User login
Younger patients with NSCLC tend to live longer
Younger patients with non–small cell lung cancer (NSCLC) may have better survival, despite higher rates of brain metastasis and driver mutations, according to results from a retrospective analysis.
“We carried out a comprehensive analysis of patient clinicopathologic features and clinical outcomes in both young (age ≤ 50 years) and older (age > 60 years) patients with NSCLC,” wrote Anna May Suidan of Tel Aviv University, and colleagues. The findings were published in the Journal of Global Oncology.
The researchers reviewed medical records of patients who were diagnosed with lung cancer at a large cancer treatment facility in Israel from 2010 to 2015. Patients were categorized into two groups according to age at cancer diagnosis, which was established based on tumor pathology.
Various clinical data were collected, including demographic information, history of malignancy, smoking history, histologic subtype, and survival data.
In all, 62 patients were included in the younger cohort (median age, 44.5 years) and 124 patients in the older cohort (median age, 68.0 years).
After analysis, the researchers found that younger patients had a higher incidence of brain metastasis (39% vs. 25%, respectively; P = .04), and increased rates of EGFR mutations (23% vs. 18%, respectively; P = .4) and ALK translocations (13% vs. 2%, respectively; P = .002) versus older patients.
“Our cohort, which was [composed] of white patients, demonstrated that younger patients harbored more targetable driver mutations compared with older patients (34% vs. 18%; P = .01),” the researchers wrote.
In addition, among those with a driver mutation, younger patients showed a trend toward better survival (median survival, 33 vs. 25 months, respectively; P = .4).
Two key limitations of the study were the small sample size and retrospective design.
“[These results] highlight the importance of genetic background assessments and considering lung cancer as a possible diagnosis in young symptomatic patients in clinical settings,” the researchers concluded.
No funding sources were reported. The authors reported financial affiliations with Astra Zeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Novartis, Roche, Teva Pharmaceuticals, and several others.
SOURCE: Suidan AM et al. J Glob Oncol. 2019 May 8. doi: 10.1200/JGO.18.00216.
Younger patients with non–small cell lung cancer (NSCLC) may have better survival, despite higher rates of brain metastasis and driver mutations, according to results from a retrospective analysis.
“We carried out a comprehensive analysis of patient clinicopathologic features and clinical outcomes in both young (age ≤ 50 years) and older (age > 60 years) patients with NSCLC,” wrote Anna May Suidan of Tel Aviv University, and colleagues. The findings were published in the Journal of Global Oncology.
The researchers reviewed medical records of patients who were diagnosed with lung cancer at a large cancer treatment facility in Israel from 2010 to 2015. Patients were categorized into two groups according to age at cancer diagnosis, which was established based on tumor pathology.
Various clinical data were collected, including demographic information, history of malignancy, smoking history, histologic subtype, and survival data.
In all, 62 patients were included in the younger cohort (median age, 44.5 years) and 124 patients in the older cohort (median age, 68.0 years).
After analysis, the researchers found that younger patients had a higher incidence of brain metastasis (39% vs. 25%, respectively; P = .04), and increased rates of EGFR mutations (23% vs. 18%, respectively; P = .4) and ALK translocations (13% vs. 2%, respectively; P = .002) versus older patients.
“Our cohort, which was [composed] of white patients, demonstrated that younger patients harbored more targetable driver mutations compared with older patients (34% vs. 18%; P = .01),” the researchers wrote.
In addition, among those with a driver mutation, younger patients showed a trend toward better survival (median survival, 33 vs. 25 months, respectively; P = .4).
Two key limitations of the study were the small sample size and retrospective design.
“[These results] highlight the importance of genetic background assessments and considering lung cancer as a possible diagnosis in young symptomatic patients in clinical settings,” the researchers concluded.
No funding sources were reported. The authors reported financial affiliations with Astra Zeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Novartis, Roche, Teva Pharmaceuticals, and several others.
SOURCE: Suidan AM et al. J Glob Oncol. 2019 May 8. doi: 10.1200/JGO.18.00216.
Younger patients with non–small cell lung cancer (NSCLC) may have better survival, despite higher rates of brain metastasis and driver mutations, according to results from a retrospective analysis.
“We carried out a comprehensive analysis of patient clinicopathologic features and clinical outcomes in both young (age ≤ 50 years) and older (age > 60 years) patients with NSCLC,” wrote Anna May Suidan of Tel Aviv University, and colleagues. The findings were published in the Journal of Global Oncology.
The researchers reviewed medical records of patients who were diagnosed with lung cancer at a large cancer treatment facility in Israel from 2010 to 2015. Patients were categorized into two groups according to age at cancer diagnosis, which was established based on tumor pathology.
Various clinical data were collected, including demographic information, history of malignancy, smoking history, histologic subtype, and survival data.
In all, 62 patients were included in the younger cohort (median age, 44.5 years) and 124 patients in the older cohort (median age, 68.0 years).
After analysis, the researchers found that younger patients had a higher incidence of brain metastasis (39% vs. 25%, respectively; P = .04), and increased rates of EGFR mutations (23% vs. 18%, respectively; P = .4) and ALK translocations (13% vs. 2%, respectively; P = .002) versus older patients.
“Our cohort, which was [composed] of white patients, demonstrated that younger patients harbored more targetable driver mutations compared with older patients (34% vs. 18%; P = .01),” the researchers wrote.
In addition, among those with a driver mutation, younger patients showed a trend toward better survival (median survival, 33 vs. 25 months, respectively; P = .4).
Two key limitations of the study were the small sample size and retrospective design.
“[These results] highlight the importance of genetic background assessments and considering lung cancer as a possible diagnosis in young symptomatic patients in clinical settings,” the researchers concluded.
No funding sources were reported. The authors reported financial affiliations with Astra Zeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Novartis, Roche, Teva Pharmaceuticals, and several others.
SOURCE: Suidan AM et al. J Glob Oncol. 2019 May 8. doi: 10.1200/JGO.18.00216.
FROM THE JOURNAL OF GLOBAL ONCOLOGY
Infections within first year of life predicted IBD
according to the findings of a large population-based study.
It remains unclear whether the risk reflects infections in themselves or the use of antibiotic therapy, wrote Charles N. Bernstein, MD, of the University of Manitoba, Winnipeg, and associates. Infections did not appear to be a proxy for immunodeficiency disorders, which were similarly infrequent among cases and controls, they noted. Limiting antibiotic usage, while desirable, would be difficult to do for infections as serious as many in the study. Hence, they suggested research to determine “exactly what antibiotic intake does to infant gut microflora or intestinal or systemic immune responses,” and whether giving probiotics or prebiotics after antibiotic therapy helps attenuate the risk of inflammatory bowel disease (IBD) and other autoimmune disorders. The findings were published in Gastroenterology.
IBD is probably multifactorial, but specific causal factors remain unclear. Based on mounting evidence for the role of gut dysbiosis, the researchers explored whether IBD is associated with higher rates of infections and other critical events during the neonatal period and the first year of life by comparing 825 patients with IBD and 5,999 controls matched by age, sex, and area of residence. The data source was the University of Manitoba IBD Epidemiology Database, which includes all Manitobans diagnosed with IBD from 1984 to 2010. The researchers also compared patients with 1,740 unaffected siblings.
Gastrointestinal infections, gastrointestinal disease, and abdominal pain during the first year of life did not predict subsequent IBD. Maternal IBD was the strongest risk factor (odds ratio, 4.5; 95% confidence interval, 3.1-6.7). Among neonatal events, the only significant risk factor was being in the highest versus the lowest socioeconomic quintile (OR, 1.35; 95% CI, 1.01-1.79). This association persisted during the first year of life.
Infections during the first year of life were a significant risk factor for IBD before age 10 (OR, 3.1; 95% CI, 1.1-8.8) and age 20 years (OR, 1.6; 95% CI, 1.2-2.2) in the population-based analysis. In contrast, patients and their unaffected siblings had similar rates of infection during early life. The study may have missed differences in exposures between these groups, or perhaps patients lack certain protective genes possessed by healthy siblings, the researchers wrote.
Numbers of antibiotic prescriptions during the first year and the first decade of life did not significantly differ between 33 cases and 270 controls with available data. However, there was a trend toward more antibiotics prescribed to patients versus controls.
“Together with our past reports that neither cesarean section birth nor antenatal or perinatal maternal use of antibiotics predict ultimate development of IBD, it seems that neonatal changes to the microbiome are subsumed by those occurring in the first year of life,” the investigators concluded. They recommended studying the infant gut microbiome before and for several months after infections and antibiotic exposure to determine which shifts in microbiota predict IBD onset.
The Manitoba Centre for Health Policy provided access to the Population Health Research Data Repository. Dr. Bernstein is supported by the Bingham Chair in Gastroenterology. He reported ties to AbbVie Canada, Ferring Canada, Janssen Canada, Shire Canada, Takeda Canada, Pfizer Canada, Napo Pharmaceuticals, 4D Pharma, and Mylan.
SOURCE: Bernstein CN et al. Gastroenterology. 2019 Feb 14. doi: 10.1053/j.gastro.2019.02.004.
Understanding and exploring factors that could impact inflammatory bowel disease (IBD) development is imperative. This study by Bernstein et al. evaluated whether environmental factors in the first year of life may impact subsequent diagnosis of IBD using population-based cohort data with robust and detailed health information. Maternal history of IBD was the most predictive factor in development of IBD, further evidence of a genetic component to disease pathogenesis. However, environmental factors such as high socioeconomic status within the first year of life were predictive of diagnosis of IBD later in life, possibly lending further support to the “hygiene hypothesis.”
Also, significant infections identified in the clinical setting or requiring hospitalization were predictive of subsequent IBD diagnosis. This is particularly interesting as gut microbiome perturbations increasingly take the stage as a possible pathway of significance in IBD. Could infection within the first year of life or the subsequent antibiotic use required affect the gut microbiome so significantly and perhaps permanently to affect development of later childhood or adult IBD?
Sara Horst, MD, MPH, is an associate professor of medicine in the department of gastroenterology, hepatology, and medicine at Vanderbilt University, Nashville, Tenn. She has consulted for Janssen, UCB, and Boehringer Ingelheim.
Understanding and exploring factors that could impact inflammatory bowel disease (IBD) development is imperative. This study by Bernstein et al. evaluated whether environmental factors in the first year of life may impact subsequent diagnosis of IBD using population-based cohort data with robust and detailed health information. Maternal history of IBD was the most predictive factor in development of IBD, further evidence of a genetic component to disease pathogenesis. However, environmental factors such as high socioeconomic status within the first year of life were predictive of diagnosis of IBD later in life, possibly lending further support to the “hygiene hypothesis.”
Also, significant infections identified in the clinical setting or requiring hospitalization were predictive of subsequent IBD diagnosis. This is particularly interesting as gut microbiome perturbations increasingly take the stage as a possible pathway of significance in IBD. Could infection within the first year of life or the subsequent antibiotic use required affect the gut microbiome so significantly and perhaps permanently to affect development of later childhood or adult IBD?
Sara Horst, MD, MPH, is an associate professor of medicine in the department of gastroenterology, hepatology, and medicine at Vanderbilt University, Nashville, Tenn. She has consulted for Janssen, UCB, and Boehringer Ingelheim.
Understanding and exploring factors that could impact inflammatory bowel disease (IBD) development is imperative. This study by Bernstein et al. evaluated whether environmental factors in the first year of life may impact subsequent diagnosis of IBD using population-based cohort data with robust and detailed health information. Maternal history of IBD was the most predictive factor in development of IBD, further evidence of a genetic component to disease pathogenesis. However, environmental factors such as high socioeconomic status within the first year of life were predictive of diagnosis of IBD later in life, possibly lending further support to the “hygiene hypothesis.”
Also, significant infections identified in the clinical setting or requiring hospitalization were predictive of subsequent IBD diagnosis. This is particularly interesting as gut microbiome perturbations increasingly take the stage as a possible pathway of significance in IBD. Could infection within the first year of life or the subsequent antibiotic use required affect the gut microbiome so significantly and perhaps permanently to affect development of later childhood or adult IBD?
Sara Horst, MD, MPH, is an associate professor of medicine in the department of gastroenterology, hepatology, and medicine at Vanderbilt University, Nashville, Tenn. She has consulted for Janssen, UCB, and Boehringer Ingelheim.
according to the findings of a large population-based study.
It remains unclear whether the risk reflects infections in themselves or the use of antibiotic therapy, wrote Charles N. Bernstein, MD, of the University of Manitoba, Winnipeg, and associates. Infections did not appear to be a proxy for immunodeficiency disorders, which were similarly infrequent among cases and controls, they noted. Limiting antibiotic usage, while desirable, would be difficult to do for infections as serious as many in the study. Hence, they suggested research to determine “exactly what antibiotic intake does to infant gut microflora or intestinal or systemic immune responses,” and whether giving probiotics or prebiotics after antibiotic therapy helps attenuate the risk of inflammatory bowel disease (IBD) and other autoimmune disorders. The findings were published in Gastroenterology.
IBD is probably multifactorial, but specific causal factors remain unclear. Based on mounting evidence for the role of gut dysbiosis, the researchers explored whether IBD is associated with higher rates of infections and other critical events during the neonatal period and the first year of life by comparing 825 patients with IBD and 5,999 controls matched by age, sex, and area of residence. The data source was the University of Manitoba IBD Epidemiology Database, which includes all Manitobans diagnosed with IBD from 1984 to 2010. The researchers also compared patients with 1,740 unaffected siblings.
Gastrointestinal infections, gastrointestinal disease, and abdominal pain during the first year of life did not predict subsequent IBD. Maternal IBD was the strongest risk factor (odds ratio, 4.5; 95% confidence interval, 3.1-6.7). Among neonatal events, the only significant risk factor was being in the highest versus the lowest socioeconomic quintile (OR, 1.35; 95% CI, 1.01-1.79). This association persisted during the first year of life.
Infections during the first year of life were a significant risk factor for IBD before age 10 (OR, 3.1; 95% CI, 1.1-8.8) and age 20 years (OR, 1.6; 95% CI, 1.2-2.2) in the population-based analysis. In contrast, patients and their unaffected siblings had similar rates of infection during early life. The study may have missed differences in exposures between these groups, or perhaps patients lack certain protective genes possessed by healthy siblings, the researchers wrote.
Numbers of antibiotic prescriptions during the first year and the first decade of life did not significantly differ between 33 cases and 270 controls with available data. However, there was a trend toward more antibiotics prescribed to patients versus controls.
“Together with our past reports that neither cesarean section birth nor antenatal or perinatal maternal use of antibiotics predict ultimate development of IBD, it seems that neonatal changes to the microbiome are subsumed by those occurring in the first year of life,” the investigators concluded. They recommended studying the infant gut microbiome before and for several months after infections and antibiotic exposure to determine which shifts in microbiota predict IBD onset.
The Manitoba Centre for Health Policy provided access to the Population Health Research Data Repository. Dr. Bernstein is supported by the Bingham Chair in Gastroenterology. He reported ties to AbbVie Canada, Ferring Canada, Janssen Canada, Shire Canada, Takeda Canada, Pfizer Canada, Napo Pharmaceuticals, 4D Pharma, and Mylan.
SOURCE: Bernstein CN et al. Gastroenterology. 2019 Feb 14. doi: 10.1053/j.gastro.2019.02.004.
according to the findings of a large population-based study.
It remains unclear whether the risk reflects infections in themselves or the use of antibiotic therapy, wrote Charles N. Bernstein, MD, of the University of Manitoba, Winnipeg, and associates. Infections did not appear to be a proxy for immunodeficiency disorders, which were similarly infrequent among cases and controls, they noted. Limiting antibiotic usage, while desirable, would be difficult to do for infections as serious as many in the study. Hence, they suggested research to determine “exactly what antibiotic intake does to infant gut microflora or intestinal or systemic immune responses,” and whether giving probiotics or prebiotics after antibiotic therapy helps attenuate the risk of inflammatory bowel disease (IBD) and other autoimmune disorders. The findings were published in Gastroenterology.
IBD is probably multifactorial, but specific causal factors remain unclear. Based on mounting evidence for the role of gut dysbiosis, the researchers explored whether IBD is associated with higher rates of infections and other critical events during the neonatal period and the first year of life by comparing 825 patients with IBD and 5,999 controls matched by age, sex, and area of residence. The data source was the University of Manitoba IBD Epidemiology Database, which includes all Manitobans diagnosed with IBD from 1984 to 2010. The researchers also compared patients with 1,740 unaffected siblings.
Gastrointestinal infections, gastrointestinal disease, and abdominal pain during the first year of life did not predict subsequent IBD. Maternal IBD was the strongest risk factor (odds ratio, 4.5; 95% confidence interval, 3.1-6.7). Among neonatal events, the only significant risk factor was being in the highest versus the lowest socioeconomic quintile (OR, 1.35; 95% CI, 1.01-1.79). This association persisted during the first year of life.
Infections during the first year of life were a significant risk factor for IBD before age 10 (OR, 3.1; 95% CI, 1.1-8.8) and age 20 years (OR, 1.6; 95% CI, 1.2-2.2) in the population-based analysis. In contrast, patients and their unaffected siblings had similar rates of infection during early life. The study may have missed differences in exposures between these groups, or perhaps patients lack certain protective genes possessed by healthy siblings, the researchers wrote.
Numbers of antibiotic prescriptions during the first year and the first decade of life did not significantly differ between 33 cases and 270 controls with available data. However, there was a trend toward more antibiotics prescribed to patients versus controls.
“Together with our past reports that neither cesarean section birth nor antenatal or perinatal maternal use of antibiotics predict ultimate development of IBD, it seems that neonatal changes to the microbiome are subsumed by those occurring in the first year of life,” the investigators concluded. They recommended studying the infant gut microbiome before and for several months after infections and antibiotic exposure to determine which shifts in microbiota predict IBD onset.
The Manitoba Centre for Health Policy provided access to the Population Health Research Data Repository. Dr. Bernstein is supported by the Bingham Chair in Gastroenterology. He reported ties to AbbVie Canada, Ferring Canada, Janssen Canada, Shire Canada, Takeda Canada, Pfizer Canada, Napo Pharmaceuticals, 4D Pharma, and Mylan.
SOURCE: Bernstein CN et al. Gastroenterology. 2019 Feb 14. doi: 10.1053/j.gastro.2019.02.004.
FROM GASTROENTEROLOGY
Suicide Attempts Among Persons with Migraine
Persons with migraine had a much higher prevalence of ever attempting suicide than those without migraine, a recent study found. The study, a nationally representative analysis of the 2012 Canadian Community Health Survey – Mental Health, identified the gender-specific prevalence of suicide attempts among those with migraine and examined the factors associated with suicide attempts among migraineurs. Among the details:
- Of 21,744 respondents, 2223 had migraine.
- Those with migraine had a much higher prevalence of ever attempting suicide vs those without migraine (men: 7.5% vs 1.9%; women: 9.3% vs 2.7%).
- Among migraineurs, the odds of suicide attempts were higher among poorer respondents, those in chronic pain and those with a history of childhood adversities, substance dependence and/or mental illness.
Fuller-Thomson E, Hodgins GA. Suicide attempts among those with migraine: Finding from a nationally representative Canadian study. [Published online ahead of print April 4, 2019]. Arch Suicide Res. doi: 10.1080/13811118.2019.1578710.
