User login
Key Information Sessions, Speakers, Networking Opportunities for Hospitalists Lined up at HM15

Efren Manjarrez, MD, SFHM, exudes excitement for HM15.
As the chair of SHM’s Annual Meeting Committee and course director for the four-day assembly (March 29-April 1) at the Gaylord National Resort and Convention Center in National Harbor, Md., he just can’t help but sound like a proud papa.
“There’s no greater source of information about our profession, period,” Dr. Manjarrez boasts. “This annual meeting is chock full of the best speakers, the most up-to-date information—and let’s not forget that this is just the greatest opportunity for networking that we have annually as a profession.”
This year’s meeting is on pace to draw at least 2,500 attendees, a tally that tops even the 2014 meeting in Las Vegas. Dr. Manjarrez says there’s plenty to keep a few thousand of his colleagues busy. Highlights this year will include:
- Seven pre-courses on March 29, all of which can be applied toward CME credits. A new offering this year, “Enhancing Communication Skills to Improve the Patient and Provider Experience,” aims to give participants hands-on lessons.
- A new “Young Hospitalists” educational track on March 30 features sessions on “Career Pathways in Hospital Medicine” and “Making the Most of Your Mentoring Relationships.”
- The largest Research, Innovation, and Clinical Vignette (RIV) poster competition in history, with nearly 1,300 abstracts submitted for judging.
- Plenary sessions from patient safety guru Peter Pronovost, MD, PhD, FCCM; hospital medicine pioneer Robert Wachter, MD, MHM; and Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement.
With all of that to choose from, Dr. Manjarrez chatted with The Hospitalist about what he thinks of the annual meeting.
Question: How important is it to bring new people into the meeting, not just attendees, but also those who are driving and shaping the content of the meeting?
Answer: We want to make sure that we’ve got a diversity of faculty that is representative of the SHM membership. There are well-established people within SHM who have performed very well at the annual meeting. At the same time, we have to make sure that we’re opening the pipeline for new talent to come through; just as SHM rotates people in and out of the board, as well as all of the committees, it does the same thing with the annual meeting.

Q: Engaging the next generation of hospitalists seems to be a recent focus, as well as an important one. How do you view that?
A: The person who lit my fire on this was [SHM President] Eric Howell. So, as the annual meeting committee was doing its due diligence, we saw that other specialty societies like the ACP [American College of Physicians] and the American College of Emergency Physicians also had course content in the main meeting to pull in the next generation of general internists and emergency physicians. We thought that the time was right for SHM to do the exact same thing. And, of course, we were meeting our past president’s mission in doing this.
Q: How much do you enjoy the RIV competition? Why is the RIV such an important piece of the meeting?
A: The research and innovation piece allows [interaction for] every single grade of hospitalist, whether you’re an established superstar like a Sanjay Saint, or whether you’re a medical student or resident who’s just getting your feet wet and you have a passion for hospital medicine. It sort of levels the playing field, because when you have that competition and you’ve got that poster session, everybody’s on a first-name basis. That’s where you’re able to network and create more research and innovation within our field. I myself submitted three abstracts, two of which were with my learners.
Q: Congratulations on that.
A: Thanks, and I expect to take at least one learner with me to the annual meeting. To piggyback on that, we’re asking every single clinician educator coming to the meeting to bring at least one learner with you, one medical student or resident with you, to feel the passion for HM15, and hopefully to present a poster.
Q: Why do you want them to bring someone?
A: We view the society as pulling in the next generation of hospitalists, not hoping that the next generation finds us. This is our way to actively increase our membership and pull people into our great profession.
Q: How important is it to have healthcare leaders as keynote addresses, as opposed to just HM leaders?
A: Having somebody like these individuals who are at the forefront of patient safety and quality improvement, No. 1, speaking to us, but No. 2, they have the opportunity to see our passion as well when they come to our sessions, when they come to our posters, and they’re going to see that this profession is on fire. They’re going to get to see that firsthand. So I think it’s a two-way street: We get to see them, but they get to see us, and I wouldn’t discount that second point one bit.
Richard Quinn is a freelance writer in New Jersey.
Efren Manjarrez, MD, SFHM, exudes excitement for HM15.
As the chair of SHM’s Annual Meeting Committee and course director for the four-day assembly (March 29-April 1) at the Gaylord National Resort and Convention Center in National Harbor, Md., he just can’t help but sound like a proud papa.
“There’s no greater source of information about our profession, period,” Dr. Manjarrez boasts. “This annual meeting is chock full of the best speakers, the most up-to-date information—and let’s not forget that this is just the greatest opportunity for networking that we have annually as a profession.”
This year’s meeting is on pace to draw at least 2,500 attendees, a tally that tops even the 2014 meeting in Las Vegas. Dr. Manjarrez says there’s plenty to keep a few thousand of his colleagues busy. Highlights this year will include:
- Seven pre-courses on March 29, all of which can be applied toward CME credits. A new offering this year, “Enhancing Communication Skills to Improve the Patient and Provider Experience,” aims to give participants hands-on lessons.
- A new “Young Hospitalists” educational track on March 30 features sessions on “Career Pathways in Hospital Medicine” and “Making the Most of Your Mentoring Relationships.”
- The largest Research, Innovation, and Clinical Vignette (RIV) poster competition in history, with nearly 1,300 abstracts submitted for judging.
- Plenary sessions from patient safety guru Peter Pronovost, MD, PhD, FCCM; hospital medicine pioneer Robert Wachter, MD, MHM; and Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement.
With all of that to choose from, Dr. Manjarrez chatted with The Hospitalist about what he thinks of the annual meeting.
Question: How important is it to bring new people into the meeting, not just attendees, but also those who are driving and shaping the content of the meeting?
Answer: We want to make sure that we’ve got a diversity of faculty that is representative of the SHM membership. There are well-established people within SHM who have performed very well at the annual meeting. At the same time, we have to make sure that we’re opening the pipeline for new talent to come through; just as SHM rotates people in and out of the board, as well as all of the committees, it does the same thing with the annual meeting.
Q: Engaging the next generation of hospitalists seems to be a recent focus, as well as an important one. How do you view that?
A: The person who lit my fire on this was [SHM President] Eric Howell. So, as the annual meeting committee was doing its due diligence, we saw that other specialty societies like the ACP [American College of Physicians] and the American College of Emergency Physicians also had course content in the main meeting to pull in the next generation of general internists and emergency physicians. We thought that the time was right for SHM to do the exact same thing. And, of course, we were meeting our past president’s mission in doing this.
Q: How much do you enjoy the RIV competition? Why is the RIV such an important piece of the meeting?
A: The research and innovation piece allows [interaction for] every single grade of hospitalist, whether you’re an established superstar like a Sanjay Saint, or whether you’re a medical student or resident who’s just getting your feet wet and you have a passion for hospital medicine. It sort of levels the playing field, because when you have that competition and you’ve got that poster session, everybody’s on a first-name basis. That’s where you’re able to network and create more research and innovation within our field. I myself submitted three abstracts, two of which were with my learners.
Q: Congratulations on that.
A: Thanks, and I expect to take at least one learner with me to the annual meeting. To piggyback on that, we’re asking every single clinician educator coming to the meeting to bring at least one learner with you, one medical student or resident with you, to feel the passion for HM15, and hopefully to present a poster.
Q: Why do you want them to bring someone?
A: We view the society as pulling in the next generation of hospitalists, not hoping that the next generation finds us. This is our way to actively increase our membership and pull people into our great profession.
Q: How important is it to have healthcare leaders as keynote addresses, as opposed to just HM leaders?
A: Having somebody like these individuals who are at the forefront of patient safety and quality improvement, No. 1, speaking to us, but No. 2, they have the opportunity to see our passion as well when they come to our sessions, when they come to our posters, and they’re going to see that this profession is on fire. They’re going to get to see that firsthand. So I think it’s a two-way street: We get to see them, but they get to see us, and I wouldn’t discount that second point one bit.
Richard Quinn is a freelance writer in New Jersey.
Efren Manjarrez, MD, SFHM, exudes excitement for HM15.
As the chair of SHM’s Annual Meeting Committee and course director for the four-day assembly (March 29-April 1) at the Gaylord National Resort and Convention Center in National Harbor, Md., he just can’t help but sound like a proud papa.
“There’s no greater source of information about our profession, period,” Dr. Manjarrez boasts. “This annual meeting is chock full of the best speakers, the most up-to-date information—and let’s not forget that this is just the greatest opportunity for networking that we have annually as a profession.”
This year’s meeting is on pace to draw at least 2,500 attendees, a tally that tops even the 2014 meeting in Las Vegas. Dr. Manjarrez says there’s plenty to keep a few thousand of his colleagues busy. Highlights this year will include:
- Seven pre-courses on March 29, all of which can be applied toward CME credits. A new offering this year, “Enhancing Communication Skills to Improve the Patient and Provider Experience,” aims to give participants hands-on lessons.
- A new “Young Hospitalists” educational track on March 30 features sessions on “Career Pathways in Hospital Medicine” and “Making the Most of Your Mentoring Relationships.”
- The largest Research, Innovation, and Clinical Vignette (RIV) poster competition in history, with nearly 1,300 abstracts submitted for judging.
- Plenary sessions from patient safety guru Peter Pronovost, MD, PhD, FCCM; hospital medicine pioneer Robert Wachter, MD, MHM; and Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement.
With all of that to choose from, Dr. Manjarrez chatted with The Hospitalist about what he thinks of the annual meeting.
Question: How important is it to bring new people into the meeting, not just attendees, but also those who are driving and shaping the content of the meeting?
Answer: We want to make sure that we’ve got a diversity of faculty that is representative of the SHM membership. There are well-established people within SHM who have performed very well at the annual meeting. At the same time, we have to make sure that we’re opening the pipeline for new talent to come through; just as SHM rotates people in and out of the board, as well as all of the committees, it does the same thing with the annual meeting.
Q: Engaging the next generation of hospitalists seems to be a recent focus, as well as an important one. How do you view that?
A: The person who lit my fire on this was [SHM President] Eric Howell. So, as the annual meeting committee was doing its due diligence, we saw that other specialty societies like the ACP [American College of Physicians] and the American College of Emergency Physicians also had course content in the main meeting to pull in the next generation of general internists and emergency physicians. We thought that the time was right for SHM to do the exact same thing. And, of course, we were meeting our past president’s mission in doing this.
Q: How much do you enjoy the RIV competition? Why is the RIV such an important piece of the meeting?
A: The research and innovation piece allows [interaction for] every single grade of hospitalist, whether you’re an established superstar like a Sanjay Saint, or whether you’re a medical student or resident who’s just getting your feet wet and you have a passion for hospital medicine. It sort of levels the playing field, because when you have that competition and you’ve got that poster session, everybody’s on a first-name basis. That’s where you’re able to network and create more research and innovation within our field. I myself submitted three abstracts, two of which were with my learners.
Q: Congratulations on that.
A: Thanks, and I expect to take at least one learner with me to the annual meeting. To piggyback on that, we’re asking every single clinician educator coming to the meeting to bring at least one learner with you, one medical student or resident with you, to feel the passion for HM15, and hopefully to present a poster.
Q: Why do you want them to bring someone?
A: We view the society as pulling in the next generation of hospitalists, not hoping that the next generation finds us. This is our way to actively increase our membership and pull people into our great profession.
Q: How important is it to have healthcare leaders as keynote addresses, as opposed to just HM leaders?
A: Having somebody like these individuals who are at the forefront of patient safety and quality improvement, No. 1, speaking to us, but No. 2, they have the opportunity to see our passion as well when they come to our sessions, when they come to our posters, and they’re going to see that this profession is on fire. They’re going to get to see that firsthand. So I think it’s a two-way street: We get to see them, but they get to see us, and I wouldn’t discount that second point one bit.
Richard Quinn is a freelance writer in New Jersey.
CLINICAL POSTER HIGHLIGHTS: Advances in Treatment of Psoriasis Vulgaris and Actinic Keratosis

CLINICAL POSTER HIGHLIGHTS: Advances in Treatment of Psoriasis Vulgaris and Actinic Keratosis
A poster review supplement to Dermatology News.
CLINICAL POSTER HIGHLIGHTS: Advances in Treatment of Psoriasis Vulgaris and Actinic Keratosis
A poster review supplement to Dermatology News.
CLINICAL POSTER HIGHLIGHTS: Advances in Treatment of Psoriasis Vulgaris and Actinic Keratosis
A poster review supplement to Dermatology News.
Pregnancy outcomes similar in kidney transplant patients, despite age
Pregnancy outcomes were similar for women who underwent kidney transplants in childhood and those who received transplants as adults, according to findings published Feb. 2 in JAMA Pediatrics.
Live births occurred in 76% of pregnancies in women who received kidney transplants as children, compared with 77% of pregnancies among women who received transplants as adults, wrote Melanie L. Wyld and her colleagues from Sydney Medical School in Australia.
The study examined a total of 101 pregnancies in 66 women who received transplants before age 18 years, and 626 pregnancies in 401 women who were adults at the time of transplant.
Mean gestational age and prematurity incidence were also similar in the two groups, with child-transplant recipients having a mean gestational age of 35 weeks, and adult-transplant recipients having a mean gestational age of 36 weeks.
Incidence of prematurity was 45% in child-transplant mothers and 53% in adult-transplant mothers, the researchers reported.
“To our knowledge, this study is the first to look at pregnancy outcomes for women who received a kidney transplant as a child,” the researchers wrote. These results should “provide comfort to such mothers and their physicians that their early onset of kidney failure and longer period of posttransplant exposure to immunosuppression do not adversely affect their pregnancy outcomes,” they added.
Read the full article at: JAMA Pediatr. 2015;169(2):e143626. (doi:10.1001/jamapediatrics.2014.3626).
Pregnancy outcomes were similar for women who underwent kidney transplants in childhood and those who received transplants as adults, according to findings published Feb. 2 in JAMA Pediatrics.
Live births occurred in 76% of pregnancies in women who received kidney transplants as children, compared with 77% of pregnancies among women who received transplants as adults, wrote Melanie L. Wyld and her colleagues from Sydney Medical School in Australia.
The study examined a total of 101 pregnancies in 66 women who received transplants before age 18 years, and 626 pregnancies in 401 women who were adults at the time of transplant.
Mean gestational age and prematurity incidence were also similar in the two groups, with child-transplant recipients having a mean gestational age of 35 weeks, and adult-transplant recipients having a mean gestational age of 36 weeks.
Incidence of prematurity was 45% in child-transplant mothers and 53% in adult-transplant mothers, the researchers reported.
“To our knowledge, this study is the first to look at pregnancy outcomes for women who received a kidney transplant as a child,” the researchers wrote. These results should “provide comfort to such mothers and their physicians that their early onset of kidney failure and longer period of posttransplant exposure to immunosuppression do not adversely affect their pregnancy outcomes,” they added.
Read the full article at: JAMA Pediatr. 2015;169(2):e143626. (doi:10.1001/jamapediatrics.2014.3626).
Pregnancy outcomes were similar for women who underwent kidney transplants in childhood and those who received transplants as adults, according to findings published Feb. 2 in JAMA Pediatrics.
Live births occurred in 76% of pregnancies in women who received kidney transplants as children, compared with 77% of pregnancies among women who received transplants as adults, wrote Melanie L. Wyld and her colleagues from Sydney Medical School in Australia.
The study examined a total of 101 pregnancies in 66 women who received transplants before age 18 years, and 626 pregnancies in 401 women who were adults at the time of transplant.
Mean gestational age and prematurity incidence were also similar in the two groups, with child-transplant recipients having a mean gestational age of 35 weeks, and adult-transplant recipients having a mean gestational age of 36 weeks.
Incidence of prematurity was 45% in child-transplant mothers and 53% in adult-transplant mothers, the researchers reported.
“To our knowledge, this study is the first to look at pregnancy outcomes for women who received a kidney transplant as a child,” the researchers wrote. These results should “provide comfort to such mothers and their physicians that their early onset of kidney failure and longer period of posttransplant exposure to immunosuppression do not adversely affect their pregnancy outcomes,” they added.
Read the full article at: JAMA Pediatr. 2015;169(2):e143626. (doi:10.1001/jamapediatrics.2014.3626).
Outcomes still dismal in PTCL, project shows
SAN FRANCISCO—Outcomes remain dismal for the majority of patients with peripheral T-cell lymphoma (PTCL), according to a speaker at the 7th Annual T-cell Lymphoma Forum.
Massimo Federico, MD, of the Università di Modena e Reggio Emilia in Italy, presented an analysis of the first 1000 patients enrolled in the prospective T-Cell Project.
The data showed no improvements in survival for these patients compared to patients included in the retrospective International Peripheral T-Cell Lymphoma
Project.
The International Peripheral T-Cell Lymphoma Project included PTCL patients treated at various institutions between 1990 and 2002.
The T-Cell Project was designed to complement this retrospective analysis, providing prospective international data on PTCL patients.
“The main aim was to verify if a prospective collection of data would allow for more accurate information to better define prognosis of the most frequent subtypes of PTCL—PTCL not otherwise specified (NOS) and angioimmunoblastic T-cell lymphoma (AITL)—and improve our knowledge of clinical and biological characteristics and outcomes of the more uncommon subtypes of PTCL,” Dr Federico said.
He reported that, as of January 12, 2015, 73 institutions were recruiting patients for the project, and 6 institutions were active but not yet recruiting.
Of the 1308 patients registered at that point, 46% were from European countries (Italy, UK, Switzerland, Slovakia, Spain, and France), 20% were from the US, 20% were from South America (Argentina, Brazil, Chile, and Uruguay), and 14% were from the Middle East or Far East (South Korea, Hong Kong, and Israel).
Dr Federico went on to present data from the first 1000 patients registered in the project. The final analysis actually included 943 patients, as some patients withdrew consent, some did not have baseline data available, and some diagnoses could not be confirmed.
So of the 943 patients, 37% had PTCL-NOS, 17% had AITL, 15% had ALK-negative anaplastic large-cell lymphoma (ALCL), 7% had ALK-positive ALCL, 11% had natural killer/T-cell lymphoma (NKTCL), 8% had T-cell receptor γδ T-cell lymphoma, and 5% had other histologies.
The patients’ median age was 56 (range, 18-89), and 61% were male. Twenty-four percent of patients had an ECOG status greater than 1, 48% had B symptoms, and 71% had disease-related discomfort. Sixty-seven percent of patients had stage III-IV disease, 27% had nodal-only disease, 6% had bulky disease, 29% had more than 1 extranodal site, and 19% had bone marrow involvement.
The median follow-up was 41 months (range, 1-91). The 5-year overall survival (OS) was 44%, and the median OS was 39 months.
The 5-year OS was 35% for patients with PTCL-NOS, 42% for those with AITL, 45% for those with ALK-negative ALCL, 80% for those with ALK-positive ALCL, 48% for those with NKTCL (56% for nasal and 33% for extranasal), and 39% for those with T-cell receptor γδ T-cell lymphoma.
In comparison, the International Peripheral T-Cell Lymphoma Project showed a 5-year OS of 32% for patients with PTCL-NOS, 70% for patients with ALK-positive ALCL, and 49% for patients with ALK-negative ALCL (K. Savage et al. Blood 2008). The 5-year OS was 40% for patients with nasal NKTCL and 15% for those with extranasal NKTCL (W. Au et al. Blood 2008).
“[T]he outcome of PTCL continues to be dismal in the majority of cases, [with] no improvement in overall survival compared to older series,” Dr Federico summarized. “Treatment remains challenging, and new therapies are welcome.”
He added that the next steps for the T-Cell Project are to continue registration (with the goal of reaching 2000 assessable cases), extend the network to additional sites (particularly in under-represented areas such as Japan, China, India, and Oceania), and expand the collection of tissue.
“In particular, we intend to create an international tissue catalogue—including paraffin-embedded samples and, if possible, frozen ones—accessible to research groups with a solid reputation in investigating PTCLs at the molecular and translation level.” ![]()
SAN FRANCISCO—Outcomes remain dismal for the majority of patients with peripheral T-cell lymphoma (PTCL), according to a speaker at the 7th Annual T-cell Lymphoma Forum.
Massimo Federico, MD, of the Università di Modena e Reggio Emilia in Italy, presented an analysis of the first 1000 patients enrolled in the prospective T-Cell Project.
The data showed no improvements in survival for these patients compared to patients included in the retrospective International Peripheral T-Cell Lymphoma
Project.
The International Peripheral T-Cell Lymphoma Project included PTCL patients treated at various institutions between 1990 and 2002.
The T-Cell Project was designed to complement this retrospective analysis, providing prospective international data on PTCL patients.
“The main aim was to verify if a prospective collection of data would allow for more accurate information to better define prognosis of the most frequent subtypes of PTCL—PTCL not otherwise specified (NOS) and angioimmunoblastic T-cell lymphoma (AITL)—and improve our knowledge of clinical and biological characteristics and outcomes of the more uncommon subtypes of PTCL,” Dr Federico said.
He reported that, as of January 12, 2015, 73 institutions were recruiting patients for the project, and 6 institutions were active but not yet recruiting.
Of the 1308 patients registered at that point, 46% were from European countries (Italy, UK, Switzerland, Slovakia, Spain, and France), 20% were from the US, 20% were from South America (Argentina, Brazil, Chile, and Uruguay), and 14% were from the Middle East or Far East (South Korea, Hong Kong, and Israel).
Dr Federico went on to present data from the first 1000 patients registered in the project. The final analysis actually included 943 patients, as some patients withdrew consent, some did not have baseline data available, and some diagnoses could not be confirmed.
So of the 943 patients, 37% had PTCL-NOS, 17% had AITL, 15% had ALK-negative anaplastic large-cell lymphoma (ALCL), 7% had ALK-positive ALCL, 11% had natural killer/T-cell lymphoma (NKTCL), 8% had T-cell receptor γδ T-cell lymphoma, and 5% had other histologies.
The patients’ median age was 56 (range, 18-89), and 61% were male. Twenty-four percent of patients had an ECOG status greater than 1, 48% had B symptoms, and 71% had disease-related discomfort. Sixty-seven percent of patients had stage III-IV disease, 27% had nodal-only disease, 6% had bulky disease, 29% had more than 1 extranodal site, and 19% had bone marrow involvement.
