User login
OsteoArthritis Research Society International (OARSI): World Congress on Osteoarthritis
Glucosamine, chondroitin combo found equal to celecoxib for severe knee OA pain
PARIS – A fixed-dose combination of glucosamine and chondroitin sulfate was as good as the cyclo-oxygenase-2 inhibitor celecoxib in relieving moderate to severe knee pain in patients with knee osteoarthritis in the double-blind, noninferiority MOVES trial.
Side effect profiles and tolerability were also similar with glucosamine/chondroitin (Droglican) and celecoxib (Celebrex), with 51% of patients overall experiencing treatment-emergent adverse events, Dr. Marc Hochberg reported at the World Congress on Osteoarthritis.

"In a group that is either contraindicated or relatively contraindicated to celecoxib, you get similar efficacy [with Droglican] at 6 months," he said in an interview.
Dr. Hochberg noted that the phase IV (MOVES) Multicentric Osteoarthritis Intervention Study enrolled patients who were consistent with the European label for celecoxib, meaning that those with prior coronary artery disease or peripheral artery disease were excluded, as were those with unstable diabetes or uncontrolled hypertension.
MOVES was designed to extend the findings of the GAIT (Glucosamine/Chondroitin Arthritis Intervention Trial), which suggested in exploratory analyses that combination 1,500 mg daily glucosamine and 1,200 mg daily chondroitin sulfate was effective in the subgroup with moderate to severe knee osteoarthritis pain, but that either agent alone or in combination was not effective in reducing osteoarthritis knee pain in the overall cohort (N. Engl. J. Med. 2006;354:795-808).
MOVES randomly assigned 606 patients in a double-blind, double-dummy fashion to receive either two capsules of Droglican (250 mg glucosamine and 200 mg chondroitin sulfate) three times daily or celecoxib 200 mg plus five placebo capsules per day. Two-thirds of patients (62.6%) had Kellgren-Lawrence grade 2 radiological changes, and 84% were female. Their mean age was 62.7 years.
At 180 days, the mean WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores in the Droglican and celecoxib groups improved from 372 and 370.6, respectively, to 185.8 and 184.7.
This corresponds to a mean difference of 1.11 units (95% confidence interval, –21.99-19.76; P = .917), which met the noninferiority margin, according to Dr. Hochberg, head of rheumatology and clinical immunology, University of Maryland, Baltimore.The results remained robust in sensitivity analyses.
There also were no significant differences between the two groups in the absolute improvement in the WOMAC stiffness and function scales and the five individual items of the WOMAC pain scale at 6 months, Dr. Hochberg reported at the meeting, sponsored by the Osteoarthritis Research Society International.
Dr. Hochberg reported no conflicts. His coauthors were employees or on the steering committee for Bioiberica, the study sponsor and maker of Droglican.
PARIS – A fixed-dose combination of glucosamine and chondroitin sulfate was as good as the cyclo-oxygenase-2 inhibitor celecoxib in relieving moderate to severe knee pain in patients with knee osteoarthritis in the double-blind, noninferiority MOVES trial.
Side effect profiles and tolerability were also similar with glucosamine/chondroitin (Droglican) and celecoxib (Celebrex), with 51% of patients overall experiencing treatment-emergent adverse events, Dr. Marc Hochberg reported at the World Congress on Osteoarthritis.
"In a group that is either contraindicated or relatively contraindicated to celecoxib, you get similar efficacy [with Droglican] at 6 months," he said in an interview.
Dr. Hochberg noted that the phase IV (MOVES) Multicentric Osteoarthritis Intervention Study enrolled patients who were consistent with the European label for celecoxib, meaning that those with prior coronary artery disease or peripheral artery disease were excluded, as were those with unstable diabetes or uncontrolled hypertension.
MOVES was designed to extend the findings of the GAIT (Glucosamine/Chondroitin Arthritis Intervention Trial), which suggested in exploratory analyses that combination 1,500 mg daily glucosamine and 1,200 mg daily chondroitin sulfate was effective in the subgroup with moderate to severe knee osteoarthritis pain, but that either agent alone or in combination was not effective in reducing osteoarthritis knee pain in the overall cohort (N. Engl. J. Med. 2006;354:795-808).
MOVES randomly assigned 606 patients in a double-blind, double-dummy fashion to receive either two capsules of Droglican (250 mg glucosamine and 200 mg chondroitin sulfate) three times daily or celecoxib 200 mg plus five placebo capsules per day. Two-thirds of patients (62.6%) had Kellgren-Lawrence grade 2 radiological changes, and 84% were female. Their mean age was 62.7 years.
At 180 days, the mean WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores in the Droglican and celecoxib groups improved from 372 and 370.6, respectively, to 185.8 and 184.7.
This corresponds to a mean difference of 1.11 units (95% confidence interval, –21.99-19.76; P = .917), which met the noninferiority margin, according to Dr. Hochberg, head of rheumatology and clinical immunology, University of Maryland, Baltimore.The results remained robust in sensitivity analyses.
There also were no significant differences between the two groups in the absolute improvement in the WOMAC stiffness and function scales and the five individual items of the WOMAC pain scale at 6 months, Dr. Hochberg reported at the meeting, sponsored by the Osteoarthritis Research Society International.
Dr. Hochberg reported no conflicts. His coauthors were employees or on the steering committee for Bioiberica, the study sponsor and maker of Droglican.
PARIS – A fixed-dose combination of glucosamine and chondroitin sulfate was as good as the cyclo-oxygenase-2 inhibitor celecoxib in relieving moderate to severe knee pain in patients with knee osteoarthritis in the double-blind, noninferiority MOVES trial.
Side effect profiles and tolerability were also similar with glucosamine/chondroitin (Droglican) and celecoxib (Celebrex), with 51% of patients overall experiencing treatment-emergent adverse events, Dr. Marc Hochberg reported at the World Congress on Osteoarthritis.
"In a group that is either contraindicated or relatively contraindicated to celecoxib, you get similar efficacy [with Droglican] at 6 months," he said in an interview.
Dr. Hochberg noted that the phase IV (MOVES) Multicentric Osteoarthritis Intervention Study enrolled patients who were consistent with the European label for celecoxib, meaning that those with prior coronary artery disease or peripheral artery disease were excluded, as were those with unstable diabetes or uncontrolled hypertension.
MOVES was designed to extend the findings of the GAIT (Glucosamine/Chondroitin Arthritis Intervention Trial), which suggested in exploratory analyses that combination 1,500 mg daily glucosamine and 1,200 mg daily chondroitin sulfate was effective in the subgroup with moderate to severe knee osteoarthritis pain, but that either agent alone or in combination was not effective in reducing osteoarthritis knee pain in the overall cohort (N. Engl. J. Med. 2006;354:795-808).
MOVES randomly assigned 606 patients in a double-blind, double-dummy fashion to receive either two capsules of Droglican (250 mg glucosamine and 200 mg chondroitin sulfate) three times daily or celecoxib 200 mg plus five placebo capsules per day. Two-thirds of patients (62.6%) had Kellgren-Lawrence grade 2 radiological changes, and 84% were female. Their mean age was 62.7 years.
At 180 days, the mean WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores in the Droglican and celecoxib groups improved from 372 and 370.6, respectively, to 185.8 and 184.7.
This corresponds to a mean difference of 1.11 units (95% confidence interval, –21.99-19.76; P = .917), which met the noninferiority margin, according to Dr. Hochberg, head of rheumatology and clinical immunology, University of Maryland, Baltimore.The results remained robust in sensitivity analyses.
There also were no significant differences between the two groups in the absolute improvement in the WOMAC stiffness and function scales and the five individual items of the WOMAC pain scale at 6 months, Dr. Hochberg reported at the meeting, sponsored by the Osteoarthritis Research Society International.
Dr. Hochberg reported no conflicts. His coauthors were employees or on the steering committee for Bioiberica, the study sponsor and maker of Droglican.
AT OARSI 2014
Key clinical point: Patients with moderate to severe knee OA pain who do not have prior coronary artery disease or peripheral artery disease or unstable diabetes or uncontrolled hypertension have similar reductions in pain with either celecoxib 200 mg daily or a combination of 250 mg glucosamine and 200 mg chondroitin sulfate three times daily.
Major finding: Mean WOMAC scores improved in the Droglican and celecoxib groups from 372 and 370.6 at baseline to 185.8 and 184.7 at 180 days.
Data source: A prospective, double-blind, double-dummy trial in 606 patients with moderate to severe knee OA pain.
Disclosures: Dr. Hochberg reported no conflicts. His coauthors were employees or on the steering committee for Bioiberica, the study sponsor and maker of Droglican.

Inflammatory ultrasound changes track with hand OA progression
PARIS – Inflammatory ultrasound features in hand osteoarthritis may point clinicians toward patients at higher risk for radiographic progression, a longitudinal study suggests.
"We found inflammatory ultrasound features are independently associated with both progressive joint space narrowing and progression of osteophytes in hand osteoarthritis. This is especially true with persistent inflammation," Dr. Marion Kortekaas said at the World Congress on Osteoarthritis.

She presented data on 56 consecutive hand OA patients who underwent baseline and 2.3-year follow-up radiographic and ultrasound assessment of all first carpometacarpal, distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first interphalangeal joints.
Radiographs were scored for osteophytes and joint space narrowing using the OARSI Atlas grading system (0-3 scale). Ultrasound synovial thickening, effusion, and power Doppler signal (PDS) were scored on a validated 3-point scale, with 3 being severe. Progression was defined as at least one grade increase of either joint space narrowing or osteophytes, explained Dr. Kortekaas, a rheumatologist at Leiden (the Netherlands) University Medical Center.
Most patients were female (86%) and their average age was 61 years. Patients with rheumatic diseases, trauma/operation, and corticosteroid use were excluded.
Of 1,680 joints at baseline, 141 (8.4%) had synovial thickening, 332 (19.8%) effusion, and 146 (8.7%) PDS.
At follow-up, progression of osteophytes and joint space narrowing was present in 120 and 96 joints, respectively, she said.
PDS, synovial thickening, and effusion were "persistent," defined as present at baseline and follow-up, in 40, 118, and 232 joints, and were "fluctuating," or present only at baseline or follow-up, in 243, 641, and 636 joints, respectively.
Using generalized estimating equations analyses, progression was independently associated with ultrasound synovial thickening (odds ratio, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7) for grade 2-3 vs. grade 0, after adjustment for age, sex, body mass index, baseline osteophytes, and joint space narrowing scores, Dr. Kortekaas said.
Joint space narrowing was also independently associated with the ultrasound features of synovial thickening (OR, 3.4), effusion (OR, 3.3), and power Doppler signal (OR, 3.1), again after adjustment and comparing grade 2-3 vs. grade 0.
Persistent inflammation showed stronger associations with radiographic progression than did fluctuating inflammatory features in comparison with no inflammatory features at all, she said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, Dr. Kortekaas said inflammatory and synovial changes are loosely related to symptoms and pain, but that the group has yet to look at an association with C-reactive protein or inflammation in other joints.
Session comoderator Dr. Gillian Hawker, professor of medicine at the University of Toronto and physician in chief of medicine at Women’s College Hospital, Toronto, commented that until recently, ultrasound for hand OA has been far more common in clinical practice in Europe than in North America.
"I think that’s exactly where the radiology community is starting to go," she said in an interview. "Would we be doing a better job, picking things up earlier if we were ultrasounding? [There’s] definitely higher sensitivity. But, we haven’t quite gotten there yet. It’s going to cost money to get ultrasound machines into practices and train physicians."
Dr. Hawker observed that the American College of Radiology has added an ultrasound course and that residents at her institution are now going through ultrasound training as part of their residency.
Dr. Kortekaas and her coauthors reported no conflicting interests.
PARIS – Inflammatory ultrasound features in hand osteoarthritis may point clinicians toward patients at higher risk for radiographic progression, a longitudinal study suggests.
"We found inflammatory ultrasound features are independently associated with both progressive joint space narrowing and progression of osteophytes in hand osteoarthritis. This is especially true with persistent inflammation," Dr. Marion Kortekaas said at the World Congress on Osteoarthritis.
She presented data on 56 consecutive hand OA patients who underwent baseline and 2.3-year follow-up radiographic and ultrasound assessment of all first carpometacarpal, distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first interphalangeal joints.
