User login
A Case of Kidney Failure
An 84-year-old woman with history of coronary artery disease, hypertension, and hyperlipidemia presented with six months of anorexia, nausea, a five-pound weight loss, weakness, and nonbloody diarrhea. Over the past one to two weeks, she noticed decreased urine output despite her use of furosemide.
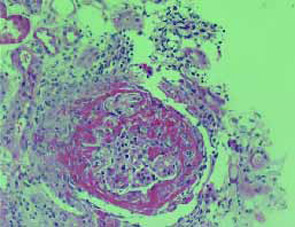
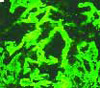
She was found to have a serum creatinine of 3.5 mg/dL on admission, increased from 1.5 mg/dL five days previously. She had no rash, dyspnea, cough, or abdominal pain. Urinalysis revealed >100 red blood cells (RBC), >100 white blood cells (WBC), occasional hyaline casts, and many gramnegative bacilli. Ciprofloxacin was started for her urinary tract infection. A renal biopsy was performed. The images shown are photomicrographs of light microscopy and immunofluorescence of the renal biopsy specimen. TH
Which of the following would be the most appropriate initial therapy for this condition?
- Increase dose of furosemide;
- Start fish oil;
- Initiate Low-dose dopamine;
- Discontinue ACE inhibitor; or
- Begin emergent plasmapheresis.
Discussion
The correct answer is e: plasmapheresis. The renal biopsy, as shown in the image at left, reveals crescents involving glomeruli on light microscopy and linear IgG staining on immunofluorescence. This patient has antiglomerular basement membrane (anti-GBM) glomerulonephritis (GN), which accounts for 10% to 20% of crescentic glomerulonephritides. It is characterized by circulating antibodies to the glomerular basement membrane with deposition of IgG or, rarely, IgA along the GBM.
The pulmonary-renal vasculitic syndrome is called Goodpasture’s syndrome, in which pulmonary hemorrhage occurs concurrently with GN. Anti-GBM disease has a bimodal distribution, with peaks in the second to third decades and the sixth to seventh decades of life.
Etiology is usually idiopathic, but hydrocarbon exposure has also been associated with the disease. Clinical presentation of renal anti-GBM disease is characterized by an acute onset of GN with severe oliguria or anuria. Urinalysis typically shows hematuria, dysmorphic red blood cells, and red blood cell casts. The diagnostic laboratory finding is circulating antibodies to GBM, specifically to the alpha-3 chain of type IV collagen; these are detected by radioimmunoassay or enzyme immunoassay in approximately 90% of patients.
The standard treatment for anti-GBM disease includes intensive plasmapheresis combined with corticosteroids and cyclophosphamide or azathioprine. Plasmapheresis consists of removal of two to four liters of plasma and replacement with fresh frozen plasma or a 5% albumin solution on a daily basis until circulating antibody levels become undetectable (usually two to three weeks). Steroids should be administered initially as pulse methylprednisolone (30 mg/kg or 1,000 mg intravenously over 20 minutes) for three doses (daily or every other day) followed by daily oral prednisone (1 mg/kg per day) for at least the first month, followed by a gradual taper. The initial cyclophosphamide dose is 2 mg/kg per day either orally or intravenously (0.5 g/m2 body surface area).
Selecting patients for treatment is based primarily on severity at presentation. Based on a large retrospective review of 71 patients treated with plasma exchange, prednisolone, and cyclophosphamide, those who presented with plasma creatinine (Cr) concentration of less than 5.7 mg/dL or those who had Cr greater than 5.7 mg/dL but did not require immediate dialysis had a favorable long-term patient and renal survival (approximately 70% to 80% at 90 months). Patients who required immediate dialysis had poor survival (approximately 35% at 90 months). Patients who had crescents in all glomeruli on renal biopsy required long-term maintenance dialysis. Therefore, plasma exchange, prednisone, and cyclophosphamide should be administered in the following settings:
- Pulmonary hemorrhage;
- Renal failure (Cr above 5-7 mg/dL) but not requiring immediate renal replacement therapy; and
- Less severe disease on renal biopsy (less than 30% to 50% crescents). Therapy is unlikely to be effective in patients who present with dialysisdependent renal failure without hemoptysis or if 100% of glomeruli have crescents on renal biopsy. In these settings, the risk of therapy may exceed the likelihood of benefit.
Fish oil is a potential therapy for IgA nephropathy, not anti-GBM disease. ACE inhibition may be useful in patients with nephrotic syndrome. IV hydration would be likely to cause volume overload and precipitate the need for acute dialysis. Low-dose dopamine has not proven effective in reversing acute renal failure. TH
REFERENCES
- Clarkson MR, Brenner BM. Pocket Companion to Brenner & Rector’s The Kidney, 7th ed. Philadelphia, Pa: Elsevier Inc; 2005:198-199.
- Rose BD, Kaplan AA, Appel GB. Treatment of anti-GBM antibody disease (Goodpasture’s syndrome). UpToDate Online. Available at: www.uptodate.com/physicians/pulmonology_toclist.asp. Last accessed August 18, 2005.
- Levy JB, Turner AN, Rees AJ, et al. Long-term outcome of anti-glomerular basement membrane antibody disease treated with plasma exchange and immunosuppression. Ann Intern Med. 2001;134:1033.
- Bolton WK. Goodpasture’s syndrome. Kidney Int. 1996;50:1753.
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int. 2003;63:1164.
An 84-year-old woman with history of coronary artery disease, hypertension, and hyperlipidemia presented with six months of anorexia, nausea, a five-pound weight loss, weakness, and nonbloody diarrhea. Over the past one to two weeks, she noticed decreased urine output despite her use of furosemide.
She was found to have a serum creatinine of 3.5 mg/dL on admission, increased from 1.5 mg/dL five days previously. She had no rash, dyspnea, cough, or abdominal pain. Urinalysis revealed >100 red blood cells (RBC), >100 white blood cells (WBC), occasional hyaline casts, and many gramnegative bacilli. Ciprofloxacin was started for her urinary tract infection. A renal biopsy was performed. The images shown are photomicrographs of light microscopy and immunofluorescence of the renal biopsy specimen. TH
Which of the following would be the most appropriate initial therapy for this condition?
- Increase dose of furosemide;
- Start fish oil;
- Initiate Low-dose dopamine;
- Discontinue ACE inhibitor; or
- Begin emergent plasmapheresis.
Discussion
The correct answer is e: plasmapheresis. The renal biopsy, as shown in the image at left, reveals crescents involving glomeruli on light microscopy and linear IgG staining on immunofluorescence. This patient has antiglomerular basement membrane (anti-GBM) glomerulonephritis (GN), which accounts for 10% to 20% of crescentic glomerulonephritides. It is characterized by circulating antibodies to the glomerular basement membrane with deposition of IgG or, rarely, IgA along the GBM.
The pulmonary-renal vasculitic syndrome is called Goodpasture’s syndrome, in which pulmonary hemorrhage occurs concurrently with GN. Anti-GBM disease has a bimodal distribution, with peaks in the second to third decades and the sixth to seventh decades of life.
Etiology is usually idiopathic, but hydrocarbon exposure has also been associated with the disease. Clinical presentation of renal anti-GBM disease is characterized by an acute onset of GN with severe oliguria or anuria. Urinalysis typically shows hematuria, dysmorphic red blood cells, and red blood cell casts. The diagnostic laboratory finding is circulating antibodies to GBM, specifically to the alpha-3 chain of type IV collagen; these are detected by radioimmunoassay or enzyme immunoassay in approximately 90% of patients.
The standard treatment for anti-GBM disease includes intensive plasmapheresis combined with corticosteroids and cyclophosphamide or azathioprine. Plasmapheresis consists of removal of two to four liters of plasma and replacement with fresh frozen plasma or a 5% albumin solution on a daily basis until circulating antibody levels become undetectable (usually two to three weeks). Steroids should be administered initially as pulse methylprednisolone (30 mg/kg or 1,000 mg intravenously over 20 minutes) for three doses (daily or every other day) followed by daily oral prednisone (1 mg/kg per day) for at least the first month, followed by a gradual taper. The initial cyclophosphamide dose is 2 mg/kg per day either orally or intravenously (0.5 g/m2 body surface area).
Selecting patients for treatment is based primarily on severity at presentation. Based on a large retrospective review of 71 patients treated with plasma exchange, prednisolone, and cyclophosphamide, those who presented with plasma creatinine (Cr) concentration of less than 5.7 mg/dL or those who had Cr greater than 5.7 mg/dL but did not require immediate dialysis had a favorable long-term patient and renal survival (approximately 70% to 80% at 90 months). Patients who required immediate dialysis had poor survival (approximately 35% at 90 months). Patients who had crescents in all glomeruli on renal biopsy required long-term maintenance dialysis. Therefore, plasma exchange, prednisone, and cyclophosphamide should be administered in the following settings:
- Pulmonary hemorrhage;
- Renal failure (Cr above 5-7 mg/dL) but not requiring immediate renal replacement therapy; and
- Less severe disease on renal biopsy (less than 30% to 50% crescents). Therapy is unlikely to be effective in patients who present with dialysisdependent renal failure without hemoptysis or if 100% of glomeruli have crescents on renal biopsy. In these settings, the risk of therapy may exceed the likelihood of benefit.
