rates all over the map, from 1% to 40%, probably in large part because they used a variety of definitions for burning mouth syndrome. The new population-based study focused on disease incidence rather than prevalence utilized a standardized definition for the diagnosis: subjective burning pain of the oral mucosa in the absence of physical findings or an identifiable extraneous cause. All cases had to be diagnosed by a physician participating in the Rochester (Minn.) Epidemiology Project, explained Mr. Kohorst, a medical student at the Mayo Medical School in Rochester.
Because burning mouth syndrome is a diagnosis of exclusion, typically a year or more goes by and three different physicians are consulted before the correct diagnosis is made.
The pathogenesis of burning mouth syndrome remains poorly understood. It is predominantly a disorder affecting postmenopausal women. In the Minnesota study, for example, women accounted for 84% of the 169 individuals diagnosed with new-onset burning mouth syndrome during the study period. The incidence among women was 18.8 cases per 100,000 person-years, compared with 3.7 per 100,000 person-years in men. The incidence climbed sharply after age 50 in both men and women, achieving a peak rate of 70.3 cases per 100,000 person-years among women age 70-79.
Some prior studies have reported a strong association between burning mouth syndrome and smoking that wasn’t evident in the Olmsted County population-based study. Only 11% of the Minnesota patients with new-onset burning mouth syndrome were current smokers and 63% were never-smokers, rates mirroring those of the county’s general population, according to Mr. Kohorst.
Eighty-eight percent of patients reported bilateral as opposed to unilateral mouth pain. The tongue was the sole involved site in 53% of cases. Forty-two percent of patients rated the pain as mild, while 13% characterized it as severe based upon a score of 8 or more on a 10-point scale. Most affected patients described the burning pain as a continuous feature throughout their day.
The next step in this research project will be to investigate the potential role of concurrent disease states and medication use in the incidence and prevalence of burning mouth syndrome in the county’s population, Mr. Kohorst said.
He reported having no financial conflicts regarding this study.
AT THE EADV CONGRESS
Key clinical point: Burning mouth syndrome occurs a lot less frequently than previously understood.
Major finding: The incidence of newly diagnosed burning mouth syndrome using standardized criteria in Olmsted County, Minn., during 2000-2010 was 18.8 cases per 100,000 person-years among women and 3.7 in men.
Data source: This first-ever population-based study of burning mouth syndrome was carried out through the Rochester Epidemiology Project.
Disclosures: The Rochester Epidemiology Project is supported by the National Institutes of Health and the Mayo Clinic. Mr. Kohorst reported having no financial conflicts.

Maintenance Tacrolimus for Eczema Boosts Quality of Life
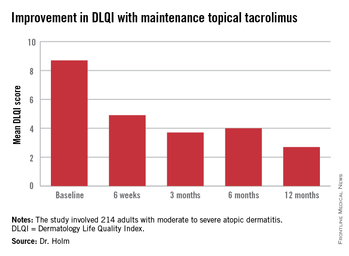
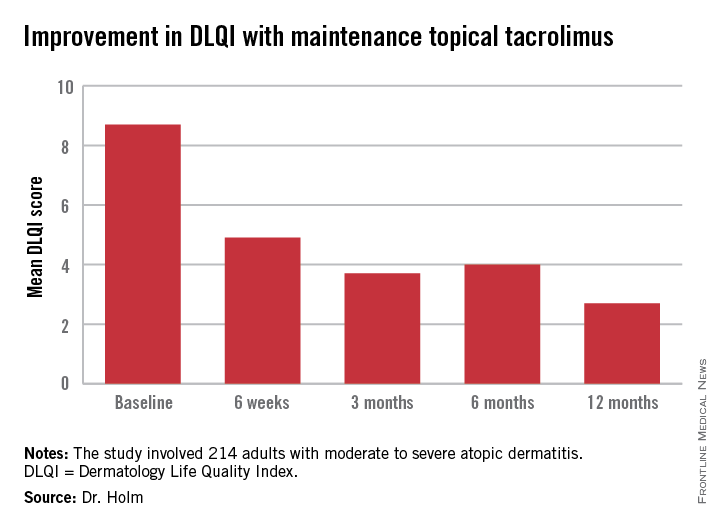
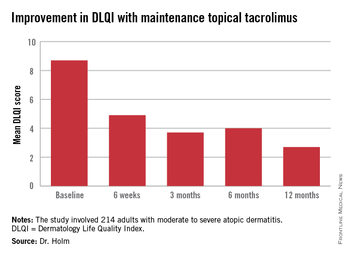
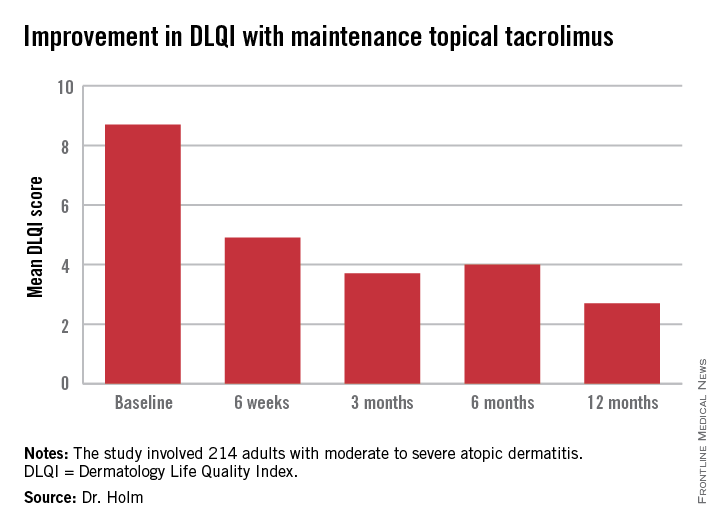
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
Continue for other outcomes >>
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
Continue for other outcomes >>
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
Continue for other outcomes >>
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AT THE EADV CONGRESS
Maintenance tacrolimus for eczema boosts quality of life
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AT THE EADV CONGRESS
Key clinical point: Twice-weekly proactive application of topical tacrolimus in adults with moderate to severe atopic dermatitis not only reduces flares, it dramatically improves patients’ self-rated quality of life.
Major finding: Mean scores on the Dermatology Life Quality Index in patients on maintenance therapy improved from 8.7 at baseline to 2.7 at 12 months, indicative of minimal disease impact upon daily life.
Data source: This was a 41-site, two-nation study involving 214 adults with moderate to severe atopic dermatitis.
Disclosures: The study was sponsored by Astellas. The presenter is a consultant to the company.
Ixekizumab linked to decrease in psoriasis-related sexual difficulties
AMSTERDAM – Patient complaints of psoriasis-related sexual difficulties decreased significantly in response to treatment with the investigational biologic agent ixekizumab in a phase 2 dose-ranging study.
Sexual problems attributed by psoriasis patients to their skin condition are a common, underappreciated, and understudied problem. Most physicians simply don’t ask. But when they do, as was done formally in this study, it turned out that at baseline roughly one-third of the 142 participating subjects with moderate to severe chronic plaque psoriasis reported some degree of sexual problems they believed due specifically to their skin disease, Dr. Lyn Guenther reported at the annual congress of the European Academy of Dermatology and Venereology.
That rate dropped precipitously and in dose-dependent fashion in response to subcutaneous therapy with ixekizumab, a super-potent psoriasis medication directed against interleukin 17A, according to Dr. Guenther, professor of dermatology at the University of Western Ontario, London.
The study entailed double-blind randomization of the 142 participants to subcutaneous injections of ixekizumab at 10, 25, 75, or 150 mg or placebo at 0, 2, 4, 8, 12, and 16 weeks. The standard primary outcome -- the proportion of patients with a PASI 75 improvement at 12 weeks -- has previously been reported as highly positive (N. Engl. J. Med. 2012;366:1190-9).
