User login
Key questions to ask atopic dermatitis patients with sleep complaints
If you don’t think it’s important to assess for sleep disorders in your patients with atopic dermatitis (AD), think again.
According to Sabra M. Abbott, MD, PhD, professor of neurology at Northwestern University, Chicago, as well as increased night kicks and nocturnal leg cramps, and a more than twofold increased risk for insomnia.
During the Revolutionizing Atopic Dermatitis symposium, she offered key questions to ask AD patients who present with sleep complaints:
When do you go to bed? “This does not refer to when you get into bed, but when do you actually go to bed with an intention to go to sleep, outside of watching television or answering emails?” Dr. Abbott said.
How long does it take for you to fall asleep?
Do you wake up in the middle of the night, and for how long? What do you do if you wake up?
When do you wake up in the morning? Is it on your own, or with an alarm clock?
Does this schedule change on nonworkdays?
Do you have daytime impairment? Meaning, do your sleep complaints impact how you function during the daytime?
Do you snore? Meaning, is there concern for sleep apnea?
Do you have uncomfortable sensations in your legs? Are they worse in the evening and improve with movement? These are signs of possible restless legs syndrome.
The Epworth Sleepiness Scale is one self-administered questionnaire to consider using for AD patients with sleep complaints. “This provides patients with several examples of typical scenarios they might encounter during the day and queries whether or not they feel that they could deal with any of those scenarios,” Dr. Abbott said. “A score of greater than 10 indicates that they are sleepy; it’s not just an overall sense of fatigue and decreased energy.”
Other brief self-assessment tools she recommended are the Insomnia Severity Index and the STOP-Bang questionnaire.
Dr. Abbott reported having no financial disclosures.
If you don’t think it’s important to assess for sleep disorders in your patients with atopic dermatitis (AD), think again.
According to Sabra M. Abbott, MD, PhD, professor of neurology at Northwestern University, Chicago, as well as increased night kicks and nocturnal leg cramps, and a more than twofold increased risk for insomnia.
During the Revolutionizing Atopic Dermatitis symposium, she offered key questions to ask AD patients who present with sleep complaints:
When do you go to bed? “This does not refer to when you get into bed, but when do you actually go to bed with an intention to go to sleep, outside of watching television or answering emails?” Dr. Abbott said.
How long does it take for you to fall asleep?
Do you wake up in the middle of the night, and for how long? What do you do if you wake up?
When do you wake up in the morning? Is it on your own, or with an alarm clock?
Does this schedule change on nonworkdays?
Do you have daytime impairment? Meaning, do your sleep complaints impact how you function during the daytime?
Do you snore? Meaning, is there concern for sleep apnea?
Do you have uncomfortable sensations in your legs? Are they worse in the evening and improve with movement? These are signs of possible restless legs syndrome.
The Epworth Sleepiness Scale is one self-administered questionnaire to consider using for AD patients with sleep complaints. “This provides patients with several examples of typical scenarios they might encounter during the day and queries whether or not they feel that they could deal with any of those scenarios,” Dr. Abbott said. “A score of greater than 10 indicates that they are sleepy; it’s not just an overall sense of fatigue and decreased energy.”
Other brief self-assessment tools she recommended are the Insomnia Severity Index and the STOP-Bang questionnaire.
Dr. Abbott reported having no financial disclosures.
If you don’t think it’s important to assess for sleep disorders in your patients with atopic dermatitis (AD), think again.
According to Sabra M. Abbott, MD, PhD, professor of neurology at Northwestern University, Chicago, as well as increased night kicks and nocturnal leg cramps, and a more than twofold increased risk for insomnia.
During the Revolutionizing Atopic Dermatitis symposium, she offered key questions to ask AD patients who present with sleep complaints:
When do you go to bed? “This does not refer to when you get into bed, but when do you actually go to bed with an intention to go to sleep, outside of watching television or answering emails?” Dr. Abbott said.
How long does it take for you to fall asleep?
Do you wake up in the middle of the night, and for how long? What do you do if you wake up?
When do you wake up in the morning? Is it on your own, or with an alarm clock?
Does this schedule change on nonworkdays?
Do you have daytime impairment? Meaning, do your sleep complaints impact how you function during the daytime?
Do you snore? Meaning, is there concern for sleep apnea?
Do you have uncomfortable sensations in your legs? Are they worse in the evening and improve with movement? These are signs of possible restless legs syndrome.
The Epworth Sleepiness Scale is one self-administered questionnaire to consider using for AD patients with sleep complaints. “This provides patients with several examples of typical scenarios they might encounter during the day and queries whether or not they feel that they could deal with any of those scenarios,” Dr. Abbott said. “A score of greater than 10 indicates that they are sleepy; it’s not just an overall sense of fatigue and decreased energy.”
Other brief self-assessment tools she recommended are the Insomnia Severity Index and the STOP-Bang questionnaire.
Dr. Abbott reported having no financial disclosures.
FROM REVOLUTIONIZING AD 2021
One doctor’s psychedelic journey to confront his cancer
Pradeep Bansal considered the five capsules he was about to swallow. Together they made up a 25-mg dose of a substance that, in another setting, could have landed him in federal prison.
The substance was psilocybin, the active ingredient in magic mushrooms. To be more exact, it was a synthetic form of psilocybin called COMP360, made to pharmaceutical standards by a company called COMPASS Pathways. He was taking it as part of an Food and Drug Administration–approved clinical study on mental health therapy for people with cancer.
Dr. Bansal, a New York gastroenterologist, was far more comfortable giving medical treatment than receiving it. But he was getting used to it.
He had already been through surgery and a number of other treatments to address the physical aspects of his cancer. The psilocybin was to address the mental aspects – the crushing anxiety and depression that had stuck with him after his diagnosis.
Dr. Bansal did not arrive at this moment lightly.
“I was extremely skeptical going into this process,” said Dr. Bansal, who during a long medical career had looked with distrust and even disdain at alternative therapies.
“I don’t have much patience for holistic medicine, homeopathy, acupuncture, or alternative medicines with claims of spiritual upliftment or altered states of mind.”
But Bansal had done his homework on psilocybin and was impressed.
according to studies published in 2011, 2014, and 2016.
One study from Johns Hopkins University tracked the effects of a single guided dose of psilocybin in terminal cancer patients with anxiety and depression. More than 80% had a “significant decrease” in symptoms – even 6 months after treatment – with more than 60% of the group remaining in the normal mood range.
For the study Dr. Bansal joined, there had been weeks of screening and consultation and preparation in a strictly controlled scientific trial.
And yet, even with all that he had learned, even with his psychiatrist-guide by his side, he was afraid. Afraid of what he might experience under the powerful effects of psilocybin. And afraid that this was all a misguided waste of time – that his mental angst would still be there when it was all over.
He knew that psilocybin, like other psychedelic substances, could take you on a “trip” – could remove you, at least for a time, from normal conscious experience.
Maybe he would feel “funny,” he thought. Maybe he would have some hallucinations. But how would that change the reality of his cancer? How would it lift the black dread and anxiety he felt about his future?
Stuck in a dark place
Dr. Bansal had first noticed blood in his urine – a lot of it – in September 2019.
Two months later, doctors diagnosed cancer in his right kidney. He would need surgery to remove the kidney and surrounding lymph nodes (an operation called radical nephrectomy).
It was a shock, said Dr. Bansal. But the diagnosis and the surgery happened so quickly that he hardly had time to think. And treatment results seemed good. The cancer was only in stage I and the CT scans showed no signs of cancer after surgery.
“We were so relieved. Everyone was so happy,” Dr. Bansal said. “They didn’t even give me chemotherapy after surgery because it seemed so early.”
But a routine scan in June 2020 revealed more cancer in his lung. Within a couple of months, it was in his bladder too.
“It was devastating,” Dr. Bansal said. “I went from thinking I was healthy again to stage IV cancer.”
As doctors scheduled surgery to remove part of his lung, Dr. Bansal started on painful immunotherapy (BCG therapy) for his bladder.
At this point, from a psychological standpoint, Dr. Bansal was reeling. As a doctor, he knew all too well the meaning of stage IV cancer.
With two adult children and a grandchild on the way, Dr. Bansal had been looking forward to retirement with his wife of almost 40 years. “Suddenly, I wasn’t sure I was going to last that long,” Bansal recalled. “I was in a very dark place. I was very anxious, very depressed from lack of sleep.”
He saw a therapist about his cancer diagnosis and maintained his regular meditation practice at home. He hired a personal trainer and tried to focus on any good news that he got about his treatment.
Those things helped, but not enough.
The basic facts were inescapable. His cancer might end everything. He couldn’t stop thinking about it. And then he couldn’t stop thinking about how he couldn’t stop thinking about it.
If the worst happened, he didn’t want to spend his last days in a state of such relentless existential angst. And it wasn’t just for himself. He wanted to be strong and mentally present for his family and his loved ones and his patients.
As he searched for something to ease his mental anguish, Dr. Bansal recalled some psychedelic research on end-of-life anxiety and depression that he’d read about in Michael Pollan’s book on psychedelics, “How to Change Your Mind” (New York, Penguin Press, 2018).
The studies were small and the research was new, but Dr. Bansal was impressed enough with the results to take a chance. He called a lead researcher of one of the studies, a fellow New York doctor, and eventually found himself accepted into a new study.
Starting the journey
By the time Dr. Bansal arrived at the Bill Richards Center for Healing at the Aquilino Cancer Center in Rockville, Md., he had already been through weeks of screening.
The main requirements for the study were a cancer diagnosis and a measurable level of depression. But study participants also had to be physically fit enough to handle the medication, and psychologically free from a personal or family history of psychosis or schizophrenia. (The study also required participants to slowly wean themselves from medications like SSRIs for depression or antianxiety medications under the strict supervision of a qualified doctor.)
Dr. Bansal’s week of treatment began almost immediately on arrival at Aquilino. Everything was carefully choreographed but not rushed. From Monday to Wednesday, doctors followed his physical health with exams, ECGs, and blood work. And most importantly, they began to prepare him for the “dosing session” on Thursday when he would take the psilocybin.
This is the careful crafting of “set and setting” stressed in so many psychedelic therapies. “Set” refers to your mindset going into the drug experience. “Setting” is the space and people around you when the drug sends you into an altered state of consciousness.
Dr. Bansal met several times with at least three therapists in the days leading up to his dosing. He attended 4-plus hours of therapist-led group sessions with other people who would get a dosing on the same day. Together, they talked about what to expect during the experience and what to do in the face of fear or panic.
He connected with a therapist who would be his personal guide. Dr. Bansal’s therapist was a military psychiatrist with over 30 years’ experience.
“He was there with me from day 1, and so we established a relationship,” Dr. Bansal said.
“He asked me a lot of personal background history – you know, my religious convictions, aspirations, all those things.”
“Trust and let go,” was a kind of mantra for the treatment repeated by his guide and other doctors.
For Dr. Bansal, a doctor and scientist accustomed to using hard facts rather than touchy-feely slogans to navigate the care of patients, it was an adjustment, to say the least.
But he did his best to set aside his doubts and embrace the journey he was about to take.
The day of the trip
Thursday morning finally arrived. The setting of the dosing room was warm and welcoming, more like a cozy home study than a hospital room.
This matters more than you might think. First, because it’s important that you feel safe, open, and comfortable enough to let go and enter into a therapeutic process. But also because though rare, it’s possible – especially with psilocybin – for people to lose track of where they are and what they’re doing and put themselves or others in danger.
The dose, 25 mg, had been carefully calibrated to induce a psychedelic experience sufficient for therapy. Much less than that, say 10 mg, isn’t enough for most people to enter this state. A double dose, 50 mg, though not physically unsafe, may leave you too incoherent to have the useful insights key to therapeutic value.
A doctor, the lead investigator of the study, brought the five capsules into the room in an intricately carved crucible with a small ceremonial cup that held the water with which to take it.
“It was very solemn,” Dr. Bansal said. “He sat down with me in a very calming way.”
The doctor said: “Don’t worry about it. Just trust and let go.”
And that’s just what he did.
Dr. Bansal swallowed the capsules and lay down. The doctor quietly left the room so that Dr. Bansal and his psychiatrist guide could begin their session together.
Special eye shades kept him in the pitch dark whether his eyes were open or closed. Headphones streamed a curated musical playlist – much of it Western classical like Strauss, Bach, Mozart, and Beethoven – but also modern electronica and other music from cultures around the globe.
Dr. Bansal would remain here, with his therapist-guide by his side, in largely this same position, for the next 7-and-a-half hours.
It took about 45 minutes for the medication to kick in.
The investigator
The doctor who brought the capsules into the dosing room was Manish Agrawal, MD, codirector of clinical research at the Aquilino Cancer Center and lead investigator of the study.
Dr. Agrawal trained at the National Cancer Institute and practiced for many years as an oncologist before developing an interest in psychedelic therapies. It was his work with cancer patients that drew him to psychedelics in the first place.
He had seen too many of his patients mentally wrecked by a cancer diagnosis, and he often felt helpless to comfort them.
“You take care of the physical aspects of the cancer, right? You talk about side effects and recommend another scan to look for recurrence.”
“But what about the psychological effects?”
They can be very serious and too often go ignored, said Dr. Agrawal. Your plans for the future suddenly become moot. You may be concerned about your ability to work or worried about the pain and suffering and financial strain that might be ahead for both you and your family. And to top it all off, you’re staring into the face of your own mortality.
So it’s no wonder, said Dr. Agrawal, that many people develop clinical levels of anxiety and depression after a cancer diagnosis.
Like Dr. Bansal, Dr. Agrawal had been impressed by early studies on psilocybin-assisted therapies for end-of-life anxiety and depression. He had tried other approaches – support groups, one-on-one therapy, religious counselors, psychiatrist-prescribed medication – but he was never really happy with the results.
To Dr. Agrawal, psilocybin-assisted therapy was the first thing that looked like it could really make a difference.
And so after his psychedelic certification at the California Institute of Integral Studies, Dr. Agrawal was determined to change his approach.
The result was the Bill Richards Center for Healing at Aquilino Cancer Center, built specifically to study psychedelic-assisted therapies for psychological distress in people with cancer. The mission of the center is to help develop safe, FDA-approved psychedelic therapies for the mental health of cancer patients, and, once approved, provide a state-of-the-art facility and staff to administer those treatments.
A trip into the unknown
Back in the dosing room, Dr. Bansal was starting to feel the effects of the medication. As the psilocybin kicked in, spectacular images swirled.
“It was as if a million stained glass windows had suddenly come to life and were dancing in front of my vision,” Dr. Bansal said.
There were moving landscapes and intricate swirling patterns and massive stages in the sky where he saw orchestras playing the music he was hearing.
Dr. Bansal saw himself being crushed by a huge machine and buried, dead, in the Earth. He died and returned to life several times, glided over the top of New York City with the skyscrapers just below him, and took in the vision of the entire universe.
“I saw this expanse of the sky that was limitless. And there was this prehistoric reptile creature that spanned galaxies in the sky ahead of me who was dying. I said: ‘My God, the universe is dying,’ but then after a few moments, the universe came to life again in a burst of stars exploding.”
All the while, Dr. Bansal said, he was well aware that it was simply his mind creating these images, thoughts, and ideas. He knew he was in a safe room wearing eyeshades and headphones.
And yet, he says, it felt true. “The images and feelings are so powerful that you cannot help but believe they are in some way a part of reality.”
“At one point, I saw this giant Ferris wheel coming towards me and it was full of giant crabs, clicking and clacking their pincers. And my brain told me: ‘That’s my cancer!’ ”
Dr. Bansal was terrified. But he and his therapist had arranged a system of signals before the session. “If I was feeling afraid, I would hold his hand and if I had other issues, I would raise my hand. If I was feeling good, I would give him a thumbs up.”
Dr. Bansal reached out to his therapist and grasped his hand. “I said, ‘My cancer is coming at me!’ ”
His therapist was clear about what to do: Stand firm and walk toward it.
“That’s what they tell you: If you see anything frightening, you face it. And that’s the whole point of this exercise. And so, I stood and walked forward, and it just blew off in a puff of smoke.”
A state of peace
Around 3 hours into the experience, Dr. Bansal started to feel an immense sense of peace, happiness, and even comfort.
“I felt like I was watching a movie or a multidimensional slideshow. I was also a part of the movie. I felt like I could tell my mind what I wanted to see, and it would show it to me. It’s almost like you can mold your own visions. It was mystical.”
After about 8 hours, as the effects of the drug wore off, Dr. Bansal removed his eyeshades and headphones. He was completely drained.
“Even though I was lying down on my back for 7 hours, I felt like I had been run over by a truck. I was exhausted beyond belief physically and mentally.”
This was partly because of the fact that he hadn’t eaten much during the session. But mostly, said Dr. Bansal, it was because of the searing emotional intensity of the experience.
After the journey
It’s hard to put into words, said Dr. Bansal, what this treatment has done for his life. He feels as if he has stumbled onto something very precious that had been right in front of him all along. He wrote of his change in perspective almost obsessively in his journal in the days and weeks after treatment. One passage reads:
“It seems that, as time is passing on, I’m becoming more relaxed and hopeful, more calm, and at peace. Family has become even more important to me now. Money, politics, material gains, alcohol, seem less important.”
And yet there was nothing “easy” about the experience. In fact, in some ways the experience demanded more from him. “I feel I need to be more compassionate and considerate – less irritable and angry, more understanding of others’ needs. I feel I need to be a better human being, a better patient, a better father, and a better doctor for my patients.”
The experience, he said, gave him something far more important than mere ease. It gave him a sense of meaning.
From his journal:
“I died, and I was reborn. If I survived this, then I can face anything and anybody in the cosmic scheme. I can become part of it.
“How many sorrows in the universe? My cancer is nothing. Life does not end with the end of life. What was will be again. Eternally.”
That’s not an unusual response, according to the namesake of the Bill Richards Center for Healing. Bill Richards, PhD, has worked in the world of psychedelic-assisted psychotherapy since 1963.
A psychologist with decades of experience, Dr. Richards and colleagues figure that, with few possible exceptions, he has helped treat more people with psychedelic therapies than anyone alive in Western medicine today. At Aquilino, he works directly with patients and oversees the therapy protocol that goes along with the psilocybin dosing sessions.
“It’s inspiring,” Dr. Richards said.
“You meet someone who’s very depressed and scared and isolating from family and having all kinds of physical complaints. And a few days later, you talk to the same person and they have a whole new lease on life.”
And the positive effects can extend deep into the family system, he said.
After psilocybin treatment, said Dr. Richards, the person with cancer can become a kind of social worker for the family. They’re often far better able to talk about death and loss and even money and family issues than their loved ones. It’s not uncommon after treatment to see the resolution of years-old resentments or grievances that have dogged a family for many years.
Plus, said Dr. Richards, the cancer patient often ends up as a kind model to other family members for how to approach death. “They can demonstrate how to live fully – right to the last breath – which is a real gift because those relatives and loved ones have to die someday too, you know.”
At 80 years old, Dr. Richards is still in active practice and hopes to spend the rest of his days working with people in end-of-life care.
After the experience
Psychedelic-assisted therapy does not end with the dosing session. Integration sessions, where you discuss what happened during the dosing session, are a key part of most treatments.
The goal is to help participants absorb and “integrate” their experience. It typically happens over two or more sessions of 60-90 minutes with a therapist. In some cases, the therapist may invite a significant other to join in the integration process.
Dr. Agrawal’s trial at the Bill Richards center added something new: group therapy. Not only did Dr. Bansal meet with his therapist, he also met with a group of three other people in the trial who had their dosing the same day.
The point, said Dr. Agrawal, is to try and determine the effect of the group on the therapy. After their private dosing sessions, they come back together to discuss their experiences.
“After the psilocybin, they feel like they’ve been to war together,” Dr. Agrawal said. “There is this profound openness and connection. They feel able to share things with each other that they wouldn’t with other people.”
It will take some time to figure out how the group affects the overall outcome, but Dr. Bansal thinks it was integral to the success of his treatment.
In fact, he continues to meet regularly with his therapy group, even though it’s long since past the requirements of the study.
Pradeep 2.0
Dr. Bansal still has tough days with his cancer. Recently, immunotherapy treatment for his bladder caused side effects – pain, bleeding, fever, and chills – for most of the night. He felt like he was “passing razor blades” when he peed.
“And yet it was somehow okay,” he said. “It was only pain.”
“It’s as if there is a part of me that is watching myself objectively, going through the painful process of treatments saying: ‘It’s all right. I will be with you through this journey, through this experience. Don’t worry.’”
Months after taking that one dose, Dr. Bansal still calls it as “the single most powerful experience of my life.”
The change in his mental outlook, Dr. Bansal said, was profound, particularly in regard to his cancer.
“I understood that I still had cancer and that it could kill me in a few weeks, or months, or years. But my perspective had shifted.”
Dr. Bansal was as surprised as anyone. “Had somebody told me going into this that I would come out a transformed being or a person with a completely different perspective on life, I would never have believed it.”
He even named his new outlook. “I call it Pradeep 2.0.”
A version of this article first appeared on WebMD.com.
Pradeep Bansal considered the five capsules he was about to swallow. Together they made up a 25-mg dose of a substance that, in another setting, could have landed him in federal prison.
The substance was psilocybin, the active ingredient in magic mushrooms. To be more exact, it was a synthetic form of psilocybin called COMP360, made to pharmaceutical standards by a company called COMPASS Pathways. He was taking it as part of an Food and Drug Administration–approved clinical study on mental health therapy for people with cancer.
Dr. Bansal, a New York gastroenterologist, was far more comfortable giving medical treatment than receiving it. But he was getting used to it.
He had already been through surgery and a number of other treatments to address the physical aspects of his cancer. The psilocybin was to address the mental aspects – the crushing anxiety and depression that had stuck with him after his diagnosis.
Dr. Bansal did not arrive at this moment lightly.
“I was extremely skeptical going into this process,” said Dr. Bansal, who during a long medical career had looked with distrust and even disdain at alternative therapies.
“I don’t have much patience for holistic medicine, homeopathy, acupuncture, or alternative medicines with claims of spiritual upliftment or altered states of mind.”
But Bansal had done his homework on psilocybin and was impressed.
according to studies published in 2011, 2014, and 2016.
One study from Johns Hopkins University tracked the effects of a single guided dose of psilocybin in terminal cancer patients with anxiety and depression. More than 80% had a “significant decrease” in symptoms – even 6 months after treatment – with more than 60% of the group remaining in the normal mood range.
For the study Dr. Bansal joined, there had been weeks of screening and consultation and preparation in a strictly controlled scientific trial.
And yet, even with all that he had learned, even with his psychiatrist-guide by his side, he was afraid. Afraid of what he might experience under the powerful effects of psilocybin. And afraid that this was all a misguided waste of time – that his mental angst would still be there when it was all over.
He knew that psilocybin, like other psychedelic substances, could take you on a “trip” – could remove you, at least for a time, from normal conscious experience.
Maybe he would feel “funny,” he thought. Maybe he would have some hallucinations. But how would that change the reality of his cancer? How would it lift the black dread and anxiety he felt about his future?
Stuck in a dark place
Dr. Bansal had first noticed blood in his urine – a lot of it – in September 2019.
Two months later, doctors diagnosed cancer in his right kidney. He would need surgery to remove the kidney and surrounding lymph nodes (an operation called radical nephrectomy).
It was a shock, said Dr. Bansal. But the diagnosis and the surgery happened so quickly that he hardly had time to think. And treatment results seemed good. The cancer was only in stage I and the CT scans showed no signs of cancer after surgery.
“We were so relieved. Everyone was so happy,” Dr. Bansal said. “They didn’t even give me chemotherapy after surgery because it seemed so early.”
But a routine scan in June 2020 revealed more cancer in his lung. Within a couple of months, it was in his bladder too.
“It was devastating,” Dr. Bansal said. “I went from thinking I was healthy again to stage IV cancer.”
As doctors scheduled surgery to remove part of his lung, Dr. Bansal started on painful immunotherapy (BCG therapy) for his bladder.
At this point, from a psychological standpoint, Dr. Bansal was reeling. As a doctor, he knew all too well the meaning of stage IV cancer.
With two adult children and a grandchild on the way, Dr. Bansal had been looking forward to retirement with his wife of almost 40 years. “Suddenly, I wasn’t sure I was going to last that long,” Bansal recalled. “I was in a very dark place. I was very anxious, very depressed from lack of sleep.”
He saw a therapist about his cancer diagnosis and maintained his regular meditation practice at home. He hired a personal trainer and tried to focus on any good news that he got about his treatment.
Those things helped, but not enough.
The basic facts were inescapable. His cancer might end everything. He couldn’t stop thinking about it. And then he couldn’t stop thinking about how he couldn’t stop thinking about it.
If the worst happened, he didn’t want to spend his last days in a state of such relentless existential angst. And it wasn’t just for himself. He wanted to be strong and mentally present for his family and his loved ones and his patients.
As he searched for something to ease his mental anguish, Dr. Bansal recalled some psychedelic research on end-of-life anxiety and depression that he’d read about in Michael Pollan’s book on psychedelics, “How to Change Your Mind” (New York, Penguin Press, 2018).
The studies were small and the research was new, but Dr. Bansal was impressed enough with the results to take a chance. He called a lead researcher of one of the studies, a fellow New York doctor, and eventually found himself accepted into a new study.
Starting the journey
By the time Dr. Bansal arrived at the Bill Richards Center for Healing at the Aquilino Cancer Center in Rockville, Md., he had already been through weeks of screening.
The main requirements for the study were a cancer diagnosis and a measurable level of depression. But study participants also had to be physically fit enough to handle the medication, and psychologically free from a personal or family history of psychosis or schizophrenia. (The study also required participants to slowly wean themselves from medications like SSRIs for depression or antianxiety medications under the strict supervision of a qualified doctor.)
Dr. Bansal’s week of treatment began almost immediately on arrival at Aquilino. Everything was carefully choreographed but not rushed. From Monday to Wednesday, doctors followed his physical health with exams, ECGs, and blood work. And most importantly, they began to prepare him for the “dosing session” on Thursday when he would take the psilocybin.
This is the careful crafting of “set and setting” stressed in so many psychedelic therapies. “Set” refers to your mindset going into the drug experience. “Setting” is the space and people around you when the drug sends you into an altered state of consciousness.
Dr. Bansal met several times with at least three therapists in the days leading up to his dosing. He attended 4-plus hours of therapist-led group sessions with other people who would get a dosing on the same day. Together, they talked about what to expect during the experience and what to do in the face of fear or panic.
He connected with a therapist who would be his personal guide. Dr. Bansal’s therapist was a military psychiatrist with over 30 years’ experience.
“He was there with me from day 1, and so we established a relationship,” Dr. Bansal said.
“He asked me a lot of personal background history – you know, my religious convictions, aspirations, all those things.”
“Trust and let go,” was a kind of mantra for the treatment repeated by his guide and other doctors.
For Dr. Bansal, a doctor and scientist accustomed to using hard facts rather than touchy-feely slogans to navigate the care of patients, it was an adjustment, to say the least.
But he did his best to set aside his doubts and embrace the journey he was about to take.
The day of the trip
Thursday morning finally arrived. The setting of the dosing room was warm and welcoming, more like a cozy home study than a hospital room.
This matters more than you might think. First, because it’s important that you feel safe, open, and comfortable enough to let go and enter into a therapeutic process. But also because though rare, it’s possible – especially with psilocybin – for people to lose track of where they are and what they’re doing and put themselves or others in danger.
The dose, 25 mg, had been carefully calibrated to induce a psychedelic experience sufficient for therapy. Much less than that, say 10 mg, isn’t enough for most people to enter this state. A double dose, 50 mg, though not physically unsafe, may leave you too incoherent to have the useful insights key to therapeutic value.
A doctor, the lead investigator of the study, brought the five capsules into the room in an intricately carved crucible with a small ceremonial cup that held the water with which to take it.
“It was very solemn,” Dr. Bansal said. “He sat down with me in a very calming way.”
The doctor said: “Don’t worry about it. Just trust and let go.”
And that’s just what he did.
Dr. Bansal swallowed the capsules and lay down. The doctor quietly left the room so that Dr. Bansal and his psychiatrist guide could begin their session together.
Special eye shades kept him in the pitch dark whether his eyes were open or closed. Headphones streamed a curated musical playlist – much of it Western classical like Strauss, Bach, Mozart, and Beethoven – but also modern electronica and other music from cultures around the globe.
Dr. Bansal would remain here, with his therapist-guide by his side, in largely this same position, for the next 7-and-a-half hours.
It took about 45 minutes for the medication to kick in.
The investigator
The doctor who brought the capsules into the dosing room was Manish Agrawal, MD, codirector of clinical research at the Aquilino Cancer Center and lead investigator of the study.
Dr. Agrawal trained at the National Cancer Institute and practiced for many years as an oncologist before developing an interest in psychedelic therapies. It was his work with cancer patients that drew him to psychedelics in the first place.
He had seen too many of his patients mentally wrecked by a cancer diagnosis, and he often felt helpless to comfort them.
“You take care of the physical aspects of the cancer, right? You talk about side effects and recommend another scan to look for recurrence.”
“But what about the psychological effects?”
They can be very serious and too often go ignored, said Dr. Agrawal. Your plans for the future suddenly become moot. You may be concerned about your ability to work or worried about the pain and suffering and financial strain that might be ahead for both you and your family. And to top it all off, you’re staring into the face of your own mortality.
So it’s no wonder, said Dr. Agrawal, that many people develop clinical levels of anxiety and depression after a cancer diagnosis.
Like Dr. Bansal, Dr. Agrawal had been impressed by early studies on psilocybin-assisted therapies for end-of-life anxiety and depression. He had tried other approaches – support groups, one-on-one therapy, religious counselors, psychiatrist-prescribed medication – but he was never really happy with the results.
To Dr. Agrawal, psilocybin-assisted therapy was the first thing that looked like it could really make a difference.
And so after his psychedelic certification at the California Institute of Integral Studies, Dr. Agrawal was determined to change his approach.
The result was the Bill Richards Center for Healing at Aquilino Cancer Center, built specifically to study psychedelic-assisted therapies for psychological distress in people with cancer. The mission of the center is to help develop safe, FDA-approved psychedelic therapies for the mental health of cancer patients, and, once approved, provide a state-of-the-art facility and staff to administer those treatments.
A trip into the unknown
Back in the dosing room, Dr. Bansal was starting to feel the effects of the medication. As the psilocybin kicked in, spectacular images swirled.
“It was as if a million stained glass windows had suddenly come to life and were dancing in front of my vision,” Dr. Bansal said.
There were moving landscapes and intricate swirling patterns and massive stages in the sky where he saw orchestras playing the music he was hearing.
Dr. Bansal saw himself being crushed by a huge machine and buried, dead, in the Earth. He died and returned to life several times, glided over the top of New York City with the skyscrapers just below him, and took in the vision of the entire universe.
“I saw this expanse of the sky that was limitless. And there was this prehistoric reptile creature that spanned galaxies in the sky ahead of me who was dying. I said: ‘My God, the universe is dying,’ but then after a few moments, the universe came to life again in a burst of stars exploding.”
All the while, Dr. Bansal said, he was well aware that it was simply his mind creating these images, thoughts, and ideas. He knew he was in a safe room wearing eyeshades and headphones.
And yet, he says, it felt true. “The images and feelings are so powerful that you cannot help but believe they are in some way a part of reality.”
“At one point, I saw this giant Ferris wheel coming towards me and it was full of giant crabs, clicking and clacking their pincers. And my brain told me: ‘That’s my cancer!’ ”
Dr. Bansal was terrified. But he and his therapist had arranged a system of signals before the session. “If I was feeling afraid, I would hold his hand and if I had other issues, I would raise my hand. If I was feeling good, I would give him a thumbs up.”
Dr. Bansal reached out to his therapist and grasped his hand. “I said, ‘My cancer is coming at me!’ ”
His therapist was clear about what to do: Stand firm and walk toward it.
“That’s what they tell you: If you see anything frightening, you face it. And that’s the whole point of this exercise. And so, I stood and walked forward, and it just blew off in a puff of smoke.”
A state of peace
Around 3 hours into the experience, Dr. Bansal started to feel an immense sense of peace, happiness, and even comfort.
“I felt like I was watching a movie or a multidimensional slideshow. I was also a part of the movie. I felt like I could tell my mind what I wanted to see, and it would show it to me. It’s almost like you can mold your own visions. It was mystical.”
After about 8 hours, as the effects of the drug wore off, Dr. Bansal removed his eyeshades and headphones. He was completely drained.
“Even though I was lying down on my back for 7 hours, I felt like I had been run over by a truck. I was exhausted beyond belief physically and mentally.”
This was partly because of the fact that he hadn’t eaten much during the session. But mostly, said Dr. Bansal, it was because of the searing emotional intensity of the experience.
After the journey
It’s hard to put into words, said Dr. Bansal, what this treatment has done for his life. He feels as if he has stumbled onto something very precious that had been right in front of him all along. He wrote of his change in perspective almost obsessively in his journal in the days and weeks after treatment. One passage reads:
“It seems that, as time is passing on, I’m becoming more relaxed and hopeful, more calm, and at peace. Family has become even more important to me now. Money, politics, material gains, alcohol, seem less important.”
And yet there was nothing “easy” about the experience. In fact, in some ways the experience demanded more from him. “I feel I need to be more compassionate and considerate – less irritable and angry, more understanding of others’ needs. I feel I need to be a better human being, a better patient, a better father, and a better doctor for my patients.”
The experience, he said, gave him something far more important than mere ease. It gave him a sense of meaning.
From his journal:
“I died, and I was reborn. If I survived this, then I can face anything and anybody in the cosmic scheme. I can become part of it.
“How many sorrows in the universe? My cancer is nothing. Life does not end with the end of life. What was will be again. Eternally.”
That’s not an unusual response, according to the namesake of the Bill Richards Center for Healing. Bill Richards, PhD, has worked in the world of psychedelic-assisted psychotherapy since 1963.
A psychologist with decades of experience, Dr. Richards and colleagues figure that, with few possible exceptions, he has helped treat more people with psychedelic therapies than anyone alive in Western medicine today. At Aquilino, he works directly with patients and oversees the therapy protocol that goes along with the psilocybin dosing sessions.
“It’s inspiring,” Dr. Richards said.
“You meet someone who’s very depressed and scared and isolating from family and having all kinds of physical complaints. And a few days later, you talk to the same person and they have a whole new lease on life.”
And the positive effects can extend deep into the family system, he said.
After psilocybin treatment, said Dr. Richards, the person with cancer can become a kind of social worker for the family. They’re often far better able to talk about death and loss and even money and family issues than their loved ones. It’s not uncommon after treatment to see the resolution of years-old resentments or grievances that have dogged a family for many years.
Plus, said Dr. Richards, the cancer patient often ends up as a kind model to other family members for how to approach death. “They can demonstrate how to live fully – right to the last breath – which is a real gift because those relatives and loved ones have to die someday too, you know.”
At 80 years old, Dr. Richards is still in active practice and hopes to spend the rest of his days working with people in end-of-life care.
After the experience
Psychedelic-assisted therapy does not end with the dosing session. Integration sessions, where you discuss what happened during the dosing session, are a key part of most treatments.
The goal is to help participants absorb and “integrate” their experience. It typically happens over two or more sessions of 60-90 minutes with a therapist. In some cases, the therapist may invite a significant other to join in the integration process.
Dr. Agrawal’s trial at the Bill Richards center added something new: group therapy. Not only did Dr. Bansal meet with his therapist, he also met with a group of three other people in the trial who had their dosing the same day.
The point, said Dr. Agrawal, is to try and determine the effect of the group on the therapy. After their private dosing sessions, they come back together to discuss their experiences.
“After the psilocybin, they feel like they’ve been to war together,” Dr. Agrawal said. “There is this profound openness and connection. They feel able to share things with each other that they wouldn’t with other people.”
It will take some time to figure out how the group affects the overall outcome, but Dr. Bansal thinks it was integral to the success of his treatment.
In fact, he continues to meet regularly with his therapy group, even though it’s long since past the requirements of the study.
Pradeep 2.0
Dr. Bansal still has tough days with his cancer. Recently, immunotherapy treatment for his bladder caused side effects – pain, bleeding, fever, and chills – for most of the night. He felt like he was “passing razor blades” when he peed.
“And yet it was somehow okay,” he said. “It was only pain.”
“It’s as if there is a part of me that is watching myself objectively, going through the painful process of treatments saying: ‘It’s all right. I will be with you through this journey, through this experience. Don’t worry.’”
Months after taking that one dose, Dr. Bansal still calls it as “the single most powerful experience of my life.”
The change in his mental outlook, Dr. Bansal said, was profound, particularly in regard to his cancer.
“I understood that I still had cancer and that it could kill me in a few weeks, or months, or years. But my perspective had shifted.”
Dr. Bansal was as surprised as anyone. “Had somebody told me going into this that I would come out a transformed being or a person with a completely different perspective on life, I would never have believed it.”
He even named his new outlook. “I call it Pradeep 2.0.”
A version of this article first appeared on WebMD.com.
Pradeep Bansal considered the five capsules he was about to swallow. Together they made up a 25-mg dose of a substance that, in another setting, could have landed him in federal prison.
The substance was psilocybin, the active ingredient in magic mushrooms. To be more exact, it was a synthetic form of psilocybin called COMP360, made to pharmaceutical standards by a company called COMPASS Pathways. He was taking it as part of an Food and Drug Administration–approved clinical study on mental health therapy for people with cancer.
Dr. Bansal, a New York gastroenterologist, was far more comfortable giving medical treatment than receiving it. But he was getting used to it.
He had already been through surgery and a number of other treatments to address the physical aspects of his cancer. The psilocybin was to address the mental aspects – the crushing anxiety and depression that had stuck with him after his diagnosis.
Dr. Bansal did not arrive at this moment lightly.
“I was extremely skeptical going into this process,” said Dr. Bansal, who during a long medical career had looked with distrust and even disdain at alternative therapies.
“I don’t have much patience for holistic medicine, homeopathy, acupuncture, or alternative medicines with claims of spiritual upliftment or altered states of mind.”
But Bansal had done his homework on psilocybin and was impressed.
according to studies published in 2011, 2014, and 2016.
One study from Johns Hopkins University tracked the effects of a single guided dose of psilocybin in terminal cancer patients with anxiety and depression. More than 80% had a “significant decrease” in symptoms – even 6 months after treatment – with more than 60% of the group remaining in the normal mood range.
For the study Dr. Bansal joined, there had been weeks of screening and consultation and preparation in a strictly controlled scientific trial.
And yet, even with all that he had learned, even with his psychiatrist-guide by his side, he was afraid. Afraid of what he might experience under the powerful effects of psilocybin. And afraid that this was all a misguided waste of time – that his mental angst would still be there when it was all over.
He knew that psilocybin, like other psychedelic substances, could take you on a “trip” – could remove you, at least for a time, from normal conscious experience.
Maybe he would feel “funny,” he thought. Maybe he would have some hallucinations. But how would that change the reality of his cancer? How would it lift the black dread and anxiety he felt about his future?
Stuck in a dark place
Dr. Bansal had first noticed blood in his urine – a lot of it – in September 2019.
Two months later, doctors diagnosed cancer in his right kidney. He would need surgery to remove the kidney and surrounding lymph nodes (an operation called radical nephrectomy).
