User login
Drumstick Digits
A 42‐year‐old man with chronic kidney disease and a history of childhood repair of Tetralogy of Fallot was admitted with pneumonia. Examination of his extremities revealed clubbing of his fingers (Figure 1) and toes (Figure 2).


Clubbing may be primary, known as pachydermoperiostosis, or secondary, due to a variety of neoplastic, pulmonary, cardiac, gastrointestinal, and infectious diseases.1 Examination reveals softening of the nail bed with loss of the normal angle between the nail and the proximal nail fold, an increase in the nail fold convexity, and thickening of the distal phalange with eventual hyperextensibility of the distal interphalangeal joint. Diagnosis is based on various criteria, such as the profile angle (Lovibond's angle) or distal phalangeal to interphalangeal depth ratio. The loss of the normal diamond‐shaped window created by placing the back surfaces of terminal phalanges of similar fingers together, also known as Schamroth's sign, was noted by Dr. Leo Schamroth when he developed endocarditis and is one of the few eponyms named after both a physician and the patient in whom it was found (Figure 3).2 Recent literature suggests that vascular endothelial growth factor (VEGF), a platelet‐derived factor induced by hypoxia, may play a role in digital clubbing.3 Processes that alter normal pulmonary circulation disrupt fragmentation of megakaryocytes in the lung into platelets. Consequently, whole megakaryocytes enter the systemic circulation and become impacted in the peripheral capillaries, where they cause stromal hypoxia and release of platelet‐derived growth factor and VEGF, leading to the vascular hyperplasia that underlies clubbing.

- ,,.Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance.J Am Acad Dermatol.2005;52:1020–1028.
- .A unique eponymous sign of finger clubbing (Schamroth sign) that is named not only after a physician who described it but also after the patient who happened to be the physician himself.Am J Cardiol.2005;96:1614–1615.
- .Exploring the cause of the most ancient clinical sign of medicine: finger clubbing.Semin Arthritis Rheum.2007;36:380–385.
A 42‐year‐old man with chronic kidney disease and a history of childhood repair of Tetralogy of Fallot was admitted with pneumonia. Examination of his extremities revealed clubbing of his fingers (Figure 1) and toes (Figure 2).
Clubbing may be primary, known as pachydermoperiostosis, or secondary, due to a variety of neoplastic, pulmonary, cardiac, gastrointestinal, and infectious diseases.1 Examination reveals softening of the nail bed with loss of the normal angle between the nail and the proximal nail fold, an increase in the nail fold convexity, and thickening of the distal phalange with eventual hyperextensibility of the distal interphalangeal joint. Diagnosis is based on various criteria, such as the profile angle (Lovibond's angle) or distal phalangeal to interphalangeal depth ratio. The loss of the normal diamond‐shaped window created by placing the back surfaces of terminal phalanges of similar fingers together, also known as Schamroth's sign, was noted by Dr. Leo Schamroth when he developed endocarditis and is one of the few eponyms named after both a physician and the patient in whom it was found (Figure 3).2 Recent literature suggests that vascular endothelial growth factor (VEGF), a platelet‐derived factor induced by hypoxia, may play a role in digital clubbing.3 Processes that alter normal pulmonary circulation disrupt fragmentation of megakaryocytes in the lung into platelets. Consequently, whole megakaryocytes enter the systemic circulation and become impacted in the peripheral capillaries, where they cause stromal hypoxia and release of platelet‐derived growth factor and VEGF, leading to the vascular hyperplasia that underlies clubbing.
A 42‐year‐old man with chronic kidney disease and a history of childhood repair of Tetralogy of Fallot was admitted with pneumonia. Examination of his extremities revealed clubbing of his fingers (Figure 1) and toes (Figure 2).
Clubbing may be primary, known as pachydermoperiostosis, or secondary, due to a variety of neoplastic, pulmonary, cardiac, gastrointestinal, and infectious diseases.1 Examination reveals softening of the nail bed with loss of the normal angle between the nail and the proximal nail fold, an increase in the nail fold convexity, and thickening of the distal phalange with eventual hyperextensibility of the distal interphalangeal joint. Diagnosis is based on various criteria, such as the profile angle (Lovibond's angle) or distal phalangeal to interphalangeal depth ratio. The loss of the normal diamond‐shaped window created by placing the back surfaces of terminal phalanges of similar fingers together, also known as Schamroth's sign, was noted by Dr. Leo Schamroth when he developed endocarditis and is one of the few eponyms named after both a physician and the patient in whom it was found (Figure 3).2 Recent literature suggests that vascular endothelial growth factor (VEGF), a platelet‐derived factor induced by hypoxia, may play a role in digital clubbing.3 Processes that alter normal pulmonary circulation disrupt fragmentation of megakaryocytes in the lung into platelets. Consequently, whole megakaryocytes enter the systemic circulation and become impacted in the peripheral capillaries, where they cause stromal hypoxia and release of platelet‐derived growth factor and VEGF, leading to the vascular hyperplasia that underlies clubbing.
- ,,.Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance.J Am Acad Dermatol.2005;52:1020–1028.
- .A unique eponymous sign of finger clubbing (Schamroth sign) that is named not only after a physician who described it but also after the patient who happened to be the physician himself.Am J Cardiol.2005;96:1614–1615.
- .Exploring the cause of the most ancient clinical sign of medicine: finger clubbing.Semin Arthritis Rheum.2007;36:380–385.
- ,,.Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance.J Am Acad Dermatol.2005;52:1020–1028.
- .A unique eponymous sign of finger clubbing (Schamroth sign) that is named not only after a physician who described it but also after the patient who happened to be the physician himself.Am J Cardiol.2005;96:1614–1615.
- .Exploring the cause of the most ancient clinical sign of medicine: finger clubbing.Semin Arthritis Rheum.2007;36:380–385.

Hyponatremia: SIADH or CSW?
An 83‐year‐old man admitted for weakness, lethargy, and mental status changes was found to have human immunodeficiency virus (HIV) disease and cryptococcal meningitis. His hospital course was complicated by worsening hyponatremia (sodium 136 mEq/L). By hospital day 6, the patient's serum sodium had declined to 127 mEq/L from his admission level of 133 mEq/L. The initial impression was that the patient had syndrome of inappropriate antidiuretic hormone (SIADH) and fluid restriction to less than 1500 mL per day was initiated. By hospital day 11, serum sodium continued to decline, to 123 mEq/L, despite fluid restriction.
The past medical history was remarkable for coronary artery disease, hypertension, hyperlipidemia, and anemia, but by self‐report he had not been taking any medications. His review of systems was positive for intermittent bouts of diarrhea.
Vital signs on day 11 included a temperature of 37.3C, blood pressure (BP) of 105/55 mm Hg, and pulse of 90 beats per minute. The BP on admission had been 145/86 mm Hg but had steadily declined with fluid restriction. On physical examination, he appeared thin and cachetic with no evidence of jugular venous distention, rales, or peripheral edema to suggest volume overload. He had been receiving 2 to 4 L of isotonic saline daily for 5 days before the fluid restriction was initiated. The urine output continuously exceeded his intake by at least 500 mL per day throughout his hospital course. His only inpatient medications were amphotericin B and flucytosine. For nutritional supplementation, he was receiving a high‐calorie supplement with free‐water flushes via a nasogastric tube.
Laboratory results revealed a serum sodium concentration of 123 mEq/L, serum potassium of 4.4 mEq/L, serum creatinine of 0.6 mg/dL, urine sodium of 139 mEq/L, serum osmolality of 272 mOsm/kg, and urine osmolality of 598 mOsm/kg (see Table 1). Urinalysis revealed a specific gravity of 1.030. A random serum cortisol level was 11.1 g/dL. A thyroid‐stimulating hormone (TSH) level was 1.32 IU/mL. Brain natriuretic peptide (BNP) was elevated, at 686 pg/mL. A fractional excretion of uric acid was also elevated, at 83.8%.
| Parameters | Day 1 | Fluid Restriction Initiated: Day 6 | Day 8 | Fluid Resuscitation Initiated: Day 11 | Day 13 | Day 15 | Day 26 | Day 37* | Day 40 | Day 44 |
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
| Na (mEq/L) | 133 | 127 | 126 | 123 | 131 | 119 | 140 | 131 | 132 | 135 |
| K (mEq/L) | 4.2 | 4.2 | ||||||||
| BUN (mg/dL) | 39 | 36 | ||||||||
| Cr (mg/dL) | 1.1 | 0.9 | ||||||||
| UNa (mEq/L) | 139 | 86 | 154 | 138 | ||||||
| UOsm (mOsm/kg) | 598 | 362 | 376 | |||||||
| SOsm (mOsm/kg) | 272 | 273 | 279 | |||||||
| BNP (pg/mL) | 686 | 900 | 222 | |||||||
| SUA (mg/dL) | 1.7 | 2.6 | 1.6 | |||||||
| UUA (mg/dL) | 38 | 11 | ||||||||
| FEUA (%) | 83.82 | 28.21 | ||||||||
| FENa (%) | 3.94 | 7.33 | ||||||||
| BP (mm Hg) | 147 | 136 | 122 | 105 | 101 | 90 | 125 | 132 | 140 | |
| Total input (mL) | 700 | NR | 1285 | 3320 | NR | 3040 | 4030 | 4240 | 3120 | 1900 |
| Urine output (mL) | 500 | NR | 2400 | 6501 | NR | 3150 | 3380 | 2950 | 1900 | 950 |
The clinical assessment was volume depletion given the high urine specific gravity, decreasing BP, and a negative fluid balance. The hyponatremia was determined to be due to sodium loss rather than dilution from inappropriate antidiuretic hormone secretion. Intravenous fluid (IVF) hydration with isotonic saline was initiated with a goal to keep the patient in positive fluid balance. The serum sodium level gradually improved to 140 mEq/L over the next 10 days. Attempts to decrease the rate of IVF resulted in a fall in serum sodium and improved when isotonic saline was increased. Eventually, the patient was placed on fludrocortisone, which normalized his urine output and serum sodium.
The response to the treatment regimen supported our diagnosis of cerebral salt wasting (CSW). The patient's serum sodium concentration upon discharge was 135 mEq/L.
Discussion
Our case illustrates the diagnostic challenge presented to physicians when they manage hyponatremia in the setting of a central nervous system (CNS) event. Hyponatremia (sodium 136 mEq/L) has been associated with confusion, lethargy, seizures, coma, and even death.1 Hyponatremia has been reported to occur in up to 30% of the patients with subarachnoid hemorrhage.2, 3
SIADH is frequently the cause of hyponatremia in a patient with a concurrent intracranial process. However, CSW is an important diagnosis to consider and differentiate from SIADH. In a retrospective review of 316 patients with subarachnoid hemorrhage and hyponatremia, 69% were determined to be due to SIADH while 6.5% were from CSW.4 Both CSW and SIADH have been reported to occur in the setting of head trauma, intracranial or metastatic neoplasm, carcinomatous or infectious meningitis, subarachnoid hemorrhage, and CNS surgery. Cryptococcal meningitis as an etiology of CSW has not been previously reported.
The main differentiating feature between SIADH and CSW is that CSW is a dysfunction of renal sodium absorption whereas in SIADH renal sodium handling is intact. This also leads to a difference in the extracellular volume status. SIADH is associated with an increased to normal volume status whereas CSW is a volume‐depleted state. Our patient exhibited a low serum osmolality and a high urine osmolality in the context of hyponatremia, which is present in both CSW and SIADH. However, the clinical course and presentation suggested volume loss, specifically the diarrhea, high urine specific gravity, declining BP, and a negative fluid balance. Some other features that are helpful in determining the volume status may include orthostatic changes, tachycardia, and skin turgor.
Our patient had a low serum uric acid, which is also present in both SIADH and CSW. The key difference between the 2 is that while uric acid will improve with resolution of hyponatremia in SIADH, it will remain low in CSW, as in our patient's uric acid levels, which remained low after normalization of the serum sodium.
Finally, the hyponatremia improved with isotonic fluid repletion, which would not occur in SIADH. The majority of the CSW patients will respond to volume repletion alone, as CSW is a transient condition that will usually resolve in 3 to 4 weeks.3 However, a few patients may require fludrocortisone, as was needed in our patient.
The renal wasting of sodium in CSW is poorly understood. Some postulated mechanisms cite the disruption of sympathetic neural input to the kidney and natriuresis induced by natriuretic peptides. Natriuretic peptides, in particular BNP, have been reported to be elevated in patients with CSW.5, 6 Natriuretic peptides cause salt wasting by inhibition of sodium reabsorption in renal tubule and intramedullary collecting.5, 6 Renin and aldosterone release can also inhibited by the natriuretic peptides. BNP levels were elevated in our patient despite volume loss and no signs of congestive heart failure. Cardiac congestion is a possible etiology for the elevated BNP levels, which peaked to 900 pg/mL on hospital day 37. However, 3 days later the BNP levels declined to 222 pg/mL despite the fact that he was continually in positive fluid balance, suggesting that the BNP elevation was due to CSW and not heart failure.
Conclusions
Our case illustrates the diagnostic and management challenge of hyponatremia in the setting of a CNS event. Both SIADH and CSW are possible etiologies but it is important to make a differentiation. Levels of natriuretic peptides and changes in fractional excretion of uric acid may help differentiate between the 2 conditions.6 The key difference mechanistically is that CSW is due to sodium‐handling deficits, whereas in SIADH sodium‐handling is intact. It is essential to establish volume status since SIADH is a euvolemic to mildly hypervolemic state vs. CSW, which is a volume‐depleted state.7
CSW is well recognized in the neurosurgical arena. The hospitalist will encounter neurosurgical patients with increasing frequency, and thus having an understanding of this disorder, including its diagnosis and treatment, is key.
- ,.Hyponatremia.N Engl J Med.2000;342(21):1581–1589.
- .Hyponatremia in acute brain disease: the cerebral salt wasting syndrome.Eur J Intern Med.2002;13(1):9–14.
- .Cerebral salt wasting syndrome: a review.Neurosurgery.1996;38(1):152–160.
- ,,, et al.The incidence and pathophysiology of hyponatraemia after subarachnoid haemorrhage.Clin Endocrinol (Oxf).2006;64(3):250–254.
- ,,.Brain natriuretic peptide and cerebral vasospasm in subarachnoid hemorrhage. Clinical and TCD correlations.Stroke.2000;31(1):118–122.
- ,,, et al.Secretion of brain natriuretic peptide in patients with aneurysmal subarachnoid haemorrhage.Lancet.1997;349(9047):245–249.
- ,,,.Clinical assessment of extracellular fluid volume in hyponatremia.Am J Med.1987;83(5):905–908.
An 83‐year‐old man admitted for weakness, lethargy, and mental status changes was found to have human immunodeficiency virus (HIV) disease and cryptococcal meningitis. His hospital course was complicated by worsening hyponatremia (sodium 136 mEq/L). By hospital day 6, the patient's serum sodium had declined to 127 mEq/L from his admission level of 133 mEq/L. The initial impression was that the patient had syndrome of inappropriate antidiuretic hormone (SIADH) and fluid restriction to less than 1500 mL per day was initiated. By hospital day 11, serum sodium continued to decline, to 123 mEq/L, despite fluid restriction.
The past medical history was remarkable for coronary artery disease, hypertension, hyperlipidemia, and anemia, but by self‐report he had not been taking any medications. His review of systems was positive for intermittent bouts of diarrhea.
Vital signs on day 11 included a temperature of 37.3C, blood pressure (BP) of 105/55 mm Hg, and pulse of 90 beats per minute. The BP on admission had been 145/86 mm Hg but had steadily declined with fluid restriction. On physical examination, he appeared thin and cachetic with no evidence of jugular venous distention, rales, or peripheral edema to suggest volume overload. He had been receiving 2 to 4 L of isotonic saline daily for 5 days before the fluid restriction was initiated. The urine output continuously exceeded his intake by at least 500 mL per day throughout his hospital course. His only inpatient medications were amphotericin B and flucytosine. For nutritional supplementation, he was receiving a high‐calorie supplement with free‐water flushes via a nasogastric tube.
Laboratory results revealed a serum sodium concentration of 123 mEq/L, serum potassium of 4.4 mEq/L, serum creatinine of 0.6 mg/dL, urine sodium of 139 mEq/L, serum osmolality of 272 mOsm/kg, and urine osmolality of 598 mOsm/kg (see Table 1). Urinalysis revealed a specific gravity of 1.030. A random serum cortisol level was 11.1 g/dL. A thyroid‐stimulating hormone (TSH) level was 1.32 IU/mL. Brain natriuretic peptide (BNP) was elevated, at 686 pg/mL. A fractional excretion of uric acid was also elevated, at 83.8%.
| Parameters | Day 1 | Fluid Restriction Initiated: Day 6 | Day 8 | Fluid Resuscitation Initiated: Day 11 | Day 13 | Day 15 | Day 26 | Day 37* | Day 40 | Day 44 |
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
| Na (mEq/L) | 133 | 127 | 126 | 123 | 131 | 119 | 140 | 131 | 132 | 135 |
| K (mEq/L) | 4.2 | 4.2 | ||||||||
| BUN (mg/dL) | 39 | 36 | ||||||||
| Cr (mg/dL) | 1.1 | 0.9 | ||||||||
| UNa (mEq/L) | 139 | 86 | 154 | 138 | ||||||
| UOsm (mOsm/kg) | 598 | 362 | 376 | |||||||
| SOsm (mOsm/kg) | 272 | 273 | 279 | |||||||
| BNP (pg/mL) | 686 | 900 | 222 | |||||||
| SUA (mg/dL) | 1.7 | 2.6 | 1.6 | |||||||
| UUA (mg/dL) | 38 | 11 | ||||||||
| FEUA (%) | 83.82 | 28.21 | ||||||||
| FENa (%) | 3.94 | 7.33 | ||||||||
| BP (mm Hg) | 147 | 136 | 122 | 105 | 101 | 90 | 125 | 132 | 140 | |
| Total input (mL) | 700 | NR | 1285 | 3320 | NR | 3040 | 4030 | 4240 | 3120 | 1900 |
| Urine output (mL) | 500 | NR | 2400 | 6501 | NR | 3150 | 3380 | 2950 | 1900 | 950 |
The clinical assessment was volume depletion given the high urine specific gravity, decreasing BP, and a negative fluid balance. The hyponatremia was determined to be due to sodium loss rather than dilution from inappropriate antidiuretic hormone secretion. Intravenous fluid (IVF) hydration with isotonic saline was initiated with a goal to keep the patient in positive fluid balance. The serum sodium level gradually improved to 140 mEq/L over the next 10 days. Attempts to decrease the rate of IVF resulted in a fall in serum sodium and improved when isotonic saline was increased. Eventually, the patient was placed on fludrocortisone, which normalized his urine output and serum sodium.
The response to the treatment regimen supported our diagnosis of cerebral salt wasting (CSW). The patient's serum sodium concentration upon discharge was 135 mEq/L.
Discussion
Our case illustrates the diagnostic challenge presented to physicians when they manage hyponatremia in the setting of a central nervous system (CNS) event. Hyponatremia (sodium 136 mEq/L) has been associated with confusion, lethargy, seizures, coma, and even death.1 Hyponatremia has been reported to occur in up to 30% of the patients with subarachnoid hemorrhage.2, 3
SIADH is frequently the cause of hyponatremia in a patient with a concurrent intracranial process. However, CSW is an important diagnosis to consider and differentiate from SIADH. In a retrospective review of 316 patients with subarachnoid hemorrhage and hyponatremia, 69% were determined to be due to SIADH while 6.5% were from CSW.4 Both CSW and SIADH have been reported to occur in the setting of head trauma, intracranial or metastatic neoplasm, carcinomatous or infectious meningitis, subarachnoid hemorrhage, and CNS surgery. Cryptococcal meningitis as an etiology of CSW has not been previously reported.
The main differentiating feature between SIADH and CSW is that CSW is a dysfunction of renal sodium absorption whereas in SIADH renal sodium handling is intact. This also leads to a difference in the extracellular volume status. SIADH is associated with an increased to normal volume status whereas CSW is a volume‐depleted state. Our patient exhibited a low serum osmolality and a high urine osmolality in the context of hyponatremia, which is present in both CSW and SIADH. However, the clinical course and presentation suggested volume loss, specifically the diarrhea, high urine specific gravity, declining BP, and a negative fluid balance. Some other features that are helpful in determining the volume status may include orthostatic changes, tachycardia, and skin turgor.
Our patient had a low serum uric acid, which is also present in both SIADH and CSW. The key difference between the 2 is that while uric acid will improve with resolution of hyponatremia in SIADH, it will remain low in CSW, as in our patient's uric acid levels, which remained low after normalization of the serum sodium.
Finally, the hyponatremia improved with isotonic fluid repletion, which would not occur in SIADH. The majority of the CSW patients will respond to volume repletion alone, as CSW is a transient condition that will usually resolve in 3 to 4 weeks.3 However, a few patients may require fludrocortisone, as was needed in our patient.
The renal wasting of sodium in CSW is poorly understood. Some postulated mechanisms cite the disruption of sympathetic neural input to the kidney and natriuresis induced by natriuretic peptides. Natriuretic peptides, in particular BNP, have been reported to be elevated in patients with CSW.5, 6 Natriuretic peptides cause salt wasting by inhibition of sodium reabsorption in renal tubule and intramedullary collecting.5, 6 Renin and aldosterone release can also inhibited by the natriuretic peptides. BNP levels were elevated in our patient despite volume loss and no signs of congestive heart failure. Cardiac congestion is a possible etiology for the elevated BNP levels, which peaked to 900 pg/mL on hospital day 37. However, 3 days later the BNP levels declined to 222 pg/mL despite the fact that he was continually in positive fluid balance, suggesting that the BNP elevation was due to CSW and not heart failure.
Conclusions
Our case illustrates the diagnostic and management challenge of hyponatremia in the setting of a CNS event. Both SIADH and CSW are possible etiologies but it is important to make a differentiation. Levels of natriuretic peptides and changes in fractional excretion of uric acid may help differentiate between the 2 conditions.6 The key difference mechanistically is that CSW is due to sodium‐handling deficits, whereas in SIADH sodium‐handling is intact. It is essential to establish volume status since SIADH is a euvolemic to mildly hypervolemic state vs. CSW, which is a volume‐depleted state.7
CSW is well recognized in the neurosurgical arena. The hospitalist will encounter neurosurgical patients with increasing frequency, and thus having an understanding of this disorder, including its diagnosis and treatment, is key.
An 83‐year‐old man admitted for weakness, lethargy, and mental status changes was found to have human immunodeficiency virus (HIV) disease and cryptococcal meningitis. His hospital course was complicated by worsening hyponatremia (sodium 136 mEq/L). By hospital day 6, the patient's serum sodium had declined to 127 mEq/L from his admission level of 133 mEq/L. The initial impression was that the patient had syndrome of inappropriate antidiuretic hormone (SIADH) and fluid restriction to less than 1500 mL per day was initiated. By hospital day 11, serum sodium continued to decline, to 123 mEq/L, despite fluid restriction.
The past medical history was remarkable for coronary artery disease, hypertension, hyperlipidemia, and anemia, but by self‐report he had not been taking any medications. His review of systems was positive for intermittent bouts of diarrhea.
Vital signs on day 11 included a temperature of 37.3C, blood pressure (BP) of 105/55 mm Hg, and pulse of 90 beats per minute. The BP on admission had been 145/86 mm Hg but had steadily declined with fluid restriction. On physical examination, he appeared thin and cachetic with no evidence of jugular venous distention, rales, or peripheral edema to suggest volume overload. He had been receiving 2 to 4 L of isotonic saline daily for 5 days before the fluid restriction was initiated. The urine output continuously exceeded his intake by at least 500 mL per day throughout his hospital course. His only inpatient medications were amphotericin B and flucytosine. For nutritional supplementation, he was receiving a high‐calorie supplement with free‐water flushes via a nasogastric tube.
Laboratory results revealed a serum sodium concentration of 123 mEq/L, serum potassium of 4.4 mEq/L, serum creatinine of 0.6 mg/dL, urine sodium of 139 mEq/L, serum osmolality of 272 mOsm/kg, and urine osmolality of 598 mOsm/kg (see Table 1). Urinalysis revealed a specific gravity of 1.030. A random serum cortisol level was 11.1 g/dL. A thyroid‐stimulating hormone (TSH) level was 1.32 IU/mL. Brain natriuretic peptide (BNP) was elevated, at 686 pg/mL. A fractional excretion of uric acid was also elevated, at 83.8%.
| Parameters | Day 1 | Fluid Restriction Initiated: Day 6 | Day 8 | Fluid Resuscitation Initiated: Day 11 | Day 13 | Day 15 | Day 26 | Day 37* | Day 40 | Day 44 |
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
| Na (mEq/L) | 133 | 127 | 126 | 123 | 131 | 119 | 140 | 131 | 132 | 135 |
| K (mEq/L) | 4.2 | 4.2 | ||||||||
| BUN (mg/dL) | 39 | 36 | ||||||||
| Cr (mg/dL) | 1.1 | 0.9 | ||||||||
| UNa (mEq/L) | 139 | 86 | 154 | 138 | ||||||
| UOsm (mOsm/kg) | 598 | 362 | 376 | |||||||
| SOsm (mOsm/kg) | 272 | 273 | 279 | |||||||
| BNP (pg/mL) | 686 | 900 | 222 | |||||||
| SUA (mg/dL) | 1.7 | 2.6 | 1.6 | |||||||
| UUA (mg/dL) | 38 | 11 | ||||||||
| FEUA (%) | 83.82 | 28.21 | ||||||||
| FENa (%) | 3.94 | 7.33 | ||||||||
| BP (mm Hg) | 147 | 136 | 122 | 105 | 101 | 90 | 125 | 132 | 140 | |
| Total input (mL) | 700 | NR | 1285 | 3320 | NR | 3040 | 4030 | 4240 | 3120 | 1900 |
| Urine output (mL) | 500 | NR | 2400 | 6501 | NR | 3150 | 3380 | 2950 | 1900 | 950 |
The clinical assessment was volume depletion given the high urine specific gravity, decreasing BP, and a negative fluid balance. The hyponatremia was determined to be due to sodium loss rather than dilution from inappropriate antidiuretic hormone secretion. Intravenous fluid (IVF) hydration with isotonic saline was initiated with a goal to keep the patient in positive fluid balance. The serum sodium level gradually improved to 140 mEq/L over the next 10 days. Attempts to decrease the rate of IVF resulted in a fall in serum sodium and improved when isotonic saline was increased. Eventually, the patient was placed on fludrocortisone, which normalized his urine output and serum sodium.
The response to the treatment regimen supported our diagnosis of cerebral salt wasting (CSW). The patient's serum sodium concentration upon discharge was 135 mEq/L.
Discussion
Our case illustrates the diagnostic challenge presented to physicians when they manage hyponatremia in the setting of a central nervous system (CNS) event. Hyponatremia (sodium 136 mEq/L) has been associated with confusion, lethargy, seizures, coma, and even death.1 Hyponatremia has been reported to occur in up to 30% of the patients with subarachnoid hemorrhage.2, 3
SIADH is frequently the cause of hyponatremia in a patient with a concurrent intracranial process. However, CSW is an important diagnosis to consider and differentiate from SIADH. In a retrospective review of 316 patients with subarachnoid hemorrhage and hyponatremia, 69% were determined to be due to SIADH while 6.5% were from CSW.4 Both CSW and SIADH have been reported to occur in the setting of head trauma, intracranial or metastatic neoplasm, carcinomatous or infectious meningitis, subarachnoid hemorrhage, and CNS surgery. Cryptococcal meningitis as an etiology of CSW has not been previously reported.
The main differentiating feature between SIADH and CSW is that CSW is a dysfunction of renal sodium absorption whereas in SIADH renal sodium handling is intact. This also leads to a difference in the extracellular volume status. SIADH is associated with an increased to normal volume status whereas CSW is a volume‐depleted state. Our patient exhibited a low serum osmolality and a high urine osmolality in the context of hyponatremia, which is present in both CSW and SIADH. However, the clinical course and presentation suggested volume loss, specifically the diarrhea, high urine specific gravity, declining BP, and a negative fluid balance. Some other features that are helpful in determining the volume status may include orthostatic changes, tachycardia, and skin turgor.
Our patient had a low serum uric acid, which is also present in both SIADH and CSW. The key difference between the 2 is that while uric acid will improve with resolution of hyponatremia in SIADH, it will remain low in CSW, as in our patient's uric acid levels, which remained low after normalization of the serum sodium.
Finally, the hyponatremia improved with isotonic fluid repletion, which would not occur in SIADH. The majority of the CSW patients will respond to volume repletion alone, as CSW is a transient condition that will usually resolve in 3 to 4 weeks.3 However, a few patients may require fludrocortisone, as was needed in our patient.
The renal wasting of sodium in CSW is poorly understood. Some postulated mechanisms cite the disruption of sympathetic neural input to the kidney and natriuresis induced by natriuretic peptides. Natriuretic peptides, in particular BNP, have been reported to be elevated in patients with CSW.5, 6 Natriuretic peptides cause salt wasting by inhibition of sodium reabsorption in renal tubule and intramedullary collecting.5, 6 Renin and aldosterone release can also inhibited by the natriuretic peptides. BNP levels were elevated in our patient despite volume loss and no signs of congestive heart failure. Cardiac congestion is a possible etiology for the elevated BNP levels, which peaked to 900 pg/mL on hospital day 37. However, 3 days later the BNP levels declined to 222 pg/mL despite the fact that he was continually in positive fluid balance, suggesting that the BNP elevation was due to CSW and not heart failure.
Conclusions
Our case illustrates the diagnostic and management challenge of hyponatremia in the setting of a CNS event. Both SIADH and CSW are possible etiologies but it is important to make a differentiation. Levels of natriuretic peptides and changes in fractional excretion of uric acid may help differentiate between the 2 conditions.6 The key difference mechanistically is that CSW is due to sodium‐handling deficits, whereas in SIADH sodium‐handling is intact. It is essential to establish volume status since SIADH is a euvolemic to mildly hypervolemic state vs. CSW, which is a volume‐depleted state.7
CSW is well recognized in the neurosurgical arena. The hospitalist will encounter neurosurgical patients with increasing frequency, and thus having an understanding of this disorder, including its diagnosis and treatment, is key.
- ,.Hyponatremia.N Engl J Med.2000;342(21):1581–1589.
- .Hyponatremia in acute brain disease: the cerebral salt wasting syndrome.Eur J Intern Med.2002;13(1):9–14.
- .Cerebral salt wasting syndrome: a review.Neurosurgery.1996;38(1):152–160.
- ,,, et al.The incidence and pathophysiology of hyponatraemia after subarachnoid haemorrhage.Clin Endocrinol (Oxf).2006;64(3):250–254.
- ,,.Brain natriuretic peptide and cerebral vasospasm in subarachnoid hemorrhage. Clinical and TCD correlations.Stroke.2000;31(1):118–122.
- ,,, et al.Secretion of brain natriuretic peptide in patients with aneurysmal subarachnoid haemorrhage.Lancet.1997;349(9047):245–249.
- ,,,.Clinical assessment of extracellular fluid volume in hyponatremia.Am J Med.1987;83(5):905–908.
- ,.Hyponatremia.N Engl J Med.2000;342(21):1581–1589.
- .Hyponatremia in acute brain disease: the cerebral salt wasting syndrome.Eur J Intern Med.2002;13(1):9–14.
- .Cerebral salt wasting syndrome: a review.Neurosurgery.1996;38(1):152–160.
- ,,, et al.The incidence and pathophysiology of hyponatraemia after subarachnoid haemorrhage.Clin Endocrinol (Oxf).2006;64(3):250–254.
- ,,.Brain natriuretic peptide and cerebral vasospasm in subarachnoid hemorrhage. Clinical and TCD correlations.Stroke.2000;31(1):118–122.
- ,,, et al.Secretion of brain natriuretic peptide in patients with aneurysmal subarachnoid haemorrhage.Lancet.1997;349(9047):245–249.
- ,,,.Clinical assessment of extracellular fluid volume in hyponatremia.Am J Med.1987;83(5):905–908.
Ethics of the Hospitalist Model
Wachter and Goldman1 first described hospitalists in 1996 as a new breed of physicians who devote blocks of time exclusively to the care of hospitalized patients. Since its definition, the hospitalist model has prompted 2 major debates. First, does the hospitalist system improve clinical efficiency, quality of care, cost effectiveness, and patient satisfaction? A series of large and small randomized trials have all but definitively proven the hospitalist model's advantage. Yet whether the hospitalist model is good for patient care has proven to remain contentious, as most recently demonstrated by the discussion between Williams2 and Centor3 and others like it.4, 5 What is clear in these exchanges is that the debate has shifted to the second great debate: does the hospitalist model pose inherent conflicts in clinical ethics? What are the implications of the purposeful discontinuity in care, the autonomy issues raised by mandatory hospitalist use, and the structural management issues that potentially pit hospitalists against patients in fiduciary and financial conflicts of interest? These important issues are certainly not new, and the hospitalist model has made much effort to address some of them.6, 7 This work aims to serve as a review of these important ethical concerns, demonstrating how some questions have been answered, while some remain unanswered.
The Hospitalist Model's Founding Premise
A growing threshold for hospital admission in the last 3 decades caused primary care physicians (PCPs) to see a diminishing number of inpatients. A survey in 1978 found that PCPs spent 40% of their time in the hospital, rounding on 10 patients per day.8 By 2001, PCPs spent 10% of their time in the hospital on average, and most PCPs rounded on fewer than 2 inpatients per day.9 The cost of inefficiencies associated with primary coordination of care in the hospital increasingly outweighed the tradeoff of preserving the patient‐PCP relationship in the hospital. Converging with increasing attention on cost controls through the restructuring of service provision, the hospitalist was born. Wachter10 argued that the hospitalist model could alleviate inpatient demands placed on PCPs while improving the outcomes and lowering the cost of care for hospitalized patients.
Early on there were setbacks to proving Wachter's10 case. Small studies found hospitalists to have higher hospital charges and longer length of stays.11 A survey of PCPs found only 56% were satisfied with communication with hospitalists and that most believed that patients generally preferred to be cared for in the hospital by their regular physician.12, 13 Meltzer and Herthko14 found 70% of people sampled said they would prefer care by their own physician to that of a hospitalist if they were hospitalized for a general medical condition. Yet this study found in a national random‐digit phone survey that only 10% of the respondents would pay $750 for their PCP to follow them to the hospital, the cost savings of the hospitalist system proven by the only 2 randomized trials performed at the time.15, 16 To 90% of respondents, the value of the PCP at the bedside was not worth the cost tradeoff to keep them there.
The meteoric rise in the number of hospitalists reflects the many studies and reviews that affirmed the premise that hospitalists improved inpatient efficiency without harmful effects on quality of care.17, 18 In a large retrospective cohort study of over 75,000 patients in 45 hospitals across the country, Lindenauer et al.19 found that hospitalists had a $268 lower cost when compared to internists, $125 lower cost when compared to family physicians, and a shorter hospital stay by about one‐half day when compared to both groups. The group found no significant difference in rates of death or readmission rates. While called modest in the text, these savings over time and volume add up for hospitals. Patients benefit from hospitalist care, researchers hypothesize, because of their familiarity with hospital systems, their increased availability to patients, and their experience with common hospital problems. Though the Lindenauer et al.19 study was criticized for design flaws, it prompted the editorialist McMahon20 to assert that the question was sufficiently answered, and it was time to move on away from the studies focusing on cost and comparing outcomes. As Wachter21 wrote, the demand for hospitalists is now relatively de‐linked from the field's original premiseefficiency advantagesand is now both more diversified and more robust. The model has become an accepted mode of care for hospitalized patients, with up to 20,000 hospitalists currently practicing in 29% of all hospitals and in over one‐half of hospitals with over 200 beds in the United States.22, 23
The Patient‐Physician Relationship
Purposeful discontinuity of care in the hospitalist system has the potential to diminish the doctor‐patient relationship.12 This relationship is built on a bond of loyalty, confidentiality, and trust. Handing off care to a hospitalist when the patient is most vulnerable can be viewed as a violation of this covenant. According to Meltzer,24 the hospitalist model pits Franicis Peabody's25 intimate personal relationship between patient and physician against Adam Smith et al.'s11 benefits of specialization. Peabody25 observed that physicians' lack of understanding of their patients as persons is especially acute in the hospital, where
one gets in the habit of using the oil immersion lamp instead of the low power, and focuses too intently in the center of the field. . . . The institutional eye tends to become focused on the lung, and it forgets that the lung is only one member of the body.
This movement toward patient‐centered medicine fits into an ever‐growing sentiment to value the social as well as the physiological, a holistic approach to the patient as a person. This emphasis was the original justification for PCPs to coordinate increasingly specialized hospital care and translate recommendations suitable to patients. Can the long‐term relationship between patient and PCP be replaced by the hospital generalist, or would hospitalists be inherently deficient in their abilities to coordinate care appropriate for patients? Hospitalized patients are frequently in no position to make complex decisions regarding their care.26 Lo7 argues that PCPs who know patients over extended periods of time are in a better position to respect patient wishes by individualizing discussions with patients and checking that patients' decisions are consistent with their core values. The long‐term relationship is also critical for designing a complex discharge plan suitable to the patients' ability and resources. Information about long‐term patient compliance with medications is much more available to PCPs. Patients trust physicians to keep promises made concerning end‐of‐life issues, and these assurances are vulnerable during handoffs of care. Pantilat et al.6 provide a case study of an outpatient Do‐Not‐Resuscitate order ineffective in the hospital. These scenarios occur because most written advance directives are unavailable in acute situations, and when they are, hospitalists unfamiliar with the patient's wishes may hesitate to act on directives not specific enough to answer the acute clinical question.27
Hospitalists' broadened responsibility to systematically improve the care of patients may potentially improve end‐of‐life care. Patient values can be better communicated to hospitalists by encouraging inpatients to complete advance directive surveys and then asking hospitalists to discuss those directives with their patients.6 Significantly, Auerbach and Pantilat28 found that end‐of‐life care was improved with hospitalist care. This chart review found hospitalists more likely to have discussions with patients and their families regarding care and providing comfort care more frequently at the time of death than community‐based physicians. The authors hypothesize that hospitalists may have better communication with dying patients and their families because they spend more time in the hospital each day, using frequent meetings to better understand the preferences of patients. These preferences often require clarification and often change after admission, making previous discussions about end‐of‐life care with PCPs moot. Greater expertise in hospital care may also allow hospitalists to better recognize patients who are nearing death and may explain the fewer symptoms documented by Auerbach and Pantilat28 at the end of life among patients cared for by hospitalists compared to community‐based physicians.
Hospital medicine has taken continuity of care issues seriously, and responded by making pragmatic recommendations to preserve the patient‐PCP relationship in the hospital and assuage the perception that patients have been dropped. Harlan et al.29 identify important issues around good communication between pediatric hospitalists and PCPs including the content and timing of communication beneficial to the patient. Hospitalists can use a standard script for introducing themselves to patients, explaining their role, and their continued coordination with the PCP.30 PCPs can still be involved in the care of their patients in hospitals through continuity visits or phone calls with patients and through better communication with hospitalists.31 Generally, reimbursing PCPs for their increased role in the hospitalist system can encourage better communication with hospitalists.19 Potential disagreements between PCPs and hospitalist regarding the care of the patient can be resolved through explicit conflict resolution procedures within the hospitalist system.6
These procedural solutions are only as successful as they are used. A large review by Kripalani et al.32 found communication between hospitalists and PCPs occurred infrequently (3%‐20%), affecting the quality of care in approximately 25% of follow‐up visits and contributing to PCP dissatisfaction. Sharma et al.33 found that continuity visits decreased from 50.5% in 1996 to 39.8% in 2006. In a survey of patients cared for in a hospitalist system, Hruby et al.34 found that 33% of hospitalized patients had some contact with their PCP directly and 66% of patients were satisfied with the contact they or their relative had with their PCP. When probed, patient satisfaction is too vague a measurement to assess the complex value of the patient‐physician relationship. Studying these issues may require relying more on individualized narratives rather than generalized statistics, or may require years of follow‐up. As Centor3 argues, we need this broader perspective of the patient's experience in order to understand the effects of the hospitalist model on patient trust in their PCP and in their overall care. Studies by Davis et al.35 and Halpert et al.36 assert that rising quality of care and patient satisfaction with the hospitalist system rebuts coordination of care concerns. Yet we need more studies investigating the relationship between improved communication and patient outcomes, as evidence is currently conflicting on this subject.32, 37, 38
The Journal of Hospital Medicine has pursued this research agenda; the April 2009 issue presents several studies describing best practices in the discharging of hospitalized patients. Manning et al.39 describe a tool to assess patient mobility after discharge, and O'Leary et al.40 used electronic health records to create a better discharge summary. Project BOOST (Better Outcomes for Older Adults Through Safe Transitions) has shown improvements in discharge transition procedures41 and the use of transition coaches for vulnerable older patients has been proven cost‐effective and has been scaled up to more than 100 healthcare organizations.42, 43
Inpatient care handoff to PCPs is not entirely novel, as surgeons, oncologists, cardiologists, and other specialists have always grappled with continuity of care. It would be prudent to investigate what can be learned from these efforts, and which practices can be best applied to the hospitalist model. More longitudinal studies need to investigate the prevalence and success of the procedural recommendations to preserve the patient‐physician relationship. We need to know more about what works and what does not. How have hospitals found novel ways in implementing these approaches, and how can they be applied to a diversity of hospital settings? We need a better outcome measurement than patient or physician satisfaction for probing the subtleties of the patient‐physician relationship. There is a sizeable population that does not have a PCP to care for them before hospitalization or after discharge, and discussions about continuity of care must address these patients. Last, these best practices and patient centered values need to be incorporated into the core competencies of residencies and fellowships for a new generation of hospitalists.
Maintaining the continuity of the physician‐patient relationship is an integral part of the original premise of the hospitalist model. Importantly, Meltzer24 found that this discontinuity within the hospital has the potential to eliminate the savings of the hospitalist system. Yet concerns about continuity of care do not sufficiently encompass the complexand at times fragilerelationship between physician and patient. The survival of the physician‐patient relationship depends on the hospitalist model's affirmation of the values of coordination and Peabody's25 approach to patient‐centered care. If the hospitalist model is to thrive, it needs to emphasize its duty as steward of the PCP‐patient relationship as much as it focuses on efficiency and cost‐effectiveness.