For her secondary analysis of psoriasis-related sexual difficulties and their response to treatment, Dr. Guenther used as her metric the patients’ response to item 9 on the Dermatology Life Quality Index, which all subjects completed at weeks 0, 8, and 16. Item 9 asks the extent to which the responder’s skin “caused any sexual difficulties” during the past week. The options range from 0 (none at all) to 3 (very much). She categorized a response of 1 or more as evidence of sexual difficulties. And because of the relatively small sample size in this study, she lumped together as the low-dose therapy group those patients assigned to ixekizumab at 10 or 25 mg, with the high-dose group being comprised of patients on 75 or
After 8 weeks on low-dose ixekizumab, the proportion of patients reporting any skin disease-related sexual difficulties within the past week fell from a baseline of 30% to 16%. After 8 weeks of high-dose ixekizumab, the figure was just 7%. Those rates remained unchanged at 16 weeks. In contrast, the placebo group remained unchanged over time, with 32% of patients still reporting sexual difficulties caused by their skin disease at week 8.
The degree to which a patient’s psoriasis improved in response to therapy with the humanized monoclonal antibody was closely related to the reduction in skin-related sexual problems. Among the 76 ixekizumab-treated patients who achieved a PASI 75 response at week 16, the rate of self-reported sexual difficulties within the previous week was 7%. For those with less than a PASI 75 response, the rate was 24%.
An impressively high 38% percent of patients on high-dose ixekizumab achieved a PASI 100 response. Only 5% of them reported any skin-related sexual difficulties at week 8, as did 9% at week 16.
Dr. Guenther also looked at the data restricting the analysis to patients with more severe baseline sexual impairment as defined by a response of 2 or 3 on item 9 of the DLQI. Among patients on high-dose izekizumab, the rate dropped from 10.5% at baseline to 1.8% at week 8 to zero at week 16. For patients on low-dose izekizumab, the progression was 13.8% to 8.8% to 3.5% at week 16. Rates remained unchanged over time in the control group.
Although this phase 2 study was limited in size, Dr. Guenther found much the same thing earlier in the much larger phase 3 PHOENIX 1 and 2 trials of ustekinumab (Stelara), which together featured 1,334 psoriasis patients randomized to the human anti-interkelukin-12/23 monoclonal antibody. In that analysis, the proportion of ustekinumab-treated patients with impaired sexual function as assessed by DLQI item 9 plunged from 22.4% at baseline to 2.7% at week 12, compared with no change in placebo-treated controls. The bigger the PASI improvement, the greater the reduction in psoriasis-related sexual dysfunction (J. Eur. Acad. Dermatol. Venereol. 2011;25:851-7).
The phase 2 ixekizumab study was funded by Eli Lilly. Dr. Guenther is a consultant to the company. Positive primary outcomes in three pivotal phase 3 clinical trials of ixekizumab totalling nearly 3,900 randomized psoriasis patients have since been reported. The company plans to apply for marketing approval of the biologic in the first half of 2015.
AMSTERDAM – Patient complaints of psoriasis-related sexual difficulties decreased significantly in response to treatment with the investigational biologic agent ixekizumab in a phase 2 dose-ranging study.
Sexual problems attributed by psoriasis patients to their skin condition are a common, underappreciated, and understudied problem. Most physicians simply don’t ask. But when they do, as was done formally in this study, it turned out that at baseline roughly one-third of the 142 participating subjects with moderate to severe chronic plaque psoriasis reported some degree of sexual problems they believed due specifically to their skin disease, Dr. Lyn Guenther reported at the annual congress of the European Academy of Dermatology and Venereology.
That rate dropped precipitously and in dose-dependent fashion in response to subcutaneous therapy with ixekizumab, a super-potent psoriasis medication directed against interleukin 17A, according to Dr. Guenther, professor of dermatology at the University of Western Ontario, London.
The study entailed double-blind randomization of the 142 participants to subcutaneous injections of ixekizumab at 10, 25, 75, or 150 mg or placebo at 0, 2, 4, 8, 12, and 16 weeks. The standard primary outcome -- the proportion of patients with a PASI 75 improvement at 12 weeks -- has previously been reported as highly positive (N. Engl. J. Med. 2012;366:1190-9).
For her secondary analysis of psoriasis-related sexual difficulties and their response to treatment, Dr. Guenther used as her metric the patients’ response to item 9 on the Dermatology Life Quality Index, which all subjects completed at weeks 0, 8, and 16. Item 9 asks the extent to which the responder’s skin “caused any sexual difficulties” during the past week. The options range from 0 (none at all) to 3 (very much). She categorized a response of 1 or more as evidence of sexual difficulties. And because of the relatively small sample size in this study, she lumped together as the low-dose therapy group those patients assigned to ixekizumab at 10 or 25 mg, with the high-dose group being comprised of patients on 75 or
After 8 weeks on low-dose ixekizumab, the proportion of patients reporting any skin disease-related sexual difficulties within the past week fell from a baseline of 30% to 16%. After 8 weeks of high-dose ixekizumab, the figure was just 7%. Those rates remained unchanged at 16 weeks. In contrast, the placebo group remained unchanged over time, with 32% of patients still reporting sexual difficulties caused by their skin disease at week 8.
The degree to which a patient’s psoriasis improved in response to therapy with the humanized monoclonal antibody was closely related to the reduction in skin-related sexual problems. Among the 76 ixekizumab-treated patients who achieved a PASI 75 response at week 16, the rate of self-reported sexual difficulties within the previous week was 7%. For those with less than a PASI 75 response, the rate was 24%.
An impressively high 38% percent of patients on high-dose ixekizumab achieved a PASI 100 response. Only 5% of them reported any skin-related sexual difficulties at week 8, as did 9% at week 16.
Dr. Guenther also looked at the data restricting the analysis to patients with more severe baseline sexual impairment as defined by a response of 2 or 3 on item 9 of the DLQI. Among patients on high-dose izekizumab, the rate dropped from 10.5% at baseline to 1.8% at week 8 to zero at week 16. For patients on low-dose izekizumab, the progression was 13.8% to 8.8% to 3.5% at week 16. Rates remained unchanged over time in the control group.
Although this phase 2 study was limited in size, Dr. Guenther found much the same thing earlier in the much larger phase 3 PHOENIX 1 and 2 trials of ustekinumab (Stelara), which together featured 1,334 psoriasis patients randomized to the human anti-interkelukin-12/23 monoclonal antibody. In that analysis, the proportion of ustekinumab-treated patients with impaired sexual function as assessed by DLQI item 9 plunged from 22.4% at baseline to 2.7% at week 12, compared with no change in placebo-treated controls. The bigger the PASI improvement, the greater the reduction in psoriasis-related sexual dysfunction (J. Eur. Acad. Dermatol. Venereol. 2011;25:851-7).
The phase 2 ixekizumab study was funded by Eli Lilly. Dr. Guenther is a consultant to the company. Positive primary outcomes in three pivotal phase 3 clinical trials of ixekizumab totalling nearly 3,900 randomized psoriasis patients have since been reported. The company plans to apply for marketing approval of the biologic in the first half of 2015.
AMSTERDAM – Patient complaints of psoriasis-related sexual difficulties decreased significantly in response to treatment with the investigational biologic agent ixekizumab in a phase 2 dose-ranging study.
Sexual problems attributed by psoriasis patients to their skin condition are a common, underappreciated, and understudied problem. Most physicians simply don’t ask. But when they do, as was done formally in this study, it turned out that at baseline roughly one-third of the 142 participating subjects with moderate to severe chronic plaque psoriasis reported some degree of sexual problems they believed due specifically to their skin disease, Dr. Lyn Guenther reported at the annual congress of the European Academy of Dermatology and Venereology.
That rate dropped precipitously and in dose-dependent fashion in response to subcutaneous therapy with ixekizumab, a super-potent psoriasis medication directed against interleukin 17A, according to Dr. Guenther, professor of dermatology at the University of Western Ontario, London.
The study entailed double-blind randomization of the 142 participants to subcutaneous injections of ixekizumab at 10, 25, 75, or 150 mg or placebo at 0, 2, 4, 8, 12, and 16 weeks. The standard primary outcome -- the proportion of patients with a PASI 75 improvement at 12 weeks -- has previously been reported as highly positive (N. Engl. J. Med. 2012;366:1190-9).
