User login
Psychiatry Innovation Lab nurtures young businesses
The future of mental health is in our own hands. As psychiatrists, we have a wealth of experience to fuel transformation in our field and improve care for our patients. What we lack is the space in which to share our ideas and turn them into tangible solutions like sustainable businesses, diagnostic devices, mobile apps, or prevention campaigns.
The Psychiatry Innovation Lab provides just that – it is an incubator nurturing early-stage ideas and ventures by investing in them through mentorship, education, funding, and collaboration opportunities within a community of mental health innovators.

The lab’s main event is on Sunday, May 6, 2018, when leaders in psychiatry will gather alongside industry leaders at the Jacob Javits Convention Center in New York City during the American Psychiatric Association meeting for this fourth annual live event . At the event, finalists will pitch ideas “Shark Tank” style to a panel of expert judges. Finalists will work closely with industry leaders and audience members to fine-tune their ideas before pitching their revisions to the judges as well as to a live, voting audience, who together select the winners of cash awards and other prizes.

The Psychiatry Innovation Lab was founded in 2015 by Nina Vasan, MD, a Stanford (Calif.) University psychiatrist and author of Do Good Well: Your Guide to Leadership, Action, and Social Innovation (San Francisco: Jossey-Bass, 2013), with the purpose of catalyzing more entrepreneurship and innovation in mental health.
“The most meaningful part of the lab has been the impact that these ventures have had on the patients that we serve,” said Dr. Vasan, chair of the Psychiatry Innovation Lab and director of Brainstorm, the Stanford Laboratory for Brain Health Innovation and Entrepreneurship. “Year after year, psychiatrists come back and tell us that they are looking at their own patient care differently now. They’re looking for ways to be innovative, and we’re giving them the tools necessary to turn their clinical expertise into successful ventures.”
Applications are currently open online to pitch an idea in this year’s lab. Applications consist of brief answers to questions and a short YouTube video. The deadline for submissions is Friday, March 9, 2018. Anyone with innovative ideas, regardless of the stage, is invited to apply. The APA Workgroup on Psychiatry Innovation, which oversees the lab, welcomes ideas from people pitching for the first time to those working on their ideas full time. They noted that past finalists have come from all experience levels and a wide range of backgrounds, including students, CEOs, engineers, and psychiatrists.
Past winners and participants have come from a range of stages, from early start-ups to established companies, including NeuroLex Labs, which uses voice samples to detect behavioral health illness; Spring, which uses machine learning to determine the best depression treatment; Muse, which creates an EEG sensing headband to aid mindfulness practice; and Overdose Recovery Bracelet, which builds a wristband to deliver naloxone to people who have overdosed on opiates.
The diversity of ideas has been remarkable; ideas in the past have ranged from traditional for-profit businesses to nonprofits, educational and public health programs, and proposals for government reform. They address problems at all parts of the health care spectrum: prevention, diagnosis, treatment, systems, EMRs, and more.
“Many past ideas have revolved around technology such as artificial intelligence, social networking, or telemedicine,” Dr. Vasan said. “. Those ideas are especially important in solving the most pressing problems in our field today.”
In addition to those competing, anyone registered to attend the APA annual meeting can attend the event as an audience member or join a team and help as an innovation leader during the coaching portion of the program. Last year alone, more than 70% of the participants in the lab said that it was better than other educational events they have attended, 95% of participants found it useful, and participants made an average of six new contacts through the event.
“The Psychiatry Innovation Lab connected me to people who continue to inspire and educate me toward making a real impact with my own endeavors,” said Cody Rall, MD, founder of the YouTube channel Techforpsych and a 2016 semifinalist.
“The lab has grown dramatically. When we started we worked hard to find just one sponsor; last year we had 10 sponsors and over $25,000 in cash and prizes.” Dr. Vasan said. “We also had our first international finalist from Pakistan. The commitment to solving problems in mental health is taking off, and we want to ensure that psychiatrists are front and center in leading the change.”
For more information about joining the innovation lab or other ways to be involved, including sponsorship and judging, visit https://www.psychiatry.org/innovation or email Nina Taylor, APA deputy director of education, at [email protected].
This article was updated January 23, 2018.
Dr. Chaudhary is a board member of the APA Psychiatry Innovation Lab and the APA Workgroup on Psychiatry Innovation; chief resident in child and adolescent psychiatry at Massachusetts General Hospital/McLean and clinical fellow at Harvard Medical School, both in Boston; and founding partner of Brainstorm: Stanford Laboratory for Brain Health Innovation and Entrepreneurship. Dr. Ghomi is a board member of the APA Psychiatry Innovation Lab and the APA Workgroup on Psychiatry Innovation; resident in psychiatry at the University of Washington, Seattle; chief medical officer at NeuroLex; and founding partner of Brainstorm: Stanford Laboratory for Brain Health Innovation and Entrepreneurship.
The future of mental health is in our own hands. As psychiatrists, we have a wealth of experience to fuel transformation in our field and improve care for our patients. What we lack is the space in which to share our ideas and turn them into tangible solutions like sustainable businesses, diagnostic devices, mobile apps, or prevention campaigns.
The Psychiatry Innovation Lab provides just that – it is an incubator nurturing early-stage ideas and ventures by investing in them through mentorship, education, funding, and collaboration opportunities within a community of mental health innovators.
The lab’s main event is on Sunday, May 6, 2018, when leaders in psychiatry will gather alongside industry leaders at the Jacob Javits Convention Center in New York City during the American Psychiatric Association meeting for this fourth annual live event . At the event, finalists will pitch ideas “Shark Tank” style to a panel of expert judges. Finalists will work closely with industry leaders and audience members to fine-tune their ideas before pitching their revisions to the judges as well as to a live, voting audience, who together select the winners of cash awards and other prizes.
The Psychiatry Innovation Lab was founded in 2015 by Nina Vasan, MD, a Stanford (Calif.) University psychiatrist and author of Do Good Well: Your Guide to Leadership, Action, and Social Innovation (San Francisco: Jossey-Bass, 2013), with the purpose of catalyzing more entrepreneurship and innovation in mental health.
“The most meaningful part of the lab has been the impact that these ventures have had on the patients that we serve,” said Dr. Vasan, chair of the Psychiatry Innovation Lab and director of Brainstorm, the Stanford Laboratory for Brain Health Innovation and Entrepreneurship. “Year after year, psychiatrists come back and tell us that they are looking at their own patient care differently now. They’re looking for ways to be innovative, and we’re giving them the tools necessary to turn their clinical expertise into successful ventures.”
Applications are currently open online to pitch an idea in this year’s lab. Applications consist of brief answers to questions and a short YouTube video. The deadline for submissions is Friday, March 9, 2018. Anyone with innovative ideas, regardless of the stage, is invited to apply. The APA Workgroup on Psychiatry Innovation, which oversees the lab, welcomes ideas from people pitching for the first time to those working on their ideas full time. They noted that past finalists have come from all experience levels and a wide range of backgrounds, including students, CEOs, engineers, and psychiatrists.
Past winners and participants have come from a range of stages, from early start-ups to established companies, including NeuroLex Labs, which uses voice samples to detect behavioral health illness; Spring, which uses machine learning to determine the best depression treatment; Muse, which creates an EEG sensing headband to aid mindfulness practice; and Overdose Recovery Bracelet, which builds a wristband to deliver naloxone to people who have overdosed on opiates.
The diversity of ideas has been remarkable; ideas in the past have ranged from traditional for-profit businesses to nonprofits, educational and public health programs, and proposals for government reform. They address problems at all parts of the health care spectrum: prevention, diagnosis, treatment, systems, EMRs, and more.
“Many past ideas have revolved around technology such as artificial intelligence, social networking, or telemedicine,” Dr. Vasan said. “. Those ideas are especially important in solving the most pressing problems in our field today.”
In addition to those competing, anyone registered to attend the APA annual meeting can attend the event as an audience member or join a team and help as an innovation leader during the coaching portion of the program. Last year alone, more than 70% of the participants in the lab said that it was better than other educational events they have attended, 95% of participants found it useful, and participants made an average of six new contacts through the event.
“The Psychiatry Innovation Lab connected me to people who continue to inspire and educate me toward making a real impact with my own endeavors,” said Cody Rall, MD, founder of the YouTube channel Techforpsych and a 2016 semifinalist.
“The lab has grown dramatically. When we started we worked hard to find just one sponsor; last year we had 10 sponsors and over $25,000 in cash and prizes.” Dr. Vasan said. “We also had our first international finalist from Pakistan. The commitment to solving problems in mental health is taking off, and we want to ensure that psychiatrists are front and center in leading the change.”
For more information about joining the innovation lab or other ways to be involved, including sponsorship and judging, visit https://www.psychiatry.org/innovation or email Nina Taylor, APA deputy director of education, at [email protected].
This article was updated January 23, 2018.
Dr. Chaudhary is a board member of the APA Psychiatry Innovation Lab and the APA Workgroup on Psychiatry Innovation; chief resident in child and adolescent psychiatry at Massachusetts General Hospital/McLean and clinical fellow at Harvard Medical School, both in Boston; and founding partner of Brainstorm: Stanford Laboratory for Brain Health Innovation and Entrepreneurship. Dr. Ghomi is a board member of the APA Psychiatry Innovation Lab and the APA Workgroup on Psychiatry Innovation; resident in psychiatry at the University of Washington, Seattle; chief medical officer at NeuroLex; and founding partner of Brainstorm: Stanford Laboratory for Brain Health Innovation and Entrepreneurship.
The future of mental health is in our own hands. As psychiatrists, we have a wealth of experience to fuel transformation in our field and improve care for our patients. What we lack is the space in which to share our ideas and turn them into tangible solutions like sustainable businesses, diagnostic devices, mobile apps, or prevention campaigns.
The Psychiatry Innovation Lab provides just that – it is an incubator nurturing early-stage ideas and ventures by investing in them through mentorship, education, funding, and collaboration opportunities within a community of mental health innovators.
The lab’s main event is on Sunday, May 6, 2018, when leaders in psychiatry will gather alongside industry leaders at the Jacob Javits Convention Center in New York City during the American Psychiatric Association meeting for this fourth annual live event . At the event, finalists will pitch ideas “Shark Tank” style to a panel of expert judges. Finalists will work closely with industry leaders and audience members to fine-tune their ideas before pitching their revisions to the judges as well as to a live, voting audience, who together select the winners of cash awards and other prizes.
The Psychiatry Innovation Lab was founded in 2015 by Nina Vasan, MD, a Stanford (Calif.) University psychiatrist and author of Do Good Well: Your Guide to Leadership, Action, and Social Innovation (San Francisco: Jossey-Bass, 2013), with the purpose of catalyzing more entrepreneurship and innovation in mental health.
“The most meaningful part of the lab has been the impact that these ventures have had on the patients that we serve,” said Dr. Vasan, chair of the Psychiatry Innovation Lab and director of Brainstorm, the Stanford Laboratory for Brain Health Innovation and Entrepreneurship. “Year after year, psychiatrists come back and tell us that they are looking at their own patient care differently now. They’re looking for ways to be innovative, and we’re giving them the tools necessary to turn their clinical expertise into successful ventures.”
Applications are currently open online to pitch an idea in this year’s lab. Applications consist of brief answers to questions and a short YouTube video. The deadline for submissions is Friday, March 9, 2018. Anyone with innovative ideas, regardless of the stage, is invited to apply. The APA Workgroup on Psychiatry Innovation, which oversees the lab, welcomes ideas from people pitching for the first time to those working on their ideas full time. They noted that past finalists have come from all experience levels and a wide range of backgrounds, including students, CEOs, engineers, and psychiatrists.
Past winners and participants have come from a range of stages, from early start-ups to established companies, including NeuroLex Labs, which uses voice samples to detect behavioral health illness; Spring, which uses machine learning to determine the best depression treatment; Muse, which creates an EEG sensing headband to aid mindfulness practice; and Overdose Recovery Bracelet, which builds a wristband to deliver naloxone to people who have overdosed on opiates.
The diversity of ideas has been remarkable; ideas in the past have ranged from traditional for-profit businesses to nonprofits, educational and public health programs, and proposals for government reform. They address problems at all parts of the health care spectrum: prevention, diagnosis, treatment, systems, EMRs, and more.
“Many past ideas have revolved around technology such as artificial intelligence, social networking, or telemedicine,” Dr. Vasan said. “. Those ideas are especially important in solving the most pressing problems in our field today.”
In addition to those competing, anyone registered to attend the APA annual meeting can attend the event as an audience member or join a team and help as an innovation leader during the coaching portion of the program. Last year alone, more than 70% of the participants in the lab said that it was better than other educational events they have attended, 95% of participants found it useful, and participants made an average of six new contacts through the event.
“The Psychiatry Innovation Lab connected me to people who continue to inspire and educate me toward making a real impact with my own endeavors,” said Cody Rall, MD, founder of the YouTube channel Techforpsych and a 2016 semifinalist.
“The lab has grown dramatically. When we started we worked hard to find just one sponsor; last year we had 10 sponsors and over $25,000 in cash and prizes.” Dr. Vasan said. “We also had our first international finalist from Pakistan. The commitment to solving problems in mental health is taking off, and we want to ensure that psychiatrists are front and center in leading the change.”
For more information about joining the innovation lab or other ways to be involved, including sponsorship and judging, visit https://www.psychiatry.org/innovation or email Nina Taylor, APA deputy director of education, at [email protected].
This article was updated January 23, 2018.
Dr. Chaudhary is a board member of the APA Psychiatry Innovation Lab and the APA Workgroup on Psychiatry Innovation; chief resident in child and adolescent psychiatry at Massachusetts General Hospital/McLean and clinical fellow at Harvard Medical School, both in Boston; and founding partner of Brainstorm: Stanford Laboratory for Brain Health Innovation and Entrepreneurship. Dr. Ghomi is a board member of the APA Psychiatry Innovation Lab and the APA Workgroup on Psychiatry Innovation; resident in psychiatry at the University of Washington, Seattle; chief medical officer at NeuroLex; and founding partner of Brainstorm: Stanford Laboratory for Brain Health Innovation and Entrepreneurship.
Isolated severe tricuspid regurgitation: An emerging disease
SNOWMASS, COLO. – that’s treatable, provided affected patients are referred for surgery before the clinical course progresses to intractable right heart disease with cirrhosis and liver failure, Rick A. Nishimura, MD, said at the Annual Cardiovascular Conference at Snowmass.
“This is an emerging disease that you’re all going to see in your practices this year. You’ve got to know what to do with these patients. Get to them early,” urged Dr. Nishimura, professor of cardiovascular sciences and hypertension at the Mayo Clinic in Rochester, Minn.
The medical textbooks don’t discuss isolated severe tricuspid regurgitation (ISTR) or its etiology. ISTR is a disorder of progressive right ventricular dilation and dysfunction whose etiology involves either longstanding atrial fibrillation or valvular disruption due to interference from a crossing lead of a permanent pacemaker or implantable cardioverter defibrillator.
“This is something different. These patients have a normal left heart and left heart valves and normal pressures, with no pulmonary hypertension. So it doesn’t fit into any of the textbook categories of tricuspid regurgitation,” the cardiologist said.
Moreover, the current American College of Cardiology/American Heart Association guidelines on valvular heart disease don’t address ISTR, either. Physicians who attempt to apply the guidelines in deciding when to refer a patient with ISTR for surgery will oftentimes find they’ve waited too long and the patient has started to develop end-stage disease, according to Dr. Nishimura.
And he should know: He was lead author of the current ACC/AHA guidelines (J Am Coll Cardiol. 2014 Jun 10;63[22]:2438-88).
Decades ago, Eugene Braunwald, MD, of Harvard Medical School, Boston, famously called the tricuspid valve “the forgotten valve.” The history of the Snowmass winter cardiology conference bears that out. During 2007-2017, the conference featured an average of 5.4 sessions per year on aortic valve disease, 4.5 sessions per year on mitral valve disease, and not a single session on tricuspid valve disease. But the tricuspid valve is forgotten no longer, Dr. Nishimura emphasized.
How ISTR presents
The affected patient has a history of either longstanding atrial fibrillation or a permanent pacemaker or ICD.
“This is something that 4 or 5 years ago people said didn’t exist. Our pacemaker people told me, ‘Nah, you can never get tricuspid regurgitation from our leads.’ Now it’s one of the leading causes of tricuspid regurgitation going to operation,” said Dr. Nishimura.
The presenting symptoms of ISTR are typically ascites, edema, and shortness of breath.
“Why should patients with a right heart problem get dyspnea? It turns out that when the right ventricle dilates it pushes the septum in, so the effective operative compliance of the left ventricle decreases and you actually see the pulmonary artery wedge pressure go up,” he explained.
On physical examination, the patient will have elevated jugular venous pressure with large V waves.
“This is a clue that something is going on. The patient will have neck veins jumping up to her ear lobes. The ear lobes are going to wiggle with every heart beat – boom, boom, boom. If you see that, you start to figure out what’s going on. You need nothing else,” Dr. Nishimura said.
The patient will likely also have a pulsatile enlarged liver and, even though this is valve disease, a murmur that’s either soft or inaudible.
Echocardiographic diagnosis
Echocardiography will show a dilated right ventricle and right atrium, a dilated inferior vena cava, and a normal left ventricle with no pulmonary hypertension. The classic sign of ISTR on continuous wave Doppler echocardiography is a dagger-shaped tricuspid regurgitation peak velocity signal of less than 2.5 meters/sec, which indicates the absence of pulmonary hypertension. This dagger shape occurs because the right atrial pressure equalizes the right ventricular pressure.
It’s also important to point the echo probe at the hepatic veins to spot another echocardiographic hallmark of ISTR: systolic reversal.
A thorough echo exam makes hemodynamic catheterization unnecessary in these patients, Dr. Nishimura added.
When to refer for tricuspid valve repair or replacement
The clinical course of ISTR is progressive, often rapidly so. It starts with elevated jugular venous pressure, then comes fatigue and shortness of breath, moving on to ascites and edema, then finally cirrhosis and renal failure. It’s a vicious cycle in which tricuspid regurgitation begets annular dilation, which causes chordal stretching and worsening tricuspid regurgitation, leading to further annular dilation.
Patients typically aren’t referred for surgery – and may not even present to a physician – until they’ve already developed end-stage disease. That’s probably why the outcomes of surgery for ISTR are so poor. Dr. Nishimura was senior investigator of a recent retrospective study of national trends and outcomes for ISTR surgery based on the National Inpatient Sample. The number of operations increased by 250% during a recent 10-year period, but the surgery is still rare: 290 operations in 2004, climbing to 780 nationwide in 2013.
In-hospital mortality remained steady over time at 8.8%, far higher than rates of in-hospital mortality for surgery for aortic and mitral valve disease, which today stand at 1%-2% or less. The adjusted risk of in-hospital mortality for tricuspid valve replacement in patients with ISTR was 1.9-fold greater than for valve repair (J Am Coll Cardiol. 2017 Dec 19;70[24]:2953-60).
“I think the reason the operative risk of valve surgery for ISTR is so high is that we’re waiting until patients have end-stage disease,” Dr. Nishimura said.
Indeed, he recommends referral for surgery as soon as the echocardiographic diagnosis of ISTR is made in a patient with huge neck veins.
“This will probably take the operative risk down by going to a time when the right ventricle can still recover,” he added.
In a patient with ISTR and pacemaker or defibrillator leads crossing the valve, tricuspid valve repair or replacement should be accompanied by exteriorization of the leads.
Dr. Nishimura reported having no financial conflicts of interest regarding his presentation.
SNOWMASS, COLO. – that’s treatable, provided affected patients are referred for surgery before the clinical course progresses to intractable right heart disease with cirrhosis and liver failure, Rick A. Nishimura, MD, said at the Annual Cardiovascular Conference at Snowmass.
“This is an emerging disease that you’re all going to see in your practices this year. You’ve got to know what to do with these patients. Get to them early,” urged Dr. Nishimura, professor of cardiovascular sciences and hypertension at the Mayo Clinic in Rochester, Minn.
The medical textbooks don’t discuss isolated severe tricuspid regurgitation (ISTR) or its etiology. ISTR is a disorder of progressive right ventricular dilation and dysfunction whose etiology involves either longstanding atrial fibrillation or valvular disruption due to interference from a crossing lead of a permanent pacemaker or implantable cardioverter defibrillator.