Radiographs were scored for osteophytes and joint space narrowing using the OARSI Atlas grading system (0-3 scale). Ultrasound synovial thickening, effusion, and power Doppler signal (PDS) were scored on a validated 3-point scale, with 3 being severe. Progression was defined as at least one grade increase of either joint space narrowing or osteophytes, explained Dr. Kortekaas, a rheumatologist at Leiden (the Netherlands) University Medical Center.
Most patients were female (86%) and their average age was 61 years. Patients with rheumatic diseases, trauma/operation, and corticosteroid use were excluded.
Of 1,680 joints at baseline, 141 (8.4%) had synovial thickening, 332 (19.8%) effusion, and 146 (8.7%) PDS.
At follow-up, progression of osteophytes and joint space narrowing was present in 120 and 96 joints, respectively, she said.
PDS, synovial thickening, and effusion were "persistent," defined as present at baseline and follow-up, in 40, 118, and 232 joints, and were "fluctuating," or present only at baseline or follow-up, in 243, 641, and 636 joints, respectively.
Using generalized estimating equations analyses, progression was independently associated with ultrasound synovial thickening (odds ratio, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7) for grade 2-3 vs. grade 0, after adjustment for age, sex, body mass index, baseline osteophytes, and joint space narrowing scores, Dr. Kortekaas said.
Joint space narrowing was also independently associated with the ultrasound features of synovial thickening (OR, 3.4), effusion (OR, 3.3), and power Doppler signal (OR, 3.1), again after adjustment and comparing grade 2-3 vs. grade 0.
Persistent inflammation showed stronger associations with radiographic progression than did fluctuating inflammatory features in comparison with no inflammatory features at all, she said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, Dr. Kortekaas said inflammatory and synovial changes are loosely related to symptoms and pain, but that the group has yet to look at an association with C-reactive protein or inflammation in other joints.
Session comoderator Dr. Gillian Hawker, professor of medicine at the University of Toronto and physician in chief of medicine at Women’s College Hospital, Toronto, commented that until recently, ultrasound for hand OA has been far more common in clinical practice in Europe than in North America.
"I think that’s exactly where the radiology community is starting to go," she said in an interview. "Would we be doing a better job, picking things up earlier if we were ultrasounding? [There’s] definitely higher sensitivity. But, we haven’t quite gotten there yet. It’s going to cost money to get ultrasound machines into practices and train physicians."
Dr. Hawker observed that the American College of Radiology has added an ultrasound course and that residents at her institution are now going through ultrasound training as part of their residency.
Dr. Kortekaas and her coauthors reported no conflicting interests.
PARIS – Inflammatory ultrasound features in hand osteoarthritis may point clinicians toward patients at higher risk for radiographic progression, a longitudinal study suggests.
"We found inflammatory ultrasound features are independently associated with both progressive joint space narrowing and progression of osteophytes in hand osteoarthritis. This is especially true with persistent inflammation," Dr. Marion Kortekaas said at the World Congress on Osteoarthritis.
She presented data on 56 consecutive hand OA patients who underwent baseline and 2.3-year follow-up radiographic and ultrasound assessment of all first carpometacarpal, distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first interphalangeal joints.
Radiographs were scored for osteophytes and joint space narrowing using the OARSI Atlas grading system (0-3 scale). Ultrasound synovial thickening, effusion, and power Doppler signal (PDS) were scored on a validated 3-point scale, with 3 being severe. Progression was defined as at least one grade increase of either joint space narrowing or osteophytes, explained Dr. Kortekaas, a rheumatologist at Leiden (the Netherlands) University Medical Center.
Most patients were female (86%) and their average age was 61 years. Patients with rheumatic diseases, trauma/operation, and corticosteroid use were excluded.
Of 1,680 joints at baseline, 141 (8.4%) had synovial thickening, 332 (19.8%) effusion, and 146 (8.7%) PDS.
At follow-up, progression of osteophytes and joint space narrowing was present in 120 and 96 joints, respectively, she said.
PDS, synovial thickening, and effusion were "persistent," defined as present at baseline and follow-up, in 40, 118, and 232 joints, and were "fluctuating," or present only at baseline or follow-up, in 243, 641, and 636 joints, respectively.
Using generalized estimating equations analyses, progression was independently associated with ultrasound synovial thickening (odds ratio, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7) for grade 2-3 vs. grade 0, after adjustment for age, sex, body mass index, baseline osteophytes, and joint space narrowing scores, Dr. Kortekaas said.
Joint space narrowing was also independently associated with the ultrasound features of synovial thickening (OR, 3.4), effusion (OR, 3.3), and power Doppler signal (OR, 3.1), again after adjustment and comparing grade 2-3 vs. grade 0.
Persistent inflammation showed stronger associations with radiographic progression than did fluctuating inflammatory features in comparison with no inflammatory features at all, she said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, Dr. Kortekaas said inflammatory and synovial changes are loosely related to symptoms and pain, but that the group has yet to look at an association with C-reactive protein or inflammation in other joints.
Session comoderator Dr. Gillian Hawker, professor of medicine at the University of Toronto and physician in chief of medicine at Women’s College Hospital, Toronto, commented that until recently, ultrasound for hand OA has been far more common in clinical practice in Europe than in North America.
"I think that’s exactly where the radiology community is starting to go," she said in an interview. "Would we be doing a better job, picking things up earlier if we were ultrasounding? [There’s] definitely higher sensitivity. But, we haven’t quite gotten there yet. It’s going to cost money to get ultrasound machines into practices and train physicians."
Dr. Hawker observed that the American College of Radiology has added an ultrasound course and that residents at her institution are now going through ultrasound training as part of their residency.
Dr. Kortekaas and her coauthors reported no conflicting interests.
AT OARSI 2014
Key clinical point: Patients with inflammatory changes in hand OA on ultrasound during follow-up are at higher risk for radiographic progression.
Major finding: In adjusted analyses, hand OA progression was independently associated with ultrasound synovial thickening (OR, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7).
Data source: A longitudinal study in 56 consecutive hand OA patients.
Disclosures: Dr. Kortekaas and her coauthors reported no conflicting interests.

Tapping office IT boosts orthopedic patient–reported outcomes
PARIS – Combining e-mail and office-based technology garnered patient-reported outcomes from more than 90% of patients receiving orthopedic care, in an analysis of 18,073 physician-patient encounters.
"Integrating [patient-reported outcomes] measurement into orthopedic standard of care without interrupting clinical practice is possible and currently in use," Xiang Zhou, Ph.D., reported at the World Congress on Osteoarthritis.
Patient-reported outcomes, or PROs, have taken center stage in recent years as a way to measure the safety and effectiveness of total joint arthroplasty, with respect to both technical and patient satisfaction.
New York University Langone Medical Center implemented an IT system in May 2012 for all nine adult orthopedic reconstructive surgeons at its Center for Musculoskeletal Care. Patients with e-mail addresses on file were sent a link to a PRO questionnaire, individualized to their clinical needs, 3 days before their appointment. A reminder e-mail was sent the day before their visit if the questionnaire was not completed. Tablets were also distributed in the waiting room for patients who did not complete via e-mail. Real-time and previous PRO scores were available in the electronic health record for physicians to review during the examination.
PRO records were captured for 83% of 8,864 patients seen in 20 months. Of those, 72% had multiple, longitudinal PRO scores recorded, according to Dr. Zhou, a research scientist in NYU Langone’s orthopedic surgery department.
Of the 18,073 physician-patient encounters, 71% included a completed PRO score. Monthly completion rates ranged from a high of 91% to a low of 56%.
"Reaching more than a 90% PRO collection rate is possible with the support of participating physicians," he noted.
Patients under age 65 had a significantly higher overall PRO completion rate than did older patients (76% vs. 65%; P less than .001), as did males vs. females (73% vs. 70%; P less than .001), Dr. Zhou reported at the meeting, sponsored by the Osteoarthritis Research Society International.
In all, 55% of patients who provided an e-mail address completed their PRO questionnaires via e-mail. In that subset, no significant differences were seen by age (55% both groups; P = .996) or gender (56% male vs. 55% female; P = .752).
PRO scores are now included in the electronic health record and routinely captured and used by physicians.
"Routine real-time and longitudinal PRO reports are a valuable tool to stimulate patient-physician communication and inform treatment decisions," the authors concluded in the poster presentation.
Dr. Zhou reported having no financial disclosures.
PARIS – Combining e-mail and office-based technology garnered patient-reported outcomes from more than 90% of patients receiving orthopedic care, in an analysis of 18,073 physician-patient encounters.
"Integrating [patient-reported outcomes] measurement into orthopedic standard of care without interrupting clinical practice is possible and currently in use," Xiang Zhou, Ph.D., reported at the World Congress on Osteoarthritis.
Patient-reported outcomes, or PROs, have taken center stage in recent years as a way to measure the safety and effectiveness of total joint arthroplasty, with respect to both technical and patient satisfaction.
New York University Langone Medical Center implemented an IT system in May 2012 for all nine adult orthopedic reconstructive surgeons at its Center for Musculoskeletal Care. Patients with e-mail addresses on file were sent a link to a PRO questionnaire, individualized to their clinical needs, 3 days before their appointment. A reminder e-mail was sent the day before their visit if the questionnaire was not completed. Tablets were also distributed in the waiting room for patients who did not complete via e-mail. Real-time and previous PRO scores were available in the electronic health record for physicians to review during the examination.
PRO records were captured for 83% of 8,864 patients seen in 20 months. Of those, 72% had multiple, longitudinal PRO scores recorded, according to Dr. Zhou, a research scientist in NYU Langone’s orthopedic surgery department.
Of the 18,073 physician-patient encounters, 71% included a completed PRO score. Monthly completion rates ranged from a high of 91% to a low of 56%.
"Reaching more than a 90% PRO collection rate is possible with the support of participating physicians," he noted.
Patients under age 65 had a significantly higher overall PRO completion rate than did older patients (76% vs. 65%; P less than .001), as did males vs. females (73% vs. 70%; P less than .001), Dr. Zhou reported at the meeting, sponsored by the Osteoarthritis Research Society International.
In all, 55% of patients who provided an e-mail address completed their PRO questionnaires via e-mail. In that subset, no significant differences were seen by age (55% both groups; P = .996) or gender (56% male vs. 55% female; P = .752).
PRO scores are now included in the electronic health record and routinely captured and used by physicians.
"Routine real-time and longitudinal PRO reports are a valuable tool to stimulate patient-physician communication and inform treatment decisions," the authors concluded in the poster presentation.
Dr. Zhou reported having no financial disclosures.
PARIS – Combining e-mail and office-based technology garnered patient-reported outcomes from more than 90% of patients receiving orthopedic care, in an analysis of 18,073 physician-patient encounters.
"Integrating [patient-reported outcomes] measurement into orthopedic standard of care without interrupting clinical practice is possible and currently in use," Xiang Zhou, Ph.D., reported at the World Congress on Osteoarthritis.
Patient-reported outcomes, or PROs, have taken center stage in recent years as a way to measure the safety and effectiveness of total joint arthroplasty, with respect to both technical and patient satisfaction.
New York University Langone Medical Center implemented an IT system in May 2012 for all nine adult orthopedic reconstructive surgeons at its Center for Musculoskeletal Care. Patients with e-mail addresses on file were sent a link to a PRO questionnaire, individualized to their clinical needs, 3 days before their appointment. A reminder e-mail was sent the day before their visit if the questionnaire was not completed. Tablets were also distributed in the waiting room for patients who did not complete via e-mail. Real-time and previous PRO scores were available in the electronic health record for physicians to review during the examination.
PRO records were captured for 83% of 8,864 patients seen in 20 months. Of those, 72% had multiple, longitudinal PRO scores recorded, according to Dr. Zhou, a research scientist in NYU Langone’s orthopedic surgery department.
Of the 18,073 physician-patient encounters, 71% included a completed PRO score. Monthly completion rates ranged from a high of 91% to a low of 56%.
"Reaching more than a 90% PRO collection rate is possible with the support of participating physicians," he noted.
Patients under age 65 had a significantly higher overall PRO completion rate than did older patients (76% vs. 65%; P less than .001), as did males vs. females (73% vs. 70%; P less than .001), Dr. Zhou reported at the meeting, sponsored by the Osteoarthritis Research Society International.
In all, 55% of patients who provided an e-mail address completed their PRO questionnaires via e-mail. In that subset, no significant differences were seen by age (55% both groups; P = .996) or gender (56% male vs. 55% female; P = .752).