Fish oil is a potential therapy for IgA nephropathy, not anti-GBM disease. ACE inhibition may be useful in patients with nephrotic syndrome. IV hydration would be likely to cause volume overload and precipitate the need for acute dialysis. Low-dose dopamine has not proven effective in reversing acute renal failure. TH
REFERENCES
- Clarkson MR, Brenner BM. Pocket Companion to Brenner & Rector’s The Kidney, 7th ed. Philadelphia, Pa: Elsevier Inc; 2005:198-199.
- Rose BD, Kaplan AA, Appel GB. Treatment of anti-GBM antibody disease (Goodpasture’s syndrome). UpToDate Online. Available at: www.uptodate.com/physicians/pulmonology_toclist.asp. Last accessed August 18, 2005.
- Levy JB, Turner AN, Rees AJ, et al. Long-term outcome of anti-glomerular basement membrane antibody disease treated with plasma exchange and immunosuppression. Ann Intern Med. 2001;134:1033.
- Bolton WK. Goodpasture’s syndrome. Kidney Int. 1996;50:1753.
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int. 2003;63:1164.
An 84-year-old woman with history of coronary artery disease, hypertension, and hyperlipidemia presented with six months of anorexia, nausea, a five-pound weight loss, weakness, and nonbloody diarrhea. Over the past one to two weeks, she noticed decreased urine output despite her use of furosemide.
She was found to have a serum creatinine of 3.5 mg/dL on admission, increased from 1.5 mg/dL five days previously. She had no rash, dyspnea, cough, or abdominal pain. Urinalysis revealed >100 red blood cells (RBC), >100 white blood cells (WBC), occasional hyaline casts, and many gramnegative bacilli. Ciprofloxacin was started for her urinary tract infection. A renal biopsy was performed. The images shown are photomicrographs of light microscopy and immunofluorescence of the renal biopsy specimen. TH
Which of the following would be the most appropriate initial therapy for this condition?
- Increase dose of furosemide;
- Start fish oil;
- Initiate Low-dose dopamine;
- Discontinue ACE inhibitor; or
- Begin emergent plasmapheresis.
Discussion
The correct answer is e: plasmapheresis. The renal biopsy, as shown in the image at left, reveals crescents involving glomeruli on light microscopy and linear IgG staining on immunofluorescence. This patient has antiglomerular basement membrane (anti-GBM) glomerulonephritis (GN), which accounts for 10% to 20% of crescentic glomerulonephritides. It is characterized by circulating antibodies to the glomerular basement membrane with deposition of IgG or, rarely, IgA along the GBM.
The pulmonary-renal vasculitic syndrome is called Goodpasture’s syndrome, in which pulmonary hemorrhage occurs concurrently with GN. Anti-GBM disease has a bimodal distribution, with peaks in the second to third decades and the sixth to seventh decades of life.
Etiology is usually idiopathic, but hydrocarbon exposure has also been associated with the disease. Clinical presentation of renal anti-GBM disease is characterized by an acute onset of GN with severe oliguria or anuria. Urinalysis typically shows hematuria, dysmorphic red blood cells, and red blood cell casts. The diagnostic laboratory finding is circulating antibodies to GBM, specifically to the alpha-3 chain of type IV collagen; these are detected by radioimmunoassay or enzyme immunoassay in approximately 90% of patients.
The standard treatment for anti-GBM disease includes intensive plasmapheresis combined with corticosteroids and cyclophosphamide or azathioprine. Plasmapheresis consists of removal of two to four liters of plasma and replacement with fresh frozen plasma or a 5% albumin solution on a daily basis until circulating antibody levels become undetectable (usually two to three weeks). Steroids should be administered initially as pulse methylprednisolone (30 mg/kg or 1,000 mg intravenously over 20 minutes) for three doses (daily or every other day) followed by daily oral prednisone (1 mg/kg per day) for at least the first month, followed by a gradual taper. The initial cyclophosphamide dose is 2 mg/kg per day either orally or intravenously (0.5 g/m2 body surface area).
Selecting patients for treatment is based primarily on severity at presentation. Based on a large retrospective review of 71 patients treated with plasma exchange, prednisolone, and cyclophosphamide, those who presented with plasma creatinine (Cr) concentration of less than 5.7 mg/dL or those who had Cr greater than 5.7 mg/dL but did not require immediate dialysis had a favorable long-term patient and renal survival (approximately 70% to 80% at 90 months). Patients who required immediate dialysis had poor survival (approximately 35% at 90 months). Patients who had crescents in all glomeruli on renal biopsy required long-term maintenance dialysis. Therefore, plasma exchange, prednisone, and cyclophosphamide should be administered in the following settings:
- Pulmonary hemorrhage;
- Renal failure (Cr above 5-7 mg/dL) but not requiring immediate renal replacement therapy; and
- Less severe disease on renal biopsy (less than 30% to 50% crescents). Therapy is unlikely to be effective in patients who present with dialysisdependent renal failure without hemoptysis or if 100% of glomeruli have crescents on renal biopsy. In these settings, the risk of therapy may exceed the likelihood of benefit.
Fish oil is a potential therapy for IgA nephropathy, not anti-GBM disease. ACE inhibition may be useful in patients with nephrotic syndrome. IV hydration would be likely to cause volume overload and precipitate the need for acute dialysis. Low-dose dopamine has not proven effective in reversing acute renal failure. TH
REFERENCES
- Clarkson MR, Brenner BM. Pocket Companion to Brenner & Rector’s The Kidney, 7th ed. Philadelphia, Pa: Elsevier Inc; 2005:198-199.
- Rose BD, Kaplan AA, Appel GB. Treatment of anti-GBM antibody disease (Goodpasture’s syndrome). UpToDate Online. Available at: www.uptodate.com/physicians/pulmonology_toclist.asp. Last accessed August 18, 2005.
- Levy JB, Turner AN, Rees AJ, et al. Long-term outcome of anti-glomerular basement membrane antibody disease treated with plasma exchange and immunosuppression. Ann Intern Med. 2001;134:1033.
- Bolton WK. Goodpasture’s syndrome. Kidney Int. 1996;50:1753.
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int. 2003;63:1164.
Added Value

At times it seems as though the solution to every problem in the medical center is for the hospitalists to do it. At the University of California at San Francisco, my hospitalist colleagues lead efforts in information technology, quality improvement, perioperative care, transfers of patients to the medical center, and chair countless medical staff committees.
SHM published a supplement (2005; vol. 9, supp. 1) to The Hospitalist detailing the ways hospitalists add value. The supplement contained articles about treating unassigned patients, leading medical staffs, providing extraordinary availability, improving resource utilization, maximizing throughput and improving patient flow, educating staff and colleagues, and improving patient safety and quality of care.
Given all these activities, it’s no wonder life as a hospitalist is busy. But these activities also add a richness and variety to work and place us at the center of the life of the hospital. As our field continues to grow, our responsibilities will continue to grow. In the years ahead, one challenge for our field will be to know when to say “no.”
At an increasing number of hospitals across the country hospitalists add value in another important way by becoming involved with starting, staffing, and using palliative care services. Hospitalists already play a central role in caring for patients with life-threatening illness by providing expert symptom management and talking with them and their families frankly and compassionately about their illness, prognosis, and preferences for care. While this opportunity to affect the care of individual patients and their families is critical, we can better improve the care of these patients by participating in and leading efforts to establish palliative care services within our institutions.
For hospitalists, the arguments that support starting a palliative care service will be familiar because they involve many of the same issues as when starting a hospitalist program. It is helpful to consider why a hospitalist would want to undertake such an endeavor and why a hospital would support it. Here are the key issues:
1) Need: Many hospitalist programs are started to care for patients for whom there was not a doctor available. While inpatients who need palliative care may already have a doctor, the same argument about need applies. Simply put, the hospital is where half of Americans die and where others with serious, chronic, and life-threatening illness spend time. If for no other reason, palliative care services, like hospitalist programs, are necessary because so many patients need this care.
2) Quality: One of the most important drivers of hospitalist programs is quality. Because hospitalists focus on the care of hospitalized patients they can develop expertise and deliver higher quality. The same holds for palliative care. Studies demonstrate widespread shortfalls in
the quality of care that seriously ill and dying patients receive.1 In addition to doing a poor job managing pain, we typically fail to elicit and respect patient preferences. Just as a hospitalist program provides clinicians focused on the care of inpatients, a palliative care team consisting of physicians, nurses, a social worker, pharmacist, and chaplain provides expertise to address the broad range of issues that arise for patients and their families in a comprehensive and high-quality way.
3) Economics: Studies show that hospitalist programs can reduce length of stay and costs at similar quality.2 While cost-cutting is never the sole reason and often not the most important reason for starting a hospitalist program, the fact that these programs can reduce costs makes them financially attractive to hospitals. Palliative care programs provide the same financial advantages, usually with improved quality.
When given a choice, patients faced with a terminal illness will often choose care focused on symptom management and quality of life rather than longevity. Most often this care requires administering simple medications such as opioids, avoiding invasive procedures, and dedicating clinicians’ time to ensure that symptoms are well-managed, and the broad range of concerns are addressed. At UCSF and elsewhere palliative care programs consistently demonstrate cost savings.3 As our chief operating officer says, “We support palliative care because it’s the right thing to do. It helps that it reduces costs, but that’s not why we do it.”
