User login
The End of General Hospitals
Where will you be in 20 years? If you’re a young hospitalist, you may work in an enormous state-of-the-art hospital complex that includes the latest technologies, the best in amenities, and a well-thought-out design that will meet your needs and those of other staff for years to come.
“There are a lot of different approaches” to designing the hospital facility of the future, says George R. Tingwald, MD, AIA, ACHA, director of healthcare design at Skidmore, Owings, and Merrill in San Francisco. “The difference depends on whether you look at it from a constructability standpoint versus a much more consumer-based focus. Though many think they have the right approach, it’s hard to say that everybody’s decided on a single solution.”
The Future Looks … Big
It’s not just the hospital facility itself that will change in the future. The number of hospitals in each community may change as well—and the hospitals will be considerably larger.
“We will probably see fewer but larger hospitals in the future,” predicts Dr. Tingwald. “We’re in an era where we’re seeing significant growth in the number of inpatients served. Because of the baby boom and increasing longevity in Americans we’re already seeing an increase, and it’s going to continue. We’ll definitely see more hospital beds in the future.”
The type of patients who fill those hospital beds will change as well.
“We’ll continue to see sicker and sicker patients in those hospital beds,” says Dr. Tingwald. “More people will be managed on an outpatient basis as more diagnostic and treatment procedures will be done as outpatients. Look at breast cancer: From initial detection to diagnosis to biopsy to lumpectomy to chemotherapy or radiation treatment, to cure, or end-of-life care, each step can now be done on an outpatient basis.”
What does this mean? “Someone can have a very significant, multiepisodic disease and never stay in the hospital—unless there are complications,” explains Dr. Tingwald. “Therefore, we’ll have only very acute patients in the hospital. The hospital will basically become an intensive care unit.”
In the past, approximately 10% of a hospital’s beds were in the ICU. That percentage is rising—an indication of things to come. That percentage is now around 20% or 30% and growing, especially in major centers. Only seriously ill people will be admitted—but even they won’t spend a lot of time in the hospital. They will die, recover to a point where they can be moved to rehabilitation or other support facility, or be sent home.
What about the prediction that there will be fewer hospitals in the future? Dr. Tingwald predicts that technology and expertise will weed out some facilities.
“We used to have a lot of what I would call general hospitals—meaning every one was the same,” he explains. “That’s changing radically. The institutions with the expertise and wherewithal to develop technical sophistication, such as university hospitals and specialty hospitals, are doing well. Those that don’t have that sophistication can’t keep up. The big centers are growing because they have the equipment and the expertise. The smaller ones are failing.”
This trend may come as a surprise to some in healthcare, in light of previous predictions. “This is different than the futurists were saying 10 or 20 years ago, when predictions were for more home-based and community-based care,” says Dr. Tingwald. “The reverse has happened. The latest equipment is not available to everyone, let alone smaller, unaffiliated hospitals. And the people that can work with that technology are few and far between.”
The addition of new technology will have some effect on the size of the hospital. “You need a lot of physical space for wiring,” admits Dr. Tingwald. “But the ‘brains’ of the technology can be offsite at a separate IT center or data center.”
Focus on Family-Centered Care
Perhaps the most noticeable differences in the hospital facility of the future will be those related to a change in services, design, and attitude toward providing amenities for patients and their families.
“Patient-centered care, or its close cousin—family-centered care—is a significant trend in healthcare design now, and that significantly impacts the design of facilities,” states Dr. Tingwald. “The most important aspect is having all private rooms. Almost no new construction includes shared patient rooms. The key element of this care is family involvement, and that includes families rooming in with patients. You can’t physically or psychologically do this in a shared room.”
He points out that this trend includes all room types: “It started in pediatrics, but has gone into general acute care settings, intensive care settings, and now neonatal intensive care units.”
What are the pros and cons of a move toward all private rooms? “It takes up room, but it’s proving not to be significantly more costly,” says Dr. Tingwald. “Private rooms are more expensive to build, but in the end they’re less expensive to operate. In an all-private room hospital you can increase your occupancy to 80% or even 90% because you’re not trying to match up patients by gender and age. Also, nursing isn’t moving patients to get the bed mixes right. Studies show that nurses spend up to 40% of their time in transfers. And finally, private rooms have increased market share considerably.”
Another aspect of family centered care is the addition of technologies and services that cater to patient comfort and even enjoyment. “Anything someone has at home or wants in a hotel, families and patients are demanding, including room service,” says Dr. Tingwald. “Patients can decide when and what they want to eat [within their prescribed diet], and families can order food. In some hospitals, patients can already order food using a plasma screen in their room. This is showing to be an economically viable alternative. There’s less food waste, and patients are much happier.”
You’ll also see patient rooms with plasma screen televisions and DVD players, equipped for movies on demand, educational content—even the ability for physicians to view X-rays and other diagnostics on screen, and for families waiting in the room to communicate with physicians in the operating room.
“These are consumer-driven things, but they’re not luxuries,” insists Dr. Tingwald. “They’re often things that save time, increase the ability for education, and significantly decrease errors.”
Another argument for adding amenities like plasma screen TVs and room service: “In healthcare you think adding this technology must be too expensive,” says Dr. Tingwald, “but if you walk into a fast-food place, the person behind the counter uses a touch screen. Everybody else has done this already. Facilities that don’t partake in these transitions are not going to survive.”
Other family-centered improvements include major changes in patient registration. “Most registration can be done from home, over the Internet,” he says. “At Northwestern Memorial Hospital [in Chicago], patients have an encoded card they swipe when they drive into the parking garage, and the receptionist knows they’re coming and gets their room ready before they arrive.”
In the future, more facilities will offer options like these to make the registration process easy and fast.
The hospital of the future will feature a friendlier environment, with landscaping and nice views from patient rooms, artwork and amenities that are important in the healing process. They will also include an emphasis on alternative treatments, says Dr. Tingwald, “from massage to aromatherapy to spaces for yoga or meditation.”
Plan for Flexibility
The key to the design of the hospital of the future will be its ability to change without building additions, remodeling, or rehabbing.
“We’re no longer planning a facility in a static way, thinking that things will not change. Flexibility and adaptability are planned from the beginning,” explains Dr. Tingwald. “You’ll see a lot more generic room types—rooms that are all a single size, but adaptable. A private patient room might be initially planned for acute care, but it can be adapted for an ICU room with minimal or no remodeling.”
This holds true for other room types as well. “In diagnostic and treatment spaces, we plan for one, or no more than two, sizes of space,” he says. “You don’t know if in the future more procedures will be surgical or non-invasive, so rooms are planned to handle both functions. Also, the kingdoms are coming down and divisions between diagnostic departments are blending.”
The Johns Hopkins Hospital (Baltimore), the University of California, Los Angeles Medical Center, and California Pacific Medical Center in San Francisco are all designing “platform floors,” where surgery, interventional imaging, cardiac catheterization, and other procedure-based services share preoperative and postoperative areas and have single access.
“These floors provide adjacency of services allowing a lot more flexibility and decreased redundancy,” explains Dr. Tingwald. “Also, there aren’t as many patient transfers, and a key to patient-centered care is less movement of the patient.”
Built-in flexibility is designed to accommodate scalability as well. “In the planning process, we anticipate higher volumes in an emergency or disaster,” he says. “We plan how to expand the emergency room, and we make rooms larger than we used to. That way, if volumes increase quickly, you could put two, three, maybe more patients in a space. Nurses hate when you say that, but we have to have timely solutions that are affordable. This approach can be considered on nursing units as well, with these ‘super singles’ able to handle a second patient during a February flu outbreak, for example. That’s better than having an entire wing of the hospital that’s only used during winter months, patients stuck in the emergency department for days, or patients in the halls.”
A Design with Built-In Patient Safety
The physical design of the hospital of the future will better address and correct issues with patient safety. “Whatever design elements can minimize errors and improve outcomes are being studied intensively right now,” says Dr. Tingwald. “For example, we used to mirror many room types so that walls could share plumbing, etc. One room would be the mirror image of the one next to it, requiring the staff to learn different layouts, which increases time of response and possible errors. Now, we try to make procedure rooms as similar as possible to reduce the potential for error.”
There are design elements that limit the possibility of hospital-borne infection, including ultraviolet light and biologic surfaces. There is also a greater emphasis on including track systems for lifts for getting patients out of bed and moving them without injury to the patient or the staff.
Consider Hospitalists and Other Staff
How will the hospital of the future accommodate hospitalists?
“We’re certainly seeing more hospitalists,” says Dr. Tingwald. “As you have sicker patients in the hospital, it’s harder for their primary care physicians to manage them, so we’re going to see even more hospitalists. This means that we have to provide space for them; both offices, because they don’t have other office space, and sleeping accommodations, which means private rooms with bath, as well as lounge space.”
Hospitals will provide appealing space for physicians because it will help them recruit hospitalists. Improving lounges and other staff spaces will be a goal of future hospital designs.
“There will be a lot more emphasis on good environments for work and for support services,” predicts Dr. Tingwald. “This will increase the attraction and retention of top staff. You’ll see things like fitness centers, and basic additions like enough parking spaces.”
As hospital facilities move toward more patient-centered care, with flexible layouts and space designed for patient safety, the working environment is certain to become more conducive to providing good care and working efficiently. It will also become more comfortable, convenient, and pleasant for hospitalists and other staff. And that is something to look forward to. TH
Writer Jane Jerrard wrote the first three installments of the “Future” series.
FLASHBACK
Cadaver Particles
—Ignaz Semmelweis, 1861
Death stalked the halls of the First Division of the Allegemeine Krankenhaus (Vienna General Hospital), a large teaching hospital in Austria. Healthy post-partum women suddenly become febrile and died from puerperal sepsis (childbed fever). In the mid-19th century, this problem was seen in hospitals across Europe, though rarely in home deliveries. It was a seemingly insoluble dilemma. Opinions varied on the etiology. Was it miasmas, the paint on the walls, were the beds too close, or was it clogged milk glands? Complacency and acceptance of status quo were, to some, the easiest solution.
In the mid-1800s Hungarian Physician Ignaz Semmelweis was given an appointment as an assistant in obstetrics at the Allegemeine Krankenhaus. He had adopted the Austrian paradigm of clinical and pathologic anatomy. The answer to any question lay in the autopsy. It seemed like the more autopsies they did, the more women died. The death of Semmelweis’ colleague, Jakob Kolletschka (who was initially injured when his knife slipped during an autopsy of a woman who died of puerperal fever and then died himself of symptoms similar to those that killed the woman) gave Semmelweis the vital clue.
He realized that something carried on unwashed surgeons’ hands from infected cadavers caused the disease to occur in the women. These “cadaver particles” were transmitted from the morning autopsies to the women on the wards by the unwashed hands of students and faculty. Adopting proper hygiene could save thousands of lives. Properly washed hands were the simple answer. This also explained the mystery of why the puerperal fever rate was lower on the midwife-run wards where they did not do autopsies.
Decades before Pasteur and Lister, accepting that their own hands brought death was a bitter pill for the great men of obstetrics to swallow. Unfortunately for Semmelweis and the women who continued to die, it was years before Oliver Wendell Holmes incontrovertibly published his essay, “The Contagiousness of Puerperal Fever” in 1843 in the New England Quarterly Journal of Medicine. That essay showed the source of puerperal fever. Despite his clinical success Semmelweis was unable to persuade his fellow physicians.
The nosocomial spread of infection on unwashed hands rings true to this day. We spend our days gloved, gowned, and masked in the battle against MRSA, VRE, and other pathogens. Whether soap or alcohol, when we scrub our hands we should remember that it is more than a ritual. It’s a duty to prevent the spread of disease.
—Jamie Newman, MD, FACP
Where will you be in 20 years? If you’re a young hospitalist, you may work in an enormous state-of-the-art hospital complex that includes the latest technologies, the best in amenities, and a well-thought-out design that will meet your needs and those of other staff for years to come.
“There are a lot of different approaches” to designing the hospital facility of the future, says George R. Tingwald, MD, AIA, ACHA, director of healthcare design at Skidmore, Owings, and Merrill in San Francisco. “The difference depends on whether you look at it from a constructability standpoint versus a much more consumer-based focus. Though many think they have the right approach, it’s hard to say that everybody’s decided on a single solution.”
The Future Looks … Big
It’s not just the hospital facility itself that will change in the future. The number of hospitals in each community may change as well—and the hospitals will be considerably larger.
“We will probably see fewer but larger hospitals in the future,” predicts Dr. Tingwald. “We’re in an era where we’re seeing significant growth in the number of inpatients served. Because of the baby boom and increasing longevity in Americans we’re already seeing an increase, and it’s going to continue. We’ll definitely see more hospital beds in the future.”
The type of patients who fill those hospital beds will change as well.
“We’ll continue to see sicker and sicker patients in those hospital beds,” says Dr. Tingwald. “More people will be managed on an outpatient basis as more diagnostic and treatment procedures will be done as outpatients. Look at breast cancer: From initial detection to diagnosis to biopsy to lumpectomy to chemotherapy or radiation treatment, to cure, or end-of-life care, each step can now be done on an outpatient basis.”
What does this mean? “Someone can have a very significant, multiepisodic disease and never stay in the hospital—unless there are complications,” explains Dr. Tingwald. “Therefore, we’ll have only very acute patients in the hospital. The hospital will basically become an intensive care unit.”
In the past, approximately 10% of a hospital’s beds were in the ICU. That percentage is rising—an indication of things to come. That percentage is now around 20% or 30% and growing, especially in major centers. Only seriously ill people will be admitted—but even they won’t spend a lot of time in the hospital. They will die, recover to a point where they can be moved to rehabilitation or other support facility, or be sent home.
What about the prediction that there will be fewer hospitals in the future? Dr. Tingwald predicts that technology and expertise will weed out some facilities.
“We used to have a lot of what I would call general hospitals—meaning every one was the same,” he explains. “That’s changing radically. The institutions with the expertise and wherewithal to develop technical sophistication, such as university hospitals and specialty hospitals, are doing well. Those that don’t have that sophistication can’t keep up. The big centers are growing because they have the equipment and the expertise. The smaller ones are failing.”
This trend may come as a surprise to some in healthcare, in light of previous predictions. “This is different than the futurists were saying 10 or 20 years ago, when predictions were for more home-based and community-based care,” says Dr. Tingwald. “The reverse has happened. The latest equipment is not available to everyone, let alone smaller, unaffiliated hospitals. And the people that can work with that technology are few and far between.”
The addition of new technology will have some effect on the size of the hospital. “You need a lot of physical space for wiring,” admits Dr. Tingwald. “But the ‘brains’ of the technology can be offsite at a separate IT center or data center.”
Focus on Family-Centered Care
Perhaps the most noticeable differences in the hospital facility of the future will be those related to a change in services, design, and attitude toward providing amenities for patients and their families.
