User login
Health Care Will Be Better and You Will Make It Happen

The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data driven with clear quality measurements, where better performance is rewarded by better compensation is coming to a hospital near you during your professional career. And SHM and hospitalists are at the center of this revolution in the care of the acutely ill patient.
Hospitals are complex organizations with many moving parts and many unique constituencies often with different and, at times, competing definitions of success. What is clear is that even though many people have been talking about rewarding quality or making the hospital work for the patient, the current system is primarily physician centered and driven by increasing units of activity rather than how well a job is done. If we had the ideal system the patient would be able to demand that the physician appear when he wanted him to and we would be paying more for the best quality of care.
In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change from the noisy centralized nurses’ station where the health professionals congregate to a place designed to have data and nurses and doctors at the bedside. This would be the first concrete step to get the important members of the team (physicians, nurses, pharmacists, therapists) closer to the patient and closer to each other. The next step is to figure out how best to use everyone’s knowledge and perspective of the patient to provide more efficient and more effective care. SHM is working with Robert Wood Johnson Foundation and others on this initiative.
We will need to shift the data we collect from being mostly about getting paid to more about measuring how good a job we are doing. And while we are at it, it would be good if we could agree on what should be measured and if we could create a constant format so we can compare performance between institutions and groups. It would also be nice if physicians would agree to even be measured, and even better if physicians would be active participants in validating and responding to the data.
Then we would need to get the payers, the businesses and the insurers, and the government to care enough about quality to put their money where their measurements are and start paying for better performance rather than for more units of service (e.g., more visits, procedures, or surgeries, no matter the indications or the outcomes).
Before you start thinking this is the raving of someone who wants manna from heaven, let me point out what is happening right now in 2005.
SHM has partnered with the Critical Care Institute of the American College of Chest Physicians (ACCP), the American Association of Critical Care Nurses (AACCN), the American Society of Health System Pharmacists (ASHP), and others to form a Critical Care Collaborative. Together these organizations represent over 100,000 healthcare professionals and through their leadership will work towards designing a more patient-focused approach that relies on communication and cooperation from the entire team responsible for delivering patient care. The goal will be to design and test models of care, as well as to increase recognition and awareness of existing models by tapping into the resources of the participating organizations. Efforts will be directed at all elements of the system including the point of care, support systems (IT), administration, payers, and regulatory bodies.
SHM is also actively participating in quality and team-based initiatives with the endocrine societies and the cardiology communities. This will lead to a new way of managing care in diabetes, heart failure, coronary artery disease, and deep vein thrombosis and pulmonary embolism.
On a national level President Bush has appointed David Brailler as the “health IT czar” with the charge to expand and integrate the information capabilities in health care. This coupled with the work being done at the National Quality Forum by Ken Kizer and others will lead to practical front line applications of standards of care and the ability to measure our performance in the reality of today’s hospital.
And even the payers are getting into the mix. The new buzz words are “pay for performance” and it is all the rage. CMS and others are well into beta test programs to see just how this would play out. Peer pressure and restriction of privileges have been the only concrete drivers to improve quality in the past. The prospect that demonstrable, measurable better care will translate into more compensation or greater market share is being tested in today’s hospital.
This is not a pipe dream or a Ralph Waldo Emerson essay. These initiatives are being driven by capable action oriented leaders who have a history of making change happen. And hospitalists, who for the most part are in the beginning of a 20 to 30-year professional career, are primed to play significant roles in this changing dynamic.
In the most basic way, today’s 12,000 hospitalists and the next 20,000 who will join us in the coming years must be much more than just willing participants to make this fly. Sure hospitalists will be the effector arm of health system change in their hospitals, but hospitalists must have
the skills and the vision to help shape this better day in health care. Hospitalists need to embrace the patient-centered, performance-driven acute care system. Hospitalists need to demand care delivered by teams and have the leadership skills to help these teams manage and lead change.
This wasn’t taught in medical school or residency, but that doesn’t matter. Hospital medicine as a new specialty has arrived coincident to (or by design at) a special moment in health care. Our patients have expectations of excellent care. There are plenty of resources available to do the best job. We just aren’t organized to be the best that we can be. But this will all be sorted out in the coming years. It is an exciting time to be a health professional, and hospitalists are at the center. And SHM has the vision and will have the programs to help our hospitalists be an important part in creating this new era of health care.
The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data driven with clear quality measurements, where better performance is rewarded by better compensation is coming to a hospital near you during your professional career. And SHM and hospitalists are at the center of this revolution in the care of the acutely ill patient.
Hospitals are complex organizations with many moving parts and many unique constituencies often with different and, at times, competing definitions of success. What is clear is that even though many people have been talking about rewarding quality or making the hospital work for the patient, the current system is primarily physician centered and driven by increasing units of activity rather than how well a job is done. If we had the ideal system the patient would be able to demand that the physician appear when he wanted him to and we would be paying more for the best quality of care.
In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change from the noisy centralized nurses’ station where the health professionals congregate to a place designed to have data and nurses and doctors at the bedside. This would be the first concrete step to get the important members of the team (physicians, nurses, pharmacists, therapists) closer to the patient and closer to each other. The next step is to figure out how best to use everyone’s knowledge and perspective of the patient to provide more efficient and more effective care. SHM is working with Robert Wood Johnson Foundation and others on this initiative.
We will need to shift the data we collect from being mostly about getting paid to more about measuring how good a job we are doing. And while we are at it, it would be good if we could agree on what should be measured and if we could create a constant format so we can compare performance between institutions and groups. It would also be nice if physicians would agree to even be measured, and even better if physicians would be active participants in validating and responding to the data.
Then we would need to get the payers, the businesses and the insurers, and the government to care enough about quality to put their money where their measurements are and start paying for better performance rather than for more units of service (e.g., more visits, procedures, or surgeries, no matter the indications or the outcomes).
Before you start thinking this is the raving of someone who wants manna from heaven, let me point out what is happening right now in 2005.
SHM has partnered with the Critical Care Institute of the American College of Chest Physicians (ACCP), the American Association of Critical Care Nurses (AACCN), the American Society of Health System Pharmacists (ASHP), and others to form a Critical Care Collaborative. Together these organizations represent over 100,000 healthcare professionals and through their leadership will work towards designing a more patient-focused approach that relies on communication and cooperation from the entire team responsible for delivering patient care. The goal will be to design and test models of care, as well as to increase recognition and awareness of existing models by tapping into the resources of the participating organizations. Efforts will be directed at all elements of the system including the point of care, support systems (IT), administration, payers, and regulatory bodies.
SHM is also actively participating in quality and team-based initiatives with the endocrine societies and the cardiology communities. This will lead to a new way of managing care in diabetes, heart failure, coronary artery disease, and deep vein thrombosis and pulmonary embolism.
On a national level President Bush has appointed David Brailler as the “health IT czar” with the charge to expand and integrate the information capabilities in health care. This coupled with the work being done at the National Quality Forum by Ken Kizer and others will lead to practical front line applications of standards of care and the ability to measure our performance in the reality of today’s hospital.
And even the payers are getting into the mix. The new buzz words are “pay for performance” and it is all the rage. CMS and others are well into beta test programs to see just how this would play out. Peer pressure and restriction of privileges have been the only concrete drivers to improve quality in the past. The prospect that demonstrable, measurable better care will translate into more compensation or greater market share is being tested in today’s hospital.
This is not a pipe dream or a Ralph Waldo Emerson essay. These initiatives are being driven by capable action oriented leaders who have a history of making change happen. And hospitalists, who for the most part are in the beginning of a 20 to 30-year professional career, are primed to play significant roles in this changing dynamic.
In the most basic way, today’s 12,000 hospitalists and the next 20,000 who will join us in the coming years must be much more than just willing participants to make this fly. Sure hospitalists will be the effector arm of health system change in their hospitals, but hospitalists must have
the skills and the vision to help shape this better day in health care. Hospitalists need to embrace the patient-centered, performance-driven acute care system. Hospitalists need to demand care delivered by teams and have the leadership skills to help these teams manage and lead change.
This wasn’t taught in medical school or residency, but that doesn’t matter. Hospital medicine as a new specialty has arrived coincident to (or by design at) a special moment in health care. Our patients have expectations of excellent care. There are plenty of resources available to do the best job. We just aren’t organized to be the best that we can be. But this will all be sorted out in the coming years. It is an exciting time to be a health professional, and hospitalists are at the center. And SHM has the vision and will have the programs to help our hospitalists be an important part in creating this new era of health care.
The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data driven with clear quality measurements, where better performance is rewarded by better compensation is coming to a hospital near you during your professional career. And SHM and hospitalists are at the center of this revolution in the care of the acutely ill patient.
Hospitals are complex organizations with many moving parts and many unique constituencies often with different and, at times, competing definitions of success. What is clear is that even though many people have been talking about rewarding quality or making the hospital work for the patient, the current system is primarily physician centered and driven by increasing units of activity rather than how well a job is done. If we had the ideal system the patient would be able to demand that the physician appear when he wanted him to and we would be paying more for the best quality of care.
In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change from the noisy centralized nurses’ station where the health professionals congregate to a place designed to have data and nurses and doctors at the bedside. This would be the first concrete step to get the important members of the team (physicians, nurses, pharmacists, therapists) closer to the patient and closer to each other. The next step is to figure out how best to use everyone’s knowledge and perspective of the patient to provide more efficient and more effective care. SHM is working with Robert Wood Johnson Foundation and others on this initiative.
We will need to shift the data we collect from being mostly about getting paid to more about measuring how good a job we are doing. And while we are at it, it would be good if we could agree on what should be measured and if we could create a constant format so we can compare performance between institutions and groups. It would also be nice if physicians would agree to even be measured, and even better if physicians would be active participants in validating and responding to the data.
Then we would need to get the payers, the businesses and the insurers, and the government to care enough about quality to put their money where their measurements are and start paying for better performance rather than for more units of service (e.g., more visits, procedures, or surgeries, no matter the indications or the outcomes).
Before you start thinking this is the raving of someone who wants manna from heaven, let me point out what is happening right now in 2005.
SHM has partnered with the Critical Care Institute of the American College of Chest Physicians (ACCP), the American Association of Critical Care Nurses (AACCN), the American Society of Health System Pharmacists (ASHP), and others to form a Critical Care Collaborative. Together these organizations represent over 100,000 healthcare professionals and through their leadership will work towards designing a more patient-focused approach that relies on communication and cooperation from the entire team responsible for delivering patient care. The goal will be to design and test models of care, as well as to increase recognition and awareness of existing models by tapping into the resources of the participating organizations. Efforts will be directed at all elements of the system including the point of care, support systems (IT), administration, payers, and regulatory bodies.
SHM is also actively participating in quality and team-based initiatives with the endocrine societies and the cardiology communities. This will lead to a new way of managing care in diabetes, heart failure, coronary artery disease, and deep vein thrombosis and pulmonary embolism.
On a national level President Bush has appointed David Brailler as the “health IT czar” with the charge to expand and integrate the information capabilities in health care. This coupled with the work being done at the National Quality Forum by Ken Kizer and others will lead to practical front line applications of standards of care and the ability to measure our performance in the reality of today’s hospital.
And even the payers are getting into the mix. The new buzz words are “pay for performance” and it is all the rage. CMS and others are well into beta test programs to see just how this would play out. Peer pressure and restriction of privileges have been the only concrete drivers to improve quality in the past. The prospect that demonstrable, measurable better care will translate into more compensation or greater market share is being tested in today’s hospital.
This is not a pipe dream or a Ralph Waldo Emerson essay. These initiatives are being driven by capable action oriented leaders who have a history of making change happen. And hospitalists, who for the most part are in the beginning of a 20 to 30-year professional career, are primed to play significant roles in this changing dynamic.
In the most basic way, today’s 12,000 hospitalists and the next 20,000 who will join us in the coming years must be much more than just willing participants to make this fly. Sure hospitalists will be the effector arm of health system change in their hospitals, but hospitalists must have
the skills and the vision to help shape this better day in health care. Hospitalists need to embrace the patient-centered, performance-driven acute care system. Hospitalists need to demand care delivered by teams and have the leadership skills to help these teams manage and lead change.
This wasn’t taught in medical school or residency, but that doesn’t matter. Hospital medicine as a new specialty has arrived coincident to (or by design at) a special moment in health care. Our patients have expectations of excellent care. There are plenty of resources available to do the best job. We just aren’t organized to be the best that we can be. But this will all be sorted out in the coming years. It is an exciting time to be a health professional, and hospitalists are at the center. And SHM has the vision and will have the programs to help our hospitalists be an important part in creating this new era of health care.
Five-Year Review of Codes Begins
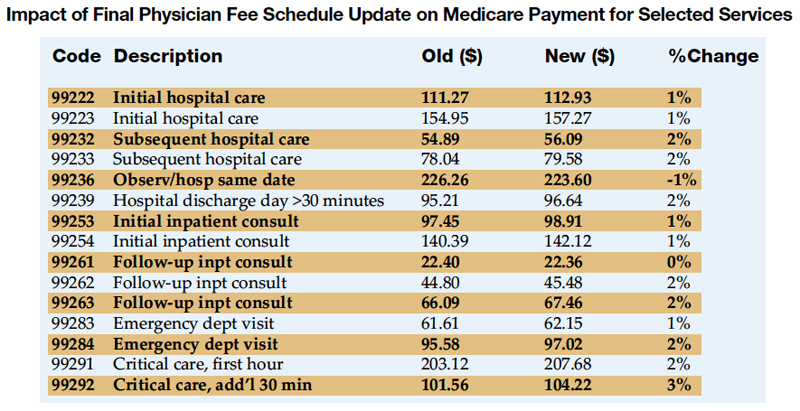
The Medicare Physician Fee Schedule indicates how much each physician service will be reimbursed by Medicare. Payment rates are a combination of three components: physician work, practice expense, and professional liability (malpractice). The Centers for Medicare and Medicaid Services (CMS) assigns relative value units (RVU) to each component, largely based on recommendations made by the Relative Value Update Committee (RUC).
Each billing code is to be reviewed at least once every 5 years to determine its RVU. The second Five-Year Review process has just begun and will review physician work RVU. By approximately March 15 this year, the American Medical Association (AMA) will have collected responses. Surveys will be sent to those specialty societies that expressed an interest in surveying the codes. Once the surveys are completed, specialty societies make their coding recommendations to the AMA. The Society of Hospitalist Medicine (SHM) will be making recommendations to the AMA in conjunction with our other colleagues who use similar codes.
In September, the recommendations are forwarded to the RUC for review. The RUC recommendations are then forwarded to CMS for consideration. Once CMS has completed their review, they typically publish a Notice of Proposed Rulemaking (NPRM) on Five-Year Review in March (in this case, March 2006). The Final Rule is expected to be released November 2006, and the new physician work RVU assignments will be implemented January 1, 2007.
Many cognitive specialty groups began to organize before the current Five-Year Review process started, in order to more efficiently coordinate efforts regarding codes of mutual interest. SHM has joined other such specialties in signing on to a unified letter to CMS regarding this Five-Year Review.
The 2005 Physician Fee Schedule was recently released. Below are the rates for selected services frequently rendered by hospitalists.
Dr. Gorman can be contacted at [email protected].
The Medicare Physician Fee Schedule indicates how much each physician service will be reimbursed by Medicare. Payment rates are a combination of three components: physician work, practice expense, and professional liability (malpractice). The Centers for Medicare and Medicaid Services (CMS) assigns relative value units (RVU) to each component, largely based on recommendations made by the Relative Value Update Committee (RUC).
Each billing code is to be reviewed at least once every 5 years to determine its RVU. The second Five-Year Review process has just begun and will review physician work RVU. By approximately March 15 this year, the American Medical Association (AMA) will have collected responses. Surveys will be sent to those specialty societies that expressed an interest in surveying the codes. Once the surveys are completed, specialty societies make their coding recommendations to the AMA. The Society of Hospitalist Medicine (SHM) will be making recommendations to the AMA in conjunction with our other colleagues who use similar codes.
In September, the recommendations are forwarded to the RUC for review. The RUC recommendations are then forwarded to CMS for consideration. Once CMS has completed their review, they typically publish a Notice of Proposed Rulemaking (NPRM) on Five-Year Review in March (in this case, March 2006). The Final Rule is expected to be released November 2006, and the new physician work RVU assignments will be implemented January 1, 2007.
Many cognitive specialty groups began to organize before the current Five-Year Review process started, in order to more efficiently coordinate efforts regarding codes of mutual interest. SHM has joined other such specialties in signing on to a unified letter to CMS regarding this Five-Year Review.
The 2005 Physician Fee Schedule was recently released. Below are the rates for selected services frequently rendered by hospitalists.
Dr. Gorman can be contacted at [email protected].
The Medicare Physician Fee Schedule indicates how much each physician service will be reimbursed by Medicare. Payment rates are a combination of three components: physician work, practice expense, and professional liability (malpractice). The Centers for Medicare and Medicaid Services (CMS) assigns relative value units (RVU) to each component, largely based on recommendations made by the Relative Value Update Committee (RUC).
Each billing code is to be reviewed at least once every 5 years to determine its RVU. The second Five-Year Review process has just begun and will review physician work RVU. By approximately March 15 this year, the American Medical Association (AMA) will have collected responses. Surveys will be sent to those specialty societies that expressed an interest in surveying the codes. Once the surveys are completed, specialty societies make their coding recommendations to the AMA. The Society of Hospitalist Medicine (SHM) will be making recommendations to the AMA in conjunction with our other colleagues who use similar codes.
In September, the recommendations are forwarded to the RUC for review. The RUC recommendations are then forwarded to CMS for consideration. Once CMS has completed their review, they typically publish a Notice of Proposed Rulemaking (NPRM) on Five-Year Review in March (in this case, March 2006). The Final Rule is expected to be released November 2006, and the new physician work RVU assignments will be implemented January 1, 2007.
Many cognitive specialty groups began to organize before the current Five-Year Review process started, in order to more efficiently coordinate efforts regarding codes of mutual interest. SHM has joined other such specialties in signing on to a unified letter to CMS regarding this Five-Year Review.
The 2005 Physician Fee Schedule was recently released. Below are the rates for selected services frequently rendered by hospitalists.
Dr. Gorman can be contacted at [email protected].
Other Pediatric Literature of Interest
1. Uehara R, Yashiro M, Nakamura Y, Yanagawa H. Clinical features of patients with Kawasaki disease whose parents had the same disease. Arch Pediatr Adolesc Med. 2004;158:1166-9.
Authors from the Department of Public Heath, Jichi Medical School and Saitama Prefectural University in Japan note that in the 35 years that have passed since the initial descriptions of Kawasaki disease some patients who had the disease have reached reproductive age and, thus, familial cases of two generations occur. Based on responses to nationwide surveys of hospitals and pediatric departments 65 cases of Kawasaki disease were identified in children whose parents had the same diagnosis. The odds for having sibling cases of Kawasaki disease were significantly increased for patients whose parents had the disease (OR, 6.94; 95% CI, 2.77–17.38). Patients with parental Kawasaki disease were also more likely to have recurrent disease, receive additional intravenous immunoglobulin administrations, and to have coronary artery abnormalities. The authors aptly discuss significant limitations to the study design; however, they conclude that these results highlight the need for exploration of a possible genetic contribution to pathogenesis of Kawasaki disease.
2. Jacobs RF, Maples HD, Aranda JV, et al. Pharmacokinetics of intravenously administered azithromycin in pediatric patients. Pediatr Infect Dis J. 2005;24:34-9.
Azithromyin is an azalide antibiotic with in vitro activity against a spectrum of bacterial pathogens commonly treated in pediatric infections. Currently intravenous (IV) azithromycin is only approved for use in adults. These researchers from three sites of the Pediatric Pharmacology Research Unit Network report results of an open-label single-dose pharmacokinetic and tolerance study of intravenous azithromycin in a pediatric population. This information will be required to facilitate approval for use in the pediatric population, as well as guide dosing for therapeutic trials. The authors studied pharmacokinetics in 29 patients ages 0.5 to <e;16 years of age and conclude that the disposition of IV administered azithromycin is comparable in patients in this age range; however, there was a tendency for increased clearance in younger children. The most common adverse effect was nausea that did not require intervention reported in 25% of the subjects.
3. Berger WE, Qaqundah PY, Blake, K, et al. Safety of budesonide inhalation suspension in infants aged six to twelve months with mild to moderate persistent asthma or recurrent wheeze. J Pediatr. 2005;146:91-5.
Current guidelines recommend inhaled corticosteroids (ICS) for long-term management of persistent asthma in children regardless of age. Currently the only nebulized ICS approved for use by the US Food and Drug Administration is budesonide. Controlled studies analyzing the safety and efficacy of budesonide exclusively in infants is lacking. Therefore, these researchers present a multicenter, randomized, double-blinded, parallel group, placebo-controlled study of 141 patients assessing the safety of once-daily administered nebulized budesonide in infants with persistent asthma. The primary outcome variable was adrenal function measured as mean changes from baseline to study end in postcosyntropin-stimulated plasma cortisol levels. The study was not powered to measure efficacy. The study concludes that the safety profile for nebulized budesonide was similar to that of placebo, with no suppression of adrenal function.
1. Uehara R, Yashiro M, Nakamura Y, Yanagawa H. Clinical features of patients with Kawasaki disease whose parents had the same disease. Arch Pediatr Adolesc Med. 2004;158:1166-9.
Authors from the Department of Public Heath, Jichi Medical School and Saitama Prefectural University in Japan note that in the 35 years that have passed since the initial descriptions of Kawasaki disease some patients who had the disease have reached reproductive age and, thus, familial cases of two generations occur. Based on responses to nationwide surveys of hospitals and pediatric departments 65 cases of Kawasaki disease were identified in children whose parents had the same diagnosis. The odds for having sibling cases of Kawasaki disease were significantly increased for patients whose parents had the disease (OR, 6.94; 95% CI, 2.77–17.38). Patients with parental Kawasaki disease were also more likely to have recurrent disease, receive additional intravenous immunoglobulin administrations, and to have coronary artery abnormalities. The authors aptly discuss significant limitations to the study design; however, they conclude that these results highlight the need for exploration of a possible genetic contribution to pathogenesis of Kawasaki disease.
2. Jacobs RF, Maples HD, Aranda JV, et al. Pharmacokinetics of intravenously administered azithromycin in pediatric patients. Pediatr Infect Dis J. 2005;24:34-9.
Azithromyin is an azalide antibiotic with in vitro activity against a spectrum of bacterial pathogens commonly treated in pediatric infections. Currently intravenous (IV) azithromycin is only approved for use in adults. These researchers from three sites of the Pediatric Pharmacology Research Unit Network report results of an open-label single-dose pharmacokinetic and tolerance study of intravenous azithromycin in a pediatric population. This information will be required to facilitate approval for use in the pediatric population, as well as guide dosing for therapeutic trials. The authors studied pharmacokinetics in 29 patients ages 0.5 to <e;16 years of age and conclude that the disposition of IV administered azithromycin is comparable in patients in this age range; however, there was a tendency for increased clearance in younger children. The most common adverse effect was nausea that did not require intervention reported in 25% of the subjects.
3. Berger WE, Qaqundah PY, Blake, K, et al. Safety of budesonide inhalation suspension in infants aged six to twelve months with mild to moderate persistent asthma or recurrent wheeze. J Pediatr. 2005;146:91-5.
Current guidelines recommend inhaled corticosteroids (ICS) for long-term management of persistent asthma in children regardless of age. Currently the only nebulized ICS approved for use by the US Food and Drug Administration is budesonide. Controlled studies analyzing the safety and efficacy of budesonide exclusively in infants is lacking. Therefore, these researchers present a multicenter, randomized, double-blinded, parallel group, placebo-controlled study of 141 patients assessing the safety of once-daily administered nebulized budesonide in infants with persistent asthma. The primary outcome variable was adrenal function measured as mean changes from baseline to study end in postcosyntropin-stimulated plasma cortisol levels. The study was not powered to measure efficacy. The study concludes that the safety profile for nebulized budesonide was similar to that of placebo, with no suppression of adrenal function.
1. Uehara R, Yashiro M, Nakamura Y, Yanagawa H. Clinical features of patients with Kawasaki disease whose parents had the same disease. Arch Pediatr Adolesc Med. 2004;158:1166-9.
Authors from the Department of Public Heath, Jichi Medical School and Saitama Prefectural University in Japan note that in the 35 years that have passed since the initial descriptions of Kawasaki disease some patients who had the disease have reached reproductive age and, thus, familial cases of two generations occur. Based on responses to nationwide surveys of hospitals and pediatric departments 65 cases of Kawasaki disease were identified in children whose parents had the same diagnosis. The odds for having sibling cases of Kawasaki disease were significantly increased for patients whose parents had the disease (OR, 6.94; 95% CI, 2.77–17.38). Patients with parental Kawasaki disease were also more likely to have recurrent disease, receive additional intravenous immunoglobulin administrations, and to have coronary artery abnormalities. The authors aptly discuss significant limitations to the study design; however, they conclude that these results highlight the need for exploration of a possible genetic contribution to pathogenesis of Kawasaki disease.
2. Jacobs RF, Maples HD, Aranda JV, et al. Pharmacokinetics of intravenously administered azithromycin in pediatric patients. Pediatr Infect Dis J. 2005;24:34-9.
Azithromyin is an azalide antibiotic with in vitro activity against a spectrum of bacterial pathogens commonly treated in pediatric infections. Currently intravenous (IV) azithromycin is only approved for use in adults. These researchers from three sites of the Pediatric Pharmacology Research Unit Network report results of an open-label single-dose pharmacokinetic and tolerance study of intravenous azithromycin in a pediatric population. This information will be required to facilitate approval for use in the pediatric population, as well as guide dosing for therapeutic trials. The authors studied pharmacokinetics in 29 patients ages 0.5 to <e;16 years of age and conclude that the disposition of IV administered azithromycin is comparable in patients in this age range; however, there was a tendency for increased clearance in younger children. The most common adverse effect was nausea that did not require intervention reported in 25% of the subjects.
3. Berger WE, Qaqundah PY, Blake, K, et al. Safety of budesonide inhalation suspension in infants aged six to twelve months with mild to moderate persistent asthma or recurrent wheeze. J Pediatr. 2005;146:91-5.
Current guidelines recommend inhaled corticosteroids (ICS) for long-term management of persistent asthma in children regardless of age. Currently the only nebulized ICS approved for use by the US Food and Drug Administration is budesonide. Controlled studies analyzing the safety and efficacy of budesonide exclusively in infants is lacking. Therefore, these researchers present a multicenter, randomized, double-blinded, parallel group, placebo-controlled study of 141 patients assessing the safety of once-daily administered nebulized budesonide in infants with persistent asthma. The primary outcome variable was adrenal function measured as mean changes from baseline to study end in postcosyntropin-stimulated plasma cortisol levels. The study was not powered to measure efficacy. The study concludes that the safety profile for nebulized budesonide was similar to that of placebo, with no suppression of adrenal function.
Pediatric in the Literature
Parents' Priorities and Satisfaction with Acute Pediatric Care
Ammentorp J, Mainz J, Sabroe S. Parents’ priorities and satisfaction with acute pediatric care. Arch Pediatr Adolesc Med. 2005;159:127-31.
Researchers from Kolding Hospital in Denmark designed this study to identify parents’ priorities of and satisfaction with care provided to pediatric patients by nurses and physicians. The cross-sectional study took place on the pediatric ward by enrolling consecutively admitted patients between 0800 and 2200 who spoke and understood Danish. The researchers designed and validated a 36 item questionnaire with input from 13 previous studies about patient satisfaction. The items were assessed using a 5-point Likert scale and were grouped into six dimensions of service: 1) Access to care and treatment, 2) Information and communication related to care and treatment, 3) Information related to practical conditions (i.e., orientation to the ward), 4) Physicians’ behavior, 5) Nurses’ behavior, and 6) Access to service. The survey consisted of two parts. Section 1 addressed priorities and was to be filled out by the parent(s) at admission. Section 2 addressed satisfaction and was to be filled out at discharge. The response rates for Section 1 and Section 2 were 84% and 67%, respectively. Statistical analysis demonstrated that parents could differentiate between priority and satisfaction.
Parents generally rated most aspects of care as important, and aspects related directly to treatment were rated highest. The three most important priorities with the assigned scores with 5 being the highest possible score were: 1) Find(ing) out what is wrong with the child (4.6), 2) Taking care of the child’s pain if it is relevant (4.6), and 3) Explanation of the diagnosis/problem (4.5). The least important items for parents in general were related to orientation of the ward. Interestingly, the least important item for parents in the study was having the child discharged the same day as admission (2.7).
