User login
FDA approves belinostat for peripheral T-cell lymphoma
Belinostat, a histone deacetylase inhibitor, has been approved for treating peripheral T-cell lymphoma, based on the results of the BELIEF study that found an overall response rate of nearly 26% among treated patients.
This is the third drug approved for this rare, aggressive form of non-Hodgkin’s lymphoma (NHL) since 2009, according to the Food and Drug Administration statement announcing the approval on July 3.
The other two drugs are pralatrexate injection (Folotyn), a folate analogue metabolic inhibitor approved in 2009 for treating relapsed or refractory peripheral T-cell lymphoma (PTCL); and romidepsin (Istodax), a histone deacetylase (HDAC) inhibitor approved in 2011 for treating PTCL in patients who have received at least one previous treatment.
This is an accelerated approval, which is based on surrogate or intermediate endpoints considered by the FDA as "reasonably likely to predict clinical benefit for patients with serious conditions with unmet medical needs." Confirmatory trials that verify the clinical benefit are required for full approval; otherwise, the approval can be withdrawn by the FDA. Belinostat will be marketed as Beleodaq by Spectrum Pharmaceuticals, which also markets Folotyn.
HDAC inhibitors "catalyze the removal of acetyl groups from the lysine residues of histones and some nonhistone proteins," and in vitro, belinostat "caused the accumulation of acetylated histones and other proteins, inducing cell cycle arrest and/or apoptosis of some transformed cells," according to a statement on the approval, issued by Spectrum on July 7. "Belinostat shows preferential cytotoxicity towards tumor cells compared to normal cells," and it "inhibited the enzymatic activity of histone deacetylases at nanomolar concentrations," the statement said.
In the BELIEF study, an open-label, single-arm, nonrandomized study, 129 patients with relapsed or refractory PTCL were treated with belinostat, administered via an IV infusion, once a day on days 1-5 of a 21-day cycle, repeated every 3 weeks until the disease progressed or adverse effects became unacceptable. The overall response rate (complete and partial responses), the primary efficacy endpoint, was 25.8%. Nausea, vomiting, fatigue, pyrexia, and anemia were the most common adverse events associated with treatment, according to the FDA.
The company said that the drug is expected to be available in less than 3 weeks of approval (before July 24). The confirmatory trial is a phase III study that will evaluate belinostat plus CHOP (cyclophosphamide, vincristine, doxorubicin, prednisone), compared with CHOP alone.
PTCL accounts for about 10%-15% of NHL cases in North America, according to the FDA, which cites National Cancer Institute estimates that 70,800 Americans will be diagnosed with NHL and 18,990 will die of NHL in 2014.
The prescribing information for belinostat is available here.
Belinostat, a histone deacetylase inhibitor, has been approved for treating peripheral T-cell lymphoma, based on the results of the BELIEF study that found an overall response rate of nearly 26% among treated patients.
This is the third drug approved for this rare, aggressive form of non-Hodgkin’s lymphoma (NHL) since 2009, according to the Food and Drug Administration statement announcing the approval on July 3.
The other two drugs are pralatrexate injection (Folotyn), a folate analogue metabolic inhibitor approved in 2009 for treating relapsed or refractory peripheral T-cell lymphoma (PTCL); and romidepsin (Istodax), a histone deacetylase (HDAC) inhibitor approved in 2011 for treating PTCL in patients who have received at least one previous treatment.
This is an accelerated approval, which is based on surrogate or intermediate endpoints considered by the FDA as "reasonably likely to predict clinical benefit for patients with serious conditions with unmet medical needs." Confirmatory trials that verify the clinical benefit are required for full approval; otherwise, the approval can be withdrawn by the FDA. Belinostat will be marketed as Beleodaq by Spectrum Pharmaceuticals, which also markets Folotyn.
HDAC inhibitors "catalyze the removal of acetyl groups from the lysine residues of histones and some nonhistone proteins," and in vitro, belinostat "caused the accumulation of acetylated histones and other proteins, inducing cell cycle arrest and/or apoptosis of some transformed cells," according to a statement on the approval, issued by Spectrum on July 7. "Belinostat shows preferential cytotoxicity towards tumor cells compared to normal cells," and it "inhibited the enzymatic activity of histone deacetylases at nanomolar concentrations," the statement said.
In the BELIEF study, an open-label, single-arm, nonrandomized study, 129 patients with relapsed or refractory PTCL were treated with belinostat, administered via an IV infusion, once a day on days 1-5 of a 21-day cycle, repeated every 3 weeks until the disease progressed or adverse effects became unacceptable. The overall response rate (complete and partial responses), the primary efficacy endpoint, was 25.8%. Nausea, vomiting, fatigue, pyrexia, and anemia were the most common adverse events associated with treatment, according to the FDA.
The company said that the drug is expected to be available in less than 3 weeks of approval (before July 24). The confirmatory trial is a phase III study that will evaluate belinostat plus CHOP (cyclophosphamide, vincristine, doxorubicin, prednisone), compared with CHOP alone.
PTCL accounts for about 10%-15% of NHL cases in North America, according to the FDA, which cites National Cancer Institute estimates that 70,800 Americans will be diagnosed with NHL and 18,990 will die of NHL in 2014.
The prescribing information for belinostat is available here.
Belinostat, a histone deacetylase inhibitor, has been approved for treating peripheral T-cell lymphoma, based on the results of the BELIEF study that found an overall response rate of nearly 26% among treated patients.
This is the third drug approved for this rare, aggressive form of non-Hodgkin’s lymphoma (NHL) since 2009, according to the Food and Drug Administration statement announcing the approval on July 3.
The other two drugs are pralatrexate injection (Folotyn), a folate analogue metabolic inhibitor approved in 2009 for treating relapsed or refractory peripheral T-cell lymphoma (PTCL); and romidepsin (Istodax), a histone deacetylase (HDAC) inhibitor approved in 2011 for treating PTCL in patients who have received at least one previous treatment.
This is an accelerated approval, which is based on surrogate or intermediate endpoints considered by the FDA as "reasonably likely to predict clinical benefit for patients with serious conditions with unmet medical needs." Confirmatory trials that verify the clinical benefit are required for full approval; otherwise, the approval can be withdrawn by the FDA. Belinostat will be marketed as Beleodaq by Spectrum Pharmaceuticals, which also markets Folotyn.
HDAC inhibitors "catalyze the removal of acetyl groups from the lysine residues of histones and some nonhistone proteins," and in vitro, belinostat "caused the accumulation of acetylated histones and other proteins, inducing cell cycle arrest and/or apoptosis of some transformed cells," according to a statement on the approval, issued by Spectrum on July 7. "Belinostat shows preferential cytotoxicity towards tumor cells compared to normal cells," and it "inhibited the enzymatic activity of histone deacetylases at nanomolar concentrations," the statement said.
In the BELIEF study, an open-label, single-arm, nonrandomized study, 129 patients with relapsed or refractory PTCL were treated with belinostat, administered via an IV infusion, once a day on days 1-5 of a 21-day cycle, repeated every 3 weeks until the disease progressed or adverse effects became unacceptable. The overall response rate (complete and partial responses), the primary efficacy endpoint, was 25.8%. Nausea, vomiting, fatigue, pyrexia, and anemia were the most common adverse events associated with treatment, according to the FDA.
The company said that the drug is expected to be available in less than 3 weeks of approval (before July 24). The confirmatory trial is a phase III study that will evaluate belinostat plus CHOP (cyclophosphamide, vincristine, doxorubicin, prednisone), compared with CHOP alone.
PTCL accounts for about 10%-15% of NHL cases in North America, according to the FDA, which cites National Cancer Institute estimates that 70,800 Americans will be diagnosed with NHL and 18,990 will die of NHL in 2014.
The prescribing information for belinostat is available here.
Hailey-Hailey Disease
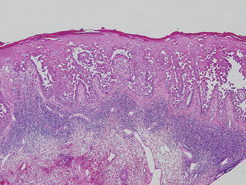
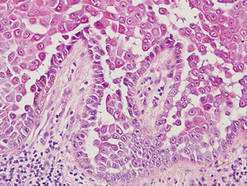
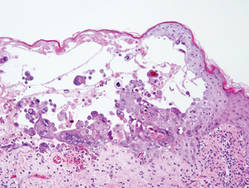
Hailey-Hailey disease (HHD), or benign familial chronic pemphigus, typically presents as suprabasal blisters with a perivascular and interstitial lymphocytic infiltrate (Figure 1).1 Villi, or elongated dermal papillae lined with a single layer of basal cells, protrude into the bullae (Figure 2). In HHD lesions, the epidermis is thickened with scale-crust, and at least the lower half of the epidermis shows acantholysis. Despite the acantholytic changes, a few intact intercellular bridges remain, giving the appearance of a dilapidated brick wall (Figure 2). There may be dyskeratotic cells among the acantholytic cells, though they are scant in many cases. These acantholytic dyskeratotic cells have eosinophilic polygonal-shaped cytoplasm. Hailey-Hailey disease typically does not show adnexal extension of the acantholysis. Direct immunofluorescence is negative in HHD.
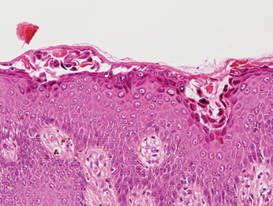
Pemphigus vulgaris is an autoimmune intraepidermal bullous disease that presents with suprabasal acantholysis (Figure 3).2 The epidermis is not thickened and acantholysis is limited to the suprabasal layer. Acantholytic cells with eosinophils and/or neutrophils are found within the bullae. Perivascular and interstitial infiltrates of lymphocytes, eosinophils, and occasionally neutrophils are seen; however, the inflammatory cell infiltrate can vary from extensive to scant. Direct immunofluorescence usually reveals IgG and/or C3 deposition on the surface of the keratinocytes throughout the epidermis.
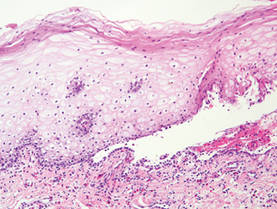
Pemphigus foliaceus is another autoimmune intraepidermal bullous disease that is characterized by acantholysis in the granular or upper spinous layers (Figure 4).3 The epidermis is not thickened. Sometimes acantholytic cells show dyskeratotic change (Figure 4). Some biopsy specimens do not contain the roof of the bullae; therefore, only erosion is seen and the diagnosis may be missed. Moreover, when only the adnexal epithelium shows acantholysis without epidermal involvement, diagnosis can be difficult.4 Acantholysis is accompanied with a superficial perivascular and interstitial inflammatory cell infiltrate consisting of lymphocytes, eosinophils, and occasionally neutrophils. The amount of inflammatory cell infiltrate may vary. Bullous impetigo and staphylococcal scalded skin syndrome reveal a similar histopathologic pattern. Direct immunofluorescence usually discloses IgG and/or C3 deposition on cell surfaces of keratinocytes in the entire or upper epidermis.
Herpesvirus infection shows ballooning (intracellular edema) of keratinocytes. Eventually acantholysis occurs and intraepidermal bullae are formed. In the bullae, virus-associated acantholytic keratinocytes, some that are multinucleated, can be easily found (Figure 5).5 These cells are larger than normal keratinocytes and have steel gray nuclei with peripheral accentuation. Some of these cells are necrotic, and the remains of necrotic multinucleated acantholytic cells are easily recognized. Adnexal epithelial cells occasionally are affected by herpesvirus infection; nuclear change is similar to the epidermis. A perivascular and interstitial infiltrate of lymphocytes and neutrophils is seen. Neutrophils accumulate within the old bullae, clinically manifesting as a pustule.
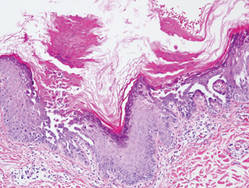
Darier disease is characterized by suprabasal clefts and acantholysis above the basal layer (Figure 6).6 Similar to HHD, villi protrude within the clefts (Figure 6). Conspicuous columns of parakeratosis above the acantholytic epidermis often are observed. Dyskeratotic cells exist among acantholytic ke-ratinocytes in the granular layer and parakeratotic column, which are known as corps ronds and crops grains, respectively. A scant to moderate lymphocytic infiltrate is found in the upper dermis.