Patient Autonomy
The mandatory transfer of patients into the hospitalist model raises serious ethical issues. A survey in 2000 of PCPs found that 23% were required to use hospitalists for all admissions.44 Other surveys found this prevalence to be as low as 2%.12 Nevertheless, several high profile cases of Health Maintenance Organizations (HMOs)Prudential HealthCareSouth Florida, Prudential, Humana, and Cigna Corporationall using mandatory hospitalists, prompted protests from professional organizations and there were even legislative efforts to ban the practice of the mandatory use of hospitalists in 2000 and 2001.45 Today, most insurance plans, as well as the Society of Hospital Medicine (SHM), support voluntary rather than mandatory hospitalist use.46 Yet while not mandatory, the hospitalist is the default provider in many settings, giving a de facto mandate for hospitalist care. As Royo et al.47 point out, the rise in physician employment by hospitals has facilitated a self‐selecting progression toward a structural network that closely resembles the mandatory model.
While PCPs and internists contested mandatory hospitalist plans as infringements on their autonomy, they overlooked the harm to the patient's autonomy. When healthy in the ambulatory setting, the patient has the opportunity to choose his or her doctor to provide longitudinal care. When the patient is admitted acutely to a hospital, the patient does not have the freedom to choose a physician; the patient is assigned to the hospitalist on duty that night. This call for patient autonomy is of utmost importance in the hospitalized patient, where patients are increasingly sicker, their diseases under a high‐powered lens, and their options diminished. This freedom of choice is integral to the patient‐physician partnership. Yet this freedom of choice is largely hindered by the employer's choice in the health plan for their employees or an individual's ability to pay for a health plan. These represent some of the many barriers to choice facing patients in the American model of health insurance.
As the hospitalist system grows to become the accepted mode of hospital care, more patients need to be informed about the transition of care to another physician and what steps are taken to ensure appropriate continuity of care. Transfers of patients from PCPs to hospitalists must be voluntary, with the decision left to patient care preferences.48 Educating patients in the outpatient setting about the hospitalist model, its benefits, risks, and alternatives, is necessary for them to make informed decisions about hospital care. This will require the collaboration of PCPs and hospitalists together. The continued success of the model depends on the nurturance of the partnership between the PCP, the hospitalist, and the patient.
Meltzer and Herthko14 have proposed that patients pay a premium for the option to choose a PCP that is not mandated to transfer their care to a hospitalist, in order to offset cost savings with the hospitalist system. Yet Meltzer and Herthko's14 study suggests that many patients could not afford to pay this premium and, in effect, patient autonomy would be preserved for the affluent. This raises the oft‐neglected professional ethic of justice for low‐income patients. Alexander and Lantos49 were resigned to see this infringement on patient autonomy as an inevitable consequence of balancing the desires of patients with the drive to lower cost and improve outcomes. If the hospitalist model grows to be the predominant mode of care, it is unclear if patient choice can survive. Investigators need to test whether the advantages of hospitalist care can coexist with voluntary programs. If it proves that they indeed cannot, then the hospitalist system will need to respond to concerned patients with honest answers and find pragmatic solutions to diminishing patient choice.
Conflict of Interest
The hospitalist system's main benefit of cost‐savings prompted Pantilat et al.6 to wonder whether hospitalists would face a conflict of interest between what is best for the patient and what financial incentives and utilization review encourage or require them to do. The financial support provided by many hospitals to meet the operating expenses of hospitalist programs is often associated with explicit or implicit incentives to reduce the length of hospital stay and costs.50 With hospitals employing hospitalists and increasingly pressuring them to decrease length of stay and discharge patients quickly, patients may have no advocate to protect them from discharge planners. Many hospitalists supplement their income by supervising discharge planners, and a dispute would put the hospitalist in the uncomfortable position of advocating for his patient against his employer and colleagues. While conflicts of interests occur in many managed care arrangements, they may be more acute in hospitalist systems. A weakened patient‐physician relationship may put the patients' best interest inferior to the employer's interests. Hospitalists do not immediately deal with adverse consequences of premature discharges in the outpatient setting and virtually no malpractice case law considers the obligations and practices of hospitalists in these settings.51
The SHM identified a core competency of hospitalists to
recommend treatment options that optimize patient care, include consideration of resource utilization, and are formulated without regard to financial incentives or other conflicts of interest.52
Ethical issues concerning conflict of interest remain unanswered, largely because no information about organizational features such as explicit incentives for reductions in length of stay is available to researchers or to patients. This is the wrong approach and only feeds the fear that hospitalists may weigh patients' best interest with financial incentives. Abbo and Volandes53 have argued that ambivalence to cost considerations is hazardous. If the hospitalist model cannot be forthright with the active considerations of costs in daily clinical practice, it is unlikely to truly make strides at cost savings, and may even raise the cost of care in the long run.
Jonsen et al.54 provide ethical standards for considering costs in clinical decisions. First, a physician's first priority should be to provide patient‐centered care that focuses on medical indications and patient preferences. Second, quality care does not mean all available care; quality care reflects what is not only diagnostically sound and technically correct, but also appropriate. Third, conflicts of interest are most vulnerable when there is a failing of the patient‐physician relationship. Health care organizations should expect physicians to argue for policies that provide all services that have a reasonable likelihood of benefiting the patient. Fourth, patient and physician autonomy and freedom of choice should be maximized within the limits of the system. Persons should be fully informed of the constraints of the system before choosing it. Plans need to disclose any financial incentive arrangements that exist between the plan and the physician. And incentive arrangements should be based on quality of care rather than on underutilization of care services. Fifth, the system should reflect principles of just distribution, ensuring that all who have a fair claim to service should receive it without discrimination. Last, capitation plans should share risks among physicians, not patients, while incentives are provided for improvements in access, prevention, and patient satisfaction.
Conflicts of interest have been a concern for as long as physicians have been paid for services. Fears about interference into the doctor‐patient relationship, whether they are from government or business, continue to stall real efforts to lower skyrocketing medical costs. The hospitalist model rebuts conflict of interest claims with improved outcomes, efficiency, and quality of care in the many reviews cited above. These arguments do prove that the hospitalist model's emphasis on medically indicated and appropriate care does address Jonsen et al.'s54 first and second standards. Yet, as Jonsen et al.54 point out, without strongly emphasizing the patient‐physician relationship and patient autonomy, it leaves itself vulnerable to creating conflicts of interest. Hospitalist systems need to be forthright about their explicit or implicit incentive structures and disclose this information to patients in a timely manner for them to make informed decisions. These incentives should be linked to quality of care and patient satisfaction, not cost savings. Last, hospitalist training programs should make ethical cost considerations a core competency of their curriculum.
Conclusions
Hospitalism was founded on the premise that it could improve the quality and reduce the cost of hospital care. Many randomized studies have all but definitively proven this original assertion. It is now time for the model to prove that these gains are not to the detriment of the patient‐physician relationship. Hospitalism must define itself as the steward of this relationship, valuing it as much as it values outcomes and costs. This is of particular concern in the United States as Medicare Part A (payment for inpatient care) is scheduled to go bankrupt in 2019, leading to potentially reasonable fears of hospital‐motivated cost containment.57
Investigators must find an outcome that encompasses the complexity of the patient‐physician relationship, and methods to improve it must be studied and improved upon. Preserving the patient‐physician relationship is a systemic issue, and full‐time hospitalists may be in the best position to implement systemic reforms to improve communication and continuity of care. Pham's56 case study of a hospitalist piecing together disparate parts of the patient's story illustrates this point. This should include more investigation into the prevalence of use and success of methods aimed at protecting the patient‐physician relationship at critical points in the handover of care. When proven successful, The SHM should propose new standards and safeguards to insure that these methods become standard practice in patient care. This effort, led by Snow et al.,57 is currently underway.
A hospitalist model that does not emphasize mitigating the effects of the diminishing patient‐physician relationship leaves itself exposed to further infringements on autonomy and choice. It is unclear whether patient autonomy and choice can coexist in a successful hospitalist system. The consequences of these unanswered ethical questions need to be explored. The professions of primary care need to be more proactive in educating patients about choice of care in hospitals, and hospitalists need to provide that choice, allowing voluntary programs in hospital care when feasible.
When combined, a wounded patient‐physician relationship and impaired patient autonomy leave the hospitalist model vulnerable to claims of financial and fiduciary conflict of interest. These concerns need not be inherent to the hospitalist systems, but hospitalists will need to be forthright and honest about incentives structures, and link them to quality of care and patient satisfaction, not to efficiency and cost savings.
It is indeed time for hospitalism to move onaway from proving its founding premise, and toward addressing these lingering ethical issues. Hospitalism's continued growth and success depends on it.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .Hospitalists and the hospital medicine system of care are good for patient care.Arch Intern Med.2008;168(12):1254–1256, discussion 1259–1260.
- .A hospitalist inpatient system does not improve patient care outcomes.Arch Intern Med.2008;168(12):1257–1258, discussion 1259–1260.
- .Are inpatients' needs better served by hospitalists than by their family doctors?: Yes.Can Fam Physician.2008;54(8):1100–1101,1104–1106.
- .Are inpatients' needs better served by hospitalists than by their family doctors?: No.Can Fam Physician.2008;54(8):1101–1103,1105–1107.
- ,,.A new doctor in the house: ethical issues in hospitalist systems.JAMA.1999;282:171–174.
- .Ethical and policy implications of hospitalist systems.Dis Mon.2002;48:281–290.
- Robert Wood Johnson Foundation.Medical Practice in the United States.Princeton, NJ:The Robert Wood Johnson Foundation;1981.
- .Response to David Meltzer's paper “Hospitalists and the doctor‐patient relationship.”J Legal Stud2001;30:615–623.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- ,,.Primary care family physicians and 2 hospitalists models: comparison of outcomes, processes, and costs.J Fam Prac.2002;51:1021–1027.
- ,,, et al.Primary care physician attitudes regarding communication with hospitalists.Dis Mon.2002;48(4):218–229.
- ,,, et al.Physician attitudes towards and prevalence of the hospitalist model of care: results of a national survey.Am J Med.2000;109:648–653.
- ,.Patients' willingness to pay for hospital care by their primary care physician versus hospitalists: results of a national survey. [Society of General Internal Medicine 23rd annual meeting. Boston, Massachusetts, USA. May 4–6, 2000. Abstracts.]J Gen Intern Med.2000;15(suppl 1):135.
- ,,, et al.Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560.
- ,,, et al.Effects of hospitalist physicians on an academic general medicine service: results of a randomized trial. [22nd Annual meeting of The Society of General Internal Medicine. San Francisco, California, USA. April 29‐May 1, 1999. Abstracts.]J Gen Intern Med.1999;14(suppl 2):112.
- ,.The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- ,.Economic and healthcare forces of hospitalist movement.Mt Sinai J Med.2008;75(5):424–429.
- ,,, et al.Outcomes of care by hospitalists, general internists, and family physicians.N Engl J Med.2007;357:2589–2600.
- .The hospitalist movement—time to move on.N Engl J Med.2007;357:2627–2629.
- .Today's New England Journal Hospitalist Study. Weblog Entry.Wachter's World: The Hospitalist.2007. Available at: http://www.the‐hospitalist.org/blogs/wachters_world/archive/2007/12/20/today‐s‐new‐england‐journal‐hospitalist‐study.aspx. Accessed July 2009.
- ,,, et al.The Rise of the Hospitalist in California.Oakland, CA:California Health Care Foundation;2007.
- ,,, et al.The status of hospital medicine groups in the United States.J Hosp Med.2006;1:75–80.
- .Hospitalists and the doctor patient relationship.J Legal Stud.2001;2:615–623.
- .Landmark article March 19, 1927: the care of the patient. By Francis W. Peabody.JAMA.1984;252:813–818.
- .The Practice of Autonomy: Patients, Doctors, and Medical Decisions.New York, NY:Oxford University Press;1998.
- ,,, et al.A prospective study of advance directives for life‐sustaining care.N Engl J Med.1991;324:882–888.
- ,.End‐of‐life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms.Am J Med.2004;116:669–675.
- ,,, et al.Pediatric hospitalists and primary care providers: a communication needs assessment.J Hosp Med.2009;4(3):187–193.
- .What should you say after “Hello”?Today's Hospitalist Apr2008. Available at: http://www.todayshospitalist.com/index.php?b=articles_read48:267–272.
- ,,, et al.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297(8):831–841.
- ,,, et al.Continuity of outpatient and inpatient care by primary care physicians for hospitalized older adults.JAMA.2009;301(16):1671–1680.
- ,,.How do patients view the role of the primary care physician in inpatient care?Dis Mon.2002;48:230–238.
- ,,, et al.Effects of hospitalists on cost, outcomes and patient satisfaction in a rural health system.Am J Med.2000;108:621–626.
- ,,, et al.The impact of an inpatient physician program on quality, utilization, and satisfaction.Am J Manag Care.2000;6:549–555.
- ,,, et al.Association of communication between hospital‐based physicians and primary care providers with patient outcomes.J Gen Intern Med.2009;24:381–386.
- ,,.Rehospitalizations among patients in the Medicare fee‐for‐service program.N Engl J Med.2009;360(14):1418–1428.
- ,,.Home alone: mobility independence before discharge.J Hosp Med.2009;4:252–254.
- ,,, et al.Creating a better discharge summary: improvement in quality and timeliness using an electronic discharge summary.J Hosp Med.2009;4:219–225.
- Society of Hospital Medicine. BOOSTing Care Transitions Resource Room. Available at: http://www.hospitalmedicine.org. Accessed July2009.
- ,,,.The care transitions intervention: results for a randomized control trial.Arch Intern Med.2006;166:1822–1828.
- Care Transitions Program. Available at: http://www.caretransitions.org. Accessed July2009.
- ,,, et al.Friend or foe? How primary care physicians perceive hospitalists.Arch Intern Med.2000;160(19):2902–2908.
- .Use of mandatory hospitalists blasted.ACP‐ASIM Observer, May1999. Available at: http://www.acpinternist.org/archives/1999/05/hosps.htm. Accessed July 2009.
- .Hospitalists: the next big thing?Trustee Magazine, May2005. Available at: http://www.trusteemag.com/trusteemag_app/jsp/articledisplay.jsp?dcrpath=TRUSTEEMAG/PubsNewsArticleGen/data/2005/0505TRU_FEA_CoverStory. Accessed July 2009.
- ,,.Hospitalist medicine: voluntary or mandatory?Virtual Mentor.2008;10(12):813–816.
- .The hospitalist model: perspectives of the patient, the internist, and internal medicine.Ann Intern Med.1999;130:368–372.
- ,.The doctor‐patient relationship in the post‐managed care era.Am J Bioeth2006;6(1):29–32.
- ,,, et al.Health care market trends and the evolution of hospitalist use and roles.J Gen Intern Med.2005;20:101–107.
- .Key legal principles for hospitalists.Dis Mon.2002;48(4):197–206.
- Society of Hospital Medicine.Professionalism and medical ethics.J Hosp Med.2006;1:90–91.
- ,.Teaching residents to consider costs in medical decision making.Am J Bioeth2006;6(4):33–34.
- ,,.Clinical Ethics: A Practical Approach to Ethical Decision in Clinical Medicine.6th ed.New York, NY:McGraw‐Hill Medical;2006.
- ,. The 2004 Medicare and Social Security trustees reports. National Center for Policy Analysis, Study No. 266.2004. Available at: http://www.ncpa.org/pub/st/st266. Accessed July 2009.
- .Dismantling Rube Goldberg: cutting through the chaos to achieve coordinated care.J Hosp Med.2009;4(4):259–260.
- ,,, et al.Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine.J Hosp Med.2009;4:364–70. [http://dx.doi.org/10.1002/jhm.510]
Wachter and Goldman1 first described hospitalists in 1996 as a new breed of physicians who devote blocks of time exclusively to the care of hospitalized patients. Since its definition, the hospitalist model has prompted 2 major debates. First, does the hospitalist system improve clinical efficiency, quality of care, cost effectiveness, and patient satisfaction? A series of large and small randomized trials have all but definitively proven the hospitalist model's advantage. Yet whether the hospitalist model is good for patient care has proven to remain contentious, as most recently demonstrated by the discussion between Williams2 and Centor3 and others like it.4, 5 What is clear in these exchanges is that the debate has shifted to the second great debate: does the hospitalist model pose inherent conflicts in clinical ethics? What are the implications of the purposeful discontinuity in care, the autonomy issues raised by mandatory hospitalist use, and the structural management issues that potentially pit hospitalists against patients in fiduciary and financial conflicts of interest? These important issues are certainly not new, and the hospitalist model has made much effort to address some of them.6, 7 This work aims to serve as a review of these important ethical concerns, demonstrating how some questions have been answered, while some remain unanswered.
The Hospitalist Model's Founding Premise
A growing threshold for hospital admission in the last 3 decades caused primary care physicians (PCPs) to see a diminishing number of inpatients. A survey in 1978 found that PCPs spent 40% of their time in the hospital, rounding on 10 patients per day.8 By 2001, PCPs spent 10% of their time in the hospital on average, and most PCPs rounded on fewer than 2 inpatients per day.9 The cost of inefficiencies associated with primary coordination of care in the hospital increasingly outweighed the tradeoff of preserving the patient‐PCP relationship in the hospital. Converging with increasing attention on cost controls through the restructuring of service provision, the hospitalist was born. Wachter10 argued that the hospitalist model could alleviate inpatient demands placed on PCPs while improving the outcomes and lowering the cost of care for hospitalized patients.
Early on there were setbacks to proving Wachter's10 case. Small studies found hospitalists to have higher hospital charges and longer length of stays.11 A survey of PCPs found only 56% were satisfied with communication with hospitalists and that most believed that patients generally preferred to be cared for in the hospital by their regular physician.12, 13 Meltzer and Herthko14 found 70% of people sampled said they would prefer care by their own physician to that of a hospitalist if they were hospitalized for a general medical condition. Yet this study found in a national random‐digit phone survey that only 10% of the respondents would pay $750 for their PCP to follow them to the hospital, the cost savings of the hospitalist system proven by the only 2 randomized trials performed at the time.15, 16 To 90% of respondents, the value of the PCP at the bedside was not worth the cost tradeoff to keep them there.
The meteoric rise in the number of hospitalists reflects the many studies and reviews that affirmed the premise that hospitalists improved inpatient efficiency without harmful effects on quality of care.17, 18 In a large retrospective cohort study of over 75,000 patients in 45 hospitals across the country, Lindenauer et al.19 found that hospitalists had a $268 lower cost when compared to internists, $125 lower cost when compared to family physicians, and a shorter hospital stay by about one‐half day when compared to both groups. The group found no significant difference in rates of death or readmission rates. While called modest in the text, these savings over time and volume add up for hospitals. Patients benefit from hospitalist care, researchers hypothesize, because of their familiarity with hospital systems, their increased availability to patients, and their experience with common hospital problems. Though the Lindenauer et al.19 study was criticized for design flaws, it prompted the editorialist McMahon20 to assert that the question was sufficiently answered, and it was time to move on away from the studies focusing on cost and comparing outcomes. As Wachter21 wrote, the demand for hospitalists is now relatively de‐linked from the field's original premiseefficiency advantagesand is now both more diversified and more robust. The model has become an accepted mode of care for hospitalized patients, with up to 20,000 hospitalists currently practicing in 29% of all hospitals and in over one‐half of hospitals with over 200 beds in the United States.22, 23
The Patient‐Physician Relationship
Purposeful discontinuity of care in the hospitalist system has the potential to diminish the doctor‐patient relationship.12 This relationship is built on a bond of loyalty, confidentiality, and trust. Handing off care to a hospitalist when the patient is most vulnerable can be viewed as a violation of this covenant. According to Meltzer,24 the hospitalist model pits Franicis Peabody's25 intimate personal relationship between patient and physician against Adam Smith et al.'s11 benefits of specialization. Peabody25 observed that physicians' lack of understanding of their patients as persons is especially acute in the hospital, where
one gets in the habit of using the oil immersion lamp instead of the low power, and focuses too intently in the center of the field. . . . The institutional eye tends to become focused on the lung, and it forgets that the lung is only one member of the body.
This movement toward patient‐centered medicine fits into an ever‐growing sentiment to value the social as well as the physiological, a holistic approach to the patient as a person. This emphasis was the original justification for PCPs to coordinate increasingly specialized hospital care and translate recommendations suitable to patients. Can the long‐term relationship between patient and PCP be replaced by the hospital generalist, or would hospitalists be inherently deficient in their abilities to coordinate care appropriate for patients? Hospitalized patients are frequently in no position to make complex decisions regarding their care.26 Lo7 argues that PCPs who know patients over extended periods of time are in a better position to respect patient wishes by individualizing discussions with patients and checking that patients' decisions are consistent with their core values. The long‐term relationship is also critical for designing a complex discharge plan suitable to the patients' ability and resources. Information about long‐term patient compliance with medications is much more available to PCPs. Patients trust physicians to keep promises made concerning end‐of‐life issues, and these assurances are vulnerable during handoffs of care. Pantilat et al.6 provide a case study of an outpatient Do‐Not‐Resuscitate order ineffective in the hospital. These scenarios occur because most written advance directives are unavailable in acute situations, and when they are, hospitalists unfamiliar with the patient's wishes may hesitate to act on directives not specific enough to answer the acute clinical question.27
Hospitalists' broadened responsibility to systematically improve the care of patients may potentially improve end‐of‐life care. Patient values can be better communicated to hospitalists by encouraging inpatients to complete advance directive surveys and then asking hospitalists to discuss those directives with their patients.6 Significantly, Auerbach and Pantilat28 found that end‐of‐life care was improved with hospitalist care. This chart review found hospitalists more likely to have discussions with patients and their families regarding care and providing comfort care more frequently at the time of death than community‐based physicians. The authors hypothesize that hospitalists may have better communication with dying patients and their families because they spend more time in the hospital each day, using frequent meetings to better understand the preferences of patients. These preferences often require clarification and often change after admission, making previous discussions about end‐of‐life care with PCPs moot. Greater expertise in hospital care may also allow hospitalists to better recognize patients who are nearing death and may explain the fewer symptoms documented by Auerbach and Pantilat28 at the end of life among patients cared for by hospitalists compared to community‐based physicians.
Hospital medicine has taken continuity of care issues seriously, and responded by making pragmatic recommendations to preserve the patient‐PCP relationship in the hospital and assuage the perception that patients have been dropped. Harlan et al.29 identify important issues around good communication between pediatric hospitalists and PCPs including the content and timing of communication beneficial to the patient. Hospitalists can use a standard script for introducing themselves to patients, explaining their role, and their continued coordination with the PCP.30 PCPs can still be involved in the care of their patients in hospitals through continuity visits or phone calls with patients and through better communication with hospitalists.31 Generally, reimbursing PCPs for their increased role in the hospitalist system can encourage better communication with hospitalists.19 Potential disagreements between PCPs and hospitalist regarding the care of the patient can be resolved through explicit conflict resolution procedures within the hospitalist system.6
These procedural solutions are only as successful as they are used. A large review by Kripalani et al.32 found communication between hospitalists and PCPs occurred infrequently (3%‐20%), affecting the quality of care in approximately 25% of follow‐up visits and contributing to PCP dissatisfaction. Sharma et al.33 found that continuity visits decreased from 50.5% in 1996 to 39.8% in 2006. In a survey of patients cared for in a hospitalist system, Hruby et al.34 found that 33% of hospitalized patients had some contact with their PCP directly and 66% of patients were satisfied with the contact they or their relative had with their PCP. When probed, patient satisfaction is too vague a measurement to assess the complex value of the patient‐physician relationship. Studying these issues may require relying more on individualized narratives rather than generalized statistics, or may require years of follow‐up. As Centor3 argues, we need this broader perspective of the patient's experience in order to understand the effects of the hospitalist model on patient trust in their PCP and in their overall care. Studies by Davis et al.35 and Halpert et al.36 assert that rising quality of care and patient satisfaction with the hospitalist system rebuts coordination of care concerns. Yet we need more studies investigating the relationship between improved communication and patient outcomes, as evidence is currently conflicting on this subject.32, 37, 38
The Journal of Hospital Medicine has pursued this research agenda; the April 2009 issue presents several studies describing best practices in the discharging of hospitalized patients. Manning et al.39 describe a tool to assess patient mobility after discharge, and O'Leary et al.40 used electronic health records to create a better discharge summary. Project BOOST (Better Outcomes for Older Adults Through Safe Transitions) has shown improvements in discharge transition procedures41 and the use of transition coaches for vulnerable older patients has been proven cost‐effective and has been scaled up to more than 100 healthcare organizations.42, 43
Inpatient care handoff to PCPs is not entirely novel, as surgeons, oncologists, cardiologists, and other specialists have always grappled with continuity of care. It would be prudent to investigate what can be learned from these efforts, and which practices can be best applied to the hospitalist model. More longitudinal studies need to investigate the prevalence and success of the procedural recommendations to preserve the patient‐physician relationship. We need to know more about what works and what does not. How have hospitals found novel ways in implementing these approaches, and how can they be applied to a diversity of hospital settings? We need a better outcome measurement than patient or physician satisfaction for probing the subtleties of the patient‐physician relationship. There is a sizeable population that does not have a PCP to care for them before hospitalization or after discharge, and discussions about continuity of care must address these patients. Last, these best practices and patient centered values need to be incorporated into the core competencies of residencies and fellowships for a new generation of hospitalists.
Maintaining the continuity of the physician‐patient relationship is an integral part of the original premise of the hospitalist model. Importantly, Meltzer24 found that this discontinuity within the hospital has the potential to eliminate the savings of the hospitalist system. Yet concerns about continuity of care do not sufficiently encompass the complexand at times fragilerelationship between physician and patient. The survival of the physician‐patient relationship depends on the hospitalist model's affirmation of the values of coordination and Peabody's25 approach to patient‐centered care. If the hospitalist model is to thrive, it needs to emphasize its duty as steward of the PCP‐patient relationship as much as it focuses on efficiency and cost‐effectiveness.
Patient Autonomy
The mandatory transfer of patients into the hospitalist model raises serious ethical issues. A survey in 2000 of PCPs found that 23% were required to use hospitalists for all admissions.44 Other surveys found this prevalence to be as low as 2%.12 Nevertheless, several high profile cases of Health Maintenance Organizations (HMOs)Prudential HealthCareSouth Florida, Prudential, Humana, and Cigna Corporationall using mandatory hospitalists, prompted protests from professional organizations and there were even legislative efforts to ban the practice of the mandatory use of hospitalists in 2000 and 2001.45 Today, most insurance plans, as well as the Society of Hospital Medicine (SHM), support voluntary rather than mandatory hospitalist use.46 Yet while not mandatory, the hospitalist is the default provider in many settings, giving a de facto mandate for hospitalist care. As Royo et al.47 point out, the rise in physician employment by hospitals has facilitated a self‐selecting progression toward a structural network that closely resembles the mandatory model.
While PCPs and internists contested mandatory hospitalist plans as infringements on their autonomy, they overlooked the harm to the patient's autonomy. When healthy in the ambulatory setting, the patient has the opportunity to choose his or her doctor to provide longitudinal care. When the patient is admitted acutely to a hospital, the patient does not have the freedom to choose a physician; the patient is assigned to the hospitalist on duty that night. This call for patient autonomy is of utmost importance in the hospitalized patient, where patients are increasingly sicker, their diseases under a high‐powered lens, and their options diminished. This freedom of choice is integral to the patient‐physician partnership. Yet this freedom of choice is largely hindered by the employer's choice in the health plan for their employees or an individual's ability to pay for a health plan. These represent some of the many barriers to choice facing patients in the American model of health insurance.
As the hospitalist system grows to become the accepted mode of hospital care, more patients need to be informed about the transition of care to another physician and what steps are taken to ensure appropriate continuity of care. Transfers of patients from PCPs to hospitalists must be voluntary, with the decision left to patient care preferences.48 Educating patients in the outpatient setting about the hospitalist model, its benefits, risks, and alternatives, is necessary for them to make informed decisions about hospital care. This will require the collaboration of PCPs and hospitalists together. The continued success of the model depends on the nurturance of the partnership between the PCP, the hospitalist, and the patient.
Meltzer and Herthko14 have proposed that patients pay a premium for the option to choose a PCP that is not mandated to transfer their care to a hospitalist, in order to offset cost savings with the hospitalist system. Yet Meltzer and Herthko's14 study suggests that many patients could not afford to pay this premium and, in effect, patient autonomy would be preserved for the affluent. This raises the oft‐neglected professional ethic of justice for low‐income patients. Alexander and Lantos49 were resigned to see this infringement on patient autonomy as an inevitable consequence of balancing the desires of patients with the drive to lower cost and improve outcomes. If the hospitalist model grows to be the predominant mode of care, it is unclear if patient choice can survive. Investigators need to test whether the advantages of hospitalist care can coexist with voluntary programs. If it proves that they indeed cannot, then the hospitalist system will need to respond to concerned patients with honest answers and find pragmatic solutions to diminishing patient choice.
Conflict of Interest
The hospitalist system's main benefit of cost‐savings prompted Pantilat et al.6 to wonder whether hospitalists would face a conflict of interest between what is best for the patient and what financial incentives and utilization review encourage or require them to do. The financial support provided by many hospitals to meet the operating expenses of hospitalist programs is often associated with explicit or implicit incentives to reduce the length of hospital stay and costs.50 With hospitals employing hospitalists and increasingly pressuring them to decrease length of stay and discharge patients quickly, patients may have no advocate to protect them from discharge planners. Many hospitalists supplement their income by supervising discharge planners, and a dispute would put the hospitalist in the uncomfortable position of advocating for his patient against his employer and colleagues. While conflicts of interests occur in many managed care arrangements, they may be more acute in hospitalist systems. A weakened patient‐physician relationship may put the patients' best interest inferior to the employer's interests. Hospitalists do not immediately deal with adverse consequences of premature discharges in the outpatient setting and virtually no malpractice case law considers the obligations and practices of hospitalists in these settings.51
The SHM identified a core competency of hospitalists to
recommend treatment options that optimize patient care, include consideration of resource utilization, and are formulated without regard to financial incentives or other conflicts of interest.52
Ethical issues concerning conflict of interest remain unanswered, largely because no information about organizational features such as explicit incentives for reductions in length of stay is available to researchers or to patients. This is the wrong approach and only feeds the fear that hospitalists may weigh patients' best interest with financial incentives. Abbo and Volandes53 have argued that ambivalence to cost considerations is hazardous. If the hospitalist model cannot be forthright with the active considerations of costs in daily clinical practice, it is unlikely to truly make strides at cost savings, and may even raise the cost of care in the long run.
Jonsen et al.54 provide ethical standards for considering costs in clinical decisions. First, a physician's first priority should be to provide patient‐centered care that focuses on medical indications and patient preferences. Second, quality care does not mean all available care; quality care reflects what is not only diagnostically sound and technically correct, but also appropriate. Third, conflicts of interest are most vulnerable when there is a failing of the patient‐physician relationship. Health care organizations should expect physicians to argue for policies that provide all services that have a reasonable likelihood of benefiting the patient. Fourth, patient and physician autonomy and freedom of choice should be maximized within the limits of the system. Persons should be fully informed of the constraints of the system before choosing it. Plans need to disclose any financial incentive arrangements that exist between the plan and the physician. And incentive arrangements should be based on quality of care rather than on underutilization of care services. Fifth, the system should reflect principles of just distribution, ensuring that all who have a fair claim to service should receive it without discrimination. Last, capitation plans should share risks among physicians, not patients, while incentives are provided for improvements in access, prevention, and patient satisfaction.
Conflicts of interest have been a concern for as long as physicians have been paid for services. Fears about interference into the doctor‐patient relationship, whether they are from government or business, continue to stall real efforts to lower skyrocketing medical costs. The hospitalist model rebuts conflict of interest claims with improved outcomes, efficiency, and quality of care in the many reviews cited above. These arguments do prove that the hospitalist model's emphasis on medically indicated and appropriate care does address Jonsen et al.'s54 first and second standards. Yet, as Jonsen et al.54 point out, without strongly emphasizing the patient‐physician relationship and patient autonomy, it leaves itself vulnerable to creating conflicts of interest. Hospitalist systems need to be forthright about their explicit or implicit incentive structures and disclose this information to patients in a timely manner for them to make informed decisions. These incentives should be linked to quality of care and patient satisfaction, not cost savings. Last, hospitalist training programs should make ethical cost considerations a core competency of their curriculum.
Conclusions
Hospitalism was founded on the premise that it could improve the quality and reduce the cost of hospital care. Many randomized studies have all but definitively proven this original assertion. It is now time for the model to prove that these gains are not to the detriment of the patient‐physician relationship. Hospitalism must define itself as the steward of this relationship, valuing it as much as it values outcomes and costs. This is of particular concern in the United States as Medicare Part A (payment for inpatient care) is scheduled to go bankrupt in 2019, leading to potentially reasonable fears of hospital‐motivated cost containment.57
Investigators must find an outcome that encompasses the complexity of the patient‐physician relationship, and methods to improve it must be studied and improved upon. Preserving the patient‐physician relationship is a systemic issue, and full‐time hospitalists may be in the best position to implement systemic reforms to improve communication and continuity of care. Pham's56 case study of a hospitalist piecing together disparate parts of the patient's story illustrates this point. This should include more investigation into the prevalence of use and success of methods aimed at protecting the patient‐physician relationship at critical points in the handover of care. When proven successful, The SHM should propose new standards and safeguards to insure that these methods become standard practice in patient care. This effort, led by Snow et al.,57 is currently underway.
A hospitalist model that does not emphasize mitigating the effects of the diminishing patient‐physician relationship leaves itself exposed to further infringements on autonomy and choice. It is unclear whether patient autonomy and choice can coexist in a successful hospitalist system. The consequences of these unanswered ethical questions need to be explored. The professions of primary care need to be more proactive in educating patients about choice of care in hospitals, and hospitalists need to provide that choice, allowing voluntary programs in hospital care when feasible.
When combined, a wounded patient‐physician relationship and impaired patient autonomy leave the hospitalist model vulnerable to claims of financial and fiduciary conflict of interest. These concerns need not be inherent to the hospitalist systems, but hospitalists will need to be forthright and honest about incentives structures, and link them to quality of care and patient satisfaction, not to efficiency and cost savings.
It is indeed time for hospitalism to move onaway from proving its founding premise, and toward addressing these lingering ethical issues. Hospitalism's continued growth and success depends on it.
Wachter and Goldman1 first described hospitalists in 1996 as a new breed of physicians who devote blocks of time exclusively to the care of hospitalized patients. Since its definition, the hospitalist model has prompted 2 major debates. First, does the hospitalist system improve clinical efficiency, quality of care, cost effectiveness, and patient satisfaction? A series of large and small randomized trials have all but definitively proven the hospitalist model's advantage. Yet whether the hospitalist model is good for patient care has proven to remain contentious, as most recently demonstrated by the discussion between Williams2 and Centor3 and others like it.4, 5 What is clear in these exchanges is that the debate has shifted to the second great debate: does the hospitalist model pose inherent conflicts in clinical ethics? What are the implications of the purposeful discontinuity in care, the autonomy issues raised by mandatory hospitalist use, and the structural management issues that potentially pit hospitalists against patients in fiduciary and financial conflicts of interest? These important issues are certainly not new, and the hospitalist model has made much effort to address some of them.6, 7 This work aims to serve as a review of these important ethical concerns, demonstrating how some questions have been answered, while some remain unanswered.
The Hospitalist Model's Founding Premise
A growing threshold for hospital admission in the last 3 decades caused primary care physicians (PCPs) to see a diminishing number of inpatients. A survey in 1978 found that PCPs spent 40% of their time in the hospital, rounding on 10 patients per day.8 By 2001, PCPs spent 10% of their time in the hospital on average, and most PCPs rounded on fewer than 2 inpatients per day.9 The cost of inefficiencies associated with primary coordination of care in the hospital increasingly outweighed the tradeoff of preserving the patient‐PCP relationship in the hospital. Converging with increasing attention on cost controls through the restructuring of service provision, the hospitalist was born. Wachter10 argued that the hospitalist model could alleviate inpatient demands placed on PCPs while improving the outcomes and lowering the cost of care for hospitalized patients.
Early on there were setbacks to proving Wachter's10 case. Small studies found hospitalists to have higher hospital charges and longer length of stays.11 A survey of PCPs found only 56% were satisfied with communication with hospitalists and that most believed that patients generally preferred to be cared for in the hospital by their regular physician.12, 13 Meltzer and Herthko14 found 70% of people sampled said they would prefer care by their own physician to that of a hospitalist if they were hospitalized for a general medical condition. Yet this study found in a national random‐digit phone survey that only 10% of the respondents would pay $750 for their PCP to follow them to the hospital, the cost savings of the hospitalist system proven by the only 2 randomized trials performed at the time.15, 16 To 90% of respondents, the value of the PCP at the bedside was not worth the cost tradeoff to keep them there.
The meteoric rise in the number of hospitalists reflects the many studies and reviews that affirmed the premise that hospitalists improved inpatient efficiency without harmful effects on quality of care.17, 18 In a large retrospective cohort study of over 75,000 patients in 45 hospitals across the country, Lindenauer et al.19 found that hospitalists had a $268 lower cost when compared to internists, $125 lower cost when compared to family physicians, and a shorter hospital stay by about one‐half day when compared to both groups. The group found no significant difference in rates of death or readmission rates. While called modest in the text, these savings over time and volume add up for hospitals. Patients benefit from hospitalist care, researchers hypothesize, because of their familiarity with hospital systems, their increased availability to patients, and their experience with common hospital problems. Though the Lindenauer et al.19 study was criticized for design flaws, it prompted the editorialist McMahon20 to assert that the question was sufficiently answered, and it was time to move on away from the studies focusing on cost and comparing outcomes. As Wachter21 wrote, the demand for hospitalists is now relatively de‐linked from the field's original premiseefficiency advantagesand is now both more diversified and more robust. The model has become an accepted mode of care for hospitalized patients, with up to 20,000 hospitalists currently practicing in 29% of all hospitals and in over one‐half of hospitals with over 200 beds in the United States.22, 23
The Patient‐Physician Relationship
Purposeful discontinuity of care in the hospitalist system has the potential to diminish the doctor‐patient relationship.12 This relationship is built on a bond of loyalty, confidentiality, and trust. Handing off care to a hospitalist when the patient is most vulnerable can be viewed as a violation of this covenant. According to Meltzer,24 the hospitalist model pits Franicis Peabody's25 intimate personal relationship between patient and physician against Adam Smith et al.'s11 benefits of specialization. Peabody25 observed that physicians' lack of understanding of their patients as persons is especially acute in the hospital, where
one gets in the habit of using the oil immersion lamp instead of the low power, and focuses too intently in the center of the field. . . . The institutional eye tends to become focused on the lung, and it forgets that the lung is only one member of the body.
This movement toward patient‐centered medicine fits into an ever‐growing sentiment to value the social as well as the physiological, a holistic approach to the patient as a person. This emphasis was the original justification for PCPs to coordinate increasingly specialized hospital care and translate recommendations suitable to patients. Can the long‐term relationship between patient and PCP be replaced by the hospital generalist, or would hospitalists be inherently deficient in their abilities to coordinate care appropriate for patients? Hospitalized patients are frequently in no position to make complex decisions regarding their care.26 Lo7 argues that PCPs who know patients over extended periods of time are in a better position to respect patient wishes by individualizing discussions with patients and checking that patients' decisions are consistent with their core values. The long‐term relationship is also critical for designing a complex discharge plan suitable to the patients' ability and resources. Information about long‐term patient compliance with medications is much more available to PCPs. Patients trust physicians to keep promises made concerning end‐of‐life issues, and these assurances are vulnerable during handoffs of care. Pantilat et al.6 provide a case study of an outpatient Do‐Not‐Resuscitate order ineffective in the hospital. These scenarios occur because most written advance directives are unavailable in acute situations, and when they are, hospitalists unfamiliar with the patient's wishes may hesitate to act on directives not specific enough to answer the acute clinical question.27
Hospitalists' broadened responsibility to systematically improve the care of patients may potentially improve end‐of‐life care. Patient values can be better communicated to hospitalists by encouraging inpatients to complete advance directive surveys and then asking hospitalists to discuss those directives with their patients.6 Significantly, Auerbach and Pantilat28 found that end‐of‐life care was improved with hospitalist care. This chart review found hospitalists more likely to have discussions with patients and their families regarding care and providing comfort care more frequently at the time of death than community‐based physicians. The authors hypothesize that hospitalists may have better communication with dying patients and their families because they spend more time in the hospital each day, using frequent meetings to better understand the preferences of patients. These preferences often require clarification and often change after admission, making previous discussions about end‐of‐life care with PCPs moot. Greater expertise in hospital care may also allow hospitalists to better recognize patients who are nearing death and may explain the fewer symptoms documented by Auerbach and Pantilat28 at the end of life among patients cared for by hospitalists compared to community‐based physicians.