Parents were most satisfied with the kindness of the nurses (4.4) and understanding the nurses information (4.3). The lowest satisfaction level was found with waiting time on the ward for medication evaluation, and this was also the greatest gap between priority and satisfaction for the parents in the study (priority 4.5, satisfaction 3.0)
The researchers present satisfaction and priority data together in a scatter plot with priority mean score on the vertical axis and satisfaction mean score on the horizontal access and in so doing create four quadrants that aid in focusing attention on improving quality on their ward. The researchers conclude that items that plot in the upper left quadrant deserve special attention as items that parents believe are important but are not satisfied with. Items differentiating between physician and nursing involvement in the same service areas were plotted as well, and results indicated that, in general, parents gave physician service higher priority but were more satisfied with nursing service.
The researchers conclude that the tool they describe is a validated questionnaire that can be used to evaluate parent priorities for and satisfaction with care provided on pediatric inpatient wards. This information can be used to guide further investigations and quality development. For the study ward this tool demonstrated that waiting time and communication with parents represented the most important areas for improvement.
Satisfaction is an important aspect of quality of care, as well an important attribute of the potential value added by physicians dedicated to inpatient medicine. Several important factors limit generalizing the specific conclusions of this study, including not including the non-Danish speaking minority and not identifying parents whose children have had multiple inpatient admissions. Regardless, the survey and scatter plot analysis with a “special attention” quadrant have obvious utility in the effort to produce quality improvement with regard to parents’ perception of the quality of care their children receive. Other interesting applications not specifically addressed in the study include measuring the priorities and satisfaction level of patients old enough to respond, including questions regarding service provided by nurse practitioners or physician’s assistants and testing to see if parents’ and/or patients’ priorities change from admission, through hospitalization, and at discharge.
Evaluation of a Staff-Only Hospitalist System in a Tertiary Care, Academic Children's Hospital
Dwight P, MacArthur C, Friedman JN, et al. Evaluation of a staff-only hospitalist system in a tertiary care, academic children’s hospital. Pediatrics. 2004;114:1545-9.
The division of pediatrics at The Hospital for Sick Children in Toronto, a tertiary care, academic center, operates a pediatric inpatient unit with approximately 4000 admissions each year. In 1995, limited resident duty hours led to a reorganization of inpatient pediatric teams to include two distinct hospitalist models: A hospitalist/housestaff model (CTU) and hospitalist staff -only model (CPU). The authors review recent research that has demonstrated the efficiency of hospitalist/housestaff systems in both adult and pediatric medicine and accurately point out that published data is lacking assessing the staff -only pediatric hospitalist model. Therefore, the authors designed a cohort study of 3807 admissions to the general inpatient pediatric unit between July 1, 1996 and June 30, 1997.
The primary outcome measure was length of stay, and secondary outcome measures included frequency of subspecialty consultation, readmission to the hospital, and death. Consultations were measured as none or >1 and readmissions were defined as admission within 7 days of discharge for the same or a related diagnosis. Clinically relevant information collected for each patient included age, gender, referral source, stay in a special care unit, most responsible diagnosis, and comorbidity. Comorbidity was defined as either an uncomplicated stay or a stay complicated by a chronic illness, series or important conditions, and/or a potentially life-threatening condition. The CTU team had a daily census of 24 to 30 patients and consisted of 1 attending pediatrician, 3 or 4 pediatric residents, and 2 medical students. CTU pediatricians attended this service 4–8 weeks each year. The CPU was staffed with 3 pediatricians who were responsible for all aspects of care Monday through Friday from 0800 to 1700 and on weekends. Medical students were included on this team. Overnight and weekends clinical fellows not part of the CPU team provided coverage. Each CPU physicians maintained a daily census of 8–10 patients. These physicians spent approximately 11 months of the year providing inpatient care.
During the study there were 3807 admissions, of which 33% were to the CPU and 67% were to the CTU. Patients admitted to the CPU were older (median age: 95 weeks vs. 69 weeks, p < .01) and less likely to have comorbidity (24% vs. 30%; p < .01). The diagnoses admitted to the two teams were not significantly different. The median length of hospital stay for the CPU team was 2.5 days (interquartile range [IQR]: 1.6–4.4 days) versus 2.9 days (IQR: 1.8–4.9) for the CTU team (p < .01). Multivariate linear regression showed a significant difference in length of stay after adjustment for age, gender and comorbidity (p < .04). The authors performed a stratified analysis of the 10 most frequent diagnoses admitted during the study period, and the median length of stay for these groups combined was shorter on the CPU team compared with the CTU team (2.1 days vs. 2.6 days, p < .01). There was no significant difference between the two teams with readmissions, frequency of consultation, or death.
The authors discuss some important limitations to the study. First, the unique characteristics of the individual unit studied inhibit the ability to generalize the results. Second, there were some differences in the baseline characteristics between the two groups, although multivariate analysis of theses differences did not change the statistical significance of the results. Finally, satisfaction of patients, families, and care providers was not measured.
These researchers conclude that within this system the hospitalist staff -only team reduced the length of stay by 14% compared with an attending staff/housestaff team. Although statistically significant, the clinical significance of this reduction in length of stay is unclear and the authors did not include financial data in the study design. Despite these facts, the authors make an important assertion that the difference in stay of 8 hours may be enough to promote throughput by decreasing wait times for admissions from the emergency departments and/or special care units. Additional studies are required to test this assertion.
Parents' Priorities and Satisfaction with Acute Pediatric Care
Ammentorp J, Mainz J, Sabroe S. Parents’ priorities and satisfaction with acute pediatric care. Arch Pediatr Adolesc Med. 2005;159:127-31.
Researchers from Kolding Hospital in Denmark designed this study to identify parents’ priorities of and satisfaction with care provided to pediatric patients by nurses and physicians. The cross-sectional study took place on the pediatric ward by enrolling consecutively admitted patients between 0800 and 2200 who spoke and understood Danish. The researchers designed and validated a 36 item questionnaire with input from 13 previous studies about patient satisfaction. The items were assessed using a 5-point Likert scale and were grouped into six dimensions of service: 1) Access to care and treatment, 2) Information and communication related to care and treatment, 3) Information related to practical conditions (i.e., orientation to the ward), 4) Physicians’ behavior, 5) Nurses’ behavior, and 6) Access to service. The survey consisted of two parts. Section 1 addressed priorities and was to be filled out by the parent(s) at admission. Section 2 addressed satisfaction and was to be filled out at discharge. The response rates for Section 1 and Section 2 were 84% and 67%, respectively. Statistical analysis demonstrated that parents could differentiate between priority and satisfaction.
Parents generally rated most aspects of care as important, and aspects related directly to treatment were rated highest. The three most important priorities with the assigned scores with 5 being the highest possible score were: 1) Find(ing) out what is wrong with the child (4.6), 2) Taking care of the child’s pain if it is relevant (4.6), and 3) Explanation of the diagnosis/problem (4.5). The least important items for parents in general were related to orientation of the ward. Interestingly, the least important item for parents in the study was having the child discharged the same day as admission (2.7).
Parents were most satisfied with the kindness of the nurses (4.4) and understanding the nurses information (4.3). The lowest satisfaction level was found with waiting time on the ward for medication evaluation, and this was also the greatest gap between priority and satisfaction for the parents in the study (priority 4.5, satisfaction 3.0)
The researchers present satisfaction and priority data together in a scatter plot with priority mean score on the vertical axis and satisfaction mean score on the horizontal access and in so doing create four quadrants that aid in focusing attention on improving quality on their ward. The researchers conclude that items that plot in the upper left quadrant deserve special attention as items that parents believe are important but are not satisfied with. Items differentiating between physician and nursing involvement in the same service areas were plotted as well, and results indicated that, in general, parents gave physician service higher priority but were more satisfied with nursing service.
The researchers conclude that the tool they describe is a validated questionnaire that can be used to evaluate parent priorities for and satisfaction with care provided on pediatric inpatient wards. This information can be used to guide further investigations and quality development. For the study ward this tool demonstrated that waiting time and communication with parents represented the most important areas for improvement.
Satisfaction is an important aspect of quality of care, as well an important attribute of the potential value added by physicians dedicated to inpatient medicine. Several important factors limit generalizing the specific conclusions of this study, including not including the non-Danish speaking minority and not identifying parents whose children have had multiple inpatient admissions. Regardless, the survey and scatter plot analysis with a “special attention” quadrant have obvious utility in the effort to produce quality improvement with regard to parents’ perception of the quality of care their children receive. Other interesting applications not specifically addressed in the study include measuring the priorities and satisfaction level of patients old enough to respond, including questions regarding service provided by nurse practitioners or physician’s assistants and testing to see if parents’ and/or patients’ priorities change from admission, through hospitalization, and at discharge.
Evaluation of a Staff-Only Hospitalist System in a Tertiary Care, Academic Children's Hospital
Dwight P, MacArthur C, Friedman JN, et al. Evaluation of a staff-only hospitalist system in a tertiary care, academic children’s hospital. Pediatrics. 2004;114:1545-9.
The division of pediatrics at The Hospital for Sick Children in Toronto, a tertiary care, academic center, operates a pediatric inpatient unit with approximately 4000 admissions each year. In 1995, limited resident duty hours led to a reorganization of inpatient pediatric teams to include two distinct hospitalist models: A hospitalist/housestaff model (CTU) and hospitalist staff -only model (CPU). The authors review recent research that has demonstrated the efficiency of hospitalist/housestaff systems in both adult and pediatric medicine and accurately point out that published data is lacking assessing the staff -only pediatric hospitalist model. Therefore, the authors designed a cohort study of 3807 admissions to the general inpatient pediatric unit between July 1, 1996 and June 30, 1997.
The primary outcome measure was length of stay, and secondary outcome measures included frequency of subspecialty consultation, readmission to the hospital, and death. Consultations were measured as none or >1 and readmissions were defined as admission within 7 days of discharge for the same or a related diagnosis. Clinically relevant information collected for each patient included age, gender, referral source, stay in a special care unit, most responsible diagnosis, and comorbidity. Comorbidity was defined as either an uncomplicated stay or a stay complicated by a chronic illness, series or important conditions, and/or a potentially life-threatening condition. The CTU team had a daily census of 24 to 30 patients and consisted of 1 attending pediatrician, 3 or 4 pediatric residents, and 2 medical students. CTU pediatricians attended this service 4–8 weeks each year. The CPU was staffed with 3 pediatricians who were responsible for all aspects of care Monday through Friday from 0800 to 1700 and on weekends. Medical students were included on this team. Overnight and weekends clinical fellows not part of the CPU team provided coverage. Each CPU physicians maintained a daily census of 8–10 patients. These physicians spent approximately 11 months of the year providing inpatient care.
During the study there were 3807 admissions, of which 33% were to the CPU and 67% were to the CTU. Patients admitted to the CPU were older (median age: 95 weeks vs. 69 weeks, p < .01) and less likely to have comorbidity (24% vs. 30%; p < .01). The diagnoses admitted to the two teams were not significantly different. The median length of hospital stay for the CPU team was 2.5 days (interquartile range [IQR]: 1.6–4.4 days) versus 2.9 days (IQR: 1.8–4.9) for the CTU team (p < .01). Multivariate linear regression showed a significant difference in length of stay after adjustment for age, gender and comorbidity (p < .04). The authors performed a stratified analysis of the 10 most frequent diagnoses admitted during the study period, and the median length of stay for these groups combined was shorter on the CPU team compared with the CTU team (2.1 days vs. 2.6 days, p < .01). There was no significant difference between the two teams with readmissions, frequency of consultation, or death.
The authors discuss some important limitations to the study. First, the unique characteristics of the individual unit studied inhibit the ability to generalize the results. Second, there were some differences in the baseline characteristics between the two groups, although multivariate analysis of theses differences did not change the statistical significance of the results. Finally, satisfaction of patients, families, and care providers was not measured.
These researchers conclude that within this system the hospitalist staff -only team reduced the length of stay by 14% compared with an attending staff/housestaff team. Although statistically significant, the clinical significance of this reduction in length of stay is unclear and the authors did not include financial data in the study design. Despite these facts, the authors make an important assertion that the difference in stay of 8 hours may be enough to promote throughput by decreasing wait times for admissions from the emergency departments and/or special care units. Additional studies are required to test this assertion.
Parents' Priorities and Satisfaction with Acute Pediatric Care
Ammentorp J, Mainz J, Sabroe S. Parents’ priorities and satisfaction with acute pediatric care. Arch Pediatr Adolesc Med. 2005;159:127-31.
Researchers from Kolding Hospital in Denmark designed this study to identify parents’ priorities of and satisfaction with care provided to pediatric patients by nurses and physicians. The cross-sectional study took place on the pediatric ward by enrolling consecutively admitted patients between 0800 and 2200 who spoke and understood Danish. The researchers designed and validated a 36 item questionnaire with input from 13 previous studies about patient satisfaction. The items were assessed using a 5-point Likert scale and were grouped into six dimensions of service: 1) Access to care and treatment, 2) Information and communication related to care and treatment, 3) Information related to practical conditions (i.e., orientation to the ward), 4) Physicians’ behavior, 5) Nurses’ behavior, and 6) Access to service. The survey consisted of two parts. Section 1 addressed priorities and was to be filled out by the parent(s) at admission. Section 2 addressed satisfaction and was to be filled out at discharge. The response rates for Section 1 and Section 2 were 84% and 67%, respectively. Statistical analysis demonstrated that parents could differentiate between priority and satisfaction.
Parents generally rated most aspects of care as important, and aspects related directly to treatment were rated highest. The three most important priorities with the assigned scores with 5 being the highest possible score were: 1) Find(ing) out what is wrong with the child (4.6), 2) Taking care of the child’s pain if it is relevant (4.6), and 3) Explanation of the diagnosis/problem (4.5). The least important items for parents in general were related to orientation of the ward. Interestingly, the least important item for parents in the study was having the child discharged the same day as admission (2.7).
Parents were most satisfied with the kindness of the nurses (4.4) and understanding the nurses information (4.3). The lowest satisfaction level was found with waiting time on the ward for medication evaluation, and this was also the greatest gap between priority and satisfaction for the parents in the study (priority 4.5, satisfaction 3.0)
The researchers present satisfaction and priority data together in a scatter plot with priority mean score on the vertical axis and satisfaction mean score on the horizontal access and in so doing create four quadrants that aid in focusing attention on improving quality on their ward. The researchers conclude that items that plot in the upper left quadrant deserve special attention as items that parents believe are important but are not satisfied with. Items differentiating between physician and nursing involvement in the same service areas were plotted as well, and results indicated that, in general, parents gave physician service higher priority but were more satisfied with nursing service.
The researchers conclude that the tool they describe is a validated questionnaire that can be used to evaluate parent priorities for and satisfaction with care provided on pediatric inpatient wards. This information can be used to guide further investigations and quality development. For the study ward this tool demonstrated that waiting time and communication with parents represented the most important areas for improvement.
Satisfaction is an important aspect of quality of care, as well an important attribute of the potential value added by physicians dedicated to inpatient medicine. Several important factors limit generalizing the specific conclusions of this study, including not including the non-Danish speaking minority and not identifying parents whose children have had multiple inpatient admissions. Regardless, the survey and scatter plot analysis with a “special attention” quadrant have obvious utility in the effort to produce quality improvement with regard to parents’ perception of the quality of care their children receive. Other interesting applications not specifically addressed in the study include measuring the priorities and satisfaction level of patients old enough to respond, including questions regarding service provided by nurse practitioners or physician’s assistants and testing to see if parents’ and/or patients’ priorities change from admission, through hospitalization, and at discharge.
Evaluation of a Staff-Only Hospitalist System in a Tertiary Care, Academic Children's Hospital
Dwight P, MacArthur C, Friedman JN, et al. Evaluation of a staff-only hospitalist system in a tertiary care, academic children’s hospital. Pediatrics. 2004;114:1545-9.
The division of pediatrics at The Hospital for Sick Children in Toronto, a tertiary care, academic center, operates a pediatric inpatient unit with approximately 4000 admissions each year. In 1995, limited resident duty hours led to a reorganization of inpatient pediatric teams to include two distinct hospitalist models: A hospitalist/housestaff model (CTU) and hospitalist staff -only model (CPU). The authors review recent research that has demonstrated the efficiency of hospitalist/housestaff systems in both adult and pediatric medicine and accurately point out that published data is lacking assessing the staff -only pediatric hospitalist model. Therefore, the authors designed a cohort study of 3807 admissions to the general inpatient pediatric unit between July 1, 1996 and June 30, 1997.
The primary outcome measure was length of stay, and secondary outcome measures included frequency of subspecialty consultation, readmission to the hospital, and death. Consultations were measured as none or >1 and readmissions were defined as admission within 7 days of discharge for the same or a related diagnosis. Clinically relevant information collected for each patient included age, gender, referral source, stay in a special care unit, most responsible diagnosis, and comorbidity. Comorbidity was defined as either an uncomplicated stay or a stay complicated by a chronic illness, series or important conditions, and/or a potentially life-threatening condition. The CTU team had a daily census of 24 to 30 patients and consisted of 1 attending pediatrician, 3 or 4 pediatric residents, and 2 medical students. CTU pediatricians attended this service 4–8 weeks each year. The CPU was staffed with 3 pediatricians who were responsible for all aspects of care Monday through Friday from 0800 to 1700 and on weekends. Medical students were included on this team. Overnight and weekends clinical fellows not part of the CPU team provided coverage. Each CPU physicians maintained a daily census of 8–10 patients. These physicians spent approximately 11 months of the year providing inpatient care.
During the study there were 3807 admissions, of which 33% were to the CPU and 67% were to the CTU. Patients admitted to the CPU were older (median age: 95 weeks vs. 69 weeks, p < .01) and less likely to have comorbidity (24% vs. 30%; p < .01). The diagnoses admitted to the two teams were not significantly different. The median length of hospital stay for the CPU team was 2.5 days (interquartile range [IQR]: 1.6–4.4 days) versus 2.9 days (IQR: 1.8–4.9) for the CTU team (p < .01). Multivariate linear regression showed a significant difference in length of stay after adjustment for age, gender and comorbidity (p < .04). The authors performed a stratified analysis of the 10 most frequent diagnoses admitted during the study period, and the median length of stay for these groups combined was shorter on the CPU team compared with the CTU team (2.1 days vs. 2.6 days, p < .01). There was no significant difference between the two teams with readmissions, frequency of consultation, or death.
The authors discuss some important limitations to the study. First, the unique characteristics of the individual unit studied inhibit the ability to generalize the results. Second, there were some differences in the baseline characteristics between the two groups, although multivariate analysis of theses differences did not change the statistical significance of the results. Finally, satisfaction of patients, families, and care providers was not measured.
These researchers conclude that within this system the hospitalist staff -only team reduced the length of stay by 14% compared with an attending staff/housestaff team. Although statistically significant, the clinical significance of this reduction in length of stay is unclear and the authors did not include financial data in the study design. Despite these facts, the authors make an important assertion that the difference in stay of 8 hours may be enough to promote throughput by decreasing wait times for admissions from the emergency departments and/or special care units. Additional studies are required to test this assertion.
TIPs Case Report
A 10-month-old Hispanic female presents to the emergency department with a chief complaint of being limp. The mother states that the first day of the child’s illness began with tactile fever. The patient did not have any diarrhea or vomiting. After presenting to the emergency department she was diagnosed with a left otitis media. At that time, intramuscular ceftriaxone was given and amoxicillin was prescribed. The second day the patient was doing well and there were no new problems. On the third day the patient woke up and was not moving her arms and legs as much as usual, did not want to sit up on her own, and was lying limp. Additionally, she had some decreased oral intake that day and one loose stool.
Upon follow up at the pediatrician’s office there was concern about how limp the child seemed and she was sent back to the emergency department for transfer to the children’s hospital. However, the emergency department did blood work, gave intravenous fluids, and after observing slight improvement in limb movement, discharged the child to home.
At home, the child spiked a temperature. She was brought to the pediatrician’s office the next day where slight improvement in movement and more alert affect were noted; however, concern remained regarding her overall decreased activity. The child was again sent to the emergency department for transport to the pediatric hospital.
Review of systems revealed one vomiting episode and one loose stool, slight runny nose, and decrease in oral intake 1 day prior to admission. They had recently returned form California from a weekend trip. There was no significant past medical history aside from an otitis media 4 months ago. The child was born full-term without any complications. The child does not take any chronic medications, but did take two doses of amoxicillin for one and a half days in addition to acetaminophen for fever. The child does not have any known allergies. Her diet includes breastmilk and table foods. Six month vaccinations are not completed, but prior vaccines had been given on schedule. The child lives with her mother only and family history was not significant. Developmentally the child rolled over at 4 months, sits without support, pulls to stand, and stands with help.
Physical exam showed a temperature of 100.5F, heart rate of 148, respiratory rate of 30, blood pressure 103/70, and a weight of 10.5 kg (90%). Patient is well developed and well nourished without any acute distress. Physical exam was pertinent for supple neck with head lag, generalized weakness with decreased muscular strength in the upper and lower extremities. Upper extremities strength was 4/5 and lower extremities were 3/5. Neck laxity was present, sitting required support, and she refused to stand. Neurologically the patient was alert with reflexes mildly decreased in the lower extremities.
Laboratory evaluation included a complete blood count with a white blood cell (WBC) count of 11.7 and of hemoglobin of 11.4. A comprehensive metabolic panel was within normal limits. Lumbar puncture showed glucose of 50, protein of 38, 2 WBCs, 2 red blood cells, and a negative gram stain. Urinalysis was negative. Erythrocyte sedimentation rate was 17, CPK was 57, and chest radiograph was negative.

At this time stool was sent for botulism toxin; however, there was no history of eating canned food or honey. While waiting for results the patient showed slight improvement in movement and activity and demonstrated good oral intake. Physical therapy and speech therapy were working with the patient and lower extremity movement was improving, but she still had diffi culty standing. At this time an MRI of the brain and cervical spine was ordered and showed an intramedullary lesion involving the cervical and upper thoracic cord with localized cord enlargement. Enhancement was seen along C5 and C6 to the T1 level without canal stenosis and normal anatomic alignment was noted (Figure 1). In the meantime, stool for botulism toxin returned negative. Treatment was started for the diagnosis of transverse myelitis and included dexamethasone 2 mg/kg once daily with a taper over 5 weeks. She had minimal improvement prior to discharge, but showed slow and steady resolution of symptoms. Follow up with neurology was to be done on an outpatient basis, as well as continuation of physical therapy and occupational therapy.
Discussion
Transverse myelitis or transverse myelopathy (TM) is a syndrome of acute or subacute inflammation involving the spinal cord with partial or complete loss of neurologic function. It is usually limited to a number of spinal segments. The incidence is 1.3 new cases per one million residents annually. It affects all ages and both sexes; however, is uncommon in children less than 10 years of age. There are three theories for the etiology: cell-mediated autoimmune inflammation and/or demyelination of the spinal cord, a direct viral infection of the cord, and a paraneoplastic remote effect of cancer.
Clinical features include abrupt onset of symptoms varying from hours to a few days. One third of patients have a preceding viral illness. An early sign is muscle weakness, especially of the lower limbs. There may be numbness at the midthoracic region, strength loss as extreme as paraplegia, loss of bowel or bladder control, or sensory loss, most commonly involves pain and temperature. Fifty percent may experience a sharp, gnawing back pain at the level of the myelitis. Progression of the disease can lead to spasticity and hyperreflexia.
There is not a confirmation of any pathophysiologic mechanism. Demyelination, neuronal injury, and incomplete or complete necrosis of neural tissue may be associated with inflammatory changes on biopsy.
Differential diagnosis includes idiopathic autoimmune transverse myelitis, acute disseminated encephalomyelitis, multiple sclerosis (MS), Guillain-Barre, viral myelitis, vasculitis, spinal cord infarction, paraneoplastic myelopathy, vascular malformations, and nutritional myelopathy. Additionally, infectious etiologies include HIV myelopathy, spirochetal infection, and poliomyelitis.
Diagnosis is by exclusion. First, a mechanical, compressive lesion must be excluded from the differential. MRI of the spine visualizes the myelin and excludes compression and is used primarily to exclude these possible etiologies. MRI of the brain is useful to diagnose multiple sclerosis. Lumbar puncture results are variable ranging from normal to nonspecifi c inflammatory changes including a mild increase in protein or leukocytosis with an increase in polymorponuclear cells. Glucose is usually normal.
It is important, especially in adolescents, to differentiate TM from MS and Guillain-Barre. In MS symptoms are more likely separated by time, with “attacks” and a relapsing and remitting presentation. MS patients typically present with numbness and weakness in more than one extremity. In Guillain-Barre syndrome the presentation may be similar to TM in that there is weakness in the lower extremity, areflexia, and a possible viral illness precedent. However, a dermatome localization of sensory loss on neurologic exam can differentiate between a spinal cord lesion and a peripheral nerve etiology.
Treatment for TM symptoms is nonspecifi c. If a specific etiology is found then specific treatment should be rendered, otherwise one must rule out infectious or systemic inflammatory disorders. Pharmacologic treatment commonly includes high dose steroids, for example methylprednisone 1 g IV daily for 3–5 days followed with an
oral steroid taper. The evidence in the literature supporting this therapeutic approach includes mostly small studies with inconsistent results. In addition, small, uncontrolled or pilot studies have demonstrated that cyclophosphamide, azathioprine and plasmapheresis alone or in addition to corticosteroids may improve outcomes. Larger scale randomized, blinded, and controlled studies are required to more clearly define the most safe and efficacious treatment for this uncommon pediatric diagnosis.
References
- Knebusch M, Strassburg HM, Reiners K. Acute myelitis in childhood: nine cases and review of the literature. Dev Med Child Neurol. 1998;40:631-9.
- Rolad L. Pathophysiology and clinical feature of Multiple sclerosis. Immune and Infectious Disease.408-11.
- Transverse Myelitis consortium working group. Proposed diagnostic and nosology of acute transverse myelitis. Neurology. 2002;59(4).
- Andronikou S, Albuquerque-Jonathan G, Wilmshurst J, Hewlett R. MRI fi nding in acute idiopathic transverse myelopathy in children. Pediatr Radiol. 2003;33:624-9.
- Corboy J, Price R. Myelitis and toxic, infl ammatory, and infectious disorders. Curr Opin Neurol Neurosurg. 1993;6:564-70.
- Rust R. Multiple sclerosis, acute disseminated encephalomyelitis, and related conditions. Semin Pediatr Neurol. 2000;7:66-90.
- Mewashingh L, Christiaens F, et al. Cervical myelitis from herpes simplex virus type 1. Pediatr Neurol. 2004;30:54-6.
- Dhiwakar M, Buxton N. Acute transverse myelitis mimicking and intramedullary neoplasm. Br J Neurosurg. 2004;18:72-3.
- Fegan, Cheng, Demmeller, Kaplan. Textbook of Pediatric Infectious Disease. 5th Ed. 2004:518-31.
- Samuels, Feske. Offi ce Practice of Neurology. 2nd Ed. 2003
A 10-month-old Hispanic female presents to the emergency department with a chief complaint of being limp. The mother states that the first day of the child’s illness began with tactile fever. The patient did not have any diarrhea or vomiting. After presenting to the emergency department she was diagnosed with a left otitis media. At that time, intramuscular ceftriaxone was given and amoxicillin was prescribed. The second day the patient was doing well and there were no new problems. On the third day the patient woke up and was not moving her arms and legs as much as usual, did not want to sit up on her own, and was lying limp. Additionally, she had some decreased oral intake that day and one loose stool.
Upon follow up at the pediatrician’s office there was concern about how limp the child seemed and she was sent back to the emergency department for transfer to the children’s hospital. However, the emergency department did blood work, gave intravenous fluids, and after observing slight improvement in limb movement, discharged the child to home.
At home, the child spiked a temperature. She was brought to the pediatrician’s office the next day where slight improvement in movement and more alert affect were noted; however, concern remained regarding her overall decreased activity. The child was again sent to the emergency department for transport to the pediatric hospital.
Review of systems revealed one vomiting episode and one loose stool, slight runny nose, and decrease in oral intake 1 day prior to admission. They had recently returned form California from a weekend trip. There was no significant past medical history aside from an otitis media 4 months ago. The child was born full-term without any complications. The child does not take any chronic medications, but did take two doses of amoxicillin for one and a half days in addition to acetaminophen for fever. The child does not have any known allergies. Her diet includes breastmilk and table foods. Six month vaccinations are not completed, but prior vaccines had been given on schedule. The child lives with her mother only and family history was not significant. Developmentally the child rolled over at 4 months, sits without support, pulls to stand, and stands with help.