Persons with migraine had a much higher prevalence of ever attempting suicide than those without migraine, a recent study found. The study, a nationally representative analysis of the 2012 Canadian Community Health Survey – Mental Health, identified the gender-specific prevalence of suicide attempts among those with migraine and examined the factors associated with suicide attempts among migraineurs. Among the details:
- Of 21,744 respondents, 2223 had migraine.
- Those with migraine had a much higher prevalence of ever attempting suicide vs those without migraine (men: 7.5% vs 1.9%; women: 9.3% vs 2.7%).
- Among migraineurs, the odds of suicide attempts were higher among poorer respondents, those in chronic pain and those with a history of childhood adversities, substance dependence and/or mental illness.
Fuller-Thomson E, Hodgins GA. Suicide attempts among those with migraine: Finding from a nationally representative Canadian study. [Published online ahead of print April 4, 2019]. Arch Suicide Res. doi: 10.1080/13811118.2019.1578710.
Persons with migraine had a much higher prevalence of ever attempting suicide than those without migraine, a recent study found. The study, a nationally representative analysis of the 2012 Canadian Community Health Survey – Mental Health, identified the gender-specific prevalence of suicide attempts among those with migraine and examined the factors associated with suicide attempts among migraineurs. Among the details:
- Of 21,744 respondents, 2223 had migraine.
- Those with migraine had a much higher prevalence of ever attempting suicide vs those without migraine (men: 7.5% vs 1.9%; women: 9.3% vs 2.7%).
- Among migraineurs, the odds of suicide attempts were higher among poorer respondents, those in chronic pain and those with a history of childhood adversities, substance dependence and/or mental illness.
Fuller-Thomson E, Hodgins GA. Suicide attempts among those with migraine: Finding from a nationally representative Canadian study. [Published online ahead of print April 4, 2019]. Arch Suicide Res. doi: 10.1080/13811118.2019.1578710.
Treatment Response Using Pharmacy Register in Migraine
Pharmacy databases are a valid source for identification of treatment response in migraine, a recent study found. In a clinical cohort, 1913 migraineurs were interviewed using a semi-structured interview to retrieve treatment response data for acute and prophylactic migraine drugs. Researchers assessed whether number or purchases at different thresholds could predict the specificity and sensitivity of treatment response. The found:
- Purchase of drugs was significantly associated with treatment response.
- Specifically, for migraine drugs, it was concluded that 10 purchases of triptans, or 4 purchases of prophylactic drugs, are sufficient to predict a positive treatment response.
- In the Danish pharmacy database, 73% of migraine patients had purchased 10 or more triptans, while 55% to 63% had purchased 1 or more of the 4 prophylactic drugs.
Hansen TF, Chalmer MA, Haspang TM, Kogelman L, Olesen J. Predicting treatment response using pharmacy register in migraine. J Headache Pain. 2019;20(1):31. doi:10.1186/s10194-019-0987-y.
Pharmacy databases are a valid source for identification of treatment response in migraine, a recent study found. In a clinical cohort, 1913 migraineurs were interviewed using a semi-structured interview to retrieve treatment response data for acute and prophylactic migraine drugs. Researchers assessed whether number or purchases at different thresholds could predict the specificity and sensitivity of treatment response. The found:
- Purchase of drugs was significantly associated with treatment response.
- Specifically, for migraine drugs, it was concluded that 10 purchases of triptans, or 4 purchases of prophylactic drugs, are sufficient to predict a positive treatment response.
- In the Danish pharmacy database, 73% of migraine patients had purchased 10 or more triptans, while 55% to 63% had purchased 1 or more of the 4 prophylactic drugs.
Hansen TF, Chalmer MA, Haspang TM, Kogelman L, Olesen J. Predicting treatment response using pharmacy register in migraine. J Headache Pain. 2019;20(1):31. doi:10.1186/s10194-019-0987-y.
Pharmacy databases are a valid source for identification of treatment response in migraine, a recent study found. In a clinical cohort, 1913 migraineurs were interviewed using a semi-structured interview to retrieve treatment response data for acute and prophylactic migraine drugs. Researchers assessed whether number or purchases at different thresholds could predict the specificity and sensitivity of treatment response. The found:
- Purchase of drugs was significantly associated with treatment response.
- Specifically, for migraine drugs, it was concluded that 10 purchases of triptans, or 4 purchases of prophylactic drugs, are sufficient to predict a positive treatment response.
- In the Danish pharmacy database, 73% of migraine patients had purchased 10 or more triptans, while 55% to 63% had purchased 1 or more of the 4 prophylactic drugs.
Hansen TF, Chalmer MA, Haspang TM, Kogelman L, Olesen J. Predicting treatment response using pharmacy register in migraine. J Headache Pain. 2019;20(1):31. doi:10.1186/s10194-019-0987-y.
Sleep Disturbances and Headaches in US Adolescents
Adolescents with migraine headaches have shorter sleep duration and wake up earlier compared to those without migraine, a new study found. The study sample included 10,123 adolescents in the National Comorbidity Survey – Adolescent Supplement, a face-to-face survey of adolescents aged 13 to 18 years in the continental United States. The cross-sectional study examined the associations of sleep patterns, symptoms, and disorders with specific headache subtypes in this population. Researchers found:
- No significant difference in bedtime between youth with and without headache was reported.
- Those with any headache, particularly migraine, had significantly more sleep disturbances than those without headache.
- Youth with migraine and aura were more likely to report difficultly maintaining sleep, early morning awakening, daytime fatigue, and persistent insomnia symptoms vs those with migraine without aura.
Lateef T, Witonsky K, He J, Merikangas KR. Headaches and sleep duration problems in US adolescents: Findings from the National Comorbidity Survey – Adolescent Supplement (NCS-A). [Published online ahead of print April 13, 2019]. Cephalalgia. doi:10.1177/0333102419835466.
Adolescents with migraine headaches have shorter sleep duration and wake up earlier compared to those without migraine, a new study found. The study sample included 10,123 adolescents in the National Comorbidity Survey – Adolescent Supplement, a face-to-face survey of adolescents aged 13 to 18 years in the continental United States. The cross-sectional study examined the associations of sleep patterns, symptoms, and disorders with specific headache subtypes in this population. Researchers found:
- No significant difference in bedtime between youth with and without headache was reported.
- Those with any headache, particularly migraine, had significantly more sleep disturbances than those without headache.
- Youth with migraine and aura were more likely to report difficultly maintaining sleep, early morning awakening, daytime fatigue, and persistent insomnia symptoms vs those with migraine without aura.
Lateef T, Witonsky K, He J, Merikangas KR. Headaches and sleep duration problems in US adolescents: Findings from the National Comorbidity Survey – Adolescent Supplement (NCS-A). [Published online ahead of print April 13, 2019]. Cephalalgia. doi:10.1177/0333102419835466.
Adolescents with migraine headaches have shorter sleep duration and wake up earlier compared to those without migraine, a new study found. The study sample included 10,123 adolescents in the National Comorbidity Survey – Adolescent Supplement, a face-to-face survey of adolescents aged 13 to 18 years in the continental United States. The cross-sectional study examined the associations of sleep patterns, symptoms, and disorders with specific headache subtypes in this population. Researchers found:
- No significant difference in bedtime between youth with and without headache was reported.
- Those with any headache, particularly migraine, had significantly more sleep disturbances than those without headache.
- Youth with migraine and aura were more likely to report difficultly maintaining sleep, early morning awakening, daytime fatigue, and persistent insomnia symptoms vs those with migraine without aura.
Lateef T, Witonsky K, He J, Merikangas KR. Headaches and sleep duration problems in US adolescents: Findings from the National Comorbidity Survey – Adolescent Supplement (NCS-A). [Published online ahead of print April 13, 2019]. Cephalalgia. doi:10.1177/0333102419835466.
Walk-in ultrasound helps to avoid unnecessary steroids for giant cell arteritis
BIRMINGHAM, England – More than half of all patients referred to a fast-track giant cell arteritis (GCA) clinic that offers a walk-in ultrasonography service avoided use of glucocorticoids, according to a report given at the annual conference of the British Society for Rheumatology.
The clinic, an initiative run by the University Hospital Coventry and Warwickshire (UHCW) NHS Trust for the past 6 years, provides same-day diagnosis and treatment for suspected GCA.
“Walk-in ultrasound helps to avoid steroids completely in a significant proportion of patients,” said study author and presenter Shirish Dubey, MBBS, a consultant rheumatologist at the UHCW NHS Trust. Of 652 patients seen at the UHCW GCA fast-track clinic between 2014 and 2017, 143 (22%) were diagnosed with GCA. Over 400 had not been exposed to glucocorticoids and 369 (57%) were able to avoid unnecessary glucocorticoid use in the cohort, Dr. Dubey reported.
The old NHS paradigm for managing patients with suspected GCA was that when they presented to their primary care physicians, they would be started on immediate glucocorticoid therapy while waiting for an urgent specialist referral. However, that referral could take anywhere from a couple of days to a couple of weeks to happen, Dr. Dubey explained. Patients would then undergo possible temporal artery biopsy (TAB) and only then, following confirmation of a GCA diagnosis, would a management plan be agreed upon.
UCHW introduced its fast-track pathway for the diagnosis of GCA in mid-2013. The pathway called for patients with suspected GCA aged 50 years or older who had two or more features present, such as an abrupt, new-onset headache or facial pain, scalp pain and tenderness, jaw claudication, or visual symptoms. Primary care physicians could make urgent referrals to the service via an on-call rheumatology trainee or ophthalmology senior house officer.
“Patients are normally steroid-naive and seen on the same day,” Dr. Dubey said. Doppler ultrasound of the temporal artery results in around 80% of diagnoses, with TAB still needed in some cases.
One of the downsides of the fast-track process perhaps is the increasing number of referrals. “One thing we find is that we have become a glorified headache service,” Dr. Dubey said. However, many patients do not have GCA and, when there is a low clinical probability and the ultrasound is negative, the patient is usually reassured and discharged with no need for glucocorticoids. Although the number of referrals have increased – 98 patients in 2014, 154 in 2015, 123 in 2016, and 277 in 2017 – the number of those diagnosed with GCA has remained around the same.
To see how ultrasound was faring in real-life practice, the UHCW NHS Trust team compared Doppler ultrasound findings against the final clinical diagnosis for the period 2014 to 2017. A sensitivity of just under 48% and specificity of 98% was recorded. The positive and negative predictive values were 87% and 88%, respectively.
The specificity of ultrasound was lower than that reported previously in the literature, the UHCW NHS Trust team pointed out in its abstract, but it does compare similarly with other real-world studies. The use of glucocorticoids affected the ultrasound results, with better sensitivity (55%) when these drugs were not used prior to the scan.
The use of TAB versus a clinical diagnosis in 100 patients seen over the same time period showed it had a sensitivity of 37% and a specificity of 100%, with positive and negative predictive values of 100% and 62%. The sensitivity of TAB is again low, Dr. Dubey said, but that could be because TAB is performed only when the diagnosis is uncertain.
This was an unselected cohort of patients, but overall there were good positive and negative predictive values. The UHCW NHS Trust team suggested that ultrasound can assist and reassure clinicians trying to diagnose or exclude GCA in their patients.
Regular multidisciplinary team meetings including rheumatology, ophthalmology, and vascular Doppler physiologists are key to the fast-track service, Dr. Dubey pointed out.
Despite the shortcomings of the retrospective study, Dr. Dubey stressed that the team was confident that none of the patients who had been ruled out as having GCA were subsequently diagnosed as having GCA.
Importantly, he said, the use of ultrasound had made a big difference in cost; the group plans to formally evaluate costs of ultrasound versus TAB.
The study received no commercial funding. Dr. Dubey had no conflicts of interest to disclose.
SOURCE: Pinnell J et al. Rheumatology. 2019;58(suppl 3):Abstract 038.
BIRMINGHAM, England – More than half of all patients referred to a fast-track giant cell arteritis (GCA) clinic that offers a walk-in ultrasonography service avoided use of glucocorticoids, according to a report given at the annual conference of the British Society for Rheumatology.
The clinic, an initiative run by the University Hospital Coventry and Warwickshire (UHCW) NHS Trust for the past 6 years, provides same-day diagnosis and treatment for suspected GCA.
“Walk-in ultrasound helps to avoid steroids completely in a significant proportion of patients,” said study author and presenter Shirish Dubey, MBBS, a consultant rheumatologist at the UHCW NHS Trust. Of 652 patients seen at the UHCW GCA fast-track clinic between 2014 and 2017, 143 (22%) were diagnosed with GCA. Over 400 had not been exposed to glucocorticoids and 369 (57%) were able to avoid unnecessary glucocorticoid use in the cohort, Dr. Dubey reported.
The old NHS paradigm for managing patients with suspected GCA was that when they presented to their primary care physicians, they would be started on immediate glucocorticoid therapy while waiting for an urgent specialist referral. However, that referral could take anywhere from a couple of days to a couple of weeks to happen, Dr. Dubey explained. Patients would then undergo possible temporal artery biopsy (TAB) and only then, following confirmation of a GCA diagnosis, would a management plan be agreed upon.
UCHW introduced its fast-track pathway for the diagnosis of GCA in mid-2013. The pathway called for patients with suspected GCA aged 50 years or older who had two or more features present, such as an abrupt, new-onset headache or facial pain, scalp pain and tenderness, jaw claudication, or visual symptoms. Primary care physicians could make urgent referrals to the service via an on-call rheumatology trainee or ophthalmology senior house officer.
“Patients are normally steroid-naive and seen on the same day,” Dr. Dubey said. Doppler ultrasound of the temporal artery results in around 80% of diagnoses, with TAB still needed in some cases.
One of the downsides of the fast-track process perhaps is the increasing number of referrals. “One thing we find is that we have become a glorified headache service,” Dr. Dubey said. However, many patients do not have GCA and, when there is a low clinical probability and the ultrasound is negative, the patient is usually reassured and discharged with no need for glucocorticoids. Although the number of referrals have increased – 98 patients in 2014, 154 in 2015, 123 in 2016, and 277 in 2017 – the number of those diagnosed with GCA has remained around the same.
To see how ultrasound was faring in real-life practice, the UHCW NHS Trust team compared Doppler ultrasound findings against the final clinical diagnosis for the period 2014 to 2017. A sensitivity of just under 48% and specificity of 98% was recorded. The positive and negative predictive values were 87% and 88%, respectively.
The specificity of ultrasound was lower than that reported previously in the literature, the UHCW NHS Trust team pointed out in its abstract, but it does compare similarly with other real-world studies. The use of glucocorticoids affected the ultrasound results, with better sensitivity (55%) when these drugs were not used prior to the scan.
The use of TAB versus a clinical diagnosis in 100 patients seen over the same time period showed it had a sensitivity of 37% and a specificity of 100%, with positive and negative predictive values of 100% and 62%. The sensitivity of TAB is again low, Dr. Dubey said, but that could be because TAB is performed only when the diagnosis is uncertain.
This was an unselected cohort of patients, but overall there were good positive and negative predictive values. The UHCW NHS Trust team suggested that ultrasound can assist and reassure clinicians trying to diagnose or exclude GCA in their patients.
Regular multidisciplinary team meetings including rheumatology, ophthalmology, and vascular Doppler physiologists are key to the fast-track service, Dr. Dubey pointed out.
Despite the shortcomings of the retrospective study, Dr. Dubey stressed that the team was confident that none of the patients who had been ruled out as having GCA were subsequently diagnosed as having GCA.
Importantly, he said, the use of ultrasound had made a big difference in cost; the group plans to formally evaluate costs of ultrasound versus TAB.
The study received no commercial funding. Dr. Dubey had no conflicts of interest to disclose.
SOURCE: Pinnell J et al. Rheumatology. 2019;58(suppl 3):Abstract 038.
BIRMINGHAM, England – More than half of all patients referred to a fast-track giant cell arteritis (GCA) clinic that offers a walk-in ultrasonography service avoided use of glucocorticoids, according to a report given at the annual conference of the British Society for Rheumatology.
The clinic, an initiative run by the University Hospital Coventry and Warwickshire (UHCW) NHS Trust for the past 6 years, provides same-day diagnosis and treatment for suspected GCA.
“Walk-in ultrasound helps to avoid steroids completely in a significant proportion of patients,” said study author and presenter Shirish Dubey, MBBS, a consultant rheumatologist at the UHCW NHS Trust. Of 652 patients seen at the UHCW GCA fast-track clinic between 2014 and 2017, 143 (22%) were diagnosed with GCA. Over 400 had not been exposed to glucocorticoids and 369 (57%) were able to avoid unnecessary glucocorticoid use in the cohort, Dr. Dubey reported.
The old NHS paradigm for managing patients with suspected GCA was that when they presented to their primary care physicians, they would be started on immediate glucocorticoid therapy while waiting for an urgent specialist referral. However, that referral could take anywhere from a couple of days to a couple of weeks to happen, Dr. Dubey explained. Patients would then undergo possible temporal artery biopsy (TAB) and only then, following confirmation of a GCA diagnosis, would a management plan be agreed upon.
UCHW introduced its fast-track pathway for the diagnosis of GCA in mid-2013. The pathway called for patients with suspected GCA aged 50 years or older who had two or more features present, such as an abrupt, new-onset headache or facial pain, scalp pain and tenderness, jaw claudication, or visual symptoms. Primary care physicians could make urgent referrals to the service via an on-call rheumatology trainee or ophthalmology senior house officer.
“Patients are normally steroid-naive and seen on the same day,” Dr. Dubey said. Doppler ultrasound of the temporal artery results in around 80% of diagnoses, with TAB still needed in some cases.
One of the downsides of the fast-track process perhaps is the increasing number of referrals. “One thing we find is that we have become a glorified headache service,” Dr. Dubey said. However, many patients do not have GCA and, when there is a low clinical probability and the ultrasound is negative, the patient is usually reassured and discharged with no need for glucocorticoids. Although the number of referrals have increased – 98 patients in 2014, 154 in 2015, 123 in 2016, and 277 in 2017 – the number of those diagnosed with GCA has remained around the same.
To see how ultrasound was faring in real-life practice, the UHCW NHS Trust team compared Doppler ultrasound findings against the final clinical diagnosis for the period 2014 to 2017. A sensitivity of just under 48% and specificity of 98% was recorded. The positive and negative predictive values were 87% and 88%, respectively.
The specificity of ultrasound was lower than that reported previously in the literature, the UHCW NHS Trust team pointed out in its abstract, but it does compare similarly with other real-world studies. The use of glucocorticoids affected the ultrasound results, with better sensitivity (55%) when these drugs were not used prior to the scan.
The use of TAB versus a clinical diagnosis in 100 patients seen over the same time period showed it had a sensitivity of 37% and a specificity of 100%, with positive and negative predictive values of 100% and 62%. The sensitivity of TAB is again low, Dr. Dubey said, but that could be because TAB is performed only when the diagnosis is uncertain.
This was an unselected cohort of patients, but overall there were good positive and negative predictive values. The UHCW NHS Trust team suggested that ultrasound can assist and reassure clinicians trying to diagnose or exclude GCA in their patients.
