User login
Syringomatous Carcinoma in a Young Patient Treated With Mohs Micrographic Surgery
Syringomatous carcinoma (SC), considered by some to be a variant of microcystic adnexal carcinoma (MAC),1 is a rare malignant neoplasm of sweat gland origin. SC encompasses a range of neoplasms with different degrees of differentiation, and its nomenclature has varied over the years. SC also has been referred to as syringoid eccrine carcinoma,2 basal cell tumor with eccrine differentiation,3 malignant syringoma,4 and sclerosing sweat duct carcinoma.5 Its diagnosis has been a dilemma in a number of reported cases, probably due to the combination of its rarity and thus limited clinical and histopathologic information, microscopic similarities to other benign and malignant neoplasms, and characteristic histologic features that may only be apparent in surgical excisions containing deeper tissue. We report a case of SC that masqueraded as an epidermoid cyst in an unusually young patient.
Case Report
A 23-year-old Asian man, who was otherwise healthy, presented with an asymptomatic slowly enlarging nodule of one year's duration on the right medial eyebrow. Prior treatment with intralesional steroid injections resulted in minimal improvement. The patient had no personal or family history of skin cancers. Physical examination results demonstrated a well-demarcated, mobile, nontender subcutaneous nodule measuring 7 mm in diameter. The clinical presentation favored a diagnosis of an epidermal inclusion cyst, and the patient underwent surgical excision of the lesion. Results of the histopathologic examination revealed a neoplasm in the dermis consisting of bands and nests of pale staining basaloid cells extending between the collagen fibers (Figure 1). There were focal areas of ductal differentiation, scattered individual necrotic cells, moderate dermal fibrosis, and chronic inflammation with numerous eo-sinophils. Moderate nuclear atypia also was present (Figure 2). Perineural involvement was not seen. Results of immunohistochemical analysis revealed positive staining for high—and low—molecular-weight cytokeratins, as well as carcinoembryonic antigen (CEA)(Figure 3). There was scattered positivity with S-100 protein in occasional cells lining lumina and in dendritic cells (Figure 4). The histopathologic findings supported the diagnosis of SC. Because the neoplasm extended to the surgical margins of the specimen, repeat surgical excision with continuous microscopic control under the Mohs micrographic technique was performed to prevent local recurrence and spare normal tissue. At the 18-month follow-up visit, no local recurrence was seen.
Comment SC is a rare, malignant sweat gland neoplasm that usually occurs in the fourth and fifth decades of life.4-8 SC typically presents as a slow-growing, solitary, painless nodule or indurated plaque on the head or neck region.6-8 It has been frequently found on the upper and lower lips; however, it also has been reported to occur on the finger and breast.9,10 Predisposing factors for the development of SC are unclear11 but may include previous radiation to the face and history of receiving an organ transplant with immunosuppressive drug therapy.12-17 Histopathologically, SC is characterized by asymmetric and deep dermal invasion of tumor cells, perineural involvement, ductal formation, keratin-filled cysts, multiple nests of basaloid or squamous cells, and desmoplasia of the surrounding dermal stroma (Table 1).5,6 Some authors consider SC to be closely related to MAC but generally describe SC as more basaloid with larger tubules and a more sclerotic stroma than MAC.18-26 If histologic examination of SC is limited to the superficial dermis, SC demonstrates similarities to other neoplasms, including syringomas, trichoadenomas, trichoepitheliomas, basal cell carcinomas, or squamous cell carcinomas. In the reported cases in which SC was initially misdiagnosed as another benign or malignant neoplasm, many misdiagnoses were due to either a benign clinical appearance of the lesion or biopsy specimens that were too superficial to contain the deeper characteristic histologic features of SC.8,9,11,27-30
Immunohistochemical studies can facilitate the diagnosis of SC and differentiate it from other neoplasms. SC stains positively for CEA, S-100 protein, epithelial membrane antigen, cyto-keratin, and gross cystic disease fluid protein 15,31 all of which aid in the confirmation of a sweat gland neoplasm (Table 2).8,32,33,39 Positivity for CEA in the ductal lining cells and the luminal contents of tumor ducts confirms sweat gland differentiation.25,33,34 This ductal immunoreactivity to CEA appears to be one of the most reliable findings to differentiate SC and MAC from other adnexal tumors, especially desmoplastic trichoepithelioma, which may be one of the more challenging histo-pathologic differential diagnoses.35 In addition, epithelial membrane antigen positivity can be found in the areas showing glandular features.35 This can assist in distinguishing SC from a desmoplastic trichoepithelioma or sclerosing type basal cell carcinoma, both of which demonstrate negativity to epithelial membrane antigen.35 S-100 protein positivity in dendritic cells, as well as in some cords and ducts in SC, further verifies dendritic differentiation toward sweat gland structures and is useful as an adjunct in the confirmation of glandular differentiation.25,33,34,36
Without proper and timely diagnosis and management, SC can cause severe patient morbidity. Although SC rarely metastasizes and can have an indolent course, it can be locally de-structive and lead to potentially disfiguring outcomes.5-7 SC can invade deeply and infiltrate into the dermis, subcutaneous fat tissue, muscle, perichondrium, periosteum, and galea.8 Goto et al9 reported a case of an SC that was initially misdiagnosed as a basal cell carcinoma of the left middle finger. The deeper, characteristic features of SC were not recognized until after the affected finger required amputation due to erosion of the bone. Hoppenreijs et al11 described an aggressive case of an SC arising at a site of previously irradiated squamous cell carcinoma of the lower eyelid. Extensive involvement of the SC in the orbit led to the recommendation of an orbital exenter-ation; however, it was not performed because of the poor clinical condition of the patient. Treatments for SC have included wide local excision and Mohs micrographic surgery (MMS). SC treatment with wide local excision often resulted in incomplete excision of the neoplasm despite having taken an adequate margin around the clinically assessable tumor.5 Cases of SC treated with wide local excision had a recurrence rate of 47%.5 The positive surgical margins following wide local excision may be due to the deep infiltration of SC, which frequently exceeds the clinically predicted size of the tumor.5 Due to the close relationship of MAC and SC, we feel that MMS treatment of SC will reduce recurrences as it has for MAC. Currently, there is strong support for the treatment of MAC with MMS as a gold standard to ensure complete clearance of the neoplasm and to reduce the local recurrence rate.12,13,17,21,22,37,38 In a study of MAC by Chiller et al,37 the authors demonstrated a median 4-fold increase in defect size when they compared the clinically estimated pretreatment size of the lesion with the MMS-determined posttreatment size of the lesion. The authors therefore suggest that, similar to the MMS-treated lesions, the lesions completely treated with wide local excision also would produce a defect size that is at least 4 times greater than the predicted pretreatment size of the lesion. Because wide local excision relies on predicted margins of the lesion, which the authors have shown can be greatly underestimated, Chiller et al37 argue that the use of MMS, which does not rely on predicted margins, is a reasonable first-line therapeutic modality for effectively treating patients with MAC. Furthermore, MMS allows for the examination of the entire peripheral and deep margins of the lesion, which is critical when considering the deep infiltrative nature of MAC. The reported local recurrence rate of MAC treated with MMS is 0% to 5%,12,13,21,26,38 which is much lower than the reported local recurrence rate following treatment with wide local excision. This reduced recurrence rate found in MAC cases treated with MMS is probably due to the ability to confirm complete removal of the neoplasm with MMS.
Conclusion To our knowledge, this case report describes the occurrence of SC, a rare sweat gland neoplasm, in the youngest reported patient and is only the second reported case of SC treated with MMS. Adequate sampling of tissue with an excisional biopsy allowed for appropriate evaluation with histologic and immunohistochemical studies to arrive at the diagnosis that could easily have been missed with a superficial biopsy. In our patient, histopathologic evaluation showed typical nests of basaloid cells, ductal differentiation, and ductal fibrosis seen in SC. However, perineural involvement that is particularly characteristic of SC was not present. This may portend a better prognosis for our patient whose tumor was completely excised after one stage of MMS and has not shown evidence of recurrence at the 18-month follow-up visit. MMS allowed for evaluation of the entire surgical margin and decreased risk of local recurrence resulting from an incomplete excision. In addition, it also allowed for sparing of normal tissue in a cosmetically sensitive area where SC commonly occurs. In summary, this case highlights the importance of including SC in the differential diagnosis of an enlarging cystic lesion in a younger patient and its successful treatment with MMS.
- Weedon D. Tumors of cutaneous appendages. In: Weedon D, ed. Skin Pathology. 2nd ed. London, England: Churchill Livingstone; 2002:897.
- Sanchez Yus E, Requena Caballero L, Garcia Salazar I, et al. Clear cell syringoid eccrine carcinoma. Am J Dermatopathol. 1987;9:225-231.
- Freeman RG, Winkelmann RK. Basal cell tumor with eccrine differentiation (eccrine epithelioma). Arch Dermatol. 1969;100:234-242.
- Glatt HJ, Proia AD, Tsoy EA, et al. Malignant syringoma of the eyelid. Ophthalmology. 1984;91:987-990.
- Cooper PH, Mills SE, Leonard DD, et al. Sclerosing sweat duct (syringomatous) carcinoma. Am J Surg Pathol. 1985;9:422-433.
- Mehregan AH, Hashimoto K, Rahbari H. Eccrine adenocarcinoma: a clinicopathologic study of 35 cases. Arch Dermatol. 1983;119:104-114.
- Wick MR, Goellner JR, Wolfe JT III, et al. Adnexal carcinomas of the skin, I: eccrine carcinomas. Cancer. 1985;56:1147-1162.
- Abenoza P, Ackerman AB. Syringomatous carcinomas. In: Abenoza P, Ackerman AB, eds. Neoplasms with Eccrine Differentiation. Philadelphia, Pa: Lea & Febiger; 1990:371-412.
- Goto M, Sonoda T, Shibuya H, et al. Digital syringomatous carcinoma mimicking basal cell carcinoma. Br J Dermatol. 2001;144:438-439.
- Urso C. Syringomatous breast carcinoma and correlated lesions. Pathologica. 1996;88:196-199.
- Hoppenreijs VP, Reuser TT, Mooy CM, et al. Syringomatous carcinoma of the eyelid and orbit: a clinical and histopathological challenge. Br J Ophthalmol. 1997;81:668-672.
- Snow S, Madjar DD, Hardy S, et al. Microcystic adnexal carcinoma: report of 13 cases and review of the literature. Dermatol Surg. 2001;27:401-408.
- Friedman PM, Friedman RH, Jiang SB, et al. Microcystic adnexal carcinoma: collaborative series review and update. J Am Acad Dermatol. 1999;41:225-231.
- Antley CA, Carney M, Smoller BR. Microcystic adnexal carcinoma arising in the setting of previous radiation therapy. J Cutan Pathol. 1999;26:48-50.
- Borenstein A, Seidman DS, Trau H, et al. Microcystic adnexal carcinoma following radiotherapy in childhood. Am J Med Sci. 1991;301:259-261.
- Fleischmann HE, Roth RJ, Wood C, et al. Microcystic adnexal carcinoma treated by microscopically controlled excision. J Dermatol Surg Oncol. 1984;10:873-875.
- Schwarze HP, Loche F, Lamant L, et al. Microcystic adnexal carcinoma induced by multiple radiation therapy. Int J Dermatol. 2000;39:369-372.
- Cooper PH, Mills SE. Microcystic adnexal carcinoma. J Am Acad Dermatol. 1984;10:908-914.
- Hamm JC, Argenta LC, Swanson NA. Microcystic adnexal carcinoma: an unpredictable aggressive neoplasm. Ann Plast Surg. 1987;19:173-180.
- Birkby CS, Argenyi ZB, Whitaker DC. Microcystic adnexal carcinoma with mandibular invasion and bone marrow replacement. J Dermatol Surg Oncol. 1989;15:308-312.
- Leibovitch I, Huilgol SC, Selva D, et al. Microcystic adnexal carcinoma: treatment with Mohs micrographic surgery. J Am Acad Dermatol. 2005;52:295-300.
- Gardner ES, Goldb
Syringomatous carcinoma (SC), considered by some to be a variant of microcystic adnexal carcinoma (MAC),1 is a rare malignant neoplasm of sweat gland origin. SC encompasses a range of neoplasms with different degrees of differentiation, and its nomenclature has varied over the years. SC also has been referred to as syringoid eccrine carcinoma,2 basal cell tumor with eccrine differentiation,3 malignant syringoma,4 and sclerosing sweat duct carcinoma.5 Its diagnosis has been a dilemma in a number of reported cases, probably due to the combination of its rarity and thus limited clinical and histopathologic information, microscopic similarities to other benign and malignant neoplasms, and characteristic histologic features that may only be apparent in surgical excisions containing deeper tissue. We report a case of SC that masqueraded as an epidermoid cyst in an unusually young patient.
Case Report
A 23-year-old Asian man, who was otherwise healthy, presented with an asymptomatic slowly enlarging nodule of one year's duration on the right medial eyebrow. Prior treatment with intralesional steroid injections resulted in minimal improvement. The patient had no personal or family history of skin cancers. Physical examination results demonstrated a well-demarcated, mobile, nontender subcutaneous nodule measuring 7 mm in diameter. The clinical presentation favored a diagnosis of an epidermal inclusion cyst, and the patient underwent surgical excision of the lesion. Results of the histopathologic examination revealed a neoplasm in the dermis consisting of bands and nests of pale staining basaloid cells extending between the collagen fibers (Figure 1). There were focal areas of ductal differentiation, scattered individual necrotic cells, moderate dermal fibrosis, and chronic inflammation with numerous eo-sinophils. Moderate nuclear atypia also was present (Figure 2). Perineural involvement was not seen. Results of immunohistochemical analysis revealed positive staining for high—and low—molecular-weight cytokeratins, as well as carcinoembryonic antigen (CEA)(Figure 3). There was scattered positivity with S-100 protein in occasional cells lining lumina and in dendritic cells (Figure 4). The histopathologic findings supported the diagnosis of SC. Because the neoplasm extended to the surgical margins of the specimen, repeat surgical excision with continuous microscopic control under the Mohs micrographic technique was performed to prevent local recurrence and spare normal tissue. At the 18-month follow-up visit, no local recurrence was seen.
Comment SC is a rare, malignant sweat gland neoplasm that usually occurs in the fourth and fifth decades of life.4-8 SC typically presents as a slow-growing, solitary, painless nodule or indurated plaque on the head or neck region.6-8 It has been frequently found on the upper and lower lips; however, it also has been reported to occur on the finger and breast.9,10 Predisposing factors for the development of SC are unclear11 but may include previous radiation to the face and history of receiving an organ transplant with immunosuppressive drug therapy.12-17 Histopathologically, SC is characterized by asymmetric and deep dermal invasion of tumor cells, perineural involvement, ductal formation, keratin-filled cysts, multiple nests of basaloid or squamous cells, and desmoplasia of the surrounding dermal stroma (Table 1).5,6 Some authors consider SC to be closely related to MAC but generally describe SC as more basaloid with larger tubules and a more sclerotic stroma than MAC.18-26 If histologic examination of SC is limited to the superficial dermis, SC demonstrates similarities to other neoplasms, including syringomas, trichoadenomas, trichoepitheliomas, basal cell carcinomas, or squamous cell carcinomas. In the reported cases in which SC was initially misdiagnosed as another benign or malignant neoplasm, many misdiagnoses were due to either a benign clinical appearance of the lesion or biopsy specimens that were too superficial to contain the deeper characteristic histologic features of SC.8,9,11,27-30
Immunohistochemical studies can facilitate the diagnosis of SC and differentiate it from other neoplasms. SC stains positively for CEA, S-100 protein, epithelial membrane antigen, cyto-keratin, and gross cystic disease fluid protein 15,31 all of which aid in the confirmation of a sweat gland neoplasm (Table 2).8,32,33,39 Positivity for CEA in the ductal lining cells and the luminal contents of tumor ducts confirms sweat gland differentiation.25,33,34 This ductal immunoreactivity to CEA appears to be one of the most reliable findings to differentiate SC and MAC from other adnexal tumors, especially desmoplastic trichoepithelioma, which may be one of the more challenging histo-pathologic differential diagnoses.35 In addition, epithelial membrane antigen positivity can be found in the areas showing glandular features.35 This can assist in distinguishing SC from a desmoplastic trichoepithelioma or sclerosing type basal cell carcinoma, both of which demonstrate negativity to epithelial membrane antigen.35 S-100 protein positivity in dendritic cells, as well as in some cords and ducts in SC, further verifies dendritic differentiation toward sweat gland structures and is useful as an adjunct in the confirmation of glandular differentiation.25,33,34,36
Without proper and timely diagnosis and management, SC can cause severe patient morbidity. Although SC rarely metastasizes and can have an indolent course, it can be locally de-structive and lead to potentially disfiguring outcomes.5-7 SC can invade deeply and infiltrate into the dermis, subcutaneous fat tissue, muscle, perichondrium, periosteum, and galea.8 Goto et al9 reported a case of an SC that was initially misdiagnosed as a basal cell carcinoma of the left middle finger. The deeper, characteristic features of SC were not recognized until after the affected finger required amputation due to erosion of the bone. Hoppenreijs et al11 described an aggressive case of an SC arising at a site of previously irradiated squamous cell carcinoma of the lower eyelid. Extensive involvement of the SC in the orbit led to the recommendation of an orbital exenter-ation; however, it was not performed because of the poor clinical condition of the patient. Treatments for SC have included wide local excision and Mohs micrographic surgery (MMS). SC treatment with wide local excision often resulted in incomplete excision of the neoplasm despite having taken an adequate margin around the clinically assessable tumor.5 Cases of SC treated with wide local excision had a recurrence rate of 47%.5 The positive surgical margins following wide local excision may be due to the deep infiltration of SC, which frequently exceeds the clinically predicted size of the tumor.5 Due to the close relationship of MAC and SC, we feel that MMS treatment of SC will reduce recurrences as it has for MAC. Currently, there is strong support for the treatment of MAC with MMS as a gold standard to ensure complete clearance of the neoplasm and to reduce the local recurrence rate.12,13,17,21,22,37,38 In a study of MAC by Chiller et al,37 the authors demonstrated a median 4-fold increase in defect size when they compared the clinically estimated pretreatment size of the lesion with the MMS-determined posttreatment size of the lesion. The authors therefore suggest that, similar to the MMS-treated lesions, the lesions completely treated with wide local excision also would produce a defect size that is at least 4 times greater than the predicted pretreatment size of the lesion. Because wide local excision relies on predicted margins of the lesion, which the authors have shown can be greatly underestimated, Chiller et al37 argue that the use of MMS, which does not rely on predicted margins, is a reasonable first-line therapeutic modality for effectively treating patients with MAC. Furthermore, MMS allows for the examination of the entire peripheral and deep margins of the lesion, which is critical when considering the deep infiltrative nature of MAC. The reported local recurrence rate of MAC treated with MMS is 0% to 5%,12,13,21,26,38 which is much lower than the reported local recurrence rate following treatment with wide local excision. This reduced recurrence rate found in MAC cases treated with MMS is probably due to the ability to confirm complete removal of the neoplasm with MMS.
Conclusion To our knowledge, this case report describes the occurrence of SC, a rare sweat gland neoplasm, in the youngest reported patient and is only the second reported case of SC treated with MMS. Adequate sampling of tissue with an excisional biopsy allowed for appropriate evaluation with histologic and immunohistochemical studies to arrive at the diagnosis that could easily have been missed with a superficial biopsy. In our patient, histopathologic evaluation showed typical nests of basaloid cells, ductal differentiation, and ductal fibrosis seen in SC. However, perineural involvement that is particularly characteristic of SC was not present. This may portend a better prognosis for our patient whose tumor was completely excised after one stage of MMS and has not shown evidence of recurrence at the 18-month follow-up visit. MMS allowed for evaluation of the entire surgical margin and decreased risk of local recurrence resulting from an incomplete excision. In addition, it also allowed for sparing of normal tissue in a cosmetically sensitive area where SC commonly occurs. In summary, this case highlights the importance of including SC in the differential diagnosis of an enlarging cystic lesion in a younger patient and its successful treatment with MMS.
Syringomatous carcinoma (SC), considered by some to be a variant of microcystic adnexal carcinoma (MAC),1 is a rare malignant neoplasm of sweat gland origin. SC encompasses a range of neoplasms with different degrees of differentiation, and its nomenclature has varied over the years. SC also has been referred to as syringoid eccrine carcinoma,2 basal cell tumor with eccrine differentiation,3 malignant syringoma,4 and sclerosing sweat duct carcinoma.5 Its diagnosis has been a dilemma in a number of reported cases, probably due to the combination of its rarity and thus limited clinical and histopathologic information, microscopic similarities to other benign and malignant neoplasms, and characteristic histologic features that may only be apparent in surgical excisions containing deeper tissue. We report a case of SC that masqueraded as an epidermoid cyst in an unusually young patient.
Case Report
A 23-year-old Asian man, who was otherwise healthy, presented with an asymptomatic slowly enlarging nodule of one year's duration on the right medial eyebrow. Prior treatment with intralesional steroid injections resulted in minimal improvement. The patient had no personal or family history of skin cancers. Physical examination results demonstrated a well-demarcated, mobile, nontender subcutaneous nodule measuring 7 mm in diameter. The clinical presentation favored a diagnosis of an epidermal inclusion cyst, and the patient underwent surgical excision of the lesion. Results of the histopathologic examination revealed a neoplasm in the dermis consisting of bands and nests of pale staining basaloid cells extending between the collagen fibers (Figure 1). There were focal areas of ductal differentiation, scattered individual necrotic cells, moderate dermal fibrosis, and chronic inflammation with numerous eo-sinophils. Moderate nuclear atypia also was present (Figure 2). Perineural involvement was not seen. Results of immunohistochemical analysis revealed positive staining for high—and low—molecular-weight cytokeratins, as well as carcinoembryonic antigen (CEA)(Figure 3). There was scattered positivity with S-100 protein in occasional cells lining lumina and in dendritic cells (Figure 4). The histopathologic findings supported the diagnosis of SC. Because the neoplasm extended to the surgical margins of the specimen, repeat surgical excision with continuous microscopic control under the Mohs micrographic technique was performed to prevent local recurrence and spare normal tissue. At the 18-month follow-up visit, no local recurrence was seen.
Comment SC is a rare, malignant sweat gland neoplasm that usually occurs in the fourth and fifth decades of life.4-8 SC typically presents as a slow-growing, solitary, painless nodule or indurated plaque on the head or neck region.6-8 It has been frequently found on the upper and lower lips; however, it also has been reported to occur on the finger and breast.9,10 Predisposing factors for the development of SC are unclear11 but may include previous radiation to the face and history of receiving an organ transplant with immunosuppressive drug therapy.12-17 Histopathologically, SC is characterized by asymmetric and deep dermal invasion of tumor cells, perineural involvement, ductal formation, keratin-filled cysts, multiple nests of basaloid or squamous cells, and desmoplasia of the surrounding dermal stroma (Table 1).5,6 Some authors consider SC to be closely related to MAC but generally describe SC as more basaloid with larger tubules and a more sclerotic stroma than MAC.18-26 If histologic examination of SC is limited to the superficial dermis, SC demonstrates similarities to other neoplasms, including syringomas, trichoadenomas, trichoepitheliomas, basal cell carcinomas, or squamous cell carcinomas. In the reported cases in which SC was initially misdiagnosed as another benign or malignant neoplasm, many misdiagnoses were due to either a benign clinical appearance of the lesion or biopsy specimens that were too superficial to contain the deeper characteristic histologic features of SC.8,9,11,27-30
Immunohistochemical studies can facilitate the diagnosis of SC and differentiate it from other neoplasms. SC stains positively for CEA, S-100 protein, epithelial membrane antigen, cyto-keratin, and gross cystic disease fluid protein 15,31 all of which aid in the confirmation of a sweat gland neoplasm (Table 2).8,32,33,39 Positivity for CEA in the ductal lining cells and the luminal contents of tumor ducts confirms sweat gland differentiation.25,33,34 This ductal immunoreactivity to CEA appears to be one of the most reliable findings to differentiate SC and MAC from other adnexal tumors, especially desmoplastic trichoepithelioma, which may be one of the more challenging histo-pathologic differential diagnoses.35 In addition, epithelial membrane antigen positivity can be found in the areas showing glandular features.35 This can assist in distinguishing SC from a desmoplastic trichoepithelioma or sclerosing type basal cell carcinoma, both of which demonstrate negativity to epithelial membrane antigen.35 S-100 protein positivity in dendritic cells, as well as in some cords and ducts in SC, further verifies dendritic differentiation toward sweat gland structures and is useful as an adjunct in the confirmation of glandular differentiation.25,33,34,36
Without proper and timely diagnosis and management, SC can cause severe patient morbidity. Although SC rarely metastasizes and can have an indolent course, it can be locally de-structive and lead to potentially disfiguring outcomes.5-7 SC can invade deeply and infiltrate into the dermis, subcutaneous fat tissue, muscle, perichondrium, periosteum, and galea.8 Goto et al9 reported a case of an SC that was initially misdiagnosed as a basal cell carcinoma of the left middle finger. The deeper, characteristic features of SC were not recognized until after the affected finger required amputation due to erosion of the bone. Hoppenreijs et al11 described an aggressive case of an SC arising at a site of previously irradiated squamous cell carcinoma of the lower eyelid. Extensive involvement of the SC in the orbit led to the recommendation of an orbital exenter-ation; however, it was not performed because of the poor clinical condition of the patient. Treatments for SC have included wide local excision and Mohs micrographic surgery (MMS). SC treatment with wide local excision often resulted in incomplete excision of the neoplasm despite having taken an adequate margin around the clinically assessable tumor.5 Cases of SC treated with wide local excision had a recurrence rate of 47%.5 The positive surgical margins following wide local excision may be due to the deep infiltration of SC, which frequently exceeds the clinically predicted size of the tumor.5 Due to the close relationship of MAC and SC, we feel that MMS treatment of SC will reduce recurrences as it has for MAC. Currently, there is strong support for the treatment of MAC with MMS as a gold standard to ensure complete clearance of the neoplasm and to reduce the local recurrence rate.12,13,17,21,22,37,38 In a study of MAC by Chiller et al,37 the authors demonstrated a median 4-fold increase in defect size when they compared the clinically estimated pretreatment size of the lesion with the MMS-determined posttreatment size of the lesion. The authors therefore suggest that, similar to the MMS-treated lesions, the lesions completely treated with wide local excision also would produce a defect size that is at least 4 times greater than the predicted pretreatment size of the lesion. Because wide local excision relies on predicted margins of the lesion, which the authors have shown can be greatly underestimated, Chiller et al37 argue that the use of MMS, which does not rely on predicted margins, is a reasonable first-line therapeutic modality for effectively treating patients with MAC. Furthermore, MMS allows for the examination of the entire peripheral and deep margins of the lesion, which is critical when considering the deep infiltrative nature of MAC. The reported local recurrence rate of MAC treated with MMS is 0% to 5%,12,13,21,26,38 which is much lower than the reported local recurrence rate following treatment with wide local excision. This reduced recurrence rate found in MAC cases treated with MMS is probably due to the ability to confirm complete removal of the neoplasm with MMS.
Conclusion To our knowledge, this case report describes the occurrence of SC, a rare sweat gland neoplasm, in the youngest reported patient and is only the second reported case of SC treated with MMS. Adequate sampling of tissue with an excisional biopsy allowed for appropriate evaluation with histologic and immunohistochemical studies to arrive at the diagnosis that could easily have been missed with a superficial biopsy. In our patient, histopathologic evaluation showed typical nests of basaloid cells, ductal differentiation, and ductal fibrosis seen in SC. However, perineural involvement that is particularly characteristic of SC was not present. This may portend a better prognosis for our patient whose tumor was completely excised after one stage of MMS and has not shown evidence of recurrence at the 18-month follow-up visit. MMS allowed for evaluation of the entire surgical margin and decreased risk of local recurrence resulting from an incomplete excision. In addition, it also allowed for sparing of normal tissue in a cosmetically sensitive area where SC commonly occurs. In summary, this case highlights the importance of including SC in the differential diagnosis of an enlarging cystic lesion in a younger patient and its successful treatment with MMS.
- Weedon D. Tumors of cutaneous appendages. In: Weedon D, ed. Skin Pathology. 2nd ed. London, England: Churchill Livingstone; 2002:897.
- Sanchez Yus E, Requena Caballero L, Garcia Salazar I, et al. Clear cell syringoid eccrine carcinoma. Am J Dermatopathol. 1987;9:225-231.
- Freeman RG, Winkelmann RK. Basal cell tumor with eccrine differentiation (eccrine epithelioma). Arch Dermatol. 1969;100:234-242.
- Glatt HJ, Proia AD, Tsoy EA, et al. Malignant syringoma of the eyelid. Ophthalmology. 1984;91:987-990.
- Cooper PH, Mills SE, Leonard DD, et al. Sclerosing sweat duct (syringomatous) carcinoma. Am J Surg Pathol. 1985;9:422-433.
- Mehregan AH, Hashimoto K, Rahbari H. Eccrine adenocarcinoma: a clinicopathologic study of 35 cases. Arch Dermatol. 1983;119:104-114.
- Wick MR, Goellner JR, Wolfe JT III, et al. Adnexal carcinomas of the skin, I: eccrine carcinomas. Cancer. 1985;56:1147-1162.
- Abenoza P, Ackerman AB. Syringomatous carcinomas. In: Abenoza P, Ackerman AB, eds. Neoplasms with Eccrine Differentiation. Philadelphia, Pa: Lea & Febiger; 1990:371-412.
- Goto M, Sonoda T, Shibuya H, et al. Digital syringomatous carcinoma mimicking basal cell carcinoma. Br J Dermatol. 2001;144:438-439.
- Urso C. Syringomatous breast carcinoma and correlated lesions. Pathologica. 1996;88:196-199.
- Hoppenreijs VP, Reuser TT, Mooy CM, et al. Syringomatous carcinoma of the eyelid and orbit: a clinical and histopathological challenge. Br J Ophthalmol. 1997;81:668-672.
- Snow S, Madjar DD, Hardy S, et al. Microcystic adnexal carcinoma: report of 13 cases and review of the literature. Dermatol Surg. 2001;27:401-408.
- Friedman PM, Friedman RH, Jiang SB, et al. Microcystic adnexal carcinoma: collaborative series review and update. J Am Acad Dermatol. 1999;41:225-231.
- Antley CA, Carney M, Smoller BR. Microcystic adnexal carcinoma arising in the setting of previous radiation therapy. J Cutan Pathol. 1999;26:48-50.
- Borenstein A, Seidman DS, Trau H, et al. Microcystic adnexal carcinoma following radiotherapy in childhood. Am J Med Sci. 1991;301:259-261.
- Fleischmann HE, Roth RJ, Wood C, et al. Microcystic adnexal carcinoma treated by microscopically controlled excision. J Dermatol Surg Oncol. 1984;10:873-875.
- Schwarze HP, Loche F, Lamant L, et al. Microcystic adnexal carcinoma induced by multiple radiation therapy. Int J Dermatol. 2000;39:369-372.
- Cooper PH, Mills SE. Microcystic adnexal carcinoma. J Am Acad Dermatol. 1984;10:908-914.
- Hamm JC, Argenta LC, Swanson NA. Microcystic adnexal carcinoma: an unpredictable aggressive neoplasm. Ann Plast Surg. 1987;19:173-180.
- Birkby CS, Argenyi ZB, Whitaker DC. Microcystic adnexal carcinoma with mandibular invasion and bone marrow replacement. J Dermatol Surg Oncol. 1989;15:308-312.
- Leibovitch I, Huilgol SC, Selva D, et al. Microcystic adnexal carcinoma: treatment with Mohs micrographic surgery. J Am Acad Dermatol. 2005;52:295-300.
- Gardner ES, Goldb
- Weedon D. Tumors of cutaneous appendages. In: Weedon D, ed. Skin Pathology. 2nd ed. London, England: Churchill Livingstone; 2002:897.
- Sanchez Yus E, Requena Caballero L, Garcia Salazar I, et al. Clear cell syringoid eccrine carcinoma. Am J Dermatopathol. 1987;9:225-231.
- Freeman RG, Winkelmann RK. Basal cell tumor with eccrine differentiation (eccrine epithelioma). Arch Dermatol. 1969;100:234-242.
- Glatt HJ, Proia AD, Tsoy EA, et al. Malignant syringoma of the eyelid. Ophthalmology. 1984;91:987-990.
- Cooper PH, Mills SE, Leonard DD, et al. Sclerosing sweat duct (syringomatous) carcinoma. Am J Surg Pathol. 1985;9:422-433.
- Mehregan AH, Hashimoto K, Rahbari H. Eccrine adenocarcinoma: a clinicopathologic study of 35 cases. Arch Dermatol. 1983;119:104-114.
- Wick MR, Goellner JR, Wolfe JT III, et al. Adnexal carcinomas of the skin, I: eccrine carcinomas. Cancer. 1985;56:1147-1162.
- Abenoza P, Ackerman AB. Syringomatous carcinomas. In: Abenoza P, Ackerman AB, eds. Neoplasms with Eccrine Differentiation. Philadelphia, Pa: Lea & Febiger; 1990:371-412.
- Goto M, Sonoda T, Shibuya H, et al. Digital syringomatous carcinoma mimicking basal cell carcinoma. Br J Dermatol. 2001;144:438-439.
- Urso C. Syringomatous breast carcinoma and correlated lesions. Pathologica. 1996;88:196-199.
- Hoppenreijs VP, Reuser TT, Mooy CM, et al. Syringomatous carcinoma of the eyelid and orbit: a clinical and histopathological challenge. Br J Ophthalmol. 1997;81:668-672.
- Snow S, Madjar DD, Hardy S, et al. Microcystic adnexal carcinoma: report of 13 cases and review of the literature. Dermatol Surg. 2001;27:401-408.
- Friedman PM, Friedman RH, Jiang SB, et al. Microcystic adnexal carcinoma: collaborative series review and update. J Am Acad Dermatol. 1999;41:225-231.
- Antley CA, Carney M, Smoller BR. Microcystic adnexal carcinoma arising in the setting of previous radiation therapy. J Cutan Pathol. 1999;26:48-50.
- Borenstein A, Seidman DS, Trau H, et al. Microcystic adnexal carcinoma following radiotherapy in childhood. Am J Med Sci. 1991;301:259-261.
- Fleischmann HE, Roth RJ, Wood C, et al. Microcystic adnexal carcinoma treated by microscopically controlled excision. J Dermatol Surg Oncol. 1984;10:873-875.
- Schwarze HP, Loche F, Lamant L, et al. Microcystic adnexal carcinoma induced by multiple radiation therapy. Int J Dermatol. 2000;39:369-372.
- Cooper PH, Mills SE. Microcystic adnexal carcinoma. J Am Acad Dermatol. 1984;10:908-914.
- Hamm JC, Argenta LC, Swanson NA. Microcystic adnexal carcinoma: an unpredictable aggressive neoplasm. Ann Plast Surg. 1987;19:173-180.
- Birkby CS, Argenyi ZB, Whitaker DC. Microcystic adnexal carcinoma with mandibular invasion and bone marrow replacement. J Dermatol Surg Oncol. 1989;15:308-312.
- Leibovitch I, Huilgol SC, Selva D, et al. Microcystic adnexal carcinoma: treatment with Mohs micrographic surgery. J Am Acad Dermatol. 2005;52:295-300.
- Gardner ES, Goldb
Alabaster Skin After CO2 Laser Resurfacing: Evidence for Suppressed Melanogenesis Rather Than Just Melanocyte Destruction
Medical problem or psychosis?
Distinguishing the cause of a patient’s psychotic symptoms can be clinically challenging in a primary care practice. This case was submitted by Matthew Rosenberg, MD, who practices family medicine at Sacramento (CA) County Primary Care Clinic. This month’s consultant is Bezalel Dantz, MD.
How would you have advised Dr. Rosenberg?
Case: ‘you’re just gonna die’
I was seeing Mr. J, age 31, weekly to monitor abdominal complaints. For 3 weeks he experienced increasing epigastric pain, and he had been evaluated twice in the emergency room for this complaint. Plain films, ultrasound, CT, and an elevated lipase reading suggested an inconclusive diagnosis of pancreatitis.
During his second office visit, Mr. J also complained of “hearing voices.” Further questioning revealed that he had been hearing voices—often male—making degrading comments for several years. The voices have increased in frequency during his illness, and their negative comments include, “What do you have to live for?” and “You’re just gonna die.”
Mr. J blames the voices on distant drug use, claiming his parents “forced” him as a young teen to take hallucinogens. He often thinks he is being followed and does not trust others. He said both parents had mental illnesses but does not know the diagnoses or seriousness of their disorders.
His thoughts are well-organized with clear content. He shows no signs of depression or mania. He plays guitar in a band and appears to be a thoughtful and high-functioning individual.
I need help with the differential diagnosis and suggestions of possible treatment options.
Dr. Dantz’s consultation
The first step in evaluating psychosis is to determine whether it indicates a medical disorder, substanceinduced disorder, or primary psychiatric illness. The chronicity and nature of Mr. J’s psychotic symptoms (auditory hallucinations and paranoid delusions), his age, and a family history of psychiatric illness suggest a primary psychiatric disorder. The elevated lipase might explain his abdominal pain but is likely independent of his psychosis.
Medical workup. Conduct a comprehensive physical exam and medical and psychiatric history. Obtain collateral information from the family about the patient’s psychiatric symptoms, family history, recreational drug use, and stressors. Acute onset, age >40, comorbid medical conditions, lack of acute psychosocial stressors, and a negative personal or family psychiatric history suggest a medical cause (The skinny on one patient’s psychosis,” November 2005.) Also assess for use of alcohol, marijuana, hallucinogens, narcotics, stimulants, and inhalants. Until any drug has been stopped for at least 1 week, its contribution to psychosis may be unclear.
Table 1
Medical conditions that may present as psychosis
| Type of condition | Examples |
|---|---|
| CNS infection | HIV, neurosyphilis, cycticercosis, encephalitis, prion disease |
| Neoplasm | Primary or metastatic, paraneoplastic syndromes |
| Endocrinopathies | Thyroid, parathyroid, adrenal |
| Degenerative diseases | Alzheimer’s disease, frontotemporal dementia, Huntington’s disease, Parkinson’s disease, Wilson’s disease, Lewy body dementia |
| Demyelinating disorders | Multiple sclerosis, adrenal leukodystrophy |
| Metabolic disorders | Cirrhosis, vitamin deficiency, uremia, porphyria, heavy metal poisoning |
| Vasculitis | Systemic lupus erythematosus |
| Others | Seizures, migraine aura, hypnagogic and hypnopompic hallucinations, neurosarcoidosis |
Lab testing. When signs or symptoms do not suggest an organic disease, laboratory tests have a low yield and are of questionable value.2 In primary care practice, however, many psychotic patients complain of somatic symptoms. Given the devastating impact of psychotic illness, one can argue that even a yield <5% justifies a workup.
A urine toxicology screen is by far the most important lab test. CBC, comprehensive metabolic panel, thyroid function tests, erythrocyte sedimentation rate, and calcium level may reveal a medical cause. Consider HIV antibody and syphilis tests in at-risk individuals.
Findings on physical exam or abnormal lab results would guide further testing. Because of Mr. J’s GI and neurologic symptoms, a 24-hour urine test may be reasonable, particularly if he has had episodes of acute intermittent porphyria.
Neuroimaging. Consider a scan when psychosis is comorbid with:
- age >40
- neurologic complaints (such as headache, numbness, vertigo, seizures)
- focal neurologic findings (such as weakness, gait abnormality, clonus, or spasticity)
- confusion, cognitive deficit, history of malignancy
- head trauma
- immunocompromised state
- atypical psychotic symptoms (such as visual or olfactory hallucinations).
Psychiatric workup. If the history and physical exam reveal no organic basis, the next step is to determine the nature of this patient’s psychosis. The two most common psychiatric conditions associated with psychosis are:
- schizophrenic spectrum disorders (such as schizophreniform, schizophrenia and schizoaffective disorder)
- affective disorders (such as psychotic depression and bipolar disorder).
Distinguishing among these conditions can be challenging (Table 2) because patients rarely present with typical syndromes.
For example, a bipolar patient may present in a mixed state with both depressive and manic features. Psychosis in schizophrenia may be brief (<6 months in schizophreniform disorder) and may be characterized by manic-like grandiose delusions or negative symptoms (flat affect, poverty of speech) that mimic affective symptoms. Finally, some patients have both an affective disorder and schizophrenia, as in schizoaffective disorder.
For Mr. J, years of uninterrupted hallucinations, longstanding paranoid delusions, and absence of prominent affective symptoms suggest schizophrenia. His hallucinations are typical of those reported in schizophrenia. Voices giving a running commentary on a person’s thoughts and actions and derogatory comments are two of the most common auditory hallucinations.
Somatic concerns are also prominent in schizophrenia. Patients may describe symptoms in bizarre terms, such as “electric shocks in my head” or “there’s a fire in my spleen.”
Supporting evidence for a schizophrenia diagnosis would include a history of social isolation, lack of interest in work, and poor social interaction. Mr. J has a supportive partner, and we are told he appears to be high-functioning and active as a guitarist in a band. These factors might support an alternate diagnosis of affective psychosis. Finally, his past drug use and somatic symptoms raise the possibility of active substance abuse.
