User login
CHIP out of cash amid government shutdown
The Children’s Health Insurance Plan remains without funding as a temporary government funding bill that included a 6-year extension of the popular bipartisan program failed to garner enough support in the Senate.
On Jan. 19, to clear that hurdle.
Other Republican senators who voted against the bill were Jeff Flake of Arizona, Lindsey Graham of South Carolina, Mike Lee of Utah, and Rand Paul of Kentucky.
Democratic senators who voted for the bill were Joe Donnelly of Indiana, Heidi Heitkamp of North Dakota, Doug Jones of Alabama, Joe Manchin of West Virginia, and Claire McCaskill of Missouri.
The continuing resolution also featured a few other health care provisions, including delays to the medical device tax and the so-called Cadillac tax on high-valued health insurance plans offered by employers.
In comments made on the Senate floor prior to the vote, Finance Committee Chairman Orrin Hatch (R-Utah) called out Democrats for failing to pass the bill.
“There’s really nothing wrong with the substance of the bill, Mr. President, or at least very few of our Democratic colleagues are complaining about what’s actually in the bill” he said. “Instead, they’re complaining about what’s not in it.”
Democrats made their stand on the absence of language on Deferred Action for Childhood Arrivals (DACA), which addresses the immigration status of young people – often called Dreamers – who were brought to this country illegally as children.
Democrats also complained that funding for community health centers was not included.
Sen. Hatch, one of the original authors of the CHIP authorizing legislation, continued to argue for the program and the overall funding bill.
“This new bill before us would reauthorize CHIP for 6 six years,” he noted. “A 6-year extension would be the longest in the history of the program. In all other respects, the bill is identical to the one the Finance Committee reported [in September] with broad bipartisan support,” although no further action was taken on it after receiving near unanimous support in committee.
Finance Committee Ranking Member Ron Wyden (D-Ore.) took exception to the characterization that Democrats were not in support of the CHIP provision.
“The Chairman and I did negotiate a CHIP extension back in September, and the Senate Finance did report it out in a near unanimous, bipartisan basis,” he said. “CHIP could have passed the Congress within days, but the House Republicans had other ideas.”
Sen. Wyden noted that CHIP reauthorization was attached to other legislative actions in the House that all failed to garner enough support instead of being sent through as a stand-alone bill that likely would have received large bipartisan support.
And even though the extension would be for 6 years, Sen. Wyden also questioned why it wasn’t receiving permanent authorization.
“Congress learned that making CHIP permanent actually saves taxpayer dollars,” he said. “It’s a better deal than a 6-year extension, less of an expense for the taxpayer. True fiscal conservatives ought to be tripping over themselves to pass a permanent bill without preconditions. But at every turn in the CHIP debate, Republican leaders have found a new hostage.”
Sen. McConnell said following the failed voted that the Senate would resume activities beginning at noon on Jan. 20 – with votes expected – in hopes of finding a solution.
The Children’s Health Insurance Plan remains without funding as a temporary government funding bill that included a 6-year extension of the popular bipartisan program failed to garner enough support in the Senate.
On Jan. 19, to clear that hurdle.
Other Republican senators who voted against the bill were Jeff Flake of Arizona, Lindsey Graham of South Carolina, Mike Lee of Utah, and Rand Paul of Kentucky.
Democratic senators who voted for the bill were Joe Donnelly of Indiana, Heidi Heitkamp of North Dakota, Doug Jones of Alabama, Joe Manchin of West Virginia, and Claire McCaskill of Missouri.
The continuing resolution also featured a few other health care provisions, including delays to the medical device tax and the so-called Cadillac tax on high-valued health insurance plans offered by employers.
In comments made on the Senate floor prior to the vote, Finance Committee Chairman Orrin Hatch (R-Utah) called out Democrats for failing to pass the bill.
“There’s really nothing wrong with the substance of the bill, Mr. President, or at least very few of our Democratic colleagues are complaining about what’s actually in the bill” he said. “Instead, they’re complaining about what’s not in it.”
Democrats made their stand on the absence of language on Deferred Action for Childhood Arrivals (DACA), which addresses the immigration status of young people – often called Dreamers – who were brought to this country illegally as children.
Democrats also complained that funding for community health centers was not included.
Sen. Hatch, one of the original authors of the CHIP authorizing legislation, continued to argue for the program and the overall funding bill.
“This new bill before us would reauthorize CHIP for 6 six years,” he noted. “A 6-year extension would be the longest in the history of the program. In all other respects, the bill is identical to the one the Finance Committee reported [in September] with broad bipartisan support,” although no further action was taken on it after receiving near unanimous support in committee.
Finance Committee Ranking Member Ron Wyden (D-Ore.) took exception to the characterization that Democrats were not in support of the CHIP provision.
“The Chairman and I did negotiate a CHIP extension back in September, and the Senate Finance did report it out in a near unanimous, bipartisan basis,” he said. “CHIP could have passed the Congress within days, but the House Republicans had other ideas.”
Sen. Wyden noted that CHIP reauthorization was attached to other legislative actions in the House that all failed to garner enough support instead of being sent through as a stand-alone bill that likely would have received large bipartisan support.
And even though the extension would be for 6 years, Sen. Wyden also questioned why it wasn’t receiving permanent authorization.
“Congress learned that making CHIP permanent actually saves taxpayer dollars,” he said. “It’s a better deal than a 6-year extension, less of an expense for the taxpayer. True fiscal conservatives ought to be tripping over themselves to pass a permanent bill without preconditions. But at every turn in the CHIP debate, Republican leaders have found a new hostage.”
Sen. McConnell said following the failed voted that the Senate would resume activities beginning at noon on Jan. 20 – with votes expected – in hopes of finding a solution.
The Children’s Health Insurance Plan remains without funding as a temporary government funding bill that included a 6-year extension of the popular bipartisan program failed to garner enough support in the Senate.
On Jan. 19, to clear that hurdle.
Other Republican senators who voted against the bill were Jeff Flake of Arizona, Lindsey Graham of South Carolina, Mike Lee of Utah, and Rand Paul of Kentucky.
Democratic senators who voted for the bill were Joe Donnelly of Indiana, Heidi Heitkamp of North Dakota, Doug Jones of Alabama, Joe Manchin of West Virginia, and Claire McCaskill of Missouri.
The continuing resolution also featured a few other health care provisions, including delays to the medical device tax and the so-called Cadillac tax on high-valued health insurance plans offered by employers.
In comments made on the Senate floor prior to the vote, Finance Committee Chairman Orrin Hatch (R-Utah) called out Democrats for failing to pass the bill.
“There’s really nothing wrong with the substance of the bill, Mr. President, or at least very few of our Democratic colleagues are complaining about what’s actually in the bill” he said. “Instead, they’re complaining about what’s not in it.”
Democrats made their stand on the absence of language on Deferred Action for Childhood Arrivals (DACA), which addresses the immigration status of young people – often called Dreamers – who were brought to this country illegally as children.
Democrats also complained that funding for community health centers was not included.
Sen. Hatch, one of the original authors of the CHIP authorizing legislation, continued to argue for the program and the overall funding bill.
“This new bill before us would reauthorize CHIP for 6 six years,” he noted. “A 6-year extension would be the longest in the history of the program. In all other respects, the bill is identical to the one the Finance Committee reported [in September] with broad bipartisan support,” although no further action was taken on it after receiving near unanimous support in committee.
Finance Committee Ranking Member Ron Wyden (D-Ore.) took exception to the characterization that Democrats were not in support of the CHIP provision.
“The Chairman and I did negotiate a CHIP extension back in September, and the Senate Finance did report it out in a near unanimous, bipartisan basis,” he said. “CHIP could have passed the Congress within days, but the House Republicans had other ideas.”
Sen. Wyden noted that CHIP reauthorization was attached to other legislative actions in the House that all failed to garner enough support instead of being sent through as a stand-alone bill that likely would have received large bipartisan support.
And even though the extension would be for 6 years, Sen. Wyden also questioned why it wasn’t receiving permanent authorization.
“Congress learned that making CHIP permanent actually saves taxpayer dollars,” he said. “It’s a better deal than a 6-year extension, less of an expense for the taxpayer. True fiscal conservatives ought to be tripping over themselves to pass a permanent bill without preconditions. But at every turn in the CHIP debate, Republican leaders have found a new hostage.”
Sen. McConnell said following the failed voted that the Senate would resume activities beginning at noon on Jan. 20 – with votes expected – in hopes of finding a solution.
Earlier treatment but shorter survival: The rurality paradox in cancer
MONTREAL – Does rurality matter in cancer treatment? According to lessons from a Scottish study, the answer may be yes, but in unexpected ways.
Patients who lived further away from a cancer treatment center were more likely to be treated within the 62 days postreferral window that the Scottish government has set as a target. Compared with those living within 15 minutes of a cancer center, the adjusted odds ratio for patients living at least an hour away to receive timely treatment was 1.42 (95% confidence interval, 1.25-1.61). For those living on remote islands, the aOR was 1.32 (95% CI, 1.09-1.59).

Dr. Murchie, speaking at the annual meeting of the North American Primary Care Research Group, shared results of an updated study that looked at the cancer population in Northeast Scotland to see how living farther from a cancer center might be associated with time to diagnosis and treatment of cancer and with 1-year survival rates.
A “seminal” work that set the background for this study, said Dr. Murchie, was the 2002 publication tracking the relationship between rural residence status and cancer survival (Br J Cancer. 2002;87[6]:585-90). Findings from that study showed that as the distance from the patient’s residence to a cancer center increased, so did the risk that the cancer wasn’t diagnosed before death. Survival, especially for prostate and lung cancer, was found to decrease with increasing distance, said Dr. Murchie.
“This study has been widely replicated in the global literature, but the mechanisms have never been satisfactorily explained,” he said.
For the present study, the primary outcome measure was whether patients achieved treatment within 62 days of referral, the target set by the Scottish government, said Dr. Murchie.
Secondary outcomes included secondary care delay – whether treatment was begun within 31 days of diagnosis – and survival at 1 year after presentation or referral by a general practitioner.
A total of 12,339 patients were included; 74% were older than 60 years. Patients were relatively affluent, with 59% in the two least-deprived quintiles according to Scottish government classification. Dr. Murchie said that this is in keeping with the geographic-socioeconomic status distribution in Scotland. Females made up 56% of the population, and 35% were classified as rural dwelling.
Nearly a third of patients (n = 3,722; 30.6%) had breast cancer. Colorectal cancer was the next most common diagnosis (n = 2,775; 22.5%), followed by prostate cancer, lung cancer, upper gastrointestinal cancer, melanoma, and cervical cancer. Most patients (n = 8,537; 62%) had a Charlson Comorbidity Index score of 0.
Dr. Murchie used the Northeast and Aberdeen Scottish Cancer and Residence Cohort (NASCAR) data gathered during 2007-2014; the cohort’s data came from a variety of sources, including the region’s cancer care pathway database. National cancer registries, morbidity records, and other nationally maintained demographic databases were also used for the NASCAR dataset.
Those building the NASCAR cohort were able to link all of the data from disparate datasets and still keep investigators blinded to patient identity via a “safe harvest” technique that created pseudonyms to harmonize the datasets.
Using patient postal codes, a geographical information systems approach was used to determine traveling time to a cancer center. Travel time, Dr. Murchie pointed out, is a better measure than straight-line distance of true accessibility for rural-dwelling patients.
In discussion, Dr. Murchie said that the correlation between longer distance and shorter time to treatment held even when he and his colleagues controlled for “the most obvious explanation – that disease was more advanced on diagnosis among remoter people.” But, he said, “This does not translate into better survival. Why?”
Hypotheses, said Dr. Murchie, include the many small and large barriers to care that rural-dwelling individuals face. They must find a way to their GP, or place a phone call, and that physician must weigh the risk of a serious complication against the burden to the patient – and that patient’s family – of travel from a remote location to a cancer center.
