User login
Introduction from the Editor
As editor of this supplement to The Hospitalist, I would like to introduce these eight papers prepared by the SHM Benchmarks Committee by identifying the unifying themes and consistent messages.
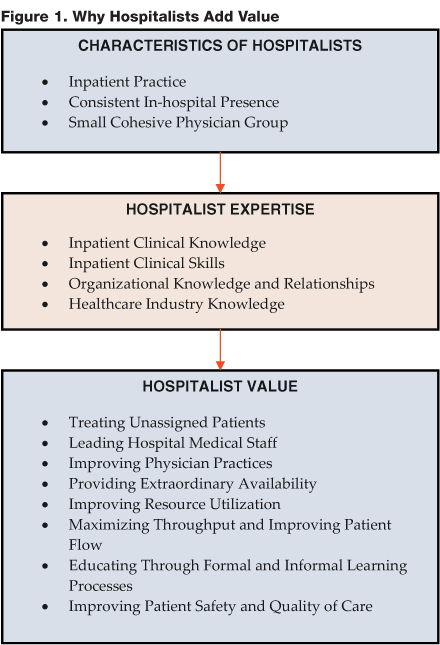
In all of the papers, the value provided by hospitalists comes across loud and clear. The authors not only cite statistics and published research studies, they provide examples and quotes from acknowledged hospitalist experts and leaders. However, perhaps more importantly, the papers convey a strong rationale as to WHY hospitalist programs provide value. Figure 1 attempts to describe this rationale. It depicts three elements:
- The characteristics of hospitalists: These are immutable attributes that uniquely define this new physician specialty.
- The expertise of hospitalists: As they practice hospital medicine, hospitalists have developed a unique combination of knowledge, skills, and relationships
- The value added by hospitalists: Hospitalists impact a wide range of issues that address the patient care, financial, and strategic goals of the hospital.
The Characteristics of Hospitalists
What attributes differentiate hospitalists from other medical specialties?
The first attribute describes what hospitalists do: they practice hospital medicine; for the most part, hospitalists have an inpatient practice. Their day consists of admitting, rounding, managing, discharging, and consulting for hospitalized patients.
The second attribute describes where hospitalists practice; they have a consistent presence in the hospital. As a consequence, hospitalists do similar things and relate to the same people in the same place on a daily basis.
The third attribute describes how hospitalists are organized. A hospitalist program is a cohesive physician group, and like any other medical group, the members develop a common organizational identity, a consistent practice philosophy, and a balance of individual and communal goals.
The Expertise of Hospitalists
What skills, knowledge, and relationships are unique to the specialty of hospital medicine?
As inpatient generalists, hospitalists continually treat the most common reasons for admission, thus acquiring exceptional clinical knowledge of these conditions and issues involved in managing patients with multiple co-morbidities. In addition, hospitalists are familiar with the clinical tools supporting the patient care process.
In addition to clinical knowledge, hospitalists have impatient clinical skills, including diagnosis, physical examination, discharge planning, medical chart recording, family meeting coordination and oversight, and the performance of technical procedures.
Through their constant presence in the hospital, hospitalists develop exceptional organizational knowledge and relationships. They are quite familiar with the flow of patients through their hospital, including hospital processes, procedures, rules, regulations, and information systems. They understand "how to get things done" in their facility and often have good relationships with other healthcare professionals and hospital departments.
Hospitalists often are the most knowledgeable inpatient clinicians with regard to a wide range of healthcare industry issues. These include comprehension of the payer/insurance rules, state and Federal regulations, public health initiatives, recently enacted or pending healthcare legislation, and financial issues facing their hospital.
The Value Added by Hospitalists
How do hospitalists add value to the major stakeholders in the healthcare industry: hospitals, physicians, and health plans?
Each of the eight papers describes a different dimension of the benefits provided by hospital medicine programs.
First, hospitalists provide an effective solution to hospital that are having a difficult time organizing their medical staff to provide on-call coverage for unassigned patient care, both in the ED and subsequent to admission.
A second issue of concern for hospitals relates to the fact that many physicians are no longer able or willing to serve on hospital committees or play a medical staff leadership role. Hospitalists have emerged as strong candidates to play this role in their hospitals.
Third, hospitalists provide value by helping to improve physician practices, including primary care physicians, surgeons, emergency physicians and specialists.
Today, most hospitals use traditional physician on-call systems to provide overnight coverage. A fourth value added by hospitalists relates to the extraordinary coverage (24/7) provided by many hospital medicine programs.
The dominant challenge facing American hospitals relates to financial pressures. Published research studies have consistently documented that hospital medicine programs generate resource utilization savings.
Improved throughput management is a sixth value added by hospitalists. Many hospitals are operating at or close to capacity, creating a crisis of bed availability. Hospitalists are uniquely qualified to address these patient flow issues.
A seventh dimension of the value provided by hospitalists relates to the formal and informal education they provide. In a formal capacity, hospitalists are teachers of clinical and non-clinical inpatient skills to medical students, residents, and fellows. In an informal role, hospitalists impart knowledge to other physicians, healthcare professionals, patients, families, and hospital administrators.
Hospitalists make major contributions to the healthcare quality and patient safety, the eighth aspect of value added by this new specialty. Hospitalists can reduce medical errors, improve the process of care, and achieve better patient outcomes.
Conclusion
Hospital medicine has developed as a specialty with unique characteristics and expertise. Hospilalists have specialized skills, knowledge, and relationships that contribute value to hospitals, physicians, patients, and health plans. These benefits include and go significantly beyond the delivery of quality patient care to hospital inpatients. The hospital medicine specialty continues to grow at a significant rate because of the broad-based positive impact made by hospitalists.
Joseph A. Miller, Editor
Mr. Miller can be contacted at [email protected]
As editor of this supplement to The Hospitalist, I would like to introduce these eight papers prepared by the SHM Benchmarks Committee by identifying the unifying themes and consistent messages.
In all of the papers, the value provided by hospitalists comes across loud and clear. The authors not only cite statistics and published research studies, they provide examples and quotes from acknowledged hospitalist experts and leaders. However, perhaps more importantly, the papers convey a strong rationale as to WHY hospitalist programs provide value. Figure 1 attempts to describe this rationale. It depicts three elements:
- The characteristics of hospitalists: These are immutable attributes that uniquely define this new physician specialty.
- The expertise of hospitalists: As they practice hospital medicine, hospitalists have developed a unique combination of knowledge, skills, and relationships
- The value added by hospitalists: Hospitalists impact a wide range of issues that address the patient care, financial, and strategic goals of the hospital.
The Characteristics of Hospitalists
What attributes differentiate hospitalists from other medical specialties?
The first attribute describes what hospitalists do: they practice hospital medicine; for the most part, hospitalists have an inpatient practice. Their day consists of admitting, rounding, managing, discharging, and consulting for hospitalized patients.
The second attribute describes where hospitalists practice; they have a consistent presence in the hospital. As a consequence, hospitalists do similar things and relate to the same people in the same place on a daily basis.
The third attribute describes how hospitalists are organized. A hospitalist program is a cohesive physician group, and like any other medical group, the members develop a common organizational identity, a consistent practice philosophy, and a balance of individual and communal goals.
The Expertise of Hospitalists
What skills, knowledge, and relationships are unique to the specialty of hospital medicine?
As inpatient generalists, hospitalists continually treat the most common reasons for admission, thus acquiring exceptional clinical knowledge of these conditions and issues involved in managing patients with multiple co-morbidities. In addition, hospitalists are familiar with the clinical tools supporting the patient care process.
In addition to clinical knowledge, hospitalists have impatient clinical skills, including diagnosis, physical examination, discharge planning, medical chart recording, family meeting coordination and oversight, and the performance of technical procedures.
Through their constant presence in the hospital, hospitalists develop exceptional organizational knowledge and relationships. They are quite familiar with the flow of patients through their hospital, including hospital processes, procedures, rules, regulations, and information systems. They understand "how to get things done" in their facility and often have good relationships with other healthcare professionals and hospital departments.
Hospitalists often are the most knowledgeable inpatient clinicians with regard to a wide range of healthcare industry issues. These include comprehension of the payer/insurance rules, state and Federal regulations, public health initiatives, recently enacted or pending healthcare legislation, and financial issues facing their hospital.
The Value Added by Hospitalists
How do hospitalists add value to the major stakeholders in the healthcare industry: hospitals, physicians, and health plans?
Each of the eight papers describes a different dimension of the benefits provided by hospital medicine programs.
First, hospitalists provide an effective solution to hospital that are having a difficult time organizing their medical staff to provide on-call coverage for unassigned patient care, both in the ED and subsequent to admission.
A second issue of concern for hospitals relates to the fact that many physicians are no longer able or willing to serve on hospital committees or play a medical staff leadership role. Hospitalists have emerged as strong candidates to play this role in their hospitals.
Third, hospitalists provide value by helping to improve physician practices, including primary care physicians, surgeons, emergency physicians and specialists.
Today, most hospitals use traditional physician on-call systems to provide overnight coverage. A fourth value added by hospitalists relates to the extraordinary coverage (24/7) provided by many hospital medicine programs.
The dominant challenge facing American hospitals relates to financial pressures. Published research studies have consistently documented that hospital medicine programs generate resource utilization savings.
Improved throughput management is a sixth value added by hospitalists. Many hospitals are operating at or close to capacity, creating a crisis of bed availability. Hospitalists are uniquely qualified to address these patient flow issues.
A seventh dimension of the value provided by hospitalists relates to the formal and informal education they provide. In a formal capacity, hospitalists are teachers of clinical and non-clinical inpatient skills to medical students, residents, and fellows. In an informal role, hospitalists impart knowledge to other physicians, healthcare professionals, patients, families, and hospital administrators.
Hospitalists make major contributions to the healthcare quality and patient safety, the eighth aspect of value added by this new specialty. Hospitalists can reduce medical errors, improve the process of care, and achieve better patient outcomes.
Conclusion
Hospital medicine has developed as a specialty with unique characteristics and expertise. Hospilalists have specialized skills, knowledge, and relationships that contribute value to hospitals, physicians, patients, and health plans. These benefits include and go significantly beyond the delivery of quality patient care to hospital inpatients. The hospital medicine specialty continues to grow at a significant rate because of the broad-based positive impact made by hospitalists.
Joseph A. Miller, Editor
Mr. Miller can be contacted at [email protected]
As editor of this supplement to The Hospitalist, I would like to introduce these eight papers prepared by the SHM Benchmarks Committee by identifying the unifying themes and consistent messages.
In all of the papers, the value provided by hospitalists comes across loud and clear. The authors not only cite statistics and published research studies, they provide examples and quotes from acknowledged hospitalist experts and leaders. However, perhaps more importantly, the papers convey a strong rationale as to WHY hospitalist programs provide value. Figure 1 attempts to describe this rationale. It depicts three elements:
- The characteristics of hospitalists: These are immutable attributes that uniquely define this new physician specialty.
- The expertise of hospitalists: As they practice hospital medicine, hospitalists have developed a unique combination of knowledge, skills, and relationships
- The value added by hospitalists: Hospitalists impact a wide range of issues that address the patient care, financial, and strategic goals of the hospital.
The Characteristics of Hospitalists
What attributes differentiate hospitalists from other medical specialties?
The first attribute describes what hospitalists do: they practice hospital medicine; for the most part, hospitalists have an inpatient practice. Their day consists of admitting, rounding, managing, discharging, and consulting for hospitalized patients.
The second attribute describes where hospitalists practice; they have a consistent presence in the hospital. As a consequence, hospitalists do similar things and relate to the same people in the same place on a daily basis.
The third attribute describes how hospitalists are organized. A hospitalist program is a cohesive physician group, and like any other medical group, the members develop a common organizational identity, a consistent practice philosophy, and a balance of individual and communal goals.
The Expertise of Hospitalists
What skills, knowledge, and relationships are unique to the specialty of hospital medicine?
As inpatient generalists, hospitalists continually treat the most common reasons for admission, thus acquiring exceptional clinical knowledge of these conditions and issues involved in managing patients with multiple co-morbidities. In addition, hospitalists are familiar with the clinical tools supporting the patient care process.
In addition to clinical knowledge, hospitalists have impatient clinical skills, including diagnosis, physical examination, discharge planning, medical chart recording, family meeting coordination and oversight, and the performance of technical procedures.
Through their constant presence in the hospital, hospitalists develop exceptional organizational knowledge and relationships. They are quite familiar with the flow of patients through their hospital, including hospital processes, procedures, rules, regulations, and information systems. They understand "how to get things done" in their facility and often have good relationships with other healthcare professionals and hospital departments.
Hospitalists often are the most knowledgeable inpatient clinicians with regard to a wide range of healthcare industry issues. These include comprehension of the payer/insurance rules, state and Federal regulations, public health initiatives, recently enacted or pending healthcare legislation, and financial issues facing their hospital.
The Value Added by Hospitalists
How do hospitalists add value to the major stakeholders in the healthcare industry: hospitals, physicians, and health plans?
Each of the eight papers describes a different dimension of the benefits provided by hospital medicine programs.
First, hospitalists provide an effective solution to hospital that are having a difficult time organizing their medical staff to provide on-call coverage for unassigned patient care, both in the ED and subsequent to admission.
A second issue of concern for hospitals relates to the fact that many physicians are no longer able or willing to serve on hospital committees or play a medical staff leadership role. Hospitalists have emerged as strong candidates to play this role in their hospitals.
Third, hospitalists provide value by helping to improve physician practices, including primary care physicians, surgeons, emergency physicians and specialists.
Today, most hospitals use traditional physician on-call systems to provide overnight coverage. A fourth value added by hospitalists relates to the extraordinary coverage (24/7) provided by many hospital medicine programs.
The dominant challenge facing American hospitals relates to financial pressures. Published research studies have consistently documented that hospital medicine programs generate resource utilization savings.
Improved throughput management is a sixth value added by hospitalists. Many hospitals are operating at or close to capacity, creating a crisis of bed availability. Hospitalists are uniquely qualified to address these patient flow issues.
A seventh dimension of the value provided by hospitalists relates to the formal and informal education they provide. In a formal capacity, hospitalists are teachers of clinical and non-clinical inpatient skills to medical students, residents, and fellows. In an informal role, hospitalists impart knowledge to other physicians, healthcare professionals, patients, families, and hospital administrators.
Hospitalists make major contributions to the healthcare quality and patient safety, the eighth aspect of value added by this new specialty. Hospitalists can reduce medical errors, improve the process of care, and achieve better patient outcomes.
Conclusion
Hospital medicine has developed as a specialty with unique characteristics and expertise. Hospilalists have specialized skills, knowledge, and relationships that contribute value to hospitals, physicians, patients, and health plans. These benefits include and go significantly beyond the delivery of quality patient care to hospital inpatients. The hospital medicine specialty continues to grow at a significant rate because of the broad-based positive impact made by hospitalists.
Joseph A. Miller, Editor
Mr. Miller can be contacted at [email protected]
The Future Role of Hospitalists
Since the mid 1990s when Robert Wachter and Lee Goldman first coined the term ''hospitalist',' we have seen the nation's hospitals and health systems open their doors to these ''specialists in inpatient medicine'' (1). We have also seen publications and academic studies that outline the benefits of implementing hospitalist programs. As the CEO of an integrated delivery system, I can recount firsthand how our hospitalist program, in existence since 1995, has improved patient care in our facilities. Not only have our hospitalists saved the system thousands of days in length of stay and reduced our costs per day, but they have also improved quality of care. In addition, members of our hospitalist groups have emerged as physician liaisons, championing education and training initiatives and serving as a bridge between the medical staff and management.
As our experience and the articles included in this supplement suggest, hospitalists add value on multiple levels and have imbedded a new model of care within the nation's hospitals. What's next? How will hospitalists continue to improve the comprehensiveness and continuity of healthcare across the patient care continuum? And, perhaps more importantly, how do we get there from here?
While hospitalist programs are burgeoning, many hospitals and health systems have yet to realize the full value added by hospitalist programs. As it relates to the healthcare industry, hospitalist programs are still in their infancy. Early adopters continue to refine and modify program models to meet changing physician and patient needs as well as to decrease the financial cost to the hospital. In addition, preliminary results of an AHA study (2) on hospitalist programs suggest that larger hospitals have a higher probability of having a hospitalist program than smaller hospitals. The same study also suggests that hospitalists have a greater impact on smaller hospitals. As a result, the population of hospitals that benefits the most from hospitalist programs has barely begun to realize the value of such programs. The message is the same for both early and late adopters. ''When you come to the fork in the road, take it'' (Yogi Berra).
In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent. In August 2004, Robert Wachter gave an interview to Health Leaders describing how hospitalists can "contribute to the notion of changing systems'' (3). In the article, The Emerging Role of ''hospitalists" in the American Health Care System, Wachter and Goldman explain that the hospitalist model "creates a core group of faculty members whose inpatient work is more than a marginal activity and who are thus committed to quality improvement in the hospital'' (1). As the work of hospitalists generates from within the hospital, they have a personal stake in the hospital systems and the improvement of these systems (1). The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process improvement initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change.
In addition to serving as change agents, hospitalists themselves may become the solution to some of the systems that need changing. They are already helping to solve on-call challenges by providing 24/7 coverage and by taking call. Hospitalists have also assumed a greater role in caring for patients in the ED by managing patients that otherwise would have been admitted by on-call medicine physicians. As more and more physicians decrease the time they spend in the hospital and as more patients are admitted with chronic care needs, the hospitalist will play an integral role in meeting these challenges.
Hospitalists may also become more involved in providing continuity to the delivery of healthcare services. Consider the opportunities that exist to involve hospitalists in improving preoperative and postoperative patient care. For example, hospitalists could play a role in the management of patients who require perioperative beta-blockers to decrease cardiac events in major non-cardiac surgery. Hospitalists may also continue to diversify their clinical roles by coordinating care in ICUs where intensivists are unavailable or by caring for patients in post-acute settings (4,5).
With the ability to manage varying aspects of a patient's care, hospitalists can help resolve the disconnect that exists as a patient moves across the continuum of care. A patient may enter the system through the ICU, followed by a transfer to a Medicine Unit, and then be discharged to his primary care physician or a nursing home. The reality of ineffective communication and incomplete hand-offs may result in poor information exchange that impacts the care of the patient. By involving a hospitalist in this process, the coordination of patient care becomes seamless and the chance for medical error decreases.
In order to expand the current hospitalist model to the clinically diverse and dynamic model of the future, all stakeholders, from management to physicians, must take proactive steps. Part of this process will involve the development of an economic model that accounts for the value that hospitalist programs bring. The more quantifiable these programs become, the easier it will be to prove their value and implement them in capital-strapped facilities. Another part of moving the hospitalist model to the future centers on relationship management. A lack of understanding of the benefits that hospitalists provide and the roles that they assume in hospitals prevents collaboration with other specialties. Lines of communication must be opened and issues of distrust resolved to facilitate the relationship between hospitalists, the medical staff, and management. Finally we must educate the community about the benefits of hospitalists in the delivery of patient care. The success of hospitalist programs is just as dependent on the development of an external support network as it is on the existence of a strong internal infrastructure.
Without a doubt, hospitalists add value to our nation's hospitals. An exciting debate is emerging about how hospitalists will continue to change the model of healthcare as we know it, and what implications this will have for our hospitals and health systems.
References
- Wachter RM Goldman L. The emerging role of ''hospitalists'' in the American healthcare system. N Engl J Med. 1996;335:514-7.
- 2003 American Hospital Association (AHA) Annual Survey (preliminary results)
- Olsen K, Wachter R. The word on medical mistakes. Healthleaders News. Aug 20, 2004.
- Pham HH, Devers K, Kuo S, Berenson R. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005;20:101-7.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287:487-94.
Since the mid 1990s when Robert Wachter and Lee Goldman first coined the term ''hospitalist',' we have seen the nation's hospitals and health systems open their doors to these ''specialists in inpatient medicine'' (1). We have also seen publications and academic studies that outline the benefits of implementing hospitalist programs. As the CEO of an integrated delivery system, I can recount firsthand how our hospitalist program, in existence since 1995, has improved patient care in our facilities. Not only have our hospitalists saved the system thousands of days in length of stay and reduced our costs per day, but they have also improved quality of care. In addition, members of our hospitalist groups have emerged as physician liaisons, championing education and training initiatives and serving as a bridge between the medical staff and management.
As our experience and the articles included in this supplement suggest, hospitalists add value on multiple levels and have imbedded a new model of care within the nation's hospitals. What's next? How will hospitalists continue to improve the comprehensiveness and continuity of healthcare across the patient care continuum? And, perhaps more importantly, how do we get there from here?
While hospitalist programs are burgeoning, many hospitals and health systems have yet to realize the full value added by hospitalist programs. As it relates to the healthcare industry, hospitalist programs are still in their infancy. Early adopters continue to refine and modify program models to meet changing physician and patient needs as well as to decrease the financial cost to the hospital. In addition, preliminary results of an AHA study (2) on hospitalist programs suggest that larger hospitals have a higher probability of having a hospitalist program than smaller hospitals. The same study also suggests that hospitalists have a greater impact on smaller hospitals. As a result, the population of hospitals that benefits the most from hospitalist programs has barely begun to realize the value of such programs. The message is the same for both early and late adopters. ''When you come to the fork in the road, take it'' (Yogi Berra).
In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent. In August 2004, Robert Wachter gave an interview to Health Leaders describing how hospitalists can "contribute to the notion of changing systems'' (3). In the article, The Emerging Role of ''hospitalists" in the American Health Care System, Wachter and Goldman explain that the hospitalist model "creates a core group of faculty members whose inpatient work is more than a marginal activity and who are thus committed to quality improvement in the hospital'' (1). As the work of hospitalists generates from within the hospital, they have a personal stake in the hospital systems and the improvement of these systems (1). The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process improvement initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change.
In addition to serving as change agents, hospitalists themselves may become the solution to some of the systems that need changing. They are already helping to solve on-call challenges by providing 24/7 coverage and by taking call. Hospitalists have also assumed a greater role in caring for patients in the ED by managing patients that otherwise would have been admitted by on-call medicine physicians. As more and more physicians decrease the time they spend in the hospital and as more patients are admitted with chronic care needs, the hospitalist will play an integral role in meeting these challenges.
Hospitalists may also become more involved in providing continuity to the delivery of healthcare services. Consider the opportunities that exist to involve hospitalists in improving preoperative and postoperative patient care. For example, hospitalists could play a role in the management of patients who require perioperative beta-blockers to decrease cardiac events in major non-cardiac surgery. Hospitalists may also continue to diversify their clinical roles by coordinating care in ICUs where intensivists are unavailable or by caring for patients in post-acute settings (4,5).
With the ability to manage varying aspects of a patient's care, hospitalists can help resolve the disconnect that exists as a patient moves across the continuum of care. A patient may enter the system through the ICU, followed by a transfer to a Medicine Unit, and then be discharged to his primary care physician or a nursing home. The reality of ineffective communication and incomplete hand-offs may result in poor information exchange that impacts the care of the patient. By involving a hospitalist in this process, the coordination of patient care becomes seamless and the chance for medical error decreases.
In order to expand the current hospitalist model to the clinically diverse and dynamic model of the future, all stakeholders, from management to physicians, must take proactive steps. Part of this process will involve the development of an economic model that accounts for the value that hospitalist programs bring. The more quantifiable these programs become, the easier it will be to prove their value and implement them in capital-strapped facilities. Another part of moving the hospitalist model to the future centers on relationship management. A lack of understanding of the benefits that hospitalists provide and the roles that they assume in hospitals prevents collaboration with other specialties. Lines of communication must be opened and issues of distrust resolved to facilitate the relationship between hospitalists, the medical staff, and management. Finally we must educate the community about the benefits of hospitalists in the delivery of patient care. The success of hospitalist programs is just as dependent on the development of an external support network as it is on the existence of a strong internal infrastructure.
Without a doubt, hospitalists add value to our nation's hospitals. An exciting debate is emerging about how hospitalists will continue to change the model of healthcare as we know it, and what implications this will have for our hospitals and health systems.
References
- Wachter RM Goldman L. The emerging role of ''hospitalists'' in the American healthcare system. N Engl J Med. 1996;335:514-7.
- 2003 American Hospital Association (AHA) Annual Survey (preliminary results)
- Olsen K, Wachter R. The word on medical mistakes. Healthleaders News. Aug 20, 2004.
- Pham HH, Devers K, Kuo S, Berenson R. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005;20:101-7.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287:487-94.
Since the mid 1990s when Robert Wachter and Lee Goldman first coined the term ''hospitalist',' we have seen the nation's hospitals and health systems open their doors to these ''specialists in inpatient medicine'' (1). We have also seen publications and academic studies that outline the benefits of implementing hospitalist programs. As the CEO of an integrated delivery system, I can recount firsthand how our hospitalist program, in existence since 1995, has improved patient care in our facilities. Not only have our hospitalists saved the system thousands of days in length of stay and reduced our costs per day, but they have also improved quality of care. In addition, members of our hospitalist groups have emerged as physician liaisons, championing education and training initiatives and serving as a bridge between the medical staff and management.
As our experience and the articles included in this supplement suggest, hospitalists add value on multiple levels and have imbedded a new model of care within the nation's hospitals. What's next? How will hospitalists continue to improve the comprehensiveness and continuity of healthcare across the patient care continuum? And, perhaps more importantly, how do we get there from here?
While hospitalist programs are burgeoning, many hospitals and health systems have yet to realize the full value added by hospitalist programs. As it relates to the healthcare industry, hospitalist programs are still in their infancy. Early adopters continue to refine and modify program models to meet changing physician and patient needs as well as to decrease the financial cost to the hospital. In addition, preliminary results of an AHA study (2) on hospitalist programs suggest that larger hospitals have a higher probability of having a hospitalist program than smaller hospitals. The same study also suggests that hospitalists have a greater impact on smaller hospitals. As a result, the population of hospitals that benefits the most from hospitalist programs has barely begun to realize the value of such programs. The message is the same for both early and late adopters. ''When you come to the fork in the road, take it'' (Yogi Berra).
In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent. In August 2004, Robert Wachter gave an interview to Health Leaders describing how hospitalists can "contribute to the notion of changing systems'' (3). In the article, The Emerging Role of ''hospitalists" in the American Health Care System, Wachter and Goldman explain that the hospitalist model "creates a core group of faculty members whose inpatient work is more than a marginal activity and who are thus committed to quality improvement in the hospital'' (1). As the work of hospitalists generates from within the hospital, they have a personal stake in the hospital systems and the improvement of these systems (1). The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process improvement initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change.
In addition to serving as change agents, hospitalists themselves may become the solution to some of the systems that need changing. They are already helping to solve on-call challenges by providing 24/7 coverage and by taking call. Hospitalists have also assumed a greater role in caring for patients in the ED by managing patients that otherwise would have been admitted by on-call medicine physicians. As more and more physicians decrease the time they spend in the hospital and as more patients are admitted with chronic care needs, the hospitalist will play an integral role in meeting these challenges.
Hospitalists may also become more involved in providing continuity to the delivery of healthcare services. Consider the opportunities that exist to involve hospitalists in improving preoperative and postoperative patient care. For example, hospitalists could play a role in the management of patients who require perioperative beta-blockers to decrease cardiac events in major non-cardiac surgery. Hospitalists may also continue to diversify their clinical roles by coordinating care in ICUs where intensivists are unavailable or by caring for patients in post-acute settings (4,5).
With the ability to manage varying aspects of a patient's care, hospitalists can help resolve the disconnect that exists as a patient moves across the continuum of care. A patient may enter the system through the ICU, followed by a transfer to a Medicine Unit, and then be discharged to his primary care physician or a nursing home. The reality of ineffective communication and incomplete hand-offs may result in poor information exchange that impacts the care of the patient. By involving a hospitalist in this process, the coordination of patient care becomes seamless and the chance for medical error decreases.
In order to expand the current hospitalist model to the clinically diverse and dynamic model of the future, all stakeholders, from management to physicians, must take proactive steps. Part of this process will involve the development of an economic model that accounts for the value that hospitalist programs bring. The more quantifiable these programs become, the easier it will be to prove their value and implement them in capital-strapped facilities. Another part of moving the hospitalist model to the future centers on relationship management. A lack of understanding of the benefits that hospitalists provide and the roles that they assume in hospitals prevents collaboration with other specialties. Lines of communication must be opened and issues of distrust resolved to facilitate the relationship between hospitalists, the medical staff, and management. Finally we must educate the community about the benefits of hospitalists in the delivery of patient care. The success of hospitalist programs is just as dependent on the development of an external support network as it is on the existence of a strong internal infrastructure.
Without a doubt, hospitalists add value to our nation's hospitals. An exciting debate is emerging about how hospitalists will continue to change the model of healthcare as we know it, and what implications this will have for our hospitals and health systems.
References
- Wachter RM Goldman L. The emerging role of ''hospitalists'' in the American healthcare system. N Engl J Med. 1996;335:514-7.
- 2003 American Hospital Association (AHA) Annual Survey (preliminary results)
- Olsen K, Wachter R. The word on medical mistakes. Healthleaders News. Aug 20, 2004.
- Pham HH, Devers K, Kuo S, Berenson R. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005;20:101-7.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287:487-94.
Publication as Patient

I was in my office perusing patient records when I got the call. I’d been selected to be the new Physician Editor of The Hospitalist. I felt surprised—and excited. Then, harsh reality set in: My first deadline was only three weeks away. I checked my pulse—117 and irregularly irregular, good. I brewed some foxglove tea, chewed on some willow bark, and prepared to work.
Deja Vu
I found myself experiencing an unusual sensation. What was the emotion I was feeling? A fine mixture of dread and excitement, with an overlay of angst. I’d had this sensation before, but when?
I looked at the May issue of The Hospitalist. How was I going to continue to produce a quality publication—and improve upon it? The people who had supported my selection as editor were counting on me; my mom was counting on me. Heck, even I was even counting on me.
I drew a blank. Where would I go with this? That’s when it hit me: the sense of being in a situation that I wanted, only to discover I wasn’t ready. The tidal forces of time and pressure descended upon me.
In a flash I knew what was happening. I was suffering from delayed post-traumatic residency syndrome. It was 1985, and I was back in Houston’s old Ben Taub Hospital. (Reminiscing is a sure sign of early senescence.) I was the intern coming on service, a very busy general medicine service. Among my new patients, I had to pick up an elderly gentleman who had been ill for years and who had been in the hospital for more than a month. His chart was missing, he was unresponsive, and his family was AWOL.
My beeper kept going off. There was a code on the other side of the hospital, and the ED was calling. Should I give the patient heparin? How do I dose it? Should I give antibiotics and, if so, which ones? Should I draw blood cultures? My circuits totally overloaded.
My resident came to my rescue, with a cup of coffee and good advice: Settle down, find the old records, obtain a history, and perform a physical exam before I even thought about therapeutic intervention.
This was exactly what I needed to do as physician editor. I turned to my current resident-equivalent, in this case Lisa Dionne from John Wiley & Sons—the editorial Yang to my Yin. She gave me the same advice my resident had decades before: Get the back issues of The Hospitalist from SHM, see where it was going, where it had been, learn the terminology, and get organized. Luckily the SHM staff is a lot more responsive then the medical records department at Ben Taub was.
Then, as with any patient, I had to ask some basic questions. What initial symptoms caused the development of The Hospitalist? How long had the publication been present? What made it better, and what made it worse? Was it progressing or was it unchanged? Was I having chest pain? What was SHM, and why did it exist? What did a hospitalist want to read? What was a hospitalist, and why would anyone want to be one?
Why I’m a Hospitalist
That final question seemed the heart of my issue. I pondered what forces drove me to become a hospitalist and why I enjoyed it so much.
When I finished my residency I went into private practice. Like most residents of the time I was totally unprepared for ambulatory care. I could run a code, knew all the latest diagnostic tests, and could even quote a few articles.
But the first time I saw a young man with chronic back pain who wanted to go on disability, or an elderly lady with osteoporosis and breast cancer who wondered if she could take quinine for leg cramps, I was lost. It only took a decade or two for me to feel vaguely competent. Meantime I did some hard time in the hospital, but my focus shifted tectonically toward the outpatient. When my running partner Mitchell Wilson decided to start one of the early hospitalist programs (at the University of Texas) my hospital time ever more rapidly receded.
At the same time, the forces of capitalism were at work: IPAs and IPOs, practice management groups, university expansions and contractions, hospital closings. This was the new shifting sand (or shifting dullness) of medical practice. I was ready for a change, but could I give up my comfortably cluttered office, my established, fairly well-tuned patients, my six-year-old National Geographic magazines in the waiting room? Would going back to the hospital feel like being a resident again? There was only one way to find out.
I said goodbye to the beach and the fire ants, loaded my truck like Jed Clampett, and moved to Rochester—Minn., that is—frozen tundra, lots of geese. Under the auspices of Jeanne Huddleston and the Mayo Clinic Inpatient Internal Medicine Team, I joined the world of hospitalists.
New Beginnings
My first impression of life as a hospitalist was that I was cold. Frigid really. Of course it was winter in Minnesota, so I guess I should have expected that. I rapidly discovered that it was a lot nicer being a member of the consulting staff than a member of the house staff. In some ways I felt like an intern again. It was difficult to believe, but hospital medicine had changed over the last decade or two; however, the patients hadn’t.
I was armed with acceptable history taking and exam skills. I had a superb support system in the nurse practitioners and physician assistants who carried my load the first few weeks. My colleagues were supportive. I muddled through and, after several years, felt like I was back to my baseline level of moderate competence.
Though my story is immensely fascinating (to me) from an autobiographical standpoint, does it answer the question of why I enjoy being a hospitalist? Usually people ask me, “What is a hospitalist?” I usually explain that I’m an internist—not an intern—though some days I feel like the latter. The taxonomy of hospitalists is fairly diverse. Some of us come straight from residency, for others it’s the resolution of a mid-career crisis.
One of my favorite things about being a hospitalist is the control I have over my schedule. As an outpatient doctor I had a timetable to keep based on the waiting patient. If I got behind, waxed conversational, or got involved with a family, my day was ruined. Patients got mad at me; my nurses were aggravated.
In the hospital, I have a body of work I must do each day. It’s predictably unpredictable at the beginning of the shift. I have a certain number of patients to see, discharge, and admit. I risk acute medical emergencies, unexpected families who want an update on their mother’s condition, and similar hospitalist activities of daily life (aka HADLs). The volume of work is variable: Some days are difficult, some aren’t. The complexity of cases is stimulating and makes continued learning a necessity. Instead of being isolated in an office I interact with other physicians and staff. The most stimulating aspect I experience is the sensation that hospital medicine is an evolving field and there are hundreds of dedicated colleagues out there trying to make it better.
My goal as physician editor is to work with SHM members to continue to produce a great source of hospitalist information. The Hospitalist readers include internists, family practitioners, pediatricians, nurse practitioners, and physician assistants. They also comprise administrators, businesspeople, and legislators. I perceive important topics to involve medical management, education, communication, economics, government regulation, ethics, and palliative care, as well as the activities of our society, chapters, and members.
With the team from John Wiley & Sons and the support of SHM administration and the members, I hope to accomplish this task. My patient all those years ago survived and left the hospital. I only can hope that The Hospitalist will thrive as well. TH
Jamie Newman, MD, FACP, is senior associate consultant, Hospital Internal Medicine, associate professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
I was in my office perusing patient records when I got the call. I’d been selected to be the new Physician Editor of The Hospitalist. I felt surprised—and excited. Then, harsh reality set in: My first deadline was only three weeks away. I checked my pulse—117 and irregularly irregular, good. I brewed some foxglove tea, chewed on some willow bark, and prepared to work.
Deja Vu
I found myself experiencing an unusual sensation. What was the emotion I was feeling? A fine mixture of dread and excitement, with an overlay of angst. I’d had this sensation before, but when?
I looked at the May issue of The Hospitalist. How was I going to continue to produce a quality publication—and improve upon it? The people who had supported my selection as editor were counting on me; my mom was counting on me. Heck, even I was even counting on me.
I drew a blank. Where would I go with this? That’s when it hit me: the sense of being in a situation that I wanted, only to discover I wasn’t ready. The tidal forces of time and pressure descended upon me.
In a flash I knew what was happening. I was suffering from delayed post-traumatic residency syndrome. It was 1985, and I was back in Houston’s old Ben Taub Hospital. (Reminiscing is a sure sign of early senescence.) I was the intern coming on service, a very busy general medicine service. Among my new patients, I had to pick up an elderly gentleman who had been ill for years and who had been in the hospital for more than a month. His chart was missing, he was unresponsive, and his family was AWOL.
My beeper kept going off. There was a code on the other side of the hospital, and the ED was calling. Should I give the patient heparin? How do I dose it? Should I give antibiotics and, if so, which ones? Should I draw blood cultures? My circuits totally overloaded.
My resident came to my rescue, with a cup of coffee and good advice: Settle down, find the old records, obtain a history, and perform a physical exam before I even thought about therapeutic intervention.
This was exactly what I needed to do as physician editor. I turned to my current resident-equivalent, in this case Lisa Dionne from John Wiley & Sons—the editorial Yang to my Yin. She gave me the same advice my resident had decades before: Get the back issues of The Hospitalist from SHM, see where it was going, where it had been, learn the terminology, and get organized. Luckily the SHM staff is a lot more responsive then the medical records department at Ben Taub was.
Then, as with any patient, I had to ask some basic questions. What initial symptoms caused the development of The Hospitalist? How long had the publication been present? What made it better, and what made it worse? Was it progressing or was it unchanged? Was I having chest pain? What was SHM, and why did it exist? What did a hospitalist want to read? What was a hospitalist, and why would anyone want to be one?
Why I’m a Hospitalist
That final question seemed the heart of my issue. I pondered what forces drove me to become a hospitalist and why I enjoyed it so much.
When I finished my residency I went into private practice. Like most residents of the time I was totally unprepared for ambulatory care. I could run a code, knew all the latest diagnostic tests, and could even quote a few articles.
But the first time I saw a young man with chronic back pain who wanted to go on disability, or an elderly lady with osteoporosis and breast cancer who wondered if she could take quinine for leg cramps, I was lost. It only took a decade or two for me to feel vaguely competent. Meantime I did some hard time in the hospital, but my focus shifted tectonically toward the outpatient. When my running partner Mitchell Wilson decided to start one of the early hospitalist programs (at the University of Texas) my hospital time ever more rapidly receded.
At the same time, the forces of capitalism were at work: IPAs and IPOs, practice management groups, university expansions and contractions, hospital closings. This was the new shifting sand (or shifting dullness) of medical practice. I was ready for a change, but could I give up my comfortably cluttered office, my established, fairly well-tuned patients, my six-year-old National Geographic magazines in the waiting room? Would going back to the hospital feel like being a resident again? There was only one way to find out.
I said goodbye to the beach and the fire ants, loaded my truck like Jed Clampett, and moved to Rochester—Minn., that is—frozen tundra, lots of geese. Under the auspices of Jeanne Huddleston and the Mayo Clinic Inpatient Internal Medicine Team, I joined the world of hospitalists.
New Beginnings
My first impression of life as a hospitalist was that I was cold. Frigid really. Of course it was winter in Minnesota, so I guess I should have expected that. I rapidly discovered that it was a lot nicer being a member of the consulting staff than a member of the house staff. In some ways I felt like an intern again. It was difficult to believe, but hospital medicine had changed over the last decade or two; however, the patients hadn’t.
I was armed with acceptable history taking and exam skills. I had a superb support system in the nurse practitioners and physician assistants who carried my load the first few weeks. My colleagues were supportive. I muddled through and, after several years, felt like I was back to my baseline level of moderate competence.
Though my story is immensely fascinating (to me) from an autobiographical standpoint, does it answer the question of why I enjoy being a hospitalist? Usually people ask me, “What is a hospitalist?” I usually explain that I’m an internist—not an intern—though some days I feel like the latter. The taxonomy of hospitalists is fairly diverse. Some of us come straight from residency, for others it’s the resolution of a mid-career crisis.
One of my favorite things about being a hospitalist is the control I have over my schedule. As an outpatient doctor I had a timetable to keep based on the waiting patient. If I got behind, waxed conversational, or got involved with a family, my day was ruined. Patients got mad at me; my nurses were aggravated.
In the hospital, I have a body of work I must do each day. It’s predictably unpredictable at the beginning of the shift. I have a certain number of patients to see, discharge, and admit. I risk acute medical emergencies, unexpected families who want an update on their mother’s condition, and similar hospitalist activities of daily life (aka HADLs). The volume of work is variable: Some days are difficult, some aren’t. The complexity of cases is stimulating and makes continued learning a necessity. Instead of being isolated in an office I interact with other physicians and staff. The most stimulating aspect I experience is the sensation that hospital medicine is an evolving field and there are hundreds of dedicated colleagues out there trying to make it better.
My goal as physician editor is to work with SHM members to continue to produce a great source of hospitalist information. The Hospitalist readers include internists, family practitioners, pediatricians, nurse practitioners, and physician assistants. They also comprise administrators, businesspeople, and legislators. I perceive important topics to involve medical management, education, communication, economics, government regulation, ethics, and palliative care, as well as the activities of our society, chapters, and members.
With the team from John Wiley & Sons and the support of SHM administration and the members, I hope to accomplish this task. My patient all those years ago survived and left the hospital. I only can hope that The Hospitalist will thrive as well. TH
Jamie Newman, MD, FACP, is senior associate consultant, Hospital Internal Medicine, associate professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
I was in my office perusing patient records when I got the call. I’d been selected to be the new Physician Editor of The Hospitalist. I felt surprised—and excited. Then, harsh reality set in: My first deadline was only three weeks away. I checked my pulse—117 and irregularly irregular, good. I brewed some foxglove tea, chewed on some willow bark, and prepared to work.
Deja Vu
I found myself experiencing an unusual sensation. What was the emotion I was feeling? A fine mixture of dread and excitement, with an overlay of angst. I’d had this sensation before, but when?
I looked at the May issue of The Hospitalist. How was I going to continue to produce a quality publication—and improve upon it? The people who had supported my selection as editor were counting on me; my mom was counting on me. Heck, even I was even counting on me.
