User login
How lymphoma affects male fertility
for semen quality testing
New research has shown that lymphoma and its treatment can impact a number of sperm characteristics, thereby reducing fertility in males.
Results also indicated that most patients eventually experience semen recovery, but the degree and timing of that recovery may depend on the patient’s diagnosis and treatment.
In this study, recovery was more likely among patients with Hodgkin lymphoma than those with non-Hodgkin lymphoma.
And recovery was both quicker and more likely among patients who did not receive alkylating chemotherapy.
On the other hand, multivariate analyses suggested that only a patient’s pre-treatment total sperm count was related to recovery.
Louis Bujan, MD, PhD, of Université de Toulouse in France, and colleagues reported these results in Fertility and Sterility.
The study included 75 patients—57 with Hodgkin lymphoma and 18 with non-Hodgkin lymphoma. The researchers collected sperm samples before patients began cancer treatment and again at later intervals: 3 months, 6 months, 12 months, and 24 months post-treatment.
The team compared patients’ sperm characteristics to those of a control group consisting of 257 healthy, fertile men.
Results revealed that lymphoma patients had impaired sperm quality even before they began treatment. Compared to fertile controls, patients had higher levels of sperm chromatin alterations and DNA fragmentation, with the only risk factor being their cancer diagnosis.
However, between 3 months and 6 months post-treatment, patients’ levels of sperm DNA fragmentation and chromatin structure damage improved. The damage level decreased relative to a patient’s own pre-treatment level of damage, while still remaining higher than damage levels in the control group.
After treatment, patients’ sperm density, total count, motility, and vitality decreased, with the lowest values seen at the 3- and 6-month marks.
Alkylating chemotherapy was more detrimental to spermatogenesis than non-alkylating drugs. Patients who received alkylating chemotherapy were more likely to cease sperm production entirely or take longer to resume sperm production than patients receiving non-alkylating chemotherapy.
Twelve months after treatment, mean sperm counts recovered to pre-treatment values for patients who had received doxorubicin, bleomycin, vinblastine, and darcarbacine (ABVD) or ABVD and radiotherapy.
But this was not the case for patients who received doxorubicin, cyclophosphamide, vincristine, and prednisone (CHOP) or mechlorethamine, oncovin, procarbazine, and prednisone (MOPP).
At the 24-month mark, 7% of patients remained azoospermic. Kaplan Meir estimates suggested that, after 24 months, most patients would recover normal sperm counts.
Recovery was projected for 92% of patients who received ABVD and radiotherapy, 90% of patients who received ABVD alone, and 61% of CHOP-treated patients. (There was no estimate for MOPP therapy, perhaps due to a low number of patients.)
A patient’s type of lymphoma appeared to impact sperm count recovery as well. Estimates suggested that, after 24 months, 86% of Hodgkin lymphoma patients would experience recovery, compared to 73% of non-Hodgkin lymphoma patients.
“While many men can look forward to their fertility returning after treatment is over, not all will be so fortunate,” said Rebecca Sokol, MD, MPH, President of the American Society for Reproductive Medicine.
“It is imperative that, prior to the initiation of therapy, counseling and sperm preservation be made available to all lymphoma patients and their partners who may want to have children in the future.” ![]()
for semen quality testing
New research has shown that lymphoma and its treatment can impact a number of sperm characteristics, thereby reducing fertility in males.
Results also indicated that most patients eventually experience semen recovery, but the degree and timing of that recovery may depend on the patient’s diagnosis and treatment.
In this study, recovery was more likely among patients with Hodgkin lymphoma than those with non-Hodgkin lymphoma.
And recovery was both quicker and more likely among patients who did not receive alkylating chemotherapy.
On the other hand, multivariate analyses suggested that only a patient’s pre-treatment total sperm count was related to recovery.
Louis Bujan, MD, PhD, of Université de Toulouse in France, and colleagues reported these results in Fertility and Sterility.
The study included 75 patients—57 with Hodgkin lymphoma and 18 with non-Hodgkin lymphoma. The researchers collected sperm samples before patients began cancer treatment and again at later intervals: 3 months, 6 months, 12 months, and 24 months post-treatment.
The team compared patients’ sperm characteristics to those of a control group consisting of 257 healthy, fertile men.
Results revealed that lymphoma patients had impaired sperm quality even before they began treatment. Compared to fertile controls, patients had higher levels of sperm chromatin alterations and DNA fragmentation, with the only risk factor being their cancer diagnosis.
However, between 3 months and 6 months post-treatment, patients’ levels of sperm DNA fragmentation and chromatin structure damage improved. The damage level decreased relative to a patient’s own pre-treatment level of damage, while still remaining higher than damage levels in the control group.
After treatment, patients’ sperm density, total count, motility, and vitality decreased, with the lowest values seen at the 3- and 6-month marks.
Alkylating chemotherapy was more detrimental to spermatogenesis than non-alkylating drugs. Patients who received alkylating chemotherapy were more likely to cease sperm production entirely or take longer to resume sperm production than patients receiving non-alkylating chemotherapy.
Twelve months after treatment, mean sperm counts recovered to pre-treatment values for patients who had received doxorubicin, bleomycin, vinblastine, and darcarbacine (ABVD) or ABVD and radiotherapy.
But this was not the case for patients who received doxorubicin, cyclophosphamide, vincristine, and prednisone (CHOP) or mechlorethamine, oncovin, procarbazine, and prednisone (MOPP).
At the 24-month mark, 7% of patients remained azoospermic. Kaplan Meir estimates suggested that, after 24 months, most patients would recover normal sperm counts.
Recovery was projected for 92% of patients who received ABVD and radiotherapy, 90% of patients who received ABVD alone, and 61% of CHOP-treated patients. (There was no estimate for MOPP therapy, perhaps due to a low number of patients.)
A patient’s type of lymphoma appeared to impact sperm count recovery as well. Estimates suggested that, after 24 months, 86% of Hodgkin lymphoma patients would experience recovery, compared to 73% of non-Hodgkin lymphoma patients.
“While many men can look forward to their fertility returning after treatment is over, not all will be so fortunate,” said Rebecca Sokol, MD, MPH, President of the American Society for Reproductive Medicine.
“It is imperative that, prior to the initiation of therapy, counseling and sperm preservation be made available to all lymphoma patients and their partners who may want to have children in the future.” ![]()
for semen quality testing
New research has shown that lymphoma and its treatment can impact a number of sperm characteristics, thereby reducing fertility in males.
Results also indicated that most patients eventually experience semen recovery, but the degree and timing of that recovery may depend on the patient’s diagnosis and treatment.
In this study, recovery was more likely among patients with Hodgkin lymphoma than those with non-Hodgkin lymphoma.
And recovery was both quicker and more likely among patients who did not receive alkylating chemotherapy.
On the other hand, multivariate analyses suggested that only a patient’s pre-treatment total sperm count was related to recovery.
Louis Bujan, MD, PhD, of Université de Toulouse in France, and colleagues reported these results in Fertility and Sterility.
The study included 75 patients—57 with Hodgkin lymphoma and 18 with non-Hodgkin lymphoma. The researchers collected sperm samples before patients began cancer treatment and again at later intervals: 3 months, 6 months, 12 months, and 24 months post-treatment.
The team compared patients’ sperm characteristics to those of a control group consisting of 257 healthy, fertile men.
Results revealed that lymphoma patients had impaired sperm quality even before they began treatment. Compared to fertile controls, patients had higher levels of sperm chromatin alterations and DNA fragmentation, with the only risk factor being their cancer diagnosis.
However, between 3 months and 6 months post-treatment, patients’ levels of sperm DNA fragmentation and chromatin structure damage improved. The damage level decreased relative to a patient’s own pre-treatment level of damage, while still remaining higher than damage levels in the control group.
After treatment, patients’ sperm density, total count, motility, and vitality decreased, with the lowest values seen at the 3- and 6-month marks.
Alkylating chemotherapy was more detrimental to spermatogenesis than non-alkylating drugs. Patients who received alkylating chemotherapy were more likely to cease sperm production entirely or take longer to resume sperm production than patients receiving non-alkylating chemotherapy.
Twelve months after treatment, mean sperm counts recovered to pre-treatment values for patients who had received doxorubicin, bleomycin, vinblastine, and darcarbacine (ABVD) or ABVD and radiotherapy.
But this was not the case for patients who received doxorubicin, cyclophosphamide, vincristine, and prednisone (CHOP) or mechlorethamine, oncovin, procarbazine, and prednisone (MOPP).
At the 24-month mark, 7% of patients remained azoospermic. Kaplan Meir estimates suggested that, after 24 months, most patients would recover normal sperm counts.
Recovery was projected for 92% of patients who received ABVD and radiotherapy, 90% of patients who received ABVD alone, and 61% of CHOP-treated patients. (There was no estimate for MOPP therapy, perhaps due to a low number of patients.)
A patient’s type of lymphoma appeared to impact sperm count recovery as well. Estimates suggested that, after 24 months, 86% of Hodgkin lymphoma patients would experience recovery, compared to 73% of non-Hodgkin lymphoma patients.
“While many men can look forward to their fertility returning after treatment is over, not all will be so fortunate,” said Rebecca Sokol, MD, MPH, President of the American Society for Reproductive Medicine.
“It is imperative that, prior to the initiation of therapy, counseling and sperm preservation be made available to all lymphoma patients and their partners who may want to have children in the future.” ![]()
Apixaban gets European approval for DVT, PE

Credit: Kevin MacKenzie
The European Commission has approved apixaban (Eliquis) to treat and prevent deep vein thrombosis (DVT) and pulmonary embolism (PE).
The approval applies to all European Union (EU) member states, as well as Iceland and Norway.
Apixaban was already approved in the EU to prevent venous thromboembolism (VTE) in adults who have undergone total hip or knee replacement surgery, and to prevent stroke and systemic embolism in adults with nonvalvular atrial fibrillation.
The new marketing authorization for apixaban follows the positive opinion issued by the European Medicines Agency’s Committee for Medicinal Products for Human Use in June and is supported by results of 2 phase 3 clinical trials, AMPLIFY and AMPLIFY-EXT.
Results of AMPLIFY
The AMPLIFY trial included 5395 patients with confirmed, symptomatic DVT or PE requiring treatment for 6 months. They had a mean age of 56.9 years, and 89.8% of randomized patients had unprovoked VTE.
About half of patients (n=2691) were randomized to receive apixaban at 10 mg twice daily for 7 days, followed by 5 mg twice daily for 6 months.
The other half (n=2704) were randomized to the standard of care, which was enoxaparin at 1 mg/kg twice daily for at least 5 days until INR ≥ 2 and warfarin (target INR range 2.0-3.0) for 6 months.
Apixaban proved noninferior to standard therapy in the combined primary endpoint of adjudicated recurrent symptomatic VTE (nonfatal DVT or PE) or VTE-related death.
This outcome occurred in 2.3% of patients in the apixaban arm and 2.7% of patients in the standard-therapy arm (P<0.0001 for noninferiority).
Apixaban also proved superior to standard therapy with regard to bleeding. The composite endpoint of major bleeding and clinically relevant, nonmajor bleeding occurred in 4.3% of patients in the apixaban arm and 9.7% of patients in the standard-therapy arm (P<0.001).
Results of AMPLIFY-EXT
The AMPLIFY-EXT trial included 2486 patients who had completed 6 to 12 months of anticoagulation treatment for DVT or PE. The mean age was 56.7 years, and 91.7% of randomized patients had unprovoked VTE.
Patients were randomized to receive apixaban at 2.5 mg (n=842), apixaban at 5 mg (n=815), or placebo (n=829).
Both apixaban doses were significantly superior to placebo (P<0.001) with regard to the primary efficacy endpoint, which was recurrent VTE or all-cause death.
During the 12-month active study period, these events occurred in 3.8% of patients in the 2.5-mg arm, 4.2% of patients in the 5-mg arm, and 11.6% of patients in the placebo arm.
The primary safety endpoint was the incidence of major bleeding, and there was no significant difference among the treatment arms. Major bleeding occurred in 0.2% of patients in the 2.5-mg arm, 0.1% of patients in the 5-mg arm, and 0.5% of patients in the placebo arm.
About apixaban
Apixaban is approved to reduce the risk of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation in the US, EU, Japan, and a number of other countries around the world.
The drug is approved to prevent VTE in adult patients who have undergone elective hip or knee replacement surgery in the US, EU, and a number of other countries.
And now, apixaban is approved for the treatment of DVT/PE and the prevention of recurrent DVT/PE in the EU. The drug is not approved for this indication in the US.
Apixaban is under joint development by Pfizer and Bristol-Myers Squibb. ![]()
Credit: Kevin MacKenzie
The European Commission has approved apixaban (Eliquis) to treat and prevent deep vein thrombosis (DVT) and pulmonary embolism (PE).
The approval applies to all European Union (EU) member states, as well as Iceland and Norway.
Apixaban was already approved in the EU to prevent venous thromboembolism (VTE) in adults who have undergone total hip or knee replacement surgery, and to prevent stroke and systemic embolism in adults with nonvalvular atrial fibrillation.
The new marketing authorization for apixaban follows the positive opinion issued by the European Medicines Agency’s Committee for Medicinal Products for Human Use in June and is supported by results of 2 phase 3 clinical trials, AMPLIFY and AMPLIFY-EXT.
Results of AMPLIFY
The AMPLIFY trial included 5395 patients with confirmed, symptomatic DVT or PE requiring treatment for 6 months. They had a mean age of 56.9 years, and 89.8% of randomized patients had unprovoked VTE.
About half of patients (n=2691) were randomized to receive apixaban at 10 mg twice daily for 7 days, followed by 5 mg twice daily for 6 months.
The other half (n=2704) were randomized to the standard of care, which was enoxaparin at 1 mg/kg twice daily for at least 5 days until INR ≥ 2 and warfarin (target INR range 2.0-3.0) for 6 months.
Apixaban proved noninferior to standard therapy in the combined primary endpoint of adjudicated recurrent symptomatic VTE (nonfatal DVT or PE) or VTE-related death.
This outcome occurred in 2.3% of patients in the apixaban arm and 2.7% of patients in the standard-therapy arm (P<0.0001 for noninferiority).
Apixaban also proved superior to standard therapy with regard to bleeding. The composite endpoint of major bleeding and clinically relevant, nonmajor bleeding occurred in 4.3% of patients in the apixaban arm and 9.7% of patients in the standard-therapy arm (P<0.001).
Results of AMPLIFY-EXT
The AMPLIFY-EXT trial included 2486 patients who had completed 6 to 12 months of anticoagulation treatment for DVT or PE. The mean age was 56.7 years, and 91.7% of randomized patients had unprovoked VTE.
Patients were randomized to receive apixaban at 2.5 mg (n=842), apixaban at 5 mg (n=815), or placebo (n=829).
Both apixaban doses were significantly superior to placebo (P<0.001) with regard to the primary efficacy endpoint, which was recurrent VTE or all-cause death.
During the 12-month active study period, these events occurred in 3.8% of patients in the 2.5-mg arm, 4.2% of patients in the 5-mg arm, and 11.6% of patients in the placebo arm.
The primary safety endpoint was the incidence of major bleeding, and there was no significant difference among the treatment arms. Major bleeding occurred in 0.2% of patients in the 2.5-mg arm, 0.1% of patients in the 5-mg arm, and 0.5% of patients in the placebo arm.
About apixaban
Apixaban is approved to reduce the risk of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation in the US, EU, Japan, and a number of other countries around the world.
The drug is approved to prevent VTE in adult patients who have undergone elective hip or knee replacement surgery in the US, EU, and a number of other countries.
And now, apixaban is approved for the treatment of DVT/PE and the prevention of recurrent DVT/PE in the EU. The drug is not approved for this indication in the US.
Apixaban is under joint development by Pfizer and Bristol-Myers Squibb. ![]()
Credit: Kevin MacKenzie
The European Commission has approved apixaban (Eliquis) to treat and prevent deep vein thrombosis (DVT) and pulmonary embolism (PE).
The approval applies to all European Union (EU) member states, as well as Iceland and Norway.
Apixaban was already approved in the EU to prevent venous thromboembolism (VTE) in adults who have undergone total hip or knee replacement surgery, and to prevent stroke and systemic embolism in adults with nonvalvular atrial fibrillation.
The new marketing authorization for apixaban follows the positive opinion issued by the European Medicines Agency’s Committee for Medicinal Products for Human Use in June and is supported by results of 2 phase 3 clinical trials, AMPLIFY and AMPLIFY-EXT.
Results of AMPLIFY
The AMPLIFY trial included 5395 patients with confirmed, symptomatic DVT or PE requiring treatment for 6 months. They had a mean age of 56.9 years, and 89.8% of randomized patients had unprovoked VTE.
About half of patients (n=2691) were randomized to receive apixaban at 10 mg twice daily for 7 days, followed by 5 mg twice daily for 6 months.
The other half (n=2704) were randomized to the standard of care, which was enoxaparin at 1 mg/kg twice daily for at least 5 days until INR ≥ 2 and warfarin (target INR range 2.0-3.0) for 6 months.
Apixaban proved noninferior to standard therapy in the combined primary endpoint of adjudicated recurrent symptomatic VTE (nonfatal DVT or PE) or VTE-related death.
This outcome occurred in 2.3% of patients in the apixaban arm and 2.7% of patients in the standard-therapy arm (P<0.0001 for noninferiority).
Apixaban also proved superior to standard therapy with regard to bleeding. The composite endpoint of major bleeding and clinically relevant, nonmajor bleeding occurred in 4.3% of patients in the apixaban arm and 9.7% of patients in the standard-therapy arm (P<0.001).
Results of AMPLIFY-EXT
The AMPLIFY-EXT trial included 2486 patients who had completed 6 to 12 months of anticoagulation treatment for DVT or PE. The mean age was 56.7 years, and 91.7% of randomized patients had unprovoked VTE.
Patients were randomized to receive apixaban at 2.5 mg (n=842), apixaban at 5 mg (n=815), or placebo (n=829).
Both apixaban doses were significantly superior to placebo (P<0.001) with regard to the primary efficacy endpoint, which was recurrent VTE or all-cause death.
During the 12-month active study period, these events occurred in 3.8% of patients in the 2.5-mg arm, 4.2% of patients in the 5-mg arm, and 11.6% of patients in the placebo arm.
The primary safety endpoint was the incidence of major bleeding, and there was no significant difference among the treatment arms. Major bleeding occurred in 0.2% of patients in the 2.5-mg arm, 0.1% of patients in the 5-mg arm, and 0.5% of patients in the placebo arm.
About apixaban
Apixaban is approved to reduce the risk of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation in the US, EU, Japan, and a number of other countries around the world.
The drug is approved to prevent VTE in adult patients who have undergone elective hip or knee replacement surgery in the US, EU, and a number of other countries.
And now, apixaban is approved for the treatment of DVT/PE and the prevention of recurrent DVT/PE in the EU. The drug is not approved for this indication in the US.
Apixaban is under joint development by Pfizer and Bristol-Myers Squibb. ![]()
Obinutuzumab approved for CLL in Europe
The European Commission has approved the anti-CD20 monoclonal antibody obinutuzumab for use in the European Union (EU).
Obinutuzumab can now be used in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia (CLL) who have comorbidities that make them ineligible to receive fludarabine-based therapy.
Obinutuzumab is already approved for this indication in the US.
Obinutuzumab is marketed as Gazyvaro in the EU and Switzerland but as Gazyva in the US and the rest of the world.
The European Commission’s approval follows a positive opinion granted by The European Medicine Agency’s Committee for Medicinal Products for Human Use in May.
The approval is based on results of the phase 3 CLL11 study, which showed that obinutuzumab plus chlorambucil improved progression-free survival (PFS), when compared to chlorambucil alone or in combination with rituximab.
This 2-stage study included 781 previously untreated CLL patients with comorbidities. In stage 1 (n=589), researchers compared obinutuzumab plus chlorambucil to chlorambucil alone and rituximab plus chlorambucil to chlorambucil alone.
Stage 2 (n=663) was a direct comparison of obinutuzumab plus chlorambucil and rituximab plus chlorambucil.
Stage 1 results were presented at ASCO 2013, stage 2 results were presented at ASH 2013, and the complete results were published in NEJM last March.
Obinutuzumab plus chlorambucil improved PFS when compared to chlorambucil alone. The median PFS was 26.7 months and 11.1 months, respectively (P<0.001).
Obinutuzumab plus chlorambucil also improved PFS when compared to rituximab plus chlorambucil. The median PFS was 26.7 months and 16.3 months, respectively (P<0.001).
Infusion-related reactions and neutropenia were more common in the obinutuzumab arm than in the rituximab arm. But obinutuzumab-treated patients did not have an increased risk of infection.
Obinutuzumab is being developed by Roche. The company said it expects to begin launching the drug in a number of European countries this year. ![]()
The European Commission has approved the anti-CD20 monoclonal antibody obinutuzumab for use in the European Union (EU).
Obinutuzumab can now be used in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia (CLL) who have comorbidities that make them ineligible to receive fludarabine-based therapy.
Obinutuzumab is already approved for this indication in the US.
Obinutuzumab is marketed as Gazyvaro in the EU and Switzerland but as Gazyva in the US and the rest of the world.
The European Commission’s approval follows a positive opinion granted by The European Medicine Agency’s Committee for Medicinal Products for Human Use in May.
The approval is based on results of the phase 3 CLL11 study, which showed that obinutuzumab plus chlorambucil improved progression-free survival (PFS), when compared to chlorambucil alone or in combination with rituximab.
This 2-stage study included 781 previously untreated CLL patients with comorbidities. In stage 1 (n=589), researchers compared obinutuzumab plus chlorambucil to chlorambucil alone and rituximab plus chlorambucil to chlorambucil alone.
Stage 2 (n=663) was a direct comparison of obinutuzumab plus chlorambucil and rituximab plus chlorambucil.
Stage 1 results were presented at ASCO 2013, stage 2 results were presented at ASH 2013, and the complete results were published in NEJM last March.
Obinutuzumab plus chlorambucil improved PFS when compared to chlorambucil alone. The median PFS was 26.7 months and 11.1 months, respectively (P<0.001).
Obinutuzumab plus chlorambucil also improved PFS when compared to rituximab plus chlorambucil. The median PFS was 26.7 months and 16.3 months, respectively (P<0.001).
Infusion-related reactions and neutropenia were more common in the obinutuzumab arm than in the rituximab arm. But obinutuzumab-treated patients did not have an increased risk of infection.
Obinutuzumab is being developed by Roche. The company said it expects to begin launching the drug in a number of European countries this year. ![]()
The European Commission has approved the anti-CD20 monoclonal antibody obinutuzumab for use in the European Union (EU).
Obinutuzumab can now be used in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia (CLL) who have comorbidities that make them ineligible to receive fludarabine-based therapy.
Obinutuzumab is already approved for this indication in the US.
Obinutuzumab is marketed as Gazyvaro in the EU and Switzerland but as Gazyva in the US and the rest of the world.
The European Commission’s approval follows a positive opinion granted by The European Medicine Agency’s Committee for Medicinal Products for Human Use in May.
The approval is based on results of the phase 3 CLL11 study, which showed that obinutuzumab plus chlorambucil improved progression-free survival (PFS), when compared to chlorambucil alone or in combination with rituximab.
This 2-stage study included 781 previously untreated CLL patients with comorbidities. In stage 1 (n=589), researchers compared obinutuzumab plus chlorambucil to chlorambucil alone and rituximab plus chlorambucil to chlorambucil alone.
Stage 2 (n=663) was a direct comparison of obinutuzumab plus chlorambucil and rituximab plus chlorambucil.
Stage 1 results were presented at ASCO 2013, stage 2 results were presented at ASH 2013, and the complete results were published in NEJM last March.
Obinutuzumab plus chlorambucil improved PFS when compared to chlorambucil alone. The median PFS was 26.7 months and 11.1 months, respectively (P<0.001).
Obinutuzumab plus chlorambucil also improved PFS when compared to rituximab plus chlorambucil. The median PFS was 26.7 months and 16.3 months, respectively (P<0.001).
Infusion-related reactions and neutropenia were more common in the obinutuzumab arm than in the rituximab arm. But obinutuzumab-treated patients did not have an increased risk of infection.
Obinutuzumab is being developed by Roche. The company said it expects to begin launching the drug in a number of European countries this year. ![]()
Is the United States a proving ground or quagmire for mobile health?
The use of mobile or wireless devices in health care continues to challenge the regulatory landscape. States increasingly are playing a role in either advancing or retracing steps previously taken at the federal level. In the spirit of Ferris Bueller, "isms" have provided a number of opportunities for discussion surrounding mobile health technologies. Federalism remains a key criterion upon which our country creates health care policy – which could serve as a double-edged sword.
On the one hand, it might encourage innovation and provide policy that satisfies the needs of specific constituents. On the other hand, it may create more complexity or even contradict previous policy. The result is often a legal quagmire of wasted time, energy, and money. While policy will never keep pace with technology and innovation, a number of stakeholders are working to bridge the gap.
