User login
Regionalized trauma care trims 30-day mortality
LAKE BUENA VISTA, FLA. – Regionalized trauma care significantly reduces long-term mortality and maintains similar functional outcomes in patients with severe traumatic brain injury, a study showed.
Regionalization of trauma care is a health care strategy that attempts to improve outcomes for trauma patients by setting up a tiered, integrated system that aims to match the injured patient with the appropriate health care facility in a timely fashion. The Northern Ohio Trauma System (NOTS) was created in 2010 to manage trauma patients using the regionalization model.
In this study of outcomes in NOTS patients, longer-term follow-up of 3,496 severe traumatic brain injury (TBI) admissions showed 30-day mortality fell from 21% to 16% after regionalization (24% relative reduction; P value < .0001) and 6-month mortality declined from 24% to 20% (17% relative reduction; P = .004).

Multivariable logistic regression only strengthened the effect of regionalization on the primary outcome, lead study author Dr. Michael Kelly said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
The odds ratio for 30-day mortality was 0.74, representing a 26% relative mortality reduction, and 0.82 for 6-month mortality, representing an 18% relative reduction.
At last year’s EAST meeting, Dr. Kelly and his colleagues reported that hospital mortality declined from 19% (262/1,359 patients) to 14% (302/2,137) in patients with severe TBI after the creation of the NOTS in 2010.
Despite bucking the current trend of rising mortality in hospitalized TBI patients, particularly those with severe brain injuries, their previous results were criticized by some as incomplete because hospital mortality was used without functional status measures or long-term mortality, he said.
To bridge the knowledge gap, the investigators identified all TBI patients older than 14 years with a Head Abbreviated Injury Scale (AIS) ≥ 3 from 2008 to 2012 in the NOTS database and matched them to the Ohio death index and the regional TBI rehabilitation database. Overall Functional Independence Measure (FIM) scores and FIM score gains were compared in 414 patients who were discharged to the regional TBI rehabilitation unit.
As a general rule of thumb, an overall FIM score of 60 is equivalent to 4 hours of personal care assistance in a nursing facility–type setting, a score of 80 equals 2 hours of personalized care in a nursing facility, more than 80 means the patient is able to receive family care at home, and ≥ 100 means minimal burdens in personal care, said Dr. Kelly of the MetroHealth Medical Center, Cleveland, and Cleveland Clinic.
A gain of 22 points is considered a minimal clinically important difference (MCID) for the overall FIM score. The MCID is 17 points for a FIM motor subscale gain, 3 for a FIM cognitive subscale gain, and has not been established for the FIM social subscale.
Overall FIM scores were similar before and after regionalization of trauma care (RT) at admission (54 vs. 48; P = .2) and at discharge (92 vs. 89; P = .1), he said.
FIM scores were similar in both groups at admission and discharge on the cognitive and social subscale domains, but were significantly lower post RT on the motor subscale at admission (38 vs. 31; P = .02) and discharge (68 vs. 65; P = .03). These differences were not clinically significant, according to Dr. Kelly and senior study author Dr. Jeffrey Claridge, NOTS medical director.
Pre- and post-RT patients had similar overall FIM score gains (37 vs. 36; P = .6), motor subscale gains (both groups 29), and social subscale gains (both groups 1). FIM cognitive subscale gains were significantly lower post RT (6 vs. 5; P = .01), but this difference was also not clinically significant.
Notably, discharges to regional TBI rehabilitation increased from 9% before RT to 14% after RT, Dr. Kelly said. The percentage of patients who were discharged to a skilled nurse facility or long-term care facility remained stable at about 30%, as did the percentage discharged home at about 40%.
“Regionalization improves long-term survival and maintains similar functional outcomes for patients with severe traumatic brain injury,” he concluded.

Discussant Dr. Jeffrey Coughenour of the University of Missouri Health System in Columbia said it appears regionalization is working, but added, “While we are saving more lives, what kind of lives are we saving? A question that has ever increasing implications for patients and payers evaluating the care we provide.”
He praised the investigators for using the FIM scale rather than the Glasgow Outcome Scale to try and answer this question, but said more information is needed on whether FIM scores improved in more challenging patients such as those with an AIS score of 4 or 5 or those entering rehabilitation after discharge to a skilled nursing or long-term care facility.
Data were not broken down for these more challenging subsets, Dr. Kelly said. The question of quality of life post regionalization was asked after the first study and that functional status was shown to be maintained in TBI patients in the follow-up study.
“Since no major changes in the hospital-based care or rehabilitation care of these TBI patients occurred, we weren’t surprised to see that functional outcomes did not improve,” he said in an interview. “The regionalization protocols were designed primarily to improve survival.”
During a discussion of the results, audience members questioned whether the investigators could be certain the results could be attributed to regionalization and not improvements in treatment of concurrent injuries or improvements in TBI treatment already underway at the time of policy change.
For the most part, these patients had isolated TBIs and no major changes in personnel or TBI care occurred during the study period, Dr. Kelly said.
Under NOTS, region-wide initiatives included use of the Centers for Disease Control and Prevention guidelines for field triage, a transfer line and transfer protocols, and a research database shared between two large hospital systems comprising the level I MetroHealth Medical Center trauma center, two level II trauma centers, and 12 nontrauma hospitals.
Dr. Kelly, his coauthors, and Dr. Coughenour reported no financial disclosures.
LAKE BUENA VISTA, FLA. – Regionalized trauma care significantly reduces long-term mortality and maintains similar functional outcomes in patients with severe traumatic brain injury, a study showed.
Regionalization of trauma care is a health care strategy that attempts to improve outcomes for trauma patients by setting up a tiered, integrated system that aims to match the injured patient with the appropriate health care facility in a timely fashion. The Northern Ohio Trauma System (NOTS) was created in 2010 to manage trauma patients using the regionalization model.
In this study of outcomes in NOTS patients, longer-term follow-up of 3,496 severe traumatic brain injury (TBI) admissions showed 30-day mortality fell from 21% to 16% after regionalization (24% relative reduction; P value < .0001) and 6-month mortality declined from 24% to 20% (17% relative reduction; P = .004).
Multivariable logistic regression only strengthened the effect of regionalization on the primary outcome, lead study author Dr. Michael Kelly said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
The odds ratio for 30-day mortality was 0.74, representing a 26% relative mortality reduction, and 0.82 for 6-month mortality, representing an 18% relative reduction.
At last year’s EAST meeting, Dr. Kelly and his colleagues reported that hospital mortality declined from 19% (262/1,359 patients) to 14% (302/2,137) in patients with severe TBI after the creation of the NOTS in 2010.
Despite bucking the current trend of rising mortality in hospitalized TBI patients, particularly those with severe brain injuries, their previous results were criticized by some as incomplete because hospital mortality was used without functional status measures or long-term mortality, he said.
To bridge the knowledge gap, the investigators identified all TBI patients older than 14 years with a Head Abbreviated Injury Scale (AIS) ≥ 3 from 2008 to 2012 in the NOTS database and matched them to the Ohio death index and the regional TBI rehabilitation database. Overall Functional Independence Measure (FIM) scores and FIM score gains were compared in 414 patients who were discharged to the regional TBI rehabilitation unit.
As a general rule of thumb, an overall FIM score of 60 is equivalent to 4 hours of personal care assistance in a nursing facility–type setting, a score of 80 equals 2 hours of personalized care in a nursing facility, more than 80 means the patient is able to receive family care at home, and ≥ 100 means minimal burdens in personal care, said Dr. Kelly of the MetroHealth Medical Center, Cleveland, and Cleveland Clinic.
A gain of 22 points is considered a minimal clinically important difference (MCID) for the overall FIM score. The MCID is 17 points for a FIM motor subscale gain, 3 for a FIM cognitive subscale gain, and has not been established for the FIM social subscale.
Overall FIM scores were similar before and after regionalization of trauma care (RT) at admission (54 vs. 48; P = .2) and at discharge (92 vs. 89; P = .1), he said.
FIM scores were similar in both groups at admission and discharge on the cognitive and social subscale domains, but were significantly lower post RT on the motor subscale at admission (38 vs. 31; P = .02) and discharge (68 vs. 65; P = .03). These differences were not clinically significant, according to Dr. Kelly and senior study author Dr. Jeffrey Claridge, NOTS medical director.
Pre- and post-RT patients had similar overall FIM score gains (37 vs. 36; P = .6), motor subscale gains (both groups 29), and social subscale gains (both groups 1). FIM cognitive subscale gains were significantly lower post RT (6 vs. 5; P = .01), but this difference was also not clinically significant.
Notably, discharges to regional TBI rehabilitation increased from 9% before RT to 14% after RT, Dr. Kelly said. The percentage of patients who were discharged to a skilled nurse facility or long-term care facility remained stable at about 30%, as did the percentage discharged home at about 40%.