It was a shock, said Dr. Bansal. But the diagnosis and the surgery happened so quickly that he hardly had time to think. And treatment results seemed good. The cancer was only in stage I and the CT scans showed no signs of cancer after surgery.
“We were so relieved. Everyone was so happy,” Dr. Bansal said. “They didn’t even give me chemotherapy after surgery because it seemed so early.”
But a routine scan in June 2020 revealed more cancer in his lung. Within a couple of months, it was in his bladder too.
“It was devastating,” Dr. Bansal said. “I went from thinking I was healthy again to stage IV cancer.”
As doctors scheduled surgery to remove part of his lung, Dr. Bansal started on painful immunotherapy (BCG therapy) for his bladder.
At this point, from a psychological standpoint, Dr. Bansal was reeling. As a doctor, he knew all too well the meaning of stage IV cancer.
With two adult children and a grandchild on the way, Dr. Bansal had been looking forward to retirement with his wife of almost 40 years. “Suddenly, I wasn’t sure I was going to last that long,” Bansal recalled. “I was in a very dark place. I was very anxious, very depressed from lack of sleep.”
He saw a therapist about his cancer diagnosis and maintained his regular meditation practice at home. He hired a personal trainer and tried to focus on any good news that he got about his treatment.
Those things helped, but not enough.
The basic facts were inescapable. His cancer might end everything. He couldn’t stop thinking about it. And then he couldn’t stop thinking about how he couldn’t stop thinking about it.
If the worst happened, he didn’t want to spend his last days in a state of such relentless existential angst. And it wasn’t just for himself. He wanted to be strong and mentally present for his family and his loved ones and his patients.
As he searched for something to ease his mental anguish, Dr. Bansal recalled some psychedelic research on end-of-life anxiety and depression that he’d read about in Michael Pollan’s book on psychedelics, “How to Change Your Mind” (New York, Penguin Press, 2018).
The studies were small and the research was new, but Dr. Bansal was impressed enough with the results to take a chance. He called a lead researcher of one of the studies, a fellow New York doctor, and eventually found himself accepted into a new study.
Starting the journey
By the time Dr. Bansal arrived at the Bill Richards Center for Healing at the Aquilino Cancer Center in Rockville, Md., he had already been through weeks of screening.
The main requirements for the study were a cancer diagnosis and a measurable level of depression. But study participants also had to be physically fit enough to handle the medication, and psychologically free from a personal or family history of psychosis or schizophrenia. (The study also required participants to slowly wean themselves from medications like SSRIs for depression or antianxiety medications under the strict supervision of a qualified doctor.)
Dr. Bansal’s week of treatment began almost immediately on arrival at Aquilino. Everything was carefully choreographed but not rushed. From Monday to Wednesday, doctors followed his physical health with exams, ECGs, and blood work. And most importantly, they began to prepare him for the “dosing session” on Thursday when he would take the psilocybin.
This is the careful crafting of “set and setting” stressed in so many psychedelic therapies. “Set” refers to your mindset going into the drug experience. “Setting” is the space and people around you when the drug sends you into an altered state of consciousness.
Dr. Bansal met several times with at least three therapists in the days leading up to his dosing. He attended 4-plus hours of therapist-led group sessions with other people who would get a dosing on the same day. Together, they talked about what to expect during the experience and what to do in the face of fear or panic.
He connected with a therapist who would be his personal guide. Dr. Bansal’s therapist was a military psychiatrist with over 30 years’ experience.
“He was there with me from day 1, and so we established a relationship,” Dr. Bansal said.
“He asked me a lot of personal background history – you know, my religious convictions, aspirations, all those things.”
“Trust and let go,” was a kind of mantra for the treatment repeated by his guide and other doctors.
For Dr. Bansal, a doctor and scientist accustomed to using hard facts rather than touchy-feely slogans to navigate the care of patients, it was an adjustment, to say the least.
But he did his best to set aside his doubts and embrace the journey he was about to take.
The day of the trip
Thursday morning finally arrived. The setting of the dosing room was warm and welcoming, more like a cozy home study than a hospital room.
This matters more than you might think. First, because it’s important that you feel safe, open, and comfortable enough to let go and enter into a therapeutic process. But also because though rare, it’s possible – especially with psilocybin – for people to lose track of where they are and what they’re doing and put themselves or others in danger.
The dose, 25 mg, had been carefully calibrated to induce a psychedelic experience sufficient for therapy. Much less than that, say 10 mg, isn’t enough for most people to enter this state. A double dose, 50 mg, though not physically unsafe, may leave you too incoherent to have the useful insights key to therapeutic value.
A doctor, the lead investigator of the study, brought the five capsules into the room in an intricately carved crucible with a small ceremonial cup that held the water with which to take it.
“It was very solemn,” Dr. Bansal said. “He sat down with me in a very calming way.”
The doctor said: “Don’t worry about it. Just trust and let go.”
And that’s just what he did.
Dr. Bansal swallowed the capsules and lay down. The doctor quietly left the room so that Dr. Bansal and his psychiatrist guide could begin their session together.
Special eye shades kept him in the pitch dark whether his eyes were open or closed. Headphones streamed a curated musical playlist – much of it Western classical like Strauss, Bach, Mozart, and Beethoven – but also modern electronica and other music from cultures around the globe.
Dr. Bansal would remain here, with his therapist-guide by his side, in largely this same position, for the next 7-and-a-half hours.
It took about 45 minutes for the medication to kick in.
The investigator
The doctor who brought the capsules into the dosing room was Manish Agrawal, MD, codirector of clinical research at the Aquilino Cancer Center and lead investigator of the study.
Dr. Agrawal trained at the National Cancer Institute and practiced for many years as an oncologist before developing an interest in psychedelic therapies. It was his work with cancer patients that drew him to psychedelics in the first place.
He had seen too many of his patients mentally wrecked by a cancer diagnosis, and he often felt helpless to comfort them.
“You take care of the physical aspects of the cancer, right? You talk about side effects and recommend another scan to look for recurrence.”
“But what about the psychological effects?”
They can be very serious and too often go ignored, said Dr. Agrawal. Your plans for the future suddenly become moot. You may be concerned about your ability to work or worried about the pain and suffering and financial strain that might be ahead for both you and your family. And to top it all off, you’re staring into the face of your own mortality.
So it’s no wonder, said Dr. Agrawal, that many people develop clinical levels of anxiety and depression after a cancer diagnosis.
Like Dr. Bansal, Dr. Agrawal had been impressed by early studies on psilocybin-assisted therapies for end-of-life anxiety and depression. He had tried other approaches – support groups, one-on-one therapy, religious counselors, psychiatrist-prescribed medication – but he was never really happy with the results.
To Dr. Agrawal, psilocybin-assisted therapy was the first thing that looked like it could really make a difference.
And so after his psychedelic certification at the California Institute of Integral Studies, Dr. Agrawal was determined to change his approach.
The result was the Bill Richards Center for Healing at Aquilino Cancer Center, built specifically to study psychedelic-assisted therapies for psychological distress in people with cancer. The mission of the center is to help develop safe, FDA-approved psychedelic therapies for the mental health of cancer patients, and, once approved, provide a state-of-the-art facility and staff to administer those treatments.
A trip into the unknown
Back in the dosing room, Dr. Bansal was starting to feel the effects of the medication. As the psilocybin kicked in, spectacular images swirled.
“It was as if a million stained glass windows had suddenly come to life and were dancing in front of my vision,” Dr. Bansal said.
There were moving landscapes and intricate swirling patterns and massive stages in the sky where he saw orchestras playing the music he was hearing.
Dr. Bansal saw himself being crushed by a huge machine and buried, dead, in the Earth. He died and returned to life several times, glided over the top of New York City with the skyscrapers just below him, and took in the vision of the entire universe.
“I saw this expanse of the sky that was limitless. And there was this prehistoric reptile creature that spanned galaxies in the sky ahead of me who was dying. I said: ‘My God, the universe is dying,’ but then after a few moments, the universe came to life again in a burst of stars exploding.”
All the while, Dr. Bansal said, he was well aware that it was simply his mind creating these images, thoughts, and ideas. He knew he was in a safe room wearing eyeshades and headphones.
And yet, he says, it felt true. “The images and feelings are so powerful that you cannot help but believe they are in some way a part of reality.”
“At one point, I saw this giant Ferris wheel coming towards me and it was full of giant crabs, clicking and clacking their pincers. And my brain told me: ‘That’s my cancer!’ ”
Dr. Bansal was terrified. But he and his therapist had arranged a system of signals before the session. “If I was feeling afraid, I would hold his hand and if I had other issues, I would raise my hand. If I was feeling good, I would give him a thumbs up.”
Dr. Bansal reached out to his therapist and grasped his hand. “I said, ‘My cancer is coming at me!’ ”
His therapist was clear about what to do: Stand firm and walk toward it.
“That’s what they tell you: If you see anything frightening, you face it. And that’s the whole point of this exercise. And so, I stood and walked forward, and it just blew off in a puff of smoke.”
A state of peace
Around 3 hours into the experience, Dr. Bansal started to feel an immense sense of peace, happiness, and even comfort.
“I felt like I was watching a movie or a multidimensional slideshow. I was also a part of the movie. I felt like I could tell my mind what I wanted to see, and it would show it to me. It’s almost like you can mold your own visions. It was mystical.”
After about 8 hours, as the effects of the drug wore off, Dr. Bansal removed his eyeshades and headphones. He was completely drained.
“Even though I was lying down on my back for 7 hours, I felt like I had been run over by a truck. I was exhausted beyond belief physically and mentally.”
This was partly because of the fact that he hadn’t eaten much during the session. But mostly, said Dr. Bansal, it was because of the searing emotional intensity of the experience.
After the journey
It’s hard to put into words, said Dr. Bansal, what this treatment has done for his life. He feels as if he has stumbled onto something very precious that had been right in front of him all along. He wrote of his change in perspective almost obsessively in his journal in the days and weeks after treatment. One passage reads:
“It seems that, as time is passing on, I’m becoming more relaxed and hopeful, more calm, and at peace. Family has become even more important to me now. Money, politics, material gains, alcohol, seem less important.”
And yet there was nothing “easy” about the experience. In fact, in some ways the experience demanded more from him. “I feel I need to be more compassionate and considerate – less irritable and angry, more understanding of others’ needs. I feel I need to be a better human being, a better patient, a better father, and a better doctor for my patients.”
The experience, he said, gave him something far more important than mere ease. It gave him a sense of meaning.
From his journal:
“I died, and I was reborn. If I survived this, then I can face anything and anybody in the cosmic scheme. I can become part of it.
“How many sorrows in the universe? My cancer is nothing. Life does not end with the end of life. What was will be again. Eternally.”
That’s not an unusual response, according to the namesake of the Bill Richards Center for Healing. Bill Richards, PhD, has worked in the world of psychedelic-assisted psychotherapy since 1963.
A psychologist with decades of experience, Dr. Richards and colleagues figure that, with few possible exceptions, he has helped treat more people with psychedelic therapies than anyone alive in Western medicine today. At Aquilino, he works directly with patients and oversees the therapy protocol that goes along with the psilocybin dosing sessions.
“It’s inspiring,” Dr. Richards said.
“You meet someone who’s very depressed and scared and isolating from family and having all kinds of physical complaints. And a few days later, you talk to the same person and they have a whole new lease on life.”
And the positive effects can extend deep into the family system, he said.
After psilocybin treatment, said Dr. Richards, the person with cancer can become a kind of social worker for the family. They’re often far better able to talk about death and loss and even money and family issues than their loved ones. It’s not uncommon after treatment to see the resolution of years-old resentments or grievances that have dogged a family for many years.
Plus, said Dr. Richards, the cancer patient often ends up as a kind model to other family members for how to approach death. “They can demonstrate how to live fully – right to the last breath – which is a real gift because those relatives and loved ones have to die someday too, you know.”
At 80 years old, Dr. Richards is still in active practice and hopes to spend the rest of his days working with people in end-of-life care.
After the experience
Psychedelic-assisted therapy does not end with the dosing session. Integration sessions, where you discuss what happened during the dosing session, are a key part of most treatments.
The goal is to help participants absorb and “integrate” their experience. It typically happens over two or more sessions of 60-90 minutes with a therapist. In some cases, the therapist may invite a significant other to join in the integration process.
Dr. Agrawal’s trial at the Bill Richards center added something new: group therapy. Not only did Dr. Bansal meet with his therapist, he also met with a group of three other people in the trial who had their dosing the same day.
The point, said Dr. Agrawal, is to try and determine the effect of the group on the therapy. After their private dosing sessions, they come back together to discuss their experiences.
“After the psilocybin, they feel like they’ve been to war together,” Dr. Agrawal said. “There is this profound openness and connection. They feel able to share things with each other that they wouldn’t with other people.”
It will take some time to figure out how the group affects the overall outcome, but Dr. Bansal thinks it was integral to the success of his treatment.
In fact, he continues to meet regularly with his therapy group, even though it’s long since past the requirements of the study.
Pradeep 2.0
Dr. Bansal still has tough days with his cancer. Recently, immunotherapy treatment for his bladder caused side effects – pain, bleeding, fever, and chills – for most of the night. He felt like he was “passing razor blades” when he peed.
“And yet it was somehow okay,” he said. “It was only pain.”
“It’s as if there is a part of me that is watching myself objectively, going through the painful process of treatments saying: ‘It’s all right. I will be with you through this journey, through this experience. Don’t worry.’”
Months after taking that one dose, Dr. Bansal still calls it as “the single most powerful experience of my life.”
The change in his mental outlook, Dr. Bansal said, was profound, particularly in regard to his cancer.
“I understood that I still had cancer and that it could kill me in a few weeks, or months, or years. But my perspective had shifted.”
Dr. Bansal was as surprised as anyone. “Had somebody told me going into this that I would come out a transformed being or a person with a completely different perspective on life, I would never have believed it.”
He even named his new outlook. “I call it Pradeep 2.0.”
A version of this article first appeared on WebMD.com.
Experts plead for more pediatric telehealth
A specialty group is asking federal and state governments to preserve and expand access to telehealth services for children with developmental and behavioral problems.
Citing the success during the COVID-19 pandemic of telehealth for these patients, the Society for Developmental and Behavioral Pediatrics (SDBP) has issued a position statement in its official journal calling for continued use of video and telephone for home-based diagnostic assessments, medication management follow-ups, and therapeutic interventions for children with autism spectrum disorder, attention-deficit/hyperactivity disorder, and other neurodevelopmental conditions.
“Telehealth offers plenty of opportunities for quick check-ins. It can offer some crisis management opportunities ... to address a parent’s concern about challenging behaviors or navigating school system issues or developmental needs,” lead author Robert D. Keder, MD, assistant professor of pediatrics at University of Connecticut, Farmington, and cochair of SDBP’s Advocacy Committee, told this news organization.
“The video visit does really offer us so much more. It’s so enriching and lets us as providers meet the child in their natural home environment. The real magic of a video visit is we haven’t done house calls as a medical society for decades. But now, literally, the power of telehealth lets us do a house call.”
In the face of the pandemic, emergency government policies allowed care to continue remotely via telehealth, including video and phone calls. The policies have allowed patients to have video visits in their own home, lifted provider licensure requirements for visits across state lines, and allowed reimbursement not only for video visits but also for telephone encounters.
As a result, the field of developmental and behavioral pediatrics (DBP) has recognized telehealth as a viable and useful model of care for children with neurodevelopmental disorders, said Neelkamal Soares, MD, a member of the society’s board and a coauthor of the position paper.
“Telehealth has been helpful in mitigating barriers families often face when attending in-person visits,” such as the lack of transportation and child care, missed work hours, and other issues, said Dr. Soares, professor of pediatric and adolescent medicine at Western Michigan University Stryker in Kalamazoo. At the same time, the growth in the use of the technology has highlighted additional obstacles to equitable access to care, including broadband connectivity, digital literacy, and the availability of interpretation and sign language services, he said.
Dr. Keder said telehealth has enabled him to better help with behavior management by observing children where they are most comfortable. Remote visits also allow him to consider information such as furniture arrangements and how that can affect the patient’s living conditions, and also sibling interactions, learning and homework, eating, and sleep.
Telemedicine conferences enable DBP specialists to facilitate care collaboration with different members of the patient’s care team. Consent from a family and a click of a button allows for therapists, early intervention specialists, teachers, school nurses, or even primary care providers the capacity to participate in a telehealth visit, he said.
Dr. Keder said the future of telehealth is uncertain. The policies from the pandemic may expire in the near term and vary from state to state. The goal of the policy statement is to advocate for legislation and policies that support ongoing, equitable, home-based telehealth care for patients seen by DBP providers while ensuring equitable access to DBP in general.
Kate Benton, PhD, a clinical psychologist with Lurie Children’s Hospital at Northwestern Medicine Central DuPage Hospital in Winfield, Ill., said the society has done an excellent job of explaining the need to maintain telehealth in light of the shortage of pediatricians, clinical psychologists, and other professionals in the field.
“Telehealth has opened new avenues for these patients who otherwise have difficulty seeing specialists. This is a population of children who without telehealth have significant challenges in getting access to care,” she said.
Wendy Fournier, mother of an autistic child and president of the National Autism Association, said telehealth can be beneficial for some individuals with the disorder.
“There are many aspects of in-person doctor visits that can be overwhelming, including bright lights, many people talking, waiting for the doctor, being comfortable with the doctor’s touch, etc.,” Ms. Fournier said in an interview. “All of these things can cause sensory and emotional dysregulation leading to overwhelming anxiety and fear.”
Visits to the doctor can be especially difficult for people who are nonverbal and unable to express their discomfort, said.
“At my daughter’s last medical appointment, she could not stay in the exam room and pulled me out the door. Thankfully, we have an understanding and compassionate physician who finished our appointment in our car. I believe that telehealth visits should remain available as a necessary and vital accommodation for people with disabilities,” Ms. Fournier said.
False equivalence?
Dr. Soares said researchers have attempted to assess the evidence of telehealth benefits in such situations as ADHD, cognitive behavioral therapy, and parent training.
“There is a paucity of published studies that specifically look at different conditions and compare in-person to telehealth visits, but these are ongoing in autism diagnostics and other areas by several SDBP members,” he said. “Stay tuned.”
Dr. Keder added that telehealth will never replace in-person visits, but the availability of this new option gives developmental pediatricians flexibility in strategies in treating and evaluating patients.
“Both are helpful and viable models. In the pandemic, we were forced out of necessity to embrace telehealth,” he said. “Because of this, we are seeing the power and benefits telehealth offers. Now many families like a mixture of alternating in person with telehealth visits.”
The policy statement cites research that finds patients are highly satisfied with telehealth and that telehealth may cost less than in-office visits.
The report stresses that equitable access to devices needed for telehealth visits is a concern because there is disproportionate access to required technology, especially in rural and underserved communities. The Federal Communications Commission has provided grants to eligible families to offset the cost, in part, for a laptop, desktop computer, or tablet. However, more is still needed, the group said.
The position paper calls for:
- Equitable access to the infrastructure and technology for telehealth, including greater access to broadband services in rural and underserved areas.
- Increased access to devices needed to connect children with neurodevelopmental disorders with critical health care services.
- Reimbursement of interpretation services for the people who are deaf and/or have limited English proficiency.
- Mitigation of geographic barriers to accessing DBP care.
- Permitting patients to access telehealth from their home or whichever physical location provides opportunities for safe and timely care, especially for established patients.
- Ensuring more engagement by state medical licensing boards to join the Interstate Medical Licensing Compact to provide care by telehealth when there is already an insufficient geographic distribution of that type of provider in a state, as is being conducted in the field of psychology.
- Ensuring ongoing reimbursement.
- Parity in reimbursement for telehealth in-person visits.
- Increased funding for research looking into outcomes, quality, and effectiveness of telehealth services at the federal and state levels.
“Our organization can work with families to educate lawmakers, insurance administrators, and organizational leaders about the value that telehealth holds in the care of their child and family,” Dr. Soares said. “We can also conduct research to add to the evidence based around the topic to further the science around telehealth outcomes and equivalency to in-person settings.”
“With the current workforce shortage in DBP and behavioral health it is more critical than ever to maintain access to care,” Dr. Keder added. “The pandemic has provided an opportunity to better harness the amazing power of telehealth to allow for access to equitable care for families. We hope that this statement moves legislators, leaders, and voters to continue to advocate for ongoing telehealth at both the state, federal, and organizational levels.”
Dr. Benton, Dr. Keder, and Dr. Soares have disclosed no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
A specialty group is asking federal and state governments to preserve and expand access to telehealth services for children with developmental and behavioral problems.
Citing the success during the COVID-19 pandemic of telehealth for these patients, the Society for Developmental and Behavioral Pediatrics (SDBP) has issued a position statement in its official journal calling for continued use of video and telephone for home-based diagnostic assessments, medication management follow-ups, and therapeutic interventions for children with autism spectrum disorder, attention-deficit/hyperactivity disorder, and other neurodevelopmental conditions.
“Telehealth offers plenty of opportunities for quick check-ins. It can offer some crisis management opportunities ... to address a parent’s concern about challenging behaviors or navigating school system issues or developmental needs,” lead author Robert D. Keder, MD, assistant professor of pediatrics at University of Connecticut, Farmington, and cochair of SDBP’s Advocacy Committee, told this news organization.
“The video visit does really offer us so much more. It’s so enriching and lets us as providers meet the child in their natural home environment. The real magic of a video visit is we haven’t done house calls as a medical society for decades. But now, literally, the power of telehealth lets us do a house call.”
In the face of the pandemic, emergency government policies allowed care to continue remotely via telehealth, including video and phone calls. The policies have allowed patients to have video visits in their own home, lifted provider licensure requirements for visits across state lines, and allowed reimbursement not only for video visits but also for telephone encounters.
As a result, the field of developmental and behavioral pediatrics (DBP) has recognized telehealth as a viable and useful model of care for children with neurodevelopmental disorders, said Neelkamal Soares, MD, a member of the society’s board and a coauthor of the position paper.
“Telehealth has been helpful in mitigating barriers families often face when attending in-person visits,” such as the lack of transportation and child care, missed work hours, and other issues, said Dr. Soares, professor of pediatric and adolescent medicine at Western Michigan University Stryker in Kalamazoo. At the same time, the growth in the use of the technology has highlighted additional obstacles to equitable access to care, including broadband connectivity, digital literacy, and the availability of interpretation and sign language services, he said.
Dr. Keder said telehealth has enabled him to better help with behavior management by observing children where they are most comfortable. Remote visits also allow him to consider information such as furniture arrangements and how that can affect the patient’s living conditions, and also sibling interactions, learning and homework, eating, and sleep.
Telemedicine conferences enable DBP specialists to facilitate care collaboration with different members of the patient’s care team. Consent from a family and a click of a button allows for therapists, early intervention specialists, teachers, school nurses, or even primary care providers the capacity to participate in a telehealth visit, he said.
Dr. Keder said the future of telehealth is uncertain. The policies from the pandemic may expire in the near term and vary from state to state. The goal of the policy statement is to advocate for legislation and policies that support ongoing, equitable, home-based telehealth care for patients seen by DBP providers while ensuring equitable access to DBP in general.
Kate Benton, PhD, a clinical psychologist with Lurie Children’s Hospital at Northwestern Medicine Central DuPage Hospital in Winfield, Ill., said the society has done an excellent job of explaining the need to maintain telehealth in light of the shortage of pediatricians, clinical psychologists, and other professionals in the field.
“Telehealth has opened new avenues for these patients who otherwise have difficulty seeing specialists. This is a population of children who without telehealth have significant challenges in getting access to care,” she said.
Wendy Fournier, mother of an autistic child and president of the National Autism Association, said telehealth can be beneficial for some individuals with the disorder.
“There are many aspects of in-person doctor visits that can be overwhelming, including bright lights, many people talking, waiting for the doctor, being comfortable with the doctor’s touch, etc.,” Ms. Fournier said in an interview. “All of these things can cause sensory and emotional dysregulation leading to overwhelming anxiety and fear.”
Visits to the doctor can be especially difficult for people who are nonverbal and unable to express their discomfort, said.
“At my daughter’s last medical appointment, she could not stay in the exam room and pulled me out the door. Thankfully, we have an understanding and compassionate physician who finished our appointment in our car. I believe that telehealth visits should remain available as a necessary and vital accommodation for people with disabilities,” Ms. Fournier said.
False equivalence?
Dr. Soares said researchers have attempted to assess the evidence of telehealth benefits in such situations as ADHD, cognitive behavioral therapy, and parent training.
“There is a paucity of published studies that specifically look at different conditions and compare in-person to telehealth visits, but these are ongoing in autism diagnostics and other areas by several SDBP members,” he said. “Stay tuned.”
Dr. Keder added that telehealth will never replace in-person visits, but the availability of this new option gives developmental pediatricians flexibility in strategies in treating and evaluating patients.
“Both are helpful and viable models. In the pandemic, we were forced out of necessity to embrace telehealth,” he said. “Because of this, we are seeing the power and benefits telehealth offers. Now many families like a mixture of alternating in person with telehealth visits.”
The policy statement cites research that finds patients are highly satisfied with telehealth and that telehealth may cost less than in-office visits.
The report stresses that equitable access to devices needed for telehealth visits is a concern because there is disproportionate access to required technology, especially in rural and underserved communities. The Federal Communications Commission has provided grants to eligible families to offset the cost, in part, for a laptop, desktop computer, or tablet. However, more is still needed, the group said.
The position paper calls for:
- Equitable access to the infrastructure and technology for telehealth, including greater access to broadband services in rural and underserved areas.
- Increased access to devices needed to connect children with neurodevelopmental disorders with critical health care services.
- Reimbursement of interpretation services for the people who are deaf and/or have limited English proficiency.
- Mitigation of geographic barriers to accessing DBP care.
- Permitting patients to access telehealth from their home or whichever physical location provides opportunities for safe and timely care, especially for established patients.
- Ensuring more engagement by state medical licensing boards to join the Interstate Medical Licensing Compact to provide care by telehealth when there is already an insufficient geographic distribution of that type of provider in a state, as is being conducted in the field of psychology.
- Ensuring ongoing reimbursement.
- Parity in reimbursement for telehealth in-person visits.
- Increased funding for research looking into outcomes, quality, and effectiveness of telehealth services at the federal and state levels.
“Our organization can work with families to educate lawmakers, insurance administrators, and organizational leaders about the value that telehealth holds in the care of their child and family,” Dr. Soares said. “We can also conduct research to add to the evidence based around the topic to further the science around telehealth outcomes and equivalency to in-person settings.”
“With the current workforce shortage in DBP and behavioral health it is more critical than ever to maintain access to care,” Dr. Keder added. “The pandemic has provided an opportunity to better harness the amazing power of telehealth to allow for access to equitable care for families. We hope that this statement moves legislators, leaders, and voters to continue to advocate for ongoing telehealth at both the state, federal, and organizational levels.”
Dr. Benton, Dr. Keder, and Dr. Soares have disclosed no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
A specialty group is asking federal and state governments to preserve and expand access to telehealth services for children with developmental and behavioral problems.
Citing the success during the COVID-19 pandemic of telehealth for these patients, the Society for Developmental and Behavioral Pediatrics (SDBP) has issued a position statement in its official journal calling for continued use of video and telephone for home-based diagnostic assessments, medication management follow-ups, and therapeutic interventions for children with autism spectrum disorder, attention-deficit/hyperactivity disorder, and other neurodevelopmental conditions.
“Telehealth offers plenty of opportunities for quick check-ins. It can offer some crisis management opportunities ... to address a parent’s concern about challenging behaviors or navigating school system issues or developmental needs,” lead author Robert D. Keder, MD, assistant professor of pediatrics at University of Connecticut, Farmington, and cochair of SDBP’s Advocacy Committee, told this news organization.
“The video visit does really offer us so much more. It’s so enriching and lets us as providers meet the child in their natural home environment. The real magic of a video visit is we haven’t done house calls as a medical society for decades. But now, literally, the power of telehealth lets us do a house call.”
In the face of the pandemic, emergency government policies allowed care to continue remotely via telehealth, including video and phone calls. The policies have allowed patients to have video visits in their own home, lifted provider licensure requirements for visits across state lines, and allowed reimbursement not only for video visits but also for telephone encounters.
As a result, the field of developmental and behavioral pediatrics (DBP) has recognized telehealth as a viable and useful model of care for children with neurodevelopmental disorders, said Neelkamal Soares, MD, a member of the society’s board and a coauthor of the position paper.
“Telehealth has been helpful in mitigating barriers families often face when attending in-person visits,” such as the lack of transportation and child care, missed work hours, and other issues, said Dr. Soares, professor of pediatric and adolescent medicine at Western Michigan University Stryker in Kalamazoo. At the same time, the growth in the use of the technology has highlighted additional obstacles to equitable access to care, including broadband connectivity, digital literacy, and the availability of interpretation and sign language services, he said.
Dr. Keder said telehealth has enabled him to better help with behavior management by observing children where they are most comfortable. Remote visits also allow him to consider information such as furniture arrangements and how that can affect the patient’s living conditions, and also sibling interactions, learning and homework, eating, and sleep.
Telemedicine conferences enable DBP specialists to facilitate care collaboration with different members of the patient’s care team. Consent from a family and a click of a button allows for therapists, early intervention specialists, teachers, school nurses, or even primary care providers the capacity to participate in a telehealth visit, he said.
Dr. Keder said the future of telehealth is uncertain. The policies from the pandemic may expire in the near term and vary from state to state. The goal of the policy statement is to advocate for legislation and policies that support ongoing, equitable, home-based telehealth care for patients seen by DBP providers while ensuring equitable access to DBP in general.
Kate Benton, PhD, a clinical psychologist with Lurie Children’s Hospital at Northwestern Medicine Central DuPage Hospital in Winfield, Ill., said the society has done an excellent job of explaining the need to maintain telehealth in light of the shortage of pediatricians, clinical psychologists, and other professionals in the field.
“Telehealth has opened new avenues for these patients who otherwise have difficulty seeing specialists. This is a population of children who without telehealth have significant challenges in getting access to care,” she said.
Wendy Fournier, mother of an autistic child and president of the National Autism Association, said telehealth can be beneficial for some individuals with the disorder.
“There are many aspects of in-person doctor visits that can be overwhelming, including bright lights, many people talking, waiting for the doctor, being comfortable with the doctor’s touch, etc.,” Ms. Fournier said in an interview. “All of these things can cause sensory and emotional dysregulation leading to overwhelming anxiety and fear.”
Visits to the doctor can be especially difficult for people who are nonverbal and unable to express their discomfort, said.
“At my daughter’s last medical appointment, she could not stay in the exam room and pulled me out the door. Thankfully, we have an understanding and compassionate physician who finished our appointment in our car. I believe that telehealth visits should remain available as a necessary and vital accommodation for people with disabilities,” Ms. Fournier said.
False equivalence?
Dr. Soares said researchers have attempted to assess the evidence of telehealth benefits in such situations as ADHD, cognitive behavioral therapy, and parent training.
“There is a paucity of published studies that specifically look at different conditions and compare in-person to telehealth visits, but these are ongoing in autism diagnostics and other areas by several SDBP members,” he said. “Stay tuned.”
Dr. Keder added that telehealth will never replace in-person visits, but the availability of this new option gives developmental pediatricians flexibility in strategies in treating and evaluating patients.
“Both are helpful and viable models. In the pandemic, we were forced out of necessity to embrace telehealth,” he said. “Because of this, we are seeing the power and benefits telehealth offers. Now many families like a mixture of alternating in person with telehealth visits.”
The policy statement cites research that finds patients are highly satisfied with telehealth and that telehealth may cost less than in-office visits.
The report stresses that equitable access to devices needed for telehealth visits is a concern because there is disproportionate access to required technology, especially in rural and underserved communities. The Federal Communications Commission has provided grants to eligible families to offset the cost, in part, for a laptop, desktop computer, or tablet. However, more is still needed, the group said.
The position paper calls for:
- Equitable access to the infrastructure and technology for telehealth, including greater access to broadband services in rural and underserved areas.
- Increased access to devices needed to connect children with neurodevelopmental disorders with critical health care services.
- Reimbursement of interpretation services for the people who are deaf and/or have limited English proficiency.
- Mitigation of geographic barriers to accessing DBP care.
- Permitting patients to access telehealth from their home or whichever physical location provides opportunities for safe and timely care, especially for established patients.
- Ensuring more engagement by state medical licensing boards to join the Interstate Medical Licensing Compact to provide care by telehealth when there is already an insufficient geographic distribution of that type of provider in a state, as is being conducted in the field of psychology.
- Ensuring ongoing reimbursement.
- Parity in reimbursement for telehealth in-person visits.
- Increased funding for research looking into outcomes, quality, and effectiveness of telehealth services at the federal and state levels.
“Our organization can work with families to educate lawmakers, insurance administrators, and organizational leaders about the value that telehealth holds in the care of their child and family,” Dr. Soares said. “We can also conduct research to add to the evidence based around the topic to further the science around telehealth outcomes and equivalency to in-person settings.”
“With the current workforce shortage in DBP and behavioral health it is more critical than ever to maintain access to care,” Dr. Keder added. “The pandemic has provided an opportunity to better harness the amazing power of telehealth to allow for access to equitable care for families. We hope that this statement moves legislators, leaders, and voters to continue to advocate for ongoing telehealth at both the state, federal, and organizational levels.”
Dr. Benton, Dr. Keder, and Dr. Soares have disclosed no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Mayo Clinic fires 700 employees for refusing COVID vaccine
The medical center, which is Minnesota’s largest employer, has major campuses in Arizona, Florida, and Minnesota and operates hospitals in Iowa and Wisconsin.
Employees had until Jan. 3 to get vaccinated or receive approval for an exemption. On Jan. 4, the hospital fired those who didn’t meet the requirement, according to Action News Jax, a CBS affiliate in Florida.
The 700 employees make up about 1% of Mayo Clinic’s 73,000-person workforce. So far, none of the employees at the campus in Jacksonville, Fla., have been affected, the news outlet reported.
“Florida staff who are not in compliance with our vaccination program remain employed pending the outcome of litigation related to the Centers for Medicare & Medicaid Services requirements,” a Mayo Clinic spokesperson told Action News Jax.
The federal government and Florida remain at odds over vaccine mandates, and several lawsuits are winding through the court system. Florida Gov. Ron DeSantis signed legislation in November that bans private Florida employers from requiring all employees to get vaccinated and calls for various exemption options, according to The Florida Times-Union. The state law clashes with a federal rule that requires vaccinations for all health care workers at hospitals that receive Medicare and Medicaid funding.
The Mayo Clinic mandate required employees to receive at least one COVID-19 vaccine dose and not be “overdue” for a second dose, according to the statement. Only medical and religious exemptions were allowed, and most medical and religious exemptions were approved.
“While Mayo Clinic is saddened to lose valuable employees, we need to take all steps necessary to keep our patients, workforce, visitors, and communities safe,” Mayo Clinic wrote in its statement. “If individuals released from employment choose to get vaccinated at a later date, the opportunity exists for them to apply and return to Mayo Clinic for future job openings.”
With the latest surge in COVID-19 cases from the Omicron variant, the Mayo Clinic also encouraged unvaccinated people to get a shot and those who are eligible for a booster to get one “as soon as possible.”
“Based on science and data, it’s clear that vaccination keeps people out of the hospital and saves lives,” according to the statement. “That’s true for everyone in our communities – and it’s especially true for the many patients with serious or complex diseases who seek care at Mayo Clinic each day.”
A version of this article first appeared on WebMD.com.
The medical center, which is Minnesota’s largest employer, has major campuses in Arizona, Florida, and Minnesota and operates hospitals in Iowa and Wisconsin.
Employees had until Jan. 3 to get vaccinated or receive approval for an exemption. On Jan. 4, the hospital fired those who didn’t meet the requirement, according to Action News Jax, a CBS affiliate in Florida.
The 700 employees make up about 1% of Mayo Clinic’s 73,000-person workforce. So far, none of the employees at the campus in Jacksonville, Fla., have been affected, the news outlet reported.
“Florida staff who are not in compliance with our vaccination program remain employed pending the outcome of litigation related to the Centers for Medicare & Medicaid Services requirements,” a Mayo Clinic spokesperson told Action News Jax.
The federal government and Florida remain at odds over vaccine mandates, and several lawsuits are winding through the court system. Florida Gov. Ron DeSantis signed legislation in November that bans private Florida employers from requiring all employees to get vaccinated and calls for various exemption options, according to The Florida Times-Union. The state law clashes with a federal rule that requires vaccinations for all health care workers at hospitals that receive Medicare and Medicaid funding.
The Mayo Clinic mandate required employees to receive at least one COVID-19 vaccine dose and not be “overdue” for a second dose, according to the statement. Only medical and religious exemptions were allowed, and most medical and religious exemptions were approved.
“While Mayo Clinic is saddened to lose valuable employees, we need to take all steps necessary to keep our patients, workforce, visitors, and communities safe,” Mayo Clinic wrote in its statement. “If individuals released from employment choose to get vaccinated at a later date, the opportunity exists for them to apply and return to Mayo Clinic for future job openings.”
With the latest surge in COVID-19 cases from the Omicron variant, the Mayo Clinic also encouraged unvaccinated people to get a shot and those who are eligible for a booster to get one “as soon as possible.”
“Based on science and data, it’s clear that vaccination keeps people out of the hospital and saves lives,” according to the statement. “That’s true for everyone in our communities – and it’s especially true for the many patients with serious or complex diseases who seek care at Mayo Clinic each day.”
A version of this article first appeared on WebMD.com.
The medical center, which is Minnesota’s largest employer, has major campuses in Arizona, Florida, and Minnesota and operates hospitals in Iowa and Wisconsin.
Employees had until Jan. 3 to get vaccinated or receive approval for an exemption. On Jan. 4, the hospital fired those who didn’t meet the requirement, according to Action News Jax, a CBS affiliate in Florida.
The 700 employees make up about 1% of Mayo Clinic’s 73,000-person workforce. So far, none of the employees at the campus in Jacksonville, Fla., have been affected, the news outlet reported.
“Florida staff who are not in compliance with our vaccination program remain employed pending the outcome of litigation related to the Centers for Medicare & Medicaid Services requirements,” a Mayo Clinic spokesperson told Action News Jax.
The federal government and Florida remain at odds over vaccine mandates, and several lawsuits are winding through the court system. Florida Gov. Ron DeSantis signed legislation in November that bans private Florida employers from requiring all employees to get vaccinated and calls for various exemption options, according to The Florida Times-Union. The state law clashes with a federal rule that requires vaccinations for all health care workers at hospitals that receive Medicare and Medicaid funding.
The Mayo Clinic mandate required employees to receive at least one COVID-19 vaccine dose and not be “overdue” for a second dose, according to the statement. Only medical and religious exemptions were allowed, and most medical and religious exemptions were approved.
“While Mayo Clinic is saddened to lose valuable employees, we need to take all steps necessary to keep our patients, workforce, visitors, and communities safe,” Mayo Clinic wrote in its statement. “If individuals released from employment choose to get vaccinated at a later date, the opportunity exists for them to apply and return to Mayo Clinic for future job openings.”
