User login
Neurology Reviews covers innovative and emerging news in neurology and neuroscience every month, with a focus on practical approaches to treating Parkinson's disease, epilepsy, headache, stroke, multiple sclerosis, Alzheimer's disease, and other neurologic disorders.
PML
Progressive multifocal leukoencephalopathy
Rituxan
The leading independent newspaper covering neurology news and commentary.
Long COVID ‘brain fog’ confounds doctors, but new research offers hope
Kate Whitley was petrified of COVID-19 from the beginning of the pandemic because she has Hashimoto disease, an autoimmune disorder that she knew put her at high risk for complications.
She was right to be worried. Two months after contracting the infection in September 2022, the 42-year-old Nashville resident was diagnosed with long COVID. For Ms. Whitley, the resulting brain fog has been the most challenging factor. She is the owner of a successful paper goods store, and she can’t remember basic aspects of her job. She can’t tolerate loud noises and gets so distracted that she has trouble remembering what she was doing.
Ms. Whitley doesn’t like the term “brain fog” because it doesn’t begin to describe the dramatic disruption to her life over the past 7 months.
Brain fog is among the most common symptoms of long COVID, and also one of the most poorly understood. A reported 46% of those diagnosed with long COVID complain of brain fog or a loss of memory. Many clinicians agree that the term is vague and often doesn’t truly represent the condition. That, in turn, makes it harder for doctors to diagnose and treat it. There are no standard tests for it, nor are there guidelines for symptom management or treatment.
“There’s a lot of imprecision in the term because it might mean different things to different patients,” said James C. Jackson, PsyD, a neuropsychiatrist at Vanderbilt University, Nashville, Tenn., and author of a new book, “Clearing the Fog: From Surviving to Thriving With Long COVID – A Practical Guide.”
Dr. Jackson, who began treating Ms. Whitley in February 2023, said that it makes more sense to call brain fog a brain impairment or an acquired brain injury (ABI) because it doesn’t occur gradually. COVID damages the brain and causes injury. For those with long COVID who were previously in the intensive care unit and may have undergone ventilation, hypoxic brain injury may result from the lack of oxygen to the brain.
Even among those with milder cases of acute COVID, there’s some evidence that persistent neuroinflammation in the brain caused by an activated immune system may also cause damage.
In both cases, the results can be debilitating. Ms. Whitley also has dysautonomia – a disorder of the autonomic nervous system that can cause dizziness, sweating, and headaches along with fatigue and heart palpitations.
She said that she’s so forgetful that when she sees people socially, she’s nervous of what she’ll say. “I feel like I’m constantly sticking my foot in my mouth because I can’t remember details of other people’s lives,” she said.
Although brain disorders such as Alzheimer’s disease and other forms of dementia are marked by a slow decline, ABI occurs more suddenly and may include a loss of executive function and attention.
“With a brain injury, you’re doing fine, and then some event happens (in this case COVID), and immediately after that, your cognitive function is different,” said Dr. Jackson.
Additionally, ABI is an actual diagnosis, whereas brain fog is not.
“With a brain injury, there’s a treatment pathway for cognitive rehabilitation,” said Dr. Jackson.
Treatments may include speech, cognitive, and occupational therapy as well as meeting with a neuropsychiatrist for treatment of the mental and behavioral disorders that may result. Dr. Jackson said that while many patients aren’t functioning cognitively or physically at 100%, they can make enough strides that they don’t have to give up things such as driving and, in some cases, their jobs.
Other experts agree that long COVID may damage the brain. An April 2022 study published in the journal Nature found strong evidence that SARS-CoV-2 infection may cause brain-related abnormalities, for example, a reduction in gray matter in certain parts of the brain, including the prefrontal cortex, hypothalamus, and amygdala.
Additionally, white matter, which is found deeper in the brain and is responsible for the exchange of information between different parts of the brain, may also be at risk of damage as a result of the virus, according to a November 2022 study published in the journal SN Comprehensive Clinical Medicine.
Calling it a “fog” makes it easier for clinicians and the general public to dismiss its severity, said Tyler Reed Bell, PhD, a researcher who specializes in viruses that cause brain injury. He is a fellow in the department of psychiatry at the University of California, San Diego. Brain fog can make driving and returning to work especially dangerous. Because of difficulty focusing, patients are much more likely to make mistakes that cause accidents.
“The COVID virus is very invasive to the brain,” Dr. Bell said.
Others contend this may be a rush to judgment. Karla L. Thompson, PhD, lead neuropsychologist at the University of North Carolina at Chapel Hill’s COVID Recovery Clinic, agrees that in more serious cases of COVID that cause a lack of oxygen to the brain, it’s reasonable to call it a brain injury. But brain fog can also be associated with other long COVID symptoms, not just damage to the brain.
Chronic fatigue and poor sleep are both commonly reported symptoms of long COVID that negatively affect brain function, she said. Sleep disturbances, cardiac problems, dysautonomia, and emotional distress could also affect the way the brain functions post COVID. Finding the right treatment requires identifying all the factors contributing to cognitive impairment.
Part of the problem in treating long COVID brain fog is that diagnostic technology is not sensitive enough to detect inflammation that could be causing damage.
Grace McComsey, MD, who leads the long COVID RECOVER study at University Hospitals Health System in Cleveland, said her team is working on identifying biomarkers that could detect brain inflammation in a way similar to the manner researchers have identified biomarkers to help diagnose chronic fatigue syndrome. Additionally, a new study published last month in JAMA for the first time clearly defined 12 symptoms of long COVID, and brain fog was listed among them. All of this contributes to the development of clear diagnostic criteria.
“It will make a big difference once we have some consistency among clinicians in diagnosing the condition,” said Dr. McComsey.
Ms. Whitley is thankful for the treatment that she’s received thus far. She’s seeing a cognitive rehabilitation therapist, who assesses her memory, cognition, and attention span and gives her tools to break up simple tasks, such as driving, so that they don’t feel overwhelming. She’s back behind the wheel and back to work.
But perhaps most importantly, Ms. Whitley joined a support group, led by Dr. Jackson, that includes other people experiencing the same symptoms she is. When she was at her darkest, they understood.
“Talking to other survivors has been the only solace in all this,” Ms. Whitley said. “Together, we grieve all that’s been lost.”
A version of this article first appeared on Medscape.com.
Kate Whitley was petrified of COVID-19 from the beginning of the pandemic because she has Hashimoto disease, an autoimmune disorder that she knew put her at high risk for complications.
She was right to be worried. Two months after contracting the infection in September 2022, the 42-year-old Nashville resident was diagnosed with long COVID. For Ms. Whitley, the resulting brain fog has been the most challenging factor. She is the owner of a successful paper goods store, and she can’t remember basic aspects of her job. She can’t tolerate loud noises and gets so distracted that she has trouble remembering what she was doing.
Ms. Whitley doesn’t like the term “brain fog” because it doesn’t begin to describe the dramatic disruption to her life over the past 7 months.
Brain fog is among the most common symptoms of long COVID, and also one of the most poorly understood. A reported 46% of those diagnosed with long COVID complain of brain fog or a loss of memory. Many clinicians agree that the term is vague and often doesn’t truly represent the condition. That, in turn, makes it harder for doctors to diagnose and treat it. There are no standard tests for it, nor are there guidelines for symptom management or treatment.
“There’s a lot of imprecision in the term because it might mean different things to different patients,” said James C. Jackson, PsyD, a neuropsychiatrist at Vanderbilt University, Nashville, Tenn., and author of a new book, “Clearing the Fog: From Surviving to Thriving With Long COVID – A Practical Guide.”
Dr. Jackson, who began treating Ms. Whitley in February 2023, said that it makes more sense to call brain fog a brain impairment or an acquired brain injury (ABI) because it doesn’t occur gradually. COVID damages the brain and causes injury. For those with long COVID who were previously in the intensive care unit and may have undergone ventilation, hypoxic brain injury may result from the lack of oxygen to the brain.
Even among those with milder cases of acute COVID, there’s some evidence that persistent neuroinflammation in the brain caused by an activated immune system may also cause damage.
In both cases, the results can be debilitating. Ms. Whitley also has dysautonomia – a disorder of the autonomic nervous system that can cause dizziness, sweating, and headaches along with fatigue and heart palpitations.
She said that she’s so forgetful that when she sees people socially, she’s nervous of what she’ll say. “I feel like I’m constantly sticking my foot in my mouth because I can’t remember details of other people’s lives,” she said.
Although brain disorders such as Alzheimer’s disease and other forms of dementia are marked by a slow decline, ABI occurs more suddenly and may include a loss of executive function and attention.
“With a brain injury, you’re doing fine, and then some event happens (in this case COVID), and immediately after that, your cognitive function is different,” said Dr. Jackson.
Additionally, ABI is an actual diagnosis, whereas brain fog is not.
“With a brain injury, there’s a treatment pathway for cognitive rehabilitation,” said Dr. Jackson.
Treatments may include speech, cognitive, and occupational therapy as well as meeting with a neuropsychiatrist for treatment of the mental and behavioral disorders that may result. Dr. Jackson said that while many patients aren’t functioning cognitively or physically at 100%, they can make enough strides that they don’t have to give up things such as driving and, in some cases, their jobs.
Other experts agree that long COVID may damage the brain. An April 2022 study published in the journal Nature found strong evidence that SARS-CoV-2 infection may cause brain-related abnormalities, for example, a reduction in gray matter in certain parts of the brain, including the prefrontal cortex, hypothalamus, and amygdala.
Additionally, white matter, which is found deeper in the brain and is responsible for the exchange of information between different parts of the brain, may also be at risk of damage as a result of the virus, according to a November 2022 study published in the journal SN Comprehensive Clinical Medicine.
Calling it a “fog” makes it easier for clinicians and the general public to dismiss its severity, said Tyler Reed Bell, PhD, a researcher who specializes in viruses that cause brain injury. He is a fellow in the department of psychiatry at the University of California, San Diego. Brain fog can make driving and returning to work especially dangerous. Because of difficulty focusing, patients are much more likely to make mistakes that cause accidents.
“The COVID virus is very invasive to the brain,” Dr. Bell said.
Others contend this may be a rush to judgment. Karla L. Thompson, PhD, lead neuropsychologist at the University of North Carolina at Chapel Hill’s COVID Recovery Clinic, agrees that in more serious cases of COVID that cause a lack of oxygen to the brain, it’s reasonable to call it a brain injury. But brain fog can also be associated with other long COVID symptoms, not just damage to the brain.
Chronic fatigue and poor sleep are both commonly reported symptoms of long COVID that negatively affect brain function, she said. Sleep disturbances, cardiac problems, dysautonomia, and emotional distress could also affect the way the brain functions post COVID. Finding the right treatment requires identifying all the factors contributing to cognitive impairment.
Part of the problem in treating long COVID brain fog is that diagnostic technology is not sensitive enough to detect inflammation that could be causing damage.
Grace McComsey, MD, who leads the long COVID RECOVER study at University Hospitals Health System in Cleveland, said her team is working on identifying biomarkers that could detect brain inflammation in a way similar to the manner researchers have identified biomarkers to help diagnose chronic fatigue syndrome. Additionally, a new study published last month in JAMA for the first time clearly defined 12 symptoms of long COVID, and brain fog was listed among them. All of this contributes to the development of clear diagnostic criteria.
“It will make a big difference once we have some consistency among clinicians in diagnosing the condition,” said Dr. McComsey.
Ms. Whitley is thankful for the treatment that she’s received thus far. She’s seeing a cognitive rehabilitation therapist, who assesses her memory, cognition, and attention span and gives her tools to break up simple tasks, such as driving, so that they don’t feel overwhelming. She’s back behind the wheel and back to work.
But perhaps most importantly, Ms. Whitley joined a support group, led by Dr. Jackson, that includes other people experiencing the same symptoms she is. When she was at her darkest, they understood.
“Talking to other survivors has been the only solace in all this,” Ms. Whitley said. “Together, we grieve all that’s been lost.”
A version of this article first appeared on Medscape.com.
Kate Whitley was petrified of COVID-19 from the beginning of the pandemic because she has Hashimoto disease, an autoimmune disorder that she knew put her at high risk for complications.
She was right to be worried. Two months after contracting the infection in September 2022, the 42-year-old Nashville resident was diagnosed with long COVID. For Ms. Whitley, the resulting brain fog has been the most challenging factor. She is the owner of a successful paper goods store, and she can’t remember basic aspects of her job. She can’t tolerate loud noises and gets so distracted that she has trouble remembering what she was doing.
Ms. Whitley doesn’t like the term “brain fog” because it doesn’t begin to describe the dramatic disruption to her life over the past 7 months.
Brain fog is among the most common symptoms of long COVID, and also one of the most poorly understood. A reported 46% of those diagnosed with long COVID complain of brain fog or a loss of memory. Many clinicians agree that the term is vague and often doesn’t truly represent the condition. That, in turn, makes it harder for doctors to diagnose and treat it. There are no standard tests for it, nor are there guidelines for symptom management or treatment.
“There’s a lot of imprecision in the term because it might mean different things to different patients,” said James C. Jackson, PsyD, a neuropsychiatrist at Vanderbilt University, Nashville, Tenn., and author of a new book, “Clearing the Fog: From Surviving to Thriving With Long COVID – A Practical Guide.”
Dr. Jackson, who began treating Ms. Whitley in February 2023, said that it makes more sense to call brain fog a brain impairment or an acquired brain injury (ABI) because it doesn’t occur gradually. COVID damages the brain and causes injury. For those with long COVID who were previously in the intensive care unit and may have undergone ventilation, hypoxic brain injury may result from the lack of oxygen to the brain.
Even among those with milder cases of acute COVID, there’s some evidence that persistent neuroinflammation in the brain caused by an activated immune system may also cause damage.
In both cases, the results can be debilitating. Ms. Whitley also has dysautonomia – a disorder of the autonomic nervous system that can cause dizziness, sweating, and headaches along with fatigue and heart palpitations.
She said that she’s so forgetful that when she sees people socially, she’s nervous of what she’ll say. “I feel like I’m constantly sticking my foot in my mouth because I can’t remember details of other people’s lives,” she said.
Although brain disorders such as Alzheimer’s disease and other forms of dementia are marked by a slow decline, ABI occurs more suddenly and may include a loss of executive function and attention.
“With a brain injury, you’re doing fine, and then some event happens (in this case COVID), and immediately after that, your cognitive function is different,” said Dr. Jackson.
Additionally, ABI is an actual diagnosis, whereas brain fog is not.
“With a brain injury, there’s a treatment pathway for cognitive rehabilitation,” said Dr. Jackson.
Treatments may include speech, cognitive, and occupational therapy as well as meeting with a neuropsychiatrist for treatment of the mental and behavioral disorders that may result. Dr. Jackson said that while many patients aren’t functioning cognitively or physically at 100%, they can make enough strides that they don’t have to give up things such as driving and, in some cases, their jobs.
Other experts agree that long COVID may damage the brain. An April 2022 study published in the journal Nature found strong evidence that SARS-CoV-2 infection may cause brain-related abnormalities, for example, a reduction in gray matter in certain parts of the brain, including the prefrontal cortex, hypothalamus, and amygdala.
Additionally, white matter, which is found deeper in the brain and is responsible for the exchange of information between different parts of the brain, may also be at risk of damage as a result of the virus, according to a November 2022 study published in the journal SN Comprehensive Clinical Medicine.
Calling it a “fog” makes it easier for clinicians and the general public to dismiss its severity, said Tyler Reed Bell, PhD, a researcher who specializes in viruses that cause brain injury. He is a fellow in the department of psychiatry at the University of California, San Diego. Brain fog can make driving and returning to work especially dangerous. Because of difficulty focusing, patients are much more likely to make mistakes that cause accidents.
