User login
Risky Business
[H]ospitalists are in a very litigation-intensive and volatile environment. … [T]hey are practicing in a niche that has not been fully accepted by the medical community. There’s a lot of tension on various specialty groups as to the role of hospitalists, the value of hospitalists, whether for a variety of reasons they are creating impediments [to] the quality of care, possibly raising competitive concerns. And so the best trained, the best intentioned, and most capable hospitalist is choosing … a dangerous area of practice from a liability perspective.
—Barry Halpern, JD, Snell and Wilmer Law Offices, expert in medical malpractice law
As hospitalists move from patient to patient, consult to consult, and decision to decision, risk management—proactively identifying, assessing, and prioritizing risks with a goal of minimizing their negative consequences—may not stay uppermost in their minds. Yet for hospitalists, by virtue of their constant location and activity in hospitals, risks lurk at every corner, and the potential for being judged at fault is real and potentially costly.
What are the hospitalist’s risks of being sued for malpractice? How can hospitalists best protect themselves against malpractice claims? Does being liable for patient care ever cause hospitalists to handicap themselves, to hold back in some ways?
What Risks Do Hospitalists Face?
“I think the issue that hospitalists are facing from a medical-legal standpoint is there is not a lot of cumulative experience with case law, precedent, in the field of hospital medicine,” says Tom Baudendistel, MD, a hospitalist and associate program director at California Pacific Medical Center in San Francisco.
Besides errors of medical practice, hospitalists are at risk when they:
- Practice beyond the scope of their specialty;
- Fail to communicate or communicate poorly with patients, families, staff, and referring physicians; and
- Fail to exercise independent medical judgment.
Hospitalists work with sicker, more complicated patients in an environment where more things can go wrong. (See The Hospitalist, July/August 2002, “Hospitalists and the Malpractice Insurance Crisis.”) All things considered, hospital-based physicians are at greater risk of being sued than their colleagues who work in offices.
Case #1: The hospitalist failed to detect a vertebral artery dissection in a younger patient. Should they have been able to detect that? It’s a rather unusual stroke presentation. A neurologist would have picked it up—and certainly would have been held liable or negligent if they’d missed that diagnosis. During their training neurologists would have certainly seen this condition as a cause of stroke in someone below age 45. But internists, in general, don’t receive good neurologic training as part of their residencies, and in community hospitals there is no set neurology service.
Neurologists have now become more office-based and allow the hospitalists to do more. By doing more, they’re also exposed to more legal risk. Should the hospitalist be held negligent for missing an unusual stroke? It depends on what you think is a hospitalist’s scope of practice.
—Dr. Baudendistel
Scope of Practice
A hospitalist’s scope of practice is somewhat difficult to define, although the classification “hospitalist” is gaining clarity (including with insurance underwriters), and the hospitalist model is becoming more recognized as a subspecialty. (See “A Malpractice Primer,” The Hospitalist, Dec. 2005, p. 1.)
One challenge in defining the hospitalist’s scope of practice is that hospitalists do a variety of things and work in different departments of the hospital: Some spend more time in acute care, some are more in general care, and some of them are mostly in trauma care.
It is generally acknowledged that healthcare practitioners must employ the same degree of diligence and skill commonly possessed by other members of the healthcare profession who are engaged in the same kind of work in similar locales. Thus, hospitalists need to be acutely aware of how other hospitalists practice in similar settings with similar resources available.
Hospitalists in rural and suburban hospitals, which have fewer and less specialized staff readily available for consults, should expect to have a different scope of practice. In time further clarification of the roles, responsibilities, and clinical skills of hospitalists will be established so that the scope of practice is more clearly defined.
Dr. Baudendistel believes that residents tracking to specialize in hospital medicine could benefit from having more education in certain areas: neurology, perioperative medicine, and critical care.
SHM has recognized the need for better risk management strategies to protect hospitalists and will provide this information and continuing education in The Core Competencies in Hospital Medicine to be published the January/February 2006 issue of the Journal of Hospital Medicine.
Case #2: A male patient came into the ED at a rural hospital with an altered mental status. He had a history of falls and the CT scan in the ED showed a large subdural hematoma.
“We need to admit this patient to the hospital,” said the ED doc. “Call the hospitalist.”
“What does neurosurgery want to do?” asked the hospitalist.
The hospitalist tried to reach the neurosurgeon. And the ED doc wasn’t able to obtain neurosurgery consult because the neurosurgeon said that he wasn’t on call for that hospital. So the hospitalist was … left responsible without neurosurgery backup.
Ultimately, the patient worsened. The hospitalist called a different neurosurgeon at a different hospital who clearly wasn’t in charge of the patient. That doctor said, “Get the patient over to us, and we’ll take care of it.”
There was a 12-hour delay, and the patient finally got transferred to the other hospital, had surgery, and did OK. But he was definitely deteriorating.
The neurosurgeon who said he wasn’t on call for that hospital was wrong. He was lying or just didn’t know of his group’s call coverage. It was a clear violation. And it left the hospital in a situation that isn’t all that unfamiliar.
In this case, the hospitalist wasn’t at fault. There was clear chart documentation [provided as evidence] that said, “I called the neurosurgeon three times and they’re not calling back. Finally they called back the fourth time and said that they’re not coming in.” —Dr. Baudendistel
Communication
Communication is crucial in a clinician’s provision of quality care and also provides a safety net to help prevent liability. Communication with patients, families, staff, and other physicians—particularly their inpatients’ primary care physicians—provides the strongest armor against malpractice assaults. Timeliness and the urgency of the issue are key to patient care and are also are examined by those who review malpractice claims.
In recent years medical malpractice claims payouts have increased substantially for both jury verdicts and settlements. For monetary awards involving doctor-patient relations, which are largely predicated upon communication, the median payout is $230,000.1
Some hot-button areas that carry higher risk and call for meticulous communication between providers include:
- Inpatient postoperative care;
- Post-discharge communication (hand-offs);
- Diagnosis and treatment of a patient for whom there is an incomplete history; and
- Acceptance for treatment of patients whose medical conditions may either be unfamiliar to hospitalists or for which they have had limited or no training.
Communication with Patients
Communication—every aspect of it—is essential for the patient’s health, attitude, and satisfaction. Interestingly, legal data show that most patients who have bad outcomes don’t file suit.2 Although patients litigate for a variety of reasons, chief among them is when they perceive they have suffered because of administrative errors, rude practitioners or support staff, or the denial of tests and referrals they had requested and thought were reasonable.3 Data from a number of studies conducted within the past two decades show that although no particular communication skills can be directly associated with reducing malpractice claims, when patients perceive that their providers treat them genuinely and fairly, and update them honestly and regularly, they are less likely to sue.4-9
One-on-One with Barry Halpern, JD

My law firm practices throughout the western United States, and one of the areas that I see as a general pattern is when … continuity of care becomes an issue. The cases that are sometimes the most troublesome are those in which the hospitalist is involved.
There’s never a real clear demarcation of responsibility between, for instance, the surgery service and the hospitalist. Orders are written and then interpreted by the nursing staff in ways that, in retrospect, even the surgical service or the hospitalist are not pleased with. Yet the physicians aren’t talking to each other, and the documentation in the medical record is intermittent … .
Those kinds of situations, particularly where there is later alleged to have been, for instance, a medication error, become very difficult to defend. Because from the perspective of the lay jury that will be looking at the case, it’s easy for a plaintiff lawyer to depict a very disjointed and uncoordinated approach to care, when—in fact—the reality of practices is that they don’t always go perfectly and things aren’t always documented the instant that they are done.
And sometimes bad things happen despite everybody’s best efforts. But when you have a rough interface between the hospitalist and the other physicians with regard to responsibility for a patient, you are inviting a legal problem.
—Halpern is an attorney with Snell and Wilmer Law Offices, Phoenix
Case #3: A 72-year-old female who was pretty healthy (she had some high blood pressure) came in with abdominal pain. The ED doctor drew the laboratories, which suggested pancreatitis, and then investigated why she had pancreatitis. The ultrasound ordered by the ED doc showed gallstones. The physician then correctly inferred that she had gallstones causing her pancreatitis.
A hospitalist was called [and] admitted the patient. Surgery and GI consultants were called. The GI consultant first ordered an endoscopic retrograde cholangiopancreatography to clean the gallstones from the common bile duct. That went fine, and the next day the patient looked a little better. The GI service said, “Anticipated to go home in a couple days.” Surgery felt the same.
Then the consensus was to remove her gallbladder because eventually she would need to have it done. And that’s when things started to go badly.
On postoperative day two, the patient started having pain out of proportion to what should be expected. The internist (the hospitalist) raised that question in his note. The surgeon said, “No, that’s still postoperative pain,” and increased the pain medicine.
The hospitalist said, “I’m really concerned about this; I’ll talk to the surgeon.”
Again the surgeon said, “There’s nothing to worry about. I’ll at least order a HIDA scan.”
Initially the patient refused the scan, but the next day—postoperative day three—she was still having pain and was clearly worse. She had a high fever; her blood pressure dropped; and her white blood cell count climbed from 10,000 to 20,000, indicating infection/inflammation. Finally the hospitalist ordered a CT scan, which shows a perforation caused by the surgery.
The patient went to surgery for repair. As was predicted, she had a rocky hospital course and ultimately died a month later.
The surgeon was clearly in the wrong. … I was consulted and was asked, “What would you do with the hospitalist? What was their role in that case? Do you think he failed to meet the standard of care?”
—Dr. Baudendistel
Communication with Other Clinicians
“Communication between physicians is critical,” says Sally Whitaker, RN, BSN, risk manager with Rex Healthcare in Raleigh, N.C. “[Hospitalists] shouldn’t just rely on knowing they’ve put their notes on the discharge summary.”
At Rex Hospital (one of Rex Healthcare’s six facilities) where Whitaker works, when seminal events (those big bad things that happen) occur and result in severe trauma or death, the appropriate people meet to backtrack through the steps and scenarios that led to the breakdown.
“Fortunately we don’t have seminal events every day, but every day we do have things that go wrong,” she says. “ … And when we look at our Group Cause Analysis meetings, three-quarters of them [involve] communication issues.”
Exercise Independent Medical Judgment
Hospitalists should read their insurance and employer contracts carefully (especially those with a managed care organization) to ensure that the contract includes a statement allowing the physician to exercise independent medical judgment in the treatment of all patients. If that statement is not present, the hospitalist should request a revision in the contract to include such a statement.
In medical residency programs, a distinction is often made between being a consultant and being a co-manager, says Dr. Baudendistel, but “you have to assume there’s no legal difference between [the two].” Case #3 , he says, was a challenge to decide because the responsibilities of the surgeon and hospitalist in postoperative care were not clearly demarcated.
“I think the surgeon was probably saying, ‘I see this all the time and this is within the realm of what happens after one of these surgeries; let’s not be too worried yet,’” he says. “And I think the internist [hospitalist] ultimately pulled the trigger correctly and the [controversy later on pertained to] whether it should have been done a day or two earlier and whether that have mattered.”
This case illustrates that, although hospitalists are members of teams and partner with consultants and primary physicians, in the end they are managers of patient care and may (we hope rarely) have to break ranks to make aggressive care decisions.
“I think that the other thing that was in [the hospitalist’s] favor,” says Dr. Baudendistel of the case, “was that he was writing very thorough notes, [and] really was discussing everything with the family and everyone was on board. He was doing a very compassionate job … trying to manage this care.”
To Dr. Baudendistel, who is the chair of SHM’s ethics committee, this went a long way toward showing good faith.
Reducing Risks: Concern for the Medical Record
If the medical record is found deficient or illuminating in a negative way, it may serve the plaintiff attorney’s strategy well for establishing negligence or wrongdoing. The chart notes documented by nurses, attending staff, consultants, other residents, and therapists could either portray a smoothly managed case or a chronology of errors and omissions. The chart should never be cosigned and never merely assumed to be accurate.
When Things Go Wrong
Whitaker advises hospitalists to keep the lines of communication open. “Especially after something unexpected has happened,” she says. “So many times I think the human tendency is to just withdraw, or you feel terrible and you don’t know what to say, or you’re afraid you’re going to get emotional while you’re talking with the family.”
This is normal human response in these circumstances, but if you act on the impulse to withdraw and avoid the patient and family, or hold back, which may eventually lead to a filed claim from a family that feels abandoned.
“Until now the number of lawsuits has been really steady and the amount that we were paying in lawsuits was increasing,” says Whitaker. “However, we’re trying to work with the families earlier on so if we make a mistake and we realize that we made a mistake then we admit that. And we try to do what we can to make it right for that patient and their family.”
This often means reaching a fair and reasonable settlement, says Whitaker, “and [examining fair and reasonable means reviewing] the communication at the time the event occurred. Did we acknowledge that we made a mistake? Did we let them know we’d be willing to work with them? And did we let them know we [have since] made these changes … so they’ll … be reassured [that] hopefully it won’t happen again?”
Who’s in Charge?
Linda Greenwald, RN, MS, editor of risk management publications at ProMutual Insurance Group in Boston, wrote in the company’s newsletter, Perspectives on Clinical Risk Management, that in prior times, the question, “Who’s in charge?” was rhetorical.10 These days any number of generalists or specialists might claim that role. And therein lies the rub: Greenwald says that in many cases involving hospitalists the lines of responsibility are unclear and one or more systems may fail. If so, Greenwald writes, the result may be a malpractice claim alleging:
- Failure to diagnose when each of two physicians assumes the other has responsibility for follow-up;
- Negligence in treatment when one physician fails to monitor on an outpatient basis the medication first prescribed by another physician when the patient was an inpatient; and/or
- Negligent care when a patient misinterprets the information one physician asks him or her to relay to another physician.10
Halpern concurs that the modern mix of professionals working as a team on hospital care can be a major challenge.
“In olden days, when a primary care physician referred to a surgeon, and the surgeon performed surgery, and the surgeon took responsibility for postoperative care, and occasionally brought in a consultant, the lines were relatively clear,” says Halpern. “When a hospitalist is injected into the mix, unless the hospital has really clear procedures and unless everybody is comfortable with the system and everybody is talking to each other and agreeing on the lines of demarcation, you’re creating a soup that plaintiff lawyers would be happy to stir.”
The more murky the communication, the greater the liability. “And when you have murky lines of communication, murky lines of responsibility, and a medical catastrophe,” says Halpern, “human nature compounds the problem by frequently causing a finger-pointing contest, where each component of the patient care team circles its own wagons [and] points in a different direction. And that is the absolute worst thing that can happen when trying to deal with a patient injury claim.”
Summary
The hospitalist’s primary risk for malpractice claims may be inadequate or absent patient follow-up resulting from a lack of communication. The best means of protection from claims is for hospitalists to incorporate a comprehensive risk management program into their practice.
Several strategies have proved successful to help prevent litigation. In general, hospitalists should make sure that their hospital has clearly delineated policies regarding responsibility for patients; clearly understand—and ensure that your coworkers, colleagues, and referring physicians understand—the hospital’s systems and protocols; exercise good communication skills; conform to the standard of care; know your own scope of care to the best of your ability; and exercise independent medical judgment, even when partnering with others. TH
Andrea Sattinger also writes the “Alliances” department for The Hospitalist.
References
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003;348:2281-2284.
- Virshup BB, Oppenberg MPH, Coleman MM. Strategic risk management: reducing malpractice claims through more effective patient-doctor communication. Am J Med Quality. 1999;14:153-159.
- Gurwitz JH, Terry S, Field TS, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289:1107-1116.
- Shapiro RS, Simpson DE, Lawrence SL, et al.. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989;149:2190-2196.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;227:558-559.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365-1370.
- Cohen JR. Apology and organizations: exploring an example from medical practice. Fordham Urban Law Journal. 2000;27:1447-1482.
- Cohen JR. Advising clients to apologize. Southern California Law Review. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care JAMA. 1994;272:1588-1591.
- Greenwald L. Who's in charge? Perspectives on Clinical Risk Management. Boston, Mass: ProMutual Group Risk Management Services; Fall 2000.
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9.
[H]ospitalists are in a very litigation-intensive and volatile environment. … [T]hey are practicing in a niche that has not been fully accepted by the medical community. There’s a lot of tension on various specialty groups as to the role of hospitalists, the value of hospitalists, whether for a variety of reasons they are creating impediments [to] the quality of care, possibly raising competitive concerns. And so the best trained, the best intentioned, and most capable hospitalist is choosing … a dangerous area of practice from a liability perspective.
—Barry Halpern, JD, Snell and Wilmer Law Offices, expert in medical malpractice law
As hospitalists move from patient to patient, consult to consult, and decision to decision, risk management—proactively identifying, assessing, and prioritizing risks with a goal of minimizing their negative consequences—may not stay uppermost in their minds. Yet for hospitalists, by virtue of their constant location and activity in hospitals, risks lurk at every corner, and the potential for being judged at fault is real and potentially costly.
What are the hospitalist’s risks of being sued for malpractice? How can hospitalists best protect themselves against malpractice claims? Does being liable for patient care ever cause hospitalists to handicap themselves, to hold back in some ways?
What Risks Do Hospitalists Face?
“I think the issue that hospitalists are facing from a medical-legal standpoint is there is not a lot of cumulative experience with case law, precedent, in the field of hospital medicine,” says Tom Baudendistel, MD, a hospitalist and associate program director at California Pacific Medical Center in San Francisco.
Besides errors of medical practice, hospitalists are at risk when they:
- Practice beyond the scope of their specialty;
- Fail to communicate or communicate poorly with patients, families, staff, and referring physicians; and
- Fail to exercise independent medical judgment.
Hospitalists work with sicker, more complicated patients in an environment where more things can go wrong. (See The Hospitalist, July/August 2002, “Hospitalists and the Malpractice Insurance Crisis.”) All things considered, hospital-based physicians are at greater risk of being sued than their colleagues who work in offices.
Case #1: The hospitalist failed to detect a vertebral artery dissection in a younger patient. Should they have been able to detect that? It’s a rather unusual stroke presentation. A neurologist would have picked it up—and certainly would have been held liable or negligent if they’d missed that diagnosis. During their training neurologists would have certainly seen this condition as a cause of stroke in someone below age 45. But internists, in general, don’t receive good neurologic training as part of their residencies, and in community hospitals there is no set neurology service.
Neurologists have now become more office-based and allow the hospitalists to do more. By doing more, they’re also exposed to more legal risk. Should the hospitalist be held negligent for missing an unusual stroke? It depends on what you think is a hospitalist’s scope of practice.
—Dr. Baudendistel
Scope of Practice
A hospitalist’s scope of practice is somewhat difficult to define, although the classification “hospitalist” is gaining clarity (including with insurance underwriters), and the hospitalist model is becoming more recognized as a subspecialty. (See “A Malpractice Primer,” The Hospitalist, Dec. 2005, p. 1.)
One challenge in defining the hospitalist’s scope of practice is that hospitalists do a variety of things and work in different departments of the hospital: Some spend more time in acute care, some are more in general care, and some of them are mostly in trauma care.
It is generally acknowledged that healthcare practitioners must employ the same degree of diligence and skill commonly possessed by other members of the healthcare profession who are engaged in the same kind of work in similar locales. Thus, hospitalists need to be acutely aware of how other hospitalists practice in similar settings with similar resources available.
Hospitalists in rural and suburban hospitals, which have fewer and less specialized staff readily available for consults, should expect to have a different scope of practice. In time further clarification of the roles, responsibilities, and clinical skills of hospitalists will be established so that the scope of practice is more clearly defined.
Dr. Baudendistel believes that residents tracking to specialize in hospital medicine could benefit from having more education in certain areas: neurology, perioperative medicine, and critical care.
SHM has recognized the need for better risk management strategies to protect hospitalists and will provide this information and continuing education in The Core Competencies in Hospital Medicine to be published the January/February 2006 issue of the Journal of Hospital Medicine.
Case #2: A male patient came into the ED at a rural hospital with an altered mental status. He had a history of falls and the CT scan in the ED showed a large subdural hematoma.
“We need to admit this patient to the hospital,” said the ED doc. “Call the hospitalist.”
“What does neurosurgery want to do?” asked the hospitalist.
The hospitalist tried to reach the neurosurgeon. And the ED doc wasn’t able to obtain neurosurgery consult because the neurosurgeon said that he wasn’t on call for that hospital. So the hospitalist was … left responsible without neurosurgery backup.
Ultimately, the patient worsened. The hospitalist called a different neurosurgeon at a different hospital who clearly wasn’t in charge of the patient. That doctor said, “Get the patient over to us, and we’ll take care of it.”
There was a 12-hour delay, and the patient finally got transferred to the other hospital, had surgery, and did OK. But he was definitely deteriorating.
The neurosurgeon who said he wasn’t on call for that hospital was wrong. He was lying or just didn’t know of his group’s call coverage. It was a clear violation. And it left the hospital in a situation that isn’t all that unfamiliar.
In this case, the hospitalist wasn’t at fault. There was clear chart documentation [provided as evidence] that said, “I called the neurosurgeon three times and they’re not calling back. Finally they called back the fourth time and said that they’re not coming in.” —Dr. Baudendistel
Communication
Communication is crucial in a clinician’s provision of quality care and also provides a safety net to help prevent liability. Communication with patients, families, staff, and other physicians—particularly their inpatients’ primary care physicians—provides the strongest armor against malpractice assaults. Timeliness and the urgency of the issue are key to patient care and are also are examined by those who review malpractice claims.
In recent years medical malpractice claims payouts have increased substantially for both jury verdicts and settlements. For monetary awards involving doctor-patient relations, which are largely predicated upon communication, the median payout is $230,000.1
Some hot-button areas that carry higher risk and call for meticulous communication between providers include:
- Inpatient postoperative care;
- Post-discharge communication (hand-offs);
- Diagnosis and treatment of a patient for whom there is an incomplete history; and
- Acceptance for treatment of patients whose medical conditions may either be unfamiliar to hospitalists or for which they have had limited or no training.
Communication with Patients
Communication—every aspect of it—is essential for the patient’s health, attitude, and satisfaction. Interestingly, legal data show that most patients who have bad outcomes don’t file suit.2 Although patients litigate for a variety of reasons, chief among them is when they perceive they have suffered because of administrative errors, rude practitioners or support staff, or the denial of tests and referrals they had requested and thought were reasonable.3 Data from a number of studies conducted within the past two decades show that although no particular communication skills can be directly associated with reducing malpractice claims, when patients perceive that their providers treat them genuinely and fairly, and update them honestly and regularly, they are less likely to sue.4-9
One-on-One with Barry Halpern, JD
My law firm practices throughout the western United States, and one of the areas that I see as a general pattern is when … continuity of care becomes an issue. The cases that are sometimes the most troublesome are those in which the hospitalist is involved.
There’s never a real clear demarcation of responsibility between, for instance, the surgery service and the hospitalist. Orders are written and then interpreted by the nursing staff in ways that, in retrospect, even the surgical service or the hospitalist are not pleased with. Yet the physicians aren’t talking to each other, and the documentation in the medical record is intermittent … .
Those kinds of situations, particularly where there is later alleged to have been, for instance, a medication error, become very difficult to defend. Because from the perspective of the lay jury that will be looking at the case, it’s easy for a plaintiff lawyer to depict a very disjointed and uncoordinated approach to care, when—in fact—the reality of practices is that they don’t always go perfectly and things aren’t always documented the instant that they are done.
And sometimes bad things happen despite everybody’s best efforts. But when you have a rough interface between the hospitalist and the other physicians with regard to responsibility for a patient, you are inviting a legal problem.
—Halpern is an attorney with Snell and Wilmer Law Offices, Phoenix
Case #3: A 72-year-old female who was pretty healthy (she had some high blood pressure) came in with abdominal pain. The ED doctor drew the laboratories, which suggested pancreatitis, and then investigated why she had pancreatitis. The ultrasound ordered by the ED doc showed gallstones. The physician then correctly inferred that she had gallstones causing her pancreatitis.
A hospitalist was called [and] admitted the patient. Surgery and GI consultants were called. The GI consultant first ordered an endoscopic retrograde cholangiopancreatography to clean the gallstones from the common bile duct. That went fine, and the next day the patient looked a little better. The GI service said, “Anticipated to go home in a couple days.” Surgery felt the same.
Then the consensus was to remove her gallbladder because eventually she would need to have it done. And that’s when things started to go badly.
On postoperative day two, the patient started having pain out of proportion to what should be expected. The internist (the hospitalist) raised that question in his note. The surgeon said, “No, that’s still postoperative pain,” and increased the pain medicine.
The hospitalist said, “I’m really concerned about this; I’ll talk to the surgeon.”
Again the surgeon said, “There’s nothing to worry about. I’ll at least order a HIDA scan.”
Initially the patient refused the scan, but the next day—postoperative day three—she was still having pain and was clearly worse. She had a high fever; her blood pressure dropped; and her white blood cell count climbed from 10,000 to 20,000, indicating infection/inflammation. Finally the hospitalist ordered a CT scan, which shows a perforation caused by the surgery.
The patient went to surgery for repair. As was predicted, she had a rocky hospital course and ultimately died a month later.
The surgeon was clearly in the wrong. … I was consulted and was asked, “What would you do with the hospitalist? What was their role in that case? Do you think he failed to meet the standard of care?”
—Dr. Baudendistel
Communication with Other Clinicians
“Communication between physicians is critical,” says Sally Whitaker, RN, BSN, risk manager with Rex Healthcare in Raleigh, N.C. “[Hospitalists] shouldn’t just rely on knowing they’ve put their notes on the discharge summary.”
At Rex Hospital (one of Rex Healthcare’s six facilities) where Whitaker works, when seminal events (those big bad things that happen) occur and result in severe trauma or death, the appropriate people meet to backtrack through the steps and scenarios that led to the breakdown.
“Fortunately we don’t have seminal events every day, but every day we do have things that go wrong,” she says. “ … And when we look at our Group Cause Analysis meetings, three-quarters of them [involve] communication issues.”
Exercise Independent Medical Judgment
Hospitalists should read their insurance and employer contracts carefully (especially those with a managed care organization) to ensure that the contract includes a statement allowing the physician to exercise independent medical judgment in the treatment of all patients. If that statement is not present, the hospitalist should request a revision in the contract to include such a statement.
In medical residency programs, a distinction is often made between being a consultant and being a co-manager, says Dr. Baudendistel, but “you have to assume there’s no legal difference between [the two].” Case #3 , he says, was a challenge to decide because the responsibilities of the surgeon and hospitalist in postoperative care were not clearly demarcated.
“I think the surgeon was probably saying, ‘I see this all the time and this is within the realm of what happens after one of these surgeries; let’s not be too worried yet,’” he says. “And I think the internist [hospitalist] ultimately pulled the trigger correctly and the [controversy later on pertained to] whether it should have been done a day or two earlier and whether that have mattered.”
This case illustrates that, although hospitalists are members of teams and partner with consultants and primary physicians, in the end they are managers of patient care and may (we hope rarely) have to break ranks to make aggressive care decisions.
“I think that the other thing that was in [the hospitalist’s] favor,” says Dr. Baudendistel of the case, “was that he was writing very thorough notes, [and] really was discussing everything with the family and everyone was on board. He was doing a very compassionate job … trying to manage this care.”
To Dr. Baudendistel, who is the chair of SHM’s ethics committee, this went a long way toward showing good faith.
Reducing Risks: Concern for the Medical Record
If the medical record is found deficient or illuminating in a negative way, it may serve the plaintiff attorney’s strategy well for establishing negligence or wrongdoing. The chart notes documented by nurses, attending staff, consultants, other residents, and therapists could either portray a smoothly managed case or a chronology of errors and omissions. The chart should never be cosigned and never merely assumed to be accurate.
When Things Go Wrong
Whitaker advises hospitalists to keep the lines of communication open. “Especially after something unexpected has happened,” she says. “So many times I think the human tendency is to just withdraw, or you feel terrible and you don’t know what to say, or you’re afraid you’re going to get emotional while you’re talking with the family.”
This is normal human response in these circumstances, but if you act on the impulse to withdraw and avoid the patient and family, or hold back, which may eventually lead to a filed claim from a family that feels abandoned.
“Until now the number of lawsuits has been really steady and the amount that we were paying in lawsuits was increasing,” says Whitaker. “However, we’re trying to work with the families earlier on so if we make a mistake and we realize that we made a mistake then we admit that. And we try to do what we can to make it right for that patient and their family.”
This often means reaching a fair and reasonable settlement, says Whitaker, “and [examining fair and reasonable means reviewing] the communication at the time the event occurred. Did we acknowledge that we made a mistake? Did we let them know we’d be willing to work with them? And did we let them know we [have since] made these changes … so they’ll … be reassured [that] hopefully it won’t happen again?”
Who’s in Charge?