Dr. Murchie encouraged international collaboration and replication of his work so that cancer researchers and primary care practitioners can reach a better understanding of the unique challenges in treating rural cancer patients.
Dr. Murchie reported that he had no relevant disclosures.
SOURCE: Murchie P. NAPCRG 2017 Abstract CR15.
MONTREAL – Does rurality matter in cancer treatment? According to lessons from a Scottish study, the answer may be yes, but in unexpected ways.
Patients who lived further away from a cancer treatment center were more likely to be treated within the 62 days postreferral window that the Scottish government has set as a target. Compared with those living within 15 minutes of a cancer center, the adjusted odds ratio for patients living at least an hour away to receive timely treatment was 1.42 (95% confidence interval, 1.25-1.61). For those living on remote islands, the aOR was 1.32 (95% CI, 1.09-1.59).
Dr. Murchie, speaking at the annual meeting of the North American Primary Care Research Group, shared results of an updated study that looked at the cancer population in Northeast Scotland to see how living farther from a cancer center might be associated with time to diagnosis and treatment of cancer and with 1-year survival rates.
A “seminal” work that set the background for this study, said Dr. Murchie, was the 2002 publication tracking the relationship between rural residence status and cancer survival (Br J Cancer. 2002;87[6]:585-90). Findings from that study showed that as the distance from the patient’s residence to a cancer center increased, so did the risk that the cancer wasn’t diagnosed before death. Survival, especially for prostate and lung cancer, was found to decrease with increasing distance, said Dr. Murchie.
“This study has been widely replicated in the global literature, but the mechanisms have never been satisfactorily explained,” he said.
For the present study, the primary outcome measure was whether patients achieved treatment within 62 days of referral, the target set by the Scottish government, said Dr. Murchie.
Secondary outcomes included secondary care delay – whether treatment was begun within 31 days of diagnosis – and survival at 1 year after presentation or referral by a general practitioner.
A total of 12,339 patients were included; 74% were older than 60 years. Patients were relatively affluent, with 59% in the two least-deprived quintiles according to Scottish government classification. Dr. Murchie said that this is in keeping with the geographic-socioeconomic status distribution in Scotland. Females made up 56% of the population, and 35% were classified as rural dwelling.
Nearly a third of patients (n = 3,722; 30.6%) had breast cancer. Colorectal cancer was the next most common diagnosis (n = 2,775; 22.5%), followed by prostate cancer, lung cancer, upper gastrointestinal cancer, melanoma, and cervical cancer. Most patients (n = 8,537; 62%) had a Charlson Comorbidity Index score of 0.
Dr. Murchie used the Northeast and Aberdeen Scottish Cancer and Residence Cohort (NASCAR) data gathered during 2007-2014; the cohort’s data came from a variety of sources, including the region’s cancer care pathway database. National cancer registries, morbidity records, and other nationally maintained demographic databases were also used for the NASCAR dataset.
Those building the NASCAR cohort were able to link all of the data from disparate datasets and still keep investigators blinded to patient identity via a “safe harvest” technique that created pseudonyms to harmonize the datasets.
Using patient postal codes, a geographical information systems approach was used to determine traveling time to a cancer center. Travel time, Dr. Murchie pointed out, is a better measure than straight-line distance of true accessibility for rural-dwelling patients.
In discussion, Dr. Murchie said that the correlation between longer distance and shorter time to treatment held even when he and his colleagues controlled for “the most obvious explanation – that disease was more advanced on diagnosis among remoter people.” But, he said, “This does not translate into better survival. Why?”
Hypotheses, said Dr. Murchie, include the many small and large barriers to care that rural-dwelling individuals face. They must find a way to their GP, or place a phone call, and that physician must weigh the risk of a serious complication against the burden to the patient – and that patient’s family – of travel from a remote location to a cancer center.
Dr. Murchie encouraged international collaboration and replication of his work so that cancer researchers and primary care practitioners can reach a better understanding of the unique challenges in treating rural cancer patients.
Dr. Murchie reported that he had no relevant disclosures.
SOURCE: Murchie P. NAPCRG 2017 Abstract CR15.
MONTREAL – Does rurality matter in cancer treatment? According to lessons from a Scottish study, the answer may be yes, but in unexpected ways.
Patients who lived further away from a cancer treatment center were more likely to be treated within the 62 days postreferral window that the Scottish government has set as a target. Compared with those living within 15 minutes of a cancer center, the adjusted odds ratio for patients living at least an hour away to receive timely treatment was 1.42 (95% confidence interval, 1.25-1.61). For those living on remote islands, the aOR was 1.32 (95% CI, 1.09-1.59).
Dr. Murchie, speaking at the annual meeting of the North American Primary Care Research Group, shared results of an updated study that looked at the cancer population in Northeast Scotland to see how living farther from a cancer center might be associated with time to diagnosis and treatment of cancer and with 1-year survival rates.
A “seminal” work that set the background for this study, said Dr. Murchie, was the 2002 publication tracking the relationship between rural residence status and cancer survival (Br J Cancer. 2002;87[6]:585-90). Findings from that study showed that as the distance from the patient’s residence to a cancer center increased, so did the risk that the cancer wasn’t diagnosed before death. Survival, especially for prostate and lung cancer, was found to decrease with increasing distance, said Dr. Murchie.
“This study has been widely replicated in the global literature, but the mechanisms have never been satisfactorily explained,” he said.
For the present study, the primary outcome measure was whether patients achieved treatment within 62 days of referral, the target set by the Scottish government, said Dr. Murchie.
Secondary outcomes included secondary care delay – whether treatment was begun within 31 days of diagnosis – and survival at 1 year after presentation or referral by a general practitioner.
A total of 12,339 patients were included; 74% were older than 60 years. Patients were relatively affluent, with 59% in the two least-deprived quintiles according to Scottish government classification. Dr. Murchie said that this is in keeping with the geographic-socioeconomic status distribution in Scotland. Females made up 56% of the population, and 35% were classified as rural dwelling.
Nearly a third of patients (n = 3,722; 30.6%) had breast cancer. Colorectal cancer was the next most common diagnosis (n = 2,775; 22.5%), followed by prostate cancer, lung cancer, upper gastrointestinal cancer, melanoma, and cervical cancer. Most patients (n = 8,537; 62%) had a Charlson Comorbidity Index score of 0.
Dr. Murchie used the Northeast and Aberdeen Scottish Cancer and Residence Cohort (NASCAR) data gathered during 2007-2014; the cohort’s data came from a variety of sources, including the region’s cancer care pathway database. National cancer registries, morbidity records, and other nationally maintained demographic databases were also used for the NASCAR dataset.
Those building the NASCAR cohort were able to link all of the data from disparate datasets and still keep investigators blinded to patient identity via a “safe harvest” technique that created pseudonyms to harmonize the datasets.
Using patient postal codes, a geographical information systems approach was used to determine traveling time to a cancer center. Travel time, Dr. Murchie pointed out, is a better measure than straight-line distance of true accessibility for rural-dwelling patients.
In discussion, Dr. Murchie said that the correlation between longer distance and shorter time to treatment held even when he and his colleagues controlled for “the most obvious explanation – that disease was more advanced on diagnosis among remoter people.” But, he said, “This does not translate into better survival. Why?”
Hypotheses, said Dr. Murchie, include the many small and large barriers to care that rural-dwelling individuals face. They must find a way to their GP, or place a phone call, and that physician must weigh the risk of a serious complication against the burden to the patient – and that patient’s family – of travel from a remote location to a cancer center.
Dr. Murchie encouraged international collaboration and replication of his work so that cancer researchers and primary care practitioners can reach a better understanding of the unique challenges in treating rural cancer patients.
Dr. Murchie reported that he had no relevant disclosures.
SOURCE: Murchie P. NAPCRG 2017 Abstract CR15.
REPORTING FROM NAPCRG 2017
Key clinical point: Rural Scottish cancer patients were treated earlier but had shorter survival.
Major finding: Rural patients had an odds ratio of 1.42 for prompt treatment after a cancer diagnosis.
Study details: Study of 12,339 rural and urban patients with cancer living in Scotland.
Disclosures: Dr. Murchie reported no conflicts of interest.
Source: Murchie P. NAPCRG 2017 Abstract CR15.
Bright light therapy improves sleep in cancer survivors

Results of a pilot study suggest that systematic bright light exposure can improve sleep in fatigued cancer survivors.
Subjects who were exposed to bright light every morning for 4 weeks had a significantly greater improvement in sleep efficiency than those who were exposed to dim light over the same period.
In fact, subjects in the bright light group were able to achieve clinically normal levels of sleep efficiency, and subjects in the dim light group were not.
Sleep efficiency is the percentage of time in bed that subjects spent sleeping.
Lisa M. Wu, PhD, of Northwestern University in Chicago, Illinois, and her colleagues reported these results in the Journal of Clinical Sleep Medicine.
The team noted that cancer patients report sleep disturbances at a significantly higher rate than the general population. Between 23% and 44% of cancer patients experience insomnia symptoms even years after treatment.
With this in mind, the researchers studied 44 individuals who had completed cancer treatment and met criteria for clinically significant fatigue at screening.
The subjects had an average age of 53.6, and 75% percent were female. Roughly 55% (n=24) had been diagnosed with a hematologic malignancy.
The subjects were randomized to a bright white light intervention or a dim red light intervention. Subjects in both treatment arms were provided with a light box and instructed to use it every morning for 30 minutes for 4 weeks. Sleep was evaluated using wrist actigraphy and the Pittsburgh Sleep Quality Index.
At baseline, 52.6% of subjects in the dim light group and 60% in the bright light group exceeded the clinical cutoff for poor sleep efficiency (≤ 85%). The mean sleep efficiency was 81.8% and 82.8%, respectively.
During the study period, sleep efficiency improved significantly more among subjects exposed to the bright light than those exposed to the dim light (P=0.003).
The mean sleep efficiency was in the clinically normal range for subjects in the bright light group at the end of the intervention (86.06%) and 3 weeks after (85.77%).
However, the cutoff for poor sleep efficiency was not reached in the dim light group, either at the end of the intervention (mean=79.35%) or 3 weeks after (mean=80.88%).
Total sleep time tended to increase over the study period for subjects in the bright light group, but there was no significant difference in total sleep time between the bright light and dim light groups.
Likewise, there was no significant between-group difference in waking after sleep onset, although this outcome tended to decrease over the study period for subjects in the bright light group.
“Systematic light exposure using bright white light is a low-cost and easily disseminated intervention that offers a feasible and potentially effective alternative to improve sleep in cancer survivors,” Dr Wu said.
However, she and her colleagues noted that larger-scale studies are needed. ![]()
Results of a pilot study suggest that systematic bright light exposure can improve sleep in fatigued cancer survivors.
Subjects who were exposed to bright light every morning for 4 weeks had a significantly greater improvement in sleep efficiency than those who were exposed to dim light over the same period.
In fact, subjects in the bright light group were able to achieve clinically normal levels of sleep efficiency, and subjects in the dim light group were not.
Sleep efficiency is the percentage of time in bed that subjects spent sleeping.
Lisa M. Wu, PhD, of Northwestern University in Chicago, Illinois, and her colleagues reported these results in the Journal of Clinical Sleep Medicine.
The team noted that cancer patients report sleep disturbances at a significantly higher rate than the general population. Between 23% and 44% of cancer patients experience insomnia symptoms even years after treatment.
With this in mind, the researchers studied 44 individuals who had completed cancer treatment and met criteria for clinically significant fatigue at screening.
The subjects had an average age of 53.6, and 75% percent were female. Roughly 55% (n=24) had been diagnosed with a hematologic malignancy.
The subjects were randomized to a bright white light intervention or a dim red light intervention. Subjects in both treatment arms were provided with a light box and instructed to use it every morning for 30 minutes for 4 weeks. Sleep was evaluated using wrist actigraphy and the Pittsburgh Sleep Quality Index.