With the latest surge in COVID-19 cases from the Omicron variant, the Mayo Clinic also encouraged unvaccinated people to get a shot and those who are eligible for a booster to get one “as soon as possible.”
“Based on science and data, it’s clear that vaccination keeps people out of the hospital and saves lives,” according to the statement. “That’s true for everyone in our communities – and it’s especially true for the many patients with serious or complex diseases who seek care at Mayo Clinic each day.”
A version of this article first appeared on WebMD.com.
Using Telehealth Rehabilitation Therapy to Treat a Finger Flexor Tendon Repair During COVID-19
Telehealth-assisted finger rehabilitat ion therapy demonstrated good functional results following repair of a zone 2 flexor tendon laceration.
In 1948, Sterling Bunnell, MD, used the term no man’s land to describe the area between the A1 pulley at the volar aspect of the metacarpophalangeal joint and the insertion of the flexor digitorum superficialis tendons on the middle phalanx (zone 2).1 Bunnell’s description referenced the area of land in World War I between the trenches of opposing armies, and his goal was to emphasize the heightened risks of performing tendon repair in this area, as these repairs were notorious for poor outcomes. In lieu of tendon repair, Bunnell advocated treatment of tendon lacerations in this area with tendon excision and grafting.
It was not until the 1960s that researchers began to advocate for acute repair of tendons in this area.2,3 Since Verdan’s and Kleinart’s work, fastidious adherence to atraumatic technique and improvements in suture technique and rehabilitation protocols have allowed hand surgeons to repair tendons in this area with some level of success. Over the ensuing decades, acute repair of flexor tendon injuries within zone 2 has become the standard of care. The importance of meticulous technique during flexor tendon repair cannot be overemphasized; however, without appropriate hand therapy, even the most meticulous repair may fail.
COVID-19 has created significant barriers to patient care. Reducing travel and limiting face-to-face patient visits have been emphasized as methods that reduce spread of the virus, but these restrictions also prevent patients from easily accessing hand therapy. Recent adoption of telemedicine and videoconferencing technologies may help to reduce some of these barriers, but few previous studies have described the use of videoconferencing technology to supplant face-to-face hand therapy visits. This case describes the use of videoconferencing technology to provide hand therapy for a patient following repair of an acute flexor tendon laceration in zone 2.
Case Presentation
A patient aged < 50 years presented to a US Department of Veterans Affairs (VA) hand surgery clinic 2 days after sustaining a laceration to the flexor digitorum profundus (FDP) in zone 2 of the small finger while cleaning a knife. During the discussion of their treatment options and the recommended postoperative hand therapy protocol, the patient noted difficulty attending postoperative appointments due to COVID-19 as well as a lack of resources. Given these limitations and following discussion with our hand therapist, we discussed the potential for telehealth follow-up with videoconferencing. Four days following the injury, the patient underwent repair of the FDP. During surgery, the laceration was present at the level of the A3 pulley. The FDP was repaired using a 6-0 polypropylene synthetic suture for the epitendinous repair and 4-strand core suture repair using 3-0 Fiberwire suture in a modified cruciate fashion. The A2 and A4 pulleys were preserved, and venting of the pulleys was not required. At the time of surgery, the flexor digitorum superficialis and radial and ulnar digital neurovascular bundles were intact. Following surgical repair of the tendon, the patient was placed into a dorsal blocking splint with a plan for follow-up within 2 to 3 days.
The patient attended the first postoperative visit in person on postoperative day 2. During this visit, the postoperative splint and dressings were removed, and a forearm-based dorsal blocking orthosis was fabricated using thermoplastic. At this visit, the veteran relayed concerns regarding psychosocial and resource barriers in addition to concerns surrounding COVID-19 that would prevent travel to and from hand therapy appointments. Due to these concerns, a passive-motion protocol was initiated using the Indiana manual as a guide.4 The patient returned to the hand clinic at 2 weeks after surgery for evaluation by the operating surgeon and suture removal. All visits after the suture removal were conducted via either telehealth with videoconferencing or by telephone (Table 1).
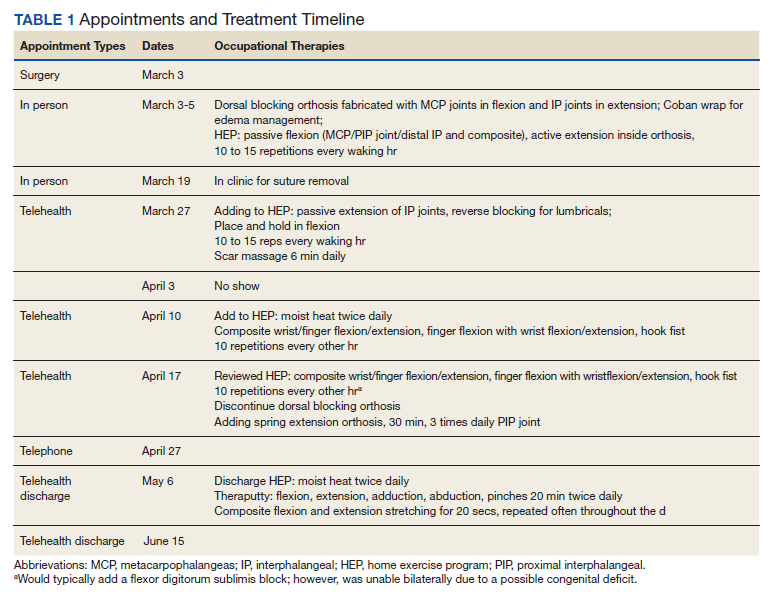
The operative team evaluated the patient 5 times following surgery. Only 2 of these visits were in-person. The patient attended 6 hand therapy sessions with 2 in-person visits to occupational therapy (Figure 1). The remaining 4 visits were conducted using videoconferencing. The patient received therapy supplies by mail as needed, and their use was reviewed in telerehabilitation sessions with videoconferencing as needed. During their postoperative course, the patient experienced little edema or scar tissue formation, and recovery was uncomplicated. The patient developed a mild extensor lag for which a proximal interphalangeal joint spring extension orthosis was provided via mail (Figure 2). The patient admitted only partial adherence with this orthosis, and at discharge, a 10-degree extensor lag remained. The patient was not concerned by this extension deficit and did not experience any associated functional deficits, demonstrated by scores on the Quick Disabilities of the Arm, Shoulder and Hand questionnaire and Patient Specific Functional Scale (Table 2).
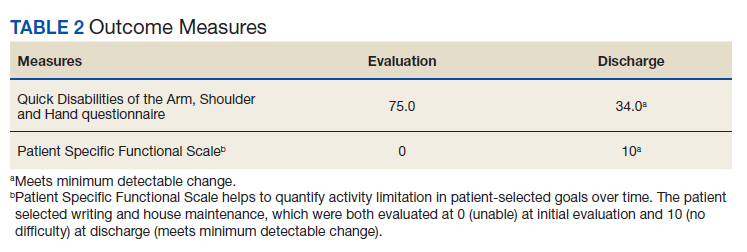

Discussion
Few studies have been published that address the efficacy of telerehabilitation after surgical management of traumatic injuries involving the upper extremity. One Australian study performed by Worboys and colleagues concluded that utilization of telehealth services for hand therapy visits may provide accurate patient assessment with favorable patient satisfaction.5 Another study performed in the UK by Gilbert and colleagues demonstrated that videoconferencing is well received by patients, as it may offer shorter wait times, improved convenience, and reduced travel cost.
The authors noted that although videoconferencing may not completely replace in-person therapy, it could act as an adjunct.6 While these in-person visits may be necessary, particularly to establish care, at least one study has demonstrated that patients may prefer follow-up via telehealth if provided the option.7 In a randomized, controlled study performed in Norway, patients were randomized to either an in-person or video consultation with an orthopedic outpatient clinic. Of patients randomized to the in-person clinic visit, 86% preferred to have follow-up via videoconferencing.7
Previous studies have demonstrated that telehealth may produce accurate patient assessment, with relatively high patient satisfaction. Given the COVID-19 pandemic and the limitations that this crisis has placed on in-person outpatient visits, clinics that previously may have been resistant to telehealth are adapting and using the technology to meet the needs of their population.8 The present case demonstrates that videoconferencing is feasible and may lead to successful results, even for cases requiring significant hand therapy follow-up, such as flexor tendon repairs.
Conclusions
Although in-person hand therapy remains the standard of care following flexor tendon repair of the hand, situations may exist in which hand therapy conducted via telehealth is better than no hand therapy at all. The present case study highlights the use of telehealth as an acceptable supplement to in-person postoperative visits.
In our case, use of a standardized protocol with an emphasis on hand function and patient satisfaction as opposed to strict range of motion measurements produced good results. Although a specific telehealth satisfaction measure was not used in this case, commonly used questionnaires may be integrated into future visits to improve telehealth implementation and patient experience. In this specific case, the veteran felt that hand function was regained and expressed general satisfaction with the telemedicine process at the conclusion of care. While telehealth was a useful adjunct in the treatment of the present patient, further study of videoconferencing should be conducted to determine whether hand therapy conducted via telehealth could be implemented more broadly following upper extremity surgery.
1. Hege JJ. History off-hand: Bunnell’s no-man’s land. Hand (NY). 2019;14(4):570-574. doi:10.1177/1558944717744337
2. Verdan C. Primary repair of flexor tendons. J Bone Joint Surg Am. 1960;42-A:647-657.
3. Kleinert HE, Kutz JE, Ashbell TS, et al. Primary repair of lacerated flexor tendon in no man’s land (abstract). J Bone Joint Surg. 1967;49A:577.
4. Cannon NM. Diagnosis and Treatment Manual for Physicians and Therapists: Upper Extremity Rehabilitation. 4th ed. Hand Rehabilitation Center of Indiana; 2001.
5. Worboys T, Brassington M, Ward EC, Cornwell PL. Delivering occupational therapy hand assessment and treatment sessions via telehealth. J Telemed Telecare. 2018;24(3):185-192. doi:10.1177/1357633X17691861
6. Gilbert AW, Jaggi A, May CR. What is the patient acceptability of real time 1:1 videoconferencing in an orthopaedics setting? A systematic review. Physiotherapy. 2018;104(2):178-186. doi:10.1016/j.physio.2017.11.217
7. Buvik A, Bugge E, Knutsen G, Smatresk A, Wilsgaard T. Patient reported outcomes with remote orthopaedic consultations by telemedicine: A randomised controlled trial. J Telemed Telecare. 2019;25(8):451-459. doi:10.1177/1357633X18783921
8. Loeb AE, Rao SS, Ficke JR, Morris CD, Riley LH 3rd, Levin AS. Departmental experience and lessons learned with accelerated introduction of telemedicine during the COVID-19 crisis. J Am Acad Orthop Surg. 2020;28(11):e469-e476. doi:10.5435/JAAOS-D-20-00380
Telehealth-assisted finger rehabilitat ion therapy demonstrated good functional results following repair of a zone 2 flexor tendon laceration.
Telehealth-assisted finger rehabilitat ion therapy demonstrated good functional results following repair of a zone 2 flexor tendon laceration.
In 1948, Sterling Bunnell, MD, used the term no man’s land to describe the area between the A1 pulley at the volar aspect of the metacarpophalangeal joint and the insertion of the flexor digitorum superficialis tendons on the middle phalanx (zone 2).1 Bunnell’s description referenced the area of land in World War I between the trenches of opposing armies, and his goal was to emphasize the heightened risks of performing tendon repair in this area, as these repairs were notorious for poor outcomes. In lieu of tendon repair, Bunnell advocated treatment of tendon lacerations in this area with tendon excision and grafting.
It was not until the 1960s that researchers began to advocate for acute repair of tendons in this area.2,3 Since Verdan’s and Kleinart’s work, fastidious adherence to atraumatic technique and improvements in suture technique and rehabilitation protocols have allowed hand surgeons to repair tendons in this area with some level of success. Over the ensuing decades, acute repair of flexor tendon injuries within zone 2 has become the standard of care. The importance of meticulous technique during flexor tendon repair cannot be overemphasized; however, without appropriate hand therapy, even the most meticulous repair may fail.
COVID-19 has created significant barriers to patient care. Reducing travel and limiting face-to-face patient visits have been emphasized as methods that reduce spread of the virus, but these restrictions also prevent patients from easily accessing hand therapy. Recent adoption of telemedicine and videoconferencing technologies may help to reduce some of these barriers, but few previous studies have described the use of videoconferencing technology to supplant face-to-face hand therapy visits. This case describes the use of videoconferencing technology to provide hand therapy for a patient following repair of an acute flexor tendon laceration in zone 2.
Case Presentation
A patient aged < 50 years presented to a US Department of Veterans Affairs (VA) hand surgery clinic 2 days after sustaining a laceration to the flexor digitorum profundus (FDP) in zone 2 of the small finger while cleaning a knife. During the discussion of their treatment options and the recommended postoperative hand therapy protocol, the patient noted difficulty attending postoperative appointments due to COVID-19 as well as a lack of resources. Given these limitations and following discussion with our hand therapist, we discussed the potential for telehealth follow-up with videoconferencing. Four days following the injury, the patient underwent repair of the FDP. During surgery, the laceration was present at the level of the A3 pulley. The FDP was repaired using a 6-0 polypropylene synthetic suture for the epitendinous repair and 4-strand core suture repair using 3-0 Fiberwire suture in a modified cruciate fashion. The A2 and A4 pulleys were preserved, and venting of the pulleys was not required. At the time of surgery, the flexor digitorum superficialis and radial and ulnar digital neurovascular bundles were intact. Following surgical repair of the tendon, the patient was placed into a dorsal blocking splint with a plan for follow-up within 2 to 3 days.
The patient attended the first postoperative visit in person on postoperative day 2. During this visit, the postoperative splint and dressings were removed, and a forearm-based dorsal blocking orthosis was fabricated using thermoplastic. At this visit, the veteran relayed concerns regarding psychosocial and resource barriers in addition to concerns surrounding COVID-19 that would prevent travel to and from hand therapy appointments. Due to these concerns, a passive-motion protocol was initiated using the Indiana manual as a guide.4 The patient returned to the hand clinic at 2 weeks after surgery for evaluation by the operating surgeon and suture removal. All visits after the suture removal were conducted via either telehealth with videoconferencing or by telephone (Table 1).
The operative team evaluated the patient 5 times following surgery. Only 2 of these visits were in-person. The patient attended 6 hand therapy sessions with 2 in-person visits to occupational therapy (Figure 1). The remaining 4 visits were conducted using videoconferencing. The patient received therapy supplies by mail as needed, and their use was reviewed in telerehabilitation sessions with videoconferencing as needed. During their postoperative course, the patient experienced little edema or scar tissue formation, and recovery was uncomplicated. The patient developed a mild extensor lag for which a proximal interphalangeal joint spring extension orthosis was provided via mail (Figure 2). The patient admitted only partial adherence with this orthosis, and at discharge, a 10-degree extensor lag remained. The patient was not concerned by this extension deficit and did not experience any associated functional deficits, demonstrated by scores on the Quick Disabilities of the Arm, Shoulder and Hand questionnaire and Patient Specific Functional Scale (Table 2).
Discussion
Few studies have been published that address the efficacy of telerehabilitation after surgical management of traumatic injuries involving the upper extremity. One Australian study performed by Worboys and colleagues concluded that utilization of telehealth services for hand therapy visits may provide accurate patient assessment with favorable patient satisfaction.5 Another study performed in the UK by Gilbert and colleagues demonstrated that videoconferencing is well received by patients, as it may offer shorter wait times, improved convenience, and reduced travel cost.
The authors noted that although videoconferencing may not completely replace in-person therapy, it could act as an adjunct.6 While these in-person visits may be necessary, particularly to establish care, at least one study has demonstrated that patients may prefer follow-up via telehealth if provided the option.7 In a randomized, controlled study performed in Norway, patients were randomized to either an in-person or video consultation with an orthopedic outpatient clinic. Of patients randomized to the in-person clinic visit, 86% preferred to have follow-up via videoconferencing.7
Previous studies have demonstrated that telehealth may produce accurate patient assessment, with relatively high patient satisfaction. Given the COVID-19 pandemic and the limitations that this crisis has placed on in-person outpatient visits, clinics that previously may have been resistant to telehealth are adapting and using the technology to meet the needs of their population.8 The present case demonstrates that videoconferencing is feasible and may lead to successful results, even for cases requiring significant hand therapy follow-up, such as flexor tendon repairs.
Conclusions
Although in-person hand therapy remains the standard of care following flexor tendon repair of the hand, situations may exist in which hand therapy conducted via telehealth is better than no hand therapy at all. The present case study highlights the use of telehealth as an acceptable supplement to in-person postoperative visits.
In our case, use of a standardized protocol with an emphasis on hand function and patient satisfaction as opposed to strict range of motion measurements produced good results. Although a specific telehealth satisfaction measure was not used in this case, commonly used questionnaires may be integrated into future visits to improve telehealth implementation and patient experience. In this specific case, the veteran felt that hand function was regained and expressed general satisfaction with the telemedicine process at the conclusion of care. While telehealth was a useful adjunct in the treatment of the present patient, further study of videoconferencing should be conducted to determine whether hand therapy conducted via telehealth could be implemented more broadly following upper extremity surgery.
In 1948, Sterling Bunnell, MD, used the term no man’s land to describe the area between the A1 pulley at the volar aspect of the metacarpophalangeal joint and the insertion of the flexor digitorum superficialis tendons on the middle phalanx (zone 2).1 Bunnell’s description referenced the area of land in World War I between the trenches of opposing armies, and his goal was to emphasize the heightened risks of performing tendon repair in this area, as these repairs were notorious for poor outcomes. In lieu of tendon repair, Bunnell advocated treatment of tendon lacerations in this area with tendon excision and grafting.
It was not until the 1960s that researchers began to advocate for acute repair of tendons in this area.2,3 Since Verdan’s and Kleinart’s work, fastidious adherence to atraumatic technique and improvements in suture technique and rehabilitation protocols have allowed hand surgeons to repair tendons in this area with some level of success. Over the ensuing decades, acute repair of flexor tendon injuries within zone 2 has become the standard of care. The importance of meticulous technique during flexor tendon repair cannot be overemphasized; however, without appropriate hand therapy, even the most meticulous repair may fail.
COVID-19 has created significant barriers to patient care. Reducing travel and limiting face-to-face patient visits have been emphasized as methods that reduce spread of the virus, but these restrictions also prevent patients from easily accessing hand therapy. Recent adoption of telemedicine and videoconferencing technologies may help to reduce some of these barriers, but few previous studies have described the use of videoconferencing technology to supplant face-to-face hand therapy visits. This case describes the use of videoconferencing technology to provide hand therapy for a patient following repair of an acute flexor tendon laceration in zone 2.
Case Presentation
A patient aged < 50 years presented to a US Department of Veterans Affairs (VA) hand surgery clinic 2 days after sustaining a laceration to the flexor digitorum profundus (FDP) in zone 2 of the small finger while cleaning a knife. During the discussion of their treatment options and the recommended postoperative hand therapy protocol, the patient noted difficulty attending postoperative appointments due to COVID-19 as well as a lack of resources. Given these limitations and following discussion with our hand therapist, we discussed the potential for telehealth follow-up with videoconferencing. Four days following the injury, the patient underwent repair of the FDP. During surgery, the laceration was present at the level of the A3 pulley. The FDP was repaired using a 6-0 polypropylene synthetic suture for the epitendinous repair and 4-strand core suture repair using 3-0 Fiberwire suture in a modified cruciate fashion. The A2 and A4 pulleys were preserved, and venting of the pulleys was not required. At the time of surgery, the flexor digitorum superficialis and radial and ulnar digital neurovascular bundles were intact. Following surgical repair of the tendon, the patient was placed into a dorsal blocking splint with a plan for follow-up within 2 to 3 days.
The patient attended the first postoperative visit in person on postoperative day 2. During this visit, the postoperative splint and dressings were removed, and a forearm-based dorsal blocking orthosis was fabricated using thermoplastic. At this visit, the veteran relayed concerns regarding psychosocial and resource barriers in addition to concerns surrounding COVID-19 that would prevent travel to and from hand therapy appointments. Due to these concerns, a passive-motion protocol was initiated using the Indiana manual as a guide.4 The patient returned to the hand clinic at 2 weeks after surgery for evaluation by the operating surgeon and suture removal. All visits after the suture removal were conducted via either telehealth with videoconferencing or by telephone (Table 1).
The operative team evaluated the patient 5 times following surgery. Only 2 of these visits were in-person. The patient attended 6 hand therapy sessions with 2 in-person visits to occupational therapy (Figure 1). The remaining 4 visits were conducted using videoconferencing. The patient received therapy supplies by mail as needed, and their use was reviewed in telerehabilitation sessions with videoconferencing as needed. During their postoperative course, the patient experienced little edema or scar tissue formation, and recovery was uncomplicated. The patient developed a mild extensor lag for which a proximal interphalangeal joint spring extension orthosis was provided via mail (Figure 2). The patient admitted only partial adherence with this orthosis, and at discharge, a 10-degree extensor lag remained. The patient was not concerned by this extension deficit and did not experience any associated functional deficits, demonstrated by scores on the Quick Disabilities of the Arm, Shoulder and Hand questionnaire and Patient Specific Functional Scale (Table 2).
Discussion
Few studies have been published that address the efficacy of telerehabilitation after surgical management of traumatic injuries involving the upper extremity. One Australian study performed by Worboys and colleagues concluded that utilization of telehealth services for hand therapy visits may provide accurate patient assessment with favorable patient satisfaction.5 Another study performed in the UK by Gilbert and colleagues demonstrated that videoconferencing is well received by patients, as it may offer shorter wait times, improved convenience, and reduced travel cost.
The authors noted that although videoconferencing may not completely replace in-person therapy, it could act as an adjunct.6 While these in-person visits may be necessary, particularly to establish care, at least one study has demonstrated that patients may prefer follow-up via telehealth if provided the option.7 In a randomized, controlled study performed in Norway, patients were randomized to either an in-person or video consultation with an orthopedic outpatient clinic. Of patients randomized to the in-person clinic visit, 86% preferred to have follow-up via videoconferencing.7
Previous studies have demonstrated that telehealth may produce accurate patient assessment, with relatively high patient satisfaction. Given the COVID-19 pandemic and the limitations that this crisis has placed on in-person outpatient visits, clinics that previously may have been resistant to telehealth are adapting and using the technology to meet the needs of their population.8 The present case demonstrates that videoconferencing is feasible and may lead to successful results, even for cases requiring significant hand therapy follow-up, such as flexor tendon repairs.
Conclusions
Although in-person hand therapy remains the standard of care following flexor tendon repair of the hand, situations may exist in which hand therapy conducted via telehealth is better than no hand therapy at all. The present case study highlights the use of telehealth as an acceptable supplement to in-person postoperative visits.
In our case, use of a standardized protocol with an emphasis on hand function and patient satisfaction as opposed to strict range of motion measurements produced good results. Although a specific telehealth satisfaction measure was not used in this case, commonly used questionnaires may be integrated into future visits to improve telehealth implementation and patient experience. In this specific case, the veteran felt that hand function was regained and expressed general satisfaction with the telemedicine process at the conclusion of care. While telehealth was a useful adjunct in the treatment of the present patient, further study of videoconferencing should be conducted to determine whether hand therapy conducted via telehealth could be implemented more broadly following upper extremity surgery.
1. Hege JJ. History off-hand: Bunnell’s no-man’s land. Hand (NY). 2019;14(4):570-574. doi:10.1177/1558944717744337
2. Verdan C. Primary repair of flexor tendons. J Bone Joint Surg Am. 1960;42-A:647-657.
3. Kleinert HE, Kutz JE, Ashbell TS, et al. Primary repair of lacerated flexor tendon in no man’s land (abstract). J Bone Joint Surg. 1967;49A:577.
4. Cannon NM. Diagnosis and Treatment Manual for Physicians and Therapists: Upper Extremity Rehabilitation. 4th ed. Hand Rehabilitation Center of Indiana; 2001.
5. Worboys T, Brassington M, Ward EC, Cornwell PL. Delivering occupational therapy hand assessment and treatment sessions via telehealth. J Telemed Telecare. 2018;24(3):185-192. doi:10.1177/1357633X17691861
6. Gilbert AW, Jaggi A, May CR. What is the patient acceptability of real time 1:1 videoconferencing in an orthopaedics setting? A systematic review. Physiotherapy. 2018;104(2):178-186. doi:10.1016/j.physio.2017.11.217
7. Buvik A, Bugge E, Knutsen G, Smatresk A, Wilsgaard T. Patient reported outcomes with remote orthopaedic consultations by telemedicine: A randomised controlled trial. J Telemed Telecare. 2019;25(8):451-459. doi:10.1177/1357633X18783921
8. Loeb AE, Rao SS, Ficke JR, Morris CD, Riley LH 3rd, Levin AS. Departmental experience and lessons learned with accelerated introduction of telemedicine during the COVID-19 crisis. J Am Acad Orthop Surg. 2020;28(11):e469-e476. doi:10.5435/JAAOS-D-20-00380
1. Hege JJ. History off-hand: Bunnell’s no-man’s land. Hand (NY). 2019;14(4):570-574. doi:10.1177/1558944717744337
2. Verdan C. Primary repair of flexor tendons. J Bone Joint Surg Am. 1960;42-A:647-657.
3. Kleinert HE, Kutz JE, Ashbell TS, et al. Primary repair of lacerated flexor tendon in no man’s land (abstract). J Bone Joint Surg. 1967;49A:577.
4. Cannon NM. Diagnosis and Treatment Manual for Physicians and Therapists: Upper Extremity Rehabilitation. 4th ed. Hand Rehabilitation Center of Indiana; 2001.
5. Worboys T, Brassington M, Ward EC, Cornwell PL. Delivering occupational therapy hand assessment and treatment sessions via telehealth. J Telemed Telecare. 2018;24(3):185-192. doi:10.1177/1357633X17691861
6. Gilbert AW, Jaggi A, May CR. What is the patient acceptability of real time 1:1 videoconferencing in an orthopaedics setting? A systematic review. Physiotherapy. 2018;104(2):178-186. doi:10.1016/j.physio.2017.11.217
7. Buvik A, Bugge E, Knutsen G, Smatresk A, Wilsgaard T. Patient reported outcomes with remote orthopaedic consultations by telemedicine: A randomised controlled trial. J Telemed Telecare. 2019;25(8):451-459. doi:10.1177/1357633X18783921
8. Loeb AE, Rao SS, Ficke JR, Morris CD, Riley LH 3rd, Levin AS. Departmental experience and lessons learned with accelerated introduction of telemedicine during the COVID-19 crisis. J Am Acad Orthop Surg. 2020;28(11):e469-e476. doi:10.5435/JAAOS-D-20-00380
Review of Efficacy and Safety of Spinal Cord Stimulation in Veterans
Lower back pain (LBP) affects an estimated 9.4% of the global population and has resulted in more years lived with disability than any other health condition.1 LBP affects a wide range of populations, but US veterans have been shown to have significantly higher rates of back pain than nonveterans. The National Institutes of Health reports that 65.6% of veterans experience chronic pain; 9.1% of veterans experience severe, chronic pain.2 Chronic back pain is treated by a range of methods, including medications, surgery, physical therapy (PT), patient education, and behavioral therapy.3 However, chronic neuropathic back pain has been shown to have limited responsiveness to medication.4
Neuropathic pain is caused by lesions in the somatosensory nervous system, resulting in spontaneous pain and amplified pain responses to both painful and nonpainful stimuli.5 The most common location for neuropathic pain is the back and legs. Between 10% and 40% of people who undergo lumbosacral spine surgery to treat neuropathic radicular pain will experience further neuropathic pain.6 This condition is referred to as failed back surgery syndrome or postlaminectomy syndrome (PLS). While neuropathic back pain has had limited responsiveness to medication and repeated lumbosacral spine surgery, spinal cord stimulation (SCS) has shown promise as an effective form of pain treatment for those experiencing PLS and other spine disorders.7-10 In addition, SCS therapy has had a very low incidence of complications, which may be on the decline with recent technological advancements.11 Patients with a diagnosis of PLS, LBP, or complex regional pain syndrome (CRPS) who have not responded to medications, therapy, and/or injections for ≥ 6 months were eligible for a trial of SCS therapy. Trial leads were placed via the percutaneous route with the battery strapped to the waistline for 3 to 5 days and were removed in clinic. Patients who experienced > 60% pain relief and functional improvement received a SCS implant.
The effectiveness of SCS has been demonstrated in a nonveteran population, but it has not been studied in a veteran population.12 US Department of Veterans Affairs (VA) health care coverage is different from Medicare and private insurance in that it is classified as a benefit and not insurance. The goals of treatment at the VA may include considerations in addition to feeling better, and patient presentations may not align with those in the private sector.
We hypothesize that SCS is both a safe and beneficial treatment option for veterans with chronic intractable spine and/or extremity pain. The purpose of this study was to determine the efficacy and safety of SCS in a veteran population.
Methods
The efficacy and safety of SCS was determined via a retrospective study. Inclusion criteria for the study consisted of any Southeastern Louisiana Veterans Health Care System (SLVHCS) patient who had an SCS trial and/or implant from 2008 to 2020. Eligible veterans must have had chronic pain for at least 6 months and had previously tried multiple medications, PT, transcutaneous nerve stimulation, facet injections, epidural steroid injections, or surgery without success. For medication therapy to be considered unsuccessful, it must have included acetaminophen, nonsteroidal anti-inflammatory drugs, and ≥ 1 adjuvant medication (gabapentin, duloxetine, amitriptyline, lidocaine, and menthol). A diagnosis of chronic LBP, PLS, cervical or lumbar spondylosis with radiculopathy, complex regional pain syndrome, or chronic pain syndrome was required for eligibility. Patients whose pain decreased by > 60% and had functional improvement in a 3- to 5-day trial received SCS implantation with percutaneous leads by a pain physician or paddle lead by a neurosurgeon.
The SLVHCS Institutional Review Board approved this study. Electronic health records were reviewed to determine patient age, anthropometric data, and date of SCS implantation. Patients were then called and interviewed to complete a survey. After obtaining verbal consent to the study, subjects were surveyed regarding whether the patient would recommend the procedure to peers, adverse effects (AEs) or complications, and the ability to decrease opiates if applicable. A verbal Pain Outcome Questionnaire (POQ) assessment of activities of daily living also was given during the phone interview regarding pain levels before SCS and at the time of the phone interview.13 (eAppendix available at doi:10.12788/fp.0204) Following the survey, a chart review was performed to corroborate the given AEs or complications and opiate use information. Before and after results of the POQ were compared via a paired sample t test, and P values < .05 were considered significant. Analyses were performed by IBM SPSS, version 26.
The primary outcome measure for this study was whether veterans would recommend SCS to their peers; in our view, this categorical outcome measure seemed to be more valuable to share with future patients who might be candidates for SCS. Since VA health care coverage and goals of treatment may be different from a nonveteran population, we opted to use this primary measure to decrease the possibility of confounding variables.
Secondary outcome measures included changes in POC scores, improvements in activities of daily living, and decreases in use of opioid pain medications.
POQ responses were recorded during the telephone interviews (0 to 10 scale). A paired sample t test was conducted to compare pain levels before and after SCS implant. Pain levels were gathered in the single phone call. Patient opioid usage, if applicable, was assessed by converting medications to morphine milligram equivalent dosing (MMED). Since patients who were on chronic opioids took multiple formulations, we changed the total daily dose to all morphine; for this study, morphine was considered equivalent to hydrocodone, and oxycodone was 1.5x morphine.
Results
Of the 90 SLVHCS patients who received an SCS implant between 2008 and 2020, 76 were reached by telephone and 65 had their responses recorded in the study. Of the 11 patients who were not included, 5 had the SCS removed; it is unclear whether these veterans would have recommended the treatment. Four were unable to quantify pain and/or SCS effects, and 2 were excluded due to a dementia diagnosis years after the implant. The mean (SD) age of participants was 63.9 (10.3) years. Forty percent of patients had a diabetes mellitus diagnosis and 1 had prediabetes. Patients’ most common qualifying diagnosis for SCS was PLS (47.7%) followed by chronic LBP (26.2%). A percutaneous 2-lead technique was the most common type of SCS type used (60.0%) followed by 1-lead (21.5%). The most common SCS manufacturer was Boston Scientific (87.7%)(Table 1). Most veterans (76.9%) recommended SCS to their peers; 13.8% did not recommend SCS; 9.2% were undecided and stated that they were unable to recommend because they did not want to persuade a peer to get SCS (Figure).

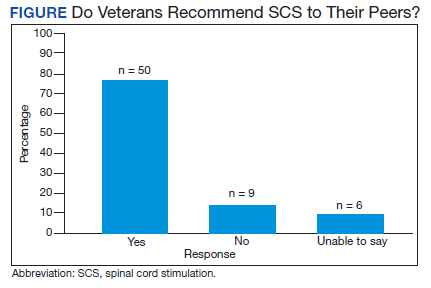
There was a statistically significant decrease in opioid use for the 40 veterans for whom pain medication was converted (P < .001)(Table 2). Six patients reported using opioids at some point but could not remember their dose, and no records were found in their chart review, so they were not included in the MMED analysis. In that group, 4 patients reported using opioids before SCS but discontinued the opioid use after SCS implantation, and 2 patients noted using opioids before SCS and concomitantly. Eighteen subjects reported no opioid use at any point before or after SCS (Table 3).
There were few life-threatening complications of SCS. Three veterans developed skin dehiscence; 2 had dehiscence at the battery/generator site, and 1 had dehiscence at the lead anchor site. Two patients with dehiscence also had morbid obesity, and the third had postoperative malnourishment. The dehiscence occurred 3 and 8 months postoperation. All 3 patients with dehiscence had the SCS explanted, though they were eager to get a new SCS implanted as soon as possible because SCS was their most successful treatment to date.
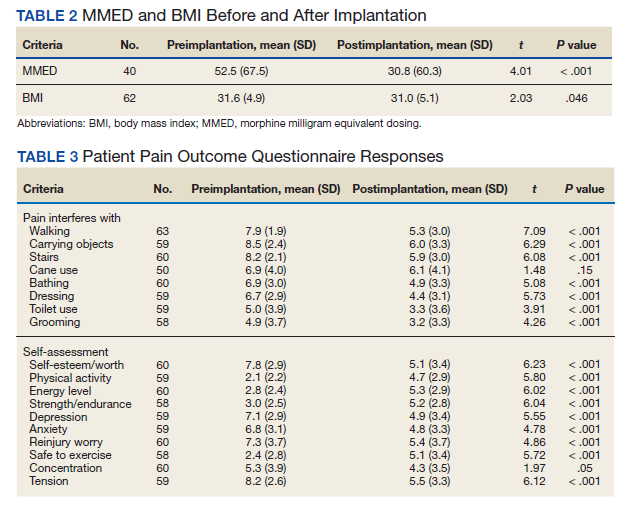
Twenty of the 64 veterans surveyed reported other complications of SCS, including lead migration, lack of pain coverage, paresthesia and numbness, soreness around generator site, SCS shocking patient when performing full thoracic spine flexion, and shingles at the battery site (Table 4). There were 11 explants among the 76 veterans contacted. The primary reason for explant was lack of pain coverage.
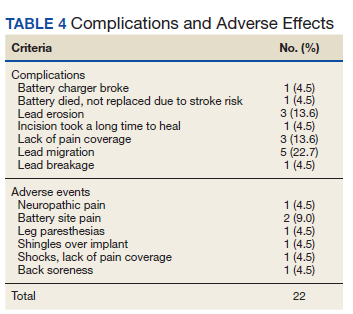
Patient concerns included pain with sitting in chairs due to tenderness around the implant, SCS helping with physical pain but not mental pain, SCS only working during the day and not helping with sleep, and patients lacking education regarding possible complications of SCS.
Discussion
In this nonrandomized retrospective review, SCS was shown to be an effective treatment for intractable spine and/or extremity pain. Veterans’ pain levels were significantly reduced following SCS implantation, and more than three-fourths of veterans recommended SCS to their peers. We used the recommendation of SCS to peers as the most important metric regarding the effectiveness of SCS, as this measure was felt to be more valuable to share with future patients; furthermore, categorical analysis has been shown to be more valuable than ordinal pain scales to measure pain.14 In addition to wanting to expand the available research to the general public, we wanted a measure that we could easily relay to our patient population regarding SCS.
The explant rate of 14.5% among surveyed veterans falls at the higher end of the normal ranges found in previous studies of long-term SCS outcomes.15-17 One possible reason for the higher rate is that we did not differentiate based on the reason for the explant (ie, no benefit, further surgery needed for underlying medical condition, or SCS-specific complications). Another possible contributing factor to the higher than expected explant rate is the geographic location in the New Orleans metro area; New Orleans is considered to have one of the highest rates of obesity in the United States and obesity typically has other diseases associated with it such as hypertension and diabetes mellitus.
Limitations
Limitations of the study include the relatively low number of subjects, subjective nature of the interview questions, and the patients’ answers. Typically the POQ has been used as a prospective assessment of pain; whether it is valid in a retrospective analysis is not clear. While there was a statistically significant decrease of opioid use after getting SCS, this study can only show correlation, not causation. During the study period, there has been a drastic change in opioid prescribing patterns and efforts to decrease the amount of opioids prescribed.
Subjects also were asked to rate their pain and quality of life before SCS. Some subjects had SCS implantation up to 10 years prior to the phone interview. The variable amount of time between SCS implantation and interview likely affected subjects’ responses. Chronic pain is a moving target. Patients have good days and bad days that would likely change opinions on SCS benefits on a single phone interview. Some patients needed battery replacements at the time of the interview (battery life averaged about 3 to 5 years in our study population) and were asked to report current levels of pain from the perspective of when their batteries were still functional, further affecting results.
Conclusions
SCS was shown to improve the quality of life of US veterans at SLVHCS across a wide variety of metrics, including activities of daily living, as well as mental and physical health. For veterans with chronic intractable pain who have tried and failed more conservative treatments, SCS is a great treatment.
1. Hoy DG, Smith E, Cross M, et al. The global burden of musculoskeletal conditions for 2010: an overview of methods. Ann Rheum Dis. 2014;73(6):982-989 doi:10.1136/annrheumdis-2013-204344
2. Nahin RL. Severe pain in veterans: the effect of age and sex, and comparisons with the general population. J Pain. 2017;18(3):247-254. doi:10.1016/j.jpain.2016.10.021
3. Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011.
4. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162-173. doi:10.1016/S1474-4422(14)70251-0
5. Costigan M, Scholz J, Woolf CJ. Neuropathic pain: a maladaptive response of the nervous system to damage. Annu Rev Neurosci. 2009;32:1-32. doi:10.1146/annurev.neuro.051508.135531
6. Wilkinson HA. The Failed Back Syndrome: Etiology and Therapy. 2nd ed. Harper & Row; 1991.
7. Kumar K, Taylor RS, Jacques L, et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007;132(1-2):179-188. doi:10.1016/j.pain.2007.07.028
8. North RB, Kidd DH, Farrokhi F, Piantadosi SA. Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial. Neurosurgery. 2005;56(1):98-107. doi:10.1227/01.neu.0000144839.65524.e0
9. Geurts JW, Smits H, Kemler MA, Brunner F, Kessels AG, van Kleef M. Spinal cord stimulation for complex regional pain syndrome type I: a prospective cohort study with long-term follow-up. Neuromodulation. 2013;16(6):523-529. doi:10.1111/ner.12024
10. Kumar K, Rizvi S, Bnurs SB. Spinal cord stimulation is effective in management of complex regional pain syndrome I: fact or fiction. Neurosurgery. 2011;69(3):566-5580. doi:10.1227/NEU.0b013e3182181e60
11. Mekhail NA, Mathews M, Nageeb F, Guirguis M, Mekhail MN, Cheng J. Retrospective review of 707 cases of spinal cord stimulation: indications and complications. Pain Pract. 2011;11(2):148-153. doi:10.1111/j.1533-2500.2010.00407.x
12. Veizi E, Hayek SM, North J, et al. Spinal cord stimulation (SCS) with anatomically guided (3D) neural targeting shows superior chronic axial low back pain relief compared to traditional SCS-LUMINA Study. Pain Med. 2017;18(8):1534-1548. doi:10.1093/pm/pnw286
13. Gordon DB, Polomano RC, Pellino TA, et al. Revised American Pain Society Patient Outcome Questionnaire (APS-POQ-R) for quality improvement of pain management in hospitalized adults: preliminary psychometric evaluation. J Pain. 2010;11(11):1172-1186. doi:10.1016/j.jpain.2010.02.012
14. Kennedy DJ, Schneider B. Lies, damn lies, and statistic: a commentary. Pain Med. 2020;21(10):2052-2054. doi:10.1093/pm/pnaa287
15. Van Buyten JP, Wille F, Smet I, et al. Therapy-related explants after spinal cord stimulation: results of an international retrospective chart review study. Neuromodulation. 2017;20(7):642-649. doi:10.1111/ner.12642
16. Hayek SM, Veizi E, Hanes M. Treatment-limiting complications of percutaneous spinal cord stimulator implants: a review of eight years of experience from an academic center database. Neuromodulation. 2015;18(7):603-609. doi:10.1111/ner.12312
17. Pope JE, Deer TR, Falowski S, et al. Multicenter retrospective study of neurostimulation with exit of therapy by explant. Neuromodulation. 2017;20(6):543-552. doi:10.1111/ner.12634
Lower back pain (LBP) affects an estimated 9.4% of the global population and has resulted in more years lived with disability than any other health condition.1 LBP affects a wide range of populations, but US veterans have been shown to have significantly higher rates of back pain than nonveterans. The National Institutes of Health reports that 65.6% of veterans experience chronic pain; 9.1% of veterans experience severe, chronic pain.2 Chronic back pain is treated by a range of methods, including medications, surgery, physical therapy (PT), patient education, and behavioral therapy.3 However, chronic neuropathic back pain has been shown to have limited responsiveness to medication.4
Neuropathic pain is caused by lesions in the somatosensory nervous system, resulting in spontaneous pain and amplified pain responses to both painful and nonpainful stimuli.5 The most common location for neuropathic pain is the back and legs. Between 10% and 40% of people who undergo lumbosacral spine surgery to treat neuropathic radicular pain will experience further neuropathic pain.6 This condition is referred to as failed back surgery syndrome or postlaminectomy syndrome (PLS). While neuropathic back pain has had limited responsiveness to medication and repeated lumbosacral spine surgery, spinal cord stimulation (SCS) has shown promise as an effective form of pain treatment for those experiencing PLS and other spine disorders.7-10 In addition, SCS therapy has had a very low incidence of complications, which may be on the decline with recent technological advancements.11 Patients with a diagnosis of PLS, LBP, or complex regional pain syndrome (CRPS) who have not responded to medications, therapy, and/or injections for ≥ 6 months were eligible for a trial of SCS therapy. Trial leads were placed via the percutaneous route with the battery strapped to the waistline for 3 to 5 days and were removed in clinic. Patients who experienced > 60% pain relief and functional improvement received a SCS implant.
The effectiveness of SCS has been demonstrated in a nonveteran population, but it has not been studied in a veteran population.12 US Department of Veterans Affairs (VA) health care coverage is different from Medicare and private insurance in that it is classified as a benefit and not insurance. The goals of treatment at the VA may include considerations in addition to feeling better, and patient presentations may not align with those in the private sector.
We hypothesize that SCS is both a safe and beneficial treatment option for veterans with chronic intractable spine and/or extremity pain. The purpose of this study was to determine the efficacy and safety of SCS in a veteran population.
Methods
The efficacy and safety of SCS was determined via a retrospective study. Inclusion criteria for the study consisted of any Southeastern Louisiana Veterans Health Care System (SLVHCS) patient who had an SCS trial and/or implant from 2008 to 2020. Eligible veterans must have had chronic pain for at least 6 months and had previously tried multiple medications, PT, transcutaneous nerve stimulation, facet injections, epidural steroid injections, or surgery without success. For medication therapy to be considered unsuccessful, it must have included acetaminophen, nonsteroidal anti-inflammatory drugs, and ≥ 1 adjuvant medication (gabapentin, duloxetine, amitriptyline, lidocaine, and menthol). A diagnosis of chronic LBP, PLS, cervical or lumbar spondylosis with radiculopathy, complex regional pain syndrome, or chronic pain syndrome was required for eligibility. Patients whose pain decreased by > 60% and had functional improvement in a 3- to 5-day trial received SCS implantation with percutaneous leads by a pain physician or paddle lead by a neurosurgeon.
The SLVHCS Institutional Review Board approved this study. Electronic health records were reviewed to determine patient age, anthropometric data, and date of SCS implantation. Patients were then called and interviewed to complete a survey. After obtaining verbal consent to the study, subjects were surveyed regarding whether the patient would recommend the procedure to peers, adverse effects (AEs) or complications, and the ability to decrease opiates if applicable. A verbal Pain Outcome Questionnaire (POQ) assessment of activities of daily living also was given during the phone interview regarding pain levels before SCS and at the time of the phone interview.13 (eAppendix available at doi:10.12788/fp.0204) Following the survey, a chart review was performed to corroborate the given AEs or complications and opiate use information. Before and after results of the POQ were compared via a paired sample t test, and P values < .05 were considered significant. Analyses were performed by IBM SPSS, version 26.
The primary outcome measure for this study was whether veterans would recommend SCS to their peers; in our view, this categorical outcome measure seemed to be more valuable to share with future patients who might be candidates for SCS. Since VA health care coverage and goals of treatment may be different from a nonveteran population, we opted to use this primary measure to decrease the possibility of confounding variables.
Secondary outcome measures included changes in POC scores, improvements in activities of daily living, and decreases in use of opioid pain medications.
POQ responses were recorded during the telephone interviews (0 to 10 scale). A paired sample t test was conducted to compare pain levels before and after SCS implant. Pain levels were gathered in the single phone call. Patient opioid usage, if applicable, was assessed by converting medications to morphine milligram equivalent dosing (MMED). Since patients who were on chronic opioids took multiple formulations, we changed the total daily dose to all morphine; for this study, morphine was considered equivalent to hydrocodone, and oxycodone was 1.5x morphine.
Results
Of the 90 SLVHCS patients who received an SCS implant between 2008 and 2020, 76 were reached by telephone and 65 had their responses recorded in the study. Of the 11 patients who were not included, 5 had the SCS removed; it is unclear whether these veterans would have recommended the treatment. Four were unable to quantify pain and/or SCS effects, and 2 were excluded due to a dementia diagnosis years after the implant. The mean (SD) age of participants was 63.9 (10.3) years. Forty percent of patients had a diabetes mellitus diagnosis and 1 had prediabetes. Patients’ most common qualifying diagnosis for SCS was PLS (47.7%) followed by chronic LBP (26.2%). A percutaneous 2-lead technique was the most common type of SCS type used (60.0%) followed by 1-lead (21.5%). The most common SCS manufacturer was Boston Scientific (87.7%)(Table 1). Most veterans (76.9%) recommended SCS to their peers; 13.8% did not recommend SCS; 9.2% were undecided and stated that they were unable to recommend because they did not want to persuade a peer to get SCS (Figure).
There was a statistically significant decrease in opioid use for the 40 veterans for whom pain medication was converted (P < .001)(Table 2). Six patients reported using opioids at some point but could not remember their dose, and no records were found in their chart review, so they were not included in the MMED analysis. In that group, 4 patients reported using opioids before SCS but discontinued the opioid use after SCS implantation, and 2 patients noted using opioids before SCS and concomitantly. Eighteen subjects reported no opioid use at any point before or after SCS (Table 3).
There were few life-threatening complications of SCS. Three veterans developed skin dehiscence; 2 had dehiscence at the battery/generator site, and 1 had dehiscence at the lead anchor site. Two patients with dehiscence also had morbid obesity, and the third had postoperative malnourishment. The dehiscence occurred 3 and 8 months postoperation. All 3 patients with dehiscence had the SCS explanted, though they were eager to get a new SCS implanted as soon as possible because SCS was their most successful treatment to date.
Twenty of the 64 veterans surveyed reported other complications of SCS, including lead migration, lack of pain coverage, paresthesia and numbness, soreness around generator site, SCS shocking patient when performing full thoracic spine flexion, and shingles at the battery site (Table 4). There were 11 explants among the 76 veterans contacted. The primary reason for explant was lack of pain coverage.
Patient concerns included pain with sitting in chairs due to tenderness around the implant, SCS helping with physical pain but not mental pain, SCS only working during the day and not helping with sleep, and patients lacking education regarding possible complications of SCS.
Discussion
In this nonrandomized retrospective review, SCS was shown to be an effective treatment for intractable spine and/or extremity pain. Veterans’ pain levels were significantly reduced following SCS implantation, and more than three-fourths of veterans recommended SCS to their peers. We used the recommendation of SCS to peers as the most important metric regarding the effectiveness of SCS, as this measure was felt to be more valuable to share with future patients; furthermore, categorical analysis has been shown to be more valuable than ordinal pain scales to measure pain.14 In addition to wanting to expand the available research to the general public, we wanted a measure that we could easily relay to our patient population regarding SCS.
The explant rate of 14.5% among surveyed veterans falls at the higher end of the normal ranges found in previous studies of long-term SCS outcomes.15-17 One possible reason for the higher rate is that we did not differentiate based on the reason for the explant (ie, no benefit, further surgery needed for underlying medical condition, or SCS-specific complications). Another possible contributing factor to the higher than expected explant rate is the geographic location in the New Orleans metro area; New Orleans is considered to have one of the highest rates of obesity in the United States and obesity typically has other diseases associated with it such as hypertension and diabetes mellitus.
Limitations
Limitations of the study include the relatively low number of subjects, subjective nature of the interview questions, and the patients’ answers. Typically the POQ has been used as a prospective assessment of pain; whether it is valid in a retrospective analysis is not clear. While there was a statistically significant decrease of opioid use after getting SCS, this study can only show correlation, not causation. During the study period, there has been a drastic change in opioid prescribing patterns and efforts to decrease the amount of opioids prescribed.
Subjects also were asked to rate their pain and quality of life before SCS. Some subjects had SCS implantation up to 10 years prior to the phone interview. The variable amount of time between SCS implantation and interview likely affected subjects’ responses. Chronic pain is a moving target. Patients have good days and bad days that would likely change opinions on SCS benefits on a single phone interview. Some patients needed battery replacements at the time of the interview (battery life averaged about 3 to 5 years in our study population) and were asked to report current levels of pain from the perspective of when their batteries were still functional, further affecting results.
Conclusions
SCS was shown to improve the quality of life of US veterans at SLVHCS across a wide variety of metrics, including activities of daily living, as well as mental and physical health. For veterans with chronic intractable pain who have tried and failed more conservative treatments, SCS is a great treatment.
Lower back pain (LBP) affects an estimated 9.4% of the global population and has resulted in more years lived with disability than any other health condition.1 LBP affects a wide range of populations, but US veterans have been shown to have significantly higher rates of back pain than nonveterans. The National Institutes of Health reports that 65.6% of veterans experience chronic pain; 9.1% of veterans experience severe, chronic pain.2 Chronic back pain is treated by a range of methods, including medications, surgery, physical therapy (PT), patient education, and behavioral therapy.3 However, chronic neuropathic back pain has been shown to have limited responsiveness to medication.4
Neuropathic pain is caused by lesions in the somatosensory nervous system, resulting in spontaneous pain and amplified pain responses to both painful and nonpainful stimuli.5 The most common location for neuropathic pain is the back and legs. Between 10% and 40% of people who undergo lumbosacral spine surgery to treat neuropathic radicular pain will experience further neuropathic pain.6 This condition is referred to as failed back surgery syndrome or postlaminectomy syndrome (PLS). While neuropathic back pain has had limited responsiveness to medication and repeated lumbosacral spine surgery, spinal cord stimulation (SCS) has shown promise as an effective form of pain treatment for those experiencing PLS and other spine disorders.7-10 In addition, SCS therapy has had a very low incidence of complications, which may be on the decline with recent technological advancements.11 Patients with a diagnosis of PLS, LBP, or complex regional pain syndrome (CRPS) who have not responded to medications, therapy, and/or injections for ≥ 6 months were eligible for a trial of SCS therapy. Trial leads were placed via the percutaneous route with the battery strapped to the waistline for 3 to 5 days and were removed in clinic. Patients who experienced > 60% pain relief and functional improvement received a SCS implant.
The effectiveness of SCS has been demonstrated in a nonveteran population, but it has not been studied in a veteran population.12 US Department of Veterans Affairs (VA) health care coverage is different from Medicare and private insurance in that it is classified as a benefit and not insurance. The goals of treatment at the VA may include considerations in addition to feeling better, and patient presentations may not align with those in the private sector.
We hypothesize that SCS is both a safe and beneficial treatment option for veterans with chronic intractable spine and/or extremity pain. The purpose of this study was to determine the efficacy and safety of SCS in a veteran population.
Methods
The efficacy and safety of SCS was determined via a retrospective study. Inclusion criteria for the study consisted of any Southeastern Louisiana Veterans Health Care System (SLVHCS) patient who had an SCS trial and/or implant from 2008 to 2020. Eligible veterans must have had chronic pain for at least 6 months and had previously tried multiple medications, PT, transcutaneous nerve stimulation, facet injections, epidural steroid injections, or surgery without success. For medication therapy to be considered unsuccessful, it must have included acetaminophen, nonsteroidal anti-inflammatory drugs, and ≥ 1 adjuvant medication (gabapentin, duloxetine, amitriptyline, lidocaine, and menthol). A diagnosis of chronic LBP, PLS, cervical or lumbar spondylosis with radiculopathy, complex regional pain syndrome, or chronic pain syndrome was required for eligibility. Patients whose pain decreased by > 60% and had functional improvement in a 3- to 5-day trial received SCS implantation with percutaneous leads by a pain physician or paddle lead by a neurosurgeon.
The SLVHCS Institutional Review Board approved this study. Electronic health records were reviewed to determine patient age, anthropometric data, and date of SCS implantation. Patients were then called and interviewed to complete a survey. After obtaining verbal consent to the study, subjects were surveyed regarding whether the patient would recommend the procedure to peers, adverse effects (AEs) or complications, and the ability to decrease opiates if applicable. A verbal Pain Outcome Questionnaire (POQ) assessment of activities of daily living also was given during the phone interview regarding pain levels before SCS and at the time of the phone interview.13 (eAppendix available at doi:10.12788/fp.0204) Following the survey, a chart review was performed to corroborate the given AEs or complications and opiate use information. Before and after results of the POQ were compared via a paired sample t test, and P values < .05 were considered significant. Analyses were performed by IBM SPSS, version 26.
The primary outcome measure for this study was whether veterans would recommend SCS to their peers; in our view, this categorical outcome measure seemed to be more valuable to share with future patients who might be candidates for SCS. Since VA health care coverage and goals of treatment may be different from a nonveteran population, we opted to use this primary measure to decrease the possibility of confounding variables.
Secondary outcome measures included changes in POC scores, improvements in activities of daily living, and decreases in use of opioid pain medications.
POQ responses were recorded during the telephone interviews (0 to 10 scale). A paired sample t test was conducted to compare pain levels before and after SCS implant. Pain levels were gathered in the single phone call. Patient opioid usage, if applicable, was assessed by converting medications to morphine milligram equivalent dosing (MMED). Since patients who were on chronic opioids took multiple formulations, we changed the total daily dose to all morphine; for this study, morphine was considered equivalent to hydrocodone, and oxycodone was 1.5x morphine.
Results
Of the 90 SLVHCS patients who received an SCS implant between 2008 and 2020, 76 were reached by telephone and 65 had their responses recorded in the study. Of the 11 patients who were not included, 5 had the SCS removed; it is unclear whether these veterans would have recommended the treatment. Four were unable to quantify pain and/or SCS effects, and 2 were excluded due to a dementia diagnosis years after the implant. The mean (SD) age of participants was 63.9 (10.3) years. Forty percent of patients had a diabetes mellitus diagnosis and 1 had prediabetes. Patients’ most common qualifying diagnosis for SCS was PLS (47.7%) followed by chronic LBP (26.2%). A percutaneous 2-lead technique was the most common type of SCS type used (60.0%) followed by 1-lead (21.5%). The most common SCS manufacturer was Boston Scientific (87.7%)(Table 1). Most veterans (76.9%) recommended SCS to their peers; 13.8% did not recommend SCS; 9.2% were undecided and stated that they were unable to recommend because they did not want to persuade a peer to get SCS (Figure).
There was a statistically significant decrease in opioid use for the 40 veterans for whom pain medication was converted (P < .001)(Table 2). Six patients reported using opioids at some point but could not remember their dose, and no records were found in their chart review, so they were not included in the MMED analysis. In that group, 4 patients reported using opioids before SCS but discontinued the opioid use after SCS implantation, and 2 patients noted using opioids before SCS and concomitantly. Eighteen subjects reported no opioid use at any point before or after SCS (Table 3).
There were few life-threatening complications of SCS. Three veterans developed skin dehiscence; 2 had dehiscence at the battery/generator site, and 1 had dehiscence at the lead anchor site. Two patients with dehiscence also had morbid obesity, and the third had postoperative malnourishment. The dehiscence occurred 3 and 8 months postoperation. All 3 patients with dehiscence had the SCS explanted, though they were eager to get a new SCS implanted as soon as possible because SCS was their most successful treatment to date.
Twenty of the 64 veterans surveyed reported other complications of SCS, including lead migration, lack of pain coverage, paresthesia and numbness, soreness around generator site, SCS shocking patient when performing full thoracic spine flexion, and shingles at the battery site (Table 4). There were 11 explants among the 76 veterans contacted. The primary reason for explant was lack of pain coverage.
Patient concerns included pain with sitting in chairs due to tenderness around the implant, SCS helping with physical pain but not mental pain, SCS only working during the day and not helping with sleep, and patients lacking education regarding possible complications of SCS.
Discussion
In this nonrandomized retrospective review, SCS was shown to be an effective treatment for intractable spine and/or extremity pain. Veterans’ pain levels were significantly reduced following SCS implantation, and more than three-fourths of veterans recommended SCS to their peers. We used the recommendation of SCS to peers as the most important metric regarding the effectiveness of SCS, as this measure was felt to be more valuable to share with future patients; furthermore, categorical analysis has been shown to be more valuable than ordinal pain scales to measure pain.14 In addition to wanting to expand the available research to the general public, we wanted a measure that we could easily relay to our patient population regarding SCS.
The explant rate of 14.5% among surveyed veterans falls at the higher end of the normal ranges found in previous studies of long-term SCS outcomes.15-17 One possible reason for the higher rate is that we did not differentiate based on the reason for the explant (ie, no benefit, further surgery needed for underlying medical condition, or SCS-specific complications). Another possible contributing factor to the higher than expected explant rate is the geographic location in the New Orleans metro area; New Orleans is considered to have one of the highest rates of obesity in the United States and obesity typically has other diseases associated with it such as hypertension and diabetes mellitus.
Limitations
Limitations of the study include the relatively low number of subjects, subjective nature of the interview questions, and the patients’ answers. Typically the POQ has been used as a prospective assessment of pain; whether it is valid in a retrospective analysis is not clear. While there was a statistically significant decrease of opioid use after getting SCS, this study can only show correlation, not causation. During the study period, there has been a drastic change in opioid prescribing patterns and efforts to decrease the amount of opioids prescribed.
Subjects also were asked to rate their pain and quality of life before SCS. Some subjects had SCS implantation up to 10 years prior to the phone interview. The variable amount of time between SCS implantation and interview likely affected subjects’ responses. Chronic pain is a moving target. Patients have good days and bad days that would likely change opinions on SCS benefits on a single phone interview. Some patients needed battery replacements at the time of the interview (battery life averaged about 3 to 5 years in our study population) and were asked to report current levels of pain from the perspective of when their batteries were still functional, further affecting results.
Conclusions
SCS was shown to improve the quality of life of US veterans at SLVHCS across a wide variety of metrics, including activities of daily living, as well as mental and physical health. For veterans with chronic intractable pain who have tried and failed more conservative treatments, SCS is a great treatment.
1. Hoy DG, Smith E, Cross M, et al. The global burden of musculoskeletal conditions for 2010: an overview of methods. Ann Rheum Dis. 2014;73(6):982-989 doi:10.1136/annrheumdis-2013-204344
2. Nahin RL. Severe pain in veterans: the effect of age and sex, and comparisons with the general population. J Pain. 2017;18(3):247-254. doi:10.1016/j.jpain.2016.10.021
3. Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011.
4. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162-173. doi:10.1016/S1474-4422(14)70251-0
5. Costigan M, Scholz J, Woolf CJ. Neuropathic pain: a maladaptive response of the nervous system to damage. Annu Rev Neurosci. 2009;32:1-32. doi:10.1146/annurev.neuro.051508.135531
6. Wilkinson HA. The Failed Back Syndrome: Etiology and Therapy. 2nd ed. Harper & Row; 1991.
7. Kumar K, Taylor RS, Jacques L, et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007;132(1-2):179-188. doi:10.1016/j.pain.2007.07.028
8. North RB, Kidd DH, Farrokhi F, Piantadosi SA. Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial. Neurosurgery. 2005;56(1):98-107. doi:10.1227/01.neu.0000144839.65524.e0
9. Geurts JW, Smits H, Kemler MA, Brunner F, Kessels AG, van Kleef M. Spinal cord stimulation for complex regional pain syndrome type I: a prospective cohort study with long-term follow-up. Neuromodulation. 2013;16(6):523-529. doi:10.1111/ner.12024
10. Kumar K, Rizvi S, Bnurs SB. Spinal cord stimulation is effective in management of complex regional pain syndrome I: fact or fiction. Neurosurgery. 2011;69(3):566-5580. doi:10.1227/NEU.0b013e3182181e60
11. Mekhail NA, Mathews M, Nageeb F, Guirguis M, Mekhail MN, Cheng J. Retrospective review of 707 cases of spinal cord stimulation: indications and complications. Pain Pract. 2011;11(2):148-153. doi:10.1111/j.1533-2500.2010.00407.x
12. Veizi E, Hayek SM, North J, et al. Spinal cord stimulation (SCS) with anatomically guided (3D) neural targeting shows superior chronic axial low back pain relief compared to traditional SCS-LUMINA Study. Pain Med. 2017;18(8):1534-1548. doi:10.1093/pm/pnw286
13. Gordon DB, Polomano RC, Pellino TA, et al. Revised American Pain Society Patient Outcome Questionnaire (APS-POQ-R) for quality improvement of pain management in hospitalized adults: preliminary psychometric evaluation. J Pain. 2010;11(11):1172-1186. doi:10.1016/j.jpain.2010.02.012
14. Kennedy DJ, Schneider B. Lies, damn lies, and statistic: a commentary. Pain Med. 2020;21(10):2052-2054. doi:10.1093/pm/pnaa287
15. Van Buyten JP, Wille F, Smet I, et al. Therapy-related explants after spinal cord stimulation: results of an international retrospective chart review study. Neuromodulation. 2017;20(7):642-649. doi:10.1111/ner.12642
16. Hayek SM, Veizi E, Hanes M. Treatment-limiting complications of percutaneous spinal cord stimulator implants: a review of eight years of experience from an academic center database. Neuromodulation. 2015;18(7):603-609. doi:10.1111/ner.12312
17. Pope JE, Deer TR, Falowski S, et al. Multicenter retrospective study of neurostimulation with exit of therapy by explant. Neuromodulation. 2017;20(6):543-552. doi:10.1111/ner.12634
1. Hoy DG, Smith E, Cross M, et al. The global burden of musculoskeletal conditions for 2010: an overview of methods. Ann Rheum Dis. 2014;73(6):982-989 doi:10.1136/annrheumdis-2013-204344
2. Nahin RL. Severe pain in veterans: the effect of age and sex, and comparisons with the general population. J Pain. 2017;18(3):247-254. doi:10.1016/j.jpain.2016.10.021
3. Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011.
4. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162-173. doi:10.1016/S1474-4422(14)70251-0
5. Costigan M, Scholz J, Woolf CJ. Neuropathic pain: a maladaptive response of the nervous system to damage. Annu Rev Neurosci. 2009;32:1-32. doi:10.1146/annurev.neuro.051508.135531
6. Wilkinson HA. The Failed Back Syndrome: Etiology and Therapy. 2nd ed. Harper & Row; 1991.
7. Kumar K, Taylor RS, Jacques L, et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007;132(1-2):179-188. doi:10.1016/j.pain.2007.07.028
8. North RB, Kidd DH, Farrokhi F, Piantadosi SA. Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial. Neurosurgery. 2005;56(1):98-107. doi:10.1227/01.neu.0000144839.65524.e0
9. Geurts JW, Smits H, Kemler MA, Brunner F, Kessels AG, van Kleef M. Spinal cord stimulation for complex regional pain syndrome type I: a prospective cohort study with long-term follow-up. Neuromodulation. 2013;16(6):523-529. doi:10.1111/ner.12024
10. Kumar K, Rizvi S, Bnurs SB. Spinal cord stimulation is effective in management of complex regional pain syndrome I: fact or fiction. Neurosurgery. 2011;69(3):566-5580. doi:10.1227/NEU.0b013e3182181e60
11. Mekhail NA, Mathews M, Nageeb F, Guirguis M, Mekhail MN, Cheng J. Retrospective review of 707 cases of spinal cord stimulation: indications and complications. Pain Pract. 2011;11(2):148-153. doi:10.1111/j.1533-2500.2010.00407.x
12. Veizi E, Hayek SM, North J, et al. Spinal cord stimulation (SCS) with anatomically guided (3D) neural targeting shows superior chronic axial low back pain relief compared to traditional SCS-LUMINA Study. Pain Med. 2017;18(8):1534-1548. doi:10.1093/pm/pnw286
13. Gordon DB, Polomano RC, Pellino TA, et al. Revised American Pain Society Patient Outcome Questionnaire (APS-POQ-R) for quality improvement of pain management in hospitalized adults: preliminary psychometric evaluation. J Pain. 2010;11(11):1172-1186. doi:10.1016/j.jpain.2010.02.012
14. Kennedy DJ, Schneider B. Lies, damn lies, and statistic: a commentary. Pain Med. 2020;21(10):2052-2054. doi:10.1093/pm/pnaa287
15. Van Buyten JP, Wille F, Smet I, et al. Therapy-related explants after spinal cord stimulation: results of an international retrospective chart review study. Neuromodulation. 2017;20(7):642-649. doi:10.1111/ner.12642
16. Hayek SM, Veizi E, Hanes M. Treatment-limiting complications of percutaneous spinal cord stimulator implants: a review of eight years of experience from an academic center database. Neuromodulation. 2015;18(7):603-609. doi:10.1111/ner.12312
17. Pope JE, Deer TR, Falowski S, et al. Multicenter retrospective study of neurostimulation with exit of therapy by explant. Neuromodulation. 2017;20(6):543-552. doi:10.1111/ner.12634
Rotating Hinge Distal Femur Replacement: A Turn for the Worse
Preoperatively periprosthetic joint infection with a postoperative complication of 180° rotation of the press-fit femoral component is a rare event, and knowledge of this possible complication is important for arthroplasty surgeons.
The use of a rotating hinge distal femur replacement (DFR) for significant bone and soft tissue defects in the setting of total knee arthroplasty (TKA) revision has become increasingly more common. Although significant advancements have been made in modern DFR components, complications and failure rates remain high. The unanticipated early failure presented serves as the first reported case in the literature to our knowledge of a 180° rotation of a press-fit DFR.
Originally, DFRs were used primarily for oncology patients with substantial bone loss following large mass excisions. The utility of DFRs has grown to include massive bone loss in the setting of TKA revision, periprosthetic fractures, and periprosthetic joint infections.1-3 DFRs help restore the joint line in the setting of significant bone loss and contain a rotating hinge mechanism that provides functional movement despite the loss of soft tissue constraints around the knee.1-3
DFRs have been associated with early postoperative mobilization and decreased need for ambulatory devices at 1 year in revision TKA and periprosthetic and geriatric distal femur fractures.4-6 Advances in prosthetic design, biomechanics, and fixation technique have led to improved survival rates.3 Despite these improvements, the overall complication rate remains high at 30 to 40%.3-7 Commonly reported complications after DFR include infection, aseptic loosening, soft tissue failure, and structural failure.3,4,7 Recent case studies also have reported on dislocation or disengagement of the rotating hinge.8-11
In this case report, we present a patient who had a DFR as the second stage of a 2-stage TKA revision due to a periprosthetic joint infection with a postoperative complication of 180° rotation of the press-fit femoral component. Although this is a rare event, knowledge of this possible complication is important for arthroplasty surgeons.
Case Presentation
A patient with a history of hypertension, osteopenia, and rheumatoid arthritis underwent a primary right TKA in 2007. Ten weeks postoperatively, the patient had a ground-level fall that resulted in a right periprosthetic supracondylar distal femur fracture that was treated with a distal femur locking plate. The patient healed, however, with a significant golf club deformity (Figure 1). The patient did well for more than a decade but in 2019 was admitted with pelvic inflammatory disease and adnexal abscess that was treated with broad-spectrum IV antibiotics. Shortly after this admission, the patient developed a right knee periprosthetic infection with cultures positive for Ureaplasma parvum.
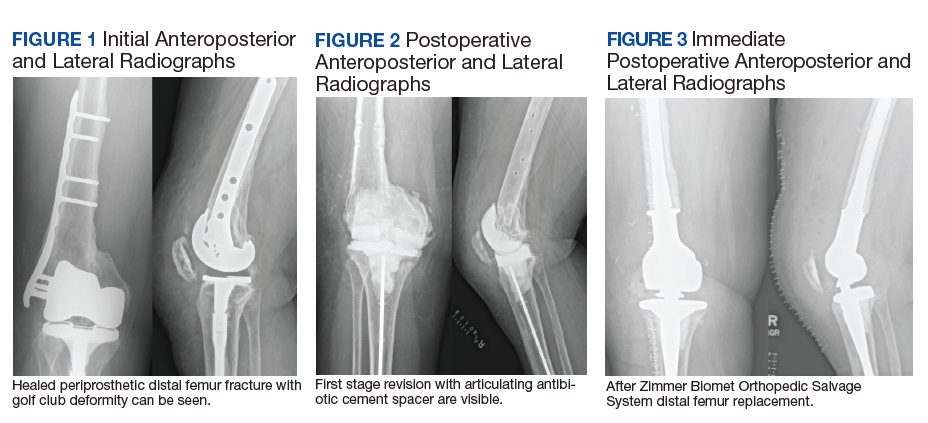
The patient then underwent a 2-stage revision of the infected TKA. Stage 1 consisted of explant of the TKA components as well as removal of the distal femur plate and screws and placement of an articulating antibiotic cement spacer (Figure 2). The patient completed 6 weeks of IV antibiotics. Following completion of the antibiotic course, we obtained a serum erythrocyte sedimentation rate, C-reactive protein level, and white blood cell count, which were all within normal limits. A knee aspiration was performed and did not show signs of residual infection. Frozen histopathology was sent during the second stage of the revision and did not show infection. After the results of the frozen histopathology returned, the antibiotic spacer was removed, and the femoral canal was thoroughly debrided. Cement and fibrous tissue in the femoral canal were carefully removed. In the setting of significant bone loss and soft tissue compromise due to the previous infection and distal femur fracture, the Zimmer Biomet Orthopedic Salvage System (OSS) with porous coated press-fit elliptical femoral stem was utilized.
The femoral canal was reamed until good cortical chatter was obtained at 16 mm. Per the Biomet OSS guide, “For bowed (curved) long and short press-fit stems, the final flexible reamer shaft diameter may need to be larger than the definitive trial and implant diameter.” After trialing, size 15.5 mm was selected for implantation. Intraoperatively the final stem was noted to have good interference fit after insertion and was stable throughout knee range of motion and varus/valgus stress testing. The patient did well with mobilization while in the hospital postoperatively and was discharged home (Figure 3).
Five days after discharge, the patient kicked the repaired knee onto a chair for rest and elevation and experienced extreme pain and was unable to flex the knee. On presentation to the emergency department, the X-rays showed 180° rotation around the longitudinal axis of the femoral component without any other obvious component failure or fracture (Figure 4). The patient was taken back to surgery the following day. Intraoperatively, the femoral stem was found to be loose and rotated 180° (Figure 5). No failure or dislocation of the tibial or rotating hinge components were identified. The press-fit femoral stem was removed and replaced with a cemented stem (Figure 6).
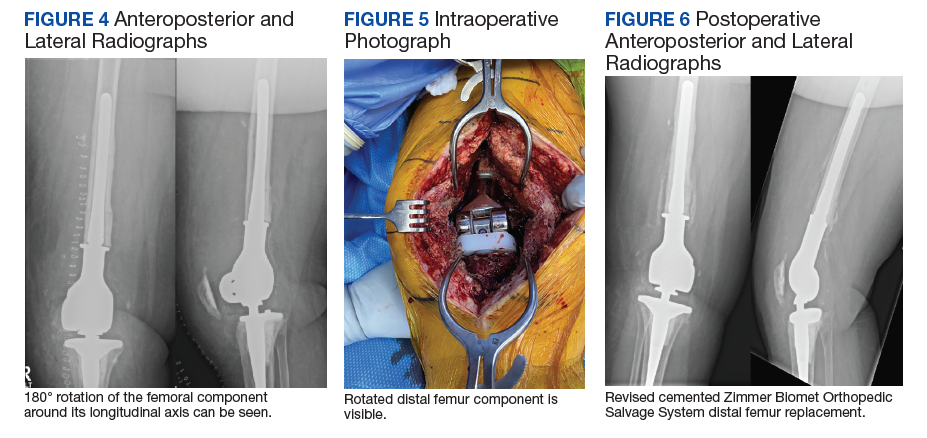
The postoperative course after the revision surgery was uneventful, and the patient is doing well clinically with no pain, functional range of motion of 5 to 105°, and has returned to regular activities without difficulty.
Discussion
Despite advancements in DFRs and increasing use in the setting of revision TKA, the procedure remains high risk with respect to postoperative complications.3-7 Vertesich and colleagues demonstrated that 43.3% of patients who underwent DFR for failed TKA developed at least 1 postoperative complication that required a return to the operating room.7Physicians need to be aware of the high rate of complications and counsel patients appropriately preoperatively.
Complications after DFR include infection, aseptic loosening, soft tissue failure, and structural failure.4,7 Soft tissue failures include insufficiency or rupture of the extensor mechanism and patella dislocation.4,7 Structural failures include fracture of the hinge mechanism, dissociation of the component from the stem, rotating hinge-bushing failure, and dislocation of the hinge.4,7 In the acute postoperative period, the most common complications are infection and rotating-hinge dislocation/failure.3,12 There are various component options available for DFRs, including straight vs curved, cemented vs cementless/press-fit, and long vs short stems.13 Studies have sought to elucidate the ideal implant to decrease the rate of complications. Lu and colleagues demonstrated that curved press-fit short stems provided a stable interface without loosening over the short term (2 years) in 42 patients.13 No implant failures or incidences of aseptic loosening occurred in their study.13
The implant used in this case was a curved press-fit short-stem DFR. It was thought that this patient was young and with good enough bone quality that a press-fit short stem would be best in preserving bone stock. Both the technique guide and literature support reaming 0 to 2 mm greater than the planned stem size to accommodate the implant curvature.13 In this case, the intramedullary canal was reamed 0.5 mm larger than the curved stem that was implanted (16 mm and 15.5 mm, respectively). Intraoperatively during the index DFR, the component was stable and seemed to have a good press-fit interface. Despite this, obvious loosening of the component occurred with a relatively low-energy mechanism when the patient kicked the leg onto a chair, causing just enough force and femoral rotation to result in 180° rotation of the component.
Conclusions
We present this case report to make surgeons aware of this rare but serious complication. Although the final implant is a porous and curved stem, careful attention should be made during trialing to use the best-fitting implant to prevent this complication. If an adequate interference fit cannot be obtained, cementing the component may be required to prevent its loosening and catastrophic failure.
1. Sculco PK, Abdel MP, Hanssen AD, Lewallen DG. The management of bone loss in revision total knee arthroplasty: rebuild, reinforce, and augment. Bone Joint J. 2016;98-B(1 suppl A):120-124. doi:10.1302/0301-620X.98B1.36345
2. Harrison RJ Jr, Thacker MM, Pitcher JD, Temple HT, Scully SP. Distal femur replacement is useful in complex total knee arthroplasty revisions. Clin Orthop Relat Res. 2006;446:113-120. doi:10.1097/01.blo.0000214433.64774.1b
3. Smith EL, Shah A, Son SJ, et al. Survivorship of megaprostheses in revision hip and knee arthroplasty for septic and aseptic indications: a retrospective, multicenter study with minimum 2-year follow-up. Arthroplast Today. 2020;6(3):475-479. Published 2020 Jun 29. doi:10.1016/j.artd.2020.05.004
4. Wyles CC, Tibbo ME, Yuan BJ, Trousdale RT, Berry DJ, Abdel MP. Long-term results of total knee arthroplasty with contemporary distal femoral replacement. J Bone Joint Surg Am. 2020;102(1):45-51. doi:10.2106/JBJS.19.00489
5. Haidukewych GJ. Role of distal femoral replacement for periprosthetic fractures above a total knee arthroplasty: when and how?, J Orthop Trauma. 2019;33(suppl 6):S33-S35. doi:10.1097/BOT.0000000000001566
6. Hart GP, Kneisl JS, Springer BD, Patt JC, Karunakar MA. Open reduction vs distal femoral replacement arthroplasty for comminuted distal femur fractures in the patients 70 years and older: J Arthroplasty. 2017;32(1):202-206. doi:10.1016/j.arth.2016.06.006
7. Vertesich K, Puchner SE, Staats K, et al. Distal femoral reconstruction following failed total knee arthroplasty is accompanied with risk for complication and reduced joint function. BMC Musculoskelet Disord. 2019 Jan 31;20(1):47-54. doi:10.1186/s12891-019-2432-4
8. Biswas D, Haughom B, Mayle RE Jr, Della Valle CJ. Case report: Failure of rotating-hinge total knee prosthesis by disengagement of the hinge-post extension. Clin Orthop Relat Res. 2013;471(4):1389-1392. doi:10.1007/s11999-012-2736-2
9. Ward WG, Haight D, Ritchie P, Gordon S, Eckardt JJ. Dislocation of rotating hinge knee prostheses. A report of four cases. J Bone Joint Surg Am. 2005;87(5):1108-1112. doi:10.2106/JBJS.00837pp
10. Pacha-Vicente D, Malik A, Castellet-Feliu E, Nardi-Vilardaga J. Dislocation of rotating-hinge knee prostheses with antidislocation mechanism. J Arthroplasty. 2008;23(2):299-303. doi:10.1016/j.arth.2006.11.020
11. Manzano G, Schwarzkopf R. Posterior dislocation of the hinge-post extension in a rotating hinge total knee prosthesis. Case Rep Orthop. 2013;2013:756538. doi:10.1155/2013/756538
12. Vaishya R., Thapa, SS, Vaish A. Non-neoplastic indications and outcomes of the proximal and distal femur megaprosthesis: a critical review. Knee Surg Relat Res. 2020;32(1):18. Published 2020 Apr 9. doi:10.1186/s43019-020-00034-7
13. Lu M, Wang J, Xiao C, et al. Uncemented, curved, short endoprosthesis stem for distal femoral reconstruction: early follow-up outcomes. World J Surg Onc. 2018;16(1):183. doi:10.1186/s12957-018-1486-3
Preoperatively periprosthetic joint infection with a postoperative complication of 180° rotation of the press-fit femoral component is a rare event, and knowledge of this possible complication is important for arthroplasty surgeons.