The median follow-up was 41 months (range, 1-91). The 5-year overall survival (OS) was 44%, and the median OS was 39 months.
The 5-year OS was 35% for patients with PTCL-NOS, 42% for those with AITL, 45% for those with ALK-negative ALCL, 80% for those with ALK-positive ALCL, 48% for those with NKTCL (56% for nasal and 33% for extranasal), and 39% for those with T-cell receptor γδ T-cell lymphoma.
In comparison, the International Peripheral T-Cell Lymphoma Project showed a 5-year OS of 32% for patients with PTCL-NOS, 70% for patients with ALK-positive ALCL, and 49% for patients with ALK-negative ALCL (K. Savage et al. Blood 2008). The 5-year OS was 40% for patients with nasal NKTCL and 15% for those with extranasal NKTCL (W. Au et al. Blood 2008).
“[T]he outcome of PTCL continues to be dismal in the majority of cases, [with] no improvement in overall survival compared to older series,” Dr Federico summarized. “Treatment remains challenging, and new therapies are welcome.”
He added that the next steps for the T-Cell Project are to continue registration (with the goal of reaching 2000 assessable cases), extend the network to additional sites (particularly in under-represented areas such as Japan, China, India, and Oceania), and expand the collection of tissue.
“In particular, we intend to create an international tissue catalogue—including paraffin-embedded samples and, if possible, frozen ones—accessible to research groups with a solid reputation in investigating PTCLs at the molecular and translation level.” ![]()
SAN FRANCISCO—Outcomes remain dismal for the majority of patients with peripheral T-cell lymphoma (PTCL), according to a speaker at the 7th Annual T-cell Lymphoma Forum.
Massimo Federico, MD, of the Università di Modena e Reggio Emilia in Italy, presented an analysis of the first 1000 patients enrolled in the prospective T-Cell Project.
The data showed no improvements in survival for these patients compared to patients included in the retrospective International Peripheral T-Cell Lymphoma
Project.
The International Peripheral T-Cell Lymphoma Project included PTCL patients treated at various institutions between 1990 and 2002.
The T-Cell Project was designed to complement this retrospective analysis, providing prospective international data on PTCL patients.
“The main aim was to verify if a prospective collection of data would allow for more accurate information to better define prognosis of the most frequent subtypes of PTCL—PTCL not otherwise specified (NOS) and angioimmunoblastic T-cell lymphoma (AITL)—and improve our knowledge of clinical and biological characteristics and outcomes of the more uncommon subtypes of PTCL,” Dr Federico said.
He reported that, as of January 12, 2015, 73 institutions were recruiting patients for the project, and 6 institutions were active but not yet recruiting.
Of the 1308 patients registered at that point, 46% were from European countries (Italy, UK, Switzerland, Slovakia, Spain, and France), 20% were from the US, 20% were from South America (Argentina, Brazil, Chile, and Uruguay), and 14% were from the Middle East or Far East (South Korea, Hong Kong, and Israel).
Dr Federico went on to present data from the first 1000 patients registered in the project. The final analysis actually included 943 patients, as some patients withdrew consent, some did not have baseline data available, and some diagnoses could not be confirmed.
So of the 943 patients, 37% had PTCL-NOS, 17% had AITL, 15% had ALK-negative anaplastic large-cell lymphoma (ALCL), 7% had ALK-positive ALCL, 11% had natural killer/T-cell lymphoma (NKTCL), 8% had T-cell receptor γδ T-cell lymphoma, and 5% had other histologies.
The patients’ median age was 56 (range, 18-89), and 61% were male. Twenty-four percent of patients had an ECOG status greater than 1, 48% had B symptoms, and 71% had disease-related discomfort. Sixty-seven percent of patients had stage III-IV disease, 27% had nodal-only disease, 6% had bulky disease, 29% had more than 1 extranodal site, and 19% had bone marrow involvement.
The median follow-up was 41 months (range, 1-91). The 5-year overall survival (OS) was 44%, and the median OS was 39 months.
The 5-year OS was 35% for patients with PTCL-NOS, 42% for those with AITL, 45% for those with ALK-negative ALCL, 80% for those with ALK-positive ALCL, 48% for those with NKTCL (56% for nasal and 33% for extranasal), and 39% for those with T-cell receptor γδ T-cell lymphoma.
In comparison, the International Peripheral T-Cell Lymphoma Project showed a 5-year OS of 32% for patients with PTCL-NOS, 70% for patients with ALK-positive ALCL, and 49% for patients with ALK-negative ALCL (K. Savage et al. Blood 2008). The 5-year OS was 40% for patients with nasal NKTCL and 15% for those with extranasal NKTCL (W. Au et al. Blood 2008).
“[T]he outcome of PTCL continues to be dismal in the majority of cases, [with] no improvement in overall survival compared to older series,” Dr Federico summarized. “Treatment remains challenging, and new therapies are welcome.”
He added that the next steps for the T-Cell Project are to continue registration (with the goal of reaching 2000 assessable cases), extend the network to additional sites (particularly in under-represented areas such as Japan, China, India, and Oceania), and expand the collection of tissue.
“In particular, we intend to create an international tissue catalogue—including paraffin-embedded samples and, if possible, frozen ones—accessible to research groups with a solid reputation in investigating PTCLs at the molecular and translation level.” ![]()
Distribution of PTCL subtypes varies by race/ethnicity

SAN FRANCISCO—The distribution of peripheral T-cell lymphoma (PTCL) subtypes in the US varies greatly according to race and ethnicity, new research suggests.
The retrospective study showed that the overall incidence of PTCL and its subtypes is lower in American Indians and Alaskan Natives than in other ethnic groups.
And the black population has a significantly higher incidence of PTCL—and the most common subtype, PTCL-not otherwise specified (NOS)—than other populations.
Andrei Shustov, MD, of the University of Washington Medical Center in Seattle, presented these and other findings at the 7th Annual T-cell Lymphoma Forum.
The findings were derived from data collected by the Surveillance, Epidemiology, and End Results (SEER) Cancer Registries, which cover 28% of the US population. The data included patients older than 15 years of age who were treated at 18 centers from 2000 through 2011.
Of all cancer patients registered over the 12-year period, 60% were non-Hispanic whites (n=470,864,199), 17% were Hispanic whites (n=134,464,006), 12% were black (n=92,294,395), 10% were Asian/Pacific Islanders (n=74,973,831), and 1% were American Indian/Alaskan Natives (n=10,802,898).
The overall incidence of PTCL was highest in blacks—2.11 per 100,000 persons per year, compared to 1.63 in non-Hispanic whites, 1.53 in Hispanic whites, 1.46 in Asian/Pacific Islanders, and 0.97 in American Indian/Alaskan Natives.
Although American Indian/Alaskan Natives appear to have the lowest overall rate of PTCLs, some cases may have been misclassified, Dr Shustov noted.
“The data collected for ethnicity in the SEER registry are self-reported, and a lot of American Indian/Alaskan Natives misreport their ethnic background,” he said.
Subtype analyses
PTCL-NOS was the most common subtype among all the racial/ethnic groups. The highest rate of PTCL-NOS (per 100,000 persons per year) was in blacks—at 0.77, compared to 0.47 in non-Hispanic whites, 0.46 in Hispanic whites, 0.45 in Asian/Pacific Islanders, and 0.28 in American Indian/Alaskan Natives.
The proportion of PTCL-NOS cases was 29.5% in non-Hispanic whites, 35.7% in blacks, 29.8% in Asian/Pacific Islanders, 27% in Hispanic whites, and 23.1% in American Indian/Alaskan Natives.
The proportion of angioimmunoblastic T-cell lymphoma cases was 9.9% in non-Hispanic whites, 5.2% in blacks, 15.3% in Asian/Pacific Islanders, 9.9% in Hispanic whites, and 2.6% in American Indian/Alaskan Natives.
The proportion of anaplastic large-cell lymphoma cases was 17.6% in non-Hispanic whites, 17.3% in blacks, 12.4% in Asian/Pacific Islanders, 21.2% in Hispanic whites, and 28.2% in American Indian/Alaskan Natives.
And the proportion of NK/T-cell lymphoma cases was 3.4% in non-Hispanic whites, 2.0% in blacks, 13.9% in Asian/Pacific Islanders, 14.6% in Hispanic whites, and 14.1% in American Indian/Alaskan Natives.
“That data indicates that, given the overall incidence of T-cell lymphoma in Natives is lower than in whites, if you’re a Native American/Alaskan Native [with] T-cell lymphoma, you’re 4 times more likely to have nasal NK-cell lymphoma than non-Hispanic whites,” Dr Shustov said.
He then showed a pairwise comparison of the percentage of PTCL subtypes. All of the racial/ethnic groups were significantly different from one another (P<0.001), except when Hispanic whites were compared to American Indian/Alaskan Natives (P=0.14).
Dr Shustov said this might be explained by the fact that these two groups have similar genetic backgrounds. ![]()
SAN FRANCISCO—The distribution of peripheral T-cell lymphoma (PTCL) subtypes in the US varies greatly according to race and ethnicity, new research suggests.
The retrospective study showed that the overall incidence of PTCL and its subtypes is lower in American Indians and Alaskan Natives than in other ethnic groups.
And the black population has a significantly higher incidence of PTCL—and the most common subtype, PTCL-not otherwise specified (NOS)—than other populations.
Andrei Shustov, MD, of the University of Washington Medical Center in Seattle, presented these and other findings at the 7th Annual T-cell Lymphoma Forum.
The findings were derived from data collected by the Surveillance, Epidemiology, and End Results (SEER) Cancer Registries, which cover 28% of the US population. The data included patients older than 15 years of age who were treated at 18 centers from 2000 through 2011.
Of all cancer patients registered over the 12-year period, 60% were non-Hispanic whites (n=470,864,199), 17% were Hispanic whites (n=134,464,006), 12% were black (n=92,294,395), 10% were Asian/Pacific Islanders (n=74,973,831), and 1% were American Indian/Alaskan Natives (n=10,802,898).
The overall incidence of PTCL was highest in blacks—2.11 per 100,000 persons per year, compared to 1.63 in non-Hispanic whites, 1.53 in Hispanic whites, 1.46 in Asian/Pacific Islanders, and 0.97 in American Indian/Alaskan Natives.
Although American Indian/Alaskan Natives appear to have the lowest overall rate of PTCLs, some cases may have been misclassified, Dr Shustov noted.
“The data collected for ethnicity in the SEER registry are self-reported, and a lot of American Indian/Alaskan Natives misreport their ethnic background,” he said.
Subtype analyses
PTCL-NOS was the most common subtype among all the racial/ethnic groups. The highest rate of PTCL-NOS (per 100,000 persons per year) was in blacks—at 0.77, compared to 0.47 in non-Hispanic whites, 0.46 in Hispanic whites, 0.45 in Asian/Pacific Islanders, and 0.28 in American Indian/Alaskan Natives.
The proportion of PTCL-NOS cases was 29.5% in non-Hispanic whites, 35.7% in blacks, 29.8% in Asian/Pacific Islanders, 27% in Hispanic whites, and 23.1% in American Indian/Alaskan Natives.
The proportion of angioimmunoblastic T-cell lymphoma cases was 9.9% in non-Hispanic whites, 5.2% in blacks, 15.3% in Asian/Pacific Islanders, 9.9% in Hispanic whites, and 2.6% in American Indian/Alaskan Natives.
The proportion of anaplastic large-cell lymphoma cases was 17.6% in non-Hispanic whites, 17.3% in blacks, 12.4% in Asian/Pacific Islanders, 21.2% in Hispanic whites, and 28.2% in American Indian/Alaskan Natives.
And the proportion of NK/T-cell lymphoma cases was 3.4% in non-Hispanic whites, 2.0% in blacks, 13.9% in Asian/Pacific Islanders, 14.6% in Hispanic whites, and 14.1% in American Indian/Alaskan Natives.
“That data indicates that, given the overall incidence of T-cell lymphoma in Natives is lower than in whites, if you’re a Native American/Alaskan Native [with] T-cell lymphoma, you’re 4 times more likely to have nasal NK-cell lymphoma than non-Hispanic whites,” Dr Shustov said.
He then showed a pairwise comparison of the percentage of PTCL subtypes. All of the racial/ethnic groups were significantly different from one another (P<0.001), except when Hispanic whites were compared to American Indian/Alaskan Natives (P=0.14).
Dr Shustov said this might be explained by the fact that these two groups have similar genetic backgrounds. ![]()
SAN FRANCISCO—The distribution of peripheral T-cell lymphoma (PTCL) subtypes in the US varies greatly according to race and ethnicity, new research suggests.
The retrospective study showed that the overall incidence of PTCL and its subtypes is lower in American Indians and Alaskan Natives than in other ethnic groups.
And the black population has a significantly higher incidence of PTCL—and the most common subtype, PTCL-not otherwise specified (NOS)—than other populations.
Andrei Shustov, MD, of the University of Washington Medical Center in Seattle, presented these and other findings at the 7th Annual T-cell Lymphoma Forum.
The findings were derived from data collected by the Surveillance, Epidemiology, and End Results (SEER) Cancer Registries, which cover 28% of the US population. The data included patients older than 15 years of age who were treated at 18 centers from 2000 through 2011.
Of all cancer patients registered over the 12-year period, 60% were non-Hispanic whites (n=470,864,199), 17% were Hispanic whites (n=134,464,006), 12% were black (n=92,294,395), 10% were Asian/Pacific Islanders (n=74,973,831), and 1% were American Indian/Alaskan Natives (n=10,802,898).
The overall incidence of PTCL was highest in blacks—2.11 per 100,000 persons per year, compared to 1.63 in non-Hispanic whites, 1.53 in Hispanic whites, 1.46 in Asian/Pacific Islanders, and 0.97 in American Indian/Alaskan Natives.
Although American Indian/Alaskan Natives appear to have the lowest overall rate of PTCLs, some cases may have been misclassified, Dr Shustov noted.
“The data collected for ethnicity in the SEER registry are self-reported, and a lot of American Indian/Alaskan Natives misreport their ethnic background,” he said.
Subtype analyses
PTCL-NOS was the most common subtype among all the racial/ethnic groups. The highest rate of PTCL-NOS (per 100,000 persons per year) was in blacks—at 0.77, compared to 0.47 in non-Hispanic whites, 0.46 in Hispanic whites, 0.45 in Asian/Pacific Islanders, and 0.28 in American Indian/Alaskan Natives.
The proportion of PTCL-NOS cases was 29.5% in non-Hispanic whites, 35.7% in blacks, 29.8% in Asian/Pacific Islanders, 27% in Hispanic whites, and 23.1% in American Indian/Alaskan Natives.
The proportion of angioimmunoblastic T-cell lymphoma cases was 9.9% in non-Hispanic whites, 5.2% in blacks, 15.3% in Asian/Pacific Islanders, 9.9% in Hispanic whites, and 2.6% in American Indian/Alaskan Natives.
The proportion of anaplastic large-cell lymphoma cases was 17.6% in non-Hispanic whites, 17.3% in blacks, 12.4% in Asian/Pacific Islanders, 21.2% in Hispanic whites, and 28.2% in American Indian/Alaskan Natives.
And the proportion of NK/T-cell lymphoma cases was 3.4% in non-Hispanic whites, 2.0% in blacks, 13.9% in Asian/Pacific Islanders, 14.6% in Hispanic whites, and 14.1% in American Indian/Alaskan Natives.
“That data indicates that, given the overall incidence of T-cell lymphoma in Natives is lower than in whites, if you’re a Native American/Alaskan Native [with] T-cell lymphoma, you’re 4 times more likely to have nasal NK-cell lymphoma than non-Hispanic whites,” Dr Shustov said.
He then showed a pairwise comparison of the percentage of PTCL subtypes. All of the racial/ethnic groups were significantly different from one another (P<0.001), except when Hispanic whites were compared to American Indian/Alaskan Natives (P=0.14).
Dr Shustov said this might be explained by the fact that these two groups have similar genetic backgrounds. ![]()
Prepackaged toddler foods often contain too much salt and sugar
Need another reason to make your toddler dinner instead of feeding him a prepackaged meal? New research shows a large number of dinners, snacks, and desserts sold in the United States that are designed for toddlers contain added sugar and salt, leaving them at risk for developing hypertension and diabetes later on in life.
Fortunately, commercial foods made for infants (vegetables, dinners, plain fruit without grains, dry cereals) sold in the United States tend to have little sugar and sodium added. But parents should still try to limit salty snacks, sweet desserts, and juice drinks, because they often contain more salt and sugar than kids need.
Approximately 79% of U.S. children aged 1-3 years eat more sodium than is recommended by the Institute of Medicine, noted Mary E. Cogswell, DrPH, a researcher from the Centers for Disease Control and Prevention in a study published in Pediatrics.

Dr. Cogswell and her team of researchers looked at package information for 1,074 food products sold in the United States in 2012 that was marketed to infants, toddlers, or both.
Seventy-two percent of toddler dinners examined contained added sodium, and 32% percent of toddler dinners contained added sugar; 52% of ready-to-serve mixed grains and fruits contained too much added sugar. The majority of dairy-based desserts (70%) and fruit juices (88%) intended for both infant and toddler consumption also contained added sugar.
Limiting how much sugar and salt your children are exposed to can go a long way in preventing obesity and high blood pressure, so parents should look carefully at labels when selecting what foods to buy for toddlers.
“Key advice for parents includes limiting juice and avoiding sugar-sweetened beverages and energy-dense, nutrient-poor snacks; if purchasing commercial toddler foods, the labels should be checked for sodium and added sugar,” the authors wrote.
Need another reason to make your toddler dinner instead of feeding him a prepackaged meal? New research shows a large number of dinners, snacks, and desserts sold in the United States that are designed for toddlers contain added sugar and salt, leaving them at risk for developing hypertension and diabetes later on in life.
Fortunately, commercial foods made for infants (vegetables, dinners, plain fruit without grains, dry cereals) sold in the United States tend to have little sugar and sodium added. But parents should still try to limit salty snacks, sweet desserts, and juice drinks, because they often contain more salt and sugar than kids need.
Approximately 79% of U.S. children aged 1-3 years eat more sodium than is recommended by the Institute of Medicine, noted Mary E. Cogswell, DrPH, a researcher from the Centers for Disease Control and Prevention in a study published in Pediatrics.
Dr. Cogswell and her team of researchers looked at package information for 1,074 food products sold in the United States in 2012 that was marketed to infants, toddlers, or both.
Seventy-two percent of toddler dinners examined contained added sodium, and 32% percent of toddler dinners contained added sugar; 52% of ready-to-serve mixed grains and fruits contained too much added sugar. The majority of dairy-based desserts (70%) and fruit juices (88%) intended for both infant and toddler consumption also contained added sugar.
Limiting how much sugar and salt your children are exposed to can go a long way in preventing obesity and high blood pressure, so parents should look carefully at labels when selecting what foods to buy for toddlers.
“Key advice for parents includes limiting juice and avoiding sugar-sweetened beverages and energy-dense, nutrient-poor snacks; if purchasing commercial toddler foods, the labels should be checked for sodium and added sugar,” the authors wrote.
Need another reason to make your toddler dinner instead of feeding him a prepackaged meal? New research shows a large number of dinners, snacks, and desserts sold in the United States that are designed for toddlers contain added sugar and salt, leaving them at risk for developing hypertension and diabetes later on in life.
Fortunately, commercial foods made for infants (vegetables, dinners, plain fruit without grains, dry cereals) sold in the United States tend to have little sugar and sodium added. But parents should still try to limit salty snacks, sweet desserts, and juice drinks, because they often contain more salt and sugar than kids need.
Approximately 79% of U.S. children aged 1-3 years eat more sodium than is recommended by the Institute of Medicine, noted Mary E. Cogswell, DrPH, a researcher from the Centers for Disease Control and Prevention in a study published in Pediatrics.
Dr. Cogswell and her team of researchers looked at package information for 1,074 food products sold in the United States in 2012 that was marketed to infants, toddlers, or both.
Seventy-two percent of toddler dinners examined contained added sodium, and 32% percent of toddler dinners contained added sugar; 52% of ready-to-serve mixed grains and fruits contained too much added sugar. The majority of dairy-based desserts (70%) and fruit juices (88%) intended for both infant and toddler consumption also contained added sugar.
Limiting how much sugar and salt your children are exposed to can go a long way in preventing obesity and high blood pressure, so parents should look carefully at labels when selecting what foods to buy for toddlers.
“Key advice for parents includes limiting juice and avoiding sugar-sweetened beverages and energy-dense, nutrient-poor snacks; if purchasing commercial toddler foods, the labels should be checked for sodium and added sugar,” the authors wrote.

Solutions for Complex Patients
The presence of hospitalists has been a major change in acute care in recent decades. The demographics of hospitalized patients also have changed, with a substantial increase in the proportion of patients aged 65 years and older to almost 50%. Older hospitalized patients represent a medically complex population, with multiple chronic conditions including cognitive impairment.[1] It is noteworthy that, in many US hospitals, the majority of older patients are now cared for by hospitalists without subspecialty training in geriatric medicine.[2] The convergence of these changes has led us to ask important questions about the best approach to caring for the growing population of hospitalized older patients.
The care of older hospitalized patients poses unique challenges both during and following a hospitalization event. This patient population tends to have multiple chronic conditions coupled with frequent healthcare utilization or transitions in care (eg, hospital to postacute care). In addition, geriatric syndromes are common among this group and may include: delirium, dementia, depression, functional impairment, falls, incontinence, pain, polypharmacy, and unintentional weight loss. It is also common for multiple geriatric syndromes to co‐occur (eg, falls and incontinence). The presence of one or more geriatric syndromes may complicate patient care and additionally impact outcomes, including hospitalization and mortality.[3, 4] An interdisciplinary geriatric team specifically diagnoses and treats these syndromes within the context of other presenting illnesses and comorbidities. Thus, a logical hypothesis would be that specialized geriatric consultation would improve outcomes of older hospitalized patients.