Linda Greenwald, RN, MS, editor of risk management publications at ProMutual Insurance Group in Boston, wrote in the company’s newsletter, Perspectives on Clinical Risk Management, that in prior times, the question, “Who’s in charge?” was rhetorical.10 These days any number of generalists or specialists might claim that role. And therein lies the rub: Greenwald says that in many cases involving hospitalists the lines of responsibility are unclear and one or more systems may fail. If so, Greenwald writes, the result may be a malpractice claim alleging:
- Failure to diagnose when each of two physicians assumes the other has responsibility for follow-up;
- Negligence in treatment when one physician fails to monitor on an outpatient basis the medication first prescribed by another physician when the patient was an inpatient; and/or
- Negligent care when a patient misinterprets the information one physician asks him or her to relay to another physician.10
Halpern concurs that the modern mix of professionals working as a team on hospital care can be a major challenge.
“In olden days, when a primary care physician referred to a surgeon, and the surgeon performed surgery, and the surgeon took responsibility for postoperative care, and occasionally brought in a consultant, the lines were relatively clear,” says Halpern. “When a hospitalist is injected into the mix, unless the hospital has really clear procedures and unless everybody is comfortable with the system and everybody is talking to each other and agreeing on the lines of demarcation, you’re creating a soup that plaintiff lawyers would be happy to stir.”
The more murky the communication, the greater the liability. “And when you have murky lines of communication, murky lines of responsibility, and a medical catastrophe,” says Halpern, “human nature compounds the problem by frequently causing a finger-pointing contest, where each component of the patient care team circles its own wagons [and] points in a different direction. And that is the absolute worst thing that can happen when trying to deal with a patient injury claim.”
Summary
The hospitalist’s primary risk for malpractice claims may be inadequate or absent patient follow-up resulting from a lack of communication. The best means of protection from claims is for hospitalists to incorporate a comprehensive risk management program into their practice.
Several strategies have proved successful to help prevent litigation. In general, hospitalists should make sure that their hospital has clearly delineated policies regarding responsibility for patients; clearly understand—and ensure that your coworkers, colleagues, and referring physicians understand—the hospital’s systems and protocols; exercise good communication skills; conform to the standard of care; know your own scope of care to the best of your ability; and exercise independent medical judgment, even when partnering with others. TH
Andrea Sattinger also writes the “Alliances” department for The Hospitalist.
References
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003;348:2281-2284.
- Virshup BB, Oppenberg MPH, Coleman MM. Strategic risk management: reducing malpractice claims through more effective patient-doctor communication. Am J Med Quality. 1999;14:153-159.
- Gurwitz JH, Terry S, Field TS, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289:1107-1116.
- Shapiro RS, Simpson DE, Lawrence SL, et al.. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989;149:2190-2196.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;227:558-559.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365-1370.
- Cohen JR. Apology and organizations: exploring an example from medical practice. Fordham Urban Law Journal. 2000;27:1447-1482.
- Cohen JR. Advising clients to apologize. Southern California Law Review. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care JAMA. 1994;272:1588-1591.
- Greenwald L. Who's in charge? Perspectives on Clinical Risk Management. Boston, Mass: ProMutual Group Risk Management Services; Fall 2000.
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9.
[H]ospitalists are in a very litigation-intensive and volatile environment. … [T]hey are practicing in a niche that has not been fully accepted by the medical community. There’s a lot of tension on various specialty groups as to the role of hospitalists, the value of hospitalists, whether for a variety of reasons they are creating impediments [to] the quality of care, possibly raising competitive concerns. And so the best trained, the best intentioned, and most capable hospitalist is choosing … a dangerous area of practice from a liability perspective.
—Barry Halpern, JD, Snell and Wilmer Law Offices, expert in medical malpractice law
As hospitalists move from patient to patient, consult to consult, and decision to decision, risk management—proactively identifying, assessing, and prioritizing risks with a goal of minimizing their negative consequences—may not stay uppermost in their minds. Yet for hospitalists, by virtue of their constant location and activity in hospitals, risks lurk at every corner, and the potential for being judged at fault is real and potentially costly.
What are the hospitalist’s risks of being sued for malpractice? How can hospitalists best protect themselves against malpractice claims? Does being liable for patient care ever cause hospitalists to handicap themselves, to hold back in some ways?
What Risks Do Hospitalists Face?
“I think the issue that hospitalists are facing from a medical-legal standpoint is there is not a lot of cumulative experience with case law, precedent, in the field of hospital medicine,” says Tom Baudendistel, MD, a hospitalist and associate program director at California Pacific Medical Center in San Francisco.
Besides errors of medical practice, hospitalists are at risk when they:
- Practice beyond the scope of their specialty;
- Fail to communicate or communicate poorly with patients, families, staff, and referring physicians; and
- Fail to exercise independent medical judgment.
Hospitalists work with sicker, more complicated patients in an environment where more things can go wrong. (See The Hospitalist, July/August 2002, “Hospitalists and the Malpractice Insurance Crisis.”) All things considered, hospital-based physicians are at greater risk of being sued than their colleagues who work in offices.
Case #1: The hospitalist failed to detect a vertebral artery dissection in a younger patient. Should they have been able to detect that? It’s a rather unusual stroke presentation. A neurologist would have picked it up—and certainly would have been held liable or negligent if they’d missed that diagnosis. During their training neurologists would have certainly seen this condition as a cause of stroke in someone below age 45. But internists, in general, don’t receive good neurologic training as part of their residencies, and in community hospitals there is no set neurology service.
Neurologists have now become more office-based and allow the hospitalists to do more. By doing more, they’re also exposed to more legal risk. Should the hospitalist be held negligent for missing an unusual stroke? It depends on what you think is a hospitalist’s scope of practice.
—Dr. Baudendistel
Scope of Practice
A hospitalist’s scope of practice is somewhat difficult to define, although the classification “hospitalist” is gaining clarity (including with insurance underwriters), and the hospitalist model is becoming more recognized as a subspecialty. (See “A Malpractice Primer,” The Hospitalist, Dec. 2005, p. 1.)
One challenge in defining the hospitalist’s scope of practice is that hospitalists do a variety of things and work in different departments of the hospital: Some spend more time in acute care, some are more in general care, and some of them are mostly in trauma care.
It is generally acknowledged that healthcare practitioners must employ the same degree of diligence and skill commonly possessed by other members of the healthcare profession who are engaged in the same kind of work in similar locales. Thus, hospitalists need to be acutely aware of how other hospitalists practice in similar settings with similar resources available.
Hospitalists in rural and suburban hospitals, which have fewer and less specialized staff readily available for consults, should expect to have a different scope of practice. In time further clarification of the roles, responsibilities, and clinical skills of hospitalists will be established so that the scope of practice is more clearly defined.
Dr. Baudendistel believes that residents tracking to specialize in hospital medicine could benefit from having more education in certain areas: neurology, perioperative medicine, and critical care.
SHM has recognized the need for better risk management strategies to protect hospitalists and will provide this information and continuing education in The Core Competencies in Hospital Medicine to be published the January/February 2006 issue of the Journal of Hospital Medicine.
Case #2: A male patient came into the ED at a rural hospital with an altered mental status. He had a history of falls and the CT scan in the ED showed a large subdural hematoma.
“We need to admit this patient to the hospital,” said the ED doc. “Call the hospitalist.”
“What does neurosurgery want to do?” asked the hospitalist.
The hospitalist tried to reach the neurosurgeon. And the ED doc wasn’t able to obtain neurosurgery consult because the neurosurgeon said that he wasn’t on call for that hospital. So the hospitalist was … left responsible without neurosurgery backup.
Ultimately, the patient worsened. The hospitalist called a different neurosurgeon at a different hospital who clearly wasn’t in charge of the patient. That doctor said, “Get the patient over to us, and we’ll take care of it.”
There was a 12-hour delay, and the patient finally got transferred to the other hospital, had surgery, and did OK. But he was definitely deteriorating.
The neurosurgeon who said he wasn’t on call for that hospital was wrong. He was lying or just didn’t know of his group’s call coverage. It was a clear violation. And it left the hospital in a situation that isn’t all that unfamiliar.
In this case, the hospitalist wasn’t at fault. There was clear chart documentation [provided as evidence] that said, “I called the neurosurgeon three times and they’re not calling back. Finally they called back the fourth time and said that they’re not coming in.” —Dr. Baudendistel
Communication
Communication is crucial in a clinician’s provision of quality care and also provides a safety net to help prevent liability. Communication with patients, families, staff, and other physicians—particularly their inpatients’ primary care physicians—provides the strongest armor against malpractice assaults. Timeliness and the urgency of the issue are key to patient care and are also are examined by those who review malpractice claims.
In recent years medical malpractice claims payouts have increased substantially for both jury verdicts and settlements. For monetary awards involving doctor-patient relations, which are largely predicated upon communication, the median payout is $230,000.1
Some hot-button areas that carry higher risk and call for meticulous communication between providers include:
- Inpatient postoperative care;
- Post-discharge communication (hand-offs);
- Diagnosis and treatment of a patient for whom there is an incomplete history; and
- Acceptance for treatment of patients whose medical conditions may either be unfamiliar to hospitalists or for which they have had limited or no training.
Communication with Patients
Communication—every aspect of it—is essential for the patient’s health, attitude, and satisfaction. Interestingly, legal data show that most patients who have bad outcomes don’t file suit.2 Although patients litigate for a variety of reasons, chief among them is when they perceive they have suffered because of administrative errors, rude practitioners or support staff, or the denial of tests and referrals they had requested and thought were reasonable.3 Data from a number of studies conducted within the past two decades show that although no particular communication skills can be directly associated with reducing malpractice claims, when patients perceive that their providers treat them genuinely and fairly, and update them honestly and regularly, they are less likely to sue.4-9
One-on-One with Barry Halpern, JD
My law firm practices throughout the western United States, and one of the areas that I see as a general pattern is when … continuity of care becomes an issue. The cases that are sometimes the most troublesome are those in which the hospitalist is involved.
There’s never a real clear demarcation of responsibility between, for instance, the surgery service and the hospitalist. Orders are written and then interpreted by the nursing staff in ways that, in retrospect, even the surgical service or the hospitalist are not pleased with. Yet the physicians aren’t talking to each other, and the documentation in the medical record is intermittent … .
Those kinds of situations, particularly where there is later alleged to have been, for instance, a medication error, become very difficult to defend. Because from the perspective of the lay jury that will be looking at the case, it’s easy for a plaintiff lawyer to depict a very disjointed and uncoordinated approach to care, when—in fact—the reality of practices is that they don’t always go perfectly and things aren’t always documented the instant that they are done.
And sometimes bad things happen despite everybody’s best efforts. But when you have a rough interface between the hospitalist and the other physicians with regard to responsibility for a patient, you are inviting a legal problem.
—Halpern is an attorney with Snell and Wilmer Law Offices, Phoenix
Case #3: A 72-year-old female who was pretty healthy (she had some high blood pressure) came in with abdominal pain. The ED doctor drew the laboratories, which suggested pancreatitis, and then investigated why she had pancreatitis. The ultrasound ordered by the ED doc showed gallstones. The physician then correctly inferred that she had gallstones causing her pancreatitis.
A hospitalist was called [and] admitted the patient. Surgery and GI consultants were called. The GI consultant first ordered an endoscopic retrograde cholangiopancreatography to clean the gallstones from the common bile duct. That went fine, and the next day the patient looked a little better. The GI service said, “Anticipated to go home in a couple days.” Surgery felt the same.
Then the consensus was to remove her gallbladder because eventually she would need to have it done. And that’s when things started to go badly.
On postoperative day two, the patient started having pain out of proportion to what should be expected. The internist (the hospitalist) raised that question in his note. The surgeon said, “No, that’s still postoperative pain,” and increased the pain medicine.
The hospitalist said, “I’m really concerned about this; I’ll talk to the surgeon.”
Again the surgeon said, “There’s nothing to worry about. I’ll at least order a HIDA scan.”
Initially the patient refused the scan, but the next day—postoperative day three—she was still having pain and was clearly worse. She had a high fever; her blood pressure dropped; and her white blood cell count climbed from 10,000 to 20,000, indicating infection/inflammation. Finally the hospitalist ordered a CT scan, which shows a perforation caused by the surgery.
The patient went to surgery for repair. As was predicted, she had a rocky hospital course and ultimately died a month later.
The surgeon was clearly in the wrong. … I was consulted and was asked, “What would you do with the hospitalist? What was their role in that case? Do you think he failed to meet the standard of care?”
—Dr. Baudendistel
Communication with Other Clinicians
“Communication between physicians is critical,” says Sally Whitaker, RN, BSN, risk manager with Rex Healthcare in Raleigh, N.C. “[Hospitalists] shouldn’t just rely on knowing they’ve put their notes on the discharge summary.”
At Rex Hospital (one of Rex Healthcare’s six facilities) where Whitaker works, when seminal events (those big bad things that happen) occur and result in severe trauma or death, the appropriate people meet to backtrack through the steps and scenarios that led to the breakdown.
“Fortunately we don’t have seminal events every day, but every day we do have things that go wrong,” she says. “ … And when we look at our Group Cause Analysis meetings, three-quarters of them [involve] communication issues.”
Exercise Independent Medical Judgment
Hospitalists should read their insurance and employer contracts carefully (especially those with a managed care organization) to ensure that the contract includes a statement allowing the physician to exercise independent medical judgment in the treatment of all patients. If that statement is not present, the hospitalist should request a revision in the contract to include such a statement.
In medical residency programs, a distinction is often made between being a consultant and being a co-manager, says Dr. Baudendistel, but “you have to assume there’s no legal difference between [the two].” Case #3 , he says, was a challenge to decide because the responsibilities of the surgeon and hospitalist in postoperative care were not clearly demarcated.
“I think the surgeon was probably saying, ‘I see this all the time and this is within the realm of what happens after one of these surgeries; let’s not be too worried yet,’” he says. “And I think the internist [hospitalist] ultimately pulled the trigger correctly and the [controversy later on pertained to] whether it should have been done a day or two earlier and whether that have mattered.”
This case illustrates that, although hospitalists are members of teams and partner with consultants and primary physicians, in the end they are managers of patient care and may (we hope rarely) have to break ranks to make aggressive care decisions.
“I think that the other thing that was in [the hospitalist’s] favor,” says Dr. Baudendistel of the case, “was that he was writing very thorough notes, [and] really was discussing everything with the family and everyone was on board. He was doing a very compassionate job … trying to manage this care.”
To Dr. Baudendistel, who is the chair of SHM’s ethics committee, this went a long way toward showing good faith.
Reducing Risks: Concern for the Medical Record
If the medical record is found deficient or illuminating in a negative way, it may serve the plaintiff attorney’s strategy well for establishing negligence or wrongdoing. The chart notes documented by nurses, attending staff, consultants, other residents, and therapists could either portray a smoothly managed case or a chronology of errors and omissions. The chart should never be cosigned and never merely assumed to be accurate.
When Things Go Wrong
Whitaker advises hospitalists to keep the lines of communication open. “Especially after something unexpected has happened,” she says. “So many times I think the human tendency is to just withdraw, or you feel terrible and you don’t know what to say, or you’re afraid you’re going to get emotional while you’re talking with the family.”
This is normal human response in these circumstances, but if you act on the impulse to withdraw and avoid the patient and family, or hold back, which may eventually lead to a filed claim from a family that feels abandoned.
“Until now the number of lawsuits has been really steady and the amount that we were paying in lawsuits was increasing,” says Whitaker. “However, we’re trying to work with the families earlier on so if we make a mistake and we realize that we made a mistake then we admit that. And we try to do what we can to make it right for that patient and their family.”
This often means reaching a fair and reasonable settlement, says Whitaker, “and [examining fair and reasonable means reviewing] the communication at the time the event occurred. Did we acknowledge that we made a mistake? Did we let them know we’d be willing to work with them? And did we let them know we [have since] made these changes … so they’ll … be reassured [that] hopefully it won’t happen again?”
Who’s in Charge?
Linda Greenwald, RN, MS, editor of risk management publications at ProMutual Insurance Group in Boston, wrote in the company’s newsletter, Perspectives on Clinical Risk Management, that in prior times, the question, “Who’s in charge?” was rhetorical.10 These days any number of generalists or specialists might claim that role. And therein lies the rub: Greenwald says that in many cases involving hospitalists the lines of responsibility are unclear and one or more systems may fail. If so, Greenwald writes, the result may be a malpractice claim alleging:
- Failure to diagnose when each of two physicians assumes the other has responsibility for follow-up;
- Negligence in treatment when one physician fails to monitor on an outpatient basis the medication first prescribed by another physician when the patient was an inpatient; and/or
- Negligent care when a patient misinterprets the information one physician asks him or her to relay to another physician.10
Halpern concurs that the modern mix of professionals working as a team on hospital care can be a major challenge.
“In olden days, when a primary care physician referred to a surgeon, and the surgeon performed surgery, and the surgeon took responsibility for postoperative care, and occasionally brought in a consultant, the lines were relatively clear,” says Halpern. “When a hospitalist is injected into the mix, unless the hospital has really clear procedures and unless everybody is comfortable with the system and everybody is talking to each other and agreeing on the lines of demarcation, you’re creating a soup that plaintiff lawyers would be happy to stir.”
The more murky the communication, the greater the liability. “And when you have murky lines of communication, murky lines of responsibility, and a medical catastrophe,” says Halpern, “human nature compounds the problem by frequently causing a finger-pointing contest, where each component of the patient care team circles its own wagons [and] points in a different direction. And that is the absolute worst thing that can happen when trying to deal with a patient injury claim.”
Summary
The hospitalist’s primary risk for malpractice claims may be inadequate or absent patient follow-up resulting from a lack of communication. The best means of protection from claims is for hospitalists to incorporate a comprehensive risk management program into their practice.
Several strategies have proved successful to help prevent litigation. In general, hospitalists should make sure that their hospital has clearly delineated policies regarding responsibility for patients; clearly understand—and ensure that your coworkers, colleagues, and referring physicians understand—the hospital’s systems and protocols; exercise good communication skills; conform to the standard of care; know your own scope of care to the best of your ability; and exercise independent medical judgment, even when partnering with others. TH
Andrea Sattinger also writes the “Alliances” department for The Hospitalist.
References
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003;348:2281-2284.
- Virshup BB, Oppenberg MPH, Coleman MM. Strategic risk management: reducing malpractice claims through more effective patient-doctor communication. Am J Med Quality. 1999;14:153-159.
- Gurwitz JH, Terry S, Field TS, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289:1107-1116.
- Shapiro RS, Simpson DE, Lawrence SL, et al.. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989;149:2190-2196.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;227:558-559.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365-1370.
- Cohen JR. Apology and organizations: exploring an example from medical practice. Fordham Urban Law Journal. 2000;27:1447-1482.
- Cohen JR. Advising clients to apologize. Southern California Law Review. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care JAMA. 1994;272:1588-1591.
- Greenwald L. Who's in charge? Perspectives on Clinical Risk Management. Boston, Mass: ProMutual Group Risk Management Services; Fall 2000.
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9.
Evaluating and managing hypogammaglobulinemia
A Patch Test Study to Evaluate the Allergenicity of a Metallic Jewelry Alloy in Patients Allergic to Cobalt
Can a vaccine prevent Alzheimer’s disease?
Deposition of amyloid-β peptide (Aβ) is believed to contribute to Alzheimer’s disease (AD) pathogenesis. Derived from a larger precursor protein, Aβ aggregates into plaques, and may promote neuronal death and, ultimately, dementia.
Current treatments alleviate symptoms without slowing underlying neurodegeneration. The prospect of harnessing the immune system to target the Aβ peptide offers an intriguing option for preventing this devastating, increasingly common disease.
Anti-a BETA antibodies
Transgenic mice bred to overexpress AD genes have responded remarkably in studies using the immune system to target the amyloid-β peptide.3 Several mouse groups have shown plaque reduction (Figure 1) and improved cognitive performance. These findings substantiate the amyloid hypothesis in AD pathogenesis.
A host could acquire anti-Aβ antibodies though two basic approaches (Figure 2):2
Figure 1 Differences in amyloid deposition between control and immunized mice
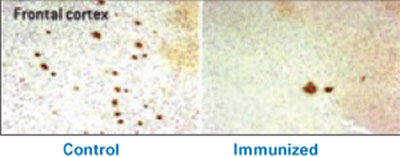
Frontal cortex of an unvaccinated mouse (left) shows more amyloid deposits (dark spots) than that of a mouse producing antibodies against the amyloid-β peptide (right).
Source: Image by Cynthia A. Lemere, PhD. Used with permission.Active immunization exposes the subject to the antigen (in this case the Aβ peptide) and allows T cells and B cells to produce anti-Aβ antibodies. This approach has been studied in humans, but adverse effects have stymied its development.
Passive immunization, which involves developing anti-Aβ antibodies in a separate source, aims to clear Aβ peptide without requiring an immunologic response from the host. Large doses of antibodies administered weekly or monthly would be needed to build adequate plasma levels in the CNS, and large quantities of circulating antibodies could cause hemorrhagic stroke.
A troublesome trial
After successful preclinical and phase 1 testing of a vaccine against the Aβ peptide (called AN-1792), a phase 2a placebo-controlled trial in 2001 followed patients with mild to moderate AD. Drug administration was halted after 18 patients (6%) developed meningoencephalitis after several months.4 However, 300 patients with AD and 72 control patients had received at least one injection, and double-blind assessments were maintained for 12 months.
Figure 2 Methods for immunizing against Aβ peptide
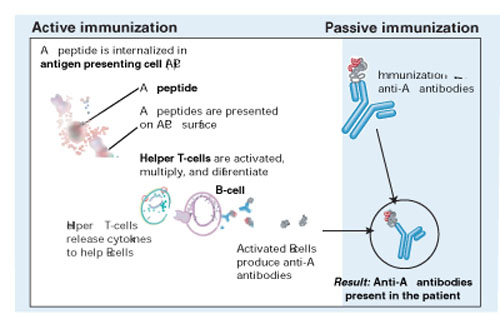
Active immunization produces anti-Aβ antibodies via immunologic response to vaccination. With passive immunization, anti-Aβ antibodies are administered directly.
Illustration by Rich LaRocco.All patients with meningoencephalitis had received the vaccine but not all developed an immune response, suggesting that something other than the antibodies—such as T cells—caused the encephalitis. Twelve patients recovered, but six had persistent cognitive and neurologic deficits.
More-optimistic news
Of the 300 patients who received an active vaccine, 20% developed an adequate antibody response.5
The responders showed no significant difference from the placebo group in most outcome measures but showed less worsening in the nine-component Neuropsychological Test Battery (NTB) (P=0.02). Of particular interest, antibody responders showed significant improvement in the NTB—s memory domain (P=0.03). Further, subjects with higher IgG antibody titers showed greater improvement than did other responders.
More work ahead
Although the outcome of this initial AN-1792 trial is disappointing because of its discontinuation and mixed results, T cell infiltration and amyloid depletion were found during postmortem examinations of two vaccine recipients.6
Pharmaceutical companies are testing two compounds for AD immunotherapy:7
- AAB-001, a human monoclonal antibody, targets all 42 Aβ amino acids via passive immunization and has entered phase 2 trials.
- ACC-001, an Aβ immuno-conjugate designed to elicit an active antibody response, began phase 1 testing last fall.
These efforts suggest that an “Alzheimer’s vaccine” could be produced, provided it could attack the Aβ peptide without inducing a significant cellular reaction.
1. Neugroschl JA, Kolevzor A, Samuels SC, Marir DB. Dementia. In: Sadock BJ, Sadock VA (eds). Kaplan & Sadock’s comprehensive text-book of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins; 2005:1068-93.
2. Schenk D. Amyloid-beta immunotherapy for Alzheimer’s disease: the end of the beginning. Nat Rev Neurosci 2002;3:824-8.
3. Schenk D, Hagen M, Seubert P. Current progress in beta-amyloid immunotherapy. Current Opin Immunol 2004;16:599-606.
4. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoen-cephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003;61:46-54.
5. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005;64:1553-62.
6. Ferrer I, Boada Rovira M, Sanchez Guerra ML, et al. Neuropathology and pathogenesis of encephalitis following amyloid-beta immunization in Alzheimer’s disease. Brain Pathology 2004;14(1):11-20.
7. Sullivan MG. Immunotherapy studies for AD back on track. Psychiatry News 2005;33(11):69.-
Deposition of amyloid-β peptide (Aβ) is believed to contribute to Alzheimer’s disease (AD) pathogenesis. Derived from a larger precursor protein, Aβ aggregates into plaques, and may promote neuronal death and, ultimately, dementia.
Current treatments alleviate symptoms without slowing underlying neurodegeneration. The prospect of harnessing the immune system to target the Aβ peptide offers an intriguing option for preventing this devastating, increasingly common disease.
Anti-a BETA antibodies
Transgenic mice bred to overexpress AD genes have responded remarkably in studies using the immune system to target the amyloid-β peptide.3 Several mouse groups have shown plaque reduction (Figure 1) and improved cognitive performance. These findings substantiate the amyloid hypothesis in AD pathogenesis.
A host could acquire anti-Aβ antibodies though two basic approaches (Figure 2):2
Figure 1 Differences in amyloid deposition between control and immunized mice
Frontal cortex of an unvaccinated mouse (left) shows more amyloid deposits (dark spots) than that of a mouse producing antibodies against the amyloid-β peptide (right).
Source: Image by Cynthia A. Lemere, PhD. Used with permission.Active immunization exposes the subject to the antigen (in this case the Aβ peptide) and allows T cells and B cells to produce anti-Aβ antibodies. This approach has been studied in humans, but adverse effects have stymied its development.
Passive immunization, which involves developing anti-Aβ antibodies in a separate source, aims to clear Aβ peptide without requiring an immunologic response from the host. Large doses of antibodies administered weekly or monthly would be needed to build adequate plasma levels in the CNS, and large quantities of circulating antibodies could cause hemorrhagic stroke.
A troublesome trial
After successful preclinical and phase 1 testing of a vaccine against the Aβ peptide (called AN-1792), a phase 2a placebo-controlled trial in 2001 followed patients with mild to moderate AD. Drug administration was halted after 18 patients (6%) developed meningoencephalitis after several months.4 However, 300 patients with AD and 72 control patients had received at least one injection, and double-blind assessments were maintained for 12 months.
Figure 2 Methods for immunizing against Aβ peptide
Active immunization produces anti-Aβ antibodies via immunologic response to vaccination. With passive immunization, anti-Aβ antibodies are administered directly.
Illustration by Rich LaRocco.All patients with meningoencephalitis had received the vaccine but not all developed an immune response, suggesting that something other than the antibodies—such as T cells—caused the encephalitis. Twelve patients recovered, but six had persistent cognitive and neurologic deficits.
More-optimistic news
Of the 300 patients who received an active vaccine, 20% developed an adequate antibody response.5
The responders showed no significant difference from the placebo group in most outcome measures but showed less worsening in the nine-component Neuropsychological Test Battery (NTB) (P=0.02). Of particular interest, antibody responders showed significant improvement in the NTB—s memory domain (P=0.03). Further, subjects with higher IgG antibody titers showed greater improvement than did other responders.
More work ahead
Although the outcome of this initial AN-1792 trial is disappointing because of its discontinuation and mixed results, T cell infiltration and amyloid depletion were found during postmortem examinations of two vaccine recipients.6
Pharmaceutical companies are testing two compounds for AD immunotherapy:7
- AAB-001, a human monoclonal antibody, targets all 42 Aβ amino acids via passive immunization and has entered phase 2 trials.
- ACC-001, an Aβ immuno-conjugate designed to elicit an active antibody response, began phase 1 testing last fall.
These efforts suggest that an “Alzheimer’s vaccine” could be produced, provided it could attack the Aβ peptide without inducing a significant cellular reaction.
Deposition of amyloid-β peptide (Aβ) is believed to contribute to Alzheimer’s disease (AD) pathogenesis. Derived from a larger precursor protein, Aβ aggregates into plaques, and may promote neuronal death and, ultimately, dementia.
Current treatments alleviate symptoms without slowing underlying neurodegeneration. The prospect of harnessing the immune system to target the Aβ peptide offers an intriguing option for preventing this devastating, increasingly common disease.
Anti-a BETA antibodies
Transgenic mice bred to overexpress AD genes have responded remarkably in studies using the immune system to target the amyloid-β peptide.3 Several mouse groups have shown plaque reduction (Figure 1) and improved cognitive performance. These findings substantiate the amyloid hypothesis in AD pathogenesis.
A host could acquire anti-Aβ antibodies though two basic approaches (Figure 2):2
Figure 1 Differences in amyloid deposition between control and immunized mice
Frontal cortex of an unvaccinated mouse (left) shows more amyloid deposits (dark spots) than that of a mouse producing antibodies against the amyloid-β peptide (right).
Source: Image by Cynthia A. Lemere, PhD. Used with permission.Active immunization exposes the subject to the antigen (in this case the Aβ peptide) and allows T cells and B cells to produce anti-Aβ antibodies. This approach has been studied in humans, but adverse effects have stymied its development.