Preoperatively periprosthetic joint infection with a postoperative complication of 180° rotation of the press-fit femoral component is a rare event, and knowledge of this possible complication is important for arthroplasty surgeons.
The use of a rotating hinge distal femur replacement (DFR) for significant bone and soft tissue defects in the setting of total knee arthroplasty (TKA) revision has become increasingly more common. Although significant advancements have been made in modern DFR components, complications and failure rates remain high. The unanticipated early failure presented serves as the first reported case in the literature to our knowledge of a 180° rotation of a press-fit DFR.
Originally, DFRs were used primarily for oncology patients with substantial bone loss following large mass excisions. The utility of DFRs has grown to include massive bone loss in the setting of TKA revision, periprosthetic fractures, and periprosthetic joint infections.1-3 DFRs help restore the joint line in the setting of significant bone loss and contain a rotating hinge mechanism that provides functional movement despite the loss of soft tissue constraints around the knee.1-3
DFRs have been associated with early postoperative mobilization and decreased need for ambulatory devices at 1 year in revision TKA and periprosthetic and geriatric distal femur fractures.4-6 Advances in prosthetic design, biomechanics, and fixation technique have led to improved survival rates.3 Despite these improvements, the overall complication rate remains high at 30 to 40%.3-7 Commonly reported complications after DFR include infection, aseptic loosening, soft tissue failure, and structural failure.3,4,7 Recent case studies also have reported on dislocation or disengagement of the rotating hinge.8-11
In this case report, we present a patient who had a DFR as the second stage of a 2-stage TKA revision due to a periprosthetic joint infection with a postoperative complication of 180° rotation of the press-fit femoral component. Although this is a rare event, knowledge of this possible complication is important for arthroplasty surgeons.
Case Presentation
A patient with a history of hypertension, osteopenia, and rheumatoid arthritis underwent a primary right TKA in 2007. Ten weeks postoperatively, the patient had a ground-level fall that resulted in a right periprosthetic supracondylar distal femur fracture that was treated with a distal femur locking plate. The patient healed, however, with a significant golf club deformity (Figure 1). The patient did well for more than a decade but in 2019 was admitted with pelvic inflammatory disease and adnexal abscess that was treated with broad-spectrum IV antibiotics. Shortly after this admission, the patient developed a right knee periprosthetic infection with cultures positive for Ureaplasma parvum.
The patient then underwent a 2-stage revision of the infected TKA. Stage 1 consisted of explant of the TKA components as well as removal of the distal femur plate and screws and placement of an articulating antibiotic cement spacer (Figure 2). The patient completed 6 weeks of IV antibiotics. Following completion of the antibiotic course, we obtained a serum erythrocyte sedimentation rate, C-reactive protein level, and white blood cell count, which were all within normal limits. A knee aspiration was performed and did not show signs of residual infection. Frozen histopathology was sent during the second stage of the revision and did not show infection. After the results of the frozen histopathology returned, the antibiotic spacer was removed, and the femoral canal was thoroughly debrided. Cement and fibrous tissue in the femoral canal were carefully removed. In the setting of significant bone loss and soft tissue compromise due to the previous infection and distal femur fracture, the Zimmer Biomet Orthopedic Salvage System (OSS) with porous coated press-fit elliptical femoral stem was utilized.
The femoral canal was reamed until good cortical chatter was obtained at 16 mm. Per the Biomet OSS guide, “For bowed (curved) long and short press-fit stems, the final flexible reamer shaft diameter may need to be larger than the definitive trial and implant diameter.” After trialing, size 15.5 mm was selected for implantation. Intraoperatively the final stem was noted to have good interference fit after insertion and was stable throughout knee range of motion and varus/valgus stress testing. The patient did well with mobilization while in the hospital postoperatively and was discharged home (Figure 3).
Five days after discharge, the patient kicked the repaired knee onto a chair for rest and elevation and experienced extreme pain and was unable to flex the knee. On presentation to the emergency department, the X-rays showed 180° rotation around the longitudinal axis of the femoral component without any other obvious component failure or fracture (Figure 4). The patient was taken back to surgery the following day. Intraoperatively, the femoral stem was found to be loose and rotated 180° (Figure 5). No failure or dislocation of the tibial or rotating hinge components were identified. The press-fit femoral stem was removed and replaced with a cemented stem (Figure 6).
The postoperative course after the revision surgery was uneventful, and the patient is doing well clinically with no pain, functional range of motion of 5 to 105°, and has returned to regular activities without difficulty.
Discussion
Despite advancements in DFRs and increasing use in the setting of revision TKA, the procedure remains high risk with respect to postoperative complications.3-7 Vertesich and colleagues demonstrated that 43.3% of patients who underwent DFR for failed TKA developed at least 1 postoperative complication that required a return to the operating room.7Physicians need to be aware of the high rate of complications and counsel patients appropriately preoperatively.
Complications after DFR include infection, aseptic loosening, soft tissue failure, and structural failure.4,7 Soft tissue failures include insufficiency or rupture of the extensor mechanism and patella dislocation.4,7 Structural failures include fracture of the hinge mechanism, dissociation of the component from the stem, rotating hinge-bushing failure, and dislocation of the hinge.4,7 In the acute postoperative period, the most common complications are infection and rotating-hinge dislocation/failure.3,12 There are various component options available for DFRs, including straight vs curved, cemented vs cementless/press-fit, and long vs short stems.13 Studies have sought to elucidate the ideal implant to decrease the rate of complications. Lu and colleagues demonstrated that curved press-fit short stems provided a stable interface without loosening over the short term (2 years) in 42 patients.13 No implant failures or incidences of aseptic loosening occurred in their study.13
The implant used in this case was a curved press-fit short-stem DFR. It was thought that this patient was young and with good enough bone quality that a press-fit short stem would be best in preserving bone stock. Both the technique guide and literature support reaming 0 to 2 mm greater than the planned stem size to accommodate the implant curvature.13 In this case, the intramedullary canal was reamed 0.5 mm larger than the curved stem that was implanted (16 mm and 15.5 mm, respectively). Intraoperatively during the index DFR, the component was stable and seemed to have a good press-fit interface. Despite this, obvious loosening of the component occurred with a relatively low-energy mechanism when the patient kicked the leg onto a chair, causing just enough force and femoral rotation to result in 180° rotation of the component.
Conclusions
We present this case report to make surgeons aware of this rare but serious complication. Although the final implant is a porous and curved stem, careful attention should be made during trialing to use the best-fitting implant to prevent this complication. If an adequate interference fit cannot be obtained, cementing the component may be required to prevent its loosening and catastrophic failure.
The use of a rotating hinge distal femur replacement (DFR) for significant bone and soft tissue defects in the setting of total knee arthroplasty (TKA) revision has become increasingly more common. Although significant advancements have been made in modern DFR components, complications and failure rates remain high. The unanticipated early failure presented serves as the first reported case in the literature to our knowledge of a 180° rotation of a press-fit DFR.
Originally, DFRs were used primarily for oncology patients with substantial bone loss following large mass excisions. The utility of DFRs has grown to include massive bone loss in the setting of TKA revision, periprosthetic fractures, and periprosthetic joint infections.1-3 DFRs help restore the joint line in the setting of significant bone loss and contain a rotating hinge mechanism that provides functional movement despite the loss of soft tissue constraints around the knee.1-3
DFRs have been associated with early postoperative mobilization and decreased need for ambulatory devices at 1 year in revision TKA and periprosthetic and geriatric distal femur fractures.4-6 Advances in prosthetic design, biomechanics, and fixation technique have led to improved survival rates.3 Despite these improvements, the overall complication rate remains high at 30 to 40%.3-7 Commonly reported complications after DFR include infection, aseptic loosening, soft tissue failure, and structural failure.3,4,7 Recent case studies also have reported on dislocation or disengagement of the rotating hinge.8-11
In this case report, we present a patient who had a DFR as the second stage of a 2-stage TKA revision due to a periprosthetic joint infection with a postoperative complication of 180° rotation of the press-fit femoral component. Although this is a rare event, knowledge of this possible complication is important for arthroplasty surgeons.
Case Presentation
A patient with a history of hypertension, osteopenia, and rheumatoid arthritis underwent a primary right TKA in 2007. Ten weeks postoperatively, the patient had a ground-level fall that resulted in a right periprosthetic supracondylar distal femur fracture that was treated with a distal femur locking plate. The patient healed, however, with a significant golf club deformity (Figure 1). The patient did well for more than a decade but in 2019 was admitted with pelvic inflammatory disease and adnexal abscess that was treated with broad-spectrum IV antibiotics. Shortly after this admission, the patient developed a right knee periprosthetic infection with cultures positive for Ureaplasma parvum.
The patient then underwent a 2-stage revision of the infected TKA. Stage 1 consisted of explant of the TKA components as well as removal of the distal femur plate and screws and placement of an articulating antibiotic cement spacer (Figure 2). The patient completed 6 weeks of IV antibiotics. Following completion of the antibiotic course, we obtained a serum erythrocyte sedimentation rate, C-reactive protein level, and white blood cell count, which were all within normal limits. A knee aspiration was performed and did not show signs of residual infection. Frozen histopathology was sent during the second stage of the revision and did not show infection. After the results of the frozen histopathology returned, the antibiotic spacer was removed, and the femoral canal was thoroughly debrided. Cement and fibrous tissue in the femoral canal were carefully removed. In the setting of significant bone loss and soft tissue compromise due to the previous infection and distal femur fracture, the Zimmer Biomet Orthopedic Salvage System (OSS) with porous coated press-fit elliptical femoral stem was utilized.
The femoral canal was reamed until good cortical chatter was obtained at 16 mm. Per the Biomet OSS guide, “For bowed (curved) long and short press-fit stems, the final flexible reamer shaft diameter may need to be larger than the definitive trial and implant diameter.” After trialing, size 15.5 mm was selected for implantation. Intraoperatively the final stem was noted to have good interference fit after insertion and was stable throughout knee range of motion and varus/valgus stress testing. The patient did well with mobilization while in the hospital postoperatively and was discharged home (Figure 3).
Five days after discharge, the patient kicked the repaired knee onto a chair for rest and elevation and experienced extreme pain and was unable to flex the knee. On presentation to the emergency department, the X-rays showed 180° rotation around the longitudinal axis of the femoral component without any other obvious component failure or fracture (Figure 4). The patient was taken back to surgery the following day. Intraoperatively, the femoral stem was found to be loose and rotated 180° (Figure 5). No failure or dislocation of the tibial or rotating hinge components were identified. The press-fit femoral stem was removed and replaced with a cemented stem (Figure 6).
The postoperative course after the revision surgery was uneventful, and the patient is doing well clinically with no pain, functional range of motion of 5 to 105°, and has returned to regular activities without difficulty.
Discussion
Despite advancements in DFRs and increasing use in the setting of revision TKA, the procedure remains high risk with respect to postoperative complications.3-7 Vertesich and colleagues demonstrated that 43.3% of patients who underwent DFR for failed TKA developed at least 1 postoperative complication that required a return to the operating room.7Physicians need to be aware of the high rate of complications and counsel patients appropriately preoperatively.
Complications after DFR include infection, aseptic loosening, soft tissue failure, and structural failure.4,7 Soft tissue failures include insufficiency or rupture of the extensor mechanism and patella dislocation.4,7 Structural failures include fracture of the hinge mechanism, dissociation of the component from the stem, rotating hinge-bushing failure, and dislocation of the hinge.4,7 In the acute postoperative period, the most common complications are infection and rotating-hinge dislocation/failure.3,12 There are various component options available for DFRs, including straight vs curved, cemented vs cementless/press-fit, and long vs short stems.13 Studies have sought to elucidate the ideal implant to decrease the rate of complications. Lu and colleagues demonstrated that curved press-fit short stems provided a stable interface without loosening over the short term (2 years) in 42 patients.13 No implant failures or incidences of aseptic loosening occurred in their study.13
The implant used in this case was a curved press-fit short-stem DFR. It was thought that this patient was young and with good enough bone quality that a press-fit short stem would be best in preserving bone stock. Both the technique guide and literature support reaming 0 to 2 mm greater than the planned stem size to accommodate the implant curvature.13 In this case, the intramedullary canal was reamed 0.5 mm larger than the curved stem that was implanted (16 mm and 15.5 mm, respectively). Intraoperatively during the index DFR, the component was stable and seemed to have a good press-fit interface. Despite this, obvious loosening of the component occurred with a relatively low-energy mechanism when the patient kicked the leg onto a chair, causing just enough force and femoral rotation to result in 180° rotation of the component.
Conclusions
We present this case report to make surgeons aware of this rare but serious complication. Although the final implant is a porous and curved stem, careful attention should be made during trialing to use the best-fitting implant to prevent this complication. If an adequate interference fit cannot be obtained, cementing the component may be required to prevent its loosening and catastrophic failure.
1. Sculco PK, Abdel MP, Hanssen AD, Lewallen DG. The management of bone loss in revision total knee arthroplasty: rebuild, reinforce, and augment. Bone Joint J. 2016;98-B(1 suppl A):120-124. doi:10.1302/0301-620X.98B1.36345
2. Harrison RJ Jr, Thacker MM, Pitcher JD, Temple HT, Scully SP. Distal femur replacement is useful in complex total knee arthroplasty revisions. Clin Orthop Relat Res. 2006;446:113-120. doi:10.1097/01.blo.0000214433.64774.1b
3. Smith EL, Shah A, Son SJ, et al. Survivorship of megaprostheses in revision hip and knee arthroplasty for septic and aseptic indications: a retrospective, multicenter study with minimum 2-year follow-up. Arthroplast Today. 2020;6(3):475-479. Published 2020 Jun 29. doi:10.1016/j.artd.2020.05.004
4. Wyles CC, Tibbo ME, Yuan BJ, Trousdale RT, Berry DJ, Abdel MP. Long-term results of total knee arthroplasty with contemporary distal femoral replacement. J Bone Joint Surg Am. 2020;102(1):45-51. doi:10.2106/JBJS.19.00489
5. Haidukewych GJ. Role of distal femoral replacement for periprosthetic fractures above a total knee arthroplasty: when and how?, J Orthop Trauma. 2019;33(suppl 6):S33-S35. doi:10.1097/BOT.0000000000001566
6. Hart GP, Kneisl JS, Springer BD, Patt JC, Karunakar MA. Open reduction vs distal femoral replacement arthroplasty for comminuted distal femur fractures in the patients 70 years and older: J Arthroplasty. 2017;32(1):202-206. doi:10.1016/j.arth.2016.06.006
7. Vertesich K, Puchner SE, Staats K, et al. Distal femoral reconstruction following failed total knee arthroplasty is accompanied with risk for complication and reduced joint function. BMC Musculoskelet Disord. 2019 Jan 31;20(1):47-54. doi:10.1186/s12891-019-2432-4
8. Biswas D, Haughom B, Mayle RE Jr, Della Valle CJ. Case report: Failure of rotating-hinge total knee prosthesis by disengagement of the hinge-post extension. Clin Orthop Relat Res. 2013;471(4):1389-1392. doi:10.1007/s11999-012-2736-2
9. Ward WG, Haight D, Ritchie P, Gordon S, Eckardt JJ. Dislocation of rotating hinge knee prostheses. A report of four cases. J Bone Joint Surg Am. 2005;87(5):1108-1112. doi:10.2106/JBJS.00837pp
10. Pacha-Vicente D, Malik A, Castellet-Feliu E, Nardi-Vilardaga J. Dislocation of rotating-hinge knee prostheses with antidislocation mechanism. J Arthroplasty. 2008;23(2):299-303. doi:10.1016/j.arth.2006.11.020
11. Manzano G, Schwarzkopf R. Posterior dislocation of the hinge-post extension in a rotating hinge total knee prosthesis. Case Rep Orthop. 2013;2013:756538. doi:10.1155/2013/756538
12. Vaishya R., Thapa, SS, Vaish A. Non-neoplastic indications and outcomes of the proximal and distal femur megaprosthesis: a critical review. Knee Surg Relat Res. 2020;32(1):18. Published 2020 Apr 9. doi:10.1186/s43019-020-00034-7
13. Lu M, Wang J, Xiao C, et al. Uncemented, curved, short endoprosthesis stem for distal femoral reconstruction: early follow-up outcomes. World J Surg Onc. 2018;16(1):183. doi:10.1186/s12957-018-1486-3
1. Sculco PK, Abdel MP, Hanssen AD, Lewallen DG. The management of bone loss in revision total knee arthroplasty: rebuild, reinforce, and augment. Bone Joint J. 2016;98-B(1 suppl A):120-124. doi:10.1302/0301-620X.98B1.36345
2. Harrison RJ Jr, Thacker MM, Pitcher JD, Temple HT, Scully SP. Distal femur replacement is useful in complex total knee arthroplasty revisions. Clin Orthop Relat Res. 2006;446:113-120. doi:10.1097/01.blo.0000214433.64774.1b
3. Smith EL, Shah A, Son SJ, et al. Survivorship of megaprostheses in revision hip and knee arthroplasty for septic and aseptic indications: a retrospective, multicenter study with minimum 2-year follow-up. Arthroplast Today. 2020;6(3):475-479. Published 2020 Jun 29. doi:10.1016/j.artd.2020.05.004
4. Wyles CC, Tibbo ME, Yuan BJ, Trousdale RT, Berry DJ, Abdel MP. Long-term results of total knee arthroplasty with contemporary distal femoral replacement. J Bone Joint Surg Am. 2020;102(1):45-51. doi:10.2106/JBJS.19.00489
5. Haidukewych GJ. Role of distal femoral replacement for periprosthetic fractures above a total knee arthroplasty: when and how?, J Orthop Trauma. 2019;33(suppl 6):S33-S35. doi:10.1097/BOT.0000000000001566
6. Hart GP, Kneisl JS, Springer BD, Patt JC, Karunakar MA. Open reduction vs distal femoral replacement arthroplasty for comminuted distal femur fractures in the patients 70 years and older: J Arthroplasty. 2017;32(1):202-206. doi:10.1016/j.arth.2016.06.006
7. Vertesich K, Puchner SE, Staats K, et al. Distal femoral reconstruction following failed total knee arthroplasty is accompanied with risk for complication and reduced joint function. BMC Musculoskelet Disord. 2019 Jan 31;20(1):47-54. doi:10.1186/s12891-019-2432-4
8. Biswas D, Haughom B, Mayle RE Jr, Della Valle CJ. Case report: Failure of rotating-hinge total knee prosthesis by disengagement of the hinge-post extension. Clin Orthop Relat Res. 2013;471(4):1389-1392. doi:10.1007/s11999-012-2736-2
9. Ward WG, Haight D, Ritchie P, Gordon S, Eckardt JJ. Dislocation of rotating hinge knee prostheses. A report of four cases. J Bone Joint Surg Am. 2005;87(5):1108-1112. doi:10.2106/JBJS.00837pp
10. Pacha-Vicente D, Malik A, Castellet-Feliu E, Nardi-Vilardaga J. Dislocation of rotating-hinge knee prostheses with antidislocation mechanism. J Arthroplasty. 2008;23(2):299-303. doi:10.1016/j.arth.2006.11.020
11. Manzano G, Schwarzkopf R. Posterior dislocation of the hinge-post extension in a rotating hinge total knee prosthesis. Case Rep Orthop. 2013;2013:756538. doi:10.1155/2013/756538
12. Vaishya R., Thapa, SS, Vaish A. Non-neoplastic indications and outcomes of the proximal and distal femur megaprosthesis: a critical review. Knee Surg Relat Res. 2020;32(1):18. Published 2020 Apr 9. doi:10.1186/s43019-020-00034-7
13. Lu M, Wang J, Xiao C, et al. Uncemented, curved, short endoprosthesis stem for distal femoral reconstruction: early follow-up outcomes. World J Surg Onc. 2018;16(1):183. doi:10.1186/s12957-018-1486-3
Nicotine and Nicotine Replacement Therapy Use During Myocardial Perfusion Imaging
Chest pain is one of the most common concerns in patients presenting to the emergency department in the United States, accounting for approximately 7.6 million visits annually.1 Given the high mortality rate associated with acute coronary syndromes, prompt evaluation of chest pain is essential.2 Even in mild cases, recognition of newly onset or worsening coronary artery disease (CAD) is crucial to ensure that patients receive optimal medication therapy.
In symptomatic patients with risk factors for CAD, such as advanced age, hypertension, hyperlipidemia, obesity, and diabetes mellitus, myocardial perfusion imaging (MPI) is frequently used as a modality to assess the presence, location, and severity of ischemic or infarcted myocardium.2 MPI requires administration of a radiopharmaceutical before and after the patient undergoes a form of stress.2 This radiopharmaceutical is then detected in the myocardium with a nuclear camera, and images are obtained of the heart to assess myocardial blood flow.2
MPI can be performed using exercise-induced stress via a treadmill, or medication-induced stress (Table 1). In both strategies, healthy coronary arteries dilate to provide the myocardium with more blood flow to meet the increasing myocardial oxygen demand during this period of stress. While healthy vessels are able to dilate appropriately, coronary arteries with flow-limiting stenoses are unable to dilate to the same extent in response to stress.2 Because radioactive isotope uptake by the myocardium is directly related to arterial blood flow, MPI is able to demonstrate a mismatch in coronary blood flow between healthy and diseased coronary arteries indicated by differences in radioisotope uptake.2 The presence of such a mismatch, in conjunction with clinical history, potentially suggests the presence of CAD.
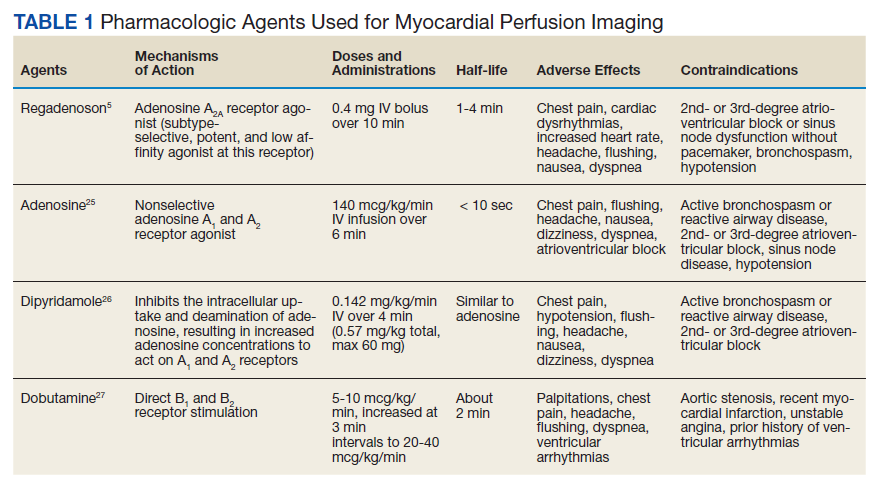
Prior to conducting MPI with a medication, certain substances should be avoided. For instance, methylxanthines, such as caffeine, aminophylline, and theophylline, antagonize adenosine receptors and can have major drug interactions with regadenoson, adenosine, and dipyridamole. Therefore, it is advised that these substances be stopped for at least 12 hours before testing.3 In some cases, other medications that can affect coronary blood flow, such as long-acting nitrates, β-blockers, and calcium channel blockers, are recommended to be avoided for 12 to 48 hours in order to obtain the most accurate depiction of underlying coronary disease.4
Because nicotine and nicotine replacement therapy (NRT) may have substantial effects on coronary circulation, a current area of controversy is whether these should be stopped prior to the use of a stress-inducing medication during MPI. To date, no formal drug interaction studies have been conducted between nicotine and regadenoson.5 Similarly, the ADVANCE MPI 2 Trial, which led to the US Food and Drug Administration approval of regadenoson, did not specify restrictions on the use of nicotine prior to stress testing in the protocol.6 However, as this trial was multicenter, investigators admit that individual study sites could have had their own restrictions on the use of nicotine prior to stress testing with regadenoson, but this information was not collected.6 The current review focuses on how the simultaneous use of nicotine or NRT during MPI with pharmacologic agents, such as regadenoson, may affect the accuracy of imaging results and the clinical impact of this interaction.
Nicotine Coronary Artery Effect
It is well documented that long-term cigarette smoking is a major risk factor for CAD.7 Compared with nonsmokers, cigarette smokers experience 2 times greater risk of morbidity and mortality from ischemic heart disease.7 There are several mechanisms by which nicotine induces damage to the myocardium (Figure). Nicotine has direct effects on both the sympathetic nervous system (SNS) and myocardial endothelium.8 Together, these factors result in reduced coronary blood flow, leading to less oxygen supply to meet an increased oxygen demand, resulting in myocardial ischemia.
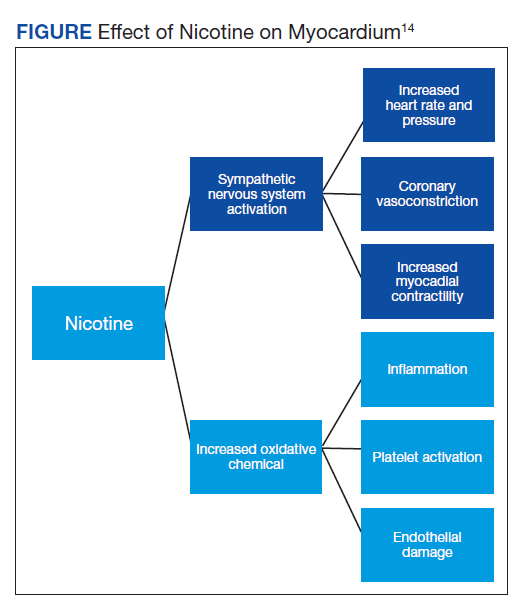
Nicotine’s effect on coronary vasomotor tone occurs primarily through noradrenergic stimulation of α and β receptors associated with coronary vasoconstriction or vasodilation, respectively.9,10 These competing influences on coronary blood flow appear to manifest differently based on whether patients are at rest or in a stressed state. A study by Czerin and colleagues demonstrated that in healthy patients with relatively short smoking histories and in a healthy nonsmoker control group, coronary blood flow increased by 25% and 40%, respectively, with nicotine use at rest.9 However, when these patients were stressed with dipyramidole and while smoking during the examination, myocardial blood flow was reduced by 11% in the study group and 14% in the control group.9 This is likely because the patients studied had relatively healthy coronary arteries that were able to maximally dilate when stressed. In this scenario, nicotine’s dilatory effects are offset by nicotine’s α-receptor–mediated vasoconstriction effects.9 Of note, patients in the study group experienced a somewhat diminished increase in coronary blood flow at rest with nicotine use, suggesting that even a short smoking history may damage the myocardial endothelium, rendering it less responsive to nicotine’s vasodilatory effects.9
These principles similarly apply to patients with underlying moderate-to-severe cardiovascular disease (CVD). With nicotine use at rest, patients with significant CAD do not experience as dramatic of an increase in coronary blood flow, which typically decreases or remains the same despite increased myocardial work.10 This may be because patients with moderate-to-severe CAD often have flow-limiting stenoses and damaged endothelium that do not allow vessels to respond as efficiently to increased myocardial demand or to nicotine’s β-receptor–mediated vasodilatory effects.10,11 Moreover, when stressed, diseased coronary arteries are not able to further dilate and nicotine’s α-receptor–mediated vasoconstriction effects dominate.10,11
In a study by Quillen and colleagues of patients with moderate-to-severe CAD, the mean diameter of proximal coronary artery segments decreased by 5%, the distal coronary diameter decreased 8%, and the coronary vascular resistance increased by 21% while smoking at rest.12 The investigators did not analyze how parameters changed when these diseased coronary arteries were stressed using a medication during MPI. However, it can be predicted that coronary arteries would have constricted to a similar or greater degree than observed in Czerin and colleagues’ study, given that the underlying myocardium was diseased and more susceptible to nicotine’s vasoconstriction effects.9 Importantly, these studies have several limitations, most notably that they are older and have small sample sizes. Additionally, while statistically significant differences were found in the degree of changes in coronary circulation with nicotine use at rest and during stress, it is unclear whether this translates to a clinically significant and impactful finding.9-12
Nicotine Replacement Therapy and Stress Testing
Given the association between cigarette smoking and CAD, medical practitioners strongly encourage patients to quit smoking to reduce their risk of adverse cardiovascular outcomes. Various smoking cessation treatments are available for patients. Common, readily accessible forms of therapy include nicotine replacement products (Table 2).
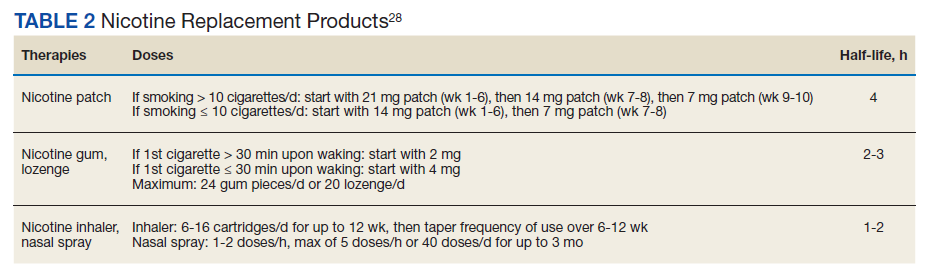
Early studies of NRT in patients with underlying CVD found an increased risk of cardiovascular events, such as myocardial infarction, presumably due to the nicotine content of these products.13,14 However, the concentration of nicotine in NRT is substantially lower than that found in cigarettes and in some formulations, such as transdermal patches, nicotine is delivered over a prolonged period of time.15 For this reason, NRT is thought to be safe in patients with underlying CVD and stable ischemic heart disease. A recent systematic review and meta-analysis found that while NRT may be associated with tachycardia, it did not increase the risk of more serious cardiovascular adverse effects (AEs).16,17
Given the lower nicotine concentration in NRT products, the associated hemodynamic effect of nicotine also is thought to be less pronounced. In a study conducted by Tzivoni and colleagues in patients with CAD using transdermal nicotine patches, no differences in blood pressure, heart rate, ischemia, or arrhythmias were found from baseline to 2 weeks.18 These findings were further confirmed in a small study by Lucini and colleagues, which found that nicotine patches produced slight hemodynamic effects, but to a lesser extent than cigarette smoking.19 For the NRT gum formulation, while a small study found that 4 mg produced coronary vasoconstriction in patients with underlying CAD, a study by Nitenberg and Antony demonstrated that healthy and diseased coronary arteries did not significantly constrict while patients were using nicotine gum both before and after a cold pressor test, suggesting a lesser degree of coronary vasoconstriction than nicotine from cigarette smoking.20,21 Similar findings have been described with the nicotine intranasal spray in a study by Keeley and colleagues, which showed no additional AEs on myocardial demand or vasoconstriction when an intranasal nicotine spray was added to cigarette smoking.22 Importantly, a review of the transdermal and gum formulations found that these less pronounced hemodynamic effects were observed across different doses of NRT; however, further studies are needed to clarify the relationship between NRT dose and cardiovascular effects.23
Overall, NRT does not seem to activate the SNS to the same degree as nicotine obtained via cigarette smoking and likely does not increase the myocardial oxygen demand as much. Additionally, by containing a lower concentration of nicotine, NRT may not impair the myocardium’s ability to supply oxygen to coronary arteries to the same extent as nicotine from cigarette smoking. Therefore, the effects of NRT on MPI using a stress-inducing medication may not be as pronounced. However, due to study limitations, results should be interpreted cautiously.18-23
Conclusions
Because of the close relationship between cigarette smoking and CAD, many patients with underlying CVD are either current smokers or may be using NRT for smoking cessation. Therefore, the question of whether to refrain from nicotine use prior to MPI is clinically relevant. Currently, there is a lack of high-quality studies demonstrating the effects of nicotine and NRT on coronary perfusion. Because of this, the impact of nicotine and NRT use on the accuracy of MPI using stress-inducing medications remains uncertain. Nevertheless, given that nicotine and NRT may largely affect the accuracy of imaging results, several institutions have adopted protocols that prohibit patients from using these drugs on the day of nuclear stress testing.
There are currently no data specifying the number of hours to hold nicotine products prior to cardiac stress testing. It is generally recommended that other medications that affect coronary blood flow be held for 5 half-lives before conducting MPI.4 Following the same guidance for nicotine and NRT may present a reasonable approach to ensure accurate imaging results. Based on the discussed literature, patients should be instructed to refrain from cigarette smoking for at least 5 to 10 hours prior to MPI, given nicotine’s half-life of about 1 to 2 hours.24
The data for NRT are less clear. While use of NRT may not be an absolute contraindication to conducting MPI, it is important to consider that this may affect the accuracy of results. Given this uncertainty, it is likely ideal to hold NRT prior to MPI, based on the specific formulation of NRT and that product's half-life. Further robust studies are needed to analyze the impact of nicotine and NRT on the accuracy of nuclear stress testing using a medication.
1. Rui P, Kang K, Ashman JJ. National Hospital Ambulatory Medical Care Survey: 2016 emergency department summary tables. Published 2016. Accessed March 30, 2020. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf
2. Lange RA. Cardiovascular testing. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10th ed. McGraw Hill; 2017.
3. Mace S. Observation Medicine: Principles and Protocols. Cambridge University Press; 2017.
4. Currie GM. Pharmacology, part 4: nuclear cardiology. J Nucl Med Technol. 2019;47(2):97-110. doi:10.2967/jnmt.118.219675
5. Regadenoson; Package insert. Astellas Pharma US Inc; 2008.
6. Iskandrian AE, Bateman TM, Belardinelli L, et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: results of the ADVANCE phase 3 multicenter international trial. J Nucl Cardiol. 2007;14(5):645-658. doi:10.1016/j.nuclcard.2007.06.114
7. Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18(3):109-114. doi:10.4103/HEARTVIEWS.HEARTVIEWS_106_17
8. Benowitz NL, Burbank AD. Cardiovascular toxicity of nicotine: implications for electronic cigarette use. Trends Cardiovasc Med. 2016;26(6):515-523. doi:10.1016/j.tcm.2016.03.001
9. Czernin J, Sun K, Brunken R, Böttcher M, Phelps M, Schelbert H. Effect of acute and long-term smoking on myocardial blood flow and flow reserve. Circulation. 1995;91:2891-2897. doi:10.1161/01.CIR.91.12.2891
10. Winniford MD, Wheelan KR, Kremers MS, et al. Smoking-induced coronary vasoconstriction in patients with atherosclerotic coronary artery disease: evidence for adrenergically mediated alterations in coronary artery tone. Circulation. 1986;73(4):662-667. doi:10.1161/01.cir.73.4.662
11. Klein LW, Ambrose J, Pichard A, Holt J, Gorlin R, Teichholz LE. Acute coronary hemodynamic response to cigarette smoking in patients with coronary artery disease. J Am Coll Cardiol. 1984;3(4):879-886. doi:10.1016/s0735-1097(84)80344-7
12. Quillen JE, Rossen JD, Oskarsson HJ, Minor RL Jr, Lopez AG, Winniford MD. Acute effect of cigarette smoking on the coronary circulation: constriction of epicardial and resistance vessels. J Am Coll Cardiol. 1993;22(3):642-647. doi:10.1016/0735-1097(93)90170-6
13. Dacosta A, Guy JM, Tardy B, et al. Myocardial infarction and nicotine patch: a contributing or causative factor?. Eur Heart J. 1993;14(12):1709-1711. doi:10.1093/eurheartj/14.12.1709
14. Ottervanger JP, Festen JM, de Vries AG, Stricker BH. Acute myocardial infarction while using the nicotine patch. Chest. 1995;107(6):1765-1766. doi:10.1378/chest.107.6.1765
15. Dollerup J, Vestbo J, Murray-Thomas T, et al. Cardiovascular risks in smokers treated with nicotine replacement therapy: a historical cohort study. Clin Epidemiol. 2017;9:231-243. Published 2017 Apr 26. doi:10.2147/CLEP.S127775
16. Mills EJ, Wu P, Lockhart I, Wilson K, Ebbert JO. Adverse events associated with nicotine replacement therapy (NRT) for smoking cessation. A systematic review and meta-analysis of one hundred and twenty studies involving 177,390 individuals. Tob Induc Dis. 2010;8(1):8. Published 2010 Jul 13. doi:10.1186/1617-9625-8-8
17. Mills EJ, Thorlund K, Eapen S, Wu P, Prochaska JJ. Cardiovascular events associated with smoking cessation pharmacotherapies: a network meta-analysis. Circulation. 2014;129(1):28-41. doi:10.1161/CIRCULATIONAHA.113.003961
18. Tzivoni D, Keren A, Meyler S, Khoury Z, Lerer T, Brunel P. Cardiovascular safety of transdermal nicotine patches in patients with coronary artery disease who try to quit smoking. Cardiovasc Drugs Ther. 1998;12(3):239-244. doi:10.1023/a:1007757530765
19. Lucini D, Bertocchi F, Malliani A, Pagani M. Autonomic effects of nicotine patch administration in habitual cigarette smokers: a double-blind, placebo-controlled study using spectral analysis of RR interval and systolic arterial pressure variabilities. J Cardiovasc Pharmacol. 1998;31(5):714-720. doi:10.1097/00005344-199805000-00010
20. Kaijser L, Berglund B. Effect of nicotine on coronary blood-flow in man. Clin Physiol. 1985;5(6):541-552. doi:10.1111/j.1475-097x.1985.tb00767.x
21. Nitenberg A, Antony I. Effects of nicotine gum on coronary vasomotor responses during sympathetic stimulation in patients with coronary artery stenosis. J Cardiovasc Pharmacol. 1999;34(5):694-699. doi:10.1097/00005344-199911000-00011
22. Keeley EC, Pirwitz MJ, Landau C, et al. Intranasal nicotine spray does not augment the adverse effects of cigarette smoking on myocardial oxygen demand or coronary arterial dimensions. Am J Med. 1996;101(4):357-363. doi:10.1016/s0002-9343(96)00237-9
23. Benowitz NL, Gourlay SG. Cardiovascular toxicity of nicotine: implications for nicotine replacement therapy. J Am Coll Cardiol. 1997;29(7):1422-1431. doi:10.1016/s0735-1097(97)00079-x
24. Flowers L. Nicotine replacement therapy. Amer J Psych. 2017;11(6):4-7.
25. Adenosine; Package insert. Astellas Pharma US Inc; 1989.
26. Dipyridamole; Package insert. Boehringer Ingelheim Pharmaceuticals Inc; 2019.
27. Dobutamine; Package insert. Baxter Healthcare Corporation; 2012.
Chest pain is one of the most common concerns in patients presenting to the emergency department in the United States, accounting for approximately 7.6 million visits annually.1 Given the high mortality rate associated with acute coronary syndromes, prompt evaluation of chest pain is essential.2 Even in mild cases, recognition of newly onset or worsening coronary artery disease (CAD) is crucial to ensure that patients receive optimal medication therapy.