4) Mission alignment: Hospitalist programs align beautifully with the mission of hospitals to provide high-quality, safe patient care at lower cost and with higher satisfaction. Many hospitals have other concerns that hospitalists help with, such as increasing throughput, managing unassigned patients, and improving care processes. Similarly palliative care programs improve the quality of care for patients with life-threatening illness, reduce costs, and increase patient and family satisfaction. Palliative care services also help with throughput by helping to transition patients to less intensive levels of care consistent with their preferences and expediting discharge to home and hospice.
5) Interdisciplinary skills: No hospitalist is an island. The effective hospitalist understands the benefits and necessity of working closely with colleagues from other disciplines to provide high-quality care. In the same way it requires an interdisciplinary palliative care team to address the range of issues facing patients from pain and symptom management to depression and anxiety to spiritual concerns to practical questions about how to get help at home and who will pay for it. The skills that hospitalists develop working with colleagues in the hospital are identical to those needed to provide palliative care.
WHY HOSPITALISTS MUST GET INVOLVED
The parallels between hospitalist programs and palliative care programs support the role of hospitalists in providing palliative care. But there are other important reasons for hospitalists to become involved with palliative care teams.
First, palliative care adds variety to work. Although it may seem that any given day already has too much variety, focusing on palliative care issues, and visiting with patients about their hopes and fears can be a welcome change from general hospitalist work. Second, palliative care can provide incredible personal rewards. Third, palliative care can add diversification to a hospitalist’s income stream through professional fees and hospital support directed at palliative care. Fourth, for the vast majority of us hospitalists who are generalists, palliative care offers the opportunity to develop special expertise and even board certification. Finally, a palliative care service in the hospital can increase the status of the institution, improving family satisfaction, addressing many JCAHO requirements, and supporting the bottom line.
As hospitalists we have many ways to get involved with a palliative care service. Those who are really motivated can lead the implementation of a palliative care service. Because only a minority of hospitals have palliative care programs, this opportunity will be available at many institutions.4,5 But even if you don’t want to lead the effort, you can still play a key role by joining an existing palliative care team or joining a team that is planning to start a program.
Palliative care programs can improve the care of seriously ill and dying patients. They address an important and unmet patient care need and mesh well with the mission and goals of nearly all hospitals. Hospitalists are perfectly positioned to participate in, lead, and use palliative care services. Such work not only helps our patients but benefits us as well by providing the rewards of helping patients and families in need. In the end, we gain not only from easing the suffering of our fellow human beings but from remembering how precious life is, how limited our time is, and how important our choices are about how we spend our time. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at UCSF.
REFERENCES
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). The SUPPORT Principal Investigators. JAMA. 1995;274(20):1591-1598.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287(4):487-494.
- Smith TJ, Coyne PJ, Cassel B, et al. A high-volume specialist palliative care unit and team may reduce in-hospital end-of-life care costs. J Palliat Med. 2003;6(5):699-705.
- Pan CX, Morrison RS, Meier DE, et al. How prevalent are hospital-based palliative care programs? Status report and future directions. J Palliat Med. 2001;4(3):315-324.
- Pantilat SZ, Billings JA. Prevalence and structure of palliative care services in California hospitals. Arch Intern Med. May 12 2003;163(9):1084-1088.
At times it seems as though the solution to every problem in the medical center is for the hospitalists to do it. At the University of California at San Francisco, my hospitalist colleagues lead efforts in information technology, quality improvement, perioperative care, transfers of patients to the medical center, and chair countless medical staff committees.
SHM published a supplement (2005; vol. 9, supp. 1) to The Hospitalist detailing the ways hospitalists add value. The supplement contained articles about treating unassigned patients, leading medical staffs, providing extraordinary availability, improving resource utilization, maximizing throughput and improving patient flow, educating staff and colleagues, and improving patient safety and quality of care.
Given all these activities, it’s no wonder life as a hospitalist is busy. But these activities also add a richness and variety to work and place us at the center of the life of the hospital. As our field continues to grow, our responsibilities will continue to grow. In the years ahead, one challenge for our field will be to know when to say “no.”
At an increasing number of hospitals across the country hospitalists add value in another important way by becoming involved with starting, staffing, and using palliative care services. Hospitalists already play a central role in caring for patients with life-threatening illness by providing expert symptom management and talking with them and their families frankly and compassionately about their illness, prognosis, and preferences for care. While this opportunity to affect the care of individual patients and their families is critical, we can better improve the care of these patients by participating in and leading efforts to establish palliative care services within our institutions.
For hospitalists, the arguments that support starting a palliative care service will be familiar because they involve many of the same issues as when starting a hospitalist program. It is helpful to consider why a hospitalist would want to undertake such an endeavor and why a hospital would support it. Here are the key issues:
1) Need: Many hospitalist programs are started to care for patients for whom there was not a doctor available. While inpatients who need palliative care may already have a doctor, the same argument about need applies. Simply put, the hospital is where half of Americans die and where others with serious, chronic, and life-threatening illness spend time. If for no other reason, palliative care services, like hospitalist programs, are necessary because so many patients need this care.
2) Quality: One of the most important drivers of hospitalist programs is quality. Because hospitalists focus on the care of hospitalized patients they can develop expertise and deliver higher quality. The same holds for palliative care. Studies demonstrate widespread shortfalls in
the quality of care that seriously ill and dying patients receive.1 In addition to doing a poor job managing pain, we typically fail to elicit and respect patient preferences. Just as a hospitalist program provides clinicians focused on the care of inpatients, a palliative care team consisting of physicians, nurses, a social worker, pharmacist, and chaplain provides expertise to address the broad range of issues that arise for patients and their families in a comprehensive and high-quality way.
3) Economics: Studies show that hospitalist programs can reduce length of stay and costs at similar quality.2 While cost-cutting is never the sole reason and often not the most important reason for starting a hospitalist program, the fact that these programs can reduce costs makes them financially attractive to hospitals. Palliative care programs provide the same financial advantages, usually with improved quality.
When given a choice, patients faced with a terminal illness will often choose care focused on symptom management and quality of life rather than longevity. Most often this care requires administering simple medications such as opioids, avoiding invasive procedures, and dedicating clinicians’ time to ensure that symptoms are well-managed, and the broad range of concerns are addressed. At UCSF and elsewhere palliative care programs consistently demonstrate cost savings.3 As our chief operating officer says, “We support palliative care because it’s the right thing to do. It helps that it reduces costs, but that’s not why we do it.”
4) Mission alignment: Hospitalist programs align beautifully with the mission of hospitals to provide high-quality, safe patient care at lower cost and with higher satisfaction. Many hospitals have other concerns that hospitalists help with, such as increasing throughput, managing unassigned patients, and improving care processes. Similarly palliative care programs improve the quality of care for patients with life-threatening illness, reduce costs, and increase patient and family satisfaction. Palliative care services also help with throughput by helping to transition patients to less intensive levels of care consistent with their preferences and expediting discharge to home and hospice.
5) Interdisciplinary skills: No hospitalist is an island. The effective hospitalist understands the benefits and necessity of working closely with colleagues from other disciplines to provide high-quality care. In the same way it requires an interdisciplinary palliative care team to address the range of issues facing patients from pain and symptom management to depression and anxiety to spiritual concerns to practical questions about how to get help at home and who will pay for it. The skills that hospitalists develop working with colleagues in the hospital are identical to those needed to provide palliative care.
WHY HOSPITALISTS MUST GET INVOLVED
The parallels between hospitalist programs and palliative care programs support the role of hospitalists in providing palliative care. But there are other important reasons for hospitalists to become involved with palliative care teams.
First, palliative care adds variety to work. Although it may seem that any given day already has too much variety, focusing on palliative care issues, and visiting with patients about their hopes and fears can be a welcome change from general hospitalist work. Second, palliative care can provide incredible personal rewards. Third, palliative care can add diversification to a hospitalist’s income stream through professional fees and hospital support directed at palliative care. Fourth, for the vast majority of us hospitalists who are generalists, palliative care offers the opportunity to develop special expertise and even board certification. Finally, a palliative care service in the hospital can increase the status of the institution, improving family satisfaction, addressing many JCAHO requirements, and supporting the bottom line.
As hospitalists we have many ways to get involved with a palliative care service. Those who are really motivated can lead the implementation of a palliative care service. Because only a minority of hospitals have palliative care programs, this opportunity will be available at many institutions.4,5 But even if you don’t want to lead the effort, you can still play a key role by joining an existing palliative care team or joining a team that is planning to start a program.
Palliative care programs can improve the care of seriously ill and dying patients. They address an important and unmet patient care need and mesh well with the mission and goals of nearly all hospitals. Hospitalists are perfectly positioned to participate in, lead, and use palliative care services. Such work not only helps our patients but benefits us as well by providing the rewards of helping patients and families in need. In the end, we gain not only from easing the suffering of our fellow human beings but from remembering how precious life is, how limited our time is, and how important our choices are about how we spend our time. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at UCSF.
REFERENCES
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). The SUPPORT Principal Investigators. JAMA. 1995;274(20):1591-1598.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287(4):487-494.