HIMSS – the Health Information Management System Society – has provided an overview of contemporary issues focused on the state level to advance the use of mobile and wireless devices in health care. Their paper titled "Mobile Health IT in the States: A Policy Perspective"sheds light on a number of potential redundancies in the regulatory system and offers some guidance on other issues.
One major issue gaining plenty of interest among physicians and lawmakers is the ability for mobile devices to facilitate the delivery of health care in a more meaningful, cost effective way. However, whenever disruptive technology begins to upset vested interests, one can expect a robust discussion.
The licensure of physicians and other providers and establishing telehealth standards of care remain substantial obstacles to overcome in the regulatory space. Federal licensure would permit physicians to care for patients across state lines via telehealth delivery systems. Some medical boards of states bordering large metropolitan areas such as Washington, D.C., have entered into reciprocal provider licensing agreements to allow for telehealth encounters.
Reimbursement represents another major obstacle to widespread adoption by providers. Telehealth is primarily a technology approved in certain rural areas under Medicaid. Enter a new age of consumerism in health care, and for a small fee, providers can engage in consultations using your mobile device.
A number of studies have examined the desire for patients to receive care on a mobile device, and not surprisingly, convenience wins out. However, a number of discordant state polices increasingly prohibit the ability to scale many of these innovative and cost-saving approaches to care delivery. The HIMSS paper encourages states to consider health IT, electronic health record (EHR) adoption, telehealth, and mobile health (mHealth) when resourcing and determining coverage for publicly funded health programs such as Medicaid, public health initiatives, and state employee health benefits programs.
Unfortunately, reimbursement for telehealth services for Medicare patients as well is also limited to rural settings defined as "originating sites."
"An originating site is the location of an eligible Medicare beneficiary at the time the service being furnished via a telecommunications system occurs. Medicare beneficiaries are eligible for telehealth services only if they are presented from an originating site located in a rural Health Professional Shortage Area, either located outside of a Metropolitan Statistical Area (MSA) or in a rural census tract, as determined by the Office of Rural Health Policy within the Health Resources and Services Administration (HRSA) or [from] a county outside of an MSA."
Telehealth reimbursement only covers certain specialties and services. Telehealth has been in existence for decades and has been the focus of many outcomes-based studies.
Extending this to mobile technologies such as medical apps remains a challenge due to the lack of evidence. However, I foresee the critical need for such applications, the rapid development of state-of-the-art sensor technologies, and the emergence of analytics to converge and make the success of mobile health technologies a welcome and accepted reality.
Dr. Scher is an electrophysiologist with the Heart Group of Lancaster (Pa.) General Health. He is also director of DLS Healthcare Consulting, Harrisburg, Pa., and clinical associate professor of medicine at the Pennsylvania State University, Hershey.
The use of mobile or wireless devices in health care continues to challenge the regulatory landscape. States increasingly are playing a role in either advancing or retracing steps previously taken at the federal level. In the spirit of Ferris Bueller, "isms" have provided a number of opportunities for discussion surrounding mobile health technologies. Federalism remains a key criterion upon which our country creates health care policy – which could serve as a double-edged sword.
On the one hand, it might encourage innovation and provide policy that satisfies the needs of specific constituents. On the other hand, it may create more complexity or even contradict previous policy. The result is often a legal quagmire of wasted time, energy, and money. While policy will never keep pace with technology and innovation, a number of stakeholders are working to bridge the gap.
HIMSS – the Health Information Management System Society – has provided an overview of contemporary issues focused on the state level to advance the use of mobile and wireless devices in health care. Their paper titled "Mobile Health IT in the States: A Policy Perspective"sheds light on a number of potential redundancies in the regulatory system and offers some guidance on other issues.
One major issue gaining plenty of interest among physicians and lawmakers is the ability for mobile devices to facilitate the delivery of health care in a more meaningful, cost effective way. However, whenever disruptive technology begins to upset vested interests, one can expect a robust discussion.
The licensure of physicians and other providers and establishing telehealth standards of care remain substantial obstacles to overcome in the regulatory space. Federal licensure would permit physicians to care for patients across state lines via telehealth delivery systems. Some medical boards of states bordering large metropolitan areas such as Washington, D.C., have entered into reciprocal provider licensing agreements to allow for telehealth encounters.
Reimbursement represents another major obstacle to widespread adoption by providers. Telehealth is primarily a technology approved in certain rural areas under Medicaid. Enter a new age of consumerism in health care, and for a small fee, providers can engage in consultations using your mobile device.
A number of studies have examined the desire for patients to receive care on a mobile device, and not surprisingly, convenience wins out. However, a number of discordant state polices increasingly prohibit the ability to scale many of these innovative and cost-saving approaches to care delivery. The HIMSS paper encourages states to consider health IT, electronic health record (EHR) adoption, telehealth, and mobile health (mHealth) when resourcing and determining coverage for publicly funded health programs such as Medicaid, public health initiatives, and state employee health benefits programs.
Unfortunately, reimbursement for telehealth services for Medicare patients as well is also limited to rural settings defined as "originating sites."
"An originating site is the location of an eligible Medicare beneficiary at the time the service being furnished via a telecommunications system occurs. Medicare beneficiaries are eligible for telehealth services only if they are presented from an originating site located in a rural Health Professional Shortage Area, either located outside of a Metropolitan Statistical Area (MSA) or in a rural census tract, as determined by the Office of Rural Health Policy within the Health Resources and Services Administration (HRSA) or [from] a county outside of an MSA."
Telehealth reimbursement only covers certain specialties and services. Telehealth has been in existence for decades and has been the focus of many outcomes-based studies.
Extending this to mobile technologies such as medical apps remains a challenge due to the lack of evidence. However, I foresee the critical need for such applications, the rapid development of state-of-the-art sensor technologies, and the emergence of analytics to converge and make the success of mobile health technologies a welcome and accepted reality.
Dr. Scher is an electrophysiologist with the Heart Group of Lancaster (Pa.) General Health. He is also director of DLS Healthcare Consulting, Harrisburg, Pa., and clinical associate professor of medicine at the Pennsylvania State University, Hershey.
The use of mobile or wireless devices in health care continues to challenge the regulatory landscape. States increasingly are playing a role in either advancing or retracing steps previously taken at the federal level. In the spirit of Ferris Bueller, "isms" have provided a number of opportunities for discussion surrounding mobile health technologies. Federalism remains a key criterion upon which our country creates health care policy – which could serve as a double-edged sword.
On the one hand, it might encourage innovation and provide policy that satisfies the needs of specific constituents. On the other hand, it may create more complexity or even contradict previous policy. The result is often a legal quagmire of wasted time, energy, and money. While policy will never keep pace with technology and innovation, a number of stakeholders are working to bridge the gap.
HIMSS – the Health Information Management System Society – has provided an overview of contemporary issues focused on the state level to advance the use of mobile and wireless devices in health care. Their paper titled "Mobile Health IT in the States: A Policy Perspective"sheds light on a number of potential redundancies in the regulatory system and offers some guidance on other issues.
One major issue gaining plenty of interest among physicians and lawmakers is the ability for mobile devices to facilitate the delivery of health care in a more meaningful, cost effective way. However, whenever disruptive technology begins to upset vested interests, one can expect a robust discussion.
The licensure of physicians and other providers and establishing telehealth standards of care remain substantial obstacles to overcome in the regulatory space. Federal licensure would permit physicians to care for patients across state lines via telehealth delivery systems. Some medical boards of states bordering large metropolitan areas such as Washington, D.C., have entered into reciprocal provider licensing agreements to allow for telehealth encounters.
Reimbursement represents another major obstacle to widespread adoption by providers. Telehealth is primarily a technology approved in certain rural areas under Medicaid. Enter a new age of consumerism in health care, and for a small fee, providers can engage in consultations using your mobile device.
A number of studies have examined the desire for patients to receive care on a mobile device, and not surprisingly, convenience wins out. However, a number of discordant state polices increasingly prohibit the ability to scale many of these innovative and cost-saving approaches to care delivery. The HIMSS paper encourages states to consider health IT, electronic health record (EHR) adoption, telehealth, and mobile health (mHealth) when resourcing and determining coverage for publicly funded health programs such as Medicaid, public health initiatives, and state employee health benefits programs.
Unfortunately, reimbursement for telehealth services for Medicare patients as well is also limited to rural settings defined as "originating sites."
"An originating site is the location of an eligible Medicare beneficiary at the time the service being furnished via a telecommunications system occurs. Medicare beneficiaries are eligible for telehealth services only if they are presented from an originating site located in a rural Health Professional Shortage Area, either located outside of a Metropolitan Statistical Area (MSA) or in a rural census tract, as determined by the Office of Rural Health Policy within the Health Resources and Services Administration (HRSA) or [from] a county outside of an MSA."
Telehealth reimbursement only covers certain specialties and services. Telehealth has been in existence for decades and has been the focus of many outcomes-based studies.
Extending this to mobile technologies such as medical apps remains a challenge due to the lack of evidence. However, I foresee the critical need for such applications, the rapid development of state-of-the-art sensor technologies, and the emergence of analytics to converge and make the success of mobile health technologies a welcome and accepted reality.
Dr. Scher is an electrophysiologist with the Heart Group of Lancaster (Pa.) General Health. He is also director of DLS Healthcare Consulting, Harrisburg, Pa., and clinical associate professor of medicine at the Pennsylvania State University, Hershey.

Access to a Behavioral Weight Loss Website With or Without Group Sessions Increased Weight Loss in Statewide Campaign
Study Overview
Objective. To determine the efficacy and cost-effectiveness of adding an evidence-based internet behavioral weight loss intervention alone or combined with optional group sessions to ShapeUp Rhode Island 2011 (SURI), a 3-month statewide wellness campaign.
Design. 3-arm randomized clinical trial.
Setting and participants. Study participants were recruited from the Rhode Island community via employers, media, and mass mailings at the time of SURI 2011 registration. Of the 3806 participants that joined the weight loss division, 1139 were willing to be contacted for research, and the first 431 were screened for study eligibility. Exclusion criteria were minimal: age < 18 years or > 70 years, body mass index (BMI) < 25 kg/m2, pregnant, nursing, or plans to become pregnant, a serious medical condition (eg, cancer), unreliable internet access, non-English speaking, current or previous participation in our weight loss studies, and planned relocation. Those who reported a medical condition that could interfere with safe participation (eg, diabetes) obtained doctor’s consent to participate. Of those screened, 230 met inclusion criteria, completed orientation procedures, and were randomized using a 1:2:2 randomization scheme to the standard SURI program (S; n = 46); SURI plus internet behavioral weight loss intervention (SI; n = 90); or SURI plus internet behavioral weight loss intervention plus optional group sessions (SIG; n = 94). To avoid contamination, individuals on the same SURI team (see below) were randomized to the same intervention.
Intervention. Participants in the standard SURI program did not receive any behavioral weight loss treatment. SURI is a self-sustaining, annual community campaign designed to help Rhode Islanders lose weight and increase their physical activity through an online, team-based competition. Participants join in teams, enter the weight loss or physical activity division or both, and compete with other teams. Throughout the 3-month program, participants have access to a reporting SURI website where they submit their weekly weight and activity data and view their personal and team progress. They also receive paper logs to record weight and activity, a pedometer, access to newsletters and community workshops, and recognition for meeting goals.
Participants in the SI arm received the 3-month SURI program plus a 3-month internet behavioral weight loss intervention. Before SURI began, SI participants attended a 1-hour group meeting during which they received their weight loss goal (lose 1 to 2 pounds per week), calorie and fat gram goal (starting weight < 250 lbs: 1200–1500 kcal/day, 40–50 g of fat; starting weight ≥ 250 lbs: 1500–1800 kcal/day, 50–60 g of fat), and activity goal (gradually increase to 200 minutes of aerobic activity per week). During this session, participants were also taught self-monitoring skills and oriented to an internet behavioral weight loss intervention website developed by the authors. The intervention website included 12 weekly, 10- to 15-minute multimedia lessons based on the Diabetes Prevention Program and a self-monitoring platform where participants tracked their daily weight, calorie, and activity information. Participants received weekly automated feedback on their progress. The intervention website also included information on meal plans, prepackaged meals, and meal replacements.
Participants in the SIG arm received everything in SI and were additionally given the option to attend weekly group meetings at Miriam Hospital’s Weight Control and Diabetes Research Center during the 3 months. The 12 weekly, optional group sessions were led by masters-level staff with extensive training in behavioral weight loss. Sessions involved private weigh-ins and covered topics that supplemented the internet intervention (eg, recipe modification, portion control).
Main outcomes measures. The main outcome was weight loss at the end of the 3-month program. Participants completed measures (ie, weight, BMI) in person at baseline and 3 months (post-treatment), and at 6- and 12-month follow-up visits. Adherence measures included reported weight and physical activity on the SURI website (S, SI, and SIG), log ins, viewed lessons, and self-monitoring entries on the intervention website (SI, SIG), and number of groups meetings attended (SIG). To measure weight loss behaviors, the authors used the Weight Control Practices questionnaire to assess engagement in core weight loss strategies targeted in treatment, and the Paffenbarger questionnaire to assess weekly kcal expended in moderate to vigorous activity. The authors also assessed costs from the payer (labor, rent, intervention materials), participant (SURI registration fee, transportation, time spent on intervention), and societal perspective (sum of payer and participant costs) in order to calculate the cost per kg of weight lost in each study arm.
Results. Participants were predominantly female, non-Hispanic white, and had a mean BMI of 34.4 kg/m2 (SE = 0.05). Groups differed only on education (P = 0.02), and attendance at post-treatment and 6- and 12-month follow-up were high (93%, 91%, and 86% respectively). The authors found that weight loss did not differ by educational attainment (P s > 0.57).
Overall, there was a significant group-by-time interaction for weight loss (P < 0.001). Percentage weight loss at 3 months differed among the 3 groups—S: 1.1% ± 0.9%; SI: 4.2% ± 0.6%; SIG: 6.1% ± 0.6% (P s ≤ 0.04). There was also an overall group effect for percentage of individuals achieving 5% weight loss (P < 0.001). SI and SIG had higher percentages of participants who achieved a 5% weight loss than the control (SI: 42%; SIG: 54%; S: 7%; P s < 0.001) but did not differ from one another (P = 0.01). Initial weight losses and percentage of participants who achieved a 5% weight loss were largely maintained through the no-treatment follow-up phase at 6-months, but the 3 groups no longer differed from one another at 12 months (S: 1.2% [SE =0.9]; SI: 2.2% [SE = 0.6]; SIG: 3.3% [SE = 0.6]; P s > 0.05).
All groups reported significant increases in physical activity over time (p < 0.001). More reporting of weight and physical activity data on the SURI website was associated with greater percentage weight loss (r = 0.25; P < 0.001). Number of log ins and lessons viewed on the intervention website were positively associated with percentage weight loss (r = 0.45; P ≤ 0.001; and r = 0.34; P ≤ 0.001 respectively). Greater attendance to group sessions was associated with better weight outcomes (r = 0.61; P ≤ 0.001). Younger age was associated with poorer adherence, including less reporting on the SURI website, viewing of lessons, and logging in to the weight loss website.
There was a significant group-by-time effect interaction for the use of behavioral weight loss strategies (P < 0.001), and increased use of these strategies was associated with greater percentage weight loss in all 3 groups post-treatment. At 12 months, however, there were no differences between groups in the use of these strategies (P s ≤ 0.07).
Cost per kg of weight loss was similar for S ($39) and SI ($35), but both were lower than SIG ($114).
Conclusion. Both intervention arms (SI and SIG) achieved more weight loss at 6 months than SURI alone. Although mean weight loss was greatest with optional group sessions (SIG), the addition of the behavioral intervention website alone (SI) was the most cost-effective method to enhance weight loss. Thus, adding a novel internet behavioral weight loss intervention to a statewide community health initiative may be a cost-effective approach to improving obesity treatment outcomes.
Commentary
Weight loss treatment is recommended for adults with a BMI of > 30 kg/m2, as well as those with BMI < 25 kg/m2 with weight-related comorbidities [1]. Intensive behavioral treatment should be the first line of intervention for overweight and obese individuals and can lead to 8% to 10% weight loss [2], particularly in initial months of treatment [3]. However, behavioral treatment is inherently challenging and time-consuming, and readily available to only a fraction of the intended population. Although weight losses achieved from intensive lifestyle interventions such as the Diabetes Prevention Program (DPP) [4] may be higher, innovative community weight loss programs that use a variety of weight loss strategies can provide opportunities to a wider population of overweight and obese individuals and at a lower cost [3].
This study built upon the authors’ previous work [5], which showed that SURI participants with behavioral weight loss strategies via email significantly improved 3-month weight losses. In this current study, they compared SURI alone to SURI with additional access to an internet behavioral weight loss website with or without optional group sessions. Since significant weight loss was not maintained at 12 months, this suggests that perhaps access to the behavioral weight loss website should have continued for longer and/or included a maintenance phase after the 3-month intervention. Weight loss often reaches its peak around 6 months, and weight regain occurs without effective maintenance therapy [6].
General strengths of the study included the use of a randomized, intention-to-treat design, dissemination of evidence-based weight loss strategies, objective outcomes measurement, adherence metrics, and strong retention of participants with clear accounting of all enrolled patients from recruitment through analysis. This study demonstrated significant weight loss in an intervention with minimal/optional health professional interaction. This intervention also placed responsibility on participants to self-monitor their diet and physical activity, participate in online lessons, and attend optional group sessions. The success of this community-based intervention suggests feasibility and scalability within a real-world setting. The authors also conducted cost-effectiveness analyses demonstrating that the SI program was more cost-effective than SIG.
However, there are weaknesses as well. In setting the sample size for each arm of this study, no justification was described for choosing a 1:2:2 randomization scheme. In randomized control trials, the allocation of participants into the different study arms is often balanced to equal numbers which maximizes statistical power [7]. However, the use of unequal randomization ratios among study arms can be beneficial and even necessary for various reasons including cost, availability of the intervention, overcoming intervention/treatment learning curves, and if a higher drop-out rate is anticipated. Providing a justification for unbalanced sample sizes would be helpful to future researchers looking to replicate the study. Additionally, participants were mostly non-Hispanic white and female, thus limiting generalizability. While representative of the broader Rhode Island population, findings based on this population this may not be applicable to vulnerable (ie, low literacy, resource-poor) or underrepresented populations (ie, minorities) [8].
Applications for Clinical Practice
An internet-based behavioral weight loss intervention, when added to a community weight management initiative, is cost-effective and can lead to short-term weight loss. Given that clinicians often lack time, training, and resources to adequately address obesity in the office [9,10], encouraging patients to enroll in similar programs may be an effective strategy to address such barriers. The study also highlights the need for maintenance interventions to help keep weight off. Findings should be replicated in more diverse communities.
—Katrina F. Mateo, MPH, and Melanie Jay, MD, MS
1. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. National Heart, Lung, and Blood Institute; 1998.
2. Wadden TA, Butryn ML, Wilson C. Lifestyle modification for the management of obesity. Gastroenterology 2007;132:2226–38.
3. Butryn ML, Webb V, Wadden TA. Behavioral treatment of obesity. Psych Clin North Am 2011;34:841–59.
4. The Diabetes Prevention Program Research Group. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002;25:2165–71.
5. Wing RR, Crane MM, Thomas JG, et al. Improving weight loss outcomes of community interventions by incorporating behavioral strategies. Am J Public Health 2010;100:2513–9.
6. Wing RR, Tate DF, Gorin A, et al. A self-regulation program for maintenance of weight loss. N Engl J Med 2006;355:1563–71.
7. Dumville JC, Hahn S, Miles JN V, Torgerson DJ. The use of unequal randomisation ratios in clinical trials: a review. Contemp Clin Trials 2006;27:1–12.
8. Marshall PL. Ethical challenges in study design and informed consent for health research in resource-poor settings. World Health Organization; 2007.
9. Jay M, Gillespie C, Ark T, et al. Do internists, pediatricians, and psychiatrists feel competent in obesity care? Using a needs assessment to drive curriculum design. J Gen Intern Med 2008;23:1066–70.
10. Loureiro ML, Nayga RM. Obesity, weight loss, and physician’s advice. Soc Sci Med 2006;62:2458–68.
Study Overview
Objective. To determine the efficacy and cost-effectiveness of adding an evidence-based internet behavioral weight loss intervention alone or combined with optional group sessions to ShapeUp Rhode Island 2011 (SURI), a 3-month statewide wellness campaign.
Design. 3-arm randomized clinical trial.
Setting and participants. Study participants were recruited from the Rhode Island community via employers, media, and mass mailings at the time of SURI 2011 registration. Of the 3806 participants that joined the weight loss division, 1139 were willing to be contacted for research, and the first 431 were screened for study eligibility. Exclusion criteria were minimal: age < 18 years or > 70 years, body mass index (BMI) < 25 kg/m2, pregnant, nursing, or plans to become pregnant, a serious medical condition (eg, cancer), unreliable internet access, non-English speaking, current or previous participation in our weight loss studies, and planned relocation. Those who reported a medical condition that could interfere with safe participation (eg, diabetes) obtained doctor’s consent to participate. Of those screened, 230 met inclusion criteria, completed orientation procedures, and were randomized using a 1:2:2 randomization scheme to the standard SURI program (S; n = 46); SURI plus internet behavioral weight loss intervention (SI; n = 90); or SURI plus internet behavioral weight loss intervention plus optional group sessions (SIG; n = 94). To avoid contamination, individuals on the same SURI team (see below) were randomized to the same intervention.
Intervention. Participants in the standard SURI program did not receive any behavioral weight loss treatment. SURI is a self-sustaining, annual community campaign designed to help Rhode Islanders lose weight and increase their physical activity through an online, team-based competition. Participants join in teams, enter the weight loss or physical activity division or both, and compete with other teams. Throughout the 3-month program, participants have access to a reporting SURI website where they submit their weekly weight and activity data and view their personal and team progress. They also receive paper logs to record weight and activity, a pedometer, access to newsletters and community workshops, and recognition for meeting goals.
Participants in the SI arm received the 3-month SURI program plus a 3-month internet behavioral weight loss intervention. Before SURI began, SI participants attended a 1-hour group meeting during which they received their weight loss goal (lose 1 to 2 pounds per week), calorie and fat gram goal (starting weight < 250 lbs: 1200–1500 kcal/day, 40–50 g of fat; starting weight ≥ 250 lbs: 1500–1800 kcal/day, 50–60 g of fat), and activity goal (gradually increase to 200 minutes of aerobic activity per week). During this session, participants were also taught self-monitoring skills and oriented to an internet behavioral weight loss intervention website developed by the authors. The intervention website included 12 weekly, 10- to 15-minute multimedia lessons based on the Diabetes Prevention Program and a self-monitoring platform where participants tracked their daily weight, calorie, and activity information. Participants received weekly automated feedback on their progress. The intervention website also included information on meal plans, prepackaged meals, and meal replacements.
Participants in the SIG arm received everything in SI and were additionally given the option to attend weekly group meetings at Miriam Hospital’s Weight Control and Diabetes Research Center during the 3 months. The 12 weekly, optional group sessions were led by masters-level staff with extensive training in behavioral weight loss. Sessions involved private weigh-ins and covered topics that supplemented the internet intervention (eg, recipe modification, portion control).
Main outcomes measures. The main outcome was weight loss at the end of the 3-month program. Participants completed measures (ie, weight, BMI) in person at baseline and 3 months (post-treatment), and at 6- and 12-month follow-up visits. Adherence measures included reported weight and physical activity on the SURI website (S, SI, and SIG), log ins, viewed lessons, and self-monitoring entries on the intervention website (SI, SIG), and number of groups meetings attended (SIG). To measure weight loss behaviors, the authors used the Weight Control Practices questionnaire to assess engagement in core weight loss strategies targeted in treatment, and the Paffenbarger questionnaire to assess weekly kcal expended in moderate to vigorous activity. The authors also assessed costs from the payer (labor, rent, intervention materials), participant (SURI registration fee, transportation, time spent on intervention), and societal perspective (sum of payer and participant costs) in order to calculate the cost per kg of weight lost in each study arm.
Results. Participants were predominantly female, non-Hispanic white, and had a mean BMI of 34.4 kg/m2 (SE = 0.05). Groups differed only on education (P = 0.02), and attendance at post-treatment and 6- and 12-month follow-up were high (93%, 91%, and 86% respectively). The authors found that weight loss did not differ by educational attainment (P s > 0.57).
Overall, there was a significant group-by-time interaction for weight loss (P < 0.001). Percentage weight loss at 3 months differed among the 3 groups—S: 1.1% ± 0.9%; SI: 4.2% ± 0.6%; SIG: 6.1% ± 0.6% (P s ≤ 0.04). There was also an overall group effect for percentage of individuals achieving 5% weight loss (P < 0.001). SI and SIG had higher percentages of participants who achieved a 5% weight loss than the control (SI: 42%; SIG: 54%; S: 7%; P s < 0.001) but did not differ from one another (P = 0.01). Initial weight losses and percentage of participants who achieved a 5% weight loss were largely maintained through the no-treatment follow-up phase at 6-months, but the 3 groups no longer differed from one another at 12 months (S: 1.2% [SE =0.9]; SI: 2.2% [SE = 0.6]; SIG: 3.3% [SE = 0.6]; P s > 0.05).