“This is something different. These patients have a normal left heart and left heart valves and normal pressures, with no pulmonary hypertension. So it doesn’t fit into any of the textbook categories of tricuspid regurgitation,” the cardiologist said.
Moreover, the current American College of Cardiology/American Heart Association guidelines on valvular heart disease don’t address ISTR, either. Physicians who attempt to apply the guidelines in deciding when to refer a patient with ISTR for surgery will oftentimes find they’ve waited too long and the patient has started to develop end-stage disease, according to Dr. Nishimura.
And he should know: He was lead author of the current ACC/AHA guidelines (J Am Coll Cardiol. 2014 Jun 10;63[22]:2438-88).
Decades ago, Eugene Braunwald, MD, of Harvard Medical School, Boston, famously called the tricuspid valve “the forgotten valve.” The history of the Snowmass winter cardiology conference bears that out. During 2007-2017, the conference featured an average of 5.4 sessions per year on aortic valve disease, 4.5 sessions per year on mitral valve disease, and not a single session on tricuspid valve disease. But the tricuspid valve is forgotten no longer, Dr. Nishimura emphasized.
How ISTR presents
The affected patient has a history of either longstanding atrial fibrillation or a permanent pacemaker or ICD.
“This is something that 4 or 5 years ago people said didn’t exist. Our pacemaker people told me, ‘Nah, you can never get tricuspid regurgitation from our leads.’ Now it’s one of the leading causes of tricuspid regurgitation going to operation,” said Dr. Nishimura.
The presenting symptoms of ISTR are typically ascites, edema, and shortness of breath.
“Why should patients with a right heart problem get dyspnea? It turns out that when the right ventricle dilates it pushes the septum in, so the effective operative compliance of the left ventricle decreases and you actually see the pulmonary artery wedge pressure go up,” he explained.
On physical examination, the patient will have elevated jugular venous pressure with large V waves.
“This is a clue that something is going on. The patient will have neck veins jumping up to her ear lobes. The ear lobes are going to wiggle with every heart beat – boom, boom, boom. If you see that, you start to figure out what’s going on. You need nothing else,” Dr. Nishimura said.
The patient will likely also have a pulsatile enlarged liver and, even though this is valve disease, a murmur that’s either soft or inaudible.
Echocardiographic diagnosis
Echocardiography will show a dilated right ventricle and right atrium, a dilated inferior vena cava, and a normal left ventricle with no pulmonary hypertension. The classic sign of ISTR on continuous wave Doppler echocardiography is a dagger-shaped tricuspid regurgitation peak velocity signal of less than 2.5 meters/sec, which indicates the absence of pulmonary hypertension. This dagger shape occurs because the right atrial pressure equalizes the right ventricular pressure.
It’s also important to point the echo probe at the hepatic veins to spot another echocardiographic hallmark of ISTR: systolic reversal.
A thorough echo exam makes hemodynamic catheterization unnecessary in these patients, Dr. Nishimura added.
When to refer for tricuspid valve repair or replacement
The clinical course of ISTR is progressive, often rapidly so. It starts with elevated jugular venous pressure, then comes fatigue and shortness of breath, moving on to ascites and edema, then finally cirrhosis and renal failure. It’s a vicious cycle in which tricuspid regurgitation begets annular dilation, which causes chordal stretching and worsening tricuspid regurgitation, leading to further annular dilation.
Patients typically aren’t referred for surgery – and may not even present to a physician – until they’ve already developed end-stage disease. That’s probably why the outcomes of surgery for ISTR are so poor. Dr. Nishimura was senior investigator of a recent retrospective study of national trends and outcomes for ISTR surgery based on the National Inpatient Sample. The number of operations increased by 250% during a recent 10-year period, but the surgery is still rare: 290 operations in 2004, climbing to 780 nationwide in 2013.
In-hospital mortality remained steady over time at 8.8%, far higher than rates of in-hospital mortality for surgery for aortic and mitral valve disease, which today stand at 1%-2% or less. The adjusted risk of in-hospital mortality for tricuspid valve replacement in patients with ISTR was 1.9-fold greater than for valve repair (J Am Coll Cardiol. 2017 Dec 19;70[24]:2953-60).
“I think the reason the operative risk of valve surgery for ISTR is so high is that we’re waiting until patients have end-stage disease,” Dr. Nishimura said.
Indeed, he recommends referral for surgery as soon as the echocardiographic diagnosis of ISTR is made in a patient with huge neck veins.
“This will probably take the operative risk down by going to a time when the right ventricle can still recover,” he added.
In a patient with ISTR and pacemaker or defibrillator leads crossing the valve, tricuspid valve repair or replacement should be accompanied by exteriorization of the leads.
Dr. Nishimura reported having no financial conflicts of interest regarding his presentation.
SNOWMASS, COLO. – that’s treatable, provided affected patients are referred for surgery before the clinical course progresses to intractable right heart disease with cirrhosis and liver failure, Rick A. Nishimura, MD, said at the Annual Cardiovascular Conference at Snowmass.
“This is an emerging disease that you’re all going to see in your practices this year. You’ve got to know what to do with these patients. Get to them early,” urged Dr. Nishimura, professor of cardiovascular sciences and hypertension at the Mayo Clinic in Rochester, Minn.
The medical textbooks don’t discuss isolated severe tricuspid regurgitation (ISTR) or its etiology. ISTR is a disorder of progressive right ventricular dilation and dysfunction whose etiology involves either longstanding atrial fibrillation or valvular disruption due to interference from a crossing lead of a permanent pacemaker or implantable cardioverter defibrillator.
“This is something different. These patients have a normal left heart and left heart valves and normal pressures, with no pulmonary hypertension. So it doesn’t fit into any of the textbook categories of tricuspid regurgitation,” the cardiologist said.
Moreover, the current American College of Cardiology/American Heart Association guidelines on valvular heart disease don’t address ISTR, either. Physicians who attempt to apply the guidelines in deciding when to refer a patient with ISTR for surgery will oftentimes find they’ve waited too long and the patient has started to develop end-stage disease, according to Dr. Nishimura.
And he should know: He was lead author of the current ACC/AHA guidelines (J Am Coll Cardiol. 2014 Jun 10;63[22]:2438-88).
Decades ago, Eugene Braunwald, MD, of Harvard Medical School, Boston, famously called the tricuspid valve “the forgotten valve.” The history of the Snowmass winter cardiology conference bears that out. During 2007-2017, the conference featured an average of 5.4 sessions per year on aortic valve disease, 4.5 sessions per year on mitral valve disease, and not a single session on tricuspid valve disease. But the tricuspid valve is forgotten no longer, Dr. Nishimura emphasized.
How ISTR presents
The affected patient has a history of either longstanding atrial fibrillation or a permanent pacemaker or ICD.
“This is something that 4 or 5 years ago people said didn’t exist. Our pacemaker people told me, ‘Nah, you can never get tricuspid regurgitation from our leads.’ Now it’s one of the leading causes of tricuspid regurgitation going to operation,” said Dr. Nishimura.
The presenting symptoms of ISTR are typically ascites, edema, and shortness of breath.
“Why should patients with a right heart problem get dyspnea? It turns out that when the right ventricle dilates it pushes the septum in, so the effective operative compliance of the left ventricle decreases and you actually see the pulmonary artery wedge pressure go up,” he explained.
On physical examination, the patient will have elevated jugular venous pressure with large V waves.
“This is a clue that something is going on. The patient will have neck veins jumping up to her ear lobes. The ear lobes are going to wiggle with every heart beat – boom, boom, boom. If you see that, you start to figure out what’s going on. You need nothing else,” Dr. Nishimura said.
The patient will likely also have a pulsatile enlarged liver and, even though this is valve disease, a murmur that’s either soft or inaudible.
Echocardiographic diagnosis
Echocardiography will show a dilated right ventricle and right atrium, a dilated inferior vena cava, and a normal left ventricle with no pulmonary hypertension. The classic sign of ISTR on continuous wave Doppler echocardiography is a dagger-shaped tricuspid regurgitation peak velocity signal of less than 2.5 meters/sec, which indicates the absence of pulmonary hypertension. This dagger shape occurs because the right atrial pressure equalizes the right ventricular pressure.
It’s also important to point the echo probe at the hepatic veins to spot another echocardiographic hallmark of ISTR: systolic reversal.
A thorough echo exam makes hemodynamic catheterization unnecessary in these patients, Dr. Nishimura added.
When to refer for tricuspid valve repair or replacement
The clinical course of ISTR is progressive, often rapidly so. It starts with elevated jugular venous pressure, then comes fatigue and shortness of breath, moving on to ascites and edema, then finally cirrhosis and renal failure. It’s a vicious cycle in which tricuspid regurgitation begets annular dilation, which causes chordal stretching and worsening tricuspid regurgitation, leading to further annular dilation.
Patients typically aren’t referred for surgery – and may not even present to a physician – until they’ve already developed end-stage disease. That’s probably why the outcomes of surgery for ISTR are so poor. Dr. Nishimura was senior investigator of a recent retrospective study of national trends and outcomes for ISTR surgery based on the National Inpatient Sample. The number of operations increased by 250% during a recent 10-year period, but the surgery is still rare: 290 operations in 2004, climbing to 780 nationwide in 2013.
In-hospital mortality remained steady over time at 8.8%, far higher than rates of in-hospital mortality for surgery for aortic and mitral valve disease, which today stand at 1%-2% or less. The adjusted risk of in-hospital mortality for tricuspid valve replacement in patients with ISTR was 1.9-fold greater than for valve repair (J Am Coll Cardiol. 2017 Dec 19;70[24]:2953-60).
“I think the reason the operative risk of valve surgery for ISTR is so high is that we’re waiting until patients have end-stage disease,” Dr. Nishimura said.
Indeed, he recommends referral for surgery as soon as the echocardiographic diagnosis of ISTR is made in a patient with huge neck veins.
“This will probably take the operative risk down by going to a time when the right ventricle can still recover,” he added.
In a patient with ISTR and pacemaker or defibrillator leads crossing the valve, tricuspid valve repair or replacement should be accompanied by exteriorization of the leads.
Dr. Nishimura reported having no financial conflicts of interest regarding his presentation.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Pilot Inpatient Pain Pharmacist Consult Service at the West Palm Beach VA Medical Center
The term pain refers to unpleasant sensory, emotional experiences associated with actual or potential tissue damage and is described in terms of such damage.1 Acute pain from neurophysiologic responses to noxious stimuli resolves upon tissue healing or stimuli removal (eg, 3-6 months); however, chronic pain lingers beyond the expected time course of the acute injury and repair process.1,2 Despite pain management advances, the under- or overtreatment of pain for different patient populations (eg, cancer and noncancer) remains an important concern.3,4
Hospitals have focused on optimizing inpatient pain management, because uncontrolled pain remains the most common reason for readmissions the first week postsurgery.5 The safe use of opioids (prescription, illicit synthetic, or heroin) poses major challenges and raises significant concerns. Rates of opioid-related hospital admissions have increased by 42% since 2009, and total overdose deaths reached a new high of 47,055 in 2014, including 28,647 (61%) from opioids.6
Opioids rank among the medications most often associated with serious adverse events (AEs), including respiratory depression and death.7 In response, the Joint Commission recommends patient assessments for opioid-related AEs, technology to monitor opioid prescribing, pharmacist consultation for opioid conversions and route of administration changes, provider education about risks of opioids, and risk screening tools for opioid-related oversedation and respiratory depression.7 Treatment guidelines strive to minimize the impact of acute pain by offering a scientific basis for practice, but evidence suggests a lack of suitable pain programs.7 Increases in opioid prescribing along with clinical guidelines and state laws recommending specialty pain service referrals for patients on high-dose opioids, have increased demand for competent pain clinicians.8
The expertise of a clinical pharmacy specialists (CPS) can help refine ineffective and potentially harmful pain medication therapy in complex patient cases. Existing literature outlines the various benefits of pharmacist participation in collaborative pain services for cancer and noncancer pain, as well as cases involving substance abuse.9-13 Various articles support pharmacists’ role as an educator and team member who can add valuable, trustworthy clinical knowledge that enhances clinical encounters and guides protocol/policy development.12,13 These efforts have improved patient satisfaction and encouraged physicians and nurses to proactively seek pharmacists’ advice for difficult cases.9
Frequent communication with interdisciplinary teams have helped considerably in establishing clinical pharmacy services that benefit patient care and offer sources of professional accomplishment.10,11 For example, pharmacists at Kaweah Delta Medical Center in Visalia, CA launched an innovative pain program that encompassed consultations and opioid stewardship, which demonstrated that pharmacists can improve patient outcomes in the front lines of pain management.14 Pain CPSs have advanced knowledge of pharmacokinetics, pharmacodynamics, and therapeutics to promote safe and effective analgesic use, as well as to identify opioid use disorders. Evidence suggests that pharmacists’ presence on interdisciplinary pain teams improves outcomes by optimizing medication selection, improving adherence, and preventing AEs.8
Following the plan-do-study-act model for quality improvement (QI), this project hoped to expand current pain programs at the West Palm Beach VAMC (WPBVAMC) by evaluating the feasibility of an inpatient pain pharmacist consult service (IPPCS) at the 301-bed teaching facility, which includes 130 acute/intensive care and 120 nursing/domiciliary beds.15 Staff provide primary- and secondary-level care to veterans in 7 counties along Florida’s southeastern coast.
In 2009, the WPBVAMC PGY-2 Pain Management and Palliative Care Program became the VA’s first accredited pain pharmacy residency. Residents train with the Physical Medicine & Rehabilitation (PMR) and Chronic Pain Management departments, which provide outpatient services from 7 pain physicians, a pain psychologist, registered nurse, chiropractor, acupuncturist, physical/occupational therapy (PT/OT), and 3 pain/palliative care CPSs.
The WPBVAMC had established interdisciplinary outpatient chronic pain clinic (OCPC) physician- and pharmacist-run services along with a pain CPS electronic consult (e-consult) program. However, no formal mechanisms for inpatient pain consultations existed. Prior to the IPPCS outlined in this study, OCPC practitioners, including 2 pain CPSs, managed impromptu inpatient pain issues as “curbside consultations” along with usual day-to-day clinic duties.
The OCPC, PMR, and Clinical Pharmacy administration recognized the need for more clinical support to manage complex analgesic issues in inpatient veterans, as these patients often have acute pain with underlying chronic pain syndromes. In a national survey, veterans were significantly more likely than were nonveterans to report painful health conditions (65.5% vs 56.4%) and to classify their pain as severe (9.1% vs 6.3%).16 The WPBVAMC administration concluded that an IPPCS would offer a more efficient means of handling such cases. The IPPCS would formally streamline inpatient pain consults, enabling CPSs to thoroughly evaluate pain-related issues to propose evidence-based recommendations.
The primary objective of this QI project was to assess the IPPCS implementation as part of multimodal care to satisfy unmet patient care needs at the WPBVAMC. Secondary objectives for program feasibility included identifying the volume and type of pain consults, categorizing pharmacist interventions, classifying providers’ satisfaction, and determining types of responses to pharmacists’ medication recommendations.
Methods
This QI project ascertained the feasibility of the IPPCS by evaluating all consults obtained during the pilot period from November 2, 2015 through May 6, 2016. The IPPCS was accessible Monday through Friday during normal business hours. Goal turnaround time for consult completion was 24 to 72 hours, given the lack of coverage on holidays and weekends. The target population included veterans hospitalized at the WPBVAMC inpatient ward or nursing home with uncontrolled pain on IV and/or oral analgesic medications. All IPPCS consults submitted during the pilot period were included in the sample.
The WPBVAMC Scientific Advisory Committee (SAC) approved this QI program prior to initiation. Following supervisory support from the OCPC, PMR, and Clinical Pharmacy departments, hospital technologists assisted in creating a consult link in the Computerized Patient Record System (CPRS), which allowed providers to submit IPPCS requests for specific patients efficiently. Consults were categorized as postoperative pain, acute or chronic pain, malignant pain, or end-of-life pain. Inpatient providers could enter requests for assistance with 1 or more of the following: opioid dose conversions, opioid taper/titration schedules, general opioid treatment recommendations, or nonopioid/adjuvant recommendations.
The Medical Records Committee approved a customized CPRS subjective-objective-assessment-recommendations (SOAR) note template, which helped standardize the pain CPS documentation. To promote consult requests and interdisciplinary collaboration, inpatient clinicians received education about the IPPCS at respective meetings (eg, General Medicine staff and Clinical Pharmacy meetings).
All CPSs involved in this project were residency-trained in direct patient care, including pain and palliative care, and maintained national board certification as pharmacotherapy specialists. Their role included reviewing patients’ electronic medical records, conducting face-to-face pain assessments, completing opioid risk assessments, evaluating analgesic regimen appropriateness, reviewing medication adherence, completing pain medication reconciliation, querying the Florida Prescription Drug Monitoring Program (PDMP), interpreting urine drug testing (UDT), and delivering provider/patient/caregiver education. Parameters used to determine the appropriateness of analgesic regimens included, but were not limited to:
- Use of oral instead of IV medications if oral dosing was feasible/possible/appropriate;
- Dose and adjustments per renal/hepatic function;
- Adequate treatment duration and titration;
- No therapeutic drug class duplications;
- Medication tolerability (eg, allergies, AEs, drug interactions); and
- Opioid risk assessment per Opioid Risk Tool (ORT) score and medical history.
Consulting providers clarified patients’ pain diagnoses prior to pharmacy consultations.
After face-to-face patient interviews, the inpatient pain CPS prepared pain management recommendations, including nonopioid/adjuvant pain medications and/or opioid dose adjustments. The IPPCS also collaborated with pain physicians for intervention procedures, nonpharmacologic recommendations, and for more complex patients who may have required additional imaging or detailed physical evaluations. Pain CPSs documented CPRS notes with the SOAR template and discussed all recommendations with appropriate inpatient teams.
Respective providers received questionnaires hosted on SurveyMonkey.com (San Mateo, CA) to gauge their satisfaction with the IPPCS at the end of the pilot period, which helped determine program utility. Data collected for the pilot included patient demographics; patient admission diagnosis; consulting inpatient service; type of pain and reason for IPPCS request; total morphine equivalent daily dose (MEDD); pertinent past medical history (ie, sleep apnea, psychiatric comorbidities, or substance use disorder [SUD]); ORT score; patients’ reported average pain severity on the 10-point Numeric Pain Rating Scale (NPRS); number of requests submitted; medications discontinued, initiated, or dose increased/decreased; and number of pharmacist recommendations, including number accepted by providers. The ORT is a 5-item questionnaire used to determine risk of opioid-related aberrant behaviors in adults to help discriminate between low-risk and high-risk individuals (Table 1).17 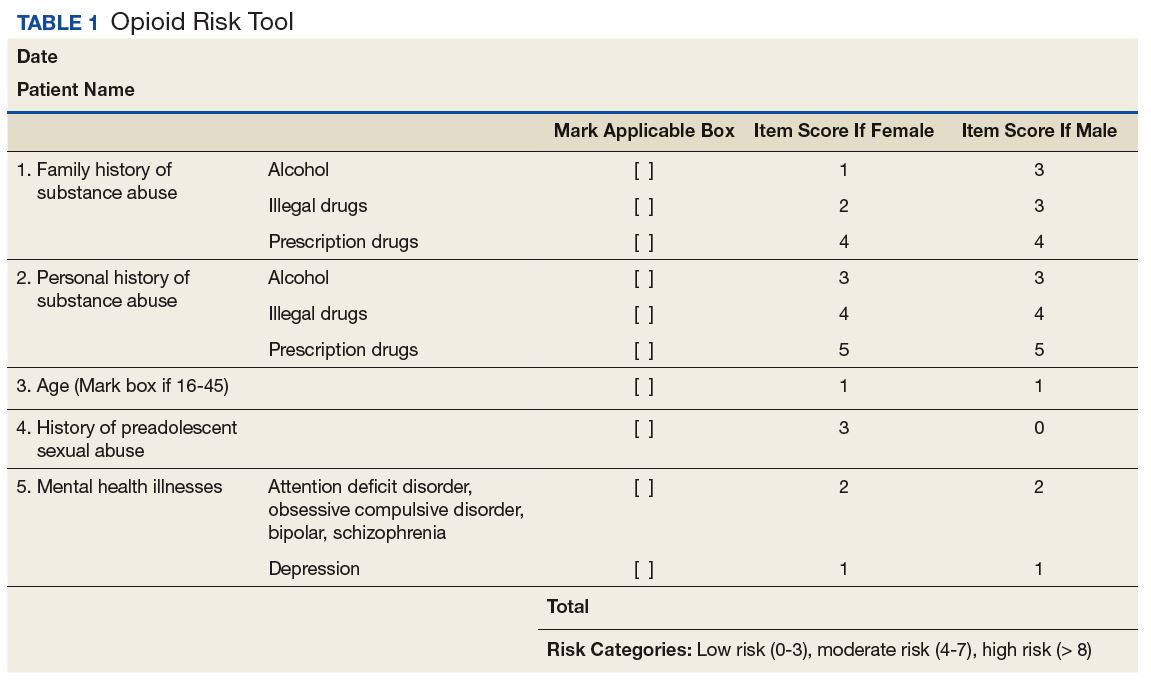
Descriptive statistics were used to evaluate the results, and a Likert scale was used to evaluate responses the from provider satisfaction questionnaires. The IPPCS collected and organized the data using Microsoft Excel (Redmond, WA).