“Patient-centered care, or its close cousin—family-centered care—is a significant trend in healthcare design now, and that significantly impacts the design of facilities,” states Dr. Tingwald. “The most important aspect is having all private rooms. Almost no new construction includes shared patient rooms. The key element of this care is family involvement, and that includes families rooming in with patients. You can’t physically or psychologically do this in a shared room.”
He points out that this trend includes all room types: “It started in pediatrics, but has gone into general acute care settings, intensive care settings, and now neonatal intensive care units.”
What are the pros and cons of a move toward all private rooms? “It takes up room, but it’s proving not to be significantly more costly,” says Dr. Tingwald. “Private rooms are more expensive to build, but in the end they’re less expensive to operate. In an all-private room hospital you can increase your occupancy to 80% or even 90% because you’re not trying to match up patients by gender and age. Also, nursing isn’t moving patients to get the bed mixes right. Studies show that nurses spend up to 40% of their time in transfers. And finally, private rooms have increased market share considerably.”
Another aspect of family centered care is the addition of technologies and services that cater to patient comfort and even enjoyment. “Anything someone has at home or wants in a hotel, families and patients are demanding, including room service,” says Dr. Tingwald. “Patients can decide when and what they want to eat [within their prescribed diet], and families can order food. In some hospitals, patients can already order food using a plasma screen in their room. This is showing to be an economically viable alternative. There’s less food waste, and patients are much happier.”
You’ll also see patient rooms with plasma screen televisions and DVD players, equipped for movies on demand, educational content—even the ability for physicians to view X-rays and other diagnostics on screen, and for families waiting in the room to communicate with physicians in the operating room.
“These are consumer-driven things, but they’re not luxuries,” insists Dr. Tingwald. “They’re often things that save time, increase the ability for education, and significantly decrease errors.”
Another argument for adding amenities like plasma screen TVs and room service: “In healthcare you think adding this technology must be too expensive,” says Dr. Tingwald, “but if you walk into a fast-food place, the person behind the counter uses a touch screen. Everybody else has done this already. Facilities that don’t partake in these transitions are not going to survive.”
Other family-centered improvements include major changes in patient registration. “Most registration can be done from home, over the Internet,” he says. “At Northwestern Memorial Hospital [in Chicago], patients have an encoded card they swipe when they drive into the parking garage, and the receptionist knows they’re coming and gets their room ready before they arrive.”
In the future, more facilities will offer options like these to make the registration process easy and fast.
The hospital of the future will feature a friendlier environment, with landscaping and nice views from patient rooms, artwork and amenities that are important in the healing process. They will also include an emphasis on alternative treatments, says Dr. Tingwald, “from massage to aromatherapy to spaces for yoga or meditation.”
Plan for Flexibility
The key to the design of the hospital of the future will be its ability to change without building additions, remodeling, or rehabbing.
“We’re no longer planning a facility in a static way, thinking that things will not change. Flexibility and adaptability are planned from the beginning,” explains Dr. Tingwald. “You’ll see a lot more generic room types—rooms that are all a single size, but adaptable. A private patient room might be initially planned for acute care, but it can be adapted for an ICU room with minimal or no remodeling.”
This holds true for other room types as well. “In diagnostic and treatment spaces, we plan for one, or no more than two, sizes of space,” he says. “You don’t know if in the future more procedures will be surgical or non-invasive, so rooms are planned to handle both functions. Also, the kingdoms are coming down and divisions between diagnostic departments are blending.”
The Johns Hopkins Hospital (Baltimore), the University of California, Los Angeles Medical Center, and California Pacific Medical Center in San Francisco are all designing “platform floors,” where surgery, interventional imaging, cardiac catheterization, and other procedure-based services share preoperative and postoperative areas and have single access.
“These floors provide adjacency of services allowing a lot more flexibility and decreased redundancy,” explains Dr. Tingwald. “Also, there aren’t as many patient transfers, and a key to patient-centered care is less movement of the patient.”
Built-in flexibility is designed to accommodate scalability as well. “In the planning process, we anticipate higher volumes in an emergency or disaster,” he says. “We plan how to expand the emergency room, and we make rooms larger than we used to. That way, if volumes increase quickly, you could put two, three, maybe more patients in a space. Nurses hate when you say that, but we have to have timely solutions that are affordable. This approach can be considered on nursing units as well, with these ‘super singles’ able to handle a second patient during a February flu outbreak, for example. That’s better than having an entire wing of the hospital that’s only used during winter months, patients stuck in the emergency department for days, or patients in the halls.”
A Design with Built-In Patient Safety
The physical design of the hospital of the future will better address and correct issues with patient safety. “Whatever design elements can minimize errors and improve outcomes are being studied intensively right now,” says Dr. Tingwald. “For example, we used to mirror many room types so that walls could share plumbing, etc. One room would be the mirror image of the one next to it, requiring the staff to learn different layouts, which increases time of response and possible errors. Now, we try to make procedure rooms as similar as possible to reduce the potential for error.”
There are design elements that limit the possibility of hospital-borne infection, including ultraviolet light and biologic surfaces. There is also a greater emphasis on including track systems for lifts for getting patients out of bed and moving them without injury to the patient or the staff.
Consider Hospitalists and Other Staff
How will the hospital of the future accommodate hospitalists?
“We’re certainly seeing more hospitalists,” says Dr. Tingwald. “As you have sicker patients in the hospital, it’s harder for their primary care physicians to manage them, so we’re going to see even more hospitalists. This means that we have to provide space for them; both offices, because they don’t have other office space, and sleeping accommodations, which means private rooms with bath, as well as lounge space.”
Hospitals will provide appealing space for physicians because it will help them recruit hospitalists. Improving lounges and other staff spaces will be a goal of future hospital designs.
“There will be a lot more emphasis on good environments for work and for support services,” predicts Dr. Tingwald. “This will increase the attraction and retention of top staff. You’ll see things like fitness centers, and basic additions like enough parking spaces.”
As hospital facilities move toward more patient-centered care, with flexible layouts and space designed for patient safety, the working environment is certain to become more conducive to providing good care and working efficiently. It will also become more comfortable, convenient, and pleasant for hospitalists and other staff. And that is something to look forward to. TH
Writer Jane Jerrard wrote the first three installments of the “Future” series.
FLASHBACK
Cadaver Particles
—Ignaz Semmelweis, 1861
Death stalked the halls of the First Division of the Allegemeine Krankenhaus (Vienna General Hospital), a large teaching hospital in Austria. Healthy post-partum women suddenly become febrile and died from puerperal sepsis (childbed fever). In the mid-19th century, this problem was seen in hospitals across Europe, though rarely in home deliveries. It was a seemingly insoluble dilemma. Opinions varied on the etiology. Was it miasmas, the paint on the walls, were the beds too close, or was it clogged milk glands? Complacency and acceptance of status quo were, to some, the easiest solution.
In the mid-1800s Hungarian Physician Ignaz Semmelweis was given an appointment as an assistant in obstetrics at the Allegemeine Krankenhaus. He had adopted the Austrian paradigm of clinical and pathologic anatomy. The answer to any question lay in the autopsy. It seemed like the more autopsies they did, the more women died. The death of Semmelweis’ colleague, Jakob Kolletschka (who was initially injured when his knife slipped during an autopsy of a woman who died of puerperal fever and then died himself of symptoms similar to those that killed the woman) gave Semmelweis the vital clue.
He realized that something carried on unwashed surgeons’ hands from infected cadavers caused the disease to occur in the women. These “cadaver particles” were transmitted from the morning autopsies to the women on the wards by the unwashed hands of students and faculty. Adopting proper hygiene could save thousands of lives. Properly washed hands were the simple answer. This also explained the mystery of why the puerperal fever rate was lower on the midwife-run wards where they did not do autopsies.
Decades before Pasteur and Lister, accepting that their own hands brought death was a bitter pill for the great men of obstetrics to swallow. Unfortunately for Semmelweis and the women who continued to die, it was years before Oliver Wendell Holmes incontrovertibly published his essay, “The Contagiousness of Puerperal Fever” in 1843 in the New England Quarterly Journal of Medicine. That essay showed the source of puerperal fever. Despite his clinical success Semmelweis was unable to persuade his fellow physicians.
The nosocomial spread of infection on unwashed hands rings true to this day. We spend our days gloved, gowned, and masked in the battle against MRSA, VRE, and other pathogens. Whether soap or alcohol, when we scrub our hands we should remember that it is more than a ritual. It’s a duty to prevent the spread of disease.
—Jamie Newman, MD, FACP
Where will you be in 20 years? If you’re a young hospitalist, you may work in an enormous state-of-the-art hospital complex that includes the latest technologies, the best in amenities, and a well-thought-out design that will meet your needs and those of other staff for years to come.
“There are a lot of different approaches” to designing the hospital facility of the future, says George R. Tingwald, MD, AIA, ACHA, director of healthcare design at Skidmore, Owings, and Merrill in San Francisco. “The difference depends on whether you look at it from a constructability standpoint versus a much more consumer-based focus. Though many think they have the right approach, it’s hard to say that everybody’s decided on a single solution.”
The Future Looks … Big
It’s not just the hospital facility itself that will change in the future. The number of hospitals in each community may change as well—and the hospitals will be considerably larger.
“We will probably see fewer but larger hospitals in the future,” predicts Dr. Tingwald. “We’re in an era where we’re seeing significant growth in the number of inpatients served. Because of the baby boom and increasing longevity in Americans we’re already seeing an increase, and it’s going to continue. We’ll definitely see more hospital beds in the future.”
The type of patients who fill those hospital beds will change as well.
“We’ll continue to see sicker and sicker patients in those hospital beds,” says Dr. Tingwald. “More people will be managed on an outpatient basis as more diagnostic and treatment procedures will be done as outpatients. Look at breast cancer: From initial detection to diagnosis to biopsy to lumpectomy to chemotherapy or radiation treatment, to cure, or end-of-life care, each step can now be done on an outpatient basis.”
What does this mean? “Someone can have a very significant, multiepisodic disease and never stay in the hospital—unless there are complications,” explains Dr. Tingwald. “Therefore, we’ll have only very acute patients in the hospital. The hospital will basically become an intensive care unit.”
In the past, approximately 10% of a hospital’s beds were in the ICU. That percentage is rising—an indication of things to come. That percentage is now around 20% or 30% and growing, especially in major centers. Only seriously ill people will be admitted—but even they won’t spend a lot of time in the hospital. They will die, recover to a point where they can be moved to rehabilitation or other support facility, or be sent home.
What about the prediction that there will be fewer hospitals in the future? Dr. Tingwald predicts that technology and expertise will weed out some facilities.
“We used to have a lot of what I would call general hospitals—meaning every one was the same,” he explains. “That’s changing radically. The institutions with the expertise and wherewithal to develop technical sophistication, such as university hospitals and specialty hospitals, are doing well. Those that don’t have that sophistication can’t keep up. The big centers are growing because they have the equipment and the expertise. The smaller ones are failing.”
This trend may come as a surprise to some in healthcare, in light of previous predictions. “This is different than the futurists were saying 10 or 20 years ago, when predictions were for more home-based and community-based care,” says Dr. Tingwald. “The reverse has happened. The latest equipment is not available to everyone, let alone smaller, unaffiliated hospitals. And the people that can work with that technology are few and far between.”
The addition of new technology will have some effect on the size of the hospital. “You need a lot of physical space for wiring,” admits Dr. Tingwald. “But the ‘brains’ of the technology can be offsite at a separate IT center or data center.”
Focus on Family-Centered Care
Perhaps the most noticeable differences in the hospital facility of the future will be those related to a change in services, design, and attitude toward providing amenities for patients and their families.
“Patient-centered care, or its close cousin—family-centered care—is a significant trend in healthcare design now, and that significantly impacts the design of facilities,” states Dr. Tingwald. “The most important aspect is having all private rooms. Almost no new construction includes shared patient rooms. The key element of this care is family involvement, and that includes families rooming in with patients. You can’t physically or psychologically do this in a shared room.”
He points out that this trend includes all room types: “It started in pediatrics, but has gone into general acute care settings, intensive care settings, and now neonatal intensive care units.”
What are the pros and cons of a move toward all private rooms? “It takes up room, but it’s proving not to be significantly more costly,” says Dr. Tingwald. “Private rooms are more expensive to build, but in the end they’re less expensive to operate. In an all-private room hospital you can increase your occupancy to 80% or even 90% because you’re not trying to match up patients by gender and age. Also, nursing isn’t moving patients to get the bed mixes right. Studies show that nurses spend up to 40% of their time in transfers. And finally, private rooms have increased market share considerably.”
Another aspect of family centered care is the addition of technologies and services that cater to patient comfort and even enjoyment. “Anything someone has at home or wants in a hotel, families and patients are demanding, including room service,” says Dr. Tingwald. “Patients can decide when and what they want to eat [within their prescribed diet], and families can order food. In some hospitals, patients can already order food using a plasma screen in their room. This is showing to be an economically viable alternative. There’s less food waste, and patients are much happier.”
You’ll also see patient rooms with plasma screen televisions and DVD players, equipped for movies on demand, educational content—even the ability for physicians to view X-rays and other diagnostics on screen, and for families waiting in the room to communicate with physicians in the operating room.
“These are consumer-driven things, but they’re not luxuries,” insists Dr. Tingwald. “They’re often things that save time, increase the ability for education, and significantly decrease errors.”
Another argument for adding amenities like plasma screen TVs and room service: “In healthcare you think adding this technology must be too expensive,” says Dr. Tingwald, “but if you walk into a fast-food place, the person behind the counter uses a touch screen. Everybody else has done this already. Facilities that don’t partake in these transitions are not going to survive.”
Other family-centered improvements include major changes in patient registration. “Most registration can be done from home, over the Internet,” he says. “At Northwestern Memorial Hospital [in Chicago], patients have an encoded card they swipe when they drive into the parking garage, and the receptionist knows they’re coming and gets their room ready before they arrive.”
In the future, more facilities will offer options like these to make the registration process easy and fast.
The hospital of the future will feature a friendlier environment, with landscaping and nice views from patient rooms, artwork and amenities that are important in the healing process. They will also include an emphasis on alternative treatments, says Dr. Tingwald, “from massage to aromatherapy to spaces for yoga or meditation.”
Plan for Flexibility
The key to the design of the hospital of the future will be its ability to change without building additions, remodeling, or rehabbing.
“We’re no longer planning a facility in a static way, thinking that things will not change. Flexibility and adaptability are planned from the beginning,” explains Dr. Tingwald. “You’ll see a lot more generic room types—rooms that are all a single size, but adaptable. A private patient room might be initially planned for acute care, but it can be adapted for an ICU room with minimal or no remodeling.”
This holds true for other room types as well. “In diagnostic and treatment spaces, we plan for one, or no more than two, sizes of space,” he says. “You don’t know if in the future more procedures will be surgical or non-invasive, so rooms are planned to handle both functions. Also, the kingdoms are coming down and divisions between diagnostic departments are blending.”