Passive immunization, which involves developing anti-Aβ antibodies in a separate source, aims to clear Aβ peptide without requiring an immunologic response from the host. Large doses of antibodies administered weekly or monthly would be needed to build adequate plasma levels in the CNS, and large quantities of circulating antibodies could cause hemorrhagic stroke.
A troublesome trial
After successful preclinical and phase 1 testing of a vaccine against the Aβ peptide (called AN-1792), a phase 2a placebo-controlled trial in 2001 followed patients with mild to moderate AD. Drug administration was halted after 18 patients (6%) developed meningoencephalitis after several months.4 However, 300 patients with AD and 72 control patients had received at least one injection, and double-blind assessments were maintained for 12 months.
Figure 2 Methods for immunizing against Aβ peptide
Active immunization produces anti-Aβ antibodies via immunologic response to vaccination. With passive immunization, anti-Aβ antibodies are administered directly.
Illustration by Rich LaRocco.All patients with meningoencephalitis had received the vaccine but not all developed an immune response, suggesting that something other than the antibodies—such as T cells—caused the encephalitis. Twelve patients recovered, but six had persistent cognitive and neurologic deficits.
More-optimistic news
Of the 300 patients who received an active vaccine, 20% developed an adequate antibody response.5
The responders showed no significant difference from the placebo group in most outcome measures but showed less worsening in the nine-component Neuropsychological Test Battery (NTB) (P=0.02). Of particular interest, antibody responders showed significant improvement in the NTB—s memory domain (P=0.03). Further, subjects with higher IgG antibody titers showed greater improvement than did other responders.
More work ahead
Although the outcome of this initial AN-1792 trial is disappointing because of its discontinuation and mixed results, T cell infiltration and amyloid depletion were found during postmortem examinations of two vaccine recipients.6
Pharmaceutical companies are testing two compounds for AD immunotherapy:7
- AAB-001, a human monoclonal antibody, targets all 42 Aβ amino acids via passive immunization and has entered phase 2 trials.
- ACC-001, an Aβ immuno-conjugate designed to elicit an active antibody response, began phase 1 testing last fall.
These efforts suggest that an “Alzheimer’s vaccine” could be produced, provided it could attack the Aβ peptide without inducing a significant cellular reaction.
1. Neugroschl JA, Kolevzor A, Samuels SC, Marir DB. Dementia. In: Sadock BJ, Sadock VA (eds). Kaplan & Sadock’s comprehensive text-book of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins; 2005:1068-93.
2. Schenk D. Amyloid-beta immunotherapy for Alzheimer’s disease: the end of the beginning. Nat Rev Neurosci 2002;3:824-8.
3. Schenk D, Hagen M, Seubert P. Current progress in beta-amyloid immunotherapy. Current Opin Immunol 2004;16:599-606.
4. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoen-cephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003;61:46-54.
5. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005;64:1553-62.
6. Ferrer I, Boada Rovira M, Sanchez Guerra ML, et al. Neuropathology and pathogenesis of encephalitis following amyloid-beta immunization in Alzheimer’s disease. Brain Pathology 2004;14(1):11-20.
7. Sullivan MG. Immunotherapy studies for AD back on track. Psychiatry News 2005;33(11):69.-
1. Neugroschl JA, Kolevzor A, Samuels SC, Marir DB. Dementia. In: Sadock BJ, Sadock VA (eds). Kaplan & Sadock’s comprehensive text-book of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins; 2005:1068-93.
2. Schenk D. Amyloid-beta immunotherapy for Alzheimer’s disease: the end of the beginning. Nat Rev Neurosci 2002;3:824-8.
3. Schenk D, Hagen M, Seubert P. Current progress in beta-amyloid immunotherapy. Current Opin Immunol 2004;16:599-606.
4. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoen-cephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003;61:46-54.
5. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005;64:1553-62.
6. Ferrer I, Boada Rovira M, Sanchez Guerra ML, et al. Neuropathology and pathogenesis of encephalitis following amyloid-beta immunization in Alzheimer’s disease. Brain Pathology 2004;14(1):11-20.
7. Sullivan MG. Immunotherapy studies for AD back on track. Psychiatry News 2005;33(11):69.-
What to tell patients about side effects
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Adult with ADHD? Try medication + psychotherapy
Mr. B, age 50, dreams of becoming a computer programmer but fears he will embarrass himself—as he has in many classrooms before. He is seeking evaluation because his teenage son was recently diagnosed with attention-deficit/hyperactivity disorder (ADHD), and he recognizes similar symptoms in himself.
Mr. B received a college degree with great difficulty, putting off assignments until the last minute and “squeaking by.” For years he has changed occupations often, never progressing beyond entry level, and now works as a personal care provider and limousine driver. He reports problems keeping up with work and managing time.
His history includes early childhood hyperactivity, difficulty sitting through classes, sloppy handwriting, disorganization, short attention span, and distractibility. He is restless, fidgety, and has trouble staying on topic. His disorganization has caused marital difficulties, for which he has sought counseling.
After careful evaluation, you determine that Mr. B meets criteria for ADHD, combined type, and for anxiety disorder not otherwise specified. His treatment goals are to increase his ability to focus; procrastinate less; improve his planning, prioritizing, and self-esteem; and to become less sensitive to criticism and less anxious about handling work demands.
Like Mr. B, adults with ADHD need treatment for the disorder’s core symptoms as well as its psychiatric comorbidities and psychosocial consequences. Comprehensive treatment with medications, cognitive-behavioral therapy (CBT), and environmental adaptations is usually recommended.
Comorbidity rules
Core symptoms. ADHD is a lifespan disorder with multiple behavioral, cognitive, and emotional manifestations that impair relationships and academic and vocational functioning. ADHD-like symptoms are seen in other conditions such as mood disorders or substance abuse, but complaints of inattention, distractibility, procrastination, restlessness, and impulsivity—particularly when pervasive and chronic—are highly indicative of ADHD.
In treating adults with ADHD, we have noticed common behavioral patterns that contribute to their psychosocial problems (Table 1). Dysfunctional coping behaviors have short-term advantages, but patients readily admit they would rather accomplish tasks through greater thought and planning.
Chronic frustrations—often associated with deep shame—are typical of adult ADHD. Many patients have maladaptive core beliefs of failure, self-mistrust, and inadequacy (Table 2).
Table 1
Common dysfunctional behavioral patterns in adults with ADHD
| Behavior | Description | Short-term gain/long-term loss |
|---|---|---|
| Anticipatory avoidance | Magnifying the difficulty of a pending task and doubts about being able to complete it; results in rationalizations to justify procrastination | Defers short-term stress, but often creates a self-fulfilling prophecy because the task looms and may seem overwhelming when facing a deadline |
| Brinksmanship | Waiting until the last moment (eg, the night before) to complete a task, often when facing an impending deadline | Deadline-associated stress can be focusing, but this tactic leaves little room for error and may yield a substandard result |
| Pseudoefficiency | Completing several low-priority, manageable tasks (eg, checking e-mail) but avoiding high-priority tasks (eg, a project for work) | Creates sense of productivity by reducing items on to-do list but defers a more difficult project |
| Juggling | Taking on new, exciting projects and feeling ‘busy’ without completing projects already started | It is easier to become motivated to start a novel project than to complete an ongoing one; pattern usually results in several incomplete projects |
Table 2
5 common maladaptive core beliefs of adults with ADHD
| Self-mistrust | ‘I cannot rely on myself to do what I need to do. I let myself down’ |
| Failure | ‘I always have failed and always will fail at what I set out to do.’ |
| Inadequacy | ‘I am basically a bad and defective person.’ |
| Incompetence | ‘I am too inept to handle life’s basic demands.’ |
| Instability | ‘My life will always be chaotic and in turmoil.’ |
Psychiatric comorbidity is the rule in adults with ADHD (Table 3). For example, among 43 patients who received combined medication and CBT at the University of Pennsylvania Adult ADHD Treatment and Research Program, 75% reported at least one comorbid condition, including:
- 27 (63%) with mood disorder
- 23 (54%) with anxiety disorder
- 5 (12%) with substance abuse.1
Other treatment studies have reported similar comorbidity rates in adults with ADHD.2-4
Table 3
Psychiatric comorbidity in adult ADHD
| Disorder | Prevalence |
|---|---|
| Mood disorders | 50% to 65% |
| Recurrent depression | |
| Bipolar disorder | |
| Cyclothymia | |
| Dysthymia | |
| Depressive disorder NOS | |
| Anxiety disorders | 40% to 55% |
| Generalized anxiety disorder | |
| Anxiety disorder NOS | |
| Others | Various |
| Substance use disorder | |
| Learning disabilities | |
| Intermittent explosive disorder | |
| Tourette syndrome | |
| Antisocial personality | |
| Borderline personality disorder | |
| Dependent personality | |
| NOS: Not otherwise specified | |
Making the diagnosis
Diagnosis of adult ADHD is based on a comprehensive assessment, including:
- careful history of presenting complaints
- thorough review of educational, occupational, and family history
- standardized rating scales (such as the Barkley ADHD Behavior Checklists, the Conners’ Adult ADHD Rating Scale, or the Brown Attention Deficit Disorder Scales)
- collateral information
- assessment of mood, anxiety, substance use, and learning/organizational skills. For details, consult references on adult ADHD.5-8
Case continued: Self-fulfilling prophesies
On standardized rating scales, Mr. B meets criteria for combined ADHD for childhood and current symptoms. Information from his wife and brother also confirms the ADHD diagnosis.
He is motivated, resilient, optimistic, and has a good support system. However, his negative automatic thoughts about his ability to succeed in school and to handle increasing time demands suggest deeper beliefs of inadequacy and failure.
Mr. B struggled academically. Without guidance about how to change his approach to difficult situations, he has repeated old thinking and behavior patterns. Believing he will embarrass himself and fail to learn required material, Mr. B procrastinates and avoids doing assignments. In class, his feelings of inadequacy make him self-conscious, which causes him to lose focus and have trouble concentrating.
See the world through the patient’s eyes
Understanding your patient. Before you start treatment, we recommend that you conceptualize how ADHD has influenced your patient’s life, including:
- developmental experiences
- family-of-origin issues, such as conflicts with parents stemming from ADHD symptoms or reciprocal interactions with an ADHD parent
- world view (“schemata”)
- patterns of coping with (or avoiding) stress
- attitudes toward self and important others
- readiness to change.
Developing a working case conceptualization is a dynamic, collaborative process. You talk with patients, and encourage them to reflect on how ADHD affects their view of themselves and their important relationships. The conceptualization takes shape as you:
- observe patients’ behaviors
- elicit how they think and feel
- assess with them the relevance and accuracies of their belief systems and response patterns.
Seeing the world “through their eyes” prepares you to help them accept the diagnosis and learn to manage ADHD symptoms. Then, by providing a blueprint to manage what patients may see as uncontrollable responses, you can help them take charge of their automatic reactions.
Psychoeducation. To set the stage for treatment, encourage patients to learn about ADHD by reading articles and books and consulting Web sites for adults with ADHD (see Related resources). Psychoeducation helps patients:
- review possible treatment approaches, including organizational (environmental) management, medication, and psychotherapy (individual or group)
- become informed participants in setting treatment goals.
Explain the relative contribution of each treatment component. For example, medications can reduce distractibility and improve attention, organizational strategies can reduce disorganization and improve time management, and structured psychotherapy can help the patient develop more effective coping skills.
Case continued: Planning combined treatment
You discuss diagnosis and treatment options with Mr. B, and he agrees to start the methylphenidate compound Concerta, initially at 18 mg/d, and weekly CBT sessions. You recommended a stimulant based on efficacy studies and your clinical experience in treating adults with ADHD. Mr. B wants a medication that will help him focus while working or studying, and he says Concerta has improved his son’s ADHD symptoms.
You instruct Mr. B to increase the dosage by 18 mg each week until he reaches 72 mg/d. You also tell him to keep a medication response log and to note any positive changes and side effects.
If an adult with ADHD expresses preference for a particular medication, we usually prescribe that one first. Most patients to whom we offer both medication and psychotherapy agree to this “top-down” and “bottom-up” approach. “Top down” means giving patients new ways of thinking to help them understand and modify their responses. “Bottom up” refers to the medication reducing their impulsivity, distractibility, and inattentiveness.
CBT for adult ADHD
Medications can ameliorate key symptoms of adult ADHD, but adjunctive interventions are needed to improve functioning and quality of life. Evidence supporting psychosocial treatment for adults with ADHD is limited, but CBT has been studied the most.1,9-13 Safren et al13 found a four-fold greater therapeutic response when patients received adjunctive CBT for residual ADHD symptoms, compared with patients who received medication alone.
We usually provide CBT weekly for 12 weeks and then taper to 8 additional sessions over 3 months (total 20 sessions). We may extend CBT with additional sessions to address complicated issues. CBT helps adults with ADHD to:
- identify dysfunctional thinking, feeling, and behaving patterns
- recognize contexts in which patterns arise
- systematically change these patterns.
CBT can reduce ADHD-associated anxiety and depression and improve coping skills and sense of well-being.1,9,11 Its flexibility allows you to address family issues with patients’ partners, children and other relatives to improve communication, reduce conflict, and develop healthier interactions.
We focus CBT sessions on finding alternate coping strategies. We might try role playing, rehearsing, creating “thought experiments,” and anticipating and preparing to modify typical patterns of avoidance. These approaches have been described elsewhere.10,11,14
We adopt an active stance during therapy to keep ADHD patients’ distractibility from disrupting our conversation. For example, we set the therapeutic agenda, provide feedback about patients’ behaviors, and encourage them to clarify rewards and consequences of using (or avoiding) problem-solving strategies.
Although we typically assign between-session homework, we expect patients to have difficulty completing it. We remain nonjudgmental and collaborative, viewing incomplete assignments as opportunities to learn about patients’ unproductive problem solving and to help them develop more-effective patterns.
Challenging maladaptive beliefs. A strong therapeutic relationship allows adults with ADHD to discuss their chronic frustrations, which often are associated with deep shame. We then shift CBT’s focus to deeper ADHD-related schemata that perpetuate dysfunctional patterns.
We work with patients to elucidate and challenge their maladaptive core beliefs and encourage new ways to view themselves and others. Allowing patients to grieve about the limitations ADHD imposes on their lives also helps to reduce chronic negative self-esteem.
Case continued: ‘less frenetic’
Mr. B achieves good results within 3 weeks of an increasing titration of stimulant medication, reporting significantly less restlessness and greater concentration without significant side effects. His wife confirms that he is less frenetic, can converse without interruptions, and is better at managing his complicated work schedule.
Which medications?
Drug therapy for adult ADHD is not as well-studied as in children and adolescents, but American Academy of Child and Adolescent Psychiatry guidelines and others15-18 recommend stimulant and nonstimulant medications. Your choice depends on the patient’s clinical profile (including risk factors and comorbid conditions), past medication use, treatment goals, preferred medication effects and dosing patterns (once-daily versus multiple times), and potential side effects. Stimulants or atomoxetine are first-line choices for adult ADHD without psychiatric comorbidity.
Stimulants work quickly and are cleared relatively rapidly from the brain without causing euphoria or dependency. They are effective (80% to 90% response rate) and well-tolerated, though long-term effects have not been studied in adults (Table 4).
Stimulants’ effect size of 0.9 is considered substantial. Effect size—a statistical method of reporting an intervention’s effect across different studies—is typically rated as:
- <0.32 very small
- 0.33 to 0.54, moderate
- >0.55, significant or very strong.
When choosing a medication, we usually try methylphenidate and amphetamine first, one after the other. We explain to the patient how stimulants work in the brain and the need for a comparative trial to determine which might work best for him or her. If the patient has tried a stimulant and found it helpful, we start with that class. Similarly, if he/she has not had good results with one type, we start with the other. Approximately one-third of our patients respond equally well to methylphenidate or amphetamine, one-third respond better to methylphenidate, and one-third respond better to amphetamine.
To determine the optimal dosage, we usually titrate up from 10 to 30 mg per dose of an immediate-release preparation. We begin with this form to help patients notice the medication’s onset and duration of action. After we find the optimal dosage, we switch to a longer-acting preparation.
Insomnia, mood instability, and euphoria are unacceptable stimulant side effects, although many patients welcome others such as appetite suppression and weight loss. Closely monitor cardiovascular effects, and review potential interactions with other medications, such as antihypertensives or bronchodilators. Because sudden death has been reported with stimulants in persons with structural cardiac lesions,19 obtain a cardiology consultation for patients with a history of heart disease.
We encourage patients to keep daily medication logs (Box), which we review at each visit and use to make dosing or medication changes. Dosing guidelines resemble those used for children and adolescents, although adults usually tolerate higher maximum dosages (such as methylphenidate, 80 to 100 mg/d).
Because of stimulants’ potential for recreational misuse and abuse, remain wary about choosing stimulants for patients with whom you lack a solid doctor-patient relationship.
Table 4
Stimulant dosages used in treating adult ADHD
| Class (brand name) | Daily dosing | Typical dosing schedule |
|---|---|---|
| Methylphenidate | ||
| Short-acting (Metadate, Ritadex, Ritalin) | Two to four times | 10 to 40 mg bid to qid |
| Intermediate-acting (Metadate SR, Ritalin SR) | Once or twice | 20 to 60 mg qd to bid |
| Extended-release (Concerta, Metadate CD, Ritalin LA) | Once or twice | 18 to 108 mg qd (Concerta) 20 to 40 mg bid (Ritalin LA, Metadate CD) |
| Dextromethylphenidate | ||
| Short-acting (Focalin) | Two to four times | 5 to 20 mg bid to qid |
| Long-acting (Focalin XR) | Once or twice | 10 to 20 mg qd or bid |
| Dextroamphetamine | ||
| Short-acting (Dexedrine) | Twice or three times | 10 to 30 mg bid or tid |
| Intermediate-acting (Dexedrine spansules) | Once or twice | 10 to 30 mg bid |
| Mixed amphetamine salts | ||
| Intermediate-acting (Adderall) | Once or twice | 10 to 30 mg bid or tid |
| Extended-release (Adderall XR) | Once or twice | 10 to 40 mg qd or bid |
Atomoxetine, a nonstimulant, norepinephrine re-uptake inhibitor, is approved for ADHD in adults.20-22 In two double-blind, controlled, randomized trials totalling 536 adults, Michaelson et al20 found significantly reduced ADHD symptoms after 10 weeks of atomoxetine treatment. Effect sizes of 0.35 and 0.40 were reported, with 10% of patients discontinuing because of side effects.
Atomoxetine has a long duration of action (>12 hours) but a more gradual onset (4 to 6 weeks) than that of stimulants. Approximately 60% of patients respond to atomoxetine, though effect sizes are less than those of stimulants. We have found atomoxetine works well for patients who:
- do not tolerate or are uncomfortable with taking stimulants
- are highly anxious
- report emotional dysregulation as a major target symptom.
To reduce risk of common side effects (nausea, GI upset, headache, sedation, reduced sex drive), we start with low dosages (such as 25 mg bid) and increase weekly by 25 mg to a target of 80 to 100 mg/d.
Treating complicated ADHD
Bupropion or tricyclic antidepressants are reasonable options for ADHD with depression. Atomoxetine, a tricyclic, or a stimulant plus a selective serotonin reuptake inhibitor (SSRI) can provide good symptom relief for adults with ADHD and comorbid anxiety and/or depression.
Bupropion. Approximately 50% of adults with ADHD respond to bupropion,23,24 with a treatment effect size of 0.6. Bupropion’s efficacy in smoking cessation adds value for those trying to quit.
We usually start extended-release bupropion at 150 mg/d and increase after 2 weeks to 300 mg/d if response is suboptimal. Headache, dry mouth, insomnia, and nausea are the most common adverse effects. Agitation or irritability is sometimes serious enough to warrant stopping bupropion.
Combining medications. Using SSRIs with stimulants can help adults with ADHD and comorbid anxiety or depression. Any SSRI can be safely combined with stimulants, though we tend to pick:
- more-sedating agents such as paroxetine or sertraline when patients report difficulty with insomnia or overactivation
- less-sedating compounds such as fluoxetine or citalopram when patients complain of being too tired or underactive.
When patients taking SSRIs seek help for ADHD, adding a stimulant usually reduces inattention, distractibility, impulsivity, and/or subjective feelings of restlessness. We prescribe usual dosages because stimulants and SSRIs do not interact. We have not seen serious side effects, but some patients report feeling oversedated.
Tricyclics. We use tricyclics when a stimulant/SSRI combination does not relieve symptoms satisfactorily or a patient complains of side effects. We usually have good results with desipramine or imipramine, 150 to 300 mg/d, or nortriptyline, 50 to 150 mg/d. Spencer et al have reported a response rate of 68% with nortriptyline or desipramine in a retrospective chart review25 and a prospective placebo-controlled trial26 of adults with ADHD.
Case continued: Closer to dream job
After 6 months of combined treatment, Mr. B reports much-improved ADHD symptoms, with minimal stimulant-related side effects. He has made some realistic plans for computer programming school and is taking preliminary courses. Keeping a schedule book has reduced his tardiness and tendency to procrastinate.
He is more comfortable in the classroom and better able to challenge self-critical thinking. When routine difficulties arise, he is using more-adaptive coping strategies. To maintain gains achieved in therapy, he chooses to continue periodic CBT booster sessions.
Long-term treatment
Even with medication and CBT, patients may require referral for organizational coaching, academic counseling, school or workplace accommodations, vocational counseling, cognitive remediation, group therapy, or social skills classes. You can help them obtain quality adjunctive care by collaborating with professionals who offer these services.
No studies have examined long-term care of adults with ADHD. In our experience, ongoing medication and intermittent therapy can sustain symptom control and coping skills for years. Most patients are initially skeptical about staying on medication, but after they experience the benefits most seem willing to continue as long as the medication helps.
Most of our patients sustain changes in thinking, feeling, and behaving that they learn through BT. They may seek additional sessions to meet a challenge, such as a new job or starting a family.
Books
- Kolberg J, Nadeau K. ADD-friendly ways to organize your life. New York: Brunner-Routledge; 2002.
- Hallowell EM, Ratey JJ. Driven to distraction. New York: Touchstone; 1994.
- Hallowell E, Ratey J. Delivered from distraction. New York: Ballantine Books; 2005.
Organizations
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). National Resource Center on AD/HD. www.chadd.org.
- Attention Deficit Disorder Association (ADDA). Resources and membership organization for adults with ADHD. www.add.org.
Drug brand names
- Amphetamine • Adderall, Dexedrine
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Imipramine • Tofranil
- Methylphenidate • Concerta, Focalin, Metadate, Ritalin
- Nortriptyline • Aventyl, Pamelor
Disclosures
Dr. Rostain is a consultant to Shire Pharamaceuticals Group and a speaker for Eli Lilly & Co. and Ortho-McNeil Pharmaceutical
Dr. Ramsay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rostain AL, Ramsay JR. A combined treatment approach for adults with attention-deficit/hyperactivity disorder. Results of an open study of 43 patients J Attention Disorders. In press.
2. Shekim WO, Asarnow RF, Hess E, et al. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Comp Psychiatry 1990;31:416-25.
3. Biederman J, Faraone SV, Spencer T, et al. Patterns of psychiatric comorbidity, cognition and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:1792-8.
4. Wilens TE, Biederman J, Spencer T. Attention-deficit/hyperactivity disorder across the lifespan. Ann Rev Medicine 2002;53:113-31.
5. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guilford Press; 1998.
6. Wender PH. ADHD: Attention-deficit hyperactivity disorder in children and adults. New York: Oxford University Press; 2000.
7. Goldstein S, Ellison AT. Clinician’s guide to adult ADHD. San Diego: Academic Press; 2000.
8. Brown TE. Attention-deficit disorder: the unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
9. Wilens TE, McDermott SP, Biederman J, et al. Cognitive therapy in the treatment of adults with ADHD: a systematic chart review of 26 cases. J Cogn Ther 1999;13:215-26.
10. Ramsay JR, Rostain AL. A cognitive therapy approach for adult attention-deficit/hyperactivity disorder. J Cogn Psychother 2003;17:319-34.
11. Safren SA, Sprich S, Chulvick S, Otto MW. Psychosocial treatments for adults with attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:349-60.
12. Ramsay JR, Rostain AL. Adapting psychotherapy to meet the needs of adults with attention-deficit/hyperactivity disorder. Psychotherapy: Theory, Research, Practice, Training 2005;42:72-84.
13. Safren SA, Otto MW, Sprich S, et al. Cognitive-behavior therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther 2005;43:831-42.
14. Ramsay JR, Rostain AL. Girl, repeatedly interrupted: The case of a young adult woman with ADHD. Clinical Case Studies 2005;4:329-46.
15. American Academy of Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;42(suppl 2):26S-49S.
16. Weiss M, Murray C, Weiss G. Adults with attention-deficit/hyperactivity disorder: Current concepts. J Psychiatr Pract 2002;8:99-111.
17. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs 2003;63:2395-411.
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol 2005;61:589-606.
19. Francis PD. Effects of psychotropic medications on the pediatric electrocardiogram and recommendations for monitoring. Curr Opin Pediatr 2002;14(2):224-30
20. Michaelson D, Adler L, Spencer T. Atomoxetine in adults: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;53:112-20.
21. Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs 2004;64:205-22.
22. Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry 2005;58:125-31.
23. Wilens TE, Spencer T, Biederman J. A controlled clinical trial of bupropion for attention-deficit/hyperactivity disorder in adults. Am J Psychiatry 2001;158:282-8.
24. Wilens TE, Haight BR, Horrigan JP, et al. Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Biol Psychiatry 2005;57:793-801.
25. Wilens TE, Biederman JB, Mick E, Spencer TJ. A systematic assessment of tricyclic antidepressants in the treatment of adult attention deficit/hyperactivity disorder. J Nerv Ment Dis 1995;183:48-50.
26. Wilens TE, Biederman JB, Prince J, et al. Six-week, double-blind, placebo-controlled study of desipramine for adult attention deficit hyperactivity disorder. Am J Psychiatry 1996;153:1147-53.
Mr. B, age 50, dreams of becoming a computer programmer but fears he will embarrass himself—as he has in many classrooms before. He is seeking evaluation because his teenage son was recently diagnosed with attention-deficit/hyperactivity disorder (ADHD), and he recognizes similar symptoms in himself.
Mr. B received a college degree with great difficulty, putting off assignments until the last minute and “squeaking by.” For years he has changed occupations often, never progressing beyond entry level, and now works as a personal care provider and limousine driver. He reports problems keeping up with work and managing time.
His history includes early childhood hyperactivity, difficulty sitting through classes, sloppy handwriting, disorganization, short attention span, and distractibility. He is restless, fidgety, and has trouble staying on topic. His disorganization has caused marital difficulties, for which he has sought counseling.
After careful evaluation, you determine that Mr. B meets criteria for ADHD, combined type, and for anxiety disorder not otherwise specified. His treatment goals are to increase his ability to focus; procrastinate less; improve his planning, prioritizing, and self-esteem; and to become less sensitive to criticism and less anxious about handling work demands.
Like Mr. B, adults with ADHD need treatment for the disorder’s core symptoms as well as its psychiatric comorbidities and psychosocial consequences. Comprehensive treatment with medications, cognitive-behavioral therapy (CBT), and environmental adaptations is usually recommended.
Comorbidity rules
Core symptoms. ADHD is a lifespan disorder with multiple behavioral, cognitive, and emotional manifestations that impair relationships and academic and vocational functioning. ADHD-like symptoms are seen in other conditions such as mood disorders or substance abuse, but complaints of inattention, distractibility, procrastination, restlessness, and impulsivity—particularly when pervasive and chronic—are highly indicative of ADHD.
In treating adults with ADHD, we have noticed common behavioral patterns that contribute to their psychosocial problems (Table 1). Dysfunctional coping behaviors have short-term advantages, but patients readily admit they would rather accomplish tasks through greater thought and planning.
Chronic frustrations—often associated with deep shame—are typical of adult ADHD. Many patients have maladaptive core beliefs of failure, self-mistrust, and inadequacy (Table 2).