The study by Nazir et al.[5] in this issue of the Journal of Hospital Medicine explores this hypothesis, but generates more questions than answers. Briefly, the study examines a cohort of older hospitalized patients with cognitive impairment (CI). The authors compare rehospitalization and mortality outcomes among 176 patients who received geriatric consultation services (GCS) and 239 patients who received usual hospital care. Although the intervention group differed from the usual care group in meaningful ways outside of the intervention, the investigators did due diligence to adjust for these differences in their analysis. After adjustment, 30‐day and 1‐year mortality outcomes were comparable between groups, and the hazard for 30‐day readmissions was higher for the GCS group.
These findings stood contrary to the authors' hypothesis and what many would expect with subspecialty involvement during hospitalization. As the authors point out, however, we should interpret these findings cautiously due to a number of factors that may contribute to the seemingly limited effect of GCS in this study. First, it is important to note that this study occurred between 2006 and 2008. The emphasis on hospital readmissions as an important clinical outcome was increasing, although it had not reached the level that followed the 2009 publication by Jencks et al.[6] This emphasis further intensified following the inclusion of the Hospital Readmissions Reduction Program (HRRP) as part of the Affordable Care Act.[7] Thus, the implementation of the GCS in this university‐affiliated hospital may have reflected this pre‐HRRP period. For example, the team‐based rounds occurred only at the time of the initial consult. If a similar GCS were designed today in the post‐HRRP period, one could imagine more intense team‐based involvement occurring throughout the hospital stay, in particular near the time of discharge. In addition, recent studies underscore the importance of supporting transitions in care for older adults, who are often in need of postacute care, home health, and other services following hospitalization.[8] As noted by Nazir and colleagues, other interventions that have shown an impact on 30‐day readmissions were multifaceted and included personnel who provide bridging between the hospital and outpatient setting. The authors also mentioned that a future component of preventing hospital readmissions was a stronger emphasis on advance care planning (ACP) discussions both during and following hospitalization. Neither of these key elements (eg, care transition personnel or proactive ACP discussions) was part of the GCS model evaluated in this study. Thus, it is unknown to what extent the higher 30‐day readmissions that occurred for the GCS group were consistent with patient/family goals of care. It is also unknown to what extent these readmissions were potentially unavoidable.
Perhaps even more importantly, this study is a reminder of the difference between efficacy and effectiveness; that is, does geriatric consultation work (efficacy) versus does a GCS as implemented at this specific hospital work (effectiveness)? The latter reflects not only aspects of what a geriatric interdisciplinary team may diagnose and recommend, but includes how patients are identified for consultation (referral process), the environment in which the consultation occurs (care coordination on unit or among team), and the fidelity to GCS recommendations. Without reported measures, it is unclear to what extent GCS achieved better recognition and treatment of geriatric syndromes, a reduction in polypharmacy, and optimal discharge planning. Theoretically, it is through the robust implementation of these components that better clinical outcomes would result. Even with a high degree of intervention implementation, 12‐month outcomes may be too far removed from the GCS intervention, especially for older patients with CI who are at high risk for decline.
Unfortunately, geriatric syndromes often go unrecognized, with high rates of polypharmacy at hospital discharge[9] and more than 50% of inpatients with unrecognized dementia,[10] delirium,[11] depression,[12] and nutritional risk.[13] Thus, our need for hospital geriatric care and expertise is greater than ever. This study highlights many of the challenges of the traditional consultative model of care and a need for innovative approaches to recognize and treat geriatric syndromes. It is likely that, given the complex nature of geriatric patients, efficacious consultative models will need to address multiple chronic conditions and extend beyond the hospital discharge period. However, based on available evidence, it is currently unclear what specific interventions are efficacious and what type of geriatric consultative model is required. No matter the method, hospitalists must recognize the unique challenges of this population and work to ensure safe hospitalization and care transitions.
Acknowledgements
The authors acknowledge John Schnelle, PhD, for his input and review of the editorial.
Disclosures: Dr. Vasilevskis is supported by the National Institutes of Health (K23AG040157) and the Tennessee Valley VA Geriatric Research, Education and Clinical Center (GRECC). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Department of Veterans' Affairs.
- , , Hospital Utilization Among Oldest Adults, 2008. HCUP statistical brief 103. Rockville, MD: Agency for Healthcare Research and Quality; 2010:1–11. Available at: http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb103.pdf. Last accessed Dec 27, 2015.
- , , , Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11):1102–1112.
- , , , , Not just specific diseases: systematic review of the association of geriatric syndromes with hospitalization or nursing home admission. Arch Gerontol Geriatr. 2013;57(1):16–26.
- , , , The association between geriatric syndromes and survival. J Am Geriatr Soc. 2012;60(5):896–904.
- , , , , , Impact of an inpatient geriatric consultative service on outcomes for cognitively impaired patients. J Hosp Med. 2015;10(5):275–280.
- , , Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360(14):1418–1428.
- Patient Protection and Affordable Care Act of 2010. Hospital Readmissions Reduction Program; 2010. Pub L No. 111‐148, 124 Stat 408, S3025.
- , , , , Transitional care interventions prevent hospital readmissions for adults with chronic illnesses. Health Aff (Millwood). 2014;33(9):1531–1539.
- , , , Epidemiology of polypharmacy among family medicine patients at hospital discharge. J Prim Care Community Health. 2013;4(2):101–105.
- , , , et al. Impact and recognition of cognitive impairment among hospitalized elders. J Hosp Med. 2010;5(2):69–75.
- , , , Detection of delirium in the acute hospital. Age Ageing. 2010;39(1):131–135.
- , , , , Recognition of depression in older medical inpatients. J Gen Intern Med. 2007;22(5):559–564.
- , , , et al. Nutritional risk and body mass index predict hospitalization, nursing home admissions, and mortality in community‐dwelling older adults: results from the UAB Study of Aging with 8.5 years of follow‐up. J Gerontol A Biol Sci Med Sci. 2014;69(9):1146–1153.
The presence of hospitalists has been a major change in acute care in recent decades. The demographics of hospitalized patients also have changed, with a substantial increase in the proportion of patients aged 65 years and older to almost 50%. Older hospitalized patients represent a medically complex population, with multiple chronic conditions including cognitive impairment.[1] It is noteworthy that, in many US hospitals, the majority of older patients are now cared for by hospitalists without subspecialty training in geriatric medicine.[2] The convergence of these changes has led us to ask important questions about the best approach to caring for the growing population of hospitalized older patients.
The care of older hospitalized patients poses unique challenges both during and following a hospitalization event. This patient population tends to have multiple chronic conditions coupled with frequent healthcare utilization or transitions in care (eg, hospital to postacute care). In addition, geriatric syndromes are common among this group and may include: delirium, dementia, depression, functional impairment, falls, incontinence, pain, polypharmacy, and unintentional weight loss. It is also common for multiple geriatric syndromes to co‐occur (eg, falls and incontinence). The presence of one or more geriatric syndromes may complicate patient care and additionally impact outcomes, including hospitalization and mortality.[3, 4] An interdisciplinary geriatric team specifically diagnoses and treats these syndromes within the context of other presenting illnesses and comorbidities. Thus, a logical hypothesis would be that specialized geriatric consultation would improve outcomes of older hospitalized patients.
The study by Nazir et al.[5] in this issue of the Journal of Hospital Medicine explores this hypothesis, but generates more questions than answers. Briefly, the study examines a cohort of older hospitalized patients with cognitive impairment (CI). The authors compare rehospitalization and mortality outcomes among 176 patients who received geriatric consultation services (GCS) and 239 patients who received usual hospital care. Although the intervention group differed from the usual care group in meaningful ways outside of the intervention, the investigators did due diligence to adjust for these differences in their analysis. After adjustment, 30‐day and 1‐year mortality outcomes were comparable between groups, and the hazard for 30‐day readmissions was higher for the GCS group.
These findings stood contrary to the authors' hypothesis and what many would expect with subspecialty involvement during hospitalization. As the authors point out, however, we should interpret these findings cautiously due to a number of factors that may contribute to the seemingly limited effect of GCS in this study. First, it is important to note that this study occurred between 2006 and 2008. The emphasis on hospital readmissions as an important clinical outcome was increasing, although it had not reached the level that followed the 2009 publication by Jencks et al.[6] This emphasis further intensified following the inclusion of the Hospital Readmissions Reduction Program (HRRP) as part of the Affordable Care Act.[7] Thus, the implementation of the GCS in this university‐affiliated hospital may have reflected this pre‐HRRP period. For example, the team‐based rounds occurred only at the time of the initial consult. If a similar GCS were designed today in the post‐HRRP period, one could imagine more intense team‐based involvement occurring throughout the hospital stay, in particular near the time of discharge. In addition, recent studies underscore the importance of supporting transitions in care for older adults, who are often in need of postacute care, home health, and other services following hospitalization.[8] As noted by Nazir and colleagues, other interventions that have shown an impact on 30‐day readmissions were multifaceted and included personnel who provide bridging between the hospital and outpatient setting. The authors also mentioned that a future component of preventing hospital readmissions was a stronger emphasis on advance care planning (ACP) discussions both during and following hospitalization. Neither of these key elements (eg, care transition personnel or proactive ACP discussions) was part of the GCS model evaluated in this study. Thus, it is unknown to what extent the higher 30‐day readmissions that occurred for the GCS group were consistent with patient/family goals of care. It is also unknown to what extent these readmissions were potentially unavoidable.
Perhaps even more importantly, this study is a reminder of the difference between efficacy and effectiveness; that is, does geriatric consultation work (efficacy) versus does a GCS as implemented at this specific hospital work (effectiveness)? The latter reflects not only aspects of what a geriatric interdisciplinary team may diagnose and recommend, but includes how patients are identified for consultation (referral process), the environment in which the consultation occurs (care coordination on unit or among team), and the fidelity to GCS recommendations. Without reported measures, it is unclear to what extent GCS achieved better recognition and treatment of geriatric syndromes, a reduction in polypharmacy, and optimal discharge planning. Theoretically, it is through the robust implementation of these components that better clinical outcomes would result. Even with a high degree of intervention implementation, 12‐month outcomes may be too far removed from the GCS intervention, especially for older patients with CI who are at high risk for decline.
Unfortunately, geriatric syndromes often go unrecognized, with high rates of polypharmacy at hospital discharge[9] and more than 50% of inpatients with unrecognized dementia,[10] delirium,[11] depression,[12] and nutritional risk.[13] Thus, our need for hospital geriatric care and expertise is greater than ever. This study highlights many of the challenges of the traditional consultative model of care and a need for innovative approaches to recognize and treat geriatric syndromes. It is likely that, given the complex nature of geriatric patients, efficacious consultative models will need to address multiple chronic conditions and extend beyond the hospital discharge period. However, based on available evidence, it is currently unclear what specific interventions are efficacious and what type of geriatric consultative model is required. No matter the method, hospitalists must recognize the unique challenges of this population and work to ensure safe hospitalization and care transitions.
Acknowledgements
The authors acknowledge John Schnelle, PhD, for his input and review of the editorial.
Disclosures: Dr. Vasilevskis is supported by the National Institutes of Health (K23AG040157) and the Tennessee Valley VA Geriatric Research, Education and Clinical Center (GRECC). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Department of Veterans' Affairs.
The presence of hospitalists has been a major change in acute care in recent decades. The demographics of hospitalized patients also have changed, with a substantial increase in the proportion of patients aged 65 years and older to almost 50%. Older hospitalized patients represent a medically complex population, with multiple chronic conditions including cognitive impairment.[1] It is noteworthy that, in many US hospitals, the majority of older patients are now cared for by hospitalists without subspecialty training in geriatric medicine.[2] The convergence of these changes has led us to ask important questions about the best approach to caring for the growing population of hospitalized older patients.
The care of older hospitalized patients poses unique challenges both during and following a hospitalization event. This patient population tends to have multiple chronic conditions coupled with frequent healthcare utilization or transitions in care (eg, hospital to postacute care). In addition, geriatric syndromes are common among this group and may include: delirium, dementia, depression, functional impairment, falls, incontinence, pain, polypharmacy, and unintentional weight loss. It is also common for multiple geriatric syndromes to co‐occur (eg, falls and incontinence). The presence of one or more geriatric syndromes may complicate patient care and additionally impact outcomes, including hospitalization and mortality.[3, 4] An interdisciplinary geriatric team specifically diagnoses and treats these syndromes within the context of other presenting illnesses and comorbidities. Thus, a logical hypothesis would be that specialized geriatric consultation would improve outcomes of older hospitalized patients.
The study by Nazir et al.[5] in this issue of the Journal of Hospital Medicine explores this hypothesis, but generates more questions than answers. Briefly, the study examines a cohort of older hospitalized patients with cognitive impairment (CI). The authors compare rehospitalization and mortality outcomes among 176 patients who received geriatric consultation services (GCS) and 239 patients who received usual hospital care. Although the intervention group differed from the usual care group in meaningful ways outside of the intervention, the investigators did due diligence to adjust for these differences in their analysis. After adjustment, 30‐day and 1‐year mortality outcomes were comparable between groups, and the hazard for 30‐day readmissions was higher for the GCS group.
These findings stood contrary to the authors' hypothesis and what many would expect with subspecialty involvement during hospitalization. As the authors point out, however, we should interpret these findings cautiously due to a number of factors that may contribute to the seemingly limited effect of GCS in this study. First, it is important to note that this study occurred between 2006 and 2008. The emphasis on hospital readmissions as an important clinical outcome was increasing, although it had not reached the level that followed the 2009 publication by Jencks et al.[6] This emphasis further intensified following the inclusion of the Hospital Readmissions Reduction Program (HRRP) as part of the Affordable Care Act.[7] Thus, the implementation of the GCS in this university‐affiliated hospital may have reflected this pre‐HRRP period. For example, the team‐based rounds occurred only at the time of the initial consult. If a similar GCS were designed today in the post‐HRRP period, one could imagine more intense team‐based involvement occurring throughout the hospital stay, in particular near the time of discharge. In addition, recent studies underscore the importance of supporting transitions in care for older adults, who are often in need of postacute care, home health, and other services following hospitalization.[8] As noted by Nazir and colleagues, other interventions that have shown an impact on 30‐day readmissions were multifaceted and included personnel who provide bridging between the hospital and outpatient setting. The authors also mentioned that a future component of preventing hospital readmissions was a stronger emphasis on advance care planning (ACP) discussions both during and following hospitalization. Neither of these key elements (eg, care transition personnel or proactive ACP discussions) was part of the GCS model evaluated in this study. Thus, it is unknown to what extent the higher 30‐day readmissions that occurred for the GCS group were consistent with patient/family goals of care. It is also unknown to what extent these readmissions were potentially unavoidable.
Perhaps even more importantly, this study is a reminder of the difference between efficacy and effectiveness; that is, does geriatric consultation work (efficacy) versus does a GCS as implemented at this specific hospital work (effectiveness)? The latter reflects not only aspects of what a geriatric interdisciplinary team may diagnose and recommend, but includes how patients are identified for consultation (referral process), the environment in which the consultation occurs (care coordination on unit or among team), and the fidelity to GCS recommendations. Without reported measures, it is unclear to what extent GCS achieved better recognition and treatment of geriatric syndromes, a reduction in polypharmacy, and optimal discharge planning. Theoretically, it is through the robust implementation of these components that better clinical outcomes would result. Even with a high degree of intervention implementation, 12‐month outcomes may be too far removed from the GCS intervention, especially for older patients with CI who are at high risk for decline.
Unfortunately, geriatric syndromes often go unrecognized, with high rates of polypharmacy at hospital discharge[9] and more than 50% of inpatients with unrecognized dementia,[10] delirium,[11] depression,[12] and nutritional risk.[13] Thus, our need for hospital geriatric care and expertise is greater than ever. This study highlights many of the challenges of the traditional consultative model of care and a need for innovative approaches to recognize and treat geriatric syndromes. It is likely that, given the complex nature of geriatric patients, efficacious consultative models will need to address multiple chronic conditions and extend beyond the hospital discharge period. However, based on available evidence, it is currently unclear what specific interventions are efficacious and what type of geriatric consultative model is required. No matter the method, hospitalists must recognize the unique challenges of this population and work to ensure safe hospitalization and care transitions.
Acknowledgements
The authors acknowledge John Schnelle, PhD, for his input and review of the editorial.
Disclosures: Dr. Vasilevskis is supported by the National Institutes of Health (K23AG040157) and the Tennessee Valley VA Geriatric Research, Education and Clinical Center (GRECC). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Department of Veterans' Affairs.
- , , Hospital Utilization Among Oldest Adults, 2008. HCUP statistical brief 103. Rockville, MD: Agency for Healthcare Research and Quality; 2010:1–11. Available at: http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb103.pdf. Last accessed Dec 27, 2015.
- , , , Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11):1102–1112.
- , , , , Not just specific diseases: systematic review of the association of geriatric syndromes with hospitalization or nursing home admission. Arch Gerontol Geriatr. 2013;57(1):16–26.
- , , , The association between geriatric syndromes and survival. J Am Geriatr Soc. 2012;60(5):896–904.
- , , , , , Impact of an inpatient geriatric consultative service on outcomes for cognitively impaired patients. J Hosp Med. 2015;10(5):275–280.
- , , Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360(14):1418–1428.
- Patient Protection and Affordable Care Act of 2010. Hospital Readmissions Reduction Program; 2010. Pub L No. 111‐148, 124 Stat 408, S3025.
- , , , , Transitional care interventions prevent hospital readmissions for adults with chronic illnesses. Health Aff (Millwood). 2014;33(9):1531–1539.
- , , , Epidemiology of polypharmacy among family medicine patients at hospital discharge. J Prim Care Community Health. 2013;4(2):101–105.
- , , , et al. Impact and recognition of cognitive impairment among hospitalized elders. J Hosp Med. 2010;5(2):69–75.
- , , , Detection of delirium in the acute hospital. Age Ageing. 2010;39(1):131–135.
- , , , , Recognition of depression in older medical inpatients. J Gen Intern Med. 2007;22(5):559–564.
- , , , et al. Nutritional risk and body mass index predict hospitalization, nursing home admissions, and mortality in community‐dwelling older adults: results from the UAB Study of Aging with 8.5 years of follow‐up. J Gerontol A Biol Sci Med Sci. 2014;69(9):1146–1153.
- , , Hospital Utilization Among Oldest Adults, 2008. HCUP statistical brief 103. Rockville, MD: Agency for Healthcare Research and Quality; 2010:1–11. Available at: http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb103.pdf. Last accessed Dec 27, 2015.
- , , , Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11):1102–1112.
- , , , , Not just specific diseases: systematic review of the association of geriatric syndromes with hospitalization or nursing home admission. Arch Gerontol Geriatr. 2013;57(1):16–26.
- , , , The association between geriatric syndromes and survival. J Am Geriatr Soc. 2012;60(5):896–904.
- , , , , , Impact of an inpatient geriatric consultative service on outcomes for cognitively impaired patients. J Hosp Med. 2015;10(5):275–280.
- , , Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360(14):1418–1428.
- Patient Protection and Affordable Care Act of 2010. Hospital Readmissions Reduction Program; 2010. Pub L No. 111‐148, 124 Stat 408, S3025.
- , , , , Transitional care interventions prevent hospital readmissions for adults with chronic illnesses. Health Aff (Millwood). 2014;33(9):1531–1539.
- , , , Epidemiology of polypharmacy among family medicine patients at hospital discharge. J Prim Care Community Health. 2013;4(2):101–105.
- , , , et al. Impact and recognition of cognitive impairment among hospitalized elders. J Hosp Med. 2010;5(2):69–75.
- , , , Detection of delirium in the acute hospital. Age Ageing. 2010;39(1):131–135.
- , , , , Recognition of depression in older medical inpatients. J Gen Intern Med. 2007;22(5):559–564.
- , , , et al. Nutritional risk and body mass index predict hospitalization, nursing home admissions, and mortality in community‐dwelling older adults: results from the UAB Study of Aging with 8.5 years of follow‐up. J Gerontol A Biol Sci Med Sci. 2014;69(9):1146–1153.
Impact of Inpatient GCS on CI Patients
Under the Patient Protection and Affordable Care Act of 2010, commonly referred to as the Affordable Care Act, hospitals face up to a 3% penalty in Medicare reimbursements for patients readmitted within 30 days of initial discharge, and measures have been proposed for modifying payments to hospitals based on their performance on this metric.[1] Cognitive impairment (CI) is considered a major risk factor for poor postdischarge outcomes including mortality and hospital readmission.[2, 3] Hospitals are seeking strategies to reduce postdischarge mortality and rehospitalization among patients with and without CI.[4] Such strategies include use of transitional care coaches, patient and caregiver education, postdischarge follow‐up, and provision of geriatric consultative services (GCS) for the care of complex patients in the hospital setting.[5, 6, 7]
GCS utilize comprehensive geriatric assessments and multidisciplinary processes to recognize and modify risk factors that may lead to poor outcomes among hospitalized patients.[8, 9, 10, 11] Implementation of GCS models including Acute Care for Elders and, recently, the Mobile Acute Care of the Elderly services have shown many benefits among older patients including a reduction in the hospital length of stay and readmission rates.[12, 13] The benefits of such services among hospitalized elders suffering from CI, however, are not well established. The objective of this article was to evaluate the impact of GCS on the readmission and mortality rates of older adults with CI within 12 months of their hospitalization to an urban, public hospital. We hypothesized that GCS will reduce both 12‐month hospital readmissions and mortality rates among this vulnerable group of older adults.
METHODS
The study was approved by the Indiana University institutional review board, and informed consent for identifiable chart review was obtained from subjects or their legally authorized representatives.
Setting
The study was conducted at Eskenazi hospital, Indianapolis, Indiana, a 340‐bed, university‐affiliated, public hospital with over 2300 admissions of patients aged 65 years or older every year.
Population
Four hundred fifteen hospitalized patients aged 65 years or older suffering from CI were enrolled into an original, randomized, controlled trial that evaluated the effect of a computerized decision support system on their quality and outcome of care between July 1, 2006 and May 30, 2008.[14] The computerized decision support included reminders for physicians to reduce the prescription of 18 anticholinergics, minimize physical restraints and Foley catheterization, and increase referral to the local GCS.[15] That previous trial neither showed an impact on quality of care nor health utilization among older patients, including mortality and hospital readmission rates. The current study uses the data from the clinical trial cohort to evaluate the effect of GCS on the 12‐month mortality and hospital readmission rates for hospitalized elders with CI (Figure 1).