For her secondary analysis of psoriasis-related sexual difficulties and their response to treatment, Dr. Guenther used as her metric the patients’ response to item 9 on the Dermatology Life Quality Index, which all subjects completed at weeks 0, 8, and 16. Item 9 asks the extent to which the responder’s skin “caused any sexual difficulties” during the past week. The options range from 0 (none at all) to 3 (very much). She categorized a response of 1 or more as evidence of sexual difficulties. And because of the relatively small sample size in this study, she lumped together as the low-dose therapy group those patients assigned to ixekizumab at 10 or 25 mg, with the high-dose group being comprised of patients on 75 or
After 8 weeks on low-dose ixekizumab, the proportion of patients reporting any skin disease-related sexual difficulties within the past week fell from a baseline of 30% to 16%. After 8 weeks of high-dose ixekizumab, the figure was just 7%. Those rates remained unchanged at 16 weeks. In contrast, the placebo group remained unchanged over time, with 32% of patients still reporting sexual difficulties caused by their skin disease at week 8.
The degree to which a patient’s psoriasis improved in response to therapy with the humanized monoclonal antibody was closely related to the reduction in skin-related sexual problems. Among the 76 ixekizumab-treated patients who achieved a PASI 75 response at week 16, the rate of self-reported sexual difficulties within the previous week was 7%. For those with less than a PASI 75 response, the rate was 24%.
An impressively high 38% percent of patients on high-dose ixekizumab achieved a PASI 100 response. Only 5% of them reported any skin-related sexual difficulties at week 8, as did 9% at week 16.
Dr. Guenther also looked at the data restricting the analysis to patients with more severe baseline sexual impairment as defined by a response of 2 or 3 on item 9 of the DLQI. Among patients on high-dose izekizumab, the rate dropped from 10.5% at baseline to 1.8% at week 8 to zero at week 16. For patients on low-dose izekizumab, the progression was 13.8% to 8.8% to 3.5% at week 16. Rates remained unchanged over time in the control group.
Although this phase 2 study was limited in size, Dr. Guenther found much the same thing earlier in the much larger phase 3 PHOENIX 1 and 2 trials of ustekinumab (Stelara), which together featured 1,334 psoriasis patients randomized to the human anti-interkelukin-12/23 monoclonal antibody. In that analysis, the proportion of ustekinumab-treated patients with impaired sexual function as assessed by DLQI item 9 plunged from 22.4% at baseline to 2.7% at week 12, compared with no change in placebo-treated controls. The bigger the PASI improvement, the greater the reduction in psoriasis-related sexual dysfunction (J. Eur. Acad. Dermatol. Venereol. 2011;25:851-7).
The phase 2 ixekizumab study was funded by Eli Lilly. Dr. Guenther is a consultant to the company. Positive primary outcomes in three pivotal phase 3 clinical trials of ixekizumab totalling nearly 3,900 randomized psoriasis patients have since been reported. The company plans to apply for marketing approval of the biologic in the first half of 2015.
AT THE EADV CONGRESS
Key clinical point: Psoriasis patients have a high rate of sexual problems they attribute to their skin disease, and which decrease with effective psoriasis therapy.
Major finding: The prevalence of self-reported psoriasis-related sexual difficulties within the previous week fell from 32% at baseline to 7% among patients with a PASI 75 response to ixekizumab at week 16.
Data source: This was a double-blind, phase 2, dose-ranging study involving 142 patients with moderate to severe chronic plaque psoriasis randomized to 16 weeks of ixekizumab or placebo.
Disclosures: The study was funded by Eli Lilly. The presenter is a consultant to the company.
Oral tofacitinib scores against psoriasis in phase III trial
AMSTERDAM – Oral tofacitinib for psoriasis proved as effective as – and in certain domains better than – subcutaneous etanercept in improving patient-reported quality of life endpoints in a phase III clinical trial.
The double-blind study included 1,101 patients with moderate to severe chronic plaque psoriasis who were randomized to 12 weeks of the oral Janus kinase inhibitor tofacitinib at 5 mg twice daily, 10 mg twice daily, subcutaneous etanercept (Enbrel) at 50 mg twice weekly, or placebo. The findings were presented by Dr. Fernando Valenzuela at the annual congress of the European Academy of Dermatology and Venereology.

Earlier in 2014, at the annual meeting of the American Academy of Dermatology in Denver, Dr. Valenzuela presented the phase III study’s primary results, in which the oral small molecule proved noninferior to the tumor necrosis factor inhibitor in improving PASI scores. At the EADV Congress in Amsterdam, he focused on the secondary outcomes, which arguably matter more to patients than do changes in PASI scores, namely, measures of quality of life and itchiness.
From a baseline Itch Severity Item score of 5, indicative of moderate to severe itching, week 12 scores fell by a mean of 3.2, 4.0, 3.5, and 0.4 points, respectively, in patients on low- or high-dose tofacitinib, etanercept, and placebo. The improvement in itch in patients randomized to tofacitinib at 10 mg twice daily was not only greater than with etanercept, it occurred faster as well, with significant reduction in itch scores documented on day 2 of therapy, reported Dr. Valenzuela, a dermatologist at the University of Chile in Santiago.
The median baseline Dermatology Life Quality Index (DLQI) score was 12. Significant improvement was seen from week 4 in all three active treatment study arms. By week 12, DLQI scores had dropped by an average of 7.3 points in patients on tofacitinib at 5 mg twice daily, 9.7 points in those on 10 mg twice daily, 9.0 points in etanercept-treated patients, and 1.9 points with placebo. Seventy-eight percent of patients on tofacitinib at 10 mg twice daily experienced a 5-point or larger drop in the DLQI by week 12, as did 75% of those on etanercept, 66% of those on low-dose tofacitinib, and 32% of those on placebo.
At baseline, 30% of patients rated their psoriasis as moderate and 70% rated their psoriasis as severe based on Patient Global Assessment. By week 12, more than 50% of patients on tofacitinib at 10 mg twice daily or etanercept rated their skin as clear or almost clear.
More than 70% of patients in all three active treatment arms indicated at week 12 that they were satisfied with their medication. Satisfaction scores were highest, and equally so, in those on high-dose tofacitinib and etanercept.
“Patients using tofacitinib at the low dose had not that good an improvement. It was better improvement than with placebo, but it doesn’t look like etanercept,” Dr. Valenzuela concluded.
Tofacitinib is approved as Xeljanz for the treatment of rheumatoid arthritis, but remains investigational for psoriasis. According to a company statement, Pfizer intends to submit a supplemental New Drug Application (sNDA) to the Food and Drug Administration by early 2015.
The study was funded by Pfizer. Dr. Valenzuela is an adviser to Pfizer, AbbVie, Eli Lilly, Janssen, Merck, and Novartis.
AMSTERDAM – Oral tofacitinib for psoriasis proved as effective as – and in certain domains better than – subcutaneous etanercept in improving patient-reported quality of life endpoints in a phase III clinical trial.
The double-blind study included 1,101 patients with moderate to severe chronic plaque psoriasis who were randomized to 12 weeks of the oral Janus kinase inhibitor tofacitinib at 5 mg twice daily, 10 mg twice daily, subcutaneous etanercept (Enbrel) at 50 mg twice weekly, or placebo. The findings were presented by Dr. Fernando Valenzuela at the annual congress of the European Academy of Dermatology and Venereology.
Earlier in 2014, at the annual meeting of the American Academy of Dermatology in Denver, Dr. Valenzuela presented the phase III study’s primary results, in which the oral small molecule proved noninferior to the tumor necrosis factor inhibitor in improving PASI scores. At the EADV Congress in Amsterdam, he focused on the secondary outcomes, which arguably matter more to patients than do changes in PASI scores, namely, measures of quality of life and itchiness.
From a baseline Itch Severity Item score of 5, indicative of moderate to severe itching, week 12 scores fell by a mean of 3.2, 4.0, 3.5, and 0.4 points, respectively, in patients on low- or high-dose tofacitinib, etanercept, and placebo. The improvement in itch in patients randomized to tofacitinib at 10 mg twice daily was not only greater than with etanercept, it occurred faster as well, with significant reduction in itch scores documented on day 2 of therapy, reported Dr. Valenzuela, a dermatologist at the University of Chile in Santiago.
