User login
Obsessive and inattentive
CASE: Perfect breath
Mr. C, a 20-year-old college student, is diagnosed with obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and tic disorder (TD). His obsessions consist of a persistent sense that he is not breathing “correctly” or “perfectly.” He compulsively holds his breath to “rush blood to my head” until “the pressure feels just right.” Mr. C says that his OCD has had longstanding, significant negative impact on his academic performance and capacity to engage in other activities. Tics have been present for years and manifest as coughing and throat-clearing. After multiple syncopal epi-sodes from breath-holding with Valsalva maneuver—some of which caused falls and head injury—Mr. C is admitted to a residential psychiatric unit specializing in treating OCD. At the time of his admission, his Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores1,2 are 23 total, 12 on the obsessions subscale, and 11 on the compulsions subscale, indicating moderate to severe illness. Cognitive-behavioral therapy (CBT) is offered, along with a combination of escitalopram, 60 mg/d, and quetiapine, 50 mg/d. Quetiapine is over-sedating at subtherapeutic doses and Mr. C’s compulsions worsen. He reports that “[it] took longer and longer to get the ‘just right’ feeling.’” Quetiapine is discontinued and risperidone, 0.5 mg/d, is started, which decreases the frequency of his tics. When he is discharged after a 36-day stay, Mr. C’s Y-BOCS scores are greatly improved at 13 total, 7 on the obsessions subscale, and 3 on the compulsions subscale.
Mr. C’s psychologist refers him to our outpatient clinic for continued psychiatric evaluation and treatment of his OCD, ADHD, and TD. At this time, he is prescribed escitalopram, 60 mg/d, and risperidone, 0.5 mg/d, along with CBT with his psychologist. We do not readminister the Y-BOCS at this time, but Mr. C reports that his OCD is “60% improved.” However, he describes prominent obsessive thoughts regarding his breathing similar to those he experienced before residential treatment. These obsessive thoughts arise in the context of specific environmental “triggers,” such as other people coughing or his own tics. The obsessions lead to compulsive urges to engage in breath-holding rituals. Mr. C experiences the thoughts and compulsions as deeply troubling and they consume 5 to 6 hours each day. Mr. C reports impaired concentration in class and during studying: “I can focus for 5 minutes, then not for 2 minutes, then for 3 minutes… I can never stay focused for more than a couple minutes,” before becoming distracted “by my OCD” or other environmental stimuli. We note on exam prominent breath-holding occurring several times per minute. Mr. C says his OCD has not impaired his ability to socialize.
Mr. C notes that he has been exposed to an array of CBT techniques, but he has difficulty using these techniques because his “mind wanders” or he lacks “motivation.” He admits he occasionally has taken a classmate’s ADHD medication (mixed amphetamine salts [MAS], dose unspecified) and found it improved his ability to focus on his academic work.
The authors’ observations
Researchers have established a relationship among OCD, ADHD, and TD across all combinations of comorbidity (OCD and ADHD,3 ADHD and TD,4 OCD and TD,5,6 and all 3 entities7). Data suggests a poorer prognosis for OCD when comorbid with either or both of these conditions.8 Researchers have raised concerns that psychostimulants could exacerbate or potentiate tic behaviors in patients with ADHD,9,10 although safe and effective use of these medications has been documented in controlled trials of patients with comorbid ADHD and tics.11-13 Furthermore, tic suppression has been reported with psychostimulants,14 as well as a differential effect of stimulants on motor vs vocal tics.15 Despite these data (Table 1),9-15 the FDA regards using psychostimulants in patients with TD as a contraindication,16 although clinicians often recognize that this practice may be unavoidable in some circumstances because of high comorbidity rates. Psychostimulants could exacerbate obsessions or compulsions in some patients because of their dopaminergic properties or through mitigation of the purported anti-obsessional properties of dopamine antagonists.17
Although there is evidence that the prevalence of prescribed psychostimulant abuse is low among ADHD patients,18 diversion of prescribed medication is a risk inherent in the use of these agents, particularly among college-age patients.19,20
Table 1
Evidence of effect of psychostimulants on tics
| Study/disorder(s) | Medication and study design | Relevant findings |
|---|---|---|
| Lipkin et al, 19949; ADHD without TD | Chart review (N = 122) to determine the incidence of tics or dyskinesias in children treated with stimulants | Approximately 9% of children developed tics or dyskinesias, which predominantly were transient, with <1% developing chronic tics or Tourette’s syndrome. Personal or family tic history and medication selection or dosage were not related to onset of tics or dyskinesias |
| Gadow et al, 199515; ADHD with TD | Methylphenidate variable dose, placebo-controlled, 2-week trials (N = 24) | All children’s ADHD symptoms improved. At a 0.1 mg/kg dose, motor tics observed in the classroom increased, but there were fewer vocal tics observed in the lunchroom |
| Castellanos et al, 199710; ADHD with Tourette’s syndrome | Methylphenidate, dextroamphetamine, variable-dose, double-blind, placebo-controlled, 9-week crossover (N = 20) | 3 patients had consistent worsening of tics while taking stimulants. Stimulants reduced hyperactivity rates compared with placebo (P = .03). Stimulants improved ADHD symptoms and had acceptable effects on tics. Methylphenidate was better tolerated than dextroamphetamine |
| Gadow et al, 199911; ADHD with TD | 34 methylphenidate-treated children, followed at 6-month intervals for 2 years | No evidence that frequency or severity of motor or vocal tics changed during maintenance therapy |
| Tourette Syndrome Study Group, 200213; ADHD with TD | Clonidine alone, methylphenidate alone, clonidine plus methylphenidate, or placebo | Worsening of tics was not reported in any group at a rate significantly higher than placebo. Tic severity was more reduced in the 2 clonidine groups than in the methylphenidate group |
| Lyon et al, 201014; ADHD with Tourette’s syndrome | Dexmethylphenidate, single-dose challenge. Ten patients with or without TSP | Acute dexmethylphenidate administration resulted in tic suppression but did not augment TSP |
| Gadow et al, 200712; ADHD with TD | Double-blind, placebo-controlled, 2-week trials each of 3 doses of methylphenidate and placebo (N = 71) | MPH-IR did not alter the overall severity of TD or OCD behaviors. Teacher ratings indicated that MPH-IR therapy decreased tic frequency and severity |
| ADHD: attention-deficit/hyperactivity disorder; MPH-IR: methylphenidate immediate release; OCD: obsessive-compulsive disorder; TD: tic disorder; TSP: tic suppression protocol | ||
TREATMENT: Weighing options
To manage impaired attention and executive function difficulties secondary to ADHD, we offer Mr. C several options, including bupropion, modafinil, and memantine augmentation. Mr. C asks for a psychostimulant because exam week is approaching and he wants a treatment with quick therapeutic effect. We discuss with Mr. C the potential for dopaminergic agents, such as psychostimulants, to exacerbate tics or OCD symptoms. Ultimately, we prescribe immediate-release MAS, 20 mg/d.
Two days later, Mr. C says he has taken 3 MAS doses and describes a marked reduction in obsessions, significant decrease in frequency of “triggers,” and greater capacity to use CBT saying, “when I am [triggered], I am able to move past the urges without doing any compulsions.” Daily time spent “stuck on” obsessions or compulsions decreases from 5 to 6 hours per day to “about 2 and a half minutes.”
Mr. C reports a modest increase in the prevalence of tics, experienced as “little throat clears and quick stuttering of breath.” He notes that, although in the past such tics would be followed by urges for “perfecting the tic and making it feel just right,” he presently “had no desire to do so.”
OUTCOME: Sharper focus
Increasing MAS immediate release from 20 mg/d to 30 mg/d suppresses Mr. C’s obsessions and compulsions for 8 hours. On the 19th day of treatment, MAS immediate release was replaced with an extended release formulation, 30 mg/d, which preserves therapeutic effect and tolerability for 16 weeks. Repeat Y-BOCS yields 9 total, 3 on obsessions subscale, and 6 on compulsions subscale scores.
One month later, Mr. C reports that his symptoms have been “improving ever since” the previous appointment. He continues to be able to access skills for managing his OCD and is doing well in his 2 accelerated summer courses, saying “I focus really well” in 3-hour class sessions. On exam, tic behaviors are nearly absent. Mr. C describes occasional bouts of anxiety associated with urges to engage in tic behaviors, in turn arising from fear of symptomatic recurrence as he worked toward stopping smoking as advised by his primary care physician and psychiatrist.
The authors’ observations
The results of the repeat Y-BOCS are consistent with improvement in obsessions but possible worsening of compulsions since Mr. C was discharged from residential treatment. Alternatively, compulsions may have worsened immediately after discharge and declined again with introduction of MAS.
A substantial body of literature describes the challenges associated with treating ADHD with comorbid tics, including the relative degree of risk of tic exacerbation associated with treating ADHD with psychostimulants. The range of FDA-approved pharmacologic options for treatment of this comorbidity is limited (Table 2),21 particularly given the risk for tardive dyskinesia associated with the typical antipsychotics haloperidol and chlorpromazine. Data support using the α-2 agonist clonidine to treat hyperactivity associated with ADHD22 and TD23 and an extended-release preparation of this medication is FDA-approved for the former but not the latter indication (an α-2A receptor subtype agonist, guanfacine, also is FDA-approved for ADHD in pediatric patients). Mr. C’s experience of robust, sustained reduction in obsessions, if not compulsions, after treatment with MAS is consistent with the few studies of stimulant use in ADHD with comorbid OCD.24,25
Effective treatment of ADHD may help Mr. C better access CBT strategies and thereby potentiate treatment of comorbid OCD.
Table 2
FDA-approved medications for ADHD, OCD, and TD
| Disorder | Medications |
|---|---|
| ADHD | Amphetamine (racemic), atomoxetine, chlorpromazine (hyperactivity), clonidine extended release, dexmethylphenidate, dextroamphetamine, guanfacine extended release, haloperidol (hyperactivity, second-line), lisdexamfetamine, methylphenidate (racemic) |
| OCD | Clomipramine, fluoxetine, fluvoxamine, paroxetine, sertraline |
| TD/Tourette’s syndrome | Haloperidol (Tourette’s), pimozide (Tourette’s) |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder; TD: tic disorder Source: Reference 21 | |
Related Resources
- Pliszka SR. Treating ADHD and comorbid disorders: psychosocial and psychopharmacological interventions. New York, NY: The Guilford Press; 2011.
- Pollak Y, Benarroch F, Kanengisser L, et al. Tourette syndrome-associated psychopathology: roles of comorbid attention-deficit hyperactivity disorder and obsessive-compulsive disorder. J Dev Behav Pediatr. 2009;30(5):413-419.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Clonidine extended release • Kapvay
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guanfacine • Intuniv, Tenex
- Haloperidol • Haldol
- Lisdexamfetamine • Vyvanse
- Memantine • Namenda
- Methylphenidate • Methylin, Ritalin
- Modafinil • Provigil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use and reliability. Arch Gen Psych. 1989;46(11):1006-1011.
2. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: II. Validity. Arch Gen Psych. 1989;46(11):1012-1016.
3. Geller DA, Biederman J, Faraone S, et al. Re-examining comorbidity of obsessive compulsive and attention-deficit hyperactivity disorder using an empirically derived taxonomy. Eur Child Adolesc Psychiatry. 2004;13(2):83-91.
4. Freeman RD. Attention deficit hyperactivity disorder in the presence of Tourette syndrome. Neurol Clin. 1997;15(2):411-420.
5. Geller DA. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr Clin North Am. 2006;29(2):353-370.
6. Eapen V, Fox-Hiley P, Banerjee S, et al. Clinical features and associated psychopathology in a Tourette syndrome cohort. Acta Neurol Scand. 2004;109(4):255-260.
7. Kano Y, Ohta M, Nagai Y, et al. Association between Tourette syndrome and comorbidities in Japan. Brain Dev. 2010;32(3):201-207.
8. Grados M, Riddle M. Do all obsessive-compulsive disorder subtypes respond to medication? Int Rev Psychiatry. 2008;20(2):189-193.
9. Lipkin PH, Goldstein IH, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 1994;148(8):859-861.
10. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry. 1997;36(5):589-596.
11. Gadow K, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry. 1999;56(4):330-333.
12. Gadow KD, Sverd J, Nolan EE, et al. Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):840-848.
13. Tourette’s Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology. 2002;58(4):527-536.
14. Lyon GJ, Samar SM, Conelea C, et al. Testing tic suppression: comparing the effects of dexmethylphenidate to no mediation in children and adolescents with attention-deficit/hyperactivity disorder and Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):283-289.
15. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry. 1995;52(6):444-455.
16. Bloch MH, Panza KE, Landerso-Weisenberger A, et al. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry. 2009;48(9):884-893.
17. McDougle CJ, Goodman WK, Price LH. Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry. 1994;55(suppl):24-31.
18. Wilens TE, Morrison NR. The intersection of attention-deficit/hyperactivity disorder and substance abuse. Curr Opin Psychiatry. 2011;24(4):280-285.
19. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
20. Schubiner H. Substance abuse in patients with attention-deficit hyperactivity disorder: therapeutic implications. CNS Drugs. 2005;19(8):643-655.
21. Stahl SM. The prescriber’s guide. Stahl’s essential psychopharmacology. 3rd ed. New York NY: Cambridge University Press; 2009.
22. Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(2):171-179.
23. Hedderick EF, Morris CM, Singer HS. Double-blind crossover study of clonidine and levetiracetam in Tourette syndrome. Pediatr Neurol. 2009;40(6):420-425.
24. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11(4):237-241.
25. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80(3):231-235.
CASE: Perfect breath
Mr. C, a 20-year-old college student, is diagnosed with obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and tic disorder (TD). His obsessions consist of a persistent sense that he is not breathing “correctly” or “perfectly.” He compulsively holds his breath to “rush blood to my head” until “the pressure feels just right.” Mr. C says that his OCD has had longstanding, significant negative impact on his academic performance and capacity to engage in other activities. Tics have been present for years and manifest as coughing and throat-clearing. After multiple syncopal epi-sodes from breath-holding with Valsalva maneuver—some of which caused falls and head injury—Mr. C is admitted to a residential psychiatric unit specializing in treating OCD. At the time of his admission, his Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores1,2 are 23 total, 12 on the obsessions subscale, and 11 on the compulsions subscale, indicating moderate to severe illness. Cognitive-behavioral therapy (CBT) is offered, along with a combination of escitalopram, 60 mg/d, and quetiapine, 50 mg/d. Quetiapine is over-sedating at subtherapeutic doses and Mr. C’s compulsions worsen. He reports that “[it] took longer and longer to get the ‘just right’ feeling.’” Quetiapine is discontinued and risperidone, 0.5 mg/d, is started, which decreases the frequency of his tics. When he is discharged after a 36-day stay, Mr. C’s Y-BOCS scores are greatly improved at 13 total, 7 on the obsessions subscale, and 3 on the compulsions subscale.
Mr. C’s psychologist refers him to our outpatient clinic for continued psychiatric evaluation and treatment of his OCD, ADHD, and TD. At this time, he is prescribed escitalopram, 60 mg/d, and risperidone, 0.5 mg/d, along with CBT with his psychologist. We do not readminister the Y-BOCS at this time, but Mr. C reports that his OCD is “60% improved.” However, he describes prominent obsessive thoughts regarding his breathing similar to those he experienced before residential treatment. These obsessive thoughts arise in the context of specific environmental “triggers,” such as other people coughing or his own tics. The obsessions lead to compulsive urges to engage in breath-holding rituals. Mr. C experiences the thoughts and compulsions as deeply troubling and they consume 5 to 6 hours each day. Mr. C reports impaired concentration in class and during studying: “I can focus for 5 minutes, then not for 2 minutes, then for 3 minutes… I can never stay focused for more than a couple minutes,” before becoming distracted “by my OCD” or other environmental stimuli. We note on exam prominent breath-holding occurring several times per minute. Mr. C says his OCD has not impaired his ability to socialize.
Mr. C notes that he has been exposed to an array of CBT techniques, but he has difficulty using these techniques because his “mind wanders” or he lacks “motivation.” He admits he occasionally has taken a classmate’s ADHD medication (mixed amphetamine salts [MAS], dose unspecified) and found it improved his ability to focus on his academic work.
The authors’ observations
Researchers have established a relationship among OCD, ADHD, and TD across all combinations of comorbidity (OCD and ADHD,3 ADHD and TD,4 OCD and TD,5,6 and all 3 entities7). Data suggests a poorer prognosis for OCD when comorbid with either or both of these conditions.8 Researchers have raised concerns that psychostimulants could exacerbate or potentiate tic behaviors in patients with ADHD,9,10 although safe and effective use of these medications has been documented in controlled trials of patients with comorbid ADHD and tics.11-13 Furthermore, tic suppression has been reported with psychostimulants,14 as well as a differential effect of stimulants on motor vs vocal tics.15 Despite these data (Table 1),9-15 the FDA regards using psychostimulants in patients with TD as a contraindication,16 although clinicians often recognize that this practice may be unavoidable in some circumstances because of high comorbidity rates. Psychostimulants could exacerbate obsessions or compulsions in some patients because of their dopaminergic properties or through mitigation of the purported anti-obsessional properties of dopamine antagonists.17
Although there is evidence that the prevalence of prescribed psychostimulant abuse is low among ADHD patients,18 diversion of prescribed medication is a risk inherent in the use of these agents, particularly among college-age patients.19,20
Table 1
Evidence of effect of psychostimulants on tics
| Study/disorder(s) | Medication and study design | Relevant findings |
|---|---|---|
| Lipkin et al, 19949; ADHD without TD | Chart review (N = 122) to determine the incidence of tics or dyskinesias in children treated with stimulants | Approximately 9% of children developed tics or dyskinesias, which predominantly were transient, with <1% developing chronic tics or Tourette’s syndrome. Personal or family tic history and medication selection or dosage were not related to onset of tics or dyskinesias |
| Gadow et al, 199515; ADHD with TD | Methylphenidate variable dose, placebo-controlled, 2-week trials (N = 24) | All children’s ADHD symptoms improved. At a 0.1 mg/kg dose, motor tics observed in the classroom increased, but there were fewer vocal tics observed in the lunchroom |
| Castellanos et al, 199710; ADHD with Tourette’s syndrome | Methylphenidate, dextroamphetamine, variable-dose, double-blind, placebo-controlled, 9-week crossover (N = 20) | 3 patients had consistent worsening of tics while taking stimulants. Stimulants reduced hyperactivity rates compared with placebo (P = .03). Stimulants improved ADHD symptoms and had acceptable effects on tics. Methylphenidate was better tolerated than dextroamphetamine |
| Gadow et al, 199911; ADHD with TD | 34 methylphenidate-treated children, followed at 6-month intervals for 2 years | No evidence that frequency or severity of motor or vocal tics changed during maintenance therapy |
| Tourette Syndrome Study Group, 200213; ADHD with TD | Clonidine alone, methylphenidate alone, clonidine plus methylphenidate, or placebo | Worsening of tics was not reported in any group at a rate significantly higher than placebo. Tic severity was more reduced in the 2 clonidine groups than in the methylphenidate group |
| Lyon et al, 201014; ADHD with Tourette’s syndrome | Dexmethylphenidate, single-dose challenge. Ten patients with or without TSP | Acute dexmethylphenidate administration resulted in tic suppression but did not augment TSP |
| Gadow et al, 200712; ADHD with TD | Double-blind, placebo-controlled, 2-week trials each of 3 doses of methylphenidate and placebo (N = 71) | MPH-IR did not alter the overall severity of TD or OCD behaviors. Teacher ratings indicated that MPH-IR therapy decreased tic frequency and severity |
| ADHD: attention-deficit/hyperactivity disorder; MPH-IR: methylphenidate immediate release; OCD: obsessive-compulsive disorder; TD: tic disorder; TSP: tic suppression protocol | ||
TREATMENT: Weighing options
To manage impaired attention and executive function difficulties secondary to ADHD, we offer Mr. C several options, including bupropion, modafinil, and memantine augmentation. Mr. C asks for a psychostimulant because exam week is approaching and he wants a treatment with quick therapeutic effect. We discuss with Mr. C the potential for dopaminergic agents, such as psychostimulants, to exacerbate tics or OCD symptoms. Ultimately, we prescribe immediate-release MAS, 20 mg/d.
Two days later, Mr. C says he has taken 3 MAS doses and describes a marked reduction in obsessions, significant decrease in frequency of “triggers,” and greater capacity to use CBT saying, “when I am [triggered], I am able to move past the urges without doing any compulsions.” Daily time spent “stuck on” obsessions or compulsions decreases from 5 to 6 hours per day to “about 2 and a half minutes.”
Mr. C reports a modest increase in the prevalence of tics, experienced as “little throat clears and quick stuttering of breath.” He notes that, although in the past such tics would be followed by urges for “perfecting the tic and making it feel just right,” he presently “had no desire to do so.”
OUTCOME: Sharper focus
Increasing MAS immediate release from 20 mg/d to 30 mg/d suppresses Mr. C’s obsessions and compulsions for 8 hours. On the 19th day of treatment, MAS immediate release was replaced with an extended release formulation, 30 mg/d, which preserves therapeutic effect and tolerability for 16 weeks. Repeat Y-BOCS yields 9 total, 3 on obsessions subscale, and 6 on compulsions subscale scores.
One month later, Mr. C reports that his symptoms have been “improving ever since” the previous appointment. He continues to be able to access skills for managing his OCD and is doing well in his 2 accelerated summer courses, saying “I focus really well” in 3-hour class sessions. On exam, tic behaviors are nearly absent. Mr. C describes occasional bouts of anxiety associated with urges to engage in tic behaviors, in turn arising from fear of symptomatic recurrence as he worked toward stopping smoking as advised by his primary care physician and psychiatrist.
The authors’ observations
The results of the repeat Y-BOCS are consistent with improvement in obsessions but possible worsening of compulsions since Mr. C was discharged from residential treatment. Alternatively, compulsions may have worsened immediately after discharge and declined again with introduction of MAS.
A substantial body of literature describes the challenges associated with treating ADHD with comorbid tics, including the relative degree of risk of tic exacerbation associated with treating ADHD with psychostimulants. The range of FDA-approved pharmacologic options for treatment of this comorbidity is limited (Table 2),21 particularly given the risk for tardive dyskinesia associated with the typical antipsychotics haloperidol and chlorpromazine. Data support using the α-2 agonist clonidine to treat hyperactivity associated with ADHD22 and TD23 and an extended-release preparation of this medication is FDA-approved for the former but not the latter indication (an α-2A receptor subtype agonist, guanfacine, also is FDA-approved for ADHD in pediatric patients). Mr. C’s experience of robust, sustained reduction in obsessions, if not compulsions, after treatment with MAS is consistent with the few studies of stimulant use in ADHD with comorbid OCD.24,25
Effective treatment of ADHD may help Mr. C better access CBT strategies and thereby potentiate treatment of comorbid OCD.
Table 2
FDA-approved medications for ADHD, OCD, and TD
| Disorder | Medications |
|---|---|
| ADHD | Amphetamine (racemic), atomoxetine, chlorpromazine (hyperactivity), clonidine extended release, dexmethylphenidate, dextroamphetamine, guanfacine extended release, haloperidol (hyperactivity, second-line), lisdexamfetamine, methylphenidate (racemic) |
| OCD | Clomipramine, fluoxetine, fluvoxamine, paroxetine, sertraline |
| TD/Tourette’s syndrome | Haloperidol (Tourette’s), pimozide (Tourette’s) |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder; TD: tic disorder Source: Reference 21 | |
Related Resources
- Pliszka SR. Treating ADHD and comorbid disorders: psychosocial and psychopharmacological interventions. New York, NY: The Guilford Press; 2011.
- Pollak Y, Benarroch F, Kanengisser L, et al. Tourette syndrome-associated psychopathology: roles of comorbid attention-deficit hyperactivity disorder and obsessive-compulsive disorder. J Dev Behav Pediatr. 2009;30(5):413-419.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Clonidine extended release • Kapvay
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guanfacine • Intuniv, Tenex
- Haloperidol • Haldol
- Lisdexamfetamine • Vyvanse
- Memantine • Namenda
- Methylphenidate • Methylin, Ritalin
- Modafinil • Provigil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Perfect breath
Mr. C, a 20-year-old college student, is diagnosed with obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and tic disorder (TD). His obsessions consist of a persistent sense that he is not breathing “correctly” or “perfectly.” He compulsively holds his breath to “rush blood to my head” until “the pressure feels just right.” Mr. C says that his OCD has had longstanding, significant negative impact on his academic performance and capacity to engage in other activities. Tics have been present for years and manifest as coughing and throat-clearing. After multiple syncopal epi-sodes from breath-holding with Valsalva maneuver—some of which caused falls and head injury—Mr. C is admitted to a residential psychiatric unit specializing in treating OCD. At the time of his admission, his Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores1,2 are 23 total, 12 on the obsessions subscale, and 11 on the compulsions subscale, indicating moderate to severe illness. Cognitive-behavioral therapy (CBT) is offered, along with a combination of escitalopram, 60 mg/d, and quetiapine, 50 mg/d. Quetiapine is over-sedating at subtherapeutic doses and Mr. C’s compulsions worsen. He reports that “[it] took longer and longer to get the ‘just right’ feeling.’” Quetiapine is discontinued and risperidone, 0.5 mg/d, is started, which decreases the frequency of his tics. When he is discharged after a 36-day stay, Mr. C’s Y-BOCS scores are greatly improved at 13 total, 7 on the obsessions subscale, and 3 on the compulsions subscale.
Mr. C’s psychologist refers him to our outpatient clinic for continued psychiatric evaluation and treatment of his OCD, ADHD, and TD. At this time, he is prescribed escitalopram, 60 mg/d, and risperidone, 0.5 mg/d, along with CBT with his psychologist. We do not readminister the Y-BOCS at this time, but Mr. C reports that his OCD is “60% improved.” However, he describes prominent obsessive thoughts regarding his breathing similar to those he experienced before residential treatment. These obsessive thoughts arise in the context of specific environmental “triggers,” such as other people coughing or his own tics. The obsessions lead to compulsive urges to engage in breath-holding rituals. Mr. C experiences the thoughts and compulsions as deeply troubling and they consume 5 to 6 hours each day. Mr. C reports impaired concentration in class and during studying: “I can focus for 5 minutes, then not for 2 minutes, then for 3 minutes… I can never stay focused for more than a couple minutes,” before becoming distracted “by my OCD” or other environmental stimuli. We note on exam prominent breath-holding occurring several times per minute. Mr. C says his OCD has not impaired his ability to socialize.
Mr. C notes that he has been exposed to an array of CBT techniques, but he has difficulty using these techniques because his “mind wanders” or he lacks “motivation.” He admits he occasionally has taken a classmate’s ADHD medication (mixed amphetamine salts [MAS], dose unspecified) and found it improved his ability to focus on his academic work.
The authors’ observations
Researchers have established a relationship among OCD, ADHD, and TD across all combinations of comorbidity (OCD and ADHD,3 ADHD and TD,4 OCD and TD,5,6 and all 3 entities7). Data suggests a poorer prognosis for OCD when comorbid with either or both of these conditions.8 Researchers have raised concerns that psychostimulants could exacerbate or potentiate tic behaviors in patients with ADHD,9,10 although safe and effective use of these medications has been documented in controlled trials of patients with comorbid ADHD and tics.11-13 Furthermore, tic suppression has been reported with psychostimulants,14 as well as a differential effect of stimulants on motor vs vocal tics.15 Despite these data (Table 1),9-15 the FDA regards using psychostimulants in patients with TD as a contraindication,16 although clinicians often recognize that this practice may be unavoidable in some circumstances because of high comorbidity rates. Psychostimulants could exacerbate obsessions or compulsions in some patients because of their dopaminergic properties or through mitigation of the purported anti-obsessional properties of dopamine antagonists.17
Although there is evidence that the prevalence of prescribed psychostimulant abuse is low among ADHD patients,18 diversion of prescribed medication is a risk inherent in the use of these agents, particularly among college-age patients.19,20
Table 1
Evidence of effect of psychostimulants on tics
| Study/disorder(s) | Medication and study design | Relevant findings |
|---|---|---|
| Lipkin et al, 19949; ADHD without TD | Chart review (N = 122) to determine the incidence of tics or dyskinesias in children treated with stimulants | Approximately 9% of children developed tics or dyskinesias, which predominantly were transient, with <1% developing chronic tics or Tourette’s syndrome. Personal or family tic history and medication selection or dosage were not related to onset of tics or dyskinesias |
| Gadow et al, 199515; ADHD with TD | Methylphenidate variable dose, placebo-controlled, 2-week trials (N = 24) | All children’s ADHD symptoms improved. At a 0.1 mg/kg dose, motor tics observed in the classroom increased, but there were fewer vocal tics observed in the lunchroom |
| Castellanos et al, 199710; ADHD with Tourette’s syndrome | Methylphenidate, dextroamphetamine, variable-dose, double-blind, placebo-controlled, 9-week crossover (N = 20) | 3 patients had consistent worsening of tics while taking stimulants. Stimulants reduced hyperactivity rates compared with placebo (P = .03). Stimulants improved ADHD symptoms and had acceptable effects on tics. Methylphenidate was better tolerated than dextroamphetamine |
| Gadow et al, 199911; ADHD with TD | 34 methylphenidate-treated children, followed at 6-month intervals for 2 years | No evidence that frequency or severity of motor or vocal tics changed during maintenance therapy |
| Tourette Syndrome Study Group, 200213; ADHD with TD | Clonidine alone, methylphenidate alone, clonidine plus methylphenidate, or placebo | Worsening of tics was not reported in any group at a rate significantly higher than placebo. Tic severity was more reduced in the 2 clonidine groups than in the methylphenidate group |
| Lyon et al, 201014; ADHD with Tourette’s syndrome | Dexmethylphenidate, single-dose challenge. Ten patients with or without TSP | Acute dexmethylphenidate administration resulted in tic suppression but did not augment TSP |
| Gadow et al, 200712; ADHD with TD | Double-blind, placebo-controlled, 2-week trials each of 3 doses of methylphenidate and placebo (N = 71) | MPH-IR did not alter the overall severity of TD or OCD behaviors. Teacher ratings indicated that MPH-IR therapy decreased tic frequency and severity |
| ADHD: attention-deficit/hyperactivity disorder; MPH-IR: methylphenidate immediate release; OCD: obsessive-compulsive disorder; TD: tic disorder; TSP: tic suppression protocol | ||
TREATMENT: Weighing options
To manage impaired attention and executive function difficulties secondary to ADHD, we offer Mr. C several options, including bupropion, modafinil, and memantine augmentation. Mr. C asks for a psychostimulant because exam week is approaching and he wants a treatment with quick therapeutic effect. We discuss with Mr. C the potential for dopaminergic agents, such as psychostimulants, to exacerbate tics or OCD symptoms. Ultimately, we prescribe immediate-release MAS, 20 mg/d.
Two days later, Mr. C says he has taken 3 MAS doses and describes a marked reduction in obsessions, significant decrease in frequency of “triggers,” and greater capacity to use CBT saying, “when I am [triggered], I am able to move past the urges without doing any compulsions.” Daily time spent “stuck on” obsessions or compulsions decreases from 5 to 6 hours per day to “about 2 and a half minutes.”
Mr. C reports a modest increase in the prevalence of tics, experienced as “little throat clears and quick stuttering of breath.” He notes that, although in the past such tics would be followed by urges for “perfecting the tic and making it feel just right,” he presently “had no desire to do so.”
OUTCOME: Sharper focus
Increasing MAS immediate release from 20 mg/d to 30 mg/d suppresses Mr. C’s obsessions and compulsions for 8 hours. On the 19th day of treatment, MAS immediate release was replaced with an extended release formulation, 30 mg/d, which preserves therapeutic effect and tolerability for 16 weeks. Repeat Y-BOCS yields 9 total, 3 on obsessions subscale, and 6 on compulsions subscale scores.
One month later, Mr. C reports that his symptoms have been “improving ever since” the previous appointment. He continues to be able to access skills for managing his OCD and is doing well in his 2 accelerated summer courses, saying “I focus really well” in 3-hour class sessions. On exam, tic behaviors are nearly absent. Mr. C describes occasional bouts of anxiety associated with urges to engage in tic behaviors, in turn arising from fear of symptomatic recurrence as he worked toward stopping smoking as advised by his primary care physician and psychiatrist.
The authors’ observations
The results of the repeat Y-BOCS are consistent with improvement in obsessions but possible worsening of compulsions since Mr. C was discharged from residential treatment. Alternatively, compulsions may have worsened immediately after discharge and declined again with introduction of MAS.
A substantial body of literature describes the challenges associated with treating ADHD with comorbid tics, including the relative degree of risk of tic exacerbation associated with treating ADHD with psychostimulants. The range of FDA-approved pharmacologic options for treatment of this comorbidity is limited (Table 2),21 particularly given the risk for tardive dyskinesia associated with the typical antipsychotics haloperidol and chlorpromazine. Data support using the α-2 agonist clonidine to treat hyperactivity associated with ADHD22 and TD23 and an extended-release preparation of this medication is FDA-approved for the former but not the latter indication (an α-2A receptor subtype agonist, guanfacine, also is FDA-approved for ADHD in pediatric patients). Mr. C’s experience of robust, sustained reduction in obsessions, if not compulsions, after treatment with MAS is consistent with the few studies of stimulant use in ADHD with comorbid OCD.24,25
Effective treatment of ADHD may help Mr. C better access CBT strategies and thereby potentiate treatment of comorbid OCD.
Table 2
FDA-approved medications for ADHD, OCD, and TD
| Disorder | Medications |
|---|---|
| ADHD | Amphetamine (racemic), atomoxetine, chlorpromazine (hyperactivity), clonidine extended release, dexmethylphenidate, dextroamphetamine, guanfacine extended release, haloperidol (hyperactivity, second-line), lisdexamfetamine, methylphenidate (racemic) |
| OCD | Clomipramine, fluoxetine, fluvoxamine, paroxetine, sertraline |
| TD/Tourette’s syndrome | Haloperidol (Tourette’s), pimozide (Tourette’s) |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder; TD: tic disorder Source: Reference 21 | |
Related Resources
- Pliszka SR. Treating ADHD and comorbid disorders: psychosocial and psychopharmacological interventions. New York, NY: The Guilford Press; 2011.