The Johns Hopkins Hospital (Baltimore), the University of California, Los Angeles Medical Center, and California Pacific Medical Center in San Francisco are all designing “platform floors,” where surgery, interventional imaging, cardiac catheterization, and other procedure-based services share preoperative and postoperative areas and have single access.
“These floors provide adjacency of services allowing a lot more flexibility and decreased redundancy,” explains Dr. Tingwald. “Also, there aren’t as many patient transfers, and a key to patient-centered care is less movement of the patient.”
Built-in flexibility is designed to accommodate scalability as well. “In the planning process, we anticipate higher volumes in an emergency or disaster,” he says. “We plan how to expand the emergency room, and we make rooms larger than we used to. That way, if volumes increase quickly, you could put two, three, maybe more patients in a space. Nurses hate when you say that, but we have to have timely solutions that are affordable. This approach can be considered on nursing units as well, with these ‘super singles’ able to handle a second patient during a February flu outbreak, for example. That’s better than having an entire wing of the hospital that’s only used during winter months, patients stuck in the emergency department for days, or patients in the halls.”
A Design with Built-In Patient Safety
The physical design of the hospital of the future will better address and correct issues with patient safety. “Whatever design elements can minimize errors and improve outcomes are being studied intensively right now,” says Dr. Tingwald. “For example, we used to mirror many room types so that walls could share plumbing, etc. One room would be the mirror image of the one next to it, requiring the staff to learn different layouts, which increases time of response and possible errors. Now, we try to make procedure rooms as similar as possible to reduce the potential for error.”
There are design elements that limit the possibility of hospital-borne infection, including ultraviolet light and biologic surfaces. There is also a greater emphasis on including track systems for lifts for getting patients out of bed and moving them without injury to the patient or the staff.
Consider Hospitalists and Other Staff
How will the hospital of the future accommodate hospitalists?
“We’re certainly seeing more hospitalists,” says Dr. Tingwald. “As you have sicker patients in the hospital, it’s harder for their primary care physicians to manage them, so we’re going to see even more hospitalists. This means that we have to provide space for them; both offices, because they don’t have other office space, and sleeping accommodations, which means private rooms with bath, as well as lounge space.”
Hospitals will provide appealing space for physicians because it will help them recruit hospitalists. Improving lounges and other staff spaces will be a goal of future hospital designs.
“There will be a lot more emphasis on good environments for work and for support services,” predicts Dr. Tingwald. “This will increase the attraction and retention of top staff. You’ll see things like fitness centers, and basic additions like enough parking spaces.”
As hospital facilities move toward more patient-centered care, with flexible layouts and space designed for patient safety, the working environment is certain to become more conducive to providing good care and working efficiently. It will also become more comfortable, convenient, and pleasant for hospitalists and other staff. And that is something to look forward to. TH
Writer Jane Jerrard wrote the first three installments of the “Future” series.
FLASHBACK
Cadaver Particles
—Ignaz Semmelweis, 1861
Death stalked the halls of the First Division of the Allegemeine Krankenhaus (Vienna General Hospital), a large teaching hospital in Austria. Healthy post-partum women suddenly become febrile and died from puerperal sepsis (childbed fever). In the mid-19th century, this problem was seen in hospitals across Europe, though rarely in home deliveries. It was a seemingly insoluble dilemma. Opinions varied on the etiology. Was it miasmas, the paint on the walls, were the beds too close, or was it clogged milk glands? Complacency and acceptance of status quo were, to some, the easiest solution.
In the mid-1800s Hungarian Physician Ignaz Semmelweis was given an appointment as an assistant in obstetrics at the Allegemeine Krankenhaus. He had adopted the Austrian paradigm of clinical and pathologic anatomy. The answer to any question lay in the autopsy. It seemed like the more autopsies they did, the more women died. The death of Semmelweis’ colleague, Jakob Kolletschka (who was initially injured when his knife slipped during an autopsy of a woman who died of puerperal fever and then died himself of symptoms similar to those that killed the woman) gave Semmelweis the vital clue.
He realized that something carried on unwashed surgeons’ hands from infected cadavers caused the disease to occur in the women. These “cadaver particles” were transmitted from the morning autopsies to the women on the wards by the unwashed hands of students and faculty. Adopting proper hygiene could save thousands of lives. Properly washed hands were the simple answer. This also explained the mystery of why the puerperal fever rate was lower on the midwife-run wards where they did not do autopsies.
Decades before Pasteur and Lister, accepting that their own hands brought death was a bitter pill for the great men of obstetrics to swallow. Unfortunately for Semmelweis and the women who continued to die, it was years before Oliver Wendell Holmes incontrovertibly published his essay, “The Contagiousness of Puerperal Fever” in 1843 in the New England Quarterly Journal of Medicine. That essay showed the source of puerperal fever. Despite his clinical success Semmelweis was unable to persuade his fellow physicians.
The nosocomial spread of infection on unwashed hands rings true to this day. We spend our days gloved, gowned, and masked in the battle against MRSA, VRE, and other pathogens. Whether soap or alcohol, when we scrub our hands we should remember that it is more than a ritual. It’s a duty to prevent the spread of disease.
—Jamie Newman, MD, FACP
An Itchy Neck
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:

- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.

This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
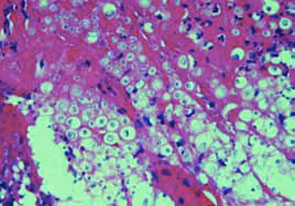
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:
- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:
- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
Career Satisfaction Toolkit
Early survey data on hospitalists, which suggest high levels of job engagement and low turnover rates, may not be as relevant as programs mature in a competitive marketplace to meet important needs such as rising census and Accreditation Council for Graduate Medical Education (ACGME) requirements. There is also a paucity of data on how different models of compensation affect hospitalists’ career satisfaction.
In 2005 the role of the hospitalist has evolved from simply improving throughput (average length of stay) to one of leadership, quality improvement, and teaching that extends beyond direct patient care. Compensation for hospitalists should not, therefore, be based solely on billing revenue. Improving the efficiency of the hospitalists work environment, which may include IT support, adequate office space, and administrative support, may not only enhance productivity but also job satisfaction. More research is needed to examine these questions.
Progress Report
One of the Career Satisfaction Task Force’s major initiatives has been developing a toolkit for the SHM membership with the purpose of providing members with an action plan for attaining a long and satisfying career in hospital medicine. The following steps are being taken in the creation of the toolkit:
- Needs assessment—questionnaire at the SHM 2005 Annual Meeting;
- Monthly conference calls;
- Timeline:
- Toolkit draft completion—Sept. 2005;
- Review SHM Membership Committee—Oct. 2005;
- Further revision;
- Submission to SHM Board for review—Nov. 2005;
- Further revision; and
- Dissemination at SHM Annual Meeting—May 2006.
- Content—four workplace domains:
- Control/Autonomy;
- Workload/Schedule;
- Community/Environment; and
- Reward/Recognition.
- Elements comprising each domain:
- Definition: specific description of workplace domain;
- Background: review of literature, expert opinion, experience-based observation, executive summary of background content;
- Guidelines: practical actionable recommendations and educational initiatives;
- Pitfalls: specific examples;
- Examples: application to different settings (community, academic, pediatric); and
- References.
Research and Timeline
In parallel to the development of the work domains for the toolkit, the Career Satisfaction Task Force is developing a questionnaire to survey hospitalist physicians on career satisfaction and “worklife.” The last survey of this type was performed in 1999. This questionnaire will allow us to assess changes in hospitalist quality of working life over time to further explore how hospitalists are faring during this critical time of rapid growth of our specialty.
The task force is developing a list of important aspects of worklife, satisfaction, and stress for hospitalists. This list will be supplemented by semi-structured interviews of SHM members and leaders in hospital medicine to include a representative viewpoint of hospitalist worklife: adult and pediatric medicine, academic and community, gender and age, directors of programs, and different employer types.
The interviews were expected to be completed in the fall of 2005. Qualitative data analysis will allow us to ascertain important themes for job performance and satisfaction to be highlighted in the survey. The questionnaire development will also consider inclusion of aspects from the prior surveys to follow results over time and when possible will use validated questions from the quality of working life literature.
We anticipate completion of the questionnaire in spring 2006 followed by surveying of a random sample of hospitalists from the SHM membership through a Web-based survey. Sampling of groups of hospitalists based on job characteristics will occur because there is significant interest and need for information about hospitalist worklife in certain work settings. The questionnaire dissemination time will overlap with the annual meeting to maximize survey response. The task force will work with SHM annual meeting committee to discuss having a dedicated computer for filling out the Web-based survey on-site.
Any SHM member who would like to participate in the questionnaire on-site, even if they were not selected for the random sample, will be encouraged to do so. Data analysis will occur in mid-late 2006. The task force will use information from the analyses to update the SHM Worklife Toolkit. We will also provide numerous forums for dissemination of the data. In particular, we plan to showcase this data at the 2007 SHM Annual Meeting followed by journal publication and Web site posting. It is our hope that this data will provide key information on the current quality of working life of hospitalist physicians to support worklife recommendations that promote sustainable, enjoyable careers in hospital medicine.
Early survey data on hospitalists, which suggest high levels of job engagement and low turnover rates, may not be as relevant as programs mature in a competitive marketplace to meet important needs such as rising census and Accreditation Council for Graduate Medical Education (ACGME) requirements. There is also a paucity of data on how different models of compensation affect hospitalists’ career satisfaction.
In 2005 the role of the hospitalist has evolved from simply improving throughput (average length of stay) to one of leadership, quality improvement, and teaching that extends beyond direct patient care. Compensation for hospitalists should not, therefore, be based solely on billing revenue. Improving the efficiency of the hospitalists work environment, which may include IT support, adequate office space, and administrative support, may not only enhance productivity but also job satisfaction. More research is needed to examine these questions.
Progress Report
One of the Career Satisfaction Task Force’s major initiatives has been developing a toolkit for the SHM membership with the purpose of providing members with an action plan for attaining a long and satisfying career in hospital medicine. The following steps are being taken in the creation of the toolkit:
- Needs assessment—questionnaire at the SHM 2005 Annual Meeting;
- Monthly conference calls;
- Timeline:
- Toolkit draft completion—Sept. 2005;
- Review SHM Membership Committee—Oct. 2005;
- Further revision;
- Submission to SHM Board for review—Nov. 2005;
- Further revision; and
- Dissemination at SHM Annual Meeting—May 2006.
- Content—four workplace domains:
- Control/Autonomy;
- Workload/Schedule;
- Community/Environment; and
- Reward/Recognition.
- Elements comprising each domain:
- Definition: specific description of workplace domain;
- Background: review of literature, expert opinion, experience-based observation, executive summary of background content;
- Guidelines: practical actionable recommendations and educational initiatives;
- Pitfalls: specific examples;
- Examples: application to different settings (community, academic, pediatric); and
- References.
Research and Timeline
In parallel to the development of the work domains for the toolkit, the Career Satisfaction Task Force is developing a questionnaire to survey hospitalist physicians on career satisfaction and “worklife.” The last survey of this type was performed in 1999. This questionnaire will allow us to assess changes in hospitalist quality of working life over time to further explore how hospitalists are faring during this critical time of rapid growth of our specialty.
The task force is developing a list of important aspects of worklife, satisfaction, and stress for hospitalists. This list will be supplemented by semi-structured interviews of SHM members and leaders in hospital medicine to include a representative viewpoint of hospitalist worklife: adult and pediatric medicine, academic and community, gender and age, directors of programs, and different employer types.
The interviews were expected to be completed in the fall of 2005. Qualitative data analysis will allow us to ascertain important themes for job performance and satisfaction to be highlighted in the survey. The questionnaire development will also consider inclusion of aspects from the prior surveys to follow results over time and when possible will use validated questions from the quality of working life literature.
We anticipate completion of the questionnaire in spring 2006 followed by surveying of a random sample of hospitalists from the SHM membership through a Web-based survey. Sampling of groups of hospitalists based on job characteristics will occur because there is significant interest and need for information about hospitalist worklife in certain work settings. The questionnaire dissemination time will overlap with the annual meeting to maximize survey response. The task force will work with SHM annual meeting committee to discuss having a dedicated computer for filling out the Web-based survey on-site.
Any SHM member who would like to participate in the questionnaire on-site, even if they were not selected for the random sample, will be encouraged to do so. Data analysis will occur in mid-late 2006. The task force will use information from the analyses to update the SHM Worklife Toolkit. We will also provide numerous forums for dissemination of the data. In particular, we plan to showcase this data at the 2007 SHM Annual Meeting followed by journal publication and Web site posting. It is our hope that this data will provide key information on the current quality of working life of hospitalist physicians to support worklife recommendations that promote sustainable, enjoyable careers in hospital medicine.
Early survey data on hospitalists, which suggest high levels of job engagement and low turnover rates, may not be as relevant as programs mature in a competitive marketplace to meet important needs such as rising census and Accreditation Council for Graduate Medical Education (ACGME) requirements. There is also a paucity of data on how different models of compensation affect hospitalists’ career satisfaction.
In 2005 the role of the hospitalist has evolved from simply improving throughput (average length of stay) to one of leadership, quality improvement, and teaching that extends beyond direct patient care. Compensation for hospitalists should not, therefore, be based solely on billing revenue. Improving the efficiency of the hospitalists work environment, which may include IT support, adequate office space, and administrative support, may not only enhance productivity but also job satisfaction. More research is needed to examine these questions.
Progress Report
One of the Career Satisfaction Task Force’s major initiatives has been developing a toolkit for the SHM membership with the purpose of providing members with an action plan for attaining a long and satisfying career in hospital medicine. The following steps are being taken in the creation of the toolkit:
- Needs assessment—questionnaire at the SHM 2005 Annual Meeting;
- Monthly conference calls;
- Timeline:
- Toolkit draft completion—Sept. 2005;
- Review SHM Membership Committee—Oct. 2005;
- Further revision;
- Submission to SHM Board for review—Nov. 2005;
- Further revision; and
- Dissemination at SHM Annual Meeting—May 2006.
- Content—four workplace domains:
- Control/Autonomy;
- Workload/Schedule;
- Community/Environment; and
- Reward/Recognition.
- Elements comprising each domain:
- Definition: specific description of workplace domain;
- Background: review of literature, expert opinion, experience-based observation, executive summary of background content;
- Guidelines: practical actionable recommendations and educational initiatives;
- Pitfalls: specific examples;
- Examples: application to different settings (community, academic, pediatric); and
- References.
Research and Timeline
In parallel to the development of the work domains for the toolkit, the Career Satisfaction Task Force is developing a questionnaire to survey hospitalist physicians on career satisfaction and “worklife.” The last survey of this type was performed in 1999. This questionnaire will allow us to assess changes in hospitalist quality of working life over time to further explore how hospitalists are faring during this critical time of rapid growth of our specialty.