I drew a blank. Where would I go with this? That’s when it hit me: the sense of being in a situation that I wanted, only to discover I wasn’t ready. The tidal forces of time and pressure descended upon me.
In a flash I knew what was happening. I was suffering from delayed post-traumatic residency syndrome. It was 1985, and I was back in Houston’s old Ben Taub Hospital. (Reminiscing is a sure sign of early senescence.) I was the intern coming on service, a very busy general medicine service. Among my new patients, I had to pick up an elderly gentleman who had been ill for years and who had been in the hospital for more than a month. His chart was missing, he was unresponsive, and his family was AWOL.
My beeper kept going off. There was a code on the other side of the hospital, and the ED was calling. Should I give the patient heparin? How do I dose it? Should I give antibiotics and, if so, which ones? Should I draw blood cultures? My circuits totally overloaded.
My resident came to my rescue, with a cup of coffee and good advice: Settle down, find the old records, obtain a history, and perform a physical exam before I even thought about therapeutic intervention.
This was exactly what I needed to do as physician editor. I turned to my current resident-equivalent, in this case Lisa Dionne from John Wiley & Sons—the editorial Yang to my Yin. She gave me the same advice my resident had decades before: Get the back issues of The Hospitalist from SHM, see where it was going, where it had been, learn the terminology, and get organized. Luckily the SHM staff is a lot more responsive then the medical records department at Ben Taub was.
Then, as with any patient, I had to ask some basic questions. What initial symptoms caused the development of The Hospitalist? How long had the publication been present? What made it better, and what made it worse? Was it progressing or was it unchanged? Was I having chest pain? What was SHM, and why did it exist? What did a hospitalist want to read? What was a hospitalist, and why would anyone want to be one?
Why I’m a Hospitalist
That final question seemed the heart of my issue. I pondered what forces drove me to become a hospitalist and why I enjoyed it so much.
When I finished my residency I went into private practice. Like most residents of the time I was totally unprepared for ambulatory care. I could run a code, knew all the latest diagnostic tests, and could even quote a few articles.
But the first time I saw a young man with chronic back pain who wanted to go on disability, or an elderly lady with osteoporosis and breast cancer who wondered if she could take quinine for leg cramps, I was lost. It only took a decade or two for me to feel vaguely competent. Meantime I did some hard time in the hospital, but my focus shifted tectonically toward the outpatient. When my running partner Mitchell Wilson decided to start one of the early hospitalist programs (at the University of Texas) my hospital time ever more rapidly receded.
At the same time, the forces of capitalism were at work: IPAs and IPOs, practice management groups, university expansions and contractions, hospital closings. This was the new shifting sand (or shifting dullness) of medical practice. I was ready for a change, but could I give up my comfortably cluttered office, my established, fairly well-tuned patients, my six-year-old National Geographic magazines in the waiting room? Would going back to the hospital feel like being a resident again? There was only one way to find out.
I said goodbye to the beach and the fire ants, loaded my truck like Jed Clampett, and moved to Rochester—Minn., that is—frozen tundra, lots of geese. Under the auspices of Jeanne Huddleston and the Mayo Clinic Inpatient Internal Medicine Team, I joined the world of hospitalists.
New Beginnings
My first impression of life as a hospitalist was that I was cold. Frigid really. Of course it was winter in Minnesota, so I guess I should have expected that. I rapidly discovered that it was a lot nicer being a member of the consulting staff than a member of the house staff. In some ways I felt like an intern again. It was difficult to believe, but hospital medicine had changed over the last decade or two; however, the patients hadn’t.
I was armed with acceptable history taking and exam skills. I had a superb support system in the nurse practitioners and physician assistants who carried my load the first few weeks. My colleagues were supportive. I muddled through and, after several years, felt like I was back to my baseline level of moderate competence.
Though my story is immensely fascinating (to me) from an autobiographical standpoint, does it answer the question of why I enjoy being a hospitalist? Usually people ask me, “What is a hospitalist?” I usually explain that I’m an internist—not an intern—though some days I feel like the latter. The taxonomy of hospitalists is fairly diverse. Some of us come straight from residency, for others it’s the resolution of a mid-career crisis.
One of my favorite things about being a hospitalist is the control I have over my schedule. As an outpatient doctor I had a timetable to keep based on the waiting patient. If I got behind, waxed conversational, or got involved with a family, my day was ruined. Patients got mad at me; my nurses were aggravated.
In the hospital, I have a body of work I must do each day. It’s predictably unpredictable at the beginning of the shift. I have a certain number of patients to see, discharge, and admit. I risk acute medical emergencies, unexpected families who want an update on their mother’s condition, and similar hospitalist activities of daily life (aka HADLs). The volume of work is variable: Some days are difficult, some aren’t. The complexity of cases is stimulating and makes continued learning a necessity. Instead of being isolated in an office I interact with other physicians and staff. The most stimulating aspect I experience is the sensation that hospital medicine is an evolving field and there are hundreds of dedicated colleagues out there trying to make it better.
My goal as physician editor is to work with SHM members to continue to produce a great source of hospitalist information. The Hospitalist readers include internists, family practitioners, pediatricians, nurse practitioners, and physician assistants. They also comprise administrators, businesspeople, and legislators. I perceive important topics to involve medical management, education, communication, economics, government regulation, ethics, and palliative care, as well as the activities of our society, chapters, and members.
With the team from John Wiley & Sons and the support of SHM administration and the members, I hope to accomplish this task. My patient all those years ago survived and left the hospital. I only can hope that The Hospitalist will thrive as well. TH
Jamie Newman, MD, FACP, is senior associate consultant, Hospital Internal Medicine, associate professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
Staph Endocarditis, METs, COPD CPGs & More
A review of staphylococcal Endocarditis
VG Fowler Jr, Miro JM, Hoen B, et al for the ICE Investigators. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA. 2005;June 22;293(24):3061-3062.
Agroup of infectious diseases experts from centers throughout the world formed the International Collaboration on Endocarditis (ICE) in 1999 to gain a global understanding of infective endocarditis. Using the Duke Criteria patients with definite infective endocarditis in a prospective manner, 275 variables were reported with these cases to a central database maintained at Duke University. The ICE-Prospective Cohort Study (ICE-PCS) enrolled 1,779 patients with infective endocarditis in 39 centers in 16 countries between June 15, 2000, and December 31, 2003, and has been described in a recent report. (Cabell CH, Abrutyn E. Infect Dis Clin North Am. 2002;16:255-72). Staphylococcus aureus was the most common cause of infective endocarditis in this group of patients (n=558; 31.6%); the authors characterized risk factors and clinical issues associated with these cases in this report.
By univariate analysis, compared with non-Staphylococcus aureus infective endocarditis, patients with infective endocarditis due to Staphylococcus aureus were more likely than patients with infective endocarditis due to other pathogens to be female (P<0.001), hemodialysis dependent (P<0.001), have diabetes mellitus (P=0.009), have other chronic illnesses (P<0.001), have a healthcare association (P<0.001), have higher rates of stroke (P<0.001), have systemic embolization (P<0.001), have persistent bacteremia (P<0.001), or die (P<0.001).
Although healthcare associated Staphylococcus aureus infective endocarditis was the most common form of Staphylococcus aureus infective endocarditis, more than 60% of healthcare-associated patients acquired the infection outside the hospital. This reflects the global trend in healthcare delivery patterns favoring ambulatory treatment (e.g., outpatient medication infusion via long-term IV access, hemodialysis)
Multivariate analysis, clinical features independently associated with Staphylococcus aureus infective endocarditis (versus non-Staphylococcus aureus infective endocarditis) were: IV drug use (OR, 9.3; 95% CI, 6.3-13.7); first clinical presentation less than one month after first symptoms (OR, 5.1; 95% CI, 3.2-8.2); healthcare-associated infection (OR, 2.9; 95% CI, 2.1-3.8), persistent bacteremia (OR, 2.3; 95% CI, 1.5-3.8), presence of a presumed intravascular device source (OR, 1.7; 95% CI, 1.2-2.6), stroke (OR, 1.6; 95% CI, 1.2-2.3), or diabetes mellitus (OR, 1.3; 95% CI, 1.1-1.8).
Patients from the United States with Staphylococcus aureus infective endocarditis were more likely to be hemodialysis-dependent, to be diabetic, to have a hemodialysis fistula or a chronic indwelling central catheter as a presumed source of infection, and to have a non-nosocomial healthcare association. Patients from the United States and Brazil were more likely to have Methicillin-resistant Staphyloccocus aureus (MRSA) than were patients from Europe, the Middle East, Australia, or New Zealand. In-hospital mortality rates were similar across regions, although American patients were significantly more likely to develop persistent bacteremia (25.6%, P<0.001).
Characteristics independently associated with mortality among patients with nonintravenous drug-use-associated Staphylococcus aureus infective endocarditis by multivariate analysis included stroke (OR, 3.67; 95% CI, 1.94-6.94), persistent bacteremia (OR, 3.06; 95% CI, 1.75-5.35), diagnosis in Southern Europe or the Middle East (OR, 3.21; 95% CI, 1.17-10.56).
This study establishes Staphylococcus aureus infective endocarditis as the leading cause of infective endocarditis in many regions of the world and spotlights the global emergence of healthcare contact as a risk factor for Staphylococcus aureus infective endocarditis. In a significant portion of these patients, an IV device was the presumed source of bacteremia; prosthetic cardiac devices (pacemakers, defibrillators, or prosthetic cardiac valves) were present in almost one-quarter of the patients.
MRSA was a significant cause of Staphylococcus aureus infective endocarditis and displayed regional variation, accounting for almost 40% of the infective endocarditis caused by Staphylococcus aureus in some regions. Patients with infective endocarditis caused by MRSA were significantly more likely to have pre-existing chronic conditions and healthcare associated infective endocarditis by both univariate and multivariate analysis. They also were often associated with persistent bacteremia. On the other hand, 20% of patients with MRSA infective endocarditis developed their infection in the absence of identifiable healthcare contact.
Limitations of this report include the fact that this is an observational study of patients from self-selected centers. Each center most likely represents a portion of the local population, making it difficult to generalize findings to the entire population centers from which this report originates. Represented hospitals were typically referral centers that have cardiac surgery programs and may have widely differing populations with varied risk factors. Advantages include the large size of this prospectively evaluated cohort and the ability to analyze regional variations between continents with a contemporary nature of the patient sample (2000-2003).
Infectious Endocarditis in Olmsted County, Minn.
Tleyjeh IM, Steckelberg JM, Murad HS, et al. Temporal trends in infective endocarditis: a population-based study in Olmsted County, Minnesota. JAMA. 2005;293:3022-3028.
Tleyjeh and colleagues at the Mayo Clinic in Rochester, Minn., retrospectively studied 102 cases of infective endocarditis that occurred in 107 Olmsted County residents from 1970-2000. Main outcome measures were incidence of infective endocarditis, proportion of patients with underlying heart disease and causative micro-organisms and clinical characteristics. The records of all Olmsted County residents with infective endocarditis were identified and reviewed in detail. The definite and possible infective endocarditis cases as defined by modified Duke Criteria were used in the analysis.
The age- and gender-adjusted incidence of infective endocarditis ranged from 5.0 to 7.0 cases per 100,000 person-years during the study period and did not change significantly over time. There were 84 (79%) cases of native valve infective endocarditis and 23 (21%) cases of prosthetic valve infective endocarditis. Valves involved: aortic—36 (24%); mitral—49 (46%), aortic and mitral—12 (11%), right-sided or bilateral—8 (7%), or unknown—8 (7%). 16 (15%) had valve surgery within 42 days and the six-month mortality was 26% (n=28).
Infective endocarditis is a disease of the older individual in this population, with a mean age ranging from 54.1 years in 1980-1984 to 67.4 years in 1995-2000 (P=0.24 for trend). There was a male predominance (67%-83%), which did not significantly change over time.
Mitral valve prolapse was the most frequent underlying valvular heart disease. Viridans streptococci were the most common causative organisms (n=47; 44%) followed by Staphylococcus aureus (n=28 cases; 26%).
The overall average crude infective endocarditis incidence of the period 1970-2000 was 4.95 per 100,000 person-years. The age- and gender-adjusted annual incidence was 6.06 per 100,000 (95% CI, 4.89-7.22). There was no time trend for either streptococcus or Staphylococcus aureus infective endocarditis: the annual adjusted incidence of viridans group streptococcal infective endocarditis was 1.7 to 3.5 cases per 100,000 person years while Staphylococcus aureus infective endocarditis had an annual adjusted incidence of 1.0-2.2 cases per 100,000. The incidence rates of viridans group streptococcal and Staphylococcus aureus infective endocarditis have not changed significantly over time in this population.
Potential limitations of this study include possible incomplete case finding or recognition of the retrospective nature of the case reviews. The homogeneity of the patient population studied (primarily elderly white males with a low prevalence of intravenous drug use) limits the ability to generalize the results. Advantages include the fact that this is a population-based study at a medical center with detailed medical records of virtually all residents of a single county. This allows us to view the clinical features and etiologic factors of primarily left-sided infective endocarditis without the referral bias that tends to taint other studies typically published out of large medical centers with larger geographic referral bases.
Computers and Adverse Drug Events
Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of adverse drug events in a highly computerized hospital. Arch Intern Med. 2005;165:1111-1116.
Adverse drug events account for a significant number of hospital admissions and the ensuing costs associated with these hospitalizations. Electronic endeavors, such as computerized physician order entry (CPOE), bar code systems, and electronic medical records attempt to reduce the preventable adverse drug events.
Nebeker, et al. attempted to assess the effects of the implementation of CPOE and other computerized medication systems on adverse drug events in a tertiary care Veterans Administration Medical Center. They used an observational study design whereby 937 out of 2,306 newly admitted patients from several hospital wards were randomly chosen and assigned to a pharmacist reviewer during a 20-week period.
They reviewed complete medical records of hospital stays every other day to document adverse drug events. Not only were traditional adverse drug events identified, but harm from overdoses and/or inappropriate dose reductions or discontinuations, as well as intolerable harm from dose titration, were documented as adverse drug events. The harms caused by the drugs were considered only if the drugs were started in the hospital.
Harms were classified based on prior literature and included standards for pharmacological typology, causality assessment, error type, event terminology, drug class, seriousness index, and medication error category indexing. Additional uncommon classifications were also used, including additional resource utilization. Consensus meetings were held weekly to confirm classification of adverse drug events. Of the admissions reviewed, 483 adverse drug events were identified of which 93% were drug reactions while 7% were due to over- or underdosing. Of the drug reactions, 90% were considered dose-dependent while 10% were considered to be idiosyncratic.
Two different indexing scales were used in classifying the harms. Using the LDS Hospital Scale, it was suggested that 91% of the adverse drug events caused moderate harm while 9% caused serious harm. Using the National Coordinating Council for Medication Error Reporting and Prevention indexing, it was suggested that 87% of the adverse drug events fell into category E (requiring treatment) and 4% into category F (requiring prolonged hospitalization). Twenty-seven percent of the total adverse drug events were thought to be due to errors, including execution and planning steps. Sixty-one percent of errors occurred with the ordering mechanism while 25% of the errors occurred in the monitoring process.
This study highlighted rates of adverse drug events five to 19 times higher than baseline. The authors explained this higher-than-expected rate in part by study elements, such as the use of clinical pharmacists as reviewers, iterative case reviews, and accessible electronic data that make adverse drug events more noticeable.
Weaknesses of this study included issues of comparability of CPOEs because there were significant feature differences among commercial software programs. In addition, this was an observational study lacking a control group. The authors felt that their study did not support the idea that the computerized patient record of the study institution had caused adverse drug events. Rather, the study supported the idea that the system increased the visibility of adverse drug events compared with a paper system. In addition, the authors recommended that the choice of CPOEs be carefully considered, with a focus on decision support features when integrated into a healthcare organization.
The Questionable Benefit of Medical Emergency Teams
Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. MERIT study investigators. Lancet. 2005;365:2091-2097.
Previous studies have reported that the MET system reduces the incidence of cardiac arrests, deaths, and unplanned ICU admissions. A MET is a preplanned group of healthcare practitioners who respond to acute patient deteriorations in hospitalized patients.
METs are usually identical to hospital code teams, with the exception that they respond prior to a patient’s developing cardiac arrest. This early response has been shown to significantly decrease unexpected hospital mortality in hospitals in the United States, Australia, and Great Britain. Even though the system has been reported since 1995, few hospitals have knowledge of or experience with METs.
Unexpected hospital deaths and cardiac arrests are often preceded by clinical warning signs. In addition, unplanned ICU admissions may be foreshadowed by abnormalities in the patient’s vital signs that may progress if appropriate interventions are not undertaken. METs assess patients with abnormal physical findings or when there is a concern about the patient’s condition. These patients have findings that may precede a serious event or cardiac arrest, but otherwise don’t meet existing criteria to call a code.
The theory is that if a MET responds to see a patient who is becoming unstable (see “Table 1: MET Calling Criteria,” at left), early interventions may reduce the likelihood of arrest. Published studies have shown a reduction in cardiac arrests and ICU length of stay in virtually all systems in which MET has been introduced (although most studies are hampered by the use of historical controls).
The MERIT study randomized 23 hospitals in Australia to continue functioning as usual (n=11) or to introduce a MET system (n=12). The study sites included a wide range of tertiary, metropolitan, and non-metropolitan hospitals in different states across Australia. The primary outcome was the composite of cardiac arrest, unexpected death, or unplanned ICU admission during the six-month study period after MET activation, using intention to treat analysis.
A four-month educational period was undertaken with the MET centers prior to initiation of the trial. Control hospitals did not receive any education about the MET concept. This was followed by a six-month trial period. Cardiac arrest teams were maintained at all hospitals. The MET consisted of at least one doctor and a nurse from the ED or ICU.
The eligible patients included those residing on a medical ward (including critical care units); the ICUs, OR, postoperative recovery areas, and ED areas were not regarded as general wards.
The primary outcome for the study was the composite outcome of the incidence (events divided by number of eligible patients admitted to the hospital and residing on a medical ward during the study period) of:
- Cardiac arrests without a pre-existing “not-for-resuscitation” (NFR) order;
- Unplanned ICU admissions; and
- Unexpected deaths (those without a pre-existing NFR order).
The results of the study:
- During the study period, the overall rate of calls for the cardiac arrest team or MET was significantly higher in intervention hospitals than in control hospitals. Calls not associated with events were more common in MET hospitals than in controls. Half of the total calls were not associated with a cardiac arrest or unexpected death, whereas in MET hospitals more than 80% of calls were not associated with a cardiac arrest or death (P<0.0001).
- In patients with documented MET calling criteria in association with cardiac arrest or unexpected death, the call rate was similar in MET and control hospitals.
- There were no significant differences between the MET and control hospitals for any outcome.
- The response to changes in vital signs was not adequate—even in MET centers.
These findings are surprising in view of previously reported findings using the MET system. Potential reasons for lack of difference between MET centers and controls include:
- Number of study sites or the duration of the study may not have been adequate for implementation or education;
- Hospitals may already be efficient in detecting and managing unstable patients;
- Patient selection criteria may have been overly restricted. For example, other studies have used 30 respirations per minute for tachypnea as a calling criterion compared with 36 breaths per minute used in this trial;
- Knowledge of the study may have leaked to control hospitals;
- Cardiac arrest teams function as METs at times: Nearly half of the calls to cardiac arrest teams in control hospitals were made without a cardiac arrest or unexpected death; and
- The selected outcomes may not be sensitive enough.
Even though this large, multicenter controlled trial was unable to show a significant benefit of METs, we should not be discouraged from performing further controlled trials in different settings. The use of METs is clearly an exciting and evolving area of medicine.
Barriers to Patient Safety
Amalberti R, Auroy Y, Berwick D, Barach P. Five system barriers to achieving ultrasafe health care. Ann Intern Med. 2005;142:756-764
Patient safety in our healthcare system is a growing concern. One area of dialogue concerning preventable healthcare-associated harms involves the comparability of the healthcare industry with non-medical industries, such as aviation and nuclear power, that have adapted successful strategies shown to provide ultrasafe environments. Amalberti, et al. discuss risk assessment in a variety of industries and explain the need for a benchmarking approach in order to optimize or achieve safety in the healthcare field.
The authors identify five systemic barriers from literature that are fundamentally connected to the ability of the healthcare field to achieve an extremely safe environment.
Barrier 1—acceptance of limitations on maximum performance: The first barrier is the type of expected performance in the field. This is illustrated by the tradeoffs associated with ultrasafety versus productivity. The amount of risk involved was directly related to the limits placed on maximum performance. The first barrier is the acceptance that every system has limits. When a producer exceeds their limit, then safety suffers. An example used is that of blood donation: The limits of collection speed are weighed against the needed screening process.
Barrier 2—abandonment of professional autonomy: The second barrier concerns the concept of professional autonomy. While more teamwork and regulations reduce individual autonomy, this appears to improve safety in the healthcare environment. The bottom line is the importance of teamwork. The example used is that of traffic on a highway: Autonomous units work together to function safely.
Barrier 3—transition from the mindset of craftsman to that of an equivalent actor: The third barrier to achieving high levels of safety includes an equivalent actor mindset. This entails establishing a reliable standard of excellent care in lieu of focusing on individuality, similar to the notion that passengers on an airline usually do not know their pilots, but have established confidence in the airline itself.
Barrier 4—the need for system-level arbitration to optimize safety strategies: The fourth barrier identified is a need for system-level arbitration to optimize safety strategies. This need results from the pressure for justice (usually through litigation) once an accident occurs. Top-down arbitration of safety will be less successful than system level design.
Barrier 5—the need to simplify professional rules and regulations: The final barrier results from the many of layers of guidelines as they serve to create an environment of excellence. This barrier necessitates the removal of these layers to simplify the environment. Existing guidelines should be distilled down to those shown to promote quality and safety. Byzantine rules can obscure the goal of safety and glorify rules, for rules sake.
Certain structural limitations within the field, such as worker shortages in the face of increasing public demands and the reliance of the field on trainees such as students, interns, and residents, create other hurdles. The authors conclude by suggesting a two-tiered system of healthcare whereby ultrasafety could be more easily accomplished in areas of medicine considered more stable (first tier), and a second tier of care that would include the more unstable conditions, and thus inherently, represent the higher risk situations where errors are more likely to occur.
Another provocative point of this article is the need to move toward educating and training teams—not individuals.
The Importance of Implementing COPD Guidelines
Harvey PA, Murphy MC, Dornom E, et al. Implementing evidence-based guidelines: inpatient management of chronic obstructive pulmonary disease. Intern Med J. 2005;35:151-155.
COPD is a common diagnosis that sometimes requires hospitalization. Evidence-based guidelines for disease management, including that of hospitalized patients, exist, but there is a paucity of knowledge about the actual quality of care delivered in the hospital as it aligns with published guidelines. This study by Harvey, et al. explores the quality of care delivered in the hospital for patients with COPD, while at the same time investigating an intervention for the medical staff in an effort to improve adherence to evidenced-based guidelines of the disease.
Using ICD-10 codes for a COPD diagnosis, the study incorporated a retrospective chart review of 49 hospital admissions prior to the intervention and 35 admissions after the intervention in a hospital in Melbourne, Australia. Data were collected pertaining to the hospital management of COPD as it compared with what the authors considered to be Level A—or the highest level of evidence summarized from several professional organizations. The intervention delivered to the medical staff included a summarized presentation of the results from the initial audit of the 49 charts, as well as an educational package that was given to them following the presentation.
Except for inappropriate use of intravenous aminophylline, of which there was a 100% concordance to Level A guidelines, the initiation of systemic steroids (intravenous and/or oral) had the highest concordance rate of 80% and 83%, pre- and postintervention respectively. Appropriate steroid duration (seven to 14 days) had the lowest concordance rates at 10% and 29%, pre- and postintervention respectively.
In addition, preintervention concordance (10%) involving steroid duration was the only rate considered significantly different in the postintervention group (29%). While concordance rates were high for the use of any type of nebulized bronchodilator (96% preintervention and 80% postintervention), the Level A guidelines the authors used suggested that beta-agonist bronchodilators should be used alone prior to the initiation of ipratropium bromide. The concordance rates for this guideline were 27% preintervention and 34% postintervention.
Largely, the authors felt their intervention failed to improve concordance rates to the Level A guidelines investigated and also that their findings of variable and lower concordance rates across the board corroborated other similar studies. The major weaknesses of this study included the small sample size and the nonrandomness of the sampling.
In addition, the authors report that the particular hospital studied included junior doctors who rotated on and off service, which likely prevented the effects of the intervention from being measured on a provider level. In spite of the weaknesses in the study, the article brings to light the need for a more effective translation of evidence-based guidelines to actual practice, especially in the practice of COPD management in the hospital. Further methods of guideline implementation in the clinic setting must be elucidated to improve the care patients with COPD receive in the hospital.
Not all Troponin Elevations Are Myocardial Infarctions
Jeremais A, Gibson CM. Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med. 2005;142:786-791.
Troponins are regulatory proteins that control the calcium-mediated interaction of actin and myosin during muscle contraction. All muscle tissue contains troponins, but cardiac troponin T and I have amino acid sequences that are different from skeletal and smooth muscle troponins, allowing them to be detectable by monoclonal antibody-based assays.
In the event of reversible or irreversible cell damage—or possibly even from transiently increased cell membrane permeability—cardiac troponins are released from myocytes into circulation. This characteristic provides a sensitive test for detecting myocardial injury and damage; however, this test is not specific for acute coronary syndromes. And any disorder that causes myocyte damage may cause an elevated troponin.
The 2002 American College of Cardiology/American Heart Association practice guidelines for unstable angina and non-ST-segment elevation myocardial infarction acknowledge that the myocardial necrosis signified by troponin elevation may not necessarily be caused by atherosclerotic coronary artery disease. Such nonthrombotic troponin elevation can be caused by four basic mechanisms, as discussed by Dr. Jeremias and Dr. Gibson.
- Demand ischemia refers to a mismatch between myocardial oxygen demand and supply in the absence of flow-limiting epicardial stenosis. Conditions such as sepsis or septic shock and the systemic inflammatory response syndrome, hypotension or hypovolemia, tachyarrhythmias, and left ventricular hypertrophy can all cause release of cardiac troponin.
- Myocardial ischemia in the absence of fixed obstructive coronary disease can be caused by coronary vasospasm, acute stroke or intracranial hemorrhage, and ingestion of sympathomimetics.
- Direct myocardial damage can be seen in cardiac contusion, direct current cardioversion, cardiac infiltrative disorders such as amyloidosis, certain chemotherapy agents, myocarditis, pericarditis, and cardiac transplantation.
- Myocardial strain occurs when volume and pressure overload of the left and/or right ventricle cause excessive wall tension. Congestive heat failure, acute pulmonary embolism, and chronic pulmonary hypertension can lead to myocardial strain and troponin elevation.
Another condition that can lead to persistently elevated cardiac troponins is end-stage renal disease. This elevation may be due to small areas of clinically silent myocardial necrosis, an increased left ventricular mass, or possibly from impaired renal troponin excretion. Although troponins are believed to be cleared by the reticuloendothelial system, recent evidence shows that troponin T is fragmented into molecules that are small enough to be renally excreted.
In summary, elevated troponin can be found in many clinical settings and is associated with impaired short- and long-term survival. TH
Classic Literature
The HATEFUL Patient

Every physician has groaned internally when seeing a certain patient’s name on his list, going out of her way to avoid a particular family, or getting hopelessly engaged and increasingly enraged in a battle over a “lost” narcotic prescription. There are certain patients with whom a doctor-patient relationship feels more like a contest than a partnership. These interactions make a physician’s daily practice difficult, and they may wreak havoc among the staff on an inpatient ward. These patients grow ever more intolerable to their caregivers, who often harbor a wish to simply make them disappear.
In his landmark 1978 article “Taking Care of the Hateful Patient,” (NEJM, 298:883-887) James Groves, MD, discussed the characteristics of these difficult patients and the sometimes difficult emotions they generate in their caregivers. He described four different groups of patients, using an illustrative case for each, and discussed the ways in which these patients’ often maddening behavior serves to mitigate their profound dependency.
Dependent clingers are those patients whose neediness is overt, who seem to regard the physician as a sow with teats to spare. Dr. Groves suggested early, firm limit-setting with these patients to prevent the formation and later shattering of the patient’s illusion of the physician as inexhaustible.
Dependency lies at the heart of an entitled demander’s behavior as well, but their fear of abandonment is expressed as hostility and arrogance rather than overt neediness. Affirming to the patient that you share in their quest for the good (but not perfect) medical care to which they are entitled allows patient and physician to rally around a common goal.
This strategy backfires with manipulative help-rejecters, who seem almost pleased to report to their physician each time they fail a new treatment attempt. Overtly expressing some doubt that the treatment will completely cure all the patient’s difficulties and providing regular follow up are recommended for this group. These strategies relieve the patient of the unconscious anxiety that he may be abandoned by his physician should his symptoms abate.
Self-destructive deniers make the physician feel powerless as they persist in behavior that undermines all efforts to improve their health. With these patients, viewing their behavior as a terminal illness and managing symptoms and exacerbations accordingly allows the physician to focus on caring for the patient without unrealistic expectations of cure on the one hand and judgmental indifference on the other.
After discussing each of these groups, Dr. Groves concluded the article by suggesting that perhaps the greatest challenge physicians face in caring for these difficult patients is the temptation to disown the negative feelings they engender. He wrote that this effort not only strains the doctor’s limits, but also wastes valuable clinical data unmasked by these feelings—data that could inform clinical care. For decades prior to Dr. Groves’ article, psychoanalysts had reflected on what Freud termed “countertransference,” or the physician’s internal emotional reaction to a patient.
In his article “Hate in the Counter-Transference,” D.W. Winnicott, MD, suggested that rather than accepting the guilt that these feelings typically engender in a caregiver, negative countertransference reactions should be regarded by the physician as valuable information in understanding the patient’s psychic world. By training and by disposition, however, most physicians considered (and continue to consider) these emotions inappropriate. They seemingly negate the sympathy, kindness, and commitment to the patient’s well-being that should be central to a physician’s vocation. Conventional wisdom held that denying the feelings was the only proper response, and if that proved impossible, transferring the patient to a willing colleague was usually recommended. In contrast, Dr. Groves freed the physician to use these feelings to improve patient care.
Now a classic and oft-cited work, “Taking Care of the Hateful Patient” distills a wealth of analytic insight into a structure and language comprehensible to the busy generalist. By explaining the reactions each group of patients induces in their physicians, Dr. Groves provides useful tools to understand a particular patient’s psychology. Suggestions for strategic approaches to each category of patient are easy to understand and to adapt to one’s own practice. He explains how judicious limit-setting can be as valuable for the patient as it is for the doctor. Perhaps most helpful is his description of the needs of these patients that lie beneath their “hateful” exterior. Armed with this understanding, a physician can reclaim the empathy that is often so elusive with these patients.—Sandra Rackley MD, Kemuel Philbrick, MD
A review of staphylococcal Endocarditis
VG Fowler Jr, Miro JM, Hoen B, et al for the ICE Investigators. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA. 2005;June 22;293(24):3061-3062.
Agroup of infectious diseases experts from centers throughout the world formed the International Collaboration on Endocarditis (ICE) in 1999 to gain a global understanding of infective endocarditis. Using the Duke Criteria patients with definite infective endocarditis in a prospective manner, 275 variables were reported with these cases to a central database maintained at Duke University. The ICE-Prospective Cohort Study (ICE-PCS) enrolled 1,779 patients with infective endocarditis in 39 centers in 16 countries between June 15, 2000, and December 31, 2003, and has been described in a recent report. (Cabell CH, Abrutyn E. Infect Dis Clin North Am. 2002;16:255-72). Staphylococcus aureus was the most common cause of infective endocarditis in this group of patients (n=558; 31.6%); the authors characterized risk factors and clinical issues associated with these cases in this report.
By univariate analysis, compared with non-Staphylococcus aureus infective endocarditis, patients with infective endocarditis due to Staphylococcus aureus were more likely than patients with infective endocarditis due to other pathogens to be female (P<0.001), hemodialysis dependent (P<0.001), have diabetes mellitus (P=0.009), have other chronic illnesses (P<0.001), have a healthcare association (P<0.001), have higher rates of stroke (P<0.001), have systemic embolization (P<0.001), have persistent bacteremia (P<0.001), or die (P<0.001).
Although healthcare associated Staphylococcus aureus infective endocarditis was the most common form of Staphylococcus aureus infective endocarditis, more than 60% of healthcare-associated patients acquired the infection outside the hospital. This reflects the global trend in healthcare delivery patterns favoring ambulatory treatment (e.g., outpatient medication infusion via long-term IV access, hemodialysis)
Multivariate analysis, clinical features independently associated with Staphylococcus aureus infective endocarditis (versus non-Staphylococcus aureus infective endocarditis) were: IV drug use (OR, 9.3; 95% CI, 6.3-13.7); first clinical presentation less than one month after first symptoms (OR, 5.1; 95% CI, 3.2-8.2); healthcare-associated infection (OR, 2.9; 95% CI, 2.1-3.8), persistent bacteremia (OR, 2.3; 95% CI, 1.5-3.8), presence of a presumed intravascular device source (OR, 1.7; 95% CI, 1.2-2.6), stroke (OR, 1.6; 95% CI, 1.2-2.3), or diabetes mellitus (OR, 1.3; 95% CI, 1.1-1.8).
Patients from the United States with Staphylococcus aureus infective endocarditis were more likely to be hemodialysis-dependent, to be diabetic, to have a hemodialysis fistula or a chronic indwelling central catheter as a presumed source of infection, and to have a non-nosocomial healthcare association. Patients from the United States and Brazil were more likely to have Methicillin-resistant Staphyloccocus aureus (MRSA) than were patients from Europe, the Middle East, Australia, or New Zealand. In-hospital mortality rates were similar across regions, although American patients were significantly more likely to develop persistent bacteremia (25.6%, P<0.001).
Characteristics independently associated with mortality among patients with nonintravenous drug-use-associated Staphylococcus aureus infective endocarditis by multivariate analysis included stroke (OR, 3.67; 95% CI, 1.94-6.94), persistent bacteremia (OR, 3.06; 95% CI, 1.75-5.35), diagnosis in Southern Europe or the Middle East (OR, 3.21; 95% CI, 1.17-10.56).
This study establishes Staphylococcus aureus infective endocarditis as the leading cause of infective endocarditis in many regions of the world and spotlights the global emergence of healthcare contact as a risk factor for Staphylococcus aureus infective endocarditis. In a significant portion of these patients, an IV device was the presumed source of bacteremia; prosthetic cardiac devices (pacemakers, defibrillators, or prosthetic cardiac valves) were present in almost one-quarter of the patients.
MRSA was a significant cause of Staphylococcus aureus infective endocarditis and displayed regional variation, accounting for almost 40% of the infective endocarditis caused by Staphylococcus aureus in some regions. Patients with infective endocarditis caused by MRSA were significantly more likely to have pre-existing chronic conditions and healthcare associated infective endocarditis by both univariate and multivariate analysis. They also were often associated with persistent bacteremia. On the other hand, 20% of patients with MRSA infective endocarditis developed their infection in the absence of identifiable healthcare contact.
Limitations of this report include the fact that this is an observational study of patients from self-selected centers. Each center most likely represents a portion of the local population, making it difficult to generalize findings to the entire population centers from which this report originates. Represented hospitals were typically referral centers that have cardiac surgery programs and may have widely differing populations with varied risk factors. Advantages include the large size of this prospectively evaluated cohort and the ability to analyze regional variations between continents with a contemporary nature of the patient sample (2000-2003).
Infectious Endocarditis in Olmsted County, Minn.
Tleyjeh IM, Steckelberg JM, Murad HS, et al. Temporal trends in infective endocarditis: a population-based study in Olmsted County, Minnesota. JAMA. 2005;293:3022-3028.
Tleyjeh and colleagues at the Mayo Clinic in Rochester, Minn., retrospectively studied 102 cases of infective endocarditis that occurred in 107 Olmsted County residents from 1970-2000. Main outcome measures were incidence of infective endocarditis, proportion of patients with underlying heart disease and causative micro-organisms and clinical characteristics. The records of all Olmsted County residents with infective endocarditis were identified and reviewed in detail. The definite and possible infective endocarditis cases as defined by modified Duke Criteria were used in the analysis.
The age- and gender-adjusted incidence of infective endocarditis ranged from 5.0 to 7.0 cases per 100,000 person-years during the study period and did not change significantly over time. There were 84 (79%) cases of native valve infective endocarditis and 23 (21%) cases of prosthetic valve infective endocarditis. Valves involved: aortic—36 (24%); mitral—49 (46%), aortic and mitral—12 (11%), right-sided or bilateral—8 (7%), or unknown—8 (7%). 16 (15%) had valve surgery within 42 days and the six-month mortality was 26% (n=28).
Infective endocarditis is a disease of the older individual in this population, with a mean age ranging from 54.1 years in 1980-1984 to 67.4 years in 1995-2000 (P=0.24 for trend). There was a male predominance (67%-83%), which did not significantly change over time.
Mitral valve prolapse was the most frequent underlying valvular heart disease. Viridans streptococci were the most common causative organisms (n=47; 44%) followed by Staphylococcus aureus (n=28 cases; 26%).
The overall average crude infective endocarditis incidence of the period 1970-2000 was 4.95 per 100,000 person-years. The age- and gender-adjusted annual incidence was 6.06 per 100,000 (95% CI, 4.89-7.22). There was no time trend for either streptococcus or Staphylococcus aureus infective endocarditis: the annual adjusted incidence of viridans group streptococcal infective endocarditis was 1.7 to 3.5 cases per 100,000 person years while Staphylococcus aureus infective endocarditis had an annual adjusted incidence of 1.0-2.2 cases per 100,000. The incidence rates of viridans group streptococcal and Staphylococcus aureus infective endocarditis have not changed significantly over time in this population.
Potential limitations of this study include possible incomplete case finding or recognition of the retrospective nature of the case reviews. The homogeneity of the patient population studied (primarily elderly white males with a low prevalence of intravenous drug use) limits the ability to generalize the results. Advantages include the fact that this is a population-based study at a medical center with detailed medical records of virtually all residents of a single county. This allows us to view the clinical features and etiologic factors of primarily left-sided infective endocarditis without the referral bias that tends to taint other studies typically published out of large medical centers with larger geographic referral bases.
Computers and Adverse Drug Events
Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of adverse drug events in a highly computerized hospital. Arch Intern Med. 2005;165:1111-1116.
Adverse drug events account for a significant number of hospital admissions and the ensuing costs associated with these hospitalizations. Electronic endeavors, such as computerized physician order entry (CPOE), bar code systems, and electronic medical records attempt to reduce the preventable adverse drug events.
Nebeker, et al. attempted to assess the effects of the implementation of CPOE and other computerized medication systems on adverse drug events in a tertiary care Veterans Administration Medical Center. They used an observational study design whereby 937 out of 2,306 newly admitted patients from several hospital wards were randomly chosen and assigned to a pharmacist reviewer during a 20-week period.
They reviewed complete medical records of hospital stays every other day to document adverse drug events. Not only were traditional adverse drug events identified, but harm from overdoses and/or inappropriate dose reductions or discontinuations, as well as intolerable harm from dose titration, were documented as adverse drug events. The harms caused by the drugs were considered only if the drugs were started in the hospital.
Harms were classified based on prior literature and included standards for pharmacological typology, causality assessment, error type, event terminology, drug class, seriousness index, and medication error category indexing. Additional uncommon classifications were also used, including additional resource utilization. Consensus meetings were held weekly to confirm classification of adverse drug events. Of the admissions reviewed, 483 adverse drug events were identified of which 93% were drug reactions while 7% were due to over- or underdosing. Of the drug reactions, 90% were considered dose-dependent while 10% were considered to be idiosyncratic.
Two different indexing scales were used in classifying the harms. Using the LDS Hospital Scale, it was suggested that 91% of the adverse drug events caused moderate harm while 9% caused serious harm. Using the National Coordinating Council for Medication Error Reporting and Prevention indexing, it was suggested that 87% of the adverse drug events fell into category E (requiring treatment) and 4% into category F (requiring prolonged hospitalization). Twenty-seven percent of the total adverse drug events were thought to be due to errors, including execution and planning steps. Sixty-one percent of errors occurred with the ordering mechanism while 25% of the errors occurred in the monitoring process.
This study highlighted rates of adverse drug events five to 19 times higher than baseline. The authors explained this higher-than-expected rate in part by study elements, such as the use of clinical pharmacists as reviewers, iterative case reviews, and accessible electronic data that make adverse drug events more noticeable.
Weaknesses of this study included issues of comparability of CPOEs because there were significant feature differences among commercial software programs. In addition, this was an observational study lacking a control group. The authors felt that their study did not support the idea that the computerized patient record of the study institution had caused adverse drug events. Rather, the study supported the idea that the system increased the visibility of adverse drug events compared with a paper system. In addition, the authors recommended that the choice of CPOEs be carefully considered, with a focus on decision support features when integrated into a healthcare organization.
The Questionable Benefit of Medical Emergency Teams
Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. MERIT study investigators. Lancet. 2005;365:2091-2097.
Previous studies have reported that the MET system reduces the incidence of cardiac arrests, deaths, and unplanned ICU admissions. A MET is a preplanned group of healthcare practitioners who respond to acute patient deteriorations in hospitalized patients.
METs are usually identical to hospital code teams, with the exception that they respond prior to a patient’s developing cardiac arrest. This early response has been shown to significantly decrease unexpected hospital mortality in hospitals in the United States, Australia, and Great Britain. Even though the system has been reported since 1995, few hospitals have knowledge of or experience with METs.
Unexpected hospital deaths and cardiac arrests are often preceded by clinical warning signs. In addition, unplanned ICU admissions may be foreshadowed by abnormalities in the patient’s vital signs that may progress if appropriate interventions are not undertaken. METs assess patients with abnormal physical findings or when there is a concern about the patient’s condition. These patients have findings that may precede a serious event or cardiac arrest, but otherwise don’t meet existing criteria to call a code.