Hospital medicine has taken continuity of care issues seriously, and responded by making pragmatic recommendations to preserve the patient‐PCP relationship in the hospital and assuage the perception that patients have been dropped. Harlan et al.29 identify important issues around good communication between pediatric hospitalists and PCPs including the content and timing of communication beneficial to the patient. Hospitalists can use a standard script for introducing themselves to patients, explaining their role, and their continued coordination with the PCP.30 PCPs can still be involved in the care of their patients in hospitals through continuity visits or phone calls with patients and through better communication with hospitalists.31 Generally, reimbursing PCPs for their increased role in the hospitalist system can encourage better communication with hospitalists.19 Potential disagreements between PCPs and hospitalist regarding the care of the patient can be resolved through explicit conflict resolution procedures within the hospitalist system.6
These procedural solutions are only as successful as they are used. A large review by Kripalani et al.32 found communication between hospitalists and PCPs occurred infrequently (3%‐20%), affecting the quality of care in approximately 25% of follow‐up visits and contributing to PCP dissatisfaction. Sharma et al.33 found that continuity visits decreased from 50.5% in 1996 to 39.8% in 2006. In a survey of patients cared for in a hospitalist system, Hruby et al.34 found that 33% of hospitalized patients had some contact with their PCP directly and 66% of patients were satisfied with the contact they or their relative had with their PCP. When probed, patient satisfaction is too vague a measurement to assess the complex value of the patient‐physician relationship. Studying these issues may require relying more on individualized narratives rather than generalized statistics, or may require years of follow‐up. As Centor3 argues, we need this broader perspective of the patient's experience in order to understand the effects of the hospitalist model on patient trust in their PCP and in their overall care. Studies by Davis et al.35 and Halpert et al.36 assert that rising quality of care and patient satisfaction with the hospitalist system rebuts coordination of care concerns. Yet we need more studies investigating the relationship between improved communication and patient outcomes, as evidence is currently conflicting on this subject.32, 37, 38
The Journal of Hospital Medicine has pursued this research agenda; the April 2009 issue presents several studies describing best practices in the discharging of hospitalized patients. Manning et al.39 describe a tool to assess patient mobility after discharge, and O'Leary et al.40 used electronic health records to create a better discharge summary. Project BOOST (Better Outcomes for Older Adults Through Safe Transitions) has shown improvements in discharge transition procedures41 and the use of transition coaches for vulnerable older patients has been proven cost‐effective and has been scaled up to more than 100 healthcare organizations.42, 43
Inpatient care handoff to PCPs is not entirely novel, as surgeons, oncologists, cardiologists, and other specialists have always grappled with continuity of care. It would be prudent to investigate what can be learned from these efforts, and which practices can be best applied to the hospitalist model. More longitudinal studies need to investigate the prevalence and success of the procedural recommendations to preserve the patient‐physician relationship. We need to know more about what works and what does not. How have hospitals found novel ways in implementing these approaches, and how can they be applied to a diversity of hospital settings? We need a better outcome measurement than patient or physician satisfaction for probing the subtleties of the patient‐physician relationship. There is a sizeable population that does not have a PCP to care for them before hospitalization or after discharge, and discussions about continuity of care must address these patients. Last, these best practices and patient centered values need to be incorporated into the core competencies of residencies and fellowships for a new generation of hospitalists.
Maintaining the continuity of the physician‐patient relationship is an integral part of the original premise of the hospitalist model. Importantly, Meltzer24 found that this discontinuity within the hospital has the potential to eliminate the savings of the hospitalist system. Yet concerns about continuity of care do not sufficiently encompass the complexand at times fragilerelationship between physician and patient. The survival of the physician‐patient relationship depends on the hospitalist model's affirmation of the values of coordination and Peabody's25 approach to patient‐centered care. If the hospitalist model is to thrive, it needs to emphasize its duty as steward of the PCP‐patient relationship as much as it focuses on efficiency and cost‐effectiveness.
Patient Autonomy
The mandatory transfer of patients into the hospitalist model raises serious ethical issues. A survey in 2000 of PCPs found that 23% were required to use hospitalists for all admissions.44 Other surveys found this prevalence to be as low as 2%.12 Nevertheless, several high profile cases of Health Maintenance Organizations (HMOs)Prudential HealthCareSouth Florida, Prudential, Humana, and Cigna Corporationall using mandatory hospitalists, prompted protests from professional organizations and there were even legislative efforts to ban the practice of the mandatory use of hospitalists in 2000 and 2001.45 Today, most insurance plans, as well as the Society of Hospital Medicine (SHM), support voluntary rather than mandatory hospitalist use.46 Yet while not mandatory, the hospitalist is the default provider in many settings, giving a de facto mandate for hospitalist care. As Royo et al.47 point out, the rise in physician employment by hospitals has facilitated a self‐selecting progression toward a structural network that closely resembles the mandatory model.
While PCPs and internists contested mandatory hospitalist plans as infringements on their autonomy, they overlooked the harm to the patient's autonomy. When healthy in the ambulatory setting, the patient has the opportunity to choose his or her doctor to provide longitudinal care. When the patient is admitted acutely to a hospital, the patient does not have the freedom to choose a physician; the patient is assigned to the hospitalist on duty that night. This call for patient autonomy is of utmost importance in the hospitalized patient, where patients are increasingly sicker, their diseases under a high‐powered lens, and their options diminished. This freedom of choice is integral to the patient‐physician partnership. Yet this freedom of choice is largely hindered by the employer's choice in the health plan for their employees or an individual's ability to pay for a health plan. These represent some of the many barriers to choice facing patients in the American model of health insurance.
As the hospitalist system grows to become the accepted mode of hospital care, more patients need to be informed about the transition of care to another physician and what steps are taken to ensure appropriate continuity of care. Transfers of patients from PCPs to hospitalists must be voluntary, with the decision left to patient care preferences.48 Educating patients in the outpatient setting about the hospitalist model, its benefits, risks, and alternatives, is necessary for them to make informed decisions about hospital care. This will require the collaboration of PCPs and hospitalists together. The continued success of the model depends on the nurturance of the partnership between the PCP, the hospitalist, and the patient.
Meltzer and Herthko14 have proposed that patients pay a premium for the option to choose a PCP that is not mandated to transfer their care to a hospitalist, in order to offset cost savings with the hospitalist system. Yet Meltzer and Herthko's14 study suggests that many patients could not afford to pay this premium and, in effect, patient autonomy would be preserved for the affluent. This raises the oft‐neglected professional ethic of justice for low‐income patients. Alexander and Lantos49 were resigned to see this infringement on patient autonomy as an inevitable consequence of balancing the desires of patients with the drive to lower cost and improve outcomes. If the hospitalist model grows to be the predominant mode of care, it is unclear if patient choice can survive. Investigators need to test whether the advantages of hospitalist care can coexist with voluntary programs. If it proves that they indeed cannot, then the hospitalist system will need to respond to concerned patients with honest answers and find pragmatic solutions to diminishing patient choice.
Conflict of Interest
The hospitalist system's main benefit of cost‐savings prompted Pantilat et al.6 to wonder whether hospitalists would face a conflict of interest between what is best for the patient and what financial incentives and utilization review encourage or require them to do. The financial support provided by many hospitals to meet the operating expenses of hospitalist programs is often associated with explicit or implicit incentives to reduce the length of hospital stay and costs.50 With hospitals employing hospitalists and increasingly pressuring them to decrease length of stay and discharge patients quickly, patients may have no advocate to protect them from discharge planners. Many hospitalists supplement their income by supervising discharge planners, and a dispute would put the hospitalist in the uncomfortable position of advocating for his patient against his employer and colleagues. While conflicts of interests occur in many managed care arrangements, they may be more acute in hospitalist systems. A weakened patient‐physician relationship may put the patients' best interest inferior to the employer's interests. Hospitalists do not immediately deal with adverse consequences of premature discharges in the outpatient setting and virtually no malpractice case law considers the obligations and practices of hospitalists in these settings.51
The SHM identified a core competency of hospitalists to
recommend treatment options that optimize patient care, include consideration of resource utilization, and are formulated without regard to financial incentives or other conflicts of interest.52
Ethical issues concerning conflict of interest remain unanswered, largely because no information about organizational features such as explicit incentives for reductions in length of stay is available to researchers or to patients. This is the wrong approach and only feeds the fear that hospitalists may weigh patients' best interest with financial incentives. Abbo and Volandes53 have argued that ambivalence to cost considerations is hazardous. If the hospitalist model cannot be forthright with the active considerations of costs in daily clinical practice, it is unlikely to truly make strides at cost savings, and may even raise the cost of care in the long run.
Jonsen et al.54 provide ethical standards for considering costs in clinical decisions. First, a physician's first priority should be to provide patient‐centered care that focuses on medical indications and patient preferences. Second, quality care does not mean all available care; quality care reflects what is not only diagnostically sound and technically correct, but also appropriate. Third, conflicts of interest are most vulnerable when there is a failing of the patient‐physician relationship. Health care organizations should expect physicians to argue for policies that provide all services that have a reasonable likelihood of benefiting the patient. Fourth, patient and physician autonomy and freedom of choice should be maximized within the limits of the system. Persons should be fully informed of the constraints of the system before choosing it. Plans need to disclose any financial incentive arrangements that exist between the plan and the physician. And incentive arrangements should be based on quality of care rather than on underutilization of care services. Fifth, the system should reflect principles of just distribution, ensuring that all who have a fair claim to service should receive it without discrimination. Last, capitation plans should share risks among physicians, not patients, while incentives are provided for improvements in access, prevention, and patient satisfaction.
Conflicts of interest have been a concern for as long as physicians have been paid for services. Fears about interference into the doctor‐patient relationship, whether they are from government or business, continue to stall real efforts to lower skyrocketing medical costs. The hospitalist model rebuts conflict of interest claims with improved outcomes, efficiency, and quality of care in the many reviews cited above. These arguments do prove that the hospitalist model's emphasis on medically indicated and appropriate care does address Jonsen et al.'s54 first and second standards. Yet, as Jonsen et al.54 point out, without strongly emphasizing the patient‐physician relationship and patient autonomy, it leaves itself vulnerable to creating conflicts of interest. Hospitalist systems need to be forthright about their explicit or implicit incentive structures and disclose this information to patients in a timely manner for them to make informed decisions. These incentives should be linked to quality of care and patient satisfaction, not cost savings. Last, hospitalist training programs should make ethical cost considerations a core competency of their curriculum.
Conclusions
Hospitalism was founded on the premise that it could improve the quality and reduce the cost of hospital care. Many randomized studies have all but definitively proven this original assertion. It is now time for the model to prove that these gains are not to the detriment of the patient‐physician relationship. Hospitalism must define itself as the steward of this relationship, valuing it as much as it values outcomes and costs. This is of particular concern in the United States as Medicare Part A (payment for inpatient care) is scheduled to go bankrupt in 2019, leading to potentially reasonable fears of hospital‐motivated cost containment.57
Investigators must find an outcome that encompasses the complexity of the patient‐physician relationship, and methods to improve it must be studied and improved upon. Preserving the patient‐physician relationship is a systemic issue, and full‐time hospitalists may be in the best position to implement systemic reforms to improve communication and continuity of care. Pham's56 case study of a hospitalist piecing together disparate parts of the patient's story illustrates this point. This should include more investigation into the prevalence of use and success of methods aimed at protecting the patient‐physician relationship at critical points in the handover of care. When proven successful, The SHM should propose new standards and safeguards to insure that these methods become standard practice in patient care. This effort, led by Snow et al.,57 is currently underway.
A hospitalist model that does not emphasize mitigating the effects of the diminishing patient‐physician relationship leaves itself exposed to further infringements on autonomy and choice. It is unclear whether patient autonomy and choice can coexist in a successful hospitalist system. The consequences of these unanswered ethical questions need to be explored. The professions of primary care need to be more proactive in educating patients about choice of care in hospitals, and hospitalists need to provide that choice, allowing voluntary programs in hospital care when feasible.
When combined, a wounded patient‐physician relationship and impaired patient autonomy leave the hospitalist model vulnerable to claims of financial and fiduciary conflict of interest. These concerns need not be inherent to the hospitalist systems, but hospitalists will need to be forthright and honest about incentives structures, and link them to quality of care and patient satisfaction, not to efficiency and cost savings.
It is indeed time for hospitalism to move onaway from proving its founding premise, and toward addressing these lingering ethical issues. Hospitalism's continued growth and success depends on it.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .Hospitalists and the hospital medicine system of care are good for patient care.Arch Intern Med.2008;168(12):1254–1256, discussion 1259–1260.
- .A hospitalist inpatient system does not improve patient care outcomes.Arch Intern Med.2008;168(12):1257–1258, discussion 1259–1260.
- .Are inpatients' needs better served by hospitalists than by their family doctors?: Yes.Can Fam Physician.2008;54(8):1100–1101,1104–1106.
- .Are inpatients' needs better served by hospitalists than by their family doctors?: No.Can Fam Physician.2008;54(8):1101–1103,1105–1107.
- ,,.A new doctor in the house: ethical issues in hospitalist systems.JAMA.1999;282:171–174.
- .Ethical and policy implications of hospitalist systems.Dis Mon.2002;48:281–290.
- Robert Wood Johnson Foundation.Medical Practice in the United States.Princeton, NJ:The Robert Wood Johnson Foundation;1981.
- .Response to David Meltzer's paper “Hospitalists and the doctor‐patient relationship.”J Legal Stud2001;30:615–623.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- ,,.Primary care family physicians and 2 hospitalists models: comparison of outcomes, processes, and costs.J Fam Prac.2002;51:1021–1027.
- ,,, et al.Primary care physician attitudes regarding communication with hospitalists.Dis Mon.2002;48(4):218–229.
- ,,, et al.Physician attitudes towards and prevalence of the hospitalist model of care: results of a national survey.Am J Med.2000;109:648–653.
- ,.Patients' willingness to pay for hospital care by their primary care physician versus hospitalists: results of a national survey. [Society of General Internal Medicine 23rd annual meeting. Boston, Massachusetts, USA. May 4–6, 2000. Abstracts.]J Gen Intern Med.2000;15(suppl 1):135.
- ,,, et al.Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560.
- ,,, et al.Effects of hospitalist physicians on an academic general medicine service: results of a randomized trial. [22nd Annual meeting of The Society of General Internal Medicine. San Francisco, California, USA. April 29‐May 1, 1999. Abstracts.]J Gen Intern Med.1999;14(suppl 2):112.
- ,.The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- ,.Economic and healthcare forces of hospitalist movement.Mt Sinai J Med.2008;75(5):424–429.
- ,,, et al.Outcomes of care by hospitalists, general internists, and family physicians.N Engl J Med.2007;357:2589–2600.
- .The hospitalist movement—time to move on.N Engl J Med.2007;357:2627–2629.
- .Today's New England Journal Hospitalist Study. Weblog Entry.Wachter's World: The Hospitalist.2007. Available at: http://www.the‐hospitalist.org/blogs/wachters_world/archive/2007/12/20/today‐s‐new‐england‐journal‐hospitalist‐study.aspx. Accessed July 2009.
- ,,, et al.The Rise of the Hospitalist in California.Oakland, CA:California Health Care Foundation;2007.
- ,,, et al.The status of hospital medicine groups in the United States.J Hosp Med.2006;1:75–80.
- .Hospitalists and the doctor patient relationship.J Legal Stud.2001;2:615–623.
- .Landmark article March 19, 1927: the care of the patient. By Francis W. Peabody.JAMA.1984;252:813–818.
- .The Practice of Autonomy: Patients, Doctors, and Medical Decisions.New York, NY:Oxford University Press;1998.
- ,,, et al.A prospective study of advance directives for life‐sustaining care.N Engl J Med.1991;324:882–888.
- ,.End‐of‐life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms.Am J Med.2004;116:669–675.
- ,,, et al.Pediatric hospitalists and primary care providers: a communication needs assessment.J Hosp Med.2009;4(3):187–193.
- .What should you say after “Hello”?Today's Hospitalist Apr2008. Available at: http://www.todayshospitalist.com/index.php?b=articles_read48:267–272.
- ,,, et al.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297(8):831–841.
- ,,, et al.Continuity of outpatient and inpatient care by primary care physicians for hospitalized older adults.JAMA.2009;301(16):1671–1680.
- ,,.How do patients view the role of the primary care physician in inpatient care?Dis Mon.2002;48:230–238.
- ,,, et al.Effects of hospitalists on cost, outcomes and patient satisfaction in a rural health system.Am J Med.2000;108:621–626.
- ,,, et al.The impact of an inpatient physician program on quality, utilization, and satisfaction.Am J Manag Care.2000;6:549–555.
- ,,, et al.Association of communication between hospital‐based physicians and primary care providers with patient outcomes.J Gen Intern Med.2009;24:381–386.
- ,,.Rehospitalizations among patients in the Medicare fee‐for‐service program.N Engl J Med.2009;360(14):1418–1428.
- ,,.Home alone: mobility independence before discharge.J Hosp Med.2009;4:252–254.
- ,,, et al.Creating a better discharge summary: improvement in quality and timeliness using an electronic discharge summary.J Hosp Med.2009;4:219–225.
- Society of Hospital Medicine. BOOSTing Care Transitions Resource Room. Available at: http://www.hospitalmedicine.org. Accessed July2009.
- ,,,.The care transitions intervention: results for a randomized control trial.Arch Intern Med.2006;166:1822–1828.
- Care Transitions Program. Available at: http://www.caretransitions.org. Accessed July2009.
- ,,, et al.Friend or foe? How primary care physicians perceive hospitalists.Arch Intern Med.2000;160(19):2902–2908.
- .Use of mandatory hospitalists blasted.ACP‐ASIM Observer, May1999. Available at: http://www.acpinternist.org/archives/1999/05/hosps.htm. Accessed July 2009.
- .Hospitalists: the next big thing?Trustee Magazine, May2005. Available at: http://www.trusteemag.com/trusteemag_app/jsp/articledisplay.jsp?dcrpath=TRUSTEEMAG/PubsNewsArticleGen/data/2005/0505TRU_FEA_CoverStory. Accessed July 2009.
- ,,.Hospitalist medicine: voluntary or mandatory?Virtual Mentor.2008;10(12):813–816.
- .The hospitalist model: perspectives of the patient, the internist, and internal medicine.Ann Intern Med.1999;130:368–372.
- ,.The doctor‐patient relationship in the post‐managed care era.Am J Bioeth2006;6(1):29–32.
- ,,, et al.Health care market trends and the evolution of hospitalist use and roles.J Gen Intern Med.2005;20:101–107.
- .Key legal principles for hospitalists.Dis Mon.2002;48(4):197–206.
- Society of Hospital Medicine.Professionalism and medical ethics.J Hosp Med.2006;1:90–91.
- ,.Teaching residents to consider costs in medical decision making.Am J Bioeth2006;6(4):33–34.
- ,,.Clinical Ethics: A Practical Approach to Ethical Decision in Clinical Medicine.6th ed.New York, NY:McGraw‐Hill Medical;2006.
- ,. The 2004 Medicare and Social Security trustees reports. National Center for Policy Analysis, Study No. 266.2004. Available at: http://www.ncpa.org/pub/st/st266. Accessed July 2009.
- .Dismantling Rube Goldberg: cutting through the chaos to achieve coordinated care.J Hosp Med.2009;4(4):259–260.
- ,,, et al.Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine.J Hosp Med.2009;4:364–70. [http://dx.doi.org/10.1002/jhm.510]
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .Hospitalists and the hospital medicine system of care are good for patient care.Arch Intern Med.2008;168(12):1254–1256, discussion 1259–1260.
- .A hospitalist inpatient system does not improve patient care outcomes.Arch Intern Med.2008;168(12):1257–1258, discussion 1259–1260.
- .Are inpatients' needs better served by hospitalists than by their family doctors?: Yes.Can Fam Physician.2008;54(8):1100–1101,1104–1106.
- .Are inpatients' needs better served by hospitalists than by their family doctors?: No.Can Fam Physician.2008;54(8):1101–1103,1105–1107.
- ,,.A new doctor in the house: ethical issues in hospitalist systems.JAMA.1999;282:171–174.
- .Ethical and policy implications of hospitalist systems.Dis Mon.2002;48:281–290.
- Robert Wood Johnson Foundation.Medical Practice in the United States.Princeton, NJ:The Robert Wood Johnson Foundation;1981.
- .Response to David Meltzer's paper “Hospitalists and the doctor‐patient relationship.”J Legal Stud2001;30:615–623.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- ,,.Primary care family physicians and 2 hospitalists models: comparison of outcomes, processes, and costs.J Fam Prac.2002;51:1021–1027.
- ,,, et al.Primary care physician attitudes regarding communication with hospitalists.Dis Mon.2002;48(4):218–229.
- ,,, et al.Physician attitudes towards and prevalence of the hospitalist model of care: results of a national survey.Am J Med.2000;109:648–653.
- ,.Patients' willingness to pay for hospital care by their primary care physician versus hospitalists: results of a national survey. [Society of General Internal Medicine 23rd annual meeting. Boston, Massachusetts, USA. May 4–6, 2000. Abstracts.]J Gen Intern Med.2000;15(suppl 1):135.
- ,,, et al.Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560.
- ,,, et al.Effects of hospitalist physicians on an academic general medicine service: results of a randomized trial. [22nd Annual meeting of The Society of General Internal Medicine. San Francisco, California, USA. April 29‐May 1, 1999. Abstracts.]J Gen Intern Med.1999;14(suppl 2):112.
- ,.The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- ,.Economic and healthcare forces of hospitalist movement.Mt Sinai J Med.2008;75(5):424–429.
- ,,, et al.Outcomes of care by hospitalists, general internists, and family physicians.N Engl J Med.2007;357:2589–2600.
- .The hospitalist movement—time to move on.N Engl J Med.2007;357:2627–2629.
- .Today's New England Journal Hospitalist Study. Weblog Entry.Wachter's World: The Hospitalist.2007. Available at: http://www.the‐hospitalist.org/blogs/wachters_world/archive/2007/12/20/today‐s‐new‐england‐journal‐hospitalist‐study.aspx. Accessed July 2009.
- ,,, et al.The Rise of the Hospitalist in California.Oakland, CA:California Health Care Foundation;2007.
- ,,, et al.The status of hospital medicine groups in the United States.J Hosp Med.2006;1:75–80.
- .Hospitalists and the doctor patient relationship.J Legal Stud.2001;2:615–623.
- .Landmark article March 19, 1927: the care of the patient. By Francis W. Peabody.JAMA.1984;252:813–818.
- .The Practice of Autonomy: Patients, Doctors, and Medical Decisions.New York, NY:Oxford University Press;1998.
- ,,, et al.A prospective study of advance directives for life‐sustaining care.N Engl J Med.1991;324:882–888.
- ,.End‐of‐life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms.Am J Med.2004;116:669–675.
- ,,, et al.Pediatric hospitalists and primary care providers: a communication needs assessment.J Hosp Med.2009;4(3):187–193.
- .What should you say after “Hello”?Today's Hospitalist Apr2008. Available at: http://www.todayshospitalist.com/index.php?b=articles_read48:267–272.
- ,,, et al.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297(8):831–841.
- ,,, et al.Continuity of outpatient and inpatient care by primary care physicians for hospitalized older adults.JAMA.2009;301(16):1671–1680.
- ,,.How do patients view the role of the primary care physician in inpatient care?Dis Mon.2002;48:230–238.
- ,,, et al.Effects of hospitalists on cost, outcomes and patient satisfaction in a rural health system.Am J Med.2000;108:621–626.
- ,,, et al.The impact of an inpatient physician program on quality, utilization, and satisfaction.Am J Manag Care.2000;6:549–555.
- ,,, et al.Association of communication between hospital‐based physicians and primary care providers with patient outcomes.J Gen Intern Med.2009;24:381–386.
- ,,.Rehospitalizations among patients in the Medicare fee‐for‐service program.N Engl J Med.2009;360(14):1418–1428.
- ,,.Home alone: mobility independence before discharge.J Hosp Med.2009;4:252–254.
- ,,, et al.Creating a better discharge summary: improvement in quality and timeliness using an electronic discharge summary.J Hosp Med.2009;4:219–225.
- Society of Hospital Medicine. BOOSTing Care Transitions Resource Room. Available at: http://www.hospitalmedicine.org. Accessed July2009.
- ,,,.The care transitions intervention: results for a randomized control trial.Arch Intern Med.2006;166:1822–1828.
- Care Transitions Program. Available at: http://www.caretransitions.org. Accessed July2009.
- ,,, et al.Friend or foe? How primary care physicians perceive hospitalists.Arch Intern Med.2000;160(19):2902–2908.
- .Use of mandatory hospitalists blasted.ACP‐ASIM Observer, May1999. Available at: http://www.acpinternist.org/archives/1999/05/hosps.htm. Accessed July 2009.
- .Hospitalists: the next big thing?Trustee Magazine, May2005. Available at: http://www.trusteemag.com/trusteemag_app/jsp/articledisplay.jsp?dcrpath=TRUSTEEMAG/PubsNewsArticleGen/data/2005/0505TRU_FEA_CoverStory. Accessed July 2009.
- ,,.Hospitalist medicine: voluntary or mandatory?Virtual Mentor.2008;10(12):813–816.
- .The hospitalist model: perspectives of the patient, the internist, and internal medicine.Ann Intern Med.1999;130:368–372.
- ,.The doctor‐patient relationship in the post‐managed care era.Am J Bioeth2006;6(1):29–32.
- ,,, et al.Health care market trends and the evolution of hospitalist use and roles.J Gen Intern Med.2005;20:101–107.
- .Key legal principles for hospitalists.Dis Mon.2002;48(4):197–206.
- Society of Hospital Medicine.Professionalism and medical ethics.J Hosp Med.2006;1:90–91.
- ,.Teaching residents to consider costs in medical decision making.Am J Bioeth2006;6(4):33–34.
- ,,.Clinical Ethics: A Practical Approach to Ethical Decision in Clinical Medicine.6th ed.New York, NY:McGraw‐Hill Medical;2006.
- ,. The 2004 Medicare and Social Security trustees reports. National Center for Policy Analysis, Study No. 266.2004. Available at: http://www.ncpa.org/pub/st/st266. Accessed July 2009.
- .Dismantling Rube Goldberg: cutting through the chaos to achieve coordinated care.J Hosp Med.2009;4(4):259–260.
- ,,, et al.Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine.J Hosp Med.2009;4:364–70. [http://dx.doi.org/10.1002/jhm.510]
Patient Hospital Financial Burden
Hospitalizations often impose a tremendous financial burden on patients and their families, adding to the stress and long‐term impact from medical illnesses. It is widely underappreciated that physicians can play an important role in substantially reducing patients' out‐of‐pocket expenses by participating in hospital‐based case review and utilization management. These topics are not a focus of most formal training curricula and unfortunately are typically viewed by medical staff as intrusive, time consuming, or only in terms of enhancing the facility's profitability. In reality, with strict rules governing insurance benefits the facility's interests are typically aligned with those of the patient.
One of the greatest impacts on a patient's financial liability is whether an admission is classified in observation vs. inpatient status, and is subject to much confusion. It is a common misperception that these are time‐based designations. Instead, they revolve around stringent medical necessity guidelines that examine the severity of the illness and the intensity of services provided.1 Inpatient stays may be brief, even a single day, if justified by medical need (although these short durations are closely scrutinized by the payors) or if involving a short list of procedures automatically triggering that status (ie, defibrillator placement).2 Conversely, observation status, although usually up to only 48 hours, can extend longer if inpatient criteria are never met and are then apt to generate large bills.
The key concept for the financial liability of patients in observation status is that their billing structure revolves around being categorized as outpatients, even though they stay overnight and are physically housed and cared for in the expensive hospital setting.3 This nonintuitive classification can culminate in unexpectedly high charges for which the patient is liable (Table 1): medications at inflated hospital pharmacy prices, especially when expensive antibiotics or immunosuppressive agents are administered (since outpatient prescriptions are not often covered by policies); ancillary services, radiology or laboratory tests with a high patient share of cost; and an hourly room charge that can easily exceed $30 per hour. The latter can be especially burdensome, as most insurance plans only cover the first 48 hours of observation. During that period the patient would be liable for just their copayment, but afterward they could be billed for the full amount. Hospitalizations well beyond the 48 hours can thus present tremendous hardships to those patients who never meet the stringent criteria for categorization as inpatients, and whose status thus must remain outpatient‐observation. Keeping patients over a weekend for procedures that are not available at the facility until the following Monday can put these individuals beyond the 48 hour observation interval and cause unintentional rapidly escalating out‐of‐pocket expenses. Other strategies to reduce the patient's financial liability include allowing patients to take their own medications from home (with pharmacy supervision and verification, per hospital guidelines), and limiting evaluations to just the admitting diagnosis (ie, pursuing other issues after discharge). In addition, an observation stay can never be ordered ahead of time for an outpatient procedure, as that type of admission is reserved for those individuals who unexpectedly need further care at the conclusion of the recovery period (typically 4 to 6 hours). Thus, the not uncommon practice of doing a patient a favor by letting them stay overnight after an outpatient procedure thereby can be a great disservice by dramatically increasing patient liability. One can well imagine how these scenarios lead to lay press exposs of the patient receiving a bill for a $25 aspirin and a night's stay 4 times more expensive than a luxury hotel. This is not to say that going home is the best or safest plan for a particular patient, but rather that the hospital is often an unnecessarily expensive (and in that sense inappropriate) location when there are alternatives. It is up to the individual hospital to determine how to handle rapidly escalating charges related to the admission status and the timeliness of a discharge. Many centers in effect write off highly select bills that are considered either uncollectible (ie, from indigent patients) or the fault of the facility's inefficiencies. So as not to have inconsistent billing policies across different insurers and patients, however, facilities are obligated to have uniform protocols for attempting to collect chargesa scenario that can be quite harsh for those individuals with significant and discoverable monetary resources.
| Observation (Outpatient Status) (Medicare Part B) | Inpatient (Medicare Part A) | |
|---|---|---|
| ||
| Room and board | Medicare deductible: $1068 per admission (waived if readmission in 60 days) | |
| 48 hours | 20% of allowable charge (APC) | |
| >48 hours | 100% hospital charges | |
| Medications | 100% hospital charges | |
| Supplies | Up to 100% hospital charges | |
| Surgical | ||
| Operating room | Typically 20% copay of APC | |
| Recovery room | Typically 20% copay of APC | |
| Diagnostic | ||
| Laboratory | 20% copay of allowable charges | |
| Radiology | 20% copay of allowable charges | |
| Ancillary | ||
| Physical therapy | 20% copay of allowable charges | |
| Occupational therapy | 20% copay of allowable charges | |
| Speech therapy | 20% copay of allowable charges | |
Working with the physician for a timely discharge, hospital case managers and social workers are likely to arrive at creative solutions in the patient's best financial interest (ie, taxicab coupons and inexpensive hotels). As many patients simply do not have the resources to cope with unplanned overnight charges, it behooves the physician to make every effort to start outpatient procedures early in the day so as to minimize the chance of logistic problems triggering a potentially expensive overnight hospital stay.
Compare the observation patient's liability to that of the typically much‐preferred status of inpatient (Table 1) in which all expenses are rolled into one diagnosis‐related group (DRG) prospective payment.3 In the case of Medicare, the patient's bill would be the inpatient deductible, and this might be covered in its entirety by a supplemental policy. One absolutely cannot, however, simply avoid using the observation status and instead make all admissions inpatients; this would cause unnecessary resource utilization and expose the hospital to denial of payment for the entire episode of care. To prevent this situation, there are nationally‐recognized guidelines that strictly define when a hospitalization warrants an inpatient level of care. Integral to the individual qualifying for their policy's inpatient benefit, however, is that the chart must reflect not just the severity of illness but also intensity of services ordered by the physician.1 Similarly, changing a patient's status (ie, from observation to inpatient) must follow rigorous guidelines wherein the justification and timing are fully described in the body of the chart to an extent that would withstand audit.
Consider the example (Table 2) of a patient with a leg fracture admitted for pain due to edema and early compartment syndrome: a scenario appropriate for inpatient status, liability of just the $1092 Medicare deductible, and eligibility for postdischarge skilled nursing facility care. Had the charting erroneously only indicated pain and need for a new cast, then observation status would have yielded a bill for $3426, plus out of pocket nursing home expenses of over $150/day.
| Patient Liability for Observation Status (Medicare Part B) | Inpatient Charges (Covered by Medicare Part A Deductible) | |
|---|---|---|
| ||
| Room and board | $1788 | $1030 |
| Medications | $755 | $1196 |
| Supplies | $106 | $528 |
| Procedures and emergency room | $229 | $1145 |
| Diagnostic | ||
| Laboratory | $72 | $359 |
| Radiology | $159 | $795 |
| Ancillary | ||
| Electrocardiogram | $22 | $110 |
| Physical therapy | $295 | $1475 |
| Patient liability for hospitalization | $3426 | $1068 deductible for total charges of $6638 |
| Patient liability for subsequent skilled nursing facility | $159 per day* | Small daily co‐pay* |
Not only does the physician need to accurately chart the reasons for admission, but it is also extremely helpful to specifically document why the patient is not amenable to outpatient therapy. Examples include a clearly articulated history of failed attempts at home or emergency room treatment, or the need for close monitoring (ie, telemetry). In this regard case managers also provide a fresh set of eyes to evaluate the clarity and completeness of medical charting. What seems like obvious decision‐making to a physician may require expanded detailed notes to satisfy a third‐party review.
The work design of the case managers and utilization review team varies between facilities. Ideally, cases are reviewed upon admission (or within the first 24 hours), and then periodically thereafter. Many medical centers have this process computerized, wherein inpatient criteria are available online and status issues can be tracked daily. This nearly real‐time information serves as the basis for interacting with the attending physician, and is necessary because the chart documentation may not be amended after discharge. Having a robust database for all admissions is also immensely helpful in those hospitals which employ a Physician Advisor (PA) as a liaison and educator to the medical staff. This newly and now nationally recognized PA position serves an important role in educating the providers not just about these patient advocacy topics, but also other issues such as length‐of‐stay. Interestingly, having the infrastructure of a criteria‐driven database to follow the intensity of inpatient services on a daily basis gives case managers an objective perspective of when a patient requires less care and is ready for transfer to a lower acuity facility or discharge home. Physician participation is important when the patient thus runs out of intensities, since there will need to be early coordination of efforts for home health or skilled nursing care, durable medical equipment supplies, or outpatient infusions. It is important that physicians not view these activities as an inappropriate rush for discharge. In our experience most patients are in fact much happier to be out of the hospital and receiving home or skilled nursing care. Those in need of physical or occupational therapy may in fact have superior care in facilities dedicated to those activities. In addition, unnecessarily prolonged hospitalizations carry their own risks, such as hospital‐acquired infections and deep venous thromboses. An additional motivator for discharge is that, just as there are insurance plan limits for outpatient benefits, there can also be caps for inpatient services. Physicians thus have a role in preserving the limited and precious number of covered inpatient days of care, beyond which time the patient would be financially totally responsible. For example, most states limit the number of inpatient days covered by Medicaid. In Florida there is a cap of only 45 days per year (unless the patient is pediatric or within the first year of a transplant4). Similarly, there have been patients and families shocked and ill‐prepared to discover that all their Medicare hospital benefits were exhausted5: a not well‐publicized possibility, as in the setting of expensive intensive care units, transplantation, or chemotherapy. Timely discharges and careful resource utilization by physicians thus not only help the hospital but also are important for the patient.
In summary, physicians need to be aware that there can be tremendous financial hardship to patients caused by inappropriate or unnecessarily long observation stays, especially in cases where an inpatient designation would have been justified by appropriate documentation. Case managers, although employed by the facility, can thus assist physicians in this regard and together play an important role as patient advocates.
- Interqual® Level of Care Criteria: Acute Care Adult.Newton, MA:McKesson Health Solutions;2009.
- Department of Health and Human Services (DHHS), Centers for Medicare and Medicaid Services (CMS).2008. Final changes to the hospital outpatient prospective payment system and CY 2009. Available at: http://www.cms.hhs.gov/HospitalOutpatientPPS/HORD/list.asp. Accessed September 2009.
- Department of Health and Human Services (DHHS), Centers for Medicare and Medicaid Services (CMS).2008. Medicare Program; Changes to the hospital inpatient prospective payment systems and fiscal year 2009 rates. Available at: http://www.cms.hhs.gov/AcuteInpatientPPS/IPPS/itemdetail.asp. Accessed September 2009.
- Florida Medicaid covered services. Available at: http://www.fdhc.state. fl.us/Medicaid/MediPass/pdf/HealthyOutcomesCoveredServicesFlyerEnglish 0606.pdf. Accessed September 2009.
- Medicare Benefit Policy Manual: Chapter 5. Lifetime reserve days. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c05.pdf. Accessed September 2009.
Hospitalizations often impose a tremendous financial burden on patients and their families, adding to the stress and long‐term impact from medical illnesses. It is widely underappreciated that physicians can play an important role in substantially reducing patients' out‐of‐pocket expenses by participating in hospital‐based case review and utilization management. These topics are not a focus of most formal training curricula and unfortunately are typically viewed by medical staff as intrusive, time consuming, or only in terms of enhancing the facility's profitability. In reality, with strict rules governing insurance benefits the facility's interests are typically aligned with those of the patient.
One of the greatest impacts on a patient's financial liability is whether an admission is classified in observation vs. inpatient status, and is subject to much confusion. It is a common misperception that these are time‐based designations. Instead, they revolve around stringent medical necessity guidelines that examine the severity of the illness and the intensity of services provided.1 Inpatient stays may be brief, even a single day, if justified by medical need (although these short durations are closely scrutinized by the payors) or if involving a short list of procedures automatically triggering that status (ie, defibrillator placement).2 Conversely, observation status, although usually up to only 48 hours, can extend longer if inpatient criteria are never met and are then apt to generate large bills.
The key concept for the financial liability of patients in observation status is that their billing structure revolves around being categorized as outpatients, even though they stay overnight and are physically housed and cared for in the expensive hospital setting.3 This nonintuitive classification can culminate in unexpectedly high charges for which the patient is liable (Table 1): medications at inflated hospital pharmacy prices, especially when expensive antibiotics or immunosuppressive agents are administered (since outpatient prescriptions are not often covered by policies); ancillary services, radiology or laboratory tests with a high patient share of cost; and an hourly room charge that can easily exceed $30 per hour. The latter can be especially burdensome, as most insurance plans only cover the first 48 hours of observation. During that period the patient would be liable for just their copayment, but afterward they could be billed for the full amount. Hospitalizations well beyond the 48 hours can thus present tremendous hardships to those patients who never meet the stringent criteria for categorization as inpatients, and whose status thus must remain outpatient‐observation. Keeping patients over a weekend for procedures that are not available at the facility until the following Monday can put these individuals beyond the 48 hour observation interval and cause unintentional rapidly escalating out‐of‐pocket expenses. Other strategies to reduce the patient's financial liability include allowing patients to take their own medications from home (with pharmacy supervision and verification, per hospital guidelines), and limiting evaluations to just the admitting diagnosis (ie, pursuing other issues after discharge). In addition, an observation stay can never be ordered ahead of time for an outpatient procedure, as that type of admission is reserved for those individuals who unexpectedly need further care at the conclusion of the recovery period (typically 4 to 6 hours). Thus, the not uncommon practice of doing a patient a favor by letting them stay overnight after an outpatient procedure thereby can be a great disservice by dramatically increasing patient liability. One can well imagine how these scenarios lead to lay press exposs of the patient receiving a bill for a $25 aspirin and a night's stay 4 times more expensive than a luxury hotel. This is not to say that going home is the best or safest plan for a particular patient, but rather that the hospital is often an unnecessarily expensive (and in that sense inappropriate) location when there are alternatives. It is up to the individual hospital to determine how to handle rapidly escalating charges related to the admission status and the timeliness of a discharge. Many centers in effect write off highly select bills that are considered either uncollectible (ie, from indigent patients) or the fault of the facility's inefficiencies. So as not to have inconsistent billing policies across different insurers and patients, however, facilities are obligated to have uniform protocols for attempting to collect chargesa scenario that can be quite harsh for those individuals with significant and discoverable monetary resources.
| Observation (Outpatient Status) (Medicare Part B) | Inpatient (Medicare Part A) | |
|---|---|---|
| ||
| Room and board | Medicare deductible: $1068 per admission (waived if readmission in 60 days) | |
| 48 hours | 20% of allowable charge (APC) | |
| >48 hours | 100% hospital charges | |
| Medications | 100% hospital charges | |
| Supplies | Up to 100% hospital charges | |
| Surgical | ||
| Operating room | Typically 20% copay of APC | |
| Recovery room | Typically 20% copay of APC | |
| Diagnostic | ||
| Laboratory | 20% copay of allowable charges | |
| Radiology | 20% copay of allowable charges | |
| Ancillary | ||
| Physical therapy | 20% copay of allowable charges | |
| Occupational therapy | 20% copay of allowable charges | |
| Speech therapy | 20% copay of allowable charges | |
Working with the physician for a timely discharge, hospital case managers and social workers are likely to arrive at creative solutions in the patient's best financial interest (ie, taxicab coupons and inexpensive hotels). As many patients simply do not have the resources to cope with unplanned overnight charges, it behooves the physician to make every effort to start outpatient procedures early in the day so as to minimize the chance of logistic problems triggering a potentially expensive overnight hospital stay.
Compare the observation patient's liability to that of the typically much‐preferred status of inpatient (Table 1) in which all expenses are rolled into one diagnosis‐related group (DRG) prospective payment.3 In the case of Medicare, the patient's bill would be the inpatient deductible, and this might be covered in its entirety by a supplemental policy. One absolutely cannot, however, simply avoid using the observation status and instead make all admissions inpatients; this would cause unnecessary resource utilization and expose the hospital to denial of payment for the entire episode of care. To prevent this situation, there are nationally‐recognized guidelines that strictly define when a hospitalization warrants an inpatient level of care. Integral to the individual qualifying for their policy's inpatient benefit, however, is that the chart must reflect not just the severity of illness but also intensity of services ordered by the physician.1 Similarly, changing a patient's status (ie, from observation to inpatient) must follow rigorous guidelines wherein the justification and timing are fully described in the body of the chart to an extent that would withstand audit.
Consider the example (Table 2) of a patient with a leg fracture admitted for pain due to edema and early compartment syndrome: a scenario appropriate for inpatient status, liability of just the $1092 Medicare deductible, and eligibility for postdischarge skilled nursing facility care. Had the charting erroneously only indicated pain and need for a new cast, then observation status would have yielded a bill for $3426, plus out of pocket nursing home expenses of over $150/day.
| Patient Liability for Observation Status (Medicare Part B) | Inpatient Charges (Covered by Medicare Part A Deductible) | |
|---|---|---|
| ||
| Room and board | $1788 | $1030 |
| Medications | $755 | $1196 |
| Supplies | $106 | $528 |
| Procedures and emergency room | $229 | $1145 |
| Diagnostic | ||
| Laboratory | $72 | $359 |
| Radiology | $159 | $795 |
| Ancillary | ||
| Electrocardiogram | $22 | $110 |
| Physical therapy | $295 | $1475 |
| Patient liability for hospitalization | $3426 | $1068 deductible for total charges of $6638 |
| Patient liability for subsequent skilled nursing facility | $159 per day* | Small daily co‐pay* |
Not only does the physician need to accurately chart the reasons for admission, but it is also extremely helpful to specifically document why the patient is not amenable to outpatient therapy. Examples include a clearly articulated history of failed attempts at home or emergency room treatment, or the need for close monitoring (ie, telemetry). In this regard case managers also provide a fresh set of eyes to evaluate the clarity and completeness of medical charting. What seems like obvious decision‐making to a physician may require expanded detailed notes to satisfy a third‐party review.