Physical exam showed a temperature of 100.5F, heart rate of 148, respiratory rate of 30, blood pressure 103/70, and a weight of 10.5 kg (90%). Patient is well developed and well nourished without any acute distress. Physical exam was pertinent for supple neck with head lag, generalized weakness with decreased muscular strength in the upper and lower extremities. Upper extremities strength was 4/5 and lower extremities were 3/5. Neck laxity was present, sitting required support, and she refused to stand. Neurologically the patient was alert with reflexes mildly decreased in the lower extremities.
Laboratory evaluation included a complete blood count with a white blood cell (WBC) count of 11.7 and of hemoglobin of 11.4. A comprehensive metabolic panel was within normal limits. Lumbar puncture showed glucose of 50, protein of 38, 2 WBCs, 2 red blood cells, and a negative gram stain. Urinalysis was negative. Erythrocyte sedimentation rate was 17, CPK was 57, and chest radiograph was negative.
At this time stool was sent for botulism toxin; however, there was no history of eating canned food or honey. While waiting for results the patient showed slight improvement in movement and activity and demonstrated good oral intake. Physical therapy and speech therapy were working with the patient and lower extremity movement was improving, but she still had diffi culty standing. At this time an MRI of the brain and cervical spine was ordered and showed an intramedullary lesion involving the cervical and upper thoracic cord with localized cord enlargement. Enhancement was seen along C5 and C6 to the T1 level without canal stenosis and normal anatomic alignment was noted (Figure 1). In the meantime, stool for botulism toxin returned negative. Treatment was started for the diagnosis of transverse myelitis and included dexamethasone 2 mg/kg once daily with a taper over 5 weeks. She had minimal improvement prior to discharge, but showed slow and steady resolution of symptoms. Follow up with neurology was to be done on an outpatient basis, as well as continuation of physical therapy and occupational therapy.
Discussion
Transverse myelitis or transverse myelopathy (TM) is a syndrome of acute or subacute inflammation involving the spinal cord with partial or complete loss of neurologic function. It is usually limited to a number of spinal segments. The incidence is 1.3 new cases per one million residents annually. It affects all ages and both sexes; however, is uncommon in children less than 10 years of age. There are three theories for the etiology: cell-mediated autoimmune inflammation and/or demyelination of the spinal cord, a direct viral infection of the cord, and a paraneoplastic remote effect of cancer.
Clinical features include abrupt onset of symptoms varying from hours to a few days. One third of patients have a preceding viral illness. An early sign is muscle weakness, especially of the lower limbs. There may be numbness at the midthoracic region, strength loss as extreme as paraplegia, loss of bowel or bladder control, or sensory loss, most commonly involves pain and temperature. Fifty percent may experience a sharp, gnawing back pain at the level of the myelitis. Progression of the disease can lead to spasticity and hyperreflexia.
There is not a confirmation of any pathophysiologic mechanism. Demyelination, neuronal injury, and incomplete or complete necrosis of neural tissue may be associated with inflammatory changes on biopsy.
Differential diagnosis includes idiopathic autoimmune transverse myelitis, acute disseminated encephalomyelitis, multiple sclerosis (MS), Guillain-Barre, viral myelitis, vasculitis, spinal cord infarction, paraneoplastic myelopathy, vascular malformations, and nutritional myelopathy. Additionally, infectious etiologies include HIV myelopathy, spirochetal infection, and poliomyelitis.
Diagnosis is by exclusion. First, a mechanical, compressive lesion must be excluded from the differential. MRI of the spine visualizes the myelin and excludes compression and is used primarily to exclude these possible etiologies. MRI of the brain is useful to diagnose multiple sclerosis. Lumbar puncture results are variable ranging from normal to nonspecifi c inflammatory changes including a mild increase in protein or leukocytosis with an increase in polymorponuclear cells. Glucose is usually normal.
It is important, especially in adolescents, to differentiate TM from MS and Guillain-Barre. In MS symptoms are more likely separated by time, with “attacks” and a relapsing and remitting presentation. MS patients typically present with numbness and weakness in more than one extremity. In Guillain-Barre syndrome the presentation may be similar to TM in that there is weakness in the lower extremity, areflexia, and a possible viral illness precedent. However, a dermatome localization of sensory loss on neurologic exam can differentiate between a spinal cord lesion and a peripheral nerve etiology.
Treatment for TM symptoms is nonspecifi c. If a specific etiology is found then specific treatment should be rendered, otherwise one must rule out infectious or systemic inflammatory disorders. Pharmacologic treatment commonly includes high dose steroids, for example methylprednisone 1 g IV daily for 3–5 days followed with an
oral steroid taper. The evidence in the literature supporting this therapeutic approach includes mostly small studies with inconsistent results. In addition, small, uncontrolled or pilot studies have demonstrated that cyclophosphamide, azathioprine and plasmapheresis alone or in addition to corticosteroids may improve outcomes. Larger scale randomized, blinded, and controlled studies are required to more clearly define the most safe and efficacious treatment for this uncommon pediatric diagnosis.
References
- Knebusch M, Strassburg HM, Reiners K. Acute myelitis in childhood: nine cases and review of the literature. Dev Med Child Neurol. 1998;40:631-9.
- Rolad L. Pathophysiology and clinical feature of Multiple sclerosis. Immune and Infectious Disease.408-11.
- Transverse Myelitis consortium working group. Proposed diagnostic and nosology of acute transverse myelitis. Neurology. 2002;59(4).
- Andronikou S, Albuquerque-Jonathan G, Wilmshurst J, Hewlett R. MRI fi nding in acute idiopathic transverse myelopathy in children. Pediatr Radiol. 2003;33:624-9.
- Corboy J, Price R. Myelitis and toxic, infl ammatory, and infectious disorders. Curr Opin Neurol Neurosurg. 1993;6:564-70.
- Rust R. Multiple sclerosis, acute disseminated encephalomyelitis, and related conditions. Semin Pediatr Neurol. 2000;7:66-90.
- Mewashingh L, Christiaens F, et al. Cervical myelitis from herpes simplex virus type 1. Pediatr Neurol. 2004;30:54-6.
- Dhiwakar M, Buxton N. Acute transverse myelitis mimicking and intramedullary neoplasm. Br J Neurosurg. 2004;18:72-3.
- Fegan, Cheng, Demmeller, Kaplan. Textbook of Pediatric Infectious Disease. 5th Ed. 2004:518-31.
- Samuels, Feske. Offi ce Practice of Neurology. 2nd Ed. 2003
A 10-month-old Hispanic female presents to the emergency department with a chief complaint of being limp. The mother states that the first day of the child’s illness began with tactile fever. The patient did not have any diarrhea or vomiting. After presenting to the emergency department she was diagnosed with a left otitis media. At that time, intramuscular ceftriaxone was given and amoxicillin was prescribed. The second day the patient was doing well and there were no new problems. On the third day the patient woke up and was not moving her arms and legs as much as usual, did not want to sit up on her own, and was lying limp. Additionally, she had some decreased oral intake that day and one loose stool.
Upon follow up at the pediatrician’s office there was concern about how limp the child seemed and she was sent back to the emergency department for transfer to the children’s hospital. However, the emergency department did blood work, gave intravenous fluids, and after observing slight improvement in limb movement, discharged the child to home.
At home, the child spiked a temperature. She was brought to the pediatrician’s office the next day where slight improvement in movement and more alert affect were noted; however, concern remained regarding her overall decreased activity. The child was again sent to the emergency department for transport to the pediatric hospital.
Review of systems revealed one vomiting episode and one loose stool, slight runny nose, and decrease in oral intake 1 day prior to admission. They had recently returned form California from a weekend trip. There was no significant past medical history aside from an otitis media 4 months ago. The child was born full-term without any complications. The child does not take any chronic medications, but did take two doses of amoxicillin for one and a half days in addition to acetaminophen for fever. The child does not have any known allergies. Her diet includes breastmilk and table foods. Six month vaccinations are not completed, but prior vaccines had been given on schedule. The child lives with her mother only and family history was not significant. Developmentally the child rolled over at 4 months, sits without support, pulls to stand, and stands with help.
Physical exam showed a temperature of 100.5F, heart rate of 148, respiratory rate of 30, blood pressure 103/70, and a weight of 10.5 kg (90%). Patient is well developed and well nourished without any acute distress. Physical exam was pertinent for supple neck with head lag, generalized weakness with decreased muscular strength in the upper and lower extremities. Upper extremities strength was 4/5 and lower extremities were 3/5. Neck laxity was present, sitting required support, and she refused to stand. Neurologically the patient was alert with reflexes mildly decreased in the lower extremities.
Laboratory evaluation included a complete blood count with a white blood cell (WBC) count of 11.7 and of hemoglobin of 11.4. A comprehensive metabolic panel was within normal limits. Lumbar puncture showed glucose of 50, protein of 38, 2 WBCs, 2 red blood cells, and a negative gram stain. Urinalysis was negative. Erythrocyte sedimentation rate was 17, CPK was 57, and chest radiograph was negative.
At this time stool was sent for botulism toxin; however, there was no history of eating canned food or honey. While waiting for results the patient showed slight improvement in movement and activity and demonstrated good oral intake. Physical therapy and speech therapy were working with the patient and lower extremity movement was improving, but she still had diffi culty standing. At this time an MRI of the brain and cervical spine was ordered and showed an intramedullary lesion involving the cervical and upper thoracic cord with localized cord enlargement. Enhancement was seen along C5 and C6 to the T1 level without canal stenosis and normal anatomic alignment was noted (Figure 1). In the meantime, stool for botulism toxin returned negative. Treatment was started for the diagnosis of transverse myelitis and included dexamethasone 2 mg/kg once daily with a taper over 5 weeks. She had minimal improvement prior to discharge, but showed slow and steady resolution of symptoms. Follow up with neurology was to be done on an outpatient basis, as well as continuation of physical therapy and occupational therapy.
Discussion
Transverse myelitis or transverse myelopathy (TM) is a syndrome of acute or subacute inflammation involving the spinal cord with partial or complete loss of neurologic function. It is usually limited to a number of spinal segments. The incidence is 1.3 new cases per one million residents annually. It affects all ages and both sexes; however, is uncommon in children less than 10 years of age. There are three theories for the etiology: cell-mediated autoimmune inflammation and/or demyelination of the spinal cord, a direct viral infection of the cord, and a paraneoplastic remote effect of cancer.
Clinical features include abrupt onset of symptoms varying from hours to a few days. One third of patients have a preceding viral illness. An early sign is muscle weakness, especially of the lower limbs. There may be numbness at the midthoracic region, strength loss as extreme as paraplegia, loss of bowel or bladder control, or sensory loss, most commonly involves pain and temperature. Fifty percent may experience a sharp, gnawing back pain at the level of the myelitis. Progression of the disease can lead to spasticity and hyperreflexia.
There is not a confirmation of any pathophysiologic mechanism. Demyelination, neuronal injury, and incomplete or complete necrosis of neural tissue may be associated with inflammatory changes on biopsy.
Differential diagnosis includes idiopathic autoimmune transverse myelitis, acute disseminated encephalomyelitis, multiple sclerosis (MS), Guillain-Barre, viral myelitis, vasculitis, spinal cord infarction, paraneoplastic myelopathy, vascular malformations, and nutritional myelopathy. Additionally, infectious etiologies include HIV myelopathy, spirochetal infection, and poliomyelitis.
Diagnosis is by exclusion. First, a mechanical, compressive lesion must be excluded from the differential. MRI of the spine visualizes the myelin and excludes compression and is used primarily to exclude these possible etiologies. MRI of the brain is useful to diagnose multiple sclerosis. Lumbar puncture results are variable ranging from normal to nonspecifi c inflammatory changes including a mild increase in protein or leukocytosis with an increase in polymorponuclear cells. Glucose is usually normal.
It is important, especially in adolescents, to differentiate TM from MS and Guillain-Barre. In MS symptoms are more likely separated by time, with “attacks” and a relapsing and remitting presentation. MS patients typically present with numbness and weakness in more than one extremity. In Guillain-Barre syndrome the presentation may be similar to TM in that there is weakness in the lower extremity, areflexia, and a possible viral illness precedent. However, a dermatome localization of sensory loss on neurologic exam can differentiate between a spinal cord lesion and a peripheral nerve etiology.
Treatment for TM symptoms is nonspecifi c. If a specific etiology is found then specific treatment should be rendered, otherwise one must rule out infectious or systemic inflammatory disorders. Pharmacologic treatment commonly includes high dose steroids, for example methylprednisone 1 g IV daily for 3–5 days followed with an
oral steroid taper. The evidence in the literature supporting this therapeutic approach includes mostly small studies with inconsistent results. In addition, small, uncontrolled or pilot studies have demonstrated that cyclophosphamide, azathioprine and plasmapheresis alone or in addition to corticosteroids may improve outcomes. Larger scale randomized, blinded, and controlled studies are required to more clearly define the most safe and efficacious treatment for this uncommon pediatric diagnosis.
References
- Knebusch M, Strassburg HM, Reiners K. Acute myelitis in childhood: nine cases and review of the literature. Dev Med Child Neurol. 1998;40:631-9.
- Rolad L. Pathophysiology and clinical feature of Multiple sclerosis. Immune and Infectious Disease.408-11.
- Transverse Myelitis consortium working group. Proposed diagnostic and nosology of acute transverse myelitis. Neurology. 2002;59(4).
- Andronikou S, Albuquerque-Jonathan G, Wilmshurst J, Hewlett R. MRI fi nding in acute idiopathic transverse myelopathy in children. Pediatr Radiol. 2003;33:624-9.
- Corboy J, Price R. Myelitis and toxic, infl ammatory, and infectious disorders. Curr Opin Neurol Neurosurg. 1993;6:564-70.
- Rust R. Multiple sclerosis, acute disseminated encephalomyelitis, and related conditions. Semin Pediatr Neurol. 2000;7:66-90.
- Mewashingh L, Christiaens F, et al. Cervical myelitis from herpes simplex virus type 1. Pediatr Neurol. 2004;30:54-6.
- Dhiwakar M, Buxton N. Acute transverse myelitis mimicking and intramedullary neoplasm. Br J Neurosurg. 2004;18:72-3.
- Fegan, Cheng, Demmeller, Kaplan. Textbook of Pediatric Infectious Disease. 5th Ed. 2004:518-31.
- Samuels, Feske. Offi ce Practice of Neurology. 2nd Ed. 2003
Other Literature of Interest
1. Dexter PR, Perkins SM, Mahany KS, Jones K, McDonald CJ. Inpatient computer-based standing orders vs. physician reminders to increase influenza and pneumococcal vaccination rates: a randomized trial. JAMA. 2004; 292: 2366-71.
Past studies have suggested that most patients admitted with severe pneumococcal infections have been hospitalized in the preceding 5 years, and simply being hospitalized is a potential risk factor for later pneumococcal infection. Likewise, hospitalization provides an opportunity to vaccinate high-risk patients against influenza, and raising pneumococcal and influenza immunization rates is a CMS quality improvement priority. Prior investigations have supported the use of labor-intensive manual standing orders as well as computerized reminders, but this prospective trial was conducted in 1998 and 1999 to assess the effectiveness of a computer-based system to screen for eligible patients and then generate orders to perform pneumonia and influenza vaccinations on inpatients at the time of discharge.
Over 13 months, a total of 3777 inpatients were entered into the study. The hospital computer identified patients eligible for vaccination based on common criteria and randomized them to one of two groups of physician teams. For one group of teams, the computer order-entry system would automatically generate vaccination orders at the time of discharge for vaccine-eligible patients; for the other group of teams, only computer reminders were provided to physicians. The outcome measure was administration of vaccine; long-term outcomes such as incidence of subsequent disease or mortality were not measured.
During the study period, 50% of all hospitalized patients were identified as eligible for influenza vaccination; 22% were eligible for pneumococcal vaccination. In each case, the “standing order” group received vaccine more often (influenza: 42% vs. 30%, p<.001; pneumococcal vaccine: 51% vs. 31%). The numbers were subsequently adjusted to allow for patients who had previously received vaccine, but the impressive differences persisted. Nurses reported reasons for non-administration in 98% of the eligible patients who were not vaccinated; the most common reason was patient refusal. It is not clear if the physicians knew that a study was being conducted. No adverse reactions were reported.
CMS has pushed for the development of institutional standing order sets as a tool to improve compliance with vaccination rate targets. Where the technology is available, computer systems that can screen eligible patients and generate automatic orders are an effective tool in implementing many quality-improvement initiatives, and hospitalists are in a crucial position to take an active role in their development and implementation.
2. Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for a trial fibrillation. Ann Intern Med. 2004; 141: 745-52.
Warfarin has been shown to reduce risk of stroke in patients with chronic and paroxysmal atrial fibrillation. Intracranial hemorrhage remains one of the most feared complications of warfarin, especially among older patients, prompting suggestions to consider lower intensity anticoagulation among patients older than 75 years who have atrial fibrillation.
This study evaluated the relationship between the intensity of anticoagulation, risk of intracranial hemorrhage, and age of patients with atrial fibrillation.
This was a retrospective case control study conducted at a tertiary care medical center. One-hundred and seventy patients on warfarin and admitted with intracranial hemorrhage from 1993 to 2002 were matched with 1020 patients who were on warfarin but without intracranial bleed. After controlling for comorbid conditions and aspirin use, authors conducted multivariable logistic regression analysis to determine the odds of intracranial hemorrhage with regard to age and INR. The risk of intracranial hemorrhage increased at 85 years of age and at INR values of 3.5 or greater. The risk of intracranial hemorrhage at INR less than 2.0 did not differ statistically from the risk at INR of 2.0–3.0.
This study shows the risk of intracranial hemorrhage is not decreased by choosing lower intensity anticoagulation, and target INR should still be kept at 2.5 among elderly patients. However, patients older than 85 years should be counseled about their higher risk of intracranial hemorrhage.
3. Heeschen C, Hamm CW, Mitrovic V, et al. N-terminal pro-B-type natriuretic peptide levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation. 2004;110: 3206-12.
Recent data demonstrate the prognostic value of assessment of neurohormonal activation in patients with acute coronary syndromes (ACS). B-type natriuretic peptide levels (BNP) and levels of the N-terminal fragment of the BNP prohormone (NT-proBNP) predict adverse long-term outcomes in patients with ACS. Investigators reviewed plasma samples of Troponin T (TnT) and NT-proBNP obtained from patients with ACS enrolled in the Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM) trial, which randomized patients to tirofiban or heparin for 48 hours and assessed mortality and myocardial infarction at 30 day follow-up. TnT and NT-proBNP determinations were available at baseline for 1791 patients, and at 48 and 72 hours from 1401 patients. Baseline NT-proBNP levels >250 ng/L were associated with significantly higher rates of death and myocardial infarction at 7 and 30 day follow-up. After adjustment for TnT and C-reactive protein levels, elevated NTproBNP levels maintained its predictive value (OR 2.7; p<.001). In patients with normal TnT levels, NT-proBNP levels identified a subgroup of patients at increased risk (OR 3.0; p=.004). However, in patients with high TnT levels (>0.1 mcg/L), NT-proBNP lost its predictive value (p=.58). More importantly, patients with normal levels of both TnT and NT-proBNP were at very low risk (0.6% event rate at 30 day follow-up).
Serial determinations of NT-proBNP levels at 48 and 72 hours were reviewed in patients without major adverse cardiac events (death or myocardial infarction); these patients were subdivided into groups with and without refractory ischemia. Patients without refractory ischemia showed a significant decline in NT-proBNP levels, whereas patients with refractory ischemia had no significant change. Persistently elevated NT-proBNP levels at 72 hours were associated with a 17.2% risk of death or MI at 30 days, compared with 0.6% risk if NT-proBNP returned to normal at 72 hours (p<.001). Neither TnT nor C-reactive protein demonstrated similar predictive value.
The study is limited by its retrospective nature, by potential selection bias by including only patients with direct evidence of coronary artery disease, and by limitations of the generalizability of its findings (e.g., to emergency department patients with chest pain).
As BNP and NT-proBNP are counter-regulatory hormones that play an active role in the response to ischemic injury, the authors suggest that NT-proBNP is a promising tool for dynamic risk assessment in patients with ACS. The authors also do not differentiate between BNP and NT-proBNP with regard to use in risk stratification, which might lead one to believe that these tests share similar predictive value. (Of note, the study was entirely funded by a company that produces an assay for NT-proBNP). Prospective trials to validate this tool are warranted
4. Heuschmann PU, Kolominsky-Rabas PL, Roether J, et al. Predictors of in-hospital mortality in patients with acute ischemic stroke treated with thrombolytic therapy. JAMA. 2004;292:1831-38.
The objective of this study was to identify factors associated with in-hospital mortality in ischemic stroke patients treated with recombinant tissue plasminogen activator (tPA). It was a prospective observational cohort study of 1658 patients conducted at 225 community and academic hospitals throughout Germany with main outcome of in-hospital mortality.
In this study 10% of patients who were treated with tPA died during their hospital stay, with 2/3 of deaths occurring in the first 7 days. Relative probability of in-hospital mortality increased with increasing patient age, with an odds ratio (OR) of 1.6 for each 10-year increment in age. Age was an independent predictor of in hospital mortality irrespective of tPA administration, with patients older than 75 years age having 4 fold higher mortality than the youngest cohort of less than 55 years age.
Other factors predicting in hospital mortality were altered level of consciousness and relative lack of experience with tPA treatment in the center. Altered level of consciousness was a predictor of stroke severity and an independent predictor of in-hospital mortality (OR 3.4). The increase in mortality in centers with limited experience with tPA administration (OR 0.97) reflected learning curve issues with these patients. The study was not designed to separate out the confounders of operator experience curve from institutional experience curves, or to derive the exact relationship between experience and outcomes.
5. McAlister FA, Bertsch K, Man J, et al. Incidence of and risk factors for pulmonary complications after non-thoracic surgery. Am J Respir Crit Care Med. 2004; published ahead of print on November 24, 2004 as doi:10.1164/rccm.200408-1069OC. Accessed January 27, 2005.
Postoperative pulmonary complications after nonthoracic surgery are a cause of significant morbidity and increased length of hospital stay. Previous studies of preoperative pulmonary assessment were limited by non-representative patient samples, conflicting results, and lack of explicit definitions of these complications. The authors conducted a prospective cohort study of 1055 patients seen in a Pre-Admission Clinic of a tertiary care university hospital. Mean age was 55 years, 50% male, and the cohort consisted of patients scheduled for intermediate risk elective surgery (upper abdominal, lower abdominal, orthopedic). They evaluated physical exam maneuvers (cough test, wheeze test, maximal laryngeal height, and forced expiratory time, all of which are described in an online data supplement) and preoperative spirometry values, and collected information on clinically significant postoperative pulmonary complications, including pneumonia, respiratory failure requiring mechanical ventilation, atelectasis requiring bronchoscopy, or pneumothorax or pleural effusion requiring percutaneous intervention. Twenty-eight patients (2.7%) suffered a pulmonary complication within 7 days of surgery, one of whom died. Length of stay was significantly prolonged in this group (mean 27.9 days vs 4.5 days, p=.006). Multivariate regression analysis revealed four variables that were independently associated with increased risk for postoperative pulmonary complications: age > 65 years, positive cough test (repeated coughing after asking the patient to inhale deeply and cough once), perioperative nasogastric tube, and anesthesia duration 2.5 hours or greater. Number of pack years smoked, FEV1, FEV1/FVC ratio, and upper abdominal surgery were associated with postoperative pulmonary complications but were not found to be independently associated by multivariate analysis.
While it is not surprising that the above risk factors are predictive of postoperative complications, this is the first study to incorporate specific exam maneuvers and spirometry into a risk prediction analysis. Limitations of this model are lack of independent validation and lack of generalizability to other populations, e.g., inpatients awaiting urgent surgery. Of note, the study further provides further support for not routinely obtaining pulmonary function testing for risk stratification prior to noncardiac surgery.
6. Mortenson, EM, Restrepo M, Anzeuto A, Pugh J. Effects of guideline-concordant antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am J Med. 2004;117:726-31.
The American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) have published guidelines for the management of community acquired pneumonia that include recommendations for antibiotic selection. This retrospective cohort study attempted to measure the association between adherence to such guidelines and 30-day mortality in patients admitted with pneumonia to two Texas hospitals.
The characteristics of the patients studied reflect a reasonable cross-section of typical pneumonia patients, with the exception that the patients were mostly (85%) men. Of the study population, 78% were admitted through the ER, 20% admitted to the ICU, and 9% were nursing home residents. Antibiotics were considered “concordant” if they were consistent with either the most recent IDSA or ATS recommendations. The “nonconcordant” group was slightly older (66 vs. 61), generally sicker (higher rate of comorbid COPD and CVD), had more cerebrovascular disease, was more likely to present with altered mental status, and less frequently received antibiotics within 8 hours of presentation. The study did not comment on patients’ vaccination status. Thirty-day mortality was 6.2% in the guideline-concordant group, versus 21.7% in the other group (p < .001). The most common “non-concordant” regimen described was use of a beta-lactam alone, although specific antibiotic regimens were not evaluated.
While the results of this study are not surprising, they provide us with both the validation to continue practice according to existing recommendations, particularly the avoidance of monotherapy with beta-lactam antibiotics. The study also provides us with the imperative to take the lead in developing evidence-based pneumonia pathways at our own hospitals.
7. Pham MX, Whooley MA, Evans GT Jr, et al. Prognostic value of low-level cardiac troponin-I elevations in patients without definite acute coronary syndromes. Am Heart J. 2004;148: 776-82.
With the availability of rapid and highly sensitive and specific troponin testing, many patients admitted to the hospital with non-cardiac diagnoses have been recognized as having abnormal serum troponin-I or troponin-T levels, often just slightly above the reference cutoff for “normal.” While the clinical assumption is often that the elevated enzyme level does not reflect an acute coronary syndrome per se, its significance regarding the patient’s underlying cardiac health is often unclear.
Pham et al. retrospectively reviewed the 1-year mortality of 366 patients who were admitted to the San Francisco VA without evidence of acute MI or ACS either clinically or by EKG, but who had low-level troponin-I elevations (up to 3.0 ng/mL—a level that the authors state was reached by institutional consensus, and which was measured by a “first-generation” assay). These patients were admitted for a broad spectrum of diagnoses ranging from CHF to COPD to sepsis. Ninety-six percent of the patients were men; their average age was 69.
Follow-up was accomplished after a mean of 288 days and included 97% of patients. The primary endpoint was MI or death due to cardiac disease at one year; secondary endpoints were revascularization or admission for unstable angina. The primary endpoint was reached by 11% of patients with cTn-I between 1.0 and 3.0 ng/mL, and 4% of the patients with cTn-I up to 1.0 ng/mL (adjusted HR 3.4, 95% CI, 1.3 to 9.4), and the higher the cTn-I, the higher the risk. However, the authors did not test for the level of risk by specific diagnosis, so they caution against overgeneralizing their findings.
The findings of this study add to the evidence that any evidence of myocardial injury implies an increased risk of underlying heart disease and accompanying long—term cardiac complications– even if such injury occurs in the absence of ACS or known heart disease. Hospitalists often see such injury in the setting of acute infection and pulmonary disease and may be the first to recognize the possibility of CHD in a given patient. To date, guidelines addressing optimal prospective risk stratification have not been developed. Until they are, hospitalists should be aware of the ramifications of “troponin leak” and be prepared to initiate necessary inpatient monitoring and treatments, and to coordinate appropriate follow-up for these patients.
8. Saposnik G, Young B, Silver B, et al. Lack of improvement in patients with acute stroke after treatment with thrombolytic therapy: predictors and association with outcome. JAMA. 2004; 292: 1839-44.
Recombinant tissue plasminogen activator (tPA) has been shown to be one of the most efficacious therapies for acute stroke treatment. This was a systematic evaluation of predictors for outcomes at 24 hours after tPA therapy and of the prognostic significance of lack of improvement at 24 hours for long-term outcomes at 3 months.
The trial was a prospective cohort study of 216 consecutive patients admitted with acute ischemic stroke to a university hospital. The decision to treat with tPA was based on the NINDS protocol with one difference: patients with involvement of more than one third of the middle cerebral artery on the baseline CT scan were excluded. A control CT scan was performed at 24 hours to determine the presence of new infarction, cortical involvement, and extension of the ischemic lesion.
Lack of improvement was defined as a difference between the NIHSS score at baseline and at 24 hours of 3 points or less. Poor outcome at 3 months was defined by a modified Rankin Scale score of 3 to 5 or death.
After adjusting for age, gender, and stroke severity, hyperglycemia at admission (glucose > 144 mg/dL), cortical involvement, and time to treatment were independent predictors of lack of improvement at 24 hours. After adjusting for age, gender, and stroke severity, lack of improvement at 24 hours was an independent predictor of poor outcome and death at 3 months. Patients with lack of improvement at 24 hours also had longer lengths of hospitalization.