The theory is that if a MET responds to see a patient who is becoming unstable (see “Table 1: MET Calling Criteria,” at left), early interventions may reduce the likelihood of arrest. Published studies have shown a reduction in cardiac arrests and ICU length of stay in virtually all systems in which MET has been introduced (although most studies are hampered by the use of historical controls).
The MERIT study randomized 23 hospitals in Australia to continue functioning as usual (n=11) or to introduce a MET system (n=12). The study sites included a wide range of tertiary, metropolitan, and non-metropolitan hospitals in different states across Australia. The primary outcome was the composite of cardiac arrest, unexpected death, or unplanned ICU admission during the six-month study period after MET activation, using intention to treat analysis.
A four-month educational period was undertaken with the MET centers prior to initiation of the trial. Control hospitals did not receive any education about the MET concept. This was followed by a six-month trial period. Cardiac arrest teams were maintained at all hospitals. The MET consisted of at least one doctor and a nurse from the ED or ICU.
The eligible patients included those residing on a medical ward (including critical care units); the ICUs, OR, postoperative recovery areas, and ED areas were not regarded as general wards.
The primary outcome for the study was the composite outcome of the incidence (events divided by number of eligible patients admitted to the hospital and residing on a medical ward during the study period) of:
- Cardiac arrests without a pre-existing “not-for-resuscitation” (NFR) order;
- Unplanned ICU admissions; and
- Unexpected deaths (those without a pre-existing NFR order).
The results of the study:
- During the study period, the overall rate of calls for the cardiac arrest team or MET was significantly higher in intervention hospitals than in control hospitals. Calls not associated with events were more common in MET hospitals than in controls. Half of the total calls were not associated with a cardiac arrest or unexpected death, whereas in MET hospitals more than 80% of calls were not associated with a cardiac arrest or death (P<0.0001).
- In patients with documented MET calling criteria in association with cardiac arrest or unexpected death, the call rate was similar in MET and control hospitals.
- There were no significant differences between the MET and control hospitals for any outcome.
- The response to changes in vital signs was not adequate—even in MET centers.
These findings are surprising in view of previously reported findings using the MET system. Potential reasons for lack of difference between MET centers and controls include:
- Number of study sites or the duration of the study may not have been adequate for implementation or education;
- Hospitals may already be efficient in detecting and managing unstable patients;
- Patient selection criteria may have been overly restricted. For example, other studies have used 30 respirations per minute for tachypnea as a calling criterion compared with 36 breaths per minute used in this trial;
- Knowledge of the study may have leaked to control hospitals;
- Cardiac arrest teams function as METs at times: Nearly half of the calls to cardiac arrest teams in control hospitals were made without a cardiac arrest or unexpected death; and
- The selected outcomes may not be sensitive enough.
Even though this large, multicenter controlled trial was unable to show a significant benefit of METs, we should not be discouraged from performing further controlled trials in different settings. The use of METs is clearly an exciting and evolving area of medicine.
Barriers to Patient Safety
Amalberti R, Auroy Y, Berwick D, Barach P. Five system barriers to achieving ultrasafe health care. Ann Intern Med. 2005;142:756-764
Patient safety in our healthcare system is a growing concern. One area of dialogue concerning preventable healthcare-associated harms involves the comparability of the healthcare industry with non-medical industries, such as aviation and nuclear power, that have adapted successful strategies shown to provide ultrasafe environments. Amalberti, et al. discuss risk assessment in a variety of industries and explain the need for a benchmarking approach in order to optimize or achieve safety in the healthcare field.
The authors identify five systemic barriers from literature that are fundamentally connected to the ability of the healthcare field to achieve an extremely safe environment.
Barrier 1—acceptance of limitations on maximum performance: The first barrier is the type of expected performance in the field. This is illustrated by the tradeoffs associated with ultrasafety versus productivity. The amount of risk involved was directly related to the limits placed on maximum performance. The first barrier is the acceptance that every system has limits. When a producer exceeds their limit, then safety suffers. An example used is that of blood donation: The limits of collection speed are weighed against the needed screening process.
Barrier 2—abandonment of professional autonomy: The second barrier concerns the concept of professional autonomy. While more teamwork and regulations reduce individual autonomy, this appears to improve safety in the healthcare environment. The bottom line is the importance of teamwork. The example used is that of traffic on a highway: Autonomous units work together to function safely.
Barrier 3—transition from the mindset of craftsman to that of an equivalent actor: The third barrier to achieving high levels of safety includes an equivalent actor mindset. This entails establishing a reliable standard of excellent care in lieu of focusing on individuality, similar to the notion that passengers on an airline usually do not know their pilots, but have established confidence in the airline itself.
Barrier 4—the need for system-level arbitration to optimize safety strategies: The fourth barrier identified is a need for system-level arbitration to optimize safety strategies. This need results from the pressure for justice (usually through litigation) once an accident occurs. Top-down arbitration of safety will be less successful than system level design.
Barrier 5—the need to simplify professional rules and regulations: The final barrier results from the many of layers of guidelines as they serve to create an environment of excellence. This barrier necessitates the removal of these layers to simplify the environment. Existing guidelines should be distilled down to those shown to promote quality and safety. Byzantine rules can obscure the goal of safety and glorify rules, for rules sake.
Certain structural limitations within the field, such as worker shortages in the face of increasing public demands and the reliance of the field on trainees such as students, interns, and residents, create other hurdles. The authors conclude by suggesting a two-tiered system of healthcare whereby ultrasafety could be more easily accomplished in areas of medicine considered more stable (first tier), and a second tier of care that would include the more unstable conditions, and thus inherently, represent the higher risk situations where errors are more likely to occur.
Another provocative point of this article is the need to move toward educating and training teams—not individuals.
The Importance of Implementing COPD Guidelines
Harvey PA, Murphy MC, Dornom E, et al. Implementing evidence-based guidelines: inpatient management of chronic obstructive pulmonary disease. Intern Med J. 2005;35:151-155.
COPD is a common diagnosis that sometimes requires hospitalization. Evidence-based guidelines for disease management, including that of hospitalized patients, exist, but there is a paucity of knowledge about the actual quality of care delivered in the hospital as it aligns with published guidelines. This study by Harvey, et al. explores the quality of care delivered in the hospital for patients with COPD, while at the same time investigating an intervention for the medical staff in an effort to improve adherence to evidenced-based guidelines of the disease.
Using ICD-10 codes for a COPD diagnosis, the study incorporated a retrospective chart review of 49 hospital admissions prior to the intervention and 35 admissions after the intervention in a hospital in Melbourne, Australia. Data were collected pertaining to the hospital management of COPD as it compared with what the authors considered to be Level A—or the highest level of evidence summarized from several professional organizations. The intervention delivered to the medical staff included a summarized presentation of the results from the initial audit of the 49 charts, as well as an educational package that was given to them following the presentation.
Except for inappropriate use of intravenous aminophylline, of which there was a 100% concordance to Level A guidelines, the initiation of systemic steroids (intravenous and/or oral) had the highest concordance rate of 80% and 83%, pre- and postintervention respectively. Appropriate steroid duration (seven to 14 days) had the lowest concordance rates at 10% and 29%, pre- and postintervention respectively.
In addition, preintervention concordance (10%) involving steroid duration was the only rate considered significantly different in the postintervention group (29%). While concordance rates were high for the use of any type of nebulized bronchodilator (96% preintervention and 80% postintervention), the Level A guidelines the authors used suggested that beta-agonist bronchodilators should be used alone prior to the initiation of ipratropium bromide. The concordance rates for this guideline were 27% preintervention and 34% postintervention.
Largely, the authors felt their intervention failed to improve concordance rates to the Level A guidelines investigated and also that their findings of variable and lower concordance rates across the board corroborated other similar studies. The major weaknesses of this study included the small sample size and the nonrandomness of the sampling.
In addition, the authors report that the particular hospital studied included junior doctors who rotated on and off service, which likely prevented the effects of the intervention from being measured on a provider level. In spite of the weaknesses in the study, the article brings to light the need for a more effective translation of evidence-based guidelines to actual practice, especially in the practice of COPD management in the hospital. Further methods of guideline implementation in the clinic setting must be elucidated to improve the care patients with COPD receive in the hospital.
Not all Troponin Elevations Are Myocardial Infarctions
Jeremais A, Gibson CM. Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med. 2005;142:786-791.
Troponins are regulatory proteins that control the calcium-mediated interaction of actin and myosin during muscle contraction. All muscle tissue contains troponins, but cardiac troponin T and I have amino acid sequences that are different from skeletal and smooth muscle troponins, allowing them to be detectable by monoclonal antibody-based assays.
In the event of reversible or irreversible cell damage—or possibly even from transiently increased cell membrane permeability—cardiac troponins are released from myocytes into circulation. This characteristic provides a sensitive test for detecting myocardial injury and damage; however, this test is not specific for acute coronary syndromes. And any disorder that causes myocyte damage may cause an elevated troponin.
The 2002 American College of Cardiology/American Heart Association practice guidelines for unstable angina and non-ST-segment elevation myocardial infarction acknowledge that the myocardial necrosis signified by troponin elevation may not necessarily be caused by atherosclerotic coronary artery disease. Such nonthrombotic troponin elevation can be caused by four basic mechanisms, as discussed by Dr. Jeremias and Dr. Gibson.
- Demand ischemia refers to a mismatch between myocardial oxygen demand and supply in the absence of flow-limiting epicardial stenosis. Conditions such as sepsis or septic shock and the systemic inflammatory response syndrome, hypotension or hypovolemia, tachyarrhythmias, and left ventricular hypertrophy can all cause release of cardiac troponin.
- Myocardial ischemia in the absence of fixed obstructive coronary disease can be caused by coronary vasospasm, acute stroke or intracranial hemorrhage, and ingestion of sympathomimetics.
- Direct myocardial damage can be seen in cardiac contusion, direct current cardioversion, cardiac infiltrative disorders such as amyloidosis, certain chemotherapy agents, myocarditis, pericarditis, and cardiac transplantation.
- Myocardial strain occurs when volume and pressure overload of the left and/or right ventricle cause excessive wall tension. Congestive heat failure, acute pulmonary embolism, and chronic pulmonary hypertension can lead to myocardial strain and troponin elevation.
Another condition that can lead to persistently elevated cardiac troponins is end-stage renal disease. This elevation may be due to small areas of clinically silent myocardial necrosis, an increased left ventricular mass, or possibly from impaired renal troponin excretion. Although troponins are believed to be cleared by the reticuloendothelial system, recent evidence shows that troponin T is fragmented into molecules that are small enough to be renally excreted.
In summary, elevated troponin can be found in many clinical settings and is associated with impaired short- and long-term survival. TH
Classic Literature
The HATEFUL Patient
Every physician has groaned internally when seeing a certain patient’s name on his list, going out of her way to avoid a particular family, or getting hopelessly engaged and increasingly enraged in a battle over a “lost” narcotic prescription. There are certain patients with whom a doctor-patient relationship feels more like a contest than a partnership. These interactions make a physician’s daily practice difficult, and they may wreak havoc among the staff on an inpatient ward. These patients grow ever more intolerable to their caregivers, who often harbor a wish to simply make them disappear.
In his landmark 1978 article “Taking Care of the Hateful Patient,” (NEJM, 298:883-887) James Groves, MD, discussed the characteristics of these difficult patients and the sometimes difficult emotions they generate in their caregivers. He described four different groups of patients, using an illustrative case for each, and discussed the ways in which these patients’ often maddening behavior serves to mitigate their profound dependency.
Dependent clingers are those patients whose neediness is overt, who seem to regard the physician as a sow with teats to spare. Dr. Groves suggested early, firm limit-setting with these patients to prevent the formation and later shattering of the patient’s illusion of the physician as inexhaustible.
Dependency lies at the heart of an entitled demander’s behavior as well, but their fear of abandonment is expressed as hostility and arrogance rather than overt neediness. Affirming to the patient that you share in their quest for the good (but not perfect) medical care to which they are entitled allows patient and physician to rally around a common goal.
This strategy backfires with manipulative help-rejecters, who seem almost pleased to report to their physician each time they fail a new treatment attempt. Overtly expressing some doubt that the treatment will completely cure all the patient’s difficulties and providing regular follow up are recommended for this group. These strategies relieve the patient of the unconscious anxiety that he may be abandoned by his physician should his symptoms abate.
Self-destructive deniers make the physician feel powerless as they persist in behavior that undermines all efforts to improve their health. With these patients, viewing their behavior as a terminal illness and managing symptoms and exacerbations accordingly allows the physician to focus on caring for the patient without unrealistic expectations of cure on the one hand and judgmental indifference on the other.
After discussing each of these groups, Dr. Groves concluded the article by suggesting that perhaps the greatest challenge physicians face in caring for these difficult patients is the temptation to disown the negative feelings they engender. He wrote that this effort not only strains the doctor’s limits, but also wastes valuable clinical data unmasked by these feelings—data that could inform clinical care. For decades prior to Dr. Groves’ article, psychoanalysts had reflected on what Freud termed “countertransference,” or the physician’s internal emotional reaction to a patient.
In his article “Hate in the Counter-Transference,” D.W. Winnicott, MD, suggested that rather than accepting the guilt that these feelings typically engender in a caregiver, negative countertransference reactions should be regarded by the physician as valuable information in understanding the patient’s psychic world. By training and by disposition, however, most physicians considered (and continue to consider) these emotions inappropriate. They seemingly negate the sympathy, kindness, and commitment to the patient’s well-being that should be central to a physician’s vocation. Conventional wisdom held that denying the feelings was the only proper response, and if that proved impossible, transferring the patient to a willing colleague was usually recommended. In contrast, Dr. Groves freed the physician to use these feelings to improve patient care.
Now a classic and oft-cited work, “Taking Care of the Hateful Patient” distills a wealth of analytic insight into a structure and language comprehensible to the busy generalist. By explaining the reactions each group of patients induces in their physicians, Dr. Groves provides useful tools to understand a particular patient’s psychology. Suggestions for strategic approaches to each category of patient are easy to understand and to adapt to one’s own practice. He explains how judicious limit-setting can be as valuable for the patient as it is for the doctor. Perhaps most helpful is his description of the needs of these patients that lie beneath their “hateful” exterior. Armed with this understanding, a physician can reclaim the empathy that is often so elusive with these patients.—Sandra Rackley MD, Kemuel Philbrick, MD
A review of staphylococcal Endocarditis
VG Fowler Jr, Miro JM, Hoen B, et al for the ICE Investigators. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA. 2005;June 22;293(24):3061-3062.
Agroup of infectious diseases experts from centers throughout the world formed the International Collaboration on Endocarditis (ICE) in 1999 to gain a global understanding of infective endocarditis. Using the Duke Criteria patients with definite infective endocarditis in a prospective manner, 275 variables were reported with these cases to a central database maintained at Duke University. The ICE-Prospective Cohort Study (ICE-PCS) enrolled 1,779 patients with infective endocarditis in 39 centers in 16 countries between June 15, 2000, and December 31, 2003, and has been described in a recent report. (Cabell CH, Abrutyn E. Infect Dis Clin North Am. 2002;16:255-72). Staphylococcus aureus was the most common cause of infective endocarditis in this group of patients (n=558; 31.6%); the authors characterized risk factors and clinical issues associated with these cases in this report.
By univariate analysis, compared with non-Staphylococcus aureus infective endocarditis, patients with infective endocarditis due to Staphylococcus aureus were more likely than patients with infective endocarditis due to other pathogens to be female (P<0.001), hemodialysis dependent (P<0.001), have diabetes mellitus (P=0.009), have other chronic illnesses (P<0.001), have a healthcare association (P<0.001), have higher rates of stroke (P<0.001), have systemic embolization (P<0.001), have persistent bacteremia (P<0.001), or die (P<0.001).
Although healthcare associated Staphylococcus aureus infective endocarditis was the most common form of Staphylococcus aureus infective endocarditis, more than 60% of healthcare-associated patients acquired the infection outside the hospital. This reflects the global trend in healthcare delivery patterns favoring ambulatory treatment (e.g., outpatient medication infusion via long-term IV access, hemodialysis)
Multivariate analysis, clinical features independently associated with Staphylococcus aureus infective endocarditis (versus non-Staphylococcus aureus infective endocarditis) were: IV drug use (OR, 9.3; 95% CI, 6.3-13.7); first clinical presentation less than one month after first symptoms (OR, 5.1; 95% CI, 3.2-8.2); healthcare-associated infection (OR, 2.9; 95% CI, 2.1-3.8), persistent bacteremia (OR, 2.3; 95% CI, 1.5-3.8), presence of a presumed intravascular device source (OR, 1.7; 95% CI, 1.2-2.6), stroke (OR, 1.6; 95% CI, 1.2-2.3), or diabetes mellitus (OR, 1.3; 95% CI, 1.1-1.8).
Patients from the United States with Staphylococcus aureus infective endocarditis were more likely to be hemodialysis-dependent, to be diabetic, to have a hemodialysis fistula or a chronic indwelling central catheter as a presumed source of infection, and to have a non-nosocomial healthcare association. Patients from the United States and Brazil were more likely to have Methicillin-resistant Staphyloccocus aureus (MRSA) than were patients from Europe, the Middle East, Australia, or New Zealand. In-hospital mortality rates were similar across regions, although American patients were significantly more likely to develop persistent bacteremia (25.6%, P<0.001).
Characteristics independently associated with mortality among patients with nonintravenous drug-use-associated Staphylococcus aureus infective endocarditis by multivariate analysis included stroke (OR, 3.67; 95% CI, 1.94-6.94), persistent bacteremia (OR, 3.06; 95% CI, 1.75-5.35), diagnosis in Southern Europe or the Middle East (OR, 3.21; 95% CI, 1.17-10.56).
This study establishes Staphylococcus aureus infective endocarditis as the leading cause of infective endocarditis in many regions of the world and spotlights the global emergence of healthcare contact as a risk factor for Staphylococcus aureus infective endocarditis. In a significant portion of these patients, an IV device was the presumed source of bacteremia; prosthetic cardiac devices (pacemakers, defibrillators, or prosthetic cardiac valves) were present in almost one-quarter of the patients.
MRSA was a significant cause of Staphylococcus aureus infective endocarditis and displayed regional variation, accounting for almost 40% of the infective endocarditis caused by Staphylococcus aureus in some regions. Patients with infective endocarditis caused by MRSA were significantly more likely to have pre-existing chronic conditions and healthcare associated infective endocarditis by both univariate and multivariate analysis. They also were often associated with persistent bacteremia. On the other hand, 20% of patients with MRSA infective endocarditis developed their infection in the absence of identifiable healthcare contact.
Limitations of this report include the fact that this is an observational study of patients from self-selected centers. Each center most likely represents a portion of the local population, making it difficult to generalize findings to the entire population centers from which this report originates. Represented hospitals were typically referral centers that have cardiac surgery programs and may have widely differing populations with varied risk factors. Advantages include the large size of this prospectively evaluated cohort and the ability to analyze regional variations between continents with a contemporary nature of the patient sample (2000-2003).
Infectious Endocarditis in Olmsted County, Minn.
Tleyjeh IM, Steckelberg JM, Murad HS, et al. Temporal trends in infective endocarditis: a population-based study in Olmsted County, Minnesota. JAMA. 2005;293:3022-3028.
Tleyjeh and colleagues at the Mayo Clinic in Rochester, Minn., retrospectively studied 102 cases of infective endocarditis that occurred in 107 Olmsted County residents from 1970-2000. Main outcome measures were incidence of infective endocarditis, proportion of patients with underlying heart disease and causative micro-organisms and clinical characteristics. The records of all Olmsted County residents with infective endocarditis were identified and reviewed in detail. The definite and possible infective endocarditis cases as defined by modified Duke Criteria were used in the analysis.
The age- and gender-adjusted incidence of infective endocarditis ranged from 5.0 to 7.0 cases per 100,000 person-years during the study period and did not change significantly over time. There were 84 (79%) cases of native valve infective endocarditis and 23 (21%) cases of prosthetic valve infective endocarditis. Valves involved: aortic—36 (24%); mitral—49 (46%), aortic and mitral—12 (11%), right-sided or bilateral—8 (7%), or unknown—8 (7%). 16 (15%) had valve surgery within 42 days and the six-month mortality was 26% (n=28).
Infective endocarditis is a disease of the older individual in this population, with a mean age ranging from 54.1 years in 1980-1984 to 67.4 years in 1995-2000 (P=0.24 for trend). There was a male predominance (67%-83%), which did not significantly change over time.
Mitral valve prolapse was the most frequent underlying valvular heart disease. Viridans streptococci were the most common causative organisms (n=47; 44%) followed by Staphylococcus aureus (n=28 cases; 26%).
The overall average crude infective endocarditis incidence of the period 1970-2000 was 4.95 per 100,000 person-years. The age- and gender-adjusted annual incidence was 6.06 per 100,000 (95% CI, 4.89-7.22). There was no time trend for either streptococcus or Staphylococcus aureus infective endocarditis: the annual adjusted incidence of viridans group streptococcal infective endocarditis was 1.7 to 3.5 cases per 100,000 person years while Staphylococcus aureus infective endocarditis had an annual adjusted incidence of 1.0-2.2 cases per 100,000. The incidence rates of viridans group streptococcal and Staphylococcus aureus infective endocarditis have not changed significantly over time in this population.
Potential limitations of this study include possible incomplete case finding or recognition of the retrospective nature of the case reviews. The homogeneity of the patient population studied (primarily elderly white males with a low prevalence of intravenous drug use) limits the ability to generalize the results. Advantages include the fact that this is a population-based study at a medical center with detailed medical records of virtually all residents of a single county. This allows us to view the clinical features and etiologic factors of primarily left-sided infective endocarditis without the referral bias that tends to taint other studies typically published out of large medical centers with larger geographic referral bases.
Computers and Adverse Drug Events
Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of adverse drug events in a highly computerized hospital. Arch Intern Med. 2005;165:1111-1116.
Adverse drug events account for a significant number of hospital admissions and the ensuing costs associated with these hospitalizations. Electronic endeavors, such as computerized physician order entry (CPOE), bar code systems, and electronic medical records attempt to reduce the preventable adverse drug events.
Nebeker, et al. attempted to assess the effects of the implementation of CPOE and other computerized medication systems on adverse drug events in a tertiary care Veterans Administration Medical Center. They used an observational study design whereby 937 out of 2,306 newly admitted patients from several hospital wards were randomly chosen and assigned to a pharmacist reviewer during a 20-week period.
They reviewed complete medical records of hospital stays every other day to document adverse drug events. Not only were traditional adverse drug events identified, but harm from overdoses and/or inappropriate dose reductions or discontinuations, as well as intolerable harm from dose titration, were documented as adverse drug events. The harms caused by the drugs were considered only if the drugs were started in the hospital.
Harms were classified based on prior literature and included standards for pharmacological typology, causality assessment, error type, event terminology, drug class, seriousness index, and medication error category indexing. Additional uncommon classifications were also used, including additional resource utilization. Consensus meetings were held weekly to confirm classification of adverse drug events. Of the admissions reviewed, 483 adverse drug events were identified of which 93% were drug reactions while 7% were due to over- or underdosing. Of the drug reactions, 90% were considered dose-dependent while 10% were considered to be idiosyncratic.
Two different indexing scales were used in classifying the harms. Using the LDS Hospital Scale, it was suggested that 91% of the adverse drug events caused moderate harm while 9% caused serious harm. Using the National Coordinating Council for Medication Error Reporting and Prevention indexing, it was suggested that 87% of the adverse drug events fell into category E (requiring treatment) and 4% into category F (requiring prolonged hospitalization). Twenty-seven percent of the total adverse drug events were thought to be due to errors, including execution and planning steps. Sixty-one percent of errors occurred with the ordering mechanism while 25% of the errors occurred in the monitoring process.
This study highlighted rates of adverse drug events five to 19 times higher than baseline. The authors explained this higher-than-expected rate in part by study elements, such as the use of clinical pharmacists as reviewers, iterative case reviews, and accessible electronic data that make adverse drug events more noticeable.
Weaknesses of this study included issues of comparability of CPOEs because there were significant feature differences among commercial software programs. In addition, this was an observational study lacking a control group. The authors felt that their study did not support the idea that the computerized patient record of the study institution had caused adverse drug events. Rather, the study supported the idea that the system increased the visibility of adverse drug events compared with a paper system. In addition, the authors recommended that the choice of CPOEs be carefully considered, with a focus on decision support features when integrated into a healthcare organization.
The Questionable Benefit of Medical Emergency Teams
Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. MERIT study investigators. Lancet. 2005;365:2091-2097.
Previous studies have reported that the MET system reduces the incidence of cardiac arrests, deaths, and unplanned ICU admissions. A MET is a preplanned group of healthcare practitioners who respond to acute patient deteriorations in hospitalized patients.
METs are usually identical to hospital code teams, with the exception that they respond prior to a patient’s developing cardiac arrest. This early response has been shown to significantly decrease unexpected hospital mortality in hospitals in the United States, Australia, and Great Britain. Even though the system has been reported since 1995, few hospitals have knowledge of or experience with METs.
Unexpected hospital deaths and cardiac arrests are often preceded by clinical warning signs. In addition, unplanned ICU admissions may be foreshadowed by abnormalities in the patient’s vital signs that may progress if appropriate interventions are not undertaken. METs assess patients with abnormal physical findings or when there is a concern about the patient’s condition. These patients have findings that may precede a serious event or cardiac arrest, but otherwise don’t meet existing criteria to call a code.
The theory is that if a MET responds to see a patient who is becoming unstable (see “Table 1: MET Calling Criteria,” at left), early interventions may reduce the likelihood of arrest. Published studies have shown a reduction in cardiac arrests and ICU length of stay in virtually all systems in which MET has been introduced (although most studies are hampered by the use of historical controls).
The MERIT study randomized 23 hospitals in Australia to continue functioning as usual (n=11) or to introduce a MET system (n=12). The study sites included a wide range of tertiary, metropolitan, and non-metropolitan hospitals in different states across Australia. The primary outcome was the composite of cardiac arrest, unexpected death, or unplanned ICU admission during the six-month study period after MET activation, using intention to treat analysis.
A four-month educational period was undertaken with the MET centers prior to initiation of the trial. Control hospitals did not receive any education about the MET concept. This was followed by a six-month trial period. Cardiac arrest teams were maintained at all hospitals. The MET consisted of at least one doctor and a nurse from the ED or ICU.
The eligible patients included those residing on a medical ward (including critical care units); the ICUs, OR, postoperative recovery areas, and ED areas were not regarded as general wards.
The primary outcome for the study was the composite outcome of the incidence (events divided by number of eligible patients admitted to the hospital and residing on a medical ward during the study period) of:
- Cardiac arrests without a pre-existing “not-for-resuscitation” (NFR) order;
- Unplanned ICU admissions; and
- Unexpected deaths (those without a pre-existing NFR order).
The results of the study:
- During the study period, the overall rate of calls for the cardiac arrest team or MET was significantly higher in intervention hospitals than in control hospitals. Calls not associated with events were more common in MET hospitals than in controls. Half of the total calls were not associated with a cardiac arrest or unexpected death, whereas in MET hospitals more than 80% of calls were not associated with a cardiac arrest or death (P<0.0001).
- In patients with documented MET calling criteria in association with cardiac arrest or unexpected death, the call rate was similar in MET and control hospitals.
- There were no significant differences between the MET and control hospitals for any outcome.
- The response to changes in vital signs was not adequate—even in MET centers.
These findings are surprising in view of previously reported findings using the MET system. Potential reasons for lack of difference between MET centers and controls include:
- Number of study sites or the duration of the study may not have been adequate for implementation or education;
- Hospitals may already be efficient in detecting and managing unstable patients;
- Patient selection criteria may have been overly restricted. For example, other studies have used 30 respirations per minute for tachypnea as a calling criterion compared with 36 breaths per minute used in this trial;
- Knowledge of the study may have leaked to control hospitals;
- Cardiac arrest teams function as METs at times: Nearly half of the calls to cardiac arrest teams in control hospitals were made without a cardiac arrest or unexpected death; and
- The selected outcomes may not be sensitive enough.
Even though this large, multicenter controlled trial was unable to show a significant benefit of METs, we should not be discouraged from performing further controlled trials in different settings. The use of METs is clearly an exciting and evolving area of medicine.
Barriers to Patient Safety
Amalberti R, Auroy Y, Berwick D, Barach P. Five system barriers to achieving ultrasafe health care. Ann Intern Med. 2005;142:756-764
Patient safety in our healthcare system is a growing concern. One area of dialogue concerning preventable healthcare-associated harms involves the comparability of the healthcare industry with non-medical industries, such as aviation and nuclear power, that have adapted successful strategies shown to provide ultrasafe environments. Amalberti, et al. discuss risk assessment in a variety of industries and explain the need for a benchmarking approach in order to optimize or achieve safety in the healthcare field.
The authors identify five systemic barriers from literature that are fundamentally connected to the ability of the healthcare field to achieve an extremely safe environment.
Barrier 1—acceptance of limitations on maximum performance: The first barrier is the type of expected performance in the field. This is illustrated by the tradeoffs associated with ultrasafety versus productivity. The amount of risk involved was directly related to the limits placed on maximum performance. The first barrier is the acceptance that every system has limits. When a producer exceeds their limit, then safety suffers. An example used is that of blood donation: The limits of collection speed are weighed against the needed screening process.
Barrier 2—abandonment of professional autonomy: The second barrier concerns the concept of professional autonomy. While more teamwork and regulations reduce individual autonomy, this appears to improve safety in the healthcare environment. The bottom line is the importance of teamwork. The example used is that of traffic on a highway: Autonomous units work together to function safely.
Barrier 3—transition from the mindset of craftsman to that of an equivalent actor: The third barrier to achieving high levels of safety includes an equivalent actor mindset. This entails establishing a reliable standard of excellent care in lieu of focusing on individuality, similar to the notion that passengers on an airline usually do not know their pilots, but have established confidence in the airline itself.
Barrier 4—the need for system-level arbitration to optimize safety strategies: The fourth barrier identified is a need for system-level arbitration to optimize safety strategies. This need results from the pressure for justice (usually through litigation) once an accident occurs. Top-down arbitration of safety will be less successful than system level design.
Barrier 5—the need to simplify professional rules and regulations: The final barrier results from the many of layers of guidelines as they serve to create an environment of excellence. This barrier necessitates the removal of these layers to simplify the environment. Existing guidelines should be distilled down to those shown to promote quality and safety. Byzantine rules can obscure the goal of safety and glorify rules, for rules sake.
Certain structural limitations within the field, such as worker shortages in the face of increasing public demands and the reliance of the field on trainees such as students, interns, and residents, create other hurdles. The authors conclude by suggesting a two-tiered system of healthcare whereby ultrasafety could be more easily accomplished in areas of medicine considered more stable (first tier), and a second tier of care that would include the more unstable conditions, and thus inherently, represent the higher risk situations where errors are more likely to occur.
Another provocative point of this article is the need to move toward educating and training teams—not individuals.
The Importance of Implementing COPD Guidelines
Harvey PA, Murphy MC, Dornom E, et al. Implementing evidence-based guidelines: inpatient management of chronic obstructive pulmonary disease. Intern Med J. 2005;35:151-155.
COPD is a common diagnosis that sometimes requires hospitalization. Evidence-based guidelines for disease management, including that of hospitalized patients, exist, but there is a paucity of knowledge about the actual quality of care delivered in the hospital as it aligns with published guidelines. This study by Harvey, et al. explores the quality of care delivered in the hospital for patients with COPD, while at the same time investigating an intervention for the medical staff in an effort to improve adherence to evidenced-based guidelines of the disease.
Using ICD-10 codes for a COPD diagnosis, the study incorporated a retrospective chart review of 49 hospital admissions prior to the intervention and 35 admissions after the intervention in a hospital in Melbourne, Australia. Data were collected pertaining to the hospital management of COPD as it compared with what the authors considered to be Level A—or the highest level of evidence summarized from several professional organizations. The intervention delivered to the medical staff included a summarized presentation of the results from the initial audit of the 49 charts, as well as an educational package that was given to them following the presentation.
Except for inappropriate use of intravenous aminophylline, of which there was a 100% concordance to Level A guidelines, the initiation of systemic steroids (intravenous and/or oral) had the highest concordance rate of 80% and 83%, pre- and postintervention respectively. Appropriate steroid duration (seven to 14 days) had the lowest concordance rates at 10% and 29%, pre- and postintervention respectively.
In addition, preintervention concordance (10%) involving steroid duration was the only rate considered significantly different in the postintervention group (29%). While concordance rates were high for the use of any type of nebulized bronchodilator (96% preintervention and 80% postintervention), the Level A guidelines the authors used suggested that beta-agonist bronchodilators should be used alone prior to the initiation of ipratropium bromide. The concordance rates for this guideline were 27% preintervention and 34% postintervention.
Largely, the authors felt their intervention failed to improve concordance rates to the Level A guidelines investigated and also that their findings of variable and lower concordance rates across the board corroborated other similar studies. The major weaknesses of this study included the small sample size and the nonrandomness of the sampling.
In addition, the authors report that the particular hospital studied included junior doctors who rotated on and off service, which likely prevented the effects of the intervention from being measured on a provider level. In spite of the weaknesses in the study, the article brings to light the need for a more effective translation of evidence-based guidelines to actual practice, especially in the practice of COPD management in the hospital. Further methods of guideline implementation in the clinic setting must be elucidated to improve the care patients with COPD receive in the hospital.
Not all Troponin Elevations Are Myocardial Infarctions
Jeremais A, Gibson CM. Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med. 2005;142:786-791.
Troponins are regulatory proteins that control the calcium-mediated interaction of actin and myosin during muscle contraction. All muscle tissue contains troponins, but cardiac troponin T and I have amino acid sequences that are different from skeletal and smooth muscle troponins, allowing them to be detectable by monoclonal antibody-based assays.
In the event of reversible or irreversible cell damage—or possibly even from transiently increased cell membrane permeability—cardiac troponins are released from myocytes into circulation. This characteristic provides a sensitive test for detecting myocardial injury and damage; however, this test is not specific for acute coronary syndromes. And any disorder that causes myocyte damage may cause an elevated troponin.
The 2002 American College of Cardiology/American Heart Association practice guidelines for unstable angina and non-ST-segment elevation myocardial infarction acknowledge that the myocardial necrosis signified by troponin elevation may not necessarily be caused by atherosclerotic coronary artery disease. Such nonthrombotic troponin elevation can be caused by four basic mechanisms, as discussed by Dr. Jeremias and Dr. Gibson.
- Demand ischemia refers to a mismatch between myocardial oxygen demand and supply in the absence of flow-limiting epicardial stenosis. Conditions such as sepsis or septic shock and the systemic inflammatory response syndrome, hypotension or hypovolemia, tachyarrhythmias, and left ventricular hypertrophy can all cause release of cardiac troponin.
- Myocardial ischemia in the absence of fixed obstructive coronary disease can be caused by coronary vasospasm, acute stroke or intracranial hemorrhage, and ingestion of sympathomimetics.
- Direct myocardial damage can be seen in cardiac contusion, direct current cardioversion, cardiac infiltrative disorders such as amyloidosis, certain chemotherapy agents, myocarditis, pericarditis, and cardiac transplantation.
- Myocardial strain occurs when volume and pressure overload of the left and/or right ventricle cause excessive wall tension. Congestive heat failure, acute pulmonary embolism, and chronic pulmonary hypertension can lead to myocardial strain and troponin elevation.
Another condition that can lead to persistently elevated cardiac troponins is end-stage renal disease. This elevation may be due to small areas of clinically silent myocardial necrosis, an increased left ventricular mass, or possibly from impaired renal troponin excretion. Although troponins are believed to be cleared by the reticuloendothelial system, recent evidence shows that troponin T is fragmented into molecules that are small enough to be renally excreted.
In summary, elevated troponin can be found in many clinical settings and is associated with impaired short- and long-term survival. TH
Classic Literature
The HATEFUL Patient
Every physician has groaned internally when seeing a certain patient’s name on his list, going out of her way to avoid a particular family, or getting hopelessly engaged and increasingly enraged in a battle over a “lost” narcotic prescription. There are certain patients with whom a doctor-patient relationship feels more like a contest than a partnership. These interactions make a physician’s daily practice difficult, and they may wreak havoc among the staff on an inpatient ward. These patients grow ever more intolerable to their caregivers, who often harbor a wish to simply make them disappear.
In his landmark 1978 article “Taking Care of the Hateful Patient,” (NEJM, 298:883-887) James Groves, MD, discussed the characteristics of these difficult patients and the sometimes difficult emotions they generate in their caregivers. He described four different groups of patients, using an illustrative case for each, and discussed the ways in which these patients’ often maddening behavior serves to mitigate their profound dependency.
Dependent clingers are those patients whose neediness is overt, who seem to regard the physician as a sow with teats to spare. Dr. Groves suggested early, firm limit-setting with these patients to prevent the formation and later shattering of the patient’s illusion of the physician as inexhaustible.
Dependency lies at the heart of an entitled demander’s behavior as well, but their fear of abandonment is expressed as hostility and arrogance rather than overt neediness. Affirming to the patient that you share in their quest for the good (but not perfect) medical care to which they are entitled allows patient and physician to rally around a common goal.
This strategy backfires with manipulative help-rejecters, who seem almost pleased to report to their physician each time they fail a new treatment attempt. Overtly expressing some doubt that the treatment will completely cure all the patient’s difficulties and providing regular follow up are recommended for this group. These strategies relieve the patient of the unconscious anxiety that he may be abandoned by his physician should his symptoms abate.
Self-destructive deniers make the physician feel powerless as they persist in behavior that undermines all efforts to improve their health. With these patients, viewing their behavior as a terminal illness and managing symptoms and exacerbations accordingly allows the physician to focus on caring for the patient without unrealistic expectations of cure on the one hand and judgmental indifference on the other.
After discussing each of these groups, Dr. Groves concluded the article by suggesting that perhaps the greatest challenge physicians face in caring for these difficult patients is the temptation to disown the negative feelings they engender. He wrote that this effort not only strains the doctor’s limits, but also wastes valuable clinical data unmasked by these feelings—data that could inform clinical care. For decades prior to Dr. Groves’ article, psychoanalysts had reflected on what Freud termed “countertransference,” or the physician’s internal emotional reaction to a patient.
In his article “Hate in the Counter-Transference,” D.W. Winnicott, MD, suggested that rather than accepting the guilt that these feelings typically engender in a caregiver, negative countertransference reactions should be regarded by the physician as valuable information in understanding the patient’s psychic world. By training and by disposition, however, most physicians considered (and continue to consider) these emotions inappropriate. They seemingly negate the sympathy, kindness, and commitment to the patient’s well-being that should be central to a physician’s vocation. Conventional wisdom held that denying the feelings was the only proper response, and if that proved impossible, transferring the patient to a willing colleague was usually recommended. In contrast, Dr. Groves freed the physician to use these feelings to improve patient care.
Now a classic and oft-cited work, “Taking Care of the Hateful Patient” distills a wealth of analytic insight into a structure and language comprehensible to the busy generalist. By explaining the reactions each group of patients induces in their physicians, Dr. Groves provides useful tools to understand a particular patient’s psychology. Suggestions for strategic approaches to each category of patient are easy to understand and to adapt to one’s own practice. He explains how judicious limit-setting can be as valuable for the patient as it is for the doctor. Perhaps most helpful is his description of the needs of these patients that lie beneath their “hateful” exterior. Armed with this understanding, a physician can reclaim the empathy that is often so elusive with these patients.—Sandra Rackley MD, Kemuel Philbrick, MD
PEDIATRIC SPECIAL SECTION: Sibling Rivalry
In the flourishing metropolitan area of Atlanta, hospitalists and community-based physicians at Children’s Healthcare of Atlanta thrive within their niches, riding waves of opportunity fueled by the region’s burgeoning population. Jay Berkelhamer, MD, senior vice president of medical affairs at Children’s Healthcare of Atlanta calls his city “one of the most dynamic growth centers in the United States. Within 10 years we are estimated to have at least 150,000 more kids in Atlanta, leading to even greater opportunities for hospitalists and private practice primary care and specialty pediatricians.”
Two Hospitals, One system
Children’s Hospital of Atlanta’s hospitalist program is, in fact, two separate programs: one at Egleston, the other at Scottish Rite. The parent organization links the two and manages each hospital’s mission, structure, hiring, compensation, and outcomes.

—David Hall, MD
The six Egleston full-time equivalent hospitalists, or “cat herders,” as Corinne Taylor, MD, Egleston’s chief of medical affairs, describes them, are employees of Emory University Medical School. Most Egleston hospitalists are parents of young children and work four days a week, allowing them a balance of career and family life. Employed by the medical school and working at an academic medical center, they receive a salary, benefits, and other support services. Side by side with interns and residents, Egleston’s hospitalists see Atlanta’s sickest, frailest, and most at-risk children: the uninsured, underinsured immigrant and local population.
At Egleston the pediatric hospitalists are like their counterparts who treat adult patients in other settings. They deal with many patients with chronic conditions that lead to repeat hospitalizations.
“We see lots of ex-preemies with multiple problems such as asthma, seizures, cerebral palsy, and gastric problems,” says Dr. Taylor. “Some are ventilator-dependent and need lots of care.”
She relishes the clinical discipline that being a hospitalist at an academic medical center presents. “I do my homework every day and enjoy the stimulation of teaching our house officers,” explains Dr. Taylor. “Working with adult learners on the chronic conditions we manage and the cases with puzzling symptoms is exciting.”
Dr. Taylor’s boss is this hospitalist program’s founder, Joseph Snitzer, MD (see “Joseph Snitzer, MD: A hospital medicine pioneer”). Being hospital-based frees Dr. Snitzer to observe an endless parade of clinical challenges, including complex rheumatology cases, lupus, tumors, infected shunts, seizures, exotic infections, oncology diagnoses, and more.
“People call us from rural hospitals and private practices for help with diagnoses,” explains Dr. Snitzer. “We’re not smarter than anyone else. We just see a lot more than most other physicians.”