Regular multidisciplinary team meetings including rheumatology, ophthalmology, and vascular Doppler physiologists are key to the fast-track service, Dr. Dubey pointed out.
Despite the shortcomings of the retrospective study, Dr. Dubey stressed that the team was confident that none of the patients who had been ruled out as having GCA were subsequently diagnosed as having GCA.
Importantly, he said, the use of ultrasound had made a big difference in cost; the group plans to formally evaluate costs of ultrasound versus TAB.
The study received no commercial funding. Dr. Dubey had no conflicts of interest to disclose.
SOURCE: Pinnell J et al. Rheumatology. 2019;58(suppl 3):Abstract 038.
REPORTING FROM BSR 2019
Are ObGyns knowledgeable about the risk factors for hepatitis C virus in pregnancy?
The American College of Obstetricians and Gynecologists (ACOG) recommends risk-based screening for hepatitis C virus (HCV) infection during pregnancy.1 However, the prevalence of HCV among pregnant women in the United States is on the rise. From 2009 to 2014, HCV infection present at delivery increased 89%.2 In addition, the risk of an HCV-infected mother transmitting the infection to her baby is about 4% to 7% per pregnancy.3 Currently, the Infectious Diseases Society of America and the American Association for the Study of Liver Diseases recommend universal HCV screening in pregnancy.4
Researchers at Tufts Medical Center in Boston, Massachusetts, a tertiary care center, presented survey findings on HCV screening among ObGyns at ACOG’s 2019 Annual Clinical and Scientific Meeting in Nashville, Tennessee.5 Katherine G. Koniares, MD, and colleagues sought to assess the opinions and clinical practices of ObGyns by emailing a 10-question electronic survey to providers. A total of 38 of 41 providers (93%) responded to the survey.
Survey results show lack of knowledge on risk factors
In response to the question, “Which pregnant patients do you believe should be screened for HCV,” 43.2% of providers stated “all pregnant women,” while 54.1% said “only pregnant women with risk factors for HCV.” A small percentage (2.7%) responded that they were not sure.
Providers also were asked which patients in their practice they screen for HCV. In response, 77.8% stated that they screen pregnant women for HCV based on risk factors, while 13.9% screen all pregnant patients for HCV; 8.3% do not screen for HCV.
When asked which risk factors providers use to screen patients for HCV, 42% to 85% said they screen for each indicated risk factor. Only 36% of providers, however, correctly identified all risk factors (for example, receiving blood products from donors who later tested positive for HCV; unexplained liver disease; and percutaneous/parenteral exposures in an unregulated setting, such as receiving tattoos outside a licensed parlor).
Further study needed on universal screening
The researchers assert that risk-based screening for HCV is not effective and that further research on universal HCV screening in pregnant patients is needed.
- American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 86: Viral hepatitis in pregnancy. Obstet Gynecol. 2007;110:941-956.
- Patrick SW, Bauer AM, Warren MD, et al. Hepatitis C virus infection among women giving birth—Tennessee and the United States, 2009-2014. MMWR Morbid Mortal Weekly Rep. 2017;66:470-473.
- Koneru A, Nelson N, Hariri S, et al. Increased hepatitis C virus (HCV) detection in women of childbearing age and potential risk for vertical transmission—United States and Kentucky, 2011-2014. MMWR Morbid Mortal Weekly Rep. 2016;65:705-710.
- American Association for the Study of Liver Diseases (AASLD) and the Infectious Diseases Society of America (IDSA). Recommendations for testing, management, and treating, hepatitis C. HCV testing and linkage to care. https://www.hcvguidelines.org/.
- Koniares KG, Fadlallah H, Kolettis DS, et al. A survey of hepatitis C virus (HCV) screening in pregnancy among ObGyns at a tertiary care center. Poster presented at: American College of Obstetricians and Gynecologists Annual Clinical and Scientific Meeting; May 3-6, 2019; Nashville, TN.
The American College of Obstetricians and Gynecologists (ACOG) recommends risk-based screening for hepatitis C virus (HCV) infection during pregnancy.1 However, the prevalence of HCV among pregnant women in the United States is on the rise. From 2009 to 2014, HCV infection present at delivery increased 89%.2 In addition, the risk of an HCV-infected mother transmitting the infection to her baby is about 4% to 7% per pregnancy.3 Currently, the Infectious Diseases Society of America and the American Association for the Study of Liver Diseases recommend universal HCV screening in pregnancy.4
Researchers at Tufts Medical Center in Boston, Massachusetts, a tertiary care center, presented survey findings on HCV screening among ObGyns at ACOG’s 2019 Annual Clinical and Scientific Meeting in Nashville, Tennessee.5 Katherine G. Koniares, MD, and colleagues sought to assess the opinions and clinical practices of ObGyns by emailing a 10-question electronic survey to providers. A total of 38 of 41 providers (93%) responded to the survey.
Survey results show lack of knowledge on risk factors
In response to the question, “Which pregnant patients do you believe should be screened for HCV,” 43.2% of providers stated “all pregnant women,” while 54.1% said “only pregnant women with risk factors for HCV.” A small percentage (2.7%) responded that they were not sure.
Providers also were asked which patients in their practice they screen for HCV. In response, 77.8% stated that they screen pregnant women for HCV based on risk factors, while 13.9% screen all pregnant patients for HCV; 8.3% do not screen for HCV.
When asked which risk factors providers use to screen patients for HCV, 42% to 85% said they screen for each indicated risk factor. Only 36% of providers, however, correctly identified all risk factors (for example, receiving blood products from donors who later tested positive for HCV; unexplained liver disease; and percutaneous/parenteral exposures in an unregulated setting, such as receiving tattoos outside a licensed parlor).
Further study needed on universal screening
The researchers assert that risk-based screening for HCV is not effective and that further research on universal HCV screening in pregnant patients is needed.
The American College of Obstetricians and Gynecologists (ACOG) recommends risk-based screening for hepatitis C virus (HCV) infection during pregnancy.1 However, the prevalence of HCV among pregnant women in the United States is on the rise. From 2009 to 2014, HCV infection present at delivery increased 89%.2 In addition, the risk of an HCV-infected mother transmitting the infection to her baby is about 4% to 7% per pregnancy.3 Currently, the Infectious Diseases Society of America and the American Association for the Study of Liver Diseases recommend universal HCV screening in pregnancy.4
Researchers at Tufts Medical Center in Boston, Massachusetts, a tertiary care center, presented survey findings on HCV screening among ObGyns at ACOG’s 2019 Annual Clinical and Scientific Meeting in Nashville, Tennessee.5 Katherine G. Koniares, MD, and colleagues sought to assess the opinions and clinical practices of ObGyns by emailing a 10-question electronic survey to providers. A total of 38 of 41 providers (93%) responded to the survey.
Survey results show lack of knowledge on risk factors
In response to the question, “Which pregnant patients do you believe should be screened for HCV,” 43.2% of providers stated “all pregnant women,” while 54.1% said “only pregnant women with risk factors for HCV.” A small percentage (2.7%) responded that they were not sure.
Providers also were asked which patients in their practice they screen for HCV. In response, 77.8% stated that they screen pregnant women for HCV based on risk factors, while 13.9% screen all pregnant patients for HCV; 8.3% do not screen for HCV.
When asked which risk factors providers use to screen patients for HCV, 42% to 85% said they screen for each indicated risk factor. Only 36% of providers, however, correctly identified all risk factors (for example, receiving blood products from donors who later tested positive for HCV; unexplained liver disease; and percutaneous/parenteral exposures in an unregulated setting, such as receiving tattoos outside a licensed parlor).
Further study needed on universal screening
The researchers assert that risk-based screening for HCV is not effective and that further research on universal HCV screening in pregnant patients is needed.
- American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 86: Viral hepatitis in pregnancy. Obstet Gynecol. 2007;110:941-956.
- Patrick SW, Bauer AM, Warren MD, et al. Hepatitis C virus infection among women giving birth—Tennessee and the United States, 2009-2014. MMWR Morbid Mortal Weekly Rep. 2017;66:470-473.
- Koneru A, Nelson N, Hariri S, et al. Increased hepatitis C virus (HCV) detection in women of childbearing age and potential risk for vertical transmission—United States and Kentucky, 2011-2014. MMWR Morbid Mortal Weekly Rep. 2016;65:705-710.
- American Association for the Study of Liver Diseases (AASLD) and the Infectious Diseases Society of America (IDSA). Recommendations for testing, management, and treating, hepatitis C. HCV testing and linkage to care. https://www.hcvguidelines.org/.
- Koniares KG, Fadlallah H, Kolettis DS, et al. A survey of hepatitis C virus (HCV) screening in pregnancy among ObGyns at a tertiary care center. Poster presented at: American College of Obstetricians and Gynecologists Annual Clinical and Scientific Meeting; May 3-6, 2019; Nashville, TN.
- American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 86: Viral hepatitis in pregnancy. Obstet Gynecol. 2007;110:941-956.
- Patrick SW, Bauer AM, Warren MD, et al. Hepatitis C virus infection among women giving birth—Tennessee and the United States, 2009-2014. MMWR Morbid Mortal Weekly Rep. 2017;66:470-473.
- Koneru A, Nelson N, Hariri S, et al. Increased hepatitis C virus (HCV) detection in women of childbearing age and potential risk for vertical transmission—United States and Kentucky, 2011-2014. MMWR Morbid Mortal Weekly Rep. 2016;65:705-710.
- American Association for the Study of Liver Diseases (AASLD) and the Infectious Diseases Society of America (IDSA). Recommendations for testing, management, and treating, hepatitis C. HCV testing and linkage to care. https://www.hcvguidelines.org/.
- Koniares KG, Fadlallah H, Kolettis DS, et al. A survey of hepatitis C virus (HCV) screening in pregnancy among ObGyns at a tertiary care center. Poster presented at: American College of Obstetricians and Gynecologists Annual Clinical and Scientific Meeting; May 3-6, 2019; Nashville, TN.
Management of Late Pulmonary Complications After Hematopoietic Stem Cell Transplantation
Hematopoietic stem cell transplantation (HSCT) is increasingly being used to treat hematologic malignancies as well as nonmalignant diseases and solid tumors. Over the past 2 decades overall survival following transplant and transplant-related mortality have improved.1 With this increased survival, there is a need to focus on late complications after transplantation. Pulmonary complications are a common but sometimes underrecognized cause of late morbidity and mortality in HSCT patients. This article, the second of 2 articles on post-HSCT pulmonary complications, reviews late-onset complications, with a focus on the evaluation and treatment of bronchiolitis obliterans syndrome (BOS), one of the most common and serious late pulmonary complications in HSCT patients. The first article reviewed the management of early-onset pulmonary complications and included a basic overview of stem cell transplantation, discussion of factors associated with pulmonary complications, and a review of methods for assessing pretransplant risk for pulmonary complications in patients undergoing HSCT.2
Case Presentation
A 40-year-old white woman with a history of acute myeloid leukemia status post peripheral blood stem cell transplant presents with dyspnea on exertion, which she states started about 1 month ago and now is limiting her with even 1 flight of stairs. She also complains of mild dry cough and a 4- to 5-lb weight loss over the past 1 to 2 months. She has an occasional runny nose, but denies gastroesophageal reflux, fevers, chills, or night sweats. She has a history of matched related sibling donor transplant with busulfan and cyclophosphamide conditioning 1 year prior to presentation. She has had significant graft-versus-host disease (GVHD), affecting the liver, gastrointestinal tract, skin, and eyes.
On physical examination, heart rate is 110 beats/min, respiratory rate is 16 breaths/min, blood pressure is 92/58 mm Hg, and the patient is afebrile. Eye exam reveals scleral injection, mouth shows dry mucous membranes with a few white plaques, and the skin has chronic changes with a rash over both arms. Cardiac exam reveals tachycardia but regular rhythm and there are no murmurs, rubs, or gallops. Lungs are clear bilaterally and abdomen shows no organomegaly.
Laboratory exam shows a white blood cell count of 7800 cells/μL, hemoglobin level of 12.4 g/dL, and platelet count of 186 × 103/μL. Liver enzymes are mildly elevated. Chest radiograph shows clear lung fields bilaterally.
- What is the differential in this patient with dyspnea 1 year after transplantation?
Late pulmonary complications are generally accepted as those occurring more than 100 days post transplant. This period of time is characterized by chronic GVHD and impaired cellular and humoral immunity. Results of longitudinal studies of infections in adult HSCT patients suggest that special attention should be paid to allogeneic HSCT recipients for post-engraftment infectious pulmonary complications.3 Encapsulated bacteria such as Haemophilus influenzae and Streptococcus pneumoniae are the most frequent bacterial organisms causing late infectious pulmonary complications. Nontuberculous mycobacteria and Nocardia should also be considered. Depending upon geographic location, social and occupational risk factors, and prevalence, tuberculosis should also enter the differential.
There are many noninfectious late-onset pulmonary complications after HSCT. Unfortunately, the literature has divided pulmonary complications after HSCT using a range of criteria and classifications based upon timing, predominant pulmonary function test (PFT) findings, and etiology. These include early versus late, obstructive versus restrictive, and infectious versus noninfectious, which makes a comprehensive literature review of late pulmonary complications difficult. The most common noninfectious late-onset complications are bronchiolitis obliterans, cryptogenic organizing pneumonia (previously referred to as bronchiolitis obliterans organizing pneumonia, or BOOP), and interstitial pneumonia. Other rarely reported complications include eosinophilic pneumonia, pulmonary alveolar proteinosis, air leak syndrome, and pulmonary hypertension.
Case Continued
Because the patient does not have symptoms of infection, PFTs are obtained. Pretransplant PFTs and current PFTs are shown in Table 1. 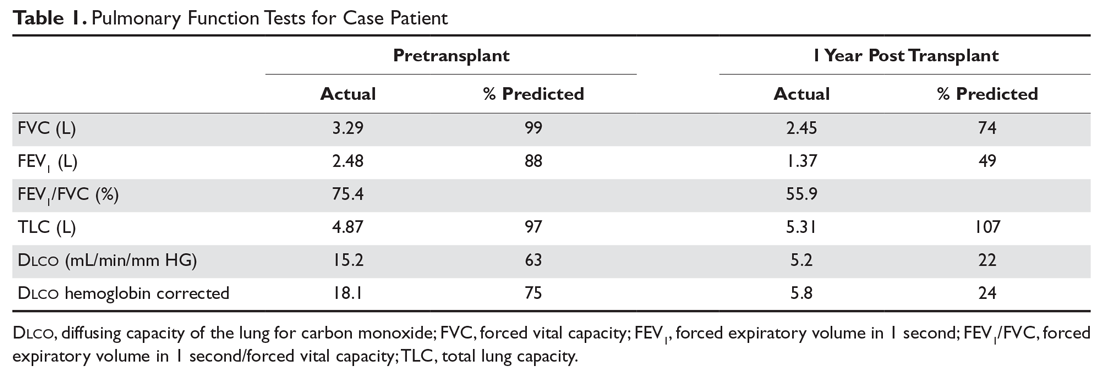
- What is the diagnosis in this case?
Bronchiolitis Obliterans
BOS is one of the most common and most serious late-onset pulmonary diseases after allogeneic transplantation. It is considered the pulmonary form of chronic GVHD. BOS was first described in 1982 in patients with chronic GVHD after bone marrow transplantation.4 Many differing definitions of bronchiolitis obliterans have been described in the literature. A recent review of the topic cites 10 different published sets of criteria for the diagnosis of bronchiolitis obliterans.5 Traditionally, bronchiolitis obliterans was thought to occur in 2% to 8% of patients undergoing allogeneic HSCT, but these findings were from older studies that used a diagnosis based on very specific pathology findings. When more liberal diagnostic criteria are used, the incidence may be as high as 26% of allogeneic HSCT patients.6
Bronchiolitis obliterans is a progressive lung disease characterized by narrowing of the terminal airways and obliteration of the terminal bronchi. Pathology may show constrictive bronchiolitis but can also show lymphocytic bronchiolitis, which may be associated with a better outcome.7 As noted, bronchiolitis obliterans has traditionally been considered a pathologic diagnosis. Current diagnostic criteria have evolved based upon the difficulty in obtaining this diagnosis through transbronchial biopsy given the patchy nature of the disease.8 The gold standard of open lung biopsy is seldom pursued in the post-HSCT population as the procedure continues to carry a worrisome risk-benefit profile.
The 2005 National Institutes of Health (NIH) consensus development project on criteria for clinical trials in chronic GVHD developed a clinical strategy for diagnosing BOS using the following criteria: absence of active infection, decreased forced expiratory volume in 1 second (FEV1) < 75%, FEV1/forced vital capacity (FVC) ratio of < 70%, and evidence of air trapping on high-resolution computed tomography (HRCT) or PFTs (residual volume > 120%). These diagnostic criteria were applied to a small series of patients with clinically identified bronchiolitis obliterans or biopsy-proven bronchiolitis obliterans. Only 18% of these patients met the requirements for the NIH consensus definition.5 A 2011 study that applied the NIH criteria found an overall prevalence of 5.5% among all transplant recipients but a prevalence of 14% in patients with GVHD.9 In 2014, the NIH consensus development group updated their recommendations. The new criteria for diagnosis of BOS require the presence of airflow obstruction (FEV1/FVC < 70% or 5th percentile of predicted), FEV1 < 75% predicted with a ≥ 10% decline in fewer than 2 years, absence of infection, and presence of air trapping (by expiratory computed tomography [CT] scan or PFT with residual volume >120% predicted) (Table 2). 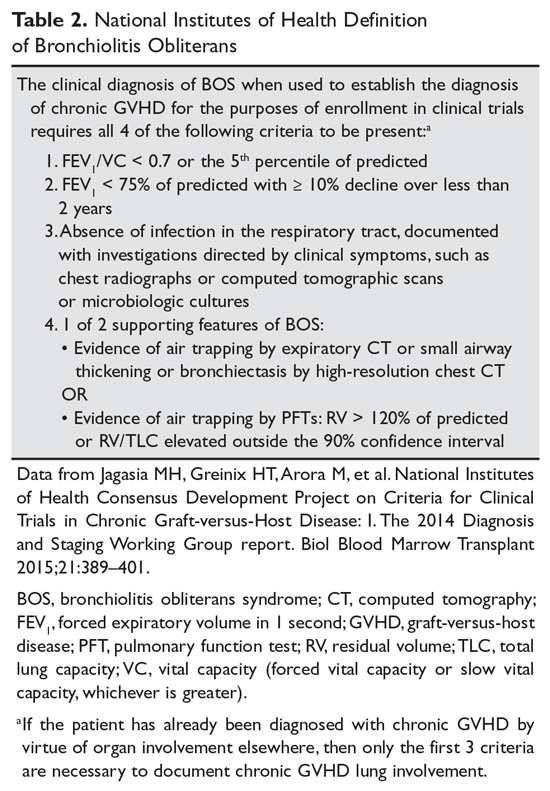
Some issues must be considered when determining airflow obstruction. The 2005 NIH working group recommends using Crapo as the reference set,11 but the National Health and Nutrition Examination Survey (NHANES) III reference values are the preferred reference set at this time12 and should be used in the United States. A recent article showed that the NHANES values were superior to older reference sets (however, they did not use Crapo as the comparison), although this study used the lower limit of normal as compared with the fixed 70% ratio.13 The 2014 NIH consensus group does not recommend a specific reference set and recognizes an FEV1/FVC ratio of 70% or less than the lower limit of normal as the cutoff value for airflow obstruction.10
Another issue in PFT interpretation is the finding of a decrease in FEV1 and FVC and normal total lung capacity, which is termed a nonspecific pattern. This pattern has been reported to occur in 9% of all PFTs and usually is associated with obstructive lung disease or obesity.14 A 2013 study described the nonspecific pattern as a BOS subgroup occurring in up to 31% of bronchiolitis obliterans patients.15
- What are the radiographic findings of BOS?