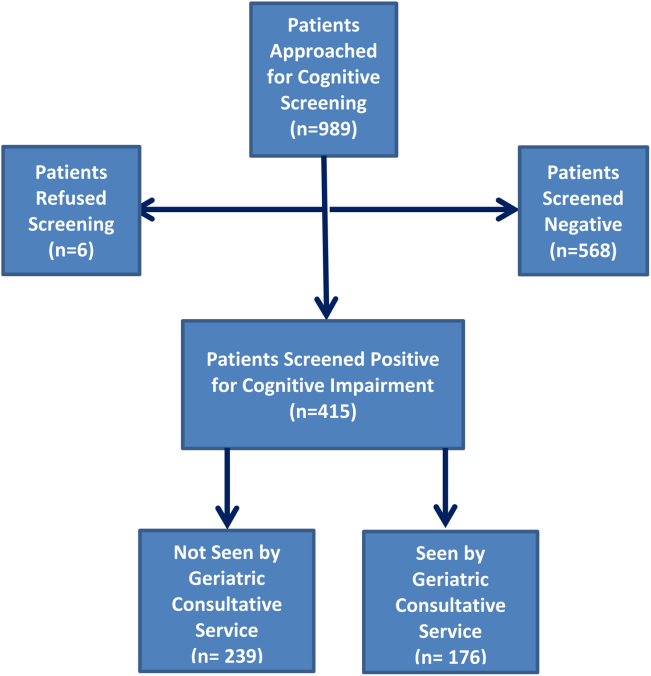
Inclusion and Exclusion Criteria
Individuals were eligible for enrollment if they were aged 65 years or older, hospitalized on a medical ward, able to speak English, and had evidence of CI within 48 hours of hospital admission. Individuals were excluded if they were previously enrolled, were aphasic, or unresponsive. The presence of CI was based on the Short Portable Mental Status Questionnaire (SPMSQ),[16] a brief 10‐item screening test with a sensitivity of 86% and specificity of 99% for dementia using a score of 7 or less (maximum possible score of 10).[16] The SPMSQ scoring process adjusts for participant educational and racial status, which was a benefit to its use given the urban setting of our hospital serving a large proportion of minority and low‐education patients. A physician‐trained research assistant administered the SPMSQ within 48 hours of hospital admission.
Geriatric Consultative Services
GCS is an interdisciplinary team of a geriatrician, a geriatric pharmacist, a case manager nurse, a social worker, a medical assistant, physical therapists, and a representative of the local Area Agency on Aging. There may be a geriatric fellow and/or medicine resident available to the team based on their rotation structure. Team‐based bedside rounds are performed on new consults only, but all patients are seen individually by the team clinicians. The team emphasizes prevention of functional decline and polypharmacy, recognition and treatment of geriatric syndromes including dementia and delirium, and early discharge/transition planning. Consensus recommendations are prepared and documented in the consult notes section of the electronic medical records. Recommendations deemed critical are discussed directly with the primary teams, but no orders are placed by the GCS team. The GCS team is available on all weekdays but not on weekends or major holidays.
Study Outcomes
For this secondary analysis, we used the Regenstrief Medical Record System (RMRS) to measure 2 outcomes: hospital readmission and mortality rates up to 1 year from discharge following index hospitalization, defined as the first admission in the original clinical trial. The RMRS is the primary instrument for processing data and monitoring patient and physician activity for the hospital.[17, 18] The RMRS is linked with a state‐wide health information exchange to capture data on hospitalization outside the hospital. The RMRS also contains death certificate information for all registered patients who die in or outside the Eskenazi hospital.
Other Data Collections
Delirium was assessed at screening and then every weekday using the Confusion Assessment Method (CAM) by a trained research assistant.[19] CAM evaluates 10 symptoms of delirium specified in the Diagnostic and Statistical Manual of Mental Disorders‐III‐Revision: acute onset, fluctuating course, inattention, disorganized thinking, altered level of consciousness, disorientation, memory impairment, perceptual disturbances, psychomotor agitation or retardation, and sleep/wake disturbance. Participant demographic characteristics, including age, sex, ethnicity, and years of education, were collected from the RMRS and from interviews performed at the time of cognitive screening. Information on length of hospital stay and discharge destination (eg, home vs facility, including skilled nursing and acute rehabilitation facilities) was also obtained from the RMRS. Charlson Comorbidity Index score was calculated using International Classification of Diseases, Ninth Revision codes gathered from 1 year before admission until the time of each participant's discharge from the hospital.[20] The Acute Physiology Score (APS) from the Acute Physiology and Chronic Health Evaluation (APACHE) III was derived from data available in the RMRS to measure the severity of illness.[21] Although the APACHE III was developed in the intensive care unit using data from the first 24 hours after admission, for our study we used the worst laboratory test value during the entire hospital stay to calculate the APS.[22]
Statistical Analysis
Baseline variables are presented as means and standard deviations for continuous variables, and percentages for binary categorical variables. Comparisons between patients receiving GCS and those who did not were performed using 2 tests for categorical variables and Kruskal‐Wallis test for continuous variables. Cox proportional hazard models were used to determine the association between receiving GCS and time to hospital readmission or mortality within 30 days or 1‐year postindex admission while adjusting for other covariates. For the models using time to readmission, patients without readmission were censored either at the endpoint (30 days or 1 year) or at time of death for those who died within the time frame in each model. Because GCS was not randomly assigned, we also conducted a propensity score analysis.[23] A logistic model for the probability of receiving GCS was conducted using patient demographic variables and information collected before and at the time of GCS. Stratified Cox proportional models using quintiles of predicted probability of receiving GCS were used in a propensity‐adjusted Cox model. All data analyses were performed using SAS version 9.3 (SAS Institute, Inc., Cary, NC).
RESULTS
Between July 1, 2006 and May 30, 2008, 415 CI patients were enrolled in the original trial, with 176 receiving the GCS. As shown in Table 1, the GCS and non‐GCS groups differed significantly. The GCS group was older (79.2 years old, 8.1 standard deviation [SD] vs 75.8 years old, 7.8 SD; P0.001), scored lower on the SPMSQ (4.7, 2.7 SD vs 5.5, 2.7 SD; P=0.002), had fewer chronic conditions with a lower mean Charlson Comorbidity Index Score (2.1, 1.86 SD vs 2.8, 2.6 SD; P=0.023), but a higher percentage of delirium (48.9% vs 29.3%), a lower percentage of being discharged home (37.5% vs 56.1%), and a higher mean length of stay (6.4 days, 6.4 SD vs 5.6 days, 5.9 SD; P=0.004). They also had a lower malignancy rate (6.2% vs 14.6%; P=0.007) and a lower number of hospitalizations in the previous year (0.5 admissions, 0.9 SD vs 0.7 admissions, 1.1 SD; P=0.035). No differences were observed in regard to gender, ethnicity, history of myocardial infarctions, chronic obstructive pulmonary disease, cerebrovascular disease, peripheral vascular disease, diabetes, and use of anticholinergic medicines.
| No GCS, n=239 | GCS, n=176 | P Value* | |
|---|---|---|---|
| |||
| Baseline characteristics | |||
| Mean age (SD) | 75.8 (7.8) | 79.2 (8.1) | <0.001 |
| % Female | 66.1 [n=158] | 68.2 [n=120] | 0.657 |
| % African American | 54.8 [n=131] | 63.6 [n=112] | 0.071 |
| Mean SPMSQ score (SD) | 5.5 (2.7) | 4.7 (2.7) | 0.002 |
| Admission diagnoses | |||
| MI | 15.5 [n=37] | 13.6 [n=24] | 0.675 |
| CHF | 38.1 [n=91] | 34.7 [n=61] | 0.475 |
| PVD | 7.1 [n=17] | 9.7 [n=17] | 0.370 |
| Cerebrovascular | 13.8 [n=33] | 19.3 [n=34] | 0.140 |
| COPD | 41.0 [n=98] | 33.0 [n=58] | 0.094 |
| Diabetes | 47.7 [n=114] | 40.9 [n=72] | 0.169 |
| Malignancy | 14.6 [n=35] | 6.2 [n=11] | 0.007 |
| Metastatic cancer | 8.8 [n=21] | 1.7 [n=3] | 0.002 |
| Mean Charlson Comorbidity (SD) | 2.8 (2.6) | 2.1 (1.8) | 0.023 |
| Mean APS (SD) | 24.5 (13.8) | 25.9 (13.5) | 0.231 |
| Definite ACB Use | 35.2 [n=84] | 27.8 [n=49] | 0.136 |
| Length of stay | 5.6 (5.9) | 6.4 (6.4) | 0.004 |
| % Any delirium | 29.3 [n=70] | 48.9 [n=156] | <0.001 |
| % Discharged home | 56.1 [n=134] | 37.5 [n=66] | <0.001 |
| No. of inpatient stays prior year | 0.7 (1.1) | 0.5 (0.9) | 0.035 |
| Follow‐up outcomes | |||
| % Readmission within 30 days | 15.1 [n=36] | 22.7 [n=40] | 0.054 |
| % Readmission within 1 year | 54.4 [n=130] | 56.3 [n=99] | 0.765 |
| % Death within 30 days | 4.2 [n=10] | 1.7 [n=3] | 0.253 |
| % Death within 1 year | 26.8 [n=64] | 23.9 [n=42] | 0.569 |
| % Readmission or death within 30 days | 18.0 [n=43] | 24.4 [n=43] | 0.113 |
| % Readmission or death within 1 year | 64.8 [n=155] | 63.1 [n=111] | 0.708 |
Table 2 describes the association of various factors with receiving GCS. Patients who were positive for delirium (odds ratio [OR]=1.65; 95% confidence interval=0.98‐2.77) and were older (OR=1.04; 95% confidence interval=1.01‐1.08) had a higher propensity to receive GCS, whereas, the presence of metastatic cancer resulted in a lower propensity (OR=0.15; 95% confidence interval=0.02‐1.16) of receiving GCS. The logistic model estimated area under the receiver operating characteristic curve was 0.707.
| Adjusted OR (95% CI) | P Value | |
|---|---|---|
| ||
| Age | 1.04 (1.011.08) | 0.006 |
| Female | 1.02 (0.641.63) | 0.942 |
| African American | 1.11 (0.711.72) | 0.657 |
| Short Portable Mental Status Questionnaire score | 1.00 (0.911.10) | 0.990 |
| Acute Physiology Score | 1.00 (0.981.02) | 0.769 |
| Charlson Comorbidity Score | 1.11 (0.841.46) | 0.471 |
| Length of hospital stay | 1.02 (0.981.07) | 0.299 |
| Definite anticholinergic use* | 0.74 (0.461.20) | 0.219 |
| Any delirium during hospital stay | 1.65 (0.982.77) | 0.061 |
| Diabetes mellitus | 0.72 (0.411.26) | 0.253 |
| Myocardial infarction | 0.83 (0.411.66) | 0.593 |
| Congestive heart failure | 0.83 (0.471.47) | 0.524 |
| Peripheral vascular disease | 1.39 (0.613.18) | 0.433 |
| Cerebrovascular disease | 1.30 (0.652.59) | 0.464 |
| Malignancy | 0.45 (0.171.21) | 0.113 |
| Metastatic cancer | 0.15 (0.021.16) | 0.069 |
| Chronic obstructive pulmonary disease | 0.91 (0.531.55) | 0.727 |
Table 3 provides results from the Cox models for receiving GCS on readmission and mortality outcomes adjusting for various sets of covariates and with the propensity score adjustment. Model 1 presents unadjusted hazard ratio (HR). Model 2 presents HRs adjusting for a common set of covariates that were significantly associated with at least 1 of the outcomes, whereas model 3 presents the results adjusting for all covariates. All 4 models yielded similar results. As evident from this table, propensity‐adjusted HR for 30‐day readmission was still significantly higher among patients receiving GCS (HR=1.75; 95% confidence interval=1.06‐2.88) but not at 1 year (HR=1.19; 95% confidence interval=0.89‐1.59). There was a trend for decreased mortality for the GCS group at 30 days (HR=0.35; 95% confidence interval=0.09‐1.35), but it disappeared at 1 year (HR=0.91; 95% confidence interval=0.59‐1.40). A composite outcome of readmissions and mortality did not show any difference between the GCS and no‐GCS groups.
| Outcome Variables | Model 1 | Model 2 | Model 3 | Propensity Adjusted | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | P Value | HR (95% CI) | P Value | HR (95% CI) | P Value | HR (95% CI) | P Value | |
| ||||||||
| Readmission within 30 days | 1.65 (1.05, 2.59) | 0.030 | 1.73 (1.08, 2.78) | 0.024 | 1.84 (1.133.00) | 0.015 | 1.75 (1.062.88) | 0.029 |
| Readmission within 1 year | 1.13 (0.87, 1.46) | 0.373 | 1.24 (0.94, 1.63) | 0.125 | 1.26 (0.941.68) | 0.117 | 1.19 (0.891.59) | 0.245 |
| Death within 30 days | 0.43 (0.12, 1.56) | 0.199 | 0.34 (0.09, 1.28) | 0.110 | 0.25 (0.061.02) | 0.053 | 0.35 (0.091.35) | 0.126 |
| Death within 1 year | 0.95 (0.65, 1.45) | 0.806 | 0.87 (0.58 1.31) | 0.506 | 0.93 (0.601.42) | 0.724 | 0.91 (0.591.40) | 0.669 |
| Readmission or Death within 30 days | 1.48 (0.97, 2.26) | 0.070 | 1.49 (0.96, 2.33) | 0.078 | 1.56 (0.982.47) | 0.061 | 1.55 (0.972.48) | 0.069 |
| Readmission or death within 1 year | 1.05 (0.82, 1.34) | 0.699 | 1.11 (0.86, 1.43) | 0.412 | 1.15 (0.881.50) | 0.318 | 1.08 (0.831.42) | 0.569 |
DISCUSSION
To our knowledge, this is the first study to analyze the impact of GCS on hospital readmission and mortality rates of CI patients. Our results did not show any short‐term or long‐term benefits of GCS for CI patients. Recent studies exploring cost benefits of the GCS have found trends toward lower readmission, but none focused on patients with CI.[6, 24, 25] It is important to note that our study did not use random allocation to assigning the patient into the GCS or control group, thus raising the possibility that patients who received GCS were sicker and were medically and socially more complex than those who did not receive the consult. Moreover, GCS consultation is preferentially sought for and completed for patients with CI and functional limitations, consistent with our finding that GCS patients more often have delirium and are less‐often discharged home.
The nature of the GCS team is another important consideration. Our GCS model did not include unit cohorting of patients, an important component of other proposed GCS models.[26] A recent meta‐analysis found that the GCS models without unit cohorting of patients did not have an impact on 1‐ or 12‐month readmission rates.[27] Low adherence to consultant recommendations (less than 33%) was thought to be a reason for such results. Importance of cohorting with regard to accomplishing recommendations by primary teams, importance of unit staff expertise in geriatric principles, and impact of a unit model on teamwork has also been highlighted by another review.[28] These findings lend to the hypothesis that unit cohorting and direct order placement by the GCS team may improve outcomes among CI patients, including a reduction in readmission rates.
Although readmissions rates were not statistically different between GCS and control groups at 1‐year postdischarge, 30‐day readmission rates were higher among the GCS group. Previous research among older heart failure patients found that a comprehensive transitional care intervention at the time of hospital discharge significantly shortened the time to readmission in the intervention group (P=0.026).[29] The factors identified by the study authors included enhanced supervision by the transitional healthcare teams along with improved awareness and education among treated patients that may have facilitated early recognition of clinical deterioration.[29] A recent study with intensive outpatient care that resulted in increased admissions among chronically ill adults provided a similar conclusion.[30]
GCS patients showed a trend toward decreased mortality as did patients enrolled in previous studies evaluating GCS models in the inpatient setting, as suggested by a recent review.[27] A caveat to note is that these trends favored ward‐styled GCS services as compared to our open GCS model,[27, 28] although the factors cited in these dedicated units affecting mortality included prompt attention to early rehabilitation, delirium management, and prevention of pressure ulcers and are also frequently implemented for patients in our GCS service model and therefore may have produced similar results.
Our neutral results in regard to the readmissions need to be interpreted with caution. First, this study was conducted in a hospital that supports expert geriatric and palliative care teams, both in the inpatient and the ambulatory settings, that provide consultative services and train medicine teams and hospital nursing staff. On the outpatient side, the presence of a robust geriatrics house‐calls program and the Geriatric Resources for Assessment and Care of Elders team results in above‐average care for the control group, and thus may also impact apparent outcomes.[31, 32] Second, 30‐day readmissions represent a complex outcome. Two recent reviews of hospital‐initiated interventions have shown that evidence regarding best strategies to decrease 30‐day readmissions is unclear.[33] Neither review included studies that targeted patients with CI only. The 2 programs that reduced 30‐day readmissions were multifaceted and included personnel who provide bridging between the hospital and the outpatient setting.[34] The GCS does include a focus on postdischarge resources, but does that on a case‐by‐case basis and no formal posthospital follow‐ups are provided. Moreover, the value of 30‐day readmission rates as a marker of quality, even though used by policymakers as an indicator of hospital quality, remains controversial.[35, 36] Broadening the outcomes of interest to include patient‐centered outcomes including satisfaction with care, that have shown to impact other health outcomes, may help improve understanding the benefits of GCS in hospitals.[37] Other comprehensive transitional care models that failed to show a benefit on 30‐day readmissions in older patients still resulted in higher satisfaction among patients.[38] Unfortunately, our evaluation did not include an assessment of patient satisfaction and quality of transitions.
Since the study period, GCS at our hospital now has incorporated a more robust focus on advance care planning (ACP) and execution of Physician Orders for Scope of Treatment that were legislated in the state in July 2013. The GCS team members are expert in carrying out complex ACP discussions and also partner with the inpatient palliative care team. It is quite possible that a study of more recent outcomes will yield more positive results for the selected outcomes. Thus, for future trials that aim to study the impact of GCS in the inpatient settings, it may be advisable to include important quality markers such as implementation of ACP and patient satisfaction along with the health utilization outcomes.
Limitations
As mentioned previously, it is possible that our risk adjustment was insufficient to account for all the medical and psychosocial differences among groups. For example, the overall anticholinergic impact of various medications such as antipsychotic medications and histamine‐2 blockers was assessed via the Anticholinergic Burden Scale on admission, but we did not have information on medication prescribing during the stay. We were further limited by lack of baseline functional status and socioeconomic details, both of which are related to 30‐day readmissions. For example, living alone, prior use of assist devices, and belonging to lower socioeconomic status are correlated with higher readmission rates.[39, 40] Patients with available social support may receive more intense supervision and may seek medical attention sooner. On the other hand, worsening health among CI patients without any approximate social support may be unnoticed for days. Absence of details of inpatient interventions may also have resulted in unmeasurable confounders that could have impacted our study outcomes. Finally, lack of information on the uptake of GCS recommendations by the primary teams is another limitation of this analysis. Future trials should include strategies to address these information gaps.
CONCLUSION
Our results comparing inpatient geriatrics consultative services with usual care in hospitalized elders having cognitive impairment failed to demonstrate an impact on readmissions and mortality. A clinical lesson learned, however, is that much work is still required to reduce readmission and mortality rates in this especially vulnerable patient population.
Disclosures
Disclosures: This work was supported by grants from a Geriatric Academic Career Award (K01HP20517) through Health Resources and Services Administration, R01AG034205 and K23‐AG043476 from the National Institute on Aging, and the John A. Hartford Foundation Center for Excellence in Geriatric Medicine. The sponsors had no role in the study design, evaluation, or manuscript development. The authors report no conflicts of interest.
- , , , et al. Relationship between hospital readmission and mortality rates for patients hospitalized with acute myocardial infarction, heart failure, or pneumonia. JAMA. 2013;309(6):587–593.
- , , , Cognitive impairment. Can it predict the course of hospitalized patients? J Am Geriatr Soc. 1986;34(8):579–585.
- , , , , , Importance of functional measures in predicting mortality among older hospitalized patients. JAMA. 1998;279(15):1187–1193.
- , Understanding preventable hospital readmissions: masqueraders, markers, and true causal factors. J Hosp Med. 2011;6(2):51–53.
- , , , et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999;340(9):669–676.
- , , , et al. Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: a randomized controlled trial of Acute Care for Elders (ACE) in a community hospital. J Am Geriatr Soc. 2000;48(12):1572–1581.
- , ; American Geriatrics Society Health Care Systems Committee. Improving the quality of transitional care for persons with complex care needs. J Am Geriatr Soc. 2003;51(4):556–557.
- , , , Development and implementation of a proactive geriatrics consultation model in collaboration with hospitalists. J Am Geriatr Soc. 2009;57(11):2139–2145.
- , , , et al. Screening of the risk of functional decline performed by an inpatient geriatric consultation team in a general hospital [in French]. Revue medicale de Bruxelles. 2013;34(6):462–468.
- , , , et al. Systematic detection and multidisciplinary care of delirium in older medical inpatients: a randomized trial. CMAJ. 2002;167(7):753–759.
- , , Potentially inappropriate prescribing for geriatric inpatients: an acute care of the elderly unit compared to a general medicine service. Consult Pharm. 2003;18(1):37–42, 47–39.
- , , , Evaluation of the Mobile Acute Care of the Elderly (MACE) service. JAMA Intern Med. 2013;173(11):990–996.
- , , , , , Effects of an acute care for elders unit on costs and 30‐day readmissions. JAMA Intern Med. 2013;173(11):981–987.
- , , , et al. Impact and recognition of cognitive impairment among hospitalized elders. J Hosp Med. 2010;5(2):69–75.
- , , , et al. Enhancing care for hospitalized older adults with cognitive impairment: a randomized controlled trial. J Gen Intern Med. 2012;27(5):561–567.