“The COVID virus is very invasive to the brain,” Dr. Bell said.
Others contend this may be a rush to judgment. Karla L. Thompson, PhD, lead neuropsychologist at the University of North Carolina at Chapel Hill’s COVID Recovery Clinic, agrees that in more serious cases of COVID that cause a lack of oxygen to the brain, it’s reasonable to call it a brain injury. But brain fog can also be associated with other long COVID symptoms, not just damage to the brain.
Chronic fatigue and poor sleep are both commonly reported symptoms of long COVID that negatively affect brain function, she said. Sleep disturbances, cardiac problems, dysautonomia, and emotional distress could also affect the way the brain functions post COVID. Finding the right treatment requires identifying all the factors contributing to cognitive impairment.
Part of the problem in treating long COVID brain fog is that diagnostic technology is not sensitive enough to detect inflammation that could be causing damage.
Grace McComsey, MD, who leads the long COVID RECOVER study at University Hospitals Health System in Cleveland, said her team is working on identifying biomarkers that could detect brain inflammation in a way similar to the manner researchers have identified biomarkers to help diagnose chronic fatigue syndrome. Additionally, a new study published last month in JAMA for the first time clearly defined 12 symptoms of long COVID, and brain fog was listed among them. All of this contributes to the development of clear diagnostic criteria.
“It will make a big difference once we have some consistency among clinicians in diagnosing the condition,” said Dr. McComsey.
Ms. Whitley is thankful for the treatment that she’s received thus far. She’s seeing a cognitive rehabilitation therapist, who assesses her memory, cognition, and attention span and gives her tools to break up simple tasks, such as driving, so that they don’t feel overwhelming. She’s back behind the wheel and back to work.
But perhaps most importantly, Ms. Whitley joined a support group, led by Dr. Jackson, that includes other people experiencing the same symptoms she is. When she was at her darkest, they understood.
“Talking to other survivors has been the only solace in all this,” Ms. Whitley said. “Together, we grieve all that’s been lost.”
A version of this article first appeared on Medscape.com.
What is the proper treatment for posttraumatic headache? Expert debate
AUSTIN, TEX – There are no guidelines available, nor is there much quality evidence to support one decision or another, according to two experts who debated the question at the annual meeting of the American Headache Society.
Early treatment
Frank Conidi, DO, spoke first, and pointed out the need to define both early treatment and the condition being treated. Is it early-treatment abortive, is it preventative, and if the patient has a concussion, is it a mild traumatic brain injury (TBI), or severe TBI?
The majority of patients with posttraumatic headache will meet criteria for migraine or probable migraine. “It can be anywhere from 58% to upwards of 90%. And if you see these patients, it makes sense, because posttraumatic headache patients are disabled by their headaches,” said Dr. Conidi, director of the Florida Center for Headache and Sports Neurology.
He argued for early treatment to reduce chronification. “We know that if headaches are left untreated, they’re going to start to spiral up and become daily. This leads to the development of peripheral and central sensitization and lowers the threshold for further migraine attacks,” said Dr. Conidi.
He noted that patients with posttraumatic headache often have comorbidities such as sleep issues, neck pain, or posttraumatic stress disorder, all of which are risk factors for chronification. Treatment does not necessarily mean medication, however. “The mainstay of posttraumatic headache treatment is actually physical and cognitive activity to tolerance. And what I call the 20/5 rule: 20 minutes of physical activity with 5-minute chill breaks. In addition, we use light sub-aerobic exercise 3 to 5 days out in concussion, [which] has been shown to improve concussion recovery time,” he said.
Dr. Conidi suggested treatment of triggers, such as neck issues and whiplash symptoms. “Probably the best treatment I’ve ever seen, and I published on this, are pericranial nerve blocks. Pericranial nerve blocks work wonderfully. If you’re going to block the pericranial nerves, block them all, not just the occipital. Block the trigeminal branches. I’ve actually been able to locate a little two-and-a-half-inch plastic Luer-lock catheter that I can hook on a 1-cc syringe with viscous lidocaine, and I can do sphenopalatine ganglion blocks on all my patients now for under 25 cents. So we’ve been combining the nerve blocks, and we’ve been using them early. Oftentimes the patients won’t have any further headaches, especially if it’s [after] a concussion,” he said.
With respect to concussion-related posttraumatic headache, he summed up: “We’re aggressive early. We’re using intervention. We’re layering our treatment. We’re using medications: prednisone, NSAIDS, and now we have gepants. We’ve been having good success with using gepants,” he said.
Treatment of TBI patients is broadly similar, with the main difference being that neurologists typically won’t see such patients early on as they may be in rehab facilities or hospitals for extended periods. “You may not be getting [to see] them for 1 or 2 months. In that case, you want to educate your neurosurgery and your [physical medicine and rehabilitation] colleagues on the treatment.
Finally, he described work that his group has done in using stimulants for posttraumatic headache. “Stimulants not only treat the cognitive symptoms, but they give the patient cognitive reserve and we find that it gets the patient through the day so they actually have less headaches. It’s a form of prevention. I know there are shortages nationally of both Adderall and Ritalin, but we have had excellent results in our posttraumatic patients using these types of medications,” said Dr. Conidi.
Delayed treatment
Amaal J. Starling, MD, offered a counterargument, but she narrowed the question down to whether preventive treatment should be used within one and a half months of the injury, which she defined as early treatment. Her argument against early preventive treatment centered around the core value of beneficence – to act for the benefit of the patient, and avoid harm.

She discussed the natural history of posttraumatic headache, which is largely self-limited. For example, an NCAA study that found 88% of concussions had symptom resolution within 1 week, and 86% of posttraumatic headache resolved within 1 week. “If individuals routinely are having a self-limited course, there is no need for early treatment with a preventive treatment option because the majority of posttraumatic headache is resolving within that one-and-a-half-month postinjury threshold. The better recommendation, as provided in evidence from Dr. Conidi’s presentation, is to provide supportive care, including acute medications or acute treatment options like nerve blocks for acute pain relief and symptom relief,” said Dr. Starling, associate professor of neurology at Mayo Clinic in Scottsdale, Ariz.
Dr. Starling expressed concern that preventive medications could lead to worsening of comorbidities. For example, posttraumatic headache is often associated with autonomic dysfunction and visual vestibular dysfunction. The former commonly occurs with concussion and is similar to postural orthostatic tachycardia syndrome (POTS), and the second most common symptom of POTS is headache, according to Dr. Starling. Posttraumatic POTS is treated similarly to idiopathic POTS, with a nonpharmacologic approach. One element of POTS management is to withdraw exacerbating medications such as beta-blockers, tricyclic antidepressants, and SNRIs. “These look strikingly similar to some of the headache preventive medications that we might consider for somebody, and so the concern is early preventive treatment with these medications to treat the posttraumatic headache may actually worsen some of these comorbidities that are present in our posttraumatic headache patients. We have to be careful about potentially exacerbating comorbidities with early preventive treatment,” she said.
Prevention medications for headache can also worsen visual vestibular dysfunction, such as dizziness. There are some data suggesting that vestibular rehabilitation and vision therapy can improve dizziness, but also headache. “We all know that many of our preventive medications for headache could potentially exacerbate visual vestibular symptoms, so we have to be careful about that. So again, first do no harm. Posttraumatic POTS is common and causes headache. Posttraumatic vestibular dysfunction is common and causes headache. Instead of initiating a headache preventive medication early, we recommend to identify these comorbidities and provide targeted treatment. Treatment of these comorbidities may, in and of itself, improve the headache. We also we have to be careful because some preventive medications may worsen the comorbidities,” said Dr. Starling.
Areas of agreement
Dr. Conidi agreed that preventative treatment is less likely to be needed for concussion patients, but said that TBI patients are more likely to require it to prevent chronification. Dr. Starling agreed that chronification is an important concern, but she noted that many posttraumatic headache patients are athletes, and preventative medications can also lead to issues that might interfere with return to play, such as decreased sweating, or weight gain or loss. This is complicated by the fact that titration and weaning periods can be long. “We have to be very careful about these medications’ side effects, especially when we don’t have the evidence to demonstrate that it is worth the potential risk of being put on these medications,” she said.
The debate led Catherin Chong, PhD, to ask about the state of the field. “There’s a posttraumatic headache special interest section here [at AHS 2023], and the question that really is coming up at every meeting is, is there some coherence in the field? Is it too early or is it time for a position statement?” asked Dr. Chong, a career scientist at Mayo Clinic (Phoenix). Dr. Chong comoderated the debate and ensuing discussion.
Dr. Starling felt it’s too early for a position statement, but a scoping review could identify research questions that could lead to a position statement. “I’m really excited about the work that’s being done to identify the cohort of individuals with acute posttraumatic headache that may chronify to persistent posttraumatic headache so that we can minimize the risk of exposing the large cohort that’s going to be likely self-limited to a treatment option. Then we can identify those individuals where that risk is worth it because they’re the ones that could lead to chronification. Figuring out if that’s looking at levels of allodynia or other factors that can [help identify those at most risk] would be important,” she said.
Dr. Conidi agreed with the need for more information on the parameters to be studied, but he expressed the belief that any position statement would be a consensus statement. “It’s not going to have any hard evidence behind it, but I do think we need [a position statement]. Even in the general neurology world, there’s a huge lack of understanding of how to treat these patients,” he said.
Dr. Conidi did not make any disclosures. Dr. Starling has consulted for AbbVie, Allergan, Amgen, Axsome Therapeutics, Everyday Health, Lundbeck, Med-IQ, Medscape, Neurolief, Satsuma, and WebMD. Dr. Chong has no relevant financial disclosures.
AUSTIN, TEX – There are no guidelines available, nor is there much quality evidence to support one decision or another, according to two experts who debated the question at the annual meeting of the American Headache Society.
Early treatment
Frank Conidi, DO, spoke first, and pointed out the need to define both early treatment and the condition being treated. Is it early-treatment abortive, is it preventative, and if the patient has a concussion, is it a mild traumatic brain injury (TBI), or severe TBI?
The majority of patients with posttraumatic headache will meet criteria for migraine or probable migraine. “It can be anywhere from 58% to upwards of 90%. And if you see these patients, it makes sense, because posttraumatic headache patients are disabled by their headaches,” said Dr. Conidi, director of the Florida Center for Headache and Sports Neurology.
He argued for early treatment to reduce chronification. “We know that if headaches are left untreated, they’re going to start to spiral up and become daily. This leads to the development of peripheral and central sensitization and lowers the threshold for further migraine attacks,” said Dr. Conidi.
He noted that patients with posttraumatic headache often have comorbidities such as sleep issues, neck pain, or posttraumatic stress disorder, all of which are risk factors for chronification. Treatment does not necessarily mean medication, however. “The mainstay of posttraumatic headache treatment is actually physical and cognitive activity to tolerance. And what I call the 20/5 rule: 20 minutes of physical activity with 5-minute chill breaks. In addition, we use light sub-aerobic exercise 3 to 5 days out in concussion, [which] has been shown to improve concussion recovery time,” he said.
Dr. Conidi suggested treatment of triggers, such as neck issues and whiplash symptoms. “Probably the best treatment I’ve ever seen, and I published on this, are pericranial nerve blocks. Pericranial nerve blocks work wonderfully. If you’re going to block the pericranial nerves, block them all, not just the occipital. Block the trigeminal branches. I’ve actually been able to locate a little two-and-a-half-inch plastic Luer-lock catheter that I can hook on a 1-cc syringe with viscous lidocaine, and I can do sphenopalatine ganglion blocks on all my patients now for under 25 cents. So we’ve been combining the nerve blocks, and we’ve been using them early. Oftentimes the patients won’t have any further headaches, especially if it’s [after] a concussion,” he said.
With respect to concussion-related posttraumatic headache, he summed up: “We’re aggressive early. We’re using intervention. We’re layering our treatment. We’re using medications: prednisone, NSAIDS, and now we have gepants. We’ve been having good success with using gepants,” he said.
Treatment of TBI patients is broadly similar, with the main difference being that neurologists typically won’t see such patients early on as they may be in rehab facilities or hospitals for extended periods. “You may not be getting [to see] them for 1 or 2 months. In that case, you want to educate your neurosurgery and your [physical medicine and rehabilitation] colleagues on the treatment.
Finally, he described work that his group has done in using stimulants for posttraumatic headache. “Stimulants not only treat the cognitive symptoms, but they give the patient cognitive reserve and we find that it gets the patient through the day so they actually have less headaches. It’s a form of prevention. I know there are shortages nationally of both Adderall and Ritalin, but we have had excellent results in our posttraumatic patients using these types of medications,” said Dr. Conidi.
Delayed treatment
Amaal J. Starling, MD, offered a counterargument, but she narrowed the question down to whether preventive treatment should be used within one and a half months of the injury, which she defined as early treatment. Her argument against early preventive treatment centered around the core value of beneficence – to act for the benefit of the patient, and avoid harm.
She discussed the natural history of posttraumatic headache, which is largely self-limited. For example, an NCAA study that found 88% of concussions had symptom resolution within 1 week, and 86% of posttraumatic headache resolved within 1 week. “If individuals routinely are having a self-limited course, there is no need for early treatment with a preventive treatment option because the majority of posttraumatic headache is resolving within that one-and-a-half-month postinjury threshold. The better recommendation, as provided in evidence from Dr. Conidi’s presentation, is to provide supportive care, including acute medications or acute treatment options like nerve blocks for acute pain relief and symptom relief,” said Dr. Starling, associate professor of neurology at Mayo Clinic in Scottsdale, Ariz.
Dr. Starling expressed concern that preventive medications could lead to worsening of comorbidities. For example, posttraumatic headache is often associated with autonomic dysfunction and visual vestibular dysfunction. The former commonly occurs with concussion and is similar to postural orthostatic tachycardia syndrome (POTS), and the second most common symptom of POTS is headache, according to Dr. Starling. Posttraumatic POTS is treated similarly to idiopathic POTS, with a nonpharmacologic approach. One element of POTS management is to withdraw exacerbating medications such as beta-blockers, tricyclic antidepressants, and SNRIs. “These look strikingly similar to some of the headache preventive medications that we might consider for somebody, and so the concern is early preventive treatment with these medications to treat the posttraumatic headache may actually worsen some of these comorbidities that are present in our posttraumatic headache patients. We have to be careful about potentially exacerbating comorbidities with early preventive treatment,” she said.
Prevention medications for headache can also worsen visual vestibular dysfunction, such as dizziness. There are some data suggesting that vestibular rehabilitation and vision therapy can improve dizziness, but also headache. “We all know that many of our preventive medications for headache could potentially exacerbate visual vestibular symptoms, so we have to be careful about that. So again, first do no harm. Posttraumatic POTS is common and causes headache. Posttraumatic vestibular dysfunction is common and causes headache. Instead of initiating a headache preventive medication early, we recommend to identify these comorbidities and provide targeted treatment. Treatment of these comorbidities may, in and of itself, improve the headache. We also we have to be careful because some preventive medications may worsen the comorbidities,” said Dr. Starling.
Areas of agreement
Dr. Conidi agreed that preventative treatment is less likely to be needed for concussion patients, but said that TBI patients are more likely to require it to prevent chronification. Dr. Starling agreed that chronification is an important concern, but she noted that many posttraumatic headache patients are athletes, and preventative medications can also lead to issues that might interfere with return to play, such as decreased sweating, or weight gain or loss. This is complicated by the fact that titration and weaning periods can be long. “We have to be very careful about these medications’ side effects, especially when we don’t have the evidence to demonstrate that it is worth the potential risk of being put on these medications,” she said.