Table 2
Differential diagnosis of primary psychosis: Typical features
| Affective disorder | Schizophrenic spectrum disorder | |
|---|---|---|
| Symptom onset | Acute or subacute | Prolonged period (months to years) of self-neglect, social isolation, odd beliefs, eccentric behaviors |
| Course | Episodic, with periods of normal social and occupational functioning between episodes | Chronic, with exacerbations superimposed on gradually deteriorating social and occupational functioning |
| Associated symptoms | Mania (irritability, insomnia, rapid speech, labile mood, psychomotor agitation, racing thoughts) | Flat or inappropriate affect, thought blocking, apathy |
| Depression (anhedonia, psychomotor retardation, sleep problems, poor appetite) |
Suicide risk. Ask psychotic patients if they think about harming themselves. Lifetime risk of suicide in schizophrenia is 10% to 15%, and rates in bipolar disorder are higher. If patients deny suicidality, ask them why. Reassuring responses include religious prohibition, hopefulness about the future, concern about suicide’s effect on a loved one, fear of dying, or lack of means.
Candidates for emergent psychiatric consultation or hospitalization include patients with violent or homicidal thoughts and any patient who has attempted suicide, has a family history of suicide, has access to means, and lacks compelling reasons against suicide. Consider immediate psychiatric evaluation and admission of patients whose delusions or behaviors put them at risk for harm.
Abdominal pain workup. Although Mr. J’s abdominal pain may be functional, also seek an organic cause. His first-time disclosure of psychotic symptoms suggests that a serious medical stressor may be exacerbating a chronic psychiatric illness. Because the elevated lipase may indicate pancreatitis, consider an endoscopic or MRI examination of the pancreas and bile ducts. In consultation with a gastroenterologist, evaluate other causes such as peptic ulcer disease, ischemic bowel (perhaps as a result of cocaine use), inflammatory bowel disease, vasculitis, porphyria, and abdominal migraine.
Managing psychosis
Psychiatric consultation is strongly recommended for patients beginning therapy for psychotic disorders who have shown a particularly high risk for suicide. Uncontrolled symptoms, unanticipated psychiatric side effects, and the humiliation that results from the insight gained through treatment may contribute to this risk.
Assuming that Mr. J does not meet criteria for acute psychiatric hospitalization, the primary care clinician can stabilize the psychotic symptoms while awaiting psychiatric referral. Any atypical antipsychotic would be appropriate (Table 3).
Table 3
Starting an atypical antipsychotic* for primary psychosis
| Drug | Starting and maintenance dosages1 | Most-common adverse effects |
|---|---|---|
| Aripiprazole | 7.5 to 15 mg daily; 15 to 30 mg daily | EPS (+), agitation (++) |
| Olanzapine | 5 to 15 mg nightly; 10 to 20 mg nightly | Sedation (+++), weight gain (++++) hyperglycemia (++++), anticholinergic |
| Quetiapine | 50 to 100 mg bid; 600 to 800 mg nightly | Sedation (++++), weight gain (+++), hyperglycemia (++) |
| Risperidone | 0.5 to 2 mg bid; 2 to 4 mg bid | EPS (++), sedation (++), weight gain (++), hyperglycemia (++), elevated prolactin |
| Ziprasidone | 20 to 40 mg bid; 60 to 80 mg bid | EPS (+), agitation (++), sedation (+), QTc prolongation2 |
| EPS: Extrapyramidal symptoms | ||
| + small risk ++ moderate risk +++ high risk ++++ most risk | ||
| * All atypical antipsychotics have been associated with rare cases of neuroleptic malignant syndrome. Tardive dyskinesia is estimated to occur in 0.5% of adults and 2.5% of geriatric patients for each year on therapy. FDA requires a warning on increased risks of hyperlipidemia, hyperglycemia, and diabetes mellitus on the labels of all atypical antipsychotics. Monitoring weight, glucose, and lipids is recommended. | ||
| 1 In clinical practice, dosages may be increased beyond maximum dosages listed. Doses may be given solely at night or bid, depending on sedation and agitation. Low dosages are recommended in geriatric patients or those with renal or hepatic disease. Review potential drug-drug interactions before dosing. | ||
| 2 Despite earlier concerns, no cases of torsade de pointes or sudden death have been reported with ziprasidone. Not recommended for patients with cardiac risk. | ||
| Source: Adapted from reference 4. | ||
Patients who refuse treatment pose a quandary. If the patient is not acutely ill, try to establish an alliance over several visits rather than endangering the therapeutic relationship through confrontation or overzealous persuasion (Table 4).
Table 4
Strategies to build a therapeutic alliance with psychotic patients
| Enlist support of the patient’s family or loved ones |
| Do not argue with the patient’s delusions |
| Focus on what is bothering the patient most, and treat identified symptoms |
| Refer to the “stress” the patient suffers because of the unusual experiences he is describing |
| Commiserate with the anxiety he feels when others (such as his family) ridicule or reject his beliefs |
| Describe the medication as a “tranquilizer” rather than an antipsychotic. Use terms such as “nerves,” “stress,” “depression,” “anxiety,” or “insomnia,” which are often preferred by psychotic patients |
| Normalize treatment by suggesting “many of my patients with fatigue or lack of sleep find this medication very helpful” |
| Use medical terms to destigmatize the illness. Suggest that the patient suffers from a chemical disturbance that can be treated, similar to patients with diabetes who require insulin |
Monitoring. The primary care physician’s role after the patient begins antipsychotic therapy is to:
- assess his or her symptoms (particularly suicidality) and adherence to psychiatric visits and treatment
- monitor for adverse effects from medications.
Atypical antipsychotics have been associated with weight gain, hyperglycemia, and hyperlipidemia. Check fasting glucose and lipids quarterly for the first year of antipsychotic therapy and annually thereafter.5 Watch for drug-drug interactions whenever a new medication is added. Monitor for abnormal movements, even though the risk of extrapyramidal symptoms and tardive dyskinesia is lower with atypical antipsychotics than with traditional agents.
For Mr. J’s psychiatric symptoms, I would:
- assess his willingness to start medication to reduce or eliminate the voices
- suggest he accept psychiatric referral
- assure him that I will remain involved in his care and continue to evaluate his abdominal symptoms.
I would also request permission to discuss his case with his partner and a family member to gather pertinent history and enlist their support for treatment. I would then start Mr. J on any drug listed in Table 3.
1. The Medical Letter. Drugs that may cause psychiatric symptoms. July 8, 2002;1134:59-62.
2. Anfinson TJ, Kathol RG. Screening laboratory evaluation in psychiatric patients: a review. Gen Hosp Psychiatry 1992;14(4):248-57.
3. Mann JJ. A current perspective of suicide and attempted suicide. Ann Intern Med 2002;136(4):302-11.
4. McIntyre RS, Konarski JZ. Tolerability profiles of atypical antipsychotics in the treatment of bipolar disorder. J Clin Psychiatry 2005;66(suppl 3):28-36.
5. Kane JM, Leucht S, Carpenter D, Docherty JP. Expert consensus guideline series. Optimizing pharmacologic treatment of psychotic disorders. Introduction: methods, commentary, and summary. J Clin Psychiatry 2003;64(suppl 12):5-19.
Dr. Dantz is a board-certified internist and psychiatrist who is assistant professor of internal medicine and psychiatry, Rush University, Chicago. He specializes in treating psychiatric disorders in the medical setting.
Distinguishing the cause of a patient’s psychotic symptoms can be clinically challenging in a primary care practice. This case was submitted by Matthew Rosenberg, MD, who practices family medicine at Sacramento (CA) County Primary Care Clinic. This month’s consultant is Bezalel Dantz, MD.
How would you have advised Dr. Rosenberg?
Case: ‘you’re just gonna die’
I was seeing Mr. J, age 31, weekly to monitor abdominal complaints. For 3 weeks he experienced increasing epigastric pain, and he had been evaluated twice in the emergency room for this complaint. Plain films, ultrasound, CT, and an elevated lipase reading suggested an inconclusive diagnosis of pancreatitis.
During his second office visit, Mr. J also complained of “hearing voices.” Further questioning revealed that he had been hearing voices—often male—making degrading comments for several years. The voices have increased in frequency during his illness, and their negative comments include, “What do you have to live for?” and “You’re just gonna die.”
Mr. J blames the voices on distant drug use, claiming his parents “forced” him as a young teen to take hallucinogens. He often thinks he is being followed and does not trust others. He said both parents had mental illnesses but does not know the diagnoses or seriousness of their disorders.
His thoughts are well-organized with clear content. He shows no signs of depression or mania. He plays guitar in a band and appears to be a thoughtful and high-functioning individual.
I need help with the differential diagnosis and suggestions of possible treatment options.
Dr. Dantz’s consultation
The first step in evaluating psychosis is to determine whether it indicates a medical disorder, substanceinduced disorder, or primary psychiatric illness. The chronicity and nature of Mr. J’s psychotic symptoms (auditory hallucinations and paranoid delusions), his age, and a family history of psychiatric illness suggest a primary psychiatric disorder. The elevated lipase might explain his abdominal pain but is likely independent of his psychosis.
Medical workup. Conduct a comprehensive physical exam and medical and psychiatric history. Obtain collateral information from the family about the patient’s psychiatric symptoms, family history, recreational drug use, and stressors. Acute onset, age >40, comorbid medical conditions, lack of acute psychosocial stressors, and a negative personal or family psychiatric history suggest a medical cause (The skinny on one patient’s psychosis,” November 2005.) Also assess for use of alcohol, marijuana, hallucinogens, narcotics, stimulants, and inhalants. Until any drug has been stopped for at least 1 week, its contribution to psychosis may be unclear.
Table 1
Medical conditions that may present as psychosis
| Type of condition | Examples |
|---|---|
| CNS infection | HIV, neurosyphilis, cycticercosis, encephalitis, prion disease |
| Neoplasm | Primary or metastatic, paraneoplastic syndromes |
| Endocrinopathies | Thyroid, parathyroid, adrenal |
| Degenerative diseases | Alzheimer’s disease, frontotemporal dementia, Huntington’s disease, Parkinson’s disease, Wilson’s disease, Lewy body dementia |
| Demyelinating disorders | Multiple sclerosis, adrenal leukodystrophy |
| Metabolic disorders | Cirrhosis, vitamin deficiency, uremia, porphyria, heavy metal poisoning |
| Vasculitis | Systemic lupus erythematosus |
| Others | Seizures, migraine aura, hypnagogic and hypnopompic hallucinations, neurosarcoidosis |
Lab testing. When signs or symptoms do not suggest an organic disease, laboratory tests have a low yield and are of questionable value.2 In primary care practice, however, many psychotic patients complain of somatic symptoms. Given the devastating impact of psychotic illness, one can argue that even a yield <5% justifies a workup.
A urine toxicology screen is by far the most important lab test. CBC, comprehensive metabolic panel, thyroid function tests, erythrocyte sedimentation rate, and calcium level may reveal a medical cause. Consider HIV antibody and syphilis tests in at-risk individuals.
Findings on physical exam or abnormal lab results would guide further testing. Because of Mr. J’s GI and neurologic symptoms, a 24-hour urine test may be reasonable, particularly if he has had episodes of acute intermittent porphyria.
Neuroimaging. Consider a scan when psychosis is comorbid with:
- age >40
- neurologic complaints (such as headache, numbness, vertigo, seizures)
- focal neurologic findings (such as weakness, gait abnormality, clonus, or spasticity)
- confusion, cognitive deficit, history of malignancy
- head trauma
- immunocompromised state
- atypical psychotic symptoms (such as visual or olfactory hallucinations).
Psychiatric workup. If the history and physical exam reveal no organic basis, the next step is to determine the nature of this patient’s psychosis. The two most common psychiatric conditions associated with psychosis are:
- schizophrenic spectrum disorders (such as schizophreniform, schizophrenia and schizoaffective disorder)
- affective disorders (such as psychotic depression and bipolar disorder).
Distinguishing among these conditions can be challenging (Table 2) because patients rarely present with typical syndromes.
For example, a bipolar patient may present in a mixed state with both depressive and manic features. Psychosis in schizophrenia may be brief (<6 months in schizophreniform disorder) and may be characterized by manic-like grandiose delusions or negative symptoms (flat affect, poverty of speech) that mimic affective symptoms. Finally, some patients have both an affective disorder and schizophrenia, as in schizoaffective disorder.
For Mr. J, years of uninterrupted hallucinations, longstanding paranoid delusions, and absence of prominent affective symptoms suggest schizophrenia. His hallucinations are typical of those reported in schizophrenia. Voices giving a running commentary on a person’s thoughts and actions and derogatory comments are two of the most common auditory hallucinations.
Somatic concerns are also prominent in schizophrenia. Patients may describe symptoms in bizarre terms, such as “electric shocks in my head” or “there’s a fire in my spleen.”
Supporting evidence for a schizophrenia diagnosis would include a history of social isolation, lack of interest in work, and poor social interaction. Mr. J has a supportive partner, and we are told he appears to be high-functioning and active as a guitarist in a band. These factors might support an alternate diagnosis of affective psychosis. Finally, his past drug use and somatic symptoms raise the possibility of active substance abuse.
Table 2
Differential diagnosis of primary psychosis: Typical features
| Affective disorder | Schizophrenic spectrum disorder | |
|---|---|---|
| Symptom onset | Acute or subacute | Prolonged period (months to years) of self-neglect, social isolation, odd beliefs, eccentric behaviors |
| Course | Episodic, with periods of normal social and occupational functioning between episodes | Chronic, with exacerbations superimposed on gradually deteriorating social and occupational functioning |
| Associated symptoms | Mania (irritability, insomnia, rapid speech, labile mood, psychomotor agitation, racing thoughts) | Flat or inappropriate affect, thought blocking, apathy |
| Depression (anhedonia, psychomotor retardation, sleep problems, poor appetite) |
Suicide risk. Ask psychotic patients if they think about harming themselves. Lifetime risk of suicide in schizophrenia is 10% to 15%, and rates in bipolar disorder are higher. If patients deny suicidality, ask them why. Reassuring responses include religious prohibition, hopefulness about the future, concern about suicide’s effect on a loved one, fear of dying, or lack of means.
Candidates for emergent psychiatric consultation or hospitalization include patients with violent or homicidal thoughts and any patient who has attempted suicide, has a family history of suicide, has access to means, and lacks compelling reasons against suicide. Consider immediate psychiatric evaluation and admission of patients whose delusions or behaviors put them at risk for harm.
Abdominal pain workup. Although Mr. J’s abdominal pain may be functional, also seek an organic cause. His first-time disclosure of psychotic symptoms suggests that a serious medical stressor may be exacerbating a chronic psychiatric illness. Because the elevated lipase may indicate pancreatitis, consider an endoscopic or MRI examination of the pancreas and bile ducts. In consultation with a gastroenterologist, evaluate other causes such as peptic ulcer disease, ischemic bowel (perhaps as a result of cocaine use), inflammatory bowel disease, vasculitis, porphyria, and abdominal migraine.
Managing psychosis
Psychiatric consultation is strongly recommended for patients beginning therapy for psychotic disorders who have shown a particularly high risk for suicide. Uncontrolled symptoms, unanticipated psychiatric side effects, and the humiliation that results from the insight gained through treatment may contribute to this risk.
Assuming that Mr. J does not meet criteria for acute psychiatric hospitalization, the primary care clinician can stabilize the psychotic symptoms while awaiting psychiatric referral. Any atypical antipsychotic would be appropriate (Table 3).
Table 3
Starting an atypical antipsychotic* for primary psychosis
| Drug | Starting and maintenance dosages1 | Most-common adverse effects |
|---|---|---|
| Aripiprazole | 7.5 to 15 mg daily; 15 to 30 mg daily | EPS (+), agitation (++) |
| Olanzapine | 5 to 15 mg nightly; 10 to 20 mg nightly | Sedation (+++), weight gain (++++) hyperglycemia (++++), anticholinergic |
| Quetiapine | 50 to 100 mg bid; 600 to 800 mg nightly | Sedation (++++), weight gain (+++), hyperglycemia (++) |
| Risperidone | 0.5 to 2 mg bid; 2 to 4 mg bid | EPS (++), sedation (++), weight gain (++), hyperglycemia (++), elevated prolactin |
| Ziprasidone | 20 to 40 mg bid; 60 to 80 mg bid | EPS (+), agitation (++), sedation (+), QTc prolongation2 |
| EPS: Extrapyramidal symptoms | ||
| + small risk ++ moderate risk +++ high risk ++++ most risk | ||
| * All atypical antipsychotics have been associated with rare cases of neuroleptic malignant syndrome. Tardive dyskinesia is estimated to occur in 0.5% of adults and 2.5% of geriatric patients for each year on therapy. FDA requires a warning on increased risks of hyperlipidemia, hyperglycemia, and diabetes mellitus on the labels of all atypical antipsychotics. Monitoring weight, glucose, and lipids is recommended. | ||
| 1 In clinical practice, dosages may be increased beyond maximum dosages listed. Doses may be given solely at night or bid, depending on sedation and agitation. Low dosages are recommended in geriatric patients or those with renal or hepatic disease. Review potential drug-drug interactions before dosing. | ||
| 2 Despite earlier concerns, no cases of torsade de pointes or sudden death have been reported with ziprasidone. Not recommended for patients with cardiac risk. | ||
| Source: Adapted from reference 4. | ||
Patients who refuse treatment pose a quandary. If the patient is not acutely ill, try to establish an alliance over several visits rather than endangering the therapeutic relationship through confrontation or overzealous persuasion (Table 4).
Table 4
Strategies to build a therapeutic alliance with psychotic patients
| Enlist support of the patient’s family or loved ones |
| Do not argue with the patient’s delusions |
| Focus on what is bothering the patient most, and treat identified symptoms |
| Refer to the “stress” the patient suffers because of the unusual experiences he is describing |
| Commiserate with the anxiety he feels when others (such as his family) ridicule or reject his beliefs |
| Describe the medication as a “tranquilizer” rather than an antipsychotic. Use terms such as “nerves,” “stress,” “depression,” “anxiety,” or “insomnia,” which are often preferred by psychotic patients |
| Normalize treatment by suggesting “many of my patients with fatigue or lack of sleep find this medication very helpful” |
| Use medical terms to destigmatize the illness. Suggest that the patient suffers from a chemical disturbance that can be treated, similar to patients with diabetes who require insulin |
Monitoring. The primary care physician’s role after the patient begins antipsychotic therapy is to:
- assess his or her symptoms (particularly suicidality) and adherence to psychiatric visits and treatment
- monitor for adverse effects from medications.
Atypical antipsychotics have been associated with weight gain, hyperglycemia, and hyperlipidemia. Check fasting glucose and lipids quarterly for the first year of antipsychotic therapy and annually thereafter.5 Watch for drug-drug interactions whenever a new medication is added. Monitor for abnormal movements, even though the risk of extrapyramidal symptoms and tardive dyskinesia is lower with atypical antipsychotics than with traditional agents.
For Mr. J’s psychiatric symptoms, I would:
- assess his willingness to start medication to reduce or eliminate the voices
- suggest he accept psychiatric referral
- assure him that I will remain involved in his care and continue to evaluate his abdominal symptoms.
I would also request permission to discuss his case with his partner and a family member to gather pertinent history and enlist their support for treatment. I would then start Mr. J on any drug listed in Table 3.
Distinguishing the cause of a patient’s psychotic symptoms can be clinically challenging in a primary care practice. This case was submitted by Matthew Rosenberg, MD, who practices family medicine at Sacramento (CA) County Primary Care Clinic. This month’s consultant is Bezalel Dantz, MD.
How would you have advised Dr. Rosenberg?
Case: ‘you’re just gonna die’
I was seeing Mr. J, age 31, weekly to monitor abdominal complaints. For 3 weeks he experienced increasing epigastric pain, and he had been evaluated twice in the emergency room for this complaint. Plain films, ultrasound, CT, and an elevated lipase reading suggested an inconclusive diagnosis of pancreatitis.
During his second office visit, Mr. J also complained of “hearing voices.” Further questioning revealed that he had been hearing voices—often male—making degrading comments for several years. The voices have increased in frequency during his illness, and their negative comments include, “What do you have to live for?” and “You’re just gonna die.”
Mr. J blames the voices on distant drug use, claiming his parents “forced” him as a young teen to take hallucinogens. He often thinks he is being followed and does not trust others. He said both parents had mental illnesses but does not know the diagnoses or seriousness of their disorders.
His thoughts are well-organized with clear content. He shows no signs of depression or mania. He plays guitar in a band and appears to be a thoughtful and high-functioning individual.
I need help with the differential diagnosis and suggestions of possible treatment options.
Dr. Dantz’s consultation
The first step in evaluating psychosis is to determine whether it indicates a medical disorder, substanceinduced disorder, or primary psychiatric illness. The chronicity and nature of Mr. J’s psychotic symptoms (auditory hallucinations and paranoid delusions), his age, and a family history of psychiatric illness suggest a primary psychiatric disorder. The elevated lipase might explain his abdominal pain but is likely independent of his psychosis.
Medical workup. Conduct a comprehensive physical exam and medical and psychiatric history. Obtain collateral information from the family about the patient’s psychiatric symptoms, family history, recreational drug use, and stressors. Acute onset, age >40, comorbid medical conditions, lack of acute psychosocial stressors, and a negative personal or family psychiatric history suggest a medical cause (The skinny on one patient’s psychosis,” November 2005.) Also assess for use of alcohol, marijuana, hallucinogens, narcotics, stimulants, and inhalants. Until any drug has been stopped for at least 1 week, its contribution to psychosis may be unclear.
Table 1
Medical conditions that may present as psychosis
| Type of condition | Examples |
|---|---|
| CNS infection | HIV, neurosyphilis, cycticercosis, encephalitis, prion disease |
| Neoplasm | Primary or metastatic, paraneoplastic syndromes |
| Endocrinopathies | Thyroid, parathyroid, adrenal |
| Degenerative diseases | Alzheimer’s disease, frontotemporal dementia, Huntington’s disease, Parkinson’s disease, Wilson’s disease, Lewy body dementia |
| Demyelinating disorders | Multiple sclerosis, adrenal leukodystrophy |
| Metabolic disorders | Cirrhosis, vitamin deficiency, uremia, porphyria, heavy metal poisoning |
| Vasculitis | Systemic lupus erythematosus |
| Others | Seizures, migraine aura, hypnagogic and hypnopompic hallucinations, neurosarcoidosis |
Lab testing. When signs or symptoms do not suggest an organic disease, laboratory tests have a low yield and are of questionable value.2 In primary care practice, however, many psychotic patients complain of somatic symptoms. Given the devastating impact of psychotic illness, one can argue that even a yield <5% justifies a workup.
A urine toxicology screen is by far the most important lab test. CBC, comprehensive metabolic panel, thyroid function tests, erythrocyte sedimentation rate, and calcium level may reveal a medical cause. Consider HIV antibody and syphilis tests in at-risk individuals.
Findings on physical exam or abnormal lab results would guide further testing. Because of Mr. J’s GI and neurologic symptoms, a 24-hour urine test may be reasonable, particularly if he has had episodes of acute intermittent porphyria.
Neuroimaging. Consider a scan when psychosis is comorbid with:
- age >40
- neurologic complaints (such as headache, numbness, vertigo, seizures)
- focal neurologic findings (such as weakness, gait abnormality, clonus, or spasticity)
- confusion, cognitive deficit, history of malignancy
- head trauma
- immunocompromised state
- atypical psychotic symptoms (such as visual or olfactory hallucinations).
Psychiatric workup. If the history and physical exam reveal no organic basis, the next step is to determine the nature of this patient’s psychosis. The two most common psychiatric conditions associated with psychosis are:
- schizophrenic spectrum disorders (such as schizophreniform, schizophrenia and schizoaffective disorder)
- affective disorders (such as psychotic depression and bipolar disorder).
Distinguishing among these conditions can be challenging (Table 2) because patients rarely present with typical syndromes.
For example, a bipolar patient may present in a mixed state with both depressive and manic features. Psychosis in schizophrenia may be brief (<6 months in schizophreniform disorder) and may be characterized by manic-like grandiose delusions or negative symptoms (flat affect, poverty of speech) that mimic affective symptoms. Finally, some patients have both an affective disorder and schizophrenia, as in schizoaffective disorder.
For Mr. J, years of uninterrupted hallucinations, longstanding paranoid delusions, and absence of prominent affective symptoms suggest schizophrenia. His hallucinations are typical of those reported in schizophrenia. Voices giving a running commentary on a person’s thoughts and actions and derogatory comments are two of the most common auditory hallucinations.
Somatic concerns are also prominent in schizophrenia. Patients may describe symptoms in bizarre terms, such as “electric shocks in my head” or “there’s a fire in my spleen.”
Supporting evidence for a schizophrenia diagnosis would include a history of social isolation, lack of interest in work, and poor social interaction. Mr. J has a supportive partner, and we are told he appears to be high-functioning and active as a guitarist in a band. These factors might support an alternate diagnosis of affective psychosis. Finally, his past drug use and somatic symptoms raise the possibility of active substance abuse.
Table 2
Differential diagnosis of primary psychosis: Typical features
| Affective disorder | Schizophrenic spectrum disorder | |
|---|---|---|
| Symptom onset | Acute or subacute | Prolonged period (months to years) of self-neglect, social isolation, odd beliefs, eccentric behaviors |
| Course | Episodic, with periods of normal social and occupational functioning between episodes | Chronic, with exacerbations superimposed on gradually deteriorating social and occupational functioning |
| Associated symptoms | Mania (irritability, insomnia, rapid speech, labile mood, psychomotor agitation, racing thoughts) | Flat or inappropriate affect, thought blocking, apathy |
| Depression (anhedonia, psychomotor retardation, sleep problems, poor appetite) |
Suicide risk. Ask psychotic patients if they think about harming themselves. Lifetime risk of suicide in schizophrenia is 10% to 15%, and rates in bipolar disorder are higher. If patients deny suicidality, ask them why. Reassuring responses include religious prohibition, hopefulness about the future, concern about suicide’s effect on a loved one, fear of dying, or lack of means.
Candidates for emergent psychiatric consultation or hospitalization include patients with violent or homicidal thoughts and any patient who has attempted suicide, has a family history of suicide, has access to means, and lacks compelling reasons against suicide. Consider immediate psychiatric evaluation and admission of patients whose delusions or behaviors put them at risk for harm.
Abdominal pain workup. Although Mr. J’s abdominal pain may be functional, also seek an organic cause. His first-time disclosure of psychotic symptoms suggests that a serious medical stressor may be exacerbating a chronic psychiatric illness. Because the elevated lipase may indicate pancreatitis, consider an endoscopic or MRI examination of the pancreas and bile ducts. In consultation with a gastroenterologist, evaluate other causes such as peptic ulcer disease, ischemic bowel (perhaps as a result of cocaine use), inflammatory bowel disease, vasculitis, porphyria, and abdominal migraine.
Managing psychosis
Psychiatric consultation is strongly recommended for patients beginning therapy for psychotic disorders who have shown a particularly high risk for suicide. Uncontrolled symptoms, unanticipated psychiatric side effects, and the humiliation that results from the insight gained through treatment may contribute to this risk.
Assuming that Mr. J does not meet criteria for acute psychiatric hospitalization, the primary care clinician can stabilize the psychotic symptoms while awaiting psychiatric referral. Any atypical antipsychotic would be appropriate (Table 3).
Table 3
Starting an atypical antipsychotic* for primary psychosis
| Drug | Starting and maintenance dosages1 | Most-common adverse effects |
|---|---|---|
| Aripiprazole | 7.5 to 15 mg daily; 15 to 30 mg daily | EPS (+), agitation (++) |
| Olanzapine | 5 to 15 mg nightly; 10 to 20 mg nightly | Sedation (+++), weight gain (++++) hyperglycemia (++++), anticholinergic |
| Quetiapine | 50 to 100 mg bid; 600 to 800 mg nightly | Sedation (++++), weight gain (+++), hyperglycemia (++) |
| Risperidone | 0.5 to 2 mg bid; 2 to 4 mg bid | EPS (++), sedation (++), weight gain (++), hyperglycemia (++), elevated prolactin |
| Ziprasidone | 20 to 40 mg bid; 60 to 80 mg bid | EPS (+), agitation (++), sedation (+), QTc prolongation2 |
| EPS: Extrapyramidal symptoms | ||
| + small risk ++ moderate risk +++ high risk ++++ most risk | ||
| * All atypical antipsychotics have been associated with rare cases of neuroleptic malignant syndrome. Tardive dyskinesia is estimated to occur in 0.5% of adults and 2.5% of geriatric patients for each year on therapy. FDA requires a warning on increased risks of hyperlipidemia, hyperglycemia, and diabetes mellitus on the labels of all atypical antipsychotics. Monitoring weight, glucose, and lipids is recommended. | ||
| 1 In clinical practice, dosages may be increased beyond maximum dosages listed. Doses may be given solely at night or bid, depending on sedation and agitation. Low dosages are recommended in geriatric patients or those with renal or hepatic disease. Review potential drug-drug interactions before dosing. | ||
| 2 Despite earlier concerns, no cases of torsade de pointes or sudden death have been reported with ziprasidone. Not recommended for patients with cardiac risk. | ||
| Source: Adapted from reference 4. | ||
Patients who refuse treatment pose a quandary. If the patient is not acutely ill, try to establish an alliance over several visits rather than endangering the therapeutic relationship through confrontation or overzealous persuasion (Table 4).
Table 4
Strategies to build a therapeutic alliance with psychotic patients
| Enlist support of the patient’s family or loved ones |
| Do not argue with the patient’s delusions |
| Focus on what is bothering the patient most, and treat identified symptoms |
| Refer to the “stress” the patient suffers because of the unusual experiences he is describing |
| Commiserate with the anxiety he feels when others (such as his family) ridicule or reject his beliefs |
| Describe the medication as a “tranquilizer” rather than an antipsychotic. Use terms such as “nerves,” “stress,” “depression,” “anxiety,” or “insomnia,” which are often preferred by psychotic patients |
| Normalize treatment by suggesting “many of my patients with fatigue or lack of sleep find this medication very helpful” |
| Use medical terms to destigmatize the illness. Suggest that the patient suffers from a chemical disturbance that can be treated, similar to patients with diabetes who require insulin |
Monitoring. The primary care physician’s role after the patient begins antipsychotic therapy is to:
- assess his or her symptoms (particularly suicidality) and adherence to psychiatric visits and treatment
- monitor for adverse effects from medications.
Atypical antipsychotics have been associated with weight gain, hyperglycemia, and hyperlipidemia. Check fasting glucose and lipids quarterly for the first year of antipsychotic therapy and annually thereafter.5 Watch for drug-drug interactions whenever a new medication is added. Monitor for abnormal movements, even though the risk of extrapyramidal symptoms and tardive dyskinesia is lower with atypical antipsychotics than with traditional agents.
For Mr. J’s psychiatric symptoms, I would:
- assess his willingness to start medication to reduce or eliminate the voices
- suggest he accept psychiatric referral
- assure him that I will remain involved in his care and continue to evaluate his abdominal symptoms.
I would also request permission to discuss his case with his partner and a family member to gather pertinent history and enlist their support for treatment. I would then start Mr. J on any drug listed in Table 3.
1. The Medical Letter. Drugs that may cause psychiatric symptoms. July 8, 2002;1134:59-62.
2. Anfinson TJ, Kathol RG. Screening laboratory evaluation in psychiatric patients: a review. Gen Hosp Psychiatry 1992;14(4):248-57.
3. Mann JJ. A current perspective of suicide and attempted suicide. Ann Intern Med 2002;136(4):302-11.
4. McIntyre RS, Konarski JZ. Tolerability profiles of atypical antipsychotics in the treatment of bipolar disorder. J Clin Psychiatry 2005;66(suppl 3):28-36.
5. Kane JM, Leucht S, Carpenter D, Docherty JP. Expert consensus guideline series. Optimizing pharmacologic treatment of psychotic disorders. Introduction: methods, commentary, and summary. J Clin Psychiatry 2003;64(suppl 12):5-19.
Dr. Dantz is a board-certified internist and psychiatrist who is assistant professor of internal medicine and psychiatry, Rush University, Chicago. He specializes in treating psychiatric disorders in the medical setting.
1. The Medical Letter. Drugs that may cause psychiatric symptoms. July 8, 2002;1134:59-62.
2. Anfinson TJ, Kathol RG. Screening laboratory evaluation in psychiatric patients: a review. Gen Hosp Psychiatry 1992;14(4):248-57.
3. Mann JJ. A current perspective of suicide and attempted suicide. Ann Intern Med 2002;136(4):302-11.
4. McIntyre RS, Konarski JZ. Tolerability profiles of atypical antipsychotics in the treatment of bipolar disorder. J Clin Psychiatry 2005;66(suppl 3):28-36.
5. Kane JM, Leucht S, Carpenter D, Docherty JP. Expert consensus guideline series. Optimizing pharmacologic treatment of psychotic disorders. Introduction: methods, commentary, and summary. J Clin Psychiatry 2003;64(suppl 12):5-19.
Dr. Dantz is a board-certified internist and psychiatrist who is assistant professor of internal medicine and psychiatry, Rush University, Chicago. He specializes in treating psychiatric disorders in the medical setting.
Malpractice Primer
Enter text here
Enter text here
Enter text here
I, Intern

Internship is a stressful and life-altering experience. Demands from patients, consulting staff, and paperwork can dehumanize the new physician and make him or her feel like an automaton. The constant exigency of being an intern is further compounded by the increasing use of algorithms and computers. Guidelines for care have existed since the Hermetic books of Thoth in ancient Egypt, but strict “cookbook” medicine limits the intern’s decision-making and individuality. Pressure for electronic record-keeping and redundant documentation further reduce the new physician into not much more than a data entry-and-retrieval terminal. With the intern spending more time with patient records than actual patients, the physician-patient relationship invariably suffers as the intern becomes a small part of the machinery. Consequently, house-staff are constantly searching for a conceptual framework to better understand and cope with their unusual existence.
Isaac Asimov, the visionary science fiction writer and one-time biochemistry professor at Boston University School of Medicine, wrote an entire corpus of work around robots and the three “Laws of Robotics” starting in the 1940s.1 It seems the laws of robotics might also apply to interns as the Three Laws of “Internotics” (original text in parenthesis):
- First Law: An intern (robot) may not injure a patient (human being), or, through inaction, allow a patient (human being) to come to harm.
- Second Law: An intern (robot) must obey orders given it by attendings (human beings) except when such orders would conflict with the First Law.*
- Third Law: An intern (robot) must protect its own existence as long as such protection does not conflict with the First or Second Law.
Ten years after the creation of these laws, Asimov developed a “Zeroth” Law: An intern (robot) may not injure humanity, or through inaction, allow humanity to come to harm.
The First Law
Isolated interpretation of the First Law is the modus operandi of robots and interns. This law is a re-wording of the basic tenet of medicine: First do no harm, or primum non nocere as quoted from Hippocrates in Epidemics. On its surface, the First Law may seem easy for the intern to interpret and follow. However, when the patient’s own perception of benefit and harm deviates from the established norms in medicine, the intern is faced with dilemma of patient autonomy versus beneficence. This may not be a novel phenomenon in the modern consumer-based healthcare system, as Will Mayo, MD, from our own institution once said during a speech at Rush Medical College in 1910: “The best interest of the patient is the only interest to be considered.”
The Second Law
The Second Law explicitly states that the intern must follow the orders of the attending physician, but much rests in the intern’s additional obligation to reconcile obligatory recommendations with their own knowledge and patients’ idiosyncrasy. This may quickly become problematic for the intern, as few orders in modern medicine are considered absolutely risk-free.
The intern must undertake two levels of risk-benefit analysis: They must first determine what type of harm the patient faces in the setting of inaction—as spelled out by the First Law—if the attending’s orders were not carried out; he then must balance such hypothetical harm with the risks associated with the attendings orders of action. If such analysis were to favor inaction, to question the attending’s order is to challenge the attending’s own interpretation of the First Law and to risk the intern’s own existence (Third Law).
Therefore, the best solution for the intern is often to not question whether such order is necessary, but to do whatever possible to protect the patient. An example might be a consultant’s request for a CAT scan in a patient at high risk for contrast-induced nephropathy. In such a case, N-acetylcystein, adequate hydration or urine alkalinization may provide optimal protection against nephropathy. As such, the intern fulfills his or her obligations to the First and Second Laws without testing the limits imposed by the Third.
The Third Law
Much of the practice of—if not the principle of—internship is a violation of the Third Law. Excessive sleepiness and stressors may lead to medical errors, substance abuse, and traffic accidents.2 Work-hour restrictions may alleviate this condition, but can also erode the already limited patient-physician relationship. Further, certain attending physicians may denigrate the performance of the intern, leading to self doubt, lower self esteem, and mental anguish.
Similarly, interaction with certain patients may challenge the intern’s physical or mental well-being. As a result, the intern juxtaposes the new physician’s self-image of competency against the hierarchical stereotype of the rookie. The Third Law allows an opportunity for the intern to be associated with the proud heritage of the caduceus. However, as most interns soon learn, an intern can possibly best ensure his or her well-being and ascent to the next level when the Third Law is not cited as regularly as the first two laws.
The Zeroth Law
The Zeroth Law may be the most challenging law for both robots and interns. While robots and interns are both proficiently trained in serving individual humans, neither positronic programming nor medical education clearly establishes how this leads to the service of humanity.
If humanity is to be defined as the collection of individuals, principles in doctoring of the individual cannot be easily duplicated onto a population. This can be demonstrated through the continuously escalating medical expenditures in the setting of limited resources. For example, if a patient presents with “atypical” chest pain, a diligent medical graduate might order a set of laboratory studies and an electrocardiogram to rule out on-going myocardial infarction despite a low likelihood of abnormality. The slightest normal variation may then involve, by the First or Second Law, observation, stress testing, or cardiac catheterization.
Even though the current economic and legal systems allow for such shotgun approach of affordable technology, such application of the First Law onto humans as a collective will exhaust the population of its limited resources and utterly defy the Zeroth Law.
Alternatively, if humanity is to mean what constitutes each person’s individuality, argument involving maleficence and beneficence must give way to autonomy in the presentation, diagnosis, and treatment of disease, despite what the intern or attending physician perceive as benefits and harm. This obviously violates the First Law in the most fundamental level. However, different from the other laws, the Zeroth Law is not prefaced with the need to comply with the other Three Laws.
Interns can and often do feel dehumanized, whether from loss of decision-making role, from lack of sleep, or as a psychological tool of survival against the rigors of life and death in the hospital. Sometimes even a perfectly beneficent act violates the First Law at a later time and haunts the practitioners. Asimov himself received surgery-related transfusion with the best intention of his treating physicians and surgeons, yet he contracted transfusion-related HIV and died years later of AIDS complications.3
While the Three Laws create a framework of the intern’s existence, it can never create the ideal intern with both the competency of the attending and frailty of the patients. The Laws of Robotics—and Internotics—remind us that just as Asimov’s “Bicentennial man” wanted to transform from robot to human, we want our interns to finish their training more human, not less so.4,** TH
*This makes the assumption that most attendings are humans in the context of this discussion—a hypothesis only. **Dr. Hu was recently a medical intern for Dr. Newman. None of the original Three Laws were violated during the course of their relationship.
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn. Dr. Hu works in the Departments of Internal Medicine and Neurology, Mayo Clinic College of Medicine, Rochester, Minn.
References
- Asimov, I. I, Robot. London: Grafton Books; 1968.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
- Asimov I, Asimov, JJ. Isaac Asimov: It’s Been a Good Life. New York: Prometheus; 2002.
- Asimov, I. The Bicentennial Man and Other Stories. New York:Doubleday and Co; 1976.
Internship is a stressful and life-altering experience. Demands from patients, consulting staff, and paperwork can dehumanize the new physician and make him or her feel like an automaton. The constant exigency of being an intern is further compounded by the increasing use of algorithms and computers. Guidelines for care have existed since the Hermetic books of Thoth in ancient Egypt, but strict “cookbook” medicine limits the intern’s decision-making and individuality. Pressure for electronic record-keeping and redundant documentation further reduce the new physician into not much more than a data entry-and-retrieval terminal. With the intern spending more time with patient records than actual patients, the physician-patient relationship invariably suffers as the intern becomes a small part of the machinery. Consequently, house-staff are constantly searching for a conceptual framework to better understand and cope with their unusual existence.
Isaac Asimov, the visionary science fiction writer and one-time biochemistry professor at Boston University School of Medicine, wrote an entire corpus of work around robots and the three “Laws of Robotics” starting in the 1940s.1 It seems the laws of robotics might also apply to interns as the Three Laws of “Internotics” (original text in parenthesis):
- First Law: An intern (robot) may not injure a patient (human being), or, through inaction, allow a patient (human being) to come to harm.
- Second Law: An intern (robot) must obey orders given it by attendings (human beings) except when such orders would conflict with the First Law.*
- Third Law: An intern (robot) must protect its own existence as long as such protection does not conflict with the First or Second Law.
Ten years after the creation of these laws, Asimov developed a “Zeroth” Law: An intern (robot) may not injure humanity, or through inaction, allow humanity to come to harm.
The First Law
Isolated interpretation of the First Law is the modus operandi of robots and interns. This law is a re-wording of the basic tenet of medicine: First do no harm, or primum non nocere as quoted from Hippocrates in Epidemics. On its surface, the First Law may seem easy for the intern to interpret and follow. However, when the patient’s own perception of benefit and harm deviates from the established norms in medicine, the intern is faced with dilemma of patient autonomy versus beneficence. This may not be a novel phenomenon in the modern consumer-based healthcare system, as Will Mayo, MD, from our own institution once said during a speech at Rush Medical College in 1910: “The best interest of the patient is the only interest to be considered.”