Chest radiograph is often normal in BOS. As discussed, air trapping can be documented using HRCT, according to the NIH clinical definition of bronchiolitis obliterans.16 A study that explored findings and trends seen on HRCT in HSCT patients with BOS found that the syndrome in these patients is characterized by central airway dilatation.17 Expiratory airway trapping on HRCT is the main finding, and this is best demonstrated on HRCT during inspiratory and expiratory phases.18 Other findings are bronchial wall thickening, parenchymal hypoattenuation, bronchiectasis, and centrilobular nodules.19
Galbán and colleagues developed a new technique called parametric response mapping that uses CT scanners to quantify normal parenchyma, functional small airway disease, emphysema, and parenchymal disease as relative lung volumes.20 This technique can detect airflow obstruction and small airway disease and was found to be a good method for detecting BOS after HSCT. In their study of parametric response mapping, the authors found that functional small airway disease affecting 28% or more of the total lung was highly indicative of bronchiolitis obliterans.20
- What therapies are used to treat BOS?
Traditionally, BOS has been treated with systemic immunosuppression. The recommended treatment had been systemic steroids at approximately 1 mg/ kg. However, it is increasingly recognized that BOS responds poorly to systemic steroids, and systemic steroids may actually be harmful and associated with increased mortality.15,21 The chronic GVHD recommendations from 2005 recommend ancillary therapy with inhaled corticosteroids and pulmonary rehabilitation.11 The updated 2011 German consensus statement lays out a clear management strategy for mild and moderate-severe disease with monitoring recommendations.22 The 2014 NIH chronic GVHD working group recommends fluticasone, azithromycin, and montelukast (ie, the FAM protocol) for treating BOS.23 FAM therapy in BOS may help lower the systemic steroid dose.24,25 Montelukast is not considered a treatment mainstay for BOS after lung transplant, but there is a study showing possible benefit in chronic GVHD.26 An evaluation of the natural history of a cohort of BOS patients treated with FAM therapy showed a rapid decline of FEV1 in the 6 months prior to diagnosis and treatment of BOS and subsequent stabilization following diagnosis and treatment.27 The benefit of high-dose inhaled corticosteroids or the combination of inhaled corticosteroids and long-acting beta-agonists has been demonstrated in small studies, which showed that these agents stabilized FEV1 and avoided the untoward side effects of systemic corticosteroids.28–30
Macrolide antibiotics have been explored as a treatment for BOS post HSCT because pilot studies suggested that azithromycin improved or stabilized FEV1 in patients with BOS after lung transplant or HSCT.31–33 Other studies of azithromycin have not shown benefit in the HSCT population after 3 months of therapy.34 A recent meta-analysis could neither support or refute the benefit of azithromycin for BOS after HSCT.35 In the lung transplant population, a study showed that patients who were started on azithromycin after transplant and continued on it 3 times a week had improved FEV1; these patients also had a reduced rate of BOS and improved overall and BOS-free survival 2 years after transplant.36 However, these benefits of azithromycin have not been observed in patients after HSCT. In fact, the ALLOZITHRO trial was stopped early because prophylactic azithromycin started at the time of the conditioning regimen with HSCT was associated with increased hematologic disease relapse, a decrease in airflow-decline-free survival, and reduced 2-year survival.30
Azithromycin is believed to exert an effect by its anti-inflammatory properties and perhaps by decreasing lung neutrophilia (it may be most beneficial in the subset of patients with high neutrophilia on bronchoalveolar lavage [BAL]).30 Adverse effects of chronic azithromycin include QT prolongation, cardiac arrhythmia, hearing loss, and antibiotic-resistant organism colonization.37,38
Other therapies include pulmonary rehabilitation, which may improve health-related quality of life and 6-minute walk distance,39 extracorporeal photopheresis,40 immunosuppression with calcineurin inhibitors or mycophenolate mofetil,21,41 and lung transplantation.42–44 A study with imatinib for the treatment of lung disease in steroid-refractory GVHD has shown promising results, but further validation with larger clinical trials is required.45
Case Continued
The patient is diagnosed with BOS and is treated for several months with prednisone 40 mg/day weaned over 3 months. She is started on inhaled corticosteroids, a proton pump inhibitor, and azithromycin 3 times per week, but she has a progressive decline in FEV1. She starts pulmonary rehabilitation but continues to functionally decline. Over the next year she develops bilateral pneumothoraces and bilateral cavitary nodules (Figure 1).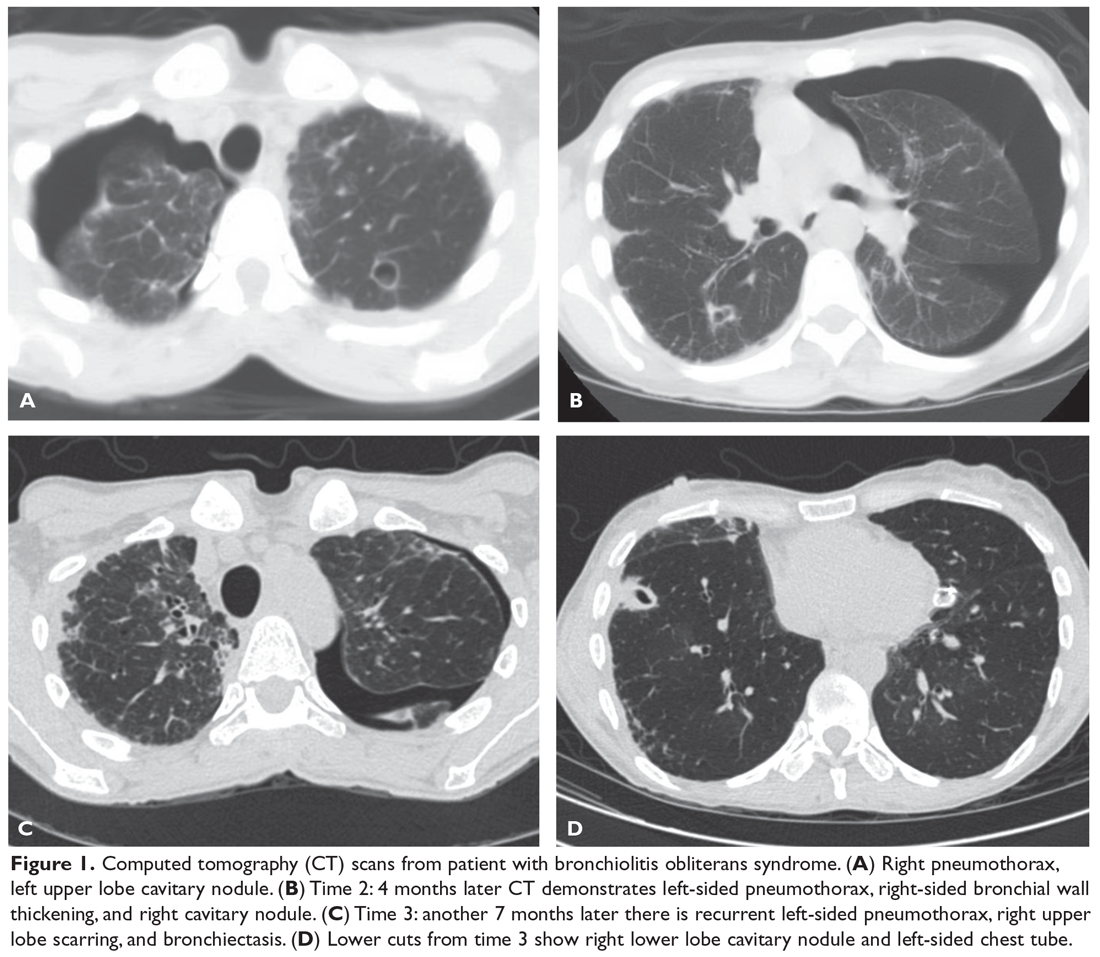
- What is causing this decline and the radiographic abnormalities?
Spontaneous air leak syndrome has been described in a little more than 1% of patients undergoing HSCT and has included pneumothorax and mediastinal and subcutaneous emphysema.46 It appears that air leak syndrome is more likely to occur in patients with chronic GVHD.47 The association between chronic GVHD and air leak syndrome could explain this patient’s recurrent pneumothoraces. The recurrent cavitary nodules are suspicious for infectious etiologies such as nontuberculous mycobacteria, tuberculosis, and fungal infections.
Case Continued
During an episode of pneumothorax, the patient undergoes chest tube placement, pleurodesis, and lung biopsy. Pathology reveals bronchiolitis obliterans as well as organizing pneumonia (Figure 2). No organisms are seen on acid-fast bacilli or GMS stains.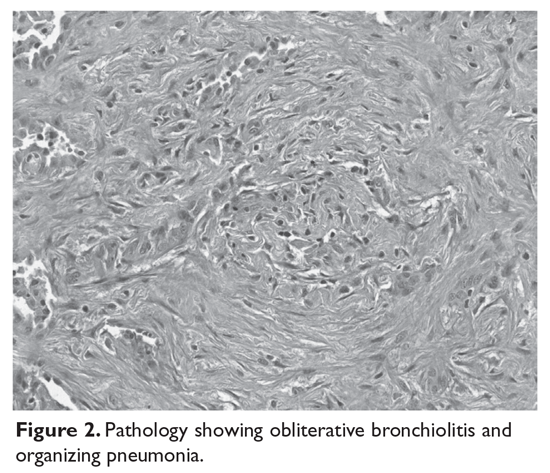
- What are the other late-onset noninfectious pulmonary complications?
Definitions of other late noninfectious pulmonary complications following HSCT are shown in Table 3.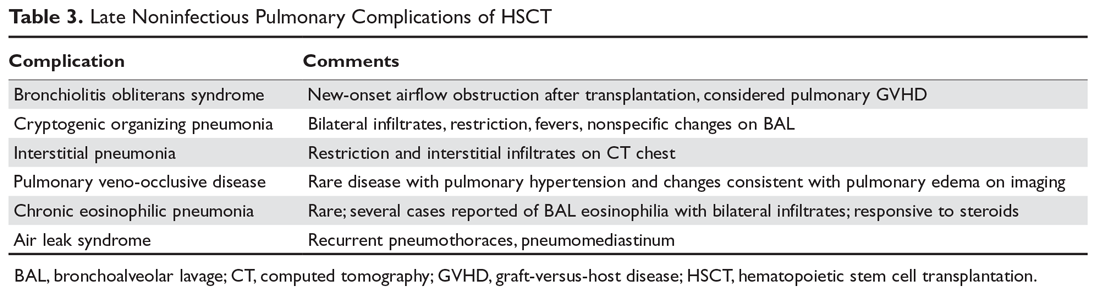
Interstitial pneumonias may represent COP or may be idiopathic pneumonia syndrome with a later onset or a nonspecific interstitial pneumonia. This syndrome is poorly defined, with a number of differing definitions of the syndrome published in the literature.50–55
A rare pulmonary complication after HSCT is pulmonary veno-occlusive disease (PVOD). Pulmonary hypertension has been reported after HSCT,56 but PVOD is a subset of pulmonary hypertension. It is associated with pleural effusions and volume overload on chest radiography.57,58 It may present early or late after transplant and is poorly understood.
Besides obstructive and restrictive PFT abnormalities, changes in small airway function59 after transplant and loss in diffusing capacity of the lungs for carbon monoxide (D
Case Conclusion
The patient’s lung function continues to worsen, but no infectious etiologies are discovered. Ultimately, she dies of respiratory failure caused by progressive bronchiolitis obliterans.
Conclusion
Late pulmonary complications occur frequently in patients who have undergone HSCT. These complications can be classified as infectious versus noninfectious etiologies. Late-onset complications are more common in allogeneic transplantations because they are associated with chronic GVHD. These complications can be manifestations of pulmonary GHVD or can be infectious complications associated with prolonged immunosuppression. Appropriate monitoring for the development of BOS is essential. Early and aggressive treatment of respiratory infections and diagnostic bronchoscopy with BAL can help elucidate most infectious causes. Still, diagnostic challenges remain and multiple causes of respiratory deterioration can be present concurrently in the post-HSCT patient. Steroid therapy remains the mainstay treatment for most noninfectious pulmonary complications and should be strongly considered once infection is effectively ruled out.
1. Remberger M, Ackefors M, Berglund S, et al. Improved survival after allogeneic hematopoietic stem cell transplantation in recent years. A single-center study. Biol Blood Marrow Transplant 2011;17:1688–97.
2. Wood KL, Esguerra VG. Management of late pulmonary complications after hematopoietic stem cell transplantation. Hosp Phys Hematology-Oncology Board Review Manual 2018;13(1):36–48.
3. Ninin E, Milpied N, Moreau P, et al. Longitudinal study of bacterial, viral, and fungal infections in adult recipients of bone marrow transplants. Clin Infect Dis 2001;33:41–7.
4. Roca J, Granena A, Rodriguez-Roisin R, et al. Fatal airway disease in an adult with chronic graft-versus-host disease. Thorax 1982;37:77–8.
5. Williams KM, Chien JW, Gladwin MT, Pavletic SZ. Bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation. JAMA 2009;302:306–14.
6. Chien JW, Martin PJ, Gooley TA, et al. Airflow obstruction after myeloablative allogeneic hematopoietic stem cell transplantation. Am J Respir Crit Care Med 2003;168:208–14.
7. Holbro A, Lehmann T, Girsberger S, et al. Lung histology predicts outcome of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2013;19:973–80.
8. Chamberlain D, Maurer J, Chaparro C, Idolor L. Evaluation of transbronchial lung biopsy specimens in the diagnosis of bronchiolitis obliterans after lung transplantation. J Heart Lung Transplant 1994;13:963–71.
9. Au BK, Au MA, Chien JW. Bronchiolitis obliterans syndrome epidemiology after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant 2011;17:1072–8.
10. Jagasia MH, Greinix HT, Arora M, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol Blood Marrow Transplant 2015;21:389–401.
11. Couriel D, Carpenter PA, Cutler C, et al. Ancillary therapy and supportive care of chronic graft-versus-host disease: national institutes of health consensus development project on criteria for clinical trials in chronic Graft-versus-host disease: V. Ancillary Therapy and Supportive Care Working Group Report. Biol Blood Marrow Transplant 2006;12:375–96.
12. Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J 2005;26:948–68.
13. Williams KM, Hnatiuk O, Mitchell SA, et al. NHANES III equations enhance early detection and mortality prediction of bronchiolitis obliterans syndrome after hematopoietic SCT. Bone Marrow Transplant 2014;49:561–6.
14. Hyatt RE, Cowl CT, Bjoraker JA, Scanlon PD. Conditions associated with an abnormal nonspecific pattern of pulmonary function tests. Chest 2009;135:419–24.
15. Bergeron A, Godet C, Chevret S, et al. Bronchiolitis obliterans syndrome after allogeneic hematopoietic SCT: phenotypes and prognosis. Bone Marrow Transplant 2013;48:819–24.
16. Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant 2005;11:945–56.
17. Gazourian L, Coronata AM, Rogers AJ, et al. Airway dilation in bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation. Respir Med 2013;107:276–83.
18. Gunn ML, Godwin JD, Kanne JP, et al. High-resolution CT findings of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. J Thorac Imaging 2008;23:244–50.
19. Sargent MA, Cairns RA, Murdoch MJ, et al. Obstructive lung disease in children after allogeneic bone marrow transplantation: evaluation with high-resolution CT. AJR Am J Roentgenol 1995;164:693–6.
20. Galban CJ, Boes JL, Bule M, et al. Parametric response mapping as an indicator of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2014;20:1592–8.
21. Meyer KC, Raghu G, Verleden GM, et al. An international ISHLT/ATS/ERS clinical practice guideline: diagnosis and management of bronchiolitis obliterans syndrome. Eur Respir J 2014;44:1479–1503.
22. Hildebrandt GC, Fazekas T, Lawitschka A, et al. Diagnosis and treatment of pulmonary chronic GVHD: report from the consensus conference on clinical practice in chronic GVHD. Bone Marrow Transplant 2011;46:1283–95.
23. Carpenter PA, Kitko CL, Elad S, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: V. The 2014 Ancillary Therapy and Supportive Care Working Group Report. Biol Blood Marrow Transplant 2015;21:1167–87.
24. Norman BC, Jacobsohn DA, Williams KM, et al. Fluticasone, azithromycin and montelukast therapy in reducing corticosteroid exposure in bronchiolitis obliterans syndrome after allogeneic hematopoietic SCT: a case series of eight patients. Bone Marrow Transplant 2011;46:1369–73.
25. Williams KM, Cheng GS, Pusic I, et al. Fluticasone, azithromycin, and montelukast treatment for new-onset bronchiolitis obliterans syndrome after hematopoietic cell transplantation. Biol Blood Marrow Transplant 2016;22:710–6.
26. Or R, Gesundheit B, Resnick I, et al. Sparing effect by montelukast treatment for chronic graft versus host disease: a pilot study. Transplantation 2007;83:577–81.
27. Cheng GS, Storer B, Chien JW, et al. Lung function trajectory in bronchiolitis obliterans syndrome after allogeneic hematopoietic cell transplant. Ann Am Thorac Soc 2016;13:1932–9.
28. Bergeron A, Belle A, Chevret S, et al. Combined inhaled steroids and bronchodilatators in obstructive airway disease after allogeneic stem cell transplantation. Bone Marrow Transplant 2007;39:547–53.
29. Bashoura L, Gupta S, Jain A, et al. Inhaled corticosteroids stabilize constrictive bronchiolitis after hematopoietic stem cell transplantation. Bone Marrow Transplant 2008;41:63–7.
30. Bergeron A, Chevret S, Granata A, et al. Effect of azithromycin on airflow decline-free survival after allogeneic hematopoietic stem cell transplant: the ALLOZITHRO randomized clinical trial. JAMA 2017;318:557–66.
31. Gerhardt SG, McDyer JF, Girgis RE, et al. Maintenance azithromycin therapy for bronchiolitis obliterans syndrome: results of a pilot study. Am J Respir Crit Care Med 2003;168:121–5.
32. Khalid M, Al Saghir A, Saleemi S, et al. Azithromycin in bronchiolitis obliterans complicating bone marrow transplantation: a preliminary study. Eur Respir J 2005;25:490–3.
33. Maimon N, Lipton JH, Chan CK, Marras TK. Macrolides in the treatment of bronchiolitis obliterans in allograft recipients. Bone Marrow Transplant 2009;44:69–73.
34. Lam DC, Lam B, Wong MK, et al. Effects of azithromycin in bronchiolitis obliterans syndrome after hematopoietic SCT--a randomized double-blinded placebo-controlled study. Bone Marrow Transplant 2011;46:1551–6.