PRO scores are now included in the electronic health record and routinely captured and used by physicians.
"Routine real-time and longitudinal PRO reports are a valuable tool to stimulate patient-physician communication and inform treatment decisions," the authors concluded in the poster presentation.
Dr. Zhou reported having no financial disclosures.
AT OARSI 2014
Major finding: Monthly completion rates of patient-reported outcomes questionnaires ranged from a high of 91% to a low of 56%.
Data source: An analysis of 18,073 orthopedic physician-patient encounters.
Disclosures: Dr. Zhou reported having no financial disclosures.
In obesity and knee OA, weight loss is a big win
PARIS – Weight loss of more than 5% produced clinically meaningful improvements in knee osteoarthritis, even when final body mass index remained high, a large, community-based study has shown.
For those patients who lost 10% body weight in the study, knee osteoarthritis symptoms improved by about 40%, consistent with the recent IDEA (Intensive Diet and Exercise for Arthritis) trial findings.
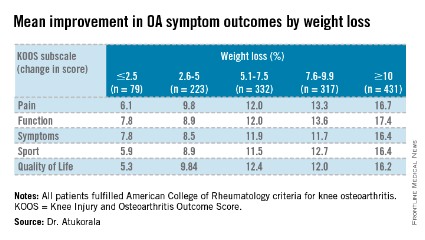
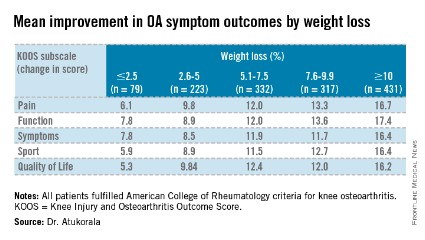
"There is a strong dose-response relationship between percentage weight loss and improvement in knee pain, function, symptoms, sport or recreation, and quality of life," Dr. Inoshi Atukorala said at the World Congress on Osteoarthritis.
Dr. Atukorala described the study as the first to examine the dose-response relationship between changes in body weight and knee osteoarthritis in a real-world, community setting.
The researchers evaluated 1,383 Australians who fulfilled the American College of Rheumatology criteria for knee osteoarthritis (OA) and were enrolled in the structured, remotely delivered "Healthy Weight for Life" knee and hip osteoarthritis management program. It integrates intensive weight loss as a component of tailored interventions, with the aim of achieving a 7%-10% body weight loss over 18 weeks, explained Dr. Atukorala, a consultant rheumatologist at the University of Colombo, Sri Lanka.
The program uses a partial very-low-calorie diet, portion management tools and devices, written healthy eating advice, and lifestyle education together with targeted telephone, e-mail, and text-message motivation and support. All participants were given the same strength, balance, and mobility exercise tools, instruction, and support.

At baseline, 81.7% of participants were obese, the average body mass index (BMI) was 34.3 kg/m2, and the mean Knee injury and Osteoarthritis Outcome Score (KOOS) pain and function subscale scores were 56.3 and 59.5. The cohort was 71% female and had an average age of 64 years.
At 18-weeks, there was a clear and significant incremental improvement in KOOS subscales across the weight-loss categories, with the greatest improvements in those losing at least 10% body weight, Dr. Atukorala said.
The weight-loss category cutoffs were chosen based on the IDEA trial (JAMA 2013;310:1263-73), as well as the weight-loss goal in the diet groups in the ADAPT study and the weight loss typically achieved in its exercise-only cohort of older adults with knee OA (Arthritis Rheum. 2004;50;1501-10), she explained.
Using repeated measures analysis of covariance, the investigators next examined the dose-response of weight loss, compared with differences in pain and function. For this analysis, the 2.5% or less weight-loss category was set as the reference.
The dose-relationship between weight loss and improvements in pain and function persisted, even after controlling for baseline age, gender, weight, height, and KOOS, Dr. Atukorala said at the meeting, sponsored by the Osteoarthritis Research Society International. The differences reached statistical significance on all KOOS subscales for the two highest weight-loss categories and on all but one subscale (KOOS sport) for those losing 5.1%-7.5% body weight.
"We are limited by the fact that the program did not assess the magnitude of exercise interventions in each weight-loss category, but it confirms the dose-response benefit of weight loss as a therapeutic intervention in knee osteoarthritis," Dr. Atukorala concluded. "And, it demonstrates the effectiveness of disseminating and implementing intensive weight-loss intervention in a community-based setting."
Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
PARIS – Weight loss of more than 5% produced clinically meaningful improvements in knee osteoarthritis, even when final body mass index remained high, a large, community-based study has shown.
For those patients who lost 10% body weight in the study, knee osteoarthritis symptoms improved by about 40%, consistent with the recent IDEA (Intensive Diet and Exercise for Arthritis) trial findings.
"There is a strong dose-response relationship between percentage weight loss and improvement in knee pain, function, symptoms, sport or recreation, and quality of life," Dr. Inoshi Atukorala said at the World Congress on Osteoarthritis.
Dr. Atukorala described the study as the first to examine the dose-response relationship between changes in body weight and knee osteoarthritis in a real-world, community setting.
The researchers evaluated 1,383 Australians who fulfilled the American College of Rheumatology criteria for knee osteoarthritis (OA) and were enrolled in the structured, remotely delivered "Healthy Weight for Life" knee and hip osteoarthritis management program. It integrates intensive weight loss as a component of tailored interventions, with the aim of achieving a 7%-10% body weight loss over 18 weeks, explained Dr. Atukorala, a consultant rheumatologist at the University of Colombo, Sri Lanka.
The program uses a partial very-low-calorie diet, portion management tools and devices, written healthy eating advice, and lifestyle education together with targeted telephone, e-mail, and text-message motivation and support. All participants were given the same strength, balance, and mobility exercise tools, instruction, and support.
At baseline, 81.7% of participants were obese, the average body mass index (BMI) was 34.3 kg/m2, and the mean Knee injury and Osteoarthritis Outcome Score (KOOS) pain and function subscale scores were 56.3 and 59.5. The cohort was 71% female and had an average age of 64 years.
At 18-weeks, there was a clear and significant incremental improvement in KOOS subscales across the weight-loss categories, with the greatest improvements in those losing at least 10% body weight, Dr. Atukorala said.
The weight-loss category cutoffs were chosen based on the IDEA trial (JAMA 2013;310:1263-73), as well as the weight-loss goal in the diet groups in the ADAPT study and the weight loss typically achieved in its exercise-only cohort of older adults with knee OA (Arthritis Rheum. 2004;50;1501-10), she explained.
Using repeated measures analysis of covariance, the investigators next examined the dose-response of weight loss, compared with differences in pain and function. For this analysis, the 2.5% or less weight-loss category was set as the reference.
The dose-relationship between weight loss and improvements in pain and function persisted, even after controlling for baseline age, gender, weight, height, and KOOS, Dr. Atukorala said at the meeting, sponsored by the Osteoarthritis Research Society International. The differences reached statistical significance on all KOOS subscales for the two highest weight-loss categories and on all but one subscale (KOOS sport) for those losing 5.1%-7.5% body weight.
"We are limited by the fact that the program did not assess the magnitude of exercise interventions in each weight-loss category, but it confirms the dose-response benefit of weight loss as a therapeutic intervention in knee osteoarthritis," Dr. Atukorala concluded. "And, it demonstrates the effectiveness of disseminating and implementing intensive weight-loss intervention in a community-based setting."
Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
PARIS – Weight loss of more than 5% produced clinically meaningful improvements in knee osteoarthritis, even when final body mass index remained high, a large, community-based study has shown.
For those patients who lost 10% body weight in the study, knee osteoarthritis symptoms improved by about 40%, consistent with the recent IDEA (Intensive Diet and Exercise for Arthritis) trial findings.
"There is a strong dose-response relationship between percentage weight loss and improvement in knee pain, function, symptoms, sport or recreation, and quality of life," Dr. Inoshi Atukorala said at the World Congress on Osteoarthritis.
Dr. Atukorala described the study as the first to examine the dose-response relationship between changes in body weight and knee osteoarthritis in a real-world, community setting.
The researchers evaluated 1,383 Australians who fulfilled the American College of Rheumatology criteria for knee osteoarthritis (OA) and were enrolled in the structured, remotely delivered "Healthy Weight for Life" knee and hip osteoarthritis management program. It integrates intensive weight loss as a component of tailored interventions, with the aim of achieving a 7%-10% body weight loss over 18 weeks, explained Dr. Atukorala, a consultant rheumatologist at the University of Colombo, Sri Lanka.
The program uses a partial very-low-calorie diet, portion management tools and devices, written healthy eating advice, and lifestyle education together with targeted telephone, e-mail, and text-message motivation and support. All participants were given the same strength, balance, and mobility exercise tools, instruction, and support.
At baseline, 81.7% of participants were obese, the average body mass index (BMI) was 34.3 kg/m2, and the mean Knee injury and Osteoarthritis Outcome Score (KOOS) pain and function subscale scores were 56.3 and 59.5. The cohort was 71% female and had an average age of 64 years.
At 18-weeks, there was a clear and significant incremental improvement in KOOS subscales across the weight-loss categories, with the greatest improvements in those losing at least 10% body weight, Dr. Atukorala said.
The weight-loss category cutoffs were chosen based on the IDEA trial (JAMA 2013;310:1263-73), as well as the weight-loss goal in the diet groups in the ADAPT study and the weight loss typically achieved in its exercise-only cohort of older adults with knee OA (Arthritis Rheum. 2004;50;1501-10), she explained.
Using repeated measures analysis of covariance, the investigators next examined the dose-response of weight loss, compared with differences in pain and function. For this analysis, the 2.5% or less weight-loss category was set as the reference.
The dose-relationship between weight loss and improvements in pain and function persisted, even after controlling for baseline age, gender, weight, height, and KOOS, Dr. Atukorala said at the meeting, sponsored by the Osteoarthritis Research Society International. The differences reached statistical significance on all KOOS subscales for the two highest weight-loss categories and on all but one subscale (KOOS sport) for those losing 5.1%-7.5% body weight.
"We are limited by the fact that the program did not assess the magnitude of exercise interventions in each weight-loss category, but it confirms the dose-response benefit of weight loss as a therapeutic intervention in knee osteoarthritis," Dr. Atukorala concluded. "And, it demonstrates the effectiveness of disseminating and implementing intensive weight-loss intervention in a community-based setting."
Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
AT OARSI 2014
Major finding: Participants who lost at least 10% body weight (mean 12.5%) had mean improvements on the KOOS pain, function, symptoms, sport, and quality of life subscales of 16.7, 17.4, 16.4, 16.4, and 16.2 points (P =.000).
Data source: Analysis of 1,383 consecutive knee OA participants in a knee and hip OA management program.
Disclosures: Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
Poor vibratory sense contributes to OA knee instability
PARIS – Impaired vibratory sense and muscle strength may be important risk factors for knee instability in persons with or at risk for symptomatic knee osteoarthritis, according to an analysis of a large, longitudinal cohort.
"Buckling is commonly been thought of as a mechanical phenomenon, but no one really knows the risk factors," Dr. Najia Shakoor said in an interview at the World Congress on Osteoarthritis. "For many, sensory input may be important. If you have greater sensory input, in this case, greater vibratory sense, perhaps you can protect yourself from buckling."
Knee instability is common in persons with knee osteoarthritis (OA) and has been found in studies to be associated with muscle weakness. None have examined whether weakness predicts onset or worsening of knee instability, she said.

It is also unknown whether decreased vibratory sense, often seen in older adults with knee OA, may distort one’s sense of knee position and increase the risk of instability.
For the current analysis, unilateral knee extensor strength and bilateral vibratory perception thresholds (VPT) were evaluated in 2,212 participants with or at risk for knee OA in the Multicenter Osteoarthritis Study (MOST). VPT was measured using a biothesiometer, with the tip placed on the tibial tuberosity and the voltage increased by 1 volt/sec from 0 until the participant acknowledged sensation.
The mean age of study participants was 68 years, mean body mass index (BMI) was 31 kg/m2, and 60% were women.
At the 60-month visit, 17% of participants reported knee buckling in the past 3 months, 29% reported slipping or "shifting, slipping, or going to give way, but didn’t actually do so," and 37% reported instability (buckling and/or slipping), said Dr. Shakoor, a rheumatologist with Rush University Medical Center, Chicago.