The Second Law
The Second Law explicitly states that the intern must follow the orders of the attending physician, but much rests in the intern’s additional obligation to reconcile obligatory recommendations with their own knowledge and patients’ idiosyncrasy. This may quickly become problematic for the intern, as few orders in modern medicine are considered absolutely risk-free.
The intern must undertake two levels of risk-benefit analysis: They must first determine what type of harm the patient faces in the setting of inaction—as spelled out by the First Law—if the attending’s orders were not carried out; he then must balance such hypothetical harm with the risks associated with the attendings orders of action. If such analysis were to favor inaction, to question the attending’s order is to challenge the attending’s own interpretation of the First Law and to risk the intern’s own existence (Third Law).
Therefore, the best solution for the intern is often to not question whether such order is necessary, but to do whatever possible to protect the patient. An example might be a consultant’s request for a CAT scan in a patient at high risk for contrast-induced nephropathy. In such a case, N-acetylcystein, adequate hydration or urine alkalinization may provide optimal protection against nephropathy. As such, the intern fulfills his or her obligations to the First and Second Laws without testing the limits imposed by the Third.
The Third Law
Much of the practice of—if not the principle of—internship is a violation of the Third Law. Excessive sleepiness and stressors may lead to medical errors, substance abuse, and traffic accidents.2 Work-hour restrictions may alleviate this condition, but can also erode the already limited patient-physician relationship. Further, certain attending physicians may denigrate the performance of the intern, leading to self doubt, lower self esteem, and mental anguish.
Similarly, interaction with certain patients may challenge the intern’s physical or mental well-being. As a result, the intern juxtaposes the new physician’s self-image of competency against the hierarchical stereotype of the rookie. The Third Law allows an opportunity for the intern to be associated with the proud heritage of the caduceus. However, as most interns soon learn, an intern can possibly best ensure his or her well-being and ascent to the next level when the Third Law is not cited as regularly as the first two laws.
The Zeroth Law
The Zeroth Law may be the most challenging law for both robots and interns. While robots and interns are both proficiently trained in serving individual humans, neither positronic programming nor medical education clearly establishes how this leads to the service of humanity.
If humanity is to be defined as the collection of individuals, principles in doctoring of the individual cannot be easily duplicated onto a population. This can be demonstrated through the continuously escalating medical expenditures in the setting of limited resources. For example, if a patient presents with “atypical” chest pain, a diligent medical graduate might order a set of laboratory studies and an electrocardiogram to rule out on-going myocardial infarction despite a low likelihood of abnormality. The slightest normal variation may then involve, by the First or Second Law, observation, stress testing, or cardiac catheterization.
Even though the current economic and legal systems allow for such shotgun approach of affordable technology, such application of the First Law onto humans as a collective will exhaust the population of its limited resources and utterly defy the Zeroth Law.
Alternatively, if humanity is to mean what constitutes each person’s individuality, argument involving maleficence and beneficence must give way to autonomy in the presentation, diagnosis, and treatment of disease, despite what the intern or attending physician perceive as benefits and harm. This obviously violates the First Law in the most fundamental level. However, different from the other laws, the Zeroth Law is not prefaced with the need to comply with the other Three Laws.
Interns can and often do feel dehumanized, whether from loss of decision-making role, from lack of sleep, or as a psychological tool of survival against the rigors of life and death in the hospital. Sometimes even a perfectly beneficent act violates the First Law at a later time and haunts the practitioners. Asimov himself received surgery-related transfusion with the best intention of his treating physicians and surgeons, yet he contracted transfusion-related HIV and died years later of AIDS complications.3
While the Three Laws create a framework of the intern’s existence, it can never create the ideal intern with both the competency of the attending and frailty of the patients. The Laws of Robotics—and Internotics—remind us that just as Asimov’s “Bicentennial man” wanted to transform from robot to human, we want our interns to finish their training more human, not less so.4,** TH
*This makes the assumption that most attendings are humans in the context of this discussion—a hypothesis only. **Dr. Hu was recently a medical intern for Dr. Newman. None of the original Three Laws were violated during the course of their relationship.
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn. Dr. Hu works in the Departments of Internal Medicine and Neurology, Mayo Clinic College of Medicine, Rochester, Minn.
References
- Asimov, I. I, Robot. London: Grafton Books; 1968.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
- Asimov I, Asimov, JJ. Isaac Asimov: It’s Been a Good Life. New York: Prometheus; 2002.
- Asimov, I. The Bicentennial Man and Other Stories. New York:Doubleday and Co; 1976.
Internship is a stressful and life-altering experience. Demands from patients, consulting staff, and paperwork can dehumanize the new physician and make him or her feel like an automaton. The constant exigency of being an intern is further compounded by the increasing use of algorithms and computers. Guidelines for care have existed since the Hermetic books of Thoth in ancient Egypt, but strict “cookbook” medicine limits the intern’s decision-making and individuality. Pressure for electronic record-keeping and redundant documentation further reduce the new physician into not much more than a data entry-and-retrieval terminal. With the intern spending more time with patient records than actual patients, the physician-patient relationship invariably suffers as the intern becomes a small part of the machinery. Consequently, house-staff are constantly searching for a conceptual framework to better understand and cope with their unusual existence.
Isaac Asimov, the visionary science fiction writer and one-time biochemistry professor at Boston University School of Medicine, wrote an entire corpus of work around robots and the three “Laws of Robotics” starting in the 1940s.1 It seems the laws of robotics might also apply to interns as the Three Laws of “Internotics” (original text in parenthesis):
- First Law: An intern (robot) may not injure a patient (human being), or, through inaction, allow a patient (human being) to come to harm.
- Second Law: An intern (robot) must obey orders given it by attendings (human beings) except when such orders would conflict with the First Law.*
- Third Law: An intern (robot) must protect its own existence as long as such protection does not conflict with the First or Second Law.
Ten years after the creation of these laws, Asimov developed a “Zeroth” Law: An intern (robot) may not injure humanity, or through inaction, allow humanity to come to harm.
The First Law
Isolated interpretation of the First Law is the modus operandi of robots and interns. This law is a re-wording of the basic tenet of medicine: First do no harm, or primum non nocere as quoted from Hippocrates in Epidemics. On its surface, the First Law may seem easy for the intern to interpret and follow. However, when the patient’s own perception of benefit and harm deviates from the established norms in medicine, the intern is faced with dilemma of patient autonomy versus beneficence. This may not be a novel phenomenon in the modern consumer-based healthcare system, as Will Mayo, MD, from our own institution once said during a speech at Rush Medical College in 1910: “The best interest of the patient is the only interest to be considered.”
The Second Law
The Second Law explicitly states that the intern must follow the orders of the attending physician, but much rests in the intern’s additional obligation to reconcile obligatory recommendations with their own knowledge and patients’ idiosyncrasy. This may quickly become problematic for the intern, as few orders in modern medicine are considered absolutely risk-free.
The intern must undertake two levels of risk-benefit analysis: They must first determine what type of harm the patient faces in the setting of inaction—as spelled out by the First Law—if the attending’s orders were not carried out; he then must balance such hypothetical harm with the risks associated with the attendings orders of action. If such analysis were to favor inaction, to question the attending’s order is to challenge the attending’s own interpretation of the First Law and to risk the intern’s own existence (Third Law).
Therefore, the best solution for the intern is often to not question whether such order is necessary, but to do whatever possible to protect the patient. An example might be a consultant’s request for a CAT scan in a patient at high risk for contrast-induced nephropathy. In such a case, N-acetylcystein, adequate hydration or urine alkalinization may provide optimal protection against nephropathy. As such, the intern fulfills his or her obligations to the First and Second Laws without testing the limits imposed by the Third.
The Third Law
Much of the practice of—if not the principle of—internship is a violation of the Third Law. Excessive sleepiness and stressors may lead to medical errors, substance abuse, and traffic accidents.2 Work-hour restrictions may alleviate this condition, but can also erode the already limited patient-physician relationship. Further, certain attending physicians may denigrate the performance of the intern, leading to self doubt, lower self esteem, and mental anguish.
Similarly, interaction with certain patients may challenge the intern’s physical or mental well-being. As a result, the intern juxtaposes the new physician’s self-image of competency against the hierarchical stereotype of the rookie. The Third Law allows an opportunity for the intern to be associated with the proud heritage of the caduceus. However, as most interns soon learn, an intern can possibly best ensure his or her well-being and ascent to the next level when the Third Law is not cited as regularly as the first two laws.
The Zeroth Law
The Zeroth Law may be the most challenging law for both robots and interns. While robots and interns are both proficiently trained in serving individual humans, neither positronic programming nor medical education clearly establishes how this leads to the service of humanity.
If humanity is to be defined as the collection of individuals, principles in doctoring of the individual cannot be easily duplicated onto a population. This can be demonstrated through the continuously escalating medical expenditures in the setting of limited resources. For example, if a patient presents with “atypical” chest pain, a diligent medical graduate might order a set of laboratory studies and an electrocardiogram to rule out on-going myocardial infarction despite a low likelihood of abnormality. The slightest normal variation may then involve, by the First or Second Law, observation, stress testing, or cardiac catheterization.
Even though the current economic and legal systems allow for such shotgun approach of affordable technology, such application of the First Law onto humans as a collective will exhaust the population of its limited resources and utterly defy the Zeroth Law.
Alternatively, if humanity is to mean what constitutes each person’s individuality, argument involving maleficence and beneficence must give way to autonomy in the presentation, diagnosis, and treatment of disease, despite what the intern or attending physician perceive as benefits and harm. This obviously violates the First Law in the most fundamental level. However, different from the other laws, the Zeroth Law is not prefaced with the need to comply with the other Three Laws.
Interns can and often do feel dehumanized, whether from loss of decision-making role, from lack of sleep, or as a psychological tool of survival against the rigors of life and death in the hospital. Sometimes even a perfectly beneficent act violates the First Law at a later time and haunts the practitioners. Asimov himself received surgery-related transfusion with the best intention of his treating physicians and surgeons, yet he contracted transfusion-related HIV and died years later of AIDS complications.3
While the Three Laws create a framework of the intern’s existence, it can never create the ideal intern with both the competency of the attending and frailty of the patients. The Laws of Robotics—and Internotics—remind us that just as Asimov’s “Bicentennial man” wanted to transform from robot to human, we want our interns to finish their training more human, not less so.4,** TH
*This makes the assumption that most attendings are humans in the context of this discussion—a hypothesis only. **Dr. Hu was recently a medical intern for Dr. Newman. None of the original Three Laws were violated during the course of their relationship.
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn. Dr. Hu works in the Departments of Internal Medicine and Neurology, Mayo Clinic College of Medicine, Rochester, Minn.
References
- Asimov, I. I, Robot. London: Grafton Books; 1968.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
- Asimov I, Asimov, JJ. Isaac Asimov: It’s Been a Good Life. New York: Prometheus; 2002.
- Asimov, I. The Bicentennial Man and Other Stories. New York:Doubleday and Co; 1976.
Hospitalists Effects on Outcomes, Costs, Point-of-Care HIV Testing, and More
Community Teaching
Halasyamani L, Valenstein P, Friedlander M. et al. A comparison of two hospitalist models with traditional care in a community teaching hospital. Am J Med. 2005;118:536-543.
Background: A growing body of literature has demonstrated the effects of hospitalists on reducing inpatient length of stay and cost of care, with some literature showing a decreased in-hospital and 30-day mortality. However, most prior studies were conducted in academic medical centers or health maintenance organizations where one group of hospitalists, employed by the institution within which they worked, was compared with traditional primary care physicians. Direct comparisons between different hospitalist models practicing within a single institution have not been published. As a result, the impact of different hospitalist characteristics, including employment status and reimbursement incentives, on inpatient resource utilization and patient care outcomes is unknown.
Methods: Halasyamani and colleagues conducted a retrospective cohort study of 10,595 patients in a tertiary care community-based teaching hospital in which private hospitalists, academic hospitalists, and community physicians all practice. They measured risk-adjusted length of stay, variable costs, 30-day readmission rates, and in-hospital and 30-day mortality for patients treated by each of these three groups, controlling for potentially confounding variables. Community physicians belonged to 21 rounding groups, most of which were private or solo. Two of the community physicians groups were hospital-owned practices reimbursed by a relative value unit system. The private hospitalist group was self-employed with no financial relationship to the hospital and worked an average of 40 weeks per year. Community physicians and private hospitalists worked Monday-Friday and covered weekends or holidays about 25% of the time. Academic hospitalists worked with internal medicine residents and students on a teaching service. They were employed by the hospital using a relative value unit system. They worked an average of 14 weeks per year as an inpatient attending in half-month rotations, which included weekend coverage.
Results: There was a 20% reduction (-0.72 days absolute difference) in length of stay on the academic hospitalist service (P<0.0001) and 8% (-0.28 days absolute difference) on the private hospitalist service (P=0.049) compared with community physicians. Case-mix adjusted relative total costs were 10% less ($173 absolute difference) on the academic (P<0.0001) and 6% less ($109 absolute difference) on the private hospitalist services (P=0.02) compared with community physicians. There were no differences in 30-day readmission, in-hospital and 30-day mortality between the three groups.
Discussion: This study is the first to look at the effects of two separate hospitalist models on resource utilization and patient outcomes within the same institution. Although both the academic and private hospitalist groups demonstrated improved resource utilization as compared with the community physicians, the magnitude of benefit was much greater for the academic hospitalist group.
As the authors point out, one major difference between the two groups was employment status, with the academic hospitalists employed directly by the hospital and the private hospitalists receiving all payment directly from payers. Previous studies have also focused on hospitalists, which were employed by the institution at which they worked, raising the question of whether alignment of employee and employer incentives is an important factor affecting resource utilization outcomes.
Results of this study highlight the need for more studies which seek to clarify specific physician-level, group-level, and organization-level characteristics of hospitalists that result in improved resource utilization and patient care outcomes.
The Last Few Hours
Bailey FA, Burgio KL, Woodby LL, et al. Improving the processes of hospital care during the last hours of life. Arch Int Med. 2005;165(15):1722-1727.
Background: End-of-life care in the acute care inpatient setting is often not initiated until very late in the dying process and may be related to inadequate early recognition of dying patients as well as difficulty transitioning from disease-modifying treatments to palliative measures. Additional barriers exist, including lack of familiarity of hospital staff with initiation and implementation of hospice care. Education about end-of-life care and introduction of a physician-led palliative care team available for consultation within acute care hospitals may help promote better recognition of the dying patient by staff and allow for a “good death.”
Methods: A single hospital within the Veterans Affairs (VA) medical system (Birmingham, Ala., VA Medical Center) was chosen as a pilot center for initiation of a physician-led Inpatient Comfort Care Program (ICCP). The study was framed as a “before-after intervention trial” and analyzed all inpatient deaths identified by the Computerized Patient Recognition System during a six-month period before and substantially after the introduction of the ICCP. A structured chart abstraction tool was used and data was obtained from the last seven days of hospitalization analyzing variables associated with recognition of the dying patient and initiation of palliative care. Education of hospital staff on both hospice care and case identification was initiated during the intervention phase of the study. Additionally, a flexible comfort care order set was introduced.
Results: Two hundred and three veterans were identified (98% men, average age 68) and no significant differences in clinical characteristics were noted between the two groups, pre-intervention and post-intervention. Post-intervention, 59.3% of patients had formal palliative care consultation. Significant findings (P<0.01) following implementation of ICCP were increased documentation of end-of-life symptoms, increased documentation of care plans, increased utilization of opioids (57.1% to 87.2%), increased initiation of do-not-resuscitate orders (61.9% to 85.1%) with a concurrent decrease in cardiopulmonary resuscitation at death (34.4% to 15.4%), and a surprising increase in restraint use (6.0% to 22.6%).
Discussion: Data on hospice care patients indicate that 10% to 30% die in an acute care hospital, identifying a need for increased education and training in palliative medicine. This study demonstrates the positive outcomes of implementation of an inpatient palliative care service both for heightened awareness of identifying the dying patient as well as initiation of end-of-life care. The increased use of opioid medications is an important marker given that many patients experience pain and dyspnea at the end of life. This study is limited by its single site and further validation at other centers implementing similar protocols and assessing similar outcomes is needed. While this intervention had important clinical benefits, additional studies examining the cost implications of this system would be helpful.
Education alone has not been shown to be entirely effective in creating change. This single-site implementation of a palliative care consultation service successfully integrated an education program with on-site consultants. Distributing pocket cards with clinical findings identifying the dying patient aided in recognition of those patients and pre-printed order sets facilitated initiation of end-of-life care. The intervention initiated is possible for many medical centers and promotes an environment allowing for a “good death” for dying patients.
Computers, Doctors, and Errors
Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293(10):1197-1203
For physicians, computerized physician order entry (CPOE) has become an important topic of discussion as many hospitals and health systems embark on the complex and lengthy process of implementing new enterprise clinical systems. Though there are undoubtedly benefits to such systems, practicing clinicians are apt to remain skeptical of the grandiose pictures the more vocal advocates of CPOE may paint. This is not to say that the promises of CPOE are empty; to the contrary, there have been substantial successes, notably in the realm of medication error prevention.
At the same time, CPOE is a mixture of complex technologies that interface in complicated ways with the culture of clinical medicine. The view that medical informatics is a technical problem that has been solved long ago is simplistic and naïve. The article by Koppel, et al, has two important implications: 1) It is critical to look at clinical information systems in the social milieu in which it functions, and 2) there are often unintended consequences that may not beneficial.
This article examines a widely used, commercial CPOE system in use at the University of Pennsylvania (Philadelphia) using both quantitative and qualitative methods. The researchers conducted focus groups and expert interviews in addition to field observations of physicians (house officers and attendings), nurses, and pharmacists in order to identify themes relating to work with the order entry system. This work helped to guide the creation of a survey instrument subsequently used to survey house staff about working conditions and sources of error and stress. There was an 85%-90% response rate that primarily included house staff who ordered more than nine medication orders per month.
Researchers found two broad categories of errors that were fostered in this environment. The first category, which they termed “information errors” were generated by fragmentation of data and the failure to integrate the hospitals various systems both electronic and paper. Examples of this type of error include antibiotic renewal failures. A common way this failure would occur is that renewal reminder stickers would be placed in the patients’ charts, but the house staff would overlook these because medication orders occurred electronically. Another example is assumed dose errors, where house staff would assume that the default dose displayed was the recommended starting dose, when in fact this was the smallest dose unit available. Physicians were assuming decision support was available when it was not.
The second type of error, human-machine interface flaws, occurred when machine rules did not correspond to work behaviors. An example of this is when patients were listed alphabetically rather than by service, making it easy to select the wrong patient. In another instance, many screens (up to 20) were required to view all of a patient’s medications, making it difficult to choose a correct medication for editing.
This study has been criticized by industry advocates for focusing on an older set of technologies or because a number of these issues related to training or “user factors.” At the other extreme, this study has been cited as a cautionary tale about the risks of CPOE. Both types of criticism miss the point. This study demonstrates that CPOE and the social environment in which it sits is a complex entity and that careful design, proper support, and maintenance are critical ingredients to the success of an incredibly complex but vital new component of hospital medicine.
Point-of-Care HIV Testing in Inpatients
Lubelchek R, Kroc K, Hota B, et al. The role of rapid vs conventional human immunodeficiency virus testing for inpatients: effects on quality of care. Arch Intern Med. 2005;165:1956-1960.
Despite advances in treatment, infection with HIV and AIDS remains a public health problem in the United States. According to the CDC the rate of new diagnosis of HIV infection has remained steady from 2000 to 2003 at about 20 per 100,000 people. (Centers for Disease Control and Prevention. Diagnosis of HIV/AIDS–32 states, 2009-2003. MMWR Morb Mortal Wkly Rep. 2004;53:1106-1110). Currently, about 850,000 to 950,000 people are believed to be living with HIV infection, and it is estimated that 180,000 to 280,000 are unaware of their diagnosis. (Fleming P, Byers RH, Sweeney PA, et al., HIV prevalence in the United States, 2000 [Abstract 11]. Presented at the Ninth Conference on Retroviruses and Opportunistic Infections, Seattle; February 24–28, 2002). These patients are not only at risk for disease progression, but can undermine efforts at disease prevention if they continue to engage in unsafe activities. Thus, increasing awareness of HIV status is an important aspect of disease prevention.
HIV testing remains a challenge. Conventional testing with enzyme immunoassay (EIA) and confirmatory Western blot requires patient follow-up for results, which approximately 25% of patients in various outpatient testing sites fail to do. (Centers for Disease Control and Prevention. Update: HIV counseling and testing using rapid tests, United States, 1995. MMWR Morb Mortal Wkly Rep. 1998;47:211-215). Given the difficulties inherent in the transition of care from the inpatient to outpatient setting, conventional testing in the inpatient setting presents additional barriers to appropriate notification. As various point-of-care HIV tests have been developed for commercial use, the possibility of rapid HIV testing presents an opportunity to reduce notification failure and improve patient care. While not replacing traditional testing, the CDC has endorsed rapid HIV testing as a means to initiate therapy and provide counseling with a particular focus on preventing further disease transmission. In this retrospective study, Lubelchek and colleagues present the effects of a rapid HIV test utilized in the emergency department on various inpatient quality of care measures for those patients who received a positive rapid HIV test later confirmed by Western blot as compared with those patients who were diagnosed after admission by traditional diagnostic methods. This study took place in the context of CDC-funded study of the use of OraQuick (OraSure Technologies, Bethlehem, Pa.) rapid HIV testing in the emergency department at Cook County Hospital in Chicago.
The manufacturer claims the product has a sensitivity of 99.6% and a specificity of 100% as compared with conventional testing. (OraQuick rapid HIV-1 antibody test summary of safety and effectiveness. November 7, 2002. Accessed October 1, 2005, at www.fda.gov/cber/pma/P010047.htm). In the initial study, two of the three emergency department’s treatment pods were equipped to provide HIV screening utilizing the point-of-care technology to consenting patients. Patients in the third pod could be referred to rapid testing based on symptoms or risk factors. All patients who received the rapid test also submitted specimens for conventional EIA and confirmatory Western blot testing. All positive rapid HIV tests were confirmed by Western blot.
In this study, patients who were not known to be infected and were subsequently admitted on non-obstetric or surgical services over 17 months from 2003 to 2004 and confirmed to be HIV positive by Western blot were identified utilizing administrative records. Where possible, charts were reviewed to confirm no prior diagnosis of HIV. Patients who received rapid HIV testing were compared with those who only received conventional testing. Endpoints included time to primary inpatient care service awareness of HIV diagnosis, time to admission or transfer to the inpatient HIV service, time to empiric treatment of diagnosis of opportunistic infection, length of stay, discharge with appropriate prophylactic medications, discharge with patient knowledge of HIV diagnosis, and initial engagement in outpatient care. Length of stay was adjusted by multivariate regression on co-morbid diagnoses (congestive heart failure, end-stage renal disease, cirrhosis, chronic obstructive pulmonary disease, and diabetes), opportunistic infections, ICU admission, need for mechanical ventilation, and CD4 count.
A total of 103 patients were identified with complete chart review completed on 86 of them. All patients except one were admitted through the emergency department. Forty-eight patients were diagnosed initially with the rapid HIV test with 58% of these specifically referred for testing by the emergency department physician, and 55 were diagnosed with conventional testing. Overall, 78% were male, 62% African American, and 20% Hispanic. The two groups were comparable in terms of age, sex, ethnicity, history of substance abuse, HIV risk factors, psychiatric diagnoses, homelessness, CD4 count, presence of opportunistic infections, mechanical ventilation, and co-morbidities. However, conventionally tested patients were more likely to require an ICU stay (31% vs. 10%, P=.01).
Patients in the rapid test group were more quickly documented in the chart as having HIV (.8 vs. 6.4 days, p<.001), placed on an HIV service sooner (1.4 versus 6.9 days, P<.001), initiated outpatient follow-up sooner (21.5 versus 49.5 days, p=.05), and had less unawareness of their HIV status (0 vs. 16%, P=.002). There was no significant difference between the two groups in time from admission to empiric treatment or diagnosis of an opportunistic infection. Patients who received the rapid test did have a lower length of stay (6.4 versus 13.2 days, P<.001). Although much of this difference was due to higher number of ICU stays in the conventional group, in multivariate analysis conventional testing still increased length of stay significantly, OR 5.4 days (2.5, 8.3).
This study suggests that patients who are tested with rapid HIV testing can lead to more efficient inpatient treatment of the complications of HIV, improved patient awareness of HIV status, and quicker outpatient follow-up. These findings have ramifications not just to the inpatient management of patients with HIV but to general public health efforts to reduce the spread of HIV infection.
Nevertheless, these results must be interpreted with caution. They reflect the experience of one institution situated in an area with a high prevalence of HIV. Some degree of selection bias is suggested by the higher presence of ICU admissions in the conventional testing group. The multivariate analysis attempted to control for confounding factors, but the possibility remains that other unrecognized factors may have influenced results. The authors do note that an analysis of patients in the rapid test group stratified by whether the test was performed for screening or by referral of the physician did not demonstrate a statistically significant difference in length of stay. This finding provides further support that the sicker patients which triggered the rapid test had shorter lengths of stay on account of the rapid test and not simply because they were sicker.
As recognized by the authors, physicians in routine practice rely on surrogate markers of HIV infection, most notably a patient’s CD4 count, and thus it is not surprising that the rapid test did not affect time to empiric treatment or diagnosis of opportunistic infection. If treatment did not differ, then explaining the longer length of stay remains an unexplained puzzle. The fact that the two groups were equally matched socially and psychiatrically leaves open the possibility that it was actual knowledge of the HIV test result—and not its effect on treatment—that drove the longer length of stay.
One possibility not suggested by the authors is that definitive knowledge of HIV status helped to mobilize patient discharge. If there were legitimate concerns of follow-up, physicians may have delayed discharge in order to receive HIV test results. Alternatively, some patients may have resisted discharge until receiving test results and the development of a more concrete plan. It would be interesting to know if the time to follow-up for the two groups would be the same if the 16% who did not know their HIV status at discharge were excluded. This suggests that knowledge of HIV status drives follow-up time and would lend some support to the notion that patient discharge was delayed for test results and clarification of the follow-up treatment plan.
Even putting aside the difference in length of stay, the difference of rapid testing on improved knowledge of HIV status and quicker follow-up is likely real and meaningful. Although this study was not designed to assess the impact of this knowledge on patient behavior, immediate knowledge of HIV status during hospitalization may translate to decreased transmission as patients alter their behavior and lends further credibility to the utility of rapid HIV testing in conjunction with conventional methods in the management of inpatients. TH
Community Teaching
Halasyamani L, Valenstein P, Friedlander M. et al. A comparison of two hospitalist models with traditional care in a community teaching hospital. Am J Med. 2005;118:536-543.
Background: A growing body of literature has demonstrated the effects of hospitalists on reducing inpatient length of stay and cost of care, with some literature showing a decreased in-hospital and 30-day mortality. However, most prior studies were conducted in academic medical centers or health maintenance organizations where one group of hospitalists, employed by the institution within which they worked, was compared with traditional primary care physicians. Direct comparisons between different hospitalist models practicing within a single institution have not been published. As a result, the impact of different hospitalist characteristics, including employment status and reimbursement incentives, on inpatient resource utilization and patient care outcomes is unknown.
Methods: Halasyamani and colleagues conducted a retrospective cohort study of 10,595 patients in a tertiary care community-based teaching hospital in which private hospitalists, academic hospitalists, and community physicians all practice. They measured risk-adjusted length of stay, variable costs, 30-day readmission rates, and in-hospital and 30-day mortality for patients treated by each of these three groups, controlling for potentially confounding variables. Community physicians belonged to 21 rounding groups, most of which were private or solo. Two of the community physicians groups were hospital-owned practices reimbursed by a relative value unit system. The private hospitalist group was self-employed with no financial relationship to the hospital and worked an average of 40 weeks per year. Community physicians and private hospitalists worked Monday-Friday and covered weekends or holidays about 25% of the time. Academic hospitalists worked with internal medicine residents and students on a teaching service. They were employed by the hospital using a relative value unit system. They worked an average of 14 weeks per year as an inpatient attending in half-month rotations, which included weekend coverage.
Results: There was a 20% reduction (-0.72 days absolute difference) in length of stay on the academic hospitalist service (P<0.0001) and 8% (-0.28 days absolute difference) on the private hospitalist service (P=0.049) compared with community physicians. Case-mix adjusted relative total costs were 10% less ($173 absolute difference) on the academic (P<0.0001) and 6% less ($109 absolute difference) on the private hospitalist services (P=0.02) compared with community physicians. There were no differences in 30-day readmission, in-hospital and 30-day mortality between the three groups.
Discussion: This study is the first to look at the effects of two separate hospitalist models on resource utilization and patient outcomes within the same institution. Although both the academic and private hospitalist groups demonstrated improved resource utilization as compared with the community physicians, the magnitude of benefit was much greater for the academic hospitalist group.
As the authors point out, one major difference between the two groups was employment status, with the academic hospitalists employed directly by the hospital and the private hospitalists receiving all payment directly from payers. Previous studies have also focused on hospitalists, which were employed by the institution at which they worked, raising the question of whether alignment of employee and employer incentives is an important factor affecting resource utilization outcomes.
Results of this study highlight the need for more studies which seek to clarify specific physician-level, group-level, and organization-level characteristics of hospitalists that result in improved resource utilization and patient care outcomes.
The Last Few Hours
Bailey FA, Burgio KL, Woodby LL, et al. Improving the processes of hospital care during the last hours of life. Arch Int Med. 2005;165(15):1722-1727.
Background: End-of-life care in the acute care inpatient setting is often not initiated until very late in the dying process and may be related to inadequate early recognition of dying patients as well as difficulty transitioning from disease-modifying treatments to palliative measures. Additional barriers exist, including lack of familiarity of hospital staff with initiation and implementation of hospice care. Education about end-of-life care and introduction of a physician-led palliative care team available for consultation within acute care hospitals may help promote better recognition of the dying patient by staff and allow for a “good death.”
Methods: A single hospital within the Veterans Affairs (VA) medical system (Birmingham, Ala., VA Medical Center) was chosen as a pilot center for initiation of a physician-led Inpatient Comfort Care Program (ICCP). The study was framed as a “before-after intervention trial” and analyzed all inpatient deaths identified by the Computerized Patient Recognition System during a six-month period before and substantially after the introduction of the ICCP. A structured chart abstraction tool was used and data was obtained from the last seven days of hospitalization analyzing variables associated with recognition of the dying patient and initiation of palliative care. Education of hospital staff on both hospice care and case identification was initiated during the intervention phase of the study. Additionally, a flexible comfort care order set was introduced.
Results: Two hundred and three veterans were identified (98% men, average age 68) and no significant differences in clinical characteristics were noted between the two groups, pre-intervention and post-intervention. Post-intervention, 59.3% of patients had formal palliative care consultation. Significant findings (P<0.01) following implementation of ICCP were increased documentation of end-of-life symptoms, increased documentation of care plans, increased utilization of opioids (57.1% to 87.2%), increased initiation of do-not-resuscitate orders (61.9% to 85.1%) with a concurrent decrease in cardiopulmonary resuscitation at death (34.4% to 15.4%), and a surprising increase in restraint use (6.0% to 22.6%).
Discussion: Data on hospice care patients indicate that 10% to 30% die in an acute care hospital, identifying a need for increased education and training in palliative medicine. This study demonstrates the positive outcomes of implementation of an inpatient palliative care service both for heightened awareness of identifying the dying patient as well as initiation of end-of-life care. The increased use of opioid medications is an important marker given that many patients experience pain and dyspnea at the end of life. This study is limited by its single site and further validation at other centers implementing similar protocols and assessing similar outcomes is needed. While this intervention had important clinical benefits, additional studies examining the cost implications of this system would be helpful.
Education alone has not been shown to be entirely effective in creating change. This single-site implementation of a palliative care consultation service successfully integrated an education program with on-site consultants. Distributing pocket cards with clinical findings identifying the dying patient aided in recognition of those patients and pre-printed order sets facilitated initiation of end-of-life care. The intervention initiated is possible for many medical centers and promotes an environment allowing for a “good death” for dying patients.
Computers, Doctors, and Errors
Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293(10):1197-1203
For physicians, computerized physician order entry (CPOE) has become an important topic of discussion as many hospitals and health systems embark on the complex and lengthy process of implementing new enterprise clinical systems. Though there are undoubtedly benefits to such systems, practicing clinicians are apt to remain skeptical of the grandiose pictures the more vocal advocates of CPOE may paint. This is not to say that the promises of CPOE are empty; to the contrary, there have been substantial successes, notably in the realm of medication error prevention.
At the same time, CPOE is a mixture of complex technologies that interface in complicated ways with the culture of clinical medicine. The view that medical informatics is a technical problem that has been solved long ago is simplistic and naïve. The article by Koppel, et al, has two important implications: 1) It is critical to look at clinical information systems in the social milieu in which it functions, and 2) there are often unintended consequences that may not beneficial.
This article examines a widely used, commercial CPOE system in use at the University of Pennsylvania (Philadelphia) using both quantitative and qualitative methods. The researchers conducted focus groups and expert interviews in addition to field observations of physicians (house officers and attendings), nurses, and pharmacists in order to identify themes relating to work with the order entry system. This work helped to guide the creation of a survey instrument subsequently used to survey house staff about working conditions and sources of error and stress. There was an 85%-90% response rate that primarily included house staff who ordered more than nine medication orders per month.
Researchers found two broad categories of errors that were fostered in this environment. The first category, which they termed “information errors” were generated by fragmentation of data and the failure to integrate the hospitals various systems both electronic and paper. Examples of this type of error include antibiotic renewal failures. A common way this failure would occur is that renewal reminder stickers would be placed in the patients’ charts, but the house staff would overlook these because medication orders occurred electronically. Another example is assumed dose errors, where house staff would assume that the default dose displayed was the recommended starting dose, when in fact this was the smallest dose unit available. Physicians were assuming decision support was available when it was not.
The second type of error, human-machine interface flaws, occurred when machine rules did not correspond to work behaviors. An example of this is when patients were listed alphabetically rather than by service, making it easy to select the wrong patient. In another instance, many screens (up to 20) were required to view all of a patient’s medications, making it difficult to choose a correct medication for editing.
This study has been criticized by industry advocates for focusing on an older set of technologies or because a number of these issues related to training or “user factors.” At the other extreme, this study has been cited as a cautionary tale about the risks of CPOE. Both types of criticism miss the point. This study demonstrates that CPOE and the social environment in which it sits is a complex entity and that careful design, proper support, and maintenance are critical ingredients to the success of an incredibly complex but vital new component of hospital medicine.
Point-of-Care HIV Testing in Inpatients
Lubelchek R, Kroc K, Hota B, et al. The role of rapid vs conventional human immunodeficiency virus testing for inpatients: effects on quality of care. Arch Intern Med. 2005;165:1956-1960.
Despite advances in treatment, infection with HIV and AIDS remains a public health problem in the United States. According to the CDC the rate of new diagnosis of HIV infection has remained steady from 2000 to 2003 at about 20 per 100,000 people. (Centers for Disease Control and Prevention. Diagnosis of HIV/AIDS–32 states, 2009-2003. MMWR Morb Mortal Wkly Rep. 2004;53:1106-1110). Currently, about 850,000 to 950,000 people are believed to be living with HIV infection, and it is estimated that 180,000 to 280,000 are unaware of their diagnosis. (Fleming P, Byers RH, Sweeney PA, et al., HIV prevalence in the United States, 2000 [Abstract 11]. Presented at the Ninth Conference on Retroviruses and Opportunistic Infections, Seattle; February 24–28, 2002). These patients are not only at risk for disease progression, but can undermine efforts at disease prevention if they continue to engage in unsafe activities. Thus, increasing awareness of HIV status is an important aspect of disease prevention.
HIV testing remains a challenge. Conventional testing with enzyme immunoassay (EIA) and confirmatory Western blot requires patient follow-up for results, which approximately 25% of patients in various outpatient testing sites fail to do. (Centers for Disease Control and Prevention. Update: HIV counseling and testing using rapid tests, United States, 1995. MMWR Morb Mortal Wkly Rep. 1998;47:211-215). Given the difficulties inherent in the transition of care from the inpatient to outpatient setting, conventional testing in the inpatient setting presents additional barriers to appropriate notification. As various point-of-care HIV tests have been developed for commercial use, the possibility of rapid HIV testing presents an opportunity to reduce notification failure and improve patient care. While not replacing traditional testing, the CDC has endorsed rapid HIV testing as a means to initiate therapy and provide counseling with a particular focus on preventing further disease transmission. In this retrospective study, Lubelchek and colleagues present the effects of a rapid HIV test utilized in the emergency department on various inpatient quality of care measures for those patients who received a positive rapid HIV test later confirmed by Western blot as compared with those patients who were diagnosed after admission by traditional diagnostic methods. This study took place in the context of CDC-funded study of the use of OraQuick (OraSure Technologies, Bethlehem, Pa.) rapid HIV testing in the emergency department at Cook County Hospital in Chicago.
The manufacturer claims the product has a sensitivity of 99.6% and a specificity of 100% as compared with conventional testing. (OraQuick rapid HIV-1 antibody test summary of safety and effectiveness. November 7, 2002. Accessed October 1, 2005, at www.fda.gov/cber/pma/P010047.htm). In the initial study, two of the three emergency department’s treatment pods were equipped to provide HIV screening utilizing the point-of-care technology to consenting patients. Patients in the third pod could be referred to rapid testing based on symptoms or risk factors. All patients who received the rapid test also submitted specimens for conventional EIA and confirmatory Western blot testing. All positive rapid HIV tests were confirmed by Western blot.
In this study, patients who were not known to be infected and were subsequently admitted on non-obstetric or surgical services over 17 months from 2003 to 2004 and confirmed to be HIV positive by Western blot were identified utilizing administrative records. Where possible, charts were reviewed to confirm no prior diagnosis of HIV. Patients who received rapid HIV testing were compared with those who only received conventional testing. Endpoints included time to primary inpatient care service awareness of HIV diagnosis, time to admission or transfer to the inpatient HIV service, time to empiric treatment of diagnosis of opportunistic infection, length of stay, discharge with appropriate prophylactic medications, discharge with patient knowledge of HIV diagnosis, and initial engagement in outpatient care. Length of stay was adjusted by multivariate regression on co-morbid diagnoses (congestive heart failure, end-stage renal disease, cirrhosis, chronic obstructive pulmonary disease, and diabetes), opportunistic infections, ICU admission, need for mechanical ventilation, and CD4 count.
A total of 103 patients were identified with complete chart review completed on 86 of them. All patients except one were admitted through the emergency department. Forty-eight patients were diagnosed initially with the rapid HIV test with 58% of these specifically referred for testing by the emergency department physician, and 55 were diagnosed with conventional testing. Overall, 78% were male, 62% African American, and 20% Hispanic. The two groups were comparable in terms of age, sex, ethnicity, history of substance abuse, HIV risk factors, psychiatric diagnoses, homelessness, CD4 count, presence of opportunistic infections, mechanical ventilation, and co-morbidities. However, conventionally tested patients were more likely to require an ICU stay (31% vs. 10%, P=.01).
Patients in the rapid test group were more quickly documented in the chart as having HIV (.8 vs. 6.4 days, p<.001), placed on an HIV service sooner (1.4 versus 6.9 days, P<.001), initiated outpatient follow-up sooner (21.5 versus 49.5 days, p=.05), and had less unawareness of their HIV status (0 vs. 16%, P=.002). There was no significant difference between the two groups in time from admission to empiric treatment or diagnosis of an opportunistic infection. Patients who received the rapid test did have a lower length of stay (6.4 versus 13.2 days, P<.001). Although much of this difference was due to higher number of ICU stays in the conventional group, in multivariate analysis conventional testing still increased length of stay significantly, OR 5.4 days (2.5, 8.3).
This study suggests that patients who are tested with rapid HIV testing can lead to more efficient inpatient treatment of the complications of HIV, improved patient awareness of HIV status, and quicker outpatient follow-up. These findings have ramifications not just to the inpatient management of patients with HIV but to general public health efforts to reduce the spread of HIV infection.
Nevertheless, these results must be interpreted with caution. They reflect the experience of one institution situated in an area with a high prevalence of HIV. Some degree of selection bias is suggested by the higher presence of ICU admissions in the conventional testing group. The multivariate analysis attempted to control for confounding factors, but the possibility remains that other unrecognized factors may have influenced results. The authors do note that an analysis of patients in the rapid test group stratified by whether the test was performed for screening or by referral of the physician did not demonstrate a statistically significant difference in length of stay. This finding provides further support that the sicker patients which triggered the rapid test had shorter lengths of stay on account of the rapid test and not simply because they were sicker.
As recognized by the authors, physicians in routine practice rely on surrogate markers of HIV infection, most notably a patient’s CD4 count, and thus it is not surprising that the rapid test did not affect time to empiric treatment or diagnosis of opportunistic infection. If treatment did not differ, then explaining the longer length of stay remains an unexplained puzzle. The fact that the two groups were equally matched socially and psychiatrically leaves open the possibility that it was actual knowledge of the HIV test result—and not its effect on treatment—that drove the longer length of stay.
