User login
Beyond Cash: Using Rewards to Motivate Physicians
SAN DIEGO – Cash is king, but it’s probably not the best way to make physicians feel appreciated. A flat-screen TV, a vacation, or a chance to take a professional development course, on the other hand, are all good ways for practices to recognize high-quality work and motivate physicians, according to Dr. John Nelson.
Dr. Nelson, a principal at Nelson Flores Hospital Medicine Consultants and a past president of the Society of Hospital Medicine, said it’s important to compensate hospitalists well. But just adding on cash bonuses doesn’t do much to energize employees and convince them to stay with a group," he said at the annual meeting of the Society of Hospital Medicine.
"Cash compensation is generally seen as an entitlement, so in most cases it doesn’t wind up being much of a motivator," he said in an interview. "It might help encourage someone to take a position in your practice, but it probably won’t do a lot to change their performance."
Base salary, health benefits, vacation time, seniority-based pay, and cost of living adjustments are all standard compensation that physicians expect to receive.
Practice leaders should instead consider offering nonmonetary incentives to their physicians, Dr. Nelson said. While cash bonuses can be viewed as cold or unemotional, nonmonetary awards have the potential to be memorable and special for employees. And while $100 is always just $100, a nonmonetary award can often have a higher perceived value.
Here are some nonmonetary incentive options:
• Write a note of thanks for doing a good job.
• Award a trophy for work in improving quality of care.
• Offer a promotion or a new title.
• Pay for attendance at a professional-development course.
• Provide a chance to contribute ideas to the group or hospital through one-on-one meeting with leadership or by leading special projects.
• Offer gifts such as vacations, televisions, or gift cards.
There are a number of different ways that these types of awards can be structured, said Dr. Nelson, who is also director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. They can be offered as recognition to teams or individuals. They can also be set up to celebrate milestones or to honor important achievements.
When designing a plan, Dr. Nelson said it’s important not to set up a reward system that creates a feeling of unfairness and produces strife within the group. Group leaders also need to keep in mind that nonmonetary awards, such as trips or gift cards, still count as compensation under the Stark Law and anti-kickback regulations. This is especially important for physicians who contract with, but are not directly employed by a hospital.
These types of awards do carry some cost for employers, but not nearly as much as a cost of living raise, for example. Exactly how much to spend will vary, Dr. Nelson said, but it should be a small percentage of the physicians’ overall salary, as low as 1%.
"If structured in the form of a nonmonetary reward, such as recognition, promotion, [or] professional development, that might be enough to inspire and encourage good performance on the part of the hospitalist," Dr. Nelson said.
SAN DIEGO – Cash is king, but it’s probably not the best way to make physicians feel appreciated. A flat-screen TV, a vacation, or a chance to take a professional development course, on the other hand, are all good ways for practices to recognize high-quality work and motivate physicians, according to Dr. John Nelson.
Dr. Nelson, a principal at Nelson Flores Hospital Medicine Consultants and a past president of the Society of Hospital Medicine, said it’s important to compensate hospitalists well. But just adding on cash bonuses doesn’t do much to energize employees and convince them to stay with a group," he said at the annual meeting of the Society of Hospital Medicine.
"Cash compensation is generally seen as an entitlement, so in most cases it doesn’t wind up being much of a motivator," he said in an interview. "It might help encourage someone to take a position in your practice, but it probably won’t do a lot to change their performance."
Base salary, health benefits, vacation time, seniority-based pay, and cost of living adjustments are all standard compensation that physicians expect to receive.
Practice leaders should instead consider offering nonmonetary incentives to their physicians, Dr. Nelson said. While cash bonuses can be viewed as cold or unemotional, nonmonetary awards have the potential to be memorable and special for employees. And while $100 is always just $100, a nonmonetary award can often have a higher perceived value.
Here are some nonmonetary incentive options:
• Write a note of thanks for doing a good job.
• Award a trophy for work in improving quality of care.
• Offer a promotion or a new title.
• Pay for attendance at a professional-development course.
• Provide a chance to contribute ideas to the group or hospital through one-on-one meeting with leadership or by leading special projects.
• Offer gifts such as vacations, televisions, or gift cards.
There are a number of different ways that these types of awards can be structured, said Dr. Nelson, who is also director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. They can be offered as recognition to teams or individuals. They can also be set up to celebrate milestones or to honor important achievements.
When designing a plan, Dr. Nelson said it’s important not to set up a reward system that creates a feeling of unfairness and produces strife within the group. Group leaders also need to keep in mind that nonmonetary awards, such as trips or gift cards, still count as compensation under the Stark Law and anti-kickback regulations. This is especially important for physicians who contract with, but are not directly employed by a hospital.
These types of awards do carry some cost for employers, but not nearly as much as a cost of living raise, for example. Exactly how much to spend will vary, Dr. Nelson said, but it should be a small percentage of the physicians’ overall salary, as low as 1%.
"If structured in the form of a nonmonetary reward, such as recognition, promotion, [or] professional development, that might be enough to inspire and encourage good performance on the part of the hospitalist," Dr. Nelson said.
SAN DIEGO – Cash is king, but it’s probably not the best way to make physicians feel appreciated. A flat-screen TV, a vacation, or a chance to take a professional development course, on the other hand, are all good ways for practices to recognize high-quality work and motivate physicians, according to Dr. John Nelson.
Dr. Nelson, a principal at Nelson Flores Hospital Medicine Consultants and a past president of the Society of Hospital Medicine, said it’s important to compensate hospitalists well. But just adding on cash bonuses doesn’t do much to energize employees and convince them to stay with a group," he said at the annual meeting of the Society of Hospital Medicine.
"Cash compensation is generally seen as an entitlement, so in most cases it doesn’t wind up being much of a motivator," he said in an interview. "It might help encourage someone to take a position in your practice, but it probably won’t do a lot to change their performance."
Base salary, health benefits, vacation time, seniority-based pay, and cost of living adjustments are all standard compensation that physicians expect to receive.
Practice leaders should instead consider offering nonmonetary incentives to their physicians, Dr. Nelson said. While cash bonuses can be viewed as cold or unemotional, nonmonetary awards have the potential to be memorable and special for employees. And while $100 is always just $100, a nonmonetary award can often have a higher perceived value.
Here are some nonmonetary incentive options:
• Write a note of thanks for doing a good job.
• Award a trophy for work in improving quality of care.
• Offer a promotion or a new title.
• Pay for attendance at a professional-development course.
• Provide a chance to contribute ideas to the group or hospital through one-on-one meeting with leadership or by leading special projects.
• Offer gifts such as vacations, televisions, or gift cards.
There are a number of different ways that these types of awards can be structured, said Dr. Nelson, who is also director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. They can be offered as recognition to teams or individuals. They can also be set up to celebrate milestones or to honor important achievements.
When designing a plan, Dr. Nelson said it’s important not to set up a reward system that creates a feeling of unfairness and produces strife within the group. Group leaders also need to keep in mind that nonmonetary awards, such as trips or gift cards, still count as compensation under the Stark Law and anti-kickback regulations. This is especially important for physicians who contract with, but are not directly employed by a hospital.
These types of awards do carry some cost for employers, but not nearly as much as a cost of living raise, for example. Exactly how much to spend will vary, Dr. Nelson said, but it should be a small percentage of the physicians’ overall salary, as low as 1%.
"If structured in the form of a nonmonetary reward, such as recognition, promotion, [or] professional development, that might be enough to inspire and encourage good performance on the part of the hospitalist," Dr. Nelson said.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Acetaminophen Safe in Alcoholics, Analysis Suggests
SAN DIEGO – Giving acetaminophen to patients who reported consuming ethanol did not adversely affect markers of liver damage in a meta-analysis of randomized, controlled trials.
"One of the questions we often get asked is the role of acetaminophen in patients with liver disease," said Dr. Kennon J. Heard, an emergency medicine physician at the University of Colorado and director of the Medical Toxicology Fellowship at the Rocky Mountain Poison and Drug Center, Denver.

The findings of the meta-analysis suggest that "acetaminophen is safe in alcoholics," he said at the annual meeting of the Society of Hospital Medicine.
The meta-analysis included five trials involving 901 subjects (including patients who reported drinking ethanol) who were randomized to receive acetaminophen or placebo. Dr. Heard and his associates looked at daily ALT measurements out to a mean of 4 days, a time period for which most of the studies had data. They also looked for any evidence of liver injury or dysfunction, hepatotoxicity, or death.
The alanine aminotransferase (ALT) levels changed by a mean of 0.04 IU/L after starting acetaminophen or placebo, "less than a tenth of a point in ALT," reported Dr. Heard. "Essentially, in this group of patients who consume alcohol, if you give them acetaminophen for 4 days, you don’t see any change in their ALT."
The study is to be published in the journal Pharmacotherapy.
When acetaminophen consumption continued beyond 4 days, ALT levels increased in most patients who consumed alcohol but also increased in 60% of non-drinkers. "The changes in the alcoholics look exactly like the changes in the non-alcoholics," he said. The median increase in ALT was between 10-20 IU/L.
Among patients who drink alcohol, the highest ALT level in the acetaminophen group was 312 IU/L, "which is pretty impressive until you see that in the placebo group, somebody went up 288" IU/L, he said. The biggest increase in ALT was in a healthy nondrinking patient on acetaminophen, whose ALT increased by 638 IU/L.
Most importantly, none of the 551 people who received acetaminophen in those trials developed an increase in International Normalized Ratio, bilirubin level, or symptomatic liver injury, he added.
Dr. Heard and his associates are now finishing a separate study that appears to confirm that these are asymptomatic, self-limiting elevations in ALT that will go away even if people stay on acetaminophen.
"It is worth knowing that if you have someone who has an ALT elevation while taking acetaminophen, it may be the cause, and it is reasonable to stop the acetaminophen and see if their ALT elevations go away rather than do an extensive workup for hepatitis," he said.
Dr. Heard has been a consultant or received research grants from Cadence Pharmaceuticals, McNeil Consumer Healthcare, and Cumberland Pharmaceuticals.
SAN DIEGO – Giving acetaminophen to patients who reported consuming ethanol did not adversely affect markers of liver damage in a meta-analysis of randomized, controlled trials.
"One of the questions we often get asked is the role of acetaminophen in patients with liver disease," said Dr. Kennon J. Heard, an emergency medicine physician at the University of Colorado and director of the Medical Toxicology Fellowship at the Rocky Mountain Poison and Drug Center, Denver.
The findings of the meta-analysis suggest that "acetaminophen is safe in alcoholics," he said at the annual meeting of the Society of Hospital Medicine.
The meta-analysis included five trials involving 901 subjects (including patients who reported drinking ethanol) who were randomized to receive acetaminophen or placebo. Dr. Heard and his associates looked at daily ALT measurements out to a mean of 4 days, a time period for which most of the studies had data. They also looked for any evidence of liver injury or dysfunction, hepatotoxicity, or death.
The alanine aminotransferase (ALT) levels changed by a mean of 0.04 IU/L after starting acetaminophen or placebo, "less than a tenth of a point in ALT," reported Dr. Heard. "Essentially, in this group of patients who consume alcohol, if you give them acetaminophen for 4 days, you don’t see any change in their ALT."
The study is to be published in the journal Pharmacotherapy.
When acetaminophen consumption continued beyond 4 days, ALT levels increased in most patients who consumed alcohol but also increased in 60% of non-drinkers. "The changes in the alcoholics look exactly like the changes in the non-alcoholics," he said. The median increase in ALT was between 10-20 IU/L.