Scottish Rite
Across town at Scottish Rite, a nonprofit hospital, the hospitalists cope with the demands of a steady influx of new Atlantans. David Hall, MD, is Scottish Rite’s medical director. He was a former Egleston hospitalist and a private practitioner for 10 years in Baltimore before he relocated to Atlanta.
“We don’t have house officers, and there is a resident on call only one night a week,” says Dr. Hall. “Pediatricians in the community need to have their patients admitted 24/7, and we also have to admit from the emergency department at night. With our hospitalists taking calls at night and working all the next day, sometimes they would be on for 36 hours straight. As our service has grown, we’ve realized that this model was not sustainable.”
To reduce the burnout from their growing patient loads, the hospitalists changed their model. As of August 1, 2005, hospitalists at Scottish Rite began working either eight- or 12-hour shifts.
“Until we gain some experience with the shift system, we know we will struggle with continuity and handoffs,” adds Dr. Hall. Scottish Rite is also increasing its complement of moonlighting private practice pediatricians who want to keep their hospital skills current by covering the heavy workload.
Dr. Hall says recruiting new hospitalists isn’t a problem. Many local physicians want to do this work—especially right after residency. Comparing being a hospitalist with his 10 years in private practice, he says, “In my office practice I’d be sitting 20 feet away from a colleague, and there wasn’t much interaction. Now I’m learning something new every day and discussing interesting patients with other doctors. Building these ongoing relationships is great.”
Benefits, Culture, and More
The compensation and benefits packages at Egleston and Scottish Rite reflect that they are two separate hospitals in one system. Egleston’s hospitalists are employed by the medical school and receive a straight salary, with no incentive or at risk components. Scottish Rite’s hospitalists are hospital employees and have 20% of their salary at risk with productivity, quality improvement, and patient satisfaction incentives.
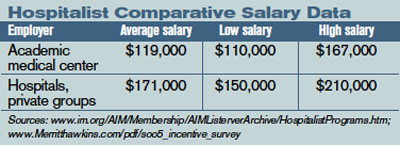
Although the different compensation systems may lead to discrepancies in pay, Dr. Berkelhamer explains that the policy of Children’s Hospital of Atlanta is to offer market-based salaries to all hospitalists. “Part of my job is to ensure that Dr. Snitzer and Dr. Hall are empowered to hire the physicians they want,” he says.
The hospitals have different corporate cultures as well. “The Scottish Rite group is very comfortable with lots of hands-on work while those at Egleston like to spend more time teaching,” says Dr. Berkelhamer.
Dr. Taylor, who trained with Dr. Snitzer and had a private practice in Atlanta for five years before becoming a full-time Egleston hospitalist in 1993, also acknowledges the different cultures at Egleston and Scottish Rite.
“We are two hospitals that come to the table and work together,” she observes. “Although we are in separate locations and may approach things differently, we practice the same type of medicine.”
Dr. Berkelhamer, who works with both sets of hospitalists, reinforces the observation that their clinical practices are consistent: “Surveys on patient and community physician satisfaction are the same, as are outcomes and productivity data.”
Special Issues for Both Hospitals
As part of a growing medical specialty in a dynamic region of the country, hospitalists at Children’s Hospital of Atlanta must confront a number of issues—some unique to them, others that reflect national trends. With different compensation and productivity systems, the two sets of hospitalists must collaborate to practice one brand of medicine.
An important formal step in their collaboration is the computerized medical and order entry system scheduled for spring 2006 implementation. The hospitalists are working together to develop clinical pathways and standardized orders based on their culling through best practices and evidence-based medicine guidelines. A newly appointed chief quality officer will keep the project on track.
Atlanta’s growth presents other issues for the hospitalists. With a constant influx of new community-based pediatricians Dr. Taylor finds that the hospitalists sometimes have trouble communicating with them to coordinate care.
“There are now at least 1,000 primary care and subspecialty pediatricians in Atlanta,” she says. “Trying to build trust and to track personal preferences with so many doctors is difficult. Fortunately we have electronic medical records so we can share important data with them.”
The hospitals’ social workers and case managers represent added glue to hold the communication together. Another of Atlanta’s challenges: It has only two medical schools from which to draw local hospitalists and other pediatricians, Emory University and the smaller Morehouse University. While not insurmountable, it means that most pediatricians practicing in the area must relocate to Atlanta.
What the Future Holds
And then there are issues that transcend Atlanta. Dr. Snitzer feels the national movement for hospitalists to become a specialty will happen sooner rather than later. In line with that movement, Children’s Hospital of Atlanta will have its first hospitalist fellowship in 2007. (For more information on pediatric hospital medicine fellowships, see “Pediatric Fellowship Offered,” below.)
For Dr. Hall, hospitalist compensation in a boomtown rankles. “People can’t really make money being hospitalists,” he explains. “Most need some subsidy to keep the programs going.”
The pay issues are being addressed, albeit slowly. Dr. Hall is encouraged by the campaign of pediatric intensivists to have coding and payment upgrades; he sees it as a template for higher hospitalist reimbursement schedules. “We only get paid for one visit a day, but we often see a patient several times a day,” he says. “Reimbursement should reflect what we really do.”
Both hospitals will have new buildings, each with 250 beds, more surgical suites, and expanded emergency departments by early 2007. That should lead to more hospitalist hiring—not surprising for a hospital that pioneered having inpatient physicians more than 20 years ago. TH
Writer Marlene Piturro is based in New York.
Joseph Snitzer, MD: A hospital medicine pioneer

In 1983—13 years before Robert Wachter, MD, FACP, coined the term “hospitalist”—Egleston Children’s Hospital Department of Pediatrics Chairman Joseph Patterson, MD, asked a former trainee to establish an in-house general pediatric service. That young doctor, Joseph Snitzer III, had been splitting his time equally between a private practice and teaching at Egleston through his affiliation with the Emory University School of Medicine. He said yes to the new assignment.
Since becoming a full-time hospitalist more than two decades ago, Dr. Snitzer relishes both his time working with interns and residents and an ever-changing mix of treatment and diagnostic mysteries. He is now the chief, Division of General Pediatrics, Children’s Healthcare of Atlanta at Egleston, and professor of pediatrics, Emory School of Medicine.
“We see everything here, from Kawasaki syndrome to neonatal apnea, seizure disorders, tumors, dehydration, jaundice, and all kinds of infections,” he explains. “About 50% of the children admitted have chronic conditions and the rest have various acute illnesses. There are unique challenges every day.”
Dr. Snitzer trained both Dr. Hall and Dr. Taylor, transmitting knowledge from one generation of physicians to the next. His hospitalist team maintains excellent relationships with the community’s doctors, both general pediatricians and specialists.
What is the main strength of Dr. Snitzer and the other hospitalists? Coordination with Atlanta’s pediatricians on getting things done in the hospital. Phone consultations with Atlanta’s physicians and those in rural areas seeking Children’s Hospital of Atlanta’s expertise on complex diagnoses and cases also keep him busy.
“Our experience with complexity is overwhelming,” he says. “Perhaps we can’t offer a great deal with simple diagnoses, such as diarrhea or simple skin infections, but we can with tough cases.” —MP
PEDIATRIC SPECIAL SECTION:
NEWS
Pediatric Fellowship Offered
Children’s Hospitalists of San Diego offers program

The Pediatric Hospitalist program at Children’s Hospital and Health Center of San Diego (CHHC) began in 1978. The current hospitalists are employed by Children’s Specialists of San Diego (CSSD), a 180-member pediatric-only specialty medical group. Inpatient care is provided for 75% of all general pediatric patients at the 233-bed tertiary care CHHC. Program consultation is offered at nearby Palomar Medical Center, a 23-bed unit within a larger 319-bed community hospital with a trauma center.
The hospitalists are the primary teaching faculty for the house staff and medical students who come from the University of California San Diego (UCSD), Balboa Naval Hospital, Pendleton Naval Medical Center, and Scripps Family Medicine. All hospitalists are board-certified pediatricians and have additional degrees or postresidency training, such as chief residency or fellowship experience.
Hospitalists fulfill many leadership roles in the hospital and community when not on service. A detailed list is available in a previous issue of The Hospitalist (Nov/Dec 2004;8(6):59-60). Current research includes an Agency for Healthcare Research and Quality (AHRQ) safety grant on medication errors, a bronchiolitis clinical trial, juvenile justice research on hepatitis B, a Hispanic cultural competency grant from the California Endowment, spiratory syncytial virus immunoprophylaxis outcomes in a managed population, and primary care perceptions of pediatric dentistry. Thus the hospitalist program has a long history of strong commitment to children and the core aspects of pediatric hospital medicine.
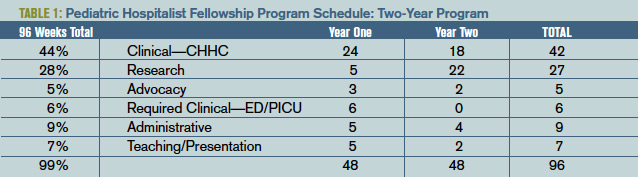
The Fellowship
The CSSD Pediatric Hospitalist Fellowship Program goal is to train highly motivated pediatricians for careers in academic and clinical hospital medicine. Over a two-year period instruction is provided in clinical, advocacy, administrative, teaching, and research aspects of pediatric hospital medicine. Clinical education emphasizes inpatient acute care, including intensive care and emergency transport at the busy main campus at CHHC. Outpatient clinical care offers experiences in adolescent juvenile hall medicine, hospice, and child protection. The diverse clinical exposure, teaching from local and national leaders, and volume of patients ensure graduates of this program are well prepared for any clinical hospitalist position.
The staff gains administrative experience via both hospital and medical group quality improvement activities. This work is directed by the medical director for CSSD and the physician advisor for quality management for CHHC, both of whom are CSSD pediatric hospitalists. Skills in process improvement, continuous quality improvement, risk management, organizational management and leadership are honed during the fellowship. Opportunity exists to take courses through the American College of Physician Executives if the trainee desires a future in administrative hospitalist medicine.
Academics and teaching are a core value of the pediatric hospitalist service. The fellow participates in the monthly division journal club and internal case review. Daily teaching while on the clinical service includes bedside rounds, management rounds, and attending rounds. Pediatric hospitalists are the primary inpatient teaching staff and as such have a significant responsibility for daily house staff education. The fellow participates in noon conferences and other educational venues under the guidance of the director of inpatient teaching (also a pediatric hospitalist).
Advocacy skills are learned through experiences in the juvenile hall system, Center for Child Protection, the American Academy of Pediatrics (AAP), and at the local and state level for children’s services funding. Under the leadership of the medical directors for the Center for Child Protection and the A.B. and Jessie Polinsky Center for Abused Children, the fellow participates in case review and observes expert child abuse testimony in court. Discussions with legislators in Sacramento focus upon protection of the California Children’s Services system, which supports critically ill state-funded children. The fellow learns AAP local and national structure, participating in conferences and chapter events.
Research is expected during this two-year fellowship program. Formal clinical research training is part of the first year curriculum of UCSD’s Clinical Research Enhancement through Supplemental Training (CREST) program. The first year of this two-year CREST program includes weekly classes covering epidemiology, patient-oriented research, health services research, and informatics. Those dedicated to completion of a master’s degree during the two-year program may integrate this training with a more intense curriculum schedule. A research project and mentor is chosen after the first quarter of the first year. Research may be in any area of pediatric hospitalist medicine. Research is presented at either Pediatric Academic Societies, Society of Hospital Medicine, or other similar forum upon completion.
The schedule is flexible, but follows the template. (See Table 1, p. 30: “Pediatric Hospitalist Fellowship Program Schedule.”)
One fellowship position is offered every year, with application submissions accepted through Dec. 1, interviews granted Dec. 15-Feb. 1 and final selection by Feb. 15. You can obtain an application from the CSSD Web site “Fellowships” page (http://childrensspecialists. com/body.cfm?id=580) or by e-mailing Fellowship Coordinator Susan Stafford at [email protected].
PEDIATRIC SPECIAL SECTION:
IN THE LITERATURE
Retrospective Study Attempts Criteria for Diagnosing MAS
Reviews by Julia Simmons, MD
Ravelli A, Magni-Manzoni S, Pistorio A, et al. Preliminary diagnostic guidelines for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. J Pediatr. 2005;146(5):598-604.
Macrophage activating syndrome (MAS) is a complication of connective tissue disorders, most often associated with active systemic juvenile idiopathic arthritis (S-JIA). It is a rare disorder and the exact incidence is unknown. It is characterized by uncontrolled activation and proliferation of T-lymphocytes and macrophages. If not recognized and treated aggressively, MAS can be life threatening.
In this article, the authors’ purpose was to review the available clinical, laboratory, and histopathologic data in patients with active S-JIA and in those with active S-JIA complicated by MAS. The goal was to develop criteria to diagnose MAS.
The retrospective study was designed using the classification, criteria approach. The index cases included patients with MAS complicating S-JIA. The “confusable” condition was active S-JIA. There were 74 patients in the index cases. Seventeen of the cases were observed at the authors’ institution. These patients were diagnosed with S-JIA using the International League of Association for Rheumatology criteria. They were identified using a database search. Fifty-seven of the cases were obtained from a Medline search. Of these 74 patients, eight were disqualified because they did not meet the definition of S-JIA, and 11 were excluded because of insufficient data. The control group contained 37 patients observed at the authors’ sites. The sensitivity rate, specificity rate, area under receiver operating characteristic curve, and diagnostic odds ratio were applied to the data to differentiate MAS complicating S-JIA from S-JIA.
The study results found hemorrhages and central nervous dysfunction were the strongest clinical discriminating factors. The strongest laboratory discriminators included thrombocytopenia, leukopenia, elevated aspartate aminotransferase, and hypofibrinogenemia. Histopathological criterion included evidence of macrophage hemophagocytosis in the bone marrow aspirate. Other useful discriminators included hypertriglyceridemia, elevated ferritin, hepatomegaly, hand hyponatremia. Final guidelines were developed after analyzing the statistics and determining the clinical importance: “The diagnosis of MAS requires the presence of any two or more laboratory criteria or of any two or three or more clinical and/or laboratory criteria. A bone marrow aspirate for the demonstration of hemophagocytosis may be required only in doubtful cases.”
In summary, MAS complicating S-JIA is a disorder without concrete diagnostic criteria. The authors have performed preliminary studies to diagnose MAS. They appropriately recognized the need for prospective larger clinical studies.
HNL Helps Distinguish Infections
Fjaertoft G, Foucard T, Xu S, et al. Human neutrophil lipocalin (HNL) as a diagnostic tool in children with acute infections: a study of the kinetics. Acta Pediatrica costarricense. 2005;94:661-666.
In pediatrics, the clinician is often faced with the diagnostic challenge of differentiating a bacterial infectious process from a viral infection. History, physical exam, and laboratory data make the distinction. In this article, the authors’ purpose was to assess the kinetics of HNL with viral and bacterial infections. Further, they assess the response of HNL when the infection is treated with antibiotics. The response of HNL is compared with that of C-reactive protein.
In the study, 92 patients with a median age of 26 months were hospitalized because they required systemic antibiotics or because of the severity of their medical condition. Upon admission and on hospital days one, two, and three, the C-reactive protein, white blood cell count with differential, and HNL were measured. The patients were retrospectively classified into five groups: true bacterial infection (n=28), true viral infection (n=4), suspected bacterial infection (n=18), suspected viral (n=34), and other.
A true bacterial infection required bacterial isolation from blood, urine, or cerebrospinal fluid culture, or radiographic demonstration of pneumonia. Patients were classified as having a suspected bacterial infection if they had a nonspecific diagnosis, but an elevated C-reactive protein and erythrocyte sedimentation rate. A true viral infection required isolation of a virus. If a patient did not meet any of the above criteria, the person was classified as having a suspected viral infection. Those patients in the “other” group were diagnosed with Kawasaki disease, Borrelia meningitis, and one undiagnosed patient. The patients were classified using history, exam, and laboratory values including white blood cell count, erythrocyte sedimentation rate, C-reactive protein, and cultures. HNL values were not used in the classification.
The results demonstrated that both C-reactive protein and HNL are elevated with true bacterial infections compared with viral illnesses. Neither C-reactive protein nor HNL were significantly different in true bacterial infections versus suspected bacterial infections. The optimal cut-off for C-reactive protein was 59 mg/L with 93% sensitivity and 68% specificity. The optimal cutoff for HNL was 217 micrograms/L with 90% sensitivity and 74% specificity. In patients with true bacterial infections, HNL was highest at admission and decreased one day after admission. In contrast, the C-reactive protein values were similar on the day of admission and on hospital day one. C-reactive protein decreased significantly on days two and three of hospitalization. After hospital day one, HNL was elevated in only 11% of patients with true bacterial infection in contrast to 83% patients with elevated C-reactive protein.
In summary, HNL may be a useful marker to distinguish bacterial and viral illnesses. In comparison with C-reactive protein, it normalizes more rapidly after appropriate antibiotic therapy is initiated. In the future, HNL may be a useful marker in monitoring the response to antibiotic therapy.
CEDKA in Peds
Lawrence SE, Cummings EA, Gaboury I, et al. Population-based study of incidence and risk factors for cerebral edema in pediatric diabetic ketoacidosis. . 2005;146:688-692.
New onset insulin dependent diabetes mellitus is complicated by diabetic ketoacidosis (DKA) in 15% to 67% of patients. The incidence of cerebral edema in diabetic ketoacidosis (CEDKA) has been reported as 0.4-3.1. In the article, the authors seek to determine the incidence, outcome, and risk factors for cerebral edema in DKA in patients younger than 16.
The study was case-controlled with an active Canadian surveillance study. The authors surveyed pediatricians for a two-year period. During this time in Canada, all physicians were requested to submit reports monthly on patients with CEDKA younger than 16.
Thirteen cases were identified and the incidence of CEDKA was 0.51%. Overall mortality from cerebral edema was 0.15%. Increased blood urea nitrogen, degree of dehydration, hyperglycemia, and lower initial bicarbonate were associated with CEDKA. TH
In the flourishing metropolitan area of Atlanta, hospitalists and community-based physicians at Children’s Healthcare of Atlanta thrive within their niches, riding waves of opportunity fueled by the region’s burgeoning population. Jay Berkelhamer, MD, senior vice president of medical affairs at Children’s Healthcare of Atlanta calls his city “one of the most dynamic growth centers in the United States. Within 10 years we are estimated to have at least 150,000 more kids in Atlanta, leading to even greater opportunities for hospitalists and private practice primary care and specialty pediatricians.”
Two Hospitals, One system
Children’s Hospital of Atlanta’s hospitalist program is, in fact, two separate programs: one at Egleston, the other at Scottish Rite. The parent organization links the two and manages each hospital’s mission, structure, hiring, compensation, and outcomes.
—David Hall, MD
The six Egleston full-time equivalent hospitalists, or “cat herders,” as Corinne Taylor, MD, Egleston’s chief of medical affairs, describes them, are employees of Emory University Medical School. Most Egleston hospitalists are parents of young children and work four days a week, allowing them a balance of career and family life. Employed by the medical school and working at an academic medical center, they receive a salary, benefits, and other support services. Side by side with interns and residents, Egleston’s hospitalists see Atlanta’s sickest, frailest, and most at-risk children: the uninsured, underinsured immigrant and local population.
At Egleston the pediatric hospitalists are like their counterparts who treat adult patients in other settings. They deal with many patients with chronic conditions that lead to repeat hospitalizations.
“We see lots of ex-preemies with multiple problems such as asthma, seizures, cerebral palsy, and gastric problems,” says Dr. Taylor. “Some are ventilator-dependent and need lots of care.”
She relishes the clinical discipline that being a hospitalist at an academic medical center presents. “I do my homework every day and enjoy the stimulation of teaching our house officers,” explains Dr. Taylor. “Working with adult learners on the chronic conditions we manage and the cases with puzzling symptoms is exciting.”
Dr. Taylor’s boss is this hospitalist program’s founder, Joseph Snitzer, MD (see “Joseph Snitzer, MD: A hospital medicine pioneer”). Being hospital-based frees Dr. Snitzer to observe an endless parade of clinical challenges, including complex rheumatology cases, lupus, tumors, infected shunts, seizures, exotic infections, oncology diagnoses, and more.
“People call us from rural hospitals and private practices for help with diagnoses,” explains Dr. Snitzer. “We’re not smarter than anyone else. We just see a lot more than most other physicians.”
Scottish Rite
Across town at Scottish Rite, a nonprofit hospital, the hospitalists cope with the demands of a steady influx of new Atlantans. David Hall, MD, is Scottish Rite’s medical director. He was a former Egleston hospitalist and a private practitioner for 10 years in Baltimore before he relocated to Atlanta.
“We don’t have house officers, and there is a resident on call only one night a week,” says Dr. Hall. “Pediatricians in the community need to have their patients admitted 24/7, and we also have to admit from the emergency department at night. With our hospitalists taking calls at night and working all the next day, sometimes they would be on for 36 hours straight. As our service has grown, we’ve realized that this model was not sustainable.”
To reduce the burnout from their growing patient loads, the hospitalists changed their model. As of August 1, 2005, hospitalists at Scottish Rite began working either eight- or 12-hour shifts.
“Until we gain some experience with the shift system, we know we will struggle with continuity and handoffs,” adds Dr. Hall. Scottish Rite is also increasing its complement of moonlighting private practice pediatricians who want to keep their hospital skills current by covering the heavy workload.
Dr. Hall says recruiting new hospitalists isn’t a problem. Many local physicians want to do this work—especially right after residency. Comparing being a hospitalist with his 10 years in private practice, he says, “In my office practice I’d be sitting 20 feet away from a colleague, and there wasn’t much interaction. Now I’m learning something new every day and discussing interesting patients with other doctors. Building these ongoing relationships is great.”
Benefits, Culture, and More
The compensation and benefits packages at Egleston and Scottish Rite reflect that they are two separate hospitals in one system. Egleston’s hospitalists are employed by the medical school and receive a straight salary, with no incentive or at risk components. Scottish Rite’s hospitalists are hospital employees and have 20% of their salary at risk with productivity, quality improvement, and patient satisfaction incentives.
Although the different compensation systems may lead to discrepancies in pay, Dr. Berkelhamer explains that the policy of Children’s Hospital of Atlanta is to offer market-based salaries to all hospitalists. “Part of my job is to ensure that Dr. Snitzer and Dr. Hall are empowered to hire the physicians they want,” he says.
The hospitals have different corporate cultures as well. “The Scottish Rite group is very comfortable with lots of hands-on work while those at Egleston like to spend more time teaching,” says Dr. Berkelhamer.
Dr. Taylor, who trained with Dr. Snitzer and had a private practice in Atlanta for five years before becoming a full-time Egleston hospitalist in 1993, also acknowledges the different cultures at Egleston and Scottish Rite.
“We are two hospitals that come to the table and work together,” she observes. “Although we are in separate locations and may approach things differently, we practice the same type of medicine.”
Dr. Berkelhamer, who works with both sets of hospitalists, reinforces the observation that their clinical practices are consistent: “Surveys on patient and community physician satisfaction are the same, as are outcomes and productivity data.”
Special Issues for Both Hospitals
As part of a growing medical specialty in a dynamic region of the country, hospitalists at Children’s Hospital of Atlanta must confront a number of issues—some unique to them, others that reflect national trends. With different compensation and productivity systems, the two sets of hospitalists must collaborate to practice one brand of medicine.
An important formal step in their collaboration is the computerized medical and order entry system scheduled for spring 2006 implementation. The hospitalists are working together to develop clinical pathways and standardized orders based on their culling through best practices and evidence-based medicine guidelines. A newly appointed chief quality officer will keep the project on track.
Atlanta’s growth presents other issues for the hospitalists. With a constant influx of new community-based pediatricians Dr. Taylor finds that the hospitalists sometimes have trouble communicating with them to coordinate care.
“There are now at least 1,000 primary care and subspecialty pediatricians in Atlanta,” she says. “Trying to build trust and to track personal preferences with so many doctors is difficult. Fortunately we have electronic medical records so we can share important data with them.”
The hospitals’ social workers and case managers represent added glue to hold the communication together. Another of Atlanta’s challenges: It has only two medical schools from which to draw local hospitalists and other pediatricians, Emory University and the smaller Morehouse University. While not insurmountable, it means that most pediatricians practicing in the area must relocate to Atlanta.
What the Future Holds
And then there are issues that transcend Atlanta. Dr. Snitzer feels the national movement for hospitalists to become a specialty will happen sooner rather than later. In line with that movement, Children’s Hospital of Atlanta will have its first hospitalist fellowship in 2007. (For more information on pediatric hospital medicine fellowships, see “Pediatric Fellowship Offered,” below.)
For Dr. Hall, hospitalist compensation in a boomtown rankles. “People can’t really make money being hospitalists,” he explains. “Most need some subsidy to keep the programs going.”
The pay issues are being addressed, albeit slowly. Dr. Hall is encouraged by the campaign of pediatric intensivists to have coding and payment upgrades; he sees it as a template for higher hospitalist reimbursement schedules. “We only get paid for one visit a day, but we often see a patient several times a day,” he says. “Reimbursement should reflect what we really do.”
Both hospitals will have new buildings, each with 250 beds, more surgical suites, and expanded emergency departments by early 2007. That should lead to more hospitalist hiring—not surprising for a hospital that pioneered having inpatient physicians more than 20 years ago. TH
Writer Marlene Piturro is based in New York.
Joseph Snitzer, MD: A hospital medicine pioneer
In 1983—13 years before Robert Wachter, MD, FACP, coined the term “hospitalist”—Egleston Children’s Hospital Department of Pediatrics Chairman Joseph Patterson, MD, asked a former trainee to establish an in-house general pediatric service. That young doctor, Joseph Snitzer III, had been splitting his time equally between a private practice and teaching at Egleston through his affiliation with the Emory University School of Medicine. He said yes to the new assignment.
Since becoming a full-time hospitalist more than two decades ago, Dr. Snitzer relishes both his time working with interns and residents and an ever-changing mix of treatment and diagnostic mysteries. He is now the chief, Division of General Pediatrics, Children’s Healthcare of Atlanta at Egleston, and professor of pediatrics, Emory School of Medicine.
“We see everything here, from Kawasaki syndrome to neonatal apnea, seizure disorders, tumors, dehydration, jaundice, and all kinds of infections,” he explains. “About 50% of the children admitted have chronic conditions and the rest have various acute illnesses. There are unique challenges every day.”
Dr. Snitzer trained both Dr. Hall and Dr. Taylor, transmitting knowledge from one generation of physicians to the next. His hospitalist team maintains excellent relationships with the community’s doctors, both general pediatricians and specialists.
What is the main strength of Dr. Snitzer and the other hospitalists? Coordination with Atlanta’s pediatricians on getting things done in the hospital. Phone consultations with Atlanta’s physicians and those in rural areas seeking Children’s Hospital of Atlanta’s expertise on complex diagnoses and cases also keep him busy.
“Our experience with complexity is overwhelming,” he says. “Perhaps we can’t offer a great deal with simple diagnoses, such as diarrhea or simple skin infections, but we can with tough cases.” —MP
PEDIATRIC SPECIAL SECTION:
NEWS
Pediatric Fellowship Offered
Children’s Hospitalists of San Diego offers program
The Pediatric Hospitalist program at Children’s Hospital and Health Center of San Diego (CHHC) began in 1978. The current hospitalists are employed by Children’s Specialists of San Diego (CSSD), a 180-member pediatric-only specialty medical group. Inpatient care is provided for 75% of all general pediatric patients at the 233-bed tertiary care CHHC. Program consultation is offered at nearby Palomar Medical Center, a 23-bed unit within a larger 319-bed community hospital with a trauma center.
The hospitalists are the primary teaching faculty for the house staff and medical students who come from the University of California San Diego (UCSD), Balboa Naval Hospital, Pendleton Naval Medical Center, and Scripps Family Medicine. All hospitalists are board-certified pediatricians and have additional degrees or postresidency training, such as chief residency or fellowship experience.
Hospitalists fulfill many leadership roles in the hospital and community when not on service. A detailed list is available in a previous issue of The Hospitalist (Nov/Dec 2004;8(6):59-60). Current research includes an Agency for Healthcare Research and Quality (AHRQ) safety grant on medication errors, a bronchiolitis clinical trial, juvenile justice research on hepatitis B, a Hispanic cultural competency grant from the California Endowment, spiratory syncytial virus immunoprophylaxis outcomes in a managed population, and primary care perceptions of pediatric dentistry. Thus the hospitalist program has a long history of strong commitment to children and the core aspects of pediatric hospital medicine.
The Fellowship
The CSSD Pediatric Hospitalist Fellowship Program goal is to train highly motivated pediatricians for careers in academic and clinical hospital medicine. Over a two-year period instruction is provided in clinical, advocacy, administrative, teaching, and research aspects of pediatric hospital medicine. Clinical education emphasizes inpatient acute care, including intensive care and emergency transport at the busy main campus at CHHC. Outpatient clinical care offers experiences in adolescent juvenile hall medicine, hospice, and child protection. The diverse clinical exposure, teaching from local and national leaders, and volume of patients ensure graduates of this program are well prepared for any clinical hospitalist position.
The staff gains administrative experience via both hospital and medical group quality improvement activities. This work is directed by the medical director for CSSD and the physician advisor for quality management for CHHC, both of whom are CSSD pediatric hospitalists. Skills in process improvement, continuous quality improvement, risk management, organizational management and leadership are honed during the fellowship. Opportunity exists to take courses through the American College of Physician Executives if the trainee desires a future in administrative hospitalist medicine.
Academics and teaching are a core value of the pediatric hospitalist service. The fellow participates in the monthly division journal club and internal case review. Daily teaching while on the clinical service includes bedside rounds, management rounds, and attending rounds. Pediatric hospitalists are the primary inpatient teaching staff and as such have a significant responsibility for daily house staff education. The fellow participates in noon conferences and other educational venues under the guidance of the director of inpatient teaching (also a pediatric hospitalist).
Advocacy skills are learned through experiences in the juvenile hall system, Center for Child Protection, the American Academy of Pediatrics (AAP), and at the local and state level for children’s services funding. Under the leadership of the medical directors for the Center for Child Protection and the A.B. and Jessie Polinsky Center for Abused Children, the fellow participates in case review and observes expert child abuse testimony in court. Discussions with legislators in Sacramento focus upon protection of the California Children’s Services system, which supports critically ill state-funded children. The fellow learns AAP local and national structure, participating in conferences and chapter events.
Research is expected during this two-year fellowship program. Formal clinical research training is part of the first year curriculum of UCSD’s Clinical Research Enhancement through Supplemental Training (CREST) program. The first year of this two-year CREST program includes weekly classes covering epidemiology, patient-oriented research, health services research, and informatics. Those dedicated to completion of a master’s degree during the two-year program may integrate this training with a more intense curriculum schedule. A research project and mentor is chosen after the first quarter of the first year. Research may be in any area of pediatric hospitalist medicine. Research is presented at either Pediatric Academic Societies, Society of Hospital Medicine, or other similar forum upon completion.
The schedule is flexible, but follows the template. (See Table 1, p. 30: “Pediatric Hospitalist Fellowship Program Schedule.”)
One fellowship position is offered every year, with application submissions accepted through Dec. 1, interviews granted Dec. 15-Feb. 1 and final selection by Feb. 15. You can obtain an application from the CSSD Web site “Fellowships” page (http://childrensspecialists. com/body.cfm?id=580) or by e-mailing Fellowship Coordinator Susan Stafford at [email protected].
PEDIATRIC SPECIAL SECTION:
IN THE LITERATURE
Retrospective Study Attempts Criteria for Diagnosing MAS
Reviews by Julia Simmons, MD
Ravelli A, Magni-Manzoni S, Pistorio A, et al. Preliminary diagnostic guidelines for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. J Pediatr. 2005;146(5):598-604.
Macrophage activating syndrome (MAS) is a complication of connective tissue disorders, most often associated with active systemic juvenile idiopathic arthritis (S-JIA). It is a rare disorder and the exact incidence is unknown. It is characterized by uncontrolled activation and proliferation of T-lymphocytes and macrophages. If not recognized and treated aggressively, MAS can be life threatening.
In this article, the authors’ purpose was to review the available clinical, laboratory, and histopathologic data in patients with active S-JIA and in those with active S-JIA complicated by MAS. The goal was to develop criteria to diagnose MAS.
The retrospective study was designed using the classification, criteria approach. The index cases included patients with MAS complicating S-JIA. The “confusable” condition was active S-JIA. There were 74 patients in the index cases. Seventeen of the cases were observed at the authors’ institution. These patients were diagnosed with S-JIA using the International League of Association for Rheumatology criteria. They were identified using a database search. Fifty-seven of the cases were obtained from a Medline search. Of these 74 patients, eight were disqualified because they did not meet the definition of S-JIA, and 11 were excluded because of insufficient data. The control group contained 37 patients observed at the authors’ sites. The sensitivity rate, specificity rate, area under receiver operating characteristic curve, and diagnostic odds ratio were applied to the data to differentiate MAS complicating S-JIA from S-JIA.
The study results found hemorrhages and central nervous dysfunction were the strongest clinical discriminating factors. The strongest laboratory discriminators included thrombocytopenia, leukopenia, elevated aspartate aminotransferase, and hypofibrinogenemia. Histopathological criterion included evidence of macrophage hemophagocytosis in the bone marrow aspirate. Other useful discriminators included hypertriglyceridemia, elevated ferritin, hepatomegaly, hand hyponatremia. Final guidelines were developed after analyzing the statistics and determining the clinical importance: “The diagnosis of MAS requires the presence of any two or more laboratory criteria or of any two or three or more clinical and/or laboratory criteria. A bone marrow aspirate for the demonstration of hemophagocytosis may be required only in doubtful cases.”
In summary, MAS complicating S-JIA is a disorder without concrete diagnostic criteria. The authors have performed preliminary studies to diagnose MAS. They appropriately recognized the need for prospective larger clinical studies.
HNL Helps Distinguish Infections
Fjaertoft G, Foucard T, Xu S, et al. Human neutrophil lipocalin (HNL) as a diagnostic tool in children with acute infections: a study of the kinetics. Acta Pediatrica costarricense. 2005;94:661-666.
In pediatrics, the clinician is often faced with the diagnostic challenge of differentiating a bacterial infectious process from a viral infection. History, physical exam, and laboratory data make the distinction. In this article, the authors’ purpose was to assess the kinetics of HNL with viral and bacterial infections. Further, they assess the response of HNL when the infection is treated with antibiotics. The response of HNL is compared with that of C-reactive protein.
In the study, 92 patients with a median age of 26 months were hospitalized because they required systemic antibiotics or because of the severity of their medical condition. Upon admission and on hospital days one, two, and three, the C-reactive protein, white blood cell count with differential, and HNL were measured. The patients were retrospectively classified into five groups: true bacterial infection (n=28), true viral infection (n=4), suspected bacterial infection (n=18), suspected viral (n=34), and other.
A true bacterial infection required bacterial isolation from blood, urine, or cerebrospinal fluid culture, or radiographic demonstration of pneumonia. Patients were classified as having a suspected bacterial infection if they had a nonspecific diagnosis, but an elevated C-reactive protein and erythrocyte sedimentation rate. A true viral infection required isolation of a virus. If a patient did not meet any of the above criteria, the person was classified as having a suspected viral infection. Those patients in the “other” group were diagnosed with Kawasaki disease, Borrelia meningitis, and one undiagnosed patient. The patients were classified using history, exam, and laboratory values including white blood cell count, erythrocyte sedimentation rate, C-reactive protein, and cultures. HNL values were not used in the classification.
The results demonstrated that both C-reactive protein and HNL are elevated with true bacterial infections compared with viral illnesses. Neither C-reactive protein nor HNL were significantly different in true bacterial infections versus suspected bacterial infections. The optimal cut-off for C-reactive protein was 59 mg/L with 93% sensitivity and 68% specificity. The optimal cutoff for HNL was 217 micrograms/L with 90% sensitivity and 74% specificity. In patients with true bacterial infections, HNL was highest at admission and decreased one day after admission. In contrast, the C-reactive protein values were similar on the day of admission and on hospital day one. C-reactive protein decreased significantly on days two and three of hospitalization. After hospital day one, HNL was elevated in only 11% of patients with true bacterial infection in contrast to 83% patients with elevated C-reactive protein.
In summary, HNL may be a useful marker to distinguish bacterial and viral illnesses. In comparison with C-reactive protein, it normalizes more rapidly after appropriate antibiotic therapy is initiated. In the future, HNL may be a useful marker in monitoring the response to antibiotic therapy.
CEDKA in Peds
Lawrence SE, Cummings EA, Gaboury I, et al. Population-based study of incidence and risk factors for cerebral edema in pediatric diabetic ketoacidosis. . 2005;146:688-692.
New onset insulin dependent diabetes mellitus is complicated by diabetic ketoacidosis (DKA) in 15% to 67% of patients. The incidence of cerebral edema in diabetic ketoacidosis (CEDKA) has been reported as 0.4-3.1. In the article, the authors seek to determine the incidence, outcome, and risk factors for cerebral edema in DKA in patients younger than 16.
The study was case-controlled with an active Canadian surveillance study. The authors surveyed pediatricians for a two-year period. During this time in Canada, all physicians were requested to submit reports monthly on patients with CEDKA younger than 16.
Thirteen cases were identified and the incidence of CEDKA was 0.51%. Overall mortality from cerebral edema was 0.15%. Increased blood urea nitrogen, degree of dehydration, hyperglycemia, and lower initial bicarbonate were associated with CEDKA. TH
In the flourishing metropolitan area of Atlanta, hospitalists and community-based physicians at Children’s Healthcare of Atlanta thrive within their niches, riding waves of opportunity fueled by the region’s burgeoning population. Jay Berkelhamer, MD, senior vice president of medical affairs at Children’s Healthcare of Atlanta calls his city “one of the most dynamic growth centers in the United States. Within 10 years we are estimated to have at least 150,000 more kids in Atlanta, leading to even greater opportunities for hospitalists and private practice primary care and specialty pediatricians.”
Two Hospitals, One system
Children’s Hospital of Atlanta’s hospitalist program is, in fact, two separate programs: one at Egleston, the other at Scottish Rite. The parent organization links the two and manages each hospital’s mission, structure, hiring, compensation, and outcomes.
—David Hall, MD
The six Egleston full-time equivalent hospitalists, or “cat herders,” as Corinne Taylor, MD, Egleston’s chief of medical affairs, describes them, are employees of Emory University Medical School. Most Egleston hospitalists are parents of young children and work four days a week, allowing them a balance of career and family life. Employed by the medical school and working at an academic medical center, they receive a salary, benefits, and other support services. Side by side with interns and residents, Egleston’s hospitalists see Atlanta’s sickest, frailest, and most at-risk children: the uninsured, underinsured immigrant and local population.
At Egleston the pediatric hospitalists are like their counterparts who treat adult patients in other settings. They deal with many patients with chronic conditions that lead to repeat hospitalizations.
“We see lots of ex-preemies with multiple problems such as asthma, seizures, cerebral palsy, and gastric problems,” says Dr. Taylor. “Some are ventilator-dependent and need lots of care.”
She relishes the clinical discipline that being a hospitalist at an academic medical center presents. “I do my homework every day and enjoy the stimulation of teaching our house officers,” explains Dr. Taylor. “Working with adult learners on the chronic conditions we manage and the cases with puzzling symptoms is exciting.”
Dr. Taylor’s boss is this hospitalist program’s founder, Joseph Snitzer, MD (see “Joseph Snitzer, MD: A hospital medicine pioneer”). Being hospital-based frees Dr. Snitzer to observe an endless parade of clinical challenges, including complex rheumatology cases, lupus, tumors, infected shunts, seizures, exotic infections, oncology diagnoses, and more.
“People call us from rural hospitals and private practices for help with diagnoses,” explains Dr. Snitzer. “We’re not smarter than anyone else. We just see a lot more than most other physicians.”
Scottish Rite
Across town at Scottish Rite, a nonprofit hospital, the hospitalists cope with the demands of a steady influx of new Atlantans. David Hall, MD, is Scottish Rite’s medical director. He was a former Egleston hospitalist and a private practitioner for 10 years in Baltimore before he relocated to Atlanta.
“We don’t have house officers, and there is a resident on call only one night a week,” says Dr. Hall. “Pediatricians in the community need to have their patients admitted 24/7, and we also have to admit from the emergency department at night. With our hospitalists taking calls at night and working all the next day, sometimes they would be on for 36 hours straight. As our service has grown, we’ve realized that this model was not sustainable.”
To reduce the burnout from their growing patient loads, the hospitalists changed their model. As of August 1, 2005, hospitalists at Scottish Rite began working either eight- or 12-hour shifts.
“Until we gain some experience with the shift system, we know we will struggle with continuity and handoffs,” adds Dr. Hall. Scottish Rite is also increasing its complement of moonlighting private practice pediatricians who want to keep their hospital skills current by covering the heavy workload.
Dr. Hall says recruiting new hospitalists isn’t a problem. Many local physicians want to do this work—especially right after residency. Comparing being a hospitalist with his 10 years in private practice, he says, “In my office practice I’d be sitting 20 feet away from a colleague, and there wasn’t much interaction. Now I’m learning something new every day and discussing interesting patients with other doctors. Building these ongoing relationships is great.”
Benefits, Culture, and More
The compensation and benefits packages at Egleston and Scottish Rite reflect that they are two separate hospitals in one system. Egleston’s hospitalists are employed by the medical school and receive a straight salary, with no incentive or at risk components. Scottish Rite’s hospitalists are hospital employees and have 20% of their salary at risk with productivity, quality improvement, and patient satisfaction incentives.
Although the different compensation systems may lead to discrepancies in pay, Dr. Berkelhamer explains that the policy of Children’s Hospital of Atlanta is to offer market-based salaries to all hospitalists. “Part of my job is to ensure that Dr. Snitzer and Dr. Hall are empowered to hire the physicians they want,” he says.
The hospitals have different corporate cultures as well. “The Scottish Rite group is very comfortable with lots of hands-on work while those at Egleston like to spend more time teaching,” says Dr. Berkelhamer.