The median baseline Dermatology Life Quality Index (DLQI) score was 12. Significant improvement was seen from week 4 in all three active treatment study arms. By week 12, DLQI scores had dropped by an average of 7.3 points in patients on tofacitinib at 5 mg twice daily, 9.7 points in those on 10 mg twice daily, 9.0 points in etanercept-treated patients, and 1.9 points with placebo. Seventy-eight percent of patients on tofacitinib at 10 mg twice daily experienced a 5-point or larger drop in the DLQI by week 12, as did 75% of those on etanercept, 66% of those on low-dose tofacitinib, and 32% of those on placebo.
At baseline, 30% of patients rated their psoriasis as moderate and 70% rated their psoriasis as severe based on Patient Global Assessment. By week 12, more than 50% of patients on tofacitinib at 10 mg twice daily or etanercept rated their skin as clear or almost clear.
More than 70% of patients in all three active treatment arms indicated at week 12 that they were satisfied with their medication. Satisfaction scores were highest, and equally so, in those on high-dose tofacitinib and etanercept.
“Patients using tofacitinib at the low dose had not that good an improvement. It was better improvement than with placebo, but it doesn’t look like etanercept,” Dr. Valenzuela concluded.
Tofacitinib is approved as Xeljanz for the treatment of rheumatoid arthritis, but remains investigational for psoriasis. According to a company statement, Pfizer intends to submit a supplemental New Drug Application (sNDA) to the Food and Drug Administration by early 2015.
The study was funded by Pfizer. Dr. Valenzuela is an adviser to Pfizer, AbbVie, Eli Lilly, Janssen, Merck, and Novartis.
AMSTERDAM – Oral tofacitinib for psoriasis proved as effective as – and in certain domains better than – subcutaneous etanercept in improving patient-reported quality of life endpoints in a phase III clinical trial.
The double-blind study included 1,101 patients with moderate to severe chronic plaque psoriasis who were randomized to 12 weeks of the oral Janus kinase inhibitor tofacitinib at 5 mg twice daily, 10 mg twice daily, subcutaneous etanercept (Enbrel) at 50 mg twice weekly, or placebo. The findings were presented by Dr. Fernando Valenzuela at the annual congress of the European Academy of Dermatology and Venereology.
Earlier in 2014, at the annual meeting of the American Academy of Dermatology in Denver, Dr. Valenzuela presented the phase III study’s primary results, in which the oral small molecule proved noninferior to the tumor necrosis factor inhibitor in improving PASI scores. At the EADV Congress in Amsterdam, he focused on the secondary outcomes, which arguably matter more to patients than do changes in PASI scores, namely, measures of quality of life and itchiness.
From a baseline Itch Severity Item score of 5, indicative of moderate to severe itching, week 12 scores fell by a mean of 3.2, 4.0, 3.5, and 0.4 points, respectively, in patients on low- or high-dose tofacitinib, etanercept, and placebo. The improvement in itch in patients randomized to tofacitinib at 10 mg twice daily was not only greater than with etanercept, it occurred faster as well, with significant reduction in itch scores documented on day 2 of therapy, reported Dr. Valenzuela, a dermatologist at the University of Chile in Santiago.
The median baseline Dermatology Life Quality Index (DLQI) score was 12. Significant improvement was seen from week 4 in all three active treatment study arms. By week 12, DLQI scores had dropped by an average of 7.3 points in patients on tofacitinib at 5 mg twice daily, 9.7 points in those on 10 mg twice daily, 9.0 points in etanercept-treated patients, and 1.9 points with placebo. Seventy-eight percent of patients on tofacitinib at 10 mg twice daily experienced a 5-point or larger drop in the DLQI by week 12, as did 75% of those on etanercept, 66% of those on low-dose tofacitinib, and 32% of those on placebo.
At baseline, 30% of patients rated their psoriasis as moderate and 70% rated their psoriasis as severe based on Patient Global Assessment. By week 12, more than 50% of patients on tofacitinib at 10 mg twice daily or etanercept rated their skin as clear or almost clear.
More than 70% of patients in all three active treatment arms indicated at week 12 that they were satisfied with their medication. Satisfaction scores were highest, and equally so, in those on high-dose tofacitinib and etanercept.
“Patients using tofacitinib at the low dose had not that good an improvement. It was better improvement than with placebo, but it doesn’t look like etanercept,” Dr. Valenzuela concluded.
Tofacitinib is approved as Xeljanz for the treatment of rheumatoid arthritis, but remains investigational for psoriasis. According to a company statement, Pfizer intends to submit a supplemental New Drug Application (sNDA) to the Food and Drug Administration by early 2015.
The study was funded by Pfizer. Dr. Valenzuela is an adviser to Pfizer, AbbVie, Eli Lilly, Janssen, Merck, and Novartis.
AT THE EADV CONGRESS
Key clinical point: Multiple measures of quality of life and disease burden improved similarly in psoriasis patients regardless of whether they were on subcutaneous etanercept or the oral Janus kinase inhibitor tofacitinib.
Major finding: From a median baseline Dermatology Life Quality Index score of 12, scores improved by an average of 7.3 points after 12 weeks of tofacitinib at 5 mg twice daily, 9.7 points with tofacitinib at 10 mg twice daily, 9.0 points with etanercept at 50 mg twice weekly, and 1.9 points with placebo.
Data source: A phase III randomized, double-blind prospective study involving 1,101 patients with moderate to severe chronic plaque psoriasis.
Disclosures: The presenter is an adviser to Pfizer, which sponsored the study, and other pharmaceutical companies.

Novel oral prophylaxis tames hereditary angioedema
AMSTERDAM – A targeted oral medication for the prevention of potentially life-threatening episodes of hereditary angioedema produced a clinically meaningful reduction in attack frequency in a double-blind, placebo-controlled phase II study.
“This is very exciting. Without exaggeration, this is one of the deadliest and most challenging diseases that we deal with as dermatologists. What these patients want is oral prophylaxis, and we’ve got proof of concept with this trial. This is a bright new future for patients with hereditary angioedema, ” Dr. Marcus Maurer said in presenting the results of the OPuS-1 (Oral Prophylaxis for Hereditary Angioedema) trial at the annual congress of the European Academy of Dermatology and Venereology.

The investigational agent BCX4161 is a potent oral inhibitor of plasma kallikrein, which plays a key role in hereditary angioedema (HAE) by inducing vasodilation, edema, and nonvascular smooth muscle contraction.
OPuS-1 was a double-blind, randomized crossover study in which 24 patients with severe HAE were assigned to 4 weeks of BCX4161 at 400 mg or placebo three times daily, then switched to 4 weeks of the other regimen after a washout period. Participants averaged 42 years of age with a mean 32-year duration of HAE. At enrollment, they averaged 1.5 attacks per week, and they had a mean of 1.2 emergency department visits for HAE during the previous year. Twenty of the 24 patients had a history of one or more laryngeal attacks, the most serious manifestation of HAE, which eventually results in death by strangulation in roughly 30% of affected individuals, explained Dr. Maurer, professor of dermatology and allergy at Charité University Hospital in Berlin.
The primary outcome was the adjudicated attack rate, which was 1.27 attacks per week with placebo and a significantly lower 0.82 per week while patients were on BCX4161. Attacks averaged 20-23 hours in duration. Three patients were attack free on BCX4161; none was attack free during the placebo phase.
The novel agent also resulted in significant improvement on the secondary endpoints of quality of life and disease activity. Quality of life, as measured by the Angioedema Quality of Life questionnaire, improved by 8.4 points from baseline during active treatment, compared with 0.5 points with placebo. Disease activity, as assessed by the Angioedema Activity Score, or AA28, decreased while patients were on BCX4161, with a mean score of 21.4 vs. 28.8 with placebo.
The tolerability and side effects of BCX4161 were the same as with placebo. The rate of treatment compliance was 98%.
HAE is a rare and debilitating genetic disease with an estimated prevalence of 1 in 50,000. The most common symptoms include asymmetric swelling of the hands, feet, face, genitals, airway, and GI tract. HAE is caused by a deficiency of the C1 inhibitor, with resultant accumulation of bradykinin. By inhibiting plasma kallikrein, BCX4161 curbs bradykinin production.