- Hernandez-Perez E. Familial benign chronic pemphigus. Cutis. 1987;39:75-77.
- Venugopal SS, Murrell DF. Diagnosis and clinical features of pemphigus vulgaris. Dermatol Clin. 2011;29:373-380, vii.
- Dasher D, Rubenstein D, Diaz LA. Pemphigus foliaceus. Curr Dir Autoimmun. 2008;10:182-194.
- Ohata C, Akamatsu K, Imai N, et al. Localized pemphigus foliaceus exclusively involving the follicular infundibulum: a novel peau d’orange appearance. Eur J Dermatol. 2011;21:392-395.
- King DF, King LA. Giant cells in lesions of varicella and herpes zoster. Am J Dermatopathol. 1986;8:456-458.
- Burge S. Management of Darier’s disease. Clin Exp Dermatol. 1999;24:53-56.
Hailey-Hailey disease (HHD), or benign familial chronic pemphigus, typically presents as suprabasal blisters with a perivascular and interstitial lymphocytic infiltrate (Figure 1).1 Villi, or elongated dermal papillae lined with a single layer of basal cells, protrude into the bullae (Figure 2). In HHD lesions, the epidermis is thickened with scale-crust, and at least the lower half of the epidermis shows acantholysis. Despite the acantholytic changes, a few intact intercellular bridges remain, giving the appearance of a dilapidated brick wall (Figure 2). There may be dyskeratotic cells among the acantholytic cells, though they are scant in many cases. These acantholytic dyskeratotic cells have eosinophilic polygonal-shaped cytoplasm. Hailey-Hailey disease typically does not show adnexal extension of the acantholysis. Direct immunofluorescence is negative in HHD.
Pemphigus vulgaris is an autoimmune intraepidermal bullous disease that presents with suprabasal acantholysis (Figure 3).2 The epidermis is not thickened and acantholysis is limited to the suprabasal layer. Acantholytic cells with eosinophils and/or neutrophils are found within the bullae. Perivascular and interstitial infiltrates of lymphocytes, eosinophils, and occasionally neutrophils are seen; however, the inflammatory cell infiltrate can vary from extensive to scant. Direct immunofluorescence usually reveals IgG and/or C3 deposition on the surface of the keratinocytes throughout the epidermis.
Pemphigus foliaceus is another autoimmune intraepidermal bullous disease that is characterized by acantholysis in the granular or upper spinous layers (Figure 4).3 The epidermis is not thickened. Sometimes acantholytic cells show dyskeratotic change (Figure 4). Some biopsy specimens do not contain the roof of the bullae; therefore, only erosion is seen and the diagnosis may be missed. Moreover, when only the adnexal epithelium shows acantholysis without epidermal involvement, diagnosis can be difficult.4 Acantholysis is accompanied with a superficial perivascular and interstitial inflammatory cell infiltrate consisting of lymphocytes, eosinophils, and occasionally neutrophils. The amount of inflammatory cell infiltrate may vary. Bullous impetigo and staphylococcal scalded skin syndrome reveal a similar histopathologic pattern. Direct immunofluorescence usually discloses IgG and/or C3 deposition on cell surfaces of keratinocytes in the entire or upper epidermis.
Herpesvirus infection shows ballooning (intracellular edema) of keratinocytes. Eventually acantholysis occurs and intraepidermal bullae are formed. In the bullae, virus-associated acantholytic keratinocytes, some that are multinucleated, can be easily found (Figure 5).5 These cells are larger than normal keratinocytes and have steel gray nuclei with peripheral accentuation. Some of these cells are necrotic, and the remains of necrotic multinucleated acantholytic cells are easily recognized. Adnexal epithelial cells occasionally are affected by herpesvirus infection; nuclear change is similar to the epidermis. A perivascular and interstitial infiltrate of lymphocytes and neutrophils is seen. Neutrophils accumulate within the old bullae, clinically manifesting as a pustule.
Darier disease is characterized by suprabasal clefts and acantholysis above the basal layer (Figure 6).6 Similar to HHD, villi protrude within the clefts (Figure 6). Conspicuous columns of parakeratosis above the acantholytic epidermis often are observed. Dyskeratotic cells exist among acantholytic ke-ratinocytes in the granular layer and parakeratotic column, which are known as corps ronds and crops grains, respectively. A scant to moderate lymphocytic infiltrate is found in the upper dermis.
Hailey-Hailey disease (HHD), or benign familial chronic pemphigus, typically presents as suprabasal blisters with a perivascular and interstitial lymphocytic infiltrate (Figure 1).1 Villi, or elongated dermal papillae lined with a single layer of basal cells, protrude into the bullae (Figure 2). In HHD lesions, the epidermis is thickened with scale-crust, and at least the lower half of the epidermis shows acantholysis. Despite the acantholytic changes, a few intact intercellular bridges remain, giving the appearance of a dilapidated brick wall (Figure 2). There may be dyskeratotic cells among the acantholytic cells, though they are scant in many cases. These acantholytic dyskeratotic cells have eosinophilic polygonal-shaped cytoplasm. Hailey-Hailey disease typically does not show adnexal extension of the acantholysis. Direct immunofluorescence is negative in HHD.
Pemphigus vulgaris is an autoimmune intraepidermal bullous disease that presents with suprabasal acantholysis (Figure 3).2 The epidermis is not thickened and acantholysis is limited to the suprabasal layer. Acantholytic cells with eosinophils and/or neutrophils are found within the bullae. Perivascular and interstitial infiltrates of lymphocytes, eosinophils, and occasionally neutrophils are seen; however, the inflammatory cell infiltrate can vary from extensive to scant. Direct immunofluorescence usually reveals IgG and/or C3 deposition on the surface of the keratinocytes throughout the epidermis.
Pemphigus foliaceus is another autoimmune intraepidermal bullous disease that is characterized by acantholysis in the granular or upper spinous layers (Figure 4).3 The epidermis is not thickened. Sometimes acantholytic cells show dyskeratotic change (Figure 4). Some biopsy specimens do not contain the roof of the bullae; therefore, only erosion is seen and the diagnosis may be missed. Moreover, when only the adnexal epithelium shows acantholysis without epidermal involvement, diagnosis can be difficult.4 Acantholysis is accompanied with a superficial perivascular and interstitial inflammatory cell infiltrate consisting of lymphocytes, eosinophils, and occasionally neutrophils. The amount of inflammatory cell infiltrate may vary. Bullous impetigo and staphylococcal scalded skin syndrome reveal a similar histopathologic pattern. Direct immunofluorescence usually discloses IgG and/or C3 deposition on cell surfaces of keratinocytes in the entire or upper epidermis.
Herpesvirus infection shows ballooning (intracellular edema) of keratinocytes. Eventually acantholysis occurs and intraepidermal bullae are formed. In the bullae, virus-associated acantholytic keratinocytes, some that are multinucleated, can be easily found (Figure 5).5 These cells are larger than normal keratinocytes and have steel gray nuclei with peripheral accentuation. Some of these cells are necrotic, and the remains of necrotic multinucleated acantholytic cells are easily recognized. Adnexal epithelial cells occasionally are affected by herpesvirus infection; nuclear change is similar to the epidermis. A perivascular and interstitial infiltrate of lymphocytes and neutrophils is seen. Neutrophils accumulate within the old bullae, clinically manifesting as a pustule.
Darier disease is characterized by suprabasal clefts and acantholysis above the basal layer (Figure 6).6 Similar to HHD, villi protrude within the clefts (Figure 6). Conspicuous columns of parakeratosis above the acantholytic epidermis often are observed. Dyskeratotic cells exist among acantholytic ke-ratinocytes in the granular layer and parakeratotic column, which are known as corps ronds and crops grains, respectively. A scant to moderate lymphocytic infiltrate is found in the upper dermis.
- Hernandez-Perez E. Familial benign chronic pemphigus. Cutis. 1987;39:75-77.
- Venugopal SS, Murrell DF. Diagnosis and clinical features of pemphigus vulgaris. Dermatol Clin. 2011;29:373-380, vii.
- Dasher D, Rubenstein D, Diaz LA. Pemphigus foliaceus. Curr Dir Autoimmun. 2008;10:182-194.
- Ohata C, Akamatsu K, Imai N, et al. Localized pemphigus foliaceus exclusively involving the follicular infundibulum: a novel peau d’orange appearance. Eur J Dermatol. 2011;21:392-395.
- King DF, King LA. Giant cells in lesions of varicella and herpes zoster. Am J Dermatopathol. 1986;8:456-458.
- Burge S. Management of Darier’s disease. Clin Exp Dermatol. 1999;24:53-56.
- Hernandez-Perez E. Familial benign chronic pemphigus. Cutis. 1987;39:75-77.
- Venugopal SS, Murrell DF. Diagnosis and clinical features of pemphigus vulgaris. Dermatol Clin. 2011;29:373-380, vii.
- Dasher D, Rubenstein D, Diaz LA. Pemphigus foliaceus. Curr Dir Autoimmun. 2008;10:182-194.
- Ohata C, Akamatsu K, Imai N, et al. Localized pemphigus foliaceus exclusively involving the follicular infundibulum: a novel peau d’orange appearance. Eur J Dermatol. 2011;21:392-395.
- King DF, King LA. Giant cells in lesions of varicella and herpes zoster. Am J Dermatopathol. 1986;8:456-458.
- Burge S. Management of Darier’s disease. Clin Exp Dermatol. 1999;24:53-56.

Efficacy, safety seen with transcatheter pulmonary valve
WASHINGTON - A transcatheter pulmonary valve system that provides a new right ventricle to pulmonary artery conduit to congenital heart disease patients without the need for open heart surgery performed a little better in a real-world registry at 10 U.S. centers than it had in the pivotal trial that led to the system's 2010 FDA approval.
The new results "confirm the strong performance of the Melody transcatheter pulmonary valve achieved by real-world providers with results comparable to the U.S. investigational device exemption [IDE] trial," Dr. Aimee K. Armstrong said at the annual meeting of the American College of Cardiology. The "high level" of 97% freedom from transcatheter pulmonary valve (TPV) dysfunction at 1 year "was better than in the IDE trial," where the level reached 94%, noted Dr. Armstrong of the University of Michigan in Ann Arbor.

The registry study, which the FDA mandated when it approved the Melody valve in 2010, ran during July 2010 to July 2012 at 10 U.S. centers that had not participated in the pivotal trial. The 99 patients who received an implant that stayed in place for at least 1 day ranged from 5 to 45 years old, with an average age of 20 years. Although patient follow-up averaged 22 months, the study's primary endpoint was acceptable hemodynamic function within the conduit at 6 months, with a prespecified performance goal of 75% of patients achieving this outcome. The outcome actually occurred in 97% of the 90 evaluable patients at 6 months, and in 88% of all 99 patients who received a conduit. The difference between each of these rates and the performance goal was statistically significant, Dr. Armstrong said.
The transcatheter valve showed excellent performance by other criteria as well. Acceptable hemodynamic function continued through 1 year in 94% of the 87 implanted patients with evaluable data at 12 months, which translated to 83% of the entire 99 patients in the implanted group. Severe or moderate pulmonary valve regurgitation existed in 85% of the patients before treatment; after treatment no patient had severe or moderate regurgitation, and after 1 year 63% had no regurgitation, 24% had trace, and 12% had mild regurgitation (figures total 99% because of rounding). The 1-year rate of 97% of patients free from dysfunction of their implanted valve appeared to surpass the 94% rate seen in the pivotal trial (Circulation 2010;122:507-16).
The results also showed that high right ventricular pressure prior to valve placement was the only variable independently associated with subsequent valve dysfunction. "Patients who go into the procedure with a very stenotic conduit are probably at higher risk for transcatheter pulmonary valve dysfunction down the road," she said.
The study was sponsored by Medtronic, which markets the Melody transcatheter pulmonary valve. Dr. Armstrong said she has received research funding from Medtronic and Edwards Lifesciences.