One possibility not suggested by the authors is that definitive knowledge of HIV status helped to mobilize patient discharge. If there were legitimate concerns of follow-up, physicians may have delayed discharge in order to receive HIV test results. Alternatively, some patients may have resisted discharge until receiving test results and the development of a more concrete plan. It would be interesting to know if the time to follow-up for the two groups would be the same if the 16% who did not know their HIV status at discharge were excluded. This suggests that knowledge of HIV status drives follow-up time and would lend some support to the notion that patient discharge was delayed for test results and clarification of the follow-up treatment plan.
Even putting aside the difference in length of stay, the difference of rapid testing on improved knowledge of HIV status and quicker follow-up is likely real and meaningful. Although this study was not designed to assess the impact of this knowledge on patient behavior, immediate knowledge of HIV status during hospitalization may translate to decreased transmission as patients alter their behavior and lends further credibility to the utility of rapid HIV testing in conjunction with conventional methods in the management of inpatients. TH
Community Teaching
Halasyamani L, Valenstein P, Friedlander M. et al. A comparison of two hospitalist models with traditional care in a community teaching hospital. Am J Med. 2005;118:536-543.
Background: A growing body of literature has demonstrated the effects of hospitalists on reducing inpatient length of stay and cost of care, with some literature showing a decreased in-hospital and 30-day mortality. However, most prior studies were conducted in academic medical centers or health maintenance organizations where one group of hospitalists, employed by the institution within which they worked, was compared with traditional primary care physicians. Direct comparisons between different hospitalist models practicing within a single institution have not been published. As a result, the impact of different hospitalist characteristics, including employment status and reimbursement incentives, on inpatient resource utilization and patient care outcomes is unknown.
Methods: Halasyamani and colleagues conducted a retrospective cohort study of 10,595 patients in a tertiary care community-based teaching hospital in which private hospitalists, academic hospitalists, and community physicians all practice. They measured risk-adjusted length of stay, variable costs, 30-day readmission rates, and in-hospital and 30-day mortality for patients treated by each of these three groups, controlling for potentially confounding variables. Community physicians belonged to 21 rounding groups, most of which were private or solo. Two of the community physicians groups were hospital-owned practices reimbursed by a relative value unit system. The private hospitalist group was self-employed with no financial relationship to the hospital and worked an average of 40 weeks per year. Community physicians and private hospitalists worked Monday-Friday and covered weekends or holidays about 25% of the time. Academic hospitalists worked with internal medicine residents and students on a teaching service. They were employed by the hospital using a relative value unit system. They worked an average of 14 weeks per year as an inpatient attending in half-month rotations, which included weekend coverage.
Results: There was a 20% reduction (-0.72 days absolute difference) in length of stay on the academic hospitalist service (P<0.0001) and 8% (-0.28 days absolute difference) on the private hospitalist service (P=0.049) compared with community physicians. Case-mix adjusted relative total costs were 10% less ($173 absolute difference) on the academic (P<0.0001) and 6% less ($109 absolute difference) on the private hospitalist services (P=0.02) compared with community physicians. There were no differences in 30-day readmission, in-hospital and 30-day mortality between the three groups.
Discussion: This study is the first to look at the effects of two separate hospitalist models on resource utilization and patient outcomes within the same institution. Although both the academic and private hospitalist groups demonstrated improved resource utilization as compared with the community physicians, the magnitude of benefit was much greater for the academic hospitalist group.
As the authors point out, one major difference between the two groups was employment status, with the academic hospitalists employed directly by the hospital and the private hospitalists receiving all payment directly from payers. Previous studies have also focused on hospitalists, which were employed by the institution at which they worked, raising the question of whether alignment of employee and employer incentives is an important factor affecting resource utilization outcomes.
Results of this study highlight the need for more studies which seek to clarify specific physician-level, group-level, and organization-level characteristics of hospitalists that result in improved resource utilization and patient care outcomes.
The Last Few Hours
Bailey FA, Burgio KL, Woodby LL, et al. Improving the processes of hospital care during the last hours of life. Arch Int Med. 2005;165(15):1722-1727.
Background: End-of-life care in the acute care inpatient setting is often not initiated until very late in the dying process and may be related to inadequate early recognition of dying patients as well as difficulty transitioning from disease-modifying treatments to palliative measures. Additional barriers exist, including lack of familiarity of hospital staff with initiation and implementation of hospice care. Education about end-of-life care and introduction of a physician-led palliative care team available for consultation within acute care hospitals may help promote better recognition of the dying patient by staff and allow for a “good death.”
Methods: A single hospital within the Veterans Affairs (VA) medical system (Birmingham, Ala., VA Medical Center) was chosen as a pilot center for initiation of a physician-led Inpatient Comfort Care Program (ICCP). The study was framed as a “before-after intervention trial” and analyzed all inpatient deaths identified by the Computerized Patient Recognition System during a six-month period before and substantially after the introduction of the ICCP. A structured chart abstraction tool was used and data was obtained from the last seven days of hospitalization analyzing variables associated with recognition of the dying patient and initiation of palliative care. Education of hospital staff on both hospice care and case identification was initiated during the intervention phase of the study. Additionally, a flexible comfort care order set was introduced.
Results: Two hundred and three veterans were identified (98% men, average age 68) and no significant differences in clinical characteristics were noted between the two groups, pre-intervention and post-intervention. Post-intervention, 59.3% of patients had formal palliative care consultation. Significant findings (P<0.01) following implementation of ICCP were increased documentation of end-of-life symptoms, increased documentation of care plans, increased utilization of opioids (57.1% to 87.2%), increased initiation of do-not-resuscitate orders (61.9% to 85.1%) with a concurrent decrease in cardiopulmonary resuscitation at death (34.4% to 15.4%), and a surprising increase in restraint use (6.0% to 22.6%).
Discussion: Data on hospice care patients indicate that 10% to 30% die in an acute care hospital, identifying a need for increased education and training in palliative medicine. This study demonstrates the positive outcomes of implementation of an inpatient palliative care service both for heightened awareness of identifying the dying patient as well as initiation of end-of-life care. The increased use of opioid medications is an important marker given that many patients experience pain and dyspnea at the end of life. This study is limited by its single site and further validation at other centers implementing similar protocols and assessing similar outcomes is needed. While this intervention had important clinical benefits, additional studies examining the cost implications of this system would be helpful.
Education alone has not been shown to be entirely effective in creating change. This single-site implementation of a palliative care consultation service successfully integrated an education program with on-site consultants. Distributing pocket cards with clinical findings identifying the dying patient aided in recognition of those patients and pre-printed order sets facilitated initiation of end-of-life care. The intervention initiated is possible for many medical centers and promotes an environment allowing for a “good death” for dying patients.
Computers, Doctors, and Errors
Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293(10):1197-1203
For physicians, computerized physician order entry (CPOE) has become an important topic of discussion as many hospitals and health systems embark on the complex and lengthy process of implementing new enterprise clinical systems. Though there are undoubtedly benefits to such systems, practicing clinicians are apt to remain skeptical of the grandiose pictures the more vocal advocates of CPOE may paint. This is not to say that the promises of CPOE are empty; to the contrary, there have been substantial successes, notably in the realm of medication error prevention.
At the same time, CPOE is a mixture of complex technologies that interface in complicated ways with the culture of clinical medicine. The view that medical informatics is a technical problem that has been solved long ago is simplistic and naïve. The article by Koppel, et al, has two important implications: 1) It is critical to look at clinical information systems in the social milieu in which it functions, and 2) there are often unintended consequences that may not beneficial.
This article examines a widely used, commercial CPOE system in use at the University of Pennsylvania (Philadelphia) using both quantitative and qualitative methods. The researchers conducted focus groups and expert interviews in addition to field observations of physicians (house officers and attendings), nurses, and pharmacists in order to identify themes relating to work with the order entry system. This work helped to guide the creation of a survey instrument subsequently used to survey house staff about working conditions and sources of error and stress. There was an 85%-90% response rate that primarily included house staff who ordered more than nine medication orders per month.
Researchers found two broad categories of errors that were fostered in this environment. The first category, which they termed “information errors” were generated by fragmentation of data and the failure to integrate the hospitals various systems both electronic and paper. Examples of this type of error include antibiotic renewal failures. A common way this failure would occur is that renewal reminder stickers would be placed in the patients’ charts, but the house staff would overlook these because medication orders occurred electronically. Another example is assumed dose errors, where house staff would assume that the default dose displayed was the recommended starting dose, when in fact this was the smallest dose unit available. Physicians were assuming decision support was available when it was not.
The second type of error, human-machine interface flaws, occurred when machine rules did not correspond to work behaviors. An example of this is when patients were listed alphabetically rather than by service, making it easy to select the wrong patient. In another instance, many screens (up to 20) were required to view all of a patient’s medications, making it difficult to choose a correct medication for editing.
This study has been criticized by industry advocates for focusing on an older set of technologies or because a number of these issues related to training or “user factors.” At the other extreme, this study has been cited as a cautionary tale about the risks of CPOE. Both types of criticism miss the point. This study demonstrates that CPOE and the social environment in which it sits is a complex entity and that careful design, proper support, and maintenance are critical ingredients to the success of an incredibly complex but vital new component of hospital medicine.
Point-of-Care HIV Testing in Inpatients
Lubelchek R, Kroc K, Hota B, et al. The role of rapid vs conventional human immunodeficiency virus testing for inpatients: effects on quality of care. Arch Intern Med. 2005;165:1956-1960.
Despite advances in treatment, infection with HIV and AIDS remains a public health problem in the United States. According to the CDC the rate of new diagnosis of HIV infection has remained steady from 2000 to 2003 at about 20 per 100,000 people. (Centers for Disease Control and Prevention. Diagnosis of HIV/AIDS–32 states, 2009-2003. MMWR Morb Mortal Wkly Rep. 2004;53:1106-1110). Currently, about 850,000 to 950,000 people are believed to be living with HIV infection, and it is estimated that 180,000 to 280,000 are unaware of their diagnosis. (Fleming P, Byers RH, Sweeney PA, et al., HIV prevalence in the United States, 2000 [Abstract 11]. Presented at the Ninth Conference on Retroviruses and Opportunistic Infections, Seattle; February 24–28, 2002). These patients are not only at risk for disease progression, but can undermine efforts at disease prevention if they continue to engage in unsafe activities. Thus, increasing awareness of HIV status is an important aspect of disease prevention.
HIV testing remains a challenge. Conventional testing with enzyme immunoassay (EIA) and confirmatory Western blot requires patient follow-up for results, which approximately 25% of patients in various outpatient testing sites fail to do. (Centers for Disease Control and Prevention. Update: HIV counseling and testing using rapid tests, United States, 1995. MMWR Morb Mortal Wkly Rep. 1998;47:211-215). Given the difficulties inherent in the transition of care from the inpatient to outpatient setting, conventional testing in the inpatient setting presents additional barriers to appropriate notification. As various point-of-care HIV tests have been developed for commercial use, the possibility of rapid HIV testing presents an opportunity to reduce notification failure and improve patient care. While not replacing traditional testing, the CDC has endorsed rapid HIV testing as a means to initiate therapy and provide counseling with a particular focus on preventing further disease transmission. In this retrospective study, Lubelchek and colleagues present the effects of a rapid HIV test utilized in the emergency department on various inpatient quality of care measures for those patients who received a positive rapid HIV test later confirmed by Western blot as compared with those patients who were diagnosed after admission by traditional diagnostic methods. This study took place in the context of CDC-funded study of the use of OraQuick (OraSure Technologies, Bethlehem, Pa.) rapid HIV testing in the emergency department at Cook County Hospital in Chicago.
The manufacturer claims the product has a sensitivity of 99.6% and a specificity of 100% as compared with conventional testing. (OraQuick rapid HIV-1 antibody test summary of safety and effectiveness. November 7, 2002. Accessed October 1, 2005, at www.fda.gov/cber/pma/P010047.htm). In the initial study, two of the three emergency department’s treatment pods were equipped to provide HIV screening utilizing the point-of-care technology to consenting patients. Patients in the third pod could be referred to rapid testing based on symptoms or risk factors. All patients who received the rapid test also submitted specimens for conventional EIA and confirmatory Western blot testing. All positive rapid HIV tests were confirmed by Western blot.
In this study, patients who were not known to be infected and were subsequently admitted on non-obstetric or surgical services over 17 months from 2003 to 2004 and confirmed to be HIV positive by Western blot were identified utilizing administrative records. Where possible, charts were reviewed to confirm no prior diagnosis of HIV. Patients who received rapid HIV testing were compared with those who only received conventional testing. Endpoints included time to primary inpatient care service awareness of HIV diagnosis, time to admission or transfer to the inpatient HIV service, time to empiric treatment of diagnosis of opportunistic infection, length of stay, discharge with appropriate prophylactic medications, discharge with patient knowledge of HIV diagnosis, and initial engagement in outpatient care. Length of stay was adjusted by multivariate regression on co-morbid diagnoses (congestive heart failure, end-stage renal disease, cirrhosis, chronic obstructive pulmonary disease, and diabetes), opportunistic infections, ICU admission, need for mechanical ventilation, and CD4 count.
A total of 103 patients were identified with complete chart review completed on 86 of them. All patients except one were admitted through the emergency department. Forty-eight patients were diagnosed initially with the rapid HIV test with 58% of these specifically referred for testing by the emergency department physician, and 55 were diagnosed with conventional testing. Overall, 78% were male, 62% African American, and 20% Hispanic. The two groups were comparable in terms of age, sex, ethnicity, history of substance abuse, HIV risk factors, psychiatric diagnoses, homelessness, CD4 count, presence of opportunistic infections, mechanical ventilation, and co-morbidities. However, conventionally tested patients were more likely to require an ICU stay (31% vs. 10%, P=.01).
Patients in the rapid test group were more quickly documented in the chart as having HIV (.8 vs. 6.4 days, p<.001), placed on an HIV service sooner (1.4 versus 6.9 days, P<.001), initiated outpatient follow-up sooner (21.5 versus 49.5 days, p=.05), and had less unawareness of their HIV status (0 vs. 16%, P=.002). There was no significant difference between the two groups in time from admission to empiric treatment or diagnosis of an opportunistic infection. Patients who received the rapid test did have a lower length of stay (6.4 versus 13.2 days, P<.001). Although much of this difference was due to higher number of ICU stays in the conventional group, in multivariate analysis conventional testing still increased length of stay significantly, OR 5.4 days (2.5, 8.3).
This study suggests that patients who are tested with rapid HIV testing can lead to more efficient inpatient treatment of the complications of HIV, improved patient awareness of HIV status, and quicker outpatient follow-up. These findings have ramifications not just to the inpatient management of patients with HIV but to general public health efforts to reduce the spread of HIV infection.
Nevertheless, these results must be interpreted with caution. They reflect the experience of one institution situated in an area with a high prevalence of HIV. Some degree of selection bias is suggested by the higher presence of ICU admissions in the conventional testing group. The multivariate analysis attempted to control for confounding factors, but the possibility remains that other unrecognized factors may have influenced results. The authors do note that an analysis of patients in the rapid test group stratified by whether the test was performed for screening or by referral of the physician did not demonstrate a statistically significant difference in length of stay. This finding provides further support that the sicker patients which triggered the rapid test had shorter lengths of stay on account of the rapid test and not simply because they were sicker.
As recognized by the authors, physicians in routine practice rely on surrogate markers of HIV infection, most notably a patient’s CD4 count, and thus it is not surprising that the rapid test did not affect time to empiric treatment or diagnosis of opportunistic infection. If treatment did not differ, then explaining the longer length of stay remains an unexplained puzzle. The fact that the two groups were equally matched socially and psychiatrically leaves open the possibility that it was actual knowledge of the HIV test result—and not its effect on treatment—that drove the longer length of stay.
One possibility not suggested by the authors is that definitive knowledge of HIV status helped to mobilize patient discharge. If there were legitimate concerns of follow-up, physicians may have delayed discharge in order to receive HIV test results. Alternatively, some patients may have resisted discharge until receiving test results and the development of a more concrete plan. It would be interesting to know if the time to follow-up for the two groups would be the same if the 16% who did not know their HIV status at discharge were excluded. This suggests that knowledge of HIV status drives follow-up time and would lend some support to the notion that patient discharge was delayed for test results and clarification of the follow-up treatment plan.
Even putting aside the difference in length of stay, the difference of rapid testing on improved knowledge of HIV status and quicker follow-up is likely real and meaningful. Although this study was not designed to assess the impact of this knowledge on patient behavior, immediate knowledge of HIV status during hospitalization may translate to decreased transmission as patients alter their behavior and lends further credibility to the utility of rapid HIV testing in conjunction with conventional methods in the management of inpatients. TH
The Constant and Familiar Face
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Nancy Perovic, RN, BSN, quality improvement and innovations coordinator with the hospitalist program at the University of Chicago Medical Center, says this quote from In Our Hands: How Hospital Leaders Can Build a Thriving Workforce is a statement she refers to often in her work and teaching: “Mutual respect between nurses and physicians for each other’s knowledge and competence, coupled with a mutual concern that quality patient care will be provided, are key organizational elements of work environments that attract and retain nurses.”1
In hospitals around the United States, in efforts to improve patient safety and in other initiatives including nurse recruitment and retention, one consistent element is optimizing communication among providers.2-4 Barbara Blakeney, MS, RN, president of the American Nurses Association, interviewed for the publication Web Morbidity and Mortality by its editor, hospitalist Robert Wachter, MD, says that when nurses are not properly supported in the work environment by other staff, and when there are not enough nurses, “it becomes a catch-22—the fewer nurses you have, the more difficult is the working environment, which leads to fewer nurses.”5
Blakeney recommends mutual training for physicians and nurses to improve patient care and safety focus on a number of key areas:
- Understanding and appreciating each other’s skill sets and knowledge base;
- Properly handing off patients and information; and
- Nurturing “a culture in which safety is considered a problem-solving situation and not a punishment situation.”6
“Nurses comprise the surveillance system in hospitals for errors and adverse occurrences,” emphasizes Blakeney, and “the effectiveness of nurse surveillance is influenced by factors that include the quality of the work environment.”5
As essential members of hospital teams, hospitalists play a big role in nurses’ work environments, and mutual support between hospitalists and nurses affects patient care and outcomes, and physician and nurse job satisfaction.6,7 In general, nurses give hospitalists high marks for communication, nurse support, and teamwork.
“From a communication perspective, working with hospitalists makes patient care a lot safer because you don’t have to think of everything that you need to tell attending physicians when they are making their daily rounds,” says Scarlett Blue, RNC, MSN, administrative director, Hospitalist Services for FirstHealth of the Carolinas, Pinehurst, N.C. “With hospitalists you know you can do real-time communication, real-time information. That’s not saying you can’t do that with other physicians who are not in the hospital, but it certainly does make it a lot easier when they’re right here.”
Make Contact
One way that hospitalists support their nurse colleagues is by their ready availability to answer questions about patient care. Julie Koppel, RN, BSN, patient care manager on the General Medicine floor at the University of California at San Francisco Medical Center, has worked exclusively with the hospitalist model in her five years of nursing. She is complimentary about hospitalists’ communication skills and refers to them as “the constant and familiar face.” Koppel relates an instance where the attending hospitalist was already off service and yet she still paged him. “He got back to me promptly and still addressed the issues even though he wasn’t on service anymore and it was about something that had happened a month ago. I still feel hospitalists are available when they’re not even here.”
Many nurses don’t have a second thought about calling a hospitalist about a patient care issue, but may still be afraid of “bothering” the hospitalist when he or she is busy. Blue says her colleagues have worked with their nursing staff to overcome that reluctance. “Call them because if they’re talking with a family or if they’re in the middle of a physical exam or if it’s something where they can’t talk, they’re going to put the hold button on,” she tells her staff. “So when you hear the Muzak, the elevator music, then you know that you need to call them back. And it’s worked.”
It’s especially important, Blue says, that nurses surmount any reluctance they feel to initiate a call so that they will do so easily in urgent situations such as alerting rapid response teams and reporting medical errors.4 Blue believes the following anecdote illustrates the perspective of most hospitalists about this issue.
“We just started rapid response teams here,” she says, “And I heard one of the hospitalists say, ‘We’ve had five rapid response team calls so far and we were looking at whether or not the calls met the criteria and were appropriate.’ And one of the other hospitalists said, ‘You know, this really wasn’t a rapid response team call, but I want the nurses to feel free to call and I think that when we’re first starting out, we just want them to call. And then we can work on fine tuning it later. I don’t want to stifle them so they feel they cannot call.”

—Mark Williams, MD
Clear and to the Point
What are the best means to improve communication between hospitalists and nurses? Three major areas for attention include developing relationships, defining communication strategies, and packaging information for clarity.7
Blue often advises nurses to speak with clarity. “Probably the best thing from a hospitalist’s perspective is to be real clear about what you are asking or what it is that you need,” she says. “The clearer that you can be in your requests, the better off you’re going to be in the long run.”
But, Blue says “hospitalists have to understand that one of the greatest benefits from a nurse’s perspective about the hospitalist program is access, immediate access, and dealing with a nurse who does not communicate well might sometimes come along with it.”
The mismatched communication styles of most physicians and nurses are well recognized by a committee at the University of Chicago in which Nancy Perovic is involved. Vineet Arora, MD, MA, a hospitalist and associate program director for the Internal Medicine Residency Program at the University of Chicago, is one of the three hospitalist members on a committee working to improve nurse-physician communication.
“We know that nurses and physicians communicate differently,” says Dr. Arora. “Physicians communicate in more of a task-oriented way and nurses are trained to communicate in a descriptive way. And that’s part of the problem, because nurses might report that physicians don’t respond to them when they need to be responded to; they might not prioritize a patient that the nurse believes is very sick. And a physician might say, ‘I didn’t know that patient was really sick’ because he was given a description such as, ‘They’re not doing OK.’”
Also, Dr. Arora says, “part of the problem that nurses and physicians may have in communicating with each other can be traced to a difference in how they were trained. Physicians are trained to interact with other physicians and nurses are trained by other nurses.”
The committee at Chicago has adopted what is referred to as the Situation-Background-Assessment-Recommendation (SBAR) technique, a tool that the U.S. Navy has used to improve communication on aircraft carriers.8 Developed by Michael Leonard, MD, physician coordinator of clinical informatics, and others at Kaiser Permanente of Colorado, the SBAR technique has been implemented widely at health systems to provide a standard framework for members of the healthcare team when communicating about a patient’s condition.
“What nurses are not very good at is being assertive,” says Perovic. “We’re getting better as we’re getting more modern, but sometimes nurses talk in a more holistic, narrative fashion and doctors just want: what’s the problem, pinpoint it, let me know what it is.”
Chicago’s Perovic and her colleagues plan to educate nurses to use the SBAR technique so they can “talk in the way that doctors are trained to accept information and respond,” she says. “For example, this might sound like, ‘This is this patient with this diagnosis and these vital signs; this is what’s happening: they’re going down, their blood pressure’s dropped, I’m really concerned, this is a different change, I suggest that we do this and that, and I need you here in 10 minutes.’”
Perovic says nurses are then instructed to “make a recommendation; so the hospitalist can prioritize from all the other patients he has to see, to answer the questions: What does this patient need right now? When do I need to see this patient? and What can the nurse do until I get there?”
Literature on the SBAR technique and the tool itself are available online at www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/Tools/SBARTechniqueforCommunicationASituationalBriefingModel.htm.8
Heedful Versus Heedless Interrelating
Exactly how hospitalists affect outcomes and influence system issues is being addressed in research led by Mark V. Williams, MD, and Tracy Scott, PhD, at Emory University Medical Center, Atlanta. Dr. Williams, who is the director of the medicine unit at Emory Hospital, the editor-in-chief of the Journal of Hospital Medicine, and a past president of SHM, spoke to The Hospitalist about the exploratory research his team is doing to assess the impact hospitalists have in nurse-physician relationships in two hospitals in Atlanta, and to particularly examine how these relationships affect patient safety.
High Reliability Organization theory, which elucidates causal pathways between work relationships and reduced error, may provide a framework for how hospitalists affect hospital functioning. “Heedful interrelating,” the theory postulates, creates an organization “mind” and through facilitating teamwork is more alert to and capable of dealing with unexpected occurrences. In fact, says Dr. Williams, data from operating rooms, emergency departments, and ICUs suggest that a lack of teamwork adversely affects patient care and increases medical errors. Research along this vein has been absent on general medical floors.
The research design explores the degree of “heedful interrelating” as opposed to “heedless interrelating” between physicians and nurses and whether hospitalists have different relationships with nurses than do other physicians.
“In heedful interrelating,” explains Dr. Williams, “the physician heeds what the nurse is saying and doing and, likewise, the nurse heeds what the physician is saying and doing.” To date, the investigators have interviewed 45 nurses (half in a university hospital setting and half in a community hospital) and 24 physicians of whom half are hospitalists.
The study examines multiple components, but an example is that “heedful interrelating is based on true mutual respect, which is almost more important over agreement,” says Dr. Williams. “And in heedless interrelating, only one view of the situation is considered correct. It represents your classic arrogant physician.”
Another example of heedful interrelating is that “it advances the goals of the whole team; in heedless interrelating, you think only of your own role,” he says. Nurses in the study reported that compared with other physicians hospitalists are more accessible, more approachable, and more appreciative of the value of the nurse’s role.
The investigators conclude that hospitalists improve the nurse-physician relationship through heedful interrelating and thereby may improve patient safety. In addition, “the nurses emphasized the need for more collaboration and perceived that physicians were not proactive in asking them about their knowledge of the patient, and lacked a holistic view of the patient’s needs. Most importantly, about half the nurses mentioned specific instances where problems in their communication with physicians led directly to problems in patient care.
Dr. Williams believes that the ideal system for communication between hospitalists and nurses would include a means for them to do their patient rounds together. Nurses want hospitalists to develop a system to deliver the patient care plans quickly and reliably, include them in formal and informal educational efforts, and acknowledge them.
Timely Distribution of Care Plans
Blue says that hospitalists at her institution, FirstHealth Moore Regional Hospital (Pinehurst, N.C.), a 385-bed acute care, nonprofit hospital that serves as the referral center for a 15-county region in the mid-Carolinas, work often and closely with the nurses on issues of outcomes. “And outcomes here are like discharge planning utilization review,” she says. “We have a report every morning and there’s a representative from that department who’s online sending out the plans for the patients for the day to the other outcomes managers. That’s already in the works, and we’re not waiting for the hospitalist to get up to the floor to see the patient.”
Overall, however, nurses in other (e.g., larger) settings may not have as good a system in place to distribute care plans. Perovic says that in focus groups she facilitates, she often hears frustration from nurses because “doctors in general—although hospitalists are better at it—do not give nurses the plan of the day or the plan of care in a timely, organized fashion so they can do their care appropriately and prepare themselves and the patient.”
Some of the problem is due to the systems of an academic medical center, Perovic says, where “doctors make rounds at various times of the day and sometimes one team can make four rounds a day. What happens is that the plan for patient care changes each time new rounds are completed because you either get new information or discover you didn’t do something.” But although the team doctors are good at communicating plan modifications among themselves, she says, “what they fail to do is always communicate that well to the nurses.”
Perovic says there is an ideal and then a real solution. “Ideally, it would be great if patient rounds were at a certain time of the day every day so that the nurse can pass her meds and then be available for rounding,” she says. “You could say to nurses, ‘Rounds are between 10 and 11; take care of your patients’ needs and then be on call and ready to go to your rounds when possible.’ Or another solution is what we do in the pediatric hospital: We have a charge nurse who has no patients and she is able to round with all the teams and all the doctors and then give the individual nurse that plan for her patients.”
Hiring a charge nurse in this vein is a human resource issue, Perovic says, and an individual hospital has to decide that it wants to pay a nurse to not have patients. In that case, she says, it is an expensive but good fix. However, accommodating nurses to accompany hospitalists on rounds is logistically almost impossible. “Because if a nurse on the general medicine ward has five patients,” Perovic says, “she might have five different teams of doctors. But depending on the diagnosis of each patient, it won’t be the same team of doctors rounding on them. She might not catch A, B, and C at the same time that D and E are making their rounds. And she could be doing a blood draw on patient D when D team comes, or giving a bath to patient A when team E comes.”
Perovic and her coworkers have tried the call light method, where the doctor comes into the room, the attending presses the call light, and the nurse knows rounds are happening and to join them at that room. But that, as well as other avenues they tried, failed because neither the nurse nor the team can necessarily count on their times of availability coinciding. Still, Dr. Arora says, “we learned a lot about trying to work together and how to understand each other. And we used some of that information to continue thinking about how to best improve physician-nurse communication.”
The team at Chicago is now considering how to design and evaluate “an intervention for more of an interdisciplinary educational process where physicians and nurses would be trained on how to communicate with each other using this standard language,” says Dr. Arora. “Nurses would understand that they could potentially use the SBAR tool to communicate with physicians, and physicians would understand that the nurses need to be included in the plan for the day and would make time to incorporate nurse suggestions and input for the plan.”
Acknowledgment
In some hospital settings what has been described as a two-class system can exist for providers.9 A culture that encourages patient safety is threatened by the nature of the hierarchy or the segregation that is established, even subtly, where nurses are treated as unequals.6,9 In the hospital culture, the “invisibility of nursing” has historically been perpetuated by a number of factors, not the least of which are differences in gender and income.6 In this atmosphere, nurses are not as likely to share from their skills and knowledge. Their lack of assertiveness with hospitalists or other physicians may take its toll in many ways, including increased risks to patient outcomes and to provider morale and satisfaction.7
Linda Aiken, PhD, FAAN, FRCN, RN, the Claire M. Fagin Leadership Professor of Nursing and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania (Philadelphia), has extensively investigated the dynamics between nurses and their co-workers. “Nurse-physician relationships are one of the most important drivers of the work environment,”9 she writes. There are also data that demonstrate the association of nurse-doctor relationships on cost, lower morbidity and mortality, retention of nurses, higher quality of care, and improved hospital reimbursement and/or market share.9
In other words, “healthy nurse-physician relationships are not just a nice thing to have,” writes Dr. Aiken. “They are a competitive advantage.”
Given the association of these relationships to so many outcomes, it is unfortunate that many nurses crave greater acknowledgment for what they bring to their work. One benefit for nursing is that because hospitalists are around the hospital more than an average attending, they know the nurses better.
“As a nurse, what I need from hospitalists is for them to recognize and teach their residents and interns that the nurse is a constant player at the bedside in the hospital, with many more years of experience,” says Perovic. “Even though she doesn’t have as much medical training as a doctor or resident, she has enough clinical-nursing hospital experience. Doctors need to appreciate that nurses are experts at hospital care and bedside care, and [doctors] need to show that respect when we’re teaching our residents because we can learn a lot from the nurses, and the nurses can actually make the doctors’ lives easier.”
In a study of a multidisciplinary intervention tested on an acute inpatient medical unit, the effect of the intervention—to improve communication and collaboration—was strongest among house staff, who reported significant increases in collaborative efforts with nurses.10 This finding underlines the importance for hospitalists to serve as models to students, interns, and residents because the most effective time to learn collaborative practice is during early training when experienced nurses can assist inexperienced interns.10 Hospitalists can also consciously reject the traditional “doctor-nurse game,” whereby patterns of behavior suggest that doctors are the dominant players and nurses must defer to them.
“Ask nurses for their opinion,” advises Blue. “Treat them like an equal, which is another one of the beauties of this program, because hospitalists certainly do that. When it comes down to it, people want to be appreciated, respected, and acknowledged for their contribution.”
Blue and her team also encourage hospitalists to share with the nurses if they happen to hear news of their patients’ progress. “If we have follow-up on somebody from the primary care provider after that patient has left the hospital, for example, we try to share that with the nursing staff because they’re our patients. They’re not just my patients and they’re not your patients; they’re our patients.”
Conclusion
The quality of the nurse-hospitalist relationship is central to patient care. The methods, means, and styles of individual and team communication all influence the effectiveness of a hospital team. Retraining providers to traverse the gap of different communication styles is a way to approach the issues that exist. Mutual training for physicians and nurses, as well as training nurses to communicate in ways that more approximate how physicians communicate, will better serve patient and provider needs.
Hospitalists can encourage nurses to overcome hesitancies to initiate calls, clarify their preferences for how nurses should contact them, and work with nurses to seek workable ways to perform patient rounds in concert. Most of all, nurses need timely care plan distribution and acknowledgment for their contributions to teamwork and patient care. TH
Writer Andrea Sattinger will write about occupational therapists’ experiences with hospitalists in the January issue.
References
- ANA Commission on Workforce for Hospitals and Health Systems. In our hands: how hospital leaders can build a thriving workforce. American Hospital Association; Chicago; 2002;55:30-31.
- Aiken LH. The unfinished patient safety agenda. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web: Agency for Healthcare Research and Quality; 2005. Accessed August. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=7&searchStr=The+unfinished+patient+safety+agenda
- Aiken LH, Clarke SP, Sloane DM. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002;14:5-13.
- Friesen MA, Farquhar MB, Hughes R. The nurse’s role in promoting a culture of safety: American Nurses Association Continuing Education, Center for American Nurses; 2005.
- Wachter R. In conversation with … Barbara A. Blakeney, MS, RN. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web. Agency for Healthcare Research and Quality; 2005. Accessed Aug. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=8&searchStr=Blakeney
- Lindeke LL, Sieckert AM. Nurse-physician workplace collaboration. Online J Issues Nurs. 2005;10:5.
- Burke M, Boal J, Mitchell R. Communicating for better care: improving nurse-physician communication. Am J Nurs. 2004;104:40-47
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12:40-41.
- Smith AP. Partners at the bedside: the importance of nurse-physician relationships. Nurs Econ. 2004;22:161-164.
- Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71-77.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Nancy Perovic, RN, BSN, quality improvement and innovations coordinator with the hospitalist program at the University of Chicago Medical Center, says this quote from In Our Hands: How Hospital Leaders Can Build a Thriving Workforce is a statement she refers to often in her work and teaching: “Mutual respect between nurses and physicians for each other’s knowledge and competence, coupled with a mutual concern that quality patient care will be provided, are key organizational elements of work environments that attract and retain nurses.”1
In hospitals around the United States, in efforts to improve patient safety and in other initiatives including nurse recruitment and retention, one consistent element is optimizing communication among providers.2-4 Barbara Blakeney, MS, RN, president of the American Nurses Association, interviewed for the publication Web Morbidity and Mortality by its editor, hospitalist Robert Wachter, MD, says that when nurses are not properly supported in the work environment by other staff, and when there are not enough nurses, “it becomes a catch-22—the fewer nurses you have, the more difficult is the working environment, which leads to fewer nurses.”5
Blakeney recommends mutual training for physicians and nurses to improve patient care and safety focus on a number of key areas:
- Understanding and appreciating each other’s skill sets and knowledge base;
- Properly handing off patients and information; and
- Nurturing “a culture in which safety is considered a problem-solving situation and not a punishment situation.”6
“Nurses comprise the surveillance system in hospitals for errors and adverse occurrences,” emphasizes Blakeney, and “the effectiveness of nurse surveillance is influenced by factors that include the quality of the work environment.”5
As essential members of hospital teams, hospitalists play a big role in nurses’ work environments, and mutual support between hospitalists and nurses affects patient care and outcomes, and physician and nurse job satisfaction.6,7 In general, nurses give hospitalists high marks for communication, nurse support, and teamwork.
“From a communication perspective, working with hospitalists makes patient care a lot safer because you don’t have to think of everything that you need to tell attending physicians when they are making their daily rounds,” says Scarlett Blue, RNC, MSN, administrative director, Hospitalist Services for FirstHealth of the Carolinas, Pinehurst, N.C. “With hospitalists you know you can do real-time communication, real-time information. That’s not saying you can’t do that with other physicians who are not in the hospital, but it certainly does make it a lot easier when they’re right here.”
Make Contact
One way that hospitalists support their nurse colleagues is by their ready availability to answer questions about patient care. Julie Koppel, RN, BSN, patient care manager on the General Medicine floor at the University of California at San Francisco Medical Center, has worked exclusively with the hospitalist model in her five years of nursing. She is complimentary about hospitalists’ communication skills and refers to them as “the constant and familiar face.” Koppel relates an instance where the attending hospitalist was already off service and yet she still paged him. “He got back to me promptly and still addressed the issues even though he wasn’t on service anymore and it was about something that had happened a month ago. I still feel hospitalists are available when they’re not even here.”
Many nurses don’t have a second thought about calling a hospitalist about a patient care issue, but may still be afraid of “bothering” the hospitalist when he or she is busy. Blue says her colleagues have worked with their nursing staff to overcome that reluctance. “Call them because if they’re talking with a family or if they’re in the middle of a physical exam or if it’s something where they can’t talk, they’re going to put the hold button on,” she tells her staff. “So when you hear the Muzak, the elevator music, then you know that you need to call them back. And it’s worked.”
It’s especially important, Blue says, that nurses surmount any reluctance they feel to initiate a call so that they will do so easily in urgent situations such as alerting rapid response teams and reporting medical errors.4 Blue believes the following anecdote illustrates the perspective of most hospitalists about this issue.
“We just started rapid response teams here,” she says, “And I heard one of the hospitalists say, ‘We’ve had five rapid response team calls so far and we were looking at whether or not the calls met the criteria and were appropriate.’ And one of the other hospitalists said, ‘You know, this really wasn’t a rapid response team call, but I want the nurses to feel free to call and I think that when we’re first starting out, we just want them to call. And then we can work on fine tuning it later. I don’t want to stifle them so they feel they cannot call.”
—Mark Williams, MD
Clear and to the Point
What are the best means to improve communication between hospitalists and nurses? Three major areas for attention include developing relationships, defining communication strategies, and packaging information for clarity.7
Blue often advises nurses to speak with clarity. “Probably the best thing from a hospitalist’s perspective is to be real clear about what you are asking or what it is that you need,” she says. “The clearer that you can be in your requests, the better off you’re going to be in the long run.”
But, Blue says “hospitalists have to understand that one of the greatest benefits from a nurse’s perspective about the hospitalist program is access, immediate access, and dealing with a nurse who does not communicate well might sometimes come along with it.”
The mismatched communication styles of most physicians and nurses are well recognized by a committee at the University of Chicago in which Nancy Perovic is involved. Vineet Arora, MD, MA, a hospitalist and associate program director for the Internal Medicine Residency Program at the University of Chicago, is one of the three hospitalist members on a committee working to improve nurse-physician communication.
“We know that nurses and physicians communicate differently,” says Dr. Arora. “Physicians communicate in more of a task-oriented way and nurses are trained to communicate in a descriptive way. And that’s part of the problem, because nurses might report that physicians don’t respond to them when they need to be responded to; they might not prioritize a patient that the nurse believes is very sick. And a physician might say, ‘I didn’t know that patient was really sick’ because he was given a description such as, ‘They’re not doing OK.’”
Also, Dr. Arora says, “part of the problem that nurses and physicians may have in communicating with each other can be traced to a difference in how they were trained. Physicians are trained to interact with other physicians and nurses are trained by other nurses.”
The committee at Chicago has adopted what is referred to as the Situation-Background-Assessment-Recommendation (SBAR) technique, a tool that the U.S. Navy has used to improve communication on aircraft carriers.8 Developed by Michael Leonard, MD, physician coordinator of clinical informatics, and others at Kaiser Permanente of Colorado, the SBAR technique has been implemented widely at health systems to provide a standard framework for members of the healthcare team when communicating about a patient’s condition.
“What nurses are not very good at is being assertive,” says Perovic. “We’re getting better as we’re getting more modern, but sometimes nurses talk in a more holistic, narrative fashion and doctors just want: what’s the problem, pinpoint it, let me know what it is.”
Chicago’s Perovic and her colleagues plan to educate nurses to use the SBAR technique so they can “talk in the way that doctors are trained to accept information and respond,” she says. “For example, this might sound like, ‘This is this patient with this diagnosis and these vital signs; this is what’s happening: they’re going down, their blood pressure’s dropped, I’m really concerned, this is a different change, I suggest that we do this and that, and I need you here in 10 minutes.’”
Perovic says nurses are then instructed to “make a recommendation; so the hospitalist can prioritize from all the other patients he has to see, to answer the questions: What does this patient need right now? When do I need to see this patient? and What can the nurse do until I get there?”
Literature on the SBAR technique and the tool itself are available online at www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/Tools/SBARTechniqueforCommunicationASituationalBriefingModel.htm.8
Heedful Versus Heedless Interrelating
Exactly how hospitalists affect outcomes and influence system issues is being addressed in research led by Mark V. Williams, MD, and Tracy Scott, PhD, at Emory University Medical Center, Atlanta. Dr. Williams, who is the director of the medicine unit at Emory Hospital, the editor-in-chief of the Journal of Hospital Medicine, and a past president of SHM, spoke to The Hospitalist about the exploratory research his team is doing to assess the impact hospitalists have in nurse-physician relationships in two hospitals in Atlanta, and to particularly examine how these relationships affect patient safety.
High Reliability Organization theory, which elucidates causal pathways between work relationships and reduced error, may provide a framework for how hospitalists affect hospital functioning. “Heedful interrelating,” the theory postulates, creates an organization “mind” and through facilitating teamwork is more alert to and capable of dealing with unexpected occurrences. In fact, says Dr. Williams, data from operating rooms, emergency departments, and ICUs suggest that a lack of teamwork adversely affects patient care and increases medical errors. Research along this vein has been absent on general medical floors.
The research design explores the degree of “heedful interrelating” as opposed to “heedless interrelating” between physicians and nurses and whether hospitalists have different relationships with nurses than do other physicians.
“In heedful interrelating,” explains Dr. Williams, “the physician heeds what the nurse is saying and doing and, likewise, the nurse heeds what the physician is saying and doing.” To date, the investigators have interviewed 45 nurses (half in a university hospital setting and half in a community hospital) and 24 physicians of whom half are hospitalists.
