User login
ASCO: Eribulin results ‘a giant step for sarcoma’
CHICAGO – For the first time ever, a new drug has shown a survival advantage – albeit a small one – in metastatic soft tissue sarcomas, diseases that are almost without exception unresponsive to medical therapies and rapidly fatal.
In a randomized, phase III trial, median overall survival for patients with metastatic leiomyosarcoma or liposarcoma treated with eribulin (Halaven) was 13.5 months compared with 11.5 months for patients treated with dacarbazine.

“For me as a clinical oncologist, this a clinically meaningful result given the unmet need in this rare, hard-to-treat family of diseases,” said lead investigator Dr. Patrick Schöffski, professor of medicine and head of experimental oncology lab at University Hospitals in Leuven, Belgium, at the annual meeting of the American Society of Clinical Oncology.
“I’ve been an oncologist for over 20 years, and there has never been a positive sarcoma study for survival – ever,” said ASCO expert Dr. Gary K. Schwartz, chief of hematology and oncology at Columbia University, New York, who was not involved in the study. “This is the first positive sarcoma study showing a survival benefit with any chemotherapy in the history of medical oncology.”
The findings represent “a small step for cancer, and a giant step for sarcoma.” Dr. Schwartz said at a press briefing.
In an interview, he added that he was “shocked” when he found out that the survival benefit with eribulin was seen in patients with liposarcoma as well as leiomyosarcoma. “I thought that the benefit would only be in patients with leiomyosarcoma,” he said.
Leiomyosarcoma and liposarcoma, also called adipocytic sarcoma, are two of the most common histologic subtypes of highly uncommon soft tissue sarcomas. Patients with advanced metastatic sarcomas generally have a very poor prognosis and precious few treatment options.
Eribulin is a synthetic analogue of halichondrin B, a macrolide antibiotic isolated from a sea sponge that has strong cytotoxic properties. In preclinical studies, it was shown to kill cancer cells via anti-mitotic effects. It is approved in the United States for treatment of patients with metastatic breast cancer for whom at least two other lines of therapy have failed.
Dr. Schöffski and colleagues in centers in the United States, Europe, and Korea randomly assigned patients with metastatic intermediate or high-grade leiomyosarcoma or liposarcoma to receive either eribulin 1.4 mg/m2 on days 1 and 8 of 21-day cycles (228 patients), or conventional therapy with dacarbazine 850, 1,000, or 1,200 mg/m2 on day 1 of every 21 day cycle (224 patients).
The majority of patients had undergone at least two prior regimens for advanced disease.
The trial met its primary endpoint of an overall survival advantage, with median OS of 13.5 months for patients on eribulin, compared with 11.5 months for those on dacarbazine. The hazard ratio (HR) was 0.768 favoring eirbulin (P = .0169).
The median progression-free survival was 2.6 months in each group.
In all, 26% of patients on eribulin and 14% on dacarbazine required dose reductions, and 8% and 5%, respectively, discontinued therapy because of treatment-emergent adverse events.
The most common grade 3 or greater toxicities in each arm were neutropenia, fatigue, and nausea. The adverse events in general were in line with known safety profiles for each agent, Dr. Schöffski said.
There were 10 deaths among patients on eribulin, two of which were attributed to the drug (1 neutropenic sepsis and one sepsis). There were three deaths among patients on dacarbazine, none attributed to therapy.
In an interview, Dr. Schöffski noted that he has treated one patient, a man with dedifferentiated liposarcoma, with 46 cycles of eribulin, “so we see activity in a tumor type that is notoriously resistant to established drugs.”
He said that moving forward, investigators may wish to test eribulin in combination with other drugs, such as therapies targeted to genetic mutations, immunotherapies, or other approaches.
The study was sponsored by Eisai, Inc. Dr. Schöffski and Dr. Schwartz reported having no relevant conflicts of interest.
CHICAGO – For the first time ever, a new drug has shown a survival advantage – albeit a small one – in metastatic soft tissue sarcomas, diseases that are almost without exception unresponsive to medical therapies and rapidly fatal.
In a randomized, phase III trial, median overall survival for patients with metastatic leiomyosarcoma or liposarcoma treated with eribulin (Halaven) was 13.5 months compared with 11.5 months for patients treated with dacarbazine.
“For me as a clinical oncologist, this a clinically meaningful result given the unmet need in this rare, hard-to-treat family of diseases,” said lead investigator Dr. Patrick Schöffski, professor of medicine and head of experimental oncology lab at University Hospitals in Leuven, Belgium, at the annual meeting of the American Society of Clinical Oncology.
“I’ve been an oncologist for over 20 years, and there has never been a positive sarcoma study for survival – ever,” said ASCO expert Dr. Gary K. Schwartz, chief of hematology and oncology at Columbia University, New York, who was not involved in the study. “This is the first positive sarcoma study showing a survival benefit with any chemotherapy in the history of medical oncology.”
The findings represent “a small step for cancer, and a giant step for sarcoma.” Dr. Schwartz said at a press briefing.
In an interview, he added that he was “shocked” when he found out that the survival benefit with eribulin was seen in patients with liposarcoma as well as leiomyosarcoma. “I thought that the benefit would only be in patients with leiomyosarcoma,” he said.
Leiomyosarcoma and liposarcoma, also called adipocytic sarcoma, are two of the most common histologic subtypes of highly uncommon soft tissue sarcomas. Patients with advanced metastatic sarcomas generally have a very poor prognosis and precious few treatment options.
Eribulin is a synthetic analogue of halichondrin B, a macrolide antibiotic isolated from a sea sponge that has strong cytotoxic properties. In preclinical studies, it was shown to kill cancer cells via anti-mitotic effects. It is approved in the United States for treatment of patients with metastatic breast cancer for whom at least two other lines of therapy have failed.
Dr. Schöffski and colleagues in centers in the United States, Europe, and Korea randomly assigned patients with metastatic intermediate or high-grade leiomyosarcoma or liposarcoma to receive either eribulin 1.4 mg/m2 on days 1 and 8 of 21-day cycles (228 patients), or conventional therapy with dacarbazine 850, 1,000, or 1,200 mg/m2 on day 1 of every 21 day cycle (224 patients).
The majority of patients had undergone at least two prior regimens for advanced disease.
The trial met its primary endpoint of an overall survival advantage, with median OS of 13.5 months for patients on eribulin, compared with 11.5 months for those on dacarbazine. The hazard ratio (HR) was 0.768 favoring eirbulin (P = .0169).
The median progression-free survival was 2.6 months in each group.
In all, 26% of patients on eribulin and 14% on dacarbazine required dose reductions, and 8% and 5%, respectively, discontinued therapy because of treatment-emergent adverse events.
The most common grade 3 or greater toxicities in each arm were neutropenia, fatigue, and nausea. The adverse events in general were in line with known safety profiles for each agent, Dr. Schöffski said.
There were 10 deaths among patients on eribulin, two of which were attributed to the drug (1 neutropenic sepsis and one sepsis). There were three deaths among patients on dacarbazine, none attributed to therapy.
In an interview, Dr. Schöffski noted that he has treated one patient, a man with dedifferentiated liposarcoma, with 46 cycles of eribulin, “so we see activity in a tumor type that is notoriously resistant to established drugs.”
He said that moving forward, investigators may wish to test eribulin in combination with other drugs, such as therapies targeted to genetic mutations, immunotherapies, or other approaches.
The study was sponsored by Eisai, Inc. Dr. Schöffski and Dr. Schwartz reported having no relevant conflicts of interest.
CHICAGO – For the first time ever, a new drug has shown a survival advantage – albeit a small one – in metastatic soft tissue sarcomas, diseases that are almost without exception unresponsive to medical therapies and rapidly fatal.
In a randomized, phase III trial, median overall survival for patients with metastatic leiomyosarcoma or liposarcoma treated with eribulin (Halaven) was 13.5 months compared with 11.5 months for patients treated with dacarbazine.
“For me as a clinical oncologist, this a clinically meaningful result given the unmet need in this rare, hard-to-treat family of diseases,” said lead investigator Dr. Patrick Schöffski, professor of medicine and head of experimental oncology lab at University Hospitals in Leuven, Belgium, at the annual meeting of the American Society of Clinical Oncology.
“I’ve been an oncologist for over 20 years, and there has never been a positive sarcoma study for survival – ever,” said ASCO expert Dr. Gary K. Schwartz, chief of hematology and oncology at Columbia University, New York, who was not involved in the study. “This is the first positive sarcoma study showing a survival benefit with any chemotherapy in the history of medical oncology.”
The findings represent “a small step for cancer, and a giant step for sarcoma.” Dr. Schwartz said at a press briefing.
In an interview, he added that he was “shocked” when he found out that the survival benefit with eribulin was seen in patients with liposarcoma as well as leiomyosarcoma. “I thought that the benefit would only be in patients with leiomyosarcoma,” he said.
Leiomyosarcoma and liposarcoma, also called adipocytic sarcoma, are two of the most common histologic subtypes of highly uncommon soft tissue sarcomas. Patients with advanced metastatic sarcomas generally have a very poor prognosis and precious few treatment options.
Eribulin is a synthetic analogue of halichondrin B, a macrolide antibiotic isolated from a sea sponge that has strong cytotoxic properties. In preclinical studies, it was shown to kill cancer cells via anti-mitotic effects. It is approved in the United States for treatment of patients with metastatic breast cancer for whom at least two other lines of therapy have failed.
Dr. Schöffski and colleagues in centers in the United States, Europe, and Korea randomly assigned patients with metastatic intermediate or high-grade leiomyosarcoma or liposarcoma to receive either eribulin 1.4 mg/m2 on days 1 and 8 of 21-day cycles (228 patients), or conventional therapy with dacarbazine 850, 1,000, or 1,200 mg/m2 on day 1 of every 21 day cycle (224 patients).
The majority of patients had undergone at least two prior regimens for advanced disease.
The trial met its primary endpoint of an overall survival advantage, with median OS of 13.5 months for patients on eribulin, compared with 11.5 months for those on dacarbazine. The hazard ratio (HR) was 0.768 favoring eirbulin (P = .0169).
The median progression-free survival was 2.6 months in each group.
In all, 26% of patients on eribulin and 14% on dacarbazine required dose reductions, and 8% and 5%, respectively, discontinued therapy because of treatment-emergent adverse events.
The most common grade 3 or greater toxicities in each arm were neutropenia, fatigue, and nausea. The adverse events in general were in line with known safety profiles for each agent, Dr. Schöffski said.
There were 10 deaths among patients on eribulin, two of which were attributed to the drug (1 neutropenic sepsis and one sepsis). There were three deaths among patients on dacarbazine, none attributed to therapy.
In an interview, Dr. Schöffski noted that he has treated one patient, a man with dedifferentiated liposarcoma, with 46 cycles of eribulin, “so we see activity in a tumor type that is notoriously resistant to established drugs.”
He said that moving forward, investigators may wish to test eribulin in combination with other drugs, such as therapies targeted to genetic mutations, immunotherapies, or other approaches.
The study was sponsored by Eisai, Inc. Dr. Schöffski and Dr. Schwartz reported having no relevant conflicts of interest.
AT ASCO 2015
Key clinical point: Eribulin is the first drug shown in a clinical trial to offer a survival advantage over existing therapies for metastatic soft-tissue sarcomas.
Major finding: Median overall survival was 13.5 months for patients treated with eribulin vs. 11.5 months for those treated with dacarbazine.
Data source: Randomized clinical trial in 452 patients with metastatic leiomyosarcoma or liposarcoma.
Disclosures: The study was sponsored by Eisai, Inc. Dr. Schöffski reported having no relevant conflicts of interest.

Drug improves upon standard therapy for relapsed CLL/SLL, speaker says

Chanan-Khan, MD
© ASCO/Zach Boyden-Holmes
CHICAGO—Interim results of the phase 3 HELIOS trial suggest that adding ibrutinib to treatment with bendamustine and rituximab (BR) improves outcomes for patients with relapsed chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL).
Patients who received ibrutinib and BR had significantly higher response rates and a significantly longer progression-free survival than patients who received BR with placebo.
There was no significant difference between the arms with regard to overall survival, but the researchers said these results were confounded by the fact that 31% of patients in the placebo arm crossed over to the ibrutinib arm after they progressed.
“We found that ibrutinib can be safely paired with existing therapy to powerfully prolong remissions and improve patients’ well-being,” said study investigator Asher Alban Akmal Chanan-Khan, MD, of the Mayo Clinic in Jacksonville, Florida.
Dr Chanan-Khan presented these findings at the 2015 ASCO Annual Meeting (abstract LBA7005). The research was funded by Janssen Research & Development, LLC, the company co-developing ibrutinib with Pharmacyclics.
The study included 578 patients with previously treated CLL/SLL, excluding those with del(17p). The patients were randomized to receive 6 cycles of BR plus once-daily ibrutinib (n=289) or 6 cycles of BR plus placebo (n=289). Ibrutinib and placebo were given until disease progression or unacceptable toxicity.
Dr Chanan-Khan said baseline characteristics were comparable between the treatment arms. For each arm, the median number of prior treatments was 2, more than 50% of patients had bulky disease, and about 80% of patients had unmutated IGVH.
“[However,] advanced Rai-stage disease was observed in a slightly [greater] proportion of patients in the control arm versus the ibrutinib arm,” Dr Chanan-Khan noted. “Conversely, a higher proportion of patients with del(11q) was noted in the ibrutinib-containing arm.”
Ultimately, 81.9% (n=235) of patients in the ibrutinib arm and 77.4% (n=222) of those in the placebo arm received their assigned 6 cycles of BR. At the time of analysis, the rate of treatment discontinuation was 29.1% (n=84) in the ibrutinib arm and 64.7% in the placebo arm (n=187).
Those patients who progressed on placebo were allowed to cross over to the ibrutinib arm, and 90 patients had crossed over at the time of the interim analysis.
Response and survival
The study’s primary endpoint was progression-free survival, as assessed by an independent review committee (IRC), in the intent-to-treat population (n=289 in each arm).
At a median follow-up of 17 months, progression-free survival was 13.3 months in the placebo arm and was not reached in the ibrutinib arm (P<0.0001).
“The hazard ratio on this particular survival curve is 0.20, which translates into a reduced risk of progression or death by 80%,” Dr Chanan-Khan said. “This is remarkable. You cannot get a better hazard ratio than this.”
Dr Chanan-Khan also noted that the overall response rate was significantly higher in the ibrutinib arm than the placebo arm. The rates were 82.7% and 67.8%, respectively (P<0.0001), according to the IRC, and 86.2% and 68.9%, respectively (P<0.0001), according to investigator assessment.
The rate of complete response plus complete response with incomplete blood count recovery was 10.4% in the ibrutinib arm and 2.8% in the placebo arm, according to the IRC. According to investigator assessment, the rates were 21.4% and 5.9%, respectively.
The median overall survival was not reached in either arm, and the hazard ratio was 0.628 (P=0.0598).
Adverse events
Dr Chanan-Kahn said the safety profile of the ibrutinib-BR combination was consistent with the safety profiles of each individual drug.
The incidence of adverse events was 70.7% in the ibrutinib-BR arm and 70% in the placebo-BR arm. The most common events were neutropenia (58.2% and 54.7%, respectively), nausea (36.9% vs 35.2%), diarrhea (35.5% vs 23.7%), thrombocytopenia (30.7% vs 24.4%), pyrexia (24.7% vs 22%), anemia (22.6% vs 28.9%), and fatigue (21.6% vs 22.6%).
The incidence of grade 3/4 adverse events was 28.9% in the ibrutinib arm and 25% in the placebo arm. The most common of these were neutropenia (53.7% vs 50.5%) and thrombocytopenia (15% in both arms).
Atrial fibrillation was seen in 7.3% of patients in the ibrutinib arm and 2.8% in the placebo arm. Grade 3/4 atrial fibrillation occurred in 2.8% and 0.7% of patients, respectively. The incidence of tumor lysis syndrome was 3.5% in both arms.
The rate of bleeding was 31% in the ibrutinib arm and 14.6% in the placebo arm. And the rates of major hemorrhage were 3.8% and 1.7%, respectively.
Adverse events were the primary reason for discontinuation in patients who received ibrutinib—14.2%, compared to 11.8% of patients who received placebo. The primary reason for discontinuation in the placebo arm was progressive disease or relapse—45%, compared to 4.8% in the ibrutinib arm.
Taken together, the results of this trial suggest treatment with ibrutinib and BR is superior to standard BR therapy in patients with relapsed CLL/SLL, Dr Chanan-Kahn said.
“This was one of the most rigorous clinical trials ever conducted in CLL,” he said, “and it truly validates ibrutinib as an important drug for this cancer.” ![]()
Chanan-Khan, MD
© ASCO/Zach Boyden-Holmes
CHICAGO—Interim results of the phase 3 HELIOS trial suggest that adding ibrutinib to treatment with bendamustine and rituximab (BR) improves outcomes for patients with relapsed chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL).
Patients who received ibrutinib and BR had significantly higher response rates and a significantly longer progression-free survival than patients who received BR with placebo.
There was no significant difference between the arms with regard to overall survival, but the researchers said these results were confounded by the fact that 31% of patients in the placebo arm crossed over to the ibrutinib arm after they progressed.
“We found that ibrutinib can be safely paired with existing therapy to powerfully prolong remissions and improve patients’ well-being,” said study investigator Asher Alban Akmal Chanan-Khan, MD, of the Mayo Clinic in Jacksonville, Florida.
Dr Chanan-Khan presented these findings at the 2015 ASCO Annual Meeting (abstract LBA7005). The research was funded by Janssen Research & Development, LLC, the company co-developing ibrutinib with Pharmacyclics.
The study included 578 patients with previously treated CLL/SLL, excluding those with del(17p). The patients were randomized to receive 6 cycles of BR plus once-daily ibrutinib (n=289) or 6 cycles of BR plus placebo (n=289). Ibrutinib and placebo were given until disease progression or unacceptable toxicity.
Dr Chanan-Khan said baseline characteristics were comparable between the treatment arms. For each arm, the median number of prior treatments was 2, more than 50% of patients had bulky disease, and about 80% of patients had unmutated IGVH.
“[However,] advanced Rai-stage disease was observed in a slightly [greater] proportion of patients in the control arm versus the ibrutinib arm,” Dr Chanan-Khan noted. “Conversely, a higher proportion of patients with del(11q) was noted in the ibrutinib-containing arm.”
Ultimately, 81.9% (n=235) of patients in the ibrutinib arm and 77.4% (n=222) of those in the placebo arm received their assigned 6 cycles of BR. At the time of analysis, the rate of treatment discontinuation was 29.1% (n=84) in the ibrutinib arm and 64.7% in the placebo arm (n=187).
Those patients who progressed on placebo were allowed to cross over to the ibrutinib arm, and 90 patients had crossed over at the time of the interim analysis.
Response and survival
The study’s primary endpoint was progression-free survival, as assessed by an independent review committee (IRC), in the intent-to-treat population (n=289 in each arm).
At a median follow-up of 17 months, progression-free survival was 13.3 months in the placebo arm and was not reached in the ibrutinib arm (P<0.0001).
“The hazard ratio on this particular survival curve is 0.20, which translates into a reduced risk of progression or death by 80%,” Dr Chanan-Khan said. “This is remarkable. You cannot get a better hazard ratio than this.”
Dr Chanan-Khan also noted that the overall response rate was significantly higher in the ibrutinib arm than the placebo arm. The rates were 82.7% and 67.8%, respectively (P<0.0001), according to the IRC, and 86.2% and 68.9%, respectively (P<0.0001), according to investigator assessment.
The rate of complete response plus complete response with incomplete blood count recovery was 10.4% in the ibrutinib arm and 2.8% in the placebo arm, according to the IRC. According to investigator assessment, the rates were 21.4% and 5.9%, respectively.
The median overall survival was not reached in either arm, and the hazard ratio was 0.628 (P=0.0598).
Adverse events
Dr Chanan-Kahn said the safety profile of the ibrutinib-BR combination was consistent with the safety profiles of each individual drug.
The incidence of adverse events was 70.7% in the ibrutinib-BR arm and 70% in the placebo-BR arm. The most common events were neutropenia (58.2% and 54.7%, respectively), nausea (36.9% vs 35.2%), diarrhea (35.5% vs 23.7%), thrombocytopenia (30.7% vs 24.4%), pyrexia (24.7% vs 22%), anemia (22.6% vs 28.9%), and fatigue (21.6% vs 22.6%).
The incidence of grade 3/4 adverse events was 28.9% in the ibrutinib arm and 25% in the placebo arm. The most common of these were neutropenia (53.7% vs 50.5%) and thrombocytopenia (15% in both arms).
Atrial fibrillation was seen in 7.3% of patients in the ibrutinib arm and 2.8% in the placebo arm. Grade 3/4 atrial fibrillation occurred in 2.8% and 0.7% of patients, respectively. The incidence of tumor lysis syndrome was 3.5% in both arms.
The rate of bleeding was 31% in the ibrutinib arm and 14.6% in the placebo arm. And the rates of major hemorrhage were 3.8% and 1.7%, respectively.
Adverse events were the primary reason for discontinuation in patients who received ibrutinib—14.2%, compared to 11.8% of patients who received placebo. The primary reason for discontinuation in the placebo arm was progressive disease or relapse—45%, compared to 4.8% in the ibrutinib arm.
Taken together, the results of this trial suggest treatment with ibrutinib and BR is superior to standard BR therapy in patients with relapsed CLL/SLL, Dr Chanan-Kahn said.
“This was one of the most rigorous clinical trials ever conducted in CLL,” he said, “and it truly validates ibrutinib as an important drug for this cancer.” ![]()
Chanan-Khan, MD
© ASCO/Zach Boyden-Holmes
CHICAGO—Interim results of the phase 3 HELIOS trial suggest that adding ibrutinib to treatment with bendamustine and rituximab (BR) improves outcomes for patients with relapsed chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL).
Patients who received ibrutinib and BR had significantly higher response rates and a significantly longer progression-free survival than patients who received BR with placebo.
There was no significant difference between the arms with regard to overall survival, but the researchers said these results were confounded by the fact that 31% of patients in the placebo arm crossed over to the ibrutinib arm after they progressed.
“We found that ibrutinib can be safely paired with existing therapy to powerfully prolong remissions and improve patients’ well-being,” said study investigator Asher Alban Akmal Chanan-Khan, MD, of the Mayo Clinic in Jacksonville, Florida.
Dr Chanan-Khan presented these findings at the 2015 ASCO Annual Meeting (abstract LBA7005). The research was funded by Janssen Research & Development, LLC, the company co-developing ibrutinib with Pharmacyclics.
The study included 578 patients with previously treated CLL/SLL, excluding those with del(17p). The patients were randomized to receive 6 cycles of BR plus once-daily ibrutinib (n=289) or 6 cycles of BR plus placebo (n=289). Ibrutinib and placebo were given until disease progression or unacceptable toxicity.