The debate led Catherin Chong, PhD, to ask about the state of the field. “There’s a posttraumatic headache special interest section here [at AHS 2023], and the question that really is coming up at every meeting is, is there some coherence in the field? Is it too early or is it time for a position statement?” asked Dr. Chong, a career scientist at Mayo Clinic (Phoenix). Dr. Chong comoderated the debate and ensuing discussion.
Dr. Starling felt it’s too early for a position statement, but a scoping review could identify research questions that could lead to a position statement. “I’m really excited about the work that’s being done to identify the cohort of individuals with acute posttraumatic headache that may chronify to persistent posttraumatic headache so that we can minimize the risk of exposing the large cohort that’s going to be likely self-limited to a treatment option. Then we can identify those individuals where that risk is worth it because they’re the ones that could lead to chronification. Figuring out if that’s looking at levels of allodynia or other factors that can [help identify those at most risk] would be important,” she said.
Dr. Conidi agreed with the need for more information on the parameters to be studied, but he expressed the belief that any position statement would be a consensus statement. “It’s not going to have any hard evidence behind it, but I do think we need [a position statement]. Even in the general neurology world, there’s a huge lack of understanding of how to treat these patients,” he said.
Dr. Conidi did not make any disclosures. Dr. Starling has consulted for AbbVie, Allergan, Amgen, Axsome Therapeutics, Everyday Health, Lundbeck, Med-IQ, Medscape, Neurolief, Satsuma, and WebMD. Dr. Chong has no relevant financial disclosures.
AUSTIN, TEX – There are no guidelines available, nor is there much quality evidence to support one decision or another, according to two experts who debated the question at the annual meeting of the American Headache Society.
Early treatment
Frank Conidi, DO, spoke first, and pointed out the need to define both early treatment and the condition being treated. Is it early-treatment abortive, is it preventative, and if the patient has a concussion, is it a mild traumatic brain injury (TBI), or severe TBI?
The majority of patients with posttraumatic headache will meet criteria for migraine or probable migraine. “It can be anywhere from 58% to upwards of 90%. And if you see these patients, it makes sense, because posttraumatic headache patients are disabled by their headaches,” said Dr. Conidi, director of the Florida Center for Headache and Sports Neurology.
He argued for early treatment to reduce chronification. “We know that if headaches are left untreated, they’re going to start to spiral up and become daily. This leads to the development of peripheral and central sensitization and lowers the threshold for further migraine attacks,” said Dr. Conidi.
He noted that patients with posttraumatic headache often have comorbidities such as sleep issues, neck pain, or posttraumatic stress disorder, all of which are risk factors for chronification. Treatment does not necessarily mean medication, however. “The mainstay of posttraumatic headache treatment is actually physical and cognitive activity to tolerance. And what I call the 20/5 rule: 20 minutes of physical activity with 5-minute chill breaks. In addition, we use light sub-aerobic exercise 3 to 5 days out in concussion, [which] has been shown to improve concussion recovery time,” he said.
Dr. Conidi suggested treatment of triggers, such as neck issues and whiplash symptoms. “Probably the best treatment I’ve ever seen, and I published on this, are pericranial nerve blocks. Pericranial nerve blocks work wonderfully. If you’re going to block the pericranial nerves, block them all, not just the occipital. Block the trigeminal branches. I’ve actually been able to locate a little two-and-a-half-inch plastic Luer-lock catheter that I can hook on a 1-cc syringe with viscous lidocaine, and I can do sphenopalatine ganglion blocks on all my patients now for under 25 cents. So we’ve been combining the nerve blocks, and we’ve been using them early. Oftentimes the patients won’t have any further headaches, especially if it’s [after] a concussion,” he said.
With respect to concussion-related posttraumatic headache, he summed up: “We’re aggressive early. We’re using intervention. We’re layering our treatment. We’re using medications: prednisone, NSAIDS, and now we have gepants. We’ve been having good success with using gepants,” he said.
Treatment of TBI patients is broadly similar, with the main difference being that neurologists typically won’t see such patients early on as they may be in rehab facilities or hospitals for extended periods. “You may not be getting [to see] them for 1 or 2 months. In that case, you want to educate your neurosurgery and your [physical medicine and rehabilitation] colleagues on the treatment.
Finally, he described work that his group has done in using stimulants for posttraumatic headache. “Stimulants not only treat the cognitive symptoms, but they give the patient cognitive reserve and we find that it gets the patient through the day so they actually have less headaches. It’s a form of prevention. I know there are shortages nationally of both Adderall and Ritalin, but we have had excellent results in our posttraumatic patients using these types of medications,” said Dr. Conidi.
Delayed treatment
Amaal J. Starling, MD, offered a counterargument, but she narrowed the question down to whether preventive treatment should be used within one and a half months of the injury, which she defined as early treatment. Her argument against early preventive treatment centered around the core value of beneficence – to act for the benefit of the patient, and avoid harm.
She discussed the natural history of posttraumatic headache, which is largely self-limited. For example, an NCAA study that found 88% of concussions had symptom resolution within 1 week, and 86% of posttraumatic headache resolved within 1 week. “If individuals routinely are having a self-limited course, there is no need for early treatment with a preventive treatment option because the majority of posttraumatic headache is resolving within that one-and-a-half-month postinjury threshold. The better recommendation, as provided in evidence from Dr. Conidi’s presentation, is to provide supportive care, including acute medications or acute treatment options like nerve blocks for acute pain relief and symptom relief,” said Dr. Starling, associate professor of neurology at Mayo Clinic in Scottsdale, Ariz.
Dr. Starling expressed concern that preventive medications could lead to worsening of comorbidities. For example, posttraumatic headache is often associated with autonomic dysfunction and visual vestibular dysfunction. The former commonly occurs with concussion and is similar to postural orthostatic tachycardia syndrome (POTS), and the second most common symptom of POTS is headache, according to Dr. Starling. Posttraumatic POTS is treated similarly to idiopathic POTS, with a nonpharmacologic approach. One element of POTS management is to withdraw exacerbating medications such as beta-blockers, tricyclic antidepressants, and SNRIs. “These look strikingly similar to some of the headache preventive medications that we might consider for somebody, and so the concern is early preventive treatment with these medications to treat the posttraumatic headache may actually worsen some of these comorbidities that are present in our posttraumatic headache patients. We have to be careful about potentially exacerbating comorbidities with early preventive treatment,” she said.
Prevention medications for headache can also worsen visual vestibular dysfunction, such as dizziness. There are some data suggesting that vestibular rehabilitation and vision therapy can improve dizziness, but also headache. “We all know that many of our preventive medications for headache could potentially exacerbate visual vestibular symptoms, so we have to be careful about that. So again, first do no harm. Posttraumatic POTS is common and causes headache. Posttraumatic vestibular dysfunction is common and causes headache. Instead of initiating a headache preventive medication early, we recommend to identify these comorbidities and provide targeted treatment. Treatment of these comorbidities may, in and of itself, improve the headache. We also we have to be careful because some preventive medications may worsen the comorbidities,” said Dr. Starling.
Areas of agreement
Dr. Conidi agreed that preventative treatment is less likely to be needed for concussion patients, but said that TBI patients are more likely to require it to prevent chronification. Dr. Starling agreed that chronification is an important concern, but she noted that many posttraumatic headache patients are athletes, and preventative medications can also lead to issues that might interfere with return to play, such as decreased sweating, or weight gain or loss. This is complicated by the fact that titration and weaning periods can be long. “We have to be very careful about these medications’ side effects, especially when we don’t have the evidence to demonstrate that it is worth the potential risk of being put on these medications,” she said.
The debate led Catherin Chong, PhD, to ask about the state of the field. “There’s a posttraumatic headache special interest section here [at AHS 2023], and the question that really is coming up at every meeting is, is there some coherence in the field? Is it too early or is it time for a position statement?” asked Dr. Chong, a career scientist at Mayo Clinic (Phoenix). Dr. Chong comoderated the debate and ensuing discussion.
Dr. Starling felt it’s too early for a position statement, but a scoping review could identify research questions that could lead to a position statement. “I’m really excited about the work that’s being done to identify the cohort of individuals with acute posttraumatic headache that may chronify to persistent posttraumatic headache so that we can minimize the risk of exposing the large cohort that’s going to be likely self-limited to a treatment option. Then we can identify those individuals where that risk is worth it because they’re the ones that could lead to chronification. Figuring out if that’s looking at levels of allodynia or other factors that can [help identify those at most risk] would be important,” she said.
Dr. Conidi agreed with the need for more information on the parameters to be studied, but he expressed the belief that any position statement would be a consensus statement. “It’s not going to have any hard evidence behind it, but I do think we need [a position statement]. Even in the general neurology world, there’s a huge lack of understanding of how to treat these patients,” he said.
Dr. Conidi did not make any disclosures. Dr. Starling has consulted for AbbVie, Allergan, Amgen, Axsome Therapeutics, Everyday Health, Lundbeck, Med-IQ, Medscape, Neurolief, Satsuma, and WebMD. Dr. Chong has no relevant financial disclosures.
AT AHS 2023
Prodrome treatment with ubrogepant prevents migraines
AUSTIN, TEX – , according to results from a new randomized, crossover study. Researchers took pains to identify migraineurs who could predict an ensuing headache 75% of the time based on prodromal symptoms. Those who could make such predictions were allowed into the randomized study.
Patients are quite good at predicting ensuing headaches when encouraged to do so, according to Peter J. Goadsby, MBBS, MD, PhD, who presented the study findings at the annual meeting of the American Headache Society.

“I find it quite useful to ask patients about these [symptoms]: Have you got cognitive clouding? Do you pass more urine? Have you got mood change? Do you feel fatigue? Associated with the attack, is how I phrase it. Get them first into the idea of thinking about the symptoms, and then get them to think about when they’re occurring. Certainly with things like brain fog, many patients will tell you that it happens. If you ask them whether they’re 100% [certain] when that’s happening, they will tell you [they’re] not. This is part of taking a history and building a relationship with the patient,” Dr. Goadsby, professor of neurology at the University of California, Los Angeles, said during the Q&A after his presentation.
‘Significant’ finding
“This is a significant finding because what patients really want is not to develop their headache and no medication has been shown to prevent a headache during the prodrome,” said Alan M. Rapoport, MD, a board certified neurologist and headache expert, as well as clinical professor of neurology at the University of California, Los Angeles, and editor-in-chief of Neurology Reviews. Successful treatment during the prodrome treatment could eliminate the need for use of preventive medication, which might decrease the patient’s adverse effects, he said.
Session comoderator Jason J. Sico, MD, took note of the patient experience during the prodrome period. “One of many noteworthy things is the large percentage of people that reported disability during prodrome before the headache. I just find that staggering, though not surprising to many of us,” he said during the session. Dr. Sico is associate professor of neurology and internal medicine at Yale University, New Haven, Conn.
Dr. Rapoport and Dr. Sico were not involved in the study.
Probing the prodrome
The study included a 60-day screening period, which had to include between 3 and 16 recorded prodrome events. Headaches had to occur within 1-6 hours in at least 75% of prodrome events. Study subjects were then randomized to 100 mg ubrogepant or placebo for up to 60 days. After their first prodrome event, they entered a 7-day washout period, and then crossed over to the other group until they experienced a second prodrome event.
During the screening period, 81.5% of prodromal events identified by patients were followed by a headache within 1-6 hours of onset. Nearly 10% of the time headache occurred in 1 hour or less, 81.5% between 1 and 6 hours, and 4.5% between 6 and 24 hours after prodrome. Commonly reported prodromal symptoms included sensitivity to light (57.2%), fatigue (50.1%), neck pain (41.9%), sensitivity to sound (33.9%), and dizziness (27.8%).
The study included 247 patients in the first sequence, and 233 in the second sequence. Patient characteristics were similar in both. Ubrogepant treatment led to a greater absence of moderate- or severe-intensity headache within 24 hours of the dose (45.5% vs. 28.6% headache-free; odds ratio [OR], 2.09; P < .0001). They were also more likely to report normal functioning over 24 hours (OR, 1.66; P < .0001) and to have absence of headache within 24 hours (23.7% vs. 13.9%; OR, 1.93; P < .0001).
Between 73% and 75% of participants reported at least mild functional disability before taking medication. Two hours after a dose, ubrogepant led to a higher rate of normal functioning (37.0% vs. 26.1%; P < .001). Ubrogepant had a similar positive effect on sensitivity to light, fatigue, neck pain, sensitivity to sound, and dizziness. Adverse events were higher during ubrogepant treatment (13.2% vs. 9.1%), and included nausea, dizziness, fatigue, and somnolence, all of which were mild. “One is really scraping the barrel [to identify adverse events]. There were no serious adverse events,” said Dr. Goadsby.
A unique result?
One questioner asked if other medications used during the prodrome might yield similar results. Dr. Goadsby expressed doubt. “I think the evidence for other treatments is not terribly good. The triptan evidence is really poor. There is no randomized, placebo-controlled trial of a triptan explicitly in promontory symptomatology. There are randomized placebo controlled trials of triptans during the aura phase. The best one was the injected sumatriptan study, and it failed. So, as far as I can see from the randomized-controlled data, triptans don’t do this, and we don’t have good data for nonsteroidals and other therapies,” said Dr. Goadsby.
The researchers showed that you could treat a patient in advance of the headache to actually prevent the headache a significant number of times; it also reduced the prodromal events and it got patients back to normal functioning to a greater extent.
Dr. Goadsby was asked how many patients are typically able to identify prodrome periods on their own. He estimated that about one in three can do it initially. “I think if you teach people how to do this, it becomes very common. I would say four out of five people in my practice are able to talk about this, but you have to introduce the topic. They’ve had [prodrome symptoms], but they haven’t thought about it for a while. This is one of the things where headache doctors can offer real benefit in helping educate patients,” said Dr. Goadsby.
Dr. Sico did not disclose any conflicts of interest. Dr. Rapoport advises AbbVie, Biohaven, Cala Health, Dr. Reddy’s, Pfizer, Satsuma, Teva Pharmaceutical Industries, and Theranica. He is on the speakers bureau of AbbVie, Dr. Reddy’s, Impel, Pfizer and Teva Pharmaceutical Industries. He is editor-in-chief of Neurology Reviews and on the Editorial Board of CNS Drugs. Dr. Goadsby has financial ties to Amgen, Eli Lilly, Alder Biopharmaceuticals, Allergan, Autonomic Technologies Inc., Biohaven Pharmaceuticals Inc., Dr. Reddy’s Laboratories, Electrocore, eNeura, Massachusetts Medical Society, MedicoLegal work, Novartis, Oxford University Press, Teva Pharmaceuticals, Trigemina, Up-to-Date, and Wolters Kluwer. He has a patent for headache assigned to eNeura without fee.
AUSTIN, TEX – , according to results from a new randomized, crossover study. Researchers took pains to identify migraineurs who could predict an ensuing headache 75% of the time based on prodromal symptoms. Those who could make such predictions were allowed into the randomized study.
Patients are quite good at predicting ensuing headaches when encouraged to do so, according to Peter J. Goadsby, MBBS, MD, PhD, who presented the study findings at the annual meeting of the American Headache Society.
“I find it quite useful to ask patients about these [symptoms]: Have you got cognitive clouding? Do you pass more urine? Have you got mood change? Do you feel fatigue? Associated with the attack, is how I phrase it. Get them first into the idea of thinking about the symptoms, and then get them to think about when they’re occurring. Certainly with things like brain fog, many patients will tell you that it happens. If you ask them whether they’re 100% [certain] when that’s happening, they will tell you [they’re] not. This is part of taking a history and building a relationship with the patient,” Dr. Goadsby, professor of neurology at the University of California, Los Angeles, said during the Q&A after his presentation.