“Regionalization improves long-term survival and maintains similar functional outcomes for patients with severe traumatic brain injury,” he concluded.
Discussant Dr. Jeffrey Coughenour of the University of Missouri Health System in Columbia said it appears regionalization is working, but added, “While we are saving more lives, what kind of lives are we saving? A question that has ever increasing implications for patients and payers evaluating the care we provide.”
He praised the investigators for using the FIM scale rather than the Glasgow Outcome Scale to try and answer this question, but said more information is needed on whether FIM scores improved in more challenging patients such as those with an AIS score of 4 or 5 or those entering rehabilitation after discharge to a skilled nursing or long-term care facility.
Data were not broken down for these more challenging subsets, Dr. Kelly said. The question of quality of life post regionalization was asked after the first study and that functional status was shown to be maintained in TBI patients in the follow-up study.
“Since no major changes in the hospital-based care or rehabilitation care of these TBI patients occurred, we weren’t surprised to see that functional outcomes did not improve,” he said in an interview. “The regionalization protocols were designed primarily to improve survival.”
During a discussion of the results, audience members questioned whether the investigators could be certain the results could be attributed to regionalization and not improvements in treatment of concurrent injuries or improvements in TBI treatment already underway at the time of policy change.
For the most part, these patients had isolated TBIs and no major changes in personnel or TBI care occurred during the study period, Dr. Kelly said.
Under NOTS, region-wide initiatives included use of the Centers for Disease Control and Prevention guidelines for field triage, a transfer line and transfer protocols, and a research database shared between two large hospital systems comprising the level I MetroHealth Medical Center trauma center, two level II trauma centers, and 12 nontrauma hospitals.
Dr. Kelly, his coauthors, and Dr. Coughenour reported no financial disclosures.
LAKE BUENA VISTA, FLA. – Regionalized trauma care significantly reduces long-term mortality and maintains similar functional outcomes in patients with severe traumatic brain injury, a study showed.
Regionalization of trauma care is a health care strategy that attempts to improve outcomes for trauma patients by setting up a tiered, integrated system that aims to match the injured patient with the appropriate health care facility in a timely fashion. The Northern Ohio Trauma System (NOTS) was created in 2010 to manage trauma patients using the regionalization model.
In this study of outcomes in NOTS patients, longer-term follow-up of 3,496 severe traumatic brain injury (TBI) admissions showed 30-day mortality fell from 21% to 16% after regionalization (24% relative reduction; P value < .0001) and 6-month mortality declined from 24% to 20% (17% relative reduction; P = .004).
Multivariable logistic regression only strengthened the effect of regionalization on the primary outcome, lead study author Dr. Michael Kelly said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
The odds ratio for 30-day mortality was 0.74, representing a 26% relative mortality reduction, and 0.82 for 6-month mortality, representing an 18% relative reduction.
At last year’s EAST meeting, Dr. Kelly and his colleagues reported that hospital mortality declined from 19% (262/1,359 patients) to 14% (302/2,137) in patients with severe TBI after the creation of the NOTS in 2010.
Despite bucking the current trend of rising mortality in hospitalized TBI patients, particularly those with severe brain injuries, their previous results were criticized by some as incomplete because hospital mortality was used without functional status measures or long-term mortality, he said.
To bridge the knowledge gap, the investigators identified all TBI patients older than 14 years with a Head Abbreviated Injury Scale (AIS) ≥ 3 from 2008 to 2012 in the NOTS database and matched them to the Ohio death index and the regional TBI rehabilitation database. Overall Functional Independence Measure (FIM) scores and FIM score gains were compared in 414 patients who were discharged to the regional TBI rehabilitation unit.
As a general rule of thumb, an overall FIM score of 60 is equivalent to 4 hours of personal care assistance in a nursing facility–type setting, a score of 80 equals 2 hours of personalized care in a nursing facility, more than 80 means the patient is able to receive family care at home, and ≥ 100 means minimal burdens in personal care, said Dr. Kelly of the MetroHealth Medical Center, Cleveland, and Cleveland Clinic.
A gain of 22 points is considered a minimal clinically important difference (MCID) for the overall FIM score. The MCID is 17 points for a FIM motor subscale gain, 3 for a FIM cognitive subscale gain, and has not been established for the FIM social subscale.
Overall FIM scores were similar before and after regionalization of trauma care (RT) at admission (54 vs. 48; P = .2) and at discharge (92 vs. 89; P = .1), he said.
FIM scores were similar in both groups at admission and discharge on the cognitive and social subscale domains, but were significantly lower post RT on the motor subscale at admission (38 vs. 31; P = .02) and discharge (68 vs. 65; P = .03). These differences were not clinically significant, according to Dr. Kelly and senior study author Dr. Jeffrey Claridge, NOTS medical director.
Pre- and post-RT patients had similar overall FIM score gains (37 vs. 36; P = .6), motor subscale gains (both groups 29), and social subscale gains (both groups 1). FIM cognitive subscale gains were significantly lower post RT (6 vs. 5; P = .01), but this difference was also not clinically significant.
Notably, discharges to regional TBI rehabilitation increased from 9% before RT to 14% after RT, Dr. Kelly said. The percentage of patients who were discharged to a skilled nurse facility or long-term care facility remained stable at about 30%, as did the percentage discharged home at about 40%.
“Regionalization improves long-term survival and maintains similar functional outcomes for patients with severe traumatic brain injury,” he concluded.
Discussant Dr. Jeffrey Coughenour of the University of Missouri Health System in Columbia said it appears regionalization is working, but added, “While we are saving more lives, what kind of lives are we saving? A question that has ever increasing implications for patients and payers evaluating the care we provide.”
He praised the investigators for using the FIM scale rather than the Glasgow Outcome Scale to try and answer this question, but said more information is needed on whether FIM scores improved in more challenging patients such as those with an AIS score of 4 or 5 or those entering rehabilitation after discharge to a skilled nursing or long-term care facility.
Data were not broken down for these more challenging subsets, Dr. Kelly said. The question of quality of life post regionalization was asked after the first study and that functional status was shown to be maintained in TBI patients in the follow-up study.
“Since no major changes in the hospital-based care or rehabilitation care of these TBI patients occurred, we weren’t surprised to see that functional outcomes did not improve,” he said in an interview. “The regionalization protocols were designed primarily to improve survival.”
During a discussion of the results, audience members questioned whether the investigators could be certain the results could be attributed to regionalization and not improvements in treatment of concurrent injuries or improvements in TBI treatment already underway at the time of policy change.
For the most part, these patients had isolated TBIs and no major changes in personnel or TBI care occurred during the study period, Dr. Kelly said.
Under NOTS, region-wide initiatives included use of the Centers for Disease Control and Prevention guidelines for field triage, a transfer line and transfer protocols, and a research database shared between two large hospital systems comprising the level I MetroHealth Medical Center trauma center, two level II trauma centers, and 12 nontrauma hospitals.
Dr. Kelly, his coauthors, and Dr. Coughenour reported no financial disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: Regionalized trauma care reduces long-term mortality and maintains functional outcomes in patients with severe TBI.
Major finding: RT reduced 30-day mortality from 21% to 16% (P < .0001) and 6-month mortality from 24% to 20% (P = .004).
Data source: Analysis of 3,496 patients with severe TBI.
Disclosures: Dr. Kelly, his coauthors, and Dr. Coughenour reported no financial disclosures.

Guideline clarifies first-line treatment for allergic rhinitis
First-line treatment for allergic rhinitis should include intranasal steroids, as well as less-sedating second-generation oral antihistamines for patients whose primary complaints are sneezing and itching, according to a new clinical practice guideline published online Feb. 2 in Otolaryngology–Head and Neck Surgery.
In contrast, sinonasal imaging should not be routine when patients first present with symptoms consistent with allergic rhinitis, and oral leukotriene receptor antagonists are not recommended as first-line therapy, said Dr. Michael D. Seidman of Henry Ford West Bloomfield (Mich.) Hospital and chair of the guideline working group, and his associates.
Dr. Seidman and a panel of 20 experts in otolaryngology, allergy and immunology, internal medicine, family medicine, pediatrics, sleep medicine, advanced practice nursing, complementary and alternative medicine, and consumer advocacy developed the new practice guideline to enable clinicians in all settings to improve patient care and reduce harmful or unnecessary variations in care for allergic rhinitis.
“The guideline is intended to focus on a limited number of quality improvement opportunities deemed most important by the working group and is not intended to be a comprehensive reference for diagnosing and managing allergic rhinitis,” the authors noted.
During the course of 1 year, the working group reviewed 1,605 randomized, controlled trials, 31 existing clinical practice guidelines, and 390 systematic reviews of the literature regarding allergic rhinitis in adults and children older than age 2 years. They then compiled 14 key recommendations that underwent extensive peer review, which have been published online and as a supplement to the February issue (Otolaryngol. Head Neck Surg. 2015;152:S1-S43).