- , , , Short Portable Mental Status Questionnaire as a screening test for dementia and delirium among the elderly. J Am Geriatr Soc. 1987;35(5):412–416.
- , , , et al. The Regenstrief Medical Record System: a quarter century experience. Int J Med Inform. 1999;54(3):225–253.
- , , , , , Factors determining the decision to institutionalize dementing individuals: a prospective study. Gerontologist. 1993;33(6):714–720.
- , , , , , Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948.
- , , , , , Resuscitation: how do we decide? A prospective study of physicians' preferences and the clinical course of hospitalized patients. JAMA. 1986;255(10):1316–1322.
- , , , et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100(6):1619–1636.
- , , , et al. Interaction between cognitive impairment and discharge destination and its effect on rehospitalization. J Am Geriatr Soc. 2013;61(11):1958–1963.
- , , , , , Propensity scores in intensive care and anaesthesiology literature: a systematic review. Intensive Care Med. 2010;36(12):1993–2003.
- , , , et al. Improving functional outcomes in older patients: lessons from an acute care for elders unit. Jt Comm J Qual Improv. 1998;24(2):63–76.
- , , , et al. Developing a stroke unit using the acute care for elders intervention and model of care. J Am Geriatr Soc. 2003;51(11):1660–1667.
- , , , A medical unit for the acute care of the elderly. J Am Geriatr Soc. 1994;42(5):545–552.
- , , , , Impact of geriatric consultation teams on clinical outcome in acute hospitals: a systematic review and meta‐analysis. BMC Med. 2013;11:48.
- , , , , Comprehensive geriatric assessment for older adults admitted to hospital: meta‐analysis of randomised controlled trials. BMJ. 2011;343:d6553.
- , , , et al. Prevention of readmission in elderly patients with congestive heart failure: results of a prospective, randomized pilot study. J Gen Intern Med. 1993;8(11):585–590.
- , , , et al. Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial. Ann Intern Med. 2012;157(1):1–10.
- , , , , House calls for seniors: building and sustaining a model of care for homebound seniors. J Am Geriatr Soc. 2009;57(6):1103–1109.
- , , , et al. Geriatric care management for low‐income seniors: a randomized controlled trial. JAMA. 2007;298(22):2623–2633.
- , , , , Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- , The effects of a discharge planning and home follow‐up intervention on elders hospitalized with common medical and surgical cardiac conditions. J Cardiovasc Nurs. 1999;14(1):44–54.
- Readmission to hospital: a measure of quality or outcome? Qual Saf Health Care. 2004;13(1):10–11.
- , , , , , Unintended consequences of steps to cut readmissions and reform payment may threaten care of vulnerable older adults. Health Aff (Millwood). 2012;31(7):1623–1632.
- , , Analyzing the effects of shared decision‐making, empathy and team interaction on patient satisfaction and treatment acceptance in medical rehabilitation using a structural equation modeling approach. Patient Educ Couns. 2013;91(2):167–175.
- , , , The Care Transitions Innovation (C‐TraIn) for Socioeconomically Disadvantaged Adults: results of a cluster randomized controlled trial. J Gen Intern Med. 2014;29(11):1460–1467.
- , , , Risk factors for early hospital readmission in low‐income elderly adults. J Am Geriatr Soc. 2014;62(3):489–494.
- , , , , , Understanding why patients of low socioeconomic status prefer hospitals over ambulatory care. Health Aff (Millwood). 2013;32(7):1196–1203.
Under the Patient Protection and Affordable Care Act of 2010, commonly referred to as the Affordable Care Act, hospitals face up to a 3% penalty in Medicare reimbursements for patients readmitted within 30 days of initial discharge, and measures have been proposed for modifying payments to hospitals based on their performance on this metric.[1] Cognitive impairment (CI) is considered a major risk factor for poor postdischarge outcomes including mortality and hospital readmission.[2, 3] Hospitals are seeking strategies to reduce postdischarge mortality and rehospitalization among patients with and without CI.[4] Such strategies include use of transitional care coaches, patient and caregiver education, postdischarge follow‐up, and provision of geriatric consultative services (GCS) for the care of complex patients in the hospital setting.[5, 6, 7]
GCS utilize comprehensive geriatric assessments and multidisciplinary processes to recognize and modify risk factors that may lead to poor outcomes among hospitalized patients.[8, 9, 10, 11] Implementation of GCS models including Acute Care for Elders and, recently, the Mobile Acute Care of the Elderly services have shown many benefits among older patients including a reduction in the hospital length of stay and readmission rates.[12, 13] The benefits of such services among hospitalized elders suffering from CI, however, are not well established. The objective of this article was to evaluate the impact of GCS on the readmission and mortality rates of older adults with CI within 12 months of their hospitalization to an urban, public hospital. We hypothesized that GCS will reduce both 12‐month hospital readmissions and mortality rates among this vulnerable group of older adults.
METHODS
The study was approved by the Indiana University institutional review board, and informed consent for identifiable chart review was obtained from subjects or their legally authorized representatives.
Setting
The study was conducted at Eskenazi hospital, Indianapolis, Indiana, a 340‐bed, university‐affiliated, public hospital with over 2300 admissions of patients aged 65 years or older every year.
Population
Four hundred fifteen hospitalized patients aged 65 years or older suffering from CI were enrolled into an original, randomized, controlled trial that evaluated the effect of a computerized decision support system on their quality and outcome of care between July 1, 2006 and May 30, 2008.[14] The computerized decision support included reminders for physicians to reduce the prescription of 18 anticholinergics, minimize physical restraints and Foley catheterization, and increase referral to the local GCS.[15] That previous trial neither showed an impact on quality of care nor health utilization among older patients, including mortality and hospital readmission rates. The current study uses the data from the clinical trial cohort to evaluate the effect of GCS on the 12‐month mortality and hospital readmission rates for hospitalized elders with CI (Figure 1).
Inclusion and Exclusion Criteria
Individuals were eligible for enrollment if they were aged 65 years or older, hospitalized on a medical ward, able to speak English, and had evidence of CI within 48 hours of hospital admission. Individuals were excluded if they were previously enrolled, were aphasic, or unresponsive. The presence of CI was based on the Short Portable Mental Status Questionnaire (SPMSQ),[16] a brief 10‐item screening test with a sensitivity of 86% and specificity of 99% for dementia using a score of 7 or less (maximum possible score of 10).[16] The SPMSQ scoring process adjusts for participant educational and racial status, which was a benefit to its use given the urban setting of our hospital serving a large proportion of minority and low‐education patients. A physician‐trained research assistant administered the SPMSQ within 48 hours of hospital admission.
Geriatric Consultative Services
GCS is an interdisciplinary team of a geriatrician, a geriatric pharmacist, a case manager nurse, a social worker, a medical assistant, physical therapists, and a representative of the local Area Agency on Aging. There may be a geriatric fellow and/or medicine resident available to the team based on their rotation structure. Team‐based bedside rounds are performed on new consults only, but all patients are seen individually by the team clinicians. The team emphasizes prevention of functional decline and polypharmacy, recognition and treatment of geriatric syndromes including dementia and delirium, and early discharge/transition planning. Consensus recommendations are prepared and documented in the consult notes section of the electronic medical records. Recommendations deemed critical are discussed directly with the primary teams, but no orders are placed by the GCS team. The GCS team is available on all weekdays but not on weekends or major holidays.
Study Outcomes
For this secondary analysis, we used the Regenstrief Medical Record System (RMRS) to measure 2 outcomes: hospital readmission and mortality rates up to 1 year from discharge following index hospitalization, defined as the first admission in the original clinical trial. The RMRS is the primary instrument for processing data and monitoring patient and physician activity for the hospital.[17, 18] The RMRS is linked with a state‐wide health information exchange to capture data on hospitalization outside the hospital. The RMRS also contains death certificate information for all registered patients who die in or outside the Eskenazi hospital.
Other Data Collections
Delirium was assessed at screening and then every weekday using the Confusion Assessment Method (CAM) by a trained research assistant.[19] CAM evaluates 10 symptoms of delirium specified in the Diagnostic and Statistical Manual of Mental Disorders‐III‐Revision: acute onset, fluctuating course, inattention, disorganized thinking, altered level of consciousness, disorientation, memory impairment, perceptual disturbances, psychomotor agitation or retardation, and sleep/wake disturbance. Participant demographic characteristics, including age, sex, ethnicity, and years of education, were collected from the RMRS and from interviews performed at the time of cognitive screening. Information on length of hospital stay and discharge destination (eg, home vs facility, including skilled nursing and acute rehabilitation facilities) was also obtained from the RMRS. Charlson Comorbidity Index score was calculated using International Classification of Diseases, Ninth Revision codes gathered from 1 year before admission until the time of each participant's discharge from the hospital.[20] The Acute Physiology Score (APS) from the Acute Physiology and Chronic Health Evaluation (APACHE) III was derived from data available in the RMRS to measure the severity of illness.[21] Although the APACHE III was developed in the intensive care unit using data from the first 24 hours after admission, for our study we used the worst laboratory test value during the entire hospital stay to calculate the APS.[22]
Statistical Analysis
Baseline variables are presented as means and standard deviations for continuous variables, and percentages for binary categorical variables. Comparisons between patients receiving GCS and those who did not were performed using 2 tests for categorical variables and Kruskal‐Wallis test for continuous variables. Cox proportional hazard models were used to determine the association between receiving GCS and time to hospital readmission or mortality within 30 days or 1‐year postindex admission while adjusting for other covariates. For the models using time to readmission, patients without readmission were censored either at the endpoint (30 days or 1 year) or at time of death for those who died within the time frame in each model. Because GCS was not randomly assigned, we also conducted a propensity score analysis.[23] A logistic model for the probability of receiving GCS was conducted using patient demographic variables and information collected before and at the time of GCS. Stratified Cox proportional models using quintiles of predicted probability of receiving GCS were used in a propensity‐adjusted Cox model. All data analyses were performed using SAS version 9.3 (SAS Institute, Inc., Cary, NC).
RESULTS
Between July 1, 2006 and May 30, 2008, 415 CI patients were enrolled in the original trial, with 176 receiving the GCS. As shown in Table 1, the GCS and non‐GCS groups differed significantly. The GCS group was older (79.2 years old, 8.1 standard deviation [SD] vs 75.8 years old, 7.8 SD; P0.001), scored lower on the SPMSQ (4.7, 2.7 SD vs 5.5, 2.7 SD; P=0.002), had fewer chronic conditions with a lower mean Charlson Comorbidity Index Score (2.1, 1.86 SD vs 2.8, 2.6 SD; P=0.023), but a higher percentage of delirium (48.9% vs 29.3%), a lower percentage of being discharged home (37.5% vs 56.1%), and a higher mean length of stay (6.4 days, 6.4 SD vs 5.6 days, 5.9 SD; P=0.004). They also had a lower malignancy rate (6.2% vs 14.6%; P=0.007) and a lower number of hospitalizations in the previous year (0.5 admissions, 0.9 SD vs 0.7 admissions, 1.1 SD; P=0.035). No differences were observed in regard to gender, ethnicity, history of myocardial infarctions, chronic obstructive pulmonary disease, cerebrovascular disease, peripheral vascular disease, diabetes, and use of anticholinergic medicines.
| No GCS, n=239 | GCS, n=176 | P Value* | |
|---|---|---|---|
| |||
| Baseline characteristics | |||
| Mean age (SD) | 75.8 (7.8) | 79.2 (8.1) | <0.001 |
| % Female | 66.1 [n=158] | 68.2 [n=120] | 0.657 |
| % African American | 54.8 [n=131] | 63.6 [n=112] | 0.071 |
| Mean SPMSQ score (SD) | 5.5 (2.7) | 4.7 (2.7) | 0.002 |
| Admission diagnoses | |||
| MI | 15.5 [n=37] | 13.6 [n=24] | 0.675 |
| CHF | 38.1 [n=91] | 34.7 [n=61] | 0.475 |
| PVD | 7.1 [n=17] | 9.7 [n=17] | 0.370 |
| Cerebrovascular | 13.8 [n=33] | 19.3 [n=34] | 0.140 |
| COPD | 41.0 [n=98] | 33.0 [n=58] | 0.094 |
| Diabetes | 47.7 [n=114] | 40.9 [n=72] | 0.169 |
| Malignancy | 14.6 [n=35] | 6.2 [n=11] | 0.007 |
| Metastatic cancer | 8.8 [n=21] | 1.7 [n=3] | 0.002 |
| Mean Charlson Comorbidity (SD) | 2.8 (2.6) | 2.1 (1.8) | 0.023 |
| Mean APS (SD) | 24.5 (13.8) | 25.9 (13.5) | 0.231 |
| Definite ACB Use | 35.2 [n=84] | 27.8 [n=49] | 0.136 |
| Length of stay | 5.6 (5.9) | 6.4 (6.4) | 0.004 |
| % Any delirium | 29.3 [n=70] | 48.9 [n=156] | <0.001 |
| % Discharged home | 56.1 [n=134] | 37.5 [n=66] | <0.001 |
| No. of inpatient stays prior year | 0.7 (1.1) | 0.5 (0.9) | 0.035 |
| Follow‐up outcomes | |||
| % Readmission within 30 days | 15.1 [n=36] | 22.7 [n=40] | 0.054 |
| % Readmission within 1 year | 54.4 [n=130] | 56.3 [n=99] | 0.765 |
| % Death within 30 days | 4.2 [n=10] | 1.7 [n=3] | 0.253 |
| % Death within 1 year | 26.8 [n=64] | 23.9 [n=42] | 0.569 |
| % Readmission or death within 30 days | 18.0 [n=43] | 24.4 [n=43] | 0.113 |
| % Readmission or death within 1 year | 64.8 [n=155] | 63.1 [n=111] | 0.708 |
Table 2 describes the association of various factors with receiving GCS. Patients who were positive for delirium (odds ratio [OR]=1.65; 95% confidence interval=0.98‐2.77) and were older (OR=1.04; 95% confidence interval=1.01‐1.08) had a higher propensity to receive GCS, whereas, the presence of metastatic cancer resulted in a lower propensity (OR=0.15; 95% confidence interval=0.02‐1.16) of receiving GCS. The logistic model estimated area under the receiver operating characteristic curve was 0.707.
| Adjusted OR (95% CI) | P Value | |
|---|---|---|
| ||
| Age | 1.04 (1.011.08) | 0.006 |
| Female | 1.02 (0.641.63) | 0.942 |
| African American | 1.11 (0.711.72) | 0.657 |
| Short Portable Mental Status Questionnaire score | 1.00 (0.911.10) | 0.990 |
| Acute Physiology Score | 1.00 (0.981.02) | 0.769 |
| Charlson Comorbidity Score | 1.11 (0.841.46) | 0.471 |
| Length of hospital stay | 1.02 (0.981.07) | 0.299 |
| Definite anticholinergic use* | 0.74 (0.461.20) | 0.219 |
| Any delirium during hospital stay | 1.65 (0.982.77) | 0.061 |
| Diabetes mellitus | 0.72 (0.411.26) | 0.253 |
| Myocardial infarction | 0.83 (0.411.66) | 0.593 |
| Congestive heart failure | 0.83 (0.471.47) | 0.524 |
| Peripheral vascular disease | 1.39 (0.613.18) | 0.433 |
| Cerebrovascular disease | 1.30 (0.652.59) | 0.464 |
| Malignancy | 0.45 (0.171.21) | 0.113 |
| Metastatic cancer | 0.15 (0.021.16) | 0.069 |
| Chronic obstructive pulmonary disease | 0.91 (0.531.55) | 0.727 |
Table 3 provides results from the Cox models for receiving GCS on readmission and mortality outcomes adjusting for various sets of covariates and with the propensity score adjustment. Model 1 presents unadjusted hazard ratio (HR). Model 2 presents HRs adjusting for a common set of covariates that were significantly associated with at least 1 of the outcomes, whereas model 3 presents the results adjusting for all covariates. All 4 models yielded similar results. As evident from this table, propensity‐adjusted HR for 30‐day readmission was still significantly higher among patients receiving GCS (HR=1.75; 95% confidence interval=1.06‐2.88) but not at 1 year (HR=1.19; 95% confidence interval=0.89‐1.59). There was a trend for decreased mortality for the GCS group at 30 days (HR=0.35; 95% confidence interval=0.09‐1.35), but it disappeared at 1 year (HR=0.91; 95% confidence interval=0.59‐1.40). A composite outcome of readmissions and mortality did not show any difference between the GCS and no‐GCS groups.
| Outcome Variables | Model 1 | Model 2 | Model 3 | Propensity Adjusted | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | P Value | HR (95% CI) | P Value | HR (95% CI) | P Value | HR (95% CI) | P Value | |
| ||||||||
| Readmission within 30 days | 1.65 (1.05, 2.59) | 0.030 | 1.73 (1.08, 2.78) | 0.024 | 1.84 (1.133.00) | 0.015 | 1.75 (1.062.88) | 0.029 |
| Readmission within 1 year | 1.13 (0.87, 1.46) | 0.373 | 1.24 (0.94, 1.63) | 0.125 | 1.26 (0.941.68) | 0.117 | 1.19 (0.891.59) | 0.245 |
| Death within 30 days | 0.43 (0.12, 1.56) | 0.199 | 0.34 (0.09, 1.28) | 0.110 | 0.25 (0.061.02) | 0.053 | 0.35 (0.091.35) | 0.126 |
| Death within 1 year | 0.95 (0.65, 1.45) | 0.806 | 0.87 (0.58 1.31) | 0.506 | 0.93 (0.601.42) | 0.724 | 0.91 (0.591.40) | 0.669 |
| Readmission or Death within 30 days | 1.48 (0.97, 2.26) | 0.070 | 1.49 (0.96, 2.33) | 0.078 | 1.56 (0.982.47) | 0.061 | 1.55 (0.972.48) | 0.069 |
| Readmission or death within 1 year | 1.05 (0.82, 1.34) | 0.699 | 1.11 (0.86, 1.43) | 0.412 | 1.15 (0.881.50) | 0.318 | 1.08 (0.831.42) | 0.569 |
DISCUSSION
To our knowledge, this is the first study to analyze the impact of GCS on hospital readmission and mortality rates of CI patients. Our results did not show any short‐term or long‐term benefits of GCS for CI patients. Recent studies exploring cost benefits of the GCS have found trends toward lower readmission, but none focused on patients with CI.[6, 24, 25] It is important to note that our study did not use random allocation to assigning the patient into the GCS or control group, thus raising the possibility that patients who received GCS were sicker and were medically and socially more complex than those who did not receive the consult. Moreover, GCS consultation is preferentially sought for and completed for patients with CI and functional limitations, consistent with our finding that GCS patients more often have delirium and are less‐often discharged home.
The nature of the GCS team is another important consideration. Our GCS model did not include unit cohorting of patients, an important component of other proposed GCS models.[26] A recent meta‐analysis found that the GCS models without unit cohorting of patients did not have an impact on 1‐ or 12‐month readmission rates.[27] Low adherence to consultant recommendations (less than 33%) was thought to be a reason for such results. Importance of cohorting with regard to accomplishing recommendations by primary teams, importance of unit staff expertise in geriatric principles, and impact of a unit model on teamwork has also been highlighted by another review.[28] These findings lend to the hypothesis that unit cohorting and direct order placement by the GCS team may improve outcomes among CI patients, including a reduction in readmission rates.
Although readmissions rates were not statistically different between GCS and control groups at 1‐year postdischarge, 30‐day readmission rates were higher among the GCS group. Previous research among older heart failure patients found that a comprehensive transitional care intervention at the time of hospital discharge significantly shortened the time to readmission in the intervention group (P=0.026).[29] The factors identified by the study authors included enhanced supervision by the transitional healthcare teams along with improved awareness and education among treated patients that may have facilitated early recognition of clinical deterioration.[29] A recent study with intensive outpatient care that resulted in increased admissions among chronically ill adults provided a similar conclusion.[30]
GCS patients showed a trend toward decreased mortality as did patients enrolled in previous studies evaluating GCS models in the inpatient setting, as suggested by a recent review.[27] A caveat to note is that these trends favored ward‐styled GCS services as compared to our open GCS model,[27, 28] although the factors cited in these dedicated units affecting mortality included prompt attention to early rehabilitation, delirium management, and prevention of pressure ulcers and are also frequently implemented for patients in our GCS service model and therefore may have produced similar results.
Our neutral results in regard to the readmissions need to be interpreted with caution. First, this study was conducted in a hospital that supports expert geriatric and palliative care teams, both in the inpatient and the ambulatory settings, that provide consultative services and train medicine teams and hospital nursing staff. On the outpatient side, the presence of a robust geriatrics house‐calls program and the Geriatric Resources for Assessment and Care of Elders team results in above‐average care for the control group, and thus may also impact apparent outcomes.[31, 32] Second, 30‐day readmissions represent a complex outcome. Two recent reviews of hospital‐initiated interventions have shown that evidence regarding best strategies to decrease 30‐day readmissions is unclear.[33] Neither review included studies that targeted patients with CI only. The 2 programs that reduced 30‐day readmissions were multifaceted and included personnel who provide bridging between the hospital and the outpatient setting.[34] The GCS does include a focus on postdischarge resources, but does that on a case‐by‐case basis and no formal posthospital follow‐ups are provided. Moreover, the value of 30‐day readmission rates as a marker of quality, even though used by policymakers as an indicator of hospital quality, remains controversial.[35, 36] Broadening the outcomes of interest to include patient‐centered outcomes including satisfaction with care, that have shown to impact other health outcomes, may help improve understanding the benefits of GCS in hospitals.[37] Other comprehensive transitional care models that failed to show a benefit on 30‐day readmissions in older patients still resulted in higher satisfaction among patients.[38] Unfortunately, our evaluation did not include an assessment of patient satisfaction and quality of transitions.
Since the study period, GCS at our hospital now has incorporated a more robust focus on advance care planning (ACP) and execution of Physician Orders for Scope of Treatment that were legislated in the state in July 2013. The GCS team members are expert in carrying out complex ACP discussions and also partner with the inpatient palliative care team. It is quite possible that a study of more recent outcomes will yield more positive results for the selected outcomes. Thus, for future trials that aim to study the impact of GCS in the inpatient settings, it may be advisable to include important quality markers such as implementation of ACP and patient satisfaction along with the health utilization outcomes.