Results
By the end of the pilot period in May 2016, the IPPCS had received 100 consult requests and completed 81% (Figure). The remaining consults included 11% forwarded to other disciplines. The service discontinued 8% of the requests, given patients’ hospital discharge prior to IPPCS review. 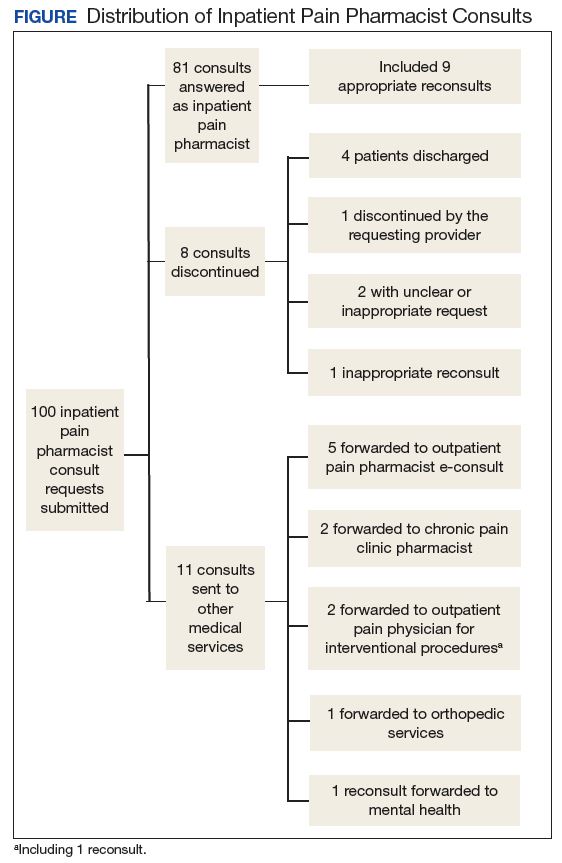
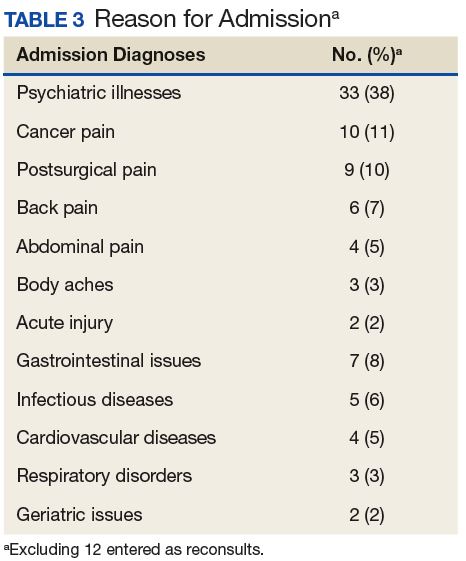
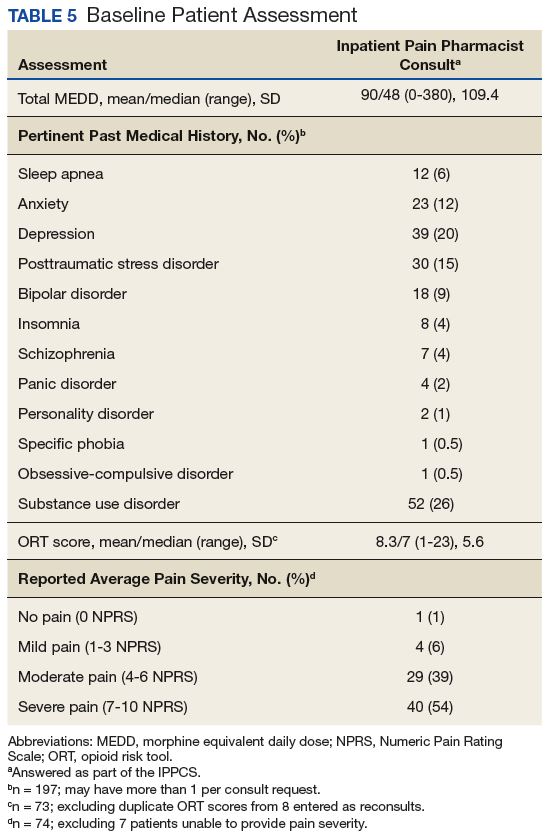
Baseline patient data are outlined in Tables 2, 3, 4, and 5. For each of the 100 consults, providers could select more than 1 reason for the request. The nonopioid/adjuvant treatment recommendations were the most common at 49% (62/128). Patients could have more than 1 pertinent medical comorbidity, with psychiatric illnesses the most prevalent at 68% (133/197). A mean ORT score of 8.1 indicated a high risk for opioid-related aberrant behavior. Overall, half the patients (37/73) were high risk, 25% (18/73) were medium risk (ORT 4-7), and 25% (18/73) were low risk (ORT 0-3). Patients’ reported average pain was often severe (NPRS 7-10) at 54% (40/74) or moderate (NPRS 4-6) at 39% (29/74). 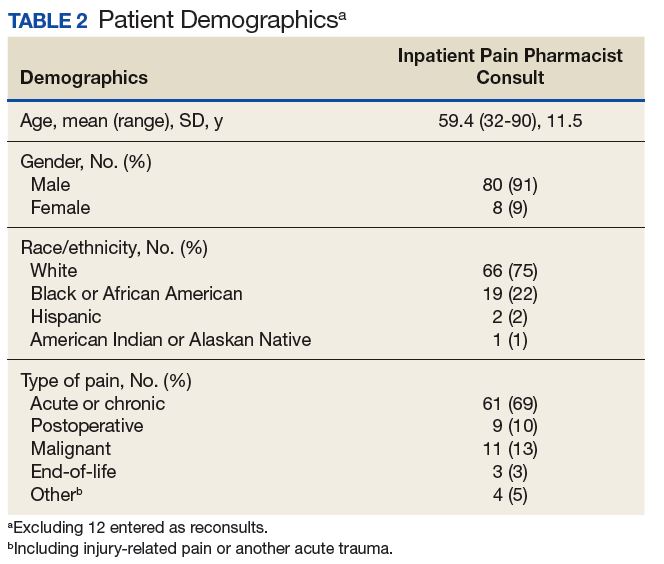
The IPPCS recommended various medications for initiation, discontinuation, or dosage changes (Table 6). For example, the IPPCS recommended initiation of topical agents in 38% (48/128) of cases. The inpatient pain CPS offered opioid initiation in 17% (22/128) of cases, with immediate-release oral morphine as the most predominant. Notably, opioids remained the most common medications suggested for discontinuation at 74% (38/51), including 47% (18/38) for IV hydromorphone. Dose titration recommendations mainly included anticonvulsants at 33% (16/48), and most dose reductions involved opioids at 78% (7/9), namely, oxycodone/acetaminophen and IV hydromorphone. 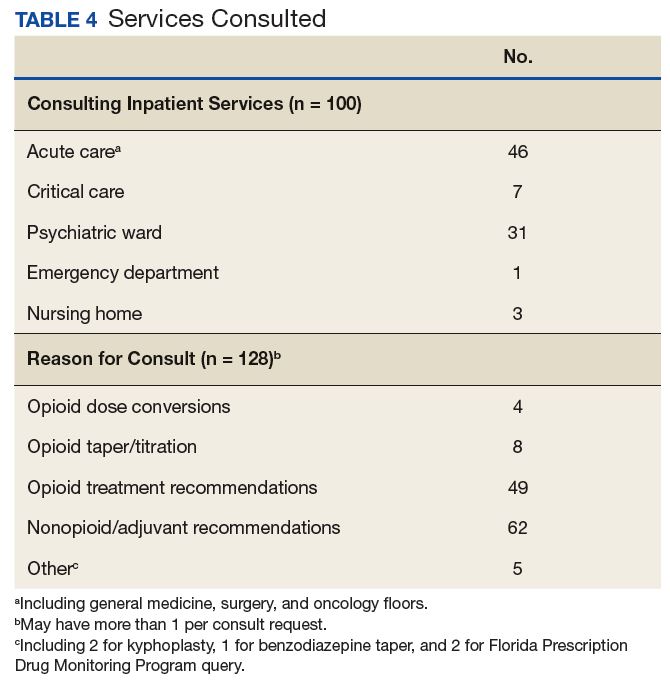
Providers accepted 76% (179/234) of IPPCS pharmacist medication recommendations. The most common included initiation/optimization of adjuvant therapy (eg, anticonvulsants, serotonin-norepinephrine reuptake inhibitors [SNRIs], and topical agents) at 46% (83/179), followed by opioid discontinuation (eg, IV hydromorphone) at 22% (40/179). Although this project primarily tracked medication interventions, examples of accepted nonpharmacologic recommendations included UDT and referrals to other programs (eg, pain psychology, substance abuse, mental health, acupuncture, chiropractor, PT/OT/PMR, and interventional pain management), which received support from each respective discipline. Declined pharmacologic recommendations mostly included topicals (eg, lidocaine, trolamine, and capsaicin cream) at 35% (19/55). However, findings also show that providers implemented 100% of medication recommendations in whole for 58% (47/81) of consults.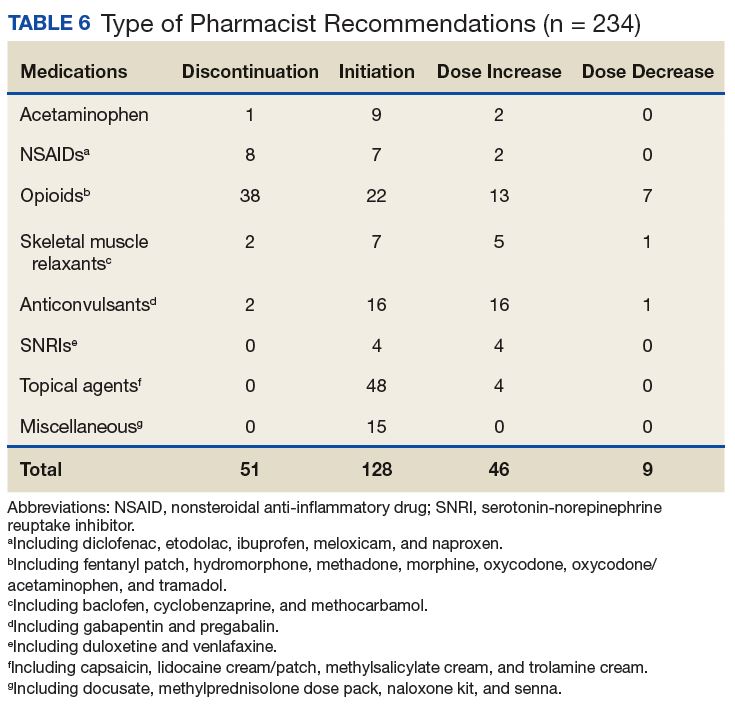
Likert scale satisfaction questionnaires offered insight into providers’ perception of the IPPCS (Table 7). One provider felt “neutral” about the consult submission process, given the time needed to complete the CPRS requests, but all other providers “agreed” or “strongly agreed” that the IPPCS was user-friendly. More importantly, 100% (15/15) “agreed” or “strongly agreed” that the inpatient pain CPS answered consults promptly with reasonable, evidence-based recommendations. All respondents declared that they would recommend the IPPCS to other practitioners and felt comfortable entering requests for future patients. 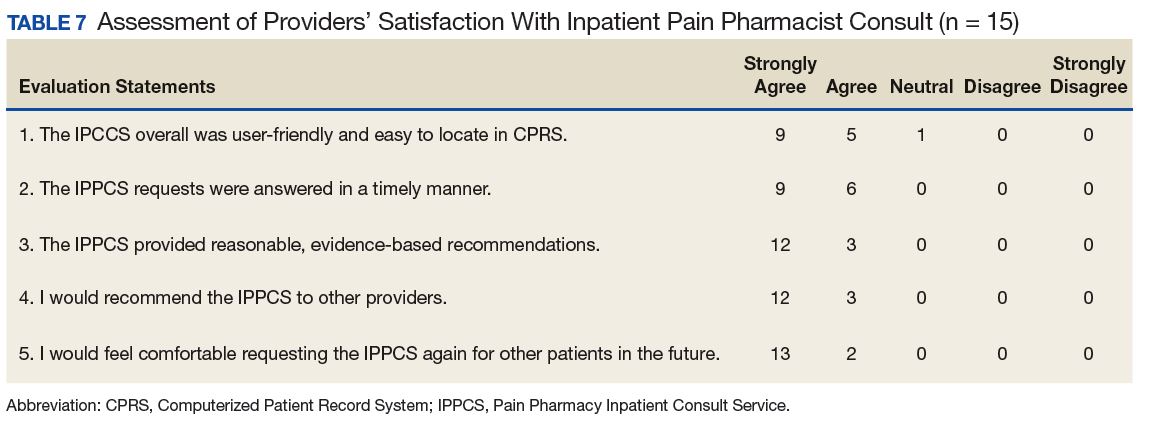
Discussion
The IPPCS achieved a total of 100 consults, which served as the sample for the pilot program. With support from the OCPC, PMR, and Clinical Pharmacy Department Administration, the IPPCS operated from November 2, 2015 through May 6, 2016. Results suggested that this new service could assist in managing inpatient pain issues in collaboration with inpatient multidisciplinary teams.
The most popular reason for IPPCS consults was acute on chronic pain. Given national efforts to improve opioid prescribing through the VA Opioid Safety Initiative (OSI) and the 2016 CDC Guideline for Opioid Prescribing, most pain consults requested nonopioid/adjuvant recommendations.18,19 Despite the wide MEDD range in this sample, the median/mean generally remained below recommended limits per current guidelines.18,19 However, the small sample size and lack of patient diversity (mostly white male veterans) limited the generalizability to non-VA medical facilities. Veterans often experienced both chronic pain and psychiatric disturbances, which explained the significant number of underlying mental health comorbidities observed. This affirmed the close interrelationship between pain and psychiatric issues described in the literature.20
Providers’ acceptance of pharmacologic and nonpharmacologic treatment modalities supported a comprehensive, multidisciplinary, and biopsychosocial approach to effective analgesic management. During this pilot, the most common pharmacy medication recommendations, namely, discontinuation of inappropriate opioids (eg, IV hydromorphone in patients who are controlled on and/or able to tolerate oral medications) and dose titration of adjuvant medications (eg, anticonvulsants for neuropathic pain), revealed that the IPPCS provided needed expertise and alternatives for complex pain patients. The IPPCS was well received, as inpatient providers accepted and implemented a large proportion of pharmacist recommendations. Despite risks of bias with a nonvalidated questionnaire, providers offered positive feedback. In the future, distributing satisfaction evaluations to patients also would provide more insight into how others perceived the IPPCS.
Limitations
Reasons for unaccepted recommendations included perceived limited effectiveness and/or feasibility of topical agents for acute pain, as providers seemed to favor systemic therapy for supposedly more immediate analgesia. Prescriber preference may explain why inpatient teams sometimes declined adjuvant therapy recommendations. However, the 2016 American Pain Society Guidelines on the Management of Postoperative Pain support a multimodal approach and confirm that adjuvants can reduce patients’ opioid requirements.21
Consulting teams did not execute some opioid recommendations, which may be due to various factors, including patient-related or provider-related factors in the inpatient vs outpatient setting. Lack of retrospective analysis for comparison of results pre- and post-IPPCS implementation also limited the outcomes. However, this project was piloted as a QI initiative after providers identified significant needs for inpatient pain management at the WPBVAMC. No retrospective analysis was undertaken, as this project analyzed only responses during the pilot program.
Other obstacles of the IPPCS included request appropriateness and triaging. The inpatient pain CPS deferred management of some consults to other disciplines (eg, gastroenterology) for more appropriate care. The IPPCS deferred certain cases of acute pancreatic pain or generalized abdominal pain for further workup to address patients’ underlying issues. The inpatient pain CPS relayed pertinent information regarding appropriate consults to inpatient teams. In the future, developing more specific inclusion/exclusion criteria and delivering provider education about proper IPPCS requests may resolve this issue.
Challenges with pain consults from inpatient psychiatry stemmed from patients’ skepticism and unwillingness to accept nonopioid/adjuvant therapies. Additionally, comorbid psychiatric disorders are often associated with SUDs and potentially opioid-related aberrant behavior. More than 40% of opioid-dependent individuals have comorbid psychiatric disorders, especially depression, anxiety, and bipolar disorder.22 Poorly-managed pain also drives SUD, as 80% of these patients illegally obtain prescription opioids. Thus, undertreatment of pain may push individuals to secure pain medications from illegal/illicit sources to achieve analgesia.23 Following pain physician consultation, the IPPCS continued inpatient opioids for 12% (10/81) of patients with a SUD history, including 5 with postoperative pain or other acute processes, since patients were kept in a monitored health care environment. The remaining included 4 with malignant pain and 1 with end-of-life pain. Overall, the IPPCS recommended that inpatient teams discharge these patients on as little opioids as possible, as well as to make referrals to substance abuse programs when necessary. Effective pain management of patients with aberrant behavior requires a comprehensive interdisciplinary team approach. To mitigate risk, effectively treat pain, and maintain patient safety, clinicians must recognize biologic, chemical, social, and psychiatric aspects of substance abuse.21
Another limitation during this pilot was an inability to promptly assess the impact of recommendations, given limited opportunities to reevaluate patients. In the future, more dedicated time for the inpatient pain CPSs to respond to consults may allow for better follow-up rather than initial consults only. Providers sometimes discharged patients within 24 hours of submitting consults as well, which left no time for the inpatient pain CPS consultation. However, the IPPCS forwarded appropriate requests to pain CPS e-consult services for chart review recommendations. Encouraging providers to submit consults earlier in patients’ hospital admissions may help reduce the number of incomplete IPPCS requests. Although expanding service hours would require more dedicated CPS staffing resources, it is another option for quicker consult completion and prompt follow-up.
Future Directions
Future efforts to expand this project include ensuring patient safety through judicious opioid use. Smooth transitions of care will particularly help to improve the quality of pain management. Current WPBVAMC policies stated that the primary care provider (PCP) alone must agree to continue prescribing outpatient analgesic medications, including opioids, prescribed from the OCPC once patients return to Primary Care. Continued provider education would ideally promote efficient utilization of the IPPCS and OCPC.
The pain pharmacy SOAR note template also could undergo additional edits/revisions, including the addition of opioid overdose risk assessments. For improved documentation and standardization, the template could autopopulate patient-specific information when the inpatient pain CPS chooses the designated note title. The IPPCS also hoped to streamline the CPRS consult link for more convenience and ease of use. Ultimately, the IPPCS wished to provide ongoing provider education, inpatient opioid therapy, and other topics upon request.
Conclusion
The IPPCS received positive provider feedback and collected 100 consults (averaging 4 per week) during the 6-month pilot QI project. Most consults were for acute or chronic pain and requested nonopioid/adjuvant recommendations. The new service intended to fulfill unmet needs at the WPBVAMC by expanding the facility’s current pain programs. Prescribers reported a high level of satisfaction and a willingness to not only refer other clinicians to the program, but also continue using the consult. Providers unanimously agreed that the pain CPS provided reasonable, evidence-based recommendations. This project demonstrated that the IPPCS can aid in meeting new demands amid the challenging landscape of pain practice.