- Smith TJ, Coyne PJ, Cassel B, et al. A high-volume specialist palliative care unit and team may reduce in-hospital end-of-life care costs. J Palliat Med. 2003;6(5):699-705.
- Pan CX, Morrison RS, Meier DE, et al. How prevalent are hospital-based palliative care programs? Status report and future directions. J Palliat Med. 2001;4(3):315-324.
- Pantilat SZ, Billings JA. Prevalence and structure of palliative care services in California hospitals. Arch Intern Med. May 12 2003;163(9):1084-1088.
At times it seems as though the solution to every problem in the medical center is for the hospitalists to do it. At the University of California at San Francisco, my hospitalist colleagues lead efforts in information technology, quality improvement, perioperative care, transfers of patients to the medical center, and chair countless medical staff committees.
SHM published a supplement (2005; vol. 9, supp. 1) to The Hospitalist detailing the ways hospitalists add value. The supplement contained articles about treating unassigned patients, leading medical staffs, providing extraordinary availability, improving resource utilization, maximizing throughput and improving patient flow, educating staff and colleagues, and improving patient safety and quality of care.
Given all these activities, it’s no wonder life as a hospitalist is busy. But these activities also add a richness and variety to work and place us at the center of the life of the hospital. As our field continues to grow, our responsibilities will continue to grow. In the years ahead, one challenge for our field will be to know when to say “no.”
At an increasing number of hospitals across the country hospitalists add value in another important way by becoming involved with starting, staffing, and using palliative care services. Hospitalists already play a central role in caring for patients with life-threatening illness by providing expert symptom management and talking with them and their families frankly and compassionately about their illness, prognosis, and preferences for care. While this opportunity to affect the care of individual patients and their families is critical, we can better improve the care of these patients by participating in and leading efforts to establish palliative care services within our institutions.
For hospitalists, the arguments that support starting a palliative care service will be familiar because they involve many of the same issues as when starting a hospitalist program. It is helpful to consider why a hospitalist would want to undertake such an endeavor and why a hospital would support it. Here are the key issues:
1) Need: Many hospitalist programs are started to care for patients for whom there was not a doctor available. While inpatients who need palliative care may already have a doctor, the same argument about need applies. Simply put, the hospital is where half of Americans die and where others with serious, chronic, and life-threatening illness spend time. If for no other reason, palliative care services, like hospitalist programs, are necessary because so many patients need this care.
2) Quality: One of the most important drivers of hospitalist programs is quality. Because hospitalists focus on the care of hospitalized patients they can develop expertise and deliver higher quality. The same holds for palliative care. Studies demonstrate widespread shortfalls in
the quality of care that seriously ill and dying patients receive.1 In addition to doing a poor job managing pain, we typically fail to elicit and respect patient preferences. Just as a hospitalist program provides clinicians focused on the care of inpatients, a palliative care team consisting of physicians, nurses, a social worker, pharmacist, and chaplain provides expertise to address the broad range of issues that arise for patients and their families in a comprehensive and high-quality way.
3) Economics: Studies show that hospitalist programs can reduce length of stay and costs at similar quality.2 While cost-cutting is never the sole reason and often not the most important reason for starting a hospitalist program, the fact that these programs can reduce costs makes them financially attractive to hospitals. Palliative care programs provide the same financial advantages, usually with improved quality.
When given a choice, patients faced with a terminal illness will often choose care focused on symptom management and quality of life rather than longevity. Most often this care requires administering simple medications such as opioids, avoiding invasive procedures, and dedicating clinicians’ time to ensure that symptoms are well-managed, and the broad range of concerns are addressed. At UCSF and elsewhere palliative care programs consistently demonstrate cost savings.3 As our chief operating officer says, “We support palliative care because it’s the right thing to do. It helps that it reduces costs, but that’s not why we do it.”
4) Mission alignment: Hospitalist programs align beautifully with the mission of hospitals to provide high-quality, safe patient care at lower cost and with higher satisfaction. Many hospitals have other concerns that hospitalists help with, such as increasing throughput, managing unassigned patients, and improving care processes. Similarly palliative care programs improve the quality of care for patients with life-threatening illness, reduce costs, and increase patient and family satisfaction. Palliative care services also help with throughput by helping to transition patients to less intensive levels of care consistent with their preferences and expediting discharge to home and hospice.
5) Interdisciplinary skills: No hospitalist is an island. The effective hospitalist understands the benefits and necessity of working closely with colleagues from other disciplines to provide high-quality care. In the same way it requires an interdisciplinary palliative care team to address the range of issues facing patients from pain and symptom management to depression and anxiety to spiritual concerns to practical questions about how to get help at home and who will pay for it. The skills that hospitalists develop working with colleagues in the hospital are identical to those needed to provide palliative care.
WHY HOSPITALISTS MUST GET INVOLVED
The parallels between hospitalist programs and palliative care programs support the role of hospitalists in providing palliative care. But there are other important reasons for hospitalists to become involved with palliative care teams.
First, palliative care adds variety to work. Although it may seem that any given day already has too much variety, focusing on palliative care issues, and visiting with patients about their hopes and fears can be a welcome change from general hospitalist work. Second, palliative care can provide incredible personal rewards. Third, palliative care can add diversification to a hospitalist’s income stream through professional fees and hospital support directed at palliative care. Fourth, for the vast majority of us hospitalists who are generalists, palliative care offers the opportunity to develop special expertise and even board certification. Finally, a palliative care service in the hospital can increase the status of the institution, improving family satisfaction, addressing many JCAHO requirements, and supporting the bottom line.
As hospitalists we have many ways to get involved with a palliative care service. Those who are really motivated can lead the implementation of a palliative care service. Because only a minority of hospitals have palliative care programs, this opportunity will be available at many institutions.4,5 But even if you don’t want to lead the effort, you can still play a key role by joining an existing palliative care team or joining a team that is planning to start a program.
Palliative care programs can improve the care of seriously ill and dying patients. They address an important and unmet patient care need and mesh well with the mission and goals of nearly all hospitals. Hospitalists are perfectly positioned to participate in, lead, and use palliative care services. Such work not only helps our patients but benefits us as well by providing the rewards of helping patients and families in need. In the end, we gain not only from easing the suffering of our fellow human beings but from remembering how precious life is, how limited our time is, and how important our choices are about how we spend our time. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at UCSF.
REFERENCES
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). The SUPPORT Principal Investigators. JAMA. 1995;274(20):1591-1598.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287(4):487-494.
- Smith TJ, Coyne PJ, Cassel B, et al. A high-volume specialist palliative care unit and team may reduce in-hospital end-of-life care costs. J Palliat Med. 2003;6(5):699-705.
- Pan CX, Morrison RS, Meier DE, et al. How prevalent are hospital-based palliative care programs? Status report and future directions. J Palliat Med. 2001;4(3):315-324.
- Pantilat SZ, Billings JA. Prevalence and structure of palliative care services in California hospitals. Arch Intern Med. May 12 2003;163(9):1084-1088.
Eye of the Storm
Editors’ note: When a disaster strikes—whether manmade or natural—we are wrenched from our normal existence into another realm entirely. The petty concerns of daily life fade from sight in the wake of destruction and death.
For the practitioner of medicine, this is a time of great challenge to demonstrate the highest ideals of medicine. The people of the Gulf Coast must now face a dawn where the life they knew is gone and must be built anew. In this issue we’re proud to include the memoirs of two New Orleans physicians who worked through this catastrophe.
For more information on how you can help with the recovery effort, visit www.hospitalmedicine.org.
Despite the best preparations and planning, many aspects of managing a physician practice change rapidly, and many new problems arise immediately following a disaster. Below, we present our experiences as a large hospitalist program in a tertiary-care referral center during the days before and the seven days after Hurricane Katrina, a category IV storm, devastated New Orleans.

PREPARATION
Ochsner Clinic Foundation (OCF) is an integrated medical institution with more than 700 physicians and 24 clinics throughout Southeast Louisiana, including Northshore and Baton Rouge. For nearly 60 years, Ochsner has cared for residents in the greater New Orleans communities at the Ochsner Main Campus, which includes a multispecialty clinic, a 500-bed hospital, and residency training programs. The Main Campus is located by the Mississippi River at the parish line between Orleans Parish and Jefferson Parish—areas protected from flooding under the levee system.
The Hospitalist Program at the Ochsner Main Campus has 18 physicians and four nurse practitioners. Approximately 60% of our patients are managed by Internal Medicine Residency teaching services and the rest by staff physicians. Prior to the landing of Hurricane Katrina, we cared for 60% of the hospitalized patients. Our past hurricane experience led us to develop a two-team system for disasters. Team A has four hospitalists who are required to stay on campus;
Team B is available within a week later to relieve Team A.
We tracked Hurricane Katrina following its exit from the Florida area. The decision analysis for our essential medical team was based on the category of the hurricane, staff location, and projected path. On Saturday, August 27, we were informed that Hurricane Katrina was reaching category V status and expected to hit New Orleans early Monday morning. This unexpected arrival required us to mobilize the hurricane emergency preparedness team rapidly. Hence both teams A and B were requested to remain on premise—preferably without family and pets. On the facility side, we had four generators on site and started to request other generators from around the country on the news of changing course of the hurricane.