During follow-up, 32% of patients developed incident instability, 20% incident buckling, 11% worsening instability, and 21% worsening buckling.
In Poisson regression person-based analyses, the risk of incident knee instability was significantly less in those with greater quadriceps strength (relative risk, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024), after adjustment for age, sex, BMI, race, clinic site, Kellgren-Lawrence OA grade, Western Ontario and McMaster Osteoarthritis Index knee pain, and both predictors.
Better vibratory sense also protected against worsening of both knee instability (RR, 0.42; P = .021) and buckling (RR, 0.67; P = .020), Dr. Shakoor reported in the poster presentation at the meeting, sponsored by the Osteoarthritis Research Society International.
Although it’s not known whether vibratory sense can be improved, muscle strength can be. "So these are potentially modifiable risk factors for a common problem," she said.
Prior work by the group has found that vibratory sense is impaired in hip as well as knee OA, compared with healthy controls.
The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
PARIS – Impaired vibratory sense and muscle strength may be important risk factors for knee instability in persons with or at risk for symptomatic knee osteoarthritis, according to an analysis of a large, longitudinal cohort.
"Buckling is commonly been thought of as a mechanical phenomenon, but no one really knows the risk factors," Dr. Najia Shakoor said in an interview at the World Congress on Osteoarthritis. "For many, sensory input may be important. If you have greater sensory input, in this case, greater vibratory sense, perhaps you can protect yourself from buckling."
Knee instability is common in persons with knee osteoarthritis (OA) and has been found in studies to be associated with muscle weakness. None have examined whether weakness predicts onset or worsening of knee instability, she said.
It is also unknown whether decreased vibratory sense, often seen in older adults with knee OA, may distort one’s sense of knee position and increase the risk of instability.
For the current analysis, unilateral knee extensor strength and bilateral vibratory perception thresholds (VPT) were evaluated in 2,212 participants with or at risk for knee OA in the Multicenter Osteoarthritis Study (MOST). VPT was measured using a biothesiometer, with the tip placed on the tibial tuberosity and the voltage increased by 1 volt/sec from 0 until the participant acknowledged sensation.
The mean age of study participants was 68 years, mean body mass index (BMI) was 31 kg/m2, and 60% were women.
At the 60-month visit, 17% of participants reported knee buckling in the past 3 months, 29% reported slipping or "shifting, slipping, or going to give way, but didn’t actually do so," and 37% reported instability (buckling and/or slipping), said Dr. Shakoor, a rheumatologist with Rush University Medical Center, Chicago.
During follow-up, 32% of patients developed incident instability, 20% incident buckling, 11% worsening instability, and 21% worsening buckling.
In Poisson regression person-based analyses, the risk of incident knee instability was significantly less in those with greater quadriceps strength (relative risk, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024), after adjustment for age, sex, BMI, race, clinic site, Kellgren-Lawrence OA grade, Western Ontario and McMaster Osteoarthritis Index knee pain, and both predictors.
Better vibratory sense also protected against worsening of both knee instability (RR, 0.42; P = .021) and buckling (RR, 0.67; P = .020), Dr. Shakoor reported in the poster presentation at the meeting, sponsored by the Osteoarthritis Research Society International.
Although it’s not known whether vibratory sense can be improved, muscle strength can be. "So these are potentially modifiable risk factors for a common problem," she said.
Prior work by the group has found that vibratory sense is impaired in hip as well as knee OA, compared with healthy controls.
The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
PARIS – Impaired vibratory sense and muscle strength may be important risk factors for knee instability in persons with or at risk for symptomatic knee osteoarthritis, according to an analysis of a large, longitudinal cohort.
"Buckling is commonly been thought of as a mechanical phenomenon, but no one really knows the risk factors," Dr. Najia Shakoor said in an interview at the World Congress on Osteoarthritis. "For many, sensory input may be important. If you have greater sensory input, in this case, greater vibratory sense, perhaps you can protect yourself from buckling."
Knee instability is common in persons with knee osteoarthritis (OA) and has been found in studies to be associated with muscle weakness. None have examined whether weakness predicts onset or worsening of knee instability, she said.
It is also unknown whether decreased vibratory sense, often seen in older adults with knee OA, may distort one’s sense of knee position and increase the risk of instability.
For the current analysis, unilateral knee extensor strength and bilateral vibratory perception thresholds (VPT) were evaluated in 2,212 participants with or at risk for knee OA in the Multicenter Osteoarthritis Study (MOST). VPT was measured using a biothesiometer, with the tip placed on the tibial tuberosity and the voltage increased by 1 volt/sec from 0 until the participant acknowledged sensation.
The mean age of study participants was 68 years, mean body mass index (BMI) was 31 kg/m2, and 60% were women.
At the 60-month visit, 17% of participants reported knee buckling in the past 3 months, 29% reported slipping or "shifting, slipping, or going to give way, but didn’t actually do so," and 37% reported instability (buckling and/or slipping), said Dr. Shakoor, a rheumatologist with Rush University Medical Center, Chicago.
During follow-up, 32% of patients developed incident instability, 20% incident buckling, 11% worsening instability, and 21% worsening buckling.
In Poisson regression person-based analyses, the risk of incident knee instability was significantly less in those with greater quadriceps strength (relative risk, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024), after adjustment for age, sex, BMI, race, clinic site, Kellgren-Lawrence OA grade, Western Ontario and McMaster Osteoarthritis Index knee pain, and both predictors.
Better vibratory sense also protected against worsening of both knee instability (RR, 0.42; P = .021) and buckling (RR, 0.67; P = .020), Dr. Shakoor reported in the poster presentation at the meeting, sponsored by the Osteoarthritis Research Society International.
Although it’s not known whether vibratory sense can be improved, muscle strength can be. "So these are potentially modifiable risk factors for a common problem," she said.
Prior work by the group has found that vibratory sense is impaired in hip as well as knee OA, compared with healthy controls.
The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
AT OARSI 2014
Key clinical point: Working to increase quadriceps strength may reduce knee instability in OA patients.
Major finding: The risk of incident knee instability was significantly less in those with greater quadriceps strength (RR, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024).
Data source: A longitudinal analysis of 2,212 patients with knee OA.
Disclosures: The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.

Vigorous exercise hastens knee OA progression
PARIS – Vigorous, but not moderate, physical exercise was associated with a significantly greater risk of knee osteoarthritis progression over 1 year in a longitudinal analysis of 99 patients.
Engaging in vigorous activity was associated with a 1.38-times increased risk for progression (95% confidence intervals, 1.04-1.83; P = .025), defined as an increase in either cartilage or meniscus defect scores at 1 year.

The odds ratios were not significantly increased for moderate activity (OR, 0.78; 95% CI, 0.47-1.28; P = .322) but were close to significance for walking activity (OR, 1.50; 95% CI, 1-2.25; P = .052), lead author Deepak Kumar, Ph.D., said at the World Congress on Osteoarthritis.
The analyses adjusted for age, body mass index, sex, pain, Kellgren-Lawrence (KL) score, and modified Whole Organ Magnetic Resonance Scores for cartilage and meniscus in the first block, and International Physical Activity Questionnaire (IPAQ) scores in the second block.
"We did not see that moderate activity was associated with progression, and this indicates that we need to further investigate the optimal dosage of physical activity for someone with knee osteoarthritis," said Dr. Kumar, a postdoctoral scholar, radiology department, University of California, San Francisco.
Although greater physical activity has been shown to reduce pain and improve function, the results support more recent work suggesting that certain types of activity may be associated with disease progression. Walking 10,000 steps or more per day was found to increase the risk of meniscus and cartilage lesions on MRI in people with knee OA (Ann. Rheum. Dis. 2013;72:1170-5), while high and very low levels of self-reported activity were associated with greater cartilage relaxation times on 2T MRI at 4 years in data from the Osteoarthritis Initiative (Osteoarthritis Cartilage 2013;12:1558-66).
For the current analysis, 99 participants in the ongoing, longitudinal Cartilage Loading and Unloading (CLOC) knee OA study underwent 3T MRI of the knee using a sagittal, high-resolution 3D fast spin-echo Cube sequence at baseline, which was repeated 1 year later. Cartilage and meniscus defects were graded by experienced radiologists. Participants with OA had a baseline radiographic KL score of more than 1 and were symptomatic; controls had a KL of 0 or 1 and no knee symptoms.
By 1 year, 35 participants showed progression (14 with OA and 21 controls) and 64 did not. Surprisingly, there was greater progression in the lateral compartment (11 lateral menisci, 12 lateral tibiae) and, more expectedly, in the patella in 12 persons, Dr. Kumar said at the meeting, sponsored by the Osteoarthritis Research Society International.
No significant baseline differences existed between nonprogressors and progressors with respect to age (53.2 years vs. 50.8 years), body mass index (24.4 kg/m2 vs. 24.5 kg/m2), and sex (62.5% vs. 48.5% female), he said.
Knee injury and Osteoarthritis Outcome Score subscale scores were also similar for pain (85.7 vs. 82.4) and symptoms (84.5 vs. 83.4).
Progressors had engaged, however, in significantly more metabolic equivalent-minutes per week of vigorous exercise than did nonprogressors (2,410.6 vs. 1,413.1; P = .046), Dr. Kumar said. Metabolic equivalent-minutes per week were similar for moderate activity (1,094.1 vs. 858.7; P = .396) and walking (1,646.2 vs. 1,245.1; P = .151).
During the discussion following the formal presentation, an attendee said the study is potentially very valuable because it suggests that something all clinicians want to do is "dangerous" but questioned whether some of the MRI data were "overread" given the almost 40% rate of progression in a relatively fit cohort. A Danish attendee also remarked that her group has experienced so many problems with patients filling out the IPAQ questionnaire that they no longer trust the data.
Dr. Kumar responded that the MRI readings were performed by expert radiologists and were reliable, and that more stringent definitions of progression are being explored. His group is also working on a new questionnaire to better define physical activity levels.
Data are also being analyzed from the rest of the cohort (160 participants) and over a longer, 3-year follow-up, he said in an interview.
"We are also identifying quantitative MRI and biomechanical metrics that may be more sensitive to disease progression in knee OA. These will help us understand the factors that are related to worsening of knee OA and develop therapies."
The National Institutes of Health–National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the work. Dr. Kumar and his coauthors reported no conflicting interests.
PARIS – Vigorous, but not moderate, physical exercise was associated with a significantly greater risk of knee osteoarthritis progression over 1 year in a longitudinal analysis of 99 patients.
Engaging in vigorous activity was associated with a 1.38-times increased risk for progression (95% confidence intervals, 1.04-1.83; P = .025), defined as an increase in either cartilage or meniscus defect scores at 1 year.
The odds ratios were not significantly increased for moderate activity (OR, 0.78; 95% CI, 0.47-1.28; P = .322) but were close to significance for walking activity (OR, 1.50; 95% CI, 1-2.25; P = .052), lead author Deepak Kumar, Ph.D., said at the World Congress on Osteoarthritis.
The analyses adjusted for age, body mass index, sex, pain, Kellgren-Lawrence (KL) score, and modified Whole Organ Magnetic Resonance Scores for cartilage and meniscus in the first block, and International Physical Activity Questionnaire (IPAQ) scores in the second block.
"We did not see that moderate activity was associated with progression, and this indicates that we need to further investigate the optimal dosage of physical activity for someone with knee osteoarthritis," said Dr. Kumar, a postdoctoral scholar, radiology department, University of California, San Francisco.
Although greater physical activity has been shown to reduce pain and improve function, the results support more recent work suggesting that certain types of activity may be associated with disease progression. Walking 10,000 steps or more per day was found to increase the risk of meniscus and cartilage lesions on MRI in people with knee OA (Ann. Rheum. Dis. 2013;72:1170-5), while high and very low levels of self-reported activity were associated with greater cartilage relaxation times on 2T MRI at 4 years in data from the Osteoarthritis Initiative (Osteoarthritis Cartilage 2013;12:1558-66).
For the current analysis, 99 participants in the ongoing, longitudinal Cartilage Loading and Unloading (CLOC) knee OA study underwent 3T MRI of the knee using a sagittal, high-resolution 3D fast spin-echo Cube sequence at baseline, which was repeated 1 year later. Cartilage and meniscus defects were graded by experienced radiologists. Participants with OA had a baseline radiographic KL score of more than 1 and were symptomatic; controls had a KL of 0 or 1 and no knee symptoms.