The task force is developing a list of important aspects of worklife, satisfaction, and stress for hospitalists. This list will be supplemented by semi-structured interviews of SHM members and leaders in hospital medicine to include a representative viewpoint of hospitalist worklife: adult and pediatric medicine, academic and community, gender and age, directors of programs, and different employer types.
The interviews were expected to be completed in the fall of 2005. Qualitative data analysis will allow us to ascertain important themes for job performance and satisfaction to be highlighted in the survey. The questionnaire development will also consider inclusion of aspects from the prior surveys to follow results over time and when possible will use validated questions from the quality of working life literature.
We anticipate completion of the questionnaire in spring 2006 followed by surveying of a random sample of hospitalists from the SHM membership through a Web-based survey. Sampling of groups of hospitalists based on job characteristics will occur because there is significant interest and need for information about hospitalist worklife in certain work settings. The questionnaire dissemination time will overlap with the annual meeting to maximize survey response. The task force will work with SHM annual meeting committee to discuss having a dedicated computer for filling out the Web-based survey on-site.
Any SHM member who would like to participate in the questionnaire on-site, even if they were not selected for the random sample, will be encouraged to do so. Data analysis will occur in mid-late 2006. The task force will use information from the analyses to update the SHM Worklife Toolkit. We will also provide numerous forums for dissemination of the data. In particular, we plan to showcase this data at the 2007 SHM Annual Meeting followed by journal publication and Web site posting. It is our hope that this data will provide key information on the current quality of working life of hospitalist physicians to support worklife recommendations that promote sustainable, enjoyable careers in hospital medicine.
Quality Will Be Job One

One of the potential benefits of hospital medicine is the tangible opportunity to change healthcare in a meaningful way. Although much of the initial ballyhoo for hospital medicine has been around service-related issues, that is about to change.
Hospitalists have been willing to take on the inpatient responsibilities for primarily outpatient-based internists, family practitioners, and pediatricians. We have been available to admit and manage the patients who present to emergency rooms with acute illnesses and who have no physician of record. We have actively worked with surgeons and subspecialists to co-manage their patient’s medical problems.
In addition, because hospitalists are much more readily available to acutely ill inpatients, because we have more expertise with these medical problems, and because practice generally makes for better performance, hospitalists have been expected to provide more effective and more efficient care.
But that is just the front end of what is creating the enormous energy behind the hospital medicine movement. We are moving into an era of measurement of defined patient outcomes and expectations from insurance companies, Medicare, the business community, and—yes—even our patients. That era will require us to step up and deliver higher quality healthcare.
This is the driver to the pay-for-performance movement and a shift from just rewarding physicians and hospitals for doing the procedure or “visiting” the patient and moving to where those who can demonstrate expertise and performance are rewarded financially and by reputation.
Hospitalists and SHM take this very seriously and are creating alliances and programs to help hospitalists become leaders in the quality and performance arenas.
Walking through the approach that SHM is taking in improving glycemic control in hospitalized patients (see below) will serve as a template for other activities SHM has planned in heart failure, VTE, hospitalized infections, and other illnesses hospitalists see and treat every day.
In a practical way, hospitals and health professionals finally came into the performance era with the first publication of the individual hospital performance results to performance measures developed by JCAHO and co-promoted with CMS in their Hospital Compare Web site. This was promulgated widely, especially at www.hospitalcompare.hhs.gov.
Because Hospital Compare was picked up by The New York Times, the Los Angeles Times, and many local papers, hospitals were soon trying to explain why their performance in heart failure, pneumonia, and heart attack looked like a failing grade. Now that the public is involved, hospitals are scrambling to quickly improve their performance rather than attacking the data.
Looking to the future, SHM is working with JCAHO to develop performance standards for glycemic control for inpatients as a way to assess how our hospitals and physicians are doing in managing diabetes. SHM is also allying with many other key stakeholders to form a steering committee for this project. These standards will take almost three years to develop, test, and implement. So the first reporting of how every hospital is doing in diabetes is most likely a 2008 or 2009 event.
Expecting that many hospitals will improve their performance in diabetic care during 2008 and 2009, SHM is now developing the tools and the training to allow hospitalists to be ready with practical solutions.
In October 2005 SHM convened a Working Group on Inpatient Glycemic Control in Chicago. This meeting under the leadership of Greg Maynard, MD, associate clinical professor of medicine, chief of the division of hospital medicine, University of California at San Diego, brought together nationally recognized diabetologists and endocrinologists with hospitalist leaders, as well as experts in the field of nursing, case management, pharmacy, risk management, and nutrition. The end result is an understanding of what constitutes an ideal management of inpatient diabetes and what role hospitalists can play.
This work group now is analyzing what resources currently exist and what gaps need to be filled. Next SHM will develop an implementation plan to get this information out to our nation’s hospitalists.
SHM has some experience in developing quality improvement tools, as you can see in our Resource Rooms on the SHM Web site. For a current working example, take a look at the DVT Quality Improvement Resource Room at www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312.
But SHM plans a more aggressive approach with proposed training sessions at the SHM Annual Meeting quality pre-course and taking these tools and approaches out to our hospitalists at local meetings throughout the country. SHM is also looking into creating a network of quality mentors that will work with individual hospitalists groups as they put SHM quality improvement tools into the workflow at their hospitals. SHM will also develop strategies for baseline measurement, ongoing data collection, involvement of team members, and procurement of local resources. SHM hopes to support research to further develop best practices and approaches.
The game plan goes something like this: SHM will develop the resources hospitalists need to improve management of inpatient diabetes in 2006. In 2007 and 2008 SHM will roll out this strategy to as many hospitalists as we can train. By 2008 JCAHO and CMS will have deployed their Performance Measures in Diabetes. When the first scores show the same deficiencies as we have seen this year in MI and heart failure, our nation’s hospitalists will be well armed to provide practical tangible solutions to improve quality.
And the beauty of this approach is that SHM is working on similar strategies right now for heart failure, DVT, pneumonia, and other key clinical conditions.
Those who pay for and receive care in our hospitals are looking at our current performance and demanding improvements. For the first time hospitals and those with resources are ready to make measurable quality a high priority. The presence of hospitalists in more than 2,000 hospitals (and more in the near future) ideally positions hospitalists to be a key change agent. The tools SHM is developing will give hospitalists the strategies and the expertise to make this happen.
This is a watershed moment in American healthcare. There is a palpable swing in the priorities of our patients. Hospitalists can help the healthcare team find real solutions. SHM has the vision and the plan to provide you with as much help as you need. Together we will do great things. TH
Dr. Wellikson has been CEO of SHM since 2000.
One of the potential benefits of hospital medicine is the tangible opportunity to change healthcare in a meaningful way. Although much of the initial ballyhoo for hospital medicine has been around service-related issues, that is about to change.
Hospitalists have been willing to take on the inpatient responsibilities for primarily outpatient-based internists, family practitioners, and pediatricians. We have been available to admit and manage the patients who present to emergency rooms with acute illnesses and who have no physician of record. We have actively worked with surgeons and subspecialists to co-manage their patient’s medical problems.
In addition, because hospitalists are much more readily available to acutely ill inpatients, because we have more expertise with these medical problems, and because practice generally makes for better performance, hospitalists have been expected to provide more effective and more efficient care.
But that is just the front end of what is creating the enormous energy behind the hospital medicine movement. We are moving into an era of measurement of defined patient outcomes and expectations from insurance companies, Medicare, the business community, and—yes—even our patients. That era will require us to step up and deliver higher quality healthcare.
This is the driver to the pay-for-performance movement and a shift from just rewarding physicians and hospitals for doing the procedure or “visiting” the patient and moving to where those who can demonstrate expertise and performance are rewarded financially and by reputation.
Hospitalists and SHM take this very seriously and are creating alliances and programs to help hospitalists become leaders in the quality and performance arenas.
Walking through the approach that SHM is taking in improving glycemic control in hospitalized patients (see below) will serve as a template for other activities SHM has planned in heart failure, VTE, hospitalized infections, and other illnesses hospitalists see and treat every day.
In a practical way, hospitals and health professionals finally came into the performance era with the first publication of the individual hospital performance results to performance measures developed by JCAHO and co-promoted with CMS in their Hospital Compare Web site. This was promulgated widely, especially at www.hospitalcompare.hhs.gov.
Because Hospital Compare was picked up by The New York Times, the Los Angeles Times, and many local papers, hospitals were soon trying to explain why their performance in heart failure, pneumonia, and heart attack looked like a failing grade. Now that the public is involved, hospitals are scrambling to quickly improve their performance rather than attacking the data.
Looking to the future, SHM is working with JCAHO to develop performance standards for glycemic control for inpatients as a way to assess how our hospitals and physicians are doing in managing diabetes. SHM is also allying with many other key stakeholders to form a steering committee for this project. These standards will take almost three years to develop, test, and implement. So the first reporting of how every hospital is doing in diabetes is most likely a 2008 or 2009 event.
Expecting that many hospitals will improve their performance in diabetic care during 2008 and 2009, SHM is now developing the tools and the training to allow hospitalists to be ready with practical solutions.
In October 2005 SHM convened a Working Group on Inpatient Glycemic Control in Chicago. This meeting under the leadership of Greg Maynard, MD, associate clinical professor of medicine, chief of the division of hospital medicine, University of California at San Diego, brought together nationally recognized diabetologists and endocrinologists with hospitalist leaders, as well as experts in the field of nursing, case management, pharmacy, risk management, and nutrition. The end result is an understanding of what constitutes an ideal management of inpatient diabetes and what role hospitalists can play.
This work group now is analyzing what resources currently exist and what gaps need to be filled. Next SHM will develop an implementation plan to get this information out to our nation’s hospitalists.
SHM has some experience in developing quality improvement tools, as you can see in our Resource Rooms on the SHM Web site. For a current working example, take a look at the DVT Quality Improvement Resource Room at www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312.
But SHM plans a more aggressive approach with proposed training sessions at the SHM Annual Meeting quality pre-course and taking these tools and approaches out to our hospitalists at local meetings throughout the country. SHM is also looking into creating a network of quality mentors that will work with individual hospitalists groups as they put SHM quality improvement tools into the workflow at their hospitals. SHM will also develop strategies for baseline measurement, ongoing data collection, involvement of team members, and procurement of local resources. SHM hopes to support research to further develop best practices and approaches.
The game plan goes something like this: SHM will develop the resources hospitalists need to improve management of inpatient diabetes in 2006. In 2007 and 2008 SHM will roll out this strategy to as many hospitalists as we can train. By 2008 JCAHO and CMS will have deployed their Performance Measures in Diabetes. When the first scores show the same deficiencies as we have seen this year in MI and heart failure, our nation’s hospitalists will be well armed to provide practical tangible solutions to improve quality.
And the beauty of this approach is that SHM is working on similar strategies right now for heart failure, DVT, pneumonia, and other key clinical conditions.
Those who pay for and receive care in our hospitals are looking at our current performance and demanding improvements. For the first time hospitals and those with resources are ready to make measurable quality a high priority. The presence of hospitalists in more than 2,000 hospitals (and more in the near future) ideally positions hospitalists to be a key change agent. The tools SHM is developing will give hospitalists the strategies and the expertise to make this happen.
This is a watershed moment in American healthcare. There is a palpable swing in the priorities of our patients. Hospitalists can help the healthcare team find real solutions. SHM has the vision and the plan to provide you with as much help as you need. Together we will do great things. TH
Dr. Wellikson has been CEO of SHM since 2000.
One of the potential benefits of hospital medicine is the tangible opportunity to change healthcare in a meaningful way. Although much of the initial ballyhoo for hospital medicine has been around service-related issues, that is about to change.
Hospitalists have been willing to take on the inpatient responsibilities for primarily outpatient-based internists, family practitioners, and pediatricians. We have been available to admit and manage the patients who present to emergency rooms with acute illnesses and who have no physician of record. We have actively worked with surgeons and subspecialists to co-manage their patient’s medical problems.
In addition, because hospitalists are much more readily available to acutely ill inpatients, because we have more expertise with these medical problems, and because practice generally makes for better performance, hospitalists have been expected to provide more effective and more efficient care.
But that is just the front end of what is creating the enormous energy behind the hospital medicine movement. We are moving into an era of measurement of defined patient outcomes and expectations from insurance companies, Medicare, the business community, and—yes—even our patients. That era will require us to step up and deliver higher quality healthcare.
This is the driver to the pay-for-performance movement and a shift from just rewarding physicians and hospitals for doing the procedure or “visiting” the patient and moving to where those who can demonstrate expertise and performance are rewarded financially and by reputation.
Hospitalists and SHM take this very seriously and are creating alliances and programs to help hospitalists become leaders in the quality and performance arenas.
Walking through the approach that SHM is taking in improving glycemic control in hospitalized patients (see below) will serve as a template for other activities SHM has planned in heart failure, VTE, hospitalized infections, and other illnesses hospitalists see and treat every day.
In a practical way, hospitals and health professionals finally came into the performance era with the first publication of the individual hospital performance results to performance measures developed by JCAHO and co-promoted with CMS in their Hospital Compare Web site. This was promulgated widely, especially at www.hospitalcompare.hhs.gov.
Because Hospital Compare was picked up by The New York Times, the Los Angeles Times, and many local papers, hospitals were soon trying to explain why their performance in heart failure, pneumonia, and heart attack looked like a failing grade. Now that the public is involved, hospitals are scrambling to quickly improve their performance rather than attacking the data.
Looking to the future, SHM is working with JCAHO to develop performance standards for glycemic control for inpatients as a way to assess how our hospitals and physicians are doing in managing diabetes. SHM is also allying with many other key stakeholders to form a steering committee for this project. These standards will take almost three years to develop, test, and implement. So the first reporting of how every hospital is doing in diabetes is most likely a 2008 or 2009 event.
Expecting that many hospitals will improve their performance in diabetic care during 2008 and 2009, SHM is now developing the tools and the training to allow hospitalists to be ready with practical solutions.
In October 2005 SHM convened a Working Group on Inpatient Glycemic Control in Chicago. This meeting under the leadership of Greg Maynard, MD, associate clinical professor of medicine, chief of the division of hospital medicine, University of California at San Diego, brought together nationally recognized diabetologists and endocrinologists with hospitalist leaders, as well as experts in the field of nursing, case management, pharmacy, risk management, and nutrition. The end result is an understanding of what constitutes an ideal management of inpatient diabetes and what role hospitalists can play.
This work group now is analyzing what resources currently exist and what gaps need to be filled. Next SHM will develop an implementation plan to get this information out to our nation’s hospitalists.
SHM has some experience in developing quality improvement tools, as you can see in our Resource Rooms on the SHM Web site. For a current working example, take a look at the DVT Quality Improvement Resource Room at www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312.