SUNDAY, AUGUST 28:
The Day before Katrina Landed
New Orleans Mayor Ray Nagin ordered a mandatory evacuation of the city for the first time in history. At Ochsner, all essential personnel were expected to report to their stations by 7 p.m. The arrival of the hurricane gave little time to our staff to arrange alternative living arrangements for their significant others and pets. Consequently many non-medical dependents and pets arrived at the facility even though we didn’t have adequate supplies to be self-sufficient for more than a few days. Many expected our organization to have ample resources to accommodate all needs—food, shelter, and support. A hurricane disaster phone line was created to update the status of OCF following the hurricane.
MONDAY, AUGUST 29:
Katrina Lands in New Orleans
OCF lost power in the early morning of August 29. Our facility sustained water and roof damage on the top floors of the hospital and unexpected ceiling glass breaks in the walkways. The howling of the intense wind created an ominous feeling among all of those sheltered in the facility. Fortunately, only minor flooding occurred around the institution.
In contrast, major flooding was reported throughout metropolitan New Orleans—especially in New Orleans East and surrounding low-lying parishes. Major wind damage was seen in buildings in the central business district, and 100% of the power was out in that area.
Downtown New Orleans and the French Quarter were dry thanks to the pumping system. Disturbingly, though, breaches in the levee system protecting New Orleans were reported in the 17th Street Canal.
By Monday afternoon, our entire facility was running on emergency generators, which provided energy only for essential equipment and left the institution with no air-conditioning, minimal lighting, and no plumbing. Physicians used flashlights to see patients, and the rooms became unbearably hot and humid; the heat index outside was 105 degrees Fahrenheit.
All regular communications went off service, including telephone lines, cell phones, and outside pagers. Fortunately OCF had invested in Spectralink phones in the past few years; this internal, antenna-based phone system continued to function. We were even able to dial long-distance intermittently. Our information system also went down, but we kept generator power for intermittent use of the Internet and Intranet to allow our employees to access information and contact with the outside world. At night—from the towers of our hospital—it was strange to see our former city of lights in total darkness.
TUESDAY, AUGUST 30:
Hurricane Aftermath Day 1
Reports of catastrophic flooding and heroic rooftop rescues in New Orleans East and other parishes were announced on the radio and via the Internet. Unfortunately the levee breach at the 17th Street Canal became uncontrolled, and water began flowing from Lake Pontchartrain into New Orleans, ultimately flooding 80% of the city of New Orleans. The Superdome and the Convention Center began to fill with thousands of refugees.
The lack of electricity, inadequate food and water supplies, overcrowding, lack of adequate sanitary conditions, and—later—security concerns exponentially created a humanitarian crisis. We were devastated by the plight of our fellow New Orleans residents, whose only crime was, largely, being too poor to evacuate. Approximately 300,000 people never evacuated, and this posed an interminable challenge for city, state, and federal governments. Unfortunately the acts of a few heartless gangs tarnished the beautiful and friendly image of the Big Easy.
At Ochsner we began to conserve our resources because of the commitment to care for more than 500 people onsite. Our dietary department provided approximately 1,600 meals daily, working in hot and sweaty conditions. In the hospital the heat began to take a physical toll on everyone. We also suffered the psychological toll of not knowing what had happened to our families, friends, and belongings. We lost the ability to run most laboratory studies. We concentrated our efforts in preserving human lives with only basic means.
With no working elevators, navigating 11 floors of the hospital was a challenge for all. Our survival tactics included not just adequate fluid hydration, but electrolyte replacement. Unexpectedly, we discovered that OCF had invested in a deep-well water system separate
from the county water supply in the hospital. Thus the hospital continued to have water for at least the first three floors. The cool well water provided much-needed refreshing showers and maintained adequate sanitary conditions.
One of our hospitalists evacuated from OCF (along with several of our team’s family members) to Houston. On their way, they passed downed power-lines, a daiquiri shop in flames, and cars carrying boats on their roofs into New Orleans to help rescue stranded people.
WEDNESDAY, AUGUST 31:
Hurricane Aftermath Day 2
Conditions in downtown New Orleans became increasing dire with rising floodwater, hunger, thirst, and reports of looting and unrest. Rumors started to spread about the status and safety of OCF. One stated that OCF had looted a nearby Wal-Mart for food and supplies even though, in fact, senior executives of Wal-Mart personally inventoried the items and generously donated them to our institution.
There were also rumors about looters approaching from downtown. Family members outside the city were urging our employees to leave because of the danger of continued flooding and civil unrest. OCF administrators (under the leadership of the CEO Patrick Quinlan, MD, President and COO Warner Thomas, MD, and Medical Director Richard Guthrie, MD) actively addressed these issues to stop the rumors with scheduled and mandatory open forums. During the next few days, OCF was in a lock-down mode with the National Guard and our own security department providing security.
Not knowing the capability of our facility in this time of extreme uncertainly, we proceeded to discharge and move patients to other centers, such as Memorial Hermann Hospital in Houston and Summit Hospital in Baton Rouge via both helicopter and ambulance.
Simultaneously we focused on patients who were stable and ready for discharge to increase our organization capacity to create a plan for providing resource for both the east and west banks of the Mississippi River.
THURSDAY, SEPTEMBER 1:
Hurricane Aftermath Day 3
With the city of New Orleans under marshal law, OCF continued in lock-down mode. During the aftermath, a high priority was to contact all the evacuated employees. An employee outreach program was implemented in which each department accounted for the whereabouts of all personnel. As for our hospitalist program, we started to meet twice daily immediately after the hurricane to address concerns of emergency department volumes, maintain open communications, provide mutual psychological support, and foster a spirit of teamwork. During these meetings we believed that our department had cemented a bond that could not be created in normal circumstances. Our efforts through the storm and the unimaginable adversity were nothing short of extraordinary.
Our medical colleagues in Charity Hospital in downtown New Orleans faced unprecedented challenges caring for patients with minimal supplies. We heard reports of doctors giving each other IV hydration and medical personnel bagging ventilator patients in shifts. With no communication except the Internet, they resorted to e-mailing CNN for help.
FRIDAY, SEPTEMBER 2:
Hurricane Aftermath Day 4
President Bush arrived to visit New Orleans and other devastated areas in the Gulf region. With the National Guard moving in to provide security and relief efforts, Mayor Nagin declared the day a turning point for the city. After the hurricane, it was uncertain how many patients would require medical care in the community. From the Hurricane Ivan experience in Pensacola, Fla., we were advised that 10 days after the disaster, one could anticipate a doubling of the highest emergency department volume for several weeks.
We were uncertain that the evacuation of the whole city could provide such volume. To offer quality clinical care and remain in sound mind under such conditions, we hospitalists unanimously agreed to care for our patients 24/7 in weekly rotation. Our hospital census during this period was at 60% of usual and the admission was running at 40% of normal. We decreased the residents from three members per team to two in order to provide a five-day rotation of three teams. We utilized the staging center of Ochsner Baton Rouge to organize our employees and provide transportation to and from New Orleans. Employees were discouraged from driving in
their own vehicles due to gasoline shortage and safety concerns.
SATURDAY, SEPTEMBER 3:
Hurricane Aftermath Day 5
Conditions in New Orleans improved rapidly with better security. Evacuees were steadily transported out of the Superdome and Convention Center. Hurricane Katrina disasters posed new challenges in providing care. We saw patients with
- Severe dehydration;
- Exhaustion caused by the lack of use or incorrect use of their medications for days resulting in exacerbation of chronic conditions such as COPD;
- Water-borne illnesses from prolonged immersion in toxic water;
- Reactive airway diseases from environmental allergens;
- Cellulitis from cuts and bruises in evacuees, as well as people attempting home repairs;
- Carbon monoxide poisoning from generators used incorrectly inside homes; and
- Withdrawals from illicit drug uses.
SUNDAY, SEPTEMBER 4:
Hurricane Aftermath Day 6
During the Sunday ad-hoc church service at Ochsner, doctors, nurses, employees, patients, and families came together in spiritual healing. We sang praises of hope and optimism for our community. We were grateful for our status in this unbelievable disaster and offered prayers and hope for those who had lost so much. We had never been so proud of the efforts of every individual in our institution for maintaining this facility for patient care in such dire situations and promised to be optimistic about our future.
Fortunately, with the help of the Jefferson Parish emergency utility crews, power was restored to our institution. We became fully functional to take on the challenges of the community.
MONDAY, SEPTEMBER 5:
Hurricane Aftermath Day 7
The 17th Street Canal breach was controlled and the water pump back in operation. Residents of Jefferson Parish were allowed to return to take their personal items from their houses but were still under voluntary evacuation, while Orleans Parish was still closed. To plan the demand for medical care in the wake of gradual recovery, OCF began to maintain all of our employees through strategic deployments in various satellite clinics and hospitals according to the needs of the population in New Orleans and other areas.
LESSONS LEARNED
We have learned so much from this disaster. The key to overcome such adverse conditions entails strong psychosocial support from colleagues and family. Strong leadership is crucial to maintain a sense of serenity and an optimistic outlook in times of uncertainty. We experienced a sense of camaraderie after seeing all medical personnel participating in activities beyond of the boundary of usual roles.