Table 1
Common dysfunctional behavioral patterns in adults with ADHD
| Behavior | Description | Short-term gain/long-term loss |
|---|---|---|
| Anticipatory avoidance | Magnifying the difficulty of a pending task and doubts about being able to complete it; results in rationalizations to justify procrastination | Defers short-term stress, but often creates a self-fulfilling prophecy because the task looms and may seem overwhelming when facing a deadline |
| Brinksmanship | Waiting until the last moment (eg, the night before) to complete a task, often when facing an impending deadline | Deadline-associated stress can be focusing, but this tactic leaves little room for error and may yield a substandard result |
| Pseudoefficiency | Completing several low-priority, manageable tasks (eg, checking e-mail) but avoiding high-priority tasks (eg, a project for work) | Creates sense of productivity by reducing items on to-do list but defers a more difficult project |
| Juggling | Taking on new, exciting projects and feeling ‘busy’ without completing projects already started | It is easier to become motivated to start a novel project than to complete an ongoing one; pattern usually results in several incomplete projects |
Table 2
5 common maladaptive core beliefs of adults with ADHD
| Self-mistrust | ‘I cannot rely on myself to do what I need to do. I let myself down’ |
| Failure | ‘I always have failed and always will fail at what I set out to do.’ |
| Inadequacy | ‘I am basically a bad and defective person.’ |
| Incompetence | ‘I am too inept to handle life’s basic demands.’ |
| Instability | ‘My life will always be chaotic and in turmoil.’ |
Psychiatric comorbidity is the rule in adults with ADHD (Table 3). For example, among 43 patients who received combined medication and CBT at the University of Pennsylvania Adult ADHD Treatment and Research Program, 75% reported at least one comorbid condition, including:
- 27 (63%) with mood disorder
- 23 (54%) with anxiety disorder
- 5 (12%) with substance abuse.1
Other treatment studies have reported similar comorbidity rates in adults with ADHD.2-4
Table 3
Psychiatric comorbidity in adult ADHD
| Disorder | Prevalence |
|---|---|
| Mood disorders | 50% to 65% |
| Recurrent depression | |
| Bipolar disorder | |
| Cyclothymia | |
| Dysthymia | |
| Depressive disorder NOS | |
| Anxiety disorders | 40% to 55% |
| Generalized anxiety disorder | |
| Anxiety disorder NOS | |
| Others | Various |
| Substance use disorder | |
| Learning disabilities | |
| Intermittent explosive disorder | |
| Tourette syndrome | |
| Antisocial personality | |
| Borderline personality disorder | |
| Dependent personality | |
| NOS: Not otherwise specified | |
Making the diagnosis
Diagnosis of adult ADHD is based on a comprehensive assessment, including:
- careful history of presenting complaints
- thorough review of educational, occupational, and family history
- standardized rating scales (such as the Barkley ADHD Behavior Checklists, the Conners’ Adult ADHD Rating Scale, or the Brown Attention Deficit Disorder Scales)
- collateral information
- assessment of mood, anxiety, substance use, and learning/organizational skills. For details, consult references on adult ADHD.5-8
Case continued: Self-fulfilling prophesies
On standardized rating scales, Mr. B meets criteria for combined ADHD for childhood and current symptoms. Information from his wife and brother also confirms the ADHD diagnosis.
He is motivated, resilient, optimistic, and has a good support system. However, his negative automatic thoughts about his ability to succeed in school and to handle increasing time demands suggest deeper beliefs of inadequacy and failure.
Mr. B struggled academically. Without guidance about how to change his approach to difficult situations, he has repeated old thinking and behavior patterns. Believing he will embarrass himself and fail to learn required material, Mr. B procrastinates and avoids doing assignments. In class, his feelings of inadequacy make him self-conscious, which causes him to lose focus and have trouble concentrating.
See the world through the patient’s eyes
Understanding your patient. Before you start treatment, we recommend that you conceptualize how ADHD has influenced your patient’s life, including:
- developmental experiences
- family-of-origin issues, such as conflicts with parents stemming from ADHD symptoms or reciprocal interactions with an ADHD parent
- world view (“schemata”)
- patterns of coping with (or avoiding) stress
- attitudes toward self and important others
- readiness to change.
Developing a working case conceptualization is a dynamic, collaborative process. You talk with patients, and encourage them to reflect on how ADHD affects their view of themselves and their important relationships. The conceptualization takes shape as you:
- observe patients’ behaviors
- elicit how they think and feel
- assess with them the relevance and accuracies of their belief systems and response patterns.
Seeing the world “through their eyes” prepares you to help them accept the diagnosis and learn to manage ADHD symptoms. Then, by providing a blueprint to manage what patients may see as uncontrollable responses, you can help them take charge of their automatic reactions.
Psychoeducation. To set the stage for treatment, encourage patients to learn about ADHD by reading articles and books and consulting Web sites for adults with ADHD (see Related resources). Psychoeducation helps patients:
- review possible treatment approaches, including organizational (environmental) management, medication, and psychotherapy (individual or group)
- become informed participants in setting treatment goals.
Explain the relative contribution of each treatment component. For example, medications can reduce distractibility and improve attention, organizational strategies can reduce disorganization and improve time management, and structured psychotherapy can help the patient develop more effective coping skills.
Case continued: Planning combined treatment
You discuss diagnosis and treatment options with Mr. B, and he agrees to start the methylphenidate compound Concerta, initially at 18 mg/d, and weekly CBT sessions. You recommended a stimulant based on efficacy studies and your clinical experience in treating adults with ADHD. Mr. B wants a medication that will help him focus while working or studying, and he says Concerta has improved his son’s ADHD symptoms.
You instruct Mr. B to increase the dosage by 18 mg each week until he reaches 72 mg/d. You also tell him to keep a medication response log and to note any positive changes and side effects.
If an adult with ADHD expresses preference for a particular medication, we usually prescribe that one first. Most patients to whom we offer both medication and psychotherapy agree to this “top-down” and “bottom-up” approach. “Top down” means giving patients new ways of thinking to help them understand and modify their responses. “Bottom up” refers to the medication reducing their impulsivity, distractibility, and inattentiveness.
CBT for adult ADHD
Medications can ameliorate key symptoms of adult ADHD, but adjunctive interventions are needed to improve functioning and quality of life. Evidence supporting psychosocial treatment for adults with ADHD is limited, but CBT has been studied the most.1,9-13 Safren et al13 found a four-fold greater therapeutic response when patients received adjunctive CBT for residual ADHD symptoms, compared with patients who received medication alone.
We usually provide CBT weekly for 12 weeks and then taper to 8 additional sessions over 3 months (total 20 sessions). We may extend CBT with additional sessions to address complicated issues. CBT helps adults with ADHD to:
- identify dysfunctional thinking, feeling, and behaving patterns
- recognize contexts in which patterns arise
- systematically change these patterns.
CBT can reduce ADHD-associated anxiety and depression and improve coping skills and sense of well-being.1,9,11 Its flexibility allows you to address family issues with patients’ partners, children and other relatives to improve communication, reduce conflict, and develop healthier interactions.
We focus CBT sessions on finding alternate coping strategies. We might try role playing, rehearsing, creating “thought experiments,” and anticipating and preparing to modify typical patterns of avoidance. These approaches have been described elsewhere.10,11,14
We adopt an active stance during therapy to keep ADHD patients’ distractibility from disrupting our conversation. For example, we set the therapeutic agenda, provide feedback about patients’ behaviors, and encourage them to clarify rewards and consequences of using (or avoiding) problem-solving strategies.
Although we typically assign between-session homework, we expect patients to have difficulty completing it. We remain nonjudgmental and collaborative, viewing incomplete assignments as opportunities to learn about patients’ unproductive problem solving and to help them develop more-effective patterns.
Challenging maladaptive beliefs. A strong therapeutic relationship allows adults with ADHD to discuss their chronic frustrations, which often are associated with deep shame. We then shift CBT’s focus to deeper ADHD-related schemata that perpetuate dysfunctional patterns.
We work with patients to elucidate and challenge their maladaptive core beliefs and encourage new ways to view themselves and others. Allowing patients to grieve about the limitations ADHD imposes on their lives also helps to reduce chronic negative self-esteem.
Case continued: ‘less frenetic’
Mr. B achieves good results within 3 weeks of an increasing titration of stimulant medication, reporting significantly less restlessness and greater concentration without significant side effects. His wife confirms that he is less frenetic, can converse without interruptions, and is better at managing his complicated work schedule.
Which medications?
Drug therapy for adult ADHD is not as well-studied as in children and adolescents, but American Academy of Child and Adolescent Psychiatry guidelines and others15-18 recommend stimulant and nonstimulant medications. Your choice depends on the patient’s clinical profile (including risk factors and comorbid conditions), past medication use, treatment goals, preferred medication effects and dosing patterns (once-daily versus multiple times), and potential side effects. Stimulants or atomoxetine are first-line choices for adult ADHD without psychiatric comorbidity.
Stimulants work quickly and are cleared relatively rapidly from the brain without causing euphoria or dependency. They are effective (80% to 90% response rate) and well-tolerated, though long-term effects have not been studied in adults (Table 4).
Stimulants’ effect size of 0.9 is considered substantial. Effect size—a statistical method of reporting an intervention’s effect across different studies—is typically rated as:
- <0.32 very small
- 0.33 to 0.54, moderate
- >0.55, significant or very strong.
When choosing a medication, we usually try methylphenidate and amphetamine first, one after the other. We explain to the patient how stimulants work in the brain and the need for a comparative trial to determine which might work best for him or her. If the patient has tried a stimulant and found it helpful, we start with that class. Similarly, if he/she has not had good results with one type, we start with the other. Approximately one-third of our patients respond equally well to methylphenidate or amphetamine, one-third respond better to methylphenidate, and one-third respond better to amphetamine.
To determine the optimal dosage, we usually titrate up from 10 to 30 mg per dose of an immediate-release preparation. We begin with this form to help patients notice the medication’s onset and duration of action. After we find the optimal dosage, we switch to a longer-acting preparation.
Insomnia, mood instability, and euphoria are unacceptable stimulant side effects, although many patients welcome others such as appetite suppression and weight loss. Closely monitor cardiovascular effects, and review potential interactions with other medications, such as antihypertensives or bronchodilators. Because sudden death has been reported with stimulants in persons with structural cardiac lesions,19 obtain a cardiology consultation for patients with a history of heart disease.
We encourage patients to keep daily medication logs (Box), which we review at each visit and use to make dosing or medication changes. Dosing guidelines resemble those used for children and adolescents, although adults usually tolerate higher maximum dosages (such as methylphenidate, 80 to 100 mg/d).
Because of stimulants’ potential for recreational misuse and abuse, remain wary about choosing stimulants for patients with whom you lack a solid doctor-patient relationship.
Table 4
Stimulant dosages used in treating adult ADHD
| Class (brand name) | Daily dosing | Typical dosing schedule |
|---|---|---|
| Methylphenidate | ||
| Short-acting (Metadate, Ritadex, Ritalin) | Two to four times | 10 to 40 mg bid to qid |
| Intermediate-acting (Metadate SR, Ritalin SR) | Once or twice | 20 to 60 mg qd to bid |
| Extended-release (Concerta, Metadate CD, Ritalin LA) | Once or twice | 18 to 108 mg qd (Concerta) 20 to 40 mg bid (Ritalin LA, Metadate CD) |
| Dextromethylphenidate | ||
| Short-acting (Focalin) | Two to four times | 5 to 20 mg bid to qid |
| Long-acting (Focalin XR) | Once or twice | 10 to 20 mg qd or bid |
| Dextroamphetamine | ||
| Short-acting (Dexedrine) | Twice or three times | 10 to 30 mg bid or tid |
| Intermediate-acting (Dexedrine spansules) | Once or twice | 10 to 30 mg bid |
| Mixed amphetamine salts | ||
| Intermediate-acting (Adderall) | Once or twice | 10 to 30 mg bid or tid |
| Extended-release (Adderall XR) | Once or twice | 10 to 40 mg qd or bid |
Atomoxetine, a nonstimulant, norepinephrine re-uptake inhibitor, is approved for ADHD in adults.20-22 In two double-blind, controlled, randomized trials totalling 536 adults, Michaelson et al20 found significantly reduced ADHD symptoms after 10 weeks of atomoxetine treatment. Effect sizes of 0.35 and 0.40 were reported, with 10% of patients discontinuing because of side effects.
Atomoxetine has a long duration of action (>12 hours) but a more gradual onset (4 to 6 weeks) than that of stimulants. Approximately 60% of patients respond to atomoxetine, though effect sizes are less than those of stimulants. We have found atomoxetine works well for patients who:
- do not tolerate or are uncomfortable with taking stimulants
- are highly anxious
- report emotional dysregulation as a major target symptom.
To reduce risk of common side effects (nausea, GI upset, headache, sedation, reduced sex drive), we start with low dosages (such as 25 mg bid) and increase weekly by 25 mg to a target of 80 to 100 mg/d.
Treating complicated ADHD
Bupropion or tricyclic antidepressants are reasonable options for ADHD with depression. Atomoxetine, a tricyclic, or a stimulant plus a selective serotonin reuptake inhibitor (SSRI) can provide good symptom relief for adults with ADHD and comorbid anxiety and/or depression.
Bupropion. Approximately 50% of adults with ADHD respond to bupropion,23,24 with a treatment effect size of 0.6. Bupropion’s efficacy in smoking cessation adds value for those trying to quit.
We usually start extended-release bupropion at 150 mg/d and increase after 2 weeks to 300 mg/d if response is suboptimal. Headache, dry mouth, insomnia, and nausea are the most common adverse effects. Agitation or irritability is sometimes serious enough to warrant stopping bupropion.
Combining medications. Using SSRIs with stimulants can help adults with ADHD and comorbid anxiety or depression. Any SSRI can be safely combined with stimulants, though we tend to pick:
- more-sedating agents such as paroxetine or sertraline when patients report difficulty with insomnia or overactivation
- less-sedating compounds such as fluoxetine or citalopram when patients complain of being too tired or underactive.
When patients taking SSRIs seek help for ADHD, adding a stimulant usually reduces inattention, distractibility, impulsivity, and/or subjective feelings of restlessness. We prescribe usual dosages because stimulants and SSRIs do not interact. We have not seen serious side effects, but some patients report feeling oversedated.
Tricyclics. We use tricyclics when a stimulant/SSRI combination does not relieve symptoms satisfactorily or a patient complains of side effects. We usually have good results with desipramine or imipramine, 150 to 300 mg/d, or nortriptyline, 50 to 150 mg/d. Spencer et al have reported a response rate of 68% with nortriptyline or desipramine in a retrospective chart review25 and a prospective placebo-controlled trial26 of adults with ADHD.
Case continued: Closer to dream job
After 6 months of combined treatment, Mr. B reports much-improved ADHD symptoms, with minimal stimulant-related side effects. He has made some realistic plans for computer programming school and is taking preliminary courses. Keeping a schedule book has reduced his tardiness and tendency to procrastinate.
He is more comfortable in the classroom and better able to challenge self-critical thinking. When routine difficulties arise, he is using more-adaptive coping strategies. To maintain gains achieved in therapy, he chooses to continue periodic CBT booster sessions.
Long-term treatment
Even with medication and CBT, patients may require referral for organizational coaching, academic counseling, school or workplace accommodations, vocational counseling, cognitive remediation, group therapy, or social skills classes. You can help them obtain quality adjunctive care by collaborating with professionals who offer these services.
No studies have examined long-term care of adults with ADHD. In our experience, ongoing medication and intermittent therapy can sustain symptom control and coping skills for years. Most patients are initially skeptical about staying on medication, but after they experience the benefits most seem willing to continue as long as the medication helps.
Most of our patients sustain changes in thinking, feeling, and behaving that they learn through BT. They may seek additional sessions to meet a challenge, such as a new job or starting a family.
Books
- Kolberg J, Nadeau K. ADD-friendly ways to organize your life. New York: Brunner-Routledge; 2002.
- Hallowell EM, Ratey JJ. Driven to distraction. New York: Touchstone; 1994.
- Hallowell E, Ratey J. Delivered from distraction. New York: Ballantine Books; 2005.
Organizations
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). National Resource Center on AD/HD. www.chadd.org.
- Attention Deficit Disorder Association (ADDA). Resources and membership organization for adults with ADHD. www.add.org.
Drug brand names
- Amphetamine • Adderall, Dexedrine
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Imipramine • Tofranil
- Methylphenidate • Concerta, Focalin, Metadate, Ritalin
- Nortriptyline • Aventyl, Pamelor
Disclosures
Dr. Rostain is a consultant to Shire Pharamaceuticals Group and a speaker for Eli Lilly & Co. and Ortho-McNeil Pharmaceutical
Dr. Ramsay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. B, age 50, dreams of becoming a computer programmer but fears he will embarrass himself—as he has in many classrooms before. He is seeking evaluation because his teenage son was recently diagnosed with attention-deficit/hyperactivity disorder (ADHD), and he recognizes similar symptoms in himself.
Mr. B received a college degree with great difficulty, putting off assignments until the last minute and “squeaking by.” For years he has changed occupations often, never progressing beyond entry level, and now works as a personal care provider and limousine driver. He reports problems keeping up with work and managing time.
His history includes early childhood hyperactivity, difficulty sitting through classes, sloppy handwriting, disorganization, short attention span, and distractibility. He is restless, fidgety, and has trouble staying on topic. His disorganization has caused marital difficulties, for which he has sought counseling.
After careful evaluation, you determine that Mr. B meets criteria for ADHD, combined type, and for anxiety disorder not otherwise specified. His treatment goals are to increase his ability to focus; procrastinate less; improve his planning, prioritizing, and self-esteem; and to become less sensitive to criticism and less anxious about handling work demands.
Like Mr. B, adults with ADHD need treatment for the disorder’s core symptoms as well as its psychiatric comorbidities and psychosocial consequences. Comprehensive treatment with medications, cognitive-behavioral therapy (CBT), and environmental adaptations is usually recommended.
Comorbidity rules
Core symptoms. ADHD is a lifespan disorder with multiple behavioral, cognitive, and emotional manifestations that impair relationships and academic and vocational functioning. ADHD-like symptoms are seen in other conditions such as mood disorders or substance abuse, but complaints of inattention, distractibility, procrastination, restlessness, and impulsivity—particularly when pervasive and chronic—are highly indicative of ADHD.
In treating adults with ADHD, we have noticed common behavioral patterns that contribute to their psychosocial problems (Table 1). Dysfunctional coping behaviors have short-term advantages, but patients readily admit they would rather accomplish tasks through greater thought and planning.
Chronic frustrations—often associated with deep shame—are typical of adult ADHD. Many patients have maladaptive core beliefs of failure, self-mistrust, and inadequacy (Table 2).
Table 1
Common dysfunctional behavioral patterns in adults with ADHD
| Behavior | Description | Short-term gain/long-term loss |
|---|---|---|
| Anticipatory avoidance | Magnifying the difficulty of a pending task and doubts about being able to complete it; results in rationalizations to justify procrastination | Defers short-term stress, but often creates a self-fulfilling prophecy because the task looms and may seem overwhelming when facing a deadline |
| Brinksmanship | Waiting until the last moment (eg, the night before) to complete a task, often when facing an impending deadline | Deadline-associated stress can be focusing, but this tactic leaves little room for error and may yield a substandard result |
| Pseudoefficiency | Completing several low-priority, manageable tasks (eg, checking e-mail) but avoiding high-priority tasks (eg, a project for work) | Creates sense of productivity by reducing items on to-do list but defers a more difficult project |
| Juggling | Taking on new, exciting projects and feeling ‘busy’ without completing projects already started | It is easier to become motivated to start a novel project than to complete an ongoing one; pattern usually results in several incomplete projects |
Table 2
5 common maladaptive core beliefs of adults with ADHD
| Self-mistrust | ‘I cannot rely on myself to do what I need to do. I let myself down’ |
| Failure | ‘I always have failed and always will fail at what I set out to do.’ |
| Inadequacy | ‘I am basically a bad and defective person.’ |
| Incompetence | ‘I am too inept to handle life’s basic demands.’ |
| Instability | ‘My life will always be chaotic and in turmoil.’ |
Psychiatric comorbidity is the rule in adults with ADHD (Table 3). For example, among 43 patients who received combined medication and CBT at the University of Pennsylvania Adult ADHD Treatment and Research Program, 75% reported at least one comorbid condition, including:
- 27 (63%) with mood disorder
- 23 (54%) with anxiety disorder
- 5 (12%) with substance abuse.1
Other treatment studies have reported similar comorbidity rates in adults with ADHD.2-4
Table 3
Psychiatric comorbidity in adult ADHD
| Disorder | Prevalence |
|---|---|
| Mood disorders | 50% to 65% |
| Recurrent depression | |
| Bipolar disorder | |
| Cyclothymia | |
| Dysthymia | |
| Depressive disorder NOS | |
| Anxiety disorders | 40% to 55% |
| Generalized anxiety disorder | |
| Anxiety disorder NOS | |
| Others | Various |
| Substance use disorder | |
| Learning disabilities | |
| Intermittent explosive disorder | |
| Tourette syndrome | |
| Antisocial personality | |
| Borderline personality disorder | |
| Dependent personality | |
| NOS: Not otherwise specified | |
Making the diagnosis
Diagnosis of adult ADHD is based on a comprehensive assessment, including:
- careful history of presenting complaints
- thorough review of educational, occupational, and family history
- standardized rating scales (such as the Barkley ADHD Behavior Checklists, the Conners’ Adult ADHD Rating Scale, or the Brown Attention Deficit Disorder Scales)
- collateral information
- assessment of mood, anxiety, substance use, and learning/organizational skills. For details, consult references on adult ADHD.5-8
Case continued: Self-fulfilling prophesies
On standardized rating scales, Mr. B meets criteria for combined ADHD for childhood and current symptoms. Information from his wife and brother also confirms the ADHD diagnosis.
He is motivated, resilient, optimistic, and has a good support system. However, his negative automatic thoughts about his ability to succeed in school and to handle increasing time demands suggest deeper beliefs of inadequacy and failure.
Mr. B struggled academically. Without guidance about how to change his approach to difficult situations, he has repeated old thinking and behavior patterns. Believing he will embarrass himself and fail to learn required material, Mr. B procrastinates and avoids doing assignments. In class, his feelings of inadequacy make him self-conscious, which causes him to lose focus and have trouble concentrating.
See the world through the patient’s eyes
Understanding your patient. Before you start treatment, we recommend that you conceptualize how ADHD has influenced your patient’s life, including:
- developmental experiences
- family-of-origin issues, such as conflicts with parents stemming from ADHD symptoms or reciprocal interactions with an ADHD parent
- world view (“schemata”)
- patterns of coping with (or avoiding) stress
- attitudes toward self and important others
- readiness to change.
Developing a working case conceptualization is a dynamic, collaborative process. You talk with patients, and encourage them to reflect on how ADHD affects their view of themselves and their important relationships. The conceptualization takes shape as you:
- observe patients’ behaviors
- elicit how they think and feel
- assess with them the relevance and accuracies of their belief systems and response patterns.
Seeing the world “through their eyes” prepares you to help them accept the diagnosis and learn to manage ADHD symptoms. Then, by providing a blueprint to manage what patients may see as uncontrollable responses, you can help them take charge of their automatic reactions.
Psychoeducation. To set the stage for treatment, encourage patients to learn about ADHD by reading articles and books and consulting Web sites for adults with ADHD (see Related resources). Psychoeducation helps patients:
- review possible treatment approaches, including organizational (environmental) management, medication, and psychotherapy (individual or group)
- become informed participants in setting treatment goals.
Explain the relative contribution of each treatment component. For example, medications can reduce distractibility and improve attention, organizational strategies can reduce disorganization and improve time management, and structured psychotherapy can help the patient develop more effective coping skills.
Case continued: Planning combined treatment
You discuss diagnosis and treatment options with Mr. B, and he agrees to start the methylphenidate compound Concerta, initially at 18 mg/d, and weekly CBT sessions. You recommended a stimulant based on efficacy studies and your clinical experience in treating adults with ADHD. Mr. B wants a medication that will help him focus while working or studying, and he says Concerta has improved his son’s ADHD symptoms.
You instruct Mr. B to increase the dosage by 18 mg each week until he reaches 72 mg/d. You also tell him to keep a medication response log and to note any positive changes and side effects.
If an adult with ADHD expresses preference for a particular medication, we usually prescribe that one first. Most patients to whom we offer both medication and psychotherapy agree to this “top-down” and “bottom-up” approach. “Top down” means giving patients new ways of thinking to help them understand and modify their responses. “Bottom up” refers to the medication reducing their impulsivity, distractibility, and inattentiveness.
CBT for adult ADHD
Medications can ameliorate key symptoms of adult ADHD, but adjunctive interventions are needed to improve functioning and quality of life. Evidence supporting psychosocial treatment for adults with ADHD is limited, but CBT has been studied the most.1,9-13 Safren et al13 found a four-fold greater therapeutic response when patients received adjunctive CBT for residual ADHD symptoms, compared with patients who received medication alone.
We usually provide CBT weekly for 12 weeks and then taper to 8 additional sessions over 3 months (total 20 sessions). We may extend CBT with additional sessions to address complicated issues. CBT helps adults with ADHD to:
- identify dysfunctional thinking, feeling, and behaving patterns
- recognize contexts in which patterns arise
- systematically change these patterns.
CBT can reduce ADHD-associated anxiety and depression and improve coping skills and sense of well-being.1,9,11 Its flexibility allows you to address family issues with patients’ partners, children and other relatives to improve communication, reduce conflict, and develop healthier interactions.
We focus CBT sessions on finding alternate coping strategies. We might try role playing, rehearsing, creating “thought experiments,” and anticipating and preparing to modify typical patterns of avoidance. These approaches have been described elsewhere.10,11,14
We adopt an active stance during therapy to keep ADHD patients’ distractibility from disrupting our conversation. For example, we set the therapeutic agenda, provide feedback about patients’ behaviors, and encourage them to clarify rewards and consequences of using (or avoiding) problem-solving strategies.
Although we typically assign between-session homework, we expect patients to have difficulty completing it. We remain nonjudgmental and collaborative, viewing incomplete assignments as opportunities to learn about patients’ unproductive problem solving and to help them develop more-effective patterns.
Challenging maladaptive beliefs. A strong therapeutic relationship allows adults with ADHD to discuss their chronic frustrations, which often are associated with deep shame. We then shift CBT’s focus to deeper ADHD-related schemata that perpetuate dysfunctional patterns.
We work with patients to elucidate and challenge their maladaptive core beliefs and encourage new ways to view themselves and others. Allowing patients to grieve about the limitations ADHD imposes on their lives also helps to reduce chronic negative self-esteem.
Case continued: ‘less frenetic’
Mr. B achieves good results within 3 weeks of an increasing titration of stimulant medication, reporting significantly less restlessness and greater concentration without significant side effects. His wife confirms that he is less frenetic, can converse without interruptions, and is better at managing his complicated work schedule.
Which medications?
Drug therapy for adult ADHD is not as well-studied as in children and adolescents, but American Academy of Child and Adolescent Psychiatry guidelines and others15-18 recommend stimulant and nonstimulant medications. Your choice depends on the patient’s clinical profile (including risk factors and comorbid conditions), past medication use, treatment goals, preferred medication effects and dosing patterns (once-daily versus multiple times), and potential side effects. Stimulants or atomoxetine are first-line choices for adult ADHD without psychiatric comorbidity.
Stimulants work quickly and are cleared relatively rapidly from the brain without causing euphoria or dependency. They are effective (80% to 90% response rate) and well-tolerated, though long-term effects have not been studied in adults (Table 4).
Stimulants’ effect size of 0.9 is considered substantial. Effect size—a statistical method of reporting an intervention’s effect across different studies—is typically rated as:
- <0.32 very small
- 0.33 to 0.54, moderate
- >0.55, significant or very strong.
When choosing a medication, we usually try methylphenidate and amphetamine first, one after the other. We explain to the patient how stimulants work in the brain and the need for a comparative trial to determine which might work best for him or her. If the patient has tried a stimulant and found it helpful, we start with that class. Similarly, if he/she has not had good results with one type, we start with the other. Approximately one-third of our patients respond equally well to methylphenidate or amphetamine, one-third respond better to methylphenidate, and one-third respond better to amphetamine.
To determine the optimal dosage, we usually titrate up from 10 to 30 mg per dose of an immediate-release preparation. We begin with this form to help patients notice the medication’s onset and duration of action. After we find the optimal dosage, we switch to a longer-acting preparation.
Insomnia, mood instability, and euphoria are unacceptable stimulant side effects, although many patients welcome others such as appetite suppression and weight loss. Closely monitor cardiovascular effects, and review potential interactions with other medications, such as antihypertensives or bronchodilators. Because sudden death has been reported with stimulants in persons with structural cardiac lesions,19 obtain a cardiology consultation for patients with a history of heart disease.
We encourage patients to keep daily medication logs (Box), which we review at each visit and use to make dosing or medication changes. Dosing guidelines resemble those used for children and adolescents, although adults usually tolerate higher maximum dosages (such as methylphenidate, 80 to 100 mg/d).
Because of stimulants’ potential for recreational misuse and abuse, remain wary about choosing stimulants for patients with whom you lack a solid doctor-patient relationship.