In addition to the recommendations noted above, the guideline advises:
* Clinicians should diagnose allergic rhinitis when patients present with a history and physical exam consistent with the disorder (including clear rhinorrhea, nasal congestion, pale discoloration of the nasal mucosa, and red, watery eyes) plus symptoms of nasal congestion, runny nose, itchy nose, or sneezing.
* Clinicians should perform and interpret (or refer patients for) specific IgE allergy testing for allergic rhinitis that doesn’t respond to empiric treatment, or when the diagnosis is uncertain, or when identifying the specific causative allergen would allow targeted therapy.
* Clinicians should assess diagnosed patients for associated conditions such as asthma, atopic dermatitis, sleep-disordered breathing, conjunctivitis, rhinosinusitis, and otitis media, and should document that in the medical record.
* Clinicians should offer (or refer patients for) sublingual or subcutaneous immunotherapy when allergic rhinitis doesn’t respond adequately to pharmacologic therapy.
* Clinicians may advise avoidance of known allergens or controlling the patient’s environment by such measures as removing pets, using air filtration systems, using dust-mite–reducing covers for bedding, and using acaricides.
* Clinicians may offer intranasal antihistamines for patients with seasonal, perennial or episodic allergic rhinitis.*
* Clinicians may offer (or refer patients for) reduction of the inferior turbinates for patients who have nasal airway obstruction or enlarged turbinates.
* Clinicians may offer (or refer patient for) acupuncture if they are interested in nonpharmacologic therapy.
*Clinicians may offer combination pharmacologic therapy in patients with allergic rhinitis who have inadequate response to pharmacologic monotherapy.
The working group offered no recommendations concerning herbal therapy for allergic rhinitis, because of the limited literature on those substances and concern about their safety.
The full text of the guideline and its supporting data are available free of charge at www.entnet.org. In addition, an algorithm of the guideline’s action statements and a table of common allergic rhinitis clinical scenarios are available as quick reference guides for clinicians.
The American Academy of Otolaryngology–Head and Neck Surgery Foundation funded the guideline. Dr. Seidman reported being medical director of the Scientific Advisory Board of Visalus, founder of the Body Language Vitamin, and holder of six patents related to dietary supplements, aircraft, and middle ear and brain implants. His associates reported ties to Acclarent/Johnson/Johnson, FirstLine Medical, GlaxoSmithKline, Intersect, MEDA, Medtronic, Merck, Mylan, Novartis, TEVA, Transit of Venus, Sanofi, Sunovion Pharmaceuticals, and WellPoint.
*Correction, 2/18/2015: An earlier version of this story misstated the guideline for the use of intranasal antihistamines.
First-line treatment for allergic rhinitis should include intranasal steroids, as well as less-sedating second-generation oral antihistamines for patients whose primary complaints are sneezing and itching, according to a new clinical practice guideline published online Feb. 2 in Otolaryngology–Head and Neck Surgery.
In contrast, sinonasal imaging should not be routine when patients first present with symptoms consistent with allergic rhinitis, and oral leukotriene receptor antagonists are not recommended as first-line therapy, said Dr. Michael D. Seidman of Henry Ford West Bloomfield (Mich.) Hospital and chair of the guideline working group, and his associates.
Dr. Seidman and a panel of 20 experts in otolaryngology, allergy and immunology, internal medicine, family medicine, pediatrics, sleep medicine, advanced practice nursing, complementary and alternative medicine, and consumer advocacy developed the new practice guideline to enable clinicians in all settings to improve patient care and reduce harmful or unnecessary variations in care for allergic rhinitis.
“The guideline is intended to focus on a limited number of quality improvement opportunities deemed most important by the working group and is not intended to be a comprehensive reference for diagnosing and managing allergic rhinitis,” the authors noted.
During the course of 1 year, the working group reviewed 1,605 randomized, controlled trials, 31 existing clinical practice guidelines, and 390 systematic reviews of the literature regarding allergic rhinitis in adults and children older than age 2 years. They then compiled 14 key recommendations that underwent extensive peer review, which have been published online and as a supplement to the February issue (Otolaryngol. Head Neck Surg. 2015;152:S1-S43).
In addition to the recommendations noted above, the guideline advises:
* Clinicians should diagnose allergic rhinitis when patients present with a history and physical exam consistent with the disorder (including clear rhinorrhea, nasal congestion, pale discoloration of the nasal mucosa, and red, watery eyes) plus symptoms of nasal congestion, runny nose, itchy nose, or sneezing.
* Clinicians should perform and interpret (or refer patients for) specific IgE allergy testing for allergic rhinitis that doesn’t respond to empiric treatment, or when the diagnosis is uncertain, or when identifying the specific causative allergen would allow targeted therapy.
* Clinicians should assess diagnosed patients for associated conditions such as asthma, atopic dermatitis, sleep-disordered breathing, conjunctivitis, rhinosinusitis, and otitis media, and should document that in the medical record.
* Clinicians should offer (or refer patients for) sublingual or subcutaneous immunotherapy when allergic rhinitis doesn’t respond adequately to pharmacologic therapy.
* Clinicians may advise avoidance of known allergens or controlling the patient’s environment by such measures as removing pets, using air filtration systems, using dust-mite–reducing covers for bedding, and using acaricides.
* Clinicians may offer intranasal antihistamines for patients with seasonal, perennial or episodic allergic rhinitis.*
* Clinicians may offer (or refer patients for) reduction of the inferior turbinates for patients who have nasal airway obstruction or enlarged turbinates.
* Clinicians may offer (or refer patient for) acupuncture if they are interested in nonpharmacologic therapy.
*Clinicians may offer combination pharmacologic therapy in patients with allergic rhinitis who have inadequate response to pharmacologic monotherapy.
The working group offered no recommendations concerning herbal therapy for allergic rhinitis, because of the limited literature on those substances and concern about their safety.
The full text of the guideline and its supporting data are available free of charge at www.entnet.org. In addition, an algorithm of the guideline’s action statements and a table of common allergic rhinitis clinical scenarios are available as quick reference guides for clinicians.
The American Academy of Otolaryngology–Head and Neck Surgery Foundation funded the guideline. Dr. Seidman reported being medical director of the Scientific Advisory Board of Visalus, founder of the Body Language Vitamin, and holder of six patents related to dietary supplements, aircraft, and middle ear and brain implants. His associates reported ties to Acclarent/Johnson/Johnson, FirstLine Medical, GlaxoSmithKline, Intersect, MEDA, Medtronic, Merck, Mylan, Novartis, TEVA, Transit of Venus, Sanofi, Sunovion Pharmaceuticals, and WellPoint.
*Correction, 2/18/2015: An earlier version of this story misstated the guideline for the use of intranasal antihistamines.
First-line treatment for allergic rhinitis should include intranasal steroids, as well as less-sedating second-generation oral antihistamines for patients whose primary complaints are sneezing and itching, according to a new clinical practice guideline published online Feb. 2 in Otolaryngology–Head and Neck Surgery.
In contrast, sinonasal imaging should not be routine when patients first present with symptoms consistent with allergic rhinitis, and oral leukotriene receptor antagonists are not recommended as first-line therapy, said Dr. Michael D. Seidman of Henry Ford West Bloomfield (Mich.) Hospital and chair of the guideline working group, and his associates.
Dr. Seidman and a panel of 20 experts in otolaryngology, allergy and immunology, internal medicine, family medicine, pediatrics, sleep medicine, advanced practice nursing, complementary and alternative medicine, and consumer advocacy developed the new practice guideline to enable clinicians in all settings to improve patient care and reduce harmful or unnecessary variations in care for allergic rhinitis.
“The guideline is intended to focus on a limited number of quality improvement opportunities deemed most important by the working group and is not intended to be a comprehensive reference for diagnosing and managing allergic rhinitis,” the authors noted.
During the course of 1 year, the working group reviewed 1,605 randomized, controlled trials, 31 existing clinical practice guidelines, and 390 systematic reviews of the literature regarding allergic rhinitis in adults and children older than age 2 years. They then compiled 14 key recommendations that underwent extensive peer review, which have been published online and as a supplement to the February issue (Otolaryngol. Head Neck Surg. 2015;152:S1-S43).
In addition to the recommendations noted above, the guideline advises:
* Clinicians should diagnose allergic rhinitis when patients present with a history and physical exam consistent with the disorder (including clear rhinorrhea, nasal congestion, pale discoloration of the nasal mucosa, and red, watery eyes) plus symptoms of nasal congestion, runny nose, itchy nose, or sneezing.
* Clinicians should perform and interpret (or refer patients for) specific IgE allergy testing for allergic rhinitis that doesn’t respond to empiric treatment, or when the diagnosis is uncertain, or when identifying the specific causative allergen would allow targeted therapy.