1. D’Arcy Y. Treating acute pain in the hospitalized patient. Nurse Pract. 2012;37(8):22-30.
2. Marks AD, Rodgers PE. Diagnosis and management of acute pain in the hospitalized patient. Am J Med. 2014;3(3):e396-e408.
3. Paice JA, Von Roenn JH. Under- or overtreatment of pain in the patient with cancer: how to achieve proper balance. J Clin Oncol. 2014;32(16):1721-1726.
4. Mafi JN, McCarthy EP, Davis RB, Landon BE. Worsening trends in the management and treatment of back pain. JAMA Intern Med. 2013;173(17):1573-1581.
5. Palomano RC, Rathmell JP, Krenzischek DA, Dunwoody CJ. Emerging trends and new approaches to acute pain management. J Perianesth Nurs. 2008;23(suppl 1):S43-S53.
6. U.S. Department of Health & Human Services, Office of the Surgeon General. Facing addiction in America: the surgeon general’s report on alcohol, drugs, and health, executive summary. https://addiction.surgeongeneral.gov/executive-summary.pdf. Published November 2016. Accessed November 1, 2017.
7. Bagian JP, Cohen M, Barnsteiner JH, et al. Safe use of opioids in hospitals. Sentinel Event Alert. 2012;49:1-5.
8. Atkinson TJ, Gulum AH, Forkum WG. The future of pain pharmacy: directed by need. Integrated Pharm Res Pract. 2016;2016(5):33-42.
9. Lothian ST, Fotis MA, Von Gutten CF, et al. Cancer pain management through a pharmacist-based analgesic dosing service. Am J Health Syst Pharm. 1999;56:1119-1125.
10. Lynn MA. Pharmacist interventions in pain management. Am J Health Syst Pharm. 2004;61(14):1487-1489.
11. Strickland JM, Huskey A, Brushwood DB. Pharmacist-physician collaboration in pain management practice. J Opioid Manag. 2007;3(6):295-301.
12. Fan T and Elgourt T. Pain management pharmacy service in a community hospital. Am J Health Syst Pharm. 2008;65(16):1560-1565.
13. Andrews LB, Bridgeman MB, Dalal KS, et al. Implementation of a pharmacist-directed pain management consultation service for hospitalised adults with a history of substance abuse. Int J Clin Pract. 2013;67(12):1342-1349.
14. Poirier RH, Brown CS, Garcia YT, Gann NY, Sandoval RA, McNulty JR. Implementation of a pharmacist directed pain management service in the inpatient setting. http://www.ashpadvantage.com/bestpractices/2014_papers/Kaweah-Delta.htm. Published 2014. Accessed November 1, 2017.
15. Langley GL, Moen R, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. 2nded. San Francisco, CA: Jossey-Bass; 2009.
16. Nahin, RL. Severe pain in veterans: the effect of age and sex, and comparisons with the general population. J Pain. 2017;18(3):247-254.
17. Webster LR, Webster RM. Predicting aberrant behaviors in opioid-treated patients: preliminary validation of the opioid risk tool. Pain Med. 2005;6(6):432-442.
18. Nazario M. Opioid therapy risk management: the VA opioid safety and naloxone distribution initiatives. http://jfpsmeeting.pharmacist.com/sites/default/files/slides/Opioid%20Therapy%20Risk%20Management.pdf. Published October 15, 2015. Accessed November 1, 2017.
19. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain – United States, 2016. MMWR Rep. 2016;65(1):1-49.
20. Outcalt SD, Kroenke K, Krebs EE, et al. Chronic pain and comorbid mental health conditions: independent associations of posttraumatic stress disorder and depression with pain, disability, and quality of life. J Behav Med. 2015;38:535.
21. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131-157.
22. NIDA/SAMHSA Blending Initiative. https://www.drugabuse.gov/nidasamhsa-blending-initiative. Updated November 2015. Accessed November 1, 2017.
23. Alford DP, German JS, Samet JH, Cheng DM, Lloyd-Travaglini CA, Saitz R. Primary care patients with drug use report chronic pain and self-medicate with alcohol and other drugs. J Gen Intern Med. 2016;31(5):486-491.
The term pain refers to unpleasant sensory, emotional experiences associated with actual or potential tissue damage and is described in terms of such damage.1 Acute pain from neurophysiologic responses to noxious stimuli resolves upon tissue healing or stimuli removal (eg, 3-6 months); however, chronic pain lingers beyond the expected time course of the acute injury and repair process.1,2 Despite pain management advances, the under- or overtreatment of pain for different patient populations (eg, cancer and noncancer) remains an important concern.3,4
Hospitals have focused on optimizing inpatient pain management, because uncontrolled pain remains the most common reason for readmissions the first week postsurgery.5 The safe use of opioids (prescription, illicit synthetic, or heroin) poses major challenges and raises significant concerns. Rates of opioid-related hospital admissions have increased by 42% since 2009, and total overdose deaths reached a new high of 47,055 in 2014, including 28,647 (61%) from opioids.6
Opioids rank among the medications most often associated with serious adverse events (AEs), including respiratory depression and death.7 In response, the Joint Commission recommends patient assessments for opioid-related AEs, technology to monitor opioid prescribing, pharmacist consultation for opioid conversions and route of administration changes, provider education about risks of opioids, and risk screening tools for opioid-related oversedation and respiratory depression.7 Treatment guidelines strive to minimize the impact of acute pain by offering a scientific basis for practice, but evidence suggests a lack of suitable pain programs.7 Increases in opioid prescribing along with clinical guidelines and state laws recommending specialty pain service referrals for patients on high-dose opioids, have increased demand for competent pain clinicians.8
The expertise of a clinical pharmacy specialists (CPS) can help refine ineffective and potentially harmful pain medication therapy in complex patient cases. Existing literature outlines the various benefits of pharmacist participation in collaborative pain services for cancer and noncancer pain, as well as cases involving substance abuse.9-13 Various articles support pharmacists’ role as an educator and team member who can add valuable, trustworthy clinical knowledge that enhances clinical encounters and guides protocol/policy development.12,13 These efforts have improved patient satisfaction and encouraged physicians and nurses to proactively seek pharmacists’ advice for difficult cases.9
Frequent communication with interdisciplinary teams have helped considerably in establishing clinical pharmacy services that benefit patient care and offer sources of professional accomplishment.10,11 For example, pharmacists at Kaweah Delta Medical Center in Visalia, CA launched an innovative pain program that encompassed consultations and opioid stewardship, which demonstrated that pharmacists can improve patient outcomes in the front lines of pain management.14 Pain CPSs have advanced knowledge of pharmacokinetics, pharmacodynamics, and therapeutics to promote safe and effective analgesic use, as well as to identify opioid use disorders. Evidence suggests that pharmacists’ presence on interdisciplinary pain teams improves outcomes by optimizing medication selection, improving adherence, and preventing AEs.8
Following the plan-do-study-act model for quality improvement (QI), this project hoped to expand current pain programs at the West Palm Beach VAMC (WPBVAMC) by evaluating the feasibility of an inpatient pain pharmacist consult service (IPPCS) at the 301-bed teaching facility, which includes 130 acute/intensive care and 120 nursing/domiciliary beds.15 Staff provide primary- and secondary-level care to veterans in 7 counties along Florida’s southeastern coast.
In 2009, the WPBVAMC PGY-2 Pain Management and Palliative Care Program became the VA’s first accredited pain pharmacy residency. Residents train with the Physical Medicine & Rehabilitation (PMR) and Chronic Pain Management departments, which provide outpatient services from 7 pain physicians, a pain psychologist, registered nurse, chiropractor, acupuncturist, physical/occupational therapy (PT/OT), and 3 pain/palliative care CPSs.
The WPBVAMC had established interdisciplinary outpatient chronic pain clinic (OCPC) physician- and pharmacist-run services along with a pain CPS electronic consult (e-consult) program. However, no formal mechanisms for inpatient pain consultations existed. Prior to the IPPCS outlined in this study, OCPC practitioners, including 2 pain CPSs, managed impromptu inpatient pain issues as “curbside consultations” along with usual day-to-day clinic duties.
The OCPC, PMR, and Clinical Pharmacy administration recognized the need for more clinical support to manage complex analgesic issues in inpatient veterans, as these patients often have acute pain with underlying chronic pain syndromes. In a national survey, veterans were significantly more likely than were nonveterans to report painful health conditions (65.5% vs 56.4%) and to classify their pain as severe (9.1% vs 6.3%).16 The WPBVAMC administration concluded that an IPPCS would offer a more efficient means of handling such cases. The IPPCS would formally streamline inpatient pain consults, enabling CPSs to thoroughly evaluate pain-related issues to propose evidence-based recommendations.
The primary objective of this QI project was to assess the IPPCS implementation as part of multimodal care to satisfy unmet patient care needs at the WPBVAMC. Secondary objectives for program feasibility included identifying the volume and type of pain consults, categorizing pharmacist interventions, classifying providers’ satisfaction, and determining types of responses to pharmacists’ medication recommendations.
Methods
This QI project ascertained the feasibility of the IPPCS by evaluating all consults obtained during the pilot period from November 2, 2015 through May 6, 2016. The IPPCS was accessible Monday through Friday during normal business hours. Goal turnaround time for consult completion was 24 to 72 hours, given the lack of coverage on holidays and weekends. The target population included veterans hospitalized at the WPBVAMC inpatient ward or nursing home with uncontrolled pain on IV and/or oral analgesic medications. All IPPCS consults submitted during the pilot period were included in the sample.
The WPBVAMC Scientific Advisory Committee (SAC) approved this QI program prior to initiation. Following supervisory support from the OCPC, PMR, and Clinical Pharmacy departments, hospital technologists assisted in creating a consult link in the Computerized Patient Record System (CPRS), which allowed providers to submit IPPCS requests for specific patients efficiently. Consults were categorized as postoperative pain, acute or chronic pain, malignant pain, or end-of-life pain. Inpatient providers could enter requests for assistance with 1 or more of the following: opioid dose conversions, opioid taper/titration schedules, general opioid treatment recommendations, or nonopioid/adjuvant recommendations.
The Medical Records Committee approved a customized CPRS subjective-objective-assessment-recommendations (SOAR) note template, which helped standardize the pain CPS documentation. To promote consult requests and interdisciplinary collaboration, inpatient clinicians received education about the IPPCS at respective meetings (eg, General Medicine staff and Clinical Pharmacy meetings).
All CPSs involved in this project were residency-trained in direct patient care, including pain and palliative care, and maintained national board certification as pharmacotherapy specialists. Their role included reviewing patients’ electronic medical records, conducting face-to-face pain assessments, completing opioid risk assessments, evaluating analgesic regimen appropriateness, reviewing medication adherence, completing pain medication reconciliation, querying the Florida Prescription Drug Monitoring Program (PDMP), interpreting urine drug testing (UDT), and delivering provider/patient/caregiver education. Parameters used to determine the appropriateness of analgesic regimens included, but were not limited to:
- Use of oral instead of IV medications if oral dosing was feasible/possible/appropriate;
- Dose and adjustments per renal/hepatic function;
- Adequate treatment duration and titration;
- No therapeutic drug class duplications;
- Medication tolerability (eg, allergies, AEs, drug interactions); and
- Opioid risk assessment per Opioid Risk Tool (ORT) score and medical history.
Consulting providers clarified patients’ pain diagnoses prior to pharmacy consultations.
After face-to-face patient interviews, the inpatient pain CPS prepared pain management recommendations, including nonopioid/adjuvant pain medications and/or opioid dose adjustments. The IPPCS also collaborated with pain physicians for intervention procedures, nonpharmacologic recommendations, and for more complex patients who may have required additional imaging or detailed physical evaluations. Pain CPSs documented CPRS notes with the SOAR template and discussed all recommendations with appropriate inpatient teams.
Respective providers received questionnaires hosted on SurveyMonkey.com (San Mateo, CA) to gauge their satisfaction with the IPPCS at the end of the pilot period, which helped determine program utility. Data collected for the pilot included patient demographics; patient admission diagnosis; consulting inpatient service; type of pain and reason for IPPCS request; total morphine equivalent daily dose (MEDD); pertinent past medical history (ie, sleep apnea, psychiatric comorbidities, or substance use disorder [SUD]); ORT score; patients’ reported average pain severity on the 10-point Numeric Pain Rating Scale (NPRS); number of requests submitted; medications discontinued, initiated, or dose increased/decreased; and number of pharmacist recommendations, including number accepted by providers. The ORT is a 5-item questionnaire used to determine risk of opioid-related aberrant behaviors in adults to help discriminate between low-risk and high-risk individuals (Table 1).17
Descriptive statistics were used to evaluate the results, and a Likert scale was used to evaluate responses the from provider satisfaction questionnaires. The IPPCS collected and organized the data using Microsoft Excel (Redmond, WA).
Results
By the end of the pilot period in May 2016, the IPPCS had received 100 consult requests and completed 81% (Figure). The remaining consults included 11% forwarded to other disciplines. The service discontinued 8% of the requests, given patients’ hospital discharge prior to IPPCS review.
Baseline patient data are outlined in Tables 2, 3, 4, and 5. For each of the 100 consults, providers could select more than 1 reason for the request. The nonopioid/adjuvant treatment recommendations were the most common at 49% (62/128). Patients could have more than 1 pertinent medical comorbidity, with psychiatric illnesses the most prevalent at 68% (133/197). A mean ORT score of 8.1 indicated a high risk for opioid-related aberrant behavior. Overall, half the patients (37/73) were high risk, 25% (18/73) were medium risk (ORT 4-7), and 25% (18/73) were low risk (ORT 0-3). Patients’ reported average pain was often severe (NPRS 7-10) at 54% (40/74) or moderate (NPRS 4-6) at 39% (29/74).
The IPPCS recommended various medications for initiation, discontinuation, or dosage changes (Table 6). For example, the IPPCS recommended initiation of topical agents in 38% (48/128) of cases. The inpatient pain CPS offered opioid initiation in 17% (22/128) of cases, with immediate-release oral morphine as the most predominant. Notably, opioids remained the most common medications suggested for discontinuation at 74% (38/51), including 47% (18/38) for IV hydromorphone. Dose titration recommendations mainly included anticonvulsants at 33% (16/48), and most dose reductions involved opioids at 78% (7/9), namely, oxycodone/acetaminophen and IV hydromorphone.
Providers accepted 76% (179/234) of IPPCS pharmacist medication recommendations. The most common included initiation/optimization of adjuvant therapy (eg, anticonvulsants, serotonin-norepinephrine reuptake inhibitors [SNRIs], and topical agents) at 46% (83/179), followed by opioid discontinuation (eg, IV hydromorphone) at 22% (40/179). Although this project primarily tracked medication interventions, examples of accepted nonpharmacologic recommendations included UDT and referrals to other programs (eg, pain psychology, substance abuse, mental health, acupuncture, chiropractor, PT/OT/PMR, and interventional pain management), which received support from each respective discipline. Declined pharmacologic recommendations mostly included topicals (eg, lidocaine, trolamine, and capsaicin cream) at 35% (19/55). However, findings also show that providers implemented 100% of medication recommendations in whole for 58% (47/81) of consults.
Likert scale satisfaction questionnaires offered insight into providers’ perception of the IPPCS (Table 7). One provider felt “neutral” about the consult submission process, given the time needed to complete the CPRS requests, but all other providers “agreed” or “strongly agreed” that the IPPCS was user-friendly. More importantly, 100% (15/15) “agreed” or “strongly agreed” that the inpatient pain CPS answered consults promptly with reasonable, evidence-based recommendations. All respondents declared that they would recommend the IPPCS to other practitioners and felt comfortable entering requests for future patients.
Discussion
The IPPCS achieved a total of 100 consults, which served as the sample for the pilot program. With support from the OCPC, PMR, and Clinical Pharmacy Department Administration, the IPPCS operated from November 2, 2015 through May 6, 2016. Results suggested that this new service could assist in managing inpatient pain issues in collaboration with inpatient multidisciplinary teams.
The most popular reason for IPPCS consults was acute on chronic pain. Given national efforts to improve opioid prescribing through the VA Opioid Safety Initiative (OSI) and the 2016 CDC Guideline for Opioid Prescribing, most pain consults requested nonopioid/adjuvant recommendations.18,19 Despite the wide MEDD range in this sample, the median/mean generally remained below recommended limits per current guidelines.18,19 However, the small sample size and lack of patient diversity (mostly white male veterans) limited the generalizability to non-VA medical facilities. Veterans often experienced both chronic pain and psychiatric disturbances, which explained the significant number of underlying mental health comorbidities observed. This affirmed the close interrelationship between pain and psychiatric issues described in the literature.20
Providers’ acceptance of pharmacologic and nonpharmacologic treatment modalities supported a comprehensive, multidisciplinary, and biopsychosocial approach to effective analgesic management. During this pilot, the most common pharmacy medication recommendations, namely, discontinuation of inappropriate opioids (eg, IV hydromorphone in patients who are controlled on and/or able to tolerate oral medications) and dose titration of adjuvant medications (eg, anticonvulsants for neuropathic pain), revealed that the IPPCS provided needed expertise and alternatives for complex pain patients. The IPPCS was well received, as inpatient providers accepted and implemented a large proportion of pharmacist recommendations. Despite risks of bias with a nonvalidated questionnaire, providers offered positive feedback. In the future, distributing satisfaction evaluations to patients also would provide more insight into how others perceived the IPPCS.
Limitations
Reasons for unaccepted recommendations included perceived limited effectiveness and/or feasibility of topical agents for acute pain, as providers seemed to favor systemic therapy for supposedly more immediate analgesia. Prescriber preference may explain why inpatient teams sometimes declined adjuvant therapy recommendations. However, the 2016 American Pain Society Guidelines on the Management of Postoperative Pain support a multimodal approach and confirm that adjuvants can reduce patients’ opioid requirements.21
Consulting teams did not execute some opioid recommendations, which may be due to various factors, including patient-related or provider-related factors in the inpatient vs outpatient setting. Lack of retrospective analysis for comparison of results pre- and post-IPPCS implementation also limited the outcomes. However, this project was piloted as a QI initiative after providers identified significant needs for inpatient pain management at the WPBVAMC. No retrospective analysis was undertaken, as this project analyzed only responses during the pilot program.
Other obstacles of the IPPCS included request appropriateness and triaging. The inpatient pain CPS deferred management of some consults to other disciplines (eg, gastroenterology) for more appropriate care. The IPPCS deferred certain cases of acute pancreatic pain or generalized abdominal pain for further workup to address patients’ underlying issues. The inpatient pain CPS relayed pertinent information regarding appropriate consults to inpatient teams. In the future, developing more specific inclusion/exclusion criteria and delivering provider education about proper IPPCS requests may resolve this issue.
Challenges with pain consults from inpatient psychiatry stemmed from patients’ skepticism and unwillingness to accept nonopioid/adjuvant therapies. Additionally, comorbid psychiatric disorders are often associated with SUDs and potentially opioid-related aberrant behavior. More than 40% of opioid-dependent individuals have comorbid psychiatric disorders, especially depression, anxiety, and bipolar disorder.22 Poorly-managed pain also drives SUD, as 80% of these patients illegally obtain prescription opioids. Thus, undertreatment of pain may push individuals to secure pain medications from illegal/illicit sources to achieve analgesia.23 Following pain physician consultation, the IPPCS continued inpatient opioids for 12% (10/81) of patients with a SUD history, including 5 with postoperative pain or other acute processes, since patients were kept in a monitored health care environment. The remaining included 4 with malignant pain and 1 with end-of-life pain. Overall, the IPPCS recommended that inpatient teams discharge these patients on as little opioids as possible, as well as to make referrals to substance abuse programs when necessary. Effective pain management of patients with aberrant behavior requires a comprehensive interdisciplinary team approach. To mitigate risk, effectively treat pain, and maintain patient safety, clinicians must recognize biologic, chemical, social, and psychiatric aspects of substance abuse.21
Another limitation during this pilot was an inability to promptly assess the impact of recommendations, given limited opportunities to reevaluate patients. In the future, more dedicated time for the inpatient pain CPSs to respond to consults may allow for better follow-up rather than initial consults only. Providers sometimes discharged patients within 24 hours of submitting consults as well, which left no time for the inpatient pain CPS consultation. However, the IPPCS forwarded appropriate requests to pain CPS e-consult services for chart review recommendations. Encouraging providers to submit consults earlier in patients’ hospital admissions may help reduce the number of incomplete IPPCS requests. Although expanding service hours would require more dedicated CPS staffing resources, it is another option for quicker consult completion and prompt follow-up.