Table 4
Stimulant dosages used in treating adult ADHD
| Class (brand name) | Daily dosing | Typical dosing schedule |
|---|---|---|
| Methylphenidate | ||
| Short-acting (Metadate, Ritadex, Ritalin) | Two to four times | 10 to 40 mg bid to qid |
| Intermediate-acting (Metadate SR, Ritalin SR) | Once or twice | 20 to 60 mg qd to bid |
| Extended-release (Concerta, Metadate CD, Ritalin LA) | Once or twice | 18 to 108 mg qd (Concerta) 20 to 40 mg bid (Ritalin LA, Metadate CD) |
| Dextromethylphenidate | ||
| Short-acting (Focalin) | Two to four times | 5 to 20 mg bid to qid |
| Long-acting (Focalin XR) | Once or twice | 10 to 20 mg qd or bid |
| Dextroamphetamine | ||
| Short-acting (Dexedrine) | Twice or three times | 10 to 30 mg bid or tid |
| Intermediate-acting (Dexedrine spansules) | Once or twice | 10 to 30 mg bid |
| Mixed amphetamine salts | ||
| Intermediate-acting (Adderall) | Once or twice | 10 to 30 mg bid or tid |
| Extended-release (Adderall XR) | Once or twice | 10 to 40 mg qd or bid |
Atomoxetine, a nonstimulant, norepinephrine re-uptake inhibitor, is approved for ADHD in adults.20-22 In two double-blind, controlled, randomized trials totalling 536 adults, Michaelson et al20 found significantly reduced ADHD symptoms after 10 weeks of atomoxetine treatment. Effect sizes of 0.35 and 0.40 were reported, with 10% of patients discontinuing because of side effects.
Atomoxetine has a long duration of action (>12 hours) but a more gradual onset (4 to 6 weeks) than that of stimulants. Approximately 60% of patients respond to atomoxetine, though effect sizes are less than those of stimulants. We have found atomoxetine works well for patients who:
- do not tolerate or are uncomfortable with taking stimulants
- are highly anxious
- report emotional dysregulation as a major target symptom.
To reduce risk of common side effects (nausea, GI upset, headache, sedation, reduced sex drive), we start with low dosages (such as 25 mg bid) and increase weekly by 25 mg to a target of 80 to 100 mg/d.
Treating complicated ADHD
Bupropion or tricyclic antidepressants are reasonable options for ADHD with depression. Atomoxetine, a tricyclic, or a stimulant plus a selective serotonin reuptake inhibitor (SSRI) can provide good symptom relief for adults with ADHD and comorbid anxiety and/or depression.
Bupropion. Approximately 50% of adults with ADHD respond to bupropion,23,24 with a treatment effect size of 0.6. Bupropion’s efficacy in smoking cessation adds value for those trying to quit.
We usually start extended-release bupropion at 150 mg/d and increase after 2 weeks to 300 mg/d if response is suboptimal. Headache, dry mouth, insomnia, and nausea are the most common adverse effects. Agitation or irritability is sometimes serious enough to warrant stopping bupropion.
Combining medications. Using SSRIs with stimulants can help adults with ADHD and comorbid anxiety or depression. Any SSRI can be safely combined with stimulants, though we tend to pick:
- more-sedating agents such as paroxetine or sertraline when patients report difficulty with insomnia or overactivation
- less-sedating compounds such as fluoxetine or citalopram when patients complain of being too tired or underactive.
When patients taking SSRIs seek help for ADHD, adding a stimulant usually reduces inattention, distractibility, impulsivity, and/or subjective feelings of restlessness. We prescribe usual dosages because stimulants and SSRIs do not interact. We have not seen serious side effects, but some patients report feeling oversedated.
Tricyclics. We use tricyclics when a stimulant/SSRI combination does not relieve symptoms satisfactorily or a patient complains of side effects. We usually have good results with desipramine or imipramine, 150 to 300 mg/d, or nortriptyline, 50 to 150 mg/d. Spencer et al have reported a response rate of 68% with nortriptyline or desipramine in a retrospective chart review25 and a prospective placebo-controlled trial26 of adults with ADHD.
Case continued: Closer to dream job
After 6 months of combined treatment, Mr. B reports much-improved ADHD symptoms, with minimal stimulant-related side effects. He has made some realistic plans for computer programming school and is taking preliminary courses. Keeping a schedule book has reduced his tardiness and tendency to procrastinate.
He is more comfortable in the classroom and better able to challenge self-critical thinking. When routine difficulties arise, he is using more-adaptive coping strategies. To maintain gains achieved in therapy, he chooses to continue periodic CBT booster sessions.
Long-term treatment
Even with medication and CBT, patients may require referral for organizational coaching, academic counseling, school or workplace accommodations, vocational counseling, cognitive remediation, group therapy, or social skills classes. You can help them obtain quality adjunctive care by collaborating with professionals who offer these services.
No studies have examined long-term care of adults with ADHD. In our experience, ongoing medication and intermittent therapy can sustain symptom control and coping skills for years. Most patients are initially skeptical about staying on medication, but after they experience the benefits most seem willing to continue as long as the medication helps.
Most of our patients sustain changes in thinking, feeling, and behaving that they learn through BT. They may seek additional sessions to meet a challenge, such as a new job or starting a family.
Books
- Kolberg J, Nadeau K. ADD-friendly ways to organize your life. New York: Brunner-Routledge; 2002.
- Hallowell EM, Ratey JJ. Driven to distraction. New York: Touchstone; 1994.
- Hallowell E, Ratey J. Delivered from distraction. New York: Ballantine Books; 2005.
Organizations
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). National Resource Center on AD/HD. www.chadd.org.
- Attention Deficit Disorder Association (ADDA). Resources and membership organization for adults with ADHD. www.add.org.
Drug brand names
- Amphetamine • Adderall, Dexedrine
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Imipramine • Tofranil
- Methylphenidate • Concerta, Focalin, Metadate, Ritalin
- Nortriptyline • Aventyl, Pamelor
Disclosures
Dr. Rostain is a consultant to Shire Pharamaceuticals Group and a speaker for Eli Lilly & Co. and Ortho-McNeil Pharmaceutical
Dr. Ramsay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rostain AL, Ramsay JR. A combined treatment approach for adults with attention-deficit/hyperactivity disorder. Results of an open study of 43 patients J Attention Disorders. In press.
2. Shekim WO, Asarnow RF, Hess E, et al. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Comp Psychiatry 1990;31:416-25.
3. Biederman J, Faraone SV, Spencer T, et al. Patterns of psychiatric comorbidity, cognition and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:1792-8.
4. Wilens TE, Biederman J, Spencer T. Attention-deficit/hyperactivity disorder across the lifespan. Ann Rev Medicine 2002;53:113-31.
5. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guilford Press; 1998.
6. Wender PH. ADHD: Attention-deficit hyperactivity disorder in children and adults. New York: Oxford University Press; 2000.
7. Goldstein S, Ellison AT. Clinician’s guide to adult ADHD. San Diego: Academic Press; 2000.
8. Brown TE. Attention-deficit disorder: the unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
9. Wilens TE, McDermott SP, Biederman J, et al. Cognitive therapy in the treatment of adults with ADHD: a systematic chart review of 26 cases. J Cogn Ther 1999;13:215-26.
10. Ramsay JR, Rostain AL. A cognitive therapy approach for adult attention-deficit/hyperactivity disorder. J Cogn Psychother 2003;17:319-34.
11. Safren SA, Sprich S, Chulvick S, Otto MW. Psychosocial treatments for adults with attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:349-60.
12. Ramsay JR, Rostain AL. Adapting psychotherapy to meet the needs of adults with attention-deficit/hyperactivity disorder. Psychotherapy: Theory, Research, Practice, Training 2005;42:72-84.
13. Safren SA, Otto MW, Sprich S, et al. Cognitive-behavior therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther 2005;43:831-42.
14. Ramsay JR, Rostain AL. Girl, repeatedly interrupted: The case of a young adult woman with ADHD. Clinical Case Studies 2005;4:329-46.
15. American Academy of Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;42(suppl 2):26S-49S.
16. Weiss M, Murray C, Weiss G. Adults with attention-deficit/hyperactivity disorder: Current concepts. J Psychiatr Pract 2002;8:99-111.
17. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs 2003;63:2395-411.
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol 2005;61:589-606.
19. Francis PD. Effects of psychotropic medications on the pediatric electrocardiogram and recommendations for monitoring. Curr Opin Pediatr 2002;14(2):224-30
20. Michaelson D, Adler L, Spencer T. Atomoxetine in adults: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;53:112-20.
21. Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs 2004;64:205-22.
22. Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry 2005;58:125-31.
23. Wilens TE, Spencer T, Biederman J. A controlled clinical trial of bupropion for attention-deficit/hyperactivity disorder in adults. Am J Psychiatry 2001;158:282-8.
24. Wilens TE, Haight BR, Horrigan JP, et al. Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Biol Psychiatry 2005;57:793-801.
25. Wilens TE, Biederman JB, Mick E, Spencer TJ. A systematic assessment of tricyclic antidepressants in the treatment of adult attention deficit/hyperactivity disorder. J Nerv Ment Dis 1995;183:48-50.
26. Wilens TE, Biederman JB, Prince J, et al. Six-week, double-blind, placebo-controlled study of desipramine for adult attention deficit hyperactivity disorder. Am J Psychiatry 1996;153:1147-53.
1. Rostain AL, Ramsay JR. A combined treatment approach for adults with attention-deficit/hyperactivity disorder. Results of an open study of 43 patients J Attention Disorders. In press.
2. Shekim WO, Asarnow RF, Hess E, et al. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Comp Psychiatry 1990;31:416-25.
3. Biederman J, Faraone SV, Spencer T, et al. Patterns of psychiatric comorbidity, cognition and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:1792-8.
4. Wilens TE, Biederman J, Spencer T. Attention-deficit/hyperactivity disorder across the lifespan. Ann Rev Medicine 2002;53:113-31.
5. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guilford Press; 1998.
6. Wender PH. ADHD: Attention-deficit hyperactivity disorder in children and adults. New York: Oxford University Press; 2000.
7. Goldstein S, Ellison AT. Clinician’s guide to adult ADHD. San Diego: Academic Press; 2000.
8. Brown TE. Attention-deficit disorder: the unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
9. Wilens TE, McDermott SP, Biederman J, et al. Cognitive therapy in the treatment of adults with ADHD: a systematic chart review of 26 cases. J Cogn Ther 1999;13:215-26.
10. Ramsay JR, Rostain AL. A cognitive therapy approach for adult attention-deficit/hyperactivity disorder. J Cogn Psychother 2003;17:319-34.
11. Safren SA, Sprich S, Chulvick S, Otto MW. Psychosocial treatments for adults with attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:349-60.
12. Ramsay JR, Rostain AL. Adapting psychotherapy to meet the needs of adults with attention-deficit/hyperactivity disorder. Psychotherapy: Theory, Research, Practice, Training 2005;42:72-84.
13. Safren SA, Otto MW, Sprich S, et al. Cognitive-behavior therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther 2005;43:831-42.
14. Ramsay JR, Rostain AL. Girl, repeatedly interrupted: The case of a young adult woman with ADHD. Clinical Case Studies 2005;4:329-46.
15. American Academy of Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;42(suppl 2):26S-49S.
16. Weiss M, Murray C, Weiss G. Adults with attention-deficit/hyperactivity disorder: Current concepts. J Psychiatr Pract 2002;8:99-111.
17. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs 2003;63:2395-411.
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol 2005;61:589-606.
19. Francis PD. Effects of psychotropic medications on the pediatric electrocardiogram and recommendations for monitoring. Curr Opin Pediatr 2002;14(2):224-30
20. Michaelson D, Adler L, Spencer T. Atomoxetine in adults: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;53:112-20.
21. Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs 2004;64:205-22.
22. Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry 2005;58:125-31.
23. Wilens TE, Spencer T, Biederman J. A controlled clinical trial of bupropion for attention-deficit/hyperactivity disorder in adults. Am J Psychiatry 2001;158:282-8.
24. Wilens TE, Haight BR, Horrigan JP, et al. Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Biol Psychiatry 2005;57:793-801.
25. Wilens TE, Biederman JB, Mick E, Spencer TJ. A systematic assessment of tricyclic antidepressants in the treatment of adult attention deficit/hyperactivity disorder. J Nerv Ment Dis 1995;183:48-50.
26. Wilens TE, Biederman JB, Prince J, et al. Six-week, double-blind, placebo-controlled study of desipramine for adult attention deficit hyperactivity disorder. Am J Psychiatry 1996;153:1147-53.
Moby Doc

Chapter 1: Loomings
Call me Dr. Ishmael. Some years ago—never mind how long precisely—having little or no money in my purse and nothing particular to interest me, I thought I would go to medical school. I wanted to feel an enlarged spleen and learn the circulation.
Chapter 2: A Bosom Friend
It was the evening before the start of a long rotation, and I had to find quarters. I had been assigned to share a call room with another student. It was late and I dimmed the lights and fell into a disturbed sleep. Suddenly the lights flashed on, and a sight unlike any I had imagined came before my bleary eyes. It was a huge man, covered in tattoos, with strange piercings and wires sticking from his ears.
“Nizetameetya,” he mumbled. He pulled off his shirt, and I could see a large caduceus motif filled the canvas of his back.
“Watchaheerfaw?” he asked. It was some time before I could translate his strange island dialect. His name was Queequeg and he was from the island of Long. Before the sun had risen, we were best of friends. Better yet, we had been assigned to the same medicine service.
Chapter 3: The Hospital
A strange old building was the Pequod Hospital, an outreach of the Nantucket General Hospital. It was a hospital of the old school. The wooden floors were shiny with use and the walls a dim yellow. It had the distinct odor of disinfectant with a trace of stale urine; it smelled like a hospital. The spirits of patients lingered in the air.
Chapter 4: The Warning
As we entered the lobby, a student in a short white coat stumbled by us. Bedraggled, he was splattered with nameless filth. His name tag read “ELISA.”
“Doing a rotation are you? At the Pequod? You on Ahab’s team are you? It’s not too late to switch services. Not too late. Too late,” he said as he staggered off.
Chapter 5: Two Squires
We entered the ward and met an intern, Dr. Flask. A short, ruddy young fellow. Very pugnacious concerning scut. He was bent over a patient’s arm prodding for a vessel. He looked at Queequeg.
“Oh lord what have we here, are you a medical student or a freak show?” he barked. Queequeg pushed him aside, pulled a needle from a loaded pocket, and without hesitation plunged it into the patient’s arm, hitting the vein instantly. He turned toward Flask, who was now smiling broadly.
Several minutes later, a second intern named Dr. Stubb walked in. A mellow dude, neither serious nor intense. He was calm in a code; fearless in the face of an angry family. He constantly twirled a drug company pen, revolving endlessly around the fingers of his left hand. During rounds, while taking a history, perhaps while asleep, that ballpoint spun continually on a journey nowhere. It was hypnotizing.
Chapter 6: A Knight
I smelled him before I saw him. It was a scent of the islands, of roasted beans and cinnamon. It was Dr. Starbuck. He held the largest cup of coffee I had ever seen.
He caught my eye and rightly read my thoughts. “It’s a triple soy latte with a twist,” he said between sips. I never saw him without a cup in his hand. Lattes, espressos, cappuccinos—cold or scalding, frothy or black, Kona or Colombian—these were his passions. It was only about the divine essence of the bean that I saw him show his true emotions.
Chapter 7: Rounds
And so the strange rotation began to take shape. We headed down the long old ward, the patient’s beds in groups of two. For those of you who never rounded in these days gone by, not corrupted by the mighty powers of Microsoft, it was an odd sight. A mass of physicians huddled around a chart rack. From this rack were pulled clipboards: long wood or plastic holders with strange colored papers barely held in place, waiting to fall out and flutter to the floor, their normal order destroyed. The rack was our lifeboat, our master, and our servant. We went from room to room to see patients, discuss them, make a diagnostic plan. Then the resident turned to the interns and began to grill them. And Lord help the student who could not withstand the devious pimpage.
Knight Starbuck was no exception to this rule. He would scour the physiology and pharmacologic depths of our souls between sips of Jamaican roast. When we did not know, he would turn to Flask or Stubb. Stubb would generally answer, his pen incessantly turning.
Something felt wrong about this service, though. Some foreboding. Some hint of disaster to come. I realized then we were a ship without a rudder, dismasted without our leader, our attending physician. We heard footsteps coming our way. I could not say precisely how, but the air seemed to become charged, as if before a storm.
Chapter 8: Enter Ahab
Dr. Ahab strode upon the ward. His whole broad form was bronzed from some strange ailment or weeks at the beach. A large scar ran along the anterior part of his neck, white against the dark skin. A mark of some desperate wound or endarterectomy. But it was not this that left me speechless in his presence; it was his great white coat.
Each of us, except Queequeg who rejected such formalities, wore a white coat. Mine was short (in measure to my educational rank), filled to the brim with anything I thought might be of value. I was not one to be found wanting when an item was needed. The residents wore longer versions, their pockets stuffed with their own totems of power.
But Ahab’s white coat was of another dimension entirely. To call it pristine would fall short of its purity: It was incandescent. A wrinkle would have expired of loneliness. It was starched and unbending, like Dr. Ahab himself. It went nearly to the floor, the tops of his wing tips barely visible beneath. It was his armor, his shield, it was Ahab.
“Do you know what I’m looking for team?” he asked each of us in turn, as the hair rose on the back of my neck. “It’s evidence I’m looking for. And not just any, but Grade A-1 that we’ll be seeking”
Chapter 9: The Chase for Evidence
And so rounds began again. Each patient in their turn was prodded and poked. The medicines were reviewed; the care plan discussed. With each case Ahab became more agitated. He demanded proof that our therapies were supported by the literature. He worshipfully spoke of articles and references like they had a life of their own, a hierarchy of existence.
As we came to the last patient, Ahab began to pace nervously. It was Stubb’s turn to present.
“The next patient is a morbidly obese 74-year-old with a DVT and PE, on heparin. We are starting Coumadin now,” began Stubb.
Suddenly Ahab erupted: “Why is this patient in the hospital? Why isn’t he on LMWH and home already?”
“I thought he needed heparinization, and I’m concerned about hypoxia,” stammered Stubb.
“Aye, but what’s your evidence that inpatient is better than outpatient treatment? Can you drive blindfolded? Are your thoughts and concerns worth the wasted resources?” hissed Ahab.
The pen fell from Stubb’s hand and lay lifeless on the floor.
Suddenly the nurse ran from the patient’s room, calling a code. We rushed into the room. The patient was a huge man—a leviathan—his flesh an off-white in the fluorescent light. Flask jumped on his chest and began to pump; Stubb intubated and bagged, while Starbuck sipped his coffee. Queequeg plunged a needle into the patient’s femoral artery for a blood gas and a central line in his subclavian before I could move my feet. A small jet of blood streamed out while Queequeg positioned the tubing. The patient was resuscitated and wheeled to the ICU. I stood helplessly, thinking about evidence.
I then noticed that Ahab, who seemed shaken, was rooted to the floor. He stared at his own chest, a streak of clotted blood across his perfect white coat.
“Oh, lonely stats of death and life. Toward thee I strive, thou all-consuming data. From a cohort’s heart I randomize thee; to the last I graph with thee; for evidence sake I control my last study.” He stumbled from the room.
Chapter 10: Epilogue
I watched Ahab head to the elevator, his perfect coat tinged now with red. He waved to me three times, beckoning me to follow. But I leaned against the chart rack; it was solid. It kept me afloat. I stood there until the other team came by and joined them for their teaching rounds. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
Chapter 1: Loomings
Call me Dr. Ishmael. Some years ago—never mind how long precisely—having little or no money in my purse and nothing particular to interest me, I thought I would go to medical school. I wanted to feel an enlarged spleen and learn the circulation.
Chapter 2: A Bosom Friend
It was the evening before the start of a long rotation, and I had to find quarters. I had been assigned to share a call room with another student. It was late and I dimmed the lights and fell into a disturbed sleep. Suddenly the lights flashed on, and a sight unlike any I had imagined came before my bleary eyes. It was a huge man, covered in tattoos, with strange piercings and wires sticking from his ears.
“Nizetameetya,” he mumbled. He pulled off his shirt, and I could see a large caduceus motif filled the canvas of his back.
“Watchaheerfaw?” he asked. It was some time before I could translate his strange island dialect. His name was Queequeg and he was from the island of Long. Before the sun had risen, we were best of friends. Better yet, we had been assigned to the same medicine service.
Chapter 3: The Hospital
A strange old building was the Pequod Hospital, an outreach of the Nantucket General Hospital. It was a hospital of the old school. The wooden floors were shiny with use and the walls a dim yellow. It had the distinct odor of disinfectant with a trace of stale urine; it smelled like a hospital. The spirits of patients lingered in the air.
Chapter 4: The Warning
As we entered the lobby, a student in a short white coat stumbled by us. Bedraggled, he was splattered with nameless filth. His name tag read “ELISA.”
“Doing a rotation are you? At the Pequod? You on Ahab’s team are you? It’s not too late to switch services. Not too late. Too late,” he said as he staggered off.
Chapter 5: Two Squires
We entered the ward and met an intern, Dr. Flask. A short, ruddy young fellow. Very pugnacious concerning scut. He was bent over a patient’s arm prodding for a vessel. He looked at Queequeg.
“Oh lord what have we here, are you a medical student or a freak show?” he barked. Queequeg pushed him aside, pulled a needle from a loaded pocket, and without hesitation plunged it into the patient’s arm, hitting the vein instantly. He turned toward Flask, who was now smiling broadly.
Several minutes later, a second intern named Dr. Stubb walked in. A mellow dude, neither serious nor intense. He was calm in a code; fearless in the face of an angry family. He constantly twirled a drug company pen, revolving endlessly around the fingers of his left hand. During rounds, while taking a history, perhaps while asleep, that ballpoint spun continually on a journey nowhere. It was hypnotizing.
Chapter 6: A Knight
I smelled him before I saw him. It was a scent of the islands, of roasted beans and cinnamon. It was Dr. Starbuck. He held the largest cup of coffee I had ever seen.
He caught my eye and rightly read my thoughts. “It’s a triple soy latte with a twist,” he said between sips. I never saw him without a cup in his hand. Lattes, espressos, cappuccinos—cold or scalding, frothy or black, Kona or Colombian—these were his passions. It was only about the divine essence of the bean that I saw him show his true emotions.
Chapter 7: Rounds
And so the strange rotation began to take shape. We headed down the long old ward, the patient’s beds in groups of two. For those of you who never rounded in these days gone by, not corrupted by the mighty powers of Microsoft, it was an odd sight. A mass of physicians huddled around a chart rack. From this rack were pulled clipboards: long wood or plastic holders with strange colored papers barely held in place, waiting to fall out and flutter to the floor, their normal order destroyed. The rack was our lifeboat, our master, and our servant. We went from room to room to see patients, discuss them, make a diagnostic plan. Then the resident turned to the interns and began to grill them. And Lord help the student who could not withstand the devious pimpage.
Knight Starbuck was no exception to this rule. He would scour the physiology and pharmacologic depths of our souls between sips of Jamaican roast. When we did not know, he would turn to Flask or Stubb. Stubb would generally answer, his pen incessantly turning.
Something felt wrong about this service, though. Some foreboding. Some hint of disaster to come. I realized then we were a ship without a rudder, dismasted without our leader, our attending physician. We heard footsteps coming our way. I could not say precisely how, but the air seemed to become charged, as if before a storm.
Chapter 8: Enter Ahab
Dr. Ahab strode upon the ward. His whole broad form was bronzed from some strange ailment or weeks at the beach. A large scar ran along the anterior part of his neck, white against the dark skin. A mark of some desperate wound or endarterectomy. But it was not this that left me speechless in his presence; it was his great white coat.
Each of us, except Queequeg who rejected such formalities, wore a white coat. Mine was short (in measure to my educational rank), filled to the brim with anything I thought might be of value. I was not one to be found wanting when an item was needed. The residents wore longer versions, their pockets stuffed with their own totems of power.
But Ahab’s white coat was of another dimension entirely. To call it pristine would fall short of its purity: It was incandescent. A wrinkle would have expired of loneliness. It was starched and unbending, like Dr. Ahab himself. It went nearly to the floor, the tops of his wing tips barely visible beneath. It was his armor, his shield, it was Ahab.
“Do you know what I’m looking for team?” he asked each of us in turn, as the hair rose on the back of my neck. “It’s evidence I’m looking for. And not just any, but Grade A-1 that we’ll be seeking”
Chapter 9: The Chase for Evidence
And so rounds began again. Each patient in their turn was prodded and poked. The medicines were reviewed; the care plan discussed. With each case Ahab became more agitated. He demanded proof that our therapies were supported by the literature. He worshipfully spoke of articles and references like they had a life of their own, a hierarchy of existence.
As we came to the last patient, Ahab began to pace nervously. It was Stubb’s turn to present.
“The next patient is a morbidly obese 74-year-old with a DVT and PE, on heparin. We are starting Coumadin now,” began Stubb.
Suddenly Ahab erupted: “Why is this patient in the hospital? Why isn’t he on LMWH and home already?”
“I thought he needed heparinization, and I’m concerned about hypoxia,” stammered Stubb.
“Aye, but what’s your evidence that inpatient is better than outpatient treatment? Can you drive blindfolded? Are your thoughts and concerns worth the wasted resources?” hissed Ahab.
The pen fell from Stubb’s hand and lay lifeless on the floor.
Suddenly the nurse ran from the patient’s room, calling a code. We rushed into the room. The patient was a huge man—a leviathan—his flesh an off-white in the fluorescent light. Flask jumped on his chest and began to pump; Stubb intubated and bagged, while Starbuck sipped his coffee. Queequeg plunged a needle into the patient’s femoral artery for a blood gas and a central line in his subclavian before I could move my feet. A small jet of blood streamed out while Queequeg positioned the tubing. The patient was resuscitated and wheeled to the ICU. I stood helplessly, thinking about evidence.
I then noticed that Ahab, who seemed shaken, was rooted to the floor. He stared at his own chest, a streak of clotted blood across his perfect white coat.
“Oh, lonely stats of death and life. Toward thee I strive, thou all-consuming data. From a cohort’s heart I randomize thee; to the last I graph with thee; for evidence sake I control my last study.” He stumbled from the room.
Chapter 10: Epilogue
I watched Ahab head to the elevator, his perfect coat tinged now with red. He waved to me three times, beckoning me to follow. But I leaned against the chart rack; it was solid. It kept me afloat. I stood there until the other team came by and joined them for their teaching rounds. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
Chapter 1: Loomings
Call me Dr. Ishmael. Some years ago—never mind how long precisely—having little or no money in my purse and nothing particular to interest me, I thought I would go to medical school. I wanted to feel an enlarged spleen and learn the circulation.
Chapter 2: A Bosom Friend
It was the evening before the start of a long rotation, and I had to find quarters. I had been assigned to share a call room with another student. It was late and I dimmed the lights and fell into a disturbed sleep. Suddenly the lights flashed on, and a sight unlike any I had imagined came before my bleary eyes. It was a huge man, covered in tattoos, with strange piercings and wires sticking from his ears.
“Nizetameetya,” he mumbled. He pulled off his shirt, and I could see a large caduceus motif filled the canvas of his back.
“Watchaheerfaw?” he asked. It was some time before I could translate his strange island dialect. His name was Queequeg and he was from the island of Long. Before the sun had risen, we were best of friends. Better yet, we had been assigned to the same medicine service.
Chapter 3: The Hospital
A strange old building was the Pequod Hospital, an outreach of the Nantucket General Hospital. It was a hospital of the old school. The wooden floors were shiny with use and the walls a dim yellow. It had the distinct odor of disinfectant with a trace of stale urine; it smelled like a hospital. The spirits of patients lingered in the air.
Chapter 4: The Warning
As we entered the lobby, a student in a short white coat stumbled by us. Bedraggled, he was splattered with nameless filth. His name tag read “ELISA.”
“Doing a rotation are you? At the Pequod? You on Ahab’s team are you? It’s not too late to switch services. Not too late. Too late,” he said as he staggered off.
Chapter 5: Two Squires
We entered the ward and met an intern, Dr. Flask. A short, ruddy young fellow. Very pugnacious concerning scut. He was bent over a patient’s arm prodding for a vessel. He looked at Queequeg.
“Oh lord what have we here, are you a medical student or a freak show?” he barked. Queequeg pushed him aside, pulled a needle from a loaded pocket, and without hesitation plunged it into the patient’s arm, hitting the vein instantly. He turned toward Flask, who was now smiling broadly.
Several minutes later, a second intern named Dr. Stubb walked in. A mellow dude, neither serious nor intense. He was calm in a code; fearless in the face of an angry family. He constantly twirled a drug company pen, revolving endlessly around the fingers of his left hand. During rounds, while taking a history, perhaps while asleep, that ballpoint spun continually on a journey nowhere. It was hypnotizing.
Chapter 6: A Knight
I smelled him before I saw him. It was a scent of the islands, of roasted beans and cinnamon. It was Dr. Starbuck. He held the largest cup of coffee I had ever seen.
He caught my eye and rightly read my thoughts. “It’s a triple soy latte with a twist,” he said between sips. I never saw him without a cup in his hand. Lattes, espressos, cappuccinos—cold or scalding, frothy or black, Kona or Colombian—these were his passions. It was only about the divine essence of the bean that I saw him show his true emotions.