* Clinicians should assess diagnosed patients for associated conditions such as asthma, atopic dermatitis, sleep-disordered breathing, conjunctivitis, rhinosinusitis, and otitis media, and should document that in the medical record.
* Clinicians should offer (or refer patients for) sublingual or subcutaneous immunotherapy when allergic rhinitis doesn’t respond adequately to pharmacologic therapy.
* Clinicians may advise avoidance of known allergens or controlling the patient’s environment by such measures as removing pets, using air filtration systems, using dust-mite–reducing covers for bedding, and using acaricides.
* Clinicians may offer intranasal antihistamines for patients with seasonal, perennial or episodic allergic rhinitis.*
* Clinicians may offer (or refer patients for) reduction of the inferior turbinates for patients who have nasal airway obstruction or enlarged turbinates.
* Clinicians may offer (or refer patient for) acupuncture if they are interested in nonpharmacologic therapy.
*Clinicians may offer combination pharmacologic therapy in patients with allergic rhinitis who have inadequate response to pharmacologic monotherapy.
The working group offered no recommendations concerning herbal therapy for allergic rhinitis, because of the limited literature on those substances and concern about their safety.
The full text of the guideline and its supporting data are available free of charge at www.entnet.org. In addition, an algorithm of the guideline’s action statements and a table of common allergic rhinitis clinical scenarios are available as quick reference guides for clinicians.
The American Academy of Otolaryngology–Head and Neck Surgery Foundation funded the guideline. Dr. Seidman reported being medical director of the Scientific Advisory Board of Visalus, founder of the Body Language Vitamin, and holder of six patents related to dietary supplements, aircraft, and middle ear and brain implants. His associates reported ties to Acclarent/Johnson/Johnson, FirstLine Medical, GlaxoSmithKline, Intersect, MEDA, Medtronic, Merck, Mylan, Novartis, TEVA, Transit of Venus, Sanofi, Sunovion Pharmaceuticals, and WellPoint.
*Correction, 2/18/2015: An earlier version of this story misstated the guideline for the use of intranasal antihistamines.
FROM OTOLARYNGOLOGY–HEAD AND NECK SURGERY
Key clinical point: First-line treatment for allergic rhinitis should include intranasal steroids and second-generation oral antihistamines, and should not include leukotriene receptor antagonists or sinonasal imaging studies.
Major finding: A panel of 20 experts took 1 year to review the literature and develop action items focusing on a limited number of quality improvement opportunities they deemed most important to improve patient care.
Data source: A review of 1,605 randomized, controlled trials, 31 sets of practice guidelines, and 390 systematic reviews regarding allergic rhinitis, and a compilation of 14 recommendations for managing the disorder.
Disclosures: The American Academy of Otolaryngology–Head and Neck Surgery Foundation funded the guideline. Dr. Seidman reported being medical director of the Scientific Advisory Board of Visalus, founder of the Body Language Vitamin, and holder of six patents related to dietary supplements, aircraft, and middle ear and brain implants. His associates reported ties to Acclarent/Johnson/Johnson, FirstLine Medical, GlaxoSmithKline, Intersect, MEDA, Medtronic, Merck, Mylan, Novartis, TEVA, Transit of Venus, Sanofi, Sunovion Pharmaceuticals, and WellPoint.
LISTEN NOW: Highlights of the February 2015 Issue of The Hospitalist
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/01/2015-February-Hospitalist-Highlights.mp3"][/audio]
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/01/2015-February-Hospitalist-Highlights.mp3"][/audio]
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/01/2015-February-Hospitalist-Highlights.mp3"][/audio]
Society of Hospital Medicine's 2015 Annual Meeting Preview

And, naturally, SHM is planning hundreds of meetings with legislators and their staffers to spread the gospel of hospital medicine.
“I’ll be honest. I’m exhausted when I get back,” says course director Efren Manjarrez, MD, SFHM, but “it’s the most uplifting exhaustion you could ever have.”
Richard Quinn is a freelance writer in New Jersey.
And, naturally, SHM is planning hundreds of meetings with legislators and their staffers to spread the gospel of hospital medicine.
“I’ll be honest. I’m exhausted when I get back,” says course director Efren Manjarrez, MD, SFHM, but “it’s the most uplifting exhaustion you could ever have.”
Richard Quinn is a freelance writer in New Jersey.
And, naturally, SHM is planning hundreds of meetings with legislators and their staffers to spread the gospel of hospital medicine.
“I’ll be honest. I’m exhausted when I get back,” says course director Efren Manjarrez, MD, SFHM, but “it’s the most uplifting exhaustion you could ever have.”
Richard Quinn is a freelance writer in New Jersey.

{kind=link}
Much Ado about Hospital Quality
I have reported previously on major incentive programs under Medicare and the Affordable Care Act that affect hospitals and, by extension, their affiliated hospitalists. I’d like to provide you with an update on these programs. The bad news is that hospitals have more revenue than ever that is at risk based on performance. The good news is that such risk, and its mitigation, centers on performance measures in the sweet spot of hospitalists and the teams they work with to improve patient care.

Hospital-Acquired Conditions
On Dec. 17, 2014, the Centers for Medicare and Medicaid Services (CMS) announced that 724 U.S. hospitals—the lowest quartile—will have 1% of their reimbursement docked effective Oct. 1, 2014, as part of the Hospital-Acquired Condition Reduction Program (HACRP). The HACRP is divided into the following domains:
- 35%, Agency for Healthcare Research and Quality Patient Safety Indicators (PSI-90). This is a composite of eight claims-based harm measures.
- 65%, CDC National Health Safety Network measures. These are clinically derived metrics, currently central line-associated blood stream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI).
The HACRP program, which debuted in October 2014, will continue at least through 2020. The 65% weight domain will change in FY16 with the addition of surgical site infections (colon, hysterectomy) and in FY17 with the addition of MRSA and Clostridium difficile infections.
The full list of U.S. hospitals and their performance in the HACRP and the Hospital Value-Based Purchasing (VBP) program is available at www.modernhealthcare.com/article/20141108/INFO/141109959.
Just two weeks prior to the CMS announcement, AHRQ announced some major accomplishments in efforts to address patient safety at U.S. hospitals. The agency reported that the number of hospital-acquired conditions in the Partnership for Patients (PfP) program in the U.S. declined 9% over a one-year period (2012 to 2013) and 17% over a three-year period (2010 to 2013). Hospital-acquired conditions are defined somewhat differently in the PfP than in the HACRP, with PfP targeting certain hospital-acquired infections, pressure ulcers, falls, and adverse drug effects.
The report noted that reductions in adverse drug events and pressure ulcers were the largest contributors to a reported 50,000 fewer in-hospital deaths over the 2010-2013 period.
Hospital Value-Based Purchasing
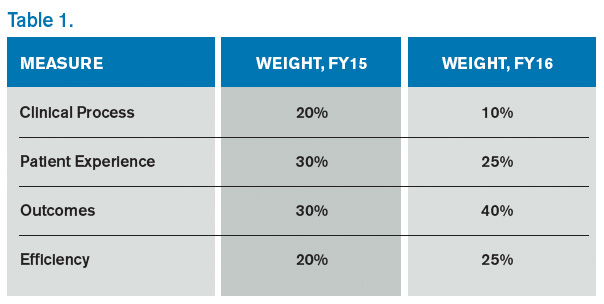
The Hospital VBP program continues to evolve. See Table 1 for a breakdown of the program for the next two years.
Unlike the HACRP and the Hospital Readmissions Reduction Program, which are pure penalty programs, VBP has hospitals at risk for 1.5% (for 2015) of Medicare payments, but they may earn back some, all, or an amount in excess of the 1.5% based on performance. For the years noted above, the VBP program metrics are as follows:
- Clinical Process: selected heart failure (HF), pneumonia (PN), myocardial infarction (MI), and surgical care measures.
- Patient Experience: a subset of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions.
- Outcomes: HF, PN, MI, 30-day mortality, CLABSI, and PSI-90.
- Efficiency: Medicare spending per beneficiary (spending from three days prior to an inpatient hospital admission through 30 days after discharge)
Readmission Penalties
CMS announced that in the latest round of the Hospital Readmissions Reduction Program, 2,610 hospitals were penalized in total, while 39 hospitals will receive the largest penalty allowed. For FY15, the program added chronic obstructive pulmonary disease and hip and knee arthroplasty to HF, PN, and MI as the conditions counting toward excess readmissions.
For FY15, the number of hospitals penalized and the amount of the penalty are expected to increase. In addition, 1% of hospitals are anticipated to receive the maximum penalty, while 77% are expected to have some penalty, and 22% will likely have no penalty. The maximum penalty has topped out at 3% of Medicare inpatient payments.