The study examines multiple components, but an example is that “heedful interrelating is based on true mutual respect, which is almost more important over agreement,” says Dr. Williams. “And in heedless interrelating, only one view of the situation is considered correct. It represents your classic arrogant physician.”
Another example of heedful interrelating is that “it advances the goals of the whole team; in heedless interrelating, you think only of your own role,” he says. Nurses in the study reported that compared with other physicians hospitalists are more accessible, more approachable, and more appreciative of the value of the nurse’s role.
The investigators conclude that hospitalists improve the nurse-physician relationship through heedful interrelating and thereby may improve patient safety. In addition, “the nurses emphasized the need for more collaboration and perceived that physicians were not proactive in asking them about their knowledge of the patient, and lacked a holistic view of the patient’s needs. Most importantly, about half the nurses mentioned specific instances where problems in their communication with physicians led directly to problems in patient care.
Dr. Williams believes that the ideal system for communication between hospitalists and nurses would include a means for them to do their patient rounds together. Nurses want hospitalists to develop a system to deliver the patient care plans quickly and reliably, include them in formal and informal educational efforts, and acknowledge them.
Timely Distribution of Care Plans
Blue says that hospitalists at her institution, FirstHealth Moore Regional Hospital (Pinehurst, N.C.), a 385-bed acute care, nonprofit hospital that serves as the referral center for a 15-county region in the mid-Carolinas, work often and closely with the nurses on issues of outcomes. “And outcomes here are like discharge planning utilization review,” she says. “We have a report every morning and there’s a representative from that department who’s online sending out the plans for the patients for the day to the other outcomes managers. That’s already in the works, and we’re not waiting for the hospitalist to get up to the floor to see the patient.”
Overall, however, nurses in other (e.g., larger) settings may not have as good a system in place to distribute care plans. Perovic says that in focus groups she facilitates, she often hears frustration from nurses because “doctors in general—although hospitalists are better at it—do not give nurses the plan of the day or the plan of care in a timely, organized fashion so they can do their care appropriately and prepare themselves and the patient.”
Some of the problem is due to the systems of an academic medical center, Perovic says, where “doctors make rounds at various times of the day and sometimes one team can make four rounds a day. What happens is that the plan for patient care changes each time new rounds are completed because you either get new information or discover you didn’t do something.” But although the team doctors are good at communicating plan modifications among themselves, she says, “what they fail to do is always communicate that well to the nurses.”
Perovic says there is an ideal and then a real solution. “Ideally, it would be great if patient rounds were at a certain time of the day every day so that the nurse can pass her meds and then be available for rounding,” she says. “You could say to nurses, ‘Rounds are between 10 and 11; take care of your patients’ needs and then be on call and ready to go to your rounds when possible.’ Or another solution is what we do in the pediatric hospital: We have a charge nurse who has no patients and she is able to round with all the teams and all the doctors and then give the individual nurse that plan for her patients.”
Hiring a charge nurse in this vein is a human resource issue, Perovic says, and an individual hospital has to decide that it wants to pay a nurse to not have patients. In that case, she says, it is an expensive but good fix. However, accommodating nurses to accompany hospitalists on rounds is logistically almost impossible. “Because if a nurse on the general medicine ward has five patients,” Perovic says, “she might have five different teams of doctors. But depending on the diagnosis of each patient, it won’t be the same team of doctors rounding on them. She might not catch A, B, and C at the same time that D and E are making their rounds. And she could be doing a blood draw on patient D when D team comes, or giving a bath to patient A when team E comes.”
Perovic and her coworkers have tried the call light method, where the doctor comes into the room, the attending presses the call light, and the nurse knows rounds are happening and to join them at that room. But that, as well as other avenues they tried, failed because neither the nurse nor the team can necessarily count on their times of availability coinciding. Still, Dr. Arora says, “we learned a lot about trying to work together and how to understand each other. And we used some of that information to continue thinking about how to best improve physician-nurse communication.”
The team at Chicago is now considering how to design and evaluate “an intervention for more of an interdisciplinary educational process where physicians and nurses would be trained on how to communicate with each other using this standard language,” says Dr. Arora. “Nurses would understand that they could potentially use the SBAR tool to communicate with physicians, and physicians would understand that the nurses need to be included in the plan for the day and would make time to incorporate nurse suggestions and input for the plan.”
Acknowledgment
In some hospital settings what has been described as a two-class system can exist for providers.9 A culture that encourages patient safety is threatened by the nature of the hierarchy or the segregation that is established, even subtly, where nurses are treated as unequals.6,9 In the hospital culture, the “invisibility of nursing” has historically been perpetuated by a number of factors, not the least of which are differences in gender and income.6 In this atmosphere, nurses are not as likely to share from their skills and knowledge. Their lack of assertiveness with hospitalists or other physicians may take its toll in many ways, including increased risks to patient outcomes and to provider morale and satisfaction.7
Linda Aiken, PhD, FAAN, FRCN, RN, the Claire M. Fagin Leadership Professor of Nursing and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania (Philadelphia), has extensively investigated the dynamics between nurses and their co-workers. “Nurse-physician relationships are one of the most important drivers of the work environment,”9 she writes. There are also data that demonstrate the association of nurse-doctor relationships on cost, lower morbidity and mortality, retention of nurses, higher quality of care, and improved hospital reimbursement and/or market share.9
In other words, “healthy nurse-physician relationships are not just a nice thing to have,” writes Dr. Aiken. “They are a competitive advantage.”
Given the association of these relationships to so many outcomes, it is unfortunate that many nurses crave greater acknowledgment for what they bring to their work. One benefit for nursing is that because hospitalists are around the hospital more than an average attending, they know the nurses better.
“As a nurse, what I need from hospitalists is for them to recognize and teach their residents and interns that the nurse is a constant player at the bedside in the hospital, with many more years of experience,” says Perovic. “Even though she doesn’t have as much medical training as a doctor or resident, she has enough clinical-nursing hospital experience. Doctors need to appreciate that nurses are experts at hospital care and bedside care, and [doctors] need to show that respect when we’re teaching our residents because we can learn a lot from the nurses, and the nurses can actually make the doctors’ lives easier.”
In a study of a multidisciplinary intervention tested on an acute inpatient medical unit, the effect of the intervention—to improve communication and collaboration—was strongest among house staff, who reported significant increases in collaborative efforts with nurses.10 This finding underlines the importance for hospitalists to serve as models to students, interns, and residents because the most effective time to learn collaborative practice is during early training when experienced nurses can assist inexperienced interns.10 Hospitalists can also consciously reject the traditional “doctor-nurse game,” whereby patterns of behavior suggest that doctors are the dominant players and nurses must defer to them.
“Ask nurses for their opinion,” advises Blue. “Treat them like an equal, which is another one of the beauties of this program, because hospitalists certainly do that. When it comes down to it, people want to be appreciated, respected, and acknowledged for their contribution.”
Blue and her team also encourage hospitalists to share with the nurses if they happen to hear news of their patients’ progress. “If we have follow-up on somebody from the primary care provider after that patient has left the hospital, for example, we try to share that with the nursing staff because they’re our patients. They’re not just my patients and they’re not your patients; they’re our patients.”
Conclusion
The quality of the nurse-hospitalist relationship is central to patient care. The methods, means, and styles of individual and team communication all influence the effectiveness of a hospital team. Retraining providers to traverse the gap of different communication styles is a way to approach the issues that exist. Mutual training for physicians and nurses, as well as training nurses to communicate in ways that more approximate how physicians communicate, will better serve patient and provider needs.
Hospitalists can encourage nurses to overcome hesitancies to initiate calls, clarify their preferences for how nurses should contact them, and work with nurses to seek workable ways to perform patient rounds in concert. Most of all, nurses need timely care plan distribution and acknowledgment for their contributions to teamwork and patient care. TH
Writer Andrea Sattinger will write about occupational therapists’ experiences with hospitalists in the January issue.
References
- ANA Commission on Workforce for Hospitals and Health Systems. In our hands: how hospital leaders can build a thriving workforce. American Hospital Association; Chicago; 2002;55:30-31.
- Aiken LH. The unfinished patient safety agenda. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web: Agency for Healthcare Research and Quality; 2005. Accessed August. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=7&searchStr=The+unfinished+patient+safety+agenda
- Aiken LH, Clarke SP, Sloane DM. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002;14:5-13.
- Friesen MA, Farquhar MB, Hughes R. The nurse’s role in promoting a culture of safety: American Nurses Association Continuing Education, Center for American Nurses; 2005.
- Wachter R. In conversation with … Barbara A. Blakeney, MS, RN. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web. Agency for Healthcare Research and Quality; 2005. Accessed Aug. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=8&searchStr=Blakeney
- Lindeke LL, Sieckert AM. Nurse-physician workplace collaboration. Online J Issues Nurs. 2005;10:5.
- Burke M, Boal J, Mitchell R. Communicating for better care: improving nurse-physician communication. Am J Nurs. 2004;104:40-47
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12:40-41.
- Smith AP. Partners at the bedside: the importance of nurse-physician relationships. Nurs Econ. 2004;22:161-164.
- Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71-77.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Nancy Perovic, RN, BSN, quality improvement and innovations coordinator with the hospitalist program at the University of Chicago Medical Center, says this quote from In Our Hands: How Hospital Leaders Can Build a Thriving Workforce is a statement she refers to often in her work and teaching: “Mutual respect between nurses and physicians for each other’s knowledge and competence, coupled with a mutual concern that quality patient care will be provided, are key organizational elements of work environments that attract and retain nurses.”1
In hospitals around the United States, in efforts to improve patient safety and in other initiatives including nurse recruitment and retention, one consistent element is optimizing communication among providers.2-4 Barbara Blakeney, MS, RN, president of the American Nurses Association, interviewed for the publication Web Morbidity and Mortality by its editor, hospitalist Robert Wachter, MD, says that when nurses are not properly supported in the work environment by other staff, and when there are not enough nurses, “it becomes a catch-22—the fewer nurses you have, the more difficult is the working environment, which leads to fewer nurses.”5
Blakeney recommends mutual training for physicians and nurses to improve patient care and safety focus on a number of key areas:
- Understanding and appreciating each other’s skill sets and knowledge base;
- Properly handing off patients and information; and
- Nurturing “a culture in which safety is considered a problem-solving situation and not a punishment situation.”6
“Nurses comprise the surveillance system in hospitals for errors and adverse occurrences,” emphasizes Blakeney, and “the effectiveness of nurse surveillance is influenced by factors that include the quality of the work environment.”5
As essential members of hospital teams, hospitalists play a big role in nurses’ work environments, and mutual support between hospitalists and nurses affects patient care and outcomes, and physician and nurse job satisfaction.6,7 In general, nurses give hospitalists high marks for communication, nurse support, and teamwork.
“From a communication perspective, working with hospitalists makes patient care a lot safer because you don’t have to think of everything that you need to tell attending physicians when they are making their daily rounds,” says Scarlett Blue, RNC, MSN, administrative director, Hospitalist Services for FirstHealth of the Carolinas, Pinehurst, N.C. “With hospitalists you know you can do real-time communication, real-time information. That’s not saying you can’t do that with other physicians who are not in the hospital, but it certainly does make it a lot easier when they’re right here.”
Make Contact
One way that hospitalists support their nurse colleagues is by their ready availability to answer questions about patient care. Julie Koppel, RN, BSN, patient care manager on the General Medicine floor at the University of California at San Francisco Medical Center, has worked exclusively with the hospitalist model in her five years of nursing. She is complimentary about hospitalists’ communication skills and refers to them as “the constant and familiar face.” Koppel relates an instance where the attending hospitalist was already off service and yet she still paged him. “He got back to me promptly and still addressed the issues even though he wasn’t on service anymore and it was about something that had happened a month ago. I still feel hospitalists are available when they’re not even here.”
Many nurses don’t have a second thought about calling a hospitalist about a patient care issue, but may still be afraid of “bothering” the hospitalist when he or she is busy. Blue says her colleagues have worked with their nursing staff to overcome that reluctance. “Call them because if they’re talking with a family or if they’re in the middle of a physical exam or if it’s something where they can’t talk, they’re going to put the hold button on,” she tells her staff. “So when you hear the Muzak, the elevator music, then you know that you need to call them back. And it’s worked.”
It’s especially important, Blue says, that nurses surmount any reluctance they feel to initiate a call so that they will do so easily in urgent situations such as alerting rapid response teams and reporting medical errors.4 Blue believes the following anecdote illustrates the perspective of most hospitalists about this issue.
“We just started rapid response teams here,” she says, “And I heard one of the hospitalists say, ‘We’ve had five rapid response team calls so far and we were looking at whether or not the calls met the criteria and were appropriate.’ And one of the other hospitalists said, ‘You know, this really wasn’t a rapid response team call, but I want the nurses to feel free to call and I think that when we’re first starting out, we just want them to call. And then we can work on fine tuning it later. I don’t want to stifle them so they feel they cannot call.”
—Mark Williams, MD
Clear and to the Point
What are the best means to improve communication between hospitalists and nurses? Three major areas for attention include developing relationships, defining communication strategies, and packaging information for clarity.7
Blue often advises nurses to speak with clarity. “Probably the best thing from a hospitalist’s perspective is to be real clear about what you are asking or what it is that you need,” she says. “The clearer that you can be in your requests, the better off you’re going to be in the long run.”
But, Blue says “hospitalists have to understand that one of the greatest benefits from a nurse’s perspective about the hospitalist program is access, immediate access, and dealing with a nurse who does not communicate well might sometimes come along with it.”
The mismatched communication styles of most physicians and nurses are well recognized by a committee at the University of Chicago in which Nancy Perovic is involved. Vineet Arora, MD, MA, a hospitalist and associate program director for the Internal Medicine Residency Program at the University of Chicago, is one of the three hospitalist members on a committee working to improve nurse-physician communication.
“We know that nurses and physicians communicate differently,” says Dr. Arora. “Physicians communicate in more of a task-oriented way and nurses are trained to communicate in a descriptive way. And that’s part of the problem, because nurses might report that physicians don’t respond to them when they need to be responded to; they might not prioritize a patient that the nurse believes is very sick. And a physician might say, ‘I didn’t know that patient was really sick’ because he was given a description such as, ‘They’re not doing OK.’”
Also, Dr. Arora says, “part of the problem that nurses and physicians may have in communicating with each other can be traced to a difference in how they were trained. Physicians are trained to interact with other physicians and nurses are trained by other nurses.”
The committee at Chicago has adopted what is referred to as the Situation-Background-Assessment-Recommendation (SBAR) technique, a tool that the U.S. Navy has used to improve communication on aircraft carriers.8 Developed by Michael Leonard, MD, physician coordinator of clinical informatics, and others at Kaiser Permanente of Colorado, the SBAR technique has been implemented widely at health systems to provide a standard framework for members of the healthcare team when communicating about a patient’s condition.
“What nurses are not very good at is being assertive,” says Perovic. “We’re getting better as we’re getting more modern, but sometimes nurses talk in a more holistic, narrative fashion and doctors just want: what’s the problem, pinpoint it, let me know what it is.”
Chicago’s Perovic and her colleagues plan to educate nurses to use the SBAR technique so they can “talk in the way that doctors are trained to accept information and respond,” she says. “For example, this might sound like, ‘This is this patient with this diagnosis and these vital signs; this is what’s happening: they’re going down, their blood pressure’s dropped, I’m really concerned, this is a different change, I suggest that we do this and that, and I need you here in 10 minutes.’”
Perovic says nurses are then instructed to “make a recommendation; so the hospitalist can prioritize from all the other patients he has to see, to answer the questions: What does this patient need right now? When do I need to see this patient? and What can the nurse do until I get there?”
Literature on the SBAR technique and the tool itself are available online at www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/Tools/SBARTechniqueforCommunicationASituationalBriefingModel.htm.8
Heedful Versus Heedless Interrelating
Exactly how hospitalists affect outcomes and influence system issues is being addressed in research led by Mark V. Williams, MD, and Tracy Scott, PhD, at Emory University Medical Center, Atlanta. Dr. Williams, who is the director of the medicine unit at Emory Hospital, the editor-in-chief of the Journal of Hospital Medicine, and a past president of SHM, spoke to The Hospitalist about the exploratory research his team is doing to assess the impact hospitalists have in nurse-physician relationships in two hospitals in Atlanta, and to particularly examine how these relationships affect patient safety.
High Reliability Organization theory, which elucidates causal pathways between work relationships and reduced error, may provide a framework for how hospitalists affect hospital functioning. “Heedful interrelating,” the theory postulates, creates an organization “mind” and through facilitating teamwork is more alert to and capable of dealing with unexpected occurrences. In fact, says Dr. Williams, data from operating rooms, emergency departments, and ICUs suggest that a lack of teamwork adversely affects patient care and increases medical errors. Research along this vein has been absent on general medical floors.
The research design explores the degree of “heedful interrelating” as opposed to “heedless interrelating” between physicians and nurses and whether hospitalists have different relationships with nurses than do other physicians.
“In heedful interrelating,” explains Dr. Williams, “the physician heeds what the nurse is saying and doing and, likewise, the nurse heeds what the physician is saying and doing.” To date, the investigators have interviewed 45 nurses (half in a university hospital setting and half in a community hospital) and 24 physicians of whom half are hospitalists.
The study examines multiple components, but an example is that “heedful interrelating is based on true mutual respect, which is almost more important over agreement,” says Dr. Williams. “And in heedless interrelating, only one view of the situation is considered correct. It represents your classic arrogant physician.”
Another example of heedful interrelating is that “it advances the goals of the whole team; in heedless interrelating, you think only of your own role,” he says. Nurses in the study reported that compared with other physicians hospitalists are more accessible, more approachable, and more appreciative of the value of the nurse’s role.
The investigators conclude that hospitalists improve the nurse-physician relationship through heedful interrelating and thereby may improve patient safety. In addition, “the nurses emphasized the need for more collaboration and perceived that physicians were not proactive in asking them about their knowledge of the patient, and lacked a holistic view of the patient’s needs. Most importantly, about half the nurses mentioned specific instances where problems in their communication with physicians led directly to problems in patient care.
Dr. Williams believes that the ideal system for communication between hospitalists and nurses would include a means for them to do their patient rounds together. Nurses want hospitalists to develop a system to deliver the patient care plans quickly and reliably, include them in formal and informal educational efforts, and acknowledge them.
Timely Distribution of Care Plans
Blue says that hospitalists at her institution, FirstHealth Moore Regional Hospital (Pinehurst, N.C.), a 385-bed acute care, nonprofit hospital that serves as the referral center for a 15-county region in the mid-Carolinas, work often and closely with the nurses on issues of outcomes. “And outcomes here are like discharge planning utilization review,” she says. “We have a report every morning and there’s a representative from that department who’s online sending out the plans for the patients for the day to the other outcomes managers. That’s already in the works, and we’re not waiting for the hospitalist to get up to the floor to see the patient.”
Overall, however, nurses in other (e.g., larger) settings may not have as good a system in place to distribute care plans. Perovic says that in focus groups she facilitates, she often hears frustration from nurses because “doctors in general—although hospitalists are better at it—do not give nurses the plan of the day or the plan of care in a timely, organized fashion so they can do their care appropriately and prepare themselves and the patient.”
Some of the problem is due to the systems of an academic medical center, Perovic says, where “doctors make rounds at various times of the day and sometimes one team can make four rounds a day. What happens is that the plan for patient care changes each time new rounds are completed because you either get new information or discover you didn’t do something.” But although the team doctors are good at communicating plan modifications among themselves, she says, “what they fail to do is always communicate that well to the nurses.”
Perovic says there is an ideal and then a real solution. “Ideally, it would be great if patient rounds were at a certain time of the day every day so that the nurse can pass her meds and then be available for rounding,” she says. “You could say to nurses, ‘Rounds are between 10 and 11; take care of your patients’ needs and then be on call and ready to go to your rounds when possible.’ Or another solution is what we do in the pediatric hospital: We have a charge nurse who has no patients and she is able to round with all the teams and all the doctors and then give the individual nurse that plan for her patients.”
Hiring a charge nurse in this vein is a human resource issue, Perovic says, and an individual hospital has to decide that it wants to pay a nurse to not have patients. In that case, she says, it is an expensive but good fix. However, accommodating nurses to accompany hospitalists on rounds is logistically almost impossible. “Because if a nurse on the general medicine ward has five patients,” Perovic says, “she might have five different teams of doctors. But depending on the diagnosis of each patient, it won’t be the same team of doctors rounding on them. She might not catch A, B, and C at the same time that D and E are making their rounds. And she could be doing a blood draw on patient D when D team comes, or giving a bath to patient A when team E comes.”
Perovic and her coworkers have tried the call light method, where the doctor comes into the room, the attending presses the call light, and the nurse knows rounds are happening and to join them at that room. But that, as well as other avenues they tried, failed because neither the nurse nor the team can necessarily count on their times of availability coinciding. Still, Dr. Arora says, “we learned a lot about trying to work together and how to understand each other. And we used some of that information to continue thinking about how to best improve physician-nurse communication.”
The team at Chicago is now considering how to design and evaluate “an intervention for more of an interdisciplinary educational process where physicians and nurses would be trained on how to communicate with each other using this standard language,” says Dr. Arora. “Nurses would understand that they could potentially use the SBAR tool to communicate with physicians, and physicians would understand that the nurses need to be included in the plan for the day and would make time to incorporate nurse suggestions and input for the plan.”
Acknowledgment
In some hospital settings what has been described as a two-class system can exist for providers.9 A culture that encourages patient safety is threatened by the nature of the hierarchy or the segregation that is established, even subtly, where nurses are treated as unequals.6,9 In the hospital culture, the “invisibility of nursing” has historically been perpetuated by a number of factors, not the least of which are differences in gender and income.6 In this atmosphere, nurses are not as likely to share from their skills and knowledge. Their lack of assertiveness with hospitalists or other physicians may take its toll in many ways, including increased risks to patient outcomes and to provider morale and satisfaction.7
Linda Aiken, PhD, FAAN, FRCN, RN, the Claire M. Fagin Leadership Professor of Nursing and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania (Philadelphia), has extensively investigated the dynamics between nurses and their co-workers. “Nurse-physician relationships are one of the most important drivers of the work environment,”9 she writes. There are also data that demonstrate the association of nurse-doctor relationships on cost, lower morbidity and mortality, retention of nurses, higher quality of care, and improved hospital reimbursement and/or market share.9
In other words, “healthy nurse-physician relationships are not just a nice thing to have,” writes Dr. Aiken. “They are a competitive advantage.”
Given the association of these relationships to so many outcomes, it is unfortunate that many nurses crave greater acknowledgment for what they bring to their work. One benefit for nursing is that because hospitalists are around the hospital more than an average attending, they know the nurses better.
“As a nurse, what I need from hospitalists is for them to recognize and teach their residents and interns that the nurse is a constant player at the bedside in the hospital, with many more years of experience,” says Perovic. “Even though she doesn’t have as much medical training as a doctor or resident, she has enough clinical-nursing hospital experience. Doctors need to appreciate that nurses are experts at hospital care and bedside care, and [doctors] need to show that respect when we’re teaching our residents because we can learn a lot from the nurses, and the nurses can actually make the doctors’ lives easier.”
In a study of a multidisciplinary intervention tested on an acute inpatient medical unit, the effect of the intervention—to improve communication and collaboration—was strongest among house staff, who reported significant increases in collaborative efforts with nurses.10 This finding underlines the importance for hospitalists to serve as models to students, interns, and residents because the most effective time to learn collaborative practice is during early training when experienced nurses can assist inexperienced interns.10 Hospitalists can also consciously reject the traditional “doctor-nurse game,” whereby patterns of behavior suggest that doctors are the dominant players and nurses must defer to them.
“Ask nurses for their opinion,” advises Blue. “Treat them like an equal, which is another one of the beauties of this program, because hospitalists certainly do that. When it comes down to it, people want to be appreciated, respected, and acknowledged for their contribution.”
Blue and her team also encourage hospitalists to share with the nurses if they happen to hear news of their patients’ progress. “If we have follow-up on somebody from the primary care provider after that patient has left the hospital, for example, we try to share that with the nursing staff because they’re our patients. They’re not just my patients and they’re not your patients; they’re our patients.”
Conclusion
The quality of the nurse-hospitalist relationship is central to patient care. The methods, means, and styles of individual and team communication all influence the effectiveness of a hospital team. Retraining providers to traverse the gap of different communication styles is a way to approach the issues that exist. Mutual training for physicians and nurses, as well as training nurses to communicate in ways that more approximate how physicians communicate, will better serve patient and provider needs.
Hospitalists can encourage nurses to overcome hesitancies to initiate calls, clarify their preferences for how nurses should contact them, and work with nurses to seek workable ways to perform patient rounds in concert. Most of all, nurses need timely care plan distribution and acknowledgment for their contributions to teamwork and patient care. TH
Writer Andrea Sattinger will write about occupational therapists’ experiences with hospitalists in the January issue.
References
- ANA Commission on Workforce for Hospitals and Health Systems. In our hands: how hospital leaders can build a thriving workforce. American Hospital Association; Chicago; 2002;55:30-31.
- Aiken LH. The unfinished patient safety agenda. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web: Agency for Healthcare Research and Quality; 2005. Accessed August. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=7&searchStr=The+unfinished+patient+safety+agenda
- Aiken LH, Clarke SP, Sloane DM. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002;14:5-13.
- Friesen MA, Farquhar MB, Hughes R. The nurse’s role in promoting a culture of safety: American Nurses Association Continuing Education, Center for American Nurses; 2005.
- Wachter R. In conversation with … Barbara A. Blakeney, MS, RN. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web. Agency for Healthcare Research and Quality; 2005. Accessed Aug. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=8&searchStr=Blakeney
- Lindeke LL, Sieckert AM. Nurse-physician workplace collaboration. Online J Issues Nurs. 2005;10:5.
- Burke M, Boal J, Mitchell R. Communicating for better care: improving nurse-physician communication. Am J Nurs. 2004;104:40-47
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12:40-41.
- Smith AP. Partners at the bedside: the importance of nurse-physician relationships. Nurs Econ. 2004;22:161-164.
- Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71-77.
One-Month-Old UTI Patient
Scenario: A 32-day-old female presents with vomiting and jaundice, and the mother reports that the child is irritable and not eating as well as usual. The pediatric hospitalist suspects a UTI and orders a dipstick/urinalysis and urine culture. The dipstick/urinalysis results are positive for nitrite and leukocyte esterase, indicating antibiotic therapy for presumed UTI.
Introduction
UTI is one of the most common bacterial infections in infants and young children. To prevent progression to pyelonephritis and avoid potential renal scarring or failure, early recognition and prompt treatment are critical.
Clinical signs and symptoms of UTI in newborns include jaundice, sepsis, failure to thrive, poor feeding, vomiting, and fever. In infants and preschoolers, hospitalists should also suspect UTI in the presence of diarrhea, strong-smelling urine, abdominal or flank pain, and new onset urinary incontinence.1
Treatment recommendations, which are age-dependent, include antibiotic therapy initiated upon an abnormal dipstick/urinalysis. If a urine culture is positive, a seven- to 14-day course of antibiotic therapy is recommended, followed by prophylactic antibiotics until results of imaging studies are available.1 According to a study by Hoberman and Wald, treatment of UTI with oral antibiotics alone is generally effective, even for young children with pyelonephritis.2
Imaging recommendations for a first UTI include ultrasound, cystogram, and renal cortical scan.
Up to this point, there’s been very little disagreement about the management of UTI. However, the question of whether the one-month-old patient in our scenario should be admitted or sent home with strict instructions on the administration of antibiotics remains controversial. The pediatric UTI guideline from Cincinnati Children’s Hospital Medical Center recommends routine hospital admission if the infant is under 30 days old.1 On the other hand, Santen and Altieri, among others, recommend, “Sick children and infants less than three months should be treated as inpatients, and healthy children and older infants may be treated as outpatients.”3,4
—Jeffrey M. Simmons, MD
The Set-Up
We asked several pediatric hospitalists across the country—including an instructor of pediatrics at Cincinnati Children’s Hospital Medical Center—to respond to this simple scenario, posing the following questions: “What recommendation would you follow? Would you admit the one-month-old infant in our scenario or send her home? Why?”
Predictably, admission criteria varied, but most agreed that this infant should be admitted. No one based their response on age.
Automatic Admission Cut-off Not Well Supported
Jeffrey M. Simmons, MD, instructor of pediatrics, Division of General and Community Pediatrics, Cincinnati Children’s Hospital Medical Center, responds: “My perspective on the UTI scenario is that the only dogma that applies is that the infant needs antibiotics. Because [the scenario] mentions vomiting, I would, therefore, most likely give parenteral antibiotics and admit.
“An issue within this scenario that I don’t believe the literature answers clearly is once a UTI is identified by the U/A, what risk remains of bacteremia or meningitis in the over 30-day-old infant? We are taught that infants don’t ‘localize’ infections well (i.e., a serious bacterial infection in one place can rapidly lead to disseminated infection). I sense a growing consensus that after 30 days or so this concern is less at issue. However, for clarity, I would prefer to obtain blood and CSF cultures on this infant prior to initiating antibiotic therapy. Without those cultures, and the screening tests that go with them (i.e., serum WBC count, CSF cell count, and glucose), I would be uncomfortable sending the infant home.
“However, if the WBC count was between 5 and 15, the CSF reassuring, the parents in agreement and reliable with good primary care follow-up the next morning, I think such an infant could be managed with one dose of IV/IM antibiotics after cultures are obtained and sent home. The following day, depending on culture results and the clinical situation, this infant might either be admitted, given another dose of parenteral antibiotics pending final blood culture, or switched to oral antibiotics.
“Such a plan is complex, so if the primary care physician or family was at all uncomfortable, admission to accomplish that plan would clearly be appropriate.
“A final issue not adequately addressed within the scenario is an assessment of the infant’s hydration—potentially an issue due to the vomiting. If the infant was mildly to moderately dehydrated with persistent vomiting, I would also then admit until this improved.
“In regard to the cited evidence, I would say that clearly an arbitrary cut-off of automatic admission under three months is not well supported by current literature, but is certainly many practitioners’ ‘style.’ Oral antibiotics are clearly efficacious for pyelonephritis, but the clinician needs to be confident the family can give them and the infant will keep them down. I believe most practitioners would agree with admission for an infant under 30 days, but where to precisely draw that line needs to be better established through investigation. Potential concomitant bacteremia and meningitis lead me to support obtaining blood and CSF cultures on any infant under 60 days for which I plan to initiate antibiotics for UTI.”
Possibility of Dehydration Indicates Admission
Michael P. Fullmer, DO, Central Iowa Pediatric Hospitalists, Mercy Medical Center, Des Moines, Iowa, responds: “This patient is not febrile, but does have other systemic symptoms, including poor feeding, irritability, jaundice, and vomiting. These systemic symptoms could be indicative of a serious bacterial infection like UTI, bacteremia, or meningitis. This patient most likely has a UTI. These symptoms may suggest pyelonephritis rather than lower UTI, but the distinction is not necessary for our decision here.
“Bacteremia is present in up to 22.7% of infants less than two months old with a UTI. This adds to the complexity of the issue, and a blood culture is probably indicated. Meningitis should be considered, but a lumbar puncture is probably not indicated in this scenario.
“A one-month-old with a UTI should be admitted to the hospital and started on parenteral antibiotics. There are several reasons for admission. First, the presence of vomiting makes oral antibiotic administration impractical (if not impossible). Intramuscular antibiotic injection may be an option, but the IV route gives the provider more options and is usually better accepted by parents. Next, if the patient is not already dehydrated, the poor feeding and vomiting could lead to dehydration. This alone would be an indication for admission. Finally, admission would give the physician time to observe the infant for clinical improvement. This may be subtle in the absence of fever.
“Another consideration is the recommended imaging for all children less than two years old. The AAP has recommended a renal ultrasound and VCUG for all infants and young children with their first UTI. This is important for discovery of urinary tract anomalies that predispose the patient to recurrent UTIs and eventual renal scarring and dysfunction. The imaging should be performed at the earliest convenient time if the patient is responding to therapy. In our practice, we generally have the renal ultrasound performed while the patient is in the hospital and arrange the VCUG as an outpatient [exam] prior to completion of the course of antibiotics.
“Patients are discharged when they are afebrile for 24 hours, have adequate oral intake and are able to take oral antibiotics. Please refer to the AAP Clinical Practice Guideline for more detail.5,6
—Michael Fullmer, DO
Admission Criteria Must Take Fever Into Account
John W. Graef, MD, chief, Services Office at Children’s Hospital, Harvard Vanguard Services Office, Boston, responds: “The presence or absence of fever is an important variable. Dipstick urines are shortcuts and don’t provide such information as the presence or absence of casts, although the fact that the child is vomiting and irritable is suggestive of pyelonephritis as opposed to a simple UTI/cystitis. [The scenario doesn’t] mention how the urine is obtained. Presumably it is a cath specimen, but that needs to be specified.
“Jaundice can occur with a UTI, but usually in the first week or so of life. A 32-day-old infant with pyelo is unlikely to be jaundiced unless for some other reason.
“I certainly agree with routine admission of a febrile infant up to one month, but not necessarily an otherwise well female infant. The presence of vomiting and irritability with or without fever might prompt a full septic work-up, in which case the decision to admit an afebrile infant would depend on the results of the CBC/UA and probably an LP. A blood culture and CBC should be drawn in the ED.
“In other words, one can’t have it both ways. If the irritability and vomiting are due to pyelo, a septic work-up is warranted. If all parameters are normal, the only reason for admission is hydration of a vomiting infant. If the infant was afebrile and had an uncomplicated UTI, I would not automatically admit an otherwise well 32-day-old.
“Poor PO (per OS, i.e., oral, by mouth) intake in an infant with a UTI warrants IV fluid regardless of age.”
—John W. Graef, MD
True Emesis With Decreased Oral Intake Indicates Admission
Erin R. Stucky, MD, pediatric hospitalist, Children’s Hospital and Health Center San Diego, associate professor, UCSD Pediatrics, responds: “The decision to admit or discharge this one-month-old with vomiting, jaundice, poor eating, and irritability should include consideration of hydration status, toxicity, sepsis potential, and ability to secure close follow-up. We will make the assumption that the infant is term, with no past medical history, family history, or prenatal evaluation that would put the infant at greater risk for sepsis or likelihood of underlying anatomic genitourinary abnormality. In addition we will assume that the urinalysis was performed by catheterization in a non-pretreated infant.
“A careful history should elicit the change in urine output, frequency, and volume of emesis to contrast with small ‘spit-ups,’ and change in feeding duration or volume. Observation of a feeding in the office or emergency department can be of great value in determining likelihood of ability to maintain hydration at home. Feeding type should be confirmed [because] parents may dilute or alternately concentrate formula in response to vomiting. In this scenario, true emesis in an infant with decreased oral intake would be grounds for admission, intravenous hydration, and evaluation of electrolytes.
“A newly irritable infant evokes a visceral sensation for all pediatric hospitalists. An irritable one-month-old may be suffering from a single system infection, electrolyte imbalance, or other insult, but unfortunately may just as easily have multisystem involvement. Vital signs and physical exam findings of toxicity, such as tachycardia and delayed capillary refill, are not known to us. The presence of jaundice raises concern for cholestasis induced by E. coli or possibly rarer metabolic disease, such as galactosemia. Admission would allow for evaluation and monitoring of the more likely causes of irritability in our index patient, which include sepsis, meningitis, and electrolyte and acid-base imbalances.
“The urinalysis in this infant is suggestive of a urinary tract infection, although infants may have no abnormalities noted on initial urinalysis.7,8 The risk of bacteremia in infants under 60 days with documented urinary tract infection is significant. A number of studies support the need to treat infants less than 30 days with parenteral antibiotics.9-14 Addition of C-reactive protein testing at this time does not aid in distinguishing those who are bacteremic in this age group.15 The often quoted study by Hoberman of 306 children included only 13 under the age of two months.16 Of the 13 reported positive blood cultures, 10 were in children under age six months. Daily intramuscular ceftriaxone treatment would cover a majority of the typical neonatal UTI organisms, can be administered in the outpatient setting, and is proven to be as effective as intravenous delivery. The clinical response to bacteremia is, however, unpredictable in young infants. The sepsis potential in this infant requires admission for physiologic monitoring and support as needed.
“Final, but not inconsequential, concerns are barriers to follow-up. These include parental experience and coping skills with feeding and monitoring an ill infant, ability to educate on the illness and reasons for follow-up, transportation, and operational issues, such as weekend clinic hours or holiday office closures. For the index patient these issues are overshadowed by the clinical criteria for admission but would be of great importance for discharge.”
Conclusion
Based on these responses, admitting a suspected UTI patient on the basis of age alone, as suggested by Santen and Altieri, is likely inappropriate. Many other factors must be weighed and would likely indicate admission for the patient in the scenario, regardless of the infant’s age. In short, until there’s better evidence for age-based admission criteria, clinical judgment based on the individual patient presentation must continue to drive care and treatment decisions.
Keri Losavio is a medical journalist with more than 10 years’ experience.
References
- UTI Guideline Team, Cincinnati Children’s Hospital Medical Center. “Evidence based clinical practice guideline for children 12 years of age or less with acute first time urinary tract infection.” www.cincinnatichildrens.org/svc/dept-div/health-policy/ev-based/uti.htm. Guideline 7, pages 1–20, April 2005.
- Hoberman A, Wald ER. Treatment of urinary tract infections. Pediatr Infect Dis J. 1999;18(11):1020–1021.
- Santen SA, Altieri MF. Pediatric urinary tract infection. Emerg Med Clin North Am. 200119(3):675–690.
- Egland AG, Egland TK. Pyelonephritis. eMedicine. www.emedicine.com/emerg/topic769.htm. Accessed Oct. 16, 2005.
- No authors listed. Practice parameter: the diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. American Academy of Pediatrics. Committee on Quality Improvement. Subcommittee on Urinary Tract Infection. Pediatrics. 1999;103(4):843–852.
- Pitetti RD, Choi S. Utility of blood cultures in febrile children with UTI. Am J Emerg Med. 2002;20:271–274.
- Dayan PS, Bennett J, Best R, et al. Test characteristics of the urine Gram stain in infants 60 days of age with fever. Pediatr Emerg Care. 2002;18(1):12–14.
- Huicho L, Campos-Sanchez M, Alamo C. Meta-analysis of urine screening tests for determining the risk of urinary tract infection in children. Pediatr Infect Dis J. 2002;21 (1):1-11.
- Byington C L, Enriquez F, Hoff C, et al. Serious bacterial infections in febrile infants 1 to 90 days old with and without viral infections. Pediatrics. 2004; 113(6):1662–1666.
- Baraff L. Management of fever without source in infants and children. Ann Emerg Med. 2000;36(6):602–614.
- Baraff LJ, Oslund SA, Schriger DL, Stephen ML. Probability of bacterial infections in febrile infants less than three months of age: A meta-analysis. Pediatr Infect Dis J. 1992;11(4):257–264.
- Klein JO. Management of the febrile child without a focus of infection in the era of universal pneumococcal immunization. Pediatr Infect Dis J. 2002;21(6):584–588.
- Syrogiannopoulos G, Grieva I, Anastassiou E, et al. Sterile cerebrospinal fluid pleocytosis in young infants with urinary tract infections. Pediatr Infect Dis J. 2001;20(10):927–930.
- Jaskiewicz JA, McCarthy CA, Richardson AC, et al. Febrile infants at low risk for serious bacterial infection—an appraisal of the Rochester criteria and implications for management. Febrile Collaborative Study Group. Pediatrics. 1994;94(3):390–396.
- Malik A, Hui C, Pennie RA, Kirpalani H. Beyond the complete blood cell count and C-reactive protein: A systematic review of modern diagnostic tests for neonatal sepsis. Arch Pediatr Adolesc Med. 2003;157(6):511–516.
- Hoberman A, Wald ER, Hickey RW, et al. Oral versus intravenous therapy for urinary tract Infections in young children. Pediatrics.1999;104:79–86
PEDIATRIC SPECIAL SECTION
IN THE LITERATURE
Utilize Clinical and Demographic Factors to Diagnose UTIs in Young Febrile Infants
Review by Sara E. Gardner, MD
Zorc JJ, Levine DA, Platt SL, et al. Clinical and demographic factors associated with urinary tract infections in young febrile infants. Pediatrics. 2000;116(3):644-648.
UTI is a common cause of serious bacterial infection in the febrile infant <60 days of age. Standard urinalysis and urine dipstick techniques, commonly used to diagnose UTI, have relatively low sensitivity increasing the possibility of a missed diagnosis. An accurate initial diagnosis is critical in this age group for whom complications from UTI include bacteremia and renal scarring.
To describe the demographic and clinical factors associated with UTI in infants ≤60 days of age with fever, these authors conducted a prospective cross sectional study from October 1999 to March 2001. Patients were enrolled at eight different institutions after presentation to an emergency department. One-thousand-twenty-five patients age 60 days or younger (mean age 35.5 days, 60.5% male) were enrolled with either reported or documented fever >38. Routine testing for all children included respiratory syncytial virus (RSV) sampling and bladder catheterization or suprapubic aspiration for urinalysis and culture.
A positive urinalysis was defined as a trace or greater result for leukocyte esterase and/or nitrite on dipstick or greater than or equal to five WBCs per high power field (hpf) on urine microscopy. UTI was defined as growth of a single pathogen of ≥1,000 colony forming units (cfu)/mL for urine cultures obtained by suprapubic catheterization, ≥50,000 cfu/mL from a catheterized specimen, or ≥10,000 cfu/ml from a catheterized specimen with a positive urinalysis.