Among patients who drink alcohol, the highest ALT level in the acetaminophen group was 312 IU/L, "which is pretty impressive until you see that in the placebo group, somebody went up 288" IU/L, he said. The biggest increase in ALT was in a healthy nondrinking patient on acetaminophen, whose ALT increased by 638 IU/L.
Most importantly, none of the 551 people who received acetaminophen in those trials developed an increase in International Normalized Ratio, bilirubin level, or symptomatic liver injury, he added.
Dr. Heard and his associates are now finishing a separate study that appears to confirm that these are asymptomatic, self-limiting elevations in ALT that will go away even if people stay on acetaminophen.
"It is worth knowing that if you have someone who has an ALT elevation while taking acetaminophen, it may be the cause, and it is reasonable to stop the acetaminophen and see if their ALT elevations go away rather than do an extensive workup for hepatitis," he said.
Dr. Heard has been a consultant or received research grants from Cadence Pharmaceuticals, McNeil Consumer Healthcare, and Cumberland Pharmaceuticals.
SAN DIEGO – Giving acetaminophen to patients who reported consuming ethanol did not adversely affect markers of liver damage in a meta-analysis of randomized, controlled trials.
"One of the questions we often get asked is the role of acetaminophen in patients with liver disease," said Dr. Kennon J. Heard, an emergency medicine physician at the University of Colorado and director of the Medical Toxicology Fellowship at the Rocky Mountain Poison and Drug Center, Denver.
The findings of the meta-analysis suggest that "acetaminophen is safe in alcoholics," he said at the annual meeting of the Society of Hospital Medicine.
The meta-analysis included five trials involving 901 subjects (including patients who reported drinking ethanol) who were randomized to receive acetaminophen or placebo. Dr. Heard and his associates looked at daily ALT measurements out to a mean of 4 days, a time period for which most of the studies had data. They also looked for any evidence of liver injury or dysfunction, hepatotoxicity, or death.
The alanine aminotransferase (ALT) levels changed by a mean of 0.04 IU/L after starting acetaminophen or placebo, "less than a tenth of a point in ALT," reported Dr. Heard. "Essentially, in this group of patients who consume alcohol, if you give them acetaminophen for 4 days, you don’t see any change in their ALT."
The study is to be published in the journal Pharmacotherapy.
When acetaminophen consumption continued beyond 4 days, ALT levels increased in most patients who consumed alcohol but also increased in 60% of non-drinkers. "The changes in the alcoholics look exactly like the changes in the non-alcoholics," he said. The median increase in ALT was between 10-20 IU/L.
Among patients who drink alcohol, the highest ALT level in the acetaminophen group was 312 IU/L, "which is pretty impressive until you see that in the placebo group, somebody went up 288" IU/L, he said. The biggest increase in ALT was in a healthy nondrinking patient on acetaminophen, whose ALT increased by 638 IU/L.
Most importantly, none of the 551 people who received acetaminophen in those trials developed an increase in International Normalized Ratio, bilirubin level, or symptomatic liver injury, he added.
Dr. Heard and his associates are now finishing a separate study that appears to confirm that these are asymptomatic, self-limiting elevations in ALT that will go away even if people stay on acetaminophen.
"It is worth knowing that if you have someone who has an ALT elevation while taking acetaminophen, it may be the cause, and it is reasonable to stop the acetaminophen and see if their ALT elevations go away rather than do an extensive workup for hepatitis," he said.
Dr. Heard has been a consultant or received research grants from Cadence Pharmaceuticals, McNeil Consumer Healthcare, and Cumberland Pharmaceuticals.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Major Finding: ALT levels changed by a median of 0.04 IU/L in alcohol drinkers and nondrinkers after taking acetaminophen for 4 days, with no significant difference between subjects on acetaminophen or placebo.
Data Source: The meta-analysis of five randomized, controlled trials included 901 subjects.
Disclosures: Dr. Heard has been a consultant or received research grants from Cadence Pharmaceuticals, McNeil Consumer Healthcare, and Cumberland Pharmaceuticals.
Inappropriate Bronchiolitis Care Plummets With Peer Networking
SAN DIEGO – Inappropriate use of bronchodilators to treat pediatric bronchiolitis declined from 70% of patients in 2007 to 58% in 2010, thanks to benchmarking and peer-to-peer collaborative efforts of the Value in Inpatient Pediatrics Network at hospitals in 14 states.
Bronchodilator utilization decreased by 45% as measured by doses per patient, from 7.6 doses/patient in 2007 to 4.2 doses/patient in 2010, Dr. Shawn Ralston and her associates reported at the annual meeting of the Society of Hospital Medicine.
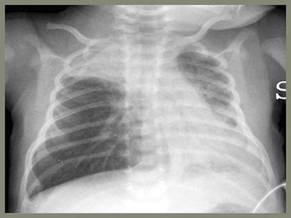
Inappropriate use of chest physiotherapy to treat pediatric bronchiolitis also declined, from 14% of cases in 2007 to 4.2% in 2010, said Dr. Ralston, chief of the division of inpatient pediatrics at the University of Texas Health Science Center, San Antonio.
The investigators had hoped to see declines as well in the inappropriate use of chest x-rays, steroids, and testing for respiratory syncytial virus, but mild declines in these categories did not reach statistical significance.
Bronchiolitis is the most common reason for hospitalizing infants and toddlers, with wide variation in care. Practice guidelines from the American Academy of Pediatrics (AAP) in 2006 recommend treating pediatric bronchiolitis with nothing but supportive care. Bronchodilator therapy and steroid therapy have been shown to have no benefit for these cases in repeated meta-analyses over the past 15 and 12 years, respectively.
"None of the things we all do frequently have any support" in the literature for managing pediatric bronchiolitis, Dr. Ralston, a steering committee member of the Value in Inpatient Pediatrics (VIP) Network.
The VIP Network, formed out of an AAP section on hospital medicine, pulled together physicians who were frustrated with the lack of pediatric resources for quality improvement in smaller academic and community hospitals. The VIP Network chose bronchiolitis as its first target to see if it could start to change management by providing a peer group for local leaders to share resources and benchmark progress within the group.

The VIP Network functions as a virtual community with yearly meetings that adopted group norms for appropriate bronchiolitis care. Its website offers handouts, bibliographies, and other resources, and network members provided peer-to-peer coaching on quality improvement.
Members produced yearly benchmarking reports using hospital billing data for diagnostic codes 466.11 or 466.19 starting in 2008 (with some 2007 data serving as additional baseline data). Dr. Ralston said that 90% of data came from non-freestanding children’s facilities. In all, 70% of participating facilities did not have a guideline for pediatric bronchiolitis management prior to joining the Network, Dr. Ralston said. A total of 30% of facilities were in urban locations.
The results show that an all-volunteer group with no source of specific funding and no new resources can make real-world changes that improve the quality of care, she said.
"The caveat is that it has to be something the physicians really care about," she said. "Clinicians are significantly more motivated for this kind of work than researchers."
Dr. Ralston reported having no financial disclosures. She receives funds from the American Academy of Pediatrics to be editor of the journal Hospital Pediatrics.
SAN DIEGO – Inappropriate use of bronchodilators to treat pediatric bronchiolitis declined from 70% of patients in 2007 to 58% in 2010, thanks to benchmarking and peer-to-peer collaborative efforts of the Value in Inpatient Pediatrics Network at hospitals in 14 states.
Bronchodilator utilization decreased by 45% as measured by doses per patient, from 7.6 doses/patient in 2007 to 4.2 doses/patient in 2010, Dr. Shawn Ralston and her associates reported at the annual meeting of the Society of Hospital Medicine.
Inappropriate use of chest physiotherapy to treat pediatric bronchiolitis also declined, from 14% of cases in 2007 to 4.2% in 2010, said Dr. Ralston, chief of the division of inpatient pediatrics at the University of Texas Health Science Center, San Antonio.
The investigators had hoped to see declines as well in the inappropriate use of chest x-rays, steroids, and testing for respiratory syncytial virus, but mild declines in these categories did not reach statistical significance.
Bronchiolitis is the most common reason for hospitalizing infants and toddlers, with wide variation in care. Practice guidelines from the American Academy of Pediatrics (AAP) in 2006 recommend treating pediatric bronchiolitis with nothing but supportive care. Bronchodilator therapy and steroid therapy have been shown to have no benefit for these cases in repeated meta-analyses over the past 15 and 12 years, respectively.
"None of the things we all do frequently have any support" in the literature for managing pediatric bronchiolitis, Dr. Ralston, a steering committee member of the Value in Inpatient Pediatrics (VIP) Network.
The VIP Network, formed out of an AAP section on hospital medicine, pulled together physicians who were frustrated with the lack of pediatric resources for quality improvement in smaller academic and community hospitals. The VIP Network chose bronchiolitis as its first target to see if it could start to change management by providing a peer group for local leaders to share resources and benchmark progress within the group.
The VIP Network functions as a virtual community with yearly meetings that adopted group norms for appropriate bronchiolitis care. Its website offers handouts, bibliographies, and other resources, and network members provided peer-to-peer coaching on quality improvement.
Members produced yearly benchmarking reports using hospital billing data for diagnostic codes 466.11 or 466.19 starting in 2008 (with some 2007 data serving as additional baseline data). Dr. Ralston said that 90% of data came from non-freestanding children’s facilities. In all, 70% of participating facilities did not have a guideline for pediatric bronchiolitis management prior to joining the Network, Dr. Ralston said. A total of 30% of facilities were in urban locations.
The results show that an all-volunteer group with no source of specific funding and no new resources can make real-world changes that improve the quality of care, she said.
"The caveat is that it has to be something the physicians really care about," she said. "Clinicians are significantly more motivated for this kind of work than researchers."
Dr. Ralston reported having no financial disclosures. She receives funds from the American Academy of Pediatrics to be editor of the journal Hospital Pediatrics.
SAN DIEGO – Inappropriate use of bronchodilators to treat pediatric bronchiolitis declined from 70% of patients in 2007 to 58% in 2010, thanks to benchmarking and peer-to-peer collaborative efforts of the Value in Inpatient Pediatrics Network at hospitals in 14 states.
Bronchodilator utilization decreased by 45% as measured by doses per patient, from 7.6 doses/patient in 2007 to 4.2 doses/patient in 2010, Dr. Shawn Ralston and her associates reported at the annual meeting of the Society of Hospital Medicine.
Inappropriate use of chest physiotherapy to treat pediatric bronchiolitis also declined, from 14% of cases in 2007 to 4.2% in 2010, said Dr. Ralston, chief of the division of inpatient pediatrics at the University of Texas Health Science Center, San Antonio.
The investigators had hoped to see declines as well in the inappropriate use of chest x-rays, steroids, and testing for respiratory syncytial virus, but mild declines in these categories did not reach statistical significance.
Bronchiolitis is the most common reason for hospitalizing infants and toddlers, with wide variation in care. Practice guidelines from the American Academy of Pediatrics (AAP) in 2006 recommend treating pediatric bronchiolitis with nothing but supportive care. Bronchodilator therapy and steroid therapy have been shown to have no benefit for these cases in repeated meta-analyses over the past 15 and 12 years, respectively.
"None of the things we all do frequently have any support" in the literature for managing pediatric bronchiolitis, Dr. Ralston, a steering committee member of the Value in Inpatient Pediatrics (VIP) Network.
The VIP Network, formed out of an AAP section on hospital medicine, pulled together physicians who were frustrated with the lack of pediatric resources for quality improvement in smaller academic and community hospitals. The VIP Network chose bronchiolitis as its first target to see if it could start to change management by providing a peer group for local leaders to share resources and benchmark progress within the group.