Limitations
As mentioned previously, it is possible that our risk adjustment was insufficient to account for all the medical and psychosocial differences among groups. For example, the overall anticholinergic impact of various medications such as antipsychotic medications and histamine‐2 blockers was assessed via the Anticholinergic Burden Scale on admission, but we did not have information on medication prescribing during the stay. We were further limited by lack of baseline functional status and socioeconomic details, both of which are related to 30‐day readmissions. For example, living alone, prior use of assist devices, and belonging to lower socioeconomic status are correlated with higher readmission rates.[39, 40] Patients with available social support may receive more intense supervision and may seek medical attention sooner. On the other hand, worsening health among CI patients without any approximate social support may be unnoticed for days. Absence of details of inpatient interventions may also have resulted in unmeasurable confounders that could have impacted our study outcomes. Finally, lack of information on the uptake of GCS recommendations by the primary teams is another limitation of this analysis. Future trials should include strategies to address these information gaps.
CONCLUSION
Our results comparing inpatient geriatrics consultative services with usual care in hospitalized elders having cognitive impairment failed to demonstrate an impact on readmissions and mortality. A clinical lesson learned, however, is that much work is still required to reduce readmission and mortality rates in this especially vulnerable patient population.
Disclosures
Disclosures: This work was supported by grants from a Geriatric Academic Career Award (K01HP20517) through Health Resources and Services Administration, R01AG034205 and K23‐AG043476 from the National Institute on Aging, and the John A. Hartford Foundation Center for Excellence in Geriatric Medicine. The sponsors had no role in the study design, evaluation, or manuscript development. The authors report no conflicts of interest.
Under the Patient Protection and Affordable Care Act of 2010, commonly referred to as the Affordable Care Act, hospitals face up to a 3% penalty in Medicare reimbursements for patients readmitted within 30 days of initial discharge, and measures have been proposed for modifying payments to hospitals based on their performance on this metric.[1] Cognitive impairment (CI) is considered a major risk factor for poor postdischarge outcomes including mortality and hospital readmission.[2, 3] Hospitals are seeking strategies to reduce postdischarge mortality and rehospitalization among patients with and without CI.[4] Such strategies include use of transitional care coaches, patient and caregiver education, postdischarge follow‐up, and provision of geriatric consultative services (GCS) for the care of complex patients in the hospital setting.[5, 6, 7]
GCS utilize comprehensive geriatric assessments and multidisciplinary processes to recognize and modify risk factors that may lead to poor outcomes among hospitalized patients.[8, 9, 10, 11] Implementation of GCS models including Acute Care for Elders and, recently, the Mobile Acute Care of the Elderly services have shown many benefits among older patients including a reduction in the hospital length of stay and readmission rates.[12, 13] The benefits of such services among hospitalized elders suffering from CI, however, are not well established. The objective of this article was to evaluate the impact of GCS on the readmission and mortality rates of older adults with CI within 12 months of their hospitalization to an urban, public hospital. We hypothesized that GCS will reduce both 12‐month hospital readmissions and mortality rates among this vulnerable group of older adults.
METHODS
The study was approved by the Indiana University institutional review board, and informed consent for identifiable chart review was obtained from subjects or their legally authorized representatives.
Setting
The study was conducted at Eskenazi hospital, Indianapolis, Indiana, a 340‐bed, university‐affiliated, public hospital with over 2300 admissions of patients aged 65 years or older every year.
Population
Four hundred fifteen hospitalized patients aged 65 years or older suffering from CI were enrolled into an original, randomized, controlled trial that evaluated the effect of a computerized decision support system on their quality and outcome of care between July 1, 2006 and May 30, 2008.[14] The computerized decision support included reminders for physicians to reduce the prescription of 18 anticholinergics, minimize physical restraints and Foley catheterization, and increase referral to the local GCS.[15] That previous trial neither showed an impact on quality of care nor health utilization among older patients, including mortality and hospital readmission rates. The current study uses the data from the clinical trial cohort to evaluate the effect of GCS on the 12‐month mortality and hospital readmission rates for hospitalized elders with CI (Figure 1).
Inclusion and Exclusion Criteria
Individuals were eligible for enrollment if they were aged 65 years or older, hospitalized on a medical ward, able to speak English, and had evidence of CI within 48 hours of hospital admission. Individuals were excluded if they were previously enrolled, were aphasic, or unresponsive. The presence of CI was based on the Short Portable Mental Status Questionnaire (SPMSQ),[16] a brief 10‐item screening test with a sensitivity of 86% and specificity of 99% for dementia using a score of 7 or less (maximum possible score of 10).[16] The SPMSQ scoring process adjusts for participant educational and racial status, which was a benefit to its use given the urban setting of our hospital serving a large proportion of minority and low‐education patients. A physician‐trained research assistant administered the SPMSQ within 48 hours of hospital admission.
Geriatric Consultative Services
GCS is an interdisciplinary team of a geriatrician, a geriatric pharmacist, a case manager nurse, a social worker, a medical assistant, physical therapists, and a representative of the local Area Agency on Aging. There may be a geriatric fellow and/or medicine resident available to the team based on their rotation structure. Team‐based bedside rounds are performed on new consults only, but all patients are seen individually by the team clinicians. The team emphasizes prevention of functional decline and polypharmacy, recognition and treatment of geriatric syndromes including dementia and delirium, and early discharge/transition planning. Consensus recommendations are prepared and documented in the consult notes section of the electronic medical records. Recommendations deemed critical are discussed directly with the primary teams, but no orders are placed by the GCS team. The GCS team is available on all weekdays but not on weekends or major holidays.
Study Outcomes
For this secondary analysis, we used the Regenstrief Medical Record System (RMRS) to measure 2 outcomes: hospital readmission and mortality rates up to 1 year from discharge following index hospitalization, defined as the first admission in the original clinical trial. The RMRS is the primary instrument for processing data and monitoring patient and physician activity for the hospital.[17, 18] The RMRS is linked with a state‐wide health information exchange to capture data on hospitalization outside the hospital. The RMRS also contains death certificate information for all registered patients who die in or outside the Eskenazi hospital.
Other Data Collections
Delirium was assessed at screening and then every weekday using the Confusion Assessment Method (CAM) by a trained research assistant.[19] CAM evaluates 10 symptoms of delirium specified in the Diagnostic and Statistical Manual of Mental Disorders‐III‐Revision: acute onset, fluctuating course, inattention, disorganized thinking, altered level of consciousness, disorientation, memory impairment, perceptual disturbances, psychomotor agitation or retardation, and sleep/wake disturbance. Participant demographic characteristics, including age, sex, ethnicity, and years of education, were collected from the RMRS and from interviews performed at the time of cognitive screening. Information on length of hospital stay and discharge destination (eg, home vs facility, including skilled nursing and acute rehabilitation facilities) was also obtained from the RMRS. Charlson Comorbidity Index score was calculated using International Classification of Diseases, Ninth Revision codes gathered from 1 year before admission until the time of each participant's discharge from the hospital.[20] The Acute Physiology Score (APS) from the Acute Physiology and Chronic Health Evaluation (APACHE) III was derived from data available in the RMRS to measure the severity of illness.[21] Although the APACHE III was developed in the intensive care unit using data from the first 24 hours after admission, for our study we used the worst laboratory test value during the entire hospital stay to calculate the APS.[22]
Statistical Analysis
Baseline variables are presented as means and standard deviations for continuous variables, and percentages for binary categorical variables. Comparisons between patients receiving GCS and those who did not were performed using 2 tests for categorical variables and Kruskal‐Wallis test for continuous variables. Cox proportional hazard models were used to determine the association between receiving GCS and time to hospital readmission or mortality within 30 days or 1‐year postindex admission while adjusting for other covariates. For the models using time to readmission, patients without readmission were censored either at the endpoint (30 days or 1 year) or at time of death for those who died within the time frame in each model. Because GCS was not randomly assigned, we also conducted a propensity score analysis.[23] A logistic model for the probability of receiving GCS was conducted using patient demographic variables and information collected before and at the time of GCS. Stratified Cox proportional models using quintiles of predicted probability of receiving GCS were used in a propensity‐adjusted Cox model. All data analyses were performed using SAS version 9.3 (SAS Institute, Inc., Cary, NC).
RESULTS
Between July 1, 2006 and May 30, 2008, 415 CI patients were enrolled in the original trial, with 176 receiving the GCS. As shown in Table 1, the GCS and non‐GCS groups differed significantly. The GCS group was older (79.2 years old, 8.1 standard deviation [SD] vs 75.8 years old, 7.8 SD; P0.001), scored lower on the SPMSQ (4.7, 2.7 SD vs 5.5, 2.7 SD; P=0.002), had fewer chronic conditions with a lower mean Charlson Comorbidity Index Score (2.1, 1.86 SD vs 2.8, 2.6 SD; P=0.023), but a higher percentage of delirium (48.9% vs 29.3%), a lower percentage of being discharged home (37.5% vs 56.1%), and a higher mean length of stay (6.4 days, 6.4 SD vs 5.6 days, 5.9 SD; P=0.004). They also had a lower malignancy rate (6.2% vs 14.6%; P=0.007) and a lower number of hospitalizations in the previous year (0.5 admissions, 0.9 SD vs 0.7 admissions, 1.1 SD; P=0.035). No differences were observed in regard to gender, ethnicity, history of myocardial infarctions, chronic obstructive pulmonary disease, cerebrovascular disease, peripheral vascular disease, diabetes, and use of anticholinergic medicines.
| No GCS, n=239 | GCS, n=176 | P Value* | |
|---|---|---|---|
| |||
| Baseline characteristics | |||
| Mean age (SD) | 75.8 (7.8) | 79.2 (8.1) | <0.001 |
| % Female | 66.1 [n=158] | 68.2 [n=120] | 0.657 |
| % African American | 54.8 [n=131] | 63.6 [n=112] | 0.071 |
| Mean SPMSQ score (SD) | 5.5 (2.7) | 4.7 (2.7) | 0.002 |
| Admission diagnoses | |||
| MI | 15.5 [n=37] | 13.6 [n=24] | 0.675 |
| CHF | 38.1 [n=91] | 34.7 [n=61] | 0.475 |
| PVD | 7.1 [n=17] | 9.7 [n=17] | 0.370 |
| Cerebrovascular | 13.8 [n=33] | 19.3 [n=34] | 0.140 |
| COPD | 41.0 [n=98] | 33.0 [n=58] | 0.094 |
| Diabetes | 47.7 [n=114] | 40.9 [n=72] | 0.169 |
| Malignancy | 14.6 [n=35] | 6.2 [n=11] | 0.007 |
| Metastatic cancer | 8.8 [n=21] | 1.7 [n=3] | 0.002 |
| Mean Charlson Comorbidity (SD) | 2.8 (2.6) | 2.1 (1.8) | 0.023 |
| Mean APS (SD) | 24.5 (13.8) | 25.9 (13.5) | 0.231 |
| Definite ACB Use | 35.2 [n=84] | 27.8 [n=49] | 0.136 |
| Length of stay | 5.6 (5.9) | 6.4 (6.4) | 0.004 |
| % Any delirium | 29.3 [n=70] | 48.9 [n=156] | <0.001 |
| % Discharged home | 56.1 [n=134] | 37.5 [n=66] | <0.001 |
| No. of inpatient stays prior year | 0.7 (1.1) | 0.5 (0.9) | 0.035 |
| Follow‐up outcomes | |||
| % Readmission within 30 days | 15.1 [n=36] | 22.7 [n=40] | 0.054 |
| % Readmission within 1 year | 54.4 [n=130] | 56.3 [n=99] | 0.765 |
| % Death within 30 days | 4.2 [n=10] | 1.7 [n=3] | 0.253 |
| % Death within 1 year | 26.8 [n=64] | 23.9 [n=42] | 0.569 |
| % Readmission or death within 30 days | 18.0 [n=43] | 24.4 [n=43] | 0.113 |
| % Readmission or death within 1 year | 64.8 [n=155] | 63.1 [n=111] | 0.708 |
Table 2 describes the association of various factors with receiving GCS. Patients who were positive for delirium (odds ratio [OR]=1.65; 95% confidence interval=0.98‐2.77) and were older (OR=1.04; 95% confidence interval=1.01‐1.08) had a higher propensity to receive GCS, whereas, the presence of metastatic cancer resulted in a lower propensity (OR=0.15; 95% confidence interval=0.02‐1.16) of receiving GCS. The logistic model estimated area under the receiver operating characteristic curve was 0.707.
| Adjusted OR (95% CI) | P Value | |
|---|---|---|
| ||
| Age | 1.04 (1.011.08) | 0.006 |
| Female | 1.02 (0.641.63) | 0.942 |
| African American | 1.11 (0.711.72) | 0.657 |
| Short Portable Mental Status Questionnaire score | 1.00 (0.911.10) | 0.990 |
| Acute Physiology Score | 1.00 (0.981.02) | 0.769 |
| Charlson Comorbidity Score | 1.11 (0.841.46) | 0.471 |
| Length of hospital stay | 1.02 (0.981.07) | 0.299 |
| Definite anticholinergic use* | 0.74 (0.461.20) | 0.219 |
| Any delirium during hospital stay | 1.65 (0.982.77) | 0.061 |
| Diabetes mellitus | 0.72 (0.411.26) | 0.253 |
| Myocardial infarction | 0.83 (0.411.66) | 0.593 |
| Congestive heart failure | 0.83 (0.471.47) | 0.524 |
| Peripheral vascular disease | 1.39 (0.613.18) | 0.433 |
| Cerebrovascular disease | 1.30 (0.652.59) | 0.464 |
| Malignancy | 0.45 (0.171.21) | 0.113 |
| Metastatic cancer | 0.15 (0.021.16) | 0.069 |
| Chronic obstructive pulmonary disease | 0.91 (0.531.55) | 0.727 |
Table 3 provides results from the Cox models for receiving GCS on readmission and mortality outcomes adjusting for various sets of covariates and with the propensity score adjustment. Model 1 presents unadjusted hazard ratio (HR). Model 2 presents HRs adjusting for a common set of covariates that were significantly associated with at least 1 of the outcomes, whereas model 3 presents the results adjusting for all covariates. All 4 models yielded similar results. As evident from this table, propensity‐adjusted HR for 30‐day readmission was still significantly higher among patients receiving GCS (HR=1.75; 95% confidence interval=1.06‐2.88) but not at 1 year (HR=1.19; 95% confidence interval=0.89‐1.59). There was a trend for decreased mortality for the GCS group at 30 days (HR=0.35; 95% confidence interval=0.09‐1.35), but it disappeared at 1 year (HR=0.91; 95% confidence interval=0.59‐1.40). A composite outcome of readmissions and mortality did not show any difference between the GCS and no‐GCS groups.
| Outcome Variables | Model 1 | Model 2 | Model 3 | Propensity Adjusted | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | P Value | HR (95% CI) | P Value | HR (95% CI) | P Value | HR (95% CI) | P Value | |
| ||||||||
| Readmission within 30 days | 1.65 (1.05, 2.59) | 0.030 | 1.73 (1.08, 2.78) | 0.024 | 1.84 (1.133.00) | 0.015 | 1.75 (1.062.88) | 0.029 |
| Readmission within 1 year | 1.13 (0.87, 1.46) | 0.373 | 1.24 (0.94, 1.63) | 0.125 | 1.26 (0.941.68) | 0.117 | 1.19 (0.891.59) | 0.245 |
| Death within 30 days | 0.43 (0.12, 1.56) | 0.199 | 0.34 (0.09, 1.28) | 0.110 | 0.25 (0.061.02) | 0.053 | 0.35 (0.091.35) | 0.126 |
| Death within 1 year | 0.95 (0.65, 1.45) | 0.806 | 0.87 (0.58 1.31) | 0.506 | 0.93 (0.601.42) | 0.724 | 0.91 (0.591.40) | 0.669 |
| Readmission or Death within 30 days | 1.48 (0.97, 2.26) | 0.070 | 1.49 (0.96, 2.33) | 0.078 | 1.56 (0.982.47) | 0.061 | 1.55 (0.972.48) | 0.069 |
| Readmission or death within 1 year | 1.05 (0.82, 1.34) | 0.699 | 1.11 (0.86, 1.43) | 0.412 | 1.15 (0.881.50) | 0.318 | 1.08 (0.831.42) | 0.569 |
DISCUSSION
To our knowledge, this is the first study to analyze the impact of GCS on hospital readmission and mortality rates of CI patients. Our results did not show any short‐term or long‐term benefits of GCS for CI patients. Recent studies exploring cost benefits of the GCS have found trends toward lower readmission, but none focused on patients with CI.[6, 24, 25] It is important to note that our study did not use random allocation to assigning the patient into the GCS or control group, thus raising the possibility that patients who received GCS were sicker and were medically and socially more complex than those who did not receive the consult. Moreover, GCS consultation is preferentially sought for and completed for patients with CI and functional limitations, consistent with our finding that GCS patients more often have delirium and are less‐often discharged home.
The nature of the GCS team is another important consideration. Our GCS model did not include unit cohorting of patients, an important component of other proposed GCS models.[26] A recent meta‐analysis found that the GCS models without unit cohorting of patients did not have an impact on 1‐ or 12‐month readmission rates.[27] Low adherence to consultant recommendations (less than 33%) was thought to be a reason for such results. Importance of cohorting with regard to accomplishing recommendations by primary teams, importance of unit staff expertise in geriatric principles, and impact of a unit model on teamwork has also been highlighted by another review.[28] These findings lend to the hypothesis that unit cohorting and direct order placement by the GCS team may improve outcomes among CI patients, including a reduction in readmission rates.
Although readmissions rates were not statistically different between GCS and control groups at 1‐year postdischarge, 30‐day readmission rates were higher among the GCS group. Previous research among older heart failure patients found that a comprehensive transitional care intervention at the time of hospital discharge significantly shortened the time to readmission in the intervention group (P=0.026).[29] The factors identified by the study authors included enhanced supervision by the transitional healthcare teams along with improved awareness and education among treated patients that may have facilitated early recognition of clinical deterioration.[29] A recent study with intensive outpatient care that resulted in increased admissions among chronically ill adults provided a similar conclusion.[30]
GCS patients showed a trend toward decreased mortality as did patients enrolled in previous studies evaluating GCS models in the inpatient setting, as suggested by a recent review.[27] A caveat to note is that these trends favored ward‐styled GCS services as compared to our open GCS model,[27, 28] although the factors cited in these dedicated units affecting mortality included prompt attention to early rehabilitation, delirium management, and prevention of pressure ulcers and are also frequently implemented for patients in our GCS service model and therefore may have produced similar results.
Our neutral results in regard to the readmissions need to be interpreted with caution. First, this study was conducted in a hospital that supports expert geriatric and palliative care teams, both in the inpatient and the ambulatory settings, that provide consultative services and train medicine teams and hospital nursing staff. On the outpatient side, the presence of a robust geriatrics house‐calls program and the Geriatric Resources for Assessment and Care of Elders team results in above‐average care for the control group, and thus may also impact apparent outcomes.[31, 32] Second, 30‐day readmissions represent a complex outcome. Two recent reviews of hospital‐initiated interventions have shown that evidence regarding best strategies to decrease 30‐day readmissions is unclear.[33] Neither review included studies that targeted patients with CI only. The 2 programs that reduced 30‐day readmissions were multifaceted and included personnel who provide bridging between the hospital and the outpatient setting.[34] The GCS does include a focus on postdischarge resources, but does that on a case‐by‐case basis and no formal posthospital follow‐ups are provided. Moreover, the value of 30‐day readmission rates as a marker of quality, even though used by policymakers as an indicator of hospital quality, remains controversial.[35, 36] Broadening the outcomes of interest to include patient‐centered outcomes including satisfaction with care, that have shown to impact other health outcomes, may help improve understanding the benefits of GCS in hospitals.[37] Other comprehensive transitional care models that failed to show a benefit on 30‐day readmissions in older patients still resulted in higher satisfaction among patients.[38] Unfortunately, our evaluation did not include an assessment of patient satisfaction and quality of transitions.
Since the study period, GCS at our hospital now has incorporated a more robust focus on advance care planning (ACP) and execution of Physician Orders for Scope of Treatment that were legislated in the state in July 2013. The GCS team members are expert in carrying out complex ACP discussions and also partner with the inpatient palliative care team. It is quite possible that a study of more recent outcomes will yield more positive results for the selected outcomes. Thus, for future trials that aim to study the impact of GCS in the inpatient settings, it may be advisable to include important quality markers such as implementation of ACP and patient satisfaction along with the health utilization outcomes.
Limitations
As mentioned previously, it is possible that our risk adjustment was insufficient to account for all the medical and psychosocial differences among groups. For example, the overall anticholinergic impact of various medications such as antipsychotic medications and histamine‐2 blockers was assessed via the Anticholinergic Burden Scale on admission, but we did not have information on medication prescribing during the stay. We were further limited by lack of baseline functional status and socioeconomic details, both of which are related to 30‐day readmissions. For example, living alone, prior use of assist devices, and belonging to lower socioeconomic status are correlated with higher readmission rates.[39, 40] Patients with available social support may receive more intense supervision and may seek medical attention sooner. On the other hand, worsening health among CI patients without any approximate social support may be unnoticed for days. Absence of details of inpatient interventions may also have resulted in unmeasurable confounders that could have impacted our study outcomes. Finally, lack of information on the uptake of GCS recommendations by the primary teams is another limitation of this analysis. Future trials should include strategies to address these information gaps.
CONCLUSION
Our results comparing inpatient geriatrics consultative services with usual care in hospitalized elders having cognitive impairment failed to demonstrate an impact on readmissions and mortality. A clinical lesson learned, however, is that much work is still required to reduce readmission and mortality rates in this especially vulnerable patient population.
Disclosures
Disclosures: This work was supported by grants from a Geriatric Academic Career Award (K01HP20517) through Health Resources and Services Administration, R01AG034205 and K23‐AG043476 from the National Institute on Aging, and the John A. Hartford Foundation Center for Excellence in Geriatric Medicine. The sponsors had no role in the study design, evaluation, or manuscript development. The authors report no conflicts of interest.