‘Significant’ finding
“This is a significant finding because what patients really want is not to develop their headache and no medication has been shown to prevent a headache during the prodrome,” said Alan M. Rapoport, MD, a board certified neurologist and headache expert, as well as clinical professor of neurology at the University of California, Los Angeles, and editor-in-chief of Neurology Reviews. Successful treatment during the prodrome treatment could eliminate the need for use of preventive medication, which might decrease the patient’s adverse effects, he said.
Session comoderator Jason J. Sico, MD, took note of the patient experience during the prodrome period. “One of many noteworthy things is the large percentage of people that reported disability during prodrome before the headache. I just find that staggering, though not surprising to many of us,” he said during the session. Dr. Sico is associate professor of neurology and internal medicine at Yale University, New Haven, Conn.
Dr. Rapoport and Dr. Sico were not involved in the study.
Probing the prodrome
The study included a 60-day screening period, which had to include between 3 and 16 recorded prodrome events. Headaches had to occur within 1-6 hours in at least 75% of prodrome events. Study subjects were then randomized to 100 mg ubrogepant or placebo for up to 60 days. After their first prodrome event, they entered a 7-day washout period, and then crossed over to the other group until they experienced a second prodrome event.
During the screening period, 81.5% of prodromal events identified by patients were followed by a headache within 1-6 hours of onset. Nearly 10% of the time headache occurred in 1 hour or less, 81.5% between 1 and 6 hours, and 4.5% between 6 and 24 hours after prodrome. Commonly reported prodromal symptoms included sensitivity to light (57.2%), fatigue (50.1%), neck pain (41.9%), sensitivity to sound (33.9%), and dizziness (27.8%).
The study included 247 patients in the first sequence, and 233 in the second sequence. Patient characteristics were similar in both. Ubrogepant treatment led to a greater absence of moderate- or severe-intensity headache within 24 hours of the dose (45.5% vs. 28.6% headache-free; odds ratio [OR], 2.09; P < .0001). They were also more likely to report normal functioning over 24 hours (OR, 1.66; P < .0001) and to have absence of headache within 24 hours (23.7% vs. 13.9%; OR, 1.93; P < .0001).
Between 73% and 75% of participants reported at least mild functional disability before taking medication. Two hours after a dose, ubrogepant led to a higher rate of normal functioning (37.0% vs. 26.1%; P < .001). Ubrogepant had a similar positive effect on sensitivity to light, fatigue, neck pain, sensitivity to sound, and dizziness. Adverse events were higher during ubrogepant treatment (13.2% vs. 9.1%), and included nausea, dizziness, fatigue, and somnolence, all of which were mild. “One is really scraping the barrel [to identify adverse events]. There were no serious adverse events,” said Dr. Goadsby.
A unique result?
One questioner asked if other medications used during the prodrome might yield similar results. Dr. Goadsby expressed doubt. “I think the evidence for other treatments is not terribly good. The triptan evidence is really poor. There is no randomized, placebo-controlled trial of a triptan explicitly in promontory symptomatology. There are randomized placebo controlled trials of triptans during the aura phase. The best one was the injected sumatriptan study, and it failed. So, as far as I can see from the randomized-controlled data, triptans don’t do this, and we don’t have good data for nonsteroidals and other therapies,” said Dr. Goadsby.
The researchers showed that you could treat a patient in advance of the headache to actually prevent the headache a significant number of times; it also reduced the prodromal events and it got patients back to normal functioning to a greater extent.
Dr. Goadsby was asked how many patients are typically able to identify prodrome periods on their own. He estimated that about one in three can do it initially. “I think if you teach people how to do this, it becomes very common. I would say four out of five people in my practice are able to talk about this, but you have to introduce the topic. They’ve had [prodrome symptoms], but they haven’t thought about it for a while. This is one of the things where headache doctors can offer real benefit in helping educate patients,” said Dr. Goadsby.
Dr. Sico did not disclose any conflicts of interest. Dr. Rapoport advises AbbVie, Biohaven, Cala Health, Dr. Reddy’s, Pfizer, Satsuma, Teva Pharmaceutical Industries, and Theranica. He is on the speakers bureau of AbbVie, Dr. Reddy’s, Impel, Pfizer and Teva Pharmaceutical Industries. He is editor-in-chief of Neurology Reviews and on the Editorial Board of CNS Drugs. Dr. Goadsby has financial ties to Amgen, Eli Lilly, Alder Biopharmaceuticals, Allergan, Autonomic Technologies Inc., Biohaven Pharmaceuticals Inc., Dr. Reddy’s Laboratories, Electrocore, eNeura, Massachusetts Medical Society, MedicoLegal work, Novartis, Oxford University Press, Teva Pharmaceuticals, Trigemina, Up-to-Date, and Wolters Kluwer. He has a patent for headache assigned to eNeura without fee.
AUSTIN, TEX – , according to results from a new randomized, crossover study. Researchers took pains to identify migraineurs who could predict an ensuing headache 75% of the time based on prodromal symptoms. Those who could make such predictions were allowed into the randomized study.
Patients are quite good at predicting ensuing headaches when encouraged to do so, according to Peter J. Goadsby, MBBS, MD, PhD, who presented the study findings at the annual meeting of the American Headache Society.
“I find it quite useful to ask patients about these [symptoms]: Have you got cognitive clouding? Do you pass more urine? Have you got mood change? Do you feel fatigue? Associated with the attack, is how I phrase it. Get them first into the idea of thinking about the symptoms, and then get them to think about when they’re occurring. Certainly with things like brain fog, many patients will tell you that it happens. If you ask them whether they’re 100% [certain] when that’s happening, they will tell you [they’re] not. This is part of taking a history and building a relationship with the patient,” Dr. Goadsby, professor of neurology at the University of California, Los Angeles, said during the Q&A after his presentation.
‘Significant’ finding
“This is a significant finding because what patients really want is not to develop their headache and no medication has been shown to prevent a headache during the prodrome,” said Alan M. Rapoport, MD, a board certified neurologist and headache expert, as well as clinical professor of neurology at the University of California, Los Angeles, and editor-in-chief of Neurology Reviews. Successful treatment during the prodrome treatment could eliminate the need for use of preventive medication, which might decrease the patient’s adverse effects, he said.
Session comoderator Jason J. Sico, MD, took note of the patient experience during the prodrome period. “One of many noteworthy things is the large percentage of people that reported disability during prodrome before the headache. I just find that staggering, though not surprising to many of us,” he said during the session. Dr. Sico is associate professor of neurology and internal medicine at Yale University, New Haven, Conn.
Dr. Rapoport and Dr. Sico were not involved in the study.
Probing the prodrome
The study included a 60-day screening period, which had to include between 3 and 16 recorded prodrome events. Headaches had to occur within 1-6 hours in at least 75% of prodrome events. Study subjects were then randomized to 100 mg ubrogepant or placebo for up to 60 days. After their first prodrome event, they entered a 7-day washout period, and then crossed over to the other group until they experienced a second prodrome event.
During the screening period, 81.5% of prodromal events identified by patients were followed by a headache within 1-6 hours of onset. Nearly 10% of the time headache occurred in 1 hour or less, 81.5% between 1 and 6 hours, and 4.5% between 6 and 24 hours after prodrome. Commonly reported prodromal symptoms included sensitivity to light (57.2%), fatigue (50.1%), neck pain (41.9%), sensitivity to sound (33.9%), and dizziness (27.8%).
The study included 247 patients in the first sequence, and 233 in the second sequence. Patient characteristics were similar in both. Ubrogepant treatment led to a greater absence of moderate- or severe-intensity headache within 24 hours of the dose (45.5% vs. 28.6% headache-free; odds ratio [OR], 2.09; P < .0001). They were also more likely to report normal functioning over 24 hours (OR, 1.66; P < .0001) and to have absence of headache within 24 hours (23.7% vs. 13.9%; OR, 1.93; P < .0001).
Between 73% and 75% of participants reported at least mild functional disability before taking medication. Two hours after a dose, ubrogepant led to a higher rate of normal functioning (37.0% vs. 26.1%; P < .001). Ubrogepant had a similar positive effect on sensitivity to light, fatigue, neck pain, sensitivity to sound, and dizziness. Adverse events were higher during ubrogepant treatment (13.2% vs. 9.1%), and included nausea, dizziness, fatigue, and somnolence, all of which were mild. “One is really scraping the barrel [to identify adverse events]. There were no serious adverse events,” said Dr. Goadsby.
A unique result?
One questioner asked if other medications used during the prodrome might yield similar results. Dr. Goadsby expressed doubt. “I think the evidence for other treatments is not terribly good. The triptan evidence is really poor. There is no randomized, placebo-controlled trial of a triptan explicitly in promontory symptomatology. There are randomized placebo controlled trials of triptans during the aura phase. The best one was the injected sumatriptan study, and it failed. So, as far as I can see from the randomized-controlled data, triptans don’t do this, and we don’t have good data for nonsteroidals and other therapies,” said Dr. Goadsby.
The researchers showed that you could treat a patient in advance of the headache to actually prevent the headache a significant number of times; it also reduced the prodromal events and it got patients back to normal functioning to a greater extent.
Dr. Goadsby was asked how many patients are typically able to identify prodrome periods on their own. He estimated that about one in three can do it initially. “I think if you teach people how to do this, it becomes very common. I would say four out of five people in my practice are able to talk about this, but you have to introduce the topic. They’ve had [prodrome symptoms], but they haven’t thought about it for a while. This is one of the things where headache doctors can offer real benefit in helping educate patients,” said Dr. Goadsby.
Dr. Sico did not disclose any conflicts of interest. Dr. Rapoport advises AbbVie, Biohaven, Cala Health, Dr. Reddy’s, Pfizer, Satsuma, Teva Pharmaceutical Industries, and Theranica. He is on the speakers bureau of AbbVie, Dr. Reddy’s, Impel, Pfizer and Teva Pharmaceutical Industries. He is editor-in-chief of Neurology Reviews and on the Editorial Board of CNS Drugs. Dr. Goadsby has financial ties to Amgen, Eli Lilly, Alder Biopharmaceuticals, Allergan, Autonomic Technologies Inc., Biohaven Pharmaceuticals Inc., Dr. Reddy’s Laboratories, Electrocore, eNeura, Massachusetts Medical Society, MedicoLegal work, Novartis, Oxford University Press, Teva Pharmaceuticals, Trigemina, Up-to-Date, and Wolters Kluwer. He has a patent for headache assigned to eNeura without fee.
FROM AHS 2023
Medical cannabis does not reduce use of prescription meds
TOPLINE:
, according to a new study published in Annals of Internal Medicine.
METHODOLOGY:
- Cannabis advocates suggest that legal medical cannabis can be a partial solution to the opioid overdose crisis in the United States, which claimed more than 80,000 lives in 2021.
- Current research on how legalized cannabis reduces dependence on prescription pain medication is inconclusive.
- Researchers examined insurance data for the period 2010-2022 from 583,820 adults with chronic noncancer pain.
- They drew from 12 states in which medical cannabis is legal and from 17 in which it is not legal to create a hypothetical randomized trial. The control group simulated prescription rates where medical cannabis was not available.
- Authors evaluated prescription rates for opioids, nonopioid painkillers, and pain interventions, such as physical therapy.
TAKEAWAY:
In a given month during the first 3 years after legalization, for states with medical cannabis, the investigators found the following:
- There was an average decrease of 1.07 percentage points in the proportion of patients who received any opioid prescription, compared to a 1.12 percentage point decrease in the control group.
- There was an average increase of 1.14 percentage points in the proportion of patients who received any nonopioid prescription painkiller, compared to a 1.19 percentage point increase in the control group.
- There was a 0.17 percentage point decrease in the proportion of patients who received any pain procedure, compared to a 0.001 percentage point decrease in the control group.
IN PRACTICE:
“This study did not identify important effects of medical cannabis laws on receipt of opioid or nonopioid pain treatment among patients with chronic noncancer pain,” according to the researchers.
SOURCE:
The study was led by Emma E. McGinty, PhD, of Weill Cornell Medicine, New York, and was funded by the National Institute on Drug Abuse.
LIMITATIONS:
The investigators used a simulated, hypothetical control group that was based on untestable assumptions. They also drew data solely from insured individuals, so the study does not necessarily represent uninsured populations.
DISCLOSURES:
Dr. McGinty reports receiving a grant from NIDA. Her coauthors reported receiving support from NIDA and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
TOPLINE:
, according to a new study published in Annals of Internal Medicine.
METHODOLOGY:
- Cannabis advocates suggest that legal medical cannabis can be a partial solution to the opioid overdose crisis in the United States, which claimed more than 80,000 lives in 2021.
- Current research on how legalized cannabis reduces dependence on prescription pain medication is inconclusive.
- Researchers examined insurance data for the period 2010-2022 from 583,820 adults with chronic noncancer pain.
- They drew from 12 states in which medical cannabis is legal and from 17 in which it is not legal to create a hypothetical randomized trial. The control group simulated prescription rates where medical cannabis was not available.
- Authors evaluated prescription rates for opioids, nonopioid painkillers, and pain interventions, such as physical therapy.
TAKEAWAY:
In a given month during the first 3 years after legalization, for states with medical cannabis, the investigators found the following:
- There was an average decrease of 1.07 percentage points in the proportion of patients who received any opioid prescription, compared to a 1.12 percentage point decrease in the control group.
- There was an average increase of 1.14 percentage points in the proportion of patients who received any nonopioid prescription painkiller, compared to a 1.19 percentage point increase in the control group.
- There was a 0.17 percentage point decrease in the proportion of patients who received any pain procedure, compared to a 0.001 percentage point decrease in the control group.
IN PRACTICE:
“This study did not identify important effects of medical cannabis laws on receipt of opioid or nonopioid pain treatment among patients with chronic noncancer pain,” according to the researchers.
SOURCE:
The study was led by Emma E. McGinty, PhD, of Weill Cornell Medicine, New York, and was funded by the National Institute on Drug Abuse.
LIMITATIONS:
The investigators used a simulated, hypothetical control group that was based on untestable assumptions. They also drew data solely from insured individuals, so the study does not necessarily represent uninsured populations.
DISCLOSURES:
Dr. McGinty reports receiving a grant from NIDA. Her coauthors reported receiving support from NIDA and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
TOPLINE:
, according to a new study published in Annals of Internal Medicine.
METHODOLOGY:
- Cannabis advocates suggest that legal medical cannabis can be a partial solution to the opioid overdose crisis in the United States, which claimed more than 80,000 lives in 2021.
- Current research on how legalized cannabis reduces dependence on prescription pain medication is inconclusive.
- Researchers examined insurance data for the period 2010-2022 from 583,820 adults with chronic noncancer pain.
- They drew from 12 states in which medical cannabis is legal and from 17 in which it is not legal to create a hypothetical randomized trial. The control group simulated prescription rates where medical cannabis was not available.
- Authors evaluated prescription rates for opioids, nonopioid painkillers, and pain interventions, such as physical therapy.
TAKEAWAY:
In a given month during the first 3 years after legalization, for states with medical cannabis, the investigators found the following:
- There was an average decrease of 1.07 percentage points in the proportion of patients who received any opioid prescription, compared to a 1.12 percentage point decrease in the control group.
- There was an average increase of 1.14 percentage points in the proportion of patients who received any nonopioid prescription painkiller, compared to a 1.19 percentage point increase in the control group.
- There was a 0.17 percentage point decrease in the proportion of patients who received any pain procedure, compared to a 0.001 percentage point decrease in the control group.
IN PRACTICE:
“This study did not identify important effects of medical cannabis laws on receipt of opioid or nonopioid pain treatment among patients with chronic noncancer pain,” according to the researchers.
SOURCE:
The study was led by Emma E. McGinty, PhD, of Weill Cornell Medicine, New York, and was funded by the National Institute on Drug Abuse.