- Pollak Y, Benarroch F, Kanengisser L, et al. Tourette syndrome-associated psychopathology: roles of comorbid attention-deficit hyperactivity disorder and obsessive-compulsive disorder. J Dev Behav Pediatr. 2009;30(5):413-419.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Clonidine extended release • Kapvay
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guanfacine • Intuniv, Tenex
- Haloperidol • Haldol
- Lisdexamfetamine • Vyvanse
- Memantine • Namenda
- Methylphenidate • Methylin, Ritalin
- Modafinil • Provigil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use and reliability. Arch Gen Psych. 1989;46(11):1006-1011.
2. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: II. Validity. Arch Gen Psych. 1989;46(11):1012-1016.
3. Geller DA, Biederman J, Faraone S, et al. Re-examining comorbidity of obsessive compulsive and attention-deficit hyperactivity disorder using an empirically derived taxonomy. Eur Child Adolesc Psychiatry. 2004;13(2):83-91.
4. Freeman RD. Attention deficit hyperactivity disorder in the presence of Tourette syndrome. Neurol Clin. 1997;15(2):411-420.
5. Geller DA. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr Clin North Am. 2006;29(2):353-370.
6. Eapen V, Fox-Hiley P, Banerjee S, et al. Clinical features and associated psychopathology in a Tourette syndrome cohort. Acta Neurol Scand. 2004;109(4):255-260.
7. Kano Y, Ohta M, Nagai Y, et al. Association between Tourette syndrome and comorbidities in Japan. Brain Dev. 2010;32(3):201-207.
8. Grados M, Riddle M. Do all obsessive-compulsive disorder subtypes respond to medication? Int Rev Psychiatry. 2008;20(2):189-193.
9. Lipkin PH, Goldstein IH, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 1994;148(8):859-861.
10. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry. 1997;36(5):589-596.
11. Gadow K, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry. 1999;56(4):330-333.
12. Gadow KD, Sverd J, Nolan EE, et al. Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):840-848.
13. Tourette’s Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology. 2002;58(4):527-536.
14. Lyon GJ, Samar SM, Conelea C, et al. Testing tic suppression: comparing the effects of dexmethylphenidate to no mediation in children and adolescents with attention-deficit/hyperactivity disorder and Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):283-289.
15. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry. 1995;52(6):444-455.
16. Bloch MH, Panza KE, Landerso-Weisenberger A, et al. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry. 2009;48(9):884-893.
17. McDougle CJ, Goodman WK, Price LH. Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry. 1994;55(suppl):24-31.
18. Wilens TE, Morrison NR. The intersection of attention-deficit/hyperactivity disorder and substance abuse. Curr Opin Psychiatry. 2011;24(4):280-285.
19. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
20. Schubiner H. Substance abuse in patients with attention-deficit hyperactivity disorder: therapeutic implications. CNS Drugs. 2005;19(8):643-655.
21. Stahl SM. The prescriber’s guide. Stahl’s essential psychopharmacology. 3rd ed. New York NY: Cambridge University Press; 2009.
22. Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(2):171-179.
23. Hedderick EF, Morris CM, Singer HS. Double-blind crossover study of clonidine and levetiracetam in Tourette syndrome. Pediatr Neurol. 2009;40(6):420-425.
24. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11(4):237-241.
25. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80(3):231-235.
1. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use and reliability. Arch Gen Psych. 1989;46(11):1006-1011.
2. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: II. Validity. Arch Gen Psych. 1989;46(11):1012-1016.
3. Geller DA, Biederman J, Faraone S, et al. Re-examining comorbidity of obsessive compulsive and attention-deficit hyperactivity disorder using an empirically derived taxonomy. Eur Child Adolesc Psychiatry. 2004;13(2):83-91.
4. Freeman RD. Attention deficit hyperactivity disorder in the presence of Tourette syndrome. Neurol Clin. 1997;15(2):411-420.
5. Geller DA. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr Clin North Am. 2006;29(2):353-370.
6. Eapen V, Fox-Hiley P, Banerjee S, et al. Clinical features and associated psychopathology in a Tourette syndrome cohort. Acta Neurol Scand. 2004;109(4):255-260.
7. Kano Y, Ohta M, Nagai Y, et al. Association between Tourette syndrome and comorbidities in Japan. Brain Dev. 2010;32(3):201-207.
8. Grados M, Riddle M. Do all obsessive-compulsive disorder subtypes respond to medication? Int Rev Psychiatry. 2008;20(2):189-193.
9. Lipkin PH, Goldstein IH, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 1994;148(8):859-861.
10. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry. 1997;36(5):589-596.
11. Gadow K, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry. 1999;56(4):330-333.
12. Gadow KD, Sverd J, Nolan EE, et al. Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):840-848.
13. Tourette’s Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology. 2002;58(4):527-536.
14. Lyon GJ, Samar SM, Conelea C, et al. Testing tic suppression: comparing the effects of dexmethylphenidate to no mediation in children and adolescents with attention-deficit/hyperactivity disorder and Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):283-289.
15. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry. 1995;52(6):444-455.
16. Bloch MH, Panza KE, Landerso-Weisenberger A, et al. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry. 2009;48(9):884-893.
17. McDougle CJ, Goodman WK, Price LH. Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry. 1994;55(suppl):24-31.
18. Wilens TE, Morrison NR. The intersection of attention-deficit/hyperactivity disorder and substance abuse. Curr Opin Psychiatry. 2011;24(4):280-285.
19. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
20. Schubiner H. Substance abuse in patients with attention-deficit hyperactivity disorder: therapeutic implications. CNS Drugs. 2005;19(8):643-655.
21. Stahl SM. The prescriber’s guide. Stahl’s essential psychopharmacology. 3rd ed. New York NY: Cambridge University Press; 2009.
22. Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(2):171-179.
23. Hedderick EF, Morris CM, Singer HS. Double-blind crossover study of clonidine and levetiracetam in Tourette syndrome. Pediatr Neurol. 2009;40(6):420-425.
24. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11(4):237-241.
25. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80(3):231-235.
P-glycoprotein: Why this drug transporter may be clinically important
Discuss this article at www.facebook.com/CurrentPsychiatry
• Venlafaxine has been shown to decrease indinavir concentrations in cellular models and healthy individuals in a controlled trial.
• It is not known if this effect would occur with other protease inhibitors; however, most protease inhibitors are P-glycoprotein substrates.
• In preliminary cellular models, desvenlafaxine did not have the same effect.
• It is not known if other psychotropics have the same effect on P-glycoprotein or other efflux proteins.
Mr. B, age 32, was diagnosed with human immunodeficiency virus (HIV) approximately 10 years ago. His current HIV regimen is highly active antiretroviral therapy, which includes the protease inhibitor (PI) indinavir and the combination product lamivudine and zidovudine, 2 nucleoside reverse transcriptase inhibitors. He shows no symptoms and his viral load has been undetectable for 9 years.
Several months ago, Mr. B reported to his primary care physician feelings of depressed mood, anhedonia, significant weight loss, fatigue, and feelings of worthlessness. He was diagnosed with major depressive disorder and started venlafaxine, 150 mg/d. The depressive episode is now in remission and the only major side effect he experiences is lethargy. His physician decides to check Mr. B’s viral load, which is 1,100 copies/mL. This viral load value indicates a significant elevation from the baseline (<48 copies/mL), which although still low, is considered virologic failure.1 To rule out a lab error the viral load test is replicated, but the result is the same.
Mr. B’s case may represent an interaction between his antidepressant and one of his antiviral drugs that is a P-glycoprotein substrate. This protein transports a variety of drug substrates across cell membranes and affects the distribution and elimination of many prescription and nonprescription medications. Whether a drug induces or inhibits P-glycoprotein can affect plasma and cellular concentrations of drugs and can lead to unexpected increases or decreases in plasma concentrations of the affected drug. Understanding P-glycoprotein’s role can help you choose effective psychotropics for patients such as Mr. B.
Change in drug effect
Because depression is common among patients with HIV, my colleagues and I evaluated the pharmacokinetic effects of indinavir on venlafaxine and venlafaxine on indinavir to determine if venlafaxine would be safe to use in a patient taking a PI because of potential cytochrome P450 (CYP450) drug interactions in both classes of medications.2 Adding venlafaxine resulted in a 36% decrease in maximum concentrations for indinavir and a 28% decrease in area under the curve Figure.2 Study participants were healthy individuals; however, we concluded that had we studied patients with HIV, indinavir efficacy could decrease, resulting in an increased viral load. After this study, the manufacturer of venlafaxine included a caution about this combination in the product labeling.3 Because the extended-release formulation includes the same compound, the same effect could be expected and was included in the most recent version of the extended-release venlafaxine prescribing information.4
What is interesting about the venlafaxine-indinavir interaction is that there was no change in either agent’s half-life and therefore no reason to assume this effect was a traditional CYP450 drug interaction. The investigators considered other types of drug interactions and focused on mechanisms that could be presystemic, ie, affecting the absorption and bioavailability of indinavir. This led investigators to believe that the mechanism involved a drug transport protein such as P-glycoprotein, which is present in gut lumen. Subsequent studies have shown in a cellular model that venlafaxine—but not desvenlafaxine—is an inducer of P-glycoprotein and breast cancer resistant protein (BCRP).5,6 Researchers are conducting animal studies to attempt to duplicate the cellular models. However, it could be presumed that the study of venlafaxine and indinavir in healthy individuals already had demonstrated this effect.2
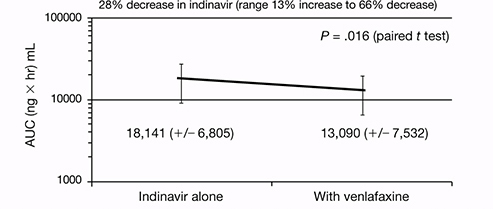
Figure: Indinavir area under the curve before and after steady state venlafaxine
Decrease in area under the curve (AUC) for indinavir when healthy individuals achieved steady state dosing of venlafaxine
Source: Reference 2
Cause and effect
P-glycoprotein transports drugs or other foreign compounds out of the cells (efflux) of the target tissue so they can be further metabolized by metabolic enzymes for elimination. These proteins are called efflux proteins. There are many efflux proteins in addition to P-glycoprotein; a common one is BCRP, which confers resistance to some anticancer drugs. In addition to the gut lumen and breast tissue, efflux proteins are present in most tissues throughout the body, including the blood-brain barrier.
If drug A inhibits an efflux protein, then drug B would be able to enter the target tissue with greater ease and not be “kicked out” because the efflux system would be disabled. This could result in higher-than-expected tissue concentrations of drug B. Pharmaceutical companies often perform P-glycoprotein inhibition studies before a drug is marketed and include this data in the prescribing information.
If, on the other hand, drug A induces an efflux protein, then drug B would be “kicked out” at a greater rate than normal because the efflux system would be working in overdrive. In this case, tissue concentrations of drug B would be lower than expected and could lead to therapeutic failure. Typically, pharmaceutical companies either do not conduct these induction studies, or if they are performed, they often are not described in prescribing information. This lack of efficacy has been well documented with chemotherapeutic failure caused by drug efflux by BCRP.7 It is likely that Mr. B’s viral load increased when venlafaxine was added to his regimen—the antidepressant induced P-glycoprotein, which reduced indinavir concentrations and subsequent therapeutic effect.
Clinicians should review specific medications they are considering using if the drugs have a narrow therapeutic index or if therapeutic failure from subtherapeutic or supratherapeutic doses would be considered problematic Table.8 Kim9 provides a comprehensive list of P-glycoprotein substrates, inhibitors, and inducers. However, keep in mind that the list of substrates, inhibitors, and inducers changes regularly as new research becomes available.
Table
Selected psychotropics that affect P-glycoprotein
| Substrates | |
| Amitriptyline | Paroxetine |
| Carbamazepine | Quetiapine |
| Chlorpromazine | Risperidone |
| Citalopram | Sertraline |
| Doxepin | Topiramate |
| Nortriptyline | Venlafaxine |
| Olanzapine | |
| Inhibitors | |
| Amitriptyline | Imipramine |
| Carbamazepine | Nefazodone |
| Chlorpromazine | Paroxetine |
| Desipramine | Sertraline |
| Disulfiram | Thioridazine |
| Fluoxetine | Trifluoperazine |
| Fluvoxamine | Trimipramine |
| Haloperidol | |
| Inducersa | |
| Amitriptyline | Phenothiazines |
| Nefazodone | Trazodone |
| aData supporting induction is limited Source: Reference 8 | |
- Linnet K, Ejsing TB. A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol. 2008;18(3):157-169.
- Weiss J, Dormann SM, Martin-Facklam M, et al. Inhibition of P-glycoprotein by newer antidepressants. J Pharmacol Exp Ther. 2003;305(1):197-204.
Drug Brand Names
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Desipramine • Norpramin
- Desvenlafaxine • Pristiq
- Disulfiram • Antabuse
- Doxepin • Adapin, Silenor
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Indinavir • Crixivan
- Lamivudine and zidovudine • Combivir
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Melleril
- Topiramate • Topamax
- Trazodone • Desyrel, Oleptro
- Trifluoperazine • Stelazine
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Disclosure
Dr. Levin receives grant/research support from Pfizer.
1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington DC: Department of Health and Human Services; January 10, 2011;1-166.
2. Levin GM, Nelson LA, DeVane CL, et al. A pharmacokinetic drug-drug interaction study of venlafaxine and indinavir. Psychopharmacol Bull. 2001;35(2):62-71.
3. Effexor [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2010.
4. Effexor XR [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2011.
5. Ehret MJ, Levin GM, Narasimhan M, et al. Venlafaxine induces P-glycoprotein in human Caco-2 cells. Hum Psychopharmacol. 2007;22(1):49-53.
6. Bachmeier CJ, Beaulieu-Abdelahad D, Ganey NJ, et al. Induction of drug efflux protein expression by venlafaxine but not desvenlafaxine. Biopharm Drug Dispos. 2011;32(4):233-244.
7. Rosenberg MF, Bikadi Z, Chan J, et al. The human breast cancer resistance protein (BCRP/ABCG2) shows conformational changes with mitoxantrone. Structure. 2010;18(4):482-493.
8. Oesterheld J. P-glycoprotein (PGP) table - the effect of drugs and foods. http://www.genemedrx.com/PGPtable.php. Accessed February 3 2012.
9. Kim RB. Drugs as P-glycoprotein substrates inhibitors, and inducers. Drug Metab Rev. 2002;34(1-2):47-54.
Gary M. Levin, PharmD, BCPP, FCCP
Dr. Levin is Associate Dean for Clinical Programs and Professor of Pharmacy Practice, College of Pharmacy, Roseman University of Health Sciences, Henderson, NV.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Gary M. Levin, PharmD, BCPP, FCCP
Dr. Levin is Associate Dean for Clinical Programs and Professor of Pharmacy Practice, College of Pharmacy, Roseman University of Health Sciences, Henderson, NV.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Gary M. Levin, PharmD, BCPP, FCCP
Dr. Levin is Associate Dean for Clinical Programs and Professor of Pharmacy Practice, College of Pharmacy, Roseman University of Health Sciences, Henderson, NV.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Discuss this article at www.facebook.com/CurrentPsychiatry
• Venlafaxine has been shown to decrease indinavir concentrations in cellular models and healthy individuals in a controlled trial.
• It is not known if this effect would occur with other protease inhibitors; however, most protease inhibitors are P-glycoprotein substrates.
• In preliminary cellular models, desvenlafaxine did not have the same effect.
• It is not known if other psychotropics have the same effect on P-glycoprotein or other efflux proteins.
Mr. B, age 32, was diagnosed with human immunodeficiency virus (HIV) approximately 10 years ago. His current HIV regimen is highly active antiretroviral therapy, which includes the protease inhibitor (PI) indinavir and the combination product lamivudine and zidovudine, 2 nucleoside reverse transcriptase inhibitors. He shows no symptoms and his viral load has been undetectable for 9 years.
Several months ago, Mr. B reported to his primary care physician feelings of depressed mood, anhedonia, significant weight loss, fatigue, and feelings of worthlessness. He was diagnosed with major depressive disorder and started venlafaxine, 150 mg/d. The depressive episode is now in remission and the only major side effect he experiences is lethargy. His physician decides to check Mr. B’s viral load, which is 1,100 copies/mL. This viral load value indicates a significant elevation from the baseline (<48 copies/mL), which although still low, is considered virologic failure.1 To rule out a lab error the viral load test is replicated, but the result is the same.
Mr. B’s case may represent an interaction between his antidepressant and one of his antiviral drugs that is a P-glycoprotein substrate. This protein transports a variety of drug substrates across cell membranes and affects the distribution and elimination of many prescription and nonprescription medications. Whether a drug induces or inhibits P-glycoprotein can affect plasma and cellular concentrations of drugs and can lead to unexpected increases or decreases in plasma concentrations of the affected drug. Understanding P-glycoprotein’s role can help you choose effective psychotropics for patients such as Mr. B.
Change in drug effect
Because depression is common among patients with HIV, my colleagues and I evaluated the pharmacokinetic effects of indinavir on venlafaxine and venlafaxine on indinavir to determine if venlafaxine would be safe to use in a patient taking a PI because of potential cytochrome P450 (CYP450) drug interactions in both classes of medications.2 Adding venlafaxine resulted in a 36% decrease in maximum concentrations for indinavir and a 28% decrease in area under the curve Figure.2 Study participants were healthy individuals; however, we concluded that had we studied patients with HIV, indinavir efficacy could decrease, resulting in an increased viral load. After this study, the manufacturer of venlafaxine included a caution about this combination in the product labeling.3 Because the extended-release formulation includes the same compound, the same effect could be expected and was included in the most recent version of the extended-release venlafaxine prescribing information.4
What is interesting about the venlafaxine-indinavir interaction is that there was no change in either agent’s half-life and therefore no reason to assume this effect was a traditional CYP450 drug interaction. The investigators considered other types of drug interactions and focused on mechanisms that could be presystemic, ie, affecting the absorption and bioavailability of indinavir. This led investigators to believe that the mechanism involved a drug transport protein such as P-glycoprotein, which is present in gut lumen. Subsequent studies have shown in a cellular model that venlafaxine—but not desvenlafaxine—is an inducer of P-glycoprotein and breast cancer resistant protein (BCRP).5,6 Researchers are conducting animal studies to attempt to duplicate the cellular models. However, it could be presumed that the study of venlafaxine and indinavir in healthy individuals already had demonstrated this effect.2
Figure: Indinavir area under the curve before and after steady state venlafaxine
Decrease in area under the curve (AUC) for indinavir when healthy individuals achieved steady state dosing of venlafaxine
Source: Reference 2
Cause and effect
P-glycoprotein transports drugs or other foreign compounds out of the cells (efflux) of the target tissue so they can be further metabolized by metabolic enzymes for elimination. These proteins are called efflux proteins. There are many efflux proteins in addition to P-glycoprotein; a common one is BCRP, which confers resistance to some anticancer drugs. In addition to the gut lumen and breast tissue, efflux proteins are present in most tissues throughout the body, including the blood-brain barrier.
If drug A inhibits an efflux protein, then drug B would be able to enter the target tissue with greater ease and not be “kicked out” because the efflux system would be disabled. This could result in higher-than-expected tissue concentrations of drug B. Pharmaceutical companies often perform P-glycoprotein inhibition studies before a drug is marketed and include this data in the prescribing information.
If, on the other hand, drug A induces an efflux protein, then drug B would be “kicked out” at a greater rate than normal because the efflux system would be working in overdrive. In this case, tissue concentrations of drug B would be lower than expected and could lead to therapeutic failure. Typically, pharmaceutical companies either do not conduct these induction studies, or if they are performed, they often are not described in prescribing information. This lack of efficacy has been well documented with chemotherapeutic failure caused by drug efflux by BCRP.7 It is likely that Mr. B’s viral load increased when venlafaxine was added to his regimen—the antidepressant induced P-glycoprotein, which reduced indinavir concentrations and subsequent therapeutic effect.
Clinicians should review specific medications they are considering using if the drugs have a narrow therapeutic index or if therapeutic failure from subtherapeutic or supratherapeutic doses would be considered problematic Table.8 Kim9 provides a comprehensive list of P-glycoprotein substrates, inhibitors, and inducers. However, keep in mind that the list of substrates, inhibitors, and inducers changes regularly as new research becomes available.
Table
Selected psychotropics that affect P-glycoprotein
| Substrates | |
| Amitriptyline | Paroxetine |
| Carbamazepine | Quetiapine |
| Chlorpromazine | Risperidone |
| Citalopram | Sertraline |
| Doxepin | Topiramate |
| Nortriptyline | Venlafaxine |
| Olanzapine | |
| Inhibitors | |
| Amitriptyline | Imipramine |
| Carbamazepine | Nefazodone |
| Chlorpromazine | Paroxetine |
| Desipramine | Sertraline |
| Disulfiram | Thioridazine |
| Fluoxetine | Trifluoperazine |
| Fluvoxamine | Trimipramine |
| Haloperidol | |
| Inducersa | |
| Amitriptyline | Phenothiazines |
| Nefazodone | Trazodone |
| aData supporting induction is limited Source: Reference 8 | |
- Linnet K, Ejsing TB. A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol. 2008;18(3):157-169.
- Weiss J, Dormann SM, Martin-Facklam M, et al. Inhibition of P-glycoprotein by newer antidepressants. J Pharmacol Exp Ther. 2003;305(1):197-204.
Drug Brand Names
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Desipramine • Norpramin
- Desvenlafaxine • Pristiq
- Disulfiram • Antabuse
- Doxepin • Adapin, Silenor
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Indinavir • Crixivan
- Lamivudine and zidovudine • Combivir
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Melleril
- Topiramate • Topamax
- Trazodone • Desyrel, Oleptro
- Trifluoperazine • Stelazine
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Disclosure
Dr. Levin receives grant/research support from Pfizer.
Discuss this article at www.facebook.com/CurrentPsychiatry
• Venlafaxine has been shown to decrease indinavir concentrations in cellular models and healthy individuals in a controlled trial.
• It is not known if this effect would occur with other protease inhibitors; however, most protease inhibitors are P-glycoprotein substrates.
• In preliminary cellular models, desvenlafaxine did not have the same effect.
• It is not known if other psychotropics have the same effect on P-glycoprotein or other efflux proteins.
Mr. B, age 32, was diagnosed with human immunodeficiency virus (HIV) approximately 10 years ago. His current HIV regimen is highly active antiretroviral therapy, which includes the protease inhibitor (PI) indinavir and the combination product lamivudine and zidovudine, 2 nucleoside reverse transcriptase inhibitors. He shows no symptoms and his viral load has been undetectable for 9 years.
Several months ago, Mr. B reported to his primary care physician feelings of depressed mood, anhedonia, significant weight loss, fatigue, and feelings of worthlessness. He was diagnosed with major depressive disorder and started venlafaxine, 150 mg/d. The depressive episode is now in remission and the only major side effect he experiences is lethargy. His physician decides to check Mr. B’s viral load, which is 1,100 copies/mL. This viral load value indicates a significant elevation from the baseline (<48 copies/mL), which although still low, is considered virologic failure.1 To rule out a lab error the viral load test is replicated, but the result is the same.
Mr. B’s case may represent an interaction between his antidepressant and one of his antiviral drugs that is a P-glycoprotein substrate. This protein transports a variety of drug substrates across cell membranes and affects the distribution and elimination of many prescription and nonprescription medications. Whether a drug induces or inhibits P-glycoprotein can affect plasma and cellular concentrations of drugs and can lead to unexpected increases or decreases in plasma concentrations of the affected drug. Understanding P-glycoprotein’s role can help you choose effective psychotropics for patients such as Mr. B.
Change in drug effect
Because depression is common among patients with HIV, my colleagues and I evaluated the pharmacokinetic effects of indinavir on venlafaxine and venlafaxine on indinavir to determine if venlafaxine would be safe to use in a patient taking a PI because of potential cytochrome P450 (CYP450) drug interactions in both classes of medications.2 Adding venlafaxine resulted in a 36% decrease in maximum concentrations for indinavir and a 28% decrease in area under the curve Figure.2 Study participants were healthy individuals; however, we concluded that had we studied patients with HIV, indinavir efficacy could decrease, resulting in an increased viral load. After this study, the manufacturer of venlafaxine included a caution about this combination in the product labeling.3 Because the extended-release formulation includes the same compound, the same effect could be expected and was included in the most recent version of the extended-release venlafaxine prescribing information.4
What is interesting about the venlafaxine-indinavir interaction is that there was no change in either agent’s half-life and therefore no reason to assume this effect was a traditional CYP450 drug interaction. The investigators considered other types of drug interactions and focused on mechanisms that could be presystemic, ie, affecting the absorption and bioavailability of indinavir. This led investigators to believe that the mechanism involved a drug transport protein such as P-glycoprotein, which is present in gut lumen. Subsequent studies have shown in a cellular model that venlafaxine—but not desvenlafaxine—is an inducer of P-glycoprotein and breast cancer resistant protein (BCRP).5,6 Researchers are conducting animal studies to attempt to duplicate the cellular models. However, it could be presumed that the study of venlafaxine and indinavir in healthy individuals already had demonstrated this effect.2
Figure: Indinavir area under the curve before and after steady state venlafaxine
Decrease in area under the curve (AUC) for indinavir when healthy individuals achieved steady state dosing of venlafaxine
Source: Reference 2
Cause and effect
P-glycoprotein transports drugs or other foreign compounds out of the cells (efflux) of the target tissue so they can be further metabolized by metabolic enzymes for elimination. These proteins are called efflux proteins. There are many efflux proteins in addition to P-glycoprotein; a common one is BCRP, which confers resistance to some anticancer drugs. In addition to the gut lumen and breast tissue, efflux proteins are present in most tissues throughout the body, including the blood-brain barrier.
If drug A inhibits an efflux protein, then drug B would be able to enter the target tissue with greater ease and not be “kicked out” because the efflux system would be disabled. This could result in higher-than-expected tissue concentrations of drug B. Pharmaceutical companies often perform P-glycoprotein inhibition studies before a drug is marketed and include this data in the prescribing information.
If, on the other hand, drug A induces an efflux protein, then drug B would be “kicked out” at a greater rate than normal because the efflux system would be working in overdrive. In this case, tissue concentrations of drug B would be lower than expected and could lead to therapeutic failure. Typically, pharmaceutical companies either do not conduct these induction studies, or if they are performed, they often are not described in prescribing information. This lack of efficacy has been well documented with chemotherapeutic failure caused by drug efflux by BCRP.7 It is likely that Mr. B’s viral load increased when venlafaxine was added to his regimen—the antidepressant induced P-glycoprotein, which reduced indinavir concentrations and subsequent therapeutic effect.
Clinicians should review specific medications they are considering using if the drugs have a narrow therapeutic index or if therapeutic failure from subtherapeutic or supratherapeutic doses would be considered problematic Table.8 Kim9 provides a comprehensive list of P-glycoprotein substrates, inhibitors, and inducers. However, keep in mind that the list of substrates, inhibitors, and inducers changes regularly as new research becomes available.
Table
Selected psychotropics that affect P-glycoprotein
| Substrates | |
| Amitriptyline | Paroxetine |
| Carbamazepine | Quetiapine |
| Chlorpromazine | Risperidone |
| Citalopram | Sertraline |
| Doxepin | Topiramate |
| Nortriptyline | Venlafaxine |
| Olanzapine | |
| Inhibitors | |
| Amitriptyline | Imipramine |
| Carbamazepine | Nefazodone |
| Chlorpromazine | Paroxetine |
| Desipramine | Sertraline |
| Disulfiram | Thioridazine |
| Fluoxetine | Trifluoperazine |
| Fluvoxamine | Trimipramine |
| Haloperidol | |
| Inducersa | |
| Amitriptyline | Phenothiazines |
| Nefazodone | Trazodone |
| aData supporting induction is limited Source: Reference 8 | |
- Linnet K, Ejsing TB. A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol. 2008;18(3):157-169.
- Weiss J, Dormann SM, Martin-Facklam M, et al. Inhibition of P-glycoprotein by newer antidepressants. J Pharmacol Exp Ther. 2003;305(1):197-204.
Drug Brand Names
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Desipramine • Norpramin
- Desvenlafaxine • Pristiq
- Disulfiram • Antabuse
- Doxepin • Adapin, Silenor
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Indinavir • Crixivan
- Lamivudine and zidovudine • Combivir
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Melleril
- Topiramate • Topamax
- Trazodone • Desyrel, Oleptro
- Trifluoperazine • Stelazine
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Disclosure
Dr. Levin receives grant/research support from Pfizer.
1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington DC: Department of Health and Human Services; January 10, 2011;1-166.
2. Levin GM, Nelson LA, DeVane CL, et al. A pharmacokinetic drug-drug interaction study of venlafaxine and indinavir. Psychopharmacol Bull. 2001;35(2):62-71.
3. Effexor [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2010.
4. Effexor XR [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2011.
5. Ehret MJ, Levin GM, Narasimhan M, et al. Venlafaxine induces P-glycoprotein in human Caco-2 cells. Hum Psychopharmacol. 2007;22(1):49-53.
6. Bachmeier CJ, Beaulieu-Abdelahad D, Ganey NJ, et al. Induction of drug efflux protein expression by venlafaxine but not desvenlafaxine. Biopharm Drug Dispos. 2011;32(4):233-244.
7. Rosenberg MF, Bikadi Z, Chan J, et al. The human breast cancer resistance protein (BCRP/ABCG2) shows conformational changes with mitoxantrone. Structure. 2010;18(4):482-493.
8. Oesterheld J. P-glycoprotein (PGP) table - the effect of drugs and foods. http://www.genemedrx.com/PGPtable.php. Accessed February 3 2012.
9. Kim RB. Drugs as P-glycoprotein substrates inhibitors, and inducers. Drug Metab Rev. 2002;34(1-2):47-54.
1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington DC: Department of Health and Human Services; January 10, 2011;1-166.
2. Levin GM, Nelson LA, DeVane CL, et al. A pharmacokinetic drug-drug interaction study of venlafaxine and indinavir. Psychopharmacol Bull. 2001;35(2):62-71.
3. Effexor [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2010.
4. Effexor XR [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2011.
5. Ehret MJ, Levin GM, Narasimhan M, et al. Venlafaxine induces P-glycoprotein in human Caco-2 cells. Hum Psychopharmacol. 2007;22(1):49-53.
6. Bachmeier CJ, Beaulieu-Abdelahad D, Ganey NJ, et al. Induction of drug efflux protein expression by venlafaxine but not desvenlafaxine. Biopharm Drug Dispos. 2011;32(4):233-244.
7. Rosenberg MF, Bikadi Z, Chan J, et al. The human breast cancer resistance protein (BCRP/ABCG2) shows conformational changes with mitoxantrone. Structure. 2010;18(4):482-493.
8. Oesterheld J. P-glycoprotein (PGP) table - the effect of drugs and foods. http://www.genemedrx.com/PGPtable.php. Accessed February 3 2012.
9. Kim RB. Drugs as P-glycoprotein substrates inhibitors, and inducers. Drug Metab Rev. 2002;34(1-2):47-54.
A paranoid, violent teenager
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Sleepless and paranoid
Ms. V, age 16, is referred to our psychiatric hospital from a juvenile detention center after she is charged with killing her sister with a hammer. She reports paranoid delusions, including believing that her sister was poisoning her food. Ms. V’s troubling behavior increased in the 6 months before the murder. She began to ask her mother to smell her food for possible poison. Her school grades dropped and she experienced decreased sleep and appetite. According to her mother, Ms. V’s insomnia worsened recently because of her paranoid thinking, which was evident when she noticed that her daughter slept with a hammer. Ms. V stopped socializing with her peers and no longer went to the gym.
Ms. V’s mother describes her daughter’s negative symptoms as consisting of social isolation and a flat affect. There was no evidence of auditory or visual hallucinations. After noticing the change in her daughter’s behavior, Ms. V’s mother attempted to schedule an appointment with a mental health professional, but there was a 2-month waiting list.
Ms. V cleaned her room before the murder, which was uncharacteristic of her routine behavior. On the day of the murder, Ms. V approached her sister while she was sleeping on the sofa and struck her on the head several times with a hammer. After the sister died, neighbors spotted Ms. V washing blood off her hands in their backyard with a sprinkler. Soaked in blood, she approached one of the neighbors and said that someone had been killed in the house. The neighbors called the police and Ms. V was arrested. She did not express remorse. She did not exhibit physical aggression toward others before the murder. Ms. V’s sense of entitlement and grandiosity persisted after the murder.
The authors’ observations
Paranoid delusions are fixed false beliefs with severe fears of others that may impair functioning at school or work, in personal relationships, and in other social dimensions. Paranoid thinking can have diverse presentations, ranging from social concerns such as fear of rejection to severe threat perceptions of people trying to cause substantial physical harm.1 Paranoid thoughts can be a result of misinterpretation of language, a personality disorder, anxiety, or psychosis.
Feelings of low self-esteem2 and anger1 may develop in a patient experiencing paranoid ideations. When anger begins to escalate, it may erupt into violent behavior. In Ms. V’s case, her paranoid ideations increased until she killed her younger sister. Ms. V’s case is similar to a mass shooting near Tucson, AZ on January 8, 2011 in that it possibly could have been prevented with earlier psychiatric intervention (Box).3-6
On January 8, 2011, a mass shooting occurred near Tucson, AZ that killed 6 and wounded 13. The suspect, 22-year-old Jared Lee Loughner, refused to cooperate with authorities by invoking his right to remain silent.3 Although the motives behind this crime remain undisclosed, mental illness appears to be a contributing factor.