All groups reported significant increases in physical activity over time (p < 0.001). More reporting of weight and physical activity data on the SURI website was associated with greater percentage weight loss (r = 0.25; P < 0.001). Number of log ins and lessons viewed on the intervention website were positively associated with percentage weight loss (r = 0.45; P ≤ 0.001; and r = 0.34; P ≤ 0.001 respectively). Greater attendance to group sessions was associated with better weight outcomes (r = 0.61; P ≤ 0.001). Younger age was associated with poorer adherence, including less reporting on the SURI website, viewing of lessons, and logging in to the weight loss website.
There was a significant group-by-time effect interaction for the use of behavioral weight loss strategies (P < 0.001), and increased use of these strategies was associated with greater percentage weight loss in all 3 groups post-treatment. At 12 months, however, there were no differences between groups in the use of these strategies (P s ≤ 0.07).
Cost per kg of weight loss was similar for S ($39) and SI ($35), but both were lower than SIG ($114).
Conclusion. Both intervention arms (SI and SIG) achieved more weight loss at 6 months than SURI alone. Although mean weight loss was greatest with optional group sessions (SIG), the addition of the behavioral intervention website alone (SI) was the most cost-effective method to enhance weight loss. Thus, adding a novel internet behavioral weight loss intervention to a statewide community health initiative may be a cost-effective approach to improving obesity treatment outcomes.
Commentary
Weight loss treatment is recommended for adults with a BMI of > 30 kg/m2, as well as those with BMI < 25 kg/m2 with weight-related comorbidities [1]. Intensive behavioral treatment should be the first line of intervention for overweight and obese individuals and can lead to 8% to 10% weight loss [2], particularly in initial months of treatment [3]. However, behavioral treatment is inherently challenging and time-consuming, and readily available to only a fraction of the intended population. Although weight losses achieved from intensive lifestyle interventions such as the Diabetes Prevention Program (DPP) [4] may be higher, innovative community weight loss programs that use a variety of weight loss strategies can provide opportunities to a wider population of overweight and obese individuals and at a lower cost [3].
This study built upon the authors’ previous work [5], which showed that SURI participants with behavioral weight loss strategies via email significantly improved 3-month weight losses. In this current study, they compared SURI alone to SURI with additional access to an internet behavioral weight loss website with or without optional group sessions. Since significant weight loss was not maintained at 12 months, this suggests that perhaps access to the behavioral weight loss website should have continued for longer and/or included a maintenance phase after the 3-month intervention. Weight loss often reaches its peak around 6 months, and weight regain occurs without effective maintenance therapy [6].
General strengths of the study included the use of a randomized, intention-to-treat design, dissemination of evidence-based weight loss strategies, objective outcomes measurement, adherence metrics, and strong retention of participants with clear accounting of all enrolled patients from recruitment through analysis. This study demonstrated significant weight loss in an intervention with minimal/optional health professional interaction. This intervention also placed responsibility on participants to self-monitor their diet and physical activity, participate in online lessons, and attend optional group sessions. The success of this community-based intervention suggests feasibility and scalability within a real-world setting. The authors also conducted cost-effectiveness analyses demonstrating that the SI program was more cost-effective than SIG.
However, there are weaknesses as well. In setting the sample size for each arm of this study, no justification was described for choosing a 1:2:2 randomization scheme. In randomized control trials, the allocation of participants into the different study arms is often balanced to equal numbers which maximizes statistical power [7]. However, the use of unequal randomization ratios among study arms can be beneficial and even necessary for various reasons including cost, availability of the intervention, overcoming intervention/treatment learning curves, and if a higher drop-out rate is anticipated. Providing a justification for unbalanced sample sizes would be helpful to future researchers looking to replicate the study. Additionally, participants were mostly non-Hispanic white and female, thus limiting generalizability. While representative of the broader Rhode Island population, findings based on this population this may not be applicable to vulnerable (ie, low literacy, resource-poor) or underrepresented populations (ie, minorities) [8].
Applications for Clinical Practice
An internet-based behavioral weight loss intervention, when added to a community weight management initiative, is cost-effective and can lead to short-term weight loss. Given that clinicians often lack time, training, and resources to adequately address obesity in the office [9,10], encouraging patients to enroll in similar programs may be an effective strategy to address such barriers. The study also highlights the need for maintenance interventions to help keep weight off. Findings should be replicated in more diverse communities.
—Katrina F. Mateo, MPH, and Melanie Jay, MD, MS
Study Overview
Objective. To determine the efficacy and cost-effectiveness of adding an evidence-based internet behavioral weight loss intervention alone or combined with optional group sessions to ShapeUp Rhode Island 2011 (SURI), a 3-month statewide wellness campaign.
Design. 3-arm randomized clinical trial.
Setting and participants. Study participants were recruited from the Rhode Island community via employers, media, and mass mailings at the time of SURI 2011 registration. Of the 3806 participants that joined the weight loss division, 1139 were willing to be contacted for research, and the first 431 were screened for study eligibility. Exclusion criteria were minimal: age < 18 years or > 70 years, body mass index (BMI) < 25 kg/m2, pregnant, nursing, or plans to become pregnant, a serious medical condition (eg, cancer), unreliable internet access, non-English speaking, current or previous participation in our weight loss studies, and planned relocation. Those who reported a medical condition that could interfere with safe participation (eg, diabetes) obtained doctor’s consent to participate. Of those screened, 230 met inclusion criteria, completed orientation procedures, and were randomized using a 1:2:2 randomization scheme to the standard SURI program (S; n = 46); SURI plus internet behavioral weight loss intervention (SI; n = 90); or SURI plus internet behavioral weight loss intervention plus optional group sessions (SIG; n = 94). To avoid contamination, individuals on the same SURI team (see below) were randomized to the same intervention.
Intervention. Participants in the standard SURI program did not receive any behavioral weight loss treatment. SURI is a self-sustaining, annual community campaign designed to help Rhode Islanders lose weight and increase their physical activity through an online, team-based competition. Participants join in teams, enter the weight loss or physical activity division or both, and compete with other teams. Throughout the 3-month program, participants have access to a reporting SURI website where they submit their weekly weight and activity data and view their personal and team progress. They also receive paper logs to record weight and activity, a pedometer, access to newsletters and community workshops, and recognition for meeting goals.
Participants in the SI arm received the 3-month SURI program plus a 3-month internet behavioral weight loss intervention. Before SURI began, SI participants attended a 1-hour group meeting during which they received their weight loss goal (lose 1 to 2 pounds per week), calorie and fat gram goal (starting weight < 250 lbs: 1200–1500 kcal/day, 40–50 g of fat; starting weight ≥ 250 lbs: 1500–1800 kcal/day, 50–60 g of fat), and activity goal (gradually increase to 200 minutes of aerobic activity per week). During this session, participants were also taught self-monitoring skills and oriented to an internet behavioral weight loss intervention website developed by the authors. The intervention website included 12 weekly, 10- to 15-minute multimedia lessons based on the Diabetes Prevention Program and a self-monitoring platform where participants tracked their daily weight, calorie, and activity information. Participants received weekly automated feedback on their progress. The intervention website also included information on meal plans, prepackaged meals, and meal replacements.
Participants in the SIG arm received everything in SI and were additionally given the option to attend weekly group meetings at Miriam Hospital’s Weight Control and Diabetes Research Center during the 3 months. The 12 weekly, optional group sessions were led by masters-level staff with extensive training in behavioral weight loss. Sessions involved private weigh-ins and covered topics that supplemented the internet intervention (eg, recipe modification, portion control).
Main outcomes measures. The main outcome was weight loss at the end of the 3-month program. Participants completed measures (ie, weight, BMI) in person at baseline and 3 months (post-treatment), and at 6- and 12-month follow-up visits. Adherence measures included reported weight and physical activity on the SURI website (S, SI, and SIG), log ins, viewed lessons, and self-monitoring entries on the intervention website (SI, SIG), and number of groups meetings attended (SIG). To measure weight loss behaviors, the authors used the Weight Control Practices questionnaire to assess engagement in core weight loss strategies targeted in treatment, and the Paffenbarger questionnaire to assess weekly kcal expended in moderate to vigorous activity. The authors also assessed costs from the payer (labor, rent, intervention materials), participant (SURI registration fee, transportation, time spent on intervention), and societal perspective (sum of payer and participant costs) in order to calculate the cost per kg of weight lost in each study arm.
Results. Participants were predominantly female, non-Hispanic white, and had a mean BMI of 34.4 kg/m2 (SE = 0.05). Groups differed only on education (P = 0.02), and attendance at post-treatment and 6- and 12-month follow-up were high (93%, 91%, and 86% respectively). The authors found that weight loss did not differ by educational attainment (P s > 0.57).
Overall, there was a significant group-by-time interaction for weight loss (P < 0.001). Percentage weight loss at 3 months differed among the 3 groups—S: 1.1% ± 0.9%; SI: 4.2% ± 0.6%; SIG: 6.1% ± 0.6% (P s ≤ 0.04). There was also an overall group effect for percentage of individuals achieving 5% weight loss (P < 0.001). SI and SIG had higher percentages of participants who achieved a 5% weight loss than the control (SI: 42%; SIG: 54%; S: 7%; P s < 0.001) but did not differ from one another (P = 0.01). Initial weight losses and percentage of participants who achieved a 5% weight loss were largely maintained through the no-treatment follow-up phase at 6-months, but the 3 groups no longer differed from one another at 12 months (S: 1.2% [SE =0.9]; SI: 2.2% [SE = 0.6]; SIG: 3.3% [SE = 0.6]; P s > 0.05).
All groups reported significant increases in physical activity over time (p < 0.001). More reporting of weight and physical activity data on the SURI website was associated with greater percentage weight loss (r = 0.25; P < 0.001). Number of log ins and lessons viewed on the intervention website were positively associated with percentage weight loss (r = 0.45; P ≤ 0.001; and r = 0.34; P ≤ 0.001 respectively). Greater attendance to group sessions was associated with better weight outcomes (r = 0.61; P ≤ 0.001). Younger age was associated with poorer adherence, including less reporting on the SURI website, viewing of lessons, and logging in to the weight loss website.
There was a significant group-by-time effect interaction for the use of behavioral weight loss strategies (P < 0.001), and increased use of these strategies was associated with greater percentage weight loss in all 3 groups post-treatment. At 12 months, however, there were no differences between groups in the use of these strategies (P s ≤ 0.07).
Cost per kg of weight loss was similar for S ($39) and SI ($35), but both were lower than SIG ($114).
Conclusion. Both intervention arms (SI and SIG) achieved more weight loss at 6 months than SURI alone. Although mean weight loss was greatest with optional group sessions (SIG), the addition of the behavioral intervention website alone (SI) was the most cost-effective method to enhance weight loss. Thus, adding a novel internet behavioral weight loss intervention to a statewide community health initiative may be a cost-effective approach to improving obesity treatment outcomes.
Commentary
Weight loss treatment is recommended for adults with a BMI of > 30 kg/m2, as well as those with BMI < 25 kg/m2 with weight-related comorbidities [1]. Intensive behavioral treatment should be the first line of intervention for overweight and obese individuals and can lead to 8% to 10% weight loss [2], particularly in initial months of treatment [3]. However, behavioral treatment is inherently challenging and time-consuming, and readily available to only a fraction of the intended population. Although weight losses achieved from intensive lifestyle interventions such as the Diabetes Prevention Program (DPP) [4] may be higher, innovative community weight loss programs that use a variety of weight loss strategies can provide opportunities to a wider population of overweight and obese individuals and at a lower cost [3].
This study built upon the authors’ previous work [5], which showed that SURI participants with behavioral weight loss strategies via email significantly improved 3-month weight losses. In this current study, they compared SURI alone to SURI with additional access to an internet behavioral weight loss website with or without optional group sessions. Since significant weight loss was not maintained at 12 months, this suggests that perhaps access to the behavioral weight loss website should have continued for longer and/or included a maintenance phase after the 3-month intervention. Weight loss often reaches its peak around 6 months, and weight regain occurs without effective maintenance therapy [6].
General strengths of the study included the use of a randomized, intention-to-treat design, dissemination of evidence-based weight loss strategies, objective outcomes measurement, adherence metrics, and strong retention of participants with clear accounting of all enrolled patients from recruitment through analysis. This study demonstrated significant weight loss in an intervention with minimal/optional health professional interaction. This intervention also placed responsibility on participants to self-monitor their diet and physical activity, participate in online lessons, and attend optional group sessions. The success of this community-based intervention suggests feasibility and scalability within a real-world setting. The authors also conducted cost-effectiveness analyses demonstrating that the SI program was more cost-effective than SIG.
However, there are weaknesses as well. In setting the sample size for each arm of this study, no justification was described for choosing a 1:2:2 randomization scheme. In randomized control trials, the allocation of participants into the different study arms is often balanced to equal numbers which maximizes statistical power [7]. However, the use of unequal randomization ratios among study arms can be beneficial and even necessary for various reasons including cost, availability of the intervention, overcoming intervention/treatment learning curves, and if a higher drop-out rate is anticipated. Providing a justification for unbalanced sample sizes would be helpful to future researchers looking to replicate the study. Additionally, participants were mostly non-Hispanic white and female, thus limiting generalizability. While representative of the broader Rhode Island population, findings based on this population this may not be applicable to vulnerable (ie, low literacy, resource-poor) or underrepresented populations (ie, minorities) [8].
Applications for Clinical Practice
An internet-based behavioral weight loss intervention, when added to a community weight management initiative, is cost-effective and can lead to short-term weight loss. Given that clinicians often lack time, training, and resources to adequately address obesity in the office [9,10], encouraging patients to enroll in similar programs may be an effective strategy to address such barriers. The study also highlights the need for maintenance interventions to help keep weight off. Findings should be replicated in more diverse communities.
—Katrina F. Mateo, MPH, and Melanie Jay, MD, MS
1. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. National Heart, Lung, and Blood Institute; 1998.
2. Wadden TA, Butryn ML, Wilson C. Lifestyle modification for the management of obesity. Gastroenterology 2007;132:2226–38.
3. Butryn ML, Webb V, Wadden TA. Behavioral treatment of obesity. Psych Clin North Am 2011;34:841–59.
4. The Diabetes Prevention Program Research Group. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002;25:2165–71.
5. Wing RR, Crane MM, Thomas JG, et al. Improving weight loss outcomes of community interventions by incorporating behavioral strategies. Am J Public Health 2010;100:2513–9.
6. Wing RR, Tate DF, Gorin A, et al. A self-regulation program for maintenance of weight loss. N Engl J Med 2006;355:1563–71.
7. Dumville JC, Hahn S, Miles JN V, Torgerson DJ. The use of unequal randomisation ratios in clinical trials: a review. Contemp Clin Trials 2006;27:1–12.
8. Marshall PL. Ethical challenges in study design and informed consent for health research in resource-poor settings. World Health Organization; 2007.
9. Jay M, Gillespie C, Ark T, et al. Do internists, pediatricians, and psychiatrists feel competent in obesity care? Using a needs assessment to drive curriculum design. J Gen Intern Med 2008;23:1066–70.
10. Loureiro ML, Nayga RM. Obesity, weight loss, and physician’s advice. Soc Sci Med 2006;62:2458–68.
1. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. National Heart, Lung, and Blood Institute; 1998.
2. Wadden TA, Butryn ML, Wilson C. Lifestyle modification for the management of obesity. Gastroenterology 2007;132:2226–38.
3. Butryn ML, Webb V, Wadden TA. Behavioral treatment of obesity. Psych Clin North Am 2011;34:841–59.
4. The Diabetes Prevention Program Research Group. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002;25:2165–71.
5. Wing RR, Crane MM, Thomas JG, et al. Improving weight loss outcomes of community interventions by incorporating behavioral strategies. Am J Public Health 2010;100:2513–9.
6. Wing RR, Tate DF, Gorin A, et al. A self-regulation program for maintenance of weight loss. N Engl J Med 2006;355:1563–71.
7. Dumville JC, Hahn S, Miles JN V, Torgerson DJ. The use of unequal randomisation ratios in clinical trials: a review. Contemp Clin Trials 2006;27:1–12.
8. Marshall PL. Ethical challenges in study design and informed consent for health research in resource-poor settings. World Health Organization; 2007.
9. Jay M, Gillespie C, Ark T, et al. Do internists, pediatricians, and psychiatrists feel competent in obesity care? Using a needs assessment to drive curriculum design. J Gen Intern Med 2008;23:1066–70.
10. Loureiro ML, Nayga RM. Obesity, weight loss, and physician’s advice. Soc Sci Med 2006;62:2458–68.
Epidural Steroid Injections for Spinal Stenosis Back Pain Simply Don’t Work
Study Overview
Objective. To determine the effectiveness of epidural injections of glucocorticoids plus anesthetic compared with injections of anesthetic alone in patients with lumbar spinal stenosis.
Design. The LESS (Lumbar Epidural Steroid Injection for Spinal Stenosis) trial—a double-blind, multisite, randomized controlled trial.
Setting and participants. The study was conducted at 16 sites in the United States and enrolled 400 patients between April 2011 and June 2013. Patients at least 50 years of age with spinal stenosis as evidenced by magnetic resonance imaging (MRI) or computed tomography (CT) were invited to participate. Additional eligibility criteria included an average pain rating of more than 4 on a scale of 0 to 10 (0 being the lowest score) for back, buttock, or leg pain. Patients were excluded if they did not have stenosis of the central canal, had spondylolisthesis requiring surgery, or had received epidural glucocorticoid injections within the previous 6 months. Patients were randomly assigned to receive a standard epidural injection of glucocorticoids plus lidocaine or lidocaine alone. At the 3-week follow-up they could choose to receive a repeat injection. At the 6-week assessment they were allowed to cross over to the other treatment group. Patients were blinded throughout the study. The treating physicians were also blinded through the use of 2 opaque prefilled syringes provided by the study staff—one marked “inject” and one marked “discard.”
Main outcome measures. The 2 outcomes, measured at 6 weeks, were the Roland-Morris Disability Questionnaire (RMDQ) score (range, 0 to 24, with higher scores indicating greater physical disability) and the patient’s rating of average buttock, hip, or leg pain in the previous week (scale of 0 to 10 with 0 indicating no pain and 10 indicating “pain as bad as you can imagine”).
Eight secondary patient-oriented outcomes were also measured: (1) at least minimal clinically meaningful improvement (≥ 30%), (2) substantial clinically meaningful improvement (≥ 50%), (3) average back pain in the previous week, and scores on the (4) Brief Pain Inventory (BPI) interference scale, (5) 8-question Patient Health Questionnaire (PHQ-8), (6) Generalized Anxiety Disorder 7 scale (GAD-7), (7) EQ-5D (a health status measure) and (8) Swiss Spinal Stenosis Questionnaire (SSSQ).
Main results. The 2 groups were similar with respect to baseline characteristics, except that the duration of pain was shorter in the lidocaine-alone group. At 6 weeks, both groups had improved RMDQ scores (glucocorticoid –4.2 points vs. no glucocorticoid –3.1 points, respectively). However, the difference in RMDQ score between the 2 groups was not statistically significant (–1.0 points [95% CI, –2.1 to 0.1]; P = 0.07). In addition, there was no difference in treatment effect at 6 weeks as measured by patient’s reported leg pain (–0.2 points [95% CI, –0.8 to 0.4]; P = 0.48). Furthermore, there were no significant differences in the secondary outcomes of clinically meaningful improvement, BPI, SSSQ symptoms and physical function, EQ-5D, and GAD-7 scales at 6 weeks. Among the secondary outcomes, only symptoms of depression and patient satisfaction showed a statistically significant improvement in the glucocorticoid plus lidocaine group. Of note, though not statistically significant, there were more adverse events in the glucocorticoid plus lidocaine group compared to the lidocaine alone group (21.5% vs. 15.5%, respectively). Finally, the glucocorticoid plus lidocaine group also had a significantly higher proportion of patients with cortisol serum suppression compared to the lidocaine alone group.
Conclusion. The authors concluded that there was no difference in pain-related functional disability (as measured by the RMDQ score) and pain intensity between patients receiving fluoroscopically guided epidural injections with glucocorticoids plus lidocaine compared with lidocaine alone for lumbar spinal stenosis. The injection of glucocorticoid should be avoided due to its potentially systemic effects, including suppression of the hypothalamic-pituitary axis and reduction in bone mineral density, which may increase the risk of fracture.
Commentary
Lumbar spinal stenosis is one of the most common causes of spine-related back and leg pain; it disproportionally affects older adults due to degenerative changes resulting in narrowing of the spinal canal and nerve-root. Epidural glucocorticoid injections containing a glucocorticoid and an anesthetic are commonly used to relieve symptoms of lumbar stenosis. While this treatment approach is controversial, more than 2.2 million lumbar epidural glucocorticoid injections are performed in the Medicare population each year [1,2]. Previous uncontrolled studies suggest that epidural glucocorticoid injections provide short-term pain relief for some patients with spinal stenosis [3]. While complications from the procedure are rare, a multistate outbreak of fungal meningitis due to contaminated glucocorticoid injections affected at least 751 patients with 64 deaths in 2012 [4].
The purpose of the current study by Friedly et al was to determine whether adding a glucocorticoid to an anesthetic in epidural spinal injections is superior to anesthetic alone for symptom relief and functional improvement in patients with lumbar spinal stenosis. In contrast to previous studies, the authors defined short-term results as 3 weeks after injection, and long-term results as 6 weeks after injection. Despite the shorter follow-up period, results were similar to previous studies, in that adding glucocorticoid to anesthetic in epidural spinal injection reduced pain and improved patient’s functionality short-term, but improvements were not sustained long-term. Based on these results, the authors concluded that there is no benefit in adding glucocorticoid epidural injections for back pain arising from lumbar spinal stenosis.
One major limitation of this study is the lack of a placebo arm. Because of the lack of a placebo arm, it cannot be ascertained whether epidural injection with lidocaine alone conferred a benefit. However, this study provides robust evidence that epidural steroid injections are not beneficial for treatment of back and leg pain associated with lumbar spinal stenosis.
Applications for Clinical Practice
Epidural steroid injection is long accepted in medical communities as a safe and effective treatment for lumbar spinal stenosis symptoms. In light of the potential dangers of epidural steroid injections, including meningitis, coupled with the increasing cost of the procedure, other potential side effects, and demonstrated ineffectiveness of the treatment, providers should stop recommending epidural steroid injections for lumbar spinal stenosis.
—Ka Ming Gordon Ngai, MD, MPH
1. Manchikanti L, Pampati V, Boswell MV, et al. Analysis of the growth of epidural injections and costs in the Medicare population: a comparative evaluation of 1997, 2002, and 2006 data. Pain Physician 2010;13:199–212.
2. Manchikanti L, Pampati V, Falco FJ, et al. Assessment of the growth of epidural injections in the medicare population from 2000 to 2011. Pain Physician 2013;16:E349–364.
3. Shamliyan TA, Staal JB, Goldmann D, et al. Epidural steroid injections for radicular lumbosacral pain: a systematic review. Phys Med Rehabil Clin North Am 2014;25:471–89.
4. CDC. Multistate outbreak of fungal meningitis and other infections. 23 Oct 2013. Accessed 9 Jul 2014 at www.cdc.gov/hai/outbreaks/meningitis.html.
Study Overview
Objective. To determine the effectiveness of epidural injections of glucocorticoids plus anesthetic compared with injections of anesthetic alone in patients with lumbar spinal stenosis.
Design. The LESS (Lumbar Epidural Steroid Injection for Spinal Stenosis) trial—a double-blind, multisite, randomized controlled trial.
Setting and participants. The study was conducted at 16 sites in the United States and enrolled 400 patients between April 2011 and June 2013. Patients at least 50 years of age with spinal stenosis as evidenced by magnetic resonance imaging (MRI) or computed tomography (CT) were invited to participate. Additional eligibility criteria included an average pain rating of more than 4 on a scale of 0 to 10 (0 being the lowest score) for back, buttock, or leg pain. Patients were excluded if they did not have stenosis of the central canal, had spondylolisthesis requiring surgery, or had received epidural glucocorticoid injections within the previous 6 months. Patients were randomly assigned to receive a standard epidural injection of glucocorticoids plus lidocaine or lidocaine alone. At the 3-week follow-up they could choose to receive a repeat injection. At the 6-week assessment they were allowed to cross over to the other treatment group. Patients were blinded throughout the study. The treating physicians were also blinded through the use of 2 opaque prefilled syringes provided by the study staff—one marked “inject” and one marked “discard.”