At baseline, 52.6% of subjects in the dim light group and 60% in the bright light group exceeded the clinical cutoff for poor sleep efficiency (≤ 85%). The mean sleep efficiency was 81.8% and 82.8%, respectively.
During the study period, sleep efficiency improved significantly more among subjects exposed to the bright light than those exposed to the dim light (P=0.003).
The mean sleep efficiency was in the clinically normal range for subjects in the bright light group at the end of the intervention (86.06%) and 3 weeks after (85.77%).
However, the cutoff for poor sleep efficiency was not reached in the dim light group, either at the end of the intervention (mean=79.35%) or 3 weeks after (mean=80.88%).
Total sleep time tended to increase over the study period for subjects in the bright light group, but there was no significant difference in total sleep time between the bright light and dim light groups.
Likewise, there was no significant between-group difference in waking after sleep onset, although this outcome tended to decrease over the study period for subjects in the bright light group.
“Systematic light exposure using bright white light is a low-cost and easily disseminated intervention that offers a feasible and potentially effective alternative to improve sleep in cancer survivors,” Dr Wu said.
However, she and her colleagues noted that larger-scale studies are needed. ![]()
Results of a pilot study suggest that systematic bright light exposure can improve sleep in fatigued cancer survivors.
Subjects who were exposed to bright light every morning for 4 weeks had a significantly greater improvement in sleep efficiency than those who were exposed to dim light over the same period.
In fact, subjects in the bright light group were able to achieve clinically normal levels of sleep efficiency, and subjects in the dim light group were not.
Sleep efficiency is the percentage of time in bed that subjects spent sleeping.
Lisa M. Wu, PhD, of Northwestern University in Chicago, Illinois, and her colleagues reported these results in the Journal of Clinical Sleep Medicine.
The team noted that cancer patients report sleep disturbances at a significantly higher rate than the general population. Between 23% and 44% of cancer patients experience insomnia symptoms even years after treatment.
With this in mind, the researchers studied 44 individuals who had completed cancer treatment and met criteria for clinically significant fatigue at screening.
The subjects had an average age of 53.6, and 75% percent were female. Roughly 55% (n=24) had been diagnosed with a hematologic malignancy.
The subjects were randomized to a bright white light intervention or a dim red light intervention. Subjects in both treatment arms were provided with a light box and instructed to use it every morning for 30 minutes for 4 weeks. Sleep was evaluated using wrist actigraphy and the Pittsburgh Sleep Quality Index.
At baseline, 52.6% of subjects in the dim light group and 60% in the bright light group exceeded the clinical cutoff for poor sleep efficiency (≤ 85%). The mean sleep efficiency was 81.8% and 82.8%, respectively.
During the study period, sleep efficiency improved significantly more among subjects exposed to the bright light than those exposed to the dim light (P=0.003).
The mean sleep efficiency was in the clinically normal range for subjects in the bright light group at the end of the intervention (86.06%) and 3 weeks after (85.77%).
However, the cutoff for poor sleep efficiency was not reached in the dim light group, either at the end of the intervention (mean=79.35%) or 3 weeks after (mean=80.88%).
Total sleep time tended to increase over the study period for subjects in the bright light group, but there was no significant difference in total sleep time between the bright light and dim light groups.
Likewise, there was no significant between-group difference in waking after sleep onset, although this outcome tended to decrease over the study period for subjects in the bright light group.
“Systematic light exposure using bright white light is a low-cost and easily disseminated intervention that offers a feasible and potentially effective alternative to improve sleep in cancer survivors,” Dr Wu said.
However, she and her colleagues noted that larger-scale studies are needed. ![]()
STUDY: More mammograms after cost-sharing elimination
More women received recommended mammograms after cost sharing for the service was eliminated under the Affordable Care Act, a study shows.
In health plans that eliminated cost sharing, such as copays, deductibles, or other out-of-pocket costs, the rate of biennial screening mammography increased from 60% in the 2-year period before the cost-sharing elimination to 65% in the 2-year period following the new regulation, according to an analysis in the New England Journal of Medicine.
In addition to the increased rate of mammograms in the first group, results showed the rates of biennial mammography in the second group were 73.1% (95% confidence interval, 69.2-77.0) and 72.8% (95% CI, 69.7-76.0) during the same periods, yielding a difference in differences of 5.7 percentage points. Investigators also found the difference in differences was 9.8 percentage points among women living in areas with the highest quartile of educational attainment, compared with 4.3 percentage points among women in the lowest quartile. After the elimination of cost sharing, the rate of biennial mammography rose by 6.5 percentage points for white women and 8.4 percentage points for black women, the study found. The rate was nearly unchanged for Hispanic women.
The findings extend that of past studies that show older women who need mammograms are sensitive to out-of-pocket costs and the presence of supplemental coverage, the authors conclude. If the cost-sharing provisions of the ACA are rescinded, the results also “raise concern that fewer older women will receive recommended breast-cancer screening.”
However, the authors also note that since mammogram rates in the health plans that eliminated cost sharing remained below those in plans with full coverage and less than three-quarters of women in control plans received biennial breast cancer screenings, that “the removal of out-of-pocket payments alone may not raise screening rates to desired levels.”
SOURCE: Trivedi A et al. N Engl J Med. 2018 Jan 18;378:262-9.
More women received recommended mammograms after cost sharing for the service was eliminated under the Affordable Care Act, a study shows.
In health plans that eliminated cost sharing, such as copays, deductibles, or other out-of-pocket costs, the rate of biennial screening mammography increased from 60% in the 2-year period before the cost-sharing elimination to 65% in the 2-year period following the new regulation, according to an analysis in the New England Journal of Medicine.
In addition to the increased rate of mammograms in the first group, results showed the rates of biennial mammography in the second group were 73.1% (95% confidence interval, 69.2-77.0) and 72.8% (95% CI, 69.7-76.0) during the same periods, yielding a difference in differences of 5.7 percentage points. Investigators also found the difference in differences was 9.8 percentage points among women living in areas with the highest quartile of educational attainment, compared with 4.3 percentage points among women in the lowest quartile. After the elimination of cost sharing, the rate of biennial mammography rose by 6.5 percentage points for white women and 8.4 percentage points for black women, the study found. The rate was nearly unchanged for Hispanic women.
The findings extend that of past studies that show older women who need mammograms are sensitive to out-of-pocket costs and the presence of supplemental coverage, the authors conclude. If the cost-sharing provisions of the ACA are rescinded, the results also “raise concern that fewer older women will receive recommended breast-cancer screening.”
However, the authors also note that since mammogram rates in the health plans that eliminated cost sharing remained below those in plans with full coverage and less than three-quarters of women in control plans received biennial breast cancer screenings, that “the removal of out-of-pocket payments alone may not raise screening rates to desired levels.”
SOURCE: Trivedi A et al. N Engl J Med. 2018 Jan 18;378:262-9.
More women received recommended mammograms after cost sharing for the service was eliminated under the Affordable Care Act, a study shows.
In health plans that eliminated cost sharing, such as copays, deductibles, or other out-of-pocket costs, the rate of biennial screening mammography increased from 60% in the 2-year period before the cost-sharing elimination to 65% in the 2-year period following the new regulation, according to an analysis in the New England Journal of Medicine.
In addition to the increased rate of mammograms in the first group, results showed the rates of biennial mammography in the second group were 73.1% (95% confidence interval, 69.2-77.0) and 72.8% (95% CI, 69.7-76.0) during the same periods, yielding a difference in differences of 5.7 percentage points. Investigators also found the difference in differences was 9.8 percentage points among women living in areas with the highest quartile of educational attainment, compared with 4.3 percentage points among women in the lowest quartile. After the elimination of cost sharing, the rate of biennial mammography rose by 6.5 percentage points for white women and 8.4 percentage points for black women, the study found. The rate was nearly unchanged for Hispanic women.
The findings extend that of past studies that show older women who need mammograms are sensitive to out-of-pocket costs and the presence of supplemental coverage, the authors conclude. If the cost-sharing provisions of the ACA are rescinded, the results also “raise concern that fewer older women will receive recommended breast-cancer screening.”
However, the authors also note that since mammogram rates in the health plans that eliminated cost sharing remained below those in plans with full coverage and less than three-quarters of women in control plans received biennial breast cancer screenings, that “the removal of out-of-pocket payments alone may not raise screening rates to desired levels.”
SOURCE: Trivedi A et al. N Engl J Med. 2018 Jan 18;378:262-9.
Key clinical point:
Major finding: In plans that eliminated cost sharing, the rate of biennial screening mammography increased from 60% to 65% in the 2-year period thereafter.
Study details: A difference-in-differences study of biennial screening mammography among 15,085 women aged 65-74 years in 24 Medicare Advantage plans.
Disclosures: Dr. Trivedi reported personal fees from Merck Foundation outside the submitted work. Authors reported no other disclosures.
Source: Trivedi A et al. N Engl J Med. 2018 Jan 18;378:262-9.
Surgery or Medical Management for Refractory Pediatric Epilepsy?
Children and adolescents with drug-resistant epilepsy who undergo surgery appear to have significantly higher rates of seizure freedom and better quality of life and behavior scores at 12 months than those who receive medical therapy alone, according to a study published in the October 26, 2017, issue of the New England Journal of Medicine. Serious anticipated adverse events may occur after surgery, however.
“The improvements that were observed in other cognitive, behavioral, and quality of life scores in the surgery group may have been due to a reduction in the frequency of seizures; conversely, the deterioration in these measures in the medical-therapy group may be attributed to a continuation of seizures,” said Rekha Dwivedi, PhD, a postdoctoral fellow at the All India Institute of Medical Sciences in New Delhi, and colleagues.

Comparing Methods Intended to Improve Outcomes
Children and adolescents with drug-resistant epilepsy have an increased risk of poor long-term intellectual and psychosocial outcomes, along with a poor health-related quality of life. Neurosurgical treatment may improve seizures in children and adolescents with drug-resistant epilepsy, but evidence of benefit from randomized trials in this age group is limited.
A meta-analysis of uncontrolled studies comparing seizure outcomes of surgeries in children indicated that 74% of patients with brain lesions and 45% without lesions had become seizure-free at one year of follow-up. In a retrospective analysis involving 142 children and adolescents with drug-resistant epilepsy who had undergone surgery, 79.3% of patients were free from disabling seizures after a mean follow-up of approximately four years.
To investigate the effects of surgery further, Dr. Dwivedi and colleagues performed a single-center trial. They sought to compare epilepsy surgery with continued medical therapy alone in patients on a waiting list for surgery.
Researchers randomized 116 patients age 18 or younger with drug-resistant epilepsy to brain surgery appropriate to the underlying cause of epilepsy, along with appropriate medical therapy, or to medical therapy alone. Patients for whom there was no consensus regarding the location of an epileptic focus, patients who had any other systemic illness, and patients with a history of status epilepticus were excluded.
Participants assigned to the surgery group underwent the procedure within a month after randomization. Those assigned to the medical-therapy group remained on a waiting list. Surgery for these patients was scheduled for one year or longer after randomization. The primary outcome was seizure freedom at 12 months. Secondary outcomes included the Hague Seizure Severity scale score, the Binet–Kamat intelligence quotient or the social quotient on the Vineland Social Maturity Scale, the T score on the Child Behavior Checklist, and the Pediatric Quality of Life Inventory score.
Most of the Surgery Group Became Seizure-Free at 12 Months
Median age was 9 in the surgery group and 10 in the medical-therapy group. In all, 14 patients had temporal lobe resections, 12 patients had resection of a lesion in a lobe other than the temporal lobe, 15 patients had hemispherotomy, 10 patients had a corpus callosotomy, and six patients had a disconnection or resection of hypothalamic hamartoma.