Future Directions
Future efforts to expand this project include ensuring patient safety through judicious opioid use. Smooth transitions of care will particularly help to improve the quality of pain management. Current WPBVAMC policies stated that the primary care provider (PCP) alone must agree to continue prescribing outpatient analgesic medications, including opioids, prescribed from the OCPC once patients return to Primary Care. Continued provider education would ideally promote efficient utilization of the IPPCS and OCPC.
The pain pharmacy SOAR note template also could undergo additional edits/revisions, including the addition of opioid overdose risk assessments. For improved documentation and standardization, the template could autopopulate patient-specific information when the inpatient pain CPS chooses the designated note title. The IPPCS also hoped to streamline the CPRS consult link for more convenience and ease of use. Ultimately, the IPPCS wished to provide ongoing provider education, inpatient opioid therapy, and other topics upon request.
Conclusion
The IPPCS received positive provider feedback and collected 100 consults (averaging 4 per week) during the 6-month pilot QI project. Most consults were for acute or chronic pain and requested nonopioid/adjuvant recommendations. The new service intended to fulfill unmet needs at the WPBVAMC by expanding the facility’s current pain programs. Prescribers reported a high level of satisfaction and a willingness to not only refer other clinicians to the program, but also continue using the consult. Providers unanimously agreed that the pain CPS provided reasonable, evidence-based recommendations. This project demonstrated that the IPPCS can aid in meeting new demands amid the challenging landscape of pain practice.
The term pain refers to unpleasant sensory, emotional experiences associated with actual or potential tissue damage and is described in terms of such damage.1 Acute pain from neurophysiologic responses to noxious stimuli resolves upon tissue healing or stimuli removal (eg, 3-6 months); however, chronic pain lingers beyond the expected time course of the acute injury and repair process.1,2 Despite pain management advances, the under- or overtreatment of pain for different patient populations (eg, cancer and noncancer) remains an important concern.3,4
Hospitals have focused on optimizing inpatient pain management, because uncontrolled pain remains the most common reason for readmissions the first week postsurgery.5 The safe use of opioids (prescription, illicit synthetic, or heroin) poses major challenges and raises significant concerns. Rates of opioid-related hospital admissions have increased by 42% since 2009, and total overdose deaths reached a new high of 47,055 in 2014, including 28,647 (61%) from opioids.6
Opioids rank among the medications most often associated with serious adverse events (AEs), including respiratory depression and death.7 In response, the Joint Commission recommends patient assessments for opioid-related AEs, technology to monitor opioid prescribing, pharmacist consultation for opioid conversions and route of administration changes, provider education about risks of opioids, and risk screening tools for opioid-related oversedation and respiratory depression.7 Treatment guidelines strive to minimize the impact of acute pain by offering a scientific basis for practice, but evidence suggests a lack of suitable pain programs.7 Increases in opioid prescribing along with clinical guidelines and state laws recommending specialty pain service referrals for patients on high-dose opioids, have increased demand for competent pain clinicians.8
The expertise of a clinical pharmacy specialists (CPS) can help refine ineffective and potentially harmful pain medication therapy in complex patient cases. Existing literature outlines the various benefits of pharmacist participation in collaborative pain services for cancer and noncancer pain, as well as cases involving substance abuse.9-13 Various articles support pharmacists’ role as an educator and team member who can add valuable, trustworthy clinical knowledge that enhances clinical encounters and guides protocol/policy development.12,13 These efforts have improved patient satisfaction and encouraged physicians and nurses to proactively seek pharmacists’ advice for difficult cases.9
Frequent communication with interdisciplinary teams have helped considerably in establishing clinical pharmacy services that benefit patient care and offer sources of professional accomplishment.10,11 For example, pharmacists at Kaweah Delta Medical Center in Visalia, CA launched an innovative pain program that encompassed consultations and opioid stewardship, which demonstrated that pharmacists can improve patient outcomes in the front lines of pain management.14 Pain CPSs have advanced knowledge of pharmacokinetics, pharmacodynamics, and therapeutics to promote safe and effective analgesic use, as well as to identify opioid use disorders. Evidence suggests that pharmacists’ presence on interdisciplinary pain teams improves outcomes by optimizing medication selection, improving adherence, and preventing AEs.8
Following the plan-do-study-act model for quality improvement (QI), this project hoped to expand current pain programs at the West Palm Beach VAMC (WPBVAMC) by evaluating the feasibility of an inpatient pain pharmacist consult service (IPPCS) at the 301-bed teaching facility, which includes 130 acute/intensive care and 120 nursing/domiciliary beds.15 Staff provide primary- and secondary-level care to veterans in 7 counties along Florida’s southeastern coast.
In 2009, the WPBVAMC PGY-2 Pain Management and Palliative Care Program became the VA’s first accredited pain pharmacy residency. Residents train with the Physical Medicine & Rehabilitation (PMR) and Chronic Pain Management departments, which provide outpatient services from 7 pain physicians, a pain psychologist, registered nurse, chiropractor, acupuncturist, physical/occupational therapy (PT/OT), and 3 pain/palliative care CPSs.
The WPBVAMC had established interdisciplinary outpatient chronic pain clinic (OCPC) physician- and pharmacist-run services along with a pain CPS electronic consult (e-consult) program. However, no formal mechanisms for inpatient pain consultations existed. Prior to the IPPCS outlined in this study, OCPC practitioners, including 2 pain CPSs, managed impromptu inpatient pain issues as “curbside consultations” along with usual day-to-day clinic duties.
The OCPC, PMR, and Clinical Pharmacy administration recognized the need for more clinical support to manage complex analgesic issues in inpatient veterans, as these patients often have acute pain with underlying chronic pain syndromes. In a national survey, veterans were significantly more likely than were nonveterans to report painful health conditions (65.5% vs 56.4%) and to classify their pain as severe (9.1% vs 6.3%).16 The WPBVAMC administration concluded that an IPPCS would offer a more efficient means of handling such cases. The IPPCS would formally streamline inpatient pain consults, enabling CPSs to thoroughly evaluate pain-related issues to propose evidence-based recommendations.
The primary objective of this QI project was to assess the IPPCS implementation as part of multimodal care to satisfy unmet patient care needs at the WPBVAMC. Secondary objectives for program feasibility included identifying the volume and type of pain consults, categorizing pharmacist interventions, classifying providers’ satisfaction, and determining types of responses to pharmacists’ medication recommendations.
Methods
This QI project ascertained the feasibility of the IPPCS by evaluating all consults obtained during the pilot period from November 2, 2015 through May 6, 2016. The IPPCS was accessible Monday through Friday during normal business hours. Goal turnaround time for consult completion was 24 to 72 hours, given the lack of coverage on holidays and weekends. The target population included veterans hospitalized at the WPBVAMC inpatient ward or nursing home with uncontrolled pain on IV and/or oral analgesic medications. All IPPCS consults submitted during the pilot period were included in the sample.
The WPBVAMC Scientific Advisory Committee (SAC) approved this QI program prior to initiation. Following supervisory support from the OCPC, PMR, and Clinical Pharmacy departments, hospital technologists assisted in creating a consult link in the Computerized Patient Record System (CPRS), which allowed providers to submit IPPCS requests for specific patients efficiently. Consults were categorized as postoperative pain, acute or chronic pain, malignant pain, or end-of-life pain. Inpatient providers could enter requests for assistance with 1 or more of the following: opioid dose conversions, opioid taper/titration schedules, general opioid treatment recommendations, or nonopioid/adjuvant recommendations.
The Medical Records Committee approved a customized CPRS subjective-objective-assessment-recommendations (SOAR) note template, which helped standardize the pain CPS documentation. To promote consult requests and interdisciplinary collaboration, inpatient clinicians received education about the IPPCS at respective meetings (eg, General Medicine staff and Clinical Pharmacy meetings).
All CPSs involved in this project were residency-trained in direct patient care, including pain and palliative care, and maintained national board certification as pharmacotherapy specialists. Their role included reviewing patients’ electronic medical records, conducting face-to-face pain assessments, completing opioid risk assessments, evaluating analgesic regimen appropriateness, reviewing medication adherence, completing pain medication reconciliation, querying the Florida Prescription Drug Monitoring Program (PDMP), interpreting urine drug testing (UDT), and delivering provider/patient/caregiver education. Parameters used to determine the appropriateness of analgesic regimens included, but were not limited to:
- Use of oral instead of IV medications if oral dosing was feasible/possible/appropriate;
- Dose and adjustments per renal/hepatic function;
- Adequate treatment duration and titration;
- No therapeutic drug class duplications;
- Medication tolerability (eg, allergies, AEs, drug interactions); and
- Opioid risk assessment per Opioid Risk Tool (ORT) score and medical history.
Consulting providers clarified patients’ pain diagnoses prior to pharmacy consultations.
After face-to-face patient interviews, the inpatient pain CPS prepared pain management recommendations, including nonopioid/adjuvant pain medications and/or opioid dose adjustments. The IPPCS also collaborated with pain physicians for intervention procedures, nonpharmacologic recommendations, and for more complex patients who may have required additional imaging or detailed physical evaluations. Pain CPSs documented CPRS notes with the SOAR template and discussed all recommendations with appropriate inpatient teams.
Respective providers received questionnaires hosted on SurveyMonkey.com (San Mateo, CA) to gauge their satisfaction with the IPPCS at the end of the pilot period, which helped determine program utility. Data collected for the pilot included patient demographics; patient admission diagnosis; consulting inpatient service; type of pain and reason for IPPCS request; total morphine equivalent daily dose (MEDD); pertinent past medical history (ie, sleep apnea, psychiatric comorbidities, or substance use disorder [SUD]); ORT score; patients’ reported average pain severity on the 10-point Numeric Pain Rating Scale (NPRS); number of requests submitted; medications discontinued, initiated, or dose increased/decreased; and number of pharmacist recommendations, including number accepted by providers. The ORT is a 5-item questionnaire used to determine risk of opioid-related aberrant behaviors in adults to help discriminate between low-risk and high-risk individuals (Table 1).17
Descriptive statistics were used to evaluate the results, and a Likert scale was used to evaluate responses the from provider satisfaction questionnaires. The IPPCS collected and organized the data using Microsoft Excel (Redmond, WA).
Results
By the end of the pilot period in May 2016, the IPPCS had received 100 consult requests and completed 81% (Figure). The remaining consults included 11% forwarded to other disciplines. The service discontinued 8% of the requests, given patients’ hospital discharge prior to IPPCS review.
Baseline patient data are outlined in Tables 2, 3, 4, and 5. For each of the 100 consults, providers could select more than 1 reason for the request. The nonopioid/adjuvant treatment recommendations were the most common at 49% (62/128). Patients could have more than 1 pertinent medical comorbidity, with psychiatric illnesses the most prevalent at 68% (133/197). A mean ORT score of 8.1 indicated a high risk for opioid-related aberrant behavior. Overall, half the patients (37/73) were high risk, 25% (18/73) were medium risk (ORT 4-7), and 25% (18/73) were low risk (ORT 0-3). Patients’ reported average pain was often severe (NPRS 7-10) at 54% (40/74) or moderate (NPRS 4-6) at 39% (29/74).
The IPPCS recommended various medications for initiation, discontinuation, or dosage changes (Table 6). For example, the IPPCS recommended initiation of topical agents in 38% (48/128) of cases. The inpatient pain CPS offered opioid initiation in 17% (22/128) of cases, with immediate-release oral morphine as the most predominant. Notably, opioids remained the most common medications suggested for discontinuation at 74% (38/51), including 47% (18/38) for IV hydromorphone. Dose titration recommendations mainly included anticonvulsants at 33% (16/48), and most dose reductions involved opioids at 78% (7/9), namely, oxycodone/acetaminophen and IV hydromorphone.
Providers accepted 76% (179/234) of IPPCS pharmacist medication recommendations. The most common included initiation/optimization of adjuvant therapy (eg, anticonvulsants, serotonin-norepinephrine reuptake inhibitors [SNRIs], and topical agents) at 46% (83/179), followed by opioid discontinuation (eg, IV hydromorphone) at 22% (40/179). Although this project primarily tracked medication interventions, examples of accepted nonpharmacologic recommendations included UDT and referrals to other programs (eg, pain psychology, substance abuse, mental health, acupuncture, chiropractor, PT/OT/PMR, and interventional pain management), which received support from each respective discipline. Declined pharmacologic recommendations mostly included topicals (eg, lidocaine, trolamine, and capsaicin cream) at 35% (19/55). However, findings also show that providers implemented 100% of medication recommendations in whole for 58% (47/81) of consults.
Likert scale satisfaction questionnaires offered insight into providers’ perception of the IPPCS (Table 7). One provider felt “neutral” about the consult submission process, given the time needed to complete the CPRS requests, but all other providers “agreed” or “strongly agreed” that the IPPCS was user-friendly. More importantly, 100% (15/15) “agreed” or “strongly agreed” that the inpatient pain CPS answered consults promptly with reasonable, evidence-based recommendations. All respondents declared that they would recommend the IPPCS to other practitioners and felt comfortable entering requests for future patients.
Discussion
The IPPCS achieved a total of 100 consults, which served as the sample for the pilot program. With support from the OCPC, PMR, and Clinical Pharmacy Department Administration, the IPPCS operated from November 2, 2015 through May 6, 2016. Results suggested that this new service could assist in managing inpatient pain issues in collaboration with inpatient multidisciplinary teams.
The most popular reason for IPPCS consults was acute on chronic pain. Given national efforts to improve opioid prescribing through the VA Opioid Safety Initiative (OSI) and the 2016 CDC Guideline for Opioid Prescribing, most pain consults requested nonopioid/adjuvant recommendations.18,19 Despite the wide MEDD range in this sample, the median/mean generally remained below recommended limits per current guidelines.18,19 However, the small sample size and lack of patient diversity (mostly white male veterans) limited the generalizability to non-VA medical facilities. Veterans often experienced both chronic pain and psychiatric disturbances, which explained the significant number of underlying mental health comorbidities observed. This affirmed the close interrelationship between pain and psychiatric issues described in the literature.20
Providers’ acceptance of pharmacologic and nonpharmacologic treatment modalities supported a comprehensive, multidisciplinary, and biopsychosocial approach to effective analgesic management. During this pilot, the most common pharmacy medication recommendations, namely, discontinuation of inappropriate opioids (eg, IV hydromorphone in patients who are controlled on and/or able to tolerate oral medications) and dose titration of adjuvant medications (eg, anticonvulsants for neuropathic pain), revealed that the IPPCS provided needed expertise and alternatives for complex pain patients. The IPPCS was well received, as inpatient providers accepted and implemented a large proportion of pharmacist recommendations. Despite risks of bias with a nonvalidated questionnaire, providers offered positive feedback. In the future, distributing satisfaction evaluations to patients also would provide more insight into how others perceived the IPPCS.
Limitations
Reasons for unaccepted recommendations included perceived limited effectiveness and/or feasibility of topical agents for acute pain, as providers seemed to favor systemic therapy for supposedly more immediate analgesia. Prescriber preference may explain why inpatient teams sometimes declined adjuvant therapy recommendations. However, the 2016 American Pain Society Guidelines on the Management of Postoperative Pain support a multimodal approach and confirm that adjuvants can reduce patients’ opioid requirements.21
Consulting teams did not execute some opioid recommendations, which may be due to various factors, including patient-related or provider-related factors in the inpatient vs outpatient setting. Lack of retrospective analysis for comparison of results pre- and post-IPPCS implementation also limited the outcomes. However, this project was piloted as a QI initiative after providers identified significant needs for inpatient pain management at the WPBVAMC. No retrospective analysis was undertaken, as this project analyzed only responses during the pilot program.
Other obstacles of the IPPCS included request appropriateness and triaging. The inpatient pain CPS deferred management of some consults to other disciplines (eg, gastroenterology) for more appropriate care. The IPPCS deferred certain cases of acute pancreatic pain or generalized abdominal pain for further workup to address patients’ underlying issues. The inpatient pain CPS relayed pertinent information regarding appropriate consults to inpatient teams. In the future, developing more specific inclusion/exclusion criteria and delivering provider education about proper IPPCS requests may resolve this issue.
Challenges with pain consults from inpatient psychiatry stemmed from patients’ skepticism and unwillingness to accept nonopioid/adjuvant therapies. Additionally, comorbid psychiatric disorders are often associated with SUDs and potentially opioid-related aberrant behavior. More than 40% of opioid-dependent individuals have comorbid psychiatric disorders, especially depression, anxiety, and bipolar disorder.22 Poorly-managed pain also drives SUD, as 80% of these patients illegally obtain prescription opioids. Thus, undertreatment of pain may push individuals to secure pain medications from illegal/illicit sources to achieve analgesia.23 Following pain physician consultation, the IPPCS continued inpatient opioids for 12% (10/81) of patients with a SUD history, including 5 with postoperative pain or other acute processes, since patients were kept in a monitored health care environment. The remaining included 4 with malignant pain and 1 with end-of-life pain. Overall, the IPPCS recommended that inpatient teams discharge these patients on as little opioids as possible, as well as to make referrals to substance abuse programs when necessary. Effective pain management of patients with aberrant behavior requires a comprehensive interdisciplinary team approach. To mitigate risk, effectively treat pain, and maintain patient safety, clinicians must recognize biologic, chemical, social, and psychiatric aspects of substance abuse.21
Another limitation during this pilot was an inability to promptly assess the impact of recommendations, given limited opportunities to reevaluate patients. In the future, more dedicated time for the inpatient pain CPSs to respond to consults may allow for better follow-up rather than initial consults only. Providers sometimes discharged patients within 24 hours of submitting consults as well, which left no time for the inpatient pain CPS consultation. However, the IPPCS forwarded appropriate requests to pain CPS e-consult services for chart review recommendations. Encouraging providers to submit consults earlier in patients’ hospital admissions may help reduce the number of incomplete IPPCS requests. Although expanding service hours would require more dedicated CPS staffing resources, it is another option for quicker consult completion and prompt follow-up.
Future Directions
Future efforts to expand this project include ensuring patient safety through judicious opioid use. Smooth transitions of care will particularly help to improve the quality of pain management. Current WPBVAMC policies stated that the primary care provider (PCP) alone must agree to continue prescribing outpatient analgesic medications, including opioids, prescribed from the OCPC once patients return to Primary Care. Continued provider education would ideally promote efficient utilization of the IPPCS and OCPC.
The pain pharmacy SOAR note template also could undergo additional edits/revisions, including the addition of opioid overdose risk assessments. For improved documentation and standardization, the template could autopopulate patient-specific information when the inpatient pain CPS chooses the designated note title. The IPPCS also hoped to streamline the CPRS consult link for more convenience and ease of use. Ultimately, the IPPCS wished to provide ongoing provider education, inpatient opioid therapy, and other topics upon request.
Conclusion
The IPPCS received positive provider feedback and collected 100 consults (averaging 4 per week) during the 6-month pilot QI project. Most consults were for acute or chronic pain and requested nonopioid/adjuvant recommendations. The new service intended to fulfill unmet needs at the WPBVAMC by expanding the facility’s current pain programs. Prescribers reported a high level of satisfaction and a willingness to not only refer other clinicians to the program, but also continue using the consult. Providers unanimously agreed that the pain CPS provided reasonable, evidence-based recommendations. This project demonstrated that the IPPCS can aid in meeting new demands amid the challenging landscape of pain practice.
1. D’Arcy Y. Treating acute pain in the hospitalized patient. Nurse Pract. 2012;37(8):22-30.
2. Marks AD, Rodgers PE. Diagnosis and management of acute pain in the hospitalized patient. Am J Med. 2014;3(3):e396-e408.
3. Paice JA, Von Roenn JH. Under- or overtreatment of pain in the patient with cancer: how to achieve proper balance. J Clin Oncol. 2014;32(16):1721-1726.
4. Mafi JN, McCarthy EP, Davis RB, Landon BE. Worsening trends in the management and treatment of back pain. JAMA Intern Med. 2013;173(17):1573-1581.
5. Palomano RC, Rathmell JP, Krenzischek DA, Dunwoody CJ. Emerging trends and new approaches to acute pain management. J Perianesth Nurs. 2008;23(suppl 1):S43-S53.