The VIP Network functions as a virtual community with yearly meetings that adopted group norms for appropriate bronchiolitis care. Its website offers handouts, bibliographies, and other resources, and network members provided peer-to-peer coaching on quality improvement.
Members produced yearly benchmarking reports using hospital billing data for diagnostic codes 466.11 or 466.19 starting in 2008 (with some 2007 data serving as additional baseline data). Dr. Ralston said that 90% of data came from non-freestanding children’s facilities. In all, 70% of participating facilities did not have a guideline for pediatric bronchiolitis management prior to joining the Network, Dr. Ralston said. A total of 30% of facilities were in urban locations.
The results show that an all-volunteer group with no source of specific funding and no new resources can make real-world changes that improve the quality of care, she said.
"The caveat is that it has to be something the physicians really care about," she said. "Clinicians are significantly more motivated for this kind of work than researchers."
Dr. Ralston reported having no financial disclosures. She receives funds from the American Academy of Pediatrics to be editor of the journal Hospital Pediatrics.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Major Finding: Use of bronchodilators for pediatric bronchiolitis declined from 70% of cases to 58%, and bronchodilator doses per patient decreased by 45% from 2007 to 2010.
Data Source: Data came from an analysis of hospital billing data from participating sites in the Value in Inpatient Pediatrics Network.
Disclosures: Dr. Ralston reported having no relevant financial disclosures. She receives funds from the American Academy of Pediatrics to be editor of the journal Hospital Pediatrics.
Follow Clinical End Points, Not Clock, for Acetaminophen Overdose
SAN DIEGO – The clock has run out on 20-hour and 72-hour protocols for treating acetaminophen overdose. Clinical end points such as acetaminophen concentration and AST or ALT levels now determine when to end therapy.
In the mid-2000s, a 20-hour protocol for treatment with intravenous acetylcysteine generally replaced the traditional 72-hour protocol for treatment with oral acetylcysteine, but the 20-hour protocol has proved insufficient in rare cases of overdose on very, very large amounts of acetaminophen, Dr. Kennon J. Heard said.

In some of these patients, so much acetaminophen gets stored in the GI tract that the patient continues to absorb acetaminophen during the 20 hours of treatment. If treatment stops at 20 hours, "they’re going to have another overdose. They’re going to go on and get sick," he said at the annual meeting of the Society of Hospital Medicine.
Most toxicologists now prefer to end treatment based on clinical end points instead of time-based protocols. The new approach gets nearly all patients with acetaminophen overdose out of the hospital before 72 hours, and most patients still get treated for only 20 hours, said Dr. Heard, an emergency medicine physician at the University of Colorado and director of the Medical Toxicology Fellowship at the Rocky Mountain Poison and Drug Center, Denver.
Follow serum acetaminophen levels until all of the drug has been metabolized, indicated by serum levels below 10 mg/L or, ideally, undetectable levels. Make sure that markers of liver injury –ALT, (alanine aminotransferase), AST (aspartate aminotransferase) International Normalized Ratio, and creatinine – are improving or at least stable before ending therapy, he advised.
"If their AST or ALT starts out normal and stays normal, you can stop at 20 hours. If the AST or ALT is going up, we like to see it clearly start to go down or at least stabilizing at 20 hours, or sometimes even sooner," he said. "As long as the patient is clinically well, the ALT and AST are improving and they don’t have any acetaminophen on board, you can stop treatment."
In cases of massive overdose, in which the patient presents with a serum acetaminophen level greater than 500 mg/L or has a level greater than 75 mg/L after 20 hours of treatment, consult with your local poison center experts, Dr. Heard added.
Prolonged treatment may be needed, and some experts have suggested giving higher doses of acetylcysteine because the very high levels of acetaminophen may exceed the ability of acetylcysteine to detoxify the patient, he said.
"These cases are rare. We usually have one or two of them a year," Dr. Heard said.
Historically, the 72-hour protocol for treatment with oral acetylcysteine was developed before acetaminophen assays were routinely available in the United States. Patients were hospitalized for 3 days, "drinking stuff that smelled terrible, and generally, it was probably a waste of a lot of resources" because studies have subsequently shown that most patients don’t need 72 hours of treatment, he said.
With oral therapy, it seemed that as long as patients started treatment within 10-20 hours of overdose, they would recover. After development of intravenous acetylcysteine and shortening of the protocol to 20 hours, however, these rare cases of treatment failure began showing up.
Dr. Heard has been a consultant or received research grants from Cadence Pharmaceuticals, McNeil Consumer Healthcare, and Cumberland Pharmaceuticals.
SAN DIEGO – The clock has run out on 20-hour and 72-hour protocols for treating acetaminophen overdose. Clinical end points such as acetaminophen concentration and AST or ALT levels now determine when to end therapy.
In the mid-2000s, a 20-hour protocol for treatment with intravenous acetylcysteine generally replaced the traditional 72-hour protocol for treatment with oral acetylcysteine, but the 20-hour protocol has proved insufficient in rare cases of overdose on very, very large amounts of acetaminophen, Dr. Kennon J. Heard said.
In some of these patients, so much acetaminophen gets stored in the GI tract that the patient continues to absorb acetaminophen during the 20 hours of treatment. If treatment stops at 20 hours, "they’re going to have another overdose. They’re going to go on and get sick," he said at the annual meeting of the Society of Hospital Medicine.
Most toxicologists now prefer to end treatment based on clinical end points instead of time-based protocols. The new approach gets nearly all patients with acetaminophen overdose out of the hospital before 72 hours, and most patients still get treated for only 20 hours, said Dr. Heard, an emergency medicine physician at the University of Colorado and director of the Medical Toxicology Fellowship at the Rocky Mountain Poison and Drug Center, Denver.
Follow serum acetaminophen levels until all of the drug has been metabolized, indicated by serum levels below 10 mg/L or, ideally, undetectable levels. Make sure that markers of liver injury –ALT, (alanine aminotransferase), AST (aspartate aminotransferase) International Normalized Ratio, and creatinine – are improving or at least stable before ending therapy, he advised.
"If their AST or ALT starts out normal and stays normal, you can stop at 20 hours. If the AST or ALT is going up, we like to see it clearly start to go down or at least stabilizing at 20 hours, or sometimes even sooner," he said. "As long as the patient is clinically well, the ALT and AST are improving and they don’t have any acetaminophen on board, you can stop treatment."
In cases of massive overdose, in which the patient presents with a serum acetaminophen level greater than 500 mg/L or has a level greater than 75 mg/L after 20 hours of treatment, consult with your local poison center experts, Dr. Heard added.
Prolonged treatment may be needed, and some experts have suggested giving higher doses of acetylcysteine because the very high levels of acetaminophen may exceed the ability of acetylcysteine to detoxify the patient, he said.
"These cases are rare. We usually have one or two of them a year," Dr. Heard said.
Historically, the 72-hour protocol for treatment with oral acetylcysteine was developed before acetaminophen assays were routinely available in the United States. Patients were hospitalized for 3 days, "drinking stuff that smelled terrible, and generally, it was probably a waste of a lot of resources" because studies have subsequently shown that most patients don’t need 72 hours of treatment, he said.
With oral therapy, it seemed that as long as patients started treatment within 10-20 hours of overdose, they would recover. After development of intravenous acetylcysteine and shortening of the protocol to 20 hours, however, these rare cases of treatment failure began showing up.
Dr. Heard has been a consultant or received research grants from Cadence Pharmaceuticals, McNeil Consumer Healthcare, and Cumberland Pharmaceuticals.
SAN DIEGO – The clock has run out on 20-hour and 72-hour protocols for treating acetaminophen overdose. Clinical end points such as acetaminophen concentration and AST or ALT levels now determine when to end therapy.
In the mid-2000s, a 20-hour protocol for treatment with intravenous acetylcysteine generally replaced the traditional 72-hour protocol for treatment with oral acetylcysteine, but the 20-hour protocol has proved insufficient in rare cases of overdose on very, very large amounts of acetaminophen, Dr. Kennon J. Heard said.
In some of these patients, so much acetaminophen gets stored in the GI tract that the patient continues to absorb acetaminophen during the 20 hours of treatment. If treatment stops at 20 hours, "they’re going to have another overdose. They’re going to go on and get sick," he said at the annual meeting of the Society of Hospital Medicine.
Most toxicologists now prefer to end treatment based on clinical end points instead of time-based protocols. The new approach gets nearly all patients with acetaminophen overdose out of the hospital before 72 hours, and most patients still get treated for only 20 hours, said Dr. Heard, an emergency medicine physician at the University of Colorado and director of the Medical Toxicology Fellowship at the Rocky Mountain Poison and Drug Center, Denver.
Follow serum acetaminophen levels until all of the drug has been metabolized, indicated by serum levels below 10 mg/L or, ideally, undetectable levels. Make sure that markers of liver injury –ALT, (alanine aminotransferase), AST (aspartate aminotransferase) International Normalized Ratio, and creatinine – are improving or at least stable before ending therapy, he advised.
"If their AST or ALT starts out normal and stays normal, you can stop at 20 hours. If the AST or ALT is going up, we like to see it clearly start to go down or at least stabilizing at 20 hours, or sometimes even sooner," he said. "As long as the patient is clinically well, the ALT and AST are improving and they don’t have any acetaminophen on board, you can stop treatment."
In cases of massive overdose, in which the patient presents with a serum acetaminophen level greater than 500 mg/L or has a level greater than 75 mg/L after 20 hours of treatment, consult with your local poison center experts, Dr. Heard added.
Prolonged treatment may be needed, and some experts have suggested giving higher doses of acetylcysteine because the very high levels of acetaminophen may exceed the ability of acetylcysteine to detoxify the patient, he said.
"These cases are rare. We usually have one or two of them a year," Dr. Heard said.
Historically, the 72-hour protocol for treatment with oral acetylcysteine was developed before acetaminophen assays were routinely available in the United States. Patients were hospitalized for 3 days, "drinking stuff that smelled terrible, and generally, it was probably a waste of a lot of resources" because studies have subsequently shown that most patients don’t need 72 hours of treatment, he said.
With oral therapy, it seemed that as long as patients started treatment within 10-20 hours of overdose, they would recover. After development of intravenous acetylcysteine and shortening of the protocol to 20 hours, however, these rare cases of treatment failure began showing up.
Dr. Heard has been a consultant or received research grants from Cadence Pharmaceuticals, McNeil Consumer Healthcare, and Cumberland Pharmaceuticals.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Teamwork Mandate Headed for MOC
SAN DIEGO – Hospitalists undergoing maintenance of certification may soon be required to complete a module focused on team-based care, but be allowed drop one requirement related to practice improvement.
Currently, hospitalists who choose to recertify using the focused practice in hospital medicine maintenance of certification (MOC) program through the American Board of Internal Medicine have the option of substituting a teamwork module for 1 of the 2 required practice improvement modules, according to Dr. Jeffrey G. Wiese, past president of the Society of Hospital Medicine and associate dean for graduate medical education at Tulane University in New Orleans.
"The eventual goal will be to have the teamwork module a required part of the hospital medicine MOC process," he said. "We are hoping this will occur in 2014."
Hospitalists are dedicated to team-based care and the change reflects that focus, Dr. Wiese said.
Dr. Wiese, who spoke about the MOC process during the SHM annual meeting, addressed some of the confusion around the differences between MOC for hospital medicine vs. standard internal medicine. "This is not as confusing as it may first look," Dr. Wiese said.
