User login
Cold Urticaria: A Case Report and Review of the Literature
Case Report
An otherwise healthy 9-year-old Filipino girl presented with a complaint of urticaria precipitated by cold exposure over the preceding 5 weeks. She had no recent illnesses and normal results of a school physical examination performed 2 weeks prior to symptom onset. The patient's medical history was significant only for cat allergy; however, she noted that on multiple occasions, erythema and pruritus appeared on her arms and face after walking through the freezer aisle of a grocery store. Urticaria subsequently developed on regions where she scratched and spontaneously resolved 2 to 3 hours later. On one occasion, urticaria appeared diffusely on the patient while she showered after swimming; it resolved within a few hours after she was given diphenhydramine by her mother. Three days prior to presentation, the patient experienced upper lip angioedema with erythema, globus sensation, and difficulty swallowing after drinking a strawberry slushy. She denied having respiratory complaints at that time, and her symptoms again resolved spontaneously. A day later, the patient tolerated ice cream with no complaints. Her family history was significant for a maternal history of seasonal allergies.
On physical examination, the patient appeared to be well. She had 2 to 3 discrete urticarial lesions on the distal posterior aspect of each calf that, according to her mother, recently began appearing on "cold and rainy" days. The mother attributed them to her daughter's lower legs being exposed because of the length of her pants. Results of the remainder of the examination were unremarkable, and dermatographism was absent.
Laboratory evaluation consisted of a strawberry radioallergosorbent test and cryoglobulins test, both of which had negative results. An ice cube wrapped in plastic was applied to the volar surface of the patient's right forearm for 5 minutes. A 9X6-cm wheal was noted 3 minutes after ice removal (Figure).
PLEASE REFER TO THE PDF TO VIEW THE FIGURE
A diagnosis of cold urticaria with associated angioedema was made. The patient's mother opted for her daughter to use only diphenhydramine as needed; additionally, an epinephrine autoinjector was dispensed. By 3 months after symptom onset, the patient's only complaint was pruritus of her hands if they became too cold. No urticaria was noted. At 6-month follow-up, the patient denied having had symptoms for the preceding 2 months, and the results of an ice cube test were negative.
Comment
Cold urticaria is a form of physical urticaria that is notable for the development of urticaria and/or angioedema after cold exposure.1 Cold urticaria syndromes were first described in the 19th century2 and are uncommon. However, it has been observed that approximately one third of adult3 and pediatric4 patients with cold urticaria have systemic reactions that are mostly hypotensive episodes associated with aquatic activities. Thus, identification of these patients should be a priority.
The prevalence of cold urticaria is not well defined. Cold urticaria is most commonly noted in young adults, with only 11% of cases noted in children under 10 years of age.3 Most forms of cold urticaria are idiopathic (Table); however, some forms can be secondary to underlying conditions such as malignancies, vasculitides, and infectious diseases.8 Cryoglobulinemia (primary and secondary to malignancy) often is cited as a cause of secondary cold urticaria.3,8-11 Mounting evidence indicates that a possible autoimmune mechanism underlies the idiopathic form of this disorder in many patients.12
PLEASE REFER TO THE PDF TO VIEW THE TABLE
Although most forms of cold urticaria are considered to be acquired, familial forms have been described,7,13 some of which have been classified within the hereditary periodic fever syndromes.12 Diagnosis of cold urticaria primarily is made by evaluating the patient's clinical history; the diagnosis may be confirmed by applying a cold stimulus, most commonly an ice cube wrapped in plastic and applied to the volar aspect of the patient's forearm. A positive reaction is noted by the formation of a wheal during rewarming of the skin. The length of time that a cold stimulus is applied is not standardized; commonly, 3-, 5-, and 10-minute applications are used. Visitsuntorn et al14 observed the effectiveness of 3- or 5-minute applications in children who had not taken antihistamines for at least 5 days prior. The authors also noted that false-positive results (defined as reddening of the skin and minimal edema) were possible with 10- and 20-minute applications in patients with chronic urticaria not induced by cold. Other studies have observed that the length of time necessary for a cold stimulus to induce wheal formation inversely may be related to the patient's risk of having a systemic reaction.1,8,12 Specifically, patients who demonstrated wheal formation after the application of a cold stimulus for 3 minutes or less were noted to experience cold-induced hypotension more frequently. Regardless, it should be recognized that all patients with cold urticaria are at risk for hypotensive reactions.
Approximately 20% of patients with cold urticaria lack an immediate response to cold stimulus with an ice cube; these patients have so-called atypical acquired cold urticaria syndromes1,12 (eg, cold-dependant dermatographism, delayed cold urticaria, systemic cold urticaria). Other forms of cold stimulus testing that can be considered include partially immersing a limb of the patient's in cold water3 or placing the patient in a cold room15; however, these forms of cold stimulus may put the patient at increased risk for a systemic reaction. Finally, scratching the skin prior to cooling or during cooling also may be of diagnostic value in cases of cold-dependant dermatographism.9,15
Additional testing should be guided by a patient's history. To determine if a secondary cause is responsible for the clinical presentation of cold urticaria, laboratory studies could include complete blood count, erythrocyte sedimentation rate, antinuclear antibodies titer, infectious mononucleosis serology, syphilis serology, rheumatoid factor, total complement, cold agglutinins, cold hemolysin, cryofibrinogen, and cryoglobulin.12 Of note, approximately 4% of patients with cold urticaria have been observed to have cryoglobulinemia. Thus, testing for cryoglobulinemia is the most likely laboratory study to yield positive results.1,16 Beyond evaluation for cryoprecipitates, however, an extensive search for etiology is not indicated unless additional clinical findings warrant investigation.16
Treatment of patients with cold urticaria can be difficult. Patients and their families should be counseled on the risks of aquatic activities and should be instructed on the proper use of an epinephrine autoinjector. In severe cases, patients may elect to move to warmer climates. Antihistamines sometimes provide benefit, especially at high doses and/or with the more potent formulations, such as doxepin. Cyproheptadine has been shown to be more effective than chlorpheniramine.17 Second-generation antihistamines also may be considered to minimize sedation. Cetirizine, loratadine, and desloratadine have been shown to be effective and well-tolerated options for treatment.18,19 Additionally, leukotriene receptor antagonists may have a role in treatment.5 Bonadonna et al6 demonstrated that cetirizine and zafirlukast in combination are more effective than either drug alone. Adjusting the level of medication so that the patient requires more than 3 minutes of cold stimulus testing before having a wheal response is a recommended goal of therapy that is aimed at minimizing the patient's risk of having a hypotensive reaction.12
Cold urticaria is an uncommon disorder that can put patients at significant risk. Taking a thorough history and confirming the condition through the use of cold stimulation tests can lead to a diagnosis in most cases. Although most forms of cold urticaria are idiopathic and acquired, familial and secondary forms also must be kept in mind when considering this diagnosis. In addition to antihistamine therapy, an epinephrine autoinjector and preventive measures play an important role in treating patients with cold urticaria.
- Wanderer AA, Grandel KE, Wasserman SI, et al. Clinical characteristics of cold-induced systemic reactions in acquired cold urticaria syndromes: recommendations for prevention of this complication and a proposal for a diagnostic classification of cold urticaria. J Allergy Clin Immunol. 1986;78:417-423.
- Bourdon H. Note Sur L'uticaire intermittente. Bull Mem Soc Med Hop Paris. 1866;3:259-262.
- Neittaanmaki H. Cold urticaria. clinical findings in 220 patients. J Am Acad Dermatol. 1985;13:636-644.
- Alangari AA, Twarog FJ, Shih MC, et al. Clinical features and anaphylaxis in children with cold urticaria. Pediatrics. 2004;113:e313-e317.
- Hani N, Hartmann K, Casper C, et al. Improvement of cold urticaria by treatment with the leukotriene receptor antagonist montelukast [letter]. Acta Derm Venereol. 2000;80:229.
- Bonadonna P, Lombardi C, Gianenrico S, et al. Treatment of acquired cold urticaria with cetirizine and zafirlukast in combination. J Am Acad Dermatol. 2003;49:714-716.
- Soter NA, Joshi NP, Twarog FJ, et al. Delayed cold-induced urticaria: a dominantly inherited disorder. J Allergy Clin Immunol. 1977;59:294-297.
- Wanderer A. Cold urticaria syndromes: historical background, diagnostic classification, clinical and laboratory characteristics, pathogenesis, and management. J Allergy Clin Immunol. 1990;85:965-981.
- Costanzi JJ, Coltman CA. Kappa chain cold precipitable immunoglobulin G (IgG) associated with cold urticaria, I: clinical observations. Clin Exp Immunol. 1967;2:167-178.
- Rawnsley HM, Shelley WB. Cold urticaria with cryoglobulinemia in a patient with chronic lymphocytic leukemia. Arch Dermatol. 1968;98:12-17.
- Hauptmann G, Lang JM, North ML, et al. Lymphosarcoma, cold urticaria, IgG1 monoclonal cryoglobulin, and compliment abnormalities. Scand J Haematol. 1975;15:22-26.
- Wanderer AA, Hoffman HM. The spectrum of acquired and familial cold-induced urticaria/urticaria-like syndromes. Immunol Allergy Clin North Am. 2004;24:259-286.
- Hoffman HM, Wright FA, Broide DH, et al. Identification of a locus on chromosome 1q44 for familial cold urticaria. Am J Hum Genet. 2000;66:1693-1698.
- Visitsuntorn N, Tuchinda M, Arunyanark N, et al. Ice cube test in children with cold urticaria. Asian Pac J Allergy Immunol. 1992;10:111-115.
- Kaplan AP. Unusual cold-induced disorders: cold-dependant dermatographism and systemic cold urticaria. J Allergy Clin Immunol. 1984;73:453-456.
- Koeppel MC, Bertrand S, Abitan R, et al. Urticaria caused by cold. 104 cases [in French]. Ann Dermatol Venereol. 1996;123:627-632.
- Wanderer AA, St Pierre JP, Ellis EF. Primary acquired cold urticaria. double-blind comparative study of treatment with cyproheptadine, chlorpheniramine, and placebo. Arch Dermatol. 1977;113:1375-1377.
- Villas Martinez F, Contreras FJ, Lopez Cazana JM, et al. A comparison of new nonsedating and classical antihistamines in the treatment of primary acquired cold urticaria (ACU). J Investig Allergol Clin Immunol. 1992;2:258-262.
- Juhlin L. Inhibition of cold urticaria by desloratidine. J Dermatolog Treat. 2004;15:51-59.
Case Report
An otherwise healthy 9-year-old Filipino girl presented with a complaint of urticaria precipitated by cold exposure over the preceding 5 weeks. She had no recent illnesses and normal results of a school physical examination performed 2 weeks prior to symptom onset. The patient's medical history was significant only for cat allergy; however, she noted that on multiple occasions, erythema and pruritus appeared on her arms and face after walking through the freezer aisle of a grocery store. Urticaria subsequently developed on regions where she scratched and spontaneously resolved 2 to 3 hours later. On one occasion, urticaria appeared diffusely on the patient while she showered after swimming; it resolved within a few hours after she was given diphenhydramine by her mother. Three days prior to presentation, the patient experienced upper lip angioedema with erythema, globus sensation, and difficulty swallowing after drinking a strawberry slushy. She denied having respiratory complaints at that time, and her symptoms again resolved spontaneously. A day later, the patient tolerated ice cream with no complaints. Her family history was significant for a maternal history of seasonal allergies.
On physical examination, the patient appeared to be well. She had 2 to 3 discrete urticarial lesions on the distal posterior aspect of each calf that, according to her mother, recently began appearing on "cold and rainy" days. The mother attributed them to her daughter's lower legs being exposed because of the length of her pants. Results of the remainder of the examination were unremarkable, and dermatographism was absent.
Laboratory evaluation consisted of a strawberry radioallergosorbent test and cryoglobulins test, both of which had negative results. An ice cube wrapped in plastic was applied to the volar surface of the patient's right forearm for 5 minutes. A 9X6-cm wheal was noted 3 minutes after ice removal (Figure).
PLEASE REFER TO THE PDF TO VIEW THE FIGURE
A diagnosis of cold urticaria with associated angioedema was made. The patient's mother opted for her daughter to use only diphenhydramine as needed; additionally, an epinephrine autoinjector was dispensed. By 3 months after symptom onset, the patient's only complaint was pruritus of her hands if they became too cold. No urticaria was noted. At 6-month follow-up, the patient denied having had symptoms for the preceding 2 months, and the results of an ice cube test were negative.
Comment
Cold urticaria is a form of physical urticaria that is notable for the development of urticaria and/or angioedema after cold exposure.1 Cold urticaria syndromes were first described in the 19th century2 and are uncommon. However, it has been observed that approximately one third of adult3 and pediatric4 patients with cold urticaria have systemic reactions that are mostly hypotensive episodes associated with aquatic activities. Thus, identification of these patients should be a priority.
The prevalence of cold urticaria is not well defined. Cold urticaria is most commonly noted in young adults, with only 11% of cases noted in children under 10 years of age.3 Most forms of cold urticaria are idiopathic (Table); however, some forms can be secondary to underlying conditions such as malignancies, vasculitides, and infectious diseases.8 Cryoglobulinemia (primary and secondary to malignancy) often is cited as a cause of secondary cold urticaria.3,8-11 Mounting evidence indicates that a possible autoimmune mechanism underlies the idiopathic form of this disorder in many patients.12
PLEASE REFER TO THE PDF TO VIEW THE TABLE
Although most forms of cold urticaria are considered to be acquired, familial forms have been described,7,13 some of which have been classified within the hereditary periodic fever syndromes.12 Diagnosis of cold urticaria primarily is made by evaluating the patient's clinical history; the diagnosis may be confirmed by applying a cold stimulus, most commonly an ice cube wrapped in plastic and applied to the volar aspect of the patient's forearm. A positive reaction is noted by the formation of a wheal during rewarming of the skin. The length of time that a cold stimulus is applied is not standardized; commonly, 3-, 5-, and 10-minute applications are used. Visitsuntorn et al14 observed the effectiveness of 3- or 5-minute applications in children who had not taken antihistamines for at least 5 days prior. The authors also noted that false-positive results (defined as reddening of the skin and minimal edema) were possible with 10- and 20-minute applications in patients with chronic urticaria not induced by cold. Other studies have observed that the length of time necessary for a cold stimulus to induce wheal formation inversely may be related to the patient's risk of having a systemic reaction.1,8,12 Specifically, patients who demonstrated wheal formation after the application of a cold stimulus for 3 minutes or less were noted to experience cold-induced hypotension more frequently. Regardless, it should be recognized that all patients with cold urticaria are at risk for hypotensive reactions.
Approximately 20% of patients with cold urticaria lack an immediate response to cold stimulus with an ice cube; these patients have so-called atypical acquired cold urticaria syndromes1,12 (eg, cold-dependant dermatographism, delayed cold urticaria, systemic cold urticaria). Other forms of cold stimulus testing that can be considered include partially immersing a limb of the patient's in cold water3 or placing the patient in a cold room15; however, these forms of cold stimulus may put the patient at increased risk for a systemic reaction. Finally, scratching the skin prior to cooling or during cooling also may be of diagnostic value in cases of cold-dependant dermatographism.9,15
Additional testing should be guided by a patient's history. To determine if a secondary cause is responsible for the clinical presentation of cold urticaria, laboratory studies could include complete blood count, erythrocyte sedimentation rate, antinuclear antibodies titer, infectious mononucleosis serology, syphilis serology, rheumatoid factor, total complement, cold agglutinins, cold hemolysin, cryofibrinogen, and cryoglobulin.12 Of note, approximately 4% of patients with cold urticaria have been observed to have cryoglobulinemia. Thus, testing for cryoglobulinemia is the most likely laboratory study to yield positive results.1,16 Beyond evaluation for cryoprecipitates, however, an extensive search for etiology is not indicated unless additional clinical findings warrant investigation.16
Treatment of patients with cold urticaria can be difficult. Patients and their families should be counseled on the risks of aquatic activities and should be instructed on the proper use of an epinephrine autoinjector. In severe cases, patients may elect to move to warmer climates. Antihistamines sometimes provide benefit, especially at high doses and/or with the more potent formulations, such as doxepin. Cyproheptadine has been shown to be more effective than chlorpheniramine.17 Second-generation antihistamines also may be considered to minimize sedation. Cetirizine, loratadine, and desloratadine have been shown to be effective and well-tolerated options for treatment.18,19 Additionally, leukotriene receptor antagonists may have a role in treatment.5 Bonadonna et al6 demonstrated that cetirizine and zafirlukast in combination are more effective than either drug alone. Adjusting the level of medication so that the patient requires more than 3 minutes of cold stimulus testing before having a wheal response is a recommended goal of therapy that is aimed at minimizing the patient's risk of having a hypotensive reaction.12
Cold urticaria is an uncommon disorder that can put patients at significant risk. Taking a thorough history and confirming the condition through the use of cold stimulation tests can lead to a diagnosis in most cases. Although most forms of cold urticaria are idiopathic and acquired, familial and secondary forms also must be kept in mind when considering this diagnosis. In addition to antihistamine therapy, an epinephrine autoinjector and preventive measures play an important role in treating patients with cold urticaria.
Case Report
An otherwise healthy 9-year-old Filipino girl presented with a complaint of urticaria precipitated by cold exposure over the preceding 5 weeks. She had no recent illnesses and normal results of a school physical examination performed 2 weeks prior to symptom onset. The patient's medical history was significant only for cat allergy; however, she noted that on multiple occasions, erythema and pruritus appeared on her arms and face after walking through the freezer aisle of a grocery store. Urticaria subsequently developed on regions where she scratched and spontaneously resolved 2 to 3 hours later. On one occasion, urticaria appeared diffusely on the patient while she showered after swimming; it resolved within a few hours after she was given diphenhydramine by her mother. Three days prior to presentation, the patient experienced upper lip angioedema with erythema, globus sensation, and difficulty swallowing after drinking a strawberry slushy. She denied having respiratory complaints at that time, and her symptoms again resolved spontaneously. A day later, the patient tolerated ice cream with no complaints. Her family history was significant for a maternal history of seasonal allergies.
On physical examination, the patient appeared to be well. She had 2 to 3 discrete urticarial lesions on the distal posterior aspect of each calf that, according to her mother, recently began appearing on "cold and rainy" days. The mother attributed them to her daughter's lower legs being exposed because of the length of her pants. Results of the remainder of the examination were unremarkable, and dermatographism was absent.
Laboratory evaluation consisted of a strawberry radioallergosorbent test and cryoglobulins test, both of which had negative results. An ice cube wrapped in plastic was applied to the volar surface of the patient's right forearm for 5 minutes. A 9X6-cm wheal was noted 3 minutes after ice removal (Figure).
PLEASE REFER TO THE PDF TO VIEW THE FIGURE
A diagnosis of cold urticaria with associated angioedema was made. The patient's mother opted for her daughter to use only diphenhydramine as needed; additionally, an epinephrine autoinjector was dispensed. By 3 months after symptom onset, the patient's only complaint was pruritus of her hands if they became too cold. No urticaria was noted. At 6-month follow-up, the patient denied having had symptoms for the preceding 2 months, and the results of an ice cube test were negative.
Comment
Cold urticaria is a form of physical urticaria that is notable for the development of urticaria and/or angioedema after cold exposure.1 Cold urticaria syndromes were first described in the 19th century2 and are uncommon. However, it has been observed that approximately one third of adult3 and pediatric4 patients with cold urticaria have systemic reactions that are mostly hypotensive episodes associated with aquatic activities. Thus, identification of these patients should be a priority.
The prevalence of cold urticaria is not well defined. Cold urticaria is most commonly noted in young adults, with only 11% of cases noted in children under 10 years of age.3 Most forms of cold urticaria are idiopathic (Table); however, some forms can be secondary to underlying conditions such as malignancies, vasculitides, and infectious diseases.8 Cryoglobulinemia (primary and secondary to malignancy) often is cited as a cause of secondary cold urticaria.3,8-11 Mounting evidence indicates that a possible autoimmune mechanism underlies the idiopathic form of this disorder in many patients.12
PLEASE REFER TO THE PDF TO VIEW THE TABLE
Although most forms of cold urticaria are considered to be acquired, familial forms have been described,7,13 some of which have been classified within the hereditary periodic fever syndromes.12 Diagnosis of cold urticaria primarily is made by evaluating the patient's clinical history; the diagnosis may be confirmed by applying a cold stimulus, most commonly an ice cube wrapped in plastic and applied to the volar aspect of the patient's forearm. A positive reaction is noted by the formation of a wheal during rewarming of the skin. The length of time that a cold stimulus is applied is not standardized; commonly, 3-, 5-, and 10-minute applications are used. Visitsuntorn et al14 observed the effectiveness of 3- or 5-minute applications in children who had not taken antihistamines for at least 5 days prior. The authors also noted that false-positive results (defined as reddening of the skin and minimal edema) were possible with 10- and 20-minute applications in patients with chronic urticaria not induced by cold. Other studies have observed that the length of time necessary for a cold stimulus to induce wheal formation inversely may be related to the patient's risk of having a systemic reaction.1,8,12 Specifically, patients who demonstrated wheal formation after the application of a cold stimulus for 3 minutes or less were noted to experience cold-induced hypotension more frequently. Regardless, it should be recognized that all patients with cold urticaria are at risk for hypotensive reactions.
Approximately 20% of patients with cold urticaria lack an immediate response to cold stimulus with an ice cube; these patients have so-called atypical acquired cold urticaria syndromes1,12 (eg, cold-dependant dermatographism, delayed cold urticaria, systemic cold urticaria). Other forms of cold stimulus testing that can be considered include partially immersing a limb of the patient's in cold water3 or placing the patient in a cold room15; however, these forms of cold stimulus may put the patient at increased risk for a systemic reaction. Finally, scratching the skin prior to cooling or during cooling also may be of diagnostic value in cases of cold-dependant dermatographism.9,15
Additional testing should be guided by a patient's history. To determine if a secondary cause is responsible for the clinical presentation of cold urticaria, laboratory studies could include complete blood count, erythrocyte sedimentation rate, antinuclear antibodies titer, infectious mononucleosis serology, syphilis serology, rheumatoid factor, total complement, cold agglutinins, cold hemolysin, cryofibrinogen, and cryoglobulin.12 Of note, approximately 4% of patients with cold urticaria have been observed to have cryoglobulinemia. Thus, testing for cryoglobulinemia is the most likely laboratory study to yield positive results.1,16 Beyond evaluation for cryoprecipitates, however, an extensive search for etiology is not indicated unless additional clinical findings warrant investigation.16
Treatment of patients with cold urticaria can be difficult. Patients and their families should be counseled on the risks of aquatic activities and should be instructed on the proper use of an epinephrine autoinjector. In severe cases, patients may elect to move to warmer climates. Antihistamines sometimes provide benefit, especially at high doses and/or with the more potent formulations, such as doxepin. Cyproheptadine has been shown to be more effective than chlorpheniramine.17 Second-generation antihistamines also may be considered to minimize sedation. Cetirizine, loratadine, and desloratadine have been shown to be effective and well-tolerated options for treatment.18,19 Additionally, leukotriene receptor antagonists may have a role in treatment.5 Bonadonna et al6 demonstrated that cetirizine and zafirlukast in combination are more effective than either drug alone. Adjusting the level of medication so that the patient requires more than 3 minutes of cold stimulus testing before having a wheal response is a recommended goal of therapy that is aimed at minimizing the patient's risk of having a hypotensive reaction.12
Cold urticaria is an uncommon disorder that can put patients at significant risk. Taking a thorough history and confirming the condition through the use of cold stimulation tests can lead to a diagnosis in most cases. Although most forms of cold urticaria are idiopathic and acquired, familial and secondary forms also must be kept in mind when considering this diagnosis. In addition to antihistamine therapy, an epinephrine autoinjector and preventive measures play an important role in treating patients with cold urticaria.
- Wanderer AA, Grandel KE, Wasserman SI, et al. Clinical characteristics of cold-induced systemic reactions in acquired cold urticaria syndromes: recommendations for prevention of this complication and a proposal for a diagnostic classification of cold urticaria. J Allergy Clin Immunol. 1986;78:417-423.
- Bourdon H. Note Sur L'uticaire intermittente. Bull Mem Soc Med Hop Paris. 1866;3:259-262.
- Neittaanmaki H. Cold urticaria. clinical findings in 220 patients. J Am Acad Dermatol. 1985;13:636-644.
- Alangari AA, Twarog FJ, Shih MC, et al. Clinical features and anaphylaxis in children with cold urticaria. Pediatrics. 2004;113:e313-e317.
- Hani N, Hartmann K, Casper C, et al. Improvement of cold urticaria by treatment with the leukotriene receptor antagonist montelukast [letter]. Acta Derm Venereol. 2000;80:229.
- Bonadonna P, Lombardi C, Gianenrico S, et al. Treatment of acquired cold urticaria with cetirizine and zafirlukast in combination. J Am Acad Dermatol. 2003;49:714-716.
- Soter NA, Joshi NP, Twarog FJ, et al. Delayed cold-induced urticaria: a dominantly inherited disorder. J Allergy Clin Immunol. 1977;59:294-297.
- Wanderer A. Cold urticaria syndromes: historical background, diagnostic classification, clinical and laboratory characteristics, pathogenesis, and management. J Allergy Clin Immunol. 1990;85:965-981.
- Costanzi JJ, Coltman CA. Kappa chain cold precipitable immunoglobulin G (IgG) associated with cold urticaria, I: clinical observations. Clin Exp Immunol. 1967;2:167-178.
- Rawnsley HM, Shelley WB. Cold urticaria with cryoglobulinemia in a patient with chronic lymphocytic leukemia. Arch Dermatol. 1968;98:12-17.
- Hauptmann G, Lang JM, North ML, et al. Lymphosarcoma, cold urticaria, IgG1 monoclonal cryoglobulin, and compliment abnormalities. Scand J Haematol. 1975;15:22-26.
- Wanderer AA, Hoffman HM. The spectrum of acquired and familial cold-induced urticaria/urticaria-like syndromes. Immunol Allergy Clin North Am. 2004;24:259-286.
- Hoffman HM, Wright FA, Broide DH, et al. Identification of a locus on chromosome 1q44 for familial cold urticaria. Am J Hum Genet. 2000;66:1693-1698.
- Visitsuntorn N, Tuchinda M, Arunyanark N, et al. Ice cube test in children with cold urticaria. Asian Pac J Allergy Immunol. 1992;10:111-115.
- Kaplan AP. Unusual cold-induced disorders: cold-dependant dermatographism and systemic cold urticaria. J Allergy Clin Immunol. 1984;73:453-456.
- Koeppel MC, Bertrand S, Abitan R, et al. Urticaria caused by cold. 104 cases [in French]. Ann Dermatol Venereol. 1996;123:627-632.
- Wanderer AA, St Pierre JP, Ellis EF. Primary acquired cold urticaria. double-blind comparative study of treatment with cyproheptadine, chlorpheniramine, and placebo. Arch Dermatol. 1977;113:1375-1377.
- Villas Martinez F, Contreras FJ, Lopez Cazana JM, et al. A comparison of new nonsedating and classical antihistamines in the treatment of primary acquired cold urticaria (ACU). J Investig Allergol Clin Immunol. 1992;2:258-262.
- Juhlin L. Inhibition of cold urticaria by desloratidine. J Dermatolog Treat. 2004;15:51-59.
- Wanderer AA, Grandel KE, Wasserman SI, et al. Clinical characteristics of cold-induced systemic reactions in acquired cold urticaria syndromes: recommendations for prevention of this complication and a proposal for a diagnostic classification of cold urticaria. J Allergy Clin Immunol. 1986;78:417-423.
- Bourdon H. Note Sur L'uticaire intermittente. Bull Mem Soc Med Hop Paris. 1866;3:259-262.
- Neittaanmaki H. Cold urticaria. clinical findings in 220 patients. J Am Acad Dermatol. 1985;13:636-644.
- Alangari AA, Twarog FJ, Shih MC, et al. Clinical features and anaphylaxis in children with cold urticaria. Pediatrics. 2004;113:e313-e317.
- Hani N, Hartmann K, Casper C, et al. Improvement of cold urticaria by treatment with the leukotriene receptor antagonist montelukast [letter]. Acta Derm Venereol. 2000;80:229.
- Bonadonna P, Lombardi C, Gianenrico S, et al. Treatment of acquired cold urticaria with cetirizine and zafirlukast in combination. J Am Acad Dermatol. 2003;49:714-716.
- Soter NA, Joshi NP, Twarog FJ, et al. Delayed cold-induced urticaria: a dominantly inherited disorder. J Allergy Clin Immunol. 1977;59:294-297.
- Wanderer A. Cold urticaria syndromes: historical background, diagnostic classification, clinical and laboratory characteristics, pathogenesis, and management. J Allergy Clin Immunol. 1990;85:965-981.
- Costanzi JJ, Coltman CA. Kappa chain cold precipitable immunoglobulin G (IgG) associated with cold urticaria, I: clinical observations. Clin Exp Immunol. 1967;2:167-178.
- Rawnsley HM, Shelley WB. Cold urticaria with cryoglobulinemia in a patient with chronic lymphocytic leukemia. Arch Dermatol. 1968;98:12-17.
- Hauptmann G, Lang JM, North ML, et al. Lymphosarcoma, cold urticaria, IgG1 monoclonal cryoglobulin, and compliment abnormalities. Scand J Haematol. 1975;15:22-26.
- Wanderer AA, Hoffman HM. The spectrum of acquired and familial cold-induced urticaria/urticaria-like syndromes. Immunol Allergy Clin North Am. 2004;24:259-286.
- Hoffman HM, Wright FA, Broide DH, et al. Identification of a locus on chromosome 1q44 for familial cold urticaria. Am J Hum Genet. 2000;66:1693-1698.
- Visitsuntorn N, Tuchinda M, Arunyanark N, et al. Ice cube test in children with cold urticaria. Asian Pac J Allergy Immunol. 1992;10:111-115.
- Kaplan AP. Unusual cold-induced disorders: cold-dependant dermatographism and systemic cold urticaria. J Allergy Clin Immunol. 1984;73:453-456.
- Koeppel MC, Bertrand S, Abitan R, et al. Urticaria caused by cold. 104 cases [in French]. Ann Dermatol Venereol. 1996;123:627-632.
- Wanderer AA, St Pierre JP, Ellis EF. Primary acquired cold urticaria. double-blind comparative study of treatment with cyproheptadine, chlorpheniramine, and placebo. Arch Dermatol. 1977;113:1375-1377.
- Villas Martinez F, Contreras FJ, Lopez Cazana JM, et al. A comparison of new nonsedating and classical antihistamines in the treatment of primary acquired cold urticaria (ACU). J Investig Allergol Clin Immunol. 1992;2:258-262.
- Juhlin L. Inhibition of cold urticaria by desloratidine. J Dermatolog Treat. 2004;15:51-59.
Enhancing the Care and Treatment of Skin of Color, Part 1: The Broad Scope of Pigmentary Disorders
The Vitamin D and Sunlight Controversy—We Will Wait and See [editorial]
Beyond the mirror: Treating body dysmorphic disorder
Identifying which came first—body dysmorphic disorder (BDD) or comorbid anxiety or depressive disorders—can be as complex as treating the disorder’s delusional thinking and high suicide risk. To help you when working alone or with a psychotherapist, we offer strategies we have found useful for:
- diagnosing BDD
- educating patients and families about it
- choosing and dosing medications
- addressing inaccurate perceptions with targeted cognitive-behavioral therapies.
Though many recommendations are based on published data, we also draw on our clinical experience because research on effective BDD treatments is limited.
Body dysmorphic disorder (BDD) is preoccupation with an imagined defect in physical appearance or excessive concern about a slight physical anomaly that causes significant distress or impairs social, occupational, or other functioning.1 BDD patients have obsessive thoughts about their “flaws” and engage in compulsive behaviors and avoidances related to how they perceive their appearance, similar to behavior seen in obsessive-compulsive disorder. BDD causes great distress and disability, often accompanied by depression and suicidality.2
BDD occurs in an estimated 0.7% of the general population3 and in 6 to 14% of persons receiving treatment for anxiety or depressive disorders.4,5 These estimates may be low, however, as persons with BDD often do not seek treatment. Men and women are equally affected.6 Average age of onset is 16, although diagnosis often doesn’t occur for another 10 to 15 years.7
Assessment
BDD causes patients great distress and disability—often accompanied by major depression—but is easy to miss or misdiagnose (Box).1-7 Even when suicidal, BDD patients often do not reveal their symptoms to clinicians,2 probably because of poor insight or shame about their appearance. When a patient describes being unable to stop thinking about specific aspects of his or her appearance, assess further for BDD.
BDD patients’ conviction that their appearance is defective ranges from good insight to mildly overvalued ideation to frankly delusional.8 They often have ideas of reference (such as thinking others may be looking at their “defective” body part) and delusions of reference (such as being convinced others are talking about their “defective” body part). Asking a patient the questions in Table 1 can help establish the diagnosis. BDD also is included in the Structured Clinical Interview for DSM-IV (SCID). Useful assessment tools include:
- Body Dysmorphic Disorder Questionnaire,9 a 5-minute, patient-rated scale for screening
- Body Dysmorphic Disorder Examination,10 to diagnose BDD, survey BDD symptoms, and measure severity
- Yale-Brown Obsessive-Compulsive Scale modified for Body Dysmorphic Disorder (BDD-YBOCS),11 for measuring symptom severity and changes over time.
Comorbidity. Psychiatric comorbidity is common in BDD (Table 2),6,7,12-14 and deciding which disorder to address first can be difficult. If there is acute mania or non-BDD psychosis, we suggest that you stabilize these before treating BDD. Suicidality or severe substance dependence or abuse may result from BDD and therefore needs to be treated in conjunction with BDD.
If comorbid obsessive-compulsive disorder (OCD) or social phobia symptoms are interconnected with the patient’s BDD, treat concurrently; if not, address sequentially, starting with the more-severe symptoms. For example, symptoms that suggest social phobia (such as fear of public speaking) may be related to BDD, and treatment should focus on BDD. A patient with obsessive fears about how “contaminants” will affect her skin’s appearance may need to have the OCD and BDD addressed concurrently.
For other comorbidities, the treatment hierarchy is less clear. Major depression, for example, may be caused by severe BDD and might not improve until BDD improves. Even when a patient has several concurrent Axis I disorders, don’t over-look treating BDD; otherwise, the patient may remain quite impaired.
Assess suicide risk, as ≥ 25% of BDD patients may attempt suicide in their lifetimes.2 Safety measures include frequent monitoring, medication, family involvement, and—if necessary—hospitalization.
Table 1
Patient interview: Questions to help diagnose BDD
| Are you concerned about specific parts of your appearance that you believe are ugly or defective? |
| Do you find it difficult to stop thinking about parts of your appearance? |
| Do you avoid certain situations, places, or being seen in general because of your appearance? |
| Do you feel anxious, ashamed, disgusted, or depressed by specific aspects of your appearance? |
| Are any of your behaviors influenced by your appearance, such as trying to hide parts of your appearance or taking a long time getting ready to leave your residence? |
| Does your preoccupation cause you a lot of distress, anxiety, disgust, and/or shame? |
| Is preoccupation with your appearance interfering with your social life, ability to work, job performance, or other important areas of your life? |
| Do you tend to use mirrors very often or avoid them? |
| Does what you see in the mirror determine your mood that day? |
| How important do you think appearance is in life? |
| Do you use any oral or topical medications for dermatologic reasons or to prevent hair loss? |
| Have you ever had cosmetic surgery? If so, how satisfied were you with the outcome? Did you have any revisions? |
Table 2
Lifetime prevalence (%) of comorbid Axis I disorders in BDD
| Study | N | Major depression | Social phobia | OCD | Substance use disorders |
|---|---|---|---|---|---|
| Gunstad and Phillips (2003)*12 | 175 | 75 | 37 | 30 | 30 |
| Zimmerman and Mattia (1998)14 | 16 | 69 | 69 | 38 | 6 |
| Perugi et al (1997)13 | 58 | 41 | 12 | 41 | † |
| Veale et al (1996)7 | 50 | 8 | 16 | 6 | 2 |
| Hollander et al (1993)6 | 50 | 68 | 12 | 78 | 22 |
| N: number of study subjects | |||||
| OCD: obsessive-compulsive disorder | |||||
| * Phenomenology group | |||||
| † not reported | |||||
| Source: Adapted and reprinted with permission from reference 12. | |||||
Patient education
Improving insight. Educate patients that BDD is a brain disorder that creates faulty, inaccurate thoughts and perceptions about appearance. Many patients initially resist a BDD diagnosis; delusional thinking and poor insight lead them to assume the “flaw” they see is an accurate perception. They may need to hear about other persons with similar concerns to realize that a psychiatric disorder is causing their distress.
Other helpful resources for improving insight include:
- group therapy
- The Broken Mirror, by Katharine A. Phillips, MD,15 which contains case examples to which BDD sufferers may relate
- Websites and online forums (see Related resources).
Explaining BDD. Discuss possible causes of BDD, giving patients alternate explanations for the physical defects they perceive. Contributing factors may include:
- neurobiological abnormalities and genetic factors16
- a history since childhood of shyness, perfectionism, or anxious temperament
- being teased, abused, or in poor family and peer relationships.17
Emphasize that multiple, different, converging factors cause BDD for each individual.
The obsessive-compulsive cycle. Explain that thoughts create distressing emotions, and that persons with BDD try to relieve or prevent these emotions by performing compulsive behaviors. Compulsions then strengthen the association between intrusive thoughts about appearance “defects” and negative feelings about appearance.
Review a list of common compulsions (Table 3) with BDD patients, as many have engaged in these behaviors for years without realizing they are compulsions.
Table 3
Common BDD compulsions and avoidances
| Excessive grooming |
| Excessive checking or avoidance of mirrors and other reflective surfaces |
| Asking for reassurance about appearance |
| “Camouflaging” (hiding or covering up) supposed defects |
| Scrutinizing the appearance of other people and comparing to oneself |
| Avoiding social interactions |
| Avoidance of certain lighting conditions |
| Skin-picking to “fix” perceived flaws |
| Having repeated cosmetic or dermatological procedures, such as dermabrasion, cosmetic surgery, etc. |
Pharmacotherapy
BDD is a severe and complex disorder that often requires multimodal treatment using cognitive-behavioral therapy (CBT) and medication (algorithm).18 In our experience, most BDD patients need medication for the disorder and for common comorbidities. We recommend starting medications before or when beginning CBT for patients with moderate to severe BDD (BDD YBOCs ≥ 20).
Serotonin reuptake inhibitors (SRIs) have reduced BDD symptoms in open-label19,20 and controlled trials.21,22 As first-line treatments, SRIs decrease distress, compulsions, and frequency and intensity of obsessions about perceived defects; they also can improve insight.21-24 SRIs appear equally effective for delusional and nondelusional patients;21,23 whether CBT is similarly effective is unclear.
Relatively high dosages are usually necessary, according to published flexible-dosing trials in BDD,19-23 a retrospective chart review24 and our experience. Try dosages similar to those used for OCD (Table 4) as tolerated, and monitor for side effects. Twelve to 16 weeks of treatment are often needed for a full therapeutic effect.20-21
Augmentation. Consider adding another agent if a full SRI trial achieves partial symptom relief. One open-label trial of 13 BDD patients found that 6 (46%) improved when buspirone (mean dosage 48.3 mg/d) was added to SRI therapy.25 In a chart review, Phillips et al24 reported variable response rates of BDD patients treated with augmentation trials of clomipramine (4/9), buspirone (12/36), lithium (1/5), methylphenidate (1/6), and antipsychotics (2/13).
Very few studies have examined antipsychotic use in BDD. Placebo-controlled data are available only for pimozide.27 Conventional antipsychotics are unlikely to be effective, either as monotherapy26 or augmentation.27 As for the atypicals, olanzapine augmentation showed little to no efficacy in one small trial, although the average dosage used was low (4.6 mg/d).28 In our experience, atypicals—such as aripiprazole, 5 to 30 mg/d; quetiapine 100 to 300 mg/d; olanzapine, 7.5 to 15 mg/d; or risperidone, 1 to 3 mg/d—can improve BDD core symptoms and improve insight.
Benzodiazepines can be useful for acute anxiety or agitation. Carefully monitor benzodiazepine use, however, as substance abuse is relatively common in BDD patients.29
Table 4
Recommended SRI dosages for treating BDD*†
| Drug | Dosage range (mg/d) |
|---|---|
| Citalopram | 40 to 100 |
| Clomipramine | 150 to 250 |
| Escitalopram | 20 to 50 |
| Fluoxetine | 40 to 100 |
| Fluvoxamine | 200 to 400 |
| Paroxetine | 40 to 100 |
| Sertraline | 150 to 400 |
| * Off-label use. | |
| † May exceed FDA-recommended maximum dosages. | |
Specialized cbt techniques
Cognitive restructuring. Trying to convince BDD patients there is nothing wrong with their appearance will not be successful. Instead, we use cognitive restructuring to challenge the rationality of their thoughts and beliefs and to find alternate, more rational ones:
Therapist: “I know I cannot convince you that your (body area) is not defective, but can you give me evidence of how this ‘defect’ has affected your life?”
BDD patient: “Well, I haven’t had a date for a long time. I think this is evidence that my (body part) must be ugly, and that no one wants to date me because of it.”
Therapist: “What are some other possible reasons why you haven’t had a date in a long time? You admitted that you have barely left your house for many months. Is it possible that you have not had a date for a long time because you rarely go outside?”
With cognitive restructuring, patients learn to:
- identify automatic thoughts and beliefs that provoke distress
- examine evidence supporting or refuting these beliefs
- de-catastrophize (such as “What is the worst thing that could happen if you left the house today without checking your [body part]? Do you think you would eventually be able to cope with that?”)
- learn to more accurately assess the probability of feared negative consequences
- arrive at rational responses.
In our experience—which is supported by OCD literature—participating in CBT is very hard for patients with frank delusions, and insight determines how effective cognitive restructuring can be.30 If a patient is convinced a body part is defective, she is unlikely to stay in treatment—much less be open to restructuring her thoughts. Even unsuccessful attempts can help you gauge the intensity of patients’ beliefs, however.
During cognitive restructuring, it is important to uncover patients’ core beliefs (underlying, organizing principles they hold about themselves, others, and the world). BDD patients commonly believe that appearance is of utmost importance and that no one could love them because of their “defect.” The therapist can then help the patient challenge the rationality of those core beliefs.
Behavioral therapy. Basic behavioral therapy attempts to normalize excessive response to appearance concerns and to prepare patients for exposure and response prevention therapy (ERP). Having identified their compulsions, the next step is to guide patients in changing these behaviors, such as by:
- decreasing reassurance-seeking
- reducing avoidance of social situations
- decreasing opportunities to use the mirror
- reducing time spent on the Internet seeking cosmetic solutions
- increasing eye contact in social situations
- decreasing scanning of others’ physical features.
For example, suggest that BDD patients stand at least an arm’s length away when using a mirror for normal grooming. Then, instead of focusing on their body part, they will view it within the context of their entire face and body.
Exposure and response prevention
ERP exposes the patient to situations that evoke negative emotions—primarily shame and anxiety in BDD—so that they gradually habituate to these feelings. Individualize exposure exercises, targeting the body parts each person believes are defective. Because these exercises are intended to induce the discomfort patients usually experience, do not attempt ERP until the patient has had extensive education, developed insight, and has consented to treatment.
Create a hierarchy of ERP tasks (Table 5), ranking situations from low- to high-distress. Address items lower on the hierarchy first, and progress to higher items as the lower ones become easier to perform. Do not attempt the highest-distress items until the patient has improved insight and is not severely ill and suicidal.
During exposures, patients must remain in distress-provoking situations—without performing compulsive behaviors—until their negative feelings decrease by at least 50% of the initial subjective, self-rated distress level. Leaving the situation before stress diminishes may reinforce shame and discomfort. Performing compulsive behaviors during or after an exposure will negate the exposure’s effect.
Mirrors and ERP. Some therapists use mirrors for exposure exercises, but this is a complex issue. Mirror-checking is a common BDD compulsion that provides temporary relief but ultimately reinforces negative, intrusive thoughts about the disliked body area. How BDD patients perceive themselves changes from moment to moment; they may stare at and analyze any reflective surface in hopes that their “defect” will not appear as deformed or ugly that day. Thus, one cannot predict whether looking in the mirror at any one time is an exposure or a compulsion.
ERP exercises for BDD need to emphasize behaviors that involve interactions with the outside world, rather than reinforcing the importance of appearance. Using the mirror for ERP could promote checking compulsions and may send the message that appearance is the focal point of treatment. On the other hand, for patients with persistent mirror avoidance, gradual mirror exposures may be useful. A technique called mirror retraining helps patients objectively view their appearance and has been used with success in some individuals.
Table 5
Exposure and response therapy: a BDD patient’s sample hierarchy
| High-distress tasks | Subjective distress rating (scale of 0 to 100) |
| 1. Purposely creating the appearance of acne/skin defects | 100 |
| 2. Intentionally messing up my hair before going in public | 100 |
| 3. Standing under bright or fluorescent lighting in public | 90 |
| 4. Sitting in a position where others can directly see my face for an extended period | 85 |
| 5. Highlighting my face with a flashlight or bright light, while sitting in front of my therapist or another person. | 80 |
| Lower-distress tasks | |
| 6. Intentionally going outside in daylight hours, instead of only after dark | 70 |
| 7. Not turning away from others in an attempt to prevent them from seeing my face | 65 |
| 8. Standing close to people when talking to them, rather than standing at a distance | 50 |
| 9. Going out in public without camouflaging my hair with hats or scarves | 40 |
Psychosocial development
BDD therapy challenges the disorder’s core theme—that appearance is one’s only important attribute—and helps patients identify and develop qualities not related to appearance. Through social interactions, the BDD patient can:
- develop a multidimensional sense of self
- receive nonappearance-related positive feedback from the outside world.
Explore psychosocial development during the assessment phase and when a patient shows little progress in CBT. In some patients, for example, BDD onset in childhood or adolescence interferes with developmental transition to adulthood.
In our experience, some patients may resist treatment because of conscious and unconscious fears of adult responsibilities and relationships. We focus therapy on making them aware of these phenomena, exploring fears of development, and encouraging them to seek new relationships and responsibilities.
Because a BDD patient’s symptoms often create conflict and distress at home, offer the family support and education about the disorder. Occasionally, forces within the family seem to be working against the individual’s recovery and/or independence.
In some families, an individual with BDD may become the “identified patient,” diverting attention from other dysfunctional family members or relationships. During therapy, the BDD patient’s goal to develop a sense of self that is not appearance-based may run counter to the family’s need to keep him or her in the “sick” role.
If therapy is to succeed, talk to the patient about these dynamics. Consider family therapy if resistance to change is strong. When a patient is not progressing well with CBT, we find understanding the family system can be useful to comprehensive BDD treatment, although this observation remains to be validated.
Preventing and treating relapse
Educate patients that BDD is usually chronic, even when treated with psychotherapy and medication.31 Relapse often occurs, especially when patients discontinue medications on their own24 or drop out of therapy early. No guidelines exist, but based on our experience:
- we continue medication for at least 1 year after a patient improves
- psychotherapy is more variable but may need to last 6 to 12 months or more.
When therapy ends, we encourage patients to practice and reinforce everything they learned during treatment. Casting BDD resurgence as normal—and not as failure—will help patients who relapse to resist the downward spiral of low self-esteem, shame, and turning to the mirror for reassurance. Identifying BDD symptom triggers and developing plans to cope with them may also prevent relapse. CBT “booster sessions” scheduled monthly for 3 to 6 months may help patients who have completed therapy.
FOR CLINICIANS:
- Phillips KA. “I’m as ugly as the elephant man:” How to recognize and treat body dysmorphic disorder. Current Psychiatry. 2002;1(1):58-65.
- Cororve MB, Gleaves DH. Body dysmorphic disorder: a review of conceptualizations, assessment, and treatment strategies. Clin Psychol Rev. 2001;21(6):949-70.
FOR PATIENTS AND FAMILIES:
- Phillips KA. The broken mirror. New York: Oxford University Press; 2005.
- BDD and body image program, Butler Hospital, Providence, RI. BDD education and support. www.BDDcentral.com.
- Winograd A. Director, Accurate Reflections, Los Angeles, CA. Support group and information on BDD and obsessive compulsive spectrum disorders. www.AccurateReflections.com
Drug brand names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Buspirone • BuSpar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lithium • Lithobid, others
- Methylphenidate • Ritalin, Concerta
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders (4th ed. text rev.). Washington, DC: American Psychiatric Association; 2000.
2. Phillips KA, Coles ME, Menard W, et al. Suicidal ideation and suicide attempts in body dysmorphic disorder. J Clin Psychiatry 2005;66(6):717-25.
3. Otto MW, Wilhelm S, Cohen LS, Harlow BL. Prevalence of body dysmorphic disorder in a community sample of women. Am J Psychiatry 2001;158(12):2061-3.
4. Wilhelm S, Otto MW, Zucker BG, Pollack MH. Prevalence of body dysmorphic disorder in patients with anxiety disorders. J Anxiety Disord 1997;11(5):499-502.
5. Phillips KA, Nierenberg AA, Brendel G, Fava M. Prevalence and clinical features of body dysmorphic disorder in atypical major depression. J Nerv Ment Dis 1996;184(2):125-9.