The work design of the case managers and utilization review team varies between facilities. Ideally, cases are reviewed upon admission (or within the first 24 hours), and then periodically thereafter. Many medical centers have this process computerized, wherein inpatient criteria are available online and status issues can be tracked daily. This nearly real‐time information serves as the basis for interacting with the attending physician, and is necessary because the chart documentation may not be amended after discharge. Having a robust database for all admissions is also immensely helpful in those hospitals which employ a Physician Advisor (PA) as a liaison and educator to the medical staff. This newly and now nationally recognized PA position serves an important role in educating the providers not just about these patient advocacy topics, but also other issues such as length‐of‐stay. Interestingly, having the infrastructure of a criteria‐driven database to follow the intensity of inpatient services on a daily basis gives case managers an objective perspective of when a patient requires less care and is ready for transfer to a lower acuity facility or discharge home. Physician participation is important when the patient thus runs out of intensities, since there will need to be early coordination of efforts for home health or skilled nursing care, durable medical equipment supplies, or outpatient infusions. It is important that physicians not view these activities as an inappropriate rush for discharge. In our experience most patients are in fact much happier to be out of the hospital and receiving home or skilled nursing care. Those in need of physical or occupational therapy may in fact have superior care in facilities dedicated to those activities. In addition, unnecessarily prolonged hospitalizations carry their own risks, such as hospital‐acquired infections and deep venous thromboses. An additional motivator for discharge is that, just as there are insurance plan limits for outpatient benefits, there can also be caps for inpatient services. Physicians thus have a role in preserving the limited and precious number of covered inpatient days of care, beyond which time the patient would be financially totally responsible. For example, most states limit the number of inpatient days covered by Medicaid. In Florida there is a cap of only 45 days per year (unless the patient is pediatric or within the first year of a transplant4). Similarly, there have been patients and families shocked and ill‐prepared to discover that all their Medicare hospital benefits were exhausted5: a not well‐publicized possibility, as in the setting of expensive intensive care units, transplantation, or chemotherapy. Timely discharges and careful resource utilization by physicians thus not only help the hospital but also are important for the patient.
In summary, physicians need to be aware that there can be tremendous financial hardship to patients caused by inappropriate or unnecessarily long observation stays, especially in cases where an inpatient designation would have been justified by appropriate documentation. Case managers, although employed by the facility, can thus assist physicians in this regard and together play an important role as patient advocates.
Hospitalizations often impose a tremendous financial burden on patients and their families, adding to the stress and long‐term impact from medical illnesses. It is widely underappreciated that physicians can play an important role in substantially reducing patients' out‐of‐pocket expenses by participating in hospital‐based case review and utilization management. These topics are not a focus of most formal training curricula and unfortunately are typically viewed by medical staff as intrusive, time consuming, or only in terms of enhancing the facility's profitability. In reality, with strict rules governing insurance benefits the facility's interests are typically aligned with those of the patient.
One of the greatest impacts on a patient's financial liability is whether an admission is classified in observation vs. inpatient status, and is subject to much confusion. It is a common misperception that these are time‐based designations. Instead, they revolve around stringent medical necessity guidelines that examine the severity of the illness and the intensity of services provided.1 Inpatient stays may be brief, even a single day, if justified by medical need (although these short durations are closely scrutinized by the payors) or if involving a short list of procedures automatically triggering that status (ie, defibrillator placement).2 Conversely, observation status, although usually up to only 48 hours, can extend longer if inpatient criteria are never met and are then apt to generate large bills.
The key concept for the financial liability of patients in observation status is that their billing structure revolves around being categorized as outpatients, even though they stay overnight and are physically housed and cared for in the expensive hospital setting.3 This nonintuitive classification can culminate in unexpectedly high charges for which the patient is liable (Table 1): medications at inflated hospital pharmacy prices, especially when expensive antibiotics or immunosuppressive agents are administered (since outpatient prescriptions are not often covered by policies); ancillary services, radiology or laboratory tests with a high patient share of cost; and an hourly room charge that can easily exceed $30 per hour. The latter can be especially burdensome, as most insurance plans only cover the first 48 hours of observation. During that period the patient would be liable for just their copayment, but afterward they could be billed for the full amount. Hospitalizations well beyond the 48 hours can thus present tremendous hardships to those patients who never meet the stringent criteria for categorization as inpatients, and whose status thus must remain outpatient‐observation. Keeping patients over a weekend for procedures that are not available at the facility until the following Monday can put these individuals beyond the 48 hour observation interval and cause unintentional rapidly escalating out‐of‐pocket expenses. Other strategies to reduce the patient's financial liability include allowing patients to take their own medications from home (with pharmacy supervision and verification, per hospital guidelines), and limiting evaluations to just the admitting diagnosis (ie, pursuing other issues after discharge). In addition, an observation stay can never be ordered ahead of time for an outpatient procedure, as that type of admission is reserved for those individuals who unexpectedly need further care at the conclusion of the recovery period (typically 4 to 6 hours). Thus, the not uncommon practice of doing a patient a favor by letting them stay overnight after an outpatient procedure thereby can be a great disservice by dramatically increasing patient liability. One can well imagine how these scenarios lead to lay press exposs of the patient receiving a bill for a $25 aspirin and a night's stay 4 times more expensive than a luxury hotel. This is not to say that going home is the best or safest plan for a particular patient, but rather that the hospital is often an unnecessarily expensive (and in that sense inappropriate) location when there are alternatives. It is up to the individual hospital to determine how to handle rapidly escalating charges related to the admission status and the timeliness of a discharge. Many centers in effect write off highly select bills that are considered either uncollectible (ie, from indigent patients) or the fault of the facility's inefficiencies. So as not to have inconsistent billing policies across different insurers and patients, however, facilities are obligated to have uniform protocols for attempting to collect chargesa scenario that can be quite harsh for those individuals with significant and discoverable monetary resources.
| Observation (Outpatient Status) (Medicare Part B) | Inpatient (Medicare Part A) | |
|---|---|---|
| ||
| Room and board | Medicare deductible: $1068 per admission (waived if readmission in 60 days) | |
| 48 hours | 20% of allowable charge (APC) | |
| >48 hours | 100% hospital charges | |
| Medications | 100% hospital charges | |
| Supplies | Up to 100% hospital charges | |
| Surgical | ||
| Operating room | Typically 20% copay of APC | |
| Recovery room | Typically 20% copay of APC | |
| Diagnostic | ||
| Laboratory | 20% copay of allowable charges | |
| Radiology | 20% copay of allowable charges | |
| Ancillary | ||
| Physical therapy | 20% copay of allowable charges | |
| Occupational therapy | 20% copay of allowable charges | |
| Speech therapy | 20% copay of allowable charges | |
Working with the physician for a timely discharge, hospital case managers and social workers are likely to arrive at creative solutions in the patient's best financial interest (ie, taxicab coupons and inexpensive hotels). As many patients simply do not have the resources to cope with unplanned overnight charges, it behooves the physician to make every effort to start outpatient procedures early in the day so as to minimize the chance of logistic problems triggering a potentially expensive overnight hospital stay.
Compare the observation patient's liability to that of the typically much‐preferred status of inpatient (Table 1) in which all expenses are rolled into one diagnosis‐related group (DRG) prospective payment.3 In the case of Medicare, the patient's bill would be the inpatient deductible, and this might be covered in its entirety by a supplemental policy. One absolutely cannot, however, simply avoid using the observation status and instead make all admissions inpatients; this would cause unnecessary resource utilization and expose the hospital to denial of payment for the entire episode of care. To prevent this situation, there are nationally‐recognized guidelines that strictly define when a hospitalization warrants an inpatient level of care. Integral to the individual qualifying for their policy's inpatient benefit, however, is that the chart must reflect not just the severity of illness but also intensity of services ordered by the physician.1 Similarly, changing a patient's status (ie, from observation to inpatient) must follow rigorous guidelines wherein the justification and timing are fully described in the body of the chart to an extent that would withstand audit.
Consider the example (Table 2) of a patient with a leg fracture admitted for pain due to edema and early compartment syndrome: a scenario appropriate for inpatient status, liability of just the $1092 Medicare deductible, and eligibility for postdischarge skilled nursing facility care. Had the charting erroneously only indicated pain and need for a new cast, then observation status would have yielded a bill for $3426, plus out of pocket nursing home expenses of over $150/day.
| Patient Liability for Observation Status (Medicare Part B) | Inpatient Charges (Covered by Medicare Part A Deductible) | |
|---|---|---|
| ||
| Room and board | $1788 | $1030 |
| Medications | $755 | $1196 |
| Supplies | $106 | $528 |
| Procedures and emergency room | $229 | $1145 |
| Diagnostic | ||
| Laboratory | $72 | $359 |
| Radiology | $159 | $795 |
| Ancillary | ||
| Electrocardiogram | $22 | $110 |
| Physical therapy | $295 | $1475 |
| Patient liability for hospitalization | $3426 | $1068 deductible for total charges of $6638 |
| Patient liability for subsequent skilled nursing facility | $159 per day* | Small daily co‐pay* |
Not only does the physician need to accurately chart the reasons for admission, but it is also extremely helpful to specifically document why the patient is not amenable to outpatient therapy. Examples include a clearly articulated history of failed attempts at home or emergency room treatment, or the need for close monitoring (ie, telemetry). In this regard case managers also provide a fresh set of eyes to evaluate the clarity and completeness of medical charting. What seems like obvious decision‐making to a physician may require expanded detailed notes to satisfy a third‐party review.
The work design of the case managers and utilization review team varies between facilities. Ideally, cases are reviewed upon admission (or within the first 24 hours), and then periodically thereafter. Many medical centers have this process computerized, wherein inpatient criteria are available online and status issues can be tracked daily. This nearly real‐time information serves as the basis for interacting with the attending physician, and is necessary because the chart documentation may not be amended after discharge. Having a robust database for all admissions is also immensely helpful in those hospitals which employ a Physician Advisor (PA) as a liaison and educator to the medical staff. This newly and now nationally recognized PA position serves an important role in educating the providers not just about these patient advocacy topics, but also other issues such as length‐of‐stay. Interestingly, having the infrastructure of a criteria‐driven database to follow the intensity of inpatient services on a daily basis gives case managers an objective perspective of when a patient requires less care and is ready for transfer to a lower acuity facility or discharge home. Physician participation is important when the patient thus runs out of intensities, since there will need to be early coordination of efforts for home health or skilled nursing care, durable medical equipment supplies, or outpatient infusions. It is important that physicians not view these activities as an inappropriate rush for discharge. In our experience most patients are in fact much happier to be out of the hospital and receiving home or skilled nursing care. Those in need of physical or occupational therapy may in fact have superior care in facilities dedicated to those activities. In addition, unnecessarily prolonged hospitalizations carry their own risks, such as hospital‐acquired infections and deep venous thromboses. An additional motivator for discharge is that, just as there are insurance plan limits for outpatient benefits, there can also be caps for inpatient services. Physicians thus have a role in preserving the limited and precious number of covered inpatient days of care, beyond which time the patient would be financially totally responsible. For example, most states limit the number of inpatient days covered by Medicaid. In Florida there is a cap of only 45 days per year (unless the patient is pediatric or within the first year of a transplant4). Similarly, there have been patients and families shocked and ill‐prepared to discover that all their Medicare hospital benefits were exhausted5: a not well‐publicized possibility, as in the setting of expensive intensive care units, transplantation, or chemotherapy. Timely discharges and careful resource utilization by physicians thus not only help the hospital but also are important for the patient.
In summary, physicians need to be aware that there can be tremendous financial hardship to patients caused by inappropriate or unnecessarily long observation stays, especially in cases where an inpatient designation would have been justified by appropriate documentation. Case managers, although employed by the facility, can thus assist physicians in this regard and together play an important role as patient advocates.
- Interqual® Level of Care Criteria: Acute Care Adult.Newton, MA:McKesson Health Solutions;2009.
- Department of Health and Human Services (DHHS), Centers for Medicare and Medicaid Services (CMS).2008. Final changes to the hospital outpatient prospective payment system and CY 2009. Available at: http://www.cms.hhs.gov/HospitalOutpatientPPS/HORD/list.asp. Accessed September 2009.
- Department of Health and Human Services (DHHS), Centers for Medicare and Medicaid Services (CMS).2008. Medicare Program; Changes to the hospital inpatient prospective payment systems and fiscal year 2009 rates. Available at: http://www.cms.hhs.gov/AcuteInpatientPPS/IPPS/itemdetail.asp. Accessed September 2009.
- Florida Medicaid covered services. Available at: http://www.fdhc.state. fl.us/Medicaid/MediPass/pdf/HealthyOutcomesCoveredServicesFlyerEnglish 0606.pdf. Accessed September 2009.
- Medicare Benefit Policy Manual: Chapter 5. Lifetime reserve days. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c05.pdf. Accessed September 2009.
- Interqual® Level of Care Criteria: Acute Care Adult.Newton, MA:McKesson Health Solutions;2009.
- Department of Health and Human Services (DHHS), Centers for Medicare and Medicaid Services (CMS).2008. Final changes to the hospital outpatient prospective payment system and CY 2009. Available at: http://www.cms.hhs.gov/HospitalOutpatientPPS/HORD/list.asp. Accessed September 2009.
- Department of Health and Human Services (DHHS), Centers for Medicare and Medicaid Services (CMS).2008. Medicare Program; Changes to the hospital inpatient prospective payment systems and fiscal year 2009 rates. Available at: http://www.cms.hhs.gov/AcuteInpatientPPS/IPPS/itemdetail.asp. Accessed September 2009.
- Florida Medicaid covered services. Available at: http://www.fdhc.state. fl.us/Medicaid/MediPass/pdf/HealthyOutcomesCoveredServicesFlyerEnglish 0606.pdf. Accessed September 2009.
- Medicare Benefit Policy Manual: Chapter 5. Lifetime reserve days. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c05.pdf. Accessed September 2009.
Myelofibrosis with Hepatosplenomegaly
An 83‐year‐old man with a 7‐year history of myelofibrosis presented to the hospital with progressive weakness and fatigue, which resulted in him tripping and falling onto his left hand and arm 1 day prior to admission. His past medical history was significant for transfusion‐dependent anemia and hypertension. His current treatment regimen for myelofibrosis included thalidomide and darbopoetin alfa.
Physical examination revealed a pale and edematous man who was holding his injured arm to his chest, but in no distress. He had massive hepatosplenomegaly (Figure 1) and pitting edema of the lower extremities that extended to his abdomen.

Laboratory studies showed a white blood count of 5000, hematocrit of 29%, and platelets of 218,000. The peripheral blood smear (Figure 2) showed marked anisocytosis, poikilocytosis, and teardrop cells (Figure 2; arrow).
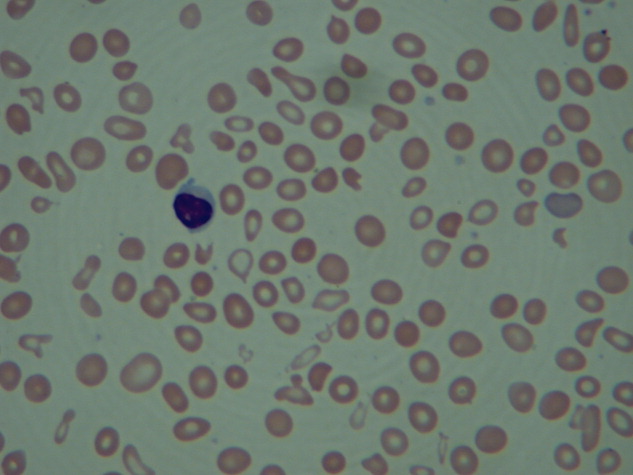
Imaging of the left arm and hand was significant for a third metacarpal fracture and first phalanx fracture. Of note, these x‐rays also revealed numerous round lucencies within the osseous structures of the left hand, wrist, and forearm (Figure 3; arrow).

The patient's hospital course was uncomplicated and included casting of the left arm, treatment of his lower extremity edema, and transfusion for a slowly declining hematocrit. He was discharged home after several days but died 1 month later.
Primary myelofibrosis is a myeloproliferative disease that consists of 2 phases. The first phase is the growth and proliferation of abnormal bone marrow stem cells, which leads to ineffective erythropoiesis. This is followed by reactive myelofibrosis and extramedullary hematopoiesis.1 These 2 phases of the disease can lead to a constellation of findings, as illustrated in these images. The median length of survival from diagnosis is 3 to 5 years, with the main causes of death being infection, hemorrhage, cardiac failure, and leukemic transformation.1 Presenting signs, symptoms, and laboratory results may include cachexia, splenomegaly, anemia, an increased or decreased white blood cell count and/or platelet count, and an increase in lactate dehydrogenase. Radiographically, the most common findings are marked splenomegaly and osteosclerosis.2
Osteosclerotic lesions are found in 30% to 70% of patients with myelofibrosis and are a result of marrow fibrosis, which leads to the appearance of diffuse, patchy increases in bone density.2 Osteolytic lesions, as seen in this case, are much less common. They appear in the literature in case reports, but are not considered to be a typical finding. They are usually painful and have been reported as a poor prognostic indicator.3, 4
- Myelofibrosis with myeloid metaplasia.N Engl J Med.2000;342(17):1255‒1265.
- ,,,,.Imaging findings in patients with myelofibrosis.Eur Radiol.1999;9:1366‒1375.
- ,,, et al.Unusual radiological findings in a case of myelofibrosis secondary to polycythemia vera.Ann Hematol.2006;85:555‒556.
- ,,.Osteolytic bone lesions in a patient with idiopathic myelofibrosis and bronchial carcinoma.J Clin Pathol.1995;48:867‒868.
An 83‐year‐old man with a 7‐year history of myelofibrosis presented to the hospital with progressive weakness and fatigue, which resulted in him tripping and falling onto his left hand and arm 1 day prior to admission. His past medical history was significant for transfusion‐dependent anemia and hypertension. His current treatment regimen for myelofibrosis included thalidomide and darbopoetin alfa.
Physical examination revealed a pale and edematous man who was holding his injured arm to his chest, but in no distress. He had massive hepatosplenomegaly (Figure 1) and pitting edema of the lower extremities that extended to his abdomen.
Laboratory studies showed a white blood count of 5000, hematocrit of 29%, and platelets of 218,000. The peripheral blood smear (Figure 2) showed marked anisocytosis, poikilocytosis, and teardrop cells (Figure 2; arrow).
Imaging of the left arm and hand was significant for a third metacarpal fracture and first phalanx fracture. Of note, these x‐rays also revealed numerous round lucencies within the osseous structures of the left hand, wrist, and forearm (Figure 3; arrow).
The patient's hospital course was uncomplicated and included casting of the left arm, treatment of his lower extremity edema, and transfusion for a slowly declining hematocrit. He was discharged home after several days but died 1 month later.
Primary myelofibrosis is a myeloproliferative disease that consists of 2 phases. The first phase is the growth and proliferation of abnormal bone marrow stem cells, which leads to ineffective erythropoiesis. This is followed by reactive myelofibrosis and extramedullary hematopoiesis.1 These 2 phases of the disease can lead to a constellation of findings, as illustrated in these images. The median length of survival from diagnosis is 3 to 5 years, with the main causes of death being infection, hemorrhage, cardiac failure, and leukemic transformation.1 Presenting signs, symptoms, and laboratory results may include cachexia, splenomegaly, anemia, an increased or decreased white blood cell count and/or platelet count, and an increase in lactate dehydrogenase. Radiographically, the most common findings are marked splenomegaly and osteosclerosis.2
Osteosclerotic lesions are found in 30% to 70% of patients with myelofibrosis and are a result of marrow fibrosis, which leads to the appearance of diffuse, patchy increases in bone density.2 Osteolytic lesions, as seen in this case, are much less common. They appear in the literature in case reports, but are not considered to be a typical finding. They are usually painful and have been reported as a poor prognostic indicator.3, 4
An 83‐year‐old man with a 7‐year history of myelofibrosis presented to the hospital with progressive weakness and fatigue, which resulted in him tripping and falling onto his left hand and arm 1 day prior to admission. His past medical history was significant for transfusion‐dependent anemia and hypertension. His current treatment regimen for myelofibrosis included thalidomide and darbopoetin alfa.
Physical examination revealed a pale and edematous man who was holding his injured arm to his chest, but in no distress. He had massive hepatosplenomegaly (Figure 1) and pitting edema of the lower extremities that extended to his abdomen.
Laboratory studies showed a white blood count of 5000, hematocrit of 29%, and platelets of 218,000. The peripheral blood smear (Figure 2) showed marked anisocytosis, poikilocytosis, and teardrop cells (Figure 2; arrow).
Imaging of the left arm and hand was significant for a third metacarpal fracture and first phalanx fracture. Of note, these x‐rays also revealed numerous round lucencies within the osseous structures of the left hand, wrist, and forearm (Figure 3; arrow).
The patient's hospital course was uncomplicated and included casting of the left arm, treatment of his lower extremity edema, and transfusion for a slowly declining hematocrit. He was discharged home after several days but died 1 month later.
Primary myelofibrosis is a myeloproliferative disease that consists of 2 phases. The first phase is the growth and proliferation of abnormal bone marrow stem cells, which leads to ineffective erythropoiesis. This is followed by reactive myelofibrosis and extramedullary hematopoiesis.1 These 2 phases of the disease can lead to a constellation of findings, as illustrated in these images. The median length of survival from diagnosis is 3 to 5 years, with the main causes of death being infection, hemorrhage, cardiac failure, and leukemic transformation.1 Presenting signs, symptoms, and laboratory results may include cachexia, splenomegaly, anemia, an increased or decreased white blood cell count and/or platelet count, and an increase in lactate dehydrogenase. Radiographically, the most common findings are marked splenomegaly and osteosclerosis.2
Osteosclerotic lesions are found in 30% to 70% of patients with myelofibrosis and are a result of marrow fibrosis, which leads to the appearance of diffuse, patchy increases in bone density.2 Osteolytic lesions, as seen in this case, are much less common. They appear in the literature in case reports, but are not considered to be a typical finding. They are usually painful and have been reported as a poor prognostic indicator.3, 4
- Myelofibrosis with myeloid metaplasia.N Engl J Med.2000;342(17):1255‒1265.
- ,,,,.Imaging findings in patients with myelofibrosis.Eur Radiol.1999;9:1366‒1375.
- ,,, et al.Unusual radiological findings in a case of myelofibrosis secondary to polycythemia vera.Ann Hematol.2006;85:555‒556.
- ,,.Osteolytic bone lesions in a patient with idiopathic myelofibrosis and bronchial carcinoma.J Clin Pathol.1995;48:867‒868.
- Myelofibrosis with myeloid metaplasia.N Engl J Med.2000;342(17):1255‒1265.
- ,,,,.Imaging findings in patients with myelofibrosis.Eur Radiol.1999;9:1366‒1375.
- ,,, et al.Unusual radiological findings in a case of myelofibrosis secondary to polycythemia vera.Ann Hematol.2006;85:555‒556.
- ,,.Osteolytic bone lesions in a patient with idiopathic myelofibrosis and bronchial carcinoma.J Clin Pathol.1995;48:867‒868.

Disseminated Sporotrichosis
A 61‐year‐old healthy man presented with recurrent right wrist pain. The patient underwent unsuccessful carpal tunnel surgery and pathology revealed granulomatous inflammation. With worsening pain and new nodular inflammation, prednisone and azathioprine were prescribed for presumed sarcoidosis. Subsequently, right arm ulceration developed (Figure 1), and wound and blood cultures revealed Sporothrix schenkii. Immunosuppressive medications were stopped, but the ulceration progressed and ultimately involved the entire arm (Figure 2). New lower‐extremity fluid collections seen on the magnetic resonance imaging (MRI) MRI (Figures 3, 4) prompted several surgical debridements. Multiple abscesses formed in all extremities despite amphotericin and itraconazole therapy. The patient was eventually discharged with ongoing amphotericin and plans for surveillance imaging and repeated debridements.



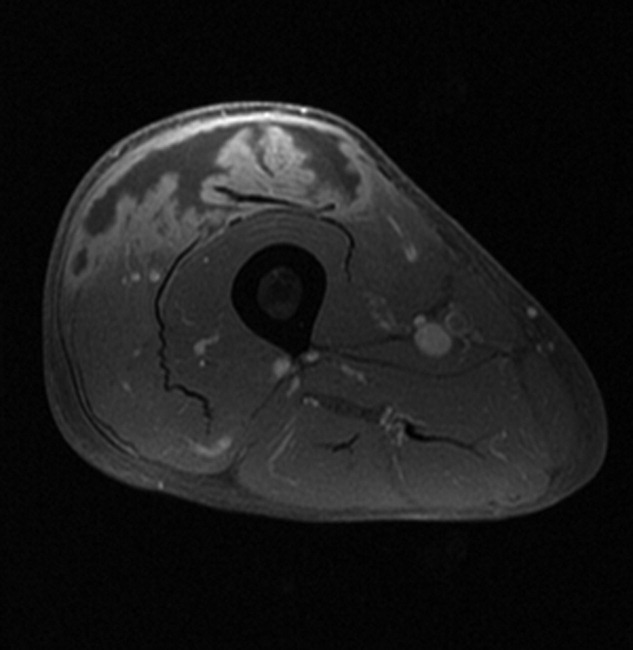
Sporothrix schenckii is a dimorphic fungus often associated with cutaneous infections of the extremities in gardeners. These infections are definitively treated with oral azole medications or topical potassium iodide. Disseminated sporotrichosis is almost exclusively seen in immunosuppressed patients including those with human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS)1 and hematologic malignancies.2 Iatrogenic immunosuppression from chemotherapy or corticosteroids can also place a patient at risk for disseminated disease. Disseminated sporotrichosis is extremely difficult to manage with significant morbidity and mortality; fatal cases are commonly reported in the literature.3
- ,,,.Cutaneous and meningeal sporotrichosis in a HIV patient.Rev Iberoam Micol.2007;24(2):161–163.
- ,,.Systemic sporotrichosis.Ann Intern Med.1970;73(1):23–30.
- ,,,,.Fatal sporotrichosis.Cutis.2006;78(4):253–256.
A 61‐year‐old healthy man presented with recurrent right wrist pain. The patient underwent unsuccessful carpal tunnel surgery and pathology revealed granulomatous inflammation. With worsening pain and new nodular inflammation, prednisone and azathioprine were prescribed for presumed sarcoidosis. Subsequently, right arm ulceration developed (Figure 1), and wound and blood cultures revealed Sporothrix schenkii. Immunosuppressive medications were stopped, but the ulceration progressed and ultimately involved the entire arm (Figure 2). New lower‐extremity fluid collections seen on the magnetic resonance imaging (MRI) MRI (Figures 3, 4) prompted several surgical debridements. Multiple abscesses formed in all extremities despite amphotericin and itraconazole therapy. The patient was eventually discharged with ongoing amphotericin and plans for surveillance imaging and repeated debridements.
Sporothrix schenckii is a dimorphic fungus often associated with cutaneous infections of the extremities in gardeners. These infections are definitively treated with oral azole medications or topical potassium iodide. Disseminated sporotrichosis is almost exclusively seen in immunosuppressed patients including those with human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS)1 and hematologic malignancies.2 Iatrogenic immunosuppression from chemotherapy or corticosteroids can also place a patient at risk for disseminated disease. Disseminated sporotrichosis is extremely difficult to manage with significant morbidity and mortality; fatal cases are commonly reported in the literature.3
A 61‐year‐old healthy man presented with recurrent right wrist pain. The patient underwent unsuccessful carpal tunnel surgery and pathology revealed granulomatous inflammation. With worsening pain and new nodular inflammation, prednisone and azathioprine were prescribed for presumed sarcoidosis. Subsequently, right arm ulceration developed (Figure 1), and wound and blood cultures revealed Sporothrix schenkii. Immunosuppressive medications were stopped, but the ulceration progressed and ultimately involved the entire arm (Figure 2). New lower‐extremity fluid collections seen on the magnetic resonance imaging (MRI) MRI (Figures 3, 4) prompted several surgical debridements. Multiple abscesses formed in all extremities despite amphotericin and itraconazole therapy. The patient was eventually discharged with ongoing amphotericin and plans for surveillance imaging and repeated debridements.
Sporothrix schenckii is a dimorphic fungus often associated with cutaneous infections of the extremities in gardeners. These infections are definitively treated with oral azole medications or topical potassium iodide. Disseminated sporotrichosis is almost exclusively seen in immunosuppressed patients including those with human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS)1 and hematologic malignancies.2 Iatrogenic immunosuppression from chemotherapy or corticosteroids can also place a patient at risk for disseminated disease. Disseminated sporotrichosis is extremely difficult to manage with significant morbidity and mortality; fatal cases are commonly reported in the literature.3
- ,,,.Cutaneous and meningeal sporotrichosis in a HIV patient.Rev Iberoam Micol.2007;24(2):161–163.
- ,,.Systemic sporotrichosis.Ann Intern Med.1970;73(1):23–30.
- ,,,,.Fatal sporotrichosis.Cutis.2006;78(4):253–256.
- ,,,.Cutaneous and meningeal sporotrichosis in a HIV patient.Rev Iberoam Micol.2007;24(2):161–163.
- ,,.Systemic sporotrichosis.Ann Intern Med.1970;73(1):23–30.
- ,,,,.Fatal sporotrichosis.Cutis.2006;78(4):253–256.

Cefepime: Underrecognized Cause of NCSE
Hospitalized patients with sepsis or severe nosocomial infections are frequently treated empirically with broad‐spectrum antibiotics. Cefepime hydrochloride, a fourth‐generation cephalosporin, is a common antibiotic of first choice. Its proconvulsant properties are well described in the literature,1, 2 but its importance as a potential cause of change in mental status is probably underestimated. We report a case of change in mental status related to nonconvulsive status epilepticus (NCSE) caused by the use of cefepime in an elderly, hospitalized patient. Our goal is to raise awareness about this uncommon and still underrecognized complication.
Case Report
A 72‐year‐old woman with stage III chronic kidney disease secondary to hypertension with a stable creatinine of 1.5 mg/dL (glomerular filtration rate (GFR) estimated by the modification of diet in renal disease (MDRD) at 36 mL/minute/1.73 m2) was admitted to the hospital for worsening of her chronic back pain. She had a past medical history significant for hyperlipidemia, asthma, and peripheral vascular disease, with breast cancer in remission since 1989. She had no history of seizures or cerebrovascular disease. Her medications were ibuprofen, oxycontin, cilastazol, acetaminophen/oxycodone, and an albuterol/empratropium inhaler. Her physical examination was remarkable only for decreased strength in the right lower extremity. Magnetic resonance imaging (MRI) of the lumbosacral spine showed signs consistent with an inflammatory process at the level of L4‐L5. A computed tomography (CT)‐guided biopsy was performed and confirmed a diagnosis of osteomyelitis on biopsy. Cultures from the biopsy grew Pseudomonas aeruginosa and treatment with intravenous cefepime at a dose of 1 g every 12 hours was initiated. Over the next 3 days, the patient had a gradual worsening of her mental status, leading to pronounced somnolence with occasional episodes of agitation during which she had no focal motor deficits. Her mental status declined to the point of unresponsiveness to simple verbal commands. She had not received any new medications other than cefepime. Her creatinine level was stable throughout this time period at 1.6 mg/dL. No other abnormalities were found on laboratory evaluation or on CT and MRI scans of the brain. An electroencephalogram (EEG) was markedly abnormal due to a generalized background slowing and disorganization with frequent bilateral paroxysmal epileptiform discharges, confirming the clinical diagnosis of subclinical generalized status epilepticus. Given that there were no other intrinsic neurological or metabolic reasons for this mental status change, and given that cefepime was the only new medication added before the patient started deteriorating, cefepime was discontinued and treatment for seizures was started with intravenous benzodiazepines. Over the next 2 days, her mental status returned to normal. She was soon discharged to a rehabilitation center.
Discussion
Beta‐lactam antibiotics have been described to induce seizures due to their direct and/or indirect inhibition of the gamma‐aminobutyric acid (GABA) system.1, 3 Previous experiments have shown a dose‐dependent effect on seizures, and suggest that the cephalosporin with the most pronounced proconvulsant effect is cefazolin.1, 3
Cefepime has been associated with neurological side effects such as headache, confusion, hallucinations, agitation, myoclonus, ataxia, seizures, and coma. Another underrecognized but critical side effect is NSCE. This is defined as seizure activity for more than 30 minutes, with cognitive and behavioral changes, but without convulsive clinical manifestations. This complication has been reported in the literature, but it is probably underrecognized.3‐7 The tendency for cefepime to produce more subclinical activity than the other cephalosporins is not well understood.
Cefepime is mainly eliminated though renal excretion (85%) and displays linear pharmacokinetic properties, thus its dose needs to be adjusted according to renal function. Consequently, in the case of renal dysfunction, accumulation of the drug is proportional to the degree of renal impairment. For NSCE, the most important risk factor is renal impairment, although cases in patients with normal kidney function have been described.36 Age, preexisting central nervous system (CNS) disease, sepsis, and cardiopulmonary bypass have also been reported as possible risk factors for NCSE.1
Cefepime can accumulate in the cerebrospinal fluid (CSF) in the setting of renal dysfunction, decreased protein‐binding capacity (as is sometimes seen in the elderly), and increased blood‐brain permeability in the setting of CNS infections. Accumulation of the drug in the CSF can lead to blockade of the GABA‐A receptor through a mechanism of competitive antagonism1, 8
The onset of NSCE varies between 1 and 16 days after initiation of cefepime therapy.3‐5, 7 It is frequently confused with delirium, since hospitalized patients treated with broad‐spectrum antibiotics such as cefepime frequently have other comorbidities and risk factors for delirium.
This can delay the diagnosis of NSCE due to a lack of awareness of this critical complication in the setting of renal dysfunction. In order to quantify the likelihood that the NSCE was related to cefepime and not to other causes, we calculated a Naranjo adverse drug events probability score, which consists of 9 questions on the relationship between the adverse event and the incriminated drug.9 Each answer is scored from 1 to +2 points. This score was designed to quantify the strength of the association between any adverse event and a pharmacological agent.
In our patient, the Naranjo score was 7 points, suggesting that the diagnosis of cefepime‐induced NCSE was probable.
The diagnosis of NCSE is made through a combination of a high index of clinical suspicion, specific findings on EEG, and improvement with withdrawal of the drug. Fatal outcomes have been reported.5, 6 Early and prompt recognition of the condition is crucial for the prevention of its morbidity and mortality.
The mainstay of treatment is prompt withdrawal of antibiotics and symptomatic treatment with benzodiazepines or barbiturates. Very severe cases with refractory seizures have been treated with hemodialysis. Phenytoin should be avoided as a treatment of this condition due to its lack of GABA‐agonist activity.
Conclusion
Cefepime can cause NCSE, predominantly in patients with renal dysfunction. Its frequency is probably underestimated in hospitalized patients with multiple comorbid conditions. Hospitalists should be aware of this unusual but critical relationship, especially in patients with renal failure. A high level of clinical suspicion and an emergency EEG are essential to obtain a prompt and accurate diagnosis.
- .Antibiotic‐induced convulsions.Crit Care Clin.1997;13:741‐762.
- ,.Cefepime neurotoxicity: case report, pharmacokinetic considerations, and literature review.Pharmacotherapy.2006;26(8):1169‐1174.
- ,,,,.Relationship between structure and convulsant properties of some β‐lactams antibiotics following intracerebroventricular microinjections in rats.Antimicrob Agents Chemother.1995;39:232‐237.
- ,,,,,.Cefepime‐ and cefixime‐induced encephalopathy in a patient with normal renal function.Neurology.2005;65(11):1840.
- ,,, et al.Cefepime induced neurotoxicity: an underestimated complication of antibiotherapy in patients with acute renal failure.Intensive Care Med.2002;28:214‐217.
- ,,,.Nonconvulsive status epilepticus due to cefepime in a patient with normal renal function.Epilepsy Behav.2006;8(1):312‐314.
- ,,, et al.Nonconvulsive status epilepticus associated with cephalosporins in patients with renal failure.Am J Med.2001;111(2):115‐119.
- ,,, et al.Evidence for the involvement of GABA(A) receptor blockade in convulsions induced by cephalosporins.Neuropharmacology.2003;45(3):304‐314.
- ,,, et al.A method for estimating the probability of adverse drug reactions.Clin Pharmacol Ther.1981;30(2):239‐245.
Hospitalized patients with sepsis or severe nosocomial infections are frequently treated empirically with broad‐spectrum antibiotics. Cefepime hydrochloride, a fourth‐generation cephalosporin, is a common antibiotic of first choice. Its proconvulsant properties are well described in the literature,1, 2 but its importance as a potential cause of change in mental status is probably underestimated. We report a case of change in mental status related to nonconvulsive status epilepticus (NCSE) caused by the use of cefepime in an elderly, hospitalized patient. Our goal is to raise awareness about this uncommon and still underrecognized complication.
Case Report
A 72‐year‐old woman with stage III chronic kidney disease secondary to hypertension with a stable creatinine of 1.5 mg/dL (glomerular filtration rate (GFR) estimated by the modification of diet in renal disease (MDRD) at 36 mL/minute/1.73 m2) was admitted to the hospital for worsening of her chronic back pain. She had a past medical history significant for hyperlipidemia, asthma, and peripheral vascular disease, with breast cancer in remission since 1989. She had no history of seizures or cerebrovascular disease. Her medications were ibuprofen, oxycontin, cilastazol, acetaminophen/oxycodone, and an albuterol/empratropium inhaler. Her physical examination was remarkable only for decreased strength in the right lower extremity. Magnetic resonance imaging (MRI) of the lumbosacral spine showed signs consistent with an inflammatory process at the level of L4‐L5. A computed tomography (CT)‐guided biopsy was performed and confirmed a diagnosis of osteomyelitis on biopsy. Cultures from the biopsy grew Pseudomonas aeruginosa and treatment with intravenous cefepime at a dose of 1 g every 12 hours was initiated. Over the next 3 days, the patient had a gradual worsening of her mental status, leading to pronounced somnolence with occasional episodes of agitation during which she had no focal motor deficits. Her mental status declined to the point of unresponsiveness to simple verbal commands. She had not received any new medications other than cefepime. Her creatinine level was stable throughout this time period at 1.6 mg/dL. No other abnormalities were found on laboratory evaluation or on CT and MRI scans of the brain. An electroencephalogram (EEG) was markedly abnormal due to a generalized background slowing and disorganization with frequent bilateral paroxysmal epileptiform discharges, confirming the clinical diagnosis of subclinical generalized status epilepticus. Given that there were no other intrinsic neurological or metabolic reasons for this mental status change, and given that cefepime was the only new medication added before the patient started deteriorating, cefepime was discontinued and treatment for seizures was started with intravenous benzodiazepines. Over the next 2 days, her mental status returned to normal. She was soon discharged to a rehabilitation center.
Discussion
Beta‐lactam antibiotics have been described to induce seizures due to their direct and/or indirect inhibition of the gamma‐aminobutyric acid (GABA) system.1, 3 Previous experiments have shown a dose‐dependent effect on seizures, and suggest that the cephalosporin with the most pronounced proconvulsant effect is cefazolin.1, 3
Cefepime has been associated with neurological side effects such as headache, confusion, hallucinations, agitation, myoclonus, ataxia, seizures, and coma. Another underrecognized but critical side effect is NSCE. This is defined as seizure activity for more than 30 minutes, with cognitive and behavioral changes, but without convulsive clinical manifestations. This complication has been reported in the literature, but it is probably underrecognized.3‐7 The tendency for cefepime to produce more subclinical activity than the other cephalosporins is not well understood.
Cefepime is mainly eliminated though renal excretion (85%) and displays linear pharmacokinetic properties, thus its dose needs to be adjusted according to renal function. Consequently, in the case of renal dysfunction, accumulation of the drug is proportional to the degree of renal impairment. For NSCE, the most important risk factor is renal impairment, although cases in patients with normal kidney function have been described.36 Age, preexisting central nervous system (CNS) disease, sepsis, and cardiopulmonary bypass have also been reported as possible risk factors for NCSE.1
Cefepime can accumulate in the cerebrospinal fluid (CSF) in the setting of renal dysfunction, decreased protein‐binding capacity (as is sometimes seen in the elderly), and increased blood‐brain permeability in the setting of CNS infections. Accumulation of the drug in the CSF can lead to blockade of the GABA‐A receptor through a mechanism of competitive antagonism1, 8
The onset of NSCE varies between 1 and 16 days after initiation of cefepime therapy.3‐5, 7 It is frequently confused with delirium, since hospitalized patients treated with broad‐spectrum antibiotics such as cefepime frequently have other comorbidities and risk factors for delirium.
This can delay the diagnosis of NSCE due to a lack of awareness of this critical complication in the setting of renal dysfunction. In order to quantify the likelihood that the NSCE was related to cefepime and not to other causes, we calculated a Naranjo adverse drug events probability score, which consists of 9 questions on the relationship between the adverse event and the incriminated drug.9 Each answer is scored from 1 to +2 points. This score was designed to quantify the strength of the association between any adverse event and a pharmacological agent.
In our patient, the Naranjo score was 7 points, suggesting that the diagnosis of cefepime‐induced NCSE was probable.
The diagnosis of NCSE is made through a combination of a high index of clinical suspicion, specific findings on EEG, and improvement with withdrawal of the drug. Fatal outcomes have been reported.5, 6 Early and prompt recognition of the condition is crucial for the prevention of its morbidity and mortality.
The mainstay of treatment is prompt withdrawal of antibiotics and symptomatic treatment with benzodiazepines or barbiturates. Very severe cases with refractory seizures have been treated with hemodialysis. Phenytoin should be avoided as a treatment of this condition due to its lack of GABA‐agonist activity.
Conclusion
Cefepime can cause NCSE, predominantly in patients with renal dysfunction. Its frequency is probably underestimated in hospitalized patients with multiple comorbid conditions. Hospitalists should be aware of this unusual but critical relationship, especially in patients with renal failure. A high level of clinical suspicion and an emergency EEG are essential to obtain a prompt and accurate diagnosis.
Hospitalized patients with sepsis or severe nosocomial infections are frequently treated empirically with broad‐spectrum antibiotics. Cefepime hydrochloride, a fourth‐generation cephalosporin, is a common antibiotic of first choice. Its proconvulsant properties are well described in the literature,1, 2 but its importance as a potential cause of change in mental status is probably underestimated. We report a case of change in mental status related to nonconvulsive status epilepticus (NCSE) caused by the use of cefepime in an elderly, hospitalized patient. Our goal is to raise awareness about this uncommon and still underrecognized complication.