Dr. Taylor, who trained with Dr. Snitzer and had a private practice in Atlanta for five years before becoming a full-time Egleston hospitalist in 1993, also acknowledges the different cultures at Egleston and Scottish Rite.
“We are two hospitals that come to the table and work together,” she observes. “Although we are in separate locations and may approach things differently, we practice the same type of medicine.”
Dr. Berkelhamer, who works with both sets of hospitalists, reinforces the observation that their clinical practices are consistent: “Surveys on patient and community physician satisfaction are the same, as are outcomes and productivity data.”
Special Issues for Both Hospitals
As part of a growing medical specialty in a dynamic region of the country, hospitalists at Children’s Hospital of Atlanta must confront a number of issues—some unique to them, others that reflect national trends. With different compensation and productivity systems, the two sets of hospitalists must collaborate to practice one brand of medicine.
An important formal step in their collaboration is the computerized medical and order entry system scheduled for spring 2006 implementation. The hospitalists are working together to develop clinical pathways and standardized orders based on their culling through best practices and evidence-based medicine guidelines. A newly appointed chief quality officer will keep the project on track.
Atlanta’s growth presents other issues for the hospitalists. With a constant influx of new community-based pediatricians Dr. Taylor finds that the hospitalists sometimes have trouble communicating with them to coordinate care.
“There are now at least 1,000 primary care and subspecialty pediatricians in Atlanta,” she says. “Trying to build trust and to track personal preferences with so many doctors is difficult. Fortunately we have electronic medical records so we can share important data with them.”
The hospitals’ social workers and case managers represent added glue to hold the communication together. Another of Atlanta’s challenges: It has only two medical schools from which to draw local hospitalists and other pediatricians, Emory University and the smaller Morehouse University. While not insurmountable, it means that most pediatricians practicing in the area must relocate to Atlanta.
What the Future Holds
And then there are issues that transcend Atlanta. Dr. Snitzer feels the national movement for hospitalists to become a specialty will happen sooner rather than later. In line with that movement, Children’s Hospital of Atlanta will have its first hospitalist fellowship in 2007. (For more information on pediatric hospital medicine fellowships, see “Pediatric Fellowship Offered,” below.)
For Dr. Hall, hospitalist compensation in a boomtown rankles. “People can’t really make money being hospitalists,” he explains. “Most need some subsidy to keep the programs going.”
The pay issues are being addressed, albeit slowly. Dr. Hall is encouraged by the campaign of pediatric intensivists to have coding and payment upgrades; he sees it as a template for higher hospitalist reimbursement schedules. “We only get paid for one visit a day, but we often see a patient several times a day,” he says. “Reimbursement should reflect what we really do.”
Both hospitals will have new buildings, each with 250 beds, more surgical suites, and expanded emergency departments by early 2007. That should lead to more hospitalist hiring—not surprising for a hospital that pioneered having inpatient physicians more than 20 years ago. TH
Writer Marlene Piturro is based in New York.
Joseph Snitzer, MD: A hospital medicine pioneer
In 1983—13 years before Robert Wachter, MD, FACP, coined the term “hospitalist”—Egleston Children’s Hospital Department of Pediatrics Chairman Joseph Patterson, MD, asked a former trainee to establish an in-house general pediatric service. That young doctor, Joseph Snitzer III, had been splitting his time equally between a private practice and teaching at Egleston through his affiliation with the Emory University School of Medicine. He said yes to the new assignment.
Since becoming a full-time hospitalist more than two decades ago, Dr. Snitzer relishes both his time working with interns and residents and an ever-changing mix of treatment and diagnostic mysteries. He is now the chief, Division of General Pediatrics, Children’s Healthcare of Atlanta at Egleston, and professor of pediatrics, Emory School of Medicine.
“We see everything here, from Kawasaki syndrome to neonatal apnea, seizure disorders, tumors, dehydration, jaundice, and all kinds of infections,” he explains. “About 50% of the children admitted have chronic conditions and the rest have various acute illnesses. There are unique challenges every day.”
Dr. Snitzer trained both Dr. Hall and Dr. Taylor, transmitting knowledge from one generation of physicians to the next. His hospitalist team maintains excellent relationships with the community’s doctors, both general pediatricians and specialists.
What is the main strength of Dr. Snitzer and the other hospitalists? Coordination with Atlanta’s pediatricians on getting things done in the hospital. Phone consultations with Atlanta’s physicians and those in rural areas seeking Children’s Hospital of Atlanta’s expertise on complex diagnoses and cases also keep him busy.
“Our experience with complexity is overwhelming,” he says. “Perhaps we can’t offer a great deal with simple diagnoses, such as diarrhea or simple skin infections, but we can with tough cases.” —MP
PEDIATRIC SPECIAL SECTION:
NEWS
Pediatric Fellowship Offered
Children’s Hospitalists of San Diego offers program
The Pediatric Hospitalist program at Children’s Hospital and Health Center of San Diego (CHHC) began in 1978. The current hospitalists are employed by Children’s Specialists of San Diego (CSSD), a 180-member pediatric-only specialty medical group. Inpatient care is provided for 75% of all general pediatric patients at the 233-bed tertiary care CHHC. Program consultation is offered at nearby Palomar Medical Center, a 23-bed unit within a larger 319-bed community hospital with a trauma center.
The hospitalists are the primary teaching faculty for the house staff and medical students who come from the University of California San Diego (UCSD), Balboa Naval Hospital, Pendleton Naval Medical Center, and Scripps Family Medicine. All hospitalists are board-certified pediatricians and have additional degrees or postresidency training, such as chief residency or fellowship experience.
Hospitalists fulfill many leadership roles in the hospital and community when not on service. A detailed list is available in a previous issue of The Hospitalist (Nov/Dec 2004;8(6):59-60). Current research includes an Agency for Healthcare Research and Quality (AHRQ) safety grant on medication errors, a bronchiolitis clinical trial, juvenile justice research on hepatitis B, a Hispanic cultural competency grant from the California Endowment, spiratory syncytial virus immunoprophylaxis outcomes in a managed population, and primary care perceptions of pediatric dentistry. Thus the hospitalist program has a long history of strong commitment to children and the core aspects of pediatric hospital medicine.
The Fellowship
The CSSD Pediatric Hospitalist Fellowship Program goal is to train highly motivated pediatricians for careers in academic and clinical hospital medicine. Over a two-year period instruction is provided in clinical, advocacy, administrative, teaching, and research aspects of pediatric hospital medicine. Clinical education emphasizes inpatient acute care, including intensive care and emergency transport at the busy main campus at CHHC. Outpatient clinical care offers experiences in adolescent juvenile hall medicine, hospice, and child protection. The diverse clinical exposure, teaching from local and national leaders, and volume of patients ensure graduates of this program are well prepared for any clinical hospitalist position.
The staff gains administrative experience via both hospital and medical group quality improvement activities. This work is directed by the medical director for CSSD and the physician advisor for quality management for CHHC, both of whom are CSSD pediatric hospitalists. Skills in process improvement, continuous quality improvement, risk management, organizational management and leadership are honed during the fellowship. Opportunity exists to take courses through the American College of Physician Executives if the trainee desires a future in administrative hospitalist medicine.
Academics and teaching are a core value of the pediatric hospitalist service. The fellow participates in the monthly division journal club and internal case review. Daily teaching while on the clinical service includes bedside rounds, management rounds, and attending rounds. Pediatric hospitalists are the primary inpatient teaching staff and as such have a significant responsibility for daily house staff education. The fellow participates in noon conferences and other educational venues under the guidance of the director of inpatient teaching (also a pediatric hospitalist).
Advocacy skills are learned through experiences in the juvenile hall system, Center for Child Protection, the American Academy of Pediatrics (AAP), and at the local and state level for children’s services funding. Under the leadership of the medical directors for the Center for Child Protection and the A.B. and Jessie Polinsky Center for Abused Children, the fellow participates in case review and observes expert child abuse testimony in court. Discussions with legislators in Sacramento focus upon protection of the California Children’s Services system, which supports critically ill state-funded children. The fellow learns AAP local and national structure, participating in conferences and chapter events.
Research is expected during this two-year fellowship program. Formal clinical research training is part of the first year curriculum of UCSD’s Clinical Research Enhancement through Supplemental Training (CREST) program. The first year of this two-year CREST program includes weekly classes covering epidemiology, patient-oriented research, health services research, and informatics. Those dedicated to completion of a master’s degree during the two-year program may integrate this training with a more intense curriculum schedule. A research project and mentor is chosen after the first quarter of the first year. Research may be in any area of pediatric hospitalist medicine. Research is presented at either Pediatric Academic Societies, Society of Hospital Medicine, or other similar forum upon completion.
The schedule is flexible, but follows the template. (See Table 1, p. 30: “Pediatric Hospitalist Fellowship Program Schedule.”)
One fellowship position is offered every year, with application submissions accepted through Dec. 1, interviews granted Dec. 15-Feb. 1 and final selection by Feb. 15. You can obtain an application from the CSSD Web site “Fellowships” page (http://childrensspecialists. com/body.cfm?id=580) or by e-mailing Fellowship Coordinator Susan Stafford at [email protected].
PEDIATRIC SPECIAL SECTION:
IN THE LITERATURE
Retrospective Study Attempts Criteria for Diagnosing MAS
Reviews by Julia Simmons, MD
Ravelli A, Magni-Manzoni S, Pistorio A, et al. Preliminary diagnostic guidelines for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. J Pediatr. 2005;146(5):598-604.
Macrophage activating syndrome (MAS) is a complication of connective tissue disorders, most often associated with active systemic juvenile idiopathic arthritis (S-JIA). It is a rare disorder and the exact incidence is unknown. It is characterized by uncontrolled activation and proliferation of T-lymphocytes and macrophages. If not recognized and treated aggressively, MAS can be life threatening.
In this article, the authors’ purpose was to review the available clinical, laboratory, and histopathologic data in patients with active S-JIA and in those with active S-JIA complicated by MAS. The goal was to develop criteria to diagnose MAS.
The retrospective study was designed using the classification, criteria approach. The index cases included patients with MAS complicating S-JIA. The “confusable” condition was active S-JIA. There were 74 patients in the index cases. Seventeen of the cases were observed at the authors’ institution. These patients were diagnosed with S-JIA using the International League of Association for Rheumatology criteria. They were identified using a database search. Fifty-seven of the cases were obtained from a Medline search. Of these 74 patients, eight were disqualified because they did not meet the definition of S-JIA, and 11 were excluded because of insufficient data. The control group contained 37 patients observed at the authors’ sites. The sensitivity rate, specificity rate, area under receiver operating characteristic curve, and diagnostic odds ratio were applied to the data to differentiate MAS complicating S-JIA from S-JIA.
The study results found hemorrhages and central nervous dysfunction were the strongest clinical discriminating factors. The strongest laboratory discriminators included thrombocytopenia, leukopenia, elevated aspartate aminotransferase, and hypofibrinogenemia. Histopathological criterion included evidence of macrophage hemophagocytosis in the bone marrow aspirate. Other useful discriminators included hypertriglyceridemia, elevated ferritin, hepatomegaly, hand hyponatremia. Final guidelines were developed after analyzing the statistics and determining the clinical importance: “The diagnosis of MAS requires the presence of any two or more laboratory criteria or of any two or three or more clinical and/or laboratory criteria. A bone marrow aspirate for the demonstration of hemophagocytosis may be required only in doubtful cases.”
In summary, MAS complicating S-JIA is a disorder without concrete diagnostic criteria. The authors have performed preliminary studies to diagnose MAS. They appropriately recognized the need for prospective larger clinical studies.
HNL Helps Distinguish Infections
Fjaertoft G, Foucard T, Xu S, et al. Human neutrophil lipocalin (HNL) as a diagnostic tool in children with acute infections: a study of the kinetics. Acta Pediatrica costarricense. 2005;94:661-666.
In pediatrics, the clinician is often faced with the diagnostic challenge of differentiating a bacterial infectious process from a viral infection. History, physical exam, and laboratory data make the distinction. In this article, the authors’ purpose was to assess the kinetics of HNL with viral and bacterial infections. Further, they assess the response of HNL when the infection is treated with antibiotics. The response of HNL is compared with that of C-reactive protein.
In the study, 92 patients with a median age of 26 months were hospitalized because they required systemic antibiotics or because of the severity of their medical condition. Upon admission and on hospital days one, two, and three, the C-reactive protein, white blood cell count with differential, and HNL were measured. The patients were retrospectively classified into five groups: true bacterial infection (n=28), true viral infection (n=4), suspected bacterial infection (n=18), suspected viral (n=34), and other.
A true bacterial infection required bacterial isolation from blood, urine, or cerebrospinal fluid culture, or radiographic demonstration of pneumonia. Patients were classified as having a suspected bacterial infection if they had a nonspecific diagnosis, but an elevated C-reactive protein and erythrocyte sedimentation rate. A true viral infection required isolation of a virus. If a patient did not meet any of the above criteria, the person was classified as having a suspected viral infection. Those patients in the “other” group were diagnosed with Kawasaki disease, Borrelia meningitis, and one undiagnosed patient. The patients were classified using history, exam, and laboratory values including white blood cell count, erythrocyte sedimentation rate, C-reactive protein, and cultures. HNL values were not used in the classification.
The results demonstrated that both C-reactive protein and HNL are elevated with true bacterial infections compared with viral illnesses. Neither C-reactive protein nor HNL were significantly different in true bacterial infections versus suspected bacterial infections. The optimal cut-off for C-reactive protein was 59 mg/L with 93% sensitivity and 68% specificity. The optimal cutoff for HNL was 217 micrograms/L with 90% sensitivity and 74% specificity. In patients with true bacterial infections, HNL was highest at admission and decreased one day after admission. In contrast, the C-reactive protein values were similar on the day of admission and on hospital day one. C-reactive protein decreased significantly on days two and three of hospitalization. After hospital day one, HNL was elevated in only 11% of patients with true bacterial infection in contrast to 83% patients with elevated C-reactive protein.
In summary, HNL may be a useful marker to distinguish bacterial and viral illnesses. In comparison with C-reactive protein, it normalizes more rapidly after appropriate antibiotic therapy is initiated. In the future, HNL may be a useful marker in monitoring the response to antibiotic therapy.
CEDKA in Peds
Lawrence SE, Cummings EA, Gaboury I, et al. Population-based study of incidence and risk factors for cerebral edema in pediatric diabetic ketoacidosis. . 2005;146:688-692.
New onset insulin dependent diabetes mellitus is complicated by diabetic ketoacidosis (DKA) in 15% to 67% of patients. The incidence of cerebral edema in diabetic ketoacidosis (CEDKA) has been reported as 0.4-3.1. In the article, the authors seek to determine the incidence, outcome, and risk factors for cerebral edema in DKA in patients younger than 16.
The study was case-controlled with an active Canadian surveillance study. The authors surveyed pediatricians for a two-year period. During this time in Canada, all physicians were requested to submit reports monthly on patients with CEDKA younger than 16.
Thirteen cases were identified and the incidence of CEDKA was 0.51%. Overall mortality from cerebral edema was 0.15%. Increased blood urea nitrogen, degree of dehydration, hyperglycemia, and lower initial bicarbonate were associated with CEDKA. TH
The Role of Hospitalists in Stroke Management
Distinguishing the evolving role of the hospitalist in managing patients with stroke requires exploring a number of challenges, a couple of controversies, and some clear opportunities.
Challenges
Hospitalists and their specialist colleagues face a number of challenges associated with stroke management, including the nature of provider teamwork, whether patients present within the window of time for thrombolytic administration, whether hospitalists should administer those agents, and also the care of patients with intracerebral hemorrhage (ICH).
Specialty Support
Traditionally the neurologist has been the key clinician involved in the diagnosis and treatment of patients with stroke. And because a great many neurologists prefer to practice almost exclusively in the outpatient setting, a team of providers in the hospital must handle the current stroke care volume.
“Coming to the hospital can be a challenge for some of them, although there is a subset of neurologists who really like to be inside the hospital and look after acute issues with respect to neurology,” says Sandeep Sachdeva, MD, Swedish Medical Center in Seattle. “In our institution we’ve had enough neurologists, but most of them are busy with their outpatient practices so they’re not able to spend substantial time [in the hospital]. By default we have to look at the hospitalist program here as a resource for taking care of stroke patients.”1
Emergent evaluation and treatment of acute ischemic stroke is a hot-button issue, especially for community-based hospitals. Some neurologists can leave their office and attend to an acute ischemic stroke presenting to the emergency department, while others can’t. To address this issue some hospitals have developed stroke teams that usually consist of highly trained nurses/advanced registered nurse practitioners (ARNPs) working under the direction of a neurologist, as is the case at Swedish Medical Center. These stroke teams respond to acute strokes presenting in the emergency department and then assist the emergency department physician in expediting the patient evaluation and ensuring that no protocol violation occurs while emergent therapy, such as IV tPA, is administered.
The final decision for administering this medication rests with the emergency department physician and, in some instances, with the neurologist if he or she is able to evaluate the patient in the emergency department. Hospitalists must evaluate their comfort level, knowledge, and experience—and then discuss with their neurologists and emergency department physicians the development of—a care algorithm commensurate with national and local standards of care as it pertains to caring for patients who present with acute stroke.
With relatively little specialty support available, it becomes more important for communication between providers to be clear and reliable; and practitioners must determine the local standard of care.
“I think with stroke it’s a particularly vexing issue, especially when you get outside of metropolitan areas,” says Larry Goldstein, MD, director of the Duke University Stroke Center, Durham, N.C. “In metropolitan areas there may be hospitals with different capabilities that are not too far from one another. And it may make sense in that situation for one hospital to decide on their own: ‘We just don’t have the resources to be able to treat a specific condition, … and it might be better … for patients to not come here for that since we can’t offer the appropriate level of care for that condition.’”
But in rural and other less populated areas, he says “ … that community hospital may be the only game in town. And even though they … wouldn’t have everything that a tertiary care [or] quaternary care academic center would have, they could identify areas that are critically important for the acute care patients they are serving and develop the appropriate levels of competency in that area.”
Administering Thrombolytics
What is the standard by which an individual hospitalist is expected to practice, especially concerning the administration of tPA?
In that regard—without a doubt—patient safety comes first. “Whenever there’s confusion in my mind, I always think … first, do no harm,” says Dr. Sachdeva. “If this is an urban area and other hospitalists are not [administering] tPA, then they are not expected to do so and that may not meet the standard of care for that area. Rural hospitals have successfully been giving tPA to patients with acute ischemic stroke.
The caveat here is that appropriate planning as well as training of caregivers has to take place prior to starting IV tPA administration. “Rural hospitals that have the IV tPA capability usually do so in collaboration with larger regional institutions, academic or otherwise, where services of neurologists and neurosurgeons are available,” says Dr. Sachdeva. “Size of the institution should not be an impediment to IV tPA administration.”
As baby boomers age, the demand for better stroke care will increase, and hospitals as well as caregivers need to be prepared to meet the expectations of patients.
David Thurber, MD, medical director of the Cary Hospital Medicine Service, a division of Wake Medical Center, Cary, N.C., speaks of the need for specialty backup at community hospitals.
“For those people who practice in community hospitals, including myself,” he says, “it’s like being the pitcher on a baseball team: If you can’t field the outfield, you shouldn’t be pitching the ball because there’s nobody out there to catch it. So if you can’t get the backup of a neurologist, or of a neurosurgeon in the case of hemorrhagic stroke, in my opinion you have no business pushing tPA. Your obligation is to try, as many community hospitals have done with invasive cardiac procedures, such as emergent use of percutaneous coronary artery intervention, to transfer the patient to a facility where those can be done in a timely fashion.”
What should hospitalists do if they are expected to administer tPA and are unsure of their skill level?
“I would take this issue back to the administration of the hospital,” says Dr. Sachdeva, “and come up with a plan where the neurologists or the emergency department physicians feel motivated to give tPA.”
The most important element to consider when making the decision of whether to administer tPA is the quality of the history. “If there is any doubt about the time or the mechanism of stroke onset, then as practitioners we are very well justified in not giving tPA,” says Dr. Sachdeva, who believes there are more lawsuits for not giving tPA than for giving it. But if you withhold tPA and justify the decision with appropriate reasoning, that certainly places the individual on steadier legal ground.
Training and Competence
Stroke management is not a universally strong topic in medical education. “Not every medical school requires a rotation in the neurosciences or exposure to stroke treatment,” says Dr. Goldstein, “and it’s the same thing in residency programs, depending on which residency program you go through, be it as an internist or as an emergency physician. … So it begins in medical school and follows through residency, but as we know, our training only begins in those formal settings. In medicine, training is a lifelong activity. Things change all the time. And it would [take] appropriate levels of continuing education directly related to cerebrovascular disease to be able to understand modern diagnosis and modern therapeutics.”
Another issue is whether an institution will receive patients for stroke treatment. “Just as hospitals credential people to [perform] procedures, not every hospital can offer every therapy to every patient at the same level,” says Dr. Goldstein. “The thing that is inappropriate is to force people to do things for which they’re not trained.”
Although that is also partially an institutional decision, “institutions can’t have it both ways,” he explains. “They can’t say well, we’re going to be taking care of patients with X, Y, or Z, but then not have the facilities and personnel available to be able to acutely treat and stabilize patients even if they do require more advanced care somewhere else.”
Dr. Sachdeva’s team had to cover a considerable knowledge gap to bring his colleagues up to speed and competence by talking directly to the hospitalists and arranging CMEs for them, as well as by encouraging them to get certified in using the National Institutes of Health (NIH) stroke scale.
“The key is for hospitalists to make sure when they’re taking on an area of patient care that they feel comfortable doing that and not themselves be the default for any medical or surgical conditions,” says David Likosky, MD, who is board certified in neurology and internal medicine, and is the director of the Stroke Program of Evergreen Healthcare, Kirkland, Wash.
One way to become better prepared to manage stroke is to familiarize oneself with the National Institutes of Health (NIH) stroke scale. Online training for the NIH Stroke Scale (approved for two hours of category 1 CME credit from the NIH) is available at www.ninds.nih.gov/doctors/NIH_Stroke_Scale.pdf.).
Excellent resources for developing protocols include the American Stroke Association/American Heart Association, the work of the Brain Attack Coalition (a group of professional, voluntary, and governmental entities dedicated to reducing the occurrence, disabilities, and death associated with stroke—www.stroke-site.org/), and the Web site (www.strokecenter.org), produced out of Washington University in St. Louis. SHM (www.hospitalmedicine.org), which is in the process of creating a Web-based stroke resource room, which—at press time—was scheduled to be live by August 1.
—David Thurber, MD
Systems and Monitoring
Having the right systems in place enables smooth patient assessment and treatment. First establish a means for education in stroke care for hospitalists and all support staff. Other important systems include having protocols for admitting [patients] for stroke care; setting up communication pathways for various disciplines involved in stroke care; having systems to gather, analyze, and monitor data; and having particularly good teamwork and response time.
William Likosky, MD, director of the Stroke Program at the Swedish Medical Center, Seattle, strongly believes in systems and processes of care, whereby a well-designed system should not only be able to prevent mistakes by an individual caregiver, but also to facilitate optimal evidence-based care in every case. As an institution Swedish Medical draws inspiration from the Institute of Healthcare Improvement’s campaign to prevent 100,000 avoidable deaths nationwide in its hospitalized patients. Since its inception at Swedish Medical two years ago, the stroke program is credited with preventing 22 deaths.
Of course any protocol’s worth will vary according to the effectiveness with which it is implemented. Developing protocols and care pathways is an avenue for hospitalists to take a leadership role in implementing evidence-based care, in co-ordinating care between different services, and eventually affecting resource utilization, quality of care, and patient satisfaction positively.
Protocols or pathways fail when they’re not patient-centered, when input isn’t solicited from other caregivers during the development phase, or when their implementation is not monitored. To Dr. Sachdeva, “the main issue is how you implement [the protocol], how you monitor the implementation, and how you fix the glitches or the problems that usually ensue when you’re rolling out a new protocol.”
Response and Feedback
Another imperative of any stroke program is its response time. “We monitor very closely our emergency department evaluation times for patients coming in within the window for giving tPA,” says Dr. Sachdeva. “We are strict about this because we want every patient to be evaluated within 45 minutes—anybody who is a candidate for possible intervention with acute thrombolytics—either IV or IA. Those times are monitored, and any time that 45-minute window is missed, we have an individual conversation with the people who were responsible, not as a confrontation, but [to ask], ‘What can we do to help you?’ And each time we do that we learn something new.
“Usually in these cases, there were things that were happening that were out of control and sometimes you can control them and sometimes you can’t,” he says. “Next time we try to manage the variables better. So we do have a hands-on continuous monitoring process that is not intrusive, and it gives us an idea of how we are holding up with certain quality parameters.”
Teamwork and Communication
One of the important systems is how well all involved work as a team. “Most of the time, IV tPA is given in the emergency department and the emergency department doctors now are very comfortable giving IV tPA with the telephonic help from a neurologist,” says Dr. Sachdeva. “But they also receive assistance from the stroke nurse, who consults on every stroke patient who is a candidate for emergent intervention in the emergency department.”
Swedish Medical maintains dedicated stroke nurses who act as facilitators to ensure everybody holds up their end of the bargain in stroke care. This includes a combination of nurses and nurse practitioners. But ultimately it is the emergency department physician’s decision in consultation with the neurologist by phone.
Part of their facilitation involves negotiating to cut down on time. “We don’t … rush our patients, but we cut down on avoidable delays,” says Dr. Sachdeva. “We try to get all the pertinent workup done as fast as we can, and then collate the data, make sure the data are disseminated to the parties that need the data, and decisions are made and appropriate treatment algorithms applied.”
These dedicated nurses are available in person for any acute stroke that falls within the window for an emergent intervention. “But if it is [an] acute stroke outside the window,” says Dr. Sachdeva, “they will consult telephonically to help you get certain things started, and then consult on the patient the next business day. They are available 24/7 both to the emergency department and to any floor area of the hospital. Anyplace that stroke can happen … they are there in a heartbeat. And the stroke nurses have been invaluable in assisting the hospitalists in day-to-day care of the stroke patients as well as in educating patients and their families.”
Controversies in Stroke Management
Although many hospitalists are uncomfortable treating ischemic strokes, far more may show discomfort at the idea of treating hemorrhagic strokes.
“Bleeding within the head carries a morbidity and mortality that sometimes is exaggerated in terms of its perception,” he says, “and once again, one has to look at the training that was given to most hospitalists during their residency. It was insufficient with respect to managing intracranial hemorrhages.”
Treating hemorrhagic strokes has traditionally been the preserve of neurosurgeons. “Some neurosurgeons are of the opinion that if there is no indication for surgical intervention for a particular ICH case, then the patient should be on the medical service,” says Dr. Sachdeva. “The medical side is feeling thoroughly unprepared to handle these.”
His team is looking at this issue at their institution to come up with appropriate algorithms regarding triage and care of patients with ICH.
Hospitalists and Stroke Management: Opportunities
One advantage of the hospitalist system in managing stroke is that hospitalists are readily available. Monitoring patients’ recovery for any emergent complications is also an important role for the hospitalist. Most often these complications are urinary tract infections, aspiration pneumonia, and deep venous thrombosis.
The team at Swedish refers to these high-risk complications as “dashboards,” likening them to the dashboard of an automobile that must be carefully watched.
Swedish Medical has seven markers for quality of care that the stroke team monitors. They have a statistician, people who gather the data, people who analyze the data, and those who then put the data in a graph format for the team to review trends reflecting quality of care.
This secondary prevention comes into play while coordinating care at the time of discharge. Hospitalists can start the ball rolling so a primary care physician or the facility to which the patient may next be transferred will continue the appropriate care for these patients.
Hospitalists could also take leadership role within their institutions in formulating pathways for emergent evaluation of strokes that occur in hospitalized patients.
“This is what most hospitalists should be able to do with adequate training,” says Dr. Sachdeva. “At the very least, hospitalists can positively impact stroke care by setting into place protocols, processes, and systems of care to ensure prevention DVTs, UTIs, aspiration pneumonias, and initiation of appropriate secondary prevention modalities for patients admitted with a diagnosis of stroke.”
Any institution that prevents these complications from developing should see an automatic benefit of those quality parameters in decreased length of stay, decreased utilization of resources, and improved patient satisfaction.
Follow-Up and Compliance
Having the undivided attention of the patient and his or her family at the time of hospitalization is a golden opportunity.
“We start patients on a vigorous, evidence-based secondary prevention regimen and by opening a dialogue with the patient and the family,” says Dr. Sachdeva. “Realize you’ve started something good; it needs to be followed up and reinforced on a regular basis either through their primary care provider or through a dedicated stroke follow-up clinic.”
The plan for handling a potential future brain attack is also outlined. One of the most noteworthy programs for secondary prevention of strokes is the one out of the University of California, Los Angeles called PROTECT—Preventing Recurrence of Thromboembolic Events through Coordinated Treatment (http://strokeprotect.mednet.ucla.edu/). (See p. 22.)2
Dr. Thurber, who is also president of the Piedmont Chapter of SHM, hopes that secondary prevention work by stroke teams around the country and the results of public education campaigns can help reduce the number of patients who present for stroke treatment outside the time window for thrombolytic therapy.
Communication with PCPs
If you have a dedicated group of primary care physicians that you work with, then they are, in effect, your customers. They should develop that program so they can give their input as how they would like communication and they can know what kind of care their patients will receive once admitted to the hospitalists or the hospitalist-neurologist team.
Call the primary care physicians at the time of discharge in order to convey the highlights of hospitalization and review key follow-up issues. Information can fall through the cracks, but the PROTECT program shows that this is rare if you use the tools provided as part of the program.1 Their data show that initiating secondary prevention modalities while the patient is hospitalized is important, but following up on them is just as important to good outcomes.
The discharging physician must partner with the primary care providers to maintain the momentum with respect to secondary prevention, re-enforcing education, and monitoring for development of side effects from the medications initiated during hospitalization.
Future Trends
Given the trends of an expanding hospitalist system, increasing time limitations for specialists, the relative dearth of neurologists, and uninviting circumstances for practice and compensation, neurologists will need to partner with a group of physicians who are structured to be available 24/7.
In his coauthored letter to the editor of Stroke, published in June 2005, Dr. Likosky challenged neurologists to avoid being “asleep at the wheel” in stroke prevention.1 “If neurologists want to be the ones taking care of stroke patients,” he said, “then they need to decide what role they want to play, because otherwise it’s going to be taken over by hospitalists, which may be the most appropriate thing.”
Conclusion
Challenges and opportunities characterize the work of hospitalists involved in stroke care. Good, ongoing training is imperative as are effective institutional systems and efficient monitoring of those systems. Protocols can be adapted to best serve an individual institution; the nature of their implementation and the teamwork or lack thereof will make the difference in the benefit to medical and institutional outcomes.
Recommendations for best performance in stroke care include keeping open channels of communication and good feedback systems, discussing controversies in order to seek resolutions and improve systems, and using the advantage of access to patients and their families to best begin follow-up and secondary prevention efforts. TH
Writer Andrea M. Sattinger will cover the malpractice crisis in healthcare in future issues of The Hospitalist.
References
- Likosky DJ. Who will care for our hospitalized patients? Stroke. 2005;36:1113-1114.
- Ovbiagele B, Saver JL, Fredieu A, et al. PROTECT: A coordinated stroke treatment program to prevent recurrent thromboembolic events. Neurology. 2004;63:1217-1222.
Distinguishing the evolving role of the hospitalist in managing patients with stroke requires exploring a number of challenges, a couple of controversies, and some clear opportunities.
Challenges
Hospitalists and their specialist colleagues face a number of challenges associated with stroke management, including the nature of provider teamwork, whether patients present within the window of time for thrombolytic administration, whether hospitalists should administer those agents, and also the care of patients with intracerebral hemorrhage (ICH).
Specialty Support
Traditionally the neurologist has been the key clinician involved in the diagnosis and treatment of patients with stroke. And because a great many neurologists prefer to practice almost exclusively in the outpatient setting, a team of providers in the hospital must handle the current stroke care volume.
“Coming to the hospital can be a challenge for some of them, although there is a subset of neurologists who really like to be inside the hospital and look after acute issues with respect to neurology,” says Sandeep Sachdeva, MD, Swedish Medical Center in Seattle. “In our institution we’ve had enough neurologists, but most of them are busy with their outpatient practices so they’re not able to spend substantial time [in the hospital]. By default we have to look at the hospitalist program here as a resource for taking care of stroke patients.”1
Emergent evaluation and treatment of acute ischemic stroke is a hot-button issue, especially for community-based hospitals. Some neurologists can leave their office and attend to an acute ischemic stroke presenting to the emergency department, while others can’t. To address this issue some hospitals have developed stroke teams that usually consist of highly trained nurses/advanced registered nurse practitioners (ARNPs) working under the direction of a neurologist, as is the case at Swedish Medical Center. These stroke teams respond to acute strokes presenting in the emergency department and then assist the emergency department physician in expediting the patient evaluation and ensuring that no protocol violation occurs while emergent therapy, such as IV tPA, is administered.
The final decision for administering this medication rests with the emergency department physician and, in some instances, with the neurologist if he or she is able to evaluate the patient in the emergency department. Hospitalists must evaluate their comfort level, knowledge, and experience—and then discuss with their neurologists and emergency department physicians the development of—a care algorithm commensurate with national and local standards of care as it pertains to caring for patients who present with acute stroke.
With relatively little specialty support available, it becomes more important for communication between providers to be clear and reliable; and practitioners must determine the local standard of care.
“I think with stroke it’s a particularly vexing issue, especially when you get outside of metropolitan areas,” says Larry Goldstein, MD, director of the Duke University Stroke Center, Durham, N.C. “In metropolitan areas there may be hospitals with different capabilities that are not too far from one another. And it may make sense in that situation for one hospital to decide on their own: ‘We just don’t have the resources to be able to treat a specific condition, … and it might be better … for patients to not come here for that since we can’t offer the appropriate level of care for that condition.’”
But in rural and other less populated areas, he says “ … that community hospital may be the only game in town. And even though they … wouldn’t have everything that a tertiary care [or] quaternary care academic center would have, they could identify areas that are critically important for the acute care patients they are serving and develop the appropriate levels of competency in that area.”
Administering Thrombolytics
What is the standard by which an individual hospitalist is expected to practice, especially concerning the administration of tPA?
In that regard—without a doubt—patient safety comes first. “Whenever there’s confusion in my mind, I always think … first, do no harm,” says Dr. Sachdeva. “If this is an urban area and other hospitalists are not [administering] tPA, then they are not expected to do so and that may not meet the standard of care for that area. Rural hospitals have successfully been giving tPA to patients with acute ischemic stroke.
The caveat here is that appropriate planning as well as training of caregivers has to take place prior to starting IV tPA administration. “Rural hospitals that have the IV tPA capability usually do so in collaboration with larger regional institutions, academic or otherwise, where services of neurologists and neurosurgeons are available,” says Dr. Sachdeva. “Size of the institution should not be an impediment to IV tPA administration.”
As baby boomers age, the demand for better stroke care will increase, and hospitals as well as caregivers need to be prepared to meet the expectations of patients.
David Thurber, MD, medical director of the Cary Hospital Medicine Service, a division of Wake Medical Center, Cary, N.C., speaks of the need for specialty backup at community hospitals.
“For those people who practice in community hospitals, including myself,” he says, “it’s like being the pitcher on a baseball team: If you can’t field the outfield, you shouldn’t be pitching the ball because there’s nobody out there to catch it. So if you can’t get the backup of a neurologist, or of a neurosurgeon in the case of hemorrhagic stroke, in my opinion you have no business pushing tPA. Your obligation is to try, as many community hospitals have done with invasive cardiac procedures, such as emergent use of percutaneous coronary artery intervention, to transfer the patient to a facility where those can be done in a timely fashion.”
What should hospitalists do if they are expected to administer tPA and are unsure of their skill level?
“I would take this issue back to the administration of the hospital,” says Dr. Sachdeva, “and come up with a plan where the neurologists or the emergency department physicians feel motivated to give tPA.”
The most important element to consider when making the decision of whether to administer tPA is the quality of the history. “If there is any doubt about the time or the mechanism of stroke onset, then as practitioners we are very well justified in not giving tPA,” says Dr. Sachdeva, who believes there are more lawsuits for not giving tPA than for giving it. But if you withhold tPA and justify the decision with appropriate reasoning, that certainly places the individual on steadier legal ground.
Training and Competence
Stroke management is not a universally strong topic in medical education. “Not every medical school requires a rotation in the neurosciences or exposure to stroke treatment,” says Dr. Goldstein, “and it’s the same thing in residency programs, depending on which residency program you go through, be it as an internist or as an emergency physician. … So it begins in medical school and follows through residency, but as we know, our training only begins in those formal settings. In medicine, training is a lifelong activity. Things change all the time. And it would [take] appropriate levels of continuing education directly related to cerebrovascular disease to be able to understand modern diagnosis and modern therapeutics.”
Another issue is whether an institution will receive patients for stroke treatment. “Just as hospitals credential people to [perform] procedures, not every hospital can offer every therapy to every patient at the same level,” says Dr. Goldstein. “The thing that is inappropriate is to force people to do things for which they’re not trained.”
Although that is also partially an institutional decision, “institutions can’t have it both ways,” he explains. “They can’t say well, we’re going to be taking care of patients with X, Y, or Z, but then not have the facilities and personnel available to be able to acutely treat and stabilize patients even if they do require more advanced care somewhere else.”
Dr. Sachdeva’s team had to cover a considerable knowledge gap to bring his colleagues up to speed and competence by talking directly to the hospitalists and arranging CMEs for them, as well as by encouraging them to get certified in using the National Institutes of Health (NIH) stroke scale.
“The key is for hospitalists to make sure when they’re taking on an area of patient care that they feel comfortable doing that and not themselves be the default for any medical or surgical conditions,” says David Likosky, MD, who is board certified in neurology and internal medicine, and is the director of the Stroke Program of Evergreen Healthcare, Kirkland, Wash.
One way to become better prepared to manage stroke is to familiarize oneself with the National Institutes of Health (NIH) stroke scale. Online training for the NIH Stroke Scale (approved for two hours of category 1 CME credit from the NIH) is available at www.ninds.nih.gov/doctors/NIH_Stroke_Scale.pdf.).
Excellent resources for developing protocols include the American Stroke Association/American Heart Association, the work of the Brain Attack Coalition (a group of professional, voluntary, and governmental entities dedicated to reducing the occurrence, disabilities, and death associated with stroke—www.stroke-site.org/), and the Web site (www.strokecenter.org), produced out of Washington University in St. Louis. SHM (www.hospitalmedicine.org), which is in the process of creating a Web-based stroke resource room, which—at press time—was scheduled to be live by August 1.
—David Thurber, MD
Systems and Monitoring
Having the right systems in place enables smooth patient assessment and treatment. First establish a means for education in stroke care for hospitalists and all support staff. Other important systems include having protocols for admitting [patients] for stroke care; setting up communication pathways for various disciplines involved in stroke care; having systems to gather, analyze, and monitor data; and having particularly good teamwork and response time.
William Likosky, MD, director of the Stroke Program at the Swedish Medical Center, Seattle, strongly believes in systems and processes of care, whereby a well-designed system should not only be able to prevent mistakes by an individual caregiver, but also to facilitate optimal evidence-based care in every case. As an institution Swedish Medical draws inspiration from the Institute of Healthcare Improvement’s campaign to prevent 100,000 avoidable deaths nationwide in its hospitalized patients. Since its inception at Swedish Medical two years ago, the stroke program is credited with preventing 22 deaths.
Of course any protocol’s worth will vary according to the effectiveness with which it is implemented. Developing protocols and care pathways is an avenue for hospitalists to take a leadership role in implementing evidence-based care, in co-ordinating care between different services, and eventually affecting resource utilization, quality of care, and patient satisfaction positively.
Protocols or pathways fail when they’re not patient-centered, when input isn’t solicited from other caregivers during the development phase, or when their implementation is not monitored. To Dr. Sachdeva, “the main issue is how you implement [the protocol], how you monitor the implementation, and how you fix the glitches or the problems that usually ensue when you’re rolling out a new protocol.”
Response and Feedback
Another imperative of any stroke program is its response time. “We monitor very closely our emergency department evaluation times for patients coming in within the window for giving tPA,” says Dr. Sachdeva. “We are strict about this because we want every patient to be evaluated within 45 minutes—anybody who is a candidate for possible intervention with acute thrombolytics—either IV or IA. Those times are monitored, and any time that 45-minute window is missed, we have an individual conversation with the people who were responsible, not as a confrontation, but [to ask], ‘What can we do to help you?’ And each time we do that we learn something new.
“Usually in these cases, there were things that were happening that were out of control and sometimes you can control them and sometimes you can’t,” he says. “Next time we try to manage the variables better. So we do have a hands-on continuous monitoring process that is not intrusive, and it gives us an idea of how we are holding up with certain quality parameters.”
Teamwork and Communication
One of the important systems is how well all involved work as a team. “Most of the time, IV tPA is given in the emergency department and the emergency department doctors now are very comfortable giving IV tPA with the telephonic help from a neurologist,” says Dr. Sachdeva. “But they also receive assistance from the stroke nurse, who consults on every stroke patient who is a candidate for emergent intervention in the emergency department.”
Swedish Medical maintains dedicated stroke nurses who act as facilitators to ensure everybody holds up their end of the bargain in stroke care. This includes a combination of nurses and nurse practitioners. But ultimately it is the emergency department physician’s decision in consultation with the neurologist by phone.
Part of their facilitation involves negotiating to cut down on time. “We don’t … rush our patients, but we cut down on avoidable delays,” says Dr. Sachdeva. “We try to get all the pertinent workup done as fast as we can, and then collate the data, make sure the data are disseminated to the parties that need the data, and decisions are made and appropriate treatment algorithms applied.”