6. Hollander E, Cohen L, Simeon D. Body dysmorphic disorder. Psychiatr Ann 1993;23:359-64.
7. Veale D, Boocock A, Gournay K, et al. Body dysmorphic disorder. survey of fifty cases. Br J Psychiatry 1996;169(2):196-201.
8. Phillips KA. Psychosis in body dysmorphic disorder. J Psychiatr Res 2004;38(1):63-72.
9. Dufresne RG, Phillips KA, Vittorio CC, Wilkel CS. A screening questionnaire for body dysmorphic disorder in a cosmetic dermatologic surgery practice. Dermatol Surg 2001;27(5):457-62.
10. Rosen JC, Reiter J. Development of the body dysmorphic disorder examination. Behav Res Ther 1996;34(9):755-66.
11. Phillips KA, Hollander E, Rasmussen SA, et al. A severity rating scale for body dysmorphic disorder: development, reliability, and validity of a modified version of the Yale-Brown Obsessive Compulsive Scale. Psychopharmacol Bull 1997;33(1):17-22.
12. Gunstad J, Phillips KA. Axis I comorbidity in body dysmorphic disorder. Compr Psychiatry 2003;44(4):270-6.
13. Perugi G, Akiskal HS, Giannotti D, et al. Gender-related differences in body dysmorphic disorder (dysmorphophobia). J Nerv Ment Dis 1997;185(9):578-82.
14. Zimmerman M, Mattia JI. Body dysmorphic disorder in psychiatric outpatients: recognition, prevalence, comorbidity, demographic, and clinical correlates. Compr Psychiatry 1998;39(5):265-70.
15. Phillips KA. The broken mirror. New York: Oxford University Press; 2005.
16. Rauch SL, Phillips KA, Segal E, et al. A preliminary morphometric magnetic resonance imaging study of regional brain volumes in body dysmorphic disorder. Psychiatry Res 2003;122(1):13-19.
17. Veale D. Body dysmorphic disorder. Postgrad Med J 2004;80(940):67-71.
18. Saxena S, Winograd A, Dunkin JJ, et al. A retrospective review of clinical characteristics and treatment response in body dysmorphic disorder versus obsessive-compulsive disorder. J Clin Psychiatry 2001;62:67-72.
19. Phillips KA, Najjar F. An open-label study of citalopram in body dysmorphic disorder. J Clin Psychiatry 2003;64(6):715-20.
20. Phillips KA, Dwight MM, McElroy SL. Efficacy and safety of fluvoxamine in body dysmorphic disorder. J Clin Psychiatry 1998;59(4):165-71.
21. Phillips KA, Albertini RS, Rasmussen SA. A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder. Arch Gen Psychiatry 2002;59(4):381-8.
22. Hollander E, Allen A, Kwon J, et al. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: Selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch Gen Psychiatry 1999;56(11):1033-9.
23. Phillips KA, McElroy SL, Dwight MM, et al. Delusionality and response to open-label fluvoxamine in body dysmorphic disorder. J Clin Psychiatry 2001;62(2):87-91.
24. Phillips KA, Albertini RS, Siniscalchi JM, et al. Effectiveness of pharmacotherapy for body dysmorphic disorder: a chart-review study. J Clin Psychiatry 2001;62(9):721-7.
25. Phillips KA. An open study of buspirone augmentation of serotonin-reuptake inhibitors in body dysmorphic disorder. Psychopharmacol Bull 1996;32(1):175-80.
26. Phillips KA, McElroy SL, Keck PE, Jr, et al. A comparison of delusional and nondelusional body dysmorphic disorder in 100 cases. Psychopharmacol Bull 1994;30(2):179-86.
27. Phillips KA. Placebo-controlled study of pimozide augmentation of fluoxetine in body dysmorphic disorder. Am J Psychiatry 2005;162(2):377-9.
28. Phillips KA. Olanzapine augmentation of fluoxetine in body dysmorphic disorder. Am J Psychiatry 2005;162(5):1022-3.
29. Grant JE, Menard W, Pagano ME, et al. Substance use disorders in individuals with body dysmorphic disorder. J Clin Psychiatry 2005;66(3):309-16.
30. Foa EB. Failures in treating obsessive-compulsives. Behav Res Ther 1979;17:169-76.
31. Phillips KA, McElroy SL, Keck PE, Jr, et al. Body dysmorphic disorder: 30 cases of imagined ugliness. Am J Psychiatry 1993;150(2):302-8.
Identifying which came first—body dysmorphic disorder (BDD) or comorbid anxiety or depressive disorders—can be as complex as treating the disorder’s delusional thinking and high suicide risk. To help you when working alone or with a psychotherapist, we offer strategies we have found useful for:
- diagnosing BDD
- educating patients and families about it
- choosing and dosing medications
- addressing inaccurate perceptions with targeted cognitive-behavioral therapies.
Though many recommendations are based on published data, we also draw on our clinical experience because research on effective BDD treatments is limited.
Body dysmorphic disorder (BDD) is preoccupation with an imagined defect in physical appearance or excessive concern about a slight physical anomaly that causes significant distress or impairs social, occupational, or other functioning.1 BDD patients have obsessive thoughts about their “flaws” and engage in compulsive behaviors and avoidances related to how they perceive their appearance, similar to behavior seen in obsessive-compulsive disorder. BDD causes great distress and disability, often accompanied by depression and suicidality.2
BDD occurs in an estimated 0.7% of the general population3 and in 6 to 14% of persons receiving treatment for anxiety or depressive disorders.4,5 These estimates may be low, however, as persons with BDD often do not seek treatment. Men and women are equally affected.6 Average age of onset is 16, although diagnosis often doesn’t occur for another 10 to 15 years.7
Assessment
BDD causes patients great distress and disability—often accompanied by major depression—but is easy to miss or misdiagnose (Box).1-7 Even when suicidal, BDD patients often do not reveal their symptoms to clinicians,2 probably because of poor insight or shame about their appearance. When a patient describes being unable to stop thinking about specific aspects of his or her appearance, assess further for BDD.
BDD patients’ conviction that their appearance is defective ranges from good insight to mildly overvalued ideation to frankly delusional.8 They often have ideas of reference (such as thinking others may be looking at their “defective” body part) and delusions of reference (such as being convinced others are talking about their “defective” body part). Asking a patient the questions in Table 1 can help establish the diagnosis. BDD also is included in the Structured Clinical Interview for DSM-IV (SCID). Useful assessment tools include:
- Body Dysmorphic Disorder Questionnaire,9 a 5-minute, patient-rated scale for screening
- Body Dysmorphic Disorder Examination,10 to diagnose BDD, survey BDD symptoms, and measure severity
- Yale-Brown Obsessive-Compulsive Scale modified for Body Dysmorphic Disorder (BDD-YBOCS),11 for measuring symptom severity and changes over time.
Comorbidity. Psychiatric comorbidity is common in BDD (Table 2),6,7,12-14 and deciding which disorder to address first can be difficult. If there is acute mania or non-BDD psychosis, we suggest that you stabilize these before treating BDD. Suicidality or severe substance dependence or abuse may result from BDD and therefore needs to be treated in conjunction with BDD.
If comorbid obsessive-compulsive disorder (OCD) or social phobia symptoms are interconnected with the patient’s BDD, treat concurrently; if not, address sequentially, starting with the more-severe symptoms. For example, symptoms that suggest social phobia (such as fear of public speaking) may be related to BDD, and treatment should focus on BDD. A patient with obsessive fears about how “contaminants” will affect her skin’s appearance may need to have the OCD and BDD addressed concurrently.
For other comorbidities, the treatment hierarchy is less clear. Major depression, for example, may be caused by severe BDD and might not improve until BDD improves. Even when a patient has several concurrent Axis I disorders, don’t over-look treating BDD; otherwise, the patient may remain quite impaired.
Assess suicide risk, as ≥ 25% of BDD patients may attempt suicide in their lifetimes.2 Safety measures include frequent monitoring, medication, family involvement, and—if necessary—hospitalization.
Table 1
Patient interview: Questions to help diagnose BDD
| Are you concerned about specific parts of your appearance that you believe are ugly or defective? |
| Do you find it difficult to stop thinking about parts of your appearance? |
| Do you avoid certain situations, places, or being seen in general because of your appearance? |
| Do you feel anxious, ashamed, disgusted, or depressed by specific aspects of your appearance? |
| Are any of your behaviors influenced by your appearance, such as trying to hide parts of your appearance or taking a long time getting ready to leave your residence? |
| Does your preoccupation cause you a lot of distress, anxiety, disgust, and/or shame? |
| Is preoccupation with your appearance interfering with your social life, ability to work, job performance, or other important areas of your life? |
| Do you tend to use mirrors very often or avoid them? |
| Does what you see in the mirror determine your mood that day? |
| How important do you think appearance is in life? |
| Do you use any oral or topical medications for dermatologic reasons or to prevent hair loss? |
| Have you ever had cosmetic surgery? If so, how satisfied were you with the outcome? Did you have any revisions? |
Table 2
Lifetime prevalence (%) of comorbid Axis I disorders in BDD
| Study | N | Major depression | Social phobia | OCD | Substance use disorders |
|---|---|---|---|---|---|
| Gunstad and Phillips (2003)*12 | 175 | 75 | 37 | 30 | 30 |
| Zimmerman and Mattia (1998)14 | 16 | 69 | 69 | 38 | 6 |
| Perugi et al (1997)13 | 58 | 41 | 12 | 41 | † |
| Veale et al (1996)7 | 50 | 8 | 16 | 6 | 2 |
| Hollander et al (1993)6 | 50 | 68 | 12 | 78 | 22 |
| N: number of study subjects | |||||
| OCD: obsessive-compulsive disorder | |||||
| * Phenomenology group | |||||
| † not reported | |||||
| Source: Adapted and reprinted with permission from reference 12. | |||||
Patient education
Improving insight. Educate patients that BDD is a brain disorder that creates faulty, inaccurate thoughts and perceptions about appearance. Many patients initially resist a BDD diagnosis; delusional thinking and poor insight lead them to assume the “flaw” they see is an accurate perception. They may need to hear about other persons with similar concerns to realize that a psychiatric disorder is causing their distress.
Other helpful resources for improving insight include:
- group therapy
- The Broken Mirror, by Katharine A. Phillips, MD,15 which contains case examples to which BDD sufferers may relate
- Websites and online forums (see Related resources).
Explaining BDD. Discuss possible causes of BDD, giving patients alternate explanations for the physical defects they perceive. Contributing factors may include:
- neurobiological abnormalities and genetic factors16
- a history since childhood of shyness, perfectionism, or anxious temperament
- being teased, abused, or in poor family and peer relationships.17
Emphasize that multiple, different, converging factors cause BDD for each individual.
The obsessive-compulsive cycle. Explain that thoughts create distressing emotions, and that persons with BDD try to relieve or prevent these emotions by performing compulsive behaviors. Compulsions then strengthen the association between intrusive thoughts about appearance “defects” and negative feelings about appearance.
Review a list of common compulsions (Table 3) with BDD patients, as many have engaged in these behaviors for years without realizing they are compulsions.
Table 3
Common BDD compulsions and avoidances
| Excessive grooming |
| Excessive checking or avoidance of mirrors and other reflective surfaces |
| Asking for reassurance about appearance |
| “Camouflaging” (hiding or covering up) supposed defects |
| Scrutinizing the appearance of other people and comparing to oneself |
| Avoiding social interactions |
| Avoidance of certain lighting conditions |
| Skin-picking to “fix” perceived flaws |
| Having repeated cosmetic or dermatological procedures, such as dermabrasion, cosmetic surgery, etc. |
Pharmacotherapy
BDD is a severe and complex disorder that often requires multimodal treatment using cognitive-behavioral therapy (CBT) and medication (algorithm).18 In our experience, most BDD patients need medication for the disorder and for common comorbidities. We recommend starting medications before or when beginning CBT for patients with moderate to severe BDD (BDD YBOCs ≥ 20).
Serotonin reuptake inhibitors (SRIs) have reduced BDD symptoms in open-label19,20 and controlled trials.21,22 As first-line treatments, SRIs decrease distress, compulsions, and frequency and intensity of obsessions about perceived defects; they also can improve insight.21-24 SRIs appear equally effective for delusional and nondelusional patients;21,23 whether CBT is similarly effective is unclear.
Relatively high dosages are usually necessary, according to published flexible-dosing trials in BDD,19-23 a retrospective chart review24 and our experience. Try dosages similar to those used for OCD (Table 4) as tolerated, and monitor for side effects. Twelve to 16 weeks of treatment are often needed for a full therapeutic effect.20-21
Augmentation. Consider adding another agent if a full SRI trial achieves partial symptom relief. One open-label trial of 13 BDD patients found that 6 (46%) improved when buspirone (mean dosage 48.3 mg/d) was added to SRI therapy.25 In a chart review, Phillips et al24 reported variable response rates of BDD patients treated with augmentation trials of clomipramine (4/9), buspirone (12/36), lithium (1/5), methylphenidate (1/6), and antipsychotics (2/13).
Very few studies have examined antipsychotic use in BDD. Placebo-controlled data are available only for pimozide.27 Conventional antipsychotics are unlikely to be effective, either as monotherapy26 or augmentation.27 As for the atypicals, olanzapine augmentation showed little to no efficacy in one small trial, although the average dosage used was low (4.6 mg/d).28 In our experience, atypicals—such as aripiprazole, 5 to 30 mg/d; quetiapine 100 to 300 mg/d; olanzapine, 7.5 to 15 mg/d; or risperidone, 1 to 3 mg/d—can improve BDD core symptoms and improve insight.
Benzodiazepines can be useful for acute anxiety or agitation. Carefully monitor benzodiazepine use, however, as substance abuse is relatively common in BDD patients.29
Table 4
Recommended SRI dosages for treating BDD*†
| Drug | Dosage range (mg/d) |
|---|---|
| Citalopram | 40 to 100 |
| Clomipramine | 150 to 250 |
| Escitalopram | 20 to 50 |
| Fluoxetine | 40 to 100 |
| Fluvoxamine | 200 to 400 |
| Paroxetine | 40 to 100 |
| Sertraline | 150 to 400 |
| * Off-label use. | |
| † May exceed FDA-recommended maximum dosages. | |
Specialized cbt techniques
Cognitive restructuring. Trying to convince BDD patients there is nothing wrong with their appearance will not be successful. Instead, we use cognitive restructuring to challenge the rationality of their thoughts and beliefs and to find alternate, more rational ones:
Therapist: “I know I cannot convince you that your (body area) is not defective, but can you give me evidence of how this ‘defect’ has affected your life?”
BDD patient: “Well, I haven’t had a date for a long time. I think this is evidence that my (body part) must be ugly, and that no one wants to date me because of it.”
Therapist: “What are some other possible reasons why you haven’t had a date in a long time? You admitted that you have barely left your house for many months. Is it possible that you have not had a date for a long time because you rarely go outside?”
With cognitive restructuring, patients learn to:
- identify automatic thoughts and beliefs that provoke distress
- examine evidence supporting or refuting these beliefs
- de-catastrophize (such as “What is the worst thing that could happen if you left the house today without checking your [body part]? Do you think you would eventually be able to cope with that?”)
- learn to more accurately assess the probability of feared negative consequences
- arrive at rational responses.
In our experience—which is supported by OCD literature—participating in CBT is very hard for patients with frank delusions, and insight determines how effective cognitive restructuring can be.30 If a patient is convinced a body part is defective, she is unlikely to stay in treatment—much less be open to restructuring her thoughts. Even unsuccessful attempts can help you gauge the intensity of patients’ beliefs, however.
During cognitive restructuring, it is important to uncover patients’ core beliefs (underlying, organizing principles they hold about themselves, others, and the world). BDD patients commonly believe that appearance is of utmost importance and that no one could love them because of their “defect.” The therapist can then help the patient challenge the rationality of those core beliefs.
Behavioral therapy. Basic behavioral therapy attempts to normalize excessive response to appearance concerns and to prepare patients for exposure and response prevention therapy (ERP). Having identified their compulsions, the next step is to guide patients in changing these behaviors, such as by:
- decreasing reassurance-seeking
- reducing avoidance of social situations
- decreasing opportunities to use the mirror
- reducing time spent on the Internet seeking cosmetic solutions
- increasing eye contact in social situations
- decreasing scanning of others’ physical features.
For example, suggest that BDD patients stand at least an arm’s length away when using a mirror for normal grooming. Then, instead of focusing on their body part, they will view it within the context of their entire face and body.
Exposure and response prevention
ERP exposes the patient to situations that evoke negative emotions—primarily shame and anxiety in BDD—so that they gradually habituate to these feelings. Individualize exposure exercises, targeting the body parts each person believes are defective. Because these exercises are intended to induce the discomfort patients usually experience, do not attempt ERP until the patient has had extensive education, developed insight, and has consented to treatment.
Create a hierarchy of ERP tasks (Table 5), ranking situations from low- to high-distress. Address items lower on the hierarchy first, and progress to higher items as the lower ones become easier to perform. Do not attempt the highest-distress items until the patient has improved insight and is not severely ill and suicidal.
During exposures, patients must remain in distress-provoking situations—without performing compulsive behaviors—until their negative feelings decrease by at least 50% of the initial subjective, self-rated distress level. Leaving the situation before stress diminishes may reinforce shame and discomfort. Performing compulsive behaviors during or after an exposure will negate the exposure’s effect.
Mirrors and ERP. Some therapists use mirrors for exposure exercises, but this is a complex issue. Mirror-checking is a common BDD compulsion that provides temporary relief but ultimately reinforces negative, intrusive thoughts about the disliked body area. How BDD patients perceive themselves changes from moment to moment; they may stare at and analyze any reflective surface in hopes that their “defect” will not appear as deformed or ugly that day. Thus, one cannot predict whether looking in the mirror at any one time is an exposure or a compulsion.
ERP exercises for BDD need to emphasize behaviors that involve interactions with the outside world, rather than reinforcing the importance of appearance. Using the mirror for ERP could promote checking compulsions and may send the message that appearance is the focal point of treatment. On the other hand, for patients with persistent mirror avoidance, gradual mirror exposures may be useful. A technique called mirror retraining helps patients objectively view their appearance and has been used with success in some individuals.
Table 5
Exposure and response therapy: a BDD patient’s sample hierarchy
| High-distress tasks | Subjective distress rating (scale of 0 to 100) |
| 1. Purposely creating the appearance of acne/skin defects | 100 |
| 2. Intentionally messing up my hair before going in public | 100 |
| 3. Standing under bright or fluorescent lighting in public | 90 |
| 4. Sitting in a position where others can directly see my face for an extended period | 85 |
| 5. Highlighting my face with a flashlight or bright light, while sitting in front of my therapist or another person. | 80 |
| Lower-distress tasks | |
| 6. Intentionally going outside in daylight hours, instead of only after dark | 70 |
| 7. Not turning away from others in an attempt to prevent them from seeing my face | 65 |
| 8. Standing close to people when talking to them, rather than standing at a distance | 50 |
| 9. Going out in public without camouflaging my hair with hats or scarves | 40 |
Psychosocial development
BDD therapy challenges the disorder’s core theme—that appearance is one’s only important attribute—and helps patients identify and develop qualities not related to appearance. Through social interactions, the BDD patient can:
- develop a multidimensional sense of self
- receive nonappearance-related positive feedback from the outside world.
Explore psychosocial development during the assessment phase and when a patient shows little progress in CBT. In some patients, for example, BDD onset in childhood or adolescence interferes with developmental transition to adulthood.
In our experience, some patients may resist treatment because of conscious and unconscious fears of adult responsibilities and relationships. We focus therapy on making them aware of these phenomena, exploring fears of development, and encouraging them to seek new relationships and responsibilities.
Because a BDD patient’s symptoms often create conflict and distress at home, offer the family support and education about the disorder. Occasionally, forces within the family seem to be working against the individual’s recovery and/or independence.
In some families, an individual with BDD may become the “identified patient,” diverting attention from other dysfunctional family members or relationships. During therapy, the BDD patient’s goal to develop a sense of self that is not appearance-based may run counter to the family’s need to keep him or her in the “sick” role.
If therapy is to succeed, talk to the patient about these dynamics. Consider family therapy if resistance to change is strong. When a patient is not progressing well with CBT, we find understanding the family system can be useful to comprehensive BDD treatment, although this observation remains to be validated.
Preventing and treating relapse
Educate patients that BDD is usually chronic, even when treated with psychotherapy and medication.31 Relapse often occurs, especially when patients discontinue medications on their own24 or drop out of therapy early. No guidelines exist, but based on our experience:
- we continue medication for at least 1 year after a patient improves
- psychotherapy is more variable but may need to last 6 to 12 months or more.
When therapy ends, we encourage patients to practice and reinforce everything they learned during treatment. Casting BDD resurgence as normal—and not as failure—will help patients who relapse to resist the downward spiral of low self-esteem, shame, and turning to the mirror for reassurance. Identifying BDD symptom triggers and developing plans to cope with them may also prevent relapse. CBT “booster sessions” scheduled monthly for 3 to 6 months may help patients who have completed therapy.
FOR CLINICIANS:
- Phillips KA. “I’m as ugly as the elephant man:” How to recognize and treat body dysmorphic disorder. Current Psychiatry. 2002;1(1):58-65.
- Cororve MB, Gleaves DH. Body dysmorphic disorder: a review of conceptualizations, assessment, and treatment strategies. Clin Psychol Rev. 2001;21(6):949-70.
FOR PATIENTS AND FAMILIES:
- Phillips KA. The broken mirror. New York: Oxford University Press; 2005.
- BDD and body image program, Butler Hospital, Providence, RI. BDD education and support. www.BDDcentral.com.
- Winograd A. Director, Accurate Reflections, Los Angeles, CA. Support group and information on BDD and obsessive compulsive spectrum disorders. www.AccurateReflections.com
Drug brand names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Buspirone • BuSpar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lithium • Lithobid, others
- Methylphenidate • Ritalin, Concerta
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Identifying which came first—body dysmorphic disorder (BDD) or comorbid anxiety or depressive disorders—can be as complex as treating the disorder’s delusional thinking and high suicide risk. To help you when working alone or with a psychotherapist, we offer strategies we have found useful for:
- diagnosing BDD
- educating patients and families about it
- choosing and dosing medications
- addressing inaccurate perceptions with targeted cognitive-behavioral therapies.
Though many recommendations are based on published data, we also draw on our clinical experience because research on effective BDD treatments is limited.
Body dysmorphic disorder (BDD) is preoccupation with an imagined defect in physical appearance or excessive concern about a slight physical anomaly that causes significant distress or impairs social, occupational, or other functioning.1 BDD patients have obsessive thoughts about their “flaws” and engage in compulsive behaviors and avoidances related to how they perceive their appearance, similar to behavior seen in obsessive-compulsive disorder. BDD causes great distress and disability, often accompanied by depression and suicidality.2
BDD occurs in an estimated 0.7% of the general population3 and in 6 to 14% of persons receiving treatment for anxiety or depressive disorders.4,5 These estimates may be low, however, as persons with BDD often do not seek treatment. Men and women are equally affected.6 Average age of onset is 16, although diagnosis often doesn’t occur for another 10 to 15 years.7
Assessment
BDD causes patients great distress and disability—often accompanied by major depression—but is easy to miss or misdiagnose (Box).1-7 Even when suicidal, BDD patients often do not reveal their symptoms to clinicians,2 probably because of poor insight or shame about their appearance. When a patient describes being unable to stop thinking about specific aspects of his or her appearance, assess further for BDD.
BDD patients’ conviction that their appearance is defective ranges from good insight to mildly overvalued ideation to frankly delusional.8 They often have ideas of reference (such as thinking others may be looking at their “defective” body part) and delusions of reference (such as being convinced others are talking about their “defective” body part). Asking a patient the questions in Table 1 can help establish the diagnosis. BDD also is included in the Structured Clinical Interview for DSM-IV (SCID). Useful assessment tools include:
- Body Dysmorphic Disorder Questionnaire,9 a 5-minute, patient-rated scale for screening
- Body Dysmorphic Disorder Examination,10 to diagnose BDD, survey BDD symptoms, and measure severity
- Yale-Brown Obsessive-Compulsive Scale modified for Body Dysmorphic Disorder (BDD-YBOCS),11 for measuring symptom severity and changes over time.
Comorbidity. Psychiatric comorbidity is common in BDD (Table 2),6,7,12-14 and deciding which disorder to address first can be difficult. If there is acute mania or non-BDD psychosis, we suggest that you stabilize these before treating BDD. Suicidality or severe substance dependence or abuse may result from BDD and therefore needs to be treated in conjunction with BDD.
If comorbid obsessive-compulsive disorder (OCD) or social phobia symptoms are interconnected with the patient’s BDD, treat concurrently; if not, address sequentially, starting with the more-severe symptoms. For example, symptoms that suggest social phobia (such as fear of public speaking) may be related to BDD, and treatment should focus on BDD. A patient with obsessive fears about how “contaminants” will affect her skin’s appearance may need to have the OCD and BDD addressed concurrently.
For other comorbidities, the treatment hierarchy is less clear. Major depression, for example, may be caused by severe BDD and might not improve until BDD improves. Even when a patient has several concurrent Axis I disorders, don’t over-look treating BDD; otherwise, the patient may remain quite impaired.
Assess suicide risk, as ≥ 25% of BDD patients may attempt suicide in their lifetimes.2 Safety measures include frequent monitoring, medication, family involvement, and—if necessary—hospitalization.
Table 1
Patient interview: Questions to help diagnose BDD
| Are you concerned about specific parts of your appearance that you believe are ugly or defective? |
| Do you find it difficult to stop thinking about parts of your appearance? |
| Do you avoid certain situations, places, or being seen in general because of your appearance? |
| Do you feel anxious, ashamed, disgusted, or depressed by specific aspects of your appearance? |
| Are any of your behaviors influenced by your appearance, such as trying to hide parts of your appearance or taking a long time getting ready to leave your residence? |
| Does your preoccupation cause you a lot of distress, anxiety, disgust, and/or shame? |
| Is preoccupation with your appearance interfering with your social life, ability to work, job performance, or other important areas of your life? |
| Do you tend to use mirrors very often or avoid them? |
| Does what you see in the mirror determine your mood that day? |
| How important do you think appearance is in life? |
| Do you use any oral or topical medications for dermatologic reasons or to prevent hair loss? |
| Have you ever had cosmetic surgery? If so, how satisfied were you with the outcome? Did you have any revisions? |
Table 2
Lifetime prevalence (%) of comorbid Axis I disorders in BDD
| Study | N | Major depression | Social phobia | OCD | Substance use disorders |
|---|---|---|---|---|---|
| Gunstad and Phillips (2003)*12 | 175 | 75 | 37 | 30 | 30 |
| Zimmerman and Mattia (1998)14 | 16 | 69 | 69 | 38 | 6 |
| Perugi et al (1997)13 | 58 | 41 | 12 | 41 | † |
| Veale et al (1996)7 | 50 | 8 | 16 | 6 | 2 |
| Hollander et al (1993)6 | 50 | 68 | 12 | 78 | 22 |
| N: number of study subjects | |||||
| OCD: obsessive-compulsive disorder | |||||
| * Phenomenology group | |||||
| † not reported | |||||
| Source: Adapted and reprinted with permission from reference 12. | |||||
Patient education
Improving insight. Educate patients that BDD is a brain disorder that creates faulty, inaccurate thoughts and perceptions about appearance. Many patients initially resist a BDD diagnosis; delusional thinking and poor insight lead them to assume the “flaw” they see is an accurate perception. They may need to hear about other persons with similar concerns to realize that a psychiatric disorder is causing their distress.
Other helpful resources for improving insight include:
- group therapy
- The Broken Mirror, by Katharine A. Phillips, MD,15 which contains case examples to which BDD sufferers may relate
- Websites and online forums (see Related resources).
Explaining BDD. Discuss possible causes of BDD, giving patients alternate explanations for the physical defects they perceive. Contributing factors may include:
- neurobiological abnormalities and genetic factors16
- a history since childhood of shyness, perfectionism, or anxious temperament
- being teased, abused, or in poor family and peer relationships.17
Emphasize that multiple, different, converging factors cause BDD for each individual.
The obsessive-compulsive cycle. Explain that thoughts create distressing emotions, and that persons with BDD try to relieve or prevent these emotions by performing compulsive behaviors. Compulsions then strengthen the association between intrusive thoughts about appearance “defects” and negative feelings about appearance.
Review a list of common compulsions (Table 3) with BDD patients, as many have engaged in these behaviors for years without realizing they are compulsions.
Table 3
Common BDD compulsions and avoidances
| Excessive grooming |
| Excessive checking or avoidance of mirrors and other reflective surfaces |
| Asking for reassurance about appearance |
| “Camouflaging” (hiding or covering up) supposed defects |
| Scrutinizing the appearance of other people and comparing to oneself |
| Avoiding social interactions |
| Avoidance of certain lighting conditions |
| Skin-picking to “fix” perceived flaws |
| Having repeated cosmetic or dermatological procedures, such as dermabrasion, cosmetic surgery, etc. |
Pharmacotherapy
BDD is a severe and complex disorder that often requires multimodal treatment using cognitive-behavioral therapy (CBT) and medication (algorithm).18 In our experience, most BDD patients need medication for the disorder and for common comorbidities. We recommend starting medications before or when beginning CBT for patients with moderate to severe BDD (BDD YBOCs ≥ 20).
Serotonin reuptake inhibitors (SRIs) have reduced BDD symptoms in open-label19,20 and controlled trials.21,22 As first-line treatments, SRIs decrease distress, compulsions, and frequency and intensity of obsessions about perceived defects; they also can improve insight.21-24 SRIs appear equally effective for delusional and nondelusional patients;21,23 whether CBT is similarly effective is unclear.
Relatively high dosages are usually necessary, according to published flexible-dosing trials in BDD,19-23 a retrospective chart review24 and our experience. Try dosages similar to those used for OCD (Table 4) as tolerated, and monitor for side effects. Twelve to 16 weeks of treatment are often needed for a full therapeutic effect.20-21
Augmentation. Consider adding another agent if a full SRI trial achieves partial symptom relief. One open-label trial of 13 BDD patients found that 6 (46%) improved when buspirone (mean dosage 48.3 mg/d) was added to SRI therapy.25 In a chart review, Phillips et al24 reported variable response rates of BDD patients treated with augmentation trials of clomipramine (4/9), buspirone (12/36), lithium (1/5), methylphenidate (1/6), and antipsychotics (2/13).
Very few studies have examined antipsychotic use in BDD. Placebo-controlled data are available only for pimozide.27 Conventional antipsychotics are unlikely to be effective, either as monotherapy26 or augmentation.27 As for the atypicals, olanzapine augmentation showed little to no efficacy in one small trial, although the average dosage used was low (4.6 mg/d).28 In our experience, atypicals—such as aripiprazole, 5 to 30 mg/d; quetiapine 100 to 300 mg/d; olanzapine, 7.5 to 15 mg/d; or risperidone, 1 to 3 mg/d—can improve BDD core symptoms and improve insight.
Benzodiazepines can be useful for acute anxiety or agitation. Carefully monitor benzodiazepine use, however, as substance abuse is relatively common in BDD patients.29
Table 4
Recommended SRI dosages for treating BDD*†
| Drug | Dosage range (mg/d) |
|---|---|
| Citalopram | 40 to 100 |
| Clomipramine | 150 to 250 |
| Escitalopram | 20 to 50 |
| Fluoxetine | 40 to 100 |
| Fluvoxamine | 200 to 400 |
| Paroxetine | 40 to 100 |
| Sertraline | 150 to 400 |
| * Off-label use. | |
| † May exceed FDA-recommended maximum dosages. | |
Specialized cbt techniques
Cognitive restructuring. Trying to convince BDD patients there is nothing wrong with their appearance will not be successful. Instead, we use cognitive restructuring to challenge the rationality of their thoughts and beliefs and to find alternate, more rational ones:
Therapist: “I know I cannot convince you that your (body area) is not defective, but can you give me evidence of how this ‘defect’ has affected your life?”
BDD patient: “Well, I haven’t had a date for a long time. I think this is evidence that my (body part) must be ugly, and that no one wants to date me because of it.”
Therapist: “What are some other possible reasons why you haven’t had a date in a long time? You admitted that you have barely left your house for many months. Is it possible that you have not had a date for a long time because you rarely go outside?”
With cognitive restructuring, patients learn to:
- identify automatic thoughts and beliefs that provoke distress
- examine evidence supporting or refuting these beliefs
- de-catastrophize (such as “What is the worst thing that could happen if you left the house today without checking your [body part]? Do you think you would eventually be able to cope with that?”)
- learn to more accurately assess the probability of feared negative consequences
- arrive at rational responses.
In our experience—which is supported by OCD literature—participating in CBT is very hard for patients with frank delusions, and insight determines how effective cognitive restructuring can be.30 If a patient is convinced a body part is defective, she is unlikely to stay in treatment—much less be open to restructuring her thoughts. Even unsuccessful attempts can help you gauge the intensity of patients’ beliefs, however.
During cognitive restructuring, it is important to uncover patients’ core beliefs (underlying, organizing principles they hold about themselves, others, and the world). BDD patients commonly believe that appearance is of utmost importance and that no one could love them because of their “defect.” The therapist can then help the patient challenge the rationality of those core beliefs.
Behavioral therapy. Basic behavioral therapy attempts to normalize excessive response to appearance concerns and to prepare patients for exposure and response prevention therapy (ERP). Having identified their compulsions, the next step is to guide patients in changing these behaviors, such as by:
- decreasing reassurance-seeking
- reducing avoidance of social situations
- decreasing opportunities to use the mirror
- reducing time spent on the Internet seeking cosmetic solutions
- increasing eye contact in social situations
- decreasing scanning of others’ physical features.
For example, suggest that BDD patients stand at least an arm’s length away when using a mirror for normal grooming. Then, instead of focusing on their body part, they will view it within the context of their entire face and body.
Exposure and response prevention
ERP exposes the patient to situations that evoke negative emotions—primarily shame and anxiety in BDD—so that they gradually habituate to these feelings. Individualize exposure exercises, targeting the body parts each person believes are defective. Because these exercises are intended to induce the discomfort patients usually experience, do not attempt ERP until the patient has had extensive education, developed insight, and has consented to treatment.
Create a hierarchy of ERP tasks (Table 5), ranking situations from low- to high-distress. Address items lower on the hierarchy first, and progress to higher items as the lower ones become easier to perform. Do not attempt the highest-distress items until the patient has improved insight and is not severely ill and suicidal.
During exposures, patients must remain in distress-provoking situations—without performing compulsive behaviors—until their negative feelings decrease by at least 50% of the initial subjective, self-rated distress level. Leaving the situation before stress diminishes may reinforce shame and discomfort. Performing compulsive behaviors during or after an exposure will negate the exposure’s effect.
Mirrors and ERP. Some therapists use mirrors for exposure exercises, but this is a complex issue. Mirror-checking is a common BDD compulsion that provides temporary relief but ultimately reinforces negative, intrusive thoughts about the disliked body area. How BDD patients perceive themselves changes from moment to moment; they may stare at and analyze any reflective surface in hopes that their “defect” will not appear as deformed or ugly that day. Thus, one cannot predict whether looking in the mirror at any one time is an exposure or a compulsion.
ERP exercises for BDD need to emphasize behaviors that involve interactions with the outside world, rather than reinforcing the importance of appearance. Using the mirror for ERP could promote checking compulsions and may send the message that appearance is the focal point of treatment. On the other hand, for patients with persistent mirror avoidance, gradual mirror exposures may be useful. A technique called mirror retraining helps patients objectively view their appearance and has been used with success in some individuals.
Table 5
Exposure and response therapy: a BDD patient’s sample hierarchy
| High-distress tasks | Subjective distress rating (scale of 0 to 100) |
| 1. Purposely creating the appearance of acne/skin defects | 100 |
| 2. Intentionally messing up my hair before going in public | 100 |
| 3. Standing under bright or fluorescent lighting in public | 90 |
| 4. Sitting in a position where others can directly see my face for an extended period | 85 |
| 5. Highlighting my face with a flashlight or bright light, while sitting in front of my therapist or another person. | 80 |
| Lower-distress tasks | |
| 6. Intentionally going outside in daylight hours, instead of only after dark | 70 |
| 7. Not turning away from others in an attempt to prevent them from seeing my face | 65 |
| 8. Standing close to people when talking to them, rather than standing at a distance | 50 |
| 9. Going out in public without camouflaging my hair with hats or scarves | 40 |
Psychosocial development
BDD therapy challenges the disorder’s core theme—that appearance is one’s only important attribute—and helps patients identify and develop qualities not related to appearance. Through social interactions, the BDD patient can:
- develop a multidimensional sense of self
- receive nonappearance-related positive feedback from the outside world.
Explore psychosocial development during the assessment phase and when a patient shows little progress in CBT. In some patients, for example, BDD onset in childhood or adolescence interferes with developmental transition to adulthood.
In our experience, some patients may resist treatment because of conscious and unconscious fears of adult responsibilities and relationships. We focus therapy on making them aware of these phenomena, exploring fears of development, and encouraging them to seek new relationships and responsibilities.
Because a BDD patient’s symptoms often create conflict and distress at home, offer the family support and education about the disorder. Occasionally, forces within the family seem to be working against the individual’s recovery and/or independence.
In some families, an individual with BDD may become the “identified patient,” diverting attention from other dysfunctional family members or relationships. During therapy, the BDD patient’s goal to develop a sense of self that is not appearance-based may run counter to the family’s need to keep him or her in the “sick” role.
If therapy is to succeed, talk to the patient about these dynamics. Consider family therapy if resistance to change is strong. When a patient is not progressing well with CBT, we find understanding the family system can be useful to comprehensive BDD treatment, although this observation remains to be validated.
Preventing and treating relapse
Educate patients that BDD is usually chronic, even when treated with psychotherapy and medication.31 Relapse often occurs, especially when patients discontinue medications on their own24 or drop out of therapy early. No guidelines exist, but based on our experience:
- we continue medication for at least 1 year after a patient improves
- psychotherapy is more variable but may need to last 6 to 12 months or more.
When therapy ends, we encourage patients to practice and reinforce everything they learned during treatment. Casting BDD resurgence as normal—and not as failure—will help patients who relapse to resist the downward spiral of low self-esteem, shame, and turning to the mirror for reassurance. Identifying BDD symptom triggers and developing plans to cope with them may also prevent relapse. CBT “booster sessions” scheduled monthly for 3 to 6 months may help patients who have completed therapy.
FOR CLINICIANS:
- Phillips KA. “I’m as ugly as the elephant man:” How to recognize and treat body dysmorphic disorder. Current Psychiatry. 2002;1(1):58-65.
- Cororve MB, Gleaves DH. Body dysmorphic disorder: a review of conceptualizations, assessment, and treatment strategies. Clin Psychol Rev. 2001;21(6):949-70.
FOR PATIENTS AND FAMILIES:
- Phillips KA. The broken mirror. New York: Oxford University Press; 2005.
- BDD and body image program, Butler Hospital, Providence, RI. BDD education and support. www.BDDcentral.com.
- Winograd A. Director, Accurate Reflections, Los Angeles, CA. Support group and information on BDD and obsessive compulsive spectrum disorders. www.AccurateReflections.com
Drug brand names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Buspirone • BuSpar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lithium • Lithobid, others
- Methylphenidate • Ritalin, Concerta
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders (4th ed. text rev.). Washington, DC: American Psychiatric Association; 2000.
2. Phillips KA, Coles ME, Menard W, et al. Suicidal ideation and suicide attempts in body dysmorphic disorder. J Clin Psychiatry 2005;66(6):717-25.
3. Otto MW, Wilhelm S, Cohen LS, Harlow BL. Prevalence of body dysmorphic disorder in a community sample of women. Am J Psychiatry 2001;158(12):2061-3.
4. Wilhelm S, Otto MW, Zucker BG, Pollack MH. Prevalence of body dysmorphic disorder in patients with anxiety disorders. J Anxiety Disord 1997;11(5):499-502.
5. Phillips KA, Nierenberg AA, Brendel G, Fava M. Prevalence and clinical features of body dysmorphic disorder in atypical major depression. J Nerv Ment Dis 1996;184(2):125-9.
6. Hollander E, Cohen L, Simeon D. Body dysmorphic disorder. Psychiatr Ann 1993;23:359-64.
7. Veale D, Boocock A, Gournay K, et al. Body dysmorphic disorder. survey of fifty cases. Br J Psychiatry 1996;169(2):196-201.
8. Phillips KA. Psychosis in body dysmorphic disorder. J Psychiatr Res 2004;38(1):63-72.
9. Dufresne RG, Phillips KA, Vittorio CC, Wilkel CS. A screening questionnaire for body dysmorphic disorder in a cosmetic dermatologic surgery practice. Dermatol Surg 2001;27(5):457-62.
10. Rosen JC, Reiter J. Development of the body dysmorphic disorder examination. Behav Res Ther 1996;34(9):755-66.
11. Phillips KA, Hollander E, Rasmussen SA, et al. A severity rating scale for body dysmorphic disorder: development, reliability, and validity of a modified version of the Yale-Brown Obsessive Compulsive Scale. Psychopharmacol Bull 1997;33(1):17-22.
12. Gunstad J, Phillips KA. Axis I comorbidity in body dysmorphic disorder. Compr Psychiatry 2003;44(4):270-6.
13. Perugi G, Akiskal HS, Giannotti D, et al. Gender-related differences in body dysmorphic disorder (dysmorphophobia). J Nerv Ment Dis 1997;185(9):578-82.
14. Zimmerman M, Mattia JI. Body dysmorphic disorder in psychiatric outpatients: recognition, prevalence, comorbidity, demographic, and clinical correlates. Compr Psychiatry 1998;39(5):265-70.
15. Phillips KA. The broken mirror. New York: Oxford University Press; 2005.
16. Rauch SL, Phillips KA, Segal E, et al. A preliminary morphometric magnetic resonance imaging study of regional brain volumes in body dysmorphic disorder. Psychiatry Res 2003;122(1):13-19.
17. Veale D. Body dysmorphic disorder. Postgrad Med J 2004;80(940):67-71.
18. Saxena S, Winograd A, Dunkin JJ, et al. A retrospective review of clinical characteristics and treatment response in body dysmorphic disorder versus obsessive-compulsive disorder. J Clin Psychiatry 2001;62:67-72.
19. Phillips KA, Najjar F. An open-label study of citalopram in body dysmorphic disorder. J Clin Psychiatry 2003;64(6):715-20.
20. Phillips KA, Dwight MM, McElroy SL. Efficacy and safety of fluvoxamine in body dysmorphic disorder. J Clin Psychiatry 1998;59(4):165-71.
21. Phillips KA, Albertini RS, Rasmussen SA. A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder. Arch Gen Psychiatry 2002;59(4):381-8.
22. Hollander E, Allen A, Kwon J, et al. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: Selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch Gen Psychiatry 1999;56(11):1033-9.
23. Phillips KA, McElroy SL, Dwight MM, et al. Delusionality and response to open-label fluvoxamine in body dysmorphic disorder. J Clin Psychiatry 2001;62(2):87-91.
24. Phillips KA, Albertini RS, Siniscalchi JM, et al. Effectiveness of pharmacotherapy for body dysmorphic disorder: a chart-review study. J Clin Psychiatry 2001;62(9):721-7.
25. Phillips KA. An open study of buspirone augmentation of serotonin-reuptake inhibitors in body dysmorphic disorder. Psychopharmacol Bull 1996;32(1):175-80.
26. Phillips KA, McElroy SL, Keck PE, Jr, et al. A comparison of delusional and nondelusional body dysmorphic disorder in 100 cases. Psychopharmacol Bull 1994;30(2):179-86.
27. Phillips KA. Placebo-controlled study of pimozide augmentation of fluoxetine in body dysmorphic disorder. Am J Psychiatry 2005;162(2):377-9.
28. Phillips KA. Olanzapine augmentation of fluoxetine in body dysmorphic disorder. Am J Psychiatry 2005;162(5):1022-3.
29. Grant JE, Menard W, Pagano ME, et al. Substance use disorders in individuals with body dysmorphic disorder. J Clin Psychiatry 2005;66(3):309-16.
30. Foa EB. Failures in treating obsessive-compulsives. Behav Res Ther 1979;17:169-76.
31. Phillips KA, McElroy SL, Keck PE, Jr, et al. Body dysmorphic disorder: 30 cases of imagined ugliness. Am J Psychiatry 1993;150(2):302-8.
1. Diagnostic and statistical manual of mental disorders (4th ed. text rev.). Washington, DC: American Psychiatric Association; 2000.
2. Phillips KA, Coles ME, Menard W, et al. Suicidal ideation and suicide attempts in body dysmorphic disorder. J Clin Psychiatry 2005;66(6):717-25.
3. Otto MW, Wilhelm S, Cohen LS, Harlow BL. Prevalence of body dysmorphic disorder in a community sample of women. Am J Psychiatry 2001;158(12):2061-3.
4. Wilhelm S, Otto MW, Zucker BG, Pollack MH. Prevalence of body dysmorphic disorder in patients with anxiety disorders. J Anxiety Disord 1997;11(5):499-502.
5. Phillips KA, Nierenberg AA, Brendel G, Fava M. Prevalence and clinical features of body dysmorphic disorder in atypical major depression. J Nerv Ment Dis 1996;184(2):125-9.
6. Hollander E, Cohen L, Simeon D. Body dysmorphic disorder. Psychiatr Ann 1993;23:359-64.
7. Veale D, Boocock A, Gournay K, et al. Body dysmorphic disorder. survey of fifty cases. Br J Psychiatry 1996;169(2):196-201.
8. Phillips KA. Psychosis in body dysmorphic disorder. J Psychiatr Res 2004;38(1):63-72.
9. Dufresne RG, Phillips KA, Vittorio CC, Wilkel CS. A screening questionnaire for body dysmorphic disorder in a cosmetic dermatologic surgery practice. Dermatol Surg 2001;27(5):457-62.
10. Rosen JC, Reiter J. Development of the body dysmorphic disorder examination. Behav Res Ther 1996;34(9):755-66.
11. Phillips KA, Hollander E, Rasmussen SA, et al. A severity rating scale for body dysmorphic disorder: development, reliability, and validity of a modified version of the Yale-Brown Obsessive Compulsive Scale. Psychopharmacol Bull 1997;33(1):17-22.
12. Gunstad J, Phillips KA. Axis I comorbidity in body dysmorphic disorder. Compr Psychiatry 2003;44(4):270-6.
13. Perugi G, Akiskal HS, Giannotti D, et al. Gender-related differences in body dysmorphic disorder (dysmorphophobia). J Nerv Ment Dis 1997;185(9):578-82.
14. Zimmerman M, Mattia JI. Body dysmorphic disorder in psychiatric outpatients: recognition, prevalence, comorbidity, demographic, and clinical correlates. Compr Psychiatry 1998;39(5):265-70.
15. Phillips KA. The broken mirror. New York: Oxford University Press; 2005.
16. Rauch SL, Phillips KA, Segal E, et al. A preliminary morphometric magnetic resonance imaging study of regional brain volumes in body dysmorphic disorder. Psychiatry Res 2003;122(1):13-19.
17. Veale D. Body dysmorphic disorder. Postgrad Med J 2004;80(940):67-71.
18. Saxena S, Winograd A, Dunkin JJ, et al. A retrospective review of clinical characteristics and treatment response in body dysmorphic disorder versus obsessive-compulsive disorder. J Clin Psychiatry 2001;62:67-72.
19. Phillips KA, Najjar F. An open-label study of citalopram in body dysmorphic disorder. J Clin Psychiatry 2003;64(6):715-20.
20. Phillips KA, Dwight MM, McElroy SL. Efficacy and safety of fluvoxamine in body dysmorphic disorder. J Clin Psychiatry 1998;59(4):165-71.
21. Phillips KA, Albertini RS, Rasmussen SA. A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder. Arch Gen Psychiatry 2002;59(4):381-8.
22. Hollander E, Allen A, Kwon J, et al. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: Selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch Gen Psychiatry 1999;56(11):1033-9.
23. Phillips KA, McElroy SL, Dwight MM, et al. Delusionality and response to open-label fluvoxamine in body dysmorphic disorder. J Clin Psychiatry 2001;62(2):87-91.
24. Phillips KA, Albertini RS, Siniscalchi JM, et al. Effectiveness of pharmacotherapy for body dysmorphic disorder: a chart-review study. J Clin Psychiatry 2001;62(9):721-7.
25. Phillips KA. An open study of buspirone augmentation of serotonin-reuptake inhibitors in body dysmorphic disorder. Psychopharmacol Bull 1996;32(1):175-80.
26. Phillips KA, McElroy SL, Keck PE, Jr, et al. A comparison of delusional and nondelusional body dysmorphic disorder in 100 cases. Psychopharmacol Bull 1994;30(2):179-86.
27. Phillips KA. Placebo-controlled study of pimozide augmentation of fluoxetine in body dysmorphic disorder. Am J Psychiatry 2005;162(2):377-9.
28. Phillips KA. Olanzapine augmentation of fluoxetine in body dysmorphic disorder. Am J Psychiatry 2005;162(5):1022-3.
29. Grant JE, Menard W, Pagano ME, et al. Substance use disorders in individuals with body dysmorphic disorder. J Clin Psychiatry 2005;66(3):309-16.