Of the patients enrolled in the study, 92 were found to have UTI by these diagnostic criteria. Using the chi-squared test and calculated odds ratios with 95% confidence intervals, uncircumcised male (OR: 10.4; 95% CI: 4.7-31.4) and maximum temperature of ≥39º C (OR: 2.4 per degree C; 95% CI: 1.5-3.6) were found to be statistically significant variables for predicting UTI. These risk factors remained statistically significant after multivariable analysis controlling for other factors.
Interestingly of the above 92 patients diagnosed with UTI, 85 grew ≥50,000 cfu of a single pathogen, but six (8%) grew 10,000-49,000 cfu with a positive UA based on the study criteria. Zorc, et al. included these patients with >10,000 cfu and >5 WBC/hpf in this study despite previous studies that have established a definition of positive urinalysis to be ≥10 WBC/hpf. Zorc, et al. acknowledge the conservative definition applied in their current study, but assert that the overall results of the study would have been similar had 10,000 or 50,000 cfu/mL thresholds been chosen. To support this assertion, Zorc, et al. retrospectively applied enhanced urinalysis, a sensitive form of urinalysis including hemocytometric cell count and gram stain described by Hoberman, et al. to study patients with low bacteria counts. Based on Hoberman’s study, enhanced urinalysis can differentiate acute infection from asymptomatic bacteriuria in patients with bacterial growth between 10,000 to 50,000 cfu/mL.
Another significant limitation of this study was failure to enroll one-third of eligible patients to the study. In addition, the authors note that missed patients had a lower rate of UTI compared with enrolled patients.
Although this study design prohibits generalization to patient care areas outside the emergency department, the findings can assist the hospitalist in the evaluation of the febrile infant during RSV season and potentially guide decisions regarding empiric antibiotic therapy as part of evaluations to diagnose or exclude serious bacterial infection. Additionally, this study raises the question of need for better methods of urinalysis for febrile, uncircumcised male infants.
Back to the Basics: A Clinical Approach to Excluding Acute Appendicitis
Review by Jane G. Buss, MD
Kharbanda AB, Taylor GA, Fishman SJ, et al. A clinical decision rule to identify children at low risk for appendicitis. Pediatrics. 2005;116(3):709-16.
Appendicitis is the most common condition requiring emergency abdominal surgery in the pediatric population. To diagnosis appendicitis, clinicians typically utilize clinical findings, imaging studies, and laboratory testing. The use of clinical scoring systems to improve the diagnosis of appendicitis in children has been limited, mostly resulting from unacceptably low sensitivities/specificities, or the lack of validation. The use of CT scan to aid in the evaluation of children with appendicitis has become widespread. Concerns remain, however, regarding long-term radiation effects and increased healthcare costs associated with this approach.
The authors of this study sought to develop clinical scores for children to predict which of those with acute abdominal pain do not have appendicitis. Additionally, they hoped to lessen the use of CT scanning. Their goal was to identify those groups of children who have significant abdominal pain without appendicitis who could be safely observed without CT scan or possible surgery.
This prospective cohort study enrolled 601 eligible children ages three to 18 with suspected appendicitis who presented to the emergency department over a 15-month period. Two low-risk clinical decision rules were developed using logistic regression and recursive partitioning. Using logistic regression, six factors were identified from analysis of 425 patients in the derivation set significantly associated with an increased likelihood of appendicitis. The score components include:
- Nausea (2 points);
- History of focal right lower quadrant pain (RLQ) (2 points);
- Migration of pain (1 point);
- Difficulty walking (1 point);
- Rebound tenderness (2 points); and
- Absolute neutrophil count (ANC) >6.75 x 103/uL (6 points).
When tested with data from the 176 patients in the validation set, a score of less than or equal to five had a sensitivity of 96.3%, and a negative predictive value of 95.6% for excluding appendicitis.
The authors then derived a second clinical low-risk decision rule by recursive partitioning. They determined that a combination of ANC <6.75 X 10 to the third/microliter, absence of nausea (or emesis or anorexia), and absence of maximal tenderness in the RLQ essentially excluded appendicitis in the derivation and validation groups. This rule had a sensitivity of 98.1%, and a negative predictive value of 97.5%.
In summary, these authors derived two clinical decision rules giving the clinician the option of a clinical score (logistic regression) or a decision tree (recursive partitioning) to identify children at low risk for appendicitis. Their findings suggest application of either low-risk rule would lead to decreased reliance on CT scan. Applying these clinical rules to their patients could have reduced the rate of CT scan by 20%. They conclude that pediatric patients who have suspected appendicitis and are at low risk by either model should be considered for observation rather than undergo CT scan or operative care.
Epidemiology of Fungal Infection in the Tertiary Care Inpatient Setting
Review by Brandan P. Kennedy, MD
Abelson, JA, Moore T, Bruckner D, et al. Frequency of fungemia in hospitalized pediatric inpatients over 11 years at a tertiary care institution. Pediatrics. 2005;116(1):611-617.
Fungal organisms are relatively uncommon causes of blood infections in the pediatric population. When they do occur, they cause significant morbidity and mortality. The incidence of fungal blood infections appears to be rising at a faster rate than that of other pathogens. Authors from the University of California performed this study to describe those rate changes, and to evaluate whether treatment has improved in the past 11 years.
This retrospective cohort study involved children admitted to Mattel Children’s Hospital in Los Angeles, California, during an 11-year period from January 1991 to December 2001. Information obtained on all positive fungal cultures from all body sites included date and site of culture, demographics, and fungal etiology. Additionally, data regarding underlying illness, hospital course, outcome, and antimicrobial treatment were considered.
Study results demonstrated a significant increase in diagnosed fungemia in children. There was a 15% increase in overall pediatric admissions in the study period, and a 23% increase in positive fungal cultures in the same period. Of 272 blood cultures, 97 were positive for fungus. Although this is a relatively small number of total infections, data demonstrated a 91% increase in fungemia during the study period. Candida species were the organisms most frequently isolated from any body site with 85% of the total isolates. Of the total positive isolates, it appeared that approximately 78% reflected colonization as opposed to infection.
Outcomes for fungal infections improved only marginally in the study period. Fifty percent of patients with fungemia died between 1991 and 1996, and 45% died between 1997 and 2001. The mortality rate for immunocompromised conditions was 57%. The cost effectiveness of fungal screening cultures was also evaluated, which demonstrated that fungal cultures identified 14 patients independent of bacterial blood cultures at a cost of $560,000, which resulted in a cost of $40,000 per identified patient.
The study reaches several significant conclusions. First there has been a significant increase in fungal infections that exceeds the increase in overall pediatric hospital admissions. However, it is important to recognize the increase in immunocompromised conditions during the study period, which may account for the higher incidence of fungemia.
Second the addition of fungal blood cultures to bacterial blood cultures as part of a routine workup for febrile patients appeared to yield limited clinical information at a very high cost. Third this study highlights the serious threat fungal infections pose to immunocompromised hosts who have a significantly higher incidence of infection, as well as higher morbidity and mortality. Fourth the use of broad spectrum antibiotics may be increasing fungal colonization in patients and consequently increasing the risk for pathologic fungal infection. Finally morbidity and mortality rates for fungal infections did not greatly improve, despite significant improvements in supportive care made during the study period
This study demonstrates a need for better diagnostic markers for fungal infections, especially those that might provide earlier detection and diagnosis at less cost. The importance of judicious use of antibiotics is underscored while the need for a broader base of therapeutic agents is highlighted. These issues may be key ingredients needed to reduce adverse outcomes from fungal infections, especially in the immunocompromised host.
Rotavirus Vaccine Revisited
Salinas B, Perez Schael I, Linhares AC, et al. Evaluation of safety, immunogenicity and efficacy of an attenuated rotavirus vaccine, RIX4414. Ped Infect Dis J. 2005;24(9):807-816.
Rotavirus is the leading cause of severe gastroenteritis among children worldwide. In the United States, rotavirus is responsible for approximately 5%-10% of all diarrhea among children older than five and accounts for approximately 50,000 hospitalizations each year. An estimated one in 200,000 children with rotavirus diarrhea dies from complications of infection. The immunizing effect of rotavirus infection stimulated the development of live attenuated vaccines. In 1998, a three-dose regimen of a tetravalent rhesus-human reassortant vaccine (RotaShield: Wyeth Laboratories,) was licensed for infant immunization in the United States. Within the first year of use, it was withdrawn due to an observed risk of intussusception. The current study was designed to evaluate immunogenicity and efficacy of a live attenuated monovalent human rotavirus vaccine, RIX4414.
A double-blind, randomized, placebo-controlled design was utilized with the RIX4414 rotavirus vaccine administered at three different virus concentrations. Infants were randomly assigned to one of the three study groups or the placebo group. Infants in the vaccine groups received two oral doses of the vaccine at the age of two and four months. An identical placebo containing the same constituents as the vaccine except for the vaccine virus was used as the control. The vaccine was given concomitantly with other routine vaccinations. To determine immunogenicity, blood samples were obtained from all infants immediately before the first vaccination to exclude previous rotavirus infection. Blood samples were obtained two months after the first second vaccine doses and again at one year to measure anti-rotavirus IgA antibodies. Additionally, stool was obtained from 25% of the study sample and tested for rotavirus viral shedding, with differentiation between wild type and vaccine also being performed.
There were 2,155 infants enrolled in this study from three countries in South America, allowing for slightly more than 500 infants in each group. The study began in May 2001, and the final one-year follow-up was completed in April 2003. The anti-rotavirus IgA seroconversion rates two months after first and second doses were 38%-43% and 61%-65%, respectively. This compared with a 5.3% seroconversion rate in the control group, which was determined to be a wild type virus. Vaccine take after two doses was shown in all three vaccine study groups, ranging from 65% to 75% for the lowest to highest vaccine concentration groups. Reactogenicity and safety was evaluated by monitoring incidences of fever, diarrhea, vomiting, irritability, and loss of appetite during the 15 days after vaccine administration. The results were similar for the four study groups suggesting no significant reactogenicity. There were 220 serious adverse events reported including one intussusception. However, none of these events was determined to be related to the vaccine. The RIX4414 vaccine was demonstrated to effectively protect against severe gastroenteritis caused by G1 type rotavirus and also was shown to provide some cross protection to other serotypes.
This well-designed study demonstrated a statistically significant reduction in gastroenteritis due to rotavirus infection, especially of the predominant G1 serotype, after two doses of the RIX4414 human rotavirus vaccine. Objective measures of viral shedding and IgA seroconversion support the efficacy of the vaccine. This study provided a large sample population with good controls.
An important and possibly confounding variable not addressed by the study was breastfeeding status of the infants. There is clinical evidence demonstrating the protective properties of secretory IgA in human milk against rotavirus infection, and this could have influenced the observed severity of disease in the sample population. It would have been interesting to isolate breastfeeding status as a study variable and note any effect on the results of the study.
Aside from this observation, this study appears to show a promising new oral rotavirus vaccine. As further research on the RIX4414 vaccine continues, there is hope that this vaccine could make a significant positive impact on morbidity and hospitalization rates for rotavirus infections worldwide. TH
Scenario: A 32-day-old female presents with vomiting and jaundice, and the mother reports that the child is irritable and not eating as well as usual. The pediatric hospitalist suspects a UTI and orders a dipstick/urinalysis and urine culture. The dipstick/urinalysis results are positive for nitrite and leukocyte esterase, indicating antibiotic therapy for presumed UTI.
Introduction
UTI is one of the most common bacterial infections in infants and young children. To prevent progression to pyelonephritis and avoid potential renal scarring or failure, early recognition and prompt treatment are critical.
Clinical signs and symptoms of UTI in newborns include jaundice, sepsis, failure to thrive, poor feeding, vomiting, and fever. In infants and preschoolers, hospitalists should also suspect UTI in the presence of diarrhea, strong-smelling urine, abdominal or flank pain, and new onset urinary incontinence.1
Treatment recommendations, which are age-dependent, include antibiotic therapy initiated upon an abnormal dipstick/urinalysis. If a urine culture is positive, a seven- to 14-day course of antibiotic therapy is recommended, followed by prophylactic antibiotics until results of imaging studies are available.1 According to a study by Hoberman and Wald, treatment of UTI with oral antibiotics alone is generally effective, even for young children with pyelonephritis.2
Imaging recommendations for a first UTI include ultrasound, cystogram, and renal cortical scan.
Up to this point, there’s been very little disagreement about the management of UTI. However, the question of whether the one-month-old patient in our scenario should be admitted or sent home with strict instructions on the administration of antibiotics remains controversial. The pediatric UTI guideline from Cincinnati Children’s Hospital Medical Center recommends routine hospital admission if the infant is under 30 days old.1 On the other hand, Santen and Altieri, among others, recommend, “Sick children and infants less than three months should be treated as inpatients, and healthy children and older infants may be treated as outpatients.”3,4
—Jeffrey M. Simmons, MD
The Set-Up
We asked several pediatric hospitalists across the country—including an instructor of pediatrics at Cincinnati Children’s Hospital Medical Center—to respond to this simple scenario, posing the following questions: “What recommendation would you follow? Would you admit the one-month-old infant in our scenario or send her home? Why?”
Predictably, admission criteria varied, but most agreed that this infant should be admitted. No one based their response on age.
Automatic Admission Cut-off Not Well Supported
Jeffrey M. Simmons, MD, instructor of pediatrics, Division of General and Community Pediatrics, Cincinnati Children’s Hospital Medical Center, responds: “My perspective on the UTI scenario is that the only dogma that applies is that the infant needs antibiotics. Because [the scenario] mentions vomiting, I would, therefore, most likely give parenteral antibiotics and admit.
“An issue within this scenario that I don’t believe the literature answers clearly is once a UTI is identified by the U/A, what risk remains of bacteremia or meningitis in the over 30-day-old infant? We are taught that infants don’t ‘localize’ infections well (i.e., a serious bacterial infection in one place can rapidly lead to disseminated infection). I sense a growing consensus that after 30 days or so this concern is less at issue. However, for clarity, I would prefer to obtain blood and CSF cultures on this infant prior to initiating antibiotic therapy. Without those cultures, and the screening tests that go with them (i.e., serum WBC count, CSF cell count, and glucose), I would be uncomfortable sending the infant home.
“However, if the WBC count was between 5 and 15, the CSF reassuring, the parents in agreement and reliable with good primary care follow-up the next morning, I think such an infant could be managed with one dose of IV/IM antibiotics after cultures are obtained and sent home. The following day, depending on culture results and the clinical situation, this infant might either be admitted, given another dose of parenteral antibiotics pending final blood culture, or switched to oral antibiotics.
“Such a plan is complex, so if the primary care physician or family was at all uncomfortable, admission to accomplish that plan would clearly be appropriate.
“A final issue not adequately addressed within the scenario is an assessment of the infant’s hydration—potentially an issue due to the vomiting. If the infant was mildly to moderately dehydrated with persistent vomiting, I would also then admit until this improved.
“In regard to the cited evidence, I would say that clearly an arbitrary cut-off of automatic admission under three months is not well supported by current literature, but is certainly many practitioners’ ‘style.’ Oral antibiotics are clearly efficacious for pyelonephritis, but the clinician needs to be confident the family can give them and the infant will keep them down. I believe most practitioners would agree with admission for an infant under 30 days, but where to precisely draw that line needs to be better established through investigation. Potential concomitant bacteremia and meningitis lead me to support obtaining blood and CSF cultures on any infant under 60 days for which I plan to initiate antibiotics for UTI.”
Possibility of Dehydration Indicates Admission
Michael P. Fullmer, DO, Central Iowa Pediatric Hospitalists, Mercy Medical Center, Des Moines, Iowa, responds: “This patient is not febrile, but does have other systemic symptoms, including poor feeding, irritability, jaundice, and vomiting. These systemic symptoms could be indicative of a serious bacterial infection like UTI, bacteremia, or meningitis. This patient most likely has a UTI. These symptoms may suggest pyelonephritis rather than lower UTI, but the distinction is not necessary for our decision here.
“Bacteremia is present in up to 22.7% of infants less than two months old with a UTI. This adds to the complexity of the issue, and a blood culture is probably indicated. Meningitis should be considered, but a lumbar puncture is probably not indicated in this scenario.
“A one-month-old with a UTI should be admitted to the hospital and started on parenteral antibiotics. There are several reasons for admission. First, the presence of vomiting makes oral antibiotic administration impractical (if not impossible). Intramuscular antibiotic injection may be an option, but the IV route gives the provider more options and is usually better accepted by parents. Next, if the patient is not already dehydrated, the poor feeding and vomiting could lead to dehydration. This alone would be an indication for admission. Finally, admission would give the physician time to observe the infant for clinical improvement. This may be subtle in the absence of fever.
“Another consideration is the recommended imaging for all children less than two years old. The AAP has recommended a renal ultrasound and VCUG for all infants and young children with their first UTI. This is important for discovery of urinary tract anomalies that predispose the patient to recurrent UTIs and eventual renal scarring and dysfunction. The imaging should be performed at the earliest convenient time if the patient is responding to therapy. In our practice, we generally have the renal ultrasound performed while the patient is in the hospital and arrange the VCUG as an outpatient [exam] prior to completion of the course of antibiotics.
“Patients are discharged when they are afebrile for 24 hours, have adequate oral intake and are able to take oral antibiotics. Please refer to the AAP Clinical Practice Guideline for more detail.5,6
—Michael Fullmer, DO
Admission Criteria Must Take Fever Into Account
John W. Graef, MD, chief, Services Office at Children’s Hospital, Harvard Vanguard Services Office, Boston, responds: “The presence or absence of fever is an important variable. Dipstick urines are shortcuts and don’t provide such information as the presence or absence of casts, although the fact that the child is vomiting and irritable is suggestive of pyelonephritis as opposed to a simple UTI/cystitis. [The scenario doesn’t] mention how the urine is obtained. Presumably it is a cath specimen, but that needs to be specified.
“Jaundice can occur with a UTI, but usually in the first week or so of life. A 32-day-old infant with pyelo is unlikely to be jaundiced unless for some other reason.
“I certainly agree with routine admission of a febrile infant up to one month, but not necessarily an otherwise well female infant. The presence of vomiting and irritability with or without fever might prompt a full septic work-up, in which case the decision to admit an afebrile infant would depend on the results of the CBC/UA and probably an LP. A blood culture and CBC should be drawn in the ED.
“In other words, one can’t have it both ways. If the irritability and vomiting are due to pyelo, a septic work-up is warranted. If all parameters are normal, the only reason for admission is hydration of a vomiting infant. If the infant was afebrile and had an uncomplicated UTI, I would not automatically admit an otherwise well 32-day-old.
“Poor PO (per OS, i.e., oral, by mouth) intake in an infant with a UTI warrants IV fluid regardless of age.”
—John W. Graef, MD
True Emesis With Decreased Oral Intake Indicates Admission
Erin R. Stucky, MD, pediatric hospitalist, Children’s Hospital and Health Center San Diego, associate professor, UCSD Pediatrics, responds: “The decision to admit or discharge this one-month-old with vomiting, jaundice, poor eating, and irritability should include consideration of hydration status, toxicity, sepsis potential, and ability to secure close follow-up. We will make the assumption that the infant is term, with no past medical history, family history, or prenatal evaluation that would put the infant at greater risk for sepsis or likelihood of underlying anatomic genitourinary abnormality. In addition we will assume that the urinalysis was performed by catheterization in a non-pretreated infant.
“A careful history should elicit the change in urine output, frequency, and volume of emesis to contrast with small ‘spit-ups,’ and change in feeding duration or volume. Observation of a feeding in the office or emergency department can be of great value in determining likelihood of ability to maintain hydration at home. Feeding type should be confirmed [because] parents may dilute or alternately concentrate formula in response to vomiting. In this scenario, true emesis in an infant with decreased oral intake would be grounds for admission, intravenous hydration, and evaluation of electrolytes.
“A newly irritable infant evokes a visceral sensation for all pediatric hospitalists. An irritable one-month-old may be suffering from a single system infection, electrolyte imbalance, or other insult, but unfortunately may just as easily have multisystem involvement. Vital signs and physical exam findings of toxicity, such as tachycardia and delayed capillary refill, are not known to us. The presence of jaundice raises concern for cholestasis induced by E. coli or possibly rarer metabolic disease, such as galactosemia. Admission would allow for evaluation and monitoring of the more likely causes of irritability in our index patient, which include sepsis, meningitis, and electrolyte and acid-base imbalances.
“The urinalysis in this infant is suggestive of a urinary tract infection, although infants may have no abnormalities noted on initial urinalysis.7,8 The risk of bacteremia in infants under 60 days with documented urinary tract infection is significant. A number of studies support the need to treat infants less than 30 days with parenteral antibiotics.9-14 Addition of C-reactive protein testing at this time does not aid in distinguishing those who are bacteremic in this age group.15 The often quoted study by Hoberman of 306 children included only 13 under the age of two months.16 Of the 13 reported positive blood cultures, 10 were in children under age six months. Daily intramuscular ceftriaxone treatment would cover a majority of the typical neonatal UTI organisms, can be administered in the outpatient setting, and is proven to be as effective as intravenous delivery. The clinical response to bacteremia is, however, unpredictable in young infants. The sepsis potential in this infant requires admission for physiologic monitoring and support as needed.
“Final, but not inconsequential, concerns are barriers to follow-up. These include parental experience and coping skills with feeding and monitoring an ill infant, ability to educate on the illness and reasons for follow-up, transportation, and operational issues, such as weekend clinic hours or holiday office closures. For the index patient these issues are overshadowed by the clinical criteria for admission but would be of great importance for discharge.”
Conclusion
Based on these responses, admitting a suspected UTI patient on the basis of age alone, as suggested by Santen and Altieri, is likely inappropriate. Many other factors must be weighed and would likely indicate admission for the patient in the scenario, regardless of the infant’s age. In short, until there’s better evidence for age-based admission criteria, clinical judgment based on the individual patient presentation must continue to drive care and treatment decisions.
Keri Losavio is a medical journalist with more than 10 years’ experience.
References
- UTI Guideline Team, Cincinnati Children’s Hospital Medical Center. “Evidence based clinical practice guideline for children 12 years of age or less with acute first time urinary tract infection.” www.cincinnatichildrens.org/svc/dept-div/health-policy/ev-based/uti.htm. Guideline 7, pages 1–20, April 2005.
- Hoberman A, Wald ER. Treatment of urinary tract infections. Pediatr Infect Dis J. 1999;18(11):1020–1021.
- Santen SA, Altieri MF. Pediatric urinary tract infection. Emerg Med Clin North Am. 200119(3):675–690.
- Egland AG, Egland TK. Pyelonephritis. eMedicine. www.emedicine.com/emerg/topic769.htm. Accessed Oct. 16, 2005.
- No authors listed. Practice parameter: the diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. American Academy of Pediatrics. Committee on Quality Improvement. Subcommittee on Urinary Tract Infection. Pediatrics. 1999;103(4):843–852.
- Pitetti RD, Choi S. Utility of blood cultures in febrile children with UTI. Am J Emerg Med. 2002;20:271–274.
- Dayan PS, Bennett J, Best R, et al. Test characteristics of the urine Gram stain in infants 60 days of age with fever. Pediatr Emerg Care. 2002;18(1):12–14.
- Huicho L, Campos-Sanchez M, Alamo C. Meta-analysis of urine screening tests for determining the risk of urinary tract infection in children. Pediatr Infect Dis J. 2002;21 (1):1-11.
- Byington C L, Enriquez F, Hoff C, et al. Serious bacterial infections in febrile infants 1 to 90 days old with and without viral infections. Pediatrics. 2004; 113(6):1662–1666.
- Baraff L. Management of fever without source in infants and children. Ann Emerg Med. 2000;36(6):602–614.
- Baraff LJ, Oslund SA, Schriger DL, Stephen ML. Probability of bacterial infections in febrile infants less than three months of age: A meta-analysis. Pediatr Infect Dis J. 1992;11(4):257–264.
- Klein JO. Management of the febrile child without a focus of infection in the era of universal pneumococcal immunization. Pediatr Infect Dis J. 2002;21(6):584–588.
- Syrogiannopoulos G, Grieva I, Anastassiou E, et al. Sterile cerebrospinal fluid pleocytosis in young infants with urinary tract infections. Pediatr Infect Dis J. 2001;20(10):927–930.
- Jaskiewicz JA, McCarthy CA, Richardson AC, et al. Febrile infants at low risk for serious bacterial infection—an appraisal of the Rochester criteria and implications for management. Febrile Collaborative Study Group. Pediatrics. 1994;94(3):390–396.
- Malik A, Hui C, Pennie RA, Kirpalani H. Beyond the complete blood cell count and C-reactive protein: A systematic review of modern diagnostic tests for neonatal sepsis. Arch Pediatr Adolesc Med. 2003;157(6):511–516.
- Hoberman A, Wald ER, Hickey RW, et al. Oral versus intravenous therapy for urinary tract Infections in young children. Pediatrics.1999;104:79–86
PEDIATRIC SPECIAL SECTION
IN THE LITERATURE
Utilize Clinical and Demographic Factors to Diagnose UTIs in Young Febrile Infants
Review by Sara E. Gardner, MD
Zorc JJ, Levine DA, Platt SL, et al. Clinical and demographic factors associated with urinary tract infections in young febrile infants. Pediatrics. 2000;116(3):644-648.
UTI is a common cause of serious bacterial infection in the febrile infant <60 days of age. Standard urinalysis and urine dipstick techniques, commonly used to diagnose UTI, have relatively low sensitivity increasing the possibility of a missed diagnosis. An accurate initial diagnosis is critical in this age group for whom complications from UTI include bacteremia and renal scarring.
To describe the demographic and clinical factors associated with UTI in infants ≤60 days of age with fever, these authors conducted a prospective cross sectional study from October 1999 to March 2001. Patients were enrolled at eight different institutions after presentation to an emergency department. One-thousand-twenty-five patients age 60 days or younger (mean age 35.5 days, 60.5% male) were enrolled with either reported or documented fever >38. Routine testing for all children included respiratory syncytial virus (RSV) sampling and bladder catheterization or suprapubic aspiration for urinalysis and culture.
A positive urinalysis was defined as a trace or greater result for leukocyte esterase and/or nitrite on dipstick or greater than or equal to five WBCs per high power field (hpf) on urine microscopy. UTI was defined as growth of a single pathogen of ≥1,000 colony forming units (cfu)/mL for urine cultures obtained by suprapubic catheterization, ≥50,000 cfu/mL from a catheterized specimen, or ≥10,000 cfu/ml from a catheterized specimen with a positive urinalysis.
Of the patients enrolled in the study, 92 were found to have UTI by these diagnostic criteria. Using the chi-squared test and calculated odds ratios with 95% confidence intervals, uncircumcised male (OR: 10.4; 95% CI: 4.7-31.4) and maximum temperature of ≥39º C (OR: 2.4 per degree C; 95% CI: 1.5-3.6) were found to be statistically significant variables for predicting UTI. These risk factors remained statistically significant after multivariable analysis controlling for other factors.
Interestingly of the above 92 patients diagnosed with UTI, 85 grew ≥50,000 cfu of a single pathogen, but six (8%) grew 10,000-49,000 cfu with a positive UA based on the study criteria. Zorc, et al. included these patients with >10,000 cfu and >5 WBC/hpf in this study despite previous studies that have established a definition of positive urinalysis to be ≥10 WBC/hpf. Zorc, et al. acknowledge the conservative definition applied in their current study, but assert that the overall results of the study would have been similar had 10,000 or 50,000 cfu/mL thresholds been chosen. To support this assertion, Zorc, et al. retrospectively applied enhanced urinalysis, a sensitive form of urinalysis including hemocytometric cell count and gram stain described by Hoberman, et al. to study patients with low bacteria counts. Based on Hoberman’s study, enhanced urinalysis can differentiate acute infection from asymptomatic bacteriuria in patients with bacterial growth between 10,000 to 50,000 cfu/mL.
Another significant limitation of this study was failure to enroll one-third of eligible patients to the study. In addition, the authors note that missed patients had a lower rate of UTI compared with enrolled patients.
Although this study design prohibits generalization to patient care areas outside the emergency department, the findings can assist the hospitalist in the evaluation of the febrile infant during RSV season and potentially guide decisions regarding empiric antibiotic therapy as part of evaluations to diagnose or exclude serious bacterial infection. Additionally, this study raises the question of need for better methods of urinalysis for febrile, uncircumcised male infants.
Back to the Basics: A Clinical Approach to Excluding Acute Appendicitis
Review by Jane G. Buss, MD
Kharbanda AB, Taylor GA, Fishman SJ, et al. A clinical decision rule to identify children at low risk for appendicitis. Pediatrics. 2005;116(3):709-16.
Appendicitis is the most common condition requiring emergency abdominal surgery in the pediatric population. To diagnosis appendicitis, clinicians typically utilize clinical findings, imaging studies, and laboratory testing. The use of clinical scoring systems to improve the diagnosis of appendicitis in children has been limited, mostly resulting from unacceptably low sensitivities/specificities, or the lack of validation. The use of CT scan to aid in the evaluation of children with appendicitis has become widespread. Concerns remain, however, regarding long-term radiation effects and increased healthcare costs associated with this approach.
The authors of this study sought to develop clinical scores for children to predict which of those with acute abdominal pain do not have appendicitis. Additionally, they hoped to lessen the use of CT scanning. Their goal was to identify those groups of children who have significant abdominal pain without appendicitis who could be safely observed without CT scan or possible surgery.
This prospective cohort study enrolled 601 eligible children ages three to 18 with suspected appendicitis who presented to the emergency department over a 15-month period. Two low-risk clinical decision rules were developed using logistic regression and recursive partitioning. Using logistic regression, six factors were identified from analysis of 425 patients in the derivation set significantly associated with an increased likelihood of appendicitis. The score components include:
- Nausea (2 points);
- History of focal right lower quadrant pain (RLQ) (2 points);
- Migration of pain (1 point);
- Difficulty walking (1 point);
- Rebound tenderness (2 points); and
- Absolute neutrophil count (ANC) >6.75 x 103/uL (6 points).
When tested with data from the 176 patients in the validation set, a score of less than or equal to five had a sensitivity of 96.3%, and a negative predictive value of 95.6% for excluding appendicitis.
The authors then derived a second clinical low-risk decision rule by recursive partitioning. They determined that a combination of ANC <6.75 X 10 to the third/microliter, absence of nausea (or emesis or anorexia), and absence of maximal tenderness in the RLQ essentially excluded appendicitis in the derivation and validation groups. This rule had a sensitivity of 98.1%, and a negative predictive value of 97.5%.
In summary, these authors derived two clinical decision rules giving the clinician the option of a clinical score (logistic regression) or a decision tree (recursive partitioning) to identify children at low risk for appendicitis. Their findings suggest application of either low-risk rule would lead to decreased reliance on CT scan. Applying these clinical rules to their patients could have reduced the rate of CT scan by 20%. They conclude that pediatric patients who have suspected appendicitis and are at low risk by either model should be considered for observation rather than undergo CT scan or operative care.
Epidemiology of Fungal Infection in the Tertiary Care Inpatient Setting
Review by Brandan P. Kennedy, MD
Abelson, JA, Moore T, Bruckner D, et al. Frequency of fungemia in hospitalized pediatric inpatients over 11 years at a tertiary care institution. Pediatrics. 2005;116(1):611-617.
Fungal organisms are relatively uncommon causes of blood infections in the pediatric population. When they do occur, they cause significant morbidity and mortality. The incidence of fungal blood infections appears to be rising at a faster rate than that of other pathogens. Authors from the University of California performed this study to describe those rate changes, and to evaluate whether treatment has improved in the past 11 years.
This retrospective cohort study involved children admitted to Mattel Children’s Hospital in Los Angeles, California, during an 11-year period from January 1991 to December 2001. Information obtained on all positive fungal cultures from all body sites included date and site of culture, demographics, and fungal etiology. Additionally, data regarding underlying illness, hospital course, outcome, and antimicrobial treatment were considered.
Study results demonstrated a significant increase in diagnosed fungemia in children. There was a 15% increase in overall pediatric admissions in the study period, and a 23% increase in positive fungal cultures in the same period. Of 272 blood cultures, 97 were positive for fungus. Although this is a relatively small number of total infections, data demonstrated a 91% increase in fungemia during the study period. Candida species were the organisms most frequently isolated from any body site with 85% of the total isolates. Of the total positive isolates, it appeared that approximately 78% reflected colonization as opposed to infection.
Outcomes for fungal infections improved only marginally in the study period. Fifty percent of patients with fungemia died between 1991 and 1996, and 45% died between 1997 and 2001. The mortality rate for immunocompromised conditions was 57%. The cost effectiveness of fungal screening cultures was also evaluated, which demonstrated that fungal cultures identified 14 patients independent of bacterial blood cultures at a cost of $560,000, which resulted in a cost of $40,000 per identified patient.
The study reaches several significant conclusions. First there has been a significant increase in fungal infections that exceeds the increase in overall pediatric hospital admissions. However, it is important to recognize the increase in immunocompromised conditions during the study period, which may account for the higher incidence of fungemia.
Second the addition of fungal blood cultures to bacterial blood cultures as part of a routine workup for febrile patients appeared to yield limited clinical information at a very high cost. Third this study highlights the serious threat fungal infections pose to immunocompromised hosts who have a significantly higher incidence of infection, as well as higher morbidity and mortality. Fourth the use of broad spectrum antibiotics may be increasing fungal colonization in patients and consequently increasing the risk for pathologic fungal infection. Finally morbidity and mortality rates for fungal infections did not greatly improve, despite significant improvements in supportive care made during the study period
This study demonstrates a need for better diagnostic markers for fungal infections, especially those that might provide earlier detection and diagnosis at less cost. The importance of judicious use of antibiotics is underscored while the need for a broader base of therapeutic agents is highlighted. These issues may be key ingredients needed to reduce adverse outcomes from fungal infections, especially in the immunocompromised host.
Rotavirus Vaccine Revisited
Salinas B, Perez Schael I, Linhares AC, et al. Evaluation of safety, immunogenicity and efficacy of an attenuated rotavirus vaccine, RIX4414. Ped Infect Dis J. 2005;24(9):807-816.
Rotavirus is the leading cause of severe gastroenteritis among children worldwide. In the United States, rotavirus is responsible for approximately 5%-10% of all diarrhea among children older than five and accounts for approximately 50,000 hospitalizations each year. An estimated one in 200,000 children with rotavirus diarrhea dies from complications of infection. The immunizing effect of rotavirus infection stimulated the development of live attenuated vaccines. In 1998, a three-dose regimen of a tetravalent rhesus-human reassortant vaccine (RotaShield: Wyeth Laboratories,) was licensed for infant immunization in the United States. Within the first year of use, it was withdrawn due to an observed risk of intussusception. The current study was designed to evaluate immunogenicity and efficacy of a live attenuated monovalent human rotavirus vaccine, RIX4414.
A double-blind, randomized, placebo-controlled design was utilized with the RIX4414 rotavirus vaccine administered at three different virus concentrations. Infants were randomly assigned to one of the three study groups or the placebo group. Infants in the vaccine groups received two oral doses of the vaccine at the age of two and four months. An identical placebo containing the same constituents as the vaccine except for the vaccine virus was used as the control. The vaccine was given concomitantly with other routine vaccinations. To determine immunogenicity, blood samples were obtained from all infants immediately before the first vaccination to exclude previous rotavirus infection. Blood samples were obtained two months after the first second vaccine doses and again at one year to measure anti-rotavirus IgA antibodies. Additionally, stool was obtained from 25% of the study sample and tested for rotavirus viral shedding, with differentiation between wild type and vaccine also being performed.
There were 2,155 infants enrolled in this study from three countries in South America, allowing for slightly more than 500 infants in each group. The study began in May 2001, and the final one-year follow-up was completed in April 2003. The anti-rotavirus IgA seroconversion rates two months after first and second doses were 38%-43% and 61%-65%, respectively. This compared with a 5.3% seroconversion rate in the control group, which was determined to be a wild type virus. Vaccine take after two doses was shown in all three vaccine study groups, ranging from 65% to 75% for the lowest to highest vaccine concentration groups. Reactogenicity and safety was evaluated by monitoring incidences of fever, diarrhea, vomiting, irritability, and loss of appetite during the 15 days after vaccine administration. The results were similar for the four study groups suggesting no significant reactogenicity. There were 220 serious adverse events reported including one intussusception. However, none of these events was determined to be related to the vaccine. The RIX4414 vaccine was demonstrated to effectively protect against severe gastroenteritis caused by G1 type rotavirus and also was shown to provide some cross protection to other serotypes.
This well-designed study demonstrated a statistically significant reduction in gastroenteritis due to rotavirus infection, especially of the predominant G1 serotype, after two doses of the RIX4414 human rotavirus vaccine. Objective measures of viral shedding and IgA seroconversion support the efficacy of the vaccine. This study provided a large sample population with good controls.
An important and possibly confounding variable not addressed by the study was breastfeeding status of the infants. There is clinical evidence demonstrating the protective properties of secretory IgA in human milk against rotavirus infection, and this could have influenced the observed severity of disease in the sample population. It would have been interesting to isolate breastfeeding status as a study variable and note any effect on the results of the study.
Aside from this observation, this study appears to show a promising new oral rotavirus vaccine. As further research on the RIX4414 vaccine continues, there is hope that this vaccine could make a significant positive impact on morbidity and hospitalization rates for rotavirus infections worldwide. TH
Scenario: A 32-day-old female presents with vomiting and jaundice, and the mother reports that the child is irritable and not eating as well as usual. The pediatric hospitalist suspects a UTI and orders a dipstick/urinalysis and urine culture. The dipstick/urinalysis results are positive for nitrite and leukocyte esterase, indicating antibiotic therapy for presumed UTI.
Introduction
UTI is one of the most common bacterial infections in infants and young children. To prevent progression to pyelonephritis and avoid potential renal scarring or failure, early recognition and prompt treatment are critical.
Clinical signs and symptoms of UTI in newborns include jaundice, sepsis, failure to thrive, poor feeding, vomiting, and fever. In infants and preschoolers, hospitalists should also suspect UTI in the presence of diarrhea, strong-smelling urine, abdominal or flank pain, and new onset urinary incontinence.1
Treatment recommendations, which are age-dependent, include antibiotic therapy initiated upon an abnormal dipstick/urinalysis. If a urine culture is positive, a seven- to 14-day course of antibiotic therapy is recommended, followed by prophylactic antibiotics until results of imaging studies are available.1 According to a study by Hoberman and Wald, treatment of UTI with oral antibiotics alone is generally effective, even for young children with pyelonephritis.2
Imaging recommendations for a first UTI include ultrasound, cystogram, and renal cortical scan.
Up to this point, there’s been very little disagreement about the management of UTI. However, the question of whether the one-month-old patient in our scenario should be admitted or sent home with strict instructions on the administration of antibiotics remains controversial. The pediatric UTI guideline from Cincinnati Children’s Hospital Medical Center recommends routine hospital admission if the infant is under 30 days old.1 On the other hand, Santen and Altieri, among others, recommend, “Sick children and infants less than three months should be treated as inpatients, and healthy children and older infants may be treated as outpatients.”3,4
—Jeffrey M. Simmons, MD
The Set-Up
We asked several pediatric hospitalists across the country—including an instructor of pediatrics at Cincinnati Children’s Hospital Medical Center—to respond to this simple scenario, posing the following questions: “What recommendation would you follow? Would you admit the one-month-old infant in our scenario or send her home? Why?”
Predictably, admission criteria varied, but most agreed that this infant should be admitted. No one based their response on age.
Automatic Admission Cut-off Not Well Supported
Jeffrey M. Simmons, MD, instructor of pediatrics, Division of General and Community Pediatrics, Cincinnati Children’s Hospital Medical Center, responds: “My perspective on the UTI scenario is that the only dogma that applies is that the infant needs antibiotics. Because [the scenario] mentions vomiting, I would, therefore, most likely give parenteral antibiotics and admit.
“An issue within this scenario that I don’t believe the literature answers clearly is once a UTI is identified by the U/A, what risk remains of bacteremia or meningitis in the over 30-day-old infant? We are taught that infants don’t ‘localize’ infections well (i.e., a serious bacterial infection in one place can rapidly lead to disseminated infection). I sense a growing consensus that after 30 days or so this concern is less at issue. However, for clarity, I would prefer to obtain blood and CSF cultures on this infant prior to initiating antibiotic therapy. Without those cultures, and the screening tests that go with them (i.e., serum WBC count, CSF cell count, and glucose), I would be uncomfortable sending the infant home.
“However, if the WBC count was between 5 and 15, the CSF reassuring, the parents in agreement and reliable with good primary care follow-up the next morning, I think such an infant could be managed with one dose of IV/IM antibiotics after cultures are obtained and sent home. The following day, depending on culture results and the clinical situation, this infant might either be admitted, given another dose of parenteral antibiotics pending final blood culture, or switched to oral antibiotics.
“Such a plan is complex, so if the primary care physician or family was at all uncomfortable, admission to accomplish that plan would clearly be appropriate.
“A final issue not adequately addressed within the scenario is an assessment of the infant’s hydration—potentially an issue due to the vomiting. If the infant was mildly to moderately dehydrated with persistent vomiting, I would also then admit until this improved.