By 1 year, 35 participants showed progression (14 with OA and 21 controls) and 64 did not. Surprisingly, there was greater progression in the lateral compartment (11 lateral menisci, 12 lateral tibiae) and, more expectedly, in the patella in 12 persons, Dr. Kumar said at the meeting, sponsored by the Osteoarthritis Research Society International.
No significant baseline differences existed between nonprogressors and progressors with respect to age (53.2 years vs. 50.8 years), body mass index (24.4 kg/m2 vs. 24.5 kg/m2), and sex (62.5% vs. 48.5% female), he said.
Knee injury and Osteoarthritis Outcome Score subscale scores were also similar for pain (85.7 vs. 82.4) and symptoms (84.5 vs. 83.4).
Progressors had engaged, however, in significantly more metabolic equivalent-minutes per week of vigorous exercise than did nonprogressors (2,410.6 vs. 1,413.1; P = .046), Dr. Kumar said. Metabolic equivalent-minutes per week were similar for moderate activity (1,094.1 vs. 858.7; P = .396) and walking (1,646.2 vs. 1,245.1; P = .151).
During the discussion following the formal presentation, an attendee said the study is potentially very valuable because it suggests that something all clinicians want to do is "dangerous" but questioned whether some of the MRI data were "overread" given the almost 40% rate of progression in a relatively fit cohort. A Danish attendee also remarked that her group has experienced so many problems with patients filling out the IPAQ questionnaire that they no longer trust the data.
Dr. Kumar responded that the MRI readings were performed by expert radiologists and were reliable, and that more stringent definitions of progression are being explored. His group is also working on a new questionnaire to better define physical activity levels.
Data are also being analyzed from the rest of the cohort (160 participants) and over a longer, 3-year follow-up, he said in an interview.
"We are also identifying quantitative MRI and biomechanical metrics that may be more sensitive to disease progression in knee OA. These will help us understand the factors that are related to worsening of knee OA and develop therapies."
The National Institutes of Health–National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the work. Dr. Kumar and his coauthors reported no conflicting interests.
PARIS – Vigorous, but not moderate, physical exercise was associated with a significantly greater risk of knee osteoarthritis progression over 1 year in a longitudinal analysis of 99 patients.
Engaging in vigorous activity was associated with a 1.38-times increased risk for progression (95% confidence intervals, 1.04-1.83; P = .025), defined as an increase in either cartilage or meniscus defect scores at 1 year.
The odds ratios were not significantly increased for moderate activity (OR, 0.78; 95% CI, 0.47-1.28; P = .322) but were close to significance for walking activity (OR, 1.50; 95% CI, 1-2.25; P = .052), lead author Deepak Kumar, Ph.D., said at the World Congress on Osteoarthritis.
The analyses adjusted for age, body mass index, sex, pain, Kellgren-Lawrence (KL) score, and modified Whole Organ Magnetic Resonance Scores for cartilage and meniscus in the first block, and International Physical Activity Questionnaire (IPAQ) scores in the second block.
"We did not see that moderate activity was associated with progression, and this indicates that we need to further investigate the optimal dosage of physical activity for someone with knee osteoarthritis," said Dr. Kumar, a postdoctoral scholar, radiology department, University of California, San Francisco.
Although greater physical activity has been shown to reduce pain and improve function, the results support more recent work suggesting that certain types of activity may be associated with disease progression. Walking 10,000 steps or more per day was found to increase the risk of meniscus and cartilage lesions on MRI in people with knee OA (Ann. Rheum. Dis. 2013;72:1170-5), while high and very low levels of self-reported activity were associated with greater cartilage relaxation times on 2T MRI at 4 years in data from the Osteoarthritis Initiative (Osteoarthritis Cartilage 2013;12:1558-66).
For the current analysis, 99 participants in the ongoing, longitudinal Cartilage Loading and Unloading (CLOC) knee OA study underwent 3T MRI of the knee using a sagittal, high-resolution 3D fast spin-echo Cube sequence at baseline, which was repeated 1 year later. Cartilage and meniscus defects were graded by experienced radiologists. Participants with OA had a baseline radiographic KL score of more than 1 and were symptomatic; controls had a KL of 0 or 1 and no knee symptoms.
By 1 year, 35 participants showed progression (14 with OA and 21 controls) and 64 did not. Surprisingly, there was greater progression in the lateral compartment (11 lateral menisci, 12 lateral tibiae) and, more expectedly, in the patella in 12 persons, Dr. Kumar said at the meeting, sponsored by the Osteoarthritis Research Society International.
No significant baseline differences existed between nonprogressors and progressors with respect to age (53.2 years vs. 50.8 years), body mass index (24.4 kg/m2 vs. 24.5 kg/m2), and sex (62.5% vs. 48.5% female), he said.
Knee injury and Osteoarthritis Outcome Score subscale scores were also similar for pain (85.7 vs. 82.4) and symptoms (84.5 vs. 83.4).
Progressors had engaged, however, in significantly more metabolic equivalent-minutes per week of vigorous exercise than did nonprogressors (2,410.6 vs. 1,413.1; P = .046), Dr. Kumar said. Metabolic equivalent-minutes per week were similar for moderate activity (1,094.1 vs. 858.7; P = .396) and walking (1,646.2 vs. 1,245.1; P = .151).
During the discussion following the formal presentation, an attendee said the study is potentially very valuable because it suggests that something all clinicians want to do is "dangerous" but questioned whether some of the MRI data were "overread" given the almost 40% rate of progression in a relatively fit cohort. A Danish attendee also remarked that her group has experienced so many problems with patients filling out the IPAQ questionnaire that they no longer trust the data.
Dr. Kumar responded that the MRI readings were performed by expert radiologists and were reliable, and that more stringent definitions of progression are being explored. His group is also working on a new questionnaire to better define physical activity levels.
Data are also being analyzed from the rest of the cohort (160 participants) and over a longer, 3-year follow-up, he said in an interview.
"We are also identifying quantitative MRI and biomechanical metrics that may be more sensitive to disease progression in knee OA. These will help us understand the factors that are related to worsening of knee OA and develop therapies."
The National Institutes of Health–National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the work. Dr. Kumar and his coauthors reported no conflicting interests.
AT OARSI 2014
Major finding: Vigorous activity was associated with a 1.38 times increased risk for progression (95% CI, 1.04-1.83; P = .025).
Data source: Longitudinal analysis of 99 participants in the ongoing CLOC knee OA study.
Disclosures: The National Institutes of Health–National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the work. Dr. Kumar and his coauthors reported no conflicting interests.

Recent knee injuries spark rapid cascade to joint failure
PARIS – Recent knee injuries are strongly associated with accelerated knee osteoarthritis, according to an analysis from the prospective, multicenter Osteoarthritis Initiative.
"Certain injuries may initiate or coincide with an accelerated cascade towards joint failure in as little as 12 months," Jeffrey Driban, Ph.D., said at the World Congress on Osteoarthritis. "In fact, 76% of individuals with an injury and accelerated knee osteoarthritis experienced their injury in the 12 months prior to the study outcome."
The study defined accelerated knee OA as progression from a Kellgren-Lawrence grade 0 or 1 on baseline bilateral radiographs to end-stage KL grade 3 or 4 within 48 months.
Although knee OA typically has been a slowly progressive disorder, 5%-17% of patients now experience accelerated forms of OA.
"If we can better characterize this phenomenon and its potential risk factors, we can provide more insights into the nature of progression in hopes of identifying an at-risk subset," said Dr. Driban of the division of rheumatology at Tufts Medical Center, Boston.
The study by Dr. Driban and his colleagues was published in Arthritis Care & Research (2014 April 29 [doi:10.1002/acr.22359]).
A total of 1,930 participants in the Osteoarthritis Initiative, all with a KL grade of 0 or 1 on baseline bilateral radiographs, were asked at baseline and at each annual visit whether they had ever been "injured enough to limit ability to walk for at least 2 days."
On follow-up, 1,325 had no knee OA, 54 had accelerated knee OA, and 187 had typical knee OA, defined as at least one knee increased in radiographic scoring within 48 months (excluding accelerated OA).
After exclusion of 12 patients with missing data, 30% of the accelerated OA group, 28% in the typical OA group, and 35% in the no OA group had a history of knee injury before baseline. A new knee injury was reported by 32%, 13%, and 11%, respectively, with data missing from 59 persons.
In univariate analyses, participants with accelerated knee OA were significantly older than were those with typical OA or no OA (61.8 years vs. 58 years vs. 59.2 years; P = .023) and had a greater body mass index (28.9 kg/m2 vs. 27.9 kg/m2 vs. 27.1 kg/m2; P = .002), Dr. Driban said.
In multinomial logistic regression analyses that adjusted for age, sex, BMI, presence of static knee malalignment, and systolic blood pressure, there was no association between prior knee injury and accelerated OA (odds ratio, 0.84) or typical OA (OR, 0.76).
However, when the investigators looked further, participants with accelerated OA were almost 3.5 times more likely to report a recent knee injury during the observation period (OR, 3.37; 95% confidence interval, 1.82-6.25) than were those with typical OA (OR, 0.99) or no OA (reference), he said.
Moreover, if a participant experienced a knee injury 1 year before the study outcome, the risk of accelerated OA increased ninefold (OR, 9.22; CI, 4.50-18.90) versus threefold for typical OA (OR, 3.04; CI, 1.66-5.58).
Despite the focus on injuries leading to accelerated OA, the analyses can’t rule out that accelerated OA may also cause an injury or that there could be a "vicious cycle," in which an injury can cause accelerated OA, associated with joint space loss, increased symptoms, and increased risk for subsequent injury, Dr. Driban said.
This line of thought helps explain why prior injury was not associated with accelerated knee OA, but recent injury was. As patients were free of radiographic OA at baseline, those with a history of a prior injury that could cause accelerated knee OA would already have been eliminated from the study, he explained in an interview.
Secondly, if accelerated knee OA can increase the risk of injury, knee injuries from years ago would not be related to accelerated knee OA because the disorder did not exist at the time of the injury.
Finally, there also could be a recall bias, as patients often have a hard time recalling injuries that may have happened years ago.
Despite the limitations of self-reported injuries and insufficient data regarding the type, severity, status of the meniscus, mechanism, or subsequent treatment of the knee injury, the findings represent an important "starting point" in understanding the association between injuries and accelerated osteoarthritis, Dr. Driban said.
"We need to monitor older adults who report an injury, as this may initiate accelerated OA or indicate an individual experiencing accelerated OA, and we need to determine which injuries may be related to accelerated osteoarthritis," he said at the meeting, sponsored by the Osteoarthritis Research Society International.
During the discussion following the formal presentation, Dr. David Felson, professor of medicine and epidemiology at Boston University, said, "I think what you are saying is exactly right," but suggested that the investigators exclude patients with spontaneous osteonecrosis of the knee and osteochondritis dissecans, as both conditions are more common than anticipated and can drive very rapid development of OA. Conversely, inclusion of patients with osteophyte-only knee OA would increase the number likely identified with accelerated OA, he said.
Dr. Driban reported no conflicting interests.
PARIS – Recent knee injuries are strongly associated with accelerated knee osteoarthritis, according to an analysis from the prospective, multicenter Osteoarthritis Initiative.
"Certain injuries may initiate or coincide with an accelerated cascade towards joint failure in as little as 12 months," Jeffrey Driban, Ph.D., said at the World Congress on Osteoarthritis. "In fact, 76% of individuals with an injury and accelerated knee osteoarthritis experienced their injury in the 12 months prior to the study outcome."
The study defined accelerated knee OA as progression from a Kellgren-Lawrence grade 0 or 1 on baseline bilateral radiographs to end-stage KL grade 3 or 4 within 48 months.
Although knee OA typically has been a slowly progressive disorder, 5%-17% of patients now experience accelerated forms of OA.
"If we can better characterize this phenomenon and its potential risk factors, we can provide more insights into the nature of progression in hopes of identifying an at-risk subset," said Dr. Driban of the division of rheumatology at Tufts Medical Center, Boston.
The study by Dr. Driban and his colleagues was published in Arthritis Care & Research (2014 April 29 [doi:10.1002/acr.22359]).
A total of 1,930 participants in the Osteoarthritis Initiative, all with a KL grade of 0 or 1 on baseline bilateral radiographs, were asked at baseline and at each annual visit whether they had ever been "injured enough to limit ability to walk for at least 2 days."