30. Foa EB. Failures in treating obsessive-compulsives. Behav Res Ther 1979;17:169-76.
31. Phillips KA, McElroy SL, Keck PE, Jr, et al. Body dysmorphic disorder: 30 cases of imagined ugliness. Am J Psychiatry 1993;150(2):302-8.
Rituximab Found Effective in Tx-Refractory SLE
VIENNA — Rituximab successfully induced remission of severe extrarenal systemic lupus erythematosus previously unresponsive to cyclophosphamide and/or mycophenolate in five of six treated patients in a small series, Constantine K. Saadeh, M.D., reported at the annual European congress of rheumatology.
Previous studies of rituximab in SLE have focused on the agent's utility in patients with refractory lupus nephritis. But in Dr. Saadeh's six-patient series, the anti-CD20 chimeric monoclonal antibody targeting mature B cells induced remission in patients with lupus skin, lung, and synovial disease.
All five responders to two 500-mg doses of rituximab given a week apart experienced disease remissions lasting at least 3 months. All five experienced a transient 2- to 3-week drop in their globulin fraction beginning roughly a week after treatment.
The sole rituximab nonresponder had mixed lupus nephritis and chronic glomerulonephritis that continued to deteriorate, requiring hemodialysis, added Dr. Saadeh, an Amarillo, Tex., rheumatologist.
The rituximab nonresponder was also the only one of the six patients who did not have depressed complement levels at baseline. It's possible that this agent requires depressed complement levels in order to be effective in SLE, although that hypothesis will require further investigation, the physician noted at the meeting, which was sponsored by the European League Against Rheumatism.
VIENNA — Rituximab successfully induced remission of severe extrarenal systemic lupus erythematosus previously unresponsive to cyclophosphamide and/or mycophenolate in five of six treated patients in a small series, Constantine K. Saadeh, M.D., reported at the annual European congress of rheumatology.
Previous studies of rituximab in SLE have focused on the agent's utility in patients with refractory lupus nephritis. But in Dr. Saadeh's six-patient series, the anti-CD20 chimeric monoclonal antibody targeting mature B cells induced remission in patients with lupus skin, lung, and synovial disease.
All five responders to two 500-mg doses of rituximab given a week apart experienced disease remissions lasting at least 3 months. All five experienced a transient 2- to 3-week drop in their globulin fraction beginning roughly a week after treatment.
The sole rituximab nonresponder had mixed lupus nephritis and chronic glomerulonephritis that continued to deteriorate, requiring hemodialysis, added Dr. Saadeh, an Amarillo, Tex., rheumatologist.
The rituximab nonresponder was also the only one of the six patients who did not have depressed complement levels at baseline. It's possible that this agent requires depressed complement levels in order to be effective in SLE, although that hypothesis will require further investigation, the physician noted at the meeting, which was sponsored by the European League Against Rheumatism.
VIENNA — Rituximab successfully induced remission of severe extrarenal systemic lupus erythematosus previously unresponsive to cyclophosphamide and/or mycophenolate in five of six treated patients in a small series, Constantine K. Saadeh, M.D., reported at the annual European congress of rheumatology.
Previous studies of rituximab in SLE have focused on the agent's utility in patients with refractory lupus nephritis. But in Dr. Saadeh's six-patient series, the anti-CD20 chimeric monoclonal antibody targeting mature B cells induced remission in patients with lupus skin, lung, and synovial disease.
All five responders to two 500-mg doses of rituximab given a week apart experienced disease remissions lasting at least 3 months. All five experienced a transient 2- to 3-week drop in their globulin fraction beginning roughly a week after treatment.
The sole rituximab nonresponder had mixed lupus nephritis and chronic glomerulonephritis that continued to deteriorate, requiring hemodialysis, added Dr. Saadeh, an Amarillo, Tex., rheumatologist.
The rituximab nonresponder was also the only one of the six patients who did not have depressed complement levels at baseline. It's possible that this agent requires depressed complement levels in order to be effective in SLE, although that hypothesis will require further investigation, the physician noted at the meeting, which was sponsored by the European League Against Rheumatism.
Combination Drug Therapy Soothes Scleroderma
A combination of oral methotrexate and pulsed high-dose corticosteroids significantly improved the visible inflammation in 15 adults with severe localized scleroderma, wrote Alexander Kreuter, M.D., of Ruhr-University Bochum (Germany) and his colleagues.
In a prospective, nonrandomized pilot study, nine women and six men received a weekly oral methotrexate dose of 15 mg. They also received an intravenous methylprednisolone sodium succinate dose of 1,000 mg for 3 consecutive days each month.
Patients were treated for at least 6 months, and the mean treatment duration was 9.8 months (Arch. Dermatol. 2005; 141:847–52). The two treatments have shown effectiveness against severe localized scleroderma when used separately, the researchers noted.
On average, the modified skin scores of the patients dropped significantly, from 10.9 to 5.5, and signs of improvement were visible after 2 months. In addition, the visual analog scores (VAS) for tightness improved in 12 patients. On average, the VAS for tightness decreased significantly, from 65.3 to 27.5.
Follow-up visits occurred every 4 weeks, and a modified skin score was used to assess skin involvement. Ultrasonography was performed at the end of the study to confirm the clinical improvement, and it showed a significant decrease in skin thickness between baseline and the study's end.
The patients also demonstrated significant increases in dermal density at the end of the study, and the dermal collagen structure had returned to normal or near normal levels.
The patients' ages ranged from 18 to 73 years, and the duration of illness ranged from 1 to 36 years. Prior to the study, 11 patients had been treated unsuccessfully with other methods.
Adverse effects included mild nausea and headache in three patients, diabetes mellitus in two patients, and weight gain in one patient, but these effects normalized after treatment ended. None of the patients showed signs of relapse over 6 months of follow-up.
Although the study was limited by its small size and lack of placebo controls, the favorable response and moderate side effects suggest that combination therapy for localized scleroderma merits further study and that the treatment may be effective in less severe cases as well.
A combination of oral methotrexate and pulsed high-dose corticosteroids significantly improved the visible inflammation in 15 adults with severe localized scleroderma, wrote Alexander Kreuter, M.D., of Ruhr-University Bochum (Germany) and his colleagues.
In a prospective, nonrandomized pilot study, nine women and six men received a weekly oral methotrexate dose of 15 mg. They also received an intravenous methylprednisolone sodium succinate dose of 1,000 mg for 3 consecutive days each month.
Patients were treated for at least 6 months, and the mean treatment duration was 9.8 months (Arch. Dermatol. 2005; 141:847–52). The two treatments have shown effectiveness against severe localized scleroderma when used separately, the researchers noted.
On average, the modified skin scores of the patients dropped significantly, from 10.9 to 5.5, and signs of improvement were visible after 2 months. In addition, the visual analog scores (VAS) for tightness improved in 12 patients. On average, the VAS for tightness decreased significantly, from 65.3 to 27.5.
Follow-up visits occurred every 4 weeks, and a modified skin score was used to assess skin involvement. Ultrasonography was performed at the end of the study to confirm the clinical improvement, and it showed a significant decrease in skin thickness between baseline and the study's end.
The patients also demonstrated significant increases in dermal density at the end of the study, and the dermal collagen structure had returned to normal or near normal levels.
The patients' ages ranged from 18 to 73 years, and the duration of illness ranged from 1 to 36 years. Prior to the study, 11 patients had been treated unsuccessfully with other methods.
Adverse effects included mild nausea and headache in three patients, diabetes mellitus in two patients, and weight gain in one patient, but these effects normalized after treatment ended. None of the patients showed signs of relapse over 6 months of follow-up.
Although the study was limited by its small size and lack of placebo controls, the favorable response and moderate side effects suggest that combination therapy for localized scleroderma merits further study and that the treatment may be effective in less severe cases as well.
A combination of oral methotrexate and pulsed high-dose corticosteroids significantly improved the visible inflammation in 15 adults with severe localized scleroderma, wrote Alexander Kreuter, M.D., of Ruhr-University Bochum (Germany) and his colleagues.
In a prospective, nonrandomized pilot study, nine women and six men received a weekly oral methotrexate dose of 15 mg. They also received an intravenous methylprednisolone sodium succinate dose of 1,000 mg for 3 consecutive days each month.
Patients were treated for at least 6 months, and the mean treatment duration was 9.8 months (Arch. Dermatol. 2005; 141:847–52). The two treatments have shown effectiveness against severe localized scleroderma when used separately, the researchers noted.
On average, the modified skin scores of the patients dropped significantly, from 10.9 to 5.5, and signs of improvement were visible after 2 months. In addition, the visual analog scores (VAS) for tightness improved in 12 patients. On average, the VAS for tightness decreased significantly, from 65.3 to 27.5.
Follow-up visits occurred every 4 weeks, and a modified skin score was used to assess skin involvement. Ultrasonography was performed at the end of the study to confirm the clinical improvement, and it showed a significant decrease in skin thickness between baseline and the study's end.
The patients also demonstrated significant increases in dermal density at the end of the study, and the dermal collagen structure had returned to normal or near normal levels.
The patients' ages ranged from 18 to 73 years, and the duration of illness ranged from 1 to 36 years. Prior to the study, 11 patients had been treated unsuccessfully with other methods.
Adverse effects included mild nausea and headache in three patients, diabetes mellitus in two patients, and weight gain in one patient, but these effects normalized after treatment ended. None of the patients showed signs of relapse over 6 months of follow-up.
Although the study was limited by its small size and lack of placebo controls, the favorable response and moderate side effects suggest that combination therapy for localized scleroderma merits further study and that the treatment may be effective in less severe cases as well.
Infectious Arthritis of Native and Prosthetic Joints
Introduction
Acute bacterial arthritis is a potentially serious and rapidly progressive infection that may involve native or prosthetic joints. The epidemiology, pathophysiology, repertoire of potential infecting pathogens, clinical presentation and treatment differ for these two forms of infectious arthritis, but both are associated with significant morbidity and mortality. Infectious arthritis of native and prosthetic joints may be caused by viruses, or fungi, but the most common cause is bacteria.
Acute Bacterial Arthritis
Epidemiology
The burden of septic arthritis in the general population is considerable. The incidence of native joint septic arthritis is approximately 5 cases per 100,000 persons per year and is much higher in patients with rheumatoid arthritis (1,2). Between 1% and 5% of joints with indwelling prostheses become infected and the total number of infections per year is increasing due to a rise in the number of patients who have had prosthetic replacement surgery (3). The mortality from joint infection is difficult to estimate due to differing comorbidity in afflicted patients, but is likely between 15% and 30% (4-6). There is substantial morbidity from these infections because of decreased joint function and mobility, and in cases involving joint prostheses from the excisional or exchange arthroplastic surgery that is often required for treatment.
The most common route of infection for native joint infection is hematogenous (1), but may also be a result of direct inoculation of bacteria through trauma or joint surgery (including arthrocentesis, corticosteroid injection, or arthroscopy) (7), or via contiguous spread from adjacent infected soft tissue or bone (1,8). While hematogenous infection of prosthetic joints occurs, the majority of these infections are the result of joint contamination in the course of implantation surgery or post-surgical wound infection (3). Host factors that increase the risk of septic arthritis include pre-existing joint disease (especially rheumatoid arthritis), immunosuppression, diabetes mellitus, malignancy, chronic renal failure, intravenous drug use, severe skin diseases, and advanced age (1,2,4,6). The extent of joint injury resulting from infection depends on the virulence of the infecting pathogen and degree of host immune response (9).
Microbiology
Native Joint
The most common causes of bacterial septic arthritis are outlined in Table 1. In adults, the most frequent etiology is S. aureus (37–65% of cases) (1,4,6,8,12,15,16) followed by Streptococcus sp. (12,15). An increasing percentage of S. aureus isolated from septic joints are resistant to antistaphylococcal penicillins and cephalosporins (methicillin-resistant S. aureus, MRSA). In adults with diabetes, malignancy, and genitourinary structural abnormalities, group B Streptococcus is a frequently isolated pathogen (5,6,17). Gram-negative bacilli are commonly found in neonates, intravenous drug users, and immunocompromised hosts (18). N. gonorrhoeae is a significant cause of bacterial arthritis in sexually active adults and adolescents (19) and Kingella kingae and Haemophilus influenzae are likely pediatric isolates (20,21). Joint infections that follow bite trauma usually are seen in the small joints of the hand and involve Pasteurella multocida in the case of animal bites, and Eikenella corrodens in the case of humans bites (22-24). Polymicrobial floras are found in up to 8% of cases of septic arthritis.
Prosthetic Joint
The bacteria that cause prosthetic joint arthritis vary depending on the stage of infection as defined by the elapsed time after implantation surgery (Table 1 on page 31). The coagulase negative staphylococci are the most common (30–43% of cases) (3,10), followed by S. aureus (12–23%) (25).
Nonbacterial Pathogens
Nonbacterial pathogens that may cause septic arthritis include viruses, fungi, and mycobacteria. Viral arthritis is often associated with a systemic febrile illness and other manifestations of infection such as rash. Parvovirus B19 is the most common viral arthritide, presenting as a symmetric polyarticular arthritis involving the joints of the hand as well as larger joints (26). The classic red “slapped cheeks” associated with this viral infection in children is usually not present in adults, although a faint lacy reticular rash may be seen.
Fungi and mycobacteria usually cause a subacute or chronic mono- or oligoarticular arthritis (27). Candida species are an increasing cause of both native and prosthetic joint septic arthritis. Risk factors for this infection include loss of skin integrity, diabetes, malignancy, intravenous drug use, and immunosuppressive therapy including glucocorticoids (28). Patients are often chronically ill and have exposure to broad-spectrum antimicrobials, hyperalimentation fluid, and/or indwelling central intravenous catheters. Other fungi, including Cryptococcus, Blastomyces, Histoplasma, Coccidioides, and Sporothrix are rare causes of septic arthritis (29,30). Mycobacterium tuberculosis is the most common cause of mycobacterial arthritis worldwide and should be considered in a patient presenting with chronic arthritis with risk factors for tuberculosis, including being foreign-born (31).

Clinical Features
The clinical manifestations, severity, treatment, and prognosis of septic arthritis are dependent on the identity and virulence of the bacterium, source of joint infection, and underlying host factors. Nongonococcal septic arthritis is monoarticular in 80% to 90% of cases. The knee is usually affected (50% of cases) (27) followed by the hip, wrists, and ankles (2). In adults, the majority of hip infections involve prosthetic or osteosynthetic material (1). Arthritis of the small joints of the foot is most often seen in diabetic patients and is usually secondary to contiguous skin and soft tissue ulcerations or adjacent osteomyelitis.
Gonococcal arthritis may present as febrile monoarticular arthritis, usually of the knees, wrists, and ankles (27), or as one of the manifestations of disseminated gonococcal infection. The latter is characterized by fever, dermatitis, tenosynovitis, and migratory polyarthralgia or polyarthritis (19). Skin lesions are often pustular and occur simultaneously with tenosynovitis, predominately affecting the fingers, hands, wrists, or feet. Concomitant mucosal infection of the urethra or cervix is often present but usually asymptomatic. Urethral and cervical cultures or a nucleic amplification test will frequently yield N. gonorrhoeae (19,32).
Symptoms of acute septic arthritis include pain and loss of joint function. Fever and chills are often present. The acutely infected native joint is usually red, warm, and swollen with an obvious effusion. Range of motion is limited and extremely painful. For deep and axial joint, pain is often the only focal symptom. More subtle symptoms and signs may result in a delay of diagnosis and are particularly seen in patients receiving systemic or intra-articular steroids, and in those with immunocompromised status, advanced comorbidities (including rheumatoid arthritis), and extreme age (33). A thorough physical examination may reveal a distant source of joint infection in up to 50% of patients (27).

Prosthetic joint infection may present acutely as above, particularly in early stage infection, or more indolently with progressive joint pain, minimal swelling or effusion, and absence of fever (34). In late infection a cutaneous draining sinus tract may be present. Rarely, the involved prosthesis may be visible beneath an ulceration or focus of soft-tissue breakdown.
Diseases that can mimic septic arthritis are crystalinduced arthritis, rheumatoid arthritis, systemic lupus erythematosus, spondyloarthropathy, Still’s disease, rheumatic fever, and Kawasaki syndrome.
Diagnostic Approach
A diagnostic approach to acute native joint arthritis is outlined in Figure 1 on page 32 (35,36). Important aspects include exclusion of other causes of arthritis including trauma, rheumatic diseases, and crystalline arthritis. The most important diagnostic test upon which management hinges is diagnostic arthrocentesis. Fluoroscopic or CT-guided arthrocentesis is indicated for axial and deep joints (e.g., sacroiliac or pubic symphysis) or in the event of a “dry tap” of a peripheral joint. Synovial fluid analysis will often suggest whether an acutely painful joint is due to noninflammatory, sterile inflammatory, or septic causes (Table 2 on page 33). In addition, it will provide fluid for culture and gram stain, a rapid test that can guide early empiric antibiotic therapy. Bacterial, fungal, and mycobacterial cultures should always be performed in order to direct pathogen-specific antimicrobial therapy, which is often given as a prolonged course. Antimicrobial therapy should be delayed until arthrocentesis and other appropriate diagnostic cultures are obtained unless the patient shows signs of sepsis.
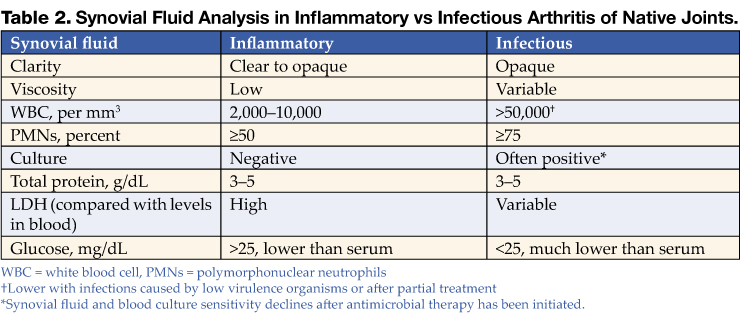
For prosthetic joint infections the diagnostic approach is essentially the same although early radiographic imaging is more important than in native joint infection as it may show signs of prosthesis failure or loosening (seen in many late prosthesis infections). Additionally, the synovial fluid white blood cell (WBC) is often lower than in nativejoint infection, with a diagnostic cutoff suggested as greater than 1,700 cells/mm3 or >65% neutrophils (37).
Nonspecific blood tests such as a white blood count, erythrocyte sedimentation rate, or C-reactive protein argue against joint infection if they are normal, but do not specifically suggest septic arthritis if elevated. Other important diagnostic tests include blood cultures (positive in 50–70% of acute bacterial arthritides) (27), but in only 30% or less of gonococcal arthritis cases) (38), wound cultures (although these often correlate poorly with synovial fluid culture results, except when the pathogen is S. aureus), and serologic testing for B. burgdorferi in selected cases with clinical features of Lyme arthritis in endemic areas. If gonococcal arthritis is suspected urethral and cervical specimens should be sent for N. gonorrhoeae culture and nucleic acid amplification tests. Radiographic and scintillographic imaging may yield additional information that will assist in identifying preexisting joint disease or for confirming a diagnosis of native or prosthetic joint infection or its complications (Table 3 on page 33).
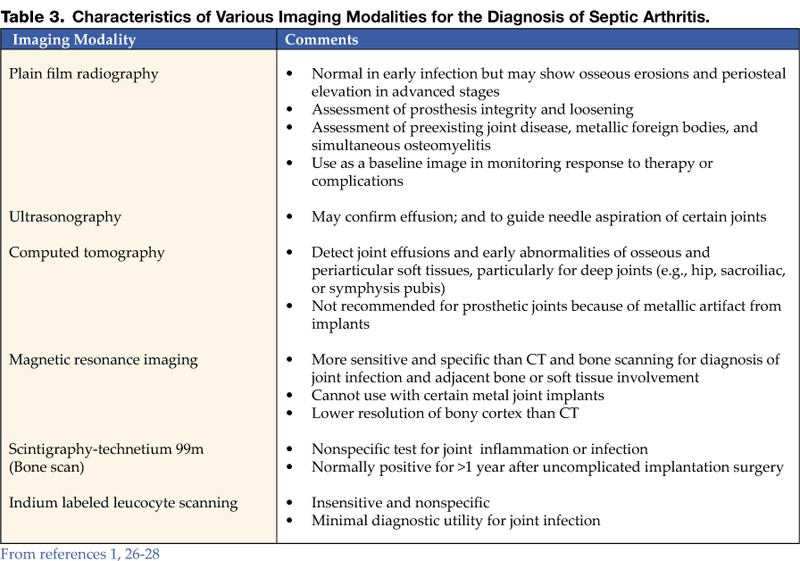
Treatment
Native joint
Prompt joint drainage and antimicrobial therapy are the mainstays of treatment in bacterial, fungal, or mycobacterial joint infection. Drainage can be through closed needle aspiration performed daily, or arthroscopy. The former modality allows direct visual inspection of the joint with concomitant irrigation, lysis of adhesions, and removal of necrotic tissue and purulent material (42). Open surgical drainage is recommended for septic arthritis of the hip and when less invasive methods fail to control infection.
Initial antimicrobial therapy should be withheld until synovial fluid has been obtained and should be based on synovial fluid gram staining (Table 4). In the case of a nondiagnostic gram stain, empiric antimicrobial coverage of likely infecting pathogens is indicated. Therapy should be narrowed based on identification and antimicrobial susceptibility testing of bacteria cultured from synovial fluid, blood, or in some cases from ancillary cultures. For patients with MRSA-related infection who are allergic to or intolerant of vancomycin, linezolid or daptomycin are potential alternatives, although not approved by the U.S. Food and Drug Administration for this indication. Linezolid is a potentially attractive option for treatment as it is available as an oral tablet, but for bone and joint infection treatment experience is limited. For septic arthritis related to animal or human bites ampicillin-sulbactam or amoxicillin-clavulanate (clindamycin plus ciprofloxacin in penicillin-allergic patients) provides activity against Pasteurella multocida and other oral bacteria. Gonococcal arthritis is best treated initially with ceftriaxone or cefotaxime; oral ciprofloxacin or levofloxacin may be substituted in regions without fluoroquinolone resistance as the patient improves (Table 4). Septic arthritis due to Candida sp. should be treated initially with an amphotericin B preparation followed by a prolonged course of fluconazole if susceptibility testing confirms activity against the cultured yeast isolate (43).
Duration of intravenous antimicrobials for bacterial joint infections is usually 2 to 4 weeks, while for gonococcal arthritis 2 weeks is sufficient. Antimicrobial therapy that continues for 2 weeks or longer should have weekly followup and laboratory monitoring for hematologic, renal, and liver toxicity.
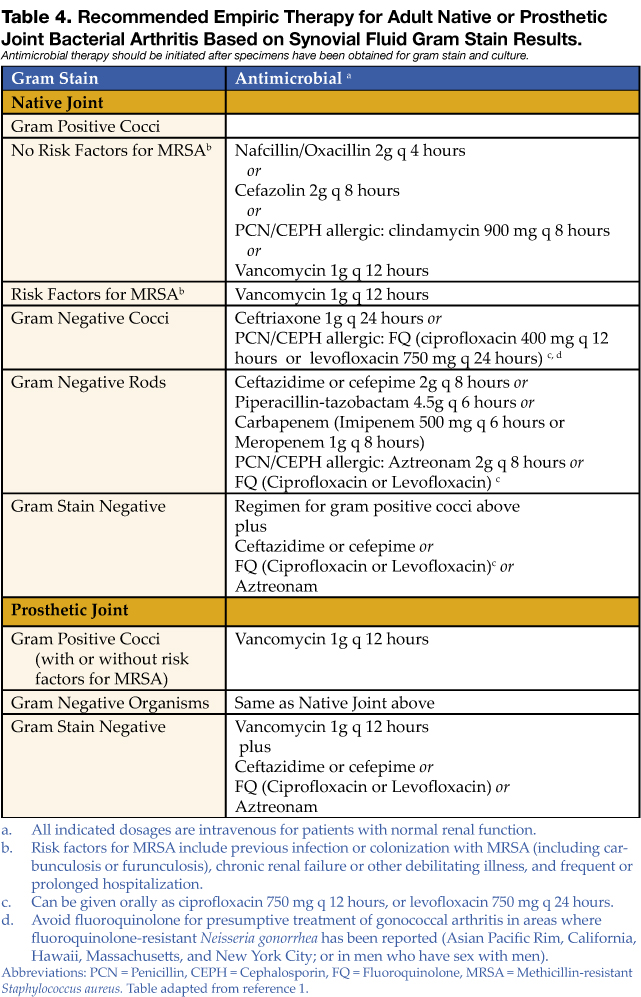
Prosthetic Joint
Treatment of prosthetic joint septic arthritis is complex, and early consultation with an orthopedic surgeon and infectious diseases physician is recommended. Extensive surgical debridement of the afflicted joint and effective, prolonged antimicrobial therapy is necessary in almost all cases. In order to achieve an optimal synovial fluid and tissue culture yield, antimicrobial therapy should be delayed until the time of debridement surgery unless the patient is septic or exhibiting serious systemic complications of infection. Suggestions for early empiric therapy while awaiting culture results are given in Table 4. Final antimicrobial choices should be based on culture results with assistance from an infectious diseases consultant.
Carefully selected cases of prosthetic joint infection may be treated with simple surgical debridement of the joint with prosthesis retention and at least 3 months of antimicrobial therapy that includes rifampin if the organism is gram positive (44). Patients who present with a short duration of symptoms within 1 month of joint implantation, or those with acute hematogenous infection, are the best candidates for such a treatment strategy. Unfortunately, relapse is common in these cases, particularly if the infection is due to S. aureus, gram-negative bacilli, or drug-resistant pathogens. Thus, the optimal treatment protocols involve surgical excision of the infected prosthesis and prolonged antimicrobial therapy.
Surgical prosthesis extraction and reimplantation can be performed in either a one- or two-stage approach. The two-stage procedure is the more successful strategy and involves removal of the prosthesis and cement followed by a 6-week course of bactericidal antimicrobial therapy. Subsequently a new prosthesis is reimplanted. Using this approach, a 90% to 96% success rate in total hip replacement infections and a 97% success rate in total knee infections has been realized (45-47). An alternative tactic is a one-stage surgical procedure that excises the infected prosthesis with immediate reimplantation of a new joint using antibiotic-impregnated methacrylate cement. This method is effective in 77% to 83% of cases (48-50). Higher failure rates are observed for S. aureus and gram-negative bacillary infections (51). One-stage procedures are often used for elderly or infirm patients who might not tolerate protracted bed rest and a second major operation (52). A recent review article by Zimmerli et al. provides an excellent overview of antimicrobial and surgical treatment options for prosthetic joint infections (34).
Suppressive Antibiotic Therapy
Lifelong oral antimicrobial therapy plays a limited role for definitive therapy but is useful when a surgical approach is not possible because of medical or surgical contraindications. The goal of suppressive therapy is to control the infection and retain prosthesis function. It is important that patients and their families understand that the intention of such treatment is not to cure but to suppress the infection. Generally, oral suppressive therapy is initiated after a course of intravenous therapy. Goulet et al. (53) demonstrated a 63% success rate in maintaining function of hip arthroplasty in patients who met 5 criteria: 1) prostheses removal is not possible, 2) the pathogen is avirulent, 3) the pathogen is sensitive to oral antibiotics, 4) the patient is adherent to and tolerates antibiotics, and 5) the prosthesis is not loose. Patients being treated with lifelong suppressive therapy are at risk for the development of antibiotic resistance (in either the joint infecting pathogen or other commensal organism), local or systemic progression of infection, and adverse effects from chronic antibiotic usage.
Antimicrobial Prophylaxis to Prevent Joint Prosthesis Infection
Patients undergoing elective total joint replacement surgery should be evaluated for symptoms or signs of local infection that predispose to occult or overt bacteremia (particularly odontogenic, urologic, and dermatologic). Surgery should be delayed until such infections and coexisting medical conditions have been treated. Perioperative antibiotic prophylaxis has been shown to reduce deep wound infection and prosthetic joint infection in joint reimplant surgery but should not be continued for more than 24 hours after the preoperative dose (54,55). In order to decrease the risk of hematogenous seeding of established implants, early recognition and treatment of overt infection is crucial. The use of prophylactic antibiotics for patients with joint implants prior to or after dental or other procedures such as colonoscopy or cystoscopy is controversial. The American Academy of Orthopedic Surgeons recommends that a single dose of prophylactic antibiotic be given to certain patients undergoing urologic instrumentation or dental procedures that are accompanied by significant bleeding (56,57). Patients who are candidates for such prophylaxis include those with rheumatoid arthritis or other inflammatory arthropathy, immunosuppression, diabetes, malnutrition, hemophilia, or who have had a previous joint infection.
Dr. Ohl can be contacted at [email protected].
References
- Kaandorp CJ, Dinant HJ, van de Laar MA, Moens HJ, Prins AP, Dijkmans BA. Incidence and sources of native and prosthetic joint infection: a community based prospective survey. Ann Rheum Dis. 1997;56:470-5.
- Ohl C. Infectious arthritis of native joints. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and Practice of Infectious Diseases. 6th ed. Philadelphia: Elsevier, 2005:1311-1322.
- Brause B. Infections with prostheses in bones and joints. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and Practices of Infectious Diseases. 6th ed. Philadelphia: Elsevier, 2005:1332-7.
- Gupta MN, Sturrock RD, Field M. A prospective 2-year study of 75 patients with adult-onset septic arthritis. Rheumatology (Oxford). 2001;40:24-30.
- Nolla JM, Gomez-Vaquero C, Fiter J, et al. Pyarthrosis in patients with rheumatoid arthritis: a detailed analysis of 10 cases and literature review. Semin Arthritis Rheum 2000;30: 121-6.
- Weston VC, Jones AC, Bradbury N, Fawthrop F, Doherty M. Clinical features and outcome of septic arthritis in a single UK Health District 1982-1991. Ann Rheum Dis 1999;58:214-219.
- Kuzmanova SI, Atanassov AN, Andreev SA, Solakov PT. Minor and major complications of arthroscopic synovectomy of the knee joint performed by rheumatologist. Folia Med (Plovdiv). 2003;45:55-9.
- Morgan DS, Fisher D, Merianos A, Currie BJ. An 18 year clinical review of septic arthritis from tropical Australia. Epidemiol Infect 1996;117:423-8.
- Mader JT, Shirtliff M, Calhoun JH. The host and the skeletal infection: classification and pathogenesis of acute bacterial bone and joint sepsis. Baillieres Best Pract Res Clin Rheumatol 1999;13:1-20.
- Berendt A. Infections of prosthetic joints and related problems. In: Cohen J, Powderly W, eds. Infectious Diseases. Edinburgh: Mosby, 2005: 583-589.
- Raymond NJ, Henry J, Workowski KA. Enterococcal arthritis: case report and review. Clin Infect Dis. 1995;21: 516-522.
- Ross JJ, Saltzman CL, Carling P, Shapiro DS. Pneumococcal septic arthritis: review of 190 cases. Clin Infect Dis. 2003;36:319-27.
- Kortekangas P, Aro HT, Tuominen J, Toivanen A. Synovial fluid leukocytosis in bacterial arthritis vs. reactive arthritis and rheumatoid arthritis in the adult knee. Scand J Rheumatol. 1992;21:283-8.
- Sack K. Monarthritis: differential diagnosis. Am J Med. 1997; 102(1A):30S-34S.
- Dubost JJ, Soubrier M, De Champs C, Ristori JM, Bussiere JL, Sauvezie B. No changes in the distribution of organisms responsible for septic arthritis over a 20 year period. Ann Rheum Dis. 2002;61:267-9.
- Ryan MJ, Kavanagh R, Wall PG, Hazleman BL. Bacterial joint infections in England and Wales: analysis of bacterial isolates over a four year period. Br J Rheumatol. 1997;36:370-3.
- Nolla JM, Gomez-Vaquero C, Corbella X, et al. Group B streptococcus (Streptococcus agalactiae) pyogenic arthritis in nonpregnant adults. Medicine (Baltimore). 2003;82: 119-28.
- Shirtliff ME, Mader JT. Acute septic arthritis. Clin Microbiol Rev. 2002;15:527-44.
- Bardin T. Gonococcal arthritis. Best Pract Res Clin Rheumatol. 2003;17:201-8.
- Yagupsky P, Dagan R. Kingella kingae: an emerging cause of invasive infections in young children. Clin Infect Dis. 1997;24:860-66.
- Bowerman SG, Green NE, Mencio GA. Decline of bone and joint infections attributable to haemophilus influenzae type b. Clin Orthop. 1997;(341):128-33.
- Ewing R, Fainstein V, Musher DM, Lidsky M, Clarridge J. Articular and skeletal infections caused by Pasteurella multocida. South Med J. 1980;73:1349-52.
- Murray PM. Septic arthritis of the hand and wrist. Hand Clin. 1998;14:579-87, viii.
- Resnick D, Pineda CJ, Weisman MH, Kerr R. Osteomyelitis and septic arthritis of the hand following human bites. Skeletal Radiol. 1985;14:263-6.
- Murdoch DR, Roberts SA, Fowler JV Jr, et al. Infection of orthopedic prostheses after Staphylococcus aureus bacteremia. Clin Infect Dis. 2001;32:647-9.
- Woolf AD, Campion GV, Chishick A, et al. Clinical manifestations of human parvovirus B19 in adults. Arch Intern Med. 1989;149:1153-6.
- Goldenberg DL. Septic arthritis. Lancet 1998; 351:197-202.
- Silveira LH, Cuellar ML, Citera G, Cabrera GE, Scopelitis E, Espinoza LR. Candida arthritis. Rheum Dis Clin North Am. 1993;19:427-37.
- Cuellar ML, Silveira LH, Espinoza LR. Fungal arthritis. Ann Rheum Dis. 1992;51:690-7.
- Cuellar ML, Silveira LH, Citera G, Cabrera GE, Valle R. Other fungal arthritides. Rheum Dis Clin North Am. 1993;19:439-55.
- Malaviya AN, Kotwal PP. Arthritis associated with tuberculosis. Best Pract Res Clin Rheumatol. 2003;17:319-43.
- Van Der PB, Ferrero DV, Buck-Barrington L, et al. Multicenter evaluation of the BDProbeTec ET System for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in urine specimens, female endocervical swabs, and male urethral swabs. J Clin Microbiol. 2001;39:1008-16.
- Kaandorp CJ, van Schaardenburg D, Krijnen P, Habbema JD, van de Laar MA. Risk factors for septic arthritis in patients with joint disease: a prospective study. Arthritis Rheum. 1995;38:1819-25.
- Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. N Engl J Med. 2004;351:1645-54.
- Guidelines for the initial evaluation of the adult patient with acute musculoskeletal symptoms. American College of Rheumatology Ad Hoc Committee on Clinical Guidelines. Arthritis Rheum. 1996;39:1-8.
- Siva C, Velazquez C, Mody A, Brasington R. Diagnosing acute monoarthritis in adults: a practical approach for the family physician. Am Fam Physician. 2003;68:83-90.
- Trampuz A, Hanssen AD, Osmon DR, Mandrekar J, Steckelberg JM, Patel R. Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med. 2004; 117:556-62.
- Cucurull E, Espinoza LR. Gonococcal arthritis. Rheum Dis Clin North Am. 1998; 24:305-22.
- Chhem RK, Kaplan PA, Dussault RG. Ultrasonography of the musculoskeletal system. Radiol Clin North Am. 1994;32:275-289.
- Learch TJ, Farooki S. Magnetic resonance imaging of septic arthritis. Clin Imaging. 2000;24:236-42.
- Mohana-Borges AV, Chung CB, Resnick D. Monoarticular arthritis. Radiol Clin North Am. 2004;42:135-49.
- Donatto KC. Orthopedic management of septic arthritis. Rheum Dis Clin North Am. 1998;24:275-86.
- Pappas PG, Rex JH, Sobel JD, et al. Guidelines for treatment of candidiasis. Clin Infect Dis. 2004;38:161-89.
- Zimmerli W, Widmer AF, Blatter M, Frei R, Ochsner PE. Role of rifampin for treatment of orthopedic implant-related staphylococcal infections: a randomized controlled trial. Foreign-Body Infection (FBI) Study Group. JAMA. 1998;279:1537-41.
- Garvin KL, Salvati EA, Brause BD. Role of gentamicin-impregnated cement in total joint arthroplasty. Orthop Clin North Am. 1988;19:605-10.
- Lieberman JR, Callaway GH, Salvati EA, Pellicci PM, Brause BD. Treatment of the infected total hip arthroplasty with a two-stage reimplantation protocol. Clin Orthop Relat Res. 1994;205-12.
- Windsor RE, Insall JN, Urs WK, Miller DV, Brause BD. Twostage reimplantation for the salvage of total knee arthroplasty complicated by infection. Further follow-up and refinement of indications. J Bone Joint Surg Am. 1990;72:272-8.
- Buchholz HW, Elson RA, Engelbrecht E, Lodenkamper H, Rottger J, Siegel A. Management of deep infection of total hip replacement. J Bone Joint Surg Br. 1981; 63-B(3):342-53.
- Carlsson AS, Josefsson G, Lindberg L. Revision with gentamicin-impregnated cement for deep infections in total hip arthroplasties. J Bone Joint Surg Am. 1978;60:1059-64.
- Jackson WO, Schmalzried TP. Limited role of direct exchange arthroplasty in the treatment of infected total hip replacements. Clin Orthop Relat Res. 2000;(381):101-5.
- Fitzgerald RH Jr, Jones DR. Hip implant infection. Treatment with resection arthroplasty and late total hip arthroplasty. Am J Med. 1985; 78(6B):225-8.
- Garvin KL, Hanssen AD. Infection after total hip arthroplasty. Past, present, and future. J Bone Joint Surg Am. 1995;77:1576-88.
- Goulet JA, Pellicci PM, Brause BD, Salvati EM. Prolonged suppression of infection in total hip arthroplasty. J Arthroplasty. 1988; 3:109-16.
- Engesaeter LB, Lie SA, Espehaug B, Furnes O, Vollset SE, Havelin LI. Antibiotic prophylaxis in total hip arthroplasty: effects of antibiotic prophylaxis systemically and in bone cement on the revision rate of 22,170 primary hip replacements followed 0-14 years in the Norwegian Arthroplasty Register. Acta Orthop Scand. 2003; 74:644-51.
- Norden CW. A critical review of antibiotic prophylaxis in orthopedic surgery. Rev Infect Dis 1983;5:928-32.
- Antibiotic prophylaxis for urological patients with total joint replacements. J Urol. 2003; 169:1796-7.
- Antibiotic prophylaxis for dental patients with total joint replacements. J Am Dent Assoc. 2003; 134:895-9.
Introduction
Acute bacterial arthritis is a potentially serious and rapidly progressive infection that may involve native or prosthetic joints. The epidemiology, pathophysiology, repertoire of potential infecting pathogens, clinical presentation and treatment differ for these two forms of infectious arthritis, but both are associated with significant morbidity and mortality. Infectious arthritis of native and prosthetic joints may be caused by viruses, or fungi, but the most common cause is bacteria.
Acute Bacterial Arthritis
Epidemiology
The burden of septic arthritis in the general population is considerable. The incidence of native joint septic arthritis is approximately 5 cases per 100,000 persons per year and is much higher in patients with rheumatoid arthritis (1,2). Between 1% and 5% of joints with indwelling prostheses become infected and the total number of infections per year is increasing due to a rise in the number of patients who have had prosthetic replacement surgery (3). The mortality from joint infection is difficult to estimate due to differing comorbidity in afflicted patients, but is likely between 15% and 30% (4-6). There is substantial morbidity from these infections because of decreased joint function and mobility, and in cases involving joint prostheses from the excisional or exchange arthroplastic surgery that is often required for treatment.
The most common route of infection for native joint infection is hematogenous (1), but may also be a result of direct inoculation of bacteria through trauma or joint surgery (including arthrocentesis, corticosteroid injection, or arthroscopy) (7), or via contiguous spread from adjacent infected soft tissue or bone (1,8). While hematogenous infection of prosthetic joints occurs, the majority of these infections are the result of joint contamination in the course of implantation surgery or post-surgical wound infection (3). Host factors that increase the risk of septic arthritis include pre-existing joint disease (especially rheumatoid arthritis), immunosuppression, diabetes mellitus, malignancy, chronic renal failure, intravenous drug use, severe skin diseases, and advanced age (1,2,4,6). The extent of joint injury resulting from infection depends on the virulence of the infecting pathogen and degree of host immune response (9).
Microbiology
Native Joint
The most common causes of bacterial septic arthritis are outlined in Table 1. In adults, the most frequent etiology is S. aureus (37–65% of cases) (1,4,6,8,12,15,16) followed by Streptococcus sp. (12,15). An increasing percentage of S. aureus isolated from septic joints are resistant to antistaphylococcal penicillins and cephalosporins (methicillin-resistant S. aureus, MRSA). In adults with diabetes, malignancy, and genitourinary structural abnormalities, group B Streptococcus is a frequently isolated pathogen (5,6,17). Gram-negative bacilli are commonly found in neonates, intravenous drug users, and immunocompromised hosts (18). N. gonorrhoeae is a significant cause of bacterial arthritis in sexually active adults and adolescents (19) and Kingella kingae and Haemophilus influenzae are likely pediatric isolates (20,21). Joint infections that follow bite trauma usually are seen in the small joints of the hand and involve Pasteurella multocida in the case of animal bites, and Eikenella corrodens in the case of humans bites (22-24). Polymicrobial floras are found in up to 8% of cases of septic arthritis.
Prosthetic Joint
The bacteria that cause prosthetic joint arthritis vary depending on the stage of infection as defined by the elapsed time after implantation surgery (Table 1 on page 31). The coagulase negative staphylococci are the most common (30–43% of cases) (3,10), followed by S. aureus (12–23%) (25).
Nonbacterial Pathogens
Nonbacterial pathogens that may cause septic arthritis include viruses, fungi, and mycobacteria. Viral arthritis is often associated with a systemic febrile illness and other manifestations of infection such as rash. Parvovirus B19 is the most common viral arthritide, presenting as a symmetric polyarticular arthritis involving the joints of the hand as well as larger joints (26). The classic red “slapped cheeks” associated with this viral infection in children is usually not present in adults, although a faint lacy reticular rash may be seen.
Fungi and mycobacteria usually cause a subacute or chronic mono- or oligoarticular arthritis (27). Candida species are an increasing cause of both native and prosthetic joint septic arthritis. Risk factors for this infection include loss of skin integrity, diabetes, malignancy, intravenous drug use, and immunosuppressive therapy including glucocorticoids (28). Patients are often chronically ill and have exposure to broad-spectrum antimicrobials, hyperalimentation fluid, and/or indwelling central intravenous catheters. Other fungi, including Cryptococcus, Blastomyces, Histoplasma, Coccidioides, and Sporothrix are rare causes of septic arthritis (29,30). Mycobacterium tuberculosis is the most common cause of mycobacterial arthritis worldwide and should be considered in a patient presenting with chronic arthritis with risk factors for tuberculosis, including being foreign-born (31).
Clinical Features
The clinical manifestations, severity, treatment, and prognosis of septic arthritis are dependent on the identity and virulence of the bacterium, source of joint infection, and underlying host factors. Nongonococcal septic arthritis is monoarticular in 80% to 90% of cases. The knee is usually affected (50% of cases) (27) followed by the hip, wrists, and ankles (2). In adults, the majority of hip infections involve prosthetic or osteosynthetic material (1). Arthritis of the small joints of the foot is most often seen in diabetic patients and is usually secondary to contiguous skin and soft tissue ulcerations or adjacent osteomyelitis.
Gonococcal arthritis may present as febrile monoarticular arthritis, usually of the knees, wrists, and ankles (27), or as one of the manifestations of disseminated gonococcal infection. The latter is characterized by fever, dermatitis, tenosynovitis, and migratory polyarthralgia or polyarthritis (19). Skin lesions are often pustular and occur simultaneously with tenosynovitis, predominately affecting the fingers, hands, wrists, or feet. Concomitant mucosal infection of the urethra or cervix is often present but usually asymptomatic. Urethral and cervical cultures or a nucleic amplification test will frequently yield N. gonorrhoeae (19,32).
Symptoms of acute septic arthritis include pain and loss of joint function. Fever and chills are often present. The acutely infected native joint is usually red, warm, and swollen with an obvious effusion. Range of motion is limited and extremely painful. For deep and axial joint, pain is often the only focal symptom. More subtle symptoms and signs may result in a delay of diagnosis and are particularly seen in patients receiving systemic or intra-articular steroids, and in those with immunocompromised status, advanced comorbidities (including rheumatoid arthritis), and extreme age (33). A thorough physical examination may reveal a distant source of joint infection in up to 50% of patients (27).
Prosthetic joint infection may present acutely as above, particularly in early stage infection, or more indolently with progressive joint pain, minimal swelling or effusion, and absence of fever (34). In late infection a cutaneous draining sinus tract may be present. Rarely, the involved prosthesis may be visible beneath an ulceration or focus of soft-tissue breakdown.
Diseases that can mimic septic arthritis are crystalinduced arthritis, rheumatoid arthritis, systemic lupus erythematosus, spondyloarthropathy, Still’s disease, rheumatic fever, and Kawasaki syndrome.
Diagnostic Approach
A diagnostic approach to acute native joint arthritis is outlined in Figure 1 on page 32 (35,36). Important aspects include exclusion of other causes of arthritis including trauma, rheumatic diseases, and crystalline arthritis. The most important diagnostic test upon which management hinges is diagnostic arthrocentesis. Fluoroscopic or CT-guided arthrocentesis is indicated for axial and deep joints (e.g., sacroiliac or pubic symphysis) or in the event of a “dry tap” of a peripheral joint. Synovial fluid analysis will often suggest whether an acutely painful joint is due to noninflammatory, sterile inflammatory, or septic causes (Table 2 on page 33). In addition, it will provide fluid for culture and gram stain, a rapid test that can guide early empiric antibiotic therapy. Bacterial, fungal, and mycobacterial cultures should always be performed in order to direct pathogen-specific antimicrobial therapy, which is often given as a prolonged course. Antimicrobial therapy should be delayed until arthrocentesis and other appropriate diagnostic cultures are obtained unless the patient shows signs of sepsis.
For prosthetic joint infections the diagnostic approach is essentially the same although early radiographic imaging is more important than in native joint infection as it may show signs of prosthesis failure or loosening (seen in many late prosthesis infections). Additionally, the synovial fluid white blood cell (WBC) is often lower than in nativejoint infection, with a diagnostic cutoff suggested as greater than 1,700 cells/mm3 or >65% neutrophils (37).
Nonspecific blood tests such as a white blood count, erythrocyte sedimentation rate, or C-reactive protein argue against joint infection if they are normal, but do not specifically suggest septic arthritis if elevated. Other important diagnostic tests include blood cultures (positive in 50–70% of acute bacterial arthritides) (27), but in only 30% or less of gonococcal arthritis cases) (38), wound cultures (although these often correlate poorly with synovial fluid culture results, except when the pathogen is S. aureus), and serologic testing for B. burgdorferi in selected cases with clinical features of Lyme arthritis in endemic areas. If gonococcal arthritis is suspected urethral and cervical specimens should be sent for N. gonorrhoeae culture and nucleic acid amplification tests. Radiographic and scintillographic imaging may yield additional information that will assist in identifying preexisting joint disease or for confirming a diagnosis of native or prosthetic joint infection or its complications (Table 3 on page 33).
Treatment
Native joint
Prompt joint drainage and antimicrobial therapy are the mainstays of treatment in bacterial, fungal, or mycobacterial joint infection. Drainage can be through closed needle aspiration performed daily, or arthroscopy. The former modality allows direct visual inspection of the joint with concomitant irrigation, lysis of adhesions, and removal of necrotic tissue and purulent material (42). Open surgical drainage is recommended for septic arthritis of the hip and when less invasive methods fail to control infection.
Initial antimicrobial therapy should be withheld until synovial fluid has been obtained and should be based on synovial fluid gram staining (Table 4). In the case of a nondiagnostic gram stain, empiric antimicrobial coverage of likely infecting pathogens is indicated. Therapy should be narrowed based on identification and antimicrobial susceptibility testing of bacteria cultured from synovial fluid, blood, or in some cases from ancillary cultures. For patients with MRSA-related infection who are allergic to or intolerant of vancomycin, linezolid or daptomycin are potential alternatives, although not approved by the U.S. Food and Drug Administration for this indication. Linezolid is a potentially attractive option for treatment as it is available as an oral tablet, but for bone and joint infection treatment experience is limited. For septic arthritis related to animal or human bites ampicillin-sulbactam or amoxicillin-clavulanate (clindamycin plus ciprofloxacin in penicillin-allergic patients) provides activity against Pasteurella multocida and other oral bacteria. Gonococcal arthritis is best treated initially with ceftriaxone or cefotaxime; oral ciprofloxacin or levofloxacin may be substituted in regions without fluoroquinolone resistance as the patient improves (Table 4). Septic arthritis due to Candida sp. should be treated initially with an amphotericin B preparation followed by a prolonged course of fluconazole if susceptibility testing confirms activity against the cultured yeast isolate (43).