35. Yadav H, Peters SG, Keogh KA, et al. Azithromycin for the treatment of obliterative bronchiolitis after hematopoietic stem cell transplantation: a systematic review and meta-analysis. Biol Blood Marrow Transplant 2016;22:2264–9.
36. Vos R, Vanaudenaerde BM, Verleden SE, et al. A randomised controlled trial of azithromycin to prevent chronic rejection after lung transplantation. Eur Respir J 2011;37:164–72.
37. Svanstrom H, Pasternak B, Hviid A. Use of azithromycin and death from cardiovascular causes. N Engl J Med 2013;368:1704–12.
38. Albert RK, Connett J, Bailey WC, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med 2011;365:689–98.
39. Tran J, Norder EE, Diaz PT, et al. Pulmonary rehabilitation for bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2012;18:1250–4.
40. Lucid CE, Savani BN, Engelhardt BG, et al. Extracorporeal photopheresis in patients with refractory bronchiolitis obliterans developing after allo-SCT. Bone Marrow Transplant 2011;46:426–9.
41. Hostettler KE, Halter JP, Gerull S, et al. Calcineurin inhibitors in bronchiolitis obliterans syndrome following stem cell transplantation. Eur Respir J 2014;43:221–32.
42. Holm AM, Riise GC, Brinch L, et al. Lung transplantation for bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation: unresolved questions. Transplantation 2013;96:e21–22.
43. Cheng GS, Edelman JD, Madtes DK, et al. Outcomes of lung transplantation after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2014;20:1169–75.
44. Okumura H, Ohtake S, Ontachi Y, et al. Living-donor lobar lung transplantation for broncho-bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation: does bronchiolitis obliterans recur in transplanted lungs? Int J Hematol 2007;86:369–73.
45. Olivieri A, Cimminiello M, Corradini P, et al. Long-term outcome and prospective validation of NIH response criteria in 39 patients receiving imatinib for steroid-refractory chronic GVHD. Blood 2013;122:4111–8.
46. Rahmanian S, Wood KL. Bronchiolitis obliterans and the risk of pneumothorax after transbronchial biopsy. Respiratory Medicine CME 2010;3:87–9.
47. Sakai R, Kanamori H, Nakaseko C, et al. Air-leak syndrome following allo-SCT in adult patients: report from the Kanto Study Group for Cell Therapy in Japan. Bone Marrow Transplant 2011;46:379–84.
48. Visscher DW, Myers JL. Histologic spectrum of idiopathic interstitial pneumonias. Proc Am Thorac Soc 2006;3:322–9.
49. Cordier JF. Cryptogenic organising pneumonia. Eur Respir J 2006;28:422–46.
50. Nishio N, Yagasaki H, Takahashi Y, et al. Late-onset non-infectious pulmonary complications following allogeneic hematopoietic stem cell transplantation in children. Bone Marrow Transplant 2009;44:303–8.
51. Ueda K, Watadani T, Maeda E, et al. Outcome and treatment of late-onset noninfectious pulmonary complications after allogeneic haematopoietic SCT. Bone Marrow Transplant 2010;45:1719–27.
52. Schlemmer F, Chevret S, Lorillon G, et al. Late-onset noninfectious interstitial lung disease after allogeneic hematopoietic stem cell transplantation. Respir Med 2014;108:1525–33.
53. Palmas A, Tefferi A, Myers JL, et al. Late-onset noninfectious pulmonary complications after allogeneic bone marrow transplantation. Br J Haematol 1998;100:680–7.
54. Sakaida E, Nakaseko C, Harima A, et al. Late-onset noninfectious pulmonary complications after allogeneic stem cell transplantation are significantly associated with chronic graft-versus-host disease and with the graft-versus-leukemia effect. Blood 2003;102:4236–42.
55. Solh M, Arat M, Cao Q, et al. Late-onset noninfectious pulmonary complications in adult allogeneic hematopoietic cell transplant recipients. Transplantation 2011;91:798–803.
56. Dandoy CE, Hirsch R, Chima R, et al. Pulmonary hypertension after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2013;19:1546–56.
57. Bunte MC, Patnaik MM, Pritzker MR, Burns LJ. Pulmonary veno-occlusive disease following hematopoietic stem cell transplantation: a rare model of endothelial dysfunction. Bone Marrow Transplant 2008;41:677–86.
58. Troussard X, Bernaudin JF, Cordonnier C, et al. Pulmonary veno-occlusive disease after bone marrow transplantation. Thorax 1984;39:956–7.
59. Lahzami S, Schoeffel RE, Pechey V, et al. Small airways function declines after allogeneic haematopoietic stem cell transplantation. Eur Respir J 2011;38:1180–8.
60. Jain NA, Pophali PA, Klotz JK, et al. Repair of impaired pulmonary function is possible in very-long-term allogeneic stem cell transplantation survivors. Biol Blood Marrow Transplant 2014;20:209–13.
61. Barisione G, Bacigalupo A, Crimi E, et al. Changes in lung volumes and airway responsiveness following haematopoietic stem cell transplantation. Eur Respir J 2008;32:1576–82.
62. Kovalszki A, Schumaker GL, Klein A, et al. Reduced respiratory and skeletal muscle strength in survivors of sibling or unrelated donor hematopoietic stem cell transplantation. Bone Marrow Transplant 2008;41:965–9.
63. Mathiesen S, Uhlving HH, Buchvald F, et al. Aerobic exercise capacity at long-term follow-up after paediatric allogeneic haematopoietic SCT. Bone Marrow Transplant 2014;49:1393–9.
Hematopoietic stem cell transplantation (HSCT) is increasingly being used to treat hematologic malignancies as well as nonmalignant diseases and solid tumors. Over the past 2 decades overall survival following transplant and transplant-related mortality have improved.1 With this increased survival, there is a need to focus on late complications after transplantation. Pulmonary complications are a common but sometimes underrecognized cause of late morbidity and mortality in HSCT patients. This article, the second of 2 articles on post-HSCT pulmonary complications, reviews late-onset complications, with a focus on the evaluation and treatment of bronchiolitis obliterans syndrome (BOS), one of the most common and serious late pulmonary complications in HSCT patients. The first article reviewed the management of early-onset pulmonary complications and included a basic overview of stem cell transplantation, discussion of factors associated with pulmonary complications, and a review of methods for assessing pretransplant risk for pulmonary complications in patients undergoing HSCT.2
Case Presentation
A 40-year-old white woman with a history of acute myeloid leukemia status post peripheral blood stem cell transplant presents with dyspnea on exertion, which she states started about 1 month ago and now is limiting her with even 1 flight of stairs. She also complains of mild dry cough and a 4- to 5-lb weight loss over the past 1 to 2 months. She has an occasional runny nose, but denies gastroesophageal reflux, fevers, chills, or night sweats. She has a history of matched related sibling donor transplant with busulfan and cyclophosphamide conditioning 1 year prior to presentation. She has had significant graft-versus-host disease (GVHD), affecting the liver, gastrointestinal tract, skin, and eyes.
On physical examination, heart rate is 110 beats/min, respiratory rate is 16 breaths/min, blood pressure is 92/58 mm Hg, and the patient is afebrile. Eye exam reveals scleral injection, mouth shows dry mucous membranes with a few white plaques, and the skin has chronic changes with a rash over both arms. Cardiac exam reveals tachycardia but regular rhythm and there are no murmurs, rubs, or gallops. Lungs are clear bilaterally and abdomen shows no organomegaly.
Laboratory exam shows a white blood cell count of 7800 cells/μL, hemoglobin level of 12.4 g/dL, and platelet count of 186 × 103/μL. Liver enzymes are mildly elevated. Chest radiograph shows clear lung fields bilaterally.
- What is the differential in this patient with dyspnea 1 year after transplantation?
Late pulmonary complications are generally accepted as those occurring more than 100 days post transplant. This period of time is characterized by chronic GVHD and impaired cellular and humoral immunity. Results of longitudinal studies of infections in adult HSCT patients suggest that special attention should be paid to allogeneic HSCT recipients for post-engraftment infectious pulmonary complications.3 Encapsulated bacteria such as Haemophilus influenzae and Streptococcus pneumoniae are the most frequent bacterial organisms causing late infectious pulmonary complications. Nontuberculous mycobacteria and Nocardia should also be considered. Depending upon geographic location, social and occupational risk factors, and prevalence, tuberculosis should also enter the differential.
There are many noninfectious late-onset pulmonary complications after HSCT. Unfortunately, the literature has divided pulmonary complications after HSCT using a range of criteria and classifications based upon timing, predominant pulmonary function test (PFT) findings, and etiology. These include early versus late, obstructive versus restrictive, and infectious versus noninfectious, which makes a comprehensive literature review of late pulmonary complications difficult. The most common noninfectious late-onset complications are bronchiolitis obliterans, cryptogenic organizing pneumonia (previously referred to as bronchiolitis obliterans organizing pneumonia, or BOOP), and interstitial pneumonia. Other rarely reported complications include eosinophilic pneumonia, pulmonary alveolar proteinosis, air leak syndrome, and pulmonary hypertension.
Case Continued
Because the patient does not have symptoms of infection, PFTs are obtained. Pretransplant PFTs and current PFTs are shown in Table 1.
- What is the diagnosis in this case?
Bronchiolitis Obliterans
BOS is one of the most common and most serious late-onset pulmonary diseases after allogeneic transplantation. It is considered the pulmonary form of chronic GVHD. BOS was first described in 1982 in patients with chronic GVHD after bone marrow transplantation.4 Many differing definitions of bronchiolitis obliterans have been described in the literature. A recent review of the topic cites 10 different published sets of criteria for the diagnosis of bronchiolitis obliterans.5 Traditionally, bronchiolitis obliterans was thought to occur in 2% to 8% of patients undergoing allogeneic HSCT, but these findings were from older studies that used a diagnosis based on very specific pathology findings. When more liberal diagnostic criteria are used, the incidence may be as high as 26% of allogeneic HSCT patients.6
Bronchiolitis obliterans is a progressive lung disease characterized by narrowing of the terminal airways and obliteration of the terminal bronchi. Pathology may show constrictive bronchiolitis but can also show lymphocytic bronchiolitis, which may be associated with a better outcome.7 As noted, bronchiolitis obliterans has traditionally been considered a pathologic diagnosis. Current diagnostic criteria have evolved based upon the difficulty in obtaining this diagnosis through transbronchial biopsy given the patchy nature of the disease.8 The gold standard of open lung biopsy is seldom pursued in the post-HSCT population as the procedure continues to carry a worrisome risk-benefit profile.
The 2005 National Institutes of Health (NIH) consensus development project on criteria for clinical trials in chronic GVHD developed a clinical strategy for diagnosing BOS using the following criteria: absence of active infection, decreased forced expiratory volume in 1 second (FEV1) < 75%, FEV1/forced vital capacity (FVC) ratio of < 70%, and evidence of air trapping on high-resolution computed tomography (HRCT) or PFTs (residual volume > 120%). These diagnostic criteria were applied to a small series of patients with clinically identified bronchiolitis obliterans or biopsy-proven bronchiolitis obliterans. Only 18% of these patients met the requirements for the NIH consensus definition.5 A 2011 study that applied the NIH criteria found an overall prevalence of 5.5% among all transplant recipients but a prevalence of 14% in patients with GVHD.9 In 2014, the NIH consensus development group updated their recommendations. The new criteria for diagnosis of BOS require the presence of airflow obstruction (FEV1/FVC < 70% or 5th percentile of predicted), FEV1 < 75% predicted with a ≥ 10% decline in fewer than 2 years, absence of infection, and presence of air trapping (by expiratory computed tomography [CT] scan or PFT with residual volume >120% predicted) (Table 2).
Some issues must be considered when determining airflow obstruction. The 2005 NIH working group recommends using Crapo as the reference set,11 but the National Health and Nutrition Examination Survey (NHANES) III reference values are the preferred reference set at this time12 and should be used in the United States. A recent article showed that the NHANES values were superior to older reference sets (however, they did not use Crapo as the comparison), although this study used the lower limit of normal as compared with the fixed 70% ratio.13 The 2014 NIH consensus group does not recommend a specific reference set and recognizes an FEV1/FVC ratio of 70% or less than the lower limit of normal as the cutoff value for airflow obstruction.10
Another issue in PFT interpretation is the finding of a decrease in FEV1 and FVC and normal total lung capacity, which is termed a nonspecific pattern. This pattern has been reported to occur in 9% of all PFTs and usually is associated with obstructive lung disease or obesity.14 A 2013 study described the nonspecific pattern as a BOS subgroup occurring in up to 31% of bronchiolitis obliterans patients.15
- What are the radiographic findings of BOS?
Chest radiograph is often normal in BOS. As discussed, air trapping can be documented using HRCT, according to the NIH clinical definition of bronchiolitis obliterans.16 A study that explored findings and trends seen on HRCT in HSCT patients with BOS found that the syndrome in these patients is characterized by central airway dilatation.17 Expiratory airway trapping on HRCT is the main finding, and this is best demonstrated on HRCT during inspiratory and expiratory phases.18 Other findings are bronchial wall thickening, parenchymal hypoattenuation, bronchiectasis, and centrilobular nodules.19
Galbán and colleagues developed a new technique called parametric response mapping that uses CT scanners to quantify normal parenchyma, functional small airway disease, emphysema, and parenchymal disease as relative lung volumes.20 This technique can detect airflow obstruction and small airway disease and was found to be a good method for detecting BOS after HSCT. In their study of parametric response mapping, the authors found that functional small airway disease affecting 28% or more of the total lung was highly indicative of bronchiolitis obliterans.20
- What therapies are used to treat BOS?
Traditionally, BOS has been treated with systemic immunosuppression. The recommended treatment had been systemic steroids at approximately 1 mg/ kg. However, it is increasingly recognized that BOS responds poorly to systemic steroids, and systemic steroids may actually be harmful and associated with increased mortality.15,21 The chronic GVHD recommendations from 2005 recommend ancillary therapy with inhaled corticosteroids and pulmonary rehabilitation.11 The updated 2011 German consensus statement lays out a clear management strategy for mild and moderate-severe disease with monitoring recommendations.22 The 2014 NIH chronic GVHD working group recommends fluticasone, azithromycin, and montelukast (ie, the FAM protocol) for treating BOS.23 FAM therapy in BOS may help lower the systemic steroid dose.24,25 Montelukast is not considered a treatment mainstay for BOS after lung transplant, but there is a study showing possible benefit in chronic GVHD.26 An evaluation of the natural history of a cohort of BOS patients treated with FAM therapy showed a rapid decline of FEV1 in the 6 months prior to diagnosis and treatment of BOS and subsequent stabilization following diagnosis and treatment.27 The benefit of high-dose inhaled corticosteroids or the combination of inhaled corticosteroids and long-acting beta-agonists has been demonstrated in small studies, which showed that these agents stabilized FEV1 and avoided the untoward side effects of systemic corticosteroids.28–30
Macrolide antibiotics have been explored as a treatment for BOS post HSCT because pilot studies suggested that azithromycin improved or stabilized FEV1 in patients with BOS after lung transplant or HSCT.31–33 Other studies of azithromycin have not shown benefit in the HSCT population after 3 months of therapy.34 A recent meta-analysis could neither support or refute the benefit of azithromycin for BOS after HSCT.35 In the lung transplant population, a study showed that patients who were started on azithromycin after transplant and continued on it 3 times a week had improved FEV1; these patients also had a reduced rate of BOS and improved overall and BOS-free survival 2 years after transplant.36 However, these benefits of azithromycin have not been observed in patients after HSCT. In fact, the ALLOZITHRO trial was stopped early because prophylactic azithromycin started at the time of the conditioning regimen with HSCT was associated with increased hematologic disease relapse, a decrease in airflow-decline-free survival, and reduced 2-year survival.30
Azithromycin is believed to exert an effect by its anti-inflammatory properties and perhaps by decreasing lung neutrophilia (it may be most beneficial in the subset of patients with high neutrophilia on bronchoalveolar lavage [BAL]).30 Adverse effects of chronic azithromycin include QT prolongation, cardiac arrhythmia, hearing loss, and antibiotic-resistant organism colonization.37,38
Other therapies include pulmonary rehabilitation, which may improve health-related quality of life and 6-minute walk distance,39 extracorporeal photopheresis,40 immunosuppression with calcineurin inhibitors or mycophenolate mofetil,21,41 and lung transplantation.42–44 A study with imatinib for the treatment of lung disease in steroid-refractory GVHD has shown promising results, but further validation with larger clinical trials is required.45
Case Continued
The patient is diagnosed with BOS and is treated for several months with prednisone 40 mg/day weaned over 3 months. She is started on inhaled corticosteroids, a proton pump inhibitor, and azithromycin 3 times per week, but she has a progressive decline in FEV1. She starts pulmonary rehabilitation but continues to functionally decline. Over the next year she develops bilateral pneumothoraces and bilateral cavitary nodules (Figure 1).
- What is causing this decline and the radiographic abnormalities?
Spontaneous air leak syndrome has been described in a little more than 1% of patients undergoing HSCT and has included pneumothorax and mediastinal and subcutaneous emphysema.46 It appears that air leak syndrome is more likely to occur in patients with chronic GVHD.47 The association between chronic GVHD and air leak syndrome could explain this patient’s recurrent pneumothoraces. The recurrent cavitary nodules are suspicious for infectious etiologies such as nontuberculous mycobacteria, tuberculosis, and fungal infections.
Case Continued
During an episode of pneumothorax, the patient undergoes chest tube placement, pleurodesis, and lung biopsy. Pathology reveals bronchiolitis obliterans as well as organizing pneumonia (Figure 2). No organisms are seen on acid-fast bacilli or GMS stains.
- What are the other late-onset noninfectious pulmonary complications?
Definitions of other late noninfectious pulmonary complications following HSCT are shown in Table 3.
Interstitial pneumonias may represent COP or may be idiopathic pneumonia syndrome with a later onset or a nonspecific interstitial pneumonia. This syndrome is poorly defined, with a number of differing definitions of the syndrome published in the literature.50–55
A rare pulmonary complication after HSCT is pulmonary veno-occlusive disease (PVOD). Pulmonary hypertension has been reported after HSCT,56 but PVOD is a subset of pulmonary hypertension. It is associated with pleural effusions and volume overload on chest radiography.57,58 It may present early or late after transplant and is poorly understood.
Besides obstructive and restrictive PFT abnormalities, changes in small airway function59 after transplant and loss in diffusing capacity of the lungs for carbon monoxide (D
Case Conclusion
The patient’s lung function continues to worsen, but no infectious etiologies are discovered. Ultimately, she dies of respiratory failure caused by progressive bronchiolitis obliterans.
Conclusion
Late pulmonary complications occur frequently in patients who have undergone HSCT. These complications can be classified as infectious versus noninfectious etiologies. Late-onset complications are more common in allogeneic transplantations because they are associated with chronic GVHD. These complications can be manifestations of pulmonary GHVD or can be infectious complications associated with prolonged immunosuppression. Appropriate monitoring for the development of BOS is essential. Early and aggressive treatment of respiratory infections and diagnostic bronchoscopy with BAL can help elucidate most infectious causes. Still, diagnostic challenges remain and multiple causes of respiratory deterioration can be present concurrently in the post-HSCT patient. Steroid therapy remains the mainstay treatment for most noninfectious pulmonary complications and should be strongly considered once infection is effectively ruled out.