Reports indicate that Mr. Loughner was abusing drugs and those close to him had noticed personality changes.4,5 The college he was attending advised Mr. Loughner to undergo a mental health evaluation, but he refused and dropped out of school.4,5 While in custody after the shooting, Mr. Loughner was diagnosed with paranoid schizophrenia, deemed incompetent to stand trial, and ordered to receive psychiatric treatment.6
This tragic mass shooting and similar incidents have led to questions regarding the adequacy of the mental health care infrastructure in United States. Experts suggest that this tragedy could have been prevented with more aggressive psychiatric prevention and intervention. Critical analysis of similar recent cases and expert opinions are needed to address this problem effectively.
EVALUATION: Remorseless
At admission, Ms. V’s affect is restricted and, at times, inappropriate. She is guarded about discussing the homicide but describes paranoid thoughts about her sister poisoning her. She is eager to learn if the police had found poison in her food. Her speech is soft with good articulation. Based on her presentation, her intelligence is average. She shows no evidence of remorse and is preoccupied with her sister poisoning her.
The Rorschach Inkblot Technique reveals positive evidence for a severe thought disorder. Ms. V’s thinking seems regressed. Ms. V’s medical workup, including MRI, electroencephalogram, and laboratory tests, are all within normal limits.
In the 5th grade, Ms. V’s primary care provider prescribed amphetamine and dextroamphetamine for attention-deficit/hyperactivity disorder, but she discontinued the drug after 1 year. Ms. V has never been hospitalized for psychiatric illness. She had no chronic medical conditions and no developmental delays.
Ms. V also has a history of periodic temper problems characterized by verbal aggression such as threatening the assistant principal at her school, and throwing her cellphone at her mother a few weeks before the murder, but no other aggressive episodes. Ms. V’s history does not suggest conduct disorder. She has no history of suicidal ideation or suicide attempts. Ms. V has used alcohol since age 15, but her mother reports that she was not a heavy or frequent user. Her last reported alcohol use was 10 days before the murder. A maternal uncle had been diagnosed with schizophrenia.
Before the murder, Ms. V lived with her sister and mother. Her parents were divorced. At age 9, Ms. V was sexually abused by a soccer coach; however, she denied symptoms of posttraumatic stress disorder related to the sexual abuse. She had no criminal history before the murder.
The authors’ observations
Based on Ms. V’s presentation and history, schizophrenia, paranoid type seems to be the most likely diagnosis because of her negative symptoms, including affective flattening, positive family history for schizophrenia, and paranoid delusions leading to dysfunction (Table).7 Delusional disorder seems less likely because Ms. V is young and has negative symptoms. Because she is generally healthy and her medical workup is negative, psychotic disorder due to a general medical condition is ruled out. She does not appear to be over-reporting, malingering, or exaggerating symptoms. In the context of psychosis, adolescent psychopathy does not seem likely even though there is evidence of grandiosity and a lack of remorse.
Table
DSM-IV-TR criteria for schizophrenia
A. Characteristic symptoms: ≥2 of the following, each present for a significant portion of time during a 1-month period:
|
| B. Social/occupational dysfunction: For a significant portion of the time since the onset of the disturbance, ≥1 major areas of functioning such as work, interpersonal relations, or self-care are markedly below the level achieved prior to the onset |
| C. Duration: Continuous signs of the disturbance persist for at least 6 months. This 6-month period must include at least 1 month of symptoms that meet Criterion A and may include periods of prodromal or residual symptoms |
| D. Schizoaffective and mood disorder exclusion: Schizoaffective disorder and mood disorder with psychotic features have been ruled out because either (1) no major depressive, manic, or mixed episodes have occurred concurrently with the active-phase symptoms; or (2) if mood episodes have occurred during active-phase symptoms, their total duration has been brief relative to the duration of the active and residual periods |
| E. Substance/general medical condition exclusion: The disturbance is not due to the direct physiological effects of a substance or a general medical condition |
| F. Relationship to a pervasive developmental disorder: If there is a history of autistic disorder or another pervasive developmental disorder, the additional diagnosis of schizophrenia is made only if prominent delusions or hallucinations are also present for at least 1 month |
| Diagnostic criteria for paranoid type: A type of schizophrenia in which the following criteria are met: A. Preoccupation with ≥1 delusions or frequent auditory hallucinations B. None of the following are prominent: disorganized speech, disorganized or catatonic behavior, or flat or inappropriate affect |
| Source: Reference 7 |
The authors’ observations
Various treatments can be used for paranoia with aggression, but the severity of the paranoia should be assessed before initiating treatment. Although categorizing paranoid ideations as mild, moderate, and severe is mainly a clinical judgment, Freeman et al1 have attempted to design a paranoia hierarchy from social concerns to severe threats. CBT8 and antipsychotic medication may help reduce mild to moderate paranoid delusions, particularly those associated with schizophrenia or mood disorders. For severe paranoia, hospitalization should carefully be considered.
When a patient exhibits moderate paranoia, the probability of progressing to severe symptoms or improving to mild symptoms depends on several variables. Pharmacologic treatment, family insight, and social support may be important variables in such circumstances. Psychoeducation for the family is vital.
In patients experiencing paranoia, violence may be prevented by proper assessment and treatment. The patient’s family should be educated about paranoid ideation and the need for treatment to improve symptoms and ensure safety. The long-term effects of untreated paranoia and types of treatment modalities available should be discussed with the family and the patient. During these teaching sessions, focus on improving the overall insight of the family and the patient about the psychotic illness to improve treatment adherence.9 This step may be challenging if the family is resistant to the patient receiving mental health treatment.
Gaining a detailed clinical history of a patient’s paranoia is important. A clinician should look for changes in behavior, such as the patient becoming quieter or more hostile, and impaired academic or social functioning. After gathering sufficient evidence contrary to the delusion, clinicians can help patients improve their reality testing.
Rule out medical and neurologic conditions that may be contributing to paranoia and aggression.
TREATMENT: Some improvement
Ms. V is started on risperidone, 1 mg/d, which leads to a partial response. She starts interacting more with staff and her peers on the unit, but her delusions of her sister poisioning her persist. Given the severity of the crime, Ms. V is sent to adult court, where she is found not guilty by reason of insanity and committed to a state hospital.
The authors’ observations
New-onset paranoia is a serious symptom that requires immediate evaluation and treatment. We recommend an approach presened in a flowchart (Figure) that highlights the importance of early intervention and aggressive treatment.
The MacArthur Violence Risk Assessment Study10 indicated that a “suspicious” attitude toward others can be a precipitating cause for increased violence in some cases. In light of ongoing controversy regarding the link between violence and mental illnesses such as schizophrenia,10-12 addressing an individual’s psychiatric illness early is preferable to prevent possible complications such as violent crimes. Because patients with paranoid ideations may have severely impaired ego control, they may be at risk for acting out aggressive and/or destructive urges. Therefore, new-onset paranoia should be thought of as a medical emergency similar to chest pain. Although accurately predicting and preventing violence may be impossible, in Ms. V’s case, earlier mental health treatment and intervention may have been able to prevent a murder.
Figure: Paranoia: A suggested approach to treatment
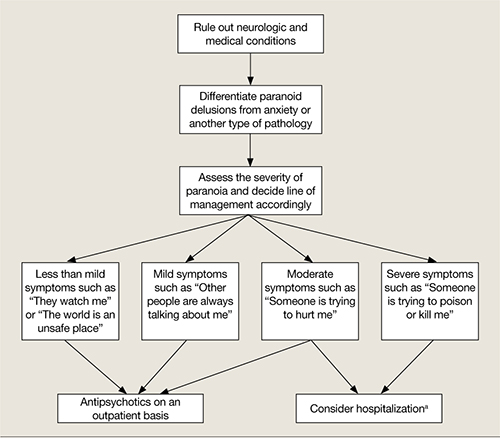
aBased on clinical judgment and extent of social support
Symptoms may become less severe or more severe (bidirectional). Strong social support has a positive effect on all levels and complements therapy. Regular counseling sessions and enhanced family insight about the patient’s paranoia helps strengthen social support
- Marneros A, Pillmann F, Wustmann T. Delusional disorders—are they simply paranoid schizophrenia? [published online ahead of print November 15, 2010]. Schizophr Bull. doi: 10.1093/schbul/sbq125.
Drug Brand Names
Amphetamine and dextroamphetamine • Adderall
Risperidone • Risperdal
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Personal and clinical details of this case were altered to maintain patient confidentiality.
1. Freeman D, Garety PA, Bebbington PE, et al. Psychological investigation of the structure of paranoia in a non-clinical population. Br J Psychiatry. 2005;186:427-435.
2. Kendler KS, Hays P. Paranoid psychosis (delusional disorder) and schizophrenia. A family history study. Arch Gen Psychiatry. 1981;38(5):547-551.
3. CNN Wire Staff. Police “actively pursuing” second person in Tucson shooting. CNN. http://us.cnn.com/2011/CRIME/01/08/arizona.shooting. Published January 9 2011. Accessed January 9, 2012.
4. Lipton E, Savage C, Shane S. Arizona suspect’s recent acts offer hints of alienation. The New York Times. January 8 2011:A8. http://www.nytimes.com/2011/01/09/us/politics/09shooter.html. Accessed January 10, 2012.
5. Berger J. Mental health warnings preceded rampage as Arizona gunman likely went untreated. http://www.foxnews.com/us/2011/01/10/mental-health-warnings-preceded-arizona-rampage-evidence-gunman-sought. Published January 10, 2011. Accessed January 11, 2012.
6. Lacey M. Suspect in shooting of Giffords ruled unfit for trial. The New York Times. May 25 2011:A1. http://www.nytimes.com/2011/05/26/us/26loughner.html. Accessed January 5, 2012.
7. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
8. Turkington D, Kingdon D, Weiden PJ. Cognitive behavior therapy for schizophrenia. Am J Psychiatry. 2006;163(3):365-373.
9. Smith CM, Barzman DH, Pristach CA. Effect of patient and family insight on compliance of schizophrenic patients. J Clin Pharmacol. 1997;37(2):147-154.
10. Appelbaum PS, Robbins PC, Monahan J. Violence and delusions: data from the MacArthur Violence Risk Assessment Study. Am J Psychiatry. 2000;157(4):566-572.
11. Mullen PE. A reassessment of the link between mental disorder and violent behaviour and its implications for clinical practice. Aust N Z J Psychiatry. 1997;31(1):3-11.
12. Fazel S, Gulati G, Linsell L, et al. Schizophrenia and violence: systematic review and meta-analysis. PLoS Med. 2009;6(8):e1000120.-
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Sleepless and paranoid
Ms. V, age 16, is referred to our psychiatric hospital from a juvenile detention center after she is charged with killing her sister with a hammer. She reports paranoid delusions, including believing that her sister was poisoning her food. Ms. V’s troubling behavior increased in the 6 months before the murder. She began to ask her mother to smell her food for possible poison. Her school grades dropped and she experienced decreased sleep and appetite. According to her mother, Ms. V’s insomnia worsened recently because of her paranoid thinking, which was evident when she noticed that her daughter slept with a hammer. Ms. V stopped socializing with her peers and no longer went to the gym.
Ms. V’s mother describes her daughter’s negative symptoms as consisting of social isolation and a flat affect. There was no evidence of auditory or visual hallucinations. After noticing the change in her daughter’s behavior, Ms. V’s mother attempted to schedule an appointment with a mental health professional, but there was a 2-month waiting list.
Ms. V cleaned her room before the murder, which was uncharacteristic of her routine behavior. On the day of the murder, Ms. V approached her sister while she was sleeping on the sofa and struck her on the head several times with a hammer. After the sister died, neighbors spotted Ms. V washing blood off her hands in their backyard with a sprinkler. Soaked in blood, she approached one of the neighbors and said that someone had been killed in the house. The neighbors called the police and Ms. V was arrested. She did not express remorse. She did not exhibit physical aggression toward others before the murder. Ms. V’s sense of entitlement and grandiosity persisted after the murder.
The authors’ observations
Paranoid delusions are fixed false beliefs with severe fears of others that may impair functioning at school or work, in personal relationships, and in other social dimensions. Paranoid thinking can have diverse presentations, ranging from social concerns such as fear of rejection to severe threat perceptions of people trying to cause substantial physical harm.1 Paranoid thoughts can be a result of misinterpretation of language, a personality disorder, anxiety, or psychosis.
Feelings of low self-esteem2 and anger1 may develop in a patient experiencing paranoid ideations. When anger begins to escalate, it may erupt into violent behavior. In Ms. V’s case, her paranoid ideations increased until she killed her younger sister. Ms. V’s case is similar to a mass shooting near Tucson, AZ on January 8, 2011 in that it possibly could have been prevented with earlier psychiatric intervention (Box).3-6
On January 8, 2011, a mass shooting occurred near Tucson, AZ that killed 6 and wounded 13. The suspect, 22-year-old Jared Lee Loughner, refused to cooperate with authorities by invoking his right to remain silent.3 Although the motives behind this crime remain undisclosed, mental illness appears to be a contributing factor.
Reports indicate that Mr. Loughner was abusing drugs and those close to him had noticed personality changes.4,5 The college he was attending advised Mr. Loughner to undergo a mental health evaluation, but he refused and dropped out of school.4,5 While in custody after the shooting, Mr. Loughner was diagnosed with paranoid schizophrenia, deemed incompetent to stand trial, and ordered to receive psychiatric treatment.6
This tragic mass shooting and similar incidents have led to questions regarding the adequacy of the mental health care infrastructure in United States. Experts suggest that this tragedy could have been prevented with more aggressive psychiatric prevention and intervention. Critical analysis of similar recent cases and expert opinions are needed to address this problem effectively.
EVALUATION: Remorseless
At admission, Ms. V’s affect is restricted and, at times, inappropriate. She is guarded about discussing the homicide but describes paranoid thoughts about her sister poisoning her. She is eager to learn if the police had found poison in her food. Her speech is soft with good articulation. Based on her presentation, her intelligence is average. She shows no evidence of remorse and is preoccupied with her sister poisoning her.
The Rorschach Inkblot Technique reveals positive evidence for a severe thought disorder. Ms. V’s thinking seems regressed. Ms. V’s medical workup, including MRI, electroencephalogram, and laboratory tests, are all within normal limits.
In the 5th grade, Ms. V’s primary care provider prescribed amphetamine and dextroamphetamine for attention-deficit/hyperactivity disorder, but she discontinued the drug after 1 year. Ms. V has never been hospitalized for psychiatric illness. She had no chronic medical conditions and no developmental delays.
Ms. V also has a history of periodic temper problems characterized by verbal aggression such as threatening the assistant principal at her school, and throwing her cellphone at her mother a few weeks before the murder, but no other aggressive episodes. Ms. V’s history does not suggest conduct disorder. She has no history of suicidal ideation or suicide attempts. Ms. V has used alcohol since age 15, but her mother reports that she was not a heavy or frequent user. Her last reported alcohol use was 10 days before the murder. A maternal uncle had been diagnosed with schizophrenia.
Before the murder, Ms. V lived with her sister and mother. Her parents were divorced. At age 9, Ms. V was sexually abused by a soccer coach; however, she denied symptoms of posttraumatic stress disorder related to the sexual abuse. She had no criminal history before the murder.
The authors’ observations
Based on Ms. V’s presentation and history, schizophrenia, paranoid type seems to be the most likely diagnosis because of her negative symptoms, including affective flattening, positive family history for schizophrenia, and paranoid delusions leading to dysfunction (Table).7 Delusional disorder seems less likely because Ms. V is young and has negative symptoms. Because she is generally healthy and her medical workup is negative, psychotic disorder due to a general medical condition is ruled out. She does not appear to be over-reporting, malingering, or exaggerating symptoms. In the context of psychosis, adolescent psychopathy does not seem likely even though there is evidence of grandiosity and a lack of remorse.
Table
DSM-IV-TR criteria for schizophrenia
A. Characteristic symptoms: ≥2 of the following, each present for a significant portion of time during a 1-month period:
|
| B. Social/occupational dysfunction: For a significant portion of the time since the onset of the disturbance, ≥1 major areas of functioning such as work, interpersonal relations, or self-care are markedly below the level achieved prior to the onset |
| C. Duration: Continuous signs of the disturbance persist for at least 6 months. This 6-month period must include at least 1 month of symptoms that meet Criterion A and may include periods of prodromal or residual symptoms |
| D. Schizoaffective and mood disorder exclusion: Schizoaffective disorder and mood disorder with psychotic features have been ruled out because either (1) no major depressive, manic, or mixed episodes have occurred concurrently with the active-phase symptoms; or (2) if mood episodes have occurred during active-phase symptoms, their total duration has been brief relative to the duration of the active and residual periods |
| E. Substance/general medical condition exclusion: The disturbance is not due to the direct physiological effects of a substance or a general medical condition |
| F. Relationship to a pervasive developmental disorder: If there is a history of autistic disorder or another pervasive developmental disorder, the additional diagnosis of schizophrenia is made only if prominent delusions or hallucinations are also present for at least 1 month |
| Diagnostic criteria for paranoid type: A type of schizophrenia in which the following criteria are met: A. Preoccupation with ≥1 delusions or frequent auditory hallucinations B. None of the following are prominent: disorganized speech, disorganized or catatonic behavior, or flat or inappropriate affect |
| Source: Reference 7 |
The authors’ observations
Various treatments can be used for paranoia with aggression, but the severity of the paranoia should be assessed before initiating treatment. Although categorizing paranoid ideations as mild, moderate, and severe is mainly a clinical judgment, Freeman et al1 have attempted to design a paranoia hierarchy from social concerns to severe threats. CBT8 and antipsychotic medication may help reduce mild to moderate paranoid delusions, particularly those associated with schizophrenia or mood disorders. For severe paranoia, hospitalization should carefully be considered.
When a patient exhibits moderate paranoia, the probability of progressing to severe symptoms or improving to mild symptoms depends on several variables. Pharmacologic treatment, family insight, and social support may be important variables in such circumstances. Psychoeducation for the family is vital.
In patients experiencing paranoia, violence may be prevented by proper assessment and treatment. The patient’s family should be educated about paranoid ideation and the need for treatment to improve symptoms and ensure safety. The long-term effects of untreated paranoia and types of treatment modalities available should be discussed with the family and the patient. During these teaching sessions, focus on improving the overall insight of the family and the patient about the psychotic illness to improve treatment adherence.9 This step may be challenging if the family is resistant to the patient receiving mental health treatment.
Gaining a detailed clinical history of a patient’s paranoia is important. A clinician should look for changes in behavior, such as the patient becoming quieter or more hostile, and impaired academic or social functioning. After gathering sufficient evidence contrary to the delusion, clinicians can help patients improve their reality testing.
Rule out medical and neurologic conditions that may be contributing to paranoia and aggression.
TREATMENT: Some improvement
Ms. V is started on risperidone, 1 mg/d, which leads to a partial response. She starts interacting more with staff and her peers on the unit, but her delusions of her sister poisioning her persist. Given the severity of the crime, Ms. V is sent to adult court, where she is found not guilty by reason of insanity and committed to a state hospital.
The authors’ observations
New-onset paranoia is a serious symptom that requires immediate evaluation and treatment. We recommend an approach presened in a flowchart (Figure) that highlights the importance of early intervention and aggressive treatment.
The MacArthur Violence Risk Assessment Study10 indicated that a “suspicious” attitude toward others can be a precipitating cause for increased violence in some cases. In light of ongoing controversy regarding the link between violence and mental illnesses such as schizophrenia,10-12 addressing an individual’s psychiatric illness early is preferable to prevent possible complications such as violent crimes. Because patients with paranoid ideations may have severely impaired ego control, they may be at risk for acting out aggressive and/or destructive urges. Therefore, new-onset paranoia should be thought of as a medical emergency similar to chest pain. Although accurately predicting and preventing violence may be impossible, in Ms. V’s case, earlier mental health treatment and intervention may have been able to prevent a murder.
Figure: Paranoia: A suggested approach to treatment
aBased on clinical judgment and extent of social support
Symptoms may become less severe or more severe (bidirectional). Strong social support has a positive effect on all levels and complements therapy. Regular counseling sessions and enhanced family insight about the patient’s paranoia helps strengthen social support
- Marneros A, Pillmann F, Wustmann T. Delusional disorders—are they simply paranoid schizophrenia? [published online ahead of print November 15, 2010]. Schizophr Bull. doi: 10.1093/schbul/sbq125.
Drug Brand Names
Amphetamine and dextroamphetamine • Adderall
Risperidone • Risperdal
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Personal and clinical details of this case were altered to maintain patient confidentiality.
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Sleepless and paranoid
Ms. V, age 16, is referred to our psychiatric hospital from a juvenile detention center after she is charged with killing her sister with a hammer. She reports paranoid delusions, including believing that her sister was poisoning her food. Ms. V’s troubling behavior increased in the 6 months before the murder. She began to ask her mother to smell her food for possible poison. Her school grades dropped and she experienced decreased sleep and appetite. According to her mother, Ms. V’s insomnia worsened recently because of her paranoid thinking, which was evident when she noticed that her daughter slept with a hammer. Ms. V stopped socializing with her peers and no longer went to the gym.
Ms. V’s mother describes her daughter’s negative symptoms as consisting of social isolation and a flat affect. There was no evidence of auditory or visual hallucinations. After noticing the change in her daughter’s behavior, Ms. V’s mother attempted to schedule an appointment with a mental health professional, but there was a 2-month waiting list.
Ms. V cleaned her room before the murder, which was uncharacteristic of her routine behavior. On the day of the murder, Ms. V approached her sister while she was sleeping on the sofa and struck her on the head several times with a hammer. After the sister died, neighbors spotted Ms. V washing blood off her hands in their backyard with a sprinkler. Soaked in blood, she approached one of the neighbors and said that someone had been killed in the house. The neighbors called the police and Ms. V was arrested. She did not express remorse. She did not exhibit physical aggression toward others before the murder. Ms. V’s sense of entitlement and grandiosity persisted after the murder.
The authors’ observations
Paranoid delusions are fixed false beliefs with severe fears of others that may impair functioning at school or work, in personal relationships, and in other social dimensions. Paranoid thinking can have diverse presentations, ranging from social concerns such as fear of rejection to severe threat perceptions of people trying to cause substantial physical harm.1 Paranoid thoughts can be a result of misinterpretation of language, a personality disorder, anxiety, or psychosis.
Feelings of low self-esteem2 and anger1 may develop in a patient experiencing paranoid ideations. When anger begins to escalate, it may erupt into violent behavior. In Ms. V’s case, her paranoid ideations increased until she killed her younger sister. Ms. V’s case is similar to a mass shooting near Tucson, AZ on January 8, 2011 in that it possibly could have been prevented with earlier psychiatric intervention (Box).3-6
On January 8, 2011, a mass shooting occurred near Tucson, AZ that killed 6 and wounded 13. The suspect, 22-year-old Jared Lee Loughner, refused to cooperate with authorities by invoking his right to remain silent.3 Although the motives behind this crime remain undisclosed, mental illness appears to be a contributing factor.
Reports indicate that Mr. Loughner was abusing drugs and those close to him had noticed personality changes.4,5 The college he was attending advised Mr. Loughner to undergo a mental health evaluation, but he refused and dropped out of school.4,5 While in custody after the shooting, Mr. Loughner was diagnosed with paranoid schizophrenia, deemed incompetent to stand trial, and ordered to receive psychiatric treatment.6
This tragic mass shooting and similar incidents have led to questions regarding the adequacy of the mental health care infrastructure in United States. Experts suggest that this tragedy could have been prevented with more aggressive psychiatric prevention and intervention. Critical analysis of similar recent cases and expert opinions are needed to address this problem effectively.
EVALUATION: Remorseless
At admission, Ms. V’s affect is restricted and, at times, inappropriate. She is guarded about discussing the homicide but describes paranoid thoughts about her sister poisoning her. She is eager to learn if the police had found poison in her food. Her speech is soft with good articulation. Based on her presentation, her intelligence is average. She shows no evidence of remorse and is preoccupied with her sister poisoning her.
The Rorschach Inkblot Technique reveals positive evidence for a severe thought disorder. Ms. V’s thinking seems regressed. Ms. V’s medical workup, including MRI, electroencephalogram, and laboratory tests, are all within normal limits.
In the 5th grade, Ms. V’s primary care provider prescribed amphetamine and dextroamphetamine for attention-deficit/hyperactivity disorder, but she discontinued the drug after 1 year. Ms. V has never been hospitalized for psychiatric illness. She had no chronic medical conditions and no developmental delays.
Ms. V also has a history of periodic temper problems characterized by verbal aggression such as threatening the assistant principal at her school, and throwing her cellphone at her mother a few weeks before the murder, but no other aggressive episodes. Ms. V’s history does not suggest conduct disorder. She has no history of suicidal ideation or suicide attempts. Ms. V has used alcohol since age 15, but her mother reports that she was not a heavy or frequent user. Her last reported alcohol use was 10 days before the murder. A maternal uncle had been diagnosed with schizophrenia.
Before the murder, Ms. V lived with her sister and mother. Her parents were divorced. At age 9, Ms. V was sexually abused by a soccer coach; however, she denied symptoms of posttraumatic stress disorder related to the sexual abuse. She had no criminal history before the murder.
The authors’ observations
Based on Ms. V’s presentation and history, schizophrenia, paranoid type seems to be the most likely diagnosis because of her negative symptoms, including affective flattening, positive family history for schizophrenia, and paranoid delusions leading to dysfunction (Table).7 Delusional disorder seems less likely because Ms. V is young and has negative symptoms. Because she is generally healthy and her medical workup is negative, psychotic disorder due to a general medical condition is ruled out. She does not appear to be over-reporting, malingering, or exaggerating symptoms. In the context of psychosis, adolescent psychopathy does not seem likely even though there is evidence of grandiosity and a lack of remorse.
Table
DSM-IV-TR criteria for schizophrenia
A. Characteristic symptoms: ≥2 of the following, each present for a significant portion of time during a 1-month period:
|
| B. Social/occupational dysfunction: For a significant portion of the time since the onset of the disturbance, ≥1 major areas of functioning such as work, interpersonal relations, or self-care are markedly below the level achieved prior to the onset |
| C. Duration: Continuous signs of the disturbance persist for at least 6 months. This 6-month period must include at least 1 month of symptoms that meet Criterion A and may include periods of prodromal or residual symptoms |
| D. Schizoaffective and mood disorder exclusion: Schizoaffective disorder and mood disorder with psychotic features have been ruled out because either (1) no major depressive, manic, or mixed episodes have occurred concurrently with the active-phase symptoms; or (2) if mood episodes have occurred during active-phase symptoms, their total duration has been brief relative to the duration of the active and residual periods |
| E. Substance/general medical condition exclusion: The disturbance is not due to the direct physiological effects of a substance or a general medical condition |
| F. Relationship to a pervasive developmental disorder: If there is a history of autistic disorder or another pervasive developmental disorder, the additional diagnosis of schizophrenia is made only if prominent delusions or hallucinations are also present for at least 1 month |
| Diagnostic criteria for paranoid type: A type of schizophrenia in which the following criteria are met: A. Preoccupation with ≥1 delusions or frequent auditory hallucinations B. None of the following are prominent: disorganized speech, disorganized or catatonic behavior, or flat or inappropriate affect |
| Source: Reference 7 |
The authors’ observations
Various treatments can be used for paranoia with aggression, but the severity of the paranoia should be assessed before initiating treatment. Although categorizing paranoid ideations as mild, moderate, and severe is mainly a clinical judgment, Freeman et al1 have attempted to design a paranoia hierarchy from social concerns to severe threats. CBT8 and antipsychotic medication may help reduce mild to moderate paranoid delusions, particularly those associated with schizophrenia or mood disorders. For severe paranoia, hospitalization should carefully be considered.
When a patient exhibits moderate paranoia, the probability of progressing to severe symptoms or improving to mild symptoms depends on several variables. Pharmacologic treatment, family insight, and social support may be important variables in such circumstances. Psychoeducation for the family is vital.
In patients experiencing paranoia, violence may be prevented by proper assessment and treatment. The patient’s family should be educated about paranoid ideation and the need for treatment to improve symptoms and ensure safety. The long-term effects of untreated paranoia and types of treatment modalities available should be discussed with the family and the patient. During these teaching sessions, focus on improving the overall insight of the family and the patient about the psychotic illness to improve treatment adherence.9 This step may be challenging if the family is resistant to the patient receiving mental health treatment.
Gaining a detailed clinical history of a patient’s paranoia is important. A clinician should look for changes in behavior, such as the patient becoming quieter or more hostile, and impaired academic or social functioning. After gathering sufficient evidence contrary to the delusion, clinicians can help patients improve their reality testing.
Rule out medical and neurologic conditions that may be contributing to paranoia and aggression.
TREATMENT: Some improvement
Ms. V is started on risperidone, 1 mg/d, which leads to a partial response. She starts interacting more with staff and her peers on the unit, but her delusions of her sister poisioning her persist. Given the severity of the crime, Ms. V is sent to adult court, where she is found not guilty by reason of insanity and committed to a state hospital.
The authors’ observations
New-onset paranoia is a serious symptom that requires immediate evaluation and treatment. We recommend an approach presened in a flowchart (Figure) that highlights the importance of early intervention and aggressive treatment.
The MacArthur Violence Risk Assessment Study10 indicated that a “suspicious” attitude toward others can be a precipitating cause for increased violence in some cases. In light of ongoing controversy regarding the link between violence and mental illnesses such as schizophrenia,10-12 addressing an individual’s psychiatric illness early is preferable to prevent possible complications such as violent crimes. Because patients with paranoid ideations may have severely impaired ego control, they may be at risk for acting out aggressive and/or destructive urges. Therefore, new-onset paranoia should be thought of as a medical emergency similar to chest pain. Although accurately predicting and preventing violence may be impossible, in Ms. V’s case, earlier mental health treatment and intervention may have been able to prevent a murder.
Figure: Paranoia: A suggested approach to treatment
aBased on clinical judgment and extent of social support
Symptoms may become less severe or more severe (bidirectional). Strong social support has a positive effect on all levels and complements therapy. Regular counseling sessions and enhanced family insight about the patient’s paranoia helps strengthen social support
- Marneros A, Pillmann F, Wustmann T. Delusional disorders—are they simply paranoid schizophrenia? [published online ahead of print November 15, 2010]. Schizophr Bull. doi: 10.1093/schbul/sbq125.
Drug Brand Names
Amphetamine and dextroamphetamine • Adderall
Risperidone • Risperdal
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Personal and clinical details of this case were altered to maintain patient confidentiality.
1. Freeman D, Garety PA, Bebbington PE, et al. Psychological investigation of the structure of paranoia in a non-clinical population. Br J Psychiatry. 2005;186:427-435.
2. Kendler KS, Hays P. Paranoid psychosis (delusional disorder) and schizophrenia. A family history study. Arch Gen Psychiatry. 1981;38(5):547-551.
3. CNN Wire Staff. Police “actively pursuing” second person in Tucson shooting. CNN. http://us.cnn.com/2011/CRIME/01/08/arizona.shooting. Published January 9 2011. Accessed January 9, 2012.
4. Lipton E, Savage C, Shane S. Arizona suspect’s recent acts offer hints of alienation. The New York Times. January 8 2011:A8. http://www.nytimes.com/2011/01/09/us/politics/09shooter.html. Accessed January 10, 2012.
5. Berger J. Mental health warnings preceded rampage as Arizona gunman likely went untreated. http://www.foxnews.com/us/2011/01/10/mental-health-warnings-preceded-arizona-rampage-evidence-gunman-sought. Published January 10, 2011. Accessed January 11, 2012.
6. Lacey M. Suspect in shooting of Giffords ruled unfit for trial. The New York Times. May 25 2011:A1. http://www.nytimes.com/2011/05/26/us/26loughner.html. Accessed January 5, 2012.
7. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
8. Turkington D, Kingdon D, Weiden PJ. Cognitive behavior therapy for schizophrenia. Am J Psychiatry. 2006;163(3):365-373.
9. Smith CM, Barzman DH, Pristach CA. Effect of patient and family insight on compliance of schizophrenic patients. J Clin Pharmacol. 1997;37(2):147-154.
10. Appelbaum PS, Robbins PC, Monahan J. Violence and delusions: data from the MacArthur Violence Risk Assessment Study. Am J Psychiatry. 2000;157(4):566-572.
11. Mullen PE. A reassessment of the link between mental disorder and violent behaviour and its implications for clinical practice. Aust N Z J Psychiatry. 1997;31(1):3-11.
12. Fazel S, Gulati G, Linsell L, et al. Schizophrenia and violence: systematic review and meta-analysis. PLoS Med. 2009;6(8):e1000120.-
1. Freeman D, Garety PA, Bebbington PE, et al. Psychological investigation of the structure of paranoia in a non-clinical population. Br J Psychiatry. 2005;186:427-435.
2. Kendler KS, Hays P. Paranoid psychosis (delusional disorder) and schizophrenia. A family history study. Arch Gen Psychiatry. 1981;38(5):547-551.
3. CNN Wire Staff. Police “actively pursuing” second person in Tucson shooting. CNN. http://us.cnn.com/2011/CRIME/01/08/arizona.shooting. Published January 9 2011. Accessed January 9, 2012.
4. Lipton E, Savage C, Shane S. Arizona suspect’s recent acts offer hints of alienation. The New York Times. January 8 2011:A8. http://www.nytimes.com/2011/01/09/us/politics/09shooter.html. Accessed January 10, 2012.
5. Berger J. Mental health warnings preceded rampage as Arizona gunman likely went untreated. http://www.foxnews.com/us/2011/01/10/mental-health-warnings-preceded-arizona-rampage-evidence-gunman-sought. Published January 10, 2011. Accessed January 11, 2012.
6. Lacey M. Suspect in shooting of Giffords ruled unfit for trial. The New York Times. May 25 2011:A1. http://www.nytimes.com/2011/05/26/us/26loughner.html. Accessed January 5, 2012.
7. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
8. Turkington D, Kingdon D, Weiden PJ. Cognitive behavior therapy for schizophrenia. Am J Psychiatry. 2006;163(3):365-373.
9. Smith CM, Barzman DH, Pristach CA. Effect of patient and family insight on compliance of schizophrenic patients. J Clin Pharmacol. 1997;37(2):147-154.
10. Appelbaum PS, Robbins PC, Monahan J. Violence and delusions: data from the MacArthur Violence Risk Assessment Study. Am J Psychiatry. 2000;157(4):566-572.
11. Mullen PE. A reassessment of the link between mental disorder and violent behaviour and its implications for clinical practice. Aust N Z J Psychiatry. 1997;31(1):3-11.
12. Fazel S, Gulati G, Linsell L, et al. Schizophrenia and violence: systematic review and meta-analysis. PLoS Med. 2009;6(8):e1000120.-
Contact Allergy to Dimethacrylate
The delirious substance abuser
CASE: Hurt and confused
Emergency medical services (EMS) are called to Ms. K’s apartment after her roommate found her lying on the floor moaning. The roommate tells EMS that Ms. K, age 29, appeared confused and was slurring her words, and reports that this change in her awareness progressed rapidly over a few hours. EMS personnel find that Ms. K has multiple contusions on her arms and face, which they presume to be self-inflicted. A marijuana pipe is discovered at Ms. K’s apartment.
In the emergency room (ER), Ms. K is inattentive and has difficulty following simple commands. Her speech is mumbled and her thoughts are disorganized. She displays psychomotor restlessness in the form of combativeness. Ms. K cannot provide meaningful historical data and is disoriented to place and time. The ER staff requests a psychiatric consultation.
Family members reveal that Ms. K has no preexisting medical conditions, is not taking prescription medications, but has a history of substance abuse (sporadic cocaine and cannabis use). Her family is unaware of recent substance use.
Physical examination reveals tachycardia (heart rate 110 to 120 beats per minute), hypotension (blood pressure 78/49 mm Hg), hypothermia (temperature 88ºF), and peripheral pulse oximetry of 84%. Her pupils are dilated and reactive to light; no conjunctival injection is noted. Her lung fields are clear on auscultation, but she is noted to have a rapid, irregular heartbeat. The abdomen is positive for bowel sounds, soft on palpation, and without any repositioning or notable overt signs of tenderness. Ms. K’s toes show purple discoloration with poor capillary refill. The dorsalis pedis pulses are reported to be 1+ bilaterally; however, the remainder of the arterial pulse examination is normal.
Her sodium, potassium, and chloride values are normal, but she has an abnormal anion gap (28.1 mEq/L), blood urea nitrogen (53 mg/dL), creatinine (2.9 mg/dL), creatine kinase (10,857 U/L), creatine kinase MB (432.6 ng/mL), and hyperglycemia (glucose 425 mg/dL). Arterial blood gas reveals hypoxia (Po2 of 55 mm Hg), with metabolic acidosis (sodium bicarbonate 10 with compensatory Pco2 of 33 mm Hg). Her urine is cloudy, positive for protein, ketones, hemoglobin, and glucose. She is thought to have a high anion gap acidosis related to dehydration, lactic acidosis (lactic acid 20 mEq/L), and hyperglycemia. Urine toxicology is positive for cannabinoids; ethylene glycol and methanol screen negatively, which rules these out as potential contributors to her high anion gap acidosis.
Ms. K is intubated and IV fluids are initiated for rhabdomyolysis and acute renal failure. Dialysis is implemented on a short-term basis. Her mental state improves gradually over 3 days.
The authors’ observations
Based on the abrupt onset of inattention and confusion, disorganized speech, memory impairments, and psychomotor agitation, we made an initial diagnosis of delirium; however, the precise etiology remained unclear. DSM-IV-TR diagnostic criteria for delirium are described in Table 1. Although delirium due to multiple etiologies does not have a DSM-IV-TR coding designation, we speculated that multiple causes contributed to Ms. K’s presentation. Acute renal failure secondary to dehydration as well as rhabdomyolysis, hypoxia, and hyperglycemia were implicated as general medical conditions etiologically linked to delirium. Because Ms. K has no preexisting medical conditions and her roommate and family stated she had a history of substance abuse, we also considered a presumptive diagnosis of substance-induced delirium. The medical team speculated that, based on information provided by her family, Ms. K may have had a seizure or may have fallen, which would account for her multiple contusions, and could have led to muscle injury and breakdown and the resultant rhabdomyolysis.
The possibility of cannabinoid-induced delirium has been reported, albeit rarely.1-3 However, Ms. K’s presentation—hypothermia, variable heart rate, lack of dry mucous membranes—was not consistent with significant anticholinergic toxicity or cannabinoid intoxication (Table 2).
By contrast, cocaine-induced delirium has been reported and initially appeared to be a plausible cause of Ms. K’s symptoms (Table 2). Delirium related to excess ingestion of cocaine may be related to the drug’s secondary effects resulting in rhabdomyolysis and renal dysfunction.4-6 Although several mechanisms underlying this relationship have been proposed, no single specific mechanism has been identified. The basis for cocaine ingestion and the resultant metabolic and renal effects, as observed in Ms. K’s case, likely are multifactorial. Mechanisms of the rhabdomyolysis might include:
- blockade of synaptic catecholamine reuptake and induction of adrenergic agonism, resulting in vasoconstriction and ischemia and leading to muscle damage
- cocaine-induced seizures and/or prolonged unconsciousness, leading to muscle compression and breakdown of muscle tissue
- a period of exertion induced by cocaine, precipitating an excited delirium and associated rhabdomyolysis
- a surge in dopamine concentrations, similar to neuroleptic malignant syndrome, precipitates hyperthermia, muscle rigidity, and psychomotor agitation, disrupting neuromuscular homeostasis and leading to rhabdomyolysis.
We were uncertain about the plausibility that acute cocaine intoxication caused Ms. K’s medical sequelae, in light of her toxicology findings. If cocaine use was the inciting event, and because the delirium reportedly had developed over several hours, we would expect cocaine to be detected in the toxicology screen. However, it was not detected. Cocaine can remain detectable in urine for 2 to 4 days,7 which raised our speculation that remote cocaine abuse could account for Ms. K’s current presentation and the timeline the roommate initially relayed to EMS personnel was inaccurate. We needed to clarify the timeline and progression of Ms. K’s symptoms with the roommate. In addition, we suggested to the medical team that alternative substances of abuse could be causing Ms. K’s symptoms and the roommate might be the only person who could unveil this possibility.
Table 1
DSM-IV-TR criteria for delirium due to multiple etiologies
| A. Disturbance of consciousness (ie, reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention |
| B. A change in cognition (such as memory deficit, disorientation, language disturbances) or the development of a perceptual disturbance that is not better accounted for by a preexisting, established, or evolving dementia |
| C. The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate during the course of the day |
| D. There is evidence from the history, physical examination, or laboratory findings that the delirium has >1 etiology (eg, >1 etiological general medical condition, a general medical condition plus substance intoxication or medication side effect) |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Table 2
Diagnostic criteria for cannabis and cocaine intoxication
| Diagnostic criteria | Cannabis intoxication | Cocaine intoxication |
|---|---|---|
| Recurrent use | + | + |
| Symptom onset | During or shortly after use | During or shortly after use |
| Behavioral changes | Impaired motor coordination | Hypervigilance, stereotyped behaviors |
| Psychological changes | Euphoria, anxiety, sensation of slowed time, social withdrawal, impaired judgment | Euphoria, anxiety, tension, anger, changes in sociability, interpersonal sensitivity, impaired social or occupational functioning |
| Associated criteria (≥2) | Conjunctival injection, increased appetite, dry mouth, tachycardia | Tachycardia or bradycardia, papillary dilation, elevated or lowered blood pressure, chills/perspiration, nausea/vomiting, evidence of weight loss, psychomotor changes, muscular weakness, chest pain, cardiac arrhythmias, seizure, dyskinesia, dystonia, delirium, coma |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 | ||
HISTORY: Unknown substance
Ms. K’s roommate is contacted for supplemental history. The roommate reports that recently he observed Ms. K “snorting” a brown/tan-colored substance. He had not seen her use this substance previously, and when he asked her what it was, she reportedly said that it was “PeeVee” (also called “bath salts”) purchased over the Internet.
The authors’ observations
MDPV is a novel chemical compound that is used as a recreational drug (Table 3).8 It commonly is acquired from Internet sources and sold as “bath salts.” Its use first emerged in approximately 2004, and its popularity has been increasing because of its easy availability and relatively low cost.9 The American Association of Poison Control Centers received 302 calls related to MDPV toxicity in 2010 and 5,625 calls related to MDPV use between January 1 and October 31, 2011.10,11
MDPV has psychoactive properties, with stimulant effects acting as a norepinephrine-dopamine reuptake inhibitor.8,9,12 When snorted, ingested orally, or inserted rectally, the agent produces effects comparable to cocaine or psychostimulants such as methylphenidate or dextroamphetamine.
Acute effects of MDPV include heightened alertness, diminished need for sleep, hyperarousal, and euphoria.8,9 These symptoms often are accompanied by increases in heart rate and blood pressure, sweating, and peripheral vasoconstriction. Individuals may abuse MDPV to acquire sustained attention, reduce their need for sleep, or for aphrodisiac effects. In many cases, anxiety and irritability can accompany the desired euphoric effects. For some, the euphoric effects can be superseded by anxiety or agitation. Mood and attention effects are estimated to last 3 to 4 hours; however, tachycardia and hypertension can persist for 6 to 8 hours.
MDPV use can trigger cravings and lead to binging. Euphoric stimulation with MDPV can become dysphoric as the dose and duration of use increase. Extended use has been associated with agitation, irritability, aggression, panic and marked anxiety, psychosis, and delirium.8,9 Anxiety can range from mild dysphoric stimulation to extreme panic-like states. In moderate forms, a state of sympathetic discharge can occur, producing physiologic effects resembling panic attacks, including hypertension, tachycardia, sweating, and peripheral vasoconstriction. In more severe cases, users may experience a feeling of impending doom, marked distress, and frank psychosis. Patients may experience disorientation and unsystematized paranoid delusions. Case reports of intoxication have described self-injurious behaviors, such as cutting, which may account for the contusions observed on Ms. K’s face and arms. Increasingly, MDPV use has resulted in ER presentations with patients manifesting abrupt onset confusion, anxiety, and self-injurious behaviors.
The mechanisms underlying MDPV-induced delirium have not been definitively identified. Given the similarities in mechanism of action between MDPV and cocaine, causes for delirium related to MDPV are similarly presumed to be multifactorial. The course of delirium associated with MDPV intoxication is self-limited and requires supportive measures.8,9
Suspect MDPV abuse in patients who present with signs or symptoms of stimulant intoxication but have a negative toxicology screen for cocaine and other psychostimulants. MDPV is not detected on routine toxicology assessments; however, it can be identified through laboratories with gas chromatography/mass spectroscopy capabilities. However, the time needed to obtain the results may exceed the clinical course of the patient’s delirium. One of the limitations in Ms. K’s case was the lack of gas chromatography/mass spectroscopy to confirm MDPV ingestion. Ms. K’s roommate could not locate any unused brown powder within their apartment to bring in for laboratory investigations. Recently, screening assessments for MDPV have become commercially available (see Related Resources).
Table 3
Overview of MDPV features
| Chemical name | 3,4-methylenedioxypyrovalerone |
| Popular names | MDPV, PV, PeeVee, Super coke, Magic |
| Sources | Sold as “bath salts” by Internet sources, “head shops,” and gas stations |
| Mode of use | Oral, snorting, smoking, rectal insertion, intravenous |
| Acute effects | Increased energy, perception of heightened alertness/attention, aphrodisiac properties, increased sociability |
| Adverse psychological effects | Anxiety (panic attacks), irritability, agitation, confusion, suicidal ideations, visual distortions |
| Adverse physical effects | Insomnia/overstimulation, bruxism, muscle twitching, pupil dilation/blurred vision, anorexia, headache, nausea/vomiting, hyperthermia, irregular heart beat, tachycardia, dyspnea, fatigue |
| Effects of protracted use | Dysphoria, depression, anhedonia |
| LD50 | Unknown |
| LD50: lethal dose; MDPV: methylenedioxypyrovalerone Source: Reference 8 | |
OUTCOME: Referral to treatment
Dialysis is discontinued within 1 day of hospitalization. Ms. K’s peripheral arterial perfusion improves, as does her thermoregulatory status. Her mental status improvements coincide with improvements in her physical and metabolic status.
Ms. K is able to sustain attention when speaking with interviewers. She is aware of her surroundings and is no longer distracted by extraneous stimuli. Her speech is articulate and her thoughts are linear. There is no evidence of any residual thought disorganization, delusions, or hallucinations.
Initially, Ms. K is reluctant to acknowledge her substance use, but eventually, she concedes to acquiring a stimulant from an Internet source and abusing it in undetermined amounts. She had no experience with using MDPV and did not know how to avoid ingesting dangerous amounts. We educate Ms. K about the dangers she faced during this hospitalization and the potential life-threatening outcomes. She is amenable to pursuing outpatient substance abuse treatment. Her roommate is enlisted to facilitate her follow-up with this treatment.
The authors’ observations
Managing MDPV toxicity presents a diagnostic dilemma for medical personnel and psychiatrists when evaluating and managing acute delirium. MDPV ingestion may go unrecognized in clinical settings because toxicology assessments for it are not readily available and patients’ historical information may be unreliable.
Because of the seriousness of sequelae associated with MDPV use, state and federal agencies have intervened. Until recently, bath salts did not have a controlled substance designation. In October 2011, the US Drug Enforcement Administration (DEA) ruled to make MDPV a controlled substance for 1 year, with the possibility of a 6-month extension.13 Although this ruling is temporary, it makes possession, sale, or distribution of these chemicals, or the products that contain them, illegal in the United States. In the interim, the DEA and the US Department of Health and Human Services will determine whether MDPV should remain a controlled substance.
- American Screening Corp. (MDPV screening). www.americanscreeningcorp.com.
- U.S. Drug Enforcement Administration. 3, 4-Methylenedioxypyrovalerone (MDPV). www.deadiversion.usdoj.gov/drugs_concern/mdpv.pdf.
- Prosser JM, Nelson LS. The toxicology of bath salts: a review of synthetic cathinones [published online ahead of print November 23, 2011]. J Med Toxicol. doi: 10.1007/s13181-011-0193-z.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. André C, Jaber-Filho JA, Bento RM, et al. Delirium following ingestion of marijuana in chocolate cookies. CNS Spectr. 2006;11(4):262-264.
2. Hollister LE. Health aspects of cannabis. Pharmacol Rev. 1986;38(1):1-20.
3. Meyer ME. Psychiatric consequences of marijuana use: the state of the evidence. In: Tinklenberg JR ed. Marijuana and health hazards: methodologic issues in current research. New York, NY: Academic Press; 1975:33–152.
4. Ruttenber AJ, Lawler-Heavner J, Yin M, et al. Fatal excited delirium following cocaine use: epidemiologic findings provide new evidence for mechanisms of cocaine toxicity. J Forensic Sci. 1997;42(1):25-31.
5. Ruttenber AJ, McAnally HB, Wetli CV. Cocaine-associated rhabdomyolysis and excited delirium: different stages of the same syndrome. Am J Forensic Med Pathol. 1999;20(2):120-127.
6. Singhal PC, Rubin RB, Peters A, et al. Rhabdomyolysis and acute renal failure associated with cocaine abuse. J Toxicol Clin Toxicol. 1990;28(3):321-330.
7. Moeller KE, Lee KC, Kissack JC. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83(1):66-76.
8. Psychonaut WebMapping Research Group. MDPV report. London United Kingdom: Institute of Psychiatry, King’s College. http://www.psychonautproject.eu/documents/reports/MDPV.pdf. Accessed November 23, 2011.
9. Ross EA, Watson M, Goldberger B. “Bath salts” intoxication. N Engl J Med. 2011;365(10):967-968.
10. American Association of Poison Control Centers. Bath salts data. http://www.aapcc.org/dnn/Portals/0/Bath%20Salts%20Data%20for%20Website%2011.03.2011.pdf. Updated November 3 2011. Accessed November 23, 2011.
11. Centers for Disease Control and Prevention. Emergency department visits after use of a drug sold as “bath salts”—Michigan November 13, 2010-March 31, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(19):624-627.
12. Westphal F, Junge T, Rösner P, et al. Mass and NMR spectroscopic characterization of 3, 4-methylenedioxypyrovalerone: a designer drug with α-pyrrolidinophenone structure. Forensic Sci Int. 2009;190(1-3):1-8.
13. U.S. Drug Enforcement Administration. Chemicals used in “bath salts” now under federal control and regulation. http://www.justice.gov/dea/pubs/pressrel/pr102111.html. Accessed November 23, 2011.
CASE: Hurt and confused
Emergency medical services (EMS) are called to Ms. K’s apartment after her roommate found her lying on the floor moaning. The roommate tells EMS that Ms. K, age 29, appeared confused and was slurring her words, and reports that this change in her awareness progressed rapidly over a few hours. EMS personnel find that Ms. K has multiple contusions on her arms and face, which they presume to be self-inflicted. A marijuana pipe is discovered at Ms. K’s apartment.
In the emergency room (ER), Ms. K is inattentive and has difficulty following simple commands. Her speech is mumbled and her thoughts are disorganized. She displays psychomotor restlessness in the form of combativeness. Ms. K cannot provide meaningful historical data and is disoriented to place and time. The ER staff requests a psychiatric consultation.
Family members reveal that Ms. K has no preexisting medical conditions, is not taking prescription medications, but has a history of substance abuse (sporadic cocaine and cannabis use). Her family is unaware of recent substance use.
Physical examination reveals tachycardia (heart rate 110 to 120 beats per minute), hypotension (blood pressure 78/49 mm Hg), hypothermia (temperature 88ºF), and peripheral pulse oximetry of 84%. Her pupils are dilated and reactive to light; no conjunctival injection is noted. Her lung fields are clear on auscultation, but she is noted to have a rapid, irregular heartbeat. The abdomen is positive for bowel sounds, soft on palpation, and without any repositioning or notable overt signs of tenderness. Ms. K’s toes show purple discoloration with poor capillary refill. The dorsalis pedis pulses are reported to be 1+ bilaterally; however, the remainder of the arterial pulse examination is normal.
Her sodium, potassium, and chloride values are normal, but she has an abnormal anion gap (28.1 mEq/L), blood urea nitrogen (53 mg/dL), creatinine (2.9 mg/dL), creatine kinase (10,857 U/L), creatine kinase MB (432.6 ng/mL), and hyperglycemia (glucose 425 mg/dL). Arterial blood gas reveals hypoxia (Po2 of 55 mm Hg), with metabolic acidosis (sodium bicarbonate 10 with compensatory Pco2 of 33 mm Hg). Her urine is cloudy, positive for protein, ketones, hemoglobin, and glucose. She is thought to have a high anion gap acidosis related to dehydration, lactic acidosis (lactic acid 20 mEq/L), and hyperglycemia. Urine toxicology is positive for cannabinoids; ethylene glycol and methanol screen negatively, which rules these out as potential contributors to her high anion gap acidosis.
Ms. K is intubated and IV fluids are initiated for rhabdomyolysis and acute renal failure. Dialysis is implemented on a short-term basis. Her mental state improves gradually over 3 days.
The authors’ observations
Based on the abrupt onset of inattention and confusion, disorganized speech, memory impairments, and psychomotor agitation, we made an initial diagnosis of delirium; however, the precise etiology remained unclear. DSM-IV-TR diagnostic criteria for delirium are described in Table 1. Although delirium due to multiple etiologies does not have a DSM-IV-TR coding designation, we speculated that multiple causes contributed to Ms. K’s presentation. Acute renal failure secondary to dehydration as well as rhabdomyolysis, hypoxia, and hyperglycemia were implicated as general medical conditions etiologically linked to delirium. Because Ms. K has no preexisting medical conditions and her roommate and family stated she had a history of substance abuse, we also considered a presumptive diagnosis of substance-induced delirium. The medical team speculated that, based on information provided by her family, Ms. K may have had a seizure or may have fallen, which would account for her multiple contusions, and could have led to muscle injury and breakdown and the resultant rhabdomyolysis.
The possibility of cannabinoid-induced delirium has been reported, albeit rarely.1-3 However, Ms. K’s presentation—hypothermia, variable heart rate, lack of dry mucous membranes—was not consistent with significant anticholinergic toxicity or cannabinoid intoxication (Table 2).
By contrast, cocaine-induced delirium has been reported and initially appeared to be a plausible cause of Ms. K’s symptoms (Table 2). Delirium related to excess ingestion of cocaine may be related to the drug’s secondary effects resulting in rhabdomyolysis and renal dysfunction.4-6 Although several mechanisms underlying this relationship have been proposed, no single specific mechanism has been identified. The basis for cocaine ingestion and the resultant metabolic and renal effects, as observed in Ms. K’s case, likely are multifactorial. Mechanisms of the rhabdomyolysis might include:
- blockade of synaptic catecholamine reuptake and induction of adrenergic agonism, resulting in vasoconstriction and ischemia and leading to muscle damage
- cocaine-induced seizures and/or prolonged unconsciousness, leading to muscle compression and breakdown of muscle tissue
- a period of exertion induced by cocaine, precipitating an excited delirium and associated rhabdomyolysis
- a surge in dopamine concentrations, similar to neuroleptic malignant syndrome, precipitates hyperthermia, muscle rigidity, and psychomotor agitation, disrupting neuromuscular homeostasis and leading to rhabdomyolysis.
We were uncertain about the plausibility that acute cocaine intoxication caused Ms. K’s medical sequelae, in light of her toxicology findings. If cocaine use was the inciting event, and because the delirium reportedly had developed over several hours, we would expect cocaine to be detected in the toxicology screen. However, it was not detected. Cocaine can remain detectable in urine for 2 to 4 days,7 which raised our speculation that remote cocaine abuse could account for Ms. K’s current presentation and the timeline the roommate initially relayed to EMS personnel was inaccurate. We needed to clarify the timeline and progression of Ms. K’s symptoms with the roommate. In addition, we suggested to the medical team that alternative substances of abuse could be causing Ms. K’s symptoms and the roommate might be the only person who could unveil this possibility.
Table 1
DSM-IV-TR criteria for delirium due to multiple etiologies
| A. Disturbance of consciousness (ie, reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention |
| B. A change in cognition (such as memory deficit, disorientation, language disturbances) or the development of a perceptual disturbance that is not better accounted for by a preexisting, established, or evolving dementia |
| C. The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate during the course of the day |
| D. There is evidence from the history, physical examination, or laboratory findings that the delirium has >1 etiology (eg, >1 etiological general medical condition, a general medical condition plus substance intoxication or medication side effect) |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Table 2
Diagnostic criteria for cannabis and cocaine intoxication
| Diagnostic criteria | Cannabis intoxication | Cocaine intoxication |
|---|---|---|
| Recurrent use | + | + |
| Symptom onset | During or shortly after use | During or shortly after use |
| Behavioral changes | Impaired motor coordination | Hypervigilance, stereotyped behaviors |
| Psychological changes | Euphoria, anxiety, sensation of slowed time, social withdrawal, impaired judgment | Euphoria, anxiety, tension, anger, changes in sociability, interpersonal sensitivity, impaired social or occupational functioning |
| Associated criteria (≥2) | Conjunctival injection, increased appetite, dry mouth, tachycardia | Tachycardia or bradycardia, papillary dilation, elevated or lowered blood pressure, chills/perspiration, nausea/vomiting, evidence of weight loss, psychomotor changes, muscular weakness, chest pain, cardiac arrhythmias, seizure, dyskinesia, dystonia, delirium, coma |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 | ||
HISTORY: Unknown substance
Ms. K’s roommate is contacted for supplemental history. The roommate reports that recently he observed Ms. K “snorting” a brown/tan-colored substance. He had not seen her use this substance previously, and when he asked her what it was, she reportedly said that it was “PeeVee” (also called “bath salts”) purchased over the Internet.
The authors’ observations
MDPV is a novel chemical compound that is used as a recreational drug (Table 3).8 It commonly is acquired from Internet sources and sold as “bath salts.” Its use first emerged in approximately 2004, and its popularity has been increasing because of its easy availability and relatively low cost.9 The American Association of Poison Control Centers received 302 calls related to MDPV toxicity in 2010 and 5,625 calls related to MDPV use between January 1 and October 31, 2011.10,11
MDPV has psychoactive properties, with stimulant effects acting as a norepinephrine-dopamine reuptake inhibitor.8,9,12 When snorted, ingested orally, or inserted rectally, the agent produces effects comparable to cocaine or psychostimulants such as methylphenidate or dextroamphetamine.
Acute effects of MDPV include heightened alertness, diminished need for sleep, hyperarousal, and euphoria.8,9 These symptoms often are accompanied by increases in heart rate and blood pressure, sweating, and peripheral vasoconstriction. Individuals may abuse MDPV to acquire sustained attention, reduce their need for sleep, or for aphrodisiac effects. In many cases, anxiety and irritability can accompany the desired euphoric effects. For some, the euphoric effects can be superseded by anxiety or agitation. Mood and attention effects are estimated to last 3 to 4 hours; however, tachycardia and hypertension can persist for 6 to 8 hours.
MDPV use can trigger cravings and lead to binging. Euphoric stimulation with MDPV can become dysphoric as the dose and duration of use increase. Extended use has been associated with agitation, irritability, aggression, panic and marked anxiety, psychosis, and delirium.8,9 Anxiety can range from mild dysphoric stimulation to extreme panic-like states. In moderate forms, a state of sympathetic discharge can occur, producing physiologic effects resembling panic attacks, including hypertension, tachycardia, sweating, and peripheral vasoconstriction. In more severe cases, users may experience a feeling of impending doom, marked distress, and frank psychosis. Patients may experience disorientation and unsystematized paranoid delusions. Case reports of intoxication have described self-injurious behaviors, such as cutting, which may account for the contusions observed on Ms. K’s face and arms. Increasingly, MDPV use has resulted in ER presentations with patients manifesting abrupt onset confusion, anxiety, and self-injurious behaviors.
The mechanisms underlying MDPV-induced delirium have not been definitively identified. Given the similarities in mechanism of action between MDPV and cocaine, causes for delirium related to MDPV are similarly presumed to be multifactorial. The course of delirium associated with MDPV intoxication is self-limited and requires supportive measures.8,9
Suspect MDPV abuse in patients who present with signs or symptoms of stimulant intoxication but have a negative toxicology screen for cocaine and other psychostimulants. MDPV is not detected on routine toxicology assessments; however, it can be identified through laboratories with gas chromatography/mass spectroscopy capabilities. However, the time needed to obtain the results may exceed the clinical course of the patient’s delirium. One of the limitations in Ms. K’s case was the lack of gas chromatography/mass spectroscopy to confirm MDPV ingestion. Ms. K’s roommate could not locate any unused brown powder within their apartment to bring in for laboratory investigations. Recently, screening assessments for MDPV have become commercially available (see Related Resources).
Table 3
Overview of MDPV features
| Chemical name | 3,4-methylenedioxypyrovalerone |
| Popular names | MDPV, PV, PeeVee, Super coke, Magic |
| Sources | Sold as “bath salts” by Internet sources, “head shops,” and gas stations |
| Mode of use | Oral, snorting, smoking, rectal insertion, intravenous |
| Acute effects | Increased energy, perception of heightened alertness/attention, aphrodisiac properties, increased sociability |
| Adverse psychological effects | Anxiety (panic attacks), irritability, agitation, confusion, suicidal ideations, visual distortions |
| Adverse physical effects | Insomnia/overstimulation, bruxism, muscle twitching, pupil dilation/blurred vision, anorexia, headache, nausea/vomiting, hyperthermia, irregular heart beat, tachycardia, dyspnea, fatigue |
| Effects of protracted use | Dysphoria, depression, anhedonia |
| LD50 | Unknown |
| LD50: lethal dose; MDPV: methylenedioxypyrovalerone Source: Reference 8 | |
OUTCOME: Referral to treatment
Dialysis is discontinued within 1 day of hospitalization. Ms. K’s peripheral arterial perfusion improves, as does her thermoregulatory status. Her mental status improvements coincide with improvements in her physical and metabolic status.
Ms. K is able to sustain attention when speaking with interviewers. She is aware of her surroundings and is no longer distracted by extraneous stimuli. Her speech is articulate and her thoughts are linear. There is no evidence of any residual thought disorganization, delusions, or hallucinations.
Initially, Ms. K is reluctant to acknowledge her substance use, but eventually, she concedes to acquiring a stimulant from an Internet source and abusing it in undetermined amounts. She had no experience with using MDPV and did not know how to avoid ingesting dangerous amounts. We educate Ms. K about the dangers she faced during this hospitalization and the potential life-threatening outcomes. She is amenable to pursuing outpatient substance abuse treatment. Her roommate is enlisted to facilitate her follow-up with this treatment.
The authors’ observations
Managing MDPV toxicity presents a diagnostic dilemma for medical personnel and psychiatrists when evaluating and managing acute delirium. MDPV ingestion may go unrecognized in clinical settings because toxicology assessments for it are not readily available and patients’ historical information may be unreliable.
Because of the seriousness of sequelae associated with MDPV use, state and federal agencies have intervened. Until recently, bath salts did not have a controlled substance designation. In October 2011, the US Drug Enforcement Administration (DEA) ruled to make MDPV a controlled substance for 1 year, with the possibility of a 6-month extension.13 Although this ruling is temporary, it makes possession, sale, or distribution of these chemicals, or the products that contain them, illegal in the United States. In the interim, the DEA and the US Department of Health and Human Services will determine whether MDPV should remain a controlled substance.
- American Screening Corp. (MDPV screening). www.americanscreeningcorp.com.
- U.S. Drug Enforcement Administration. 3, 4-Methylenedioxypyrovalerone (MDPV). www.deadiversion.usdoj.gov/drugs_concern/mdpv.pdf.
- Prosser JM, Nelson LS. The toxicology of bath salts: a review of synthetic cathinones [published online ahead of print November 23, 2011]. J Med Toxicol. doi: 10.1007/s13181-011-0193-z.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Hurt and confused
Emergency medical services (EMS) are called to Ms. K’s apartment after her roommate found her lying on the floor moaning. The roommate tells EMS that Ms. K, age 29, appeared confused and was slurring her words, and reports that this change in her awareness progressed rapidly over a few hours. EMS personnel find that Ms. K has multiple contusions on her arms and face, which they presume to be self-inflicted. A marijuana pipe is discovered at Ms. K’s apartment.
In the emergency room (ER), Ms. K is inattentive and has difficulty following simple commands. Her speech is mumbled and her thoughts are disorganized. She displays psychomotor restlessness in the form of combativeness. Ms. K cannot provide meaningful historical data and is disoriented to place and time. The ER staff requests a psychiatric consultation.
Family members reveal that Ms. K has no preexisting medical conditions, is not taking prescription medications, but has a history of substance abuse (sporadic cocaine and cannabis use). Her family is unaware of recent substance use.
Physical examination reveals tachycardia (heart rate 110 to 120 beats per minute), hypotension (blood pressure 78/49 mm Hg), hypothermia (temperature 88ºF), and peripheral pulse oximetry of 84%. Her pupils are dilated and reactive to light; no conjunctival injection is noted. Her lung fields are clear on auscultation, but she is noted to have a rapid, irregular heartbeat. The abdomen is positive for bowel sounds, soft on palpation, and without any repositioning or notable overt signs of tenderness. Ms. K’s toes show purple discoloration with poor capillary refill. The dorsalis pedis pulses are reported to be 1+ bilaterally; however, the remainder of the arterial pulse examination is normal.
Her sodium, potassium, and chloride values are normal, but she has an abnormal anion gap (28.1 mEq/L), blood urea nitrogen (53 mg/dL), creatinine (2.9 mg/dL), creatine kinase (10,857 U/L), creatine kinase MB (432.6 ng/mL), and hyperglycemia (glucose 425 mg/dL). Arterial blood gas reveals hypoxia (Po2 of 55 mm Hg), with metabolic acidosis (sodium bicarbonate 10 with compensatory Pco2 of 33 mm Hg). Her urine is cloudy, positive for protein, ketones, hemoglobin, and glucose. She is thought to have a high anion gap acidosis related to dehydration, lactic acidosis (lactic acid 20 mEq/L), and hyperglycemia. Urine toxicology is positive for cannabinoids; ethylene glycol and methanol screen negatively, which rules these out as potential contributors to her high anion gap acidosis.
Ms. K is intubated and IV fluids are initiated for rhabdomyolysis and acute renal failure. Dialysis is implemented on a short-term basis. Her mental state improves gradually over 3 days.
The authors’ observations
Based on the abrupt onset of inattention and confusion, disorganized speech, memory impairments, and psychomotor agitation, we made an initial diagnosis of delirium; however, the precise etiology remained unclear. DSM-IV-TR diagnostic criteria for delirium are described in Table 1. Although delirium due to multiple etiologies does not have a DSM-IV-TR coding designation, we speculated that multiple causes contributed to Ms. K’s presentation. Acute renal failure secondary to dehydration as well as rhabdomyolysis, hypoxia, and hyperglycemia were implicated as general medical conditions etiologically linked to delirium. Because Ms. K has no preexisting medical conditions and her roommate and family stated she had a history of substance abuse, we also considered a presumptive diagnosis of substance-induced delirium. The medical team speculated that, based on information provided by her family, Ms. K may have had a seizure or may have fallen, which would account for her multiple contusions, and could have led to muscle injury and breakdown and the resultant rhabdomyolysis.
The possibility of cannabinoid-induced delirium has been reported, albeit rarely.1-3 However, Ms. K’s presentation—hypothermia, variable heart rate, lack of dry mucous membranes—was not consistent with significant anticholinergic toxicity or cannabinoid intoxication (Table 2).