The expansion of the essential personnel team list to include social workers and discharge planners is crucial to focus on the unique and nonconventional logistical challenges post-disaster. Intense focus on group dynamics was essential to avoid physical and emotional burnout. Frequent and predictably scheduled face-to-face communication was also important in disseminating accurate, unadulterated information because our decision-making changed hour-to-hour immediately after Hurricane Katrina, day-to-day in the few days afterward, and week-to-week just one week post-disaster.
Obviously the financial implications are immense for our city and our institution. We are developing financial plans, a relief fund, and other resources to assist our employees who have been severely affected by the hurricane. TH
Dr. Deitelzweig and Dr. Lee work at the Ochsner Clinic Foundation, Department of Hospital-Based Internal Medicine, New Orleans. You can contact Dr. Deitelzweig by phone at (504) 842-5766; his e-mail is [email protected]
Editors’ note: When a disaster strikes—whether manmade or natural—we are wrenched from our normal existence into another realm entirely. The petty concerns of daily life fade from sight in the wake of destruction and death.
For the practitioner of medicine, this is a time of great challenge to demonstrate the highest ideals of medicine. The people of the Gulf Coast must now face a dawn where the life they knew is gone and must be built anew. In this issue we’re proud to include the memoirs of two New Orleans physicians who worked through this catastrophe.
For more information on how you can help with the recovery effort, visit www.hospitalmedicine.org.
Despite the best preparations and planning, many aspects of managing a physician practice change rapidly, and many new problems arise immediately following a disaster. Below, we present our experiences as a large hospitalist program in a tertiary-care referral center during the days before and the seven days after Hurricane Katrina, a category IV storm, devastated New Orleans.
PREPARATION
Ochsner Clinic Foundation (OCF) is an integrated medical institution with more than 700 physicians and 24 clinics throughout Southeast Louisiana, including Northshore and Baton Rouge. For nearly 60 years, Ochsner has cared for residents in the greater New Orleans communities at the Ochsner Main Campus, which includes a multispecialty clinic, a 500-bed hospital, and residency training programs. The Main Campus is located by the Mississippi River at the parish line between Orleans Parish and Jefferson Parish—areas protected from flooding under the levee system.
The Hospitalist Program at the Ochsner Main Campus has 18 physicians and four nurse practitioners. Approximately 60% of our patients are managed by Internal Medicine Residency teaching services and the rest by staff physicians. Prior to the landing of Hurricane Katrina, we cared for 60% of the hospitalized patients. Our past hurricane experience led us to develop a two-team system for disasters. Team A has four hospitalists who are required to stay on campus;
Team B is available within a week later to relieve Team A.
We tracked Hurricane Katrina following its exit from the Florida area. The decision analysis for our essential medical team was based on the category of the hurricane, staff location, and projected path. On Saturday, August 27, we were informed that Hurricane Katrina was reaching category V status and expected to hit New Orleans early Monday morning. This unexpected arrival required us to mobilize the hurricane emergency preparedness team rapidly. Hence both teams A and B were requested to remain on premise—preferably without family and pets. On the facility side, we had four generators on site and started to request other generators from around the country on the news of changing course of the hurricane.
SUNDAY, AUGUST 28:
The Day before Katrina Landed
New Orleans Mayor Ray Nagin ordered a mandatory evacuation of the city for the first time in history. At Ochsner, all essential personnel were expected to report to their stations by 7 p.m. The arrival of the hurricane gave little time to our staff to arrange alternative living arrangements for their significant others and pets. Consequently many non-medical dependents and pets arrived at the facility even though we didn’t have adequate supplies to be self-sufficient for more than a few days. Many expected our organization to have ample resources to accommodate all needs—food, shelter, and support. A hurricane disaster phone line was created to update the status of OCF following the hurricane.
MONDAY, AUGUST 29:
Katrina Lands in New Orleans
OCF lost power in the early morning of August 29. Our facility sustained water and roof damage on the top floors of the hospital and unexpected ceiling glass breaks in the walkways. The howling of the intense wind created an ominous feeling among all of those sheltered in the facility. Fortunately, only minor flooding occurred around the institution.
In contrast, major flooding was reported throughout metropolitan New Orleans—especially in New Orleans East and surrounding low-lying parishes. Major wind damage was seen in buildings in the central business district, and 100% of the power was out in that area.
Downtown New Orleans and the French Quarter were dry thanks to the pumping system. Disturbingly, though, breaches in the levee system protecting New Orleans were reported in the 17th Street Canal.
By Monday afternoon, our entire facility was running on emergency generators, which provided energy only for essential equipment and left the institution with no air-conditioning, minimal lighting, and no plumbing. Physicians used flashlights to see patients, and the rooms became unbearably hot and humid; the heat index outside was 105 degrees Fahrenheit.
All regular communications went off service, including telephone lines, cell phones, and outside pagers. Fortunately OCF had invested in Spectralink phones in the past few years; this internal, antenna-based phone system continued to function. We were even able to dial long-distance intermittently. Our information system also went down, but we kept generator power for intermittent use of the Internet and Intranet to allow our employees to access information and contact with the outside world. At night—from the towers of our hospital—it was strange to see our former city of lights in total darkness.
TUESDAY, AUGUST 30:
Hurricane Aftermath Day 1
Reports of catastrophic flooding and heroic rooftop rescues in New Orleans East and other parishes were announced on the radio and via the Internet. Unfortunately the levee breach at the 17th Street Canal became uncontrolled, and water began flowing from Lake Pontchartrain into New Orleans, ultimately flooding 80% of the city of New Orleans. The Superdome and the Convention Center began to fill with thousands of refugees.
The lack of electricity, inadequate food and water supplies, overcrowding, lack of adequate sanitary conditions, and—later—security concerns exponentially created a humanitarian crisis. We were devastated by the plight of our fellow New Orleans residents, whose only crime was, largely, being too poor to evacuate. Approximately 300,000 people never evacuated, and this posed an interminable challenge for city, state, and federal governments. Unfortunately the acts of a few heartless gangs tarnished the beautiful and friendly image of the Big Easy.
At Ochsner we began to conserve our resources because of the commitment to care for more than 500 people onsite. Our dietary department provided approximately 1,600 meals daily, working in hot and sweaty conditions. In the hospital the heat began to take a physical toll on everyone. We also suffered the psychological toll of not knowing what had happened to our families, friends, and belongings. We lost the ability to run most laboratory studies. We concentrated our efforts in preserving human lives with only basic means.
With no working elevators, navigating 11 floors of the hospital was a challenge for all. Our survival tactics included not just adequate fluid hydration, but electrolyte replacement. Unexpectedly, we discovered that OCF had invested in a deep-well water system separate
from the county water supply in the hospital. Thus the hospital continued to have water for at least the first three floors. The cool well water provided much-needed refreshing showers and maintained adequate sanitary conditions.
One of our hospitalists evacuated from OCF (along with several of our team’s family members) to Houston. On their way, they passed downed power-lines, a daiquiri shop in flames, and cars carrying boats on their roofs into New Orleans to help rescue stranded people.
WEDNESDAY, AUGUST 31:
Hurricane Aftermath Day 2
Conditions in downtown New Orleans became increasing dire with rising floodwater, hunger, thirst, and reports of looting and unrest. Rumors started to spread about the status and safety of OCF. One stated that OCF had looted a nearby Wal-Mart for food and supplies even though, in fact, senior executives of Wal-Mart personally inventoried the items and generously donated them to our institution.
There were also rumors about looters approaching from downtown. Family members outside the city were urging our employees to leave because of the danger of continued flooding and civil unrest. OCF administrators (under the leadership of the CEO Patrick Quinlan, MD, President and COO Warner Thomas, MD, and Medical Director Richard Guthrie, MD) actively addressed these issues to stop the rumors with scheduled and mandatory open forums. During the next few days, OCF was in a lock-down mode with the National Guard and our own security department providing security.
Not knowing the capability of our facility in this time of extreme uncertainly, we proceeded to discharge and move patients to other centers, such as Memorial Hermann Hospital in Houston and Summit Hospital in Baton Rouge via both helicopter and ambulance.
Simultaneously we focused on patients who were stable and ready for discharge to increase our organization capacity to create a plan for providing resource for both the east and west banks of the Mississippi River.
THURSDAY, SEPTEMBER 1:
Hurricane Aftermath Day 3
With the city of New Orleans under marshal law, OCF continued in lock-down mode. During the aftermath, a high priority was to contact all the evacuated employees. An employee outreach program was implemented in which each department accounted for the whereabouts of all personnel. As for our hospitalist program, we started to meet twice daily immediately after the hurricane to address concerns of emergency department volumes, maintain open communications, provide mutual psychological support, and foster a spirit of teamwork. During these meetings we believed that our department had cemented a bond that could not be created in normal circumstances. Our efforts through the storm and the unimaginable adversity were nothing short of extraordinary.
Our medical colleagues in Charity Hospital in downtown New Orleans faced unprecedented challenges caring for patients with minimal supplies. We heard reports of doctors giving each other IV hydration and medical personnel bagging ventilator patients in shifts. With no communication except the Internet, they resorted to e-mailing CNN for help.