Requirements for the two MOC pathways are very similar, he said. For instance, both pathways have the same four elements, and beginning this summer, both pathways will have the same renewal frequency for the various required elements.
Both pathways share the requirement that physicians be board certified and have a valid license to practice medicine. Physicians in the hospital medicine pathway are also required to attest to being a hospitalist by meeting a threshold of inpatient encounters and to be Advanced Cardiac Life Support (ACLS) certified.
The second element is the secure examination. Physicians in both pathways must take a secure exam every 10 years, but the content on the two exams is different. Dr. Wiese said hospitalists will find that the hospital medicine exam is "focused on content that you actually use as a hospitalist."
The third element is the self-evaluation requirement. The standard internal medicine MOC requires physicians to complete 1 practice improvement module every 5 years. The hospital medicine MOC currently requires completion of 2 practice improvement modules every 5 years, with the option of using the team-based module as a substitute for one of the practice improvement modules. The eventual goal, anticipated for 2014, is that the hospital medicine MOC pathway will require completion of the team-based module, and the practice improvement requirement will drop from two to one, making the requirements for practice improvement the same in both the hospitalist and internal medicine MOC pathways.

Currently, physicians in the hospital medicine focused practice MOC pathway are also required to complete one less medical knowledge module than their counterparts in the standard internal medicine MOC pathway.
Hospitalists have many good reasons to pay attention to the MOC process, said Dr. Patrick J. Torcson, chair of SHM’s Performance Measurement and Reporting Committee. In addition to the professional satisfaction that comes with being up-to-date on medical knowledge, payers are beginning to recognize the process. Medicare is offering a 0.5% bonus payment on allowable Medicare charges for physicians who participate in the MOC process. "For the typical hospitalist, that’s about $700 over the 10-year cycle, allowing them to defray part of the cost of the MOC or continuing medical education," said Dr. Torcson, who is the director of hospital medicine at St. Tammany Parish Hospital in Covington, La.
"I think it’s really the right thing to do for our developing specialty," he said. "We really have to distinguish ourselves and there’s really no better brand distinction than a professional designation based on board certification and maintenance of certification."
recertify, MOC, American Board of Internal Medicine, Dr. Jeffrey G. Wiese, the Society of Hospital Medicine,
SAN DIEGO – Hospitalists undergoing maintenance of certification may soon be required to complete a module focused on team-based care, but be allowed drop one requirement related to practice improvement.
Currently, hospitalists who choose to recertify using the focused practice in hospital medicine maintenance of certification (MOC) program through the American Board of Internal Medicine have the option of substituting a teamwork module for 1 of the 2 required practice improvement modules, according to Dr. Jeffrey G. Wiese, past president of the Society of Hospital Medicine and associate dean for graduate medical education at Tulane University in New Orleans.
"The eventual goal will be to have the teamwork module a required part of the hospital medicine MOC process," he said. "We are hoping this will occur in 2014."
Hospitalists are dedicated to team-based care and the change reflects that focus, Dr. Wiese said.
Dr. Wiese, who spoke about the MOC process during the SHM annual meeting, addressed some of the confusion around the differences between MOC for hospital medicine vs. standard internal medicine. "This is not as confusing as it may first look," Dr. Wiese said.
Requirements for the two MOC pathways are very similar, he said. For instance, both pathways have the same four elements, and beginning this summer, both pathways will have the same renewal frequency for the various required elements.
Both pathways share the requirement that physicians be board certified and have a valid license to practice medicine. Physicians in the hospital medicine pathway are also required to attest to being a hospitalist by meeting a threshold of inpatient encounters and to be Advanced Cardiac Life Support (ACLS) certified.
The second element is the secure examination. Physicians in both pathways must take a secure exam every 10 years, but the content on the two exams is different. Dr. Wiese said hospitalists will find that the hospital medicine exam is "focused on content that you actually use as a hospitalist."
The third element is the self-evaluation requirement. The standard internal medicine MOC requires physicians to complete 1 practice improvement module every 5 years. The hospital medicine MOC currently requires completion of 2 practice improvement modules every 5 years, with the option of using the team-based module as a substitute for one of the practice improvement modules. The eventual goal, anticipated for 2014, is that the hospital medicine MOC pathway will require completion of the team-based module, and the practice improvement requirement will drop from two to one, making the requirements for practice improvement the same in both the hospitalist and internal medicine MOC pathways.
Currently, physicians in the hospital medicine focused practice MOC pathway are also required to complete one less medical knowledge module than their counterparts in the standard internal medicine MOC pathway.
Hospitalists have many good reasons to pay attention to the MOC process, said Dr. Patrick J. Torcson, chair of SHM’s Performance Measurement and Reporting Committee. In addition to the professional satisfaction that comes with being up-to-date on medical knowledge, payers are beginning to recognize the process. Medicare is offering a 0.5% bonus payment on allowable Medicare charges for physicians who participate in the MOC process. "For the typical hospitalist, that’s about $700 over the 10-year cycle, allowing them to defray part of the cost of the MOC or continuing medical education," said Dr. Torcson, who is the director of hospital medicine at St. Tammany Parish Hospital in Covington, La.
"I think it’s really the right thing to do for our developing specialty," he said. "We really have to distinguish ourselves and there’s really no better brand distinction than a professional designation based on board certification and maintenance of certification."
SAN DIEGO – Hospitalists undergoing maintenance of certification may soon be required to complete a module focused on team-based care, but be allowed drop one requirement related to practice improvement.
Currently, hospitalists who choose to recertify using the focused practice in hospital medicine maintenance of certification (MOC) program through the American Board of Internal Medicine have the option of substituting a teamwork module for 1 of the 2 required practice improvement modules, according to Dr. Jeffrey G. Wiese, past president of the Society of Hospital Medicine and associate dean for graduate medical education at Tulane University in New Orleans.
"The eventual goal will be to have the teamwork module a required part of the hospital medicine MOC process," he said. "We are hoping this will occur in 2014."
Hospitalists are dedicated to team-based care and the change reflects that focus, Dr. Wiese said.
Dr. Wiese, who spoke about the MOC process during the SHM annual meeting, addressed some of the confusion around the differences between MOC for hospital medicine vs. standard internal medicine. "This is not as confusing as it may first look," Dr. Wiese said.
Requirements for the two MOC pathways are very similar, he said. For instance, both pathways have the same four elements, and beginning this summer, both pathways will have the same renewal frequency for the various required elements.
Both pathways share the requirement that physicians be board certified and have a valid license to practice medicine. Physicians in the hospital medicine pathway are also required to attest to being a hospitalist by meeting a threshold of inpatient encounters and to be Advanced Cardiac Life Support (ACLS) certified.
The second element is the secure examination. Physicians in both pathways must take a secure exam every 10 years, but the content on the two exams is different. Dr. Wiese said hospitalists will find that the hospital medicine exam is "focused on content that you actually use as a hospitalist."
The third element is the self-evaluation requirement. The standard internal medicine MOC requires physicians to complete 1 practice improvement module every 5 years. The hospital medicine MOC currently requires completion of 2 practice improvement modules every 5 years, with the option of using the team-based module as a substitute for one of the practice improvement modules. The eventual goal, anticipated for 2014, is that the hospital medicine MOC pathway will require completion of the team-based module, and the practice improvement requirement will drop from two to one, making the requirements for practice improvement the same in both the hospitalist and internal medicine MOC pathways.
Currently, physicians in the hospital medicine focused practice MOC pathway are also required to complete one less medical knowledge module than their counterparts in the standard internal medicine MOC pathway.
Hospitalists have many good reasons to pay attention to the MOC process, said Dr. Patrick J. Torcson, chair of SHM’s Performance Measurement and Reporting Committee. In addition to the professional satisfaction that comes with being up-to-date on medical knowledge, payers are beginning to recognize the process. Medicare is offering a 0.5% bonus payment on allowable Medicare charges for physicians who participate in the MOC process. "For the typical hospitalist, that’s about $700 over the 10-year cycle, allowing them to defray part of the cost of the MOC or continuing medical education," said Dr. Torcson, who is the director of hospital medicine at St. Tammany Parish Hospital in Covington, La.
"I think it’s really the right thing to do for our developing specialty," he said. "We really have to distinguish ourselves and there’s really no better brand distinction than a professional designation based on board certification and maintenance of certification."
recertify, MOC, American Board of Internal Medicine, Dr. Jeffrey G. Wiese, the Society of Hospital Medicine,
recertify, MOC, American Board of Internal Medicine, Dr. Jeffrey G. Wiese, the Society of Hospital Medicine,
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Experts Weigh In on Decoding Care Transitions
SAN DIEGO – Thinking through how to better prepare patients to go from the hospital to home occupies an increasing amount of time for the typical hospitalist. Aside from the fact that transitions of care are a core competency in the specialty, Medicare is also turning up the heat with its plan to impose financial penalties on hospitals with excessive readmission rates. Those penalties will take effect this October.
At the annual meeting of the Society of Hospital Medicine, Dr. Mark V. Williams, chief of hospital medicine at Northwestern University in Chicago and principal investigator for Project BOOST (Better Outcomes for Older Adults Through Safe Transitions) joined Dr. Eric A. Coleman, professor of medicine and director of the Care Transitions Program at the University of Colorado in Denver, for a freewheeling question-and-answer session.

The hourlong exchange covered everything from the state of research in the field to how to avoid Medicare penalties.
One take-home message from the discussion is that reducing preventable readmissions will be a focus for virtually every hospitalist, even though some of the key research questions that could help improve care transitions are still unanswered. For instance, there have been many prediction scales that have looked at risk for readmission. But the scales don’t work very well in practice.
"[The scales] come out to be okay, but not great," said Dr. Coleman, who has tried to develop a more reliable risk prediction tool as part of his own research efforts.
But the real lesson from the lukewarm success of existing risk prediction tools is that researchers and clinicians may be focusing on the wrong variables. "I’m not exactly sure that what we think we’re after is what we’re after," Dr. Coleman said.
Dr. Coleman said when he speaks to patients at the bedside about why they think they have been readmitted to the hospital multiple times, it’s not necessarily about organ systems function. And that supports the findings of some research he was involved in that found that factors such as cognition and literacy were the biggest predictors in whether patients would actually follow through on their discharge instructions. "These are not necessarily things that we routinely collect and screen for," he said.
Dr. Williams agreed that there’s a need to routinely collect more data, beyond whether or not patients have specific comorbidities. Quantitative data on the patient’s socioeconomic status, health literacy level, occupation status, and social support could shed a lot of light on whether they will be capable of following through on their care when they return home. Dr. Williams said one of the hospitalists who has been involved in Project BOOST once told him that when he sees a patient he always asks, "Do you have a daughter?" And if the patient says yes, he can relax because now he knows that there’s great social support at home.
While improving care transitions is good for patient care, it will soon also be good business for hospitals. Under a new readmission program from the Centers for Medicare and Medicaid Services, Medicare officials will cut payments to hospitals whose readmission rates for acute myocardial infarction, congestive heart failure, and pneumonia are considered too high. But what many hospitalists may not appreciate, Dr. Williams said, is that CMS officials will be basing that determination on the hospital’s 3-year average performance from fiscal year 2009 through 2011. The next year, the CMS will use data collected from fiscal years 2010-2012.
While reducing preventable readmissions is now a focus for most hospitals, they really should have started that work years ago, Dr. Williams said.

"We need to have been working on this for awhile because the clock is ticking; data are being collected," he said. "And very importantly, it will take awhile to improve those numbers unless you’re able to make staggering changes right off the bat because it’s a 3-year rolling average."