|
| Dr. Robert Jaquiss |
This study is an important post-approval demonstration that the excellent early results obtained in the original IDE trial in the United States can be reproduced or even exceeded with a broader rollout of the Melody valve to many more centers. The next set of data, which is eagerly anticipated, is the mid-term and longer results for the Melody valve, which will begin to answer questions about the durability of valve competence. Additional information about the performance of the valve in alternative anatomic settings, such as in failing stented bioprostheses - so-called "valve-in-valve" usage - is also beginning to accumulate.
Dr. Robert Jaquiss is professor of surgery and pediatrics and chief of pediatric heart surgery at Duke University School of Medicine and an associate medical editor for Vascular Specialist.
|
|
| Dr. Robert Jaquiss |
This study is an important post-approval demonstration that the excellent early results obtained in the original IDE trial in the United States can be reproduced or even exceeded with a broader rollout of the Melody valve to many more centers. The next set of data, which is eagerly anticipated, is the mid-term and longer results for the Melody valve, which will begin to answer questions about the durability of valve competence. Additional information about the performance of the valve in alternative anatomic settings, such as in failing stented bioprostheses - so-called "valve-in-valve" usage - is also beginning to accumulate.
Dr. Robert Jaquiss is professor of surgery and pediatrics and chief of pediatric heart surgery at Duke University School of Medicine and an associate medical editor for Vascular Specialist.
|
|
| Dr. Robert Jaquiss |
This study is an important post-approval demonstration that the excellent early results obtained in the original IDE trial in the United States can be reproduced or even exceeded with a broader rollout of the Melody valve to many more centers. The next set of data, which is eagerly anticipated, is the mid-term and longer results for the Melody valve, which will begin to answer questions about the durability of valve competence. Additional information about the performance of the valve in alternative anatomic settings, such as in failing stented bioprostheses - so-called "valve-in-valve" usage - is also beginning to accumulate.
Dr. Robert Jaquiss is professor of surgery and pediatrics and chief of pediatric heart surgery at Duke University School of Medicine and an associate medical editor for Vascular Specialist.
WASHINGTON - A transcatheter pulmonary valve system that provides a new right ventricle to pulmonary artery conduit to congenital heart disease patients without the need for open heart surgery performed a little better in a real-world registry at 10 U.S. centers than it had in the pivotal trial that led to the system's 2010 FDA approval.
The new results "confirm the strong performance of the Melody transcatheter pulmonary valve achieved by real-world providers with results comparable to the U.S. investigational device exemption [IDE] trial," Dr. Aimee K. Armstrong said at the annual meeting of the American College of Cardiology. The "high level" of 97% freedom from transcatheter pulmonary valve (TPV) dysfunction at 1 year "was better than in the IDE trial," where the level reached 94%, noted Dr. Armstrong of the University of Michigan in Ann Arbor.
The registry study, which the FDA mandated when it approved the Melody valve in 2010, ran during July 2010 to July 2012 at 10 U.S. centers that had not participated in the pivotal trial. The 99 patients who received an implant that stayed in place for at least 1 day ranged from 5 to 45 years old, with an average age of 20 years. Although patient follow-up averaged 22 months, the study's primary endpoint was acceptable hemodynamic function within the conduit at 6 months, with a prespecified performance goal of 75% of patients achieving this outcome. The outcome actually occurred in 97% of the 90 evaluable patients at 6 months, and in 88% of all 99 patients who received a conduit. The difference between each of these rates and the performance goal was statistically significant, Dr. Armstrong said.
The transcatheter valve showed excellent performance by other criteria as well. Acceptable hemodynamic function continued through 1 year in 94% of the 87 implanted patients with evaluable data at 12 months, which translated to 83% of the entire 99 patients in the implanted group. Severe or moderate pulmonary valve regurgitation existed in 85% of the patients before treatment; after treatment no patient had severe or moderate regurgitation, and after 1 year 63% had no regurgitation, 24% had trace, and 12% had mild regurgitation (figures total 99% because of rounding). The 1-year rate of 97% of patients free from dysfunction of their implanted valve appeared to surpass the 94% rate seen in the pivotal trial (Circulation 2010;122:507-16).
The results also showed that high right ventricular pressure prior to valve placement was the only variable independently associated with subsequent valve dysfunction. "Patients who go into the procedure with a very stenotic conduit are probably at higher risk for transcatheter pulmonary valve dysfunction down the road," she said.
The study was sponsored by Medtronic, which markets the Melody transcatheter pulmonary valve. Dr. Armstrong said she has received research funding from Medtronic and Edwards Lifesciences.
WASHINGTON - A transcatheter pulmonary valve system that provides a new right ventricle to pulmonary artery conduit to congenital heart disease patients without the need for open heart surgery performed a little better in a real-world registry at 10 U.S. centers than it had in the pivotal trial that led to the system's 2010 FDA approval.
The new results "confirm the strong performance of the Melody transcatheter pulmonary valve achieved by real-world providers with results comparable to the U.S. investigational device exemption [IDE] trial," Dr. Aimee K. Armstrong said at the annual meeting of the American College of Cardiology. The "high level" of 97% freedom from transcatheter pulmonary valve (TPV) dysfunction at 1 year "was better than in the IDE trial," where the level reached 94%, noted Dr. Armstrong of the University of Michigan in Ann Arbor.
The registry study, which the FDA mandated when it approved the Melody valve in 2010, ran during July 2010 to July 2012 at 10 U.S. centers that had not participated in the pivotal trial. The 99 patients who received an implant that stayed in place for at least 1 day ranged from 5 to 45 years old, with an average age of 20 years. Although patient follow-up averaged 22 months, the study's primary endpoint was acceptable hemodynamic function within the conduit at 6 months, with a prespecified performance goal of 75% of patients achieving this outcome. The outcome actually occurred in 97% of the 90 evaluable patients at 6 months, and in 88% of all 99 patients who received a conduit. The difference between each of these rates and the performance goal was statistically significant, Dr. Armstrong said.
The transcatheter valve showed excellent performance by other criteria as well. Acceptable hemodynamic function continued through 1 year in 94% of the 87 implanted patients with evaluable data at 12 months, which translated to 83% of the entire 99 patients in the implanted group. Severe or moderate pulmonary valve regurgitation existed in 85% of the patients before treatment; after treatment no patient had severe or moderate regurgitation, and after 1 year 63% had no regurgitation, 24% had trace, and 12% had mild regurgitation (figures total 99% because of rounding). The 1-year rate of 97% of patients free from dysfunction of their implanted valve appeared to surpass the 94% rate seen in the pivotal trial (Circulation 2010;122:507-16).
The results also showed that high right ventricular pressure prior to valve placement was the only variable independently associated with subsequent valve dysfunction. "Patients who go into the procedure with a very stenotic conduit are probably at higher risk for transcatheter pulmonary valve dysfunction down the road," she said.
The study was sponsored by Medtronic, which markets the Melody transcatheter pulmonary valve. Dr. Armstrong said she has received research funding from Medtronic and Edwards Lifesciences.
Key clinical point: The Melody transcatheter pulmonary valve system worked as well in a real world registry as it did in its pivotal trial as a conduit between the right ventricle and pulmonary artery.
Major finding: Acceptable hemodynamic function at 6 months occurred in 88% of implanted patients, significantly surpassing the 75% performance goal.
Data source: A series of 99 patients who received a transcatheter pulmonary valve at any of 10 participating U.S. centers.
Disclosures: The study was sponsored by Medtronic, which markets the Melody transcatheter pulmonary valve. Dr. Armstrong said that she has received consultant fees and honoraria from Siemens Healthcare and St. Jude Medical, and has received research funding from Medtronic and Edwards Lifesciences.

Subclinical seizures a risk during cardiac surgery
TORONTO – Routine EEG monitoring after surgery with cardiopulmonary bypass in neonates revealed a seizure incidence of 8% in a recent study. In most cases (85%), seizure activity was detectable only on EEG and would not have been identified or treated without EEG monitoring, reported Dr. Maryam Y. Naim, of Children’s Hospital of Philadelphia, during the AATS Annual Meeting.
Of concern, status epilepticus was noted in 62% of neonates with seizures, and mortality was higher in babies with seizures versus those without (38% vs. 3%; P less than .01). "Postoperative seizures are associated with worse neurological outcomes," said Dr. Naim. In addition to being a biomarker of underlying brain injury, there is some evidence that the seizures themselves may cause secondary brain injury.
A total of 161 neonates had 48-hours of EEG monitoring begun within 6 hours of cardiac surgery with CPB. The median gestational age of the cohort was 39 weeks, 16% were premature, and 13% had identified genetic defects. The median age at surgery was 5 days. Deep hypothermic circulatory arrest was used in 48% of surgeries (median time, 48 minutes), 16% had open chest with delayed sternal closure, and 9% had a cardiac arrest.
Seizures were detected in 13 (8%), with a median onset of 20 hours after return to the cardiac ICU (CICU) from surgery. Seizures were subclinical, or EEG only, in 11 patients (85%), electroclinical in the other 2 (15%), and status epilepticus was seen in 8 (62%). When seizures occurred, the patient was treated with antiseizure medications. Abnormal vital signs or movements suggestive of seizure activity were noted at the bedside; although such events were recorded in 32 patients (22%), none had EEG correlates consistent with seizure activity.
"Neonates with all types of heart disease had seizures ... " said Dr. Naim. " ... with a highest percentage occurring in those with single ventricles and arch obstruction."
Neuroimaging studies were reviewed by a neurologist to determine any association between injury and seizure location. Although neonates with and without seizures had similar CICU lengths of stay, mortality was higher in those with seizures (38% vs. 3%; P less than .01). No predictors of seizures were identified on multivariable analysis.
"Based on these data, we are continuing routine postoperative EEG monitoring in all neonates following surgery with CPB," she said.
While not discredited in any way, Dr. Naim’s data were met with a fair amount of pushback from the gathered group of pediatric cardiothoracic surgical experts. An informal poll of the audience showed that 80%-90% do not routinely monitor neonates for seizures post-CPB despite ACNS recommendations, and several of the comments questioned the technical and financial feasibility of routine EEG monitoring.
Said the invited discussant, Dr. Frank Pigula, a cardiac surgeon from Boston Children’s Hospital, "In all the groups that have studied this, in all patients who have had a seizure, there were documented brain abnormalities. So, the ways I picture these data are that a seizure is a sign of an underlying brain injury, much like a fever is a sign of an underlying infection.
"And you’ve made a good case for the routine postoperative surveillance for seizures; I’m sure everyone would agree that treating seizures is a good thing, but is there any evidence showing us that the early identification and treatment of seizures improves outcomes, either developmental delays or mortality?
In response, Dr. Naim noted that all the CHOP seizure sufferers were treated, whether they had EEG only or clinical seizures, and, at the 4-year mark, they are showing fewer neurodevelopmental issues than previous cohorts of untreated neonates.
"I think one thing that is very concerning is emerging evidence that the seizures themselves cause secondary brain injury," she said.
Dr. Naim and Dr. Pigula reported having no financial disclosures.
TORONTO – Routine EEG monitoring after surgery with cardiopulmonary bypass in neonates revealed a seizure incidence of 8% in a recent study. In most cases (85%), seizure activity was detectable only on EEG and would not have been identified or treated without EEG monitoring, reported Dr. Maryam Y. Naim, of Children’s Hospital of Philadelphia, during the AATS Annual Meeting.
Of concern, status epilepticus was noted in 62% of neonates with seizures, and mortality was higher in babies with seizures versus those without (38% vs. 3%; P less than .01). "Postoperative seizures are associated with worse neurological outcomes," said Dr. Naim. In addition to being a biomarker of underlying brain injury, there is some evidence that the seizures themselves may cause secondary brain injury.
A total of 161 neonates had 48-hours of EEG monitoring begun within 6 hours of cardiac surgery with CPB. The median gestational age of the cohort was 39 weeks, 16% were premature, and 13% had identified genetic defects. The median age at surgery was 5 days. Deep hypothermic circulatory arrest was used in 48% of surgeries (median time, 48 minutes), 16% had open chest with delayed sternal closure, and 9% had a cardiac arrest.
Seizures were detected in 13 (8%), with a median onset of 20 hours after return to the cardiac ICU (CICU) from surgery. Seizures were subclinical, or EEG only, in 11 patients (85%), electroclinical in the other 2 (15%), and status epilepticus was seen in 8 (62%). When seizures occurred, the patient was treated with antiseizure medications. Abnormal vital signs or movements suggestive of seizure activity were noted at the bedside; although such events were recorded in 32 patients (22%), none had EEG correlates consistent with seizure activity.