At 12 months, 44 of 57 patients (77%) in the surgery group became seizure-free, compared with four of 59 patients (7%) in the medical-therapy group. Furthermore, 21 patients (37%) in the surgery group were completely seizure-free during the entire 12-month period.
All patients who had undergone temporal lobectomy or hypothalamic hamartoma surgeries were seizure-free at the last follow-up. Of the patients who had undergone extratemporal resection or hemispherotomy, 11 of 12 patients (92%) and 13 of 15 (87%), had complete freedom from seizures, respectively.
Two of 15 patients (13%) in the medical-therapy group who were on the waiting list for a temporal lobectomy were seizure-free at 12 months, along with one of 19 patients (5%) who were on a waiting list for extratemporal resection and one of 16 patients (6%) who were waiting for a corpus callostomy. Patients with a planned hemispherotomy or intervention for hypothalamic hamartoma were not seizure-free at 12 months.
In addition, between-group differences in the change from baseline to 12 months significantly favored surgery with respect to the Hague Seizure Severity scale score, the Child Behavior Checklist, the Pediatric Quality of Life Inventory, and the Vineland Social Maturity Scale, but not the Binet–Kamat intelligence quotient, said the researchers.
Adverse Events and Study Limitations
Serious adverse events occurred in 19 patients (33%) in the surgery group and no patients in the medical-therapy group. Monoparesis occurred in two patients who had undergone temporal lobectomy or resection of parietal focal cortical dysplasia. Hemiparesis occurred in 15 patients who had undergone hemispherotomy. Finally, generalized hypotonia and language deficits occurred in one patient who had undergone frontal lobectomy.
Ten patients in the medical-therapy group had physical injuries associated with seizures (eg, cuts, burns, and fractures). One patient had an adverse event associated with an antiepileptic drug, and autistic features developed in another patient. No deaths occurred in either group.
One study limitation was that patients included in this trial underwent many types of epilepsy surgeries to treat various underlying pathologic causes of seizures. Another limitation was that there was an overrepresentation of hypothalamic hamartomas, compared with some other series, said the researchers.
—Erica Tricarico
Suggested Reading
Dwivedi R, Ramanujam B, Chandra PS, et al. Surgery for drug-resistant epilepsy in children. N Engl J Med. 2017;377(17):1639-1647.
Children and adolescents with drug-resistant epilepsy who undergo surgery appear to have significantly higher rates of seizure freedom and better quality of life and behavior scores at 12 months than those who receive medical therapy alone, according to a study published in the October 26, 2017, issue of the New England Journal of Medicine. Serious anticipated adverse events may occur after surgery, however.
“The improvements that were observed in other cognitive, behavioral, and quality of life scores in the surgery group may have been due to a reduction in the frequency of seizures; conversely, the deterioration in these measures in the medical-therapy group may be attributed to a continuation of seizures,” said Rekha Dwivedi, PhD, a postdoctoral fellow at the All India Institute of Medical Sciences in New Delhi, and colleagues.
Comparing Methods Intended to Improve Outcomes
Children and adolescents with drug-resistant epilepsy have an increased risk of poor long-term intellectual and psychosocial outcomes, along with a poor health-related quality of life. Neurosurgical treatment may improve seizures in children and adolescents with drug-resistant epilepsy, but evidence of benefit from randomized trials in this age group is limited.
A meta-analysis of uncontrolled studies comparing seizure outcomes of surgeries in children indicated that 74% of patients with brain lesions and 45% without lesions had become seizure-free at one year of follow-up. In a retrospective analysis involving 142 children and adolescents with drug-resistant epilepsy who had undergone surgery, 79.3% of patients were free from disabling seizures after a mean follow-up of approximately four years.
To investigate the effects of surgery further, Dr. Dwivedi and colleagues performed a single-center trial. They sought to compare epilepsy surgery with continued medical therapy alone in patients on a waiting list for surgery.
Researchers randomized 116 patients age 18 or younger with drug-resistant epilepsy to brain surgery appropriate to the underlying cause of epilepsy, along with appropriate medical therapy, or to medical therapy alone. Patients for whom there was no consensus regarding the location of an epileptic focus, patients who had any other systemic illness, and patients with a history of status epilepticus were excluded.
Participants assigned to the surgery group underwent the procedure within a month after randomization. Those assigned to the medical-therapy group remained on a waiting list. Surgery for these patients was scheduled for one year or longer after randomization. The primary outcome was seizure freedom at 12 months. Secondary outcomes included the Hague Seizure Severity scale score, the Binet–Kamat intelligence quotient or the social quotient on the Vineland Social Maturity Scale, the T score on the Child Behavior Checklist, and the Pediatric Quality of Life Inventory score.
Most of the Surgery Group Became Seizure-Free at 12 Months
Median age was 9 in the surgery group and 10 in the medical-therapy group. In all, 14 patients had temporal lobe resections, 12 patients had resection of a lesion in a lobe other than the temporal lobe, 15 patients had hemispherotomy, 10 patients had a corpus callosotomy, and six patients had a disconnection or resection of hypothalamic hamartoma.
At 12 months, 44 of 57 patients (77%) in the surgery group became seizure-free, compared with four of 59 patients (7%) in the medical-therapy group. Furthermore, 21 patients (37%) in the surgery group were completely seizure-free during the entire 12-month period.
All patients who had undergone temporal lobectomy or hypothalamic hamartoma surgeries were seizure-free at the last follow-up. Of the patients who had undergone extratemporal resection or hemispherotomy, 11 of 12 patients (92%) and 13 of 15 (87%), had complete freedom from seizures, respectively.
Two of 15 patients (13%) in the medical-therapy group who were on the waiting list for a temporal lobectomy were seizure-free at 12 months, along with one of 19 patients (5%) who were on a waiting list for extratemporal resection and one of 16 patients (6%) who were waiting for a corpus callostomy. Patients with a planned hemispherotomy or intervention for hypothalamic hamartoma were not seizure-free at 12 months.
In addition, between-group differences in the change from baseline to 12 months significantly favored surgery with respect to the Hague Seizure Severity scale score, the Child Behavior Checklist, the Pediatric Quality of Life Inventory, and the Vineland Social Maturity Scale, but not the Binet–Kamat intelligence quotient, said the researchers.
Adverse Events and Study Limitations
Serious adverse events occurred in 19 patients (33%) in the surgery group and no patients in the medical-therapy group. Monoparesis occurred in two patients who had undergone temporal lobectomy or resection of parietal focal cortical dysplasia. Hemiparesis occurred in 15 patients who had undergone hemispherotomy. Finally, generalized hypotonia and language deficits occurred in one patient who had undergone frontal lobectomy.
Ten patients in the medical-therapy group had physical injuries associated with seizures (eg, cuts, burns, and fractures). One patient had an adverse event associated with an antiepileptic drug, and autistic features developed in another patient. No deaths occurred in either group.
One study limitation was that patients included in this trial underwent many types of epilepsy surgeries to treat various underlying pathologic causes of seizures. Another limitation was that there was an overrepresentation of hypothalamic hamartomas, compared with some other series, said the researchers.
—Erica Tricarico
Suggested Reading
Dwivedi R, Ramanujam B, Chandra PS, et al. Surgery for drug-resistant epilepsy in children. N Engl J Med. 2017;377(17):1639-1647.
Children and adolescents with drug-resistant epilepsy who undergo surgery appear to have significantly higher rates of seizure freedom and better quality of life and behavior scores at 12 months than those who receive medical therapy alone, according to a study published in the October 26, 2017, issue of the New England Journal of Medicine. Serious anticipated adverse events may occur after surgery, however.
“The improvements that were observed in other cognitive, behavioral, and quality of life scores in the surgery group may have been due to a reduction in the frequency of seizures; conversely, the deterioration in these measures in the medical-therapy group may be attributed to a continuation of seizures,” said Rekha Dwivedi, PhD, a postdoctoral fellow at the All India Institute of Medical Sciences in New Delhi, and colleagues.
Comparing Methods Intended to Improve Outcomes
Children and adolescents with drug-resistant epilepsy have an increased risk of poor long-term intellectual and psychosocial outcomes, along with a poor health-related quality of life. Neurosurgical treatment may improve seizures in children and adolescents with drug-resistant epilepsy, but evidence of benefit from randomized trials in this age group is limited.
A meta-analysis of uncontrolled studies comparing seizure outcomes of surgeries in children indicated that 74% of patients with brain lesions and 45% without lesions had become seizure-free at one year of follow-up. In a retrospective analysis involving 142 children and adolescents with drug-resistant epilepsy who had undergone surgery, 79.3% of patients were free from disabling seizures after a mean follow-up of approximately four years.
To investigate the effects of surgery further, Dr. Dwivedi and colleagues performed a single-center trial. They sought to compare epilepsy surgery with continued medical therapy alone in patients on a waiting list for surgery.
Researchers randomized 116 patients age 18 or younger with drug-resistant epilepsy to brain surgery appropriate to the underlying cause of epilepsy, along with appropriate medical therapy, or to medical therapy alone. Patients for whom there was no consensus regarding the location of an epileptic focus, patients who had any other systemic illness, and patients with a history of status epilepticus were excluded.
Participants assigned to the surgery group underwent the procedure within a month after randomization. Those assigned to the medical-therapy group remained on a waiting list. Surgery for these patients was scheduled for one year or longer after randomization. The primary outcome was seizure freedom at 12 months. Secondary outcomes included the Hague Seizure Severity scale score, the Binet–Kamat intelligence quotient or the social quotient on the Vineland Social Maturity Scale, the T score on the Child Behavior Checklist, and the Pediatric Quality of Life Inventory score.
Most of the Surgery Group Became Seizure-Free at 12 Months
Median age was 9 in the surgery group and 10 in the medical-therapy group. In all, 14 patients had temporal lobe resections, 12 patients had resection of a lesion in a lobe other than the temporal lobe, 15 patients had hemispherotomy, 10 patients had a corpus callosotomy, and six patients had a disconnection or resection of hypothalamic hamartoma.
At 12 months, 44 of 57 patients (77%) in the surgery group became seizure-free, compared with four of 59 patients (7%) in the medical-therapy group. Furthermore, 21 patients (37%) in the surgery group were completely seizure-free during the entire 12-month period.
All patients who had undergone temporal lobectomy or hypothalamic hamartoma surgeries were seizure-free at the last follow-up. Of the patients who had undergone extratemporal resection or hemispherotomy, 11 of 12 patients (92%) and 13 of 15 (87%), had complete freedom from seizures, respectively.
Two of 15 patients (13%) in the medical-therapy group who were on the waiting list for a temporal lobectomy were seizure-free at 12 months, along with one of 19 patients (5%) who were on a waiting list for extratemporal resection and one of 16 patients (6%) who were waiting for a corpus callostomy. Patients with a planned hemispherotomy or intervention for hypothalamic hamartoma were not seizure-free at 12 months.
In addition, between-group differences in the change from baseline to 12 months significantly favored surgery with respect to the Hague Seizure Severity scale score, the Child Behavior Checklist, the Pediatric Quality of Life Inventory, and the Vineland Social Maturity Scale, but not the Binet–Kamat intelligence quotient, said the researchers.
Adverse Events and Study Limitations
Serious adverse events occurred in 19 patients (33%) in the surgery group and no patients in the medical-therapy group. Monoparesis occurred in two patients who had undergone temporal lobectomy or resection of parietal focal cortical dysplasia. Hemiparesis occurred in 15 patients who had undergone hemispherotomy. Finally, generalized hypotonia and language deficits occurred in one patient who had undergone frontal lobectomy.
Ten patients in the medical-therapy group had physical injuries associated with seizures (eg, cuts, burns, and fractures). One patient had an adverse event associated with an antiepileptic drug, and autistic features developed in another patient. No deaths occurred in either group.
One study limitation was that patients included in this trial underwent many types of epilepsy surgeries to treat various underlying pathologic causes of seizures. Another limitation was that there was an overrepresentation of hypothalamic hamartomas, compared with some other series, said the researchers.