Duration of intravenous antimicrobials for bacterial joint infections is usually 2 to 4 weeks, while for gonococcal arthritis 2 weeks is sufficient. Antimicrobial therapy that continues for 2 weeks or longer should have weekly followup and laboratory monitoring for hematologic, renal, and liver toxicity.
Prosthetic Joint
Treatment of prosthetic joint septic arthritis is complex, and early consultation with an orthopedic surgeon and infectious diseases physician is recommended. Extensive surgical debridement of the afflicted joint and effective, prolonged antimicrobial therapy is necessary in almost all cases. In order to achieve an optimal synovial fluid and tissue culture yield, antimicrobial therapy should be delayed until the time of debridement surgery unless the patient is septic or exhibiting serious systemic complications of infection. Suggestions for early empiric therapy while awaiting culture results are given in Table 4. Final antimicrobial choices should be based on culture results with assistance from an infectious diseases consultant.
Carefully selected cases of prosthetic joint infection may be treated with simple surgical debridement of the joint with prosthesis retention and at least 3 months of antimicrobial therapy that includes rifampin if the organism is gram positive (44). Patients who present with a short duration of symptoms within 1 month of joint implantation, or those with acute hematogenous infection, are the best candidates for such a treatment strategy. Unfortunately, relapse is common in these cases, particularly if the infection is due to S. aureus, gram-negative bacilli, or drug-resistant pathogens. Thus, the optimal treatment protocols involve surgical excision of the infected prosthesis and prolonged antimicrobial therapy.
Surgical prosthesis extraction and reimplantation can be performed in either a one- or two-stage approach. The two-stage procedure is the more successful strategy and involves removal of the prosthesis and cement followed by a 6-week course of bactericidal antimicrobial therapy. Subsequently a new prosthesis is reimplanted. Using this approach, a 90% to 96% success rate in total hip replacement infections and a 97% success rate in total knee infections has been realized (45-47). An alternative tactic is a one-stage surgical procedure that excises the infected prosthesis with immediate reimplantation of a new joint using antibiotic-impregnated methacrylate cement. This method is effective in 77% to 83% of cases (48-50). Higher failure rates are observed for S. aureus and gram-negative bacillary infections (51). One-stage procedures are often used for elderly or infirm patients who might not tolerate protracted bed rest and a second major operation (52). A recent review article by Zimmerli et al. provides an excellent overview of antimicrobial and surgical treatment options for prosthetic joint infections (34).
Suppressive Antibiotic Therapy
Lifelong oral antimicrobial therapy plays a limited role for definitive therapy but is useful when a surgical approach is not possible because of medical or surgical contraindications. The goal of suppressive therapy is to control the infection and retain prosthesis function. It is important that patients and their families understand that the intention of such treatment is not to cure but to suppress the infection. Generally, oral suppressive therapy is initiated after a course of intravenous therapy. Goulet et al. (53) demonstrated a 63% success rate in maintaining function of hip arthroplasty in patients who met 5 criteria: 1) prostheses removal is not possible, 2) the pathogen is avirulent, 3) the pathogen is sensitive to oral antibiotics, 4) the patient is adherent to and tolerates antibiotics, and 5) the prosthesis is not loose. Patients being treated with lifelong suppressive therapy are at risk for the development of antibiotic resistance (in either the joint infecting pathogen or other commensal organism), local or systemic progression of infection, and adverse effects from chronic antibiotic usage.
Antimicrobial Prophylaxis to Prevent Joint Prosthesis Infection
Patients undergoing elective total joint replacement surgery should be evaluated for symptoms or signs of local infection that predispose to occult or overt bacteremia (particularly odontogenic, urologic, and dermatologic). Surgery should be delayed until such infections and coexisting medical conditions have been treated. Perioperative antibiotic prophylaxis has been shown to reduce deep wound infection and prosthetic joint infection in joint reimplant surgery but should not be continued for more than 24 hours after the preoperative dose (54,55). In order to decrease the risk of hematogenous seeding of established implants, early recognition and treatment of overt infection is crucial. The use of prophylactic antibiotics for patients with joint implants prior to or after dental or other procedures such as colonoscopy or cystoscopy is controversial. The American Academy of Orthopedic Surgeons recommends that a single dose of prophylactic antibiotic be given to certain patients undergoing urologic instrumentation or dental procedures that are accompanied by significant bleeding (56,57). Patients who are candidates for such prophylaxis include those with rheumatoid arthritis or other inflammatory arthropathy, immunosuppression, diabetes, malnutrition, hemophilia, or who have had a previous joint infection.
Dr. Ohl can be contacted at [email protected].
References
- Kaandorp CJ, Dinant HJ, van de Laar MA, Moens HJ, Prins AP, Dijkmans BA. Incidence and sources of native and prosthetic joint infection: a community based prospective survey. Ann Rheum Dis. 1997;56:470-5.
- Ohl C. Infectious arthritis of native joints. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and Practice of Infectious Diseases. 6th ed. Philadelphia: Elsevier, 2005:1311-1322.
- Brause B. Infections with prostheses in bones and joints. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and Practices of Infectious Diseases. 6th ed. Philadelphia: Elsevier, 2005:1332-7.
- Gupta MN, Sturrock RD, Field M. A prospective 2-year study of 75 patients with adult-onset septic arthritis. Rheumatology (Oxford). 2001;40:24-30.
- Nolla JM, Gomez-Vaquero C, Fiter J, et al. Pyarthrosis in patients with rheumatoid arthritis: a detailed analysis of 10 cases and literature review. Semin Arthritis Rheum 2000;30: 121-6.
- Weston VC, Jones AC, Bradbury N, Fawthrop F, Doherty M. Clinical features and outcome of septic arthritis in a single UK Health District 1982-1991. Ann Rheum Dis 1999;58:214-219.
- Kuzmanova SI, Atanassov AN, Andreev SA, Solakov PT. Minor and major complications of arthroscopic synovectomy of the knee joint performed by rheumatologist. Folia Med (Plovdiv). 2003;45:55-9.
- Morgan DS, Fisher D, Merianos A, Currie BJ. An 18 year clinical review of septic arthritis from tropical Australia. Epidemiol Infect 1996;117:423-8.
- Mader JT, Shirtliff M, Calhoun JH. The host and the skeletal infection: classification and pathogenesis of acute bacterial bone and joint sepsis. Baillieres Best Pract Res Clin Rheumatol 1999;13:1-20.
- Berendt A. Infections of prosthetic joints and related problems. In: Cohen J, Powderly W, eds. Infectious Diseases. Edinburgh: Mosby, 2005: 583-589.
- Raymond NJ, Henry J, Workowski KA. Enterococcal arthritis: case report and review. Clin Infect Dis. 1995;21: 516-522.
- Ross JJ, Saltzman CL, Carling P, Shapiro DS. Pneumococcal septic arthritis: review of 190 cases. Clin Infect Dis. 2003;36:319-27.
- Kortekangas P, Aro HT, Tuominen J, Toivanen A. Synovial fluid leukocytosis in bacterial arthritis vs. reactive arthritis and rheumatoid arthritis in the adult knee. Scand J Rheumatol. 1992;21:283-8.
- Sack K. Monarthritis: differential diagnosis. Am J Med. 1997; 102(1A):30S-34S.
- Dubost JJ, Soubrier M, De Champs C, Ristori JM, Bussiere JL, Sauvezie B. No changes in the distribution of organisms responsible for septic arthritis over a 20 year period. Ann Rheum Dis. 2002;61:267-9.
- Ryan MJ, Kavanagh R, Wall PG, Hazleman BL. Bacterial joint infections in England and Wales: analysis of bacterial isolates over a four year period. Br J Rheumatol. 1997;36:370-3.
- Nolla JM, Gomez-Vaquero C, Corbella X, et al. Group B streptococcus (Streptococcus agalactiae) pyogenic arthritis in nonpregnant adults. Medicine (Baltimore). 2003;82: 119-28.
- Shirtliff ME, Mader JT. Acute septic arthritis. Clin Microbiol Rev. 2002;15:527-44.
- Bardin T. Gonococcal arthritis. Best Pract Res Clin Rheumatol. 2003;17:201-8.
- Yagupsky P, Dagan R. Kingella kingae: an emerging cause of invasive infections in young children. Clin Infect Dis. 1997;24:860-66.
- Bowerman SG, Green NE, Mencio GA. Decline of bone and joint infections attributable to haemophilus influenzae type b. Clin Orthop. 1997;(341):128-33.
- Ewing R, Fainstein V, Musher DM, Lidsky M, Clarridge J. Articular and skeletal infections caused by Pasteurella multocida. South Med J. 1980;73:1349-52.
- Murray PM. Septic arthritis of the hand and wrist. Hand Clin. 1998;14:579-87, viii.
- Resnick D, Pineda CJ, Weisman MH, Kerr R. Osteomyelitis and septic arthritis of the hand following human bites. Skeletal Radiol. 1985;14:263-6.
- Murdoch DR, Roberts SA, Fowler JV Jr, et al. Infection of orthopedic prostheses after Staphylococcus aureus bacteremia. Clin Infect Dis. 2001;32:647-9.
- Woolf AD, Campion GV, Chishick A, et al. Clinical manifestations of human parvovirus B19 in adults. Arch Intern Med. 1989;149:1153-6.
- Goldenberg DL. Septic arthritis. Lancet 1998; 351:197-202.
- Silveira LH, Cuellar ML, Citera G, Cabrera GE, Scopelitis E, Espinoza LR. Candida arthritis. Rheum Dis Clin North Am. 1993;19:427-37.
- Cuellar ML, Silveira LH, Espinoza LR. Fungal arthritis. Ann Rheum Dis. 1992;51:690-7.
- Cuellar ML, Silveira LH, Citera G, Cabrera GE, Valle R. Other fungal arthritides. Rheum Dis Clin North Am. 1993;19:439-55.
- Malaviya AN, Kotwal PP. Arthritis associated with tuberculosis. Best Pract Res Clin Rheumatol. 2003;17:319-43.
- Van Der PB, Ferrero DV, Buck-Barrington L, et al. Multicenter evaluation of the BDProbeTec ET System for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in urine specimens, female endocervical swabs, and male urethral swabs. J Clin Microbiol. 2001;39:1008-16.
- Kaandorp CJ, van Schaardenburg D, Krijnen P, Habbema JD, van de Laar MA. Risk factors for septic arthritis in patients with joint disease: a prospective study. Arthritis Rheum. 1995;38:1819-25.
- Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. N Engl J Med. 2004;351:1645-54.
- Guidelines for the initial evaluation of the adult patient with acute musculoskeletal symptoms. American College of Rheumatology Ad Hoc Committee on Clinical Guidelines. Arthritis Rheum. 1996;39:1-8.
- Siva C, Velazquez C, Mody A, Brasington R. Diagnosing acute monoarthritis in adults: a practical approach for the family physician. Am Fam Physician. 2003;68:83-90.
- Trampuz A, Hanssen AD, Osmon DR, Mandrekar J, Steckelberg JM, Patel R. Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med. 2004; 117:556-62.
- Cucurull E, Espinoza LR. Gonococcal arthritis. Rheum Dis Clin North Am. 1998; 24:305-22.
- Chhem RK, Kaplan PA, Dussault RG. Ultrasonography of the musculoskeletal system. Radiol Clin North Am. 1994;32:275-289.
- Learch TJ, Farooki S. Magnetic resonance imaging of septic arthritis. Clin Imaging. 2000;24:236-42.
- Mohana-Borges AV, Chung CB, Resnick D. Monoarticular arthritis. Radiol Clin North Am. 2004;42:135-49.
- Donatto KC. Orthopedic management of septic arthritis. Rheum Dis Clin North Am. 1998;24:275-86.
- Pappas PG, Rex JH, Sobel JD, et al. Guidelines for treatment of candidiasis. Clin Infect Dis. 2004;38:161-89.
- Zimmerli W, Widmer AF, Blatter M, Frei R, Ochsner PE. Role of rifampin for treatment of orthopedic implant-related staphylococcal infections: a randomized controlled trial. Foreign-Body Infection (FBI) Study Group. JAMA. 1998;279:1537-41.
- Garvin KL, Salvati EA, Brause BD. Role of gentamicin-impregnated cement in total joint arthroplasty. Orthop Clin North Am. 1988;19:605-10.
- Lieberman JR, Callaway GH, Salvati EA, Pellicci PM, Brause BD. Treatment of the infected total hip arthroplasty with a two-stage reimplantation protocol. Clin Orthop Relat Res. 1994;205-12.
- Windsor RE, Insall JN, Urs WK, Miller DV, Brause BD. Twostage reimplantation for the salvage of total knee arthroplasty complicated by infection. Further follow-up and refinement of indications. J Bone Joint Surg Am. 1990;72:272-8.
- Buchholz HW, Elson RA, Engelbrecht E, Lodenkamper H, Rottger J, Siegel A. Management of deep infection of total hip replacement. J Bone Joint Surg Br. 1981; 63-B(3):342-53.
- Carlsson AS, Josefsson G, Lindberg L. Revision with gentamicin-impregnated cement for deep infections in total hip arthroplasties. J Bone Joint Surg Am. 1978;60:1059-64.
- Jackson WO, Schmalzried TP. Limited role of direct exchange arthroplasty in the treatment of infected total hip replacements. Clin Orthop Relat Res. 2000;(381):101-5.
- Fitzgerald RH Jr, Jones DR. Hip implant infection. Treatment with resection arthroplasty and late total hip arthroplasty. Am J Med. 1985; 78(6B):225-8.
- Garvin KL, Hanssen AD. Infection after total hip arthroplasty. Past, present, and future. J Bone Joint Surg Am. 1995;77:1576-88.
- Goulet JA, Pellicci PM, Brause BD, Salvati EM. Prolonged suppression of infection in total hip arthroplasty. J Arthroplasty. 1988; 3:109-16.
- Engesaeter LB, Lie SA, Espehaug B, Furnes O, Vollset SE, Havelin LI. Antibiotic prophylaxis in total hip arthroplasty: effects of antibiotic prophylaxis systemically and in bone cement on the revision rate of 22,170 primary hip replacements followed 0-14 years in the Norwegian Arthroplasty Register. Acta Orthop Scand. 2003; 74:644-51.
- Norden CW. A critical review of antibiotic prophylaxis in orthopedic surgery. Rev Infect Dis 1983;5:928-32.
- Antibiotic prophylaxis for urological patients with total joint replacements. J Urol. 2003; 169:1796-7.
- Antibiotic prophylaxis for dental patients with total joint replacements. J Am Dent Assoc. 2003; 134:895-9.
Introduction
Acute bacterial arthritis is a potentially serious and rapidly progressive infection that may involve native or prosthetic joints. The epidemiology, pathophysiology, repertoire of potential infecting pathogens, clinical presentation and treatment differ for these two forms of infectious arthritis, but both are associated with significant morbidity and mortality. Infectious arthritis of native and prosthetic joints may be caused by viruses, or fungi, but the most common cause is bacteria.
Acute Bacterial Arthritis
Epidemiology
The burden of septic arthritis in the general population is considerable. The incidence of native joint septic arthritis is approximately 5 cases per 100,000 persons per year and is much higher in patients with rheumatoid arthritis (1,2). Between 1% and 5% of joints with indwelling prostheses become infected and the total number of infections per year is increasing due to a rise in the number of patients who have had prosthetic replacement surgery (3). The mortality from joint infection is difficult to estimate due to differing comorbidity in afflicted patients, but is likely between 15% and 30% (4-6). There is substantial morbidity from these infections because of decreased joint function and mobility, and in cases involving joint prostheses from the excisional or exchange arthroplastic surgery that is often required for treatment.
The most common route of infection for native joint infection is hematogenous (1), but may also be a result of direct inoculation of bacteria through trauma or joint surgery (including arthrocentesis, corticosteroid injection, or arthroscopy) (7), or via contiguous spread from adjacent infected soft tissue or bone (1,8). While hematogenous infection of prosthetic joints occurs, the majority of these infections are the result of joint contamination in the course of implantation surgery or post-surgical wound infection (3). Host factors that increase the risk of septic arthritis include pre-existing joint disease (especially rheumatoid arthritis), immunosuppression, diabetes mellitus, malignancy, chronic renal failure, intravenous drug use, severe skin diseases, and advanced age (1,2,4,6). The extent of joint injury resulting from infection depends on the virulence of the infecting pathogen and degree of host immune response (9).
Microbiology
Native Joint
The most common causes of bacterial septic arthritis are outlined in Table 1. In adults, the most frequent etiology is S. aureus (37–65% of cases) (1,4,6,8,12,15,16) followed by Streptococcus sp. (12,15). An increasing percentage of S. aureus isolated from septic joints are resistant to antistaphylococcal penicillins and cephalosporins (methicillin-resistant S. aureus, MRSA). In adults with diabetes, malignancy, and genitourinary structural abnormalities, group B Streptococcus is a frequently isolated pathogen (5,6,17). Gram-negative bacilli are commonly found in neonates, intravenous drug users, and immunocompromised hosts (18). N. gonorrhoeae is a significant cause of bacterial arthritis in sexually active adults and adolescents (19) and Kingella kingae and Haemophilus influenzae are likely pediatric isolates (20,21). Joint infections that follow bite trauma usually are seen in the small joints of the hand and involve Pasteurella multocida in the case of animal bites, and Eikenella corrodens in the case of humans bites (22-24). Polymicrobial floras are found in up to 8% of cases of septic arthritis.
Prosthetic Joint
The bacteria that cause prosthetic joint arthritis vary depending on the stage of infection as defined by the elapsed time after implantation surgery (Table 1 on page 31). The coagulase negative staphylococci are the most common (30–43% of cases) (3,10), followed by S. aureus (12–23%) (25).
Nonbacterial Pathogens
Nonbacterial pathogens that may cause septic arthritis include viruses, fungi, and mycobacteria. Viral arthritis is often associated with a systemic febrile illness and other manifestations of infection such as rash. Parvovirus B19 is the most common viral arthritide, presenting as a symmetric polyarticular arthritis involving the joints of the hand as well as larger joints (26). The classic red “slapped cheeks” associated with this viral infection in children is usually not present in adults, although a faint lacy reticular rash may be seen.
Fungi and mycobacteria usually cause a subacute or chronic mono- or oligoarticular arthritis (27). Candida species are an increasing cause of both native and prosthetic joint septic arthritis. Risk factors for this infection include loss of skin integrity, diabetes, malignancy, intravenous drug use, and immunosuppressive therapy including glucocorticoids (28). Patients are often chronically ill and have exposure to broad-spectrum antimicrobials, hyperalimentation fluid, and/or indwelling central intravenous catheters. Other fungi, including Cryptococcus, Blastomyces, Histoplasma, Coccidioides, and Sporothrix are rare causes of septic arthritis (29,30). Mycobacterium tuberculosis is the most common cause of mycobacterial arthritis worldwide and should be considered in a patient presenting with chronic arthritis with risk factors for tuberculosis, including being foreign-born (31).
Clinical Features
The clinical manifestations, severity, treatment, and prognosis of septic arthritis are dependent on the identity and virulence of the bacterium, source of joint infection, and underlying host factors. Nongonococcal septic arthritis is monoarticular in 80% to 90% of cases. The knee is usually affected (50% of cases) (27) followed by the hip, wrists, and ankles (2). In adults, the majority of hip infections involve prosthetic or osteosynthetic material (1). Arthritis of the small joints of the foot is most often seen in diabetic patients and is usually secondary to contiguous skin and soft tissue ulcerations or adjacent osteomyelitis.
Gonococcal arthritis may present as febrile monoarticular arthritis, usually of the knees, wrists, and ankles (27), or as one of the manifestations of disseminated gonococcal infection. The latter is characterized by fever, dermatitis, tenosynovitis, and migratory polyarthralgia or polyarthritis (19). Skin lesions are often pustular and occur simultaneously with tenosynovitis, predominately affecting the fingers, hands, wrists, or feet. Concomitant mucosal infection of the urethra or cervix is often present but usually asymptomatic. Urethral and cervical cultures or a nucleic amplification test will frequently yield N. gonorrhoeae (19,32).
Symptoms of acute septic arthritis include pain and loss of joint function. Fever and chills are often present. The acutely infected native joint is usually red, warm, and swollen with an obvious effusion. Range of motion is limited and extremely painful. For deep and axial joint, pain is often the only focal symptom. More subtle symptoms and signs may result in a delay of diagnosis and are particularly seen in patients receiving systemic or intra-articular steroids, and in those with immunocompromised status, advanced comorbidities (including rheumatoid arthritis), and extreme age (33). A thorough physical examination may reveal a distant source of joint infection in up to 50% of patients (27).
Prosthetic joint infection may present acutely as above, particularly in early stage infection, or more indolently with progressive joint pain, minimal swelling or effusion, and absence of fever (34). In late infection a cutaneous draining sinus tract may be present. Rarely, the involved prosthesis may be visible beneath an ulceration or focus of soft-tissue breakdown.
Diseases that can mimic septic arthritis are crystalinduced arthritis, rheumatoid arthritis, systemic lupus erythematosus, spondyloarthropathy, Still’s disease, rheumatic fever, and Kawasaki syndrome.
Diagnostic Approach
A diagnostic approach to acute native joint arthritis is outlined in Figure 1 on page 32 (35,36). Important aspects include exclusion of other causes of arthritis including trauma, rheumatic diseases, and crystalline arthritis. The most important diagnostic test upon which management hinges is diagnostic arthrocentesis. Fluoroscopic or CT-guided arthrocentesis is indicated for axial and deep joints (e.g., sacroiliac or pubic symphysis) or in the event of a “dry tap” of a peripheral joint. Synovial fluid analysis will often suggest whether an acutely painful joint is due to noninflammatory, sterile inflammatory, or septic causes (Table 2 on page 33). In addition, it will provide fluid for culture and gram stain, a rapid test that can guide early empiric antibiotic therapy. Bacterial, fungal, and mycobacterial cultures should always be performed in order to direct pathogen-specific antimicrobial therapy, which is often given as a prolonged course. Antimicrobial therapy should be delayed until arthrocentesis and other appropriate diagnostic cultures are obtained unless the patient shows signs of sepsis.
For prosthetic joint infections the diagnostic approach is essentially the same although early radiographic imaging is more important than in native joint infection as it may show signs of prosthesis failure or loosening (seen in many late prosthesis infections). Additionally, the synovial fluid white blood cell (WBC) is often lower than in nativejoint infection, with a diagnostic cutoff suggested as greater than 1,700 cells/mm3 or >65% neutrophils (37).
Nonspecific blood tests such as a white blood count, erythrocyte sedimentation rate, or C-reactive protein argue against joint infection if they are normal, but do not specifically suggest septic arthritis if elevated. Other important diagnostic tests include blood cultures (positive in 50–70% of acute bacterial arthritides) (27), but in only 30% or less of gonococcal arthritis cases) (38), wound cultures (although these often correlate poorly with synovial fluid culture results, except when the pathogen is S. aureus), and serologic testing for B. burgdorferi in selected cases with clinical features of Lyme arthritis in endemic areas. If gonococcal arthritis is suspected urethral and cervical specimens should be sent for N. gonorrhoeae culture and nucleic acid amplification tests. Radiographic and scintillographic imaging may yield additional information that will assist in identifying preexisting joint disease or for confirming a diagnosis of native or prosthetic joint infection or its complications (Table 3 on page 33).
Treatment
Native joint
Prompt joint drainage and antimicrobial therapy are the mainstays of treatment in bacterial, fungal, or mycobacterial joint infection. Drainage can be through closed needle aspiration performed daily, or arthroscopy. The former modality allows direct visual inspection of the joint with concomitant irrigation, lysis of adhesions, and removal of necrotic tissue and purulent material (42). Open surgical drainage is recommended for septic arthritis of the hip and when less invasive methods fail to control infection.
Initial antimicrobial therapy should be withheld until synovial fluid has been obtained and should be based on synovial fluid gram staining (Table 4). In the case of a nondiagnostic gram stain, empiric antimicrobial coverage of likely infecting pathogens is indicated. Therapy should be narrowed based on identification and antimicrobial susceptibility testing of bacteria cultured from synovial fluid, blood, or in some cases from ancillary cultures. For patients with MRSA-related infection who are allergic to or intolerant of vancomycin, linezolid or daptomycin are potential alternatives, although not approved by the U.S. Food and Drug Administration for this indication. Linezolid is a potentially attractive option for treatment as it is available as an oral tablet, but for bone and joint infection treatment experience is limited. For septic arthritis related to animal or human bites ampicillin-sulbactam or amoxicillin-clavulanate (clindamycin plus ciprofloxacin in penicillin-allergic patients) provides activity against Pasteurella multocida and other oral bacteria. Gonococcal arthritis is best treated initially with ceftriaxone or cefotaxime; oral ciprofloxacin or levofloxacin may be substituted in regions without fluoroquinolone resistance as the patient improves (Table 4). Septic arthritis due to Candida sp. should be treated initially with an amphotericin B preparation followed by a prolonged course of fluconazole if susceptibility testing confirms activity against the cultured yeast isolate (43).
Duration of intravenous antimicrobials for bacterial joint infections is usually 2 to 4 weeks, while for gonococcal arthritis 2 weeks is sufficient. Antimicrobial therapy that continues for 2 weeks or longer should have weekly followup and laboratory monitoring for hematologic, renal, and liver toxicity.
Prosthetic Joint
Treatment of prosthetic joint septic arthritis is complex, and early consultation with an orthopedic surgeon and infectious diseases physician is recommended. Extensive surgical debridement of the afflicted joint and effective, prolonged antimicrobial therapy is necessary in almost all cases. In order to achieve an optimal synovial fluid and tissue culture yield, antimicrobial therapy should be delayed until the time of debridement surgery unless the patient is septic or exhibiting serious systemic complications of infection. Suggestions for early empiric therapy while awaiting culture results are given in Table 4. Final antimicrobial choices should be based on culture results with assistance from an infectious diseases consultant.
Carefully selected cases of prosthetic joint infection may be treated with simple surgical debridement of the joint with prosthesis retention and at least 3 months of antimicrobial therapy that includes rifampin if the organism is gram positive (44). Patients who present with a short duration of symptoms within 1 month of joint implantation, or those with acute hematogenous infection, are the best candidates for such a treatment strategy. Unfortunately, relapse is common in these cases, particularly if the infection is due to S. aureus, gram-negative bacilli, or drug-resistant pathogens. Thus, the optimal treatment protocols involve surgical excision of the infected prosthesis and prolonged antimicrobial therapy.
Surgical prosthesis extraction and reimplantation can be performed in either a one- or two-stage approach. The two-stage procedure is the more successful strategy and involves removal of the prosthesis and cement followed by a 6-week course of bactericidal antimicrobial therapy. Subsequently a new prosthesis is reimplanted. Using this approach, a 90% to 96% success rate in total hip replacement infections and a 97% success rate in total knee infections has been realized (45-47). An alternative tactic is a one-stage surgical procedure that excises the infected prosthesis with immediate reimplantation of a new joint using antibiotic-impregnated methacrylate cement. This method is effective in 77% to 83% of cases (48-50). Higher failure rates are observed for S. aureus and gram-negative bacillary infections (51). One-stage procedures are often used for elderly or infirm patients who might not tolerate protracted bed rest and a second major operation (52). A recent review article by Zimmerli et al. provides an excellent overview of antimicrobial and surgical treatment options for prosthetic joint infections (34).
Suppressive Antibiotic Therapy
Lifelong oral antimicrobial therapy plays a limited role for definitive therapy but is useful when a surgical approach is not possible because of medical or surgical contraindications. The goal of suppressive therapy is to control the infection and retain prosthesis function. It is important that patients and their families understand that the intention of such treatment is not to cure but to suppress the infection. Generally, oral suppressive therapy is initiated after a course of intravenous therapy. Goulet et al. (53) demonstrated a 63% success rate in maintaining function of hip arthroplasty in patients who met 5 criteria: 1) prostheses removal is not possible, 2) the pathogen is avirulent, 3) the pathogen is sensitive to oral antibiotics, 4) the patient is adherent to and tolerates antibiotics, and 5) the prosthesis is not loose. Patients being treated with lifelong suppressive therapy are at risk for the development of antibiotic resistance (in either the joint infecting pathogen or other commensal organism), local or systemic progression of infection, and adverse effects from chronic antibiotic usage.
Antimicrobial Prophylaxis to Prevent Joint Prosthesis Infection
Patients undergoing elective total joint replacement surgery should be evaluated for symptoms or signs of local infection that predispose to occult or overt bacteremia (particularly odontogenic, urologic, and dermatologic). Surgery should be delayed until such infections and coexisting medical conditions have been treated. Perioperative antibiotic prophylaxis has been shown to reduce deep wound infection and prosthetic joint infection in joint reimplant surgery but should not be continued for more than 24 hours after the preoperative dose (54,55). In order to decrease the risk of hematogenous seeding of established implants, early recognition and treatment of overt infection is crucial. The use of prophylactic antibiotics for patients with joint implants prior to or after dental or other procedures such as colonoscopy or cystoscopy is controversial. The American Academy of Orthopedic Surgeons recommends that a single dose of prophylactic antibiotic be given to certain patients undergoing urologic instrumentation or dental procedures that are accompanied by significant bleeding (56,57). Patients who are candidates for such prophylaxis include those with rheumatoid arthritis or other inflammatory arthropathy, immunosuppression, diabetes, malnutrition, hemophilia, or who have had a previous joint infection.
Dr. Ohl can be contacted at [email protected].
References
- Kaandorp CJ, Dinant HJ, van de Laar MA, Moens HJ, Prins AP, Dijkmans BA. Incidence and sources of native and prosthetic joint infection: a community based prospective survey. Ann Rheum Dis. 1997;56:470-5.
- Ohl C. Infectious arthritis of native joints. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and Practice of Infectious Diseases. 6th ed. Philadelphia: Elsevier, 2005:1311-1322.
- Brause B. Infections with prostheses in bones and joints. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and Practices of Infectious Diseases. 6th ed. Philadelphia: Elsevier, 2005:1332-7.
- Gupta MN, Sturrock RD, Field M. A prospective 2-year study of 75 patients with adult-onset septic arthritis. Rheumatology (Oxford). 2001;40:24-30.
- Nolla JM, Gomez-Vaquero C, Fiter J, et al. Pyarthrosis in patients with rheumatoid arthritis: a detailed analysis of 10 cases and literature review. Semin Arthritis Rheum 2000;30: 121-6.
- Weston VC, Jones AC, Bradbury N, Fawthrop F, Doherty M. Clinical features and outcome of septic arthritis in a single UK Health District 1982-1991. Ann Rheum Dis 1999;58:214-219.
- Kuzmanova SI, Atanassov AN, Andreev SA, Solakov PT. Minor and major complications of arthroscopic synovectomy of the knee joint performed by rheumatologist. Folia Med (Plovdiv). 2003;45:55-9.
- Morgan DS, Fisher D, Merianos A, Currie BJ. An 18 year clinical review of septic arthritis from tropical Australia. Epidemiol Infect 1996;117:423-8.
- Mader JT, Shirtliff M, Calhoun JH. The host and the skeletal infection: classification and pathogenesis of acute bacterial bone and joint sepsis. Baillieres Best Pract Res Clin Rheumatol 1999;13:1-20.
- Berendt A. Infections of prosthetic joints and related problems. In: Cohen J, Powderly W, eds. Infectious Diseases. Edinburgh: Mosby, 2005: 583-589.
- Raymond NJ, Henry J, Workowski KA. Enterococcal arthritis: case report and review. Clin Infect Dis. 1995;21: 516-522.
- Ross JJ, Saltzman CL, Carling P, Shapiro DS. Pneumococcal septic arthritis: review of 190 cases. Clin Infect Dis. 2003;36:319-27.
- Kortekangas P, Aro HT, Tuominen J, Toivanen A. Synovial fluid leukocytosis in bacterial arthritis vs. reactive arthritis and rheumatoid arthritis in the adult knee. Scand J Rheumatol. 1992;21:283-8.
- Sack K. Monarthritis: differential diagnosis. Am J Med. 1997; 102(1A):30S-34S.
- Dubost JJ, Soubrier M, De Champs C, Ristori JM, Bussiere JL, Sauvezie B. No changes in the distribution of organisms responsible for septic arthritis over a 20 year period. Ann Rheum Dis. 2002;61:267-9.
- Ryan MJ, Kavanagh R, Wall PG, Hazleman BL. Bacterial joint infections in England and Wales: analysis of bacterial isolates over a four year period. Br J Rheumatol. 1997;36:370-3.
- Nolla JM, Gomez-Vaquero C, Corbella X, et al. Group B streptococcus (Streptococcus agalactiae) pyogenic arthritis in nonpregnant adults. Medicine (Baltimore). 2003;82: 119-28.
- Shirtliff ME, Mader JT. Acute septic arthritis. Clin Microbiol Rev. 2002;15:527-44.
- Bardin T. Gonococcal arthritis. Best Pract Res Clin Rheumatol. 2003;17:201-8.
- Yagupsky P, Dagan R. Kingella kingae: an emerging cause of invasive infections in young children. Clin Infect Dis. 1997;24:860-66.
- Bowerman SG, Green NE, Mencio GA. Decline of bone and joint infections attributable to haemophilus influenzae type b. Clin Orthop. 1997;(341):128-33.
- Ewing R, Fainstein V, Musher DM, Lidsky M, Clarridge J. Articular and skeletal infections caused by Pasteurella multocida. South Med J. 1980;73:1349-52.
- Murray PM. Septic arthritis of the hand and wrist. Hand Clin. 1998;14:579-87, viii.
- Resnick D, Pineda CJ, Weisman MH, Kerr R. Osteomyelitis and septic arthritis of the hand following human bites. Skeletal Radiol. 1985;14:263-6.
- Murdoch DR, Roberts SA, Fowler JV Jr, et al. Infection of orthopedic prostheses after Staphylococcus aureus bacteremia. Clin Infect Dis. 2001;32:647-9.
- Woolf AD, Campion GV, Chishick A, et al. Clinical manifestations of human parvovirus B19 in adults. Arch Intern Med. 1989;149:1153-6.
- Goldenberg DL. Septic arthritis. Lancet 1998; 351:197-202.
- Silveira LH, Cuellar ML, Citera G, Cabrera GE, Scopelitis E, Espinoza LR. Candida arthritis. Rheum Dis Clin North Am. 1993;19:427-37.
- Cuellar ML, Silveira LH, Espinoza LR. Fungal arthritis. Ann Rheum Dis. 1992;51:690-7.
- Cuellar ML, Silveira LH, Citera G, Cabrera GE, Valle R. Other fungal arthritides. Rheum Dis Clin North Am. 1993;19:439-55.
- Malaviya AN, Kotwal PP. Arthritis associated with tuberculosis. Best Pract Res Clin Rheumatol. 2003;17:319-43.
- Van Der PB, Ferrero DV, Buck-Barrington L, et al. Multicenter evaluation of the BDProbeTec ET System for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in urine specimens, female endocervical swabs, and male urethral swabs. J Clin Microbiol. 2001;39:1008-16.
- Kaandorp CJ, van Schaardenburg D, Krijnen P, Habbema JD, van de Laar MA. Risk factors for septic arthritis in patients with joint disease: a prospective study. Arthritis Rheum. 1995;38:1819-25.
- Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. N Engl J Med. 2004;351:1645-54.
- Guidelines for the initial evaluation of the adult patient with acute musculoskeletal symptoms. American College of Rheumatology Ad Hoc Committee on Clinical Guidelines. Arthritis Rheum. 1996;39:1-8.
- Siva C, Velazquez C, Mody A, Brasington R. Diagnosing acute monoarthritis in adults: a practical approach for the family physician. Am Fam Physician. 2003;68:83-90.
- Trampuz A, Hanssen AD, Osmon DR, Mandrekar J, Steckelberg JM, Patel R. Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med. 2004; 117:556-62.
- Cucurull E, Espinoza LR. Gonococcal arthritis. Rheum Dis Clin North Am. 1998; 24:305-22.
- Chhem RK, Kaplan PA, Dussault RG. Ultrasonography of the musculoskeletal system. Radiol Clin North Am. 1994;32:275-289.
- Learch TJ, Farooki S. Magnetic resonance imaging of septic arthritis. Clin Imaging. 2000;24:236-42.
- Mohana-Borges AV, Chung CB, Resnick D. Monoarticular arthritis. Radiol Clin North Am. 2004;42:135-49.
- Donatto KC. Orthopedic management of septic arthritis. Rheum Dis Clin North Am. 1998;24:275-86.
- Pappas PG, Rex JH, Sobel JD, et al. Guidelines for treatment of candidiasis. Clin Infect Dis. 2004;38:161-89.
- Zimmerli W, Widmer AF, Blatter M, Frei R, Ochsner PE. Role of rifampin for treatment of orthopedic implant-related staphylococcal infections: a randomized controlled trial. Foreign-Body Infection (FBI) Study Group. JAMA. 1998;279:1537-41.
- Garvin KL, Salvati EA, Brause BD. Role of gentamicin-impregnated cement in total joint arthroplasty. Orthop Clin North Am. 1988;19:605-10.
- Lieberman JR, Callaway GH, Salvati EA, Pellicci PM, Brause BD. Treatment of the infected total hip arthroplasty with a two-stage reimplantation protocol. Clin Orthop Relat Res. 1994;205-12.
- Windsor RE, Insall JN, Urs WK, Miller DV, Brause BD. Twostage reimplantation for the salvage of total knee arthroplasty complicated by infection. Further follow-up and refinement of indications. J Bone Joint Surg Am. 1990;72:272-8.
- Buchholz HW, Elson RA, Engelbrecht E, Lodenkamper H, Rottger J, Siegel A. Management of deep infection of total hip replacement. J Bone Joint Surg Br. 1981; 63-B(3):342-53.
- Carlsson AS, Josefsson G, Lindberg L. Revision with gentamicin-impregnated cement for deep infections in total hip arthroplasties. J Bone Joint Surg Am. 1978;60:1059-64.
- Jackson WO, Schmalzried TP. Limited role of direct exchange arthroplasty in the treatment of infected total hip replacements. Clin Orthop Relat Res. 2000;(381):101-5.
- Fitzgerald RH Jr, Jones DR. Hip implant infection. Treatment with resection arthroplasty and late total hip arthroplasty. Am J Med. 1985; 78(6B):225-8.
- Garvin KL, Hanssen AD. Infection after total hip arthroplasty. Past, present, and future. J Bone Joint Surg Am. 1995;77:1576-88.
- Goulet JA, Pellicci PM, Brause BD, Salvati EM. Prolonged suppression of infection in total hip arthroplasty. J Arthroplasty. 1988; 3:109-16.
- Engesaeter LB, Lie SA, Espehaug B, Furnes O, Vollset SE, Havelin LI. Antibiotic prophylaxis in total hip arthroplasty: effects of antibiotic prophylaxis systemically and in bone cement on the revision rate of 22,170 primary hip replacements followed 0-14 years in the Norwegian Arthroplasty Register. Acta Orthop Scand. 2003; 74:644-51.
- Norden CW. A critical review of antibiotic prophylaxis in orthopedic surgery. Rev Infect Dis 1983;5:928-32.
- Antibiotic prophylaxis for urological patients with total joint replacements. J Urol. 2003; 169:1796-7.
- Antibiotic prophylaxis for dental patients with total joint replacements. J Am Dent Assoc. 2003; 134:895-9.
Reducing Antimicrobial Resistance and Hospital-Associated Infections: The Role of the Hospitalist
While infections that develop during hospitalization may appear to be an uncommon but recognized risk of hospital care today, the incidence of these infections has been increasing dramatically during the last 2 to 3 decades, and the risk of acquiring an organism that is resistant to 1 or more antibiotics is becoming increasingly common. Recent studies estimate that approximately 2 million patients contract healthcare-associated infections each year (1). These infections are the most common type of serious adverse event in health care, affecting up to 5–10% of hospitalized patients, leading to approximately 90,000 deaths annually, and adding approximately $5 billion to annual healthcare costs (1-3). Increasingly, healthcare-associated infection risk is viewed as a patient safety issue, as many of these infections may be avoidable or preventable by following evidence-based best practices in infection control and patient care while patients are hospitalized. This article will summarize some of the overlap between patient safety and infection control, explain some of the pressures that have led to development and cultivation of antimicrobial resistance, and describe the Centers for Disease Control and Prevention (CDC) campaign for prevention of healthcare-associated infections and antimicrobial resistance, as well as the role of hospitalists in such prevention.
Patient Safety
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) specifically identifies in its 2005 National Patient Safety Goals that hospitals and clinicians reduce the risk of healthcare-associated infections. The goals encourage clinicians to comply with current CDC hand hygiene guidelines and that hospitals and clinicians manage as sentinel events all identified cases of unanticipated death or permanent loss of function associated with a heathcare-associated infection. A sentinel event is defined by JCAHO as an unexpected occurrence involving death or serious physical or psychological injury. Such an event signals the need for immediate investigation and response by the institution. By including healthcare-associated infections in this category of high-risk event, with potential morbidity and mortality, JCAHO highlights the frequency and importance of infections acquired in our healthcare system today.
Further, the Agency for Healthcare Research and Quality (AHRQ) recently published an evidence-based report, developed and written primarily by hospitalists, delineating 79 patient safety practices, of which 22 (28%) involved infection control (4). At least 5 of these 22 infection control practices were considered valuable enough, and with sufficiently strong supporting evidence, to mandate widespread implementation. Additionally, the Institute for Healthcare Improvement (IHI; www.ihi.org) recently launched its 100,000 Lives Campaign, enlisting hundreds of hospitals around the United States in a commitment to implement changes that have been proven to prevent avoidable deaths. Three of their first 6 interventions involve the reduction of healthcare-associated infections, including central-line infections, surgical-site infections, and hospital-acquired pneumonia.
Increasingly, hospital-onset infections have become a patient safety issue, and they will remain under public and institutional scrutiny while hospitals take efforts to reduce their incidence and improve care quality. Hospitalists have evolved to serve a unique role as advocate of both patients and hospitals. They should therefore foster quality improvement in the hospital, as well as lead and support initiatives that reduce hospital-acquired infections and resistance.
Healthcare-Associated Infections and Development of Resistance
Bacteria have developed multiple microbiologic and genetic mechanisms to elude antimicrobial agents. Certain practices in medical care, whether intentional or not, can promote persistence or spread of resistant microbes that can cause infections. Such practices may include:
- Inattention to basic infection control measures (e.g., hand washing)
- Unrecognized colonization (e.g., treating colonized urinary or vascular catheters, without evidence of infection)
- Unrecognized reservoirs (e.g., environmental)
- Selective pressure from overuse or inappropriate use of antibiotics
- Movement of patients and staff within a single institution and between institutions
Inappropriate use or overuse of antibiotics can actually remove or “select” the sensitive microbes and promote overgrowth of resistant organisms when present. Each of these practices may serve as a focus for quality improvement interventions to reduce resistance.
Most healthcare-associated infections (more than 80%) originate from 4 specific patient sites: urinary tract, surgical-site (wound), bloodstream, and lung (pneumonia) (5). It is not coincidental that these infection sites are frequently associated with invasive procedures, and many times with indwelling invasive devices that may be used during the course of inpatient care. For example, urinary tract infections, the most common hospital-acquired infections, are usually associated with urinary catheter use. Similarly, bloodstream infections are usually associated with intravascular catheters, and hospital-acquired pneumonia is usually associated with ventilator use.
Because many of the invasive devices that are utilized during the course of inpatient care carry significant risk, including infection risk, it is incumbent upon hospitalists to be aware of these risks, to explain these risks to their patients, and to take all steps at their disposal to help reduce such risk in their patients. Dr. Julie Gerberding, Director of the CDC, has emphasized that the 2 greatest predictors of infection risk in the hospital are length of stay and use of invasive devices (6). While excellent evidence already demonstrates that hospitalists reduce length of stay (7), they should also spearhead the efforts to minimize the use of invasive devices whenever possible, and lead evidence-based efforts to minimize infection in hospitalized patients when invasive devices must be used.
Prevention of Resistance: Best Practices
CDC/SHM Collaboration
In September 2003, the Society of Hospital Medicine (SHM) and the CDC entered into a collaborative agreement to educate hospitalists about the reduction of hospital-acquired infections and the prevention of antimicrobial resistance. The long-term goals of this agreement include developing quality-improvement initiatives and research in the area of antimicrobial resistance reduction. The short-term goals include development of educational materials and resources for hospitalists aimed at reducing hospital-acquired infections and resistance. SHM has provided instruction in the reduction of hospital-acquired infections and antimicrobial resistance, in workshop format, to its membership at national, regional, and local chapter meetings. SHM has also developed an Internet-based educational tool for antimicrobial resistance on its Web site, which will soon be transformed into a new Web-based Resource Room to educate membership on antimicrobial resistance and reduction of hospital-acquired infections.
CDC Campaign
(www.cdc.gov/drugresistance/healthcare/)
The CDC, in collaboration with the National Institutes of Health (NIH) and the Food and Drug Administration (FDA), as well as professional societies, healthcare organizations, public health agencies, and corporate partners, has developed its Campaign to Prevent Antimicrobial Resistance to facilitate the implementation of educational and behavioral interventions that will assist clinicians in appropriate antimicrobial prescribing. The goals of these intervention programs are to improve clinician practices and prevent antimicrobial resistance. The campaign focuses on 4 main strategies: prevent infection, diagnose and treat infection, use antimicrobials wisely, and prevent transmission. Multiple 12-step programs have been developed (or are in the process of development), targeting specific patient populations, including hospitalized adults, dialysis patients, surgical patients, hospitalized children, and long-term-care patients. Each of these patient populations is relevant to the practicing hospitalist, who may access the educational materials and resources cost-free on the Internet. The CDC provides on-line resources (Web site listed above), including a downloadable slide-set, a 12-step fact sheet, and tips for patients. The program translates existing scientific evidence and national guidelines into action steps that can be taken now to prevent antimicrobial resistance.
The 12 Steps to Prevent Antimicrobial Resistance in Hospitalized Adults was the first intervention program to be initiated, because hospital patients are at especially high risk for serious antimicrobial-resistant infections. The rate of multiple drug-resistant organisms causing infection within our hospitals is increasing at a rapid rate. Currently, national data demonstrate that more than 50% of Staphylococcus aureus isolates causing infections in intensive care units (ICUs) are resistant to methicillin (MRSA), while more than 40% are resistant in other non-ICU hospital units (9). Similarly, gram-negative organisms have developed resistance, with more than 25% of Pseudomonas aeruginosa ICU isolates now resistant to fluoroquinolones (9), with a much higher percentage resistant at some institutions. This rapidly growing problem has led the CDC to develop the following 12 Steps to Prevent Antimicrobial Resistance in Hospitalized Adults:
- Vaccinate
- Get the catheters out
- Target the pathogen
- Access the experts
- Practice antimicrobial control
- Use local data
- Treat infection, not contamination
- Treat infection, not colonization
- Know when to say “no” to vanco
- Stop treatment when infection is cured or unlikely
- Isolate the pathogen
- Break the chain of contagion
Prevent Infection
Diagnose and Treat Infection Effectively
Use Antimicrobials Wisely
Prevent Transmission
These steps are designed to optimize patient safety and the outcome of infectious disease management, and hospitalists have the ability to utilize these recommendations to improve the care of their patients.
Hospitalists must employ efforts to prevent infections that may occur during hospitalization as well as those that may bring patients back to the hospital. Such efforts include predischarge influenza and pneumococcal vaccination when indicated, to reduce the more than 100,000 hospitalizations and 20,000 deaths due to influenza and the more than 12,000 deaths due to Streptococcus pneumoniae (10). Clinicians should get annual influenza vaccines as well, to reduce transmission to patients and to other healthcare workers.
Because catheters and other invasive devices are the No. 1 cause of hospital-acquired infections, evidence-based efforts must be utilized to reduce the likelihood of such infections. An estimated 250,000 catheter-related bloodstream infections (CR-BSI) occur each year, with an attributable cost of at least $25,000 per infection and an attributable mortality of 12–25% (11). Because of this, the CDC has recommended adherence to performance indicators for reducing bloodstream infections (8,12). Such performance indicators are based on strong evidence (13-15) and include the following:
- Appropriate site selection for catheter placement (i.e., subclavian over femoral or internal jugular) (14)
- Appropriate hand hygiene and aseptic technique (including use of maximal sterile barriers) during catheter placement
- Adequate skin asepsis (using chlorhexidine preferentially over iodine or alcohol based solutions) (15)
- Catheter discontinuation when no longer essential
- Antibiotic-impregnated catheters in high-risk patients
Recent studies have demonstrated that CR-BSI can be significantly reduced or even virtually eliminated with educational efforts combined with strict adherence to evidence based guidelines for prevention, as well as efforts to remove catheters early (16).
To diagnose and treat infections effectively, hospitalists must obtain appropriate cultures, target empiric therapy to the likely pathogens and local antibiogram data, and target final therapy to the known pathogens and antimicrobial susceptibility test results. The correct regimen, timing, dosage, route, and duration of antibiotic can impact morbidity and mortality in patients presenting with infectious diseases. Therefore, careful selection becomes crucial, and accessing infectious disease expertise in complex or critically ill patients with infectious diseases can be lifesaving.