6. U.S. Department of Health & Human Services, Office of the Surgeon General. Facing addiction in America: the surgeon general’s report on alcohol, drugs, and health, executive summary. https://addiction.surgeongeneral.gov/executive-summary.pdf. Published November 2016. Accessed November 1, 2017.
7. Bagian JP, Cohen M, Barnsteiner JH, et al. Safe use of opioids in hospitals. Sentinel Event Alert. 2012;49:1-5.
8. Atkinson TJ, Gulum AH, Forkum WG. The future of pain pharmacy: directed by need. Integrated Pharm Res Pract. 2016;2016(5):33-42.
9. Lothian ST, Fotis MA, Von Gutten CF, et al. Cancer pain management through a pharmacist-based analgesic dosing service. Am J Health Syst Pharm. 1999;56:1119-1125.
10. Lynn MA. Pharmacist interventions in pain management. Am J Health Syst Pharm. 2004;61(14):1487-1489.
11. Strickland JM, Huskey A, Brushwood DB. Pharmacist-physician collaboration in pain management practice. J Opioid Manag. 2007;3(6):295-301.
12. Fan T and Elgourt T. Pain management pharmacy service in a community hospital. Am J Health Syst Pharm. 2008;65(16):1560-1565.
13. Andrews LB, Bridgeman MB, Dalal KS, et al. Implementation of a pharmacist-directed pain management consultation service for hospitalised adults with a history of substance abuse. Int J Clin Pract. 2013;67(12):1342-1349.
14. Poirier RH, Brown CS, Garcia YT, Gann NY, Sandoval RA, McNulty JR. Implementation of a pharmacist directed pain management service in the inpatient setting. http://www.ashpadvantage.com/bestpractices/2014_papers/Kaweah-Delta.htm. Published 2014. Accessed November 1, 2017.
15. Langley GL, Moen R, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. 2nded. San Francisco, CA: Jossey-Bass; 2009.
16. Nahin, RL. Severe pain in veterans: the effect of age and sex, and comparisons with the general population. J Pain. 2017;18(3):247-254.
17. Webster LR, Webster RM. Predicting aberrant behaviors in opioid-treated patients: preliminary validation of the opioid risk tool. Pain Med. 2005;6(6):432-442.
18. Nazario M. Opioid therapy risk management: the VA opioid safety and naloxone distribution initiatives. http://jfpsmeeting.pharmacist.com/sites/default/files/slides/Opioid%20Therapy%20Risk%20Management.pdf. Published October 15, 2015. Accessed November 1, 2017.
19. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain – United States, 2016. MMWR Rep. 2016;65(1):1-49.
20. Outcalt SD, Kroenke K, Krebs EE, et al. Chronic pain and comorbid mental health conditions: independent associations of posttraumatic stress disorder and depression with pain, disability, and quality of life. J Behav Med. 2015;38:535.
21. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131-157.
22. NIDA/SAMHSA Blending Initiative. https://www.drugabuse.gov/nidasamhsa-blending-initiative. Updated November 2015. Accessed November 1, 2017.
23. Alford DP, German JS, Samet JH, Cheng DM, Lloyd-Travaglini CA, Saitz R. Primary care patients with drug use report chronic pain and self-medicate with alcohol and other drugs. J Gen Intern Med. 2016;31(5):486-491.
1. D’Arcy Y. Treating acute pain in the hospitalized patient. Nurse Pract. 2012;37(8):22-30.
2. Marks AD, Rodgers PE. Diagnosis and management of acute pain in the hospitalized patient. Am J Med. 2014;3(3):e396-e408.
3. Paice JA, Von Roenn JH. Under- or overtreatment of pain in the patient with cancer: how to achieve proper balance. J Clin Oncol. 2014;32(16):1721-1726.
4. Mafi JN, McCarthy EP, Davis RB, Landon BE. Worsening trends in the management and treatment of back pain. JAMA Intern Med. 2013;173(17):1573-1581.
5. Palomano RC, Rathmell JP, Krenzischek DA, Dunwoody CJ. Emerging trends and new approaches to acute pain management. J Perianesth Nurs. 2008;23(suppl 1):S43-S53.
6. U.S. Department of Health & Human Services, Office of the Surgeon General. Facing addiction in America: the surgeon general’s report on alcohol, drugs, and health, executive summary. https://addiction.surgeongeneral.gov/executive-summary.pdf. Published November 2016. Accessed November 1, 2017.
7. Bagian JP, Cohen M, Barnsteiner JH, et al. Safe use of opioids in hospitals. Sentinel Event Alert. 2012;49:1-5.
8. Atkinson TJ, Gulum AH, Forkum WG. The future of pain pharmacy: directed by need. Integrated Pharm Res Pract. 2016;2016(5):33-42.
9. Lothian ST, Fotis MA, Von Gutten CF, et al. Cancer pain management through a pharmacist-based analgesic dosing service. Am J Health Syst Pharm. 1999;56:1119-1125.
10. Lynn MA. Pharmacist interventions in pain management. Am J Health Syst Pharm. 2004;61(14):1487-1489.
11. Strickland JM, Huskey A, Brushwood DB. Pharmacist-physician collaboration in pain management practice. J Opioid Manag. 2007;3(6):295-301.
12. Fan T and Elgourt T. Pain management pharmacy service in a community hospital. Am J Health Syst Pharm. 2008;65(16):1560-1565.
13. Andrews LB, Bridgeman MB, Dalal KS, et al. Implementation of a pharmacist-directed pain management consultation service for hospitalised adults with a history of substance abuse. Int J Clin Pract. 2013;67(12):1342-1349.
14. Poirier RH, Brown CS, Garcia YT, Gann NY, Sandoval RA, McNulty JR. Implementation of a pharmacist directed pain management service in the inpatient setting. http://www.ashpadvantage.com/bestpractices/2014_papers/Kaweah-Delta.htm. Published 2014. Accessed November 1, 2017.
15. Langley GL, Moen R, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. 2nded. San Francisco, CA: Jossey-Bass; 2009.
16. Nahin, RL. Severe pain in veterans: the effect of age and sex, and comparisons with the general population. J Pain. 2017;18(3):247-254.
17. Webster LR, Webster RM. Predicting aberrant behaviors in opioid-treated patients: preliminary validation of the opioid risk tool. Pain Med. 2005;6(6):432-442.
18. Nazario M. Opioid therapy risk management: the VA opioid safety and naloxone distribution initiatives. http://jfpsmeeting.pharmacist.com/sites/default/files/slides/Opioid%20Therapy%20Risk%20Management.pdf. Published October 15, 2015. Accessed November 1, 2017.
19. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain – United States, 2016. MMWR Rep. 2016;65(1):1-49.
20. Outcalt SD, Kroenke K, Krebs EE, et al. Chronic pain and comorbid mental health conditions: independent associations of posttraumatic stress disorder and depression with pain, disability, and quality of life. J Behav Med. 2015;38:535.
21. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131-157.
22. NIDA/SAMHSA Blending Initiative. https://www.drugabuse.gov/nidasamhsa-blending-initiative. Updated November 2015. Accessed November 1, 2017.
23. Alford DP, German JS, Samet JH, Cheng DM, Lloyd-Travaglini CA, Saitz R. Primary care patients with drug use report chronic pain and self-medicate with alcohol and other drugs. J Gen Intern Med. 2016;31(5):486-491.
EC authorizes brentuximab vedotin for CTCL

The European Commission (EC) has extended the conditional marketing authorization for brentuximab vedotin (Adcetris®).
The drug is now approved for use in adults with CD30-positive cutaneous T-cell lymphoma (CTCL) who have received at least 1 prior systemic therapy.
Brentuximab vedotin can be marketed for this indication in the member states of the European Union as well as in Norway, Liechtenstein, and Iceland.
Conditional marketing authorization from the EC is valid for 1 year and is reviewed annually.
With conditional authorization, drug developers are required to provide comprehensive data confirming a drug’s benefit-risk balance is positive. Once these data are available, a conditional marketing authorization may be converted to a standard marketing authorization.
Drugs are eligible for conditional marketing authorization if they are designated as orphan medicines, intended for use in emergency situations, or designed to treat, prevent, or diagnose seriously debilitating or life-threatening diseases.
The EC previously granted brentuximab vedotin conditional marketing authorization for the treatment of:
- Adults with CD30+ Hodgkin lymphoma who are at an increased risk of relapse or progression following autologous hematopoietic stem cell transplant (auto-HSCT)
- Adults with relapsed or refractory CD30+ Hodgkin lymphoma after auto-HSCT or after at least 2 prior therapies when auto-HSCT or multi-agent chemotherapy is not a treatment option
- Adults with relapsed or refractory systemic anaplastic large-cell lymphoma.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
Phase 3 data
The EC’s latest authorization for brentuximab vedotin is based on data from the phase 3 ALCANZA trial.
Updated results from ALCANZA were presented at the 2017 ASH Annual Meeting in December. Results were previously presented at the 9th Annual T-cell Lymphoma Forum in January 2017 and published in The Lancet in June 2017.
The trial included 128 evaluable patients with CD30-positive CTCL who had received at least 1 prior systemic therapy.
Sixty-four patients were assigned to receive brentuximab vedotin, and 64 were assigned to receive the investigator’s choice of methotrexate or bexarotene (control arm). Patients received treatment for up to 1 year.
For the update, the median follow-up was 33.9 months.
There was a significant improvement in the rate of objective response lasting at least 4 months (ORR4) in the brentuximab vedotin arm compared to the control arm. The ORR4 was 60.9% and 7.8%, respectively (P<0.001). The complete response rate was 18.8% and 0%, respectively (P<0.001).
The median progression-free survival was 15.8 months in the brentuximab vedotin arm and 3.6 months in the control arm (hazard ratio=0.373; 95% CI, 0.245-0.569; P<0.001).
At time of analysis, 73% of patients in the brentuximab vedotin arm and 75% in the control arm had received 1 or more subsequent skin-directed or systemic therapies. The median time to next treatment was 14.2 months in the brentuximab vedotin arm and 6.1 months in the control arm (P<0.001).
Peripheral neuropathy was the most commonly reported adverse event in patients who received brentuximab vedotin. The incidence was 67% in these patients and 6% in controls.
In the brentuximab arm, 86% of patients reported resolution or improvement in peripheral neuropathy. Eighteen patients had ongoing peripheral neuropathy events, including 15 patients with grade 1 and 3 patients with grade 2 events. ![]()
The European Commission (EC) has extended the conditional marketing authorization for brentuximab vedotin (Adcetris®).
The drug is now approved for use in adults with CD30-positive cutaneous T-cell lymphoma (CTCL) who have received at least 1 prior systemic therapy.
Brentuximab vedotin can be marketed for this indication in the member states of the European Union as well as in Norway, Liechtenstein, and Iceland.
Conditional marketing authorization from the EC is valid for 1 year and is reviewed annually.
With conditional authorization, drug developers are required to provide comprehensive data confirming a drug’s benefit-risk balance is positive. Once these data are available, a conditional marketing authorization may be converted to a standard marketing authorization.
Drugs are eligible for conditional marketing authorization if they are designated as orphan medicines, intended for use in emergency situations, or designed to treat, prevent, or diagnose seriously debilitating or life-threatening diseases.
The EC previously granted brentuximab vedotin conditional marketing authorization for the treatment of:
- Adults with CD30+ Hodgkin lymphoma who are at an increased risk of relapse or progression following autologous hematopoietic stem cell transplant (auto-HSCT)
- Adults with relapsed or refractory CD30+ Hodgkin lymphoma after auto-HSCT or after at least 2 prior therapies when auto-HSCT or multi-agent chemotherapy is not a treatment option
- Adults with relapsed or refractory systemic anaplastic large-cell lymphoma.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
Phase 3 data
The EC’s latest authorization for brentuximab vedotin is based on data from the phase 3 ALCANZA trial.
Updated results from ALCANZA were presented at the 2017 ASH Annual Meeting in December. Results were previously presented at the 9th Annual T-cell Lymphoma Forum in January 2017 and published in The Lancet in June 2017.
The trial included 128 evaluable patients with CD30-positive CTCL who had received at least 1 prior systemic therapy.
Sixty-four patients were assigned to receive brentuximab vedotin, and 64 were assigned to receive the investigator’s choice of methotrexate or bexarotene (control arm). Patients received treatment for up to 1 year.
For the update, the median follow-up was 33.9 months.
There was a significant improvement in the rate of objective response lasting at least 4 months (ORR4) in the brentuximab vedotin arm compared to the control arm. The ORR4 was 60.9% and 7.8%, respectively (P<0.001). The complete response rate was 18.8% and 0%, respectively (P<0.001).
The median progression-free survival was 15.8 months in the brentuximab vedotin arm and 3.6 months in the control arm (hazard ratio=0.373; 95% CI, 0.245-0.569; P<0.001).
At time of analysis, 73% of patients in the brentuximab vedotin arm and 75% in the control arm had received 1 or more subsequent skin-directed or systemic therapies. The median time to next treatment was 14.2 months in the brentuximab vedotin arm and 6.1 months in the control arm (P<0.001).
Peripheral neuropathy was the most commonly reported adverse event in patients who received brentuximab vedotin. The incidence was 67% in these patients and 6% in controls.
In the brentuximab arm, 86% of patients reported resolution or improvement in peripheral neuropathy. Eighteen patients had ongoing peripheral neuropathy events, including 15 patients with grade 1 and 3 patients with grade 2 events. ![]()
The European Commission (EC) has extended the conditional marketing authorization for brentuximab vedotin (Adcetris®).
The drug is now approved for use in adults with CD30-positive cutaneous T-cell lymphoma (CTCL) who have received at least 1 prior systemic therapy.
Brentuximab vedotin can be marketed for this indication in the member states of the European Union as well as in Norway, Liechtenstein, and Iceland.
Conditional marketing authorization from the EC is valid for 1 year and is reviewed annually.
With conditional authorization, drug developers are required to provide comprehensive data confirming a drug’s benefit-risk balance is positive. Once these data are available, a conditional marketing authorization may be converted to a standard marketing authorization.
Drugs are eligible for conditional marketing authorization if they are designated as orphan medicines, intended for use in emergency situations, or designed to treat, prevent, or diagnose seriously debilitating or life-threatening diseases.
The EC previously granted brentuximab vedotin conditional marketing authorization for the treatment of:
- Adults with CD30+ Hodgkin lymphoma who are at an increased risk of relapse or progression following autologous hematopoietic stem cell transplant (auto-HSCT)
- Adults with relapsed or refractory CD30+ Hodgkin lymphoma after auto-HSCT or after at least 2 prior therapies when auto-HSCT or multi-agent chemotherapy is not a treatment option
- Adults with relapsed or refractory systemic anaplastic large-cell lymphoma.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
Phase 3 data
The EC’s latest authorization for brentuximab vedotin is based on data from the phase 3 ALCANZA trial.
Updated results from ALCANZA were presented at the 2017 ASH Annual Meeting in December. Results were previously presented at the 9th Annual T-cell Lymphoma Forum in January 2017 and published in The Lancet in June 2017.
The trial included 128 evaluable patients with CD30-positive CTCL who had received at least 1 prior systemic therapy.
Sixty-four patients were assigned to receive brentuximab vedotin, and 64 were assigned to receive the investigator’s choice of methotrexate or bexarotene (control arm). Patients received treatment for up to 1 year.
For the update, the median follow-up was 33.9 months.
There was a significant improvement in the rate of objective response lasting at least 4 months (ORR4) in the brentuximab vedotin arm compared to the control arm. The ORR4 was 60.9% and 7.8%, respectively (P<0.001). The complete response rate was 18.8% and 0%, respectively (P<0.001).
The median progression-free survival was 15.8 months in the brentuximab vedotin arm and 3.6 months in the control arm (hazard ratio=0.373; 95% CI, 0.245-0.569; P<0.001).
At time of analysis, 73% of patients in the brentuximab vedotin arm and 75% in the control arm had received 1 or more subsequent skin-directed or systemic therapies. The median time to next treatment was 14.2 months in the brentuximab vedotin arm and 6.1 months in the control arm (P<0.001).
Peripheral neuropathy was the most commonly reported adverse event in patients who received brentuximab vedotin. The incidence was 67% in these patients and 6% in controls.
In the brentuximab arm, 86% of patients reported resolution or improvement in peripheral neuropathy. Eighteen patients had ongoing peripheral neuropathy events, including 15 patients with grade 1 and 3 patients with grade 2 events. ![]()
Ofatumumab to be pulled from non-US markets

Novartis is planning to stop marketing ofatumumab (Arzerra®) outside the US, but the drug will still be available for certain patients.
The company plans to work with regulatory authorities to establish compassionate use programs for chronic lymphocytic leukemia (CLL) patients outside the US who are currently receiving ofatumumab.
Patients accessing these programs will be offered continued treatment with ofatumumab for as long as they benefit from it, free of charge.
And Novartis will continue to market ofatumumab for CLL in the US.
“Novartis’s intention to transition Arzerra to compassionate use programs in the non-US markets reflects the fact that many more drugs have become available for CLL over the last 5 years and that there is a low number of patients using Arzerra outside of the US market,” said Jan van de Winkel, PhD, chief executive officer of Genmab.
Ofatumumab is marketed under a collaboration agreement between Genmab and Novartis.
Because Novartis has decided to pull ofatumumab from non-US markets, the company will pay Genmab a lump sum of $50 million (USD) for lost potential milestones and royalties. Royalties will continue to be earned on net sales of the drug.
Novartis intends to start the transition to compassionate use programs as soon as the company and regulatory authorities have agreed to a plan.
The two phase 3 studies of ofatumumab in relapsing multiple sclerosis and the study in indolent non-Hodgkin lymphoma will not be affected by this change. All 3 trials will continue.
About ofatumumab
Ofatumumab is a monoclonal antibody designed to target CD20 on the surface of CLL cells and normal B lymphocytes.
In more than 60 countries worldwide, including the US and European Union member countries, ofatumumab is approved as monotherapy for CLL patients who are refractory to treatment with fludarabine and alemtuzumab.
Other approved indications for ofatumumab in the European Union include:
- In combination with chlorambucil or bendamustine to treat CLL patients who have not received prior therapy and are not eligible for fludarabine-based therapy
- In combination with fludarabine and cyclophosphamide to treat adults with relapsed CLL.
Other approved indications for ofatumumab in the US include:
- In combination with chlorambucil to treat previously untreated CLL patients for whom fludarabine-based therapy is considered inappropriate
- In combination with fludarabine and cyclophosphamide to treat patients with relapsed CLL
- For extended treatment of patients who are in complete or partial response after at least 2 lines of therapy for recurrent or progressive CLL.

Novartis is planning to stop marketing ofatumumab (Arzerra®) outside the US, but the drug will still be available for certain patients.
The company plans to work with regulatory authorities to establish compassionate use programs for chronic lymphocytic leukemia (CLL) patients outside the US who are currently receiving ofatumumab.
Patients accessing these programs will be offered continued treatment with ofatumumab for as long as they benefit from it, free of charge.
And Novartis will continue to market ofatumumab for CLL in the US.
“Novartis’s intention to transition Arzerra to compassionate use programs in the non-US markets reflects the fact that many more drugs have become available for CLL over the last 5 years and that there is a low number of patients using Arzerra outside of the US market,” said Jan van de Winkel, PhD, chief executive officer of Genmab.
Ofatumumab is marketed under a collaboration agreement between Genmab and Novartis.
Because Novartis has decided to pull ofatumumab from non-US markets, the company will pay Genmab a lump sum of $50 million (USD) for lost potential milestones and royalties. Royalties will continue to be earned on net sales of the drug.
Novartis intends to start the transition to compassionate use programs as soon as the company and regulatory authorities have agreed to a plan.
The two phase 3 studies of ofatumumab in relapsing multiple sclerosis and the study in indolent non-Hodgkin lymphoma will not be affected by this change. All 3 trials will continue.
About ofatumumab
Ofatumumab is a monoclonal antibody designed to target CD20 on the surface of CLL cells and normal B lymphocytes.
In more than 60 countries worldwide, including the US and European Union member countries, ofatumumab is approved as monotherapy for CLL patients who are refractory to treatment with fludarabine and alemtuzumab.
Other approved indications for ofatumumab in the European Union include:
- In combination with chlorambucil or bendamustine to treat CLL patients who have not received prior therapy and are not eligible for fludarabine-based therapy
- In combination with fludarabine and cyclophosphamide to treat adults with relapsed CLL.