HCAHPS Star Ratings
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures. The initial ratings will be based on discharges during the period ranging from July 2013 through June 2014.
What’s a Hospitalist to Do?
The latest version of CMS incentive programs should serve to reinforce your hospital medicine group’s strategy to be agents of collaboration and change. Link up with your quality department to align priorities, and make sure you have hospitalist representatives on key patient safety, patient experience, and quality improvement committees.
Because dollars are at stake for your hospital, have a clear understanding of the value your hospitalist group brings to the table, so you can secure the appropriate financial support for the time and work expended on these initiatives.
And don’t forget to keep the patient at the center of your efforts.

I have reported previously on major incentive programs under Medicare and the Affordable Care Act that affect hospitals and, by extension, their affiliated hospitalists. I’d like to provide you with an update on these programs. The bad news is that hospitals have more revenue than ever that is at risk based on performance. The good news is that such risk, and its mitigation, centers on performance measures in the sweet spot of hospitalists and the teams they work with to improve patient care.
Hospital-Acquired Conditions
On Dec. 17, 2014, the Centers for Medicare and Medicaid Services (CMS) announced that 724 U.S. hospitals—the lowest quartile—will have 1% of their reimbursement docked effective Oct. 1, 2014, as part of the Hospital-Acquired Condition Reduction Program (HACRP). The HACRP is divided into the following domains:
- 35%, Agency for Healthcare Research and Quality Patient Safety Indicators (PSI-90). This is a composite of eight claims-based harm measures.
- 65%, CDC National Health Safety Network measures. These are clinically derived metrics, currently central line-associated blood stream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI).
The HACRP program, which debuted in October 2014, will continue at least through 2020. The 65% weight domain will change in FY16 with the addition of surgical site infections (colon, hysterectomy) and in FY17 with the addition of MRSA and Clostridium difficile infections.
The full list of U.S. hospitals and their performance in the HACRP and the Hospital Value-Based Purchasing (VBP) program is available at www.modernhealthcare.com/article/20141108/INFO/141109959.
Just two weeks prior to the CMS announcement, AHRQ announced some major accomplishments in efforts to address patient safety at U.S. hospitals. The agency reported that the number of hospital-acquired conditions in the Partnership for Patients (PfP) program in the U.S. declined 9% over a one-year period (2012 to 2013) and 17% over a three-year period (2010 to 2013). Hospital-acquired conditions are defined somewhat differently in the PfP than in the HACRP, with PfP targeting certain hospital-acquired infections, pressure ulcers, falls, and adverse drug effects.
The report noted that reductions in adverse drug events and pressure ulcers were the largest contributors to a reported 50,000 fewer in-hospital deaths over the 2010-2013 period.
Hospital Value-Based Purchasing
The Hospital VBP program continues to evolve. See Table 1 for a breakdown of the program for the next two years.
Unlike the HACRP and the Hospital Readmissions Reduction Program, which are pure penalty programs, VBP has hospitals at risk for 1.5% (for 2015) of Medicare payments, but they may earn back some, all, or an amount in excess of the 1.5% based on performance. For the years noted above, the VBP program metrics are as follows:
- Clinical Process: selected heart failure (HF), pneumonia (PN), myocardial infarction (MI), and surgical care measures.
- Patient Experience: a subset of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions.
- Outcomes: HF, PN, MI, 30-day mortality, CLABSI, and PSI-90.
- Efficiency: Medicare spending per beneficiary (spending from three days prior to an inpatient hospital admission through 30 days after discharge)
Readmission Penalties
CMS announced that in the latest round of the Hospital Readmissions Reduction Program, 2,610 hospitals were penalized in total, while 39 hospitals will receive the largest penalty allowed. For FY15, the program added chronic obstructive pulmonary disease and hip and knee arthroplasty to HF, PN, and MI as the conditions counting toward excess readmissions.
For FY15, the number of hospitals penalized and the amount of the penalty are expected to increase. In addition, 1% of hospitals are anticipated to receive the maximum penalty, while 77% are expected to have some penalty, and 22% will likely have no penalty. The maximum penalty has topped out at 3% of Medicare inpatient payments.
HCAHPS Star Ratings
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures. The initial ratings will be based on discharges during the period ranging from July 2013 through June 2014.
What’s a Hospitalist to Do?
The latest version of CMS incentive programs should serve to reinforce your hospital medicine group’s strategy to be agents of collaboration and change. Link up with your quality department to align priorities, and make sure you have hospitalist representatives on key patient safety, patient experience, and quality improvement committees.
Because dollars are at stake for your hospital, have a clear understanding of the value your hospitalist group brings to the table, so you can secure the appropriate financial support for the time and work expended on these initiatives.
And don’t forget to keep the patient at the center of your efforts.
I have reported previously on major incentive programs under Medicare and the Affordable Care Act that affect hospitals and, by extension, their affiliated hospitalists. I’d like to provide you with an update on these programs. The bad news is that hospitals have more revenue than ever that is at risk based on performance. The good news is that such risk, and its mitigation, centers on performance measures in the sweet spot of hospitalists and the teams they work with to improve patient care.
Hospital-Acquired Conditions
On Dec. 17, 2014, the Centers for Medicare and Medicaid Services (CMS) announced that 724 U.S. hospitals—the lowest quartile—will have 1% of their reimbursement docked effective Oct. 1, 2014, as part of the Hospital-Acquired Condition Reduction Program (HACRP). The HACRP is divided into the following domains:
- 35%, Agency for Healthcare Research and Quality Patient Safety Indicators (PSI-90). This is a composite of eight claims-based harm measures.
- 65%, CDC National Health Safety Network measures. These are clinically derived metrics, currently central line-associated blood stream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI).
The HACRP program, which debuted in October 2014, will continue at least through 2020. The 65% weight domain will change in FY16 with the addition of surgical site infections (colon, hysterectomy) and in FY17 with the addition of MRSA and Clostridium difficile infections.
The full list of U.S. hospitals and their performance in the HACRP and the Hospital Value-Based Purchasing (VBP) program is available at www.modernhealthcare.com/article/20141108/INFO/141109959.
Just two weeks prior to the CMS announcement, AHRQ announced some major accomplishments in efforts to address patient safety at U.S. hospitals. The agency reported that the number of hospital-acquired conditions in the Partnership for Patients (PfP) program in the U.S. declined 9% over a one-year period (2012 to 2013) and 17% over a three-year period (2010 to 2013). Hospital-acquired conditions are defined somewhat differently in the PfP than in the HACRP, with PfP targeting certain hospital-acquired infections, pressure ulcers, falls, and adverse drug effects.
The report noted that reductions in adverse drug events and pressure ulcers were the largest contributors to a reported 50,000 fewer in-hospital deaths over the 2010-2013 period.
Hospital Value-Based Purchasing
The Hospital VBP program continues to evolve. See Table 1 for a breakdown of the program for the next two years.
Unlike the HACRP and the Hospital Readmissions Reduction Program, which are pure penalty programs, VBP has hospitals at risk for 1.5% (for 2015) of Medicare payments, but they may earn back some, all, or an amount in excess of the 1.5% based on performance. For the years noted above, the VBP program metrics are as follows:
- Clinical Process: selected heart failure (HF), pneumonia (PN), myocardial infarction (MI), and surgical care measures.
- Patient Experience: a subset of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions.
- Outcomes: HF, PN, MI, 30-day mortality, CLABSI, and PSI-90.
- Efficiency: Medicare spending per beneficiary (spending from three days prior to an inpatient hospital admission through 30 days after discharge)
Readmission Penalties
CMS announced that in the latest round of the Hospital Readmissions Reduction Program, 2,610 hospitals were penalized in total, while 39 hospitals will receive the largest penalty allowed. For FY15, the program added chronic obstructive pulmonary disease and hip and knee arthroplasty to HF, PN, and MI as the conditions counting toward excess readmissions.
For FY15, the number of hospitals penalized and the amount of the penalty are expected to increase. In addition, 1% of hospitals are anticipated to receive the maximum penalty, while 77% are expected to have some penalty, and 22% will likely have no penalty. The maximum penalty has topped out at 3% of Medicare inpatient payments.
HCAHPS Star Ratings
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures. The initial ratings will be based on discharges during the period ranging from July 2013 through June 2014.
What’s a Hospitalist to Do?
The latest version of CMS incentive programs should serve to reinforce your hospital medicine group’s strategy to be agents of collaboration and change. Link up with your quality department to align priorities, and make sure you have hospitalist representatives on key patient safety, patient experience, and quality improvement committees.
Because dollars are at stake for your hospital, have a clear understanding of the value your hospitalist group brings to the table, so you can secure the appropriate financial support for the time and work expended on these initiatives.
And don’t forget to keep the patient at the center of your efforts.