“This disease has nothing to do with histamine or mast cells. This is not allergy or urticaria,” Dr. Maurer noted.
OPuS-2, a larger 12-week trial, is planned.
AMSTERDAM – A targeted oral medication for the prevention of potentially life-threatening episodes of hereditary angioedema produced a clinically meaningful reduction in attack frequency in a double-blind, placebo-controlled phase II study.
“This is very exciting. Without exaggeration, this is one of the deadliest and most challenging diseases that we deal with as dermatologists. What these patients want is oral prophylaxis, and we’ve got proof of concept with this trial. This is a bright new future for patients with hereditary angioedema, ” Dr. Marcus Maurer said in presenting the results of the OPuS-1 (Oral Prophylaxis for Hereditary Angioedema) trial at the annual congress of the European Academy of Dermatology and Venereology.
The investigational agent BCX4161 is a potent oral inhibitor of plasma kallikrein, which plays a key role in hereditary angioedema (HAE) by inducing vasodilation, edema, and nonvascular smooth muscle contraction.
OPuS-1 was a double-blind, randomized crossover study in which 24 patients with severe HAE were assigned to 4 weeks of BCX4161 at 400 mg or placebo three times daily, then switched to 4 weeks of the other regimen after a washout period. Participants averaged 42 years of age with a mean 32-year duration of HAE. At enrollment, they averaged 1.5 attacks per week, and they had a mean of 1.2 emergency department visits for HAE during the previous year. Twenty of the 24 patients had a history of one or more laryngeal attacks, the most serious manifestation of HAE, which eventually results in death by strangulation in roughly 30% of affected individuals, explained Dr. Maurer, professor of dermatology and allergy at Charité University Hospital in Berlin.
The primary outcome was the adjudicated attack rate, which was 1.27 attacks per week with placebo and a significantly lower 0.82 per week while patients were on BCX4161. Attacks averaged 20-23 hours in duration. Three patients were attack free on BCX4161; none was attack free during the placebo phase.
The novel agent also resulted in significant improvement on the secondary endpoints of quality of life and disease activity. Quality of life, as measured by the Angioedema Quality of Life questionnaire, improved by 8.4 points from baseline during active treatment, compared with 0.5 points with placebo. Disease activity, as assessed by the Angioedema Activity Score, or AA28, decreased while patients were on BCX4161, with a mean score of 21.4 vs. 28.8 with placebo.
The tolerability and side effects of BCX4161 were the same as with placebo. The rate of treatment compliance was 98%.
HAE is a rare and debilitating genetic disease with an estimated prevalence of 1 in 50,000. The most common symptoms include asymmetric swelling of the hands, feet, face, genitals, airway, and GI tract. HAE is caused by a deficiency of the C1 inhibitor, with resultant accumulation of bradykinin. By inhibiting plasma kallikrein, BCX4161 curbs bradykinin production.
“This disease has nothing to do with histamine or mast cells. This is not allergy or urticaria,” Dr. Maurer noted.
OPuS-2, a larger 12-week trial, is planned.
AMSTERDAM – A targeted oral medication for the prevention of potentially life-threatening episodes of hereditary angioedema produced a clinically meaningful reduction in attack frequency in a double-blind, placebo-controlled phase II study.
“This is very exciting. Without exaggeration, this is one of the deadliest and most challenging diseases that we deal with as dermatologists. What these patients want is oral prophylaxis, and we’ve got proof of concept with this trial. This is a bright new future for patients with hereditary angioedema, ” Dr. Marcus Maurer said in presenting the results of the OPuS-1 (Oral Prophylaxis for Hereditary Angioedema) trial at the annual congress of the European Academy of Dermatology and Venereology.
The investigational agent BCX4161 is a potent oral inhibitor of plasma kallikrein, which plays a key role in hereditary angioedema (HAE) by inducing vasodilation, edema, and nonvascular smooth muscle contraction.
OPuS-1 was a double-blind, randomized crossover study in which 24 patients with severe HAE were assigned to 4 weeks of BCX4161 at 400 mg or placebo three times daily, then switched to 4 weeks of the other regimen after a washout period. Participants averaged 42 years of age with a mean 32-year duration of HAE. At enrollment, they averaged 1.5 attacks per week, and they had a mean of 1.2 emergency department visits for HAE during the previous year. Twenty of the 24 patients had a history of one or more laryngeal attacks, the most serious manifestation of HAE, which eventually results in death by strangulation in roughly 30% of affected individuals, explained Dr. Maurer, professor of dermatology and allergy at Charité University Hospital in Berlin.
The primary outcome was the adjudicated attack rate, which was 1.27 attacks per week with placebo and a significantly lower 0.82 per week while patients were on BCX4161. Attacks averaged 20-23 hours in duration. Three patients were attack free on BCX4161; none was attack free during the placebo phase.
The novel agent also resulted in significant improvement on the secondary endpoints of quality of life and disease activity. Quality of life, as measured by the Angioedema Quality of Life questionnaire, improved by 8.4 points from baseline during active treatment, compared with 0.5 points with placebo. Disease activity, as assessed by the Angioedema Activity Score, or AA28, decreased while patients were on BCX4161, with a mean score of 21.4 vs. 28.8 with placebo.
The tolerability and side effects of BCX4161 were the same as with placebo. The rate of treatment compliance was 98%.
HAE is a rare and debilitating genetic disease with an estimated prevalence of 1 in 50,000. The most common symptoms include asymmetric swelling of the hands, feet, face, genitals, airway, and GI tract. HAE is caused by a deficiency of the C1 inhibitor, with resultant accumulation of bradykinin. By inhibiting plasma kallikrein, BCX4161 curbs bradykinin production.
“This disease has nothing to do with histamine or mast cells. This is not allergy or urticaria,” Dr. Maurer noted.
OPuS-2, a larger 12-week trial, is planned.
AT THE EADV CONGRESS
Key clinical point: A safe and effective oral daily drug for reducing the frequency of hereditary angioedema attacks is in the works.
Major finding: The mean angioedema attack rate was 1.27 episodes per week while patients were on placebo and significantly less at 0.82 attacks per week while they were on BCX4161.
Data source: OPuS-1, a randomized, double-blind, placebo-controlled crossover study, including 24 patients with severe hereditary angioedema.
Disclosures: The study was sponsored by BioCryst Pharmaceuticals. Dr. Maurer is a consultant to the company.

Adapalene/benzoyl peroxide + doxycycline outscores oral isotretinoin
AMSTERDAM – The combination of fixed-dose adapalene/benzoyl peroxide plus oral doxycyline is a reasonable alternative to oral isotretinoin in patients with severe nodular acne, according to the findings of a phase IIIb randomized head-to-head comparative study.
The topical/oral combination is a particularly attractive option for those patients who aren’t candidates for the potent oral retinoid, are unwilling to take it, or can’t tolerate its side effects, Dr. Jerry Tan said at the annual congress of the European Academy of Dermatology and Venereology.
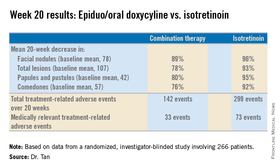
Dr. Tan presented the results of the phase IIIb POWER trial, a 20-week, multicenter, randomized investigator-blinded study involving 266 patients with an average age of 19 years. Participants were randomized to adapalene 0.1%/benzoyl peroxide 2.5% gel (Epiduo)plus oral doxycyline hyclate at 200 mg/day or to placebo gel plus oral isotretinoin at 0.5 mg/kg per day for the first 4 weeks and 1.0 mg/kg per day for the remaining 16 weeks.
At 2 weeks, patients in the combination treatment group averaged a 40% reduction in facial nodules, compared with baseline, versus a 24% decrease with isotretinoin. The combination treatment group also averaged a 27% reduction in facial papules and pustules, an effect size twice that seen in the isotretinoin group at that point. The combination therapy group had a 13% decrease in comedones, compared with 6% with isotretinoin, reported Dr. Tan, a dermatologist at the University of Western Ontario, London.