Hospitals that have been doing well for the past 3 years are probably in pretty good shape, Dr. Williams said. Those that have been doing poorly will have to play catch up. "I think right now every site ought to be looking at their care transitions process," he said.
Hospitalists can try to partner with physicians and other health care providers in the community, said Dr. Coleman.
"When you look at some of the more successful collaborations going on across the country that have been able to significantly reduce their readmission rates and subsequent admission rate as well, it is because of these developing partnerships and realizing that hospitals can’t do it all on their own," he said.
Dr. Coleman encouraged hospitalists to learn more about the Community-Based Care Transition Program, an initiative created under the Affordable Care Act, which provides grants for hospitals to collaborate with community partners. "I think that this is an opportunity for not only hospitals, but hospitalists, to begin taking an even greater leadership role" in what the hospitals can do and what hospitals can do very well with their partners, he said.
Dr. Williams agreed that partnerships with community physicians are a big part of the future of hospital medicine. But payers will have to step up and begin to reimburse physicians for doing that work, he said. For instance, insurers could pay hospitalists to call primary care physicians. "It would be fascinating to have some experiments with this to see how they impact continuity of care and utilization overall," Dr. Williams said.
SAN DIEGO – Thinking through how to better prepare patients to go from the hospital to home occupies an increasing amount of time for the typical hospitalist. Aside from the fact that transitions of care are a core competency in the specialty, Medicare is also turning up the heat with its plan to impose financial penalties on hospitals with excessive readmission rates. Those penalties will take effect this October.
At the annual meeting of the Society of Hospital Medicine, Dr. Mark V. Williams, chief of hospital medicine at Northwestern University in Chicago and principal investigator for Project BOOST (Better Outcomes for Older Adults Through Safe Transitions) joined Dr. Eric A. Coleman, professor of medicine and director of the Care Transitions Program at the University of Colorado in Denver, for a freewheeling question-and-answer session.
The hourlong exchange covered everything from the state of research in the field to how to avoid Medicare penalties.
One take-home message from the discussion is that reducing preventable readmissions will be a focus for virtually every hospitalist, even though some of the key research questions that could help improve care transitions are still unanswered. For instance, there have been many prediction scales that have looked at risk for readmission. But the scales don’t work very well in practice.
"[The scales] come out to be okay, but not great," said Dr. Coleman, who has tried to develop a more reliable risk prediction tool as part of his own research efforts.
But the real lesson from the lukewarm success of existing risk prediction tools is that researchers and clinicians may be focusing on the wrong variables. "I’m not exactly sure that what we think we’re after is what we’re after," Dr. Coleman said.
Dr. Coleman said when he speaks to patients at the bedside about why they think they have been readmitted to the hospital multiple times, it’s not necessarily about organ systems function. And that supports the findings of some research he was involved in that found that factors such as cognition and literacy were the biggest predictors in whether patients would actually follow through on their discharge instructions. "These are not necessarily things that we routinely collect and screen for," he said.
Dr. Williams agreed that there’s a need to routinely collect more data, beyond whether or not patients have specific comorbidities. Quantitative data on the patient’s socioeconomic status, health literacy level, occupation status, and social support could shed a lot of light on whether they will be capable of following through on their care when they return home. Dr. Williams said one of the hospitalists who has been involved in Project BOOST once told him that when he sees a patient he always asks, "Do you have a daughter?" And if the patient says yes, he can relax because now he knows that there’s great social support at home.
While improving care transitions is good for patient care, it will soon also be good business for hospitals. Under a new readmission program from the Centers for Medicare and Medicaid Services, Medicare officials will cut payments to hospitals whose readmission rates for acute myocardial infarction, congestive heart failure, and pneumonia are considered too high. But what many hospitalists may not appreciate, Dr. Williams said, is that CMS officials will be basing that determination on the hospital’s 3-year average performance from fiscal year 2009 through 2011. The next year, the CMS will use data collected from fiscal years 2010-2012.
While reducing preventable readmissions is now a focus for most hospitals, they really should have started that work years ago, Dr. Williams said.
"We need to have been working on this for awhile because the clock is ticking; data are being collected," he said. "And very importantly, it will take awhile to improve those numbers unless you’re able to make staggering changes right off the bat because it’s a 3-year rolling average."
Hospitals that have been doing well for the past 3 years are probably in pretty good shape, Dr. Williams said. Those that have been doing poorly will have to play catch up. "I think right now every site ought to be looking at their care transitions process," he said.
Hospitalists can try to partner with physicians and other health care providers in the community, said Dr. Coleman.
"When you look at some of the more successful collaborations going on across the country that have been able to significantly reduce their readmission rates and subsequent admission rate as well, it is because of these developing partnerships and realizing that hospitals can’t do it all on their own," he said.
Dr. Coleman encouraged hospitalists to learn more about the Community-Based Care Transition Program, an initiative created under the Affordable Care Act, which provides grants for hospitals to collaborate with community partners. "I think that this is an opportunity for not only hospitals, but hospitalists, to begin taking an even greater leadership role" in what the hospitals can do and what hospitals can do very well with their partners, he said.
Dr. Williams agreed that partnerships with community physicians are a big part of the future of hospital medicine. But payers will have to step up and begin to reimburse physicians for doing that work, he said. For instance, insurers could pay hospitalists to call primary care physicians. "It would be fascinating to have some experiments with this to see how they impact continuity of care and utilization overall," Dr. Williams said.
SAN DIEGO – Thinking through how to better prepare patients to go from the hospital to home occupies an increasing amount of time for the typical hospitalist. Aside from the fact that transitions of care are a core competency in the specialty, Medicare is also turning up the heat with its plan to impose financial penalties on hospitals with excessive readmission rates. Those penalties will take effect this October.
At the annual meeting of the Society of Hospital Medicine, Dr. Mark V. Williams, chief of hospital medicine at Northwestern University in Chicago and principal investigator for Project BOOST (Better Outcomes for Older Adults Through Safe Transitions) joined Dr. Eric A. Coleman, professor of medicine and director of the Care Transitions Program at the University of Colorado in Denver, for a freewheeling question-and-answer session.
The hourlong exchange covered everything from the state of research in the field to how to avoid Medicare penalties.
One take-home message from the discussion is that reducing preventable readmissions will be a focus for virtually every hospitalist, even though some of the key research questions that could help improve care transitions are still unanswered. For instance, there have been many prediction scales that have looked at risk for readmission. But the scales don’t work very well in practice.
"[The scales] come out to be okay, but not great," said Dr. Coleman, who has tried to develop a more reliable risk prediction tool as part of his own research efforts.
But the real lesson from the lukewarm success of existing risk prediction tools is that researchers and clinicians may be focusing on the wrong variables. "I’m not exactly sure that what we think we’re after is what we’re after," Dr. Coleman said.
Dr. Coleman said when he speaks to patients at the bedside about why they think they have been readmitted to the hospital multiple times, it’s not necessarily about organ systems function. And that supports the findings of some research he was involved in that found that factors such as cognition and literacy were the biggest predictors in whether patients would actually follow through on their discharge instructions. "These are not necessarily things that we routinely collect and screen for," he said.
Dr. Williams agreed that there’s a need to routinely collect more data, beyond whether or not patients have specific comorbidities. Quantitative data on the patient’s socioeconomic status, health literacy level, occupation status, and social support could shed a lot of light on whether they will be capable of following through on their care when they return home. Dr. Williams said one of the hospitalists who has been involved in Project BOOST once told him that when he sees a patient he always asks, "Do you have a daughter?" And if the patient says yes, he can relax because now he knows that there’s great social support at home.
While improving care transitions is good for patient care, it will soon also be good business for hospitals. Under a new readmission program from the Centers for Medicare and Medicaid Services, Medicare officials will cut payments to hospitals whose readmission rates for acute myocardial infarction, congestive heart failure, and pneumonia are considered too high. But what many hospitalists may not appreciate, Dr. Williams said, is that CMS officials will be basing that determination on the hospital’s 3-year average performance from fiscal year 2009 through 2011. The next year, the CMS will use data collected from fiscal years 2010-2012.
While reducing preventable readmissions is now a focus for most hospitals, they really should have started that work years ago, Dr. Williams said.
"We need to have been working on this for awhile because the clock is ticking; data are being collected," he said. "And very importantly, it will take awhile to improve those numbers unless you’re able to make staggering changes right off the bat because it’s a 3-year rolling average."
Hospitals that have been doing well for the past 3 years are probably in pretty good shape, Dr. Williams said. Those that have been doing poorly will have to play catch up. "I think right now every site ought to be looking at their care transitions process," he said.
Hospitalists can try to partner with physicians and other health care providers in the community, said Dr. Coleman.
"When you look at some of the more successful collaborations going on across the country that have been able to significantly reduce their readmission rates and subsequent admission rate as well, it is because of these developing partnerships and realizing that hospitals can’t do it all on their own," he said.
Dr. Coleman encouraged hospitalists to learn more about the Community-Based Care Transition Program, an initiative created under the Affordable Care Act, which provides grants for hospitals to collaborate with community partners. "I think that this is an opportunity for not only hospitals, but hospitalists, to begin taking an even greater leadership role" in what the hospitals can do and what hospitals can do very well with their partners, he said.
Dr. Williams agreed that partnerships with community physicians are a big part of the future of hospital medicine. But payers will have to step up and begin to reimburse physicians for doing that work, he said. For instance, insurers could pay hospitalists to call primary care physicians. "It would be fascinating to have some experiments with this to see how they impact continuity of care and utilization overall," Dr. Williams said.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Work-Life Balance: Keeping Burnout at Bay
SAN DIEGO – Hospitalists arrived in hope and in unabashed need of hearing about balancing work and home lives.
One said he was looking for tips on balancing the competing demands of work and home. "It’s never balanced," lamented another, a female hospitalist with a full-time physician husband and three children.
Someone else said he wanted to find ways to prevent burnout. "I’m already burned out," said another at the annual meeting of the Society of Hospital Medicine.
An office-based physician in private practice said he was wondering if hospital medicine might offer a "better," more balanced way to practice. "I just quit my job" due to burnout, one hospitalist admitted.

Work-life balance boils down to one’s relationships not only with others but with one’s self, said session moderator Dr. Carole Warde. She encouraged everyone to translate some of the same core competencies expected of hospitalists professionally to manage these relationships, including "be engaged," "listen actively," "work in teams," and "resolve conflicts."
"Relationships never come easy. They always come from a place of work," said Dr. Warde, who recently joined the Greater Los Angeles Veterans Affairs Health System to practice as a primary care physician and to set up the VA’s version of patient-centered medical homes.
She adapted a passage from the book by Parker J. Palmer, "The Courage to Teach: Exploring the Inner Landscape of a Teacher’s Life" (10th anniversary edition, Wiley, 2007) as it might apply to physicians: "As I practice, I project the condition of my soul onto my patients, colleagues, family, and friends and our way of being together. Doctoring holds a mirror to the soul. If I am willing to look at that mirror, I have a chance to gain self-knowledge. Knowing myself is as crucial to good doctoring as knowing my patients and my subject," Dr. Warde said.
"This isn’t something that anybody told me in medical school," she said. Physicians who don’t pay attention to their well-being risk emotionally withdrawing into a self-protective shell, which reduces their ability to understand patients’ needs, impairs clinical decision making, and leads to inattentiveness, loss of meaning, and burnout, she said.
A panel of three hospitalists at the session described their own attempts to balance work and home life.
Dr. Diana Childers, an academic hospitalist at the University of California, San Diego, said that with a husband in the U.S. Navy, two children, and her own diagnosis of type 1 diabetes to manage, "time off seems to disappear." She plans her exercise a week in advance. "If I can exercise three to four times a week, that’s good," she said.