Dr Chanan-Khan said baseline characteristics were comparable between the treatment arms. For each arm, the median number of prior treatments was 2, more than 50% of patients had bulky disease, and about 80% of patients had unmutated IGVH.
“[However,] advanced Rai-stage disease was observed in a slightly [greater] proportion of patients in the control arm versus the ibrutinib arm,” Dr Chanan-Khan noted. “Conversely, a higher proportion of patients with del(11q) was noted in the ibrutinib-containing arm.”
Ultimately, 81.9% (n=235) of patients in the ibrutinib arm and 77.4% (n=222) of those in the placebo arm received their assigned 6 cycles of BR. At the time of analysis, the rate of treatment discontinuation was 29.1% (n=84) in the ibrutinib arm and 64.7% in the placebo arm (n=187).
Those patients who progressed on placebo were allowed to cross over to the ibrutinib arm, and 90 patients had crossed over at the time of the interim analysis.
Response and survival
The study’s primary endpoint was progression-free survival, as assessed by an independent review committee (IRC), in the intent-to-treat population (n=289 in each arm).
At a median follow-up of 17 months, progression-free survival was 13.3 months in the placebo arm and was not reached in the ibrutinib arm (P<0.0001).
“The hazard ratio on this particular survival curve is 0.20, which translates into a reduced risk of progression or death by 80%,” Dr Chanan-Khan said. “This is remarkable. You cannot get a better hazard ratio than this.”
Dr Chanan-Khan also noted that the overall response rate was significantly higher in the ibrutinib arm than the placebo arm. The rates were 82.7% and 67.8%, respectively (P<0.0001), according to the IRC, and 86.2% and 68.9%, respectively (P<0.0001), according to investigator assessment.
The rate of complete response plus complete response with incomplete blood count recovery was 10.4% in the ibrutinib arm and 2.8% in the placebo arm, according to the IRC. According to investigator assessment, the rates were 21.4% and 5.9%, respectively.
The median overall survival was not reached in either arm, and the hazard ratio was 0.628 (P=0.0598).
Adverse events
Dr Chanan-Kahn said the safety profile of the ibrutinib-BR combination was consistent with the safety profiles of each individual drug.
The incidence of adverse events was 70.7% in the ibrutinib-BR arm and 70% in the placebo-BR arm. The most common events were neutropenia (58.2% and 54.7%, respectively), nausea (36.9% vs 35.2%), diarrhea (35.5% vs 23.7%), thrombocytopenia (30.7% vs 24.4%), pyrexia (24.7% vs 22%), anemia (22.6% vs 28.9%), and fatigue (21.6% vs 22.6%).
The incidence of grade 3/4 adverse events was 28.9% in the ibrutinib arm and 25% in the placebo arm. The most common of these were neutropenia (53.7% vs 50.5%) and thrombocytopenia (15% in both arms).
Atrial fibrillation was seen in 7.3% of patients in the ibrutinib arm and 2.8% in the placebo arm. Grade 3/4 atrial fibrillation occurred in 2.8% and 0.7% of patients, respectively. The incidence of tumor lysis syndrome was 3.5% in both arms.
The rate of bleeding was 31% in the ibrutinib arm and 14.6% in the placebo arm. And the rates of major hemorrhage were 3.8% and 1.7%, respectively.
Adverse events were the primary reason for discontinuation in patients who received ibrutinib—14.2%, compared to 11.8% of patients who received placebo. The primary reason for discontinuation in the placebo arm was progressive disease or relapse—45%, compared to 4.8% in the ibrutinib arm.
Taken together, the results of this trial suggest treatment with ibrutinib and BR is superior to standard BR therapy in patients with relapsed CLL/SLL, Dr Chanan-Kahn said.
“This was one of the most rigorous clinical trials ever conducted in CLL,” he said, “and it truly validates ibrutinib as an important drug for this cancer.” ![]()
Carotid artery stenosis guidelines need modernizing
VIENNA – Guidelines used around the world for the management of carotid stenosis, both in asymptomatic and symptomatic cases, are often outdated and do not match current evidence, according to the results of a systematic review undertaken by an international group of experts.*
Furthermore, the qualifying statements used to back up the recommendations are often confused and too simplistic, being based only on the degree of randomized data used.

“Other problems were that the guidelines often didn’t even define asymptomatic carotid artery stenosis or symptomatic carotid artery stenosis or they left out procedural standards,” said Dr. Anne Abbott, who presented the findings at the annual European Stroke Conference.
“A number of important discoveries have been made in recent years to better inform treatment decisions for patients with carotid stenosis,” Dr. Abbott, a neurologist at Monash University in Melbourne, Australia, observed.
For instance, based on evidence available today, it is clear that medical therapy alone is best for patients with moderate or severe (50%-99%) asymptomatic disease. Surgery in these patients might actually be harmful, she noted, and it is unknown if or by how much carotid endarterectomy improves stroke prevention versus medical therapy alone.
“We just haven’t done the studies, and this is where we should be concentrating our efforts with respect to randomized, placebo-controlled trials,” Dr. Abbott proposed. “But we do know that the 6% 30-day stroke/death rate [with endarterectomy] is really now too high.”
It’s also now apparent that carotid angioplasty or stenting is more harmful than carotid endarterectomy in asymptomatic patients and “shouldn’t be recommended for routine practice.” Many of the guidelines were still supporting this as an option, she observed, based on the supposed counterbalancing argument that surgical intervention was more likely to increase the risk for heart attacks than stenting. However, the evidence shows that the greatest risk to patients in the periprocedural period is the stroke risk, which is increased by stenting.
Dr. Abbott explained how the team of 16 experts had reviewed all the latest available guidelines for asymptomatic and symptomatic carotid stenosis that they could find from published from January 2008 until January 2015. She noted that guidelines were often difficult to access were often only found because the team knew of their existence through their professional networks.
A total of 34 guidelines from 23 regions or countries in six languages were identified and included in the review. Each of these was independently assessed by two to six of the team, looking at the clinical scenarios covered, the nature of the recommendations made and what evidence was being used to support the recommendations.
Of 28 guidelines that gave recommendations for asymptomatic carotid stenosis, surgery was endorsed for patients at average surgical risk and only one (4%) endorsed medical treatment alone. Eighteen (64%) recommended that stenting be performed or considered, and 24 (86%) supported the use of endarterectomy. “This is despite current evidence that these procedures are now more likely to harm than help patients,” Dr. Abbott said.
“Of major concern I think is that a high proportion, about half, of these guidelines are recommending stenting for high surgical risk asymptomatic patients, she cautioned. “This includes patients with major medical comorbidities – heart failure, respiratory failure – who have a very short life expectancy and are least likely to benefit and are more likely to be at risk from the procedures.”
Somewhat similar findings were seen regarding the use of stenting and surgery in the 33 guidelines that gave recommendations for the management of symptomatic carotid stenosis. Endarterectomy was recommended for average-surgical-risk symptomatic patients by 31 (94%) guidelines and, worryingly, stenting was still being advocated in 19 (58%) guidelines with only nine (27%) saying that stenting should not be used. Stenting was also being endorsed in symptomatic patients at high surgical risk.
Dr. Abbott said that the guidelines were hard to compare because they used a variety of qualifying statements to try to advise on the degree to which a procedure was recommended. There was no consistency or standardization: six guidelines did not use any qualifying statements or were not defined in two guidelines, 10 guidelines used class or grade to denote the strength of the recommendation being made, and 27 guidelines used class, grade, or other means to denote the strength of the evidence the recommendations were being based on.
All this means, however, that there are many opportunities to modernize the guidelines and bring them up-to-date with current knowledge. They shouldn’t be recommending stenting over surgery, for example, and they need to standardize what the recommendations are based on.
“The guidelines should always define their target population properly and that comes straight from randomized trials usually,” Dr. Abbott noted. Procedural standards also need to be given. “Guidelines also need to be consistent throughout, self-contained, and be more accessible.”
Dr. Abbott had no relevant disclosures.
*CORRECTION: 6/21/2015 An error in identification of the stent was corrected.
VIENNA – Guidelines used around the world for the management of carotid stenosis, both in asymptomatic and symptomatic cases, are often outdated and do not match current evidence, according to the results of a systematic review undertaken by an international group of experts.*
Furthermore, the qualifying statements used to back up the recommendations are often confused and too simplistic, being based only on the degree of randomized data used.
“Other problems were that the guidelines often didn’t even define asymptomatic carotid artery stenosis or symptomatic carotid artery stenosis or they left out procedural standards,” said Dr. Anne Abbott, who presented the findings at the annual European Stroke Conference.
“A number of important discoveries have been made in recent years to better inform treatment decisions for patients with carotid stenosis,” Dr. Abbott, a neurologist at Monash University in Melbourne, Australia, observed.
For instance, based on evidence available today, it is clear that medical therapy alone is best for patients with moderate or severe (50%-99%) asymptomatic disease. Surgery in these patients might actually be harmful, she noted, and it is unknown if or by how much carotid endarterectomy improves stroke prevention versus medical therapy alone.
“We just haven’t done the studies, and this is where we should be concentrating our efforts with respect to randomized, placebo-controlled trials,” Dr. Abbott proposed. “But we do know that the 6% 30-day stroke/death rate [with endarterectomy] is really now too high.”
It’s also now apparent that carotid angioplasty or stenting is more harmful than carotid endarterectomy in asymptomatic patients and “shouldn’t be recommended for routine practice.” Many of the guidelines were still supporting this as an option, she observed, based on the supposed counterbalancing argument that surgical intervention was more likely to increase the risk for heart attacks than stenting. However, the evidence shows that the greatest risk to patients in the periprocedural period is the stroke risk, which is increased by stenting.
Dr. Abbott explained how the team of 16 experts had reviewed all the latest available guidelines for asymptomatic and symptomatic carotid stenosis that they could find from published from January 2008 until January 2015. She noted that guidelines were often difficult to access were often only found because the team knew of their existence through their professional networks.
A total of 34 guidelines from 23 regions or countries in six languages were identified and included in the review. Each of these was independently assessed by two to six of the team, looking at the clinical scenarios covered, the nature of the recommendations made and what evidence was being used to support the recommendations.
Of 28 guidelines that gave recommendations for asymptomatic carotid stenosis, surgery was endorsed for patients at average surgical risk and only one (4%) endorsed medical treatment alone. Eighteen (64%) recommended that stenting be performed or considered, and 24 (86%) supported the use of endarterectomy. “This is despite current evidence that these procedures are now more likely to harm than help patients,” Dr. Abbott said.
“Of major concern I think is that a high proportion, about half, of these guidelines are recommending stenting for high surgical risk asymptomatic patients, she cautioned. “This includes patients with major medical comorbidities – heart failure, respiratory failure – who have a very short life expectancy and are least likely to benefit and are more likely to be at risk from the procedures.”
Somewhat similar findings were seen regarding the use of stenting and surgery in the 33 guidelines that gave recommendations for the management of symptomatic carotid stenosis. Endarterectomy was recommended for average-surgical-risk symptomatic patients by 31 (94%) guidelines and, worryingly, stenting was still being advocated in 19 (58%) guidelines with only nine (27%) saying that stenting should not be used. Stenting was also being endorsed in symptomatic patients at high surgical risk.
Dr. Abbott said that the guidelines were hard to compare because they used a variety of qualifying statements to try to advise on the degree to which a procedure was recommended. There was no consistency or standardization: six guidelines did not use any qualifying statements or were not defined in two guidelines, 10 guidelines used class or grade to denote the strength of the recommendation being made, and 27 guidelines used class, grade, or other means to denote the strength of the evidence the recommendations were being based on.
All this means, however, that there are many opportunities to modernize the guidelines and bring them up-to-date with current knowledge. They shouldn’t be recommending stenting over surgery, for example, and they need to standardize what the recommendations are based on.
“The guidelines should always define their target population properly and that comes straight from randomized trials usually,” Dr. Abbott noted. Procedural standards also need to be given. “Guidelines also need to be consistent throughout, self-contained, and be more accessible.”
Dr. Abbott had no relevant disclosures.
*CORRECTION: 6/21/2015 An error in identification of the stent was corrected.
VIENNA – Guidelines used around the world for the management of carotid stenosis, both in asymptomatic and symptomatic cases, are often outdated and do not match current evidence, according to the results of a systematic review undertaken by an international group of experts.*
Furthermore, the qualifying statements used to back up the recommendations are often confused and too simplistic, being based only on the degree of randomized data used.
“Other problems were that the guidelines often didn’t even define asymptomatic carotid artery stenosis or symptomatic carotid artery stenosis or they left out procedural standards,” said Dr. Anne Abbott, who presented the findings at the annual European Stroke Conference.
“A number of important discoveries have been made in recent years to better inform treatment decisions for patients with carotid stenosis,” Dr. Abbott, a neurologist at Monash University in Melbourne, Australia, observed.
For instance, based on evidence available today, it is clear that medical therapy alone is best for patients with moderate or severe (50%-99%) asymptomatic disease. Surgery in these patients might actually be harmful, she noted, and it is unknown if or by how much carotid endarterectomy improves stroke prevention versus medical therapy alone.
“We just haven’t done the studies, and this is where we should be concentrating our efforts with respect to randomized, placebo-controlled trials,” Dr. Abbott proposed. “But we do know that the 6% 30-day stroke/death rate [with endarterectomy] is really now too high.”
It’s also now apparent that carotid angioplasty or stenting is more harmful than carotid endarterectomy in asymptomatic patients and “shouldn’t be recommended for routine practice.” Many of the guidelines were still supporting this as an option, she observed, based on the supposed counterbalancing argument that surgical intervention was more likely to increase the risk for heart attacks than stenting. However, the evidence shows that the greatest risk to patients in the periprocedural period is the stroke risk, which is increased by stenting.
Dr. Abbott explained how the team of 16 experts had reviewed all the latest available guidelines for asymptomatic and symptomatic carotid stenosis that they could find from published from January 2008 until January 2015. She noted that guidelines were often difficult to access were often only found because the team knew of their existence through their professional networks.
A total of 34 guidelines from 23 regions or countries in six languages were identified and included in the review. Each of these was independently assessed by two to six of the team, looking at the clinical scenarios covered, the nature of the recommendations made and what evidence was being used to support the recommendations.
Of 28 guidelines that gave recommendations for asymptomatic carotid stenosis, surgery was endorsed for patients at average surgical risk and only one (4%) endorsed medical treatment alone. Eighteen (64%) recommended that stenting be performed or considered, and 24 (86%) supported the use of endarterectomy. “This is despite current evidence that these procedures are now more likely to harm than help patients,” Dr. Abbott said.
“Of major concern I think is that a high proportion, about half, of these guidelines are recommending stenting for high surgical risk asymptomatic patients, she cautioned. “This includes patients with major medical comorbidities – heart failure, respiratory failure – who have a very short life expectancy and are least likely to benefit and are more likely to be at risk from the procedures.”
Somewhat similar findings were seen regarding the use of stenting and surgery in the 33 guidelines that gave recommendations for the management of symptomatic carotid stenosis. Endarterectomy was recommended for average-surgical-risk symptomatic patients by 31 (94%) guidelines and, worryingly, stenting was still being advocated in 19 (58%) guidelines with only nine (27%) saying that stenting should not be used. Stenting was also being endorsed in symptomatic patients at high surgical risk.
Dr. Abbott said that the guidelines were hard to compare because they used a variety of qualifying statements to try to advise on the degree to which a procedure was recommended. There was no consistency or standardization: six guidelines did not use any qualifying statements or were not defined in two guidelines, 10 guidelines used class or grade to denote the strength of the recommendation being made, and 27 guidelines used class, grade, or other means to denote the strength of the evidence the recommendations were being based on.
All this means, however, that there are many opportunities to modernize the guidelines and bring them up-to-date with current knowledge. They shouldn’t be recommending stenting over surgery, for example, and they need to standardize what the recommendations are based on.
“The guidelines should always define their target population properly and that comes straight from randomized trials usually,” Dr. Abbott noted. Procedural standards also need to be given. “Guidelines also need to be consistent throughout, self-contained, and be more accessible.”
Dr. Abbott had no relevant disclosures.
*CORRECTION: 6/21/2015 An error in identification of the stent was corrected.
AT THE EUROPEAN STROKE CONFERENCE
Key clinical point: Guidelines for carotid stenosis need reviewing and updating in line with modern evidence and practice.
Major finding: Carotid angiography/stenting was recommended for both asymptomatic and symptomatic patients despite current evidence showing that it is more likely to cause harm than provide benefit.
Data source: Systematic review of 33 guidelines for asymptomatic and symptomatic carotid stenosis.
Disclosures: Dr. Abbott had no relevant disclosures.

Paclitaxel balloon achieves unprecedented success in complex PAD
PARIS – A proprietary drug-coated percutaneous angioplasty balloon has achieved unprecedented clinical success in treating long lesions in the superficial femoral arteries.
“The 360-day primary patency rate of 91.1% and clinically driven target lesion revascularization rate of 6% are unmatched for this complex patient subgroup,” Dr. Dierk Scheinert declared in presenting the results of the IN.PACT Global Study Long Lesion Imaging Cohort at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

The 157 patients who comprise the long lesion cohort are among 1,538 patients with various forms of complex peripheral arterial disease being treated at 64 sites on four continents under the IN.PACT Global Clinical Study, which focuses on the use of Medtronic’s Admiral paclitaxel-coated balloon for percutaneous transluminal angioplasty. Upon balloon inflation, the paclitaxel binds to the vessel wall, penetrating deep into the adventitia in order to interfere with smooth muscle cell proliferation and neointimal hyperplasia. The drug remains in the vessel wall at therapeutic levels for up to 6 months.
The Food and Drug Administration approved the balloon for lesions up to 18 cm in length in native superficial femoral or popliteal arteries. Dr. Scheinert presented a study that sought to broaden that indication: The average lesion length in the 157 participants was 26.4 cm.
The majority of the target lesions, 83%, were de novo, 60% were total occlusions, and 72% featured calcification. These were patients with substantial comorbidities: 41% had diabetes, 88% hypertension, 52% coronary heart disease, 77% dyslipidemia, and 34% were current smokers, noted Dr. Scheinert, professor and chairman of the department of vascular medicine and angiology at the University of Leipzig (Germany).
The mean diameter of the target stenosis was 90% predilatation and 39% afterwards. Provisional stents were implanted in 33% of the 100 patients with lesion lengths of 15-25 cm and 53% in those with lesions longer than 25 cm.
The 12-month primary patency rate, defined as freedom from clinically driven target lesion revascularization and restenosis as determined by a central core lab, varied by lesion length: 97.7% for 15- to 25-cm-long lesions compared with 79.2% for longer ones.
The major adverse event rate – a composite of all-cause mortality, major target limb amputation, clinically driven target vessel revascularization, or thrombosis – was 11.9%.
Of note, the impressive 91.1% primary patency rate at 12 months fell off sharply to 80.7% at 390 days, prompting comment from session cochair Dr. Elazer Edelman.
“I am struck by what happened to these patients at the end of 1 year. Not to detract in any way from the value and importance of what you’ve shown, but the fact that at 1 year we get this precipitous decline is something we as a group ought to be investigating,” said Dr. Edelman, a cardiologist who is professor of health sciences and technology at the Massachusetts Institute of Technology, professor of medicine at Harvard University, and director of the Harvard-MIT Biomedical Engineering Center.
“We have to be a little bit patient,” Dr. Scheinert replied. “We’re going to see some long-term follow-up data beginning this fall. The positive message here is that at 6 months we see almost no events, which is an achievement because typically we already see the first step down in the results curve by then. And we see patency results at 12 months that we haven’t seen with any other therapy so far.”
Dr. Edelman retorted that while it’s clear this innovative therapy has delayed the period of vulnerability to patency loss, “Your work cannot continue to be impactful if we don’t focus on where the loss of patency occurs.”
“When we talk about adjunctive therapy, we need to think now about something innovative. We need to start thinking about how to give drugs from 6 to 12 to 18 months,” he asserted.
Dr. Scheinert is on the scientific advisory board for Medtronic, which funded the study, as well as on advisory boards for more than a dozen other medical companies.
PARIS – A proprietary drug-coated percutaneous angioplasty balloon has achieved unprecedented clinical success in treating long lesions in the superficial femoral arteries.
“The 360-day primary patency rate of 91.1% and clinically driven target lesion revascularization rate of 6% are unmatched for this complex patient subgroup,” Dr. Dierk Scheinert declared in presenting the results of the IN.PACT Global Study Long Lesion Imaging Cohort at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The 157 patients who comprise the long lesion cohort are among 1,538 patients with various forms of complex peripheral arterial disease being treated at 64 sites on four continents under the IN.PACT Global Clinical Study, which focuses on the use of Medtronic’s Admiral paclitaxel-coated balloon for percutaneous transluminal angioplasty. Upon balloon inflation, the paclitaxel binds to the vessel wall, penetrating deep into the adventitia in order to interfere with smooth muscle cell proliferation and neointimal hyperplasia. The drug remains in the vessel wall at therapeutic levels for up to 6 months.
The Food and Drug Administration approved the balloon for lesions up to 18 cm in length in native superficial femoral or popliteal arteries. Dr. Scheinert presented a study that sought to broaden that indication: The average lesion length in the 157 participants was 26.4 cm.
The majority of the target lesions, 83%, were de novo, 60% were total occlusions, and 72% featured calcification. These were patients with substantial comorbidities: 41% had diabetes, 88% hypertension, 52% coronary heart disease, 77% dyslipidemia, and 34% were current smokers, noted Dr. Scheinert, professor and chairman of the department of vascular medicine and angiology at the University of Leipzig (Germany).
The mean diameter of the target stenosis was 90% predilatation and 39% afterwards. Provisional stents were implanted in 33% of the 100 patients with lesion lengths of 15-25 cm and 53% in those with lesions longer than 25 cm.
The 12-month primary patency rate, defined as freedom from clinically driven target lesion revascularization and restenosis as determined by a central core lab, varied by lesion length: 97.7% for 15- to 25-cm-long lesions compared with 79.2% for longer ones.
The major adverse event rate – a composite of all-cause mortality, major target limb amputation, clinically driven target vessel revascularization, or thrombosis – was 11.9%.
Of note, the impressive 91.1% primary patency rate at 12 months fell off sharply to 80.7% at 390 days, prompting comment from session cochair Dr. Elazer Edelman.
“I am struck by what happened to these patients at the end of 1 year. Not to detract in any way from the value and importance of what you’ve shown, but the fact that at 1 year we get this precipitous decline is something we as a group ought to be investigating,” said Dr. Edelman, a cardiologist who is professor of health sciences and technology at the Massachusetts Institute of Technology, professor of medicine at Harvard University, and director of the Harvard-MIT Biomedical Engineering Center.
“We have to be a little bit patient,” Dr. Scheinert replied. “We’re going to see some long-term follow-up data beginning this fall. The positive message here is that at 6 months we see almost no events, which is an achievement because typically we already see the first step down in the results curve by then. And we see patency results at 12 months that we haven’t seen with any other therapy so far.”