9. Taylor AL, Ziesche S, Yancy C, et al. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. 2004;351:2049-57.
Neurohormonal changes, endothelial dysfunction, impaired nitric oxide availability, and oxidant stress all contribute to the structural remodeling of the left ventricle in congestive heart failure. The combination of isosorbide dinitrate, an organic nitrate that stimulates nitric oxide signaling, and the antioxidant and vasodilator hydralazine improves survival in heart failure. Based on more recent data that black patients have a clinically significant response to this combination therapy, the authors of the African-American Heart Failure Trial (A-HeFT) evaluated 1050 black patients with congestive heart failure in a randomized, double-blind, placebo controlled trial. Patients were randomized to fixed doses of isosorbide dinitrate and hydralazine plus background therapy (i.e., digoxin, ACE inhibitors, beta-blockers, diuretics, angiotensin receptor blockers) or to placebo plus background therapy. After 18 months, the trial was stopped due to a significantly higher mortality rate in the placebo group (10.2% in the placebo group vs. 6.2% with combination
therapy, p=.02); survival differences emerged at 180 days and increased progressively thereafter. The combination therapy group reported more headache and dizziness but suffered fewer exacerbations of congestive heart failure and reported improvement in subjective assessments of quality of life as measured by questionnaires. Accompanying editorials discuss the role of nitric oxide and prevention of oxidative stress in the treatment of heart failure, as well as the controversial issues surrounding race-based therapeutics.
1. Dexter PR, Perkins SM, Mahany KS, Jones K, McDonald CJ. Inpatient computer-based standing orders vs. physician reminders to increase influenza and pneumococcal vaccination rates: a randomized trial. JAMA. 2004; 292: 2366-71.
Past studies have suggested that most patients admitted with severe pneumococcal infections have been hospitalized in the preceding 5 years, and simply being hospitalized is a potential risk factor for later pneumococcal infection. Likewise, hospitalization provides an opportunity to vaccinate high-risk patients against influenza, and raising pneumococcal and influenza immunization rates is a CMS quality improvement priority. Prior investigations have supported the use of labor-intensive manual standing orders as well as computerized reminders, but this prospective trial was conducted in 1998 and 1999 to assess the effectiveness of a computer-based system to screen for eligible patients and then generate orders to perform pneumonia and influenza vaccinations on inpatients at the time of discharge.
Over 13 months, a total of 3777 inpatients were entered into the study. The hospital computer identified patients eligible for vaccination based on common criteria and randomized them to one of two groups of physician teams. For one group of teams, the computer order-entry system would automatically generate vaccination orders at the time of discharge for vaccine-eligible patients; for the other group of teams, only computer reminders were provided to physicians. The outcome measure was administration of vaccine; long-term outcomes such as incidence of subsequent disease or mortality were not measured.
During the study period, 50% of all hospitalized patients were identified as eligible for influenza vaccination; 22% were eligible for pneumococcal vaccination. In each case, the “standing order” group received vaccine more often (influenza: 42% vs. 30%, p<.001; pneumococcal vaccine: 51% vs. 31%). The numbers were subsequently adjusted to allow for patients who had previously received vaccine, but the impressive differences persisted. Nurses reported reasons for non-administration in 98% of the eligible patients who were not vaccinated; the most common reason was patient refusal. It is not clear if the physicians knew that a study was being conducted. No adverse reactions were reported.
CMS has pushed for the development of institutional standing order sets as a tool to improve compliance with vaccination rate targets. Where the technology is available, computer systems that can screen eligible patients and generate automatic orders are an effective tool in implementing many quality-improvement initiatives, and hospitalists are in a crucial position to take an active role in their development and implementation.
2. Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for a trial fibrillation. Ann Intern Med. 2004; 141: 745-52.
Warfarin has been shown to reduce risk of stroke in patients with chronic and paroxysmal atrial fibrillation. Intracranial hemorrhage remains one of the most feared complications of warfarin, especially among older patients, prompting suggestions to consider lower intensity anticoagulation among patients older than 75 years who have atrial fibrillation.
This study evaluated the relationship between the intensity of anticoagulation, risk of intracranial hemorrhage, and age of patients with atrial fibrillation.
This was a retrospective case control study conducted at a tertiary care medical center. One-hundred and seventy patients on warfarin and admitted with intracranial hemorrhage from 1993 to 2002 were matched with 1020 patients who were on warfarin but without intracranial bleed. After controlling for comorbid conditions and aspirin use, authors conducted multivariable logistic regression analysis to determine the odds of intracranial hemorrhage with regard to age and INR. The risk of intracranial hemorrhage increased at 85 years of age and at INR values of 3.5 or greater. The risk of intracranial hemorrhage at INR less than 2.0 did not differ statistically from the risk at INR of 2.0–3.0.
This study shows the risk of intracranial hemorrhage is not decreased by choosing lower intensity anticoagulation, and target INR should still be kept at 2.5 among elderly patients. However, patients older than 85 years should be counseled about their higher risk of intracranial hemorrhage.
3. Heeschen C, Hamm CW, Mitrovic V, et al. N-terminal pro-B-type natriuretic peptide levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation. 2004;110: 3206-12.
Recent data demonstrate the prognostic value of assessment of neurohormonal activation in patients with acute coronary syndromes (ACS). B-type natriuretic peptide levels (BNP) and levels of the N-terminal fragment of the BNP prohormone (NT-proBNP) predict adverse long-term outcomes in patients with ACS. Investigators reviewed plasma samples of Troponin T (TnT) and NT-proBNP obtained from patients with ACS enrolled in the Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM) trial, which randomized patients to tirofiban or heparin for 48 hours and assessed mortality and myocardial infarction at 30 day follow-up. TnT and NT-proBNP determinations were available at baseline for 1791 patients, and at 48 and 72 hours from 1401 patients. Baseline NT-proBNP levels >250 ng/L were associated with significantly higher rates of death and myocardial infarction at 7 and 30 day follow-up. After adjustment for TnT and C-reactive protein levels, elevated NTproBNP levels maintained its predictive value (OR 2.7; p<.001). In patients with normal TnT levels, NT-proBNP levels identified a subgroup of patients at increased risk (OR 3.0; p=.004). However, in patients with high TnT levels (>0.1 mcg/L), NT-proBNP lost its predictive value (p=.58). More importantly, patients with normal levels of both TnT and NT-proBNP were at very low risk (0.6% event rate at 30 day follow-up).
Serial determinations of NT-proBNP levels at 48 and 72 hours were reviewed in patients without major adverse cardiac events (death or myocardial infarction); these patients were subdivided into groups with and without refractory ischemia. Patients without refractory ischemia showed a significant decline in NT-proBNP levels, whereas patients with refractory ischemia had no significant change. Persistently elevated NT-proBNP levels at 72 hours were associated with a 17.2% risk of death or MI at 30 days, compared with 0.6% risk if NT-proBNP returned to normal at 72 hours (p<.001). Neither TnT nor C-reactive protein demonstrated similar predictive value.
The study is limited by its retrospective nature, by potential selection bias by including only patients with direct evidence of coronary artery disease, and by limitations of the generalizability of its findings (e.g., to emergency department patients with chest pain).
As BNP and NT-proBNP are counter-regulatory hormones that play an active role in the response to ischemic injury, the authors suggest that NT-proBNP is a promising tool for dynamic risk assessment in patients with ACS. The authors also do not differentiate between BNP and NT-proBNP with regard to use in risk stratification, which might lead one to believe that these tests share similar predictive value. (Of note, the study was entirely funded by a company that produces an assay for NT-proBNP). Prospective trials to validate this tool are warranted
4. Heuschmann PU, Kolominsky-Rabas PL, Roether J, et al. Predictors of in-hospital mortality in patients with acute ischemic stroke treated with thrombolytic therapy. JAMA. 2004;292:1831-38.
The objective of this study was to identify factors associated with in-hospital mortality in ischemic stroke patients treated with recombinant tissue plasminogen activator (tPA). It was a prospective observational cohort study of 1658 patients conducted at 225 community and academic hospitals throughout Germany with main outcome of in-hospital mortality.
In this study 10% of patients who were treated with tPA died during their hospital stay, with 2/3 of deaths occurring in the first 7 days. Relative probability of in-hospital mortality increased with increasing patient age, with an odds ratio (OR) of 1.6 for each 10-year increment in age. Age was an independent predictor of in hospital mortality irrespective of tPA administration, with patients older than 75 years age having 4 fold higher mortality than the youngest cohort of less than 55 years age.
Other factors predicting in hospital mortality were altered level of consciousness and relative lack of experience with tPA treatment in the center. Altered level of consciousness was a predictor of stroke severity and an independent predictor of in-hospital mortality (OR 3.4). The increase in mortality in centers with limited experience with tPA administration (OR 0.97) reflected learning curve issues with these patients. The study was not designed to separate out the confounders of operator experience curve from institutional experience curves, or to derive the exact relationship between experience and outcomes.
5. McAlister FA, Bertsch K, Man J, et al. Incidence of and risk factors for pulmonary complications after non-thoracic surgery. Am J Respir Crit Care Med. 2004; published ahead of print on November 24, 2004 as doi:10.1164/rccm.200408-1069OC. Accessed January 27, 2005.
Postoperative pulmonary complications after nonthoracic surgery are a cause of significant morbidity and increased length of hospital stay. Previous studies of preoperative pulmonary assessment were limited by non-representative patient samples, conflicting results, and lack of explicit definitions of these complications. The authors conducted a prospective cohort study of 1055 patients seen in a Pre-Admission Clinic of a tertiary care university hospital. Mean age was 55 years, 50% male, and the cohort consisted of patients scheduled for intermediate risk elective surgery (upper abdominal, lower abdominal, orthopedic). They evaluated physical exam maneuvers (cough test, wheeze test, maximal laryngeal height, and forced expiratory time, all of which are described in an online data supplement) and preoperative spirometry values, and collected information on clinically significant postoperative pulmonary complications, including pneumonia, respiratory failure requiring mechanical ventilation, atelectasis requiring bronchoscopy, or pneumothorax or pleural effusion requiring percutaneous intervention. Twenty-eight patients (2.7%) suffered a pulmonary complication within 7 days of surgery, one of whom died. Length of stay was significantly prolonged in this group (mean 27.9 days vs 4.5 days, p=.006). Multivariate regression analysis revealed four variables that were independently associated with increased risk for postoperative pulmonary complications: age > 65 years, positive cough test (repeated coughing after asking the patient to inhale deeply and cough once), perioperative nasogastric tube, and anesthesia duration 2.5 hours or greater. Number of pack years smoked, FEV1, FEV1/FVC ratio, and upper abdominal surgery were associated with postoperative pulmonary complications but were not found to be independently associated by multivariate analysis.
While it is not surprising that the above risk factors are predictive of postoperative complications, this is the first study to incorporate specific exam maneuvers and spirometry into a risk prediction analysis. Limitations of this model are lack of independent validation and lack of generalizability to other populations, e.g., inpatients awaiting urgent surgery. Of note, the study further provides further support for not routinely obtaining pulmonary function testing for risk stratification prior to noncardiac surgery.
6. Mortenson, EM, Restrepo M, Anzeuto A, Pugh J. Effects of guideline-concordant antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am J Med. 2004;117:726-31.
The American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) have published guidelines for the management of community acquired pneumonia that include recommendations for antibiotic selection. This retrospective cohort study attempted to measure the association between adherence to such guidelines and 30-day mortality in patients admitted with pneumonia to two Texas hospitals.
The characteristics of the patients studied reflect a reasonable cross-section of typical pneumonia patients, with the exception that the patients were mostly (85%) men. Of the study population, 78% were admitted through the ER, 20% admitted to the ICU, and 9% were nursing home residents. Antibiotics were considered “concordant” if they were consistent with either the most recent IDSA or ATS recommendations. The “nonconcordant” group was slightly older (66 vs. 61), generally sicker (higher rate of comorbid COPD and CVD), had more cerebrovascular disease, was more likely to present with altered mental status, and less frequently received antibiotics within 8 hours of presentation. The study did not comment on patients’ vaccination status. Thirty-day mortality was 6.2% in the guideline-concordant group, versus 21.7% in the other group (p < .001). The most common “non-concordant” regimen described was use of a beta-lactam alone, although specific antibiotic regimens were not evaluated.
While the results of this study are not surprising, they provide us with both the validation to continue practice according to existing recommendations, particularly the avoidance of monotherapy with beta-lactam antibiotics. The study also provides us with the imperative to take the lead in developing evidence-based pneumonia pathways at our own hospitals.
7. Pham MX, Whooley MA, Evans GT Jr, et al. Prognostic value of low-level cardiac troponin-I elevations in patients without definite acute coronary syndromes. Am Heart J. 2004;148: 776-82.
With the availability of rapid and highly sensitive and specific troponin testing, many patients admitted to the hospital with non-cardiac diagnoses have been recognized as having abnormal serum troponin-I or troponin-T levels, often just slightly above the reference cutoff for “normal.” While the clinical assumption is often that the elevated enzyme level does not reflect an acute coronary syndrome per se, its significance regarding the patient’s underlying cardiac health is often unclear.
Pham et al. retrospectively reviewed the 1-year mortality of 366 patients who were admitted to the San Francisco VA without evidence of acute MI or ACS either clinically or by EKG, but who had low-level troponin-I elevations (up to 3.0 ng/mL—a level that the authors state was reached by institutional consensus, and which was measured by a “first-generation” assay). These patients were admitted for a broad spectrum of diagnoses ranging from CHF to COPD to sepsis. Ninety-six percent of the patients were men; their average age was 69.
Follow-up was accomplished after a mean of 288 days and included 97% of patients. The primary endpoint was MI or death due to cardiac disease at one year; secondary endpoints were revascularization or admission for unstable angina. The primary endpoint was reached by 11% of patients with cTn-I between 1.0 and 3.0 ng/mL, and 4% of the patients with cTn-I up to 1.0 ng/mL (adjusted HR 3.4, 95% CI, 1.3 to 9.4), and the higher the cTn-I, the higher the risk. However, the authors did not test for the level of risk by specific diagnosis, so they caution against overgeneralizing their findings.
The findings of this study add to the evidence that any evidence of myocardial injury implies an increased risk of underlying heart disease and accompanying long—term cardiac complications– even if such injury occurs in the absence of ACS or known heart disease. Hospitalists often see such injury in the setting of acute infection and pulmonary disease and may be the first to recognize the possibility of CHD in a given patient. To date, guidelines addressing optimal prospective risk stratification have not been developed. Until they are, hospitalists should be aware of the ramifications of “troponin leak” and be prepared to initiate necessary inpatient monitoring and treatments, and to coordinate appropriate follow-up for these patients.
8. Saposnik G, Young B, Silver B, et al. Lack of improvement in patients with acute stroke after treatment with thrombolytic therapy: predictors and association with outcome. JAMA. 2004; 292: 1839-44.
Recombinant tissue plasminogen activator (tPA) has been shown to be one of the most efficacious therapies for acute stroke treatment. This was a systematic evaluation of predictors for outcomes at 24 hours after tPA therapy and of the prognostic significance of lack of improvement at 24 hours for long-term outcomes at 3 months.
The trial was a prospective cohort study of 216 consecutive patients admitted with acute ischemic stroke to a university hospital. The decision to treat with tPA was based on the NINDS protocol with one difference: patients with involvement of more than one third of the middle cerebral artery on the baseline CT scan were excluded. A control CT scan was performed at 24 hours to determine the presence of new infarction, cortical involvement, and extension of the ischemic lesion.
Lack of improvement was defined as a difference between the NIHSS score at baseline and at 24 hours of 3 points or less. Poor outcome at 3 months was defined by a modified Rankin Scale score of 3 to 5 or death.
After adjusting for age, gender, and stroke severity, hyperglycemia at admission (glucose > 144 mg/dL), cortical involvement, and time to treatment were independent predictors of lack of improvement at 24 hours. After adjusting for age, gender, and stroke severity, lack of improvement at 24 hours was an independent predictor of poor outcome and death at 3 months. Patients with lack of improvement at 24 hours also had longer lengths of hospitalization.
9. Taylor AL, Ziesche S, Yancy C, et al. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. 2004;351:2049-57.
Neurohormonal changes, endothelial dysfunction, impaired nitric oxide availability, and oxidant stress all contribute to the structural remodeling of the left ventricle in congestive heart failure. The combination of isosorbide dinitrate, an organic nitrate that stimulates nitric oxide signaling, and the antioxidant and vasodilator hydralazine improves survival in heart failure. Based on more recent data that black patients have a clinically significant response to this combination therapy, the authors of the African-American Heart Failure Trial (A-HeFT) evaluated 1050 black patients with congestive heart failure in a randomized, double-blind, placebo controlled trial. Patients were randomized to fixed doses of isosorbide dinitrate and hydralazine plus background therapy (i.e., digoxin, ACE inhibitors, beta-blockers, diuretics, angiotensin receptor blockers) or to placebo plus background therapy. After 18 months, the trial was stopped due to a significantly higher mortality rate in the placebo group (10.2% in the placebo group vs. 6.2% with combination
therapy, p=.02); survival differences emerged at 180 days and increased progressively thereafter. The combination therapy group reported more headache and dizziness but suffered fewer exacerbations of congestive heart failure and reported improvement in subjective assessments of quality of life as measured by questionnaires. Accompanying editorials discuss the role of nitric oxide and prevention of oxidative stress in the treatment of heart failure, as well as the controversial issues surrounding race-based therapeutics.
1. Dexter PR, Perkins SM, Mahany KS, Jones K, McDonald CJ. Inpatient computer-based standing orders vs. physician reminders to increase influenza and pneumococcal vaccination rates: a randomized trial. JAMA. 2004; 292: 2366-71.
Past studies have suggested that most patients admitted with severe pneumococcal infections have been hospitalized in the preceding 5 years, and simply being hospitalized is a potential risk factor for later pneumococcal infection. Likewise, hospitalization provides an opportunity to vaccinate high-risk patients against influenza, and raising pneumococcal and influenza immunization rates is a CMS quality improvement priority. Prior investigations have supported the use of labor-intensive manual standing orders as well as computerized reminders, but this prospective trial was conducted in 1998 and 1999 to assess the effectiveness of a computer-based system to screen for eligible patients and then generate orders to perform pneumonia and influenza vaccinations on inpatients at the time of discharge.
Over 13 months, a total of 3777 inpatients were entered into the study. The hospital computer identified patients eligible for vaccination based on common criteria and randomized them to one of two groups of physician teams. For one group of teams, the computer order-entry system would automatically generate vaccination orders at the time of discharge for vaccine-eligible patients; for the other group of teams, only computer reminders were provided to physicians. The outcome measure was administration of vaccine; long-term outcomes such as incidence of subsequent disease or mortality were not measured.
During the study period, 50% of all hospitalized patients were identified as eligible for influenza vaccination; 22% were eligible for pneumococcal vaccination. In each case, the “standing order” group received vaccine more often (influenza: 42% vs. 30%, p<.001; pneumococcal vaccine: 51% vs. 31%). The numbers were subsequently adjusted to allow for patients who had previously received vaccine, but the impressive differences persisted. Nurses reported reasons for non-administration in 98% of the eligible patients who were not vaccinated; the most common reason was patient refusal. It is not clear if the physicians knew that a study was being conducted. No adverse reactions were reported.
CMS has pushed for the development of institutional standing order sets as a tool to improve compliance with vaccination rate targets. Where the technology is available, computer systems that can screen eligible patients and generate automatic orders are an effective tool in implementing many quality-improvement initiatives, and hospitalists are in a crucial position to take an active role in their development and implementation.
2. Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for a trial fibrillation. Ann Intern Med. 2004; 141: 745-52.
Warfarin has been shown to reduce risk of stroke in patients with chronic and paroxysmal atrial fibrillation. Intracranial hemorrhage remains one of the most feared complications of warfarin, especially among older patients, prompting suggestions to consider lower intensity anticoagulation among patients older than 75 years who have atrial fibrillation.
This study evaluated the relationship between the intensity of anticoagulation, risk of intracranial hemorrhage, and age of patients with atrial fibrillation.
This was a retrospective case control study conducted at a tertiary care medical center. One-hundred and seventy patients on warfarin and admitted with intracranial hemorrhage from 1993 to 2002 were matched with 1020 patients who were on warfarin but without intracranial bleed. After controlling for comorbid conditions and aspirin use, authors conducted multivariable logistic regression analysis to determine the odds of intracranial hemorrhage with regard to age and INR. The risk of intracranial hemorrhage increased at 85 years of age and at INR values of 3.5 or greater. The risk of intracranial hemorrhage at INR less than 2.0 did not differ statistically from the risk at INR of 2.0–3.0.
This study shows the risk of intracranial hemorrhage is not decreased by choosing lower intensity anticoagulation, and target INR should still be kept at 2.5 among elderly patients. However, patients older than 85 years should be counseled about their higher risk of intracranial hemorrhage.
3. Heeschen C, Hamm CW, Mitrovic V, et al. N-terminal pro-B-type natriuretic peptide levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation. 2004;110: 3206-12.
Recent data demonstrate the prognostic value of assessment of neurohormonal activation in patients with acute coronary syndromes (ACS). B-type natriuretic peptide levels (BNP) and levels of the N-terminal fragment of the BNP prohormone (NT-proBNP) predict adverse long-term outcomes in patients with ACS. Investigators reviewed plasma samples of Troponin T (TnT) and NT-proBNP obtained from patients with ACS enrolled in the Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM) trial, which randomized patients to tirofiban or heparin for 48 hours and assessed mortality and myocardial infarction at 30 day follow-up. TnT and NT-proBNP determinations were available at baseline for 1791 patients, and at 48 and 72 hours from 1401 patients. Baseline NT-proBNP levels >250 ng/L were associated with significantly higher rates of death and myocardial infarction at 7 and 30 day follow-up. After adjustment for TnT and C-reactive protein levels, elevated NTproBNP levels maintained its predictive value (OR 2.7; p<.001). In patients with normal TnT levels, NT-proBNP levels identified a subgroup of patients at increased risk (OR 3.0; p=.004). However, in patients with high TnT levels (>0.1 mcg/L), NT-proBNP lost its predictive value (p=.58). More importantly, patients with normal levels of both TnT and NT-proBNP were at very low risk (0.6% event rate at 30 day follow-up).
Serial determinations of NT-proBNP levels at 48 and 72 hours were reviewed in patients without major adverse cardiac events (death or myocardial infarction); these patients were subdivided into groups with and without refractory ischemia. Patients without refractory ischemia showed a significant decline in NT-proBNP levels, whereas patients with refractory ischemia had no significant change. Persistently elevated NT-proBNP levels at 72 hours were associated with a 17.2% risk of death or MI at 30 days, compared with 0.6% risk if NT-proBNP returned to normal at 72 hours (p<.001). Neither TnT nor C-reactive protein demonstrated similar predictive value.
The study is limited by its retrospective nature, by potential selection bias by including only patients with direct evidence of coronary artery disease, and by limitations of the generalizability of its findings (e.g., to emergency department patients with chest pain).
As BNP and NT-proBNP are counter-regulatory hormones that play an active role in the response to ischemic injury, the authors suggest that NT-proBNP is a promising tool for dynamic risk assessment in patients with ACS. The authors also do not differentiate between BNP and NT-proBNP with regard to use in risk stratification, which might lead one to believe that these tests share similar predictive value. (Of note, the study was entirely funded by a company that produces an assay for NT-proBNP). Prospective trials to validate this tool are warranted
4. Heuschmann PU, Kolominsky-Rabas PL, Roether J, et al. Predictors of in-hospital mortality in patients with acute ischemic stroke treated with thrombolytic therapy. JAMA. 2004;292:1831-38.
The objective of this study was to identify factors associated with in-hospital mortality in ischemic stroke patients treated with recombinant tissue plasminogen activator (tPA). It was a prospective observational cohort study of 1658 patients conducted at 225 community and academic hospitals throughout Germany with main outcome of in-hospital mortality.
In this study 10% of patients who were treated with tPA died during their hospital stay, with 2/3 of deaths occurring in the first 7 days. Relative probability of in-hospital mortality increased with increasing patient age, with an odds ratio (OR) of 1.6 for each 10-year increment in age. Age was an independent predictor of in hospital mortality irrespective of tPA administration, with patients older than 75 years age having 4 fold higher mortality than the youngest cohort of less than 55 years age.
Other factors predicting in hospital mortality were altered level of consciousness and relative lack of experience with tPA treatment in the center. Altered level of consciousness was a predictor of stroke severity and an independent predictor of in-hospital mortality (OR 3.4). The increase in mortality in centers with limited experience with tPA administration (OR 0.97) reflected learning curve issues with these patients. The study was not designed to separate out the confounders of operator experience curve from institutional experience curves, or to derive the exact relationship between experience and outcomes.
5. McAlister FA, Bertsch K, Man J, et al. Incidence of and risk factors for pulmonary complications after non-thoracic surgery. Am J Respir Crit Care Med. 2004; published ahead of print on November 24, 2004 as doi:10.1164/rccm.200408-1069OC. Accessed January 27, 2005.
Postoperative pulmonary complications after nonthoracic surgery are a cause of significant morbidity and increased length of hospital stay. Previous studies of preoperative pulmonary assessment were limited by non-representative patient samples, conflicting results, and lack of explicit definitions of these complications. The authors conducted a prospective cohort study of 1055 patients seen in a Pre-Admission Clinic of a tertiary care university hospital. Mean age was 55 years, 50% male, and the cohort consisted of patients scheduled for intermediate risk elective surgery (upper abdominal, lower abdominal, orthopedic). They evaluated physical exam maneuvers (cough test, wheeze test, maximal laryngeal height, and forced expiratory time, all of which are described in an online data supplement) and preoperative spirometry values, and collected information on clinically significant postoperative pulmonary complications, including pneumonia, respiratory failure requiring mechanical ventilation, atelectasis requiring bronchoscopy, or pneumothorax or pleural effusion requiring percutaneous intervention. Twenty-eight patients (2.7%) suffered a pulmonary complication within 7 days of surgery, one of whom died. Length of stay was significantly prolonged in this group (mean 27.9 days vs 4.5 days, p=.006). Multivariate regression analysis revealed four variables that were independently associated with increased risk for postoperative pulmonary complications: age > 65 years, positive cough test (repeated coughing after asking the patient to inhale deeply and cough once), perioperative nasogastric tube, and anesthesia duration 2.5 hours or greater. Number of pack years smoked, FEV1, FEV1/FVC ratio, and upper abdominal surgery were associated with postoperative pulmonary complications but were not found to be independently associated by multivariate analysis.
While it is not surprising that the above risk factors are predictive of postoperative complications, this is the first study to incorporate specific exam maneuvers and spirometry into a risk prediction analysis. Limitations of this model are lack of independent validation and lack of generalizability to other populations, e.g., inpatients awaiting urgent surgery. Of note, the study further provides further support for not routinely obtaining pulmonary function testing for risk stratification prior to noncardiac surgery.
6. Mortenson, EM, Restrepo M, Anzeuto A, Pugh J. Effects of guideline-concordant antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am J Med. 2004;117:726-31.
The American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) have published guidelines for the management of community acquired pneumonia that include recommendations for antibiotic selection. This retrospective cohort study attempted to measure the association between adherence to such guidelines and 30-day mortality in patients admitted with pneumonia to two Texas hospitals.
The characteristics of the patients studied reflect a reasonable cross-section of typical pneumonia patients, with the exception that the patients were mostly (85%) men. Of the study population, 78% were admitted through the ER, 20% admitted to the ICU, and 9% were nursing home residents. Antibiotics were considered “concordant” if they were consistent with either the most recent IDSA or ATS recommendations. The “nonconcordant” group was slightly older (66 vs. 61), generally sicker (higher rate of comorbid COPD and CVD), had more cerebrovascular disease, was more likely to present with altered mental status, and less frequently received antibiotics within 8 hours of presentation. The study did not comment on patients’ vaccination status. Thirty-day mortality was 6.2% in the guideline-concordant group, versus 21.7% in the other group (p < .001). The most common “non-concordant” regimen described was use of a beta-lactam alone, although specific antibiotic regimens were not evaluated.
While the results of this study are not surprising, they provide us with both the validation to continue practice according to existing recommendations, particularly the avoidance of monotherapy with beta-lactam antibiotics. The study also provides us with the imperative to take the lead in developing evidence-based pneumonia pathways at our own hospitals.
7. Pham MX, Whooley MA, Evans GT Jr, et al. Prognostic value of low-level cardiac troponin-I elevations in patients without definite acute coronary syndromes. Am Heart J. 2004;148: 776-82.