—Erica Tricarico
Suggested Reading
Dwivedi R, Ramanujam B, Chandra PS, et al. Surgery for drug-resistant epilepsy in children. N Engl J Med. 2017;377(17):1639-1647.
Flu season takes another turn for the worse
By one measure at least – the proportion of outpatient visits for influenza-like illness (ILI) – this flu season is now the worst in almost a decade, according to data from the Centers for Disease Control and Prevention.
which hit an early peak of 7.7% in October of 2009. The slight pause that occurred in the first week of January as the rate only rose from 5.7% to 5.8% now looks more like the earlier trend from December, when the level of outpatient visits more than doubled over a 3-week period, data from the CDC FluView website show.
“The geographic spread of influenza in Puerto Rico and 49 states was reported as widespread” for the week ending Jan. 13, and 24 states had the highest level of ILI activity on the CDC’s 1-10 scale, the CDC influenza division reported Jan 19.
There were 10 flu-related pediatric deaths reported during the week, with two occurring in the week ending Jan. 13. A total of 30 deaths in children have been associated with influenza so far for the 2017-2018 season, the CDC said.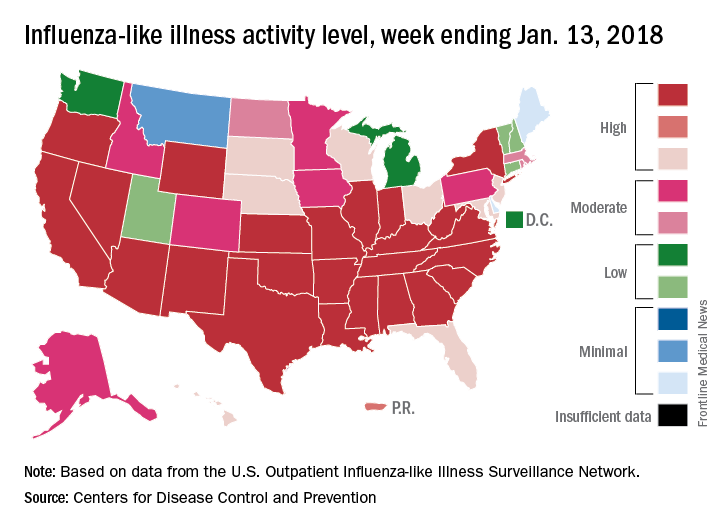
By one measure at least – the proportion of outpatient visits for influenza-like illness (ILI) – this flu season is now the worst in almost a decade, according to data from the Centers for Disease Control and Prevention.
which hit an early peak of 7.7% in October of 2009. The slight pause that occurred in the first week of January as the rate only rose from 5.7% to 5.8% now looks more like the earlier trend from December, when the level of outpatient visits more than doubled over a 3-week period, data from the CDC FluView website show.
“The geographic spread of influenza in Puerto Rico and 49 states was reported as widespread” for the week ending Jan. 13, and 24 states had the highest level of ILI activity on the CDC’s 1-10 scale, the CDC influenza division reported Jan 19.
There were 10 flu-related pediatric deaths reported during the week, with two occurring in the week ending Jan. 13. A total of 30 deaths in children have been associated with influenza so far for the 2017-2018 season, the CDC said.
By one measure at least – the proportion of outpatient visits for influenza-like illness (ILI) – this flu season is now the worst in almost a decade, according to data from the Centers for Disease Control and Prevention.
which hit an early peak of 7.7% in October of 2009. The slight pause that occurred in the first week of January as the rate only rose from 5.7% to 5.8% now looks more like the earlier trend from December, when the level of outpatient visits more than doubled over a 3-week period, data from the CDC FluView website show.
“The geographic spread of influenza in Puerto Rico and 49 states was reported as widespread” for the week ending Jan. 13, and 24 states had the highest level of ILI activity on the CDC’s 1-10 scale, the CDC influenza division reported Jan 19.
There were 10 flu-related pediatric deaths reported during the week, with two occurring in the week ending Jan. 13. A total of 30 deaths in children have been associated with influenza so far for the 2017-2018 season, the CDC said.
New multi-analyte blood test shows promise in screening for several common solid tumors
Imagine a single blood test that would cost less than $500 and could screen for at least eight cancer types.
It’s early days for the technology, called CancerSEEK, but the test had a sensitivity of 69%-98%, depending on the cancer type, and a specificity of 99% in a cohort of 1,005 patients with stage I-III cancers and 850 healthy controls, wrote Joshua D. Cohen of the Ludwig Center for Cancer Genetics and Therapeutics at Johns Hopkins University, Baltimore, and his colleagues. The report was published in Science.
CancerSEEK tests for mutations in 2,001 genomic positions and eight proteins. The researchers examined a 61-amplicon panel with each amplicon analyzing an average of 33 base pairs within a gene. They theorized the test could detect between 41% and 95% of the cancers in the Catalog of Somatic Mutations in Cancer dataset. They next used multiplex-PCR techniques to minimize errors associated with large sequencing and identified protein biomarkers for early stage cancers that may not release detectable ctDNA.
The researchers used the technology to examine blood samples from 1,005 patients with stage I (20%), stage II (49%), or stage III (31%) cancers of the ovary, liver, stomach, pancreas, esophagus, colorectum, lung, or breast prior to undergoing neoadjuvant chemotherapy. Participants had a median age of 64 years (range of 22-93 years). The healthy controls did not have a history of cancer, chronic kidney disease, autoimmune disease, or high-grade dysplasia.
The sensitivity of the test ranged from 98% in ovarian cancer to 33% in breast cancer, but the specificity was greater than 99% with only 7 of 812 control participants having a positive result. “We could not be certain that the few ‘false positive’ individuals identified among the healthy cohort did not actually have an as-yet undetected cancer, but classifying them as false positives provided the most conservative approach to classification and interpretation of the data,” the authors wrote.
Based on cancer stage, sensitivity for stage I cancers was 43%, for stage II 73%, and for stage III 78%. Again, sensitivity varied depending on cancer type, with 100% sensitivity for stage I liver cancer and 20% sensitivity for stage I esophageal cancer.
When tumor tissue samples from 153 patients with statistically significant ctDNA levels were analyzed, identical mutations were found in the plasma and tumor in 90% (138) of all cases.
The protein markers in the CancerSEEK test might also be able to anatomically locate malignancies. Using machine learning to analyze patients testing positive with CancerSEEK, the results narrowed the source of the cancer to two possible anatomical sites in approximately 83% of patients and to one anatomical site in approximately 63% of patients. Accuracy was highest for colorectal cancer and lowest for lung cancer.
As the study included otherwise healthy patients with known malignancies, the results need to be confirmed with prospective studies of incidence cancer types in a large population. Patients in the screening setting may have less advanced disease and other comorbidities that could impact the sensitivity and specificity of the CancerSEEK test, the researchers wrote.
The study was funded by multiple sources including grants from the National Institutes of Health. The authors reported various disclosures involving diagnostics and pharmaceutical companies.
SOURCE: Cohen JD et al., Science 2018 Jan 18. doi: 10.1126/science.aar3247.
Molecular panels are here to stay – and the GI community will in some shape or form be impacted, be it in performing diagnostic procedures on test-positive patients, or risk-stratifying patients prior to testing.
The conceptual challenge is that it is not about what any given test measures – various panels use separate combination of markers from epigenetics to DNA mutations as well as whole or truncated proteins – but how well a specific test with its somewhat arbitrarily chosen components and cutoffs performs. And, more importantly, what the clinical implications of positive or negative test results are. And no one knows that. At least for now.
A recent report in Science from a group from the Ludwig Center for Cancer Genetics at Johns Hopkins proposes a new cancer blood test based on a very systematic and thoughtful approach to include select mutations in cell-free DNA and circulating proteins associated with various solid organ tumors. For validation, they used healthy and advanced but nonmetastatic cancer cohorts. Through stringent controls and a series of validations, the authors present a range of sensitivities for the various cancer types with an impressive specificity. This is a technically very strong approach with many nifty and thoughtful additions to give this test a very promising first foray – did anybody watch CNN?
While not ready for prime time, which is a tall order for a first report, the authors dutifully point out the need for a prospective real life cohort validation. In the meantime, regardless of the outcome of this particular test, it is a repeated reminder that we need to stay abreast of the advances and the details of each molecular test, especially with a likely very diverse and distinct group of tests to choose from.

Many of us will be part of interpreting results and determining further management. Just as with hereditary cancer genetic panel testing, our technical ability may have stretched beyond our ability to fully understand the implications. Many questions will arise: What about true false positives? False negatives? Intervals? Can such tests replace other screening? How to choose any given test over the other? Should tests be combined or alternated? The tests will be technically refined and are here to stay – we need to get to work on finding answers to the clinically relevant questions.
Barbara Jung, MD, AGAF, is the Thomas J. Layden Endowed Professor and chief of the division of gastroenterology and hepatology, University of Chicago.
Molecular panels are here to stay – and the GI community will in some shape or form be impacted, be it in performing diagnostic procedures on test-positive patients, or risk-stratifying patients prior to testing.
The conceptual challenge is that it is not about what any given test measures – various panels use separate combination of markers from epigenetics to DNA mutations as well as whole or truncated proteins – but how well a specific test with its somewhat arbitrarily chosen components and cutoffs performs. And, more importantly, what the clinical implications of positive or negative test results are. And no one knows that. At least for now.
A recent report in Science from a group from the Ludwig Center for Cancer Genetics at Johns Hopkins proposes a new cancer blood test based on a very systematic and thoughtful approach to include select mutations in cell-free DNA and circulating proteins associated with various solid organ tumors. For validation, they used healthy and advanced but nonmetastatic cancer cohorts. Through stringent controls and a series of validations, the authors present a range of sensitivities for the various cancer types with an impressive specificity. This is a technically very strong approach with many nifty and thoughtful additions to give this test a very promising first foray – did anybody watch CNN?
While not ready for prime time, which is a tall order for a first report, the authors dutifully point out the need for a prospective real life cohort validation. In the meantime, regardless of the outcome of this particular test, it is a repeated reminder that we need to stay abreast of the advances and the details of each molecular test, especially with a likely very diverse and distinct group of tests to choose from.
Many of us will be part of interpreting results and determining further management. Just as with hereditary cancer genetic panel testing, our technical ability may have stretched beyond our ability to fully understand the implications. Many questions will arise: What about true false positives? False negatives? Intervals? Can such tests replace other screening? How to choose any given test over the other? Should tests be combined or alternated? The tests will be technically refined and are here to stay – we need to get to work on finding answers to the clinically relevant questions.
Barbara Jung, MD, AGAF, is the Thomas J. Layden Endowed Professor and chief of the division of gastroenterology and hepatology, University of Chicago.
Molecular panels are here to stay – and the GI community will in some shape or form be impacted, be it in performing diagnostic procedures on test-positive patients, or risk-stratifying patients prior to testing.
The conceptual challenge is that it is not about what any given test measures – various panels use separate combination of markers from epigenetics to DNA mutations as well as whole or truncated proteins – but how well a specific test with its somewhat arbitrarily chosen components and cutoffs performs. And, more importantly, what the clinical implications of positive or negative test results are. And no one knows that. At least for now.
A recent report in Science from a group from the Ludwig Center for Cancer Genetics at Johns Hopkins proposes a new cancer blood test based on a very systematic and thoughtful approach to include select mutations in cell-free DNA and circulating proteins associated with various solid organ tumors. For validation, they used healthy and advanced but nonmetastatic cancer cohorts. Through stringent controls and a series of validations, the authors present a range of sensitivities for the various cancer types with an impressive specificity. This is a technically very strong approach with many nifty and thoughtful additions to give this test a very promising first foray – did anybody watch CNN?