Chapter 7: Rounds
And so the strange rotation began to take shape. We headed down the long old ward, the patient’s beds in groups of two. For those of you who never rounded in these days gone by, not corrupted by the mighty powers of Microsoft, it was an odd sight. A mass of physicians huddled around a chart rack. From this rack were pulled clipboards: long wood or plastic holders with strange colored papers barely held in place, waiting to fall out and flutter to the floor, their normal order destroyed. The rack was our lifeboat, our master, and our servant. We went from room to room to see patients, discuss them, make a diagnostic plan. Then the resident turned to the interns and began to grill them. And Lord help the student who could not withstand the devious pimpage.
Knight Starbuck was no exception to this rule. He would scour the physiology and pharmacologic depths of our souls between sips of Jamaican roast. When we did not know, he would turn to Flask or Stubb. Stubb would generally answer, his pen incessantly turning.
Something felt wrong about this service, though. Some foreboding. Some hint of disaster to come. I realized then we were a ship without a rudder, dismasted without our leader, our attending physician. We heard footsteps coming our way. I could not say precisely how, but the air seemed to become charged, as if before a storm.
Chapter 8: Enter Ahab
Dr. Ahab strode upon the ward. His whole broad form was bronzed from some strange ailment or weeks at the beach. A large scar ran along the anterior part of his neck, white against the dark skin. A mark of some desperate wound or endarterectomy. But it was not this that left me speechless in his presence; it was his great white coat.
Each of us, except Queequeg who rejected such formalities, wore a white coat. Mine was short (in measure to my educational rank), filled to the brim with anything I thought might be of value. I was not one to be found wanting when an item was needed. The residents wore longer versions, their pockets stuffed with their own totems of power.
But Ahab’s white coat was of another dimension entirely. To call it pristine would fall short of its purity: It was incandescent. A wrinkle would have expired of loneliness. It was starched and unbending, like Dr. Ahab himself. It went nearly to the floor, the tops of his wing tips barely visible beneath. It was his armor, his shield, it was Ahab.
“Do you know what I’m looking for team?” he asked each of us in turn, as the hair rose on the back of my neck. “It’s evidence I’m looking for. And not just any, but Grade A-1 that we’ll be seeking”
Chapter 9: The Chase for Evidence
And so rounds began again. Each patient in their turn was prodded and poked. The medicines were reviewed; the care plan discussed. With each case Ahab became more agitated. He demanded proof that our therapies were supported by the literature. He worshipfully spoke of articles and references like they had a life of their own, a hierarchy of existence.
As we came to the last patient, Ahab began to pace nervously. It was Stubb’s turn to present.
“The next patient is a morbidly obese 74-year-old with a DVT and PE, on heparin. We are starting Coumadin now,” began Stubb.
Suddenly Ahab erupted: “Why is this patient in the hospital? Why isn’t he on LMWH and home already?”
“I thought he needed heparinization, and I’m concerned about hypoxia,” stammered Stubb.
“Aye, but what’s your evidence that inpatient is better than outpatient treatment? Can you drive blindfolded? Are your thoughts and concerns worth the wasted resources?” hissed Ahab.
The pen fell from Stubb’s hand and lay lifeless on the floor.
Suddenly the nurse ran from the patient’s room, calling a code. We rushed into the room. The patient was a huge man—a leviathan—his flesh an off-white in the fluorescent light. Flask jumped on his chest and began to pump; Stubb intubated and bagged, while Starbuck sipped his coffee. Queequeg plunged a needle into the patient’s femoral artery for a blood gas and a central line in his subclavian before I could move my feet. A small jet of blood streamed out while Queequeg positioned the tubing. The patient was resuscitated and wheeled to the ICU. I stood helplessly, thinking about evidence.
I then noticed that Ahab, who seemed shaken, was rooted to the floor. He stared at his own chest, a streak of clotted blood across his perfect white coat.
“Oh, lonely stats of death and life. Toward thee I strive, thou all-consuming data. From a cohort’s heart I randomize thee; to the last I graph with thee; for evidence sake I control my last study.” He stumbled from the room.
Chapter 10: Epilogue
I watched Ahab head to the elevator, his perfect coat tinged now with red. He waved to me three times, beckoning me to follow. But I leaned against the chart rack; it was solid. It kept me afloat. I stood there until the other team came by and joined them for their teaching rounds. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
Help Me. I Can’t Speak.
Each week in the United States, child protective services and agencies receive reports of more than 50,000 suspected child abuse incidents. In 2002, 2.6 million incidents involving 4.5 million children were reported. Approximately four children die every day as a result of abuse or neglect.1 But numbers don’t tell the whole story. Behind every number is a child at risk.
“I can picture right now in my mind a young baby who was about six months of age with a belly that was protruded and distended,” says Erin R. Stucky, MD, a pediatric hospitalist at Children’s Hospital and Health Center San Diego, and an associate professor of pediatrics at the University of California San Diego. “[She had] no bowel sounds, and the arms and legs were so thin, had no fat whatsoever. The skin was rolling. The face looked dysmorphic, but it was simply because the eyes were so white, and there was no fat on the face at all. The baby had an irritated cry. The hair was thin. [She] had a look of anxiety, true anxiety [in her] eyes. It was impressive, as though this infant was saying, ‘Help me. I can’t speak.’ [She] was very socially engaged, but tired. If you had to qualify the look further, it would be something like, ‘I’m in pain. Protect me. Please don’t walk out the door.’
“The child had been admitted from the emergency department at an outside facility. They had been focused, appropriately to some extent, on the fact that the belly was distended and that the baby had no bowel sounds. They were focused on the fact that the parent’s history [of the child] was of vomiting during the day, but it clearly did not equate whatsoever with the way the child looked. It was immediately clear, simply looking at the baby while walking in the room, that something very bad was wrong and that the parents’ answers and explanations did not fit.”
What It Is
Child abuse manifests in many forms, including physical abuse, sexual abuse, emotional abuse, and neglect, with a “child” typically defined as a person under 18. Legal definitions of the forms of child abuse vary, but, in general, they reflect societal views of actions deemed improper and unacceptable because they place a child at risk of physical or emotional harm.2 The federal Child Abuse Prevention and Treatment Act (CAPTA) defines child abuse and neglect as:
- Any recent act or failure to act on the part of a parent or caretaker that results in death, serious physical or emotional harm, sexual abuse, or exploitation; or
- An act or failure to act that presents an imminent risk of serious harm.3
States must include these minimum standards in their statutes in order to receive federal funds.
Neglect is the most common form of child abuse.2 Although definitions of neglect vary by state, they share characteristics. Minnesota defines neglect as inadequate food, shelter, clothing, or medical care. California includes both overt acts and omissions in the definition of neglect, defining general neglect as a lack of food, clothing, or medical care and severe neglect as malnutrition, failure to thrive, or willfully putting a child in danger. And Rhode Island’s neglect definition goes even further, including the above acts and omissions as well as the failure to provide a minimum degree of care or proper supervision or guardianship due to unwillingness, social problems, mental incompetency, or the use of a drug, drugs or alcohol, desertion, or abandonment. Rhode Island also includes the failure to take financial responsibility for a child.4
According to Georgia Berrenberg, esq., deputy district attorney, Second Judicial District of New Mexico, sexual abuse is the most common type that goes to trial. Berrenberg, who has been a prosecutor since 1984 and was in the child abuse division from 1996–2005, estimates that approximately 70% of cases involve sexual abuse compared with 30% that involve physical abuse.
However, pediatric hospitalists will most commonly see neglect, presenting as malnutrition or failure to thrive, in a child admitted to the hospital.4
Recognize Abuse and Neglect
Pediatric hospitalists are in a unique position to recognize child abuse and neglect, intervene appropriately, and help families avoid ultimate tragedy. They are trained to consider the entire child—no matter the presenting condition—to look at general issues and to think about development and nutrition every time they examine a child.
“When someone says, ‘This child has pneumonia,’ my job is to not think pneumonia; my job is to think, ‘What’s causing this child to breathe fast?’ to make sure I don’t miss anything,” says Dr. Stucky. “If the history doesn’t fit the examination and my first, second, [and] third thoughts are child abuse/neglect. It’s my job to work on that, but it’s also my job to push my own buttons to make sure that it’s not anything else medically going on. The child that never has a bruise or fracture is the odd one out. The key [to recognizing abuse] is history.”
Don’t jump to conclusions. Hospitalists need to consider the history reported by the parent in light of the physical exam of the child. For example, if the parent tells you that the child fell headfirst off a tricycle and landed on his face, note the pattern of the bruising. If the child has bruising around the eye then that could be consistent with the history, but if the child’s eyelid is cut or bruised and there’s no bruising around the eye, that’s another matter. The eyebrow and cheekbone will protect the eye when you fall and land on your face.
“Pay attention to what you hear and see in those first few minutes and hours with that family because stories are going to change,” says Berrenberg. “Be very, very clear about the initial things that are said.”
Dealing with the medical issues that led to the admission is paramount, and it’s important for the hospitalist to communicate effectively with the parent to ensure that the child receives the most appropriate treatment. Asking open-ended questions while you take the history can be revealing:
- Can you tell me how long this has been happening?
- What do you think might be contributing to this?
- Can you tell me how you’ve been dealing with these issues at home?
- Run me through a typical day at home with your baby.
In addition to the history, consider the parent/child interaction. “Most kids, even when they’re stressed and in pain are very attentive to where their parents are,” says Dr. Stucky. “They want to be with them no matter what. They may be angry and battling. They may respond to pain differently, but that relationship is very important. As you watch it you can really get a good sense [of whether] this child’s anger outburst is because they’re in pain, they’re confused, they have autism, or they are really angry with their parent and this is the way they’re protecting themselves.”
The hospitalist has to be up front with the parent about what the next step in their child’s treatment is going to be. “It’s a delicate discussion, but an honest one,” says Dr. Stucky. “It’s important to say to the parent, overtly, ‘I’m very concerned about your baby’s weight loss. I’m very concerned that this has happened over the past several months and that it has taken this long for your baby to be seen by a doctor. I’m very concerned, and I want you to understand that your baby has a critical condition right now. It’s so malnourished that the body’s organs aren’t working properly. ... Because of this concern, I’m going to call social workers. Because of this concern I’ll use [work with] a team of people to help me to take care of your baby. They’ll ask a lot of questions, and it’s very important that you answer honestly so we can do the best for your baby and make sure that the whole family can get whatever help is needed to take care of the problem.’ ”
Reporting Requirements
In most states healthcare workers not only have a moral responsibility to report suspected abuse, they are required by law to do so. In fact, New Mexico’s statute requires anyone who suspects child abuse to report it and makes failure to do so a misdemeanor. Hospitalists should know in advance to whom to report the suspected abuse.
Consider making a call to a social worker your first step. “Social workers are invaluable,” says Dr. Stucky. “They’re there for the families. They ask the harder questions that allow us to have that medical relationship and continue to care for the child’s needs. They can look up information that we can’t. They can look up child protection history, whether the parent has been incarcerated, things that support the possibility of abuse. They can file the CPS report, allowing the hospitalist to continue caring medically for the child.”
According to Berrenberg, the police should be your second call.
Dealing with child abuse and neglect is a team effort. In addition to the police and a social worker, you need to involve the nutritionist and the primary care pediatrician (if they have one). If you’re lucky, your hospital may have a child abuse specialist on staff. “Be ready to deal with a whole variety of people who may or may not know what else has already happened,” says Berrenberg.
After the Hospital Stay
Although child abuse is all too common, most pediatric hospitalists won’t often see the inside of a courtroom. Dr. Stucky says that cases with which she’s been involved have gone to trial twice during her 10 years as a pediatric hospitalist. And Berrenberg says, “Failure to thrive is not something we charge very often. That’s a difficult thing to prove.”
That said, prepare for the possibility of being called as a fact witness. According to Berrenberg, physicians may be asked to report on not just their observations of the child, but also on statements made in their presence.
“Statements made to physicians and to healthcare personnel are critical—be it by parents, caretakers, or the child themselves in the case of sexual abuse,” she says. “If statements are made in the course of diagnosis and treatment, then those statements can come in under hearsay exceptions. ... The doctor can testify about those statements.”
Remember it’s the doctor/patient relationship that’s important. Your patient’s parents have no doctor/patient relationship.
Berrenberg offers the following advice for physicians preparing to testify: “Be patient. Read everything you have on your case. Expect everything to change. When you’re told that you’re going to trial on Monday, expect that to change. If you’ve testified before and there are transcripts available, expect the defense to know about that previous testimony. If you’re basing your opinion on literature, expect the defense attorney to have found that literature and be familiar with it.
“Work with your prosecutor. Know what they want you for. They might only want you for a limited piece; they might want you for the whole gamut. They will tell you what they’re going to expect of you. Spend as much time as you can with them, with the photos, with the file. It’s always what you don’t expect to come up that comes up.”
Pediatric hospitalists should also be prepared for old cases to come back. “We’ll bring you from wherever you are—even if you’re out of the country,” says Berrenberg. “We’ll bring you back if we need you to testify. We’ll find you. If you’re the one who saw the child and were the initial responder, so to speak, no one else can say what you saw.”
Conclusion
What happened to the six-month-old baby Dr. Stucky remembers so clearly?
“I only know what happened during the hospital stay,” she says. “This family clearly needed help and guidance. There was an overwhelming, clear [indication] that the mother had significant, major depression. She wasn’t feeding the baby. She was completely ignoring the child, and she acknowledged that. ... The father was at work and thought that perhaps this baby was just ill or sickly. He was told that the baby was being taken to the doctor, and that wasn’t happening. He was naive and innocent in thinking that things were being dealt with and thinking that their baby was simply a baby who cried a lot and wasn’t gaining weight well.
“Once this was all [addressed], he jumped at the opportunity to have the mother in therapy and on medications. The mother herself was completely willing to give up the care. ... In this case, the paternal grandmother took over the care of this child. The father would drop off the baby at her house during the day and pick up the baby at night. On weekends they would share the duties. That was the plan at discharge. ... I can’t guarantee it, but it’s my sense that this worked very well.”
Keri Losavio is a medical journalist with more than 10 years’ experience.
References
- National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov/topics/prevention/index.cfm.
- “What Is Child Maltreatment?” From A Coordinated Response to Child Abuse and Neglect: The Foundation for Practice. National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov.
- Child Abuse Prevention and Treatment Act. Download the complete text from the Cornell University Legal Information Institute: www4.law.cornell.edu/uscode/42/ch67.html.
- “Monitoring Child Neglect.” Summary of discussions at a meeting co-sponsored by the Centers for Disease Control and Prevention (CDC) and Prevent Child Abuse America (PCA America), March 29, 2002.
PEDIATRIC SPECIAL SECTION
In the Literature
Optimizing Management of GERD: Medical therapy or surgical intervention?
Hassall E. Outcomes of fundoplication: causes for concern, newer options. Arch Dis Child. 2005;90:1047-1052.
Review by Ray Chan, MD
This narrative review provides a concise overview of gastroesophageal reflux disease (GERD) while specifically addressing surgical treatment. The author focuses on the potential complications of surgical treatment and cites several studies demonstrating a high rate of complications and patient dissatisfaction with their outcomes. In contrast, the review does cite several sources that concluded good outcomes; however, the article questions the conclusions of these studies due to study designs with poorly defined and subjective outcome measures.
In contrast to the discussion on fundoplication, the review offers a more favorable description of proton pump inhibitor therapy. In the concluding remarks Hassall argues that medical therapy options should be exhausted prior to surgical therapy. The author states that the risk of mortality and morbidity combined with less than desirable efficacy of fundoplication should caution clinicians from being too eager in recommending fundoplication.
Clinically significant GERD is a common inpatient problem. This article provides a good review of the pathophysiology of this disease and available treatment options. Unfortunately, this narrative review does not utilize a systematic method of identifying relevant studies nor does it include a systematic approach for critical appraisal of these studies. Nevertheless the caution it raises about fundoplication is a worthy one that should be explored further. It is interesting to note that prior to this review the author has received grant support and was a paid consultant for AstraZeneca and TAP Pharmaceutical Products Inc.
Support for Bag UA Screening During Evaluation for UTI
McGillivray D, Mok E, Mulrooney E, et al. A head-to-head comparison: “clean-void” bag versus catheter urinalysis in the diagnosis of urinary tract infection in young children. J Pediatr. 2005;147(4):451-456.
Review by Jenny Geheb, RN, CPNP
Early detection of urinary tract infection (UTI) can be especially important in children. This study uses a cross-sectional design to compare the validity of the urinalysis on clean-voided bag versus catheter urine specimens using the catheter culture as the “gold” standard. This study looked at 303 non-toilet-trained children under age three at risk for UTI who presented to a children’s hospital emergency department. Paired bag and catheter specimens were obtained from each child and sent for dipstick and microscopic urinalysis. Sensitivity and specificity were compared using McNemar’s [chi]2 test for paired specimens and the ordinary [chi]2 test for unpaired comparisons.
The study, which was conducted at the Montreal Children’s Hospital, found that the bag dipstick was more sensitive than the catheter dipstick for the entire study sample: 0.85 (95% confidence interval [CI] = 0.78 to 0.93) versus 0.71 (95% CI= 0.95 to 0.99), respectively. Both bag and catheter dipstick sensitivities were lower in infants <90 days old. Specificity was consistently lower for the bag specimens than for the catheter specimens.
A child at high risk for UTI (previous history of UTI, anatomic abnormalities, immunosuppressed, or presence of urinary symptoms) should be catheterized to obtain both a UA and culture; however, in children older than 90 days with fever without source and at low risk for UTI, a “selective catheterization” approach, as outlined in the American Academy of Pediatrics practice parameter, appears to be reasonable.
In low-risk children, serious consequences of infection are less likely, and the authors propose that the risks of missing a UTI are likely to be outweighed by the risks of catheterization, including pain, false-positive result, trauma, introduction of infection, test resistance by staff, and parental concern.
In summary, the provider may choose to use a bag urine screening strategy to reduce the number of unnecessary catheterizations in children who are considered low risk and over 90 days old. Further studies are needed to analyze the cost-benefit ratio of this approach as well as to confirm these findings with larger populations.
Short-Course Antibiotic Treatment for Streptococcal Pharyngitis
Casey JR, Pichichero ME. Meta-analysis of short course antibiotic treatment for group A streptococcal tonsillopharyngitis. Ped Infect Dis J. 2005;24(10):909-917.
Review by Jenny Geheb, RN, CPNP
Group A streptococcal (GAS) tonsillopharyngitis is a common cause for antibiotic treatment in children. Researchers at the University of Rochester Medical Center (N.Y.) performed a meta-analysis of current data to compare bacterial and clinical cure rates in patients with GAS tonsillopharyngitis treated with short course antibiotic treatment with oral [beta]-lactam or macrolide antibiotics for four to five days with standard 10-day treatment courses. Medline, Embase, reference lists, and abstract searches were all used to identify applicable publications. Trials were included if there was bacteriologic confirmation of GAS tonsillopharyngitis, random assignment to antibiotic therapy for a [beta]-lactam or macrolide antibiotic of shortened course versus a 10-day course, and assessment of bacteriologic outcome using a throat culture.
Twenty-two trials involving 7,470 patients were included in four separate analyses. Trials were grouped by a short course of cephalosporins (n=14), macrolides (other than azithromycin) (n=6), penicillin (n=2), and amoxicillin (n=2). Cephalosporin trials were further grouped by penicillin (n=12) or the same cephalosporin (n=3). Five trials were conducted in the United States with the remainder conducted in Europe.
Meta-analysis showed that short course cephalosporin treatment was superior for bacterial cure rate compared with 10 days of penicillin (OR 1.47; 95% CI, 1.06-2.03). Short-course penicillin therapy was inferior in achieving bacterial cure versus 10 days of penicillin. Clinical cure rate mirrored the bacterial cure rate results. Small sample size limited the statistical power and conclusions of the short course macrolide trials as well as trials of four or five days of cephalosporin therapy compared with 10 days of the same.
This meta-analysis shows that short-course treatment of GAS tonsillopharyngitis can be more effective when prescribing four or five days of cefdinir, cefpodoxime, or cefuroxime treatment than standard 10-day treatment of penicillin. In the United States cefdinir, cefpodoxime, and azithromycin are indicated for short-course treatment. As prescribing practitioners, it is important for us to consider the advantages of shortened antibiotic courses, including improved patient compliance, fewer adverse effects, and reduced impact on development of antibiotic resistance and nasopharyngeal colonization with resistant bacteria. However, the authors emphasize that caution must be used in interpretation of the results of this meta-analysis.
For example, the trials were grouped according to class of antibiotics so that the cephalosporin group included seven different cephalosporins (one first generation, two second generation, and four third generation). In addition, there was much variability in the quality and design of compared studies, which makes it difficult to make strong conclusions. Repeat studies are needed, especially in regard to short-course macrolide or amoxicillin treatment.
Each week in the United States, child protective services and agencies receive reports of more than 50,000 suspected child abuse incidents. In 2002, 2.6 million incidents involving 4.5 million children were reported. Approximately four children die every day as a result of abuse or neglect.1 But numbers don’t tell the whole story. Behind every number is a child at risk.
“I can picture right now in my mind a young baby who was about six months of age with a belly that was protruded and distended,” says Erin R. Stucky, MD, a pediatric hospitalist at Children’s Hospital and Health Center San Diego, and an associate professor of pediatrics at the University of California San Diego. “[She had] no bowel sounds, and the arms and legs were so thin, had no fat whatsoever. The skin was rolling. The face looked dysmorphic, but it was simply because the eyes were so white, and there was no fat on the face at all. The baby had an irritated cry. The hair was thin. [She] had a look of anxiety, true anxiety [in her] eyes. It was impressive, as though this infant was saying, ‘Help me. I can’t speak.’ [She] was very socially engaged, but tired. If you had to qualify the look further, it would be something like, ‘I’m in pain. Protect me. Please don’t walk out the door.’
“The child had been admitted from the emergency department at an outside facility. They had been focused, appropriately to some extent, on the fact that the belly was distended and that the baby had no bowel sounds. They were focused on the fact that the parent’s history [of the child] was of vomiting during the day, but it clearly did not equate whatsoever with the way the child looked. It was immediately clear, simply looking at the baby while walking in the room, that something very bad was wrong and that the parents’ answers and explanations did not fit.”
What It Is
Child abuse manifests in many forms, including physical abuse, sexual abuse, emotional abuse, and neglect, with a “child” typically defined as a person under 18. Legal definitions of the forms of child abuse vary, but, in general, they reflect societal views of actions deemed improper and unacceptable because they place a child at risk of physical or emotional harm.2 The federal Child Abuse Prevention and Treatment Act (CAPTA) defines child abuse and neglect as:
- Any recent act or failure to act on the part of a parent or caretaker that results in death, serious physical or emotional harm, sexual abuse, or exploitation; or
- An act or failure to act that presents an imminent risk of serious harm.3
States must include these minimum standards in their statutes in order to receive federal funds.
Neglect is the most common form of child abuse.2 Although definitions of neglect vary by state, they share characteristics. Minnesota defines neglect as inadequate food, shelter, clothing, or medical care. California includes both overt acts and omissions in the definition of neglect, defining general neglect as a lack of food, clothing, or medical care and severe neglect as malnutrition, failure to thrive, or willfully putting a child in danger. And Rhode Island’s neglect definition goes even further, including the above acts and omissions as well as the failure to provide a minimum degree of care or proper supervision or guardianship due to unwillingness, social problems, mental incompetency, or the use of a drug, drugs or alcohol, desertion, or abandonment. Rhode Island also includes the failure to take financial responsibility for a child.4
According to Georgia Berrenberg, esq., deputy district attorney, Second Judicial District of New Mexico, sexual abuse is the most common type that goes to trial. Berrenberg, who has been a prosecutor since 1984 and was in the child abuse division from 1996–2005, estimates that approximately 70% of cases involve sexual abuse compared with 30% that involve physical abuse.
However, pediatric hospitalists will most commonly see neglect, presenting as malnutrition or failure to thrive, in a child admitted to the hospital.4
Recognize Abuse and Neglect
Pediatric hospitalists are in a unique position to recognize child abuse and neglect, intervene appropriately, and help families avoid ultimate tragedy. They are trained to consider the entire child—no matter the presenting condition—to look at general issues and to think about development and nutrition every time they examine a child.
“When someone says, ‘This child has pneumonia,’ my job is to not think pneumonia; my job is to think, ‘What’s causing this child to breathe fast?’ to make sure I don’t miss anything,” says Dr. Stucky. “If the history doesn’t fit the examination and my first, second, [and] third thoughts are child abuse/neglect. It’s my job to work on that, but it’s also my job to push my own buttons to make sure that it’s not anything else medically going on. The child that never has a bruise or fracture is the odd one out. The key [to recognizing abuse] is history.”
Don’t jump to conclusions. Hospitalists need to consider the history reported by the parent in light of the physical exam of the child. For example, if the parent tells you that the child fell headfirst off a tricycle and landed on his face, note the pattern of the bruising. If the child has bruising around the eye then that could be consistent with the history, but if the child’s eyelid is cut or bruised and there’s no bruising around the eye, that’s another matter. The eyebrow and cheekbone will protect the eye when you fall and land on your face.
“Pay attention to what you hear and see in those first few minutes and hours with that family because stories are going to change,” says Berrenberg. “Be very, very clear about the initial things that are said.”
Dealing with the medical issues that led to the admission is paramount, and it’s important for the hospitalist to communicate effectively with the parent to ensure that the child receives the most appropriate treatment. Asking open-ended questions while you take the history can be revealing:
- Can you tell me how long this has been happening?
- What do you think might be contributing to this?
- Can you tell me how you’ve been dealing with these issues at home?
- Run me through a typical day at home with your baby.
In addition to the history, consider the parent/child interaction. “Most kids, even when they’re stressed and in pain are very attentive to where their parents are,” says Dr. Stucky. “They want to be with them no matter what. They may be angry and battling. They may respond to pain differently, but that relationship is very important. As you watch it you can really get a good sense [of whether] this child’s anger outburst is because they’re in pain, they’re confused, they have autism, or they are really angry with their parent and this is the way they’re protecting themselves.”
The hospitalist has to be up front with the parent about what the next step in their child’s treatment is going to be. “It’s a delicate discussion, but an honest one,” says Dr. Stucky. “It’s important to say to the parent, overtly, ‘I’m very concerned about your baby’s weight loss. I’m very concerned that this has happened over the past several months and that it has taken this long for your baby to be seen by a doctor. I’m very concerned, and I want you to understand that your baby has a critical condition right now. It’s so malnourished that the body’s organs aren’t working properly. ... Because of this concern, I’m going to call social workers. Because of this concern I’ll use [work with] a team of people to help me to take care of your baby. They’ll ask a lot of questions, and it’s very important that you answer honestly so we can do the best for your baby and make sure that the whole family can get whatever help is needed to take care of the problem.’ ”
Reporting Requirements
In most states healthcare workers not only have a moral responsibility to report suspected abuse, they are required by law to do so. In fact, New Mexico’s statute requires anyone who suspects child abuse to report it and makes failure to do so a misdemeanor. Hospitalists should know in advance to whom to report the suspected abuse.
Consider making a call to a social worker your first step. “Social workers are invaluable,” says Dr. Stucky. “They’re there for the families. They ask the harder questions that allow us to have that medical relationship and continue to care for the child’s needs. They can look up information that we can’t. They can look up child protection history, whether the parent has been incarcerated, things that support the possibility of abuse. They can file the CPS report, allowing the hospitalist to continue caring medically for the child.”
According to Berrenberg, the police should be your second call.
Dealing with child abuse and neglect is a team effort. In addition to the police and a social worker, you need to involve the nutritionist and the primary care pediatrician (if they have one). If you’re lucky, your hospital may have a child abuse specialist on staff. “Be ready to deal with a whole variety of people who may or may not know what else has already happened,” says Berrenberg.
After the Hospital Stay
Although child abuse is all too common, most pediatric hospitalists won’t often see the inside of a courtroom. Dr. Stucky says that cases with which she’s been involved have gone to trial twice during her 10 years as a pediatric hospitalist. And Berrenberg says, “Failure to thrive is not something we charge very often. That’s a difficult thing to prove.”
That said, prepare for the possibility of being called as a fact witness. According to Berrenberg, physicians may be asked to report on not just their observations of the child, but also on statements made in their presence.
“Statements made to physicians and to healthcare personnel are critical—be it by parents, caretakers, or the child themselves in the case of sexual abuse,” she says. “If statements are made in the course of diagnosis and treatment, then those statements can come in under hearsay exceptions. ... The doctor can testify about those statements.”
Remember it’s the doctor/patient relationship that’s important. Your patient’s parents have no doctor/patient relationship.
Berrenberg offers the following advice for physicians preparing to testify: “Be patient. Read everything you have on your case. Expect everything to change. When you’re told that you’re going to trial on Monday, expect that to change. If you’ve testified before and there are transcripts available, expect the defense to know about that previous testimony. If you’re basing your opinion on literature, expect the defense attorney to have found that literature and be familiar with it.