"Neonates with all types of heart disease had seizures ... " said Dr. Naim. " ... with a highest percentage occurring in those with single ventricles and arch obstruction."
Neuroimaging studies were reviewed by a neurologist to determine any association between injury and seizure location. Although neonates with and without seizures had similar CICU lengths of stay, mortality was higher in those with seizures (38% vs. 3%; P less than .01). No predictors of seizures were identified on multivariable analysis.
"Based on these data, we are continuing routine postoperative EEG monitoring in all neonates following surgery with CPB," she said.
While not discredited in any way, Dr. Naim’s data were met with a fair amount of pushback from the gathered group of pediatric cardiothoracic surgical experts. An informal poll of the audience showed that 80%-90% do not routinely monitor neonates for seizures post-CPB despite ACNS recommendations, and several of the comments questioned the technical and financial feasibility of routine EEG monitoring.
Said the invited discussant, Dr. Frank Pigula, a cardiac surgeon from Boston Children’s Hospital, "In all the groups that have studied this, in all patients who have had a seizure, there were documented brain abnormalities. So, the ways I picture these data are that a seizure is a sign of an underlying brain injury, much like a fever is a sign of an underlying infection.
"And you’ve made a good case for the routine postoperative surveillance for seizures; I’m sure everyone would agree that treating seizures is a good thing, but is there any evidence showing us that the early identification and treatment of seizures improves outcomes, either developmental delays or mortality?
In response, Dr. Naim noted that all the CHOP seizure sufferers were treated, whether they had EEG only or clinical seizures, and, at the 4-year mark, they are showing fewer neurodevelopmental issues than previous cohorts of untreated neonates.
"I think one thing that is very concerning is emerging evidence that the seizures themselves cause secondary brain injury," she said.
Dr. Naim and Dr. Pigula reported having no financial disclosures.
TORONTO – Routine EEG monitoring after surgery with cardiopulmonary bypass in neonates revealed a seizure incidence of 8% in a recent study. In most cases (85%), seizure activity was detectable only on EEG and would not have been identified or treated without EEG monitoring, reported Dr. Maryam Y. Naim, of Children’s Hospital of Philadelphia, during the AATS Annual Meeting.
Of concern, status epilepticus was noted in 62% of neonates with seizures, and mortality was higher in babies with seizures versus those without (38% vs. 3%; P less than .01). "Postoperative seizures are associated with worse neurological outcomes," said Dr. Naim. In addition to being a biomarker of underlying brain injury, there is some evidence that the seizures themselves may cause secondary brain injury.
A total of 161 neonates had 48-hours of EEG monitoring begun within 6 hours of cardiac surgery with CPB. The median gestational age of the cohort was 39 weeks, 16% were premature, and 13% had identified genetic defects. The median age at surgery was 5 days. Deep hypothermic circulatory arrest was used in 48% of surgeries (median time, 48 minutes), 16% had open chest with delayed sternal closure, and 9% had a cardiac arrest.
Seizures were detected in 13 (8%), with a median onset of 20 hours after return to the cardiac ICU (CICU) from surgery. Seizures were subclinical, or EEG only, in 11 patients (85%), electroclinical in the other 2 (15%), and status epilepticus was seen in 8 (62%). When seizures occurred, the patient was treated with antiseizure medications. Abnormal vital signs or movements suggestive of seizure activity were noted at the bedside; although such events were recorded in 32 patients (22%), none had EEG correlates consistent with seizure activity.
"Neonates with all types of heart disease had seizures ... " said Dr. Naim. " ... with a highest percentage occurring in those with single ventricles and arch obstruction."
Neuroimaging studies were reviewed by a neurologist to determine any association between injury and seizure location. Although neonates with and without seizures had similar CICU lengths of stay, mortality was higher in those with seizures (38% vs. 3%; P less than .01). No predictors of seizures were identified on multivariable analysis.
"Based on these data, we are continuing routine postoperative EEG monitoring in all neonates following surgery with CPB," she said.
While not discredited in any way, Dr. Naim’s data were met with a fair amount of pushback from the gathered group of pediatric cardiothoracic surgical experts. An informal poll of the audience showed that 80%-90% do not routinely monitor neonates for seizures post-CPB despite ACNS recommendations, and several of the comments questioned the technical and financial feasibility of routine EEG monitoring.
Said the invited discussant, Dr. Frank Pigula, a cardiac surgeon from Boston Children’s Hospital, "In all the groups that have studied this, in all patients who have had a seizure, there were documented brain abnormalities. So, the ways I picture these data are that a seizure is a sign of an underlying brain injury, much like a fever is a sign of an underlying infection.
"And you’ve made a good case for the routine postoperative surveillance for seizures; I’m sure everyone would agree that treating seizures is a good thing, but is there any evidence showing us that the early identification and treatment of seizures improves outcomes, either developmental delays or mortality?
In response, Dr. Naim noted that all the CHOP seizure sufferers were treated, whether they had EEG only or clinical seizures, and, at the 4-year mark, they are showing fewer neurodevelopmental issues than previous cohorts of untreated neonates.
"I think one thing that is very concerning is emerging evidence that the seizures themselves cause secondary brain injury," she said.
Dr. Naim and Dr. Pigula reported having no financial disclosures.
Breathe2Relax

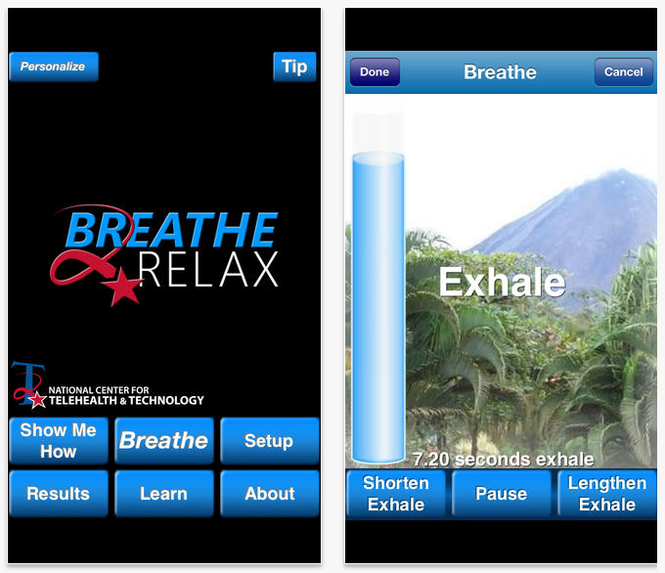
The Breathe2Relax app is centered around the basic concept that breathing into the belly—diaphragmatic breathing—provides deeper relaxation than does breathing into the chest. Designed for use by individuals with PTSD and TBI, the app helps with mood stabilization, anger control, and anxiety management. It is a portable stress management tool with breathing exercises documented to decrease the body’s “fight-or-flight” stress response.
Setup
Although you can jump right into the guided breathing exercises, you may find a richer experience by exploring the setup menu of the app before beginning. (TIP: Skip the Personalize button and go straight to Setup.) Setting up the app to your personal preferences will reduce the chances of growing agitated when you begin the breathing exercises.
Almost every element you encounter while using the app can be modified: scenery (eg, mountain meadows or the cosmos), background music (mostly instrumental and earth sounds, plus a choice for no music at all), inhale and exhale lengths set to tenths of a second, whether a breathing metronome and visual prompts will display during the exercise, and whether a voice will prompt breathing instructions. Additional modifications include how many cycles of inhalations/exhalations will be provided, whether you want to track your stress levels (these can be graphed later and tracked over time), and, importantly, whether you want this data to be saved and transmitted to T2 for survey data (there is a choice to remain anonymous) or to disenroll from the study and delete all stored information.
Breathe
Once all of your preferences are set, they will remain saved in the app until you change them. If you already know how to breathe diaphragmatically, click “Breathe” to begin a breathing session. If you are uncertain or need a refresher, click “Show Me How” to watch a 2-minute instructional video. As noted during this instruction, “Be patient. Although breathing sounds like it should be easy to do, diaphragmatic breathing takes practice.” It is recommended that this practice be done every day for maximum benefit, and it is okay to practice when you’re already feeling relaxed.
When you are ready to work through the breathing session, begin by rating your stress level. If you want to skip this step, go ahead and hit “Skip.” If you never want to enter this information when you enter the breathing session portion of the app, click the box that reads “Do Not Show Again” or return to the Setup menu and select “OFF” under Stress Tracking Information. However, by taking just a moment to note stress levels before (and after), you will see over time how you are performing and whether or not this is a beneficial exercise for you. Oftentimes, we don’t accurately perceive our own emotions and reactions, so graphing this output can help limit personal bias.
If you are following the breathing metronome, you will see it rise and fall with each breath until the session is complete. You will then be prompted to record your ending stress level and can click “Finish” to return to the home screen.
Results
The benefit of tracking stress levels during breathing sessions is revealed in a simple line graph. A thin line is produced using starting stress levels and a thick line is produced using ending stress levels. Sometimes the breathing session will result in a dramatic shift in stress level reduction, sometimes an insignificant reduction, and sometimes it may seemingly increase stress levels. If the latter happens, it is possible you were unable to focus on the exercise enough to properly engage in diaphragmatic breathing, or maybe one of the app settings has agitated you and it’s time to update your settings in the Setup menu.

Learning
Read about or watch information on stress by selecting 1 of 3 topics. “Biology of Stress” covers what happens in the body during stress, the consequences of stress on the body, how breathing can help control the stress response, and the resilience of the mind and body after handling a stressful episode. “Diaphragmatic Breathing” explains what the diaphragm is, the difference in oxygen levels supplied to the body during chest breathing and diaphragmatic breathing, and how to determine what kind of a breather you are. Access the Body Scanner under “Effects of Stress on the Body” to learn about the effects of stress on 10 different areas of the body.
Wellness Tips
On the home screen is a button called “Tip.” Tucked away in this little, unsuspecting corner of the app are wellness tips, such as “If you’re feeling guilty about something, remember that self-forgiveness means recognizing mistakes and accepting shortcomings” and “Don’t believe everything you think: Challenge your negative thoughts. Is there evidence to support the way you perceive the situation?” These tips don’t rotate frequently, but it’s a nice surprise when a new one displays.
Final Thoughts
This app can be used in several different ways, serving as a stand-alone stress management tool or in tandem with clinical care directed by a health care provider. As is noted by T2, “Due to its portability, this guided exercise is easily accessible when it is needed most.” And although the app was designed for individuals with PTSD and TBI, anybody who wants to feel more relaxed can access this free tool and reap the many benefits provided through diaphragmatic breathing.
The Breathe2Relax app is centered around the basic concept that breathing into the belly—diaphragmatic breathing—provides deeper relaxation than does breathing into the chest. Designed for use by individuals with PTSD and TBI, the app helps with mood stabilization, anger control, and anxiety management. It is a portable stress management tool with breathing exercises documented to decrease the body’s “fight-or-flight” stress response.
Setup
Although you can jump right into the guided breathing exercises, you may find a richer experience by exploring the setup menu of the app before beginning. (TIP: Skip the Personalize button and go straight to Setup.) Setting up the app to your personal preferences will reduce the chances of growing agitated when you begin the breathing exercises.
Almost every element you encounter while using the app can be modified: scenery (eg, mountain meadows or the cosmos), background music (mostly instrumental and earth sounds, plus a choice for no music at all), inhale and exhale lengths set to tenths of a second, whether a breathing metronome and visual prompts will display during the exercise, and whether a voice will prompt breathing instructions. Additional modifications include how many cycles of inhalations/exhalations will be provided, whether you want to track your stress levels (these can be graphed later and tracked over time), and, importantly, whether you want this data to be saved and transmitted to T2 for survey data (there is a choice to remain anonymous) or to disenroll from the study and delete all stored information.
Breathe
Once all of your preferences are set, they will remain saved in the app until you change them. If you already know how to breathe diaphragmatically, click “Breathe” to begin a breathing session. If you are uncertain or need a refresher, click “Show Me How” to watch a 2-minute instructional video. As noted during this instruction, “Be patient. Although breathing sounds like it should be easy to do, diaphragmatic breathing takes practice.” It is recommended that this practice be done every day for maximum benefit, and it is okay to practice when you’re already feeling relaxed.