“In regard to the cited evidence, I would say that clearly an arbitrary cut-off of automatic admission under three months is not well supported by current literature, but is certainly many practitioners’ ‘style.’ Oral antibiotics are clearly efficacious for pyelonephritis, but the clinician needs to be confident the family can give them and the infant will keep them down. I believe most practitioners would agree with admission for an infant under 30 days, but where to precisely draw that line needs to be better established through investigation. Potential concomitant bacteremia and meningitis lead me to support obtaining blood and CSF cultures on any infant under 60 days for which I plan to initiate antibiotics for UTI.”
Possibility of Dehydration Indicates Admission
Michael P. Fullmer, DO, Central Iowa Pediatric Hospitalists, Mercy Medical Center, Des Moines, Iowa, responds: “This patient is not febrile, but does have other systemic symptoms, including poor feeding, irritability, jaundice, and vomiting. These systemic symptoms could be indicative of a serious bacterial infection like UTI, bacteremia, or meningitis. This patient most likely has a UTI. These symptoms may suggest pyelonephritis rather than lower UTI, but the distinction is not necessary for our decision here.
“Bacteremia is present in up to 22.7% of infants less than two months old with a UTI. This adds to the complexity of the issue, and a blood culture is probably indicated. Meningitis should be considered, but a lumbar puncture is probably not indicated in this scenario.
“A one-month-old with a UTI should be admitted to the hospital and started on parenteral antibiotics. There are several reasons for admission. First, the presence of vomiting makes oral antibiotic administration impractical (if not impossible). Intramuscular antibiotic injection may be an option, but the IV route gives the provider more options and is usually better accepted by parents. Next, if the patient is not already dehydrated, the poor feeding and vomiting could lead to dehydration. This alone would be an indication for admission. Finally, admission would give the physician time to observe the infant for clinical improvement. This may be subtle in the absence of fever.
“Another consideration is the recommended imaging for all children less than two years old. The AAP has recommended a renal ultrasound and VCUG for all infants and young children with their first UTI. This is important for discovery of urinary tract anomalies that predispose the patient to recurrent UTIs and eventual renal scarring and dysfunction. The imaging should be performed at the earliest convenient time if the patient is responding to therapy. In our practice, we generally have the renal ultrasound performed while the patient is in the hospital and arrange the VCUG as an outpatient [exam] prior to completion of the course of antibiotics.
“Patients are discharged when they are afebrile for 24 hours, have adequate oral intake and are able to take oral antibiotics. Please refer to the AAP Clinical Practice Guideline for more detail.5,6
—Michael Fullmer, DO
Admission Criteria Must Take Fever Into Account
John W. Graef, MD, chief, Services Office at Children’s Hospital, Harvard Vanguard Services Office, Boston, responds: “The presence or absence of fever is an important variable. Dipstick urines are shortcuts and don’t provide such information as the presence or absence of casts, although the fact that the child is vomiting and irritable is suggestive of pyelonephritis as opposed to a simple UTI/cystitis. [The scenario doesn’t] mention how the urine is obtained. Presumably it is a cath specimen, but that needs to be specified.
“Jaundice can occur with a UTI, but usually in the first week or so of life. A 32-day-old infant with pyelo is unlikely to be jaundiced unless for some other reason.
“I certainly agree with routine admission of a febrile infant up to one month, but not necessarily an otherwise well female infant. The presence of vomiting and irritability with or without fever might prompt a full septic work-up, in which case the decision to admit an afebrile infant would depend on the results of the CBC/UA and probably an LP. A blood culture and CBC should be drawn in the ED.
“In other words, one can’t have it both ways. If the irritability and vomiting are due to pyelo, a septic work-up is warranted. If all parameters are normal, the only reason for admission is hydration of a vomiting infant. If the infant was afebrile and had an uncomplicated UTI, I would not automatically admit an otherwise well 32-day-old.
“Poor PO (per OS, i.e., oral, by mouth) intake in an infant with a UTI warrants IV fluid regardless of age.”
—John W. Graef, MD
True Emesis With Decreased Oral Intake Indicates Admission
Erin R. Stucky, MD, pediatric hospitalist, Children’s Hospital and Health Center San Diego, associate professor, UCSD Pediatrics, responds: “The decision to admit or discharge this one-month-old with vomiting, jaundice, poor eating, and irritability should include consideration of hydration status, toxicity, sepsis potential, and ability to secure close follow-up. We will make the assumption that the infant is term, with no past medical history, family history, or prenatal evaluation that would put the infant at greater risk for sepsis or likelihood of underlying anatomic genitourinary abnormality. In addition we will assume that the urinalysis was performed by catheterization in a non-pretreated infant.
“A careful history should elicit the change in urine output, frequency, and volume of emesis to contrast with small ‘spit-ups,’ and change in feeding duration or volume. Observation of a feeding in the office or emergency department can be of great value in determining likelihood of ability to maintain hydration at home. Feeding type should be confirmed [because] parents may dilute or alternately concentrate formula in response to vomiting. In this scenario, true emesis in an infant with decreased oral intake would be grounds for admission, intravenous hydration, and evaluation of electrolytes.
“A newly irritable infant evokes a visceral sensation for all pediatric hospitalists. An irritable one-month-old may be suffering from a single system infection, electrolyte imbalance, or other insult, but unfortunately may just as easily have multisystem involvement. Vital signs and physical exam findings of toxicity, such as tachycardia and delayed capillary refill, are not known to us. The presence of jaundice raises concern for cholestasis induced by E. coli or possibly rarer metabolic disease, such as galactosemia. Admission would allow for evaluation and monitoring of the more likely causes of irritability in our index patient, which include sepsis, meningitis, and electrolyte and acid-base imbalances.
“The urinalysis in this infant is suggestive of a urinary tract infection, although infants may have no abnormalities noted on initial urinalysis.7,8 The risk of bacteremia in infants under 60 days with documented urinary tract infection is significant. A number of studies support the need to treat infants less than 30 days with parenteral antibiotics.9-14 Addition of C-reactive protein testing at this time does not aid in distinguishing those who are bacteremic in this age group.15 The often quoted study by Hoberman of 306 children included only 13 under the age of two months.16 Of the 13 reported positive blood cultures, 10 were in children under age six months. Daily intramuscular ceftriaxone treatment would cover a majority of the typical neonatal UTI organisms, can be administered in the outpatient setting, and is proven to be as effective as intravenous delivery. The clinical response to bacteremia is, however, unpredictable in young infants. The sepsis potential in this infant requires admission for physiologic monitoring and support as needed.
“Final, but not inconsequential, concerns are barriers to follow-up. These include parental experience and coping skills with feeding and monitoring an ill infant, ability to educate on the illness and reasons for follow-up, transportation, and operational issues, such as weekend clinic hours or holiday office closures. For the index patient these issues are overshadowed by the clinical criteria for admission but would be of great importance for discharge.”
Conclusion
Based on these responses, admitting a suspected UTI patient on the basis of age alone, as suggested by Santen and Altieri, is likely inappropriate. Many other factors must be weighed and would likely indicate admission for the patient in the scenario, regardless of the infant’s age. In short, until there’s better evidence for age-based admission criteria, clinical judgment based on the individual patient presentation must continue to drive care and treatment decisions.
Keri Losavio is a medical journalist with more than 10 years’ experience.
References
- UTI Guideline Team, Cincinnati Children’s Hospital Medical Center. “Evidence based clinical practice guideline for children 12 years of age or less with acute first time urinary tract infection.” www.cincinnatichildrens.org/svc/dept-div/health-policy/ev-based/uti.htm. Guideline 7, pages 1–20, April 2005.
- Hoberman A, Wald ER. Treatment of urinary tract infections. Pediatr Infect Dis J. 1999;18(11):1020–1021.
- Santen SA, Altieri MF. Pediatric urinary tract infection. Emerg Med Clin North Am. 200119(3):675–690.
- Egland AG, Egland TK. Pyelonephritis. eMedicine. www.emedicine.com/emerg/topic769.htm. Accessed Oct. 16, 2005.
- No authors listed. Practice parameter: the diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. American Academy of Pediatrics. Committee on Quality Improvement. Subcommittee on Urinary Tract Infection. Pediatrics. 1999;103(4):843–852.
- Pitetti RD, Choi S. Utility of blood cultures in febrile children with UTI. Am J Emerg Med. 2002;20:271–274.
- Dayan PS, Bennett J, Best R, et al. Test characteristics of the urine Gram stain in infants 60 days of age with fever. Pediatr Emerg Care. 2002;18(1):12–14.
- Huicho L, Campos-Sanchez M, Alamo C. Meta-analysis of urine screening tests for determining the risk of urinary tract infection in children. Pediatr Infect Dis J. 2002;21 (1):1-11.
- Byington C L, Enriquez F, Hoff C, et al. Serious bacterial infections in febrile infants 1 to 90 days old with and without viral infections. Pediatrics. 2004; 113(6):1662–1666.
- Baraff L. Management of fever without source in infants and children. Ann Emerg Med. 2000;36(6):602–614.
- Baraff LJ, Oslund SA, Schriger DL, Stephen ML. Probability of bacterial infections in febrile infants less than three months of age: A meta-analysis. Pediatr Infect Dis J. 1992;11(4):257–264.
- Klein JO. Management of the febrile child without a focus of infection in the era of universal pneumococcal immunization. Pediatr Infect Dis J. 2002;21(6):584–588.
- Syrogiannopoulos G, Grieva I, Anastassiou E, et al. Sterile cerebrospinal fluid pleocytosis in young infants with urinary tract infections. Pediatr Infect Dis J. 2001;20(10):927–930.
- Jaskiewicz JA, McCarthy CA, Richardson AC, et al. Febrile infants at low risk for serious bacterial infection—an appraisal of the Rochester criteria and implications for management. Febrile Collaborative Study Group. Pediatrics. 1994;94(3):390–396.
- Malik A, Hui C, Pennie RA, Kirpalani H. Beyond the complete blood cell count and C-reactive protein: A systematic review of modern diagnostic tests for neonatal sepsis. Arch Pediatr Adolesc Med. 2003;157(6):511–516.
- Hoberman A, Wald ER, Hickey RW, et al. Oral versus intravenous therapy for urinary tract Infections in young children. Pediatrics.1999;104:79–86
PEDIATRIC SPECIAL SECTION
IN THE LITERATURE
Utilize Clinical and Demographic Factors to Diagnose UTIs in Young Febrile Infants
Review by Sara E. Gardner, MD
Zorc JJ, Levine DA, Platt SL, et al. Clinical and demographic factors associated with urinary tract infections in young febrile infants. Pediatrics. 2000;116(3):644-648.
UTI is a common cause of serious bacterial infection in the febrile infant <60 days of age. Standard urinalysis and urine dipstick techniques, commonly used to diagnose UTI, have relatively low sensitivity increasing the possibility of a missed diagnosis. An accurate initial diagnosis is critical in this age group for whom complications from UTI include bacteremia and renal scarring.
To describe the demographic and clinical factors associated with UTI in infants ≤60 days of age with fever, these authors conducted a prospective cross sectional study from October 1999 to March 2001. Patients were enrolled at eight different institutions after presentation to an emergency department. One-thousand-twenty-five patients age 60 days or younger (mean age 35.5 days, 60.5% male) were enrolled with either reported or documented fever >38. Routine testing for all children included respiratory syncytial virus (RSV) sampling and bladder catheterization or suprapubic aspiration for urinalysis and culture.
A positive urinalysis was defined as a trace or greater result for leukocyte esterase and/or nitrite on dipstick or greater than or equal to five WBCs per high power field (hpf) on urine microscopy. UTI was defined as growth of a single pathogen of ≥1,000 colony forming units (cfu)/mL for urine cultures obtained by suprapubic catheterization, ≥50,000 cfu/mL from a catheterized specimen, or ≥10,000 cfu/ml from a catheterized specimen with a positive urinalysis.
Of the patients enrolled in the study, 92 were found to have UTI by these diagnostic criteria. Using the chi-squared test and calculated odds ratios with 95% confidence intervals, uncircumcised male (OR: 10.4; 95% CI: 4.7-31.4) and maximum temperature of ≥39º C (OR: 2.4 per degree C; 95% CI: 1.5-3.6) were found to be statistically significant variables for predicting UTI. These risk factors remained statistically significant after multivariable analysis controlling for other factors.
Interestingly of the above 92 patients diagnosed with UTI, 85 grew ≥50,000 cfu of a single pathogen, but six (8%) grew 10,000-49,000 cfu with a positive UA based on the study criteria. Zorc, et al. included these patients with >10,000 cfu and >5 WBC/hpf in this study despite previous studies that have established a definition of positive urinalysis to be ≥10 WBC/hpf. Zorc, et al. acknowledge the conservative definition applied in their current study, but assert that the overall results of the study would have been similar had 10,000 or 50,000 cfu/mL thresholds been chosen. To support this assertion, Zorc, et al. retrospectively applied enhanced urinalysis, a sensitive form of urinalysis including hemocytometric cell count and gram stain described by Hoberman, et al. to study patients with low bacteria counts. Based on Hoberman’s study, enhanced urinalysis can differentiate acute infection from asymptomatic bacteriuria in patients with bacterial growth between 10,000 to 50,000 cfu/mL.
Another significant limitation of this study was failure to enroll one-third of eligible patients to the study. In addition, the authors note that missed patients had a lower rate of UTI compared with enrolled patients.
Although this study design prohibits generalization to patient care areas outside the emergency department, the findings can assist the hospitalist in the evaluation of the febrile infant during RSV season and potentially guide decisions regarding empiric antibiotic therapy as part of evaluations to diagnose or exclude serious bacterial infection. Additionally, this study raises the question of need for better methods of urinalysis for febrile, uncircumcised male infants.
Back to the Basics: A Clinical Approach to Excluding Acute Appendicitis
Review by Jane G. Buss, MD
Kharbanda AB, Taylor GA, Fishman SJ, et al. A clinical decision rule to identify children at low risk for appendicitis. Pediatrics. 2005;116(3):709-16.
Appendicitis is the most common condition requiring emergency abdominal surgery in the pediatric population. To diagnosis appendicitis, clinicians typically utilize clinical findings, imaging studies, and laboratory testing. The use of clinical scoring systems to improve the diagnosis of appendicitis in children has been limited, mostly resulting from unacceptably low sensitivities/specificities, or the lack of validation. The use of CT scan to aid in the evaluation of children with appendicitis has become widespread. Concerns remain, however, regarding long-term radiation effects and increased healthcare costs associated with this approach.
The authors of this study sought to develop clinical scores for children to predict which of those with acute abdominal pain do not have appendicitis. Additionally, they hoped to lessen the use of CT scanning. Their goal was to identify those groups of children who have significant abdominal pain without appendicitis who could be safely observed without CT scan or possible surgery.
This prospective cohort study enrolled 601 eligible children ages three to 18 with suspected appendicitis who presented to the emergency department over a 15-month period. Two low-risk clinical decision rules were developed using logistic regression and recursive partitioning. Using logistic regression, six factors were identified from analysis of 425 patients in the derivation set significantly associated with an increased likelihood of appendicitis. The score components include:
- Nausea (2 points);
- History of focal right lower quadrant pain (RLQ) (2 points);
- Migration of pain (1 point);
- Difficulty walking (1 point);
- Rebound tenderness (2 points); and
- Absolute neutrophil count (ANC) >6.75 x 103/uL (6 points).
When tested with data from the 176 patients in the validation set, a score of less than or equal to five had a sensitivity of 96.3%, and a negative predictive value of 95.6% for excluding appendicitis.
The authors then derived a second clinical low-risk decision rule by recursive partitioning. They determined that a combination of ANC <6.75 X 10 to the third/microliter, absence of nausea (or emesis or anorexia), and absence of maximal tenderness in the RLQ essentially excluded appendicitis in the derivation and validation groups. This rule had a sensitivity of 98.1%, and a negative predictive value of 97.5%.
In summary, these authors derived two clinical decision rules giving the clinician the option of a clinical score (logistic regression) or a decision tree (recursive partitioning) to identify children at low risk for appendicitis. Their findings suggest application of either low-risk rule would lead to decreased reliance on CT scan. Applying these clinical rules to their patients could have reduced the rate of CT scan by 20%. They conclude that pediatric patients who have suspected appendicitis and are at low risk by either model should be considered for observation rather than undergo CT scan or operative care.
Epidemiology of Fungal Infection in the Tertiary Care Inpatient Setting
Review by Brandan P. Kennedy, MD
Abelson, JA, Moore T, Bruckner D, et al. Frequency of fungemia in hospitalized pediatric inpatients over 11 years at a tertiary care institution. Pediatrics. 2005;116(1):611-617.
Fungal organisms are relatively uncommon causes of blood infections in the pediatric population. When they do occur, they cause significant morbidity and mortality. The incidence of fungal blood infections appears to be rising at a faster rate than that of other pathogens. Authors from the University of California performed this study to describe those rate changes, and to evaluate whether treatment has improved in the past 11 years.
This retrospective cohort study involved children admitted to Mattel Children’s Hospital in Los Angeles, California, during an 11-year period from January 1991 to December 2001. Information obtained on all positive fungal cultures from all body sites included date and site of culture, demographics, and fungal etiology. Additionally, data regarding underlying illness, hospital course, outcome, and antimicrobial treatment were considered.
Study results demonstrated a significant increase in diagnosed fungemia in children. There was a 15% increase in overall pediatric admissions in the study period, and a 23% increase in positive fungal cultures in the same period. Of 272 blood cultures, 97 were positive for fungus. Although this is a relatively small number of total infections, data demonstrated a 91% increase in fungemia during the study period. Candida species were the organisms most frequently isolated from any body site with 85% of the total isolates. Of the total positive isolates, it appeared that approximately 78% reflected colonization as opposed to infection.
Outcomes for fungal infections improved only marginally in the study period. Fifty percent of patients with fungemia died between 1991 and 1996, and 45% died between 1997 and 2001. The mortality rate for immunocompromised conditions was 57%. The cost effectiveness of fungal screening cultures was also evaluated, which demonstrated that fungal cultures identified 14 patients independent of bacterial blood cultures at a cost of $560,000, which resulted in a cost of $40,000 per identified patient.
The study reaches several significant conclusions. First there has been a significant increase in fungal infections that exceeds the increase in overall pediatric hospital admissions. However, it is important to recognize the increase in immunocompromised conditions during the study period, which may account for the higher incidence of fungemia.
Second the addition of fungal blood cultures to bacterial blood cultures as part of a routine workup for febrile patients appeared to yield limited clinical information at a very high cost. Third this study highlights the serious threat fungal infections pose to immunocompromised hosts who have a significantly higher incidence of infection, as well as higher morbidity and mortality. Fourth the use of broad spectrum antibiotics may be increasing fungal colonization in patients and consequently increasing the risk for pathologic fungal infection. Finally morbidity and mortality rates for fungal infections did not greatly improve, despite significant improvements in supportive care made during the study period
This study demonstrates a need for better diagnostic markers for fungal infections, especially those that might provide earlier detection and diagnosis at less cost. The importance of judicious use of antibiotics is underscored while the need for a broader base of therapeutic agents is highlighted. These issues may be key ingredients needed to reduce adverse outcomes from fungal infections, especially in the immunocompromised host.
Rotavirus Vaccine Revisited
Salinas B, Perez Schael I, Linhares AC, et al. Evaluation of safety, immunogenicity and efficacy of an attenuated rotavirus vaccine, RIX4414. Ped Infect Dis J. 2005;24(9):807-816.
Rotavirus is the leading cause of severe gastroenteritis among children worldwide. In the United States, rotavirus is responsible for approximately 5%-10% of all diarrhea among children older than five and accounts for approximately 50,000 hospitalizations each year. An estimated one in 200,000 children with rotavirus diarrhea dies from complications of infection. The immunizing effect of rotavirus infection stimulated the development of live attenuated vaccines. In 1998, a three-dose regimen of a tetravalent rhesus-human reassortant vaccine (RotaShield: Wyeth Laboratories,) was licensed for infant immunization in the United States. Within the first year of use, it was withdrawn due to an observed risk of intussusception. The current study was designed to evaluate immunogenicity and efficacy of a live attenuated monovalent human rotavirus vaccine, RIX4414.
A double-blind, randomized, placebo-controlled design was utilized with the RIX4414 rotavirus vaccine administered at three different virus concentrations. Infants were randomly assigned to one of the three study groups or the placebo group. Infants in the vaccine groups received two oral doses of the vaccine at the age of two and four months. An identical placebo containing the same constituents as the vaccine except for the vaccine virus was used as the control. The vaccine was given concomitantly with other routine vaccinations. To determine immunogenicity, blood samples were obtained from all infants immediately before the first vaccination to exclude previous rotavirus infection. Blood samples were obtained two months after the first second vaccine doses and again at one year to measure anti-rotavirus IgA antibodies. Additionally, stool was obtained from 25% of the study sample and tested for rotavirus viral shedding, with differentiation between wild type and vaccine also being performed.
There were 2,155 infants enrolled in this study from three countries in South America, allowing for slightly more than 500 infants in each group. The study began in May 2001, and the final one-year follow-up was completed in April 2003. The anti-rotavirus IgA seroconversion rates two months after first and second doses were 38%-43% and 61%-65%, respectively. This compared with a 5.3% seroconversion rate in the control group, which was determined to be a wild type virus. Vaccine take after two doses was shown in all three vaccine study groups, ranging from 65% to 75% for the lowest to highest vaccine concentration groups. Reactogenicity and safety was evaluated by monitoring incidences of fever, diarrhea, vomiting, irritability, and loss of appetite during the 15 days after vaccine administration. The results were similar for the four study groups suggesting no significant reactogenicity. There were 220 serious adverse events reported including one intussusception. However, none of these events was determined to be related to the vaccine. The RIX4414 vaccine was demonstrated to effectively protect against severe gastroenteritis caused by G1 type rotavirus and also was shown to provide some cross protection to other serotypes.
This well-designed study demonstrated a statistically significant reduction in gastroenteritis due to rotavirus infection, especially of the predominant G1 serotype, after two doses of the RIX4414 human rotavirus vaccine. Objective measures of viral shedding and IgA seroconversion support the efficacy of the vaccine. This study provided a large sample population with good controls.
An important and possibly confounding variable not addressed by the study was breastfeeding status of the infants. There is clinical evidence demonstrating the protective properties of secretory IgA in human milk against rotavirus infection, and this could have influenced the observed severity of disease in the sample population. It would have been interesting to isolate breastfeeding status as a study variable and note any effect on the results of the study.
Aside from this observation, this study appears to show a promising new oral rotavirus vaccine. As further research on the RIX4414 vaccine continues, there is hope that this vaccine could make a significant positive impact on morbidity and hospitalization rates for rotavirus infections worldwide. TH
Say What?
Mack Lipkin, MD, the founding president of the American Academy on Physician and Patient, a society dedicated to research, education, and professional standards in patient-physician communication, reported some interesting data in a PowerPoint presentation he gave in 2000 at the working conference on Diversity and Communication in Healthcare sponsored in part by the U.S. Office of Minority Health. Dr. Lipkin said that physicians’ lowest level of communication skills are reached during their medical residencies; even medical students’ skills were rated higher. Dr. Lipkin, who is also director of the Division of Primary Care in the Department of Medicine at New York University School of Medicine, New York City, went on to explain that, typically, physicians will recover some capacity with communication as they enter practice and years of experience ensue, but they never reach the level they possessed before they entered medical school.
While some hospitalists may consider this a startling claim, few are likely to find it shocking. Although hospitalists believe using good communication skills is an important part of their work, their skills may not necessarily match their beliefs or intentions. Research in progress by hospitalist Paul Mueller, MD, and his colleagues at the Mayo Clinic College of Medicine, Rochester, Minn., reveals that a majority of new internal medicine faculty—regardless of years in practice or background—believe they could benefit from and desire additional training in communication; yet these individuals teach communication skills to medical students (personal communication, 2005).
Medical education curriculum experts nationwide are pumping up their coverage of physician-patient communication to supply the demand stemming from a surge of interest in this topic in recent decades. Some reasons for this include reports and investigations into medical errors, an explosion of medical and health information easily accessible to patients and families, the rise of a vital consumer advocacy and empowerment movement, the reliance on outcomes assessments that include patient satisfaction ratings, a growing emphasis on patient- or relationship-centered care, and the reduced time for medical encounters caused at least in part by cost-containment initiatives.
The relationship between communication and medical outcomes is being increasingly explored, including the effects on physician satisfaction.1-5 But what are the further, personal effects to the individual hospitalist when he or she perpetuates poor communication skills?
—Robert Trowbridge, MD
Communication With Patients And Families
The work of hospitalists depends acutely on communication.
“It’s part of the role of the hospitalist to explain and help shepherd [patients] through the healthcare system,” says Robert Trowbridge, MD, a hospitalist and assistant professor of medicine, University of Vermont College of Medicine, Maine Medical Center, Portland.
Professionals whose medical practice is based on short clinical visits or performing procedures may or may not be good communicators, but it’s probably not as integral to the way they or the situations their patients are going through will be perceived. The conventional wisdom in professional and lay circles tends to be, “He may be a lousy communicator, but he’s a hellava surgeon,” says Dr. Trowbridge.
But most patients expect good communication from their primary care physician and because they are serving that function when a patient is hospitalized, hospitalists should understand that patients and families expect those skills of them. “And if the [hospitalists] don’t do well [in communicating], there can be much more stress on the patients and physicians,” explains Dr. Trowbridge.
What Constitutes Poor Communication?
“First, on one level, poor communication skills are inefficient in talking with patients,” says Steven Pantilat, MD, SHM president. “So, I think it makes your work harder.”
Some examples of communication inefficiency (or ineffectiveness) for a clinician include:2,4,5,6-8
- Lacking the ability to articulate ideas adequately;
- Transferring insufficient information between the provider and the patient, including inadequate elicitation of key facts from the patient;
- Failing to assess the current level of information before supplying new information;
- Taking too much or too little time in regard to the needs of the situation;
- Overusing medical terms and not recognizing when patients cannot decipher them;
- Using little eye contact and appropriate touch;
- Using closed body language;
- Being inattentive to the patient’s body language;
- Using inappropriately open or closed questions when the circumstance calls for the opposite;
- Not using a patient’s own words when doing so would be helpful to diagnosis or management;
- Exhibiting a lack of empathy, compassion, understanding, and support;
- Being inattentive or insensitive to a patient’s feelings;
- Being inattentive to cognitive, psychosocial, and affective needs;
- Disregarding the need for shared decision-making;
- Lacking the skill for or failing to use active listening;
- Failing to use timeliness in feedback or reporting test results;
- Neglecting to seek feedback regarding whether cultural, regional, or language/accent differences (both the doctor’s and the patient’s) impede communication; or
- Using an angry, anxious, or dominant tone of voice.
The second effect of poor communication that Dr. Pantilat cites is that “patients are less satisfied with their care and … to the extent that the relationship with the physician actually has an impact on how patients feel, patients may not ‘get better,’ ” he says. “And I don’t mean, for instance, that with a patient who has pneumonia, their pneumonia won’t get better; but there are a lot of other conditions where feeling like someone is listening to you, feeling like you’ve been heard, feeling like someone has communicated clearly can make you feel better.”7 (See also The Hospitalist, “Patient Satisfaction: The Hospitalist’s Role,” July/August 2005.)8
Inpatient communication tends to be a different kind of communication than that used in some other medical settings—more intense in a shorter time period and conducted between people who are strangers at the time of the patient’s admission. “It’s not that the stakes are higher, but it’s actually just the intensity of it is different,” says Arpana Vidyarthi, MD, a hospitalist who is the director of quality inpatient medicine at the University of California, San Francisco Medical Center.
“Time constraints are a major reason for poor communication skills happening,” says Dr. Trowbridge, whose hospitalist practice involves 60% clinical work with the Maine Hospitalist Group and 40% administrative work involving medical students and faculty development with the Department of Medicine at Maine Medical Center. “Relationships are really what many physicians most enjoy in medicine: with colleagues, … with patients, … with families. Having poor communication skills has a huge impact on job satisfaction and then personal satisfaction,” in many instances because of the heightened levels of stress.
“People are not here because they’re trying to get their lipids down,” says Dr. Vidyarthi. “They’re here because they’re [acutely ill]. When people are very, very ill, or when they’re having an intense experience, they tend to hang on every word.”
For the physician, she says, “there are so many things to communicate and because it is often very complicated, the relationship and the trust have to be built quickly, and information has to be transferred very quickly. Poor communication will lead to potentially not being able to build that alliance with the patient during that short period of time of their hospital experience.”
Hospitalists must be on the lookout for how the constraints of time affect the way they practice and relate to their patients because every nuance of behavior or tone of voice can make a difference to how a patient perceives his or her doctor.
For example, in a study conducted at Harvard University in 2002, investigators used audiotapes of 57 surgeons, 36 of whom had had two or more malpractice claims filed against them.9 Patients were asked to listen to two 20-second clips of audio between these surgeons and two patients. Those surgeons who were judged by the tone of their voices as “high dominance” and “low concern/anxiety” correlated with those who had had previous malpractice claims.
Because there is no continuity of relationship to help steady what might be an emotional response when things go wrong in the patient’s treatment or when patients and families are upset by circumstances, hospitalists may be subjected to blame, resentment, fear, and displaced anger concerning their communications with patients and families.
“Especially if you’re harried in an incredible time crunch, if you don’t [communicate] with patients and patient families [about] what is going on [in their care], those relationships very quickly can turn antagonistic,” says Dr. Trowbridge. “And then the very thing most of us like about medicine—relationships with patients and families—becomes something that people tend to avoid.”
Dr. Trowbridge says that this can become somewhat of a vicious cycle whereby a certain extent of inadvertently “avoiding the patient and family may lead to further communication faults.” On the flip side, using good communication can be a circular process but in a positive way: A good communicator may experience better well-being, which in turn, leads to better communication skills.2,5 Also, on a practical level, the data are clear that bad communication puts you at risk for malpractice litigation.9,10
Communication with Colleagues
“People that don’t have very good communication skills tend not to be successful,” says Dr. Vidyarthi, who practices with the hospitalist group at UCSF and is also an assistant professor there. Her definition of success is closely linked to the quality of relationships; that is, “being well liked by the nurses, building working relationships with … the nurses,” as well as others, including the hospital administrator. “Hospitalists are almost always … doing quality work or performance improvement,” she explained. “They’re on committees. That is the nature of what we do. … Not learning what those [communication skills] are and [not] being able to communicate at [effective] levels would … be a detriment to one’s personal job advancement, but absolutely to one’s job satisfaction as well.”
Collegiality, in fact, is one component cited as a “powerful engine of socialization” in organizational structures more likely to foster the lifelong learning and commitment that are inherent to medical professionalism.1,3-5,11,12
Many of the components of effective communication with colleagues parallel those that are best used with patients. “Communication is what holds that team together,” says Dr. Vidyarthi, whose interests include information transfer and communication as a form for team-building. “In academic medicine, poor communication can impact the teaching environment, the experience of the students and the residents, and that team cohesion. And that can lead to poor patient care, it can definitely lead to a poor educational experience, and it is not enjoyable, so job satisfaction suffers.”
Dr. Pantilat, who is associate professor of clinical medicine and director, Palliative Care Service and Palliative Care Leadership Center at UCSF, theorizes that when interacting with colleagues such as other hospitalists and physicians, nurses, social workers, case managers, and pharmacists, poor communication skills can make the physician’s work tougher. “Poor communication makes your life difficult with your colleagues,” says Dr. Pantilat. “People don’t like talking to you or interacting with you … and your job can generally be more difficult.”
Post-Discharge Communication
In the traditional medical model, a primary care physician would see patients in her/his office, the hospital, or rehabilitation. With the expansion in hospital medicine, patients are now “handed off” and seen by a number of providers. Hand-off fumbles can mean critical information may be lost, leading to poorer outcomes and greater readmission rates.13-15
Forging and maintaining effective communication with colleagues following the discharge of patients is an area where few in-house physicians do well, says Dr. Vidyarthi, who has it on her agenda to tackle this “huge problem” for her institution in the coming year. There are two pieces to that problem, she says. One is to accurately identify the patients’ primary care physicians and the other is to make contact with them.
“You could page them, but they’re in clinic, and they can’t take five minutes out when you can’t take five minutes out,” says Dr. Vidyarthi. “The communication with the primary care physician is actually a field in and of itself.”15
Part of her plan is to devise some means of “physician-independent generated communication,” perhaps a letter or e-mail sent from the hospital to report to a primary care physician that his/her patient has been admitted to the hospital.
“That raises a flag to that primary so they can try to find the hospitalist, which is usually very easy … because we’re always in the hospital,” says Dr. Vidyarthi. “And it’s the first stage of the communication: Now that person is aware. If I can find them, if I can access them, they’ll be able to take that time out, because they know their patient’s there.”
In her work as a senior fellow at the Center for Health Professions at UCSF, Dr. Vidyarthi strives to “embed communication into the larger framework of organizational change.” And what does a hospitalist do if an institution’s post-discharge communications system is not up to par? There are three basic things you can do to help overcome this source of frustration, she says. The first is to continually build relationships with primary care providers.
“If I send an e-mail to somebody and they know who I am, they are much more likely to respond to that because they know me,” says Dr. Vidyarthi.
Next, find a system that works for you. “Don’t wait for the rest of the systems to be put in place,” she says. “This is about personal practice. And if that means you take five minutes in the morning to send an e-mail or five minutes in the evening, whatever it is, find [a system] that really works and figure out a way to evaluate it.”
A good way to do this, Dr. Vidyarthi suggests, is to take a quick survey in the midst of talking to that primary care physician to ask whether the medium, content, and timing that you used to contact him/her worked well.
“Then,” she says, “if you have five primaries that you talked to [who] maybe said, ‘Yes, that was helpful to me,’ or ‘Not so much really, I had all that info already,’ at least you have data. Asking ‘Do you think this will help your patients when they come to see you in the office?’ is a great question [to solidify] performance improvement. In other words, find out if what you’re doing is being effective.”
The final step to overcome a lack of an effective institutional system for post-discharge communication is to share what you’ve learned with others. “These little pieces can really empower others to make a difference,” says Dr. Vidyarthi. “Trying to change and overhaul an entire system will turn off even the most motivated of people who want to improve the system, so focus on your own personal practice models. Change it, figure out what works, and then try to disseminate it. That makes it feel and seem much more doable.”
Conclusion
Hospitalists who exercise poor communication skills with patients, families, and colleagues can experience multiple negative effects, including poor patient-related outcomes and an increased risk of malpractice litigation. Personally, consistently using poor communication may make work more difficult, reduce job satisfaction, and reduce work success and enjoyment with hospital teams and primary care physicians. TH
Contributor Andrea Sattinger makes good communication a priority every day.
References
- Finset KB, Gude T, Hem E, et al. Which young physicians are satisfied with their work? A prospective nationwide study in Norway. BMC Med Educ. 2005;5:19.
- Roter DL, Stewart M, Putnam SM, et al. Communication patterns of primary care physicians. JAMA. 1997;277:350-356.
- Konrad TR, Williams ES, Linzer M, et al. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Measuring physician job satisfaction in a changing workplace and a challenging environment. Med Care. 1999;37:1174-1182.
- Shanafelt TD, West C, Zhao X, et al. Relationship between increased personal well-being and enhanced empathy among internal medicine residents. J Gen Intern Med. 2005;20:559-564.
- Shanafelt TD, Sloan JA, Habermann TM. The well-being of physicians. Am J Med. 2003;114:513-519.
- Novack DH, Suchman AL, Clark W, et al. Calibrating the physician. Personal awareness and effective patient care. Working Group on Promoting Physician Personal Awareness, American Academy on Physician and Patient. JAMA. 1997;278:502-509.
- Greenfield S, Kaplan S, Ware WE Jr. Expanding patient involvement in care: effects on patient outcomes. Ann Intern Med. 1985;102:520-528.
- Torcson PJ. Patient satisfaction: the hospitalist’s role. The Hospitalist. 2005;July/Aug:27-30.
- Ambady N, LaPlante D, Nguyen T. Surgeons’ tone of voice: a clue to malpractice history. Surgery. 2002;132:5-9.
- Levinson W, Roter DL, Mullooly JP. Physician-patient communication. The relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277:553-559.
- Frankford DM, Patterson MA, Konrad TR. Transforming practice organizations to foster lifelong learning and commitment to medical professionalism. Acad Med. 2000;75:708-17.
- Falkum E, Vaglum P. The relationship between interpersonal problems and occupational stress in physicians. Gen Hosp Psychiatry. 2005;27:285-291.
- Coleman EA, Smith JD, Min SJ, et al. Post-hospital medicine discrepancies; prevalence, types, and contributing factors. Paper presented at the Society of Hospital Medicine Annual Meeting; April 29-30; Chicago, Illinois: Society of Hospital Medicine 2005.
- Burniske GM, Burnett A, Greenwald J, et al. Post-discharge follow-up telephone call by a pharmacist and impact on patient care. Paper presented at the Society of Hospital Medicine Annual Meeting. April 29-30; Chicago.
- Wachter R, Shojania K. Internal Bleeding: The Truth Behind America's Terrifying Epidemic of Medical Mistakes. New York, NY: Rugged Land; 2004.
Mack Lipkin, MD, the founding president of the American Academy on Physician and Patient, a society dedicated to research, education, and professional standards in patient-physician communication, reported some interesting data in a PowerPoint presentation he gave in 2000 at the working conference on Diversity and Communication in Healthcare sponsored in part by the U.S. Office of Minority Health. Dr. Lipkin said that physicians’ lowest level of communication skills are reached during their medical residencies; even medical students’ skills were rated higher. Dr. Lipkin, who is also director of the Division of Primary Care in the Department of Medicine at New York University School of Medicine, New York City, went on to explain that, typically, physicians will recover some capacity with communication as they enter practice and years of experience ensue, but they never reach the level they possessed before they entered medical school.
While some hospitalists may consider this a startling claim, few are likely to find it shocking. Although hospitalists believe using good communication skills is an important part of their work, their skills may not necessarily match their beliefs or intentions. Research in progress by hospitalist Paul Mueller, MD, and his colleagues at the Mayo Clinic College of Medicine, Rochester, Minn., reveals that a majority of new internal medicine faculty—regardless of years in practice or background—believe they could benefit from and desire additional training in communication; yet these individuals teach communication skills to medical students (personal communication, 2005).
Medical education curriculum experts nationwide are pumping up their coverage of physician-patient communication to supply the demand stemming from a surge of interest in this topic in recent decades. Some reasons for this include reports and investigations into medical errors, an explosion of medical and health information easily accessible to patients and families, the rise of a vital consumer advocacy and empowerment movement, the reliance on outcomes assessments that include patient satisfaction ratings, a growing emphasis on patient- or relationship-centered care, and the reduced time for medical encounters caused at least in part by cost-containment initiatives.
The relationship between communication and medical outcomes is being increasingly explored, including the effects on physician satisfaction.1-5 But what are the further, personal effects to the individual hospitalist when he or she perpetuates poor communication skills?
—Robert Trowbridge, MD
Communication With Patients And Families
The work of hospitalists depends acutely on communication.
“It’s part of the role of the hospitalist to explain and help shepherd [patients] through the healthcare system,” says Robert Trowbridge, MD, a hospitalist and assistant professor of medicine, University of Vermont College of Medicine, Maine Medical Center, Portland.
Professionals whose medical practice is based on short clinical visits or performing procedures may or may not be good communicators, but it’s probably not as integral to the way they or the situations their patients are going through will be perceived. The conventional wisdom in professional and lay circles tends to be, “He may be a lousy communicator, but he’s a hellava surgeon,” says Dr. Trowbridge.
But most patients expect good communication from their primary care physician and because they are serving that function when a patient is hospitalized, hospitalists should understand that patients and families expect those skills of them. “And if the [hospitalists] don’t do well [in communicating], there can be much more stress on the patients and physicians,” explains Dr. Trowbridge.
What Constitutes Poor Communication?
“First, on one level, poor communication skills are inefficient in talking with patients,” says Steven Pantilat, MD, SHM president. “So, I think it makes your work harder.”
Some examples of communication inefficiency (or ineffectiveness) for a clinician include:2,4,5,6-8
- Lacking the ability to articulate ideas adequately;
- Transferring insufficient information between the provider and the patient, including inadequate elicitation of key facts from the patient;
- Failing to assess the current level of information before supplying new information;
- Taking too much or too little time in regard to the needs of the situation;
- Overusing medical terms and not recognizing when patients cannot decipher them;
- Using little eye contact and appropriate touch;
- Using closed body language;
- Being inattentive to the patient’s body language;
- Using inappropriately open or closed questions when the circumstance calls for the opposite;
- Not using a patient’s own words when doing so would be helpful to diagnosis or management;
- Exhibiting a lack of empathy, compassion, understanding, and support;
- Being inattentive or insensitive to a patient’s feelings;
- Being inattentive to cognitive, psychosocial, and affective needs;
- Disregarding the need for shared decision-making;
- Lacking the skill for or failing to use active listening;
- Failing to use timeliness in feedback or reporting test results;
- Neglecting to seek feedback regarding whether cultural, regional, or language/accent differences (both the doctor’s and the patient’s) impede communication; or
- Using an angry, anxious, or dominant tone of voice.