Wise or appropriate use of antimicrobials can be facilitated by multiple efforts within hospitals. First, practicing antimicrobial control at the institutional level may involve use of standardized antimicrobial order forms, formulary restrictions, prior approval to start or continue specific antimicrobials, pharmacy substitution or switch, multidisciplinary drug utilization evaluation, provider performance feedback, or computerized decision support ordering systems. Many of these efforts can reduce costs while improving outcomes. Second, because the prevalence of resistance can vary by location, patient population, hospital unit, and length of stay, knowledge of the inpatient population that one treats (e.g., community vs. tertiary care, immunocompetent vs. immunosuppressed, or ICU vs. non-ICU) as well as the local antibiogram can help clinicians make decisions regarding initial antimicrobial selections.
Third, curbing antimicrobial overuse can be fostered by avoiding treatment of contamination or colonization. Contaminated cultures may be reduced by using and advocating proper antisepsis for blood cultures and other culture specimens. Recognition of organisms unlikely to represent true bacteremia (e.g., Corynebacterium), as well as those very likely to represent true bacteremia (e.g., Staphylococcus aureus or Entero-bacteriaceae), and interpreting culture results within clinical context help clinicians effectively treat positive cultures when indicated and avoid treating contaminants. Additionally, recognizing when cultures from urinary catheters, intravascular catheters, and endotracheal tubes represent colonization rather than infection and taking active steps to obtain accurate (rather than colonized) cultures can further curb nonindicated antibiotic use. For example, routinely sending catheter tips for culture is not indicated. Also, urinalysis should always accompany urine cultures sent from urinary catheters. Fourth, stopping antimicrobial therapy when infections are cured, cultures are negative and infection unlikely, or when infection is not diagnosed also limits antimicrobial overuse.
Finally, prevention of infection transmission from patient to patient or from healthcare worker to patient can be accomplished by use of standard infection control precautions, use of appropriate isolation precautions and handling of bodily fluids, and accessing infection control experts when questions arise. Frequent and effective hand hygiene as well as empowering all hospital staff to take part in and enforce infection control measures will help reduce transmission of infection by healthcare personnel.
In summary, antimicrobial resistance and hospital-acquired infections represent an enormous issue for patients, providers, hospitals, and the public. Hospitalists are positioned to take a large role in improving patient safety by supporting, following, and advocating the recommended guidelines and evidence-based measures to reduce the incidence of hospital-acquired infections at the local and national levels. Great investment of time, resources, and efforts in quality-improvement initiatives are necessary to reduce resistance, reduce infection, and improve overall outcomes for our patients.
References
- Burke JP. Infection control—a problem for patient safety. N Engl J Med. 2003; 348:651-6.
- Jarvis WR. Infection control and changing health-care delivery systems. Emerg Infect Dis. 2001;7:170-3.
- Stone PW, Larson E, Kawar LN. A systematic audit of economic evidence linking nosocomial infections and infection control interventions: 1990–2000. Am J Infect Control. 2002;30:145-52.
- Shojania KG, Duncan BW, McDonald KM, Wachter RM, Markowitz AJ. making health care safer: a critical analysis of patient safety practices. Evid Rep Technol Assess. 2001;43: i-x, 1-668. Review. Full report available at www.ahrq.gov.
- National Nosocomial Infections Surveillance (NNIS) system report, data summary from October 1986- April 1996, issued May 1996. A report from the National Nosocomial Infections Surveillance (NNIS) system. Am J Infect Control. 1996;24:380-8.
- Gerberding JL. Hospital-onset infections: a patient safety issue. Ann Intern Med. 2002;137:665-70.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287:487-94.
- O’Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter infections. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2002;51:1-29.
- National Nosocomial Infections Surveillance (NNIS) system report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control. 2004;32: 470-85.
- Influenza and Pneumococcal Vaccination Levels Among Persons Aged ≥65 Years--United States, 1999. MMWR Morb Mortal Wkly Rep. 2001;50:532-7.
- Kluger DM, Maki DG. The relative risk of intravascular device related bloodstream infections in adults. Abstracts of the 39th Interscience Conference on Antimicrob Agents Chemother. 1999:514.
- Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med. 2000;132:391-402.
- McGee DC, Gould MK. Preventing Complications of Central Venous Catheterization. N Engl J Med. 2003;348:1123-33.
- Merrer J, De Jonghe B, Golliot F, et al. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. JAMA. 2001;286:700-7.
- Chaiyakunapruk N, Veenstra DL, Lipsky BA, Saint S. Chlorhexidine compared with povidone-iodine solution for vascular catheter-site care: a meta-analysis. Ann Intern Med. 2002;136:792-801.
- Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-20.
While infections that develop during hospitalization may appear to be an uncommon but recognized risk of hospital care today, the incidence of these infections has been increasing dramatically during the last 2 to 3 decades, and the risk of acquiring an organism that is resistant to 1 or more antibiotics is becoming increasingly common. Recent studies estimate that approximately 2 million patients contract healthcare-associated infections each year (1). These infections are the most common type of serious adverse event in health care, affecting up to 5–10% of hospitalized patients, leading to approximately 90,000 deaths annually, and adding approximately $5 billion to annual healthcare costs (1-3). Increasingly, healthcare-associated infection risk is viewed as a patient safety issue, as many of these infections may be avoidable or preventable by following evidence-based best practices in infection control and patient care while patients are hospitalized. This article will summarize some of the overlap between patient safety and infection control, explain some of the pressures that have led to development and cultivation of antimicrobial resistance, and describe the Centers for Disease Control and Prevention (CDC) campaign for prevention of healthcare-associated infections and antimicrobial resistance, as well as the role of hospitalists in such prevention.
Patient Safety
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) specifically identifies in its 2005 National Patient Safety Goals that hospitals and clinicians reduce the risk of healthcare-associated infections. The goals encourage clinicians to comply with current CDC hand hygiene guidelines and that hospitals and clinicians manage as sentinel events all identified cases of unanticipated death or permanent loss of function associated with a heathcare-associated infection. A sentinel event is defined by JCAHO as an unexpected occurrence involving death or serious physical or psychological injury. Such an event signals the need for immediate investigation and response by the institution. By including healthcare-associated infections in this category of high-risk event, with potential morbidity and mortality, JCAHO highlights the frequency and importance of infections acquired in our healthcare system today.
Further, the Agency for Healthcare Research and Quality (AHRQ) recently published an evidence-based report, developed and written primarily by hospitalists, delineating 79 patient safety practices, of which 22 (28%) involved infection control (4). At least 5 of these 22 infection control practices were considered valuable enough, and with sufficiently strong supporting evidence, to mandate widespread implementation. Additionally, the Institute for Healthcare Improvement (IHI; www.ihi.org) recently launched its 100,000 Lives Campaign, enlisting hundreds of hospitals around the United States in a commitment to implement changes that have been proven to prevent avoidable deaths. Three of their first 6 interventions involve the reduction of healthcare-associated infections, including central-line infections, surgical-site infections, and hospital-acquired pneumonia.
Increasingly, hospital-onset infections have become a patient safety issue, and they will remain under public and institutional scrutiny while hospitals take efforts to reduce their incidence and improve care quality. Hospitalists have evolved to serve a unique role as advocate of both patients and hospitals. They should therefore foster quality improvement in the hospital, as well as lead and support initiatives that reduce hospital-acquired infections and resistance.
Healthcare-Associated Infections and Development of Resistance
Bacteria have developed multiple microbiologic and genetic mechanisms to elude antimicrobial agents. Certain practices in medical care, whether intentional or not, can promote persistence or spread of resistant microbes that can cause infections. Such practices may include:
- Inattention to basic infection control measures (e.g., hand washing)
- Unrecognized colonization (e.g., treating colonized urinary or vascular catheters, without evidence of infection)
- Unrecognized reservoirs (e.g., environmental)
- Selective pressure from overuse or inappropriate use of antibiotics
- Movement of patients and staff within a single institution and between institutions
Inappropriate use or overuse of antibiotics can actually remove or “select” the sensitive microbes and promote overgrowth of resistant organisms when present. Each of these practices may serve as a focus for quality improvement interventions to reduce resistance.
Most healthcare-associated infections (more than 80%) originate from 4 specific patient sites: urinary tract, surgical-site (wound), bloodstream, and lung (pneumonia) (5). It is not coincidental that these infection sites are frequently associated with invasive procedures, and many times with indwelling invasive devices that may be used during the course of inpatient care. For example, urinary tract infections, the most common hospital-acquired infections, are usually associated with urinary catheter use. Similarly, bloodstream infections are usually associated with intravascular catheters, and hospital-acquired pneumonia is usually associated with ventilator use.
Because many of the invasive devices that are utilized during the course of inpatient care carry significant risk, including infection risk, it is incumbent upon hospitalists to be aware of these risks, to explain these risks to their patients, and to take all steps at their disposal to help reduce such risk in their patients. Dr. Julie Gerberding, Director of the CDC, has emphasized that the 2 greatest predictors of infection risk in the hospital are length of stay and use of invasive devices (6). While excellent evidence already demonstrates that hospitalists reduce length of stay (7), they should also spearhead the efforts to minimize the use of invasive devices whenever possible, and lead evidence-based efforts to minimize infection in hospitalized patients when invasive devices must be used.
Prevention of Resistance: Best Practices
CDC/SHM Collaboration
In September 2003, the Society of Hospital Medicine (SHM) and the CDC entered into a collaborative agreement to educate hospitalists about the reduction of hospital-acquired infections and the prevention of antimicrobial resistance. The long-term goals of this agreement include developing quality-improvement initiatives and research in the area of antimicrobial resistance reduction. The short-term goals include development of educational materials and resources for hospitalists aimed at reducing hospital-acquired infections and resistance. SHM has provided instruction in the reduction of hospital-acquired infections and antimicrobial resistance, in workshop format, to its membership at national, regional, and local chapter meetings. SHM has also developed an Internet-based educational tool for antimicrobial resistance on its Web site, which will soon be transformed into a new Web-based Resource Room to educate membership on antimicrobial resistance and reduction of hospital-acquired infections.
CDC Campaign
(www.cdc.gov/drugresistance/healthcare/)
The CDC, in collaboration with the National Institutes of Health (NIH) and the Food and Drug Administration (FDA), as well as professional societies, healthcare organizations, public health agencies, and corporate partners, has developed its Campaign to Prevent Antimicrobial Resistance to facilitate the implementation of educational and behavioral interventions that will assist clinicians in appropriate antimicrobial prescribing. The goals of these intervention programs are to improve clinician practices and prevent antimicrobial resistance. The campaign focuses on 4 main strategies: prevent infection, diagnose and treat infection, use antimicrobials wisely, and prevent transmission. Multiple 12-step programs have been developed (or are in the process of development), targeting specific patient populations, including hospitalized adults, dialysis patients, surgical patients, hospitalized children, and long-term-care patients. Each of these patient populations is relevant to the practicing hospitalist, who may access the educational materials and resources cost-free on the Internet. The CDC provides on-line resources (Web site listed above), including a downloadable slide-set, a 12-step fact sheet, and tips for patients. The program translates existing scientific evidence and national guidelines into action steps that can be taken now to prevent antimicrobial resistance.
The 12 Steps to Prevent Antimicrobial Resistance in Hospitalized Adults was the first intervention program to be initiated, because hospital patients are at especially high risk for serious antimicrobial-resistant infections. The rate of multiple drug-resistant organisms causing infection within our hospitals is increasing at a rapid rate. Currently, national data demonstrate that more than 50% of Staphylococcus aureus isolates causing infections in intensive care units (ICUs) are resistant to methicillin (MRSA), while more than 40% are resistant in other non-ICU hospital units (9). Similarly, gram-negative organisms have developed resistance, with more than 25% of Pseudomonas aeruginosa ICU isolates now resistant to fluoroquinolones (9), with a much higher percentage resistant at some institutions. This rapidly growing problem has led the CDC to develop the following 12 Steps to Prevent Antimicrobial Resistance in Hospitalized Adults:
- Vaccinate
- Get the catheters out
- Target the pathogen
- Access the experts
- Practice antimicrobial control
- Use local data
- Treat infection, not contamination
- Treat infection, not colonization
- Know when to say “no” to vanco
- Stop treatment when infection is cured or unlikely
- Isolate the pathogen
- Break the chain of contagion
Prevent Infection
Diagnose and Treat Infection Effectively
Use Antimicrobials Wisely
Prevent Transmission
These steps are designed to optimize patient safety and the outcome of infectious disease management, and hospitalists have the ability to utilize these recommendations to improve the care of their patients.
Hospitalists must employ efforts to prevent infections that may occur during hospitalization as well as those that may bring patients back to the hospital. Such efforts include predischarge influenza and pneumococcal vaccination when indicated, to reduce the more than 100,000 hospitalizations and 20,000 deaths due to influenza and the more than 12,000 deaths due to Streptococcus pneumoniae (10). Clinicians should get annual influenza vaccines as well, to reduce transmission to patients and to other healthcare workers.
Because catheters and other invasive devices are the No. 1 cause of hospital-acquired infections, evidence-based efforts must be utilized to reduce the likelihood of such infections. An estimated 250,000 catheter-related bloodstream infections (CR-BSI) occur each year, with an attributable cost of at least $25,000 per infection and an attributable mortality of 12–25% (11). Because of this, the CDC has recommended adherence to performance indicators for reducing bloodstream infections (8,12). Such performance indicators are based on strong evidence (13-15) and include the following:
- Appropriate site selection for catheter placement (i.e., subclavian over femoral or internal jugular) (14)
- Appropriate hand hygiene and aseptic technique (including use of maximal sterile barriers) during catheter placement
- Adequate skin asepsis (using chlorhexidine preferentially over iodine or alcohol based solutions) (15)
- Catheter discontinuation when no longer essential
- Antibiotic-impregnated catheters in high-risk patients
Recent studies have demonstrated that CR-BSI can be significantly reduced or even virtually eliminated with educational efforts combined with strict adherence to evidence based guidelines for prevention, as well as efforts to remove catheters early (16).
To diagnose and treat infections effectively, hospitalists must obtain appropriate cultures, target empiric therapy to the likely pathogens and local antibiogram data, and target final therapy to the known pathogens and antimicrobial susceptibility test results. The correct regimen, timing, dosage, route, and duration of antibiotic can impact morbidity and mortality in patients presenting with infectious diseases. Therefore, careful selection becomes crucial, and accessing infectious disease expertise in complex or critically ill patients with infectious diseases can be lifesaving.
Wise or appropriate use of antimicrobials can be facilitated by multiple efforts within hospitals. First, practicing antimicrobial control at the institutional level may involve use of standardized antimicrobial order forms, formulary restrictions, prior approval to start or continue specific antimicrobials, pharmacy substitution or switch, multidisciplinary drug utilization evaluation, provider performance feedback, or computerized decision support ordering systems. Many of these efforts can reduce costs while improving outcomes. Second, because the prevalence of resistance can vary by location, patient population, hospital unit, and length of stay, knowledge of the inpatient population that one treats (e.g., community vs. tertiary care, immunocompetent vs. immunosuppressed, or ICU vs. non-ICU) as well as the local antibiogram can help clinicians make decisions regarding initial antimicrobial selections.
Third, curbing antimicrobial overuse can be fostered by avoiding treatment of contamination or colonization. Contaminated cultures may be reduced by using and advocating proper antisepsis for blood cultures and other culture specimens. Recognition of organisms unlikely to represent true bacteremia (e.g., Corynebacterium), as well as those very likely to represent true bacteremia (e.g., Staphylococcus aureus or Entero-bacteriaceae), and interpreting culture results within clinical context help clinicians effectively treat positive cultures when indicated and avoid treating contaminants. Additionally, recognizing when cultures from urinary catheters, intravascular catheters, and endotracheal tubes represent colonization rather than infection and taking active steps to obtain accurate (rather than colonized) cultures can further curb nonindicated antibiotic use. For example, routinely sending catheter tips for culture is not indicated. Also, urinalysis should always accompany urine cultures sent from urinary catheters. Fourth, stopping antimicrobial therapy when infections are cured, cultures are negative and infection unlikely, or when infection is not diagnosed also limits antimicrobial overuse.
Finally, prevention of infection transmission from patient to patient or from healthcare worker to patient can be accomplished by use of standard infection control precautions, use of appropriate isolation precautions and handling of bodily fluids, and accessing infection control experts when questions arise. Frequent and effective hand hygiene as well as empowering all hospital staff to take part in and enforce infection control measures will help reduce transmission of infection by healthcare personnel.
In summary, antimicrobial resistance and hospital-acquired infections represent an enormous issue for patients, providers, hospitals, and the public. Hospitalists are positioned to take a large role in improving patient safety by supporting, following, and advocating the recommended guidelines and evidence-based measures to reduce the incidence of hospital-acquired infections at the local and national levels. Great investment of time, resources, and efforts in quality-improvement initiatives are necessary to reduce resistance, reduce infection, and improve overall outcomes for our patients.
References
- Burke JP. Infection control—a problem for patient safety. N Engl J Med. 2003; 348:651-6.
- Jarvis WR. Infection control and changing health-care delivery systems. Emerg Infect Dis. 2001;7:170-3.
- Stone PW, Larson E, Kawar LN. A systematic audit of economic evidence linking nosocomial infections and infection control interventions: 1990–2000. Am J Infect Control. 2002;30:145-52.
- Shojania KG, Duncan BW, McDonald KM, Wachter RM, Markowitz AJ. making health care safer: a critical analysis of patient safety practices. Evid Rep Technol Assess. 2001;43: i-x, 1-668. Review. Full report available at www.ahrq.gov.
- National Nosocomial Infections Surveillance (NNIS) system report, data summary from October 1986- April 1996, issued May 1996. A report from the National Nosocomial Infections Surveillance (NNIS) system. Am J Infect Control. 1996;24:380-8.
- Gerberding JL. Hospital-onset infections: a patient safety issue. Ann Intern Med. 2002;137:665-70.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287:487-94.
- O’Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter infections. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2002;51:1-29.
- National Nosocomial Infections Surveillance (NNIS) system report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control. 2004;32: 470-85.
- Influenza and Pneumococcal Vaccination Levels Among Persons Aged ≥65 Years--United States, 1999. MMWR Morb Mortal Wkly Rep. 2001;50:532-7.
- Kluger DM, Maki DG. The relative risk of intravascular device related bloodstream infections in adults. Abstracts of the 39th Interscience Conference on Antimicrob Agents Chemother. 1999:514.
- Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med. 2000;132:391-402.
- McGee DC, Gould MK. Preventing Complications of Central Venous Catheterization. N Engl J Med. 2003;348:1123-33.
- Merrer J, De Jonghe B, Golliot F, et al. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. JAMA. 2001;286:700-7.
- Chaiyakunapruk N, Veenstra DL, Lipsky BA, Saint S. Chlorhexidine compared with povidone-iodine solution for vascular catheter-site care: a meta-analysis. Ann Intern Med. 2002;136:792-801.
- Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-20.
While infections that develop during hospitalization may appear to be an uncommon but recognized risk of hospital care today, the incidence of these infections has been increasing dramatically during the last 2 to 3 decades, and the risk of acquiring an organism that is resistant to 1 or more antibiotics is becoming increasingly common. Recent studies estimate that approximately 2 million patients contract healthcare-associated infections each year (1). These infections are the most common type of serious adverse event in health care, affecting up to 5–10% of hospitalized patients, leading to approximately 90,000 deaths annually, and adding approximately $5 billion to annual healthcare costs (1-3). Increasingly, healthcare-associated infection risk is viewed as a patient safety issue, as many of these infections may be avoidable or preventable by following evidence-based best practices in infection control and patient care while patients are hospitalized. This article will summarize some of the overlap between patient safety and infection control, explain some of the pressures that have led to development and cultivation of antimicrobial resistance, and describe the Centers for Disease Control and Prevention (CDC) campaign for prevention of healthcare-associated infections and antimicrobial resistance, as well as the role of hospitalists in such prevention.
Patient Safety
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) specifically identifies in its 2005 National Patient Safety Goals that hospitals and clinicians reduce the risk of healthcare-associated infections. The goals encourage clinicians to comply with current CDC hand hygiene guidelines and that hospitals and clinicians manage as sentinel events all identified cases of unanticipated death or permanent loss of function associated with a heathcare-associated infection. A sentinel event is defined by JCAHO as an unexpected occurrence involving death or serious physical or psychological injury. Such an event signals the need for immediate investigation and response by the institution. By including healthcare-associated infections in this category of high-risk event, with potential morbidity and mortality, JCAHO highlights the frequency and importance of infections acquired in our healthcare system today.
Further, the Agency for Healthcare Research and Quality (AHRQ) recently published an evidence-based report, developed and written primarily by hospitalists, delineating 79 patient safety practices, of which 22 (28%) involved infection control (4). At least 5 of these 22 infection control practices were considered valuable enough, and with sufficiently strong supporting evidence, to mandate widespread implementation. Additionally, the Institute for Healthcare Improvement (IHI; www.ihi.org) recently launched its 100,000 Lives Campaign, enlisting hundreds of hospitals around the United States in a commitment to implement changes that have been proven to prevent avoidable deaths. Three of their first 6 interventions involve the reduction of healthcare-associated infections, including central-line infections, surgical-site infections, and hospital-acquired pneumonia.
Increasingly, hospital-onset infections have become a patient safety issue, and they will remain under public and institutional scrutiny while hospitals take efforts to reduce their incidence and improve care quality. Hospitalists have evolved to serve a unique role as advocate of both patients and hospitals. They should therefore foster quality improvement in the hospital, as well as lead and support initiatives that reduce hospital-acquired infections and resistance.
Healthcare-Associated Infections and Development of Resistance
Bacteria have developed multiple microbiologic and genetic mechanisms to elude antimicrobial agents. Certain practices in medical care, whether intentional or not, can promote persistence or spread of resistant microbes that can cause infections. Such practices may include:
- Inattention to basic infection control measures (e.g., hand washing)
- Unrecognized colonization (e.g., treating colonized urinary or vascular catheters, without evidence of infection)
- Unrecognized reservoirs (e.g., environmental)
- Selective pressure from overuse or inappropriate use of antibiotics
- Movement of patients and staff within a single institution and between institutions
Inappropriate use or overuse of antibiotics can actually remove or “select” the sensitive microbes and promote overgrowth of resistant organisms when present. Each of these practices may serve as a focus for quality improvement interventions to reduce resistance.
Most healthcare-associated infections (more than 80%) originate from 4 specific patient sites: urinary tract, surgical-site (wound), bloodstream, and lung (pneumonia) (5). It is not coincidental that these infection sites are frequently associated with invasive procedures, and many times with indwelling invasive devices that may be used during the course of inpatient care. For example, urinary tract infections, the most common hospital-acquired infections, are usually associated with urinary catheter use. Similarly, bloodstream infections are usually associated with intravascular catheters, and hospital-acquired pneumonia is usually associated with ventilator use.
Because many of the invasive devices that are utilized during the course of inpatient care carry significant risk, including infection risk, it is incumbent upon hospitalists to be aware of these risks, to explain these risks to their patients, and to take all steps at their disposal to help reduce such risk in their patients. Dr. Julie Gerberding, Director of the CDC, has emphasized that the 2 greatest predictors of infection risk in the hospital are length of stay and use of invasive devices (6). While excellent evidence already demonstrates that hospitalists reduce length of stay (7), they should also spearhead the efforts to minimize the use of invasive devices whenever possible, and lead evidence-based efforts to minimize infection in hospitalized patients when invasive devices must be used.
Prevention of Resistance: Best Practices
CDC/SHM Collaboration
In September 2003, the Society of Hospital Medicine (SHM) and the CDC entered into a collaborative agreement to educate hospitalists about the reduction of hospital-acquired infections and the prevention of antimicrobial resistance. The long-term goals of this agreement include developing quality-improvement initiatives and research in the area of antimicrobial resistance reduction. The short-term goals include development of educational materials and resources for hospitalists aimed at reducing hospital-acquired infections and resistance. SHM has provided instruction in the reduction of hospital-acquired infections and antimicrobial resistance, in workshop format, to its membership at national, regional, and local chapter meetings. SHM has also developed an Internet-based educational tool for antimicrobial resistance on its Web site, which will soon be transformed into a new Web-based Resource Room to educate membership on antimicrobial resistance and reduction of hospital-acquired infections.
CDC Campaign
(www.cdc.gov/drugresistance/healthcare/)
The CDC, in collaboration with the National Institutes of Health (NIH) and the Food and Drug Administration (FDA), as well as professional societies, healthcare organizations, public health agencies, and corporate partners, has developed its Campaign to Prevent Antimicrobial Resistance to facilitate the implementation of educational and behavioral interventions that will assist clinicians in appropriate antimicrobial prescribing. The goals of these intervention programs are to improve clinician practices and prevent antimicrobial resistance. The campaign focuses on 4 main strategies: prevent infection, diagnose and treat infection, use antimicrobials wisely, and prevent transmission. Multiple 12-step programs have been developed (or are in the process of development), targeting specific patient populations, including hospitalized adults, dialysis patients, surgical patients, hospitalized children, and long-term-care patients. Each of these patient populations is relevant to the practicing hospitalist, who may access the educational materials and resources cost-free on the Internet. The CDC provides on-line resources (Web site listed above), including a downloadable slide-set, a 12-step fact sheet, and tips for patients. The program translates existing scientific evidence and national guidelines into action steps that can be taken now to prevent antimicrobial resistance.
The 12 Steps to Prevent Antimicrobial Resistance in Hospitalized Adults was the first intervention program to be initiated, because hospital patients are at especially high risk for serious antimicrobial-resistant infections. The rate of multiple drug-resistant organisms causing infection within our hospitals is increasing at a rapid rate. Currently, national data demonstrate that more than 50% of Staphylococcus aureus isolates causing infections in intensive care units (ICUs) are resistant to methicillin (MRSA), while more than 40% are resistant in other non-ICU hospital units (9). Similarly, gram-negative organisms have developed resistance, with more than 25% of Pseudomonas aeruginosa ICU isolates now resistant to fluoroquinolones (9), with a much higher percentage resistant at some institutions. This rapidly growing problem has led the CDC to develop the following 12 Steps to Prevent Antimicrobial Resistance in Hospitalized Adults:
- Vaccinate
- Get the catheters out
- Target the pathogen
- Access the experts
- Practice antimicrobial control
- Use local data
- Treat infection, not contamination
- Treat infection, not colonization
- Know when to say “no” to vanco
- Stop treatment when infection is cured or unlikely
- Isolate the pathogen
- Break the chain of contagion
Prevent Infection
Diagnose and Treat Infection Effectively
Use Antimicrobials Wisely
Prevent Transmission
These steps are designed to optimize patient safety and the outcome of infectious disease management, and hospitalists have the ability to utilize these recommendations to improve the care of their patients.
Hospitalists must employ efforts to prevent infections that may occur during hospitalization as well as those that may bring patients back to the hospital. Such efforts include predischarge influenza and pneumococcal vaccination when indicated, to reduce the more than 100,000 hospitalizations and 20,000 deaths due to influenza and the more than 12,000 deaths due to Streptococcus pneumoniae (10). Clinicians should get annual influenza vaccines as well, to reduce transmission to patients and to other healthcare workers.
Because catheters and other invasive devices are the No. 1 cause of hospital-acquired infections, evidence-based efforts must be utilized to reduce the likelihood of such infections. An estimated 250,000 catheter-related bloodstream infections (CR-BSI) occur each year, with an attributable cost of at least $25,000 per infection and an attributable mortality of 12–25% (11). Because of this, the CDC has recommended adherence to performance indicators for reducing bloodstream infections (8,12). Such performance indicators are based on strong evidence (13-15) and include the following:
- Appropriate site selection for catheter placement (i.e., subclavian over femoral or internal jugular) (14)
- Appropriate hand hygiene and aseptic technique (including use of maximal sterile barriers) during catheter placement
- Adequate skin asepsis (using chlorhexidine preferentially over iodine or alcohol based solutions) (15)
- Catheter discontinuation when no longer essential
- Antibiotic-impregnated catheters in high-risk patients
Recent studies have demonstrated that CR-BSI can be significantly reduced or even virtually eliminated with educational efforts combined with strict adherence to evidence based guidelines for prevention, as well as efforts to remove catheters early (16).
To diagnose and treat infections effectively, hospitalists must obtain appropriate cultures, target empiric therapy to the likely pathogens and local antibiogram data, and target final therapy to the known pathogens and antimicrobial susceptibility test results. The correct regimen, timing, dosage, route, and duration of antibiotic can impact morbidity and mortality in patients presenting with infectious diseases. Therefore, careful selection becomes crucial, and accessing infectious disease expertise in complex or critically ill patients with infectious diseases can be lifesaving.
Wise or appropriate use of antimicrobials can be facilitated by multiple efforts within hospitals. First, practicing antimicrobial control at the institutional level may involve use of standardized antimicrobial order forms, formulary restrictions, prior approval to start or continue specific antimicrobials, pharmacy substitution or switch, multidisciplinary drug utilization evaluation, provider performance feedback, or computerized decision support ordering systems. Many of these efforts can reduce costs while improving outcomes. Second, because the prevalence of resistance can vary by location, patient population, hospital unit, and length of stay, knowledge of the inpatient population that one treats (e.g., community vs. tertiary care, immunocompetent vs. immunosuppressed, or ICU vs. non-ICU) as well as the local antibiogram can help clinicians make decisions regarding initial antimicrobial selections.
Third, curbing antimicrobial overuse can be fostered by avoiding treatment of contamination or colonization. Contaminated cultures may be reduced by using and advocating proper antisepsis for blood cultures and other culture specimens. Recognition of organisms unlikely to represent true bacteremia (e.g., Corynebacterium), as well as those very likely to represent true bacteremia (e.g., Staphylococcus aureus or Entero-bacteriaceae), and interpreting culture results within clinical context help clinicians effectively treat positive cultures when indicated and avoid treating contaminants. Additionally, recognizing when cultures from urinary catheters, intravascular catheters, and endotracheal tubes represent colonization rather than infection and taking active steps to obtain accurate (rather than colonized) cultures can further curb nonindicated antibiotic use. For example, routinely sending catheter tips for culture is not indicated. Also, urinalysis should always accompany urine cultures sent from urinary catheters. Fourth, stopping antimicrobial therapy when infections are cured, cultures are negative and infection unlikely, or when infection is not diagnosed also limits antimicrobial overuse.
Finally, prevention of infection transmission from patient to patient or from healthcare worker to patient can be accomplished by use of standard infection control precautions, use of appropriate isolation precautions and handling of bodily fluids, and accessing infection control experts when questions arise. Frequent and effective hand hygiene as well as empowering all hospital staff to take part in and enforce infection control measures will help reduce transmission of infection by healthcare personnel.
In summary, antimicrobial resistance and hospital-acquired infections represent an enormous issue for patients, providers, hospitals, and the public. Hospitalists are positioned to take a large role in improving patient safety by supporting, following, and advocating the recommended guidelines and evidence-based measures to reduce the incidence of hospital-acquired infections at the local and national levels. Great investment of time, resources, and efforts in quality-improvement initiatives are necessary to reduce resistance, reduce infection, and improve overall outcomes for our patients.
References
- Burke JP. Infection control—a problem for patient safety. N Engl J Med. 2003; 348:651-6.
- Jarvis WR. Infection control and changing health-care delivery systems. Emerg Infect Dis. 2001;7:170-3.
- Stone PW, Larson E, Kawar LN. A systematic audit of economic evidence linking nosocomial infections and infection control interventions: 1990–2000. Am J Infect Control. 2002;30:145-52.
- Shojania KG, Duncan BW, McDonald KM, Wachter RM, Markowitz AJ. making health care safer: a critical analysis of patient safety practices. Evid Rep Technol Assess. 2001;43: i-x, 1-668. Review. Full report available at www.ahrq.gov.
- National Nosocomial Infections Surveillance (NNIS) system report, data summary from October 1986- April 1996, issued May 1996. A report from the National Nosocomial Infections Surveillance (NNIS) system. Am J Infect Control. 1996;24:380-8.
- Gerberding JL. Hospital-onset infections: a patient safety issue. Ann Intern Med. 2002;137:665-70.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287:487-94.
- O’Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter infections. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2002;51:1-29.
- National Nosocomial Infections Surveillance (NNIS) system report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control. 2004;32: 470-85.
- Influenza and Pneumococcal Vaccination Levels Among Persons Aged ≥65 Years--United States, 1999. MMWR Morb Mortal Wkly Rep. 2001;50:532-7.
- Kluger DM, Maki DG. The relative risk of intravascular device related bloodstream infections in adults. Abstracts of the 39th Interscience Conference on Antimicrob Agents Chemother. 1999:514.
- Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med. 2000;132:391-402.
- McGee DC, Gould MK. Preventing Complications of Central Venous Catheterization. N Engl J Med. 2003;348:1123-33.
- Merrer J, De Jonghe B, Golliot F, et al. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. JAMA. 2001;286:700-7.
- Chaiyakunapruk N, Veenstra DL, Lipsky BA, Saint S. Chlorhexidine compared with povidone-iodine solution for vascular catheter-site care: a meta-analysis. Ann Intern Med. 2002;136:792-801.
- Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-20.
The Inpatient with AIDS: What the Hospitalist Needs to Know
The opinions and assertions contained herein are those of the authors and are not to be construed as official or as reflecting the views of the Department of Defense, the Department of the Navy, or the naval services at large.
Introduction
An estimated 850,000 to 950,000 persons in the United States are living with human immunodeficiency virus (HIV), 280,000 of whom are unaware of their infection and another 43,000 of whom meet the definition of acquired immunodeficiency syndrome (AIDS) (www.cdc.gov). The use of highly active antiretroviral therapy (HAART) has produced significant declines in morbidity and mortality from AIDS. Compared with the first 2 decades of the HIV pandemic, the number of HIV-related hospital admissions has declined. However, recently, this rate of decline has markedly slowed (1-3). The reasons for this plateau are many including a steady number of admissions for complications related to HAART, treatment failures, and the overall increased prevalence of HIV infection. Not only will HIV-infected patients still frequently require admission to the hospital, but the complexity of their inpatient care will continue to increase with the advancements in multiple drug regimens, aging of the HIV-infected population, and the interaction of HIV infection with medical comorbidities, many of which are attributable to HAART.
The hospitalist caring for the inpatient with AIDS is presented with several challenges including not only the diagnosis and management of opportunistic infections, but also the complications of HAART. In this article we review the guidelines for the initiation and continuation of HAART in the hospital, review important clinical complications of antiretroviral therapy, and review conditions that may result in the hospitalization of AIDS patients.
Initiation of HAART in the Hospital
In those who do not have access to health care, the initial diagnosis of HIV infection frequently occurs during a hospitalization for an AIDS-defining illness. Initiation of antiretrovirals is contingent on several issues, including CD4 count, viral load, clinical status, likelihood of continued adherence, and the concurrent treatment of opportunistic infections (OIs). All patients with HIV infection and a CD4 count <200 cells/mm3 or an AIDS-defining illness should receive antiretroviral therapy. Controversy exists as to whether a patient admitted for the treatment of an opportunistic infection should begin antiretroviral therapy immediately, or whether this therapy should be deferred until after acute treatment of the OI. The potential detrimental effects of drug-drug interactions, the need for treatment interruptions, and drug-related toxicity between antiretrovirals and OI-specific therapy may support initiating HAART after control of an OI is achieved. Conversely, for some opportunistic infections, such as cryptosporidiosis, the use of HAART is essential for successful treatment of the infection.
An ongoing randomized controlled trial initiated within the Adult AIDS Clinical Trials Group (ACTG) comparing outcomes between patients who start HAART immediately after presentation with an acute OI and patients who start HAART at least 4 weeks after the OI has resolved should help identify the factors supporting early or delayed initiation of antiretrovirals (4).
Generally speaking, HAART can be administered by combining either a protease inhibitor (PI) or a nonnucleoside reverse transcriptase inhibitor (NNRTI) with 2 nucleoside reverse transcriptase inhibitors (NRTIs). There are currently more than 20 FDA-approved antiretrovirals. Frequent updates on the guidelines for the use of antiretroviral agents in HIV-infected adults are available at www.AIDSinfo.nih.gov, and a discussion of this topic is beyond the scope of this review.
Continuation of HAART in the Hospital
In most cases, every effort should be made to minimize interruption of HAART during a hospitalization. Although some investigators are examining the virologic and immunologic safety of interrupting HAART as a treatment strategy, there are few data on viral replication, CD4 cell count decline, and rate of acquisition of new mutations in hospitalized patients who have unexpected treatment interruptions (5). The long half-life of some antiretrovirals promotes the emergence of resistance once HAART is stopped. For example, once NNRTIs are stopped, subtherapeutic levels remain in the plasma and cells for several days. HIV then replicates in a milieu that may select for resistance mutations.
Because zidovudine is the only antiretroviral available in a parenteral preparation, it is often difficult to continue HAART when a patient cannot take medications by mouth. Drugs given by the enteral route in a hospitalized patient may also be poorly absorbed, and few data exist on the absorption of antiretrovirals administered through a gastrostomy or jejunostomy tube (6).
Prescribing HAART in the Hospital
Antiretroviral prescribing errors occur frequently in the hospitalized AIDS patient. The most common errors include overdosing or underdosing, missing components of multidrug regimens, or missing critical drug-drug interactions (7). Underdosing may lead to resistance, and overdosing contributes to increased toxicity. In one report, prescribing errors occurred in 12% of admissions in the post-HAART era (1998) compared with 2% of admissions in the pre-HAART era (1996) (7). The NRTIs, including didanosine, emtricitabine, lamivudine, stavudine, and zidovudine, require decreased dosing in renal insufficiency. Tenofovir is not recommended for use if the creatine clearance is less than 60 mL/minute. Dosage adjustments in hepatic disease are recommended for amprenavir, fosamprenavir, delavirdine, efavirenz, and nevirapine.
Immune Reconstitution Syndrome
The widespread use of HAART has produced sustained suppression of HIV replication and recovery of CD4 cell counts. It also became evident that HAART resulted in not only a numerical increase in CD4 cells, but also in a functional immune recovery (8-10). This improved T-cell response to antigens results in adequate protection against specific opportunistic infections, allowing for discontinuation of primary and secondary prophylaxis in HIV-infected patients. Immune reconstitution syndrome (IRS), an inflammatory syndrome, is recognized as a potential complication that can occur days to months after starting HAART. The onset of IRS is characterized by a paradoxical worsening of clinical or laboratory parameters despite a favorable response in CD4 cell counts and the suppression of viral replication (9,11,12). IRS has been reported to occur in 10–25% of patients who receive HAART and more commonly in those whose CD4 cell counts are <50 cells/mm3 at the start of HAART (9,11). It is postulated that the inflammatory response is triggered by the recognition of antigens associated with ongoing infection or recognition of persisting antigens associated with past (nonreplicating) infections. Mycobacterial antigens, frequently implicated in IRS, are responsible for about one third of cases. Other antigens associated with IRS include cytomegalovirus and hepatitis B and C (11). In most circumstances, with the management of IRS, HAART should be continued, while specific antimicrobial therapy and steroids should be considered (10).
Medical Conditions that Should Prompt HIV Screening
There are several medical conditions that should prompt screening for HIV infection. Generally, anyone presenting with a fever of unknown etiology who is sexually active or had a blood transfusion prior to 1985 should be screened for HIV infection. Symptoms consistent with acute retroviral syndrome (fever, sore throat, malaise, and skin rash) may be more commonly recognized by clinicians now than previously, and this remains a “golden opportunity” to intervene. Frequently, acute retroviral syndrome will be attributed to Epstein-Barr virus; however, caution should be used in the diagnosis of mononucleosis in those other than teenage populations. It is recommended that all persons presenting with any sexually transmitted disease, unexplained generalized lymphadenopathy, oral candidiasis, or tuberculosis should also be tested. Other conditions where HIV infection should be considered include enigmatic pneumonia, acute hepatitis B infection, herpes zoster infection (particularly in younger, seemingly immunocompetent individuals), idiopathic thrombocytopenic purpura, and nephropathy of unknown cause.
Drug Interactions
Drug interactions are an important consideration in the treatment of HIV infection. Interactions between HAART and other drugs used for the treatment or prophylaxis of opportunistic infections along with those used for the treatment of drug-induced endocrinopathies (hyperlipidemia, diabetes mellitus) are virtually unavoidable. Drug interactions occur either because of drug metabolism or absorption. The multiple metabolic pathways of some drugs make it difficult to predict the outcome of drug interactions. All protease inhibitors and non-nucleoside reverse transcriptase inhibitors are metabolized by the cytochrome P-450 enzyme system and each of these drugs may alter the metabolism of other antiretrovirals and concomitantly administered drugs (13,14). A decrease in trough plasma concentrations of the protease inhibitors to a level below the in vitro concentration required to inhibit replication of 50% of viral strains (IC50) may lead to development of resistance. Because nucleoside analogue reverse transcriptase inhibitors are primarily eliminated by the kidney, they do not interact with other drugs through the cytochrome P-450 system.
One noteworthy interaction that the clinician caring for HIV-infected patients should be aware of is the interaction of ribavirin with zidovudine. Ribavirin decreases the phosphorylation of zidovudine and stavudine in vitro, resulting in decreased concentrations of the active compound. HIV-infected patients who are coinfected with hepatitis C may be treated with regimens that include ribavirin, which may reduce the efficacy of zidovudine (15). Another important interaction is the effect of nevirapine or efavirenz on plasma methadone concentrations. Both drugs can decrease methadone plasma levels by 50%, and patients receiving chronic therapy may need increased methadone doses to prevent withdrawal symptoms (16).
Protease inhibitors are associated with numerous interactions including certain antiarrhythmics, sedatives, hypnotics, ergot derivatives, and several lipid-lowering agents (statins). Not only do protease inhibitors affect the metabolism of certain drugs, but also their own metabolism is altered by other inducers or inhibitors of cytochrome activity that can cause clinically important decreases in serum levels of protease inhibitors. One widely recognized interaction is that of rifampin, which may decrease levels of some protease inhibitors by 80%. The resulting low plasma concentrations may promote viral resistance and result in treatment failure. Patients being treated for tuberculosis, who are also receiving protease inhibitors should be treated with a four-drug regimen that includes rifabutin (at half dose) instead of rifampin. Updated guidelines for the use of rifabutin or rifampin in HIV-infected patients receiving antiretroviral agents have been reviewed recently (17).
Other potent inducers such as phenytoin, phenobarbital, and carbamazepine can cause similar reductions in serum levels of protease inhibitors. Azole antifungal drugs and macrolides also have important interactions that complicate both the treatment and prophylaxis of opportunistic infections.
Interactions that interfere with absorption can also affect plasma drug concentrations. For example, the absorption of fluconazole is unaffected by variations in gastric pH, while itraconazole and ketoconazole require an acidic environment for optimal absorption. The protease inhibitor, atazanavir, also requires a low pH for absorption and thus is contraindicated with the use of proton pump inhibitors; taking atazanavir with acidic beverages is not sufficient to overcome this (18).
New information about drug interactions becomes known on almost a daily basis in patients with HIV infection. The number of documented and theoretical interactions can become overwhelming to the clinician. Clinicians should suspect potential drug interactions in a patient who is failing therapy but who is adherent to HAART. Fortunately, there are extensive tables on Web sites (www.hivatis.org) and product information to aid in the recognition and management of drug interactions.
Complications of HAART
Diabetes mellitus, hyperlipidemias, lipodystrophy, and insulin resistance are among the many complex metabolic abnormalities attributable to the use of HAART. For the most part, these complications are managed conservatively and usually do not mandate the discontinuation of HAART. Pancreatitis, hepatic steatosis, and lactic acidosis are wellrecognized complications of NRTIs. These are usually more acute and may result in hospitalization and necessitate the discontinuation of medications. Cessation of the offending agent (didanosine [ddI], stavudine [d4T], and zalcitabine [ddC) usually results in resolution of pancreatitis, but the episode may limit use of these agents in the future. Hepatic steatosis and lactic acidosis are rare but life-threatening adverse effects associated with the mitochondrial toxicity seen with the NRTIs. Symptoms usually develop insidiously with nausea, vomiting, abdominal pain, weight loss, or dyspnea and can progress rapidly to fatal lactic acidosis. Hepatomegaly, ascites, elevated liver associated enzymes, and an increased anion gap with lactic acidemia are usually present (19,20). Discontinuation of antiretroivirals is imperative.
There is an accumulating body of evidence that suggests that HIV-infected patients receiving HAART may be at risk for accelerated coronary disease (21). In addition, some cohort studies have reported an increased incidence of myocardial infarction (MI) following the introduction of HAART and the risk for MI rose progressively with the number of years on antiretroviral therapy (22,23). However, it is important to note that many traditional risk factors for coronary artery disease contribute more substantially to the risk for a cardiovascular event than does HAART. Therefore, aggressive modification of primary cardiac risk factors is warranted.
Hypersensitivity Drug Reactions
Drug hypersensitivity reactions are life-threatening reactions that result in a systemic illness that usually includes fever and maculopapular rash accompanied by constitutional symptoms (fatigue, myalgias, and arthralgias), visceral involvement (lymphadenopathy, mucositis, pneumonitis, myocarditis, hepatitis, and interstitial nephritis), and hematologic abnormalities (eosinophilia) (24).
Abacavir, an NRTI, is a relatively new antiretroviral agent used in many HAART regimens. Abacavir is associated with a hypersensitivity reaction, which can be fatal if abacavir use is continued despite the reaction, or if re-challenge with the drug takes place after the reaction (25). The overall incidence of this reaction appears to be around 4% (25). Prior antiretroviral experience and being of African descent are associated with a nearly 40% reduction in the risk of this hypersensitivity reaction, while patients of white race are at a significantly greater risk. CD4 cell counts do not appear to be significantly related to abacavir hypersensitivity (26). The exact metabolite that is likely responsible for abacavir hypersensitivity is unknown.
The most common symptoms of abacavir hypersensitivity reaction are fever, rash, nausea, vomiting, and abdominal pain. Occasionally, respiratory symptoms will be present and can mimic influenza. However, gastrointestinal symptoms are the most prominent complaints after fever and rash and help to distinguish between influenza and abacavir hypersensitivity. More than 90% of hypersensitivity reactions occur during the first 6 weeks of treatment, with a median time to development of 8 days. A fever that develops within a few weeks after the initiation of therapy with abacavir may be due to causes other than hypersensitivity. One of the most common situations is the simultaneous initiation of treatment with other drugs, such as trimethoprimsulfamethxazole, efavirenz, or nevirapine, all of which are associated with a higher incidence of hypersensitivity than abacavir (27,28). Symptoms may be sudden and worsen over a few days if abacavir is continued. Symptoms tend to improve in 48 hours after abacavir is discontinued. Supportive therapy includes intravenous hydration and withdrawal of abacavir as well as all other antiretrovirals. Early in the use of this medication, 20% of patients who were re-challenged with the drug experienced unanticipated life-threatening events manifesting as an anaphylactic or immediate type hypersensitivity reaction. Hypotension, renal insufficiency, and bronchospasm have resulted in death. Rechallenge symptoms have been seen with the first dose (29). A discussion of the potential for this hypersensitivity is warranted when prescribing this agent. In the United States, a patient information card warning of this hypersensitivity reaction is distributed to the patient with each bottle of abacavir. Prednisone does not prevent the development of hypersensitivity reaction.
Symptoms of toxicity from TMP-SMX are more likely to occur in the HIV infected than in patients without HIV infection. Fever and rash can occur in up to 50% of HIV-infected patients. The rash can be treatment limiting or severe in up to 20% of HIV-infected patients who receive it. Life-threatening reactions may occur, including fatal Stevens Johnson-type exfoliative skin reactions. Most toxicity in HIV-infected patients appears to be related to metabolites of the sulfamethoxazole component and decreased levels of glutathione. There have been reports of severe systemic reactions that resemble anaphylaxis or septic shock occurring in HIV-infected patients who are re-challenged with TMP-SMX after experiencing toxicity within the previous 6–8 weeks (30).
The NNRTIf nevirapine and efavirenz can cause a delayed hypersensitivity reaction similar to that seen with abacavir. Cutaneous involvement is a prominent component of both nevirapine and efavirenz hypersensitivity reaction, with rash more likely to occur with the use of nevirapine. In addition, female patients have a higher propensity of developing Stevens-Johnson syndrome and symptomatic hepatic events from nevirapine (28,31).
Laboratory Abnormalities Related to Drugs
Hyperbilirubinemia and Atazanavir and Indinavir
Atazanavir, a protease inhibitor, is metabolized by the liver via CYP3A and also inhibits both CTP3A and UGT1A1. UGT1A1 is required for conjugation of bilirubin and inhibition of this enzyme results in elevated levels of unconjugated bilirubin. This effect is similar to what is observed in Gilbert’s syndrome. Asymptomatic indirect hyperbilirubemia may be seen in up to 60% of patients receiving atazanavir. Total bilirubin levels may rise to greater than 5 mg/dL, and more than 17% of patients may experience jaundice (18). Concurrent elevations in hepatic serum transaminases should not be attributed to atazanavir and alternative etiologies for these elevations should be sought. This hyperbilirubinemia is reversible upon discontinuation of the atazanavir.
Similarly, but to a lesser degree, asymptomatic unconjugated hyperbilirubinemia (>2 mg/dL) has been reported in up to 14% of patients treated with indinavir. Elevated serum transaminases were seen in less than 1%.