When you are ready to work through the breathing session, begin by rating your stress level. If you want to skip this step, go ahead and hit “Skip.” If you never want to enter this information when you enter the breathing session portion of the app, click the box that reads “Do Not Show Again” or return to the Setup menu and select “OFF” under Stress Tracking Information. However, by taking just a moment to note stress levels before (and after), you will see over time how you are performing and whether or not this is a beneficial exercise for you. Oftentimes, we don’t accurately perceive our own emotions and reactions, so graphing this output can help limit personal bias.
If you are following the breathing metronome, you will see it rise and fall with each breath until the session is complete. You will then be prompted to record your ending stress level and can click “Finish” to return to the home screen.
Results
The benefit of tracking stress levels during breathing sessions is revealed in a simple line graph. A thin line is produced using starting stress levels and a thick line is produced using ending stress levels. Sometimes the breathing session will result in a dramatic shift in stress level reduction, sometimes an insignificant reduction, and sometimes it may seemingly increase stress levels. If the latter happens, it is possible you were unable to focus on the exercise enough to properly engage in diaphragmatic breathing, or maybe one of the app settings has agitated you and it’s time to update your settings in the Setup menu.
Learning
Read about or watch information on stress by selecting 1 of 3 topics. “Biology of Stress” covers what happens in the body during stress, the consequences of stress on the body, how breathing can help control the stress response, and the resilience of the mind and body after handling a stressful episode. “Diaphragmatic Breathing” explains what the diaphragm is, the difference in oxygen levels supplied to the body during chest breathing and diaphragmatic breathing, and how to determine what kind of a breather you are. Access the Body Scanner under “Effects of Stress on the Body” to learn about the effects of stress on 10 different areas of the body.
Wellness Tips
On the home screen is a button called “Tip.” Tucked away in this little, unsuspecting corner of the app are wellness tips, such as “If you’re feeling guilty about something, remember that self-forgiveness means recognizing mistakes and accepting shortcomings” and “Don’t believe everything you think: Challenge your negative thoughts. Is there evidence to support the way you perceive the situation?” These tips don’t rotate frequently, but it’s a nice surprise when a new one displays.
Final Thoughts
This app can be used in several different ways, serving as a stand-alone stress management tool or in tandem with clinical care directed by a health care provider. As is noted by T2, “Due to its portability, this guided exercise is easily accessible when it is needed most.” And although the app was designed for individuals with PTSD and TBI, anybody who wants to feel more relaxed can access this free tool and reap the many benefits provided through diaphragmatic breathing.
The Breathe2Relax app is centered around the basic concept that breathing into the belly—diaphragmatic breathing—provides deeper relaxation than does breathing into the chest. Designed for use by individuals with PTSD and TBI, the app helps with mood stabilization, anger control, and anxiety management. It is a portable stress management tool with breathing exercises documented to decrease the body’s “fight-or-flight” stress response.
Setup
Although you can jump right into the guided breathing exercises, you may find a richer experience by exploring the setup menu of the app before beginning. (TIP: Skip the Personalize button and go straight to Setup.) Setting up the app to your personal preferences will reduce the chances of growing agitated when you begin the breathing exercises.
Almost every element you encounter while using the app can be modified: scenery (eg, mountain meadows or the cosmos), background music (mostly instrumental and earth sounds, plus a choice for no music at all), inhale and exhale lengths set to tenths of a second, whether a breathing metronome and visual prompts will display during the exercise, and whether a voice will prompt breathing instructions. Additional modifications include how many cycles of inhalations/exhalations will be provided, whether you want to track your stress levels (these can be graphed later and tracked over time), and, importantly, whether you want this data to be saved and transmitted to T2 for survey data (there is a choice to remain anonymous) or to disenroll from the study and delete all stored information.
Breathe
Once all of your preferences are set, they will remain saved in the app until you change them. If you already know how to breathe diaphragmatically, click “Breathe” to begin a breathing session. If you are uncertain or need a refresher, click “Show Me How” to watch a 2-minute instructional video. As noted during this instruction, “Be patient. Although breathing sounds like it should be easy to do, diaphragmatic breathing takes practice.” It is recommended that this practice be done every day for maximum benefit, and it is okay to practice when you’re already feeling relaxed.
When you are ready to work through the breathing session, begin by rating your stress level. If you want to skip this step, go ahead and hit “Skip.” If you never want to enter this information when you enter the breathing session portion of the app, click the box that reads “Do Not Show Again” or return to the Setup menu and select “OFF” under Stress Tracking Information. However, by taking just a moment to note stress levels before (and after), you will see over time how you are performing and whether or not this is a beneficial exercise for you. Oftentimes, we don’t accurately perceive our own emotions and reactions, so graphing this output can help limit personal bias.
If you are following the breathing metronome, you will see it rise and fall with each breath until the session is complete. You will then be prompted to record your ending stress level and can click “Finish” to return to the home screen.
Results
The benefit of tracking stress levels during breathing sessions is revealed in a simple line graph. A thin line is produced using starting stress levels and a thick line is produced using ending stress levels. Sometimes the breathing session will result in a dramatic shift in stress level reduction, sometimes an insignificant reduction, and sometimes it may seemingly increase stress levels. If the latter happens, it is possible you were unable to focus on the exercise enough to properly engage in diaphragmatic breathing, or maybe one of the app settings has agitated you and it’s time to update your settings in the Setup menu.
Learning
Read about or watch information on stress by selecting 1 of 3 topics. “Biology of Stress” covers what happens in the body during stress, the consequences of stress on the body, how breathing can help control the stress response, and the resilience of the mind and body after handling a stressful episode. “Diaphragmatic Breathing” explains what the diaphragm is, the difference in oxygen levels supplied to the body during chest breathing and diaphragmatic breathing, and how to determine what kind of a breather you are. Access the Body Scanner under “Effects of Stress on the Body” to learn about the effects of stress on 10 different areas of the body.
Wellness Tips
On the home screen is a button called “Tip.” Tucked away in this little, unsuspecting corner of the app are wellness tips, such as “If you’re feeling guilty about something, remember that self-forgiveness means recognizing mistakes and accepting shortcomings” and “Don’t believe everything you think: Challenge your negative thoughts. Is there evidence to support the way you perceive the situation?” These tips don’t rotate frequently, but it’s a nice surprise when a new one displays.
Final Thoughts
This app can be used in several different ways, serving as a stand-alone stress management tool or in tandem with clinical care directed by a health care provider. As is noted by T2, “Due to its portability, this guided exercise is easily accessible when it is needed most.” And although the app was designed for individuals with PTSD and TBI, anybody who wants to feel more relaxed can access this free tool and reap the many benefits provided through diaphragmatic breathing.
Biochemical cascade can lead to MPNs

Credit: Indiana University
Preclinical research has revealed a cascade of molecular events in the bone marrow that produce high levels of inflammation, disrupt hematopoiesis, and lead to the development of myeloproliferative neoplasms (MPNs).
The discovery points the way to potential new strategies for treating MPNs and leukemias and further illuminates the relationship between inflammation and cancer, according to Nadia Carlesso, MD, PhD, of the Indiana University School of Medicine in Indianapolis.
Dr Carlesso and her colleagues described the discovery in Cell Stem Cell.
The team used a mouse model to elucidate the role of Notch in hematopoiesis. And they found that loss of Notch function in the microenvironment causes a chain of molecular events that result in excess production of inflammatory factors.
“Some of these inflammatory molecules are cytokines that induce uncontrolled proliferation of myeloid cells and lead to myeloproliferative disorders,” Dr Carlesso said. “[However,] loss of Notch has to occur in specific cells of the bone marrow microenvironment, like endothelial cells, to really be capable to trigger such a high inflammatory status.”
Specifically, Dr Carlesso and her colleagues showed that Notch signaling represses expression of the microRNA miR-155 by promoting binding of RBPJ, a nonredundant downstream effector of the canonical Notch signaling cascade, to the miR-155 promoter.
Loss of Notch/RBPJ signaling upregulates miR-155 in bone marrow endothelial cells. And this leads to miR-155-mediated targeting of the NF-kB inhibitor kB-Ras1, NF-kB activation, increased proinflammatory cytokine production, and the development of an MPN-like disorder.
But when the researchers deleted miR-155 in the stroma of RBPJ_/_ mice, they were able to prevent cytokine induction and the MPN-like disease.
The team also discovered elevated levels of miR-155 in samples from humans with MPNs. This suggests that developing drugs to target the inflammatory reaction at key points could be a promising strategy to limit the development of MPNs in humans.
Dr Carlesso noted that a key finding of this research was that the molecular cascade leading to inflammation was not occurring directly in hematopoietic stem cells but in cells of the bone marrow microenvironment.
“This work indicates that we need to target not only the tumor cells but also the inflammatory microenvironment that surrounds them and may contribute to their generation,” she said. “We believe that this combined strategy will be more effective in preventing myeloproliferative disease progression and transformation in acute leukemias.”
Dr Carlesso also pointed out that, because Notch is an oncogene, it is often targeted by therapies for other types of cancer. But this research suggests targeting Notch can have adverse effects on hematopoiesis, and clinicians should be aware of this risk. ![]()
Credit: Indiana University
Preclinical research has revealed a cascade of molecular events in the bone marrow that produce high levels of inflammation, disrupt hematopoiesis, and lead to the development of myeloproliferative neoplasms (MPNs).
The discovery points the way to potential new strategies for treating MPNs and leukemias and further illuminates the relationship between inflammation and cancer, according to Nadia Carlesso, MD, PhD, of the Indiana University School of Medicine in Indianapolis.
Dr Carlesso and her colleagues described the discovery in Cell Stem Cell.
The team used a mouse model to elucidate the role of Notch in hematopoiesis. And they found that loss of Notch function in the microenvironment causes a chain of molecular events that result in excess production of inflammatory factors.
“Some of these inflammatory molecules are cytokines that induce uncontrolled proliferation of myeloid cells and lead to myeloproliferative disorders,” Dr Carlesso said. “[However,] loss of Notch has to occur in specific cells of the bone marrow microenvironment, like endothelial cells, to really be capable to trigger such a high inflammatory status.”
Specifically, Dr Carlesso and her colleagues showed that Notch signaling represses expression of the microRNA miR-155 by promoting binding of RBPJ, a nonredundant downstream effector of the canonical Notch signaling cascade, to the miR-155 promoter.
Loss of Notch/RBPJ signaling upregulates miR-155 in bone marrow endothelial cells. And this leads to miR-155-mediated targeting of the NF-kB inhibitor kB-Ras1, NF-kB activation, increased proinflammatory cytokine production, and the development of an MPN-like disorder.
But when the researchers deleted miR-155 in the stroma of RBPJ_/_ mice, they were able to prevent cytokine induction and the MPN-like disease.
The team also discovered elevated levels of miR-155 in samples from humans with MPNs. This suggests that developing drugs to target the inflammatory reaction at key points could be a promising strategy to limit the development of MPNs in humans.
Dr Carlesso noted that a key finding of this research was that the molecular cascade leading to inflammation was not occurring directly in hematopoietic stem cells but in cells of the bone marrow microenvironment.
“This work indicates that we need to target not only the tumor cells but also the inflammatory microenvironment that surrounds them and may contribute to their generation,” she said. “We believe that this combined strategy will be more effective in preventing myeloproliferative disease progression and transformation in acute leukemias.”
Dr Carlesso also pointed out that, because Notch is an oncogene, it is often targeted by therapies for other types of cancer. But this research suggests targeting Notch can have adverse effects on hematopoiesis, and clinicians should be aware of this risk. ![]()
Credit: Indiana University
Preclinical research has revealed a cascade of molecular events in the bone marrow that produce high levels of inflammation, disrupt hematopoiesis, and lead to the development of myeloproliferative neoplasms (MPNs).
The discovery points the way to potential new strategies for treating MPNs and leukemias and further illuminates the relationship between inflammation and cancer, according to Nadia Carlesso, MD, PhD, of the Indiana University School of Medicine in Indianapolis.