In symptomatic patients with risk factors for CAD, such as advanced age, hypertension, hyperlipidemia, obesity, and diabetes mellitus, myocardial perfusion imaging (MPI) is frequently used as a modality to assess the presence, location, and severity of ischemic or infarcted myocardium.2 MPI requires administration of a radiopharmaceutical before and after the patient undergoes a form of stress.2 This radiopharmaceutical is then detected in the myocardium with a nuclear camera, and images are obtained of the heart to assess myocardial blood flow.2
MPI can be performed using exercise-induced stress via a treadmill, or medication-induced stress (Table 1). In both strategies, healthy coronary arteries dilate to provide the myocardium with more blood flow to meet the increasing myocardial oxygen demand during this period of stress. While healthy vessels are able to dilate appropriately, coronary arteries with flow-limiting stenoses are unable to dilate to the same extent in response to stress.2 Because radioactive isotope uptake by the myocardium is directly related to arterial blood flow, MPI is able to demonstrate a mismatch in coronary blood flow between healthy and diseased coronary arteries indicated by differences in radioisotope uptake.2 The presence of such a mismatch, in conjunction with clinical history, potentially suggests the presence of CAD.
Prior to conducting MPI with a medication, certain substances should be avoided. For instance, methylxanthines, such as caffeine, aminophylline, and theophylline, antagonize adenosine receptors and can have major drug interactions with regadenoson, adenosine, and dipyridamole. Therefore, it is advised that these substances be stopped for at least 12 hours before testing.3 In some cases, other medications that can affect coronary blood flow, such as long-acting nitrates, β-blockers, and calcium channel blockers, are recommended to be avoided for 12 to 48 hours in order to obtain the most accurate depiction of underlying coronary disease.4
Because nicotine and nicotine replacement therapy (NRT) may have substantial effects on coronary circulation, a current area of controversy is whether these should be stopped prior to the use of a stress-inducing medication during MPI. To date, no formal drug interaction studies have been conducted between nicotine and regadenoson.5 Similarly, the ADVANCE MPI 2 Trial, which led to the US Food and Drug Administration approval of regadenoson, did not specify restrictions on the use of nicotine prior to stress testing in the protocol.6 However, as this trial was multicenter, investigators admit that individual study sites could have had their own restrictions on the use of nicotine prior to stress testing with regadenoson, but this information was not collected.6 The current review focuses on how the simultaneous use of nicotine or NRT during MPI with pharmacologic agents, such as regadenoson, may affect the accuracy of imaging results and the clinical impact of this interaction.
Nicotine Coronary Artery Effect
It is well documented that long-term cigarette smoking is a major risk factor for CAD.7 Compared with nonsmokers, cigarette smokers experience 2 times greater risk of morbidity and mortality from ischemic heart disease.7 There are several mechanisms by which nicotine induces damage to the myocardium (Figure). Nicotine has direct effects on both the sympathetic nervous system (SNS) and myocardial endothelium.8 Together, these factors result in reduced coronary blood flow, leading to less oxygen supply to meet an increased oxygen demand, resulting in myocardial ischemia.
Nicotine’s effect on coronary vasomotor tone occurs primarily through noradrenergic stimulation of α and β receptors associated with coronary vasoconstriction or vasodilation, respectively.9,10 These competing influences on coronary blood flow appear to manifest differently based on whether patients are at rest or in a stressed state. A study by Czerin and colleagues demonstrated that in healthy patients with relatively short smoking histories and in a healthy nonsmoker control group, coronary blood flow increased by 25% and 40%, respectively, with nicotine use at rest.9 However, when these patients were stressed with dipyramidole and while smoking during the examination, myocardial blood flow was reduced by 11% in the study group and 14% in the control group.9 This is likely because the patients studied had relatively healthy coronary arteries that were able to maximally dilate when stressed. In this scenario, nicotine’s dilatory effects are offset by nicotine’s α-receptor–mediated vasoconstriction effects.9 Of note, patients in the study group experienced a somewhat diminished increase in coronary blood flow at rest with nicotine use, suggesting that even a short smoking history may damage the myocardial endothelium, rendering it less responsive to nicotine’s vasodilatory effects.9
These principles similarly apply to patients with underlying moderate-to-severe cardiovascular disease (CVD). With nicotine use at rest, patients with significant CAD do not experience as dramatic of an increase in coronary blood flow, which typically decreases or remains the same despite increased myocardial work.10 This may be because patients with moderate-to-severe CAD often have flow-limiting stenoses and damaged endothelium that do not allow vessels to respond as efficiently to increased myocardial demand or to nicotine’s β-receptor–mediated vasodilatory effects.10,11 Moreover, when stressed, diseased coronary arteries are not able to further dilate and nicotine’s α-receptor–mediated vasoconstriction effects dominate.10,11
In a study by Quillen and colleagues of patients with moderate-to-severe CAD, the mean diameter of proximal coronary artery segments decreased by 5%, the distal coronary diameter decreased 8%, and the coronary vascular resistance increased by 21% while smoking at rest.12 The investigators did not analyze how parameters changed when these diseased coronary arteries were stressed using a medication during MPI. However, it can be predicted that coronary arteries would have constricted to a similar or greater degree than observed in Czerin and colleagues’ study, given that the underlying myocardium was diseased and more susceptible to nicotine’s vasoconstriction effects.9 Importantly, these studies have several limitations, most notably that they are older and have small sample sizes. Additionally, while statistically significant differences were found in the degree of changes in coronary circulation with nicotine use at rest and during stress, it is unclear whether this translates to a clinically significant and impactful finding.9-12
Nicotine Replacement Therapy and Stress Testing
Given the association between cigarette smoking and CAD, medical practitioners strongly encourage patients to quit smoking to reduce their risk of adverse cardiovascular outcomes. Various smoking cessation treatments are available for patients. Common, readily accessible forms of therapy include nicotine replacement products (Table 2).
Early studies of NRT in patients with underlying CVD found an increased risk of cardiovascular events, such as myocardial infarction, presumably due to the nicotine content of these products.13,14 However, the concentration of nicotine in NRT is substantially lower than that found in cigarettes and in some formulations, such as transdermal patches, nicotine is delivered over a prolonged period of time.15 For this reason, NRT is thought to be safe in patients with underlying CVD and stable ischemic heart disease. A recent systematic review and meta-analysis found that while NRT may be associated with tachycardia, it did not increase the risk of more serious cardiovascular adverse effects (AEs).16,17
Given the lower nicotine concentration in NRT products, the associated hemodynamic effect of nicotine also is thought to be less pronounced. In a study conducted by Tzivoni and colleagues in patients with CAD using transdermal nicotine patches, no differences in blood pressure, heart rate, ischemia, or arrhythmias were found from baseline to 2 weeks.18 These findings were further confirmed in a small study by Lucini and colleagues, which found that nicotine patches produced slight hemodynamic effects, but to a lesser extent than cigarette smoking.19 For the NRT gum formulation, while a small study found that 4 mg produced coronary vasoconstriction in patients with underlying CAD, a study by Nitenberg and Antony demonstrated that healthy and diseased coronary arteries did not significantly constrict while patients were using nicotine gum both before and after a cold pressor test, suggesting a lesser degree of coronary vasoconstriction than nicotine from cigarette smoking.20,21 Similar findings have been described with the nicotine intranasal spray in a study by Keeley and colleagues, which showed no additional AEs on myocardial demand or vasoconstriction when an intranasal nicotine spray was added to cigarette smoking.22 Importantly, a review of the transdermal and gum formulations found that these less pronounced hemodynamic effects were observed across different doses of NRT; however, further studies are needed to clarify the relationship between NRT dose and cardiovascular effects.23
Overall, NRT does not seem to activate the SNS to the same degree as nicotine obtained via cigarette smoking and likely does not increase the myocardial oxygen demand as much. Additionally, by containing a lower concentration of nicotine, NRT may not impair the myocardium’s ability to supply oxygen to coronary arteries to the same extent as nicotine from cigarette smoking. Therefore, the effects of NRT on MPI using a stress-inducing medication may not be as pronounced. However, due to study limitations, results should be interpreted cautiously.18-23
Conclusions
Because of the close relationship between cigarette smoking and CAD, many patients with underlying CVD are either current smokers or may be using NRT for smoking cessation. Therefore, the question of whether to refrain from nicotine use prior to MPI is clinically relevant. Currently, there is a lack of high-quality studies demonstrating the effects of nicotine and NRT on coronary perfusion. Because of this, the impact of nicotine and NRT use on the accuracy of MPI using stress-inducing medications remains uncertain. Nevertheless, given that nicotine and NRT may largely affect the accuracy of imaging results, several institutions have adopted protocols that prohibit patients from using these drugs on the day of nuclear stress testing.
There are currently no data specifying the number of hours to hold nicotine products prior to cardiac stress testing. It is generally recommended that other medications that affect coronary blood flow be held for 5 half-lives before conducting MPI.4 Following the same guidance for nicotine and NRT may present a reasonable approach to ensure accurate imaging results. Based on the discussed literature, patients should be instructed to refrain from cigarette smoking for at least 5 to 10 hours prior to MPI, given nicotine’s half-life of about 1 to 2 hours.24
The data for NRT are less clear. While use of NRT may not be an absolute contraindication to conducting MPI, it is important to consider that this may affect the accuracy of results. Given this uncertainty, it is likely ideal to hold NRT prior to MPI, based on the specific formulation of NRT and that product's half-life. Further robust studies are needed to analyze the impact of nicotine and NRT on the accuracy of nuclear stress testing using a medication.
Chest pain is one of the most common concerns in patients presenting to the emergency department in the United States, accounting for approximately 7.6 million visits annually.1 Given the high mortality rate associated with acute coronary syndromes, prompt evaluation of chest pain is essential.2 Even in mild cases, recognition of newly onset or worsening coronary artery disease (CAD) is crucial to ensure that patients receive optimal medication therapy.
In symptomatic patients with risk factors for CAD, such as advanced age, hypertension, hyperlipidemia, obesity, and diabetes mellitus, myocardial perfusion imaging (MPI) is frequently used as a modality to assess the presence, location, and severity of ischemic or infarcted myocardium.2 MPI requires administration of a radiopharmaceutical before and after the patient undergoes a form of stress.2 This radiopharmaceutical is then detected in the myocardium with a nuclear camera, and images are obtained of the heart to assess myocardial blood flow.2
MPI can be performed using exercise-induced stress via a treadmill, or medication-induced stress (Table 1). In both strategies, healthy coronary arteries dilate to provide the myocardium with more blood flow to meet the increasing myocardial oxygen demand during this period of stress. While healthy vessels are able to dilate appropriately, coronary arteries with flow-limiting stenoses are unable to dilate to the same extent in response to stress.2 Because radioactive isotope uptake by the myocardium is directly related to arterial blood flow, MPI is able to demonstrate a mismatch in coronary blood flow between healthy and diseased coronary arteries indicated by differences in radioisotope uptake.2 The presence of such a mismatch, in conjunction with clinical history, potentially suggests the presence of CAD.
Prior to conducting MPI with a medication, certain substances should be avoided. For instance, methylxanthines, such as caffeine, aminophylline, and theophylline, antagonize adenosine receptors and can have major drug interactions with regadenoson, adenosine, and dipyridamole. Therefore, it is advised that these substances be stopped for at least 12 hours before testing.3 In some cases, other medications that can affect coronary blood flow, such as long-acting nitrates, β-blockers, and calcium channel blockers, are recommended to be avoided for 12 to 48 hours in order to obtain the most accurate depiction of underlying coronary disease.4
Because nicotine and nicotine replacement therapy (NRT) may have substantial effects on coronary circulation, a current area of controversy is whether these should be stopped prior to the use of a stress-inducing medication during MPI. To date, no formal drug interaction studies have been conducted between nicotine and regadenoson.5 Similarly, the ADVANCE MPI 2 Trial, which led to the US Food and Drug Administration approval of regadenoson, did not specify restrictions on the use of nicotine prior to stress testing in the protocol.6 However, as this trial was multicenter, investigators admit that individual study sites could have had their own restrictions on the use of nicotine prior to stress testing with regadenoson, but this information was not collected.6 The current review focuses on how the simultaneous use of nicotine or NRT during MPI with pharmacologic agents, such as regadenoson, may affect the accuracy of imaging results and the clinical impact of this interaction.
Nicotine Coronary Artery Effect
It is well documented that long-term cigarette smoking is a major risk factor for CAD.7 Compared with nonsmokers, cigarette smokers experience 2 times greater risk of morbidity and mortality from ischemic heart disease.7 There are several mechanisms by which nicotine induces damage to the myocardium (Figure). Nicotine has direct effects on both the sympathetic nervous system (SNS) and myocardial endothelium.8 Together, these factors result in reduced coronary blood flow, leading to less oxygen supply to meet an increased oxygen demand, resulting in myocardial ischemia.
Nicotine’s effect on coronary vasomotor tone occurs primarily through noradrenergic stimulation of α and β receptors associated with coronary vasoconstriction or vasodilation, respectively.9,10 These competing influences on coronary blood flow appear to manifest differently based on whether patients are at rest or in a stressed state. A study by Czerin and colleagues demonstrated that in healthy patients with relatively short smoking histories and in a healthy nonsmoker control group, coronary blood flow increased by 25% and 40%, respectively, with nicotine use at rest.9 However, when these patients were stressed with dipyramidole and while smoking during the examination, myocardial blood flow was reduced by 11% in the study group and 14% in the control group.9 This is likely because the patients studied had relatively healthy coronary arteries that were able to maximally dilate when stressed. In this scenario, nicotine’s dilatory effects are offset by nicotine’s α-receptor–mediated vasoconstriction effects.9 Of note, patients in the study group experienced a somewhat diminished increase in coronary blood flow at rest with nicotine use, suggesting that even a short smoking history may damage the myocardial endothelium, rendering it less responsive to nicotine’s vasodilatory effects.9
These principles similarly apply to patients with underlying moderate-to-severe cardiovascular disease (CVD). With nicotine use at rest, patients with significant CAD do not experience as dramatic of an increase in coronary blood flow, which typically decreases or remains the same despite increased myocardial work.10 This may be because patients with moderate-to-severe CAD often have flow-limiting stenoses and damaged endothelium that do not allow vessels to respond as efficiently to increased myocardial demand or to nicotine’s β-receptor–mediated vasodilatory effects.10,11 Moreover, when stressed, diseased coronary arteries are not able to further dilate and nicotine’s α-receptor–mediated vasoconstriction effects dominate.10,11
In a study by Quillen and colleagues of patients with moderate-to-severe CAD, the mean diameter of proximal coronary artery segments decreased by 5%, the distal coronary diameter decreased 8%, and the coronary vascular resistance increased by 21% while smoking at rest.12 The investigators did not analyze how parameters changed when these diseased coronary arteries were stressed using a medication during MPI. However, it can be predicted that coronary arteries would have constricted to a similar or greater degree than observed in Czerin and colleagues’ study, given that the underlying myocardium was diseased and more susceptible to nicotine’s vasoconstriction effects.9 Importantly, these studies have several limitations, most notably that they are older and have small sample sizes. Additionally, while statistically significant differences were found in the degree of changes in coronary circulation with nicotine use at rest and during stress, it is unclear whether this translates to a clinically significant and impactful finding.9-12
Nicotine Replacement Therapy and Stress Testing
Given the association between cigarette smoking and CAD, medical practitioners strongly encourage patients to quit smoking to reduce their risk of adverse cardiovascular outcomes. Various smoking cessation treatments are available for patients. Common, readily accessible forms of therapy include nicotine replacement products (Table 2).
Early studies of NRT in patients with underlying CVD found an increased risk of cardiovascular events, such as myocardial infarction, presumably due to the nicotine content of these products.13,14 However, the concentration of nicotine in NRT is substantially lower than that found in cigarettes and in some formulations, such as transdermal patches, nicotine is delivered over a prolonged period of time.15 For this reason, NRT is thought to be safe in patients with underlying CVD and stable ischemic heart disease. A recent systematic review and meta-analysis found that while NRT may be associated with tachycardia, it did not increase the risk of more serious cardiovascular adverse effects (AEs).16,17
Given the lower nicotine concentration in NRT products, the associated hemodynamic effect of nicotine also is thought to be less pronounced. In a study conducted by Tzivoni and colleagues in patients with CAD using transdermal nicotine patches, no differences in blood pressure, heart rate, ischemia, or arrhythmias were found from baseline to 2 weeks.18 These findings were further confirmed in a small study by Lucini and colleagues, which found that nicotine patches produced slight hemodynamic effects, but to a lesser extent than cigarette smoking.19 For the NRT gum formulation, while a small study found that 4 mg produced coronary vasoconstriction in patients with underlying CAD, a study by Nitenberg and Antony demonstrated that healthy and diseased coronary arteries did not significantly constrict while patients were using nicotine gum both before and after a cold pressor test, suggesting a lesser degree of coronary vasoconstriction than nicotine from cigarette smoking.20,21 Similar findings have been described with the nicotine intranasal spray in a study by Keeley and colleagues, which showed no additional AEs on myocardial demand or vasoconstriction when an intranasal nicotine spray was added to cigarette smoking.22 Importantly, a review of the transdermal and gum formulations found that these less pronounced hemodynamic effects were observed across different doses of NRT; however, further studies are needed to clarify the relationship between NRT dose and cardiovascular effects.23
Overall, NRT does not seem to activate the SNS to the same degree as nicotine obtained via cigarette smoking and likely does not increase the myocardial oxygen demand as much. Additionally, by containing a lower concentration of nicotine, NRT may not impair the myocardium’s ability to supply oxygen to coronary arteries to the same extent as nicotine from cigarette smoking. Therefore, the effects of NRT on MPI using a stress-inducing medication may not be as pronounced. However, due to study limitations, results should be interpreted cautiously.18-23
Conclusions
Because of the close relationship between cigarette smoking and CAD, many patients with underlying CVD are either current smokers or may be using NRT for smoking cessation. Therefore, the question of whether to refrain from nicotine use prior to MPI is clinically relevant. Currently, there is a lack of high-quality studies demonstrating the effects of nicotine and NRT on coronary perfusion. Because of this, the impact of nicotine and NRT use on the accuracy of MPI using stress-inducing medications remains uncertain. Nevertheless, given that nicotine and NRT may largely affect the accuracy of imaging results, several institutions have adopted protocols that prohibit patients from using these drugs on the day of nuclear stress testing.
There are currently no data specifying the number of hours to hold nicotine products prior to cardiac stress testing. It is generally recommended that other medications that affect coronary blood flow be held for 5 half-lives before conducting MPI.4 Following the same guidance for nicotine and NRT may present a reasonable approach to ensure accurate imaging results. Based on the discussed literature, patients should be instructed to refrain from cigarette smoking for at least 5 to 10 hours prior to MPI, given nicotine’s half-life of about 1 to 2 hours.24
The data for NRT are less clear. While use of NRT may not be an absolute contraindication to conducting MPI, it is important to consider that this may affect the accuracy of results. Given this uncertainty, it is likely ideal to hold NRT prior to MPI, based on the specific formulation of NRT and that product's half-life. Further robust studies are needed to analyze the impact of nicotine and NRT on the accuracy of nuclear stress testing using a medication.
1. Rui P, Kang K, Ashman JJ. National Hospital Ambulatory Medical Care Survey: 2016 emergency department summary tables. Published 2016. Accessed March 30, 2020. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf
2. Lange RA. Cardiovascular testing. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10th ed. McGraw Hill; 2017.
3. Mace S. Observation Medicine: Principles and Protocols. Cambridge University Press; 2017.
4. Currie GM. Pharmacology, part 4: nuclear cardiology. J Nucl Med Technol. 2019;47(2):97-110. doi:10.2967/jnmt.118.219675
5. Regadenoson; Package insert. Astellas Pharma US Inc; 2008.
6. Iskandrian AE, Bateman TM, Belardinelli L, et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: results of the ADVANCE phase 3 multicenter international trial. J Nucl Cardiol. 2007;14(5):645-658. doi:10.1016/j.nuclcard.2007.06.114
7. Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18(3):109-114. doi:10.4103/HEARTVIEWS.HEARTVIEWS_106_17
8. Benowitz NL, Burbank AD. Cardiovascular toxicity of nicotine: implications for electronic cigarette use. Trends Cardiovasc Med. 2016;26(6):515-523. doi:10.1016/j.tcm.2016.03.001
9. Czernin J, Sun K, Brunken R, Böttcher M, Phelps M, Schelbert H. Effect of acute and long-term smoking on myocardial blood flow and flow reserve. Circulation. 1995;91:2891-2897. doi:10.1161/01.CIR.91.12.2891
10. Winniford MD, Wheelan KR, Kremers MS, et al. Smoking-induced coronary vasoconstriction in patients with atherosclerotic coronary artery disease: evidence for adrenergically mediated alterations in coronary artery tone. Circulation. 1986;73(4):662-667. doi:10.1161/01.cir.73.4.662
11. Klein LW, Ambrose J, Pichard A, Holt J, Gorlin R, Teichholz LE. Acute coronary hemodynamic response to cigarette smoking in patients with coronary artery disease. J Am Coll Cardiol. 1984;3(4):879-886. doi:10.1016/s0735-1097(84)80344-7
12. Quillen JE, Rossen JD, Oskarsson HJ, Minor RL Jr, Lopez AG, Winniford MD. Acute effect of cigarette smoking on the coronary circulation: constriction of epicardial and resistance vessels. J Am Coll Cardiol. 1993;22(3):642-647. doi:10.1016/0735-1097(93)90170-6
13. Dacosta A, Guy JM, Tardy B, et al. Myocardial infarction and nicotine patch: a contributing or causative factor?. Eur Heart J. 1993;14(12):1709-1711. doi:10.1093/eurheartj/14.12.1709
14. Ottervanger JP, Festen JM, de Vries AG, Stricker BH. Acute myocardial infarction while using the nicotine patch. Chest. 1995;107(6):1765-1766. doi:10.1378/chest.107.6.1765
15. Dollerup J, Vestbo J, Murray-Thomas T, et al. Cardiovascular risks in smokers treated with nicotine replacement therapy: a historical cohort study. Clin Epidemiol. 2017;9:231-243. Published 2017 Apr 26. doi:10.2147/CLEP.S127775
16. Mills EJ, Wu P, Lockhart I, Wilson K, Ebbert JO. Adverse events associated with nicotine replacement therapy (NRT) for smoking cessation. A systematic review and meta-analysis of one hundred and twenty studies involving 177,390 individuals. Tob Induc Dis. 2010;8(1):8. Published 2010 Jul 13. doi:10.1186/1617-9625-8-8
17. Mills EJ, Thorlund K, Eapen S, Wu P, Prochaska JJ. Cardiovascular events associated with smoking cessation pharmacotherapies: a network meta-analysis. Circulation. 2014;129(1):28-41. doi:10.1161/CIRCULATIONAHA.113.003961
18. Tzivoni D, Keren A, Meyler S, Khoury Z, Lerer T, Brunel P. Cardiovascular safety of transdermal nicotine patches in patients with coronary artery disease who try to quit smoking. Cardiovasc Drugs Ther. 1998;12(3):239-244. doi:10.1023/a:1007757530765
19. Lucini D, Bertocchi F, Malliani A, Pagani M. Autonomic effects of nicotine patch administration in habitual cigarette smokers: a double-blind, placebo-controlled study using spectral analysis of RR interval and systolic arterial pressure variabilities. J Cardiovasc Pharmacol. 1998;31(5):714-720. doi:10.1097/00005344-199805000-00010
20. Kaijser L, Berglund B. Effect of nicotine on coronary blood-flow in man. Clin Physiol. 1985;5(6):541-552. doi:10.1111/j.1475-097x.1985.tb00767.x
21. Nitenberg A, Antony I. Effects of nicotine gum on coronary vasomotor responses during sympathetic stimulation in patients with coronary artery stenosis. J Cardiovasc Pharmacol. 1999;34(5):694-699. doi:10.1097/00005344-199911000-00011
22. Keeley EC, Pirwitz MJ, Landau C, et al. Intranasal nicotine spray does not augment the adverse effects of cigarette smoking on myocardial oxygen demand or coronary arterial dimensions. Am J Med. 1996;101(4):357-363. doi:10.1016/s0002-9343(96)00237-9
23. Benowitz NL, Gourlay SG. Cardiovascular toxicity of nicotine: implications for nicotine replacement therapy. J Am Coll Cardiol. 1997;29(7):1422-1431. doi:10.1016/s0735-1097(97)00079-x
24. Flowers L. Nicotine replacement therapy. Amer J Psych. 2017;11(6):4-7.
25. Adenosine; Package insert. Astellas Pharma US Inc; 1989.
26. Dipyridamole; Package insert. Boehringer Ingelheim Pharmaceuticals Inc; 2019.
27. Dobutamine; Package insert. Baxter Healthcare Corporation; 2012.
1. Rui P, Kang K, Ashman JJ. National Hospital Ambulatory Medical Care Survey: 2016 emergency department summary tables. Published 2016. Accessed March 30, 2020. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf
2. Lange RA. Cardiovascular testing. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10th ed. McGraw Hill; 2017.
3. Mace S. Observation Medicine: Principles and Protocols. Cambridge University Press; 2017.
4. Currie GM. Pharmacology, part 4: nuclear cardiology. J Nucl Med Technol. 2019;47(2):97-110. doi:10.2967/jnmt.118.219675
5. Regadenoson; Package insert. Astellas Pharma US Inc; 2008.
6. Iskandrian AE, Bateman TM, Belardinelli L, et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: results of the ADVANCE phase 3 multicenter international trial. J Nucl Cardiol. 2007;14(5):645-658. doi:10.1016/j.nuclcard.2007.06.114
7. Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18(3):109-114. doi:10.4103/HEARTVIEWS.HEARTVIEWS_106_17
8. Benowitz NL, Burbank AD. Cardiovascular toxicity of nicotine: implications for electronic cigarette use. Trends Cardiovasc Med. 2016;26(6):515-523. doi:10.1016/j.tcm.2016.03.001
9. Czernin J, Sun K, Brunken R, Böttcher M, Phelps M, Schelbert H. Effect of acute and long-term smoking on myocardial blood flow and flow reserve. Circulation. 1995;91:2891-2897. doi:10.1161/01.CIR.91.12.2891
10. Winniford MD, Wheelan KR, Kremers MS, et al. Smoking-induced coronary vasoconstriction in patients with atherosclerotic coronary artery disease: evidence for adrenergically mediated alterations in coronary artery tone. Circulation. 1986;73(4):662-667. doi:10.1161/01.cir.73.4.662
11. Klein LW, Ambrose J, Pichard A, Holt J, Gorlin R, Teichholz LE. Acute coronary hemodynamic response to cigarette smoking in patients with coronary artery disease. J Am Coll Cardiol. 1984;3(4):879-886. doi:10.1016/s0735-1097(84)80344-7
12. Quillen JE, Rossen JD, Oskarsson HJ, Minor RL Jr, Lopez AG, Winniford MD. Acute effect of cigarette smoking on the coronary circulation: constriction of epicardial and resistance vessels. J Am Coll Cardiol. 1993;22(3):642-647. doi:10.1016/0735-1097(93)90170-6
13. Dacosta A, Guy JM, Tardy B, et al. Myocardial infarction and nicotine patch: a contributing or causative factor?. Eur Heart J. 1993;14(12):1709-1711. doi:10.1093/eurheartj/14.12.1709
14. Ottervanger JP, Festen JM, de Vries AG, Stricker BH. Acute myocardial infarction while using the nicotine patch. Chest. 1995;107(6):1765-1766. doi:10.1378/chest.107.6.1765
15. Dollerup J, Vestbo J, Murray-Thomas T, et al. Cardiovascular risks in smokers treated with nicotine replacement therapy: a historical cohort study. Clin Epidemiol. 2017;9:231-243. Published 2017 Apr 26. doi:10.2147/CLEP.S127775
16. Mills EJ, Wu P, Lockhart I, Wilson K, Ebbert JO. Adverse events associated with nicotine replacement therapy (NRT) for smoking cessation. A systematic review and meta-analysis of one hundred and twenty studies involving 177,390 individuals. Tob Induc Dis. 2010;8(1):8. Published 2010 Jul 13. doi:10.1186/1617-9625-8-8
17. Mills EJ, Thorlund K, Eapen S, Wu P, Prochaska JJ. Cardiovascular events associated with smoking cessation pharmacotherapies: a network meta-analysis. Circulation. 2014;129(1):28-41. doi:10.1161/CIRCULATIONAHA.113.003961
18. Tzivoni D, Keren A, Meyler S, Khoury Z, Lerer T, Brunel P. Cardiovascular safety of transdermal nicotine patches in patients with coronary artery disease who try to quit smoking. Cardiovasc Drugs Ther. 1998;12(3):239-244. doi:10.1023/a:1007757530765
19. Lucini D, Bertocchi F, Malliani A, Pagani M. Autonomic effects of nicotine patch administration in habitual cigarette smokers: a double-blind, placebo-controlled study using spectral analysis of RR interval and systolic arterial pressure variabilities. J Cardiovasc Pharmacol. 1998;31(5):714-720. doi:10.1097/00005344-199805000-00010
20. Kaijser L, Berglund B. Effect of nicotine on coronary blood-flow in man. Clin Physiol. 1985;5(6):541-552. doi:10.1111/j.1475-097x.1985.tb00767.x
21. Nitenberg A, Antony I. Effects of nicotine gum on coronary vasomotor responses during sympathetic stimulation in patients with coronary artery stenosis. J Cardiovasc Pharmacol. 1999;34(5):694-699. doi:10.1097/00005344-199911000-00011
22. Keeley EC, Pirwitz MJ, Landau C, et al. Intranasal nicotine spray does not augment the adverse effects of cigarette smoking on myocardial oxygen demand or coronary arterial dimensions. Am J Med. 1996;101(4):357-363. doi:10.1016/s0002-9343(96)00237-9
23. Benowitz NL, Gourlay SG. Cardiovascular toxicity of nicotine: implications for nicotine replacement therapy. J Am Coll Cardiol. 1997;29(7):1422-1431. doi:10.1016/s0735-1097(97)00079-x
24. Flowers L. Nicotine replacement therapy. Amer J Psych. 2017;11(6):4-7.
25. Adenosine; Package insert. Astellas Pharma US Inc; 1989.
26. Dipyridamole; Package insert. Boehringer Ingelheim Pharmaceuticals Inc; 2019.
27. Dobutamine; Package insert. Baxter Healthcare Corporation; 2012.
A 1-Year Review of a Nationally Led Intervention to Improve Suicide Prevention Screening at a Large Homeless Veterans Clinic
Suicide is a national public health concern that affects thousands of US individuals and families, with repercussions that reverberate through entire communities. In 2019, there were 47,500 US deaths by suicide, which accounted for about 1 death every 11 minutes.1 Suicide remains the tenth leading cause of death in the United States and has been part of the top 12 leading causes of death since 1975.2 Unfortunately, this trend has worsened; suicide rates have increased by 35% from 1999 to 2018.3 One particularly vulnerable population is US veterans who accounted for 13.8% of all suicide deaths in 2018.4 Among veterans, the suicide death average increased from 16.6 per day in 2005 to 17.6 in 2018.4 Furthermore, veterans experiencing homelessness are 5 times more likely to attempt suicide and 2.5 times more likely to have suicidal ideation compared with veterans without a history of homelessness.4 Suicide is a significant issue among veterans experiencing homelessness: Veterans account for about 11% of the overall US homeless population.5
Recent data suggest opportunities for suicide risk assessment in the primary care setting. A study from the Veterans Health Administration (VHA) Office for Suicide Prevention found that in 2014 an average of 20 veterans died by suicide every day and 6 of the 20 (30%) on average used VHA services within the prior year.6 Similarly, a review of 40 studies on suicide found that 45% of suicide victims had contact with their primary care practitioner (PCP) within 1 month of suicide, and 75% of victims had contact within the year of suicide.7 An analysis of depression screening in 2008/2009 using Patient Health Questionnaire-2 (PHQ-2) or Patient Health Questionnaire-9 (PHQ-9) at 3 large western US Department of Veterans Affairs (VA) medical centers found that 55% were screened for depression.8 The VA has made suicide prevention a top priority and supports the established US goal of reducing annual suicide deaths by 20% by 2025.9 Given key opportunities for suicide risk assessment in the primary care setting, the VHA Office of Mental Health and Suicide Prevention implemented a national, standardized process for suicide risk assessment on October 1, 2018.10,11
The VA approach to suicide screening, evaluation, and documentation has evolved over time. Between October 2018 and December 2020, the process was augmented to include 3 stages embedded into the electronic health record (EHR): a primary screen (PHQ-2 with Item 9 from the PHQ-9 [PHQ-2+I9]), a secondary screen (Columbia-Suicide Severity Rating Scale [C-SSRS]), and a tertiary screen (Comprehensive Suicide Risk Evaluation [CSRE]). The primary screen consisted of the depression screening using the PHQ-2 with the addition of I9 asking about suicidal ideation. The secondary screening, or C-SSRS, included 8 questions to elaborate on suicidal ideation, intent, plan, and any history of suicidal attempts or preparatory behaviors. The tertiary screen consisted of the CSRE, a questionnaire developed internally by the VA in 2018 to further evaluate the veteran’s suicidal thoughts, attempts, warning signs, risk factors, protective factors, and reasons for living. The goal of the screenings was to identify veterans at risk of suicide, assess risk severity, and to individually tailor risk mitigation strategies for safe disposition. These risk categories were developed by the regional Mental Illness Research, Education and Clinical Center, which suggested treatment strategies, such as hospitalization or close outpatient follow-up.12,13
The Homeless Patient Aligned Care Team (HPACT) clinic at the West Los Angeles VA Medical Center (WLAVAMC) in California, one of the largest VA homeless clinics in the country and 1 of 7 national VA Office of Academic Affiliation Centers of Excellence in Primary Care Education training programs implemented the standardized tools for suicide risk screening and quality improvement (QI). The HPACT clinic is an interprofessional team, including primary care, mental health, social work, pharmacy, and peer support, that is adjacent to the WLAVAMC general primary care clinics. The team collaboratively addresses both medical and psychosocial needs of veterans with a focus on the Housing First Model, an approach that prioritizes ending homelessness while addressing all factors associated with veterans' health and well-being. After 1 year of stable housing, veterans graduate to the WLAVAMC general primary care clinics.
Given the vulnerability of veterans experiencing homelessness, the clinic leadership identified suicide risk screening as a high priority initiative and created a taskforce to oversee effective implementation of clinic screening efforts. An interprofessional team of nurse practitioners (NPs), pharmacists, physicians, psychologists, social workers (SWs), and trainees formed to improve screening efforts and use the QI principles to guide analysis and intervention. The team wrote the following SMART (Specific, Measurable, Achievable, Relevant, and Time-bound) Aim statements: (1) ensure > 90% of eligible patients receive a primary screen; (2) ensure > 90% of positive primary I9 screens receive subsequent screenings within 24 hours; and (3) increase staff comfort and familiarity using the screening tools. This article examines the results of the screening initiative 1-year postimplementation, describes difficulties faced, and suggests strategies that might be used to overcome those challenges.
Methods
This QI analysis was exempt from institutional review board review. Prior to the standardized national suicide risk assessment rollout of October 1, 2018, the QI team met to review and understand the workflow to be implemented into the HPACT clinic. To describe the initial screening process, the new suicide risk assessment consisted of primary, secondary, and tertiary screens that would warrant subsequent intervention by clinicians if positive (Figure 1). The primary screen included the PHQ-2+I9 questionnaire (PHQ-2 for depression and I9 for suicidal ideation). If either were positive, follow-up questionnaires were required. Of note, patients with a prior depression diagnosis, cognitive impairment defined at a severity of moderate or greater based on clinician evaluation and judgement, or life expectancy < 6 months were exempt from screening because, by definition, they had theoretically already been screened and classified as under surveillance.
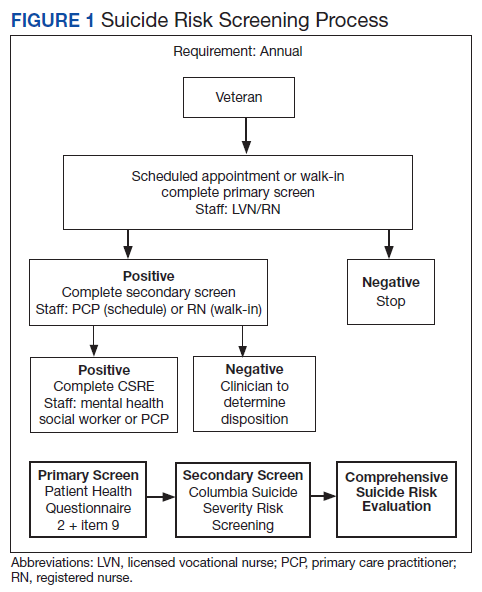
A positive I9 response prompted a secondary screen using C-SSRS. A positive secondary screen prompted a tertiary screen using CSRE. If the PHQ-2 screening was positive but I9 was negative, the standard follow-up depression clinical reminder was used. Any clinical staff member could perform the primary screen, including licensed vocational nurses (LVNs), registered nurses (RNs), and SWs in any setting (eg, emergency department, primary care, inpatient services). The secondary and tertiary screens required completion by a licensed clinician. RNs were able to perform the secondary screen but not the tertiary screen.
The HPACT clinic serves approximately 3000 patients by 50 staff and trainees divided into 2 teams. LVNs and RNs were tasked to conduct the primary screen as part of their initial clinic check-in. If the primary screen was positive for scheduled patients, LVNs notified a PCP to complete the secondary screen. For unscheduled patients, RNs conducted a primary screen and, if positive, a secondary screen. If the secondary screen was positive, a tertiary screen was performed by mental health practitioners or SWs, or PCPs if the former were unavailable. SWs, mental health practitioners, and PCPs were colocated in the clinic, which allowed for safe and convenient warm handoffs between clinicians.