On follow-up, 1,325 had no knee OA, 54 had accelerated knee OA, and 187 had typical knee OA, defined as at least one knee increased in radiographic scoring within 48 months (excluding accelerated OA).
After exclusion of 12 patients with missing data, 30% of the accelerated OA group, 28% in the typical OA group, and 35% in the no OA group had a history of knee injury before baseline. A new knee injury was reported by 32%, 13%, and 11%, respectively, with data missing from 59 persons.
In univariate analyses, participants with accelerated knee OA were significantly older than were those with typical OA or no OA (61.8 years vs. 58 years vs. 59.2 years; P = .023) and had a greater body mass index (28.9 kg/m2 vs. 27.9 kg/m2 vs. 27.1 kg/m2; P = .002), Dr. Driban said.
In multinomial logistic regression analyses that adjusted for age, sex, BMI, presence of static knee malalignment, and systolic blood pressure, there was no association between prior knee injury and accelerated OA (odds ratio, 0.84) or typical OA (OR, 0.76).
However, when the investigators looked further, participants with accelerated OA were almost 3.5 times more likely to report a recent knee injury during the observation period (OR, 3.37; 95% confidence interval, 1.82-6.25) than were those with typical OA (OR, 0.99) or no OA (reference), he said.
Moreover, if a participant experienced a knee injury 1 year before the study outcome, the risk of accelerated OA increased ninefold (OR, 9.22; CI, 4.50-18.90) versus threefold for typical OA (OR, 3.04; CI, 1.66-5.58).
Despite the focus on injuries leading to accelerated OA, the analyses can’t rule out that accelerated OA may also cause an injury or that there could be a "vicious cycle," in which an injury can cause accelerated OA, associated with joint space loss, increased symptoms, and increased risk for subsequent injury, Dr. Driban said.
This line of thought helps explain why prior injury was not associated with accelerated knee OA, but recent injury was. As patients were free of radiographic OA at baseline, those with a history of a prior injury that could cause accelerated knee OA would already have been eliminated from the study, he explained in an interview.
Secondly, if accelerated knee OA can increase the risk of injury, knee injuries from years ago would not be related to accelerated knee OA because the disorder did not exist at the time of the injury.
Finally, there also could be a recall bias, as patients often have a hard time recalling injuries that may have happened years ago.
Despite the limitations of self-reported injuries and insufficient data regarding the type, severity, status of the meniscus, mechanism, or subsequent treatment of the knee injury, the findings represent an important "starting point" in understanding the association between injuries and accelerated osteoarthritis, Dr. Driban said.
"We need to monitor older adults who report an injury, as this may initiate accelerated OA or indicate an individual experiencing accelerated OA, and we need to determine which injuries may be related to accelerated osteoarthritis," he said at the meeting, sponsored by the Osteoarthritis Research Society International.
During the discussion following the formal presentation, Dr. David Felson, professor of medicine and epidemiology at Boston University, said, "I think what you are saying is exactly right," but suggested that the investigators exclude patients with spontaneous osteonecrosis of the knee and osteochondritis dissecans, as both conditions are more common than anticipated and can drive very rapid development of OA. Conversely, inclusion of patients with osteophyte-only knee OA would increase the number likely identified with accelerated OA, he said.
Dr. Driban reported no conflicting interests.
PARIS – Recent knee injuries are strongly associated with accelerated knee osteoarthritis, according to an analysis from the prospective, multicenter Osteoarthritis Initiative.
"Certain injuries may initiate or coincide with an accelerated cascade towards joint failure in as little as 12 months," Jeffrey Driban, Ph.D., said at the World Congress on Osteoarthritis. "In fact, 76% of individuals with an injury and accelerated knee osteoarthritis experienced their injury in the 12 months prior to the study outcome."
The study defined accelerated knee OA as progression from a Kellgren-Lawrence grade 0 or 1 on baseline bilateral radiographs to end-stage KL grade 3 or 4 within 48 months.
Although knee OA typically has been a slowly progressive disorder, 5%-17% of patients now experience accelerated forms of OA.
"If we can better characterize this phenomenon and its potential risk factors, we can provide more insights into the nature of progression in hopes of identifying an at-risk subset," said Dr. Driban of the division of rheumatology at Tufts Medical Center, Boston.
The study by Dr. Driban and his colleagues was published in Arthritis Care & Research (2014 April 29 [doi:10.1002/acr.22359]).
A total of 1,930 participants in the Osteoarthritis Initiative, all with a KL grade of 0 or 1 on baseline bilateral radiographs, were asked at baseline and at each annual visit whether they had ever been "injured enough to limit ability to walk for at least 2 days."
On follow-up, 1,325 had no knee OA, 54 had accelerated knee OA, and 187 had typical knee OA, defined as at least one knee increased in radiographic scoring within 48 months (excluding accelerated OA).
After exclusion of 12 patients with missing data, 30% of the accelerated OA group, 28% in the typical OA group, and 35% in the no OA group had a history of knee injury before baseline. A new knee injury was reported by 32%, 13%, and 11%, respectively, with data missing from 59 persons.
In univariate analyses, participants with accelerated knee OA were significantly older than were those with typical OA or no OA (61.8 years vs. 58 years vs. 59.2 years; P = .023) and had a greater body mass index (28.9 kg/m2 vs. 27.9 kg/m2 vs. 27.1 kg/m2; P = .002), Dr. Driban said.
In multinomial logistic regression analyses that adjusted for age, sex, BMI, presence of static knee malalignment, and systolic blood pressure, there was no association between prior knee injury and accelerated OA (odds ratio, 0.84) or typical OA (OR, 0.76).
However, when the investigators looked further, participants with accelerated OA were almost 3.5 times more likely to report a recent knee injury during the observation period (OR, 3.37; 95% confidence interval, 1.82-6.25) than were those with typical OA (OR, 0.99) or no OA (reference), he said.
Moreover, if a participant experienced a knee injury 1 year before the study outcome, the risk of accelerated OA increased ninefold (OR, 9.22; CI, 4.50-18.90) versus threefold for typical OA (OR, 3.04; CI, 1.66-5.58).
Despite the focus on injuries leading to accelerated OA, the analyses can’t rule out that accelerated OA may also cause an injury or that there could be a "vicious cycle," in which an injury can cause accelerated OA, associated with joint space loss, increased symptoms, and increased risk for subsequent injury, Dr. Driban said.
This line of thought helps explain why prior injury was not associated with accelerated knee OA, but recent injury was. As patients were free of radiographic OA at baseline, those with a history of a prior injury that could cause accelerated knee OA would already have been eliminated from the study, he explained in an interview.
Secondly, if accelerated knee OA can increase the risk of injury, knee injuries from years ago would not be related to accelerated knee OA because the disorder did not exist at the time of the injury.
Finally, there also could be a recall bias, as patients often have a hard time recalling injuries that may have happened years ago.
Despite the limitations of self-reported injuries and insufficient data regarding the type, severity, status of the meniscus, mechanism, or subsequent treatment of the knee injury, the findings represent an important "starting point" in understanding the association between injuries and accelerated osteoarthritis, Dr. Driban said.
"We need to monitor older adults who report an injury, as this may initiate accelerated OA or indicate an individual experiencing accelerated OA, and we need to determine which injuries may be related to accelerated osteoarthritis," he said at the meeting, sponsored by the Osteoarthritis Research Society International.
During the discussion following the formal presentation, Dr. David Felson, professor of medicine and epidemiology at Boston University, said, "I think what you are saying is exactly right," but suggested that the investigators exclude patients with spontaneous osteonecrosis of the knee and osteochondritis dissecans, as both conditions are more common than anticipated and can drive very rapid development of OA. Conversely, inclusion of patients with osteophyte-only knee OA would increase the number likely identified with accelerated OA, he said.
Dr. Driban reported no conflicting interests.
AT OARSI 2014
Key clinical point: Older adults who report a knee injury should be monitored for accelerated knee OA.
Major finding: Knee injury within 1 year of the study outcome increased the odds of accelerated OA ninefold (OR, 9.22; CI, 4.50-18.90).
Data source: Person-based analyses of 1,930 participants in the Osteoarthritis Initiative.
Disclosures: Dr. Driban reported no conflicting interests.
Childhood sports knee injuries carry heavy burden
PARIS – Knee trauma from a childhood sports injury can have serious consequences in young adults, judging from preliminary results from a historical cohort.
When assessed 3-10 years after the sports injury, at an average age of 22 years, young adults appear to be at higher risk of abnormalities visible on MRI that are consistent with future arthropathy and have poorer knee-related quality of life and more knee symptoms.
They are at higher risk of having structural asymmetry of the vastus medialis muscle and being categorized as being overweight or obese.
There also appears to be some trends for increased percent body fat and reduced participation in physical activity, Jackie L. Whittaker, Ph.D., said at the World Congress on Osteoarthritis.
She stressed that these are preliminary findings and that the group hopes to quadruple the size of the cohort this year in order to better understand the relationships they’ve identified.
"With that being said, if we are seeing what we think we’re seeing, there may be some clinical, structural, physiologic, and behavioral markers that can be used to identify individuals who are at risk and target them with secondary prevention strategies at an earlier age," said Dr. Whittaker, a postdoctoral fellow and physiotherapist, University of Calgary Sport Injury Prevention Research Centre, Alberta, Canada.
The historical cohort study involved 25 patients recruited from previous sports injury epidemiology studies who had an intra-articular knee injury in ice hockey (male and female), soccer, basketball, or other sports that required medical attention and time off play, and 25 uninjured controls matched on age, sex, and sport. The median age at injury was 15 years (range 9-18 years). Eight patients in the injured group had contralateral knee surgeries, in addition to surgery on the primary knee. The median age in both groups was 22 years.
Using the Knee injury and Osteoarthritis Outcome Scores (KOOS) outcome, injured participants scored significantly lower, indicating worse function, on all five, 100-point subscales: pain (mean 93 vs. 97), symptoms (mean 82.9 vs. 92.4), activities of daily living (mean 96.3 vs. 99.3), sport/recreation (mean 90.6 vs. 97.4), and knee-related quality of life (mean 89.7 vs. 97.7), Dr. Whittaker said.
Further, in a subsample of 10 matched pairs, injured participants were three times more likely to have an MRI Osteoarthritis Score (MOAKS) of one than were matched controls, according to the study, led by her colleague Carolyn Emery, Ph.D.
Although there was no difference in quadriceps strength between groups, injured participants were 3.8 times more likely to have a difference in the cross-sectional area of the vastus medialis muscle greater than 15%.
"We think that this may be clinically relevant, as there has been some recent prospective work (Arthritis Rheum. 2012;64:3917-25) that has shown a temporal relationship between a decrease in size of the vastus medialis muscle and progression or loss of tibial joint cartilage," she said.
Within 3-10 years after their knee trauma, injured participants have a significantly higher mean body mass index (BMI) than do uninjured participants (25.4 kg/m2 vs. 23.2 kg/m2) and a trend for more body fat (20.8% vs. 18.7%).
Not surprisingly, these troubling findings were coupled with a trend for injured participants to spend less time each week participating in moderate to strenuous activity (97.8 minutes vs. 101.4 minutes) and also fewer participated in sports in the previous year (4% vs. 16%).
"If we dichotomize BMI, what we see is that those individuals in the injured group are two times more likely to have a BMI that is [classified as] overweight or obese," Dr. Whittaker said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, the suggestion was made to stratify future data by age at injury, as puberty has an influence on response to injury.
Dr. Whittaker reported funding from the Alberta Children’s Hospital Foundation, Alberta Innovates Health Solutions Alberta Team Osteoarthritis, Canadian Institutes of Health Research, and the University of Calgary Sport Injury Prevention Research Centre.
PARIS – Knee trauma from a childhood sports injury can have serious consequences in young adults, judging from preliminary results from a historical cohort.
When assessed 3-10 years after the sports injury, at an average age of 22 years, young adults appear to be at higher risk of abnormalities visible on MRI that are consistent with future arthropathy and have poorer knee-related quality of life and more knee symptoms.
They are at higher risk of having structural asymmetry of the vastus medialis muscle and being categorized as being overweight or obese.
There also appears to be some trends for increased percent body fat and reduced participation in physical activity, Jackie L. Whittaker, Ph.D., said at the World Congress on Osteoarthritis.