Dr Carlesso and her colleagues described the discovery in Cell Stem Cell.
The team used a mouse model to elucidate the role of Notch in hematopoiesis. And they found that loss of Notch function in the microenvironment causes a chain of molecular events that result in excess production of inflammatory factors.
“Some of these inflammatory molecules are cytokines that induce uncontrolled proliferation of myeloid cells and lead to myeloproliferative disorders,” Dr Carlesso said. “[However,] loss of Notch has to occur in specific cells of the bone marrow microenvironment, like endothelial cells, to really be capable to trigger such a high inflammatory status.”
Specifically, Dr Carlesso and her colleagues showed that Notch signaling represses expression of the microRNA miR-155 by promoting binding of RBPJ, a nonredundant downstream effector of the canonical Notch signaling cascade, to the miR-155 promoter.
Loss of Notch/RBPJ signaling upregulates miR-155 in bone marrow endothelial cells. And this leads to miR-155-mediated targeting of the NF-kB inhibitor kB-Ras1, NF-kB activation, increased proinflammatory cytokine production, and the development of an MPN-like disorder.
But when the researchers deleted miR-155 in the stroma of RBPJ_/_ mice, they were able to prevent cytokine induction and the MPN-like disease.
The team also discovered elevated levels of miR-155 in samples from humans with MPNs. This suggests that developing drugs to target the inflammatory reaction at key points could be a promising strategy to limit the development of MPNs in humans.
Dr Carlesso noted that a key finding of this research was that the molecular cascade leading to inflammation was not occurring directly in hematopoietic stem cells but in cells of the bone marrow microenvironment.
“This work indicates that we need to target not only the tumor cells but also the inflammatory microenvironment that surrounds them and may contribute to their generation,” she said. “We believe that this combined strategy will be more effective in preventing myeloproliferative disease progression and transformation in acute leukemias.”
Dr Carlesso also pointed out that, because Notch is an oncogene, it is often targeted by therapies for other types of cancer. But this research suggests targeting Notch can have adverse effects on hematopoiesis, and clinicians should be aware of this risk. ![]()
Adipose-derived SCs can resist methotrexate

A new study indicates that adipose-derived stem cells (ASCs) are highly resistant to the chemotherapy drug methotrexate (MTX).
Cultured ASCs and tissue samples that included ASCs were able to withstand exposure to MTX quite well. The drug had little or no effect on ASC viability, division, senescence, or differentiation.
The researchers believe these findings could prove significant for cancer patients, particularly children with acute lymphoblastic leukemia.
“Kids undergo chemotherapy at such an important time, when they should be growing, but, instead, they are introduced to this very harsh environment where bone cells are damaged with these drugs,” said study author Olivia Beane, a graduate student at Brown University in Providence, Rhode Island.
“That leads to major long-term side effects, including osteoporosis and bone defects. If we found a stem cell that was resistant to the chemotherapeutic agent and could promote bone growth by becoming bone itself, then maybe they wouldn’t have these issues.”
Beane’s work, which appears in Experimental Cell Research, grew out of more basic research. She was originally looking for chemicals that could help purify ASCs from mixed cell cultures to encourage their proliferation.
Among other things, she tried chemotherapy drugs, speculating that ASCs might withstand a drug that other cells could not. The idea that this could help cancer patients did not come until later.
To explore potential cancer applications, Beane and her colleagues exposed pure human ASC cultures, stromal vascular fraction (SVF) tissue samples (which include ASCs and several other cell types), and cultures of human fibroblast cells to medically relevant concentrations of chemotherapy drugs for 24 hours.
The researchers then measured how those cell populations fared over the next 10 days. They also measured the ability of MTX-exposed ASCs, both alone and in SVF, to proliferate and differentiate.
In contrast to the fibroblast controls, the ASCs withstood a variety of MTX doses. The drug had little or no effect on ASC viability, cell division, senescence, or differentiation. ASCs also resisted vincristine to an extent, but they could not withstand exposure to cytarabine or etoposide.
The SVF tissue samples withstood MTX doses well too. That is significant, according to the researchers, because the tissue would be clinically useful if an ASC-based therapy were ever developed for cancer patients. Hypothetically, fresh SVF could be harvested from the fat of a donor and injected into bone tissue, delivering ASCs to the site.
To understand why ASCs resist MTX, the researchers conducted further tests. MTX shuts down DNA biosynthesis by binding the protein dihydrofolate reductase so it is unavailable to assist in that essential task.
The testing showed that ASCs ramped up dihydrofolate reductase levels upon exposure to the drug. They produced enough to overcome a clinically relevant dose of MTX.
Now, the researchers are eager to see if they can translate these findings to deliver a medical benefit for cancer patients. To that end, the team is planning several more experiments.
One is to test ASC survival and performance after 48- and 72-hour exposures to MTX. Another is to begin examining how the cells fare in mouse models of chemotherapy. The researchers plan to directly compare ASCs and bone marrow-derived stem cells exposed to various chemotherapies. ![]()
A new study indicates that adipose-derived stem cells (ASCs) are highly resistant to the chemotherapy drug methotrexate (MTX).
Cultured ASCs and tissue samples that included ASCs were able to withstand exposure to MTX quite well. The drug had little or no effect on ASC viability, division, senescence, or differentiation.
The researchers believe these findings could prove significant for cancer patients, particularly children with acute lymphoblastic leukemia.
“Kids undergo chemotherapy at such an important time, when they should be growing, but, instead, they are introduced to this very harsh environment where bone cells are damaged with these drugs,” said study author Olivia Beane, a graduate student at Brown University in Providence, Rhode Island.
“That leads to major long-term side effects, including osteoporosis and bone defects. If we found a stem cell that was resistant to the chemotherapeutic agent and could promote bone growth by becoming bone itself, then maybe they wouldn’t have these issues.”
Beane’s work, which appears in Experimental Cell Research, grew out of more basic research. She was originally looking for chemicals that could help purify ASCs from mixed cell cultures to encourage their proliferation.
Among other things, she tried chemotherapy drugs, speculating that ASCs might withstand a drug that other cells could not. The idea that this could help cancer patients did not come until later.
To explore potential cancer applications, Beane and her colleagues exposed pure human ASC cultures, stromal vascular fraction (SVF) tissue samples (which include ASCs and several other cell types), and cultures of human fibroblast cells to medically relevant concentrations of chemotherapy drugs for 24 hours.
The researchers then measured how those cell populations fared over the next 10 days. They also measured the ability of MTX-exposed ASCs, both alone and in SVF, to proliferate and differentiate.
In contrast to the fibroblast controls, the ASCs withstood a variety of MTX doses. The drug had little or no effect on ASC viability, cell division, senescence, or differentiation. ASCs also resisted vincristine to an extent, but they could not withstand exposure to cytarabine or etoposide.
The SVF tissue samples withstood MTX doses well too. That is significant, according to the researchers, because the tissue would be clinically useful if an ASC-based therapy were ever developed for cancer patients. Hypothetically, fresh SVF could be harvested from the fat of a donor and injected into bone tissue, delivering ASCs to the site.
To understand why ASCs resist MTX, the researchers conducted further tests. MTX shuts down DNA biosynthesis by binding the protein dihydrofolate reductase so it is unavailable to assist in that essential task.
The testing showed that ASCs ramped up dihydrofolate reductase levels upon exposure to the drug. They produced enough to overcome a clinically relevant dose of MTX.
Now, the researchers are eager to see if they can translate these findings to deliver a medical benefit for cancer patients. To that end, the team is planning several more experiments.
One is to test ASC survival and performance after 48- and 72-hour exposures to MTX. Another is to begin examining how the cells fare in mouse models of chemotherapy. The researchers plan to directly compare ASCs and bone marrow-derived stem cells exposed to various chemotherapies. ![]()
A new study indicates that adipose-derived stem cells (ASCs) are highly resistant to the chemotherapy drug methotrexate (MTX).
Cultured ASCs and tissue samples that included ASCs were able to withstand exposure to MTX quite well. The drug had little or no effect on ASC viability, division, senescence, or differentiation.
The researchers believe these findings could prove significant for cancer patients, particularly children with acute lymphoblastic leukemia.
“Kids undergo chemotherapy at such an important time, when they should be growing, but, instead, they are introduced to this very harsh environment where bone cells are damaged with these drugs,” said study author Olivia Beane, a graduate student at Brown University in Providence, Rhode Island.
“That leads to major long-term side effects, including osteoporosis and bone defects. If we found a stem cell that was resistant to the chemotherapeutic agent and could promote bone growth by becoming bone itself, then maybe they wouldn’t have these issues.”
Beane’s work, which appears in Experimental Cell Research, grew out of more basic research. She was originally looking for chemicals that could help purify ASCs from mixed cell cultures to encourage their proliferation.
Among other things, she tried chemotherapy drugs, speculating that ASCs might withstand a drug that other cells could not. The idea that this could help cancer patients did not come until later.
To explore potential cancer applications, Beane and her colleagues exposed pure human ASC cultures, stromal vascular fraction (SVF) tissue samples (which include ASCs and several other cell types), and cultures of human fibroblast cells to medically relevant concentrations of chemotherapy drugs for 24 hours.
The researchers then measured how those cell populations fared over the next 10 days. They also measured the ability of MTX-exposed ASCs, both alone and in SVF, to proliferate and differentiate.
In contrast to the fibroblast controls, the ASCs withstood a variety of MTX doses. The drug had little or no effect on ASC viability, cell division, senescence, or differentiation. ASCs also resisted vincristine to an extent, but they could not withstand exposure to cytarabine or etoposide.
The SVF tissue samples withstood MTX doses well too. That is significant, according to the researchers, because the tissue would be clinically useful if an ASC-based therapy were ever developed for cancer patients. Hypothetically, fresh SVF could be harvested from the fat of a donor and injected into bone tissue, delivering ASCs to the site.
To understand why ASCs resist MTX, the researchers conducted further tests. MTX shuts down DNA biosynthesis by binding the protein dihydrofolate reductase so it is unavailable to assist in that essential task.
The testing showed that ASCs ramped up dihydrofolate reductase levels upon exposure to the drug. They produced enough to overcome a clinically relevant dose of MTX.
Now, the researchers are eager to see if they can translate these findings to deliver a medical benefit for cancer patients. To that end, the team is planning several more experiments.
One is to test ASC survival and performance after 48- and 72-hour exposures to MTX. Another is to begin examining how the cells fare in mouse models of chemotherapy. The researchers plan to directly compare ASCs and bone marrow-derived stem cells exposed to various chemotherapies. ![]()
Factor affects thrombus size and content

Credit: Kevin MacKenzie
The activity of transglutaminase factor XIII is critical for retaining red blood cells in a thrombus and therefore affects the clot’s size, investigators have reported in the Journal of Clinical Investigation.
The team showed that mice deficient in factor XIII had smaller thrombi containing fewer red blood cells than wild-type mice. And the same phenomenon occurred in humans.
According to the researchers, this discovery could aid the development of a safer alternative to anticoagulants.
“If we can develop a treatment that exploits this discovery to reduce the size of blood clots, it would represent a whole new approach to treating thrombosis that’s different from anything else on the market,” said study author Alisa Wolberg, PhD, of the University of North Carolina at Chapel Hill.
“We think reducing factor XIII activity could be helpful to a large number of people, perhaps including some who cannot take existing blood-thinning medications.”
Dr Wolberg and her colleagues examined the role of factor XIII in clot formation, first in mice and then in human samples. To their surprise, the team found that mice incapable of producing factor XIII formed thrombi that were half the size of the clots produced by wild-type mice.
“That difference in itself was extremely striking,” said study author Maria Aleman, PhD, also of the University of North Carolina at Chapel Hill.
“Then, the second surprise was discovering that the size difference was actually due to a reduced number of red blood cells in the clot. Since no previous studies had suggested that it was possible to manipulate the number of red blood cells, we knew we had found something new.”
Factor XIII appears to play a crucial role in helping the fibrin matrix keep its integrity during thrombus formation. Normally, the fibrin matrix forms a strong mesh in and around the clot, trapping red blood cells within. Without factor XIII, some red blood cells are squeezed out, resulting in a much smaller clot.