Dr. Edelman retorted that while it’s clear this innovative therapy has delayed the period of vulnerability to patency loss, “Your work cannot continue to be impactful if we don’t focus on where the loss of patency occurs.”
“When we talk about adjunctive therapy, we need to think now about something innovative. We need to start thinking about how to give drugs from 6 to 12 to 18 months,” he asserted.
Dr. Scheinert is on the scientific advisory board for Medtronic, which funded the study, as well as on advisory boards for more than a dozen other medical companies.
PARIS – A proprietary drug-coated percutaneous angioplasty balloon has achieved unprecedented clinical success in treating long lesions in the superficial femoral arteries.
“The 360-day primary patency rate of 91.1% and clinically driven target lesion revascularization rate of 6% are unmatched for this complex patient subgroup,” Dr. Dierk Scheinert declared in presenting the results of the IN.PACT Global Study Long Lesion Imaging Cohort at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The 157 patients who comprise the long lesion cohort are among 1,538 patients with various forms of complex peripheral arterial disease being treated at 64 sites on four continents under the IN.PACT Global Clinical Study, which focuses on the use of Medtronic’s Admiral paclitaxel-coated balloon for percutaneous transluminal angioplasty. Upon balloon inflation, the paclitaxel binds to the vessel wall, penetrating deep into the adventitia in order to interfere with smooth muscle cell proliferation and neointimal hyperplasia. The drug remains in the vessel wall at therapeutic levels for up to 6 months.
The Food and Drug Administration approved the balloon for lesions up to 18 cm in length in native superficial femoral or popliteal arteries. Dr. Scheinert presented a study that sought to broaden that indication: The average lesion length in the 157 participants was 26.4 cm.
The majority of the target lesions, 83%, were de novo, 60% were total occlusions, and 72% featured calcification. These were patients with substantial comorbidities: 41% had diabetes, 88% hypertension, 52% coronary heart disease, 77% dyslipidemia, and 34% were current smokers, noted Dr. Scheinert, professor and chairman of the department of vascular medicine and angiology at the University of Leipzig (Germany).
The mean diameter of the target stenosis was 90% predilatation and 39% afterwards. Provisional stents were implanted in 33% of the 100 patients with lesion lengths of 15-25 cm and 53% in those with lesions longer than 25 cm.
The 12-month primary patency rate, defined as freedom from clinically driven target lesion revascularization and restenosis as determined by a central core lab, varied by lesion length: 97.7% for 15- to 25-cm-long lesions compared with 79.2% for longer ones.
The major adverse event rate – a composite of all-cause mortality, major target limb amputation, clinically driven target vessel revascularization, or thrombosis – was 11.9%.
Of note, the impressive 91.1% primary patency rate at 12 months fell off sharply to 80.7% at 390 days, prompting comment from session cochair Dr. Elazer Edelman.
“I am struck by what happened to these patients at the end of 1 year. Not to detract in any way from the value and importance of what you’ve shown, but the fact that at 1 year we get this precipitous decline is something we as a group ought to be investigating,” said Dr. Edelman, a cardiologist who is professor of health sciences and technology at the Massachusetts Institute of Technology, professor of medicine at Harvard University, and director of the Harvard-MIT Biomedical Engineering Center.
“We have to be a little bit patient,” Dr. Scheinert replied. “We’re going to see some long-term follow-up data beginning this fall. The positive message here is that at 6 months we see almost no events, which is an achievement because typically we already see the first step down in the results curve by then. And we see patency results at 12 months that we haven’t seen with any other therapy so far.”
Dr. Edelman retorted that while it’s clear this innovative therapy has delayed the period of vulnerability to patency loss, “Your work cannot continue to be impactful if we don’t focus on where the loss of patency occurs.”
“When we talk about adjunctive therapy, we need to think now about something innovative. We need to start thinking about how to give drugs from 6 to 12 to 18 months,” he asserted.
Dr. Scheinert is on the scientific advisory board for Medtronic, which funded the study, as well as on advisory boards for more than a dozen other medical companies.
AT EuroPCR
Key clinical point: A paclitaxel-coated angioplasty balloon results in 12-month patency rates never before seen in patients with peripheral arterial disease involving long lesions in the superficial femoral arteries.
Major finding: The 12-month primary patency rate was 91.1% in patients whose average lesion length was 26.4 cm.
Data source: This prospective, multinational study included 157 subjects with complex superficial femoral artery lesions at least 15 cm in length.
Disclosures: The IN.PACT Global Study is funded by Medtronic. The presenter is on the company’s scientific advisory board.

APA: DSM-5 leaves one-third of soldiers with subthreshold PTSD in limbo, expert says
TORONTO – The most effective ways to diagnose and treat posttraumatic stress disorder in military populations is at issue after the results of a recent study showed that a third of soldiers who previously would have qualified for the diagnosis do not under updated criteria. The matter is far from settled, however, and continues to be a matter of debate.
Data from a randomized, controlled study published last year (Lancet Psychiatry 2014;1:269-77)* and presented at the annual meeting of the American Psychiatric Association indicate that about a third of soldiers who would have received a clinical diagnosis of PTSD under the DSM-IV criteria do not meet the standard under the DSM-5, released in 2013.
The DSM-5 definition added criteria denoting a person’s efforts to avoid any person, place, or thing that causes them to remember details or feelings experienced during a specific traumatic event. According to former Army psychiatrist Col. (Ret.) Charles W. Hoge, this kind of emotional suppression is exactly what military, law enforcement, and first responder personnel are trained to do in order to accomplish their duties. Indeed, his study indicated that most of the soldiers who did not meet the clinical threshold for PTSD failed criterion C, the section that addresses avoidance.
“The reason to change a definition is to improve clinical utility or improve specificity, but what we’ve done is just shifted the deck chairs,” said Dr. Hoge during his presentation at the meeting.
Not so, said Dr. Matthew J. Friedman, who served on the DSM-5 Work Group that addressed PTSD, and recently retired as executive director of the Veterans Affairs’ National Center for PTSD. In an interview, Dr. Friedman disagreed with framing the findings in terms of clinical utility, particularly if the diagnostic criteria are seen as “easily and reliably utilized by different clinicians.” In that case, Dr. Friedman said in the DSM-5 field trials conducted prior to the manual’s release, the proposed PTSD criteria proved to be among the “best.”
Rather than view the findings merely as a shuffling of seats, Dr. Friedman suggested the findings could lead to a deeper line of inquiry around whether there is in fact a response bias in military personnel who might be less likely to “endorse avoidance symptoms. If the study had been done by a structured interview with a trained clinician instead of by self-report, would the results have looked the same?”
In addition to increasing the number of criteria for PTSD from 17 to 20 symptoms, including the avoidant criteria, the DSM-5 reworded 8 symptoms, and further specified symptom clusters from three groups to four, with the addition of alterations in cognitions and mood to the third cluster, and alterations in arousal and reactivity becoming the fourth. The DSM-5 also reclassified the disorder from one of anxiety to one of trauma and stress.
Dr. Hoge, currently a researcher at the Center for Psychiatry and Neuroscience at Walter Reed Army Institute of Research in Silver Spring, Md., and his colleagues conducted a head-to-head comparison of the number of PTSD diagnoses obtained according to criteria in either the DSM-IV or the DSM-5. They surveyed 1,822 infantry soldiers for a single brigade combat team, more than half of whom had been deployed to Iraq or Afghanistan. Each survey included items from both the DSM-IV’s PTSD Check List, specific for “stressful experiences,” as well as the PCL-5 from the DSM-5. The questions from each were separated in the same survey by several other health-related items. Two versions of the survey were created and distributed randomly across the cohort; one version of the study listed the DSM-IV PCL-S questions first, the other survey had the PCL-5 version first.
The demographic and health outcomes in each group were essentially identical: Respondents were almost entirely male, aged 18-25 years, and roughly half of each group was married. Nearly one-fifth of each group was found by the survey to have moderate to severe general anxiety disorder.
The prevalence rates of PTSD in both survey groups were nearly identical: 12.9% vs. 12.2%, respectively; however, 30% of those surveyed who previously would have met the criteria for PTSD in the DSM-IV did not meet the DSM-5 criteria. Meanwhile, 28% of those who met DSM-5 criteria would not have met the DSM-IV criteria.
Dr. Friedman said the method used in Dr. Hoge’s study did not specifically explore the effect of the A criteria that identify the level of actual exposure to a traumatic event and a person’s immediate reaction to it. The DSM-IV stipulated in criterion A2 that a person experience “fear, helplessness, or horror” directly after a traumatic event. “One of the things that we found is that many soldiers who have all of the PTSD symptoms were ineligible for a PTSD diagnosis because they did not meet the A2 criterion.”
Dr. Friedman did not say whether this necessarily was the result of one’s crisis response training but noted that based on an evidence review, his work group dropped the criterion, and that now many people previously considered subclinical receive a PTSD diagnosis. “Had the A criteria been included in [Dr. Hoge’s] exploration, then a soldier who would not have met the A criteria in DSM-VI would make it in DSM-5, so it becomes a different ball game,” said Dr. Friedman, senior adviser at the National Center for PTSD, and professor of psychiatry and of pharmacology and toxicology at the Geisel School of Medicine at Dartmouth, Hanover, N.H.
In the study, Dr. Hoge and his coauthors wrote, “there is good evidence lending support to removal of the criterion A2,” yet during his presentation, he emphasized that just as service members learn to override fear, hopelessness, or horror, “they also learn to override avoidance symptoms as part of their training.” He concluded that because the prevalence rates are virtually the same between the fourth and fifth editions of the DSM, but for different reasons, there is no clinical utility in the new criteria. “Technically, [these soldiers] don’t meet the new definition, but clearly, they are individuals who need trauma-focused therapy and would have met the previous definition.”
Former Army psychiatrist Col. (Ret.) Elspeth Cameron Ritchie, meanwhile, said in an interview that Dr. Hoge and Dr. Friedman are “both world-renowned researchers in the field of PTSD and other related injuries of war.”
“All of us are struggling with the right way to diagnose PTSD, especially after almost 14 years of war and hundreds of thousands of wounded service members,” Dr. Ritchie said. “In addition, PTSD is not a simple, uniform diagnosis. It probably is many overlapping diagnoses.”
She has warned clinicians to proceed with caution, since how military personnel are diagnosed can have serious implications for their careers and benefits.
Currently, the VA and the Department of Defense support the status quo for any personnel previously diagnosed according to DSM-IV criteria, but how subclinical cases should be handled is still at issue. The DSM-5 recommendation for subthreshold symptoms is to consider them an adjustment disorder.
Dr. Hoge rejected this as unhelpful, noting that a failure to adjust or adapt in the military setting has a “pejorative connotation.”
Dr. Friedman and the National Center for PTSD currently recommend using 308.89 from the DSM-5, which is “other specified trauma and stressor-related disorder.” Using “chronic adjustment disorder” is not appropriate, said Dr. Friedman, “because it has a 6-month time limit.” Dr. Friedman also noted that 308.89 in the DSM-5 is the same as the DSM-IV anxiety not otherwise specified, which prior to the DSM-5 was what was used for subthreshold PTSD. According to Dr. Hoge, however, 308.89 is linked in military electronic health records to “adjustment reaction with aggression antisocial behavior/destructiveness” and “aggressor identified syndrome,” both of which could have similar deleterious effects to a soldier as an “adjustment disorder.”
The current U.S. Army Medical Command policy allows physicians to continue diagnosing PTSD according to DSM-IV standards or to apply an unspecified anxiety code (ICD-9 300.00) for any subthreshold PTSD patients.
The fractious approach to diagnosis, according to Dr. Hoge, might be simplified by implementation later this year of the ICD-10, although he said early indications of the ICD-11 in Europe do not show better specificity when compared with the DSM-IV. He noted that the ICD-11 is simpler and has fewer symptom criteria. Here in the United States, he said, “We are not going in the right direction.”
Dr. Hoge said his presentation was based on his own findings and does not represent the opinions or policies of the U.S. Army.
On Twitter @whitneymcknight
*Correction, 6/2/2014: An earlier version of this article misattributed a reference to Lancet Psychiatry.
TORONTO – The most effective ways to diagnose and treat posttraumatic stress disorder in military populations is at issue after the results of a recent study showed that a third of soldiers who previously would have qualified for the diagnosis do not under updated criteria. The matter is far from settled, however, and continues to be a matter of debate.
Data from a randomized, controlled study published last year (Lancet Psychiatry 2014;1:269-77)* and presented at the annual meeting of the American Psychiatric Association indicate that about a third of soldiers who would have received a clinical diagnosis of PTSD under the DSM-IV criteria do not meet the standard under the DSM-5, released in 2013.
The DSM-5 definition added criteria denoting a person’s efforts to avoid any person, place, or thing that causes them to remember details or feelings experienced during a specific traumatic event. According to former Army psychiatrist Col. (Ret.) Charles W. Hoge, this kind of emotional suppression is exactly what military, law enforcement, and first responder personnel are trained to do in order to accomplish their duties. Indeed, his study indicated that most of the soldiers who did not meet the clinical threshold for PTSD failed criterion C, the section that addresses avoidance.
“The reason to change a definition is to improve clinical utility or improve specificity, but what we’ve done is just shifted the deck chairs,” said Dr. Hoge during his presentation at the meeting.
Not so, said Dr. Matthew J. Friedman, who served on the DSM-5 Work Group that addressed PTSD, and recently retired as executive director of the Veterans Affairs’ National Center for PTSD. In an interview, Dr. Friedman disagreed with framing the findings in terms of clinical utility, particularly if the diagnostic criteria are seen as “easily and reliably utilized by different clinicians.” In that case, Dr. Friedman said in the DSM-5 field trials conducted prior to the manual’s release, the proposed PTSD criteria proved to be among the “best.”
Rather than view the findings merely as a shuffling of seats, Dr. Friedman suggested the findings could lead to a deeper line of inquiry around whether there is in fact a response bias in military personnel who might be less likely to “endorse avoidance symptoms. If the study had been done by a structured interview with a trained clinician instead of by self-report, would the results have looked the same?”
In addition to increasing the number of criteria for PTSD from 17 to 20 symptoms, including the avoidant criteria, the DSM-5 reworded 8 symptoms, and further specified symptom clusters from three groups to four, with the addition of alterations in cognitions and mood to the third cluster, and alterations in arousal and reactivity becoming the fourth. The DSM-5 also reclassified the disorder from one of anxiety to one of trauma and stress.
Dr. Hoge, currently a researcher at the Center for Psychiatry and Neuroscience at Walter Reed Army Institute of Research in Silver Spring, Md., and his colleagues conducted a head-to-head comparison of the number of PTSD diagnoses obtained according to criteria in either the DSM-IV or the DSM-5. They surveyed 1,822 infantry soldiers for a single brigade combat team, more than half of whom had been deployed to Iraq or Afghanistan. Each survey included items from both the DSM-IV’s PTSD Check List, specific for “stressful experiences,” as well as the PCL-5 from the DSM-5. The questions from each were separated in the same survey by several other health-related items. Two versions of the survey were created and distributed randomly across the cohort; one version of the study listed the DSM-IV PCL-S questions first, the other survey had the PCL-5 version first.
The demographic and health outcomes in each group were essentially identical: Respondents were almost entirely male, aged 18-25 years, and roughly half of each group was married. Nearly one-fifth of each group was found by the survey to have moderate to severe general anxiety disorder.
The prevalence rates of PTSD in both survey groups were nearly identical: 12.9% vs. 12.2%, respectively; however, 30% of those surveyed who previously would have met the criteria for PTSD in the DSM-IV did not meet the DSM-5 criteria. Meanwhile, 28% of those who met DSM-5 criteria would not have met the DSM-IV criteria.
Dr. Friedman said the method used in Dr. Hoge’s study did not specifically explore the effect of the A criteria that identify the level of actual exposure to a traumatic event and a person’s immediate reaction to it. The DSM-IV stipulated in criterion A2 that a person experience “fear, helplessness, or horror” directly after a traumatic event. “One of the things that we found is that many soldiers who have all of the PTSD symptoms were ineligible for a PTSD diagnosis because they did not meet the A2 criterion.”
Dr. Friedman did not say whether this necessarily was the result of one’s crisis response training but noted that based on an evidence review, his work group dropped the criterion, and that now many people previously considered subclinical receive a PTSD diagnosis. “Had the A criteria been included in [Dr. Hoge’s] exploration, then a soldier who would not have met the A criteria in DSM-VI would make it in DSM-5, so it becomes a different ball game,” said Dr. Friedman, senior adviser at the National Center for PTSD, and professor of psychiatry and of pharmacology and toxicology at the Geisel School of Medicine at Dartmouth, Hanover, N.H.
In the study, Dr. Hoge and his coauthors wrote, “there is good evidence lending support to removal of the criterion A2,” yet during his presentation, he emphasized that just as service members learn to override fear, hopelessness, or horror, “they also learn to override avoidance symptoms as part of their training.” He concluded that because the prevalence rates are virtually the same between the fourth and fifth editions of the DSM, but for different reasons, there is no clinical utility in the new criteria. “Technically, [these soldiers] don’t meet the new definition, but clearly, they are individuals who need trauma-focused therapy and would have met the previous definition.”
Former Army psychiatrist Col. (Ret.) Elspeth Cameron Ritchie, meanwhile, said in an interview that Dr. Hoge and Dr. Friedman are “both world-renowned researchers in the field of PTSD and other related injuries of war.”
“All of us are struggling with the right way to diagnose PTSD, especially after almost 14 years of war and hundreds of thousands of wounded service members,” Dr. Ritchie said. “In addition, PTSD is not a simple, uniform diagnosis. It probably is many overlapping diagnoses.”
She has warned clinicians to proceed with caution, since how military personnel are diagnosed can have serious implications for their careers and benefits.
Currently, the VA and the Department of Defense support the status quo for any personnel previously diagnosed according to DSM-IV criteria, but how subclinical cases should be handled is still at issue. The DSM-5 recommendation for subthreshold symptoms is to consider them an adjustment disorder.
Dr. Hoge rejected this as unhelpful, noting that a failure to adjust or adapt in the military setting has a “pejorative connotation.”
Dr. Friedman and the National Center for PTSD currently recommend using 308.89 from the DSM-5, which is “other specified trauma and stressor-related disorder.” Using “chronic adjustment disorder” is not appropriate, said Dr. Friedman, “because it has a 6-month time limit.” Dr. Friedman also noted that 308.89 in the DSM-5 is the same as the DSM-IV anxiety not otherwise specified, which prior to the DSM-5 was what was used for subthreshold PTSD. According to Dr. Hoge, however, 308.89 is linked in military electronic health records to “adjustment reaction with aggression antisocial behavior/destructiveness” and “aggressor identified syndrome,” both of which could have similar deleterious effects to a soldier as an “adjustment disorder.”
The current U.S. Army Medical Command policy allows physicians to continue diagnosing PTSD according to DSM-IV standards or to apply an unspecified anxiety code (ICD-9 300.00) for any subthreshold PTSD patients.
The fractious approach to diagnosis, according to Dr. Hoge, might be simplified by implementation later this year of the ICD-10, although he said early indications of the ICD-11 in Europe do not show better specificity when compared with the DSM-IV. He noted that the ICD-11 is simpler and has fewer symptom criteria. Here in the United States, he said, “We are not going in the right direction.”
Dr. Hoge said his presentation was based on his own findings and does not represent the opinions or policies of the U.S. Army.
On Twitter @whitneymcknight
*Correction, 6/2/2014: An earlier version of this article misattributed a reference to Lancet Psychiatry.
TORONTO – The most effective ways to diagnose and treat posttraumatic stress disorder in military populations is at issue after the results of a recent study showed that a third of soldiers who previously would have qualified for the diagnosis do not under updated criteria. The matter is far from settled, however, and continues to be a matter of debate.
Data from a randomized, controlled study published last year (Lancet Psychiatry 2014;1:269-77)* and presented at the annual meeting of the American Psychiatric Association indicate that about a third of soldiers who would have received a clinical diagnosis of PTSD under the DSM-IV criteria do not meet the standard under the DSM-5, released in 2013.
The DSM-5 definition added criteria denoting a person’s efforts to avoid any person, place, or thing that causes them to remember details or feelings experienced during a specific traumatic event. According to former Army psychiatrist Col. (Ret.) Charles W. Hoge, this kind of emotional suppression is exactly what military, law enforcement, and first responder personnel are trained to do in order to accomplish their duties. Indeed, his study indicated that most of the soldiers who did not meet the clinical threshold for PTSD failed criterion C, the section that addresses avoidance.
“The reason to change a definition is to improve clinical utility or improve specificity, but what we’ve done is just shifted the deck chairs,” said Dr. Hoge during his presentation at the meeting.
Not so, said Dr. Matthew J. Friedman, who served on the DSM-5 Work Group that addressed PTSD, and recently retired as executive director of the Veterans Affairs’ National Center for PTSD. In an interview, Dr. Friedman disagreed with framing the findings in terms of clinical utility, particularly if the diagnostic criteria are seen as “easily and reliably utilized by different clinicians.” In that case, Dr. Friedman said in the DSM-5 field trials conducted prior to the manual’s release, the proposed PTSD criteria proved to be among the “best.”
Rather than view the findings merely as a shuffling of seats, Dr. Friedman suggested the findings could lead to a deeper line of inquiry around whether there is in fact a response bias in military personnel who might be less likely to “endorse avoidance symptoms. If the study had been done by a structured interview with a trained clinician instead of by self-report, would the results have looked the same?”
In addition to increasing the number of criteria for PTSD from 17 to 20 symptoms, including the avoidant criteria, the DSM-5 reworded 8 symptoms, and further specified symptom clusters from three groups to four, with the addition of alterations in cognitions and mood to the third cluster, and alterations in arousal and reactivity becoming the fourth. The DSM-5 also reclassified the disorder from one of anxiety to one of trauma and stress.
Dr. Hoge, currently a researcher at the Center for Psychiatry and Neuroscience at Walter Reed Army Institute of Research in Silver Spring, Md., and his colleagues conducted a head-to-head comparison of the number of PTSD diagnoses obtained according to criteria in either the DSM-IV or the DSM-5. They surveyed 1,822 infantry soldiers for a single brigade combat team, more than half of whom had been deployed to Iraq or Afghanistan. Each survey included items from both the DSM-IV’s PTSD Check List, specific for “stressful experiences,” as well as the PCL-5 from the DSM-5. The questions from each were separated in the same survey by several other health-related items. Two versions of the survey were created and distributed randomly across the cohort; one version of the study listed the DSM-IV PCL-S questions first, the other survey had the PCL-5 version first.
The demographic and health outcomes in each group were essentially identical: Respondents were almost entirely male, aged 18-25 years, and roughly half of each group was married. Nearly one-fifth of each group was found by the survey to have moderate to severe general anxiety disorder.