FRIDAY, SEPTEMBER 2:
Hurricane Aftermath Day 4
President Bush arrived to visit New Orleans and other devastated areas in the Gulf region. With the National Guard moving in to provide security and relief efforts, Mayor Nagin declared the day a turning point for the city. After the hurricane, it was uncertain how many patients would require medical care in the community. From the Hurricane Ivan experience in Pensacola, Fla., we were advised that 10 days after the disaster, one could anticipate a doubling of the highest emergency department volume for several weeks.
We were uncertain that the evacuation of the whole city could provide such volume. To offer quality clinical care and remain in sound mind under such conditions, we hospitalists unanimously agreed to care for our patients 24/7 in weekly rotation. Our hospital census during this period was at 60% of usual and the admission was running at 40% of normal. We decreased the residents from three members per team to two in order to provide a five-day rotation of three teams. We utilized the staging center of Ochsner Baton Rouge to organize our employees and provide transportation to and from New Orleans. Employees were discouraged from driving in
their own vehicles due to gasoline shortage and safety concerns.
SATURDAY, SEPTEMBER 3:
Hurricane Aftermath Day 5
Conditions in New Orleans improved rapidly with better security. Evacuees were steadily transported out of the Superdome and Convention Center. Hurricane Katrina disasters posed new challenges in providing care. We saw patients with
- Severe dehydration;
- Exhaustion caused by the lack of use or incorrect use of their medications for days resulting in exacerbation of chronic conditions such as COPD;
- Water-borne illnesses from prolonged immersion in toxic water;
- Reactive airway diseases from environmental allergens;
- Cellulitis from cuts and bruises in evacuees, as well as people attempting home repairs;
- Carbon monoxide poisoning from generators used incorrectly inside homes; and
- Withdrawals from illicit drug uses.
SUNDAY, SEPTEMBER 4:
Hurricane Aftermath Day 6
During the Sunday ad-hoc church service at Ochsner, doctors, nurses, employees, patients, and families came together in spiritual healing. We sang praises of hope and optimism for our community. We were grateful for our status in this unbelievable disaster and offered prayers and hope for those who had lost so much. We had never been so proud of the efforts of every individual in our institution for maintaining this facility for patient care in such dire situations and promised to be optimistic about our future.
Fortunately, with the help of the Jefferson Parish emergency utility crews, power was restored to our institution. We became fully functional to take on the challenges of the community.
MONDAY, SEPTEMBER 5:
Hurricane Aftermath Day 7
The 17th Street Canal breach was controlled and the water pump back in operation. Residents of Jefferson Parish were allowed to return to take their personal items from their houses but were still under voluntary evacuation, while Orleans Parish was still closed. To plan the demand for medical care in the wake of gradual recovery, OCF began to maintain all of our employees through strategic deployments in various satellite clinics and hospitals according to the needs of the population in New Orleans and other areas.
LESSONS LEARNED
We have learned so much from this disaster. The key to overcome such adverse conditions entails strong psychosocial support from colleagues and family. Strong leadership is crucial to maintain a sense of serenity and an optimistic outlook in times of uncertainty. We experienced a sense of camaraderie after seeing all medical personnel participating in activities beyond of the boundary of usual roles.
The expansion of the essential personnel team list to include social workers and discharge planners is crucial to focus on the unique and nonconventional logistical challenges post-disaster. Intense focus on group dynamics was essential to avoid physical and emotional burnout. Frequent and predictably scheduled face-to-face communication was also important in disseminating accurate, unadulterated information because our decision-making changed hour-to-hour immediately after Hurricane Katrina, day-to-day in the few days afterward, and week-to-week just one week post-disaster.
Obviously the financial implications are immense for our city and our institution. We are developing financial plans, a relief fund, and other resources to assist our employees who have been severely affected by the hurricane. TH
Dr. Deitelzweig and Dr. Lee work at the Ochsner Clinic Foundation, Department of Hospital-Based Internal Medicine, New Orleans. You can contact Dr. Deitelzweig by phone at (504) 842-5766; his e-mail is [email protected]
Editors’ note: When a disaster strikes—whether manmade or natural—we are wrenched from our normal existence into another realm entirely. The petty concerns of daily life fade from sight in the wake of destruction and death.
For the practitioner of medicine, this is a time of great challenge to demonstrate the highest ideals of medicine. The people of the Gulf Coast must now face a dawn where the life they knew is gone and must be built anew. In this issue we’re proud to include the memoirs of two New Orleans physicians who worked through this catastrophe.
For more information on how you can help with the recovery effort, visit www.hospitalmedicine.org.
Despite the best preparations and planning, many aspects of managing a physician practice change rapidly, and many new problems arise immediately following a disaster. Below, we present our experiences as a large hospitalist program in a tertiary-care referral center during the days before and the seven days after Hurricane Katrina, a category IV storm, devastated New Orleans.
PREPARATION
Ochsner Clinic Foundation (OCF) is an integrated medical institution with more than 700 physicians and 24 clinics throughout Southeast Louisiana, including Northshore and Baton Rouge. For nearly 60 years, Ochsner has cared for residents in the greater New Orleans communities at the Ochsner Main Campus, which includes a multispecialty clinic, a 500-bed hospital, and residency training programs. The Main Campus is located by the Mississippi River at the parish line between Orleans Parish and Jefferson Parish—areas protected from flooding under the levee system.
The Hospitalist Program at the Ochsner Main Campus has 18 physicians and four nurse practitioners. Approximately 60% of our patients are managed by Internal Medicine Residency teaching services and the rest by staff physicians. Prior to the landing of Hurricane Katrina, we cared for 60% of the hospitalized patients. Our past hurricane experience led us to develop a two-team system for disasters. Team A has four hospitalists who are required to stay on campus;
Team B is available within a week later to relieve Team A.
We tracked Hurricane Katrina following its exit from the Florida area. The decision analysis for our essential medical team was based on the category of the hurricane, staff location, and projected path. On Saturday, August 27, we were informed that Hurricane Katrina was reaching category V status and expected to hit New Orleans early Monday morning. This unexpected arrival required us to mobilize the hurricane emergency preparedness team rapidly. Hence both teams A and B were requested to remain on premise—preferably without family and pets. On the facility side, we had four generators on site and started to request other generators from around the country on the news of changing course of the hurricane.
SUNDAY, AUGUST 28:
The Day before Katrina Landed
New Orleans Mayor Ray Nagin ordered a mandatory evacuation of the city for the first time in history. At Ochsner, all essential personnel were expected to report to their stations by 7 p.m. The arrival of the hurricane gave little time to our staff to arrange alternative living arrangements for their significant others and pets. Consequently many non-medical dependents and pets arrived at the facility even though we didn’t have adequate supplies to be self-sufficient for more than a few days. Many expected our organization to have ample resources to accommodate all needs—food, shelter, and support. A hurricane disaster phone line was created to update the status of OCF following the hurricane.
MONDAY, AUGUST 29:
Katrina Lands in New Orleans
OCF lost power in the early morning of August 29. Our facility sustained water and roof damage on the top floors of the hospital and unexpected ceiling glass breaks in the walkways. The howling of the intense wind created an ominous feeling among all of those sheltered in the facility. Fortunately, only minor flooding occurred around the institution.
In contrast, major flooding was reported throughout metropolitan New Orleans—especially in New Orleans East and surrounding low-lying parishes. Major wind damage was seen in buildings in the central business district, and 100% of the power was out in that area.
Downtown New Orleans and the French Quarter were dry thanks to the pumping system. Disturbingly, though, breaches in the levee system protecting New Orleans were reported in the 17th Street Canal.
By Monday afternoon, our entire facility was running on emergency generators, which provided energy only for essential equipment and left the institution with no air-conditioning, minimal lighting, and no plumbing. Physicians used flashlights to see patients, and the rooms became unbearably hot and humid; the heat index outside was 105 degrees Fahrenheit.
All regular communications went off service, including telephone lines, cell phones, and outside pagers. Fortunately OCF had invested in Spectralink phones in the past few years; this internal, antenna-based phone system continued to function. We were even able to dial long-distance intermittently. Our information system also went down, but we kept generator power for intermittent use of the Internet and Intranet to allow our employees to access information and contact with the outside world. At night—from the towers of our hospital—it was strange to see our former city of lights in total darkness.
TUESDAY, AUGUST 30:
Hurricane Aftermath Day 1
Reports of catastrophic flooding and heroic rooftop rescues in New Orleans East and other parishes were announced on the radio and via the Internet. Unfortunately the levee breach at the 17th Street Canal became uncontrolled, and water began flowing from Lake Pontchartrain into New Orleans, ultimately flooding 80% of the city of New Orleans. The Superdome and the Convention Center began to fill with thousands of refugees.
The lack of electricity, inadequate food and water supplies, overcrowding, lack of adequate sanitary conditions, and—later—security concerns exponentially created a humanitarian crisis. We were devastated by the plight of our fellow New Orleans residents, whose only crime was, largely, being too poor to evacuate. Approximately 300,000 people never evacuated, and this posed an interminable challenge for city, state, and federal governments. Unfortunately the acts of a few heartless gangs tarnished the beautiful and friendly image of the Big Easy.
At Ochsner we began to conserve our resources because of the commitment to care for more than 500 people onsite. Our dietary department provided approximately 1,600 meals daily, working in hot and sweaty conditions. In the hospital the heat began to take a physical toll on everyone. We also suffered the psychological toll of not knowing what had happened to our families, friends, and belongings. We lost the ability to run most laboratory studies. We concentrated our efforts in preserving human lives with only basic means.