By contrast, cocaine-induced delirium has been reported and initially appeared to be a plausible cause of Ms. K’s symptoms (Table 2). Delirium related to excess ingestion of cocaine may be related to the drug’s secondary effects resulting in rhabdomyolysis and renal dysfunction.4-6 Although several mechanisms underlying this relationship have been proposed, no single specific mechanism has been identified. The basis for cocaine ingestion and the resultant metabolic and renal effects, as observed in Ms. K’s case, likely are multifactorial. Mechanisms of the rhabdomyolysis might include:
- blockade of synaptic catecholamine reuptake and induction of adrenergic agonism, resulting in vasoconstriction and ischemia and leading to muscle damage
- cocaine-induced seizures and/or prolonged unconsciousness, leading to muscle compression and breakdown of muscle tissue
- a period of exertion induced by cocaine, precipitating an excited delirium and associated rhabdomyolysis
- a surge in dopamine concentrations, similar to neuroleptic malignant syndrome, precipitates hyperthermia, muscle rigidity, and psychomotor agitation, disrupting neuromuscular homeostasis and leading to rhabdomyolysis.
We were uncertain about the plausibility that acute cocaine intoxication caused Ms. K’s medical sequelae, in light of her toxicology findings. If cocaine use was the inciting event, and because the delirium reportedly had developed over several hours, we would expect cocaine to be detected in the toxicology screen. However, it was not detected. Cocaine can remain detectable in urine for 2 to 4 days,7 which raised our speculation that remote cocaine abuse could account for Ms. K’s current presentation and the timeline the roommate initially relayed to EMS personnel was inaccurate. We needed to clarify the timeline and progression of Ms. K’s symptoms with the roommate. In addition, we suggested to the medical team that alternative substances of abuse could be causing Ms. K’s symptoms and the roommate might be the only person who could unveil this possibility.
Table 1
DSM-IV-TR criteria for delirium due to multiple etiologies
| A. Disturbance of consciousness (ie, reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention |
| B. A change in cognition (such as memory deficit, disorientation, language disturbances) or the development of a perceptual disturbance that is not better accounted for by a preexisting, established, or evolving dementia |
| C. The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate during the course of the day |
| D. There is evidence from the history, physical examination, or laboratory findings that the delirium has >1 etiology (eg, >1 etiological general medical condition, a general medical condition plus substance intoxication or medication side effect) |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Table 2
Diagnostic criteria for cannabis and cocaine intoxication
| Diagnostic criteria | Cannabis intoxication | Cocaine intoxication |
|---|---|---|
| Recurrent use | + | + |
| Symptom onset | During or shortly after use | During or shortly after use |
| Behavioral changes | Impaired motor coordination | Hypervigilance, stereotyped behaviors |
| Psychological changes | Euphoria, anxiety, sensation of slowed time, social withdrawal, impaired judgment | Euphoria, anxiety, tension, anger, changes in sociability, interpersonal sensitivity, impaired social or occupational functioning |
| Associated criteria (≥2) | Conjunctival injection, increased appetite, dry mouth, tachycardia | Tachycardia or bradycardia, papillary dilation, elevated or lowered blood pressure, chills/perspiration, nausea/vomiting, evidence of weight loss, psychomotor changes, muscular weakness, chest pain, cardiac arrhythmias, seizure, dyskinesia, dystonia, delirium, coma |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 | ||
HISTORY: Unknown substance
Ms. K’s roommate is contacted for supplemental history. The roommate reports that recently he observed Ms. K “snorting” a brown/tan-colored substance. He had not seen her use this substance previously, and when he asked her what it was, she reportedly said that it was “PeeVee” (also called “bath salts”) purchased over the Internet.
The authors’ observations
MDPV is a novel chemical compound that is used as a recreational drug (Table 3).8 It commonly is acquired from Internet sources and sold as “bath salts.” Its use first emerged in approximately 2004, and its popularity has been increasing because of its easy availability and relatively low cost.9 The American Association of Poison Control Centers received 302 calls related to MDPV toxicity in 2010 and 5,625 calls related to MDPV use between January 1 and October 31, 2011.10,11
MDPV has psychoactive properties, with stimulant effects acting as a norepinephrine-dopamine reuptake inhibitor.8,9,12 When snorted, ingested orally, or inserted rectally, the agent produces effects comparable to cocaine or psychostimulants such as methylphenidate or dextroamphetamine.
Acute effects of MDPV include heightened alertness, diminished need for sleep, hyperarousal, and euphoria.8,9 These symptoms often are accompanied by increases in heart rate and blood pressure, sweating, and peripheral vasoconstriction. Individuals may abuse MDPV to acquire sustained attention, reduce their need for sleep, or for aphrodisiac effects. In many cases, anxiety and irritability can accompany the desired euphoric effects. For some, the euphoric effects can be superseded by anxiety or agitation. Mood and attention effects are estimated to last 3 to 4 hours; however, tachycardia and hypertension can persist for 6 to 8 hours.
MDPV use can trigger cravings and lead to binging. Euphoric stimulation with MDPV can become dysphoric as the dose and duration of use increase. Extended use has been associated with agitation, irritability, aggression, panic and marked anxiety, psychosis, and delirium.8,9 Anxiety can range from mild dysphoric stimulation to extreme panic-like states. In moderate forms, a state of sympathetic discharge can occur, producing physiologic effects resembling panic attacks, including hypertension, tachycardia, sweating, and peripheral vasoconstriction. In more severe cases, users may experience a feeling of impending doom, marked distress, and frank psychosis. Patients may experience disorientation and unsystematized paranoid delusions. Case reports of intoxication have described self-injurious behaviors, such as cutting, which may account for the contusions observed on Ms. K’s face and arms. Increasingly, MDPV use has resulted in ER presentations with patients manifesting abrupt onset confusion, anxiety, and self-injurious behaviors.
The mechanisms underlying MDPV-induced delirium have not been definitively identified. Given the similarities in mechanism of action between MDPV and cocaine, causes for delirium related to MDPV are similarly presumed to be multifactorial. The course of delirium associated with MDPV intoxication is self-limited and requires supportive measures.8,9
Suspect MDPV abuse in patients who present with signs or symptoms of stimulant intoxication but have a negative toxicology screen for cocaine and other psychostimulants. MDPV is not detected on routine toxicology assessments; however, it can be identified through laboratories with gas chromatography/mass spectroscopy capabilities. However, the time needed to obtain the results may exceed the clinical course of the patient’s delirium. One of the limitations in Ms. K’s case was the lack of gas chromatography/mass spectroscopy to confirm MDPV ingestion. Ms. K’s roommate could not locate any unused brown powder within their apartment to bring in for laboratory investigations. Recently, screening assessments for MDPV have become commercially available (see Related Resources).
Table 3
Overview of MDPV features
| Chemical name | 3,4-methylenedioxypyrovalerone |
| Popular names | MDPV, PV, PeeVee, Super coke, Magic |
| Sources | Sold as “bath salts” by Internet sources, “head shops,” and gas stations |
| Mode of use | Oral, snorting, smoking, rectal insertion, intravenous |
| Acute effects | Increased energy, perception of heightened alertness/attention, aphrodisiac properties, increased sociability |
| Adverse psychological effects | Anxiety (panic attacks), irritability, agitation, confusion, suicidal ideations, visual distortions |
| Adverse physical effects | Insomnia/overstimulation, bruxism, muscle twitching, pupil dilation/blurred vision, anorexia, headache, nausea/vomiting, hyperthermia, irregular heart beat, tachycardia, dyspnea, fatigue |
| Effects of protracted use | Dysphoria, depression, anhedonia |
| LD50 | Unknown |
| LD50: lethal dose; MDPV: methylenedioxypyrovalerone Source: Reference 8 | |
OUTCOME: Referral to treatment
Dialysis is discontinued within 1 day of hospitalization. Ms. K’s peripheral arterial perfusion improves, as does her thermoregulatory status. Her mental status improvements coincide with improvements in her physical and metabolic status.
Ms. K is able to sustain attention when speaking with interviewers. She is aware of her surroundings and is no longer distracted by extraneous stimuli. Her speech is articulate and her thoughts are linear. There is no evidence of any residual thought disorganization, delusions, or hallucinations.
Initially, Ms. K is reluctant to acknowledge her substance use, but eventually, she concedes to acquiring a stimulant from an Internet source and abusing it in undetermined amounts. She had no experience with using MDPV and did not know how to avoid ingesting dangerous amounts. We educate Ms. K about the dangers she faced during this hospitalization and the potential life-threatening outcomes. She is amenable to pursuing outpatient substance abuse treatment. Her roommate is enlisted to facilitate her follow-up with this treatment.
The authors’ observations
Managing MDPV toxicity presents a diagnostic dilemma for medical personnel and psychiatrists when evaluating and managing acute delirium. MDPV ingestion may go unrecognized in clinical settings because toxicology assessments for it are not readily available and patients’ historical information may be unreliable.
Because of the seriousness of sequelae associated with MDPV use, state and federal agencies have intervened. Until recently, bath salts did not have a controlled substance designation. In October 2011, the US Drug Enforcement Administration (DEA) ruled to make MDPV a controlled substance for 1 year, with the possibility of a 6-month extension.13 Although this ruling is temporary, it makes possession, sale, or distribution of these chemicals, or the products that contain them, illegal in the United States. In the interim, the DEA and the US Department of Health and Human Services will determine whether MDPV should remain a controlled substance.
- American Screening Corp. (MDPV screening). www.americanscreeningcorp.com.
- U.S. Drug Enforcement Administration. 3, 4-Methylenedioxypyrovalerone (MDPV). www.deadiversion.usdoj.gov/drugs_concern/mdpv.pdf.
- Prosser JM, Nelson LS. The toxicology of bath salts: a review of synthetic cathinones [published online ahead of print November 23, 2011]. J Med Toxicol. doi: 10.1007/s13181-011-0193-z.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. André C, Jaber-Filho JA, Bento RM, et al. Delirium following ingestion of marijuana in chocolate cookies. CNS Spectr. 2006;11(4):262-264.
2. Hollister LE. Health aspects of cannabis. Pharmacol Rev. 1986;38(1):1-20.
3. Meyer ME. Psychiatric consequences of marijuana use: the state of the evidence. In: Tinklenberg JR ed. Marijuana and health hazards: methodologic issues in current research. New York, NY: Academic Press; 1975:33–152.
4. Ruttenber AJ, Lawler-Heavner J, Yin M, et al. Fatal excited delirium following cocaine use: epidemiologic findings provide new evidence for mechanisms of cocaine toxicity. J Forensic Sci. 1997;42(1):25-31.
5. Ruttenber AJ, McAnally HB, Wetli CV. Cocaine-associated rhabdomyolysis and excited delirium: different stages of the same syndrome. Am J Forensic Med Pathol. 1999;20(2):120-127.
6. Singhal PC, Rubin RB, Peters A, et al. Rhabdomyolysis and acute renal failure associated with cocaine abuse. J Toxicol Clin Toxicol. 1990;28(3):321-330.
7. Moeller KE, Lee KC, Kissack JC. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83(1):66-76.
8. Psychonaut WebMapping Research Group. MDPV report. London United Kingdom: Institute of Psychiatry, King’s College. http://www.psychonautproject.eu/documents/reports/MDPV.pdf. Accessed November 23, 2011.
9. Ross EA, Watson M, Goldberger B. “Bath salts” intoxication. N Engl J Med. 2011;365(10):967-968.
10. American Association of Poison Control Centers. Bath salts data. http://www.aapcc.org/dnn/Portals/0/Bath%20Salts%20Data%20for%20Website%2011.03.2011.pdf. Updated November 3 2011. Accessed November 23, 2011.
11. Centers for Disease Control and Prevention. Emergency department visits after use of a drug sold as “bath salts”—Michigan November 13, 2010-March 31, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(19):624-627.
12. Westphal F, Junge T, Rösner P, et al. Mass and NMR spectroscopic characterization of 3, 4-methylenedioxypyrovalerone: a designer drug with α-pyrrolidinophenone structure. Forensic Sci Int. 2009;190(1-3):1-8.
13. U.S. Drug Enforcement Administration. Chemicals used in “bath salts” now under federal control and regulation. http://www.justice.gov/dea/pubs/pressrel/pr102111.html. Accessed November 23, 2011.
1. André C, Jaber-Filho JA, Bento RM, et al. Delirium following ingestion of marijuana in chocolate cookies. CNS Spectr. 2006;11(4):262-264.
2. Hollister LE. Health aspects of cannabis. Pharmacol Rev. 1986;38(1):1-20.
3. Meyer ME. Psychiatric consequences of marijuana use: the state of the evidence. In: Tinklenberg JR ed. Marijuana and health hazards: methodologic issues in current research. New York, NY: Academic Press; 1975:33–152.
4. Ruttenber AJ, Lawler-Heavner J, Yin M, et al. Fatal excited delirium following cocaine use: epidemiologic findings provide new evidence for mechanisms of cocaine toxicity. J Forensic Sci. 1997;42(1):25-31.
5. Ruttenber AJ, McAnally HB, Wetli CV. Cocaine-associated rhabdomyolysis and excited delirium: different stages of the same syndrome. Am J Forensic Med Pathol. 1999;20(2):120-127.
6. Singhal PC, Rubin RB, Peters A, et al. Rhabdomyolysis and acute renal failure associated with cocaine abuse. J Toxicol Clin Toxicol. 1990;28(3):321-330.
7. Moeller KE, Lee KC, Kissack JC. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83(1):66-76.
8. Psychonaut WebMapping Research Group. MDPV report. London United Kingdom: Institute of Psychiatry, King’s College. http://www.psychonautproject.eu/documents/reports/MDPV.pdf. Accessed November 23, 2011.
9. Ross EA, Watson M, Goldberger B. “Bath salts” intoxication. N Engl J Med. 2011;365(10):967-968.
10. American Association of Poison Control Centers. Bath salts data. http://www.aapcc.org/dnn/Portals/0/Bath%20Salts%20Data%20for%20Website%2011.03.2011.pdf. Updated November 3 2011. Accessed November 23, 2011.
11. Centers for Disease Control and Prevention. Emergency department visits after use of a drug sold as “bath salts”—Michigan November 13, 2010-March 31, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(19):624-627.
12. Westphal F, Junge T, Rösner P, et al. Mass and NMR spectroscopic characterization of 3, 4-methylenedioxypyrovalerone: a designer drug with α-pyrrolidinophenone structure. Forensic Sci Int. 2009;190(1-3):1-8.
13. U.S. Drug Enforcement Administration. Chemicals used in “bath salts” now under federal control and regulation. http://www.justice.gov/dea/pubs/pressrel/pr102111.html. Accessed November 23, 2011.
Smoking cessation: What to tell patients about over-the-counter treatments
Discuss this article at www.facebook.com/CurrentPsychiatry
• Over-the-counter smoking cessation products likely will be the most appropriate first-line choice for many individuals before trying prescription products.
• Instruct patients to avoid smoking while using nicotine replacement therapy and educate them about the immediate and long-term benefits of quitting.
• Encourage patients to seek psychosocial counseling along with pharmacotherapy.
• Urge patients to engage in other quitting strategies by referring them to online and telephone resources (Related Resources). Also, encourage them to attend follow-up appointments to assess cessation therapy.
Mr. T, age 56, has major depressive disorder that is well controlled with fluoxetine, 40 mg/d. He has smoked ≥1 packs of cigarettes per day for the last 25 years. On a recent visit, he indicates that he has begun using a 21-mg nicotine patch as advised by his pharmacist and that things are going OK, although he has had some “slip ups.” He is on week 7 of his quitting regimen and now is stepping down the patch dosage.
Upon further questioning he says that he has been cutting the 21-mg patches in half to save money. Mr. T also explains that occasionally he has given in to a strong urge to smoke because it was “too much to handle.” He states that he does not think this is a big deal because he uses electronic cigarettes and has heard that these products don’t contain “the bad cancer stuff.” At the end of Mr. T’s visit, he asks for something to help him sleep because has been unable to sleep consistently and has been having vivid dreams since starting the patch. He also wants to know how to reduce itching from the patch.
Approximately 46 million Americans smoke and cigarette smoking accounts for 1 of every 5 deaths in the United States each year.1 Since the advent of “Stop Smoking” campaigns, bans on smoking in public buildings, over-the-counter (OTC) nicotine replacement products, and Surgeon General recommendations, discussing smoking cessation with patients has become standard practice.
Research suggests that treatment to quit smoking should include a combination of pharmacotherapy and counseling, such as cognitive-behavioral strategies, support groups, and quitting hotlines.2 Pharmacotherapy consists of OTC nicotine replacement therapy (NRT) products and prescription medications. This article briefly highlights how to counsel patients about using OTC NRT products (Table 1).2-5 See Table 2 for a summary of prescription smoking cessation agents
Table 1
Over-the-counter nicotine replacement therapy products
| Product | Dosage | Side effects | Amount of nicotine | Costa | Comments |
|---|---|---|---|---|---|
| Nicotine transdermal patches | For patients who smoked >.5 PPD: 21 mg/d for 6 weeks; 14 mg/d for 2 weeks; 7 mg/d for 2 weeks | Local skin irritation, sleep disturbances, and vivid dreams | 7, 14, or 21 mg /d | 21 mg: $32 for 14 patches 14 mg: $32 for 14 patches 7 mg: $19 for 7 patches | Alternate sites. Do not cut. Do not leave on skin for longer than life of patch (24 hours). Washing, bathing, swimming are OK. Remove patch if undergoing MRI because of reports of burns |
| For patients who smoked <.5 PPD: 14 mg/d for 6 weeks; 7 mg/d for 2 weeks | |||||
| Nicotine polacrilex gum | For patients who smoked ≥1.25 PPD: 4 mg | Unpleasant taste, jaw soreness, hiccups, dyspepsia, hypersalivation, and nausea (from chewing gum too quickly) | 2 or 4 mg per piece | 4 mg: $50 for 170 pieces 2 mg: $50 for 170 pieces | Use “chew and park” method. As part of combination therapy, use only as needed. No more than 24 pieces per day; use caution with patients with jaw or mouth conditions |
| For patients who smoked <1.25 PPD: 2 mg Weeks 1 to 6: 1 piece every 1 to 2 hours Weeks 7 to 9: 1 piece every 2 to 4 hours Weeks 10 to 12: 1 piece every 4 to 8 hours | |||||
| Nicotine polacrilex lozenge | For patients who smoked 1st cigarette within 30 minutes of waking: 4 mg | Mouth irritation, hiccups, nausea, cough, and insomnia | 2 or 4 mg per lozenge | 4 mg: $43 for 72 lozenges 2 mg: $43 for 72 lozenges | Dissolve lozenge in mouth for 20 to 30 minutes. Rotate lozenge to different parts of mouth occasionally. Do not chew. No more than 5 lozenges in 6 hours or 20 per day. Same taper schedule as nicotine gum |
| For patients who smoked 1st cigarette >30 minutes after waking: 2 mg | |||||
| aAll prices taken from drugstore.com on September 26, 2011 PPD: packs per day Source: References 2-5 | |||||
Patches
Nicotine replacement patches are best used for maintenance treatment of nicotine cravings. They deliver a fixed amount of nicotine over 24 hours.3 Patches have a specially formulated transdermal matrix system and should not be cut. Doing so damages the drug delivery system and could lead to drug evaporation from the cut edges.4 Mr. T’s psychiatrist advises him not to cut patches but instead purchase the 14-mg patch because he is at this step of the smoking cessation regimen.
Skin irritation caused by adhesive is a common adverse event from nicotine patches. Rotating the location of each patch to a different hairless body area is the best way to prevent or combat skin irritation. If rotating the location of the patch does not relieve irritation, patients can apply a thin layer of an OTC hydrocortisone 1% cream to the affected site 2 to 4 times a day after gently washing the area.5 Instruct patients to avoid using occlusive dressings over the topical application.
Nicotine replacement patches also have been reported to cause vivid dreams and insomnia.3 These side effects may be caused by nighttime nicotine absorption, which might be avoided by switching to a different NRT product or removing the 24-hour patch when going to bed.4
Combining treatments
Many patients experience nicotine cravings while using the nicotine replacement patch. Stressful situations and events can trigger a patient’s desire for nicotine and withdrawal symptoms that a patch that delivers a continuous amount of nicotine over 24 hours cannot alleviate. Combining different forms of treatment could combat these symptoms.2,3,5
Combination therapy might consist of using sustained-release bupropion or a nicotine patch with rapid-acting NRT products such as a lozenge, gum, nasal spray, or inhaler. In Mr. T’s case, clinicians recommend that he use nicotine polacrilex gum in addition to the patch to quell his cravings. Also, he is instructed to stop using electronic cigarettes because they are considered tobacco products, are not regulated by the FDA, and may contain toxic substances.6
Instruct patients who use nicotine gum to employ the “chew and park” method.4 First, they should chew the gum very slowly until they notice a minty taste or tingling feeling, then “park” the gum between the cheek and gums for 1 to 2 minutes to allow nicotine to be absorbed across the gum lining. After 2 minutes or when tingling ceases, patients should slowly resume chewing until a tingling or minty taste returns and then “park” the gum again in a different area of the gums. Tell patients to repeat the “chew and park” method until there is no more taste or tingling (approximately 30 minutes). Explain that chewing the gum too fast may result in nausea or lightheadedness and patients should refrain from eating or drinking 15 minutes before or while using the gum. Mr. T is instructed to use the gum only when the urge to smoke is overbearing, and not regularly.
The nicotine polacrilex gum is more viscous than ordinary chewing gum and may stick to or possibly damage dental work such as fillings, dentures, crowns, and braces. An acceptable alternative is the nicotine polacrilex lozenge. Advise patients who want to try lozenges to:
- place the lozenge in the mouth and allow it to dissolve slowly over 20 to 30 minutes (during this time patients may experience a tingling sensation as nicotine is released)
- rotate the lozenge to different areas of the mouth every few minutes to lessen irritation
- avoid chewing or swallowing the lozenge because doing so will lead to improper release of nicotine and side effects, including nausea, hiccups, and heartburn
- refrain from eating or drinking 15 minutes before or while using the lozenge.
For many patients, the breadth of pharmacologic agents available for smoking cessation has made quitting a more attainable goal. OTC smoking cessation products are available in most drug stores, which gives smokers easy access to taking this important step. Counseling patients on the proper use of OTC products may help them successfully stop smoking.7
Although a patient’s medical history, including cardiac status, must be considered before starting specific agents, in many instances patient preference is the prevailing factor when choosing therapy. Often, the risks of continued smoking outweigh the risks of using smoking cessation products. OTC smoking cessation products may be an appropriate first-line treatment for many individuals before trying prescription medications, such as bupropion or varenicline.
For patients
- Treat Tobacco. www.treatobacco.net.
- Smokefree.gov mobile application. http://smokefree.gov/apps.
- Medline Plus. Quitting smoking. www.nlm.nih.gov/medlineplus/quittingsmoking.html.
- Quit for Life Program. www.quitnow.net.
- American Lung Association. Stop Smoking. www.lungusa.org/stop-smoking.
For clinicians
- Agency for Health Research and Quality. Treating tobacco use and dependence: 2008 update. www.ahrq.gov/path/tobacco.htm#clinicians.
Drug Brand Names
- Bupropion SR • Zyban, Wellbutrin SR
- Fluoxetine • Prozac
- Varenicline • Chantix
Disclosure
Dr. Ellingrod receives grant/research support from the National Institute of Mental Health.
Dr. Burghardt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table 2
Prescription smoking cessation productsa
| Product | Dosage | Side effects | Amount of nicotine | Costb | Notes |
|---|---|---|---|---|---|
| Nicotine inhaler | 6 to 16 cartridges/d | Throat/mouth irritation and cough | 10 mg cartridges deliver 4 mg of nicotine | 10 mg inhaler with 168 cartridges: $213 | Vapor, not smoke, is released and deposited in mouth. Similar mechanism of action to nicotine gum. Continuously puff for ~20 minutes. Gradually reduce dosage over 12 weeks. Helps with patients who need the “action” of smoking. Caution in patients who have a history of bronchospastic disease because of potential airway irritation |
| Nicotine nasal spray | 10 mg/ml bottle 8 to 40 doses/d One dose is a spray to each nostril | Initial (~10 week) watery eyes, coughing, and nasal and throat irritation | 0.5 mg/spray | 10 ml bottle: $186 | Fastest delivery of nicotine vs other products. Tilt head back slightly when delivering spray. Do not sniff, swallow, or inhale through the nose. Continue treatment for 3 to 6 months with an individualized reduction in usage |
| Bupropion SR | 150 mg/d for 3 days, then 300 mg/d for 7 to 12 weeks or longer | Weight change, constipation, confusion, headache, and insomnia | N/A | 60 tablets: $106 | Patients should stop smoking during the second week of treatment. Combination treatment has achieved higher cessation rates. Avoid bedtime dosing to minimize insomnia (eg, 7 AM and 3 PM dosing strategy). Avoid in patients with seizure disorders |
| Varenicline | Days 1 to 3: 0.5 mg/d Days 4 to 7: 1 mg/d Day 8 to end of treatment: 2 mg/d Start treatment 1 week before quitting and continue for 3 to 6 months | Constipation, flatulence, nausea, vomiting, insomnia, and headache | N/A | Starting pack: $179 Continuing pack: $177 | Partial agonist of nicotinic acetylcholine receptor. Superiority to placebo has been shown but more studies are needed to show superiority to NRT. Safety and efficacy of combination therapy has not been established. Pack titrates dosage to 2 mg/d to decrease nausea. Take with water and food. Has a “black-box” warning for serious neuropsychiatric events, including suicidal ideations and behavior |
1. Centers for Disease Control and Prevention Smoking and Tobacco Use. Adult cigarette smoking in the United States: current estimate. http://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm. Accessed November 29 2011.
2. Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel, Liaisons, and Staff. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
3. Physicians’ Desk Reference. 64th ed. Montvale, NJ: Thomson PDR; 2010.
4. Kroon LA, Hudmon KS, Corelli RL. Smoking cessation. In: Berardi RR Ferreri SP, Hume AL, et al, eds. Handbook of nonprescription drugs: an interactive approach to self-care. 16th ed. Washington, DC: American Pharmacists Association; 2009:883–916.
5. Doering PL, Kennedy WK, Boothby LA. Substance-related disorders: alcohol nicotine, and caffeine. In: DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: a pathophysiologic approach. 7th ed. New York, NY: McGraw-Hill; 2008:1083–1098.
6. U.S. Food and Drug Administration. Electronic cigarettes. http://www.fda.gov/NewsEvents/PublicHealthFocus/ucm172906.htm. Accessed November 29, 2011.
7. Prokhorov AV, Hudmon KS, Marani S, et al. Engaging physicians and pharmacists in providing smoking cessation counseling. Arch Intern Med. 2010;170(18):1640-1646.
Kyle Burghardt, PharmD
Dr. Burghardt is a Research Fellow, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Dr. Ellingrod is Associate Professor, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Kyle Burghardt, PharmD
Dr. Burghardt is a Research Fellow, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Dr. Ellingrod is Associate Professor, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Kyle Burghardt, PharmD
Dr. Burghardt is a Research Fellow, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Dr. Ellingrod is Associate Professor, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Discuss this article at www.facebook.com/CurrentPsychiatry
• Over-the-counter smoking cessation products likely will be the most appropriate first-line choice for many individuals before trying prescription products.
• Instruct patients to avoid smoking while using nicotine replacement therapy and educate them about the immediate and long-term benefits of quitting.
• Encourage patients to seek psychosocial counseling along with pharmacotherapy.
• Urge patients to engage in other quitting strategies by referring them to online and telephone resources (Related Resources). Also, encourage them to attend follow-up appointments to assess cessation therapy.
Mr. T, age 56, has major depressive disorder that is well controlled with fluoxetine, 40 mg/d. He has smoked ≥1 packs of cigarettes per day for the last 25 years. On a recent visit, he indicates that he has begun using a 21-mg nicotine patch as advised by his pharmacist and that things are going OK, although he has had some “slip ups.” He is on week 7 of his quitting regimen and now is stepping down the patch dosage.
Upon further questioning he says that he has been cutting the 21-mg patches in half to save money. Mr. T also explains that occasionally he has given in to a strong urge to smoke because it was “too much to handle.” He states that he does not think this is a big deal because he uses electronic cigarettes and has heard that these products don’t contain “the bad cancer stuff.” At the end of Mr. T’s visit, he asks for something to help him sleep because has been unable to sleep consistently and has been having vivid dreams since starting the patch. He also wants to know how to reduce itching from the patch.
Approximately 46 million Americans smoke and cigarette smoking accounts for 1 of every 5 deaths in the United States each year.1 Since the advent of “Stop Smoking” campaigns, bans on smoking in public buildings, over-the-counter (OTC) nicotine replacement products, and Surgeon General recommendations, discussing smoking cessation with patients has become standard practice.
Research suggests that treatment to quit smoking should include a combination of pharmacotherapy and counseling, such as cognitive-behavioral strategies, support groups, and quitting hotlines.2 Pharmacotherapy consists of OTC nicotine replacement therapy (NRT) products and prescription medications. This article briefly highlights how to counsel patients about using OTC NRT products (Table 1).2-5 See Table 2 for a summary of prescription smoking cessation agents
Table 1
Over-the-counter nicotine replacement therapy products
| Product | Dosage | Side effects | Amount of nicotine | Costa | Comments |
|---|---|---|---|---|---|
| Nicotine transdermal patches | For patients who smoked >.5 PPD: 21 mg/d for 6 weeks; 14 mg/d for 2 weeks; 7 mg/d for 2 weeks | Local skin irritation, sleep disturbances, and vivid dreams | 7, 14, or 21 mg /d | 21 mg: $32 for 14 patches 14 mg: $32 for 14 patches 7 mg: $19 for 7 patches | Alternate sites. Do not cut. Do not leave on skin for longer than life of patch (24 hours). Washing, bathing, swimming are OK. Remove patch if undergoing MRI because of reports of burns |
| For patients who smoked <.5 PPD: 14 mg/d for 6 weeks; 7 mg/d for 2 weeks | |||||
| Nicotine polacrilex gum | For patients who smoked ≥1.25 PPD: 4 mg | Unpleasant taste, jaw soreness, hiccups, dyspepsia, hypersalivation, and nausea (from chewing gum too quickly) | 2 or 4 mg per piece | 4 mg: $50 for 170 pieces 2 mg: $50 for 170 pieces | Use “chew and park” method. As part of combination therapy, use only as needed. No more than 24 pieces per day; use caution with patients with jaw or mouth conditions |
| For patients who smoked <1.25 PPD: 2 mg Weeks 1 to 6: 1 piece every 1 to 2 hours Weeks 7 to 9: 1 piece every 2 to 4 hours Weeks 10 to 12: 1 piece every 4 to 8 hours | |||||
| Nicotine polacrilex lozenge | For patients who smoked 1st cigarette within 30 minutes of waking: 4 mg | Mouth irritation, hiccups, nausea, cough, and insomnia | 2 or 4 mg per lozenge | 4 mg: $43 for 72 lozenges 2 mg: $43 for 72 lozenges | Dissolve lozenge in mouth for 20 to 30 minutes. Rotate lozenge to different parts of mouth occasionally. Do not chew. No more than 5 lozenges in 6 hours or 20 per day. Same taper schedule as nicotine gum |
| For patients who smoked 1st cigarette >30 minutes after waking: 2 mg | |||||
| aAll prices taken from drugstore.com on September 26, 2011 PPD: packs per day Source: References 2-5 | |||||
Patches
Nicotine replacement patches are best used for maintenance treatment of nicotine cravings. They deliver a fixed amount of nicotine over 24 hours.3 Patches have a specially formulated transdermal matrix system and should not be cut. Doing so damages the drug delivery system and could lead to drug evaporation from the cut edges.4 Mr. T’s psychiatrist advises him not to cut patches but instead purchase the 14-mg patch because he is at this step of the smoking cessation regimen.
Skin irritation caused by adhesive is a common adverse event from nicotine patches. Rotating the location of each patch to a different hairless body area is the best way to prevent or combat skin irritation. If rotating the location of the patch does not relieve irritation, patients can apply a thin layer of an OTC hydrocortisone 1% cream to the affected site 2 to 4 times a day after gently washing the area.5 Instruct patients to avoid using occlusive dressings over the topical application.
Nicotine replacement patches also have been reported to cause vivid dreams and insomnia.3 These side effects may be caused by nighttime nicotine absorption, which might be avoided by switching to a different NRT product or removing the 24-hour patch when going to bed.4
Combining treatments
Many patients experience nicotine cravings while using the nicotine replacement patch. Stressful situations and events can trigger a patient’s desire for nicotine and withdrawal symptoms that a patch that delivers a continuous amount of nicotine over 24 hours cannot alleviate. Combining different forms of treatment could combat these symptoms.2,3,5
Combination therapy might consist of using sustained-release bupropion or a nicotine patch with rapid-acting NRT products such as a lozenge, gum, nasal spray, or inhaler. In Mr. T’s case, clinicians recommend that he use nicotine polacrilex gum in addition to the patch to quell his cravings. Also, he is instructed to stop using electronic cigarettes because they are considered tobacco products, are not regulated by the FDA, and may contain toxic substances.6
Instruct patients who use nicotine gum to employ the “chew and park” method.4 First, they should chew the gum very slowly until they notice a minty taste or tingling feeling, then “park” the gum between the cheek and gums for 1 to 2 minutes to allow nicotine to be absorbed across the gum lining. After 2 minutes or when tingling ceases, patients should slowly resume chewing until a tingling or minty taste returns and then “park” the gum again in a different area of the gums. Tell patients to repeat the “chew and park” method until there is no more taste or tingling (approximately 30 minutes). Explain that chewing the gum too fast may result in nausea or lightheadedness and patients should refrain from eating or drinking 15 minutes before or while using the gum. Mr. T is instructed to use the gum only when the urge to smoke is overbearing, and not regularly.