Renal Abnormalities and Indinavir
Several renal syndromes have been associated with indinavir use, ranging from obstructive uropathy and acute renal failure to asymptomatic pyuria. The range of clinical syndromes is a consequence of indinavir crystals aggregating within or irritating the urinary tract (32). Symptomatic nephrolithiasis (indinavir crystallization) has been reported to affect up to 12% (range, 5–35 %) of patients who receive indinavir, while up to 67% of patients will have asymptomatic crystalluria. The cumulative frequency of nephrolithiasis events increases with increasing exposure to indinavir. Therapy may be continued or interrupted for a few days. Adequate hydration is necessary with the administration of indinavir. Indinavir associated pyuria is frequently associated with interstitial nephritis or urothelial inflammation. Discontinuation of indinavir will lead to resolution of urine abnormalities.
Elevated Mean Corpuscular Volume (MCV) and NRTIs
Elevation of MCV or macrocytosis occurs in more than 90% of patients treated with zidovudine, but is not correlated with the development of anemia. Macrocytosis (MCV values exceeding 110/fl) develops within 2 weeks following the initiation of zidovudine therapy, and its presence can be used as a marker for medical adherence. When anemia does occur it is associated with a dose related bone marrow toxicity manifested as a macrocytic anemia. Serum B12 and folate levels are normal. Stavudine use is also associated with macrocytosis, in non-zidovudine-containing regimens (33).
Drug Screens and Efavirenz
The use of efavirenz, a potent non-nucleoside reverse transcriptase inhibitor, can cause a false-positive urine drug screen for cannabinoid. Efavirenz does not bind to cannabinoid receptors. The false-positive test results are specific to the assay kit used (34).
Evaluation of the AIDS Patient with Fever
Fever is a common symptom in HIV-infected patients, the etiology of which can be identified in more than 80% of cases (35,36). The AIDS patient with fever poses a considerable challenge given that the expanded differential may include a wide range of OIs. The CD4 cell count remains a valuable predictor of risk for infection. Patients with CD4 cell counts greater than 500 cells/mm3 should be evaluated as if immunocompetent. Patients with CD4 cell counts between 200 and 500 cells/mm3 are at increased risk for upper and lower bacterial respiratory infections, tuberculosis, and sinusitis, but overall their risk for opportunistic infection is not increased. In patients with CD4 counts less than 200 cells/mm3, Pneumocystis jiroveci pneumonia, formerly known as Pneumocystis carinii pneumonia, is the most common cause of fever in those not receiving primary prophylaxis. As the CD4 cell count decreases below 100 cells/mm3, the risk for disseminated MAC, toxoplasmosis, CMV, disseminated fungal infections, and lymphoma should be considered possible causes of fever. HIV itself is usually not the cause of fever in patients with advanced immunosuppression (37).
In patients with CD4 counts >200 cells/mm3, the clinician can usually construct a laboratory and radiographic evaluation guided by symptoms, while in patients with severe immunosuppression a broader evaluation is required. A serum cryptococcal antigen should be obtained, as it has high sensitivity and specificity for both systemic disease as well as meningitis (38). Bacterial, mycobacterial, and fungal isolator blood cultures should be performed, as well as a urine culture, despite lack of symptoms. Urine AFB cultures can be added if there is a suspicion for tuberculosis. Sputum should be evaluated with gram stain, AFB smear, and culture, as well as PCP direct fluorescent antibody. If diarrhea is present, stool studies should include bacterial culture, ova and parasites evaluation, an assay for C. difficile, and Cryptosporidia and Giardia stool antigen assays. A serum LDH may be elevated in PCP, disseminated histoplasmosis, or lymphoma. A serum CMV antigen may be useful in the patient with fever and diarrhea, hepatitis, or retinitis.
A chest radiograph should be performed in all febrile AIDS patients. Chest films may be normal in 5–10% of HIV-infected patients with tuberculosis (TB). The typical radiographic appearance of Pneumocystis jiroveci pneumonia is a bilateral interstitial pattern characterized by reticular or ground-glass opacities. However, normal chest radiographs may be seen in one third of AIDS patients with active PCP. High-resolution computed tomography (HRCT) of the chest should be obtained if there is still a clinical suspicion for Pneumocystis. HRCT has been shown in several reports to have a 100% negative predictive value in the evaluation for PCP (39,40).
A lumbar puncture should be performed if the patient is symptomatic or if the serum cryptococcal antigen is reactive. A bone marrow biopsy and culture is also useful particularly in the evaluation of the patient with cytopenias. Bacterial, fungal, and AFB cultures may yield disseminated mycobacterial or fungal disease. Histopathologic evaluation may reveal granulomas with organisms or lymphoma. Bronchoscopy may be pursued in cases of high suspicion for TB or PCP.
Guidelines for the management of opportunistic infections associated with human immunodeficiency virus are available at www.AIDSinfo.nih.gov.
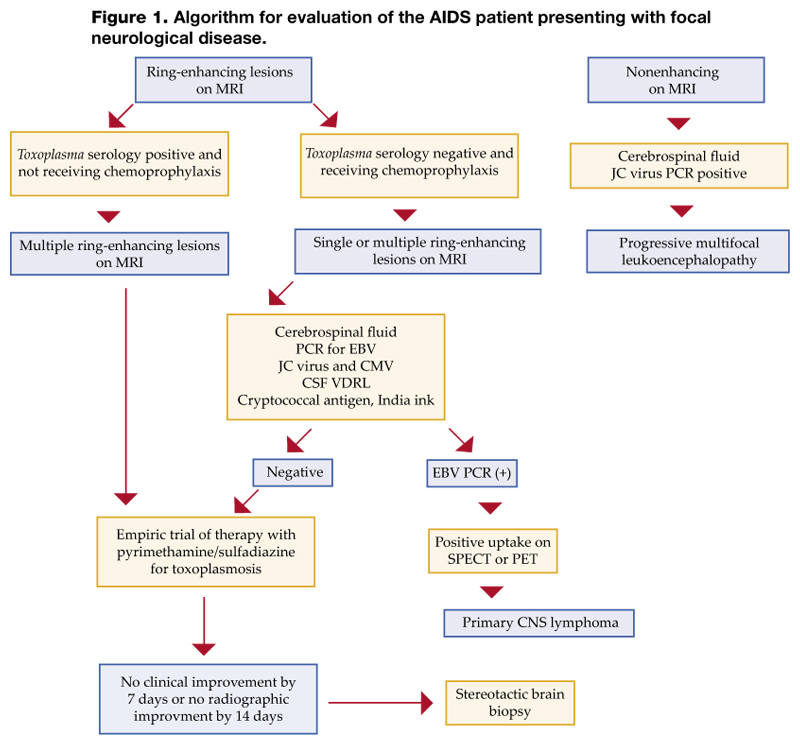
Evaluation of the AIDS Patient with Focal Neurological Disease
Toxoplasma encephalitis (TE) may be distinguished from primary CNS lymphoma without a brain biopsy. TE is caused by reactivation of latent infection by the protozoan Toxoplasma gondii. Almost 90% of patients have CD4 counts less than 200 cells/mm3 and 75% have CD4 counts less than 100 cells/mm3. Serum anti-Toxoplasma IgG antibodies are detected in more than 90% of patients with TE. Lesions on CT or MRI (a more sensitive modality) are typically multiple ring-enhancing lesions with a predilection for the basal ganglia. An emipiric trial of therapy is recommended, and a response confirms a diagnosis in the patient who has a positive Toxoplasma antibody and is not receiving trimethoprim-sulfamethoxazole prophylaxis. A lumbar puncture in this setting is not necessary and maybe ill advised if cerebral edema is present (Figure 1, page 24).
Primary CNS lymphoma (PCNSL) has a similar radiographic appearance as TE. Solitary lesions are more frequent in PCNSL. Positron emission tomography (PET) and single photon emission CT (SPECT) are useful adjunctive imaging modalities as they are positive in PCNSL due to the increased metabolic activity of the tumor. Cytologic analysis of the CSF may show lymphomatous cells. Epstein-Barr virus (EBV) DNA is uniformly detected in PCNSL in AIDS patients and detection of EBV DNA by PCR on the CSF has a sensitivity of 90–100% and a specificity of 87–98% for the diagnosis of PCNSL (41,42). Combining SPECT imaging and EBV PCR provides 100% sensitivity and 100% negative predictive value in the evaluation of AIDS-related primary CNS lymphoma (43), obviating the need for brain biopsy.
Progressive multifocal leukoencephalopathy (PML) is characterized radiographically by multiple and bilateral hypodense lesions of the white matter without mass effect or enhancement on CT. MRI demonstrates areas of hypointensity on T1-weighted images and increased intensity on T2-weighted images. JC virus DNA can be detected by PCR of CSF or brain tissue with sensitivity of approximately 80% and specificity of 95%. Because of the high positive predictive value of a positive PCR, a patient with AIDS who also has a compatible MRI can be diagnosed with PML (44,45).
Other focal neurologic disease seen in AIDS patients includes cryptococcomas, tuberculomas, CMV encephalitis, neurosyphilis, Nocardia and Aspergillus infection, and bacterial brain abscesses (46).
Conclusion
As survival of the HIV-infected population improves, more patients may require hospitalization for HAART treatment failures or complications attributed to antiretroviral therapy. The hospitalist should be familiar with the complications of antiretroviral agents, the interactions between HAART and medications used to treat opportunistic infections, and medical conditions induced by HAART. Evaluation of the HIV-infected patient presenting with fever can be based on the CD4 cell count, which predicts risk for opportunistic infections. Finally, using combined diagnostic approaches along with modern imaging and laboratory assays may preclude the need for more invasive procedures in the HIV-infected hospitalized patient.
Dr. Decker may be reached at [email protected].
References
- Torres RA, Barr M. Impact of combination therapy for HIV infection on inpatient census. N Engl J Med. 1997;336:1531-2.
- Fleishman JA, Hellinger FJ. Trends in HIV-related inpatient admissions from 1993 to 1997: a seven-state study. J Acquir Immune Defic Syndr. 2001;28:73-80.
- Fleishman JA, Hellinger FH. Recent trends in HIV-related inpatient admissions 1996-2000: a 7-state study. J Acquir Immune Defic Syndr. 2003;34:102-10.
- Powderly WG. Should patients with an acute opportunistic infection receive antiretroviral therapy immediately? Advanced Studies in Medicine. 2005;5:S111-S116.
- Fagard C, Oxenius A, Gunthard H, et al. A prospective trial of structured treatment interruptions in human immunodeficiency virus infection. Arch Intern Med. 2003;163:1220-6.
- Soni N, Pozniak A. Continuing HIV therapy in the ICU. Crit Care. 2001;5:247-8.
- Purdy BD, Raymond AM, Lesar TS. Antiretroviral prescribing errors in hospitalized patients. Ann Pharmacother. 2000;34:833-8.
- Autran B, Carcelain G, Li TS, et al. Positive effects of combined antiretroviral therapy on CD4+ T cell homeostasis and function in advanced HIV disease. Science. 1997;277:112-6.
- Cooney EL. Clinical indicators of immune restoration following highly active antiretroviral therapy. Clin Infect Dis. 2002;34:224-33.
- Hirsch HH, Kaufmann G, Sendi P, BaĴegay M. Immune reconstitution in HIV-infected patients. Clin Infect Dis. 2004;38:1159-66.
- Cheng VC, Yuen KY, Chan WM, Wong SS, Ma ES, Chan RM. Immunorestitution disease involving the innate and adaptive response. Clin Infect Dis. 2000;30:882-92.
- Fishman JE, Saraf-Lavi E, Narita M, Hollender ES, Ramsinghani R, Ashkin D. Pulmonary tuberculosis in AIDS patients: transient chest radiographic worsening after initiation of antiretroviral therapy. AJR Am J Roentgenol. 2000;174:43-9.
- Piscitelli SC, Gallicano KD. Interactions among drugs for HIV and opportunistic infections. N Engl J Med. 2001;344:984-96.
- Barry M, Mulcahy F, Merry C, Gibbons S, Back D. Pharmacokinetics and potential interactions amongst antiretroviral agents used to treat patients with HIV infection. Clin Pharmacokinet. 1999;36:289-304.
- Sim SM, Hoggard PG, Sales SD, Phiboonbanakit D, Hart CA, Back DJ. Effect of ribavirin on zidovudine efficacy and toxicity in vitro: a concentration-dependent interaction. AIDS Res Hum Retroviruses. 1998;14:1661-7.
- Clarke SM, Mulcahy FM, Tjia J, et al. The pharmacokinetics of methadone in HIV-positive patients receiving the non-nucleoside reverse transcriptase inhibitor efavirenz. Br J Clin Pharmacol. 2001;51:213-7.
- Centers for Disease Control and Prevention. Updated guidelines for the use of rifabutin or rifampin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors. Morb Mortal Wkly Rep. 2000;49:185-9.
- Havlir DV, O’Marro SD. Atazanavir: new option for treatment of HIV infection. Clin Infect Dis. 2004;38:1599-604.
- Sheng WH, Hsieh SM, Lee SC, et al. Fatal lactic acidosis associated with highly active antiretroviral therapy in patients with advanced human immunodeficiency virus infection in Taiwan. Int J STD AIDS. 2004;15:249-53.
- Herman JS, Easterbrook PJ. The metabolic toxicities of antiretroviral therapy. Int J STD AIDS. 2001;12:555-62;quiz 563-4.
- Behrens G, Schmidt H, Meyer D, Stoll M, Schmidt RE. Vascular complications associated with use of HIV protease inhibitors. Lancet. 1998;351:1958.
- Klein D, Hurley LB, Sidney S. Cardiovascular Disease and HIV Infection. N Engl J Med. 2003;349:1869-70; author reply 1869-70.
- Friis-Moller N, Sabin CA, Weber R, et al. Combination antiretroviral therapy and the risk of myocardial infarction. N Engl J Med. 2003;349:1993-2003.
- Anderson JA, Adkinson NF Jr. Allergic reactions to drugs and biologic agents. JAMA. 1987;258:2891-9.
- Hewitt RG. Abacavir hypersensitivity reaction. Clin Infect Dis. 2002;34:1137-42.
- Hetherington S, Hughes AR, Mosteller M, et al. Genetic variations in HLA-B region and hypersensitivity reactions to abacavir. Lancet. 2002;359:1121-2.
- Bossi P, Colin D, Bricaire F, Caumes E. Hypersensitivity syndrome associated with efavirenz therapy. Clin Infect Dis. 2000;30:227-8.
- Bourezane Y, Salard D, Hoen B, Vandel S, Drobacheff C, Laurent R. DRESS (drug rash with eosinophilia and systemic symptoms) syndrome associated with nevirapine therapy. Clin Infect Dis. 1998;27:1321-2.
- Walensky RP, Goldberg JH, Daily JP. Anaphylaxis after rechallenge with abacavir. AIDS. 1999;13:999-1000.
- Martin GJ, Paparello SF, Decker CF. A severe systemic reaction to trimethoprim-sulfamethoxazole in a patient infected with the human immunodeficiency virus. Clin Infect Dis. 1993;16:175-6.
- Bersoff-Matcha SJ, Miller WC, Aberg JA, et al. Sex differences in nevirapine rash. Clin Infect Dis. 2001;32:124-9.
- Kopp JB, Falloon J, Filie A, et al. Indinavir-associated interstitial nephritis and urothelial inflammation: clinical and cytologic findings. Clin Infect Dis. 2002;34:1122-8.
- Geene D, Sudre P, Anwar D, Goehring C, Saaidia A, Hirschel B. Causes of macrocytosis in HIV-infected patients not treated with zidovudine. Swiss HIV Cohort Study. J Infect. 2000;40:160-3.
- Gottesman L. Sustiva may cause false positive on marijuana test. WORLD. 1999:7.
- Sepkowitz KA, Telzak EE, Carrow M, Armstrong D. Fever among outpatients with advanced human immunodeficiency virus infection. Arch Intern Med. 1993;153: 1909-12.
- Barat LM, Gunn JE, Steger KA, Perkins CJ, Craven DE. Causes of fever in patients infected with human immunodeficiency virus who were admitted to Boston City Hospital. Clin Infect Dis. 1996;23:320-8.
- Sepkowitz KA. FUO and AIDS. Curr Clin Top Infect Dis. 1999;19:1-15.
- Asawavichienjinda T, Sitthi-Amorn C, Tanyanont V. Serum cyrptococcal antigen: diagnostic value in the diagnosis of AIDS-related cryptococcal meningitis. J Med Assoc Thai. 1999;82:65-71.
- Richards PJ, Riddell L, Reznek RH, Armstrong P, Pinching AJ, Parkin JM. High resolution computed tomography in HIV patients with suspected Pneumocystis carinii pneumonia and a normal chest radiograph. Clin Radiol. 1996;51:689-93.
- Gruden JF, Huang L, Turner J, et al. High-resolution CT in the evaluation of clinically suspected Pneumocystis carinii pneumonia in AIDS patients with normal, equivocal, or nonspecific radiographic findings. AJR Am J Roentgenol. 1997;169:967-75.
- MacMahon EM, Glass JD, Hayward SD, et al. Association of Epstein-Barr virus with primary central nervous system lymphoma in AIDS. AIDS Res Hum Retroviruses. 1992;8:740-2.
- Rao CR, Jain K, Bhatia K, Laksmaiah KC, Shankar SK. Association of primary central nervous system lymphomas with the Epstein-Barr virus. Neurol India. 2003;51:237-40.
- Antinori A, De Rossi G, Ammassari A, et al. Value of combined approach with thallium-201 single-photon emission computed tomography and Epstein-Barr virus DNA polymerase chain reaction in CSF for the diagnosis of AIDS-related primary CNS lymphoma. J Clin Oncol. 1999;17:554-60.
- Post MJ, Yiannoutsos C, Simpson D, et al. Progressive multifocal leukoencephalopathy in AIDS: are there any MR findings useful to patient management and predictive of patient survival? AIDS Clinical Trials Group, 243 Team. AJNR Am J Neuroradiol. 1999;20:1896-906.
- Weber T. Cerebrospinal fluid analysis for the diagnosis of human immunodeficiency virus-related neurologic diseases. Semin Neurol. 1999;19:223-33.
- Skiest DJ. Focal neurological disease in patients with acquired immunodeficiency syndrome. Clin Infect Dis. 2002;34:103-15.
The opinions and assertions contained herein are those of the authors and are not to be construed as official or as reflecting the views of the Department of Defense, the Department of the Navy, or the naval services at large.
Introduction
An estimated 850,000 to 950,000 persons in the United States are living with human immunodeficiency virus (HIV), 280,000 of whom are unaware of their infection and another 43,000 of whom meet the definition of acquired immunodeficiency syndrome (AIDS) (www.cdc.gov). The use of highly active antiretroviral therapy (HAART) has produced significant declines in morbidity and mortality from AIDS. Compared with the first 2 decades of the HIV pandemic, the number of HIV-related hospital admissions has declined. However, recently, this rate of decline has markedly slowed (1-3). The reasons for this plateau are many including a steady number of admissions for complications related to HAART, treatment failures, and the overall increased prevalence of HIV infection. Not only will HIV-infected patients still frequently require admission to the hospital, but the complexity of their inpatient care will continue to increase with the advancements in multiple drug regimens, aging of the HIV-infected population, and the interaction of HIV infection with medical comorbidities, many of which are attributable to HAART.
The hospitalist caring for the inpatient with AIDS is presented with several challenges including not only the diagnosis and management of opportunistic infections, but also the complications of HAART. In this article we review the guidelines for the initiation and continuation of HAART in the hospital, review important clinical complications of antiretroviral therapy, and review conditions that may result in the hospitalization of AIDS patients.
Initiation of HAART in the Hospital
In those who do not have access to health care, the initial diagnosis of HIV infection frequently occurs during a hospitalization for an AIDS-defining illness. Initiation of antiretrovirals is contingent on several issues, including CD4 count, viral load, clinical status, likelihood of continued adherence, and the concurrent treatment of opportunistic infections (OIs). All patients with HIV infection and a CD4 count <200 cells/mm3 or an AIDS-defining illness should receive antiretroviral therapy. Controversy exists as to whether a patient admitted for the treatment of an opportunistic infection should begin antiretroviral therapy immediately, or whether this therapy should be deferred until after acute treatment of the OI. The potential detrimental effects of drug-drug interactions, the need for treatment interruptions, and drug-related toxicity between antiretrovirals and OI-specific therapy may support initiating HAART after control of an OI is achieved. Conversely, for some opportunistic infections, such as cryptosporidiosis, the use of HAART is essential for successful treatment of the infection.
An ongoing randomized controlled trial initiated within the Adult AIDS Clinical Trials Group (ACTG) comparing outcomes between patients who start HAART immediately after presentation with an acute OI and patients who start HAART at least 4 weeks after the OI has resolved should help identify the factors supporting early or delayed initiation of antiretrovirals (4).
Generally speaking, HAART can be administered by combining either a protease inhibitor (PI) or a nonnucleoside reverse transcriptase inhibitor (NNRTI) with 2 nucleoside reverse transcriptase inhibitors (NRTIs). There are currently more than 20 FDA-approved antiretrovirals. Frequent updates on the guidelines for the use of antiretroviral agents in HIV-infected adults are available at www.AIDSinfo.nih.gov, and a discussion of this topic is beyond the scope of this review.
Continuation of HAART in the Hospital
In most cases, every effort should be made to minimize interruption of HAART during a hospitalization. Although some investigators are examining the virologic and immunologic safety of interrupting HAART as a treatment strategy, there are few data on viral replication, CD4 cell count decline, and rate of acquisition of new mutations in hospitalized patients who have unexpected treatment interruptions (5). The long half-life of some antiretrovirals promotes the emergence of resistance once HAART is stopped. For example, once NNRTIs are stopped, subtherapeutic levels remain in the plasma and cells for several days. HIV then replicates in a milieu that may select for resistance mutations.
Because zidovudine is the only antiretroviral available in a parenteral preparation, it is often difficult to continue HAART when a patient cannot take medications by mouth. Drugs given by the enteral route in a hospitalized patient may also be poorly absorbed, and few data exist on the absorption of antiretrovirals administered through a gastrostomy or jejunostomy tube (6).
Prescribing HAART in the Hospital
Antiretroviral prescribing errors occur frequently in the hospitalized AIDS patient. The most common errors include overdosing or underdosing, missing components of multidrug regimens, or missing critical drug-drug interactions (7). Underdosing may lead to resistance, and overdosing contributes to increased toxicity. In one report, prescribing errors occurred in 12% of admissions in the post-HAART era (1998) compared with 2% of admissions in the pre-HAART era (1996) (7). The NRTIs, including didanosine, emtricitabine, lamivudine, stavudine, and zidovudine, require decreased dosing in renal insufficiency. Tenofovir is not recommended for use if the creatine clearance is less than 60 mL/minute. Dosage adjustments in hepatic disease are recommended for amprenavir, fosamprenavir, delavirdine, efavirenz, and nevirapine.
Immune Reconstitution Syndrome
The widespread use of HAART has produced sustained suppression of HIV replication and recovery of CD4 cell counts. It also became evident that HAART resulted in not only a numerical increase in CD4 cells, but also in a functional immune recovery (8-10). This improved T-cell response to antigens results in adequate protection against specific opportunistic infections, allowing for discontinuation of primary and secondary prophylaxis in HIV-infected patients. Immune reconstitution syndrome (IRS), an inflammatory syndrome, is recognized as a potential complication that can occur days to months after starting HAART. The onset of IRS is characterized by a paradoxical worsening of clinical or laboratory parameters despite a favorable response in CD4 cell counts and the suppression of viral replication (9,11,12). IRS has been reported to occur in 10–25% of patients who receive HAART and more commonly in those whose CD4 cell counts are <50 cells/mm3 at the start of HAART (9,11). It is postulated that the inflammatory response is triggered by the recognition of antigens associated with ongoing infection or recognition of persisting antigens associated with past (nonreplicating) infections. Mycobacterial antigens, frequently implicated in IRS, are responsible for about one third of cases. Other antigens associated with IRS include cytomegalovirus and hepatitis B and C (11). In most circumstances, with the management of IRS, HAART should be continued, while specific antimicrobial therapy and steroids should be considered (10).
Medical Conditions that Should Prompt HIV Screening
There are several medical conditions that should prompt screening for HIV infection. Generally, anyone presenting with a fever of unknown etiology who is sexually active or had a blood transfusion prior to 1985 should be screened for HIV infection. Symptoms consistent with acute retroviral syndrome (fever, sore throat, malaise, and skin rash) may be more commonly recognized by clinicians now than previously, and this remains a “golden opportunity” to intervene. Frequently, acute retroviral syndrome will be attributed to Epstein-Barr virus; however, caution should be used in the diagnosis of mononucleosis in those other than teenage populations. It is recommended that all persons presenting with any sexually transmitted disease, unexplained generalized lymphadenopathy, oral candidiasis, or tuberculosis should also be tested. Other conditions where HIV infection should be considered include enigmatic pneumonia, acute hepatitis B infection, herpes zoster infection (particularly in younger, seemingly immunocompetent individuals), idiopathic thrombocytopenic purpura, and nephropathy of unknown cause.
Drug Interactions
Drug interactions are an important consideration in the treatment of HIV infection. Interactions between HAART and other drugs used for the treatment or prophylaxis of opportunistic infections along with those used for the treatment of drug-induced endocrinopathies (hyperlipidemia, diabetes mellitus) are virtually unavoidable. Drug interactions occur either because of drug metabolism or absorption. The multiple metabolic pathways of some drugs make it difficult to predict the outcome of drug interactions. All protease inhibitors and non-nucleoside reverse transcriptase inhibitors are metabolized by the cytochrome P-450 enzyme system and each of these drugs may alter the metabolism of other antiretrovirals and concomitantly administered drugs (13,14). A decrease in trough plasma concentrations of the protease inhibitors to a level below the in vitro concentration required to inhibit replication of 50% of viral strains (IC50) may lead to development of resistance. Because nucleoside analogue reverse transcriptase inhibitors are primarily eliminated by the kidney, they do not interact with other drugs through the cytochrome P-450 system.
One noteworthy interaction that the clinician caring for HIV-infected patients should be aware of is the interaction of ribavirin with zidovudine. Ribavirin decreases the phosphorylation of zidovudine and stavudine in vitro, resulting in decreased concentrations of the active compound. HIV-infected patients who are coinfected with hepatitis C may be treated with regimens that include ribavirin, which may reduce the efficacy of zidovudine (15). Another important interaction is the effect of nevirapine or efavirenz on plasma methadone concentrations. Both drugs can decrease methadone plasma levels by 50%, and patients receiving chronic therapy may need increased methadone doses to prevent withdrawal symptoms (16).
Protease inhibitors are associated with numerous interactions including certain antiarrhythmics, sedatives, hypnotics, ergot derivatives, and several lipid-lowering agents (statins). Not only do protease inhibitors affect the metabolism of certain drugs, but also their own metabolism is altered by other inducers or inhibitors of cytochrome activity that can cause clinically important decreases in serum levels of protease inhibitors. One widely recognized interaction is that of rifampin, which may decrease levels of some protease inhibitors by 80%. The resulting low plasma concentrations may promote viral resistance and result in treatment failure. Patients being treated for tuberculosis, who are also receiving protease inhibitors should be treated with a four-drug regimen that includes rifabutin (at half dose) instead of rifampin. Updated guidelines for the use of rifabutin or rifampin in HIV-infected patients receiving antiretroviral agents have been reviewed recently (17).
Other potent inducers such as phenytoin, phenobarbital, and carbamazepine can cause similar reductions in serum levels of protease inhibitors. Azole antifungal drugs and macrolides also have important interactions that complicate both the treatment and prophylaxis of opportunistic infections.
Interactions that interfere with absorption can also affect plasma drug concentrations. For example, the absorption of fluconazole is unaffected by variations in gastric pH, while itraconazole and ketoconazole require an acidic environment for optimal absorption. The protease inhibitor, atazanavir, also requires a low pH for absorption and thus is contraindicated with the use of proton pump inhibitors; taking atazanavir with acidic beverages is not sufficient to overcome this (18).
New information about drug interactions becomes known on almost a daily basis in patients with HIV infection. The number of documented and theoretical interactions can become overwhelming to the clinician. Clinicians should suspect potential drug interactions in a patient who is failing therapy but who is adherent to HAART. Fortunately, there are extensive tables on Web sites (www.hivatis.org) and product information to aid in the recognition and management of drug interactions.
Complications of HAART
Diabetes mellitus, hyperlipidemias, lipodystrophy, and insulin resistance are among the many complex metabolic abnormalities attributable to the use of HAART. For the most part, these complications are managed conservatively and usually do not mandate the discontinuation of HAART. Pancreatitis, hepatic steatosis, and lactic acidosis are wellrecognized complications of NRTIs. These are usually more acute and may result in hospitalization and necessitate the discontinuation of medications. Cessation of the offending agent (didanosine [ddI], stavudine [d4T], and zalcitabine [ddC) usually results in resolution of pancreatitis, but the episode may limit use of these agents in the future. Hepatic steatosis and lactic acidosis are rare but life-threatening adverse effects associated with the mitochondrial toxicity seen with the NRTIs. Symptoms usually develop insidiously with nausea, vomiting, abdominal pain, weight loss, or dyspnea and can progress rapidly to fatal lactic acidosis. Hepatomegaly, ascites, elevated liver associated enzymes, and an increased anion gap with lactic acidemia are usually present (19,20). Discontinuation of antiretroivirals is imperative.
There is an accumulating body of evidence that suggests that HIV-infected patients receiving HAART may be at risk for accelerated coronary disease (21). In addition, some cohort studies have reported an increased incidence of myocardial infarction (MI) following the introduction of HAART and the risk for MI rose progressively with the number of years on antiretroviral therapy (22,23). However, it is important to note that many traditional risk factors for coronary artery disease contribute more substantially to the risk for a cardiovascular event than does HAART. Therefore, aggressive modification of primary cardiac risk factors is warranted.
Hypersensitivity Drug Reactions
Drug hypersensitivity reactions are life-threatening reactions that result in a systemic illness that usually includes fever and maculopapular rash accompanied by constitutional symptoms (fatigue, myalgias, and arthralgias), visceral involvement (lymphadenopathy, mucositis, pneumonitis, myocarditis, hepatitis, and interstitial nephritis), and hematologic abnormalities (eosinophilia) (24).
Abacavir, an NRTI, is a relatively new antiretroviral agent used in many HAART regimens. Abacavir is associated with a hypersensitivity reaction, which can be fatal if abacavir use is continued despite the reaction, or if re-challenge with the drug takes place after the reaction (25). The overall incidence of this reaction appears to be around 4% (25). Prior antiretroviral experience and being of African descent are associated with a nearly 40% reduction in the risk of this hypersensitivity reaction, while patients of white race are at a significantly greater risk. CD4 cell counts do not appear to be significantly related to abacavir hypersensitivity (26). The exact metabolite that is likely responsible for abacavir hypersensitivity is unknown.
The most common symptoms of abacavir hypersensitivity reaction are fever, rash, nausea, vomiting, and abdominal pain. Occasionally, respiratory symptoms will be present and can mimic influenza. However, gastrointestinal symptoms are the most prominent complaints after fever and rash and help to distinguish between influenza and abacavir hypersensitivity. More than 90% of hypersensitivity reactions occur during the first 6 weeks of treatment, with a median time to development of 8 days. A fever that develops within a few weeks after the initiation of therapy with abacavir may be due to causes other than hypersensitivity. One of the most common situations is the simultaneous initiation of treatment with other drugs, such as trimethoprimsulfamethxazole, efavirenz, or nevirapine, all of which are associated with a higher incidence of hypersensitivity than abacavir (27,28). Symptoms may be sudden and worsen over a few days if abacavir is continued. Symptoms tend to improve in 48 hours after abacavir is discontinued. Supportive therapy includes intravenous hydration and withdrawal of abacavir as well as all other antiretrovirals. Early in the use of this medication, 20% of patients who were re-challenged with the drug experienced unanticipated life-threatening events manifesting as an anaphylactic or immediate type hypersensitivity reaction. Hypotension, renal insufficiency, and bronchospasm have resulted in death. Rechallenge symptoms have been seen with the first dose (29). A discussion of the potential for this hypersensitivity is warranted when prescribing this agent. In the United States, a patient information card warning of this hypersensitivity reaction is distributed to the patient with each bottle of abacavir. Prednisone does not prevent the development of hypersensitivity reaction.
Symptoms of toxicity from TMP-SMX are more likely to occur in the HIV infected than in patients without HIV infection. Fever and rash can occur in up to 50% of HIV-infected patients. The rash can be treatment limiting or severe in up to 20% of HIV-infected patients who receive it. Life-threatening reactions may occur, including fatal Stevens Johnson-type exfoliative skin reactions. Most toxicity in HIV-infected patients appears to be related to metabolites of the sulfamethoxazole component and decreased levels of glutathione. There have been reports of severe systemic reactions that resemble anaphylaxis or septic shock occurring in HIV-infected patients who are re-challenged with TMP-SMX after experiencing toxicity within the previous 6–8 weeks (30).
The NNRTIf nevirapine and efavirenz can cause a delayed hypersensitivity reaction similar to that seen with abacavir. Cutaneous involvement is a prominent component of both nevirapine and efavirenz hypersensitivity reaction, with rash more likely to occur with the use of nevirapine. In addition, female patients have a higher propensity of developing Stevens-Johnson syndrome and symptomatic hepatic events from nevirapine (28,31).
Laboratory Abnormalities Related to Drugs
Hyperbilirubinemia and Atazanavir and Indinavir
Atazanavir, a protease inhibitor, is metabolized by the liver via CYP3A and also inhibits both CTP3A and UGT1A1. UGT1A1 is required for conjugation of bilirubin and inhibition of this enzyme results in elevated levels of unconjugated bilirubin. This effect is similar to what is observed in Gilbert’s syndrome. Asymptomatic indirect hyperbilirubemia may be seen in up to 60% of patients receiving atazanavir. Total bilirubin levels may rise to greater than 5 mg/dL, and more than 17% of patients may experience jaundice (18). Concurrent elevations in hepatic serum transaminases should not be attributed to atazanavir and alternative etiologies for these elevations should be sought. This hyperbilirubinemia is reversible upon discontinuation of the atazanavir.
Similarly, but to a lesser degree, asymptomatic unconjugated hyperbilirubinemia (>2 mg/dL) has been reported in up to 14% of patients treated with indinavir. Elevated serum transaminases were seen in less than 1%.
Renal Abnormalities and Indinavir
Several renal syndromes have been associated with indinavir use, ranging from obstructive uropathy and acute renal failure to asymptomatic pyuria. The range of clinical syndromes is a consequence of indinavir crystals aggregating within or irritating the urinary tract (32). Symptomatic nephrolithiasis (indinavir crystallization) has been reported to affect up to 12% (range, 5–35 %) of patients who receive indinavir, while up to 67% of patients will have asymptomatic crystalluria. The cumulative frequency of nephrolithiasis events increases with increasing exposure to indinavir. Therapy may be continued or interrupted for a few days. Adequate hydration is necessary with the administration of indinavir. Indinavir associated pyuria is frequently associated with interstitial nephritis or urothelial inflammation. Discontinuation of indinavir will lead to resolution of urine abnormalities.
Elevated Mean Corpuscular Volume (MCV) and NRTIs
Elevation of MCV or macrocytosis occurs in more than 90% of patients treated with zidovudine, but is not correlated with the development of anemia. Macrocytosis (MCV values exceeding 110/fl) develops within 2 weeks following the initiation of zidovudine therapy, and its presence can be used as a marker for medical adherence. When anemia does occur it is associated with a dose related bone marrow toxicity manifested as a macrocytic anemia. Serum B12 and folate levels are normal. Stavudine use is also associated with macrocytosis, in non-zidovudine-containing regimens (33).
Drug Screens and Efavirenz
The use of efavirenz, a potent non-nucleoside reverse transcriptase inhibitor, can cause a false-positive urine drug screen for cannabinoid. Efavirenz does not bind to cannabinoid receptors. The false-positive test results are specific to the assay kit used (34).
Evaluation of the AIDS Patient with Fever
Fever is a common symptom in HIV-infected patients, the etiology of which can be identified in more than 80% of cases (35,36). The AIDS patient with fever poses a considerable challenge given that the expanded differential may include a wide range of OIs. The CD4 cell count remains a valuable predictor of risk for infection. Patients with CD4 cell counts greater than 500 cells/mm3 should be evaluated as if immunocompetent. Patients with CD4 cell counts between 200 and 500 cells/mm3 are at increased risk for upper and lower bacterial respiratory infections, tuberculosis, and sinusitis, but overall their risk for opportunistic infection is not increased. In patients with CD4 counts less than 200 cells/mm3, Pneumocystis jiroveci pneumonia, formerly known as Pneumocystis carinii pneumonia, is the most common cause of fever in those not receiving primary prophylaxis. As the CD4 cell count decreases below 100 cells/mm3, the risk for disseminated MAC, toxoplasmosis, CMV, disseminated fungal infections, and lymphoma should be considered possible causes of fever. HIV itself is usually not the cause of fever in patients with advanced immunosuppression (37).
In patients with CD4 counts >200 cells/mm3, the clinician can usually construct a laboratory and radiographic evaluation guided by symptoms, while in patients with severe immunosuppression a broader evaluation is required. A serum cryptococcal antigen should be obtained, as it has high sensitivity and specificity for both systemic disease as well as meningitis (38). Bacterial, mycobacterial, and fungal isolator blood cultures should be performed, as well as a urine culture, despite lack of symptoms. Urine AFB cultures can be added if there is a suspicion for tuberculosis. Sputum should be evaluated with gram stain, AFB smear, and culture, as well as PCP direct fluorescent antibody. If diarrhea is present, stool studies should include bacterial culture, ova and parasites evaluation, an assay for C. difficile, and Cryptosporidia and Giardia stool antigen assays. A serum LDH may be elevated in PCP, disseminated histoplasmosis, or lymphoma. A serum CMV antigen may be useful in the patient with fever and diarrhea, hepatitis, or retinitis.
A chest radiograph should be performed in all febrile AIDS patients. Chest films may be normal in 5–10% of HIV-infected patients with tuberculosis (TB). The typical radiographic appearance of Pneumocystis jiroveci pneumonia is a bilateral interstitial pattern characterized by reticular or ground-glass opacities. However, normal chest radiographs may be seen in one third of AIDS patients with active PCP. High-resolution computed tomography (HRCT) of the chest should be obtained if there is still a clinical suspicion for Pneumocystis. HRCT has been shown in several reports to have a 100% negative predictive value in the evaluation for PCP (39,40).
A lumbar puncture should be performed if the patient is symptomatic or if the serum cryptococcal antigen is reactive. A bone marrow biopsy and culture is also useful particularly in the evaluation of the patient with cytopenias. Bacterial, fungal, and AFB cultures may yield disseminated mycobacterial or fungal disease. Histopathologic evaluation may reveal granulomas with organisms or lymphoma. Bronchoscopy may be pursued in cases of high suspicion for TB or PCP.
Guidelines for the management of opportunistic infections associated with human immunodeficiency virus are available at www.AIDSinfo.nih.gov.
Evaluation of the AIDS Patient with Focal Neurological Disease
Toxoplasma encephalitis (TE) may be distinguished from primary CNS lymphoma without a brain biopsy. TE is caused by reactivation of latent infection by the protozoan Toxoplasma gondii. Almost 90% of patients have CD4 counts less than 200 cells/mm3 and 75% have CD4 counts less than 100 cells/mm3. Serum anti-Toxoplasma IgG antibodies are detected in more than 90% of patients with TE. Lesions on CT or MRI (a more sensitive modality) are typically multiple ring-enhancing lesions with a predilection for the basal ganglia. An emipiric trial of therapy is recommended, and a response confirms a diagnosis in the patient who has a positive Toxoplasma antibody and is not receiving trimethoprim-sulfamethoxazole prophylaxis. A lumbar puncture in this setting is not necessary and maybe ill advised if cerebral edema is present (Figure 1, page 24).
Primary CNS lymphoma (PCNSL) has a similar radiographic appearance as TE. Solitary lesions are more frequent in PCNSL. Positron emission tomography (PET) and single photon emission CT (SPECT) are useful adjunctive imaging modalities as they are positive in PCNSL due to the increased metabolic activity of the tumor. Cytologic analysis of the CSF may show lymphomatous cells. Epstein-Barr virus (EBV) DNA is uniformly detected in PCNSL in AIDS patients and detection of EBV DNA by PCR on the CSF has a sensitivity of 90–100% and a specificity of 87–98% for the diagnosis of PCNSL (41,42). Combining SPECT imaging and EBV PCR provides 100% sensitivity and 100% negative predictive value in the evaluation of AIDS-related primary CNS lymphoma (43), obviating the need for brain biopsy.
Progressive multifocal leukoencephalopathy (PML) is characterized radiographically by multiple and bilateral hypodense lesions of the white matter without mass effect or enhancement on CT. MRI demonstrates areas of hypointensity on T1-weighted images and increased intensity on T2-weighted images. JC virus DNA can be detected by PCR of CSF or brain tissue with sensitivity of approximately 80% and specificity of 95%. Because of the high positive predictive value of a positive PCR, a patient with AIDS who also has a compatible MRI can be diagnosed with PML (44,45).
Other focal neurologic disease seen in AIDS patients includes cryptococcomas, tuberculomas, CMV encephalitis, neurosyphilis, Nocardia and Aspergillus infection, and bacterial brain abscesses (46).
Conclusion
As survival of the HIV-infected population improves, more patients may require hospitalization for HAART treatment failures or complications attributed to antiretroviral therapy. The hospitalist should be familiar with the complications of antiretroviral agents, the interactions between HAART and medications used to treat opportunistic infections, and medical conditions induced by HAART. Evaluation of the HIV-infected patient presenting with fever can be based on the CD4 cell count, which predicts risk for opportunistic infections. Finally, using combined diagnostic approaches along with modern imaging and laboratory assays may preclude the need for more invasive procedures in the HIV-infected hospitalized patient.
Dr. Decker may be reached at [email protected].
References
- Torres RA, Barr M. Impact of combination therapy for HIV infection on inpatient census. N Engl J Med. 1997;336:1531-2.
- Fleishman JA, Hellinger FJ. Trends in HIV-related inpatient admissions from 1993 to 1997: a seven-state study. J Acquir Immune Defic Syndr. 2001;28:73-80.
- Fleishman JA, Hellinger FH. Recent trends in HIV-related inpatient admissions 1996-2000: a 7-state study. J Acquir Immune Defic Syndr. 2003;34:102-10.
- Powderly WG. Should patients with an acute opportunistic infection receive antiretroviral therapy immediately? Advanced Studies in Medicine. 2005;5:S111-S116.
- Fagard C, Oxenius A, Gunthard H, et al. A prospective trial of structured treatment interruptions in human immunodeficiency virus infection. Arch Intern Med. 2003;163:1220-6.
- Soni N, Pozniak A. Continuing HIV therapy in the ICU. Crit Care. 2001;5:247-8.
- Purdy BD, Raymond AM, Lesar TS. Antiretroviral prescribing errors in hospitalized patients. Ann Pharmacother. 2000;34:833-8.
- Autran B, Carcelain G, Li TS, et al. Positive effects of combined antiretroviral therapy on CD4+ T cell homeostasis and function in advanced HIV disease. Science. 1997;277:112-6.
- Cooney EL. Clinical indicators of immune restoration following highly active antiretroviral therapy. Clin Infect Dis. 2002;34:224-33.
- Hirsch HH, Kaufmann G, Sendi P, BaĴegay M. Immune reconstitution in HIV-infected patients. Clin Infect Dis. 2004;38:1159-66.
- Cheng VC, Yuen KY, Chan WM, Wong SS, Ma ES, Chan RM. Immunorestitution disease involving the innate and adaptive response. Clin Infect Dis. 2000;30:882-92.
- Fishman JE, Saraf-Lavi E, Narita M, Hollender ES, Ramsinghani R, Ashkin D. Pulmonary tuberculosis in AIDS patients: transient chest radiographic worsening after initiation of antiretroviral therapy. AJR Am J Roentgenol. 2000;174:43-9.
- Piscitelli SC, Gallicano KD. Interactions among drugs for HIV and opportunistic infections. N Engl J Med. 2001;344:984-96.
- Barry M, Mulcahy F, Merry C, Gibbons S, Back D. Pharmacokinetics and potential interactions amongst antiretroviral agents used to treat patients with HIV infection. Clin Pharmacokinet. 1999;36:289-304.
- Sim SM, Hoggard PG, Sales SD, Phiboonbanakit D, Hart CA, Back DJ. Effect of ribavirin on zidovudine efficacy and toxicity in vitro: a concentration-dependent interaction. AIDS Res Hum Retroviruses. 1998;14:1661-7.
- Clarke SM, Mulcahy FM, Tjia J, et al. The pharmacokinetics of methadone in HIV-positive patients receiving the non-nucleoside reverse transcriptase inhibitor efavirenz. Br J Clin Pharmacol. 2001;51:213-7.
- Centers for Disease Control and Prevention. Updated guidelines for the use of rifabutin or rifampin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors. Morb Mortal Wkly Rep. 2000;49:185-9.
- Havlir DV, O’Marro SD. Atazanavir: new option for treatment of HIV infection. Clin Infect Dis. 2004;38:1599-604.
- Sheng WH, Hsieh SM, Lee SC, et al. Fatal lactic acidosis associated with highly active antiretroviral therapy in patients with advanced human immunodeficiency virus infection in Taiwan. Int J STD AIDS. 2004;15:249-53.
- Herman JS, Easterbrook PJ. The metabolic toxicities of antiretroviral therapy. Int J STD AIDS. 2001;12:555-62;quiz 563-4.
- Behrens G, Schmidt H, Meyer D, Stoll M, Schmidt RE. Vascular complications associated with use of HIV protease inhibitors. Lancet. 1998;351:1958.
- Klein D, Hurley LB, Sidney S. Cardiovascular Disease and HIV Infection. N Engl J Med. 2003;349:1869-70; author reply 1869-70.
- Friis-Moller N, Sabin CA, Weber R, et al. Combination antiretroviral therapy and the risk of myocardial infarction. N Engl J Med. 2003;349:1993-2003.
- Anderson JA, Adkinson NF Jr. Allergic reactions to drugs and biologic agents. JAMA. 1987;258:2891-9.
- Hewitt RG. Abacavir hypersensitivity reaction. Clin Infect Dis. 2002;34:1137-42.
- Hetherington S, Hughes AR, Mosteller M, et al. Genetic variations in HLA-B region and hypersensitivity reactions to abacavir. Lancet. 2002;359:1121-2.
- Bossi P, Colin D, Bricaire F, Caumes E. Hypersensitivity syndrome associated with efavirenz therapy. Clin Infect Dis. 2000;30:227-8.
- Bourezane Y, Salard D, Hoen B, Vandel S, Drobacheff C, Laurent R. DRESS (drug rash with eosinophilia and systemic symptoms) syndrome associated with nevirapine therapy. Clin Infect Dis. 1998;27:1321-2.
- Walensky RP, Goldberg JH, Daily JP. Anaphylaxis after rechallenge with abacavir. AIDS. 1999;13:999-1000.
- Martin GJ, Paparello SF, Decker CF. A severe systemic reaction to trimethoprim-sulfamethoxazole in a patient infected with the human immunodeficiency virus. Clin Infect Dis. 1993;16:175-6.
- Bersoff-Matcha SJ, Miller WC, Aberg JA, et al. Sex differences in nevirapine rash. Clin Infect Dis. 2001;32:124-9.
- Kopp JB, Falloon J, Filie A, et al. Indinavir-associated interstitial nephritis and urothelial inflammation: clinical and cytologic findings. Clin Infect Dis. 2002;34:1122-8.
- Geene D, Sudre P, Anwar D, Goehring C, Saaidia A, Hirschel B. Causes of macrocytosis in HIV-infected patients not treated with zidovudine. Swiss HIV Cohort Study. J Infect. 2000;40:160-3.
- Gottesman L. Sustiva may cause false positive on marijuana test. WORLD. 1999:7.
- Sepkowitz KA, Telzak EE, Carrow M, Armstrong D. Fever among outpatients with advanced human immunodeficiency virus infection. Arch Intern Med. 1993;153: 1909-12.
- Barat LM, Gunn JE, Steger KA, Perkins CJ, Craven DE. Causes of fever in patients infected with human immunodeficiency virus who were admitted to Boston City Hospital. Clin Infect Dis. 1996;23:320-8.
- Sepkowitz KA. FUO and AIDS. Curr Clin Top Infect Dis. 1999;19:1-15.
- Asawavichienjinda T, Sitthi-Amorn C, Tanyanont V. Serum cyrptococcal antigen: diagnostic value in the diagnosis of AIDS-related cryptococcal meningitis. J Med Assoc Thai. 1999;82:65-71.
- Richards PJ, Riddell L, Reznek RH, Armstrong P, Pinching AJ, Parkin JM. High resolution computed tomography in HIV patients with suspected Pneumocystis carinii pneumonia and a normal chest radiograph. Clin Radiol. 1996;51:689-93.
- Gruden JF, Huang L, Turner J, et al. High-resolution CT in the evaluation of clinically suspected Pneumocystis carinii pneumonia in AIDS patients with normal, equivocal, or nonspecific radiographic findings. AJR Am J Roentgenol. 1997;169:967-75.