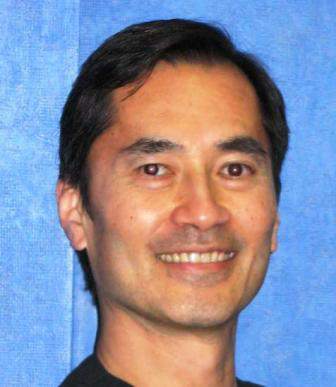
By the study’s end at week 20, however, isotretinoin showed superior efficacy. But this came at the cost of a significantly worse safety profile. Indeed, the only truly serious treatment-related adverse event seen in the study – a case of Stevens-Johnson syndrome requiring hospitalization – occurred in a patient on isotretinoin.
In an effort to capture both the strengths and drawbacks of each treatment strategy in a single metric, Dr. Tan and his coinvestigators came up with a prespecified novel endpoint they termed “the composite success rate.” They defined it as at least a 75% reduction in a patient’s nodule count, plus the absence of treatment-related, medically relevant adverse events. Based on this measure, the fixed-dose topical plus oral doxycycline regimen was more effective, with a 74% composite success rate, compared with 58% for isotretinoin.
The trial was funded by Galderma. Dr. Tan disclosed serving as a paid researcher for and consultant to Galderma and other pharmaceutical companies.
AMSTERDAM – The combination of fixed-dose adapalene/benzoyl peroxide plus oral doxycyline is a reasonable alternative to oral isotretinoin in patients with severe nodular acne, according to the findings of a phase IIIb randomized head-to-head comparative study.
The topical/oral combination is a particularly attractive option for those patients who aren’t candidates for the potent oral retinoid, are unwilling to take it, or can’t tolerate its side effects, Dr. Jerry Tan said at the annual congress of the European Academy of Dermatology and Venereology.
Dr. Tan presented the results of the phase IIIb POWER trial, a 20-week, multicenter, randomized investigator-blinded study involving 266 patients with an average age of 19 years. Participants were randomized to adapalene 0.1%/benzoyl peroxide 2.5% gel (Epiduo)plus oral doxycyline hyclate at 200 mg/day or to placebo gel plus oral isotretinoin at 0.5 mg/kg per day for the first 4 weeks and 1.0 mg/kg per day for the remaining 16 weeks.
At 2 weeks, patients in the combination treatment group averaged a 40% reduction in facial nodules, compared with baseline, versus a 24% decrease with isotretinoin. The combination treatment group also averaged a 27% reduction in facial papules and pustules, an effect size twice that seen in the isotretinoin group at that point. The combination therapy group had a 13% decrease in comedones, compared with 6% with isotretinoin, reported Dr. Tan, a dermatologist at the University of Western Ontario, London.
By the study’s end at week 20, however, isotretinoin showed superior efficacy. But this came at the cost of a significantly worse safety profile. Indeed, the only truly serious treatment-related adverse event seen in the study – a case of Stevens-Johnson syndrome requiring hospitalization – occurred in a patient on isotretinoin.
In an effort to capture both the strengths and drawbacks of each treatment strategy in a single metric, Dr. Tan and his coinvestigators came up with a prespecified novel endpoint they termed “the composite success rate.” They defined it as at least a 75% reduction in a patient’s nodule count, plus the absence of treatment-related, medically relevant adverse events. Based on this measure, the fixed-dose topical plus oral doxycycline regimen was more effective, with a 74% composite success rate, compared with 58% for isotretinoin.
The trial was funded by Galderma. Dr. Tan disclosed serving as a paid researcher for and consultant to Galderma and other pharmaceutical companies.
AMSTERDAM – The combination of fixed-dose adapalene/benzoyl peroxide plus oral doxycyline is a reasonable alternative to oral isotretinoin in patients with severe nodular acne, according to the findings of a phase IIIb randomized head-to-head comparative study.
The topical/oral combination is a particularly attractive option for those patients who aren’t candidates for the potent oral retinoid, are unwilling to take it, or can’t tolerate its side effects, Dr. Jerry Tan said at the annual congress of the European Academy of Dermatology and Venereology.
Dr. Tan presented the results of the phase IIIb POWER trial, a 20-week, multicenter, randomized investigator-blinded study involving 266 patients with an average age of 19 years. Participants were randomized to adapalene 0.1%/benzoyl peroxide 2.5% gel (Epiduo)plus oral doxycyline hyclate at 200 mg/day or to placebo gel plus oral isotretinoin at 0.5 mg/kg per day for the first 4 weeks and 1.0 mg/kg per day for the remaining 16 weeks.
At 2 weeks, patients in the combination treatment group averaged a 40% reduction in facial nodules, compared with baseline, versus a 24% decrease with isotretinoin. The combination treatment group also averaged a 27% reduction in facial papules and pustules, an effect size twice that seen in the isotretinoin group at that point. The combination therapy group had a 13% decrease in comedones, compared with 6% with isotretinoin, reported Dr. Tan, a dermatologist at the University of Western Ontario, London.
By the study’s end at week 20, however, isotretinoin showed superior efficacy. But this came at the cost of a significantly worse safety profile. Indeed, the only truly serious treatment-related adverse event seen in the study – a case of Stevens-Johnson syndrome requiring hospitalization – occurred in a patient on isotretinoin.
In an effort to capture both the strengths and drawbacks of each treatment strategy in a single metric, Dr. Tan and his coinvestigators came up with a prespecified novel endpoint they termed “the composite success rate.” They defined it as at least a 75% reduction in a patient’s nodule count, plus the absence of treatment-related, medically relevant adverse events. Based on this measure, the fixed-dose topical plus oral doxycycline regimen was more effective, with a 74% composite success rate, compared with 58% for isotretinoin.
The trial was funded by Galderma. Dr. Tan disclosed serving as a paid researcher for and consultant to Galderma and other pharmaceutical companies.
AT THE EADV CONGRESS
Key clinical point: The combination of fixed-dose adapalene/benzoyl peroxide plus oral doxycyline is an alternative to oral isotretinoin in patients with severe nodular acne.
Major finding: The composite success rate – a novel metric balancing efficacy and safety – was 74% in acne patients treated for 20 weeks with fixed-dose adapalene/benzoyl peroxide gel plus oral doxycycline, compared with 58% in those treated with oral isotretinoin.
Data source: A 20-week, multicenter, randomized, placebo-controlled, investigator-blinded, phase IIIb clinical trial involving 266 patients with severe nodular acne.
Disclosures: The POWER study was funded by Galderma. The presenter has received research grants from and serves as a consultant to Galderma and other pharmaceutical companies.
Psoriasis: Brodalumab maintains efficacy through 144 weeks
AMSTERDAM – The majority of psoriasis patients placed on the investigational biologic agent brodalumab maintained a PASI 100 response throughout 144 weeks in a long-term, open-label extension of a phase II study.
“The benefit/risk ratio of brodalumab remains very favorable, and warrants continued development of this anti–interleukin-17 receptor A human monoclonal antibody as a potential treatment for psoriasis,” Dr. Kim Papp declared in presenting the study results at the annual congress of the European Academy of Dermatology and Venereology.
Large phase III clinical trials of brodalumab for the treatment of moderate to severe plaque psoriasis are ongoing.
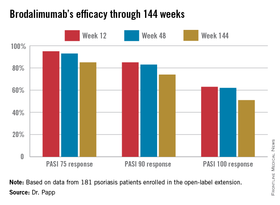
The parent phase II study was 16 weeks long, double blinded, and placebo controlled. At the study’s end, 181 participants enrolled in the open-label extension, in which they received subcutaneous brodalumab at 210 mg every 2 weeks. The study protocol was amended after about a year, with the dose reduced to 140 mg every 2 weeks in the 119 patients weighing 100 kg or less. Six of those patients subsequently had an inadequate response to the lower dose, and were returned to the higher-dose regimen, explained Dr. Papp of Probity Medical Research in Waterloo, Ont.
Roughly 95% of patients became PASI 75 responders within the first few weeks. There was very little drop-off over time. The PASI 75 response rate was 95% at week 12, 93% at week 48, and 85% at week 144.
At week 144, roughly two-thirds of subjects were deemed clear or almost clear according to Physician Global Assessment.
No new safety signals emerged during this long-term study. The most common adverse events were minor upper respiratory infections. Two percent of patients developed a grade 2 absolute neutrophil count of less than 1,500 per 109/L; however, these were transitory events that resolved without a change in treatment.