With the availability of rapid and highly sensitive and specific troponin testing, many patients admitted to the hospital with non-cardiac diagnoses have been recognized as having abnormal serum troponin-I or troponin-T levels, often just slightly above the reference cutoff for “normal.” While the clinical assumption is often that the elevated enzyme level does not reflect an acute coronary syndrome per se, its significance regarding the patient’s underlying cardiac health is often unclear.
Pham et al. retrospectively reviewed the 1-year mortality of 366 patients who were admitted to the San Francisco VA without evidence of acute MI or ACS either clinically or by EKG, but who had low-level troponin-I elevations (up to 3.0 ng/mL—a level that the authors state was reached by institutional consensus, and which was measured by a “first-generation” assay). These patients were admitted for a broad spectrum of diagnoses ranging from CHF to COPD to sepsis. Ninety-six percent of the patients were men; their average age was 69.
Follow-up was accomplished after a mean of 288 days and included 97% of patients. The primary endpoint was MI or death due to cardiac disease at one year; secondary endpoints were revascularization or admission for unstable angina. The primary endpoint was reached by 11% of patients with cTn-I between 1.0 and 3.0 ng/mL, and 4% of the patients with cTn-I up to 1.0 ng/mL (adjusted HR 3.4, 95% CI, 1.3 to 9.4), and the higher the cTn-I, the higher the risk. However, the authors did not test for the level of risk by specific diagnosis, so they caution against overgeneralizing their findings.
The findings of this study add to the evidence that any evidence of myocardial injury implies an increased risk of underlying heart disease and accompanying long—term cardiac complications– even if such injury occurs in the absence of ACS or known heart disease. Hospitalists often see such injury in the setting of acute infection and pulmonary disease and may be the first to recognize the possibility of CHD in a given patient. To date, guidelines addressing optimal prospective risk stratification have not been developed. Until they are, hospitalists should be aware of the ramifications of “troponin leak” and be prepared to initiate necessary inpatient monitoring and treatments, and to coordinate appropriate follow-up for these patients.
8. Saposnik G, Young B, Silver B, et al. Lack of improvement in patients with acute stroke after treatment with thrombolytic therapy: predictors and association with outcome. JAMA. 2004; 292: 1839-44.
Recombinant tissue plasminogen activator (tPA) has been shown to be one of the most efficacious therapies for acute stroke treatment. This was a systematic evaluation of predictors for outcomes at 24 hours after tPA therapy and of the prognostic significance of lack of improvement at 24 hours for long-term outcomes at 3 months.
The trial was a prospective cohort study of 216 consecutive patients admitted with acute ischemic stroke to a university hospital. The decision to treat with tPA was based on the NINDS protocol with one difference: patients with involvement of more than one third of the middle cerebral artery on the baseline CT scan were excluded. A control CT scan was performed at 24 hours to determine the presence of new infarction, cortical involvement, and extension of the ischemic lesion.
Lack of improvement was defined as a difference between the NIHSS score at baseline and at 24 hours of 3 points or less. Poor outcome at 3 months was defined by a modified Rankin Scale score of 3 to 5 or death.
After adjusting for age, gender, and stroke severity, hyperglycemia at admission (glucose > 144 mg/dL), cortical involvement, and time to treatment were independent predictors of lack of improvement at 24 hours. After adjusting for age, gender, and stroke severity, lack of improvement at 24 hours was an independent predictor of poor outcome and death at 3 months. Patients with lack of improvement at 24 hours also had longer lengths of hospitalization.
9. Taylor AL, Ziesche S, Yancy C, et al. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. 2004;351:2049-57.
Neurohormonal changes, endothelial dysfunction, impaired nitric oxide availability, and oxidant stress all contribute to the structural remodeling of the left ventricle in congestive heart failure. The combination of isosorbide dinitrate, an organic nitrate that stimulates nitric oxide signaling, and the antioxidant and vasodilator hydralazine improves survival in heart failure. Based on more recent data that black patients have a clinically significant response to this combination therapy, the authors of the African-American Heart Failure Trial (A-HeFT) evaluated 1050 black patients with congestive heart failure in a randomized, double-blind, placebo controlled trial. Patients were randomized to fixed doses of isosorbide dinitrate and hydralazine plus background therapy (i.e., digoxin, ACE inhibitors, beta-blockers, diuretics, angiotensin receptor blockers) or to placebo plus background therapy. After 18 months, the trial was stopped due to a significantly higher mortality rate in the placebo group (10.2% in the placebo group vs. 6.2% with combination
therapy, p=.02); survival differences emerged at 180 days and increased progressively thereafter. The combination therapy group reported more headache and dizziness but suffered fewer exacerbations of congestive heart failure and reported improvement in subjective assessments of quality of life as measured by questionnaires. Accompanying editorials discuss the role of nitric oxide and prevention of oxidative stress in the treatment of heart failure, as well as the controversial issues surrounding race-based therapeutics.
In the Literature
CARP Trial Suggests No Benefit to Revascularization Before Vascular Surgery
McFalls, EO, Ward HB, Mortiz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med. 2004;351:2795-2804.
Recent studies have presented evidence that treatment with beta-blockers for patients with CAD could reduce the risk of perioperative cardiac complications. Beta-blockers have since become a critical part of the management plan for the perioperative patient. Evidence-based practice guidelines for cardiac risk assessment have been published by both the American College of Physicians and the American College of Cardiology/American Heart Association. However, practice patterns continue to vary between physicians and cardiologists, particularly for patients clinically stratified into the intermediate-risk category. Some physicians feel comfortable with a conservative approach of medical optimization even in the setting of established CAD, while others favor more aggressive treatment, even though the prospective data supporting cardiac revascularization before major surgery has been lacking. The study investigators sought to clarify this uncertainty.
The prospective trial enrolled 510 patients at 18 VA centers. Patients scheduled for major vascular operations were eligible, and were preoperatively assessed via clinical criteria, stress imaging, and angiography when appropriate. Eligible patients had significant (at least 70%) stenosis of at least one coronary artery. High-risk patients (i.e., those with left main disease, severe aortic stenosis, and LVEF <20%) were excluded. Patients were then randomized to one
of two groups. The first group underwent revascularization with PTCA or CABG plus medical optimization; the second group received only medical optimization. Most patients in both groups received beta-blockers, and more than half in each received statins. The patient populations were appropriately randomized, although overwhelmingly male (98%). Most patients had one- or two-vessel CAD. The primary endpoint was long-term mortality. Secondary endpoints included MI, stroke, renal failure requiring dialysis, and limb loss. Follow-up rates were similar in both groups (86% and 85%).
The major finding of the study was the lack of difference in mortality between the two groups at an average follow-up of 2.7 years (22% vs. 23%, RR= 0.98, 95% CI 0.70 to 1.37, p = 0.92). Analyzing by “treatment-received” instead of “intention-to-treat” did not significantly change this result. Of note, ten patients in the revascularization arm died between the revascularization procedure and the vascular surgery. Not surprisingly, revascularization also delayed the time to surgery for patients in that arm of the study. In the authors’ analysis, the patients were also divided into subgroups based on high-risk variables (prior CABG, category of Revised Cardiac Risk Index, etc.), but the study was not powered to detect mortality differences between the two arms within these subgroups. The authors concluded that there was no benefit to revascularization in patients with stable coronary syndromes prior to elective vascular surgeries.
The results of this study validate the conservative practice recommended by the existing guidelines— that is, to perform revascularization procedures in the preoperative setting only when indicated by clinical criteria such as unstable ischemic symptoms, and if likely to improve long-term survival. Beta-blockers, and based on recent studies probably “statins,” should continue to be the mainstay of perioperative risk optimization for patients with stable coronary disease.
There were, however, several important considerations: first, the study group was exclusively male, although there is little reason to believe that women would have better outcomes from revascularization. And second, the highest-risk patients were excluded, and therefore the results should not be extrapolated to that population. Prospective identification of the group of patients who may benefit from aggressive intervention should remain a target of risk assessment and further research. (BH)
Blood Transfusion May Increase Mortality in Acute Coronary Syndrome
Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004;292:1555-62.
The increased use of invasive procedures and anticoagulant and fibrinolytic drugs in patients with ischemic heart disease in recent years predictably increases the potential for bleeding and perceived need for transfusion. Studies evaluating the association between transfusion and mortality have produced mixed results. A more pertinent clinical question is whether transfusion is beneficial or harmful in patients with acute coronary syndromes who acutely develop anemia during their hospitalization.
The authors used clinical data from three large international trials of patients with acute coronary syndromes (GUSTO IIb, PURSUIT, and PARAGON B) to determine the association between blood transfusion and outcomes among patients who developed moderate to severe bleeding, anemia, or both during their hospitalization.
Assessment of clinically significant bleeding complications was based on the GUSTO definition of severe (intracranial hemorrhage or hemodynamic compromise and requiring intervention) or moderate (hemodynamically stable but requiring blood transfusion) bleeding. The GUSTO IIb and PURSUIT trials used the above definition; PARAGON B categorized bleeding as “major or life threatening” (intracranial hemorrhage or bleeding leading to hemodynamic compromise requiring intervention) or “intermediate” (requiring transfusion or a decrease in hemoglobin of 5 g/dL or more, or a decrease in hematocrit ( 15%). Major or life-threatening bleeding episodes and intermediate bleeding episodes in PARAGON B were deemed equivalent to severe and moderate bleeding episodes in GUSTO.
Data were collected on the date, time, severity, and location of each bleeding event, and on the date and number of units of packed red blood cells and whole blood transfused. The primary end-point was 30-day all-cause mortality. Secondary end-points were occurrence of the composite of 30-day death or MI.
The unadjusted rates of 30-day death, MI, and composite death/MI were significantly higher among patients who received a transfusion (30-day death, 8.00% vs. 3.08%; p<.001; 30-day MI, 25.16% vs. 8.16%; p<.001; 30-day composite death/MI, 29.24% vs. 10.02%; p<.001).
After adjustment for baseline characteristics, bleeding and transfusion propensity, and nadir hematocrit, blood transfusion was associated with a hazard ratio for death of 3.94 (95% confidence interval, 3.26–4.75).
No significant association was found between transfusion and 30-day mortality at a nadir hematocrit of 25% or less (adjusted OR 1.13; 95% CI 0.70-1.82). However, at a nadir hematocrit higher than 25%, transfusion was associated with significantly higher odds of 30-day death, even after excluding patients who underwent CABG or those who died within the first 5 days of follow-up.
These findings differ from the findings of Wu et al. (1) who noted that blood transfusion was associated with lower 30-day mortality among elderly patients with MI if the admission hematocrit was 30% or lower. The current authors propose that their data is more robust due to meticulous collection through clinical trial records, and that their analysis accounts for timing of transfusion and indications for transfusion.
Many clinicians logically believe that augmentation of oxygen carrying capacity via transfusion would be beneficial to patients with active ischemia. However, the authors note that red blood cells in stored blood may be depleted of both 2,3-diphosphoglyceric acid and nitric oxide, both of which are critical components to oxygen delivery and exchange. These cells then function as nitric oxide “sinks,” promoting vasoconstriction, platelet aggregation, and impaired oxygen delivery to tissues. In addition, inflammatory mediators associated with exacerbation of myocardial ischemia may remain in transfused blood, potentially contributing to adverse outcomes.
As this is a nonrandomized, post hoc observational study, further prescriptive conclusions regarding transfusion cannot be made. However, the authors, along with an accompanying editorial, call for prospective randomized trials of transfusion in anemic patients with acute coronary syndromes to better define the role of this commonly used therapy. (CW)
- Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001;345:1230-6.
Cost-effectiveness of Rhythm Versus Rate Control in Atrial Fibrillation
Marshall DA, Levy AR, Vidaillet H, et al. Cost-effectiveness of rhythm versus rate control in atrial fibrillation. Ann Intern Med. 2004;141:653-61.
Atrial fibrillation is the most common arrhythmia treated by physicians. It afflicts nearly 10% of patients age 80 years or older. There are two primary modalities of managing patients with atrial fibrillation; rate control versus cardioversion into sinus rhythm.
AFFIRM was a multicenter randomized controlled trial involving 213 centers in USA and Canada that compared rate versus rhythm control in 4060 patients. These patients had a mean age of 70 years. Sixty-one percent of the enrolled patients were men, and 66% had recurrent atrial fibrillation. Seventy-one percent of patients had hypertension, 39% had coronary artery disease, and 9% had congestive heart failure. Patients were block randomized by center to either rate control or rhythm control and followed for an average of 3.5 years. AFFIRM results showed no significant mortality difference between the two groups (hazard ratio for rate versus rhythm control, 0.87 with 95% CI, 0.75 to 1.01).
Primary data on survival and resource utilization were used to conduct the economic analysis from a third party payer perspective. Authors used intention to treat data for the economic analysis.
For resource utilization estimates, US healthcare cost figures for the year 2002 were used. All earlier costs were appropriately adjusted using Consumer Price Index, Medical Care component to estimate their nominal values in year 2002. Hospital costs were taken as the mean charges per day from Healthcare Cost and Utilization Project statistics for Diseases of the Circulatory System for patients older than 18 years age. Low and high end of these costs were assumed to be equivalent to 25th and 75th percentiles of the mean costs, respectively. Physician costs were assumed to be equivalent to be the average of all carriers’ payments for the relative value units of the services rendered based on a generic current procedural terminology code. Sensitivity analysis was conducted on these physician costs using minimum payment among these carriers as the low cost estimate and the standard charges for Marshfield Clinic for the high end. Costs of pacemaker and implantable cardioverter defibrillators were based on manufacturers’ list prices. For sensitivity analysis, hardware costs were excluded for low cost estimates and the maximum manufacturers’ list price for the high estimate was used.
At each follow-up visit during the AFFIRM trial, the number of cardioversion attempts since the prior visit was recorded. Costs of cardioversion were based on average payment to Marshfield Clinic for outpatient electrical cardioversion for the year 2002. Authors assigned no costs for low cost estimate and used billed charges for high costs for sensitivity analysis.
At each follow-up visit, the number of short stay and emergency department visits since the prior visit was recorded. Weighted average Medicare costs for level I and II facilities were used as the baseline estimate for these visits. Estimates for sensitivity analysis were the minimum and maximum Medicare payments for these visits. Physician fees were based on level III emergency department visit with low and high cost estimates assigned as described above.
Medication costs were based on the least average wholesale price (AWP) for a generic medication. Low and high cost estimates were taken from lowest quoted US Internet pharmacy price and highest AWP for the most expensive drug in the class respectively. Only medications used for atrial fibrillation and anticoagulation were considered for analysis.
The authors calculated the mean cost per patient In the Literature (continued) and the mean survival time between the two interventions. Future costs were discounted by 3%. For the base estimate, rhythm control was more expensive and less effective than rate control, i.e., dominated by the rate control. Rate control dominated rhythm control even for high and low estimates of the sensitivity analysis demonstrating stability of the results. Authors used 10,000 simulations to perform non-parametric bootstrapping analysis to find the 95% credible intervals around the base estimate. The bootstrap results showed that for 95% of the results rate control had higher survival time and was less costly than rhythm control. These simulation results clearly showed rate control is more cost-effective for patient population resembling that of AFFIRM trial.
The study has some limitations. These results are robust for patients similar to those in AFFIRM trial, i.e., older patients with cardiovascular defects that are at risk of cerebrovascular embolism. However these results may not be applicable to younger patients and those with “lone atrial fibrillation.” The study had a follow-up period of 3.5 years, and the cost-effectiveness analysis is confined to this period. It is difficult to determine mortality advantage of one treatment over another within the limited duration of the AFFIRM study. Most of the patients were on multiple pharmacologic agents for rhythm control and had a high incidence of cross-over from rhythm control to rate control reflecting modest benefits of the current agents. These results may not be applicable to patients whose atrial fibrillation is well controlled by a single agent or by non-pharmacological treatment. Patients on rhythm control agents had, as expected, more hospitalization days from the side effects and treatment protocols of the agents (especially pharmacologic) used to control the rhythm. With advances in both pharmacologic as well as nonpharmacologic methods for rhythm control generating safer and more efficacious technologies, the results of this analysis may become less valid in the future. The analysis was conducted from a third-party payer perspective, without accounting for the quality of life. Thus patients who have symptomatic atrial fibrillation and those with diastolic dysfunction may have improved quality of life from rhythm control over just rate control. The results may not be applicable to these patients. (SS)
CARP Trial Suggests No Benefit to Revascularization Before Vascular Surgery
McFalls, EO, Ward HB, Mortiz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med. 2004;351:2795-2804.
Recent studies have presented evidence that treatment with beta-blockers for patients with CAD could reduce the risk of perioperative cardiac complications. Beta-blockers have since become a critical part of the management plan for the perioperative patient. Evidence-based practice guidelines for cardiac risk assessment have been published by both the American College of Physicians and the American College of Cardiology/American Heart Association. However, practice patterns continue to vary between physicians and cardiologists, particularly for patients clinically stratified into the intermediate-risk category. Some physicians feel comfortable with a conservative approach of medical optimization even in the setting of established CAD, while others favor more aggressive treatment, even though the prospective data supporting cardiac revascularization before major surgery has been lacking. The study investigators sought to clarify this uncertainty.
The prospective trial enrolled 510 patients at 18 VA centers. Patients scheduled for major vascular operations were eligible, and were preoperatively assessed via clinical criteria, stress imaging, and angiography when appropriate. Eligible patients had significant (at least 70%) stenosis of at least one coronary artery. High-risk patients (i.e., those with left main disease, severe aortic stenosis, and LVEF <20%) were excluded. Patients were then randomized to one
of two groups. The first group underwent revascularization with PTCA or CABG plus medical optimization; the second group received only medical optimization. Most patients in both groups received beta-blockers, and more than half in each received statins. The patient populations were appropriately randomized, although overwhelmingly male (98%). Most patients had one- or two-vessel CAD. The primary endpoint was long-term mortality. Secondary endpoints included MI, stroke, renal failure requiring dialysis, and limb loss. Follow-up rates were similar in both groups (86% and 85%).
The major finding of the study was the lack of difference in mortality between the two groups at an average follow-up of 2.7 years (22% vs. 23%, RR= 0.98, 95% CI 0.70 to 1.37, p = 0.92). Analyzing by “treatment-received” instead of “intention-to-treat” did not significantly change this result. Of note, ten patients in the revascularization arm died between the revascularization procedure and the vascular surgery. Not surprisingly, revascularization also delayed the time to surgery for patients in that arm of the study. In the authors’ analysis, the patients were also divided into subgroups based on high-risk variables (prior CABG, category of Revised Cardiac Risk Index, etc.), but the study was not powered to detect mortality differences between the two arms within these subgroups. The authors concluded that there was no benefit to revascularization in patients with stable coronary syndromes prior to elective vascular surgeries.
The results of this study validate the conservative practice recommended by the existing guidelines— that is, to perform revascularization procedures in the preoperative setting only when indicated by clinical criteria such as unstable ischemic symptoms, and if likely to improve long-term survival. Beta-blockers, and based on recent studies probably “statins,” should continue to be the mainstay of perioperative risk optimization for patients with stable coronary disease.
There were, however, several important considerations: first, the study group was exclusively male, although there is little reason to believe that women would have better outcomes from revascularization. And second, the highest-risk patients were excluded, and therefore the results should not be extrapolated to that population. Prospective identification of the group of patients who may benefit from aggressive intervention should remain a target of risk assessment and further research. (BH)
Blood Transfusion May Increase Mortality in Acute Coronary Syndrome
Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004;292:1555-62.
The increased use of invasive procedures and anticoagulant and fibrinolytic drugs in patients with ischemic heart disease in recent years predictably increases the potential for bleeding and perceived need for transfusion. Studies evaluating the association between transfusion and mortality have produced mixed results. A more pertinent clinical question is whether transfusion is beneficial or harmful in patients with acute coronary syndromes who acutely develop anemia during their hospitalization.
The authors used clinical data from three large international trials of patients with acute coronary syndromes (GUSTO IIb, PURSUIT, and PARAGON B) to determine the association between blood transfusion and outcomes among patients who developed moderate to severe bleeding, anemia, or both during their hospitalization.
Assessment of clinically significant bleeding complications was based on the GUSTO definition of severe (intracranial hemorrhage or hemodynamic compromise and requiring intervention) or moderate (hemodynamically stable but requiring blood transfusion) bleeding. The GUSTO IIb and PURSUIT trials used the above definition; PARAGON B categorized bleeding as “major or life threatening” (intracranial hemorrhage or bleeding leading to hemodynamic compromise requiring intervention) or “intermediate” (requiring transfusion or a decrease in hemoglobin of 5 g/dL or more, or a decrease in hematocrit ( 15%). Major or life-threatening bleeding episodes and intermediate bleeding episodes in PARAGON B were deemed equivalent to severe and moderate bleeding episodes in GUSTO.
Data were collected on the date, time, severity, and location of each bleeding event, and on the date and number of units of packed red blood cells and whole blood transfused. The primary end-point was 30-day all-cause mortality. Secondary end-points were occurrence of the composite of 30-day death or MI.
The unadjusted rates of 30-day death, MI, and composite death/MI were significantly higher among patients who received a transfusion (30-day death, 8.00% vs. 3.08%; p<.001; 30-day MI, 25.16% vs. 8.16%; p<.001; 30-day composite death/MI, 29.24% vs. 10.02%; p<.001).
After adjustment for baseline characteristics, bleeding and transfusion propensity, and nadir hematocrit, blood transfusion was associated with a hazard ratio for death of 3.94 (95% confidence interval, 3.26–4.75).
No significant association was found between transfusion and 30-day mortality at a nadir hematocrit of 25% or less (adjusted OR 1.13; 95% CI 0.70-1.82). However, at a nadir hematocrit higher than 25%, transfusion was associated with significantly higher odds of 30-day death, even after excluding patients who underwent CABG or those who died within the first 5 days of follow-up.
These findings differ from the findings of Wu et al. (1) who noted that blood transfusion was associated with lower 30-day mortality among elderly patients with MI if the admission hematocrit was 30% or lower. The current authors propose that their data is more robust due to meticulous collection through clinical trial records, and that their analysis accounts for timing of transfusion and indications for transfusion.
Many clinicians logically believe that augmentation of oxygen carrying capacity via transfusion would be beneficial to patients with active ischemia. However, the authors note that red blood cells in stored blood may be depleted of both 2,3-diphosphoglyceric acid and nitric oxide, both of which are critical components to oxygen delivery and exchange. These cells then function as nitric oxide “sinks,” promoting vasoconstriction, platelet aggregation, and impaired oxygen delivery to tissues. In addition, inflammatory mediators associated with exacerbation of myocardial ischemia may remain in transfused blood, potentially contributing to adverse outcomes.
As this is a nonrandomized, post hoc observational study, further prescriptive conclusions regarding transfusion cannot be made. However, the authors, along with an accompanying editorial, call for prospective randomized trials of transfusion in anemic patients with acute coronary syndromes to better define the role of this commonly used therapy. (CW)
- Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001;345:1230-6.
Cost-effectiveness of Rhythm Versus Rate Control in Atrial Fibrillation
Marshall DA, Levy AR, Vidaillet H, et al. Cost-effectiveness of rhythm versus rate control in atrial fibrillation. Ann Intern Med. 2004;141:653-61.
Atrial fibrillation is the most common arrhythmia treated by physicians. It afflicts nearly 10% of patients age 80 years or older. There are two primary modalities of managing patients with atrial fibrillation; rate control versus cardioversion into sinus rhythm.
AFFIRM was a multicenter randomized controlled trial involving 213 centers in USA and Canada that compared rate versus rhythm control in 4060 patients. These patients had a mean age of 70 years. Sixty-one percent of the enrolled patients were men, and 66% had recurrent atrial fibrillation. Seventy-one percent of patients had hypertension, 39% had coronary artery disease, and 9% had congestive heart failure. Patients were block randomized by center to either rate control or rhythm control and followed for an average of 3.5 years. AFFIRM results showed no significant mortality difference between the two groups (hazard ratio for rate versus rhythm control, 0.87 with 95% CI, 0.75 to 1.01).
Primary data on survival and resource utilization were used to conduct the economic analysis from a third party payer perspective. Authors used intention to treat data for the economic analysis.
For resource utilization estimates, US healthcare cost figures for the year 2002 were used. All earlier costs were appropriately adjusted using Consumer Price Index, Medical Care component to estimate their nominal values in year 2002. Hospital costs were taken as the mean charges per day from Healthcare Cost and Utilization Project statistics for Diseases of the Circulatory System for patients older than 18 years age. Low and high end of these costs were assumed to be equivalent to 25th and 75th percentiles of the mean costs, respectively. Physician costs were assumed to be equivalent to be the average of all carriers’ payments for the relative value units of the services rendered based on a generic current procedural terminology code. Sensitivity analysis was conducted on these physician costs using minimum payment among these carriers as the low cost estimate and the standard charges for Marshfield Clinic for the high end. Costs of pacemaker and implantable cardioverter defibrillators were based on manufacturers’ list prices. For sensitivity analysis, hardware costs were excluded for low cost estimates and the maximum manufacturers’ list price for the high estimate was used.
At each follow-up visit during the AFFIRM trial, the number of cardioversion attempts since the prior visit was recorded. Costs of cardioversion were based on average payment to Marshfield Clinic for outpatient electrical cardioversion for the year 2002. Authors assigned no costs for low cost estimate and used billed charges for high costs for sensitivity analysis.
At each follow-up visit, the number of short stay and emergency department visits since the prior visit was recorded. Weighted average Medicare costs for level I and II facilities were used as the baseline estimate for these visits. Estimates for sensitivity analysis were the minimum and maximum Medicare payments for these visits. Physician fees were based on level III emergency department visit with low and high cost estimates assigned as described above.
Medication costs were based on the least average wholesale price (AWP) for a generic medication. Low and high cost estimates were taken from lowest quoted US Internet pharmacy price and highest AWP for the most expensive drug in the class respectively. Only medications used for atrial fibrillation and anticoagulation were considered for analysis.
The authors calculated the mean cost per patient In the Literature (continued) and the mean survival time between the two interventions. Future costs were discounted by 3%. For the base estimate, rhythm control was more expensive and less effective than rate control, i.e., dominated by the rate control. Rate control dominated rhythm control even for high and low estimates of the sensitivity analysis demonstrating stability of the results. Authors used 10,000 simulations to perform non-parametric bootstrapping analysis to find the 95% credible intervals around the base estimate. The bootstrap results showed that for 95% of the results rate control had higher survival time and was less costly than rhythm control. These simulation results clearly showed rate control is more cost-effective for patient population resembling that of AFFIRM trial.
The study has some limitations. These results are robust for patients similar to those in AFFIRM trial, i.e., older patients with cardiovascular defects that are at risk of cerebrovascular embolism. However these results may not be applicable to younger patients and those with “lone atrial fibrillation.” The study had a follow-up period of 3.5 years, and the cost-effectiveness analysis is confined to this period. It is difficult to determine mortality advantage of one treatment over another within the limited duration of the AFFIRM study. Most of the patients were on multiple pharmacologic agents for rhythm control and had a high incidence of cross-over from rhythm control to rate control reflecting modest benefits of the current agents. These results may not be applicable to patients whose atrial fibrillation is well controlled by a single agent or by non-pharmacological treatment. Patients on rhythm control agents had, as expected, more hospitalization days from the side effects and treatment protocols of the agents (especially pharmacologic) used to control the rhythm. With advances in both pharmacologic as well as nonpharmacologic methods for rhythm control generating safer and more efficacious technologies, the results of this analysis may become less valid in the future. The analysis was conducted from a third-party payer perspective, without accounting for the quality of life. Thus patients who have symptomatic atrial fibrillation and those with diastolic dysfunction may have improved quality of life from rhythm control over just rate control. The results may not be applicable to these patients. (SS)
CARP Trial Suggests No Benefit to Revascularization Before Vascular Surgery
McFalls, EO, Ward HB, Mortiz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med. 2004;351:2795-2804.
Recent studies have presented evidence that treatment with beta-blockers for patients with CAD could reduce the risk of perioperative cardiac complications. Beta-blockers have since become a critical part of the management plan for the perioperative patient. Evidence-based practice guidelines for cardiac risk assessment have been published by both the American College of Physicians and the American College of Cardiology/American Heart Association. However, practice patterns continue to vary between physicians and cardiologists, particularly for patients clinically stratified into the intermediate-risk category. Some physicians feel comfortable with a conservative approach of medical optimization even in the setting of established CAD, while others favor more aggressive treatment, even though the prospective data supporting cardiac revascularization before major surgery has been lacking. The study investigators sought to clarify this uncertainty.