Hospitalists Lead Efforts To Reduce Care Costs, Improve Patient Care
In 2015, reimbursement for physicians in large groups is subject to a value modifier that takes into account the cost and quality of services performed under the Medicare Physician Fee Schedule. By 2017, the modifier will apply to all physicians participating in fee-for-service Medicare.
It’s one more way the Centers for Medicare and Medicaid Services (CMS) and the federal government are attempting to tip the scales on skyrocketing healthcare costs. Their end goal is a focus on better efficiency and less waste in the healthcare system.
But in an environment of top-down measures, hospitalists on the front lines are leading the charge to reduce overuse and overtreatment, slow cost growth, and improve both the quality of care and outcomes for their patients.
“I think the hospitalist movement has prided itself on quality improvement and patient safety in the hospital,” says Chris Moriates, MD, assistant clinical professor in the division of hospital medicine at the University of California San Francisco (UCSF) and co-creator of the cost awareness curriculum for UCSF’s internal medicine residents. “Over the last few years…they are more focused and enthusiastic about looking at value.”
Dr. Moriates leads the UCSF hospitalist division’s High Value Care Committee and is director of implementation initiatives at Costs of Care. He’s also part of a UCSF program that invites all employees to submit ideas for cutting waste in the hospital while maintaining or improving patient care quality. Last year, the winning project tackled unnecessary blood transfusions and at the same time realized $1 million in savings due to lower transfusion rates. This year, the hospital will focus on decreasing money spent on surgical supplies, potentially saving millions of dollars, he says.
A 2012 article in the Journal of the American Medical Association (JAMA) estimates wasteful spending costs the U.S. healthcare system at least $600 billion and potentially more than a trillion dollars annually due to such issues as care coordination and care delivery failures and overtreatment.1 Numerous studies also indicate overtreatment can lead to patient harm.2
“Say a patient gets a prophylactic scan for abdominal pain,” says Vineet Arora, MD, MAPP, a hospitalist on faculty in the University of Chicago’s department of medicine and director of education initiatives for Costs of Care. “The patient gets better, but an incidental finding of the scan is a renal mass. Now, there is a work-up of that mass, the patient gets a biopsy, and they have a bleed. A lot of testing leads to more testing, and more testing can lead to harm.”
—LeRoi S. Hicks, MD, MPH
Doing less is often better, says John Bulger, DO, MBA, SFHM, chief quality officer for the Geisinger Health System in Danville, Pa. Dr. Bulger, who has led SHM’s participation in the Choosing Wisely campaign, cites a September 2014 study in JAMA Internal Medicine, in which Christiana Care Health System—an 1,100-bed tertiary care center in northern Delaware—built best practice telemetry guidelines into its electronic ordering system to help physicians determine when monitoring was appropriate.3 The health system also assembled multidisciplinary teams, which identified when medications warranted telemetry, and equipped nurses with tools to determine when telemetry should be stopped.
Appropriate use of telemetry is one of SHM’s five Choosing Wisely recommendations for adult patient care.
In addition to an overall 70% reduction in telemetry use without negative impact to patient safety, Christiana Care saved $4.8 million. Throughout its inpatient units, Christiana Care utilizes a multidisciplinary team approach to coordinate patient care. Daily rounds are attended by hospitalists, nurses, pharmacists, case managers, social workers, and others to ensure timely and appropriate patient care. The health system’s Value Institute evaluates hospital efforts and assesses process design to improve efficiency and, ultimately, outcomes.
“This is preparing for war in a time of peace, essentially,” says LeRoi S. Hicks, MD, MPH, a hospitalist, researcher, and educator at Christiana Care. “The goal will be, as we move to bundled payment and population health approaches, to minimize the time patients spend in the hospitals and limit the growth curve in spending on the hospital side. We are doing this and not taking on financial risk.”
Dr. Hicks adds that in its most simple form the project “reduces variation in the care we deliver” while improving efficiency and outcomes.
For many physicians, the best way to start is to begin a dialogue with patients who might also be at risk of financial harm due to unnecessary care, Dr. Arora says. “Patients are willing to change their minds and go with the more affordable and more evidence-based treatment and forgo expensive ones if they have that conversation,” she says.
Many resources exist for physicians interested in driving the frontline charge to improve healthcare quality and value. The Costs of Care curriculum provides training and tools for physicians at teachingvalue.org, as do SHM’s Center for Quality Innovation and the Institute for Healthcare Improvement. Dr. Moriates and Dr. Arora also have co-authored a book, along with Neel Shah, MD, founder and executive director of Costs of Care, called “Understanding Value Based Healthcare.” The book will be available this spring.
“We shouldn’t sit by the side of the road waiting for things to pass by,” Dr. Arora says. “I think the key is, we know the needle is shifting in Washington, we know system innovation models are being tested. It would be silly for us to say we’re going to continue the status quo and not look at ways to contribute as physicians.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA. 2012;307(14):1513-1516.
- Morgan DJ, Wright SM, Dhruva S. Update on medical overuse. JAMA Intern Med. 2015;175(1):120-124.
- Dressler R, Dryer MM, Coletti C, Mahoney D, Doorey AJ. Altering overuse of cardiac telemetry in non-intensive care unit settings by hardwiring the use of American Heart Association guidelines. JAMA Intern Med. 2014;174(11):1852-1854.
In 2015, reimbursement for physicians in large groups is subject to a value modifier that takes into account the cost and quality of services performed under the Medicare Physician Fee Schedule. By 2017, the modifier will apply to all physicians participating in fee-for-service Medicare.
It’s one more way the Centers for Medicare and Medicaid Services (CMS) and the federal government are attempting to tip the scales on skyrocketing healthcare costs. Their end goal is a focus on better efficiency and less waste in the healthcare system.
But in an environment of top-down measures, hospitalists on the front lines are leading the charge to reduce overuse and overtreatment, slow cost growth, and improve both the quality of care and outcomes for their patients.
“I think the hospitalist movement has prided itself on quality improvement and patient safety in the hospital,” says Chris Moriates, MD, assistant clinical professor in the division of hospital medicine at the University of California San Francisco (UCSF) and co-creator of the cost awareness curriculum for UCSF’s internal medicine residents. “Over the last few years…they are more focused and enthusiastic about looking at value.”
Dr. Moriates leads the UCSF hospitalist division’s High Value Care Committee and is director of implementation initiatives at Costs of Care. He’s also part of a UCSF program that invites all employees to submit ideas for cutting waste in the hospital while maintaining or improving patient care quality. Last year, the winning project tackled unnecessary blood transfusions and at the same time realized $1 million in savings due to lower transfusion rates. This year, the hospital will focus on decreasing money spent on surgical supplies, potentially saving millions of dollars, he says.
A 2012 article in the Journal of the American Medical Association (JAMA) estimates wasteful spending costs the U.S. healthcare system at least $600 billion and potentially more than a trillion dollars annually due to such issues as care coordination and care delivery failures and overtreatment.1 Numerous studies also indicate overtreatment can lead to patient harm.2
“Say a patient gets a prophylactic scan for abdominal pain,” says Vineet Arora, MD, MAPP, a hospitalist on faculty in the University of Chicago’s department of medicine and director of education initiatives for Costs of Care. “The patient gets better, but an incidental finding of the scan is a renal mass. Now, there is a work-up of that mass, the patient gets a biopsy, and they have a bleed. A lot of testing leads to more testing, and more testing can lead to harm.”
—LeRoi S. Hicks, MD, MPH
Doing less is often better, says John Bulger, DO, MBA, SFHM, chief quality officer for the Geisinger Health System in Danville, Pa. Dr. Bulger, who has led SHM’s participation in the Choosing Wisely campaign, cites a September 2014 study in JAMA Internal Medicine, in which Christiana Care Health System—an 1,100-bed tertiary care center in northern Delaware—built best practice telemetry guidelines into its electronic ordering system to help physicians determine when monitoring was appropriate.3 The health system also assembled multidisciplinary teams, which identified when medications warranted telemetry, and equipped nurses with tools to determine when telemetry should be stopped.
Appropriate use of telemetry is one of SHM’s five Choosing Wisely recommendations for adult patient care.
In addition to an overall 70% reduction in telemetry use without negative impact to patient safety, Christiana Care saved $4.8 million. Throughout its inpatient units, Christiana Care utilizes a multidisciplinary team approach to coordinate patient care. Daily rounds are attended by hospitalists, nurses, pharmacists, case managers, social workers, and others to ensure timely and appropriate patient care. The health system’s Value Institute evaluates hospital efforts and assesses process design to improve efficiency and, ultimately, outcomes.
“This is preparing for war in a time of peace, essentially,” says LeRoi S. Hicks, MD, MPH, a hospitalist, researcher, and educator at Christiana Care. “The goal will be, as we move to bundled payment and population health approaches, to minimize the time patients spend in the hospitals and limit the growth curve in spending on the hospital side. We are doing this and not taking on financial risk.”