Main outcome measures. The 2 outcomes, measured at 6 weeks, were the Roland-Morris Disability Questionnaire (RMDQ) score (range, 0 to 24, with higher scores indicating greater physical disability) and the patient’s rating of average buttock, hip, or leg pain in the previous week (scale of 0 to 10 with 0 indicating no pain and 10 indicating “pain as bad as you can imagine”).
Eight secondary patient-oriented outcomes were also measured: (1) at least minimal clinically meaningful improvement (≥ 30%), (2) substantial clinically meaningful improvement (≥ 50%), (3) average back pain in the previous week, and scores on the (4) Brief Pain Inventory (BPI) interference scale, (5) 8-question Patient Health Questionnaire (PHQ-8), (6) Generalized Anxiety Disorder 7 scale (GAD-7), (7) EQ-5D (a health status measure) and (8) Swiss Spinal Stenosis Questionnaire (SSSQ).
Main results. The 2 groups were similar with respect to baseline characteristics, except that the duration of pain was shorter in the lidocaine-alone group. At 6 weeks, both groups had improved RMDQ scores (glucocorticoid –4.2 points vs. no glucocorticoid –3.1 points, respectively). However, the difference in RMDQ score between the 2 groups was not statistically significant (–1.0 points [95% CI, –2.1 to 0.1]; P = 0.07). In addition, there was no difference in treatment effect at 6 weeks as measured by patient’s reported leg pain (–0.2 points [95% CI, –0.8 to 0.4]; P = 0.48). Furthermore, there were no significant differences in the secondary outcomes of clinically meaningful improvement, BPI, SSSQ symptoms and physical function, EQ-5D, and GAD-7 scales at 6 weeks. Among the secondary outcomes, only symptoms of depression and patient satisfaction showed a statistically significant improvement in the glucocorticoid plus lidocaine group. Of note, though not statistically significant, there were more adverse events in the glucocorticoid plus lidocaine group compared to the lidocaine alone group (21.5% vs. 15.5%, respectively). Finally, the glucocorticoid plus lidocaine group also had a significantly higher proportion of patients with cortisol serum suppression compared to the lidocaine alone group.
Conclusion. The authors concluded that there was no difference in pain-related functional disability (as measured by the RMDQ score) and pain intensity between patients receiving fluoroscopically guided epidural injections with glucocorticoids plus lidocaine compared with lidocaine alone for lumbar spinal stenosis. The injection of glucocorticoid should be avoided due to its potentially systemic effects, including suppression of the hypothalamic-pituitary axis and reduction in bone mineral density, which may increase the risk of fracture.
Commentary
Lumbar spinal stenosis is one of the most common causes of spine-related back and leg pain; it disproportionally affects older adults due to degenerative changes resulting in narrowing of the spinal canal and nerve-root. Epidural glucocorticoid injections containing a glucocorticoid and an anesthetic are commonly used to relieve symptoms of lumbar stenosis. While this treatment approach is controversial, more than 2.2 million lumbar epidural glucocorticoid injections are performed in the Medicare population each year [1,2]. Previous uncontrolled studies suggest that epidural glucocorticoid injections provide short-term pain relief for some patients with spinal stenosis [3]. While complications from the procedure are rare, a multistate outbreak of fungal meningitis due to contaminated glucocorticoid injections affected at least 751 patients with 64 deaths in 2012 [4].
The purpose of the current study by Friedly et al was to determine whether adding a glucocorticoid to an anesthetic in epidural spinal injections is superior to anesthetic alone for symptom relief and functional improvement in patients with lumbar spinal stenosis. In contrast to previous studies, the authors defined short-term results as 3 weeks after injection, and long-term results as 6 weeks after injection. Despite the shorter follow-up period, results were similar to previous studies, in that adding glucocorticoid to anesthetic in epidural spinal injection reduced pain and improved patient’s functionality short-term, but improvements were not sustained long-term. Based on these results, the authors concluded that there is no benefit in adding glucocorticoid epidural injections for back pain arising from lumbar spinal stenosis.
One major limitation of this study is the lack of a placebo arm. Because of the lack of a placebo arm, it cannot be ascertained whether epidural injection with lidocaine alone conferred a benefit. However, this study provides robust evidence that epidural steroid injections are not beneficial for treatment of back and leg pain associated with lumbar spinal stenosis.
Applications for Clinical Practice
Epidural steroid injection is long accepted in medical communities as a safe and effective treatment for lumbar spinal stenosis symptoms. In light of the potential dangers of epidural steroid injections, including meningitis, coupled with the increasing cost of the procedure, other potential side effects, and demonstrated ineffectiveness of the treatment, providers should stop recommending epidural steroid injections for lumbar spinal stenosis.
—Ka Ming Gordon Ngai, MD, MPH
Study Overview
Objective. To determine the effectiveness of epidural injections of glucocorticoids plus anesthetic compared with injections of anesthetic alone in patients with lumbar spinal stenosis.
Design. The LESS (Lumbar Epidural Steroid Injection for Spinal Stenosis) trial—a double-blind, multisite, randomized controlled trial.
Setting and participants. The study was conducted at 16 sites in the United States and enrolled 400 patients between April 2011 and June 2013. Patients at least 50 years of age with spinal stenosis as evidenced by magnetic resonance imaging (MRI) or computed tomography (CT) were invited to participate. Additional eligibility criteria included an average pain rating of more than 4 on a scale of 0 to 10 (0 being the lowest score) for back, buttock, or leg pain. Patients were excluded if they did not have stenosis of the central canal, had spondylolisthesis requiring surgery, or had received epidural glucocorticoid injections within the previous 6 months. Patients were randomly assigned to receive a standard epidural injection of glucocorticoids plus lidocaine or lidocaine alone. At the 3-week follow-up they could choose to receive a repeat injection. At the 6-week assessment they were allowed to cross over to the other treatment group. Patients were blinded throughout the study. The treating physicians were also blinded through the use of 2 opaque prefilled syringes provided by the study staff—one marked “inject” and one marked “discard.”
Main outcome measures. The 2 outcomes, measured at 6 weeks, were the Roland-Morris Disability Questionnaire (RMDQ) score (range, 0 to 24, with higher scores indicating greater physical disability) and the patient’s rating of average buttock, hip, or leg pain in the previous week (scale of 0 to 10 with 0 indicating no pain and 10 indicating “pain as bad as you can imagine”).
Eight secondary patient-oriented outcomes were also measured: (1) at least minimal clinically meaningful improvement (≥ 30%), (2) substantial clinically meaningful improvement (≥ 50%), (3) average back pain in the previous week, and scores on the (4) Brief Pain Inventory (BPI) interference scale, (5) 8-question Patient Health Questionnaire (PHQ-8), (6) Generalized Anxiety Disorder 7 scale (GAD-7), (7) EQ-5D (a health status measure) and (8) Swiss Spinal Stenosis Questionnaire (SSSQ).
Main results. The 2 groups were similar with respect to baseline characteristics, except that the duration of pain was shorter in the lidocaine-alone group. At 6 weeks, both groups had improved RMDQ scores (glucocorticoid –4.2 points vs. no glucocorticoid –3.1 points, respectively). However, the difference in RMDQ score between the 2 groups was not statistically significant (–1.0 points [95% CI, –2.1 to 0.1]; P = 0.07). In addition, there was no difference in treatment effect at 6 weeks as measured by patient’s reported leg pain (–0.2 points [95% CI, –0.8 to 0.4]; P = 0.48). Furthermore, there were no significant differences in the secondary outcomes of clinically meaningful improvement, BPI, SSSQ symptoms and physical function, EQ-5D, and GAD-7 scales at 6 weeks. Among the secondary outcomes, only symptoms of depression and patient satisfaction showed a statistically significant improvement in the glucocorticoid plus lidocaine group. Of note, though not statistically significant, there were more adverse events in the glucocorticoid plus lidocaine group compared to the lidocaine alone group (21.5% vs. 15.5%, respectively). Finally, the glucocorticoid plus lidocaine group also had a significantly higher proportion of patients with cortisol serum suppression compared to the lidocaine alone group.
Conclusion. The authors concluded that there was no difference in pain-related functional disability (as measured by the RMDQ score) and pain intensity between patients receiving fluoroscopically guided epidural injections with glucocorticoids plus lidocaine compared with lidocaine alone for lumbar spinal stenosis. The injection of glucocorticoid should be avoided due to its potentially systemic effects, including suppression of the hypothalamic-pituitary axis and reduction in bone mineral density, which may increase the risk of fracture.
Commentary
Lumbar spinal stenosis is one of the most common causes of spine-related back and leg pain; it disproportionally affects older adults due to degenerative changes resulting in narrowing of the spinal canal and nerve-root. Epidural glucocorticoid injections containing a glucocorticoid and an anesthetic are commonly used to relieve symptoms of lumbar stenosis. While this treatment approach is controversial, more than 2.2 million lumbar epidural glucocorticoid injections are performed in the Medicare population each year [1,2]. Previous uncontrolled studies suggest that epidural glucocorticoid injections provide short-term pain relief for some patients with spinal stenosis [3]. While complications from the procedure are rare, a multistate outbreak of fungal meningitis due to contaminated glucocorticoid injections affected at least 751 patients with 64 deaths in 2012 [4].
The purpose of the current study by Friedly et al was to determine whether adding a glucocorticoid to an anesthetic in epidural spinal injections is superior to anesthetic alone for symptom relief and functional improvement in patients with lumbar spinal stenosis. In contrast to previous studies, the authors defined short-term results as 3 weeks after injection, and long-term results as 6 weeks after injection. Despite the shorter follow-up period, results were similar to previous studies, in that adding glucocorticoid to anesthetic in epidural spinal injection reduced pain and improved patient’s functionality short-term, but improvements were not sustained long-term. Based on these results, the authors concluded that there is no benefit in adding glucocorticoid epidural injections for back pain arising from lumbar spinal stenosis.
One major limitation of this study is the lack of a placebo arm. Because of the lack of a placebo arm, it cannot be ascertained whether epidural injection with lidocaine alone conferred a benefit. However, this study provides robust evidence that epidural steroid injections are not beneficial for treatment of back and leg pain associated with lumbar spinal stenosis.
Applications for Clinical Practice
Epidural steroid injection is long accepted in medical communities as a safe and effective treatment for lumbar spinal stenosis symptoms. In light of the potential dangers of epidural steroid injections, including meningitis, coupled with the increasing cost of the procedure, other potential side effects, and demonstrated ineffectiveness of the treatment, providers should stop recommending epidural steroid injections for lumbar spinal stenosis.
—Ka Ming Gordon Ngai, MD, MPH
1. Manchikanti L, Pampati V, Boswell MV, et al. Analysis of the growth of epidural injections and costs in the Medicare population: a comparative evaluation of 1997, 2002, and 2006 data. Pain Physician 2010;13:199–212.
2. Manchikanti L, Pampati V, Falco FJ, et al. Assessment of the growth of epidural injections in the medicare population from 2000 to 2011. Pain Physician 2013;16:E349–364.
3. Shamliyan TA, Staal JB, Goldmann D, et al. Epidural steroid injections for radicular lumbosacral pain: a systematic review. Phys Med Rehabil Clin North Am 2014;25:471–89.
4. CDC. Multistate outbreak of fungal meningitis and other infections. 23 Oct 2013. Accessed 9 Jul 2014 at www.cdc.gov/hai/outbreaks/meningitis.html.
1. Manchikanti L, Pampati V, Boswell MV, et al. Analysis of the growth of epidural injections and costs in the Medicare population: a comparative evaluation of 1997, 2002, and 2006 data. Pain Physician 2010;13:199–212.
2. Manchikanti L, Pampati V, Falco FJ, et al. Assessment of the growth of epidural injections in the medicare population from 2000 to 2011. Pain Physician 2013;16:E349–364.
3. Shamliyan TA, Staal JB, Goldmann D, et al. Epidural steroid injections for radicular lumbosacral pain: a systematic review. Phys Med Rehabil Clin North Am 2014;25:471–89.
4. CDC. Multistate outbreak of fungal meningitis and other infections. 23 Oct 2013. Accessed 9 Jul 2014 at www.cdc.gov/hai/outbreaks/meningitis.html.
Supporting Primary Care Patient-Centered Medical Homes with Community Care Teams: Findings from a Pilot Study
From the Lehigh Valley Health Network, Allentown, PA.
Abstract
- Objective: With the growing recognition that team-based care might help meet the country’s primary care needs, this study’s objective was to evaluate the preliminary effectiveness of multidisciplinary community care teams (CCTs) deployed to primary care practices transforming into patient-centered medical homes (PCMHs).
- Methods: A nonrandomized longitudinal study design was used contrasting the CCT practices/patients with non-CCT comparison groups. Outcomes included utilization (ED/hospital use), quality indicators (QIs), practice joy, and patient satisfaction. Two CCTs (consisting of nurse care manager, behavioral health specialist, social worker, and pharmacist) were deployed to 6 primary care practices and provided services to 406 patients. Practice level analyses compared patients from the 6 CCT practices not receiving team services (29,881 patients) to 3 non-CCT practices (22,350 patients) that were also transforming toward PCMH. The comparison group for the patient level analyses (patients who received CCT services) was patients from the same CCT practice who did not receive CCT services.
- Results: At the practice level, there were significant improvements in QIs for practices both with and without CCTs. However, reductions in the probability of an admission and readmission occurred only for high-risk patients in CCT practices. At the patient level, the probability of an unplanned admission was reduced for CCT and non-CCT patients, but the probability of a readmission was only reduced in CCT patients receiving hospital discharge reconciliation calls from CCT staff.
- Conclusion: Preliminary results suggest possible added benefit of CCTs over PCMHs alone for reducing hospitalization.
As health care organizations move from a fee-for-service model to a value-based model in an accountable care environment, the transformation of primary care to patient-centered medical homes (PCMHs) is one of the fundamental strategies for achieving higher quality care at lower cost [1–3]. The core tenets of the PCMH are a commitment to high quality and safe care that is accessible, comprehensive, and coordinated across the health continuum, as well as patient-centered [4,5]. Newer to the PCMH model has been shifting the paradigm of care from individual encounters to using elements of population health management to proactively manage a panel of patients [1,3,6]. Given the array of patients seen in a primary care setting and the complexity of care required by many patients in a panel, particularly those with chronic conditions, a team approach to care capitalizes on multidisciplinary skills to collectively take responsibility for the ongoing care of the patients to improve health outcomes [7].
Multidisciplinary team-based care is considered a crucial strategy for meeting our society’s health care needs [8], especially in light of the expected shortage of primary care physicians coupled with the anticipated growth of the patient population due to the Affordable Care Act. Several different types of team-based care have been pursued. In 2003, for example, the State of Vermont pioneered health care reform through Vermont’s Blueprint for Health using principles of the PCMH that included team-based care [9]. The goal of the program was to deliver comprehensive and coordinated care to improve health outcomes for state residents. Vermont community health teams worked with primary care providers to manage short-term care for high-needs patients with an emphasis on better self-management, care coordination, chronic care management, and social and behavioral support services. An analysis of the first pilot program found significant decreases in hospital admissions and emergency department (ED) visits, and a per-person per-month reduction in costs [9].
The Lehigh Valley Health Network adapted the Vermont health improvement model to meet the unique needs of its practices that were transforming into PCMHs. When asked by leadership what would be most helpful in this transformational process, the practices cited additional staff resources to manage their high-risk patients. In response, the network enhanced support to the practices by implementing multidisciplinary teams called community care teams (CCTs), which were deployed to the practices to help manage their high-risk patients. The purpose of this study is to evaluate the effectiveness of CCTs within the PCMH model by examining key utilization, quality, and process measures. The CCTs were expected to increase the overall practice effectiveness and efficiency (practice level outcomes) by offsetting some of the workload regarding the management of high-risk patients and improving the outcomes of patients directly managed by the CCT (patient level outcomes).
Methods
Setting
Serving 5 counties, the Lehigh Valley Health Network is a large health care delivery system in southeastern PA that currently operates in a fee-for-service environment but is moving towards becoming an accountable care organization. The concept of using CCTs to support practices’ PCMH development originated with network leadership. Leadership approached 7 primary care practices with the most extensive PCMH involvement to pilot the CCT initiative (1 practice declined participation). More specifically, the practices were selected based upon their prior 3-year experience with practice transformation as a result of participating in the South Central PA Chronic Care Initiative [10] and having achieved National Committee for Quality Assurance level 3 PCMH recognition. Practice selection was also based on the results of a network-wide comprehensive practice assessment which included TransforMed’s MHIQ survey [11] of PCMH capabilities and in-house surveys to capture practice characteristics and readiness for change.
Program Design
The CCTs were designed to support 3 to 4 primary care practices in the short-term management of high-risk patients with chronic disease. Much like the Vermont community health team model, each team consisted of a RN care manager who functioned as the team lead, a behavioral health specialist, and a social worker. A clinical pharmacist was added to the CCT program shortly after implementing the project and was shared between 2 teams. The team engaged in population health management for patients identified as high-risk for poor outcomes by supporting the further development of disease self-management and goal setting skills, addressing behavioral health, social, and economic problems, and connecting the patient to other Network and community resources as needed. Furthermore, given the growing evidence demonstrating the positive impact of coordinated and continuity of care post hospital discharge on patient outcomes [12,13], the CCT also played a vital role in supporting the PCMH transition care program for high-risk patients, which involved contacting patients via the telephone within 48 business hours of discharge from the hospital to reconcile medications, assess and identify issues for follow-up, answer patient questions and coordinate appropriate appointments.
As a pilot program, 2 CCTs were deployed to 6 primary care practices (3 family medicine, 2 internal medicine, and 1 pediatric) in July 2012. Prior to engaging the practice and patients, each team member participated in an extensive orientation, which presented essential evidence-based knowledge on the CCT and PCMH models and provided application training and support in information systems, network resources, and care management.
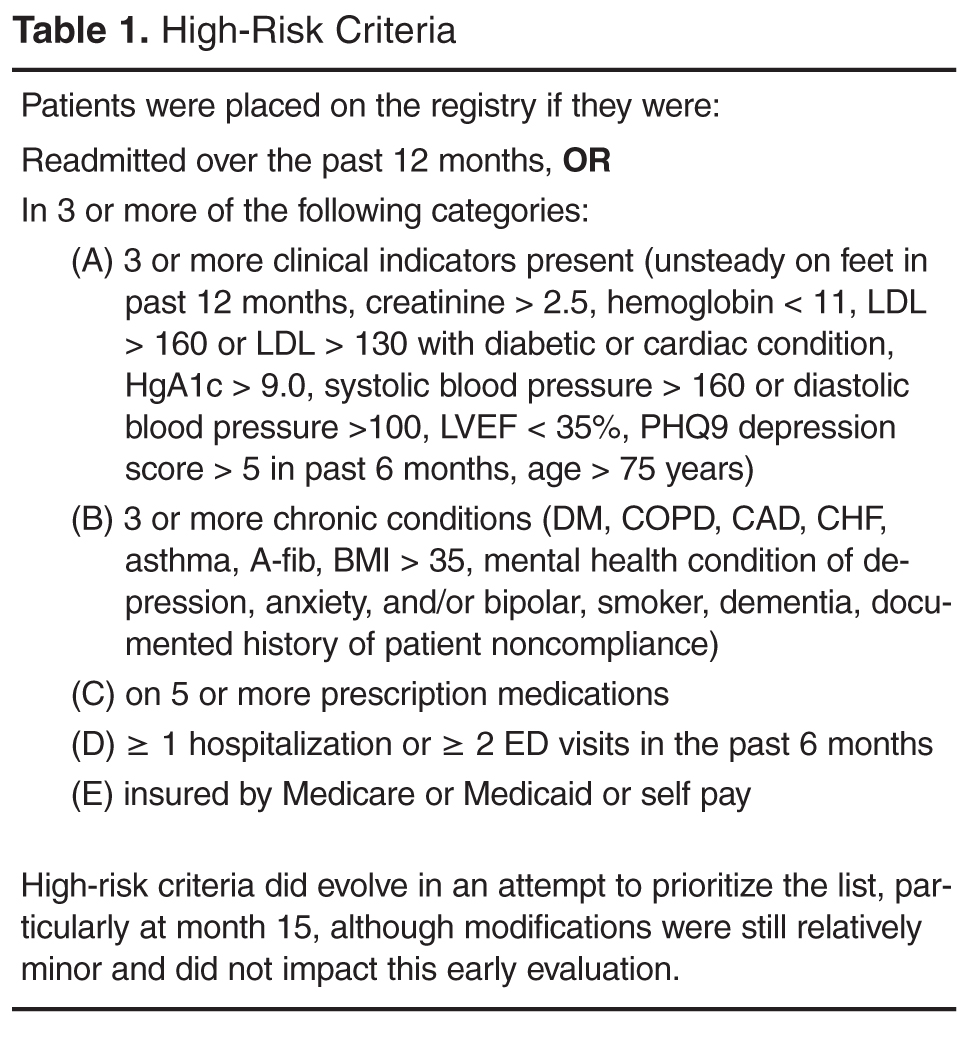
Initially the CCT care managers forwarded the high-risk registry to each provider to review and identify the top patients for proactive care management outreach. CCT care managers then called the identified patients and/or coordinated outreach with patients through office appointments scheduled in the near future. At the same time as the registry outreach began, on-site clinician referrals to the CCT and hospital discharge reconciliation calls to patients by the CCT care manager commenced. Clinician referrals did not have to meet any formal criteria in order for that patient to receive CCT services. Ideally, the program was designed to service high-risk patients on the registry; however, the majority of patient contacts for care management emerged through day-to-day clinician referrals (not necessarily high-risk) and discharge reconciliation calls to high-risk patients for months 2 through 8 of the pilot phase. Patients' care was managed with continued, ongoing services until either patient goals were met or the patient was transferred to another practice or nursing home, expired, or declined further care management assistance. The CCT behavioral health specialist addressed short-term issues or bridged the gap or need until long-term services could be coordinated, sometimes requiring 6 to 8 meetings with a patient. CCT social worker services were assigned on a case-by-case basis and occasionally provided longer-term or intermittent need management, such as medication assistance.
Study Design and Sample
A naturalistic longitudinal study design was used to evaluate the CCT’s preliminary effectiveness. The CCTs were evaluated at 2 levels. First, based on the assumption that the CCT would off-set some of the practice workload and allow the practices to proactively manage more of their patient population, the effectiveness of the CCTs was evaluated at the practice level, ie, patients who did not receive CCT services but belonged to practices with CCTs. Second, the effectiveness of the CCTs was evaluated at the patient level, ie, patients receiving CCT services. At both levels, the CCT groups were contrasted with “non-CCT” comparison groups of convenience.
![]()
Measures
Primary outcome measures were utilization: ED visits, all-cause unplanned admissions, and 30-day readmissions. Secondary outcome measures included 2 types of quality indicators(QIs, see Appendix for scoring): (a) gaps in care measures that captured whether providers were following standards of care for diabetes, ischemic vascular disease, and prevention; and (b) patient composites which reflected patient illness severity for diabetes and cardiac disease. Higher scores indicated more gaps in care or greater disease severity. Both types of QI measures required at least a 12-month window and thus could not be computed for patients engaged with the CCT who had only a 6-month follow-up period (as their scores could reflect their pre-CCT status). In addition, comprehensive care was denoted by the provision of depression screening on the PHQ-2 [14], and whether HgA1c was greater or equal to 9.0 in diabetics served as an additional patient outcome measure. Other secondary outcome measures included practice joy via the Well-Being in the Workplace Questionnaire (WWQ) [15] and patient satisfaction from CAHPS-CG 12-month survey with PCMH items [16].
Data Collection
Utilization and quality data were extracted from the network’s hospital and outpatient electronic medical records (EMR). Practice staff were emailed every 6 months and asked to anonymously complete the WWQ via Survey Monkey [17]. At baseline, patient satisfaction surveys were distributed in the practice, and patients had the option of anonymously completing them during their visit or returning them in a prepaid envelop. While not recommended for CAHPS, this procedure had been internally used with success previously. At 12 months, the same survey was mailed to a random sample of patients with a prepaid return envelope.
At the practice level, utilization and QI data were only available for patients from 4 of the 6 practices: data were not available for 1 non-EMR practice and there was negligible variation in utilization from the pediatric practice. For the patient level analyses, utilization was available for patients in all 6 practices.
Statistical Analyses
To test whether outcomes were improved relative to a comparison group following the introduction of CCTs into the practices (practice level analyses) or CCT engagement (patient level analyses), mixed models analyses of variance with repeated measures on Time (pre- vs. post-CCT) were conducted with SAS [18] PROC MIXED and PROC GENMOD for continuous and dichotomous outcomes, respectively. To determine whether there was greater improvement in the CCT groups, all models included the interaction between Time and Group (CCT versus no CCT) in addition to their main effects. At the practice level, high-risk and non-high-risk patients were analyzed separately. And, at the patient level, CCT-MNGT and CCT-DCREC patients were analyzed separately with results adjusted for patient’s age. Some variables were not normally distributed. The quality variables were able to be normalized with natural log transformations, but utilization variables had to be dichotomized into “any” versus “none” due to severe skewness, inflated 0s and larger-valued counts. Practice joy and patient satisfaction can only be reported at the practice level (responses were aggregated within each practice because anonymous responses do not permit linking specific respondents over time and different patients were sampled across measurement occasions) and non-parametric tests (Wilcoxon signed ranked tests and tests of dependent proportions) were used to test for change over time given the small sample size (n = 6).