These dedicated nurses are available in person for any acute stroke that falls within the window for an emergent intervention. “But if it is [an] acute stroke outside the window,” says Dr. Sachdeva, “they will consult telephonically to help you get certain things started, and then consult on the patient the next business day. They are available 24/7 both to the emergency department and to any floor area of the hospital. Anyplace that stroke can happen … they are there in a heartbeat. And the stroke nurses have been invaluable in assisting the hospitalists in day-to-day care of the stroke patients as well as in educating patients and their families.”
Controversies in Stroke Management
Although many hospitalists are uncomfortable treating ischemic strokes, far more may show discomfort at the idea of treating hemorrhagic strokes.
“Bleeding within the head carries a morbidity and mortality that sometimes is exaggerated in terms of its perception,” he says, “and once again, one has to look at the training that was given to most hospitalists during their residency. It was insufficient with respect to managing intracranial hemorrhages.”
Treating hemorrhagic strokes has traditionally been the preserve of neurosurgeons. “Some neurosurgeons are of the opinion that if there is no indication for surgical intervention for a particular ICH case, then the patient should be on the medical service,” says Dr. Sachdeva. “The medical side is feeling thoroughly unprepared to handle these.”
His team is looking at this issue at their institution to come up with appropriate algorithms regarding triage and care of patients with ICH.
Hospitalists and Stroke Management: Opportunities
One advantage of the hospitalist system in managing stroke is that hospitalists are readily available. Monitoring patients’ recovery for any emergent complications is also an important role for the hospitalist. Most often these complications are urinary tract infections, aspiration pneumonia, and deep venous thrombosis.
The team at Swedish refers to these high-risk complications as “dashboards,” likening them to the dashboard of an automobile that must be carefully watched.
Swedish Medical has seven markers for quality of care that the stroke team monitors. They have a statistician, people who gather the data, people who analyze the data, and those who then put the data in a graph format for the team to review trends reflecting quality of care.
This secondary prevention comes into play while coordinating care at the time of discharge. Hospitalists can start the ball rolling so a primary care physician or the facility to which the patient may next be transferred will continue the appropriate care for these patients.
Hospitalists could also take leadership role within their institutions in formulating pathways for emergent evaluation of strokes that occur in hospitalized patients.
“This is what most hospitalists should be able to do with adequate training,” says Dr. Sachdeva. “At the very least, hospitalists can positively impact stroke care by setting into place protocols, processes, and systems of care to ensure prevention DVTs, UTIs, aspiration pneumonias, and initiation of appropriate secondary prevention modalities for patients admitted with a diagnosis of stroke.”
Any institution that prevents these complications from developing should see an automatic benefit of those quality parameters in decreased length of stay, decreased utilization of resources, and improved patient satisfaction.
Follow-Up and Compliance
Having the undivided attention of the patient and his or her family at the time of hospitalization is a golden opportunity.
“We start patients on a vigorous, evidence-based secondary prevention regimen and by opening a dialogue with the patient and the family,” says Dr. Sachdeva. “Realize you’ve started something good; it needs to be followed up and reinforced on a regular basis either through their primary care provider or through a dedicated stroke follow-up clinic.”
The plan for handling a potential future brain attack is also outlined. One of the most noteworthy programs for secondary prevention of strokes is the one out of the University of California, Los Angeles called PROTECT—Preventing Recurrence of Thromboembolic Events through Coordinated Treatment (http://strokeprotect.mednet.ucla.edu/). (See p. 22.)2
Dr. Thurber, who is also president of the Piedmont Chapter of SHM, hopes that secondary prevention work by stroke teams around the country and the results of public education campaigns can help reduce the number of patients who present for stroke treatment outside the time window for thrombolytic therapy.
Communication with PCPs
If you have a dedicated group of primary care physicians that you work with, then they are, in effect, your customers. They should develop that program so they can give their input as how they would like communication and they can know what kind of care their patients will receive once admitted to the hospitalists or the hospitalist-neurologist team.
Call the primary care physicians at the time of discharge in order to convey the highlights of hospitalization and review key follow-up issues. Information can fall through the cracks, but the PROTECT program shows that this is rare if you use the tools provided as part of the program.1 Their data show that initiating secondary prevention modalities while the patient is hospitalized is important, but following up on them is just as important to good outcomes.
The discharging physician must partner with the primary care providers to maintain the momentum with respect to secondary prevention, re-enforcing education, and monitoring for development of side effects from the medications initiated during hospitalization.
Future Trends
Given the trends of an expanding hospitalist system, increasing time limitations for specialists, the relative dearth of neurologists, and uninviting circumstances for practice and compensation, neurologists will need to partner with a group of physicians who are structured to be available 24/7.
In his coauthored letter to the editor of Stroke, published in June 2005, Dr. Likosky challenged neurologists to avoid being “asleep at the wheel” in stroke prevention.1 “If neurologists want to be the ones taking care of stroke patients,” he said, “then they need to decide what role they want to play, because otherwise it’s going to be taken over by hospitalists, which may be the most appropriate thing.”
Conclusion
Challenges and opportunities characterize the work of hospitalists involved in stroke care. Good, ongoing training is imperative as are effective institutional systems and efficient monitoring of those systems. Protocols can be adapted to best serve an individual institution; the nature of their implementation and the teamwork or lack thereof will make the difference in the benefit to medical and institutional outcomes.
Recommendations for best performance in stroke care include keeping open channels of communication and good feedback systems, discussing controversies in order to seek resolutions and improve systems, and using the advantage of access to patients and their families to best begin follow-up and secondary prevention efforts. TH
Writer Andrea M. Sattinger will cover the malpractice crisis in healthcare in future issues of The Hospitalist.
References
- Likosky DJ. Who will care for our hospitalized patients? Stroke. 2005;36:1113-1114.
- Ovbiagele B, Saver JL, Fredieu A, et al. PROTECT: A coordinated stroke treatment program to prevent recurrent thromboembolic events. Neurology. 2004;63:1217-1222.
Distinguishing the evolving role of the hospitalist in managing patients with stroke requires exploring a number of challenges, a couple of controversies, and some clear opportunities.
Challenges
Hospitalists and their specialist colleagues face a number of challenges associated with stroke management, including the nature of provider teamwork, whether patients present within the window of time for thrombolytic administration, whether hospitalists should administer those agents, and also the care of patients with intracerebral hemorrhage (ICH).
Specialty Support
Traditionally the neurologist has been the key clinician involved in the diagnosis and treatment of patients with stroke. And because a great many neurologists prefer to practice almost exclusively in the outpatient setting, a team of providers in the hospital must handle the current stroke care volume.
“Coming to the hospital can be a challenge for some of them, although there is a subset of neurologists who really like to be inside the hospital and look after acute issues with respect to neurology,” says Sandeep Sachdeva, MD, Swedish Medical Center in Seattle. “In our institution we’ve had enough neurologists, but most of them are busy with their outpatient practices so they’re not able to spend substantial time [in the hospital]. By default we have to look at the hospitalist program here as a resource for taking care of stroke patients.”1
Emergent evaluation and treatment of acute ischemic stroke is a hot-button issue, especially for community-based hospitals. Some neurologists can leave their office and attend to an acute ischemic stroke presenting to the emergency department, while others can’t. To address this issue some hospitals have developed stroke teams that usually consist of highly trained nurses/advanced registered nurse practitioners (ARNPs) working under the direction of a neurologist, as is the case at Swedish Medical Center. These stroke teams respond to acute strokes presenting in the emergency department and then assist the emergency department physician in expediting the patient evaluation and ensuring that no protocol violation occurs while emergent therapy, such as IV tPA, is administered.
The final decision for administering this medication rests with the emergency department physician and, in some instances, with the neurologist if he or she is able to evaluate the patient in the emergency department. Hospitalists must evaluate their comfort level, knowledge, and experience—and then discuss with their neurologists and emergency department physicians the development of—a care algorithm commensurate with national and local standards of care as it pertains to caring for patients who present with acute stroke.
With relatively little specialty support available, it becomes more important for communication between providers to be clear and reliable; and practitioners must determine the local standard of care.
“I think with stroke it’s a particularly vexing issue, especially when you get outside of metropolitan areas,” says Larry Goldstein, MD, director of the Duke University Stroke Center, Durham, N.C. “In metropolitan areas there may be hospitals with different capabilities that are not too far from one another. And it may make sense in that situation for one hospital to decide on their own: ‘We just don’t have the resources to be able to treat a specific condition, … and it might be better … for patients to not come here for that since we can’t offer the appropriate level of care for that condition.’”
But in rural and other less populated areas, he says “ … that community hospital may be the only game in town. And even though they … wouldn’t have everything that a tertiary care [or] quaternary care academic center would have, they could identify areas that are critically important for the acute care patients they are serving and develop the appropriate levels of competency in that area.”
Administering Thrombolytics
What is the standard by which an individual hospitalist is expected to practice, especially concerning the administration of tPA?
In that regard—without a doubt—patient safety comes first. “Whenever there’s confusion in my mind, I always think … first, do no harm,” says Dr. Sachdeva. “If this is an urban area and other hospitalists are not [administering] tPA, then they are not expected to do so and that may not meet the standard of care for that area. Rural hospitals have successfully been giving tPA to patients with acute ischemic stroke.
The caveat here is that appropriate planning as well as training of caregivers has to take place prior to starting IV tPA administration. “Rural hospitals that have the IV tPA capability usually do so in collaboration with larger regional institutions, academic or otherwise, where services of neurologists and neurosurgeons are available,” says Dr. Sachdeva. “Size of the institution should not be an impediment to IV tPA administration.”
As baby boomers age, the demand for better stroke care will increase, and hospitals as well as caregivers need to be prepared to meet the expectations of patients.
David Thurber, MD, medical director of the Cary Hospital Medicine Service, a division of Wake Medical Center, Cary, N.C., speaks of the need for specialty backup at community hospitals.
“For those people who practice in community hospitals, including myself,” he says, “it’s like being the pitcher on a baseball team: If you can’t field the outfield, you shouldn’t be pitching the ball because there’s nobody out there to catch it. So if you can’t get the backup of a neurologist, or of a neurosurgeon in the case of hemorrhagic stroke, in my opinion you have no business pushing tPA. Your obligation is to try, as many community hospitals have done with invasive cardiac procedures, such as emergent use of percutaneous coronary artery intervention, to transfer the patient to a facility where those can be done in a timely fashion.”
What should hospitalists do if they are expected to administer tPA and are unsure of their skill level?
“I would take this issue back to the administration of the hospital,” says Dr. Sachdeva, “and come up with a plan where the neurologists or the emergency department physicians feel motivated to give tPA.”
The most important element to consider when making the decision of whether to administer tPA is the quality of the history. “If there is any doubt about the time or the mechanism of stroke onset, then as practitioners we are very well justified in not giving tPA,” says Dr. Sachdeva, who believes there are more lawsuits for not giving tPA than for giving it. But if you withhold tPA and justify the decision with appropriate reasoning, that certainly places the individual on steadier legal ground.
Training and Competence
Stroke management is not a universally strong topic in medical education. “Not every medical school requires a rotation in the neurosciences or exposure to stroke treatment,” says Dr. Goldstein, “and it’s the same thing in residency programs, depending on which residency program you go through, be it as an internist or as an emergency physician. … So it begins in medical school and follows through residency, but as we know, our training only begins in those formal settings. In medicine, training is a lifelong activity. Things change all the time. And it would [take] appropriate levels of continuing education directly related to cerebrovascular disease to be able to understand modern diagnosis and modern therapeutics.”
Another issue is whether an institution will receive patients for stroke treatment. “Just as hospitals credential people to [perform] procedures, not every hospital can offer every therapy to every patient at the same level,” says Dr. Goldstein. “The thing that is inappropriate is to force people to do things for which they’re not trained.”
Although that is also partially an institutional decision, “institutions can’t have it both ways,” he explains. “They can’t say well, we’re going to be taking care of patients with X, Y, or Z, but then not have the facilities and personnel available to be able to acutely treat and stabilize patients even if they do require more advanced care somewhere else.”
Dr. Sachdeva’s team had to cover a considerable knowledge gap to bring his colleagues up to speed and competence by talking directly to the hospitalists and arranging CMEs for them, as well as by encouraging them to get certified in using the National Institutes of Health (NIH) stroke scale.
“The key is for hospitalists to make sure when they’re taking on an area of patient care that they feel comfortable doing that and not themselves be the default for any medical or surgical conditions,” says David Likosky, MD, who is board certified in neurology and internal medicine, and is the director of the Stroke Program of Evergreen Healthcare, Kirkland, Wash.
One way to become better prepared to manage stroke is to familiarize oneself with the National Institutes of Health (NIH) stroke scale. Online training for the NIH Stroke Scale (approved for two hours of category 1 CME credit from the NIH) is available at www.ninds.nih.gov/doctors/NIH_Stroke_Scale.pdf.).
Excellent resources for developing protocols include the American Stroke Association/American Heart Association, the work of the Brain Attack Coalition (a group of professional, voluntary, and governmental entities dedicated to reducing the occurrence, disabilities, and death associated with stroke—www.stroke-site.org/), and the Web site (www.strokecenter.org), produced out of Washington University in St. Louis. SHM (www.hospitalmedicine.org), which is in the process of creating a Web-based stroke resource room, which—at press time—was scheduled to be live by August 1.
—David Thurber, MD
Systems and Monitoring
Having the right systems in place enables smooth patient assessment and treatment. First establish a means for education in stroke care for hospitalists and all support staff. Other important systems include having protocols for admitting [patients] for stroke care; setting up communication pathways for various disciplines involved in stroke care; having systems to gather, analyze, and monitor data; and having particularly good teamwork and response time.
William Likosky, MD, director of the Stroke Program at the Swedish Medical Center, Seattle, strongly believes in systems and processes of care, whereby a well-designed system should not only be able to prevent mistakes by an individual caregiver, but also to facilitate optimal evidence-based care in every case. As an institution Swedish Medical draws inspiration from the Institute of Healthcare Improvement’s campaign to prevent 100,000 avoidable deaths nationwide in its hospitalized patients. Since its inception at Swedish Medical two years ago, the stroke program is credited with preventing 22 deaths.
Of course any protocol’s worth will vary according to the effectiveness with which it is implemented. Developing protocols and care pathways is an avenue for hospitalists to take a leadership role in implementing evidence-based care, in co-ordinating care between different services, and eventually affecting resource utilization, quality of care, and patient satisfaction positively.
Protocols or pathways fail when they’re not patient-centered, when input isn’t solicited from other caregivers during the development phase, or when their implementation is not monitored. To Dr. Sachdeva, “the main issue is how you implement [the protocol], how you monitor the implementation, and how you fix the glitches or the problems that usually ensue when you’re rolling out a new protocol.”
Response and Feedback
Another imperative of any stroke program is its response time. “We monitor very closely our emergency department evaluation times for patients coming in within the window for giving tPA,” says Dr. Sachdeva. “We are strict about this because we want every patient to be evaluated within 45 minutes—anybody who is a candidate for possible intervention with acute thrombolytics—either IV or IA. Those times are monitored, and any time that 45-minute window is missed, we have an individual conversation with the people who were responsible, not as a confrontation, but [to ask], ‘What can we do to help you?’ And each time we do that we learn something new.
“Usually in these cases, there were things that were happening that were out of control and sometimes you can control them and sometimes you can’t,” he says. “Next time we try to manage the variables better. So we do have a hands-on continuous monitoring process that is not intrusive, and it gives us an idea of how we are holding up with certain quality parameters.”
Teamwork and Communication
One of the important systems is how well all involved work as a team. “Most of the time, IV tPA is given in the emergency department and the emergency department doctors now are very comfortable giving IV tPA with the telephonic help from a neurologist,” says Dr. Sachdeva. “But they also receive assistance from the stroke nurse, who consults on every stroke patient who is a candidate for emergent intervention in the emergency department.”
Swedish Medical maintains dedicated stroke nurses who act as facilitators to ensure everybody holds up their end of the bargain in stroke care. This includes a combination of nurses and nurse practitioners. But ultimately it is the emergency department physician’s decision in consultation with the neurologist by phone.
Part of their facilitation involves negotiating to cut down on time. “We don’t … rush our patients, but we cut down on avoidable delays,” says Dr. Sachdeva. “We try to get all the pertinent workup done as fast as we can, and then collate the data, make sure the data are disseminated to the parties that need the data, and decisions are made and appropriate treatment algorithms applied.”
These dedicated nurses are available in person for any acute stroke that falls within the window for an emergent intervention. “But if it is [an] acute stroke outside the window,” says Dr. Sachdeva, “they will consult telephonically to help you get certain things started, and then consult on the patient the next business day. They are available 24/7 both to the emergency department and to any floor area of the hospital. Anyplace that stroke can happen … they are there in a heartbeat. And the stroke nurses have been invaluable in assisting the hospitalists in day-to-day care of the stroke patients as well as in educating patients and their families.”
Controversies in Stroke Management
Although many hospitalists are uncomfortable treating ischemic strokes, far more may show discomfort at the idea of treating hemorrhagic strokes.
“Bleeding within the head carries a morbidity and mortality that sometimes is exaggerated in terms of its perception,” he says, “and once again, one has to look at the training that was given to most hospitalists during their residency. It was insufficient with respect to managing intracranial hemorrhages.”
Treating hemorrhagic strokes has traditionally been the preserve of neurosurgeons. “Some neurosurgeons are of the opinion that if there is no indication for surgical intervention for a particular ICH case, then the patient should be on the medical service,” says Dr. Sachdeva. “The medical side is feeling thoroughly unprepared to handle these.”
His team is looking at this issue at their institution to come up with appropriate algorithms regarding triage and care of patients with ICH.
Hospitalists and Stroke Management: Opportunities
One advantage of the hospitalist system in managing stroke is that hospitalists are readily available. Monitoring patients’ recovery for any emergent complications is also an important role for the hospitalist. Most often these complications are urinary tract infections, aspiration pneumonia, and deep venous thrombosis.
The team at Swedish refers to these high-risk complications as “dashboards,” likening them to the dashboard of an automobile that must be carefully watched.
Swedish Medical has seven markers for quality of care that the stroke team monitors. They have a statistician, people who gather the data, people who analyze the data, and those who then put the data in a graph format for the team to review trends reflecting quality of care.
This secondary prevention comes into play while coordinating care at the time of discharge. Hospitalists can start the ball rolling so a primary care physician or the facility to which the patient may next be transferred will continue the appropriate care for these patients.
Hospitalists could also take leadership role within their institutions in formulating pathways for emergent evaluation of strokes that occur in hospitalized patients.
“This is what most hospitalists should be able to do with adequate training,” says Dr. Sachdeva. “At the very least, hospitalists can positively impact stroke care by setting into place protocols, processes, and systems of care to ensure prevention DVTs, UTIs, aspiration pneumonias, and initiation of appropriate secondary prevention modalities for patients admitted with a diagnosis of stroke.”
Any institution that prevents these complications from developing should see an automatic benefit of those quality parameters in decreased length of stay, decreased utilization of resources, and improved patient satisfaction.
Follow-Up and Compliance
Having the undivided attention of the patient and his or her family at the time of hospitalization is a golden opportunity.
“We start patients on a vigorous, evidence-based secondary prevention regimen and by opening a dialogue with the patient and the family,” says Dr. Sachdeva. “Realize you’ve started something good; it needs to be followed up and reinforced on a regular basis either through their primary care provider or through a dedicated stroke follow-up clinic.”
The plan for handling a potential future brain attack is also outlined. One of the most noteworthy programs for secondary prevention of strokes is the one out of the University of California, Los Angeles called PROTECT—Preventing Recurrence of Thromboembolic Events through Coordinated Treatment (http://strokeprotect.mednet.ucla.edu/). (See p. 22.)2
Dr. Thurber, who is also president of the Piedmont Chapter of SHM, hopes that secondary prevention work by stroke teams around the country and the results of public education campaigns can help reduce the number of patients who present for stroke treatment outside the time window for thrombolytic therapy.
Communication with PCPs
If you have a dedicated group of primary care physicians that you work with, then they are, in effect, your customers. They should develop that program so they can give their input as how they would like communication and they can know what kind of care their patients will receive once admitted to the hospitalists or the hospitalist-neurologist team.
Call the primary care physicians at the time of discharge in order to convey the highlights of hospitalization and review key follow-up issues. Information can fall through the cracks, but the PROTECT program shows that this is rare if you use the tools provided as part of the program.1 Their data show that initiating secondary prevention modalities while the patient is hospitalized is important, but following up on them is just as important to good outcomes.
The discharging physician must partner with the primary care providers to maintain the momentum with respect to secondary prevention, re-enforcing education, and monitoring for development of side effects from the medications initiated during hospitalization.
Future Trends
Given the trends of an expanding hospitalist system, increasing time limitations for specialists, the relative dearth of neurologists, and uninviting circumstances for practice and compensation, neurologists will need to partner with a group of physicians who are structured to be available 24/7.
In his coauthored letter to the editor of Stroke, published in June 2005, Dr. Likosky challenged neurologists to avoid being “asleep at the wheel” in stroke prevention.1 “If neurologists want to be the ones taking care of stroke patients,” he said, “then they need to decide what role they want to play, because otherwise it’s going to be taken over by hospitalists, which may be the most appropriate thing.”
Conclusion
Challenges and opportunities characterize the work of hospitalists involved in stroke care. Good, ongoing training is imperative as are effective institutional systems and efficient monitoring of those systems. Protocols can be adapted to best serve an individual institution; the nature of their implementation and the teamwork or lack thereof will make the difference in the benefit to medical and institutional outcomes.
Recommendations for best performance in stroke care include keeping open channels of communication and good feedback systems, discussing controversies in order to seek resolutions and improve systems, and using the advantage of access to patients and their families to best begin follow-up and secondary prevention efforts. TH
Writer Andrea M. Sattinger will cover the malpractice crisis in healthcare in future issues of The Hospitalist.
References
- Likosky DJ. Who will care for our hospitalized patients? Stroke. 2005;36:1113-1114.
- Ovbiagele B, Saver JL, Fredieu A, et al. PROTECT: A coordinated stroke treatment program to prevent recurrent thromboembolic events. Neurology. 2004;63:1217-1222.
The Hospital of the Future
What will the hospital of the future look like? How will it function differently than it does today? What will the patient’s experience be like? What role will hospitalists play?
Imagining the hospital of the future may be an exercise in idealism for many of us, but specialists around the world are currently at work redesigning and improving many different components of the modern hospital, from changing how medical professionals work together to introducing new technologies such as “smart clothing” that house a patient’s medication history and needs.
What’s more, hospital-centric organizations, experts, and participants are moving ahead with new approaches, theories, and technology. As time passes, we’ll see which ideas and theories shake out as the best and most practical.
—Larry Wellikson, MD, FACP
What a Hospital will Look Like
The Hospitalist began focusing on what the future will look like earlier this year. “The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data- driven with clear quality measurements, where better performance is rewarded by better compensation, is coming to a hospital near you during your professional career,” wrote SHM CEO Larry Wellikson, MD, FACP, in our March/April 2005 issue.1
Dr. Wellikson then pointed out that “the current system is primarily physician-centered and driven by increasing units of activity rather than how well the job is done. … In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change … .”
Other healthcare professionals have specific dreams or goals for the future. Robin Orr, MPH, president of The Robin Orr Group, Tiburon, Calif., works with healthcare organizations to affect patient-centered care.
“You have to look at an entire culture to truly affect lasting change,” she explains. “This change will encompass the physical environment of the hospital, the patient’s access to information, and, of course, the human side—everyone from doctors to the guy who sweeps the floor.”
Sean Thomas, MD, assistant professor and chief, Division of Medical Informatics, Department of Medicine, John A. Burns School of Medicine, University of Hawaii at Manoa (Honolulu), envisions changing the way physicians review and interpret patient information.
“There’s a constant increase in the amount and complexity of clinical information collected on each patient, and this will only continue to grow,” says Dr. Thomas. “Right now the chart consists of static, self-contained narratives on the care of patients. Little bits of important information are buried in the prose of physician notes ... H&Ps, progress notes, study interpretations—pathology, imaging studies, etc.
“In order to find these bits of info, a physician must read—or likely scan—these documents and pull out what is important,” he continues. “This is a time-consuming process, and the physician runs the risk of missing vital information.”
Dr. Thomas has a vision of “smart” computer software that can pull information into a clinical abstract that provides a dynamic view of the patient’s status. This change calls for re-education of physicians and advances in technology—both of which are realistically attainable.
Regardless of their specific goals for change, most healthcare professionals agree: Improving patient care is the first priority, but so are heightening efficiency, improving costs, and reducing errors in hospitals.
Works in Progress
Numerous professional organizations are working to advance some or all aspects of hospital medicine and administration. Some of the work that is currently underway includes:
- The Institute for Healthcare Improvement (IHI) hosted the 1st Annual International Summit on Redesigning Hospital Care, June 2005 in San Diego, where medical professionals and hospital executives attended sessions on critical care, patient safety, flow, and workforce development.
- The Agency for Healthcare Research and Quality (AHRQ) awarded 108 grants totaling $139 million to advance the use of information technology in healthcare to reduce medical errors, improve the quality of patient care, and reduce the cost of healthcare.
AHRQ also created a National Resource Center for Health Information Technology and is facilitating expert and peer-to-peer collaborative learning and fostering the growth of online communities who are planning, implementing, and researching health information technology (IT).
- Denver Health (DH) has received a $350,000 hospital redesign grant—an Integrated Delivery System Research Network Project Award, which is part of the AHRQ. Its focus will be removing silos of care, or independent treatment groups, between and across hospital disciplines. DH is redesigning its internal and external processes, as well as its infrastructure.
DH is receiving input from operational, organizational, and regulatory experts (among them representatives from the Joint Commission on Accreditation of Healthcare Organizations, CMS, IHI, Microsoft, Siemens, and Ritz Carlton), providers and administrators, patients and their families. DH is creating a hospital command center to collect, control, and disperse information from a central location. It’s also focusing on improving operating room turnover time to accommodate more surgeries.
Hospitalists as Change Agents
Who will be involved in redesigning the hospital? Currently the major players in designing and implementing change include professional, nonprofit, and government associations (such as those listed above), universities, and independent healthcare consulting groups. Many groups work directly with hospitals on pilot programs for change.
Once change reaches the hospital level, different professionals can become involved, including administrators, physicians, and nursing staff.
But what role can (and should) hospitalists play in getting their institution to become a hospital of the future? “In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent,” says David L. Bernd in “The Future Role of Hospitalists.”2 “The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process management initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change. … hospitalists themselves may become the solution to some of the systems that need changing.”
Dr. Wellikson agrees: “Hospitalists, who for the most part are in the beginning of a 20- to 30-year professional career, are primed to play significant roles in this changing dynamic.
Next Month: an In-depth Look
In a series of articles over the next year or so, The Hospitalist will examine specific aspects of the hospital of the future. Experts and leading thinkers will provide their perspectives and plans regarding everything from what the hospital of the future will look like in terms of its physical layout, to how the admissions process might work, to the role that specialty hospitals will play.
Our series will envision the future of medical records and medications, critical care, patient flow, and how teamwork and collaboration might change the way medical personnel work.
In addition, each month we’ll contrast this vision of the future with a look into the distant past of hospitals (see “Flashback: The power of words,” below), providing a glimpse of the earliest beginnings of the institution and the medical profession.
This series on the hospital of the future is designed to encourage you to think progressively and plan ahead. Change waits for no one in hospital medicine, as we all know. Hospitalists must be poised to become active participants in those changes. So stay tuned; the future is coming. TH
Jane Jerrard is an editorial change agent based in Chicago.
References
- Wellikson L. SHM point of view. The Hospitalist. 2005;2:5.
- Bernd DL. The future role of hospitalists. How hospitalists add value. The Hospitalist. 2005;9(S1):4.
What will the hospital of the future look like? How will it function differently than it does today? What will the patient’s experience be like? What role will hospitalists play?
Imagining the hospital of the future may be an exercise in idealism for many of us, but specialists around the world are currently at work redesigning and improving many different components of the modern hospital, from changing how medical professionals work together to introducing new technologies such as “smart clothing” that house a patient’s medication history and needs.
What’s more, hospital-centric organizations, experts, and participants are moving ahead with new approaches, theories, and technology. As time passes, we’ll see which ideas and theories shake out as the best and most practical.
—Larry Wellikson, MD, FACP
What a Hospital will Look Like
The Hospitalist began focusing on what the future will look like earlier this year. “The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data- driven with clear quality measurements, where better performance is rewarded by better compensation, is coming to a hospital near you during your professional career,” wrote SHM CEO Larry Wellikson, MD, FACP, in our March/April 2005 issue.1
Dr. Wellikson then pointed out that “the current system is primarily physician-centered and driven by increasing units of activity rather than how well the job is done. … In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change … .”
Other healthcare professionals have specific dreams or goals for the future. Robin Orr, MPH, president of The Robin Orr Group, Tiburon, Calif., works with healthcare organizations to affect patient-centered care.
“You have to look at an entire culture to truly affect lasting change,” she explains. “This change will encompass the physical environment of the hospital, the patient’s access to information, and, of course, the human side—everyone from doctors to the guy who sweeps the floor.”
Sean Thomas, MD, assistant professor and chief, Division of Medical Informatics, Department of Medicine, John A. Burns School of Medicine, University of Hawaii at Manoa (Honolulu), envisions changing the way physicians review and interpret patient information.
“There’s a constant increase in the amount and complexity of clinical information collected on each patient, and this will only continue to grow,” says Dr. Thomas. “Right now the chart consists of static, self-contained narratives on the care of patients. Little bits of important information are buried in the prose of physician notes ... H&Ps, progress notes, study interpretations—pathology, imaging studies, etc.
“In order to find these bits of info, a physician must read—or likely scan—these documents and pull out what is important,” he continues. “This is a time-consuming process, and the physician runs the risk of missing vital information.”
Dr. Thomas has a vision of “smart” computer software that can pull information into a clinical abstract that provides a dynamic view of the patient’s status. This change calls for re-education of physicians and advances in technology—both of which are realistically attainable.
Regardless of their specific goals for change, most healthcare professionals agree: Improving patient care is the first priority, but so are heightening efficiency, improving costs, and reducing errors in hospitals.
Works in Progress
Numerous professional organizations are working to advance some or all aspects of hospital medicine and administration. Some of the work that is currently underway includes:
- The Institute for Healthcare Improvement (IHI) hosted the 1st Annual International Summit on Redesigning Hospital Care, June 2005 in San Diego, where medical professionals and hospital executives attended sessions on critical care, patient safety, flow, and workforce development.
- The Agency for Healthcare Research and Quality (AHRQ) awarded 108 grants totaling $139 million to advance the use of information technology in healthcare to reduce medical errors, improve the quality of patient care, and reduce the cost of healthcare.
AHRQ also created a National Resource Center for Health Information Technology and is facilitating expert and peer-to-peer collaborative learning and fostering the growth of online communities who are planning, implementing, and researching health information technology (IT).
- Denver Health (DH) has received a $350,000 hospital redesign grant—an Integrated Delivery System Research Network Project Award, which is part of the AHRQ. Its focus will be removing silos of care, or independent treatment groups, between and across hospital disciplines. DH is redesigning its internal and external processes, as well as its infrastructure.
DH is receiving input from operational, organizational, and regulatory experts (among them representatives from the Joint Commission on Accreditation of Healthcare Organizations, CMS, IHI, Microsoft, Siemens, and Ritz Carlton), providers and administrators, patients and their families. DH is creating a hospital command center to collect, control, and disperse information from a central location. It’s also focusing on improving operating room turnover time to accommodate more surgeries.
Hospitalists as Change Agents
Who will be involved in redesigning the hospital? Currently the major players in designing and implementing change include professional, nonprofit, and government associations (such as those listed above), universities, and independent healthcare consulting groups. Many groups work directly with hospitals on pilot programs for change.
Once change reaches the hospital level, different professionals can become involved, including administrators, physicians, and nursing staff.
But what role can (and should) hospitalists play in getting their institution to become a hospital of the future? “In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent,” says David L. Bernd in “The Future Role of Hospitalists.”2 “The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process management initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change. … hospitalists themselves may become the solution to some of the systems that need changing.”
Dr. Wellikson agrees: “Hospitalists, who for the most part are in the beginning of a 20- to 30-year professional career, are primed to play significant roles in this changing dynamic.
Next Month: an In-depth Look
In a series of articles over the next year or so, The Hospitalist will examine specific aspects of the hospital of the future. Experts and leading thinkers will provide their perspectives and plans regarding everything from what the hospital of the future will look like in terms of its physical layout, to how the admissions process might work, to the role that specialty hospitals will play.
Our series will envision the future of medical records and medications, critical care, patient flow, and how teamwork and collaboration might change the way medical personnel work.
In addition, each month we’ll contrast this vision of the future with a look into the distant past of hospitals (see “Flashback: The power of words,” below), providing a glimpse of the earliest beginnings of the institution and the medical profession.
This series on the hospital of the future is designed to encourage you to think progressively and plan ahead. Change waits for no one in hospital medicine, as we all know. Hospitalists must be poised to become active participants in those changes. So stay tuned; the future is coming. TH
Jane Jerrard is an editorial change agent based in Chicago.
References
- Wellikson L. SHM point of view. The Hospitalist. 2005;2:5.
- Bernd DL. The future role of hospitalists. How hospitalists add value. The Hospitalist. 2005;9(S1):4.
What will the hospital of the future look like? How will it function differently than it does today? What will the patient’s experience be like? What role will hospitalists play?
Imagining the hospital of the future may be an exercise in idealism for many of us, but specialists around the world are currently at work redesigning and improving many different components of the modern hospital, from changing how medical professionals work together to introducing new technologies such as “smart clothing” that house a patient’s medication history and needs.
What’s more, hospital-centric organizations, experts, and participants are moving ahead with new approaches, theories, and technology. As time passes, we’ll see which ideas and theories shake out as the best and most practical.
—Larry Wellikson, MD, FACP
What a Hospital will Look Like
The Hospitalist began focusing on what the future will look like earlier this year. “The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data- driven with clear quality measurements, where better performance is rewarded by better compensation, is coming to a hospital near you during your professional career,” wrote SHM CEO Larry Wellikson, MD, FACP, in our March/April 2005 issue.1
Dr. Wellikson then pointed out that “the current system is primarily physician-centered and driven by increasing units of activity rather than how well the job is done. … In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change … .”
Other healthcare professionals have specific dreams or goals for the future. Robin Orr, MPH, president of The Robin Orr Group, Tiburon, Calif., works with healthcare organizations to affect patient-centered care.
“You have to look at an entire culture to truly affect lasting change,” she explains. “This change will encompass the physical environment of the hospital, the patient’s access to information, and, of course, the human side—everyone from doctors to the guy who sweeps the floor.”
Sean Thomas, MD, assistant professor and chief, Division of Medical Informatics, Department of Medicine, John A. Burns School of Medicine, University of Hawaii at Manoa (Honolulu), envisions changing the way physicians review and interpret patient information.
“There’s a constant increase in the amount and complexity of clinical information collected on each patient, and this will only continue to grow,” says Dr. Thomas. “Right now the chart consists of static, self-contained narratives on the care of patients. Little bits of important information are buried in the prose of physician notes ... H&Ps, progress notes, study interpretations—pathology, imaging studies, etc.
“In order to find these bits of info, a physician must read—or likely scan—these documents and pull out what is important,” he continues. “This is a time-consuming process, and the physician runs the risk of missing vital information.”
Dr. Thomas has a vision of “smart” computer software that can pull information into a clinical abstract that provides a dynamic view of the patient’s status. This change calls for re-education of physicians and advances in technology—both of which are realistically attainable.
Regardless of their specific goals for change, most healthcare professionals agree: Improving patient care is the first priority, but so are heightening efficiency, improving costs, and reducing errors in hospitals.
Works in Progress
Numerous professional organizations are working to advance some or all aspects of hospital medicine and administration. Some of the work that is currently underway includes:
- The Institute for Healthcare Improvement (IHI) hosted the 1st Annual International Summit on Redesigning Hospital Care, June 2005 in San Diego, where medical professionals and hospital executives attended sessions on critical care, patient safety, flow, and workforce development.
- The Agency for Healthcare Research and Quality (AHRQ) awarded 108 grants totaling $139 million to advance the use of information technology in healthcare to reduce medical errors, improve the quality of patient care, and reduce the cost of healthcare.
AHRQ also created a National Resource Center for Health Information Technology and is facilitating expert and peer-to-peer collaborative learning and fostering the growth of online communities who are planning, implementing, and researching health information technology (IT).
- Denver Health (DH) has received a $350,000 hospital redesign grant—an Integrated Delivery System Research Network Project Award, which is part of the AHRQ. Its focus will be removing silos of care, or independent treatment groups, between and across hospital disciplines. DH is redesigning its internal and external processes, as well as its infrastructure.
DH is receiving input from operational, organizational, and regulatory experts (among them representatives from the Joint Commission on Accreditation of Healthcare Organizations, CMS, IHI, Microsoft, Siemens, and Ritz Carlton), providers and administrators, patients and their families. DH is creating a hospital command center to collect, control, and disperse information from a central location. It’s also focusing on improving operating room turnover time to accommodate more surgeries.
Hospitalists as Change Agents
Who will be involved in redesigning the hospital? Currently the major players in designing and implementing change include professional, nonprofit, and government associations (such as those listed above), universities, and independent healthcare consulting groups. Many groups work directly with hospitals on pilot programs for change.
Once change reaches the hospital level, different professionals can become involved, including administrators, physicians, and nursing staff.
But what role can (and should) hospitalists play in getting their institution to become a hospital of the future? “In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent,” says David L. Bernd in “The Future Role of Hospitalists.”2 “The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process management initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change. … hospitalists themselves may become the solution to some of the systems that need changing.”
Dr. Wellikson agrees: “Hospitalists, who for the most part are in the beginning of a 20- to 30-year professional career, are primed to play significant roles in this changing dynamic.
Next Month: an In-depth Look
In a series of articles over the next year or so, The Hospitalist will examine specific aspects of the hospital of the future. Experts and leading thinkers will provide their perspectives and plans regarding everything from what the hospital of the future will look like in terms of its physical layout, to how the admissions process might work, to the role that specialty hospitals will play.
Our series will envision the future of medical records and medications, critical care, patient flow, and how teamwork and collaboration might change the way medical personnel work.
In addition, each month we’ll contrast this vision of the future with a look into the distant past of hospitals (see “Flashback: The power of words,” below), providing a glimpse of the earliest beginnings of the institution and the medical profession.
This series on the hospital of the future is designed to encourage you to think progressively and plan ahead. Change waits for no one in hospital medicine, as we all know. Hospitalists must be poised to become active participants in those changes. So stay tuned; the future is coming. TH
Jane Jerrard is an editorial change agent based in Chicago.
References
- Wellikson L. SHM point of view. The Hospitalist. 2005;2:5.
- Bernd DL. The future role of hospitalists. How hospitalists add value. The Hospitalist. 2005;9(S1):4.
Magic Bullets

Patients with acute stroke or transient ischemic attack (TIA) should be admitted to a hospital for initial care and assessment; however, a substantial number of these patients will never be seen by a neurologist because of the limited number of physicians in this specialty area. Currently there is only one neurologist per 26,000 people in the United States, and most neurologists prefer to practice in the outpatient setting.1 According to one study, only 11.3% of stroke patients are attended exclusively by a neurologist.2 Hospitalists play a vital role in overcoming this lack of specialized care for stroke patients.
Pharmacotherapy
A significant body of evidence supports secondary prevention as a critical intervention strategy in reducing stroke risk. Identifying specific risk factors remains pivotal to successful secondary prevention. Managing hypertension, diabetes, and hyperlipidemia serves as an effective preventive role; however, preventive management with antithrombotic agents is an important part of the drug regimen for secondary prevention of recurrent ischemic stroke (IS).3
The choice of pharmacologic agents is based on stroke etiology. Anticoagulants such as warfarin are restricted to patients with stroke due to a cardioembolic source, whereas antiplatelet agents are mainly used to treat noncardioembolic and lacunar strokes.4 Currently, four oral antiplatelet agents may be used as therapy to prevent secondary IS: aspirin (acetylsalicylic acid or ASA), ticlopidine, clopidogrel, and ASA plus extended-release dipyridamole.
Aspirin
ASA is the most widely used and cost-effective antiplatelet agent. A salicylate, it blocks platelet activation by inhibiting the cyclo-oxygenase enzymes (COX-1 and COX-2). In several primary prevention trials ASA was associated with a statistically significant reduction in risk of first myocardial infarction (MI). Neither overall cardiovascular mortality nor total number of strokes was reduced by long-term ASA prophylaxis, however.5
ASA was shown to be effective in secondary prevention of noncardioembolic stroke (offering equivalent or better efficacy compared with warfarin) in the Stroke Prevention in Reversible Ischemia Trial and the Warfarin-Aspirin Recurrent Stroke Study.6 The Swedish Aspirin Low-Dose Trial, Dutch TIA Trial, and United Kingdom Transient Ischaemic Attack Aspirin Trial consistently demonstrated the efficacy and reduced gastric toxicity of low-dose ASA.7 A meta-analysis of 197 randomized trials versus control and 90 randomized comparisons between antiplatelet regimens show risk reduction with ASA of approximately 23% in combined vascular events (MI, stroke, and vascular death).8
Ticlopidine
Ticlopidine hydrochloride (thienopyridine) blocks platelet activation by inhibiting adenosine diphosphate-induced fibrinogen binding.7 Ticlopidine was superior to placebo and high-dose ASA in reducing the occurrence of stroke, MI, or vascular death in patients of both genders who had recent cerebral ischemia. This was demonstrated in two major phase 3 multicenter trials: the Ticlopidine Aspirin Stroke Study and the Canadian American Ticlopidine Study.9 Despite ticlopidine’s efficacy in these trials, the drug has been associated with severe adverse effects, including life-threatening neutropenia (1%) and thrombocytopenic purpura (one per 1,600 to 5,000 patients treated).3
Clopidogrel
The ticlopidine analogue clopidogrel is a potent inhibitor of platelet aggregation induced by adenosine diphosphate.7 The efficacy and safety of clopidogrel was evaluated in a randomized, double-blind, multicenter study—the Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events trial, the largest clinical study of clopidogrel—of 19,000 patients with stroke, MI, or peripheral arterial disease.10
In this study, clopidogrel showed a more favorable safety and tolerability profile than ticlopidine; however, compared with ASA clopidogrel offered only a modest benefit of 8.7% for all cardiovascular events and showed no significant benefit over ASA for recurrent stroke.