The second effect of poor communication that Dr. Pantilat cites is that “patients are less satisfied with their care and … to the extent that the relationship with the physician actually has an impact on how patients feel, patients may not ‘get better,’ ” he says. “And I don’t mean, for instance, that with a patient who has pneumonia, their pneumonia won’t get better; but there are a lot of other conditions where feeling like someone is listening to you, feeling like you’ve been heard, feeling like someone has communicated clearly can make you feel better.”7 (See also The Hospitalist, “Patient Satisfaction: The Hospitalist’s Role,” July/August 2005.)8
Inpatient communication tends to be a different kind of communication than that used in some other medical settings—more intense in a shorter time period and conducted between people who are strangers at the time of the patient’s admission. “It’s not that the stakes are higher, but it’s actually just the intensity of it is different,” says Arpana Vidyarthi, MD, a hospitalist who is the director of quality inpatient medicine at the University of California, San Francisco Medical Center.
“Time constraints are a major reason for poor communication skills happening,” says Dr. Trowbridge, whose hospitalist practice involves 60% clinical work with the Maine Hospitalist Group and 40% administrative work involving medical students and faculty development with the Department of Medicine at Maine Medical Center. “Relationships are really what many physicians most enjoy in medicine: with colleagues, … with patients, … with families. Having poor communication skills has a huge impact on job satisfaction and then personal satisfaction,” in many instances because of the heightened levels of stress.
“People are not here because they’re trying to get their lipids down,” says Dr. Vidyarthi. “They’re here because they’re [acutely ill]. When people are very, very ill, or when they’re having an intense experience, they tend to hang on every word.”
For the physician, she says, “there are so many things to communicate and because it is often very complicated, the relationship and the trust have to be built quickly, and information has to be transferred very quickly. Poor communication will lead to potentially not being able to build that alliance with the patient during that short period of time of their hospital experience.”
Hospitalists must be on the lookout for how the constraints of time affect the way they practice and relate to their patients because every nuance of behavior or tone of voice can make a difference to how a patient perceives his or her doctor.
For example, in a study conducted at Harvard University in 2002, investigators used audiotapes of 57 surgeons, 36 of whom had had two or more malpractice claims filed against them.9 Patients were asked to listen to two 20-second clips of audio between these surgeons and two patients. Those surgeons who were judged by the tone of their voices as “high dominance” and “low concern/anxiety” correlated with those who had had previous malpractice claims.
Because there is no continuity of relationship to help steady what might be an emotional response when things go wrong in the patient’s treatment or when patients and families are upset by circumstances, hospitalists may be subjected to blame, resentment, fear, and displaced anger concerning their communications with patients and families.
“Especially if you’re harried in an incredible time crunch, if you don’t [communicate] with patients and patient families [about] what is going on [in their care], those relationships very quickly can turn antagonistic,” says Dr. Trowbridge. “And then the very thing most of us like about medicine—relationships with patients and families—becomes something that people tend to avoid.”
Dr. Trowbridge says that this can become somewhat of a vicious cycle whereby a certain extent of inadvertently “avoiding the patient and family may lead to further communication faults.” On the flip side, using good communication can be a circular process but in a positive way: A good communicator may experience better well-being, which in turn, leads to better communication skills.2,5 Also, on a practical level, the data are clear that bad communication puts you at risk for malpractice litigation.9,10
Communication with Colleagues
“People that don’t have very good communication skills tend not to be successful,” says Dr. Vidyarthi, who practices with the hospitalist group at UCSF and is also an assistant professor there. Her definition of success is closely linked to the quality of relationships; that is, “being well liked by the nurses, building working relationships with … the nurses,” as well as others, including the hospital administrator. “Hospitalists are almost always … doing quality work or performance improvement,” she explained. “They’re on committees. That is the nature of what we do. … Not learning what those [communication skills] are and [not] being able to communicate at [effective] levels would … be a detriment to one’s personal job advancement, but absolutely to one’s job satisfaction as well.”
Collegiality, in fact, is one component cited as a “powerful engine of socialization” in organizational structures more likely to foster the lifelong learning and commitment that are inherent to medical professionalism.1,3-5,11,12
Many of the components of effective communication with colleagues parallel those that are best used with patients. “Communication is what holds that team together,” says Dr. Vidyarthi, whose interests include information transfer and communication as a form for team-building. “In academic medicine, poor communication can impact the teaching environment, the experience of the students and the residents, and that team cohesion. And that can lead to poor patient care, it can definitely lead to a poor educational experience, and it is not enjoyable, so job satisfaction suffers.”
Dr. Pantilat, who is associate professor of clinical medicine and director, Palliative Care Service and Palliative Care Leadership Center at UCSF, theorizes that when interacting with colleagues such as other hospitalists and physicians, nurses, social workers, case managers, and pharmacists, poor communication skills can make the physician’s work tougher. “Poor communication makes your life difficult with your colleagues,” says Dr. Pantilat. “People don’t like talking to you or interacting with you … and your job can generally be more difficult.”
Post-Discharge Communication
In the traditional medical model, a primary care physician would see patients in her/his office, the hospital, or rehabilitation. With the expansion in hospital medicine, patients are now “handed off” and seen by a number of providers. Hand-off fumbles can mean critical information may be lost, leading to poorer outcomes and greater readmission rates.13-15
Forging and maintaining effective communication with colleagues following the discharge of patients is an area where few in-house physicians do well, says Dr. Vidyarthi, who has it on her agenda to tackle this “huge problem” for her institution in the coming year. There are two pieces to that problem, she says. One is to accurately identify the patients’ primary care physicians and the other is to make contact with them.
“You could page them, but they’re in clinic, and they can’t take five minutes out when you can’t take five minutes out,” says Dr. Vidyarthi. “The communication with the primary care physician is actually a field in and of itself.”15
Part of her plan is to devise some means of “physician-independent generated communication,” perhaps a letter or e-mail sent from the hospital to report to a primary care physician that his/her patient has been admitted to the hospital.
“That raises a flag to that primary so they can try to find the hospitalist, which is usually very easy … because we’re always in the hospital,” says Dr. Vidyarthi. “And it’s the first stage of the communication: Now that person is aware. If I can find them, if I can access them, they’ll be able to take that time out, because they know their patient’s there.”
In her work as a senior fellow at the Center for Health Professions at UCSF, Dr. Vidyarthi strives to “embed communication into the larger framework of organizational change.” And what does a hospitalist do if an institution’s post-discharge communications system is not up to par? There are three basic things you can do to help overcome this source of frustration, she says. The first is to continually build relationships with primary care providers.
“If I send an e-mail to somebody and they know who I am, they are much more likely to respond to that because they know me,” says Dr. Vidyarthi.
Next, find a system that works for you. “Don’t wait for the rest of the systems to be put in place,” she says. “This is about personal practice. And if that means you take five minutes in the morning to send an e-mail or five minutes in the evening, whatever it is, find [a system] that really works and figure out a way to evaluate it.”
A good way to do this, Dr. Vidyarthi suggests, is to take a quick survey in the midst of talking to that primary care physician to ask whether the medium, content, and timing that you used to contact him/her worked well.
“Then,” she says, “if you have five primaries that you talked to [who] maybe said, ‘Yes, that was helpful to me,’ or ‘Not so much really, I had all that info already,’ at least you have data. Asking ‘Do you think this will help your patients when they come to see you in the office?’ is a great question [to solidify] performance improvement. In other words, find out if what you’re doing is being effective.”
The final step to overcome a lack of an effective institutional system for post-discharge communication is to share what you’ve learned with others. “These little pieces can really empower others to make a difference,” says Dr. Vidyarthi. “Trying to change and overhaul an entire system will turn off even the most motivated of people who want to improve the system, so focus on your own personal practice models. Change it, figure out what works, and then try to disseminate it. That makes it feel and seem much more doable.”
Conclusion
Hospitalists who exercise poor communication skills with patients, families, and colleagues can experience multiple negative effects, including poor patient-related outcomes and an increased risk of malpractice litigation. Personally, consistently using poor communication may make work more difficult, reduce job satisfaction, and reduce work success and enjoyment with hospital teams and primary care physicians. TH
Contributor Andrea Sattinger makes good communication a priority every day.
References
- Finset KB, Gude T, Hem E, et al. Which young physicians are satisfied with their work? A prospective nationwide study in Norway. BMC Med Educ. 2005;5:19.
- Roter DL, Stewart M, Putnam SM, et al. Communication patterns of primary care physicians. JAMA. 1997;277:350-356.
- Konrad TR, Williams ES, Linzer M, et al. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Measuring physician job satisfaction in a changing workplace and a challenging environment. Med Care. 1999;37:1174-1182.
- Shanafelt TD, West C, Zhao X, et al. Relationship between increased personal well-being and enhanced empathy among internal medicine residents. J Gen Intern Med. 2005;20:559-564.
- Shanafelt TD, Sloan JA, Habermann TM. The well-being of physicians. Am J Med. 2003;114:513-519.
- Novack DH, Suchman AL, Clark W, et al. Calibrating the physician. Personal awareness and effective patient care. Working Group on Promoting Physician Personal Awareness, American Academy on Physician and Patient. JAMA. 1997;278:502-509.
- Greenfield S, Kaplan S, Ware WE Jr. Expanding patient involvement in care: effects on patient outcomes. Ann Intern Med. 1985;102:520-528.
- Torcson PJ. Patient satisfaction: the hospitalist’s role. The Hospitalist. 2005;July/Aug:27-30.
- Ambady N, LaPlante D, Nguyen T. Surgeons’ tone of voice: a clue to malpractice history. Surgery. 2002;132:5-9.
- Levinson W, Roter DL, Mullooly JP. Physician-patient communication. The relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277:553-559.
- Frankford DM, Patterson MA, Konrad TR. Transforming practice organizations to foster lifelong learning and commitment to medical professionalism. Acad Med. 2000;75:708-17.
- Falkum E, Vaglum P. The relationship between interpersonal problems and occupational stress in physicians. Gen Hosp Psychiatry. 2005;27:285-291.
- Coleman EA, Smith JD, Min SJ, et al. Post-hospital medicine discrepancies; prevalence, types, and contributing factors. Paper presented at the Society of Hospital Medicine Annual Meeting; April 29-30; Chicago, Illinois: Society of Hospital Medicine 2005.
- Burniske GM, Burnett A, Greenwald J, et al. Post-discharge follow-up telephone call by a pharmacist and impact on patient care. Paper presented at the Society of Hospital Medicine Annual Meeting. April 29-30; Chicago.
- Wachter R, Shojania K. Internal Bleeding: The Truth Behind America's Terrifying Epidemic of Medical Mistakes. New York, NY: Rugged Land; 2004.
Mack Lipkin, MD, the founding president of the American Academy on Physician and Patient, a society dedicated to research, education, and professional standards in patient-physician communication, reported some interesting data in a PowerPoint presentation he gave in 2000 at the working conference on Diversity and Communication in Healthcare sponsored in part by the U.S. Office of Minority Health. Dr. Lipkin said that physicians’ lowest level of communication skills are reached during their medical residencies; even medical students’ skills were rated higher. Dr. Lipkin, who is also director of the Division of Primary Care in the Department of Medicine at New York University School of Medicine, New York City, went on to explain that, typically, physicians will recover some capacity with communication as they enter practice and years of experience ensue, but they never reach the level they possessed before they entered medical school.
While some hospitalists may consider this a startling claim, few are likely to find it shocking. Although hospitalists believe using good communication skills is an important part of their work, their skills may not necessarily match their beliefs or intentions. Research in progress by hospitalist Paul Mueller, MD, and his colleagues at the Mayo Clinic College of Medicine, Rochester, Minn., reveals that a majority of new internal medicine faculty—regardless of years in practice or background—believe they could benefit from and desire additional training in communication; yet these individuals teach communication skills to medical students (personal communication, 2005).
Medical education curriculum experts nationwide are pumping up their coverage of physician-patient communication to supply the demand stemming from a surge of interest in this topic in recent decades. Some reasons for this include reports and investigations into medical errors, an explosion of medical and health information easily accessible to patients and families, the rise of a vital consumer advocacy and empowerment movement, the reliance on outcomes assessments that include patient satisfaction ratings, a growing emphasis on patient- or relationship-centered care, and the reduced time for medical encounters caused at least in part by cost-containment initiatives.
The relationship between communication and medical outcomes is being increasingly explored, including the effects on physician satisfaction.1-5 But what are the further, personal effects to the individual hospitalist when he or she perpetuates poor communication skills?
—Robert Trowbridge, MD
Communication With Patients And Families
The work of hospitalists depends acutely on communication.
“It’s part of the role of the hospitalist to explain and help shepherd [patients] through the healthcare system,” says Robert Trowbridge, MD, a hospitalist and assistant professor of medicine, University of Vermont College of Medicine, Maine Medical Center, Portland.
Professionals whose medical practice is based on short clinical visits or performing procedures may or may not be good communicators, but it’s probably not as integral to the way they or the situations their patients are going through will be perceived. The conventional wisdom in professional and lay circles tends to be, “He may be a lousy communicator, but he’s a hellava surgeon,” says Dr. Trowbridge.
But most patients expect good communication from their primary care physician and because they are serving that function when a patient is hospitalized, hospitalists should understand that patients and families expect those skills of them. “And if the [hospitalists] don’t do well [in communicating], there can be much more stress on the patients and physicians,” explains Dr. Trowbridge.
What Constitutes Poor Communication?
“First, on one level, poor communication skills are inefficient in talking with patients,” says Steven Pantilat, MD, SHM president. “So, I think it makes your work harder.”
Some examples of communication inefficiency (or ineffectiveness) for a clinician include:2,4,5,6-8
- Lacking the ability to articulate ideas adequately;
- Transferring insufficient information between the provider and the patient, including inadequate elicitation of key facts from the patient;
- Failing to assess the current level of information before supplying new information;
- Taking too much or too little time in regard to the needs of the situation;
- Overusing medical terms and not recognizing when patients cannot decipher them;
- Using little eye contact and appropriate touch;
- Using closed body language;
- Being inattentive to the patient’s body language;
- Using inappropriately open or closed questions when the circumstance calls for the opposite;
- Not using a patient’s own words when doing so would be helpful to diagnosis or management;
- Exhibiting a lack of empathy, compassion, understanding, and support;
- Being inattentive or insensitive to a patient’s feelings;
- Being inattentive to cognitive, psychosocial, and affective needs;
- Disregarding the need for shared decision-making;
- Lacking the skill for or failing to use active listening;
- Failing to use timeliness in feedback or reporting test results;
- Neglecting to seek feedback regarding whether cultural, regional, or language/accent differences (both the doctor’s and the patient’s) impede communication; or
- Using an angry, anxious, or dominant tone of voice.
The second effect of poor communication that Dr. Pantilat cites is that “patients are less satisfied with their care and … to the extent that the relationship with the physician actually has an impact on how patients feel, patients may not ‘get better,’ ” he says. “And I don’t mean, for instance, that with a patient who has pneumonia, their pneumonia won’t get better; but there are a lot of other conditions where feeling like someone is listening to you, feeling like you’ve been heard, feeling like someone has communicated clearly can make you feel better.”7 (See also The Hospitalist, “Patient Satisfaction: The Hospitalist’s Role,” July/August 2005.)8
Inpatient communication tends to be a different kind of communication than that used in some other medical settings—more intense in a shorter time period and conducted between people who are strangers at the time of the patient’s admission. “It’s not that the stakes are higher, but it’s actually just the intensity of it is different,” says Arpana Vidyarthi, MD, a hospitalist who is the director of quality inpatient medicine at the University of California, San Francisco Medical Center.
“Time constraints are a major reason for poor communication skills happening,” says Dr. Trowbridge, whose hospitalist practice involves 60% clinical work with the Maine Hospitalist Group and 40% administrative work involving medical students and faculty development with the Department of Medicine at Maine Medical Center. “Relationships are really what many physicians most enjoy in medicine: with colleagues, … with patients, … with families. Having poor communication skills has a huge impact on job satisfaction and then personal satisfaction,” in many instances because of the heightened levels of stress.
“People are not here because they’re trying to get their lipids down,” says Dr. Vidyarthi. “They’re here because they’re [acutely ill]. When people are very, very ill, or when they’re having an intense experience, they tend to hang on every word.”
For the physician, she says, “there are so many things to communicate and because it is often very complicated, the relationship and the trust have to be built quickly, and information has to be transferred very quickly. Poor communication will lead to potentially not being able to build that alliance with the patient during that short period of time of their hospital experience.”
Hospitalists must be on the lookout for how the constraints of time affect the way they practice and relate to their patients because every nuance of behavior or tone of voice can make a difference to how a patient perceives his or her doctor.
For example, in a study conducted at Harvard University in 2002, investigators used audiotapes of 57 surgeons, 36 of whom had had two or more malpractice claims filed against them.9 Patients were asked to listen to two 20-second clips of audio between these surgeons and two patients. Those surgeons who were judged by the tone of their voices as “high dominance” and “low concern/anxiety” correlated with those who had had previous malpractice claims.
Because there is no continuity of relationship to help steady what might be an emotional response when things go wrong in the patient’s treatment or when patients and families are upset by circumstances, hospitalists may be subjected to blame, resentment, fear, and displaced anger concerning their communications with patients and families.
“Especially if you’re harried in an incredible time crunch, if you don’t [communicate] with patients and patient families [about] what is going on [in their care], those relationships very quickly can turn antagonistic,” says Dr. Trowbridge. “And then the very thing most of us like about medicine—relationships with patients and families—becomes something that people tend to avoid.”
Dr. Trowbridge says that this can become somewhat of a vicious cycle whereby a certain extent of inadvertently “avoiding the patient and family may lead to further communication faults.” On the flip side, using good communication can be a circular process but in a positive way: A good communicator may experience better well-being, which in turn, leads to better communication skills.2,5 Also, on a practical level, the data are clear that bad communication puts you at risk for malpractice litigation.9,10
Communication with Colleagues
“People that don’t have very good communication skills tend not to be successful,” says Dr. Vidyarthi, who practices with the hospitalist group at UCSF and is also an assistant professor there. Her definition of success is closely linked to the quality of relationships; that is, “being well liked by the nurses, building working relationships with … the nurses,” as well as others, including the hospital administrator. “Hospitalists are almost always … doing quality work or performance improvement,” she explained. “They’re on committees. That is the nature of what we do. … Not learning what those [communication skills] are and [not] being able to communicate at [effective] levels would … be a detriment to one’s personal job advancement, but absolutely to one’s job satisfaction as well.”
Collegiality, in fact, is one component cited as a “powerful engine of socialization” in organizational structures more likely to foster the lifelong learning and commitment that are inherent to medical professionalism.1,3-5,11,12
Many of the components of effective communication with colleagues parallel those that are best used with patients. “Communication is what holds that team together,” says Dr. Vidyarthi, whose interests include information transfer and communication as a form for team-building. “In academic medicine, poor communication can impact the teaching environment, the experience of the students and the residents, and that team cohesion. And that can lead to poor patient care, it can definitely lead to a poor educational experience, and it is not enjoyable, so job satisfaction suffers.”
Dr. Pantilat, who is associate professor of clinical medicine and director, Palliative Care Service and Palliative Care Leadership Center at UCSF, theorizes that when interacting with colleagues such as other hospitalists and physicians, nurses, social workers, case managers, and pharmacists, poor communication skills can make the physician’s work tougher. “Poor communication makes your life difficult with your colleagues,” says Dr. Pantilat. “People don’t like talking to you or interacting with you … and your job can generally be more difficult.”
Post-Discharge Communication
In the traditional medical model, a primary care physician would see patients in her/his office, the hospital, or rehabilitation. With the expansion in hospital medicine, patients are now “handed off” and seen by a number of providers. Hand-off fumbles can mean critical information may be lost, leading to poorer outcomes and greater readmission rates.13-15
Forging and maintaining effective communication with colleagues following the discharge of patients is an area where few in-house physicians do well, says Dr. Vidyarthi, who has it on her agenda to tackle this “huge problem” for her institution in the coming year. There are two pieces to that problem, she says. One is to accurately identify the patients’ primary care physicians and the other is to make contact with them.
“You could page them, but they’re in clinic, and they can’t take five minutes out when you can’t take five minutes out,” says Dr. Vidyarthi. “The communication with the primary care physician is actually a field in and of itself.”15
Part of her plan is to devise some means of “physician-independent generated communication,” perhaps a letter or e-mail sent from the hospital to report to a primary care physician that his/her patient has been admitted to the hospital.
“That raises a flag to that primary so they can try to find the hospitalist, which is usually very easy … because we’re always in the hospital,” says Dr. Vidyarthi. “And it’s the first stage of the communication: Now that person is aware. If I can find them, if I can access them, they’ll be able to take that time out, because they know their patient’s there.”
In her work as a senior fellow at the Center for Health Professions at UCSF, Dr. Vidyarthi strives to “embed communication into the larger framework of organizational change.” And what does a hospitalist do if an institution’s post-discharge communications system is not up to par? There are three basic things you can do to help overcome this source of frustration, she says. The first is to continually build relationships with primary care providers.
“If I send an e-mail to somebody and they know who I am, they are much more likely to respond to that because they know me,” says Dr. Vidyarthi.
Next, find a system that works for you. “Don’t wait for the rest of the systems to be put in place,” she says. “This is about personal practice. And if that means you take five minutes in the morning to send an e-mail or five minutes in the evening, whatever it is, find [a system] that really works and figure out a way to evaluate it.”
A good way to do this, Dr. Vidyarthi suggests, is to take a quick survey in the midst of talking to that primary care physician to ask whether the medium, content, and timing that you used to contact him/her worked well.
“Then,” she says, “if you have five primaries that you talked to [who] maybe said, ‘Yes, that was helpful to me,’ or ‘Not so much really, I had all that info already,’ at least you have data. Asking ‘Do you think this will help your patients when they come to see you in the office?’ is a great question [to solidify] performance improvement. In other words, find out if what you’re doing is being effective.”
The final step to overcome a lack of an effective institutional system for post-discharge communication is to share what you’ve learned with others. “These little pieces can really empower others to make a difference,” says Dr. Vidyarthi. “Trying to change and overhaul an entire system will turn off even the most motivated of people who want to improve the system, so focus on your own personal practice models. Change it, figure out what works, and then try to disseminate it. That makes it feel and seem much more doable.”
Conclusion
Hospitalists who exercise poor communication skills with patients, families, and colleagues can experience multiple negative effects, including poor patient-related outcomes and an increased risk of malpractice litigation. Personally, consistently using poor communication may make work more difficult, reduce job satisfaction, and reduce work success and enjoyment with hospital teams and primary care physicians. TH
Contributor Andrea Sattinger makes good communication a priority every day.
References
- Finset KB, Gude T, Hem E, et al. Which young physicians are satisfied with their work? A prospective nationwide study in Norway. BMC Med Educ. 2005;5:19.
- Roter DL, Stewart M, Putnam SM, et al. Communication patterns of primary care physicians. JAMA. 1997;277:350-356.
- Konrad TR, Williams ES, Linzer M, et al. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Measuring physician job satisfaction in a changing workplace and a challenging environment. Med Care. 1999;37:1174-1182.
- Shanafelt TD, West C, Zhao X, et al. Relationship between increased personal well-being and enhanced empathy among internal medicine residents. J Gen Intern Med. 2005;20:559-564.
- Shanafelt TD, Sloan JA, Habermann TM. The well-being of physicians. Am J Med. 2003;114:513-519.
- Novack DH, Suchman AL, Clark W, et al. Calibrating the physician. Personal awareness and effective patient care. Working Group on Promoting Physician Personal Awareness, American Academy on Physician and Patient. JAMA. 1997;278:502-509.
- Greenfield S, Kaplan S, Ware WE Jr. Expanding patient involvement in care: effects on patient outcomes. Ann Intern Med. 1985;102:520-528.
- Torcson PJ. Patient satisfaction: the hospitalist’s role. The Hospitalist. 2005;July/Aug:27-30.
- Ambady N, LaPlante D, Nguyen T. Surgeons’ tone of voice: a clue to malpractice history. Surgery. 2002;132:5-9.
- Levinson W, Roter DL, Mullooly JP. Physician-patient communication. The relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277:553-559.
- Frankford DM, Patterson MA, Konrad TR. Transforming practice organizations to foster lifelong learning and commitment to medical professionalism. Acad Med. 2000;75:708-17.
- Falkum E, Vaglum P. The relationship between interpersonal problems and occupational stress in physicians. Gen Hosp Psychiatry. 2005;27:285-291.
- Coleman EA, Smith JD, Min SJ, et al. Post-hospital medicine discrepancies; prevalence, types, and contributing factors. Paper presented at the Society of Hospital Medicine Annual Meeting; April 29-30; Chicago, Illinois: Society of Hospital Medicine 2005.
- Burniske GM, Burnett A, Greenwald J, et al. Post-discharge follow-up telephone call by a pharmacist and impact on patient care. Paper presented at the Society of Hospital Medicine Annual Meeting. April 29-30; Chicago.
- Wachter R, Shojania K. Internal Bleeding: The Truth Behind America's Terrifying Epidemic of Medical Mistakes. New York, NY: Rugged Land; 2004.
Evidence Based Medicine for The Hospitalist
The first step in finding an answer to a clinical question is to ask an effective question. This was the subject of the previous installment in this series, in which the PICOT question format was introduced (see The Hospitalist, Nov. 2005, p. 32). This format leads naturally to effective search strategies, so we optimize our chances of finding quality answers if they exist. There are many possible sources of information that can be searched, however, and the type of question asked can provide valuable guidance as to which sources should be first up for review.
Types of Questions and Where to Look for Answers
Many clinical questions pertain to basic medical knowledge rather than cutting-edge current research. These so-called background questions typically involve such issues as the underlying pathophysiology of a disease, the incidence of the disease, the general treatment considerations for the disease, and overall prognosis for patients with the disease. These questions usually do not require evaluation of the most recent medical literature and can often be answered by reviewing sources of established medical knowledge such as medical textbooks, MD Consult, or UpToDate. In fact, searching for basic knowledge in the current research literature can be exhausting because the focus of most papers is necessarily narrow and therefore too restrictive to properly address knowledge of a general nature.
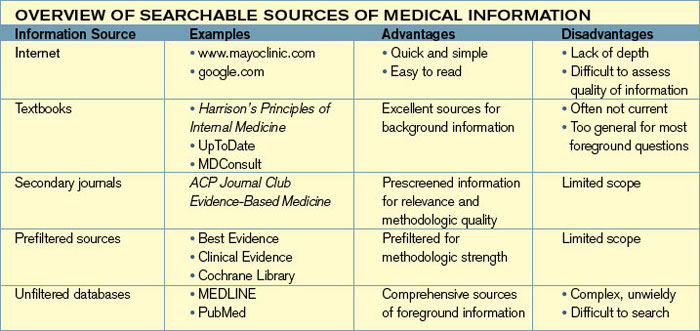
The main limitation of these more general sources is that it takes years for medical knowledge to become established, so the most current results will seldom be incorporated. For background questions this is usually acceptable, but if a major breakthrough in our understanding of a disease occurs it is unlikely to be found in these sources. An additional limitation is that the statements found in these sources are often not truly evidence-based—at least not in a transparent or reproducible manner. These limitations are becoming less problematic as resources such as UpToDate strive to add evidence-based reviews and quality measures to their summaries, and also begin to update information much more rapidly as online materials become more standard.
In contrast to background clinical questions, foreground clinical questions are more likely to relate to the management of an individual patient in a specific clinical setting, and are therefore too narrow in scope to be addressed well by the sources best suited for background questions. For example, consider the question posed in the last installment of this series, “Among men over the age of 65 with Stage II renal cell carcinoma, does post-resection chemotherapy result in greater five-year survival than nephrectomy alone?” No textbook will answer a question with this narrow focus. To find an answer we need to be able to sift through the current medical research literature.

How to Search Research Databases
The number of medical journals has increased dramatically in the past 20 years. As a result, while it may be more likely that your question has been addressed somewhere, it can be more difficult to locate the paper you need. One approach to this problem is to become skilled in developing search strategies. We will return to this, but an alternative is to utilize secondary journals such as ACP Journal Club (www.acponline.org) or prefiltered sources such as the Cochrane Library (www.cochrane.org).
Secondary journals typically screen articles for both clinical relevance and methodologic quality, making them efficient resources for busy clinicians. The Cochrane Library focuses mainly on systematic reviews of controlled trials of therapeutic interventions. The main downside of these sources is that they may not address your particular question. Therefore, one effective search strategy is to first search a secondary journal or prefiltered source and stop if you find what you need. If you don’t find what you are looking for, you will need to enter the world of the large medical research database armed with a search strategy.
Constructing effective search strategies is perhaps even more of an art than constructing effective clinical questions. Luckily, medical librarians are experts at this and should be your first stop. Not only can skilled medical librarians help you with your searches, they can also teach you efficient ways to conduct simple searches yourself. I will mention a few of these strategies, but these are truly only the tip of the iceberg.
The key elements of searching the large medical information databases such as MEDLINE include an understanding of Medical Subject Headings (MeSH), text-word searching, and combining searches. Mapping to a MeSH term and clicking the “explode” option on the search page will gather not just those papers indexed to the term of interest, but also papers referencing more specific aspects of that term. Clicking on the search term itself will reveal the “tree” of terms related to your chosen search term. For example, try searching MEDLINE for “cancer.” You will be mapped to “neoplasms,” and if you click on that term, you will see a tree of related terms. If you select “explode” for your initial search, you will include each of these related terms, expanding your search. You could also narrow your search by selecting “neoplasms by site” or another subheading, and further refining your approach from there.
To begin a search, it is helpful to first enter in relevant keywords from your clinical question. Following our previous example, these could include renal cell carcinoma, chemotherapy, and survival. Then you could perform one search for each term, combining them using the search window options. Alternatively, each term could be linked in one search using the AND/OR operators. Further restrictions such as looking only at randomized controlled trials or for specific authors are also possible. Finally, many MEDLINE sites have a collection of saved search strategies for common clinical question types. For example, a saved search strategy for articles on diagnosis (or therapy, prognosis, or any other question type) can provide an effective searching technique based on the expertise of your resident search professional.
Because many of these approaches rely on the way in which an article has been indexed, searching for synonyms can also be helpful. You may search for temporal arteritis and miss articles indexed only under giant cell arteritis, for example. MEDLINE does a good job of mapping these terms to each other, but this can fall short, particularly if you search by text word alone. Being clever with synonyms can be the difference between finding and missing the one key article that will answer your clinical question.
Searchable Sources of Medical Information
“Overview of Searchable Sources of Medical Information” (p. 18) presents a brief overview of searchable sources of information. Becoming a searching expert takes considerable dedication, but fortunately the basic strategies are not overly complicated. Additionally, significant efforts are being made to simplify the steps needed to answer clinical questions, as can be seen in the growing number of secondary journals available for both general medicine and subspecialties.
Summary
Searching for the answers to well-constructed clinical questions is obviously a crucial step in the EBM process. Well-built questions suggest efficient search strategies, simplifying what can be a complex and daunting process. Many resources are available to help with this step, including medical librarians, prefiltered searches, and saved searches for common query types. Once you locate an article addressing your clinical question, the next step is to critically appraise the article to determine whether its results are applicable to your patient. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
The first step in finding an answer to a clinical question is to ask an effective question. This was the subject of the previous installment in this series, in which the PICOT question format was introduced (see The Hospitalist, Nov. 2005, p. 32). This format leads naturally to effective search strategies, so we optimize our chances of finding quality answers if they exist. There are many possible sources of information that can be searched, however, and the type of question asked can provide valuable guidance as to which sources should be first up for review.
Types of Questions and Where to Look for Answers
Many clinical questions pertain to basic medical knowledge rather than cutting-edge current research. These so-called background questions typically involve such issues as the underlying pathophysiology of a disease, the incidence of the disease, the general treatment considerations for the disease, and overall prognosis for patients with the disease. These questions usually do not require evaluation of the most recent medical literature and can often be answered by reviewing sources of established medical knowledge such as medical textbooks, MD Consult, or UpToDate. In fact, searching for basic knowledge in the current research literature can be exhausting because the focus of most papers is necessarily narrow and therefore too restrictive to properly address knowledge of a general nature.
The main limitation of these more general sources is that it takes years for medical knowledge to become established, so the most current results will seldom be incorporated. For background questions this is usually acceptable, but if a major breakthrough in our understanding of a disease occurs it is unlikely to be found in these sources. An additional limitation is that the statements found in these sources are often not truly evidence-based—at least not in a transparent or reproducible manner. These limitations are becoming less problematic as resources such as UpToDate strive to add evidence-based reviews and quality measures to their summaries, and also begin to update information much more rapidly as online materials become more standard.
In contrast to background clinical questions, foreground clinical questions are more likely to relate to the management of an individual patient in a specific clinical setting, and are therefore too narrow in scope to be addressed well by the sources best suited for background questions. For example, consider the question posed in the last installment of this series, “Among men over the age of 65 with Stage II renal cell carcinoma, does post-resection chemotherapy result in greater five-year survival than nephrectomy alone?” No textbook will answer a question with this narrow focus. To find an answer we need to be able to sift through the current medical research literature.
How to Search Research Databases
The number of medical journals has increased dramatically in the past 20 years. As a result, while it may be more likely that your question has been addressed somewhere, it can be more difficult to locate the paper you need. One approach to this problem is to become skilled in developing search strategies. We will return to this, but an alternative is to utilize secondary journals such as ACP Journal Club (www.acponline.org) or prefiltered sources such as the Cochrane Library (www.cochrane.org).
Secondary journals typically screen articles for both clinical relevance and methodologic quality, making them efficient resources for busy clinicians. The Cochrane Library focuses mainly on systematic reviews of controlled trials of therapeutic interventions. The main downside of these sources is that they may not address your particular question. Therefore, one effective search strategy is to first search a secondary journal or prefiltered source and stop if you find what you need. If you don’t find what you are looking for, you will need to enter the world of the large medical research database armed with a search strategy.
Constructing effective search strategies is perhaps even more of an art than constructing effective clinical questions. Luckily, medical librarians are experts at this and should be your first stop. Not only can skilled medical librarians help you with your searches, they can also teach you efficient ways to conduct simple searches yourself. I will mention a few of these strategies, but these are truly only the tip of the iceberg.
The key elements of searching the large medical information databases such as MEDLINE include an understanding of Medical Subject Headings (MeSH), text-word searching, and combining searches. Mapping to a MeSH term and clicking the “explode” option on the search page will gather not just those papers indexed to the term of interest, but also papers referencing more specific aspects of that term. Clicking on the search term itself will reveal the “tree” of terms related to your chosen search term. For example, try searching MEDLINE for “cancer.” You will be mapped to “neoplasms,” and if you click on that term, you will see a tree of related terms. If you select “explode” for your initial search, you will include each of these related terms, expanding your search. You could also narrow your search by selecting “neoplasms by site” or another subheading, and further refining your approach from there.
To begin a search, it is helpful to first enter in relevant keywords from your clinical question. Following our previous example, these could include renal cell carcinoma, chemotherapy, and survival. Then you could perform one search for each term, combining them using the search window options. Alternatively, each term could be linked in one search using the AND/OR operators. Further restrictions such as looking only at randomized controlled trials or for specific authors are also possible. Finally, many MEDLINE sites have a collection of saved search strategies for common clinical question types. For example, a saved search strategy for articles on diagnosis (or therapy, prognosis, or any other question type) can provide an effective searching technique based on the expertise of your resident search professional.
Because many of these approaches rely on the way in which an article has been indexed, searching for synonyms can also be helpful. You may search for temporal arteritis and miss articles indexed only under giant cell arteritis, for example. MEDLINE does a good job of mapping these terms to each other, but this can fall short, particularly if you search by text word alone. Being clever with synonyms can be the difference between finding and missing the one key article that will answer your clinical question.
Searchable Sources of Medical Information
“Overview of Searchable Sources of Medical Information” (p. 18) presents a brief overview of searchable sources of information. Becoming a searching expert takes considerable dedication, but fortunately the basic strategies are not overly complicated. Additionally, significant efforts are being made to simplify the steps needed to answer clinical questions, as can be seen in the growing number of secondary journals available for both general medicine and subspecialties.
Summary
Searching for the answers to well-constructed clinical questions is obviously a crucial step in the EBM process. Well-built questions suggest efficient search strategies, simplifying what can be a complex and daunting process. Many resources are available to help with this step, including medical librarians, prefiltered searches, and saved searches for common query types. Once you locate an article addressing your clinical question, the next step is to critically appraise the article to determine whether its results are applicable to your patient. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
The first step in finding an answer to a clinical question is to ask an effective question. This was the subject of the previous installment in this series, in which the PICOT question format was introduced (see The Hospitalist, Nov. 2005, p. 32). This format leads naturally to effective search strategies, so we optimize our chances of finding quality answers if they exist. There are many possible sources of information that can be searched, however, and the type of question asked can provide valuable guidance as to which sources should be first up for review.
Types of Questions and Where to Look for Answers
Many clinical questions pertain to basic medical knowledge rather than cutting-edge current research. These so-called background questions typically involve such issues as the underlying pathophysiology of a disease, the incidence of the disease, the general treatment considerations for the disease, and overall prognosis for patients with the disease. These questions usually do not require evaluation of the most recent medical literature and can often be answered by reviewing sources of established medical knowledge such as medical textbooks, MD Consult, or UpToDate. In fact, searching for basic knowledge in the current research literature can be exhausting because the focus of most papers is necessarily narrow and therefore too restrictive to properly address knowledge of a general nature.
The main limitation of these more general sources is that it takes years for medical knowledge to become established, so the most current results will seldom be incorporated. For background questions this is usually acceptable, but if a major breakthrough in our understanding of a disease occurs it is unlikely to be found in these sources. An additional limitation is that the statements found in these sources are often not truly evidence-based—at least not in a transparent or reproducible manner. These limitations are becoming less problematic as resources such as UpToDate strive to add evidence-based reviews and quality measures to their summaries, and also begin to update information much more rapidly as online materials become more standard.
In contrast to background clinical questions, foreground clinical questions are more likely to relate to the management of an individual patient in a specific clinical setting, and are therefore too narrow in scope to be addressed well by the sources best suited for background questions. For example, consider the question posed in the last installment of this series, “Among men over the age of 65 with Stage II renal cell carcinoma, does post-resection chemotherapy result in greater five-year survival than nephrectomy alone?” No textbook will answer a question with this narrow focus. To find an answer we need to be able to sift through the current medical research literature.
How to Search Research Databases
The number of medical journals has increased dramatically in the past 20 years. As a result, while it may be more likely that your question has been addressed somewhere, it can be more difficult to locate the paper you need. One approach to this problem is to become skilled in developing search strategies. We will return to this, but an alternative is to utilize secondary journals such as ACP Journal Club (www.acponline.org) or prefiltered sources such as the Cochrane Library (www.cochrane.org).
Secondary journals typically screen articles for both clinical relevance and methodologic quality, making them efficient resources for busy clinicians. The Cochrane Library focuses mainly on systematic reviews of controlled trials of therapeutic interventions. The main downside of these sources is that they may not address your particular question. Therefore, one effective search strategy is to first search a secondary journal or prefiltered source and stop if you find what you need. If you don’t find what you are looking for, you will need to enter the world of the large medical research database armed with a search strategy.
Constructing effective search strategies is perhaps even more of an art than constructing effective clinical questions. Luckily, medical librarians are experts at this and should be your first stop. Not only can skilled medical librarians help you with your searches, they can also teach you efficient ways to conduct simple searches yourself. I will mention a few of these strategies, but these are truly only the tip of the iceberg.
The key elements of searching the large medical information databases such as MEDLINE include an understanding of Medical Subject Headings (MeSH), text-word searching, and combining searches. Mapping to a MeSH term and clicking the “explode” option on the search page will gather not just those papers indexed to the term of interest, but also papers referencing more specific aspects of that term. Clicking on the search term itself will reveal the “tree” of terms related to your chosen search term. For example, try searching MEDLINE for “cancer.” You will be mapped to “neoplasms,” and if you click on that term, you will see a tree of related terms. If you select “explode” for your initial search, you will include each of these related terms, expanding your search. You could also narrow your search by selecting “neoplasms by site” or another subheading, and further refining your approach from there.
To begin a search, it is helpful to first enter in relevant keywords from your clinical question. Following our previous example, these could include renal cell carcinoma, chemotherapy, and survival. Then you could perform one search for each term, combining them using the search window options. Alternatively, each term could be linked in one search using the AND/OR operators. Further restrictions such as looking only at randomized controlled trials or for specific authors are also possible. Finally, many MEDLINE sites have a collection of saved search strategies for common clinical question types. For example, a saved search strategy for articles on diagnosis (or therapy, prognosis, or any other question type) can provide an effective searching technique based on the expertise of your resident search professional.
Because many of these approaches rely on the way in which an article has been indexed, searching for synonyms can also be helpful. You may search for temporal arteritis and miss articles indexed only under giant cell arteritis, for example. MEDLINE does a good job of mapping these terms to each other, but this can fall short, particularly if you search by text word alone. Being clever with synonyms can be the difference between finding and missing the one key article that will answer your clinical question.
Searchable Sources of Medical Information
“Overview of Searchable Sources of Medical Information” (p. 18) presents a brief overview of searchable sources of information. Becoming a searching expert takes considerable dedication, but fortunately the basic strategies are not overly complicated. Additionally, significant efforts are being made to simplify the steps needed to answer clinical questions, as can be seen in the growing number of secondary journals available for both general medicine and subspecialties.
Summary
Searching for the answers to well-constructed clinical questions is obviously a crucial step in the EBM process. Well-built questions suggest efficient search strategies, simplifying what can be a complex and daunting process. Many resources are available to help with this step, including medical librarians, prefiltered searches, and saved searches for common query types. Once you locate an article addressing your clinical question, the next step is to critically appraise the article to determine whether its results are applicable to your patient. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.