Results
Patient Characteristics
Practice samples had slightly more women than men (55.2%), were largely white (95.0%) and 50 years of age on average (mean = 49.53, SD = 20.18). The prevalence of diabetes (10.2%) and cardiac disease (10.4%) was relatively low. The percentage of women (56.3%) and whites (96.4%) for the patient level analytic samples was similar to the practice samples, whereas the prevalence of diabetes (33.6% ) and cardiac disease (44.6%) was notable higher and patients were more than 10 years older on average (mean = 61.62, SD = 23.96).
Practice Level Outcomes
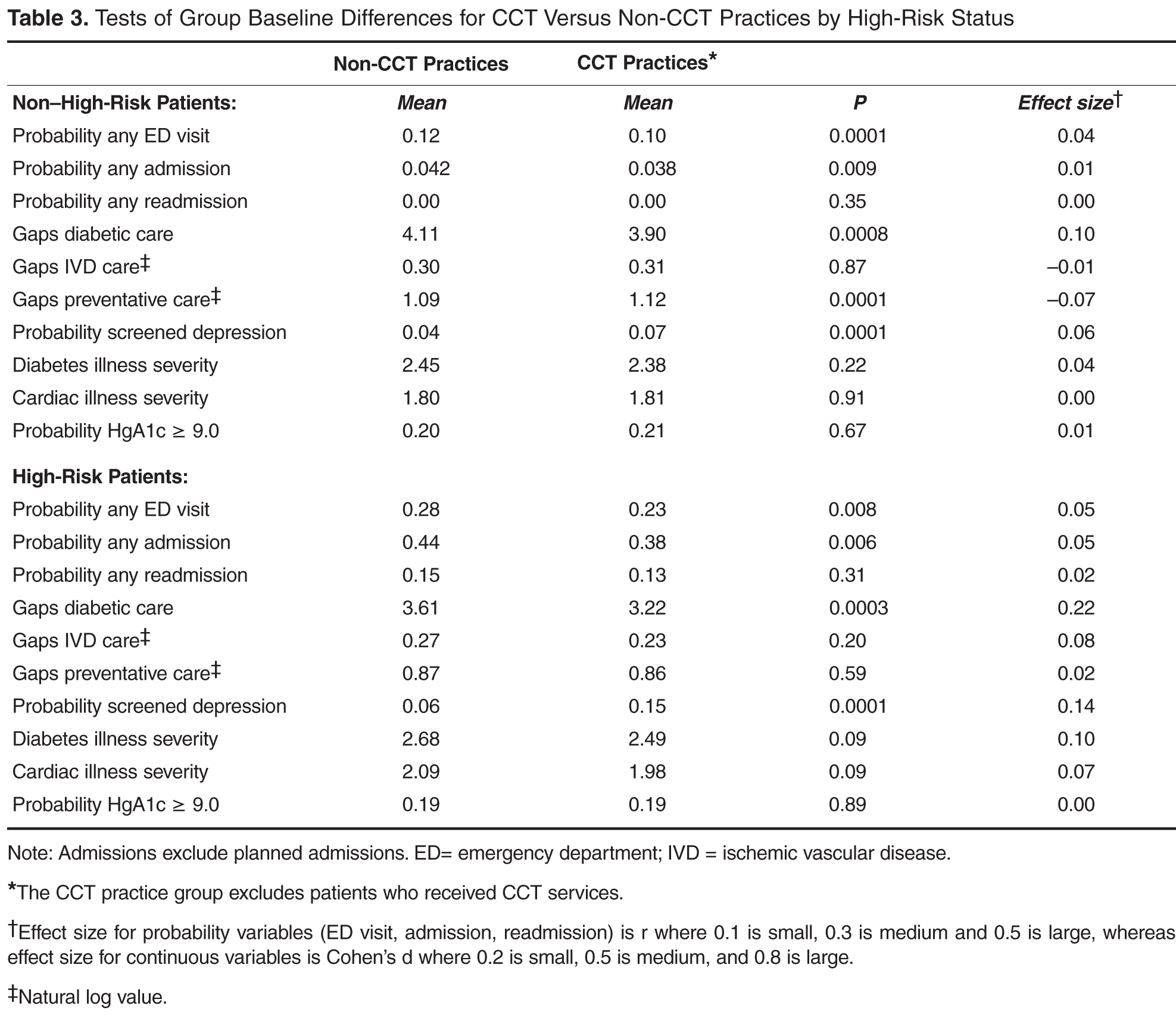
Given these group baseline differences and only one instance where the Time by Group interaction was significant where group baseline differences were absent (see below), simple pre-post analyses were conducted for each group separately (Table 4). The results for non-high-risk patients indicated that, in both CCT and non-CCT practices, there was no improvement in utilization, but there were significant reductions in gaps in diabetic and preventative care and cardiac illness severity and significant increases in depression screening, although effect sizes for the latter 2 outcomes were small to negligible. 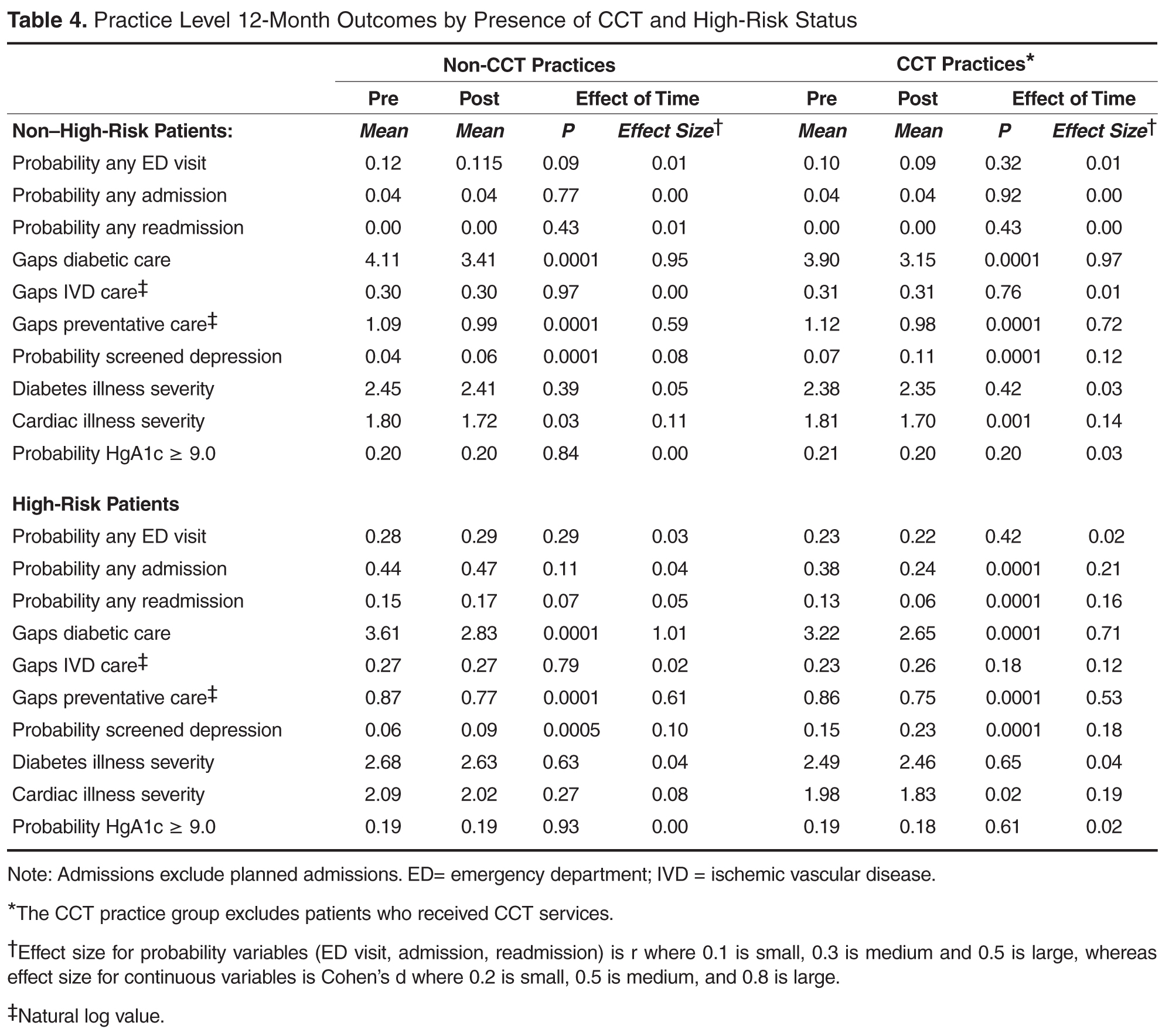
Practice joy fell in the medium range [19] at all time-points, with no notable change over time (see Appendix in the online version of this article). There was also no change in patient satisfaction (see Appendix, online), although after 12 months the “always” response for following up on lab tests was no longer higher than the national comparison and helpfulness of staff rated “never/sometimes” was below the national comparison.
Patient Level Outcomes
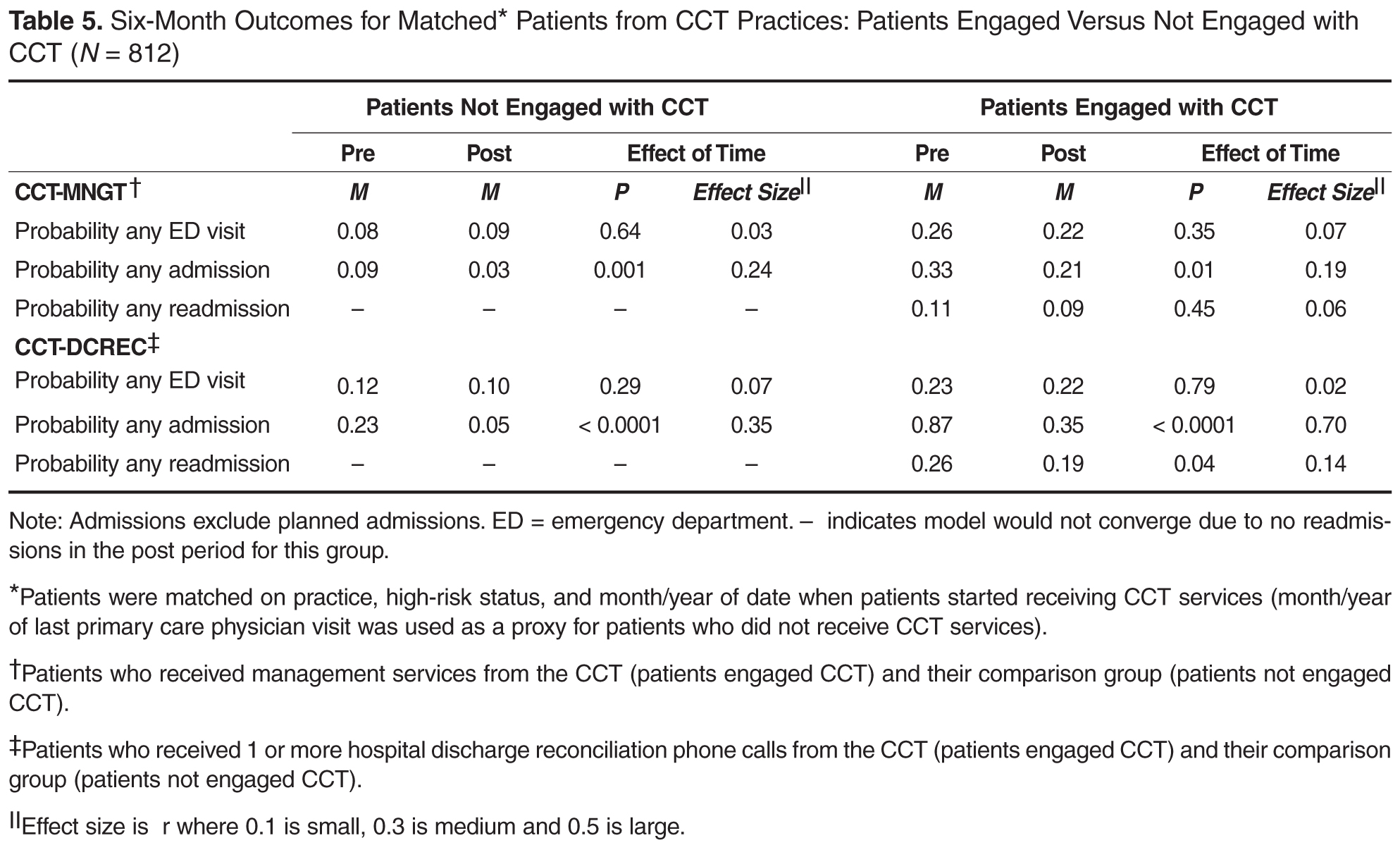
Discussion
The empirical literature indicates that PCMH practice transformation is a long, effortful process, the effects of which are not quick to manifest [20–22]. In this context, the results of the preliminary evaluation of the CCT pilot were encouraging: team-based care in the form of CCTs can be effectively used to support population health management. Overall, the results at the practice level suggest that PCMH transformation alone may be effective in creating improvements in patient care and cardiac disease (there were improvements in 3 out of 4 care gap measures and 1 disease measure for both CCT and non-CCT practices), but the presence of CCT appears necessary to reduce unplanned admissions and readmissions, at least among high-risk patients. Of course, this reduced utilization at the practice level could also be due to selection bias (practices with the longest PCMH involvement were selected for the CCT pilot) and it awaits to be seen if this finding holds as CCTs are deployed to more practices. Still, similar evidence for the CCT was found at the patient level. The probability of an unplanned admission was reduced for all groups of patients from CCT practices; however, this effect was notably large only for patients who received hospital discharge reconciliation calls from the CCT. Moreover, the only group that had a significant reduction in the probability of a 30-day readmission was also patients who received hospital discharge reconciliation calls from the CCT. Both results suggest an added benefit of CCT engagement. Although there was no change in the probability of an ED visit for any group, the CCT staff indicated that there was a substantial minority of CCT-engaged patients who were not accessing the ED when they should have been and it might be that increased appropriate use by this minority due to CCT coaching therefore cancelled out expected reductions in ED use among other CCT patients.
The intent of the current endeavor was to perform a formative evaluation [23,24] of the CCTs effectiveness. We recognized there would be analytic challenges and limits to such early-stage analyses. Nonetheless, we believed it was vital, especially given the cost of the CCTs and the growing financial pressure on health care networks more globally, to determine the preliminary effectiveness of the CCTs’, care management interventions and, if possible, suggest improvements to the intervention. As intended in formative evaluations, the evaluation is ongoing. Future analyses will bring more rigor to the evaluation and solve the data and analytic obstacles that affected the results of this first round of analyses.
A major learning of the early-stage analyses was the difficulty in developing comparison groups that are equivalent to the intervention groups at baseline. A number of matching schemes were attempted at the patient level in addition to the one presented here, but they were equally problematic. Avenues for creating more valid comparison groups in the future include the use of propensity score matching as well as drawing comparison groups from data from other networks. In addition, as time passes and more than 1 follow-up point is available for analysis, multilevel modeling can be employed which can specify different intercepts (baseline values) for groups. Still, it’s worth noting that constructing appropriate comparison groups is challenging even with those approaches: most health networks do not collect data on the most relevant matching variables (eg, health literacy, social economic status, social isolation/support) due to their cost and burden to both practices and patients.
Another major gap revealed by the early-stage analyses was the need to improve the strategy used for selecting patients for CCT intervention. In addition to many physician referrals, there was a large number of patients on the high-risk registry who required intervention relative to the small CCT staff. Various strategies to prioritize the list were attempted, including cost-related analyses. As plagued the formation of comparisons groups, it seemed the variables most critical to risk stratification were unavailable in administrative datasets. Appreciating that data collection is costly and patients and busy practices already have survey fatigue, the evaluation team examined the empirical literature for a single useful tool for ranking patients as well as constructing better matched comparison groups. This search indicated that a measure of patient activation [25–27] would be particularly helpful not only for selecting the riskiest and costliest patients for CCT intervention but also for tailoring CCT services to different types of patients. Since the implementation of the CCTs the network has also contracted with a predictive analytics company to provide risk scores for the patients.
The current formative evaluation was an important learning journey, laying important ground work for better evaluating the CCTs’ effectiveness specifically and eventually becoming an accountable care provider more generally. If the network is to provide health care more effectively and efficiently, it will need to bring greater rigor to evaluations of its various interventions and other ACO endeavors. The current formative evaluation was a valuable demonstration to non-scientists of the weakness of single group pre-post designs and how more rigorous evaluations, which include comparison groups and address confounding variables, can enhance the validity of the analytic results. This learning journey also highlighted the limitations of administrative databases and the necessity of both primary data collection and mixed methods. For example, it seems that some practices may require educational interventions to take full advantage of the CCT and qualitative assessments on practice readiness seem a necessary addition to the quantitative practice assessment to identify the specific characteristics that need strengthening. In addition, the evaluation team also recently added a qualitative sub-study on high-risk patients’ experience with the CCT to overcome locally low CAHPS response rates and capture themes broader than patient satisfaction. Upcoming rounds of analyses will also tackle other aspects of formative evaluations including the study of the CCT implementation as more practices receive CCTs and determining if process and fidelity measures of the PCMH pillars are linked to better outcomes. Furthermore, future analytic plans include identifying the active ingredients and optimal doses of the CCT intervention as well as determine the most effective matches between different types of patients and different CCT interventions (eg, behavioral, care management, social, pharmacy). While we appreciate that barriers still remain and require solutions, we hope the current evaluation highlights the utility of performing such formative evaluations.
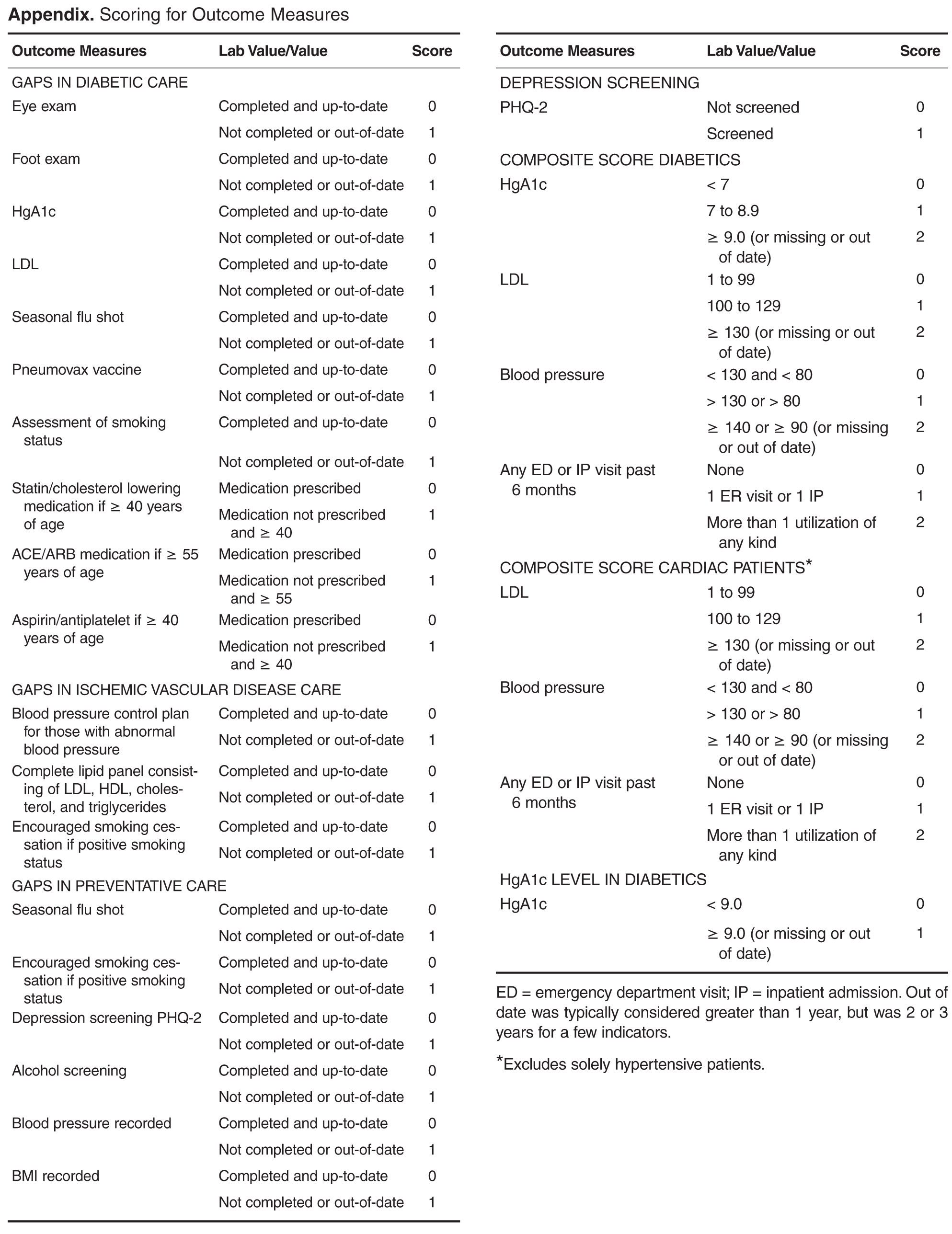
Corresponding author: Carol Foltz, PhD, Lehigh Valley Health Network, Allentown, PA, [email protected].
Funding/support: The evaluation was funded internally by Lehigh Valley Health Network and a close affiliate, the Lehigh Valley Physician Hospital Organization. The funding organizations had no role in any part of the study.
Financial disclosures: None.
1. Rittenhouse DR, Shortell SM, Fisher ES. Primary care and accountable care—two essential elements of delivery-system reform. N Engl J Med 2009;361:2301–3.
2. American Academy of Family Physicians. Primary care for the 21st century: Ensuring a quality, physician-led team for every patient. September 2012. Accessed at www.aafp.org/dam/AAFP/documents/about_us/initiatives/AAFP-PCMHWhitePaper.pdf.
3. Agency for Healthcare Research and Quality. The patient-centered medical home: Strategies to put patients at the center of primary care, February 2011. Accessed at http://pcmh.ahrq.gov/sites/default/files/attachments/Strategies%20to%20Put%20Patients%20at%20the%20Center%20of%20Primary%20Care.pdf.
4. Agency for Healthcare Research and Quality. Defining the PCMH. Accessed at http://pcmh.ahrq.gov/page/defining-pcmh.
5. Patient-Centered Primary Care Collaborative. Defining the medical home: A patient-centered philosophy that drives primary care excellence. Accessed at http://pcmh.ahrq.gov/page/defining-pcmh.
6. Margolius D, Bodenheimer T. Transforming primary care: From past practice to the practice of the future. Health Aff 2010;29:779–84.
7. Robert Graham Center. The patient centered medical home: History, seven core features, evidence and transformational change, 2007. Accessed at www.graham-center.org/online/etc/medialib/graham/documents/publications/mongraphs-books/2007/rgcmo-medical-home.Par.0001.File.tmp/rgcmo-medical-home.pdf.
8. Goldberg A. It matters how we define health care equity. Institute of Medicine. Accessed at www.iom.edu/~/media/Files/Perspectives-Files/2013/Commentaries/BPH-It-Matters-How-we-define-Health-Equity.pdf.
9. Bielaszka-DuVernay C. Vermont’s blueprint for medical homes, community health teams, and better health at lower cost. Health Aff 2011;30:383–6.
10. Bricker PL, Baron RJ, Scheirer JJ. Collaboration in Pennsylvania: rapidly spreading improved chronic care for patients to practices. J Cont Educ Health Prof 2010;30:114–25.
11.TransforMed. What does your medical home look like? A jumble of unconnected pieces or a coherent structure? Accessed at www.transformed.com/mhiq/welcome.cfm .
12. Health policy brief: care transitions. Health Aff 2012. Accessed at http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_76.pdf.
13. Greenwald J, Denham C, Jack B. The hospital discharge: A review of a high-risk care transition with highlights of a reengineered discharge process. J Patient Saf 2007;3:97–106.
14. Kroenke K, Spitzer R, Williams W. The patient health questionnaire-2: validity of a two-item depression screener. Med Care 2003;41:1284–94.
15. Parker GB, Hyett MP. Measurement of well-being in the workplace: The development of the Work Well-Being Questionnaire. Nerv Ment Dis 2011;199:394-97.
16. Agency for Healthcare Research and Quality. Clinician & group expanded 12-month survey with CAHPS patient-centered medical home (PCMH) items. Accessed at https://cahps.ahrq.gov/surveys-guidance/cg/pcmh/index.html.