Unlike existing drugs that reduce the formation of fibrin, a drug that reduces factor XIII could potentially cut the body’s ability to produce large, dangerous thrombi without sacrificing the ability to produce small, beneficial clots.
“What’s needed is a drug that reduces the risk of forming large clots but still allows you to form a clot when you need one to stanch bleeding,” Dr Wolberg said. “The biological pathway we’ve discovered may make it possible to strike that balance.” ![]()
Credit: Kevin MacKenzie
The activity of transglutaminase factor XIII is critical for retaining red blood cells in a thrombus and therefore affects the clot’s size, investigators have reported in the Journal of Clinical Investigation.
The team showed that mice deficient in factor XIII had smaller thrombi containing fewer red blood cells than wild-type mice. And the same phenomenon occurred in humans.
According to the researchers, this discovery could aid the development of a safer alternative to anticoagulants.
“If we can develop a treatment that exploits this discovery to reduce the size of blood clots, it would represent a whole new approach to treating thrombosis that’s different from anything else on the market,” said study author Alisa Wolberg, PhD, of the University of North Carolina at Chapel Hill.
“We think reducing factor XIII activity could be helpful to a large number of people, perhaps including some who cannot take existing blood-thinning medications.”
Dr Wolberg and her colleagues examined the role of factor XIII in clot formation, first in mice and then in human samples. To their surprise, the team found that mice incapable of producing factor XIII formed thrombi that were half the size of the clots produced by wild-type mice.
“That difference in itself was extremely striking,” said study author Maria Aleman, PhD, also of the University of North Carolina at Chapel Hill.
“Then, the second surprise was discovering that the size difference was actually due to a reduced number of red blood cells in the clot. Since no previous studies had suggested that it was possible to manipulate the number of red blood cells, we knew we had found something new.”
Factor XIII appears to play a crucial role in helping the fibrin matrix keep its integrity during thrombus formation. Normally, the fibrin matrix forms a strong mesh in and around the clot, trapping red blood cells within. Without factor XIII, some red blood cells are squeezed out, resulting in a much smaller clot.
Unlike existing drugs that reduce the formation of fibrin, a drug that reduces factor XIII could potentially cut the body’s ability to produce large, dangerous thrombi without sacrificing the ability to produce small, beneficial clots.
“What’s needed is a drug that reduces the risk of forming large clots but still allows you to form a clot when you need one to stanch bleeding,” Dr Wolberg said. “The biological pathway we’ve discovered may make it possible to strike that balance.” ![]()
Credit: Kevin MacKenzie
The activity of transglutaminase factor XIII is critical for retaining red blood cells in a thrombus and therefore affects the clot’s size, investigators have reported in the Journal of Clinical Investigation.
The team showed that mice deficient in factor XIII had smaller thrombi containing fewer red blood cells than wild-type mice. And the same phenomenon occurred in humans.
According to the researchers, this discovery could aid the development of a safer alternative to anticoagulants.
“If we can develop a treatment that exploits this discovery to reduce the size of blood clots, it would represent a whole new approach to treating thrombosis that’s different from anything else on the market,” said study author Alisa Wolberg, PhD, of the University of North Carolina at Chapel Hill.
“We think reducing factor XIII activity could be helpful to a large number of people, perhaps including some who cannot take existing blood-thinning medications.”
Dr Wolberg and her colleagues examined the role of factor XIII in clot formation, first in mice and then in human samples. To their surprise, the team found that mice incapable of producing factor XIII formed thrombi that were half the size of the clots produced by wild-type mice.
“That difference in itself was extremely striking,” said study author Maria Aleman, PhD, also of the University of North Carolina at Chapel Hill.
“Then, the second surprise was discovering that the size difference was actually due to a reduced number of red blood cells in the clot. Since no previous studies had suggested that it was possible to manipulate the number of red blood cells, we knew we had found something new.”
Factor XIII appears to play a crucial role in helping the fibrin matrix keep its integrity during thrombus formation. Normally, the fibrin matrix forms a strong mesh in and around the clot, trapping red blood cells within. Without factor XIII, some red blood cells are squeezed out, resulting in a much smaller clot.
Unlike existing drugs that reduce the formation of fibrin, a drug that reduces factor XIII could potentially cut the body’s ability to produce large, dangerous thrombi without sacrificing the ability to produce small, beneficial clots.
“What’s needed is a drug that reduces the risk of forming large clots but still allows you to form a clot when you need one to stanch bleeding,” Dr Wolberg said. “The biological pathway we’ve discovered may make it possible to strike that balance.” ![]()
EC expands indication for ofatumumab

Credit: Linda Bartlett
The European Commission (EC) has expanded the indication for the anti-CD20 monoclonal antibody ofatumumab (Arzerra).
The EC granted conditional approval for ofatumumab in combination with chlorambucil or bendamustine to treat patients with chronic lymphocytic leukemia (CLL) who have not received prior therapy and are not eligible for fludarabine-based therapy.
In 2010, the EC granted ofatumumab conditional approval to treat CLL patients who are refractory to fludarabine and alemtuzumab.
Ofatumumab received conditional approval because the drug’s benefits appear to outweigh the risks it poses. Ofatumumab will not receive full approval until the drug’s developers, GlaxoSmithKline and GenMab, submit results of additional research to the EC.
Trial results
The EC’s new approval of ofatumumab, for previously untreated CLL patients, is based on results from 2 trials, COMPLEMENT 1 and OMB115991.
The phase 3 COMPLEMENT 1 trial was a comparison of ofatumumab plus chlorambucil (n=221) with chlorambucil alone (n=226) in CLL patients for whom fludarabine-based treatment was considered inappropriate.
In this study, ofatumumab plus chlorambucil improved progression-free survival compared to chlorambucil alone. The median times were 22.4 months and 13.1 months, respectively, and the hazard ratio was 0.57 (P<0.001).
In the phase 2 trial known as OMB115991, researchers evaluated ofatumumab in combination with bendamustine in 44 patients with previously untreated CLL for whom fludarabine-based treatment was considered inappropriate.
The combination elicited an overall response rate of 95% and a complete response rate of 43%.
The overall safety profile of ofatumumab in CLL (previously untreated and relapsed/refractory) is based on data from 511 patients in clinical trials.
This includes 250 patients with relapsed/refractory CLL who were treated with ofatumumab alone and 261 patients with previously untreated CLL who were treated in combination with an alkylating agent.
The most common adverse effects associated with ofatumumab were infusion reactions, neutropenia, anemia, febrile neutropenia, thrombocytopenia, leukopenia, lower respiratory tract infection (including pneumonia), upper respiratory tract infection, sepsis (including neutropenic sepsis and septic shock), herpes virus infection, and urinary tract infection. ![]()
Credit: Linda Bartlett
The European Commission (EC) has expanded the indication for the anti-CD20 monoclonal antibody ofatumumab (Arzerra).
The EC granted conditional approval for ofatumumab in combination with chlorambucil or bendamustine to treat patients with chronic lymphocytic leukemia (CLL) who have not received prior therapy and are not eligible for fludarabine-based therapy.
In 2010, the EC granted ofatumumab conditional approval to treat CLL patients who are refractory to fludarabine and alemtuzumab.
Ofatumumab received conditional approval because the drug’s benefits appear to outweigh the risks it poses. Ofatumumab will not receive full approval until the drug’s developers, GlaxoSmithKline and GenMab, submit results of additional research to the EC.
Trial results
The EC’s new approval of ofatumumab, for previously untreated CLL patients, is based on results from 2 trials, COMPLEMENT 1 and OMB115991.
The phase 3 COMPLEMENT 1 trial was a comparison of ofatumumab plus chlorambucil (n=221) with chlorambucil alone (n=226) in CLL patients for whom fludarabine-based treatment was considered inappropriate.
In this study, ofatumumab plus chlorambucil improved progression-free survival compared to chlorambucil alone. The median times were 22.4 months and 13.1 months, respectively, and the hazard ratio was 0.57 (P<0.001).
In the phase 2 trial known as OMB115991, researchers evaluated ofatumumab in combination with bendamustine in 44 patients with previously untreated CLL for whom fludarabine-based treatment was considered inappropriate.
The combination elicited an overall response rate of 95% and a complete response rate of 43%.
The overall safety profile of ofatumumab in CLL (previously untreated and relapsed/refractory) is based on data from 511 patients in clinical trials.
This includes 250 patients with relapsed/refractory CLL who were treated with ofatumumab alone and 261 patients with previously untreated CLL who were treated in combination with an alkylating agent.
The most common adverse effects associated with ofatumumab were infusion reactions, neutropenia, anemia, febrile neutropenia, thrombocytopenia, leukopenia, lower respiratory tract infection (including pneumonia), upper respiratory tract infection, sepsis (including neutropenic sepsis and septic shock), herpes virus infection, and urinary tract infection. ![]()
Credit: Linda Bartlett
The European Commission (EC) has expanded the indication for the anti-CD20 monoclonal antibody ofatumumab (Arzerra).
The EC granted conditional approval for ofatumumab in combination with chlorambucil or bendamustine to treat patients with chronic lymphocytic leukemia (CLL) who have not received prior therapy and are not eligible for fludarabine-based therapy.
In 2010, the EC granted ofatumumab conditional approval to treat CLL patients who are refractory to fludarabine and alemtuzumab.
Ofatumumab received conditional approval because the drug’s benefits appear to outweigh the risks it poses. Ofatumumab will not receive full approval until the drug’s developers, GlaxoSmithKline and GenMab, submit results of additional research to the EC.
Trial results
The EC’s new approval of ofatumumab, for previously untreated CLL patients, is based on results from 2 trials, COMPLEMENT 1 and OMB115991.
The phase 3 COMPLEMENT 1 trial was a comparison of ofatumumab plus chlorambucil (n=221) with chlorambucil alone (n=226) in CLL patients for whom fludarabine-based treatment was considered inappropriate.
In this study, ofatumumab plus chlorambucil improved progression-free survival compared to chlorambucil alone. The median times were 22.4 months and 13.1 months, respectively, and the hazard ratio was 0.57 (P<0.001).
In the phase 2 trial known as OMB115991, researchers evaluated ofatumumab in combination with bendamustine in 44 patients with previously untreated CLL for whom fludarabine-based treatment was considered inappropriate.
The combination elicited an overall response rate of 95% and a complete response rate of 43%.
The overall safety profile of ofatumumab in CLL (previously untreated and relapsed/refractory) is based on data from 511 patients in clinical trials.
This includes 250 patients with relapsed/refractory CLL who were treated with ofatumumab alone and 261 patients with previously untreated CLL who were treated in combination with an alkylating agent.
The most common adverse effects associated with ofatumumab were infusion reactions, neutropenia, anemia, febrile neutropenia, thrombocytopenia, leukopenia, lower respiratory tract infection (including pneumonia), upper respiratory tract infection, sepsis (including neutropenic sepsis and septic shock), herpes virus infection, and urinary tract infection. ![]()
USPSTF: Don’t screen general population for carotid stenosis
Asymptomatic adults in the general population who have no history of stroke, transient ischemic attack, or neurologic signs or symptoms should not be screened for carotid artery stenosis, according to a U.S. Preventive Services Task Force recommendation published online July 7 in Annals of Internal Medicine.
All screening strategies, even a noninvasive one that has minimal harmful effects such as ultrasonography, are insufficiently sensitive for detecting the condition. And all of them can lead to unnecessary treatment or can themselves induce serious harms including death, stroke, and myocardial infarction. Therefore, at this time, "the harms of screening for asymptomatic carotid artery stenosis outweigh the benefits," said Dr. Michael L. LeFevre of the University of Missouri, Columbia, and his associates with the USPSTF.
The recommendation is an update of the previous one issued in 2007, which also concluded that screening the general population for carotid stenosis was unwarranted. For this update, the USPSTF performed an exhaustive review and meta-analysis of the data that have accrued since that time, which addressed advances in screening tests, risk stratification tools, both screening and treatment using carotid endarterectomy (CEA) and carotid angioplasty and stenting (CAAS), and optimal medical therapies.