But SHM plans a more aggressive approach with proposed training sessions at the SHM Annual Meeting quality pre-course and taking these tools and approaches out to our hospitalists at local meetings throughout the country. SHM is also looking into creating a network of quality mentors that will work with individual hospitalists groups as they put SHM quality improvement tools into the workflow at their hospitals. SHM will also develop strategies for baseline measurement, ongoing data collection, involvement of team members, and procurement of local resources. SHM hopes to support research to further develop best practices and approaches.
The game plan goes something like this: SHM will develop the resources hospitalists need to improve management of inpatient diabetes in 2006. In 2007 and 2008 SHM will roll out this strategy to as many hospitalists as we can train. By 2008 JCAHO and CMS will have deployed their Performance Measures in Diabetes. When the first scores show the same deficiencies as we have seen this year in MI and heart failure, our nation’s hospitalists will be well armed to provide practical tangible solutions to improve quality.
And the beauty of this approach is that SHM is working on similar strategies right now for heart failure, DVT, pneumonia, and other key clinical conditions.
Those who pay for and receive care in our hospitals are looking at our current performance and demanding improvements. For the first time hospitals and those with resources are ready to make measurable quality a high priority. The presence of hospitalists in more than 2,000 hospitals (and more in the near future) ideally positions hospitalists to be a key change agent. The tools SHM is developing will give hospitalists the strategies and the expertise to make this happen.
This is a watershed moment in American healthcare. There is a palpable swing in the priorities of our patients. Hospitalists can help the healthcare team find real solutions. SHM has the vision and the plan to provide you with as much help as you need. Together we will do great things. TH
Dr. Wellikson has been CEO of SHM since 2000.
Hospitalists Defined—Officially

When I was a kid I remember saying that “ain’t ain’t a word because ain’t ain’t in the dictionary.” I just found “ain’t” in my online dictionary, which warned against using “ain’t” because it “does not form a part of standard English and should not be used in formal contexts.”
If the dictionary is the final arbiter of what is and is not a word, then finally “hospitalist” is a word (as we reported last month, see Nov. The Hospitalist, p. 17). Of course we have been using the word since Bob Wachter and Lee Goldman first coined it in their paper in the New England Journal of Medicine in 1996.1 But the 2005 update of the Eleventh Edition of Merriam-Webster’s Collegiate Dictionary defines a “hospitalist” as “a physician who specializes in treating hospitalized patients of other physicians in order to minimize the number of hospital visits by other physicians.”
While I am delighted that our specialty is in the dictionary, I would argue that the role of a hospitalist is about more than saving other physicians’ commute time. In fact SHM published an entire supplement that catalogued the many roles of hospitalists and how we add value.2 But even if the dictionary didn’t get the definition quite right, the presence of the word hospitalist is yet more evidence of the increasing importance and growth of our field. I want to share with you some of the exciting projects that the SHM is working on to further define our field.
Board Certification
We have been in discussion with the American Board of Internal Medicine and other societies that represent important interests in internal medicine regarding board certification for hospitalists. At this point I cannot tell you what certification will look like, how it will be conferred, or when it will come about; however, SHM is committed to developing a process that recognizes the expertise and experience of hospitalists and supports high quality care for patients. As you might imagine, any process of certification for hospitalists has huge implications for all physicians who practice internal medicine, and we are working to consider these issues carefully as we move ahead. Board certification, and the process of making it come about, marks another step along the path in the maturing of our field.
Journal of Hospital Medicine and Research
More evidence of our growth as a field is the coming publication of the Journal of Hospital Medicine. Under the editorship of Mark Williams, MD, the journal will be the first dedicated to hospital medicine and the care of hospitalized patients. I still remember the early discussions at the SHM Board of Directors meetings where we first discussed having a journal. At the time there were only three or four hospitalist researchers and our major concern was whether there would be sufficient content to fill a journal once let alone six or more times a year; however, at the time we also saw where our field was headed. We knew that in order to continue to define the field of hospital medicine a journal was key.
Perhaps our decision several years ago was hubris, perhaps it was blind optimism, but I like to think it was faith in our members and our society and a belief that hospital medicine was here to stay and would only get bigger. Next month SHM will proudly publish the first volume of the Journal of Hospital Medicine. I am happy to report that we have plenty of high quality content to fill the journal. Our field has continued to expand and with it more and more researchers are focusing on hospital medicine. One walk around the poster session at our annual meeting is enough to demonstrate all of the outstanding academic work that hospitalists at academic centers and community hospitals are doing.
Hand in hand with the publication of our journal has been our research initiative. I firmly believe that in order for SHM to lead hospital medicine, we must also lead in the area of research. In order to coordinate and expand our efforts in research, we recently brought Kathleen Kerr on board at SHM as a senior advisor to lead our research initiative. Kathleen brings a new level of rigor and enthusiasm to our research initiative and helps support the outstanding work of our research committee led by Andy Auerbach, MD. At SHM research reflects our members and includes hospitalists from all settings. I invite you to present your work at our annual meeting (we are currently accepting submissions through Jan. 6, 2006, for the Research, Innovations and Clinical Vignettes competition for the 2006 annual meeting) so we can all benefit and learn from the work we are doing. I also invite you to submit your work for publication in the Journal of Hospital Medicine.
Core Competency
Yet another sign of our maturing as a field will be the publication of the Core Competencies in Hospital Medicine as a supplement to the first volume of the Journal of Hospital Medicine. The core competencies reflect hundreds of hours of work by a dedicated group of hospitalists and SHM staff led by Tina Budnitz MPH, to define the core of what hospitalists need to know. Yes, hospitalists are more than just timesavers for other physicians. The core competencies in hospital medicine will outline what hospital medicine is about and serve as the foundation for educational programs, curricula, and initiatives in hospital medicine. The core competencies will also form the basis for certification of hospitalists by defining the key attitudes and skills needed to be a hospitalist. Look for the core competencies in early 2006 along with your first volume of the journal.
Evolution of Other “Ists”
If imitation is the finest form of flattery, then hospitalists should be very flattered by the proliferation of other “-ists.” Within our own field we find “nocurnists,” hospitalists who care for patients in the hospital overnight. Although it is not clear whether being a nocturnist is a permanent state in which you work only nights or a title that you hold temporarily, it is clear that “hospitalist” is leading to a wide use of the “-ist” suffix to describe the practice of physicians.
Even more interesting is the emergence of hospitalists in other fields such as surgery and obstetrics (see our related coverage in The Hospitalist—“What Is a Laborist,” Oct. 2005, p. 6; “Trendwatch: The specialization of hospital medicine,” Oct. 2005, p. 27; and “The Doctor Is In: The role of psychiatric hospitalists,” Oct. 2005, p. 30). Because the “ist” doesn’t work well universally (neither “surgicalist” nor “obstetricist” sounds right and neither does “deliverist”) the terms being used are “surgical hospitalist” or “OB hospitalist.” In either case the idea is that there is a physician, surgeon, or an obstetrician who sees patients in the hospital instead of the patients’ primary physician. Typically these physicians are employed by the hospital to care for unassigned patients admitted through the emergency department. The adoption of “hospitalist” by other fields in medicine to describe clinicians whose professional identity revolves around the hospital is a testament to the acceptance—and even normalization—of hospitalists and to the profound change in the way we care for hospitalized patients brought about by our field.
We certainly have come a long way from the days when our newly formed society decided not to use the word hospitalist or hospital or anything like it in our name for fear of inciting animosity. In just a few short years we find a world where hospitalist is in the dictionary and other physicians begin to use the term to describe themselves. Reflecting this maturing of our field, SHM is involved in several initiatives including certification, research, a journal, and core competencies to further define hospital medicine.
If you have been thinking about getting more involved in the SHM, do so now. Become an active member; volunteer for committees. Help shape our field and the world of hospital medicine in the future. This ride certainly ain’t over. In fact, it’s just beginning. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
References
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514-517.
- Pile J. How hospitalists add value. The Hospitalist. 2005;9:Supplement 1.
When I was a kid I remember saying that “ain’t ain’t a word because ain’t ain’t in the dictionary.” I just found “ain’t” in my online dictionary, which warned against using “ain’t” because it “does not form a part of standard English and should not be used in formal contexts.”
If the dictionary is the final arbiter of what is and is not a word, then finally “hospitalist” is a word (as we reported last month, see Nov. The Hospitalist, p. 17). Of course we have been using the word since Bob Wachter and Lee Goldman first coined it in their paper in the New England Journal of Medicine in 1996.1 But the 2005 update of the Eleventh Edition of Merriam-Webster’s Collegiate Dictionary defines a “hospitalist” as “a physician who specializes in treating hospitalized patients of other physicians in order to minimize the number of hospital visits by other physicians.”
While I am delighted that our specialty is in the dictionary, I would argue that the role of a hospitalist is about more than saving other physicians’ commute time. In fact SHM published an entire supplement that catalogued the many roles of hospitalists and how we add value.2 But even if the dictionary didn’t get the definition quite right, the presence of the word hospitalist is yet more evidence of the increasing importance and growth of our field. I want to share with you some of the exciting projects that the SHM is working on to further define our field.
Board Certification
We have been in discussion with the American Board of Internal Medicine and other societies that represent important interests in internal medicine regarding board certification for hospitalists. At this point I cannot tell you what certification will look like, how it will be conferred, or when it will come about; however, SHM is committed to developing a process that recognizes the expertise and experience of hospitalists and supports high quality care for patients. As you might imagine, any process of certification for hospitalists has huge implications for all physicians who practice internal medicine, and we are working to consider these issues carefully as we move ahead. Board certification, and the process of making it come about, marks another step along the path in the maturing of our field.
Journal of Hospital Medicine and Research
More evidence of our growth as a field is the coming publication of the Journal of Hospital Medicine. Under the editorship of Mark Williams, MD, the journal will be the first dedicated to hospital medicine and the care of hospitalized patients. I still remember the early discussions at the SHM Board of Directors meetings where we first discussed having a journal. At the time there were only three or four hospitalist researchers and our major concern was whether there would be sufficient content to fill a journal once let alone six or more times a year; however, at the time we also saw where our field was headed. We knew that in order to continue to define the field of hospital medicine a journal was key.
Perhaps our decision several years ago was hubris, perhaps it was blind optimism, but I like to think it was faith in our members and our society and a belief that hospital medicine was here to stay and would only get bigger. Next month SHM will proudly publish the first volume of the Journal of Hospital Medicine. I am happy to report that we have plenty of high quality content to fill the journal. Our field has continued to expand and with it more and more researchers are focusing on hospital medicine. One walk around the poster session at our annual meeting is enough to demonstrate all of the outstanding academic work that hospitalists at academic centers and community hospitals are doing.
Hand in hand with the publication of our journal has been our research initiative. I firmly believe that in order for SHM to lead hospital medicine, we must also lead in the area of research. In order to coordinate and expand our efforts in research, we recently brought Kathleen Kerr on board at SHM as a senior advisor to lead our research initiative. Kathleen brings a new level of rigor and enthusiasm to our research initiative and helps support the outstanding work of our research committee led by Andy Auerbach, MD. At SHM research reflects our members and includes hospitalists from all settings. I invite you to present your work at our annual meeting (we are currently accepting submissions through Jan. 6, 2006, for the Research, Innovations and Clinical Vignettes competition for the 2006 annual meeting) so we can all benefit and learn from the work we are doing. I also invite you to submit your work for publication in the Journal of Hospital Medicine.
Core Competency
Yet another sign of our maturing as a field will be the publication of the Core Competencies in Hospital Medicine as a supplement to the first volume of the Journal of Hospital Medicine. The core competencies reflect hundreds of hours of work by a dedicated group of hospitalists and SHM staff led by Tina Budnitz MPH, to define the core of what hospitalists need to know. Yes, hospitalists are more than just timesavers for other physicians. The core competencies in hospital medicine will outline what hospital medicine is about and serve as the foundation for educational programs, curricula, and initiatives in hospital medicine. The core competencies will also form the basis for certification of hospitalists by defining the key attitudes and skills needed to be a hospitalist. Look for the core competencies in early 2006 along with your first volume of the journal.
Evolution of Other “Ists”
If imitation is the finest form of flattery, then hospitalists should be very flattered by the proliferation of other “-ists.” Within our own field we find “nocurnists,” hospitalists who care for patients in the hospital overnight. Although it is not clear whether being a nocturnist is a permanent state in which you work only nights or a title that you hold temporarily, it is clear that “hospitalist” is leading to a wide use of the “-ist” suffix to describe the practice of physicians.
Even more interesting is the emergence of hospitalists in other fields such as surgery and obstetrics (see our related coverage in The Hospitalist—“What Is a Laborist,” Oct. 2005, p. 6; “Trendwatch: The specialization of hospital medicine,” Oct. 2005, p. 27; and “The Doctor Is In: The role of psychiatric hospitalists,” Oct. 2005, p. 30). Because the “ist” doesn’t work well universally (neither “surgicalist” nor “obstetricist” sounds right and neither does “deliverist”) the terms being used are “surgical hospitalist” or “OB hospitalist.” In either case the idea is that there is a physician, surgeon, or an obstetrician who sees patients in the hospital instead of the patients’ primary physician. Typically these physicians are employed by the hospital to care for unassigned patients admitted through the emergency department. The adoption of “hospitalist” by other fields in medicine to describe clinicians whose professional identity revolves around the hospital is a testament to the acceptance—and even normalization—of hospitalists and to the profound change in the way we care for hospitalized patients brought about by our field.
We certainly have come a long way from the days when our newly formed society decided not to use the word hospitalist or hospital or anything like it in our name for fear of inciting animosity. In just a few short years we find a world where hospitalist is in the dictionary and other physicians begin to use the term to describe themselves. Reflecting this maturing of our field, SHM is involved in several initiatives including certification, research, a journal, and core competencies to further define hospital medicine.
If you have been thinking about getting more involved in the SHM, do so now. Become an active member; volunteer for committees. Help shape our field and the world of hospital medicine in the future. This ride certainly ain’t over. In fact, it’s just beginning. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
References
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514-517.
- Pile J. How hospitalists add value. The Hospitalist. 2005;9:Supplement 1.
When I was a kid I remember saying that “ain’t ain’t a word because ain’t ain’t in the dictionary.” I just found “ain’t” in my online dictionary, which warned against using “ain’t” because it “does not form a part of standard English and should not be used in formal contexts.”
If the dictionary is the final arbiter of what is and is not a word, then finally “hospitalist” is a word (as we reported last month, see Nov. The Hospitalist, p. 17). Of course we have been using the word since Bob Wachter and Lee Goldman first coined it in their paper in the New England Journal of Medicine in 1996.1 But the 2005 update of the Eleventh Edition of Merriam-Webster’s Collegiate Dictionary defines a “hospitalist” as “a physician who specializes in treating hospitalized patients of other physicians in order to minimize the number of hospital visits by other physicians.”