Case Report
A 72‐year‐old woman with stage III chronic kidney disease secondary to hypertension with a stable creatinine of 1.5 mg/dL (glomerular filtration rate (GFR) estimated by the modification of diet in renal disease (MDRD) at 36 mL/minute/1.73 m2) was admitted to the hospital for worsening of her chronic back pain. She had a past medical history significant for hyperlipidemia, asthma, and peripheral vascular disease, with breast cancer in remission since 1989. She had no history of seizures or cerebrovascular disease. Her medications were ibuprofen, oxycontin, cilastazol, acetaminophen/oxycodone, and an albuterol/empratropium inhaler. Her physical examination was remarkable only for decreased strength in the right lower extremity. Magnetic resonance imaging (MRI) of the lumbosacral spine showed signs consistent with an inflammatory process at the level of L4‐L5. A computed tomography (CT)‐guided biopsy was performed and confirmed a diagnosis of osteomyelitis on biopsy. Cultures from the biopsy grew Pseudomonas aeruginosa and treatment with intravenous cefepime at a dose of 1 g every 12 hours was initiated. Over the next 3 days, the patient had a gradual worsening of her mental status, leading to pronounced somnolence with occasional episodes of agitation during which she had no focal motor deficits. Her mental status declined to the point of unresponsiveness to simple verbal commands. She had not received any new medications other than cefepime. Her creatinine level was stable throughout this time period at 1.6 mg/dL. No other abnormalities were found on laboratory evaluation or on CT and MRI scans of the brain. An electroencephalogram (EEG) was markedly abnormal due to a generalized background slowing and disorganization with frequent bilateral paroxysmal epileptiform discharges, confirming the clinical diagnosis of subclinical generalized status epilepticus. Given that there were no other intrinsic neurological or metabolic reasons for this mental status change, and given that cefepime was the only new medication added before the patient started deteriorating, cefepime was discontinued and treatment for seizures was started with intravenous benzodiazepines. Over the next 2 days, her mental status returned to normal. She was soon discharged to a rehabilitation center.
Discussion
Beta‐lactam antibiotics have been described to induce seizures due to their direct and/or indirect inhibition of the gamma‐aminobutyric acid (GABA) system.1, 3 Previous experiments have shown a dose‐dependent effect on seizures, and suggest that the cephalosporin with the most pronounced proconvulsant effect is cefazolin.1, 3
Cefepime has been associated with neurological side effects such as headache, confusion, hallucinations, agitation, myoclonus, ataxia, seizures, and coma. Another underrecognized but critical side effect is NSCE. This is defined as seizure activity for more than 30 minutes, with cognitive and behavioral changes, but without convulsive clinical manifestations. This complication has been reported in the literature, but it is probably underrecognized.3‐7 The tendency for cefepime to produce more subclinical activity than the other cephalosporins is not well understood.
Cefepime is mainly eliminated though renal excretion (85%) and displays linear pharmacokinetic properties, thus its dose needs to be adjusted according to renal function. Consequently, in the case of renal dysfunction, accumulation of the drug is proportional to the degree of renal impairment. For NSCE, the most important risk factor is renal impairment, although cases in patients with normal kidney function have been described.36 Age, preexisting central nervous system (CNS) disease, sepsis, and cardiopulmonary bypass have also been reported as possible risk factors for NCSE.1
Cefepime can accumulate in the cerebrospinal fluid (CSF) in the setting of renal dysfunction, decreased protein‐binding capacity (as is sometimes seen in the elderly), and increased blood‐brain permeability in the setting of CNS infections. Accumulation of the drug in the CSF can lead to blockade of the GABA‐A receptor through a mechanism of competitive antagonism1, 8
The onset of NSCE varies between 1 and 16 days after initiation of cefepime therapy.3‐5, 7 It is frequently confused with delirium, since hospitalized patients treated with broad‐spectrum antibiotics such as cefepime frequently have other comorbidities and risk factors for delirium.
This can delay the diagnosis of NSCE due to a lack of awareness of this critical complication in the setting of renal dysfunction. In order to quantify the likelihood that the NSCE was related to cefepime and not to other causes, we calculated a Naranjo adverse drug events probability score, which consists of 9 questions on the relationship between the adverse event and the incriminated drug.9 Each answer is scored from 1 to +2 points. This score was designed to quantify the strength of the association between any adverse event and a pharmacological agent.
In our patient, the Naranjo score was 7 points, suggesting that the diagnosis of cefepime‐induced NCSE was probable.
The diagnosis of NCSE is made through a combination of a high index of clinical suspicion, specific findings on EEG, and improvement with withdrawal of the drug. Fatal outcomes have been reported.5, 6 Early and prompt recognition of the condition is crucial for the prevention of its morbidity and mortality.
The mainstay of treatment is prompt withdrawal of antibiotics and symptomatic treatment with benzodiazepines or barbiturates. Very severe cases with refractory seizures have been treated with hemodialysis. Phenytoin should be avoided as a treatment of this condition due to its lack of GABA‐agonist activity.
Conclusion
Cefepime can cause NCSE, predominantly in patients with renal dysfunction. Its frequency is probably underestimated in hospitalized patients with multiple comorbid conditions. Hospitalists should be aware of this unusual but critical relationship, especially in patients with renal failure. A high level of clinical suspicion and an emergency EEG are essential to obtain a prompt and accurate diagnosis.
- .Antibiotic‐induced convulsions.Crit Care Clin.1997;13:741‐762.
- ,.Cefepime neurotoxicity: case report, pharmacokinetic considerations, and literature review.Pharmacotherapy.2006;26(8):1169‐1174.
- ,,,,.Relationship between structure and convulsant properties of some β‐lactams antibiotics following intracerebroventricular microinjections in rats.Antimicrob Agents Chemother.1995;39:232‐237.
- ,,,,,.Cefepime‐ and cefixime‐induced encephalopathy in a patient with normal renal function.Neurology.2005;65(11):1840.
- ,,, et al.Cefepime induced neurotoxicity: an underestimated complication of antibiotherapy in patients with acute renal failure.Intensive Care Med.2002;28:214‐217.
- ,,,.Nonconvulsive status epilepticus due to cefepime in a patient with normal renal function.Epilepsy Behav.2006;8(1):312‐314.
- ,,, et al.Nonconvulsive status epilepticus associated with cephalosporins in patients with renal failure.Am J Med.2001;111(2):115‐119.
- ,,, et al.Evidence for the involvement of GABA(A) receptor blockade in convulsions induced by cephalosporins.Neuropharmacology.2003;45(3):304‐314.
- ,,, et al.A method for estimating the probability of adverse drug reactions.Clin Pharmacol Ther.1981;30(2):239‐245.
- .Antibiotic‐induced convulsions.Crit Care Clin.1997;13:741‐762.
- ,.Cefepime neurotoxicity: case report, pharmacokinetic considerations, and literature review.Pharmacotherapy.2006;26(8):1169‐1174.
- ,,,,.Relationship between structure and convulsant properties of some β‐lactams antibiotics following intracerebroventricular microinjections in rats.Antimicrob Agents Chemother.1995;39:232‐237.
- ,,,,,.Cefepime‐ and cefixime‐induced encephalopathy in a patient with normal renal function.Neurology.2005;65(11):1840.
- ,,, et al.Cefepime induced neurotoxicity: an underestimated complication of antibiotherapy in patients with acute renal failure.Intensive Care Med.2002;28:214‐217.
- ,,,.Nonconvulsive status epilepticus due to cefepime in a patient with normal renal function.Epilepsy Behav.2006;8(1):312‐314.
- ,,, et al.Nonconvulsive status epilepticus associated with cephalosporins in patients with renal failure.Am J Med.2001;111(2):115‐119.
- ,,, et al.Evidence for the involvement of GABA(A) receptor blockade in convulsions induced by cephalosporins.Neuropharmacology.2003;45(3):304‐314.
- ,,, et al.A method for estimating the probability of adverse drug reactions.Clin Pharmacol Ther.1981;30(2):239‐245.
A case of optic neuritis and transverse myelitis in a postpartum Ghanaian female
Rapid onset visual loss with limb involvement in a postpartum female invites a number of differential diagnoses, including infectious encephalomyelitis, vasculitis, an acute demyelinating disorder, and arterial/venous sinus thrombosis. We report an interesting, but initially puzzling, case of rapidly progressive optic neuritis and transverse myelitis in a postpartum Ghanaian female, later diagnosed as neuromyelitis optica (NMO).
Case Report
A 33‐year‐old Ghanaian female presented with bilateral eye pain worsened by eye movement, rapid visual loss, bifrontal headache, and right leg weakness for 48 hours. She was 8 weeks postpartum, with labor having been induced at 35 weeks due to hypertension; she was discharged on labetolol and no other medications. There was no other relevant past medical or family history, or illicit drug use.
On admission, her blood pressure was 148/99 mm Hg, pulse rate 92 beats per minute, temperature 37.8C, oxygen saturation 97% on room air, respiratory rate 14 breaths per minute, and Glasgow coma scale 15/15. Cranial nerve examination showed absent light perception in the right eye with a relative afferent pupillary defect, 20/30 Snellen visual acuity in the left eye, bilateral optic disc edema (worse on the right) and grade 1 hypertensive retinopathy, and slight facial asymmetry but otherwise grossly intact cranial nerves. Neurological examination of the limbs showed 5/5 power in upper limbs, but flexion was weaker (3/5) than extension (4/5) in lower limbs. There was hyperreflexia in the right arm and right leg with positive Babinski sign. Sensation, proprioception, and coordination were normal in both upper and lower limbs; a Romberg test was negative.
Other systems examinations were unremarkable. Complete blood count, standard electrolytes, erythrocyte sedimentation rate, C‐reactive protein, urinalysis, chest x‐ray, and an urgent head computed tomography (CT) with contrast were all noncontributory.
To cover a broad range of possible infective processes, ceftriaxone and acyclovir were started. In view of the rapid progression of her presentation she was transferred urgently to a specialty neurology hospital. There she was started on intravenous methylprednisolone to cover possible inflammatory causes, such as multiple sclerosis (MS) and vasculitis. However, her lower limb weakness progressed and she developed urinary retention. Lumbar puncture was performed; the opening pressure was 160 mm H2O. Cerebrospinal fluid (CSF) analysis demonstrated elevated protein level (121 mg/dL), 16/mm3 lymphocytosis, normal glucose, and negative gram stain and culture. Conventional CSF polymerase chain reaction for herpes simplex, Epstein‐Barr, varicella‐zoster, cytomegalovirus, John Cunningham virus (to rule out progressive multifocal leukoencephalopathy), human herpesvirus 6 viruses, and toxoplasma were negative. Antinuclear antibody, anticytoplasmic antibody, antiganglioside antibodies (GM1, GQ1b), thrombophilia screen (activated protein C resistance ratio, lupus anticoagulant and anticardiolipin antibodies, antithrombin III, protein C, and S deficiency), B12, folate, ferritin, and human immunodeficiency virus (HIV) screen were also negative. Brain magnetic resonance imaging (MRI), including venography, was normal. However, T2‐weighted MRI images of the orbit showed signal hyperintensity of the left optic chiasm and optic nerves, and T2‐weighted images of the spinal cord showed hyperintensity within the upper 4 and lower 4 thoracic levels. The diagnosis of NMO was entertained.
Following intravenous steroids, the patient was treated with a tapering course of oral steroids. She began to make a slow recovery with the aid of intense physiotherapy. Having walked in at her initial admission, she returned home needing crutches 4 weeks later and the visual acuity in her right eye remained 20/120 at best. Her requirement for intermittent urinary self‐catheterization and rectal enemas decreased with time. She continued to be rehabilitated at home with input from the community physiotherapy team and remains in remission at 12 months.
Discussion
First described by Eugene Devic in 1894, NMO is a rare, chronic inflammatory, demyelinating disease of the central nervous system.1 It is more common among Asians and Africans, with a female predominance (females comprise over two‐thirds of patients and more than 80% of those with the relapsing form of the disease).2 The mean age of onset is 35 to 47 years.2 The prevalence and incidence of NMO has not been established, partly because the disease is underrecognized and often confused with MS.
Pathophysiology and Clinical Features
NMO is a nonhereditary autoimmune condition distinct from MS. It is characterized by antibodies (NMOimmunoglobulin G [IgG]) against aquaporin 4 in myelin within astrocytes, which form part of the blood‐brain barrier.2 The damage in the spinal cord can range from inflammatory demyelination to necrosis. The inflammatory lesions in NMO have been classified as type II lesions (complement‐mediated demyelination)they differ from MS in their prominent perivascular distribution.
NMO presents with attacks of acute optic neuritis, usually bilateral, associated with severe transverse myelopathy occurring at the same time as or following the optic neuritis within a few days, weeks, or occasionally months. The following characteristics help to differentiate NMO from MS3:
-
The presence of transverse myelitis, bilateral neurological signs, and longitudinal extensive necrotic lesions on spine MRI point toward NMO.
-
Clinical involvement beyond the spinal cord and optic nerves, presence of oligoclonal bands in CSF, white matter lesions on brain MRI, and multiple small peripheral lesions on spine MRI point toward MS.
-
Acute severe presentation and rapid deterioration of neurological signs are more likely with NMO.
Diagnosis
Revised criteria proposed by the Mayo Clinic for diagnosis of NMO require 2 absolute criteria plus at least 2 supportive criteria4:
-
Absolute criteria:
-
Optic neuritis.
-
Acute myelitis.
-
Supportive criteria:
-
Brain MRI not meeting criteria for MS at disease onset.
-
Spinal cord MRI with contiguous T2‐weighted signal abnormality extending over 3 or more vertebral segments, indicating a relatively large lesion in the spinal cord.
-
NMO‐IgG seropositive status.
The criteria incorporate the recently developed NMO‐IgG test, which is currently available through centers such as the Mayo Clinic (Minnesota) and John Radcliffe Hospital (Oxford, United Kingdom). Our patient was not tested for NMO‐IgG when the assay became available because it is not known whether the test may be falsely negative during remission.
Management
Unlike MS, NMO rarely has a secondary progressive phase in which patients have increasing neurologic decline between attacks without remission. Instead, disabilities arise from the acute attacks.2 NMO may follow 1 of 3 courses:
-
Monophasic (single episode with permanent remission; approximately 20% of patients have permanent visual loss and 30% have permanent paralysis in 1 or both legs).
-
Relapsing (at least 85% of cases are characterized by 1 or more relapses, which usually occur early, with about 55% of patients having a relapse in the first year and 90% in the first 5 years).2
-
Progressive downhill course to death during first attack. Recovery is typically poor, possibly due to necrosis, with an estimated 50% death rate.1
Little is known about the effect of pregnancy on the disease progression of NMO. There are 3 other case reports of first presentation of NMO during pregnancy. In 1 case the patient was a known systemic lupus erythematosus (SLE) sufferer and NMO relapsed postpartum.5
In the acute phase, high‐dose intravenous steroid and plasmapheresis are useful. No controlled trials have established the effectiveness of treatments for the prevention of attacks. There is often steroid‐dependence, meaning that relapses are not uncommon during steroid withdrawal. Long‐term immunosuppressants are required to reduce the frequency and severity of attacks; these include azathioprine plus prednisone, mycophenolate mofetil plus prednisone, mitoxantrone, and cyclophosphamide. Rituximab, a monoclonal antibody, is currently under study. There are also case reports of monthly maintenance doses of intravenous gamma globulin resulting in prevention of relapses at 12 months.6
- .Neuromyelitis optica.Arch Neurol.2003;60(9):1336.
- .Neuromyelitis optica.Int MS J.2006;13(2):42–50.
- .Neuromyelitis optica: what it is and what it might be.Lancet.2003;361(9361):889–890.
- ,,,,.Revised diagnostic criteria for neuromyelitis optica.Neurology.2006;66:1485–1489.
- ,,, et al.Devic's neuromyelitis optica during pregnancy in a patient with systemic lupus erythematosus.Lupus.1999;8(3):244–247.
- ,.Devic's neuromyelitis optica treated with intravenous gamma globulin.Can J Neurol Sci.2004;31(2):265–267.
Rapid onset visual loss with limb involvement in a postpartum female invites a number of differential diagnoses, including infectious encephalomyelitis, vasculitis, an acute demyelinating disorder, and arterial/venous sinus thrombosis. We report an interesting, but initially puzzling, case of rapidly progressive optic neuritis and transverse myelitis in a postpartum Ghanaian female, later diagnosed as neuromyelitis optica (NMO).
Case Report
A 33‐year‐old Ghanaian female presented with bilateral eye pain worsened by eye movement, rapid visual loss, bifrontal headache, and right leg weakness for 48 hours. She was 8 weeks postpartum, with labor having been induced at 35 weeks due to hypertension; she was discharged on labetolol and no other medications. There was no other relevant past medical or family history, or illicit drug use.
On admission, her blood pressure was 148/99 mm Hg, pulse rate 92 beats per minute, temperature 37.8C, oxygen saturation 97% on room air, respiratory rate 14 breaths per minute, and Glasgow coma scale 15/15. Cranial nerve examination showed absent light perception in the right eye with a relative afferent pupillary defect, 20/30 Snellen visual acuity in the left eye, bilateral optic disc edema (worse on the right) and grade 1 hypertensive retinopathy, and slight facial asymmetry but otherwise grossly intact cranial nerves. Neurological examination of the limbs showed 5/5 power in upper limbs, but flexion was weaker (3/5) than extension (4/5) in lower limbs. There was hyperreflexia in the right arm and right leg with positive Babinski sign. Sensation, proprioception, and coordination were normal in both upper and lower limbs; a Romberg test was negative.
Other systems examinations were unremarkable. Complete blood count, standard electrolytes, erythrocyte sedimentation rate, C‐reactive protein, urinalysis, chest x‐ray, and an urgent head computed tomography (CT) with contrast were all noncontributory.
To cover a broad range of possible infective processes, ceftriaxone and acyclovir were started. In view of the rapid progression of her presentation she was transferred urgently to a specialty neurology hospital. There she was started on intravenous methylprednisolone to cover possible inflammatory causes, such as multiple sclerosis (MS) and vasculitis. However, her lower limb weakness progressed and she developed urinary retention. Lumbar puncture was performed; the opening pressure was 160 mm H2O. Cerebrospinal fluid (CSF) analysis demonstrated elevated protein level (121 mg/dL), 16/mm3 lymphocytosis, normal glucose, and negative gram stain and culture. Conventional CSF polymerase chain reaction for herpes simplex, Epstein‐Barr, varicella‐zoster, cytomegalovirus, John Cunningham virus (to rule out progressive multifocal leukoencephalopathy), human herpesvirus 6 viruses, and toxoplasma were negative. Antinuclear antibody, anticytoplasmic antibody, antiganglioside antibodies (GM1, GQ1b), thrombophilia screen (activated protein C resistance ratio, lupus anticoagulant and anticardiolipin antibodies, antithrombin III, protein C, and S deficiency), B12, folate, ferritin, and human immunodeficiency virus (HIV) screen were also negative. Brain magnetic resonance imaging (MRI), including venography, was normal. However, T2‐weighted MRI images of the orbit showed signal hyperintensity of the left optic chiasm and optic nerves, and T2‐weighted images of the spinal cord showed hyperintensity within the upper 4 and lower 4 thoracic levels. The diagnosis of NMO was entertained.
Following intravenous steroids, the patient was treated with a tapering course of oral steroids. She began to make a slow recovery with the aid of intense physiotherapy. Having walked in at her initial admission, she returned home needing crutches 4 weeks later and the visual acuity in her right eye remained 20/120 at best. Her requirement for intermittent urinary self‐catheterization and rectal enemas decreased with time. She continued to be rehabilitated at home with input from the community physiotherapy team and remains in remission at 12 months.
Discussion
First described by Eugene Devic in 1894, NMO is a rare, chronic inflammatory, demyelinating disease of the central nervous system.1 It is more common among Asians and Africans, with a female predominance (females comprise over two‐thirds of patients and more than 80% of those with the relapsing form of the disease).2 The mean age of onset is 35 to 47 years.2 The prevalence and incidence of NMO has not been established, partly because the disease is underrecognized and often confused with MS.
Pathophysiology and Clinical Features
NMO is a nonhereditary autoimmune condition distinct from MS. It is characterized by antibodies (NMOimmunoglobulin G [IgG]) against aquaporin 4 in myelin within astrocytes, which form part of the blood‐brain barrier.2 The damage in the spinal cord can range from inflammatory demyelination to necrosis. The inflammatory lesions in NMO have been classified as type II lesions (complement‐mediated demyelination)they differ from MS in their prominent perivascular distribution.
NMO presents with attacks of acute optic neuritis, usually bilateral, associated with severe transverse myelopathy occurring at the same time as or following the optic neuritis within a few days, weeks, or occasionally months. The following characteristics help to differentiate NMO from MS3:
-
The presence of transverse myelitis, bilateral neurological signs, and longitudinal extensive necrotic lesions on spine MRI point toward NMO.
-
Clinical involvement beyond the spinal cord and optic nerves, presence of oligoclonal bands in CSF, white matter lesions on brain MRI, and multiple small peripheral lesions on spine MRI point toward MS.
-
Acute severe presentation and rapid deterioration of neurological signs are more likely with NMO.
Diagnosis
Revised criteria proposed by the Mayo Clinic for diagnosis of NMO require 2 absolute criteria plus at least 2 supportive criteria4:
-
Absolute criteria:
-
Optic neuritis.
-
Acute myelitis.
-
Supportive criteria:
-
Brain MRI not meeting criteria for MS at disease onset.
-
Spinal cord MRI with contiguous T2‐weighted signal abnormality extending over 3 or more vertebral segments, indicating a relatively large lesion in the spinal cord.
-
NMO‐IgG seropositive status.
The criteria incorporate the recently developed NMO‐IgG test, which is currently available through centers such as the Mayo Clinic (Minnesota) and John Radcliffe Hospital (Oxford, United Kingdom). Our patient was not tested for NMO‐IgG when the assay became available because it is not known whether the test may be falsely negative during remission.
Management
Unlike MS, NMO rarely has a secondary progressive phase in which patients have increasing neurologic decline between attacks without remission. Instead, disabilities arise from the acute attacks.2 NMO may follow 1 of 3 courses:
-
Monophasic (single episode with permanent remission; approximately 20% of patients have permanent visual loss and 30% have permanent paralysis in 1 or both legs).
-
Relapsing (at least 85% of cases are characterized by 1 or more relapses, which usually occur early, with about 55% of patients having a relapse in the first year and 90% in the first 5 years).2
-
Progressive downhill course to death during first attack. Recovery is typically poor, possibly due to necrosis, with an estimated 50% death rate.1
Little is known about the effect of pregnancy on the disease progression of NMO. There are 3 other case reports of first presentation of NMO during pregnancy. In 1 case the patient was a known systemic lupus erythematosus (SLE) sufferer and NMO relapsed postpartum.5
In the acute phase, high‐dose intravenous steroid and plasmapheresis are useful. No controlled trials have established the effectiveness of treatments for the prevention of attacks. There is often steroid‐dependence, meaning that relapses are not uncommon during steroid withdrawal. Long‐term immunosuppressants are required to reduce the frequency and severity of attacks; these include azathioprine plus prednisone, mycophenolate mofetil plus prednisone, mitoxantrone, and cyclophosphamide. Rituximab, a monoclonal antibody, is currently under study. There are also case reports of monthly maintenance doses of intravenous gamma globulin resulting in prevention of relapses at 12 months.6
Rapid onset visual loss with limb involvement in a postpartum female invites a number of differential diagnoses, including infectious encephalomyelitis, vasculitis, an acute demyelinating disorder, and arterial/venous sinus thrombosis. We report an interesting, but initially puzzling, case of rapidly progressive optic neuritis and transverse myelitis in a postpartum Ghanaian female, later diagnosed as neuromyelitis optica (NMO).
Case Report
A 33‐year‐old Ghanaian female presented with bilateral eye pain worsened by eye movement, rapid visual loss, bifrontal headache, and right leg weakness for 48 hours. She was 8 weeks postpartum, with labor having been induced at 35 weeks due to hypertension; she was discharged on labetolol and no other medications. There was no other relevant past medical or family history, or illicit drug use.
On admission, her blood pressure was 148/99 mm Hg, pulse rate 92 beats per minute, temperature 37.8C, oxygen saturation 97% on room air, respiratory rate 14 breaths per minute, and Glasgow coma scale 15/15. Cranial nerve examination showed absent light perception in the right eye with a relative afferent pupillary defect, 20/30 Snellen visual acuity in the left eye, bilateral optic disc edema (worse on the right) and grade 1 hypertensive retinopathy, and slight facial asymmetry but otherwise grossly intact cranial nerves. Neurological examination of the limbs showed 5/5 power in upper limbs, but flexion was weaker (3/5) than extension (4/5) in lower limbs. There was hyperreflexia in the right arm and right leg with positive Babinski sign. Sensation, proprioception, and coordination were normal in both upper and lower limbs; a Romberg test was negative.
Other systems examinations were unremarkable. Complete blood count, standard electrolytes, erythrocyte sedimentation rate, C‐reactive protein, urinalysis, chest x‐ray, and an urgent head computed tomography (CT) with contrast were all noncontributory.
To cover a broad range of possible infective processes, ceftriaxone and acyclovir were started. In view of the rapid progression of her presentation she was transferred urgently to a specialty neurology hospital. There she was started on intravenous methylprednisolone to cover possible inflammatory causes, such as multiple sclerosis (MS) and vasculitis. However, her lower limb weakness progressed and she developed urinary retention. Lumbar puncture was performed; the opening pressure was 160 mm H2O. Cerebrospinal fluid (CSF) analysis demonstrated elevated protein level (121 mg/dL), 16/mm3 lymphocytosis, normal glucose, and negative gram stain and culture. Conventional CSF polymerase chain reaction for herpes simplex, Epstein‐Barr, varicella‐zoster, cytomegalovirus, John Cunningham virus (to rule out progressive multifocal leukoencephalopathy), human herpesvirus 6 viruses, and toxoplasma were negative. Antinuclear antibody, anticytoplasmic antibody, antiganglioside antibodies (GM1, GQ1b), thrombophilia screen (activated protein C resistance ratio, lupus anticoagulant and anticardiolipin antibodies, antithrombin III, protein C, and S deficiency), B12, folate, ferritin, and human immunodeficiency virus (HIV) screen were also negative. Brain magnetic resonance imaging (MRI), including venography, was normal. However, T2‐weighted MRI images of the orbit showed signal hyperintensity of the left optic chiasm and optic nerves, and T2‐weighted images of the spinal cord showed hyperintensity within the upper 4 and lower 4 thoracic levels. The diagnosis of NMO was entertained.
Following intravenous steroids, the patient was treated with a tapering course of oral steroids. She began to make a slow recovery with the aid of intense physiotherapy. Having walked in at her initial admission, she returned home needing crutches 4 weeks later and the visual acuity in her right eye remained 20/120 at best. Her requirement for intermittent urinary self‐catheterization and rectal enemas decreased with time. She continued to be rehabilitated at home with input from the community physiotherapy team and remains in remission at 12 months.
Discussion
First described by Eugene Devic in 1894, NMO is a rare, chronic inflammatory, demyelinating disease of the central nervous system.1 It is more common among Asians and Africans, with a female predominance (females comprise over two‐thirds of patients and more than 80% of those with the relapsing form of the disease).2 The mean age of onset is 35 to 47 years.2 The prevalence and incidence of NMO has not been established, partly because the disease is underrecognized and often confused with MS.
Pathophysiology and Clinical Features
NMO is a nonhereditary autoimmune condition distinct from MS. It is characterized by antibodies (NMOimmunoglobulin G [IgG]) against aquaporin 4 in myelin within astrocytes, which form part of the blood‐brain barrier.2 The damage in the spinal cord can range from inflammatory demyelination to necrosis. The inflammatory lesions in NMO have been classified as type II lesions (complement‐mediated demyelination)they differ from MS in their prominent perivascular distribution.
NMO presents with attacks of acute optic neuritis, usually bilateral, associated with severe transverse myelopathy occurring at the same time as or following the optic neuritis within a few days, weeks, or occasionally months. The following characteristics help to differentiate NMO from MS3:
-
The presence of transverse myelitis, bilateral neurological signs, and longitudinal extensive necrotic lesions on spine MRI point toward NMO.
-
Clinical involvement beyond the spinal cord and optic nerves, presence of oligoclonal bands in CSF, white matter lesions on brain MRI, and multiple small peripheral lesions on spine MRI point toward MS.
-
Acute severe presentation and rapid deterioration of neurological signs are more likely with NMO.
Diagnosis
Revised criteria proposed by the Mayo Clinic for diagnosis of NMO require 2 absolute criteria plus at least 2 supportive criteria4:
-
Absolute criteria:
-
Optic neuritis.
-
Acute myelitis.
-
Supportive criteria:
-
Brain MRI not meeting criteria for MS at disease onset.
-
Spinal cord MRI with contiguous T2‐weighted signal abnormality extending over 3 or more vertebral segments, indicating a relatively large lesion in the spinal cord.
-
NMO‐IgG seropositive status.
The criteria incorporate the recently developed NMO‐IgG test, which is currently available through centers such as the Mayo Clinic (Minnesota) and John Radcliffe Hospital (Oxford, United Kingdom). Our patient was not tested for NMO‐IgG when the assay became available because it is not known whether the test may be falsely negative during remission.
Management
Unlike MS, NMO rarely has a secondary progressive phase in which patients have increasing neurologic decline between attacks without remission. Instead, disabilities arise from the acute attacks.2 NMO may follow 1 of 3 courses:
-
Monophasic (single episode with permanent remission; approximately 20% of patients have permanent visual loss and 30% have permanent paralysis in 1 or both legs).
-
Relapsing (at least 85% of cases are characterized by 1 or more relapses, which usually occur early, with about 55% of patients having a relapse in the first year and 90% in the first 5 years).2
-
Progressive downhill course to death during first attack. Recovery is typically poor, possibly due to necrosis, with an estimated 50% death rate.1
Little is known about the effect of pregnancy on the disease progression of NMO. There are 3 other case reports of first presentation of NMO during pregnancy. In 1 case the patient was a known systemic lupus erythematosus (SLE) sufferer and NMO relapsed postpartum.5
In the acute phase, high‐dose intravenous steroid and plasmapheresis are useful. No controlled trials have established the effectiveness of treatments for the prevention of attacks. There is often steroid‐dependence, meaning that relapses are not uncommon during steroid withdrawal. Long‐term immunosuppressants are required to reduce the frequency and severity of attacks; these include azathioprine plus prednisone, mycophenolate mofetil plus prednisone, mitoxantrone, and cyclophosphamide. Rituximab, a monoclonal antibody, is currently under study. There are also case reports of monthly maintenance doses of intravenous gamma globulin resulting in prevention of relapses at 12 months.6
- .Neuromyelitis optica.Arch Neurol.2003;60(9):1336.
- .Neuromyelitis optica.Int MS J.2006;13(2):42–50.
- .Neuromyelitis optica: what it is and what it might be.Lancet.2003;361(9361):889–890.
- ,,,,.Revised diagnostic criteria for neuromyelitis optica.Neurology.2006;66:1485–1489.
- ,,, et al.Devic's neuromyelitis optica during pregnancy in a patient with systemic lupus erythematosus.Lupus.1999;8(3):244–247.
- ,.Devic's neuromyelitis optica treated with intravenous gamma globulin.Can J Neurol Sci.2004;31(2):265–267.
- .Neuromyelitis optica.Arch Neurol.2003;60(9):1336.
- .Neuromyelitis optica.Int MS J.2006;13(2):42–50.
- .Neuromyelitis optica: what it is and what it might be.Lancet.2003;361(9361):889–890.
- ,,,,.Revised diagnostic criteria for neuromyelitis optica.Neurology.2006;66:1485–1489.
- ,,, et al.Devic's neuromyelitis optica during pregnancy in a patient with systemic lupus erythematosus.Lupus.1999;8(3):244–247.
- ,.Devic's neuromyelitis optica treated with intravenous gamma globulin.Can J Neurol Sci.2004;31(2):265–267.
Pediatric OUs in the United States
The first observation units were implemented more than 40 years ago with the goal of reducing the number and duration of inpatient stays. Since then, observation units (OUs) have evolved as a safe alternative to hospitalization14 for the delivery of finite periods of care, typically less than 24 hours.58 Observation services allow for time to determine the need for hospitalization in cases that are unclear after their initial evaluation and treatment.9 Observation status is an administrative classification related to reimbursement that can be applied to patients whose diagnosis, treatment, stabilization, and discharge can reasonably be expected within 24 hours.10, 11 The site of care for observation is dependent in part upon existing facility structures; some institutions utilize virtual OUs within the emergency department (ED) or hospital ward, while others have dedicated, geographically distinct OUs, which may function as an extension of either the ED or inpatient settings.9
OUs have been instrumental in providing care to adult patients with chest pain, asthma, and acute infections.1218 Recently, there has been an increase in the number of publications from pediatric OUs in the United States and abroad. Observation may be a preferred model of care for select pediatric patients, as hospitalized children often experience brief stays.1921 Previous reviews on this model of care have combined adult and pediatric literature and have included research from countries with healthcare structures that differ considerably from the United States.2224 To date, no systematic review has summarized the pediatric OU literature with a focus on the US healthcare system.
As payers and hospitals seek cost‐effective alternatives to traditional inpatient care, geographically distinct OUs may become integral to the future of healthcare delivery for children. This systematic review provides a descriptive overview of the structure and function of pediatric OUs in the United States. We also scrutinize the outcome measures presented in the included publications and propose future directions for research to improve both observation unit care, as well as the care delivered to patients under observation status within general inpatient or ED settings.
Methods
Literature Search
With the assistance of a health services librarian, a search of the following electronic databases from January 1, 1950 through February 5, 2009 was conducted: Medline, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Health Care Advisory Board (HCAB), Lexis‐Nexis, National Guideline Clearinghouse, and Cochrane Reviews. Key words used for the Boolean search are included in Appendix A. In addition, we conducted a manual search of reference lists from reviews, guidelines, and articles meeting inclusion criteria.
We included English language peer‐reviewed publications that reported on pediatric OU care in the United States. Studies were included if they reported outcomes including lengths of stay, admission from observation rates, return visit rates, costs or charges. Descriptive publications of pediatric OU structure and function were also included. Studies were excluded if they were conducted outside the United States, evaluated psychiatric or intensive care, reported on observation status in an ED without an OU or observation status on a traditional inpatient ward. Two reviewers (M.M. and C.K.) identified articles for inclusion. Any disagreements between the reviewers were resolved by discussion and consensus agreement. Interrater reliability was assessed using the kappa statistic.
Quality Assessment
The quality of each study was rated using the Oxford Centre for Evidence‐based Medicine levels of evidence.25 With this system, levels of evidence range from 1a (homogeneous systematic review of randomized, controlled trials) to 5 (expert opinion without explicit critical appraisal).
Data Synthesis
Data on study design, OU characteristics, patient populations, and outcomes were extracted using a standardized form. Heterogeneity of study design, interventions, and outcomes precluded the ability to conduct meta‐analyses.
Results
A systematic search of the electronic databases identified 222 unique citations (Figure 1). A total of 107 abstracts were evaluated. We identified 48 articles for full‐text review, of which 18 met inclusion criteria. Hand search of references yielded 24 additional articles, of which 3 met inclusion criteria. Interrater agreement for selected articles was high at 98% (kappa = 0.85).
Observation Unit Characteristics
The majority of research on OUs has been conducted at large academic pediatric centers. One publication was from a community hospital.26 These studies present data on more than 22,000 children cared for in OUs of 11 hospitals over a 32‐year time span. Most studies were level 2 evidence: 2b, retrospective cohort studies and low‐quality randomized, controlled trials; or 2c, outcomes research. Three were descriptive and not assigned a formal evidence level.2729
Table 1 highlights general features of U.S. pediatric OUs. Five institutions renovated or expanded clinical space in order to open the OU.27, 2932 Units ranged in size from 3 to 23 beds. The OU was located in or near the ED in all but 2 hospitals, which had ward‐based units. The ED was the primary entry point into the OU with only 2 open model units accepting patients from other settings.5, 32 The annual number of observation cases ranged from 1000 to 3000 in children's hospitals. Approximately 500 ward‐based observation cases per year were cared for in the single community hospital studied. Three reports included time trends showing increased OU utilization over study years.5, 30, 31
| Publication (Year); Condition | Study Design; Level of Evidence; Time Frame; Sample Size | Hospital; Observation Setting; Year Opened | Site | Beds | Entry Point | Staffing; Physicians; Nurses |
|---|---|---|---|---|---|---|
| ||||||
| Gururaj et al.43 (1972); all conditions | Retrospective cohort; 2c; 1 year; 437 cases under observation | King's County Downstate Brooklyn; short‐stay unit | ED | 3 | Not reported | Pediatric residents; general pediatricians |
| Ellerstein and Sullivan,32 (1980); all conditions | Retrospective cohort; 2c; 6 years; 5858 cases of unscheduled care plus 1403 elective surgery cases | Children's Hospital Buffalo; observation unit; 1972 | ED | 8 | ED, clinic, procedure/OR | Primary care pediatricians; other specialists; pediatric residents |
| O'Brien et al.37 (1980); asthma | Retrospective cohort; 2c; 1 month; 434 cases of asthma, 328 discharged directly from ED, 106 treated in holding unit | Children's National DC; holding unit | ED | 6 | ED | 1‐2 pediatric residents; 1‐2 nurses |
| Willert et al.35 (1985); asthma | Randomized*; 2b; 578 cases of asthma; 166 cases 1.5 hours postaminophylline, 103 randomized, 52 to holding unit | Children's Memorial Chicago; holding room | ED | 5 | ED | General pediatricians; pediatric residents; PEM nurses |
| Listernick et al.38 (1986); dehydration | Randomized; 2b; 29 cases of dehydration; 22 to holding unit | Children's Memorial Chicago | ||||
| Balik et al.31 (1988); all conditions | Descriptive; none given | Minneapolis Children's; short‐stay unit observation area; 1985 | Day surgery area adjacent to ED | Not reported | Not reported | General pediatricians; pediatric nurses (shared with ED) |
| Marks et al.7 (1997); all conditions | Retrospective cohort; 2c; 5 months; 968 cases in short‐stay unit | Children's Hospital Boston; short‐stay unit; 1994 | Ward | 4‐18 | ED | Primary care pediatricians; PEM physicians; pediatric residents; pediatric nurses; 1:6 nurse:patient ratio |
| Marks et al.7 (1997); asthma | Pre‐post; 2b; 400 cases of asthma; 102 pre/298 post short‐stay unit | Children's Hospital Boston | ||||
| Wiley et al.6 (1998); all conditions | Retrospective cohort; 2c; 1 year; 805 cases of unscheduled observation; plus 595 scheduled cases | Connecticut Children's; outpatient extended treatment site | ED | 10 | Not reported | PEM physicians; other specialists; 1:5 nurse:patient ratio |
| Scribano et al.65 (2001); all conditions | Retrospective cohort; 2b; 2 years; 1798 cases under observation | Connecticut Children's | ||||
| Leduc et al.30 (2002); all conditions | Retrospective cohort; 2c; 6 months; 686 cases under observation (4.8% of ED visits) | Children's Hospital Denver; OU | ED | 6 | Not reported | Not reported |
| Bajaj and Roback,30 (2003); intussusception | Retrospective cohort; 2b; 4.5 years; 78 cases of intussusception (51 under observation) | Children's Hospital Denver | ||||
| Wathen et al.36 (2004); dehydration | Convenience sample; 2c; 10 months; 182 cases of dehydration (48 under observation) | Children's Hospital Denver | ||||
| Crocetti et al.26 (2004); all conditions | Retrospective cohort; 2b; 2 years; 956 cases under observation | John Hopkin's Bayview; observation status beds; 1997 | Ward | Not reported | 99% ED 1% other location | General pediatricians covering ED and ward |
| Silvestri et al.29 (2005); all conditions | Descriptive; none given | Children's Hospital of Philadelphia; OU; 1999 | ED | 12 | ED | PEM physicians; PEM fellows; urgent care pediatricians; ED nurse practitioner; inpatient nurses |
| Alpern et al.34 (2008); all conditions | Prospective cohort; 1b; 30 months; 4453 cases under observation | Children's Hospital of Philadelphia | ||||
| Thomas27 (2000); all conditions | Descriptive; none given | Primary Children's Medical Center; RTU; 1999 | ED | 22‐26 | ED, clinic, procedure/OR | PEM physicians; general pediatricians; other specialists; no residents |
| Zebrack et al.25 (2005); all conditions | Retrospective cohort; 2b; 2 years; 4189 cases of unscheduled observation plus 2288 scheduled cases | Primary Children's Medical Center | PEM nurses; 1:4 nurse:patient ratio | |||
| Miescier et al.40 (2005); asthma | Retrospective cohort; 2b; 2 years; 3029 asthma visits; 384 admitted, 301 observed, 161cases met inclusion | Primary Children's Medical Center | ||||
| Holsti et al.41 (2005); head injury | Retrospective cohort; 2b; 2 years; 827 CHI visits, 273 admitted, 285 observed, 284 cases met inclusion | Primary Children's Medical Center | ||||
| Greenberg et al.42 (2006); croup | Retrospective pre‐post; 2b; 1 year each; 694 croup cases pre‐RTU, 66 admitted; 789 croup cases post‐RTU, 33 admitted; 76 observed | Primary Children's Medical Center | ||||
| Mallory et al.33 (2006); dehydration | Retrospective cohort; 2b; 1 year; 430 dehydration cases under observation | Primary Children's Medical Center | ||||
Staffing and Workflow
Staffing models varied and have undergone transitions over time. Prior to 1997, general pediatricians primarily provided physician services. In more recent years, OUs have utilized pediatric emergency medicine (PEM) providers. Three of the 11 units allowed for direct patient care by subspecialists.5, 6, 32 One OU was staffed by nurse practitioners.29 OU nursing backgrounds included pediatrics, emergency medicine, or PEM.
Five institutions assembled multidisciplinary teams to define the unit's role and establish policies and procedures.7, 27, 2931 Workflow in the OU focused on optimizing efficiency through standardized orders, condition‐specific treatment protocols, and bedside charting.7, 26, 33 Several units emphasized the importance of ongoing evaluations by attending physicians who could immediately respond to patient needs. Rounds occurred as often as every 4 hours.5, 7 Two centers utilized combined physician‐nursing rounds to enhance provider communication.7, 34 No publications reported on patient transitions between sites of care or at shift changes.