Dr. Hicks adds that in its most simple form the project “reduces variation in the care we deliver” while improving efficiency and outcomes.
For many physicians, the best way to start is to begin a dialogue with patients who might also be at risk of financial harm due to unnecessary care, Dr. Arora says. “Patients are willing to change their minds and go with the more affordable and more evidence-based treatment and forgo expensive ones if they have that conversation,” she says.
Many resources exist for physicians interested in driving the frontline charge to improve healthcare quality and value. The Costs of Care curriculum provides training and tools for physicians at teachingvalue.org, as do SHM’s Center for Quality Innovation and the Institute for Healthcare Improvement. Dr. Moriates and Dr. Arora also have co-authored a book, along with Neel Shah, MD, founder and executive director of Costs of Care, called “Understanding Value Based Healthcare.” The book will be available this spring.
“We shouldn’t sit by the side of the road waiting for things to pass by,” Dr. Arora says. “I think the key is, we know the needle is shifting in Washington, we know system innovation models are being tested. It would be silly for us to say we’re going to continue the status quo and not look at ways to contribute as physicians.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA. 2012;307(14):1513-1516.
- Morgan DJ, Wright SM, Dhruva S. Update on medical overuse. JAMA Intern Med. 2015;175(1):120-124.
- Dressler R, Dryer MM, Coletti C, Mahoney D, Doorey AJ. Altering overuse of cardiac telemetry in non-intensive care unit settings by hardwiring the use of American Heart Association guidelines. JAMA Intern Med. 2014;174(11):1852-1854.
In 2015, reimbursement for physicians in large groups is subject to a value modifier that takes into account the cost and quality of services performed under the Medicare Physician Fee Schedule. By 2017, the modifier will apply to all physicians participating in fee-for-service Medicare.
It’s one more way the Centers for Medicare and Medicaid Services (CMS) and the federal government are attempting to tip the scales on skyrocketing healthcare costs. Their end goal is a focus on better efficiency and less waste in the healthcare system.
But in an environment of top-down measures, hospitalists on the front lines are leading the charge to reduce overuse and overtreatment, slow cost growth, and improve both the quality of care and outcomes for their patients.
“I think the hospitalist movement has prided itself on quality improvement and patient safety in the hospital,” says Chris Moriates, MD, assistant clinical professor in the division of hospital medicine at the University of California San Francisco (UCSF) and co-creator of the cost awareness curriculum for UCSF’s internal medicine residents. “Over the last few years…they are more focused and enthusiastic about looking at value.”
Dr. Moriates leads the UCSF hospitalist division’s High Value Care Committee and is director of implementation initiatives at Costs of Care. He’s also part of a UCSF program that invites all employees to submit ideas for cutting waste in the hospital while maintaining or improving patient care quality. Last year, the winning project tackled unnecessary blood transfusions and at the same time realized $1 million in savings due to lower transfusion rates. This year, the hospital will focus on decreasing money spent on surgical supplies, potentially saving millions of dollars, he says.
A 2012 article in the Journal of the American Medical Association (JAMA) estimates wasteful spending costs the U.S. healthcare system at least $600 billion and potentially more than a trillion dollars annually due to such issues as care coordination and care delivery failures and overtreatment.1 Numerous studies also indicate overtreatment can lead to patient harm.2
“Say a patient gets a prophylactic scan for abdominal pain,” says Vineet Arora, MD, MAPP, a hospitalist on faculty in the University of Chicago’s department of medicine and director of education initiatives for Costs of Care. “The patient gets better, but an incidental finding of the scan is a renal mass. Now, there is a work-up of that mass, the patient gets a biopsy, and they have a bleed. A lot of testing leads to more testing, and more testing can lead to harm.”
—LeRoi S. Hicks, MD, MPH
Doing less is often better, says John Bulger, DO, MBA, SFHM, chief quality officer for the Geisinger Health System in Danville, Pa. Dr. Bulger, who has led SHM’s participation in the Choosing Wisely campaign, cites a September 2014 study in JAMA Internal Medicine, in which Christiana Care Health System—an 1,100-bed tertiary care center in northern Delaware—built best practice telemetry guidelines into its electronic ordering system to help physicians determine when monitoring was appropriate.3 The health system also assembled multidisciplinary teams, which identified when medications warranted telemetry, and equipped nurses with tools to determine when telemetry should be stopped.
Appropriate use of telemetry is one of SHM’s five Choosing Wisely recommendations for adult patient care.
In addition to an overall 70% reduction in telemetry use without negative impact to patient safety, Christiana Care saved $4.8 million. Throughout its inpatient units, Christiana Care utilizes a multidisciplinary team approach to coordinate patient care. Daily rounds are attended by hospitalists, nurses, pharmacists, case managers, social workers, and others to ensure timely and appropriate patient care. The health system’s Value Institute evaluates hospital efforts and assesses process design to improve efficiency and, ultimately, outcomes.
“This is preparing for war in a time of peace, essentially,” says LeRoi S. Hicks, MD, MPH, a hospitalist, researcher, and educator at Christiana Care. “The goal will be, as we move to bundled payment and population health approaches, to minimize the time patients spend in the hospitals and limit the growth curve in spending on the hospital side. We are doing this and not taking on financial risk.”
Dr. Hicks adds that in its most simple form the project “reduces variation in the care we deliver” while improving efficiency and outcomes.
For many physicians, the best way to start is to begin a dialogue with patients who might also be at risk of financial harm due to unnecessary care, Dr. Arora says. “Patients are willing to change their minds and go with the more affordable and more evidence-based treatment and forgo expensive ones if they have that conversation,” she says.
Many resources exist for physicians interested in driving the frontline charge to improve healthcare quality and value. The Costs of Care curriculum provides training and tools for physicians at teachingvalue.org, as do SHM’s Center for Quality Innovation and the Institute for Healthcare Improvement. Dr. Moriates and Dr. Arora also have co-authored a book, along with Neel Shah, MD, founder and executive director of Costs of Care, called “Understanding Value Based Healthcare.” The book will be available this spring.
“We shouldn’t sit by the side of the road waiting for things to pass by,” Dr. Arora says. “I think the key is, we know the needle is shifting in Washington, we know system innovation models are being tested. It would be silly for us to say we’re going to continue the status quo and not look at ways to contribute as physicians.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA. 2012;307(14):1513-1516.
- Morgan DJ, Wright SM, Dhruva S. Update on medical overuse. JAMA Intern Med. 2015;175(1):120-124.
- Dressler R, Dryer MM, Coletti C, Mahoney D, Doorey AJ. Altering overuse of cardiac telemetry in non-intensive care unit settings by hardwiring the use of American Heart Association guidelines. JAMA Intern Med. 2014;174(11):1852-1854.
Society of Hospital Medicine Connects Physicians in Training with Specialty
SHM is introducing the Student Hospitalist Scholar Grant, an award of $500 a week for the summer to cover salary support for a student project related to patient safety/quality improvement or other areas relevant to the field of hospital medicine.
For medical students, residents, and physicians early in their careers, there has never been a better time to explore a career as a hospitalist. For details, check out SHM’s new website for physicians in training.
The demand for hospitalists continues to be high across the country, and job opportunities abound. SHM is helping to connect physicians in training with the fastest-growing medical specialty in healthcare. Here’s how:
- Local events nationwide. Together with the leading medical schools in the country and its local chapters, SHM is organizing events to introduce hospital medicine to medical students and residents. Scheduled locations in 2015 include Philadelphia, Chicago, and Los Angeles, and the list will be updated throughout the year. Events in 2014 were made possible by TeamHealth, Sound Physicians, and Cogent Healthcare.
- Special tracks at HM15. For the first time, SHM’s annual meeting includes an entire track dedicated to the topics that matter the most to young physicians and physicians-to-be, including working with mentors effectively, optimizing quality improvement, and making the most of your CV.
- Student Hospitalist Scholar Grant. SHM is introducing the Student Hospitalist Scholar Grant, an award of $500 a week for the summer to cover salary support for a student project related to patient safety/quality improvement or other areas relevant to the field of hospital medicine. The project should be conducted during the summer between the first/second years (or second/third, if possible) of medical school. The deadline for applications is Feb. 15.
SHM is introducing the Student Hospitalist Scholar Grant, an award of $500 a week for the summer to cover salary support for a student project related to patient safety/quality improvement or other areas relevant to the field of hospital medicine.
For medical students, residents, and physicians early in their careers, there has never been a better time to explore a career as a hospitalist. For details, check out SHM’s new website for physicians in training.