The prospective trial enrolled 510 patients at 18 VA centers. Patients scheduled for major vascular operations were eligible, and were preoperatively assessed via clinical criteria, stress imaging, and angiography when appropriate. Eligible patients had significant (at least 70%) stenosis of at least one coronary artery. High-risk patients (i.e., those with left main disease, severe aortic stenosis, and LVEF <20%) were excluded. Patients were then randomized to one
of two groups. The first group underwent revascularization with PTCA or CABG plus medical optimization; the second group received only medical optimization. Most patients in both groups received beta-blockers, and more than half in each received statins. The patient populations were appropriately randomized, although overwhelmingly male (98%). Most patients had one- or two-vessel CAD. The primary endpoint was long-term mortality. Secondary endpoints included MI, stroke, renal failure requiring dialysis, and limb loss. Follow-up rates were similar in both groups (86% and 85%).
The major finding of the study was the lack of difference in mortality between the two groups at an average follow-up of 2.7 years (22% vs. 23%, RR= 0.98, 95% CI 0.70 to 1.37, p = 0.92). Analyzing by “treatment-received” instead of “intention-to-treat” did not significantly change this result. Of note, ten patients in the revascularization arm died between the revascularization procedure and the vascular surgery. Not surprisingly, revascularization also delayed the time to surgery for patients in that arm of the study. In the authors’ analysis, the patients were also divided into subgroups based on high-risk variables (prior CABG, category of Revised Cardiac Risk Index, etc.), but the study was not powered to detect mortality differences between the two arms within these subgroups. The authors concluded that there was no benefit to revascularization in patients with stable coronary syndromes prior to elective vascular surgeries.
The results of this study validate the conservative practice recommended by the existing guidelines— that is, to perform revascularization procedures in the preoperative setting only when indicated by clinical criteria such as unstable ischemic symptoms, and if likely to improve long-term survival. Beta-blockers, and based on recent studies probably “statins,” should continue to be the mainstay of perioperative risk optimization for patients with stable coronary disease.
There were, however, several important considerations: first, the study group was exclusively male, although there is little reason to believe that women would have better outcomes from revascularization. And second, the highest-risk patients were excluded, and therefore the results should not be extrapolated to that population. Prospective identification of the group of patients who may benefit from aggressive intervention should remain a target of risk assessment and further research. (BH)
Blood Transfusion May Increase Mortality in Acute Coronary Syndrome
Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004;292:1555-62.
The increased use of invasive procedures and anticoagulant and fibrinolytic drugs in patients with ischemic heart disease in recent years predictably increases the potential for bleeding and perceived need for transfusion. Studies evaluating the association between transfusion and mortality have produced mixed results. A more pertinent clinical question is whether transfusion is beneficial or harmful in patients with acute coronary syndromes who acutely develop anemia during their hospitalization.
The authors used clinical data from three large international trials of patients with acute coronary syndromes (GUSTO IIb, PURSUIT, and PARAGON B) to determine the association between blood transfusion and outcomes among patients who developed moderate to severe bleeding, anemia, or both during their hospitalization.
Assessment of clinically significant bleeding complications was based on the GUSTO definition of severe (intracranial hemorrhage or hemodynamic compromise and requiring intervention) or moderate (hemodynamically stable but requiring blood transfusion) bleeding. The GUSTO IIb and PURSUIT trials used the above definition; PARAGON B categorized bleeding as “major or life threatening” (intracranial hemorrhage or bleeding leading to hemodynamic compromise requiring intervention) or “intermediate” (requiring transfusion or a decrease in hemoglobin of 5 g/dL or more, or a decrease in hematocrit ( 15%). Major or life-threatening bleeding episodes and intermediate bleeding episodes in PARAGON B were deemed equivalent to severe and moderate bleeding episodes in GUSTO.
Data were collected on the date, time, severity, and location of each bleeding event, and on the date and number of units of packed red blood cells and whole blood transfused. The primary end-point was 30-day all-cause mortality. Secondary end-points were occurrence of the composite of 30-day death or MI.
The unadjusted rates of 30-day death, MI, and composite death/MI were significantly higher among patients who received a transfusion (30-day death, 8.00% vs. 3.08%; p<.001; 30-day MI, 25.16% vs. 8.16%; p<.001; 30-day composite death/MI, 29.24% vs. 10.02%; p<.001).
After adjustment for baseline characteristics, bleeding and transfusion propensity, and nadir hematocrit, blood transfusion was associated with a hazard ratio for death of 3.94 (95% confidence interval, 3.26–4.75).
No significant association was found between transfusion and 30-day mortality at a nadir hematocrit of 25% or less (adjusted OR 1.13; 95% CI 0.70-1.82). However, at a nadir hematocrit higher than 25%, transfusion was associated with significantly higher odds of 30-day death, even after excluding patients who underwent CABG or those who died within the first 5 days of follow-up.
These findings differ from the findings of Wu et al. (1) who noted that blood transfusion was associated with lower 30-day mortality among elderly patients with MI if the admission hematocrit was 30% or lower. The current authors propose that their data is more robust due to meticulous collection through clinical trial records, and that their analysis accounts for timing of transfusion and indications for transfusion.
Many clinicians logically believe that augmentation of oxygen carrying capacity via transfusion would be beneficial to patients with active ischemia. However, the authors note that red blood cells in stored blood may be depleted of both 2,3-diphosphoglyceric acid and nitric oxide, both of which are critical components to oxygen delivery and exchange. These cells then function as nitric oxide “sinks,” promoting vasoconstriction, platelet aggregation, and impaired oxygen delivery to tissues. In addition, inflammatory mediators associated with exacerbation of myocardial ischemia may remain in transfused blood, potentially contributing to adverse outcomes.
As this is a nonrandomized, post hoc observational study, further prescriptive conclusions regarding transfusion cannot be made. However, the authors, along with an accompanying editorial, call for prospective randomized trials of transfusion in anemic patients with acute coronary syndromes to better define the role of this commonly used therapy. (CW)
- Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001;345:1230-6.
Cost-effectiveness of Rhythm Versus Rate Control in Atrial Fibrillation
Marshall DA, Levy AR, Vidaillet H, et al. Cost-effectiveness of rhythm versus rate control in atrial fibrillation. Ann Intern Med. 2004;141:653-61.
Atrial fibrillation is the most common arrhythmia treated by physicians. It afflicts nearly 10% of patients age 80 years or older. There are two primary modalities of managing patients with atrial fibrillation; rate control versus cardioversion into sinus rhythm.
AFFIRM was a multicenter randomized controlled trial involving 213 centers in USA and Canada that compared rate versus rhythm control in 4060 patients. These patients had a mean age of 70 years. Sixty-one percent of the enrolled patients were men, and 66% had recurrent atrial fibrillation. Seventy-one percent of patients had hypertension, 39% had coronary artery disease, and 9% had congestive heart failure. Patients were block randomized by center to either rate control or rhythm control and followed for an average of 3.5 years. AFFIRM results showed no significant mortality difference between the two groups (hazard ratio for rate versus rhythm control, 0.87 with 95% CI, 0.75 to 1.01).
Primary data on survival and resource utilization were used to conduct the economic analysis from a third party payer perspective. Authors used intention to treat data for the economic analysis.
For resource utilization estimates, US healthcare cost figures for the year 2002 were used. All earlier costs were appropriately adjusted using Consumer Price Index, Medical Care component to estimate their nominal values in year 2002. Hospital costs were taken as the mean charges per day from Healthcare Cost and Utilization Project statistics for Diseases of the Circulatory System for patients older than 18 years age. Low and high end of these costs were assumed to be equivalent to 25th and 75th percentiles of the mean costs, respectively. Physician costs were assumed to be equivalent to be the average of all carriers’ payments for the relative value units of the services rendered based on a generic current procedural terminology code. Sensitivity analysis was conducted on these physician costs using minimum payment among these carriers as the low cost estimate and the standard charges for Marshfield Clinic for the high end. Costs of pacemaker and implantable cardioverter defibrillators were based on manufacturers’ list prices. For sensitivity analysis, hardware costs were excluded for low cost estimates and the maximum manufacturers’ list price for the high estimate was used.
At each follow-up visit during the AFFIRM trial, the number of cardioversion attempts since the prior visit was recorded. Costs of cardioversion were based on average payment to Marshfield Clinic for outpatient electrical cardioversion for the year 2002. Authors assigned no costs for low cost estimate and used billed charges for high costs for sensitivity analysis.
At each follow-up visit, the number of short stay and emergency department visits since the prior visit was recorded. Weighted average Medicare costs for level I and II facilities were used as the baseline estimate for these visits. Estimates for sensitivity analysis were the minimum and maximum Medicare payments for these visits. Physician fees were based on level III emergency department visit with low and high cost estimates assigned as described above.
Medication costs were based on the least average wholesale price (AWP) for a generic medication. Low and high cost estimates were taken from lowest quoted US Internet pharmacy price and highest AWP for the most expensive drug in the class respectively. Only medications used for atrial fibrillation and anticoagulation were considered for analysis.
The authors calculated the mean cost per patient In the Literature (continued) and the mean survival time between the two interventions. Future costs were discounted by 3%. For the base estimate, rhythm control was more expensive and less effective than rate control, i.e., dominated by the rate control. Rate control dominated rhythm control even for high and low estimates of the sensitivity analysis demonstrating stability of the results. Authors used 10,000 simulations to perform non-parametric bootstrapping analysis to find the 95% credible intervals around the base estimate. The bootstrap results showed that for 95% of the results rate control had higher survival time and was less costly than rhythm control. These simulation results clearly showed rate control is more cost-effective for patient population resembling that of AFFIRM trial.
The study has some limitations. These results are robust for patients similar to those in AFFIRM trial, i.e., older patients with cardiovascular defects that are at risk of cerebrovascular embolism. However these results may not be applicable to younger patients and those with “lone atrial fibrillation.” The study had a follow-up period of 3.5 years, and the cost-effectiveness analysis is confined to this period. It is difficult to determine mortality advantage of one treatment over another within the limited duration of the AFFIRM study. Most of the patients were on multiple pharmacologic agents for rhythm control and had a high incidence of cross-over from rhythm control to rate control reflecting modest benefits of the current agents. These results may not be applicable to patients whose atrial fibrillation is well controlled by a single agent or by non-pharmacological treatment. Patients on rhythm control agents had, as expected, more hospitalization days from the side effects and treatment protocols of the agents (especially pharmacologic) used to control the rhythm. With advances in both pharmacologic as well as nonpharmacologic methods for rhythm control generating safer and more efficacious technologies, the results of this analysis may become less valid in the future. The analysis was conducted from a third-party payer perspective, without accounting for the quality of life. Thus patients who have symptomatic atrial fibrillation and those with diastolic dysfunction may have improved quality of life from rhythm control over just rate control. The results may not be applicable to these patients. (SS)
Practice Profile
Contact
Michael J. Pistoria, DO
Medical Director, Lehigh Valley Hospitalist Services
Associate Program Director, Internal Medicine Residency
Assistant Professor of Medicine, Penn State College of Medicine
Kevin Flynn, MS, Administrative Director
Lehigh Valley Hospital
Cedar Crest Boulevard and I-78
Allentown, PA 18105
Phone: 610-402-8045
Fax: 610-402-1675
Website: www.lvhhn.org
E-mail: [email protected]
Start Up
July 2003
Practitioners
Lehigh Valley Hospital - Cedar Crest
Ardeth Copeland, MD
Shoban Dave, MD
John Davidyock, MD
William Ford, MD
Arvind Gupta, MD (site leader)
Kweku Hayford, MD
Lehigh Valley Hospital - Muhlenberg
Donna Dowlatshahi, Coordinator
Jeff rey Faidley, MD
Melissa Geitz, DO
Wayne Howard, DO (site leader)
Melissa Liu, MD
Dan Mulcahy, DO
Gonzalo Pimentel, MD
Deborah Sterner, Coordinator
Training
All ABIM certified
Employed By
Lehigh Valley Physician Group and Specialty Physicians of LVHHN, PC
Lehigh Valley Hospital and Health Network (LVHHN) is one of the largest teaching facilities in Pennsylvania. LVHHN consists of three clinical campuses, two of which focus on inpatient care: Lehigh Valley Hospital-Cedar Crest (LVHCC) and Lehigh Valley Hospital-Muhlenberg (LVH-M). The Network has more than 1,100 physicians and is a major clinical campus for Penn State’s College of Medicine. LVH-M opens a new patient care, tower in March 2005 and has approximately 200 inpatient beds on campus. The campus offers cardiac catheterization and open heart surgery capabilities, and its intensive care unit is augmented by a tele-intensivist system. A 24/7 hospitalist program was launched at LVH-M in July 2003 and is presently staffed by six full-time physicians.
The LVH-CC campus is preparing to undergo a major expansion that will bring its total beds to approximately 800 by 2007. This campus is a tertiary care center, featuring medical and surgical intensive care, a Level I trauma unit, a burn center, open heart surgery, perinatal care and renal transplantation services. LVHHN also boasts active teaching programs, with residencies in internal medicine, surgery, OB/GYN, family medicine, and emergency medicine. There are also fellowships in cardiology, pulmonary/critical care, and hematology/oncology. The LVHCC hospitalist program provides 24/7 service staffed by six physicians and was launched in July 2004.
Finances
All LVHS physicians are salaried employees. A bonus was paid to the physicians at LVH-M at the end of the first year of services. A bonus structure is being defined for both campuses, focusing on clinical, quality, and service measures. Each hospitalist receives 4 weeks vacation and 5 days of CME. A stipend is also provided for CME. Hospitalists receive malpractice coverage and reimbursement for licensure expenses. Physicians are also entitled to a benefits package that includes disability insurance, a supplemental retirement plan, and a 401(k)/403(b).
Chart abstraction and billing is done by the employer. At the end of each shift, the hospitalist submits a list of the patients seen and/or admitted. Each campus has a program coordinator certified in coding who reviews the charts for documentation and submits for the appropriate level of care. This system has worked well in ensuring proper billing and in allowing prompt feedback to the hospitalists regarding their documentation.
Referrals
LVH-M: The LVH-M hospitalist program was developed to provide a resource for primary care physicians in the community who wished to focus on outpatient care. Primary care physicians were identified and ranked in terms of their willingness to refer patients to the hospitalist program. Care was taken not to target groups who already had referral patterns to existing LVH-M groups to minimize the adverse impact of the hospitalist program on these groups. Hospitalists then made visits to these offices to explain the hospitalist program and answer questions from the PCPs. The program quickly became successful and now has a well-established referral base.
LVH-CC: The major driver of the hospitalist program at the Cedar Crest campus was assisting with the residency program. The existing faculty group staffed two of the five inpatient teaching services and was becoming increasingly busy as a result of new referrals. The hospitalist program helped decompress some of the volume from the existing faculty services by taking over one of the other inpatient teaching slots and establishing an overflow service. The program also seeks referrals from physicians outside the hospital’s traditional referral radius. The hospitalists have also worked with the medical and surgical subspecialists, developing standards for admission of subspecialty patients to the hospitalist service.
Teaching
LVH-CC: The LVH-CC hospitalists are intimately involved in the internal medicine residency program. They staff one of five inpatient teaching services during the morning. In the afternoon and overnight hours, the hospitalists cover their own service and the two pre-existing academic inpatient services. The hospitalists round either formally or informally with the residents of these three teams in the afternoon. They also review each new admission between noon and 8 a.m. to the three inpatient teams and provide bedside teaching on these patients.
A second daytime hospitalist also staff s an overflow service to ensure compliance with Residency Review Committee guidelines regarding service and admission caps. If the three teaching services hit their respective caps, any new patients are admitted by the hospitalists to this overflow service. In addition to rounding on the overflow patients, the second hospitalist staff s a consultative medicine service with a PGY-2 or PGY-3 resident.
The hospitalists participate in morning report and the resident lectures. The hospitalists are also involved in faculty development with the academic general internists as well as other residency initiatives.
LVH-M: Hospitalists at the LVH-M campus have no formal involvement in the teaching programs (osteopathic rotating internship and emergency medicine residency) at that campus. They are an available resource for housestaff, however, and have received many positive compliments from the housestaff for their assistance with difficult patients.
Schedule
LVH-M: The primary rounding hospitalist works Monday through Friday from 7 a.m. to 3 p.m. A second hospitalist works Monday through Friday from 10 a.m. to 7 p.m. and is available on Saturday if the census is high. This hospitalist also works the Sunday night shift beginning at 7 p.m. and ending 7 a.m. Monday. The overnight hospitalist works from 7 p.m. to 7 a.m. Monday through Saturday. There is always a back-up hospitalist available in case of emergency or significant influx of patients that overwhelms the system. The hospitalists work an average of 16 shifts per month.
LVH-CC: There are two hospitalists scheduled during the daytime hours. The hospitalist rounding with the resident team works 7 a.m. to 7 p.m. Monday through Sunday. The overflow/consult hospitalist works 8 a.m. to 8 p.m. Monday through Friday and 7 p.m. to 7 a.m. Saturday and Sunday. The overnight hospitalist works 7 p.m. to 7 a.m. Monday through Friday. The hospitalists work an average of 16 shifts per month.
Future Directions
LVH-M: As the campus continues to grow, the hospitalists aim to become more intricately involved in process improvement and quality-improvement measures. The program is exploring ways of becoming active in the teaching program, either with residents and medical students or with physician assistant students. Additionally, as the Network’s tele-intensivist initiative develops, the hospitalists are working closely with their critical care colleagues to provide top-quality ICU care for patients.
LVH-CC: The LVH-CC hospitalists are becoming increasingly involved in efforts to maximize institutional efficiency and throughput. This program is also seeking to establish itself as a premier research program, in both the educational and clinical realms.
Hospitalists at both campuses are becoming involved in various hospital committees such as Therapeutics and Quality Assurance. Their expertise has also been utilized in various throughput initiatives such as an automated discharge instruction process and electronic signout development.
Given the rapid growth of both programs, staffing needs are expected to increase considerably. One long-term goal is to make it possible for hospitalists to rotate between the two campuses to allow them a variety of experiences. A hospital medicine elective is being developed for PGY-3 residents interested in a career in hospital medicine. There has also been some preliminary discussion of a hospital medicine fellowship that would emphasize teaching, research, and palliative care.
Contact
Michael J. Pistoria, DO
Medical Director, Lehigh Valley Hospitalist Services
Associate Program Director, Internal Medicine Residency
Assistant Professor of Medicine, Penn State College of Medicine
Kevin Flynn, MS, Administrative Director
Lehigh Valley Hospital
Cedar Crest Boulevard and I-78
Allentown, PA 18105
Phone: 610-402-8045
Fax: 610-402-1675
Website: www.lvhhn.org
E-mail: [email protected]
Start Up
July 2003
Practitioners
Lehigh Valley Hospital - Cedar Crest
Ardeth Copeland, MD
Shoban Dave, MD
John Davidyock, MD
William Ford, MD
Arvind Gupta, MD (site leader)
Kweku Hayford, MD
Lehigh Valley Hospital - Muhlenberg
Donna Dowlatshahi, Coordinator
Jeff rey Faidley, MD
Melissa Geitz, DO
Wayne Howard, DO (site leader)
Melissa Liu, MD
Dan Mulcahy, DO
Gonzalo Pimentel, MD
Deborah Sterner, Coordinator
Training
All ABIM certified
Employed By
Lehigh Valley Physician Group and Specialty Physicians of LVHHN, PC
Lehigh Valley Hospital and Health Network (LVHHN) is one of the largest teaching facilities in Pennsylvania. LVHHN consists of three clinical campuses, two of which focus on inpatient care: Lehigh Valley Hospital-Cedar Crest (LVHCC) and Lehigh Valley Hospital-Muhlenberg (LVH-M). The Network has more than 1,100 physicians and is a major clinical campus for Penn State’s College of Medicine. LVH-M opens a new patient care, tower in March 2005 and has approximately 200 inpatient beds on campus. The campus offers cardiac catheterization and open heart surgery capabilities, and its intensive care unit is augmented by a tele-intensivist system. A 24/7 hospitalist program was launched at LVH-M in July 2003 and is presently staffed by six full-time physicians.
The LVH-CC campus is preparing to undergo a major expansion that will bring its total beds to approximately 800 by 2007. This campus is a tertiary care center, featuring medical and surgical intensive care, a Level I trauma unit, a burn center, open heart surgery, perinatal care and renal transplantation services. LVHHN also boasts active teaching programs, with residencies in internal medicine, surgery, OB/GYN, family medicine, and emergency medicine. There are also fellowships in cardiology, pulmonary/critical care, and hematology/oncology. The LVHCC hospitalist program provides 24/7 service staffed by six physicians and was launched in July 2004.
Finances
All LVHS physicians are salaried employees. A bonus was paid to the physicians at LVH-M at the end of the first year of services. A bonus structure is being defined for both campuses, focusing on clinical, quality, and service measures. Each hospitalist receives 4 weeks vacation and 5 days of CME. A stipend is also provided for CME. Hospitalists receive malpractice coverage and reimbursement for licensure expenses. Physicians are also entitled to a benefits package that includes disability insurance, a supplemental retirement plan, and a 401(k)/403(b).
Chart abstraction and billing is done by the employer. At the end of each shift, the hospitalist submits a list of the patients seen and/or admitted. Each campus has a program coordinator certified in coding who reviews the charts for documentation and submits for the appropriate level of care. This system has worked well in ensuring proper billing and in allowing prompt feedback to the hospitalists regarding their documentation.
Referrals
LVH-M: The LVH-M hospitalist program was developed to provide a resource for primary care physicians in the community who wished to focus on outpatient care. Primary care physicians were identified and ranked in terms of their willingness to refer patients to the hospitalist program. Care was taken not to target groups who already had referral patterns to existing LVH-M groups to minimize the adverse impact of the hospitalist program on these groups. Hospitalists then made visits to these offices to explain the hospitalist program and answer questions from the PCPs. The program quickly became successful and now has a well-established referral base.
LVH-CC: The major driver of the hospitalist program at the Cedar Crest campus was assisting with the residency program. The existing faculty group staffed two of the five inpatient teaching services and was becoming increasingly busy as a result of new referrals. The hospitalist program helped decompress some of the volume from the existing faculty services by taking over one of the other inpatient teaching slots and establishing an overflow service. The program also seeks referrals from physicians outside the hospital’s traditional referral radius. The hospitalists have also worked with the medical and surgical subspecialists, developing standards for admission of subspecialty patients to the hospitalist service.
Teaching
LVH-CC: The LVH-CC hospitalists are intimately involved in the internal medicine residency program. They staff one of five inpatient teaching services during the morning. In the afternoon and overnight hours, the hospitalists cover their own service and the two pre-existing academic inpatient services. The hospitalists round either formally or informally with the residents of these three teams in the afternoon. They also review each new admission between noon and 8 a.m. to the three inpatient teams and provide bedside teaching on these patients.
A second daytime hospitalist also staff s an overflow service to ensure compliance with Residency Review Committee guidelines regarding service and admission caps. If the three teaching services hit their respective caps, any new patients are admitted by the hospitalists to this overflow service. In addition to rounding on the overflow patients, the second hospitalist staff s a consultative medicine service with a PGY-2 or PGY-3 resident.
The hospitalists participate in morning report and the resident lectures. The hospitalists are also involved in faculty development with the academic general internists as well as other residency initiatives.
LVH-M: Hospitalists at the LVH-M campus have no formal involvement in the teaching programs (osteopathic rotating internship and emergency medicine residency) at that campus. They are an available resource for housestaff, however, and have received many positive compliments from the housestaff for their assistance with difficult patients.
Schedule
LVH-M: The primary rounding hospitalist works Monday through Friday from 7 a.m. to 3 p.m. A second hospitalist works Monday through Friday from 10 a.m. to 7 p.m. and is available on Saturday if the census is high. This hospitalist also works the Sunday night shift beginning at 7 p.m. and ending 7 a.m. Monday. The overnight hospitalist works from 7 p.m. to 7 a.m. Monday through Saturday. There is always a back-up hospitalist available in case of emergency or significant influx of patients that overwhelms the system. The hospitalists work an average of 16 shifts per month.
LVH-CC: There are two hospitalists scheduled during the daytime hours. The hospitalist rounding with the resident team works 7 a.m. to 7 p.m. Monday through Sunday. The overflow/consult hospitalist works 8 a.m. to 8 p.m. Monday through Friday and 7 p.m. to 7 a.m. Saturday and Sunday. The overnight hospitalist works 7 p.m. to 7 a.m. Monday through Friday. The hospitalists work an average of 16 shifts per month.
Future Directions
LVH-M: As the campus continues to grow, the hospitalists aim to become more intricately involved in process improvement and quality-improvement measures. The program is exploring ways of becoming active in the teaching program, either with residents and medical students or with physician assistant students. Additionally, as the Network’s tele-intensivist initiative develops, the hospitalists are working closely with their critical care colleagues to provide top-quality ICU care for patients.
LVH-CC: The LVH-CC hospitalists are becoming increasingly involved in efforts to maximize institutional efficiency and throughput. This program is also seeking to establish itself as a premier research program, in both the educational and clinical realms.
Hospitalists at both campuses are becoming involved in various hospital committees such as Therapeutics and Quality Assurance. Their expertise has also been utilized in various throughput initiatives such as an automated discharge instruction process and electronic signout development.
Given the rapid growth of both programs, staffing needs are expected to increase considerably. One long-term goal is to make it possible for hospitalists to rotate between the two campuses to allow them a variety of experiences. A hospital medicine elective is being developed for PGY-3 residents interested in a career in hospital medicine. There has also been some preliminary discussion of a hospital medicine fellowship that would emphasize teaching, research, and palliative care.
Contact
Michael J. Pistoria, DO
Medical Director, Lehigh Valley Hospitalist Services
Associate Program Director, Internal Medicine Residency
Assistant Professor of Medicine, Penn State College of Medicine
Kevin Flynn, MS, Administrative Director
Lehigh Valley Hospital
Cedar Crest Boulevard and I-78
Allentown, PA 18105
Phone: 610-402-8045
Fax: 610-402-1675
Website: www.lvhhn.org
E-mail: [email protected]
Start Up
July 2003
Practitioners
Lehigh Valley Hospital - Cedar Crest
Ardeth Copeland, MD
Shoban Dave, MD
John Davidyock, MD
William Ford, MD
Arvind Gupta, MD (site leader)
Kweku Hayford, MD
Lehigh Valley Hospital - Muhlenberg
Donna Dowlatshahi, Coordinator
Jeff rey Faidley, MD
Melissa Geitz, DO
Wayne Howard, DO (site leader)
Melissa Liu, MD
Dan Mulcahy, DO
Gonzalo Pimentel, MD
Deborah Sterner, Coordinator
Training
All ABIM certified
Employed By
Lehigh Valley Physician Group and Specialty Physicians of LVHHN, PC
Lehigh Valley Hospital and Health Network (LVHHN) is one of the largest teaching facilities in Pennsylvania. LVHHN consists of three clinical campuses, two of which focus on inpatient care: Lehigh Valley Hospital-Cedar Crest (LVHCC) and Lehigh Valley Hospital-Muhlenberg (LVH-M). The Network has more than 1,100 physicians and is a major clinical campus for Penn State’s College of Medicine. LVH-M opens a new patient care, tower in March 2005 and has approximately 200 inpatient beds on campus. The campus offers cardiac catheterization and open heart surgery capabilities, and its intensive care unit is augmented by a tele-intensivist system. A 24/7 hospitalist program was launched at LVH-M in July 2003 and is presently staffed by six full-time physicians.
The LVH-CC campus is preparing to undergo a major expansion that will bring its total beds to approximately 800 by 2007. This campus is a tertiary care center, featuring medical and surgical intensive care, a Level I trauma unit, a burn center, open heart surgery, perinatal care and renal transplantation services. LVHHN also boasts active teaching programs, with residencies in internal medicine, surgery, OB/GYN, family medicine, and emergency medicine. There are also fellowships in cardiology, pulmonary/critical care, and hematology/oncology. The LVHCC hospitalist program provides 24/7 service staffed by six physicians and was launched in July 2004.
Finances
All LVHS physicians are salaried employees. A bonus was paid to the physicians at LVH-M at the end of the first year of services. A bonus structure is being defined for both campuses, focusing on clinical, quality, and service measures. Each hospitalist receives 4 weeks vacation and 5 days of CME. A stipend is also provided for CME. Hospitalists receive malpractice coverage and reimbursement for licensure expenses. Physicians are also entitled to a benefits package that includes disability insurance, a supplemental retirement plan, and a 401(k)/403(b).
Chart abstraction and billing is done by the employer. At the end of each shift, the hospitalist submits a list of the patients seen and/or admitted. Each campus has a program coordinator certified in coding who reviews the charts for documentation and submits for the appropriate level of care. This system has worked well in ensuring proper billing and in allowing prompt feedback to the hospitalists regarding their documentation.