The nicotine polacrilex gum is more viscous than ordinary chewing gum and may stick to or possibly damage dental work such as fillings, dentures, crowns, and braces. An acceptable alternative is the nicotine polacrilex lozenge. Advise patients who want to try lozenges to:
- place the lozenge in the mouth and allow it to dissolve slowly over 20 to 30 minutes (during this time patients may experience a tingling sensation as nicotine is released)
- rotate the lozenge to different areas of the mouth every few minutes to lessen irritation
- avoid chewing or swallowing the lozenge because doing so will lead to improper release of nicotine and side effects, including nausea, hiccups, and heartburn
- refrain from eating or drinking 15 minutes before or while using the lozenge.
For many patients, the breadth of pharmacologic agents available for smoking cessation has made quitting a more attainable goal. OTC smoking cessation products are available in most drug stores, which gives smokers easy access to taking this important step. Counseling patients on the proper use of OTC products may help them successfully stop smoking.7
Although a patient’s medical history, including cardiac status, must be considered before starting specific agents, in many instances patient preference is the prevailing factor when choosing therapy. Often, the risks of continued smoking outweigh the risks of using smoking cessation products. OTC smoking cessation products may be an appropriate first-line treatment for many individuals before trying prescription medications, such as bupropion or varenicline.
For patients
- Treat Tobacco. www.treatobacco.net.
- Smokefree.gov mobile application. http://smokefree.gov/apps.
- Medline Plus. Quitting smoking. www.nlm.nih.gov/medlineplus/quittingsmoking.html.
- Quit for Life Program. www.quitnow.net.
- American Lung Association. Stop Smoking. www.lungusa.org/stop-smoking.
For clinicians
- Agency for Health Research and Quality. Treating tobacco use and dependence: 2008 update. www.ahrq.gov/path/tobacco.htm#clinicians.
Drug Brand Names
- Bupropion SR • Zyban, Wellbutrin SR
- Fluoxetine • Prozac
- Varenicline • Chantix
Disclosure
Dr. Ellingrod receives grant/research support from the National Institute of Mental Health.
Dr. Burghardt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table 2
Prescription smoking cessation productsa
| Product | Dosage | Side effects | Amount of nicotine | Costb | Notes |
|---|---|---|---|---|---|
| Nicotine inhaler | 6 to 16 cartridges/d | Throat/mouth irritation and cough | 10 mg cartridges deliver 4 mg of nicotine | 10 mg inhaler with 168 cartridges: $213 | Vapor, not smoke, is released and deposited in mouth. Similar mechanism of action to nicotine gum. Continuously puff for ~20 minutes. Gradually reduce dosage over 12 weeks. Helps with patients who need the “action” of smoking. Caution in patients who have a history of bronchospastic disease because of potential airway irritation |
| Nicotine nasal spray | 10 mg/ml bottle 8 to 40 doses/d One dose is a spray to each nostril | Initial (~10 week) watery eyes, coughing, and nasal and throat irritation | 0.5 mg/spray | 10 ml bottle: $186 | Fastest delivery of nicotine vs other products. Tilt head back slightly when delivering spray. Do not sniff, swallow, or inhale through the nose. Continue treatment for 3 to 6 months with an individualized reduction in usage |
| Bupropion SR | 150 mg/d for 3 days, then 300 mg/d for 7 to 12 weeks or longer | Weight change, constipation, confusion, headache, and insomnia | N/A | 60 tablets: $106 | Patients should stop smoking during the second week of treatment. Combination treatment has achieved higher cessation rates. Avoid bedtime dosing to minimize insomnia (eg, 7 AM and 3 PM dosing strategy). Avoid in patients with seizure disorders |
| Varenicline | Days 1 to 3: 0.5 mg/d Days 4 to 7: 1 mg/d Day 8 to end of treatment: 2 mg/d Start treatment 1 week before quitting and continue for 3 to 6 months | Constipation, flatulence, nausea, vomiting, insomnia, and headache | N/A | Starting pack: $179 Continuing pack: $177 | Partial agonist of nicotinic acetylcholine receptor. Superiority to placebo has been shown but more studies are needed to show superiority to NRT. Safety and efficacy of combination therapy has not been established. Pack titrates dosage to 2 mg/d to decrease nausea. Take with water and food. Has a “black-box” warning for serious neuropsychiatric events, including suicidal ideations and behavior |
Discuss this article at www.facebook.com/CurrentPsychiatry
• Over-the-counter smoking cessation products likely will be the most appropriate first-line choice for many individuals before trying prescription products.
• Instruct patients to avoid smoking while using nicotine replacement therapy and educate them about the immediate and long-term benefits of quitting.
• Encourage patients to seek psychosocial counseling along with pharmacotherapy.
• Urge patients to engage in other quitting strategies by referring them to online and telephone resources (Related Resources). Also, encourage them to attend follow-up appointments to assess cessation therapy.
Mr. T, age 56, has major depressive disorder that is well controlled with fluoxetine, 40 mg/d. He has smoked ≥1 packs of cigarettes per day for the last 25 years. On a recent visit, he indicates that he has begun using a 21-mg nicotine patch as advised by his pharmacist and that things are going OK, although he has had some “slip ups.” He is on week 7 of his quitting regimen and now is stepping down the patch dosage.
Upon further questioning he says that he has been cutting the 21-mg patches in half to save money. Mr. T also explains that occasionally he has given in to a strong urge to smoke because it was “too much to handle.” He states that he does not think this is a big deal because he uses electronic cigarettes and has heard that these products don’t contain “the bad cancer stuff.” At the end of Mr. T’s visit, he asks for something to help him sleep because has been unable to sleep consistently and has been having vivid dreams since starting the patch. He also wants to know how to reduce itching from the patch.
Approximately 46 million Americans smoke and cigarette smoking accounts for 1 of every 5 deaths in the United States each year.1 Since the advent of “Stop Smoking” campaigns, bans on smoking in public buildings, over-the-counter (OTC) nicotine replacement products, and Surgeon General recommendations, discussing smoking cessation with patients has become standard practice.
Research suggests that treatment to quit smoking should include a combination of pharmacotherapy and counseling, such as cognitive-behavioral strategies, support groups, and quitting hotlines.2 Pharmacotherapy consists of OTC nicotine replacement therapy (NRT) products and prescription medications. This article briefly highlights how to counsel patients about using OTC NRT products (Table 1).2-5 See Table 2 for a summary of prescription smoking cessation agents
Table 1
Over-the-counter nicotine replacement therapy products
| Product | Dosage | Side effects | Amount of nicotine | Costa | Comments |
|---|---|---|---|---|---|
| Nicotine transdermal patches | For patients who smoked >.5 PPD: 21 mg/d for 6 weeks; 14 mg/d for 2 weeks; 7 mg/d for 2 weeks | Local skin irritation, sleep disturbances, and vivid dreams | 7, 14, or 21 mg /d | 21 mg: $32 for 14 patches 14 mg: $32 for 14 patches 7 mg: $19 for 7 patches | Alternate sites. Do not cut. Do not leave on skin for longer than life of patch (24 hours). Washing, bathing, swimming are OK. Remove patch if undergoing MRI because of reports of burns |
| For patients who smoked <.5 PPD: 14 mg/d for 6 weeks; 7 mg/d for 2 weeks | |||||
| Nicotine polacrilex gum | For patients who smoked ≥1.25 PPD: 4 mg | Unpleasant taste, jaw soreness, hiccups, dyspepsia, hypersalivation, and nausea (from chewing gum too quickly) | 2 or 4 mg per piece | 4 mg: $50 for 170 pieces 2 mg: $50 for 170 pieces | Use “chew and park” method. As part of combination therapy, use only as needed. No more than 24 pieces per day; use caution with patients with jaw or mouth conditions |
| For patients who smoked <1.25 PPD: 2 mg Weeks 1 to 6: 1 piece every 1 to 2 hours Weeks 7 to 9: 1 piece every 2 to 4 hours Weeks 10 to 12: 1 piece every 4 to 8 hours | |||||
| Nicotine polacrilex lozenge | For patients who smoked 1st cigarette within 30 minutes of waking: 4 mg | Mouth irritation, hiccups, nausea, cough, and insomnia | 2 or 4 mg per lozenge | 4 mg: $43 for 72 lozenges 2 mg: $43 for 72 lozenges | Dissolve lozenge in mouth for 20 to 30 minutes. Rotate lozenge to different parts of mouth occasionally. Do not chew. No more than 5 lozenges in 6 hours or 20 per day. Same taper schedule as nicotine gum |
| For patients who smoked 1st cigarette >30 minutes after waking: 2 mg | |||||
| aAll prices taken from drugstore.com on September 26, 2011 PPD: packs per day Source: References 2-5 | |||||
Patches
Nicotine replacement patches are best used for maintenance treatment of nicotine cravings. They deliver a fixed amount of nicotine over 24 hours.3 Patches have a specially formulated transdermal matrix system and should not be cut. Doing so damages the drug delivery system and could lead to drug evaporation from the cut edges.4 Mr. T’s psychiatrist advises him not to cut patches but instead purchase the 14-mg patch because he is at this step of the smoking cessation regimen.
Skin irritation caused by adhesive is a common adverse event from nicotine patches. Rotating the location of each patch to a different hairless body area is the best way to prevent or combat skin irritation. If rotating the location of the patch does not relieve irritation, patients can apply a thin layer of an OTC hydrocortisone 1% cream to the affected site 2 to 4 times a day after gently washing the area.5 Instruct patients to avoid using occlusive dressings over the topical application.
Nicotine replacement patches also have been reported to cause vivid dreams and insomnia.3 These side effects may be caused by nighttime nicotine absorption, which might be avoided by switching to a different NRT product or removing the 24-hour patch when going to bed.4
Combining treatments
Many patients experience nicotine cravings while using the nicotine replacement patch. Stressful situations and events can trigger a patient’s desire for nicotine and withdrawal symptoms that a patch that delivers a continuous amount of nicotine over 24 hours cannot alleviate. Combining different forms of treatment could combat these symptoms.2,3,5
Combination therapy might consist of using sustained-release bupropion or a nicotine patch with rapid-acting NRT products such as a lozenge, gum, nasal spray, or inhaler. In Mr. T’s case, clinicians recommend that he use nicotine polacrilex gum in addition to the patch to quell his cravings. Also, he is instructed to stop using electronic cigarettes because they are considered tobacco products, are not regulated by the FDA, and may contain toxic substances.6
Instruct patients who use nicotine gum to employ the “chew and park” method.4 First, they should chew the gum very slowly until they notice a minty taste or tingling feeling, then “park” the gum between the cheek and gums for 1 to 2 minutes to allow nicotine to be absorbed across the gum lining. After 2 minutes or when tingling ceases, patients should slowly resume chewing until a tingling or minty taste returns and then “park” the gum again in a different area of the gums. Tell patients to repeat the “chew and park” method until there is no more taste or tingling (approximately 30 minutes). Explain that chewing the gum too fast may result in nausea or lightheadedness and patients should refrain from eating or drinking 15 minutes before or while using the gum. Mr. T is instructed to use the gum only when the urge to smoke is overbearing, and not regularly.
The nicotine polacrilex gum is more viscous than ordinary chewing gum and may stick to or possibly damage dental work such as fillings, dentures, crowns, and braces. An acceptable alternative is the nicotine polacrilex lozenge. Advise patients who want to try lozenges to:
- place the lozenge in the mouth and allow it to dissolve slowly over 20 to 30 minutes (during this time patients may experience a tingling sensation as nicotine is released)
- rotate the lozenge to different areas of the mouth every few minutes to lessen irritation
- avoid chewing or swallowing the lozenge because doing so will lead to improper release of nicotine and side effects, including nausea, hiccups, and heartburn
- refrain from eating or drinking 15 minutes before or while using the lozenge.
For many patients, the breadth of pharmacologic agents available for smoking cessation has made quitting a more attainable goal. OTC smoking cessation products are available in most drug stores, which gives smokers easy access to taking this important step. Counseling patients on the proper use of OTC products may help them successfully stop smoking.7
Although a patient’s medical history, including cardiac status, must be considered before starting specific agents, in many instances patient preference is the prevailing factor when choosing therapy. Often, the risks of continued smoking outweigh the risks of using smoking cessation products. OTC smoking cessation products may be an appropriate first-line treatment for many individuals before trying prescription medications, such as bupropion or varenicline.
For patients
- Treat Tobacco. www.treatobacco.net.
- Smokefree.gov mobile application. http://smokefree.gov/apps.
- Medline Plus. Quitting smoking. www.nlm.nih.gov/medlineplus/quittingsmoking.html.
- Quit for Life Program. www.quitnow.net.
- American Lung Association. Stop Smoking. www.lungusa.org/stop-smoking.
For clinicians
- Agency for Health Research and Quality. Treating tobacco use and dependence: 2008 update. www.ahrq.gov/path/tobacco.htm#clinicians.
Drug Brand Names
- Bupropion SR • Zyban, Wellbutrin SR
- Fluoxetine • Prozac
- Varenicline • Chantix
Disclosure
Dr. Ellingrod receives grant/research support from the National Institute of Mental Health.
Dr. Burghardt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table 2
Prescription smoking cessation productsa
| Product | Dosage | Side effects | Amount of nicotine | Costb | Notes |
|---|---|---|---|---|---|
| Nicotine inhaler | 6 to 16 cartridges/d | Throat/mouth irritation and cough | 10 mg cartridges deliver 4 mg of nicotine | 10 mg inhaler with 168 cartridges: $213 | Vapor, not smoke, is released and deposited in mouth. Similar mechanism of action to nicotine gum. Continuously puff for ~20 minutes. Gradually reduce dosage over 12 weeks. Helps with patients who need the “action” of smoking. Caution in patients who have a history of bronchospastic disease because of potential airway irritation |
| Nicotine nasal spray | 10 mg/ml bottle 8 to 40 doses/d One dose is a spray to each nostril | Initial (~10 week) watery eyes, coughing, and nasal and throat irritation | 0.5 mg/spray | 10 ml bottle: $186 | Fastest delivery of nicotine vs other products. Tilt head back slightly when delivering spray. Do not sniff, swallow, or inhale through the nose. Continue treatment for 3 to 6 months with an individualized reduction in usage |
| Bupropion SR | 150 mg/d for 3 days, then 300 mg/d for 7 to 12 weeks or longer | Weight change, constipation, confusion, headache, and insomnia | N/A | 60 tablets: $106 | Patients should stop smoking during the second week of treatment. Combination treatment has achieved higher cessation rates. Avoid bedtime dosing to minimize insomnia (eg, 7 AM and 3 PM dosing strategy). Avoid in patients with seizure disorders |
| Varenicline | Days 1 to 3: 0.5 mg/d Days 4 to 7: 1 mg/d Day 8 to end of treatment: 2 mg/d Start treatment 1 week before quitting and continue for 3 to 6 months | Constipation, flatulence, nausea, vomiting, insomnia, and headache | N/A | Starting pack: $179 Continuing pack: $177 | Partial agonist of nicotinic acetylcholine receptor. Superiority to placebo has been shown but more studies are needed to show superiority to NRT. Safety and efficacy of combination therapy has not been established. Pack titrates dosage to 2 mg/d to decrease nausea. Take with water and food. Has a “black-box” warning for serious neuropsychiatric events, including suicidal ideations and behavior |
1. Centers for Disease Control and Prevention Smoking and Tobacco Use. Adult cigarette smoking in the United States: current estimate. http://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm. Accessed November 29 2011.
2. Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel, Liaisons, and Staff. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
3. Physicians’ Desk Reference. 64th ed. Montvale, NJ: Thomson PDR; 2010.
4. Kroon LA, Hudmon KS, Corelli RL. Smoking cessation. In: Berardi RR Ferreri SP, Hume AL, et al, eds. Handbook of nonprescription drugs: an interactive approach to self-care. 16th ed. Washington, DC: American Pharmacists Association; 2009:883–916.
5. Doering PL, Kennedy WK, Boothby LA. Substance-related disorders: alcohol nicotine, and caffeine. In: DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: a pathophysiologic approach. 7th ed. New York, NY: McGraw-Hill; 2008:1083–1098.
6. U.S. Food and Drug Administration. Electronic cigarettes. http://www.fda.gov/NewsEvents/PublicHealthFocus/ucm172906.htm. Accessed November 29, 2011.
7. Prokhorov AV, Hudmon KS, Marani S, et al. Engaging physicians and pharmacists in providing smoking cessation counseling. Arch Intern Med. 2010;170(18):1640-1646.
1. Centers for Disease Control and Prevention Smoking and Tobacco Use. Adult cigarette smoking in the United States: current estimate. http://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm. Accessed November 29 2011.
2. Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel, Liaisons, and Staff. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
3. Physicians’ Desk Reference. 64th ed. Montvale, NJ: Thomson PDR; 2010.
4. Kroon LA, Hudmon KS, Corelli RL. Smoking cessation. In: Berardi RR Ferreri SP, Hume AL, et al, eds. Handbook of nonprescription drugs: an interactive approach to self-care. 16th ed. Washington, DC: American Pharmacists Association; 2009:883–916.
5. Doering PL, Kennedy WK, Boothby LA. Substance-related disorders: alcohol nicotine, and caffeine. In: DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: a pathophysiologic approach. 7th ed. New York, NY: McGraw-Hill; 2008:1083–1098.
6. U.S. Food and Drug Administration. Electronic cigarettes. http://www.fda.gov/NewsEvents/PublicHealthFocus/ucm172906.htm. Accessed November 29, 2011.
7. Prokhorov AV, Hudmon KS, Marani S, et al. Engaging physicians and pharmacists in providing smoking cessation counseling. Arch Intern Med. 2010;170(18):1640-1646.
Disoriented and forgetful
CASE: Disoriented and delusional
Ms. P, a 53-year-old registered nurse, is admitted to the inpatient psychiatric unit with confusion, markedly disorganized thought processes, delayed verbal responsiveness, mood lability, and persecutory delusions. Shortly before hospitalization, Ms. P traveled approximately 360 miles from her daughter’s home with a male companion. Noting changes in her mental status, the man brought Ms. P to the local hospital. She was then transferred to our facility.
At admission, Ms. P is not oriented to time. She denies auditory or visual hallucinations and does not display psychomotor agitation or retardation. She reports her mood as sad and her affect is mildly labile. Insight and judgment are considered poor.
Five years ago, Ms. P and her mother were diagnosed with Fabry’s disease (FD) based on genetic analysis. Both women are carriers for the mutations and Ms. P’s mother was found to have almost absent galactosidase activity.
The authors’ observations
FD is an X-linked recessive glycolipid storage disease caused by deficient activity of the lysosomal storage enzyme α-galactosidase A. The disorder affects both men and women and leads to progressive intracellular accumulation of globotriaosylceramide and other related glycosphingolipids.1,2 The earliest FD symptoms—burning pain and acroparesthesias—typically appear in childhood (Table 1).2 FD often is misdiagnosed in women because women tend to display neurologic symptoms later than men, with typical symptom onset in the teenage years.3,4 Often, these symptoms are confused with psychiatric disorders or vague neurologic or pain syndromes.5 In patients with no family history of FD, accurate diagnosis may not be made until adulthood.
Laboratory, dermatologic, and genetic tests can accurately determine the presence of FD.1 However, because multiple organ systems are involved, initially attributing symptoms to FD is challenging, particularly in women.1,3,5 For men, diagnosis can be established by measuring plasma or urinary globotriaosylceramide or plasma α-galactosidase A in addition to genetic analysis. In women, genetic analysis is a better diagnosis strategy because elevations in globotriaosylceramide or α-galactosidase A may not be prominent. An algorithm for diagnosing and assessing patients with FD has been proposed.2
Table 1
Typical signs and symptoms of Fabry’s disease
| Typical time at onset | Signs/symptoms |
|---|---|
| Childhood and adolescence (age ≤16) | Neuropathic pain Ophthalmologic abnormalities (cornea verticillata and tortuous retinal blood vessels) Hearing impairment Dyshidrosis (hypohidrosis and hyperhidrosis) Hypersensitivity to heat and cold Gastrointestinal disturbances and abdominal pain Lethargy and tiredness Angiokeratomas Onset of renal and cardiac signs (eg, microalbuminuria, proteinuria, abnormal heart rate variability) |
| Early adulthood (age 17 to 30) | Extension of any of the above Proteinuria and progressive renal failure Cardiomyopathy Transient ischemic attacks, strokes Facial dysmorphism |
| Later adulthood (age >30) | Worsening of any of the above Heart disease (eg, left ventricular hypertrophy, angina, arrhythmia, and dyspnea) Transient ischemic attacks, strokes Osteopenia and osteoporosis |
| Source: Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659, by permission of Oxford University Press | |
HISTORY: Cognitive deterioration
Ms. P has had psychiatric symptoms such as depression and anxiety since childhood. However, 3 years ago she started to experience psychological and cognitive deterioration. Medical records indicate that Ms. P described memory and concentration problems over the previous few years. She also reported pain, weakness, and numbness in her left leg after surgery for a work-related back injury, for which she received a financial settlement through workers’ compensation. Shortly thereafter, Ms. P separated from her third husband, moved in with her parents, and found work as a psychiatric nurse. She was dismissed after 6 weeks because she could not learn the electronic medical record system and had difficulty with memory and attention. Her performance on the Mini-Mental State Exam6 at that time was 28 out of 30, which was within normal limits.
After her parents died 3 years ago, Ms. P lived with her daughter, who became her primary caregiver and legal guardian. Ms. P’s daughter notes that her mother’s impulsive and risky behaviors grew more pronounced. Ms. P went on shopping sprees and became sexually promiscuous.
Ms. P’s psychiatric history includes childhood sexual abuse, hospitalization for a suicide attempt at age 19, and courses of psychotherapy and pharmacotherapy. In addition to FD, Ms. P’s medical history consists of coronary artery disease, type 2 diabetes mellitus, hypercholesterolemia, obesity, arthritis, back pain, fibromyalgia, and gastroesophageal reflux disease. Her family history is notable for alcohol abuse (both parents and a brother), lung cancer (mother), myocardial infarction (father), and Alzheimer’s disease (father).
The authors’ observations
Because α-galactosidase A is ubiquitous throughout the body, in addition to neurologic symptoms, FD involves multiple organ systems, with possible dermatologic, renal, gastrointestinal, cardiac, and cerebrovascular dysfunction. Despite growth in FD research, including the Fabry Outcomes Survey,3 the psychosocial and neuropsychiatric implications of the disease remain unclear.7 Behavioral presentations are idiosyncratic and unstable over time, depending on the structures impacted by progressive glycosphingolipid accumulation. Premature cardiovascular events (onset between age 30 and 40 for women), greater incidence of ischemic stroke or transient ischemic attack (7% to 30%), and frequent evidence of white matter lesions put FD patients at greater risk for developing presenile vascular dementia.1,3 Nearly all male FD patients with dementia show some evidence of stroke or transient ischemic attack; cognitive functioning has not been well explored in female patients.4 In a heterogeneous sample of 15 FD patients age 7 to 61, Segal et al8 noted deficits in attention, processing speed, and executive function .75 to 1.95 standard deviations below normative means. No patients in this study had a history of stroke or transient ischemic attack; neuroimaging studies were not reported. Kolodny and Pastores9 suggested multiple mechanisms for cognitive disruption, suggesting that mild dementia late in the disease course could be secondary to diffuse leukomalacia, multiple strokes, or possibly to lipid storage in hippocampal and frontal lobe neurons.
Psychiatric comorbidity
Psychiatric illness, such as depression or a personality disorder, may be comorbid with FD, although pathologic mechanisms remain unclear.7,10,11 Hypothesized mechanisms include:
- psychosocial stress from chronic disease
- white matter changes
- disruption of impaired L-arginine-nitric oxide pathways.7,12
Crosbie et al13 noted that FD patients presented with greater psychological distress as measured by the Minnesota Multiphasic Personality Inventory-2 than patients with Gaucher disease or chronic heart disease. However, no significant differences were found between patients with FD and those diagnosed with a pain disorder. In the Segal et al study, out of 11 adult FD patients, 4 were diagnosed with major depressive disorder, 1 with schizophrenia, 2 with schizotypal personality disorder, and 1 with borderline personality disorder.8
EVALUATION: Brain abnormalities
Head CT scans (conducted 2 years ago and 6 months ago) revealed prominent cortical sulci likely caused by underlying volume loss, especially in bifrontal areas. A brain MRI performed 2 months ago indicated a moderate degree of subcortical atrophy in bilateral frontal and parietal regions. These radiology findings suggest mild to moderate frontal atrophy, mild degree of white matter changes, and slightly enlarged ventricles. An EEG showed background slowing and lack of an alpha rhythm, indicative of cerebral cortical dysfunction.
Ms. P’s α-galactosidase A level was within normal limits; however, normal enzyme levels frequently are reported in symptomatic and asymptomatic female FD patients.14 A dermatology consult confirmed the presence of skin findings characteristic of FD (ie, multiple cherry red papules extensively distributed throughout Ms. P’s chest, abdomen, and back, as well as upper and lower extremities).
Ms. P completed 2 neuropsychological assessments separated by 5 months. For a summary of the results of these tests, see the table titled “Ms. P’s neuropsychological assessment results”. Both assessments revealed grossly impaired intellectual capacity, memory, processing speed, and motor functioning. During the assessment, Ms. P could understand all directions with minimal changes from standardized protocols. Ms. P became insistent that she would not be able to complete memory tasks successfully. She gave up prematurely on tasks, saying they were too difficult. She admitted to guessing on several items because she did not want to continue the task.
Ms. P’s performance on tasks measuring effort and validity of a person’s neuropsychological presentation was consistent with someone exaggerating neurologic symptoms. A person with true dementia may perform as poorly as Ms. P did. However, Ms. P’s scores likely underestimated her level of functioning, even if she was experiencing dementia. Ms. P could not complete tasks individuals with severe dementia complete successfully, such as simple addition and subtraction and digit repetition. Ms. P recalled several recent and remote events, such as her breakfast menu and location of her first assessment, but could not recall words practiced multiple times. Although Ms. P’s scores on a complex card-sorting task were in the impaired range, a detailed review of her pattern indicated that although Ms. P could not generate any correct sorting categories, she made few repetitive responses and errors. This pattern is consistent with someone who understands task requirements, but deliberately avoids answering correctly. This suggests that she retained some ability for hypotheses generation and problem solving; however, because she exaggerated her symptoms, specific deficits could not be determined.
The authors’ observations
Ms. P presented with an interesting manifestation of neuropsychiatric symptoms in the context of FD; however, common cardiac and cerebrovascular features of the disease were not fully developed. Ms. P experienced progressive cognitive and behavioral changes for 2 years before her admission (Table 2), which may represent a prodromal period leading up to what appeared to be a frontally mediated dementia syndrome. Müller et al15 described a patient with FD who displayed a behavioral profile similar to Ms. P’s that included increasingly unstable mood for at least 3 years, borderline personality disorder features, and rapidly fluctuating mood. A case study reported that risperidone, 1 mg/d, used to treat psychosis in a male FD patient caused extrapyramidal symptoms.16
Ms. P presented with no evidence of stroke or transient ischemic attacks, which is atypical for FD patients with cognitive impairment. However, neuroimaging did reveal frontal atrophy that may be associated with her impulse control deficits, risk-taking behavior, emotional instability, and poor judgment. Her cognitive testing was notable for impairment and exaggeration of symptoms consistent with personality disorder symptoms. Possible reasons for exaggeration include a desire to maintain the sick role or secondary gain related to obtaining disability income.
Ms. P’s behavior pattern could be caused by dementia with frontal features, possibly secondary to FD, in combination with personality and psychiatric pathology.
The mainstay of FD treatment is enzyme replacement therapy (ERT), which addresses the underlying enzyme deficiency. Available research indicates that ERT may reduce symptom severity and slow disease progression; however, further studies are needed to determine if it will reduce outcomes such as stroke, ischemic heart disease, or renal disease.2
Table 2
Symptoms that preceded Ms. P’s admission
| Time frame | Symptoms |
|---|---|
| 24 months before admission | Depressed mood Decreased ability to manage independent activities of daily living (eg, finances, cooking) Minimal objective cognitive impairment |
| 12 months before admission | Increased depression Mild to moderate decline in cognitive functioning Visual and auditory hallucinations Impulsivity/poor impulse control Irrational decision-making Increased risky behavior |
| 6 months before admission | Severe cognitive decline with cognitive symptom exaggeration Psychiatric symptom exaggeration Disorganized thinking Continued risky behavior and poor decision-making |
TREATMENT: Persistent deficits
Ms. P is started on risperidone rapidly titrated to 4 mg/d for delusional thinking and behavioral disturbance. After initially improving, she develops delirium when risperidone is increased to 4 mg/d. She has visual hallucinations, marked confusion with disorientation, worsened short-term memory, and an unsteady, shuffling gait. Risperidone is tapered and discontinued and Ms. P’s motor symptoms resolve within 2 days; however, she remains confused and delusional. We start her on quetiapine, 25 mg/d titrated to 50 mg/d, and her agitation and delusional thinking progressively decline. Memantine, titrated to 20 mg/d, and rivastigmine, started at 3 mg/d titrated to 9 mg/d, are added to address her cognitive symptoms.
Over several weeks, Ms. P’s mental status slowly improves and her drug-induced delirium completely resolves. However, she has persistent cognitive impairment characterized by compromised short-term memory and poor insight into her medical and psychological condition. She maintains unrealistic expectations about her ability to live independently and return to the workforce. The treatment team recommends that Ms. P’s daughter pursue guardianship and that she receive around-the-clock supervision after discharge from the hospital.
Table
Ms. P’s neuropsychological assessment results
| June | November | |
|---|---|---|
| Intellectual functioning | ||
| Wechsler Adult Intelligence Scale-III | ||
| FSIQ | 60 | |
| VIQ | 68 | |
| PIQ | 56 | |
| Ravens Colored Progressive Matrices | 70 | |
| Premorbid intellectual functioning estimates | ||
| Peabody Picture Vocabulary Test-2 | 89 | |
| Barona Demographic Estimate | 104 | 104 |
| North American Adult Reading Test | 99 | |
| Memory functioning | ||
| Wechsler Memory Scale-III | ||
| Immediate memory | 45 | |
| General delay memory | 47 | |
| Auditory recognition delay | 55 | |
| California Verbal Learning Test-II | ||
| Trial 1 (immediate recall) | <60 (raw = 3) | |
| Trial 5 | <60 (raw = 3) | |
| Total Words Learned | <60 (raw = 15) | |
| Short Delay Free Recall | <60 (raw = 2) | |
| Long Delay Free Recall | <60 (raw = 4) | |
| Executive functioning | ||
| Trail Making Test A | 88 | 88 |
| Trail Making Test B | failed to understand | failed to understand |
| Wisconsin Card Sort-64 | ||
| Number of categories | <60 (raw = 0) | |
| Errors | 81 | |
| Percent conceptual level responses | 74 | |
| Perseverative responses | 107 | |
| Perseverative errors | 108 | |
| COWAT FAS | 65 | 69 |
| Category exemplar | 69 | 80 |
| Motor functioning | ||
| Finger Tapping Dominant Hand | 68 | |
| Finger Tapping Non-Dominant Hand | 62 | |
| Invalidity/effort | ||
| TOMM | ||
| Trial 1 | raw = 34 | raw = 37 |
| Trial 2 | raw = 42 | raw = 45 |
| Recognition | raw = 44 | |
| MSVT verbal | fail | |
| MSVT nonverbal | fail | |
| Scores provided are standardized (mean = 100; SD = 15). Raw scores are also provided when indicated. COWAT: Controlled oral word association test; FSIQ: Full Scale IQ; MSVT: Medical Symptom Validity Test; PIQ: Performance IQ; TOMM: Test of Memory Malingering; VIQ: Verbal IQ | ||
Related Resources
- National Institute of Neurological Disorders and Stroke. Fabry disease information page. www.ninds.nih.gov/disorders/fabrys/fabrys.htm.
- National Fabry Disease Foundation. www.thenfdf.org.
- Rozenfeld P, Neumann PM. Treatment of Fabry disease: current and emerging strategies. Curr Pharm Biotechnol. 2011;12(6):916-922.
Drug Brand Names
- Donepezil • Aricept
- Memantine • Namenda
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Eng CM, Germain DP, Banikazemi M, et al. Fabry disease: guidelines for the evaluation and management of multi-organ system involvement. Genet Med. 2006;8(9):539-548.
2. Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659.
3. Deegan PB, Baehner AF, Barba Romero MA, et al. Natural history of Fabry disease in females in the Fabry Outcome Survey. J Med Genet. 2006;43(4):347-352.
4. Fellgiebel A, Müller MJ, Ginsberg L. CNS manifestations of Fabry’s disease. Lancet Neurol. 2006;5(9):791-795.
5. Møller AT, Jensen TS. Neurological manifestations in Fabry’s disease. Nat Clin Pract Neurol. 2007;3(2):95-106.
6. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198.
7. Müller MJ. Neuropsychiatric and psychosocial aspects of Fabry disease. In: Mehta A Beck M, Sunder-Plassman G, eds. Fabry disease: perspectives from 5 years of FOS. Oxford, United Kingdom: Oxford PharmaGenesis Ltd; 2006. http://www.ncbi.nlm.nih.gov/books/nbk11618. Accessed October 31, 2011.
8. Segal P, Kohn Y, Pollak Y, et al. Psychiatric and cognitive profile in Anderson-Fabry patients: a preliminary study. J Inherit Metab Dis. 2010;33(4):429-436.
9. Kolodny EH, Pastores GM. Anderson-Fabry disease: Extrarenal neurologic manifestations. J Am Soc Nephrol. 2002;13(suppl 2):S150-153.
10. Grewal RP. Psychiatric disorders in patients with Fabry disease. Int J Psychiatry Med. 1993;23(3):307-312.
11. Müller MJ, Müller KM, Dascalescu A, et al. Psychiatric and neuropsychological signs and symptoms in patients with Fabry disease: literature review [in German]. Fortschr Neurol Psychiatr. 2005;73(11):687-693.