While I am delighted that our specialty is in the dictionary, I would argue that the role of a hospitalist is about more than saving other physicians’ commute time. In fact SHM published an entire supplement that catalogued the many roles of hospitalists and how we add value.2 But even if the dictionary didn’t get the definition quite right, the presence of the word hospitalist is yet more evidence of the increasing importance and growth of our field. I want to share with you some of the exciting projects that the SHM is working on to further define our field.
Board Certification
We have been in discussion with the American Board of Internal Medicine and other societies that represent important interests in internal medicine regarding board certification for hospitalists. At this point I cannot tell you what certification will look like, how it will be conferred, or when it will come about; however, SHM is committed to developing a process that recognizes the expertise and experience of hospitalists and supports high quality care for patients. As you might imagine, any process of certification for hospitalists has huge implications for all physicians who practice internal medicine, and we are working to consider these issues carefully as we move ahead. Board certification, and the process of making it come about, marks another step along the path in the maturing of our field.
Journal of Hospital Medicine and Research
More evidence of our growth as a field is the coming publication of the Journal of Hospital Medicine. Under the editorship of Mark Williams, MD, the journal will be the first dedicated to hospital medicine and the care of hospitalized patients. I still remember the early discussions at the SHM Board of Directors meetings where we first discussed having a journal. At the time there were only three or four hospitalist researchers and our major concern was whether there would be sufficient content to fill a journal once let alone six or more times a year; however, at the time we also saw where our field was headed. We knew that in order to continue to define the field of hospital medicine a journal was key.
Perhaps our decision several years ago was hubris, perhaps it was blind optimism, but I like to think it was faith in our members and our society and a belief that hospital medicine was here to stay and would only get bigger. Next month SHM will proudly publish the first volume of the Journal of Hospital Medicine. I am happy to report that we have plenty of high quality content to fill the journal. Our field has continued to expand and with it more and more researchers are focusing on hospital medicine. One walk around the poster session at our annual meeting is enough to demonstrate all of the outstanding academic work that hospitalists at academic centers and community hospitals are doing.
Hand in hand with the publication of our journal has been our research initiative. I firmly believe that in order for SHM to lead hospital medicine, we must also lead in the area of research. In order to coordinate and expand our efforts in research, we recently brought Kathleen Kerr on board at SHM as a senior advisor to lead our research initiative. Kathleen brings a new level of rigor and enthusiasm to our research initiative and helps support the outstanding work of our research committee led by Andy Auerbach, MD. At SHM research reflects our members and includes hospitalists from all settings. I invite you to present your work at our annual meeting (we are currently accepting submissions through Jan. 6, 2006, for the Research, Innovations and Clinical Vignettes competition for the 2006 annual meeting) so we can all benefit and learn from the work we are doing. I also invite you to submit your work for publication in the Journal of Hospital Medicine.
Core Competency
Yet another sign of our maturing as a field will be the publication of the Core Competencies in Hospital Medicine as a supplement to the first volume of the Journal of Hospital Medicine. The core competencies reflect hundreds of hours of work by a dedicated group of hospitalists and SHM staff led by Tina Budnitz MPH, to define the core of what hospitalists need to know. Yes, hospitalists are more than just timesavers for other physicians. The core competencies in hospital medicine will outline what hospital medicine is about and serve as the foundation for educational programs, curricula, and initiatives in hospital medicine. The core competencies will also form the basis for certification of hospitalists by defining the key attitudes and skills needed to be a hospitalist. Look for the core competencies in early 2006 along with your first volume of the journal.
Evolution of Other “Ists”
If imitation is the finest form of flattery, then hospitalists should be very flattered by the proliferation of other “-ists.” Within our own field we find “nocurnists,” hospitalists who care for patients in the hospital overnight. Although it is not clear whether being a nocturnist is a permanent state in which you work only nights or a title that you hold temporarily, it is clear that “hospitalist” is leading to a wide use of the “-ist” suffix to describe the practice of physicians.
Even more interesting is the emergence of hospitalists in other fields such as surgery and obstetrics (see our related coverage in The Hospitalist—“What Is a Laborist,” Oct. 2005, p. 6; “Trendwatch: The specialization of hospital medicine,” Oct. 2005, p. 27; and “The Doctor Is In: The role of psychiatric hospitalists,” Oct. 2005, p. 30). Because the “ist” doesn’t work well universally (neither “surgicalist” nor “obstetricist” sounds right and neither does “deliverist”) the terms being used are “surgical hospitalist” or “OB hospitalist.” In either case the idea is that there is a physician, surgeon, or an obstetrician who sees patients in the hospital instead of the patients’ primary physician. Typically these physicians are employed by the hospital to care for unassigned patients admitted through the emergency department. The adoption of “hospitalist” by other fields in medicine to describe clinicians whose professional identity revolves around the hospital is a testament to the acceptance—and even normalization—of hospitalists and to the profound change in the way we care for hospitalized patients brought about by our field.
We certainly have come a long way from the days when our newly formed society decided not to use the word hospitalist or hospital or anything like it in our name for fear of inciting animosity. In just a few short years we find a world where hospitalist is in the dictionary and other physicians begin to use the term to describe themselves. Reflecting this maturing of our field, SHM is involved in several initiatives including certification, research, a journal, and core competencies to further define hospital medicine.
If you have been thinking about getting more involved in the SHM, do so now. Become an active member; volunteer for committees. Help shape our field and the world of hospital medicine in the future. This ride certainly ain’t over. In fact, it’s just beginning. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
References
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514-517.
- Pile J. How hospitalists add value. The Hospitalist. 2005;9:Supplement 1.
A Malpractice Primer
In a 2001 Hospital Practice article Robert Wachter, MD, named malpractice as one of the top 10 issues that require consideration as it relates to the hospitalist movement.1 There are many areas to consider when looking at malpractice insurance for hospitalists as opposed to other physician specialties. Just one area being reviewed by insurance carriers: Underwriters are grouping hospitalists with internal medicine physicians because hospitalists do not yet have their own classification code.
“When physicians spend 85% to 100% of their time in the office,” wrote Dr. Wachter, “it seems prudent to base assessments of competence on the quality of the office practice rather than that of the hospital practice. As in other situations, the hospitalist movement has exposed the inadequacies of the earlier system.” This assessment seems applicable to the area of insurance as well. There may be a need to create means by which hospitalists can be better protected from malpractice risk and coverage inadequacy. This area, like all others associated with hospital medicine, is evolving.
In this article we highlight malpractice insurance for hospitalists: what you should consider now and in the future regarding policy coverage. policies Available to Hospitalists
The types of malpractice insurance available to hospitalists include:
- Policies provided under your employer’s policy or purchased for yourself;
- Policies that cover you when any event actually occurs or when the claim is filed; and
- Policies purchased by hospitals where the payouts for claims are made either by the insurance company (the carrier) or by the employer (the hospital).
Most hospitalists are covered by institutional or group employers. In most cases, hospitalists are hired directly by hospitals or by an agency that contracts with hospitalists and administrates this relationship with the hospital.
“We recommend that the hospitals employ the hospitalists and that they put them on their hospital malpractice policy,” says Pam Kirks, insurance broker with the Gallagher Health Insurance Company in Raleigh, N.C., “because that’s the cheapest way to go for the hospitalist. There are different types of coverage out there that they can get; they can get their own coverage certainly. But I think the majority of them are becoming hospital employees.”
Occurrence or Claims Made
The types of medical malpractice insurance available to hospitalists are either “occurrence” or “claims-made” policies. An occurrence policy is one in which the policy that responds to a claim is the one that was in effect when the incident actually occurred. A claims-made policy that responds to a claim is the one that is in effect when the claim is made—provided that you also had continuous coverage from the time that the incident occurred.
Joe Zorola, director of underwriting at ProMutual Insurance Company in Boston, further explains the claims-made policy. “For instance, let’s say you have a policy this year and something happens tomorrow and five years down the line [the patient] file[s] a claim because of what happened tomorrow,” he explains. “You should have continued this policy through the next five years so that there’s no lapse of coverage, but the policy that will respond will be the policy five years from now.”
Of the 52 hospitals and 14,000 people that ProMutual insures, half of the policies are individual policies and half are group policies.
“The majority of [policies] are in Massachusetts and so are written under an occurrence basis,” says Zorola. “The ones outside of Massachusetts—and those are the group policies that we do have—are claims made.”
Physicians and insurance carriers each have preferences between the two types. “The occurrence policy is the policy that a lot of physicians like because they understand that if they did something today, [they can think] ‘I never have to worry about having insurance in the future for it,’” says Zorola. “The claims-made policy is the one that we as [insurance] companies like because it allows us to close our books on each policy year much sooner because we know that we aren’t going to have any more claims attached to the policy this year or in another year or two.”
Fully Insured or Self Insured?
Malpractice policies available through employers are either fully insured or self insured. The difference between the two types involves who is responsible for the claims payouts. With fully insured plans, the employer pays a premium to an insurer and the insurer pays claims out of the pool of premiums it collects from everyone it insures. Under a self-insured plan, the employer is responsible for paying all claims out of company assets. The Employee Retirement Income Security Act (ERISA) regulates self-insured plans; the plans are then under the jurisdiction of the U.S. Department of Labor.
“The hospitalists that we do [under]write [fully insured policies] for tend to be in the smaller community hospitals, which may not necessarily have the huge need for hospitalists; whereas the larger institutions may have a larger need for hospitalists [and] they usually tend to be self-insured,” says Zorola.
Controlled Risk Insurance Company of Vermont, known as CRICO and located in Cambridge, Mass, is one example of a self-insured system. “We only have one [malpractice insurance] product for a closed system where our clients are the Harvard teaching hospitals” says Karen O’Rourke, senior vice president of CRICO.
Individual Policies for Certain Circumstances
Hospitalists who take out individual policies are usually practicing part-time or moonlighting and have another policy with a carrier that is covering their primary practice. “And this is true across the country,” says Zorola. “Most carriers will have some sort of part-time credit that they will provide [to] the people who come to them for policies. Now there are some carriers, and these are usually the large hospital carriers, who won’t provide individual policies to physicians. They only provide coverage for the hospital and the hospital’s employees.”
Hospitalists who take out their own individual policies usually get coverage from one of the local Physician Insurers Association of America carriers.
Why Are Hospitalists Sued?
In general, hospitalists are infrequently sued for medical malpractice. They may be named in initial claims, but many are dropped before the case is resolved. However, while experts report that lawsuits against hospitalists are scarce, they also reference the lack of classification code specifically created for the hospitalist and his/her duties. Without it, it’s impossible to distinguish in data to learn when and in how many cases hospitalists were named.
O’Rourke says that internists in ambulatory or outpatient practice settings are usually at risk for claims of failure to diagnose—mostly failure to diagnose cancer or myocardial infarctions. In contrast, “the hospitalists’ failures come in the communication area,” she says, “because that’s primarily what they’re there for is to make sure that the patient receives the medical care that they’re supposed to in a hospital setting.”
O’Rourke, who directs the management of underwriting claims as part of her work at CRICO, believes there is a vast difference between the reasons for claims for internists versus hospitalists.3
“We receive so many failure-to-diagnose cases with internal medicine physicians,” she elaborates. “There have been huge losses associated with them throughout other systems that we’ve seen—some of our own, such as increases in [the rates of] breast cancer or colorectal cancer. You’re not going to see that with a hospitalist unless there’s a post-op complication—bleeding that isn’t caught and failure to diagnose—that kind of issue—soon enough. But they’re still under a surgeon’s care normally.”
O’Rourke recognizes that the care of the hospital patient is a team effort. “So it’s going to be a question of how the hospital defines the hospitalist role for each and every condition or [for] surgical patients,” she says.
If the Hospitalist Sees the Patient
A new claim that ProMutual recently received involves a hospitalist. The allegation is “failure to monitor a patient for suicide.” The claim states that the patient attempted suicide twice by trying to hang herself. The patient was admitted to the psychiatric unit of the hospital. Although a medical consultation must be done any time a patient is admitted, the hospitalist was not consulted to assess for suicide precautions. The hospitalist’s next involvement was after the attempted suicide when she responded to the code and admitted the patient to the ICU.
Given the lines of protocol, it is likely to be decided that the named psychiatrist was responsible for noting the risks with this patient and the hospitalist’s name will be dropped from the claim. The important thing for hospitalists to know is that because the hospitalist was listed as seeing the patient, she was named in the claim and this is customary procedure.
“A lot of times the plaintiff attorney will note every doctor who has seen the patient over the last number of years,” says Zorola, “because they probably don’t know a lot about the claim either, at that point. So until the investigation is done, and you can perform the depositions and find out exactly who was responsible for what,” the hospitalist will be a part of this process.
The Classification of Hospitalists
The growing trend is that insurance underwriters are creating a separate hospitalist classification. ProMutual underwriters established a classification for hospitalist and placed it in the same rate group as internal medicine physicians. But then the underwriters listened to what some of the hospitalists were saying: that because they are more specialized and are seeing patients who are more aware of the care that should be provided in the hospital, being grouped with physicians who spend most of the their time in office practice was not an accurate way to classify them.
Zorola and his colleagues now see that “setting up a separate classification for [hospitalists] allows us in the future to review their experience and determine whether they ought to be grouped with internal medicines or whether they belong in a lower or higher classification.” Hospitalists might belong in a higher, risk-associated classification “because they are seeing sick patients whereas internal medicine and family practice doctors have a mixture of sick and well patients,” he notes.
In fact, the common assumption is that hospitalists are doing riskier work simply because they work in places in which they have more opportunities to encounter risk. O’Rourke can’t say definitively how many hospitalists CRICO insures. But she can say that few claims involve hospitalists.
“We thought they were a riskier group for a while, but we couldn’t find any evidence of that in our data,” she explains. “We had a couple of claims involving people who were hospitalists, but nothing of concern.”
Whether hospitalists prove to be a riskier group in future research will depend on first determining more precisely what hospitalists do.
What Do Hospitalists Really Do?
“I can imagine that some of [the answer to this question] is that you go find out what works best for the systems you already have in place and develop systems that are needed to really quantify what [hospitalists] are supposed to do,” says O’Rourke. “And that will vary from institution to institution depending on whether it’s a teaching hospital or not.”
But there are other factors and issues at play, some of which are entirely out of control of the insured hospitalist. Barry Halpern, an attorney with Snell and Wilmer Law Firm, whose insured clients are spread over the western half of the United States, says “malpractice insurers, for a variety of reasons, … have many, many classifications for underwriting purposes and others [have] not very many at all. There are marketing issues associated with that and they don’t have a lot to do with the aspects of the specialty.”4
Your Policy Type May Matter
“[A]s you look at this from an insurance perspective, there are pros and cons for having separate insurance for hospitalists and the hospital,” says Halpern. “Where there is separate insurance, there is sometimes greater potential for conflict tension among the provider team than when the insurance is provided on an entity basis, particularly when entity claims against hospitals are a [somewhat] growing trend.”