Hematopoietic stem cell transplantation (HSCT) is increasingly being used to treat hematologic malignancies as well as nonmalignant diseases and solid tumors. Over the past 2 decades overall survival following transplant and transplant-related mortality have improved.1 With this increased survival, there is a need to focus on late complications after transplantation. Pulmonary complications are a common but sometimes underrecognized cause of late morbidity and mortality in HSCT patients. This article, the second of 2 articles on post-HSCT pulmonary complications, reviews late-onset complications, with a focus on the evaluation and treatment of bronchiolitis obliterans syndrome (BOS), one of the most common and serious late pulmonary complications in HSCT patients. The first article reviewed the management of early-onset pulmonary complications and included a basic overview of stem cell transplantation, discussion of factors associated with pulmonary complications, and a review of methods for assessing pretransplant risk for pulmonary complications in patients undergoing HSCT.2
Case Presentation
A 40-year-old white woman with a history of acute myeloid leukemia status post peripheral blood stem cell transplant presents with dyspnea on exertion, which she states started about 1 month ago and now is limiting her with even 1 flight of stairs. She also complains of mild dry cough and a 4- to 5-lb weight loss over the past 1 to 2 months. She has an occasional runny nose, but denies gastroesophageal reflux, fevers, chills, or night sweats. She has a history of matched related sibling donor transplant with busulfan and cyclophosphamide conditioning 1 year prior to presentation. She has had significant graft-versus-host disease (GVHD), affecting the liver, gastrointestinal tract, skin, and eyes.
On physical examination, heart rate is 110 beats/min, respiratory rate is 16 breaths/min, blood pressure is 92/58 mm Hg, and the patient is afebrile. Eye exam reveals scleral injection, mouth shows dry mucous membranes with a few white plaques, and the skin has chronic changes with a rash over both arms. Cardiac exam reveals tachycardia but regular rhythm and there are no murmurs, rubs, or gallops. Lungs are clear bilaterally and abdomen shows no organomegaly.
Laboratory exam shows a white blood cell count of 7800 cells/μL, hemoglobin level of 12.4 g/dL, and platelet count of 186 × 103/μL. Liver enzymes are mildly elevated. Chest radiograph shows clear lung fields bilaterally.
- What is the differential in this patient with dyspnea 1 year after transplantation?
Late pulmonary complications are generally accepted as those occurring more than 100 days post transplant. This period of time is characterized by chronic GVHD and impaired cellular and humoral immunity. Results of longitudinal studies of infections in adult HSCT patients suggest that special attention should be paid to allogeneic HSCT recipients for post-engraftment infectious pulmonary complications.3 Encapsulated bacteria such as Haemophilus influenzae and Streptococcus pneumoniae are the most frequent bacterial organisms causing late infectious pulmonary complications. Nontuberculous mycobacteria and Nocardia should also be considered. Depending upon geographic location, social and occupational risk factors, and prevalence, tuberculosis should also enter the differential.
There are many noninfectious late-onset pulmonary complications after HSCT. Unfortunately, the literature has divided pulmonary complications after HSCT using a range of criteria and classifications based upon timing, predominant pulmonary function test (PFT) findings, and etiology. These include early versus late, obstructive versus restrictive, and infectious versus noninfectious, which makes a comprehensive literature review of late pulmonary complications difficult. The most common noninfectious late-onset complications are bronchiolitis obliterans, cryptogenic organizing pneumonia (previously referred to as bronchiolitis obliterans organizing pneumonia, or BOOP), and interstitial pneumonia. Other rarely reported complications include eosinophilic pneumonia, pulmonary alveolar proteinosis, air leak syndrome, and pulmonary hypertension.
Case Continued
Because the patient does not have symptoms of infection, PFTs are obtained. Pretransplant PFTs and current PFTs are shown in Table 1.
- What is the diagnosis in this case?
Bronchiolitis Obliterans
BOS is one of the most common and most serious late-onset pulmonary diseases after allogeneic transplantation. It is considered the pulmonary form of chronic GVHD. BOS was first described in 1982 in patients with chronic GVHD after bone marrow transplantation.4 Many differing definitions of bronchiolitis obliterans have been described in the literature. A recent review of the topic cites 10 different published sets of criteria for the diagnosis of bronchiolitis obliterans.5 Traditionally, bronchiolitis obliterans was thought to occur in 2% to 8% of patients undergoing allogeneic HSCT, but these findings were from older studies that used a diagnosis based on very specific pathology findings. When more liberal diagnostic criteria are used, the incidence may be as high as 26% of allogeneic HSCT patients.6
Bronchiolitis obliterans is a progressive lung disease characterized by narrowing of the terminal airways and obliteration of the terminal bronchi. Pathology may show constrictive bronchiolitis but can also show lymphocytic bronchiolitis, which may be associated with a better outcome.7 As noted, bronchiolitis obliterans has traditionally been considered a pathologic diagnosis. Current diagnostic criteria have evolved based upon the difficulty in obtaining this diagnosis through transbronchial biopsy given the patchy nature of the disease.8 The gold standard of open lung biopsy is seldom pursued in the post-HSCT population as the procedure continues to carry a worrisome risk-benefit profile.
The 2005 National Institutes of Health (NIH) consensus development project on criteria for clinical trials in chronic GVHD developed a clinical strategy for diagnosing BOS using the following criteria: absence of active infection, decreased forced expiratory volume in 1 second (FEV1) < 75%, FEV1/forced vital capacity (FVC) ratio of < 70%, and evidence of air trapping on high-resolution computed tomography (HRCT) or PFTs (residual volume > 120%). These diagnostic criteria were applied to a small series of patients with clinically identified bronchiolitis obliterans or biopsy-proven bronchiolitis obliterans. Only 18% of these patients met the requirements for the NIH consensus definition.5 A 2011 study that applied the NIH criteria found an overall prevalence of 5.5% among all transplant recipients but a prevalence of 14% in patients with GVHD.9 In 2014, the NIH consensus development group updated their recommendations. The new criteria for diagnosis of BOS require the presence of airflow obstruction (FEV1/FVC < 70% or 5th percentile of predicted), FEV1 < 75% predicted with a ≥ 10% decline in fewer than 2 years, absence of infection, and presence of air trapping (by expiratory computed tomography [CT] scan or PFT with residual volume >120% predicted) (Table 2).
Some issues must be considered when determining airflow obstruction. The 2005 NIH working group recommends using Crapo as the reference set,11 but the National Health and Nutrition Examination Survey (NHANES) III reference values are the preferred reference set at this time12 and should be used in the United States. A recent article showed that the NHANES values were superior to older reference sets (however, they did not use Crapo as the comparison), although this study used the lower limit of normal as compared with the fixed 70% ratio.13 The 2014 NIH consensus group does not recommend a specific reference set and recognizes an FEV1/FVC ratio of 70% or less than the lower limit of normal as the cutoff value for airflow obstruction.10
Another issue in PFT interpretation is the finding of a decrease in FEV1 and FVC and normal total lung capacity, which is termed a nonspecific pattern. This pattern has been reported to occur in 9% of all PFTs and usually is associated with obstructive lung disease or obesity.14 A 2013 study described the nonspecific pattern as a BOS subgroup occurring in up to 31% of bronchiolitis obliterans patients.15
- What are the radiographic findings of BOS?
Chest radiograph is often normal in BOS. As discussed, air trapping can be documented using HRCT, according to the NIH clinical definition of bronchiolitis obliterans.16 A study that explored findings and trends seen on HRCT in HSCT patients with BOS found that the syndrome in these patients is characterized by central airway dilatation.17 Expiratory airway trapping on HRCT is the main finding, and this is best demonstrated on HRCT during inspiratory and expiratory phases.18 Other findings are bronchial wall thickening, parenchymal hypoattenuation, bronchiectasis, and centrilobular nodules.19
Galbán and colleagues developed a new technique called parametric response mapping that uses CT scanners to quantify normal parenchyma, functional small airway disease, emphysema, and parenchymal disease as relative lung volumes.20 This technique can detect airflow obstruction and small airway disease and was found to be a good method for detecting BOS after HSCT. In their study of parametric response mapping, the authors found that functional small airway disease affecting 28% or more of the total lung was highly indicative of bronchiolitis obliterans.20
- What therapies are used to treat BOS?
Traditionally, BOS has been treated with systemic immunosuppression. The recommended treatment had been systemic steroids at approximately 1 mg/ kg. However, it is increasingly recognized that BOS responds poorly to systemic steroids, and systemic steroids may actually be harmful and associated with increased mortality.15,21 The chronic GVHD recommendations from 2005 recommend ancillary therapy with inhaled corticosteroids and pulmonary rehabilitation.11 The updated 2011 German consensus statement lays out a clear management strategy for mild and moderate-severe disease with monitoring recommendations.22 The 2014 NIH chronic GVHD working group recommends fluticasone, azithromycin, and montelukast (ie, the FAM protocol) for treating BOS.23 FAM therapy in BOS may help lower the systemic steroid dose.24,25 Montelukast is not considered a treatment mainstay for BOS after lung transplant, but there is a study showing possible benefit in chronic GVHD.26 An evaluation of the natural history of a cohort of BOS patients treated with FAM therapy showed a rapid decline of FEV1 in the 6 months prior to diagnosis and treatment of BOS and subsequent stabilization following diagnosis and treatment.27 The benefit of high-dose inhaled corticosteroids or the combination of inhaled corticosteroids and long-acting beta-agonists has been demonstrated in small studies, which showed that these agents stabilized FEV1 and avoided the untoward side effects of systemic corticosteroids.28–30
Macrolide antibiotics have been explored as a treatment for BOS post HSCT because pilot studies suggested that azithromycin improved or stabilized FEV1 in patients with BOS after lung transplant or HSCT.31–33 Other studies of azithromycin have not shown benefit in the HSCT population after 3 months of therapy.34 A recent meta-analysis could neither support or refute the benefit of azithromycin for BOS after HSCT.35 In the lung transplant population, a study showed that patients who were started on azithromycin after transplant and continued on it 3 times a week had improved FEV1; these patients also had a reduced rate of BOS and improved overall and BOS-free survival 2 years after transplant.36 However, these benefits of azithromycin have not been observed in patients after HSCT. In fact, the ALLOZITHRO trial was stopped early because prophylactic azithromycin started at the time of the conditioning regimen with HSCT was associated with increased hematologic disease relapse, a decrease in airflow-decline-free survival, and reduced 2-year survival.30
Azithromycin is believed to exert an effect by its anti-inflammatory properties and perhaps by decreasing lung neutrophilia (it may be most beneficial in the subset of patients with high neutrophilia on bronchoalveolar lavage [BAL]).30 Adverse effects of chronic azithromycin include QT prolongation, cardiac arrhythmia, hearing loss, and antibiotic-resistant organism colonization.37,38
Other therapies include pulmonary rehabilitation, which may improve health-related quality of life and 6-minute walk distance,39 extracorporeal photopheresis,40 immunosuppression with calcineurin inhibitors or mycophenolate mofetil,21,41 and lung transplantation.42–44 A study with imatinib for the treatment of lung disease in steroid-refractory GVHD has shown promising results, but further validation with larger clinical trials is required.45
Case Continued
The patient is diagnosed with BOS and is treated for several months with prednisone 40 mg/day weaned over 3 months. She is started on inhaled corticosteroids, a proton pump inhibitor, and azithromycin 3 times per week, but she has a progressive decline in FEV1. She starts pulmonary rehabilitation but continues to functionally decline. Over the next year she develops bilateral pneumothoraces and bilateral cavitary nodules (Figure 1).
- What is causing this decline and the radiographic abnormalities?
Spontaneous air leak syndrome has been described in a little more than 1% of patients undergoing HSCT and has included pneumothorax and mediastinal and subcutaneous emphysema.46 It appears that air leak syndrome is more likely to occur in patients with chronic GVHD.47 The association between chronic GVHD and air leak syndrome could explain this patient’s recurrent pneumothoraces. The recurrent cavitary nodules are suspicious for infectious etiologies such as nontuberculous mycobacteria, tuberculosis, and fungal infections.
Case Continued
During an episode of pneumothorax, the patient undergoes chest tube placement, pleurodesis, and lung biopsy. Pathology reveals bronchiolitis obliterans as well as organizing pneumonia (Figure 2). No organisms are seen on acid-fast bacilli or GMS stains.
- What are the other late-onset noninfectious pulmonary complications?
Definitions of other late noninfectious pulmonary complications following HSCT are shown in Table 3.
Interstitial pneumonias may represent COP or may be idiopathic pneumonia syndrome with a later onset or a nonspecific interstitial pneumonia. This syndrome is poorly defined, with a number of differing definitions of the syndrome published in the literature.50–55
A rare pulmonary complication after HSCT is pulmonary veno-occlusive disease (PVOD). Pulmonary hypertension has been reported after HSCT,56 but PVOD is a subset of pulmonary hypertension. It is associated with pleural effusions and volume overload on chest radiography.57,58 It may present early or late after transplant and is poorly understood.
Besides obstructive and restrictive PFT abnormalities, changes in small airway function59 after transplant and loss in diffusing capacity of the lungs for carbon monoxide (D
Case Conclusion
The patient’s lung function continues to worsen, but no infectious etiologies are discovered. Ultimately, she dies of respiratory failure caused by progressive bronchiolitis obliterans.
Conclusion
Late pulmonary complications occur frequently in patients who have undergone HSCT. These complications can be classified as infectious versus noninfectious etiologies. Late-onset complications are more common in allogeneic transplantations because they are associated with chronic GVHD. These complications can be manifestations of pulmonary GHVD or can be infectious complications associated with prolonged immunosuppression. Appropriate monitoring for the development of BOS is essential. Early and aggressive treatment of respiratory infections and diagnostic bronchoscopy with BAL can help elucidate most infectious causes. Still, diagnostic challenges remain and multiple causes of respiratory deterioration can be present concurrently in the post-HSCT patient. Steroid therapy remains the mainstay treatment for most noninfectious pulmonary complications and should be strongly considered once infection is effectively ruled out.
1. Remberger M, Ackefors M, Berglund S, et al. Improved survival after allogeneic hematopoietic stem cell transplantation in recent years. A single-center study. Biol Blood Marrow Transplant 2011;17:1688–97.
2. Wood KL, Esguerra VG. Management of late pulmonary complications after hematopoietic stem cell transplantation. Hosp Phys Hematology-Oncology Board Review Manual 2018;13(1):36–48.
3. Ninin E, Milpied N, Moreau P, et al. Longitudinal study of bacterial, viral, and fungal infections in adult recipients of bone marrow transplants. Clin Infect Dis 2001;33:41–7.
4. Roca J, Granena A, Rodriguez-Roisin R, et al. Fatal airway disease in an adult with chronic graft-versus-host disease. Thorax 1982;37:77–8.
5. Williams KM, Chien JW, Gladwin MT, Pavletic SZ. Bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation. JAMA 2009;302:306–14.
6. Chien JW, Martin PJ, Gooley TA, et al. Airflow obstruction after myeloablative allogeneic hematopoietic stem cell transplantation. Am J Respir Crit Care Med 2003;168:208–14.
7. Holbro A, Lehmann T, Girsberger S, et al. Lung histology predicts outcome of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2013;19:973–80.
8. Chamberlain D, Maurer J, Chaparro C, Idolor L. Evaluation of transbronchial lung biopsy specimens in the diagnosis of bronchiolitis obliterans after lung transplantation. J Heart Lung Transplant 1994;13:963–71.
9. Au BK, Au MA, Chien JW. Bronchiolitis obliterans syndrome epidemiology after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant 2011;17:1072–8.
10. Jagasia MH, Greinix HT, Arora M, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol Blood Marrow Transplant 2015;21:389–401.
11. Couriel D, Carpenter PA, Cutler C, et al. Ancillary therapy and supportive care of chronic graft-versus-host disease: national institutes of health consensus development project on criteria for clinical trials in chronic Graft-versus-host disease: V. Ancillary Therapy and Supportive Care Working Group Report. Biol Blood Marrow Transplant 2006;12:375–96.
12. Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J 2005;26:948–68.
13. Williams KM, Hnatiuk O, Mitchell SA, et al. NHANES III equations enhance early detection and mortality prediction of bronchiolitis obliterans syndrome after hematopoietic SCT. Bone Marrow Transplant 2014;49:561–6.
14. Hyatt RE, Cowl CT, Bjoraker JA, Scanlon PD. Conditions associated with an abnormal nonspecific pattern of pulmonary function tests. Chest 2009;135:419–24.
15. Bergeron A, Godet C, Chevret S, et al. Bronchiolitis obliterans syndrome after allogeneic hematopoietic SCT: phenotypes and prognosis. Bone Marrow Transplant 2013;48:819–24.
16. Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant 2005;11:945–56.
17. Gazourian L, Coronata AM, Rogers AJ, et al. Airway dilation in bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation. Respir Med 2013;107:276–83.
18. Gunn ML, Godwin JD, Kanne JP, et al. High-resolution CT findings of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. J Thorac Imaging 2008;23:244–50.
19. Sargent MA, Cairns RA, Murdoch MJ, et al. Obstructive lung disease in children after allogeneic bone marrow transplantation: evaluation with high-resolution CT. AJR Am J Roentgenol 1995;164:693–6.
20. Galban CJ, Boes JL, Bule M, et al. Parametric response mapping as an indicator of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2014;20:1592–8.
21. Meyer KC, Raghu G, Verleden GM, et al. An international ISHLT/ATS/ERS clinical practice guideline: diagnosis and management of bronchiolitis obliterans syndrome. Eur Respir J 2014;44:1479–1503.
22. Hildebrandt GC, Fazekas T, Lawitschka A, et al. Diagnosis and treatment of pulmonary chronic GVHD: report from the consensus conference on clinical practice in chronic GVHD. Bone Marrow Transplant 2011;46:1283–95.
23. Carpenter PA, Kitko CL, Elad S, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: V. The 2014 Ancillary Therapy and Supportive Care Working Group Report. Biol Blood Marrow Transplant 2015;21:1167–87.
24. Norman BC, Jacobsohn DA, Williams KM, et al. Fluticasone, azithromycin and montelukast therapy in reducing corticosteroid exposure in bronchiolitis obliterans syndrome after allogeneic hematopoietic SCT: a case series of eight patients. Bone Marrow Transplant 2011;46:1369–73.
25. Williams KM, Cheng GS, Pusic I, et al. Fluticasone, azithromycin, and montelukast treatment for new-onset bronchiolitis obliterans syndrome after hematopoietic cell transplantation. Biol Blood Marrow Transplant 2016;22:710–6.
26. Or R, Gesundheit B, Resnick I, et al. Sparing effect by montelukast treatment for chronic graft versus host disease: a pilot study. Transplantation 2007;83:577–81.
27. Cheng GS, Storer B, Chien JW, et al. Lung function trajectory in bronchiolitis obliterans syndrome after allogeneic hematopoietic cell transplant. Ann Am Thorac Soc 2016;13:1932–9.
28. Bergeron A, Belle A, Chevret S, et al. Combined inhaled steroids and bronchodilatators in obstructive airway disease after allogeneic stem cell transplantation. Bone Marrow Transplant 2007;39:547–53.