- MacMahon EM, Glass JD, Hayward SD, et al. Association of Epstein-Barr virus with primary central nervous system lymphoma in AIDS. AIDS Res Hum Retroviruses. 1992;8:740-2.
- Rao CR, Jain K, Bhatia K, Laksmaiah KC, Shankar SK. Association of primary central nervous system lymphomas with the Epstein-Barr virus. Neurol India. 2003;51:237-40.
- Antinori A, De Rossi G, Ammassari A, et al. Value of combined approach with thallium-201 single-photon emission computed tomography and Epstein-Barr virus DNA polymerase chain reaction in CSF for the diagnosis of AIDS-related primary CNS lymphoma. J Clin Oncol. 1999;17:554-60.
- Post MJ, Yiannoutsos C, Simpson D, et al. Progressive multifocal leukoencephalopathy in AIDS: are there any MR findings useful to patient management and predictive of patient survival? AIDS Clinical Trials Group, 243 Team. AJNR Am J Neuroradiol. 1999;20:1896-906.
- Weber T. Cerebrospinal fluid analysis for the diagnosis of human immunodeficiency virus-related neurologic diseases. Semin Neurol. 1999;19:223-33.
- Skiest DJ. Focal neurological disease in patients with acquired immunodeficiency syndrome. Clin Infect Dis. 2002;34:103-15.
The opinions and assertions contained herein are those of the authors and are not to be construed as official or as reflecting the views of the Department of Defense, the Department of the Navy, or the naval services at large.
Introduction
An estimated 850,000 to 950,000 persons in the United States are living with human immunodeficiency virus (HIV), 280,000 of whom are unaware of their infection and another 43,000 of whom meet the definition of acquired immunodeficiency syndrome (AIDS) (www.cdc.gov). The use of highly active antiretroviral therapy (HAART) has produced significant declines in morbidity and mortality from AIDS. Compared with the first 2 decades of the HIV pandemic, the number of HIV-related hospital admissions has declined. However, recently, this rate of decline has markedly slowed (1-3). The reasons for this plateau are many including a steady number of admissions for complications related to HAART, treatment failures, and the overall increased prevalence of HIV infection. Not only will HIV-infected patients still frequently require admission to the hospital, but the complexity of their inpatient care will continue to increase with the advancements in multiple drug regimens, aging of the HIV-infected population, and the interaction of HIV infection with medical comorbidities, many of which are attributable to HAART.
The hospitalist caring for the inpatient with AIDS is presented with several challenges including not only the diagnosis and management of opportunistic infections, but also the complications of HAART. In this article we review the guidelines for the initiation and continuation of HAART in the hospital, review important clinical complications of antiretroviral therapy, and review conditions that may result in the hospitalization of AIDS patients.
Initiation of HAART in the Hospital
In those who do not have access to health care, the initial diagnosis of HIV infection frequently occurs during a hospitalization for an AIDS-defining illness. Initiation of antiretrovirals is contingent on several issues, including CD4 count, viral load, clinical status, likelihood of continued adherence, and the concurrent treatment of opportunistic infections (OIs). All patients with HIV infection and a CD4 count <200 cells/mm3 or an AIDS-defining illness should receive antiretroviral therapy. Controversy exists as to whether a patient admitted for the treatment of an opportunistic infection should begin antiretroviral therapy immediately, or whether this therapy should be deferred until after acute treatment of the OI. The potential detrimental effects of drug-drug interactions, the need for treatment interruptions, and drug-related toxicity between antiretrovirals and OI-specific therapy may support initiating HAART after control of an OI is achieved. Conversely, for some opportunistic infections, such as cryptosporidiosis, the use of HAART is essential for successful treatment of the infection.
An ongoing randomized controlled trial initiated within the Adult AIDS Clinical Trials Group (ACTG) comparing outcomes between patients who start HAART immediately after presentation with an acute OI and patients who start HAART at least 4 weeks after the OI has resolved should help identify the factors supporting early or delayed initiation of antiretrovirals (4).
Generally speaking, HAART can be administered by combining either a protease inhibitor (PI) or a nonnucleoside reverse transcriptase inhibitor (NNRTI) with 2 nucleoside reverse transcriptase inhibitors (NRTIs). There are currently more than 20 FDA-approved antiretrovirals. Frequent updates on the guidelines for the use of antiretroviral agents in HIV-infected adults are available at www.AIDSinfo.nih.gov, and a discussion of this topic is beyond the scope of this review.
Continuation of HAART in the Hospital
In most cases, every effort should be made to minimize interruption of HAART during a hospitalization. Although some investigators are examining the virologic and immunologic safety of interrupting HAART as a treatment strategy, there are few data on viral replication, CD4 cell count decline, and rate of acquisition of new mutations in hospitalized patients who have unexpected treatment interruptions (5). The long half-life of some antiretrovirals promotes the emergence of resistance once HAART is stopped. For example, once NNRTIs are stopped, subtherapeutic levels remain in the plasma and cells for several days. HIV then replicates in a milieu that may select for resistance mutations.
Because zidovudine is the only antiretroviral available in a parenteral preparation, it is often difficult to continue HAART when a patient cannot take medications by mouth. Drugs given by the enteral route in a hospitalized patient may also be poorly absorbed, and few data exist on the absorption of antiretrovirals administered through a gastrostomy or jejunostomy tube (6).
Prescribing HAART in the Hospital
Antiretroviral prescribing errors occur frequently in the hospitalized AIDS patient. The most common errors include overdosing or underdosing, missing components of multidrug regimens, or missing critical drug-drug interactions (7). Underdosing may lead to resistance, and overdosing contributes to increased toxicity. In one report, prescribing errors occurred in 12% of admissions in the post-HAART era (1998) compared with 2% of admissions in the pre-HAART era (1996) (7). The NRTIs, including didanosine, emtricitabine, lamivudine, stavudine, and zidovudine, require decreased dosing in renal insufficiency. Tenofovir is not recommended for use if the creatine clearance is less than 60 mL/minute. Dosage adjustments in hepatic disease are recommended for amprenavir, fosamprenavir, delavirdine, efavirenz, and nevirapine.
Immune Reconstitution Syndrome
The widespread use of HAART has produced sustained suppression of HIV replication and recovery of CD4 cell counts. It also became evident that HAART resulted in not only a numerical increase in CD4 cells, but also in a functional immune recovery (8-10). This improved T-cell response to antigens results in adequate protection against specific opportunistic infections, allowing for discontinuation of primary and secondary prophylaxis in HIV-infected patients. Immune reconstitution syndrome (IRS), an inflammatory syndrome, is recognized as a potential complication that can occur days to months after starting HAART. The onset of IRS is characterized by a paradoxical worsening of clinical or laboratory parameters despite a favorable response in CD4 cell counts and the suppression of viral replication (9,11,12). IRS has been reported to occur in 10–25% of patients who receive HAART and more commonly in those whose CD4 cell counts are <50 cells/mm3 at the start of HAART (9,11). It is postulated that the inflammatory response is triggered by the recognition of antigens associated with ongoing infection or recognition of persisting antigens associated with past (nonreplicating) infections. Mycobacterial antigens, frequently implicated in IRS, are responsible for about one third of cases. Other antigens associated with IRS include cytomegalovirus and hepatitis B and C (11). In most circumstances, with the management of IRS, HAART should be continued, while specific antimicrobial therapy and steroids should be considered (10).
Medical Conditions that Should Prompt HIV Screening
There are several medical conditions that should prompt screening for HIV infection. Generally, anyone presenting with a fever of unknown etiology who is sexually active or had a blood transfusion prior to 1985 should be screened for HIV infection. Symptoms consistent with acute retroviral syndrome (fever, sore throat, malaise, and skin rash) may be more commonly recognized by clinicians now than previously, and this remains a “golden opportunity” to intervene. Frequently, acute retroviral syndrome will be attributed to Epstein-Barr virus; however, caution should be used in the diagnosis of mononucleosis in those other than teenage populations. It is recommended that all persons presenting with any sexually transmitted disease, unexplained generalized lymphadenopathy, oral candidiasis, or tuberculosis should also be tested. Other conditions where HIV infection should be considered include enigmatic pneumonia, acute hepatitis B infection, herpes zoster infection (particularly in younger, seemingly immunocompetent individuals), idiopathic thrombocytopenic purpura, and nephropathy of unknown cause.
Drug Interactions
Drug interactions are an important consideration in the treatment of HIV infection. Interactions between HAART and other drugs used for the treatment or prophylaxis of opportunistic infections along with those used for the treatment of drug-induced endocrinopathies (hyperlipidemia, diabetes mellitus) are virtually unavoidable. Drug interactions occur either because of drug metabolism or absorption. The multiple metabolic pathways of some drugs make it difficult to predict the outcome of drug interactions. All protease inhibitors and non-nucleoside reverse transcriptase inhibitors are metabolized by the cytochrome P-450 enzyme system and each of these drugs may alter the metabolism of other antiretrovirals and concomitantly administered drugs (13,14). A decrease in trough plasma concentrations of the protease inhibitors to a level below the in vitro concentration required to inhibit replication of 50% of viral strains (IC50) may lead to development of resistance. Because nucleoside analogue reverse transcriptase inhibitors are primarily eliminated by the kidney, they do not interact with other drugs through the cytochrome P-450 system.
One noteworthy interaction that the clinician caring for HIV-infected patients should be aware of is the interaction of ribavirin with zidovudine. Ribavirin decreases the phosphorylation of zidovudine and stavudine in vitro, resulting in decreased concentrations of the active compound. HIV-infected patients who are coinfected with hepatitis C may be treated with regimens that include ribavirin, which may reduce the efficacy of zidovudine (15). Another important interaction is the effect of nevirapine or efavirenz on plasma methadone concentrations. Both drugs can decrease methadone plasma levels by 50%, and patients receiving chronic therapy may need increased methadone doses to prevent withdrawal symptoms (16).
Protease inhibitors are associated with numerous interactions including certain antiarrhythmics, sedatives, hypnotics, ergot derivatives, and several lipid-lowering agents (statins). Not only do protease inhibitors affect the metabolism of certain drugs, but also their own metabolism is altered by other inducers or inhibitors of cytochrome activity that can cause clinically important decreases in serum levels of protease inhibitors. One widely recognized interaction is that of rifampin, which may decrease levels of some protease inhibitors by 80%. The resulting low plasma concentrations may promote viral resistance and result in treatment failure. Patients being treated for tuberculosis, who are also receiving protease inhibitors should be treated with a four-drug regimen that includes rifabutin (at half dose) instead of rifampin. Updated guidelines for the use of rifabutin or rifampin in HIV-infected patients receiving antiretroviral agents have been reviewed recently (17).
Other potent inducers such as phenytoin, phenobarbital, and carbamazepine can cause similar reductions in serum levels of protease inhibitors. Azole antifungal drugs and macrolides also have important interactions that complicate both the treatment and prophylaxis of opportunistic infections.
Interactions that interfere with absorption can also affect plasma drug concentrations. For example, the absorption of fluconazole is unaffected by variations in gastric pH, while itraconazole and ketoconazole require an acidic environment for optimal absorption. The protease inhibitor, atazanavir, also requires a low pH for absorption and thus is contraindicated with the use of proton pump inhibitors; taking atazanavir with acidic beverages is not sufficient to overcome this (18).
New information about drug interactions becomes known on almost a daily basis in patients with HIV infection. The number of documented and theoretical interactions can become overwhelming to the clinician. Clinicians should suspect potential drug interactions in a patient who is failing therapy but who is adherent to HAART. Fortunately, there are extensive tables on Web sites (www.hivatis.org) and product information to aid in the recognition and management of drug interactions.
Complications of HAART
Diabetes mellitus, hyperlipidemias, lipodystrophy, and insulin resistance are among the many complex metabolic abnormalities attributable to the use of HAART. For the most part, these complications are managed conservatively and usually do not mandate the discontinuation of HAART. Pancreatitis, hepatic steatosis, and lactic acidosis are wellrecognized complications of NRTIs. These are usually more acute and may result in hospitalization and necessitate the discontinuation of medications. Cessation of the offending agent (didanosine [ddI], stavudine [d4T], and zalcitabine [ddC) usually results in resolution of pancreatitis, but the episode may limit use of these agents in the future. Hepatic steatosis and lactic acidosis are rare but life-threatening adverse effects associated with the mitochondrial toxicity seen with the NRTIs. Symptoms usually develop insidiously with nausea, vomiting, abdominal pain, weight loss, or dyspnea and can progress rapidly to fatal lactic acidosis. Hepatomegaly, ascites, elevated liver associated enzymes, and an increased anion gap with lactic acidemia are usually present (19,20). Discontinuation of antiretroivirals is imperative.
There is an accumulating body of evidence that suggests that HIV-infected patients receiving HAART may be at risk for accelerated coronary disease (21). In addition, some cohort studies have reported an increased incidence of myocardial infarction (MI) following the introduction of HAART and the risk for MI rose progressively with the number of years on antiretroviral therapy (22,23). However, it is important to note that many traditional risk factors for coronary artery disease contribute more substantially to the risk for a cardiovascular event than does HAART. Therefore, aggressive modification of primary cardiac risk factors is warranted.
Hypersensitivity Drug Reactions
Drug hypersensitivity reactions are life-threatening reactions that result in a systemic illness that usually includes fever and maculopapular rash accompanied by constitutional symptoms (fatigue, myalgias, and arthralgias), visceral involvement (lymphadenopathy, mucositis, pneumonitis, myocarditis, hepatitis, and interstitial nephritis), and hematologic abnormalities (eosinophilia) (24).
Abacavir, an NRTI, is a relatively new antiretroviral agent used in many HAART regimens. Abacavir is associated with a hypersensitivity reaction, which can be fatal if abacavir use is continued despite the reaction, or if re-challenge with the drug takes place after the reaction (25). The overall incidence of this reaction appears to be around 4% (25). Prior antiretroviral experience and being of African descent are associated with a nearly 40% reduction in the risk of this hypersensitivity reaction, while patients of white race are at a significantly greater risk. CD4 cell counts do not appear to be significantly related to abacavir hypersensitivity (26). The exact metabolite that is likely responsible for abacavir hypersensitivity is unknown.
The most common symptoms of abacavir hypersensitivity reaction are fever, rash, nausea, vomiting, and abdominal pain. Occasionally, respiratory symptoms will be present and can mimic influenza. However, gastrointestinal symptoms are the most prominent complaints after fever and rash and help to distinguish between influenza and abacavir hypersensitivity. More than 90% of hypersensitivity reactions occur during the first 6 weeks of treatment, with a median time to development of 8 days. A fever that develops within a few weeks after the initiation of therapy with abacavir may be due to causes other than hypersensitivity. One of the most common situations is the simultaneous initiation of treatment with other drugs, such as trimethoprimsulfamethxazole, efavirenz, or nevirapine, all of which are associated with a higher incidence of hypersensitivity than abacavir (27,28). Symptoms may be sudden and worsen over a few days if abacavir is continued. Symptoms tend to improve in 48 hours after abacavir is discontinued. Supportive therapy includes intravenous hydration and withdrawal of abacavir as well as all other antiretrovirals. Early in the use of this medication, 20% of patients who were re-challenged with the drug experienced unanticipated life-threatening events manifesting as an anaphylactic or immediate type hypersensitivity reaction. Hypotension, renal insufficiency, and bronchospasm have resulted in death. Rechallenge symptoms have been seen with the first dose (29). A discussion of the potential for this hypersensitivity is warranted when prescribing this agent. In the United States, a patient information card warning of this hypersensitivity reaction is distributed to the patient with each bottle of abacavir. Prednisone does not prevent the development of hypersensitivity reaction.
Symptoms of toxicity from TMP-SMX are more likely to occur in the HIV infected than in patients without HIV infection. Fever and rash can occur in up to 50% of HIV-infected patients. The rash can be treatment limiting or severe in up to 20% of HIV-infected patients who receive it. Life-threatening reactions may occur, including fatal Stevens Johnson-type exfoliative skin reactions. Most toxicity in HIV-infected patients appears to be related to metabolites of the sulfamethoxazole component and decreased levels of glutathione. There have been reports of severe systemic reactions that resemble anaphylaxis or septic shock occurring in HIV-infected patients who are re-challenged with TMP-SMX after experiencing toxicity within the previous 6–8 weeks (30).
The NNRTIf nevirapine and efavirenz can cause a delayed hypersensitivity reaction similar to that seen with abacavir. Cutaneous involvement is a prominent component of both nevirapine and efavirenz hypersensitivity reaction, with rash more likely to occur with the use of nevirapine. In addition, female patients have a higher propensity of developing Stevens-Johnson syndrome and symptomatic hepatic events from nevirapine (28,31).
Laboratory Abnormalities Related to Drugs
Hyperbilirubinemia and Atazanavir and Indinavir
Atazanavir, a protease inhibitor, is metabolized by the liver via CYP3A and also inhibits both CTP3A and UGT1A1. UGT1A1 is required for conjugation of bilirubin and inhibition of this enzyme results in elevated levels of unconjugated bilirubin. This effect is similar to what is observed in Gilbert’s syndrome. Asymptomatic indirect hyperbilirubemia may be seen in up to 60% of patients receiving atazanavir. Total bilirubin levels may rise to greater than 5 mg/dL, and more than 17% of patients may experience jaundice (18). Concurrent elevations in hepatic serum transaminases should not be attributed to atazanavir and alternative etiologies for these elevations should be sought. This hyperbilirubinemia is reversible upon discontinuation of the atazanavir.
Similarly, but to a lesser degree, asymptomatic unconjugated hyperbilirubinemia (>2 mg/dL) has been reported in up to 14% of patients treated with indinavir. Elevated serum transaminases were seen in less than 1%.
Renal Abnormalities and Indinavir
Several renal syndromes have been associated with indinavir use, ranging from obstructive uropathy and acute renal failure to asymptomatic pyuria. The range of clinical syndromes is a consequence of indinavir crystals aggregating within or irritating the urinary tract (32). Symptomatic nephrolithiasis (indinavir crystallization) has been reported to affect up to 12% (range, 5–35 %) of patients who receive indinavir, while up to 67% of patients will have asymptomatic crystalluria. The cumulative frequency of nephrolithiasis events increases with increasing exposure to indinavir. Therapy may be continued or interrupted for a few days. Adequate hydration is necessary with the administration of indinavir. Indinavir associated pyuria is frequently associated with interstitial nephritis or urothelial inflammation. Discontinuation of indinavir will lead to resolution of urine abnormalities.
Elevated Mean Corpuscular Volume (MCV) and NRTIs
Elevation of MCV or macrocytosis occurs in more than 90% of patients treated with zidovudine, but is not correlated with the development of anemia. Macrocytosis (MCV values exceeding 110/fl) develops within 2 weeks following the initiation of zidovudine therapy, and its presence can be used as a marker for medical adherence. When anemia does occur it is associated with a dose related bone marrow toxicity manifested as a macrocytic anemia. Serum B12 and folate levels are normal. Stavudine use is also associated with macrocytosis, in non-zidovudine-containing regimens (33).
Drug Screens and Efavirenz
The use of efavirenz, a potent non-nucleoside reverse transcriptase inhibitor, can cause a false-positive urine drug screen for cannabinoid. Efavirenz does not bind to cannabinoid receptors. The false-positive test results are specific to the assay kit used (34).
Evaluation of the AIDS Patient with Fever
Fever is a common symptom in HIV-infected patients, the etiology of which can be identified in more than 80% of cases (35,36). The AIDS patient with fever poses a considerable challenge given that the expanded differential may include a wide range of OIs. The CD4 cell count remains a valuable predictor of risk for infection. Patients with CD4 cell counts greater than 500 cells/mm3 should be evaluated as if immunocompetent. Patients with CD4 cell counts between 200 and 500 cells/mm3 are at increased risk for upper and lower bacterial respiratory infections, tuberculosis, and sinusitis, but overall their risk for opportunistic infection is not increased. In patients with CD4 counts less than 200 cells/mm3, Pneumocystis jiroveci pneumonia, formerly known as Pneumocystis carinii pneumonia, is the most common cause of fever in those not receiving primary prophylaxis. As the CD4 cell count decreases below 100 cells/mm3, the risk for disseminated MAC, toxoplasmosis, CMV, disseminated fungal infections, and lymphoma should be considered possible causes of fever. HIV itself is usually not the cause of fever in patients with advanced immunosuppression (37).
In patients with CD4 counts >200 cells/mm3, the clinician can usually construct a laboratory and radiographic evaluation guided by symptoms, while in patients with severe immunosuppression a broader evaluation is required. A serum cryptococcal antigen should be obtained, as it has high sensitivity and specificity for both systemic disease as well as meningitis (38). Bacterial, mycobacterial, and fungal isolator blood cultures should be performed, as well as a urine culture, despite lack of symptoms. Urine AFB cultures can be added if there is a suspicion for tuberculosis. Sputum should be evaluated with gram stain, AFB smear, and culture, as well as PCP direct fluorescent antibody. If diarrhea is present, stool studies should include bacterial culture, ova and parasites evaluation, an assay for C. difficile, and Cryptosporidia and Giardia stool antigen assays. A serum LDH may be elevated in PCP, disseminated histoplasmosis, or lymphoma. A serum CMV antigen may be useful in the patient with fever and diarrhea, hepatitis, or retinitis.
A chest radiograph should be performed in all febrile AIDS patients. Chest films may be normal in 5–10% of HIV-infected patients with tuberculosis (TB). The typical radiographic appearance of Pneumocystis jiroveci pneumonia is a bilateral interstitial pattern characterized by reticular or ground-glass opacities. However, normal chest radiographs may be seen in one third of AIDS patients with active PCP. High-resolution computed tomography (HRCT) of the chest should be obtained if there is still a clinical suspicion for Pneumocystis. HRCT has been shown in several reports to have a 100% negative predictive value in the evaluation for PCP (39,40).
A lumbar puncture should be performed if the patient is symptomatic or if the serum cryptococcal antigen is reactive. A bone marrow biopsy and culture is also useful particularly in the evaluation of the patient with cytopenias. Bacterial, fungal, and AFB cultures may yield disseminated mycobacterial or fungal disease. Histopathologic evaluation may reveal granulomas with organisms or lymphoma. Bronchoscopy may be pursued in cases of high suspicion for TB or PCP.
Guidelines for the management of opportunistic infections associated with human immunodeficiency virus are available at www.AIDSinfo.nih.gov.
Evaluation of the AIDS Patient with Focal Neurological Disease
Toxoplasma encephalitis (TE) may be distinguished from primary CNS lymphoma without a brain biopsy. TE is caused by reactivation of latent infection by the protozoan Toxoplasma gondii. Almost 90% of patients have CD4 counts less than 200 cells/mm3 and 75% have CD4 counts less than 100 cells/mm3. Serum anti-Toxoplasma IgG antibodies are detected in more than 90% of patients with TE. Lesions on CT or MRI (a more sensitive modality) are typically multiple ring-enhancing lesions with a predilection for the basal ganglia. An emipiric trial of therapy is recommended, and a response confirms a diagnosis in the patient who has a positive Toxoplasma antibody and is not receiving trimethoprim-sulfamethoxazole prophylaxis. A lumbar puncture in this setting is not necessary and maybe ill advised if cerebral edema is present (Figure 1, page 24).
Primary CNS lymphoma (PCNSL) has a similar radiographic appearance as TE. Solitary lesions are more frequent in PCNSL. Positron emission tomography (PET) and single photon emission CT (SPECT) are useful adjunctive imaging modalities as they are positive in PCNSL due to the increased metabolic activity of the tumor. Cytologic analysis of the CSF may show lymphomatous cells. Epstein-Barr virus (EBV) DNA is uniformly detected in PCNSL in AIDS patients and detection of EBV DNA by PCR on the CSF has a sensitivity of 90–100% and a specificity of 87–98% for the diagnosis of PCNSL (41,42). Combining SPECT imaging and EBV PCR provides 100% sensitivity and 100% negative predictive value in the evaluation of AIDS-related primary CNS lymphoma (43), obviating the need for brain biopsy.
Progressive multifocal leukoencephalopathy (PML) is characterized radiographically by multiple and bilateral hypodense lesions of the white matter without mass effect or enhancement on CT. MRI demonstrates areas of hypointensity on T1-weighted images and increased intensity on T2-weighted images. JC virus DNA can be detected by PCR of CSF or brain tissue with sensitivity of approximately 80% and specificity of 95%. Because of the high positive predictive value of a positive PCR, a patient with AIDS who also has a compatible MRI can be diagnosed with PML (44,45).
Other focal neurologic disease seen in AIDS patients includes cryptococcomas, tuberculomas, CMV encephalitis, neurosyphilis, Nocardia and Aspergillus infection, and bacterial brain abscesses (46).
Conclusion
As survival of the HIV-infected population improves, more patients may require hospitalization for HAART treatment failures or complications attributed to antiretroviral therapy. The hospitalist should be familiar with the complications of antiretroviral agents, the interactions between HAART and medications used to treat opportunistic infections, and medical conditions induced by HAART. Evaluation of the HIV-infected patient presenting with fever can be based on the CD4 cell count, which predicts risk for opportunistic infections. Finally, using combined diagnostic approaches along with modern imaging and laboratory assays may preclude the need for more invasive procedures in the HIV-infected hospitalized patient.
Dr. Decker may be reached at [email protected].
References
- Torres RA, Barr M. Impact of combination therapy for HIV infection on inpatient census. N Engl J Med. 1997;336:1531-2.
- Fleishman JA, Hellinger FJ. Trends in HIV-related inpatient admissions from 1993 to 1997: a seven-state study. J Acquir Immune Defic Syndr. 2001;28:73-80.
- Fleishman JA, Hellinger FH. Recent trends in HIV-related inpatient admissions 1996-2000: a 7-state study. J Acquir Immune Defic Syndr. 2003;34:102-10.
- Powderly WG. Should patients with an acute opportunistic infection receive antiretroviral therapy immediately? Advanced Studies in Medicine. 2005;5:S111-S116.
- Fagard C, Oxenius A, Gunthard H, et al. A prospective trial of structured treatment interruptions in human immunodeficiency virus infection. Arch Intern Med. 2003;163:1220-6.
- Soni N, Pozniak A. Continuing HIV therapy in the ICU. Crit Care. 2001;5:247-8.
- Purdy BD, Raymond AM, Lesar TS. Antiretroviral prescribing errors in hospitalized patients. Ann Pharmacother. 2000;34:833-8.
- Autran B, Carcelain G, Li TS, et al. Positive effects of combined antiretroviral therapy on CD4+ T cell homeostasis and function in advanced HIV disease. Science. 1997;277:112-6.
- Cooney EL. Clinical indicators of immune restoration following highly active antiretroviral therapy. Clin Infect Dis. 2002;34:224-33.
- Hirsch HH, Kaufmann G, Sendi P, BaĴegay M. Immune reconstitution in HIV-infected patients. Clin Infect Dis. 2004;38:1159-66.
- Cheng VC, Yuen KY, Chan WM, Wong SS, Ma ES, Chan RM. Immunorestitution disease involving the innate and adaptive response. Clin Infect Dis. 2000;30:882-92.
- Fishman JE, Saraf-Lavi E, Narita M, Hollender ES, Ramsinghani R, Ashkin D. Pulmonary tuberculosis in AIDS patients: transient chest radiographic worsening after initiation of antiretroviral therapy. AJR Am J Roentgenol. 2000;174:43-9.
- Piscitelli SC, Gallicano KD. Interactions among drugs for HIV and opportunistic infections. N Engl J Med. 2001;344:984-96.
- Barry M, Mulcahy F, Merry C, Gibbons S, Back D. Pharmacokinetics and potential interactions amongst antiretroviral agents used to treat patients with HIV infection. Clin Pharmacokinet. 1999;36:289-304.
- Sim SM, Hoggard PG, Sales SD, Phiboonbanakit D, Hart CA, Back DJ. Effect of ribavirin on zidovudine efficacy and toxicity in vitro: a concentration-dependent interaction. AIDS Res Hum Retroviruses. 1998;14:1661-7.
- Clarke SM, Mulcahy FM, Tjia J, et al. The pharmacokinetics of methadone in HIV-positive patients receiving the non-nucleoside reverse transcriptase inhibitor efavirenz. Br J Clin Pharmacol. 2001;51:213-7.
- Centers for Disease Control and Prevention. Updated guidelines for the use of rifabutin or rifampin for the treatment and prevention of tuberculosis among HIV-infected patients taking protease inhibitors or nonnucleoside reverse transcriptase inhibitors. Morb Mortal Wkly Rep. 2000;49:185-9.
- Havlir DV, O’Marro SD. Atazanavir: new option for treatment of HIV infection. Clin Infect Dis. 2004;38:1599-604.
- Sheng WH, Hsieh SM, Lee SC, et al. Fatal lactic acidosis associated with highly active antiretroviral therapy in patients with advanced human immunodeficiency virus infection in Taiwan. Int J STD AIDS. 2004;15:249-53.
- Herman JS, Easterbrook PJ. The metabolic toxicities of antiretroviral therapy. Int J STD AIDS. 2001;12:555-62;quiz 563-4.
- Behrens G, Schmidt H, Meyer D, Stoll M, Schmidt RE. Vascular complications associated with use of HIV protease inhibitors. Lancet. 1998;351:1958.
- Klein D, Hurley LB, Sidney S. Cardiovascular Disease and HIV Infection. N Engl J Med. 2003;349:1869-70; author reply 1869-70.
- Friis-Moller N, Sabin CA, Weber R, et al. Combination antiretroviral therapy and the risk of myocardial infarction. N Engl J Med. 2003;349:1993-2003.
- Anderson JA, Adkinson NF Jr. Allergic reactions to drugs and biologic agents. JAMA. 1987;258:2891-9.
- Hewitt RG. Abacavir hypersensitivity reaction. Clin Infect Dis. 2002;34:1137-42.
- Hetherington S, Hughes AR, Mosteller M, et al. Genetic variations in HLA-B region and hypersensitivity reactions to abacavir. Lancet. 2002;359:1121-2.
- Bossi P, Colin D, Bricaire F, Caumes E. Hypersensitivity syndrome associated with efavirenz therapy. Clin Infect Dis. 2000;30:227-8.
- Bourezane Y, Salard D, Hoen B, Vandel S, Drobacheff C, Laurent R. DRESS (drug rash with eosinophilia and systemic symptoms) syndrome associated with nevirapine therapy. Clin Infect Dis. 1998;27:1321-2.
- Walensky RP, Goldberg JH, Daily JP. Anaphylaxis after rechallenge with abacavir. AIDS. 1999;13:999-1000.
- Martin GJ, Paparello SF, Decker CF. A severe systemic reaction to trimethoprim-sulfamethoxazole in a patient infected with the human immunodeficiency virus. Clin Infect Dis. 1993;16:175-6.
- Bersoff-Matcha SJ, Miller WC, Aberg JA, et al. Sex differences in nevirapine rash. Clin Infect Dis. 2001;32:124-9.
- Kopp JB, Falloon J, Filie A, et al. Indinavir-associated interstitial nephritis and urothelial inflammation: clinical and cytologic findings. Clin Infect Dis. 2002;34:1122-8.
- Geene D, Sudre P, Anwar D, Goehring C, Saaidia A, Hirschel B. Causes of macrocytosis in HIV-infected patients not treated with zidovudine. Swiss HIV Cohort Study. J Infect. 2000;40:160-3.
- Gottesman L. Sustiva may cause false positive on marijuana test. WORLD. 1999:7.
- Sepkowitz KA, Telzak EE, Carrow M, Armstrong D. Fever among outpatients with advanced human immunodeficiency virus infection. Arch Intern Med. 1993;153: 1909-12.
- Barat LM, Gunn JE, Steger KA, Perkins CJ, Craven DE. Causes of fever in patients infected with human immunodeficiency virus who were admitted to Boston City Hospital. Clin Infect Dis. 1996;23:320-8.
- Sepkowitz KA. FUO and AIDS. Curr Clin Top Infect Dis. 1999;19:1-15.
- Asawavichienjinda T, Sitthi-Amorn C, Tanyanont V. Serum cyrptococcal antigen: diagnostic value in the diagnosis of AIDS-related cryptococcal meningitis. J Med Assoc Thai. 1999;82:65-71.
- Richards PJ, Riddell L, Reznek RH, Armstrong P, Pinching AJ, Parkin JM. High resolution computed tomography in HIV patients with suspected Pneumocystis carinii pneumonia and a normal chest radiograph. Clin Radiol. 1996;51:689-93.
- Gruden JF, Huang L, Turner J, et al. High-resolution CT in the evaluation of clinically suspected Pneumocystis carinii pneumonia in AIDS patients with normal, equivocal, or nonspecific radiographic findings. AJR Am J Roentgenol. 1997;169:967-75.
- MacMahon EM, Glass JD, Hayward SD, et al. Association of Epstein-Barr virus with primary central nervous system lymphoma in AIDS. AIDS Res Hum Retroviruses. 1992;8:740-2.
- Rao CR, Jain K, Bhatia K, Laksmaiah KC, Shankar SK. Association of primary central nervous system lymphomas with the Epstein-Barr virus. Neurol India. 2003;51:237-40.
- Antinori A, De Rossi G, Ammassari A, et al. Value of combined approach with thallium-201 single-photon emission computed tomography and Epstein-Barr virus DNA polymerase chain reaction in CSF for the diagnosis of AIDS-related primary CNS lymphoma. J Clin Oncol. 1999;17:554-60.
- Post MJ, Yiannoutsos C, Simpson D, et al. Progressive multifocal leukoencephalopathy in AIDS: are there any MR findings useful to patient management and predictive of patient survival? AIDS Clinical Trials Group, 243 Team. AJNR Am J Neuroradiol. 1999;20:1896-906.
- Weber T. Cerebrospinal fluid analysis for the diagnosis of human immunodeficiency virus-related neurologic diseases. Semin Neurol. 1999;19:223-33.
- Skiest DJ. Focal neurological disease in patients with acquired immunodeficiency syndrome. Clin Infect Dis. 2002;34:103-15.
Nosocomial Pneumonia
(This chapter has been reprinted with permission from Williams MV, Hayward R: Comprehensive Hospital Medicine, 1st edition. Philadelphia, WB Saunders, in press.)
Background
Nosocomial pneumonia (NP) is the leading cause of mortality among patients who die from hospital-acquired infections. Defined as pneumonia occurring 48 hours or more after hospital admission, NP also includes the subset of ventilator-associated pneumonia (VAP), defined as pneumonia developing 48 to 72 hours after initiation of mechanical ventilation. The incidence of NP is between 5 and 15 cases per 1000 hospital admissions. Healthcare-associated pneumonia (HCAP), part of the continuum of NP, describes an increasingly common proportion of pneumonia developing outside the hospital (Table I) (1). Typically afflicting people in a nursing home or assisted living setting, these patients are at risk for antibiotic-resistant-organisms and should be approached similarly to cases of nosocomial pneumonia rather than community-acquired pneumonia. Most of the data informing our diagnostic and treatment decisions about NP come from studies performed in mechanically ventilated patients and are extrapolated to make recommendations for non-ventilated patients.
Mortality attributable to NP is debated, but may be as high as 30%. The presence of nosocomial pneumonia increases hospital length of stay an average of 7–10 days, and in the case of VAP, is estimated to cost between $10,000 and $40,000 per case (2).
Assessment
Clinical Presentation
Signs and Symptoms
Nosocomial pneumonia is usually diagnosed based on clinical grounds. Typical symptoms and signs consist of fever, cough with sputum, and shortness of breath in the setting of hypoxia and a new infiltrate on chest radiograph (CXR). In the elderly, signs may be more subtle and delirium, fever, or leukocytosis in the absence of cough should trigger its consideration. The likelihood of NP increases among patients with risk factors for microaspiration, oropharyngeal colonization, or overgrowth of resistant organisms (Table II) (3).
Differential Diagnosis
Prior to settling on a diagnosis of NP, alternative causes of fever, hypoxia, and pulmonary infiltrates should be considered. Most commonly, these include pulmonary embolus, pulmonary edema, or atelectasis. Alternative infectious sources, such as urinary tract, skin and soft-tissue infections, and device-related infections (i.e., central venous catheters) are common in hospitalized patients and should be ruled out before diagnosing nosocomial pneumonia.
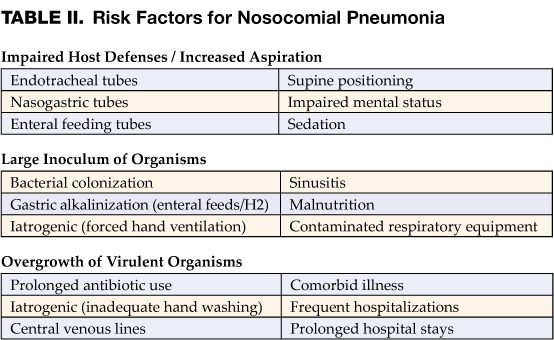
Diagnosis
Diagnostic strategies for NP seek to confirm the diagnosis and identify an etiologic pathogen, thus allowing timely, effective, and streamlined antibiotic therapy. Unfortunately, no consensus exists on the best approach to diagnosing nosocomial pneumonia. After obtaining a complete blood count and blood cultures, you can choose between a clinical or microbiologic diagnostic approach to diagnosis. A clinical diagnosis relies on a new or progressive radiographic infiltrate along with signs of infection such as fever, leukocytosis, or purulent sputum. Clinical diagnosis is sensitive, but is likely to lead to antibiotic overuse. The microbiologic approach requires sampling of secretions from the respiratory tract and may reduce inappropriate antibiotic use, but takes longer and may not be available in all hospitals.
Preferred Studies
The microbiologic approach to diagnosis relies on the use of quantitative or semi-quantitative cultures to create thresholds for antibiotic treatment. Bacterial cultures that demonstrate a level of growth above the thresholds described below warrant treatment, while those below it should trigger withholding or discontinuation of antibiotics.
Bronchoscopic Approaches: Bronchoalveolar lavage (BAL) with a cutoff of 10 (4) organisms/mL or protected specimen brush (PSB) with a cutoff of 10 (3) organisms/mL are felt to be the most specific diagnostic tests when performed prior to initiating antibiotics, or prior to changing antibiotics if a patient is already receiving them. In clinically stable patients, antibiotics can be safely discontinued if bacterial growth falls below the thresholds. If cultures are positive, antibiotic therapy should be tailored to target the organism identified. The bronchoscopic approach is favored in patients who are mechanically ventilated, develop their pneumonia late in the hospital stay (>5–7 days), are at risk for unusual pathogens, are failing therapy or suspected of having an alternative diagnosis.
Non-Bronchoscopic Approaches: Qualitative endotracheal aspirates (ETA) have been shown to be quite sensitive in ventilated patients, regularly identify organisms that may be subsequently found by BAL or PSB, and if negative, should result in withholding antibiotics. Quantitative endotracheal aspirates with a cutoff of 10 (6) organisms/mL are often encouraged to reduce antibiotic overuse, but results should be interpreted cautiously as they only have a sensitivity and specificity of about 75% (1). Consideration should be given to withholding antibiotics in a clinically stable patient with a negative quantitative ETA if antibiotics have not been changed in the preceding 72 hours. Many ICUs have begun to perform blinded sampling of lower respiratory tract secretions with suction catheters (blind PSB, blind mini-BAL). These techniques can be performed at all hours by trained respiratory therapists or nurses, provide culture data similar to that of bronchoscopy, and may be safer and less costly than bronchoscopy. In general, non-bronchoscopic techniques are preferred in patients who are not mechanically ventilated. Sputum sampling, while easy to obtain, has not been well studied in NP. However, in patients in whom bronchoscopic or other non-bronchoscopic techniques are not feasible, sputum sampling may be performed to identify potentially resistant organisms and help tailor therapy.
Alternative Options
Clinical Pulmonary Infection Score—Combining Clinical and Microbiologic Approaches
The clinical diagnosis of nosocomial pneumonia (new infiltrate + fever, leukocytosis, or purulent sputum) likely leads to antibiotic overuse, yet pursuing a bronchoscopic diagnosis is invasive, costly, and requires technical expertise. The quantitative ETA, blind PSB, and blind BAL discussed above are examples of some compromises that avoid the need for bronchoscopy, yet add microbiologic data in an attempt to prevent excess antibiotic therapy. Formally combining diagnostic approaches (clinical + microbiologic) may also be useful. One such option is the use of the clinical pulmonary infection score (CPIS), which combines clinical, radiographic, physiological, and microbiologic data into a numerical result. Scores >6 have been shown to correlate well with quantitative BAL (4). More recent studies, however, have suggested a lower specificity which could still result in antibiotic overuse, but this approach remains more accurate than a general clinical approach. Using the CPIS serially at the time NP is suspected and again at 72 hours may be more useful. Patients with an initial low clinical suspicion for pneumonia (CPIS of 6 or less) could have antibiotics safely discontinued at 72 hours if the CPIS remains low (5). Such a strategy may be useful in settings where more sophisticated diagnostic modalities are not available.
Multiple studies of biological markers of infection have attempted to find a non-invasive, rapid, accurate means of determining who needs antibiotics for presumed NP. Unfortunately, the results have largely been disappointing. More recently, measurement of a soluble triggering receptor expressed on myeloid cells (sTREM-1) that is upregulated in the setting of infection has been shown to improve our ability to diagnose NP accurately. Measurement of sTREM-1 was 98% sensitive and 90% specific for the diagnosis of pneumonia in mechanically ventilated patients (6). While promising, more data is needed before this test can be recommended for routine use.
Management
Initial Treatment
Early initiation of adequate empiric antibiotic therapy (i.e., the antibiotics administered are shown to be active against all organisms isolated) is associated with improved survival compared with initial inadequate therapy (1,7). Antibiotics should be started immediately after obtaining blood and sputum samples for culture and should not be withheld in the event of delay in diagnostic testing. The need to choose antibiotics quickly and expeditiously drives the use of broad spectrum antibiotics. In an effort to avoid unnecessary overuse of broad spectrum antibiotics, therapy should be based on risk for multidrug-resistant (MDR) pathogens. Identifying patients at low risk for MDR pathogens by clinical criteria allows for more narrow, but effective, antibiotic therapy. Low risk patients include those who develop their pneumonia early in the hospitalization (<5–7 days), are not immunocompromised, have not had prior broad spectrum antibiotics, and do not have risk factors for HCAP (Table I) (1,7). In these patients antibiotics should target common community-acquired organisms (Table III–low risk pathogens). Appropriate initial antibiotic therapy could include a third generation cephalosporin or a beta-lactam/beta-lactamase inhibitor. In some communities or hospital wards the incidence of methicillin-resistance among Staphylococcus aureus isolates (MRSA) may be high enough to warrant initial empiric therapy with vancomycin or linezolid.
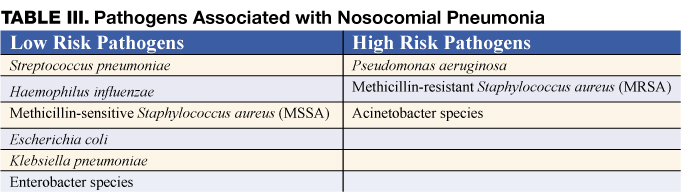
Unfortunately, today’s increasingly complex hospitalized patients are unlikely to be “low risk,” especially in intensive care units.
Patients not meeting low risk criteria are considered to be at high risk for MDR pathogens (Table III–high risk pathogens). Initial empiric therapy needs to be broad and should include one antipseudomonal agent (cefepime or imipenem or beta-lactam/beta-lactamase inhibitor) plus a fluoroquinolone or aminoglycoside plus vancomycin or linezolid. The specific initial empiric therapy should be dictated by local resistance patterns, cost, and availability of preferred agents. When such broad spectrum therapy is initiated, it becomes imperative that antibiotics are “de-escalated” to limit antibiotic overuse. De-escalation therapy focuses on narrowing the antibiotic spectrum based on culture results, and limiting the overall duration of therapy. Hospitalists should aim to accomplish such de-escalation within 48–72 hours of initiating broad-spectrum antibiotics.
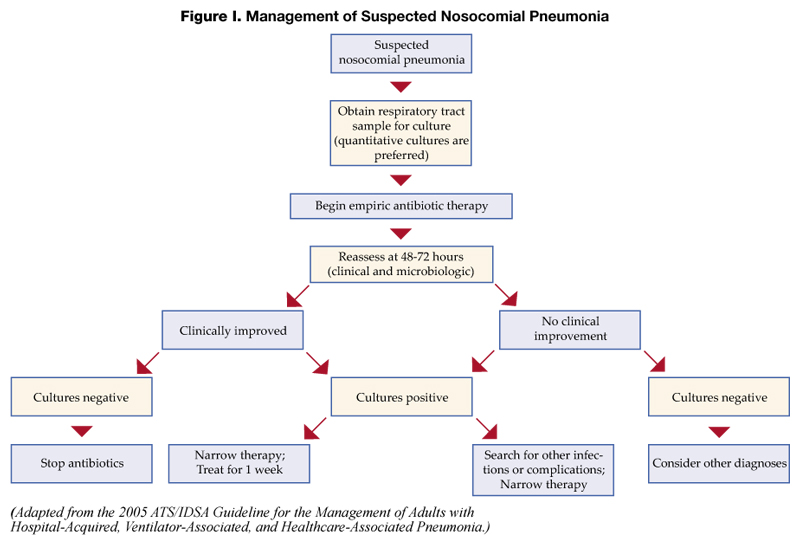
Subsequent Treatment
Patients started on initial empiric antibiotic therapy for presumed nosocomial pneumonia should be reassessed at 48–72 hours. Specifically, cultures should be checked and the clinical response to treatment evaluated. Figure I describes an algorithm for guiding treatment (1). In patients who are clinically stable and have negative lower respiratory tract cultures, antibiotics can be stopped. Patients with positive cultures should have antibiotics tailored, or “de-escalated” based on the organisms identified. In general, the most narrow spectrum antibiotic that is active against the bacteria isolated should be used. The use of combination therapy for gram negative organisms (two or more antibiotics active against a bacterial isolate) is widely practiced to achieve synergy, or prevent the development of resistance. However, in the absence of neutropenia, combination therapy has not been shown to be superior to monotherapyy (8), and monotherapy is preferred. The isolation of MRSA from a respiratory sample should also result in use of monotherapy. While some studies have suggested that linezolid may be superior to vancomycin for MRSA pneumonia, this finding needs validation in prospective studies.
A second component of de-escalation is shortening the total duration of therapy. The CPIS may be used to shorten the duration of therapy in patients at low risk for pneumonia. Investigators at a Veterans Affairs medical center randomized patients suspected of having NP, but who had a CPIS score < 6, to either treatment for 10–21 days, or short course therapy. Patients receiving short course therapy were reassessed at day 3, and if their CPIS score remained < 6, antibiotics were stopped (5). The short course therapy group had no difference in mortality when compared to the standard treatment group, but had less antibiotic use, shorter ICU stays, and was less likely to develop a superinfection or infection with a resistant organism. If the CPIS is not used, or if patients are felt to be at higher risk or convincingly demonstrated to have NP, a shorter course of therapy may still be preferred. A large randomized trial showed that 8 days of antibiotic therapy for patients with VAP resulted in similar clinical outcomes when compared to 15 days of therapy. Additionally, shorter duration antibiotic therapy was associated with lower likelihood of developing subsequent infections with multi-resistant pathogens. A subset of patients in the 8 day treatment group infected with non-fermenting gram negative bacilli (e.g., Pseudomonas aeruginosa) did have a higher pulmonary infection recurrence rate, but due to aggressive surveillance, this did not translate into a higher mortality risk in this subset of patients (9).
In summary, treatment of patients with suspected NP starts with immediate initiation of antibiotics and collection of respiratory secretions. While low risk patients can receive narrower spectrum therapy, most patients will require broad initial empiric therapy. The antibiotic regimen, however, should be narrowed at 48–72 hours based on microbiological results if the patient is improving. Overall treatment duration of 1 week is safe and effective with less chance of promoting growth of resistant organisms. In the subset of patients with pseudomonal infections, treatment of 1 week duration should be followed by active surveillance for recurrence, or alternatively, treatment can be extended to two weeks.
Prognosis
Once treatment for NP is initiated, clinical improvement is usually seen by 48–72 hours. There is little support for following either microbiologic response (clearance of positive cultures) or the response by chest radiography. The chest radiograph often lags behind the clinical response, however, a markedly worsening CXR (>50% increase in infiltrate) within the first 48 hours may indicate treatment failure. Clinical resolution as measured by temperature, white blood cell count, and oxygenation usually occurs by 6–7 days (10). Failure of oxygenation to improve by 72 hours has been shown to be predictive of treatment failure.
The overall mortality in patients with NP is as high as 30–70%, largely due to severe comorbid disease in the at risk population. Higher mortality rates are seen in patients with VAP and resistant organisms. The mortality attributable to the episode of NP is about 30%, and can be reduced to <15% with appropriate antibiotic therapy (1).
Prevention
Preventive strategies are either directed at reducing the overall incidence of infectious complications in hospitalized patients, or they are specifically targeted at reducing the incidence of nosocomial pneumonia (3). The majority of the data supporting preventive strategies is limited to patients in the ICU, and in particular, patients receiving mechanical ventilation. However, many of the preventive principles can be extrapolated to the non-ICU population. The preventive strategies are highlighted in Table IV (page 18).