Halpern notes that, in general, the courts are delivering their verdicts without considering the actual relationship between a hospital and a staff physician.3 “Of course,” he adds, “the courts are hunting for ways to make hospitals responsible on an entity basis rather than specifically for negligence in credentialing, or negligence in supervising, or negligence in providing staff and tools.”
Halpern thinks that in lawsuits where any staff physician is considered as part of the entity of the hospital institution, “it may make sense for the hospitalist to be insured under the hospital’s coverage, so that you minimize the potential for finger-pointing within the hospital-based team.” Besides creating potential tension within the group, Halpern says, “there may be indemnity agreements entered into between the hospitalists and the hospital that shift legal responsibility in a way that is sometimes not as carefully considered at the front end of an arrangement than at the back end, when a problem occurs.”
Halpern says that those kinds of situations must be looked at carefully. “[T]hose kinds of indemnity agreements can lead to a whole world of collateral claims litigation and can sometimes compromise insurance coverage,” he says. “For instance, if a hospitalist group signs an indemnity contract with the hospital without clearing it with the hospitalist’s insurer, the insurer might look at that and say, ‘We didn’t underwrite that additional obligation to defend and pay damages for the benefit of the hospital. And therefore, we deny coverage.’”
What Should Hospitalists Do?
If you are an individual hospitalist and your hospital provides your coverage, our experts have some suggestions on how to best protect yourself from surprises later about your liability insurance.
“[Y]ou certainly ought to get a copy of the policy,” says Halpern, and “focus very carefully on several things: 1) what’s covered, 2) what’s excluded, 3) what are the limits, and 4) who’s providing the coverage?”
You need to be able to feel that you can say “yes” to the question, “Is this a company that I can be confident will be there when it’s needed?”
If after a careful review of your policy, you have areas you would like to discuss with the hospital, it’s a matter of negotiation. And when you have the “negotiation muscle” to get what you need for protection, says Halpern, you’re in a better position.
“Frankly, most hospitals are interested in maintaining quality staff, quality relations with physicians—both employed and on the consulting staff,” says Halpern. “[They] are not typically in the business of muscling people and treating them badly. So if the hospitalist finds a legitimate gap in coverage or a concern, by and large hospitals look to be fair in working those things out. If they’re not, there are two basic approaches, and one is to not continue in the relationship.” (In other words, quit). “The second [approach] is to insure over the gap by going to an insurance broker and seeing if you can find coverage.”
Conclusion
Although most hospitalists are covered under their hospital policies, all hospitalists would benefit from understanding the specifics of their malpractice coverage. The dynamics of the hospitalist model will require changes in many areas including malpractice insurance. The trend of insurance carriers to establish a separate classification for hospitalists is likely to provide more precisely written coverage that accounts for the particulars of hospital medicine practice TH
Writer Andrea Sattinger will write about risk management for hospitalists in the Jan. ’06 issue.
References
- Wachter RM. The hospitalist movement: ten issues to consider. Hosp Pract. 1999;34(2):104-106.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care JAMA. 1994;272:1588-1591.
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9.
- Pham HH, Devers KJ, Kuo S, et al. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005;20:101-107.
In a 2001 Hospital Practice article Robert Wachter, MD, named malpractice as one of the top 10 issues that require consideration as it relates to the hospitalist movement.1 There are many areas to consider when looking at malpractice insurance for hospitalists as opposed to other physician specialties. Just one area being reviewed by insurance carriers: Underwriters are grouping hospitalists with internal medicine physicians because hospitalists do not yet have their own classification code.
“When physicians spend 85% to 100% of their time in the office,” wrote Dr. Wachter, “it seems prudent to base assessments of competence on the quality of the office practice rather than that of the hospital practice. As in other situations, the hospitalist movement has exposed the inadequacies of the earlier system.” This assessment seems applicable to the area of insurance as well. There may be a need to create means by which hospitalists can be better protected from malpractice risk and coverage inadequacy. This area, like all others associated with hospital medicine, is evolving.
In this article we highlight malpractice insurance for hospitalists: what you should consider now and in the future regarding policy coverage. policies Available to Hospitalists
The types of malpractice insurance available to hospitalists include:
- Policies provided under your employer’s policy or purchased for yourself;
- Policies that cover you when any event actually occurs or when the claim is filed; and
- Policies purchased by hospitals where the payouts for claims are made either by the insurance company (the carrier) or by the employer (the hospital).
Most hospitalists are covered by institutional or group employers. In most cases, hospitalists are hired directly by hospitals or by an agency that contracts with hospitalists and administrates this relationship with the hospital.
“We recommend that the hospitals employ the hospitalists and that they put them on their hospital malpractice policy,” says Pam Kirks, insurance broker with the Gallagher Health Insurance Company in Raleigh, N.C., “because that’s the cheapest way to go for the hospitalist. There are different types of coverage out there that they can get; they can get their own coverage certainly. But I think the majority of them are becoming hospital employees.”
Occurrence or Claims Made
The types of medical malpractice insurance available to hospitalists are either “occurrence” or “claims-made” policies. An occurrence policy is one in which the policy that responds to a claim is the one that was in effect when the incident actually occurred. A claims-made policy that responds to a claim is the one that is in effect when the claim is made—provided that you also had continuous coverage from the time that the incident occurred.
Joe Zorola, director of underwriting at ProMutual Insurance Company in Boston, further explains the claims-made policy. “For instance, let’s say you have a policy this year and something happens tomorrow and five years down the line [the patient] file[s] a claim because of what happened tomorrow,” he explains. “You should have continued this policy through the next five years so that there’s no lapse of coverage, but the policy that will respond will be the policy five years from now.”
Of the 52 hospitals and 14,000 people that ProMutual insures, half of the policies are individual policies and half are group policies.
“The majority of [policies] are in Massachusetts and so are written under an occurrence basis,” says Zorola. “The ones outside of Massachusetts—and those are the group policies that we do have—are claims made.”
Physicians and insurance carriers each have preferences between the two types. “The occurrence policy is the policy that a lot of physicians like because they understand that if they did something today, [they can think] ‘I never have to worry about having insurance in the future for it,’” says Zorola. “The claims-made policy is the one that we as [insurance] companies like because it allows us to close our books on each policy year much sooner because we know that we aren’t going to have any more claims attached to the policy this year or in another year or two.”
Fully Insured or Self Insured?
Malpractice policies available through employers are either fully insured or self insured. The difference between the two types involves who is responsible for the claims payouts. With fully insured plans, the employer pays a premium to an insurer and the insurer pays claims out of the pool of premiums it collects from everyone it insures. Under a self-insured plan, the employer is responsible for paying all claims out of company assets. The Employee Retirement Income Security Act (ERISA) regulates self-insured plans; the plans are then under the jurisdiction of the U.S. Department of Labor.
“The hospitalists that we do [under]write [fully insured policies] for tend to be in the smaller community hospitals, which may not necessarily have the huge need for hospitalists; whereas the larger institutions may have a larger need for hospitalists [and] they usually tend to be self-insured,” says Zorola.
Controlled Risk Insurance Company of Vermont, known as CRICO and located in Cambridge, Mass, is one example of a self-insured system. “We only have one [malpractice insurance] product for a closed system where our clients are the Harvard teaching hospitals” says Karen O’Rourke, senior vice president of CRICO.
Individual Policies for Certain Circumstances
Hospitalists who take out individual policies are usually practicing part-time or moonlighting and have another policy with a carrier that is covering their primary practice. “And this is true across the country,” says Zorola. “Most carriers will have some sort of part-time credit that they will provide [to] the people who come to them for policies. Now there are some carriers, and these are usually the large hospital carriers, who won’t provide individual policies to physicians. They only provide coverage for the hospital and the hospital’s employees.”
Hospitalists who take out their own individual policies usually get coverage from one of the local Physician Insurers Association of America carriers.
Why Are Hospitalists Sued?
In general, hospitalists are infrequently sued for medical malpractice. They may be named in initial claims, but many are dropped before the case is resolved. However, while experts report that lawsuits against hospitalists are scarce, they also reference the lack of classification code specifically created for the hospitalist and his/her duties. Without it, it’s impossible to distinguish in data to learn when and in how many cases hospitalists were named.
O’Rourke says that internists in ambulatory or outpatient practice settings are usually at risk for claims of failure to diagnose—mostly failure to diagnose cancer or myocardial infarctions. In contrast, “the hospitalists’ failures come in the communication area,” she says, “because that’s primarily what they’re there for is to make sure that the patient receives the medical care that they’re supposed to in a hospital setting.”
O’Rourke, who directs the management of underwriting claims as part of her work at CRICO, believes there is a vast difference between the reasons for claims for internists versus hospitalists.3
“We receive so many failure-to-diagnose cases with internal medicine physicians,” she elaborates. “There have been huge losses associated with them throughout other systems that we’ve seen—some of our own, such as increases in [the rates of] breast cancer or colorectal cancer. You’re not going to see that with a hospitalist unless there’s a post-op complication—bleeding that isn’t caught and failure to diagnose—that kind of issue—soon enough. But they’re still under a surgeon’s care normally.”
O’Rourke recognizes that the care of the hospital patient is a team effort. “So it’s going to be a question of how the hospital defines the hospitalist role for each and every condition or [for] surgical patients,” she says.
If the Hospitalist Sees the Patient
A new claim that ProMutual recently received involves a hospitalist. The allegation is “failure to monitor a patient for suicide.” The claim states that the patient attempted suicide twice by trying to hang herself. The patient was admitted to the psychiatric unit of the hospital. Although a medical consultation must be done any time a patient is admitted, the hospitalist was not consulted to assess for suicide precautions. The hospitalist’s next involvement was after the attempted suicide when she responded to the code and admitted the patient to the ICU.
Given the lines of protocol, it is likely to be decided that the named psychiatrist was responsible for noting the risks with this patient and the hospitalist’s name will be dropped from the claim. The important thing for hospitalists to know is that because the hospitalist was listed as seeing the patient, she was named in the claim and this is customary procedure.
“A lot of times the plaintiff attorney will note every doctor who has seen the patient over the last number of years,” says Zorola, “because they probably don’t know a lot about the claim either, at that point. So until the investigation is done, and you can perform the depositions and find out exactly who was responsible for what,” the hospitalist will be a part of this process.
The Classification of Hospitalists
The growing trend is that insurance underwriters are creating a separate hospitalist classification. ProMutual underwriters established a classification for hospitalist and placed it in the same rate group as internal medicine physicians. But then the underwriters listened to what some of the hospitalists were saying: that because they are more specialized and are seeing patients who are more aware of the care that should be provided in the hospital, being grouped with physicians who spend most of the their time in office practice was not an accurate way to classify them.
Zorola and his colleagues now see that “setting up a separate classification for [hospitalists] allows us in the future to review their experience and determine whether they ought to be grouped with internal medicines or whether they belong in a lower or higher classification.” Hospitalists might belong in a higher, risk-associated classification “because they are seeing sick patients whereas internal medicine and family practice doctors have a mixture of sick and well patients,” he notes.
In fact, the common assumption is that hospitalists are doing riskier work simply because they work in places in which they have more opportunities to encounter risk. O’Rourke can’t say definitively how many hospitalists CRICO insures. But she can say that few claims involve hospitalists.
“We thought they were a riskier group for a while, but we couldn’t find any evidence of that in our data,” she explains. “We had a couple of claims involving people who were hospitalists, but nothing of concern.”
Whether hospitalists prove to be a riskier group in future research will depend on first determining more precisely what hospitalists do.
What Do Hospitalists Really Do?
“I can imagine that some of [the answer to this question] is that you go find out what works best for the systems you already have in place and develop systems that are needed to really quantify what [hospitalists] are supposed to do,” says O’Rourke. “And that will vary from institution to institution depending on whether it’s a teaching hospital or not.”
But there are other factors and issues at play, some of which are entirely out of control of the insured hospitalist. Barry Halpern, an attorney with Snell and Wilmer Law Firm, whose insured clients are spread over the western half of the United States, says “malpractice insurers, for a variety of reasons, … have many, many classifications for underwriting purposes and others [have] not very many at all. There are marketing issues associated with that and they don’t have a lot to do with the aspects of the specialty.”4
Your Policy Type May Matter
“[A]s you look at this from an insurance perspective, there are pros and cons for having separate insurance for hospitalists and the hospital,” says Halpern. “Where there is separate insurance, there is sometimes greater potential for conflict tension among the provider team than when the insurance is provided on an entity basis, particularly when entity claims against hospitals are a [somewhat] growing trend.”
Halpern notes that, in general, the courts are delivering their verdicts without considering the actual relationship between a hospital and a staff physician.3 “Of course,” he adds, “the courts are hunting for ways to make hospitals responsible on an entity basis rather than specifically for negligence in credentialing, or negligence in supervising, or negligence in providing staff and tools.”
Halpern thinks that in lawsuits where any staff physician is considered as part of the entity of the hospital institution, “it may make sense for the hospitalist to be insured under the hospital’s coverage, so that you minimize the potential for finger-pointing within the hospital-based team.” Besides creating potential tension within the group, Halpern says, “there may be indemnity agreements entered into between the hospitalists and the hospital that shift legal responsibility in a way that is sometimes not as carefully considered at the front end of an arrangement than at the back end, when a problem occurs.”
Halpern says that those kinds of situations must be looked at carefully. “[T]hose kinds of indemnity agreements can lead to a whole world of collateral claims litigation and can sometimes compromise insurance coverage,” he says. “For instance, if a hospitalist group signs an indemnity contract with the hospital without clearing it with the hospitalist’s insurer, the insurer might look at that and say, ‘We didn’t underwrite that additional obligation to defend and pay damages for the benefit of the hospital. And therefore, we deny coverage.’”
What Should Hospitalists Do?
If you are an individual hospitalist and your hospital provides your coverage, our experts have some suggestions on how to best protect yourself from surprises later about your liability insurance.
“[Y]ou certainly ought to get a copy of the policy,” says Halpern, and “focus very carefully on several things: 1) what’s covered, 2) what’s excluded, 3) what are the limits, and 4) who’s providing the coverage?”
You need to be able to feel that you can say “yes” to the question, “Is this a company that I can be confident will be there when it’s needed?”
If after a careful review of your policy, you have areas you would like to discuss with the hospital, it’s a matter of negotiation. And when you have the “negotiation muscle” to get what you need for protection, says Halpern, you’re in a better position.
“Frankly, most hospitals are interested in maintaining quality staff, quality relations with physicians—both employed and on the consulting staff,” says Halpern. “[They] are not typically in the business of muscling people and treating them badly. So if the hospitalist finds a legitimate gap in coverage or a concern, by and large hospitals look to be fair in working those things out. If they’re not, there are two basic approaches, and one is to not continue in the relationship.” (In other words, quit). “The second [approach] is to insure over the gap by going to an insurance broker and seeing if you can find coverage.”