Criteria for Observation
All 11 hospitals have developed protocols to guide OU admissions (Table 2). Nine publications from 4 OUs commented on treatments delivered prior to observation.33, 3542 The most commonly cited criteria for admission was approval by the unit's supervising physician. Utilization review was not mentioned as an element in the OU admission decision. Common OU exclusions were the need for intensive care or monitoring while awaiting an inpatient bed; however, these were not universal. Eight centers placed bounds around the duration of OU stays, with minimum stays of 2 hours and maximum stays of 8 to 24 hours.
| Hospital | Entry Criteria | Age Range | Time | Exclusion Criteria |
|---|---|---|---|---|
| ||||
| King's County, Downstate Brooklyn | Otherwise required inpatient admission | 0‐13 years | Maximum 24 hours | Not reported |
| Acute problem of uncertain severity | ||||
| Acute problem not readily diagnosed | ||||
| Short course periodic treatment | ||||
| Diagnostic procedures impractical as outpatient | ||||
| Children's Hospital, Buffalo | Admission from any source | 0‐21 years | Maximum 24 hours | Intensive care needs |
| Short stay elective surgery | Routine diagnostic tests | |||
| Estimated length of stay 24 hours | Holding prior to admission | |||
| Children's National, Washington, DC | Inadequate response to 3 subcutaneous epinephrine injections | 8 months to 19 years | Not reported | Not reported |
| Children's Memorial, Chicago | Asthma: | |||
| Available parentAsthma score 5Inadequate response to ED treatment | >1 year | Maximum 24 hours | Past history of BPD, CF, CHD, other debilitating disease | |
| Dehydration: | ||||
| Cases receiving oral hydration | 3‐24 months | 12 hours for oral | Intensive care need | |
| Parent preference if given IV hydration | 8 to 12 hours for IV | Hypernatremia | ||
| Minneapolis Children's | Conditions listed in Table 3 | Not reported | Maximum 10 hours | Not reported |
| Children's Hospital, Boston | Straightforward diagnoses as determined by ED staff | Not reported | Not reported | Other complex medical issues |
| Bed availability | ||||
| Connecticut Children's | PEM attending discretionLimited severity of illnessUsually confined to a single organ systemClearly identified plan of care | Not reported | After 3‐4 hours in ED Low likelihood of requiring extended care >23 hours | Asthma: no supplemental O2 need, nebulized treatments >Q2 hourCroup: no supplemental O2 need, 2 racemic epinephrine treatmentsDehydration: inability to tolerate orals, bicarbonate >10, 40 mL/kg IVFSeizure: partial or generalized, postictal, unable to tolerate oralsPoisoning: mild or no symptoms, poison control recommendation |
| Children's Hospital, Denver | Intussusception: following reduction | 0‐18 years | After 3‐4 hours in ED | Not reported |
| Dehydration: based on clinical status | ||||
| Johns Hopkins, Bayview | Consultation with on‐duty pediatrician | 0‐18 years | Minimum of 2 hours | Patients requiring subspecialty or intensive care services |
| High likelihood of discharge at 24 hours | ||||
| Children's Hospital of Philadelphia | Sole discretion of the ED attending | Not reported | Minimum 4 hours | No direct admissions |
| Single focused acute condition | Maximum 23 hours | Diagnostic dilemmas | ||
| Clinical conditions appropriate for observation | Underlying complex medical problems | |||
| Primary Children's Medical Center | Observation unit attending discretion | 0‐21 years | Minimum 3 hours | Admission holds |
| Scheduled procedures as space available | Maximum 24 hours | Intensive care needs | ||
| ED admit after consult with OU doctor | Complicated, multisystem disease | |||
| Clear patient care goals | Need for multiple specialty consults | |||
| Limited severity of illness | Psychiatric patients | |||
| Diagnostic evaluation | ||||
Ages of Children Under Observation
Seven of 11 hospitals reported the age range of patients accepted in their OU (Table 2). All but 1 unit accepted children from infants to young adults, 18 to 21 years of age.43 In the 6 units that reported the age distribution of their OU population, roughly 20% were 1 year, more than 50% were 5 years, and fewer than 30% fell into an adolescent age range.5, 6, 26, 32, 34, 43
Conditions Under Observation
Many conditions under observation were common across time and location (Table 3). The list of conditions cared for in OUs has expanded in recent years. Medical conditions predominated over surgical. While the majority of observation cases required acute care, nearly one‐half of the units accepted children with scheduled care needs (eg, routine postoperative care, procedures requiring sedation, infusions, and extended evaluations such as electroencephalograms or pH probes). These scheduled cases, cared for within the OU structure, provided more steady demand for OU services.
| King's County, Downstate Brooklyn | Children's Hospital, Buffalo | Minneapolis Children's | Children's Hospital, Boston | Connecticut Children's | Children's Hospital, Denver | Johns Hopkins, Bayview | Children's Hospital of Philadelphia | Primary Children's Medical Center, Salt Lake City | |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Respiratory | |||||||||
| Asthma | |||||||||
| Pneumonia | |||||||||
| Bronchiolitis | |||||||||
| Croup | |||||||||
| Allergic reaction | |||||||||
| Cardiology | |||||||||
| Gastrointestinal | |||||||||
| Vomiting | |||||||||
| Gastro/dehydration | |||||||||
| Abdominal pain | |||||||||
| Constipation | |||||||||
| Diabetes | |||||||||
| Neurologic | |||||||||
| Seizure | |||||||||
| Head injury | |||||||||
| Infection | |||||||||
| Sepsis evaluation | |||||||||
| UTI/pyelonephritis | |||||||||
| Cellulitis | |||||||||
| Fever | |||||||||
| Pharyngitis | |||||||||
| Otitis media | |||||||||
| Adenitis | |||||||||
| Ingestion/poisoning | |||||||||
| Hematologic | |||||||||
| Sickle cell disease | |||||||||
| Transfusion/emnfusion | |||||||||
| Psychological/social | |||||||||
| Dental | |||||||||
| Surgical conditions | |||||||||
| Foreign body | |||||||||
| Trauma | |||||||||
| Burn | |||||||||
| Orthopaedic injury | |||||||||
| Postoperative complication | |||||||||
| Scheduled care | |||||||||
| Diagnostic workup | |||||||||
| Procedures/sedation | |||||||||
| Elective surgery | |||||||||
Reimbursement
One publication highlighted the special billing rules that must be considered for observation care.27 In 3 studies, payers recognized cost‐savings associated with the OU's ability to provide outpatient management for cases that would traditionally require inpatient care.31, 35, 38
Observation Unit Outcomes
Outcomes reported for pediatric OU stays fall into 4 major categories: length of stay (LOS), admission rates, return visit rates, and costs. Despite these seemingly straightforward groupings, there was significant heterogeneity in reporting these outcomes.
Length of Stay
The start time for OU length of stay (LOS) is not clearly defined in the articles included in this review. While the start of an observation period is assumed to begin at the time the order for observation is placed, it is possible that the LOS reported in these publications began at the time of ED arrival or the time the patient was physically transferred to the OU. The average LOS for individual OUs ranged from 10 to 15 hours.5, 6, 26, 30, 35, 38, 40, 41, 43 One ward‐based and 1 ED‐based unit reported LOS extending beyond 24 hours,7, 30 with averages of 35 and 9 hours, respectively. Two units limited the duration of care to 10 hours.31, 38
For studies that included a comparison group, OU stays were consistently shorter than a traditional inpatient stay by 6 to 110 hours.7, 36, 38, 39, 42 No significant differences in clinical parameters between groups were reported. There was appreciable variation in the average LOS across institutions for similar conditions, 12 to 35 hours for asthma,5, 7, 34, 35 and 9 to 18 hours for dehydration.5, 34, 36, 38
Admission Rates
Rates of hospital admission after observation from the 9 OUs reporting this outcome are presented in Table 4. Three publications from a single institution counted hospital admission in the 48 to 72 hours following discharge from the OU as though the patient were admitted to the hospital directly from the index OU stay.33, 40, 41 Conditions with the lowest admission rates, 10%, included croup, neurologic conditions, ingestions, trauma, and orthopedic injuries. The highest admission rates, >50%, were for respiratory conditions including asthma, pneumonia, and bronchiolitis.
| King's County, Downstate Brooklyn (%) | Children's Hospital, Buffalo (%) | Connecticut Children's (%) | Johns Hopkins, Bayview (%) | Children's Hospital of Philadelphia (%) | Primary Children's Medical Center, Salt Lake City (%) | |
|---|---|---|---|---|---|---|
| ||||||
| Unscheduled care | 42 | 17 | 11 | 25 | 25 | 15 |
| Respiratory | 32 | |||||
| Asthma | 57 | 16 | 26 | 22 | 22‐25* | |
| Pneumonia | 50 | 23 | 30‐48 | |||
| Bronchiolitis | 46 | 32 | 43 | |||
| Croup | 9 | 17 | 9 | 4‐6 | ||
| Allergic reaction | 3 | |||||
| Cardiology | 22 | |||||
| Gastrointestinal | 43 | 19 | ||||
| Vomiting | 5 | 22 | ||||
| Gastro/dehydration | 23 | 15/21 | 16* | |||
| Abdominal pain | 9 | 17 | 27 | |||
| Constipation | 9 | |||||
| Diabetes | 17 | |||||
| Neurologic | 10 | |||||
| Seizure | 19 | 8 | 17 | 18 | ||
| Head injury | 7 | 5* | ||||
| Infection | 19 | 34 | ||||
| Sepsis evaluation | 25 | 22 | ||||
| UTI/pyelonephritis | 25 | 16 | ||||
| Cellulitis | 15 | |||||
| Fever | 16 | 26 | ||||
| Pharyngitis | 13 | |||||
| Otitis media | 21 | |||||
| Ingestion/poisoning | 9 | 4 | 4 | 9 | 10 | 5 |
| Hematologic | 23 | |||||
| Transfusion/emnfusion | 2 | |||||
| Psychological/social | 21 | 80 | 17 | |||
| Dental | 14 | |||||
| Surgical conditions | ||||||
| Foreign body | ||||||
| Trauma | 13 | 2 | 53 | 5 | ||
| Burn | 13 | |||||
| Orthopedic injury | 22 | 3 | ||||
| Postoperative complication | 26 | 16 | ||||
| Scheduled care | ||||||
| Diagnostic workup | 0‐5 | |||||
| Procedures/sedation | 0.1‐9.0 | |||||
| Elective surgery | 13 | 0‐5 | ||||
Return Visit Rates
Unscheduled return visit rates were reported in 9 publications from 6 institutions and ranged from 0.01% to 5%.7, 26, 33, 3537, 3941 Follow‐up timeframes ranged from 48 hours to 1 month. Return visits were inconsistently defined. In most studies, rates were measured in terms of ED visits.26, 33, 3537, 39, 41 One ward‐based unit counted only hospital readmissions toward return visit rates.7 Three publications, from ED‐based units, counted hospital readmissions in the 2 to 5 days following observation toward admission rates and not as return visits.33, 40, 41 In most studies, data on return visits were collected from patient logs or patient tracking systems. Three studies contacted patients by phone and counted return visits to the clinic.3537 No studies reported on adherence to scheduled visits following observation.
Costs
Seven studies reported financial benefits of OU care when compared with traditional hospital care.7, 30, 31, 35, 37, 38, 42 Two centers admitted patients to inpatient care if their observation period reached a set time limit, after which cost savings were no longer realized.31, 35 Cost savings associated with the OU treatment of asthma and dehydration were attributed to lower charges for an OU bed.35, 38 Decreased charges for the OU treatment of croup were related to shorter LOS.42
Discussion
In the 40 years since the first studies of pediatric OUs, several US health systems have extended observation services to children. This model of care may be expanding, as suggested by an increase in the number of publications in the past 10 years. However, the number of centers within the US reporting on their OU experience remains small. Our systematic review identified a recurrent theme related to OUsthe opportunity to improve operational processes of care compared with the traditional inpatient alternative. We have identified the need to standardize OU outcomes and propose measures for future OU research.
Observation Unit Operations
The OU care model expands outpatient management of acute conditions to include children who are neither ready for discharge nor clear candidates for inpatient admission. OUs have demonstrated the ability to care for patients across the pediatric age spectrum. Over the decades spanning these publications, advances in medical therapy such as antiemetics for gastroenteritis and early administration of systemic steroids for asthma may have resulted in lower admission rates or shorter time to recovery.44, 45 Despite these advances, there are marked consistencies in the conditions cared for within OUs over time. The data summarized here may help guide institutions as they consider specific pediatric conditions amenable to observation care.
The hospitals included in this review either added physical space or revised services within existing structures to establish their OU. Hospitals facing physical constraints may look to underutilized areas, such as recovery rooms, to provide observation care, as observation does not require the use of licensed inpatient beds. Several units have responded to daily fluctuations in unscheduled observation cases by also serving patients who require outpatient procedures, brief therapeutic interventions, and diagnostic testing. By caring for patients with these scheduled care needs during the day, there is a more steady flow of patients into the OU. While hospitals traditionally have used postanesthesia care units and treatment rooms for scheduled cases, OUs appear to benefit from the consistent resource allocation associated with a constant demand for services.
To date, the vast majority of pediatric OUs in the published literature have emerged as an extension of ED services. Now, with the expansion of pediatric hospitalist services and movement toward 24/7 inpatient physician coverage, there may be increased development of ward‐based OUs and the designation of inpatient observation status. While ward‐based OUs managed by pediatric hospitalists may be well established, we were not able to identify published reports on this structure of care. A national survey of health systems should be undertaken to gather information regarding the current state of pediatric observation services.
When creating policies and procedures for OUs, input should be sought from stakeholders including hospitalists, PEM providers, primary care providers, subspecialists, mid‐level providers, nurses, and ancillary staff. As patients requiring observation level of care do not neatly fit an outpatient or inpatient designation, they present an opportunity for hospitalist and PEM physician groups to collaborate.4648 Calling on the clinical experiences of inpatient and ED providers could offer unique perspectives leading to the development of innovative observation care models.
This review focused on institutions with dedicated observation services, which in all but 1 study26 consisted of a defined geographic unit. It is possible that the practices implemented in an OU could have hospital‐wide impact. For example, 1 study reported reduction in LOS for all asthma cases after opening a ward‐based unit.7 Further, pediatric hospitalist services have been associated with shorter LOS49 and increased use of observation status beds compared with traditional ward services.50 As pediatric hospitalists expand their scope of practice to include both observation and inpatient care, clinical practice may be enhanced across these care areas. It follows that the impact of observation protocols on care in the ward setting should be independently evaluated.
The costs associated with the establishment and daily operations of an OU were not addressed in the reviewed publications. Assertions that observation provides a cost‐effective alternative to inpatient care4, 7, 23, 42 should be balanced by the possibility that OUs extend care for patients who could otherwise be discharged directly home. Studies have not evaluated the cost of OU care compared with ED care alone. Research is also needed to assess variations in testing and treatment intensity in OUs compared with the ED and inpatient alternatives. Reimbursement for observation is dependent in part upon institutional contracts with payers. A full discussion of reimbursement issues around observation services is beyond the scope of this review.
Observation Unit Outcomes
Length of Stay
Although most studies reported LOS, direct comparisons across institutions are difficult given the lack of a consistently referenced start to the observation period. Without this, LOS could begin at the time of ED arrival, time of first treatment, or time of admission to the OU. Identifying and reporting the elements contributing to LOS for observation care is necessary. The time of OU admission is important for billing considerations; the time of first treatment is important to understanding the patient's response to medical interventions; the time of ED arrival is important to evaluating ED efficiency. Each of these LOS measures should be reported in future studies.
Direct comparisons of LOS are further complicated by variability in the maximum permissible duration of an OU stay, ranging from 8 to 24 hours in the included studies. Despite these limits, some OU care will extend beyond set limits due to structural bottlenecks. For example, once the inpatient setting reaches capacity, observation LOS for patients who require admission will be prolonged. The best evaluation of LOS would come from prospective study design utilizing either randomization or quality improvement methods.
Defining Success and Failure in Observation Care
In the reviewed literature, observation failures have been defined in terms of admission after observation and unscheduled return visit rates. Admission rates are heavily dependent on appropriate selection of cases for observation. Although some observation cases are expected to require inpatient admission, OUs should question the validity of their unit's acceptance guidelines if the rate of admission is >30%.51 High rates could be the result of inadequate treatment or the selection of children too sick to improve within 24 hours. Low rates could indicate overutilization of observation for children who could be discharged directly home. Full reporting on the number of children presenting with a given condition and the different disposition pathways for each is needed to evaluate the success of OUs. Condition‐specific benchmarks for admission after observation rates could guide hospitals in their continuous improvement processes.
Unscheduled return visits may reflect premature discharge from care, diagnostic errors, or development of a new illness. OU care may influence patient adherence to scheduled follow‐up care but this has not been evaluated to date. In future research, both scheduled and unscheduled return visits following ED visits, observation stays, and brief inpatient admissions for similar disease states should be reported for comparison. Standard methodology for identifying return visits should include medical record review, claims analyses, and direct patient contact.
As hospitals function at or near capacity,52, 53 it becomes important to delineate the appropriate length of time to monitor for response to treatments in a given setting. Limited capacity was a frequently cited reason for opening a pediatric OU; however, the impact of OUs on capacity has not yet been evaluated. Operations research methods could be used to model OU services' potential to expand hospital capacity. This research could be guided by evaluation of administrative data from across institutions to identify current best practices for pediatric OU and observation status care.
OU benchmarking in the United States has begun with a small number of adult units participating in the ED OU Benchmark Alliance (EDOBA).54 In Table 5, we propose dashboard measures for pediatric OU continuous quality improvement. The proposed measures emphasize the role of observation along the continuum of care for acute conditions, from the ED through the OU with or without an inpatient stay to clinic follow‐up. Depending on the structure of observation services, individual institutions may select to monitor different dashboard measures from the proposed list. Patient safety and quality of care measures for the conditions commonly receiving pediatric OU care should also be developed.
| ED |
OU |
Inpatient |
Clinic | |
|---|---|---|---|---|
| ||||
| Length of stay* | ED arrival to OU admission | OU admit to disposition | Inpatient admit to discharge | |
| ED arrival to discharge home from OU | ||||
| ED arrival to discharge from inpatient following OU care | ||||
| OU admission to discharge home from inpatient care | ||||
| Admission* | % ED census admitted inpatient | % OU census admitted | ||
| % ED census that is observed | ||||
| Unscheduled return visits* | To ED | Requiring OU admission | Requiring inpatient admission | |
| Scheduled follow‐up* | To ED | To primary care or subspecialist office | ||
| Capacity | ED crowding scales | Unable to accept transfers | ||
| ED left before evaluation rates | Inpatient occupancy | |||
| Ambulance diversion | ||||
| Satisfaction | Patient/Parent | |||
| ED providers | OU providers | Inpatient providers | Follow‐up providers | |
| Cost | ED care | OU care | Inpatient care | |
| Total encounter | ||||
Limitations
The most important limitations to this review are the heterogeneity in interventions and reporting of outcomes, which precluded our ability to combine data or conduct meta‐analyses. We attempted to organize the outcomes data into clear and consistent groupings. However, we could not compare the performance of 1 center with another due to differences in OU structure, function, and design.
In order to focus this systematic review, we chose to include only peer reviewed publications that describe pediatric OUs within the United States. This excludes expert guidelines, which may be of value to institutions developing observation services.
Our search found only a small number of centers that utilize OUs and have published their experience. Thus, our review is likely subject to publication bias. Along this line, we identified 9 additional publications where children were cared for alongside adults within a general OU.5563 This suggests an unmeasured group of children under observation in general EDs, where more than 90% of US children receive acute care.64 These articles were excluded because we were unable to distinguish pediatric specific outcomes from the larger study population.
Finally, retrospective study design is subject to information bias. Without a comparable control group, it is difficult to understand the effects of OUs. Patients directly admitted or discharged from the ED and patients who require admission after observation all differ from patients discharged from observation in ways that should be controlled for with a randomized study design.
Conclusions
OUs have emerged to provide treatment at the intersection of outpatient and inpatient care during a time of dramatic change in both emergency and hospital medicine. As hospitalists expand their scope of practice to include observation care, opportunities will arise to collaborate with ED physicians and share their growing expertise in quality and efficiency of hospital care delivery to improve observation services for children. OUs have been established with laudable goalsto reduce inpatient admissions, increase patient safety, improve efficiency, and control costs. The current evidence is not adequate to determine if this model of healthcare delivery achieves these goals for children. Through synthesis of existing data, we have identified a need for standard reporting for OU outcomes and propose consistent measures for future observation care research. Only through prospective evaluation of comparable outcomes can we appraise the performance of pediatric OUs across institutions.
- .Observation medicine.Acad Emerg Med.1994;1(2):152–154.
- ,.Principles of observation medicine.Emerg Med Clin North Am.2001;19(1):1–17.
- ,,, et al.Emergency department observation beds improve patient care: Society for Academic Emergency Medicine debate.Ann Emerg Med.1992;21(8):967–975.
- .Pediatric observation medicine.Emerg Med Clin North Am.2001;19(1):239–254.
- ,,.The pediatric hybrid observation unit: an analysis of 6477 consecutive patient encounters.Pediatrics.2005;115(5):e535–e542.
- ,,, et al.Observation units: the role of an outpatient extended treatment site in pediatric care.Pediatr Emerg Care.1998;14(6):444–447.
- ,,, et al.Impact of a short stay unit on asthma patients admitted to a tertiary pediatric hospital.Qual Manag Health Care.1997;6(1):14–22.
- ,,, et al.Management of observation units. American College of Emergency Physicians.Ann Emerg Med.1995;25(6):823–830.
- ,,, et al. The observation unit: an operational overview for the hospitalist. Society of Hospital Medicine White Paper 2009; Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Publications/WhitePapers/White_Papers.htm. Accessed July2009.
- Acute Criteria Pediatric InterQual Level of Care.San Francisco, CA:McKesson Corporation;2006.
- Observation Status Related to U.S. Hospital Records.Healthcare Cost and Utilization Project. HCUP Methods Series Report #2002‐3. Rockville, MD: Agency for Healthcare Research and Quality;2002.
- ,,, et al.Emergency department observation unit versus hospital inpatient care for a chronic asthmatic population: a randomized trial of health status outcome and cost.Med Care.1998;36(4):599–609.
- ,,, et al.Costs of an emergency department‐based accelerated diagnostic protocol vs hospitalization in patients with chest pain: a randomized controlled trial.JAMA.1997;278(20):1670–1676.
- .Management of patients with infectious diseases in an emergency department observation unit.Emerg Med Clin North Am.2001;19(1):187–207.
- ,,, et al.A comparison between emergency diagnostic and treatment unit and inpatient care in the management of acute asthma.Arch Intern Med.1997;157(18):2055–2062.
- .Chest pain observation units.Emerg Med J.2001;18(2):148.
- ,,, et al.Randomised controlled trial and economic evaluation of a chest pain observation unit compared with routine care.BMJ.2004;328(7434):254.
- ,,, et al.A cooperative care model: cardiologists and hospitalists reduce length of stay in a chest pain observation. In:5th Scientific Forum on Quality of Care and Outcomes Research in Cardiovascular Disease and Stroke, Washington, DC, May 15‐17, 2003.Philadelphia, PA:Lippincott Williams 2003. p.P186.
- ,.Observation unit management of pediatric emergencies.Emerg Med Clin North Am.1991;9(3):669–676.
- .A short stay or 23‐hour ward in a general and academic children's hospital: are they effective?Pediatr Emerg Care.2000;16(4):223–229.
- ,,, et al.Trends in high turnover stays among children hospitalized in the United States, 1993 through 2003.Pediatrics.2009;123:996–1002.
- .Hospital based alternatives to acute paediatric admission: a systematic review.Arch Dis Child.2005;90(2):138–142.
- ,,.Short‐stay units and observation medicine: a systematic review.Med J Aust.2003;178(11):559–563.
- ,,.Use of emergency observation and assessment wards: a systematic literature review.Emerg Med J.2003;20(2):138–142.
- Oxford Centre for Evidence‐Based Medicine. Levels of evidence and grades of recommendation (May 2001). Available at: http://www.cebm.net/levels_of_evidence.asp. Accessed July2009.
- ,,, et al.Pediatric observation status beds on an inpatient unit: an integrated care model.Pediatr Emerg Care.2004;20(1):17–21.
- .Pediatric update. Our new rapid treatment unit: an innovative adaptation of the “less than 24‐hour stay” holding unit.J Emerg Nurs.2000;26(5):507.
- ,,.Use of an observation unit by a pediatric emergency department for common pediatric illnesses.Pediatr Emerg Care.2001;17(5):321–323.
- ,,, et al.Observation medicine: the expanded role of the nurse practitioner in a pediatric emergency department extended care unit.Pediatr Emerg Care.2005;21(3):199–202.
- ,,.An observation unit in a pediatric emergency department: one children's hospital's experience.J Emerg Nurs.2002;28(5):407–413.
- ,,.When the patient requires observation not hospitalization.J Nurs Admin.1988;18(10):20–23.
- ,.Observation unit in Children's Hospital—Adjunct to delivery and teaching of ambulatory pediatric care.N Y State J Med.1980;80(11):1684–1686.
- ,,, et al.Use of pediatric observation unit for treatment of children with dehydration caused by gastroenteritis.Pediatr Emerg Care.2006;22(1):1–6.
- ,,, et al.Utilization and unexpected hospitalization rates of a pediatric emergency department 23‐hour observation unit.Pediatr Emerg Care.2008;24(9):589–594.
- ,,, et al.Short‐term holding room treatment of asthmatic‐children.J Pediatr.1985;106(5):707–711.
- ,,.Usefulness of the serum electrolyte panel in the management of pediatric dehydration treated with intravenously administered fluids.Pediatrics.2004;114(5):1227–1234.
- ,,.Treatment of acute asthmatic attacks in a holding unit of a pediatric emergency room.Ann Allergy.1980;45(3):159–162.
- ,,.Outpatient oral rehydration in the United States.Am J Dis Child.1986;140(3):211–215.
- ,.Postreduction management of intussusception in a children's hospital emergency department.Pediatrics.2003;112(6 Pt 1):1302–1307.
- ,,, et al.Children with asthma admitted to a pediatric observation unit.Pediatr Emerg Care.2005;21(10):645–649.
- ,,, et al.Pediatric closed head injuries treated in an observation unit.Pediatr Emerg Care.2005;21(10):639–644.
- ,,.A reduction in hospitalization, length of stay, and hospital charges for croup with the institution of a pediatric observation unit.Am J Emerg Med.2006;24(7):818–821.
- ,,.Short stay in an outpatient department. An alternative to hospitalization.Am J Dis Child.1972;123(2):128–132.
- ,,.The role of oral ondansetron in children with vomiting as a result of acute gastritis/gastroenteritis who have failed oral rehydration therapy: a randomized controlled trial.Ann Emerg Med.2008;52(1):22–29.e6.
- ,,, et al.Oral ondansetron for gastroenteritis in a pediatric emergency department.N Engl J Med.2006;354(16):1698–1705.
- ,,, et al.Integrated hospital emergency care improves efficiency.Emerg Med J.2008;25(2):78–82.
- ,,, et al.Redefining the community pediatric hospitalist: the combined pediatric ED/inpatient unit.Pediatr Emerg Care.2007;23(1):33–37.
- ,,, et al.Program description: a hospitalist‐run, medical short‐stay unit in a teaching hospital.CMAJ.2000;163(11):1477–1480.
- ,.Evaluation of a pediatric hospitalist service: impact on length of stay and hospital charges.Pediatrics.2000;105(3 Pt 1):478–484.
- ,,, et al.Restructuring an academic pediatric inpatient service using concepts developed by hospitalists.Clin Pediatr (Phila).2001;40(12):653–660; discussion 661‐662.
- ,,, et al.American College of Emergency Physicians (ACEP).Practice Management Committee, American College of Emergency Physicians. Management of Observation Units. Irving, TX: American College of Emergency Physicians; July1994.
- Overcrowding crisis in our nation's emergency departments:is our safety net unraveling?Pediatrics.2004;114(3):878–888.
- ,.Emergency department overcrowding in the United States: an emerging threat to patient safety and public health.Emerg Med J.2003;20(5):402–405.
- ,,, et al.Characteristics of high volume teaching hospital observation units: data from the Emergency Department Observation Unit Benchmark Alliance (EDOBA).Acad Emerg Med.2009;16(s1):Abstract 628.
- ,,.Use of the emergency department observation unit in the treatment of acute asthma.Ann Emerg Med.1982;11(2):77–83.
- ,,, et al.Management of acute pyelonephritis in an emergency department observation unit.[see Comment].Ann Emerg Med.1991;20(3):253–257.
- ,,, et al.Patterns of use of an emergency department‐based observation unit.Am J Ther.2002;9(6):499–502.
- ,,, et al.Emergency department observation of poisoned patients: how long is necessary?[see Comment].Acad Emerg Med.1999;6(9):887–894.
- ,,, et al.False‐negative and false‐positive errors in abdominal pain evaluation: failure to diagnose acute appendicitis and unnecessary surgery.Acad Emerg Med.2000;7(11):1244–1255.
- .Resource use by younger versus older patients.Fam Pract Res J.1993;13(3):283–290.
- ,,, et al.Trauma 24‐hour observation critical path.J Trauma.1998;45(1):147–150.
- ,,, et al.The role of an emergency department observation unit in the management of trauma patients.J Emerg Med.1985;2(5):325–333.
- ,.Observation unit impact on ED admission for asthma.Am J Emerg Med.1994;12(1):11–14.
- ,.Emergency care for children in pediatric and general emergency departments.Pediatr Emerg Care.2007;23(2):94–102.
The first observation units were implemented more than 40 years ago with the goal of reducing the number and duration of inpatient stays. Since then, observation units (OUs) have evolved as a safe alternative to hospitalization14 for the delivery of finite periods of care, typically less than 24 hours.58 Observation services allow for time to determine the need for hospitalization in cases that are unclear after their initial evaluation and treatment.9 Observation status is an administrative classification related to reimbursement that can be applied to patients whose diagnosis, treatment, stabilization, and discharge can reasonably be expected within 24 hours.10, 11 The site of care for observation is dependent in part upon existing facility structures; some institutions utilize virtual OUs within the emergency department (ED) or hospital ward, while others have dedicated, geographically distinct OUs, which may function as an extension of either the ED or inpatient settings.9
OUs have been instrumental in providing care to adult patients with chest pain, asthma, and acute infections.1218 Recently, there has been an increase in the number of publications from pediatric OUs in the United States and abroad. Observation may be a preferred model of care for select pediatric patients, as hospitalized children often experience brief stays.1921 Previous reviews on this model of care have combined adult and pediatric literature and have included research from countries with healthcare structures that differ considerably from the United States.2224 To date, no systematic review has summarized the pediatric OU literature with a focus on the US healthcare system.
As payers and hospitals seek cost‐effective alternatives to traditional inpatient care, geographically distinct OUs may become integral to the future of healthcare delivery for children. This systematic review provides a descriptive overview of the structure and function of pediatric OUs in the United States. We also scrutinize the outcome measures presented in the included publications and propose future directions for research to improve both observation unit care, as well as the care delivered to patients under observation status within general inpatient or ED settings.
Methods
Literature Search
With the assistance of a health services librarian, a search of the following electronic databases from January 1, 1950 through February 5, 2009 was conducted: Medline, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Health Care Advisory Board (HCAB), Lexis‐Nexis, National Guideline Clearinghouse, and Cochrane Reviews. Key words used for the Boolean search are included in Appendix A. In addition, we conducted a manual search of reference lists from reviews, guidelines, and articles meeting inclusion criteria.
We included English language peer‐reviewed publications that reported on pediatric OU care in the United States. Studies were included if they reported outcomes including lengths of stay, admission from observation rates, return visit rates, costs or charges. Descriptive publications of pediatric OU structure and function were also included. Studies were excluded if they were conducted outside the United States, evaluated psychiatric or intensive care, reported on observation status in an ED without an OU or observation status on a traditional inpatient ward. Two reviewers (M.M. and C.K.) identified articles for inclusion. Any disagreements between the reviewers were resolved by discussion and consensus agreement. Interrater reliability was assessed using the kappa statistic.
Quality Assessment
The quality of each study was rated using the Oxford Centre for Evidence‐based Medicine levels of evidence.25 With this system, levels of evidence range from 1a (homogeneous systematic review of randomized, controlled trials) to 5 (expert opinion without explicit critical appraisal).
Data Synthesis
Data on study design, OU characteristics, patient populations, and outcomes were extracted using a standardized form. Heterogeneity of study design, interventions, and outcomes precluded the ability to conduct meta‐analyses.
Results
A systematic search of the electronic databases identified 222 unique citations (Figure 1). A total of 107 abstracts were evaluated. We identified 48 articles for full‐text review, of which 18 met inclusion criteria. Hand search of references yielded 24 additional articles, of which 3 met inclusion criteria. Interrater agreement for selected articles was high at 98% (kappa = 0.85).
Observation Unit Characteristics
The majority of research on OUs has been conducted at large academic pediatric centers. One publication was from a community hospital.26 These studies present data on more than 22,000 children cared for in OUs of 11 hospitals over a 32‐year time span. Most studies were level 2 evidence: 2b, retrospective cohort studies and low‐quality randomized, controlled trials; or 2c, outcomes research. Three were descriptive and not assigned a formal evidence level.2729
Table 1 highlights general features of U.S. pediatric OUs. Five institutions renovated or expanded clinical space in order to open the OU.27, 2932 Units ranged in size from 3 to 23 beds. The OU was located in or near the ED in all but 2 hospitals, which had ward‐based units. The ED was the primary entry point into the OU with only 2 open model units accepting patients from other settings.5, 32 The annual number of observation cases ranged from 1000 to 3000 in children's hospitals. Approximately 500 ward‐based observation cases per year were cared for in the single community hospital studied. Three reports included time trends showing increased OU utilization over study years.5, 30, 31
| Publication (Year); Condition | Study Design; Level of Evidence; Time Frame; Sample Size | Hospital; Observation Setting; Year Opened | Site | Beds | Entry Point | Staffing; Physicians; Nurses |
|---|---|---|---|---|---|---|
| ||||||
| Gururaj et al.43 (1972); all conditions | Retrospective cohort; 2c; 1 year; 437 cases under observation | King's County Downstate Brooklyn; short‐stay unit | ED | 3 | Not reported | Pediatric residents; general pediatricians |
| Ellerstein and Sullivan,32 (1980); all conditions | Retrospective cohort; 2c; 6 years; 5858 cases of unscheduled care plus 1403 elective surgery cases | Children's Hospital Buffalo; observation unit; 1972 | ED | 8 | ED, clinic, procedure/OR | Primary care pediatricians; other specialists; pediatric residents |
| O'Brien et al.37 (1980); asthma | Retrospective cohort; 2c; 1 month; 434 cases of asthma, 328 discharged directly from ED, 106 treated in holding unit | Children's National DC; holding unit | ED | 6 | ED | 1‐2 pediatric residents; 1‐2 nurses |
| Willert et al.35 (1985); asthma | Randomized*; 2b; 578 cases of asthma; 166 cases 1.5 hours postaminophylline, 103 randomized, 52 to holding unit | Children's Memorial Chicago; holding room | ED | 5 | ED | General pediatricians; pediatric residents; PEM nurses |
| Listernick et al.38 (1986); dehydration | Randomized; 2b; 29 cases of dehydration; 22 to holding unit | Children's Memorial Chicago | ||||
| Balik et al.31 (1988); all conditions | Descriptive; none given | Minneapolis Children's; short‐stay unit observation area; 1985 | Day surgery area adjacent to ED | Not reported | Not reported | General pediatricians; pediatric nurses (shared with ED) |
| Marks et al.7 (1997); all conditions | Retrospective cohort; 2c; 5 months; 968 cases in short‐stay unit | Children's Hospital Boston; short‐stay unit; 1994 | Ward | 4‐18 | ED | Primary care pediatricians; PEM physicians; pediatric residents; pediatric nurses; 1:6 nurse:patient ratio |
| Marks et al.7 (1997); asthma | Pre‐post; 2b; 400 cases of asthma; 102 pre/298 post short‐stay unit | Children's Hospital Boston | ||||
| Wiley et al.6 (1998); all conditions | Retrospective cohort; 2c; 1 year; 805 cases of unscheduled observation; plus 595 scheduled cases | Connecticut Children's; outpatient extended treatment site | ED | 10 | Not reported | PEM physicians; other specialists; 1:5 nurse:patient ratio |
| Scribano et al.65 (2001); all conditions | Retrospective cohort; 2b; 2 years; 1798 cases under observation | Connecticut Children's | ||||
| Leduc et al.30 (2002); all conditions | Retrospective cohort; 2c; 6 months; 686 cases under observation (4.8% of ED visits) | Children's Hospital Denver; OU | ED | 6 | Not reported | Not reported |
| Bajaj and Roback,30 (2003); intussusception | Retrospective cohort; 2b; 4.5 years; 78 cases of intussusception (51 under observation) | Children's Hospital Denver | ||||
| Wathen et al.36 (2004); dehydration | Convenience sample; 2c; 10 months; 182 cases of dehydration (48 under observation) | Children's Hospital Denver | ||||
| Crocetti et al.26 (2004); all conditions | Retrospective cohort; 2b; 2 years; 956 cases under observation | John Hopkin's Bayview; observation status beds; 1997 | Ward | Not reported | 99% ED 1% other location | General pediatricians covering ED and ward |
| Silvestri et al.29 (2005); all conditions | Descriptive; none given | Children's Hospital of Philadelphia; OU; 1999 | ED | 12 | ED | PEM physicians; PEM fellows; urgent care pediatricians; ED nurse practitioner; inpatient nurses |
| Alpern et al.34 (2008); all conditions | Prospective cohort; 1b; 30 months; 4453 cases under observation | Children's Hospital of Philadelphia | ||||
| Thomas27 (2000); all conditions | Descriptive; none given | Primary Children's Medical Center; RTU; 1999 | ED | 22‐26 | ED, clinic, procedure/OR | PEM physicians; general pediatricians; other specialists; no residents |
| Zebrack et al.25 (2005); all conditions | Retrospective cohort; 2b; 2 years; 4189 cases of unscheduled observation plus 2288 scheduled cases | Primary Children's Medical Center | PEM nurses; 1:4 nurse:patient ratio | |||
| Miescier et al.40 (2005); asthma | Retrospective cohort; 2b; 2 years; 3029 asthma visits; 384 admitted, 301 observed, 161cases met inclusion | Primary Children's Medical Center | ||||
| Holsti et al.41 (2005); head injury | Retrospective cohort; 2b; 2 years; 827 CHI visits, 273 admitted, 285 observed, 284 cases met inclusion | Primary Children's Medical Center | ||||
| Greenberg et al.42 (2006); croup | Retrospective pre‐post; 2b; 1 year each; 694 croup cases pre‐RTU, 66 admitted; 789 croup cases post‐RTU, 33 admitted; 76 observed | Primary Children's Medical Center | ||||
| Mallory et al.33 (2006); dehydration | Retrospective cohort; 2b; 1 year; 430 dehydration cases under observation | Primary Children's Medical Center | ||||
Staffing and Workflow
Staffing models varied and have undergone transitions over time. Prior to 1997, general pediatricians primarily provided physician services. In more recent years, OUs have utilized pediatric emergency medicine (PEM) providers. Three of the 11 units allowed for direct patient care by subspecialists.5, 6, 32 One OU was staffed by nurse practitioners.29 OU nursing backgrounds included pediatrics, emergency medicine, or PEM.
Five institutions assembled multidisciplinary teams to define the unit's role and establish policies and procedures.7, 27, 2931 Workflow in the OU focused on optimizing efficiency through standardized orders, condition‐specific treatment protocols, and bedside charting.7, 26, 33 Several units emphasized the importance of ongoing evaluations by attending physicians who could immediately respond to patient needs. Rounds occurred as often as every 4 hours.5, 7 Two centers utilized combined physician‐nursing rounds to enhance provider communication.7, 34 No publications reported on patient transitions between sites of care or at shift changes.