The prevalence rates of PTSD in both survey groups were nearly identical: 12.9% vs. 12.2%, respectively; however, 30% of those surveyed who previously would have met the criteria for PTSD in the DSM-IV did not meet the DSM-5 criteria. Meanwhile, 28% of those who met DSM-5 criteria would not have met the DSM-IV criteria.
Dr. Friedman said the method used in Dr. Hoge’s study did not specifically explore the effect of the A criteria that identify the level of actual exposure to a traumatic event and a person’s immediate reaction to it. The DSM-IV stipulated in criterion A2 that a person experience “fear, helplessness, or horror” directly after a traumatic event. “One of the things that we found is that many soldiers who have all of the PTSD symptoms were ineligible for a PTSD diagnosis because they did not meet the A2 criterion.”
Dr. Friedman did not say whether this necessarily was the result of one’s crisis response training but noted that based on an evidence review, his work group dropped the criterion, and that now many people previously considered subclinical receive a PTSD diagnosis. “Had the A criteria been included in [Dr. Hoge’s] exploration, then a soldier who would not have met the A criteria in DSM-VI would make it in DSM-5, so it becomes a different ball game,” said Dr. Friedman, senior adviser at the National Center for PTSD, and professor of psychiatry and of pharmacology and toxicology at the Geisel School of Medicine at Dartmouth, Hanover, N.H.
In the study, Dr. Hoge and his coauthors wrote, “there is good evidence lending support to removal of the criterion A2,” yet during his presentation, he emphasized that just as service members learn to override fear, hopelessness, or horror, “they also learn to override avoidance symptoms as part of their training.” He concluded that because the prevalence rates are virtually the same between the fourth and fifth editions of the DSM, but for different reasons, there is no clinical utility in the new criteria. “Technically, [these soldiers] don’t meet the new definition, but clearly, they are individuals who need trauma-focused therapy and would have met the previous definition.”
Former Army psychiatrist Col. (Ret.) Elspeth Cameron Ritchie, meanwhile, said in an interview that Dr. Hoge and Dr. Friedman are “both world-renowned researchers in the field of PTSD and other related injuries of war.”
“All of us are struggling with the right way to diagnose PTSD, especially after almost 14 years of war and hundreds of thousands of wounded service members,” Dr. Ritchie said. “In addition, PTSD is not a simple, uniform diagnosis. It probably is many overlapping diagnoses.”
She has warned clinicians to proceed with caution, since how military personnel are diagnosed can have serious implications for their careers and benefits.
Currently, the VA and the Department of Defense support the status quo for any personnel previously diagnosed according to DSM-IV criteria, but how subclinical cases should be handled is still at issue. The DSM-5 recommendation for subthreshold symptoms is to consider them an adjustment disorder.
Dr. Hoge rejected this as unhelpful, noting that a failure to adjust or adapt in the military setting has a “pejorative connotation.”
Dr. Friedman and the National Center for PTSD currently recommend using 308.89 from the DSM-5, which is “other specified trauma and stressor-related disorder.” Using “chronic adjustment disorder” is not appropriate, said Dr. Friedman, “because it has a 6-month time limit.” Dr. Friedman also noted that 308.89 in the DSM-5 is the same as the DSM-IV anxiety not otherwise specified, which prior to the DSM-5 was what was used for subthreshold PTSD. According to Dr. Hoge, however, 308.89 is linked in military electronic health records to “adjustment reaction with aggression antisocial behavior/destructiveness” and “aggressor identified syndrome,” both of which could have similar deleterious effects to a soldier as an “adjustment disorder.”
The current U.S. Army Medical Command policy allows physicians to continue diagnosing PTSD according to DSM-IV standards or to apply an unspecified anxiety code (ICD-9 300.00) for any subthreshold PTSD patients.
The fractious approach to diagnosis, according to Dr. Hoge, might be simplified by implementation later this year of the ICD-10, although he said early indications of the ICD-11 in Europe do not show better specificity when compared with the DSM-IV. He noted that the ICD-11 is simpler and has fewer symptom criteria. Here in the United States, he said, “We are not going in the right direction.”
Dr. Hoge said his presentation was based on his own findings and does not represent the opinions or policies of the U.S. Army.
On Twitter @whitneymcknight
*Correction, 6/2/2014: An earlier version of this article misattributed a reference to Lancet Psychiatry.
AT THE APA ANNUAL MEETING
Key clinical point: The DSM-5 definition of posttraumatic stress disorder disqualifies a third of soldiers who once qualified for the diagnosis.
Major finding: Thirty percent of soldiers who previously would have met the criteria for PTSD in the DSM-IV did not meet the DSM-5 criteria.
Data source: Randomized, controlled study of 1,822 infantry soldiers for a single brigade combat team, half of whom had been deployed in war zones.
Disclosures: Dr. Hoge said his presentation was based on his own findings and does not represent the opinions or policies of the U.S. Army.
Team calls for change in warfarin dosing algorithms

Photo courtesy of NIGMS
Investigators have proposed the use of race-stratified algorithms to help clinicians better calculate the appropriate warfarin dose for a patient.
The team’s study, published in Blood, showed that clinical and genetic factors affecting warfarin dose requirements vary by race.
“As the outcomes of disease can vary by race, so can response to medications,” said Nita Limdi, PhD, PharmD, of the University of Alabama at Birmingham.
“Therefore, warfarin dosing equations that combine race groups for analysis (race-adjusted analysis) assume that the effect of variables—such as age and genetics—are the same across race groups, which may compromise dose prediction among patients of both races.”
To better understand how genetics and clinical factors influence warfarin dosing across race groups, Dr Limdi and her colleagues analyzed 1357 patients—595 African American and 762 European American—treated with warfarin.
The team calculated and compared dose recommendations according to both race-adjusted dosing models and race-stratified dosing models. They found that race-stratified analysis improved dose prediction in both racial groups, as compared to race- adjusted analysis.
Race-stratified analysis showed that European Americans with the CYP2C9*2 variant required less warfarin than European Americans with wild-type CYP2C9. But the same was not true for African Americans.
And although all participants who carried VKORC1 required lower doses, regardless of race, the proportional dose reduction was greater among European Americans.
The investigators therefore concluded that the influence of genetic and clinical factors on warfarin dose differs by race. So race-stratified algorithms, rather than race-adjusted algorithms, should be used to guide warfarin dosing.
“Our findings highlight the need for adequate racial representation in warfarin dosing studies to improve our understanding of how the factors that influence warfarin dose differ according to race,” Dr Limdi said. “This is the first step to developing race-specific algorithms to personalize therapy.” ![]()
Photo courtesy of NIGMS
Investigators have proposed the use of race-stratified algorithms to help clinicians better calculate the appropriate warfarin dose for a patient.
The team’s study, published in Blood, showed that clinical and genetic factors affecting warfarin dose requirements vary by race.
“As the outcomes of disease can vary by race, so can response to medications,” said Nita Limdi, PhD, PharmD, of the University of Alabama at Birmingham.
“Therefore, warfarin dosing equations that combine race groups for analysis (race-adjusted analysis) assume that the effect of variables—such as age and genetics—are the same across race groups, which may compromise dose prediction among patients of both races.”
To better understand how genetics and clinical factors influence warfarin dosing across race groups, Dr Limdi and her colleagues analyzed 1357 patients—595 African American and 762 European American—treated with warfarin.
The team calculated and compared dose recommendations according to both race-adjusted dosing models and race-stratified dosing models. They found that race-stratified analysis improved dose prediction in both racial groups, as compared to race- adjusted analysis.
Race-stratified analysis showed that European Americans with the CYP2C9*2 variant required less warfarin than European Americans with wild-type CYP2C9. But the same was not true for African Americans.
And although all participants who carried VKORC1 required lower doses, regardless of race, the proportional dose reduction was greater among European Americans.
The investigators therefore concluded that the influence of genetic and clinical factors on warfarin dose differs by race. So race-stratified algorithms, rather than race-adjusted algorithms, should be used to guide warfarin dosing.
“Our findings highlight the need for adequate racial representation in warfarin dosing studies to improve our understanding of how the factors that influence warfarin dose differ according to race,” Dr Limdi said. “This is the first step to developing race-specific algorithms to personalize therapy.” ![]()
Photo courtesy of NIGMS
Investigators have proposed the use of race-stratified algorithms to help clinicians better calculate the appropriate warfarin dose for a patient.
The team’s study, published in Blood, showed that clinical and genetic factors affecting warfarin dose requirements vary by race.
“As the outcomes of disease can vary by race, so can response to medications,” said Nita Limdi, PhD, PharmD, of the University of Alabama at Birmingham.
“Therefore, warfarin dosing equations that combine race groups for analysis (race-adjusted analysis) assume that the effect of variables—such as age and genetics—are the same across race groups, which may compromise dose prediction among patients of both races.”
To better understand how genetics and clinical factors influence warfarin dosing across race groups, Dr Limdi and her colleagues analyzed 1357 patients—595 African American and 762 European American—treated with warfarin.
The team calculated and compared dose recommendations according to both race-adjusted dosing models and race-stratified dosing models. They found that race-stratified analysis improved dose prediction in both racial groups, as compared to race- adjusted analysis.
Race-stratified analysis showed that European Americans with the CYP2C9*2 variant required less warfarin than European Americans with wild-type CYP2C9. But the same was not true for African Americans.
And although all participants who carried VKORC1 required lower doses, regardless of race, the proportional dose reduction was greater among European Americans.
The investigators therefore concluded that the influence of genetic and clinical factors on warfarin dose differs by race. So race-stratified algorithms, rather than race-adjusted algorithms, should be used to guide warfarin dosing.
“Our findings highlight the need for adequate racial representation in warfarin dosing studies to improve our understanding of how the factors that influence warfarin dose differ according to race,” Dr Limdi said. “This is the first step to developing race-specific algorithms to personalize therapy.” ![]()
Surgical removal of malpositioned IUDs
Today’s intrauterine devices (IUDs) represent an excellent form of long-acting reversible contraception. Depending on the type of IUD, many also are used to help alleviate such gynecologic symptoms as abnormal uterine bleeding. Approximately 10% of IUD insertions are complicated by malpositioning, which can include embedding, translocation, or perforation. Malpositioned IUDs are often amenable to office removal but, occasionally, hysteroscopy or laparoscopy is necessary.
In this video, we begin by reviewing techniques for complicated office IUD removal. Then we present 4 cases of malpositioned IUDs that required surgical intervention; hysteroscopic, laparoscopic, or combined techniques were used in each case. This video highlights how preoperative imaging often is not sufficient to determine the necessary surgical approach. Therefore, patients should be counseled on the potential need for hysteroscopy or laparoscopy to surgically remove a malpositioned IUD.
Although risk factors for malpositioned IUDs are not well studied in the literature, understanding proper placement and identification of complications at the time of IUD placement are essential to malpositioning prevention.
My colleagues and I hope you enjoy this video.
—Dr. Arnold Advincula
Share your thoughts on this video! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Today’s intrauterine devices (IUDs) represent an excellent form of long-acting reversible contraception. Depending on the type of IUD, many also are used to help alleviate such gynecologic symptoms as abnormal uterine bleeding. Approximately 10% of IUD insertions are complicated by malpositioning, which can include embedding, translocation, or perforation. Malpositioned IUDs are often amenable to office removal but, occasionally, hysteroscopy or laparoscopy is necessary.
In this video, we begin by reviewing techniques for complicated office IUD removal. Then we present 4 cases of malpositioned IUDs that required surgical intervention; hysteroscopic, laparoscopic, or combined techniques were used in each case. This video highlights how preoperative imaging often is not sufficient to determine the necessary surgical approach. Therefore, patients should be counseled on the potential need for hysteroscopy or laparoscopy to surgically remove a malpositioned IUD.
Although risk factors for malpositioned IUDs are not well studied in the literature, understanding proper placement and identification of complications at the time of IUD placement are essential to malpositioning prevention.
My colleagues and I hope you enjoy this video.
—Dr. Arnold Advincula
Share your thoughts on this video! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Today’s intrauterine devices (IUDs) represent an excellent form of long-acting reversible contraception. Depending on the type of IUD, many also are used to help alleviate such gynecologic symptoms as abnormal uterine bleeding. Approximately 10% of IUD insertions are complicated by malpositioning, which can include embedding, translocation, or perforation. Malpositioned IUDs are often amenable to office removal but, occasionally, hysteroscopy or laparoscopy is necessary.
In this video, we begin by reviewing techniques for complicated office IUD removal. Then we present 4 cases of malpositioned IUDs that required surgical intervention; hysteroscopic, laparoscopic, or combined techniques were used in each case. This video highlights how preoperative imaging often is not sufficient to determine the necessary surgical approach. Therefore, patients should be counseled on the potential need for hysteroscopy or laparoscopy to surgically remove a malpositioned IUD.
Although risk factors for malpositioned IUDs are not well studied in the literature, understanding proper placement and identification of complications at the time of IUD placement are essential to malpositioning prevention.
My colleagues and I hope you enjoy this video.
—Dr. Arnold Advincula
Share your thoughts on this video! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Knee Extensor Mechanism Reconstruction With Complete Extensor Allograft After Failure of Patellar Tendon Repair
The extensor mechanism of the knee comprises the quadriceps tendon, the patella, and the patellar tendon. The extensor mechanism may be damaged by injury to these structures, with consequences such as the inability to actively extend the knee and hemarthrosis.1,2 Disruption of this mechanism is rare, and the most common injury pattern is an eccentric contraction of the quadriceps tendon on a flexed knee causing a tendon (quadriceps or patellar) rupture or a patella fracture.1,2
Patellar tendon ruptures are more common in persons younger than 40 years.1 Treatment is surgical, regardless of age and physical activity. In the acute setting, repair can be end-to-end suture or transosseous tunnel insertion. End-to-end suturing is difficult in chronic patellar tendon ruptures because of patella alta secondary to quadriceps contraction.3 Treatment options for chronic ruptures may involve transpatellar traction4 or tendon reinforcement with fascia lata, a semitendinosus band, or synthetic materials.3-5 Alternatively, tendon autograft and allografts have also been recommended, especially in extreme situations.1,6 Furthermore, animal experiments have shown that a compact platelet-rich fibrin scaffold (CPFS) has the potential to accelerate healing of patellar tendon defects and to act as a bioscaffold for graft augmentation.7
We describe the case of a 30-year-old man who underwent extensor mechanism reconstruction with cadaveric tendon–patellar tendon–bone allograft for failure of an infected primary end-to-end repair. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 30-year-old healthy man landed on an empty glass fish tank, resulting in a traumatic right-knee arthrotomy. On initial evaluation, the patient had a negative straight-leg-raise test and impaired knee extension. The patient was taken urgently to the operating room for irrigation and débridement and concurrent repair of the patellar tendon laceration. Antibiotic prophylaxis with 2 g of intravenous (IV) cefazolin was given in the emergency room.
Intraoperatively, after visualizing the patellar tendon laceration and excluding any associated chondral lesions, we proceeded with extensive débridement and irrigation using 9 L of normal saline pulse lavage. After we achieved a clean site, we proceeded to repair the patellar tendon using No. 2 FiberWire sutures (Arthrex, Naples, Florida) with a classic Krackow repair8 consisting of 2 sutures run in a 4-row fashion through the patella and the patellar tendon. The suture was securely tightened and then tested for stability to at least 90° of knee flexion. The retinaculum was repaired using No. 0 Vicryl sutures (Ethicon, Somerville, New Jersey). After wound closure and dressing, the patient was placed in a hinged knee brace locked in extension at all times after surgery. Antibiotic treatment with IV cefazolin was administered for 48 hours.
Postoperative management consisted of weight-bearing as tolerated on the operative limb and appropriate deep venous thrombosis prophylaxis. The patient followed up in clinic 2 weeks and 4 weeks after surgery. At 4 weeks, the patient was noted to have a secondary wound infection with superficial dehiscence and serosanguineous drainage. No wound opening was noticed, and local wound care was performed with a 1-week course of oral cephalexin. The patient was scheduled to follow up a few weeks later but did not follow up for a year.
At 1-year follow-up, the patient reported that he had had a steady progression of his knee range of motion (ROM) with decreased pain. However, over time, the patient noted subjective instability of the knee, with frequent falls occurring close to his 1-year follow-up. Examination of his knee showed that his active ROM ranged from 20° in extension to 120° in flexion, with a weak extensor mechanism. Passively, his knee could be brought to full extension. His incision was well healed, but it had an area of bogginess in the middle. Radiographs showed patella alta on the affected knee, with a lengthening of the patellar tendon of 7.70 cm on the right compared with 5.18 cm on the left. Magnetic resonance imaging (MRI) showed moderate-to-severe patellar tendinosis with small fluid pockets around the surgical material and evidence of acute patellar enthesopathy. The laboratory values showed a white blood cell count of 7580/μL (normal, 4500-11,000/μL), an erythrocyte sedimentation rate of 2 mm/h (normal, 1-15 mm/h), and a C-reactive protein level of 1.93 mg/dL (normal, 0.00-0.29 mg/dL). Based on the clinical examination and imaging findings, there was a concern for a possible chronic deep-tissue infection, in addition to failure of the primary patellar tendon repair. Operative versus nonoperative management options were discussed with the patient, and he elected to undergo surgery.
During surgery, the patellar laxity was confirmed, and the patellar tendon was noticed to be chronically thickened and surrounded by unhealthy tissue. Initially, an extensive soft-tissue débridement was performed, and all patellar tendon loculations visualized on the preoperative MRI were drained; a solid purulent-like fluid was expressed. Unfortunately, the extensive and required débridement did not allow the preservation of the patellar tendon. Appropriate cultures were taken and sent for immediate Gram-stain analysis, which returned negative. Tissue samples from the patellar tendon were also sent to the pathology department for analysis. Intraoperatively, the infrapatellar defect was filled temporarily with a tobramycin cement spacer mixed with 2 g of vancomycin in a manner similar to that of the Masquelet technique used for infected long-bone nonunions with bone loss.9,10 This technique is a 2-stage procedure that promotes the formation of a biologic membrane that allows bone healing in the reconstruction of long-bone defects. The first stage consists of a radical débridement with soft-tissue repair by flaps when needed, with the insertion of a polymethylmethacrylate cement spacer into the bone defect. The second stage is usually performed 6 to 8 weeks later, with removal of the spacer and preservation of the induced membrane, which is filled with iliac crest bone autograft augmented (if necessary) with demineralized allograft.
The incision was closed primarily, and after surgery, the patient was allowed to bear weight as tolerated in a hinged knee brace locked in extension. Final laboratory analysis from cultures and tissue samples revealed acute and chronic inflammation with more than 20 neutrophils per high-powered field. No organisms grew from aerobic, anaerobic, fungal, or mycobacterial cultures. The infectious disease service was consulted and recommended oral cephalexin.
Because all cultures were negative, all laboratory examinations did not indicate any residual infections, and no bony involvement was noticed intraoperatively or in the preoperative knee MRI, we decided to proceed with the second stage of the Masquelet technique after 2 weeks. The patient returned to the operating room for final reconstruction of his patellar tendon using a custom-ordered cadaveric tendon–patellar tendon–bone allograft, the length of which was determined by measuring the contralateral patellar tendon, ie, 5.18 cm (Figure 1A). The previous anterior knee incision was reopened and extended distally past the tibial tuberosity and proximally toward the quadriceps tendon. The antibiotic spacer was removed. We proceeded with a repeat irrigation and débridement and the allograft transfer. The selected allograft was customized by reducing the tibial bone component to an approximately 1×2-cm bone block and by reducing the allograft patellar thickness with an oscillating saw, leaving an approximately 2-mm thick patellar bone graft attached to the patellar tendon. In a similar technique using an oscillating saw, we shaved off the anterior cortex of the patient’s patella to accommodate, in a sandwich fashion, the patellar allograft. Proximally, the quadriceps tendon insertion was split longitudinally and partially separated from the superior pole of the patellar tendon to allow seating and fixation of the modified quadriceps allograft tendon component.
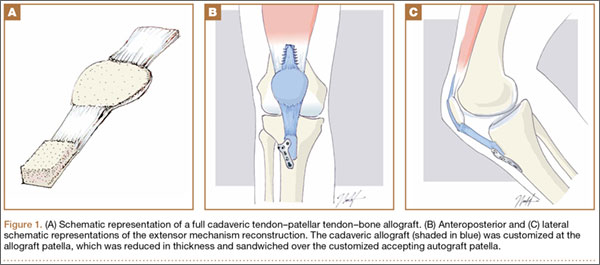
We proceeded with the fixation of the allograft first distally on the patella. The anterior cortex of the tibial tuberosity was resected to allow the perfect seating of the bone block allograft. The graft was secured with a 4.0-mm fully threaded cancellous lag screw and reinforced with a 2.4-mm, 3-hole T-volar buttress plate (Synthes, Paoli, Pennsylvania). The plate was contoured to better fit the patient’s tibia. We sutured the patellar allograft tendon to the patella using two No. 2-0 FiberWire sutures in Krackow suture technique8 (Figures 1B, 1C). We obtained good fixation of the patellar tendon, and the distance between the patellar insertion and the inferior patellar pole was the same as before surgery: 5.57 cm and comparable to the contralateral side (Figures 2A-2C). The patellar allograft and autograft sandwich were secured with additional No. 2-0 FiberWire sutures, and the quadriceps allograft and autograft were secured with the cross-stitch technique with the same material. Fine suturing of the quadriceps tendon was done with No. 0 Vicryl sutures. After the fixation was completed, we tested the stability of the reconstruction and found good flexion up to 120°.
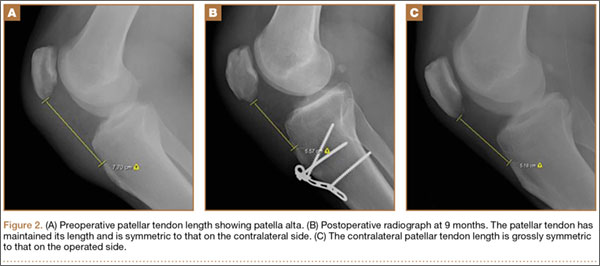
The postoperative protocol consisted of weight-bearing as tolerated in full extension and passive knee ROM, using a continuous passive ROM machine from 0° to 45° for the first 4 weeks, followed by active ROM, increased as tolerated, during the next 8 weeks.
The patient was seen in clinic 3 and 9 months after surgery. At the 3-month follow-up appointment, the patient’s examination showed knee ROM from 0° extension to 130° of flexion, no secondary infection signs, and radiographic evidence of a well-healing patellar allograft with symmetric patellar tendon length to the contralateral side. At 9-month follow-up, the patient’s active ROM was from 0° extension to 140° flexion (Figures 3A, 3B), and he had returned to his preinjury level of functioning.