“Work with your prosecutor. Know what they want you for. They might only want you for a limited piece; they might want you for the whole gamut. They will tell you what they’re going to expect of you. Spend as much time as you can with them, with the photos, with the file. It’s always what you don’t expect to come up that comes up.”
Pediatric hospitalists should also be prepared for old cases to come back. “We’ll bring you from wherever you are—even if you’re out of the country,” says Berrenberg. “We’ll bring you back if we need you to testify. We’ll find you. If you’re the one who saw the child and were the initial responder, so to speak, no one else can say what you saw.”
Conclusion
What happened to the six-month-old baby Dr. Stucky remembers so clearly?
“I only know what happened during the hospital stay,” she says. “This family clearly needed help and guidance. There was an overwhelming, clear [indication] that the mother had significant, major depression. She wasn’t feeding the baby. She was completely ignoring the child, and she acknowledged that. ... The father was at work and thought that perhaps this baby was just ill or sickly. He was told that the baby was being taken to the doctor, and that wasn’t happening. He was naive and innocent in thinking that things were being dealt with and thinking that their baby was simply a baby who cried a lot and wasn’t gaining weight well.
“Once this was all [addressed], he jumped at the opportunity to have the mother in therapy and on medications. The mother herself was completely willing to give up the care. ... In this case, the paternal grandmother took over the care of this child. The father would drop off the baby at her house during the day and pick up the baby at night. On weekends they would share the duties. That was the plan at discharge. ... I can’t guarantee it, but it’s my sense that this worked very well.”
Keri Losavio is a medical journalist with more than 10 years’ experience.
References
- National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov/topics/prevention/index.cfm.
- “What Is Child Maltreatment?” From A Coordinated Response to Child Abuse and Neglect: The Foundation for Practice. National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov.
- Child Abuse Prevention and Treatment Act. Download the complete text from the Cornell University Legal Information Institute: www4.law.cornell.edu/uscode/42/ch67.html.
- “Monitoring Child Neglect.” Summary of discussions at a meeting co-sponsored by the Centers for Disease Control and Prevention (CDC) and Prevent Child Abuse America (PCA America), March 29, 2002.
PEDIATRIC SPECIAL SECTION
In the Literature
Optimizing Management of GERD: Medical therapy or surgical intervention?
Hassall E. Outcomes of fundoplication: causes for concern, newer options. Arch Dis Child. 2005;90:1047-1052.
Review by Ray Chan, MD
This narrative review provides a concise overview of gastroesophageal reflux disease (GERD) while specifically addressing surgical treatment. The author focuses on the potential complications of surgical treatment and cites several studies demonstrating a high rate of complications and patient dissatisfaction with their outcomes. In contrast, the review does cite several sources that concluded good outcomes; however, the article questions the conclusions of these studies due to study designs with poorly defined and subjective outcome measures.
In contrast to the discussion on fundoplication, the review offers a more favorable description of proton pump inhibitor therapy. In the concluding remarks Hassall argues that medical therapy options should be exhausted prior to surgical therapy. The author states that the risk of mortality and morbidity combined with less than desirable efficacy of fundoplication should caution clinicians from being too eager in recommending fundoplication.
Clinically significant GERD is a common inpatient problem. This article provides a good review of the pathophysiology of this disease and available treatment options. Unfortunately, this narrative review does not utilize a systematic method of identifying relevant studies nor does it include a systematic approach for critical appraisal of these studies. Nevertheless the caution it raises about fundoplication is a worthy one that should be explored further. It is interesting to note that prior to this review the author has received grant support and was a paid consultant for AstraZeneca and TAP Pharmaceutical Products Inc.
Support for Bag UA Screening During Evaluation for UTI
McGillivray D, Mok E, Mulrooney E, et al. A head-to-head comparison: “clean-void” bag versus catheter urinalysis in the diagnosis of urinary tract infection in young children. J Pediatr. 2005;147(4):451-456.
Review by Jenny Geheb, RN, CPNP
Early detection of urinary tract infection (UTI) can be especially important in children. This study uses a cross-sectional design to compare the validity of the urinalysis on clean-voided bag versus catheter urine specimens using the catheter culture as the “gold” standard. This study looked at 303 non-toilet-trained children under age three at risk for UTI who presented to a children’s hospital emergency department. Paired bag and catheter specimens were obtained from each child and sent for dipstick and microscopic urinalysis. Sensitivity and specificity were compared using McNemar’s [chi]2 test for paired specimens and the ordinary [chi]2 test for unpaired comparisons.
The study, which was conducted at the Montreal Children’s Hospital, found that the bag dipstick was more sensitive than the catheter dipstick for the entire study sample: 0.85 (95% confidence interval [CI] = 0.78 to 0.93) versus 0.71 (95% CI= 0.95 to 0.99), respectively. Both bag and catheter dipstick sensitivities were lower in infants <90 days old. Specificity was consistently lower for the bag specimens than for the catheter specimens.
A child at high risk for UTI (previous history of UTI, anatomic abnormalities, immunosuppressed, or presence of urinary symptoms) should be catheterized to obtain both a UA and culture; however, in children older than 90 days with fever without source and at low risk for UTI, a “selective catheterization” approach, as outlined in the American Academy of Pediatrics practice parameter, appears to be reasonable.
In low-risk children, serious consequences of infection are less likely, and the authors propose that the risks of missing a UTI are likely to be outweighed by the risks of catheterization, including pain, false-positive result, trauma, introduction of infection, test resistance by staff, and parental concern.
In summary, the provider may choose to use a bag urine screening strategy to reduce the number of unnecessary catheterizations in children who are considered low risk and over 90 days old. Further studies are needed to analyze the cost-benefit ratio of this approach as well as to confirm these findings with larger populations.
Short-Course Antibiotic Treatment for Streptococcal Pharyngitis
Casey JR, Pichichero ME. Meta-analysis of short course antibiotic treatment for group A streptococcal tonsillopharyngitis. Ped Infect Dis J. 2005;24(10):909-917.
Review by Jenny Geheb, RN, CPNP
Group A streptococcal (GAS) tonsillopharyngitis is a common cause for antibiotic treatment in children. Researchers at the University of Rochester Medical Center (N.Y.) performed a meta-analysis of current data to compare bacterial and clinical cure rates in patients with GAS tonsillopharyngitis treated with short course antibiotic treatment with oral [beta]-lactam or macrolide antibiotics for four to five days with standard 10-day treatment courses. Medline, Embase, reference lists, and abstract searches were all used to identify applicable publications. Trials were included if there was bacteriologic confirmation of GAS tonsillopharyngitis, random assignment to antibiotic therapy for a [beta]-lactam or macrolide antibiotic of shortened course versus a 10-day course, and assessment of bacteriologic outcome using a throat culture.
Twenty-two trials involving 7,470 patients were included in four separate analyses. Trials were grouped by a short course of cephalosporins (n=14), macrolides (other than azithromycin) (n=6), penicillin (n=2), and amoxicillin (n=2). Cephalosporin trials were further grouped by penicillin (n=12) or the same cephalosporin (n=3). Five trials were conducted in the United States with the remainder conducted in Europe.
Meta-analysis showed that short course cephalosporin treatment was superior for bacterial cure rate compared with 10 days of penicillin (OR 1.47; 95% CI, 1.06-2.03). Short-course penicillin therapy was inferior in achieving bacterial cure versus 10 days of penicillin. Clinical cure rate mirrored the bacterial cure rate results. Small sample size limited the statistical power and conclusions of the short course macrolide trials as well as trials of four or five days of cephalosporin therapy compared with 10 days of the same.
This meta-analysis shows that short-course treatment of GAS tonsillopharyngitis can be more effective when prescribing four or five days of cefdinir, cefpodoxime, or cefuroxime treatment than standard 10-day treatment of penicillin. In the United States cefdinir, cefpodoxime, and azithromycin are indicated for short-course treatment. As prescribing practitioners, it is important for us to consider the advantages of shortened antibiotic courses, including improved patient compliance, fewer adverse effects, and reduced impact on development of antibiotic resistance and nasopharyngeal colonization with resistant bacteria. However, the authors emphasize that caution must be used in interpretation of the results of this meta-analysis.
For example, the trials were grouped according to class of antibiotics so that the cephalosporin group included seven different cephalosporins (one first generation, two second generation, and four third generation). In addition, there was much variability in the quality and design of compared studies, which makes it difficult to make strong conclusions. Repeat studies are needed, especially in regard to short-course macrolide or amoxicillin treatment.
Each week in the United States, child protective services and agencies receive reports of more than 50,000 suspected child abuse incidents. In 2002, 2.6 million incidents involving 4.5 million children were reported. Approximately four children die every day as a result of abuse or neglect.1 But numbers don’t tell the whole story. Behind every number is a child at risk.
“I can picture right now in my mind a young baby who was about six months of age with a belly that was protruded and distended,” says Erin R. Stucky, MD, a pediatric hospitalist at Children’s Hospital and Health Center San Diego, and an associate professor of pediatrics at the University of California San Diego. “[She had] no bowel sounds, and the arms and legs were so thin, had no fat whatsoever. The skin was rolling. The face looked dysmorphic, but it was simply because the eyes were so white, and there was no fat on the face at all. The baby had an irritated cry. The hair was thin. [She] had a look of anxiety, true anxiety [in her] eyes. It was impressive, as though this infant was saying, ‘Help me. I can’t speak.’ [She] was very socially engaged, but tired. If you had to qualify the look further, it would be something like, ‘I’m in pain. Protect me. Please don’t walk out the door.’
“The child had been admitted from the emergency department at an outside facility. They had been focused, appropriately to some extent, on the fact that the belly was distended and that the baby had no bowel sounds. They were focused on the fact that the parent’s history [of the child] was of vomiting during the day, but it clearly did not equate whatsoever with the way the child looked. It was immediately clear, simply looking at the baby while walking in the room, that something very bad was wrong and that the parents’ answers and explanations did not fit.”
What It Is
Child abuse manifests in many forms, including physical abuse, sexual abuse, emotional abuse, and neglect, with a “child” typically defined as a person under 18. Legal definitions of the forms of child abuse vary, but, in general, they reflect societal views of actions deemed improper and unacceptable because they place a child at risk of physical or emotional harm.2 The federal Child Abuse Prevention and Treatment Act (CAPTA) defines child abuse and neglect as:
- Any recent act or failure to act on the part of a parent or caretaker that results in death, serious physical or emotional harm, sexual abuse, or exploitation; or
- An act or failure to act that presents an imminent risk of serious harm.3
States must include these minimum standards in their statutes in order to receive federal funds.
Neglect is the most common form of child abuse.2 Although definitions of neglect vary by state, they share characteristics. Minnesota defines neglect as inadequate food, shelter, clothing, or medical care. California includes both overt acts and omissions in the definition of neglect, defining general neglect as a lack of food, clothing, or medical care and severe neglect as malnutrition, failure to thrive, or willfully putting a child in danger. And Rhode Island’s neglect definition goes even further, including the above acts and omissions as well as the failure to provide a minimum degree of care or proper supervision or guardianship due to unwillingness, social problems, mental incompetency, or the use of a drug, drugs or alcohol, desertion, or abandonment. Rhode Island also includes the failure to take financial responsibility for a child.4
According to Georgia Berrenberg, esq., deputy district attorney, Second Judicial District of New Mexico, sexual abuse is the most common type that goes to trial. Berrenberg, who has been a prosecutor since 1984 and was in the child abuse division from 1996–2005, estimates that approximately 70% of cases involve sexual abuse compared with 30% that involve physical abuse.
However, pediatric hospitalists will most commonly see neglect, presenting as malnutrition or failure to thrive, in a child admitted to the hospital.4
Recognize Abuse and Neglect
Pediatric hospitalists are in a unique position to recognize child abuse and neglect, intervene appropriately, and help families avoid ultimate tragedy. They are trained to consider the entire child—no matter the presenting condition—to look at general issues and to think about development and nutrition every time they examine a child.
“When someone says, ‘This child has pneumonia,’ my job is to not think pneumonia; my job is to think, ‘What’s causing this child to breathe fast?’ to make sure I don’t miss anything,” says Dr. Stucky. “If the history doesn’t fit the examination and my first, second, [and] third thoughts are child abuse/neglect. It’s my job to work on that, but it’s also my job to push my own buttons to make sure that it’s not anything else medically going on. The child that never has a bruise or fracture is the odd one out. The key [to recognizing abuse] is history.”
Don’t jump to conclusions. Hospitalists need to consider the history reported by the parent in light of the physical exam of the child. For example, if the parent tells you that the child fell headfirst off a tricycle and landed on his face, note the pattern of the bruising. If the child has bruising around the eye then that could be consistent with the history, but if the child’s eyelid is cut or bruised and there’s no bruising around the eye, that’s another matter. The eyebrow and cheekbone will protect the eye when you fall and land on your face.
“Pay attention to what you hear and see in those first few minutes and hours with that family because stories are going to change,” says Berrenberg. “Be very, very clear about the initial things that are said.”
Dealing with the medical issues that led to the admission is paramount, and it’s important for the hospitalist to communicate effectively with the parent to ensure that the child receives the most appropriate treatment. Asking open-ended questions while you take the history can be revealing:
- Can you tell me how long this has been happening?
- What do you think might be contributing to this?
- Can you tell me how you’ve been dealing with these issues at home?
- Run me through a typical day at home with your baby.
In addition to the history, consider the parent/child interaction. “Most kids, even when they’re stressed and in pain are very attentive to where their parents are,” says Dr. Stucky. “They want to be with them no matter what. They may be angry and battling. They may respond to pain differently, but that relationship is very important. As you watch it you can really get a good sense [of whether] this child’s anger outburst is because they’re in pain, they’re confused, they have autism, or they are really angry with their parent and this is the way they’re protecting themselves.”
The hospitalist has to be up front with the parent about what the next step in their child’s treatment is going to be. “It’s a delicate discussion, but an honest one,” says Dr. Stucky. “It’s important to say to the parent, overtly, ‘I’m very concerned about your baby’s weight loss. I’m very concerned that this has happened over the past several months and that it has taken this long for your baby to be seen by a doctor. I’m very concerned, and I want you to understand that your baby has a critical condition right now. It’s so malnourished that the body’s organs aren’t working properly. ... Because of this concern, I’m going to call social workers. Because of this concern I’ll use [work with] a team of people to help me to take care of your baby. They’ll ask a lot of questions, and it’s very important that you answer honestly so we can do the best for your baby and make sure that the whole family can get whatever help is needed to take care of the problem.’ ”
Reporting Requirements
In most states healthcare workers not only have a moral responsibility to report suspected abuse, they are required by law to do so. In fact, New Mexico’s statute requires anyone who suspects child abuse to report it and makes failure to do so a misdemeanor. Hospitalists should know in advance to whom to report the suspected abuse.
Consider making a call to a social worker your first step. “Social workers are invaluable,” says Dr. Stucky. “They’re there for the families. They ask the harder questions that allow us to have that medical relationship and continue to care for the child’s needs. They can look up information that we can’t. They can look up child protection history, whether the parent has been incarcerated, things that support the possibility of abuse. They can file the CPS report, allowing the hospitalist to continue caring medically for the child.”
According to Berrenberg, the police should be your second call.
Dealing with child abuse and neglect is a team effort. In addition to the police and a social worker, you need to involve the nutritionist and the primary care pediatrician (if they have one). If you’re lucky, your hospital may have a child abuse specialist on staff. “Be ready to deal with a whole variety of people who may or may not know what else has already happened,” says Berrenberg.
After the Hospital Stay
Although child abuse is all too common, most pediatric hospitalists won’t often see the inside of a courtroom. Dr. Stucky says that cases with which she’s been involved have gone to trial twice during her 10 years as a pediatric hospitalist. And Berrenberg says, “Failure to thrive is not something we charge very often. That’s a difficult thing to prove.”
That said, prepare for the possibility of being called as a fact witness. According to Berrenberg, physicians may be asked to report on not just their observations of the child, but also on statements made in their presence.
“Statements made to physicians and to healthcare personnel are critical—be it by parents, caretakers, or the child themselves in the case of sexual abuse,” she says. “If statements are made in the course of diagnosis and treatment, then those statements can come in under hearsay exceptions. ... The doctor can testify about those statements.”
Remember it’s the doctor/patient relationship that’s important. Your patient’s parents have no doctor/patient relationship.
Berrenberg offers the following advice for physicians preparing to testify: “Be patient. Read everything you have on your case. Expect everything to change. When you’re told that you’re going to trial on Monday, expect that to change. If you’ve testified before and there are transcripts available, expect the defense to know about that previous testimony. If you’re basing your opinion on literature, expect the defense attorney to have found that literature and be familiar with it.
“Work with your prosecutor. Know what they want you for. They might only want you for a limited piece; they might want you for the whole gamut. They will tell you what they’re going to expect of you. Spend as much time as you can with them, with the photos, with the file. It’s always what you don’t expect to come up that comes up.”
Pediatric hospitalists should also be prepared for old cases to come back. “We’ll bring you from wherever you are—even if you’re out of the country,” says Berrenberg. “We’ll bring you back if we need you to testify. We’ll find you. If you’re the one who saw the child and were the initial responder, so to speak, no one else can say what you saw.”
Conclusion
What happened to the six-month-old baby Dr. Stucky remembers so clearly?
“I only know what happened during the hospital stay,” she says. “This family clearly needed help and guidance. There was an overwhelming, clear [indication] that the mother had significant, major depression. She wasn’t feeding the baby. She was completely ignoring the child, and she acknowledged that. ... The father was at work and thought that perhaps this baby was just ill or sickly. He was told that the baby was being taken to the doctor, and that wasn’t happening. He was naive and innocent in thinking that things were being dealt with and thinking that their baby was simply a baby who cried a lot and wasn’t gaining weight well.
“Once this was all [addressed], he jumped at the opportunity to have the mother in therapy and on medications. The mother herself was completely willing to give up the care. ... In this case, the paternal grandmother took over the care of this child. The father would drop off the baby at her house during the day and pick up the baby at night. On weekends they would share the duties. That was the plan at discharge. ... I can’t guarantee it, but it’s my sense that this worked very well.”
Keri Losavio is a medical journalist with more than 10 years’ experience.
References
- National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov/topics/prevention/index.cfm.
- “What Is Child Maltreatment?” From A Coordinated Response to Child Abuse and Neglect: The Foundation for Practice. National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov.
- Child Abuse Prevention and Treatment Act. Download the complete text from the Cornell University Legal Information Institute: www4.law.cornell.edu/uscode/42/ch67.html.
- “Monitoring Child Neglect.” Summary of discussions at a meeting co-sponsored by the Centers for Disease Control and Prevention (CDC) and Prevent Child Abuse America (PCA America), March 29, 2002.
PEDIATRIC SPECIAL SECTION
In the Literature
Optimizing Management of GERD: Medical therapy or surgical intervention?
Hassall E. Outcomes of fundoplication: causes for concern, newer options. Arch Dis Child. 2005;90:1047-1052.
Review by Ray Chan, MD
This narrative review provides a concise overview of gastroesophageal reflux disease (GERD) while specifically addressing surgical treatment. The author focuses on the potential complications of surgical treatment and cites several studies demonstrating a high rate of complications and patient dissatisfaction with their outcomes. In contrast, the review does cite several sources that concluded good outcomes; however, the article questions the conclusions of these studies due to study designs with poorly defined and subjective outcome measures.
In contrast to the discussion on fundoplication, the review offers a more favorable description of proton pump inhibitor therapy. In the concluding remarks Hassall argues that medical therapy options should be exhausted prior to surgical therapy. The author states that the risk of mortality and morbidity combined with less than desirable efficacy of fundoplication should caution clinicians from being too eager in recommending fundoplication.
Clinically significant GERD is a common inpatient problem. This article provides a good review of the pathophysiology of this disease and available treatment options. Unfortunately, this narrative review does not utilize a systematic method of identifying relevant studies nor does it include a systematic approach for critical appraisal of these studies. Nevertheless the caution it raises about fundoplication is a worthy one that should be explored further. It is interesting to note that prior to this review the author has received grant support and was a paid consultant for AstraZeneca and TAP Pharmaceutical Products Inc.
Support for Bag UA Screening During Evaluation for UTI
McGillivray D, Mok E, Mulrooney E, et al. A head-to-head comparison: “clean-void” bag versus catheter urinalysis in the diagnosis of urinary tract infection in young children. J Pediatr. 2005;147(4):451-456.
Review by Jenny Geheb, RN, CPNP
Early detection of urinary tract infection (UTI) can be especially important in children. This study uses a cross-sectional design to compare the validity of the urinalysis on clean-voided bag versus catheter urine specimens using the catheter culture as the “gold” standard. This study looked at 303 non-toilet-trained children under age three at risk for UTI who presented to a children’s hospital emergency department. Paired bag and catheter specimens were obtained from each child and sent for dipstick and microscopic urinalysis. Sensitivity and specificity were compared using McNemar’s [chi]2 test for paired specimens and the ordinary [chi]2 test for unpaired comparisons.
The study, which was conducted at the Montreal Children’s Hospital, found that the bag dipstick was more sensitive than the catheter dipstick for the entire study sample: 0.85 (95% confidence interval [CI] = 0.78 to 0.93) versus 0.71 (95% CI= 0.95 to 0.99), respectively. Both bag and catheter dipstick sensitivities were lower in infants <90 days old. Specificity was consistently lower for the bag specimens than for the catheter specimens.
A child at high risk for UTI (previous history of UTI, anatomic abnormalities, immunosuppressed, or presence of urinary symptoms) should be catheterized to obtain both a UA and culture; however, in children older than 90 days with fever without source and at low risk for UTI, a “selective catheterization” approach, as outlined in the American Academy of Pediatrics practice parameter, appears to be reasonable.
In low-risk children, serious consequences of infection are less likely, and the authors propose that the risks of missing a UTI are likely to be outweighed by the risks of catheterization, including pain, false-positive result, trauma, introduction of infection, test resistance by staff, and parental concern.
In summary, the provider may choose to use a bag urine screening strategy to reduce the number of unnecessary catheterizations in children who are considered low risk and over 90 days old. Further studies are needed to analyze the cost-benefit ratio of this approach as well as to confirm these findings with larger populations.
Short-Course Antibiotic Treatment for Streptococcal Pharyngitis
Casey JR, Pichichero ME. Meta-analysis of short course antibiotic treatment for group A streptococcal tonsillopharyngitis. Ped Infect Dis J. 2005;24(10):909-917.
Review by Jenny Geheb, RN, CPNP
Group A streptococcal (GAS) tonsillopharyngitis is a common cause for antibiotic treatment in children. Researchers at the University of Rochester Medical Center (N.Y.) performed a meta-analysis of current data to compare bacterial and clinical cure rates in patients with GAS tonsillopharyngitis treated with short course antibiotic treatment with oral [beta]-lactam or macrolide antibiotics for four to five days with standard 10-day treatment courses. Medline, Embase, reference lists, and abstract searches were all used to identify applicable publications. Trials were included if there was bacteriologic confirmation of GAS tonsillopharyngitis, random assignment to antibiotic therapy for a [beta]-lactam or macrolide antibiotic of shortened course versus a 10-day course, and assessment of bacteriologic outcome using a throat culture.
Twenty-two trials involving 7,470 patients were included in four separate analyses. Trials were grouped by a short course of cephalosporins (n=14), macrolides (other than azithromycin) (n=6), penicillin (n=2), and amoxicillin (n=2). Cephalosporin trials were further grouped by penicillin (n=12) or the same cephalosporin (n=3). Five trials were conducted in the United States with the remainder conducted in Europe.
Meta-analysis showed that short course cephalosporin treatment was superior for bacterial cure rate compared with 10 days of penicillin (OR 1.47; 95% CI, 1.06-2.03). Short-course penicillin therapy was inferior in achieving bacterial cure versus 10 days of penicillin. Clinical cure rate mirrored the bacterial cure rate results. Small sample size limited the statistical power and conclusions of the short course macrolide trials as well as trials of four or five days of cephalosporin therapy compared with 10 days of the same.
This meta-analysis shows that short-course treatment of GAS tonsillopharyngitis can be more effective when prescribing four or five days of cefdinir, cefpodoxime, or cefuroxime treatment than standard 10-day treatment of penicillin. In the United States cefdinir, cefpodoxime, and azithromycin are indicated for short-course treatment. As prescribing practitioners, it is important for us to consider the advantages of shortened antibiotic courses, including improved patient compliance, fewer adverse effects, and reduced impact on development of antibiotic resistance and nasopharyngeal colonization with resistant bacteria. However, the authors emphasize that caution must be used in interpretation of the results of this meta-analysis.
For example, the trials were grouped according to class of antibiotics so that the cephalosporin group included seven different cephalosporins (one first generation, two second generation, and four third generation). In addition, there was much variability in the quality and design of compared studies, which makes it difficult to make strong conclusions. Repeat studies are needed, especially in regard to short-course macrolide or amoxicillin treatment.
Top PICS
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.


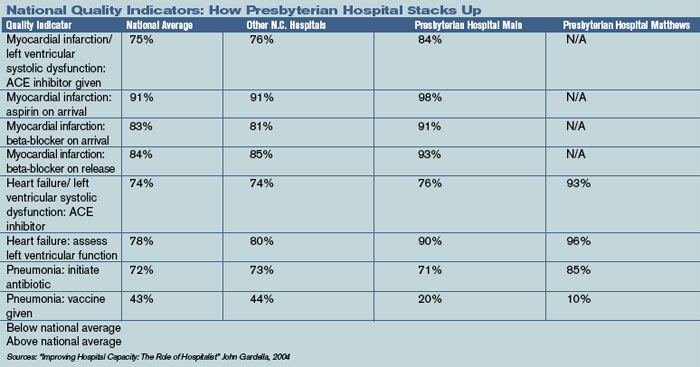
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
E-Prescribing is E-Slow
Health information technology, including e-prescribing, is “truly on the national marquee,” according to Carolyn M. Clancy, MD, director of the Agency for Healthcare Research and Technology (AHRQ). Speaking at the Annual Conference of the Healthcare Information and Management Systems Society earlier this year, she said, “Americans are quickly coming to understand how much we have to gain from health information technology (HIT). And one thing about Americans—we don’t like to wait.”
Clancy and other government officials have been pushing for widespread implementation and use of e-prescribing and other HIT in hospitals and other care settings. In 2003 the Medicare Modernization Act included a provision offering grants to physicians who implement e-prescribing systems. While all of the talk and action have stopped short of mandating the use of this technology, the handwriting is clearly on the wall. Like it or not, e-prescribing is part of healthcare’s future.
Yet despite all of these efforts on behalf of HIT few physicians are jumping on the e-prescribing bandwagon. Current estimates show that only between 5% and 18% of physicians and other clinicians use e-prescribing.
Nonetheless, while few physicians use these systems, they clearly see their value. In one survey, 78% of physicians say they believe that within the next seven years e-prescribing will account for more than half of the prescriptions written; and 75% cited reduced medication errors and time savings as two benefits of this technology.1 Another survey showed that while only 5% of physicians say they use their handheld computers for prescribing, 100% say that they use their PDAs for drug information.2
Despite the technology’s benefits, there are many reasons hospitalists and other physicians have resisted the call of e-prescribing. However, it behooves these practitioners to know about e-prescribing, consider how they might implement various technologies in their prescribing practices, and become involved in HIT initiatives at their facilities.
Money Matters: Costs Can Keep Hospitalists from E-Prescribing
E-prescribing is not widespread among hospitalists and other physicians, suggests Philip Strong, MD, IT physician liaison at El Camino Hospital and a hospitalist with the El Camino Medical Center in Mountain View, Calif.
Mark Zielzinski, chief information officer at El Camino, says that e-prescribing doesn’t really fit well with what hospitalists do.
E-prescribing is “wonderful in the physician’s office,” he explains. This is because the community-based physician writes many prescriptions every day and needs to communicate prescription information to a wide array of facilities and pharmacies.
“Hospitalists write far fewer prescriptions than attending physicians,” says Ronald Newman, MD, medical director of the hospitalist program at Beverly Hospital in Beverly, Mass. “I don’t write more than five a day.” An e-prescribing system simply isn’t practical for him.
Dr. Strong suggests, however, that the lack of enthusiasm for e-prescribing has more “to do with dollars. Systems are fairly expensive,” he says because a good system could cost as much as $150,000.
Why so much? “For a system to make sense and create more work for hospitalists, it has to interface with whatever system a hospital is using for pharmacies in the area,” explains Dr. Strong. And this can be expensive.
The cost for an individual physician or a small practice to implement e-prescribing seems much more reasonable. However, Dr. Zielzinski says that this represents only about 20% of the total cost of new technology.
“Think of what you spend when you get a home computer,” he says. “Say you spend $1,000 for the PC itself. Then you have to buy software, Internet access, a printer, and other accessories. Then you have to take the time to learn to use it all. Consider everything you spend in five years, and that $1,000 is a drop in the bucket.”