Criteria for Observation
All 11 hospitals have developed protocols to guide OU admissions (Table 2). Nine publications from 4 OUs commented on treatments delivered prior to observation.33, 3542 The most commonly cited criteria for admission was approval by the unit's supervising physician. Utilization review was not mentioned as an element in the OU admission decision. Common OU exclusions were the need for intensive care or monitoring while awaiting an inpatient bed; however, these were not universal. Eight centers placed bounds around the duration of OU stays, with minimum stays of 2 hours and maximum stays of 8 to 24 hours.
| Hospital | Entry Criteria | Age Range | Time | Exclusion Criteria |
|---|---|---|---|---|
| ||||
| King's County, Downstate Brooklyn | Otherwise required inpatient admission | 0‐13 years | Maximum 24 hours | Not reported |
| Acute problem of uncertain severity | ||||
| Acute problem not readily diagnosed | ||||
| Short course periodic treatment | ||||
| Diagnostic procedures impractical as outpatient | ||||
| Children's Hospital, Buffalo | Admission from any source | 0‐21 years | Maximum 24 hours | Intensive care needs |
| Short stay elective surgery | Routine diagnostic tests | |||
| Estimated length of stay 24 hours | Holding prior to admission | |||
| Children's National, Washington, DC | Inadequate response to 3 subcutaneous epinephrine injections | 8 months to 19 years | Not reported | Not reported |
| Children's Memorial, Chicago | Asthma: | |||
| Available parentAsthma score 5Inadequate response to ED treatment | >1 year | Maximum 24 hours | Past history of BPD, CF, CHD, other debilitating disease | |
| Dehydration: | ||||
| Cases receiving oral hydration | 3‐24 months | 12 hours for oral | Intensive care need | |
| Parent preference if given IV hydration | 8 to 12 hours for IV | Hypernatremia | ||
| Minneapolis Children's | Conditions listed in Table 3 | Not reported | Maximum 10 hours | Not reported |
| Children's Hospital, Boston | Straightforward diagnoses as determined by ED staff | Not reported | Not reported | Other complex medical issues |
| Bed availability | ||||
| Connecticut Children's | PEM attending discretionLimited severity of illnessUsually confined to a single organ systemClearly identified plan of care | Not reported | After 3‐4 hours in ED Low likelihood of requiring extended care >23 hours | Asthma: no supplemental O2 need, nebulized treatments >Q2 hourCroup: no supplemental O2 need, 2 racemic epinephrine treatmentsDehydration: inability to tolerate orals, bicarbonate >10, 40 mL/kg IVFSeizure: partial or generalized, postictal, unable to tolerate oralsPoisoning: mild or no symptoms, poison control recommendation |
| Children's Hospital, Denver | Intussusception: following reduction | 0‐18 years | After 3‐4 hours in ED | Not reported |
| Dehydration: based on clinical status | ||||
| Johns Hopkins, Bayview | Consultation with on‐duty pediatrician | 0‐18 years | Minimum of 2 hours | Patients requiring subspecialty or intensive care services |
| High likelihood of discharge at 24 hours | ||||
| Children's Hospital of Philadelphia | Sole discretion of the ED attending | Not reported | Minimum 4 hours | No direct admissions |
| Single focused acute condition | Maximum 23 hours | Diagnostic dilemmas | ||
| Clinical conditions appropriate for observation | Underlying complex medical problems | |||
| Primary Children's Medical Center | Observation unit attending discretion | 0‐21 years | Minimum 3 hours | Admission holds |
| Scheduled procedures as space available | Maximum 24 hours | Intensive care needs | ||
| ED admit after consult with OU doctor | Complicated, multisystem disease | |||
| Clear patient care goals | Need for multiple specialty consults | |||
| Limited severity of illness | Psychiatric patients | |||
| Diagnostic evaluation | ||||
Ages of Children Under Observation
Seven of 11 hospitals reported the age range of patients accepted in their OU (Table 2). All but 1 unit accepted children from infants to young adults, 18 to 21 years of age.43 In the 6 units that reported the age distribution of their OU population, roughly 20% were 1 year, more than 50% were 5 years, and fewer than 30% fell into an adolescent age range.5, 6, 26, 32, 34, 43
Conditions Under Observation
Many conditions under observation were common across time and location (Table 3). The list of conditions cared for in OUs has expanded in recent years. Medical conditions predominated over surgical. While the majority of observation cases required acute care, nearly one‐half of the units accepted children with scheduled care needs (eg, routine postoperative care, procedures requiring sedation, infusions, and extended evaluations such as electroencephalograms or pH probes). These scheduled cases, cared for within the OU structure, provided more steady demand for OU services.
| King's County, Downstate Brooklyn | Children's Hospital, Buffalo | Minneapolis Children's | Children's Hospital, Boston | Connecticut Children's | Children's Hospital, Denver | Johns Hopkins, Bayview | Children's Hospital of Philadelphia | Primary Children's Medical Center, Salt Lake City | |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Respiratory | |||||||||
| Asthma | |||||||||
| Pneumonia | |||||||||
| Bronchiolitis | |||||||||
| Croup | |||||||||
| Allergic reaction | |||||||||
| Cardiology | |||||||||
| Gastrointestinal | |||||||||
| Vomiting | |||||||||
| Gastro/dehydration | |||||||||
| Abdominal pain | |||||||||
| Constipation | |||||||||
| Diabetes | |||||||||
| Neurologic | |||||||||
| Seizure | |||||||||
| Head injury | |||||||||
| Infection | |||||||||
| Sepsis evaluation | |||||||||
| UTI/pyelonephritis | |||||||||
| Cellulitis | |||||||||
| Fever | |||||||||
| Pharyngitis | |||||||||
| Otitis media | |||||||||
| Adenitis | |||||||||
| Ingestion/poisoning | |||||||||
| Hematologic | |||||||||
| Sickle cell disease | |||||||||
| Transfusion/emnfusion | |||||||||
| Psychological/social | |||||||||
| Dental | |||||||||
| Surgical conditions | |||||||||
| Foreign body | |||||||||
| Trauma | |||||||||
| Burn | |||||||||
| Orthopaedic injury | |||||||||
| Postoperative complication | |||||||||
| Scheduled care | |||||||||
| Diagnostic workup | |||||||||
| Procedures/sedation | |||||||||
| Elective surgery | |||||||||
Reimbursement
One publication highlighted the special billing rules that must be considered for observation care.27 In 3 studies, payers recognized cost‐savings associated with the OU's ability to provide outpatient management for cases that would traditionally require inpatient care.31, 35, 38
Observation Unit Outcomes
Outcomes reported for pediatric OU stays fall into 4 major categories: length of stay (LOS), admission rates, return visit rates, and costs. Despite these seemingly straightforward groupings, there was significant heterogeneity in reporting these outcomes.
Length of Stay
The start time for OU length of stay (LOS) is not clearly defined in the articles included in this review. While the start of an observation period is assumed to begin at the time the order for observation is placed, it is possible that the LOS reported in these publications began at the time of ED arrival or the time the patient was physically transferred to the OU. The average LOS for individual OUs ranged from 10 to 15 hours.5, 6, 26, 30, 35, 38, 40, 41, 43 One ward‐based and 1 ED‐based unit reported LOS extending beyond 24 hours,7, 30 with averages of 35 and 9 hours, respectively. Two units limited the duration of care to 10 hours.31, 38
For studies that included a comparison group, OU stays were consistently shorter than a traditional inpatient stay by 6 to 110 hours.7, 36, 38, 39, 42 No significant differences in clinical parameters between groups were reported. There was appreciable variation in the average LOS across institutions for similar conditions, 12 to 35 hours for asthma,5, 7, 34, 35 and 9 to 18 hours for dehydration.5, 34, 36, 38
Admission Rates
Rates of hospital admission after observation from the 9 OUs reporting this outcome are presented in Table 4. Three publications from a single institution counted hospital admission in the 48 to 72 hours following discharge from the OU as though the patient were admitted to the hospital directly from the index OU stay.33, 40, 41 Conditions with the lowest admission rates, 10%, included croup, neurologic conditions, ingestions, trauma, and orthopedic injuries. The highest admission rates, >50%, were for respiratory conditions including asthma, pneumonia, and bronchiolitis.
| King's County, Downstate Brooklyn (%) | Children's Hospital, Buffalo (%) | Connecticut Children's (%) | Johns Hopkins, Bayview (%) | Children's Hospital of Philadelphia (%) | Primary Children's Medical Center, Salt Lake City (%) | |
|---|---|---|---|---|---|---|
| ||||||
| Unscheduled care | 42 | 17 | 11 | 25 | 25 | 15 |
| Respiratory | 32 | |||||
| Asthma | 57 | 16 | 26 | 22 | 22‐25* | |
| Pneumonia | 50 | 23 | 30‐48 | |||
| Bronchiolitis | 46 | 32 | 43 | |||
| Croup | 9 | 17 | 9 | 4‐6 | ||
| Allergic reaction | 3 | |||||
| Cardiology | 22 | |||||
| Gastrointestinal | 43 | 19 | ||||
| Vomiting | 5 | 22 | ||||
| Gastro/dehydration | 23 | 15/21 | 16* | |||
| Abdominal pain | 9 | 17 | 27 | |||
| Constipation | 9 | |||||
| Diabetes | 17 | |||||
| Neurologic | 10 | |||||
| Seizure | 19 | 8 | 17 | 18 | ||
| Head injury | 7 | 5* | ||||
| Infection | 19 | 34 | ||||
| Sepsis evaluation | 25 | 22 | ||||
| UTI/pyelonephritis | 25 | 16 | ||||
| Cellulitis | 15 | |||||
| Fever | 16 | 26 | ||||
| Pharyngitis | 13 | |||||
| Otitis media | 21 | |||||
| Ingestion/poisoning | 9 | 4 | 4 | 9 | 10 | 5 |
| Hematologic | 23 | |||||
| Transfusion/emnfusion | 2 | |||||
| Psychological/social | 21 | 80 | 17 | |||
| Dental | 14 | |||||
| Surgical conditions | ||||||
| Foreign body | ||||||
| Trauma | 13 | 2 | 53 | 5 | ||
| Burn | 13 | |||||
| Orthopedic injury | 22 | 3 | ||||
| Postoperative complication | 26 | 16 | ||||
| Scheduled care | ||||||
| Diagnostic workup | 0‐5 | |||||
| Procedures/sedation | 0.1‐9.0 | |||||
| Elective surgery | 13 | 0‐5 | ||||
Return Visit Rates
Unscheduled return visit rates were reported in 9 publications from 6 institutions and ranged from 0.01% to 5%.7, 26, 33, 3537, 3941 Follow‐up timeframes ranged from 48 hours to 1 month. Return visits were inconsistently defined. In most studies, rates were measured in terms of ED visits.26, 33, 3537, 39, 41 One ward‐based unit counted only hospital readmissions toward return visit rates.7 Three publications, from ED‐based units, counted hospital readmissions in the 2 to 5 days following observation toward admission rates and not as return visits.33, 40, 41 In most studies, data on return visits were collected from patient logs or patient tracking systems. Three studies contacted patients by phone and counted return visits to the clinic.3537 No studies reported on adherence to scheduled visits following observation.
Costs
Seven studies reported financial benefits of OU care when compared with traditional hospital care.7, 30, 31, 35, 37, 38, 42 Two centers admitted patients to inpatient care if their observation period reached a set time limit, after which cost savings were no longer realized.31, 35 Cost savings associated with the OU treatment of asthma and dehydration were attributed to lower charges for an OU bed.35, 38 Decreased charges for the OU treatment of croup were related to shorter LOS.42
Discussion
In the 40 years since the first studies of pediatric OUs, several US health systems have extended observation services to children. This model of care may be expanding, as suggested by an increase in the number of publications in the past 10 years. However, the number of centers within the US reporting on their OU experience remains small. Our systematic review identified a recurrent theme related to OUsthe opportunity to improve operational processes of care compared with the traditional inpatient alternative. We have identified the need to standardize OU outcomes and propose measures for future OU research.
Observation Unit Operations
The OU care model expands outpatient management of acute conditions to include children who are neither ready for discharge nor clear candidates for inpatient admission. OUs have demonstrated the ability to care for patients across the pediatric age spectrum. Over the decades spanning these publications, advances in medical therapy such as antiemetics for gastroenteritis and early administration of systemic steroids for asthma may have resulted in lower admission rates or shorter time to recovery.44, 45 Despite these advances, there are marked consistencies in the conditions cared for within OUs over time. The data summarized here may help guide institutions as they consider specific pediatric conditions amenable to observation care.
The hospitals included in this review either added physical space or revised services within existing structures to establish their OU. Hospitals facing physical constraints may look to underutilized areas, such as recovery rooms, to provide observation care, as observation does not require the use of licensed inpatient beds. Several units have responded to daily fluctuations in unscheduled observation cases by also serving patients who require outpatient procedures, brief therapeutic interventions, and diagnostic testing. By caring for patients with these scheduled care needs during the day, there is a more steady flow of patients into the OU. While hospitals traditionally have used postanesthesia care units and treatment rooms for scheduled cases, OUs appear to benefit from the consistent resource allocation associated with a constant demand for services.
To date, the vast majority of pediatric OUs in the published literature have emerged as an extension of ED services. Now, with the expansion of pediatric hospitalist services and movement toward 24/7 inpatient physician coverage, there may be increased development of ward‐based OUs and the designation of inpatient observation status. While ward‐based OUs managed by pediatric hospitalists may be well established, we were not able to identify published reports on this structure of care. A national survey of health systems should be undertaken to gather information regarding the current state of pediatric observation services.
When creating policies and procedures for OUs, input should be sought from stakeholders including hospitalists, PEM providers, primary care providers, subspecialists, mid‐level providers, nurses, and ancillary staff. As patients requiring observation level of care do not neatly fit an outpatient or inpatient designation, they present an opportunity for hospitalist and PEM physician groups to collaborate.4648 Calling on the clinical experiences of inpatient and ED providers could offer unique perspectives leading to the development of innovative observation care models.
This review focused on institutions with dedicated observation services, which in all but 1 study26 consisted of a defined geographic unit. It is possible that the practices implemented in an OU could have hospital‐wide impact. For example, 1 study reported reduction in LOS for all asthma cases after opening a ward‐based unit.7 Further, pediatric hospitalist services have been associated with shorter LOS49 and increased use of observation status beds compared with traditional ward services.50 As pediatric hospitalists expand their scope of practice to include both observation and inpatient care, clinical practice may be enhanced across these care areas. It follows that the impact of observation protocols on care in the ward setting should be independently evaluated.
The costs associated with the establishment and daily operations of an OU were not addressed in the reviewed publications. Assertions that observation provides a cost‐effective alternative to inpatient care4, 7, 23, 42 should be balanced by the possibility that OUs extend care for patients who could otherwise be discharged directly home. Studies have not evaluated the cost of OU care compared with ED care alone. Research is also needed to assess variations in testing and treatment intensity in OUs compared with the ED and inpatient alternatives. Reimbursement for observation is dependent in part upon institutional contracts with payers. A full discussion of reimbursement issues around observation services is beyond the scope of this review.
Observation Unit Outcomes
Length of Stay
Although most studies reported LOS, direct comparisons across institutions are difficult given the lack of a consistently referenced start to the observation period. Without this, LOS could begin at the time of ED arrival, time of first treatment, or time of admission to the OU. Identifying and reporting the elements contributing to LOS for observation care is necessary. The time of OU admission is important for billing considerations; the time of first treatment is important to understanding the patient's response to medical interventions; the time of ED arrival is important to evaluating ED efficiency. Each of these LOS measures should be reported in future studies.
Direct comparisons of LOS are further complicated by variability in the maximum permissible duration of an OU stay, ranging from 8 to 24 hours in the included studies. Despite these limits, some OU care will extend beyond set limits due to structural bottlenecks. For example, once the inpatient setting reaches capacity, observation LOS for patients who require admission will be prolonged. The best evaluation of LOS would come from prospective study design utilizing either randomization or quality improvement methods.
Defining Success and Failure in Observation Care
In the reviewed literature, observation failures have been defined in terms of admission after observation and unscheduled return visit rates. Admission rates are heavily dependent on appropriate selection of cases for observation. Although some observation cases are expected to require inpatient admission, OUs should question the validity of their unit's acceptance guidelines if the rate of admission is >30%.51 High rates could be the result of inadequate treatment or the selection of children too sick to improve within 24 hours. Low rates could indicate overutilization of observation for children who could be discharged directly home. Full reporting on the number of children presenting with a given condition and the different disposition pathways for each is needed to evaluate the success of OUs. Condition‐specific benchmarks for admission after observation rates could guide hospitals in their continuous improvement processes.
Unscheduled return visits may reflect premature discharge from care, diagnostic errors, or development of a new illness. OU care may influence patient adherence to scheduled follow‐up care but this has not been evaluated to date. In future research, both scheduled and unscheduled return visits following ED visits, observation stays, and brief inpatient admissions for similar disease states should be reported for comparison. Standard methodology for identifying return visits should include medical record review, claims analyses, and direct patient contact.
As hospitals function at or near capacity,52, 53 it becomes important to delineate the appropriate length of time to monitor for response to treatments in a given setting. Limited capacity was a frequently cited reason for opening a pediatric OU; however, the impact of OUs on capacity has not yet been evaluated. Operations research methods could be used to model OU services' potential to expand hospital capacity. This research could be guided by evaluation of administrative data from across institutions to identify current best practices for pediatric OU and observation status care.
OU benchmarking in the United States has begun with a small number of adult units participating in the ED OU Benchmark Alliance (EDOBA).54 In Table 5, we propose dashboard measures for pediatric OU continuous quality improvement. The proposed measures emphasize the role of observation along the continuum of care for acute conditions, from the ED through the OU with or without an inpatient stay to clinic follow‐up. Depending on the structure of observation services, individual institutions may select to monitor different dashboard measures from the proposed list. Patient safety and quality of care measures for the conditions commonly receiving pediatric OU care should also be developed.
| ED |
OU |
Inpatient |
Clinic | |
|---|---|---|---|---|
| ||||
| Length of stay* | ED arrival to OU admission | OU admit to disposition | Inpatient admit to discharge | |
| ED arrival to discharge home from OU | ||||
| ED arrival to discharge from inpatient following OU care | ||||
| OU admission to discharge home from inpatient care | ||||
| Admission* | % ED census admitted inpatient | % OU census admitted | ||
| % ED census that is observed | ||||
| Unscheduled return visits* | To ED | Requiring OU admission | Requiring inpatient admission | |
| Scheduled follow‐up* | To ED | To primary care or subspecialist office | ||
| Capacity | ED crowding scales | Unable to accept transfers | ||
| ED left before evaluation rates | Inpatient occupancy | |||
| Ambulance diversion | ||||
| Satisfaction | Patient/Parent | |||
| ED providers | OU providers | Inpatient providers | Follow‐up providers | |
| Cost | ED care | OU care | Inpatient care | |
| Total encounter | ||||
Limitations
The most important limitations to this review are the heterogeneity in interventions and reporting of outcomes, which precluded our ability to combine data or conduct meta‐analyses. We attempted to organize the outcomes data into clear and consistent groupings. However, we could not compare the performance of 1 center with another due to differences in OU structure, function, and design.
In order to focus this systematic review, we chose to include only peer reviewed publications that describe pediatric OUs within the United States. This excludes expert guidelines, which may be of value to institutions developing observation services.
Our search found only a small number of centers that utilize OUs and have published their experience. Thus, our review is likely subject to publication bias. Along this line, we identified 9 additional publications where children were cared for alongside adults within a general OU.5563 This suggests an unmeasured group of children under observation in general EDs, where more than 90% of US children receive acute care.64 These articles were excluded because we were unable to distinguish pediatric specific outcomes from the larger study population.
Finally, retrospective study design is subject to information bias. Without a comparable control group, it is difficult to understand the effects of OUs. Patients directly admitted or discharged from the ED and patients who require admission after observation all differ from patients discharged from observation in ways that should be controlled for with a randomized study design.
Conclusions
OUs have emerged to provide treatment at the intersection of outpatient and inpatient care during a time of dramatic change in both emergency and hospital medicine. As hospitalists expand their scope of practice to include observation care, opportunities will arise to collaborate with ED physicians and share their growing expertise in quality and efficiency of hospital care delivery to improve observation services for children. OUs have been established with laudable goalsto reduce inpatient admissions, increase patient safety, improve efficiency, and control costs. The current evidence is not adequate to determine if this model of healthcare delivery achieves these goals for children. Through synthesis of existing data, we have identified a need for standard reporting for OU outcomes and propose consistent measures for future observation care research. Only through prospective evaluation of comparable outcomes can we appraise the performance of pediatric OUs across institutions.
The first observation units were implemented more than 40 years ago with the goal of reducing the number and duration of inpatient stays. Since then, observation units (OUs) have evolved as a safe alternative to hospitalization14 for the delivery of finite periods of care, typically less than 24 hours.58 Observation services allow for time to determine the need for hospitalization in cases that are unclear after their initial evaluation and treatment.9 Observation status is an administrative classification related to reimbursement that can be applied to patients whose diagnosis, treatment, stabilization, and discharge can reasonably be expected within 24 hours.10, 11 The site of care for observation is dependent in part upon existing facility structures; some institutions utilize virtual OUs within the emergency department (ED) or hospital ward, while others have dedicated, geographically distinct OUs, which may function as an extension of either the ED or inpatient settings.9
OUs have been instrumental in providing care to adult patients with chest pain, asthma, and acute infections.1218 Recently, there has been an increase in the number of publications from pediatric OUs in the United States and abroad. Observation may be a preferred model of care for select pediatric patients, as hospitalized children often experience brief stays.1921 Previous reviews on this model of care have combined adult and pediatric literature and have included research from countries with healthcare structures that differ considerably from the United States.2224 To date, no systematic review has summarized the pediatric OU literature with a focus on the US healthcare system.
As payers and hospitals seek cost‐effective alternatives to traditional inpatient care, geographically distinct OUs may become integral to the future of healthcare delivery for children. This systematic review provides a descriptive overview of the structure and function of pediatric OUs in the United States. We also scrutinize the outcome measures presented in the included publications and propose future directions for research to improve both observation unit care, as well as the care delivered to patients under observation status within general inpatient or ED settings.
Methods
Literature Search
With the assistance of a health services librarian, a search of the following electronic databases from January 1, 1950 through February 5, 2009 was conducted: Medline, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Health Care Advisory Board (HCAB), Lexis‐Nexis, National Guideline Clearinghouse, and Cochrane Reviews. Key words used for the Boolean search are included in Appendix A. In addition, we conducted a manual search of reference lists from reviews, guidelines, and articles meeting inclusion criteria.
We included English language peer‐reviewed publications that reported on pediatric OU care in the United States. Studies were included if they reported outcomes including lengths of stay, admission from observation rates, return visit rates, costs or charges. Descriptive publications of pediatric OU structure and function were also included. Studies were excluded if they were conducted outside the United States, evaluated psychiatric or intensive care, reported on observation status in an ED without an OU or observation status on a traditional inpatient ward. Two reviewers (M.M. and C.K.) identified articles for inclusion. Any disagreements between the reviewers were resolved by discussion and consensus agreement. Interrater reliability was assessed using the kappa statistic.
Quality Assessment
The quality of each study was rated using the Oxford Centre for Evidence‐based Medicine levels of evidence.25 With this system, levels of evidence range from 1a (homogeneous systematic review of randomized, controlled trials) to 5 (expert opinion without explicit critical appraisal).
Data Synthesis
Data on study design, OU characteristics, patient populations, and outcomes were extracted using a standardized form. Heterogeneity of study design, interventions, and outcomes precluded the ability to conduct meta‐analyses.
Results
A systematic search of the electronic databases identified 222 unique citations (Figure 1). A total of 107 abstracts were evaluated. We identified 48 articles for full‐text review, of which 18 met inclusion criteria. Hand search of references yielded 24 additional articles, of which 3 met inclusion criteria. Interrater agreement for selected articles was high at 98% (kappa = 0.85).
Observation Unit Characteristics
The majority of research on OUs has been conducted at large academic pediatric centers. One publication was from a community hospital.26 These studies present data on more than 22,000 children cared for in OUs of 11 hospitals over a 32‐year time span. Most studies were level 2 evidence: 2b, retrospective cohort studies and low‐quality randomized, controlled trials; or 2c, outcomes research. Three were descriptive and not assigned a formal evidence level.2729
Table 1 highlights general features of U.S. pediatric OUs. Five institutions renovated or expanded clinical space in order to open the OU.27, 2932 Units ranged in size from 3 to 23 beds. The OU was located in or near the ED in all but 2 hospitals, which had ward‐based units. The ED was the primary entry point into the OU with only 2 open model units accepting patients from other settings.5, 32 The annual number of observation cases ranged from 1000 to 3000 in children's hospitals. Approximately 500 ward‐based observation cases per year were cared for in the single community hospital studied. Three reports included time trends showing increased OU utilization over study years.5, 30, 31
| Publication (Year); Condition | Study Design; Level of Evidence; Time Frame; Sample Size | Hospital; Observation Setting; Year Opened | Site | Beds | Entry Point | Staffing; Physicians; Nurses |
|---|---|---|---|---|---|---|
| ||||||
| Gururaj et al.43 (1972); all conditions | Retrospective cohort; 2c; 1 year; 437 cases under observation | King's County Downstate Brooklyn; short‐stay unit | ED | 3 | Not reported | Pediatric residents; general pediatricians |
| Ellerstein and Sullivan,32 (1980); all conditions | Retrospective cohort; 2c; 6 years; 5858 cases of unscheduled care plus 1403 elective surgery cases | Children's Hospital Buffalo; observation unit; 1972 | ED | 8 | ED, clinic, procedure/OR | Primary care pediatricians; other specialists; pediatric residents |
| O'Brien et al.37 (1980); asthma | Retrospective cohort; 2c; 1 month; 434 cases of asthma, 328 discharged directly from ED, 106 treated in holding unit | Children's National DC; holding unit | ED | 6 | ED | 1‐2 pediatric residents; 1‐2 nurses |
| Willert et al.35 (1985); asthma | Randomized*; 2b; 578 cases of asthma; 166 cases 1.5 hours postaminophylline, 103 randomized, 52 to holding unit | Children's Memorial Chicago; holding room | ED | 5 | ED | General pediatricians; pediatric residents; PEM nurses |
| Listernick et al.38 (1986); dehydration | Randomized; 2b; 29 cases of dehydration; 22 to holding unit | Children's Memorial Chicago | ||||
| Balik et al.31 (1988); all conditions | Descriptive; none given | Minneapolis Children's; short‐stay unit observation area; 1985 | Day surgery area adjacent to ED | Not reported | Not reported | General pediatricians; pediatric nurses (shared with ED) |
| Marks et al.7 (1997); all conditions | Retrospective cohort; 2c; 5 months; 968 cases in short‐stay unit | Children's Hospital Boston; short‐stay unit; 1994 | Ward | 4‐18 | ED | Primary care pediatricians; PEM physicians; pediatric residents; pediatric nurses; 1:6 nurse:patient ratio |
| Marks et al.7 (1997); asthma | Pre‐post; 2b; 400 cases of asthma; 102 pre/298 post short‐stay unit | Children's Hospital Boston | ||||
| Wiley et al.6 (1998); all conditions | Retrospective cohort; 2c; 1 year; 805 cases of unscheduled observation; plus 595 scheduled cases | Connecticut Children's; outpatient extended treatment site | ED | 10 | Not reported | PEM physicians; other specialists; 1:5 nurse:patient ratio |
| Scribano et al.65 (2001); all conditions | Retrospective cohort; 2b; 2 years; 1798 cases under observation | Connecticut Children's | ||||
| Leduc et al.30 (2002); all conditions | Retrospective cohort; 2c; 6 months; 686 cases under observation (4.8% of ED visits) | Children's Hospital Denver; OU | ED | 6 | Not reported | Not reported |
| Bajaj and Roback,30 (2003); intussusception | Retrospective cohort; 2b; 4.5 years; 78 cases of intussusception (51 under observation) | Children's Hospital Denver | ||||
| Wathen et al.36 (2004); dehydration | Convenience sample; 2c; 10 months; 182 cases of dehydration (48 under observation) | Children's Hospital Denver | ||||
| Crocetti et al.26 (2004); all conditions | Retrospective cohort; 2b; 2 years; 956 cases under observation | John Hopkin's Bayview; observation status beds; 1997 | Ward | Not reported | 99% ED 1% other location | General pediatricians covering ED and ward |
| Silvestri et al.29 (2005); all conditions | Descriptive; none given | Children's Hospital of Philadelphia; OU; 1999 | ED | 12 | ED | PEM physicians; PEM fellows; urgent care pediatricians; ED nurse practitioner; inpatient nurses |
| Alpern et al.34 (2008); all conditions | Prospective cohort; 1b; 30 months; 4453 cases under observation | Children's Hospital of Philadelphia | ||||
| Thomas27 (2000); all conditions | Descriptive; none given | Primary Children's Medical Center; RTU; 1999 | ED | 22‐26 | ED, clinic, procedure/OR | PEM physicians; general pediatricians; other specialists; no residents |
| Zebrack et al.25 (2005); all conditions | Retrospective cohort; 2b; 2 years; 4189 cases of unscheduled observation plus 2288 scheduled cases | Primary Children's Medical Center | PEM nurses; 1:4 nurse:patient ratio | |||
| Miescier et al.40 (2005); asthma | Retrospective cohort; 2b; 2 years; 3029 asthma visits; 384 admitted, 301 observed, 161cases met inclusion | Primary Children's Medical Center | ||||
| Holsti et al.41 (2005); head injury | Retrospective cohort; 2b; 2 years; 827 CHI visits, 273 admitted, 285 observed, 284 cases met inclusion | Primary Children's Medical Center | ||||
| Greenberg et al.42 (2006); croup | Retrospective pre‐post; 2b; 1 year each; 694 croup cases pre‐RTU, 66 admitted; 789 croup cases post‐RTU, 33 admitted; 76 observed | Primary Children's Medical Center | ||||
| Mallory et al.33 (2006); dehydration | Retrospective cohort; 2b; 1 year; 430 dehydration cases under observation | Primary Children's Medical Center | ||||
Staffing and Workflow
Staffing models varied and have undergone transitions over time. Prior to 1997, general pediatricians primarily provided physician services. In more recent years, OUs have utilized pediatric emergency medicine (PEM) providers. Three of the 11 units allowed for direct patient care by subspecialists.5, 6, 32 One OU was staffed by nurse practitioners.29 OU nursing backgrounds included pediatrics, emergency medicine, or PEM.
Five institutions assembled multidisciplinary teams to define the unit's role and establish policies and procedures.7, 27, 2931 Workflow in the OU focused on optimizing efficiency through standardized orders, condition‐specific treatment protocols, and bedside charting.7, 26, 33 Several units emphasized the importance of ongoing evaluations by attending physicians who could immediately respond to patient needs. Rounds occurred as often as every 4 hours.5, 7 Two centers utilized combined physician‐nursing rounds to enhance provider communication.7, 34 No publications reported on patient transitions between sites of care or at shift changes.
Criteria for Observation
All 11 hospitals have developed protocols to guide OU admissions (Table 2). Nine publications from 4 OUs commented on treatments delivered prior to observation.33, 3542 The most commonly cited criteria for admission was approval by the unit's supervising physician. Utilization review was not mentioned as an element in the OU admission decision. Common OU exclusions were the need for intensive care or monitoring while awaiting an inpatient bed; however, these were not universal. Eight centers placed bounds around the duration of OU stays, with minimum stays of 2 hours and maximum stays of 8 to 24 hours.
| Hospital | Entry Criteria | Age Range | Time | Exclusion Criteria |
|---|---|---|---|---|
| ||||
| King's County, Downstate Brooklyn | Otherwise required inpatient admission | 0‐13 years | Maximum 24 hours | Not reported |
| Acute problem of uncertain severity | ||||
| Acute problem not readily diagnosed | ||||
| Short course periodic treatment | ||||
| Diagnostic procedures impractical as outpatient | ||||
| Children's Hospital, Buffalo | Admission from any source | 0‐21 years | Maximum 24 hours | Intensive care needs |
| Short stay elective surgery | Routine diagnostic tests | |||
| Estimated length of stay 24 hours | Holding prior to admission | |||
| Children's National, Washington, DC | Inadequate response to 3 subcutaneous epinephrine injections | 8 months to 19 years | Not reported | Not reported |
| Children's Memorial, Chicago | Asthma: | |||
| Available parentAsthma score 5Inadequate response to ED treatment | >1 year | Maximum 24 hours | Past history of BPD, CF, CHD, other debilitating disease | |
| Dehydration: | ||||
| Cases receiving oral hydration | 3‐24 months | 12 hours for oral | Intensive care need | |
| Parent preference if given IV hydration | 8 to 12 hours for IV | Hypernatremia | ||
| Minneapolis Children's | Conditions listed in Table 3 | Not reported | Maximum 10 hours | Not reported |
| Children's Hospital, Boston | Straightforward diagnoses as determined by ED staff | Not reported | Not reported | Other complex medical issues |
| Bed availability | ||||
| Connecticut Children's | PEM attending discretionLimited severity of illnessUsually confined to a single organ systemClearly identified plan of care | Not reported | After 3‐4 hours in ED Low likelihood of requiring extended care >23 hours | Asthma: no supplemental O2 need, nebulized treatments >Q2 hourCroup: no supplemental O2 need, 2 racemic epinephrine treatmentsDehydration: inability to tolerate orals, bicarbonate >10, 40 mL/kg IVFSeizure: partial or generalized, postictal, unable to tolerate oralsPoisoning: mild or no symptoms, poison control recommendation |
| Children's Hospital, Denver | Intussusception: following reduction | 0‐18 years | After 3‐4 hours in ED | Not reported |
| Dehydration: based on clinical status | ||||
| Johns Hopkins, Bayview | Consultation with on‐duty pediatrician | 0‐18 years | Minimum of 2 hours | Patients requiring subspecialty or intensive care services |
| High likelihood of discharge at 24 hours | ||||
| Children's Hospital of Philadelphia | Sole discretion of the ED attending | Not reported | Minimum 4 hours | No direct admissions |
| Single focused acute condition | Maximum 23 hours | Diagnostic dilemmas | ||
| Clinical conditions appropriate for observation | Underlying complex medical problems | |||
| Primary Children's Medical Center | Observation unit attending discretion | 0‐21 years | Minimum 3 hours | Admission holds |
| Scheduled procedures as space available | Maximum 24 hours | Intensive care needs | ||
| ED admit after consult with OU doctor | Complicated, multisystem disease | |||
| Clear patient care goals | Need for multiple specialty consults | |||
| Limited severity of illness | Psychiatric patients | |||
| Diagnostic evaluation | ||||
Ages of Children Under Observation
Seven of 11 hospitals reported the age range of patients accepted in their OU (Table 2). All but 1 unit accepted children from infants to young adults, 18 to 21 years of age.43 In the 6 units that reported the age distribution of their OU population, roughly 20% were 1 year, more than 50% were 5 years, and fewer than 30% fell into an adolescent age range.5, 6, 26, 32, 34, 43
Conditions Under Observation
Many conditions under observation were common across time and location (Table 3). The list of conditions cared for in OUs has expanded in recent years. Medical conditions predominated over surgical. While the majority of observation cases required acute care, nearly one‐half of the units accepted children with scheduled care needs (eg, routine postoperative care, procedures requiring sedation, infusions, and extended evaluations such as electroencephalograms or pH probes). These scheduled cases, cared for within the OU structure, provided more steady demand for OU services.
| King's County, Downstate Brooklyn | Children's Hospital, Buffalo | Minneapolis Children's | Children's Hospital, Boston | Connecticut Children's | Children's Hospital, Denver | Johns Hopkins, Bayview | Children's Hospital of Philadelphia | Primary Children's Medical Center, Salt Lake City | |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Respiratory | |||||||||
| Asthma | |||||||||
| Pneumonia | |||||||||
| Bronchiolitis | |||||||||
| Croup | |||||||||
| Allergic reaction | |||||||||
| Cardiology | |||||||||
| Gastrointestinal | |||||||||
| Vomiting | |||||||||
| Gastro/dehydration | |||||||||
| Abdominal pain | |||||||||
| Constipation | |||||||||
| Diabetes | |||||||||
| Neurologic | |||||||||
| Seizure | |||||||||
| Head injury | |||||||||
| Infection | |||||||||
| Sepsis evaluation | |||||||||
| UTI/pyelonephritis | |||||||||
| Cellulitis | |||||||||
| Fever | |||||||||
| Pharyngitis | |||||||||
| Otitis media | |||||||||
| Adenitis | |||||||||
| Ingestion/poisoning | |||||||||
| Hematologic | |||||||||
| Sickle cell disease | |||||||||
| Transfusion/emnfusion | |||||||||
| Psychological/social | |||||||||
| Dental | |||||||||
| Surgical conditions | |||||||||
| Foreign body | |||||||||
| Trauma | |||||||||
| Burn | |||||||||
| Orthopaedic injury | |||||||||
| Postoperative complication | |||||||||
| Scheduled care | |||||||||
| Diagnostic workup | |||||||||
| Procedures/sedation | |||||||||
| Elective surgery | |||||||||
Reimbursement
One publication highlighted the special billing rules that must be considered for observation care.27 In 3 studies, payers recognized cost‐savings associated with the OU's ability to provide outpatient management for cases that would traditionally require inpatient care.31, 35, 38
Observation Unit Outcomes
Outcomes reported for pediatric OU stays fall into 4 major categories: length of stay (LOS), admission rates, return visit rates, and costs. Despite these seemingly straightforward groupings, there was significant heterogeneity in reporting these outcomes.
Length of Stay
The start time for OU length of stay (LOS) is not clearly defined in the articles included in this review. While the start of an observation period is assumed to begin at the time the order for observation is placed, it is possible that the LOS reported in these publications began at the time of ED arrival or the time the patient was physically transferred to the OU. The average LOS for individual OUs ranged from 10 to 15 hours.5, 6, 26, 30, 35, 38, 40, 41, 43 One ward‐based and 1 ED‐based unit reported LOS extending beyond 24 hours,7, 30 with averages of 35 and 9 hours, respectively. Two units limited the duration of care to 10 hours.31, 38
For studies that included a comparison group, OU stays were consistently shorter than a traditional inpatient stay by 6 to 110 hours.7, 36, 38, 39, 42 No significant differences in clinical parameters between groups were reported. There was appreciable variation in the average LOS across institutions for similar conditions, 12 to 35 hours for asthma,5, 7, 34, 35 and 9 to 18 hours for dehydration.5, 34, 36, 38
Admission Rates
Rates of hospital admission after observation from the 9 OUs reporting this outcome are presented in Table 4. Three publications from a single institution counted hospital admission in the 48 to 72 hours following discharge from the OU as though the patient were admitted to the hospital directly from the index OU stay.33, 40, 41 Conditions with the lowest admission rates, 10%, included croup, neurologic conditions, ingestions, trauma, and orthopedic injuries. The highest admission rates, >50%, were for respiratory conditions including asthma, pneumonia, and bronchiolitis.
| King's County, Downstate Brooklyn (%) | Children's Hospital, Buffalo (%) | Connecticut Children's (%) | Johns Hopkins, Bayview (%) | Children's Hospital of Philadelphia (%) | Primary Children's Medical Center, Salt Lake City (%) | |
|---|---|---|---|---|---|---|
| ||||||
| Unscheduled care | 42 | 17 | 11 | 25 | 25 | 15 |
| Respiratory | 32 | |||||
| Asthma | 57 | 16 | 26 | 22 | 22‐25* | |
| Pneumonia | 50 | 23 | 30‐48 | |||
| Bronchiolitis | 46 | 32 | 43 | |||
| Croup | 9 | 17 | 9 | 4‐6 | ||
| Allergic reaction | 3 | |||||
| Cardiology | 22 | |||||
| Gastrointestinal | 43 | 19 | ||||
| Vomiting | 5 | 22 | ||||
| Gastro/dehydration | 23 | 15/21 | 16* | |||
| Abdominal pain | 9 | 17 | 27 | |||
| Constipation | 9 | |||||
| Diabetes | 17 | |||||
| Neurologic | 10 | |||||
| Seizure | 19 | 8 | 17 | 18 | ||
| Head injury | 7 | 5* | ||||
| Infection | 19 | 34 | ||||
| Sepsis evaluation | 25 | 22 | ||||
| UTI/pyelonephritis | 25 | 16 | ||||
| Cellulitis | 15 | |||||
| Fever | 16 | 26 | ||||
| Pharyngitis | 13 | |||||
| Otitis media | 21 | |||||
| Ingestion/poisoning | 9 | 4 | 4 | 9 | 10 | 5 |
| Hematologic | 23 | |||||
| Transfusion/emnfusion | 2 | |||||
| Psychological/social | 21 | 80 | 17 | |||
| Dental | 14 | |||||
| Surgical conditions | ||||||
| Foreign body | ||||||
| Trauma | 13 | 2 | 53 | 5 | ||
| Burn | 13 | |||||
| Orthopedic injury | 22 | 3 | ||||
| Postoperative complication | 26 | 16 | ||||
| Scheduled care | ||||||
| Diagnostic workup | 0‐5 | |||||
| Procedures/sedation | 0.1‐9.0 | |||||
| Elective surgery | 13 | 0‐5 | ||||
Return Visit Rates
Unscheduled return visit rates were reported in 9 publications from 6 institutions and ranged from 0.01% to 5%.7, 26, 33, 3537, 3941 Follow‐up timeframes ranged from 48 hours to 1 month. Return visits were inconsistently defined. In most studies, rates were measured in terms of ED visits.26, 33, 3537, 39, 41 One ward‐based unit counted only hospital readmissions toward return visit rates.7 Three publications, from ED‐based units, counted hospital readmissions in the 2 to 5 days following observation toward admission rates and not as return visits.33, 40, 41 In most studies, data on return visits were collected from patient logs or patient tracking systems. Three studies contacted patients by phone and counted return visits to the clinic.3537 No studies reported on adherence to scheduled visits following observation.
Costs
Seven studies reported financial benefits of OU care when compared with traditional hospital care.7, 30, 31, 35, 37, 38, 42 Two centers admitted patients to inpatient care if their observation period reached a set time limit, after which cost savings were no longer realized.31, 35 Cost savings associated with the OU treatment of asthma and dehydration were attributed to lower charges for an OU bed.35, 38 Decreased charges for the OU treatment of croup were related to shorter LOS.42
Discussion
In the 40 years since the first studies of pediatric OUs, several US health systems have extended observation services to children. This model of care may be expanding, as suggested by an increase in the number of publications in the past 10 years. However, the number of centers within the US reporting on their OU experience remains small. Our systematic review identified a recurrent theme related to OUsthe opportunity to improve operational processes of care compared with the traditional inpatient alternative. We have identified the need to standardize OU outcomes and propose measures for future OU research.
Observation Unit Operations
The OU care model expands outpatient management of acute conditions to include children who are neither ready for discharge nor clear candidates for inpatient admission. OUs have demonstrated the ability to care for patients across the pediatric age spectrum. Over the decades spanning these publications, advances in medical therapy such as antiemetics for gastroenteritis and early administration of systemic steroids for asthma may have resulted in lower admission rates or shorter time to recovery.44, 45 Despite these advances, there are marked consistencies in the conditions cared for within OUs over time. The data summarized here may help guide institutions as they consider specific pediatric conditions amenable to observation care.
The hospitals included in this review either added physical space or revised services within existing structures to establish their OU. Hospitals facing physical constraints may look to underutilized areas, such as recovery rooms, to provide observation care, as observation does not require the use of licensed inpatient beds. Several units have responded to daily fluctuations in unscheduled observation cases by also serving patients who require outpatient procedures, brief therapeutic interventions, and diagnostic testing. By caring for patients with these scheduled care needs during the day, there is a more steady flow of patients into the OU. While hospitals traditionally have used postanesthesia care units and treatment rooms for scheduled cases, OUs appear to benefit from the consistent resource allocation associated with a constant demand for services.
To date, the vast majority of pediatric OUs in the published literature have emerged as an extension of ED services. Now, with the expansion of pediatric hospitalist services and movement toward 24/7 inpatient physician coverage, there may be increased development of ward‐based OUs and the designation of inpatient observation status. While ward‐based OUs managed by pediatric hospitalists may be well established, we were not able to identify published reports on this structure of care. A national survey of health systems should be undertaken to gather information regarding the current state of pediatric observation services.