Conclusion
Although most hospitalists are covered under their hospital policies, all hospitalists would benefit from understanding the specifics of their malpractice coverage. The dynamics of the hospitalist model will require changes in many areas including malpractice insurance. The trend of insurance carriers to establish a separate classification for hospitalists is likely to provide more precisely written coverage that accounts for the particulars of hospital medicine practice TH
Writer Andrea Sattinger will write about risk management for hospitalists in the Jan. ’06 issue.
References
- Wachter RM. The hospitalist movement: ten issues to consider. Hosp Pract. 1999;34(2):104-106.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care JAMA. 1994;272:1588-1591.
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9.
- Pham HH, Devers KJ, Kuo S, et al. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005;20:101-107.
In a 2001 Hospital Practice article Robert Wachter, MD, named malpractice as one of the top 10 issues that require consideration as it relates to the hospitalist movement.1 There are many areas to consider when looking at malpractice insurance for hospitalists as opposed to other physician specialties. Just one area being reviewed by insurance carriers: Underwriters are grouping hospitalists with internal medicine physicians because hospitalists do not yet have their own classification code.
“When physicians spend 85% to 100% of their time in the office,” wrote Dr. Wachter, “it seems prudent to base assessments of competence on the quality of the office practice rather than that of the hospital practice. As in other situations, the hospitalist movement has exposed the inadequacies of the earlier system.” This assessment seems applicable to the area of insurance as well. There may be a need to create means by which hospitalists can be better protected from malpractice risk and coverage inadequacy. This area, like all others associated with hospital medicine, is evolving.
In this article we highlight malpractice insurance for hospitalists: what you should consider now and in the future regarding policy coverage. policies Available to Hospitalists
The types of malpractice insurance available to hospitalists include:
- Policies provided under your employer’s policy or purchased for yourself;
- Policies that cover you when any event actually occurs or when the claim is filed; and
- Policies purchased by hospitals where the payouts for claims are made either by the insurance company (the carrier) or by the employer (the hospital).
Most hospitalists are covered by institutional or group employers. In most cases, hospitalists are hired directly by hospitals or by an agency that contracts with hospitalists and administrates this relationship with the hospital.
“We recommend that the hospitals employ the hospitalists and that they put them on their hospital malpractice policy,” says Pam Kirks, insurance broker with the Gallagher Health Insurance Company in Raleigh, N.C., “because that’s the cheapest way to go for the hospitalist. There are different types of coverage out there that they can get; they can get their own coverage certainly. But I think the majority of them are becoming hospital employees.”
Occurrence or Claims Made
The types of medical malpractice insurance available to hospitalists are either “occurrence” or “claims-made” policies. An occurrence policy is one in which the policy that responds to a claim is the one that was in effect when the incident actually occurred. A claims-made policy that responds to a claim is the one that is in effect when the claim is made—provided that you also had continuous coverage from the time that the incident occurred.
Joe Zorola, director of underwriting at ProMutual Insurance Company in Boston, further explains the claims-made policy. “For instance, let’s say you have a policy this year and something happens tomorrow and five years down the line [the patient] file[s] a claim because of what happened tomorrow,” he explains. “You should have continued this policy through the next five years so that there’s no lapse of coverage, but the policy that will respond will be the policy five years from now.”
Of the 52 hospitals and 14,000 people that ProMutual insures, half of the policies are individual policies and half are group policies.
“The majority of [policies] are in Massachusetts and so are written under an occurrence basis,” says Zorola. “The ones outside of Massachusetts—and those are the group policies that we do have—are claims made.”
Physicians and insurance carriers each have preferences between the two types. “The occurrence policy is the policy that a lot of physicians like because they understand that if they did something today, [they can think] ‘I never have to worry about having insurance in the future for it,’” says Zorola. “The claims-made policy is the one that we as [insurance] companies like because it allows us to close our books on each policy year much sooner because we know that we aren’t going to have any more claims attached to the policy this year or in another year or two.”
Fully Insured or Self Insured?
Malpractice policies available through employers are either fully insured or self insured. The difference between the two types involves who is responsible for the claims payouts. With fully insured plans, the employer pays a premium to an insurer and the insurer pays claims out of the pool of premiums it collects from everyone it insures. Under a self-insured plan, the employer is responsible for paying all claims out of company assets. The Employee Retirement Income Security Act (ERISA) regulates self-insured plans; the plans are then under the jurisdiction of the U.S. Department of Labor.
“The hospitalists that we do [under]write [fully insured policies] for tend to be in the smaller community hospitals, which may not necessarily have the huge need for hospitalists; whereas the larger institutions may have a larger need for hospitalists [and] they usually tend to be self-insured,” says Zorola.
Controlled Risk Insurance Company of Vermont, known as CRICO and located in Cambridge, Mass, is one example of a self-insured system. “We only have one [malpractice insurance] product for a closed system where our clients are the Harvard teaching hospitals” says Karen O’Rourke, senior vice president of CRICO.
Individual Policies for Certain Circumstances
Hospitalists who take out individual policies are usually practicing part-time or moonlighting and have another policy with a carrier that is covering their primary practice. “And this is true across the country,” says Zorola. “Most carriers will have some sort of part-time credit that they will provide [to] the people who come to them for policies. Now there are some carriers, and these are usually the large hospital carriers, who won’t provide individual policies to physicians. They only provide coverage for the hospital and the hospital’s employees.”
Hospitalists who take out their own individual policies usually get coverage from one of the local Physician Insurers Association of America carriers.
Why Are Hospitalists Sued?
In general, hospitalists are infrequently sued for medical malpractice. They may be named in initial claims, but many are dropped before the case is resolved. However, while experts report that lawsuits against hospitalists are scarce, they also reference the lack of classification code specifically created for the hospitalist and his/her duties. Without it, it’s impossible to distinguish in data to learn when and in how many cases hospitalists were named.
O’Rourke says that internists in ambulatory or outpatient practice settings are usually at risk for claims of failure to diagnose—mostly failure to diagnose cancer or myocardial infarctions. In contrast, “the hospitalists’ failures come in the communication area,” she says, “because that’s primarily what they’re there for is to make sure that the patient receives the medical care that they’re supposed to in a hospital setting.”
O’Rourke, who directs the management of underwriting claims as part of her work at CRICO, believes there is a vast difference between the reasons for claims for internists versus hospitalists.3
“We receive so many failure-to-diagnose cases with internal medicine physicians,” she elaborates. “There have been huge losses associated with them throughout other systems that we’ve seen—some of our own, such as increases in [the rates of] breast cancer or colorectal cancer. You’re not going to see that with a hospitalist unless there’s a post-op complication—bleeding that isn’t caught and failure to diagnose—that kind of issue—soon enough. But they’re still under a surgeon’s care normally.”
O’Rourke recognizes that the care of the hospital patient is a team effort. “So it’s going to be a question of how the hospital defines the hospitalist role for each and every condition or [for] surgical patients,” she says.
If the Hospitalist Sees the Patient
A new claim that ProMutual recently received involves a hospitalist. The allegation is “failure to monitor a patient for suicide.” The claim states that the patient attempted suicide twice by trying to hang herself. The patient was admitted to the psychiatric unit of the hospital. Although a medical consultation must be done any time a patient is admitted, the hospitalist was not consulted to assess for suicide precautions. The hospitalist’s next involvement was after the attempted suicide when she responded to the code and admitted the patient to the ICU.
Given the lines of protocol, it is likely to be decided that the named psychiatrist was responsible for noting the risks with this patient and the hospitalist’s name will be dropped from the claim. The important thing for hospitalists to know is that because the hospitalist was listed as seeing the patient, she was named in the claim and this is customary procedure.
“A lot of times the plaintiff attorney will note every doctor who has seen the patient over the last number of years,” says Zorola, “because they probably don’t know a lot about the claim either, at that point. So until the investigation is done, and you can perform the depositions and find out exactly who was responsible for what,” the hospitalist will be a part of this process.
The Classification of Hospitalists
The growing trend is that insurance underwriters are creating a separate hospitalist classification. ProMutual underwriters established a classification for hospitalist and placed it in the same rate group as internal medicine physicians. But then the underwriters listened to what some of the hospitalists were saying: that because they are more specialized and are seeing patients who are more aware of the care that should be provided in the hospital, being grouped with physicians who spend most of the their time in office practice was not an accurate way to classify them.
Zorola and his colleagues now see that “setting up a separate classification for [hospitalists] allows us in the future to review their experience and determine whether they ought to be grouped with internal medicines or whether they belong in a lower or higher classification.” Hospitalists might belong in a higher, risk-associated classification “because they are seeing sick patients whereas internal medicine and family practice doctors have a mixture of sick and well patients,” he notes.
In fact, the common assumption is that hospitalists are doing riskier work simply because they work in places in which they have more opportunities to encounter risk. O’Rourke can’t say definitively how many hospitalists CRICO insures. But she can say that few claims involve hospitalists.
“We thought they were a riskier group for a while, but we couldn’t find any evidence of that in our data,” she explains. “We had a couple of claims involving people who were hospitalists, but nothing of concern.”
Whether hospitalists prove to be a riskier group in future research will depend on first determining more precisely what hospitalists do.
What Do Hospitalists Really Do?
“I can imagine that some of [the answer to this question] is that you go find out what works best for the systems you already have in place and develop systems that are needed to really quantify what [hospitalists] are supposed to do,” says O’Rourke. “And that will vary from institution to institution depending on whether it’s a teaching hospital or not.”
But there are other factors and issues at play, some of which are entirely out of control of the insured hospitalist. Barry Halpern, an attorney with Snell and Wilmer Law Firm, whose insured clients are spread over the western half of the United States, says “malpractice insurers, for a variety of reasons, … have many, many classifications for underwriting purposes and others [have] not very many at all. There are marketing issues associated with that and they don’t have a lot to do with the aspects of the specialty.”4
Your Policy Type May Matter
“[A]s you look at this from an insurance perspective, there are pros and cons for having separate insurance for hospitalists and the hospital,” says Halpern. “Where there is separate insurance, there is sometimes greater potential for conflict tension among the provider team than when the insurance is provided on an entity basis, particularly when entity claims against hospitals are a [somewhat] growing trend.”
Halpern notes that, in general, the courts are delivering their verdicts without considering the actual relationship between a hospital and a staff physician.3 “Of course,” he adds, “the courts are hunting for ways to make hospitals responsible on an entity basis rather than specifically for negligence in credentialing, or negligence in supervising, or negligence in providing staff and tools.”
Halpern thinks that in lawsuits where any staff physician is considered as part of the entity of the hospital institution, “it may make sense for the hospitalist to be insured under the hospital’s coverage, so that you minimize the potential for finger-pointing within the hospital-based team.” Besides creating potential tension within the group, Halpern says, “there may be indemnity agreements entered into between the hospitalists and the hospital that shift legal responsibility in a way that is sometimes not as carefully considered at the front end of an arrangement than at the back end, when a problem occurs.”
Halpern says that those kinds of situations must be looked at carefully. “[T]hose kinds of indemnity agreements can lead to a whole world of collateral claims litigation and can sometimes compromise insurance coverage,” he says. “For instance, if a hospitalist group signs an indemnity contract with the hospital without clearing it with the hospitalist’s insurer, the insurer might look at that and say, ‘We didn’t underwrite that additional obligation to defend and pay damages for the benefit of the hospital. And therefore, we deny coverage.’”
What Should Hospitalists Do?
If you are an individual hospitalist and your hospital provides your coverage, our experts have some suggestions on how to best protect yourself from surprises later about your liability insurance.
“[Y]ou certainly ought to get a copy of the policy,” says Halpern, and “focus very carefully on several things: 1) what’s covered, 2) what’s excluded, 3) what are the limits, and 4) who’s providing the coverage?”
You need to be able to feel that you can say “yes” to the question, “Is this a company that I can be confident will be there when it’s needed?”
If after a careful review of your policy, you have areas you would like to discuss with the hospital, it’s a matter of negotiation. And when you have the “negotiation muscle” to get what you need for protection, says Halpern, you’re in a better position.
“Frankly, most hospitals are interested in maintaining quality staff, quality relations with physicians—both employed and on the consulting staff,” says Halpern. “[They] are not typically in the business of muscling people and treating them badly. So if the hospitalist finds a legitimate gap in coverage or a concern, by and large hospitals look to be fair in working those things out. If they’re not, there are two basic approaches, and one is to not continue in the relationship.” (In other words, quit). “The second [approach] is to insure over the gap by going to an insurance broker and seeing if you can find coverage.”
Conclusion
Although most hospitalists are covered under their hospital policies, all hospitalists would benefit from understanding the specifics of their malpractice coverage. The dynamics of the hospitalist model will require changes in many areas including malpractice insurance. The trend of insurance carriers to establish a separate classification for hospitalists is likely to provide more precisely written coverage that accounts for the particulars of hospital medicine practice TH
Writer Andrea Sattinger will write about risk management for hospitalists in the Jan. ’06 issue.
References
- Wachter RM. The hospitalist movement: ten issues to consider. Hosp Pract. 1999;34(2):104-106.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care JAMA. 1994;272:1588-1591.
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9.
- Pham HH, Devers KJ, Kuo S, et al. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005;20:101-107.
Current Concepts in Pelvic Anatomy and Reconstructive Surgery
Supplement Editor:
G. Willy Davila, MD
Contents
Preface: Sizing up the evolution of reconstructive pelvic surgery
G. Willy Davila, MD
Contemporary views on female pelvic anatomy
Matthew D. Barber, MD, MHS
Vaginal vault prolapse: Identification and surgical options
Daniel H. Biller, MD, and G. Willy Davila, MD
Anterior vaginal wall prolapse: Innovative surgical approaches
Mark D. Waters, MD, and Marie Fidela R. Paraiso, MD
Optimizing pelvic surgery outcomes
G. Willy Davila, MD
Supplement Editor:
G. Willy Davila, MD
Contents
Preface: Sizing up the evolution of reconstructive pelvic surgery
G. Willy Davila, MD
Contemporary views on female pelvic anatomy
Matthew D. Barber, MD, MHS
Vaginal vault prolapse: Identification and surgical options
Daniel H. Biller, MD, and G. Willy Davila, MD
Anterior vaginal wall prolapse: Innovative surgical approaches
Mark D. Waters, MD, and Marie Fidela R. Paraiso, MD
Optimizing pelvic surgery outcomes
G. Willy Davila, MD
Supplement Editor:
G. Willy Davila, MD
Contents
Preface: Sizing up the evolution of reconstructive pelvic surgery
G. Willy Davila, MD
Contemporary views on female pelvic anatomy
Matthew D. Barber, MD, MHS
Vaginal vault prolapse: Identification and surgical options
Daniel H. Biller, MD, and G. Willy Davila, MD
Anterior vaginal wall prolapse: Innovative surgical approaches
Mark D. Waters, MD, and Marie Fidela R. Paraiso, MD
Optimizing pelvic surgery outcomes
G. Willy Davila, MD