12. Segal P, Raas-Rothschild A. Neuropsychiatric manifestations of AFD. In: Elstein D Altarescu G, Beck M, eds. Fabry disease. New York, NY: Springer; 2010:321–324.
13. Crosbie TW, Packman W, Packman S. Psychological aspects of patients with Fabry disease. J Inherit Metab Dis. 2009;32(6):745-753.
14. Linthorst GE, Poorthuis BJ, Hollak CE. Enzyme activity for determination of presence of Fabry disease in women results in 40% false-negative results. J Am Coll Cardiol. 2008;51(21):2082.-
15. Müller MJ, Fellgiebel A, Scheurich A, et al. Recurrent brief depression in female patient with Fabry disease. Bipolar Disord. 2006;8(4):418-419.
16. Shen YC, Haw-Ming L, Lin CC, et al. Psychosis in a patient with Fabry’s disease and treatment with aripiprazole. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(3):779-780.
CASE: Disoriented and delusional
Ms. P, a 53-year-old registered nurse, is admitted to the inpatient psychiatric unit with confusion, markedly disorganized thought processes, delayed verbal responsiveness, mood lability, and persecutory delusions. Shortly before hospitalization, Ms. P traveled approximately 360 miles from her daughter’s home with a male companion. Noting changes in her mental status, the man brought Ms. P to the local hospital. She was then transferred to our facility.
At admission, Ms. P is not oriented to time. She denies auditory or visual hallucinations and does not display psychomotor agitation or retardation. She reports her mood as sad and her affect is mildly labile. Insight and judgment are considered poor.
Five years ago, Ms. P and her mother were diagnosed with Fabry’s disease (FD) based on genetic analysis. Both women are carriers for the mutations and Ms. P’s mother was found to have almost absent galactosidase activity.
The authors’ observations
FD is an X-linked recessive glycolipid storage disease caused by deficient activity of the lysosomal storage enzyme α-galactosidase A. The disorder affects both men and women and leads to progressive intracellular accumulation of globotriaosylceramide and other related glycosphingolipids.1,2 The earliest FD symptoms—burning pain and acroparesthesias—typically appear in childhood (Table 1).2 FD often is misdiagnosed in women because women tend to display neurologic symptoms later than men, with typical symptom onset in the teenage years.3,4 Often, these symptoms are confused with psychiatric disorders or vague neurologic or pain syndromes.5 In patients with no family history of FD, accurate diagnosis may not be made until adulthood.
Laboratory, dermatologic, and genetic tests can accurately determine the presence of FD.1 However, because multiple organ systems are involved, initially attributing symptoms to FD is challenging, particularly in women.1,3,5 For men, diagnosis can be established by measuring plasma or urinary globotriaosylceramide or plasma α-galactosidase A in addition to genetic analysis. In women, genetic analysis is a better diagnosis strategy because elevations in globotriaosylceramide or α-galactosidase A may not be prominent. An algorithm for diagnosing and assessing patients with FD has been proposed.2
Table 1
Typical signs and symptoms of Fabry’s disease
| Typical time at onset | Signs/symptoms |
|---|---|
| Childhood and adolescence (age ≤16) | Neuropathic pain Ophthalmologic abnormalities (cornea verticillata and tortuous retinal blood vessels) Hearing impairment Dyshidrosis (hypohidrosis and hyperhidrosis) Hypersensitivity to heat and cold Gastrointestinal disturbances and abdominal pain Lethargy and tiredness Angiokeratomas Onset of renal and cardiac signs (eg, microalbuminuria, proteinuria, abnormal heart rate variability) |
| Early adulthood (age 17 to 30) | Extension of any of the above Proteinuria and progressive renal failure Cardiomyopathy Transient ischemic attacks, strokes Facial dysmorphism |
| Later adulthood (age >30) | Worsening of any of the above Heart disease (eg, left ventricular hypertrophy, angina, arrhythmia, and dyspnea) Transient ischemic attacks, strokes Osteopenia and osteoporosis |
| Source: Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659, by permission of Oxford University Press | |
HISTORY: Cognitive deterioration
Ms. P has had psychiatric symptoms such as depression and anxiety since childhood. However, 3 years ago she started to experience psychological and cognitive deterioration. Medical records indicate that Ms. P described memory and concentration problems over the previous few years. She also reported pain, weakness, and numbness in her left leg after surgery for a work-related back injury, for which she received a financial settlement through workers’ compensation. Shortly thereafter, Ms. P separated from her third husband, moved in with her parents, and found work as a psychiatric nurse. She was dismissed after 6 weeks because she could not learn the electronic medical record system and had difficulty with memory and attention. Her performance on the Mini-Mental State Exam6 at that time was 28 out of 30, which was within normal limits.
After her parents died 3 years ago, Ms. P lived with her daughter, who became her primary caregiver and legal guardian. Ms. P’s daughter notes that her mother’s impulsive and risky behaviors grew more pronounced. Ms. P went on shopping sprees and became sexually promiscuous.
Ms. P’s psychiatric history includes childhood sexual abuse, hospitalization for a suicide attempt at age 19, and courses of psychotherapy and pharmacotherapy. In addition to FD, Ms. P’s medical history consists of coronary artery disease, type 2 diabetes mellitus, hypercholesterolemia, obesity, arthritis, back pain, fibromyalgia, and gastroesophageal reflux disease. Her family history is notable for alcohol abuse (both parents and a brother), lung cancer (mother), myocardial infarction (father), and Alzheimer’s disease (father).
The authors’ observations
Because α-galactosidase A is ubiquitous throughout the body, in addition to neurologic symptoms, FD involves multiple organ systems, with possible dermatologic, renal, gastrointestinal, cardiac, and cerebrovascular dysfunction. Despite growth in FD research, including the Fabry Outcomes Survey,3 the psychosocial and neuropsychiatric implications of the disease remain unclear.7 Behavioral presentations are idiosyncratic and unstable over time, depending on the structures impacted by progressive glycosphingolipid accumulation. Premature cardiovascular events (onset between age 30 and 40 for women), greater incidence of ischemic stroke or transient ischemic attack (7% to 30%), and frequent evidence of white matter lesions put FD patients at greater risk for developing presenile vascular dementia.1,3 Nearly all male FD patients with dementia show some evidence of stroke or transient ischemic attack; cognitive functioning has not been well explored in female patients.4 In a heterogeneous sample of 15 FD patients age 7 to 61, Segal et al8 noted deficits in attention, processing speed, and executive function .75 to 1.95 standard deviations below normative means. No patients in this study had a history of stroke or transient ischemic attack; neuroimaging studies were not reported. Kolodny and Pastores9 suggested multiple mechanisms for cognitive disruption, suggesting that mild dementia late in the disease course could be secondary to diffuse leukomalacia, multiple strokes, or possibly to lipid storage in hippocampal and frontal lobe neurons.
Psychiatric comorbidity
Psychiatric illness, such as depression or a personality disorder, may be comorbid with FD, although pathologic mechanisms remain unclear.7,10,11 Hypothesized mechanisms include:
- psychosocial stress from chronic disease
- white matter changes
- disruption of impaired L-arginine-nitric oxide pathways.7,12
Crosbie et al13 noted that FD patients presented with greater psychological distress as measured by the Minnesota Multiphasic Personality Inventory-2 than patients with Gaucher disease or chronic heart disease. However, no significant differences were found between patients with FD and those diagnosed with a pain disorder. In the Segal et al study, out of 11 adult FD patients, 4 were diagnosed with major depressive disorder, 1 with schizophrenia, 2 with schizotypal personality disorder, and 1 with borderline personality disorder.8
EVALUATION: Brain abnormalities
Head CT scans (conducted 2 years ago and 6 months ago) revealed prominent cortical sulci likely caused by underlying volume loss, especially in bifrontal areas. A brain MRI performed 2 months ago indicated a moderate degree of subcortical atrophy in bilateral frontal and parietal regions. These radiology findings suggest mild to moderate frontal atrophy, mild degree of white matter changes, and slightly enlarged ventricles. An EEG showed background slowing and lack of an alpha rhythm, indicative of cerebral cortical dysfunction.
Ms. P’s α-galactosidase A level was within normal limits; however, normal enzyme levels frequently are reported in symptomatic and asymptomatic female FD patients.14 A dermatology consult confirmed the presence of skin findings characteristic of FD (ie, multiple cherry red papules extensively distributed throughout Ms. P’s chest, abdomen, and back, as well as upper and lower extremities).
Ms. P completed 2 neuropsychological assessments separated by 5 months. For a summary of the results of these tests, see the table titled “Ms. P’s neuropsychological assessment results”. Both assessments revealed grossly impaired intellectual capacity, memory, processing speed, and motor functioning. During the assessment, Ms. P could understand all directions with minimal changes from standardized protocols. Ms. P became insistent that she would not be able to complete memory tasks successfully. She gave up prematurely on tasks, saying they were too difficult. She admitted to guessing on several items because she did not want to continue the task.
Ms. P’s performance on tasks measuring effort and validity of a person’s neuropsychological presentation was consistent with someone exaggerating neurologic symptoms. A person with true dementia may perform as poorly as Ms. P did. However, Ms. P’s scores likely underestimated her level of functioning, even if she was experiencing dementia. Ms. P could not complete tasks individuals with severe dementia complete successfully, such as simple addition and subtraction and digit repetition. Ms. P recalled several recent and remote events, such as her breakfast menu and location of her first assessment, but could not recall words practiced multiple times. Although Ms. P’s scores on a complex card-sorting task were in the impaired range, a detailed review of her pattern indicated that although Ms. P could not generate any correct sorting categories, she made few repetitive responses and errors. This pattern is consistent with someone who understands task requirements, but deliberately avoids answering correctly. This suggests that she retained some ability for hypotheses generation and problem solving; however, because she exaggerated her symptoms, specific deficits could not be determined.
The authors’ observations
Ms. P presented with an interesting manifestation of neuropsychiatric symptoms in the context of FD; however, common cardiac and cerebrovascular features of the disease were not fully developed. Ms. P experienced progressive cognitive and behavioral changes for 2 years before her admission (Table 2), which may represent a prodromal period leading up to what appeared to be a frontally mediated dementia syndrome. Müller et al15 described a patient with FD who displayed a behavioral profile similar to Ms. P’s that included increasingly unstable mood for at least 3 years, borderline personality disorder features, and rapidly fluctuating mood. A case study reported that risperidone, 1 mg/d, used to treat psychosis in a male FD patient caused extrapyramidal symptoms.16
Ms. P presented with no evidence of stroke or transient ischemic attacks, which is atypical for FD patients with cognitive impairment. However, neuroimaging did reveal frontal atrophy that may be associated with her impulse control deficits, risk-taking behavior, emotional instability, and poor judgment. Her cognitive testing was notable for impairment and exaggeration of symptoms consistent with personality disorder symptoms. Possible reasons for exaggeration include a desire to maintain the sick role or secondary gain related to obtaining disability income.
Ms. P’s behavior pattern could be caused by dementia with frontal features, possibly secondary to FD, in combination with personality and psychiatric pathology.
The mainstay of FD treatment is enzyme replacement therapy (ERT), which addresses the underlying enzyme deficiency. Available research indicates that ERT may reduce symptom severity and slow disease progression; however, further studies are needed to determine if it will reduce outcomes such as stroke, ischemic heart disease, or renal disease.2
Table 2
Symptoms that preceded Ms. P’s admission
| Time frame | Symptoms |
|---|---|
| 24 months before admission | Depressed mood Decreased ability to manage independent activities of daily living (eg, finances, cooking) Minimal objective cognitive impairment |
| 12 months before admission | Increased depression Mild to moderate decline in cognitive functioning Visual and auditory hallucinations Impulsivity/poor impulse control Irrational decision-making Increased risky behavior |
| 6 months before admission | Severe cognitive decline with cognitive symptom exaggeration Psychiatric symptom exaggeration Disorganized thinking Continued risky behavior and poor decision-making |
TREATMENT: Persistent deficits
Ms. P is started on risperidone rapidly titrated to 4 mg/d for delusional thinking and behavioral disturbance. After initially improving, she develops delirium when risperidone is increased to 4 mg/d. She has visual hallucinations, marked confusion with disorientation, worsened short-term memory, and an unsteady, shuffling gait. Risperidone is tapered and discontinued and Ms. P’s motor symptoms resolve within 2 days; however, she remains confused and delusional. We start her on quetiapine, 25 mg/d titrated to 50 mg/d, and her agitation and delusional thinking progressively decline. Memantine, titrated to 20 mg/d, and rivastigmine, started at 3 mg/d titrated to 9 mg/d, are added to address her cognitive symptoms.
Over several weeks, Ms. P’s mental status slowly improves and her drug-induced delirium completely resolves. However, she has persistent cognitive impairment characterized by compromised short-term memory and poor insight into her medical and psychological condition. She maintains unrealistic expectations about her ability to live independently and return to the workforce. The treatment team recommends that Ms. P’s daughter pursue guardianship and that she receive around-the-clock supervision after discharge from the hospital.
Table
Ms. P’s neuropsychological assessment results
| June | November | |
|---|---|---|
| Intellectual functioning | ||
| Wechsler Adult Intelligence Scale-III | ||
| FSIQ | 60 | |
| VIQ | 68 | |
| PIQ | 56 | |
| Ravens Colored Progressive Matrices | 70 | |
| Premorbid intellectual functioning estimates | ||
| Peabody Picture Vocabulary Test-2 | 89 | |
| Barona Demographic Estimate | 104 | 104 |
| North American Adult Reading Test | 99 | |
| Memory functioning | ||
| Wechsler Memory Scale-III | ||
| Immediate memory | 45 | |
| General delay memory | 47 | |
| Auditory recognition delay | 55 | |
| California Verbal Learning Test-II | ||
| Trial 1 (immediate recall) | <60 (raw = 3) | |
| Trial 5 | <60 (raw = 3) | |
| Total Words Learned | <60 (raw = 15) | |
| Short Delay Free Recall | <60 (raw = 2) | |
| Long Delay Free Recall | <60 (raw = 4) | |
| Executive functioning | ||
| Trail Making Test A | 88 | 88 |
| Trail Making Test B | failed to understand | failed to understand |
| Wisconsin Card Sort-64 | ||
| Number of categories | <60 (raw = 0) | |
| Errors | 81 | |
| Percent conceptual level responses | 74 | |
| Perseverative responses | 107 | |
| Perseverative errors | 108 | |
| COWAT FAS | 65 | 69 |
| Category exemplar | 69 | 80 |
| Motor functioning | ||
| Finger Tapping Dominant Hand | 68 | |
| Finger Tapping Non-Dominant Hand | 62 | |
| Invalidity/effort | ||
| TOMM | ||
| Trial 1 | raw = 34 | raw = 37 |
| Trial 2 | raw = 42 | raw = 45 |
| Recognition | raw = 44 | |
| MSVT verbal | fail | |
| MSVT nonverbal | fail | |
| Scores provided are standardized (mean = 100; SD = 15). Raw scores are also provided when indicated. COWAT: Controlled oral word association test; FSIQ: Full Scale IQ; MSVT: Medical Symptom Validity Test; PIQ: Performance IQ; TOMM: Test of Memory Malingering; VIQ: Verbal IQ | ||
Related Resources
- National Institute of Neurological Disorders and Stroke. Fabry disease information page. www.ninds.nih.gov/disorders/fabrys/fabrys.htm.
- National Fabry Disease Foundation. www.thenfdf.org.
- Rozenfeld P, Neumann PM. Treatment of Fabry disease: current and emerging strategies. Curr Pharm Biotechnol. 2011;12(6):916-922.
Drug Brand Names
- Donepezil • Aricept
- Memantine • Namenda
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Disoriented and delusional
Ms. P, a 53-year-old registered nurse, is admitted to the inpatient psychiatric unit with confusion, markedly disorganized thought processes, delayed verbal responsiveness, mood lability, and persecutory delusions. Shortly before hospitalization, Ms. P traveled approximately 360 miles from her daughter’s home with a male companion. Noting changes in her mental status, the man brought Ms. P to the local hospital. She was then transferred to our facility.
At admission, Ms. P is not oriented to time. She denies auditory or visual hallucinations and does not display psychomotor agitation or retardation. She reports her mood as sad and her affect is mildly labile. Insight and judgment are considered poor.
Five years ago, Ms. P and her mother were diagnosed with Fabry’s disease (FD) based on genetic analysis. Both women are carriers for the mutations and Ms. P’s mother was found to have almost absent galactosidase activity.
The authors’ observations
FD is an X-linked recessive glycolipid storage disease caused by deficient activity of the lysosomal storage enzyme α-galactosidase A. The disorder affects both men and women and leads to progressive intracellular accumulation of globotriaosylceramide and other related glycosphingolipids.1,2 The earliest FD symptoms—burning pain and acroparesthesias—typically appear in childhood (Table 1).2 FD often is misdiagnosed in women because women tend to display neurologic symptoms later than men, with typical symptom onset in the teenage years.3,4 Often, these symptoms are confused with psychiatric disorders or vague neurologic or pain syndromes.5 In patients with no family history of FD, accurate diagnosis may not be made until adulthood.
Laboratory, dermatologic, and genetic tests can accurately determine the presence of FD.1 However, because multiple organ systems are involved, initially attributing symptoms to FD is challenging, particularly in women.1,3,5 For men, diagnosis can be established by measuring plasma or urinary globotriaosylceramide or plasma α-galactosidase A in addition to genetic analysis. In women, genetic analysis is a better diagnosis strategy because elevations in globotriaosylceramide or α-galactosidase A may not be prominent. An algorithm for diagnosing and assessing patients with FD has been proposed.2
Table 1
Typical signs and symptoms of Fabry’s disease
| Typical time at onset | Signs/symptoms |
|---|---|
| Childhood and adolescence (age ≤16) | Neuropathic pain Ophthalmologic abnormalities (cornea verticillata and tortuous retinal blood vessels) Hearing impairment Dyshidrosis (hypohidrosis and hyperhidrosis) Hypersensitivity to heat and cold Gastrointestinal disturbances and abdominal pain Lethargy and tiredness Angiokeratomas Onset of renal and cardiac signs (eg, microalbuminuria, proteinuria, abnormal heart rate variability) |
| Early adulthood (age 17 to 30) | Extension of any of the above Proteinuria and progressive renal failure Cardiomyopathy Transient ischemic attacks, strokes Facial dysmorphism |
| Later adulthood (age >30) | Worsening of any of the above Heart disease (eg, left ventricular hypertrophy, angina, arrhythmia, and dyspnea) Transient ischemic attacks, strokes Osteopenia and osteoporosis |
| Source: Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659, by permission of Oxford University Press | |
HISTORY: Cognitive deterioration
Ms. P has had psychiatric symptoms such as depression and anxiety since childhood. However, 3 years ago she started to experience psychological and cognitive deterioration. Medical records indicate that Ms. P described memory and concentration problems over the previous few years. She also reported pain, weakness, and numbness in her left leg after surgery for a work-related back injury, for which she received a financial settlement through workers’ compensation. Shortly thereafter, Ms. P separated from her third husband, moved in with her parents, and found work as a psychiatric nurse. She was dismissed after 6 weeks because she could not learn the electronic medical record system and had difficulty with memory and attention. Her performance on the Mini-Mental State Exam6 at that time was 28 out of 30, which was within normal limits.
After her parents died 3 years ago, Ms. P lived with her daughter, who became her primary caregiver and legal guardian. Ms. P’s daughter notes that her mother’s impulsive and risky behaviors grew more pronounced. Ms. P went on shopping sprees and became sexually promiscuous.
Ms. P’s psychiatric history includes childhood sexual abuse, hospitalization for a suicide attempt at age 19, and courses of psychotherapy and pharmacotherapy. In addition to FD, Ms. P’s medical history consists of coronary artery disease, type 2 diabetes mellitus, hypercholesterolemia, obesity, arthritis, back pain, fibromyalgia, and gastroesophageal reflux disease. Her family history is notable for alcohol abuse (both parents and a brother), lung cancer (mother), myocardial infarction (father), and Alzheimer’s disease (father).
The authors’ observations
Because α-galactosidase A is ubiquitous throughout the body, in addition to neurologic symptoms, FD involves multiple organ systems, with possible dermatologic, renal, gastrointestinal, cardiac, and cerebrovascular dysfunction. Despite growth in FD research, including the Fabry Outcomes Survey,3 the psychosocial and neuropsychiatric implications of the disease remain unclear.7 Behavioral presentations are idiosyncratic and unstable over time, depending on the structures impacted by progressive glycosphingolipid accumulation. Premature cardiovascular events (onset between age 30 and 40 for women), greater incidence of ischemic stroke or transient ischemic attack (7% to 30%), and frequent evidence of white matter lesions put FD patients at greater risk for developing presenile vascular dementia.1,3 Nearly all male FD patients with dementia show some evidence of stroke or transient ischemic attack; cognitive functioning has not been well explored in female patients.4 In a heterogeneous sample of 15 FD patients age 7 to 61, Segal et al8 noted deficits in attention, processing speed, and executive function .75 to 1.95 standard deviations below normative means. No patients in this study had a history of stroke or transient ischemic attack; neuroimaging studies were not reported. Kolodny and Pastores9 suggested multiple mechanisms for cognitive disruption, suggesting that mild dementia late in the disease course could be secondary to diffuse leukomalacia, multiple strokes, or possibly to lipid storage in hippocampal and frontal lobe neurons.
Psychiatric comorbidity
Psychiatric illness, such as depression or a personality disorder, may be comorbid with FD, although pathologic mechanisms remain unclear.7,10,11 Hypothesized mechanisms include:
- psychosocial stress from chronic disease
- white matter changes
- disruption of impaired L-arginine-nitric oxide pathways.7,12
Crosbie et al13 noted that FD patients presented with greater psychological distress as measured by the Minnesota Multiphasic Personality Inventory-2 than patients with Gaucher disease or chronic heart disease. However, no significant differences were found between patients with FD and those diagnosed with a pain disorder. In the Segal et al study, out of 11 adult FD patients, 4 were diagnosed with major depressive disorder, 1 with schizophrenia, 2 with schizotypal personality disorder, and 1 with borderline personality disorder.8
EVALUATION: Brain abnormalities
Head CT scans (conducted 2 years ago and 6 months ago) revealed prominent cortical sulci likely caused by underlying volume loss, especially in bifrontal areas. A brain MRI performed 2 months ago indicated a moderate degree of subcortical atrophy in bilateral frontal and parietal regions. These radiology findings suggest mild to moderate frontal atrophy, mild degree of white matter changes, and slightly enlarged ventricles. An EEG showed background slowing and lack of an alpha rhythm, indicative of cerebral cortical dysfunction.
Ms. P’s α-galactosidase A level was within normal limits; however, normal enzyme levels frequently are reported in symptomatic and asymptomatic female FD patients.14 A dermatology consult confirmed the presence of skin findings characteristic of FD (ie, multiple cherry red papules extensively distributed throughout Ms. P’s chest, abdomen, and back, as well as upper and lower extremities).
Ms. P completed 2 neuropsychological assessments separated by 5 months. For a summary of the results of these tests, see the table titled “Ms. P’s neuropsychological assessment results”. Both assessments revealed grossly impaired intellectual capacity, memory, processing speed, and motor functioning. During the assessment, Ms. P could understand all directions with minimal changes from standardized protocols. Ms. P became insistent that she would not be able to complete memory tasks successfully. She gave up prematurely on tasks, saying they were too difficult. She admitted to guessing on several items because she did not want to continue the task.
Ms. P’s performance on tasks measuring effort and validity of a person’s neuropsychological presentation was consistent with someone exaggerating neurologic symptoms. A person with true dementia may perform as poorly as Ms. P did. However, Ms. P’s scores likely underestimated her level of functioning, even if she was experiencing dementia. Ms. P could not complete tasks individuals with severe dementia complete successfully, such as simple addition and subtraction and digit repetition. Ms. P recalled several recent and remote events, such as her breakfast menu and location of her first assessment, but could not recall words practiced multiple times. Although Ms. P’s scores on a complex card-sorting task were in the impaired range, a detailed review of her pattern indicated that although Ms. P could not generate any correct sorting categories, she made few repetitive responses and errors. This pattern is consistent with someone who understands task requirements, but deliberately avoids answering correctly. This suggests that she retained some ability for hypotheses generation and problem solving; however, because she exaggerated her symptoms, specific deficits could not be determined.
The authors’ observations
Ms. P presented with an interesting manifestation of neuropsychiatric symptoms in the context of FD; however, common cardiac and cerebrovascular features of the disease were not fully developed. Ms. P experienced progressive cognitive and behavioral changes for 2 years before her admission (Table 2), which may represent a prodromal period leading up to what appeared to be a frontally mediated dementia syndrome. Müller et al15 described a patient with FD who displayed a behavioral profile similar to Ms. P’s that included increasingly unstable mood for at least 3 years, borderline personality disorder features, and rapidly fluctuating mood. A case study reported that risperidone, 1 mg/d, used to treat psychosis in a male FD patient caused extrapyramidal symptoms.16
Ms. P presented with no evidence of stroke or transient ischemic attacks, which is atypical for FD patients with cognitive impairment. However, neuroimaging did reveal frontal atrophy that may be associated with her impulse control deficits, risk-taking behavior, emotional instability, and poor judgment. Her cognitive testing was notable for impairment and exaggeration of symptoms consistent with personality disorder symptoms. Possible reasons for exaggeration include a desire to maintain the sick role or secondary gain related to obtaining disability income.
Ms. P’s behavior pattern could be caused by dementia with frontal features, possibly secondary to FD, in combination with personality and psychiatric pathology.
The mainstay of FD treatment is enzyme replacement therapy (ERT), which addresses the underlying enzyme deficiency. Available research indicates that ERT may reduce symptom severity and slow disease progression; however, further studies are needed to determine if it will reduce outcomes such as stroke, ischemic heart disease, or renal disease.2
Table 2
Symptoms that preceded Ms. P’s admission
| Time frame | Symptoms |
|---|---|
| 24 months before admission | Depressed mood Decreased ability to manage independent activities of daily living (eg, finances, cooking) Minimal objective cognitive impairment |
| 12 months before admission | Increased depression Mild to moderate decline in cognitive functioning Visual and auditory hallucinations Impulsivity/poor impulse control Irrational decision-making Increased risky behavior |
| 6 months before admission | Severe cognitive decline with cognitive symptom exaggeration Psychiatric symptom exaggeration Disorganized thinking Continued risky behavior and poor decision-making |
TREATMENT: Persistent deficits
Ms. P is started on risperidone rapidly titrated to 4 mg/d for delusional thinking and behavioral disturbance. After initially improving, she develops delirium when risperidone is increased to 4 mg/d. She has visual hallucinations, marked confusion with disorientation, worsened short-term memory, and an unsteady, shuffling gait. Risperidone is tapered and discontinued and Ms. P’s motor symptoms resolve within 2 days; however, she remains confused and delusional. We start her on quetiapine, 25 mg/d titrated to 50 mg/d, and her agitation and delusional thinking progressively decline. Memantine, titrated to 20 mg/d, and rivastigmine, started at 3 mg/d titrated to 9 mg/d, are added to address her cognitive symptoms.
Over several weeks, Ms. P’s mental status slowly improves and her drug-induced delirium completely resolves. However, she has persistent cognitive impairment characterized by compromised short-term memory and poor insight into her medical and psychological condition. She maintains unrealistic expectations about her ability to live independently and return to the workforce. The treatment team recommends that Ms. P’s daughter pursue guardianship and that she receive around-the-clock supervision after discharge from the hospital.
Table
Ms. P’s neuropsychological assessment results
| June | November | |
|---|---|---|
| Intellectual functioning | ||
| Wechsler Adult Intelligence Scale-III | ||
| FSIQ | 60 | |
| VIQ | 68 | |
| PIQ | 56 | |
| Ravens Colored Progressive Matrices | 70 | |
| Premorbid intellectual functioning estimates | ||
| Peabody Picture Vocabulary Test-2 | 89 | |
| Barona Demographic Estimate | 104 | 104 |
| North American Adult Reading Test | 99 | |
| Memory functioning | ||
| Wechsler Memory Scale-III | ||
| Immediate memory | 45 | |
| General delay memory | 47 | |
| Auditory recognition delay | 55 | |
| California Verbal Learning Test-II | ||
| Trial 1 (immediate recall) | <60 (raw = 3) | |
| Trial 5 | <60 (raw = 3) | |
| Total Words Learned | <60 (raw = 15) | |
| Short Delay Free Recall | <60 (raw = 2) | |
| Long Delay Free Recall | <60 (raw = 4) | |
| Executive functioning | ||
| Trail Making Test A | 88 | 88 |
| Trail Making Test B | failed to understand | failed to understand |
| Wisconsin Card Sort-64 | ||
| Number of categories | <60 (raw = 0) | |
| Errors | 81 | |
| Percent conceptual level responses | 74 | |
| Perseverative responses | 107 | |
| Perseverative errors | 108 | |
| COWAT FAS | 65 | 69 |
| Category exemplar | 69 | 80 |
| Motor functioning | ||
| Finger Tapping Dominant Hand | 68 | |
| Finger Tapping Non-Dominant Hand | 62 | |
| Invalidity/effort | ||
| TOMM | ||
| Trial 1 | raw = 34 | raw = 37 |
| Trial 2 | raw = 42 | raw = 45 |
| Recognition | raw = 44 | |
| MSVT verbal | fail | |
| MSVT nonverbal | fail | |
| Scores provided are standardized (mean = 100; SD = 15). Raw scores are also provided when indicated. COWAT: Controlled oral word association test; FSIQ: Full Scale IQ; MSVT: Medical Symptom Validity Test; PIQ: Performance IQ; TOMM: Test of Memory Malingering; VIQ: Verbal IQ | ||
Related Resources
- National Institute of Neurological Disorders and Stroke. Fabry disease information page. www.ninds.nih.gov/disorders/fabrys/fabrys.htm.
- National Fabry Disease Foundation. www.thenfdf.org.
- Rozenfeld P, Neumann PM. Treatment of Fabry disease: current and emerging strategies. Curr Pharm Biotechnol. 2011;12(6):916-922.
Drug Brand Names
- Donepezil • Aricept
- Memantine • Namenda
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Eng CM, Germain DP, Banikazemi M, et al. Fabry disease: guidelines for the evaluation and management of multi-organ system involvement. Genet Med. 2006;8(9):539-548.
2. Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659.
3. Deegan PB, Baehner AF, Barba Romero MA, et al. Natural history of Fabry disease in females in the Fabry Outcome Survey. J Med Genet. 2006;43(4):347-352.
4. Fellgiebel A, Müller MJ, Ginsberg L. CNS manifestations of Fabry’s disease. Lancet Neurol. 2006;5(9):791-795.
5. Møller AT, Jensen TS. Neurological manifestations in Fabry’s disease. Nat Clin Pract Neurol. 2007;3(2):95-106.
6. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198.
7. Müller MJ. Neuropsychiatric and psychosocial aspects of Fabry disease. In: Mehta A Beck M, Sunder-Plassman G, eds. Fabry disease: perspectives from 5 years of FOS. Oxford, United Kingdom: Oxford PharmaGenesis Ltd; 2006. http://www.ncbi.nlm.nih.gov/books/nbk11618. Accessed October 31, 2011.
8. Segal P, Kohn Y, Pollak Y, et al. Psychiatric and cognitive profile in Anderson-Fabry patients: a preliminary study. J Inherit Metab Dis. 2010;33(4):429-436.
9. Kolodny EH, Pastores GM. Anderson-Fabry disease: Extrarenal neurologic manifestations. J Am Soc Nephrol. 2002;13(suppl 2):S150-153.
10. Grewal RP. Psychiatric disorders in patients with Fabry disease. Int J Psychiatry Med. 1993;23(3):307-312.
11. Müller MJ, Müller KM, Dascalescu A, et al. Psychiatric and neuropsychological signs and symptoms in patients with Fabry disease: literature review [in German]. Fortschr Neurol Psychiatr. 2005;73(11):687-693.
12. Segal P, Raas-Rothschild A. Neuropsychiatric manifestations of AFD. In: Elstein D Altarescu G, Beck M, eds. Fabry disease. New York, NY: Springer; 2010:321–324.
13. Crosbie TW, Packman W, Packman S. Psychological aspects of patients with Fabry disease. J Inherit Metab Dis. 2009;32(6):745-753.
14. Linthorst GE, Poorthuis BJ, Hollak CE. Enzyme activity for determination of presence of Fabry disease in women results in 40% false-negative results. J Am Coll Cardiol. 2008;51(21):2082.-
15. Müller MJ, Fellgiebel A, Scheurich A, et al. Recurrent brief depression in female patient with Fabry disease. Bipolar Disord. 2006;8(4):418-419.
16. Shen YC, Haw-Ming L, Lin CC, et al. Psychosis in a patient with Fabry’s disease and treatment with aripiprazole. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(3):779-780.
1. Eng CM, Germain DP, Banikazemi M, et al. Fabry disease: guidelines for the evaluation and management of multi-organ system involvement. Genet Med. 2006;8(9):539-548.
2. Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659.
3. Deegan PB, Baehner AF, Barba Romero MA, et al. Natural history of Fabry disease in females in the Fabry Outcome Survey. J Med Genet. 2006;43(4):347-352.
4. Fellgiebel A, Müller MJ, Ginsberg L. CNS manifestations of Fabry’s disease. Lancet Neurol. 2006;5(9):791-795.
5. Møller AT, Jensen TS. Neurological manifestations in Fabry’s disease. Nat Clin Pract Neurol. 2007;3(2):95-106.
6. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198.
7. Müller MJ. Neuropsychiatric and psychosocial aspects of Fabry disease. In: Mehta A Beck M, Sunder-Plassman G, eds. Fabry disease: perspectives from 5 years of FOS. Oxford, United Kingdom: Oxford PharmaGenesis Ltd; 2006. http://www.ncbi.nlm.nih.gov/books/nbk11618. Accessed October 31, 2011.
8. Segal P, Kohn Y, Pollak Y, et al. Psychiatric and cognitive profile in Anderson-Fabry patients: a preliminary study. J Inherit Metab Dis. 2010;33(4):429-436.