When creating policies and procedures for OUs, input should be sought from stakeholders including hospitalists, PEM providers, primary care providers, subspecialists, mid‐level providers, nurses, and ancillary staff. As patients requiring observation level of care do not neatly fit an outpatient or inpatient designation, they present an opportunity for hospitalist and PEM physician groups to collaborate.4648 Calling on the clinical experiences of inpatient and ED providers could offer unique perspectives leading to the development of innovative observation care models.
This review focused on institutions with dedicated observation services, which in all but 1 study26 consisted of a defined geographic unit. It is possible that the practices implemented in an OU could have hospital‐wide impact. For example, 1 study reported reduction in LOS for all asthma cases after opening a ward‐based unit.7 Further, pediatric hospitalist services have been associated with shorter LOS49 and increased use of observation status beds compared with traditional ward services.50 As pediatric hospitalists expand their scope of practice to include both observation and inpatient care, clinical practice may be enhanced across these care areas. It follows that the impact of observation protocols on care in the ward setting should be independently evaluated.
The costs associated with the establishment and daily operations of an OU were not addressed in the reviewed publications. Assertions that observation provides a cost‐effective alternative to inpatient care4, 7, 23, 42 should be balanced by the possibility that OUs extend care for patients who could otherwise be discharged directly home. Studies have not evaluated the cost of OU care compared with ED care alone. Research is also needed to assess variations in testing and treatment intensity in OUs compared with the ED and inpatient alternatives. Reimbursement for observation is dependent in part upon institutional contracts with payers. A full discussion of reimbursement issues around observation services is beyond the scope of this review.
Observation Unit Outcomes
Length of Stay
Although most studies reported LOS, direct comparisons across institutions are difficult given the lack of a consistently referenced start to the observation period. Without this, LOS could begin at the time of ED arrival, time of first treatment, or time of admission to the OU. Identifying and reporting the elements contributing to LOS for observation care is necessary. The time of OU admission is important for billing considerations; the time of first treatment is important to understanding the patient's response to medical interventions; the time of ED arrival is important to evaluating ED efficiency. Each of these LOS measures should be reported in future studies.
Direct comparisons of LOS are further complicated by variability in the maximum permissible duration of an OU stay, ranging from 8 to 24 hours in the included studies. Despite these limits, some OU care will extend beyond set limits due to structural bottlenecks. For example, once the inpatient setting reaches capacity, observation LOS for patients who require admission will be prolonged. The best evaluation of LOS would come from prospective study design utilizing either randomization or quality improvement methods.
Defining Success and Failure in Observation Care
In the reviewed literature, observation failures have been defined in terms of admission after observation and unscheduled return visit rates. Admission rates are heavily dependent on appropriate selection of cases for observation. Although some observation cases are expected to require inpatient admission, OUs should question the validity of their unit's acceptance guidelines if the rate of admission is >30%.51 High rates could be the result of inadequate treatment or the selection of children too sick to improve within 24 hours. Low rates could indicate overutilization of observation for children who could be discharged directly home. Full reporting on the number of children presenting with a given condition and the different disposition pathways for each is needed to evaluate the success of OUs. Condition‐specific benchmarks for admission after observation rates could guide hospitals in their continuous improvement processes.
Unscheduled return visits may reflect premature discharge from care, diagnostic errors, or development of a new illness. OU care may influence patient adherence to scheduled follow‐up care but this has not been evaluated to date. In future research, both scheduled and unscheduled return visits following ED visits, observation stays, and brief inpatient admissions for similar disease states should be reported for comparison. Standard methodology for identifying return visits should include medical record review, claims analyses, and direct patient contact.
As hospitals function at or near capacity,52, 53 it becomes important to delineate the appropriate length of time to monitor for response to treatments in a given setting. Limited capacity was a frequently cited reason for opening a pediatric OU; however, the impact of OUs on capacity has not yet been evaluated. Operations research methods could be used to model OU services' potential to expand hospital capacity. This research could be guided by evaluation of administrative data from across institutions to identify current best practices for pediatric OU and observation status care.
OU benchmarking in the United States has begun with a small number of adult units participating in the ED OU Benchmark Alliance (EDOBA).54 In Table 5, we propose dashboard measures for pediatric OU continuous quality improvement. The proposed measures emphasize the role of observation along the continuum of care for acute conditions, from the ED through the OU with or without an inpatient stay to clinic follow‐up. Depending on the structure of observation services, individual institutions may select to monitor different dashboard measures from the proposed list. Patient safety and quality of care measures for the conditions commonly receiving pediatric OU care should also be developed.
| ED |
OU |
Inpatient |
Clinic | |
|---|---|---|---|---|
| ||||
| Length of stay* | ED arrival to OU admission | OU admit to disposition | Inpatient admit to discharge | |
| ED arrival to discharge home from OU | ||||
| ED arrival to discharge from inpatient following OU care | ||||
| OU admission to discharge home from inpatient care | ||||
| Admission* | % ED census admitted inpatient | % OU census admitted | ||
| % ED census that is observed | ||||
| Unscheduled return visits* | To ED | Requiring OU admission | Requiring inpatient admission | |
| Scheduled follow‐up* | To ED | To primary care or subspecialist office | ||
| Capacity | ED crowding scales | Unable to accept transfers | ||
| ED left before evaluation rates | Inpatient occupancy | |||
| Ambulance diversion | ||||
| Satisfaction | Patient/Parent | |||
| ED providers | OU providers | Inpatient providers | Follow‐up providers | |
| Cost | ED care | OU care | Inpatient care | |
| Total encounter | ||||
Limitations
The most important limitations to this review are the heterogeneity in interventions and reporting of outcomes, which precluded our ability to combine data or conduct meta‐analyses. We attempted to organize the outcomes data into clear and consistent groupings. However, we could not compare the performance of 1 center with another due to differences in OU structure, function, and design.
In order to focus this systematic review, we chose to include only peer reviewed publications that describe pediatric OUs within the United States. This excludes expert guidelines, which may be of value to institutions developing observation services.
Our search found only a small number of centers that utilize OUs and have published their experience. Thus, our review is likely subject to publication bias. Along this line, we identified 9 additional publications where children were cared for alongside adults within a general OU.5563 This suggests an unmeasured group of children under observation in general EDs, where more than 90% of US children receive acute care.64 These articles were excluded because we were unable to distinguish pediatric specific outcomes from the larger study population.
Finally, retrospective study design is subject to information bias. Without a comparable control group, it is difficult to understand the effects of OUs. Patients directly admitted or discharged from the ED and patients who require admission after observation all differ from patients discharged from observation in ways that should be controlled for with a randomized study design.
Conclusions
OUs have emerged to provide treatment at the intersection of outpatient and inpatient care during a time of dramatic change in both emergency and hospital medicine. As hospitalists expand their scope of practice to include observation care, opportunities will arise to collaborate with ED physicians and share their growing expertise in quality and efficiency of hospital care delivery to improve observation services for children. OUs have been established with laudable goalsto reduce inpatient admissions, increase patient safety, improve efficiency, and control costs. The current evidence is not adequate to determine if this model of healthcare delivery achieves these goals for children. Through synthesis of existing data, we have identified a need for standard reporting for OU outcomes and propose consistent measures for future observation care research. Only through prospective evaluation of comparable outcomes can we appraise the performance of pediatric OUs across institutions.
- .Observation medicine.Acad Emerg Med.1994;1(2):152–154.
- ,.Principles of observation medicine.Emerg Med Clin North Am.2001;19(1):1–17.
- ,,, et al.Emergency department observation beds improve patient care: Society for Academic Emergency Medicine debate.Ann Emerg Med.1992;21(8):967–975.
- .Pediatric observation medicine.Emerg Med Clin North Am.2001;19(1):239–254.
- ,,.The pediatric hybrid observation unit: an analysis of 6477 consecutive patient encounters.Pediatrics.2005;115(5):e535–e542.
- ,,, et al.Observation units: the role of an outpatient extended treatment site in pediatric care.Pediatr Emerg Care.1998;14(6):444–447.
- ,,, et al.Impact of a short stay unit on asthma patients admitted to a tertiary pediatric hospital.Qual Manag Health Care.1997;6(1):14–22.
- ,,, et al.Management of observation units. American College of Emergency Physicians.Ann Emerg Med.1995;25(6):823–830.
- ,,, et al. The observation unit: an operational overview for the hospitalist. Society of Hospital Medicine White Paper 2009; Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Publications/WhitePapers/White_Papers.htm. Accessed July2009.
- Acute Criteria Pediatric InterQual Level of Care.San Francisco, CA:McKesson Corporation;2006.
- Observation Status Related to U.S. Hospital Records.Healthcare Cost and Utilization Project. HCUP Methods Series Report #2002‐3. Rockville, MD: Agency for Healthcare Research and Quality;2002.
- ,,, et al.Emergency department observation unit versus hospital inpatient care for a chronic asthmatic population: a randomized trial of health status outcome and cost.Med Care.1998;36(4):599–609.
- ,,, et al.Costs of an emergency department‐based accelerated diagnostic protocol vs hospitalization in patients with chest pain: a randomized controlled trial.JAMA.1997;278(20):1670–1676.
- .Management of patients with infectious diseases in an emergency department observation unit.Emerg Med Clin North Am.2001;19(1):187–207.
- ,,, et al.A comparison between emergency diagnostic and treatment unit and inpatient care in the management of acute asthma.Arch Intern Med.1997;157(18):2055–2062.
- .Chest pain observation units.Emerg Med J.2001;18(2):148.
- ,,, et al.Randomised controlled trial and economic evaluation of a chest pain observation unit compared with routine care.BMJ.2004;328(7434):254.
- ,,, et al.A cooperative care model: cardiologists and hospitalists reduce length of stay in a chest pain observation. In:5th Scientific Forum on Quality of Care and Outcomes Research in Cardiovascular Disease and Stroke, Washington, DC, May 15‐17, 2003.Philadelphia, PA:Lippincott Williams 2003. p.P186.
- ,.Observation unit management of pediatric emergencies.Emerg Med Clin North Am.1991;9(3):669–676.
- .A short stay or 23‐hour ward in a general and academic children's hospital: are they effective?Pediatr Emerg Care.2000;16(4):223–229.
- ,,, et al.Trends in high turnover stays among children hospitalized in the United States, 1993 through 2003.Pediatrics.2009;123:996–1002.
- .Hospital based alternatives to acute paediatric admission: a systematic review.Arch Dis Child.2005;90(2):138–142.
- ,,.Short‐stay units and observation medicine: a systematic review.Med J Aust.2003;178(11):559–563.
- ,,.Use of emergency observation and assessment wards: a systematic literature review.Emerg Med J.2003;20(2):138–142.
- Oxford Centre for Evidence‐Based Medicine. Levels of evidence and grades of recommendation (May 2001). Available at: http://www.cebm.net/levels_of_evidence.asp. Accessed July2009.
- ,,, et al.Pediatric observation status beds on an inpatient unit: an integrated care model.Pediatr Emerg Care.2004;20(1):17–21.
- .Pediatric update. Our new rapid treatment unit: an innovative adaptation of the “less than 24‐hour stay” holding unit.J Emerg Nurs.2000;26(5):507.
- ,,.Use of an observation unit by a pediatric emergency department for common pediatric illnesses.Pediatr Emerg Care.2001;17(5):321–323.
- ,,, et al.Observation medicine: the expanded role of the nurse practitioner in a pediatric emergency department extended care unit.Pediatr Emerg Care.2005;21(3):199–202.
- ,,.An observation unit in a pediatric emergency department: one children's hospital's experience.J Emerg Nurs.2002;28(5):407–413.
- ,,.When the patient requires observation not hospitalization.J Nurs Admin.1988;18(10):20–23.
- ,.Observation unit in Children's Hospital—Adjunct to delivery and teaching of ambulatory pediatric care.N Y State J Med.1980;80(11):1684–1686.
- ,,, et al.Use of pediatric observation unit for treatment of children with dehydration caused by gastroenteritis.Pediatr Emerg Care.2006;22(1):1–6.
- ,,, et al.Utilization and unexpected hospitalization rates of a pediatric emergency department 23‐hour observation unit.Pediatr Emerg Care.2008;24(9):589–594.
- ,,, et al.Short‐term holding room treatment of asthmatic‐children.J Pediatr.1985;106(5):707–711.
- ,,.Usefulness of the serum electrolyte panel in the management of pediatric dehydration treated with intravenously administered fluids.Pediatrics.2004;114(5):1227–1234.
- ,,.Treatment of acute asthmatic attacks in a holding unit of a pediatric emergency room.Ann Allergy.1980;45(3):159–162.
- ,,.Outpatient oral rehydration in the United States.Am J Dis Child.1986;140(3):211–215.
- ,.Postreduction management of intussusception in a children's hospital emergency department.Pediatrics.2003;112(6 Pt 1):1302–1307.
- ,,, et al.Children with asthma admitted to a pediatric observation unit.Pediatr Emerg Care.2005;21(10):645–649.
- ,,, et al.Pediatric closed head injuries treated in an observation unit.Pediatr Emerg Care.2005;21(10):639–644.
- ,,.A reduction in hospitalization, length of stay, and hospital charges for croup with the institution of a pediatric observation unit.Am J Emerg Med.2006;24(7):818–821.
- ,,.Short stay in an outpatient department. An alternative to hospitalization.Am J Dis Child.1972;123(2):128–132.
- ,,.The role of oral ondansetron in children with vomiting as a result of acute gastritis/gastroenteritis who have failed oral rehydration therapy: a randomized controlled trial.Ann Emerg Med.2008;52(1):22–29.e6.
- ,,, et al.Oral ondansetron for gastroenteritis in a pediatric emergency department.N Engl J Med.2006;354(16):1698–1705.
- ,,, et al.Integrated hospital emergency care improves efficiency.Emerg Med J.2008;25(2):78–82.
- ,,, et al.Redefining the community pediatric hospitalist: the combined pediatric ED/inpatient unit.Pediatr Emerg Care.2007;23(1):33–37.
- ,,, et al.Program description: a hospitalist‐run, medical short‐stay unit in a teaching hospital.CMAJ.2000;163(11):1477–1480.
- ,.Evaluation of a pediatric hospitalist service: impact on length of stay and hospital charges.Pediatrics.2000;105(3 Pt 1):478–484.
- ,,, et al.Restructuring an academic pediatric inpatient service using concepts developed by hospitalists.Clin Pediatr (Phila).2001;40(12):653–660; discussion 661‐662.
- ,,, et al.American College of Emergency Physicians (ACEP).Practice Management Committee, American College of Emergency Physicians. Management of Observation Units. Irving, TX: American College of Emergency Physicians; July1994.
- Overcrowding crisis in our nation's emergency departments:is our safety net unraveling?Pediatrics.2004;114(3):878–888.
- ,.Emergency department overcrowding in the United States: an emerging threat to patient safety and public health.Emerg Med J.2003;20(5):402–405.
- ,,, et al.Characteristics of high volume teaching hospital observation units: data from the Emergency Department Observation Unit Benchmark Alliance (EDOBA).Acad Emerg Med.2009;16(s1):Abstract 628.
- ,,.Use of the emergency department observation unit in the treatment of acute asthma.Ann Emerg Med.1982;11(2):77–83.
- ,,, et al.Management of acute pyelonephritis in an emergency department observation unit.[see Comment].Ann Emerg Med.1991;20(3):253–257.
- ,,, et al.Patterns of use of an emergency department‐based observation unit.Am J Ther.2002;9(6):499–502.
- ,,, et al.Emergency department observation of poisoned patients: how long is necessary?[see Comment].Acad Emerg Med.1999;6(9):887–894.
- ,,, et al.False‐negative and false‐positive errors in abdominal pain evaluation: failure to diagnose acute appendicitis and unnecessary surgery.Acad Emerg Med.2000;7(11):1244–1255.
- .Resource use by younger versus older patients.Fam Pract Res J.1993;13(3):283–290.
- ,,, et al.Trauma 24‐hour observation critical path.J Trauma.1998;45(1):147–150.
- ,,, et al.The role of an emergency department observation unit in the management of trauma patients.J Emerg Med.1985;2(5):325–333.
- ,.Observation unit impact on ED admission for asthma.Am J Emerg Med.1994;12(1):11–14.
- ,.Emergency care for children in pediatric and general emergency departments.Pediatr Emerg Care.2007;23(2):94–102.
- .Observation medicine.Acad Emerg Med.1994;1(2):152–154.
- ,.Principles of observation medicine.Emerg Med Clin North Am.2001;19(1):1–17.
- ,,, et al.Emergency department observation beds improve patient care: Society for Academic Emergency Medicine debate.Ann Emerg Med.1992;21(8):967–975.
- .Pediatric observation medicine.Emerg Med Clin North Am.2001;19(1):239–254.
- ,,.The pediatric hybrid observation unit: an analysis of 6477 consecutive patient encounters.Pediatrics.2005;115(5):e535–e542.
- ,,, et al.Observation units: the role of an outpatient extended treatment site in pediatric care.Pediatr Emerg Care.1998;14(6):444–447.
- ,,, et al.Impact of a short stay unit on asthma patients admitted to a tertiary pediatric hospital.Qual Manag Health Care.1997;6(1):14–22.
- ,,, et al.Management of observation units. American College of Emergency Physicians.Ann Emerg Med.1995;25(6):823–830.
- ,,, et al. The observation unit: an operational overview for the hospitalist. Society of Hospital Medicine White Paper 2009; Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Publications/WhitePapers/White_Papers.htm. Accessed July2009.
- Acute Criteria Pediatric InterQual Level of Care.San Francisco, CA:McKesson Corporation;2006.
- Observation Status Related to U.S. Hospital Records.Healthcare Cost and Utilization Project. HCUP Methods Series Report #2002‐3. Rockville, MD: Agency for Healthcare Research and Quality;2002.
- ,,, et al.Emergency department observation unit versus hospital inpatient care for a chronic asthmatic population: a randomized trial of health status outcome and cost.Med Care.1998;36(4):599–609.
- ,,, et al.Costs of an emergency department‐based accelerated diagnostic protocol vs hospitalization in patients with chest pain: a randomized controlled trial.JAMA.1997;278(20):1670–1676.
- .Management of patients with infectious diseases in an emergency department observation unit.Emerg Med Clin North Am.2001;19(1):187–207.
- ,,, et al.A comparison between emergency diagnostic and treatment unit and inpatient care in the management of acute asthma.Arch Intern Med.1997;157(18):2055–2062.
- .Chest pain observation units.Emerg Med J.2001;18(2):148.
- ,,, et al.Randomised controlled trial and economic evaluation of a chest pain observation unit compared with routine care.BMJ.2004;328(7434):254.
- ,,, et al.A cooperative care model: cardiologists and hospitalists reduce length of stay in a chest pain observation. In:5th Scientific Forum on Quality of Care and Outcomes Research in Cardiovascular Disease and Stroke, Washington, DC, May 15‐17, 2003.Philadelphia, PA:Lippincott Williams 2003. p.P186.
- ,.Observation unit management of pediatric emergencies.Emerg Med Clin North Am.1991;9(3):669–676.
- .A short stay or 23‐hour ward in a general and academic children's hospital: are they effective?Pediatr Emerg Care.2000;16(4):223–229.
- ,,, et al.Trends in high turnover stays among children hospitalized in the United States, 1993 through 2003.Pediatrics.2009;123:996–1002.
- .Hospital based alternatives to acute paediatric admission: a systematic review.Arch Dis Child.2005;90(2):138–142.
- ,,.Short‐stay units and observation medicine: a systematic review.Med J Aust.2003;178(11):559–563.
- ,,.Use of emergency observation and assessment wards: a systematic literature review.Emerg Med J.2003;20(2):138–142.
- Oxford Centre for Evidence‐Based Medicine. Levels of evidence and grades of recommendation (May 2001). Available at: http://www.cebm.net/levels_of_evidence.asp. Accessed July2009.
- ,,, et al.Pediatric observation status beds on an inpatient unit: an integrated care model.Pediatr Emerg Care.2004;20(1):17–21.
- .Pediatric update. Our new rapid treatment unit: an innovative adaptation of the “less than 24‐hour stay” holding unit.J Emerg Nurs.2000;26(5):507.
- ,,.Use of an observation unit by a pediatric emergency department for common pediatric illnesses.Pediatr Emerg Care.2001;17(5):321–323.
- ,,, et al.Observation medicine: the expanded role of the nurse practitioner in a pediatric emergency department extended care unit.Pediatr Emerg Care.2005;21(3):199–202.
- ,,.An observation unit in a pediatric emergency department: one children's hospital's experience.J Emerg Nurs.2002;28(5):407–413.
- ,,.When the patient requires observation not hospitalization.J Nurs Admin.1988;18(10):20–23.
- ,.Observation unit in Children's Hospital—Adjunct to delivery and teaching of ambulatory pediatric care.N Y State J Med.1980;80(11):1684–1686.
- ,,, et al.Use of pediatric observation unit for treatment of children with dehydration caused by gastroenteritis.Pediatr Emerg Care.2006;22(1):1–6.
- ,,, et al.Utilization and unexpected hospitalization rates of a pediatric emergency department 23‐hour observation unit.Pediatr Emerg Care.2008;24(9):589–594.
- ,,, et al.Short‐term holding room treatment of asthmatic‐children.J Pediatr.1985;106(5):707–711.
- ,,.Usefulness of the serum electrolyte panel in the management of pediatric dehydration treated with intravenously administered fluids.Pediatrics.2004;114(5):1227–1234.
- ,,.Treatment of acute asthmatic attacks in a holding unit of a pediatric emergency room.Ann Allergy.1980;45(3):159–162.
- ,,.Outpatient oral rehydration in the United States.Am J Dis Child.1986;140(3):211–215.
- ,.Postreduction management of intussusception in a children's hospital emergency department.Pediatrics.2003;112(6 Pt 1):1302–1307.
- ,,, et al.Children with asthma admitted to a pediatric observation unit.Pediatr Emerg Care.2005;21(10):645–649.
- ,,, et al.Pediatric closed head injuries treated in an observation unit.Pediatr Emerg Care.2005;21(10):639–644.
- ,,.A reduction in hospitalization, length of stay, and hospital charges for croup with the institution of a pediatric observation unit.Am J Emerg Med.2006;24(7):818–821.
- ,,.Short stay in an outpatient department. An alternative to hospitalization.Am J Dis Child.1972;123(2):128–132.
- ,,.The role of oral ondansetron in children with vomiting as a result of acute gastritis/gastroenteritis who have failed oral rehydration therapy: a randomized controlled trial.Ann Emerg Med.2008;52(1):22–29.e6.
- ,,, et al.Oral ondansetron for gastroenteritis in a pediatric emergency department.N Engl J Med.2006;354(16):1698–1705.
- ,,, et al.Integrated hospital emergency care improves efficiency.Emerg Med J.2008;25(2):78–82.
- ,,, et al.Redefining the community pediatric hospitalist: the combined pediatric ED/inpatient unit.Pediatr Emerg Care.2007;23(1):33–37.
- ,,, et al.Program description: a hospitalist‐run, medical short‐stay unit in a teaching hospital.CMAJ.2000;163(11):1477–1480.
- ,.Evaluation of a pediatric hospitalist service: impact on length of stay and hospital charges.Pediatrics.2000;105(3 Pt 1):478–484.
- ,,, et al.Restructuring an academic pediatric inpatient service using concepts developed by hospitalists.Clin Pediatr (Phila).2001;40(12):653–660; discussion 661‐662.
- ,,, et al.American College of Emergency Physicians (ACEP).Practice Management Committee, American College of Emergency Physicians. Management of Observation Units. Irving, TX: American College of Emergency Physicians; July1994.
- Overcrowding crisis in our nation's emergency departments:is our safety net unraveling?Pediatrics.2004;114(3):878–888.
- ,.Emergency department overcrowding in the United States: an emerging threat to patient safety and public health.Emerg Med J.2003;20(5):402–405.
- ,,, et al.Characteristics of high volume teaching hospital observation units: data from the Emergency Department Observation Unit Benchmark Alliance (EDOBA).Acad Emerg Med.2009;16(s1):Abstract 628.
- ,,.Use of the emergency department observation unit in the treatment of acute asthma.Ann Emerg Med.1982;11(2):77–83.
- ,,, et al.Management of acute pyelonephritis in an emergency department observation unit.[see Comment].Ann Emerg Med.1991;20(3):253–257.
- ,,, et al.Patterns of use of an emergency department‐based observation unit.Am J Ther.2002;9(6):499–502.
- ,,, et al.Emergency department observation of poisoned patients: how long is necessary?[see Comment].Acad Emerg Med.1999;6(9):887–894.
- ,,, et al.False‐negative and false‐positive errors in abdominal pain evaluation: failure to diagnose acute appendicitis and unnecessary surgery.Acad Emerg Med.2000;7(11):1244–1255.
- .Resource use by younger versus older patients.Fam Pract Res J.1993;13(3):283–290.
- ,,, et al.Trauma 24‐hour observation critical path.J Trauma.1998;45(1):147–150.
- ,,, et al.The role of an emergency department observation unit in the management of trauma patients.J Emerg Med.1985;2(5):325–333.
- ,.Observation unit impact on ED admission for asthma.Am J Emerg Med.1994;12(1):11–14.
- ,.Emergency care for children in pediatric and general emergency departments.Pediatr Emerg Care.2007;23(2):94–102.
Short Title
The United States spends more on healthcare than any country in the world, and it is widely believed that the Nation could spend less while achieving comparable or better outcomes. The recent debate over healthcare reform in the United States, the large Federal budget deficit in the context of the current economic recession, and the prospect of widening gaps in Medicare funding with the increasing entry of baby boomers into old age suggest that the issue of healthcare cost will remain intense for many years to come. What roles hospitalists will play in the nation's struggle to control health care costs remain to be seen. Six papers in this issue of the Journal of Hospital Medicine discuss issues related to costs, and reflect several of the ways in which hospital medicine can contribute to understanding, and ultimately, controlling healthcare costs.
Two papers, one by Whelan et al.1 examining the costs associated with upper vs. lower GI bleeding and one by Lorch et al.2 examining the costs associated with herpex simplex virus (HSV) infections among neonates with and without congenital abnormalities, focus on epidemiologic determinants of healthcare costs. Such studies can identify subgroups of patients with high costs who may be logical targets for efforts to control costs. One tension in the use of such analyses to control cost is that total cost for any patient group is the product of both the cost per patient and the number of patients falling into each group. In the case of gastrointestinal (GI) bleeding, the surprise compared to past reports is that lower GI bleeding is about as common among hospitalized patients as upper GI bleeding. This may be because pharmacotherapy for conditions that cause upper GI bleeding is reducing the rate at which disease progresses to the point where hospitalization is required. The importance of prevalence is reinforced even in the findings about HSV infection, where despite 2‐ to 3‐fold higher average costs among babies with HSV who have congenital abnormalities, the fact that 90% of babies hospitalized with HSV lack congenital abnormalities implies that the clear majority of costs are due to babies without congenital abnormalities. In seeking strategies to control costs, it is important to pay attention to both the prevalence and cost per case of specific conditions. Because hospitalists are generalist physicians who typically care for few patients with any given diagnosis, the importance of prevalence implies that disease‐specific efforts to control costs may produce smaller total gains than those that cross diseases, such as efforts to improve communication between inpatient and outpatient physicians.
Moreover, the presence of high costs for some condition does not, of course, imply that effective interventions exist to reduce those costs. Two other papers, one by Mudge et al.3 examining a disease management program for heart failure, and one by Go et al.4 examining the effects of hospitalists on the costs of hospitalization for GI bleeding, reinforce the idea that interventions to reduce hospital costs are not always as effective as hoped. Even worse, efforts to control costs can have unintended effects, such as the delays in antimicrobial administration with antimicrobial approval policies that are reported by Winters et al.5 These studies also illustrate that analyses of the effectiveness of interventions can be performed using a variety of experimental designs (eg, the before/after comparison used by Mudge et al,3 and the natural experiments based on assignment of patients to physicians based on day of admission used by Go et al.4 or based on time of day used by Winters et al.)5 The role of hospitalists as clinical leaders in hospitals often places them in positions to design and execute experiments, but the role of hospitalists as astute clinicians who can recognize the presence of natural experiments in their clinical environment can be every bit as powerful in producing valid research designs.
As society seeks strategies to control healthcare costs in the years ahead, it will almost certainly turn to the same general strategies that have been used in the past: bundling services into fixed payments for a prospectively defined episode of care, asking patients to pay more of the costs of care, and simply not paying for, or paying less for, any given type of care. Hospitalists already have dealt with many of these approaches in one form or another. Medicare's prospective payment system and the payment of fixed annual fees for the care of patients in health maintenance organizations have given all hospitalists some exposure to the pressure for lower hospital resources use under prospective payment systems. Proposals for demonstration projects within healthcare reform to study the effects of bundling inpatient and outpatient care or even hospital and professional fees suggest that hospitalists may need to be open to new incentive structures in the years to come. For example, reduced incentives for rapid discharge if costs pushed into the outpatient setting are borne by the hospital, there may be co‐management models if professional and hospital fees are bundled. Increases in patient copayments may also play some role in healthcare reform, and the paper by Ross et al.6 should be a reminder to hospitalists that we may do our patients a great disservice if we fail to recognize the effects of our decisions on their out‐of‐pocket costs. Indeed, while doctors and patient both recognize the importance of discussing out‐of‐pocket costs, they both agree that these discussions rarely occur.7 That such discussions are not reimbursed explicitly suggests one of the many challenges of controlling healthcare costs; if physician payments are decreased to control costs and physicians respond by attempting to see even more patients in any given time period, discussions of important but less urgent issues such as out‐of‐pocket costs seem likely to be reduced. Such dilemmas arise frequently as the healthcare system devises increasingly complex approaches to the control of costs and suggest to many that fundamental reform of the payment and delivery system with greater reliance on integrated health systems paid through full capitation will eventually need to become the nation's approach to healthcare cost containment.8
- ,., et al.Upper versus lower gastrointestinal bleeding: a direct comparison of clinical presentation, outcomes, and resource utilization.J Hosp Med.2010;5(3):140–146.
- ,,.Impact of congenital anomalies and treatment location on clinical outcomes and health resource use in infants hospitalized with herpes simplex virus.J Hosp Med.2010;5(3):154–158.
- ,,, et al.The paradox of readmission: effect of a quality improvement programme in hospitalised patients with heart failure.J Hosp Med.2010;5:147–152.
- ,,, et al.Do hospitalists affect clinical outcomes and efficiency for patients with acute upper gastrointestinal hemorrhage (UGIH)?J Hosp Med.2010;5(3):138–138.
- ,,.Impact of a restrictive antimicrobial policy on the process and timing of antimicrobial administration.J Hosp Med.2010;5(2):E41–E45.
- ,.Reducing patient financial liability for hospitalizations: the physician role.J Hosp Med.2010;5(3):159–161.
- ,,.Patient‐physician communication about out‐of‐pocket costs.JAMA.2003;290(7):953–958.
- ,,, et al.Toward a 21st‐century health care system: recommendations for health care reform.Ann Intern Med.2009;150:493–495.
The United States spends more on healthcare than any country in the world, and it is widely believed that the Nation could spend less while achieving comparable or better outcomes. The recent debate over healthcare reform in the United States, the large Federal budget deficit in the context of the current economic recession, and the prospect of widening gaps in Medicare funding with the increasing entry of baby boomers into old age suggest that the issue of healthcare cost will remain intense for many years to come. What roles hospitalists will play in the nation's struggle to control health care costs remain to be seen. Six papers in this issue of the Journal of Hospital Medicine discuss issues related to costs, and reflect several of the ways in which hospital medicine can contribute to understanding, and ultimately, controlling healthcare costs.
Two papers, one by Whelan et al.1 examining the costs associated with upper vs. lower GI bleeding and one by Lorch et al.2 examining the costs associated with herpex simplex virus (HSV) infections among neonates with and without congenital abnormalities, focus on epidemiologic determinants of healthcare costs. Such studies can identify subgroups of patients with high costs who may be logical targets for efforts to control costs. One tension in the use of such analyses to control cost is that total cost for any patient group is the product of both the cost per patient and the number of patients falling into each group. In the case of gastrointestinal (GI) bleeding, the surprise compared to past reports is that lower GI bleeding is about as common among hospitalized patients as upper GI bleeding. This may be because pharmacotherapy for conditions that cause upper GI bleeding is reducing the rate at which disease progresses to the point where hospitalization is required. The importance of prevalence is reinforced even in the findings about HSV infection, where despite 2‐ to 3‐fold higher average costs among babies with HSV who have congenital abnormalities, the fact that 90% of babies hospitalized with HSV lack congenital abnormalities implies that the clear majority of costs are due to babies without congenital abnormalities. In seeking strategies to control costs, it is important to pay attention to both the prevalence and cost per case of specific conditions. Because hospitalists are generalist physicians who typically care for few patients with any given diagnosis, the importance of prevalence implies that disease‐specific efforts to control costs may produce smaller total gains than those that cross diseases, such as efforts to improve communication between inpatient and outpatient physicians.
Moreover, the presence of high costs for some condition does not, of course, imply that effective interventions exist to reduce those costs. Two other papers, one by Mudge et al.3 examining a disease management program for heart failure, and one by Go et al.4 examining the effects of hospitalists on the costs of hospitalization for GI bleeding, reinforce the idea that interventions to reduce hospital costs are not always as effective as hoped. Even worse, efforts to control costs can have unintended effects, such as the delays in antimicrobial administration with antimicrobial approval policies that are reported by Winters et al.5 These studies also illustrate that analyses of the effectiveness of interventions can be performed using a variety of experimental designs (eg, the before/after comparison used by Mudge et al,3 and the natural experiments based on assignment of patients to physicians based on day of admission used by Go et al.4 or based on time of day used by Winters et al.)5 The role of hospitalists as clinical leaders in hospitals often places them in positions to design and execute experiments, but the role of hospitalists as astute clinicians who can recognize the presence of natural experiments in their clinical environment can be every bit as powerful in producing valid research designs.
As society seeks strategies to control healthcare costs in the years ahead, it will almost certainly turn to the same general strategies that have been used in the past: bundling services into fixed payments for a prospectively defined episode of care, asking patients to pay more of the costs of care, and simply not paying for, or paying less for, any given type of care. Hospitalists already have dealt with many of these approaches in one form or another. Medicare's prospective payment system and the payment of fixed annual fees for the care of patients in health maintenance organizations have given all hospitalists some exposure to the pressure for lower hospital resources use under prospective payment systems. Proposals for demonstration projects within healthcare reform to study the effects of bundling inpatient and outpatient care or even hospital and professional fees suggest that hospitalists may need to be open to new incentive structures in the years to come. For example, reduced incentives for rapid discharge if costs pushed into the outpatient setting are borne by the hospital, there may be co‐management models if professional and hospital fees are bundled. Increases in patient copayments may also play some role in healthcare reform, and the paper by Ross et al.6 should be a reminder to hospitalists that we may do our patients a great disservice if we fail to recognize the effects of our decisions on their out‐of‐pocket costs. Indeed, while doctors and patient both recognize the importance of discussing out‐of‐pocket costs, they both agree that these discussions rarely occur.7 That such discussions are not reimbursed explicitly suggests one of the many challenges of controlling healthcare costs; if physician payments are decreased to control costs and physicians respond by attempting to see even more patients in any given time period, discussions of important but less urgent issues such as out‐of‐pocket costs seem likely to be reduced. Such dilemmas arise frequently as the healthcare system devises increasingly complex approaches to the control of costs and suggest to many that fundamental reform of the payment and delivery system with greater reliance on integrated health systems paid through full capitation will eventually need to become the nation's approach to healthcare cost containment.8
The United States spends more on healthcare than any country in the world, and it is widely believed that the Nation could spend less while achieving comparable or better outcomes. The recent debate over healthcare reform in the United States, the large Federal budget deficit in the context of the current economic recession, and the prospect of widening gaps in Medicare funding with the increasing entry of baby boomers into old age suggest that the issue of healthcare cost will remain intense for many years to come. What roles hospitalists will play in the nation's struggle to control health care costs remain to be seen. Six papers in this issue of the Journal of Hospital Medicine discuss issues related to costs, and reflect several of the ways in which hospital medicine can contribute to understanding, and ultimately, controlling healthcare costs.
Two papers, one by Whelan et al.1 examining the costs associated with upper vs. lower GI bleeding and one by Lorch et al.2 examining the costs associated with herpex simplex virus (HSV) infections among neonates with and without congenital abnormalities, focus on epidemiologic determinants of healthcare costs. Such studies can identify subgroups of patients with high costs who may be logical targets for efforts to control costs. One tension in the use of such analyses to control cost is that total cost for any patient group is the product of both the cost per patient and the number of patients falling into each group. In the case of gastrointestinal (GI) bleeding, the surprise compared to past reports is that lower GI bleeding is about as common among hospitalized patients as upper GI bleeding. This may be because pharmacotherapy for conditions that cause upper GI bleeding is reducing the rate at which disease progresses to the point where hospitalization is required. The importance of prevalence is reinforced even in the findings about HSV infection, where despite 2‐ to 3‐fold higher average costs among babies with HSV who have congenital abnormalities, the fact that 90% of babies hospitalized with HSV lack congenital abnormalities implies that the clear majority of costs are due to babies without congenital abnormalities. In seeking strategies to control costs, it is important to pay attention to both the prevalence and cost per case of specific conditions. Because hospitalists are generalist physicians who typically care for few patients with any given diagnosis, the importance of prevalence implies that disease‐specific efforts to control costs may produce smaller total gains than those that cross diseases, such as efforts to improve communication between inpatient and outpatient physicians.
Moreover, the presence of high costs for some condition does not, of course, imply that effective interventions exist to reduce those costs. Two other papers, one by Mudge et al.3 examining a disease management program for heart failure, and one by Go et al.4 examining the effects of hospitalists on the costs of hospitalization for GI bleeding, reinforce the idea that interventions to reduce hospital costs are not always as effective as hoped. Even worse, efforts to control costs can have unintended effects, such as the delays in antimicrobial administration with antimicrobial approval policies that are reported by Winters et al.5 These studies also illustrate that analyses of the effectiveness of interventions can be performed using a variety of experimental designs (eg, the before/after comparison used by Mudge et al,3 and the natural experiments based on assignment of patients to physicians based on day of admission used by Go et al.4 or based on time of day used by Winters et al.)5 The role of hospitalists as clinical leaders in hospitals often places them in positions to design and execute experiments, but the role of hospitalists as astute clinicians who can recognize the presence of natural experiments in their clinical environment can be every bit as powerful in producing valid research designs.
As society seeks strategies to control healthcare costs in the years ahead, it will almost certainly turn to the same general strategies that have been used in the past: bundling services into fixed payments for a prospectively defined episode of care, asking patients to pay more of the costs of care, and simply not paying for, or paying less for, any given type of care. Hospitalists already have dealt with many of these approaches in one form or another. Medicare's prospective payment system and the payment of fixed annual fees for the care of patients in health maintenance organizations have given all hospitalists some exposure to the pressure for lower hospital resources use under prospective payment systems. Proposals for demonstration projects within healthcare reform to study the effects of bundling inpatient and outpatient care or even hospital and professional fees suggest that hospitalists may need to be open to new incentive structures in the years to come. For example, reduced incentives for rapid discharge if costs pushed into the outpatient setting are borne by the hospital, there may be co‐management models if professional and hospital fees are bundled. Increases in patient copayments may also play some role in healthcare reform, and the paper by Ross et al.6 should be a reminder to hospitalists that we may do our patients a great disservice if we fail to recognize the effects of our decisions on their out‐of‐pocket costs. Indeed, while doctors and patient both recognize the importance of discussing out‐of‐pocket costs, they both agree that these discussions rarely occur.7 That such discussions are not reimbursed explicitly suggests one of the many challenges of controlling healthcare costs; if physician payments are decreased to control costs and physicians respond by attempting to see even more patients in any given time period, discussions of important but less urgent issues such as out‐of‐pocket costs seem likely to be reduced. Such dilemmas arise frequently as the healthcare system devises increasingly complex approaches to the control of costs and suggest to many that fundamental reform of the payment and delivery system with greater reliance on integrated health systems paid through full capitation will eventually need to become the nation's approach to healthcare cost containment.8
- ,., et al.Upper versus lower gastrointestinal bleeding: a direct comparison of clinical presentation, outcomes, and resource utilization.J Hosp Med.2010;5(3):140–146.
- ,,.Impact of congenital anomalies and treatment location on clinical outcomes and health resource use in infants hospitalized with herpes simplex virus.J Hosp Med.2010;5(3):154–158.
- ,,, et al.The paradox of readmission: effect of a quality improvement programme in hospitalised patients with heart failure.J Hosp Med.2010;5:147–152.
- ,,, et al.Do hospitalists affect clinical outcomes and efficiency for patients with acute upper gastrointestinal hemorrhage (UGIH)?J Hosp Med.2010;5(3):138–138.
- ,,.Impact of a restrictive antimicrobial policy on the process and timing of antimicrobial administration.J Hosp Med.2010;5(2):E41–E45.
- ,.Reducing patient financial liability for hospitalizations: the physician role.J Hosp Med.2010;5(3):159–161.
- ,,.Patient‐physician communication about out‐of‐pocket costs.JAMA.2003;290(7):953–958.
- ,,, et al.Toward a 21st‐century health care system: recommendations for health care reform.Ann Intern Med.2009;150:493–495.
- ,., et al.Upper versus lower gastrointestinal bleeding: a direct comparison of clinical presentation, outcomes, and resource utilization.J Hosp Med.2010;5(3):140–146.
- ,,.Impact of congenital anomalies and treatment location on clinical outcomes and health resource use in infants hospitalized with herpes simplex virus.J Hosp Med.2010;5(3):154–158.
- ,,, et al.The paradox of readmission: effect of a quality improvement programme in hospitalised patients with heart failure.J Hosp Med.2010;5:147–152.
- ,,, et al.Do hospitalists affect clinical outcomes and efficiency for patients with acute upper gastrointestinal hemorrhage (UGIH)?J Hosp Med.2010;5(3):138–138.
- ,,.Impact of a restrictive antimicrobial policy on the process and timing of antimicrobial administration.J Hosp Med.2010;5(2):E41–E45.
- ,.Reducing patient financial liability for hospitalizations: the physician role.J Hosp Med.2010;5(3):159–161.
- ,,.Patient‐physician communication about out‐of‐pocket costs.JAMA.2003;290(7):953–958.
- ,,, et al.Toward a 21st‐century health care system: recommendations for health care reform.Ann Intern Med.2009;150:493–495.