Referrals
LVH-M: The LVH-M hospitalist program was developed to provide a resource for primary care physicians in the community who wished to focus on outpatient care. Primary care physicians were identified and ranked in terms of their willingness to refer patients to the hospitalist program. Care was taken not to target groups who already had referral patterns to existing LVH-M groups to minimize the adverse impact of the hospitalist program on these groups. Hospitalists then made visits to these offices to explain the hospitalist program and answer questions from the PCPs. The program quickly became successful and now has a well-established referral base.
LVH-CC: The major driver of the hospitalist program at the Cedar Crest campus was assisting with the residency program. The existing faculty group staffed two of the five inpatient teaching services and was becoming increasingly busy as a result of new referrals. The hospitalist program helped decompress some of the volume from the existing faculty services by taking over one of the other inpatient teaching slots and establishing an overflow service. The program also seeks referrals from physicians outside the hospital’s traditional referral radius. The hospitalists have also worked with the medical and surgical subspecialists, developing standards for admission of subspecialty patients to the hospitalist service.
Teaching
LVH-CC: The LVH-CC hospitalists are intimately involved in the internal medicine residency program. They staff one of five inpatient teaching services during the morning. In the afternoon and overnight hours, the hospitalists cover their own service and the two pre-existing academic inpatient services. The hospitalists round either formally or informally with the residents of these three teams in the afternoon. They also review each new admission between noon and 8 a.m. to the three inpatient teams and provide bedside teaching on these patients.
A second daytime hospitalist also staff s an overflow service to ensure compliance with Residency Review Committee guidelines regarding service and admission caps. If the three teaching services hit their respective caps, any new patients are admitted by the hospitalists to this overflow service. In addition to rounding on the overflow patients, the second hospitalist staff s a consultative medicine service with a PGY-2 or PGY-3 resident.
The hospitalists participate in morning report and the resident lectures. The hospitalists are also involved in faculty development with the academic general internists as well as other residency initiatives.
LVH-M: Hospitalists at the LVH-M campus have no formal involvement in the teaching programs (osteopathic rotating internship and emergency medicine residency) at that campus. They are an available resource for housestaff, however, and have received many positive compliments from the housestaff for their assistance with difficult patients.
Schedule
LVH-M: The primary rounding hospitalist works Monday through Friday from 7 a.m. to 3 p.m. A second hospitalist works Monday through Friday from 10 a.m. to 7 p.m. and is available on Saturday if the census is high. This hospitalist also works the Sunday night shift beginning at 7 p.m. and ending 7 a.m. Monday. The overnight hospitalist works from 7 p.m. to 7 a.m. Monday through Saturday. There is always a back-up hospitalist available in case of emergency or significant influx of patients that overwhelms the system. The hospitalists work an average of 16 shifts per month.
LVH-CC: There are two hospitalists scheduled during the daytime hours. The hospitalist rounding with the resident team works 7 a.m. to 7 p.m. Monday through Sunday. The overflow/consult hospitalist works 8 a.m. to 8 p.m. Monday through Friday and 7 p.m. to 7 a.m. Saturday and Sunday. The overnight hospitalist works 7 p.m. to 7 a.m. Monday through Friday. The hospitalists work an average of 16 shifts per month.
Future Directions
LVH-M: As the campus continues to grow, the hospitalists aim to become more intricately involved in process improvement and quality-improvement measures. The program is exploring ways of becoming active in the teaching program, either with residents and medical students or with physician assistant students. Additionally, as the Network’s tele-intensivist initiative develops, the hospitalists are working closely with their critical care colleagues to provide top-quality ICU care for patients.
LVH-CC: The LVH-CC hospitalists are becoming increasingly involved in efforts to maximize institutional efficiency and throughput. This program is also seeking to establish itself as a premier research program, in both the educational and clinical realms.
Hospitalists at both campuses are becoming involved in various hospital committees such as Therapeutics and Quality Assurance. Their expertise has also been utilized in various throughput initiatives such as an automated discharge instruction process and electronic signout development.
Given the rapid growth of both programs, staffing needs are expected to increase considerably. One long-term goal is to make it possible for hospitalists to rotate between the two campuses to allow them a variety of experiences. A hospital medicine elective is being developed for PGY-3 residents interested in a career in hospital medicine. There has also been some preliminary discussion of a hospital medicine fellowship that would emphasize teaching, research, and palliative care.
The Quality and Patient Safety Track at the 2005 SHM Annual Meeting
Quality and Patient Safety have become the cornerstone of the ways that hospitalists can improve inpatient care delivery. At this year’s annual meeting, the focus on quality and safety is represented through a series of dynamic workshops that will allow practicing hospitalists to learn practical skills in quality improvement, to contribute to the development of standards on the discharge process, and to understand emerging models of care delivery that may impact inpatient mortality. Below is a brief summary of the workshops and their objectives:
- Hospital Mortality Reduction— the Role of Rapid Response Teams: Faculty from the Institute for Healthcare Improvement and leading patient safety programs will present an overview of the concept of rapid response teams, data their effectiveness, and examples of their implementation. Hospitalists are often advocates for patient safety and quality in their institution and will be critical in the development of initiatives to reduce inpatient mortality.
- The Role of Information Technology in Quality Improvement and Safety: A dynamic team of physician leaders in quality and safety will review the literature in the use of information technology to improve quality and safety. Examples of IT approaches to improve inpatient care will be described and discussed. In addition, potential barriers in the use of IT-based approaches to quality and safety will be outlined. Hospitalists will learn about how to integrate existing IT support into quality initiatives and when IT may not be essential to process change.
- A Primer on Root Cause Analysis: Hospitalists may be asked to be part of interdisciplinary teams that review sentinel events through root cause analysis using tools such as Failure Mode Effects Analysis (FMEA). This process can often uncover system-issues that contribute to quality and safety issues. However, it is critical for hospitalists to understand the root cause analysis process, its limitations, and how to maximize the potential of FMEA to identify underlying issues critical to improving patient care and safety.
- Consensus Group/Workshop to Develop the Ideal Discharge Process: Discharging patients from the hospital is a necessary task in every hospital admission, but one that has had very little study or standardization. Hospitalists are critical agents of change in reframing the discharge process and in developing and implementing tools to make that process as safe and efficient as possible. A panel of hospitalists and experts on patient safety especially at care transition points will moderate an open forum to establish guidelines for the ideal hospital discharge. Input from participants will be used to shape guidelines and tools for discharge.
- Quality Improvement for the Clinical Hospitalist: This workshop is targeted at bringing quality improvement from the ivory tower to the practicing hospitalist. Participants will be exposed to basic quality improvement tools and strategies that can be applied in myriad settings to improve care. Examples of successful projects will be presented for discussion.
We will be evaluating participation in the quality and patients safety track at the meeting to help determine the need for more in-depth sessions such as a pre-course on quality assessment and improvement methodology. We are excited to offer such a diverse series of workshops and look forward to your active participation!
Quality and Patient Safety have become the cornerstone of the ways that hospitalists can improve inpatient care delivery. At this year’s annual meeting, the focus on quality and safety is represented through a series of dynamic workshops that will allow practicing hospitalists to learn practical skills in quality improvement, to contribute to the development of standards on the discharge process, and to understand emerging models of care delivery that may impact inpatient mortality. Below is a brief summary of the workshops and their objectives:
- Hospital Mortality Reduction— the Role of Rapid Response Teams: Faculty from the Institute for Healthcare Improvement and leading patient safety programs will present an overview of the concept of rapid response teams, data their effectiveness, and examples of their implementation. Hospitalists are often advocates for patient safety and quality in their institution and will be critical in the development of initiatives to reduce inpatient mortality.
- The Role of Information Technology in Quality Improvement and Safety: A dynamic team of physician leaders in quality and safety will review the literature in the use of information technology to improve quality and safety. Examples of IT approaches to improve inpatient care will be described and discussed. In addition, potential barriers in the use of IT-based approaches to quality and safety will be outlined. Hospitalists will learn about how to integrate existing IT support into quality initiatives and when IT may not be essential to process change.
- A Primer on Root Cause Analysis: Hospitalists may be asked to be part of interdisciplinary teams that review sentinel events through root cause analysis using tools such as Failure Mode Effects Analysis (FMEA). This process can often uncover system-issues that contribute to quality and safety issues. However, it is critical for hospitalists to understand the root cause analysis process, its limitations, and how to maximize the potential of FMEA to identify underlying issues critical to improving patient care and safety.
- Consensus Group/Workshop to Develop the Ideal Discharge Process: Discharging patients from the hospital is a necessary task in every hospital admission, but one that has had very little study or standardization. Hospitalists are critical agents of change in reframing the discharge process and in developing and implementing tools to make that process as safe and efficient as possible. A panel of hospitalists and experts on patient safety especially at care transition points will moderate an open forum to establish guidelines for the ideal hospital discharge. Input from participants will be used to shape guidelines and tools for discharge.
- Quality Improvement for the Clinical Hospitalist: This workshop is targeted at bringing quality improvement from the ivory tower to the practicing hospitalist. Participants will be exposed to basic quality improvement tools and strategies that can be applied in myriad settings to improve care. Examples of successful projects will be presented for discussion.
We will be evaluating participation in the quality and patients safety track at the meeting to help determine the need for more in-depth sessions such as a pre-course on quality assessment and improvement methodology. We are excited to offer such a diverse series of workshops and look forward to your active participation!
Quality and Patient Safety have become the cornerstone of the ways that hospitalists can improve inpatient care delivery. At this year’s annual meeting, the focus on quality and safety is represented through a series of dynamic workshops that will allow practicing hospitalists to learn practical skills in quality improvement, to contribute to the development of standards on the discharge process, and to understand emerging models of care delivery that may impact inpatient mortality. Below is a brief summary of the workshops and their objectives:
- Hospital Mortality Reduction— the Role of Rapid Response Teams: Faculty from the Institute for Healthcare Improvement and leading patient safety programs will present an overview of the concept of rapid response teams, data their effectiveness, and examples of their implementation. Hospitalists are often advocates for patient safety and quality in their institution and will be critical in the development of initiatives to reduce inpatient mortality.
- The Role of Information Technology in Quality Improvement and Safety: A dynamic team of physician leaders in quality and safety will review the literature in the use of information technology to improve quality and safety. Examples of IT approaches to improve inpatient care will be described and discussed. In addition, potential barriers in the use of IT-based approaches to quality and safety will be outlined. Hospitalists will learn about how to integrate existing IT support into quality initiatives and when IT may not be essential to process change.
- A Primer on Root Cause Analysis: Hospitalists may be asked to be part of interdisciplinary teams that review sentinel events through root cause analysis using tools such as Failure Mode Effects Analysis (FMEA). This process can often uncover system-issues that contribute to quality and safety issues. However, it is critical for hospitalists to understand the root cause analysis process, its limitations, and how to maximize the potential of FMEA to identify underlying issues critical to improving patient care and safety.
- Consensus Group/Workshop to Develop the Ideal Discharge Process: Discharging patients from the hospital is a necessary task in every hospital admission, but one that has had very little study or standardization. Hospitalists are critical agents of change in reframing the discharge process and in developing and implementing tools to make that process as safe and efficient as possible. A panel of hospitalists and experts on patient safety especially at care transition points will moderate an open forum to establish guidelines for the ideal hospital discharge. Input from participants will be used to shape guidelines and tools for discharge.
- Quality Improvement for the Clinical Hospitalist: This workshop is targeted at bringing quality improvement from the ivory tower to the practicing hospitalist. Participants will be exposed to basic quality improvement tools and strategies that can be applied in myriad settings to improve care. Examples of successful projects will be presented for discussion.
We will be evaluating participation in the quality and patients safety track at the meeting to help determine the need for more in-depth sessions such as a pre-course on quality assessment and improvement methodology. We are excited to offer such a diverse series of workshops and look forward to your active participation!
The Informed Hospitalist and the Pharmaceutical Industry
The ideal patient-physician relationship is one of choice, competence, communication, compassion, and continuity, and is free of any conflict of interest. There is heated controversy about whether the relationship between the pharmaceutical industry and medical professionals betrays this ideal. The heart of this debate lies in the fundamental difference in priorities and goals of the pharmaceutical industry and hospitalists. Hospitalists are trusted with the lives and well-being of patients. A physician is expected to make an unbiased analysis of the treatment options for a given patient and to apply that treatment to the best of his or her abilities. In contrast, the ultimate interest of the pharmaceutical industry lies with the shareholders, and the primary goal is to maximize profit. Many feel that these two goals are mutually exclusive (1,2). Medical educators believe that it is the responsibility of the medical profession, not pharmaceutical companies, to educate physicians. The entanglement of the pharmaceutical industry with physicians calls into question the credibility of information obtained from any pharmaceutical-sponsored event and casts doubt over the medical profession as a whole. Governmental regulation and legislative initiatives such as the Bayh-Dole Act (3) have furthered the commercialization of academic research and realigned academic centers’ approach to clinical research.
The pharmaceutical industry argues that its goals and the goals of the medical profession are complementary (4) and that their involvement optimizes the benefit to the patient. The pharmaceutical industry is quick to point out that pharmaceutical companies are an important source of funding for clinical trials and are the leading sponsors of continuing medical education, and that it is the most research-intensive industry in the United States supported by private funds (5). Corporate contributions to research and development in academia have increased by 900% between 1980 and 2000. The pharmaceutical industry devoted 18% of profits in 2002 to research, development, and testing activities (6). The pharmaceutical industry claims that these are designed to serve the mutual interests of the pharmaceutical industry and the medical community by providing accurate and up-to-date information to maximize patient care. The advances made as a result of commercial development have dramatically altered the landscape of research. Pharmaceutical courtship of hospitalists, who find themselves on the front line in clinical settings as prescribers or researchers, is part of an aggressive marketing campaign that some believe contributes little to the common good.
Hospitalists have increased their financial incentives with stock options, fees for consultation, speaking arrangements, and memberships on advisory boards for pharmaceutical companies. Disclosure of financial conflicts is becoming an empty ritual providing a false sense of security. Pharmaceutical research is increasingly organized by Contract Research Organizations, written up with the help of ghostwriters, and published under the name of established investigators (7,8). Not all industry-funded studies are necessarily fl awed and without scientific merit, but the fact that negative consequences can be devastating to the financial health of a corporation has to be considered.
A leading catalyst for continued pharmaceutical industry/hospitalist interaction is continuing medical education (CME). In 2003, the pharmaceutical industry provided 900 million of the one billion dollars spent on CME in the United States. Currently, the pharmaceutical industry funds approximately 60% of all CME activities in the United States (9). Information provided to physicians by a pharmaceutical representative has an inaccuracy rating of 13% (10). Not surprisingly, many of these inaccuracies favor the product being presented and casts an unfavorable light on competing drugs (10,11). This has led some to believe that this pharmaceutical representative/physician interaction is having a negative impact on patients (12) through the dissemination of inaccurate information. In addition, misleading advertisements have been found to overstate the effectiveness and minimize the risks of a given drug (11). Another form of bias is the selective publication of research studies by the pharmaceutical industry (13).
Bedside and Conference Detailing
Interactions with pharmaceutical representatives (drug detailers) often begin in medical school and proceed throughout a physician’s career (12,14). In 2003, the pharmaceutical industry spent more than 13 billion dollars on promotional activities for doctors, an average of about $10,500 per physician. There is one drug detailer for every 4.7 office-based physicians. Interactions include conferences with free lunch, personal visits by drug detailers, sponsored CME workshops/seminars, sponsored dinners, sponsored scientific conferences, sponsored research, direct gifts (e.g., cash payments for prescribing a given medication), and indirect gifts (e.g., subsidizing a trip to a medical conference). These interactions evolve from merely lunches and pens early in a physician’s career to positions as a consultant and advisory board honoree as the relationship matures. Some physicians view such exchanges as helpful and informative while others view it as unethical (2) and harmful.
Hospitalists, residents, and medical students alike believe their interactions with drug detailers, and the small gifts that they receive, do not influence their behavior (14,15). Wazana found that as physicians continue to receive gifts from drug detailers, they become even less likely to believe that the gifts can influence their behavior (16). Many physicians believe that their interactions with drug companies are beneficial not only to them but also to their patients. However, studies have found that this is in fact not the case. Physicians who interact with pharmaceutical representatives prescribe newer and more expensive drugs, rather than cheaper and equally effective generic drugs (16,17). There are a significantly higher number of prescriptions written for the drugs manufactured by pharmaceutical companies who sponsor a given CME activity than pharmaceutical companies who do not. A rise in prescription expenditures (17), as well as an increase in irrational prescribing, often follows in-house exposure to drug detailers (16).
The enormous amount spent on marketing can also be used as further proof of the pharmaceutical industry’s avarice. However, we often fail to acknowledge the role that medical educators and professionals play in this problem. Pharmaceutical companies are profitable because of our prescribing habits. For example, many medical professionals prescribe expensive “me too” drugs that often offer little if any benefit over cheaper established or prototypical drugs. Our actions encourage what we claim to be bad behavior by the pharmaceutical industry.
It is often argued by the pharmaceutical industry that these “me too” drugs have a different side effect profile, may improve compliance in long-term treatment, or will reduce cost when compared to the prototype drug. This is true in some instances, as exemplified by the wide array of anti-hypertensives and the even wider array of side effect profiles. However, there are many instances when this is far from the case. If a financial incentive did not exist for pharmaceutical companies to introduce “me too” drugs, the pharmaceutical industry would not do so unless the drug being introduced provided a substantial clinical advantage over the prototype drug. As a result, the pharmaceutical industry would be spending their time, effort, and finances on research aimed at finding new and innovative cures.
Proposed Solution to the Problem
In an effort to remedy this situation, many professional societies (as well as the pharmaceutical industry itself) have established guidelines on the interactions between the pharmaceutical industry and physicians. The AMA has established guidelines responsible for the regulation of gifts bestowed on physicians by industry (18). The Pharmaceutical Research Manufacturers of America has established similar guidelines known as the PhRMA Code (19). Increasingly, many professional organizations have taken it upon themselves to establish their own code of conduct. However, there remains a low level of awareness of the guidelines (15) that are currently in place, and some of the pharmaceutical companies have chosen not to abide by the PhRMA Code. In response to the increasing influence pharmaceutical companies are having on the medical decision-making process, many training programs are adopting policies to limit the contact between pharmaceutical representatives and physicians in training. This is being carried out at both the undergraduate and graduate medical education levels (20). The effects of such restrictions are currently unknown. McCormick found that physicians who trained in institutions with such policies were less likely to find information from pharmaceutical company representatives useful (20). However, Ferguson found that being trained in a program with a policy that limited access to pharmaceutical sales representatives did not affect the subsequent likelihood of future physician-pharmaceutical representative interactions (21).
The Informed Hospitalist in the 21st Century
The literature clearly documents that the pharmaceutical industry influences physician prescribing habits. Hospitalists can take a four-prong approach to help counteract these effects:
1. Academic Detailing
Medical educators can shield residents and medical students from the influence of pharmaceutical representatives by limiting or prohibiting contact, or they can teach trainees how to effectively manage such interactions through academic detailing. As stated above, Ferguson found that policies limiting access to drug detailers did not affect the subsequent likelihood of future physician and pharmaceutical representative interactions (21). It might be wiser to teach trainees how to manage their interactions with the drug representatives and thereby take control of the situation. In order for doctors to effectively manage such interactions, we must learn how to evaluate the literature and interpret the information given to us by representatives. Watkins found that both attendings and residents feel that they should learn how to critically evaluate promotional materials, recognize potential conflicts of interest, and consider how patients perceive physician-pharmaceutical relationships (22). Previous studies have found that educational interventions can have a significant effect on the attitudes of medical students and residents towards pharmaceutical marketing and drug detailers (23,24).
One way to evaluate pharmaceutical literature is to have academic detailing of the clinical studies and statements made by pharmaceutical detailers at sponsored events. During these academic detailing conferences the drug in question can be compared to other drugs in the class, and indications and differences should be mentioned if they exist. This should be done in the presence of both an attending who is very familiar with the drug and drug class in question and a hospital pharmacist. If this is done in a small setting, the medical students and residents can take turns critically evaluating the presentations. This approach is comparable to teaching medicine at the bedside; learners develop a deeper appreciation and understanding by experiencing various situations first-hand.
An additional benefit of critically evaluating pharmaceutical representative presentations is that when they know that the information they provide will be closely scrutinized, pharmaceutical representatives will have an incentive to provide more accurate information.
2. Cost Sensitivity
One of the many topics that can be discussed by the hospital pharmacist or attending is the price of the given drug. In discussing price, two critical points must be evaluated. The first is the price-benefit ratio of the given drug and the second is the financial situation of the patient. Physicians should always have the patient’s best interest in mind. However, this does not mean that cost should not be considered when making therapeutic decisions. Rather, a more practical therapeutic decision can be made with cost in mind. Cost is the major factor to some patients when determining whether they will fill their prescriptions. In such an instance, if cost is taken into consideration when writing the prescription, a physician is more apt to write a prescription for a less expensive medication (if one exists).
3. Three-Way Transparency
In order for hospitalists to effectively interact with the pharmaceutical industry, it must be realized that medical professionals are not victims of the marketing strategies of the pharmaceutical industry; rather, we are accomplices. We often fail to acknowledge the role medical educators and professionals play in this problem. Many years ago, Troyan Brennan called for transparency, stating “Conflict will remain with us. Physicians’ relationship with the pharmaceutical industry must be better managed” (25). However, Brennan did not offer any proposals on a better management system. Our current management system of disclosure of conflict has become obsolete. It has become a ritual practice in academia to acknowledge that one may have a conflict of interest, but this does nothing to address the real issue: the conflict of interest itself. Hospitalists can adopt a three-way transparency between the patient, colleagues, and the pharmaceutical industry where all conflicts are fully disclosed, rather than simply stating that a conflict might exist.
4. High Threshold for Rationalization
Most medical professionals, to some degree, rationalize interactions with the pharmaceutical industry. Almost all physicians insist that these interactions do not influence their judgment. The simple fact that the industry spends thousands of dollars per doctor per year indicates that we are wrong. If physicians were not being influenced, the pharmaceutical companies would not be spending such a considerable amount of money marketing to us. Patients trust physicians to make the best decision for them, they depend on researchers to publish impartial studies, and they count on educators to present unbiased truths. The cost of betrayal is paid in human lives. We should learn from the past, as well as the recent coxib debacle.
Conclusion
The interaction between hospitalists and the pharmaceutical industry continues to evolve. With increasing scrutiny from the medical profession and the government, many of the marketing practices that were considered acceptable in the past are now viewed as unacceptable and even criminal. As the relationship evolves, new conflicts are sure to arise as long as the fundamental difference between the medical profession and pharmaceutical industry continues to exist. As medical professionals, we must keep in mind that the pharmaceutical industry is a for-profit industry whose interest lies with its shareholders. It is to be expected that the pharmaceutical industry will try to maximize profits through marketing efforts directed at physicians and patients.
Medical educators must take on the responsibility of preparing medical students, residents, and fellow attendings on how to manage their interactions with the pharmaceutical industry and not just shield them from the issue. In applying the four-point approach of academic detailing, cost sensitivity, three-way transparency, and a high threshold for justification, we can better manage such interactions.
We would like to thank Dr. Anna Headly and Emily Hartsough for their constructive comments in the preparation of the manuscript.
Disclaimer: The content of the article is solely the responsibility of the authors and does not necessarily represent the official view of the Society of Hospital Medicine.
Dr. Rajput can be contacted at [email protected].
References
- Abbasi K, Smith R. No more free lunch: patients will benefit from doctors and drug companies disentangling. BMJ. 2003;326:1155-6.
- Relman AS. Separating continuing medical education from pharmaceutical marketing. JAMA. 2001;285:2009-12.
- Thursby JG, Thursby MC. Intellectual property. University licensing and the Bayh-Dole Act. Science. 2003;301:1052.
- Holmer AF. Industry strongly supports continuing medical education. JAMA. 2001;285:2012-4.
- Scherer FM. The pharmaceutical industry: price and progress. N Engl J Med. 2004;351:927-32.
- Pharmaceutical industry profiles 2003. Washinton, DC; 2003.
- Moynihan R. Who pays for the pizza? Redefining the relationships between doctors and drug companies. 2: Disentanglement. BMJ. 2003;326:1193-6.
- Smith R. Medical journals and pharmaceutical companies: uneasy bedfellows. BMJ. 2003;326:1202-5.
- Relman AS. Defending professional independence: ACCME’s proposed new guidelines for commercial support of CME. JAMA. 2003;289:2418-20.
- Ziegler MG, Lew P, Singer BC. The accuracy of drug information from pharmaceutical sales representatives. JAMA. 1995;273:1296-8.
- Gottlieb S. Congress criticises drug industry for misleading advertising. BMJ. 2002;325:1379.
- Rogers WA, Mansfield PR, Braunack-Mayer AJ, Jureidini JN. The ethics of pharmaceutical industry relationships with medical students. Med J Aust. 2004;180:411-4.
- Melander H, Ahlqvist-Rastad J, Me&er G, Beermann B. Evidence b(i)ased medicine—selective reporting from studies sponsored by pharmaceutical industry: review of studies in new drug applications. BMJ. 2003;326:1171-3.
- Lexchin J. Interactions between physician and the pharmaceutical industry: what does the literatue say? Can Med Assoc J. 1993;149:1401-7.
- Steinman MA, Shlipak MG, McPhee SJ. Of principles and pens: attitudes and practices of medicine housestaff toward pharmaceutical industry promotions. Am J Med. 2001;110:551-7.
- Wazana A. Physicians and the pharmaceutical industry: is a gift ever just a gift? JAMA. 2000;283:373-80.
- Watkins C, Moore L, Harvey I, Carthy P, Robinson E, Brawn R. Characteristics of general practitioners who frequently see drug industry representatives: national cross sectional study. BMJ. 2003;326:1178-9.
- Guidelines on gifts to physicians from industry: an update. Food Drug Law J. 2001;56:27-40.
- PhRMA CODE On Interactions with Health Care Professionals. Infectious Diseases in Clinical Practice. 2002;(11):153-4.
- McCormick BB, Tomlinson G, Brill-Edwards P, Detsky AS. Effect of restricting contact between pharmaceutical company representatives and internal medicine residents on posttraining attitudes and behavior. JAMA. 2001;286:1994-9.
- Ferguson RP, Rhim E, Belizaire W, Egede L, Carter K, Lansdale T. Encounters with pharmaceutical sales representatives among practicing internists. Am J Med. 1999;107:149-52.
- Watkins RS, Kimberly JJ. What residents don’t know about physician-pharmaceutical industry interactions. Acad Med. 2004;79:432-7.
- Wilkes MS, Hoffman JR. An innovative approach to educating medical students about pharmaceutical promotion. Acad Med. 2001;76:1271-7.
- Vinson DC, McCandless B, Hosokawa MC. Medical students’ attitudes toward pharmaceutical marketing: possibilities for change. Fam Med. 1993;25:31-3.
- Brennan TA. Buying editorials. N Engl J Med. 1994;331: 673-5; discussion 76.
The ideal patient-physician relationship is one of choice, competence, communication, compassion, and continuity, and is free of any conflict of interest. There is heated controversy about whether the relationship between the pharmaceutical industry and medical professionals betrays this ideal. The heart of this debate lies in the fundamental difference in priorities and goals of the pharmaceutical industry and hospitalists. Hospitalists are trusted with the lives and well-being of patients. A physician is expected to make an unbiased analysis of the treatment options for a given patient and to apply that treatment to the best of his or her abilities. In contrast, the ultimate interest of the pharmaceutical industry lies with the shareholders, and the primary goal is to maximize profit. Many feel that these two goals are mutually exclusive (1,2). Medical educators believe that it is the responsibility of the medical profession, not pharmaceutical companies, to educate physicians. The entanglement of the pharmaceutical industry with physicians calls into question the credibility of information obtained from any pharmaceutical-sponsored event and casts doubt over the medical profession as a whole. Governmental regulation and legislative initiatives such as the Bayh-Dole Act (3) have furthered the commercialization of academic research and realigned academic centers’ approach to clinical research.
The pharmaceutical industry argues that its goals and the goals of the medical profession are complementary (4) and that their involvement optimizes the benefit to the patient. The pharmaceutical industry is quick to point out that pharmaceutical companies are an important source of funding for clinical trials and are the leading sponsors of continuing medical education, and that it is the most research-intensive industry in the United States supported by private funds (5). Corporate contributions to research and development in academia have increased by 900% between 1980 and 2000. The pharmaceutical industry devoted 18% of profits in 2002 to research, development, and testing activities (6). The pharmaceutical industry claims that these are designed to serve the mutual interests of the pharmaceutical industry and the medical community by providing accurate and up-to-date information to maximize patient care. The advances made as a result of commercial development have dramatically altered the landscape of research. Pharmaceutical courtship of hospitalists, who find themselves on the front line in clinical settings as prescribers or researchers, is part of an aggressive marketing campaign that some believe contributes little to the common good.