She stressed that these are preliminary findings and that the group hopes to quadruple the size of the cohort this year in order to better understand the relationships they’ve identified.
"With that being said, if we are seeing what we think we’re seeing, there may be some clinical, structural, physiologic, and behavioral markers that can be used to identify individuals who are at risk and target them with secondary prevention strategies at an earlier age," said Dr. Whittaker, a postdoctoral fellow and physiotherapist, University of Calgary Sport Injury Prevention Research Centre, Alberta, Canada.
The historical cohort study involved 25 patients recruited from previous sports injury epidemiology studies who had an intra-articular knee injury in ice hockey (male and female), soccer, basketball, or other sports that required medical attention and time off play, and 25 uninjured controls matched on age, sex, and sport. The median age at injury was 15 years (range 9-18 years). Eight patients in the injured group had contralateral knee surgeries, in addition to surgery on the primary knee. The median age in both groups was 22 years.
Using the Knee injury and Osteoarthritis Outcome Scores (KOOS) outcome, injured participants scored significantly lower, indicating worse function, on all five, 100-point subscales: pain (mean 93 vs. 97), symptoms (mean 82.9 vs. 92.4), activities of daily living (mean 96.3 vs. 99.3), sport/recreation (mean 90.6 vs. 97.4), and knee-related quality of life (mean 89.7 vs. 97.7), Dr. Whittaker said.
Further, in a subsample of 10 matched pairs, injured participants were three times more likely to have an MRI Osteoarthritis Score (MOAKS) of one than were matched controls, according to the study, led by her colleague Carolyn Emery, Ph.D.
Although there was no difference in quadriceps strength between groups, injured participants were 3.8 times more likely to have a difference in the cross-sectional area of the vastus medialis muscle greater than 15%.
"We think that this may be clinically relevant, as there has been some recent prospective work (Arthritis Rheum. 2012;64:3917-25) that has shown a temporal relationship between a decrease in size of the vastus medialis muscle and progression or loss of tibial joint cartilage," she said.
Within 3-10 years after their knee trauma, injured participants have a significantly higher mean body mass index (BMI) than do uninjured participants (25.4 kg/m2 vs. 23.2 kg/m2) and a trend for more body fat (20.8% vs. 18.7%).
Not surprisingly, these troubling findings were coupled with a trend for injured participants to spend less time each week participating in moderate to strenuous activity (97.8 minutes vs. 101.4 minutes) and also fewer participated in sports in the previous year (4% vs. 16%).
"If we dichotomize BMI, what we see is that those individuals in the injured group are two times more likely to have a BMI that is [classified as] overweight or obese," Dr. Whittaker said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, the suggestion was made to stratify future data by age at injury, as puberty has an influence on response to injury.
Dr. Whittaker reported funding from the Alberta Children’s Hospital Foundation, Alberta Innovates Health Solutions Alberta Team Osteoarthritis, Canadian Institutes of Health Research, and the University of Calgary Sport Injury Prevention Research Centre.
PARIS – Knee trauma from a childhood sports injury can have serious consequences in young adults, judging from preliminary results from a historical cohort.
When assessed 3-10 years after the sports injury, at an average age of 22 years, young adults appear to be at higher risk of abnormalities visible on MRI that are consistent with future arthropathy and have poorer knee-related quality of life and more knee symptoms.
They are at higher risk of having structural asymmetry of the vastus medialis muscle and being categorized as being overweight or obese.
There also appears to be some trends for increased percent body fat and reduced participation in physical activity, Jackie L. Whittaker, Ph.D., said at the World Congress on Osteoarthritis.
She stressed that these are preliminary findings and that the group hopes to quadruple the size of the cohort this year in order to better understand the relationships they’ve identified.
"With that being said, if we are seeing what we think we’re seeing, there may be some clinical, structural, physiologic, and behavioral markers that can be used to identify individuals who are at risk and target them with secondary prevention strategies at an earlier age," said Dr. Whittaker, a postdoctoral fellow and physiotherapist, University of Calgary Sport Injury Prevention Research Centre, Alberta, Canada.
The historical cohort study involved 25 patients recruited from previous sports injury epidemiology studies who had an intra-articular knee injury in ice hockey (male and female), soccer, basketball, or other sports that required medical attention and time off play, and 25 uninjured controls matched on age, sex, and sport. The median age at injury was 15 years (range 9-18 years). Eight patients in the injured group had contralateral knee surgeries, in addition to surgery on the primary knee. The median age in both groups was 22 years.
Using the Knee injury and Osteoarthritis Outcome Scores (KOOS) outcome, injured participants scored significantly lower, indicating worse function, on all five, 100-point subscales: pain (mean 93 vs. 97), symptoms (mean 82.9 vs. 92.4), activities of daily living (mean 96.3 vs. 99.3), sport/recreation (mean 90.6 vs. 97.4), and knee-related quality of life (mean 89.7 vs. 97.7), Dr. Whittaker said.
Further, in a subsample of 10 matched pairs, injured participants were three times more likely to have an MRI Osteoarthritis Score (MOAKS) of one than were matched controls, according to the study, led by her colleague Carolyn Emery, Ph.D.
Although there was no difference in quadriceps strength between groups, injured participants were 3.8 times more likely to have a difference in the cross-sectional area of the vastus medialis muscle greater than 15%.
"We think that this may be clinically relevant, as there has been some recent prospective work (Arthritis Rheum. 2012;64:3917-25) that has shown a temporal relationship between a decrease in size of the vastus medialis muscle and progression or loss of tibial joint cartilage," she said.
Within 3-10 years after their knee trauma, injured participants have a significantly higher mean body mass index (BMI) than do uninjured participants (25.4 kg/m2 vs. 23.2 kg/m2) and a trend for more body fat (20.8% vs. 18.7%).
Not surprisingly, these troubling findings were coupled with a trend for injured participants to spend less time each week participating in moderate to strenuous activity (97.8 minutes vs. 101.4 minutes) and also fewer participated in sports in the previous year (4% vs. 16%).
"If we dichotomize BMI, what we see is that those individuals in the injured group are two times more likely to have a BMI that is [classified as] overweight or obese," Dr. Whittaker said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, the suggestion was made to stratify future data by age at injury, as puberty has an influence on response to injury.
Dr. Whittaker reported funding from the Alberta Children’s Hospital Foundation, Alberta Innovates Health Solutions Alberta Team Osteoarthritis, Canadian Institutes of Health Research, and the University of Calgary Sport Injury Prevention Research Centre.
AT OARSI 2014
Major finding: Preliminary evidence suggests that young adults with history of a sports-related knee injury differ in symptomatology, physiology, knee muscle morphology, and joint structure from uninjured controls 3-10 years post injury.
Data source: Historical cohort of 25 sport-related knee injured and 25 uninjured young adults.
Disclosures: Dr. Whittaker reported funding from the Alberta Children’s Hospital Foundation, Alberta Innovates Health Solutions Alberta Team Osteoarthritis, Canadian Institutes of Health Research, and the University of Calgary Sport Injury Prevention Research Centre.
PCPs all over the map in conservative OA therapy use
PARIS – Use of conservative, nonpharmacologic osteoarthritis therapies was relatively low and varied considerably across 10 primary care clinics within the same U.S. health care system.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were currently using pain medications such as opioids or NSAIDs to treat their symptomatic hip and/or knee OA, according to the cross-sectional analysis.
Patients received care at 1 of 10 family and internal medicine Duke Primary Care clinics in North Carolina. All were overweight and not meeting physical activity recommendations. Patients had OA symptoms for an average of 10 years, their average WOMAC (Western Ontario and McMaster Osteoarthritis Index) score was 39, and average age was 63 years.
Four of the clinics were in a rural setting (population less than 20,000), one in a medium-size town (20,000-99,999), four in small cities (100,000-250,000), and one in a large city (more than 250,000). The clinics had an average of 6.4 physicians and one nurse practitioner or physician’s assistant.
Knee brace use of any type ranged from 40%-64% across clinics, Dr. Allen reported. Use of knee braces with metal supports was even lower at 0%-18%.
The relatively low use of PT and knee braces with metal supports "may signal a need for more specific treatment recommendations or guidance for consistent application," suggested Dr. Allen, a health services researcher and exercise physiologist, Duke University Medical Center and Durham VA Medical Center, both in Durham, N.C.
Knee injections were reported by 43%-70% of patients.
Intraclass correlation coefficients (ICCs) were calculated to measure between-clinic variation in treatment use, with an ICC of more than .01 indicating considerable variation.
ICCs were 0.01 for the proportion using any pain medications, 0 for opioids, NSAIDS, knee injections and knee braces, 0.02 for metal knee braces, 0.07 for knee PT, and 0.08 for hip PT, according to Dr. Allen.
Rural clinics were typically below the median for nonpharmacologic use, possibly because of fewer resources in these areas, according to the poster presentation.
Clinics with fewer patients reporting "fair" or "poor" general health, however, tended to have higher use across treatment categories.
"These OA therapies may be more highly utilized when patients have fewer competing health problems," she suggested at the meeting, sponsored by the Osteoarthritis Research Society International.
Overall, 20% of patients in the study reported having fair or poor health, but rates ranged from a low of 10% to a high of 35%.
The study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Allen reported no conflicts of interest.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were curre
PARIS – Use of conservative, nonpharmacologic osteoarthritis therapies was relatively low and varied considerably across 10 primary care clinics within the same U.S. health care system.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were currently using pain medications such as opioids or NSAIDs to treat their symptomatic hip and/or knee OA, according to the cross-sectional analysis.
Patients received care at 1 of 10 family and internal medicine Duke Primary Care clinics in North Carolina. All were overweight and not meeting physical activity recommendations. Patients had OA symptoms for an average of 10 years, their average WOMAC (Western Ontario and McMaster Osteoarthritis Index) score was 39, and average age was 63 years.
Four of the clinics were in a rural setting (population less than 20,000), one in a medium-size town (20,000-99,999), four in small cities (100,000-250,000), and one in a large city (more than 250,000). The clinics had an average of 6.4 physicians and one nurse practitioner or physician’s assistant.
Knee brace use of any type ranged from 40%-64% across clinics, Dr. Allen reported. Use of knee braces with metal supports was even lower at 0%-18%.
The relatively low use of PT and knee braces with metal supports "may signal a need for more specific treatment recommendations or guidance for consistent application," suggested Dr. Allen, a health services researcher and exercise physiologist, Duke University Medical Center and Durham VA Medical Center, both in Durham, N.C.
Knee injections were reported by 43%-70% of patients.
Intraclass correlation coefficients (ICCs) were calculated to measure between-clinic variation in treatment use, with an ICC of more than .01 indicating considerable variation.
ICCs were 0.01 for the proportion using any pain medications, 0 for opioids, NSAIDS, knee injections and knee braces, 0.02 for metal knee braces, 0.07 for knee PT, and 0.08 for hip PT, according to Dr. Allen.
Rural clinics were typically below the median for nonpharmacologic use, possibly because of fewer resources in these areas, according to the poster presentation.
Clinics with fewer patients reporting "fair" or "poor" general health, however, tended to have higher use across treatment categories.
"These OA therapies may be more highly utilized when patients have fewer competing health problems," she suggested at the meeting, sponsored by the Osteoarthritis Research Society International.
Overall, 20% of patients in the study reported having fair or poor health, but rates ranged from a low of 10% to a high of 35%.
The study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Allen reported no conflicts of interest.
PARIS – Use of conservative, nonpharmacologic osteoarthritis therapies was relatively low and varied considerably across 10 primary care clinics within the same U.S. health care system.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were currently using pain medications such as opioids or NSAIDs to treat their symptomatic hip and/or knee OA, according to the cross-sectional analysis.
Patients received care at 1 of 10 family and internal medicine Duke Primary Care clinics in North Carolina. All were overweight and not meeting physical activity recommendations. Patients had OA symptoms for an average of 10 years, their average WOMAC (Western Ontario and McMaster Osteoarthritis Index) score was 39, and average age was 63 years.
Four of the clinics were in a rural setting (population less than 20,000), one in a medium-size town (20,000-99,999), four in small cities (100,000-250,000), and one in a large city (more than 250,000). The clinics had an average of 6.4 physicians and one nurse practitioner or physician’s assistant.
Knee brace use of any type ranged from 40%-64% across clinics, Dr. Allen reported. Use of knee braces with metal supports was even lower at 0%-18%.