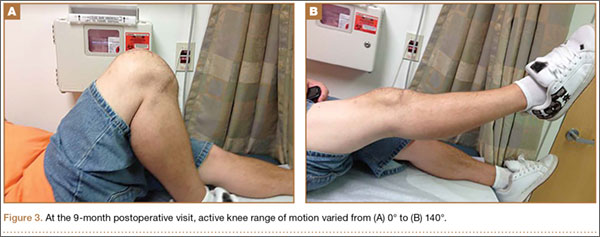
Discussion
This case report describes the successful reconstruction of a patellar tendon defect with cadaveric tendon–patellar tendon–bone allograft. Extensor mechanism injuries are uncommon in general, and the incidence of patellar tendon injury is higher in men than in women.2 Patellar tendon tears occur frequently in active patients younger than 40 years, usually as a result of sudden quadriceps contraction with the knee slightly flexed.1 Treatment of patellar tendon injury is surgical, and functional outcomes for patients with this injury are equivalent to those of patients with quadriceps tendon injuries or patellar fractures.2 Acute patellar tendon tears can be repaired by end-to-end suturing or transosseous tunnel insertion in the tibia or patella.1 Reinforcement is often added between the patella and tibial tuberosity, using a semitendinosus band or wire.1 End-to-end suture is performed using a thick resorbable suture. It is important to avoid patella alta during suturing, comparing the position of the patella with the contralateral patella with the knee in 45° of flexion. In proximal avulsion, the tendon is anchored to the bone by 2 thick nonresorbable sutures through 2 parallel bone tunnels to the proximal pole of the patella. Distal avulsion is rare in adults, but it can be managed by using staples or suture anchors.1
End-to-end suturing of chronic patellar tendon defects is difficult more than 45 days after injury primarily because of difficulties in correcting patella alta secondary to the upward force exerted by the quadriceps tendon.1,3 Extreme situations similar to the case we present warrant Achilles or patellar tendon allograft for reconstruction of the extensor mechanism.1,3,6,9
Extensor mechanism allograft also provides an effective remedy for severe quadriceps deficiency caused by loss of the patella, patellar tendon, and quadriceps tendon in total knee arthroplasty.10 However, in such cases, late failure is common, and major quadriceps deficiency occurs after removal of the allograft material.10 To improve outcome, a novel technique using the medial gastrocnemius muscle transferred to the muscular portion of the vastus medialis and lateralis flaps provides a secure and strong closure of the anterior knee, thereby restoring the extensor mechanism of the knee.10
Patellar tendon reconstruction with allograft tissue has been successfully used, especially in cases related to chronic patellar tendon ruptures11 and total knee arthroplasty.6,12-14 Crossett and colleagues12 showed that, at 2-year follow-up, the average knee score for pain, ROM, and stability had improved from 26 points (range, 6-39 points) before surgery to 81 points (range, 40-92 points). The average knee score for function had also improved: 14 points (range, 0-35 points) before surgery to 53 points (range, 30-90 points).12 Primary repair may succeed in early intervention, but in an established rupture, allograft reconstruction is often necessary. Achilles tendon is the preferred allograft, with the calcaneus fragment embedded into the proximal tibia as a new tubercle and the tendon sutured into the remaining extensor mechanism.1,11 The repair is further protected using a cable loop from the superior pole of the patella to a drill hole in the upper tibia.9 Techniques have also been described involving passage of the proximal aspect of the allograft tendon through patellar bone tunnels and suture fixation to the native quadriceps tendon.11,15 However, in our technique, we shaved off the anterior cortex of the patient’s patella to allow a sandwich-type over-position of the allograft to secure fixation to the patella.
Another alternative to allograft reconstruction involves biocompatible scaffolds. Such scaffolds incorporate the use of platelets in a fibrin framework. A CPFS, produced from blood and calcium gluconate to improve healing of patellar tendon defects, has been described in animal studies.7 In the rabbit model, CPFS acts as a provisional bioscaffold that can accelerate healing of an injured patellar tendon repair, potentially secondary to several growth factors derived from platelets.7 Platelets are biocompatible sources of growth factors, and CPFS can act as a scaffold to restore the mechanical integrity of injured soft tissue.7,16 In addition, CPFS can act to lower donor-site morbidity associated with harvesting tissue autograft.7 However, to our knowledge, such scaffolds have not been used in human trials. The LARS biocompatible ligament (Corin Group PLC, Cirencester, United Kingdom), currently not approved by the US Food and Drug Administration, is used for reconstructions of isolated or multiple knee ligament injuries.17 This graft requires the presence of healthy tissue with good blood supply from which new tendon or ligament can grow in. Sometimes it is also used for extensor mechanism reconstruction after radical tumor resection around the knee; however, good results are achieved in only 59% of cases,18 and to our knowledge, only 1 case of primary repair of a patellar tendon rupture has been published.19
Techniques involving the use of tendon–patellar tendon–bone graft with fixation via the sandwich-type over-position of the allograft for chronic patellar tendon rupture have not been described in the literature. In our patient, given the extensive patellar tendon lesion and inflammation with chronic tissue degeneration, there was no option but to use allograft. To improve the patient’s outcome, we chose the strongest possible allograft, tendon–patellar tendon–bone graft.
Conclusion
Revision patellar tendon reconstruction is a challenging, but necessary, procedure to restore the extensor mechanism of the knee, especially in young, active individuals. Various options to reconstruct the tissue defects are available. Our patient was successfully treated with a tendon–patellar tendon–bone allograft reconstruction.
1. Saragaglia D, Pison A, Rubens-Duval B. Acute and old ruptures of the extensor apparatus of the knee in adults (excluding knee replacement). Orthop Traumatol Surg Res. 2013;99(1 suppl):S67-S76.
2. Tejwani NC, Lekic N, Bechtel C, Montero N, Egol KA. Outcomes after knee joint extensor mechanism disruptions: is it better to fracture the patella or rupture the tendon? J Orthop Trauma. 2012;26(11):648-651.
3. Ecker ML, Lotke PA, Glazer RM. Late reconstruction of the patellar tendon. J Bone Joint Surg Am. 1979;61(6):884-886.
4. Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am. 1981;63(6):932-937.
5. Levy M, Goldstein J, Rosner M. A method of repair for quadriceps tendon or patellar ligament (tendon) ruptures without cast immobilization. Preliminary report. Clin Orthop Relat Res. 1987;218:297-301.
6. Burks RT, Edelson RH. Allograft reconstruction of the patellar ligament. A case report. J Bone Joint Surg Am. 1994;76(7):1077-1079.
7. Matsunaga D, Akizuki S, Takizawa T, Omae S, Kato H. Compact platelet-rich fibrin scaffold to improve healing of patellar tendon defects and for medial collateral ligament reconstruction. Knee. 2013;20(6):545-550.
8. Krackow KA, Thomas SC, Jones LC. Ligament-tendon fixation: analysis of a new stitch and comparison with standard techniques. Orthopedics. 1988;11(6):909-917.
9. Brooks P. Extensor mechanism ruptures. Orthopedics. 2009;32(9):683-684.
10. Whiteside LA. Surgical technique: muscle transfer restores extensor function after failed patella-patellar tendon allograft. Clin Orthop Relat Res. 2014;472(1):218-226.
11. Farmer K, Cosgarea AJ. Procedure 25. Acute and chronic patellar tendon ruptures. In: Miller MD, Cole BJ, Cosgarea AJ, Sekiya JK, eds. Operative Techniques: Sports Knee Surgery. Philadelphia, PA: Saunders (Elsevier); 2008:397-417.
12. Crossett LS, Sinha RK, Sechriest VF, Rubash HE. Reconstruction of a ruptured patellar tendon with achilles tendon allograft following total knee arthroplasty. J Bone Joint Surg Am. 2002;84(8):1354-1361.
13. Lahav A, Burks RT, Scholl MD. Allograft reconstruction of the patellar tendon: 12-year follow-up. Am J Orthop. 2004;33(12):623-624.
14. Yoo JH, Chang JD, Seo YJ, Baek SW. Reconstruction of a patellar tendon with Achilles tendon allograft for severe patellar infera--a case report. Knee. 2011;18(5):350-353.
15. Saldua NS, Mazurek MT. Procedure 37. Quadriceps and patellar tendon repair. In: Reider B, Terry MA, Provencher MT, eds. Operative Techniques: Sports Medicine Surgery. Philadelphia, PA: Saunders (Elsevier); 2010:623-640.
16. Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb Haemost. 2004;91(1):4-15.
17. Ibrahim SAR, Ahmad FHF, Salah M, Al Misfer ARK, Ghaffer SA, Khirat S. Surgical management of traumatic knee dislocation. Arthroscopy. 2008;24(2):178-187.
18. Dominkus M, Sabeti M, Toma C, Abdolvahab F, Trieb K, Kotz RI. Reconstructing the extensor apparatus with a new polyester ligament. Clin Orthop Relat Res. 2006;453:328-334.
19. Naim S, Gougoulias N, Griffiths D. Patellar tendon reconstruction using LARS ligament: surgical technique and case report. Strategies Trauma Limb Reconstr. 2011;6(1):39-41.
The extensor mechanism of the knee comprises the quadriceps tendon, the patella, and the patellar tendon. The extensor mechanism may be damaged by injury to these structures, with consequences such as the inability to actively extend the knee and hemarthrosis.1,2 Disruption of this mechanism is rare, and the most common injury pattern is an eccentric contraction of the quadriceps tendon on a flexed knee causing a tendon (quadriceps or patellar) rupture or a patella fracture.1,2
Patellar tendon ruptures are more common in persons younger than 40 years.1 Treatment is surgical, regardless of age and physical activity. In the acute setting, repair can be end-to-end suture or transosseous tunnel insertion. End-to-end suturing is difficult in chronic patellar tendon ruptures because of patella alta secondary to quadriceps contraction.3 Treatment options for chronic ruptures may involve transpatellar traction4 or tendon reinforcement with fascia lata, a semitendinosus band, or synthetic materials.3-5 Alternatively, tendon autograft and allografts have also been recommended, especially in extreme situations.1,6 Furthermore, animal experiments have shown that a compact platelet-rich fibrin scaffold (CPFS) has the potential to accelerate healing of patellar tendon defects and to act as a bioscaffold for graft augmentation.7
We describe the case of a 30-year-old man who underwent extensor mechanism reconstruction with cadaveric tendon–patellar tendon–bone allograft for failure of an infected primary end-to-end repair. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 30-year-old healthy man landed on an empty glass fish tank, resulting in a traumatic right-knee arthrotomy. On initial evaluation, the patient had a negative straight-leg-raise test and impaired knee extension. The patient was taken urgently to the operating room for irrigation and débridement and concurrent repair of the patellar tendon laceration. Antibiotic prophylaxis with 2 g of intravenous (IV) cefazolin was given in the emergency room.
Intraoperatively, after visualizing the patellar tendon laceration and excluding any associated chondral lesions, we proceeded with extensive débridement and irrigation using 9 L of normal saline pulse lavage. After we achieved a clean site, we proceeded to repair the patellar tendon using No. 2 FiberWire sutures (Arthrex, Naples, Florida) with a classic Krackow repair8 consisting of 2 sutures run in a 4-row fashion through the patella and the patellar tendon. The suture was securely tightened and then tested for stability to at least 90° of knee flexion. The retinaculum was repaired using No. 0 Vicryl sutures (Ethicon, Somerville, New Jersey). After wound closure and dressing, the patient was placed in a hinged knee brace locked in extension at all times after surgery. Antibiotic treatment with IV cefazolin was administered for 48 hours.
Postoperative management consisted of weight-bearing as tolerated on the operative limb and appropriate deep venous thrombosis prophylaxis. The patient followed up in clinic 2 weeks and 4 weeks after surgery. At 4 weeks, the patient was noted to have a secondary wound infection with superficial dehiscence and serosanguineous drainage. No wound opening was noticed, and local wound care was performed with a 1-week course of oral cephalexin. The patient was scheduled to follow up a few weeks later but did not follow up for a year.
At 1-year follow-up, the patient reported that he had had a steady progression of his knee range of motion (ROM) with decreased pain. However, over time, the patient noted subjective instability of the knee, with frequent falls occurring close to his 1-year follow-up. Examination of his knee showed that his active ROM ranged from 20° in extension to 120° in flexion, with a weak extensor mechanism. Passively, his knee could be brought to full extension. His incision was well healed, but it had an area of bogginess in the middle. Radiographs showed patella alta on the affected knee, with a lengthening of the patellar tendon of 7.70 cm on the right compared with 5.18 cm on the left. Magnetic resonance imaging (MRI) showed moderate-to-severe patellar tendinosis with small fluid pockets around the surgical material and evidence of acute patellar enthesopathy. The laboratory values showed a white blood cell count of 7580/μL (normal, 4500-11,000/μL), an erythrocyte sedimentation rate of 2 mm/h (normal, 1-15 mm/h), and a C-reactive protein level of 1.93 mg/dL (normal, 0.00-0.29 mg/dL). Based on the clinical examination and imaging findings, there was a concern for a possible chronic deep-tissue infection, in addition to failure of the primary patellar tendon repair. Operative versus nonoperative management options were discussed with the patient, and he elected to undergo surgery.
During surgery, the patellar laxity was confirmed, and the patellar tendon was noticed to be chronically thickened and surrounded by unhealthy tissue. Initially, an extensive soft-tissue débridement was performed, and all patellar tendon loculations visualized on the preoperative MRI were drained; a solid purulent-like fluid was expressed. Unfortunately, the extensive and required débridement did not allow the preservation of the patellar tendon. Appropriate cultures were taken and sent for immediate Gram-stain analysis, which returned negative. Tissue samples from the patellar tendon were also sent to the pathology department for analysis. Intraoperatively, the infrapatellar defect was filled temporarily with a tobramycin cement spacer mixed with 2 g of vancomycin in a manner similar to that of the Masquelet technique used for infected long-bone nonunions with bone loss.9,10 This technique is a 2-stage procedure that promotes the formation of a biologic membrane that allows bone healing in the reconstruction of long-bone defects. The first stage consists of a radical débridement with soft-tissue repair by flaps when needed, with the insertion of a polymethylmethacrylate cement spacer into the bone defect. The second stage is usually performed 6 to 8 weeks later, with removal of the spacer and preservation of the induced membrane, which is filled with iliac crest bone autograft augmented (if necessary) with demineralized allograft.
The incision was closed primarily, and after surgery, the patient was allowed to bear weight as tolerated in a hinged knee brace locked in extension. Final laboratory analysis from cultures and tissue samples revealed acute and chronic inflammation with more than 20 neutrophils per high-powered field. No organisms grew from aerobic, anaerobic, fungal, or mycobacterial cultures. The infectious disease service was consulted and recommended oral cephalexin.
Because all cultures were negative, all laboratory examinations did not indicate any residual infections, and no bony involvement was noticed intraoperatively or in the preoperative knee MRI, we decided to proceed with the second stage of the Masquelet technique after 2 weeks. The patient returned to the operating room for final reconstruction of his patellar tendon using a custom-ordered cadaveric tendon–patellar tendon–bone allograft, the length of which was determined by measuring the contralateral patellar tendon, ie, 5.18 cm (Figure 1A). The previous anterior knee incision was reopened and extended distally past the tibial tuberosity and proximally toward the quadriceps tendon. The antibiotic spacer was removed. We proceeded with a repeat irrigation and débridement and the allograft transfer. The selected allograft was customized by reducing the tibial bone component to an approximately 1×2-cm bone block and by reducing the allograft patellar thickness with an oscillating saw, leaving an approximately 2-mm thick patellar bone graft attached to the patellar tendon. In a similar technique using an oscillating saw, we shaved off the anterior cortex of the patient’s patella to accommodate, in a sandwich fashion, the patellar allograft. Proximally, the quadriceps tendon insertion was split longitudinally and partially separated from the superior pole of the patellar tendon to allow seating and fixation of the modified quadriceps allograft tendon component.
We proceeded with the fixation of the allograft first distally on the patella. The anterior cortex of the tibial tuberosity was resected to allow the perfect seating of the bone block allograft. The graft was secured with a 4.0-mm fully threaded cancellous lag screw and reinforced with a 2.4-mm, 3-hole T-volar buttress plate (Synthes, Paoli, Pennsylvania). The plate was contoured to better fit the patient’s tibia. We sutured the patellar allograft tendon to the patella using two No. 2-0 FiberWire sutures in Krackow suture technique8 (Figures 1B, 1C). We obtained good fixation of the patellar tendon, and the distance between the patellar insertion and the inferior patellar pole was the same as before surgery: 5.57 cm and comparable to the contralateral side (Figures 2A-2C). The patellar allograft and autograft sandwich were secured with additional No. 2-0 FiberWire sutures, and the quadriceps allograft and autograft were secured with the cross-stitch technique with the same material. Fine suturing of the quadriceps tendon was done with No. 0 Vicryl sutures. After the fixation was completed, we tested the stability of the reconstruction and found good flexion up to 120°.
The postoperative protocol consisted of weight-bearing as tolerated in full extension and passive knee ROM, using a continuous passive ROM machine from 0° to 45° for the first 4 weeks, followed by active ROM, increased as tolerated, during the next 8 weeks.
The patient was seen in clinic 3 and 9 months after surgery. At the 3-month follow-up appointment, the patient’s examination showed knee ROM from 0° extension to 130° of flexion, no secondary infection signs, and radiographic evidence of a well-healing patellar allograft with symmetric patellar tendon length to the contralateral side. At 9-month follow-up, the patient’s active ROM was from 0° extension to 140° flexion (Figures 3A, 3B), and he had returned to his preinjury level of functioning.
Discussion
This case report describes the successful reconstruction of a patellar tendon defect with cadaveric tendon–patellar tendon–bone allograft. Extensor mechanism injuries are uncommon in general, and the incidence of patellar tendon injury is higher in men than in women.2 Patellar tendon tears occur frequently in active patients younger than 40 years, usually as a result of sudden quadriceps contraction with the knee slightly flexed.1 Treatment of patellar tendon injury is surgical, and functional outcomes for patients with this injury are equivalent to those of patients with quadriceps tendon injuries or patellar fractures.2 Acute patellar tendon tears can be repaired by end-to-end suturing or transosseous tunnel insertion in the tibia or patella.1 Reinforcement is often added between the patella and tibial tuberosity, using a semitendinosus band or wire.1 End-to-end suture is performed using a thick resorbable suture. It is important to avoid patella alta during suturing, comparing the position of the patella with the contralateral patella with the knee in 45° of flexion. In proximal avulsion, the tendon is anchored to the bone by 2 thick nonresorbable sutures through 2 parallel bone tunnels to the proximal pole of the patella. Distal avulsion is rare in adults, but it can be managed by using staples or suture anchors.1
End-to-end suturing of chronic patellar tendon defects is difficult more than 45 days after injury primarily because of difficulties in correcting patella alta secondary to the upward force exerted by the quadriceps tendon.1,3 Extreme situations similar to the case we present warrant Achilles or patellar tendon allograft for reconstruction of the extensor mechanism.1,3,6,9
Extensor mechanism allograft also provides an effective remedy for severe quadriceps deficiency caused by loss of the patella, patellar tendon, and quadriceps tendon in total knee arthroplasty.10 However, in such cases, late failure is common, and major quadriceps deficiency occurs after removal of the allograft material.10 To improve outcome, a novel technique using the medial gastrocnemius muscle transferred to the muscular portion of the vastus medialis and lateralis flaps provides a secure and strong closure of the anterior knee, thereby restoring the extensor mechanism of the knee.10
Patellar tendon reconstruction with allograft tissue has been successfully used, especially in cases related to chronic patellar tendon ruptures11 and total knee arthroplasty.6,12-14 Crossett and colleagues12 showed that, at 2-year follow-up, the average knee score for pain, ROM, and stability had improved from 26 points (range, 6-39 points) before surgery to 81 points (range, 40-92 points). The average knee score for function had also improved: 14 points (range, 0-35 points) before surgery to 53 points (range, 30-90 points).12 Primary repair may succeed in early intervention, but in an established rupture, allograft reconstruction is often necessary. Achilles tendon is the preferred allograft, with the calcaneus fragment embedded into the proximal tibia as a new tubercle and the tendon sutured into the remaining extensor mechanism.1,11 The repair is further protected using a cable loop from the superior pole of the patella to a drill hole in the upper tibia.9 Techniques have also been described involving passage of the proximal aspect of the allograft tendon through patellar bone tunnels and suture fixation to the native quadriceps tendon.11,15 However, in our technique, we shaved off the anterior cortex of the patient’s patella to allow a sandwich-type over-position of the allograft to secure fixation to the patella.
Another alternative to allograft reconstruction involves biocompatible scaffolds. Such scaffolds incorporate the use of platelets in a fibrin framework. A CPFS, produced from blood and calcium gluconate to improve healing of patellar tendon defects, has been described in animal studies.7 In the rabbit model, CPFS acts as a provisional bioscaffold that can accelerate healing of an injured patellar tendon repair, potentially secondary to several growth factors derived from platelets.7 Platelets are biocompatible sources of growth factors, and CPFS can act as a scaffold to restore the mechanical integrity of injured soft tissue.7,16 In addition, CPFS can act to lower donor-site morbidity associated with harvesting tissue autograft.7 However, to our knowledge, such scaffolds have not been used in human trials. The LARS biocompatible ligament (Corin Group PLC, Cirencester, United Kingdom), currently not approved by the US Food and Drug Administration, is used for reconstructions of isolated or multiple knee ligament injuries.17 This graft requires the presence of healthy tissue with good blood supply from which new tendon or ligament can grow in. Sometimes it is also used for extensor mechanism reconstruction after radical tumor resection around the knee; however, good results are achieved in only 59% of cases,18 and to our knowledge, only 1 case of primary repair of a patellar tendon rupture has been published.19
Techniques involving the use of tendon–patellar tendon–bone graft with fixation via the sandwich-type over-position of the allograft for chronic patellar tendon rupture have not been described in the literature. In our patient, given the extensive patellar tendon lesion and inflammation with chronic tissue degeneration, there was no option but to use allograft. To improve the patient’s outcome, we chose the strongest possible allograft, tendon–patellar tendon–bone graft.
Conclusion
Revision patellar tendon reconstruction is a challenging, but necessary, procedure to restore the extensor mechanism of the knee, especially in young, active individuals. Various options to reconstruct the tissue defects are available. Our patient was successfully treated with a tendon–patellar tendon–bone allograft reconstruction.