29. Bashoura L, Gupta S, Jain A, et al. Inhaled corticosteroids stabilize constrictive bronchiolitis after hematopoietic stem cell transplantation. Bone Marrow Transplant 2008;41:63–7.
30. Bergeron A, Chevret S, Granata A, et al. Effect of azithromycin on airflow decline-free survival after allogeneic hematopoietic stem cell transplant: the ALLOZITHRO randomized clinical trial. JAMA 2017;318:557–66.
31. Gerhardt SG, McDyer JF, Girgis RE, et al. Maintenance azithromycin therapy for bronchiolitis obliterans syndrome: results of a pilot study. Am J Respir Crit Care Med 2003;168:121–5.
32. Khalid M, Al Saghir A, Saleemi S, et al. Azithromycin in bronchiolitis obliterans complicating bone marrow transplantation: a preliminary study. Eur Respir J 2005;25:490–3.
33. Maimon N, Lipton JH, Chan CK, Marras TK. Macrolides in the treatment of bronchiolitis obliterans in allograft recipients. Bone Marrow Transplant 2009;44:69–73.
34. Lam DC, Lam B, Wong MK, et al. Effects of azithromycin in bronchiolitis obliterans syndrome after hematopoietic SCT--a randomized double-blinded placebo-controlled study. Bone Marrow Transplant 2011;46:1551–6.
35. Yadav H, Peters SG, Keogh KA, et al. Azithromycin for the treatment of obliterative bronchiolitis after hematopoietic stem cell transplantation: a systematic review and meta-analysis. Biol Blood Marrow Transplant 2016;22:2264–9.
36. Vos R, Vanaudenaerde BM, Verleden SE, et al. A randomised controlled trial of azithromycin to prevent chronic rejection after lung transplantation. Eur Respir J 2011;37:164–72.
37. Svanstrom H, Pasternak B, Hviid A. Use of azithromycin and death from cardiovascular causes. N Engl J Med 2013;368:1704–12.
38. Albert RK, Connett J, Bailey WC, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med 2011;365:689–98.
39. Tran J, Norder EE, Diaz PT, et al. Pulmonary rehabilitation for bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2012;18:1250–4.
40. Lucid CE, Savani BN, Engelhardt BG, et al. Extracorporeal photopheresis in patients with refractory bronchiolitis obliterans developing after allo-SCT. Bone Marrow Transplant 2011;46:426–9.
41. Hostettler KE, Halter JP, Gerull S, et al. Calcineurin inhibitors in bronchiolitis obliterans syndrome following stem cell transplantation. Eur Respir J 2014;43:221–32.
42. Holm AM, Riise GC, Brinch L, et al. Lung transplantation for bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation: unresolved questions. Transplantation 2013;96:e21–22.
43. Cheng GS, Edelman JD, Madtes DK, et al. Outcomes of lung transplantation after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2014;20:1169–75.
44. Okumura H, Ohtake S, Ontachi Y, et al. Living-donor lobar lung transplantation for broncho-bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation: does bronchiolitis obliterans recur in transplanted lungs? Int J Hematol 2007;86:369–73.
45. Olivieri A, Cimminiello M, Corradini P, et al. Long-term outcome and prospective validation of NIH response criteria in 39 patients receiving imatinib for steroid-refractory chronic GVHD. Blood 2013;122:4111–8.
46. Rahmanian S, Wood KL. Bronchiolitis obliterans and the risk of pneumothorax after transbronchial biopsy. Respiratory Medicine CME 2010;3:87–9.
47. Sakai R, Kanamori H, Nakaseko C, et al. Air-leak syndrome following allo-SCT in adult patients: report from the Kanto Study Group for Cell Therapy in Japan. Bone Marrow Transplant 2011;46:379–84.
48. Visscher DW, Myers JL. Histologic spectrum of idiopathic interstitial pneumonias. Proc Am Thorac Soc 2006;3:322–9.
49. Cordier JF. Cryptogenic organising pneumonia. Eur Respir J 2006;28:422–46.
50. Nishio N, Yagasaki H, Takahashi Y, et al. Late-onset non-infectious pulmonary complications following allogeneic hematopoietic stem cell transplantation in children. Bone Marrow Transplant 2009;44:303–8.
51. Ueda K, Watadani T, Maeda E, et al. Outcome and treatment of late-onset noninfectious pulmonary complications after allogeneic haematopoietic SCT. Bone Marrow Transplant 2010;45:1719–27.
52. Schlemmer F, Chevret S, Lorillon G, et al. Late-onset noninfectious interstitial lung disease after allogeneic hematopoietic stem cell transplantation. Respir Med 2014;108:1525–33.
53. Palmas A, Tefferi A, Myers JL, et al. Late-onset noninfectious pulmonary complications after allogeneic bone marrow transplantation. Br J Haematol 1998;100:680–7.
54. Sakaida E, Nakaseko C, Harima A, et al. Late-onset noninfectious pulmonary complications after allogeneic stem cell transplantation are significantly associated with chronic graft-versus-host disease and with the graft-versus-leukemia effect. Blood 2003;102:4236–42.
55. Solh M, Arat M, Cao Q, et al. Late-onset noninfectious pulmonary complications in adult allogeneic hematopoietic cell transplant recipients. Transplantation 2011;91:798–803.
56. Dandoy CE, Hirsch R, Chima R, et al. Pulmonary hypertension after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2013;19:1546–56.
57. Bunte MC, Patnaik MM, Pritzker MR, Burns LJ. Pulmonary veno-occlusive disease following hematopoietic stem cell transplantation: a rare model of endothelial dysfunction. Bone Marrow Transplant 2008;41:677–86.
58. Troussard X, Bernaudin JF, Cordonnier C, et al. Pulmonary veno-occlusive disease after bone marrow transplantation. Thorax 1984;39:956–7.
59. Lahzami S, Schoeffel RE, Pechey V, et al. Small airways function declines after allogeneic haematopoietic stem cell transplantation. Eur Respir J 2011;38:1180–8.
60. Jain NA, Pophali PA, Klotz JK, et al. Repair of impaired pulmonary function is possible in very-long-term allogeneic stem cell transplantation survivors. Biol Blood Marrow Transplant 2014;20:209–13.
61. Barisione G, Bacigalupo A, Crimi E, et al. Changes in lung volumes and airway responsiveness following haematopoietic stem cell transplantation. Eur Respir J 2008;32:1576–82.
62. Kovalszki A, Schumaker GL, Klein A, et al. Reduced respiratory and skeletal muscle strength in survivors of sibling or unrelated donor hematopoietic stem cell transplantation. Bone Marrow Transplant 2008;41:965–9.
63. Mathiesen S, Uhlving HH, Buchvald F, et al. Aerobic exercise capacity at long-term follow-up after paediatric allogeneic haematopoietic SCT. Bone Marrow Transplant 2014;49:1393–9.
1. Remberger M, Ackefors M, Berglund S, et al. Improved survival after allogeneic hematopoietic stem cell transplantation in recent years. A single-center study. Biol Blood Marrow Transplant 2011;17:1688–97.
2. Wood KL, Esguerra VG. Management of late pulmonary complications after hematopoietic stem cell transplantation. Hosp Phys Hematology-Oncology Board Review Manual 2018;13(1):36–48.
3. Ninin E, Milpied N, Moreau P, et al. Longitudinal study of bacterial, viral, and fungal infections in adult recipients of bone marrow transplants. Clin Infect Dis 2001;33:41–7.
4. Roca J, Granena A, Rodriguez-Roisin R, et al. Fatal airway disease in an adult with chronic graft-versus-host disease. Thorax 1982;37:77–8.
5. Williams KM, Chien JW, Gladwin MT, Pavletic SZ. Bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation. JAMA 2009;302:306–14.
6. Chien JW, Martin PJ, Gooley TA, et al. Airflow obstruction after myeloablative allogeneic hematopoietic stem cell transplantation. Am J Respir Crit Care Med 2003;168:208–14.
7. Holbro A, Lehmann T, Girsberger S, et al. Lung histology predicts outcome of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2013;19:973–80.
8. Chamberlain D, Maurer J, Chaparro C, Idolor L. Evaluation of transbronchial lung biopsy specimens in the diagnosis of bronchiolitis obliterans after lung transplantation. J Heart Lung Transplant 1994;13:963–71.
9. Au BK, Au MA, Chien JW. Bronchiolitis obliterans syndrome epidemiology after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant 2011;17:1072–8.
10. Jagasia MH, Greinix HT, Arora M, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol Blood Marrow Transplant 2015;21:389–401.
11. Couriel D, Carpenter PA, Cutler C, et al. Ancillary therapy and supportive care of chronic graft-versus-host disease: national institutes of health consensus development project on criteria for clinical trials in chronic Graft-versus-host disease: V. Ancillary Therapy and Supportive Care Working Group Report. Biol Blood Marrow Transplant 2006;12:375–96.
12. Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J 2005;26:948–68.
13. Williams KM, Hnatiuk O, Mitchell SA, et al. NHANES III equations enhance early detection and mortality prediction of bronchiolitis obliterans syndrome after hematopoietic SCT. Bone Marrow Transplant 2014;49:561–6.
14. Hyatt RE, Cowl CT, Bjoraker JA, Scanlon PD. Conditions associated with an abnormal nonspecific pattern of pulmonary function tests. Chest 2009;135:419–24.
15. Bergeron A, Godet C, Chevret S, et al. Bronchiolitis obliterans syndrome after allogeneic hematopoietic SCT: phenotypes and prognosis. Bone Marrow Transplant 2013;48:819–24.
16. Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant 2005;11:945–56.
17. Gazourian L, Coronata AM, Rogers AJ, et al. Airway dilation in bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation. Respir Med 2013;107:276–83.
18. Gunn ML, Godwin JD, Kanne JP, et al. High-resolution CT findings of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. J Thorac Imaging 2008;23:244–50.
19. Sargent MA, Cairns RA, Murdoch MJ, et al. Obstructive lung disease in children after allogeneic bone marrow transplantation: evaluation with high-resolution CT. AJR Am J Roentgenol 1995;164:693–6.
20. Galban CJ, Boes JL, Bule M, et al. Parametric response mapping as an indicator of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2014;20:1592–8.
21. Meyer KC, Raghu G, Verleden GM, et al. An international ISHLT/ATS/ERS clinical practice guideline: diagnosis and management of bronchiolitis obliterans syndrome. Eur Respir J 2014;44:1479–1503.
22. Hildebrandt GC, Fazekas T, Lawitschka A, et al. Diagnosis and treatment of pulmonary chronic GVHD: report from the consensus conference on clinical practice in chronic GVHD. Bone Marrow Transplant 2011;46:1283–95.
23. Carpenter PA, Kitko CL, Elad S, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: V. The 2014 Ancillary Therapy and Supportive Care Working Group Report. Biol Blood Marrow Transplant 2015;21:1167–87.
24. Norman BC, Jacobsohn DA, Williams KM, et al. Fluticasone, azithromycin and montelukast therapy in reducing corticosteroid exposure in bronchiolitis obliterans syndrome after allogeneic hematopoietic SCT: a case series of eight patients. Bone Marrow Transplant 2011;46:1369–73.
25. Williams KM, Cheng GS, Pusic I, et al. Fluticasone, azithromycin, and montelukast treatment for new-onset bronchiolitis obliterans syndrome after hematopoietic cell transplantation. Biol Blood Marrow Transplant 2016;22:710–6.
26. Or R, Gesundheit B, Resnick I, et al. Sparing effect by montelukast treatment for chronic graft versus host disease: a pilot study. Transplantation 2007;83:577–81.
27. Cheng GS, Storer B, Chien JW, et al. Lung function trajectory in bronchiolitis obliterans syndrome after allogeneic hematopoietic cell transplant. Ann Am Thorac Soc 2016;13:1932–9.
28. Bergeron A, Belle A, Chevret S, et al. Combined inhaled steroids and bronchodilatators in obstructive airway disease after allogeneic stem cell transplantation. Bone Marrow Transplant 2007;39:547–53.
29. Bashoura L, Gupta S, Jain A, et al. Inhaled corticosteroids stabilize constrictive bronchiolitis after hematopoietic stem cell transplantation. Bone Marrow Transplant 2008;41:63–7.
30. Bergeron A, Chevret S, Granata A, et al. Effect of azithromycin on airflow decline-free survival after allogeneic hematopoietic stem cell transplant: the ALLOZITHRO randomized clinical trial. JAMA 2017;318:557–66.
31. Gerhardt SG, McDyer JF, Girgis RE, et al. Maintenance azithromycin therapy for bronchiolitis obliterans syndrome: results of a pilot study. Am J Respir Crit Care Med 2003;168:121–5.
32. Khalid M, Al Saghir A, Saleemi S, et al. Azithromycin in bronchiolitis obliterans complicating bone marrow transplantation: a preliminary study. Eur Respir J 2005;25:490–3.
33. Maimon N, Lipton JH, Chan CK, Marras TK. Macrolides in the treatment of bronchiolitis obliterans in allograft recipients. Bone Marrow Transplant 2009;44:69–73.
34. Lam DC, Lam B, Wong MK, et al. Effects of azithromycin in bronchiolitis obliterans syndrome after hematopoietic SCT--a randomized double-blinded placebo-controlled study. Bone Marrow Transplant 2011;46:1551–6.
35. Yadav H, Peters SG, Keogh KA, et al. Azithromycin for the treatment of obliterative bronchiolitis after hematopoietic stem cell transplantation: a systematic review and meta-analysis. Biol Blood Marrow Transplant 2016;22:2264–9.
36. Vos R, Vanaudenaerde BM, Verleden SE, et al. A randomised controlled trial of azithromycin to prevent chronic rejection after lung transplantation. Eur Respir J 2011;37:164–72.
37. Svanstrom H, Pasternak B, Hviid A. Use of azithromycin and death from cardiovascular causes. N Engl J Med 2013;368:1704–12.
38. Albert RK, Connett J, Bailey WC, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med 2011;365:689–98.
39. Tran J, Norder EE, Diaz PT, et al. Pulmonary rehabilitation for bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2012;18:1250–4.
40. Lucid CE, Savani BN, Engelhardt BG, et al. Extracorporeal photopheresis in patients with refractory bronchiolitis obliterans developing after allo-SCT. Bone Marrow Transplant 2011;46:426–9.
41. Hostettler KE, Halter JP, Gerull S, et al. Calcineurin inhibitors in bronchiolitis obliterans syndrome following stem cell transplantation. Eur Respir J 2014;43:221–32.
42. Holm AM, Riise GC, Brinch L, et al. Lung transplantation for bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation: unresolved questions. Transplantation 2013;96:e21–22.
43. Cheng GS, Edelman JD, Madtes DK, et al. Outcomes of lung transplantation after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2014;20:1169–75.
44. Okumura H, Ohtake S, Ontachi Y, et al. Living-donor lobar lung transplantation for broncho-bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation: does bronchiolitis obliterans recur in transplanted lungs? Int J Hematol 2007;86:369–73.
45. Olivieri A, Cimminiello M, Corradini P, et al. Long-term outcome and prospective validation of NIH response criteria in 39 patients receiving imatinib for steroid-refractory chronic GVHD. Blood 2013;122:4111–8.
46. Rahmanian S, Wood KL. Bronchiolitis obliterans and the risk of pneumothorax after transbronchial biopsy. Respiratory Medicine CME 2010;3:87–9.
47. Sakai R, Kanamori H, Nakaseko C, et al. Air-leak syndrome following allo-SCT in adult patients: report from the Kanto Study Group for Cell Therapy in Japan. Bone Marrow Transplant 2011;46:379–84.
48. Visscher DW, Myers JL. Histologic spectrum of idiopathic interstitial pneumonias. Proc Am Thorac Soc 2006;3:322–9.
49. Cordier JF. Cryptogenic organising pneumonia. Eur Respir J 2006;28:422–46.
50. Nishio N, Yagasaki H, Takahashi Y, et al. Late-onset non-infectious pulmonary complications following allogeneic hematopoietic stem cell transplantation in children. Bone Marrow Transplant 2009;44:303–8.
51. Ueda K, Watadani T, Maeda E, et al. Outcome and treatment of late-onset noninfectious pulmonary complications after allogeneic haematopoietic SCT. Bone Marrow Transplant 2010;45:1719–27.
52. Schlemmer F, Chevret S, Lorillon G, et al. Late-onset noninfectious interstitial lung disease after allogeneic hematopoietic stem cell transplantation. Respir Med 2014;108:1525–33.
53. Palmas A, Tefferi A, Myers JL, et al. Late-onset noninfectious pulmonary complications after allogeneic bone marrow transplantation. Br J Haematol 1998;100:680–7.
54. Sakaida E, Nakaseko C, Harima A, et al. Late-onset noninfectious pulmonary complications after allogeneic stem cell transplantation are significantly associated with chronic graft-versus-host disease and with the graft-versus-leukemia effect. Blood 2003;102:4236–42.
55. Solh M, Arat M, Cao Q, et al. Late-onset noninfectious pulmonary complications in adult allogeneic hematopoietic cell transplant recipients. Transplantation 2011;91:798–803.
56. Dandoy CE, Hirsch R, Chima R, et al. Pulmonary hypertension after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2013;19:1546–56.
57. Bunte MC, Patnaik MM, Pritzker MR, Burns LJ. Pulmonary veno-occlusive disease following hematopoietic stem cell transplantation: a rare model of endothelial dysfunction. Bone Marrow Transplant 2008;41:677–86.
58. Troussard X, Bernaudin JF, Cordonnier C, et al. Pulmonary veno-occlusive disease after bone marrow transplantation. Thorax 1984;39:956–7.
59. Lahzami S, Schoeffel RE, Pechey V, et al. Small airways function declines after allogeneic haematopoietic stem cell transplantation. Eur Respir J 2011;38:1180–8.
60. Jain NA, Pophali PA, Klotz JK, et al. Repair of impaired pulmonary function is possible in very-long-term allogeneic stem cell transplantation survivors. Biol Blood Marrow Transplant 2014;20:209–13.
61. Barisione G, Bacigalupo A, Crimi E, et al. Changes in lung volumes and airway responsiveness following haematopoietic stem cell transplantation. Eur Respir J 2008;32:1576–82.
62. Kovalszki A, Schumaker GL, Klein A, et al. Reduced respiratory and skeletal muscle strength in survivors of sibling or unrelated donor hematopoietic stem cell transplantation. Bone Marrow Transplant 2008;41:965–9.
63. Mathiesen S, Uhlving HH, Buchvald F, et al. Aerobic exercise capacity at long-term follow-up after paediatric allogeneic haematopoietic SCT. Bone Marrow Transplant 2014;49:1393–9.
Part 2: Why the Increase?
As established last week, there has been a startling increase in sexually transmitted infections (STIs) among older adults in the United States. The burning question on everyone’s mind (certainly mine!) is: Why? Engaging in some “educated speculation” yields many factors possibly driving this trend. For example:
1. Provider Reluctance. Older Americans may not get regular screenings for STIs because their health care providers are often reluctant to raise the issue. That may be fueled by lack of awareness on the clinician’s part: More than 60% of individuals older than 60 have sex at least once a month, yet this population is rarely considered to be “at risk” for STIs.1
2. Patient Embarrassment/awkwardness. For many older Americans, admitting that they are having sex makes them feel awkward or embarrassed. Reluctance to share intimate details means they may not seek evaluation and treatment for symptoms that seem related to their sexual health or activity.