LIMITATIONS:
The investigators used a simulated, hypothetical control group that was based on untestable assumptions. They also drew data solely from insured individuals, so the study does not necessarily represent uninsured populations.
DISCLOSURES:
Dr. McGinty reports receiving a grant from NIDA. Her coauthors reported receiving support from NIDA and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
Lean muscle mass protective against Alzheimer’s?
Investigators analyzed data on more than 450,000 participants in the UK Biobank as well as two independent samples of more than 320,000 individuals with and without AD, and more than 260,000 individuals participating in a separate genes and intelligence study.
They estimated lean muscle and fat tissue in the arms and legs and found, in adjusted analyses, over 500 genetic variants associated with lean mass.
On average, higher genetically lean mass was associated with a “modest but statistically robust” reduction in AD risk and with superior performance on cognitive tasks.
“Using human genetic data, we found evidence for a protective effect of lean mass on risk of Alzheimer’s disease,” study investigators Iyas Daghlas, MD, a resident in the department of neurology, University of California, San Francisco, said in an interview.
Although “clinical intervention studies are needed to confirm this effect, this study supports current recommendations to maintain a healthy lifestyle to prevent dementia,” he said.
The study was published online in BMJ Medicine.
Naturally randomized research
Several measures of body composition have been investigated for their potential association with AD. Lean mass – a “proxy for muscle mass, defined as the difference between total mass and fat mass” – has been shown to be reduced in patients with AD compared with controls, the researchers noted.
“Previous research studies have tested the relationship of body mass index with Alzheimer’s disease and did not find evidence for a causal effect,” Dr. Daghlas said. “We wondered whether BMI was an insufficiently granular measure and hypothesized that disaggregating body mass into lean mass and fat mass could reveal novel associations with disease.”
Most studies have used case-control designs, which might be biased by “residual confounding or reverse causality.” Naturally randomized data “may be used as an alternative to conventional observational studies to investigate causal relations between risk factors and diseases,” the researchers wrote.
In particular, the Mendelian randomization (MR) paradigm randomly allocates germline genetic variants and uses them as proxies for a specific risk factor.
MR “is a technique that permits researchers to investigate cause-and-effect relationships using human genetic data,” Dr. Daghlas explained. “In effect, we’re studying the results of a naturally randomized experiment whereby some individuals are genetically allocated to carry more lean mass.”
The current study used MR to investigate the effect of genetically proxied lean mass on the risk of AD and the “related phenotype” of cognitive performance.
Genetic proxy
As genetic proxies for lean mass, the researchers chose single nucleotide polymorphisms (genetic variants) that were associated, in a genome-wide association study (GWAS), with appendicular lean mass.
Appendicular lean mass “more accurately reflects the effects of lean mass than whole body lean mass, which includes smooth and cardiac muscle,” the authors explained.
This GWAS used phenotypic and genetic data from 450,243 participants in the UK Biobank cohort (mean age 57 years). All participants were of European ancestry.
The researchers adjusted for age, sex, and genetic ancestry. They measured appendicular lean mass using bioimpedance – an electric current that flows at different rates through the body, depending on its composition.
In addition to the UK Biobank participants, the researchers drew on an independent sample of 21,982 people with AD; a control group of 41,944 people without AD; a replication sample of 7,329 people with and 252,879 people without AD to validate the findings; and 269,867 people taking part in a genome-wide study of cognitive performance.
The researchers identified 584 variants that met criteria for use as genetic proxies for lean mass. None were located within the APOE gene region. In the aggregate, these variants explained 10.3% of the variance in appendicular lean mass.
Each standard deviation increase in genetically proxied lean mass was associated with a 12% reduction in AD risk (odds ratio [OR], 0.88; 95% confidence interval [CI], 0.82-0.95; P < .001). This finding was replicated in the independent consortium (OR, 0.91; 95% CI, 0.83-0.99; P = .02).
The findings remained “consistent” in sensitivity analyses.
A modifiable risk factor?
Higher appendicular lean mass was associated with higher levels of cognitive performance, with each SD increase in lean mass associated with an SD increase in cognitive performance (OR, 0.09; 95% CI, 0.06-0.11; P = .001).
“Adjusting for potential mediation through performance did not reduce the association between appendicular lean mass and risk of AD,” the authors wrote.
They obtained similar results using genetically proxied trunk and whole-body lean mass, after adjusting for fat mass.
The authors noted several limitations. The bioimpedance measures “only predict, but do not directly measure, lean mass.” Moreover, the approach didn’t examine whether a “critical window of risk factor timing” exists, during which lean mass might play a role in influencing AD risk and after which “interventions would no longer be effective.” Nor could the study determine whether increasing lean mass could reverse AD pathology in patients with preclinical disease or mild cognitive impairment.
Nevertheless, the findings suggest “that lean mass might be a possible modifiable protective factor for Alzheimer’s disease,” the authors wrote. “The mechanisms underlying this finding, as well as the clinical and public health implications, warrant further investigation.”
Novel strategies
In a comment, Iva Miljkovic, MD, PhD, associate professor, department of epidemiology, University of Pittsburgh, said the investigators used “very rigorous methodology.”
The finding suggesting that lean mass is associated with better cognitive function is “important, as cognitive impairment can become stable rather than progress to a pathological state; and, in some cases, can even be reversed.”
In those cases, “identifying the underlying cause – e.g., low lean mass – can significantly improve cognitive function,” said Dr. Miljkovic, senior author of a study showing muscle fat as a risk factor for cognitive decline.
More research will enable us to “expand our understanding” of the mechanisms involved and determine whether interventions aimed at preventing muscle loss and/or increasing muscle fat may have a beneficial effect on cognitive function,” she said. “This might lead to novel strategies to prevent AD.”
Dr. Daghlas is supported by the British Heart Foundation Centre of Research Excellence at Imperial College, London, and is employed part-time by Novo Nordisk. Dr. Miljkovic reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators analyzed data on more than 450,000 participants in the UK Biobank as well as two independent samples of more than 320,000 individuals with and without AD, and more than 260,000 individuals participating in a separate genes and intelligence study.
They estimated lean muscle and fat tissue in the arms and legs and found, in adjusted analyses, over 500 genetic variants associated with lean mass.
On average, higher genetically lean mass was associated with a “modest but statistically robust” reduction in AD risk and with superior performance on cognitive tasks.
“Using human genetic data, we found evidence for a protective effect of lean mass on risk of Alzheimer’s disease,” study investigators Iyas Daghlas, MD, a resident in the department of neurology, University of California, San Francisco, said in an interview.
Although “clinical intervention studies are needed to confirm this effect, this study supports current recommendations to maintain a healthy lifestyle to prevent dementia,” he said.
The study was published online in BMJ Medicine.
Naturally randomized research
Several measures of body composition have been investigated for their potential association with AD. Lean mass – a “proxy for muscle mass, defined as the difference between total mass and fat mass” – has been shown to be reduced in patients with AD compared with controls, the researchers noted.
“Previous research studies have tested the relationship of body mass index with Alzheimer’s disease and did not find evidence for a causal effect,” Dr. Daghlas said. “We wondered whether BMI was an insufficiently granular measure and hypothesized that disaggregating body mass into lean mass and fat mass could reveal novel associations with disease.”
Most studies have used case-control designs, which might be biased by “residual confounding or reverse causality.” Naturally randomized data “may be used as an alternative to conventional observational studies to investigate causal relations between risk factors and diseases,” the researchers wrote.
In particular, the Mendelian randomization (MR) paradigm randomly allocates germline genetic variants and uses them as proxies for a specific risk factor.
MR “is a technique that permits researchers to investigate cause-and-effect relationships using human genetic data,” Dr. Daghlas explained. “In effect, we’re studying the results of a naturally randomized experiment whereby some individuals are genetically allocated to carry more lean mass.”
The current study used MR to investigate the effect of genetically proxied lean mass on the risk of AD and the “related phenotype” of cognitive performance.
Genetic proxy
As genetic proxies for lean mass, the researchers chose single nucleotide polymorphisms (genetic variants) that were associated, in a genome-wide association study (GWAS), with appendicular lean mass.
Appendicular lean mass “more accurately reflects the effects of lean mass than whole body lean mass, which includes smooth and cardiac muscle,” the authors explained.
This GWAS used phenotypic and genetic data from 450,243 participants in the UK Biobank cohort (mean age 57 years). All participants were of European ancestry.
The researchers adjusted for age, sex, and genetic ancestry. They measured appendicular lean mass using bioimpedance – an electric current that flows at different rates through the body, depending on its composition.
In addition to the UK Biobank participants, the researchers drew on an independent sample of 21,982 people with AD; a control group of 41,944 people without AD; a replication sample of 7,329 people with and 252,879 people without AD to validate the findings; and 269,867 people taking part in a genome-wide study of cognitive performance.
The researchers identified 584 variants that met criteria for use as genetic proxies for lean mass. None were located within the APOE gene region. In the aggregate, these variants explained 10.3% of the variance in appendicular lean mass.
Each standard deviation increase in genetically proxied lean mass was associated with a 12% reduction in AD risk (odds ratio [OR], 0.88; 95% confidence interval [CI], 0.82-0.95; P < .001). This finding was replicated in the independent consortium (OR, 0.91; 95% CI, 0.83-0.99; P = .02).
The findings remained “consistent” in sensitivity analyses.
A modifiable risk factor?
Higher appendicular lean mass was associated with higher levels of cognitive performance, with each SD increase in lean mass associated with an SD increase in cognitive performance (OR, 0.09; 95% CI, 0.06-0.11; P = .001).
“Adjusting for potential mediation through performance did not reduce the association between appendicular lean mass and risk of AD,” the authors wrote.
They obtained similar results using genetically proxied trunk and whole-body lean mass, after adjusting for fat mass.
The authors noted several limitations. The bioimpedance measures “only predict, but do not directly measure, lean mass.” Moreover, the approach didn’t examine whether a “critical window of risk factor timing” exists, during which lean mass might play a role in influencing AD risk and after which “interventions would no longer be effective.” Nor could the study determine whether increasing lean mass could reverse AD pathology in patients with preclinical disease or mild cognitive impairment.
Nevertheless, the findings suggest “that lean mass might be a possible modifiable protective factor for Alzheimer’s disease,” the authors wrote. “The mechanisms underlying this finding, as well as the clinical and public health implications, warrant further investigation.”
Novel strategies
In a comment, Iva Miljkovic, MD, PhD, associate professor, department of epidemiology, University of Pittsburgh, said the investigators used “very rigorous methodology.”
The finding suggesting that lean mass is associated with better cognitive function is “important, as cognitive impairment can become stable rather than progress to a pathological state; and, in some cases, can even be reversed.”
In those cases, “identifying the underlying cause – e.g., low lean mass – can significantly improve cognitive function,” said Dr. Miljkovic, senior author of a study showing muscle fat as a risk factor for cognitive decline.
More research will enable us to “expand our understanding” of the mechanisms involved and determine whether interventions aimed at preventing muscle loss and/or increasing muscle fat may have a beneficial effect on cognitive function,” she said. “This might lead to novel strategies to prevent AD.”
Dr. Daghlas is supported by the British Heart Foundation Centre of Research Excellence at Imperial College, London, and is employed part-time by Novo Nordisk. Dr. Miljkovic reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators analyzed data on more than 450,000 participants in the UK Biobank as well as two independent samples of more than 320,000 individuals with and without AD, and more than 260,000 individuals participating in a separate genes and intelligence study.
They estimated lean muscle and fat tissue in the arms and legs and found, in adjusted analyses, over 500 genetic variants associated with lean mass.
On average, higher genetically lean mass was associated with a “modest but statistically robust” reduction in AD risk and with superior performance on cognitive tasks.
“Using human genetic data, we found evidence for a protective effect of lean mass on risk of Alzheimer’s disease,” study investigators Iyas Daghlas, MD, a resident in the department of neurology, University of California, San Francisco, said in an interview.
Although “clinical intervention studies are needed to confirm this effect, this study supports current recommendations to maintain a healthy lifestyle to prevent dementia,” he said.
The study was published online in BMJ Medicine.
Naturally randomized research
Several measures of body composition have been investigated for their potential association with AD. Lean mass – a “proxy for muscle mass, defined as the difference between total mass and fat mass” – has been shown to be reduced in patients with AD compared with controls, the researchers noted.
“Previous research studies have tested the relationship of body mass index with Alzheimer’s disease and did not find evidence for a causal effect,” Dr. Daghlas said. “We wondered whether BMI was an insufficiently granular measure and hypothesized that disaggregating body mass into lean mass and fat mass could reveal novel associations with disease.”
Most studies have used case-control designs, which might be biased by “residual confounding or reverse causality.” Naturally randomized data “may be used as an alternative to conventional observational studies to investigate causal relations between risk factors and diseases,” the researchers wrote.
In particular, the Mendelian randomization (MR) paradigm randomly allocates germline genetic variants and uses them as proxies for a specific risk factor.
MR “is a technique that permits researchers to investigate cause-and-effect relationships using human genetic data,” Dr. Daghlas explained. “In effect, we’re studying the results of a naturally randomized experiment whereby some individuals are genetically allocated to carry more lean mass.”
The current study used MR to investigate the effect of genetically proxied lean mass on the risk of AD and the “related phenotype” of cognitive performance.
Genetic proxy
As genetic proxies for lean mass, the researchers chose single nucleotide polymorphisms (genetic variants) that were associated, in a genome-wide association study (GWAS), with appendicular lean mass.
Appendicular lean mass “more accurately reflects the effects of lean mass than whole body lean mass, which includes smooth and cardiac muscle,” the authors explained.
This GWAS used phenotypic and genetic data from 450,243 participants in the UK Biobank cohort (mean age 57 years). All participants were of European ancestry.
The researchers adjusted for age, sex, and genetic ancestry. They measured appendicular lean mass using bioimpedance – an electric current that flows at different rates through the body, depending on its composition.
In addition to the UK Biobank participants, the researchers drew on an independent sample of 21,982 people with AD; a control group of 41,944 people without AD; a replication sample of 7,329 people with and 252,879 people without AD to validate the findings; and 269,867 people taking part in a genome-wide study of cognitive performance.
The researchers identified 584 variants that met criteria for use as genetic proxies for lean mass. None were located within the APOE gene region. In the aggregate, these variants explained 10.3% of the variance in appendicular lean mass.
Each standard deviation increase in genetically proxied lean mass was associated with a 12% reduction in AD risk (odds ratio [OR], 0.88; 95% confidence interval [CI], 0.82-0.95; P < .001). This finding was replicated in the independent consortium (OR, 0.91; 95% CI, 0.83-0.99; P = .02).
The findings remained “consistent” in sensitivity analyses.
A modifiable risk factor?
Higher appendicular lean mass was associated with higher levels of cognitive performance, with each SD increase in lean mass associated with an SD increase in cognitive performance (OR, 0.09; 95% CI, 0.06-0.11; P = .001).
“Adjusting for potential mediation through performance did not reduce the association between appendicular lean mass and risk of AD,” the authors wrote.
They obtained similar results using genetically proxied trunk and whole-body lean mass, after adjusting for fat mass.
The authors noted several limitations. The bioimpedance measures “only predict, but do not directly measure, lean mass.” Moreover, the approach didn’t examine whether a “critical window of risk factor timing” exists, during which lean mass might play a role in influencing AD risk and after which “interventions would no longer be effective.” Nor could the study determine whether increasing lean mass could reverse AD pathology in patients with preclinical disease or mild cognitive impairment.
Nevertheless, the findings suggest “that lean mass might be a possible modifiable protective factor for Alzheimer’s disease,” the authors wrote. “The mechanisms underlying this finding, as well as the clinical and public health implications, warrant further investigation.”