She is supported by her husband, a nanny, a departmental chief who "lets me complain," and colleagues who reciprocate in covering for each other when needed. Dr. Childers encouraged hospitalists to join a volunteer project in the workplace to help them find a colleague that they can connect with and talk to about their work-life challenges.
Dr. Mark Shapiro, in private hospitalist practice in San Diego, said the reciprocal relationships between colleagues in his 12-person group also helped manage the stress of work schedules. The group is considering hiring some mid-level practitioners to share the load.
"One of the variables I realized I have the most control over is how I physically feel at the end of the day. That was something that wasn’t being paid attention to," he said. Dr. Shapiro now consciously reminds himself of basic such as drinking water to stay hydrated, and avoiding hospital food when possible.

Dr. Lisa Shieh, an academic hospitalist at Stanford (Calif.) University, said that support from her department chair to address frequently-changing work hours made a big difference in stress levels. Hiring a nanny and a gardener lets her spend more time with her husband (also a physician) and children.
Finding a mentor after 5 years as a hospitalist "really helped me," Dr. Shieh said. She regularly schedules lunch with a friend at work so they can unwind together, and taps people outside her group, too. "One of my best friends is a surgeon. Sometimes I just call him and say, ‘What do you think of this?’ " Dr. Shieh said.
Stress, Quantified
The U.S. Physician Work Life Study surveyed 5,704 primary care and subspecialty physicians and found that the key factors increasing or mitigating stress were demands (such as work hours, time pressures, or a heavy case mix), control (over workplace chaos, resources, and personal life), and support from colleagues and significant others (Stress Health 2002;18:37-42).
When demands outweigh control and support, stress levels will be high, Dr. Warde said.
In a recent survey of hospitalists at 20 U.S. academic medical centers, 67% reported high stress, 57% reported having 20% or less protected academic time, 54% were satisfied with their ability to control their schedule, 63% were satisfied with the support from their division chief, and 70%-80% were satisfied with their professional relationships (Arch. Intern. Med. 2011;171:782-785).
Dr. Warde recommended an exercise for evaluating one’s work-life balance: Create a grid with three categories on the horizontal axis – Demand, Control, and Support – and three categories on the vertical axis: Personal, Family, and Professional. Fill in each column of the grid as they apply to you. "You’ll be able to identify simple ways to alter" some of the factors that you list to foster balance and reduce the stress in your life, she said.
"The thing not to do is to ignore it," Dr. Warde said.
The speakers reported having no financial disclosures.
SAN DIEGO – Hospitalists arrived in hope and in unabashed need of hearing about balancing work and home lives.
One said he was looking for tips on balancing the competing demands of work and home. "It’s never balanced," lamented another, a female hospitalist with a full-time physician husband and three children.
Someone else said he wanted to find ways to prevent burnout. "I’m already burned out," said another at the annual meeting of the Society of Hospital Medicine.
An office-based physician in private practice said he was wondering if hospital medicine might offer a "better," more balanced way to practice. "I just quit my job" due to burnout, one hospitalist admitted.
Work-life balance boils down to one’s relationships not only with others but with one’s self, said session moderator Dr. Carole Warde. She encouraged everyone to translate some of the same core competencies expected of hospitalists professionally to manage these relationships, including "be engaged," "listen actively," "work in teams," and "resolve conflicts."
"Relationships never come easy. They always come from a place of work," said Dr. Warde, who recently joined the Greater Los Angeles Veterans Affairs Health System to practice as a primary care physician and to set up the VA’s version of patient-centered medical homes.
She adapted a passage from the book by Parker J. Palmer, "The Courage to Teach: Exploring the Inner Landscape of a Teacher’s Life" (10th anniversary edition, Wiley, 2007) as it might apply to physicians: "As I practice, I project the condition of my soul onto my patients, colleagues, family, and friends and our way of being together. Doctoring holds a mirror to the soul. If I am willing to look at that mirror, I have a chance to gain self-knowledge. Knowing myself is as crucial to good doctoring as knowing my patients and my subject," Dr. Warde said.
"This isn’t something that anybody told me in medical school," she said. Physicians who don’t pay attention to their well-being risk emotionally withdrawing into a self-protective shell, which reduces their ability to understand patients’ needs, impairs clinical decision making, and leads to inattentiveness, loss of meaning, and burnout, she said.
A panel of three hospitalists at the session described their own attempts to balance work and home life.
Dr. Diana Childers, an academic hospitalist at the University of California, San Diego, said that with a husband in the U.S. Navy, two children, and her own diagnosis of type 1 diabetes to manage, "time off seems to disappear." She plans her exercise a week in advance. "If I can exercise three to four times a week, that’s good," she said.
She is supported by her husband, a nanny, a departmental chief who "lets me complain," and colleagues who reciprocate in covering for each other when needed. Dr. Childers encouraged hospitalists to join a volunteer project in the workplace to help them find a colleague that they can connect with and talk to about their work-life challenges.
Dr. Mark Shapiro, in private hospitalist practice in San Diego, said the reciprocal relationships between colleagues in his 12-person group also helped manage the stress of work schedules. The group is considering hiring some mid-level practitioners to share the load.
"One of the variables I realized I have the most control over is how I physically feel at the end of the day. That was something that wasn’t being paid attention to," he said. Dr. Shapiro now consciously reminds himself of basic such as drinking water to stay hydrated, and avoiding hospital food when possible.
Dr. Lisa Shieh, an academic hospitalist at Stanford (Calif.) University, said that support from her department chair to address frequently-changing work hours made a big difference in stress levels. Hiring a nanny and a gardener lets her spend more time with her husband (also a physician) and children.
Finding a mentor after 5 years as a hospitalist "really helped me," Dr. Shieh said. She regularly schedules lunch with a friend at work so they can unwind together, and taps people outside her group, too. "One of my best friends is a surgeon. Sometimes I just call him and say, ‘What do you think of this?’ " Dr. Shieh said.
Stress, Quantified
The U.S. Physician Work Life Study surveyed 5,704 primary care and subspecialty physicians and found that the key factors increasing or mitigating stress were demands (such as work hours, time pressures, or a heavy case mix), control (over workplace chaos, resources, and personal life), and support from colleagues and significant others (Stress Health 2002;18:37-42).
When demands outweigh control and support, stress levels will be high, Dr. Warde said.
In a recent survey of hospitalists at 20 U.S. academic medical centers, 67% reported high stress, 57% reported having 20% or less protected academic time, 54% were satisfied with their ability to control their schedule, 63% were satisfied with the support from their division chief, and 70%-80% were satisfied with their professional relationships (Arch. Intern. Med. 2011;171:782-785).
Dr. Warde recommended an exercise for evaluating one’s work-life balance: Create a grid with three categories on the horizontal axis – Demand, Control, and Support – and three categories on the vertical axis: Personal, Family, and Professional. Fill in each column of the grid as they apply to you. "You’ll be able to identify simple ways to alter" some of the factors that you list to foster balance and reduce the stress in your life, she said.
"The thing not to do is to ignore it," Dr. Warde said.
The speakers reported having no financial disclosures.
SAN DIEGO – Hospitalists arrived in hope and in unabashed need of hearing about balancing work and home lives.
One said he was looking for tips on balancing the competing demands of work and home. "It’s never balanced," lamented another, a female hospitalist with a full-time physician husband and three children.
Someone else said he wanted to find ways to prevent burnout. "I’m already burned out," said another at the annual meeting of the Society of Hospital Medicine.
An office-based physician in private practice said he was wondering if hospital medicine might offer a "better," more balanced way to practice. "I just quit my job" due to burnout, one hospitalist admitted.
Work-life balance boils down to one’s relationships not only with others but with one’s self, said session moderator Dr. Carole Warde. She encouraged everyone to translate some of the same core competencies expected of hospitalists professionally to manage these relationships, including "be engaged," "listen actively," "work in teams," and "resolve conflicts."
"Relationships never come easy. They always come from a place of work," said Dr. Warde, who recently joined the Greater Los Angeles Veterans Affairs Health System to practice as a primary care physician and to set up the VA’s version of patient-centered medical homes.
She adapted a passage from the book by Parker J. Palmer, "The Courage to Teach: Exploring the Inner Landscape of a Teacher’s Life" (10th anniversary edition, Wiley, 2007) as it might apply to physicians: "As I practice, I project the condition of my soul onto my patients, colleagues, family, and friends and our way of being together. Doctoring holds a mirror to the soul. If I am willing to look at that mirror, I have a chance to gain self-knowledge. Knowing myself is as crucial to good doctoring as knowing my patients and my subject," Dr. Warde said.
"This isn’t something that anybody told me in medical school," she said. Physicians who don’t pay attention to their well-being risk emotionally withdrawing into a self-protective shell, which reduces their ability to understand patients’ needs, impairs clinical decision making, and leads to inattentiveness, loss of meaning, and burnout, she said.
A panel of three hospitalists at the session described their own attempts to balance work and home life.
Dr. Diana Childers, an academic hospitalist at the University of California, San Diego, said that with a husband in the U.S. Navy, two children, and her own diagnosis of type 1 diabetes to manage, "time off seems to disappear." She plans her exercise a week in advance. "If I can exercise three to four times a week, that’s good," she said.
She is supported by her husband, a nanny, a departmental chief who "lets me complain," and colleagues who reciprocate in covering for each other when needed. Dr. Childers encouraged hospitalists to join a volunteer project in the workplace to help them find a colleague that they can connect with and talk to about their work-life challenges.
Dr. Mark Shapiro, in private hospitalist practice in San Diego, said the reciprocal relationships between colleagues in his 12-person group also helped manage the stress of work schedules. The group is considering hiring some mid-level practitioners to share the load.
"One of the variables I realized I have the most control over is how I physically feel at the end of the day. That was something that wasn’t being paid attention to," he said. Dr. Shapiro now consciously reminds himself of basic such as drinking water to stay hydrated, and avoiding hospital food when possible.
Dr. Lisa Shieh, an academic hospitalist at Stanford (Calif.) University, said that support from her department chair to address frequently-changing work hours made a big difference in stress levels. Hiring a nanny and a gardener lets her spend more time with her husband (also a physician) and children.
Finding a mentor after 5 years as a hospitalist "really helped me," Dr. Shieh said. She regularly schedules lunch with a friend at work so they can unwind together, and taps people outside her group, too. "One of my best friends is a surgeon. Sometimes I just call him and say, ‘What do you think of this?’ " Dr. Shieh said.
Stress, Quantified
The U.S. Physician Work Life Study surveyed 5,704 primary care and subspecialty physicians and found that the key factors increasing or mitigating stress were demands (such as work hours, time pressures, or a heavy case mix), control (over workplace chaos, resources, and personal life), and support from colleagues and significant others (Stress Health 2002;18:37-42).
When demands outweigh control and support, stress levels will be high, Dr. Warde said.
In a recent survey of hospitalists at 20 U.S. academic medical centers, 67% reported high stress, 57% reported having 20% or less protected academic time, 54% were satisfied with their ability to control their schedule, 63% were satisfied with the support from their division chief, and 70%-80% were satisfied with their professional relationships (Arch. Intern. Med. 2011;171:782-785).
Dr. Warde recommended an exercise for evaluating one’s work-life balance: Create a grid with three categories on the horizontal axis – Demand, Control, and Support – and three categories on the vertical axis: Personal, Family, and Professional. Fill in each column of the grid as they apply to you. "You’ll be able to identify simple ways to alter" some of the factors that you list to foster balance and reduce the stress in your life, she said.