General Preventive Strategies
General preventive strategies aim to avoid contamination of patients with antimicrobial resistant organisms that exist in hospitals, or mitigating the emergence of antimicrobial resistant organisms in the first place. Preventing iatrogenic spread of resistant organisms depends on careful hand hygiene. Hand washing before and after patient contact reduces the incidence of nosocomial infection. Alcohol-based hand rinses placed at the bedside may actually be superior to soap and water, and in addition, improve compliance with hand hygiene.
Minimizing the use of indwelling devices (central lines, urinary catheters) also reduces the emergence of resistant organisms. When these devices are necessary, focusing on their timely removal is critical. The control of antibiotic use has been central to many preventive strategies. Prolonged or unnecessary use of broad-spectrum antibiotics is strongly associated with development and colonization of resistant organisms. Strategies that focus on aggressive antibiotic de-escalation (described above) are a key preventive tool. Some institutions have had success with antibiotic restriction or rotation, but long term data on the effectiveness of these techniques are lacking.
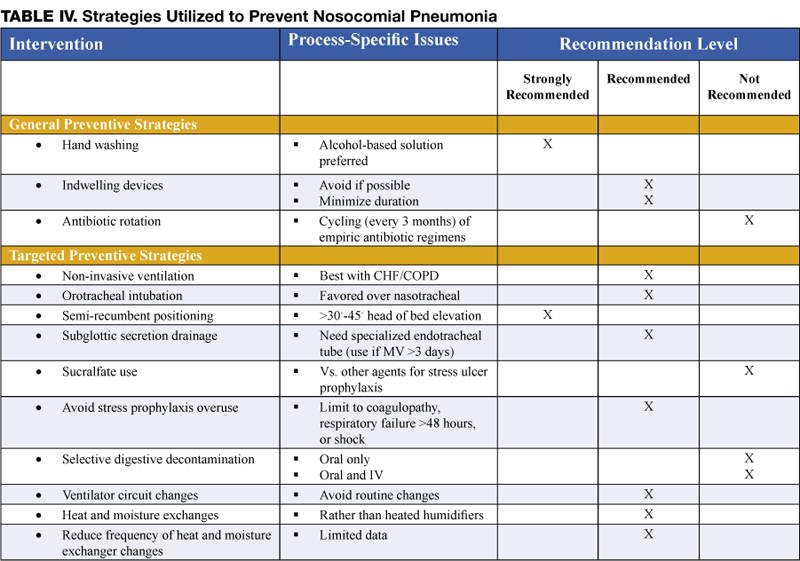
Targeted Preventive Strategies
Preventive strategies to lower the incidence of NP focus on reducing risk factors for oropharyngeal or gastric colonization and subsequent aspiration of contaminated oropharyngeal or gastric secretions (1,3,7,11).
Endotracheal intubation is one of the most important risk factors for NP in patients requiring ventilatory support. The use of non-invasive ventilation (NIV) or positive pressure mask ventilation in selected groups of patients has been effective in preventing nosocomial pneumonia. Non-invasive ventilation has been most successful in patients with acute exacerbations of chronic obstructive pulmonary disease (COPD) and pulmonary edema secondary to congestive heart failure (CHF) and should be considered in appropriately selected patients. When intubation is required the use of nasotracheal intubation should be avoided due higher rates of NP when compared to orotracheal intubation.
Supine positioning may contribute to the development of NP, likely due to an increased risk of gastric reflux and subsequent aspiration. Studies of semi-recumbent positioning (elevation of the head of the bed >45 degrees) have shown less reflux, less aspiration, and in one recent randomized control trial, a significant reduction in the rate of VAP (12). Elevation of the head of the bed is clearly indicated in mechanically ventilated patients and is also likely to benefit all patients at risk for aspiration and subsequent NP, although this technique has not been well studied in non-ventilated patients.
Subglottic secretion drainage (SSD) involves the removal of pooled secretions above the cuff of a specialized endotracheal tube that might otherwise leak into the lung. A meta-analysis of five studies evaluating this new technology showed significant reductions in the incidence of VAP. The use of SSD should be considered for use in patients requiring more than 3 days of mechanical ventilation (13).
Medications used for stress ulcer prophylaxis that increase gastric pH-such as H2 antagonists and antacids-allow for colonization of the upper gastrointestinal tract by potentially pathogenic organisms and therefore increase the risk for NP. The use of sucralfate instead of H2 antagonists is felt to lead to less alkalinization of the stomach and less bacterial overgrowth. The ability of sucralfate to prevent nosocomial pneumonia, however, has not been well demonstrated and its routine use is not recommended (14). Instead, efforts should be targeted at limiting use of stress ulcer prophylaxis to populations at high risk for clinically significant bleeding, namely patients with coagulopathy and prolonged ventilatory failure. Most patients who are not in the ICU should not receive stress ulcer prophylaxis. The risk of NP related to use of proton pump inhibitors has not been well studied.
Selective digestive decontamination (SDD) involves sterilization of the oropharynx and gastrointestinal tract in mechanically ventilated patients in order to prevent aspiration of large numbers of potentially pathogenic organisms and subsequent VAP. Most evaluations of SDD have involved oral (and sometimes gastric) application of topical polymixin, aminoglycoside, and amphotericin. In many cases, short courses of IV antibiotics have been added. At least 10 meta-analyses have shown a reduction in the risk of VAP with the use of SDD. The addition of IV antibiotics may also provide a mortality benefit. However, the long-term risk for emergence of resistant organisms, and insufficient data on the cost-effectiveness of SDD prevent its recommendation for routine use (14).
There are several preventive strategies targeted at reducing aspiration of contaminants in ventilator circuits, filters, and tubing. Recommended strategies, listed in Table III, page 16, include avoidance of routine ventilator circuit changes (change the tubing only when visibly contaminated or for a new patient), use of heat and moisture exchangers rather than heated humidifiers, and reduction in the frequency of changes of the heat and moisture exchangers (1,11,14).
Discharge/Follow-up Plans
Patients should be followed in the hospital until it is clear they are responding to therapy and clinically improving. There has been limited evaluation of strategies to rapidly transition patients to oral therapy. However, if patients are improving, are tolerating oral therapy, have a functional GI tract, and have an organism isolated that is sensitive to available oral antibiotics, the switch to oral therapy can be made. If no organism is isolated, but a patient definitely was felt to have NP, the oral antibiotics selected should have the same spectrum of activity as the previously administered IV antibiotics. In many cases, patients will have an infection with an organism that is only susceptible to IV antibiotics. These patients are likely to be ill enough to complete a full one week IV course in the hospital, but if they have no active co-morbid illness and have improved, they can have a PICC line placed (or other long-term IV access) and receive the remainder of their therapy at home or in another lower acuity setting.
In all patients who develop NP, reversible causes of aspiration should be sought, and in cases where multidrug-resistant organisms are isolated, this should be reported to any facility to which a patient is being transferred or to the primary care physician or home nurse who will assume care after discharge.
References
- Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388-416.
- Warren DK, Shukla SJ, Olsen MA, et al. Outcome and attributable cost of ventilator-associated pneumonia among intensive care unit patients in a suburban medical center. Crit Care Med. 2003;31:1312-7.
- Flanders SA, Collard HR, Saint S. Preventing Nosocomial Pneumonia. In: Lautenbach E, Woeltje K, eds. The Society for Healthcare Epidemiology of America: Practical Handbook for Healthcare Epidemiologists. Thorofare, NJ: Slack, 2004:69-78.
- Pugin J, Auckenthaler R, Mili N, Janssens JP, Lew PD, Suter PM. Diagnosis of ventilator-associated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic “blind” bronchoalveolar lavage fluid. Am Rev Respir Dis. 1991;143:1121-9.
- Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000;162:505-11.
- Gibot S, Cravoisy A, Levy B, Bene MC, Faure G, Bollaert PE. Soluble triggering receptor expressed on myeloid cells and the diagnosis of pneumonia. N Engl J Med. 2004;350:451-8.
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165:867-903.
- Paul M, Benuri-Silbiger I, Soares-Weiser K, Leibovici L. Beta lactam monotherapy versus beta lactam-aminoglycoside combination therapy for sepsis in immunocompetent patients: systematic review and metaanalysis of randomised trials. BMJ. 2004;328:668.
- Chastre J, Wolff M, Fagon JY, et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290:2588-98.
- Dennesen PJ, van der Ven AJ, Kessels AG, Ramsay G, Bonten MJ. Resolution of infectious parameters after antimicrobial therapy in patients with ventilator-associated pneumonia. Am J Respir Crit Care Med. 2001;163:1371-5.
- Collard HR, Saint S, Matthay MA. Prevention of ventilator-associated pneumonia: an evidence-based systematic review. Ann Intern Med. 2003;138:494-501.
- Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354:1851-8.
- Dezfulian C, Shojania K, Collard HR, Kim HM, Matthay MA, Saint S. Subglottic secretion drainage for preventing ventilator-associated pneumonia: a metaanalysis. Am J Med. 2005;118:11-8.
- Dodek P, Keenan S, Cook D, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305-13.
(This chapter has been reprinted with permission from Williams MV, Hayward R: Comprehensive Hospital Medicine, 1st edition. Philadelphia, WB Saunders, in press.)
Background
Nosocomial pneumonia (NP) is the leading cause of mortality among patients who die from hospital-acquired infections. Defined as pneumonia occurring 48 hours or more after hospital admission, NP also includes the subset of ventilator-associated pneumonia (VAP), defined as pneumonia developing 48 to 72 hours after initiation of mechanical ventilation. The incidence of NP is between 5 and 15 cases per 1000 hospital admissions. Healthcare-associated pneumonia (HCAP), part of the continuum of NP, describes an increasingly common proportion of pneumonia developing outside the hospital (Table I) (1). Typically afflicting people in a nursing home or assisted living setting, these patients are at risk for antibiotic-resistant-organisms and should be approached similarly to cases of nosocomial pneumonia rather than community-acquired pneumonia. Most of the data informing our diagnostic and treatment decisions about NP come from studies performed in mechanically ventilated patients and are extrapolated to make recommendations for non-ventilated patients.
Mortality attributable to NP is debated, but may be as high as 30%. The presence of nosocomial pneumonia increases hospital length of stay an average of 7–10 days, and in the case of VAP, is estimated to cost between $10,000 and $40,000 per case (2).
Assessment
Clinical Presentation
Signs and Symptoms
Nosocomial pneumonia is usually diagnosed based on clinical grounds. Typical symptoms and signs consist of fever, cough with sputum, and shortness of breath in the setting of hypoxia and a new infiltrate on chest radiograph (CXR). In the elderly, signs may be more subtle and delirium, fever, or leukocytosis in the absence of cough should trigger its consideration. The likelihood of NP increases among patients with risk factors for microaspiration, oropharyngeal colonization, or overgrowth of resistant organisms (Table II) (3).
Differential Diagnosis
Prior to settling on a diagnosis of NP, alternative causes of fever, hypoxia, and pulmonary infiltrates should be considered. Most commonly, these include pulmonary embolus, pulmonary edema, or atelectasis. Alternative infectious sources, such as urinary tract, skin and soft-tissue infections, and device-related infections (i.e., central venous catheters) are common in hospitalized patients and should be ruled out before diagnosing nosocomial pneumonia.
Diagnosis
Diagnostic strategies for NP seek to confirm the diagnosis and identify an etiologic pathogen, thus allowing timely, effective, and streamlined antibiotic therapy. Unfortunately, no consensus exists on the best approach to diagnosing nosocomial pneumonia. After obtaining a complete blood count and blood cultures, you can choose between a clinical or microbiologic diagnostic approach to diagnosis. A clinical diagnosis relies on a new or progressive radiographic infiltrate along with signs of infection such as fever, leukocytosis, or purulent sputum. Clinical diagnosis is sensitive, but is likely to lead to antibiotic overuse. The microbiologic approach requires sampling of secretions from the respiratory tract and may reduce inappropriate antibiotic use, but takes longer and may not be available in all hospitals.
Preferred Studies
The microbiologic approach to diagnosis relies on the use of quantitative or semi-quantitative cultures to create thresholds for antibiotic treatment. Bacterial cultures that demonstrate a level of growth above the thresholds described below warrant treatment, while those below it should trigger withholding or discontinuation of antibiotics.
Bronchoscopic Approaches: Bronchoalveolar lavage (BAL) with a cutoff of 10 (4) organisms/mL or protected specimen brush (PSB) with a cutoff of 10 (3) organisms/mL are felt to be the most specific diagnostic tests when performed prior to initiating antibiotics, or prior to changing antibiotics if a patient is already receiving them. In clinically stable patients, antibiotics can be safely discontinued if bacterial growth falls below the thresholds. If cultures are positive, antibiotic therapy should be tailored to target the organism identified. The bronchoscopic approach is favored in patients who are mechanically ventilated, develop their pneumonia late in the hospital stay (>5–7 days), are at risk for unusual pathogens, are failing therapy or suspected of having an alternative diagnosis.
Non-Bronchoscopic Approaches: Qualitative endotracheal aspirates (ETA) have been shown to be quite sensitive in ventilated patients, regularly identify organisms that may be subsequently found by BAL or PSB, and if negative, should result in withholding antibiotics. Quantitative endotracheal aspirates with a cutoff of 10 (6) organisms/mL are often encouraged to reduce antibiotic overuse, but results should be interpreted cautiously as they only have a sensitivity and specificity of about 75% (1). Consideration should be given to withholding antibiotics in a clinically stable patient with a negative quantitative ETA if antibiotics have not been changed in the preceding 72 hours. Many ICUs have begun to perform blinded sampling of lower respiratory tract secretions with suction catheters (blind PSB, blind mini-BAL). These techniques can be performed at all hours by trained respiratory therapists or nurses, provide culture data similar to that of bronchoscopy, and may be safer and less costly than bronchoscopy. In general, non-bronchoscopic techniques are preferred in patients who are not mechanically ventilated. Sputum sampling, while easy to obtain, has not been well studied in NP. However, in patients in whom bronchoscopic or other non-bronchoscopic techniques are not feasible, sputum sampling may be performed to identify potentially resistant organisms and help tailor therapy.
Alternative Options
Clinical Pulmonary Infection Score—Combining Clinical and Microbiologic Approaches
The clinical diagnosis of nosocomial pneumonia (new infiltrate + fever, leukocytosis, or purulent sputum) likely leads to antibiotic overuse, yet pursuing a bronchoscopic diagnosis is invasive, costly, and requires technical expertise. The quantitative ETA, blind PSB, and blind BAL discussed above are examples of some compromises that avoid the need for bronchoscopy, yet add microbiologic data in an attempt to prevent excess antibiotic therapy. Formally combining diagnostic approaches (clinical + microbiologic) may also be useful. One such option is the use of the clinical pulmonary infection score (CPIS), which combines clinical, radiographic, physiological, and microbiologic data into a numerical result. Scores >6 have been shown to correlate well with quantitative BAL (4). More recent studies, however, have suggested a lower specificity which could still result in antibiotic overuse, but this approach remains more accurate than a general clinical approach. Using the CPIS serially at the time NP is suspected and again at 72 hours may be more useful. Patients with an initial low clinical suspicion for pneumonia (CPIS of 6 or less) could have antibiotics safely discontinued at 72 hours if the CPIS remains low (5). Such a strategy may be useful in settings where more sophisticated diagnostic modalities are not available.
Multiple studies of biological markers of infection have attempted to find a non-invasive, rapid, accurate means of determining who needs antibiotics for presumed NP. Unfortunately, the results have largely been disappointing. More recently, measurement of a soluble triggering receptor expressed on myeloid cells (sTREM-1) that is upregulated in the setting of infection has been shown to improve our ability to diagnose NP accurately. Measurement of sTREM-1 was 98% sensitive and 90% specific for the diagnosis of pneumonia in mechanically ventilated patients (6). While promising, more data is needed before this test can be recommended for routine use.
Management
Initial Treatment
Early initiation of adequate empiric antibiotic therapy (i.e., the antibiotics administered are shown to be active against all organisms isolated) is associated with improved survival compared with initial inadequate therapy (1,7). Antibiotics should be started immediately after obtaining blood and sputum samples for culture and should not be withheld in the event of delay in diagnostic testing. The need to choose antibiotics quickly and expeditiously drives the use of broad spectrum antibiotics. In an effort to avoid unnecessary overuse of broad spectrum antibiotics, therapy should be based on risk for multidrug-resistant (MDR) pathogens. Identifying patients at low risk for MDR pathogens by clinical criteria allows for more narrow, but effective, antibiotic therapy. Low risk patients include those who develop their pneumonia early in the hospitalization (<5–7 days), are not immunocompromised, have not had prior broad spectrum antibiotics, and do not have risk factors for HCAP (Table I) (1,7). In these patients antibiotics should target common community-acquired organisms (Table III–low risk pathogens). Appropriate initial antibiotic therapy could include a third generation cephalosporin or a beta-lactam/beta-lactamase inhibitor. In some communities or hospital wards the incidence of methicillin-resistance among Staphylococcus aureus isolates (MRSA) may be high enough to warrant initial empiric therapy with vancomycin or linezolid.
Unfortunately, today’s increasingly complex hospitalized patients are unlikely to be “low risk,” especially in intensive care units.
Patients not meeting low risk criteria are considered to be at high risk for MDR pathogens (Table III–high risk pathogens). Initial empiric therapy needs to be broad and should include one antipseudomonal agent (cefepime or imipenem or beta-lactam/beta-lactamase inhibitor) plus a fluoroquinolone or aminoglycoside plus vancomycin or linezolid. The specific initial empiric therapy should be dictated by local resistance patterns, cost, and availability of preferred agents. When such broad spectrum therapy is initiated, it becomes imperative that antibiotics are “de-escalated” to limit antibiotic overuse. De-escalation therapy focuses on narrowing the antibiotic spectrum based on culture results, and limiting the overall duration of therapy. Hospitalists should aim to accomplish such de-escalation within 48–72 hours of initiating broad-spectrum antibiotics.
Subsequent Treatment
Patients started on initial empiric antibiotic therapy for presumed nosocomial pneumonia should be reassessed at 48–72 hours. Specifically, cultures should be checked and the clinical response to treatment evaluated. Figure I describes an algorithm for guiding treatment (1). In patients who are clinically stable and have negative lower respiratory tract cultures, antibiotics can be stopped. Patients with positive cultures should have antibiotics tailored, or “de-escalated” based on the organisms identified. In general, the most narrow spectrum antibiotic that is active against the bacteria isolated should be used. The use of combination therapy for gram negative organisms (two or more antibiotics active against a bacterial isolate) is widely practiced to achieve synergy, or prevent the development of resistance. However, in the absence of neutropenia, combination therapy has not been shown to be superior to monotherapyy (8), and monotherapy is preferred. The isolation of MRSA from a respiratory sample should also result in use of monotherapy. While some studies have suggested that linezolid may be superior to vancomycin for MRSA pneumonia, this finding needs validation in prospective studies.
A second component of de-escalation is shortening the total duration of therapy. The CPIS may be used to shorten the duration of therapy in patients at low risk for pneumonia. Investigators at a Veterans Affairs medical center randomized patients suspected of having NP, but who had a CPIS score < 6, to either treatment for 10–21 days, or short course therapy. Patients receiving short course therapy were reassessed at day 3, and if their CPIS score remained < 6, antibiotics were stopped (5). The short course therapy group had no difference in mortality when compared to the standard treatment group, but had less antibiotic use, shorter ICU stays, and was less likely to develop a superinfection or infection with a resistant organism. If the CPIS is not used, or if patients are felt to be at higher risk or convincingly demonstrated to have NP, a shorter course of therapy may still be preferred. A large randomized trial showed that 8 days of antibiotic therapy for patients with VAP resulted in similar clinical outcomes when compared to 15 days of therapy. Additionally, shorter duration antibiotic therapy was associated with lower likelihood of developing subsequent infections with multi-resistant pathogens. A subset of patients in the 8 day treatment group infected with non-fermenting gram negative bacilli (e.g., Pseudomonas aeruginosa) did have a higher pulmonary infection recurrence rate, but due to aggressive surveillance, this did not translate into a higher mortality risk in this subset of patients (9).
In summary, treatment of patients with suspected NP starts with immediate initiation of antibiotics and collection of respiratory secretions. While low risk patients can receive narrower spectrum therapy, most patients will require broad initial empiric therapy. The antibiotic regimen, however, should be narrowed at 48–72 hours based on microbiological results if the patient is improving. Overall treatment duration of 1 week is safe and effective with less chance of promoting growth of resistant organisms. In the subset of patients with pseudomonal infections, treatment of 1 week duration should be followed by active surveillance for recurrence, or alternatively, treatment can be extended to two weeks.
Prognosis
Once treatment for NP is initiated, clinical improvement is usually seen by 48–72 hours. There is little support for following either microbiologic response (clearance of positive cultures) or the response by chest radiography. The chest radiograph often lags behind the clinical response, however, a markedly worsening CXR (>50% increase in infiltrate) within the first 48 hours may indicate treatment failure. Clinical resolution as measured by temperature, white blood cell count, and oxygenation usually occurs by 6–7 days (10). Failure of oxygenation to improve by 72 hours has been shown to be predictive of treatment failure.
The overall mortality in patients with NP is as high as 30–70%, largely due to severe comorbid disease in the at risk population. Higher mortality rates are seen in patients with VAP and resistant organisms. The mortality attributable to the episode of NP is about 30%, and can be reduced to <15% with appropriate antibiotic therapy (1).
Prevention
Preventive strategies are either directed at reducing the overall incidence of infectious complications in hospitalized patients, or they are specifically targeted at reducing the incidence of nosocomial pneumonia (3). The majority of the data supporting preventive strategies is limited to patients in the ICU, and in particular, patients receiving mechanical ventilation. However, many of the preventive principles can be extrapolated to the non-ICU population. The preventive strategies are highlighted in Table IV (page 18).
General Preventive Strategies
General preventive strategies aim to avoid contamination of patients with antimicrobial resistant organisms that exist in hospitals, or mitigating the emergence of antimicrobial resistant organisms in the first place. Preventing iatrogenic spread of resistant organisms depends on careful hand hygiene. Hand washing before and after patient contact reduces the incidence of nosocomial infection. Alcohol-based hand rinses placed at the bedside may actually be superior to soap and water, and in addition, improve compliance with hand hygiene.
Minimizing the use of indwelling devices (central lines, urinary catheters) also reduces the emergence of resistant organisms. When these devices are necessary, focusing on their timely removal is critical. The control of antibiotic use has been central to many preventive strategies. Prolonged or unnecessary use of broad-spectrum antibiotics is strongly associated with development and colonization of resistant organisms. Strategies that focus on aggressive antibiotic de-escalation (described above) are a key preventive tool. Some institutions have had success with antibiotic restriction or rotation, but long term data on the effectiveness of these techniques are lacking.
Targeted Preventive Strategies
Preventive strategies to lower the incidence of NP focus on reducing risk factors for oropharyngeal or gastric colonization and subsequent aspiration of contaminated oropharyngeal or gastric secretions (1,3,7,11).
Endotracheal intubation is one of the most important risk factors for NP in patients requiring ventilatory support. The use of non-invasive ventilation (NIV) or positive pressure mask ventilation in selected groups of patients has been effective in preventing nosocomial pneumonia. Non-invasive ventilation has been most successful in patients with acute exacerbations of chronic obstructive pulmonary disease (COPD) and pulmonary edema secondary to congestive heart failure (CHF) and should be considered in appropriately selected patients. When intubation is required the use of nasotracheal intubation should be avoided due higher rates of NP when compared to orotracheal intubation.
Supine positioning may contribute to the development of NP, likely due to an increased risk of gastric reflux and subsequent aspiration. Studies of semi-recumbent positioning (elevation of the head of the bed >45 degrees) have shown less reflux, less aspiration, and in one recent randomized control trial, a significant reduction in the rate of VAP (12). Elevation of the head of the bed is clearly indicated in mechanically ventilated patients and is also likely to benefit all patients at risk for aspiration and subsequent NP, although this technique has not been well studied in non-ventilated patients.
Subglottic secretion drainage (SSD) involves the removal of pooled secretions above the cuff of a specialized endotracheal tube that might otherwise leak into the lung. A meta-analysis of five studies evaluating this new technology showed significant reductions in the incidence of VAP. The use of SSD should be considered for use in patients requiring more than 3 days of mechanical ventilation (13).
Medications used for stress ulcer prophylaxis that increase gastric pH-such as H2 antagonists and antacids-allow for colonization of the upper gastrointestinal tract by potentially pathogenic organisms and therefore increase the risk for NP. The use of sucralfate instead of H2 antagonists is felt to lead to less alkalinization of the stomach and less bacterial overgrowth. The ability of sucralfate to prevent nosocomial pneumonia, however, has not been well demonstrated and its routine use is not recommended (14). Instead, efforts should be targeted at limiting use of stress ulcer prophylaxis to populations at high risk for clinically significant bleeding, namely patients with coagulopathy and prolonged ventilatory failure. Most patients who are not in the ICU should not receive stress ulcer prophylaxis. The risk of NP related to use of proton pump inhibitors has not been well studied.
Selective digestive decontamination (SDD) involves sterilization of the oropharynx and gastrointestinal tract in mechanically ventilated patients in order to prevent aspiration of large numbers of potentially pathogenic organisms and subsequent VAP. Most evaluations of SDD have involved oral (and sometimes gastric) application of topical polymixin, aminoglycoside, and amphotericin. In many cases, short courses of IV antibiotics have been added. At least 10 meta-analyses have shown a reduction in the risk of VAP with the use of SDD. The addition of IV antibiotics may also provide a mortality benefit. However, the long-term risk for emergence of resistant organisms, and insufficient data on the cost-effectiveness of SDD prevent its recommendation for routine use (14).
There are several preventive strategies targeted at reducing aspiration of contaminants in ventilator circuits, filters, and tubing. Recommended strategies, listed in Table III, page 16, include avoidance of routine ventilator circuit changes (change the tubing only when visibly contaminated or for a new patient), use of heat and moisture exchangers rather than heated humidifiers, and reduction in the frequency of changes of the heat and moisture exchangers (1,11,14).
Discharge/Follow-up Plans
Patients should be followed in the hospital until it is clear they are responding to therapy and clinically improving. There has been limited evaluation of strategies to rapidly transition patients to oral therapy. However, if patients are improving, are tolerating oral therapy, have a functional GI tract, and have an organism isolated that is sensitive to available oral antibiotics, the switch to oral therapy can be made. If no organism is isolated, but a patient definitely was felt to have NP, the oral antibiotics selected should have the same spectrum of activity as the previously administered IV antibiotics. In many cases, patients will have an infection with an organism that is only susceptible to IV antibiotics. These patients are likely to be ill enough to complete a full one week IV course in the hospital, but if they have no active co-morbid illness and have improved, they can have a PICC line placed (or other long-term IV access) and receive the remainder of their therapy at home or in another lower acuity setting.
In all patients who develop NP, reversible causes of aspiration should be sought, and in cases where multidrug-resistant organisms are isolated, this should be reported to any facility to which a patient is being transferred or to the primary care physician or home nurse who will assume care after discharge.
References
- Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388-416.
- Warren DK, Shukla SJ, Olsen MA, et al. Outcome and attributable cost of ventilator-associated pneumonia among intensive care unit patients in a suburban medical center. Crit Care Med. 2003;31:1312-7.
- Flanders SA, Collard HR, Saint S. Preventing Nosocomial Pneumonia. In: Lautenbach E, Woeltje K, eds. The Society for Healthcare Epidemiology of America: Practical Handbook for Healthcare Epidemiologists. Thorofare, NJ: Slack, 2004:69-78.
- Pugin J, Auckenthaler R, Mili N, Janssens JP, Lew PD, Suter PM. Diagnosis of ventilator-associated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic “blind” bronchoalveolar lavage fluid. Am Rev Respir Dis. 1991;143:1121-9.
- Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000;162:505-11.
- Gibot S, Cravoisy A, Levy B, Bene MC, Faure G, Bollaert PE. Soluble triggering receptor expressed on myeloid cells and the diagnosis of pneumonia. N Engl J Med. 2004;350:451-8.
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165:867-903.
- Paul M, Benuri-Silbiger I, Soares-Weiser K, Leibovici L. Beta lactam monotherapy versus beta lactam-aminoglycoside combination therapy for sepsis in immunocompetent patients: systematic review and metaanalysis of randomised trials. BMJ. 2004;328:668.
- Chastre J, Wolff M, Fagon JY, et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290:2588-98.
- Dennesen PJ, van der Ven AJ, Kessels AG, Ramsay G, Bonten MJ. Resolution of infectious parameters after antimicrobial therapy in patients with ventilator-associated pneumonia. Am J Respir Crit Care Med. 2001;163:1371-5.
- Collard HR, Saint S, Matthay MA. Prevention of ventilator-associated pneumonia: an evidence-based systematic review. Ann Intern Med. 2003;138:494-501.
- Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354:1851-8.
- Dezfulian C, Shojania K, Collard HR, Kim HM, Matthay MA, Saint S. Subglottic secretion drainage for preventing ventilator-associated pneumonia: a metaanalysis. Am J Med. 2005;118:11-8.
- Dodek P, Keenan S, Cook D, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305-13.
(This chapter has been reprinted with permission from Williams MV, Hayward R: Comprehensive Hospital Medicine, 1st edition. Philadelphia, WB Saunders, in press.)
Background
Nosocomial pneumonia (NP) is the leading cause of mortality among patients who die from hospital-acquired infections. Defined as pneumonia occurring 48 hours or more after hospital admission, NP also includes the subset of ventilator-associated pneumonia (VAP), defined as pneumonia developing 48 to 72 hours after initiation of mechanical ventilation. The incidence of NP is between 5 and 15 cases per 1000 hospital admissions. Healthcare-associated pneumonia (HCAP), part of the continuum of NP, describes an increasingly common proportion of pneumonia developing outside the hospital (Table I) (1). Typically afflicting people in a nursing home or assisted living setting, these patients are at risk for antibiotic-resistant-organisms and should be approached similarly to cases of nosocomial pneumonia rather than community-acquired pneumonia. Most of the data informing our diagnostic and treatment decisions about NP come from studies performed in mechanically ventilated patients and are extrapolated to make recommendations for non-ventilated patients.
Mortality attributable to NP is debated, but may be as high as 30%. The presence of nosocomial pneumonia increases hospital length of stay an average of 7–10 days, and in the case of VAP, is estimated to cost between $10,000 and $40,000 per case (2).
Assessment
Clinical Presentation
Signs and Symptoms
Nosocomial pneumonia is usually diagnosed based on clinical grounds. Typical symptoms and signs consist of fever, cough with sputum, and shortness of breath in the setting of hypoxia and a new infiltrate on chest radiograph (CXR). In the elderly, signs may be more subtle and delirium, fever, or leukocytosis in the absence of cough should trigger its consideration. The likelihood of NP increases among patients with risk factors for microaspiration, oropharyngeal colonization, or overgrowth of resistant organisms (Table II) (3).
Differential Diagnosis
Prior to settling on a diagnosis of NP, alternative causes of fever, hypoxia, and pulmonary infiltrates should be considered. Most commonly, these include pulmonary embolus, pulmonary edema, or atelectasis. Alternative infectious sources, such as urinary tract, skin and soft-tissue infections, and device-related infections (i.e., central venous catheters) are common in hospitalized patients and should be ruled out before diagnosing nosocomial pneumonia.
Diagnosis
Diagnostic strategies for NP seek to confirm the diagnosis and identify an etiologic pathogen, thus allowing timely, effective, and streamlined antibiotic therapy. Unfortunately, no consensus exists on the best approach to diagnosing nosocomial pneumonia. After obtaining a complete blood count and blood cultures, you can choose between a clinical or microbiologic diagnostic approach to diagnosis. A clinical diagnosis relies on a new or progressive radiographic infiltrate along with signs of infection such as fever, leukocytosis, or purulent sputum. Clinical diagnosis is sensitive, but is likely to lead to antibiotic overuse. The microbiologic approach requires sampling of secretions from the respiratory tract and may reduce inappropriate antibiotic use, but takes longer and may not be available in all hospitals.
Preferred Studies
The microbiologic approach to diagnosis relies on the use of quantitative or semi-quantitative cultures to create thresholds for antibiotic treatment. Bacterial cultures that demonstrate a level of growth above the thresholds described below warrant treatment, while those below it should trigger withholding or discontinuation of antibiotics.
Bronchoscopic Approaches: Bronchoalveolar lavage (BAL) with a cutoff of 10 (4) organisms/mL or protected specimen brush (PSB) with a cutoff of 10 (3) organisms/mL are felt to be the most specific diagnostic tests when performed prior to initiating antibiotics, or prior to changing antibiotics if a patient is already receiving them. In clinically stable patients, antibiotics can be safely discontinued if bacterial growth falls below the thresholds. If cultures are positive, antibiotic therapy should be tailored to target the organism identified. The bronchoscopic approach is favored in patients who are mechanically ventilated, develop their pneumonia late in the hospital stay (>5–7 days), are at risk for unusual pathogens, are failing therapy or suspected of having an alternative diagnosis.
Non-Bronchoscopic Approaches: Qualitative endotracheal aspirates (ETA) have been shown to be quite sensitive in ventilated patients, regularly identify organisms that may be subsequently found by BAL or PSB, and if negative, should result in withholding antibiotics. Quantitative endotracheal aspirates with a cutoff of 10 (6) organisms/mL are often encouraged to reduce antibiotic overuse, but results should be interpreted cautiously as they only have a sensitivity and specificity of about 75% (1). Consideration should be given to withholding antibiotics in a clinically stable patient with a negative quantitative ETA if antibiotics have not been changed in the preceding 72 hours. Many ICUs have begun to perform blinded sampling of lower respiratory tract secretions with suction catheters (blind PSB, blind mini-BAL). These techniques can be performed at all hours by trained respiratory therapists or nurses, provide culture data similar to that of bronchoscopy, and may be safer and less costly than bronchoscopy. In general, non-bronchoscopic techniques are preferred in patients who are not mechanically ventilated. Sputum sampling, while easy to obtain, has not been well studied in NP. However, in patients in whom bronchoscopic or other non-bronchoscopic techniques are not feasible, sputum sampling may be performed to identify potentially resistant organisms and help tailor therapy.
Alternative Options
Clinical Pulmonary Infection Score—Combining Clinical and Microbiologic Approaches
The clinical diagnosis of nosocomial pneumonia (new infiltrate + fever, leukocytosis, or purulent sputum) likely leads to antibiotic overuse, yet pursuing a bronchoscopic diagnosis is invasive, costly, and requires technical expertise. The quantitative ETA, blind PSB, and blind BAL discussed above are examples of some compromises that avoid the need for bronchoscopy, yet add microbiologic data in an attempt to prevent excess antibiotic therapy. Formally combining diagnostic approaches (clinical + microbiologic) may also be useful. One such option is the use of the clinical pulmonary infection score (CPIS), which combines clinical, radiographic, physiological, and microbiologic data into a numerical result. Scores >6 have been shown to correlate well with quantitative BAL (4). More recent studies, however, have suggested a lower specificity which could still result in antibiotic overuse, but this approach remains more accurate than a general clinical approach. Using the CPIS serially at the time NP is suspected and again at 72 hours may be more useful. Patients with an initial low clinical suspicion for pneumonia (CPIS of 6 or less) could have antibiotics safely discontinued at 72 hours if the CPIS remains low (5). Such a strategy may be useful in settings where more sophisticated diagnostic modalities are not available.
Multiple studies of biological markers of infection have attempted to find a non-invasive, rapid, accurate means of determining who needs antibiotics for presumed NP. Unfortunately, the results have largely been disappointing. More recently, measurement of a soluble triggering receptor expressed on myeloid cells (sTREM-1) that is upregulated in the setting of infection has been shown to improve our ability to diagnose NP accurately. Measurement of sTREM-1 was 98% sensitive and 90% specific for the diagnosis of pneumonia in mechanically ventilated patients (6). While promising, more data is needed before this test can be recommended for routine use.
Management
Initial Treatment
Early initiation of adequate empiric antibiotic therapy (i.e., the antibiotics administered are shown to be active against all organisms isolated) is associated with improved survival compared with initial inadequate therapy (1,7). Antibiotics should be started immediately after obtaining blood and sputum samples for culture and should not be withheld in the event of delay in diagnostic testing. The need to choose antibiotics quickly and expeditiously drives the use of broad spectrum antibiotics. In an effort to avoid unnecessary overuse of broad spectrum antibiotics, therapy should be based on risk for multidrug-resistant (MDR) pathogens. Identifying patients at low risk for MDR pathogens by clinical criteria allows for more narrow, but effective, antibiotic therapy. Low risk patients include those who develop their pneumonia early in the hospitalization (<5–7 days), are not immunocompromised, have not had prior broad spectrum antibiotics, and do not have risk factors for HCAP (Table I) (1,7). In these patients antibiotics should target common community-acquired organisms (Table III–low risk pathogens). Appropriate initial antibiotic therapy could include a third generation cephalosporin or a beta-lactam/beta-lactamase inhibitor. In some communities or hospital wards the incidence of methicillin-resistance among Staphylococcus aureus isolates (MRSA) may be high enough to warrant initial empiric therapy with vancomycin or linezolid.
Unfortunately, today’s increasingly complex hospitalized patients are unlikely to be “low risk,” especially in intensive care units.
Patients not meeting low risk criteria are considered to be at high risk for MDR pathogens (Table III–high risk pathogens). Initial empiric therapy needs to be broad and should include one antipseudomonal agent (cefepime or imipenem or beta-lactam/beta-lactamase inhibitor) plus a fluoroquinolone or aminoglycoside plus vancomycin or linezolid. The specific initial empiric therapy should be dictated by local resistance patterns, cost, and availability of preferred agents. When such broad spectrum therapy is initiated, it becomes imperative that antibiotics are “de-escalated” to limit antibiotic overuse. De-escalation therapy focuses on narrowing the antibiotic spectrum based on culture results, and limiting the overall duration of therapy. Hospitalists should aim to accomplish such de-escalation within 48–72 hours of initiating broad-spectrum antibiotics.
Subsequent Treatment
Patients started on initial empiric antibiotic therapy for presumed nosocomial pneumonia should be reassessed at 48–72 hours. Specifically, cultures should be checked and the clinical response to treatment evaluated. Figure I describes an algorithm for guiding treatment (1). In patients who are clinically stable and have negative lower respiratory tract cultures, antibiotics can be stopped. Patients with positive cultures should have antibiotics tailored, or “de-escalated” based on the organisms identified. In general, the most narrow spectrum antibiotic that is active against the bacteria isolated should be used. The use of combination therapy for gram negative organisms (two or more antibiotics active against a bacterial isolate) is widely practiced to achieve synergy, or prevent the development of resistance. However, in the absence of neutropenia, combination therapy has not been shown to be superior to monotherapyy (8), and monotherapy is preferred. The isolation of MRSA from a respiratory sample should also result in use of monotherapy. While some studies have suggested that linezolid may be superior to vancomycin for MRSA pneumonia, this finding needs validation in prospective studies.
A second component of de-escalation is shortening the total duration of therapy. The CPIS may be used to shorten the duration of therapy in patients at low risk for pneumonia. Investigators at a Veterans Affairs medical center randomized patients suspected of having NP, but who had a CPIS score < 6, to either treatment for 10–21 days, or short course therapy. Patients receiving short course therapy were reassessed at day 3, and if their CPIS score remained < 6, antibiotics were stopped (5). The short course therapy group had no difference in mortality when compared to the standard treatment group, but had less antibiotic use, shorter ICU stays, and was less likely to develop a superinfection or infection with a resistant organism. If the CPIS is not used, or if patients are felt to be at higher risk or convincingly demonstrated to have NP, a shorter course of therapy may still be preferred. A large randomized trial showed that 8 days of antibiotic therapy for patients with VAP resulted in similar clinical outcomes when compared to 15 days of therapy. Additionally, shorter duration antibiotic therapy was associated with lower likelihood of developing subsequent infections with multi-resistant pathogens. A subset of patients in the 8 day treatment group infected with non-fermenting gram negative bacilli (e.g., Pseudomonas aeruginosa) did have a higher pulmonary infection recurrence rate, but due to aggressive surveillance, this did not translate into a higher mortality risk in this subset of patients (9).
In summary, treatment of patients with suspected NP starts with immediate initiation of antibiotics and collection of respiratory secretions. While low risk patients can receive narrower spectrum therapy, most patients will require broad initial empiric therapy. The antibiotic regimen, however, should be narrowed at 48–72 hours based on microbiological results if the patient is improving. Overall treatment duration of 1 week is safe and effective with less chance of promoting growth of resistant organisms. In the subset of patients with pseudomonal infections, treatment of 1 week duration should be followed by active surveillance for recurrence, or alternatively, treatment can be extended to two weeks.
Prognosis
Once treatment for NP is initiated, clinical improvement is usually seen by 48–72 hours. There is little support for following either microbiologic response (clearance of positive cultures) or the response by chest radiography. The chest radiograph often lags behind the clinical response, however, a markedly worsening CXR (>50% increase in infiltrate) within the first 48 hours may indicate treatment failure. Clinical resolution as measured by temperature, white blood cell count, and oxygenation usually occurs by 6–7 days (10). Failure of oxygenation to improve by 72 hours has been shown to be predictive of treatment failure.
The overall mortality in patients with NP is as high as 30–70%, largely due to severe comorbid disease in the at risk population. Higher mortality rates are seen in patients with VAP and resistant organisms. The mortality attributable to the episode of NP is about 30%, and can be reduced to <15% with appropriate antibiotic therapy (1).
Prevention
Preventive strategies are either directed at reducing the overall incidence of infectious complications in hospitalized patients, or they are specifically targeted at reducing the incidence of nosocomial pneumonia (3). The majority of the data supporting preventive strategies is limited to patients in the ICU, and in particular, patients receiving mechanical ventilation. However, many of the preventive principles can be extrapolated to the non-ICU population. The preventive strategies are highlighted in Table IV (page 18).
General Preventive Strategies
General preventive strategies aim to avoid contamination of patients with antimicrobial resistant organisms that exist in hospitals, or mitigating the emergence of antimicrobial resistant organisms in the first place. Preventing iatrogenic spread of resistant organisms depends on careful hand hygiene. Hand washing before and after patient contact reduces the incidence of nosocomial infection. Alcohol-based hand rinses placed at the bedside may actually be superior to soap and water, and in addition, improve compliance with hand hygiene.
Minimizing the use of indwelling devices (central lines, urinary catheters) also reduces the emergence of resistant organisms. When these devices are necessary, focusing on their timely removal is critical. The control of antibiotic use has been central to many preventive strategies. Prolonged or unnecessary use of broad-spectrum antibiotics is strongly associated with development and colonization of resistant organisms. Strategies that focus on aggressive antibiotic de-escalation (described above) are a key preventive tool. Some institutions have had success with antibiotic restriction or rotation, but long term data on the effectiveness of these techniques are lacking.
Targeted Preventive Strategies
Preventive strategies to lower the incidence of NP focus on reducing risk factors for oropharyngeal or gastric colonization and subsequent aspiration of contaminated oropharyngeal or gastric secretions (1,3,7,11).
Endotracheal intubation is one of the most important risk factors for NP in patients requiring ventilatory support. The use of non-invasive ventilation (NIV) or positive pressure mask ventilation in selected groups of patients has been effective in preventing nosocomial pneumonia. Non-invasive ventilation has been most successful in patients with acute exacerbations of chronic obstructive pulmonary disease (COPD) and pulmonary edema secondary to congestive heart failure (CHF) and should be considered in appropriately selected patients. When intubation is required the use of nasotracheal intubation should be avoided due higher rates of NP when compared to orotracheal intubation.
Supine positioning may contribute to the development of NP, likely due to an increased risk of gastric reflux and subsequent aspiration. Studies of semi-recumbent positioning (elevation of the head of the bed >45 degrees) have shown less reflux, less aspiration, and in one recent randomized control trial, a significant reduction in the rate of VAP (12). Elevation of the head of the bed is clearly indicated in mechanically ventilated patients and is also likely to benefit all patients at risk for aspiration and subsequent NP, although this technique has not been well studied in non-ventilated patients.
Subglottic secretion drainage (SSD) involves the removal of pooled secretions above the cuff of a specialized endotracheal tube that might otherwise leak into the lung. A meta-analysis of five studies evaluating this new technology showed significant reductions in the incidence of VAP. The use of SSD should be considered for use in patients requiring more than 3 days of mechanical ventilation (13).
Medications used for stress ulcer prophylaxis that increase gastric pH-such as H2 antagonists and antacids-allow for colonization of the upper gastrointestinal tract by potentially pathogenic organisms and therefore increase the risk for NP. The use of sucralfate instead of H2 antagonists is felt to lead to less alkalinization of the stomach and less bacterial overgrowth. The ability of sucralfate to prevent nosocomial pneumonia, however, has not been well demonstrated and its routine use is not recommended (14). Instead, efforts should be targeted at limiting use of stress ulcer prophylaxis to populations at high risk for clinically significant bleeding, namely patients with coagulopathy and prolonged ventilatory failure. Most patients who are not in the ICU should not receive stress ulcer prophylaxis. The risk of NP related to use of proton pump inhibitors has not been well studied.
Selective digestive decontamination (SDD) involves sterilization of the oropharynx and gastrointestinal tract in mechanically ventilated patients in order to prevent aspiration of large numbers of potentially pathogenic organisms and subsequent VAP. Most evaluations of SDD have involved oral (and sometimes gastric) application of topical polymixin, aminoglycoside, and amphotericin. In many cases, short courses of IV antibiotics have been added. At least 10 meta-analyses have shown a reduction in the risk of VAP with the use of SDD. The addition of IV antibiotics may also provide a mortality benefit. However, the long-term risk for emergence of resistant organisms, and insufficient data on the cost-effectiveness of SDD prevent its recommendation for routine use (14).
There are several preventive strategies targeted at reducing aspiration of contaminants in ventilator circuits, filters, and tubing. Recommended strategies, listed in Table III, page 16, include avoidance of routine ventilator circuit changes (change the tubing only when visibly contaminated or for a new patient), use of heat and moisture exchangers rather than heated humidifiers, and reduction in the frequency of changes of the heat and moisture exchangers (1,11,14).
Discharge/Follow-up Plans
Patients should be followed in the hospital until it is clear they are responding to therapy and clinically improving. There has been limited evaluation of strategies to rapidly transition patients to oral therapy. However, if patients are improving, are tolerating oral therapy, have a functional GI tract, and have an organism isolated that is sensitive to available oral antibiotics, the switch to oral therapy can be made. If no organism is isolated, but a patient definitely was felt to have NP, the oral antibiotics selected should have the same spectrum of activity as the previously administered IV antibiotics. In many cases, patients will have an infection with an organism that is only susceptible to IV antibiotics. These patients are likely to be ill enough to complete a full one week IV course in the hospital, but if they have no active co-morbid illness and have improved, they can have a PICC line placed (or other long-term IV access) and receive the remainder of their therapy at home or in another lower acuity setting.
In all patients who develop NP, reversible causes of aspiration should be sought, and in cases where multidrug-resistant organisms are isolated, this should be reported to any facility to which a patient is being transferred or to the primary care physician or home nurse who will assume care after discharge.
References
- Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388-416.
- Warren DK, Shukla SJ, Olsen MA, et al. Outcome and attributable cost of ventilator-associated pneumonia among intensive care unit patients in a suburban medical center. Crit Care Med. 2003;31:1312-7.
- Flanders SA, Collard HR, Saint S. Preventing Nosocomial Pneumonia. In: Lautenbach E, Woeltje K, eds. The Society for Healthcare Epidemiology of America: Practical Handbook for Healthcare Epidemiologists. Thorofare, NJ: Slack, 2004:69-78.
- Pugin J, Auckenthaler R, Mili N, Janssens JP, Lew PD, Suter PM. Diagnosis of ventilator-associated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic “blind” bronchoalveolar lavage fluid. Am Rev Respir Dis. 1991;143:1121-9.
- Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000;162:505-11.
- Gibot S, Cravoisy A, Levy B, Bene MC, Faure G, Bollaert PE. Soluble triggering receptor expressed on myeloid cells and the diagnosis of pneumonia. N Engl J Med. 2004;350:451-8.
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165:867-903.
- Paul M, Benuri-Silbiger I, Soares-Weiser K, Leibovici L. Beta lactam monotherapy versus beta lactam-aminoglycoside combination therapy for sepsis in immunocompetent patients: systematic review and metaanalysis of randomised trials. BMJ. 2004;328:668.
- Chastre J, Wolff M, Fagon JY, et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290:2588-98.
- Dennesen PJ, van der Ven AJ, Kessels AG, Ramsay G, Bonten MJ. Resolution of infectious parameters after antimicrobial therapy in patients with ventilator-associated pneumonia. Am J Respir Crit Care Med. 2001;163:1371-5.
- Collard HR, Saint S, Matthay MA. Prevention of ventilator-associated pneumonia: an evidence-based systematic review. Ann Intern Med. 2003;138:494-501.
- Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354:1851-8.
- Dezfulian C, Shojania K, Collard HR, Kim HM, Matthay MA, Saint S. Subglottic secretion drainage for preventing ventilator-associated pneumonia: a metaanalysis. Am J Med. 2005;118:11-8.
- Dodek P, Keenan S, Cook D, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305-13.