The relatively low use of PT and knee braces with metal supports "may signal a need for more specific treatment recommendations or guidance for consistent application," suggested Dr. Allen, a health services researcher and exercise physiologist, Duke University Medical Center and Durham VA Medical Center, both in Durham, N.C.
Knee injections were reported by 43%-70% of patients.
Intraclass correlation coefficients (ICCs) were calculated to measure between-clinic variation in treatment use, with an ICC of more than .01 indicating considerable variation.
ICCs were 0.01 for the proportion using any pain medications, 0 for opioids, NSAIDS, knee injections and knee braces, 0.02 for metal knee braces, 0.07 for knee PT, and 0.08 for hip PT, according to Dr. Allen.
Rural clinics were typically below the median for nonpharmacologic use, possibly because of fewer resources in these areas, according to the poster presentation.
Clinics with fewer patients reporting "fair" or "poor" general health, however, tended to have higher use across treatment categories.
"These OA therapies may be more highly utilized when patients have fewer competing health problems," she suggested at the meeting, sponsored by the Osteoarthritis Research Society International.
Overall, 20% of patients in the study reported having fair or poor health, but rates ranged from a low of 10% to a high of 35%.
The study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Allen reported no conflicts of interest.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were curre
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were curre
AT OARSI 2014
Data source: Cross-sectional analysis of 537 OA patients at 10 PCP clinics.
Disclosures: The study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Allen reported no conflicting interests.
Negative moods tied to OA pain flares
PARIS – Patients with knee osteoarthritis are significantly more likely to experience a flare if they report a higher negative mood in the previous 10 days.
Passive coping strategies such as "I restrict my social activities" or "I focus on the location and intensity of pain" were also significantly associated with an increased risk of flares, while more active coping strategies were protective in a Web-based, case-crossover study.

"We really need to elaborate on this, replicate it, and elucidate this connection because psychosocial factors of mood and pain coping are modifiable and ultimately may improve our patients experience of this disease, osteoarthritis," Dr. David J. Hunter said at the World Congress on Osteoarthritis.
The investigators recruited 298 patients with symptomatic knee osteoarthritis (OA) and asked them to log on to the study website if they experienced a knee pain exacerbation over 3 months of follow-up.
Daily mood (negative/positive) in the previous 10 days was assessed using the Profile of Mood States (POMS) questionnaire. The Pain Coping Inventory (PCI) was used to assess daily pain coping in the previous 30 days.
Pain exacerbation during follow-up was defined as a 2-unit increase in the patient’s visual analog knee pain score (10-point scale) from his or her mildest pain score reported at the baseline visit, said Dr. Hunter, the Florance and Cope Chair of Rheumatology, Northern Clinical School, University of Sydney, Australia.
Most of the patients were female (61%) and white (92%), and their average body mass index was 29.4 kg/m2. Their average baseline Knee injury and Osteoarthritis Outcome Score (KOOS) symptoms subscale score was 44.5 and KOOS pain subscale score 55.6.
The average POMS positive mood score was 33.9 and average negative mood (for example, distressed, irritable, nervous) score 16.5, both on a 50-point scale. The average PCI passive coping score was 8.1 on a 24-point scale, and average PCI active coping score 12.2 on a 20-point scale.
In conditional logistic regression analyses, increasing negative affect scores were significantly associated with having a pain exacerbation (P less than .001) such that patients with a score of 13-17 were nearly three times more likely to experience a flare (odds ratio, 2.77) and those with a score of 18 or more were 6.5 times more likely to do so (OR, 6.5), Dr. Hunter said.
Patients with higher PCI passive coping scores were also significantly more likely to have a pain exacerbation (OR, 1.26; P = .01), while those with more active coping strategies such as "I stay busy or active," or "I clear my mind of bothersome thoughts" were less likely to have a pain flare (OR, 0.81; P = .03).
During a discussion of the results, Dr. Hunter said they have yet to look at trajectories to see whether patients returned to their prior pain level.
Session comoderator Aileen Davis, Ph.D., senior scientist with the Toronto Western Research Institute, said the general literature recognizes there is a psychosocial component to OA pain, but that this is the first study to make the direct link with OA pain flares.
If the results can be replicated, "It means there’s a lot more we can do in terms of coping strategies and in recognizing this a lot more often," she said in an interview at the meeting, sponsored by the Osteoarthritis Research Society International.
Since many OA patients are cared for by primary care physicians, Dr. Davis suggested they may want to have a psychosocial profile of their OA patients and push management strategies or referrals to psychologists or social workers skilled in coping strategies to patients who are "fluctuators," so they can "proactively change how they’re doing things."
Dr. Hunter reported support from the Australian National Health and Medical Research Council.
Passive coping strategies, pain, active coping strategies, psychosocial factors, mood, pain, Dr. David J. Hunter, World Congress on Osteoarthritis, symptomatic knee osteoarthritis, knee pain exacerbation, Profile of Mood States questionnaire, The Pain Coping Inventory, Knee injury and Osteoarthritis Outcome Score symptoms subscale score,
PARIS – Patients with knee osteoarthritis are significantly more likely to experience a flare if they report a higher negative mood in the previous 10 days.
Passive coping strategies such as "I restrict my social activities" or "I focus on the location and intensity of pain" were also significantly associated with an increased risk of flares, while more active coping strategies were protective in a Web-based, case-crossover study.
"We really need to elaborate on this, replicate it, and elucidate this connection because psychosocial factors of mood and pain coping are modifiable and ultimately may improve our patients experience of this disease, osteoarthritis," Dr. David J. Hunter said at the World Congress on Osteoarthritis.
The investigators recruited 298 patients with symptomatic knee osteoarthritis (OA) and asked them to log on to the study website if they experienced a knee pain exacerbation over 3 months of follow-up.
Daily mood (negative/positive) in the previous 10 days was assessed using the Profile of Mood States (POMS) questionnaire. The Pain Coping Inventory (PCI) was used to assess daily pain coping in the previous 30 days.
Pain exacerbation during follow-up was defined as a 2-unit increase in the patient’s visual analog knee pain score (10-point scale) from his or her mildest pain score reported at the baseline visit, said Dr. Hunter, the Florance and Cope Chair of Rheumatology, Northern Clinical School, University of Sydney, Australia.
Most of the patients were female (61%) and white (92%), and their average body mass index was 29.4 kg/m2. Their average baseline Knee injury and Osteoarthritis Outcome Score (KOOS) symptoms subscale score was 44.5 and KOOS pain subscale score 55.6.
The average POMS positive mood score was 33.9 and average negative mood (for example, distressed, irritable, nervous) score 16.5, both on a 50-point scale. The average PCI passive coping score was 8.1 on a 24-point scale, and average PCI active coping score 12.2 on a 20-point scale.
In conditional logistic regression analyses, increasing negative affect scores were significantly associated with having a pain exacerbation (P less than .001) such that patients with a score of 13-17 were nearly three times more likely to experience a flare (odds ratio, 2.77) and those with a score of 18 or more were 6.5 times more likely to do so (OR, 6.5), Dr. Hunter said.
Patients with higher PCI passive coping scores were also significantly more likely to have a pain exacerbation (OR, 1.26; P = .01), while those with more active coping strategies such as "I stay busy or active," or "I clear my mind of bothersome thoughts" were less likely to have a pain flare (OR, 0.81; P = .03).
During a discussion of the results, Dr. Hunter said they have yet to look at trajectories to see whether patients returned to their prior pain level.
Session comoderator Aileen Davis, Ph.D., senior scientist with the Toronto Western Research Institute, said the general literature recognizes there is a psychosocial component to OA pain, but that this is the first study to make the direct link with OA pain flares.
If the results can be replicated, "It means there’s a lot more we can do in terms of coping strategies and in recognizing this a lot more often," she said in an interview at the meeting, sponsored by the Osteoarthritis Research Society International.
Since many OA patients are cared for by primary care physicians, Dr. Davis suggested they may want to have a psychosocial profile of their OA patients and push management strategies or referrals to psychologists or social workers skilled in coping strategies to patients who are "fluctuators," so they can "proactively change how they’re doing things."
Dr. Hunter reported support from the Australian National Health and Medical Research Council.
PARIS – Patients with knee osteoarthritis are significantly more likely to experience a flare if they report a higher negative mood in the previous 10 days.
Passive coping strategies such as "I restrict my social activities" or "I focus on the location and intensity of pain" were also significantly associated with an increased risk of flares, while more active coping strategies were protective in a Web-based, case-crossover study.
"We really need to elaborate on this, replicate it, and elucidate this connection because psychosocial factors of mood and pain coping are modifiable and ultimately may improve our patients experience of this disease, osteoarthritis," Dr. David J. Hunter said at the World Congress on Osteoarthritis.
The investigators recruited 298 patients with symptomatic knee osteoarthritis (OA) and asked them to log on to the study website if they experienced a knee pain exacerbation over 3 months of follow-up.
Daily mood (negative/positive) in the previous 10 days was assessed using the Profile of Mood States (POMS) questionnaire. The Pain Coping Inventory (PCI) was used to assess daily pain coping in the previous 30 days.
Pain exacerbation during follow-up was defined as a 2-unit increase in the patient’s visual analog knee pain score (10-point scale) from his or her mildest pain score reported at the baseline visit, said Dr. Hunter, the Florance and Cope Chair of Rheumatology, Northern Clinical School, University of Sydney, Australia.
Most of the patients were female (61%) and white (92%), and their average body mass index was 29.4 kg/m2. Their average baseline Knee injury and Osteoarthritis Outcome Score (KOOS) symptoms subscale score was 44.5 and KOOS pain subscale score 55.6.
The average POMS positive mood score was 33.9 and average negative mood (for example, distressed, irritable, nervous) score 16.5, both on a 50-point scale. The average PCI passive coping score was 8.1 on a 24-point scale, and average PCI active coping score 12.2 on a 20-point scale.
In conditional logistic regression analyses, increasing negative affect scores were significantly associated with having a pain exacerbation (P less than .001) such that patients with a score of 13-17 were nearly three times more likely to experience a flare (odds ratio, 2.77) and those with a score of 18 or more were 6.5 times more likely to do so (OR, 6.5), Dr. Hunter said.
Patients with higher PCI passive coping scores were also significantly more likely to have a pain exacerbation (OR, 1.26; P = .01), while those with more active coping strategies such as "I stay busy or active," or "I clear my mind of bothersome thoughts" were less likely to have a pain flare (OR, 0.81; P = .03).
During a discussion of the results, Dr. Hunter said they have yet to look at trajectories to see whether patients returned to their prior pain level.
Session comoderator Aileen Davis, Ph.D., senior scientist with the Toronto Western Research Institute, said the general literature recognizes there is a psychosocial component to OA pain, but that this is the first study to make the direct link with OA pain flares.
If the results can be replicated, "It means there’s a lot more we can do in terms of coping strategies and in recognizing this a lot more often," she said in an interview at the meeting, sponsored by the Osteoarthritis Research Society International.
Since many OA patients are cared for by primary care physicians, Dr. Davis suggested they may want to have a psychosocial profile of their OA patients and push management strategies or referrals to psychologists or social workers skilled in coping strategies to patients who are "fluctuators," so they can "proactively change how they’re doing things."
Dr. Hunter reported support from the Australian National Health and Medical Research Council.
Passive coping strategies, pain, active coping strategies, psychosocial factors, mood, pain, Dr. David J. Hunter, World Congress on Osteoarthritis, symptomatic knee osteoarthritis, knee pain exacerbation, Profile of Mood States questionnaire, The Pain Coping Inventory, Knee injury and Osteoarthritis Outcome Score symptoms subscale score,
Passive coping strategies, pain, active coping strategies, psychosocial factors, mood, pain, Dr. David J. Hunter, World Congress on Osteoarthritis, symptomatic knee osteoarthritis, knee pain exacerbation, Profile of Mood States questionnaire, The Pain Coping Inventory, Knee injury and Osteoarthritis Outcome Score symptoms subscale score,
AT OARSI 2014
Key clinical point: Clinicians may want to help OA patients with coping strategies by requesting a psychosocial profile and tailoring management strategies to it or referral to psychologists or social workers skilled in coping strategies.
Major finding: Patients with a negative affect score of 18 or more were 6.5 times more likely to experience an OA pain flare (OR, 6.5).
Data source: A case-crossover study in 298 patients with knee OA.
Disclosures: Dr. Hunter reported support from the Australian National Health and Medical Research Council.