Dr. LeFevre, a cochair of USPSTF, and his colleagues reviewed recent randomized controlled trials, meta-analyses, and cohort studies of these topics. They found that the prevalence of carotid artery stenosis is only 0.5%-1% in the general population of adults. The most feasible screen for the condition is duplex ultrasonography; but in real-world practice, even this screen yields many false-positive results in such patients, and so exposes them to harm.
There also is no evidence that another noninvasive screen for carotid artery stenosis – auscultation of the neck to detect carotid bruits – is accurate or provides any benefit. Only four studies examined this strategy; none of them used angiography as a gold standard for diagnosis, and only two involved patients from the general population.
Moreover, even when screening of asymptomatic patients leads to detection and early intervention, "the magnitude of benefit is small to none." In particular, adding medications to current optimal medical management does not appear to convey any benefit, Dr. LeFevre and his associates said.
On the other side of the benefit-to-harm scale, carotid endarterectomy is associated with a 30-day rate of stroke or mortality of approximately 2.4% overall. However, the rates are as high as 5% in low-volume medical centers and 6% in certain states. The 30-day rate of stroke or mortality associated with CAAS is 3.1%-3.8%. Those risks are far too high to counterbalance the small benefit of screening, the USPSTF reviewers noted.
Other important harms after CEA or CAAS include myocardial infarction, surgical complications, cranial nerve injury, lung embolism, pneumonia, and local hematoma requiring further surgery.
The review and meta-analysis were hampered by a dearth of high-quality data. Specifically, much more data are needed comparing patient outcomes after CEA or CAAS with those after optimal medical therapy. The planned CREST-2 (Carotid Revascularization Endarterectomy vs Stenting Trial 2) will include a comparator group on medical management alone, and should provide important findings in this regard, Dr. LeFevre and his associates said.
They added that the USPSTF recommendation against screening the general population for carotid stenosis agrees with recommendations from the American Heart Association, American Stroke Association, American College of Cardiology, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Society for Vascular Surgery, Society for Vascular Medicine, and the American Academy of Family Physicians.
More information on this recommendation – as well as recommendations for the related issues of hypertension, dyslipidemia, CHD, and diet – is available at the USPSTF website.
The USPSTF is an independent group that makes recommendations about the effectiveness of specific preventive care services and is funded by the Agency for Healthcare Research and Quality.
The available data clearly support the USPSTF’s reaffirmation of its previous recommendation against screening for asymptomatic carotid artery stenosis in the general population, yet "such screenings are offered throughout the country in health fairs and other settings," said Dr. Larry B. Goldstein.
Patients should be aware that such tests are unlikely to prevent them from having a stroke or to otherwise improve their health. The population-attributable risk for stroke related to asymptomatic CAS is only 0.7% – a figure that is dwarfed by such factors as hypertension (population-attributable risk greater than 95%), atrial fibrillation (population-attributable risk as high as 24%, depending on patient age and other factors), cigarette smoking (population-attributable risk of up to 14%), and hyperlipidemia (population-attributable risk of 9%), he noted.
Dr. Goldstein is at Duke University’s Stroke Center and Durham Veterans Affairs Medical Center in Durham, N.C. These remarks were taken from his editorial accompanying Dr. LeFevre’s report.
The available data clearly support the USPSTF’s reaffirmation of its previous recommendation against screening for asymptomatic carotid artery stenosis in the general population, yet "such screenings are offered throughout the country in health fairs and other settings," said Dr. Larry B. Goldstein.
Patients should be aware that such tests are unlikely to prevent them from having a stroke or to otherwise improve their health. The population-attributable risk for stroke related to asymptomatic CAS is only 0.7% – a figure that is dwarfed by such factors as hypertension (population-attributable risk greater than 95%), atrial fibrillation (population-attributable risk as high as 24%, depending on patient age and other factors), cigarette smoking (population-attributable risk of up to 14%), and hyperlipidemia (population-attributable risk of 9%), he noted.
Dr. Goldstein is at Duke University’s Stroke Center and Durham Veterans Affairs Medical Center in Durham, N.C. These remarks were taken from his editorial accompanying Dr. LeFevre’s report.
The available data clearly support the USPSTF’s reaffirmation of its previous recommendation against screening for asymptomatic carotid artery stenosis in the general population, yet "such screenings are offered throughout the country in health fairs and other settings," said Dr. Larry B. Goldstein.
Patients should be aware that such tests are unlikely to prevent them from having a stroke or to otherwise improve their health. The population-attributable risk for stroke related to asymptomatic CAS is only 0.7% – a figure that is dwarfed by such factors as hypertension (population-attributable risk greater than 95%), atrial fibrillation (population-attributable risk as high as 24%, depending on patient age and other factors), cigarette smoking (population-attributable risk of up to 14%), and hyperlipidemia (population-attributable risk of 9%), he noted.
Dr. Goldstein is at Duke University’s Stroke Center and Durham Veterans Affairs Medical Center in Durham, N.C. These remarks were taken from his editorial accompanying Dr. LeFevre’s report.
Asymptomatic adults in the general population who have no history of stroke, transient ischemic attack, or neurologic signs or symptoms should not be screened for carotid artery stenosis, according to a U.S. Preventive Services Task Force recommendation published online July 7 in Annals of Internal Medicine.
All screening strategies, even a noninvasive one that has minimal harmful effects such as ultrasonography, are insufficiently sensitive for detecting the condition. And all of them can lead to unnecessary treatment or can themselves induce serious harms including death, stroke, and myocardial infarction. Therefore, at this time, "the harms of screening for asymptomatic carotid artery stenosis outweigh the benefits," said Dr. Michael L. LeFevre of the University of Missouri, Columbia, and his associates with the USPSTF.
The recommendation is an update of the previous one issued in 2007, which also concluded that screening the general population for carotid stenosis was unwarranted. For this update, the USPSTF performed an exhaustive review and meta-analysis of the data that have accrued since that time, which addressed advances in screening tests, risk stratification tools, both screening and treatment using carotid endarterectomy (CEA) and carotid angioplasty and stenting (CAAS), and optimal medical therapies.
Dr. LeFevre, a cochair of USPSTF, and his colleagues reviewed recent randomized controlled trials, meta-analyses, and cohort studies of these topics. They found that the prevalence of carotid artery stenosis is only 0.5%-1% in the general population of adults. The most feasible screen for the condition is duplex ultrasonography; but in real-world practice, even this screen yields many false-positive results in such patients, and so exposes them to harm.
There also is no evidence that another noninvasive screen for carotid artery stenosis – auscultation of the neck to detect carotid bruits – is accurate or provides any benefit. Only four studies examined this strategy; none of them used angiography as a gold standard for diagnosis, and only two involved patients from the general population.
Moreover, even when screening of asymptomatic patients leads to detection and early intervention, "the magnitude of benefit is small to none." In particular, adding medications to current optimal medical management does not appear to convey any benefit, Dr. LeFevre and his associates said.
On the other side of the benefit-to-harm scale, carotid endarterectomy is associated with a 30-day rate of stroke or mortality of approximately 2.4% overall. However, the rates are as high as 5% in low-volume medical centers and 6% in certain states. The 30-day rate of stroke or mortality associated with CAAS is 3.1%-3.8%. Those risks are far too high to counterbalance the small benefit of screening, the USPSTF reviewers noted.
Other important harms after CEA or CAAS include myocardial infarction, surgical complications, cranial nerve injury, lung embolism, pneumonia, and local hematoma requiring further surgery.
The review and meta-analysis were hampered by a dearth of high-quality data. Specifically, much more data are needed comparing patient outcomes after CEA or CAAS with those after optimal medical therapy. The planned CREST-2 (Carotid Revascularization Endarterectomy vs Stenting Trial 2) will include a comparator group on medical management alone, and should provide important findings in this regard, Dr. LeFevre and his associates said.
They added that the USPSTF recommendation against screening the general population for carotid stenosis agrees with recommendations from the American Heart Association, American Stroke Association, American College of Cardiology, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Society for Vascular Surgery, Society for Vascular Medicine, and the American Academy of Family Physicians.
More information on this recommendation – as well as recommendations for the related issues of hypertension, dyslipidemia, CHD, and diet – is available at the USPSTF website.
The USPSTF is an independent group that makes recommendations about the effectiveness of specific preventive care services and is funded by the Agency for Healthcare Research and Quality.
Asymptomatic adults in the general population who have no history of stroke, transient ischemic attack, or neurologic signs or symptoms should not be screened for carotid artery stenosis, according to a U.S. Preventive Services Task Force recommendation published online July 7 in Annals of Internal Medicine.
All screening strategies, even a noninvasive one that has minimal harmful effects such as ultrasonography, are insufficiently sensitive for detecting the condition. And all of them can lead to unnecessary treatment or can themselves induce serious harms including death, stroke, and myocardial infarction. Therefore, at this time, "the harms of screening for asymptomatic carotid artery stenosis outweigh the benefits," said Dr. Michael L. LeFevre of the University of Missouri, Columbia, and his associates with the USPSTF.
The recommendation is an update of the previous one issued in 2007, which also concluded that screening the general population for carotid stenosis was unwarranted. For this update, the USPSTF performed an exhaustive review and meta-analysis of the data that have accrued since that time, which addressed advances in screening tests, risk stratification tools, both screening and treatment using carotid endarterectomy (CEA) and carotid angioplasty and stenting (CAAS), and optimal medical therapies.
Dr. LeFevre, a cochair of USPSTF, and his colleagues reviewed recent randomized controlled trials, meta-analyses, and cohort studies of these topics. They found that the prevalence of carotid artery stenosis is only 0.5%-1% in the general population of adults. The most feasible screen for the condition is duplex ultrasonography; but in real-world practice, even this screen yields many false-positive results in such patients, and so exposes them to harm.
There also is no evidence that another noninvasive screen for carotid artery stenosis – auscultation of the neck to detect carotid bruits – is accurate or provides any benefit. Only four studies examined this strategy; none of them used angiography as a gold standard for diagnosis, and only two involved patients from the general population.
Moreover, even when screening of asymptomatic patients leads to detection and early intervention, "the magnitude of benefit is small to none." In particular, adding medications to current optimal medical management does not appear to convey any benefit, Dr. LeFevre and his associates said.
On the other side of the benefit-to-harm scale, carotid endarterectomy is associated with a 30-day rate of stroke or mortality of approximately 2.4% overall. However, the rates are as high as 5% in low-volume medical centers and 6% in certain states. The 30-day rate of stroke or mortality associated with CAAS is 3.1%-3.8%. Those risks are far too high to counterbalance the small benefit of screening, the USPSTF reviewers noted.
Other important harms after CEA or CAAS include myocardial infarction, surgical complications, cranial nerve injury, lung embolism, pneumonia, and local hematoma requiring further surgery.
The review and meta-analysis were hampered by a dearth of high-quality data. Specifically, much more data are needed comparing patient outcomes after CEA or CAAS with those after optimal medical therapy. The planned CREST-2 (Carotid Revascularization Endarterectomy vs Stenting Trial 2) will include a comparator group on medical management alone, and should provide important findings in this regard, Dr. LeFevre and his associates said.
They added that the USPSTF recommendation against screening the general population for carotid stenosis agrees with recommendations from the American Heart Association, American Stroke Association, American College of Cardiology, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Society for Vascular Surgery, Society for Vascular Medicine, and the American Academy of Family Physicians.
More information on this recommendation – as well as recommendations for the related issues of hypertension, dyslipidemia, CHD, and diet – is available at the USPSTF website.
The USPSTF is an independent group that makes recommendations about the effectiveness of specific preventive care services and is funded by the Agency for Healthcare Research and Quality.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical finding: Don’t screen asymptomatic adults for carotid artery stenosis.
Major finding: The harms of screening asymptomatic adults in the general population for carotid artery stenosis outweigh the benefits, because all currently available screens "have imperfect sensitivity" and can lead to unnecessary treatment that induces serious harms, including death, stroke, myocardial infarction, cranial nerve injury, and embolism.
Data source: A comprehensive review and meta-analysis of data from randomized controlled trials, meta-analyses, and cohort studies performed since 2007 regarding CAS screening tests, risk stratification tools, for both screening and treatment using CEA and CAAS, and optimal medical therapies.
Disclosures: The USPSTF is an independent group that makes recommendations about the effectiveness of specific preventive care services and is funded by the Agency for Healthcare Research and Quality.