- , , , et al. Relationship between hospital readmission and mortality rates for patients hospitalized with acute myocardial infarction, heart failure, or pneumonia. JAMA. 2013;309(6):587–593.
- , , , Cognitive impairment. Can it predict the course of hospitalized patients? J Am Geriatr Soc. 1986;34(8):579–585.
- , , , , , Importance of functional measures in predicting mortality among older hospitalized patients. JAMA. 1998;279(15):1187–1193.
- , Understanding preventable hospital readmissions: masqueraders, markers, and true causal factors. J Hosp Med. 2011;6(2):51–53.
- , , , et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999;340(9):669–676.
- , , , et al. Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: a randomized controlled trial of Acute Care for Elders (ACE) in a community hospital. J Am Geriatr Soc. 2000;48(12):1572–1581.
- , ; American Geriatrics Society Health Care Systems Committee. Improving the quality of transitional care for persons with complex care needs. J Am Geriatr Soc. 2003;51(4):556–557.
- , , , Development and implementation of a proactive geriatrics consultation model in collaboration with hospitalists. J Am Geriatr Soc. 2009;57(11):2139–2145.
- , , , et al. Screening of the risk of functional decline performed by an inpatient geriatric consultation team in a general hospital [in French]. Revue medicale de Bruxelles. 2013;34(6):462–468.
- , , , et al. Systematic detection and multidisciplinary care of delirium in older medical inpatients: a randomized trial. CMAJ. 2002;167(7):753–759.
- , , Potentially inappropriate prescribing for geriatric inpatients: an acute care of the elderly unit compared to a general medicine service. Consult Pharm. 2003;18(1):37–42, 47–39.
- , , , Evaluation of the Mobile Acute Care of the Elderly (MACE) service. JAMA Intern Med. 2013;173(11):990–996.
- , , , , , Effects of an acute care for elders unit on costs and 30‐day readmissions. JAMA Intern Med. 2013;173(11):981–987.
- , , , et al. Impact and recognition of cognitive impairment among hospitalized elders. J Hosp Med. 2010;5(2):69–75.
- , , , et al. Enhancing care for hospitalized older adults with cognitive impairment: a randomized controlled trial. J Gen Intern Med. 2012;27(5):561–567.
- , , , Short Portable Mental Status Questionnaire as a screening test for dementia and delirium among the elderly. J Am Geriatr Soc. 1987;35(5):412–416.
- , , , et al. The Regenstrief Medical Record System: a quarter century experience. Int J Med Inform. 1999;54(3):225–253.
- , , , , , Factors determining the decision to institutionalize dementing individuals: a prospective study. Gerontologist. 1993;33(6):714–720.
- , , , , , Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948.
- , , , , , Resuscitation: how do we decide? A prospective study of physicians' preferences and the clinical course of hospitalized patients. JAMA. 1986;255(10):1316–1322.
- , , , et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100(6):1619–1636.
- , , , et al. Interaction between cognitive impairment and discharge destination and its effect on rehospitalization. J Am Geriatr Soc. 2013;61(11):1958–1963.
- , , , , , Propensity scores in intensive care and anaesthesiology literature: a systematic review. Intensive Care Med. 2010;36(12):1993–2003.
- , , , et al. Improving functional outcomes in older patients: lessons from an acute care for elders unit. Jt Comm J Qual Improv. 1998;24(2):63–76.
- , , , et al. Developing a stroke unit using the acute care for elders intervention and model of care. J Am Geriatr Soc. 2003;51(11):1660–1667.
- , , , A medical unit for the acute care of the elderly. J Am Geriatr Soc. 1994;42(5):545–552.
- , , , , Impact of geriatric consultation teams on clinical outcome in acute hospitals: a systematic review and meta‐analysis. BMC Med. 2013;11:48.
- , , , , Comprehensive geriatric assessment for older adults admitted to hospital: meta‐analysis of randomised controlled trials. BMJ. 2011;343:d6553.
- , , , et al. Prevention of readmission in elderly patients with congestive heart failure: results of a prospective, randomized pilot study. J Gen Intern Med. 1993;8(11):585–590.
- , , , et al. Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial. Ann Intern Med. 2012;157(1):1–10.
- , , , , House calls for seniors: building and sustaining a model of care for homebound seniors. J Am Geriatr Soc. 2009;57(6):1103–1109.
- , , , et al. Geriatric care management for low‐income seniors: a randomized controlled trial. JAMA. 2007;298(22):2623–2633.
- , , , , Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- , The effects of a discharge planning and home follow‐up intervention on elders hospitalized with common medical and surgical cardiac conditions. J Cardiovasc Nurs. 1999;14(1):44–54.
- Readmission to hospital: a measure of quality or outcome? Qual Saf Health Care. 2004;13(1):10–11.
- , , , , , Unintended consequences of steps to cut readmissions and reform payment may threaten care of vulnerable older adults. Health Aff (Millwood). 2012;31(7):1623–1632.
- , , Analyzing the effects of shared decision‐making, empathy and team interaction on patient satisfaction and treatment acceptance in medical rehabilitation using a structural equation modeling approach. Patient Educ Couns. 2013;91(2):167–175.
- , , , The Care Transitions Innovation (C‐TraIn) for Socioeconomically Disadvantaged Adults: results of a cluster randomized controlled trial. J Gen Intern Med. 2014;29(11):1460–1467.
- , , , Risk factors for early hospital readmission in low‐income elderly adults. J Am Geriatr Soc. 2014;62(3):489–494.
- , , , , , Understanding why patients of low socioeconomic status prefer hospitals over ambulatory care. Health Aff (Millwood). 2013;32(7):1196–1203.
- , , , et al. Relationship between hospital readmission and mortality rates for patients hospitalized with acute myocardial infarction, heart failure, or pneumonia. JAMA. 2013;309(6):587–593.
- , , , Cognitive impairment. Can it predict the course of hospitalized patients? J Am Geriatr Soc. 1986;34(8):579–585.
- , , , , , Importance of functional measures in predicting mortality among older hospitalized patients. JAMA. 1998;279(15):1187–1193.
- , Understanding preventable hospital readmissions: masqueraders, markers, and true causal factors. J Hosp Med. 2011;6(2):51–53.
- , , , et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999;340(9):669–676.
- , , , et al. Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: a randomized controlled trial of Acute Care for Elders (ACE) in a community hospital. J Am Geriatr Soc. 2000;48(12):1572–1581.
- , ; American Geriatrics Society Health Care Systems Committee. Improving the quality of transitional care for persons with complex care needs. J Am Geriatr Soc. 2003;51(4):556–557.
- , , , Development and implementation of a proactive geriatrics consultation model in collaboration with hospitalists. J Am Geriatr Soc. 2009;57(11):2139–2145.
- , , , et al. Screening of the risk of functional decline performed by an inpatient geriatric consultation team in a general hospital [in French]. Revue medicale de Bruxelles. 2013;34(6):462–468.
- , , , et al. Systematic detection and multidisciplinary care of delirium in older medical inpatients: a randomized trial. CMAJ. 2002;167(7):753–759.
- , , Potentially inappropriate prescribing for geriatric inpatients: an acute care of the elderly unit compared to a general medicine service. Consult Pharm. 2003;18(1):37–42, 47–39.
- , , , Evaluation of the Mobile Acute Care of the Elderly (MACE) service. JAMA Intern Med. 2013;173(11):990–996.
- , , , , , Effects of an acute care for elders unit on costs and 30‐day readmissions. JAMA Intern Med. 2013;173(11):981–987.
- , , , et al. Impact and recognition of cognitive impairment among hospitalized elders. J Hosp Med. 2010;5(2):69–75.
- , , , et al. Enhancing care for hospitalized older adults with cognitive impairment: a randomized controlled trial. J Gen Intern Med. 2012;27(5):561–567.
- , , , Short Portable Mental Status Questionnaire as a screening test for dementia and delirium among the elderly. J Am Geriatr Soc. 1987;35(5):412–416.
- , , , et al. The Regenstrief Medical Record System: a quarter century experience. Int J Med Inform. 1999;54(3):225–253.
- , , , , , Factors determining the decision to institutionalize dementing individuals: a prospective study. Gerontologist. 1993;33(6):714–720.
- , , , , , Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948.
- , , , , , Resuscitation: how do we decide? A prospective study of physicians' preferences and the clinical course of hospitalized patients. JAMA. 1986;255(10):1316–1322.
- , , , et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100(6):1619–1636.
- , , , et al. Interaction between cognitive impairment and discharge destination and its effect on rehospitalization. J Am Geriatr Soc. 2013;61(11):1958–1963.
- , , , , , Propensity scores in intensive care and anaesthesiology literature: a systematic review. Intensive Care Med. 2010;36(12):1993–2003.
- , , , et al. Improving functional outcomes in older patients: lessons from an acute care for elders unit. Jt Comm J Qual Improv. 1998;24(2):63–76.
- , , , et al. Developing a stroke unit using the acute care for elders intervention and model of care. J Am Geriatr Soc. 2003;51(11):1660–1667.
- , , , A medical unit for the acute care of the elderly. J Am Geriatr Soc. 1994;42(5):545–552.
- , , , , Impact of geriatric consultation teams on clinical outcome in acute hospitals: a systematic review and meta‐analysis. BMC Med. 2013;11:48.
- , , , , Comprehensive geriatric assessment for older adults admitted to hospital: meta‐analysis of randomised controlled trials. BMJ. 2011;343:d6553.
- , , , et al. Prevention of readmission in elderly patients with congestive heart failure: results of a prospective, randomized pilot study. J Gen Intern Med. 1993;8(11):585–590.
- , , , et al. Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial. Ann Intern Med. 2012;157(1):1–10.
- , , , , House calls for seniors: building and sustaining a model of care for homebound seniors. J Am Geriatr Soc. 2009;57(6):1103–1109.
- , , , et al. Geriatric care management for low‐income seniors: a randomized controlled trial. JAMA. 2007;298(22):2623–2633.
- , , , , Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- , The effects of a discharge planning and home follow‐up intervention on elders hospitalized with common medical and surgical cardiac conditions. J Cardiovasc Nurs. 1999;14(1):44–54.
- Readmission to hospital: a measure of quality or outcome? Qual Saf Health Care. 2004;13(1):10–11.
- , , , , , Unintended consequences of steps to cut readmissions and reform payment may threaten care of vulnerable older adults. Health Aff (Millwood). 2012;31(7):1623–1632.
- , , Analyzing the effects of shared decision‐making, empathy and team interaction on patient satisfaction and treatment acceptance in medical rehabilitation using a structural equation modeling approach. Patient Educ Couns. 2013;91(2):167–175.
- , , , The Care Transitions Innovation (C‐TraIn) for Socioeconomically Disadvantaged Adults: results of a cluster randomized controlled trial. J Gen Intern Med. 2014;29(11):1460–1467.
- , , , Risk factors for early hospital readmission in low‐income elderly adults. J Am Geriatr Soc. 2014;62(3):489–494.
- , , , , , Understanding why patients of low socioeconomic status prefer hospitals over ambulatory care. Health Aff (Millwood). 2013;32(7):1196–1203.
© 2015 Society of Hospital Medicine
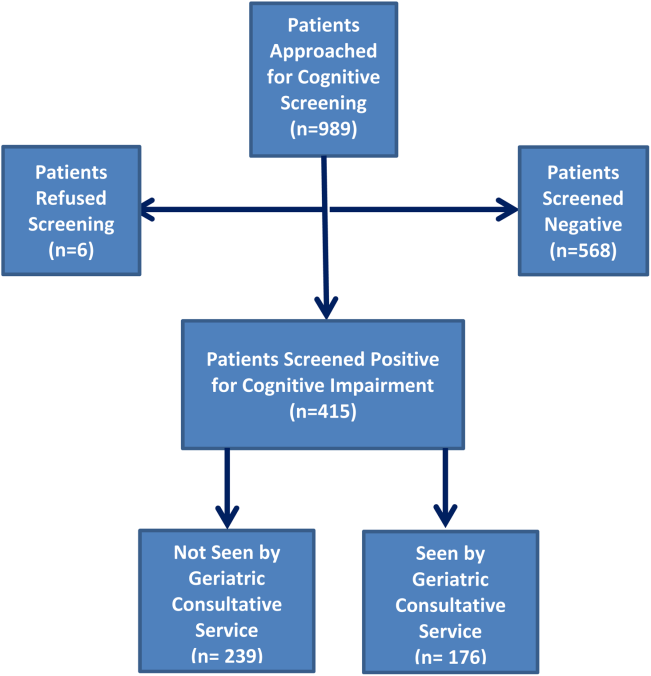
Making a diagnostic checklist more useful
I read with interest Dr. Hickner’s editorial, “How to avoid diagnostic errors” (J Fam Pract. 2014;63:625), and was fascinated by the diagnostic checklists developed by John Ely, MD, which are available at www.improvediagnosis.org/resource/resmgr/docs/diffdx.doc.
On his checklists, Dr. Ely suggests the material could be adapted for use on a handheld device, so I decided to convert Dr. Ely’s checklists from Microsoft Word to a PDF with hyperlinks so they would be easy to view on most tablets and smartphones. I kept the content exactly the same, but formatted each diagnostic problem as a “header,” which became the table of contents. Each of these table of contents headers is hyperlinked, so a user can simply tap on the item in the table of contents and jump to the correct page (“card”) in the document.
After converting Dr. Ely’s checklists to a PDF, I found them easy to use on both an iPhone and Google tablet.
Thank you again, Drs. Ely and Hickner, for your work in this area.
E. Chris Vincent, MD
Seattle, Wash
Dr. Vincent is one of the assistant editors for Clinical Inquiries, a monthly column in The Journal of Family Practice.
Dr. Hickner’s list of 7 ways to avoid diagnostic errors was excellent. I would augment his sixth tip (“Follow up, follow up, follow up, and do so in a timely manner”) with something we tell all of our patients: “Keep me informed via our online portal.” When patients have such easy access to communication with their physician, the diagnostic process is greatly enhanced.
Joseph E. Scherger, MD, MPH
Rancho Mirage, Calif
I read with interest Dr. Hickner’s editorial, “How to avoid diagnostic errors” (J Fam Pract. 2014;63:625), and was fascinated by the diagnostic checklists developed by John Ely, MD, which are available at www.improvediagnosis.org/resource/resmgr/docs/diffdx.doc.
On his checklists, Dr. Ely suggests the material could be adapted for use on a handheld device, so I decided to convert Dr. Ely’s checklists from Microsoft Word to a PDF with hyperlinks so they would be easy to view on most tablets and smartphones. I kept the content exactly the same, but formatted each diagnostic problem as a “header,” which became the table of contents. Each of these table of contents headers is hyperlinked, so a user can simply tap on the item in the table of contents and jump to the correct page (“card”) in the document.
After converting Dr. Ely’s checklists to a PDF, I found them easy to use on both an iPhone and Google tablet.
Thank you again, Drs. Ely and Hickner, for your work in this area.
E. Chris Vincent, MD
Seattle, Wash
Dr. Vincent is one of the assistant editors for Clinical Inquiries, a monthly column in The Journal of Family Practice.
Dr. Hickner’s list of 7 ways to avoid diagnostic errors was excellent. I would augment his sixth tip (“Follow up, follow up, follow up, and do so in a timely manner”) with something we tell all of our patients: “Keep me informed via our online portal.” When patients have such easy access to communication with their physician, the diagnostic process is greatly enhanced.
Joseph E. Scherger, MD, MPH
Rancho Mirage, Calif
I read with interest Dr. Hickner’s editorial, “How to avoid diagnostic errors” (J Fam Pract. 2014;63:625), and was fascinated by the diagnostic checklists developed by John Ely, MD, which are available at www.improvediagnosis.org/resource/resmgr/docs/diffdx.doc.
On his checklists, Dr. Ely suggests the material could be adapted for use on a handheld device, so I decided to convert Dr. Ely’s checklists from Microsoft Word to a PDF with hyperlinks so they would be easy to view on most tablets and smartphones. I kept the content exactly the same, but formatted each diagnostic problem as a “header,” which became the table of contents. Each of these table of contents headers is hyperlinked, so a user can simply tap on the item in the table of contents and jump to the correct page (“card”) in the document.
After converting Dr. Ely’s checklists to a PDF, I found them easy to use on both an iPhone and Google tablet.
Thank you again, Drs. Ely and Hickner, for your work in this area.
E. Chris Vincent, MD
Seattle, Wash
Dr. Vincent is one of the assistant editors for Clinical Inquiries, a monthly column in The Journal of Family Practice.
Dr. Hickner’s list of 7 ways to avoid diagnostic errors was excellent. I would augment his sixth tip (“Follow up, follow up, follow up, and do so in a timely manner”) with something we tell all of our patients: “Keep me informed via our online portal.” When patients have such easy access to communication with their physician, the diagnostic process is greatly enhanced.
Joseph E. Scherger, MD, MPH
Rancho Mirage, Calif
Skip this step when checking lipid levels
Stop requiring your patients to fast before undergoing lipid testing. Nonfasting total cholesterol (TC), high-density lipoprotein cholesterol (HDL), and low-density lipoprotein cholesterol (LDL) levels are equally predictive of cardiovascular mortality and all-cause mortality.1
Strength of recommendation
B: Based on a large, cross-sectional cohort study of adults followed for a mean of 14 years with patient-oriented outcomes.
Doran B, Guo Y, Xu J, et al. Prognostic value of fasting versus nonfasting low-density lipoprotein cholesterol levels on long-term mortality: insight from the National Health and Nutrition Examination Survey III (NHANES-III). Circulation. 2014;130:546-553.
Illustrative case
A 57-year-old man with diabetes refuses to fast before coming to the clinic for lipid testing because he’s afraid he’ll become hypoglycemic. You have not been able to obtain a lipid panel on him for more than a year and you want to determine his LDL level. Will a nonfasting lipid panel be useful?
Approximately 71 million US adults have high LDL.2 The 2013 American College of Cardiology/American Heart Association guidelines recommend fasting cholesterol checks for all adults ages 21 and older for primary prevention of cardiovascular disease.3 The US Preventive Services Task Force (USPSTF) has long recommended screening cholesterol in adults to prevent atherosclerotic vascular disease.
In 2008, the USPSTF recommended lipid screening for all men ages 35 years and older, for all men ages 20 to 35 years who are at increased risk for coronary heart disease, and for all women ages 20 years and older who are at increased risk for coronary heart disease.4 The USPSTF recommends TC and HDL as the preferred screening tests and states that these tests can be performed on fasting or nonfasting samples, but if LDL is added, a fasting sample is recommended.4 Other national and international guidelines on cholesterol management also recommend a fasting lipid panel to stratify patients’ risk and determine treatment options.5-7
LDL usually is reported as a calculated value using the Friedewald equation (LDL equals TC minus HDL minus [triglycerides divided by 5]).8 This calculation is not accurate for patients with triglyceride levels >400 mg/dL, which has prompted most authorities to recommend a fasting sample. That’s because while TC and HDL are not affected by food (and LDL may vary by only 10% or less), triglycerides can fluctuate by 20% to 30%, which would influence the calculation of a nonfasting LDL.9,10 LDL can be measured directly, but the process is generally expensive and not commonly used.11
The Centers for Disease Control and Prevention (CDC) estimates that over 20% of US adults (more than 48 million people) have not had a screening lipid panel in the previous 5 years.12 One barrier to screening is that both physicians and patients often believe that a fasting specimen is required. Yet fasting specimens are difficult to obtain because they often require a separate visit to the clinic, which can result in lost time from work and additional transportation costs.
STUDY SUMMARY: There’s no difference between fasting and nonfasting LDL
Doran et al1 used data from the NHANES-III survey to compare the prognostic value of fasting vs nonfasting LDL for all-cause mortality and cardiovascular mortality. NHANES-III is a nationally representative cross-sectional survey that was performed from 1988 to 1994.13 Doran et al1 included 16,161 US adults ages 18 years and older for whom data on fasting time were available. Participants for whom LDL calculations were not possible due to missing HDL, TC, or triglyceride levels were excluded. Those with triglycerides ≥400 mg/dL were excluded from the primary analysis.
Participants were stratified based on fasting status (≥8 hours or <8 hours) and followed for a mean of 14 (± .22) years. To control for possible cofounders, researchers used propensity score matching to identify 4299 pairs of fasting and nonfasting individuals with similar cardiovascular risk factors, including race, smoking history, prior cardiovascular disease, cholesterol medication use, diabetes, elevated TC, low HDL, hypertension, enlarged waist circumference, and low socioeconomic status. After matching, the baseline characteristics of the fasting and nonfasting groups were similar.
The primary outcome was all-cause mortality, and the secondary outcome was cardiovascular mortality. The prognostic value of fasting and nonfasting LDL for these outcomes was evaluated as the area under the receiver operator curve (ROC) using the Hosmer-Lemeshow C-statistic.14 (In this case, similar C-statistics indicate that the tests have similar prognostic values.*) Kaplan-Meier curves were used to assess survival. The association of LDL with mortality, after adjustment of potential confounders, was evaluated using Cox proportional hazard models. The groups were divided into tertiles based on LDL levels (<100 mg/dL, 100-130 mg/dL, and >130 mg/dL).
As expected, compared to individuals in the first LDL tertile (<100 mg/dL), those with a higher LDL had an increased risk of all-cause mortality (hazard ratio [HR]=1.61; 95% confidence interval [CI], 1.25-2.08 [second tertile] and HR=2.10; 95% CI, 1.70-2.61 [third tertile]). The prognostic value of fasting vs nonfasting status for predicting all-cause mortality was similar, as suggested by the C-statistics (0.59 [95% CI, 0.56-0.61] vs 0.58 [95% CI, 0.56-0.60]; P=.73).
The risk of cardiovascular mortality also increased with increasing LDL tertiles. As was the case with all-cause mortality, the prognostic value of fasting vs nonfasting status was similar for predicting cardiovascular mortality as observed by similar C-statistics (0.64 [95% CI, 0.62-0.66] vs 0.63 [95% CI, 0.60-0.65]; P=.49). In addition, fasting vs nonfasting C-statistics were similar for both diabetic and non-diabetic patients.