Dr. Zielzinski emphasizes that it’s not just the money that keeps hospitalists and other physicians from using e-prescribing. “Physicians have an intrinsic sociological resistance to change. After all, they are accustomed to evidence-based care and they are expected to have evidence to back up their decisions and actions,” he says, adding that “it takes a new clinical technique, theory, or practice an average of 17 years to get into mainstream practice. So how can we expect to accept new technology just like that?”

—Philip Strong, MD
Practical Protests: When Systems Hinder Efficiency
Another barrier to hospitalist acceptance of e-prescribing and other technology is that it sometimes takes longer to use, especially at the beginning.
“I’m part of an eight-hospitalist team, and we could use an e-prescribing system that our medical group has deployed, but we don’t,” admits Dr. Strong. “To use e-prescribing would require an extra step of work for us. We already have to dictate discharge notes and handwrite prescriptions. We don’t have the ability to substitute e-prescribing; it would just be an additional tool—and an additional step that would slow down our discharges.”
Dr. Newman agrees that physicians won’t use time-consuming technology. “Many systems take a lot of time to learn to use efficiently and effectively,” he says. “Physicians are afraid that these systems, such as e-prescribing, will slow them down and hurt their efficiency.”
He says hospitals are concerned about this and are waiting to implement systems they know physicians will use.
Eric Reines, MD, vice president of North Suburban Hospitalists PC and a hospitalist at Beverly Hospital, confesses to being a techie who enjoys this stuff. He says, however, that “most of the e-prescribing systems I’ve seen have been very poor. I like technology, but I won’t use a clunky system.”
Ease of use is essential for hospitalist acceptance of e-prescribing systems. “You can’t have a system with boxes popping up all over the screen and small black and white type that you can’t read,” says Dr. Reines. “Hospitalists and other physicians just won’t use these.”
Implementing systems that physicians don’t like is a worry that IT developers at hospitals think about about continually, confesses Dr. Zielzinski. “The biggest thing that keeps me awake at night is worrying that physicians will say, ‘This takes too long,’ ” he says, emphasizing that it’s important to educate physicians about how to use systems to make the most of their features and maximize efficiency.
While hospitals are concerned about how physicians will react to the implementation of technology, physicians’ general resistance to using e-prescribing actually could be a boon for hospitalists.
“Attending physicians aren’t likely to leave hospitals because they are required to use e-prescribing or other technology, but they might be more inclined to turn patients over to hospitalists at these facilities so that they don’t have to use these systems,” says Dr. Newman.
Vendor Vexation
Physicians often face the challenge of finding systems and software that integrate successfully with other systems and settings. Dr. Reines says vendors don’t always make widespread system compatibility a priority during product development.
Some data further suggest that e-prescribing products don’t always meet users’ needs. A report commissioned by the California Health Care Foundation evaluated 19 e-prescribing product vendors and found only four offer practical alternatives to more costly and complex prescription writing solutions.
CPOE First … Then E-Prescribing
Before you jump into e-prescribing, Dr. Strong suggests that more hospitals need to implement computerized physician order entry systems (CPOE). CPOE goes beyond prescriptions and enables physicians to electronically order everything from laboratory tests and dietary interventions to nursing care.
CPOE isn’t new; El Camino has used such a system for 30 years. “We are big-time believers in CPOE,” says Dr. Zielzinski. “It has enabled us to reduce a lot of errors.”
Dr. Strong adds that “these systems are better for overall patient through-put. The routing happens as soon as I input the order. There are no faxes, no paperwork, and no delays.”
Other groups also have long promoted the benefits of CPOE. For example, the Leapfrog Group, an organization of large healthcare purchasers, has suggested standards for CPOE systems that can intercept 50% or more of common serious prescribing errors. At the same time, a number of studies have been published documenting the value of CPOE in reducing medication errors and preventable adverse drug events.
Despite the benefits of CPOE, hospitals have been slow to implement it and many physicians oppose its use. “It’s high time we got over that,” says Dr. Strong. “We need to embrace CPOE now. If we do, e-prescribing won’t be such a shock when it comes down the pike.”
When e-prescribing piggybacks a good CPOE system, it will make more sense. “And when e-prescribing is done well, it will make more sense for physicians to embrace it,” he says. “Until then, it doesn’t make sense for most common situations.”
Dr. Zielzinski agrees that physicians and others need to get over their fear of CPOE. “I think you’ll find that CMS, JCAHO, the Leapfrog Group, and others will push more and more for this to happen. It’s the right thing to do.”
When Hospitalists Embrace High Tech
It is important to emphasize that many hospitalists and other physicians embrace technology. “The reality is that physicians come [to El Camino] because of our technology—it’s part of our culture,” says Dr. Zielzinski. When hospitalists join the El Camino staff, they go through a high-tech orientation with a physician trainer.
Pediatric Hospitalist Bettina Ackerman, MD, uses e-prescribing at her facility, Children’s Hospital of Pittsburgh (Pa.), and she likes the system. She admits that certain aspects of the technology can be cumbersome.
For example, “it’s much easier to handwrite certain information, such as complicated dosing instructions that require a lot of text,” she says. Nonetheless, she has seen the benefits as well. “It has drastically reduced medication errors in our hospital. And there is an efficiency that wasn’t there before.”
Dr. Reines stated that hospitalists are like other physicians: Some of them like e-prescribing and other technology, while others don’t. Age isn’t always a predictor, he emphasizes, noting that he is “the oldest physician in his group but I’m also the most interested in technology.” However, he suggested that hospitalists who are “fresh out of training are more used to technology such as e-prescribing. They kind of expect to use it.”
The Hospitalist’s Role … Starting Now
Dr. Strong suggests that hospitalists need to be part of the IT solution. In fact, they already are actively involved in his facility. “It is important for hospitalists to know what HIT their facilities are using and considering for purchase,” he says.
Dr. Reines agrees that physicians need to be active in IT decisions at their hospitals. “I’m on the tech committee at my facility, as are several physicians,” he explains, adding that they have strong opinions and specific input on what they want HIT programs and systems to do, what information they need, and how they expect technology to work to enhance their efficiency and benefit their patients.
Hospitalists who work at teaching hospitals can have a role in educating students about technology. “We need to look at learning opportunities that involve technology,” says Dr. Reines. “And we should encourage people not to be afraid of technology or change.”
Why Bother?
If there are so many barriers to e-prescribing and so many contraindications to its use, why should hospitalists bother with this technology?
While there is much disagreement about the use, benefits, and drawbacks of e-prescribing, there is little doubt that government agencies, regulatory bodies, and third-party payers will continue to push for the widespread implementation of such technology in the coming years.
For example, JCAHO’s establishment of the medication reconciliation process, whereby hospitals and other healthcare providers are expected to compile and use medication lists whenever patients move to a new setting will make e-prescribing more important and practical for hospitalists.
“The need to reconcile our patients’ medications at admission, during their stay, and at discharge will spur a greater need for e-prescribing,” says Dr. Zielzinski.
Dr. Ackerman urges her colleagues to learn about e-prescribing and other systems now. However, she also encourages “the powers that be” to provide more specific guidance on HIT to help physicians and others make the best use of it.
Although he doesn’t use or have a real need for e-prescribing, “I certainly think we will be seeing more hospitalists and hospitals using these systems in the coming years,” says Dr. Newman. “The opportunity—however small—to prevent certain types of errors will make it worthwhile eventually in most settings.” TH
Writer Joanne Kaldy is based in Maryland.
References
- iHealthbeat. Survey: few docs use PDAs for e-prescribing. Sept. 8, 2005. Available at ihealthbeat.org. Last accessed Sept. 14, 2005.
- Mobile Village. Docs embrace handheld e-prescribing to save time, prevent errors. Mobile & Wireless News. Feb. 7, 2003.
Health information technology, including e-prescribing, is “truly on the national marquee,” according to Carolyn M. Clancy, MD, director of the Agency for Healthcare Research and Technology (AHRQ). Speaking at the Annual Conference of the Healthcare Information and Management Systems Society earlier this year, she said, “Americans are quickly coming to understand how much we have to gain from health information technology (HIT). And one thing about Americans—we don’t like to wait.”
Clancy and other government officials have been pushing for widespread implementation and use of e-prescribing and other HIT in hospitals and other care settings. In 2003 the Medicare Modernization Act included a provision offering grants to physicians who implement e-prescribing systems. While all of the talk and action have stopped short of mandating the use of this technology, the handwriting is clearly on the wall. Like it or not, e-prescribing is part of healthcare’s future.
Yet despite all of these efforts on behalf of HIT few physicians are jumping on the e-prescribing bandwagon. Current estimates show that only between 5% and 18% of physicians and other clinicians use e-prescribing.
Nonetheless, while few physicians use these systems, they clearly see their value. In one survey, 78% of physicians say they believe that within the next seven years e-prescribing will account for more than half of the prescriptions written; and 75% cited reduced medication errors and time savings as two benefits of this technology.1 Another survey showed that while only 5% of physicians say they use their handheld computers for prescribing, 100% say that they use their PDAs for drug information.2
Despite the technology’s benefits, there are many reasons hospitalists and other physicians have resisted the call of e-prescribing. However, it behooves these practitioners to know about e-prescribing, consider how they might implement various technologies in their prescribing practices, and become involved in HIT initiatives at their facilities.
Money Matters: Costs Can Keep Hospitalists from E-Prescribing
E-prescribing is not widespread among hospitalists and other physicians, suggests Philip Strong, MD, IT physician liaison at El Camino Hospital and a hospitalist with the El Camino Medical Center in Mountain View, Calif.
Mark Zielzinski, chief information officer at El Camino, says that e-prescribing doesn’t really fit well with what hospitalists do.
E-prescribing is “wonderful in the physician’s office,” he explains. This is because the community-based physician writes many prescriptions every day and needs to communicate prescription information to a wide array of facilities and pharmacies.
“Hospitalists write far fewer prescriptions than attending physicians,” says Ronald Newman, MD, medical director of the hospitalist program at Beverly Hospital in Beverly, Mass. “I don’t write more than five a day.” An e-prescribing system simply isn’t practical for him.
Dr. Strong suggests, however, that the lack of enthusiasm for e-prescribing has more “to do with dollars. Systems are fairly expensive,” he says because a good system could cost as much as $150,000.
Why so much? “For a system to make sense and create more work for hospitalists, it has to interface with whatever system a hospital is using for pharmacies in the area,” explains Dr. Strong. And this can be expensive.
The cost for an individual physician or a small practice to implement e-prescribing seems much more reasonable. However, Dr. Zielzinski says that this represents only about 20% of the total cost of new technology.
“Think of what you spend when you get a home computer,” he says. “Say you spend $1,000 for the PC itself. Then you have to buy software, Internet access, a printer, and other accessories. Then you have to take the time to learn to use it all. Consider everything you spend in five years, and that $1,000 is a drop in the bucket.”
Dr. Zielzinski emphasizes that it’s not just the money that keeps hospitalists and other physicians from using e-prescribing. “Physicians have an intrinsic sociological resistance to change. After all, they are accustomed to evidence-based care and they are expected to have evidence to back up their decisions and actions,” he says, adding that “it takes a new clinical technique, theory, or practice an average of 17 years to get into mainstream practice. So how can we expect to accept new technology just like that?”
—Philip Strong, MD
Practical Protests: When Systems Hinder Efficiency
Another barrier to hospitalist acceptance of e-prescribing and other technology is that it sometimes takes longer to use, especially at the beginning.
“I’m part of an eight-hospitalist team, and we could use an e-prescribing system that our medical group has deployed, but we don’t,” admits Dr. Strong. “To use e-prescribing would require an extra step of work for us. We already have to dictate discharge notes and handwrite prescriptions. We don’t have the ability to substitute e-prescribing; it would just be an additional tool—and an additional step that would slow down our discharges.”
Dr. Newman agrees that physicians won’t use time-consuming technology. “Many systems take a lot of time to learn to use efficiently and effectively,” he says. “Physicians are afraid that these systems, such as e-prescribing, will slow them down and hurt their efficiency.”
He says hospitals are concerned about this and are waiting to implement systems they know physicians will use.
Eric Reines, MD, vice president of North Suburban Hospitalists PC and a hospitalist at Beverly Hospital, confesses to being a techie who enjoys this stuff. He says, however, that “most of the e-prescribing systems I’ve seen have been very poor. I like technology, but I won’t use a clunky system.”
Ease of use is essential for hospitalist acceptance of e-prescribing systems. “You can’t have a system with boxes popping up all over the screen and small black and white type that you can’t read,” says Dr. Reines. “Hospitalists and other physicians just won’t use these.”
Implementing systems that physicians don’t like is a worry that IT developers at hospitals think about about continually, confesses Dr. Zielzinski. “The biggest thing that keeps me awake at night is worrying that physicians will say, ‘This takes too long,’ ” he says, emphasizing that it’s important to educate physicians about how to use systems to make the most of their features and maximize efficiency.
While hospitals are concerned about how physicians will react to the implementation of technology, physicians’ general resistance to using e-prescribing actually could be a boon for hospitalists.
“Attending physicians aren’t likely to leave hospitals because they are required to use e-prescribing or other technology, but they might be more inclined to turn patients over to hospitalists at these facilities so that they don’t have to use these systems,” says Dr. Newman.
Vendor Vexation
Physicians often face the challenge of finding systems and software that integrate successfully with other systems and settings. Dr. Reines says vendors don’t always make widespread system compatibility a priority during product development.
Some data further suggest that e-prescribing products don’t always meet users’ needs. A report commissioned by the California Health Care Foundation evaluated 19 e-prescribing product vendors and found only four offer practical alternatives to more costly and complex prescription writing solutions.
CPOE First … Then E-Prescribing
Before you jump into e-prescribing, Dr. Strong suggests that more hospitals need to implement computerized physician order entry systems (CPOE). CPOE goes beyond prescriptions and enables physicians to electronically order everything from laboratory tests and dietary interventions to nursing care.
CPOE isn’t new; El Camino has used such a system for 30 years. “We are big-time believers in CPOE,” says Dr. Zielzinski. “It has enabled us to reduce a lot of errors.”
Dr. Strong adds that “these systems are better for overall patient through-put. The routing happens as soon as I input the order. There are no faxes, no paperwork, and no delays.”
Other groups also have long promoted the benefits of CPOE. For example, the Leapfrog Group, an organization of large healthcare purchasers, has suggested standards for CPOE systems that can intercept 50% or more of common serious prescribing errors. At the same time, a number of studies have been published documenting the value of CPOE in reducing medication errors and preventable adverse drug events.
Despite the benefits of CPOE, hospitals have been slow to implement it and many physicians oppose its use. “It’s high time we got over that,” says Dr. Strong. “We need to embrace CPOE now. If we do, e-prescribing won’t be such a shock when it comes down the pike.”
When e-prescribing piggybacks a good CPOE system, it will make more sense. “And when e-prescribing is done well, it will make more sense for physicians to embrace it,” he says. “Until then, it doesn’t make sense for most common situations.”
Dr. Zielzinski agrees that physicians and others need to get over their fear of CPOE. “I think you’ll find that CMS, JCAHO, the Leapfrog Group, and others will push more and more for this to happen. It’s the right thing to do.”
When Hospitalists Embrace High Tech
It is important to emphasize that many hospitalists and other physicians embrace technology. “The reality is that physicians come [to El Camino] because of our technology—it’s part of our culture,” says Dr. Zielzinski. When hospitalists join the El Camino staff, they go through a high-tech orientation with a physician trainer.
Pediatric Hospitalist Bettina Ackerman, MD, uses e-prescribing at her facility, Children’s Hospital of Pittsburgh (Pa.), and she likes the system. She admits that certain aspects of the technology can be cumbersome.
For example, “it’s much easier to handwrite certain information, such as complicated dosing instructions that require a lot of text,” she says. Nonetheless, she has seen the benefits as well. “It has drastically reduced medication errors in our hospital. And there is an efficiency that wasn’t there before.”
Dr. Reines stated that hospitalists are like other physicians: Some of them like e-prescribing and other technology, while others don’t. Age isn’t always a predictor, he emphasizes, noting that he is “the oldest physician in his group but I’m also the most interested in technology.” However, he suggested that hospitalists who are “fresh out of training are more used to technology such as e-prescribing. They kind of expect to use it.”
The Hospitalist’s Role … Starting Now
Dr. Strong suggests that hospitalists need to be part of the IT solution. In fact, they already are actively involved in his facility. “It is important for hospitalists to know what HIT their facilities are using and considering for purchase,” he says.
Dr. Reines agrees that physicians need to be active in IT decisions at their hospitals. “I’m on the tech committee at my facility, as are several physicians,” he explains, adding that they have strong opinions and specific input on what they want HIT programs and systems to do, what information they need, and how they expect technology to work to enhance their efficiency and benefit their patients.
Hospitalists who work at teaching hospitals can have a role in educating students about technology. “We need to look at learning opportunities that involve technology,” says Dr. Reines. “And we should encourage people not to be afraid of technology or change.”
Why Bother?
If there are so many barriers to e-prescribing and so many contraindications to its use, why should hospitalists bother with this technology?
While there is much disagreement about the use, benefits, and drawbacks of e-prescribing, there is little doubt that government agencies, regulatory bodies, and third-party payers will continue to push for the widespread implementation of such technology in the coming years.
For example, JCAHO’s establishment of the medication reconciliation process, whereby hospitals and other healthcare providers are expected to compile and use medication lists whenever patients move to a new setting will make e-prescribing more important and practical for hospitalists.
“The need to reconcile our patients’ medications at admission, during their stay, and at discharge will spur a greater need for e-prescribing,” says Dr. Zielzinski.
Dr. Ackerman urges her colleagues to learn about e-prescribing and other systems now. However, she also encourages “the powers that be” to provide more specific guidance on HIT to help physicians and others make the best use of it.
Although he doesn’t use or have a real need for e-prescribing, “I certainly think we will be seeing more hospitalists and hospitals using these systems in the coming years,” says Dr. Newman. “The opportunity—however small—to prevent certain types of errors will make it worthwhile eventually in most settings.” TH
Writer Joanne Kaldy is based in Maryland.
References
- iHealthbeat. Survey: few docs use PDAs for e-prescribing. Sept. 8, 2005. Available at ihealthbeat.org. Last accessed Sept. 14, 2005.
- Mobile Village. Docs embrace handheld e-prescribing to save time, prevent errors. Mobile & Wireless News. Feb. 7, 2003.
Health information technology, including e-prescribing, is “truly on the national marquee,” according to Carolyn M. Clancy, MD, director of the Agency for Healthcare Research and Technology (AHRQ). Speaking at the Annual Conference of the Healthcare Information and Management Systems Society earlier this year, she said, “Americans are quickly coming to understand how much we have to gain from health information technology (HIT). And one thing about Americans—we don’t like to wait.”
Clancy and other government officials have been pushing for widespread implementation and use of e-prescribing and other HIT in hospitals and other care settings. In 2003 the Medicare Modernization Act included a provision offering grants to physicians who implement e-prescribing systems. While all of the talk and action have stopped short of mandating the use of this technology, the handwriting is clearly on the wall. Like it or not, e-prescribing is part of healthcare’s future.
Yet despite all of these efforts on behalf of HIT few physicians are jumping on the e-prescribing bandwagon. Current estimates show that only between 5% and 18% of physicians and other clinicians use e-prescribing.
Nonetheless, while few physicians use these systems, they clearly see their value. In one survey, 78% of physicians say they believe that within the next seven years e-prescribing will account for more than half of the prescriptions written; and 75% cited reduced medication errors and time savings as two benefits of this technology.1 Another survey showed that while only 5% of physicians say they use their handheld computers for prescribing, 100% say that they use their PDAs for drug information.2
Despite the technology’s benefits, there are many reasons hospitalists and other physicians have resisted the call of e-prescribing. However, it behooves these practitioners to know about e-prescribing, consider how they might implement various technologies in their prescribing practices, and become involved in HIT initiatives at their facilities.
Money Matters: Costs Can Keep Hospitalists from E-Prescribing
E-prescribing is not widespread among hospitalists and other physicians, suggests Philip Strong, MD, IT physician liaison at El Camino Hospital and a hospitalist with the El Camino Medical Center in Mountain View, Calif.
Mark Zielzinski, chief information officer at El Camino, says that e-prescribing doesn’t really fit well with what hospitalists do.
E-prescribing is “wonderful in the physician’s office,” he explains. This is because the community-based physician writes many prescriptions every day and needs to communicate prescription information to a wide array of facilities and pharmacies.
“Hospitalists write far fewer prescriptions than attending physicians,” says Ronald Newman, MD, medical director of the hospitalist program at Beverly Hospital in Beverly, Mass. “I don’t write more than five a day.” An e-prescribing system simply isn’t practical for him.
Dr. Strong suggests, however, that the lack of enthusiasm for e-prescribing has more “to do with dollars. Systems are fairly expensive,” he says because a good system could cost as much as $150,000.
Why so much? “For a system to make sense and create more work for hospitalists, it has to interface with whatever system a hospital is using for pharmacies in the area,” explains Dr. Strong. And this can be expensive.
The cost for an individual physician or a small practice to implement e-prescribing seems much more reasonable. However, Dr. Zielzinski says that this represents only about 20% of the total cost of new technology.
“Think of what you spend when you get a home computer,” he says. “Say you spend $1,000 for the PC itself. Then you have to buy software, Internet access, a printer, and other accessories. Then you have to take the time to learn to use it all. Consider everything you spend in five years, and that $1,000 is a drop in the bucket.”
Dr. Zielzinski emphasizes that it’s not just the money that keeps hospitalists and other physicians from using e-prescribing. “Physicians have an intrinsic sociological resistance to change. After all, they are accustomed to evidence-based care and they are expected to have evidence to back up their decisions and actions,” he says, adding that “it takes a new clinical technique, theory, or practice an average of 17 years to get into mainstream practice. So how can we expect to accept new technology just like that?”
—Philip Strong, MD
Practical Protests: When Systems Hinder Efficiency
Another barrier to hospitalist acceptance of e-prescribing and other technology is that it sometimes takes longer to use, especially at the beginning.
“I’m part of an eight-hospitalist team, and we could use an e-prescribing system that our medical group has deployed, but we don’t,” admits Dr. Strong. “To use e-prescribing would require an extra step of work for us. We already have to dictate discharge notes and handwrite prescriptions. We don’t have the ability to substitute e-prescribing; it would just be an additional tool—and an additional step that would slow down our discharges.”
Dr. Newman agrees that physicians won’t use time-consuming technology. “Many systems take a lot of time to learn to use efficiently and effectively,” he says. “Physicians are afraid that these systems, such as e-prescribing, will slow them down and hurt their efficiency.”
He says hospitals are concerned about this and are waiting to implement systems they know physicians will use.
Eric Reines, MD, vice president of North Suburban Hospitalists PC and a hospitalist at Beverly Hospital, confesses to being a techie who enjoys this stuff. He says, however, that “most of the e-prescribing systems I’ve seen have been very poor. I like technology, but I won’t use a clunky system.”
Ease of use is essential for hospitalist acceptance of e-prescribing systems. “You can’t have a system with boxes popping up all over the screen and small black and white type that you can’t read,” says Dr. Reines. “Hospitalists and other physicians just won’t use these.”
Implementing systems that physicians don’t like is a worry that IT developers at hospitals think about about continually, confesses Dr. Zielzinski. “The biggest thing that keeps me awake at night is worrying that physicians will say, ‘This takes too long,’ ” he says, emphasizing that it’s important to educate physicians about how to use systems to make the most of their features and maximize efficiency.
While hospitals are concerned about how physicians will react to the implementation of technology, physicians’ general resistance to using e-prescribing actually could be a boon for hospitalists.
“Attending physicians aren’t likely to leave hospitals because they are required to use e-prescribing or other technology, but they might be more inclined to turn patients over to hospitalists at these facilities so that they don’t have to use these systems,” says Dr. Newman.
Vendor Vexation
Physicians often face the challenge of finding systems and software that integrate successfully with other systems and settings. Dr. Reines says vendors don’t always make widespread system compatibility a priority during product development.
Some data further suggest that e-prescribing products don’t always meet users’ needs. A report commissioned by the California Health Care Foundation evaluated 19 e-prescribing product vendors and found only four offer practical alternatives to more costly and complex prescription writing solutions.
CPOE First … Then E-Prescribing
Before you jump into e-prescribing, Dr. Strong suggests that more hospitals need to implement computerized physician order entry systems (CPOE). CPOE goes beyond prescriptions and enables physicians to electronically order everything from laboratory tests and dietary interventions to nursing care.
CPOE isn’t new; El Camino has used such a system for 30 years. “We are big-time believers in CPOE,” says Dr. Zielzinski. “It has enabled us to reduce a lot of errors.”
Dr. Strong adds that “these systems are better for overall patient through-put. The routing happens as soon as I input the order. There are no faxes, no paperwork, and no delays.”
Other groups also have long promoted the benefits of CPOE. For example, the Leapfrog Group, an organization of large healthcare purchasers, has suggested standards for CPOE systems that can intercept 50% or more of common serious prescribing errors. At the same time, a number of studies have been published documenting the value of CPOE in reducing medication errors and preventable adverse drug events.
Despite the benefits of CPOE, hospitals have been slow to implement it and many physicians oppose its use. “It’s high time we got over that,” says Dr. Strong. “We need to embrace CPOE now. If we do, e-prescribing won’t be such a shock when it comes down the pike.”
When e-prescribing piggybacks a good CPOE system, it will make more sense. “And when e-prescribing is done well, it will make more sense for physicians to embrace it,” he says. “Until then, it doesn’t make sense for most common situations.”
Dr. Zielzinski agrees that physicians and others need to get over their fear of CPOE. “I think you’ll find that CMS, JCAHO, the Leapfrog Group, and others will push more and more for this to happen. It’s the right thing to do.”
When Hospitalists Embrace High Tech
It is important to emphasize that many hospitalists and other physicians embrace technology. “The reality is that physicians come [to El Camino] because of our technology—it’s part of our culture,” says Dr. Zielzinski. When hospitalists join the El Camino staff, they go through a high-tech orientation with a physician trainer.
Pediatric Hospitalist Bettina Ackerman, MD, uses e-prescribing at her facility, Children’s Hospital of Pittsburgh (Pa.), and she likes the system. She admits that certain aspects of the technology can be cumbersome.
For example, “it’s much easier to handwrite certain information, such as complicated dosing instructions that require a lot of text,” she says. Nonetheless, she has seen the benefits as well. “It has drastically reduced medication errors in our hospital. And there is an efficiency that wasn’t there before.”
Dr. Reines stated that hospitalists are like other physicians: Some of them like e-prescribing and other technology, while others don’t. Age isn’t always a predictor, he emphasizes, noting that he is “the oldest physician in his group but I’m also the most interested in technology.” However, he suggested that hospitalists who are “fresh out of training are more used to technology such as e-prescribing. They kind of expect to use it.”
The Hospitalist’s Role … Starting Now
Dr. Strong suggests that hospitalists need to be part of the IT solution. In fact, they already are actively involved in his facility. “It is important for hospitalists to know what HIT their facilities are using and considering for purchase,” he says.
Dr. Reines agrees that physicians need to be active in IT decisions at their hospitals. “I’m on the tech committee at my facility, as are several physicians,” he explains, adding that they have strong opinions and specific input on what they want HIT programs and systems to do, what information they need, and how they expect technology to work to enhance their efficiency and benefit their patients.
Hospitalists who work at teaching hospitals can have a role in educating students about technology. “We need to look at learning opportunities that involve technology,” says Dr. Reines. “And we should encourage people not to be afraid of technology or change.”
Why Bother?
If there are so many barriers to e-prescribing and so many contraindications to its use, why should hospitalists bother with this technology?
While there is much disagreement about the use, benefits, and drawbacks of e-prescribing, there is little doubt that government agencies, regulatory bodies, and third-party payers will continue to push for the widespread implementation of such technology in the coming years.
For example, JCAHO’s establishment of the medication reconciliation process, whereby hospitals and other healthcare providers are expected to compile and use medication lists whenever patients move to a new setting will make e-prescribing more important and practical for hospitalists.
“The need to reconcile our patients’ medications at admission, during their stay, and at discharge will spur a greater need for e-prescribing,” says Dr. Zielzinski.
Dr. Ackerman urges her colleagues to learn about e-prescribing and other systems now. However, she also encourages “the powers that be” to provide more specific guidance on HIT to help physicians and others make the best use of it.
Although he doesn’t use or have a real need for e-prescribing, “I certainly think we will be seeing more hospitalists and hospitals using these systems in the coming years,” says Dr. Newman. “The opportunity—however small—to prevent certain types of errors will make it worthwhile eventually in most settings.” TH
Writer Joanne Kaldy is based in Maryland.
References
- iHealthbeat. Survey: few docs use PDAs for e-prescribing. Sept. 8, 2005. Available at ihealthbeat.org. Last accessed Sept. 14, 2005.
- Mobile Village. Docs embrace handheld e-prescribing to save time, prevent errors. Mobile & Wireless News. Feb. 7, 2003.