During this process, the interprofessional team overseeing the suicide screening implementation efforts in the HPACT clinic met in-person biweekly beginning 1 month prior to the October 1, 2018 implementation. QI tools, including flowcharts and root cause analyses, were used to analyze feedback on efficient workflow and optimize staff responsibilities. A survey assessed staff comfort and familiarity using the suicide screening tools. Informal interviews were conducted with a representative from each stage of patient care to facilitate interprofessional participation and to troubleshoot any issues. Process flowcharts that clearly delineated staff roles based on current clinic workflow and the recommendations set forth by the new process were distributed at an initial staff meeting. The process flowchart was updated after staff feedback and distributed again along with a review of the C-SSRS and CSRE at an all-staff meeting in February 2019. The QI team continued to meet to formally evaluate their SMART Aims and to identify factors driving the success and failure of the implementation.
The VA Informatics and Computing Infrastructure (VINCI) provided project data after a formal request was submitted for this analysis. At the direction of the local QI team, the VINCI team provided aggregate patient counts derived from individual patient data in the VA Corporate Data Warehouse. The data analyzed are frequencies and proportions; no bivariate or multivariate statistics were performed.
Results
During the project year, the HPACT clinic had 2932 unique patients assigned to primary care. Of those veterans, 533 (18%) were exempt from screening by protocol. Of the remainder, staff screened 1876 (64%) of eligible veterans for suicide risk (Figure 2), which did not meet the SMART Aim of screening > 90% of eligible veterans. For the follow-up screens, using a QI dashboard designed for reviewing I9 and C-SSRS results, the QI team reviewed a convenience sample of 5 provider panels and identified 34 positive I9 screens. Twenty of those 34 patients (59%) received a C-SSRS within 24 hours of the positive I9, which did not meet the SMART Aim of ensuring > 90% of primary I9 screens had subsequent C-SSRS screening within 24 hours.
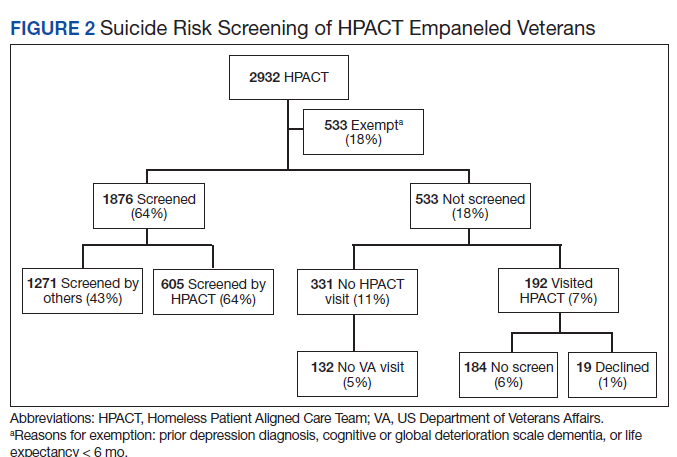
Of the veterans screened, 1,271 (43%) had their screening performed outside of the HPACT primary care team assigned, while 605 (21%) patients had their screening performed by an HPACT member. Most of the screening that occurred outside of the assigned primary care team occurred in other physical settings, including other VA facilities.
Of the 523 (18%) patients who were not screened, 331 (11%) patients had no visit to the HPACT clinic and 132 (5%) empaneled patients did not visit any VA site within the 1-year period. There were 192 (7%) patients who were not screened that had a visit to HPACT while 19 (1%) of those patients declined screening. A total of 184 (6%) patients were not screened and thus were considered true missed opportunities. This group of patients were eligible for screening but did not undergo screening in the HPACT clinic or any other VA setting despite visiting the VA.
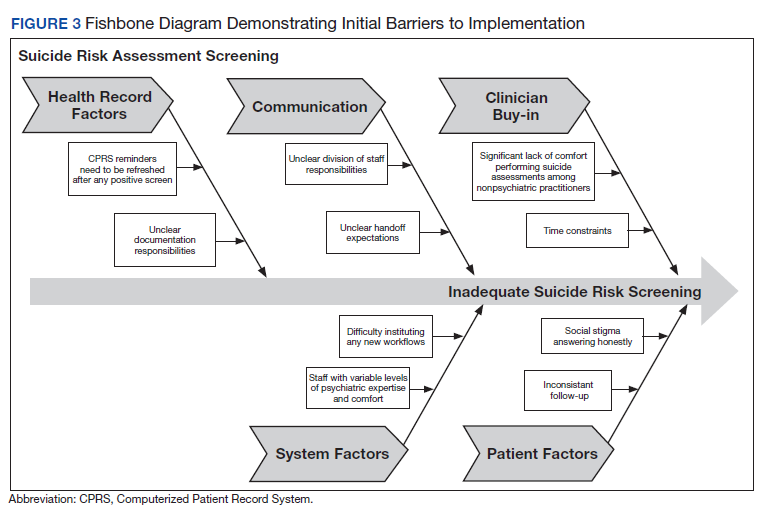
The QI team created a fishbone diagram to identify opportunities to improve screening rates and patient care (Figure 3). Using the fishbone tool, the QI team identified 5 main categories limiting complete uptake of suicide risk assessment at the HPACT clinic: health record factors, communication, clinician buy-in, system factors, and patient factors. Among the most salient barriers to use of the screening tool, the EHR system needed to be refreshed after a positive screen to be reminded of the next step, requiring close communication during patient handoffs. Handoff was confusing as there was no dedicated process to communicate positive screen information. Clinicians were concerned that completing the process, especially the tertiary screen, would be time consuming and burdensome in an already busy clinic; some clinicians were uncomfortable discussing the topic of suicide as they did not feel they had the expertise to address a positive screen. In addition, some patients were reluctant to answer the screen honestly due to past hospitalizations or concerns about stigma.
Discussion
Though the QI project failed to meet the SMART Aim of ensuring > 90% of eligible patients received a primary screen for suicide risk and > 90% of positive primary I9 screens received subsequent screenings within 24 hours, the results highlight effective practices and barriers for implementation of wide-scale EHR-based interventions for suicide assessment. Most missed screening opportunities were due to patients being lost to follow-up over the duration of the project, which is a challenge faced in this patient population. A recent analysis of the national rollout of this screening program found that 95% of eligible veterans with a visit to the VA in the first year of the program received screening.14 In a post hoc analysis using the same eligibility criteria, the rate of screening for this project was 83%. Reflecting on the data from this national cohort compared with the HPACT clinic, this brings to light potential circumstances that may be unique to veterans experiencing homelessness compared with the general veteran population, for instance, the level of engagement may be lower among veterans experiencing homelessness, though this is beyond the scope of this article. Nonetheless, promoting interprofessional collaboration, visualizing effective process flows, establishing clear lines of communication and roles for involved staff, and opening avenues for continuous feedback and troubleshooting are all potentially effective interventions to improve suicide screening rates within the veteran population.
This HPACT clinic initiative aimed to determine how a new screening process would be implemented while identifying potential areas for improvement. Surprisingly, 43% of patients who were screened had their screening performed outside of the HPACT clinic, most often in the inpatient setting at other WLAVAMC clinics or other VA systems. It is possible that due to the nature of the patient population that the HPACT clinic serves with intensive service needs, these patients have wider geographic and clinical location use than most clinic populations due to the transient nature of patients with housing insecurity. What is encouraging, however, is that through this systemwide initiative, there is an impetus to screen veterans, regardless of who performs the screening. This is particularly meaningful given that rates of depression screening may be as low as 4% among PCPs.15 During implementation, the QI team learned that nearly 18% of the empaneled HPACT patients were exempt from screening. The exempt patients do not have an active clinical reminder for depression screens. Instead, these patients are receiving mental health surveillance and specialty treatment, during which continuous monitoring and assessment for suicidal ideation and risk of suicide are performed. Additionally, an EHR-based factor that also may limit appropriate follow-up and contribute to missed opportunities is that secondary and tertiary screens do not populate until the EHR was refreshed after positive primary screens, which introduces human error in a process that could be automated. Both RNs and PCPs may occasionally miss secondary and tertiary screens due to this issue, which continues to be a barrier. Given the high risk HPACT clinic population, the QI team encouraged staff members to frequently screen patients for suicidal ideation regardless of clinical reminders. A consideration for the future would be to identify optimal frequency for screening and to continue to validate assessment methods.
Finally, while the percentage of patients who were considered missed opportunities (visited the HPACT clinic but were not screened) was relatively small at 6% of the total panel of patients, this number theoretically should be zero. Though this project was not designed to identify the specific causes for missed opportunities, future QI efforts may consider evaluating for other potential reasons. These may include differing process flows for various encounters (same-day care visits, scheduled primary care visit, RN-only visit), screening not activating at time of visit, time constraints, or other unseen reasons. Another important population is the 11% of patients who were otherwise eligible for screening but did not visit the HPACT clinic, and in some cases, no other VA location. There are a few explanatory reasons centered on the mobility of this population between health systems. However, this patient population also may be among the most vulnerable and at risk: 62% of veteran suicides in 2017 had not had a VA encounter that year.13 While there is no requirement that the veteran visit the HPACT clinic annually, future efforts may focus on increasing engagement through other means of outreach, including site visits and community care involvement, knowing the nature of the sporadic follow-up patterns in this patient population. Future work may also involve examining suicide rates by primary care clinic and triage patterns between interprofessional staff.
Limitations
Due to the limited sample size, findings cannot be generalized to all VA sites. The QI team used retrospective, administrative data. Additionally, since this is a primary care clinic focused on a specialized population, this result may not be generalizable to all primary care settings, other primary care populations, or even other homeless primary care clinics, though it may establish a benchmark when other clinics internally examine their data and processes.
Conclusions
Improving screening protocols can lead to identification of at-risk individuals who would not have otherwise been identified.16,17 As the US continues to grapple with mental health and suicide, efforts toward addressing this important issue among veterans remains a top priority.
Acknowledgments
Thank you to the VAGLAHS Center of Excellence in Primary Care Education faculty and trainees, the HPACT staff, and the VA Informatics and Computing Infrastructure (VINCI) for data support.
1. Centers for Disease Control and Prevention. Facts about suicide. Reviewed August 30, 2021. Accessed December 13, 2021. https://www.cdc.gov/suicide/facts/index.html
2. Centers for Disease Control and Prevention. Preventing suicide: a technical package of policies, programs, and practices. Published 2017. Accessed December 13, 2021. https://www.cdc.gov/violenceprevention/pdf/suicideTechnicalPackage.pdf
3. Centers for Disease Control and Prevention. Increase in suicide mortality in the United States, 1999-2018. April 8, 2020. Accessed December 13, 2021. https://www.cdc.gov/nchs/products/databriefs/db362.htm
4. US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention. 2020 National Veteran Suicide Prevention Annual Report. Published November 2020. Accessed December 13, 2021. https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Veteran-Suicide-Prevention-Annual-Report-11-2020-508.pdf
5. Culhane D, Szymkowiak D, Schinka, JA. Suicidality and the onset of homelessness: evidence for a temporal association from VHA treatment records. Psychiatr Serv. 2019;70(11):1049-1052. doi:10.1176/appi.ps.201800415
6. US Department of Housing and Urban Development. The 2015 annual homeless assessment report (AHAR) to Congress. Published November 2015. Accessed December 13, 2021. https://www.hudexchange.info/resources/documents/2015-AHAR-Part-1.pdf
7. US Department of Veterans Affairs, Office of Suicide Prevention. Suicide among veterans and other Americans 2001-2014. Published August 3, 2016. Updated August 2017. Accessed December 13, 2021. https://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf
8. Dobscha SK, Corson K, Helmer DA, et al. Brief assessment for suicidal ideation in OEF/OIF veterans with positive depression screens. Gen Hosp Psychiatry. 2013;35(3):272-278. doi:10.1016/j.genhosppsych.2012.12.001
9. Luoma JB, Martin CE, Pearson JL. Contact with mental health and primary care providers before suicide: a review of the evidence. Am J Psychiatry. 2002;159(6):909-916. doi:10.1176/appi.ajp.159.6.909
10. US Department of Veterans Affairs. National strategy for preventing veteran suicide 2018-2028. Accessed December 13, 2021. https://sprc.org/sites/default/files/resource-program/VA_National-Strategy-for-Preventing-Veterans-Suicide2018.pdf
11. US Department of Veterans Affairs. VA suicide prevention efforts. Published July 2019. Accessed December 15, 2021. https://www.mentalhealth.va.gov/suicide_prevention/docs/VA_Suicide_Prevention_Program_Fact_Sheet_508.pdf
12. Wortzel H, Matarazzo B, Homaifer B. A model for therapeutic risk management of the suicidal patient. J Psychiatr Pract. 2013;19(4):323-326. doi:10.1097/01.pra.0000432603.99211.e8
13. US Department of Veterans Affairs. VA/DoD clinical practice guidelines for the assessment and management of patients at risk for suicide. Provider summary version 2.0. Published 2019. Accessed on December 3, 2020. https://www.healthquality.va.gov/guidelines/MH/srb/VADoDSuicideRiskFullCPGFinal5088919.pdf
14. Bahraini N, Brenner LA, Barry C, et al. Assessment of rates of suicide risk screening and prevalence of positive screening results among US veterans after implementation of the Veterans Affairs suicide risk identification strategy. JAMA Netw Open. 2020;3(10):e2022531. doi:10.1001/jamanetworkopen.2020.22531
15. Akincigil A, Matthews EB. National rates and patterns of depression screening in primary care: results from 2012 and 2013. Psychiatr Serv. 2017;68(7):660-666. doi:10.1176/appi.ps.201600096
16. Posner K, Brent D, Lucas C, et al. Columbia-suicide severity rating scale (C-SSRS). Columbia University Medical Center, New York, NY. 2008. Accessed December 3, 2020. https://cssrs.columbia.edu/wp-content/uploads/C-SSRS-Screening_AU5.1_eng-USori.pdf
17. Boudreaux ED, Camargo CA Jr, Arias SA, et al. Improving suicide risk screening and detection in the emergency department. Am J Prev Med. 2016;50(4):445-453. doi:10.1016/j/amepre.2015.09.029
Suicide is a national public health concern that affects thousands of US individuals and families, with repercussions that reverberate through entire communities. In 2019, there were 47,500 US deaths by suicide, which accounted for about 1 death every 11 minutes.1 Suicide remains the tenth leading cause of death in the United States and has been part of the top 12 leading causes of death since 1975.2 Unfortunately, this trend has worsened; suicide rates have increased by 35% from 1999 to 2018.3 One particularly vulnerable population is US veterans who accounted for 13.8% of all suicide deaths in 2018.4 Among veterans, the suicide death average increased from 16.6 per day in 2005 to 17.6 in 2018.4 Furthermore, veterans experiencing homelessness are 5 times more likely to attempt suicide and 2.5 times more likely to have suicidal ideation compared with veterans without a history of homelessness.4 Suicide is a significant issue among veterans experiencing homelessness: Veterans account for about 11% of the overall US homeless population.5
Recent data suggest opportunities for suicide risk assessment in the primary care setting. A study from the Veterans Health Administration (VHA) Office for Suicide Prevention found that in 2014 an average of 20 veterans died by suicide every day and 6 of the 20 (30%) on average used VHA services within the prior year.6 Similarly, a review of 40 studies on suicide found that 45% of suicide victims had contact with their primary care practitioner (PCP) within 1 month of suicide, and 75% of victims had contact within the year of suicide.7 An analysis of depression screening in 2008/2009 using Patient Health Questionnaire-2 (PHQ-2) or Patient Health Questionnaire-9 (PHQ-9) at 3 large western US Department of Veterans Affairs (VA) medical centers found that 55% were screened for depression.8 The VA has made suicide prevention a top priority and supports the established US goal of reducing annual suicide deaths by 20% by 2025.9 Given key opportunities for suicide risk assessment in the primary care setting, the VHA Office of Mental Health and Suicide Prevention implemented a national, standardized process for suicide risk assessment on October 1, 2018.10,11
The VA approach to suicide screening, evaluation, and documentation has evolved over time. Between October 2018 and December 2020, the process was augmented to include 3 stages embedded into the electronic health record (EHR): a primary screen (PHQ-2 with Item 9 from the PHQ-9 [PHQ-2+I9]), a secondary screen (Columbia-Suicide Severity Rating Scale [C-SSRS]), and a tertiary screen (Comprehensive Suicide Risk Evaluation [CSRE]). The primary screen consisted of the depression screening using the PHQ-2 with the addition of I9 asking about suicidal ideation. The secondary screening, or C-SSRS, included 8 questions to elaborate on suicidal ideation, intent, plan, and any history of suicidal attempts or preparatory behaviors. The tertiary screen consisted of the CSRE, a questionnaire developed internally by the VA in 2018 to further evaluate the veteran’s suicidal thoughts, attempts, warning signs, risk factors, protective factors, and reasons for living. The goal of the screenings was to identify veterans at risk of suicide, assess risk severity, and to individually tailor risk mitigation strategies for safe disposition. These risk categories were developed by the regional Mental Illness Research, Education and Clinical Center, which suggested treatment strategies, such as hospitalization or close outpatient follow-up.12,13
The Homeless Patient Aligned Care Team (HPACT) clinic at the West Los Angeles VA Medical Center (WLAVAMC) in California, one of the largest VA homeless clinics in the country and 1 of 7 national VA Office of Academic Affiliation Centers of Excellence in Primary Care Education training programs implemented the standardized tools for suicide risk screening and quality improvement (QI). The HPACT clinic is an interprofessional team, including primary care, mental health, social work, pharmacy, and peer support, that is adjacent to the WLAVAMC general primary care clinics. The team collaboratively addresses both medical and psychosocial needs of veterans with a focus on the Housing First Model, an approach that prioritizes ending homelessness while addressing all factors associated with veterans' health and well-being. After 1 year of stable housing, veterans graduate to the WLAVAMC general primary care clinics.
Given the vulnerability of veterans experiencing homelessness, the clinic leadership identified suicide risk screening as a high priority initiative and created a taskforce to oversee effective implementation of clinic screening efforts. An interprofessional team of nurse practitioners (NPs), pharmacists, physicians, psychologists, social workers (SWs), and trainees formed to improve screening efforts and use the QI principles to guide analysis and intervention. The team wrote the following SMART (Specific, Measurable, Achievable, Relevant, and Time-bound) Aim statements: (1) ensure > 90% of eligible patients receive a primary screen; (2) ensure > 90% of positive primary I9 screens receive subsequent screenings within 24 hours; and (3) increase staff comfort and familiarity using the screening tools. This article examines the results of the screening initiative 1-year postimplementation, describes difficulties faced, and suggests strategies that might be used to overcome those challenges.
Methods
This QI analysis was exempt from institutional review board review. Prior to the standardized national suicide risk assessment rollout of October 1, 2018, the QI team met to review and understand the workflow to be implemented into the HPACT clinic. To describe the initial screening process, the new suicide risk assessment consisted of primary, secondary, and tertiary screens that would warrant subsequent intervention by clinicians if positive (Figure 1). The primary screen included the PHQ-2+I9 questionnaire (PHQ-2 for depression and I9 for suicidal ideation). If either were positive, follow-up questionnaires were required. Of note, patients with a prior depression diagnosis, cognitive impairment defined at a severity of moderate or greater based on clinician evaluation and judgement, or life expectancy < 6 months were exempt from screening because, by definition, they had theoretically already been screened and classified as under surveillance.
A positive I9 response prompted a secondary screen using C-SSRS. A positive secondary screen prompted a tertiary screen using CSRE. If the PHQ-2 screening was positive but I9 was negative, the standard follow-up depression clinical reminder was used. Any clinical staff member could perform the primary screen, including licensed vocational nurses (LVNs), registered nurses (RNs), and SWs in any setting (eg, emergency department, primary care, inpatient services). The secondary and tertiary screens required completion by a licensed clinician. RNs were able to perform the secondary screen but not the tertiary screen.
The HPACT clinic serves approximately 3000 patients by 50 staff and trainees divided into 2 teams. LVNs and RNs were tasked to conduct the primary screen as part of their initial clinic check-in. If the primary screen was positive for scheduled patients, LVNs notified a PCP to complete the secondary screen. For unscheduled patients, RNs conducted a primary screen and, if positive, a secondary screen. If the secondary screen was positive, a tertiary screen was performed by mental health practitioners or SWs, or PCPs if the former were unavailable. SWs, mental health practitioners, and PCPs were colocated in the clinic, which allowed for safe and convenient warm handoffs between clinicians.
During this process, the interprofessional team overseeing the suicide screening implementation efforts in the HPACT clinic met in-person biweekly beginning 1 month prior to the October 1, 2018 implementation. QI tools, including flowcharts and root cause analyses, were used to analyze feedback on efficient workflow and optimize staff responsibilities. A survey assessed staff comfort and familiarity using the suicide screening tools. Informal interviews were conducted with a representative from each stage of patient care to facilitate interprofessional participation and to troubleshoot any issues. Process flowcharts that clearly delineated staff roles based on current clinic workflow and the recommendations set forth by the new process were distributed at an initial staff meeting. The process flowchart was updated after staff feedback and distributed again along with a review of the C-SSRS and CSRE at an all-staff meeting in February 2019. The QI team continued to meet to formally evaluate their SMART Aims and to identify factors driving the success and failure of the implementation.
The VA Informatics and Computing Infrastructure (VINCI) provided project data after a formal request was submitted for this analysis. At the direction of the local QI team, the VINCI team provided aggregate patient counts derived from individual patient data in the VA Corporate Data Warehouse. The data analyzed are frequencies and proportions; no bivariate or multivariate statistics were performed.
Results
During the project year, the HPACT clinic had 2932 unique patients assigned to primary care. Of those veterans, 533 (18%) were exempt from screening by protocol. Of the remainder, staff screened 1876 (64%) of eligible veterans for suicide risk (Figure 2), which did not meet the SMART Aim of screening > 90% of eligible veterans. For the follow-up screens, using a QI dashboard designed for reviewing I9 and C-SSRS results, the QI team reviewed a convenience sample of 5 provider panels and identified 34 positive I9 screens. Twenty of those 34 patients (59%) received a C-SSRS within 24 hours of the positive I9, which did not meet the SMART Aim of ensuring > 90% of primary I9 screens had subsequent C-SSRS screening within 24 hours.
Of the veterans screened, 1,271 (43%) had their screening performed outside of the HPACT primary care team assigned, while 605 (21%) patients had their screening performed by an HPACT member. Most of the screening that occurred outside of the assigned primary care team occurred in other physical settings, including other VA facilities.
Of the 523 (18%) patients who were not screened, 331 (11%) patients had no visit to the HPACT clinic and 132 (5%) empaneled patients did not visit any VA site within the 1-year period. There were 192 (7%) patients who were not screened that had a visit to HPACT while 19 (1%) of those patients declined screening. A total of 184 (6%) patients were not screened and thus were considered true missed opportunities. This group of patients were eligible for screening but did not undergo screening in the HPACT clinic or any other VA setting despite visiting the VA.
The QI team created a fishbone diagram to identify opportunities to improve screening rates and patient care (Figure 3). Using the fishbone tool, the QI team identified 5 main categories limiting complete uptake of suicide risk assessment at the HPACT clinic: health record factors, communication, clinician buy-in, system factors, and patient factors. Among the most salient barriers to use of the screening tool, the EHR system needed to be refreshed after a positive screen to be reminded of the next step, requiring close communication during patient handoffs. Handoff was confusing as there was no dedicated process to communicate positive screen information. Clinicians were concerned that completing the process, especially the tertiary screen, would be time consuming and burdensome in an already busy clinic; some clinicians were uncomfortable discussing the topic of suicide as they did not feel they had the expertise to address a positive screen. In addition, some patients were reluctant to answer the screen honestly due to past hospitalizations or concerns about stigma.
Discussion
Though the QI project failed to meet the SMART Aim of ensuring > 90% of eligible patients received a primary screen for suicide risk and > 90% of positive primary I9 screens received subsequent screenings within 24 hours, the results highlight effective practices and barriers for implementation of wide-scale EHR-based interventions for suicide assessment. Most missed screening opportunities were due to patients being lost to follow-up over the duration of the project, which is a challenge faced in this patient population. A recent analysis of the national rollout of this screening program found that 95% of eligible veterans with a visit to the VA in the first year of the program received screening.14 In a post hoc analysis using the same eligibility criteria, the rate of screening for this project was 83%. Reflecting on the data from this national cohort compared with the HPACT clinic, this brings to light potential circumstances that may be unique to veterans experiencing homelessness compared with the general veteran population, for instance, the level of engagement may be lower among veterans experiencing homelessness, though this is beyond the scope of this article. Nonetheless, promoting interprofessional collaboration, visualizing effective process flows, establishing clear lines of communication and roles for involved staff, and opening avenues for continuous feedback and troubleshooting are all potentially effective interventions to improve suicide screening rates within the veteran population.
This HPACT clinic initiative aimed to determine how a new screening process would be implemented while identifying potential areas for improvement. Surprisingly, 43% of patients who were screened had their screening performed outside of the HPACT clinic, most often in the inpatient setting at other WLAVAMC clinics or other VA systems. It is possible that due to the nature of the patient population that the HPACT clinic serves with intensive service needs, these patients have wider geographic and clinical location use than most clinic populations due to the transient nature of patients with housing insecurity. What is encouraging, however, is that through this systemwide initiative, there is an impetus to screen veterans, regardless of who performs the screening. This is particularly meaningful given that rates of depression screening may be as low as 4% among PCPs.15 During implementation, the QI team learned that nearly 18% of the empaneled HPACT patients were exempt from screening. The exempt patients do not have an active clinical reminder for depression screens. Instead, these patients are receiving mental health surveillance and specialty treatment, during which continuous monitoring and assessment for suicidal ideation and risk of suicide are performed. Additionally, an EHR-based factor that also may limit appropriate follow-up and contribute to missed opportunities is that secondary and tertiary screens do not populate until the EHR was refreshed after positive primary screens, which introduces human error in a process that could be automated. Both RNs and PCPs may occasionally miss secondary and tertiary screens due to this issue, which continues to be a barrier. Given the high risk HPACT clinic population, the QI team encouraged staff members to frequently screen patients for suicidal ideation regardless of clinical reminders. A consideration for the future would be to identify optimal frequency for screening and to continue to validate assessment methods.
Finally, while the percentage of patients who were considered missed opportunities (visited the HPACT clinic but were not screened) was relatively small at 6% of the total panel of patients, this number theoretically should be zero. Though this project was not designed to identify the specific causes for missed opportunities, future QI efforts may consider evaluating for other potential reasons. These may include differing process flows for various encounters (same-day care visits, scheduled primary care visit, RN-only visit), screening not activating at time of visit, time constraints, or other unseen reasons. Another important population is the 11% of patients who were otherwise eligible for screening but did not visit the HPACT clinic, and in some cases, no other VA location. There are a few explanatory reasons centered on the mobility of this population between health systems. However, this patient population also may be among the most vulnerable and at risk: 62% of veteran suicides in 2017 had not had a VA encounter that year.13 While there is no requirement that the veteran visit the HPACT clinic annually, future efforts may focus on increasing engagement through other means of outreach, including site visits and community care involvement, knowing the nature of the sporadic follow-up patterns in this patient population. Future work may also involve examining suicide rates by primary care clinic and triage patterns between interprofessional staff.
Limitations
Due to the limited sample size, findings cannot be generalized to all VA sites. The QI team used retrospective, administrative data. Additionally, since this is a primary care clinic focused on a specialized population, this result may not be generalizable to all primary care settings, other primary care populations, or even other homeless primary care clinics, though it may establish a benchmark when other clinics internally examine their data and processes.
Conclusions
Improving screening protocols can lead to identification of at-risk individuals who would not have otherwise been identified.16,17 As the US continues to grapple with mental health and suicide, efforts toward addressing this important issue among veterans remains a top priority.
Acknowledgments
Thank you to the VAGLAHS Center of Excellence in Primary Care Education faculty and trainees, the HPACT staff, and the VA Informatics and Computing Infrastructure (VINCI) for data support.
Suicide is a national public health concern that affects thousands of US individuals and families, with repercussions that reverberate through entire communities. In 2019, there were 47,500 US deaths by suicide, which accounted for about 1 death every 11 minutes.1 Suicide remains the tenth leading cause of death in the United States and has been part of the top 12 leading causes of death since 1975.2 Unfortunately, this trend has worsened; suicide rates have increased by 35% from 1999 to 2018.3 One particularly vulnerable population is US veterans who accounted for 13.8% of all suicide deaths in 2018.4 Among veterans, the suicide death average increased from 16.6 per day in 2005 to 17.6 in 2018.4 Furthermore, veterans experiencing homelessness are 5 times more likely to attempt suicide and 2.5 times more likely to have suicidal ideation compared with veterans without a history of homelessness.4 Suicide is a significant issue among veterans experiencing homelessness: Veterans account for about 11% of the overall US homeless population.5
Recent data suggest opportunities for suicide risk assessment in the primary care setting. A study from the Veterans Health Administration (VHA) Office for Suicide Prevention found that in 2014 an average of 20 veterans died by suicide every day and 6 of the 20 (30%) on average used VHA services within the prior year.6 Similarly, a review of 40 studies on suicide found that 45% of suicide victims had contact with their primary care practitioner (PCP) within 1 month of suicide, and 75% of victims had contact within the year of suicide.7 An analysis of depression screening in 2008/2009 using Patient Health Questionnaire-2 (PHQ-2) or Patient Health Questionnaire-9 (PHQ-9) at 3 large western US Department of Veterans Affairs (VA) medical centers found that 55% were screened for depression.8 The VA has made suicide prevention a top priority and supports the established US goal of reducing annual suicide deaths by 20% by 2025.9 Given key opportunities for suicide risk assessment in the primary care setting, the VHA Office of Mental Health and Suicide Prevention implemented a national, standardized process for suicide risk assessment on October 1, 2018.10,11
The VA approach to suicide screening, evaluation, and documentation has evolved over time. Between October 2018 and December 2020, the process was augmented to include 3 stages embedded into the electronic health record (EHR): a primary screen (PHQ-2 with Item 9 from the PHQ-9 [PHQ-2+I9]), a secondary screen (Columbia-Suicide Severity Rating Scale [C-SSRS]), and a tertiary screen (Comprehensive Suicide Risk Evaluation [CSRE]). The primary screen consisted of the depression screening using the PHQ-2 with the addition of I9 asking about suicidal ideation. The secondary screening, or C-SSRS, included 8 questions to elaborate on suicidal ideation, intent, plan, and any history of suicidal attempts or preparatory behaviors. The tertiary screen consisted of the CSRE, a questionnaire developed internally by the VA in 2018 to further evaluate the veteran’s suicidal thoughts, attempts, warning signs, risk factors, protective factors, and reasons for living. The goal of the screenings was to identify veterans at risk of suicide, assess risk severity, and to individually tailor risk mitigation strategies for safe disposition. These risk categories were developed by the regional Mental Illness Research, Education and Clinical Center, which suggested treatment strategies, such as hospitalization or close outpatient follow-up.12,13
The Homeless Patient Aligned Care Team (HPACT) clinic at the West Los Angeles VA Medical Center (WLAVAMC) in California, one of the largest VA homeless clinics in the country and 1 of 7 national VA Office of Academic Affiliation Centers of Excellence in Primary Care Education training programs implemented the standardized tools for suicide risk screening and quality improvement (QI). The HPACT clinic is an interprofessional team, including primary care, mental health, social work, pharmacy, and peer support, that is adjacent to the WLAVAMC general primary care clinics. The team collaboratively addresses both medical and psychosocial needs of veterans with a focus on the Housing First Model, an approach that prioritizes ending homelessness while addressing all factors associated with veterans' health and well-being. After 1 year of stable housing, veterans graduate to the WLAVAMC general primary care clinics.
Given the vulnerability of veterans experiencing homelessness, the clinic leadership identified suicide risk screening as a high priority initiative and created a taskforce to oversee effective implementation of clinic screening efforts. An interprofessional team of nurse practitioners (NPs), pharmacists, physicians, psychologists, social workers (SWs), and trainees formed to improve screening efforts and use the QI principles to guide analysis and intervention. The team wrote the following SMART (Specific, Measurable, Achievable, Relevant, and Time-bound) Aim statements: (1) ensure > 90% of eligible patients receive a primary screen; (2) ensure > 90% of positive primary I9 screens receive subsequent screenings within 24 hours; and (3) increase staff comfort and familiarity using the screening tools. This article examines the results of the screening initiative 1-year postimplementation, describes difficulties faced, and suggests strategies that might be used to overcome those challenges.
Methods
This QI analysis was exempt from institutional review board review. Prior to the standardized national suicide risk assessment rollout of October 1, 2018, the QI team met to review and understand the workflow to be implemented into the HPACT clinic. To describe the initial screening process, the new suicide risk assessment consisted of primary, secondary, and tertiary screens that would warrant subsequent intervention by clinicians if positive (Figure 1). The primary screen included the PHQ-2+I9 questionnaire (PHQ-2 for depression and I9 for suicidal ideation). If either were positive, follow-up questionnaires were required. Of note, patients with a prior depression diagnosis, cognitive impairment defined at a severity of moderate or greater based on clinician evaluation and judgement, or life expectancy < 6 months were exempt from screening because, by definition, they had theoretically already been screened and classified as under surveillance.
A positive I9 response prompted a secondary screen using C-SSRS. A positive secondary screen prompted a tertiary screen using CSRE. If the PHQ-2 screening was positive but I9 was negative, the standard follow-up depression clinical reminder was used. Any clinical staff member could perform the primary screen, including licensed vocational nurses (LVNs), registered nurses (RNs), and SWs in any setting (eg, emergency department, primary care, inpatient services). The secondary and tertiary screens required completion by a licensed clinician. RNs were able to perform the secondary screen but not the tertiary screen.
The HPACT clinic serves approximately 3000 patients by 50 staff and trainees divided into 2 teams. LVNs and RNs were tasked to conduct the primary screen as part of their initial clinic check-in. If the primary screen was positive for scheduled patients, LVNs notified a PCP to complete the secondary screen. For unscheduled patients, RNs conducted a primary screen and, if positive, a secondary screen. If the secondary screen was positive, a tertiary screen was performed by mental health practitioners or SWs, or PCPs if the former were unavailable. SWs, mental health practitioners, and PCPs were colocated in the clinic, which allowed for safe and convenient warm handoffs between clinicians.
During this process, the interprofessional team overseeing the suicide screening implementation efforts in the HPACT clinic met in-person biweekly beginning 1 month prior to the October 1, 2018 implementation. QI tools, including flowcharts and root cause analyses, were used to analyze feedback on efficient workflow and optimize staff responsibilities. A survey assessed staff comfort and familiarity using the suicide screening tools. Informal interviews were conducted with a representative from each stage of patient care to facilitate interprofessional participation and to troubleshoot any issues. Process flowcharts that clearly delineated staff roles based on current clinic workflow and the recommendations set forth by the new process were distributed at an initial staff meeting. The process flowchart was updated after staff feedback and distributed again along with a review of the C-SSRS and CSRE at an all-staff meeting in February 2019. The QI team continued to meet to formally evaluate their SMART Aims and to identify factors driving the success and failure of the implementation.
The VA Informatics and Computing Infrastructure (VINCI) provided project data after a formal request was submitted for this analysis. At the direction of the local QI team, the VINCI team provided aggregate patient counts derived from individual patient data in the VA Corporate Data Warehouse. The data analyzed are frequencies and proportions; no bivariate or multivariate statistics were performed.
Results
During the project year, the HPACT clinic had 2932 unique patients assigned to primary care. Of those veterans, 533 (18%) were exempt from screening by protocol. Of the remainder, staff screened 1876 (64%) of eligible veterans for suicide risk (Figure 2), which did not meet the SMART Aim of screening > 90% of eligible veterans. For the follow-up screens, using a QI dashboard designed for reviewing I9 and C-SSRS results, the QI team reviewed a convenience sample of 5 provider panels and identified 34 positive I9 screens. Twenty of those 34 patients (59%) received a C-SSRS within 24 hours of the positive I9, which did not meet the SMART Aim of ensuring > 90% of primary I9 screens had subsequent C-SSRS screening within 24 hours.
Of the veterans screened, 1,271 (43%) had their screening performed outside of the HPACT primary care team assigned, while 605 (21%) patients had their screening performed by an HPACT member. Most of the screening that occurred outside of the assigned primary care team occurred in other physical settings, including other VA facilities.
Of the 523 (18%) patients who were not screened, 331 (11%) patients had no visit to the HPACT clinic and 132 (5%) empaneled patients did not visit any VA site within the 1-year period. There were 192 (7%) patients who were not screened that had a visit to HPACT while 19 (1%) of those patients declined screening. A total of 184 (6%) patients were not screened and thus were considered true missed opportunities. This group of patients were eligible for screening but did not undergo screening in the HPACT clinic or any other VA setting despite visiting the VA.
The QI team created a fishbone diagram to identify opportunities to improve screening rates and patient care (Figure 3). Using the fishbone tool, the QI team identified 5 main categories limiting complete uptake of suicide risk assessment at the HPACT clinic: health record factors, communication, clinician buy-in, system factors, and patient factors. Among the most salient barriers to use of the screening tool, the EHR system needed to be refreshed after a positive screen to be reminded of the next step, requiring close communication during patient handoffs. Handoff was confusing as there was no dedicated process to communicate positive screen information. Clinicians were concerned that completing the process, especially the tertiary screen, would be time consuming and burdensome in an already busy clinic; some clinicians were uncomfortable discussing the topic of suicide as they did not feel they had the expertise to address a positive screen. In addition, some patients were reluctant to answer the screen honestly due to past hospitalizations or concerns about stigma.
Discussion
Though the QI project failed to meet the SMART Aim of ensuring > 90% of eligible patients received a primary screen for suicide risk and > 90% of positive primary I9 screens received subsequent screenings within 24 hours, the results highlight effective practices and barriers for implementation of wide-scale EHR-based interventions for suicide assessment. Most missed screening opportunities were due to patients being lost to follow-up over the duration of the project, which is a challenge faced in this patient population. A recent analysis of the national rollout of this screening program found that 95% of eligible veterans with a visit to the VA in the first year of the program received screening.14 In a post hoc analysis using the same eligibility criteria, the rate of screening for this project was 83%. Reflecting on the data from this national cohort compared with the HPACT clinic, this brings to light potential circumstances that may be unique to veterans experiencing homelessness compared with the general veteran population, for instance, the level of engagement may be lower among veterans experiencing homelessness, though this is beyond the scope of this article. Nonetheless, promoting interprofessional collaboration, visualizing effective process flows, establishing clear lines of communication and roles for involved staff, and opening avenues for continuous feedback and troubleshooting are all potentially effective interventions to improve suicide screening rates within the veteran population.
This HPACT clinic initiative aimed to determine how a new screening process would be implemented while identifying potential areas for improvement. Surprisingly, 43% of patients who were screened had their screening performed outside of the HPACT clinic, most often in the inpatient setting at other WLAVAMC clinics or other VA systems. It is possible that due to the nature of the patient population that the HPACT clinic serves with intensive service needs, these patients have wider geographic and clinical location use than most clinic populations due to the transient nature of patients with housing insecurity. What is encouraging, however, is that through this systemwide initiative, there is an impetus to screen veterans, regardless of who performs the screening. This is particularly meaningful given that rates of depression screening may be as low as 4% among PCPs.15 During implementation, the QI team learned that nearly 18% of the empaneled HPACT patients were exempt from screening. The exempt patients do not have an active clinical reminder for depression screens. Instead, these patients are receiving mental health surveillance and specialty treatment, during which continuous monitoring and assessment for suicidal ideation and risk of suicide are performed. Additionally, an EHR-based factor that also may limit appropriate follow-up and contribute to missed opportunities is that secondary and tertiary screens do not populate until the EHR was refreshed after positive primary screens, which introduces human error in a process that could be automated. Both RNs and PCPs may occasionally miss secondary and tertiary screens due to this issue, which continues to be a barrier. Given the high risk HPACT clinic population, the QI team encouraged staff members to frequently screen patients for suicidal ideation regardless of clinical reminders. A consideration for the future would be to identify optimal frequency for screening and to continue to validate assessment methods.