While not ready for prime time, which is a tall order for a first report, the authors dutifully point out the need for a prospective real life cohort validation. In the meantime, regardless of the outcome of this particular test, it is a repeated reminder that we need to stay abreast of the advances and the details of each molecular test, especially with a likely very diverse and distinct group of tests to choose from.
Many of us will be part of interpreting results and determining further management. Just as with hereditary cancer genetic panel testing, our technical ability may have stretched beyond our ability to fully understand the implications. Many questions will arise: What about true false positives? False negatives? Intervals? Can such tests replace other screening? How to choose any given test over the other? Should tests be combined or alternated? The tests will be technically refined and are here to stay – we need to get to work on finding answers to the clinically relevant questions.
Barbara Jung, MD, AGAF, is the Thomas J. Layden Endowed Professor and chief of the division of gastroenterology and hepatology, University of Chicago.
Imagine a single blood test that would cost less than $500 and could screen for at least eight cancer types.
It’s early days for the technology, called CancerSEEK, but the test had a sensitivity of 69%-98%, depending on the cancer type, and a specificity of 99% in a cohort of 1,005 patients with stage I-III cancers and 850 healthy controls, wrote Joshua D. Cohen of the Ludwig Center for Cancer Genetics and Therapeutics at Johns Hopkins University, Baltimore, and his colleagues. The report was published in Science.
CancerSEEK tests for mutations in 2,001 genomic positions and eight proteins. The researchers examined a 61-amplicon panel with each amplicon analyzing an average of 33 base pairs within a gene. They theorized the test could detect between 41% and 95% of the cancers in the Catalog of Somatic Mutations in Cancer dataset. They next used multiplex-PCR techniques to minimize errors associated with large sequencing and identified protein biomarkers for early stage cancers that may not release detectable ctDNA.
The researchers used the technology to examine blood samples from 1,005 patients with stage I (20%), stage II (49%), or stage III (31%) cancers of the ovary, liver, stomach, pancreas, esophagus, colorectum, lung, or breast prior to undergoing neoadjuvant chemotherapy. Participants had a median age of 64 years (range of 22-93 years). The healthy controls did not have a history of cancer, chronic kidney disease, autoimmune disease, or high-grade dysplasia.
The sensitivity of the test ranged from 98% in ovarian cancer to 33% in breast cancer, but the specificity was greater than 99% with only 7 of 812 control participants having a positive result. “We could not be certain that the few ‘false positive’ individuals identified among the healthy cohort did not actually have an as-yet undetected cancer, but classifying them as false positives provided the most conservative approach to classification and interpretation of the data,” the authors wrote.
Based on cancer stage, sensitivity for stage I cancers was 43%, for stage II 73%, and for stage III 78%. Again, sensitivity varied depending on cancer type, with 100% sensitivity for stage I liver cancer and 20% sensitivity for stage I esophageal cancer.
When tumor tissue samples from 153 patients with statistically significant ctDNA levels were analyzed, identical mutations were found in the plasma and tumor in 90% (138) of all cases.
The protein markers in the CancerSEEK test might also be able to anatomically locate malignancies. Using machine learning to analyze patients testing positive with CancerSEEK, the results narrowed the source of the cancer to two possible anatomical sites in approximately 83% of patients and to one anatomical site in approximately 63% of patients. Accuracy was highest for colorectal cancer and lowest for lung cancer.
As the study included otherwise healthy patients with known malignancies, the results need to be confirmed with prospective studies of incidence cancer types in a large population. Patients in the screening setting may have less advanced disease and other comorbidities that could impact the sensitivity and specificity of the CancerSEEK test, the researchers wrote.
The study was funded by multiple sources including grants from the National Institutes of Health. The authors reported various disclosures involving diagnostics and pharmaceutical companies.
SOURCE: Cohen JD et al., Science 2018 Jan 18. doi: 10.1126/science.aar3247.
Imagine a single blood test that would cost less than $500 and could screen for at least eight cancer types.
It’s early days for the technology, called CancerSEEK, but the test had a sensitivity of 69%-98%, depending on the cancer type, and a specificity of 99% in a cohort of 1,005 patients with stage I-III cancers and 850 healthy controls, wrote Joshua D. Cohen of the Ludwig Center for Cancer Genetics and Therapeutics at Johns Hopkins University, Baltimore, and his colleagues. The report was published in Science.
CancerSEEK tests for mutations in 2,001 genomic positions and eight proteins. The researchers examined a 61-amplicon panel with each amplicon analyzing an average of 33 base pairs within a gene. They theorized the test could detect between 41% and 95% of the cancers in the Catalog of Somatic Mutations in Cancer dataset. They next used multiplex-PCR techniques to minimize errors associated with large sequencing and identified protein biomarkers for early stage cancers that may not release detectable ctDNA.
The researchers used the technology to examine blood samples from 1,005 patients with stage I (20%), stage II (49%), or stage III (31%) cancers of the ovary, liver, stomach, pancreas, esophagus, colorectum, lung, or breast prior to undergoing neoadjuvant chemotherapy. Participants had a median age of 64 years (range of 22-93 years). The healthy controls did not have a history of cancer, chronic kidney disease, autoimmune disease, or high-grade dysplasia.
The sensitivity of the test ranged from 98% in ovarian cancer to 33% in breast cancer, but the specificity was greater than 99% with only 7 of 812 control participants having a positive result. “We could not be certain that the few ‘false positive’ individuals identified among the healthy cohort did not actually have an as-yet undetected cancer, but classifying them as false positives provided the most conservative approach to classification and interpretation of the data,” the authors wrote.
Based on cancer stage, sensitivity for stage I cancers was 43%, for stage II 73%, and for stage III 78%. Again, sensitivity varied depending on cancer type, with 100% sensitivity for stage I liver cancer and 20% sensitivity for stage I esophageal cancer.
When tumor tissue samples from 153 patients with statistically significant ctDNA levels were analyzed, identical mutations were found in the plasma and tumor in 90% (138) of all cases.
The protein markers in the CancerSEEK test might also be able to anatomically locate malignancies. Using machine learning to analyze patients testing positive with CancerSEEK, the results narrowed the source of the cancer to two possible anatomical sites in approximately 83% of patients and to one anatomical site in approximately 63% of patients. Accuracy was highest for colorectal cancer and lowest for lung cancer.
As the study included otherwise healthy patients with known malignancies, the results need to be confirmed with prospective studies of incidence cancer types in a large population. Patients in the screening setting may have less advanced disease and other comorbidities that could impact the sensitivity and specificity of the CancerSEEK test, the researchers wrote.
The study was funded by multiple sources including grants from the National Institutes of Health. The authors reported various disclosures involving diagnostics and pharmaceutical companies.
SOURCE: Cohen JD et al., Science 2018 Jan 18. doi: 10.1126/science.aar3247.
FROM SCIENCE
Key clinical point: New blood test demonstrates ability to identify presence of eight common cancers.
Major finding: CancerSEEK demonstrated a mean sensitivity of 70% for the eight cancer types and a specificity of greater than 99%.
Data source: Retrospective study of 1,005 patients with known malignancy and 812 healthy controls.
Disclosures: The study was funded by multiple sources including grants from the National Institutes of Health. The authors reported several disclosures involving diagnostics and pharmaceutical companies.
Source: Cohen JD et al. Science 2018 Jan 18. doi: 10.1126/science.aar3247.
HHS creates new religious freedoms division
The Trump administration has announced a new division within the U.S. Health & Human Services Department that aims to protect health care providers who have religious or moral objections to performing medical services, such as abortion.
In a Jan. 18 announcement, HHS Office for Civil Rights Director Roger Severino said the new Conscience and Religious Freedom Division will focus on outreach, policy making, and vigorously enforcing existing federal laws that protect conscience and religious freedom rights. The new branch will enable health providers to file conscience and religious freedom complaints, which will then be investigated by the division.

Opinions on the new division from physicians and medical associations were mixed. The American College of Physicians (ACP) cautioned that the division’s creation must not lead to discrimination against any category of class of patients, as guided by medical professions’ ethical obligations.
“ACP would be particularly concerned if the new HHS division takes any actions that would result in denial of access to appropriate health care based on gender, gender identity, sexual orientation, race, ethnicity, or other personal characteristics,” ACP President Jack Ende, MD, said in a statement. “ACP will evaluate the newly formed division as it begins operating, informed by our ethics and public policy positions. Those state that physicians have a professional obligation to not discriminate against any class of patients, but also that a physician may have a conscientious objection to providing a specific medical service to a patient.”
The Catholic Medical Association (CMA) applauded the new HHS division, saying it’s about time that the religious and conscience rights of health providers were protected by the federal government. In the past, health providers could be drawn into medical activities in a hospital or health care system that they found moral objectionable with no recourse, said Kathleen Raviele, MD, a board member for the Catholic Medical Association and a Decatur, Ga.–based ob.gyn.
“The fact that individual health care providers are going to have a place to go if they feel they have valid complaint is really momentous,” Dr. Raviele said in an interview. “It’s respecting the rights of all of us and not just some special interest groups ... I also think [the new division] will make states [and] hospital systems less likely to try to infringe on people’s conscientious rights.”
The HIV Medicine Association called the formation of the new HHS division appalling, and said the office appears to protect health care providers who discriminate against vulnerable patients, such as women, LGBTQ patients, and minorities.
“The new division, designed to ‘protect’ health care providers who discriminate in the care and services they provide, defies the fundamental medical ethic to first do no harm,” HIV Medicine Association Chair Melanie Thompson, MD, said in a statement. “Using federal dollars to shield providers who choose to discriminate rather than protect vulnerable patients and provide services to improve their health is counter to the mission of HHS, wasteful of scarce federal funds, and will result in delayed or lack of care for vulnerable individuals, threatening their health and lives.”
The HHS Conscience and Religious Freedom Division is necessary to address the “sustained attack on conscience rights,” said Jane Orient, MD, executive director for the conservative Association of American Physicians and Surgeons.
“Many powerful and influential forces are attempting to impose their views on Americans, predominantly on Christians, forcing them to perform acts they believe to be immoral, [or risk] losing their job, their business, their livelihood, or even their life savings,” Dr. Orient said in an interview. “...We hope that the OCR will help to return our nation to its foundational principles of freedom and respect for people of conscience.”
The Trump administration has announced a new division within the U.S. Health & Human Services Department that aims to protect health care providers who have religious or moral objections to performing medical services, such as abortion.
In a Jan. 18 announcement, HHS Office for Civil Rights Director Roger Severino said the new Conscience and Religious Freedom Division will focus on outreach, policy making, and vigorously enforcing existing federal laws that protect conscience and religious freedom rights. The new branch will enable health providers to file conscience and religious freedom complaints, which will then be investigated by the division.
Opinions on the new division from physicians and medical associations were mixed. The American College of Physicians (ACP) cautioned that the division’s creation must not lead to discrimination against any category of class of patients, as guided by medical professions’ ethical obligations.
“ACP would be particularly concerned if the new HHS division takes any actions that would result in denial of access to appropriate health care based on gender, gender identity, sexual orientation, race, ethnicity, or other personal characteristics,” ACP President Jack Ende, MD, said in a statement. “ACP will evaluate the newly formed division as it begins operating, informed by our ethics and public policy positions. Those state that physicians have a professional obligation to not discriminate against any class of patients, but also that a physician may have a conscientious objection to providing a specific medical service to a patient.”
The Catholic Medical Association (CMA) applauded the new HHS division, saying it’s about time that the religious and conscience rights of health providers were protected by the federal government. In the past, health providers could be drawn into medical activities in a hospital or health care system that they found moral objectionable with no recourse, said Kathleen Raviele, MD, a board member for the Catholic Medical Association and a Decatur, Ga.–based ob.gyn.
“The fact that individual health care providers are going to have a place to go if they feel they have valid complaint is really momentous,” Dr. Raviele said in an interview. “It’s respecting the rights of all of us and not just some special interest groups ... I also think [the new division] will make states [and] hospital systems less likely to try to infringe on people’s conscientious rights.”