17. SurveyMonkey. Accessed at http://www.surveymonkey.com (last visited 06-23-2014). SurveyMonkey: Palo Alto, CA.
18. SAS [computer program]. Version 9.2. Cary, NC: SAS Institute; 2002-2008.
19. Black Dog Institute. Accessed at www.blackdoginstitute.org.au/docs/workplacewellbeingquestionnairepaperversion.pdf.
20. Jaén CR, Ferrer, RL, Miller WL, Palmer RF. Patient outcomes at 26 months in the patient-centered medical home national demonstration project. Ann Fam Med 2010;8(Suppl 1):s57–s67.
21. Solberg LI, Asche SE, Fontaine P, Flottemesch TJ. Trends in quality during medical home transformation. Ann Fam Med 2011;9:515–21.
22. Crabtree BF, Nutting PA, Miller WL, Stange KC. Summary of the national demonstration project and recommendations for the patient-centered medical home. Ann Fam Med 2010;8(Suppl 1):s80–s90.
23. Stetler CB, Legro MW, Wallace CM et al. The role of formative evaluation in implementation research and the QUERI experience. J Gen Intern Med 2006;21:S1–8.
24. Geonnotti K, Peikes D, Wang W, Smith J. Formative evaluation: fostering real-time adaptations and refinements to improve the effectiveness of patient-centered medical home models. Rockville, MD: Agency for Healthcare Research and Quality. February 2013. AHRQ Publication No. 13-0025-EF.
25. Insignia Health. Accessed at www.insigniahealth.com/solutions/patient-activation-measure.
26. Hibbard JH, Greene J, Overton V. Patients with lower activation associated with higher costs; delivery systems should know their patients’ ‘scores’. Health Aff 2013;32:216–22.
27. Hibbard JH, Greene J. What The evidence shows about patient activation: better health outcomes and care experiences fewer data on costs. Health Aff 2013;32:207–14.
From the Lehigh Valley Health Network, Allentown, PA.
Abstract
- Objective: With the growing recognition that team-based care might help meet the country’s primary care needs, this study’s objective was to evaluate the preliminary effectiveness of multidisciplinary community care teams (CCTs) deployed to primary care practices transforming into patient-centered medical homes (PCMHs).
- Methods: A nonrandomized longitudinal study design was used contrasting the CCT practices/patients with non-CCT comparison groups. Outcomes included utilization (ED/hospital use), quality indicators (QIs), practice joy, and patient satisfaction. Two CCTs (consisting of nurse care manager, behavioral health specialist, social worker, and pharmacist) were deployed to 6 primary care practices and provided services to 406 patients. Practice level analyses compared patients from the 6 CCT practices not receiving team services (29,881 patients) to 3 non-CCT practices (22,350 patients) that were also transforming toward PCMH. The comparison group for the patient level analyses (patients who received CCT services) was patients from the same CCT practice who did not receive CCT services.
- Results: At the practice level, there were significant improvements in QIs for practices both with and without CCTs. However, reductions in the probability of an admission and readmission occurred only for high-risk patients in CCT practices. At the patient level, the probability of an unplanned admission was reduced for CCT and non-CCT patients, but the probability of a readmission was only reduced in CCT patients receiving hospital discharge reconciliation calls from CCT staff.
- Conclusion: Preliminary results suggest possible added benefit of CCTs over PCMHs alone for reducing hospitalization.
As health care organizations move from a fee-for-service model to a value-based model in an accountable care environment, the transformation of primary care to patient-centered medical homes (PCMHs) is one of the fundamental strategies for achieving higher quality care at lower cost [1–3]. The core tenets of the PCMH are a commitment to high quality and safe care that is accessible, comprehensive, and coordinated across the health continuum, as well as patient-centered [4,5]. Newer to the PCMH model has been shifting the paradigm of care from individual encounters to using elements of population health management to proactively manage a panel of patients [1,3,6]. Given the array of patients seen in a primary care setting and the complexity of care required by many patients in a panel, particularly those with chronic conditions, a team approach to care capitalizes on multidisciplinary skills to collectively take responsibility for the ongoing care of the patients to improve health outcomes [7].
Multidisciplinary team-based care is considered a crucial strategy for meeting our society’s health care needs [8], especially in light of the expected shortage of primary care physicians coupled with the anticipated growth of the patient population due to the Affordable Care Act. Several different types of team-based care have been pursued. In 2003, for example, the State of Vermont pioneered health care reform through Vermont’s Blueprint for Health using principles of the PCMH that included team-based care [9]. The goal of the program was to deliver comprehensive and coordinated care to improve health outcomes for state residents. Vermont community health teams worked with primary care providers to manage short-term care for high-needs patients with an emphasis on better self-management, care coordination, chronic care management, and social and behavioral support services. An analysis of the first pilot program found significant decreases in hospital admissions and emergency department (ED) visits, and a per-person per-month reduction in costs [9].
The Lehigh Valley Health Network adapted the Vermont health improvement model to meet the unique needs of its practices that were transforming into PCMHs. When asked by leadership what would be most helpful in this transformational process, the practices cited additional staff resources to manage their high-risk patients. In response, the network enhanced support to the practices by implementing multidisciplinary teams called community care teams (CCTs), which were deployed to the practices to help manage their high-risk patients. The purpose of this study is to evaluate the effectiveness of CCTs within the PCMH model by examining key utilization, quality, and process measures. The CCTs were expected to increase the overall practice effectiveness and efficiency (practice level outcomes) by offsetting some of the workload regarding the management of high-risk patients and improving the outcomes of patients directly managed by the CCT (patient level outcomes).
Methods
Setting
Serving 5 counties, the Lehigh Valley Health Network is a large health care delivery system in southeastern PA that currently operates in a fee-for-service environment but is moving towards becoming an accountable care organization. The concept of using CCTs to support practices’ PCMH development originated with network leadership. Leadership approached 7 primary care practices with the most extensive PCMH involvement to pilot the CCT initiative (1 practice declined participation). More specifically, the practices were selected based upon their prior 3-year experience with practice transformation as a result of participating in the South Central PA Chronic Care Initiative [10] and having achieved National Committee for Quality Assurance level 3 PCMH recognition. Practice selection was also based on the results of a network-wide comprehensive practice assessment which included TransforMed’s MHIQ survey [11] of PCMH capabilities and in-house surveys to capture practice characteristics and readiness for change.
Program Design
The CCTs were designed to support 3 to 4 primary care practices in the short-term management of high-risk patients with chronic disease. Much like the Vermont community health team model, each team consisted of a RN care manager who functioned as the team lead, a behavioral health specialist, and a social worker. A clinical pharmacist was added to the CCT program shortly after implementing the project and was shared between 2 teams. The team engaged in population health management for patients identified as high-risk for poor outcomes by supporting the further development of disease self-management and goal setting skills, addressing behavioral health, social, and economic problems, and connecting the patient to other Network and community resources as needed. Furthermore, given the growing evidence demonstrating the positive impact of coordinated and continuity of care post hospital discharge on patient outcomes [12,13], the CCT also played a vital role in supporting the PCMH transition care program for high-risk patients, which involved contacting patients via the telephone within 48 business hours of discharge from the hospital to reconcile medications, assess and identify issues for follow-up, answer patient questions and coordinate appropriate appointments.
As a pilot program, 2 CCTs were deployed to 6 primary care practices (3 family medicine, 2 internal medicine, and 1 pediatric) in July 2012. Prior to engaging the practice and patients, each team member participated in an extensive orientation, which presented essential evidence-based knowledge on the CCT and PCMH models and provided application training and support in information systems, network resources, and care management.
Initially the CCT care managers forwarded the high-risk registry to each provider to review and identify the top patients for proactive care management outreach. CCT care managers then called the identified patients and/or coordinated outreach with patients through office appointments scheduled in the near future. At the same time as the registry outreach began, on-site clinician referrals to the CCT and hospital discharge reconciliation calls to patients by the CCT care manager commenced. Clinician referrals did not have to meet any formal criteria in order for that patient to receive CCT services. Ideally, the program was designed to service high-risk patients on the registry; however, the majority of patient contacts for care management emerged through day-to-day clinician referrals (not necessarily high-risk) and discharge reconciliation calls to high-risk patients for months 2 through 8 of the pilot phase. Patients' care was managed with continued, ongoing services until either patient goals were met or the patient was transferred to another practice or nursing home, expired, or declined further care management assistance. The CCT behavioral health specialist addressed short-term issues or bridged the gap or need until long-term services could be coordinated, sometimes requiring 6 to 8 meetings with a patient. CCT social worker services were assigned on a case-by-case basis and occasionally provided longer-term or intermittent need management, such as medication assistance.
Study Design and Sample
A naturalistic longitudinal study design was used to evaluate the CCT’s preliminary effectiveness. The CCTs were evaluated at 2 levels. First, based on the assumption that the CCT would off-set some of the practice workload and allow the practices to proactively manage more of their patient population, the effectiveness of the CCTs was evaluated at the practice level, ie, patients who did not receive CCT services but belonged to practices with CCTs. Second, the effectiveness of the CCTs was evaluated at the patient level, ie, patients receiving CCT services. At both levels, the CCT groups were contrasted with “non-CCT” comparison groups of convenience.
![]()
Measures
Primary outcome measures were utilization: ED visits, all-cause unplanned admissions, and 30-day readmissions. Secondary outcome measures included 2 types of quality indicators(QIs, see Appendix for scoring): (a) gaps in care measures that captured whether providers were following standards of care for diabetes, ischemic vascular disease, and prevention; and (b) patient composites which reflected patient illness severity for diabetes and cardiac disease. Higher scores indicated more gaps in care or greater disease severity. Both types of QI measures required at least a 12-month window and thus could not be computed for patients engaged with the CCT who had only a 6-month follow-up period (as their scores could reflect their pre-CCT status). In addition, comprehensive care was denoted by the provision of depression screening on the PHQ-2 [14], and whether HgA1c was greater or equal to 9.0 in diabetics served as an additional patient outcome measure. Other secondary outcome measures included practice joy via the Well-Being in the Workplace Questionnaire (WWQ) [15] and patient satisfaction from CAHPS-CG 12-month survey with PCMH items [16].
Data Collection
Utilization and quality data were extracted from the network’s hospital and outpatient electronic medical records (EMR). Practice staff were emailed every 6 months and asked to anonymously complete the WWQ via Survey Monkey [17]. At baseline, patient satisfaction surveys were distributed in the practice, and patients had the option of anonymously completing them during their visit or returning them in a prepaid envelop. While not recommended for CAHPS, this procedure had been internally used with success previously. At 12 months, the same survey was mailed to a random sample of patients with a prepaid return envelope.
At the practice level, utilization and QI data were only available for patients from 4 of the 6 practices: data were not available for 1 non-EMR practice and there was negligible variation in utilization from the pediatric practice. For the patient level analyses, utilization was available for patients in all 6 practices.
Statistical Analyses
To test whether outcomes were improved relative to a comparison group following the introduction of CCTs into the practices (practice level analyses) or CCT engagement (patient level analyses), mixed models analyses of variance with repeated measures on Time (pre- vs. post-CCT) were conducted with SAS [18] PROC MIXED and PROC GENMOD for continuous and dichotomous outcomes, respectively. To determine whether there was greater improvement in the CCT groups, all models included the interaction between Time and Group (CCT versus no CCT) in addition to their main effects. At the practice level, high-risk and non-high-risk patients were analyzed separately. And, at the patient level, CCT-MNGT and CCT-DCREC patients were analyzed separately with results adjusted for patient’s age. Some variables were not normally distributed. The quality variables were able to be normalized with natural log transformations, but utilization variables had to be dichotomized into “any” versus “none” due to severe skewness, inflated 0s and larger-valued counts. Practice joy and patient satisfaction can only be reported at the practice level (responses were aggregated within each practice because anonymous responses do not permit linking specific respondents over time and different patients were sampled across measurement occasions) and non-parametric tests (Wilcoxon signed ranked tests and tests of dependent proportions) were used to test for change over time given the small sample size (n = 6).
Results
Patient Characteristics
Practice samples had slightly more women than men (55.2%), were largely white (95.0%) and 50 years of age on average (mean = 49.53, SD = 20.18). The prevalence of diabetes (10.2%) and cardiac disease (10.4%) was relatively low. The percentage of women (56.3%) and whites (96.4%) for the patient level analytic samples was similar to the practice samples, whereas the prevalence of diabetes (33.6% ) and cardiac disease (44.6%) was notable higher and patients were more than 10 years older on average (mean = 61.62, SD = 23.96).
Practice Level Outcomes
Given these group baseline differences and only one instance where the Time by Group interaction was significant where group baseline differences were absent (see below), simple pre-post analyses were conducted for each group separately (Table 4). The results for non-high-risk patients indicated that, in both CCT and non-CCT practices, there was no improvement in utilization, but there were significant reductions in gaps in diabetic and preventative care and cardiac illness severity and significant increases in depression screening, although effect sizes for the latter 2 outcomes were small to negligible.
Practice joy fell in the medium range [19] at all time-points, with no notable change over time (see Appendix in the online version of this article). There was also no change in patient satisfaction (see Appendix, online), although after 12 months the “always” response for following up on lab tests was no longer higher than the national comparison and helpfulness of staff rated “never/sometimes” was below the national comparison.
Patient Level Outcomes
Discussion
The empirical literature indicates that PCMH practice transformation is a long, effortful process, the effects of which are not quick to manifest [20–22]. In this context, the results of the preliminary evaluation of the CCT pilot were encouraging: team-based care in the form of CCTs can be effectively used to support population health management. Overall, the results at the practice level suggest that PCMH transformation alone may be effective in creating improvements in patient care and cardiac disease (there were improvements in 3 out of 4 care gap measures and 1 disease measure for both CCT and non-CCT practices), but the presence of CCT appears necessary to reduce unplanned admissions and readmissions, at least among high-risk patients. Of course, this reduced utilization at the practice level could also be due to selection bias (practices with the longest PCMH involvement were selected for the CCT pilot) and it awaits to be seen if this finding holds as CCTs are deployed to more practices. Still, similar evidence for the CCT was found at the patient level. The probability of an unplanned admission was reduced for all groups of patients from CCT practices; however, this effect was notably large only for patients who received hospital discharge reconciliation calls from the CCT. Moreover, the only group that had a significant reduction in the probability of a 30-day readmission was also patients who received hospital discharge reconciliation calls from the CCT. Both results suggest an added benefit of CCT engagement. Although there was no change in the probability of an ED visit for any group, the CCT staff indicated that there was a substantial minority of CCT-engaged patients who were not accessing the ED when they should have been and it might be that increased appropriate use by this minority due to CCT coaching therefore cancelled out expected reductions in ED use among other CCT patients.
The intent of the current endeavor was to perform a formative evaluation [23,24] of the CCTs effectiveness. We recognized there would be analytic challenges and limits to such early-stage analyses. Nonetheless, we believed it was vital, especially given the cost of the CCTs and the growing financial pressure on health care networks more globally, to determine the preliminary effectiveness of the CCTs’, care management interventions and, if possible, suggest improvements to the intervention. As intended in formative evaluations, the evaluation is ongoing. Future analyses will bring more rigor to the evaluation and solve the data and analytic obstacles that affected the results of this first round of analyses.
A major learning of the early-stage analyses was the difficulty in developing comparison groups that are equivalent to the intervention groups at baseline. A number of matching schemes were attempted at the patient level in addition to the one presented here, but they were equally problematic. Avenues for creating more valid comparison groups in the future include the use of propensity score matching as well as drawing comparison groups from data from other networks. In addition, as time passes and more than 1 follow-up point is available for analysis, multilevel modeling can be employed which can specify different intercepts (baseline values) for groups. Still, it’s worth noting that constructing appropriate comparison groups is challenging even with those approaches: most health networks do not collect data on the most relevant matching variables (eg, health literacy, social economic status, social isolation/support) due to their cost and burden to both practices and patients.
Another major gap revealed by the early-stage analyses was the need to improve the strategy used for selecting patients for CCT intervention. In addition to many physician referrals, there was a large number of patients on the high-risk registry who required intervention relative to the small CCT staff. Various strategies to prioritize the list were attempted, including cost-related analyses. As plagued the formation of comparisons groups, it seemed the variables most critical to risk stratification were unavailable in administrative datasets. Appreciating that data collection is costly and patients and busy practices already have survey fatigue, the evaluation team examined the empirical literature for a single useful tool for ranking patients as well as constructing better matched comparison groups. This search indicated that a measure of patient activation [25–27] would be particularly helpful not only for selecting the riskiest and costliest patients for CCT intervention but also for tailoring CCT services to different types of patients. Since the implementation of the CCTs the network has also contracted with a predictive analytics company to provide risk scores for the patients.
The current formative evaluation was an important learning journey, laying important ground work for better evaluating the CCTs’ effectiveness specifically and eventually becoming an accountable care provider more generally. If the network is to provide health care more effectively and efficiently, it will need to bring greater rigor to evaluations of its various interventions and other ACO endeavors. The current formative evaluation was a valuable demonstration to non-scientists of the weakness of single group pre-post designs and how more rigorous evaluations, which include comparison groups and address confounding variables, can enhance the validity of the analytic results. This learning journey also highlighted the limitations of administrative databases and the necessity of both primary data collection and mixed methods. For example, it seems that some practices may require educational interventions to take full advantage of the CCT and qualitative assessments on practice readiness seem a necessary addition to the quantitative practice assessment to identify the specific characteristics that need strengthening. In addition, the evaluation team also recently added a qualitative sub-study on high-risk patients’ experience with the CCT to overcome locally low CAHPS response rates and capture themes broader than patient satisfaction. Upcoming rounds of analyses will also tackle other aspects of formative evaluations including the study of the CCT implementation as more practices receive CCTs and determining if process and fidelity measures of the PCMH pillars are linked to better outcomes. Furthermore, future analytic plans include identifying the active ingredients and optimal doses of the CCT intervention as well as determine the most effective matches between different types of patients and different CCT interventions (eg, behavioral, care management, social, pharmacy). While we appreciate that barriers still remain and require solutions, we hope the current evaluation highlights the utility of performing such formative evaluations.
Corresponding author: Carol Foltz, PhD, Lehigh Valley Health Network, Allentown, PA, [email protected].
Funding/support: The evaluation was funded internally by Lehigh Valley Health Network and a close affiliate, the Lehigh Valley Physician Hospital Organization. The funding organizations had no role in any part of the study.
Financial disclosures: None.
From the Lehigh Valley Health Network, Allentown, PA.
Abstract
- Objective: With the growing recognition that team-based care might help meet the country’s primary care needs, this study’s objective was to evaluate the preliminary effectiveness of multidisciplinary community care teams (CCTs) deployed to primary care practices transforming into patient-centered medical homes (PCMHs).
- Methods: A nonrandomized longitudinal study design was used contrasting the CCT practices/patients with non-CCT comparison groups. Outcomes included utilization (ED/hospital use), quality indicators (QIs), practice joy, and patient satisfaction. Two CCTs (consisting of nurse care manager, behavioral health specialist, social worker, and pharmacist) were deployed to 6 primary care practices and provided services to 406 patients. Practice level analyses compared patients from the 6 CCT practices not receiving team services (29,881 patients) to 3 non-CCT practices (22,350 patients) that were also transforming toward PCMH. The comparison group for the patient level analyses (patients who received CCT services) was patients from the same CCT practice who did not receive CCT services.
- Results: At the practice level, there were significant improvements in QIs for practices both with and without CCTs. However, reductions in the probability of an admission and readmission occurred only for high-risk patients in CCT practices. At the patient level, the probability of an unplanned admission was reduced for CCT and non-CCT patients, but the probability of a readmission was only reduced in CCT patients receiving hospital discharge reconciliation calls from CCT staff.
- Conclusion: Preliminary results suggest possible added benefit of CCTs over PCMHs alone for reducing hospitalization.
As health care organizations move from a fee-for-service model to a value-based model in an accountable care environment, the transformation of primary care to patient-centered medical homes (PCMHs) is one of the fundamental strategies for achieving higher quality care at lower cost [1–3]. The core tenets of the PCMH are a commitment to high quality and safe care that is accessible, comprehensive, and coordinated across the health continuum, as well as patient-centered [4,5]. Newer to the PCMH model has been shifting the paradigm of care from individual encounters to using elements of population health management to proactively manage a panel of patients [1,3,6]. Given the array of patients seen in a primary care setting and the complexity of care required by many patients in a panel, particularly those with chronic conditions, a team approach to care capitalizes on multidisciplinary skills to collectively take responsibility for the ongoing care of the patients to improve health outcomes [7].
Multidisciplinary team-based care is considered a crucial strategy for meeting our society’s health care needs [8], especially in light of the expected shortage of primary care physicians coupled with the anticipated growth of the patient population due to the Affordable Care Act. Several different types of team-based care have been pursued. In 2003, for example, the State of Vermont pioneered health care reform through Vermont’s Blueprint for Health using principles of the PCMH that included team-based care [9]. The goal of the program was to deliver comprehensive and coordinated care to improve health outcomes for state residents. Vermont community health teams worked with primary care providers to manage short-term care for high-needs patients with an emphasis on better self-management, care coordination, chronic care management, and social and behavioral support services. An analysis of the first pilot program found significant decreases in hospital admissions and emergency department (ED) visits, and a per-person per-month reduction in costs [9].
The Lehigh Valley Health Network adapted the Vermont health improvement model to meet the unique needs of its practices that were transforming into PCMHs. When asked by leadership what would be most helpful in this transformational process, the practices cited additional staff resources to manage their high-risk patients. In response, the network enhanced support to the practices by implementing multidisciplinary teams called community care teams (CCTs), which were deployed to the practices to help manage their high-risk patients. The purpose of this study is to evaluate the effectiveness of CCTs within the PCMH model by examining key utilization, quality, and process measures. The CCTs were expected to increase the overall practice effectiveness and efficiency (practice level outcomes) by offsetting some of the workload regarding the management of high-risk patients and improving the outcomes of patients directly managed by the CCT (patient level outcomes).
Methods
Setting
Serving 5 counties, the Lehigh Valley Health Network is a large health care delivery system in southeastern PA that currently operates in a fee-for-service environment but is moving towards becoming an accountable care organization. The concept of using CCTs to support practices’ PCMH development originated with network leadership. Leadership approached 7 primary care practices with the most extensive PCMH involvement to pilot the CCT initiative (1 practice declined participation). More specifically, the practices were selected based upon their prior 3-year experience with practice transformation as a result of participating in the South Central PA Chronic Care Initiative [10] and having achieved National Committee for Quality Assurance level 3 PCMH recognition. Practice selection was also based on the results of a network-wide comprehensive practice assessment which included TransforMed’s MHIQ survey [11] of PCMH capabilities and in-house surveys to capture practice characteristics and readiness for change.
Program Design
The CCTs were designed to support 3 to 4 primary care practices in the short-term management of high-risk patients with chronic disease. Much like the Vermont community health team model, each team consisted of a RN care manager who functioned as the team lead, a behavioral health specialist, and a social worker. A clinical pharmacist was added to the CCT program shortly after implementing the project and was shared between 2 teams. The team engaged in population health management for patients identified as high-risk for poor outcomes by supporting the further development of disease self-management and goal setting skills, addressing behavioral health, social, and economic problems, and connecting the patient to other Network and community resources as needed. Furthermore, given the growing evidence demonstrating the positive impact of coordinated and continuity of care post hospital discharge on patient outcomes [12,13], the CCT also played a vital role in supporting the PCMH transition care program for high-risk patients, which involved contacting patients via the telephone within 48 business hours of discharge from the hospital to reconcile medications, assess and identify issues for follow-up, answer patient questions and coordinate appropriate appointments.
As a pilot program, 2 CCTs were deployed to 6 primary care practices (3 family medicine, 2 internal medicine, and 1 pediatric) in July 2012. Prior to engaging the practice and patients, each team member participated in an extensive orientation, which presented essential evidence-based knowledge on the CCT and PCMH models and provided application training and support in information systems, network resources, and care management.
Initially the CCT care managers forwarded the high-risk registry to each provider to review and identify the top patients for proactive care management outreach. CCT care managers then called the identified patients and/or coordinated outreach with patients through office appointments scheduled in the near future. At the same time as the registry outreach began, on-site clinician referrals to the CCT and hospital discharge reconciliation calls to patients by the CCT care manager commenced. Clinician referrals did not have to meet any formal criteria in order for that patient to receive CCT services. Ideally, the program was designed to service high-risk patients on the registry; however, the majority of patient contacts for care management emerged through day-to-day clinician referrals (not necessarily high-risk) and discharge reconciliation calls to high-risk patients for months 2 through 8 of the pilot phase. Patients' care was managed with continued, ongoing services until either patient goals were met or the patient was transferred to another practice or nursing home, expired, or declined further care management assistance. The CCT behavioral health specialist addressed short-term issues or bridged the gap or need until long-term services could be coordinated, sometimes requiring 6 to 8 meetings with a patient. CCT social worker services were assigned on a case-by-case basis and occasionally provided longer-term or intermittent need management, such as medication assistance.