Novel strategies
In a comment, Iva Miljkovic, MD, PhD, associate professor, department of epidemiology, University of Pittsburgh, said the investigators used “very rigorous methodology.”
The finding suggesting that lean mass is associated with better cognitive function is “important, as cognitive impairment can become stable rather than progress to a pathological state; and, in some cases, can even be reversed.”
In those cases, “identifying the underlying cause – e.g., low lean mass – can significantly improve cognitive function,” said Dr. Miljkovic, senior author of a study showing muscle fat as a risk factor for cognitive decline.
More research will enable us to “expand our understanding” of the mechanisms involved and determine whether interventions aimed at preventing muscle loss and/or increasing muscle fat may have a beneficial effect on cognitive function,” she said. “This might lead to novel strategies to prevent AD.”
Dr. Daghlas is supported by the British Heart Foundation Centre of Research Excellence at Imperial College, London, and is employed part-time by Novo Nordisk. Dr. Miljkovic reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM BMJ MEDICINE
Med students, doctor groups react to SCOTUS affirmative action ban
The U.S. Supreme Court ruled on June 29 that using race as a factor in college admissions is unconstitutional, rolling back more than 40 years of affirmative action standards and changing how medical schools evaluate applicants to attract students from diverse backgrounds.
Jesse M. Ehrenfeld, MD, MPH, president of the American Medical Association, said in a prepared statement that the Supreme Court ruling will result in a less diverse physician workforce, which is “bad for health care, bad for medicine, and undermines the health of our nation.” He cited the AMA’s recent adoption of a policy advising medical schools to increase enrollment of people from racial and ethnic groups traditionally underrepresented in medicine – even if that means considering race as a factor in admissions criteria.
“Supporting racial and ethnic diversity in the health professions – spanning classrooms, labs, and clinical settings – enriches the educational experiences of all medical and health professions students and the teaching experiences of faculty, and it is essential to improving the overall health of our nation,” the Association of American Medical Colleges (AAMC) said in a prepared statement.
The American Medical Student Association also denounced the Supreme Court decision. “As future physicians committed to justice and equality, we are profoundly outraged ... We strongly support increased representation of minority students in all levels of education, including colleges and medical schools. By fostering diversity and inclusion, institutions have the power to create more empathetic and inclusive learning environments,” the organization said in a press release.
“Diversity in the health care workforce not only benefits underserved patients but improves care for all patients” by increasing understanding and empathy for people of various cultures, Omar T. Atiq, MD, president of the American College of Physicians, said in a press release.
The Supreme Court ruling stems from a lawsuit by the Students for Fair Admissions against Harvard University and the University of North Carolina. The lawsuit alleges that considering race in the college admission process constitutes discrimination and violates the Equal Protection Clause.
Chief Justice John Roberts, who delivered the court’s decision, stated that an applicant’s personal experiences should carry the most weight in admission decisions and that historically, universities have “wrongly concluded that the touchstone of an individual’s identity is not challenges bested, skills built, or lessons learned, but the color of their skin. Our constitutional history does not tolerate that choice.”
Still, Justice Roberts said the opinion does not prohibit universities from considering how race has affected an applicant’s life, “be it through discrimination, inspiration, or otherwise.”
Diversity in medical schools increased last year, with more Black, Hispanic, and female students applying and enrolling. But continued diversity efforts were expected to prove challenging with affirmative action off the table, according to an amicus brief filed last year by the AMA, the AAMC, and dozens of other professional health care organizations.
The brief supported continued use of race in college admissions, stating that eliminating that factor could slow efforts to achieve greater health equity because fewer doctors would be training and working with colleagues from diverse backgrounds.
Several universities with medical programs, such as Yale and Johns Hopkins universities, filed a separate brief citing similar concerns. After the June 29 decision, Harvard and the University of North Carolina released statements stating they would comply with the ruling.
A version of this article first appeared on Medscape.com.
The U.S. Supreme Court ruled on June 29 that using race as a factor in college admissions is unconstitutional, rolling back more than 40 years of affirmative action standards and changing how medical schools evaluate applicants to attract students from diverse backgrounds.
Jesse M. Ehrenfeld, MD, MPH, president of the American Medical Association, said in a prepared statement that the Supreme Court ruling will result in a less diverse physician workforce, which is “bad for health care, bad for medicine, and undermines the health of our nation.” He cited the AMA’s recent adoption of a policy advising medical schools to increase enrollment of people from racial and ethnic groups traditionally underrepresented in medicine – even if that means considering race as a factor in admissions criteria.
“Supporting racial and ethnic diversity in the health professions – spanning classrooms, labs, and clinical settings – enriches the educational experiences of all medical and health professions students and the teaching experiences of faculty, and it is essential to improving the overall health of our nation,” the Association of American Medical Colleges (AAMC) said in a prepared statement.
The American Medical Student Association also denounced the Supreme Court decision. “As future physicians committed to justice and equality, we are profoundly outraged ... We strongly support increased representation of minority students in all levels of education, including colleges and medical schools. By fostering diversity and inclusion, institutions have the power to create more empathetic and inclusive learning environments,” the organization said in a press release.
“Diversity in the health care workforce not only benefits underserved patients but improves care for all patients” by increasing understanding and empathy for people of various cultures, Omar T. Atiq, MD, president of the American College of Physicians, said in a press release.
The Supreme Court ruling stems from a lawsuit by the Students for Fair Admissions against Harvard University and the University of North Carolina. The lawsuit alleges that considering race in the college admission process constitutes discrimination and violates the Equal Protection Clause.
Chief Justice John Roberts, who delivered the court’s decision, stated that an applicant’s personal experiences should carry the most weight in admission decisions and that historically, universities have “wrongly concluded that the touchstone of an individual’s identity is not challenges bested, skills built, or lessons learned, but the color of their skin. Our constitutional history does not tolerate that choice.”
Still, Justice Roberts said the opinion does not prohibit universities from considering how race has affected an applicant’s life, “be it through discrimination, inspiration, or otherwise.”
Diversity in medical schools increased last year, with more Black, Hispanic, and female students applying and enrolling. But continued diversity efforts were expected to prove challenging with affirmative action off the table, according to an amicus brief filed last year by the AMA, the AAMC, and dozens of other professional health care organizations.
The brief supported continued use of race in college admissions, stating that eliminating that factor could slow efforts to achieve greater health equity because fewer doctors would be training and working with colleagues from diverse backgrounds.
Several universities with medical programs, such as Yale and Johns Hopkins universities, filed a separate brief citing similar concerns. After the June 29 decision, Harvard and the University of North Carolina released statements stating they would comply with the ruling.
A version of this article first appeared on Medscape.com.
The U.S. Supreme Court ruled on June 29 that using race as a factor in college admissions is unconstitutional, rolling back more than 40 years of affirmative action standards and changing how medical schools evaluate applicants to attract students from diverse backgrounds.
Jesse M. Ehrenfeld, MD, MPH, president of the American Medical Association, said in a prepared statement that the Supreme Court ruling will result in a less diverse physician workforce, which is “bad for health care, bad for medicine, and undermines the health of our nation.” He cited the AMA’s recent adoption of a policy advising medical schools to increase enrollment of people from racial and ethnic groups traditionally underrepresented in medicine – even if that means considering race as a factor in admissions criteria.
“Supporting racial and ethnic diversity in the health professions – spanning classrooms, labs, and clinical settings – enriches the educational experiences of all medical and health professions students and the teaching experiences of faculty, and it is essential to improving the overall health of our nation,” the Association of American Medical Colleges (AAMC) said in a prepared statement.
The American Medical Student Association also denounced the Supreme Court decision. “As future physicians committed to justice and equality, we are profoundly outraged ... We strongly support increased representation of minority students in all levels of education, including colleges and medical schools. By fostering diversity and inclusion, institutions have the power to create more empathetic and inclusive learning environments,” the organization said in a press release.
“Diversity in the health care workforce not only benefits underserved patients but improves care for all patients” by increasing understanding and empathy for people of various cultures, Omar T. Atiq, MD, president of the American College of Physicians, said in a press release.
The Supreme Court ruling stems from a lawsuit by the Students for Fair Admissions against Harvard University and the University of North Carolina. The lawsuit alleges that considering race in the college admission process constitutes discrimination and violates the Equal Protection Clause.
Chief Justice John Roberts, who delivered the court’s decision, stated that an applicant’s personal experiences should carry the most weight in admission decisions and that historically, universities have “wrongly concluded that the touchstone of an individual’s identity is not challenges bested, skills built, or lessons learned, but the color of their skin. Our constitutional history does not tolerate that choice.”
Still, Justice Roberts said the opinion does not prohibit universities from considering how race has affected an applicant’s life, “be it through discrimination, inspiration, or otherwise.”
Diversity in medical schools increased last year, with more Black, Hispanic, and female students applying and enrolling. But continued diversity efforts were expected to prove challenging with affirmative action off the table, according to an amicus brief filed last year by the AMA, the AAMC, and dozens of other professional health care organizations.
The brief supported continued use of race in college admissions, stating that eliminating that factor could slow efforts to achieve greater health equity because fewer doctors would be training and working with colleagues from diverse backgrounds.
Several universities with medical programs, such as Yale and Johns Hopkins universities, filed a separate brief citing similar concerns. After the June 29 decision, Harvard and the University of North Carolina released statements stating they would comply with the ruling.
A version of this article first appeared on Medscape.com.
Depression in People With Multiple Sclerosis
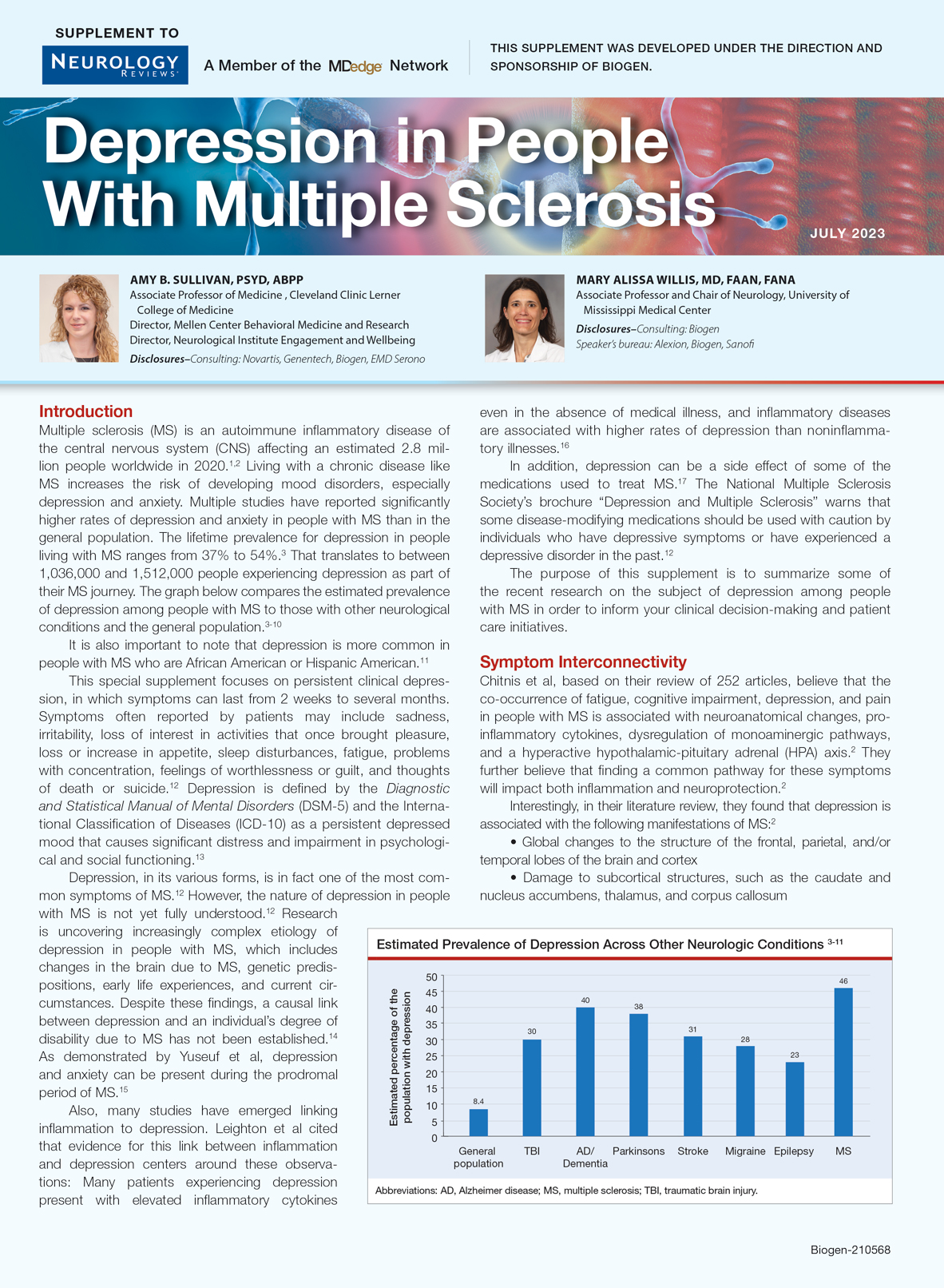
Many people believe that a diagnosis of MS and its progression can bring on depression. But is that really true?
This supplement examines the two-way connection between MS and depression. It gives you tools to actively look for signs of depression and develop techniques to more effectively communicate with and manage these individuals.
Many people believe that a diagnosis of MS and its progression can bring on depression. But is that really true?
This supplement examines the two-way connection between MS and depression. It gives you tools to actively look for signs of depression and develop techniques to more effectively communicate with and manage these individuals.
Many people believe that a diagnosis of MS and its progression can bring on depression. But is that really true?
This supplement examines the two-way connection between MS and depression. It gives you tools to actively look for signs of depression and develop techniques to more effectively communicate with and manage these individuals.
Residency match process under scrutiny again, this time by AMA
The American Medical Association is considering whether to study alternatives to the current residency matching program in an effort to improve residents’ compensation and other job-related issues. A recent call-to-action resolution by the AMA’s House of Delegates is the latest in a long string of debates about whether to change the annual process that matches future doctors with compatible residency programs.
AMA’s Resident and Fellow Section introduced the resolution in March, and the delegates approved it earlier in June at AMA’s annual meeting. The resolution states that the match process of the National Resident Matching Program (NRMP) “poses significant anticompetition concerns.” Those include preventing residents from negotiating for higher wages, better benefits, and improved working conditions, according to the approved resolution.
The full AMA board still has to consider the resolution and hasn’t set a date for that review, though it’s expected to be in the next few months, according to Jennifer Sellers, AMA’s public information officer. She said in an interview that the organization declined to comment, wanting to hold off until the board decides how to proceed.
The NRMP, which oversees the matching process, told this news organization that the AMA doesn’t play a role in the Match.
The organization doesn’t believe studying alternative placement methods benefits applicants and residents, and returning to a pre-Match environment, would harm applicants and programs, according to Donna Lamb, DHSc, MBA, BSN, president and CEO.
“The NRMP has no role in determining, publishing, or setting resident salaries nor does the NRMP have a role in the contracting or employment of residents, and it never has.”
Dr. Lamb said changing the Match would “subject applicants to undue pressure and coercion to accept an offer of training. This will exacerbate disparities in candidate selection already evident in medical education and potentially result in salary reductions in more competitive specialties and in more desirable geographic locations.”
The latest push to reform the match process dates back two decades to a 2002 class action antitrust lawsuit by residents and doctors against the NRMP and other organizations involved in the Match.
The residents argued at that time that by restraining competition among teaching hospitals, the matching system allowed hospitals to keep residents’ wages artificially low. The defendants, which included large teaching hospitals, successfully lobbied Congress for an exemption to the antitrust laws, and the case was subsequently dismissed.