Other approved indications for ofatumumab in the US include:
- In combination with chlorambucil to treat previously untreated CLL patients for whom fludarabine-based therapy is considered inappropriate
- In combination with fludarabine and cyclophosphamide to treat patients with relapsed CLL
- For extended treatment of patients who are in complete or partial response after at least 2 lines of therapy for recurrent or progressive CLL.
Novartis is planning to stop marketing ofatumumab (Arzerra®) outside the US, but the drug will still be available for certain patients.
The company plans to work with regulatory authorities to establish compassionate use programs for chronic lymphocytic leukemia (CLL) patients outside the US who are currently receiving ofatumumab.
Patients accessing these programs will be offered continued treatment with ofatumumab for as long as they benefit from it, free of charge.
And Novartis will continue to market ofatumumab for CLL in the US.
“Novartis’s intention to transition Arzerra to compassionate use programs in the non-US markets reflects the fact that many more drugs have become available for CLL over the last 5 years and that there is a low number of patients using Arzerra outside of the US market,” said Jan van de Winkel, PhD, chief executive officer of Genmab.
Ofatumumab is marketed under a collaboration agreement between Genmab and Novartis.
Because Novartis has decided to pull ofatumumab from non-US markets, the company will pay Genmab a lump sum of $50 million (USD) for lost potential milestones and royalties. Royalties will continue to be earned on net sales of the drug.
Novartis intends to start the transition to compassionate use programs as soon as the company and regulatory authorities have agreed to a plan.
The two phase 3 studies of ofatumumab in relapsing multiple sclerosis and the study in indolent non-Hodgkin lymphoma will not be affected by this change. All 3 trials will continue.
About ofatumumab
Ofatumumab is a monoclonal antibody designed to target CD20 on the surface of CLL cells and normal B lymphocytes.
In more than 60 countries worldwide, including the US and European Union member countries, ofatumumab is approved as monotherapy for CLL patients who are refractory to treatment with fludarabine and alemtuzumab.
Other approved indications for ofatumumab in the European Union include:
- In combination with chlorambucil or bendamustine to treat CLL patients who have not received prior therapy and are not eligible for fludarabine-based therapy
- In combination with fludarabine and cyclophosphamide to treat adults with relapsed CLL.
Other approved indications for ofatumumab in the US include:
- In combination with chlorambucil to treat previously untreated CLL patients for whom fludarabine-based therapy is considered inappropriate
- In combination with fludarabine and cyclophosphamide to treat patients with relapsed CLL
- For extended treatment of patients who are in complete or partial response after at least 2 lines of therapy for recurrent or progressive CLL.
Health systems plan to produce drugs themselves

A group of US health systems is planning to form a not-for-profit generic drug company with the goal of ending drug shortages and reducing prices for patients.
The company will either directly manufacture generic drugs or subcontract manufacturing to organizations it deems reputable.
“For people in the United States, there is a dangerous gap today between the demand and supply of affordable prescription drugs,” said Richard J. Gilfillan, MD, chief executive officer of Trinity Health, one of the health systems involved in this project.
“If the only way to provide our communities with affordable drugs is to produce them ourselves, then that is what we will do. We look forward to more healthcare systems around the country joining this people-centered effort.”
The organizations involved in this project include Intermountain Healthcare, Ascension, SSM Health, and Trinity Health, as well as the US Department of Veterans Affairs (although the department has not provided financial support for the project).
The 5 organizations represent more than 450 hospitals around the US, and other health systems are set to join the initiative as well.
“It’s an ambitious plan, but healthcare systems are in the best position to fix the problems in the generic drug market,” said Marc Harrison, MD, president and chief executive officer of Intermountain Healthcare.
“We witness, on a daily basis, how shortages of essential generic medications or egregious cost increases for those same drugs affect our patients. We are confident we can improve the situation for our patients by bringing much-needed competition to the generic drug market.”
The formation of this not-for-profit generic drug company will be guided by an advisory committee, which will include:
- Madhu Balachandran, retired executive vice-president of Global Operations, Amgen
- Don Berwick, MD, president emeritus and senior fellow, Institute for Healthcare Improvement; former Centers for Medicare & Medicaid Services administrator
- Clayton Christensen, professor at Harvard Business School and founder of Innosight
- Bob Kerrey, managing director, Allen & Company; former Nebraska governor and US senator
- Martin VanTrieste, retired senior vice-president and chief quality officer, Amgen
- Senior-level leaders from the organizations founding the company.
A group of US health systems is planning to form a not-for-profit generic drug company with the goal of ending drug shortages and reducing prices for patients.
The company will either directly manufacture generic drugs or subcontract manufacturing to organizations it deems reputable.
“For people in the United States, there is a dangerous gap today between the demand and supply of affordable prescription drugs,” said Richard J. Gilfillan, MD, chief executive officer of Trinity Health, one of the health systems involved in this project.
“If the only way to provide our communities with affordable drugs is to produce them ourselves, then that is what we will do. We look forward to more healthcare systems around the country joining this people-centered effort.”
The organizations involved in this project include Intermountain Healthcare, Ascension, SSM Health, and Trinity Health, as well as the US Department of Veterans Affairs (although the department has not provided financial support for the project).
The 5 organizations represent more than 450 hospitals around the US, and other health systems are set to join the initiative as well.
“It’s an ambitious plan, but healthcare systems are in the best position to fix the problems in the generic drug market,” said Marc Harrison, MD, president and chief executive officer of Intermountain Healthcare.
“We witness, on a daily basis, how shortages of essential generic medications or egregious cost increases for those same drugs affect our patients. We are confident we can improve the situation for our patients by bringing much-needed competition to the generic drug market.”
The formation of this not-for-profit generic drug company will be guided by an advisory committee, which will include:
- Madhu Balachandran, retired executive vice-president of Global Operations, Amgen
- Don Berwick, MD, president emeritus and senior fellow, Institute for Healthcare Improvement; former Centers for Medicare & Medicaid Services administrator
- Clayton Christensen, professor at Harvard Business School and founder of Innosight
- Bob Kerrey, managing director, Allen & Company; former Nebraska governor and US senator
- Martin VanTrieste, retired senior vice-president and chief quality officer, Amgen
- Senior-level leaders from the organizations founding the company.
A group of US health systems is planning to form a not-for-profit generic drug company with the goal of ending drug shortages and reducing prices for patients.
The company will either directly manufacture generic drugs or subcontract manufacturing to organizations it deems reputable.
“For people in the United States, there is a dangerous gap today between the demand and supply of affordable prescription drugs,” said Richard J. Gilfillan, MD, chief executive officer of Trinity Health, one of the health systems involved in this project.
“If the only way to provide our communities with affordable drugs is to produce them ourselves, then that is what we will do. We look forward to more healthcare systems around the country joining this people-centered effort.”
The organizations involved in this project include Intermountain Healthcare, Ascension, SSM Health, and Trinity Health, as well as the US Department of Veterans Affairs (although the department has not provided financial support for the project).
The 5 organizations represent more than 450 hospitals around the US, and other health systems are set to join the initiative as well.
“It’s an ambitious plan, but healthcare systems are in the best position to fix the problems in the generic drug market,” said Marc Harrison, MD, president and chief executive officer of Intermountain Healthcare.
“We witness, on a daily basis, how shortages of essential generic medications or egregious cost increases for those same drugs affect our patients. We are confident we can improve the situation for our patients by bringing much-needed competition to the generic drug market.”
The formation of this not-for-profit generic drug company will be guided by an advisory committee, which will include:
- Madhu Balachandran, retired executive vice-president of Global Operations, Amgen
- Don Berwick, MD, president emeritus and senior fellow, Institute for Healthcare Improvement; former Centers for Medicare & Medicaid Services administrator
- Clayton Christensen, professor at Harvard Business School and founder of Innosight
- Bob Kerrey, managing director, Allen & Company; former Nebraska governor and US senator
- Martin VanTrieste, retired senior vice-president and chief quality officer, Amgen
- Senior-level leaders from the organizations founding the company.
U.S. hospitalists estimate significant resources spent on defensive medicine
Clinical question: What percent of inpatient health care spending by hospitalists can be attributed to defensive medicine?
Background: Defensive medicine contributes an estimated $45 billion to annual U.S. health care expenditures. The prevalence of defensive medicine among hospitalists is unknown.
Setting: National survey sent to 1,753 hospitalists from all 50 states identified through the Society of Hospital Medicine database of members and meeting attendees.
Synopsis: The survey contained two primary topics: an estimation of defensive spending and liability history. The hospitalists, who had an average of 11 years in practice, completed 1,020 surveys. Participants estimated that defensive medicine accounted for 37.5% of all health care costs. Decreased estimate rates were seen among VA hospitalists (5.5% less), male respondents (36.4% vs. 39.4% for female), non-Hispanic white respondents (32.5% vs. 44.7% for other) and having more years in practice (decrease of 3% for every 10 years in practice). One in four respondents reported being sued at least once, with higher risk seen in those with greater years in practice. There was no association between liability experience and perception of defensive medicine spending. Differences between academic and community settings were not addressed. Because only 30% of practicing hospitalists are members of SHM, it may be difficult to generalize these findings.
Bottom line: Hospitalists perceive that defensive medicine is a major contributor to inpatient health care expenditures.
Citation: Saint S et al. Perception of resources spent on defensive medicine and history of being sued among hospitalists: Results from a national survey. J Hosp Med. 2017 Aug 23. doi: 10.12788/jhm.2800.
Dr. Lublin is a hospitalist at the University of Colorado School of Medicine.
Clinical question: What percent of inpatient health care spending by hospitalists can be attributed to defensive medicine?
Background: Defensive medicine contributes an estimated $45 billion to annual U.S. health care expenditures. The prevalence of defensive medicine among hospitalists is unknown.
Setting: National survey sent to 1,753 hospitalists from all 50 states identified through the Society of Hospital Medicine database of members and meeting attendees.
Synopsis: The survey contained two primary topics: an estimation of defensive spending and liability history. The hospitalists, who had an average of 11 years in practice, completed 1,020 surveys. Participants estimated that defensive medicine accounted for 37.5% of all health care costs. Decreased estimate rates were seen among VA hospitalists (5.5% less), male respondents (36.4% vs. 39.4% for female), non-Hispanic white respondents (32.5% vs. 44.7% for other) and having more years in practice (decrease of 3% for every 10 years in practice). One in four respondents reported being sued at least once, with higher risk seen in those with greater years in practice. There was no association between liability experience and perception of defensive medicine spending. Differences between academic and community settings were not addressed. Because only 30% of practicing hospitalists are members of SHM, it may be difficult to generalize these findings.
Bottom line: Hospitalists perceive that defensive medicine is a major contributor to inpatient health care expenditures.
Citation: Saint S et al. Perception of resources spent on defensive medicine and history of being sued among hospitalists: Results from a national survey. J Hosp Med. 2017 Aug 23. doi: 10.12788/jhm.2800.
Dr. Lublin is a hospitalist at the University of Colorado School of Medicine.
Clinical question: What percent of inpatient health care spending by hospitalists can be attributed to defensive medicine?
Background: Defensive medicine contributes an estimated $45 billion to annual U.S. health care expenditures. The prevalence of defensive medicine among hospitalists is unknown.
Setting: National survey sent to 1,753 hospitalists from all 50 states identified through the Society of Hospital Medicine database of members and meeting attendees.
Synopsis: The survey contained two primary topics: an estimation of defensive spending and liability history. The hospitalists, who had an average of 11 years in practice, completed 1,020 surveys. Participants estimated that defensive medicine accounted for 37.5% of all health care costs. Decreased estimate rates were seen among VA hospitalists (5.5% less), male respondents (36.4% vs. 39.4% for female), non-Hispanic white respondents (32.5% vs. 44.7% for other) and having more years in practice (decrease of 3% for every 10 years in practice). One in four respondents reported being sued at least once, with higher risk seen in those with greater years in practice. There was no association between liability experience and perception of defensive medicine spending. Differences between academic and community settings were not addressed. Because only 30% of practicing hospitalists are members of SHM, it may be difficult to generalize these findings.
Bottom line: Hospitalists perceive that defensive medicine is a major contributor to inpatient health care expenditures.
Citation: Saint S et al. Perception of resources spent on defensive medicine and history of being sued among hospitalists: Results from a national survey. J Hosp Med. 2017 Aug 23. doi: 10.12788/jhm.2800.
Dr. Lublin is a hospitalist at the University of Colorado School of Medicine.
Eradicating HCV significantly improved liver stiffness in meta-analysis
Eradicating chronic hepatitis C virus (HCV) infection led to significant decreases in liver stiffness in a systematic review and meta-analysis of nearly 3,000 patients.
Mean liver stiffness fell by 4.1 kPa (kilopascals) (95% confidence interval, 3.3-4.9 kPa) 12 or more months after patients achieved sustained virologic response to treatment, but did not significantly change in patients who did not achieve SVR, reported Siddharth Singh, MD, of the University of San Diego, La Jolla, Calif., and his associates in the January issue of Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2017.04.038). The results were especially striking among patients who received direct-acting antiviral agents (DAAs) or who had high baseline levels of inflammation, the investigators added.
SOURCE: AMERICAN GASTROENTEROLOGICAL ASSOCIATION
Based on these findings, about 47% of patients with advanced fibrosis or cirrhosis at baseline will drop below 9.5 kPa after achieving SVR, they reported. “With this decline in liver stiffness, it is conceivable that risk of liver-related complications would decrease, particularly in patients without cirrhosis,” they added. “Future research is warranted on the impact of magnitude and kinetics of decline in liver stiffness on improvement in liver-related outcomes.”
Eradicating HCV infection was known to decrease liver stiffness, but the magnitude of decline was not well understood. Therefore, the reviewers searched the literature through October 2016 for studies of HCV-infected adults who underwent liver stiffness measurement by vibration-controlled transient elastography before and at least once after completing HCV treatment. All studies also included data on median liver stiffness among patients who did and did not achieve SVR. The search identified 23 observational studies and one post hoc analysis of a randomized controlled trial, for a total of 2,934 patients, of whom 2,214 achieved SVR.
Among patients who achieved SVR, mean liver stiffness dropped by 2.4 kPa at the end of treatment (95% CI, 1.7-3.0 kPa), by 3.1 kPa 1-6 months later (95% CI, 1.6-4.7 kPa), and by 3.2 kPa 6-12 months after completing treatment (90% CI, 2.6-3.9 kPa). A year or more after finishing treatment, patients who achieved SVR had a 28% median decrease in liver stiffness (interquartile range, 22%-35%). However, liver stiffness did not significantly change among patients who did not achieve SVR, the reviewers reported.
Mean liver stiffness declined significantly more among patients who received DAAs (4.5 kPa) than among recipients of interferon-based regimens (2.6 kPa; P = .03). However, studies of DAAs included patients with greater liver stiffness at baseline, which could at least partially explain this discrepancy, the investigators said. Baseline cirrhosis also was associated with a greater decline in liver stiffness (mean, 5.1 kPa, vs. 2.8 kPa in patients without cirrhosis; P = .02), as was high baseline alanine aminotransferase level (P less than .01). Among patients whose baseline liver stiffness measurement exceeded 9.5 kPa, 47% had their liver stiffness drop to less than 9.5 kPa after achieving SVR.
Coinfection with HIV did not significantly alter the magnitude of decline in liver stiffness 6-12 months after treatment in patients who achieved SVR, the reviewers noted. “[Follow-up] assessment after SVR was relatively short; hence, long-term evolution of liver stiffness after antiviral therapy and impact of decline in liver stiffness on patient clinical outcomes could not be ascertained,” they wrote. The studies also did not consistently assess potential confounders such as nonalcoholic fatty liver disease, diabetes, and alcohol consumption.
One reviewer disclosed funding from the National Institutes of Health/National Library of Medicine. None had conflicts of interest.
The current era of new-generation direct-acting antiviral agents have revolutionized the treatment landscape of chronic hepatitis C virus infection, providing short-duration, safe, and consistently effective regimens that achieve SVR or cure in nearly 100% of patients. While achieving SVR is important, even more important is the long-term impact of SVR and whether cure translates into outcomes such as improved mortality or a reduced risk of disease progression. Although improved mortality after SVR has been demonstrated, one of the main drivers of risk of disease progression is the severity of hepatic fibrosis.

Robert J. Wong, MD, MS, is with the department of medicine and is director of research and education, division of gastroenterology and hepatology, Alameda Health System – Highland Hospital, Oakland, Calif. He has received a 2017-2019 Clinical Translational Research Award from AASLD, has received research funding from Gilead and AbbVie, and is on the speakers bureau of Gilead, Salix, and Bayer. He has also done consulting for and been an advisory board member for Gilead.
The current era of new-generation direct-acting antiviral agents have revolutionized the treatment landscape of chronic hepatitis C virus infection, providing short-duration, safe, and consistently effective regimens that achieve SVR or cure in nearly 100% of patients. While achieving SVR is important, even more important is the long-term impact of SVR and whether cure translates into outcomes such as improved mortality or a reduced risk of disease progression. Although improved mortality after SVR has been demonstrated, one of the main drivers of risk of disease progression is the severity of hepatic fibrosis.
Robert J. Wong, MD, MS, is with the department of medicine and is director of research and education, division of gastroenterology and hepatology, Alameda Health System – Highland Hospital, Oakland, Calif. He has received a 2017-2019 Clinical Translational Research Award from AASLD, has received research funding from Gilead and AbbVie, and is on the speakers bureau of Gilead, Salix, and Bayer. He has also done consulting for and been an advisory board member for Gilead.
The current era of new-generation direct-acting antiviral agents have revolutionized the treatment landscape of chronic hepatitis C virus infection, providing short-duration, safe, and consistently effective regimens that achieve SVR or cure in nearly 100% of patients. While achieving SVR is important, even more important is the long-term impact of SVR and whether cure translates into outcomes such as improved mortality or a reduced risk of disease progression. Although improved mortality after SVR has been demonstrated, one of the main drivers of risk of disease progression is the severity of hepatic fibrosis.
Robert J. Wong, MD, MS, is with the department of medicine and is director of research and education, division of gastroenterology and hepatology, Alameda Health System – Highland Hospital, Oakland, Calif. He has received a 2017-2019 Clinical Translational Research Award from AASLD, has received research funding from Gilead and AbbVie, and is on the speakers bureau of Gilead, Salix, and Bayer. He has also done consulting for and been an advisory board member for Gilead.
Eradicating chronic hepatitis C virus (HCV) infection led to significant decreases in liver stiffness in a systematic review and meta-analysis of nearly 3,000 patients.
Mean liver stiffness fell by 4.1 kPa (kilopascals) (95% confidence interval, 3.3-4.9 kPa) 12 or more months after patients achieved sustained virologic response to treatment, but did not significantly change in patients who did not achieve SVR, reported Siddharth Singh, MD, of the University of San Diego, La Jolla, Calif., and his associates in the January issue of Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2017.04.038). The results were especially striking among patients who received direct-acting antiviral agents (DAAs) or who had high baseline levels of inflammation, the investigators added.
SOURCE: AMERICAN GASTROENTEROLOGICAL ASSOCIATION
Based on these findings, about 47% of patients with advanced fibrosis or cirrhosis at baseline will drop below 9.5 kPa after achieving SVR, they reported. “With this decline in liver stiffness, it is conceivable that risk of liver-related complications would decrease, particularly in patients without cirrhosis,” they added. “Future research is warranted on the impact of magnitude and kinetics of decline in liver stiffness on improvement in liver-related outcomes.”
Eradicating HCV infection was known to decrease liver stiffness, but the magnitude of decline was not well understood. Therefore, the reviewers searched the literature through October 2016 for studies of HCV-infected adults who underwent liver stiffness measurement by vibration-controlled transient elastography before and at least once after completing HCV treatment. All studies also included data on median liver stiffness among patients who did and did not achieve SVR. The search identified 23 observational studies and one post hoc analysis of a randomized controlled trial, for a total of 2,934 patients, of whom 2,214 achieved SVR.
Among patients who achieved SVR, mean liver stiffness dropped by 2.4 kPa at the end of treatment (95% CI, 1.7-3.0 kPa), by 3.1 kPa 1-6 months later (95% CI, 1.6-4.7 kPa), and by 3.2 kPa 6-12 months after completing treatment (90% CI, 2.6-3.9 kPa). A year or more after finishing treatment, patients who achieved SVR had a 28% median decrease in liver stiffness (interquartile range, 22%-35%). However, liver stiffness did not significantly change among patients who did not achieve SVR, the reviewers reported.