The extensor mechanism of the knee comprises the quadriceps tendon, the patella, and the patellar tendon. The extensor mechanism may be damaged by injury to these structures, with consequences such as the inability to actively extend the knee and hemarthrosis.1,2 Disruption of this mechanism is rare, and the most common injury pattern is an eccentric contraction of the quadriceps tendon on a flexed knee causing a tendon (quadriceps or patellar) rupture or a patella fracture.1,2
Patellar tendon ruptures are more common in persons younger than 40 years.1 Treatment is surgical, regardless of age and physical activity. In the acute setting, repair can be end-to-end suture or transosseous tunnel insertion. End-to-end suturing is difficult in chronic patellar tendon ruptures because of patella alta secondary to quadriceps contraction.3 Treatment options for chronic ruptures may involve transpatellar traction4 or tendon reinforcement with fascia lata, a semitendinosus band, or synthetic materials.3-5 Alternatively, tendon autograft and allografts have also been recommended, especially in extreme situations.1,6 Furthermore, animal experiments have shown that a compact platelet-rich fibrin scaffold (CPFS) has the potential to accelerate healing of patellar tendon defects and to act as a bioscaffold for graft augmentation.7
We describe the case of a 30-year-old man who underwent extensor mechanism reconstruction with cadaveric tendon–patellar tendon–bone allograft for failure of an infected primary end-to-end repair. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 30-year-old healthy man landed on an empty glass fish tank, resulting in a traumatic right-knee arthrotomy. On initial evaluation, the patient had a negative straight-leg-raise test and impaired knee extension. The patient was taken urgently to the operating room for irrigation and débridement and concurrent repair of the patellar tendon laceration. Antibiotic prophylaxis with 2 g of intravenous (IV) cefazolin was given in the emergency room.
Intraoperatively, after visualizing the patellar tendon laceration and excluding any associated chondral lesions, we proceeded with extensive débridement and irrigation using 9 L of normal saline pulse lavage. After we achieved a clean site, we proceeded to repair the patellar tendon using No. 2 FiberWire sutures (Arthrex, Naples, Florida) with a classic Krackow repair8 consisting of 2 sutures run in a 4-row fashion through the patella and the patellar tendon. The suture was securely tightened and then tested for stability to at least 90° of knee flexion. The retinaculum was repaired using No. 0 Vicryl sutures (Ethicon, Somerville, New Jersey). After wound closure and dressing, the patient was placed in a hinged knee brace locked in extension at all times after surgery. Antibiotic treatment with IV cefazolin was administered for 48 hours.
Postoperative management consisted of weight-bearing as tolerated on the operative limb and appropriate deep venous thrombosis prophylaxis. The patient followed up in clinic 2 weeks and 4 weeks after surgery. At 4 weeks, the patient was noted to have a secondary wound infection with superficial dehiscence and serosanguineous drainage. No wound opening was noticed, and local wound care was performed with a 1-week course of oral cephalexin. The patient was scheduled to follow up a few weeks later but did not follow up for a year.
At 1-year follow-up, the patient reported that he had had a steady progression of his knee range of motion (ROM) with decreased pain. However, over time, the patient noted subjective instability of the knee, with frequent falls occurring close to his 1-year follow-up. Examination of his knee showed that his active ROM ranged from 20° in extension to 120° in flexion, with a weak extensor mechanism. Passively, his knee could be brought to full extension. His incision was well healed, but it had an area of bogginess in the middle. Radiographs showed patella alta on the affected knee, with a lengthening of the patellar tendon of 7.70 cm on the right compared with 5.18 cm on the left. Magnetic resonance imaging (MRI) showed moderate-to-severe patellar tendinosis with small fluid pockets around the surgical material and evidence of acute patellar enthesopathy. The laboratory values showed a white blood cell count of 7580/μL (normal, 4500-11,000/μL), an erythrocyte sedimentation rate of 2 mm/h (normal, 1-15 mm/h), and a C-reactive protein level of 1.93 mg/dL (normal, 0.00-0.29 mg/dL). Based on the clinical examination and imaging findings, there was a concern for a possible chronic deep-tissue infection, in addition to failure of the primary patellar tendon repair. Operative versus nonoperative management options were discussed with the patient, and he elected to undergo surgery.
During surgery, the patellar laxity was confirmed, and the patellar tendon was noticed to be chronically thickened and surrounded by unhealthy tissue. Initially, an extensive soft-tissue débridement was performed, and all patellar tendon loculations visualized on the preoperative MRI were drained; a solid purulent-like fluid was expressed. Unfortunately, the extensive and required débridement did not allow the preservation of the patellar tendon. Appropriate cultures were taken and sent for immediate Gram-stain analysis, which returned negative. Tissue samples from the patellar tendon were also sent to the pathology department for analysis. Intraoperatively, the infrapatellar defect was filled temporarily with a tobramycin cement spacer mixed with 2 g of vancomycin in a manner similar to that of the Masquelet technique used for infected long-bone nonunions with bone loss.9,10 This technique is a 2-stage procedure that promotes the formation of a biologic membrane that allows bone healing in the reconstruction of long-bone defects. The first stage consists of a radical débridement with soft-tissue repair by flaps when needed, with the insertion of a polymethylmethacrylate cement spacer into the bone defect. The second stage is usually performed 6 to 8 weeks later, with removal of the spacer and preservation of the induced membrane, which is filled with iliac crest bone autograft augmented (if necessary) with demineralized allograft.
The incision was closed primarily, and after surgery, the patient was allowed to bear weight as tolerated in a hinged knee brace locked in extension. Final laboratory analysis from cultures and tissue samples revealed acute and chronic inflammation with more than 20 neutrophils per high-powered field. No organisms grew from aerobic, anaerobic, fungal, or mycobacterial cultures. The infectious disease service was consulted and recommended oral cephalexin.
Because all cultures were negative, all laboratory examinations did not indicate any residual infections, and no bony involvement was noticed intraoperatively or in the preoperative knee MRI, we decided to proceed with the second stage of the Masquelet technique after 2 weeks. The patient returned to the operating room for final reconstruction of his patellar tendon using a custom-ordered cadaveric tendon–patellar tendon–bone allograft, the length of which was determined by measuring the contralateral patellar tendon, ie, 5.18 cm (Figure 1A). The previous anterior knee incision was reopened and extended distally past the tibial tuberosity and proximally toward the quadriceps tendon. The antibiotic spacer was removed. We proceeded with a repeat irrigation and débridement and the allograft transfer. The selected allograft was customized by reducing the tibial bone component to an approximately 1×2-cm bone block and by reducing the allograft patellar thickness with an oscillating saw, leaving an approximately 2-mm thick patellar bone graft attached to the patellar tendon. In a similar technique using an oscillating saw, we shaved off the anterior cortex of the patient’s patella to accommodate, in a sandwich fashion, the patellar allograft. Proximally, the quadriceps tendon insertion was split longitudinally and partially separated from the superior pole of the patellar tendon to allow seating and fixation of the modified quadriceps allograft tendon component.
We proceeded with the fixation of the allograft first distally on the patella. The anterior cortex of the tibial tuberosity was resected to allow the perfect seating of the bone block allograft. The graft was secured with a 4.0-mm fully threaded cancellous lag screw and reinforced with a 2.4-mm, 3-hole T-volar buttress plate (Synthes, Paoli, Pennsylvania). The plate was contoured to better fit the patient’s tibia. We sutured the patellar allograft tendon to the patella using two No. 2-0 FiberWire sutures in Krackow suture technique8 (Figures 1B, 1C). We obtained good fixation of the patellar tendon, and the distance between the patellar insertion and the inferior patellar pole was the same as before surgery: 5.57 cm and comparable to the contralateral side (Figures 2A-2C). The patellar allograft and autograft sandwich were secured with additional No. 2-0 FiberWire sutures, and the quadriceps allograft and autograft were secured with the cross-stitch technique with the same material. Fine suturing of the quadriceps tendon was done with No. 0 Vicryl sutures. After the fixation was completed, we tested the stability of the reconstruction and found good flexion up to 120°.
The postoperative protocol consisted of weight-bearing as tolerated in full extension and passive knee ROM, using a continuous passive ROM machine from 0° to 45° for the first 4 weeks, followed by active ROM, increased as tolerated, during the next 8 weeks.
The patient was seen in clinic 3 and 9 months after surgery. At the 3-month follow-up appointment, the patient’s examination showed knee ROM from 0° extension to 130° of flexion, no secondary infection signs, and radiographic evidence of a well-healing patellar allograft with symmetric patellar tendon length to the contralateral side. At 9-month follow-up, the patient’s active ROM was from 0° extension to 140° flexion (Figures 3A, 3B), and he had returned to his preinjury level of functioning.
Discussion
This case report describes the successful reconstruction of a patellar tendon defect with cadaveric tendon–patellar tendon–bone allograft. Extensor mechanism injuries are uncommon in general, and the incidence of patellar tendon injury is higher in men than in women.2 Patellar tendon tears occur frequently in active patients younger than 40 years, usually as a result of sudden quadriceps contraction with the knee slightly flexed.1 Treatment of patellar tendon injury is surgical, and functional outcomes for patients with this injury are equivalent to those of patients with quadriceps tendon injuries or patellar fractures.2 Acute patellar tendon tears can be repaired by end-to-end suturing or transosseous tunnel insertion in the tibia or patella.1 Reinforcement is often added between the patella and tibial tuberosity, using a semitendinosus band or wire.1 End-to-end suture is performed using a thick resorbable suture. It is important to avoid patella alta during suturing, comparing the position of the patella with the contralateral patella with the knee in 45° of flexion. In proximal avulsion, the tendon is anchored to the bone by 2 thick nonresorbable sutures through 2 parallel bone tunnels to the proximal pole of the patella. Distal avulsion is rare in adults, but it can be managed by using staples or suture anchors.1
End-to-end suturing of chronic patellar tendon defects is difficult more than 45 days after injury primarily because of difficulties in correcting patella alta secondary to the upward force exerted by the quadriceps tendon.1,3 Extreme situations similar to the case we present warrant Achilles or patellar tendon allograft for reconstruction of the extensor mechanism.1,3,6,9
Extensor mechanism allograft also provides an effective remedy for severe quadriceps deficiency caused by loss of the patella, patellar tendon, and quadriceps tendon in total knee arthroplasty.10 However, in such cases, late failure is common, and major quadriceps deficiency occurs after removal of the allograft material.10 To improve outcome, a novel technique using the medial gastrocnemius muscle transferred to the muscular portion of the vastus medialis and lateralis flaps provides a secure and strong closure of the anterior knee, thereby restoring the extensor mechanism of the knee.10
Patellar tendon reconstruction with allograft tissue has been successfully used, especially in cases related to chronic patellar tendon ruptures11 and total knee arthroplasty.6,12-14 Crossett and colleagues12 showed that, at 2-year follow-up, the average knee score for pain, ROM, and stability had improved from 26 points (range, 6-39 points) before surgery to 81 points (range, 40-92 points). The average knee score for function had also improved: 14 points (range, 0-35 points) before surgery to 53 points (range, 30-90 points).12 Primary repair may succeed in early intervention, but in an established rupture, allograft reconstruction is often necessary. Achilles tendon is the preferred allograft, with the calcaneus fragment embedded into the proximal tibia as a new tubercle and the tendon sutured into the remaining extensor mechanism.1,11 The repair is further protected using a cable loop from the superior pole of the patella to a drill hole in the upper tibia.9 Techniques have also been described involving passage of the proximal aspect of the allograft tendon through patellar bone tunnels and suture fixation to the native quadriceps tendon.11,15 However, in our technique, we shaved off the anterior cortex of the patient’s patella to allow a sandwich-type over-position of the allograft to secure fixation to the patella.
Another alternative to allograft reconstruction involves biocompatible scaffolds. Such scaffolds incorporate the use of platelets in a fibrin framework. A CPFS, produced from blood and calcium gluconate to improve healing of patellar tendon defects, has been described in animal studies.7 In the rabbit model, CPFS acts as a provisional bioscaffold that can accelerate healing of an injured patellar tendon repair, potentially secondary to several growth factors derived from platelets.7 Platelets are biocompatible sources of growth factors, and CPFS can act as a scaffold to restore the mechanical integrity of injured soft tissue.7,16 In addition, CPFS can act to lower donor-site morbidity associated with harvesting tissue autograft.7 However, to our knowledge, such scaffolds have not been used in human trials. The LARS biocompatible ligament (Corin Group PLC, Cirencester, United Kingdom), currently not approved by the US Food and Drug Administration, is used for reconstructions of isolated or multiple knee ligament injuries.17 This graft requires the presence of healthy tissue with good blood supply from which new tendon or ligament can grow in. Sometimes it is also used for extensor mechanism reconstruction after radical tumor resection around the knee; however, good results are achieved in only 59% of cases,18 and to our knowledge, only 1 case of primary repair of a patellar tendon rupture has been published.19
Techniques involving the use of tendon–patellar tendon–bone graft with fixation via the sandwich-type over-position of the allograft for chronic patellar tendon rupture have not been described in the literature. In our patient, given the extensive patellar tendon lesion and inflammation with chronic tissue degeneration, there was no option but to use allograft. To improve the patient’s outcome, we chose the strongest possible allograft, tendon–patellar tendon–bone graft.
Conclusion
Revision patellar tendon reconstruction is a challenging, but necessary, procedure to restore the extensor mechanism of the knee, especially in young, active individuals. Various options to reconstruct the tissue defects are available. Our patient was successfully treated with a tendon–patellar tendon–bone allograft reconstruction.
1. Saragaglia D, Pison A, Rubens-Duval B. Acute and old ruptures of the extensor apparatus of the knee in adults (excluding knee replacement). Orthop Traumatol Surg Res. 2013;99(1 suppl):S67-S76.
2. Tejwani NC, Lekic N, Bechtel C, Montero N, Egol KA. Outcomes after knee joint extensor mechanism disruptions: is it better to fracture the patella or rupture the tendon? J Orthop Trauma. 2012;26(11):648-651.
3. Ecker ML, Lotke PA, Glazer RM. Late reconstruction of the patellar tendon. J Bone Joint Surg Am. 1979;61(6):884-886.
4. Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am. 1981;63(6):932-937.
5. Levy M, Goldstein J, Rosner M. A method of repair for quadriceps tendon or patellar ligament (tendon) ruptures without cast immobilization. Preliminary report. Clin Orthop Relat Res. 1987;218:297-301.
6. Burks RT, Edelson RH. Allograft reconstruction of the patellar ligament. A case report. J Bone Joint Surg Am. 1994;76(7):1077-1079.
7. Matsunaga D, Akizuki S, Takizawa T, Omae S, Kato H. Compact platelet-rich fibrin scaffold to improve healing of patellar tendon defects and for medial collateral ligament reconstruction. Knee. 2013;20(6):545-550.
8. Krackow KA, Thomas SC, Jones LC. Ligament-tendon fixation: analysis of a new stitch and comparison with standard techniques. Orthopedics. 1988;11(6):909-917.
9. Brooks P. Extensor mechanism ruptures. Orthopedics. 2009;32(9):683-684.
10. Whiteside LA. Surgical technique: muscle transfer restores extensor function after failed patella-patellar tendon allograft. Clin Orthop Relat Res. 2014;472(1):218-226.
11. Farmer K, Cosgarea AJ. Procedure 25. Acute and chronic patellar tendon ruptures. In: Miller MD, Cole BJ, Cosgarea AJ, Sekiya JK, eds. Operative Techniques: Sports Knee Surgery. Philadelphia, PA: Saunders (Elsevier); 2008:397-417.
12. Crossett LS, Sinha RK, Sechriest VF, Rubash HE. Reconstruction of a ruptured patellar tendon with achilles tendon allograft following total knee arthroplasty. J Bone Joint Surg Am. 2002;84(8):1354-1361.
13. Lahav A, Burks RT, Scholl MD. Allograft reconstruction of the patellar tendon: 12-year follow-up. Am J Orthop. 2004;33(12):623-624.
14. Yoo JH, Chang JD, Seo YJ, Baek SW. Reconstruction of a patellar tendon with Achilles tendon allograft for severe patellar infera--a case report. Knee. 2011;18(5):350-353.
15. Saldua NS, Mazurek MT. Procedure 37. Quadriceps and patellar tendon repair. In: Reider B, Terry MA, Provencher MT, eds. Operative Techniques: Sports Medicine Surgery. Philadelphia, PA: Saunders (Elsevier); 2010:623-640.
16. Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb Haemost. 2004;91(1):4-15.
17. Ibrahim SAR, Ahmad FHF, Salah M, Al Misfer ARK, Ghaffer SA, Khirat S. Surgical management of traumatic knee dislocation. Arthroscopy. 2008;24(2):178-187.
18. Dominkus M, Sabeti M, Toma C, Abdolvahab F, Trieb K, Kotz RI. Reconstructing the extensor apparatus with a new polyester ligament. Clin Orthop Relat Res. 2006;453:328-334.
19. Naim S, Gougoulias N, Griffiths D. Patellar tendon reconstruction using LARS ligament: surgical technique and case report. Strategies Trauma Limb Reconstr. 2011;6(1):39-41.
1. Saragaglia D, Pison A, Rubens-Duval B. Acute and old ruptures of the extensor apparatus of the knee in adults (excluding knee replacement). Orthop Traumatol Surg Res. 2013;99(1 suppl):S67-S76.
2. Tejwani NC, Lekic N, Bechtel C, Montero N, Egol KA. Outcomes after knee joint extensor mechanism disruptions: is it better to fracture the patella or rupture the tendon? J Orthop Trauma. 2012;26(11):648-651.
3. Ecker ML, Lotke PA, Glazer RM. Late reconstruction of the patellar tendon. J Bone Joint Surg Am. 1979;61(6):884-886.
4. Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am. 1981;63(6):932-937.
5. Levy M, Goldstein J, Rosner M. A method of repair for quadriceps tendon or patellar ligament (tendon) ruptures without cast immobilization. Preliminary report. Clin Orthop Relat Res. 1987;218:297-301.
6. Burks RT, Edelson RH. Allograft reconstruction of the patellar ligament. A case report. J Bone Joint Surg Am. 1994;76(7):1077-1079.
7. Matsunaga D, Akizuki S, Takizawa T, Omae S, Kato H. Compact platelet-rich fibrin scaffold to improve healing of patellar tendon defects and for medial collateral ligament reconstruction. Knee. 2013;20(6):545-550.
8. Krackow KA, Thomas SC, Jones LC. Ligament-tendon fixation: analysis of a new stitch and comparison with standard techniques. Orthopedics. 1988;11(6):909-917.
9. Brooks P. Extensor mechanism ruptures. Orthopedics. 2009;32(9):683-684.
10. Whiteside LA. Surgical technique: muscle transfer restores extensor function after failed patella-patellar tendon allograft. Clin Orthop Relat Res. 2014;472(1):218-226.
11. Farmer K, Cosgarea AJ. Procedure 25. Acute and chronic patellar tendon ruptures. In: Miller MD, Cole BJ, Cosgarea AJ, Sekiya JK, eds. Operative Techniques: Sports Knee Surgery. Philadelphia, PA: Saunders (Elsevier); 2008:397-417.
12. Crossett LS, Sinha RK, Sechriest VF, Rubash HE. Reconstruction of a ruptured patellar tendon with achilles tendon allograft following total knee arthroplasty. J Bone Joint Surg Am. 2002;84(8):1354-1361.
13. Lahav A, Burks RT, Scholl MD. Allograft reconstruction of the patellar tendon: 12-year follow-up. Am J Orthop. 2004;33(12):623-624.
14. Yoo JH, Chang JD, Seo YJ, Baek SW. Reconstruction of a patellar tendon with Achilles tendon allograft for severe patellar infera--a case report. Knee. 2011;18(5):350-353.
15. Saldua NS, Mazurek MT. Procedure 37. Quadriceps and patellar tendon repair. In: Reider B, Terry MA, Provencher MT, eds. Operative Techniques: Sports Medicine Surgery. Philadelphia, PA: Saunders (Elsevier); 2010:623-640.
16. Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb Haemost. 2004;91(1):4-15.
17. Ibrahim SAR, Ahmad FHF, Salah M, Al Misfer ARK, Ghaffer SA, Khirat S. Surgical management of traumatic knee dislocation. Arthroscopy. 2008;24(2):178-187.
18. Dominkus M, Sabeti M, Toma C, Abdolvahab F, Trieb K, Kotz RI. Reconstructing the extensor apparatus with a new polyester ligament. Clin Orthop Relat Res. 2006;453:328-334.
19. Naim S, Gougoulias N, Griffiths D. Patellar tendon reconstruction using LARS ligament: surgical technique and case report. Strategies Trauma Limb Reconstr. 2011;6(1):39-41.

Intra-Articular Dislocation of the Patella With Associated Hoffa Fracture in a Skeletally Immature Patient
In 1887, Midelfart1 first reported on an intra-articular dislocation of the patella, and since then approximately 50 cases have been reported in the worldwide literature.2 Also known as an inferior patellar dislocation, these rare traumatic events occur when the patella dislocates intra-articularly. Because the patella commonly rotates about its horizontal axis, the articular surface is facing proximally or distally. The patella becomes lodged within the trochlea and locks the knee joint. Most cases described in the literature involved adolescent boys, with the patella difficult to reduce. Most patients required open reduction, while those who underwent successful closed reduction often needed general anesthesia.3
Similarly, coronal shear fractures of the femoral condyle (ie, Hoffa fractures) are an uncommon fracture pattern typically seen in adults. These fractures are even more infrequent in skeletally immature patients, with fewer than 5 cases documented in the literature.4-7 In our case report, we present a 14-year-old boy with a coronal shear fracture of the femoral condyle associated with an intra-articular patellar dislocation. To our knowledge, this constellation of injuries has not been reported. Additionally, closed reduction of the patella was successful after intra-articular lidocaine injection, without the need for sedation or general anesthesia. The patient’s guardian provided written informed consent for print and electronic publication of this case report.
Case Report
A 14-year-old boy presented to our institution after sustaining a direct blow to his left knee. The injury occurred as he jumped and landed on a flexed knee while playing with friends. The patient was unable to ambulate after the injury, and his left knee was locked in a slightly flexed position. Examination in the emergency department showed the knee to be held in approximately 60º of flexion, with an obvious bony prominence noted anteriorly over the femoral condyles. The patient was unable to perform a straight leg raise or any active range of motion (ROM) at the knee. Radiographs performed with the knee maintained in flexion confirmed that the patella was displaced into the knee joint and was rotated with the articular surface facing distally. Also noted was a coronal shear fracture of the lateral femoral condyle (Figures 1A, 1B).
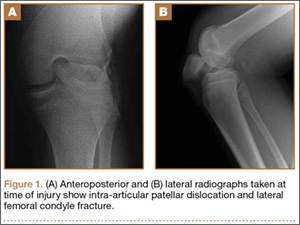
The patient received pain medication and an intra-articular lidocaine injection prior to a reduction attempt by the orthopedic resident. With the patient supine, the hip was gently flexed to relax the quadriceps muscle. As the knee was flexed up to 110º, the prominent patella was gripped between the thumb and fingers to gently free and elevate the patella out of the intercondylar notch.