In response to an audience question, Dr. Papp said antidrug antibodies did develop in some patients during the course of 144 weeks of treatment, but he had no information as to the clinical effect, if any.
“This is a fairly small study population. I think it makes sense to wait for the phase III results to see if the antibodies affect safety and/or efficacy,” he added.
Dr. Papp reported receiving research support from Amgen, which is codeveloping brodalumab with AstraZeneca/MedImmune.
AMSTERDAM – The majority of psoriasis patients placed on the investigational biologic agent brodalumab maintained a PASI 100 response throughout 144 weeks in a long-term, open-label extension of a phase II study.
“The benefit/risk ratio of brodalumab remains very favorable, and warrants continued development of this anti–interleukin-17 receptor A human monoclonal antibody as a potential treatment for psoriasis,” Dr. Kim Papp declared in presenting the study results at the annual congress of the European Academy of Dermatology and Venereology.
Large phase III clinical trials of brodalumab for the treatment of moderate to severe plaque psoriasis are ongoing.
The parent phase II study was 16 weeks long, double blinded, and placebo controlled. At the study’s end, 181 participants enrolled in the open-label extension, in which they received subcutaneous brodalumab at 210 mg every 2 weeks. The study protocol was amended after about a year, with the dose reduced to 140 mg every 2 weeks in the 119 patients weighing 100 kg or less. Six of those patients subsequently had an inadequate response to the lower dose, and were returned to the higher-dose regimen, explained Dr. Papp of Probity Medical Research in Waterloo, Ont.
Roughly 95% of patients became PASI 75 responders within the first few weeks. There was very little drop-off over time. The PASI 75 response rate was 95% at week 12, 93% at week 48, and 85% at week 144.
At week 144, roughly two-thirds of subjects were deemed clear or almost clear according to Physician Global Assessment.
No new safety signals emerged during this long-term study. The most common adverse events were minor upper respiratory infections. Two percent of patients developed a grade 2 absolute neutrophil count of less than 1,500 per 109/L; however, these were transitory events that resolved without a change in treatment.
In response to an audience question, Dr. Papp said antidrug antibodies did develop in some patients during the course of 144 weeks of treatment, but he had no information as to the clinical effect, if any.
“This is a fairly small study population. I think it makes sense to wait for the phase III results to see if the antibodies affect safety and/or efficacy,” he added.
Dr. Papp reported receiving research support from Amgen, which is codeveloping brodalumab with AstraZeneca/MedImmune.
AMSTERDAM – The majority of psoriasis patients placed on the investigational biologic agent brodalumab maintained a PASI 100 response throughout 144 weeks in a long-term, open-label extension of a phase II study.
“The benefit/risk ratio of brodalumab remains very favorable, and warrants continued development of this anti–interleukin-17 receptor A human monoclonal antibody as a potential treatment for psoriasis,” Dr. Kim Papp declared in presenting the study results at the annual congress of the European Academy of Dermatology and Venereology.
Large phase III clinical trials of brodalumab for the treatment of moderate to severe plaque psoriasis are ongoing.
The parent phase II study was 16 weeks long, double blinded, and placebo controlled. At the study’s end, 181 participants enrolled in the open-label extension, in which they received subcutaneous brodalumab at 210 mg every 2 weeks. The study protocol was amended after about a year, with the dose reduced to 140 mg every 2 weeks in the 119 patients weighing 100 kg or less. Six of those patients subsequently had an inadequate response to the lower dose, and were returned to the higher-dose regimen, explained Dr. Papp of Probity Medical Research in Waterloo, Ont.
Roughly 95% of patients became PASI 75 responders within the first few weeks. There was very little drop-off over time. The PASI 75 response rate was 95% at week 12, 93% at week 48, and 85% at week 144.
At week 144, roughly two-thirds of subjects were deemed clear or almost clear according to Physician Global Assessment.
No new safety signals emerged during this long-term study. The most common adverse events were minor upper respiratory infections. Two percent of patients developed a grade 2 absolute neutrophil count of less than 1,500 per 109/L; however, these were transitory events that resolved without a change in treatment.
In response to an audience question, Dr. Papp said antidrug antibodies did develop in some patients during the course of 144 weeks of treatment, but he had no information as to the clinical effect, if any.
“This is a fairly small study population. I think it makes sense to wait for the phase III results to see if the antibodies affect safety and/or efficacy,” he added.
Dr. Papp reported receiving research support from Amgen, which is codeveloping brodalumab with AstraZeneca/MedImmune.
AT THE EADV CONGRESS
Key clinical point: The investigational interleukin-17 receptor A inhibitor brodalumab maintained strong clinical efficacy throughout 144 weeks of psoriasis treatment.
Major finding: The PASI 90 response rate to brodalumab was 85% at week 12, 83% at week 48, and 74% at week 144.
Data source: A 181-patient, prospective, open-label extension of a phase II study.
Disclosures: Dr. Papp reported receiving financial support from Amgen, which is codeveloping brodalumab with AstraZeneca/MedImmune.
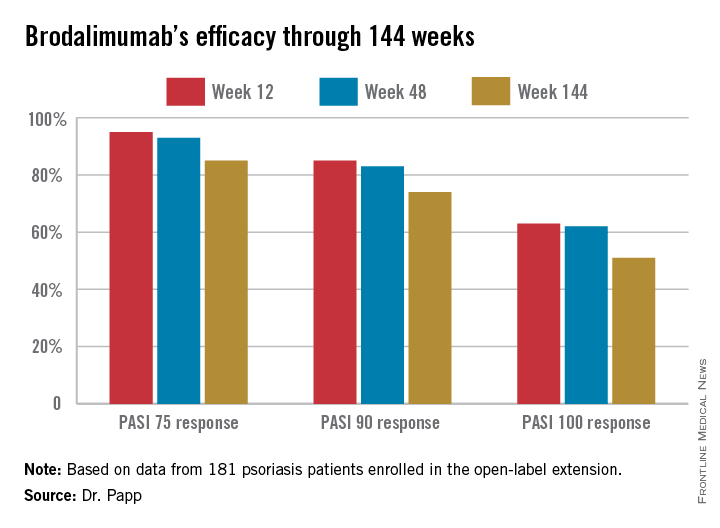
Dupilumab Advances for Severe Atopic Dermatitis
AMSTERDAM – The novel biologic agent dupilumab showed strong dose-dependent efficacy in adults with moderate to severe atopic dermatitis not adequately controlled with topical medications in a 380-patient phase IIb dose-ranging study.
“Based on the results of this study, we’ll take the top two doses further to our phase III program. We’re also planning to conduct a maintenance study. At the end of 16 weeks of treatment, we’ll investigate lower-dose regimens that may be capable of maintaining clinical response,” Dr. Marius Ardeleanu said at the annual congress of the European Academy of Dermatology and Venereology.
Dipilumab is an investigational fully human monoclonal antibody that addresses a novel target: It is directed against the interleukin-4 receptor alpha subunit (IL-4Ra). Through this effect it blocks IL-4 and IL-17, the drivers of the type 2 helper T-cell–mediated inflammation responsible for the hallmark symptoms of atopic dermatitis (AD), explained Dr. Ardeleanu of Regeneron Pharmaceuticals in Tarrytown, N.Y.
Participants in this 16-week, double-blind, international phase IIb study were randomized to placebo or one of five dupilumab dosing regimens ranging from a low of 100 mg given subcutaneously every 4 weeks to a maximum of 300 mg once weekly or every 2 weeks.
These patients had a significant disease burden. They were typically in their mid- to late 30s and had a 27-year disease history, a mean baseline SCORAD of 67 on a 0-100 scale, a baseline Eczema Area and Severity Index (EASI) score of 32, an Investigator’s Global Assessment of disease severity score of 3.5 on a 0-4 scale, and 50% body surface area involvement. Their mean average weekly self-rated itching score was 6.8 on a 0-10 scale.
The primary study endpoint was change in the EASI score from baseline to 16 weeks. The score dropped by 20% in placebo-treated controls and by significantly greater margins in all five dupilumab arms. The largest reduction in EASI score – nearly 80% – occurred in the group on 300 mg/wk, with the 300 mg every 2 weeks group showing about a 70% reduction.