WHAT’S NEW: Results suggest fasting may no longer be necessary
While obtaining a fasting lipid panel is recommended by multiple guidelines and has become traditional practice, the need for fasting originated primarily out of concern for the effect of postprandial triglycerides on calculating LDL. This is the first study that compared the prognostic value of fasting and nonfasting LDL values for predicting mortality; it demonstrated that they are essentially the same.
CAVEATS: Fasting and nonfasting measurements were taken from different patients
The fasting and nonfasting lipids were not collected from the same individuals. However, to decrease confounding, Doran et al1 factored in multiple cardiovascular risk factors as covariables.
Another caveat is that individuals with triglyceride levels >400 mg/dL were excluded. However, investigators ran a sensitivity analysis that included individuals with triglycerides >400 mg/dL and found no significant difference in C-statistics between the fasting and nonfasting groups.
CHALLENGES TO IMPLEMENTATION: Dropping the requirement to fast goes against established practice
It may be difficult for physicians to change a longstanding practice of checking fasting lipid profiles, but we see no other barriers to adopting this recommendation.
* The C-statistic is the probability that predicting the outcome is better than chance and is used to compare the goodness of fit of logistic regression models. Values for this measure range from 0.5 to 1.0. A value of 0.5 indicates that the model is no better than chance at making a prediction of membership in a group and a value of 1.0 indicates that the model perfectly identifies those within a group and those not.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Doran B, Guo Y, Xu J, et al. Prognostic value of fasting versus nonfasting low-density lipoprotein cholesterol levels on long-term mortality: insight from the National Health and Nutrition Examination Survey III (NHANES-III). Circulation. 2014;130:546-553.
2. Centers for Disease Control and Prevention (CDC). Vital signs: prevalence, treatment, and control of high levels of low-density lipoprotein cholesterol—United States, 1999-2002 and 2005-2008. MMWR Morb Mortal Wkly Rep. 2011;60:109-114.
3. Stone NJ, Robinson JG, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.
4. US Preventive Services Task Force. Final recommendation statement: Lipid disorders in adults (cholesterol, dyslipidemia): Screening. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/Page/Document/ClinicalSummaryFinal/lipid-disorders-in-adults-cholesterol-dyslipidemia-screening. Accessed January 20, 2015.
5. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143-3421.
6. De Backer G, Ambrosioni E, Borch-Johnsen K, et al; European Society of Cardiology, American Heart Association. American College of Cardiology. European guidelines on cardiovascular disease prevention in clinical practice. Third Joint Task Force of European and other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of eight societies and by invited experts). Atherosclerosis. 2004;173:381-391.
7. Genest J, McPherson R, Frohlich J, et al. 2009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult - 2009 recommendations. Can J Cardiol. 2009;25:567-579.
8. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;8:499-502.
9. Sidhu D, Naugler C. Fasting time and lipid levels in a community-based population: a cross-sectional study. Arch Intern Med. 2012;172:1707-1710.
10. Langsted A, Nordestgaard BG. Nonfasting lipids, lipoproteins, and apolipoproteins in individuals with and without diabetes: 58,434 individuals from the Copenhagen General Population Study. Clin Chem. 2001;57:482-489.
11. Mora S, Rifai N, Buring JE, et al. Comparison of LDL cholesterol concentrations by Friedewald calculation and direct measurement in relation to cardiovascular events in 27,331 women. Clin Chem. 2009;55:888-894.
12. Gillespie CD, Keenan NL, Miner JB, et al; Centers for Disease Control and Prevention (CDC). Screening for lipid disorders among adults—National Health and Nutrition Examination Survey, United States, 2005-2008. MMWR Morb Mortal Wkly Rep. 2012;61 suppl:26-31.
13. Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/nchs/nhanes/nh3data.htm. Accessed October 13, 2014.
14. Hosmer DW, Lemeshow S. Applied Logistic Regression. 2nd ed. New York, NY: John Wiley & Sons; 2000.
Stop requiring your patients to fast before undergoing lipid testing. Nonfasting total cholesterol (TC), high-density lipoprotein cholesterol (HDL), and low-density lipoprotein cholesterol (LDL) levels are equally predictive of cardiovascular mortality and all-cause mortality.1
Strength of recommendation
B: Based on a large, cross-sectional cohort study of adults followed for a mean of 14 years with patient-oriented outcomes.
Doran B, Guo Y, Xu J, et al. Prognostic value of fasting versus nonfasting low-density lipoprotein cholesterol levels on long-term mortality: insight from the National Health and Nutrition Examination Survey III (NHANES-III). Circulation. 2014;130:546-553.
Illustrative case
A 57-year-old man with diabetes refuses to fast before coming to the clinic for lipid testing because he’s afraid he’ll become hypoglycemic. You have not been able to obtain a lipid panel on him for more than a year and you want to determine his LDL level. Will a nonfasting lipid panel be useful?
Approximately 71 million US adults have high LDL.2 The 2013 American College of Cardiology/American Heart Association guidelines recommend fasting cholesterol checks for all adults ages 21 and older for primary prevention of cardiovascular disease.3 The US Preventive Services Task Force (USPSTF) has long recommended screening cholesterol in adults to prevent atherosclerotic vascular disease.
In 2008, the USPSTF recommended lipid screening for all men ages 35 years and older, for all men ages 20 to 35 years who are at increased risk for coronary heart disease, and for all women ages 20 years and older who are at increased risk for coronary heart disease.4 The USPSTF recommends TC and HDL as the preferred screening tests and states that these tests can be performed on fasting or nonfasting samples, but if LDL is added, a fasting sample is recommended.4 Other national and international guidelines on cholesterol management also recommend a fasting lipid panel to stratify patients’ risk and determine treatment options.5-7
LDL usually is reported as a calculated value using the Friedewald equation (LDL equals TC minus HDL minus [triglycerides divided by 5]).8 This calculation is not accurate for patients with triglyceride levels >400 mg/dL, which has prompted most authorities to recommend a fasting sample. That’s because while TC and HDL are not affected by food (and LDL may vary by only 10% or less), triglycerides can fluctuate by 20% to 30%, which would influence the calculation of a nonfasting LDL.9,10 LDL can be measured directly, but the process is generally expensive and not commonly used.11
The Centers for Disease Control and Prevention (CDC) estimates that over 20% of US adults (more than 48 million people) have not had a screening lipid panel in the previous 5 years.12 One barrier to screening is that both physicians and patients often believe that a fasting specimen is required. Yet fasting specimens are difficult to obtain because they often require a separate visit to the clinic, which can result in lost time from work and additional transportation costs.
STUDY SUMMARY: There’s no difference between fasting and nonfasting LDL
Doran et al1 used data from the NHANES-III survey to compare the prognostic value of fasting vs nonfasting LDL for all-cause mortality and cardiovascular mortality. NHANES-III is a nationally representative cross-sectional survey that was performed from 1988 to 1994.13 Doran et al1 included 16,161 US adults ages 18 years and older for whom data on fasting time were available. Participants for whom LDL calculations were not possible due to missing HDL, TC, or triglyceride levels were excluded. Those with triglycerides ≥400 mg/dL were excluded from the primary analysis.
Participants were stratified based on fasting status (≥8 hours or <8 hours) and followed for a mean of 14 (± .22) years. To control for possible cofounders, researchers used propensity score matching to identify 4299 pairs of fasting and nonfasting individuals with similar cardiovascular risk factors, including race, smoking history, prior cardiovascular disease, cholesterol medication use, diabetes, elevated TC, low HDL, hypertension, enlarged waist circumference, and low socioeconomic status. After matching, the baseline characteristics of the fasting and nonfasting groups were similar.
The primary outcome was all-cause mortality, and the secondary outcome was cardiovascular mortality. The prognostic value of fasting and nonfasting LDL for these outcomes was evaluated as the area under the receiver operator curve (ROC) using the Hosmer-Lemeshow C-statistic.14 (In this case, similar C-statistics indicate that the tests have similar prognostic values.*) Kaplan-Meier curves were used to assess survival. The association of LDL with mortality, after adjustment of potential confounders, was evaluated using Cox proportional hazard models. The groups were divided into tertiles based on LDL levels (<100 mg/dL, 100-130 mg/dL, and >130 mg/dL).
As expected, compared to individuals in the first LDL tertile (<100 mg/dL), those with a higher LDL had an increased risk of all-cause mortality (hazard ratio [HR]=1.61; 95% confidence interval [CI], 1.25-2.08 [second tertile] and HR=2.10; 95% CI, 1.70-2.61 [third tertile]). The prognostic value of fasting vs nonfasting status for predicting all-cause mortality was similar, as suggested by the C-statistics (0.59 [95% CI, 0.56-0.61] vs 0.58 [95% CI, 0.56-0.60]; P=.73).
The risk of cardiovascular mortality also increased with increasing LDL tertiles. As was the case with all-cause mortality, the prognostic value of fasting vs nonfasting status was similar for predicting cardiovascular mortality as observed by similar C-statistics (0.64 [95% CI, 0.62-0.66] vs 0.63 [95% CI, 0.60-0.65]; P=.49). In addition, fasting vs nonfasting C-statistics were similar for both diabetic and non-diabetic patients.
WHAT’S NEW: Results suggest fasting may no longer be necessary
While obtaining a fasting lipid panel is recommended by multiple guidelines and has become traditional practice, the need for fasting originated primarily out of concern for the effect of postprandial triglycerides on calculating LDL. This is the first study that compared the prognostic value of fasting and nonfasting LDL values for predicting mortality; it demonstrated that they are essentially the same.
CAVEATS: Fasting and nonfasting measurements were taken from different patients
The fasting and nonfasting lipids were not collected from the same individuals. However, to decrease confounding, Doran et al1 factored in multiple cardiovascular risk factors as covariables.
Another caveat is that individuals with triglyceride levels >400 mg/dL were excluded. However, investigators ran a sensitivity analysis that included individuals with triglycerides >400 mg/dL and found no significant difference in C-statistics between the fasting and nonfasting groups.
CHALLENGES TO IMPLEMENTATION: Dropping the requirement to fast goes against established practice
It may be difficult for physicians to change a longstanding practice of checking fasting lipid profiles, but we see no other barriers to adopting this recommendation.
* The C-statistic is the probability that predicting the outcome is better than chance and is used to compare the goodness of fit of logistic regression models. Values for this measure range from 0.5 to 1.0. A value of 0.5 indicates that the model is no better than chance at making a prediction of membership in a group and a value of 1.0 indicates that the model perfectly identifies those within a group and those not.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Stop requiring your patients to fast before undergoing lipid testing. Nonfasting total cholesterol (TC), high-density lipoprotein cholesterol (HDL), and low-density lipoprotein cholesterol (LDL) levels are equally predictive of cardiovascular mortality and all-cause mortality.1
Strength of recommendation
B: Based on a large, cross-sectional cohort study of adults followed for a mean of 14 years with patient-oriented outcomes.
Doran B, Guo Y, Xu J, et al. Prognostic value of fasting versus nonfasting low-density lipoprotein cholesterol levels on long-term mortality: insight from the National Health and Nutrition Examination Survey III (NHANES-III). Circulation. 2014;130:546-553.
Illustrative case
A 57-year-old man with diabetes refuses to fast before coming to the clinic for lipid testing because he’s afraid he’ll become hypoglycemic. You have not been able to obtain a lipid panel on him for more than a year and you want to determine his LDL level. Will a nonfasting lipid panel be useful?
Approximately 71 million US adults have high LDL.2 The 2013 American College of Cardiology/American Heart Association guidelines recommend fasting cholesterol checks for all adults ages 21 and older for primary prevention of cardiovascular disease.3 The US Preventive Services Task Force (USPSTF) has long recommended screening cholesterol in adults to prevent atherosclerotic vascular disease.
In 2008, the USPSTF recommended lipid screening for all men ages 35 years and older, for all men ages 20 to 35 years who are at increased risk for coronary heart disease, and for all women ages 20 years and older who are at increased risk for coronary heart disease.4 The USPSTF recommends TC and HDL as the preferred screening tests and states that these tests can be performed on fasting or nonfasting samples, but if LDL is added, a fasting sample is recommended.4 Other national and international guidelines on cholesterol management also recommend a fasting lipid panel to stratify patients’ risk and determine treatment options.5-7
LDL usually is reported as a calculated value using the Friedewald equation (LDL equals TC minus HDL minus [triglycerides divided by 5]).8 This calculation is not accurate for patients with triglyceride levels >400 mg/dL, which has prompted most authorities to recommend a fasting sample. That’s because while TC and HDL are not affected by food (and LDL may vary by only 10% or less), triglycerides can fluctuate by 20% to 30%, which would influence the calculation of a nonfasting LDL.9,10 LDL can be measured directly, but the process is generally expensive and not commonly used.11
The Centers for Disease Control and Prevention (CDC) estimates that over 20% of US adults (more than 48 million people) have not had a screening lipid panel in the previous 5 years.12 One barrier to screening is that both physicians and patients often believe that a fasting specimen is required. Yet fasting specimens are difficult to obtain because they often require a separate visit to the clinic, which can result in lost time from work and additional transportation costs.
STUDY SUMMARY: There’s no difference between fasting and nonfasting LDL
Doran et al1 used data from the NHANES-III survey to compare the prognostic value of fasting vs nonfasting LDL for all-cause mortality and cardiovascular mortality. NHANES-III is a nationally representative cross-sectional survey that was performed from 1988 to 1994.13 Doran et al1 included 16,161 US adults ages 18 years and older for whom data on fasting time were available. Participants for whom LDL calculations were not possible due to missing HDL, TC, or triglyceride levels were excluded. Those with triglycerides ≥400 mg/dL were excluded from the primary analysis.
Participants were stratified based on fasting status (≥8 hours or <8 hours) and followed for a mean of 14 (± .22) years. To control for possible cofounders, researchers used propensity score matching to identify 4299 pairs of fasting and nonfasting individuals with similar cardiovascular risk factors, including race, smoking history, prior cardiovascular disease, cholesterol medication use, diabetes, elevated TC, low HDL, hypertension, enlarged waist circumference, and low socioeconomic status. After matching, the baseline characteristics of the fasting and nonfasting groups were similar.
The primary outcome was all-cause mortality, and the secondary outcome was cardiovascular mortality. The prognostic value of fasting and nonfasting LDL for these outcomes was evaluated as the area under the receiver operator curve (ROC) using the Hosmer-Lemeshow C-statistic.14 (In this case, similar C-statistics indicate that the tests have similar prognostic values.*) Kaplan-Meier curves were used to assess survival. The association of LDL with mortality, after adjustment of potential confounders, was evaluated using Cox proportional hazard models. The groups were divided into tertiles based on LDL levels (<100 mg/dL, 100-130 mg/dL, and >130 mg/dL).
As expected, compared to individuals in the first LDL tertile (<100 mg/dL), those with a higher LDL had an increased risk of all-cause mortality (hazard ratio [HR]=1.61; 95% confidence interval [CI], 1.25-2.08 [second tertile] and HR=2.10; 95% CI, 1.70-2.61 [third tertile]). The prognostic value of fasting vs nonfasting status for predicting all-cause mortality was similar, as suggested by the C-statistics (0.59 [95% CI, 0.56-0.61] vs 0.58 [95% CI, 0.56-0.60]; P=.73).
The risk of cardiovascular mortality also increased with increasing LDL tertiles. As was the case with all-cause mortality, the prognostic value of fasting vs nonfasting status was similar for predicting cardiovascular mortality as observed by similar C-statistics (0.64 [95% CI, 0.62-0.66] vs 0.63 [95% CI, 0.60-0.65]; P=.49). In addition, fasting vs nonfasting C-statistics were similar for both diabetic and non-diabetic patients.
WHAT’S NEW: Results suggest fasting may no longer be necessary
While obtaining a fasting lipid panel is recommended by multiple guidelines and has become traditional practice, the need for fasting originated primarily out of concern for the effect of postprandial triglycerides on calculating LDL. This is the first study that compared the prognostic value of fasting and nonfasting LDL values for predicting mortality; it demonstrated that they are essentially the same.
CAVEATS: Fasting and nonfasting measurements were taken from different patients
The fasting and nonfasting lipids were not collected from the same individuals. However, to decrease confounding, Doran et al1 factored in multiple cardiovascular risk factors as covariables.
Another caveat is that individuals with triglyceride levels >400 mg/dL were excluded. However, investigators ran a sensitivity analysis that included individuals with triglycerides >400 mg/dL and found no significant difference in C-statistics between the fasting and nonfasting groups.
CHALLENGES TO IMPLEMENTATION: Dropping the requirement to fast goes against established practice
It may be difficult for physicians to change a longstanding practice of checking fasting lipid profiles, but we see no other barriers to adopting this recommendation.
* The C-statistic is the probability that predicting the outcome is better than chance and is used to compare the goodness of fit of logistic regression models. Values for this measure range from 0.5 to 1.0. A value of 0.5 indicates that the model is no better than chance at making a prediction of membership in a group and a value of 1.0 indicates that the model perfectly identifies those within a group and those not.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Doran B, Guo Y, Xu J, et al. Prognostic value of fasting versus nonfasting low-density lipoprotein cholesterol levels on long-term mortality: insight from the National Health and Nutrition Examination Survey III (NHANES-III). Circulation. 2014;130:546-553.
2. Centers for Disease Control and Prevention (CDC). Vital signs: prevalence, treatment, and control of high levels of low-density lipoprotein cholesterol—United States, 1999-2002 and 2005-2008. MMWR Morb Mortal Wkly Rep. 2011;60:109-114.
3. Stone NJ, Robinson JG, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.
4. US Preventive Services Task Force. Final recommendation statement: Lipid disorders in adults (cholesterol, dyslipidemia): Screening. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/Page/Document/ClinicalSummaryFinal/lipid-disorders-in-adults-cholesterol-dyslipidemia-screening. Accessed January 20, 2015.
5. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143-3421.
6. De Backer G, Ambrosioni E, Borch-Johnsen K, et al; European Society of Cardiology, American Heart Association. American College of Cardiology. European guidelines on cardiovascular disease prevention in clinical practice. Third Joint Task Force of European and other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of eight societies and by invited experts). Atherosclerosis. 2004;173:381-391.
7. Genest J, McPherson R, Frohlich J, et al. 2009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult - 2009 recommendations. Can J Cardiol. 2009;25:567-579.
8. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;8:499-502.
9. Sidhu D, Naugler C. Fasting time and lipid levels in a community-based population: a cross-sectional study. Arch Intern Med. 2012;172:1707-1710.
10. Langsted A, Nordestgaard BG. Nonfasting lipids, lipoproteins, and apolipoproteins in individuals with and without diabetes: 58,434 individuals from the Copenhagen General Population Study. Clin Chem. 2001;57:482-489.
11. Mora S, Rifai N, Buring JE, et al. Comparison of LDL cholesterol concentrations by Friedewald calculation and direct measurement in relation to cardiovascular events in 27,331 women. Clin Chem. 2009;55:888-894.
12. Gillespie CD, Keenan NL, Miner JB, et al; Centers for Disease Control and Prevention (CDC). Screening for lipid disorders among adults—National Health and Nutrition Examination Survey, United States, 2005-2008. MMWR Morb Mortal Wkly Rep. 2012;61 suppl:26-31.
13. Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/nchs/nhanes/nh3data.htm. Accessed October 13, 2014.
14. Hosmer DW, Lemeshow S. Applied Logistic Regression. 2nd ed. New York, NY: John Wiley & Sons; 2000.
1. Doran B, Guo Y, Xu J, et al. Prognostic value of fasting versus nonfasting low-density lipoprotein cholesterol levels on long-term mortality: insight from the National Health and Nutrition Examination Survey III (NHANES-III). Circulation. 2014;130:546-553.
2. Centers for Disease Control and Prevention (CDC). Vital signs: prevalence, treatment, and control of high levels of low-density lipoprotein cholesterol—United States, 1999-2002 and 2005-2008. MMWR Morb Mortal Wkly Rep. 2011;60:109-114.
3. Stone NJ, Robinson JG, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.
4. US Preventive Services Task Force. Final recommendation statement: Lipid disorders in adults (cholesterol, dyslipidemia): Screening. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/Page/Document/ClinicalSummaryFinal/lipid-disorders-in-adults-cholesterol-dyslipidemia-screening. Accessed January 20, 2015.
5. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143-3421.
6. De Backer G, Ambrosioni E, Borch-Johnsen K, et al; European Society of Cardiology, American Heart Association. American College of Cardiology. European guidelines on cardiovascular disease prevention in clinical practice. Third Joint Task Force of European and other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of eight societies and by invited experts). Atherosclerosis. 2004;173:381-391.
7. Genest J, McPherson R, Frohlich J, et al. 2009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult - 2009 recommendations. Can J Cardiol. 2009;25:567-579.
8. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;8:499-502.
9. Sidhu D, Naugler C. Fasting time and lipid levels in a community-based population: a cross-sectional study. Arch Intern Med. 2012;172:1707-1710.
10. Langsted A, Nordestgaard BG. Nonfasting lipids, lipoproteins, and apolipoproteins in individuals with and without diabetes: 58,434 individuals from the Copenhagen General Population Study. Clin Chem. 2001;57:482-489.
11. Mora S, Rifai N, Buring JE, et al. Comparison of LDL cholesterol concentrations by Friedewald calculation and direct measurement in relation to cardiovascular events in 27,331 women. Clin Chem. 2009;55:888-894.
12. Gillespie CD, Keenan NL, Miner JB, et al; Centers for Disease Control and Prevention (CDC). Screening for lipid disorders among adults—National Health and Nutrition Examination Survey, United States, 2005-2008. MMWR Morb Mortal Wkly Rep. 2012;61 suppl:26-31.
13. Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/nchs/nhanes/nh3data.htm. Accessed October 13, 2014.
14. Hosmer DW, Lemeshow S. Applied Logistic Regression. 2nd ed. New York, NY: John Wiley & Sons; 2000.
Copyright © 2015 Family Physicians Inquiries Network. All rights reserved.