"The thing not to do is to ignore it," Dr. Warde said.
The speakers reported having no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
'Affinity' and Beyond: Women Connect to Tackle Pay Disparities
SAN DIEGO – A plan to form "affinity groups" got off to a rousing start as participants in a women’s-interest session the enthusiastically signed up for a new listserv.
The affinity groups are designed to promote communication among members with common interests, said Dr. Janet M. Nagamine, a Society of Hospital Medicine board member who led an interest group gathering at the annual meeting. She also pumped participants for other ideas on how SHM can help address the challenges facing female hospitalists, especially the hot topic of persistent pay disparities between male and female hospitalists.

A 2011 survey by the society and the Medical Group Management Association found that female hospitalists were being paid $4,000-$29,000 less than their male counterparts were, after accounting for factors other than sex. The findings follow a previous study reporting sex-based pay disparities among hospitalists (Inquiry 2004;41:301-15) and more general studies reporting significant sex-based pay disparities among physicians (Health Aff. 2009;28:557-66 and Health Aff. 2011;30:193-201).
Anecdotes shared by women at the interest group meeting made the statistics come to life. One said she left a hospitalist position when she discovered that her two male colleagues were being paid $30,000/year more than she was. Another described complaining to her company’s CEO that male hospitalists were being paid $20,000/year more than she was, only to be brushed off by the executive – another woman – who told her that individual contracts were none of her business.
"It’s disappointing to be having this conversation," Dr. Nagamine said. "I’m appalled in this day and age to hear about things like." The solution has to be systemic, not just on a case-by-case basis, she added.
Dr. Patience E. Reich suggested ways to fight systemic gender bias during an earlier session on "Women in Hospital Medicine." Pay disparities may be the easiest for hospitalist companies to correct, by conducting self-audits assessing compensation within the company and adopting policies that promote transparency around how pay levels are set.
"Treat this as part of your business strategy," and engage male colleagues in initiatives around gender issues, said Dr. Reich, a hospitalist at Wake Forest University, Winston-Salem, N.C.
Another challenge facing women more than men is the need for flexibility in work structures. In families with two working parents, women do twice as much housework and three times as much child care as men, said Dr. Reich’s co-moderator of the session, Dr. Rachel George. The U.S. Bureau of Labor Statistics tells a similar story with its data indicating that married women spend about twice as much time on both endeavors as married men do.
Find a solution that fits your workplace, whether it’s offering part-time positions, job-sharing, child-care services, or something else, Dr. Reich said. "Please involve the top business line people when making these decisions," she added. "They will help construct something that’s workable."
A systemic lack of mentors and sponsors can negatively affect the careers of female hospitalists, who may lack access to informal networks, high-visibility assignments, and transparency around career paths. Women need to reach out to physician colleagues, male and female, inside and outside the specialty, to find mentors and sponsors. Hospitalist leaders should try to connect women with mentors and sponsors, she said.
The solutions also are personal, not just systemic, said Dr. George, regional CEO for Cogent HMG, Brentwood, Tenn., a hospitalist management group.

She urged women to step up and create opportunities. "Be part of a committee in your hospital. Participate. Show up. Speak up. Follow up," so that you and your abilities become better known, Dr. George said.
Ease up on yourself if you take a management position and not everyone likes you – that’s to be expected, she added. Lighten up, and don’t blame gender bias for every problem. Partner up with your spouse to share the load at home and/or find help for you both. Finally, "woman up" to support women’s choices in balancing work and home life, even if they don’t match your own, she said.
She suggested that SHM might compile "best practices" for facilitating a gender balance in hospitalist groups. Others suggested holding a workshop on negotiation skills, educating male colleagues about gender bias, organizing a weekend workshop on women’s issues, or even "mentored implementation of mentoring women for leadership."
"I think there’s going to be some fun work ahead," Dr. Nagamine said.
The speakers reported having no financial disclosures.
* This story was updated on Tuesday, April 10.
SAN DIEGO – A plan to form "affinity groups" got off to a rousing start as participants in a women’s-interest session the enthusiastically signed up for a new listserv.
The affinity groups are designed to promote communication among members with common interests, said Dr. Janet M. Nagamine, a Society of Hospital Medicine board member who led an interest group gathering at the annual meeting. She also pumped participants for other ideas on how SHM can help address the challenges facing female hospitalists, especially the hot topic of persistent pay disparities between male and female hospitalists.
A 2011 survey by the society and the Medical Group Management Association found that female hospitalists were being paid $4,000-$29,000 less than their male counterparts were, after accounting for factors other than sex. The findings follow a previous study reporting sex-based pay disparities among hospitalists (Inquiry 2004;41:301-15) and more general studies reporting significant sex-based pay disparities among physicians (Health Aff. 2009;28:557-66 and Health Aff. 2011;30:193-201).
Anecdotes shared by women at the interest group meeting made the statistics come to life. One said she left a hospitalist position when she discovered that her two male colleagues were being paid $30,000/year more than she was. Another described complaining to her company’s CEO that male hospitalists were being paid $20,000/year more than she was, only to be brushed off by the executive – another woman – who told her that individual contracts were none of her business.
"It’s disappointing to be having this conversation," Dr. Nagamine said. "I’m appalled in this day and age to hear about things like." The solution has to be systemic, not just on a case-by-case basis, she added.
Dr. Patience E. Reich suggested ways to fight systemic gender bias during an earlier session on "Women in Hospital Medicine." Pay disparities may be the easiest for hospitalist companies to correct, by conducting self-audits assessing compensation within the company and adopting policies that promote transparency around how pay levels are set.
"Treat this as part of your business strategy," and engage male colleagues in initiatives around gender issues, said Dr. Reich, a hospitalist at Wake Forest University, Winston-Salem, N.C.
Another challenge facing women more than men is the need for flexibility in work structures. In families with two working parents, women do twice as much housework and three times as much child care as men, said Dr. Reich’s co-moderator of the session, Dr. Rachel George. The U.S. Bureau of Labor Statistics tells a similar story with its data indicating that married women spend about twice as much time on both endeavors as married men do.
Find a solution that fits your workplace, whether it’s offering part-time positions, job-sharing, child-care services, or something else, Dr. Reich said. "Please involve the top business line people when making these decisions," she added. "They will help construct something that’s workable."
A systemic lack of mentors and sponsors can negatively affect the careers of female hospitalists, who may lack access to informal networks, high-visibility assignments, and transparency around career paths. Women need to reach out to physician colleagues, male and female, inside and outside the specialty, to find mentors and sponsors. Hospitalist leaders should try to connect women with mentors and sponsors, she said.
The solutions also are personal, not just systemic, said Dr. George, regional CEO for Cogent HMG, Brentwood, Tenn., a hospitalist management group.
She urged women to step up and create opportunities. "Be part of a committee in your hospital. Participate. Show up. Speak up. Follow up," so that you and your abilities become better known, Dr. George said.
Ease up on yourself if you take a management position and not everyone likes you – that’s to be expected, she added. Lighten up, and don’t blame gender bias for every problem. Partner up with your spouse to share the load at home and/or find help for you both. Finally, "woman up" to support women’s choices in balancing work and home life, even if they don’t match your own, she said.
She suggested that SHM might compile "best practices" for facilitating a gender balance in hospitalist groups. Others suggested holding a workshop on negotiation skills, educating male colleagues about gender bias, organizing a weekend workshop on women’s issues, or even "mentored implementation of mentoring women for leadership."
"I think there’s going to be some fun work ahead," Dr. Nagamine said.
The speakers reported having no financial disclosures.
* This story was updated on Tuesday, April 10.
SAN DIEGO – A plan to form "affinity groups" got off to a rousing start as participants in a women’s-interest session the enthusiastically signed up for a new listserv.
The affinity groups are designed to promote communication among members with common interests, said Dr. Janet M. Nagamine, a Society of Hospital Medicine board member who led an interest group gathering at the annual meeting. She also pumped participants for other ideas on how SHM can help address the challenges facing female hospitalists, especially the hot topic of persistent pay disparities between male and female hospitalists.
A 2011 survey by the society and the Medical Group Management Association found that female hospitalists were being paid $4,000-$29,000 less than their male counterparts were, after accounting for factors other than sex. The findings follow a previous study reporting sex-based pay disparities among hospitalists (Inquiry 2004;41:301-15) and more general studies reporting significant sex-based pay disparities among physicians (Health Aff. 2009;28:557-66 and Health Aff. 2011;30:193-201).
Anecdotes shared by women at the interest group meeting made the statistics come to life. One said she left a hospitalist position when she discovered that her two male colleagues were being paid $30,000/year more than she was. Another described complaining to her company’s CEO that male hospitalists were being paid $20,000/year more than she was, only to be brushed off by the executive – another woman – who told her that individual contracts were none of her business.
"It’s disappointing to be having this conversation," Dr. Nagamine said. "I’m appalled in this day and age to hear about things like." The solution has to be systemic, not just on a case-by-case basis, she added.
Dr. Patience E. Reich suggested ways to fight systemic gender bias during an earlier session on "Women in Hospital Medicine." Pay disparities may be the easiest for hospitalist companies to correct, by conducting self-audits assessing compensation within the company and adopting policies that promote transparency around how pay levels are set.
"Treat this as part of your business strategy," and engage male colleagues in initiatives around gender issues, said Dr. Reich, a hospitalist at Wake Forest University, Winston-Salem, N.C.
Another challenge facing women more than men is the need for flexibility in work structures. In families with two working parents, women do twice as much housework and three times as much child care as men, said Dr. Reich’s co-moderator of the session, Dr. Rachel George. The U.S. Bureau of Labor Statistics tells a similar story with its data indicating that married women spend about twice as much time on both endeavors as married men do.
Find a solution that fits your workplace, whether it’s offering part-time positions, job-sharing, child-care services, or something else, Dr. Reich said. "Please involve the top business line people when making these decisions," she added. "They will help construct something that’s workable."
A systemic lack of mentors and sponsors can negatively affect the careers of female hospitalists, who may lack access to informal networks, high-visibility assignments, and transparency around career paths. Women need to reach out to physician colleagues, male and female, inside and outside the specialty, to find mentors and sponsors. Hospitalist leaders should try to connect women with mentors and sponsors, she said.
The solutions also are personal, not just systemic, said Dr. George, regional CEO for Cogent HMG, Brentwood, Tenn., a hospitalist management group.
She urged women to step up and create opportunities. "Be part of a committee in your hospital. Participate. Show up. Speak up. Follow up," so that you and your abilities become better known, Dr. George said.
Ease up on yourself if you take a management position and not everyone likes you – that’s to be expected, she added. Lighten up, and don’t blame gender bias for every problem. Partner up with your spouse to share the load at home and/or find help for you both. Finally, "woman up" to support women’s choices in balancing work and home life, even if they don’t match your own, she said.
She suggested that SHM might compile "best practices" for facilitating a gender balance in hospitalist groups. Others suggested holding a workshop on negotiation skills, educating male colleagues about gender bias, organizing a weekend workshop on women’s issues, or even "mentored implementation of mentoring women for leadership."
"I think there’s going to be some fun work ahead," Dr. Nagamine said.
The speakers reported having no financial disclosures.
* This story was updated on Tuesday, April 10.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
A Hospitalist’s Call to Action
Dr. Patrick Conway is the Chief Medical Officer at the Centers for Medicare and Medicaid Services, but he also happens to be a practicing pediatric hospitalist. So when he showed up at the Society of Hospital Medicine’s annual meeting earlier this week to deliver one of the keynote addresses, he got a warm welcome from fellow hospitalists happy to see one of their own in a real position to make decisions about Medicare’s policies.