After reduction, an immediate return of normal patellar contour and patellofemoral tracking was observed as the knee was gently extended. There was no obvious defect to the patellar or quadriceps tendons, and the patient was able to perform a straight-leg raise, confirming the integrity of the extensor mechanism. Radiographs performed after the reduction confirmed relocation of the patella in correct anatomic position, as well as a lateral femoral condyle fracture (Figures 2A, 2B). Magnetic resonance imaging (MRI) of the knee confirmed no full-thickness quadriceps or patellar tendon tear. A computed tomography (CT) scan of the knee showed a comminuted fracture of the lateral femoral condyle in the coronal plane, as well as multiple bone fragments within the joint (Figures 3A, 3B). The patient was placed in a bulky soft dressing and underwent open reduction and internal fixation of the fracture.
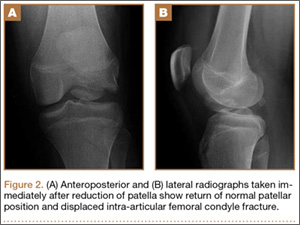
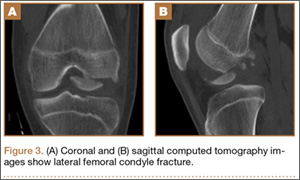
A 10-cm incision was made over the anterior aspect of the knee, and after dissection to the level of the retinaculum, a lateral parapatellar arthrotomy was performed. The patella was retracted medially to identify and free the fracture fragments. The fracture fragments were provisionally reduced and stabilized with three 0.065-in Kirschner wires. An area of osteochondral impaction proximal to the fracture was elevated and allograft bone was incorporated below the articular surface (Figures 4A, 4B). Rigid fixation of the fracture was achieved using 3 screws (2 Bio-Compression Screws [Arthrex Inc., Naples, Florida] and 1 Synthes cannulated screw [Synthes, West Chester, Pennsylvania]). The screws were placed in posteroanterior (PA) direction and inserted into the weight-bearing articular surface of the femoral condyle (Figures 4C, 4D). The screws were countersunk, and stable fixation with compression of the fracture was achieved. Reduction and screw position were verified with fluoroscopic views. The wound was closed in layers, and the patient was discharged home the next day.
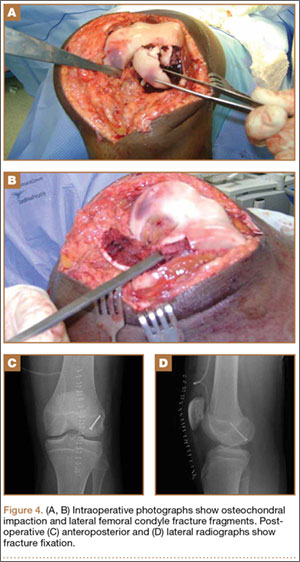
Postoperatively, the patient was non-weight-bearing on the affected limb with a hinged-knee brace to allow for knee ROM exercises immediately. He was also given a continuous passive motion device to maintain knee motion. At the 6-week mark, the patient’s fracture alignment appeared to be well-maintained and showed interval healing. Clinically, the patient was noted to have limited knee ROM. The decision was made to take the patient to the operating room primarily for a manipulation under anesthesia and resection of scar tissue from postoperative arthrofibrosis. Arthroscopic screw removal was also planned as a secondary procedure at the same time in order to prevent the possibility of chondral injury from screw migration. During the procedure, the patient was noted to have improved ROM from 5º to 85º premanipulation to 5º to 110º postoperatively. At 3 months after the initial injury, the patient was allowed to begin progressive weight-bearing on the left knee. At most recent follow-up, after 12 months, the patient was able to ambulate and bear weight on the left leg without pain. Plain radiographs show a well-healed fracture with no evidence of collapse of the femoral condyle (Figures 5A, 5B). His active ROM of the left knee was 5º to 110º without pain (Figures 5C, 5D).

Discussion
In the vast majority of patellar dislocations, the patella dislocates laterally over the trochlear groove. Inferior, or intra-articular, dislocations of the patella are rare. The mechanism of injury is usually a blow onto the patella with a flexed knee. The 2 groups commonly involved are adolescent boys and the elderly.8,9 In young men, it is thought that lax patellar attachments place adolescents at higher risk for this type of injury.10-12 While patella fractures and frank extensor mechanism ruptures are uncommon in this age group, the same mechanism of injury can lead to stripping of the deep fibers of the patellar tendon from the superior pole of the patella.3,13 The intact superficial fibers of the tendon allow the patella to hinge and displace into the joint.14
Inferior dislocations of the patella are classified into 2 types based on the orientation of the articular surface and the presence of osteophytes.15 Type I inferior dislocations occur after a direct blow to a flexed knee forces the superior pole of the patella into the intercondylar notch. Type II dislocations are caused by osteophytes on the superior pole of the patella that become wedged in the intercondylar notch and dislocate the patella inferiorly. In type I dislocations, the patella is rotated in the horizontal plane and the articular surface often faces inferiorly, but type II dislocations do not involve rotation of the articular surface. Type II injuries are seen more commonly in the elderly.
Our patient was able to tolerate a closed reduction of the patella after an intra-articular lidocaine injection, and a successful reduction was achieved without great difficulty. However, the majority of reports describe the need for an open reduction of inferior patellar dislocations.3,8 When closed reductions were a success, they were performed under general anesthesia or conscious sedation.3 It is thought that the difficulty of reduction results from the tension of the quadriceps muscle pulling the patella superiorly into intercondylar notch.11,16 However, successful closed reduction may be more likely in patients with less patellar rotation and entrapment within the intercondylar notch, as well as in patients whose knee is near full extension at presentation.17-19 Successful closed reduction is also seen in elderly patients, where dislocation is generally caused by less forceful impact and held by osteophytes. In these patients, the knee is commonly held in extension.12,15,20-22
The fracture pattern seen in this case also shows a rare fracture in skeletally immature patients, with only a few case reports in the literature. Isolated coronal plane femur fractures account for 0.65% of all femur fractures and are usually seen in adults after high-energy trauma.23 In the skeletally immature, the fracture can occur with lower-energy mechanisms. The typical mechanism is thought to be a shearing force to the femur caused by an axial load to the knee in 90° or more of flexion.4,24 A CT scan is recommended for better identification of the fracture and to plan treatment.25,26 Because of their intra-articular nature and tenuous blood supply, Hoffa fractures tend to do poorly with nonoperative treatment and are prone to displacement and nonunion.27,28 The goal of operative treatment is to obtain anatomic reduction and rigid fixation. While operative fixation techniques are varied, screw fixation with multiple smaller diameter screws has equal pullout strength compared to larger screws and may minimize damage to the articular cartilage.29-31 By preserving blood supply to the fracture, and allowing for early active mobilization, operative treatment generally provides good long-term functional outcomes in these fracture patterns.24
Conclusion
We describe a case in which the patella of an adolescent boy dislocated inferiorly into the knee joint, with an associated coronal shear fracture of the lateral femoral condyle. To our knowledge, this constellation of injuries has not been reported. For this uncommon injury pattern, we recommend a sequential treatment algorithm to minimize morbidity. We recommend first attempting a closed reduction of the patella with adequate pain control to avoid the morbidity associated with general anesthesia. After a successful reduction, an advanced imaging study (eg, MRI) is advisable to assess for concomitant soft-tissue injuries and preoperative planning, if necessary. The mechanism of injury and force required to cause a patellar dislocation of this nature leaves a high likelihood of other injuries. When a fracture is noted on plain radiographs after reduction, a CT scan can provide important information for planning surgical fixation of the fracture. Even in a skeletally immature patient, the principle of direct reduction and stable interfragmentary fixation of an articular fracture is critical for long-term function, even after a significant trauma to the knee.
1. Midelfart V. En sjelden luxation of patella. Norsk Magazin for Laegevidenskaben. 1887;4:588.
2. Kramer DE, Simoni MK. Horizontal intra-articular patellar dislocation resulting in quadriceps avulsion and medial patellofemoral ligament tear: a case report. J Pediatr Orthop B. 2013;22(4):329-332.
3. van den Broek TA, Moll PJ. Horizontal rotation of the patella. A case report with review of the literature. Acta Orthop Scand. 1985;56(5):436-438.
4. Flanagin BA, Cruz AI, Medvecky MJ. Hoffa fracture in a 14-year-old. Orthopedics. 2011;34(2):138.
5. Strauss E, Nelson JM, Abdelwahab IF. Fracture of the lateral femoral condyle. A case report. Bull Hosp Jt Dis Orthop Inst. 1984;44(1):86-90.
6. Biau DJ, Schranz PJ. Transverse Hoffa’s or deep osteochondral fracture? An unusual fracture of the lateral femoral condyle in a child. Injury. 2005;36(7):862-865.
7. McDonough PW, Bernstein RM. Nonunion of a Hoffa fracture in a child. J Orthop Trauma. 2000;14(7):519-521.
8. Brady TA, Russell D. Interarticular horizontal dislocation of the patella. A case report. J Bone Joint Surg Am. 1965;47(7):1393-1396.
9. Yuguero M, Gonzalez JA, Carma A, Huguet J. Intra-articular patellar dislocation. Orthopedics. 2003;26(5):517-518.
10. Frangakis EK. Intra-articular dislocation of the patella. A case report. J Bone Joint Surg Am. 1974;56(2):423-424.
11. Nanda R, Yadav RS, Thakur M. Intra-articular dislocation of the patella. J Trauma. 2000;48(1):159-160.
12. Choudhary RK, Tice JW. Intra-articular dislocation of the patella with incomplete rotation--two case reports and a review of the literature. Knee. 2004;11(2):125-127.
13. Chatziantoniou I, Diakos G, Pantelelli M. Horizontal dislocation of the patella. Case report. EEXOT. 2008;59(2):112-114.
14. McHugh G, Ryan E, Cleary M, Kenny P, O’Flanagan S, Keogh P. Intra-articular dislocation of the patella. Case Rep Orthop. 2013;2013:535803.
15. Bankes MJ, Eastwood DM. Inferior dislocation of the patella in the degenerate knee. Injury. 2002;33(6):528-529.
16. Theodorides A, Guo S, Case R. Intra-articular dislocation of the patella: A case report and review of the literature. Injury Extra. 2010;41(10):103-105.
17. Dimentberg RA. Intra-articular dislocation of the patella: case report and literature review. Clin J Sport Med. 1997;7(2):126-128.
18. Morin WD, Steadman JR. Case report of a successful closed reduction without anesthesia. Clin Orthop. 1993(297):179-181.
19. Murakami Y. Intra-articular dislocation of the patella. A case report. Clin Orthop. 1982;171:137-139.
20. Joshi RP. Inferior dislocation of the patella. Injury. 1997;28(5-6):389-390.
21. Garner JP, Pike JM, George CD. Intra-articular dislocation of the patella: two cases and literature review. J Trauma. 1999;47(4):780-783.
22. McCarthy TA, Quinn B, Pegum JM. Inferior dislocation of the patella: an unusual cause of a locked knee. Ir J Med Sci. 2001;170(3):209-210.
23. Manfredini M, Gildone A, Ferrante R, Bernasconi S, Massari L. Unicondylar femoral fractures: therapeutic strategy and long-term results. A review of 23 patients. Acta Orthop Belg. 2001;67(2):132-138.
24. Holmes SM, Bomback D, Baumgaertner MR. Coronal fractures of the femoral condyle: a brief report of five cases. J Orthop Trauma. 2004;18(5):316-319.
25. Nork SE, Segina DN, Aflatoon K, et al. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. J Bone Joint Surg Am. 2005;87(3):564-569.
26. Allmann KH, Altehoefer C, Wildanger G, et al. Hoffa fracture--a radiologic diagnostic approach. J Belge Radiol. 1996;79(5):201-202.
27. Oztürk A, Ozkan Y, Ozdemir RM. Nonunion of a Hoffa fracture in an adult. Chir Organi Mov. 2009;93(3):183-185.
28. Lewis SL, Pozo JL, Muirhead-Allwood WF. Coronal fractures of the lateral femoral condyle. J Bone Joint Surg Br. 1989;71(1):118-120.
29. Arastu MH, Kokke MC, Duffy PJ, Korley RE, Buckley RE. Coronal plane partial articular fractures of the distal femoral condyle: current concepts in management. Bone Joint J. 2013;95-B(9):1165-1171.
30. Westmoreland GL, McLaurin TM, Hutton WC. Screw pullout strength: a biomechanical comparison of large-fragment and small-fragment fixation in the tibial plateau. J Orthop Trauma. 2002;16(3):178-181.
31. Jarit GJ, Kummer FJ, Gibber MJ, Egol KA. A mechanical evaluation of two fixation methods using cancellous screws for coronal fractures of the lateral condyle of the distal femur (OTA type 33B). J Orthop Trauma. 2006;20(4):273-276.
In 1887, Midelfart1 first reported on an intra-articular dislocation of the patella, and since then approximately 50 cases have been reported in the worldwide literature.2 Also known as an inferior patellar dislocation, these rare traumatic events occur when the patella dislocates intra-articularly. Because the patella commonly rotates about its horizontal axis, the articular surface is facing proximally or distally. The patella becomes lodged within the trochlea and locks the knee joint. Most cases described in the literature involved adolescent boys, with the patella difficult to reduce. Most patients required open reduction, while those who underwent successful closed reduction often needed general anesthesia.3
Similarly, coronal shear fractures of the femoral condyle (ie, Hoffa fractures) are an uncommon fracture pattern typically seen in adults. These fractures are even more infrequent in skeletally immature patients, with fewer than 5 cases documented in the literature.4-7 In our case report, we present a 14-year-old boy with a coronal shear fracture of the femoral condyle associated with an intra-articular patellar dislocation. To our knowledge, this constellation of injuries has not been reported. Additionally, closed reduction of the patella was successful after intra-articular lidocaine injection, without the need for sedation or general anesthesia. The patient’s guardian provided written informed consent for print and electronic publication of this case report.
Case Report
A 14-year-old boy presented to our institution after sustaining a direct blow to his left knee. The injury occurred as he jumped and landed on a flexed knee while playing with friends. The patient was unable to ambulate after the injury, and his left knee was locked in a slightly flexed position. Examination in the emergency department showed the knee to be held in approximately 60º of flexion, with an obvious bony prominence noted anteriorly over the femoral condyles. The patient was unable to perform a straight leg raise or any active range of motion (ROM) at the knee. Radiographs performed with the knee maintained in flexion confirmed that the patella was displaced into the knee joint and was rotated with the articular surface facing distally. Also noted was a coronal shear fracture of the lateral femoral condyle (Figures 1A, 1B).
The patient received pain medication and an intra-articular lidocaine injection prior to a reduction attempt by the orthopedic resident. With the patient supine, the hip was gently flexed to relax the quadriceps muscle. As the knee was flexed up to 110º, the prominent patella was gripped between the thumb and fingers to gently free and elevate the patella out of the intercondylar notch.
After reduction, an immediate return of normal patellar contour and patellofemoral tracking was observed as the knee was gently extended. There was no obvious defect to the patellar or quadriceps tendons, and the patient was able to perform a straight-leg raise, confirming the integrity of the extensor mechanism. Radiographs performed after the reduction confirmed relocation of the patella in correct anatomic position, as well as a lateral femoral condyle fracture (Figures 2A, 2B). Magnetic resonance imaging (MRI) of the knee confirmed no full-thickness quadriceps or patellar tendon tear. A computed tomography (CT) scan of the knee showed a comminuted fracture of the lateral femoral condyle in the coronal plane, as well as multiple bone fragments within the joint (Figures 3A, 3B). The patient was placed in a bulky soft dressing and underwent open reduction and internal fixation of the fracture.
A 10-cm incision was made over the anterior aspect of the knee, and after dissection to the level of the retinaculum, a lateral parapatellar arthrotomy was performed. The patella was retracted medially to identify and free the fracture fragments. The fracture fragments were provisionally reduced and stabilized with three 0.065-in Kirschner wires. An area of osteochondral impaction proximal to the fracture was elevated and allograft bone was incorporated below the articular surface (Figures 4A, 4B). Rigid fixation of the fracture was achieved using 3 screws (2 Bio-Compression Screws [Arthrex Inc., Naples, Florida] and 1 Synthes cannulated screw [Synthes, West Chester, Pennsylvania]). The screws were placed in posteroanterior (PA) direction and inserted into the weight-bearing articular surface of the femoral condyle (Figures 4C, 4D). The screws were countersunk, and stable fixation with compression of the fracture was achieved. Reduction and screw position were verified with fluoroscopic views. The wound was closed in layers, and the patient was discharged home the next day.
Postoperatively, the patient was non-weight-bearing on the affected limb with a hinged-knee brace to allow for knee ROM exercises immediately. He was also given a continuous passive motion device to maintain knee motion. At the 6-week mark, the patient’s fracture alignment appeared to be well-maintained and showed interval healing. Clinically, the patient was noted to have limited knee ROM. The decision was made to take the patient to the operating room primarily for a manipulation under anesthesia and resection of scar tissue from postoperative arthrofibrosis. Arthroscopic screw removal was also planned as a secondary procedure at the same time in order to prevent the possibility of chondral injury from screw migration. During the procedure, the patient was noted to have improved ROM from 5º to 85º premanipulation to 5º to 110º postoperatively. At 3 months after the initial injury, the patient was allowed to begin progressive weight-bearing on the left knee. At most recent follow-up, after 12 months, the patient was able to ambulate and bear weight on the left leg without pain. Plain radiographs show a well-healed fracture with no evidence of collapse of the femoral condyle (Figures 5A, 5B). His active ROM of the left knee was 5º to 110º without pain (Figures 5C, 5D).
Discussion
In the vast majority of patellar dislocations, the patella dislocates laterally over the trochlear groove. Inferior, or intra-articular, dislocations of the patella are rare. The mechanism of injury is usually a blow onto the patella with a flexed knee. The 2 groups commonly involved are adolescent boys and the elderly.8,9 In young men, it is thought that lax patellar attachments place adolescents at higher risk for this type of injury.10-12 While patella fractures and frank extensor mechanism ruptures are uncommon in this age group, the same mechanism of injury can lead to stripping of the deep fibers of the patellar tendon from the superior pole of the patella.3,13 The intact superficial fibers of the tendon allow the patella to hinge and displace into the joint.14
Inferior dislocations of the patella are classified into 2 types based on the orientation of the articular surface and the presence of osteophytes.15 Type I inferior dislocations occur after a direct blow to a flexed knee forces the superior pole of the patella into the intercondylar notch. Type II dislocations are caused by osteophytes on the superior pole of the patella that become wedged in the intercondylar notch and dislocate the patella inferiorly. In type I dislocations, the patella is rotated in the horizontal plane and the articular surface often faces inferiorly, but type II dislocations do not involve rotation of the articular surface. Type II injuries are seen more commonly in the elderly.
Our patient was able to tolerate a closed reduction of the patella after an intra-articular lidocaine injection, and a successful reduction was achieved without great difficulty. However, the majority of reports describe the need for an open reduction of inferior patellar dislocations.3,8 When closed reductions were a success, they were performed under general anesthesia or conscious sedation.3 It is thought that the difficulty of reduction results from the tension of the quadriceps muscle pulling the patella superiorly into intercondylar notch.11,16 However, successful closed reduction may be more likely in patients with less patellar rotation and entrapment within the intercondylar notch, as well as in patients whose knee is near full extension at presentation.17-19 Successful closed reduction is also seen in elderly patients, where dislocation is generally caused by less forceful impact and held by osteophytes. In these patients, the knee is commonly held in extension.12,15,20-22
The fracture pattern seen in this case also shows a rare fracture in skeletally immature patients, with only a few case reports in the literature. Isolated coronal plane femur fractures account for 0.65% of all femur fractures and are usually seen in adults after high-energy trauma.23 In the skeletally immature, the fracture can occur with lower-energy mechanisms. The typical mechanism is thought to be a shearing force to the femur caused by an axial load to the knee in 90° or more of flexion.4,24 A CT scan is recommended for better identification of the fracture and to plan treatment.25,26 Because of their intra-articular nature and tenuous blood supply, Hoffa fractures tend to do poorly with nonoperative treatment and are prone to displacement and nonunion.27,28 The goal of operative treatment is to obtain anatomic reduction and rigid fixation. While operative fixation techniques are varied, screw fixation with multiple smaller diameter screws has equal pullout strength compared to larger screws and may minimize damage to the articular cartilage.29-31 By preserving blood supply to the fracture, and allowing for early active mobilization, operative treatment generally provides good long-term functional outcomes in these fracture patterns.24
Conclusion
We describe a case in which the patella of an adolescent boy dislocated inferiorly into the knee joint, with an associated coronal shear fracture of the lateral femoral condyle. To our knowledge, this constellation of injuries has not been reported. For this uncommon injury pattern, we recommend a sequential treatment algorithm to minimize morbidity. We recommend first attempting a closed reduction of the patella with adequate pain control to avoid the morbidity associated with general anesthesia. After a successful reduction, an advanced imaging study (eg, MRI) is advisable to assess for concomitant soft-tissue injuries and preoperative planning, if necessary. The mechanism of injury and force required to cause a patellar dislocation of this nature leaves a high likelihood of other injuries. When a fracture is noted on plain radiographs after reduction, a CT scan can provide important information for planning surgical fixation of the fracture. Even in a skeletally immature patient, the principle of direct reduction and stable interfragmentary fixation of an articular fracture is critical for long-term function, even after a significant trauma to the knee.
In 1887, Midelfart1 first reported on an intra-articular dislocation of the patella, and since then approximately 50 cases have been reported in the worldwide literature.2 Also known as an inferior patellar dislocation, these rare traumatic events occur when the patella dislocates intra-articularly. Because the patella commonly rotates about its horizontal axis, the articular surface is facing proximally or distally. The patella becomes lodged within the trochlea and locks the knee joint. Most cases described in the literature involved adolescent boys, with the patella difficult to reduce. Most patients required open reduction, while those who underwent successful closed reduction often needed general anesthesia.3
Similarly, coronal shear fractures of the femoral condyle (ie, Hoffa fractures) are an uncommon fracture pattern typically seen in adults. These fractures are even more infrequent in skeletally immature patients, with fewer than 5 cases documented in the literature.4-7 In our case report, we present a 14-year-old boy with a coronal shear fracture of the femoral condyle associated with an intra-articular patellar dislocation. To our knowledge, this constellation of injuries has not been reported. Additionally, closed reduction of the patella was successful after intra-articular lidocaine injection, without the need for sedation or general anesthesia. The patient’s guardian provided written informed consent for print and electronic publication of this case report.
Case Report
A 14-year-old boy presented to our institution after sustaining a direct blow to his left knee. The injury occurred as he jumped and landed on a flexed knee while playing with friends. The patient was unable to ambulate after the injury, and his left knee was locked in a slightly flexed position. Examination in the emergency department showed the knee to be held in approximately 60º of flexion, with an obvious bony prominence noted anteriorly over the femoral condyles. The patient was unable to perform a straight leg raise or any active range of motion (ROM) at the knee. Radiographs performed with the knee maintained in flexion confirmed that the patella was displaced into the knee joint and was rotated with the articular surface facing distally. Also noted was a coronal shear fracture of the lateral femoral condyle (Figures 1A, 1B).