Hospitalists have increased their financial incentives with stock options, fees for consultation, speaking arrangements, and memberships on advisory boards for pharmaceutical companies. Disclosure of financial conflicts is becoming an empty ritual providing a false sense of security. Pharmaceutical research is increasingly organized by Contract Research Organizations, written up with the help of ghostwriters, and published under the name of established investigators (7,8). Not all industry-funded studies are necessarily fl awed and without scientific merit, but the fact that negative consequences can be devastating to the financial health of a corporation has to be considered.
A leading catalyst for continued pharmaceutical industry/hospitalist interaction is continuing medical education (CME). In 2003, the pharmaceutical industry provided 900 million of the one billion dollars spent on CME in the United States. Currently, the pharmaceutical industry funds approximately 60% of all CME activities in the United States (9). Information provided to physicians by a pharmaceutical representative has an inaccuracy rating of 13% (10). Not surprisingly, many of these inaccuracies favor the product being presented and casts an unfavorable light on competing drugs (10,11). This has led some to believe that this pharmaceutical representative/physician interaction is having a negative impact on patients (12) through the dissemination of inaccurate information. In addition, misleading advertisements have been found to overstate the effectiveness and minimize the risks of a given drug (11). Another form of bias is the selective publication of research studies by the pharmaceutical industry (13).
Bedside and Conference Detailing
Interactions with pharmaceutical representatives (drug detailers) often begin in medical school and proceed throughout a physician’s career (12,14). In 2003, the pharmaceutical industry spent more than 13 billion dollars on promotional activities for doctors, an average of about $10,500 per physician. There is one drug detailer for every 4.7 office-based physicians. Interactions include conferences with free lunch, personal visits by drug detailers, sponsored CME workshops/seminars, sponsored dinners, sponsored scientific conferences, sponsored research, direct gifts (e.g., cash payments for prescribing a given medication), and indirect gifts (e.g., subsidizing a trip to a medical conference). These interactions evolve from merely lunches and pens early in a physician’s career to positions as a consultant and advisory board honoree as the relationship matures. Some physicians view such exchanges as helpful and informative while others view it as unethical (2) and harmful.
Hospitalists, residents, and medical students alike believe their interactions with drug detailers, and the small gifts that they receive, do not influence their behavior (14,15). Wazana found that as physicians continue to receive gifts from drug detailers, they become even less likely to believe that the gifts can influence their behavior (16). Many physicians believe that their interactions with drug companies are beneficial not only to them but also to their patients. However, studies have found that this is in fact not the case. Physicians who interact with pharmaceutical representatives prescribe newer and more expensive drugs, rather than cheaper and equally effective generic drugs (16,17). There are a significantly higher number of prescriptions written for the drugs manufactured by pharmaceutical companies who sponsor a given CME activity than pharmaceutical companies who do not. A rise in prescription expenditures (17), as well as an increase in irrational prescribing, often follows in-house exposure to drug detailers (16).
The enormous amount spent on marketing can also be used as further proof of the pharmaceutical industry’s avarice. However, we often fail to acknowledge the role that medical educators and professionals play in this problem. Pharmaceutical companies are profitable because of our prescribing habits. For example, many medical professionals prescribe expensive “me too” drugs that often offer little if any benefit over cheaper established or prototypical drugs. Our actions encourage what we claim to be bad behavior by the pharmaceutical industry.
It is often argued by the pharmaceutical industry that these “me too” drugs have a different side effect profile, may improve compliance in long-term treatment, or will reduce cost when compared to the prototype drug. This is true in some instances, as exemplified by the wide array of anti-hypertensives and the even wider array of side effect profiles. However, there are many instances when this is far from the case. If a financial incentive did not exist for pharmaceutical companies to introduce “me too” drugs, the pharmaceutical industry would not do so unless the drug being introduced provided a substantial clinical advantage over the prototype drug. As a result, the pharmaceutical industry would be spending their time, effort, and finances on research aimed at finding new and innovative cures.
Proposed Solution to the Problem
In an effort to remedy this situation, many professional societies (as well as the pharmaceutical industry itself) have established guidelines on the interactions between the pharmaceutical industry and physicians. The AMA has established guidelines responsible for the regulation of gifts bestowed on physicians by industry (18). The Pharmaceutical Research Manufacturers of America has established similar guidelines known as the PhRMA Code (19). Increasingly, many professional organizations have taken it upon themselves to establish their own code of conduct. However, there remains a low level of awareness of the guidelines (15) that are currently in place, and some of the pharmaceutical companies have chosen not to abide by the PhRMA Code. In response to the increasing influence pharmaceutical companies are having on the medical decision-making process, many training programs are adopting policies to limit the contact between pharmaceutical representatives and physicians in training. This is being carried out at both the undergraduate and graduate medical education levels (20). The effects of such restrictions are currently unknown. McCormick found that physicians who trained in institutions with such policies were less likely to find information from pharmaceutical company representatives useful (20). However, Ferguson found that being trained in a program with a policy that limited access to pharmaceutical sales representatives did not affect the subsequent likelihood of future physician-pharmaceutical representative interactions (21).
The Informed Hospitalist in the 21st Century
The literature clearly documents that the pharmaceutical industry influences physician prescribing habits. Hospitalists can take a four-prong approach to help counteract these effects:
1. Academic Detailing
Medical educators can shield residents and medical students from the influence of pharmaceutical representatives by limiting or prohibiting contact, or they can teach trainees how to effectively manage such interactions through academic detailing. As stated above, Ferguson found that policies limiting access to drug detailers did not affect the subsequent likelihood of future physician and pharmaceutical representative interactions (21). It might be wiser to teach trainees how to manage their interactions with the drug representatives and thereby take control of the situation. In order for doctors to effectively manage such interactions, we must learn how to evaluate the literature and interpret the information given to us by representatives. Watkins found that both attendings and residents feel that they should learn how to critically evaluate promotional materials, recognize potential conflicts of interest, and consider how patients perceive physician-pharmaceutical relationships (22). Previous studies have found that educational interventions can have a significant effect on the attitudes of medical students and residents towards pharmaceutical marketing and drug detailers (23,24).
One way to evaluate pharmaceutical literature is to have academic detailing of the clinical studies and statements made by pharmaceutical detailers at sponsored events. During these academic detailing conferences the drug in question can be compared to other drugs in the class, and indications and differences should be mentioned if they exist. This should be done in the presence of both an attending who is very familiar with the drug and drug class in question and a hospital pharmacist. If this is done in a small setting, the medical students and residents can take turns critically evaluating the presentations. This approach is comparable to teaching medicine at the bedside; learners develop a deeper appreciation and understanding by experiencing various situations first-hand.
An additional benefit of critically evaluating pharmaceutical representative presentations is that when they know that the information they provide will be closely scrutinized, pharmaceutical representatives will have an incentive to provide more accurate information.
2. Cost Sensitivity
One of the many topics that can be discussed by the hospital pharmacist or attending is the price of the given drug. In discussing price, two critical points must be evaluated. The first is the price-benefit ratio of the given drug and the second is the financial situation of the patient. Physicians should always have the patient’s best interest in mind. However, this does not mean that cost should not be considered when making therapeutic decisions. Rather, a more practical therapeutic decision can be made with cost in mind. Cost is the major factor to some patients when determining whether they will fill their prescriptions. In such an instance, if cost is taken into consideration when writing the prescription, a physician is more apt to write a prescription for a less expensive medication (if one exists).
3. Three-Way Transparency
In order for hospitalists to effectively interact with the pharmaceutical industry, it must be realized that medical professionals are not victims of the marketing strategies of the pharmaceutical industry; rather, we are accomplices. We often fail to acknowledge the role medical educators and professionals play in this problem. Many years ago, Troyan Brennan called for transparency, stating “Conflict will remain with us. Physicians’ relationship with the pharmaceutical industry must be better managed” (25). However, Brennan did not offer any proposals on a better management system. Our current management system of disclosure of conflict has become obsolete. It has become a ritual practice in academia to acknowledge that one may have a conflict of interest, but this does nothing to address the real issue: the conflict of interest itself. Hospitalists can adopt a three-way transparency between the patient, colleagues, and the pharmaceutical industry where all conflicts are fully disclosed, rather than simply stating that a conflict might exist.
4. High Threshold for Rationalization
Most medical professionals, to some degree, rationalize interactions with the pharmaceutical industry. Almost all physicians insist that these interactions do not influence their judgment. The simple fact that the industry spends thousands of dollars per doctor per year indicates that we are wrong. If physicians were not being influenced, the pharmaceutical companies would not be spending such a considerable amount of money marketing to us. Patients trust physicians to make the best decision for them, they depend on researchers to publish impartial studies, and they count on educators to present unbiased truths. The cost of betrayal is paid in human lives. We should learn from the past, as well as the recent coxib debacle.
Conclusion
The interaction between hospitalists and the pharmaceutical industry continues to evolve. With increasing scrutiny from the medical profession and the government, many of the marketing practices that were considered acceptable in the past are now viewed as unacceptable and even criminal. As the relationship evolves, new conflicts are sure to arise as long as the fundamental difference between the medical profession and pharmaceutical industry continues to exist. As medical professionals, we must keep in mind that the pharmaceutical industry is a for-profit industry whose interest lies with its shareholders. It is to be expected that the pharmaceutical industry will try to maximize profits through marketing efforts directed at physicians and patients.
Medical educators must take on the responsibility of preparing medical students, residents, and fellow attendings on how to manage their interactions with the pharmaceutical industry and not just shield them from the issue. In applying the four-point approach of academic detailing, cost sensitivity, three-way transparency, and a high threshold for justification, we can better manage such interactions.
We would like to thank Dr. Anna Headly and Emily Hartsough for their constructive comments in the preparation of the manuscript.
Disclaimer: The content of the article is solely the responsibility of the authors and does not necessarily represent the official view of the Society of Hospital Medicine.
Dr. Rajput can be contacted at [email protected].
References
- Abbasi K, Smith R. No more free lunch: patients will benefit from doctors and drug companies disentangling. BMJ. 2003;326:1155-6.
- Relman AS. Separating continuing medical education from pharmaceutical marketing. JAMA. 2001;285:2009-12.
- Thursby JG, Thursby MC. Intellectual property. University licensing and the Bayh-Dole Act. Science. 2003;301:1052.
- Holmer AF. Industry strongly supports continuing medical education. JAMA. 2001;285:2012-4.
- Scherer FM. The pharmaceutical industry: price and progress. N Engl J Med. 2004;351:927-32.
- Pharmaceutical industry profiles 2003. Washinton, DC; 2003.
- Moynihan R. Who pays for the pizza? Redefining the relationships between doctors and drug companies. 2: Disentanglement. BMJ. 2003;326:1193-6.
- Smith R. Medical journals and pharmaceutical companies: uneasy bedfellows. BMJ. 2003;326:1202-5.
- Relman AS. Defending professional independence: ACCME’s proposed new guidelines for commercial support of CME. JAMA. 2003;289:2418-20.
- Ziegler MG, Lew P, Singer BC. The accuracy of drug information from pharmaceutical sales representatives. JAMA. 1995;273:1296-8.
- Gottlieb S. Congress criticises drug industry for misleading advertising. BMJ. 2002;325:1379.
- Rogers WA, Mansfield PR, Braunack-Mayer AJ, Jureidini JN. The ethics of pharmaceutical industry relationships with medical students. Med J Aust. 2004;180:411-4.
- Melander H, Ahlqvist-Rastad J, Me&er G, Beermann B. Evidence b(i)ased medicine—selective reporting from studies sponsored by pharmaceutical industry: review of studies in new drug applications. BMJ. 2003;326:1171-3.
- Lexchin J. Interactions between physician and the pharmaceutical industry: what does the literatue say? Can Med Assoc J. 1993;149:1401-7.
- Steinman MA, Shlipak MG, McPhee SJ. Of principles and pens: attitudes and practices of medicine housestaff toward pharmaceutical industry promotions. Am J Med. 2001;110:551-7.
- Wazana A. Physicians and the pharmaceutical industry: is a gift ever just a gift? JAMA. 2000;283:373-80.
- Watkins C, Moore L, Harvey I, Carthy P, Robinson E, Brawn R. Characteristics of general practitioners who frequently see drug industry representatives: national cross sectional study. BMJ. 2003;326:1178-9.
- Guidelines on gifts to physicians from industry: an update. Food Drug Law J. 2001;56:27-40.
- PhRMA CODE On Interactions with Health Care Professionals. Infectious Diseases in Clinical Practice. 2002;(11):153-4.
- McCormick BB, Tomlinson G, Brill-Edwards P, Detsky AS. Effect of restricting contact between pharmaceutical company representatives and internal medicine residents on posttraining attitudes and behavior. JAMA. 2001;286:1994-9.
- Ferguson RP, Rhim E, Belizaire W, Egede L, Carter K, Lansdale T. Encounters with pharmaceutical sales representatives among practicing internists. Am J Med. 1999;107:149-52.
- Watkins RS, Kimberly JJ. What residents don’t know about physician-pharmaceutical industry interactions. Acad Med. 2004;79:432-7.
- Wilkes MS, Hoffman JR. An innovative approach to educating medical students about pharmaceutical promotion. Acad Med. 2001;76:1271-7.
- Vinson DC, McCandless B, Hosokawa MC. Medical students’ attitudes toward pharmaceutical marketing: possibilities for change. Fam Med. 1993;25:31-3.
- Brennan TA. Buying editorials. N Engl J Med. 1994;331: 673-5; discussion 76.
The ideal patient-physician relationship is one of choice, competence, communication, compassion, and continuity, and is free of any conflict of interest. There is heated controversy about whether the relationship between the pharmaceutical industry and medical professionals betrays this ideal. The heart of this debate lies in the fundamental difference in priorities and goals of the pharmaceutical industry and hospitalists. Hospitalists are trusted with the lives and well-being of patients. A physician is expected to make an unbiased analysis of the treatment options for a given patient and to apply that treatment to the best of his or her abilities. In contrast, the ultimate interest of the pharmaceutical industry lies with the shareholders, and the primary goal is to maximize profit. Many feel that these two goals are mutually exclusive (1,2). Medical educators believe that it is the responsibility of the medical profession, not pharmaceutical companies, to educate physicians. The entanglement of the pharmaceutical industry with physicians calls into question the credibility of information obtained from any pharmaceutical-sponsored event and casts doubt over the medical profession as a whole. Governmental regulation and legislative initiatives such as the Bayh-Dole Act (3) have furthered the commercialization of academic research and realigned academic centers’ approach to clinical research.
The pharmaceutical industry argues that its goals and the goals of the medical profession are complementary (4) and that their involvement optimizes the benefit to the patient. The pharmaceutical industry is quick to point out that pharmaceutical companies are an important source of funding for clinical trials and are the leading sponsors of continuing medical education, and that it is the most research-intensive industry in the United States supported by private funds (5). Corporate contributions to research and development in academia have increased by 900% between 1980 and 2000. The pharmaceutical industry devoted 18% of profits in 2002 to research, development, and testing activities (6). The pharmaceutical industry claims that these are designed to serve the mutual interests of the pharmaceutical industry and the medical community by providing accurate and up-to-date information to maximize patient care. The advances made as a result of commercial development have dramatically altered the landscape of research. Pharmaceutical courtship of hospitalists, who find themselves on the front line in clinical settings as prescribers or researchers, is part of an aggressive marketing campaign that some believe contributes little to the common good.
Hospitalists have increased their financial incentives with stock options, fees for consultation, speaking arrangements, and memberships on advisory boards for pharmaceutical companies. Disclosure of financial conflicts is becoming an empty ritual providing a false sense of security. Pharmaceutical research is increasingly organized by Contract Research Organizations, written up with the help of ghostwriters, and published under the name of established investigators (7,8). Not all industry-funded studies are necessarily fl awed and without scientific merit, but the fact that negative consequences can be devastating to the financial health of a corporation has to be considered.
A leading catalyst for continued pharmaceutical industry/hospitalist interaction is continuing medical education (CME). In 2003, the pharmaceutical industry provided 900 million of the one billion dollars spent on CME in the United States. Currently, the pharmaceutical industry funds approximately 60% of all CME activities in the United States (9). Information provided to physicians by a pharmaceutical representative has an inaccuracy rating of 13% (10). Not surprisingly, many of these inaccuracies favor the product being presented and casts an unfavorable light on competing drugs (10,11). This has led some to believe that this pharmaceutical representative/physician interaction is having a negative impact on patients (12) through the dissemination of inaccurate information. In addition, misleading advertisements have been found to overstate the effectiveness and minimize the risks of a given drug (11). Another form of bias is the selective publication of research studies by the pharmaceutical industry (13).
Bedside and Conference Detailing
Interactions with pharmaceutical representatives (drug detailers) often begin in medical school and proceed throughout a physician’s career (12,14). In 2003, the pharmaceutical industry spent more than 13 billion dollars on promotional activities for doctors, an average of about $10,500 per physician. There is one drug detailer for every 4.7 office-based physicians. Interactions include conferences with free lunch, personal visits by drug detailers, sponsored CME workshops/seminars, sponsored dinners, sponsored scientific conferences, sponsored research, direct gifts (e.g., cash payments for prescribing a given medication), and indirect gifts (e.g., subsidizing a trip to a medical conference). These interactions evolve from merely lunches and pens early in a physician’s career to positions as a consultant and advisory board honoree as the relationship matures. Some physicians view such exchanges as helpful and informative while others view it as unethical (2) and harmful.
Hospitalists, residents, and medical students alike believe their interactions with drug detailers, and the small gifts that they receive, do not influence their behavior (14,15). Wazana found that as physicians continue to receive gifts from drug detailers, they become even less likely to believe that the gifts can influence their behavior (16). Many physicians believe that their interactions with drug companies are beneficial not only to them but also to their patients. However, studies have found that this is in fact not the case. Physicians who interact with pharmaceutical representatives prescribe newer and more expensive drugs, rather than cheaper and equally effective generic drugs (16,17). There are a significantly higher number of prescriptions written for the drugs manufactured by pharmaceutical companies who sponsor a given CME activity than pharmaceutical companies who do not. A rise in prescription expenditures (17), as well as an increase in irrational prescribing, often follows in-house exposure to drug detailers (16).
The enormous amount spent on marketing can also be used as further proof of the pharmaceutical industry’s avarice. However, we often fail to acknowledge the role that medical educators and professionals play in this problem. Pharmaceutical companies are profitable because of our prescribing habits. For example, many medical professionals prescribe expensive “me too” drugs that often offer little if any benefit over cheaper established or prototypical drugs. Our actions encourage what we claim to be bad behavior by the pharmaceutical industry.
It is often argued by the pharmaceutical industry that these “me too” drugs have a different side effect profile, may improve compliance in long-term treatment, or will reduce cost when compared to the prototype drug. This is true in some instances, as exemplified by the wide array of anti-hypertensives and the even wider array of side effect profiles. However, there are many instances when this is far from the case. If a financial incentive did not exist for pharmaceutical companies to introduce “me too” drugs, the pharmaceutical industry would not do so unless the drug being introduced provided a substantial clinical advantage over the prototype drug. As a result, the pharmaceutical industry would be spending their time, effort, and finances on research aimed at finding new and innovative cures.
Proposed Solution to the Problem
In an effort to remedy this situation, many professional societies (as well as the pharmaceutical industry itself) have established guidelines on the interactions between the pharmaceutical industry and physicians. The AMA has established guidelines responsible for the regulation of gifts bestowed on physicians by industry (18). The Pharmaceutical Research Manufacturers of America has established similar guidelines known as the PhRMA Code (19). Increasingly, many professional organizations have taken it upon themselves to establish their own code of conduct. However, there remains a low level of awareness of the guidelines (15) that are currently in place, and some of the pharmaceutical companies have chosen not to abide by the PhRMA Code. In response to the increasing influence pharmaceutical companies are having on the medical decision-making process, many training programs are adopting policies to limit the contact between pharmaceutical representatives and physicians in training. This is being carried out at both the undergraduate and graduate medical education levels (20). The effects of such restrictions are currently unknown. McCormick found that physicians who trained in institutions with such policies were less likely to find information from pharmaceutical company representatives useful (20). However, Ferguson found that being trained in a program with a policy that limited access to pharmaceutical sales representatives did not affect the subsequent likelihood of future physician-pharmaceutical representative interactions (21).
The Informed Hospitalist in the 21st Century
The literature clearly documents that the pharmaceutical industry influences physician prescribing habits. Hospitalists can take a four-prong approach to help counteract these effects:
1. Academic Detailing
Medical educators can shield residents and medical students from the influence of pharmaceutical representatives by limiting or prohibiting contact, or they can teach trainees how to effectively manage such interactions through academic detailing. As stated above, Ferguson found that policies limiting access to drug detailers did not affect the subsequent likelihood of future physician and pharmaceutical representative interactions (21). It might be wiser to teach trainees how to manage their interactions with the drug representatives and thereby take control of the situation. In order for doctors to effectively manage such interactions, we must learn how to evaluate the literature and interpret the information given to us by representatives. Watkins found that both attendings and residents feel that they should learn how to critically evaluate promotional materials, recognize potential conflicts of interest, and consider how patients perceive physician-pharmaceutical relationships (22). Previous studies have found that educational interventions can have a significant effect on the attitudes of medical students and residents towards pharmaceutical marketing and drug detailers (23,24).
One way to evaluate pharmaceutical literature is to have academic detailing of the clinical studies and statements made by pharmaceutical detailers at sponsored events. During these academic detailing conferences the drug in question can be compared to other drugs in the class, and indications and differences should be mentioned if they exist. This should be done in the presence of both an attending who is very familiar with the drug and drug class in question and a hospital pharmacist. If this is done in a small setting, the medical students and residents can take turns critically evaluating the presentations. This approach is comparable to teaching medicine at the bedside; learners develop a deeper appreciation and understanding by experiencing various situations first-hand.
An additional benefit of critically evaluating pharmaceutical representative presentations is that when they know that the information they provide will be closely scrutinized, pharmaceutical representatives will have an incentive to provide more accurate information.
2. Cost Sensitivity
One of the many topics that can be discussed by the hospital pharmacist or attending is the price of the given drug. In discussing price, two critical points must be evaluated. The first is the price-benefit ratio of the given drug and the second is the financial situation of the patient. Physicians should always have the patient’s best interest in mind. However, this does not mean that cost should not be considered when making therapeutic decisions. Rather, a more practical therapeutic decision can be made with cost in mind. Cost is the major factor to some patients when determining whether they will fill their prescriptions. In such an instance, if cost is taken into consideration when writing the prescription, a physician is more apt to write a prescription for a less expensive medication (if one exists).
3. Three-Way Transparency
In order for hospitalists to effectively interact with the pharmaceutical industry, it must be realized that medical professionals are not victims of the marketing strategies of the pharmaceutical industry; rather, we are accomplices. We often fail to acknowledge the role medical educators and professionals play in this problem. Many years ago, Troyan Brennan called for transparency, stating “Conflict will remain with us. Physicians’ relationship with the pharmaceutical industry must be better managed” (25). However, Brennan did not offer any proposals on a better management system. Our current management system of disclosure of conflict has become obsolete. It has become a ritual practice in academia to acknowledge that one may have a conflict of interest, but this does nothing to address the real issue: the conflict of interest itself. Hospitalists can adopt a three-way transparency between the patient, colleagues, and the pharmaceutical industry where all conflicts are fully disclosed, rather than simply stating that a conflict might exist.
4. High Threshold for Rationalization
Most medical professionals, to some degree, rationalize interactions with the pharmaceutical industry. Almost all physicians insist that these interactions do not influence their judgment. The simple fact that the industry spends thousands of dollars per doctor per year indicates that we are wrong. If physicians were not being influenced, the pharmaceutical companies would not be spending such a considerable amount of money marketing to us. Patients trust physicians to make the best decision for them, they depend on researchers to publish impartial studies, and they count on educators to present unbiased truths. The cost of betrayal is paid in human lives. We should learn from the past, as well as the recent coxib debacle.
Conclusion
The interaction between hospitalists and the pharmaceutical industry continues to evolve. With increasing scrutiny from the medical profession and the government, many of the marketing practices that were considered acceptable in the past are now viewed as unacceptable and even criminal. As the relationship evolves, new conflicts are sure to arise as long as the fundamental difference between the medical profession and pharmaceutical industry continues to exist. As medical professionals, we must keep in mind that the pharmaceutical industry is a for-profit industry whose interest lies with its shareholders. It is to be expected that the pharmaceutical industry will try to maximize profits through marketing efforts directed at physicians and patients.
Medical educators must take on the responsibility of preparing medical students, residents, and fellow attendings on how to manage their interactions with the pharmaceutical industry and not just shield them from the issue. In applying the four-point approach of academic detailing, cost sensitivity, three-way transparency, and a high threshold for justification, we can better manage such interactions.
We would like to thank Dr. Anna Headly and Emily Hartsough for their constructive comments in the preparation of the manuscript.
Disclaimer: The content of the article is solely the responsibility of the authors and does not necessarily represent the official view of the Society of Hospital Medicine.
Dr. Rajput can be contacted at [email protected].
References
- Abbasi K, Smith R. No more free lunch: patients will benefit from doctors and drug companies disentangling. BMJ. 2003;326:1155-6.
- Relman AS. Separating continuing medical education from pharmaceutical marketing. JAMA. 2001;285:2009-12.
- Thursby JG, Thursby MC. Intellectual property. University licensing and the Bayh-Dole Act. Science. 2003;301:1052.
- Holmer AF. Industry strongly supports continuing medical education. JAMA. 2001;285:2012-4.
- Scherer FM. The pharmaceutical industry: price and progress. N Engl J Med. 2004;351:927-32.
- Pharmaceutical industry profiles 2003. Washinton, DC; 2003.
- Moynihan R. Who pays for the pizza? Redefining the relationships between doctors and drug companies. 2: Disentanglement. BMJ. 2003;326:1193-6.
- Smith R. Medical journals and pharmaceutical companies: uneasy bedfellows. BMJ. 2003;326:1202-5.
- Relman AS. Defending professional independence: ACCME’s proposed new guidelines for commercial support of CME. JAMA. 2003;289:2418-20.
- Ziegler MG, Lew P, Singer BC. The accuracy of drug information from pharmaceutical sales representatives. JAMA. 1995;273:1296-8.
- Gottlieb S. Congress criticises drug industry for misleading advertising. BMJ. 2002;325:1379.
- Rogers WA, Mansfield PR, Braunack-Mayer AJ, Jureidini JN. The ethics of pharmaceutical industry relationships with medical students. Med J Aust. 2004;180:411-4.
- Melander H, Ahlqvist-Rastad J, Me&er G, Beermann B. Evidence b(i)ased medicine—selective reporting from studies sponsored by pharmaceutical industry: review of studies in new drug applications. BMJ. 2003;326:1171-3.
- Lexchin J. Interactions between physician and the pharmaceutical industry: what does the literatue say? Can Med Assoc J. 1993;149:1401-7.
- Steinman MA, Shlipak MG, McPhee SJ. Of principles and pens: attitudes and practices of medicine housestaff toward pharmaceutical industry promotions. Am J Med. 2001;110:551-7.
- Wazana A. Physicians and the pharmaceutical industry: is a gift ever just a gift? JAMA. 2000;283:373-80.
- Watkins C, Moore L, Harvey I, Carthy P, Robinson E, Brawn R. Characteristics of general practitioners who frequently see drug industry representatives: national cross sectional study. BMJ. 2003;326:1178-9.
- Guidelines on gifts to physicians from industry: an update. Food Drug Law J. 2001;56:27-40.
- PhRMA CODE On Interactions with Health Care Professionals. Infectious Diseases in Clinical Practice. 2002;(11):153-4.
- McCormick BB, Tomlinson G, Brill-Edwards P, Detsky AS. Effect of restricting contact between pharmaceutical company representatives and internal medicine residents on posttraining attitudes and behavior. JAMA. 2001;286:1994-9.
- Ferguson RP, Rhim E, Belizaire W, Egede L, Carter K, Lansdale T. Encounters with pharmaceutical sales representatives among practicing internists. Am J Med. 1999;107:149-52.
- Watkins RS, Kimberly JJ. What residents don’t know about physician-pharmaceutical industry interactions. Acad Med. 2004;79:432-7.
- Wilkes MS, Hoffman JR. An innovative approach to educating medical students about pharmaceutical promotion. Acad Med. 2001;76:1271-7.
- Vinson DC, McCandless B, Hosokawa MC. Medical students’ attitudes toward pharmaceutical marketing: possibilities for change. Fam Med. 1993;25:31-3.
- Brennan TA. Buying editorials. N Engl J Med. 1994;331: 673-5; discussion 76.