The HIV Medicine Association called the formation of the new HHS division appalling, and said the office appears to protect health care providers who discriminate against vulnerable patients, such as women, LGBTQ patients, and minorities.
“The new division, designed to ‘protect’ health care providers who discriminate in the care and services they provide, defies the fundamental medical ethic to first do no harm,” HIV Medicine Association Chair Melanie Thompson, MD, said in a statement. “Using federal dollars to shield providers who choose to discriminate rather than protect vulnerable patients and provide services to improve their health is counter to the mission of HHS, wasteful of scarce federal funds, and will result in delayed or lack of care for vulnerable individuals, threatening their health and lives.”
The HHS Conscience and Religious Freedom Division is necessary to address the “sustained attack on conscience rights,” said Jane Orient, MD, executive director for the conservative Association of American Physicians and Surgeons.
“Many powerful and influential forces are attempting to impose their views on Americans, predominantly on Christians, forcing them to perform acts they believe to be immoral, [or risk] losing their job, their business, their livelihood, or even their life savings,” Dr. Orient said in an interview. “...We hope that the OCR will help to return our nation to its foundational principles of freedom and respect for people of conscience.”
The Trump administration has announced a new division within the U.S. Health & Human Services Department that aims to protect health care providers who have religious or moral objections to performing medical services, such as abortion.
In a Jan. 18 announcement, HHS Office for Civil Rights Director Roger Severino said the new Conscience and Religious Freedom Division will focus on outreach, policy making, and vigorously enforcing existing federal laws that protect conscience and religious freedom rights. The new branch will enable health providers to file conscience and religious freedom complaints, which will then be investigated by the division.
Opinions on the new division from physicians and medical associations were mixed. The American College of Physicians (ACP) cautioned that the division’s creation must not lead to discrimination against any category of class of patients, as guided by medical professions’ ethical obligations.
“ACP would be particularly concerned if the new HHS division takes any actions that would result in denial of access to appropriate health care based on gender, gender identity, sexual orientation, race, ethnicity, or other personal characteristics,” ACP President Jack Ende, MD, said in a statement. “ACP will evaluate the newly formed division as it begins operating, informed by our ethics and public policy positions. Those state that physicians have a professional obligation to not discriminate against any class of patients, but also that a physician may have a conscientious objection to providing a specific medical service to a patient.”
The Catholic Medical Association (CMA) applauded the new HHS division, saying it’s about time that the religious and conscience rights of health providers were protected by the federal government. In the past, health providers could be drawn into medical activities in a hospital or health care system that they found moral objectionable with no recourse, said Kathleen Raviele, MD, a board member for the Catholic Medical Association and a Decatur, Ga.–based ob.gyn.
“The fact that individual health care providers are going to have a place to go if they feel they have valid complaint is really momentous,” Dr. Raviele said in an interview. “It’s respecting the rights of all of us and not just some special interest groups ... I also think [the new division] will make states [and] hospital systems less likely to try to infringe on people’s conscientious rights.”
The HIV Medicine Association called the formation of the new HHS division appalling, and said the office appears to protect health care providers who discriminate against vulnerable patients, such as women, LGBTQ patients, and minorities.
“The new division, designed to ‘protect’ health care providers who discriminate in the care and services they provide, defies the fundamental medical ethic to first do no harm,” HIV Medicine Association Chair Melanie Thompson, MD, said in a statement. “Using federal dollars to shield providers who choose to discriminate rather than protect vulnerable patients and provide services to improve their health is counter to the mission of HHS, wasteful of scarce federal funds, and will result in delayed or lack of care for vulnerable individuals, threatening their health and lives.”
The HHS Conscience and Religious Freedom Division is necessary to address the “sustained attack on conscience rights,” said Jane Orient, MD, executive director for the conservative Association of American Physicians and Surgeons.
“Many powerful and influential forces are attempting to impose their views on Americans, predominantly on Christians, forcing them to perform acts they believe to be immoral, [or risk] losing their job, their business, their livelihood, or even their life savings,” Dr. Orient said in an interview. “...We hope that the OCR will help to return our nation to its foundational principles of freedom and respect for people of conscience.”
Are two drugs as good as three in maintaining HIV suppression?
Phase 3 clinical results show an oral, two-drug antiretroviral therapy (ART) of dolutegravir and rilpivirine to be an effective and safe alternative to a triple-drug current antiretroviral regimen (CAR) for maintaining virologic suppression of HIV-1 in adults.
Josep M Llibre, MD, from the department of infectious diseases at the Pujol University Hospital Germans Trias in Barcelona and his colleagues conducted a phase 3, randomized, parallel-group (SWORD-1 and SWORD-2), multicenter, noninferiority investigation. The pooled, open-label study reported on a total of 1,028 individuals, median age 43 years, who met a base criteria of stable viral suppression (viral load fewer than 50 copies/mL) by a first or second CAR regimen consisting of two nucleoside reverse transcriptase inhibitors (NRTIs) plus a third drug (nonnucleoside reverse transcriptase inhibitors, integrase strand transfer inhibitors, or a protease inhibitor) for a minimum of 6 months at time of screening. The overall population was 80% white, with women making up 22% of the pooled populations. Random assignment with stratification according to class, age, and planned substudy participation resulted in 512 participants continuing their CAR regimen and an intention-to-treat population of 516 participants switching to the oral, once-daily, two-drug dolutegravir/rilpivirine regimen (dolutegravir 50 mg plus rilpivirine 25 mg).
Analysis of pooled SWORD1 and SWORD2 trials at the primary 48-week endpoint showed 95% of the participants for both the intent-to-treat, two-drug dolutegravir/rilpivirine therapy and the population maintaining their standard triple-drug CAR therapy continued to have successful viral suppression as evidenced by viral loads of fewer than 50 copies/mL. This result together with an adjusted treatment difference of –2.2% (95% confidence interval, –3.0 to 2.5) supports a noninferiority with a predefined margin of –8% of the dolutegravir/rilpivirine therapy to CAR for viral suppression as reported in the Lancet.
Reports of at least one adverse event by week 48 were slightly higher for the dolutegravir/rilpivirine therapy group (77%) when compared with those in the CAR group (71%). The most commonly experienced adverse effects were nasopharyngitis (10% each for dolutegravir/rilpivirine and CAR) and headache (8% for dolutegravir/rilpivirine vs. 5% for CAR). However, adverse effects were associated with higher withdrawals from the dolutegravir/rilpivirine therapy group, compared with the CAR group (3% vs. less than 1%, respectively) by the primary 48-week endpoint.
“Once-daily oral dolutegravir/rilpivirine therapy would be the first oral two-drug regimen that provides patients with an alternative to guideline-preferred triple-drug regimens, avoids major NRTI [nucleoside reverse transcriptase inhibitor] toxicities, has limited potential for drug-drug interactions, and does not increase lipid concentrations or inflammatory biomarkers,” according to Dr. Llibre and his colleagues.
The authors disclosed associations with financial and regulatory sponsor ViiV Healthcare and partner participation by Janssen Pharmaceutica NV in the development of the dolutegravir/rilpivirine two-drug regimen.
Source: Llibre JM et al. Lancet. 2018 Jan 10. doi: 10.1016/S0140-6736(17)33095-7.
In an accompanying commentary (Lancet. 2018 Jan 10. doi: 10.1016/S0140-6736[18]30008-4), Mark A Boyd, MD, and David A Cooper, MD, of the University of Adelaide, Australia, wrote that studies done during the first 10 years of antiretroviral therapy led to the conclusion that triple therapy was the minimum required to fully maintain suppression of HIV replication. The results of this study and others make a convincing case for using dual therapy instead. “The potential pipeline for a variety of effective dual-therapy options appears rich,” they concluded.
Dr. Boyd reported receiving personal fees from Janssen-Cilag and ViiV Healthcare, while Dr. Cooper had no disclosures.
In an accompanying commentary (Lancet. 2018 Jan 10. doi: 10.1016/S0140-6736[18]30008-4), Mark A Boyd, MD, and David A Cooper, MD, of the University of Adelaide, Australia, wrote that studies done during the first 10 years of antiretroviral therapy led to the conclusion that triple therapy was the minimum required to fully maintain suppression of HIV replication. The results of this study and others make a convincing case for using dual therapy instead. “The potential pipeline for a variety of effective dual-therapy options appears rich,” they concluded.
Dr. Boyd reported receiving personal fees from Janssen-Cilag and ViiV Healthcare, while Dr. Cooper had no disclosures.
In an accompanying commentary (Lancet. 2018 Jan 10. doi: 10.1016/S0140-6736[18]30008-4), Mark A Boyd, MD, and David A Cooper, MD, of the University of Adelaide, Australia, wrote that studies done during the first 10 years of antiretroviral therapy led to the conclusion that triple therapy was the minimum required to fully maintain suppression of HIV replication. The results of this study and others make a convincing case for using dual therapy instead. “The potential pipeline for a variety of effective dual-therapy options appears rich,” they concluded.
Dr. Boyd reported receiving personal fees from Janssen-Cilag and ViiV Healthcare, while Dr. Cooper had no disclosures.
Phase 3 clinical results show an oral, two-drug antiretroviral therapy (ART) of dolutegravir and rilpivirine to be an effective and safe alternative to a triple-drug current antiretroviral regimen (CAR) for maintaining virologic suppression of HIV-1 in adults.
Josep M Llibre, MD, from the department of infectious diseases at the Pujol University Hospital Germans Trias in Barcelona and his colleagues conducted a phase 3, randomized, parallel-group (SWORD-1 and SWORD-2), multicenter, noninferiority investigation. The pooled, open-label study reported on a total of 1,028 individuals, median age 43 years, who met a base criteria of stable viral suppression (viral load fewer than 50 copies/mL) by a first or second CAR regimen consisting of two nucleoside reverse transcriptase inhibitors (NRTIs) plus a third drug (nonnucleoside reverse transcriptase inhibitors, integrase strand transfer inhibitors, or a protease inhibitor) for a minimum of 6 months at time of screening. The overall population was 80% white, with women making up 22% of the pooled populations. Random assignment with stratification according to class, age, and planned substudy participation resulted in 512 participants continuing their CAR regimen and an intention-to-treat population of 516 participants switching to the oral, once-daily, two-drug dolutegravir/rilpivirine regimen (dolutegravir 50 mg plus rilpivirine 25 mg).
Analysis of pooled SWORD1 and SWORD2 trials at the primary 48-week endpoint showed 95% of the participants for both the intent-to-treat, two-drug dolutegravir/rilpivirine therapy and the population maintaining their standard triple-drug CAR therapy continued to have successful viral suppression as evidenced by viral loads of fewer than 50 copies/mL. This result together with an adjusted treatment difference of –2.2% (95% confidence interval, –3.0 to 2.5) supports a noninferiority with a predefined margin of –8% of the dolutegravir/rilpivirine therapy to CAR for viral suppression as reported in the Lancet.
Reports of at least one adverse event by week 48 were slightly higher for the dolutegravir/rilpivirine therapy group (77%) when compared with those in the CAR group (71%). The most commonly experienced adverse effects were nasopharyngitis (10% each for dolutegravir/rilpivirine and CAR) and headache (8% for dolutegravir/rilpivirine vs. 5% for CAR). However, adverse effects were associated with higher withdrawals from the dolutegravir/rilpivirine therapy group, compared with the CAR group (3% vs. less than 1%, respectively) by the primary 48-week endpoint.
“Once-daily oral dolutegravir/rilpivirine therapy would be the first oral two-drug regimen that provides patients with an alternative to guideline-preferred triple-drug regimens, avoids major NRTI [nucleoside reverse transcriptase inhibitor] toxicities, has limited potential for drug-drug interactions, and does not increase lipid concentrations or inflammatory biomarkers,” according to Dr. Llibre and his colleagues.