The AMA was one of the defendants, so if it moves forward to review the match process, it likely would pit the organization against the NRMP.
Sherman Marek, the attorney who represented the residents, said in an interview that he was not surprised by the latest AMA resolution. “Maybe the AMA leadership has come around to the idea that it’s better for young physicians to not have the match in place,” he says. “I would applaud that sort of evolution.”
Tyler Ramsey, DO, an internal medicine resident and AMA member, said he believes the group’s current president, Jesse Ehrenfeld, MD, MPH, empathizes with doctors in training. “I think he understands [our] views and is more progressive.”
The NRMP also has considered ways to improve the match process to make it easier and more equitable for applicants. In its latest effort, the organization is studying whether programs should certify their rank order list in advance of applicants. This change would give applicants more flexibility to visit residency locations before the programs consider changing their rankings, Dr. Lamb explained. The NRMP also is mulling the possibilities of a two-phase match after deciding in 2022 not to move forward with a previous version of the proposal.
The recent House of Delegates resolution states that “residents are using other means to obtain fair wages, safe working conditions, and other benefits that are unable to be negotiated within the current system.”
Dr. Ramsey, who trains in North Carolina, said the “other means” may include negotiating through a union. “The AMA realizes that there is a problem and that people are unionizing,” he said. “Obviously, as an organization, we’re not doing something correctly, to the point where people are feeling the need to get their rights a different way.”
The Committee of Interns and Residents, which represents 30,000 members, reported a rise in medical trainee unions across the country in 2022.
Not everyone believes that ditching the Match would benefit applicants and residents. Sam Payabvash, MD, assistant professor of radiology at Yale, New Haven, Conn., School of Medicine, tweeted about the resolution as part of a larger Twitter discussion that alternatives are likely to be “more onerous and expensive for applicants.”
An advantage of the match program, Dr. Lamb argued, is that it “improves the reach of applicants into medically underserved communities through widespread program participation.”
Dr. Ramsey agreed that the match program has benefits and drawbacks, but he believes it favors programs over residents. “It comes as no surprise that numerous residents suffer from depression and our suicide rates are the highest amongst all professions due to the lack of control or negotiation of fair salary and working conditions. Overall, the way things are now, residents just do not have a lot of rights.”
A version of this article originally appeared on Medscape.com.
The American Medical Association is considering whether to study alternatives to the current residency matching program in an effort to improve residents’ compensation and other job-related issues. A recent call-to-action resolution by the AMA’s House of Delegates is the latest in a long string of debates about whether to change the annual process that matches future doctors with compatible residency programs.
AMA’s Resident and Fellow Section introduced the resolution in March, and the delegates approved it earlier in June at AMA’s annual meeting. The resolution states that the match process of the National Resident Matching Program (NRMP) “poses significant anticompetition concerns.” Those include preventing residents from negotiating for higher wages, better benefits, and improved working conditions, according to the approved resolution.
The full AMA board still has to consider the resolution and hasn’t set a date for that review, though it’s expected to be in the next few months, according to Jennifer Sellers, AMA’s public information officer. She said in an interview that the organization declined to comment, wanting to hold off until the board decides how to proceed.
The NRMP, which oversees the matching process, told this news organization that the AMA doesn’t play a role in the Match.
The organization doesn’t believe studying alternative placement methods benefits applicants and residents, and returning to a pre-Match environment, would harm applicants and programs, according to Donna Lamb, DHSc, MBA, BSN, president and CEO.
“The NRMP has no role in determining, publishing, or setting resident salaries nor does the NRMP have a role in the contracting or employment of residents, and it never has.”
Dr. Lamb said changing the Match would “subject applicants to undue pressure and coercion to accept an offer of training. This will exacerbate disparities in candidate selection already evident in medical education and potentially result in salary reductions in more competitive specialties and in more desirable geographic locations.”
The latest push to reform the match process dates back two decades to a 2002 class action antitrust lawsuit by residents and doctors against the NRMP and other organizations involved in the Match.
The residents argued at that time that by restraining competition among teaching hospitals, the matching system allowed hospitals to keep residents’ wages artificially low. The defendants, which included large teaching hospitals, successfully lobbied Congress for an exemption to the antitrust laws, and the case was subsequently dismissed.
The AMA was one of the defendants, so if it moves forward to review the match process, it likely would pit the organization against the NRMP.
Sherman Marek, the attorney who represented the residents, said in an interview that he was not surprised by the latest AMA resolution. “Maybe the AMA leadership has come around to the idea that it’s better for young physicians to not have the match in place,” he says. “I would applaud that sort of evolution.”
Tyler Ramsey, DO, an internal medicine resident and AMA member, said he believes the group’s current president, Jesse Ehrenfeld, MD, MPH, empathizes with doctors in training. “I think he understands [our] views and is more progressive.”
The NRMP also has considered ways to improve the match process to make it easier and more equitable for applicants. In its latest effort, the organization is studying whether programs should certify their rank order list in advance of applicants. This change would give applicants more flexibility to visit residency locations before the programs consider changing their rankings, Dr. Lamb explained. The NRMP also is mulling the possibilities of a two-phase match after deciding in 2022 not to move forward with a previous version of the proposal.
The recent House of Delegates resolution states that “residents are using other means to obtain fair wages, safe working conditions, and other benefits that are unable to be negotiated within the current system.”
Dr. Ramsey, who trains in North Carolina, said the “other means” may include negotiating through a union. “The AMA realizes that there is a problem and that people are unionizing,” he said. “Obviously, as an organization, we’re not doing something correctly, to the point where people are feeling the need to get their rights a different way.”
The Committee of Interns and Residents, which represents 30,000 members, reported a rise in medical trainee unions across the country in 2022.
Not everyone believes that ditching the Match would benefit applicants and residents. Sam Payabvash, MD, assistant professor of radiology at Yale, New Haven, Conn., School of Medicine, tweeted about the resolution as part of a larger Twitter discussion that alternatives are likely to be “more onerous and expensive for applicants.”
An advantage of the match program, Dr. Lamb argued, is that it “improves the reach of applicants into medically underserved communities through widespread program participation.”
Dr. Ramsey agreed that the match program has benefits and drawbacks, but he believes it favors programs over residents. “It comes as no surprise that numerous residents suffer from depression and our suicide rates are the highest amongst all professions due to the lack of control or negotiation of fair salary and working conditions. Overall, the way things are now, residents just do not have a lot of rights.”
A version of this article originally appeared on Medscape.com.
The American Medical Association is considering whether to study alternatives to the current residency matching program in an effort to improve residents’ compensation and other job-related issues. A recent call-to-action resolution by the AMA’s House of Delegates is the latest in a long string of debates about whether to change the annual process that matches future doctors with compatible residency programs.
AMA’s Resident and Fellow Section introduced the resolution in March, and the delegates approved it earlier in June at AMA’s annual meeting. The resolution states that the match process of the National Resident Matching Program (NRMP) “poses significant anticompetition concerns.” Those include preventing residents from negotiating for higher wages, better benefits, and improved working conditions, according to the approved resolution.
The full AMA board still has to consider the resolution and hasn’t set a date for that review, though it’s expected to be in the next few months, according to Jennifer Sellers, AMA’s public information officer. She said in an interview that the organization declined to comment, wanting to hold off until the board decides how to proceed.
The NRMP, which oversees the matching process, told this news organization that the AMA doesn’t play a role in the Match.
The organization doesn’t believe studying alternative placement methods benefits applicants and residents, and returning to a pre-Match environment, would harm applicants and programs, according to Donna Lamb, DHSc, MBA, BSN, president and CEO.
“The NRMP has no role in determining, publishing, or setting resident salaries nor does the NRMP have a role in the contracting or employment of residents, and it never has.”
Dr. Lamb said changing the Match would “subject applicants to undue pressure and coercion to accept an offer of training. This will exacerbate disparities in candidate selection already evident in medical education and potentially result in salary reductions in more competitive specialties and in more desirable geographic locations.”
The latest push to reform the match process dates back two decades to a 2002 class action antitrust lawsuit by residents and doctors against the NRMP and other organizations involved in the Match.
The residents argued at that time that by restraining competition among teaching hospitals, the matching system allowed hospitals to keep residents’ wages artificially low. The defendants, which included large teaching hospitals, successfully lobbied Congress for an exemption to the antitrust laws, and the case was subsequently dismissed.
The AMA was one of the defendants, so if it moves forward to review the match process, it likely would pit the organization against the NRMP.
Sherman Marek, the attorney who represented the residents, said in an interview that he was not surprised by the latest AMA resolution. “Maybe the AMA leadership has come around to the idea that it’s better for young physicians to not have the match in place,” he says. “I would applaud that sort of evolution.”
Tyler Ramsey, DO, an internal medicine resident and AMA member, said he believes the group’s current president, Jesse Ehrenfeld, MD, MPH, empathizes with doctors in training. “I think he understands [our] views and is more progressive.”
The NRMP also has considered ways to improve the match process to make it easier and more equitable for applicants. In its latest effort, the organization is studying whether programs should certify their rank order list in advance of applicants. This change would give applicants more flexibility to visit residency locations before the programs consider changing their rankings, Dr. Lamb explained. The NRMP also is mulling the possibilities of a two-phase match after deciding in 2022 not to move forward with a previous version of the proposal.
The recent House of Delegates resolution states that “residents are using other means to obtain fair wages, safe working conditions, and other benefits that are unable to be negotiated within the current system.”
Dr. Ramsey, who trains in North Carolina, said the “other means” may include negotiating through a union. “The AMA realizes that there is a problem and that people are unionizing,” he said. “Obviously, as an organization, we’re not doing something correctly, to the point where people are feeling the need to get their rights a different way.”
The Committee of Interns and Residents, which represents 30,000 members, reported a rise in medical trainee unions across the country in 2022.
Not everyone believes that ditching the Match would benefit applicants and residents. Sam Payabvash, MD, assistant professor of radiology at Yale, New Haven, Conn., School of Medicine, tweeted about the resolution as part of a larger Twitter discussion that alternatives are likely to be “more onerous and expensive for applicants.”
An advantage of the match program, Dr. Lamb argued, is that it “improves the reach of applicants into medically underserved communities through widespread program participation.”
Dr. Ramsey agreed that the match program has benefits and drawbacks, but he believes it favors programs over residents. “It comes as no surprise that numerous residents suffer from depression and our suicide rates are the highest amongst all professions due to the lack of control or negotiation of fair salary and working conditions. Overall, the way things are now, residents just do not have a lot of rights.”
A version of this article originally appeared on Medscape.com.
Migraine treatment with rimegepant linked to reduced barbiturate use
AUSTIN – , according to a real-world analysis. Butalbital is the only commonly prescribed short-acting barbiturate in the United States, according to Noah Rosen, MD, who presented the study at the annual meeting of the American Headache Society.
Despite its effectiveness, the drug carries a risk of abuse as well as neurologic side effects, and has also been linked to an increase in medication overuse headache, which in turn can affect quality of life and lead to more disability and health care costs. “Although acute treatment recommendations supported by AHS discourage the use of barbiturates for the acute treatment of migraine, butalbital and associated medications are still widely prescribed, so effective, low-risk novel abortive and preventive therapies that have potential barbiturate-sparing characteristics do have the potential to help people with migraine,” said Dr. Rosen during his presentation. He is the program director of neurology at Hofstra Northwell Health, Hempstead, N.Y.
His group previously showed an association between rimegepant initiation and a reduction in opioid use in another real-world analysis.
The present study retrospectively analyzed data from 34,486 patients drawn from the U.S.-based Longitudinal Access and Adjudication Data (LAAD) produced by IQVIA, which is an anonymized integrated commercial medical and prescription claims database. The period studied was between November 2015 and November 2022. The median age was 47 and 89% were female. Eligibility criteria included the presence of at least 6 months of baseline data before exposure to rimegepant and at least 6 months of follow-up, at least two rimegepant refills, and at least one butalbital prescription during the baseline period.
During the baseline period, the mean number of milligrams of butalbital dispensed was 1,012, and this dropped to 742 during follow-up (–26.7%). The mean number of butalbital prescription fills dropped from 0.47 to 0.32 (–32.0%). About half of patients (49.4%) had no butalbital refills after starting rimegepant. The researchers also examined triptan use and found no difference. “We saw that it actually made no significant difference with the deflection from baseline or discontinuation if they had been given a triptan or not. This seemed to concur with my own experiences with triptan use and not affecting barbiturate dosing,” said Dr. Rosen.
‘Good news’
The results are good news, according to Jason Sico, MD, who comoderated the session. “I remember being a PGY-2 neurology resident and hearing a lecture from Stew Tepper [now professor of medicine at Geisel School of Medicine at Dartmouth, Hanover, N.H.] that fiorinal and fioricet were the F words of headache medicine, so it’s really great to see a modality that could lower barbiturate use,” said Dr. Sico, who is an associate professor of neurology and internal medicine at Yale University, New Haven, Conn.
Dr. Rosen responded: “I don’t mean to malign a single chemical, because fioricet has provided many people treatment over time, but with the introduction of newer options, we would hope to see a trend toward that use.”
A listener on the virtual platform asked whether the decline in barbiturate use could be due to education by the provider on the dangers of barbiturate use when rimegepant was prescribed. “This is one of those big limitations of claims data analysis is we can speculate what the influence or the cause is, because this type of data analysis does not show causation. There are many different things that could influence the discontinuation. Education is a huge one, although you would hope that if somebody is prescribed butalbital on a regular basis, that there’s some physician contact or education that’s part of that as well. But it’s possible it plays a role,” said Dr. Rosen.
Any strategy to reduce butalbital use in migraine is important
Alan Rapoport, MD, who attended the session, was also asked to comment on the study. “Butalbital-containing medications can help headache pain but have not been approved by the FDA for a migraine indication. They can also decrease anxiety in the migraine patient, but if used frequently, they cause dependency. When used too often, butalbital-containing medications are major causes of medication overuse headache. They’re often used with other acute care medications such as triptans and over-the-counter products, and combinations of these drugs can be even more of a problem because one only needs to use any of these medicines in combination for 10 days a month or more, for at least 3 months, for a doctor to diagnose a patient with medication overuse headache. So any attempt and success to reduce the frequency of taking butalbital-containing medication is important. That can be done by counseling the patient to take fewer tablets per month, but this often does not work. This study shows a good success rate in reducing the use of these medications by treating the patient with rimegepant 75 mg ODT given once every other day. This dose has been approved by the FDA for prevention in migraine, but has not previously been shown as a treatment for overuse of butalbital or medication. Previous studies have shown that rimegepant reduced migraine days per month and the use of acute care medications monthly. It this study, rimegepant decreases the number of butalbital-containing medications taken,” said Dr. Rapoport, who is a clinical professor of neurology at the University of California, Los Angeles, and editor in chief of Neurology Reviews.
Dr. Rosen has financial ties to Allergan/Abbvie, Amgen, BioHaven, Eli Lilly, Lundbeck, Novartis, Supernus, and Teva. Dr. Sico did not disclose any conflicts of interest. Dr. Rapoport advises AbbVie, Biohaven, Cala Health, Dr. Reddy’s, Pfizer, Satsuma, Teva Pharmaceutical Industries, and Theranica. He is on the speakers bureaus of AbbVie, Dr. Reddy’s, Impel, Pfizer, and Teva Pharmaceutical Industries. He is editor in chief of Neurology Reviews and on the editorial board of CNS Drugs.
AUSTIN – , according to a real-world analysis. Butalbital is the only commonly prescribed short-acting barbiturate in the United States, according to Noah Rosen, MD, who presented the study at the annual meeting of the American Headache Society.