The demand for hospitalists continues to be high across the country, and job opportunities abound. SHM is helping to connect physicians in training with the fastest-growing medical specialty in healthcare. Here’s how:
- Local events nationwide. Together with the leading medical schools in the country and its local chapters, SHM is organizing events to introduce hospital medicine to medical students and residents. Scheduled locations in 2015 include Philadelphia, Chicago, and Los Angeles, and the list will be updated throughout the year. Events in 2014 were made possible by TeamHealth, Sound Physicians, and Cogent Healthcare.
- Special tracks at HM15. For the first time, SHM’s annual meeting includes an entire track dedicated to the topics that matter the most to young physicians and physicians-to-be, including working with mentors effectively, optimizing quality improvement, and making the most of your CV.
- Student Hospitalist Scholar Grant. SHM is introducing the Student Hospitalist Scholar Grant, an award of $500 a week for the summer to cover salary support for a student project related to patient safety/quality improvement or other areas relevant to the field of hospital medicine. The project should be conducted during the summer between the first/second years (or second/third, if possible) of medical school. The deadline for applications is Feb. 15.
SHM is introducing the Student Hospitalist Scholar Grant, an award of $500 a week for the summer to cover salary support for a student project related to patient safety/quality improvement or other areas relevant to the field of hospital medicine.
For medical students, residents, and physicians early in their careers, there has never been a better time to explore a career as a hospitalist. For details, check out SHM’s new website for physicians in training.
The demand for hospitalists continues to be high across the country, and job opportunities abound. SHM is helping to connect physicians in training with the fastest-growing medical specialty in healthcare. Here’s how:
- Local events nationwide. Together with the leading medical schools in the country and its local chapters, SHM is organizing events to introduce hospital medicine to medical students and residents. Scheduled locations in 2015 include Philadelphia, Chicago, and Los Angeles, and the list will be updated throughout the year. Events in 2014 were made possible by TeamHealth, Sound Physicians, and Cogent Healthcare.
- Special tracks at HM15. For the first time, SHM’s annual meeting includes an entire track dedicated to the topics that matter the most to young physicians and physicians-to-be, including working with mentors effectively, optimizing quality improvement, and making the most of your CV.
- Student Hospitalist Scholar Grant. SHM is introducing the Student Hospitalist Scholar Grant, an award of $500 a week for the summer to cover salary support for a student project related to patient safety/quality improvement or other areas relevant to the field of hospital medicine. The project should be conducted during the summer between the first/second years (or second/third, if possible) of medical school. The deadline for applications is Feb. 15.
Leaders in Hospital Medicine, Quality Improvement, Clinical Care to Attend HM15
Last year was a banner year for the hospital medicine movement: Hospitalist Vivek Murthy, MD, was confirmed as the U.S. Surgeon General, hospitalists across the country were recognized for their leadership of quality improvement, and a record number of hospitalists came together in Las Vegas to share successes, challenges, and knowledge at HM14, SHM’s annual conference.

This year, you can be part of the action from the very beginning. Hospital Medicine 2015 (HM15) will feature the nation’s leaders in hospital medicine, quality improvement, and clinical care.
In addition to the specialty’s leading content and experts, hospitalists flock to HM15 for the energy. The connections made—both personal and professional—empower thousands of hospitalists to bring a new enthusiasm to their hospitals and their colleagues.
Register today at www.hospitalmedicine2015.org.
Last year was a banner year for the hospital medicine movement: Hospitalist Vivek Murthy, MD, was confirmed as the U.S. Surgeon General, hospitalists across the country were recognized for their leadership of quality improvement, and a record number of hospitalists came together in Las Vegas to share successes, challenges, and knowledge at HM14, SHM’s annual conference.
This year, you can be part of the action from the very beginning. Hospital Medicine 2015 (HM15) will feature the nation’s leaders in hospital medicine, quality improvement, and clinical care.
In addition to the specialty’s leading content and experts, hospitalists flock to HM15 for the energy. The connections made—both personal and professional—empower thousands of hospitalists to bring a new enthusiasm to their hospitals and their colleagues.
Register today at www.hospitalmedicine2015.org.
Last year was a banner year for the hospital medicine movement: Hospitalist Vivek Murthy, MD, was confirmed as the U.S. Surgeon General, hospitalists across the country were recognized for their leadership of quality improvement, and a record number of hospitalists came together in Las Vegas to share successes, challenges, and knowledge at HM14, SHM’s annual conference.
This year, you can be part of the action from the very beginning. Hospital Medicine 2015 (HM15) will feature the nation’s leaders in hospital medicine, quality improvement, and clinical care.
In addition to the specialty’s leading content and experts, hospitalists flock to HM15 for the energy. The connections made—both personal and professional—empower thousands of hospitalists to bring a new enthusiasm to their hospitals and their colleagues.
Register today at www.hospitalmedicine2015.org.
Society of Hospital Medicine Offers Quality Improvement Tools for Hospitals
Whether you excel in the hospital room, the conference room, or the classroom, SHM’s quality improvement initiatives offer new tools featuring expertise from leaders in healthcare:
- Project BOOST: SHM is moving Project BOOST from an annual registration model to a rolling program, enabling hospitalists to get involved at any time of the year. As hospitals get serious about reducing readmissions and improving discharge processes, Project BOOST is a great way for hospitalists to take charge.
- Pain management and glycemic control programs: Almost every hospitalist encounters patients dealing with pain or glycemic control issues. In March, new toolkits will be available that help hospitalists lead efforts to improve the care of these patients.
- Post-Acute Care Toolbox: Managing the transition from an acute care hospital to an inpatient rehabilitation facility, long-term acute care hospital, or skilled nursing facility can be difficult. SHM’s new Post-Acute Care Toolbox enables hospitalists to go forth with confidence.
To download and share SHM’s quality improvement tools, visit www.hospitalmedicine.org/qi.
Whether you excel in the hospital room, the conference room, or the classroom, SHM’s quality improvement initiatives offer new tools featuring expertise from leaders in healthcare:
- Project BOOST: SHM is moving Project BOOST from an annual registration model to a rolling program, enabling hospitalists to get involved at any time of the year. As hospitals get serious about reducing readmissions and improving discharge processes, Project BOOST is a great way for hospitalists to take charge.
- Pain management and glycemic control programs: Almost every hospitalist encounters patients dealing with pain or glycemic control issues. In March, new toolkits will be available that help hospitalists lead efforts to improve the care of these patients.
- Post-Acute Care Toolbox: Managing the transition from an acute care hospital to an inpatient rehabilitation facility, long-term acute care hospital, or skilled nursing facility can be difficult. SHM’s new Post-Acute Care Toolbox enables hospitalists to go forth with confidence.
To download and share SHM’s quality improvement tools, visit www.hospitalmedicine.org/qi.
Whether you excel in the hospital room, the conference room, or the classroom, SHM’s quality improvement initiatives offer new tools featuring expertise from leaders in healthcare:
- Project BOOST: SHM is moving Project BOOST from an annual registration model to a rolling program, enabling hospitalists to get involved at any time of the year. As hospitals get serious about reducing readmissions and improving discharge processes, Project BOOST is a great way for hospitalists to take charge.
- Pain management and glycemic control programs: Almost every hospitalist encounters patients dealing with pain or glycemic control issues. In March, new toolkits will be available that help hospitalists lead efforts to improve the care of these patients.
- Post-Acute Care Toolbox: Managing the transition from an acute care hospital to an inpatient rehabilitation facility, long-term acute care hospital, or skilled nursing facility can be difficult. SHM’s new Post-Acute Care Toolbox enables hospitalists to go forth with confidence.
To download and share SHM’s quality improvement tools, visit www.hospitalmedicine.org/qi.
HM15 At Hand Mobile App Helps Hospitalists Plan for Annual Meeting

Hospitalists are a mobile bunch. Many were early adopters of smartphones and tablet technology. That’s why SHM is once again offering an interactive conference experience at its annual meeting. “HM15 at Hand,” the conference app for HM15, offers an interactive agenda, presentation materials, exhibitor information, maps, and more.
Be among the first to know when and where to access HM15 At Hand. Visit hm15athand to receive an email alert when the app launches on Feb. 26.
Hospitalists are a mobile bunch. Many were early adopters of smartphones and tablet technology. That’s why SHM is once again offering an interactive conference experience at its annual meeting. “HM15 at Hand,” the conference app for HM15, offers an interactive agenda, presentation materials, exhibitor information, maps, and more.
Be among the first to know when and where to access HM15 At Hand. Visit hm15athand to receive an email alert when the app launches on Feb. 26.
Hospitalists are a mobile bunch. Many were early adopters of smartphones and tablet technology. That’s why SHM is once again offering an interactive conference experience at its annual meeting. “HM15 at Hand,” the conference app for HM15, offers an interactive agenda, presentation materials, exhibitor information, maps, and more.
Be among the first to know when and where to access HM15 At Hand. Visit hm15athand to receive an email alert when the app launches on Feb. 26.