The authors disclosed associations with financial and regulatory sponsor ViiV Healthcare and partner participation by Janssen Pharmaceutica NV in the development of the dolutegravir/rilpivirine two-drug regimen.
Source: Llibre JM et al. Lancet. 2018 Jan 10. doi: 10.1016/S0140-6736(17)33095-7.
Phase 3 clinical results show an oral, two-drug antiretroviral therapy (ART) of dolutegravir and rilpivirine to be an effective and safe alternative to a triple-drug current antiretroviral regimen (CAR) for maintaining virologic suppression of HIV-1 in adults.
Josep M Llibre, MD, from the department of infectious diseases at the Pujol University Hospital Germans Trias in Barcelona and his colleagues conducted a phase 3, randomized, parallel-group (SWORD-1 and SWORD-2), multicenter, noninferiority investigation. The pooled, open-label study reported on a total of 1,028 individuals, median age 43 years, who met a base criteria of stable viral suppression (viral load fewer than 50 copies/mL) by a first or second CAR regimen consisting of two nucleoside reverse transcriptase inhibitors (NRTIs) plus a third drug (nonnucleoside reverse transcriptase inhibitors, integrase strand transfer inhibitors, or a protease inhibitor) for a minimum of 6 months at time of screening. The overall population was 80% white, with women making up 22% of the pooled populations. Random assignment with stratification according to class, age, and planned substudy participation resulted in 512 participants continuing their CAR regimen and an intention-to-treat population of 516 participants switching to the oral, once-daily, two-drug dolutegravir/rilpivirine regimen (dolutegravir 50 mg plus rilpivirine 25 mg).
Analysis of pooled SWORD1 and SWORD2 trials at the primary 48-week endpoint showed 95% of the participants for both the intent-to-treat, two-drug dolutegravir/rilpivirine therapy and the population maintaining their standard triple-drug CAR therapy continued to have successful viral suppression as evidenced by viral loads of fewer than 50 copies/mL. This result together with an adjusted treatment difference of –2.2% (95% confidence interval, –3.0 to 2.5) supports a noninferiority with a predefined margin of –8% of the dolutegravir/rilpivirine therapy to CAR for viral suppression as reported in the Lancet.
Reports of at least one adverse event by week 48 were slightly higher for the dolutegravir/rilpivirine therapy group (77%) when compared with those in the CAR group (71%). The most commonly experienced adverse effects were nasopharyngitis (10% each for dolutegravir/rilpivirine and CAR) and headache (8% for dolutegravir/rilpivirine vs. 5% for CAR). However, adverse effects were associated with higher withdrawals from the dolutegravir/rilpivirine therapy group, compared with the CAR group (3% vs. less than 1%, respectively) by the primary 48-week endpoint.
“Once-daily oral dolutegravir/rilpivirine therapy would be the first oral two-drug regimen that provides patients with an alternative to guideline-preferred triple-drug regimens, avoids major NRTI [nucleoside reverse transcriptase inhibitor] toxicities, has limited potential for drug-drug interactions, and does not increase lipid concentrations or inflammatory biomarkers,” according to Dr. Llibre and his colleagues.
The authors disclosed associations with financial and regulatory sponsor ViiV Healthcare and partner participation by Janssen Pharmaceutica NV in the development of the dolutegravir/rilpivirine two-drug regimen.
Source: Llibre JM et al. Lancet. 2018 Jan 10. doi: 10.1016/S0140-6736(17)33095-7.
FROM THE LANCET
Key clinical point: No difference was seen in maintaining virologic suppression of HIV-1 in adults switching from a traditional triple-drug regimen to a dolutegravir/rilpivirine dual-drug antiretroviral therapy.
Major finding: Of the participants in both the dual- and triple-drug groups, 95% maintained suppression to a viral load of fewer than 50 copies/mL.Study details: Two identical parallel-group studies (SWORD1 and SWORD2) of 1,024 adults participants randomly assigned in a 1:1 ratio comparing two-drug dolutegravir/rilpivirine with the active-control current triple-drug group.
Disclosures: The authors disclosed associations with financial and regulatory sponsor ViiV Healthcare and partner participation by Janssen Pharmaceutica NV in the development of the dolutegravir/rilpivirine two-drug regimen.
Source: Llibre JM et al. Lancet. 2018 Jan 10. doi: 10.1016/S0140-6736(17)33095-7.
FDA issues safety measures for all gadolinium-based contrast agents for MRI
A US Food & Drug Administration (FDA) Drug Safety Communication concerning a New Class Warning for all gadolinium-based contrast agents (GBCAs) for magnetic resonance imaging (MRI) has been released. Gadolinium has been found to remain in patients’ bodies, including the brain, for months to years.1
The FDA concluded that the benefit of all approved GBCAs outweighs any potential risks because gadolinium retention has not been directly linked to adverse health effects in patients with normal kidney function. To date, the only known adverse health effect related to gadolinium retention is a rare condition called nephrogenic systemic fibrosis that occurs in a small subgroup of patients with preexisting kidney failure. However, the FDA has recently received reports of adverse events involving multiple organ systems in patients with normal kidney function.1
After a review by the Medical Imaging Drugs Advisory Committee, the FDA is requiring several actions1:
- the development of a new Patient Medication Guide for GBCAs
- a requirement that every patient must read educational information before receiving a GBCA
- manufacturers of GBCAs must conduct human and animal studies to further assess the safety of these contrast agents.
FDA recommendations for your practice
The FDA advises that health care professionals should consider the retention characteristics of each agent when choosing a GBCA for patients who might be of higher risk for gadolinium retention.1,2 These patients include1:
- those requiring multiple lifetime doses
- pregnant women
- children
- patients with inflammatory conditions.
There are 2 types of GBCAs based on chemical structure: linear and macrocyclic. Linear GBCAs result in more retention and retention for a longer time than macrocyclic GBCAs.2 A list of FDA-approved GBCAs with their chemical structures is found here: https://www.fda.gov/Drugs/DrugSafety/ucm589213.htm.2
Recommendations also state that repeated GBCA imaging studies be minimized when possible, particularly closely spaced MRI studies. However, necessary GBCA MRI scans should not be avoided or deferred.1
Report adverse effects
Health care professionals and patients are encouraged to report adverse effects or side effects related to the use of GBCAs to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program found here: https://www.accessdata.fda.gov/scripts/medwatch/index.cfm?action=reporting.home.
- US Food & Drug Administration. Safety: Gadolinium-based Contrast Agents (GBCAs): Drug Safety Communication - Retained in Body; New Class Warnings. https://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm589580.htm. Published December 19, 2017. Accessed January 10, 2018.
- US Food & Drug Administration. Drugs: FDA Drug Safety Communication: FDA warns that gadolinium-based contrast agents (GBCAs) are retained in the body; requires new class warning. https://www.fda.gov/Drugs/DrugSafety/ucm589213.htm. Published December 19, 2017. Accessed January 10, 2018.
A US Food & Drug Administration (FDA) Drug Safety Communication concerning a New Class Warning for all gadolinium-based contrast agents (GBCAs) for magnetic resonance imaging (MRI) has been released. Gadolinium has been found to remain in patients’ bodies, including the brain, for months to years.1
The FDA concluded that the benefit of all approved GBCAs outweighs any potential risks because gadolinium retention has not been directly linked to adverse health effects in patients with normal kidney function. To date, the only known adverse health effect related to gadolinium retention is a rare condition called nephrogenic systemic fibrosis that occurs in a small subgroup of patients with preexisting kidney failure. However, the FDA has recently received reports of adverse events involving multiple organ systems in patients with normal kidney function.1
After a review by the Medical Imaging Drugs Advisory Committee, the FDA is requiring several actions1:
- the development of a new Patient Medication Guide for GBCAs
- a requirement that every patient must read educational information before receiving a GBCA
- manufacturers of GBCAs must conduct human and animal studies to further assess the safety of these contrast agents.
FDA recommendations for your practice
The FDA advises that health care professionals should consider the retention characteristics of each agent when choosing a GBCA for patients who might be of higher risk for gadolinium retention.1,2 These patients include1:
- those requiring multiple lifetime doses
- pregnant women
- children
- patients with inflammatory conditions.
There are 2 types of GBCAs based on chemical structure: linear and macrocyclic. Linear GBCAs result in more retention and retention for a longer time than macrocyclic GBCAs.2 A list of FDA-approved GBCAs with their chemical structures is found here: https://www.fda.gov/Drugs/DrugSafety/ucm589213.htm.2
Recommendations also state that repeated GBCA imaging studies be minimized when possible, particularly closely spaced MRI studies. However, necessary GBCA MRI scans should not be avoided or deferred.1
Report adverse effects
Health care professionals and patients are encouraged to report adverse effects or side effects related to the use of GBCAs to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program found here: https://www.accessdata.fda.gov/scripts/medwatch/index.cfm?action=reporting.home.
A US Food & Drug Administration (FDA) Drug Safety Communication concerning a New Class Warning for all gadolinium-based contrast agents (GBCAs) for magnetic resonance imaging (MRI) has been released. Gadolinium has been found to remain in patients’ bodies, including the brain, for months to years.1
The FDA concluded that the benefit of all approved GBCAs outweighs any potential risks because gadolinium retention has not been directly linked to adverse health effects in patients with normal kidney function. To date, the only known adverse health effect related to gadolinium retention is a rare condition called nephrogenic systemic fibrosis that occurs in a small subgroup of patients with preexisting kidney failure. However, the FDA has recently received reports of adverse events involving multiple organ systems in patients with normal kidney function.1
After a review by the Medical Imaging Drugs Advisory Committee, the FDA is requiring several actions1:
- the development of a new Patient Medication Guide for GBCAs
- a requirement that every patient must read educational information before receiving a GBCA
- manufacturers of GBCAs must conduct human and animal studies to further assess the safety of these contrast agents.
FDA recommendations for your practice
The FDA advises that health care professionals should consider the retention characteristics of each agent when choosing a GBCA for patients who might be of higher risk for gadolinium retention.1,2 These patients include1:
- those requiring multiple lifetime doses
- pregnant women
- children
- patients with inflammatory conditions.
There are 2 types of GBCAs based on chemical structure: linear and macrocyclic. Linear GBCAs result in more retention and retention for a longer time than macrocyclic GBCAs.2 A list of FDA-approved GBCAs with their chemical structures is found here: https://www.fda.gov/Drugs/DrugSafety/ucm589213.htm.2
Recommendations also state that repeated GBCA imaging studies be minimized when possible, particularly closely spaced MRI studies. However, necessary GBCA MRI scans should not be avoided or deferred.1
Report adverse effects
Health care professionals and patients are encouraged to report adverse effects or side effects related to the use of GBCAs to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program found here: https://www.accessdata.fda.gov/scripts/medwatch/index.cfm?action=reporting.home.
- US Food & Drug Administration. Safety: Gadolinium-based Contrast Agents (GBCAs): Drug Safety Communication - Retained in Body; New Class Warnings. https://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm589580.htm. Published December 19, 2017. Accessed January 10, 2018.
- US Food & Drug Administration. Drugs: FDA Drug Safety Communication: FDA warns that gadolinium-based contrast agents (GBCAs) are retained in the body; requires new class warning. https://www.fda.gov/Drugs/DrugSafety/ucm589213.htm. Published December 19, 2017. Accessed January 10, 2018.
- US Food & Drug Administration. Safety: Gadolinium-based Contrast Agents (GBCAs): Drug Safety Communication - Retained in Body; New Class Warnings. https://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm589580.htm. Published December 19, 2017. Accessed January 10, 2018.
- US Food & Drug Administration. Drugs: FDA Drug Safety Communication: FDA warns that gadolinium-based contrast agents (GBCAs) are retained in the body; requires new class warning. https://www.fda.gov/Drugs/DrugSafety/ucm589213.htm. Published December 19, 2017. Accessed January 10, 2018.