Roughly 80% of patients on 300 mg/wk or every 2 weeks showed an EASI 50 response at week 16, meaning a 50% reduction from baseline in their score, which is considered clinically meaningful improvement. One-third of patients on either of these top two–performing regimens achieved an Investigator’s Global Assessment score of 0 or 1, which is virtual remission; none of the controls did. Overall weekly average pruritus scores dropped by more than 60% with weekly treatment at 300 mg and by slightly less with biweekly therapy at 300 mg.
Safety data were similar to those from a recently published earlier phase IIa study (N. Engl. J. Med. 2014; 371:130-9). There were no dose-limiting toxicities. Headache and injection site reactions were the only adverse events more common with dupilumab than with placebo in the phase IIb trial, with the incidence of injection site reactions showing a possible dose-response relationship.
In addition to the large phase III studies now being planned, which will also evaluate step-down maintenance therapy, another study has been scheduled to investigate the use of dupilumab in combination with topical corticosteroid therapy. The earlier phase IIa study provided evidence to suggest this combination has even greater efficacy than dupilumab alone, and with modest use of the topical agent, according to Dr. Ardeleanu.
Dupilumab is also being developed as a treatment for tough-to-control moderate to severe asthma. It showed positive results in a phase II study, with reduced asthma exacerbations and improved lung function, compared with placebo (N. Engl. J. Med. 2013; 368:2455-66).
AMSTERDAM – The novel biologic agent dupilumab showed strong dose-dependent efficacy in adults with moderate to severe atopic dermatitis not adequately controlled with topical medications in a 380-patient phase IIb dose-ranging study.
“Based on the results of this study, we’ll take the top two doses further to our phase III program. We’re also planning to conduct a maintenance study. At the end of 16 weeks of treatment, we’ll investigate lower-dose regimens that may be capable of maintaining clinical response,” Dr. Marius Ardeleanu said at the annual congress of the European Academy of Dermatology and Venereology.
Dipilumab is an investigational fully human monoclonal antibody that addresses a novel target: It is directed against the interleukin-4 receptor alpha subunit (IL-4Ra). Through this effect it blocks IL-4 and IL-17, the drivers of the type 2 helper T-cell–mediated inflammation responsible for the hallmark symptoms of atopic dermatitis (AD), explained Dr. Ardeleanu of Regeneron Pharmaceuticals in Tarrytown, N.Y.
Participants in this 16-week, double-blind, international phase IIb study were randomized to placebo or one of five dupilumab dosing regimens ranging from a low of 100 mg given subcutaneously every 4 weeks to a maximum of 300 mg once weekly or every 2 weeks.
These patients had a significant disease burden. They were typically in their mid- to late 30s and had a 27-year disease history, a mean baseline SCORAD of 67 on a 0-100 scale, a baseline Eczema Area and Severity Index (EASI) score of 32, an Investigator’s Global Assessment of disease severity score of 3.5 on a 0-4 scale, and 50% body surface area involvement. Their mean average weekly self-rated itching score was 6.8 on a 0-10 scale.
The primary study endpoint was change in the EASI score from baseline to 16 weeks. The score dropped by 20% in placebo-treated controls and by significantly greater margins in all five dupilumab arms. The largest reduction in EASI score – nearly 80% – occurred in the group on 300 mg/wk, with the 300 mg every 2 weeks group showing about a 70% reduction.
Roughly 80% of patients on 300 mg/wk or every 2 weeks showed an EASI 50 response at week 16, meaning a 50% reduction from baseline in their score, which is considered clinically meaningful improvement. One-third of patients on either of these top two–performing regimens achieved an Investigator’s Global Assessment score of 0 or 1, which is virtual remission; none of the controls did. Overall weekly average pruritus scores dropped by more than 60% with weekly treatment at 300 mg and by slightly less with biweekly therapy at 300 mg.
Safety data were similar to those from a recently published earlier phase IIa study (N. Engl. J. Med. 2014; 371:130-9). There were no dose-limiting toxicities. Headache and injection site reactions were the only adverse events more common with dupilumab than with placebo in the phase IIb trial, with the incidence of injection site reactions showing a possible dose-response relationship.
In addition to the large phase III studies now being planned, which will also evaluate step-down maintenance therapy, another study has been scheduled to investigate the use of dupilumab in combination with topical corticosteroid therapy. The earlier phase IIa study provided evidence to suggest this combination has even greater efficacy than dupilumab alone, and with modest use of the topical agent, according to Dr. Ardeleanu.
Dupilumab is also being developed as a treatment for tough-to-control moderate to severe asthma. It showed positive results in a phase II study, with reduced asthma exacerbations and improved lung function, compared with placebo (N. Engl. J. Med. 2013; 368:2455-66).
AMSTERDAM – The novel biologic agent dupilumab showed strong dose-dependent efficacy in adults with moderate to severe atopic dermatitis not adequately controlled with topical medications in a 380-patient phase IIb dose-ranging study.
“Based on the results of this study, we’ll take the top two doses further to our phase III program. We’re also planning to conduct a maintenance study. At the end of 16 weeks of treatment, we’ll investigate lower-dose regimens that may be capable of maintaining clinical response,” Dr. Marius Ardeleanu said at the annual congress of the European Academy of Dermatology and Venereology.
Dipilumab is an investigational fully human monoclonal antibody that addresses a novel target: It is directed against the interleukin-4 receptor alpha subunit (IL-4Ra). Through this effect it blocks IL-4 and IL-17, the drivers of the type 2 helper T-cell–mediated inflammation responsible for the hallmark symptoms of atopic dermatitis (AD), explained Dr. Ardeleanu of Regeneron Pharmaceuticals in Tarrytown, N.Y.
Participants in this 16-week, double-blind, international phase IIb study were randomized to placebo or one of five dupilumab dosing regimens ranging from a low of 100 mg given subcutaneously every 4 weeks to a maximum of 300 mg once weekly or every 2 weeks.
These patients had a significant disease burden. They were typically in their mid- to late 30s and had a 27-year disease history, a mean baseline SCORAD of 67 on a 0-100 scale, a baseline Eczema Area and Severity Index (EASI) score of 32, an Investigator’s Global Assessment of disease severity score of 3.5 on a 0-4 scale, and 50% body surface area involvement. Their mean average weekly self-rated itching score was 6.8 on a 0-10 scale.
The primary study endpoint was change in the EASI score from baseline to 16 weeks. The score dropped by 20% in placebo-treated controls and by significantly greater margins in all five dupilumab arms. The largest reduction in EASI score – nearly 80% – occurred in the group on 300 mg/wk, with the 300 mg every 2 weeks group showing about a 70% reduction.
Roughly 80% of patients on 300 mg/wk or every 2 weeks showed an EASI 50 response at week 16, meaning a 50% reduction from baseline in their score, which is considered clinically meaningful improvement. One-third of patients on either of these top two–performing regimens achieved an Investigator’s Global Assessment score of 0 or 1, which is virtual remission; none of the controls did. Overall weekly average pruritus scores dropped by more than 60% with weekly treatment at 300 mg and by slightly less with biweekly therapy at 300 mg.
Safety data were similar to those from a recently published earlier phase IIa study (N. Engl. J. Med. 2014; 371:130-9). There were no dose-limiting toxicities. Headache and injection site reactions were the only adverse events more common with dupilumab than with placebo in the phase IIb trial, with the incidence of injection site reactions showing a possible dose-response relationship.
In addition to the large phase III studies now being planned, which will also evaluate step-down maintenance therapy, another study has been scheduled to investigate the use of dupilumab in combination with topical corticosteroid therapy. The earlier phase IIa study provided evidence to suggest this combination has even greater efficacy than dupilumab alone, and with modest use of the topical agent, according to Dr. Ardeleanu.
Dupilumab is also being developed as a treatment for tough-to-control moderate to severe asthma. It showed positive results in a phase II study, with reduced asthma exacerbations and improved lung function, compared with placebo (N. Engl. J. Med. 2013; 368:2455-66).
AT THE EADV CONGRESS