With no working elevators, navigating 11 floors of the hospital was a challenge for all. Our survival tactics included not just adequate fluid hydration, but electrolyte replacement. Unexpectedly, we discovered that OCF had invested in a deep-well water system separate
from the county water supply in the hospital. Thus the hospital continued to have water for at least the first three floors. The cool well water provided much-needed refreshing showers and maintained adequate sanitary conditions.
One of our hospitalists evacuated from OCF (along with several of our team’s family members) to Houston. On their way, they passed downed power-lines, a daiquiri shop in flames, and cars carrying boats on their roofs into New Orleans to help rescue stranded people.
WEDNESDAY, AUGUST 31:
Hurricane Aftermath Day 2
Conditions in downtown New Orleans became increasing dire with rising floodwater, hunger, thirst, and reports of looting and unrest. Rumors started to spread about the status and safety of OCF. One stated that OCF had looted a nearby Wal-Mart for food and supplies even though, in fact, senior executives of Wal-Mart personally inventoried the items and generously donated them to our institution.
There were also rumors about looters approaching from downtown. Family members outside the city were urging our employees to leave because of the danger of continued flooding and civil unrest. OCF administrators (under the leadership of the CEO Patrick Quinlan, MD, President and COO Warner Thomas, MD, and Medical Director Richard Guthrie, MD) actively addressed these issues to stop the rumors with scheduled and mandatory open forums. During the next few days, OCF was in a lock-down mode with the National Guard and our own security department providing security.
Not knowing the capability of our facility in this time of extreme uncertainly, we proceeded to discharge and move patients to other centers, such as Memorial Hermann Hospital in Houston and Summit Hospital in Baton Rouge via both helicopter and ambulance.
Simultaneously we focused on patients who were stable and ready for discharge to increase our organization capacity to create a plan for providing resource for both the east and west banks of the Mississippi River.
THURSDAY, SEPTEMBER 1:
Hurricane Aftermath Day 3
With the city of New Orleans under marshal law, OCF continued in lock-down mode. During the aftermath, a high priority was to contact all the evacuated employees. An employee outreach program was implemented in which each department accounted for the whereabouts of all personnel. As for our hospitalist program, we started to meet twice daily immediately after the hurricane to address concerns of emergency department volumes, maintain open communications, provide mutual psychological support, and foster a spirit of teamwork. During these meetings we believed that our department had cemented a bond that could not be created in normal circumstances. Our efforts through the storm and the unimaginable adversity were nothing short of extraordinary.
Our medical colleagues in Charity Hospital in downtown New Orleans faced unprecedented challenges caring for patients with minimal supplies. We heard reports of doctors giving each other IV hydration and medical personnel bagging ventilator patients in shifts. With no communication except the Internet, they resorted to e-mailing CNN for help.
FRIDAY, SEPTEMBER 2:
Hurricane Aftermath Day 4
President Bush arrived to visit New Orleans and other devastated areas in the Gulf region. With the National Guard moving in to provide security and relief efforts, Mayor Nagin declared the day a turning point for the city. After the hurricane, it was uncertain how many patients would require medical care in the community. From the Hurricane Ivan experience in Pensacola, Fla., we were advised that 10 days after the disaster, one could anticipate a doubling of the highest emergency department volume for several weeks.
We were uncertain that the evacuation of the whole city could provide such volume. To offer quality clinical care and remain in sound mind under such conditions, we hospitalists unanimously agreed to care for our patients 24/7 in weekly rotation. Our hospital census during this period was at 60% of usual and the admission was running at 40% of normal. We decreased the residents from three members per team to two in order to provide a five-day rotation of three teams. We utilized the staging center of Ochsner Baton Rouge to organize our employees and provide transportation to and from New Orleans. Employees were discouraged from driving in
their own vehicles due to gasoline shortage and safety concerns.
SATURDAY, SEPTEMBER 3:
Hurricane Aftermath Day 5
Conditions in New Orleans improved rapidly with better security. Evacuees were steadily transported out of the Superdome and Convention Center. Hurricane Katrina disasters posed new challenges in providing care. We saw patients with
- Severe dehydration;
- Exhaustion caused by the lack of use or incorrect use of their medications for days resulting in exacerbation of chronic conditions such as COPD;
- Water-borne illnesses from prolonged immersion in toxic water;
- Reactive airway diseases from environmental allergens;
- Cellulitis from cuts and bruises in evacuees, as well as people attempting home repairs;
- Carbon monoxide poisoning from generators used incorrectly inside homes; and
- Withdrawals from illicit drug uses.
SUNDAY, SEPTEMBER 4:
Hurricane Aftermath Day 6
During the Sunday ad-hoc church service at Ochsner, doctors, nurses, employees, patients, and families came together in spiritual healing. We sang praises of hope and optimism for our community. We were grateful for our status in this unbelievable disaster and offered prayers and hope for those who had lost so much. We had never been so proud of the efforts of every individual in our institution for maintaining this facility for patient care in such dire situations and promised to be optimistic about our future.
Fortunately, with the help of the Jefferson Parish emergency utility crews, power was restored to our institution. We became fully functional to take on the challenges of the community.
MONDAY, SEPTEMBER 5:
Hurricane Aftermath Day 7
The 17th Street Canal breach was controlled and the water pump back in operation. Residents of Jefferson Parish were allowed to return to take their personal items from their houses but were still under voluntary evacuation, while Orleans Parish was still closed. To plan the demand for medical care in the wake of gradual recovery, OCF began to maintain all of our employees through strategic deployments in various satellite clinics and hospitals according to the needs of the population in New Orleans and other areas.
LESSONS LEARNED
We have learned so much from this disaster. The key to overcome such adverse conditions entails strong psychosocial support from colleagues and family. Strong leadership is crucial to maintain a sense of serenity and an optimistic outlook in times of uncertainty. We experienced a sense of camaraderie after seeing all medical personnel participating in activities beyond of the boundary of usual roles.
The expansion of the essential personnel team list to include social workers and discharge planners is crucial to focus on the unique and nonconventional logistical challenges post-disaster. Intense focus on group dynamics was essential to avoid physical and emotional burnout. Frequent and predictably scheduled face-to-face communication was also important in disseminating accurate, unadulterated information because our decision-making changed hour-to-hour immediately after Hurricane Katrina, day-to-day in the few days afterward, and week-to-week just one week post-disaster.
Obviously the financial implications are immense for our city and our institution. We are developing financial plans, a relief fund, and other resources to assist our employees who have been severely affected by the hurricane. TH
Dr. Deitelzweig and Dr. Lee work at the Ochsner Clinic Foundation, Department of Hospital-Based Internal Medicine, New Orleans. You can contact Dr. Deitelzweig by phone at (504) 842-5766; his e-mail is [email protected]
Neurologic Disorders in the Older Patient
Supplement Editors:
Robert M. Palmer, MD, MPH, and Richard J. Lederman, MD, PhD
Contents
Preface: Internists and the older patient with neurologic illness
Robert M. Palmer, MD, MPH, and Richard J. Lederman, MD, PhD
The art of managing dementia in the elderly
Adam Rosenblatt, MD
Preventing ischemic stroke in the older adult
Geoffrey S.F. Ling, MD, PhD, and Shari M. Ling, MD
Seizures in the elderly: Nuances in presentation and treatment
Elizabeth Waterhouse, MD, and Alan Towne, MD
Movement disorders in the older patient: Differential diagnosis and general management
Mark S. Baron, MD
Depression in older patients with neurologic illness: Causes, recognition, management
Alan Carson, MBChB, MPhil, MD, and Richard Margolin, MD
Supplement Editors:
Robert M. Palmer, MD, MPH, and Richard J. Lederman, MD, PhD
Contents
Preface: Internists and the older patient with neurologic illness
Robert M. Palmer, MD, MPH, and Richard J. Lederman, MD, PhD
The art of managing dementia in the elderly
Adam Rosenblatt, MD
Preventing ischemic stroke in the older adult
Geoffrey S.F. Ling, MD, PhD, and Shari M. Ling, MD
Seizures in the elderly: Nuances in presentation and treatment
Elizabeth Waterhouse, MD, and Alan Towne, MD
Movement disorders in the older patient: Differential diagnosis and general management
Mark S. Baron, MD
Depression in older patients with neurologic illness: Causes, recognition, management
Alan Carson, MBChB, MPhil, MD, and Richard Margolin, MD
Supplement Editors:
Robert M. Palmer, MD, MPH, and Richard J. Lederman, MD, PhD
Contents
Preface: Internists and the older patient with neurologic illness
Robert M. Palmer, MD, MPH, and Richard J. Lederman, MD, PhD
The art of managing dementia in the elderly
Adam Rosenblatt, MD
Preventing ischemic stroke in the older adult
Geoffrey S.F. Ling, MD, PhD, and Shari M. Ling, MD
Seizures in the elderly: Nuances in presentation and treatment
Elizabeth Waterhouse, MD, and Alan Towne, MD
Movement disorders in the older patient: Differential diagnosis and general management
Mark S. Baron, MD
Depression in older patients with neurologic illness: Causes, recognition, management
Alan Carson, MBChB, MPhil, MD, and Richard Margolin, MD