The patient received pain medication and an intra-articular lidocaine injection prior to a reduction attempt by the orthopedic resident. With the patient supine, the hip was gently flexed to relax the quadriceps muscle. As the knee was flexed up to 110º, the prominent patella was gripped between the thumb and fingers to gently free and elevate the patella out of the intercondylar notch.
After reduction, an immediate return of normal patellar contour and patellofemoral tracking was observed as the knee was gently extended. There was no obvious defect to the patellar or quadriceps tendons, and the patient was able to perform a straight-leg raise, confirming the integrity of the extensor mechanism. Radiographs performed after the reduction confirmed relocation of the patella in correct anatomic position, as well as a lateral femoral condyle fracture (Figures 2A, 2B). Magnetic resonance imaging (MRI) of the knee confirmed no full-thickness quadriceps or patellar tendon tear. A computed tomography (CT) scan of the knee showed a comminuted fracture of the lateral femoral condyle in the coronal plane, as well as multiple bone fragments within the joint (Figures 3A, 3B). The patient was placed in a bulky soft dressing and underwent open reduction and internal fixation of the fracture.
A 10-cm incision was made over the anterior aspect of the knee, and after dissection to the level of the retinaculum, a lateral parapatellar arthrotomy was performed. The patella was retracted medially to identify and free the fracture fragments. The fracture fragments were provisionally reduced and stabilized with three 0.065-in Kirschner wires. An area of osteochondral impaction proximal to the fracture was elevated and allograft bone was incorporated below the articular surface (Figures 4A, 4B). Rigid fixation of the fracture was achieved using 3 screws (2 Bio-Compression Screws [Arthrex Inc., Naples, Florida] and 1 Synthes cannulated screw [Synthes, West Chester, Pennsylvania]). The screws were placed in posteroanterior (PA) direction and inserted into the weight-bearing articular surface of the femoral condyle (Figures 4C, 4D). The screws were countersunk, and stable fixation with compression of the fracture was achieved. Reduction and screw position were verified with fluoroscopic views. The wound was closed in layers, and the patient was discharged home the next day.
Postoperatively, the patient was non-weight-bearing on the affected limb with a hinged-knee brace to allow for knee ROM exercises immediately. He was also given a continuous passive motion device to maintain knee motion. At the 6-week mark, the patient’s fracture alignment appeared to be well-maintained and showed interval healing. Clinically, the patient was noted to have limited knee ROM. The decision was made to take the patient to the operating room primarily for a manipulation under anesthesia and resection of scar tissue from postoperative arthrofibrosis. Arthroscopic screw removal was also planned as a secondary procedure at the same time in order to prevent the possibility of chondral injury from screw migration. During the procedure, the patient was noted to have improved ROM from 5º to 85º premanipulation to 5º to 110º postoperatively. At 3 months after the initial injury, the patient was allowed to begin progressive weight-bearing on the left knee. At most recent follow-up, after 12 months, the patient was able to ambulate and bear weight on the left leg without pain. Plain radiographs show a well-healed fracture with no evidence of collapse of the femoral condyle (Figures 5A, 5B). His active ROM of the left knee was 5º to 110º without pain (Figures 5C, 5D).
Discussion
In the vast majority of patellar dislocations, the patella dislocates laterally over the trochlear groove. Inferior, or intra-articular, dislocations of the patella are rare. The mechanism of injury is usually a blow onto the patella with a flexed knee. The 2 groups commonly involved are adolescent boys and the elderly.8,9 In young men, it is thought that lax patellar attachments place adolescents at higher risk for this type of injury.10-12 While patella fractures and frank extensor mechanism ruptures are uncommon in this age group, the same mechanism of injury can lead to stripping of the deep fibers of the patellar tendon from the superior pole of the patella.3,13 The intact superficial fibers of the tendon allow the patella to hinge and displace into the joint.14
Inferior dislocations of the patella are classified into 2 types based on the orientation of the articular surface and the presence of osteophytes.15 Type I inferior dislocations occur after a direct blow to a flexed knee forces the superior pole of the patella into the intercondylar notch. Type II dislocations are caused by osteophytes on the superior pole of the patella that become wedged in the intercondylar notch and dislocate the patella inferiorly. In type I dislocations, the patella is rotated in the horizontal plane and the articular surface often faces inferiorly, but type II dislocations do not involve rotation of the articular surface. Type II injuries are seen more commonly in the elderly.
Our patient was able to tolerate a closed reduction of the patella after an intra-articular lidocaine injection, and a successful reduction was achieved without great difficulty. However, the majority of reports describe the need for an open reduction of inferior patellar dislocations.3,8 When closed reductions were a success, they were performed under general anesthesia or conscious sedation.3 It is thought that the difficulty of reduction results from the tension of the quadriceps muscle pulling the patella superiorly into intercondylar notch.11,16 However, successful closed reduction may be more likely in patients with less patellar rotation and entrapment within the intercondylar notch, as well as in patients whose knee is near full extension at presentation.17-19 Successful closed reduction is also seen in elderly patients, where dislocation is generally caused by less forceful impact and held by osteophytes. In these patients, the knee is commonly held in extension.12,15,20-22
The fracture pattern seen in this case also shows a rare fracture in skeletally immature patients, with only a few case reports in the literature. Isolated coronal plane femur fractures account for 0.65% of all femur fractures and are usually seen in adults after high-energy trauma.23 In the skeletally immature, the fracture can occur with lower-energy mechanisms. The typical mechanism is thought to be a shearing force to the femur caused by an axial load to the knee in 90° or more of flexion.4,24 A CT scan is recommended for better identification of the fracture and to plan treatment.25,26 Because of their intra-articular nature and tenuous blood supply, Hoffa fractures tend to do poorly with nonoperative treatment and are prone to displacement and nonunion.27,28 The goal of operative treatment is to obtain anatomic reduction and rigid fixation. While operative fixation techniques are varied, screw fixation with multiple smaller diameter screws has equal pullout strength compared to larger screws and may minimize damage to the articular cartilage.29-31 By preserving blood supply to the fracture, and allowing for early active mobilization, operative treatment generally provides good long-term functional outcomes in these fracture patterns.24
Conclusion
We describe a case in which the patella of an adolescent boy dislocated inferiorly into the knee joint, with an associated coronal shear fracture of the lateral femoral condyle. To our knowledge, this constellation of injuries has not been reported. For this uncommon injury pattern, we recommend a sequential treatment algorithm to minimize morbidity. We recommend first attempting a closed reduction of the patella with adequate pain control to avoid the morbidity associated with general anesthesia. After a successful reduction, an advanced imaging study (eg, MRI) is advisable to assess for concomitant soft-tissue injuries and preoperative planning, if necessary. The mechanism of injury and force required to cause a patellar dislocation of this nature leaves a high likelihood of other injuries. When a fracture is noted on plain radiographs after reduction, a CT scan can provide important information for planning surgical fixation of the fracture. Even in a skeletally immature patient, the principle of direct reduction and stable interfragmentary fixation of an articular fracture is critical for long-term function, even after a significant trauma to the knee.
1. Midelfart V. En sjelden luxation of patella. Norsk Magazin for Laegevidenskaben. 1887;4:588.
2. Kramer DE, Simoni MK. Horizontal intra-articular patellar dislocation resulting in quadriceps avulsion and medial patellofemoral ligament tear: a case report. J Pediatr Orthop B. 2013;22(4):329-332.
3. van den Broek TA, Moll PJ. Horizontal rotation of the patella. A case report with review of the literature. Acta Orthop Scand. 1985;56(5):436-438.
4. Flanagin BA, Cruz AI, Medvecky MJ. Hoffa fracture in a 14-year-old. Orthopedics. 2011;34(2):138.
5. Strauss E, Nelson JM, Abdelwahab IF. Fracture of the lateral femoral condyle. A case report. Bull Hosp Jt Dis Orthop Inst. 1984;44(1):86-90.
6. Biau DJ, Schranz PJ. Transverse Hoffa’s or deep osteochondral fracture? An unusual fracture of the lateral femoral condyle in a child. Injury. 2005;36(7):862-865.
7. McDonough PW, Bernstein RM. Nonunion of a Hoffa fracture in a child. J Orthop Trauma. 2000;14(7):519-521.
8. Brady TA, Russell D. Interarticular horizontal dislocation of the patella. A case report. J Bone Joint Surg Am. 1965;47(7):1393-1396.
9. Yuguero M, Gonzalez JA, Carma A, Huguet J. Intra-articular patellar dislocation. Orthopedics. 2003;26(5):517-518.
10. Frangakis EK. Intra-articular dislocation of the patella. A case report. J Bone Joint Surg Am. 1974;56(2):423-424.
11. Nanda R, Yadav RS, Thakur M. Intra-articular dislocation of the patella. J Trauma. 2000;48(1):159-160.
12. Choudhary RK, Tice JW. Intra-articular dislocation of the patella with incomplete rotation--two case reports and a review of the literature. Knee. 2004;11(2):125-127.
13. Chatziantoniou I, Diakos G, Pantelelli M. Horizontal dislocation of the patella. Case report. EEXOT. 2008;59(2):112-114.
14. McHugh G, Ryan E, Cleary M, Kenny P, O’Flanagan S, Keogh P. Intra-articular dislocation of the patella. Case Rep Orthop. 2013;2013:535803.
15. Bankes MJ, Eastwood DM. Inferior dislocation of the patella in the degenerate knee. Injury. 2002;33(6):528-529.
16. Theodorides A, Guo S, Case R. Intra-articular dislocation of the patella: A case report and review of the literature. Injury Extra. 2010;41(10):103-105.
17. Dimentberg RA. Intra-articular dislocation of the patella: case report and literature review. Clin J Sport Med. 1997;7(2):126-128.
18. Morin WD, Steadman JR. Case report of a successful closed reduction without anesthesia. Clin Orthop. 1993(297):179-181.
19. Murakami Y. Intra-articular dislocation of the patella. A case report. Clin Orthop. 1982;171:137-139.
20. Joshi RP. Inferior dislocation of the patella. Injury. 1997;28(5-6):389-390.
21. Garner JP, Pike JM, George CD. Intra-articular dislocation of the patella: two cases and literature review. J Trauma. 1999;47(4):780-783.
22. McCarthy TA, Quinn B, Pegum JM. Inferior dislocation of the patella: an unusual cause of a locked knee. Ir J Med Sci. 2001;170(3):209-210.
23. Manfredini M, Gildone A, Ferrante R, Bernasconi S, Massari L. Unicondylar femoral fractures: therapeutic strategy and long-term results. A review of 23 patients. Acta Orthop Belg. 2001;67(2):132-138.
24. Holmes SM, Bomback D, Baumgaertner MR. Coronal fractures of the femoral condyle: a brief report of five cases. J Orthop Trauma. 2004;18(5):316-319.
25. Nork SE, Segina DN, Aflatoon K, et al. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. J Bone Joint Surg Am. 2005;87(3):564-569.
26. Allmann KH, Altehoefer C, Wildanger G, et al. Hoffa fracture--a radiologic diagnostic approach. J Belge Radiol. 1996;79(5):201-202.
27. Oztürk A, Ozkan Y, Ozdemir RM. Nonunion of a Hoffa fracture in an adult. Chir Organi Mov. 2009;93(3):183-185.
28. Lewis SL, Pozo JL, Muirhead-Allwood WF. Coronal fractures of the lateral femoral condyle. J Bone Joint Surg Br. 1989;71(1):118-120.
29. Arastu MH, Kokke MC, Duffy PJ, Korley RE, Buckley RE. Coronal plane partial articular fractures of the distal femoral condyle: current concepts in management. Bone Joint J. 2013;95-B(9):1165-1171.
30. Westmoreland GL, McLaurin TM, Hutton WC. Screw pullout strength: a biomechanical comparison of large-fragment and small-fragment fixation in the tibial plateau. J Orthop Trauma. 2002;16(3):178-181.
31. Jarit GJ, Kummer FJ, Gibber MJ, Egol KA. A mechanical evaluation of two fixation methods using cancellous screws for coronal fractures of the lateral condyle of the distal femur (OTA type 33B). J Orthop Trauma. 2006;20(4):273-276.
1. Midelfart V. En sjelden luxation of patella. Norsk Magazin for Laegevidenskaben. 1887;4:588.
2. Kramer DE, Simoni MK. Horizontal intra-articular patellar dislocation resulting in quadriceps avulsion and medial patellofemoral ligament tear: a case report. J Pediatr Orthop B. 2013;22(4):329-332.
3. van den Broek TA, Moll PJ. Horizontal rotation of the patella. A case report with review of the literature. Acta Orthop Scand. 1985;56(5):436-438.
4. Flanagin BA, Cruz AI, Medvecky MJ. Hoffa fracture in a 14-year-old. Orthopedics. 2011;34(2):138.
5. Strauss E, Nelson JM, Abdelwahab IF. Fracture of the lateral femoral condyle. A case report. Bull Hosp Jt Dis Orthop Inst. 1984;44(1):86-90.
6. Biau DJ, Schranz PJ. Transverse Hoffa’s or deep osteochondral fracture? An unusual fracture of the lateral femoral condyle in a child. Injury. 2005;36(7):862-865.
7. McDonough PW, Bernstein RM. Nonunion of a Hoffa fracture in a child. J Orthop Trauma. 2000;14(7):519-521.
8. Brady TA, Russell D. Interarticular horizontal dislocation of the patella. A case report. J Bone Joint Surg Am. 1965;47(7):1393-1396.
9. Yuguero M, Gonzalez JA, Carma A, Huguet J. Intra-articular patellar dislocation. Orthopedics. 2003;26(5):517-518.
10. Frangakis EK. Intra-articular dislocation of the patella. A case report. J Bone Joint Surg Am. 1974;56(2):423-424.
11. Nanda R, Yadav RS, Thakur M. Intra-articular dislocation of the patella. J Trauma. 2000;48(1):159-160.
12. Choudhary RK, Tice JW. Intra-articular dislocation of the patella with incomplete rotation--two case reports and a review of the literature. Knee. 2004;11(2):125-127.
13. Chatziantoniou I, Diakos G, Pantelelli M. Horizontal dislocation of the patella. Case report. EEXOT. 2008;59(2):112-114.
14. McHugh G, Ryan E, Cleary M, Kenny P, O’Flanagan S, Keogh P. Intra-articular dislocation of the patella. Case Rep Orthop. 2013;2013:535803.
15. Bankes MJ, Eastwood DM. Inferior dislocation of the patella in the degenerate knee. Injury. 2002;33(6):528-529.
16. Theodorides A, Guo S, Case R. Intra-articular dislocation of the patella: A case report and review of the literature. Injury Extra. 2010;41(10):103-105.
17. Dimentberg RA. Intra-articular dislocation of the patella: case report and literature review. Clin J Sport Med. 1997;7(2):126-128.
18. Morin WD, Steadman JR. Case report of a successful closed reduction without anesthesia. Clin Orthop. 1993(297):179-181.
19. Murakami Y. Intra-articular dislocation of the patella. A case report. Clin Orthop. 1982;171:137-139.
20. Joshi RP. Inferior dislocation of the patella. Injury. 1997;28(5-6):389-390.
21. Garner JP, Pike JM, George CD. Intra-articular dislocation of the patella: two cases and literature review. J Trauma. 1999;47(4):780-783.
22. McCarthy TA, Quinn B, Pegum JM. Inferior dislocation of the patella: an unusual cause of a locked knee. Ir J Med Sci. 2001;170(3):209-210.
23. Manfredini M, Gildone A, Ferrante R, Bernasconi S, Massari L. Unicondylar femoral fractures: therapeutic strategy and long-term results. A review of 23 patients. Acta Orthop Belg. 2001;67(2):132-138.
24. Holmes SM, Bomback D, Baumgaertner MR. Coronal fractures of the femoral condyle: a brief report of five cases. J Orthop Trauma. 2004;18(5):316-319.
25. Nork SE, Segina DN, Aflatoon K, et al. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. J Bone Joint Surg Am. 2005;87(3):564-569.
26. Allmann KH, Altehoefer C, Wildanger G, et al. Hoffa fracture--a radiologic diagnostic approach. J Belge Radiol. 1996;79(5):201-202.
27. Oztürk A, Ozkan Y, Ozdemir RM. Nonunion of a Hoffa fracture in an adult. Chir Organi Mov. 2009;93(3):183-185.
28. Lewis SL, Pozo JL, Muirhead-Allwood WF. Coronal fractures of the lateral femoral condyle. J Bone Joint Surg Br. 1989;71(1):118-120.
29. Arastu MH, Kokke MC, Duffy PJ, Korley RE, Buckley RE. Coronal plane partial articular fractures of the distal femoral condyle: current concepts in management. Bone Joint J. 2013;95-B(9):1165-1171.
30. Westmoreland GL, McLaurin TM, Hutton WC. Screw pullout strength: a biomechanical comparison of large-fragment and small-fragment fixation in the tibial plateau. J Orthop Trauma. 2002;16(3):178-181.
31. Jarit GJ, Kummer FJ, Gibber MJ, Egol KA. A mechanical evaluation of two fixation methods using cancellous screws for coronal fractures of the lateral condyle of the distal femur (OTA type 33B). J Orthop Trauma. 2006;20(4):273-276.

Precaution Guidelines Updated for Visitors of Inpatients with Infectious Diseases
Hospitalists may soon see changes in precaution protocols for some hospital visitors, thanks to a revised set of guidelines published by the Society for Healthcare Epidemiology of America (SHEA). The guidelines include recommendations for visitors to patients hospitalized with infectious diseases.
"Up until now, visitors have been wearing contact precautions just like healthcare providers—gowns, gloves, masks, sometimes respirators," says lead author L. Silvia Munoz-Price, MD, PhD, enterprise epidemiologist at the Institute for Health and Society of the Medical College of Wisconsin based in Milwaukee. "We looked at the evidence for these policies. Using our judgment, a literature review, and a survey of our membership, we came up with new guidelines."
Among SHEA's recommendations are two major changes:
- Visitors of patients diagnosed with methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) don't need gowns and gloves if those pathogens are endemic in the region and the institution;
- For cases involving Clostridium difficile infection and extensively drug-resistant gram-negative organisms, contact isolation precautions are still recommended; and
- Visitors of patients under airborne isolation precautions do not need N95 respirators. Healthcare workers still need the protective masks, but because the masks only function when fitted properly to an individual, the masks loaned to visitors are probably ineffective.
"We've been asking visitors to wear N95, even though we know most likely it’s doing nothing," Dr. Munoz-Price says. "Now we're saying, stop doing that."
If visitors have had enough exposure to the patient at home, they can wear surgical masks or maybe no precautions at all, she adds. If visitors have not seen the patient for weeks, visitation may have to be restricted.
Dr. Munoz-Price notes that hospitalists should be aware of these revised guidelines and know that they apply only to visitors.
"Even though family members are not wearing contact precaution gear, that doesn't mean that hospitalists shouldn't," Dr. Munoz-Price says. "It's extremely important that hospitalists be compliant with their protocols and not be influenced by what we're doing with visitors." TH
Suzanne Bopp is a freelance writer in New Jersey.
Visit our website for more information on managing patients with infectious diseases.
Hospitalists may soon see changes in precaution protocols for some hospital visitors, thanks to a revised set of guidelines published by the Society for Healthcare Epidemiology of America (SHEA). The guidelines include recommendations for visitors to patients hospitalized with infectious diseases.
"Up until now, visitors have been wearing contact precautions just like healthcare providers—gowns, gloves, masks, sometimes respirators," says lead author L. Silvia Munoz-Price, MD, PhD, enterprise epidemiologist at the Institute for Health and Society of the Medical College of Wisconsin based in Milwaukee. "We looked at the evidence for these policies. Using our judgment, a literature review, and a survey of our membership, we came up with new guidelines."
Among SHEA's recommendations are two major changes:
- Visitors of patients diagnosed with methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) don't need gowns and gloves if those pathogens are endemic in the region and the institution;
- For cases involving Clostridium difficile infection and extensively drug-resistant gram-negative organisms, contact isolation precautions are still recommended; and
- Visitors of patients under airborne isolation precautions do not need N95 respirators. Healthcare workers still need the protective masks, but because the masks only function when fitted properly to an individual, the masks loaned to visitors are probably ineffective.
"We've been asking visitors to wear N95, even though we know most likely it’s doing nothing," Dr. Munoz-Price says. "Now we're saying, stop doing that."
If visitors have had enough exposure to the patient at home, they can wear surgical masks or maybe no precautions at all, she adds. If visitors have not seen the patient for weeks, visitation may have to be restricted.
Dr. Munoz-Price notes that hospitalists should be aware of these revised guidelines and know that they apply only to visitors.
"Even though family members are not wearing contact precaution gear, that doesn't mean that hospitalists shouldn't," Dr. Munoz-Price says. "It's extremely important that hospitalists be compliant with their protocols and not be influenced by what we're doing with visitors." TH
Suzanne Bopp is a freelance writer in New Jersey.
Visit our website for more information on managing patients with infectious diseases.
Hospitalists may soon see changes in precaution protocols for some hospital visitors, thanks to a revised set of guidelines published by the Society for Healthcare Epidemiology of America (SHEA). The guidelines include recommendations for visitors to patients hospitalized with infectious diseases.
"Up until now, visitors have been wearing contact precautions just like healthcare providers—gowns, gloves, masks, sometimes respirators," says lead author L. Silvia Munoz-Price, MD, PhD, enterprise epidemiologist at the Institute for Health and Society of the Medical College of Wisconsin based in Milwaukee. "We looked at the evidence for these policies. Using our judgment, a literature review, and a survey of our membership, we came up with new guidelines."
Among SHEA's recommendations are two major changes:
- Visitors of patients diagnosed with methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) don't need gowns and gloves if those pathogens are endemic in the region and the institution;
- For cases involving Clostridium difficile infection and extensively drug-resistant gram-negative organisms, contact isolation precautions are still recommended; and
- Visitors of patients under airborne isolation precautions do not need N95 respirators. Healthcare workers still need the protective masks, but because the masks only function when fitted properly to an individual, the masks loaned to visitors are probably ineffective.
"We've been asking visitors to wear N95, even though we know most likely it’s doing nothing," Dr. Munoz-Price says. "Now we're saying, stop doing that."
If visitors have had enough exposure to the patient at home, they can wear surgical masks or maybe no precautions at all, she adds. If visitors have not seen the patient for weeks, visitation may have to be restricted.
Dr. Munoz-Price notes that hospitalists should be aware of these revised guidelines and know that they apply only to visitors.
"Even though family members are not wearing contact precaution gear, that doesn't mean that hospitalists shouldn't," Dr. Munoz-Price says. "It's extremely important that hospitalists be compliant with their protocols and not be influenced by what we're doing with visitors." TH
Suzanne Bopp is a freelance writer in New Jersey.
Visit our website for more information on managing patients with infectious diseases.