Findings from two randomized trials—Clopidogrel in Unstable Angina to Prevent Recurrent Ischemic Events (CURE) and Clopidogrel for the Reduction of Events During Observation (CREDO)—have shown sustained benefits of clopidogrel for combined endpoints of MI, stroke, and vascular death.11-12 The incidence of stroke was very small and the risk of serious bleeding was significantly increased.
These trials provided the rationale to undertake the Management of Atherothrombosis with Clopidogrel in High-Risk Patients with Recent Transient Ischemic Attack or Ischemic Stroke study (MATCH).13 This study was designed to determine whether the addition of ASA to clopidogrel would further reduce the risk of recurrent ischemic attacks in high-risk patients after recent IS or TIA, as was observed with coronary manifestations of atherothrombosis in the CURE and CREDO trials.
MATCH, a randomized, double-blind, placebo-controlled trial, involved 7,599 patients and compared clopidogrel with low-dose ASA plus clopidogrel. During an 18-month follow-up, no significant benefit was observed for ASA plus clopidogrel versus clopidogrel monotherapy; however, there was a significant increase in the risk of life-threatening bleeding in the group receiving combined therapy (2.6% versus 1.3%, respectively). Therefore, ASA plus clopidogrel is not a recommended option for prevention of secondary stroke in cerebrovascular patients.
STROKE
The scope of the problem

Stroke is one of the most significant health problems in the United States. Approximately 700,000 strokes and occur each year. Of these, 200,000 are recurrent strokes.18 Extensive studies have identified increasing age as the leading risk factor for stroke.16
Approximately 72% of stroke patients are older than 65; on average, patients with stroke tend to be older than patients with MI.4-19 Thus, the frequency of stroke will increase dramatically with lengthening of life expectancy and advancing age of our population.
A history of TIA poses another strong risk factor for stroke. Each year approximately 300,000 Americans suffer TIAs; about one-third of these people will develop a stroke.20-21 Risk factors include hypertension, cigarette smoking, diabetes mellitus, hyperlipidemia, obesity, and heart disease.—SS
ASA Plus Extended-Release Dipyridamole
The Second European Stroke Prevention Study (ESPS-2), a randomized trial with 2,500 patients, was conducted to compare the efficacy of ASA plus dipyridamole versus placebo. Dipyridamole is a pyrimidopyrimidine derivative from the papaverine family with antithrombotic properties and vasodilatory effects on cells and vasculature.14 It inhibits phosphodiesterases, resulting in increased concentration of cyclic adenosine monophosphate (cAMP) and cyclic guanine monophosphate (cGMP), which inhibits platelet activation and adhesion.14
ESPS-2 results showed a 38% relative reduction in risk of stroke for the combination versus placebo. The study did not include an ASA-only group. Results prompted reformulation of dipyridamole into a high-dose extended-release capsule combined with low-dose ASA. The higher dose and slower release of dipyridamole combined with ASA provides a more consistent plasma level and is less affected by stomach acidity or concomitant medications.
This combination was tested versus ASA alone in the ESPS-2 trial.15 ESPS-2, a randomized, double-blind, multicenter study, enrolled 6,602 patients with prior stroke or TIA. During the two-year follow-up ASA plus extended-release dipyridamole reduced the risk of recurrent stroke by 37% compared with placebo, and by 22% compared with ASA or dipyridamole alone. Adverse events associated with this combination are similar to those observed with low-dose ASA.
These results were further substantiated by a recent post hoc analysis conducted using data from the ESPS-2 trial. ASA plus extended-release dipyridamole had greater efficacy in preventing stroke than ASA; this difference in efficacy was more pronounced in high-risk patients.16
We need further studies that include direct comparisons to verify the most effective and safe antiplatelet agent for secondary stroke prevention. The Prospective Regimen for Effectively Avoiding Second Strokes (PRoFESS) is a head-to-head trial designed to compare the combination of ASA plus extended-release dipyridamole to clopidogrel in terms of efficacy and safety. This study includes 15,500 patients in more than 20 countries at approximately 600 sites.17
Conclusions
Stroke remains a major public health concern. Hospitalists play a central role in stroke management by improving the overall quality of hospital care for stroke patients. Still, most residency programs don’t provide sufficient stroke education. Therefore, comprehensive neurology educational programs should be provided for hospitalists so they can provide efficient inpatient care; initiate effective secondary prevention strategies tailored to the specific needs of the patients, starting with appropriate antiplatelet therapy; monitor patients at poststroke rehabilitation centers during recovery period; and educate stroke patients and their caregivers about the disease and its risk factors.
Hospitalists can also initiate effective communication with outpatient primary care providers at the time of discharge to help ensure that the secondary prevention strategies initiated in the hospital are not only continued but strengthened. TH
Dr. Sachdeva is lead hospitalist in the Stroke Program at the Swedish Medical Center, Seattle, and clinical instructor at the University of Washington, Seattle.
References
- Kmietowicz Z. United Kingdom needs to double the number of neurologists. BMJ. 2001;322:1508.
- Ringel SP. The neurologist’s role in stroke management. Stroke. 1996; 27(11):1935-1936.
- Weinberger J. Adverse effects and drug interactions of antithrombotic agents used in prevention of ischaemic stroke. Drugs. 2005;65(4):461-471.
- Weinberger J. Managing and preventing ischemic stroke: Part II—risk assessment and prevention of secondary ischemic stroke. Clin Geriatr. 2004;12(8):41-46.
- Patrono C, Coller B, Dalen JF. Platelet-active drugs: the relationship among dose, effectiveness and side effects. Chest. 2001:119(suppl):39S-63S.
- Fayad P, Singh SP. Anti-thrombotic therapy for the secondary prevention of ischemic stroke. Chest. 2004;126(3):483S-512S.
- Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke. Chest. 2001;119(suppl):300S-320S.
- Antiplatelet Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;12;324(7329):71-86.
- Robert S, Miller AJ, Fagan SC. Ticlopidine: a new antiplatelet agent for cerebrovascular disease. Pharmacotherapy. 1991;11(4):317-322.
- CAPRIE Steering Committee. A randomized, blinded trial of clopidogrel versus aspirin in patients at risk for ischemic events. Lancet. 1996;348:1329-1339.
- Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345(7):494-502.
- Steinhubl SR, Berger PB, Mann JT 3rd, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288(19):2411-2420.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364(9431):331-337.
- European Stroke Prevention Study. ESPS Group. Stroke. 1990;21(8):1122-1130.20
- Diener HC, Cunha L, Forbes C, et al. European stroke prevention study. 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143(1-2):1-13.
- Sacco RL, Sivenius J, Diener HC. Efficacy of aspirin plus extended-release dipyridamole in preventing recurrent stroke in high-risk populations. Arch Neurol. 2005;62:403-408.
- PRoFESS Web site. Available at: www.profess-study.com/com/Main/newscentre/news_040604.jsp. Last accessed July 18, 2005
- Weinberger J. Managing and preventing ischemic stroke: Part I—risk assessment and treatment of primary ischemic stroke. Clin Geriatr. 2004;12(7):48-53.
- Heart Disease and Stroke Statistics—2005 Update. Dallas, Texas. American Heart Association; Dallas. 2005
- Johnston SC, Gress DR, Browner WS, et al. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901-2906.
- Feinberg WM, Albers GW, Barnett H, et al. Guidelines for the management of transient ischemic attacks. Stroke. 1994;25:1320-1335.
Patients with acute stroke or transient ischemic attack (TIA) should be admitted to a hospital for initial care and assessment; however, a substantial number of these patients will never be seen by a neurologist because of the limited number of physicians in this specialty area. Currently there is only one neurologist per 26,000 people in the United States, and most neurologists prefer to practice in the outpatient setting.1 According to one study, only 11.3% of stroke patients are attended exclusively by a neurologist.2 Hospitalists play a vital role in overcoming this lack of specialized care for stroke patients.
Pharmacotherapy
A significant body of evidence supports secondary prevention as a critical intervention strategy in reducing stroke risk. Identifying specific risk factors remains pivotal to successful secondary prevention. Managing hypertension, diabetes, and hyperlipidemia serves as an effective preventive role; however, preventive management with antithrombotic agents is an important part of the drug regimen for secondary prevention of recurrent ischemic stroke (IS).3
The choice of pharmacologic agents is based on stroke etiology. Anticoagulants such as warfarin are restricted to patients with stroke due to a cardioembolic source, whereas antiplatelet agents are mainly used to treat noncardioembolic and lacunar strokes.4 Currently, four oral antiplatelet agents may be used as therapy to prevent secondary IS: aspirin (acetylsalicylic acid or ASA), ticlopidine, clopidogrel, and ASA plus extended-release dipyridamole.
Aspirin
ASA is the most widely used and cost-effective antiplatelet agent. A salicylate, it blocks platelet activation by inhibiting the cyclo-oxygenase enzymes (COX-1 and COX-2). In several primary prevention trials ASA was associated with a statistically significant reduction in risk of first myocardial infarction (MI). Neither overall cardiovascular mortality nor total number of strokes was reduced by long-term ASA prophylaxis, however.5
ASA was shown to be effective in secondary prevention of noncardioembolic stroke (offering equivalent or better efficacy compared with warfarin) in the Stroke Prevention in Reversible Ischemia Trial and the Warfarin-Aspirin Recurrent Stroke Study.6 The Swedish Aspirin Low-Dose Trial, Dutch TIA Trial, and United Kingdom Transient Ischaemic Attack Aspirin Trial consistently demonstrated the efficacy and reduced gastric toxicity of low-dose ASA.7 A meta-analysis of 197 randomized trials versus control and 90 randomized comparisons between antiplatelet regimens show risk reduction with ASA of approximately 23% in combined vascular events (MI, stroke, and vascular death).8
Ticlopidine
Ticlopidine hydrochloride (thienopyridine) blocks platelet activation by inhibiting adenosine diphosphate-induced fibrinogen binding.7 Ticlopidine was superior to placebo and high-dose ASA in reducing the occurrence of stroke, MI, or vascular death in patients of both genders who had recent cerebral ischemia. This was demonstrated in two major phase 3 multicenter trials: the Ticlopidine Aspirin Stroke Study and the Canadian American Ticlopidine Study.9 Despite ticlopidine’s efficacy in these trials, the drug has been associated with severe adverse effects, including life-threatening neutropenia (1%) and thrombocytopenic purpura (one per 1,600 to 5,000 patients treated).3
Clopidogrel
The ticlopidine analogue clopidogrel is a potent inhibitor of platelet aggregation induced by adenosine diphosphate.7 The efficacy and safety of clopidogrel was evaluated in a randomized, double-blind, multicenter study—the Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events trial, the largest clinical study of clopidogrel—of 19,000 patients with stroke, MI, or peripheral arterial disease.10
In this study, clopidogrel showed a more favorable safety and tolerability profile than ticlopidine; however, compared with ASA clopidogrel offered only a modest benefit of 8.7% for all cardiovascular events and showed no significant benefit over ASA for recurrent stroke.
Findings from two randomized trials—Clopidogrel in Unstable Angina to Prevent Recurrent Ischemic Events (CURE) and Clopidogrel for the Reduction of Events During Observation (CREDO)—have shown sustained benefits of clopidogrel for combined endpoints of MI, stroke, and vascular death.11-12 The incidence of stroke was very small and the risk of serious bleeding was significantly increased.
These trials provided the rationale to undertake the Management of Atherothrombosis with Clopidogrel in High-Risk Patients with Recent Transient Ischemic Attack or Ischemic Stroke study (MATCH).13 This study was designed to determine whether the addition of ASA to clopidogrel would further reduce the risk of recurrent ischemic attacks in high-risk patients after recent IS or TIA, as was observed with coronary manifestations of atherothrombosis in the CURE and CREDO trials.
MATCH, a randomized, double-blind, placebo-controlled trial, involved 7,599 patients and compared clopidogrel with low-dose ASA plus clopidogrel. During an 18-month follow-up, no significant benefit was observed for ASA plus clopidogrel versus clopidogrel monotherapy; however, there was a significant increase in the risk of life-threatening bleeding in the group receiving combined therapy (2.6% versus 1.3%, respectively). Therefore, ASA plus clopidogrel is not a recommended option for prevention of secondary stroke in cerebrovascular patients.
STROKE
The scope of the problem
Stroke is one of the most significant health problems in the United States. Approximately 700,000 strokes and occur each year. Of these, 200,000 are recurrent strokes.18 Extensive studies have identified increasing age as the leading risk factor for stroke.16
Approximately 72% of stroke patients are older than 65; on average, patients with stroke tend to be older than patients with MI.4-19 Thus, the frequency of stroke will increase dramatically with lengthening of life expectancy and advancing age of our population.
A history of TIA poses another strong risk factor for stroke. Each year approximately 300,000 Americans suffer TIAs; about one-third of these people will develop a stroke.20-21 Risk factors include hypertension, cigarette smoking, diabetes mellitus, hyperlipidemia, obesity, and heart disease.—SS
ASA Plus Extended-Release Dipyridamole
The Second European Stroke Prevention Study (ESPS-2), a randomized trial with 2,500 patients, was conducted to compare the efficacy of ASA plus dipyridamole versus placebo. Dipyridamole is a pyrimidopyrimidine derivative from the papaverine family with antithrombotic properties and vasodilatory effects on cells and vasculature.14 It inhibits phosphodiesterases, resulting in increased concentration of cyclic adenosine monophosphate (cAMP) and cyclic guanine monophosphate (cGMP), which inhibits platelet activation and adhesion.14
ESPS-2 results showed a 38% relative reduction in risk of stroke for the combination versus placebo. The study did not include an ASA-only group. Results prompted reformulation of dipyridamole into a high-dose extended-release capsule combined with low-dose ASA. The higher dose and slower release of dipyridamole combined with ASA provides a more consistent plasma level and is less affected by stomach acidity or concomitant medications.
This combination was tested versus ASA alone in the ESPS-2 trial.15 ESPS-2, a randomized, double-blind, multicenter study, enrolled 6,602 patients with prior stroke or TIA. During the two-year follow-up ASA plus extended-release dipyridamole reduced the risk of recurrent stroke by 37% compared with placebo, and by 22% compared with ASA or dipyridamole alone. Adverse events associated with this combination are similar to those observed with low-dose ASA.
These results were further substantiated by a recent post hoc analysis conducted using data from the ESPS-2 trial. ASA plus extended-release dipyridamole had greater efficacy in preventing stroke than ASA; this difference in efficacy was more pronounced in high-risk patients.16
We need further studies that include direct comparisons to verify the most effective and safe antiplatelet agent for secondary stroke prevention. The Prospective Regimen for Effectively Avoiding Second Strokes (PRoFESS) is a head-to-head trial designed to compare the combination of ASA plus extended-release dipyridamole to clopidogrel in terms of efficacy and safety. This study includes 15,500 patients in more than 20 countries at approximately 600 sites.17
Conclusions
Stroke remains a major public health concern. Hospitalists play a central role in stroke management by improving the overall quality of hospital care for stroke patients. Still, most residency programs don’t provide sufficient stroke education. Therefore, comprehensive neurology educational programs should be provided for hospitalists so they can provide efficient inpatient care; initiate effective secondary prevention strategies tailored to the specific needs of the patients, starting with appropriate antiplatelet therapy; monitor patients at poststroke rehabilitation centers during recovery period; and educate stroke patients and their caregivers about the disease and its risk factors.
Hospitalists can also initiate effective communication with outpatient primary care providers at the time of discharge to help ensure that the secondary prevention strategies initiated in the hospital are not only continued but strengthened. TH
Dr. Sachdeva is lead hospitalist in the Stroke Program at the Swedish Medical Center, Seattle, and clinical instructor at the University of Washington, Seattle.
References
- Kmietowicz Z. United Kingdom needs to double the number of neurologists. BMJ. 2001;322:1508.
- Ringel SP. The neurologist’s role in stroke management. Stroke. 1996; 27(11):1935-1936.
- Weinberger J. Adverse effects and drug interactions of antithrombotic agents used in prevention of ischaemic stroke. Drugs. 2005;65(4):461-471.
- Weinberger J. Managing and preventing ischemic stroke: Part II—risk assessment and prevention of secondary ischemic stroke. Clin Geriatr. 2004;12(8):41-46.
- Patrono C, Coller B, Dalen JF. Platelet-active drugs: the relationship among dose, effectiveness and side effects. Chest. 2001:119(suppl):39S-63S.
- Fayad P, Singh SP. Anti-thrombotic therapy for the secondary prevention of ischemic stroke. Chest. 2004;126(3):483S-512S.
- Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke. Chest. 2001;119(suppl):300S-320S.
- Antiplatelet Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;12;324(7329):71-86.
- Robert S, Miller AJ, Fagan SC. Ticlopidine: a new antiplatelet agent for cerebrovascular disease. Pharmacotherapy. 1991;11(4):317-322.
- CAPRIE Steering Committee. A randomized, blinded trial of clopidogrel versus aspirin in patients at risk for ischemic events. Lancet. 1996;348:1329-1339.
- Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345(7):494-502.
- Steinhubl SR, Berger PB, Mann JT 3rd, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288(19):2411-2420.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364(9431):331-337.
- European Stroke Prevention Study. ESPS Group. Stroke. 1990;21(8):1122-1130.20
- Diener HC, Cunha L, Forbes C, et al. European stroke prevention study. 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143(1-2):1-13.
- Sacco RL, Sivenius J, Diener HC. Efficacy of aspirin plus extended-release dipyridamole in preventing recurrent stroke in high-risk populations. Arch Neurol. 2005;62:403-408.
- PRoFESS Web site. Available at: www.profess-study.com/com/Main/newscentre/news_040604.jsp. Last accessed July 18, 2005
- Weinberger J. Managing and preventing ischemic stroke: Part I—risk assessment and treatment of primary ischemic stroke. Clin Geriatr. 2004;12(7):48-53.
- Heart Disease and Stroke Statistics—2005 Update. Dallas, Texas. American Heart Association; Dallas. 2005
- Johnston SC, Gress DR, Browner WS, et al. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901-2906.
- Feinberg WM, Albers GW, Barnett H, et al. Guidelines for the management of transient ischemic attacks. Stroke. 1994;25:1320-1335.
Patients with acute stroke or transient ischemic attack (TIA) should be admitted to a hospital for initial care and assessment; however, a substantial number of these patients will never be seen by a neurologist because of the limited number of physicians in this specialty area. Currently there is only one neurologist per 26,000 people in the United States, and most neurologists prefer to practice in the outpatient setting.1 According to one study, only 11.3% of stroke patients are attended exclusively by a neurologist.2 Hospitalists play a vital role in overcoming this lack of specialized care for stroke patients.
Pharmacotherapy
A significant body of evidence supports secondary prevention as a critical intervention strategy in reducing stroke risk. Identifying specific risk factors remains pivotal to successful secondary prevention. Managing hypertension, diabetes, and hyperlipidemia serves as an effective preventive role; however, preventive management with antithrombotic agents is an important part of the drug regimen for secondary prevention of recurrent ischemic stroke (IS).3
The choice of pharmacologic agents is based on stroke etiology. Anticoagulants such as warfarin are restricted to patients with stroke due to a cardioembolic source, whereas antiplatelet agents are mainly used to treat noncardioembolic and lacunar strokes.4 Currently, four oral antiplatelet agents may be used as therapy to prevent secondary IS: aspirin (acetylsalicylic acid or ASA), ticlopidine, clopidogrel, and ASA plus extended-release dipyridamole.
Aspirin
ASA is the most widely used and cost-effective antiplatelet agent. A salicylate, it blocks platelet activation by inhibiting the cyclo-oxygenase enzymes (COX-1 and COX-2). In several primary prevention trials ASA was associated with a statistically significant reduction in risk of first myocardial infarction (MI). Neither overall cardiovascular mortality nor total number of strokes was reduced by long-term ASA prophylaxis, however.5
ASA was shown to be effective in secondary prevention of noncardioembolic stroke (offering equivalent or better efficacy compared with warfarin) in the Stroke Prevention in Reversible Ischemia Trial and the Warfarin-Aspirin Recurrent Stroke Study.6 The Swedish Aspirin Low-Dose Trial, Dutch TIA Trial, and United Kingdom Transient Ischaemic Attack Aspirin Trial consistently demonstrated the efficacy and reduced gastric toxicity of low-dose ASA.7 A meta-analysis of 197 randomized trials versus control and 90 randomized comparisons between antiplatelet regimens show risk reduction with ASA of approximately 23% in combined vascular events (MI, stroke, and vascular death).8
Ticlopidine
Ticlopidine hydrochloride (thienopyridine) blocks platelet activation by inhibiting adenosine diphosphate-induced fibrinogen binding.7 Ticlopidine was superior to placebo and high-dose ASA in reducing the occurrence of stroke, MI, or vascular death in patients of both genders who had recent cerebral ischemia. This was demonstrated in two major phase 3 multicenter trials: the Ticlopidine Aspirin Stroke Study and the Canadian American Ticlopidine Study.9 Despite ticlopidine’s efficacy in these trials, the drug has been associated with severe adverse effects, including life-threatening neutropenia (1%) and thrombocytopenic purpura (one per 1,600 to 5,000 patients treated).3
Clopidogrel
The ticlopidine analogue clopidogrel is a potent inhibitor of platelet aggregation induced by adenosine diphosphate.7 The efficacy and safety of clopidogrel was evaluated in a randomized, double-blind, multicenter study—the Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events trial, the largest clinical study of clopidogrel—of 19,000 patients with stroke, MI, or peripheral arterial disease.10
In this study, clopidogrel showed a more favorable safety and tolerability profile than ticlopidine; however, compared with ASA clopidogrel offered only a modest benefit of 8.7% for all cardiovascular events and showed no significant benefit over ASA for recurrent stroke.
Findings from two randomized trials—Clopidogrel in Unstable Angina to Prevent Recurrent Ischemic Events (CURE) and Clopidogrel for the Reduction of Events During Observation (CREDO)—have shown sustained benefits of clopidogrel for combined endpoints of MI, stroke, and vascular death.11-12 The incidence of stroke was very small and the risk of serious bleeding was significantly increased.
These trials provided the rationale to undertake the Management of Atherothrombosis with Clopidogrel in High-Risk Patients with Recent Transient Ischemic Attack or Ischemic Stroke study (MATCH).13 This study was designed to determine whether the addition of ASA to clopidogrel would further reduce the risk of recurrent ischemic attacks in high-risk patients after recent IS or TIA, as was observed with coronary manifestations of atherothrombosis in the CURE and CREDO trials.
MATCH, a randomized, double-blind, placebo-controlled trial, involved 7,599 patients and compared clopidogrel with low-dose ASA plus clopidogrel. During an 18-month follow-up, no significant benefit was observed for ASA plus clopidogrel versus clopidogrel monotherapy; however, there was a significant increase in the risk of life-threatening bleeding in the group receiving combined therapy (2.6% versus 1.3%, respectively). Therefore, ASA plus clopidogrel is not a recommended option for prevention of secondary stroke in cerebrovascular patients.
STROKE
The scope of the problem
Stroke is one of the most significant health problems in the United States. Approximately 700,000 strokes and occur each year. Of these, 200,000 are recurrent strokes.18 Extensive studies have identified increasing age as the leading risk factor for stroke.16
Approximately 72% of stroke patients are older than 65; on average, patients with stroke tend to be older than patients with MI.4-19 Thus, the frequency of stroke will increase dramatically with lengthening of life expectancy and advancing age of our population.
A history of TIA poses another strong risk factor for stroke. Each year approximately 300,000 Americans suffer TIAs; about one-third of these people will develop a stroke.20-21 Risk factors include hypertension, cigarette smoking, diabetes mellitus, hyperlipidemia, obesity, and heart disease.—SS
ASA Plus Extended-Release Dipyridamole
The Second European Stroke Prevention Study (ESPS-2), a randomized trial with 2,500 patients, was conducted to compare the efficacy of ASA plus dipyridamole versus placebo. Dipyridamole is a pyrimidopyrimidine derivative from the papaverine family with antithrombotic properties and vasodilatory effects on cells and vasculature.14 It inhibits phosphodiesterases, resulting in increased concentration of cyclic adenosine monophosphate (cAMP) and cyclic guanine monophosphate (cGMP), which inhibits platelet activation and adhesion.14
ESPS-2 results showed a 38% relative reduction in risk of stroke for the combination versus placebo. The study did not include an ASA-only group. Results prompted reformulation of dipyridamole into a high-dose extended-release capsule combined with low-dose ASA. The higher dose and slower release of dipyridamole combined with ASA provides a more consistent plasma level and is less affected by stomach acidity or concomitant medications.
This combination was tested versus ASA alone in the ESPS-2 trial.15 ESPS-2, a randomized, double-blind, multicenter study, enrolled 6,602 patients with prior stroke or TIA. During the two-year follow-up ASA plus extended-release dipyridamole reduced the risk of recurrent stroke by 37% compared with placebo, and by 22% compared with ASA or dipyridamole alone. Adverse events associated with this combination are similar to those observed with low-dose ASA.
These results were further substantiated by a recent post hoc analysis conducted using data from the ESPS-2 trial. ASA plus extended-release dipyridamole had greater efficacy in preventing stroke than ASA; this difference in efficacy was more pronounced in high-risk patients.16
We need further studies that include direct comparisons to verify the most effective and safe antiplatelet agent for secondary stroke prevention. The Prospective Regimen for Effectively Avoiding Second Strokes (PRoFESS) is a head-to-head trial designed to compare the combination of ASA plus extended-release dipyridamole to clopidogrel in terms of efficacy and safety. This study includes 15,500 patients in more than 20 countries at approximately 600 sites.17
Conclusions
Stroke remains a major public health concern. Hospitalists play a central role in stroke management by improving the overall quality of hospital care for stroke patients. Still, most residency programs don’t provide sufficient stroke education. Therefore, comprehensive neurology educational programs should be provided for hospitalists so they can provide efficient inpatient care; initiate effective secondary prevention strategies tailored to the specific needs of the patients, starting with appropriate antiplatelet therapy; monitor patients at poststroke rehabilitation centers during recovery period; and educate stroke patients and their caregivers about the disease and its risk factors.
Hospitalists can also initiate effective communication with outpatient primary care providers at the time of discharge to help ensure that the secondary prevention strategies initiated in the hospital are not only continued but strengthened. TH
Dr. Sachdeva is lead hospitalist in the Stroke Program at the Swedish Medical Center, Seattle, and clinical instructor at the University of Washington, Seattle.
References
- Kmietowicz Z. United Kingdom needs to double the number of neurologists. BMJ. 2001;322:1508.
- Ringel SP. The neurologist’s role in stroke management. Stroke. 1996; 27(11):1935-1936.
- Weinberger J. Adverse effects and drug interactions of antithrombotic agents used in prevention of ischaemic stroke. Drugs. 2005;65(4):461-471.
- Weinberger J. Managing and preventing ischemic stroke: Part II—risk assessment and prevention of secondary ischemic stroke. Clin Geriatr. 2004;12(8):41-46.
- Patrono C, Coller B, Dalen JF. Platelet-active drugs: the relationship among dose, effectiveness and side effects. Chest. 2001:119(suppl):39S-63S.
- Fayad P, Singh SP. Anti-thrombotic therapy for the secondary prevention of ischemic stroke. Chest. 2004;126(3):483S-512S.
- Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke. Chest. 2001;119(suppl):300S-320S.
- Antiplatelet Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;12;324(7329):71-86.
- Robert S, Miller AJ, Fagan SC. Ticlopidine: a new antiplatelet agent for cerebrovascular disease. Pharmacotherapy. 1991;11(4):317-322.
- CAPRIE Steering Committee. A randomized, blinded trial of clopidogrel versus aspirin in patients at risk for ischemic events. Lancet. 1996;348:1329-1339.
- Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345(7):494-502.
- Steinhubl SR, Berger PB, Mann JT 3rd, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288(19):2411-2420.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364(9431):331-337.
- European Stroke Prevention Study. ESPS Group. Stroke. 1990;21(8):1122-1130.20
- Diener HC, Cunha L, Forbes C, et al. European stroke prevention study. 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143(1-2):1-13.
- Sacco RL, Sivenius J, Diener HC. Efficacy of aspirin plus extended-release dipyridamole in preventing recurrent stroke in high-risk populations. Arch Neurol. 2005;62:403-408.
- PRoFESS Web site. Available at: www.profess-study.com/com/Main/newscentre/news_040604.jsp. Last accessed July 18, 2005
- Weinberger J. Managing and preventing ischemic stroke: Part I—risk assessment and treatment of primary ischemic stroke. Clin Geriatr. 2004;12(7):48-53.
- Heart Disease and Stroke Statistics—2005 Update. Dallas, Texas. American Heart Association; Dallas. 2005
- Johnston SC, Gress DR, Browner WS, et al. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901-2906.
- Feinberg WM, Albers GW, Barnett H, et al. Guidelines for the management of transient ischemic attacks. Stroke. 1994;25:1320-1335.
The Case of the Nonhealing Wound

An 85-year-old female developed a sore on the left foot (see image above) during the past six months. Throughout that time she underwent periodic debridement and local wound care with gentamicin ointment followed by the use of silver sulfadiazine cream dressings, an Unna Boot, and a surgical shoe with heel relief. Despite treatment her wound increased in size, bleeds easily, but it is not painful.
WHAT IS YOUR DIAGNOSIS?
- Pyogenic granuloma;
- Squamous cell carcinoma;
- Amelanotic melanoma;
- erkel cell carcinoma; or
- Hypertrophic granulation tissue?
Discussion
The correct answer is C: amelanotic melanoma. The patient’s skin biopsy revealed a nodular malignant melanoma with ulceration, Clark’s level V, Breslow thickness at least 5.8 mm. She underwent wide local excision with sentinel lymph node biopsy, which was negative for tumor. The defect was repaired with a split-thickness skin graft and temporary wound vacuum. She is being closely monitored for local recurrence and in-transit metastasis.
Melanoma classically presents as an asymmetric, irregularly hyperpigmented lesion with ill-defined borders; however, some melanomas have little to no pigment and can be easily confused with other benign or malignant entities. Amelanotic melanomas comprise about 2% to 8% of all melanomas.1-2 A seemingly amelanotic lesion may have an area of subtle pigmentation peripherally that can be a clue to the diagnosis.2-3 The prognosis of amelanotic melanomas is the same as that of pigmented melanomas and is contingent upon depth of invasion, location, and patient age and gender. Unfortunately, the diagnosis of an amelanotic melanoma is often delayed, leading to more advanced tumors. Treatment is analogous to pigmented melanomas.2
A rapidly proliferating amelanotic melanoma can be clinically confused with a pyogenic granuloma, a benign vascular hyperplasia. Pyogenic granulomas present as solitary, discrete, erythematous papules or pedunculated growths on cutaneous and mucosal surfaces. They are often friable and may ulcerate. Pyogenic granulomas are more common in children and young adults, but they can occur at any age. If a pyogenic granuloma is not surgically excised, its growth will eventually stabilize, leading to involution, necrosis, or shrinkage to a fibrotic papule.4
Hypertrophic granulation tissue is another benign entity that can resemble an amelanotic melanoma. The production of granulation tissue is a normal response in the early proliferative stage of wound healing. Granulation tissue has abundant vascular structures, which give it an erythematous, edematous, and friable appearance. As wound healing progresses, granulation tissue is replaced with new epidermis through re-epithelialization.5 Failure of a wound to show signs of progressive healing should prompt a biopsy to distinguish normal granulation tissue from malignancy. Amelanotic melanoma has been reported in cases of nonhealing diabetic foot ulcers.6
Amelanotic melanoma can also be difficult to clinically distinguish from other malignant growths, such as squamous cell carcinoma. More common in elderly patients, squamous cell carcinoma commonly presents as a pink to erythematous, scaly papule, or plaque on a sun-exposed surface. Treatment of superficial squamous cell carcinoma, such as Bowen’s disease, with cryotherapy or cautery is highly effective; however, if an amelanotic melanoma is mistakenly treated as Bowen’s disease, then the delay in eventual histological diagnosis may result in an advanced stage amelanotic melanoma.7
Merkel cell carcinoma is a highly aggressive tumor that typically presents as an erythematous to violaceous, painless, solitary nodule or plaque that grows rapidly. It usually affects older patients and commonly occurs on the head. It has a high likelihood of local recurrence, metastasis, and poor prognosis.8 Merkel cell carcinomas are rare, and they elicit the same differential diagnoses as amelanotic melanomas. Histological differentiation from amelanotic melanoma is necessary. TH
References
- Adler M, White C. Amelanotic malignant melanoma. Semin Cutan Med Surg. 1997;16:122-130.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000 May;42(5 Pt 1):731-734.
- Bono A, Maurichi A, Moglia D, et al. Clinical and dermatoscopic diagnosis of early amelanotic melanoma. Melanoma Res. 2001;11:491-494.
- Lin RL, Janniger CK. Pyogenic granuloma. Cutis. 2004 Oct;74(4):229-33.
- Freedburg IM, Eisen AZ, Klaus W, et al. Fitzpatrick’s Dermatology in General Medicine, 6th ed. New York: McGraw-Hill 2003;243.
- Gregson CL, Allain TJ. Amelanotic malignant melanoma disguised as a diabetic foot ulcer. Diabet Med. 2004 Aug;21(8):924-927.
- Holder JE, Colloby PS, Fletcher A, et al. Amelanotic superficial spreading malignant melanoma mimicking Bowen’s disease. Br J Dermatol. 1996 Mar;134(3):519-521.
- Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003 Nov;49(5):832-841.
An 85-year-old female developed a sore on the left foot (see image above) during the past six months. Throughout that time she underwent periodic debridement and local wound care with gentamicin ointment followed by the use of silver sulfadiazine cream dressings, an Unna Boot, and a surgical shoe with heel relief. Despite treatment her wound increased in size, bleeds easily, but it is not painful.
WHAT IS YOUR DIAGNOSIS?
- Pyogenic granuloma;
- Squamous cell carcinoma;
- Amelanotic melanoma;
- erkel cell carcinoma; or
- Hypertrophic granulation tissue?
Discussion
The correct answer is C: amelanotic melanoma. The patient’s skin biopsy revealed a nodular malignant melanoma with ulceration, Clark’s level V, Breslow thickness at least 5.8 mm. She underwent wide local excision with sentinel lymph node biopsy, which was negative for tumor. The defect was repaired with a split-thickness skin graft and temporary wound vacuum. She is being closely monitored for local recurrence and in-transit metastasis.
Melanoma classically presents as an asymmetric, irregularly hyperpigmented lesion with ill-defined borders; however, some melanomas have little to no pigment and can be easily confused with other benign or malignant entities. Amelanotic melanomas comprise about 2% to 8% of all melanomas.1-2 A seemingly amelanotic lesion may have an area of subtle pigmentation peripherally that can be a clue to the diagnosis.2-3 The prognosis of amelanotic melanomas is the same as that of pigmented melanomas and is contingent upon depth of invasion, location, and patient age and gender. Unfortunately, the diagnosis of an amelanotic melanoma is often delayed, leading to more advanced tumors. Treatment is analogous to pigmented melanomas.2
A rapidly proliferating amelanotic melanoma can be clinically confused with a pyogenic granuloma, a benign vascular hyperplasia. Pyogenic granulomas present as solitary, discrete, erythematous papules or pedunculated growths on cutaneous and mucosal surfaces. They are often friable and may ulcerate. Pyogenic granulomas are more common in children and young adults, but they can occur at any age. If a pyogenic granuloma is not surgically excised, its growth will eventually stabilize, leading to involution, necrosis, or shrinkage to a fibrotic papule.4
Hypertrophic granulation tissue is another benign entity that can resemble an amelanotic melanoma. The production of granulation tissue is a normal response in the early proliferative stage of wound healing. Granulation tissue has abundant vascular structures, which give it an erythematous, edematous, and friable appearance. As wound healing progresses, granulation tissue is replaced with new epidermis through re-epithelialization.5 Failure of a wound to show signs of progressive healing should prompt a biopsy to distinguish normal granulation tissue from malignancy. Amelanotic melanoma has been reported in cases of nonhealing diabetic foot ulcers.6
Amelanotic melanoma can also be difficult to clinically distinguish from other malignant growths, such as squamous cell carcinoma. More common in elderly patients, squamous cell carcinoma commonly presents as a pink to erythematous, scaly papule, or plaque on a sun-exposed surface. Treatment of superficial squamous cell carcinoma, such as Bowen’s disease, with cryotherapy or cautery is highly effective; however, if an amelanotic melanoma is mistakenly treated as Bowen’s disease, then the delay in eventual histological diagnosis may result in an advanced stage amelanotic melanoma.7
Merkel cell carcinoma is a highly aggressive tumor that typically presents as an erythematous to violaceous, painless, solitary nodule or plaque that grows rapidly. It usually affects older patients and commonly occurs on the head. It has a high likelihood of local recurrence, metastasis, and poor prognosis.8 Merkel cell carcinomas are rare, and they elicit the same differential diagnoses as amelanotic melanomas. Histological differentiation from amelanotic melanoma is necessary. TH
References
- Adler M, White C. Amelanotic malignant melanoma. Semin Cutan Med Surg. 1997;16:122-130.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000 May;42(5 Pt 1):731-734.
- Bono A, Maurichi A, Moglia D, et al. Clinical and dermatoscopic diagnosis of early amelanotic melanoma. Melanoma Res. 2001;11:491-494.
- Lin RL, Janniger CK. Pyogenic granuloma. Cutis. 2004 Oct;74(4):229-33.
- Freedburg IM, Eisen AZ, Klaus W, et al. Fitzpatrick’s Dermatology in General Medicine, 6th ed. New York: McGraw-Hill 2003;243.
- Gregson CL, Allain TJ. Amelanotic malignant melanoma disguised as a diabetic foot ulcer. Diabet Med. 2004 Aug;21(8):924-927.
- Holder JE, Colloby PS, Fletcher A, et al. Amelanotic superficial spreading malignant melanoma mimicking Bowen’s disease. Br J Dermatol. 1996 Mar;134(3):519-521.
- Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003 Nov;49(5):832-841.
An 85-year-old female developed a sore on the left foot (see image above) during the past six months. Throughout that time she underwent periodic debridement and local wound care with gentamicin ointment followed by the use of silver sulfadiazine cream dressings, an Unna Boot, and a surgical shoe with heel relief. Despite treatment her wound increased in size, bleeds easily, but it is not painful.
WHAT IS YOUR DIAGNOSIS?
- Pyogenic granuloma;
- Squamous cell carcinoma;
- Amelanotic melanoma;
- erkel cell carcinoma; or
- Hypertrophic granulation tissue?
Discussion
The correct answer is C: amelanotic melanoma. The patient’s skin biopsy revealed a nodular malignant melanoma with ulceration, Clark’s level V, Breslow thickness at least 5.8 mm. She underwent wide local excision with sentinel lymph node biopsy, which was negative for tumor. The defect was repaired with a split-thickness skin graft and temporary wound vacuum. She is being closely monitored for local recurrence and in-transit metastasis.
Melanoma classically presents as an asymmetric, irregularly hyperpigmented lesion with ill-defined borders; however, some melanomas have little to no pigment and can be easily confused with other benign or malignant entities. Amelanotic melanomas comprise about 2% to 8% of all melanomas.1-2 A seemingly amelanotic lesion may have an area of subtle pigmentation peripherally that can be a clue to the diagnosis.2-3 The prognosis of amelanotic melanomas is the same as that of pigmented melanomas and is contingent upon depth of invasion, location, and patient age and gender. Unfortunately, the diagnosis of an amelanotic melanoma is often delayed, leading to more advanced tumors. Treatment is analogous to pigmented melanomas.2
A rapidly proliferating amelanotic melanoma can be clinically confused with a pyogenic granuloma, a benign vascular hyperplasia. Pyogenic granulomas present as solitary, discrete, erythematous papules or pedunculated growths on cutaneous and mucosal surfaces. They are often friable and may ulcerate. Pyogenic granulomas are more common in children and young adults, but they can occur at any age. If a pyogenic granuloma is not surgically excised, its growth will eventually stabilize, leading to involution, necrosis, or shrinkage to a fibrotic papule.4
Hypertrophic granulation tissue is another benign entity that can resemble an amelanotic melanoma. The production of granulation tissue is a normal response in the early proliferative stage of wound healing. Granulation tissue has abundant vascular structures, which give it an erythematous, edematous, and friable appearance. As wound healing progresses, granulation tissue is replaced with new epidermis through re-epithelialization.5 Failure of a wound to show signs of progressive healing should prompt a biopsy to distinguish normal granulation tissue from malignancy. Amelanotic melanoma has been reported in cases of nonhealing diabetic foot ulcers.6
Amelanotic melanoma can also be difficult to clinically distinguish from other malignant growths, such as squamous cell carcinoma. More common in elderly patients, squamous cell carcinoma commonly presents as a pink to erythematous, scaly papule, or plaque on a sun-exposed surface. Treatment of superficial squamous cell carcinoma, such as Bowen’s disease, with cryotherapy or cautery is highly effective; however, if an amelanotic melanoma is mistakenly treated as Bowen’s disease, then the delay in eventual histological diagnosis may result in an advanced stage amelanotic melanoma.7
Merkel cell carcinoma is a highly aggressive tumor that typically presents as an erythematous to violaceous, painless, solitary nodule or plaque that grows rapidly. It usually affects older patients and commonly occurs on the head. It has a high likelihood of local recurrence, metastasis, and poor prognosis.8 Merkel cell carcinomas are rare, and they elicit the same differential diagnoses as amelanotic melanomas. Histological differentiation from amelanotic melanoma is necessary. TH
References
- Adler M, White C. Amelanotic malignant melanoma. Semin Cutan Med Surg. 1997;16:122-130.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000 May;42(5 Pt 1):731-734.