Despite its effectiveness, the drug carries a risk of abuse as well as neurologic side effects, and has also been linked to an increase in medication overuse headache, which in turn can affect quality of life and lead to more disability and health care costs. “Although acute treatment recommendations supported by AHS discourage the use of barbiturates for the acute treatment of migraine, butalbital and associated medications are still widely prescribed, so effective, low-risk novel abortive and preventive therapies that have potential barbiturate-sparing characteristics do have the potential to help people with migraine,” said Dr. Rosen during his presentation. He is the program director of neurology at Hofstra Northwell Health, Hempstead, N.Y.
His group previously showed an association between rimegepant initiation and a reduction in opioid use in another real-world analysis.
The present study retrospectively analyzed data from 34,486 patients drawn from the U.S.-based Longitudinal Access and Adjudication Data (LAAD) produced by IQVIA, which is an anonymized integrated commercial medical and prescription claims database. The period studied was between November 2015 and November 2022. The median age was 47 and 89% were female. Eligibility criteria included the presence of at least 6 months of baseline data before exposure to rimegepant and at least 6 months of follow-up, at least two rimegepant refills, and at least one butalbital prescription during the baseline period.
During the baseline period, the mean number of milligrams of butalbital dispensed was 1,012, and this dropped to 742 during follow-up (–26.7%). The mean number of butalbital prescription fills dropped from 0.47 to 0.32 (–32.0%). About half of patients (49.4%) had no butalbital refills after starting rimegepant. The researchers also examined triptan use and found no difference. “We saw that it actually made no significant difference with the deflection from baseline or discontinuation if they had been given a triptan or not. This seemed to concur with my own experiences with triptan use and not affecting barbiturate dosing,” said Dr. Rosen.
‘Good news’
The results are good news, according to Jason Sico, MD, who comoderated the session. “I remember being a PGY-2 neurology resident and hearing a lecture from Stew Tepper [now professor of medicine at Geisel School of Medicine at Dartmouth, Hanover, N.H.] that fiorinal and fioricet were the F words of headache medicine, so it’s really great to see a modality that could lower barbiturate use,” said Dr. Sico, who is an associate professor of neurology and internal medicine at Yale University, New Haven, Conn.
Dr. Rosen responded: “I don’t mean to malign a single chemical, because fioricet has provided many people treatment over time, but with the introduction of newer options, we would hope to see a trend toward that use.”
A listener on the virtual platform asked whether the decline in barbiturate use could be due to education by the provider on the dangers of barbiturate use when rimegepant was prescribed. “This is one of those big limitations of claims data analysis is we can speculate what the influence or the cause is, because this type of data analysis does not show causation. There are many different things that could influence the discontinuation. Education is a huge one, although you would hope that if somebody is prescribed butalbital on a regular basis, that there’s some physician contact or education that’s part of that as well. But it’s possible it plays a role,” said Dr. Rosen.
Any strategy to reduce butalbital use in migraine is important
Alan Rapoport, MD, who attended the session, was also asked to comment on the study. “Butalbital-containing medications can help headache pain but have not been approved by the FDA for a migraine indication. They can also decrease anxiety in the migraine patient, but if used frequently, they cause dependency. When used too often, butalbital-containing medications are major causes of medication overuse headache. They’re often used with other acute care medications such as triptans and over-the-counter products, and combinations of these drugs can be even more of a problem because one only needs to use any of these medicines in combination for 10 days a month or more, for at least 3 months, for a doctor to diagnose a patient with medication overuse headache. So any attempt and success to reduce the frequency of taking butalbital-containing medication is important. That can be done by counseling the patient to take fewer tablets per month, but this often does not work. This study shows a good success rate in reducing the use of these medications by treating the patient with rimegepant 75 mg ODT given once every other day. This dose has been approved by the FDA for prevention in migraine, but has not previously been shown as a treatment for overuse of butalbital or medication. Previous studies have shown that rimegepant reduced migraine days per month and the use of acute care medications monthly. It this study, rimegepant decreases the number of butalbital-containing medications taken,” said Dr. Rapoport, who is a clinical professor of neurology at the University of California, Los Angeles, and editor in chief of Neurology Reviews.
Dr. Rosen has financial ties to Allergan/Abbvie, Amgen, BioHaven, Eli Lilly, Lundbeck, Novartis, Supernus, and Teva. Dr. Sico did not disclose any conflicts of interest. Dr. Rapoport advises AbbVie, Biohaven, Cala Health, Dr. Reddy’s, Pfizer, Satsuma, Teva Pharmaceutical Industries, and Theranica. He is on the speakers bureaus of AbbVie, Dr. Reddy’s, Impel, Pfizer, and Teva Pharmaceutical Industries. He is editor in chief of Neurology Reviews and on the editorial board of CNS Drugs.
AUSTIN – , according to a real-world analysis. Butalbital is the only commonly prescribed short-acting barbiturate in the United States, according to Noah Rosen, MD, who presented the study at the annual meeting of the American Headache Society.
Despite its effectiveness, the drug carries a risk of abuse as well as neurologic side effects, and has also been linked to an increase in medication overuse headache, which in turn can affect quality of life and lead to more disability and health care costs. “Although acute treatment recommendations supported by AHS discourage the use of barbiturates for the acute treatment of migraine, butalbital and associated medications are still widely prescribed, so effective, low-risk novel abortive and preventive therapies that have potential barbiturate-sparing characteristics do have the potential to help people with migraine,” said Dr. Rosen during his presentation. He is the program director of neurology at Hofstra Northwell Health, Hempstead, N.Y.
His group previously showed an association between rimegepant initiation and a reduction in opioid use in another real-world analysis.
The present study retrospectively analyzed data from 34,486 patients drawn from the U.S.-based Longitudinal Access and Adjudication Data (LAAD) produced by IQVIA, which is an anonymized integrated commercial medical and prescription claims database. The period studied was between November 2015 and November 2022. The median age was 47 and 89% were female. Eligibility criteria included the presence of at least 6 months of baseline data before exposure to rimegepant and at least 6 months of follow-up, at least two rimegepant refills, and at least one butalbital prescription during the baseline period.
During the baseline period, the mean number of milligrams of butalbital dispensed was 1,012, and this dropped to 742 during follow-up (–26.7%). The mean number of butalbital prescription fills dropped from 0.47 to 0.32 (–32.0%). About half of patients (49.4%) had no butalbital refills after starting rimegepant. The researchers also examined triptan use and found no difference. “We saw that it actually made no significant difference with the deflection from baseline or discontinuation if they had been given a triptan or not. This seemed to concur with my own experiences with triptan use and not affecting barbiturate dosing,” said Dr. Rosen.
‘Good news’
The results are good news, according to Jason Sico, MD, who comoderated the session. “I remember being a PGY-2 neurology resident and hearing a lecture from Stew Tepper [now professor of medicine at Geisel School of Medicine at Dartmouth, Hanover, N.H.] that fiorinal and fioricet were the F words of headache medicine, so it’s really great to see a modality that could lower barbiturate use,” said Dr. Sico, who is an associate professor of neurology and internal medicine at Yale University, New Haven, Conn.
Dr. Rosen responded: “I don’t mean to malign a single chemical, because fioricet has provided many people treatment over time, but with the introduction of newer options, we would hope to see a trend toward that use.”
A listener on the virtual platform asked whether the decline in barbiturate use could be due to education by the provider on the dangers of barbiturate use when rimegepant was prescribed. “This is one of those big limitations of claims data analysis is we can speculate what the influence or the cause is, because this type of data analysis does not show causation. There are many different things that could influence the discontinuation. Education is a huge one, although you would hope that if somebody is prescribed butalbital on a regular basis, that there’s some physician contact or education that’s part of that as well. But it’s possible it plays a role,” said Dr. Rosen.
Any strategy to reduce butalbital use in migraine is important
Alan Rapoport, MD, who attended the session, was also asked to comment on the study. “Butalbital-containing medications can help headache pain but have not been approved by the FDA for a migraine indication. They can also decrease anxiety in the migraine patient, but if used frequently, they cause dependency. When used too often, butalbital-containing medications are major causes of medication overuse headache. They’re often used with other acute care medications such as triptans and over-the-counter products, and combinations of these drugs can be even more of a problem because one only needs to use any of these medicines in combination for 10 days a month or more, for at least 3 months, for a doctor to diagnose a patient with medication overuse headache. So any attempt and success to reduce the frequency of taking butalbital-containing medication is important. That can be done by counseling the patient to take fewer tablets per month, but this often does not work. This study shows a good success rate in reducing the use of these medications by treating the patient with rimegepant 75 mg ODT given once every other day. This dose has been approved by the FDA for prevention in migraine, but has not previously been shown as a treatment for overuse of butalbital or medication. Previous studies have shown that rimegepant reduced migraine days per month and the use of acute care medications monthly. It this study, rimegepant decreases the number of butalbital-containing medications taken,” said Dr. Rapoport, who is a clinical professor of neurology at the University of California, Los Angeles, and editor in chief of Neurology Reviews.
Dr. Rosen has financial ties to Allergan/Abbvie, Amgen, BioHaven, Eli Lilly, Lundbeck, Novartis, Supernus, and Teva. Dr. Sico did not disclose any conflicts of interest. Dr. Rapoport advises AbbVie, Biohaven, Cala Health, Dr. Reddy’s, Pfizer, Satsuma, Teva Pharmaceutical Industries, and Theranica. He is on the speakers bureaus of AbbVie, Dr. Reddy’s, Impel, Pfizer, and Teva Pharmaceutical Industries. He is editor in chief of Neurology Reviews and on the editorial board of CNS Drugs.
FROM AHS 2023
Safety first: Regulations
The word “regulations” gets a mixed response.
This is common in all industries, and certainly pharmaceuticals. On any given day there are stories on industry news sites about disputes between companies and regulatory agencies.
I’d agree that some regulation is needed. The history of pharmacy has had both remarkable successes – and failures.

Let’s look at migraines, since that’s in my field. The calcitonin gene-related peptide (CGRP) drugs have been a remarkable breakthrough, certainly the biggest one since the triptans in 1992. There are currently seven on the market for both prevention and abortive use. They’re effective and (to date) pretty safe.
But it wasn’t always that way. Look back just 14 years ago to 2009, when the first promising CGRP agent (MK-3207) had its development halted because of hepatic abnormalities. It’s cousin telcagepant (MK-0974) came to a similar end 2 years later.
Without regulations in place (and the potential for lawsuits) these might have made it to market, bringing migraine relief to some and potentially serious liver damage to others. So Merck made the right decision to axe them. Researchers learned from the experience, went back to the drawing board, and developed the current generation of far-safer drugs.
This came into sharp focus in another industry recently, when the eyes of the world were on the north Atlantic. A small tourist submarine imploded and killed five people. During the inevitable media coverage it came out that the submarine hadn’t been certified for safety by any of the agencies that handle such things, falling into a gray area in international waters where inspections aren’t required.
This isn’t to say it wasn’t safe – it had made several dives before – but obviously not safe enough. While I didn’t know the late Stockton Rush (the owner/designer) it sounds like he viewed regulations as stifling innovation, and in one interview said “at some point, safety is just pure waste.” He ignored warnings from several sides about the submersible’s ability to handle deep ocean pressure and the inevitable wear and tear repeated dives will have on the hull.
I understand there’s a margin of luck, too. Bad things can happen to any of us – or any company. Some things can’t be clearly foreseen. Some drugs don’t start to show problems until they’re on the market and reach a certain number of prescriptions.
But there’s a reason we have regulations. Pretty much every government has, going back to the Roman Empire, covering numerous things. In a perfect world we wouldn’t need them.
But people are far from perfect. And the consequences can be terrible.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The word “regulations” gets a mixed response.
This is common in all industries, and certainly pharmaceuticals. On any given day there are stories on industry news sites about disputes between companies and regulatory agencies.
I’d agree that some regulation is needed. The history of pharmacy has had both remarkable successes – and failures.
Let’s look at migraines, since that’s in my field. The calcitonin gene-related peptide (CGRP) drugs have been a remarkable breakthrough, certainly the biggest one since the triptans in 1992. There are currently seven on the market for both prevention and abortive use. They’re effective and (to date) pretty safe.
But it wasn’t always that way. Look back just 14 years ago to 2009, when the first promising CGRP agent (MK-3207) had its development halted because of hepatic abnormalities. It’s cousin telcagepant (MK-0974) came to a similar end 2 years later.
Without regulations in place (and the potential for lawsuits) these might have made it to market, bringing migraine relief to some and potentially serious liver damage to others. So Merck made the right decision to axe them. Researchers learned from the experience, went back to the drawing board, and developed the current generation of far-safer drugs.
This came into sharp focus in another industry recently, when the eyes of the world were on the north Atlantic. A small tourist submarine imploded and killed five people. During the inevitable media coverage it came out that the submarine hadn’t been certified for safety by any of the agencies that handle such things, falling into a gray area in international waters where inspections aren’t required.
This isn’t to say it wasn’t safe – it had made several dives before – but obviously not safe enough. While I didn’t know the late Stockton Rush (the owner/designer) it sounds like he viewed regulations as stifling innovation, and in one interview said “at some point, safety is just pure waste.” He ignored warnings from several sides about the submersible’s ability to handle deep ocean pressure and the inevitable wear and tear repeated dives will have on the hull.
I understand there’s a margin of luck, too. Bad things can happen to any of us – or any company. Some things can’t be clearly foreseen. Some drugs don’t start to show problems until they’re on the market and reach a certain number of prescriptions.
But there’s a reason we have regulations. Pretty much every government has, going back to the Roman Empire, covering numerous things. In a perfect world we wouldn’t need them.
But people are far from perfect. And the consequences can be terrible.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The word “regulations” gets a mixed response.
This is common in all industries, and certainly pharmaceuticals. On any given day there are stories on industry news sites about disputes between companies and regulatory agencies.
I’d agree that some regulation is needed. The history of pharmacy has had both remarkable successes – and failures.
Let’s look at migraines, since that’s in my field. The calcitonin gene-related peptide (CGRP) drugs have been a remarkable breakthrough, certainly the biggest one since the triptans in 1992. There are currently seven on the market for both prevention and abortive use. They’re effective and (to date) pretty safe.
But it wasn’t always that way. Look back just 14 years ago to 2009, when the first promising CGRP agent (MK-3207) had its development halted because of hepatic abnormalities. It’s cousin telcagepant (MK-0974) came to a similar end 2 years later.
Without regulations in place (and the potential for lawsuits) these might have made it to market, bringing migraine relief to some and potentially serious liver damage to others. So Merck made the right decision to axe them. Researchers learned from the experience, went back to the drawing board, and developed the current generation of far-safer drugs.
This came into sharp focus in another industry recently, when the eyes of the world were on the north Atlantic. A small tourist submarine imploded and killed five people. During the inevitable media coverage it came out that the submarine hadn’t been certified for safety by any of the agencies that handle such things, falling into a gray area in international waters where inspections aren’t required.
This isn’t to say it wasn’t safe – it had made several dives before – but obviously not safe enough. While I didn’t know the late Stockton Rush (the owner/designer) it sounds like he viewed regulations as stifling innovation, and in one interview said “at some point, safety is just pure waste.” He ignored warnings from several sides about the submersible’s ability to handle deep ocean pressure and the inevitable wear and tear repeated dives will have on the hull.
I understand there’s a margin of luck, too. Bad things can happen to any of us – or any company. Some things can’t be clearly foreseen. Some drugs don’t start to show problems until they’re on the market and reach a certain number of prescriptions.
But there’s a reason we have regulations. Pretty much every government has, going back to the Roman Empire, covering numerous things. In a perfect world we wouldn’t need them.
But people are far from perfect. And the consequences can be terrible.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.