Study Design and Sample
A naturalistic longitudinal study design was used to evaluate the CCT’s preliminary effectiveness. The CCTs were evaluated at 2 levels. First, based on the assumption that the CCT would off-set some of the practice workload and allow the practices to proactively manage more of their patient population, the effectiveness of the CCTs was evaluated at the practice level, ie, patients who did not receive CCT services but belonged to practices with CCTs. Second, the effectiveness of the CCTs was evaluated at the patient level, ie, patients receiving CCT services. At both levels, the CCT groups were contrasted with “non-CCT” comparison groups of convenience.
![]()
Measures
Primary outcome measures were utilization: ED visits, all-cause unplanned admissions, and 30-day readmissions. Secondary outcome measures included 2 types of quality indicators(QIs, see Appendix for scoring): (a) gaps in care measures that captured whether providers were following standards of care for diabetes, ischemic vascular disease, and prevention; and (b) patient composites which reflected patient illness severity for diabetes and cardiac disease. Higher scores indicated more gaps in care or greater disease severity. Both types of QI measures required at least a 12-month window and thus could not be computed for patients engaged with the CCT who had only a 6-month follow-up period (as their scores could reflect their pre-CCT status). In addition, comprehensive care was denoted by the provision of depression screening on the PHQ-2 [14], and whether HgA1c was greater or equal to 9.0 in diabetics served as an additional patient outcome measure. Other secondary outcome measures included practice joy via the Well-Being in the Workplace Questionnaire (WWQ) [15] and patient satisfaction from CAHPS-CG 12-month survey with PCMH items [16].
Data Collection
Utilization and quality data were extracted from the network’s hospital and outpatient electronic medical records (EMR). Practice staff were emailed every 6 months and asked to anonymously complete the WWQ via Survey Monkey [17]. At baseline, patient satisfaction surveys were distributed in the practice, and patients had the option of anonymously completing them during their visit or returning them in a prepaid envelop. While not recommended for CAHPS, this procedure had been internally used with success previously. At 12 months, the same survey was mailed to a random sample of patients with a prepaid return envelope.
At the practice level, utilization and QI data were only available for patients from 4 of the 6 practices: data were not available for 1 non-EMR practice and there was negligible variation in utilization from the pediatric practice. For the patient level analyses, utilization was available for patients in all 6 practices.
Statistical Analyses
To test whether outcomes were improved relative to a comparison group following the introduction of CCTs into the practices (practice level analyses) or CCT engagement (patient level analyses), mixed models analyses of variance with repeated measures on Time (pre- vs. post-CCT) were conducted with SAS [18] PROC MIXED and PROC GENMOD for continuous and dichotomous outcomes, respectively. To determine whether there was greater improvement in the CCT groups, all models included the interaction between Time and Group (CCT versus no CCT) in addition to their main effects. At the practice level, high-risk and non-high-risk patients were analyzed separately. And, at the patient level, CCT-MNGT and CCT-DCREC patients were analyzed separately with results adjusted for patient’s age. Some variables were not normally distributed. The quality variables were able to be normalized with natural log transformations, but utilization variables had to be dichotomized into “any” versus “none” due to severe skewness, inflated 0s and larger-valued counts. Practice joy and patient satisfaction can only be reported at the practice level (responses were aggregated within each practice because anonymous responses do not permit linking specific respondents over time and different patients were sampled across measurement occasions) and non-parametric tests (Wilcoxon signed ranked tests and tests of dependent proportions) were used to test for change over time given the small sample size (n = 6).
Results
Patient Characteristics
Practice samples had slightly more women than men (55.2%), were largely white (95.0%) and 50 years of age on average (mean = 49.53, SD = 20.18). The prevalence of diabetes (10.2%) and cardiac disease (10.4%) was relatively low. The percentage of women (56.3%) and whites (96.4%) for the patient level analytic samples was similar to the practice samples, whereas the prevalence of diabetes (33.6% ) and cardiac disease (44.6%) was notable higher and patients were more than 10 years older on average (mean = 61.62, SD = 23.96).
Practice Level Outcomes
Given these group baseline differences and only one instance where the Time by Group interaction was significant where group baseline differences were absent (see below), simple pre-post analyses were conducted for each group separately (Table 4). The results for non-high-risk patients indicated that, in both CCT and non-CCT practices, there was no improvement in utilization, but there were significant reductions in gaps in diabetic and preventative care and cardiac illness severity and significant increases in depression screening, although effect sizes for the latter 2 outcomes were small to negligible.
Practice joy fell in the medium range [19] at all time-points, with no notable change over time (see Appendix in the online version of this article). There was also no change in patient satisfaction (see Appendix, online), although after 12 months the “always” response for following up on lab tests was no longer higher than the national comparison and helpfulness of staff rated “never/sometimes” was below the national comparison.
Patient Level Outcomes
Discussion
The empirical literature indicates that PCMH practice transformation is a long, effortful process, the effects of which are not quick to manifest [20–22]. In this context, the results of the preliminary evaluation of the CCT pilot were encouraging: team-based care in the form of CCTs can be effectively used to support population health management. Overall, the results at the practice level suggest that PCMH transformation alone may be effective in creating improvements in patient care and cardiac disease (there were improvements in 3 out of 4 care gap measures and 1 disease measure for both CCT and non-CCT practices), but the presence of CCT appears necessary to reduce unplanned admissions and readmissions, at least among high-risk patients. Of course, this reduced utilization at the practice level could also be due to selection bias (practices with the longest PCMH involvement were selected for the CCT pilot) and it awaits to be seen if this finding holds as CCTs are deployed to more practices. Still, similar evidence for the CCT was found at the patient level. The probability of an unplanned admission was reduced for all groups of patients from CCT practices; however, this effect was notably large only for patients who received hospital discharge reconciliation calls from the CCT. Moreover, the only group that had a significant reduction in the probability of a 30-day readmission was also patients who received hospital discharge reconciliation calls from the CCT. Both results suggest an added benefit of CCT engagement. Although there was no change in the probability of an ED visit for any group, the CCT staff indicated that there was a substantial minority of CCT-engaged patients who were not accessing the ED when they should have been and it might be that increased appropriate use by this minority due to CCT coaching therefore cancelled out expected reductions in ED use among other CCT patients.
The intent of the current endeavor was to perform a formative evaluation [23,24] of the CCTs effectiveness. We recognized there would be analytic challenges and limits to such early-stage analyses. Nonetheless, we believed it was vital, especially given the cost of the CCTs and the growing financial pressure on health care networks more globally, to determine the preliminary effectiveness of the CCTs’, care management interventions and, if possible, suggest improvements to the intervention. As intended in formative evaluations, the evaluation is ongoing. Future analyses will bring more rigor to the evaluation and solve the data and analytic obstacles that affected the results of this first round of analyses.
A major learning of the early-stage analyses was the difficulty in developing comparison groups that are equivalent to the intervention groups at baseline. A number of matching schemes were attempted at the patient level in addition to the one presented here, but they were equally problematic. Avenues for creating more valid comparison groups in the future include the use of propensity score matching as well as drawing comparison groups from data from other networks. In addition, as time passes and more than 1 follow-up point is available for analysis, multilevel modeling can be employed which can specify different intercepts (baseline values) for groups. Still, it’s worth noting that constructing appropriate comparison groups is challenging even with those approaches: most health networks do not collect data on the most relevant matching variables (eg, health literacy, social economic status, social isolation/support) due to their cost and burden to both practices and patients.
Another major gap revealed by the early-stage analyses was the need to improve the strategy used for selecting patients for CCT intervention. In addition to many physician referrals, there was a large number of patients on the high-risk registry who required intervention relative to the small CCT staff. Various strategies to prioritize the list were attempted, including cost-related analyses. As plagued the formation of comparisons groups, it seemed the variables most critical to risk stratification were unavailable in administrative datasets. Appreciating that data collection is costly and patients and busy practices already have survey fatigue, the evaluation team examined the empirical literature for a single useful tool for ranking patients as well as constructing better matched comparison groups. This search indicated that a measure of patient activation [25–27] would be particularly helpful not only for selecting the riskiest and costliest patients for CCT intervention but also for tailoring CCT services to different types of patients. Since the implementation of the CCTs the network has also contracted with a predictive analytics company to provide risk scores for the patients.
The current formative evaluation was an important learning journey, laying important ground work for better evaluating the CCTs’ effectiveness specifically and eventually becoming an accountable care provider more generally. If the network is to provide health care more effectively and efficiently, it will need to bring greater rigor to evaluations of its various interventions and other ACO endeavors. The current formative evaluation was a valuable demonstration to non-scientists of the weakness of single group pre-post designs and how more rigorous evaluations, which include comparison groups and address confounding variables, can enhance the validity of the analytic results. This learning journey also highlighted the limitations of administrative databases and the necessity of both primary data collection and mixed methods. For example, it seems that some practices may require educational interventions to take full advantage of the CCT and qualitative assessments on practice readiness seem a necessary addition to the quantitative practice assessment to identify the specific characteristics that need strengthening. In addition, the evaluation team also recently added a qualitative sub-study on high-risk patients’ experience with the CCT to overcome locally low CAHPS response rates and capture themes broader than patient satisfaction. Upcoming rounds of analyses will also tackle other aspects of formative evaluations including the study of the CCT implementation as more practices receive CCTs and determining if process and fidelity measures of the PCMH pillars are linked to better outcomes. Furthermore, future analytic plans include identifying the active ingredients and optimal doses of the CCT intervention as well as determine the most effective matches between different types of patients and different CCT interventions (eg, behavioral, care management, social, pharmacy). While we appreciate that barriers still remain and require solutions, we hope the current evaluation highlights the utility of performing such formative evaluations.
Corresponding author: Carol Foltz, PhD, Lehigh Valley Health Network, Allentown, PA, [email protected].
Funding/support: The evaluation was funded internally by Lehigh Valley Health Network and a close affiliate, the Lehigh Valley Physician Hospital Organization. The funding organizations had no role in any part of the study.
Financial disclosures: None.
1. Rittenhouse DR, Shortell SM, Fisher ES. Primary care and accountable care—two essential elements of delivery-system reform. N Engl J Med 2009;361:2301–3.
2. American Academy of Family Physicians. Primary care for the 21st century: Ensuring a quality, physician-led team for every patient. September 2012. Accessed at www.aafp.org/dam/AAFP/documents/about_us/initiatives/AAFP-PCMHWhitePaper.pdf.
3. Agency for Healthcare Research and Quality. The patient-centered medical home: Strategies to put patients at the center of primary care, February 2011. Accessed at http://pcmh.ahrq.gov/sites/default/files/attachments/Strategies%20to%20Put%20Patients%20at%20the%20Center%20of%20Primary%20Care.pdf.
4. Agency for Healthcare Research and Quality. Defining the PCMH. Accessed at http://pcmh.ahrq.gov/page/defining-pcmh.
5. Patient-Centered Primary Care Collaborative. Defining the medical home: A patient-centered philosophy that drives primary care excellence. Accessed at http://pcmh.ahrq.gov/page/defining-pcmh.
6. Margolius D, Bodenheimer T. Transforming primary care: From past practice to the practice of the future. Health Aff 2010;29:779–84.
7. Robert Graham Center. The patient centered medical home: History, seven core features, evidence and transformational change, 2007. Accessed at www.graham-center.org/online/etc/medialib/graham/documents/publications/mongraphs-books/2007/rgcmo-medical-home.Par.0001.File.tmp/rgcmo-medical-home.pdf.
8. Goldberg A. It matters how we define health care equity. Institute of Medicine. Accessed at www.iom.edu/~/media/Files/Perspectives-Files/2013/Commentaries/BPH-It-Matters-How-we-define-Health-Equity.pdf.
9. Bielaszka-DuVernay C. Vermont’s blueprint for medical homes, community health teams, and better health at lower cost. Health Aff 2011;30:383–6.
10. Bricker PL, Baron RJ, Scheirer JJ. Collaboration in Pennsylvania: rapidly spreading improved chronic care for patients to practices. J Cont Educ Health Prof 2010;30:114–25.
11.TransforMed. What does your medical home look like? A jumble of unconnected pieces or a coherent structure? Accessed at www.transformed.com/mhiq/welcome.cfm .
12. Health policy brief: care transitions. Health Aff 2012. Accessed at http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_76.pdf.
13. Greenwald J, Denham C, Jack B. The hospital discharge: A review of a high-risk care transition with highlights of a reengineered discharge process. J Patient Saf 2007;3:97–106.
14. Kroenke K, Spitzer R, Williams W. The patient health questionnaire-2: validity of a two-item depression screener. Med Care 2003;41:1284–94.
15. Parker GB, Hyett MP. Measurement of well-being in the workplace: The development of the Work Well-Being Questionnaire. Nerv Ment Dis 2011;199:394-97.
16. Agency for Healthcare Research and Quality. Clinician & group expanded 12-month survey with CAHPS patient-centered medical home (PCMH) items. Accessed at https://cahps.ahrq.gov/surveys-guidance/cg/pcmh/index.html.
17. SurveyMonkey. Accessed at http://www.surveymonkey.com (last visited 06-23-2014). SurveyMonkey: Palo Alto, CA.
18. SAS [computer program]. Version 9.2. Cary, NC: SAS Institute; 2002-2008.
19. Black Dog Institute. Accessed at www.blackdoginstitute.org.au/docs/workplacewellbeingquestionnairepaperversion.pdf.
20. Jaén CR, Ferrer, RL, Miller WL, Palmer RF. Patient outcomes at 26 months in the patient-centered medical home national demonstration project. Ann Fam Med 2010;8(Suppl 1):s57–s67.
21. Solberg LI, Asche SE, Fontaine P, Flottemesch TJ. Trends in quality during medical home transformation. Ann Fam Med 2011;9:515–21.
22. Crabtree BF, Nutting PA, Miller WL, Stange KC. Summary of the national demonstration project and recommendations for the patient-centered medical home. Ann Fam Med 2010;8(Suppl 1):s80–s90.
23. Stetler CB, Legro MW, Wallace CM et al. The role of formative evaluation in implementation research and the QUERI experience. J Gen Intern Med 2006;21:S1–8.
24. Geonnotti K, Peikes D, Wang W, Smith J. Formative evaluation: fostering real-time adaptations and refinements to improve the effectiveness of patient-centered medical home models. Rockville, MD: Agency for Healthcare Research and Quality. February 2013. AHRQ Publication No. 13-0025-EF.
25. Insignia Health. Accessed at www.insigniahealth.com/solutions/patient-activation-measure.
26. Hibbard JH, Greene J, Overton V. Patients with lower activation associated with higher costs; delivery systems should know their patients’ ‘scores’. Health Aff 2013;32:216–22.
27. Hibbard JH, Greene J. What The evidence shows about patient activation: better health outcomes and care experiences fewer data on costs. Health Aff 2013;32:207–14.
1. Rittenhouse DR, Shortell SM, Fisher ES. Primary care and accountable care—two essential elements of delivery-system reform. N Engl J Med 2009;361:2301–3.
2. American Academy of Family Physicians. Primary care for the 21st century: Ensuring a quality, physician-led team for every patient. September 2012. Accessed at www.aafp.org/dam/AAFP/documents/about_us/initiatives/AAFP-PCMHWhitePaper.pdf.
3. Agency for Healthcare Research and Quality. The patient-centered medical home: Strategies to put patients at the center of primary care, February 2011. Accessed at http://pcmh.ahrq.gov/sites/default/files/attachments/Strategies%20to%20Put%20Patients%20at%20the%20Center%20of%20Primary%20Care.pdf.
4. Agency for Healthcare Research and Quality. Defining the PCMH. Accessed at http://pcmh.ahrq.gov/page/defining-pcmh.
5. Patient-Centered Primary Care Collaborative. Defining the medical home: A patient-centered philosophy that drives primary care excellence. Accessed at http://pcmh.ahrq.gov/page/defining-pcmh.
6. Margolius D, Bodenheimer T. Transforming primary care: From past practice to the practice of the future. Health Aff 2010;29:779–84.
7. Robert Graham Center. The patient centered medical home: History, seven core features, evidence and transformational change, 2007. Accessed at www.graham-center.org/online/etc/medialib/graham/documents/publications/mongraphs-books/2007/rgcmo-medical-home.Par.0001.File.tmp/rgcmo-medical-home.pdf.
8. Goldberg A. It matters how we define health care equity. Institute of Medicine. Accessed at www.iom.edu/~/media/Files/Perspectives-Files/2013/Commentaries/BPH-It-Matters-How-we-define-Health-Equity.pdf.
9. Bielaszka-DuVernay C. Vermont’s blueprint for medical homes, community health teams, and better health at lower cost. Health Aff 2011;30:383–6.
10. Bricker PL, Baron RJ, Scheirer JJ. Collaboration in Pennsylvania: rapidly spreading improved chronic care for patients to practices. J Cont Educ Health Prof 2010;30:114–25.
11.TransforMed. What does your medical home look like? A jumble of unconnected pieces or a coherent structure? Accessed at www.transformed.com/mhiq/welcome.cfm .
12. Health policy brief: care transitions. Health Aff 2012. Accessed at http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_76.pdf.
13. Greenwald J, Denham C, Jack B. The hospital discharge: A review of a high-risk care transition with highlights of a reengineered discharge process. J Patient Saf 2007;3:97–106.
14. Kroenke K, Spitzer R, Williams W. The patient health questionnaire-2: validity of a two-item depression screener. Med Care 2003;41:1284–94.
15. Parker GB, Hyett MP. Measurement of well-being in the workplace: The development of the Work Well-Being Questionnaire. Nerv Ment Dis 2011;199:394-97.
16. Agency for Healthcare Research and Quality. Clinician & group expanded 12-month survey with CAHPS patient-centered medical home (PCMH) items. Accessed at https://cahps.ahrq.gov/surveys-guidance/cg/pcmh/index.html.
17. SurveyMonkey. Accessed at http://www.surveymonkey.com (last visited 06-23-2014). SurveyMonkey: Palo Alto, CA.
18. SAS [computer program]. Version 9.2. Cary, NC: SAS Institute; 2002-2008.
19. Black Dog Institute. Accessed at www.blackdoginstitute.org.au/docs/workplacewellbeingquestionnairepaperversion.pdf.
20. Jaén CR, Ferrer, RL, Miller WL, Palmer RF. Patient outcomes at 26 months in the patient-centered medical home national demonstration project. Ann Fam Med 2010;8(Suppl 1):s57–s67.
21. Solberg LI, Asche SE, Fontaine P, Flottemesch TJ. Trends in quality during medical home transformation. Ann Fam Med 2011;9:515–21.
22. Crabtree BF, Nutting PA, Miller WL, Stange KC. Summary of the national demonstration project and recommendations for the patient-centered medical home. Ann Fam Med 2010;8(Suppl 1):s80–s90.
23. Stetler CB, Legro MW, Wallace CM et al. The role of formative evaluation in implementation research and the QUERI experience. J Gen Intern Med 2006;21:S1–8.
24. Geonnotti K, Peikes D, Wang W, Smith J. Formative evaluation: fostering real-time adaptations and refinements to improve the effectiveness of patient-centered medical home models. Rockville, MD: Agency for Healthcare Research and Quality. February 2013. AHRQ Publication No. 13-0025-EF.
25. Insignia Health. Accessed at www.insigniahealth.com/solutions/patient-activation-measure.
26. Hibbard JH, Greene J, Overton V. Patients with lower activation associated with higher costs; delivery systems should know their patients’ ‘scores’. Health Aff 2013;32:216–22.
27. Hibbard JH, Greene J. What The evidence shows about patient activation: better health outcomes and care experiences fewer data on costs. Health Aff 2013;32:207–14.
Understanding the spectrum of multiport and single-site robotics for hysterectomy
We present this video with the objective of demonstrating a hysterectomy performed using the robotic single-site approach in juxtaposition with a robotic multiport hysterectomy. In the video, and briefly here, we review the benefits, disadvantages, and challenges of robotic single-site hysterectomy.
The advantages of single-site robotic hysterectomy include:
- possible improved aesthetics for the patient
- allowance for surgeon independence while minimizing the need for a bedside assistant
- automatic reassignment of the robotic arm controls
- circumvention of certain limitations seen in laparoscopic single-site procedures.
The disadvantages of single-site robotic hysterectomy include:
- instrumentation is nonwristed and less robust than that of multiport instrumentation
- decreased degrees of freedom
- longer suturing time
- restricted assistant port use
- decreased applicability to a wide range of procedures as the surgical approach is limited to less complex and smaller pathology.
Related articles:
The robot is broadly accessible less than 10 years after its introduction to gynecologic surgery. Janelle Yates (News for your Practice; December 2013)
The robot is gaining ground in gynecologic surgery. Should you be using it? Arnold P. Advincula MD; Cheryl B. Iglesia MD; Rosanne M. Kho MD; Jamal Mourad, DO; Marie Fidela R. Paraiso, MD; Jason D. Wright, MD (Roundtable; April 2013)
Identify your learning curve for robotic hysterectomy. Joshua L Woelk, MD, MS, and John B. Gebhart, MD, MS (Guest Editorial; April 2013)
In general, each step of the single-port procedure has been found to be equivalent in time to a multiport approach to robotic-assisted hysterectomy—except for the step of vaginal cuff closure. Since the initial experience, aside from overcoming the learning curve of a new surgical approach, various techniques have been modified in order to surmount this challenge, such as closing the vaginal cuff vertically, using a cutting needle versus a tapered needle, addition of a “plus one” wristed multiport robotic arm, or replacing the single-site robotic needle driver with a multiport 5-mm needle driver.
Nevertheless, widespread adoption of single-site robotic gynecologic surgery still requires further technological improvements, and further research and experience is needed to determine its role, benefits, and applications in gynecologic surgery.
--Dr. Arnold Advincula, AAGL 2014 Scientific Program Chair
WE WANT TO HEAR FROM YOU!Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
We present this video with the objective of demonstrating a hysterectomy performed using the robotic single-site approach in juxtaposition with a robotic multiport hysterectomy. In the video, and briefly here, we review the benefits, disadvantages, and challenges of robotic single-site hysterectomy.
The advantages of single-site robotic hysterectomy include:
- possible improved aesthetics for the patient
- allowance for surgeon independence while minimizing the need for a bedside assistant
- automatic reassignment of the robotic arm controls
- circumvention of certain limitations seen in laparoscopic single-site procedures.
The disadvantages of single-site robotic hysterectomy include:
- instrumentation is nonwristed and less robust than that of multiport instrumentation
- decreased degrees of freedom
- longer suturing time
- restricted assistant port use
- decreased applicability to a wide range of procedures as the surgical approach is limited to less complex and smaller pathology.
Related articles:
The robot is broadly accessible less than 10 years after its introduction to gynecologic surgery. Janelle Yates (News for your Practice; December 2013)
The robot is gaining ground in gynecologic surgery. Should you be using it? Arnold P. Advincula MD; Cheryl B. Iglesia MD; Rosanne M. Kho MD; Jamal Mourad, DO; Marie Fidela R. Paraiso, MD; Jason D. Wright, MD (Roundtable; April 2013)
Identify your learning curve for robotic hysterectomy. Joshua L Woelk, MD, MS, and John B. Gebhart, MD, MS (Guest Editorial; April 2013)
In general, each step of the single-port procedure has been found to be equivalent in time to a multiport approach to robotic-assisted hysterectomy—except for the step of vaginal cuff closure. Since the initial experience, aside from overcoming the learning curve of a new surgical approach, various techniques have been modified in order to surmount this challenge, such as closing the vaginal cuff vertically, using a cutting needle versus a tapered needle, addition of a “plus one” wristed multiport robotic arm, or replacing the single-site robotic needle driver with a multiport 5-mm needle driver.
Nevertheless, widespread adoption of single-site robotic gynecologic surgery still requires further technological improvements, and further research and experience is needed to determine its role, benefits, and applications in gynecologic surgery.
--Dr. Arnold Advincula, AAGL 2014 Scientific Program Chair
WE WANT TO HEAR FROM YOU!Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
We present this video with the objective of demonstrating a hysterectomy performed using the robotic single-site approach in juxtaposition with a robotic multiport hysterectomy. In the video, and briefly here, we review the benefits, disadvantages, and challenges of robotic single-site hysterectomy.
The advantages of single-site robotic hysterectomy include:
- possible improved aesthetics for the patient
- allowance for surgeon independence while minimizing the need for a bedside assistant
- automatic reassignment of the robotic arm controls
- circumvention of certain limitations seen in laparoscopic single-site procedures.
The disadvantages of single-site robotic hysterectomy include:
- instrumentation is nonwristed and less robust than that of multiport instrumentation
- decreased degrees of freedom
- longer suturing time
- restricted assistant port use
- decreased applicability to a wide range of procedures as the surgical approach is limited to less complex and smaller pathology.