- Bono A, Maurichi A, Moglia D, et al. Clinical and dermatoscopic diagnosis of early amelanotic melanoma. Melanoma Res. 2001;11:491-494.
- Lin RL, Janniger CK. Pyogenic granuloma. Cutis. 2004 Oct;74(4):229-33.
- Freedburg IM, Eisen AZ, Klaus W, et al. Fitzpatrick’s Dermatology in General Medicine, 6th ed. New York: McGraw-Hill 2003;243.
- Gregson CL, Allain TJ. Amelanotic malignant melanoma disguised as a diabetic foot ulcer. Diabet Med. 2004 Aug;21(8):924-927.
- Holder JE, Colloby PS, Fletcher A, et al. Amelanotic superficial spreading malignant melanoma mimicking Bowen’s disease. Br J Dermatol. 1996 Mar;134(3):519-521.
- Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003 Nov;49(5):832-841.
2005 Election for SHM Board of Directors
The SHM Nominating Committee is requesting nominations for three open seats on the Board of Directors for a three-year term, beginning May 2, 2006. In addition there will be one pediatric hospitalist seat on the SHM Board for a three-year term, beginning May 2, 2006. Pediatricians may submit their nomination for either the open seats or for the specific designated pediatric seat. All SHM members will vote in both the open and pediatric board elections.
Who is eligible to be nominated? Any SHM member in good standing who is:
- Board certified in their primary specialty;
- Available to travel to board meetings twice a year;
- Prepared to respond to e-mails on a daily basis and actively participate in board list serve;
- Willing to serve on SHM committees; and
- Able to commit to a three-year term, ending in 2009.
Candidates may self-nominate or may be nominated by another SHM member. Nominated candidates must submit the following materials for consideration on the board:
- A one-page curriculum vitae (CV) (12-point font size with 1” margins);
- A one-page nominating letter (12-point font size with 1” margins);
- A recent headshot; and
- An optional additional letter of support (one page, 12-point font size with 1” margins)—although these may not come from any current SHM board members. All letters should be addressed to Steven Pantilat, MD, chair, SHM Nominations Committee. Note: The letter of support is only for Nominations Committee use, but for those candidates who are on the election ballot, the CV, headshot, and the nominating letter will be sent as submitted to all voting members of SHM. Letters will be accepted by mail or e-mail only. No faxes accepted due to potential poor quality of transmission.
The criteria used when considering nominees for ballot include:
- Duration of SHM membership;
- Activity as a hospitalist;
- Activity in or contributions to SHM;
- Activity at a local or regional level;
- Prominence as a hospitalist;
- Ability to provide skills or experience not currently found on the board; and
- Ability to add to the diversity of the board.
Timeline
Some of the critical milestone dates for the board nomination process include the following:
October 31, 2005: Deadline for submitting candidates for nomination;
November 28, 2005: Ballots mailed to SHM members
January 5, 2006: Ballots must be received at SHM offices;
January 20, 2006: Notification of candidates of results of election;
January 23, 2006: Election results posted on SHM Web site;
May 2, 2006: Elected board members take office.
If you are interested in being considered as a nominee for the SHM Board, please submit your nomination materials by October 31, 2005, to the SHM Nominations Committee, 190 N. Independence Mall West, Philadelphia, PA 19106-1572.
Questions? Send them via e-mail to [email protected] or call (800) 843-3360.
Core Competencies Are Coming!
Hospital medicine core competencies to be published in January 2006
The Society of Hospital Medicine Core Competencies project continues to move toward publication in early 2006. The goals of the project are to define hospital medicine and provide a framework for the development of hospital medicine curricula throughout the continuum of professional education and training.
The Core Competencies Task Force is chaired by Mike Pistoria, DO, with key input from Dan Dressler, MD, MSc, Sylvia McKean, MD, Alpesh Amin, MD, MBA, and staffed by Tina Budnitz, MPH.
The Core Competencies Task Force developed the methods for the project and overall template for the resulting document. The template divided topic areas into three sections: Clinical, Systems Organization, and Improvement and Procedures. Topics were selected based on the frequency with which they are seen by hospitalists and the areas in which hospitalists lend a particular expertise. The Systems Organization and Improvement section is a perfect example of the latter topics. This section consists of chapters dealing with the nonclinical issues in which a practicing hospitalist should be a proficient expert. Contributors—mostly from within SHM—were recruited to write the chapters.
Once the original chapters were received, an extensive editing process began. This process ensured consistency within and across chapters. In the initial planning process, the task force decided to utilize the Knowledge, Skills, and Attitudes (KSA) domains within each chapter. Additionally, a Systems Organization and Improvement domain was added to each chapter to reflect hospitalist efforts to promote systemwide improvements in care.
As will be detailed when the Competencies are published, the KSA domains follow established definitions in the educational literature and not those commonly used in medical literature. Competencies within each domain were carefully crafted to reflect a specific level of proficiency. In other words, for each competency, it is obvious to the reader exactly what a hospitalist should be able to do and how proficiency would be evaluated.
Another part of the editing process focused on revising each chapter to stand on its own. Given the desire that the Competencies be used for curriculum development and continuing medical education, the members of the task force felt strongly that each chapter should be self-contained so an individual could pull a chapter on Community-Acquired Pneumonia, for example, and have the relevant competencies at his or her disposal.
When the first draft of the document was completed, it was sent out for review by SHM leadership and professional medical organizations. Reviewers from the Association of American Medical Colleges, the Society of General Internal Medicine, the Society of Critical Care Medicine, and the American College of Physicians provided feedback on the Competencies. Comments from other organizations invited to participate are still pending.
The Competencies will be published as a supplement to the forthcoming Journal of Hospital Medicine (JHM) in early 2006. Several related articles are also being prepared to submit to the Journal’s review process. One article will fully detail the Competencies development, while the other will be a primer on using the Competencies. The task force and the JHM editorial staff have discussed the possibility of an ongoing series within the Journal that will highlight examples of the Competencies translated into curricula and program improvements or provide an evidence-based content outline to accompany chapters. SHM is developing several Web-based resources to provide content and training tools that support the Core Competencies.
It is important to realize the publication of the Competencies is the first of many steps to standardize and establish a core curriculum for hospital medicine. The task force recognizes the Core Competencies as a fluid document. Chapters will be added over time and specific competencies within chapters may change as medicine changes and hospitalists’ roles continue to evolve.
Over the next year, the SHM Core Curriculum Task Force will be focused on evaluating the effects of the core competencies, promoting their use, and encouraging the development of curricula based on the framework provided by the competencies. If you are interested in participating in these activities please forward your nomination to participate in the Core Curriculum Task Force to Lillian Higgins at [email protected].
COMMITTEE REPORT
How to Build a Sustainable Career in Hospital Medicine
An interim report from the SHM Career Satisfaction Task Force
By Sylvia McKean, MD, Tosha Wetterneck, MD, and Win Whitcomb, MD
In 2005 SHM recognized the importance of establishing work standards for hospitalists by charging a task force to articulate key work conditions that promote success and wellness for a career in hospital medicine. As a professional society SHM is committed to developing resources for hospitalists that facilitate long and satisfying careers in hospital medicine in diverse work settings.
Since the first SHM survey of hospitalists in 1999, the role of the hospitalist has evolved to address the needs of multiple stakeholders. Reports of stress and dissatisfaction have subsequently generated dialogue on the SHM list serve. In March a recent SHM member commented: “These messages obviously concern me, and I hope the individuals can find a reasonable solution. However, I was wondering: Are management problems like these the exception or the rule?”
As a new specialty, ill-defined and evolving job descriptions can promote burnout along with other factors. Traditional residency programs in internal medicine and pediatrics don’t adequately train physicians to become hospitalists. Lack of clarity about the hospitalist role may create a mismatch between expectations of hospital leaders and junior physicians who have not yet assumed leadership roles. Hospitalists at academic medical centers are faced with additional burdens brought on by Accreditation Council for Graduate Medical Education resident workload restrictions. The absence of career promotion tracks in medical schools may limit advancement and recognition. These issues are not unique to hospital medicine and have surfaced as problems for critical care and emergency medicine.
According to the 1999 survey, burnout in general is correlated with a lower level of perceived autonomy to perform work as one sees fit and to control the professional experience.1 Less recognition by patients, families, and other professionals for a job well done and poor integration with nonphysician team members is associated with burnout. Lacking occupational solidarity as part of a team of professionals, sharing the joys and frustrations with peers, negatively affects job satisfaction.
Although the 1999 SHM study found that burnout was not independently correlated with workload, clearly there is a ceiling beyond which physicians should not work. Consistent with what the literature says about emergency medicine, professions with high demands are more likely to experience burnout. The American College of Emergency Physicians has its own wellness section that includes consensus statements about specific work parameters.
SHM has raised awareness that the hospitalist model cannot be equivalent to office practice. It’s not feasible for hospitalists to work a volume of annual hours equivalent to those worked by primary care physicians and medical specialists How Hospitalists Add Value (a special supplement to The Hospitalist published in April 2005) reinforces the need to structure reimbursement accordingly. At the SHM 2005 Annual Meeting, Tosha Wetterneck, MD, a member of the SHM Career Satisfaction Task Force and an expert on physician burnout, led a workshop on “Burnout and Hospitalists” with Michael Williams.
Progress Report to Date
The work of the task force intersects activities of other SHM committees and task forces. Practice support, education, leadership, benchmarks, and research are fundamental to providing hospitalists with the necessary skill set to succeed. Modifiable factors in the practice (or work environment) of local hospitals will be identified in the near future to optimally support hospitalists. In addition, the SHM 2005 Education Summit identified ongoing education as critical for the development of skills required for academic and administrative advancement.
The task force is focusing on job engagement rather than burnout—its antithesis. A profile of engagement is expected to include a sustainable workload, empowered decision-making, appropriate recognition and compensation, a supportive work environment, a sense of fairness, and meaningful and valued responsibilities appropriate to level of experience.2 Learning opportunities are highly correlated with engagement. Promising approaches to career satisfaction focus on organizational changes that enhance the capacity of hospitalists to cope with the demands of caring for hospitalized patients.
Review of data specific to hospital medicine support the need to define a sustainable workload. Findings on burnout and satisfaction from an Agency for Healthcare Research and Quality-Funded Multicenter Trial of Academic Hospitalists (David Meltzer, MD, PhD, is the principle investigator) at six medical centers provide new information, but may not be applicable to other hospitalist programs. Additional research is needed to identify the key ingredients for a long and professionally rewarding career in hospital medicine and to examine the link between clinician burnout and patient safety in diverse hospital settings.
Short-Term Next Steps—By Jan. 2006
One of the major goals of the Career Satisfaction Task Force is to establish national benchmarks for sustainable work conditions for hospitalists so they are engaged in a career of hospital medicine. The task force identified the following workplace domains:
- Control/autonomy;
- Workload/schedule;
- Community/environment; and
- Reward/recognition.
The task force will:
- Articulate predictors of job satisfaction and engagement in terms of the key domains of work life;
- Define and prioritize educational outreach programs to assist in the development of Core Competencies; and
- Develop a tool kit for building engagement and identifying modifiable factors in the workplace.
Building on the work of other SHM committees, the task force will make specific recommendations about education and practice management support to promote high productivity and career satisfaction despite high workload. Value-added information will be incorporated into the recommendations to promote adequate and fair compensation. The tool kit would be an “ideal model” that SHM would support with an explanation of how to bridge the gap between existing practice and a new flexible work structure that would meet the individual needs of hospitalists. Future revisions of the tool kit would be based on research findings.
Long -Term Next Steps: Two-Year Concurrent Time Line
Dr. Wetterneck will lead an effort to survey the SHM membership about work-life, satisfaction, and burnout to further define key aspects of hospital medicine programs and work life that maximize physician career satisfaction. Information from interviews, focus groups, and prior hospitalist surveys will guide the development of a Hospitalist Worklife and Satisfaction Survey that will be administered to the SHM membership in 2006. The SHM Board has approved funding for this initiative.
The task force will:
- Promote future research into career satisfaction and engagement in hospital medicine to understand the magnitude of the problem of career satisfaction;
- Specify how to structure hospital medicine programs based on actionable data;
- Recommend how SHM can participate in improving the hospital setting as a patient care environment that not only facilitates improved patient outcomes, but also clinician workplace satisfaction for hospitalists;
- Draft a consensus statement for the peer reviewed SHM Journal of Hospital Medicine similar to the Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine;3 and
- Hold a workshop at the 2006 SHM Annual Meeting on Career Satisfaction.
The Career Satisfaction Committee Task Force welcomes your comments. Contact them at [email protected] (Sylvia McKean, MD), [email protected] (Tosha Wetterneck, MD), or [email protected] (Win Whitcomb, MD).
References
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43:72-91.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine. Ann Fam Med. 2004;2(1):S65-74.
WHAT’S ONLINE AT THE SHM WEB SITE
Improve Inpatient Outcomes with New SHM Online Resource
SHM Web site launches Quality Improvement Resource Rooms
In August SHM announced the first in a new online series to help hospitalists improve inpatient outcomes: the SHM Quality Improvement Resource Rooms. Although performance improvement is ultimately a local phenomenon, certain knowledge, approaches, methods, and tools transcend institution and disease.
When it comes to leading quality improvement in the hospital there has never been a pack-and-go road map—until now. With the launch of the SHM Resource Rooms, a hospitalist with nothing more than the motivation to lead measurable performance improvement in the hospital can do just that. The first Resource Room—focused on reducing venous thromboembolism (VTE), the leading cause of preventable hospital deaths—features a downloadable workbook and companion project outline that walks the hospitalist through every step in the improvement process (see details in “How to Use the VTE Resource Room,” below).
Hospitalists who extract the most out of the VTE Resource Room will be able to:
- Understand and use fundamental quality improvement concepts in the hospital;
- Command and teach the VTE prevention literature; and
- Engineer and lead improvement in the hospital.
The Quality Improvement Resource Rooms will support the hospitalist across domains integral to any quality improvement effort: raising collective awareness of a performance gap, knowing what evidence to put into practice, and leveraging experience with the disease as well as the improvement process.
Print and carry a ready-made workbook to guide and document your work. View a presentation depicting the key elements in quality improvement theory. Download a ready-made slide set to propel teaching of VTE prevention in the didactic setting. Adapt practical teaching tips to implement immediately. Review a listing of the pertinent literature. View and modify VTE tools shared by other hospitalists. Or post questions to a moderated forum of VTE and quality improvement experts.
By offering the new online Resource Rooms, the SHM has taken a significant step toward realizing the potential in hospital medicine: to enhance your ability to improve inpatient outcomes. The next step is yours.
At the SHM Web site, navigate to “Quality and Safety,” select “Quality Improvement Resource Rooms,” and then “Venous Thromboembolism (VTE) Resource Room.” TH
The SHM Nominating Committee is requesting nominations for three open seats on the Board of Directors for a three-year term, beginning May 2, 2006. In addition there will be one pediatric hospitalist seat on the SHM Board for a three-year term, beginning May 2, 2006. Pediatricians may submit their nomination for either the open seats or for the specific designated pediatric seat. All SHM members will vote in both the open and pediatric board elections.
Who is eligible to be nominated? Any SHM member in good standing who is:
- Board certified in their primary specialty;
- Available to travel to board meetings twice a year;
- Prepared to respond to e-mails on a daily basis and actively participate in board list serve;
- Willing to serve on SHM committees; and
- Able to commit to a three-year term, ending in 2009.
Candidates may self-nominate or may be nominated by another SHM member. Nominated candidates must submit the following materials for consideration on the board:
- A one-page curriculum vitae (CV) (12-point font size with 1” margins);
- A one-page nominating letter (12-point font size with 1” margins);
- A recent headshot; and
- An optional additional letter of support (one page, 12-point font size with 1” margins)—although these may not come from any current SHM board members. All letters should be addressed to Steven Pantilat, MD, chair, SHM Nominations Committee. Note: The letter of support is only for Nominations Committee use, but for those candidates who are on the election ballot, the CV, headshot, and the nominating letter will be sent as submitted to all voting members of SHM. Letters will be accepted by mail or e-mail only. No faxes accepted due to potential poor quality of transmission.
The criteria used when considering nominees for ballot include:
- Duration of SHM membership;
- Activity as a hospitalist;
- Activity in or contributions to SHM;
- Activity at a local or regional level;
- Prominence as a hospitalist;
- Ability to provide skills or experience not currently found on the board; and
- Ability to add to the diversity of the board.
Timeline
Some of the critical milestone dates for the board nomination process include the following:
October 31, 2005: Deadline for submitting candidates for nomination;
November 28, 2005: Ballots mailed to SHM members
January 5, 2006: Ballots must be received at SHM offices;
January 20, 2006: Notification of candidates of results of election;
January 23, 2006: Election results posted on SHM Web site;
May 2, 2006: Elected board members take office.
If you are interested in being considered as a nominee for the SHM Board, please submit your nomination materials by October 31, 2005, to the SHM Nominations Committee, 190 N. Independence Mall West, Philadelphia, PA 19106-1572.
Questions? Send them via e-mail to [email protected] or call (800) 843-3360.
Core Competencies Are Coming!
Hospital medicine core competencies to be published in January 2006
The Society of Hospital Medicine Core Competencies project continues to move toward publication in early 2006. The goals of the project are to define hospital medicine and provide a framework for the development of hospital medicine curricula throughout the continuum of professional education and training.
The Core Competencies Task Force is chaired by Mike Pistoria, DO, with key input from Dan Dressler, MD, MSc, Sylvia McKean, MD, Alpesh Amin, MD, MBA, and staffed by Tina Budnitz, MPH.
The Core Competencies Task Force developed the methods for the project and overall template for the resulting document. The template divided topic areas into three sections: Clinical, Systems Organization, and Improvement and Procedures. Topics were selected based on the frequency with which they are seen by hospitalists and the areas in which hospitalists lend a particular expertise. The Systems Organization and Improvement section is a perfect example of the latter topics. This section consists of chapters dealing with the nonclinical issues in which a practicing hospitalist should be a proficient expert. Contributors—mostly from within SHM—were recruited to write the chapters.
Once the original chapters were received, an extensive editing process began. This process ensured consistency within and across chapters. In the initial planning process, the task force decided to utilize the Knowledge, Skills, and Attitudes (KSA) domains within each chapter. Additionally, a Systems Organization and Improvement domain was added to each chapter to reflect hospitalist efforts to promote systemwide improvements in care.
As will be detailed when the Competencies are published, the KSA domains follow established definitions in the educational literature and not those commonly used in medical literature. Competencies within each domain were carefully crafted to reflect a specific level of proficiency. In other words, for each competency, it is obvious to the reader exactly what a hospitalist should be able to do and how proficiency would be evaluated.
Another part of the editing process focused on revising each chapter to stand on its own. Given the desire that the Competencies be used for curriculum development and continuing medical education, the members of the task force felt strongly that each chapter should be self-contained so an individual could pull a chapter on Community-Acquired Pneumonia, for example, and have the relevant competencies at his or her disposal.
When the first draft of the document was completed, it was sent out for review by SHM leadership and professional medical organizations. Reviewers from the Association of American Medical Colleges, the Society of General Internal Medicine, the Society of Critical Care Medicine, and the American College of Physicians provided feedback on the Competencies. Comments from other organizations invited to participate are still pending.
The Competencies will be published as a supplement to the forthcoming Journal of Hospital Medicine (JHM) in early 2006. Several related articles are also being prepared to submit to the Journal’s review process. One article will fully detail the Competencies development, while the other will be a primer on using the Competencies. The task force and the JHM editorial staff have discussed the possibility of an ongoing series within the Journal that will highlight examples of the Competencies translated into curricula and program improvements or provide an evidence-based content outline to accompany chapters. SHM is developing several Web-based resources to provide content and training tools that support the Core Competencies.
It is important to realize the publication of the Competencies is the first of many steps to standardize and establish a core curriculum for hospital medicine. The task force recognizes the Core Competencies as a fluid document. Chapters will be added over time and specific competencies within chapters may change as medicine changes and hospitalists’ roles continue to evolve.
Over the next year, the SHM Core Curriculum Task Force will be focused on evaluating the effects of the core competencies, promoting their use, and encouraging the development of curricula based on the framework provided by the competencies. If you are interested in participating in these activities please forward your nomination to participate in the Core Curriculum Task Force to Lillian Higgins at [email protected].
COMMITTEE REPORT
How to Build a Sustainable Career in Hospital Medicine
An interim report from the SHM Career Satisfaction Task Force
By Sylvia McKean, MD, Tosha Wetterneck, MD, and Win Whitcomb, MD
In 2005 SHM recognized the importance of establishing work standards for hospitalists by charging a task force to articulate key work conditions that promote success and wellness for a career in hospital medicine. As a professional society SHM is committed to developing resources for hospitalists that facilitate long and satisfying careers in hospital medicine in diverse work settings.
Since the first SHM survey of hospitalists in 1999, the role of the hospitalist has evolved to address the needs of multiple stakeholders. Reports of stress and dissatisfaction have subsequently generated dialogue on the SHM list serve. In March a recent SHM member commented: “These messages obviously concern me, and I hope the individuals can find a reasonable solution. However, I was wondering: Are management problems like these the exception or the rule?”
As a new specialty, ill-defined and evolving job descriptions can promote burnout along with other factors. Traditional residency programs in internal medicine and pediatrics don’t adequately train physicians to become hospitalists. Lack of clarity about the hospitalist role may create a mismatch between expectations of hospital leaders and junior physicians who have not yet assumed leadership roles. Hospitalists at academic medical centers are faced with additional burdens brought on by Accreditation Council for Graduate Medical Education resident workload restrictions. The absence of career promotion tracks in medical schools may limit advancement and recognition. These issues are not unique to hospital medicine and have surfaced as problems for critical care and emergency medicine.
According to the 1999 survey, burnout in general is correlated with a lower level of perceived autonomy to perform work as one sees fit and to control the professional experience.1 Less recognition by patients, families, and other professionals for a job well done and poor integration with nonphysician team members is associated with burnout. Lacking occupational solidarity as part of a team of professionals, sharing the joys and frustrations with peers, negatively affects job satisfaction.
Although the 1999 SHM study found that burnout was not independently correlated with workload, clearly there is a ceiling beyond which physicians should not work. Consistent with what the literature says about emergency medicine, professions with high demands are more likely to experience burnout. The American College of Emergency Physicians has its own wellness section that includes consensus statements about specific work parameters.
SHM has raised awareness that the hospitalist model cannot be equivalent to office practice. It’s not feasible for hospitalists to work a volume of annual hours equivalent to those worked by primary care physicians and medical specialists How Hospitalists Add Value (a special supplement to The Hospitalist published in April 2005) reinforces the need to structure reimbursement accordingly. At the SHM 2005 Annual Meeting, Tosha Wetterneck, MD, a member of the SHM Career Satisfaction Task Force and an expert on physician burnout, led a workshop on “Burnout and Hospitalists” with Michael Williams.
Progress Report to Date
The work of the task force intersects activities of other SHM committees and task forces. Practice support, education, leadership, benchmarks, and research are fundamental to providing hospitalists with the necessary skill set to succeed. Modifiable factors in the practice (or work environment) of local hospitals will be identified in the near future to optimally support hospitalists. In addition, the SHM 2005 Education Summit identified ongoing education as critical for the development of skills required for academic and administrative advancement.
The task force is focusing on job engagement rather than burnout—its antithesis. A profile of engagement is expected to include a sustainable workload, empowered decision-making, appropriate recognition and compensation, a supportive work environment, a sense of fairness, and meaningful and valued responsibilities appropriate to level of experience.2 Learning opportunities are highly correlated with engagement. Promising approaches to career satisfaction focus on organizational changes that enhance the capacity of hospitalists to cope with the demands of caring for hospitalized patients.
Review of data specific to hospital medicine support the need to define a sustainable workload. Findings on burnout and satisfaction from an Agency for Healthcare Research and Quality-Funded Multicenter Trial of Academic Hospitalists (David Meltzer, MD, PhD, is the principle investigator) at six medical centers provide new information, but may not be applicable to other hospitalist programs. Additional research is needed to identify the key ingredients for a long and professionally rewarding career in hospital medicine and to examine the link between clinician burnout and patient safety in diverse hospital settings.
Short-Term Next Steps—By Jan. 2006
One of the major goals of the Career Satisfaction Task Force is to establish national benchmarks for sustainable work conditions for hospitalists so they are engaged in a career of hospital medicine. The task force identified the following workplace domains:
- Control/autonomy;
- Workload/schedule;
- Community/environment; and
- Reward/recognition.
The task force will:
- Articulate predictors of job satisfaction and engagement in terms of the key domains of work life;
- Define and prioritize educational outreach programs to assist in the development of Core Competencies; and
- Develop a tool kit for building engagement and identifying modifiable factors in the workplace.
Building on the work of other SHM committees, the task force will make specific recommendations about education and practice management support to promote high productivity and career satisfaction despite high workload. Value-added information will be incorporated into the recommendations to promote adequate and fair compensation. The tool kit would be an “ideal model” that SHM would support with an explanation of how to bridge the gap between existing practice and a new flexible work structure that would meet the individual needs of hospitalists. Future revisions of the tool kit would be based on research findings.
Long -Term Next Steps: Two-Year Concurrent Time Line
Dr. Wetterneck will lead an effort to survey the SHM membership about work-life, satisfaction, and burnout to further define key aspects of hospital medicine programs and work life that maximize physician career satisfaction. Information from interviews, focus groups, and prior hospitalist surveys will guide the development of a Hospitalist Worklife and Satisfaction Survey that will be administered to the SHM membership in 2006. The SHM Board has approved funding for this initiative.
The task force will:
- Promote future research into career satisfaction and engagement in hospital medicine to understand the magnitude of the problem of career satisfaction;
- Specify how to structure hospital medicine programs based on actionable data;
- Recommend how SHM can participate in improving the hospital setting as a patient care environment that not only facilitates improved patient outcomes, but also clinician workplace satisfaction for hospitalists;
- Draft a consensus statement for the peer reviewed SHM Journal of Hospital Medicine similar to the Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine;3 and
- Hold a workshop at the 2006 SHM Annual Meeting on Career Satisfaction.
The Career Satisfaction Committee Task Force welcomes your comments. Contact them at [email protected] (Sylvia McKean, MD), [email protected] (Tosha Wetterneck, MD), or [email protected] (Win Whitcomb, MD).
References
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43:72-91.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine. Ann Fam Med. 2004;2(1):S65-74.
WHAT’S ONLINE AT THE SHM WEB SITE
Improve Inpatient Outcomes with New SHM Online Resource
SHM Web site launches Quality Improvement Resource Rooms
In August SHM announced the first in a new online series to help hospitalists improve inpatient outcomes: the SHM Quality Improvement Resource Rooms. Although performance improvement is ultimately a local phenomenon, certain knowledge, approaches, methods, and tools transcend institution and disease.
When it comes to leading quality improvement in the hospital there has never been a pack-and-go road map—until now. With the launch of the SHM Resource Rooms, a hospitalist with nothing more than the motivation to lead measurable performance improvement in the hospital can do just that. The first Resource Room—focused on reducing venous thromboembolism (VTE), the leading cause of preventable hospital deaths—features a downloadable workbook and companion project outline that walks the hospitalist through every step in the improvement process (see details in “How to Use the VTE Resource Room,” below).
Hospitalists who extract the most out of the VTE Resource Room will be able to:
- Understand and use fundamental quality improvement concepts in the hospital;
- Command and teach the VTE prevention literature; and
- Engineer and lead improvement in the hospital.
The Quality Improvement Resource Rooms will support the hospitalist across domains integral to any quality improvement effort: raising collective awareness of a performance gap, knowing what evidence to put into practice, and leveraging experience with the disease as well as the improvement process.
Print and carry a ready-made workbook to guide and document your work. View a presentation depicting the key elements in quality improvement theory. Download a ready-made slide set to propel teaching of VTE prevention in the didactic setting. Adapt practical teaching tips to implement immediately. Review a listing of the pertinent literature. View and modify VTE tools shared by other hospitalists. Or post questions to a moderated forum of VTE and quality improvement experts.
By offering the new online Resource Rooms, the SHM has taken a significant step toward realizing the potential in hospital medicine: to enhance your ability to improve inpatient outcomes. The next step is yours.
At the SHM Web site, navigate to “Quality and Safety,” select “Quality Improvement Resource Rooms,” and then “Venous Thromboembolism (VTE) Resource Room.” TH
The SHM Nominating Committee is requesting nominations for three open seats on the Board of Directors for a three-year term, beginning May 2, 2006. In addition there will be one pediatric hospitalist seat on the SHM Board for a three-year term, beginning May 2, 2006. Pediatricians may submit their nomination for either the open seats or for the specific designated pediatric seat. All SHM members will vote in both the open and pediatric board elections.
Who is eligible to be nominated? Any SHM member in good standing who is:
- Board certified in their primary specialty;
- Available to travel to board meetings twice a year;
- Prepared to respond to e-mails on a daily basis and actively participate in board list serve;
- Willing to serve on SHM committees; and
- Able to commit to a three-year term, ending in 2009.
Candidates may self-nominate or may be nominated by another SHM member. Nominated candidates must submit the following materials for consideration on the board:
- A one-page curriculum vitae (CV) (12-point font size with 1” margins);
- A one-page nominating letter (12-point font size with 1” margins);
- A recent headshot; and
- An optional additional letter of support (one page, 12-point font size with 1” margins)—although these may not come from any current SHM board members. All letters should be addressed to Steven Pantilat, MD, chair, SHM Nominations Committee. Note: The letter of support is only for Nominations Committee use, but for those candidates who are on the election ballot, the CV, headshot, and the nominating letter will be sent as submitted to all voting members of SHM. Letters will be accepted by mail or e-mail only. No faxes accepted due to potential poor quality of transmission.
The criteria used when considering nominees for ballot include:
- Duration of SHM membership;
- Activity as a hospitalist;
- Activity in or contributions to SHM;
- Activity at a local or regional level;
- Prominence as a hospitalist;
- Ability to provide skills or experience not currently found on the board; and
- Ability to add to the diversity of the board.
Timeline
Some of the critical milestone dates for the board nomination process include the following:
October 31, 2005: Deadline for submitting candidates for nomination;
November 28, 2005: Ballots mailed to SHM members
January 5, 2006: Ballots must be received at SHM offices;
January 20, 2006: Notification of candidates of results of election;
January 23, 2006: Election results posted on SHM Web site;
May 2, 2006: Elected board members take office.
If you are interested in being considered as a nominee for the SHM Board, please submit your nomination materials by October 31, 2005, to the SHM Nominations Committee, 190 N. Independence Mall West, Philadelphia, PA 19106-1572.
Questions? Send them via e-mail to [email protected] or call (800) 843-3360.
Core Competencies Are Coming!
Hospital medicine core competencies to be published in January 2006
The Society of Hospital Medicine Core Competencies project continues to move toward publication in early 2006. The goals of the project are to define hospital medicine and provide a framework for the development of hospital medicine curricula throughout the continuum of professional education and training.
The Core Competencies Task Force is chaired by Mike Pistoria, DO, with key input from Dan Dressler, MD, MSc, Sylvia McKean, MD, Alpesh Amin, MD, MBA, and staffed by Tina Budnitz, MPH.
The Core Competencies Task Force developed the methods for the project and overall template for the resulting document. The template divided topic areas into three sections: Clinical, Systems Organization, and Improvement and Procedures. Topics were selected based on the frequency with which they are seen by hospitalists and the areas in which hospitalists lend a particular expertise. The Systems Organization and Improvement section is a perfect example of the latter topics. This section consists of chapters dealing with the nonclinical issues in which a practicing hospitalist should be a proficient expert. Contributors—mostly from within SHM—were recruited to write the chapters.
Once the original chapters were received, an extensive editing process began. This process ensured consistency within and across chapters. In the initial planning process, the task force decided to utilize the Knowledge, Skills, and Attitudes (KSA) domains within each chapter. Additionally, a Systems Organization and Improvement domain was added to each chapter to reflect hospitalist efforts to promote systemwide improvements in care.
As will be detailed when the Competencies are published, the KSA domains follow established definitions in the educational literature and not those commonly used in medical literature. Competencies within each domain were carefully crafted to reflect a specific level of proficiency. In other words, for each competency, it is obvious to the reader exactly what a hospitalist should be able to do and how proficiency would be evaluated.
Another part of the editing process focused on revising each chapter to stand on its own. Given the desire that the Competencies be used for curriculum development and continuing medical education, the members of the task force felt strongly that each chapter should be self-contained so an individual could pull a chapter on Community-Acquired Pneumonia, for example, and have the relevant competencies at his or her disposal.
When the first draft of the document was completed, it was sent out for review by SHM leadership and professional medical organizations. Reviewers from the Association of American Medical Colleges, the Society of General Internal Medicine, the Society of Critical Care Medicine, and the American College of Physicians provided feedback on the Competencies. Comments from other organizations invited to participate are still pending.
The Competencies will be published as a supplement to the forthcoming Journal of Hospital Medicine (JHM) in early 2006. Several related articles are also being prepared to submit to the Journal’s review process. One article will fully detail the Competencies development, while the other will be a primer on using the Competencies. The task force and the JHM editorial staff have discussed the possibility of an ongoing series within the Journal that will highlight examples of the Competencies translated into curricula and program improvements or provide an evidence-based content outline to accompany chapters. SHM is developing several Web-based resources to provide content and training tools that support the Core Competencies.
It is important to realize the publication of the Competencies is the first of many steps to standardize and establish a core curriculum for hospital medicine. The task force recognizes the Core Competencies as a fluid document. Chapters will be added over time and specific competencies within chapters may change as medicine changes and hospitalists’ roles continue to evolve.
Over the next year, the SHM Core Curriculum Task Force will be focused on evaluating the effects of the core competencies, promoting their use, and encouraging the development of curricula based on the framework provided by the competencies. If you are interested in participating in these activities please forward your nomination to participate in the Core Curriculum Task Force to Lillian Higgins at [email protected].
COMMITTEE REPORT
How to Build a Sustainable Career in Hospital Medicine
An interim report from the SHM Career Satisfaction Task Force
By Sylvia McKean, MD, Tosha Wetterneck, MD, and Win Whitcomb, MD
In 2005 SHM recognized the importance of establishing work standards for hospitalists by charging a task force to articulate key work conditions that promote success and wellness for a career in hospital medicine. As a professional society SHM is committed to developing resources for hospitalists that facilitate long and satisfying careers in hospital medicine in diverse work settings.
Since the first SHM survey of hospitalists in 1999, the role of the hospitalist has evolved to address the needs of multiple stakeholders. Reports of stress and dissatisfaction have subsequently generated dialogue on the SHM list serve. In March a recent SHM member commented: “These messages obviously concern me, and I hope the individuals can find a reasonable solution. However, I was wondering: Are management problems like these the exception or the rule?”
As a new specialty, ill-defined and evolving job descriptions can promote burnout along with other factors. Traditional residency programs in internal medicine and pediatrics don’t adequately train physicians to become hospitalists. Lack of clarity about the hospitalist role may create a mismatch between expectations of hospital leaders and junior physicians who have not yet assumed leadership roles. Hospitalists at academic medical centers are faced with additional burdens brought on by Accreditation Council for Graduate Medical Education resident workload restrictions. The absence of career promotion tracks in medical schools may limit advancement and recognition. These issues are not unique to hospital medicine and have surfaced as problems for critical care and emergency medicine.
According to the 1999 survey, burnout in general is correlated with a lower level of perceived autonomy to perform work as one sees fit and to control the professional experience.1 Less recognition by patients, families, and other professionals for a job well done and poor integration with nonphysician team members is associated with burnout. Lacking occupational solidarity as part of a team of professionals, sharing the joys and frustrations with peers, negatively affects job satisfaction.
Although the 1999 SHM study found that burnout was not independently correlated with workload, clearly there is a ceiling beyond which physicians should not work. Consistent with what the literature says about emergency medicine, professions with high demands are more likely to experience burnout. The American College of Emergency Physicians has its own wellness section that includes consensus statements about specific work parameters.
SHM has raised awareness that the hospitalist model cannot be equivalent to office practice. It’s not feasible for hospitalists to work a volume of annual hours equivalent to those worked by primary care physicians and medical specialists How Hospitalists Add Value (a special supplement to The Hospitalist published in April 2005) reinforces the need to structure reimbursement accordingly. At the SHM 2005 Annual Meeting, Tosha Wetterneck, MD, a member of the SHM Career Satisfaction Task Force and an expert on physician burnout, led a workshop on “Burnout and Hospitalists” with Michael Williams.
Progress Report to Date
The work of the task force intersects activities of other SHM committees and task forces. Practice support, education, leadership, benchmarks, and research are fundamental to providing hospitalists with the necessary skill set to succeed. Modifiable factors in the practice (or work environment) of local hospitals will be identified in the near future to optimally support hospitalists. In addition, the SHM 2005 Education Summit identified ongoing education as critical for the development of skills required for academic and administrative advancement.
The task force is focusing on job engagement rather than burnout—its antithesis. A profile of engagement is expected to include a sustainable workload, empowered decision-making, appropriate recognition and compensation, a supportive work environment, a sense of fairness, and meaningful and valued responsibilities appropriate to level of experience.2 Learning opportunities are highly correlated with engagement. Promising approaches to career satisfaction focus on organizational changes that enhance the capacity of hospitalists to cope with the demands of caring for hospitalized patients.
Review of data specific to hospital medicine support the need to define a sustainable workload. Findings on burnout and satisfaction from an Agency for Healthcare Research and Quality-Funded Multicenter Trial of Academic Hospitalists (David Meltzer, MD, PhD, is the principle investigator) at six medical centers provide new information, but may not be applicable to other hospitalist programs. Additional research is needed to identify the key ingredients for a long and professionally rewarding career in hospital medicine and to examine the link between clinician burnout and patient safety in diverse hospital settings.
Short-Term Next Steps—By Jan. 2006
One of the major goals of the Career Satisfaction Task Force is to establish national benchmarks for sustainable work conditions for hospitalists so they are engaged in a career of hospital medicine. The task force identified the following workplace domains:
- Control/autonomy;
- Workload/schedule;
- Community/environment; and
- Reward/recognition.
The task force will:
- Articulate predictors of job satisfaction and engagement in terms of the key domains of work life;
- Define and prioritize educational outreach programs to assist in the development of Core Competencies; and
- Develop a tool kit for building engagement and identifying modifiable factors in the workplace.
Building on the work of other SHM committees, the task force will make specific recommendations about education and practice management support to promote high productivity and career satisfaction despite high workload. Value-added information will be incorporated into the recommendations to promote adequate and fair compensation. The tool kit would be an “ideal model” that SHM would support with an explanation of how to bridge the gap between existing practice and a new flexible work structure that would meet the individual needs of hospitalists. Future revisions of the tool kit would be based on research findings.
Long -Term Next Steps: Two-Year Concurrent Time Line
Dr. Wetterneck will lead an effort to survey the SHM membership about work-life, satisfaction, and burnout to further define key aspects of hospital medicine programs and work life that maximize physician career satisfaction. Information from interviews, focus groups, and prior hospitalist surveys will guide the development of a Hospitalist Worklife and Satisfaction Survey that will be administered to the SHM membership in 2006. The SHM Board has approved funding for this initiative.
The task force will:
- Promote future research into career satisfaction and engagement in hospital medicine to understand the magnitude of the problem of career satisfaction;
- Specify how to structure hospital medicine programs based on actionable data;
- Recommend how SHM can participate in improving the hospital setting as a patient care environment that not only facilitates improved patient outcomes, but also clinician workplace satisfaction for hospitalists;
- Draft a consensus statement for the peer reviewed SHM Journal of Hospital Medicine similar to the Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine;3 and
- Hold a workshop at the 2006 SHM Annual Meeting on Career Satisfaction.
The Career Satisfaction Committee Task Force welcomes your comments. Contact them at [email protected] (Sylvia McKean, MD), [email protected] (Tosha Wetterneck, MD), or [email protected] (Win Whitcomb, MD).
References
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43:72-91.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine. Ann Fam Med. 2004;2(1):S65-74.
WHAT’S ONLINE AT THE SHM WEB SITE
Improve Inpatient Outcomes with New SHM Online Resource
SHM Web site launches Quality Improvement Resource Rooms
In August SHM announced the first in a new online series to help hospitalists improve inpatient outcomes: the SHM Quality Improvement Resource Rooms. Although performance improvement is ultimately a local phenomenon, certain knowledge, approaches, methods, and tools transcend institution and disease.
When it comes to leading quality improvement in the hospital there has never been a pack-and-go road map—until now. With the launch of the SHM Resource Rooms, a hospitalist with nothing more than the motivation to lead measurable performance improvement in the hospital can do just that. The first Resource Room—focused on reducing venous thromboembolism (VTE), the leading cause of preventable hospital deaths—features a downloadable workbook and companion project outline that walks the hospitalist through every step in the improvement process (see details in “How to Use the VTE Resource Room,” below).
Hospitalists who extract the most out of the VTE Resource Room will be able to:
- Understand and use fundamental quality improvement concepts in the hospital;
- Command and teach the VTE prevention literature; and
- Engineer and lead improvement in the hospital.
The Quality Improvement Resource Rooms will support the hospitalist across domains integral to any quality improvement effort: raising collective awareness of a performance gap, knowing what evidence to put into practice, and leveraging experience with the disease as well as the improvement process.
Print and carry a ready-made workbook to guide and document your work. View a presentation depicting the key elements in quality improvement theory. Download a ready-made slide set to propel teaching of VTE prevention in the didactic setting. Adapt practical teaching tips to implement immediately. Review a listing of the pertinent literature. View and modify VTE tools shared by other hospitalists. Or post questions to a moderated forum of VTE and quality improvement experts.
By offering the new online Resource Rooms, the SHM has taken a significant step toward realizing the potential in hospital medicine: to enhance your ability to improve inpatient outcomes. The next step is yours.
At the SHM Web site, navigate to “Quality and Safety,” select “Quality Improvement Resource Rooms,” and then “Venous Thromboembolism (VTE) Resource Room.” TH