Finally, while the percentage of patients who were considered missed opportunities (visited the HPACT clinic but were not screened) was relatively small at 6% of the total panel of patients, this number theoretically should be zero. Though this project was not designed to identify the specific causes for missed opportunities, future QI efforts may consider evaluating for other potential reasons. These may include differing process flows for various encounters (same-day care visits, scheduled primary care visit, RN-only visit), screening not activating at time of visit, time constraints, or other unseen reasons. Another important population is the 11% of patients who were otherwise eligible for screening but did not visit the HPACT clinic, and in some cases, no other VA location. There are a few explanatory reasons centered on the mobility of this population between health systems. However, this patient population also may be among the most vulnerable and at risk: 62% of veteran suicides in 2017 had not had a VA encounter that year.13 While there is no requirement that the veteran visit the HPACT clinic annually, future efforts may focus on increasing engagement through other means of outreach, including site visits and community care involvement, knowing the nature of the sporadic follow-up patterns in this patient population. Future work may also involve examining suicide rates by primary care clinic and triage patterns between interprofessional staff.
Limitations
Due to the limited sample size, findings cannot be generalized to all VA sites. The QI team used retrospective, administrative data. Additionally, since this is a primary care clinic focused on a specialized population, this result may not be generalizable to all primary care settings, other primary care populations, or even other homeless primary care clinics, though it may establish a benchmark when other clinics internally examine their data and processes.
Conclusions
Improving screening protocols can lead to identification of at-risk individuals who would not have otherwise been identified.16,17 As the US continues to grapple with mental health and suicide, efforts toward addressing this important issue among veterans remains a top priority.
Acknowledgments
Thank you to the VAGLAHS Center of Excellence in Primary Care Education faculty and trainees, the HPACT staff, and the VA Informatics and Computing Infrastructure (VINCI) for data support.
1. Centers for Disease Control and Prevention. Facts about suicide. Reviewed August 30, 2021. Accessed December 13, 2021. https://www.cdc.gov/suicide/facts/index.html
2. Centers for Disease Control and Prevention. Preventing suicide: a technical package of policies, programs, and practices. Published 2017. Accessed December 13, 2021. https://www.cdc.gov/violenceprevention/pdf/suicideTechnicalPackage.pdf
3. Centers for Disease Control and Prevention. Increase in suicide mortality in the United States, 1999-2018. April 8, 2020. Accessed December 13, 2021. https://www.cdc.gov/nchs/products/databriefs/db362.htm
4. US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention. 2020 National Veteran Suicide Prevention Annual Report. Published November 2020. Accessed December 13, 2021. https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Veteran-Suicide-Prevention-Annual-Report-11-2020-508.pdf
5. Culhane D, Szymkowiak D, Schinka, JA. Suicidality and the onset of homelessness: evidence for a temporal association from VHA treatment records. Psychiatr Serv. 2019;70(11):1049-1052. doi:10.1176/appi.ps.201800415
6. US Department of Housing and Urban Development. The 2015 annual homeless assessment report (AHAR) to Congress. Published November 2015. Accessed December 13, 2021. https://www.hudexchange.info/resources/documents/2015-AHAR-Part-1.pdf
7. US Department of Veterans Affairs, Office of Suicide Prevention. Suicide among veterans and other Americans 2001-2014. Published August 3, 2016. Updated August 2017. Accessed December 13, 2021. https://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf
8. Dobscha SK, Corson K, Helmer DA, et al. Brief assessment for suicidal ideation in OEF/OIF veterans with positive depression screens. Gen Hosp Psychiatry. 2013;35(3):272-278. doi:10.1016/j.genhosppsych.2012.12.001
9. Luoma JB, Martin CE, Pearson JL. Contact with mental health and primary care providers before suicide: a review of the evidence. Am J Psychiatry. 2002;159(6):909-916. doi:10.1176/appi.ajp.159.6.909
10. US Department of Veterans Affairs. National strategy for preventing veteran suicide 2018-2028. Accessed December 13, 2021. https://sprc.org/sites/default/files/resource-program/VA_National-Strategy-for-Preventing-Veterans-Suicide2018.pdf
11. US Department of Veterans Affairs. VA suicide prevention efforts. Published July 2019. Accessed December 15, 2021. https://www.mentalhealth.va.gov/suicide_prevention/docs/VA_Suicide_Prevention_Program_Fact_Sheet_508.pdf
12. Wortzel H, Matarazzo B, Homaifer B. A model for therapeutic risk management of the suicidal patient. J Psychiatr Pract. 2013;19(4):323-326. doi:10.1097/01.pra.0000432603.99211.e8
13. US Department of Veterans Affairs. VA/DoD clinical practice guidelines for the assessment and management of patients at risk for suicide. Provider summary version 2.0. Published 2019. Accessed on December 3, 2020. https://www.healthquality.va.gov/guidelines/MH/srb/VADoDSuicideRiskFullCPGFinal5088919.pdf
14. Bahraini N, Brenner LA, Barry C, et al. Assessment of rates of suicide risk screening and prevalence of positive screening results among US veterans after implementation of the Veterans Affairs suicide risk identification strategy. JAMA Netw Open. 2020;3(10):e2022531. doi:10.1001/jamanetworkopen.2020.22531
15. Akincigil A, Matthews EB. National rates and patterns of depression screening in primary care: results from 2012 and 2013. Psychiatr Serv. 2017;68(7):660-666. doi:10.1176/appi.ps.201600096
16. Posner K, Brent D, Lucas C, et al. Columbia-suicide severity rating scale (C-SSRS). Columbia University Medical Center, New York, NY. 2008. Accessed December 3, 2020. https://cssrs.columbia.edu/wp-content/uploads/C-SSRS-Screening_AU5.1_eng-USori.pdf
17. Boudreaux ED, Camargo CA Jr, Arias SA, et al. Improving suicide risk screening and detection in the emergency department. Am J Prev Med. 2016;50(4):445-453. doi:10.1016/j/amepre.2015.09.029
1. Centers for Disease Control and Prevention. Facts about suicide. Reviewed August 30, 2021. Accessed December 13, 2021. https://www.cdc.gov/suicide/facts/index.html
2. Centers for Disease Control and Prevention. Preventing suicide: a technical package of policies, programs, and practices. Published 2017. Accessed December 13, 2021. https://www.cdc.gov/violenceprevention/pdf/suicideTechnicalPackage.pdf
3. Centers for Disease Control and Prevention. Increase in suicide mortality in the United States, 1999-2018. April 8, 2020. Accessed December 13, 2021. https://www.cdc.gov/nchs/products/databriefs/db362.htm
4. US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention. 2020 National Veteran Suicide Prevention Annual Report. Published November 2020. Accessed December 13, 2021. https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Veteran-Suicide-Prevention-Annual-Report-11-2020-508.pdf
5. Culhane D, Szymkowiak D, Schinka, JA. Suicidality and the onset of homelessness: evidence for a temporal association from VHA treatment records. Psychiatr Serv. 2019;70(11):1049-1052. doi:10.1176/appi.ps.201800415
6. US Department of Housing and Urban Development. The 2015 annual homeless assessment report (AHAR) to Congress. Published November 2015. Accessed December 13, 2021. https://www.hudexchange.info/resources/documents/2015-AHAR-Part-1.pdf
7. US Department of Veterans Affairs, Office of Suicide Prevention. Suicide among veterans and other Americans 2001-2014. Published August 3, 2016. Updated August 2017. Accessed December 13, 2021. https://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf
8. Dobscha SK, Corson K, Helmer DA, et al. Brief assessment for suicidal ideation in OEF/OIF veterans with positive depression screens. Gen Hosp Psychiatry. 2013;35(3):272-278. doi:10.1016/j.genhosppsych.2012.12.001
9. Luoma JB, Martin CE, Pearson JL. Contact with mental health and primary care providers before suicide: a review of the evidence. Am J Psychiatry. 2002;159(6):909-916. doi:10.1176/appi.ajp.159.6.909
10. US Department of Veterans Affairs. National strategy for preventing veteran suicide 2018-2028. Accessed December 13, 2021. https://sprc.org/sites/default/files/resource-program/VA_National-Strategy-for-Preventing-Veterans-Suicide2018.pdf
11. US Department of Veterans Affairs. VA suicide prevention efforts. Published July 2019. Accessed December 15, 2021. https://www.mentalhealth.va.gov/suicide_prevention/docs/VA_Suicide_Prevention_Program_Fact_Sheet_508.pdf
12. Wortzel H, Matarazzo B, Homaifer B. A model for therapeutic risk management of the suicidal patient. J Psychiatr Pract. 2013;19(4):323-326. doi:10.1097/01.pra.0000432603.99211.e8
13. US Department of Veterans Affairs. VA/DoD clinical practice guidelines for the assessment and management of patients at risk for suicide. Provider summary version 2.0. Published 2019. Accessed on December 3, 2020. https://www.healthquality.va.gov/guidelines/MH/srb/VADoDSuicideRiskFullCPGFinal5088919.pdf
14. Bahraini N, Brenner LA, Barry C, et al. Assessment of rates of suicide risk screening and prevalence of positive screening results among US veterans after implementation of the Veterans Affairs suicide risk identification strategy. JAMA Netw Open. 2020;3(10):e2022531. doi:10.1001/jamanetworkopen.2020.22531
15. Akincigil A, Matthews EB. National rates and patterns of depression screening in primary care: results from 2012 and 2013. Psychiatr Serv. 2017;68(7):660-666. doi:10.1176/appi.ps.201600096
16. Posner K, Brent D, Lucas C, et al. Columbia-suicide severity rating scale (C-SSRS). Columbia University Medical Center, New York, NY. 2008. Accessed December 3, 2020. https://cssrs.columbia.edu/wp-content/uploads/C-SSRS-Screening_AU5.1_eng-USori.pdf
17. Boudreaux ED, Camargo CA Jr, Arias SA, et al. Improving suicide risk screening and detection in the emergency department. Am J Prev Med. 2016;50(4):445-453. doi:10.1016/j/amepre.2015.09.029
Understanding the Intersection of Homelessness and Justice Involvement: Enhancing Veteran Suicide Prevention Through VA Programming
Despite the success of several US Department of Veterans Affairs (VA) initiatives in facilitating psychosocial functioning, rehabilitation, and re-entry among veterans experiencing homelessness and/or interactions with the criminal justice system (ie, justice-involved veterans), suicide risk among these veterans remains a significant public health concern. Rates of suicide among veterans experiencing homelessness are more than double that of veterans with no history of homelessness.1 Similarly, justice-involved veterans experience myriad mental health concerns, including elevated rates of psychiatric symptoms, suicidal thoughts, and self-directed violence relative to those with no history of criminal justice involvement.2
In addition, a bidirectional relationship between criminal justice involvement and homelessness, often called the “institutional circuit,” is well established. Criminal justice involvement can directly result in difficulty finding housing.3 For example, veterans may have their lease agreement denied based solely on their history of criminogenic behavior. Moreover, criminal justice involvement can indirectly impact a veteran’s ability to maintain housing. Indeed, justice-involved veterans can experience difficulty attaining and sustaining employment, which in turn can result in financial difficulties, including inability to afford rental or mortgage payments.
Similarly, those at risk for or experiencing housing instability may resort to criminogenic behavior to survive in the context of limited psychosocial resources.4-6 For instance, a veteran experiencing homelessness may seek refuge from inclement weather in a heated apartment stairwell and subsequently be charged with trespassing. Similarly, these veterans also may resort to theft to eat or pay bills. To this end, homelessness and justice involvement are likely a deleterious cycle that is difficult for the veteran to escape.
Unfortunately, the concurrent impact of housing insecurity and criminal justice involvement often serves to further exacerbate mental health sequelae, including suicide risk (Figure).7 In addition to precipitating frustration and helplessness among veterans who are navigating these stressors, these social determinants of health can engender a perception that the veteran is a burden to those in their support system. For example, these veterans may depend on friends or family to procure housing or transportation assistance for a job, medical appointments, and court hearings.
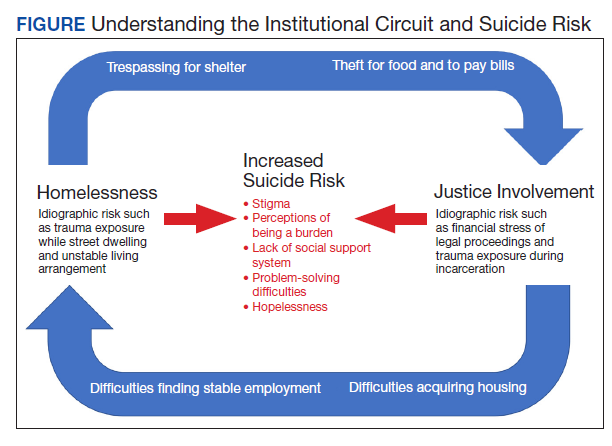
Furthermore, homelessness and justice involvement can impact veterans’ interpersonal relationships. For instance, veterans with a history of criminal justice involvement may feel stigmatized and ostracized from their social support system. Justice-involved veterans sometimes endorse being labeled an offender, which can result in perceptions that one is poorly perceived by others and generally seen as a bad person.8 In addition, the conditions of a justice-involved veteran’s probation or parole may further exacerbate social relationships. For example, veterans with histories of engaging in intimate partner violence may lose visitation rights with their children, further reinforcing negative views of self and impacting the veterans’ family network.
As such, these homeless and justice-involved veterans may lack a meaningful social support system when navigating psychosocial stressors. Because hopelessness, burdensomeness, and perceptions that one lacks a social support network are potential drivers of suicidal self-directed violence among these populations, facilitating access to and engagement in health (eg, psychotherapy, medication management) and social (eg, case management, transitional housing) services is necessary to enhance veteran suicide prevention efforts.9
Several VA homeless and justice-related programs have been developed to meet the needs of these veterans (Table). Such programs offer direct access to health and social services capable of addressing mental health symptoms and suicide risk. Moreover, these programs support veterans at various intercepts, or points at which there is an opportunity to identify those at elevated risk and provide access to evidence-based care. For instance, VA homeless programs exist tailored toward those currently, or at risk for, experiencing homelessness. Additionally, VA justice-related programs can target intercepts prior to jail or prison, such as working with crisis intervention teams or diversion courts as well as intercepts following release, such as providing services to facilitate postincarceration reentry. Even VA programs that do not directly administer mental health intervention (eg, Grant and Per Diem, Veterans Justice Outreach) serve as critical points of contact that can connect these veterans to evidence-based suicide prevention treatments (eg, Cognitive Behavioral Therapy for Suicide Prevention; pharmacotherapy) in the VA or the community.
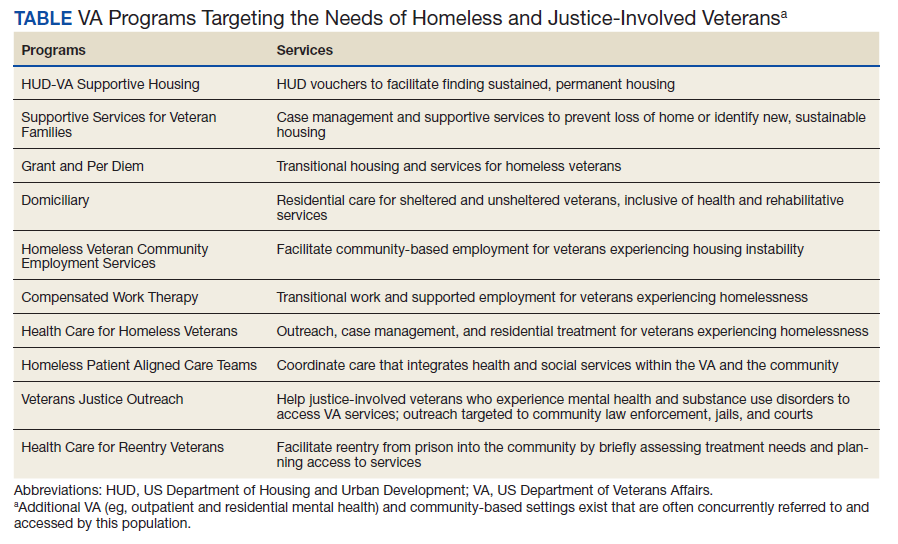
Within these programs, several suicide prevention efforts also are currently underway. In particular, the VA has mandated routine screening for suicide risk. This includes screening for the presence of elevations in acute risk (eg, suicidal intent, recent suicide attempt) and, within the context of acute risk, conducting a comprehensive risk evaluation that captures veterans’ risk and protective factors as well as access to lethal means. These clinical data are used to determine the veteran’s severity of acute and chronic risk and match them to an appropriate intervention.
Despite these ongoing efforts, several gaps in understanding exist, such as for example, elucidating the potential role of traditional VA homeless and justice-related programming in reducing risk for suicide.10 Additional research specific to suicide prevention programming among these populations also remains important.11 In particular, no examination to date has evaluated national rates of suicide risk assessment within these settings or elucidated if specific subsets of homeless and justice-involved veterans may be less likely to receive suicide risk screening. For instance, understanding whether homeless veterans accessing mental health services are more likely to be screened for suicide risk relative to homeless veterans accessing care in other VA settings (eg, emergency services). Moreover, the effectiveness of existing suicide-focused evidence-based treatments among homeless and justice-involved veterans remains unknown. Such research may reveal a need to adapt existing interventions, such as safety planning, to the idiographic needs of homeless or justice-involved veterans in order to improve effectiveness.10 Finally, social determinants of health, such as race, ethnicity, gender, and rurality may confer additional risk coupled with difficulties accessing and engaging in care within these populations.11 As such, research specific to these veteran populations and their inherent suicide prevention needs may further inform suicide prevention efforts.
Despite these gaps, it is important to acknowledge ongoing research and programmatic efforts focused on enhancing mental health and suicide prevention practices within VA settings. For example, efforts led by Temblique and colleagues acknowledge not only challenges to the execution of suicide prevention efforts in VA homeless programs, but also potential methods of enhancing care, including additional training in suicide risk screening and evaluation due to provider discomfort.12 Such quality improvement projects are paramount in their potential to identify gaps in health service delivery and thus potentially save veteran lives.
The VA currently has several programs focused on enhancing care for homeless and justice-involved veterans, and many incorporate suicide prevention initiatives. Further understanding of factors that may impact health service delivery of suicide risk assessment and intervention among these populations may be beneficial in order to enhance veteran suicide prevention efforts.
1. McCarthy JF, Bossarte RM, Katz IR, et al. Predictive modeling and concentration of the risk of suicide: implications for preventive interventions in the US Department of Veterans Affairs. Am J Public Health. 2015;105(9):1935-1942. doi:10.2105/AJPH.2015.302737
2. Holliday R, Hoffmire CA, Martin WB, Hoff RA, Monteith LL. Associations between justice involvement and PTSD and depressive symptoms, suicidal ideation, and suicide attempt among post-9/11 veterans. Psychol Trauma. 2021;13(7):730-739. doi:10.1037/tra0001038
3. Tsai J, Rosenheck RA. Risk factors for homelessness among US veterans. Epidemiol Rev. 2015;37:177-195. doi:10.1093/epirev/mxu004
4. Fischer PJ. Criminal activity among the homeless: a study of arrests in Baltimore. Hosp Community Psychiatry. 1988;39(1):46-51. doi:10.1176/ps.39.1.46
5. McCarthy B, Hagan J. Homelessness: a criminogenic situation? Br J Criminol. 1991;31(4):393–410.doi:10.1093/oxfordjournals.bjc.a048137
6. Solomon P, Draine J. Issues in serving the forensic client. Soc Work. 1995;40(1):25-33.
7. Holliday R, Forster JE, Desai A, et al. Association of lifetime homelessness and justice involvement with psychiatric symptoms, suicidal ideation, and suicide attempt among post-9/11 veterans. J Psychiatr Res. 2021;144:455-461. doi:10.1016/j.jpsychires.2021.11.007
8. Desai A, Holliday R, Borges LM, et al. Facilitating successful reentry among justice-involved veterans: the role of veteran and offender identity. J Psychiatr Pract. 2021;27(1):52-60. Published 2021 Jan 21. doi:10.1097/PRA.0000000000000520
9. Holliday R, Martin WB, Monteith LL, Clark SC, LePage JP. Suicide among justice-involved veterans: a brief overview of extant research, theoretical conceptualization, and recommendations for future research. J Soc Distress Homeless. 2021;30(1):41-49. doi: 10.1080/10530789.2019.1711306
10. Hoffberg AS, Spitzer E, Mackelprang JL, Farro SA, Brenner LA. Suicidal self-directed violence among homeless US veterans: a systematic review. Suicide Life Threat Behav. 2018;48(4):481-498. doi:10.1111/sltb.12369
11. Holliday R, Liu S, Brenner LA, et al. Preventing suicide among homeless veterans: a consensus statement by the Veterans Affairs Suicide Prevention Among Veterans Experiencing Homelessness Workgroup. Med Care. 2021;59(suppl 2):S103-S105. doi:10.1097/MLR.0000000000001399.
12. Temblique EKR, Foster K, Fujimoto J, Kopelson K, Borthick KM, et al. Addressing the mental health crisis: a one year review of a nationally-led intervention to improve suicide prevention screening at a large homeless veterans clinic. Fed Pract. 2022;39(1):12-18. doi:10.12788/fp.0215
Despite the success of several US Department of Veterans Affairs (VA) initiatives in facilitating psychosocial functioning, rehabilitation, and re-entry among veterans experiencing homelessness and/or interactions with the criminal justice system (ie, justice-involved veterans), suicide risk among these veterans remains a significant public health concern. Rates of suicide among veterans experiencing homelessness are more than double that of veterans with no history of homelessness.1 Similarly, justice-involved veterans experience myriad mental health concerns, including elevated rates of psychiatric symptoms, suicidal thoughts, and self-directed violence relative to those with no history of criminal justice involvement.2
In addition, a bidirectional relationship between criminal justice involvement and homelessness, often called the “institutional circuit,” is well established. Criminal justice involvement can directly result in difficulty finding housing.3 For example, veterans may have their lease agreement denied based solely on their history of criminogenic behavior. Moreover, criminal justice involvement can indirectly impact a veteran’s ability to maintain housing. Indeed, justice-involved veterans can experience difficulty attaining and sustaining employment, which in turn can result in financial difficulties, including inability to afford rental or mortgage payments.
Similarly, those at risk for or experiencing housing instability may resort to criminogenic behavior to survive in the context of limited psychosocial resources.4-6 For instance, a veteran experiencing homelessness may seek refuge from inclement weather in a heated apartment stairwell and subsequently be charged with trespassing. Similarly, these veterans also may resort to theft to eat or pay bills. To this end, homelessness and justice involvement are likely a deleterious cycle that is difficult for the veteran to escape.
Unfortunately, the concurrent impact of housing insecurity and criminal justice involvement often serves to further exacerbate mental health sequelae, including suicide risk (Figure).7 In addition to precipitating frustration and helplessness among veterans who are navigating these stressors, these social determinants of health can engender a perception that the veteran is a burden to those in their support system. For example, these veterans may depend on friends or family to procure housing or transportation assistance for a job, medical appointments, and court hearings.
Furthermore, homelessness and justice involvement can impact veterans’ interpersonal relationships. For instance, veterans with a history of criminal justice involvement may feel stigmatized and ostracized from their social support system. Justice-involved veterans sometimes endorse being labeled an offender, which can result in perceptions that one is poorly perceived by others and generally seen as a bad person.8 In addition, the conditions of a justice-involved veteran’s probation or parole may further exacerbate social relationships. For example, veterans with histories of engaging in intimate partner violence may lose visitation rights with their children, further reinforcing negative views of self and impacting the veterans’ family network.
As such, these homeless and justice-involved veterans may lack a meaningful social support system when navigating psychosocial stressors. Because hopelessness, burdensomeness, and perceptions that one lacks a social support network are potential drivers of suicidal self-directed violence among these populations, facilitating access to and engagement in health (eg, psychotherapy, medication management) and social (eg, case management, transitional housing) services is necessary to enhance veteran suicide prevention efforts.9
Several VA homeless and justice-related programs have been developed to meet the needs of these veterans (Table). Such programs offer direct access to health and social services capable of addressing mental health symptoms and suicide risk. Moreover, these programs support veterans at various intercepts, or points at which there is an opportunity to identify those at elevated risk and provide access to evidence-based care. For instance, VA homeless programs exist tailored toward those currently, or at risk for, experiencing homelessness. Additionally, VA justice-related programs can target intercepts prior to jail or prison, such as working with crisis intervention teams or diversion courts as well as intercepts following release, such as providing services to facilitate postincarceration reentry. Even VA programs that do not directly administer mental health intervention (eg, Grant and Per Diem, Veterans Justice Outreach) serve as critical points of contact that can connect these veterans to evidence-based suicide prevention treatments (eg, Cognitive Behavioral Therapy for Suicide Prevention; pharmacotherapy) in the VA or the community.
Within these programs, several suicide prevention efforts also are currently underway. In particular, the VA has mandated routine screening for suicide risk. This includes screening for the presence of elevations in acute risk (eg, suicidal intent, recent suicide attempt) and, within the context of acute risk, conducting a comprehensive risk evaluation that captures veterans’ risk and protective factors as well as access to lethal means. These clinical data are used to determine the veteran’s severity of acute and chronic risk and match them to an appropriate intervention.
Despite these ongoing efforts, several gaps in understanding exist, such as for example, elucidating the potential role of traditional VA homeless and justice-related programming in reducing risk for suicide.10 Additional research specific to suicide prevention programming among these populations also remains important.11 In particular, no examination to date has evaluated national rates of suicide risk assessment within these settings or elucidated if specific subsets of homeless and justice-involved veterans may be less likely to receive suicide risk screening. For instance, understanding whether homeless veterans accessing mental health services are more likely to be screened for suicide risk relative to homeless veterans accessing care in other VA settings (eg, emergency services). Moreover, the effectiveness of existing suicide-focused evidence-based treatments among homeless and justice-involved veterans remains unknown. Such research may reveal a need to adapt existing interventions, such as safety planning, to the idiographic needs of homeless or justice-involved veterans in order to improve effectiveness.10 Finally, social determinants of health, such as race, ethnicity, gender, and rurality may confer additional risk coupled with difficulties accessing and engaging in care within these populations.11 As such, research specific to these veteran populations and their inherent suicide prevention needs may further inform suicide prevention efforts.
Despite these gaps, it is important to acknowledge ongoing research and programmatic efforts focused on enhancing mental health and suicide prevention practices within VA settings. For example, efforts led by Temblique and colleagues acknowledge not only challenges to the execution of suicide prevention efforts in VA homeless programs, but also potential methods of enhancing care, including additional training in suicide risk screening and evaluation due to provider discomfort.12 Such quality improvement projects are paramount in their potential to identify gaps in health service delivery and thus potentially save veteran lives.
The VA currently has several programs focused on enhancing care for homeless and justice-involved veterans, and many incorporate suicide prevention initiatives. Further understanding of factors that may impact health service delivery of suicide risk assessment and intervention among these populations may be beneficial in order to enhance veteran suicide prevention efforts.
Despite the success of several US Department of Veterans Affairs (VA) initiatives in facilitating psychosocial functioning, rehabilitation, and re-entry among veterans experiencing homelessness and/or interactions with the criminal justice system (ie, justice-involved veterans), suicide risk among these veterans remains a significant public health concern. Rates of suicide among veterans experiencing homelessness are more than double that of veterans with no history of homelessness.1 Similarly, justice-involved veterans experience myriad mental health concerns, including elevated rates of psychiatric symptoms, suicidal thoughts, and self-directed violence relative to those with no history of criminal justice involvement.2
In addition, a bidirectional relationship between criminal justice involvement and homelessness, often called the “institutional circuit,” is well established. Criminal justice involvement can directly result in difficulty finding housing.3 For example, veterans may have their lease agreement denied based solely on their history of criminogenic behavior. Moreover, criminal justice involvement can indirectly impact a veteran’s ability to maintain housing. Indeed, justice-involved veterans can experience difficulty attaining and sustaining employment, which in turn can result in financial difficulties, including inability to afford rental or mortgage payments.
Similarly, those at risk for or experiencing housing instability may resort to criminogenic behavior to survive in the context of limited psychosocial resources.4-6 For instance, a veteran experiencing homelessness may seek refuge from inclement weather in a heated apartment stairwell and subsequently be charged with trespassing. Similarly, these veterans also may resort to theft to eat or pay bills. To this end, homelessness and justice involvement are likely a deleterious cycle that is difficult for the veteran to escape.
Unfortunately, the concurrent impact of housing insecurity and criminal justice involvement often serves to further exacerbate mental health sequelae, including suicide risk (Figure).7 In addition to precipitating frustration and helplessness among veterans who are navigating these stressors, these social determinants of health can engender a perception that the veteran is a burden to those in their support system. For example, these veterans may depend on friends or family to procure housing or transportation assistance for a job, medical appointments, and court hearings.
Furthermore, homelessness and justice involvement can impact veterans’ interpersonal relationships. For instance, veterans with a history of criminal justice involvement may feel stigmatized and ostracized from their social support system. Justice-involved veterans sometimes endorse being labeled an offender, which can result in perceptions that one is poorly perceived by others and generally seen as a bad person.8 In addition, the conditions of a justice-involved veteran’s probation or parole may further exacerbate social relationships. For example, veterans with histories of engaging in intimate partner violence may lose visitation rights with their children, further reinforcing negative views of self and impacting the veterans’ family network.
As such, these homeless and justice-involved veterans may lack a meaningful social support system when navigating psychosocial stressors. Because hopelessness, burdensomeness, and perceptions that one lacks a social support network are potential drivers of suicidal self-directed violence among these populations, facilitating access to and engagement in health (eg, psychotherapy, medication management) and social (eg, case management, transitional housing) services is necessary to enhance veteran suicide prevention efforts.9
Several VA homeless and justice-related programs have been developed to meet the needs of these veterans (Table). Such programs offer direct access to health and social services capable of addressing mental health symptoms and suicide risk. Moreover, these programs support veterans at various intercepts, or points at which there is an opportunity to identify those at elevated risk and provide access to evidence-based care. For instance, VA homeless programs exist tailored toward those currently, or at risk for, experiencing homelessness. Additionally, VA justice-related programs can target intercepts prior to jail or prison, such as working with crisis intervention teams or diversion courts as well as intercepts following release, such as providing services to facilitate postincarceration reentry. Even VA programs that do not directly administer mental health intervention (eg, Grant and Per Diem, Veterans Justice Outreach) serve as critical points of contact that can connect these veterans to evidence-based suicide prevention treatments (eg, Cognitive Behavioral Therapy for Suicide Prevention; pharmacotherapy) in the VA or the community.
Within these programs, several suicide prevention efforts also are currently underway. In particular, the VA has mandated routine screening for suicide risk. This includes screening for the presence of elevations in acute risk (eg, suicidal intent, recent suicide attempt) and, within the context of acute risk, conducting a comprehensive risk evaluation that captures veterans’ risk and protective factors as well as access to lethal means. These clinical data are used to determine the veteran’s severity of acute and chronic risk and match them to an appropriate intervention.
Despite these ongoing efforts, several gaps in understanding exist, such as for example, elucidating the potential role of traditional VA homeless and justice-related programming in reducing risk for suicide.10 Additional research specific to suicide prevention programming among these populations also remains important.11 In particular, no examination to date has evaluated national rates of suicide risk assessment within these settings or elucidated if specific subsets of homeless and justice-involved veterans may be less likely to receive suicide risk screening. For instance, understanding whether homeless veterans accessing mental health services are more likely to be screened for suicide risk relative to homeless veterans accessing care in other VA settings (eg, emergency services). Moreover, the effectiveness of existing suicide-focused evidence-based treatments among homeless and justice-involved veterans remains unknown. Such research may reveal a need to adapt existing interventions, such as safety planning, to the idiographic needs of homeless or justice-involved veterans in order to improve effectiveness.10 Finally, social determinants of health, such as race, ethnicity, gender, and rurality may confer additional risk coupled with difficulties accessing and engaging in care within these populations.11 As such, research specific to these veteran populations and their inherent suicide prevention needs may further inform suicide prevention efforts.
Despite these gaps, it is important to acknowledge ongoing research and programmatic efforts focused on enhancing mental health and suicide prevention practices within VA settings. For example, efforts led by Temblique and colleagues acknowledge not only challenges to the execution of suicide prevention efforts in VA homeless programs, but also potential methods of enhancing care, including additional training in suicide risk screening and evaluation due to provider discomfort.12 Such quality improvement projects are paramount in their potential to identify gaps in health service delivery and thus potentially save veteran lives.
The VA currently has several programs focused on enhancing care for homeless and justice-involved veterans, and many incorporate suicide prevention initiatives. Further understanding of factors that may impact health service delivery of suicide risk assessment and intervention among these populations may be beneficial in order to enhance veteran suicide prevention efforts.
1. McCarthy JF, Bossarte RM, Katz IR, et al. Predictive modeling and concentration of the risk of suicide: implications for preventive interventions in the US Department of Veterans Affairs. Am J Public Health. 2015;105(9):1935-1942. doi:10.2105/AJPH.2015.302737
2. Holliday R, Hoffmire CA, Martin WB, Hoff RA, Monteith LL. Associations between justice involvement and PTSD and depressive symptoms, suicidal ideation, and suicide attempt among post-9/11 veterans. Psychol Trauma. 2021;13(7):730-739. doi:10.1037/tra0001038
3. Tsai J, Rosenheck RA. Risk factors for homelessness among US veterans. Epidemiol Rev. 2015;37:177-195. doi:10.1093/epirev/mxu004
4. Fischer PJ. Criminal activity among the homeless: a study of arrests in Baltimore. Hosp Community Psychiatry. 1988;39(1):46-51. doi:10.1176/ps.39.1.46
5. McCarthy B, Hagan J. Homelessness: a criminogenic situation? Br J Criminol. 1991;31(4):393–410.doi:10.1093/oxfordjournals.bjc.a048137
6. Solomon P, Draine J. Issues in serving the forensic client. Soc Work. 1995;40(1):25-33.
7. Holliday R, Forster JE, Desai A, et al. Association of lifetime homelessness and justice involvement with psychiatric symptoms, suicidal ideation, and suicide attempt among post-9/11 veterans. J Psychiatr Res. 2021;144:455-461. doi:10.1016/j.jpsychires.2021.11.007
8. Desai A, Holliday R, Borges LM, et al. Facilitating successful reentry among justice-involved veterans: the role of veteran and offender identity. J Psychiatr Pract. 2021;27(1):52-60. Published 2021 Jan 21. doi:10.1097/PRA.0000000000000520
9. Holliday R, Martin WB, Monteith LL, Clark SC, LePage JP. Suicide among justice-involved veterans: a brief overview of extant research, theoretical conceptualization, and recommendations for future research. J Soc Distress Homeless. 2021;30(1):41-49. doi: 10.1080/10530789.2019.1711306
10. Hoffberg AS, Spitzer E, Mackelprang JL, Farro SA, Brenner LA. Suicidal self-directed violence among homeless US veterans: a systematic review. Suicide Life Threat Behav. 2018;48(4):481-498. doi:10.1111/sltb.12369
11. Holliday R, Liu S, Brenner LA, et al. Preventing suicide among homeless veterans: a consensus statement by the Veterans Affairs Suicide Prevention Among Veterans Experiencing Homelessness Workgroup. Med Care. 2021;59(suppl 2):S103-S105. doi:10.1097/MLR.0000000000001399.
12. Temblique EKR, Foster K, Fujimoto J, Kopelson K, Borthick KM, et al. Addressing the mental health crisis: a one year review of a nationally-led intervention to improve suicide prevention screening at a large homeless veterans clinic. Fed Pract. 2022;39(1):12-18. doi:10.12788/fp.0215
1. McCarthy JF, Bossarte RM, Katz IR, et al. Predictive modeling and concentration of the risk of suicide: implications for preventive interventions in the US Department of Veterans Affairs. Am J Public Health. 2015;105(9):1935-1942. doi:10.2105/AJPH.2015.302737
2. Holliday R, Hoffmire CA, Martin WB, Hoff RA, Monteith LL. Associations between justice involvement and PTSD and depressive symptoms, suicidal ideation, and suicide attempt among post-9/11 veterans. Psychol Trauma. 2021;13(7):730-739. doi:10.1037/tra0001038
3. Tsai J, Rosenheck RA. Risk factors for homelessness among US veterans. Epidemiol Rev. 2015;37:177-195. doi:10.1093/epirev/mxu004
4. Fischer PJ. Criminal activity among the homeless: a study of arrests in Baltimore. Hosp Community Psychiatry. 1988;39(1):46-51. doi:10.1176/ps.39.1.46
5. McCarthy B, Hagan J. Homelessness: a criminogenic situation? Br J Criminol. 1991;31(4):393–410.doi:10.1093/oxfordjournals.bjc.a048137
6. Solomon P, Draine J. Issues in serving the forensic client. Soc Work. 1995;40(1):25-33.
7. Holliday R, Forster JE, Desai A, et al. Association of lifetime homelessness and justice involvement with psychiatric symptoms, suicidal ideation, and suicide attempt among post-9/11 veterans. J Psychiatr Res. 2021;144:455-461. doi:10.1016/j.jpsychires.2021.11.007
8. Desai A, Holliday R, Borges LM, et al. Facilitating successful reentry among justice-involved veterans: the role of veteran and offender identity. J Psychiatr Pract. 2021;27(1):52-60. Published 2021 Jan 21. doi:10.1097/PRA.0000000000000520
9. Holliday R, Martin WB, Monteith LL, Clark SC, LePage JP. Suicide among justice-involved veterans: a brief overview of extant research, theoretical conceptualization, and recommendations for future research. J Soc Distress Homeless. 2021;30(1):41-49. doi: 10.1080/10530789.2019.1711306
10. Hoffberg AS, Spitzer E, Mackelprang JL, Farro SA, Brenner LA. Suicidal self-directed violence among homeless US veterans: a systematic review. Suicide Life Threat Behav. 2018;48(4):481-498. doi:10.1111/sltb.12369
11. Holliday R, Liu S, Brenner LA, et al. Preventing suicide among homeless veterans: a consensus statement by the Veterans Affairs Suicide Prevention Among Veterans Experiencing Homelessness Workgroup. Med Care. 2021;59(suppl 2):S103-S105. doi:10.1097/MLR.0000000000001399.
12. Temblique EKR, Foster K, Fujimoto J, Kopelson K, Borthick KM, et al. Addressing the mental health crisis: a one year review of a nationally-led intervention to improve suicide prevention screening at a large homeless veterans clinic. Fed Pract. 2022;39(1):12-18. doi:10.12788/fp.0215