Related articles:
The robot is broadly accessible less than 10 years after its introduction to gynecologic surgery. Janelle Yates (News for your Practice; December 2013)
The robot is gaining ground in gynecologic surgery. Should you be using it? Arnold P. Advincula MD; Cheryl B. Iglesia MD; Rosanne M. Kho MD; Jamal Mourad, DO; Marie Fidela R. Paraiso, MD; Jason D. Wright, MD (Roundtable; April 2013)
Identify your learning curve for robotic hysterectomy. Joshua L Woelk, MD, MS, and John B. Gebhart, MD, MS (Guest Editorial; April 2013)
In general, each step of the single-port procedure has been found to be equivalent in time to a multiport approach to robotic-assisted hysterectomy—except for the step of vaginal cuff closure. Since the initial experience, aside from overcoming the learning curve of a new surgical approach, various techniques have been modified in order to surmount this challenge, such as closing the vaginal cuff vertically, using a cutting needle versus a tapered needle, addition of a “plus one” wristed multiport robotic arm, or replacing the single-site robotic needle driver with a multiport 5-mm needle driver.
Nevertheless, widespread adoption of single-site robotic gynecologic surgery still requires further technological improvements, and further research and experience is needed to determine its role, benefits, and applications in gynecologic surgery.
--Dr. Arnold Advincula, AAGL 2014 Scientific Program Chair
WE WANT TO HEAR FROM YOU!Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Accountable Care Organizations: Theory and Practice
Since early 2012, a growing number of independent physician groups, physician-hospital organizations, hospitals and their employed physicians, and fully integrated health systems have entered into contracts with both CMS and commercial insurers to become accountable care organizations (ACOs). It is estimated that the health care of close to 20 million patients is now being provided under such arrangements [1].
ACOs are one manifestation of payment reform intended to slow the unsustainable cost of health care in the United States. While the details of the payment models vary widely, with many combinations of fee-for-service, bundled, and capitated arrangements, the underlying goal is consistent: ACOs are held accountable for both the cost and quality of care for a specific population. While some ACO models offer the promise of shared savings alone, others offer potential savings but also entail associated risk [2]. That pre-specified quality targets have to be met before savings can be accessed is presented as a safeguard against the perceived excesses of the managed care experience of the 1990s.
To succeed as an ACO, health care organizations face sobering structural, fiscal, and—perhaps most daunting—cultural challenges. Coordinating care between providers [3,4] and across episodes and sites of care—not a traditional strength of many provider entities—will become increasingly important. Creating equitable systems to distribute whatever savings are garnered may disrupt traditional relationships between primary care and specialist providers. Convincing organizations to make the necessary investment in an “evolved” primary care infra-structure—a prerequisite for accomplishing the goals of decreasing unnecessary and expensive health resource utilization—will be problematic in an era of shrinking overall reimbursement [5]. Finally, convincing clinicians that this model means that they are quite literally “in it together” will challenge long-standing and proud departmental and divisional identities and silos [6].
Recognizing that this grand experiment is still very much in its formative stages, we nonetheless thought that this was an opportune time to examine ACOs from several perspectives. Over the next few issues and beginning with this issue [7], we will sequentially hear from an expert in health care policy analysis, a clinician-leader working in a high-functioning patient-centered medical home practice, and a team in a large health care system charged with the overall success of population health management. We are confident that you will find these observations timely, interesting, and informative. We welcome your feedback.
1. Muhlestein D. Accountable care growth in 2014: a look ahead. Health Affairs blog. 2014 Jan 29. Available at http://healthaffairs.org/blog/2014/01/29/accountable-care-growth-in-2014-a-look-ahead/.
2. Weissman JS, Bailit M, D’Andrea G, Rosenthal MB. The design and application of shared savings programs: lessons from early adopters. Health Affairs 2012;31:1959–68.
3. Greenberg JO, Barnett ML, Spinks MA, et al. The “medical neighborhood”: integrating primary and specialty care for ambulatory patients. JAMA Intern Med 2014;174:454–7.
4. Song Z, Sequist TD, Barnett ML. Patient referrals: a linchpin for increasing the value of care. JAMA. Published online July 03, 2014. Available at http://jama.jamanetwork.com/article.aspx?articleid=1886863.
5. Rittenhouse DR, Shortell SM, Fisher ES. Primary care and accountable care – two essential elements of delivery-system reform. N Engl J Med 2009;361:2301–3.
6. Song Z, Lee TH. The era of delivery system reform begins. JAMA 2013;309:35–6.
7. Song Z. Accountable care organizations: early results and future challenges. J Clin Outcomes Manag 2014;8:364–71
Since early 2012, a growing number of independent physician groups, physician-hospital organizations, hospitals and their employed physicians, and fully integrated health systems have entered into contracts with both CMS and commercial insurers to become accountable care organizations (ACOs). It is estimated that the health care of close to 20 million patients is now being provided under such arrangements [1].
ACOs are one manifestation of payment reform intended to slow the unsustainable cost of health care in the United States. While the details of the payment models vary widely, with many combinations of fee-for-service, bundled, and capitated arrangements, the underlying goal is consistent: ACOs are held accountable for both the cost and quality of care for a specific population. While some ACO models offer the promise of shared savings alone, others offer potential savings but also entail associated risk [2]. That pre-specified quality targets have to be met before savings can be accessed is presented as a safeguard against the perceived excesses of the managed care experience of the 1990s.
To succeed as an ACO, health care organizations face sobering structural, fiscal, and—perhaps most daunting—cultural challenges. Coordinating care between providers [3,4] and across episodes and sites of care—not a traditional strength of many provider entities—will become increasingly important. Creating equitable systems to distribute whatever savings are garnered may disrupt traditional relationships between primary care and specialist providers. Convincing organizations to make the necessary investment in an “evolved” primary care infra-structure—a prerequisite for accomplishing the goals of decreasing unnecessary and expensive health resource utilization—will be problematic in an era of shrinking overall reimbursement [5]. Finally, convincing clinicians that this model means that they are quite literally “in it together” will challenge long-standing and proud departmental and divisional identities and silos [6].
Recognizing that this grand experiment is still very much in its formative stages, we nonetheless thought that this was an opportune time to examine ACOs from several perspectives. Over the next few issues and beginning with this issue [7], we will sequentially hear from an expert in health care policy analysis, a clinician-leader working in a high-functioning patient-centered medical home practice, and a team in a large health care system charged with the overall success of population health management. We are confident that you will find these observations timely, interesting, and informative. We welcome your feedback.
Since early 2012, a growing number of independent physician groups, physician-hospital organizations, hospitals and their employed physicians, and fully integrated health systems have entered into contracts with both CMS and commercial insurers to become accountable care organizations (ACOs). It is estimated that the health care of close to 20 million patients is now being provided under such arrangements [1].
ACOs are one manifestation of payment reform intended to slow the unsustainable cost of health care in the United States. While the details of the payment models vary widely, with many combinations of fee-for-service, bundled, and capitated arrangements, the underlying goal is consistent: ACOs are held accountable for both the cost and quality of care for a specific population. While some ACO models offer the promise of shared savings alone, others offer potential savings but also entail associated risk [2]. That pre-specified quality targets have to be met before savings can be accessed is presented as a safeguard against the perceived excesses of the managed care experience of the 1990s.
To succeed as an ACO, health care organizations face sobering structural, fiscal, and—perhaps most daunting—cultural challenges. Coordinating care between providers [3,4] and across episodes and sites of care—not a traditional strength of many provider entities—will become increasingly important. Creating equitable systems to distribute whatever savings are garnered may disrupt traditional relationships between primary care and specialist providers. Convincing organizations to make the necessary investment in an “evolved” primary care infra-structure—a prerequisite for accomplishing the goals of decreasing unnecessary and expensive health resource utilization—will be problematic in an era of shrinking overall reimbursement [5]. Finally, convincing clinicians that this model means that they are quite literally “in it together” will challenge long-standing and proud departmental and divisional identities and silos [6].
Recognizing that this grand experiment is still very much in its formative stages, we nonetheless thought that this was an opportune time to examine ACOs from several perspectives. Over the next few issues and beginning with this issue [7], we will sequentially hear from an expert in health care policy analysis, a clinician-leader working in a high-functioning patient-centered medical home practice, and a team in a large health care system charged with the overall success of population health management. We are confident that you will find these observations timely, interesting, and informative. We welcome your feedback.
1. Muhlestein D. Accountable care growth in 2014: a look ahead. Health Affairs blog. 2014 Jan 29. Available at http://healthaffairs.org/blog/2014/01/29/accountable-care-growth-in-2014-a-look-ahead/.
2. Weissman JS, Bailit M, D’Andrea G, Rosenthal MB. The design and application of shared savings programs: lessons from early adopters. Health Affairs 2012;31:1959–68.
3. Greenberg JO, Barnett ML, Spinks MA, et al. The “medical neighborhood”: integrating primary and specialty care for ambulatory patients. JAMA Intern Med 2014;174:454–7.
4. Song Z, Sequist TD, Barnett ML. Patient referrals: a linchpin for increasing the value of care. JAMA. Published online July 03, 2014. Available at http://jama.jamanetwork.com/article.aspx?articleid=1886863.
5. Rittenhouse DR, Shortell SM, Fisher ES. Primary care and accountable care – two essential elements of delivery-system reform. N Engl J Med 2009;361:2301–3.
6. Song Z, Lee TH. The era of delivery system reform begins. JAMA 2013;309:35–6.
7. Song Z. Accountable care organizations: early results and future challenges. J Clin Outcomes Manag 2014;8:364–71
1. Muhlestein D. Accountable care growth in 2014: a look ahead. Health Affairs blog. 2014 Jan 29. Available at http://healthaffairs.org/blog/2014/01/29/accountable-care-growth-in-2014-a-look-ahead/.
2. Weissman JS, Bailit M, D’Andrea G, Rosenthal MB. The design and application of shared savings programs: lessons from early adopters. Health Affairs 2012;31:1959–68.
3. Greenberg JO, Barnett ML, Spinks MA, et al. The “medical neighborhood”: integrating primary and specialty care for ambulatory patients. JAMA Intern Med 2014;174:454–7.
4. Song Z, Sequist TD, Barnett ML. Patient referrals: a linchpin for increasing the value of care. JAMA. Published online July 03, 2014. Available at http://jama.jamanetwork.com/article.aspx?articleid=1886863.
5. Rittenhouse DR, Shortell SM, Fisher ES. Primary care and accountable care – two essential elements of delivery-system reform. N Engl J Med 2009;361:2301–3.
6. Song Z, Lee TH. The era of delivery system reform begins. JAMA 2013;309:35–6.
7. Song Z. Accountable care organizations: early results and future challenges. J Clin Outcomes Manag 2014;8:364–71
An insider’s look at the 2014 atopic dermatitis guidelines
COEUR D’ALENE, IDAHO – The 2014 American Academy of Dermatology atopic dermatitis guidelines may already need an update, according to the cochair of the guidelines panel.
The guidelines were based upon studies published through 2012. Since then, new evidence has emerged that raises the level of uncertainty regarding several key questions the panel addressed, Dr. Robert Sidbury observed at the annual meeting of the Society for Pediatric Dermatology. Among these questions: To bathe or not to bathe? Will a child outgrow atopic dermatitis?

Serving as cochair of the guidelines committee was both a reassuring and daunting experience, according to Dr. Sidbury, chief of the division of dermatology at Seattle Children’s Hospital.
It was reassuring to note that the committee members, who included 17 atopic dermatitis experts from three countries, were free from financial conflicts as they sifted through the published data for evidence-based recommendations to inform practice. But it was daunting to learn how sketchy the supporting evidence is for some of the conventional wisdom regarding atopic dermatitis management, he explained.
By way of providing what he called "a peek behind the curtains" of the guidelines-development process, Dr. Sidbury highlighted the issue of daily bathing followed by application of emollients and moisturizers. This was among the topics the panel struggled with the most, which might come as a surprise to outsiders who consider this to be standard practice, he noted.
"It seems like a very straightforward thing. Almost everyone in this room, to a person, recommends a daily bath followed by moisturizers, yet when we examined the studies we realized that recommendation isn’t based upon much evidence," he said.
Thus, the panel concluded that bathing is "suggested" for atopic dermatitis patients, while adding that "there is no standard" for the duration or frequency of bathing. The panel rated the strength of their recommendation as C, and the level of evidence as III.
"That’s a fairly weak recommendation based upon fairly week evidence," Dr. Sidbury commented.
Moreover, since publication of the guidelines, two new studies have come forth that address the question of whether bathing plus moisturizers is beneficial in atopic dermatitis. The results conflict with each other, making recommendations even more difficult.
Data from a retrospective study of 75 patients with moderate or severe atopic dermatitis suggested that a daily 15- to 20-minute bath followed by a mid-potency topical steroid and moisturizer was indeed beneficial: 79% of subjects showed marked improvement based on Investigator’s Global Assessment at week 3, and 4% were clear (Dermatitis 2014;25:56-9).
By contrast, data from a prospective trial in which 28 children with atopic dermatitis were randomized to a daily vs. twice-weekly bath followed by appropriate care indicated that, while hydration with emollients was important, bathing frequency wasn’t (Clin. Pediatr. 2014;53:677-81).
"This paper makes me feel better about the guidelines not saying, ‘You should bathe every day,’ although that’s still my own recommendation to patients," Dr. Sidbury said.
This year also has brought two conflicting studies regarding the natural history of atopic dermatitis. A large national Taiwanese population-based cohort study of children diagnosed with atopic dermatitis within the first 2 years of life and followed from birth to age 10 years concluded that 70% of these early-onset patients eventually went into remission. A total of 19% of patients did so within the first year, and 49% in less than 4 years. The median disease duration was 4.2 years (Br. J. Dermatol. 2014;170:130-5).
On the other hand, a report from the 7,157-patient, cross-sectional, longitudinal Pediatric Eczema Elective Registry (PEER) found that by age 20, only 50% of the patients had experienced at least one symptom-free period lasting 6 months or more. The investigators concluded that atopic dermatitis is probably a lifelong disease (JAMA Dermatology 2014;150:593-600).
"That’s a provocative conclusion, and a tough thing to tell a parent," Dr. Sidbury observed. "I offer parents realistic but optimistic counsel. I tell them the tendency toward xerosis, irritancy, and infection will persist – the patient in front of you is never going to want to wear a wool sweater for the rest of their life. But the incessant itch, the need for treatment, the impact on quality of life – which is really the issue at hand – hopefully will not persist."

Since the release earlier this year of the first three of the four sections of the atopic dermatitis guidelines, Dr. Sidbury and the other panelists have received considerable feedback that the guidelines didn’t adequately address the topic of topical steroid addiction.
"Some say we missed the boat in not making coherent recommendations to parents about it. We got some very pointed comments," he conceded.
He noted that a systematic review presented at last year’s International Symposium on Atopic Dermatitis concluded that topical steroid withdrawal is a real phenomenon distinct from other topical steroid side effects. It comes in two rosacea-like variants: an erythroedematous form and a papulopustular form. An atopic dermatitis patient’s report of a burning sensation upon cessation of topical steroid therapy is a red flag.
Despite the occasional missed opportunity in drawing up the first AAD atopic guidelines in 10 years, the process was richly rewarding, Dr. Sidbury said. And although experts will continue to debate the unresolved controversies in atopic dermatitis, for him the most important lesson to emerge from the panel’s comprehensive review of the evidence was strikingly clear: "Time and time again, education trumps all. Education of patients and families leads to the best outcomes. I think that’s an important lesson to take home," he said.
Dr. Sidbury had no financial conflicts to disclose.
COEUR D’ALENE, IDAHO – The 2014 American Academy of Dermatology atopic dermatitis guidelines may already need an update, according to the cochair of the guidelines panel.
The guidelines were based upon studies published through 2012. Since then, new evidence has emerged that raises the level of uncertainty regarding several key questions the panel addressed, Dr. Robert Sidbury observed at the annual meeting of the Society for Pediatric Dermatology. Among these questions: To bathe or not to bathe? Will a child outgrow atopic dermatitis?
Serving as cochair of the guidelines committee was both a reassuring and daunting experience, according to Dr. Sidbury, chief of the division of dermatology at Seattle Children’s Hospital.
It was reassuring to note that the committee members, who included 17 atopic dermatitis experts from three countries, were free from financial conflicts as they sifted through the published data for evidence-based recommendations to inform practice. But it was daunting to learn how sketchy the supporting evidence is for some of the conventional wisdom regarding atopic dermatitis management, he explained.
By way of providing what he called "a peek behind the curtains" of the guidelines-development process, Dr. Sidbury highlighted the issue of daily bathing followed by application of emollients and moisturizers. This was among the topics the panel struggled with the most, which might come as a surprise to outsiders who consider this to be standard practice, he noted.
"It seems like a very straightforward thing. Almost everyone in this room, to a person, recommends a daily bath followed by moisturizers, yet when we examined the studies we realized that recommendation isn’t based upon much evidence," he said.
Thus, the panel concluded that bathing is "suggested" for atopic dermatitis patients, while adding that "there is no standard" for the duration or frequency of bathing. The panel rated the strength of their recommendation as C, and the level of evidence as III.
"That’s a fairly weak recommendation based upon fairly week evidence," Dr. Sidbury commented.
Moreover, since publication of the guidelines, two new studies have come forth that address the question of whether bathing plus moisturizers is beneficial in atopic dermatitis. The results conflict with each other, making recommendations even more difficult.
Data from a retrospective study of 75 patients with moderate or severe atopic dermatitis suggested that a daily 15- to 20-minute bath followed by a mid-potency topical steroid and moisturizer was indeed beneficial: 79% of subjects showed marked improvement based on Investigator’s Global Assessment at week 3, and 4% were clear (Dermatitis 2014;25:56-9).
By contrast, data from a prospective trial in which 28 children with atopic dermatitis were randomized to a daily vs. twice-weekly bath followed by appropriate care indicated that, while hydration with emollients was important, bathing frequency wasn’t (Clin. Pediatr. 2014;53:677-81).
"This paper makes me feel better about the guidelines not saying, ‘You should bathe every day,’ although that’s still my own recommendation to patients," Dr. Sidbury said.
This year also has brought two conflicting studies regarding the natural history of atopic dermatitis. A large national Taiwanese population-based cohort study of children diagnosed with atopic dermatitis within the first 2 years of life and followed from birth to age 10 years concluded that 70% of these early-onset patients eventually went into remission. A total of 19% of patients did so within the first year, and 49% in less than 4 years. The median disease duration was 4.2 years (Br. J. Dermatol. 2014;170:130-5).
On the other hand, a report from the 7,157-patient, cross-sectional, longitudinal Pediatric Eczema Elective Registry (PEER) found that by age 20, only 50% of the patients had experienced at least one symptom-free period lasting 6 months or more. The investigators concluded that atopic dermatitis is probably a lifelong disease (JAMA Dermatology 2014;150:593-600).
"That’s a provocative conclusion, and a tough thing to tell a parent," Dr. Sidbury observed. "I offer parents realistic but optimistic counsel. I tell them the tendency toward xerosis, irritancy, and infection will persist – the patient in front of you is never going to want to wear a wool sweater for the rest of their life. But the incessant itch, the need for treatment, the impact on quality of life – which is really the issue at hand – hopefully will not persist."
Since the release earlier this year of the first three of the four sections of the atopic dermatitis guidelines, Dr. Sidbury and the other panelists have received considerable feedback that the guidelines didn’t adequately address the topic of topical steroid addiction.
"Some say we missed the boat in not making coherent recommendations to parents about it. We got some very pointed comments," he conceded.
He noted that a systematic review presented at last year’s International Symposium on Atopic Dermatitis concluded that topical steroid withdrawal is a real phenomenon distinct from other topical steroid side effects. It comes in two rosacea-like variants: an erythroedematous form and a papulopustular form. An atopic dermatitis patient’s report of a burning sensation upon cessation of topical steroid therapy is a red flag.
Despite the occasional missed opportunity in drawing up the first AAD atopic guidelines in 10 years, the process was richly rewarding, Dr. Sidbury said. And although experts will continue to debate the unresolved controversies in atopic dermatitis, for him the most important lesson to emerge from the panel’s comprehensive review of the evidence was strikingly clear: "Time and time again, education trumps all. Education of patients and families leads to the best outcomes. I think that’s an important lesson to take home," he said.
Dr. Sidbury had no financial conflicts to disclose.
COEUR D’ALENE, IDAHO – The 2014 American Academy of Dermatology atopic dermatitis guidelines may already need an update, according to the cochair of the guidelines panel.
The guidelines were based upon studies published through 2012. Since then, new evidence has emerged that raises the level of uncertainty regarding several key questions the panel addressed, Dr. Robert Sidbury observed at the annual meeting of the Society for Pediatric Dermatology. Among these questions: To bathe or not to bathe? Will a child outgrow atopic dermatitis?
Serving as cochair of the guidelines committee was both a reassuring and daunting experience, according to Dr. Sidbury, chief of the division of dermatology at Seattle Children’s Hospital.
It was reassuring to note that the committee members, who included 17 atopic dermatitis experts from three countries, were free from financial conflicts as they sifted through the published data for evidence-based recommendations to inform practice. But it was daunting to learn how sketchy the supporting evidence is for some of the conventional wisdom regarding atopic dermatitis management, he explained.
By way of providing what he called "a peek behind the curtains" of the guidelines-development process, Dr. Sidbury highlighted the issue of daily bathing followed by application of emollients and moisturizers. This was among the topics the panel struggled with the most, which might come as a surprise to outsiders who consider this to be standard practice, he noted.
"It seems like a very straightforward thing. Almost everyone in this room, to a person, recommends a daily bath followed by moisturizers, yet when we examined the studies we realized that recommendation isn’t based upon much evidence," he said.
Thus, the panel concluded that bathing is "suggested" for atopic dermatitis patients, while adding that "there is no standard" for the duration or frequency of bathing. The panel rated the strength of their recommendation as C, and the level of evidence as III.
"That’s a fairly weak recommendation based upon fairly week evidence," Dr. Sidbury commented.
Moreover, since publication of the guidelines, two new studies have come forth that address the question of whether bathing plus moisturizers is beneficial in atopic dermatitis. The results conflict with each other, making recommendations even more difficult.
Data from a retrospective study of 75 patients with moderate or severe atopic dermatitis suggested that a daily 15- to 20-minute bath followed by a mid-potency topical steroid and moisturizer was indeed beneficial: 79% of subjects showed marked improvement based on Investigator’s Global Assessment at week 3, and 4% were clear (Dermatitis 2014;25:56-9).
By contrast, data from a prospective trial in which 28 children with atopic dermatitis were randomized to a daily vs. twice-weekly bath followed by appropriate care indicated that, while hydration with emollients was important, bathing frequency wasn’t (Clin. Pediatr. 2014;53:677-81).
"This paper makes me feel better about the guidelines not saying, ‘You should bathe every day,’ although that’s still my own recommendation to patients," Dr. Sidbury said.
This year also has brought two conflicting studies regarding the natural history of atopic dermatitis. A large national Taiwanese population-based cohort study of children diagnosed with atopic dermatitis within the first 2 years of life and followed from birth to age 10 years concluded that 70% of these early-onset patients eventually went into remission. A total of 19% of patients did so within the first year, and 49% in less than 4 years. The median disease duration was 4.2 years (Br. J. Dermatol. 2014;170:130-5).
On the other hand, a report from the 7,157-patient, cross-sectional, longitudinal Pediatric Eczema Elective Registry (PEER) found that by age 20, only 50% of the patients had experienced at least one symptom-free period lasting 6 months or more. The investigators concluded that atopic dermatitis is probably a lifelong disease (JAMA Dermatology 2014;150:593-600).
"That’s a provocative conclusion, and a tough thing to tell a parent," Dr. Sidbury observed. "I offer parents realistic but optimistic counsel. I tell them the tendency toward xerosis, irritancy, and infection will persist – the patient in front of you is never going to want to wear a wool sweater for the rest of their life. But the incessant itch, the need for treatment, the impact on quality of life – which is really the issue at hand – hopefully will not persist."
Since the release earlier this year of the first three of the four sections of the atopic dermatitis guidelines, Dr. Sidbury and the other panelists have received considerable feedback that the guidelines didn’t adequately address the topic of topical steroid addiction.
"Some say we missed the boat in not making coherent recommendations to parents about it. We got some very pointed comments," he conceded.
He noted that a systematic review presented at last year’s International Symposium on Atopic Dermatitis concluded that topical steroid withdrawal is a real phenomenon distinct from other topical steroid side effects. It comes in two rosacea-like variants: an erythroedematous form and a papulopustular form. An atopic dermatitis patient’s report of a burning sensation upon cessation of topical steroid therapy is a red flag.
Despite the occasional missed opportunity in drawing up the first AAD atopic guidelines in 10 years, the process was richly rewarding, Dr. Sidbury said. And although experts will continue to debate the unresolved controversies in atopic dermatitis, for him the most important lesson to emerge from the panel’s comprehensive review of the evidence was strikingly clear: "Time and time again, education trumps all. Education of patients and families leads to the best outcomes. I think that’s an important lesson to take home," he said.
Dr. Sidbury had no financial conflicts to disclose.
EXPERT OPINION FROM THE SPD ANNUAL MEETING