Dr. Conway gave the standard speech about what CMS officials are doing to transform the health care system. Then he turned to his hospitalist colleagues and gave them some things to do, too. Hospitalists need to partner with the hospital administration and their quality improvement teams. They need to understand their hospital’s performance data. And they need to take charge, he said, by leading multidisciplinary teams.

“We’re at a unique time in health care where we can drive change,” Dr. Conway said. “My challenge to you would be, please don’t sit on the sidelines.”
He urged the audience – hospitalists gathered in San Diego for continuing education and networking – to make an effort to lead some type of system improvement in their hospital. “I don’t actually care what it is, but work on some broader system changes in your local setting,” Dr. Conway said.
If hospitalists are looking for a reason to get out in front when it comes to system change, there are plenty of financial carrots and sticks coming very soon from the Medicare program. Dr. Conway outlined many of them, from Accountable Care Organizations to the readmission reduction program to the hospital value-based purchasing program. But the best reason to be active in changing the way the health system works is for the benefit of patients, he said. That’s the reason that Dr. Conway still works as a hospitalist nearly every weekend for free. “It’s about those families that you take care of,” he said.
– Mary Ellen Schneider
Dr. Patrick Conway is the Chief Medical Officer at the Centers for Medicare and Medicaid Services, but he also happens to be a practicing pediatric hospitalist. So when he showed up at the Society of Hospital Medicine’s annual meeting earlier this week to deliver one of the keynote addresses, he got a warm welcome from fellow hospitalists happy to see one of their own in a real position to make decisions about Medicare’s policies.
Dr. Conway gave the standard speech about what CMS officials are doing to transform the health care system. Then he turned to his hospitalist colleagues and gave them some things to do, too. Hospitalists need to partner with the hospital administration and their quality improvement teams. They need to understand their hospital’s performance data. And they need to take charge, he said, by leading multidisciplinary teams.
“We’re at a unique time in health care where we can drive change,” Dr. Conway said. “My challenge to you would be, please don’t sit on the sidelines.”
He urged the audience – hospitalists gathered in San Diego for continuing education and networking – to make an effort to lead some type of system improvement in their hospital. “I don’t actually care what it is, but work on some broader system changes in your local setting,” Dr. Conway said.
If hospitalists are looking for a reason to get out in front when it comes to system change, there are plenty of financial carrots and sticks coming very soon from the Medicare program. Dr. Conway outlined many of them, from Accountable Care Organizations to the readmission reduction program to the hospital value-based purchasing program. But the best reason to be active in changing the way the health system works is for the benefit of patients, he said. That’s the reason that Dr. Conway still works as a hospitalist nearly every weekend for free. “It’s about those families that you take care of,” he said.
– Mary Ellen Schneider
Dr. Patrick Conway is the Chief Medical Officer at the Centers for Medicare and Medicaid Services, but he also happens to be a practicing pediatric hospitalist. So when he showed up at the Society of Hospital Medicine’s annual meeting earlier this week to deliver one of the keynote addresses, he got a warm welcome from fellow hospitalists happy to see one of their own in a real position to make decisions about Medicare’s policies.
Dr. Conway gave the standard speech about what CMS officials are doing to transform the health care system. Then he turned to his hospitalist colleagues and gave them some things to do, too. Hospitalists need to partner with the hospital administration and their quality improvement teams. They need to understand their hospital’s performance data. And they need to take charge, he said, by leading multidisciplinary teams.
“We’re at a unique time in health care where we can drive change,” Dr. Conway said. “My challenge to you would be, please don’t sit on the sidelines.”
He urged the audience – hospitalists gathered in San Diego for continuing education and networking – to make an effort to lead some type of system improvement in their hospital. “I don’t actually care what it is, but work on some broader system changes in your local setting,” Dr. Conway said.
If hospitalists are looking for a reason to get out in front when it comes to system change, there are plenty of financial carrots and sticks coming very soon from the Medicare program. Dr. Conway outlined many of them, from Accountable Care Organizations to the readmission reduction program to the hospital value-based purchasing program. But the best reason to be active in changing the way the health system works is for the benefit of patients, he said. That’s the reason that Dr. Conway still works as a hospitalist nearly every weekend for free. “It’s about those families that you take care of,” he said.
– Mary Ellen Schneider
Gender Bias May Influence Hospitalist Pay
It’s not every day that a medical conference includes a refresher on Feminism 101, but that’s essentially what kicked off the session on "Women in Hospital Medicine: Defining Common Challenges and Strategies for Success" at the Society of Hospital Medicine annual meeting this week.
The hottest topic was the persistent pay gap between female and male physicians, as reported in study after study after study and in a recent survey by the society. But before discussion began, the 70 or so hospitalists present (including 3 men) heard a review of the gender-based basics.

"There’s an old saying: Before you try to move a fence, find out why it was put there," said Dr. Patience E. Reich, who chaired the session with Dr. Rachel George.
The studies suggest that at least some of the disparities in pay are due to gender bias, "many times unconscious," after controlling for the effects of other factors, Dr. Reich said.
She recommends the Web site of the Gender Bias Learning Project of the University of California Hastings College of Law, where visitors can play Gender Bias Bingo and find other tools for understanding gender bias in our society.
The Project identifies four gender bias patterns that many female physicians can appreciate, Dr. Reich said:
Prove it again! Men are judged by their potential, but women are judged by their accomplishments and have to prove themselves again and again. Women have to work twice as hard to get half as far as men.
The double bind. Men are perceived as assertive, but women who behave the same way are perceived as aggressive. To get ahead, women sometimes have to choose between being respected and not liked, or being liked and not respected.
The maternal wall. Mothers are considered to be uncommitted to work or incompetent. "People don’t bother hiding this one," Dr. Reich noted. She gave an example of a time when she submitted the name of a female hospitalist for an open leadership position at a hospital where she worked. A committee member dismissed the idea, saying the candidate wouldn’t want the position because "she’s trying to have another baby.” Dr. Reich countered, “Why don’t we just ask her?" When they did, the candidate said she did want the job and applied for it.
Gender wars. Internalized gender bias creates conflict between women. One example: Older female academicians who sacrificed having children in order to have a career and who now resent younger women expecting to have both, and thus refuse to mentor them.
These issues need to be addressed systemically, not just on a case-by-case basis, in order to effect change, Dr. Reich said.
At a Society of Hospital Medicine women’s interest group meeting later the same day, one doctor said Dr. Reich’s and Dr. George’s "women’s issues" session was better than similar ones she had attended at other medical conferences. "It’s important that we talk about gender bias in the open, with women and men present, and not just talk about things like work-life balance, because it’s a systemic theme," the physician said.
–Sherry Boschert (@sherryboschert on Twitter)
It’s not every day that a medical conference includes a refresher on Feminism 101, but that’s essentially what kicked off the session on "Women in Hospital Medicine: Defining Common Challenges and Strategies for Success" at the Society of Hospital Medicine annual meeting this week.
The hottest topic was the persistent pay gap between female and male physicians, as reported in study after study after study and in a recent survey by the society. But before discussion began, the 70 or so hospitalists present (including 3 men) heard a review of the gender-based basics.
"There’s an old saying: Before you try to move a fence, find out why it was put there," said Dr. Patience E. Reich, who chaired the session with Dr. Rachel George.
The studies suggest that at least some of the disparities in pay are due to gender bias, "many times unconscious," after controlling for the effects of other factors, Dr. Reich said.
She recommends the Web site of the Gender Bias Learning Project of the University of California Hastings College of Law, where visitors can play Gender Bias Bingo and find other tools for understanding gender bias in our society.
The Project identifies four gender bias patterns that many female physicians can appreciate, Dr. Reich said:
Prove it again! Men are judged by their potential, but women are judged by their accomplishments and have to prove themselves again and again. Women have to work twice as hard to get half as far as men.
The double bind. Men are perceived as assertive, but women who behave the same way are perceived as aggressive. To get ahead, women sometimes have to choose between being respected and not liked, or being liked and not respected.
The maternal wall. Mothers are considered to be uncommitted to work or incompetent. "People don’t bother hiding this one," Dr. Reich noted. She gave an example of a time when she submitted the name of a female hospitalist for an open leadership position at a hospital where she worked. A committee member dismissed the idea, saying the candidate wouldn’t want the position because "she’s trying to have another baby.” Dr. Reich countered, “Why don’t we just ask her?" When they did, the candidate said she did want the job and applied for it.
Gender wars. Internalized gender bias creates conflict between women. One example: Older female academicians who sacrificed having children in order to have a career and who now resent younger women expecting to have both, and thus refuse to mentor them.
These issues need to be addressed systemically, not just on a case-by-case basis, in order to effect change, Dr. Reich said.
At a Society of Hospital Medicine women’s interest group meeting later the same day, one doctor said Dr. Reich’s and Dr. George’s "women’s issues" session was better than similar ones she had attended at other medical conferences. "It’s important that we talk about gender bias in the open, with women and men present, and not just talk about things like work-life balance, because it’s a systemic theme," the physician said.
–Sherry Boschert (@sherryboschert on Twitter)
It’s not every day that a medical conference includes a refresher on Feminism 101, but that’s essentially what kicked off the session on "Women in Hospital Medicine: Defining Common Challenges and Strategies for Success" at the Society of Hospital Medicine annual meeting this week.
The hottest topic was the persistent pay gap between female and male physicians, as reported in study after study after study and in a recent survey by the society. But before discussion began, the 70 or so hospitalists present (including 3 men) heard a review of the gender-based basics.
"There’s an old saying: Before you try to move a fence, find out why it was put there," said Dr. Patience E. Reich, who chaired the session with Dr. Rachel George.
The studies suggest that at least some of the disparities in pay are due to gender bias, "many times unconscious," after controlling for the effects of other factors, Dr. Reich said.
She recommends the Web site of the Gender Bias Learning Project of the University of California Hastings College of Law, where visitors can play Gender Bias Bingo and find other tools for understanding gender bias in our society.
The Project identifies four gender bias patterns that many female physicians can appreciate, Dr. Reich said:
Prove it again! Men are judged by their potential, but women are judged by their accomplishments and have to prove themselves again and again. Women have to work twice as hard to get half as far as men.
The double bind. Men are perceived as assertive, but women who behave the same way are perceived as aggressive. To get ahead, women sometimes have to choose between being respected and not liked, or being liked and not respected.
The maternal wall. Mothers are considered to be uncommitted to work or incompetent. "People don’t bother hiding this one," Dr. Reich noted. She gave an example of a time when she submitted the name of a female hospitalist for an open leadership position at a hospital where she worked. A committee member dismissed the idea, saying the candidate wouldn’t want the position because "she’s trying to have another baby.” Dr. Reich countered, “Why don’t we just ask her?" When they did, the candidate said she did want the job and applied for it.
Gender wars. Internalized gender bias creates conflict between women. One example: Older female academicians who sacrificed having children in order to have a career and who now resent younger women expecting to have both, and thus refuse to mentor them.
These issues need to be addressed systemically, not just on a case-by-case basis, in order to effect change, Dr. Reich said.
At a Society of Hospital Medicine women’s interest group meeting later the same day, one doctor said Dr. Reich’s and Dr. George’s "women’s issues" session was better than similar ones she had attended at other medical conferences. "It’s important that we talk about gender bias in the open, with women and men present, and not just talk about things like work-life balance, because it’s a systemic theme," the physician said.
–Sherry Boschert (@sherryboschert on Twitter)