3. Effects of Aging. There are 2 sides to this coin: actual physiologic changes that occur with age and assumptions that all changes are just part of aging. As people get older, their immune systems tend to deteriorate, making them more vulnerable to contracting any disease—including STIs. After menopause, women's vaginal tissues thin and natural lubrication declines, increasing their risk for microtears that can leave them susceptible to infectious organisms. And let’s be honest: Some STI symptoms, such as fatigue, weakness, and changes in memory, are nonspecific and may be mistaken by clinicians for the regular progression of age.2
4. Social Changes. The world has changed since most older adults last dove into the dating pool. We now have online dating services, some of which cater to a mature audience; as a result, people may be less familiar with their partner’s sexual history. Compounding that, many older adults just aren’t accustomed to thinking of themselves or a partner as being at high risk for STIs—and if you don’t even think about it, you definitely won’t ask. Widowed or divorced adults may date more than one person at a time, raising their risk for infection after a long period of monogamy. Seniors also may not be accustomed to using a condom or do not use one because they think the risk for STIs is minimal or nonexistent. Seniors may not consider oral or anal sex as a way of contracting or transmitting STIs.3
5. Medical Advances. Compared with previous generations, today’s seniors have an easier time having sex at an older age, thanks to the availability of medications such as sildenafil (Viagra) and tadalafil (Cialis) for men with erectile dysfunction. There has also been an increase in postmenopausal women requesting and receiving bioidentical hormone replacement. With increased libido and ability to perform come more sexual encounters among the older population—and as a result, more opportunities for STIs to spread. Are there other reasons for the increase in STIs in this population? Next week we’ll consider the unique societal influences of the Baby Boom generation. In the meantime, please share your insights with me at [email protected].
1. Boskey E. STDs in the elderly community. Verywell Health. February 14, 2018. www.verywellhealth.com/stds-the-elderly-3133189. Accessed May 8, 2019.
2. East A. (2017). Seniors and STDs: common sexually transmitted diseases. CaringPeople. June 23, 2017. https://caringpeopleinc.com/blog/seniors-common-sexually-transmitted-diseases. Accessed May 8, 2019.
3. Harvard Medical School. Sexually transmitted disease? At my age? Harvard Health Letter. February 2018. www.health.harvard.edu/diseases-and-conditions/sexually-transmitted-disease-at-my-age. Accessed May 8, 2019.
As established last week, there has been a startling increase in sexually transmitted infections (STIs) among older adults in the United States. The burning question on everyone’s mind (certainly mine!) is: Why? Engaging in some “educated speculation” yields many factors possibly driving this trend. For example:
1. Provider Reluctance. Older Americans may not get regular screenings for STIs because their health care providers are often reluctant to raise the issue. That may be fueled by lack of awareness on the clinician’s part: More than 60% of individuals older than 60 have sex at least once a month, yet this population is rarely considered to be “at risk” for STIs.1
2. Patient Embarrassment/awkwardness. For many older Americans, admitting that they are having sex makes them feel awkward or embarrassed. Reluctance to share intimate details means they may not seek evaluation and treatment for symptoms that seem related to their sexual health or activity.
3. Effects of Aging. There are 2 sides to this coin: actual physiologic changes that occur with age and assumptions that all changes are just part of aging. As people get older, their immune systems tend to deteriorate, making them more vulnerable to contracting any disease—including STIs. After menopause, women's vaginal tissues thin and natural lubrication declines, increasing their risk for microtears that can leave them susceptible to infectious organisms. And let’s be honest: Some STI symptoms, such as fatigue, weakness, and changes in memory, are nonspecific and may be mistaken by clinicians for the regular progression of age.2
4. Social Changes. The world has changed since most older adults last dove into the dating pool. We now have online dating services, some of which cater to a mature audience; as a result, people may be less familiar with their partner’s sexual history. Compounding that, many older adults just aren’t accustomed to thinking of themselves or a partner as being at high risk for STIs—and if you don’t even think about it, you definitely won’t ask. Widowed or divorced adults may date more than one person at a time, raising their risk for infection after a long period of monogamy. Seniors also may not be accustomed to using a condom or do not use one because they think the risk for STIs is minimal or nonexistent. Seniors may not consider oral or anal sex as a way of contracting or transmitting STIs.3
5. Medical Advances. Compared with previous generations, today’s seniors have an easier time having sex at an older age, thanks to the availability of medications such as sildenafil (Viagra) and tadalafil (Cialis) for men with erectile dysfunction. There has also been an increase in postmenopausal women requesting and receiving bioidentical hormone replacement. With increased libido and ability to perform come more sexual encounters among the older population—and as a result, more opportunities for STIs to spread. Are there other reasons for the increase in STIs in this population? Next week we’ll consider the unique societal influences of the Baby Boom generation. In the meantime, please share your insights with me at [email protected].
As established last week, there has been a startling increase in sexually transmitted infections (STIs) among older adults in the United States. The burning question on everyone’s mind (certainly mine!) is: Why? Engaging in some “educated speculation” yields many factors possibly driving this trend. For example:
1. Provider Reluctance. Older Americans may not get regular screenings for STIs because their health care providers are often reluctant to raise the issue. That may be fueled by lack of awareness on the clinician’s part: More than 60% of individuals older than 60 have sex at least once a month, yet this population is rarely considered to be “at risk” for STIs.1
2. Patient Embarrassment/awkwardness. For many older Americans, admitting that they are having sex makes them feel awkward or embarrassed. Reluctance to share intimate details means they may not seek evaluation and treatment for symptoms that seem related to their sexual health or activity.
3. Effects of Aging. There are 2 sides to this coin: actual physiologic changes that occur with age and assumptions that all changes are just part of aging. As people get older, their immune systems tend to deteriorate, making them more vulnerable to contracting any disease—including STIs. After menopause, women's vaginal tissues thin and natural lubrication declines, increasing their risk for microtears that can leave them susceptible to infectious organisms. And let’s be honest: Some STI symptoms, such as fatigue, weakness, and changes in memory, are nonspecific and may be mistaken by clinicians for the regular progression of age.2
4. Social Changes. The world has changed since most older adults last dove into the dating pool. We now have online dating services, some of which cater to a mature audience; as a result, people may be less familiar with their partner’s sexual history. Compounding that, many older adults just aren’t accustomed to thinking of themselves or a partner as being at high risk for STIs—and if you don’t even think about it, you definitely won’t ask. Widowed or divorced adults may date more than one person at a time, raising their risk for infection after a long period of monogamy. Seniors also may not be accustomed to using a condom or do not use one because they think the risk for STIs is minimal or nonexistent. Seniors may not consider oral or anal sex as a way of contracting or transmitting STIs.3
5. Medical Advances. Compared with previous generations, today’s seniors have an easier time having sex at an older age, thanks to the availability of medications such as sildenafil (Viagra) and tadalafil (Cialis) for men with erectile dysfunction. There has also been an increase in postmenopausal women requesting and receiving bioidentical hormone replacement. With increased libido and ability to perform come more sexual encounters among the older population—and as a result, more opportunities for STIs to spread. Are there other reasons for the increase in STIs in this population? Next week we’ll consider the unique societal influences of the Baby Boom generation. In the meantime, please share your insights with me at [email protected].
1. Boskey E. STDs in the elderly community. Verywell Health. February 14, 2018. www.verywellhealth.com/stds-the-elderly-3133189. Accessed May 8, 2019.
2. East A. (2017). Seniors and STDs: common sexually transmitted diseases. CaringPeople. June 23, 2017. https://caringpeopleinc.com/blog/seniors-common-sexually-transmitted-diseases. Accessed May 8, 2019.
3. Harvard Medical School. Sexually transmitted disease? At my age? Harvard Health Letter. February 2018. www.health.harvard.edu/diseases-and-conditions/sexually-transmitted-disease-at-my-age. Accessed May 8, 2019.
1. Boskey E. STDs in the elderly community. Verywell Health. February 14, 2018. www.verywellhealth.com/stds-the-elderly-3133189. Accessed May 8, 2019.
2. East A. (2017). Seniors and STDs: common sexually transmitted diseases. CaringPeople. June 23, 2017. https://caringpeopleinc.com/blog/seniors-common-sexually-transmitted-diseases. Accessed May 8, 2019.
3. Harvard Medical School. Sexually transmitted disease? At my age? Harvard Health Letter. February 2018. www.health.harvard.edu/diseases-and-conditions/sexually-transmitted-disease-at-my-age. Accessed May 8, 2019.

High-deductible plans do not raise out-of-pocket costs for autism care
In states that mandate coverage for autism spectrum disorder (ASD) health services, families in high-deductible health plans (HDHPs) access ASD-related services without paying more out-of-pocket expenses than traditional plan enrollees, an analysis found.

Lead author Colleen L. Barry, PhD, of Johns Hopkins University, Baltimore, and colleagues examined insurance claims between 2008 and 2012 for children covered by three large U.S. insurers (United Healthcare, Aetna, and Humana) to compare the effects of ASD-related coverage mandates on health spending. At least 47 states and Washington, D.C., have enacted mandates that require insurers to cover ASD-related health services, such as diagnostic and assessment services and behavioral and functional therapies. The final study sample included 98,639 children aged 0-21 years with at least two ASD-related service claims on different days during the study period.
The investigators found that, among HDHP enrollees, coverage mandates were associated with marked increases in average monthly spending across all service categories, but not among traditional plan enrollees. Specifically for HDHP patients, ASD coverage mandates were linked to a $98 greater increase in average monthly spending for insurers on ASD-specific outpatient services, a $142 greater increase in average monthly insurer spending on all outpatient services, and a $142 greater increase in average monthly insurer spending on all health services, according to the study published in Pediatrics. Out-of-pocket spending by patients however, was not significantly different between HDHP and traditional plan enrollees in states that mandate ASD-related coverage, the study found.
Dr. Barry and associates concluded that patients in both HDHP and traditional insurance plans spend large sums on ASD-related care in coverage mandate states, but because costs likely exceed HDHP deductibles, insurers absorb any increases. They suggested that families with regularly high health care expenditures related to ASD services consider high-deductible plans in the context of mandate laws.
“Future research is needed to better understand how features of HDHPs, such as deductible size and health savings account structure, influence the ability of families to make wise choices in obtaining care, and to examine plan premiums and financial strain associated with these plans, particularly for families with children with ASD and high expenditures,” Dr. Barry and associates wrote.
The authors reported no relevant financial disclosures. The study was supported by a National Institute of Mental Health grant and funded by the National Institutes of Health.
SOURCE: Barry CL et al. Pediatrics. 2019 May 13. doi: 10.1542/peds.2018-2391.
The analysis by Barry et al. takes a deep dive into the impact of different payment models on a family’s access to autism spectrum disorder–related services, commented David Keller, MD, and Ann Reynolds, MD.
The work emphasizes the reason that “we must continue to study how interventions in behavioral economics, such as mandates and high-deductible health plans, impact access to care for our most vulnerable children,” they wrote.
These data were from 2008 to 2012, before the Affordable Care Act was implemented. As the definition of “high deductible” has changed from $3,000 annually to $10,000 annually, “have families made different choices regarding care?” they asked.
“With the implementation of value-based payments, we will be creating competing forces through the application of behavioral economics. We need to understand how the interplay of economic forces affects families and their access to essential services,” Dr. Keller and Dr. Reynolds continued.
“We need to understand how to help families make informed decisions that balance the needs of their children with the financial realities of our complex care system so that we can support them in that process,” they wrote. “Understanding the impact of behavioral economics on consumer behavior is essential to assuring that children get the right care at the right time for the right diagnosis.”
Dr. Keller is a professor and Dr. Reynolds is an associate professor at the University of Colorado at Denver, Aurora. This is an excerpt of their editorial that accompanies the study by Barry et al. (Pediatrics. 2019 May 13. doi: 10.1542/peds.2019-0926). Dr. Keller reported no relevant financial disclosures. Dr. Reynolds reported providing consultation to Ovid Therapeutics regarding evaluation of sleep severity and improvement in clinical trials.
The analysis by Barry et al. takes a deep dive into the impact of different payment models on a family’s access to autism spectrum disorder–related services, commented David Keller, MD, and Ann Reynolds, MD.
The work emphasizes the reason that “we must continue to study how interventions in behavioral economics, such as mandates and high-deductible health plans, impact access to care for our most vulnerable children,” they wrote.
These data were from 2008 to 2012, before the Affordable Care Act was implemented. As the definition of “high deductible” has changed from $3,000 annually to $10,000 annually, “have families made different choices regarding care?” they asked.
“With the implementation of value-based payments, we will be creating competing forces through the application of behavioral economics. We need to understand how the interplay of economic forces affects families and their access to essential services,” Dr. Keller and Dr. Reynolds continued.
“We need to understand how to help families make informed decisions that balance the needs of their children with the financial realities of our complex care system so that we can support them in that process,” they wrote. “Understanding the impact of behavioral economics on consumer behavior is essential to assuring that children get the right care at the right time for the right diagnosis.”
Dr. Keller is a professor and Dr. Reynolds is an associate professor at the University of Colorado at Denver, Aurora. This is an excerpt of their editorial that accompanies the study by Barry et al. (Pediatrics. 2019 May 13. doi: 10.1542/peds.2019-0926). Dr. Keller reported no relevant financial disclosures. Dr. Reynolds reported providing consultation to Ovid Therapeutics regarding evaluation of sleep severity and improvement in clinical trials.
The analysis by Barry et al. takes a deep dive into the impact of different payment models on a family’s access to autism spectrum disorder–related services, commented David Keller, MD, and Ann Reynolds, MD.
The work emphasizes the reason that “we must continue to study how interventions in behavioral economics, such as mandates and high-deductible health plans, impact access to care for our most vulnerable children,” they wrote.
These data were from 2008 to 2012, before the Affordable Care Act was implemented. As the definition of “high deductible” has changed from $3,000 annually to $10,000 annually, “have families made different choices regarding care?” they asked.
“With the implementation of value-based payments, we will be creating competing forces through the application of behavioral economics. We need to understand how the interplay of economic forces affects families and their access to essential services,” Dr. Keller and Dr. Reynolds continued.
“We need to understand how to help families make informed decisions that balance the needs of their children with the financial realities of our complex care system so that we can support them in that process,” they wrote. “Understanding the impact of behavioral economics on consumer behavior is essential to assuring that children get the right care at the right time for the right diagnosis.”
Dr. Keller is a professor and Dr. Reynolds is an associate professor at the University of Colorado at Denver, Aurora. This is an excerpt of their editorial that accompanies the study by Barry et al. (Pediatrics. 2019 May 13. doi: 10.1542/peds.2019-0926). Dr. Keller reported no relevant financial disclosures. Dr. Reynolds reported providing consultation to Ovid Therapeutics regarding evaluation of sleep severity and improvement in clinical trials.
In states that mandate coverage for autism spectrum disorder (ASD) health services, families in high-deductible health plans (HDHPs) access ASD-related services without paying more out-of-pocket expenses than traditional plan enrollees, an analysis found.
Lead author Colleen L. Barry, PhD, of Johns Hopkins University, Baltimore, and colleagues examined insurance claims between 2008 and 2012 for children covered by three large U.S. insurers (United Healthcare, Aetna, and Humana) to compare the effects of ASD-related coverage mandates on health spending. At least 47 states and Washington, D.C., have enacted mandates that require insurers to cover ASD-related health services, such as diagnostic and assessment services and behavioral and functional therapies. The final study sample included 98,639 children aged 0-21 years with at least two ASD-related service claims on different days during the study period.
The investigators found that, among HDHP enrollees, coverage mandates were associated with marked increases in average monthly spending across all service categories, but not among traditional plan enrollees. Specifically for HDHP patients, ASD coverage mandates were linked to a $98 greater increase in average monthly spending for insurers on ASD-specific outpatient services, a $142 greater increase in average monthly insurer spending on all outpatient services, and a $142 greater increase in average monthly insurer spending on all health services, according to the study published in Pediatrics. Out-of-pocket spending by patients however, was not significantly different between HDHP and traditional plan enrollees in states that mandate ASD-related coverage, the study found.
Dr. Barry and associates concluded that patients in both HDHP and traditional insurance plans spend large sums on ASD-related care in coverage mandate states, but because costs likely exceed HDHP deductibles, insurers absorb any increases. They suggested that families with regularly high health care expenditures related to ASD services consider high-deductible plans in the context of mandate laws.
“Future research is needed to better understand how features of HDHPs, such as deductible size and health savings account structure, influence the ability of families to make wise choices in obtaining care, and to examine plan premiums and financial strain associated with these plans, particularly for families with children with ASD and high expenditures,” Dr. Barry and associates wrote.
The authors reported no relevant financial disclosures. The study was supported by a National Institute of Mental Health grant and funded by the National Institutes of Health.
SOURCE: Barry CL et al. Pediatrics. 2019 May 13. doi: 10.1542/peds.2018-2391.
In states that mandate coverage for autism spectrum disorder (ASD) health services, families in high-deductible health plans (HDHPs) access ASD-related services without paying more out-of-pocket expenses than traditional plan enrollees, an analysis found.
Lead author Colleen L. Barry, PhD, of Johns Hopkins University, Baltimore, and colleagues examined insurance claims between 2008 and 2012 for children covered by three large U.S. insurers (United Healthcare, Aetna, and Humana) to compare the effects of ASD-related coverage mandates on health spending. At least 47 states and Washington, D.C., have enacted mandates that require insurers to cover ASD-related health services, such as diagnostic and assessment services and behavioral and functional therapies. The final study sample included 98,639 children aged 0-21 years with at least two ASD-related service claims on different days during the study period.
The investigators found that, among HDHP enrollees, coverage mandates were associated with marked increases in average monthly spending across all service categories, but not among traditional plan enrollees. Specifically for HDHP patients, ASD coverage mandates were linked to a $98 greater increase in average monthly spending for insurers on ASD-specific outpatient services, a $142 greater increase in average monthly insurer spending on all outpatient services, and a $142 greater increase in average monthly insurer spending on all health services, according to the study published in Pediatrics. Out-of-pocket spending by patients however, was not significantly different between HDHP and traditional plan enrollees in states that mandate ASD-related coverage, the study found.
Dr. Barry and associates concluded that patients in both HDHP and traditional insurance plans spend large sums on ASD-related care in coverage mandate states, but because costs likely exceed HDHP deductibles, insurers absorb any increases. They suggested that families with regularly high health care expenditures related to ASD services consider high-deductible plans in the context of mandate laws.
“Future research is needed to better understand how features of HDHPs, such as deductible size and health savings account structure, influence the ability of families to make wise choices in obtaining care, and to examine plan premiums and financial strain associated with these plans, particularly for families with children with ASD and high expenditures,” Dr. Barry and associates wrote.
The authors reported no relevant financial disclosures. The study was supported by a National Institute of Mental Health grant and funded by the National Institutes of Health.
SOURCE: Barry CL et al. Pediatrics. 2019 May 13. doi: 10.1542/peds.2018-2391.
FROM PEDIATRICS