Mean liver stiffness declined significantly more among patients who received DAAs (4.5 kPa) than among recipients of interferon-based regimens (2.6 kPa; P = .03). However, studies of DAAs included patients with greater liver stiffness at baseline, which could at least partially explain this discrepancy, the investigators said. Baseline cirrhosis also was associated with a greater decline in liver stiffness (mean, 5.1 kPa, vs. 2.8 kPa in patients without cirrhosis; P = .02), as was high baseline alanine aminotransferase level (P less than .01). Among patients whose baseline liver stiffness measurement exceeded 9.5 kPa, 47% had their liver stiffness drop to less than 9.5 kPa after achieving SVR.
Coinfection with HIV did not significantly alter the magnitude of decline in liver stiffness 6-12 months after treatment in patients who achieved SVR, the reviewers noted. “[Follow-up] assessment after SVR was relatively short; hence, long-term evolution of liver stiffness after antiviral therapy and impact of decline in liver stiffness on patient clinical outcomes could not be ascertained,” they wrote. The studies also did not consistently assess potential confounders such as nonalcoholic fatty liver disease, diabetes, and alcohol consumption.
One reviewer disclosed funding from the National Institutes of Health/National Library of Medicine. None had conflicts of interest.
Eradicating chronic hepatitis C virus (HCV) infection led to significant decreases in liver stiffness in a systematic review and meta-analysis of nearly 3,000 patients.
Mean liver stiffness fell by 4.1 kPa (kilopascals) (95% confidence interval, 3.3-4.9 kPa) 12 or more months after patients achieved sustained virologic response to treatment, but did not significantly change in patients who did not achieve SVR, reported Siddharth Singh, MD, of the University of San Diego, La Jolla, Calif., and his associates in the January issue of Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2017.04.038). The results were especially striking among patients who received direct-acting antiviral agents (DAAs) or who had high baseline levels of inflammation, the investigators added.
SOURCE: AMERICAN GASTROENTEROLOGICAL ASSOCIATION
Based on these findings, about 47% of patients with advanced fibrosis or cirrhosis at baseline will drop below 9.5 kPa after achieving SVR, they reported. “With this decline in liver stiffness, it is conceivable that risk of liver-related complications would decrease, particularly in patients without cirrhosis,” they added. “Future research is warranted on the impact of magnitude and kinetics of decline in liver stiffness on improvement in liver-related outcomes.”
Eradicating HCV infection was known to decrease liver stiffness, but the magnitude of decline was not well understood. Therefore, the reviewers searched the literature through October 2016 for studies of HCV-infected adults who underwent liver stiffness measurement by vibration-controlled transient elastography before and at least once after completing HCV treatment. All studies also included data on median liver stiffness among patients who did and did not achieve SVR. The search identified 23 observational studies and one post hoc analysis of a randomized controlled trial, for a total of 2,934 patients, of whom 2,214 achieved SVR.
Among patients who achieved SVR, mean liver stiffness dropped by 2.4 kPa at the end of treatment (95% CI, 1.7-3.0 kPa), by 3.1 kPa 1-6 months later (95% CI, 1.6-4.7 kPa), and by 3.2 kPa 6-12 months after completing treatment (90% CI, 2.6-3.9 kPa). A year or more after finishing treatment, patients who achieved SVR had a 28% median decrease in liver stiffness (interquartile range, 22%-35%). However, liver stiffness did not significantly change among patients who did not achieve SVR, the reviewers reported.
Mean liver stiffness declined significantly more among patients who received DAAs (4.5 kPa) than among recipients of interferon-based regimens (2.6 kPa; P = .03). However, studies of DAAs included patients with greater liver stiffness at baseline, which could at least partially explain this discrepancy, the investigators said. Baseline cirrhosis also was associated with a greater decline in liver stiffness (mean, 5.1 kPa, vs. 2.8 kPa in patients without cirrhosis; P = .02), as was high baseline alanine aminotransferase level (P less than .01). Among patients whose baseline liver stiffness measurement exceeded 9.5 kPa, 47% had their liver stiffness drop to less than 9.5 kPa after achieving SVR.
Coinfection with HIV did not significantly alter the magnitude of decline in liver stiffness 6-12 months after treatment in patients who achieved SVR, the reviewers noted. “[Follow-up] assessment after SVR was relatively short; hence, long-term evolution of liver stiffness after antiviral therapy and impact of decline in liver stiffness on patient clinical outcomes could not be ascertained,” they wrote. The studies also did not consistently assess potential confounders such as nonalcoholic fatty liver disease, diabetes, and alcohol consumption.
One reviewer disclosed funding from the National Institutes of Health/National Library of Medicine. None had conflicts of interest.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: Eradicating chronic hepatitis C virus infection led to significant decreases in liver stiffness.
Major finding: Mean liver stiffness decreased by 4.1 kPa 12 or more months after patients achieved sustained virologic response to treatment, but did not significantly improve in patients who lacked SVR.
Data source: A systematic review and meta-analysis of 2,934 patients from 23 observational studies and one post hoc analysis of a randomized controlled trial.
Disclosures: One reviewer disclosed funding from the National Institutes of Health/National Library of Medicine. The reviewers reported having no conflicts of interest.

Letter from the Editor
GI & Hepatology News is one of the most widely read publications focused on the gastroenterology community and is the official newspaper of the AGA. The New Gastroenterologist is the AGA publication targeted to trainees and early career physicians. Recognizing the strength of both digital and print communication, the AGA has consolidated its communication media.
John I. Allen, MD, MBA, AGAF
Editor in Chief of GI & Hepatology News
When The New Gastroenterologist debuted almost 3 years ago, it provided a mechanism for the AGA to condense and disseminate information in a single publication for those of us in training or in the early stages of our careers. Since then, The New Gastroenterologist has become a valuable resource for the AGA community and beyond. It is with great excitement that in 2018, The New Gastroenterologist will switch to a primarily digital format. Content will be distributed in quarterly e-newsletters, which will allow for easier distribution via social media. This will allow for the creation of a website archive of past articles that can be easily queried and accessed. Additionally, The New Gastroenterologist will debut an “In Focus” series of concise updates on pertinent topics in our field. These In Focus articles will be published on a quarterly basis in GI & Hepatology News and will undoubtedly be practical and informative features that will be of interest to all AGA members, regardless of their career stage. The first In Focus article, which appears in this issue of GI & Hepatology News, is written by Nitin Ahuja, MD, and James Reynolds, MD, and provides an enlightening overview of the evaluation and management of chronic constipation. I hope that everyone enjoys this new format of The New Gastroenterologist. As always, if you have any feedback, have interest in contributing, or have ideas that you would like to hear about, please contact me ([email protected]) or Managing Editor Ryan Farrell ([email protected]).
Bryson W. Katona, MD, PhD
Editor in Chief of The New Gastroenterologist
GI & Hepatology News is one of the most widely read publications focused on the gastroenterology community and is the official newspaper of the AGA. The New Gastroenterologist is the AGA publication targeted to trainees and early career physicians. Recognizing the strength of both digital and print communication, the AGA has consolidated its communication media.
John I. Allen, MD, MBA, AGAF
Editor in Chief of GI & Hepatology News
When The New Gastroenterologist debuted almost 3 years ago, it provided a mechanism for the AGA to condense and disseminate information in a single publication for those of us in training or in the early stages of our careers. Since then, The New Gastroenterologist has become a valuable resource for the AGA community and beyond. It is with great excitement that in 2018, The New Gastroenterologist will switch to a primarily digital format. Content will be distributed in quarterly e-newsletters, which will allow for easier distribution via social media. This will allow for the creation of a website archive of past articles that can be easily queried and accessed. Additionally, The New Gastroenterologist will debut an “In Focus” series of concise updates on pertinent topics in our field. These In Focus articles will be published on a quarterly basis in GI & Hepatology News and will undoubtedly be practical and informative features that will be of interest to all AGA members, regardless of their career stage. The first In Focus article, which appears in this issue of GI & Hepatology News, is written by Nitin Ahuja, MD, and James Reynolds, MD, and provides an enlightening overview of the evaluation and management of chronic constipation. I hope that everyone enjoys this new format of The New Gastroenterologist. As always, if you have any feedback, have interest in contributing, or have ideas that you would like to hear about, please contact me ([email protected]) or Managing Editor Ryan Farrell ([email protected]).
Bryson W. Katona, MD, PhD
Editor in Chief of The New Gastroenterologist
GI & Hepatology News is one of the most widely read publications focused on the gastroenterology community and is the official newspaper of the AGA. The New Gastroenterologist is the AGA publication targeted to trainees and early career physicians. Recognizing the strength of both digital and print communication, the AGA has consolidated its communication media.
John I. Allen, MD, MBA, AGAF
Editor in Chief of GI & Hepatology News
When The New Gastroenterologist debuted almost 3 years ago, it provided a mechanism for the AGA to condense and disseminate information in a single publication for those of us in training or in the early stages of our careers. Since then, The New Gastroenterologist has become a valuable resource for the AGA community and beyond. It is with great excitement that in 2018, The New Gastroenterologist will switch to a primarily digital format. Content will be distributed in quarterly e-newsletters, which will allow for easier distribution via social media. This will allow for the creation of a website archive of past articles that can be easily queried and accessed. Additionally, The New Gastroenterologist will debut an “In Focus” series of concise updates on pertinent topics in our field. These In Focus articles will be published on a quarterly basis in GI & Hepatology News and will undoubtedly be practical and informative features that will be of interest to all AGA members, regardless of their career stage. The first In Focus article, which appears in this issue of GI & Hepatology News, is written by Nitin Ahuja, MD, and James Reynolds, MD, and provides an enlightening overview of the evaluation and management of chronic constipation. I hope that everyone enjoys this new format of The New Gastroenterologist. As always, if you have any feedback, have interest in contributing, or have ideas that you would like to hear about, please contact me ([email protected]) or Managing Editor Ryan Farrell ([email protected]).
Bryson W. Katona, MD, PhD
Editor in Chief of The New Gastroenterologist
Outpatient Videos May Help Diagnose Psychogenic Nonepileptic Seizures
WASHINGTON, DC—Smartphone videos may help to support the clinical diagnosis of psychogenic nonepileptic seizures (PNES), according to research presented at the 71st Annual Meeting of the American Epilepsy Society. However, smartphone videos do not replace the need for video-EEG monitoring, researchers noted. “Smartphone videos are a complementary addition to medical history and physical examinations in the outpatient epilepsy clinic and can help triage hospital admission for video EEG-monitoring,” said William O. Tatum, DO, Professor of Neurology at the Mayo Clinic

Video-EEG monitoring is the standard technique for a definitive diagnosis in patients with suspected seizures. Approximately 20% to 30% of patients admitted to the video-EEG monitoring unit are misdiagnosed with epilepsy, however. In addition, expertise availability, cost, and resource utilization of video-EEG monitoring is limited. Patient-generated videos can potentially address these limitations.
A Multicenter Blinded Trial
Dr. Tatum and colleagues conducted a prospective, multicenter, blinded trial to determine the usefulness of outpatient smartphone videos in epilepsy evaluation. Investigators evaluated 41 consecutive patients with uncontrolled seizures (13 participants were male; mean age was 43.7). Patients were excluded if they were younger than 18, had an incomplete medical history and physical examination, had an atypical event, had an inadequate smartphone video, had an unconfirmed video-EEG monitoring diagnosis, or if they did not consent.
Medical history and physical examinations, smartphone videos, and video-EEG monitoring were performed from July 2014 to November 2017. Treating physicians reached a final clinical diagnosis of epilepsy, PNES, or physiologic non-epileptic events using a degree of certainty (scale: 0–10). Ten epileptologists and eight general neurology residents without a special interest in epilepsy were surveyed for a blinded smartphone video diagnosis.
Researchers shared data via HIPPA-protected data transfer utilizing web-based software. The history and physical exams, smartphone videos, and video-EEG monitoring results were obtained using survey forms and were then compared. Finally, sensitivity, specificity, and positive and negative predictive values were analyzed.
Most Smartphone Videos Showed Nonconvulsive Seizures
Epileptologists performed 310 smartphone video reads and residents performed 230 smartphone video reads. Smartphone videos were reviewed in 2.15 minutes compared with 60 minutes for medical history and physicals and 2.54 days for video-EEG monitoring. Most semiology was convulsive and most epilepsy was nonconvulsive. Physicians made a final diagnosis of PNES in 26 patients, epilepsy in 11 patients, physiologic non-epileptic events in three patients, and a PNES with physiologic non-epileptic events in one patient. Medical history and physical examination predicted a definitive diagnosis by video-EEG monitoring in 31 patients.
The median correct response for a smart phone video was 71.4% for epileptologists and 66.7% for residents. The level of confidence was similar between experts and residents, but those who made a correct diagnosis were slightly more confident. Using a level of confidence of at least five, 78% of epileptologists provided correct identification versus 68% of residents. “This suggests that a gap exists in training relative to viewing semiology for diagnostic implications and supports the ongoing need for education in patients with ’events‘”, said Dr. Tatum and colleagues.
The overall quality of smartphone videos was considered adequate for interpretation in 78% of patients. Inter-subject differences were present mainly based upon technical limitations as opposed to video quality. The primary technical limitation was lack of focus on the area of the interest. Researchers concluded that the “secure uploading, exchange, and analysis of smartphone video data in patients with paroxysmal neurological events is feasible.” No safety concerns or complications of taking smartphone videos were reported.
—Erica Tricarico
WASHINGTON, DC—Smartphone videos may help to support the clinical diagnosis of psychogenic nonepileptic seizures (PNES), according to research presented at the 71st Annual Meeting of the American Epilepsy Society. However, smartphone videos do not replace the need for video-EEG monitoring, researchers noted. “Smartphone videos are a complementary addition to medical history and physical examinations in the outpatient epilepsy clinic and can help triage hospital admission for video EEG-monitoring,” said William O. Tatum, DO, Professor of Neurology at the Mayo Clinic
Video-EEG monitoring is the standard technique for a definitive diagnosis in patients with suspected seizures. Approximately 20% to 30% of patients admitted to the video-EEG monitoring unit are misdiagnosed with epilepsy, however. In addition, expertise availability, cost, and resource utilization of video-EEG monitoring is limited. Patient-generated videos can potentially address these limitations.
A Multicenter Blinded Trial
Dr. Tatum and colleagues conducted a prospective, multicenter, blinded trial to determine the usefulness of outpatient smartphone videos in epilepsy evaluation. Investigators evaluated 41 consecutive patients with uncontrolled seizures (13 participants were male; mean age was 43.7). Patients were excluded if they were younger than 18, had an incomplete medical history and physical examination, had an atypical event, had an inadequate smartphone video, had an unconfirmed video-EEG monitoring diagnosis, or if they did not consent.
Medical history and physical examinations, smartphone videos, and video-EEG monitoring were performed from July 2014 to November 2017. Treating physicians reached a final clinical diagnosis of epilepsy, PNES, or physiologic non-epileptic events using a degree of certainty (scale: 0–10). Ten epileptologists and eight general neurology residents without a special interest in epilepsy were surveyed for a blinded smartphone video diagnosis.
Researchers shared data via HIPPA-protected data transfer utilizing web-based software. The history and physical exams, smartphone videos, and video-EEG monitoring results were obtained using survey forms and were then compared. Finally, sensitivity, specificity, and positive and negative predictive values were analyzed.
Most Smartphone Videos Showed Nonconvulsive Seizures
Epileptologists performed 310 smartphone video reads and residents performed 230 smartphone video reads. Smartphone videos were reviewed in 2.15 minutes compared with 60 minutes for medical history and physicals and 2.54 days for video-EEG monitoring. Most semiology was convulsive and most epilepsy was nonconvulsive. Physicians made a final diagnosis of PNES in 26 patients, epilepsy in 11 patients, physiologic non-epileptic events in three patients, and a PNES with physiologic non-epileptic events in one patient. Medical history and physical examination predicted a definitive diagnosis by video-EEG monitoring in 31 patients.
The median correct response for a smart phone video was 71.4% for epileptologists and 66.7% for residents. The level of confidence was similar between experts and residents, but those who made a correct diagnosis were slightly more confident. Using a level of confidence of at least five, 78% of epileptologists provided correct identification versus 68% of residents. “This suggests that a gap exists in training relative to viewing semiology for diagnostic implications and supports the ongoing need for education in patients with ’events‘”, said Dr. Tatum and colleagues.
The overall quality of smartphone videos was considered adequate for interpretation in 78% of patients. Inter-subject differences were present mainly based upon technical limitations as opposed to video quality. The primary technical limitation was lack of focus on the area of the interest. Researchers concluded that the “secure uploading, exchange, and analysis of smartphone video data in patients with paroxysmal neurological events is feasible.” No safety concerns or complications of taking smartphone videos were reported.
—Erica Tricarico
WASHINGTON, DC—Smartphone videos may help to support the clinical diagnosis of psychogenic nonepileptic seizures (PNES), according to research presented at the 71st Annual Meeting of the American Epilepsy Society. However, smartphone videos do not replace the need for video-EEG monitoring, researchers noted. “Smartphone videos are a complementary addition to medical history and physical examinations in the outpatient epilepsy clinic and can help triage hospital admission for video EEG-monitoring,” said William O. Tatum, DO, Professor of Neurology at the Mayo Clinic
Video-EEG monitoring is the standard technique for a definitive diagnosis in patients with suspected seizures. Approximately 20% to 30% of patients admitted to the video-EEG monitoring unit are misdiagnosed with epilepsy, however. In addition, expertise availability, cost, and resource utilization of video-EEG monitoring is limited. Patient-generated videos can potentially address these limitations.
A Multicenter Blinded Trial
Dr. Tatum and colleagues conducted a prospective, multicenter, blinded trial to determine the usefulness of outpatient smartphone videos in epilepsy evaluation. Investigators evaluated 41 consecutive patients with uncontrolled seizures (13 participants were male; mean age was 43.7). Patients were excluded if they were younger than 18, had an incomplete medical history and physical examination, had an atypical event, had an inadequate smartphone video, had an unconfirmed video-EEG monitoring diagnosis, or if they did not consent.
Medical history and physical examinations, smartphone videos, and video-EEG monitoring were performed from July 2014 to November 2017. Treating physicians reached a final clinical diagnosis of epilepsy, PNES, or physiologic non-epileptic events using a degree of certainty (scale: 0–10). Ten epileptologists and eight general neurology residents without a special interest in epilepsy were surveyed for a blinded smartphone video diagnosis.
Researchers shared data via HIPPA-protected data transfer utilizing web-based software. The history and physical exams, smartphone videos, and video-EEG monitoring results were obtained using survey forms and were then compared. Finally, sensitivity, specificity, and positive and negative predictive values were analyzed.
Most Smartphone Videos Showed Nonconvulsive Seizures
Epileptologists performed 310 smartphone video reads and residents performed 230 smartphone video reads. Smartphone videos were reviewed in 2.15 minutes compared with 60 minutes for medical history and physicals and 2.54 days for video-EEG monitoring. Most semiology was convulsive and most epilepsy was nonconvulsive. Physicians made a final diagnosis of PNES in 26 patients, epilepsy in 11 patients, physiologic non-epileptic events in three patients, and a PNES with physiologic non-epileptic events in one patient. Medical history and physical examination predicted a definitive diagnosis by video-EEG monitoring in 31 patients.
The median correct response for a smart phone video was 71.4% for epileptologists and 66.7% for residents. The level of confidence was similar between experts and residents, but those who made a correct diagnosis were slightly more confident. Using a level of confidence of at least five, 78% of epileptologists provided correct identification versus 68% of residents. “This suggests that a gap exists in training relative to viewing semiology for diagnostic implications and supports the ongoing need for education in patients with ’events‘”, said Dr. Tatum and colleagues.
The overall quality of smartphone videos was considered adequate for interpretation in 78% of patients. Inter-subject differences were present mainly based upon technical limitations as opposed to video quality. The primary technical limitation was lack of focus on the area of the interest. Researchers concluded that the “secure uploading, exchange, and analysis of smartphone video data in patients with paroxysmal neurological events is feasible.” No safety concerns or complications of taking smartphone videos were reported.
—Erica Tricarico