9. Kolodny EH, Pastores GM. Anderson-Fabry disease: Extrarenal neurologic manifestations. J Am Soc Nephrol. 2002;13(suppl 2):S150-153.
10. Grewal RP. Psychiatric disorders in patients with Fabry disease. Int J Psychiatry Med. 1993;23(3):307-312.
11. Müller MJ, Müller KM, Dascalescu A, et al. Psychiatric and neuropsychological signs and symptoms in patients with Fabry disease: literature review [in German]. Fortschr Neurol Psychiatr. 2005;73(11):687-693.
12. Segal P, Raas-Rothschild A. Neuropsychiatric manifestations of AFD. In: Elstein D Altarescu G, Beck M, eds. Fabry disease. New York, NY: Springer; 2010:321–324.
13. Crosbie TW, Packman W, Packman S. Psychological aspects of patients with Fabry disease. J Inherit Metab Dis. 2009;32(6):745-753.
14. Linthorst GE, Poorthuis BJ, Hollak CE. Enzyme activity for determination of presence of Fabry disease in women results in 40% false-negative results. J Am Coll Cardiol. 2008;51(21):2082.-
15. Müller MJ, Fellgiebel A, Scheurich A, et al. Recurrent brief depression in female patient with Fabry disease. Bipolar Disord. 2006;8(4):418-419.
16. Shen YC, Haw-Ming L, Lin CC, et al. Psychosis in a patient with Fabry’s disease and treatment with aripiprazole. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(3):779-780.
A questionable diagnosis
CASE: Space traveler
Mr. O, age 69, is a patient at a long-term psychiatric hospital. He has a 56-year psychiatric history, a current diagnosis of schizoaffective disorder, and suffered a torn rotator cuff approximately 5 years ago. His medication regimen is haloperidol decanoate, 100 mg IM every month, duloxetine, 60 mg/d, and naproxen, as needed for chronic pain.
He frequently lies on the floor. Attendants urge him to get up and join groups or sit with other patients but he complains of pain and soon finds another spot on the floor to use as a bed.
Eight months earlier, a homeless shelter sent Mr. O to the emergency room (ER) because he tried to eat a dollar bill and a sock. In the ER he was inattentive, with loose associations and bizarre delusions; he believed he was on a spaceship. Mr. O was admitted to the hospital, where clinicians noted that his behavior remained bizarre and he complained of insomnia. They also noted a history of setting fires, which complicated discharge planning and contributed to their decision to transfer him to our psychiatric facility for longer-term care.
During our initial interview, Mr. O readily picks himself off the floor. His responses are logical and direct but abrupt and unelaborated. His first and most vehement complaint is pain. Zolpidem, he says, is the only treatment that helps.
He says he began using zolpidem approximately 5 years ago because pain from a shoulder injury kept him awake at night. When he could not obtain the drug by prescription, he bought it on the street. One day when living in the homeless shelter, he took 30 or 40 mg of zolpidem, then “blacked out” and awoke in the ER.
His first experience with psychiatric treatment was the result of problems getting along with his single mother because of “petty things” such as shooting off a BB gun in their apartment, he says. As a teenager he was sent to a boarding school; as a young adult, to a psychiatric hospital. After his release he returned to his mother’s apartment. He worked steadily for 20 years before he obtained Social Security benefits, and then worked intermittently “off the books” until approximately 15 years ago. Mr. O lived with his mother until her death 17 years earlier, and then in her apartment alone until a fire, which he set accidentally by smoking in bed after taking zolpidem, forced him to leave 3 years ago. He says, “My whole life was in that place.” He was admitted to a psychiatric hospital for an unknown reason, which was his first psychiatric admission in 40 years. After he was released from the hospital, Mr. O lived in various homeless shelters and adult homes until his current hospitalization.
The author’s observations
An effective and well-tolerated drug with a reputation for rarely being abused, zolpidem is widely prescribed as a hypnotic. Zolpidem and benzodiazepines have different chemical structures but both act at the GABAA receptor and have comparable behavioral effects.1 The reported incidence of zolpidem abuse is much lower than the reported rate of benzodiazepine abuse when used for sleep2; however, abuse, dependence, and withdrawal have been reported.2-4 Zolpidem abuse seems to be more common among patients with a history of abusing other substances or a history of psychiatric illness.2 A French study4 found that abusers fell into 2 groups. The younger group (median age 35) used higher doses—a median of 300 mg/d—and took zolpidem in the daytime to achieve euphoria. A second, older group (median age 42) used lower doses—a median of 200 mg/d—at nighttime to sleep.
There are few reports of delirium and symptoms such as visual hallucinations and distortions associated with zolpidem use.5,6 These reactions have occurred in persons without a history of psychosis. They usually are associated with doses ≥10 mg.
In the ER Mr. O showed a disturbance in consciousness with inability to focus attention and a perceptual disturbance (he believed he was in a spaceship) that developed over hours to days. He met criteria for delirium, possibly caused by zolpidem, but his presentation also could have been attributable to an underlying psychiatric disorder.
ER and inpatient psychiatrists noted Mr. O was intoxicated with zolpidem when the shelter brought him to the ER, but both groups diagnosed schizoaffective disorder and treated him with antipsychotics. They saw his >50-year psychiatric history as evidence of an underlying, long-standing condition such as schizoaffective illness.
However, features of Mr. O’s illness are not typical of a chronic psychotic illness. He recalls psychiatric hospitalizations in his youth and recently, but not for the 40 years in between. Mr. O says he has never experienced auditory hallucinations. For these reasons, our treatment team obtains old medical records to investigate his early history (Table).
Table
Mr. O’s clinical course
| Age | Symptoms/behaviors | Diagnosis |
|---|---|---|
| 17 | Temper tantrums and destructive behaviors. No delusions or hallucinations but a flat affect and hostile attitude | Primary behavior disorder, simple adult maladjustment |
| 22 | Returned to the psychiatric hospital when his welfare payments stopped; “psychopathic” symptoms; described as defiant and resented authority and regular work | Primary behavior disorder |
| 24 | His mother complained that he stole from her and carried a weapon; while hospitalized, described as manageable and without overt psychotic symptoms | Primary behavior disorder |
| 26 | Arrested for causing property damage while intoxicated on alcohol; silly laugh, loose associations, irrelevant and incoherent speech, and believed hospital staff were against him | Psychosis with psychopathic personality |
| 66 | A fire that he set accidentally while smoking in bed after taking zolpidem destroyed his home | Diagnosis unknown |
| 68 | Transferred from a homeless shelter to the ER after he took 30 to 40 mg of zolpidem and exhibited bizarre behaviors | Schizoaffective disorder |
| 69 | More spontaneous, remains logical and relevant after haloperidol is discontinued; no delusions or hallucinations, still complains of pain | Substance use disorder and personality disorder |
| ER: emergency room | ||
HISTORY: Destructive and defiant
Mr. O’s mother reported that he had been a nervous, restless child who would scream and yell at the slightest provocation. At age 10 he became wantonly destructive. His mother bought him an expensive toy that he destroyed after a short time; he asked for another toy, which he also destroyed. When such behavior became more frequent, she took him to a city hospital, where he was treated for 6 weeks and released at age 13. He was sent to a boarding school but soon was expelled for drinking and selling beer.
Mr. O was admitted to long-term psychiatric facilities 6 times in the next 10 years, from the late 1950s to the late 1960s. He was first admitted at age 17 for temper tantrums during which he fired an air rifle and smashed windows in the home he shared with his mother. During examination he had no delusions or hallucinations but did have flat affect and a hostile attitude. Doctors documented that almost all his tantrums were as a result of interactions with his mother.
Records from this psychiatric admission state that Mr. O showed no unusual distractibility, “psychotic trends,” or paranoid thinking. After approximately 6 months in the hospital he was discharged home with the diagnosis of primary behavior disorder, simple adult maladjustment. Mr. O, who was age 18 at the time, and his mother were eager for him to complete high school and learn auto mechanics.
Nine months later, he returned to the psychiatric facility because of excessive drinking and inability to secure employment, according to his records. In the hospital, he was productive and reliable. When he was discharged home 3 months later, doctors wrote that his determination to stop drinking was firmly fixed. They encouraged Mr. O to complete high school as a night student and find employment during the day. His mother was delighted with his improvement.
A third admission, less than 2 months later, occurred after he broke a window during an argument with his mother. He had a job but quit. After 5 months he was discharged with the same diagnosis of primary behavior disorder, but his mother would not let him back in her home. He was referred to the social service department to be placed on welfare.
A year later, Mr. O had trouble managing his welfare allotment and moved repeatedly. He said he returned to the psychiatric hospital because his welfare payments had been discontinued. During this admission, doctors noted “psychopathic” symptoms; Mr. O was defiant and resented authority and regular work. Mr. O eloped from the hospital several times and brought beer into the building. After 18 months he was discharged with the same diagnosis, with plans to apply for welfare. He was not prescribed medication.
Mr. O’s fifth admission came nearly 2 years later after his mother complained that he stole from her home and carried a weapon. In the hospital he was described as manageable and without overt psychotic symptoms. When he was discharged a little more than a year after being admitted, doctors wrote that he was a psychopath who had a history of drinking, stealing, and delinquent tendencies as a teenager. His diagnosis remained primary behavior disorder.
A year after this discharge, Mr. O was arrested for causing serious property damage when he was intoxicated on alcohol. Subsequently he was readmitted.
After a few months in the hospital, Mr. O changed. He developed a silly laugh, loose associations, irrelevant and incoherent speech, and a belief that hospital staff were against him. Although Mr. O denied auditory hallucinations, a psychiatrist wrote that he seemed to be experiencing hallucinations and prescribed chlorpromazine. The next day Mr. O slashed his arms and legs in several places, requiring many sutures. His diagnosis was changed to psychosis with psychopathic personality. However, within a few months, psychiatrists determined that Mr. O had recovered, so they stopped chlorpromazine. Months later, clinicians wrote that Mr. O was idle most of the time, neat, clean, and not involved in arguments with other patients. He was discharged after 1 month in the hospital.
Over the years, psychiatrists had differing opinions about Mr. O’s diagnosis. One noted that his mental illness was characterized by emotional instability and poor judgment. He had impulsive reactions without regard for others, rapid mood swings, irritability, and depression with transient paranoia. Another clinician detected evidence of schizoid personality disorder because Mr. O did not experience hallucinations or a gross thought disorder, but did have rambling, circumstantial, autistic (unrealistic), and ambivalent thought content. Another psychiatrist wrote Mr. O best fit in the category of psychosis with psychopathic personality, which was his diagnosis at discharge from his sixth hospitalization.
The author’s observations
Mr. O’s old medical records revealed the diagnostic thinking and treatment practices of a past era. They did not demonstrate that Mr. O met current criteria for schizophrenia or schizoaffective disorder, although he may have had a brief psychotic episode. Because there was little support for a diagnosis of schizoaffective illness and haloperidol use, we stopped the drug but continued duloxetine for chronic pain. It was clear that he has a substance use disorder and perhaps met criteria for antisocial personality disorder.
OUTCOME: Further explanations
Approximately 2 months after stopping haloperidol, Mr. O is more spontaneous, logical, and relevant. He does not have delusions or hallucinations. Despite further attempts at pain management with physical therapy and increased doses of duloxetine, he still complains of pain. We do not prescribe zolpidem.
Mr. O is unwilling to discuss the incident more than 40 years ago when he cut his arms and legs except to say, “That’s the past. My life wasn’t so good at that time.” When we ask why he had been a client of Adult Protective Services 5 years before he was burned out of his apartment, he admitted that he was 21 months in arrears in his rent. “I used to do this thing called crack,” he explains. He was discharged to an adult home with a prescription for duloxetine after he promised to never smoke in his room again.
Related Resource
- Aggarwal A, Sharma DD. Zolpidem withdrawal delirium: a case report. J Neuropsychiatry Clin Neurosci. 2010;22(4):451.
Drug Brand Names
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Duloxetine • Cymbalta
- Haloperidol decanoate • Haloperidol decanoate
- Haloperidol • Haldol
- Naproxen • Naproxyn, Aleve, others
- Zolpidem • Ambien
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rush CR. Behavioral pharmacology of zolpidem relative to benzodiazepines: a review. Pharmacol Biochem Behav. 1998;61(3):253-269.
2. Hajak G, Müller WE, Wittchen HU, et al. Abuse and dependence potential for the non-benzodiazepine hypnotics zolpidem and zopiclone: a review of case reports and epidemiological data. Addiction. 2003;98(10):1371-1378.
3. Madrak LN, Rosenberg M. Zolpidem abuse. Am J Psychiatry. 2001;158(8):1330-1331.
4. Victorri-Vigneau C, Dailly E, Veyrac G, et al. Evidence of zolpidem abuse and dependence: results of the French Centre for Evaluation and Information on Pharmacodepencence (CEIP) network survey. Br J Clin Pharmacol. 2007;64(2):198-209.
5. Markowitz JS, Brewerton TD. Zolpidem-induced psychosis. Ann Clin Psychiatry. 1996;8(2):89-91.
6. Tsai MJ, Huang YB, Wu PC. A novel clinical pattern of visual hallucination after zolpidem use. J Toxicol Clin Toxicol. 2003;41(6):869-872.
CASE: Space traveler
Mr. O, age 69, is a patient at a long-term psychiatric hospital. He has a 56-year psychiatric history, a current diagnosis of schizoaffective disorder, and suffered a torn rotator cuff approximately 5 years ago. His medication regimen is haloperidol decanoate, 100 mg IM every month, duloxetine, 60 mg/d, and naproxen, as needed for chronic pain.
He frequently lies on the floor. Attendants urge him to get up and join groups or sit with other patients but he complains of pain and soon finds another spot on the floor to use as a bed.
Eight months earlier, a homeless shelter sent Mr. O to the emergency room (ER) because he tried to eat a dollar bill and a sock. In the ER he was inattentive, with loose associations and bizarre delusions; he believed he was on a spaceship. Mr. O was admitted to the hospital, where clinicians noted that his behavior remained bizarre and he complained of insomnia. They also noted a history of setting fires, which complicated discharge planning and contributed to their decision to transfer him to our psychiatric facility for longer-term care.
During our initial interview, Mr. O readily picks himself off the floor. His responses are logical and direct but abrupt and unelaborated. His first and most vehement complaint is pain. Zolpidem, he says, is the only treatment that helps.
He says he began using zolpidem approximately 5 years ago because pain from a shoulder injury kept him awake at night. When he could not obtain the drug by prescription, he bought it on the street. One day when living in the homeless shelter, he took 30 or 40 mg of zolpidem, then “blacked out” and awoke in the ER.
His first experience with psychiatric treatment was the result of problems getting along with his single mother because of “petty things” such as shooting off a BB gun in their apartment, he says. As a teenager he was sent to a boarding school; as a young adult, to a psychiatric hospital. After his release he returned to his mother’s apartment. He worked steadily for 20 years before he obtained Social Security benefits, and then worked intermittently “off the books” until approximately 15 years ago. Mr. O lived with his mother until her death 17 years earlier, and then in her apartment alone until a fire, which he set accidentally by smoking in bed after taking zolpidem, forced him to leave 3 years ago. He says, “My whole life was in that place.” He was admitted to a psychiatric hospital for an unknown reason, which was his first psychiatric admission in 40 years. After he was released from the hospital, Mr. O lived in various homeless shelters and adult homes until his current hospitalization.
The author’s observations
An effective and well-tolerated drug with a reputation for rarely being abused, zolpidem is widely prescribed as a hypnotic. Zolpidem and benzodiazepines have different chemical structures but both act at the GABAA receptor and have comparable behavioral effects.1 The reported incidence of zolpidem abuse is much lower than the reported rate of benzodiazepine abuse when used for sleep2; however, abuse, dependence, and withdrawal have been reported.2-4 Zolpidem abuse seems to be more common among patients with a history of abusing other substances or a history of psychiatric illness.2 A French study4 found that abusers fell into 2 groups. The younger group (median age 35) used higher doses—a median of 300 mg/d—and took zolpidem in the daytime to achieve euphoria. A second, older group (median age 42) used lower doses—a median of 200 mg/d—at nighttime to sleep.
There are few reports of delirium and symptoms such as visual hallucinations and distortions associated with zolpidem use.5,6 These reactions have occurred in persons without a history of psychosis. They usually are associated with doses ≥10 mg.
In the ER Mr. O showed a disturbance in consciousness with inability to focus attention and a perceptual disturbance (he believed he was in a spaceship) that developed over hours to days. He met criteria for delirium, possibly caused by zolpidem, but his presentation also could have been attributable to an underlying psychiatric disorder.
ER and inpatient psychiatrists noted Mr. O was intoxicated with zolpidem when the shelter brought him to the ER, but both groups diagnosed schizoaffective disorder and treated him with antipsychotics. They saw his >50-year psychiatric history as evidence of an underlying, long-standing condition such as schizoaffective illness.
However, features of Mr. O’s illness are not typical of a chronic psychotic illness. He recalls psychiatric hospitalizations in his youth and recently, but not for the 40 years in between. Mr. O says he has never experienced auditory hallucinations. For these reasons, our treatment team obtains old medical records to investigate his early history (Table).
Table
Mr. O’s clinical course
| Age | Symptoms/behaviors | Diagnosis |
|---|---|---|
| 17 | Temper tantrums and destructive behaviors. No delusions or hallucinations but a flat affect and hostile attitude | Primary behavior disorder, simple adult maladjustment |
| 22 | Returned to the psychiatric hospital when his welfare payments stopped; “psychopathic” symptoms; described as defiant and resented authority and regular work | Primary behavior disorder |
| 24 | His mother complained that he stole from her and carried a weapon; while hospitalized, described as manageable and without overt psychotic symptoms | Primary behavior disorder |
| 26 | Arrested for causing property damage while intoxicated on alcohol; silly laugh, loose associations, irrelevant and incoherent speech, and believed hospital staff were against him | Psychosis with psychopathic personality |
| 66 | A fire that he set accidentally while smoking in bed after taking zolpidem destroyed his home | Diagnosis unknown |
| 68 | Transferred from a homeless shelter to the ER after he took 30 to 40 mg of zolpidem and exhibited bizarre behaviors | Schizoaffective disorder |
| 69 | More spontaneous, remains logical and relevant after haloperidol is discontinued; no delusions or hallucinations, still complains of pain | Substance use disorder and personality disorder |
| ER: emergency room | ||
HISTORY: Destructive and defiant
Mr. O’s mother reported that he had been a nervous, restless child who would scream and yell at the slightest provocation. At age 10 he became wantonly destructive. His mother bought him an expensive toy that he destroyed after a short time; he asked for another toy, which he also destroyed. When such behavior became more frequent, she took him to a city hospital, where he was treated for 6 weeks and released at age 13. He was sent to a boarding school but soon was expelled for drinking and selling beer.
Mr. O was admitted to long-term psychiatric facilities 6 times in the next 10 years, from the late 1950s to the late 1960s. He was first admitted at age 17 for temper tantrums during which he fired an air rifle and smashed windows in the home he shared with his mother. During examination he had no delusions or hallucinations but did have flat affect and a hostile attitude. Doctors documented that almost all his tantrums were as a result of interactions with his mother.
Records from this psychiatric admission state that Mr. O showed no unusual distractibility, “psychotic trends,” or paranoid thinking. After approximately 6 months in the hospital he was discharged home with the diagnosis of primary behavior disorder, simple adult maladjustment. Mr. O, who was age 18 at the time, and his mother were eager for him to complete high school and learn auto mechanics.
Nine months later, he returned to the psychiatric facility because of excessive drinking and inability to secure employment, according to his records. In the hospital, he was productive and reliable. When he was discharged home 3 months later, doctors wrote that his determination to stop drinking was firmly fixed. They encouraged Mr. O to complete high school as a night student and find employment during the day. His mother was delighted with his improvement.
A third admission, less than 2 months later, occurred after he broke a window during an argument with his mother. He had a job but quit. After 5 months he was discharged with the same diagnosis of primary behavior disorder, but his mother would not let him back in her home. He was referred to the social service department to be placed on welfare.
A year later, Mr. O had trouble managing his welfare allotment and moved repeatedly. He said he returned to the psychiatric hospital because his welfare payments had been discontinued. During this admission, doctors noted “psychopathic” symptoms; Mr. O was defiant and resented authority and regular work. Mr. O eloped from the hospital several times and brought beer into the building. After 18 months he was discharged with the same diagnosis, with plans to apply for welfare. He was not prescribed medication.
Mr. O’s fifth admission came nearly 2 years later after his mother complained that he stole from her home and carried a weapon. In the hospital he was described as manageable and without overt psychotic symptoms. When he was discharged a little more than a year after being admitted, doctors wrote that he was a psychopath who had a history of drinking, stealing, and delinquent tendencies as a teenager. His diagnosis remained primary behavior disorder.
A year after this discharge, Mr. O was arrested for causing serious property damage when he was intoxicated on alcohol. Subsequently he was readmitted.
After a few months in the hospital, Mr. O changed. He developed a silly laugh, loose associations, irrelevant and incoherent speech, and a belief that hospital staff were against him. Although Mr. O denied auditory hallucinations, a psychiatrist wrote that he seemed to be experiencing hallucinations and prescribed chlorpromazine. The next day Mr. O slashed his arms and legs in several places, requiring many sutures. His diagnosis was changed to psychosis with psychopathic personality. However, within a few months, psychiatrists determined that Mr. O had recovered, so they stopped chlorpromazine. Months later, clinicians wrote that Mr. O was idle most of the time, neat, clean, and not involved in arguments with other patients. He was discharged after 1 month in the hospital.
Over the years, psychiatrists had differing opinions about Mr. O’s diagnosis. One noted that his mental illness was characterized by emotional instability and poor judgment. He had impulsive reactions without regard for others, rapid mood swings, irritability, and depression with transient paranoia. Another clinician detected evidence of schizoid personality disorder because Mr. O did not experience hallucinations or a gross thought disorder, but did have rambling, circumstantial, autistic (unrealistic), and ambivalent thought content. Another psychiatrist wrote Mr. O best fit in the category of psychosis with psychopathic personality, which was his diagnosis at discharge from his sixth hospitalization.
The author’s observations
Mr. O’s old medical records revealed the diagnostic thinking and treatment practices of a past era. They did not demonstrate that Mr. O met current criteria for schizophrenia or schizoaffective disorder, although he may have had a brief psychotic episode. Because there was little support for a diagnosis of schizoaffective illness and haloperidol use, we stopped the drug but continued duloxetine for chronic pain. It was clear that he has a substance use disorder and perhaps met criteria for antisocial personality disorder.
OUTCOME: Further explanations
Approximately 2 months after stopping haloperidol, Mr. O is more spontaneous, logical, and relevant. He does not have delusions or hallucinations. Despite further attempts at pain management with physical therapy and increased doses of duloxetine, he still complains of pain. We do not prescribe zolpidem.
Mr. O is unwilling to discuss the incident more than 40 years ago when he cut his arms and legs except to say, “That’s the past. My life wasn’t so good at that time.” When we ask why he had been a client of Adult Protective Services 5 years before he was burned out of his apartment, he admitted that he was 21 months in arrears in his rent. “I used to do this thing called crack,” he explains. He was discharged to an adult home with a prescription for duloxetine after he promised to never smoke in his room again.
Related Resource
- Aggarwal A, Sharma DD. Zolpidem withdrawal delirium: a case report. J Neuropsychiatry Clin Neurosci. 2010;22(4):451.
Drug Brand Names
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Duloxetine • Cymbalta
- Haloperidol decanoate • Haloperidol decanoate
- Haloperidol • Haldol
- Naproxen • Naproxyn, Aleve, others
- Zolpidem • Ambien
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Space traveler
Mr. O, age 69, is a patient at a long-term psychiatric hospital. He has a 56-year psychiatric history, a current diagnosis of schizoaffective disorder, and suffered a torn rotator cuff approximately 5 years ago. His medication regimen is haloperidol decanoate, 100 mg IM every month, duloxetine, 60 mg/d, and naproxen, as needed for chronic pain.
He frequently lies on the floor. Attendants urge him to get up and join groups or sit with other patients but he complains of pain and soon finds another spot on the floor to use as a bed.
Eight months earlier, a homeless shelter sent Mr. O to the emergency room (ER) because he tried to eat a dollar bill and a sock. In the ER he was inattentive, with loose associations and bizarre delusions; he believed he was on a spaceship. Mr. O was admitted to the hospital, where clinicians noted that his behavior remained bizarre and he complained of insomnia. They also noted a history of setting fires, which complicated discharge planning and contributed to their decision to transfer him to our psychiatric facility for longer-term care.
During our initial interview, Mr. O readily picks himself off the floor. His responses are logical and direct but abrupt and unelaborated. His first and most vehement complaint is pain. Zolpidem, he says, is the only treatment that helps.
He says he began using zolpidem approximately 5 years ago because pain from a shoulder injury kept him awake at night. When he could not obtain the drug by prescription, he bought it on the street. One day when living in the homeless shelter, he took 30 or 40 mg of zolpidem, then “blacked out” and awoke in the ER.
His first experience with psychiatric treatment was the result of problems getting along with his single mother because of “petty things” such as shooting off a BB gun in their apartment, he says. As a teenager he was sent to a boarding school; as a young adult, to a psychiatric hospital. After his release he returned to his mother’s apartment. He worked steadily for 20 years before he obtained Social Security benefits, and then worked intermittently “off the books” until approximately 15 years ago. Mr. O lived with his mother until her death 17 years earlier, and then in her apartment alone until a fire, which he set accidentally by smoking in bed after taking zolpidem, forced him to leave 3 years ago. He says, “My whole life was in that place.” He was admitted to a psychiatric hospital for an unknown reason, which was his first psychiatric admission in 40 years. After he was released from the hospital, Mr. O lived in various homeless shelters and adult homes until his current hospitalization.
The author’s observations
An effective and well-tolerated drug with a reputation for rarely being abused, zolpidem is widely prescribed as a hypnotic. Zolpidem and benzodiazepines have different chemical structures but both act at the GABAA receptor and have comparable behavioral effects.1 The reported incidence of zolpidem abuse is much lower than the reported rate of benzodiazepine abuse when used for sleep2; however, abuse, dependence, and withdrawal have been reported.2-4 Zolpidem abuse seems to be more common among patients with a history of abusing other substances or a history of psychiatric illness.2 A French study4 found that abusers fell into 2 groups. The younger group (median age 35) used higher doses—a median of 300 mg/d—and took zolpidem in the daytime to achieve euphoria. A second, older group (median age 42) used lower doses—a median of 200 mg/d—at nighttime to sleep.
There are few reports of delirium and symptoms such as visual hallucinations and distortions associated with zolpidem use.5,6 These reactions have occurred in persons without a history of psychosis. They usually are associated with doses ≥10 mg.
In the ER Mr. O showed a disturbance in consciousness with inability to focus attention and a perceptual disturbance (he believed he was in a spaceship) that developed over hours to days. He met criteria for delirium, possibly caused by zolpidem, but his presentation also could have been attributable to an underlying psychiatric disorder.
ER and inpatient psychiatrists noted Mr. O was intoxicated with zolpidem when the shelter brought him to the ER, but both groups diagnosed schizoaffective disorder and treated him with antipsychotics. They saw his >50-year psychiatric history as evidence of an underlying, long-standing condition such as schizoaffective illness.
However, features of Mr. O’s illness are not typical of a chronic psychotic illness. He recalls psychiatric hospitalizations in his youth and recently, but not for the 40 years in between. Mr. O says he has never experienced auditory hallucinations. For these reasons, our treatment team obtains old medical records to investigate his early history (Table).
Table
Mr. O’s clinical course
| Age | Symptoms/behaviors | Diagnosis |
|---|---|---|
| 17 | Temper tantrums and destructive behaviors. No delusions or hallucinations but a flat affect and hostile attitude | Primary behavior disorder, simple adult maladjustment |
| 22 | Returned to the psychiatric hospital when his welfare payments stopped; “psychopathic” symptoms; described as defiant and resented authority and regular work | Primary behavior disorder |
| 24 | His mother complained that he stole from her and carried a weapon; while hospitalized, described as manageable and without overt psychotic symptoms | Primary behavior disorder |
| 26 | Arrested for causing property damage while intoxicated on alcohol; silly laugh, loose associations, irrelevant and incoherent speech, and believed hospital staff were against him | Psychosis with psychopathic personality |
| 66 | A fire that he set accidentally while smoking in bed after taking zolpidem destroyed his home | Diagnosis unknown |
| 68 | Transferred from a homeless shelter to the ER after he took 30 to 40 mg of zolpidem and exhibited bizarre behaviors | Schizoaffective disorder |
| 69 | More spontaneous, remains logical and relevant after haloperidol is discontinued; no delusions or hallucinations, still complains of pain | Substance use disorder and personality disorder |
| ER: emergency room | ||
HISTORY: Destructive and defiant
Mr. O’s mother reported that he had been a nervous, restless child who would scream and yell at the slightest provocation. At age 10 he became wantonly destructive. His mother bought him an expensive toy that he destroyed after a short time; he asked for another toy, which he also destroyed. When such behavior became more frequent, she took him to a city hospital, where he was treated for 6 weeks and released at age 13. He was sent to a boarding school but soon was expelled for drinking and selling beer.
Mr. O was admitted to long-term psychiatric facilities 6 times in the next 10 years, from the late 1950s to the late 1960s. He was first admitted at age 17 for temper tantrums during which he fired an air rifle and smashed windows in the home he shared with his mother. During examination he had no delusions or hallucinations but did have flat affect and a hostile attitude. Doctors documented that almost all his tantrums were as a result of interactions with his mother.
Records from this psychiatric admission state that Mr. O showed no unusual distractibility, “psychotic trends,” or paranoid thinking. After approximately 6 months in the hospital he was discharged home with the diagnosis of primary behavior disorder, simple adult maladjustment. Mr. O, who was age 18 at the time, and his mother were eager for him to complete high school and learn auto mechanics.
Nine months later, he returned to the psychiatric facility because of excessive drinking and inability to secure employment, according to his records. In the hospital, he was productive and reliable. When he was discharged home 3 months later, doctors wrote that his determination to stop drinking was firmly fixed. They encouraged Mr. O to complete high school as a night student and find employment during the day. His mother was delighted with his improvement.
A third admission, less than 2 months later, occurred after he broke a window during an argument with his mother. He had a job but quit. After 5 months he was discharged with the same diagnosis of primary behavior disorder, but his mother would not let him back in her home. He was referred to the social service department to be placed on welfare.
A year later, Mr. O had trouble managing his welfare allotment and moved repeatedly. He said he returned to the psychiatric hospital because his welfare payments had been discontinued. During this admission, doctors noted “psychopathic” symptoms; Mr. O was defiant and resented authority and regular work. Mr. O eloped from the hospital several times and brought beer into the building. After 18 months he was discharged with the same diagnosis, with plans to apply for welfare. He was not prescribed medication.
Mr. O’s fifth admission came nearly 2 years later after his mother complained that he stole from her home and carried a weapon. In the hospital he was described as manageable and without overt psychotic symptoms. When he was discharged a little more than a year after being admitted, doctors wrote that he was a psychopath who had a history of drinking, stealing, and delinquent tendencies as a teenager. His diagnosis remained primary behavior disorder.
A year after this discharge, Mr. O was arrested for causing serious property damage when he was intoxicated on alcohol. Subsequently he was readmitted.
After a few months in the hospital, Mr. O changed. He developed a silly laugh, loose associations, irrelevant and incoherent speech, and a belief that hospital staff were against him. Although Mr. O denied auditory hallucinations, a psychiatrist wrote that he seemed to be experiencing hallucinations and prescribed chlorpromazine. The next day Mr. O slashed his arms and legs in several places, requiring many sutures. His diagnosis was changed to psychosis with psychopathic personality. However, within a few months, psychiatrists determined that Mr. O had recovered, so they stopped chlorpromazine. Months later, clinicians wrote that Mr. O was idle most of the time, neat, clean, and not involved in arguments with other patients. He was discharged after 1 month in the hospital.
Over the years, psychiatrists had differing opinions about Mr. O’s diagnosis. One noted that his mental illness was characterized by emotional instability and poor judgment. He had impulsive reactions without regard for others, rapid mood swings, irritability, and depression with transient paranoia. Another clinician detected evidence of schizoid personality disorder because Mr. O did not experience hallucinations or a gross thought disorder, but did have rambling, circumstantial, autistic (unrealistic), and ambivalent thought content. Another psychiatrist wrote Mr. O best fit in the category of psychosis with psychopathic personality, which was his diagnosis at discharge from his sixth hospitalization.
The author’s observations
Mr. O’s old medical records revealed the diagnostic thinking and treatment practices of a past era. They did not demonstrate that Mr. O met current criteria for schizophrenia or schizoaffective disorder, although he may have had a brief psychotic episode. Because there was little support for a diagnosis of schizoaffective illness and haloperidol use, we stopped the drug but continued duloxetine for chronic pain. It was clear that he has a substance use disorder and perhaps met criteria for antisocial personality disorder.
OUTCOME: Further explanations
Approximately 2 months after stopping haloperidol, Mr. O is more spontaneous, logical, and relevant. He does not have delusions or hallucinations. Despite further attempts at pain management with physical therapy and increased doses of duloxetine, he still complains of pain. We do not prescribe zolpidem.
Mr. O is unwilling to discuss the incident more than 40 years ago when he cut his arms and legs except to say, “That’s the past. My life wasn’t so good at that time.” When we ask why he had been a client of Adult Protective Services 5 years before he was burned out of his apartment, he admitted that he was 21 months in arrears in his rent. “I used to do this thing called crack,” he explains. He was discharged to an adult home with a prescription for duloxetine after he promised to never smoke in his room again.
Related Resource
- Aggarwal A, Sharma DD. Zolpidem withdrawal delirium: a case report. J Neuropsychiatry Clin Neurosci. 2010;22(4):451.
Drug Brand Names
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Duloxetine • Cymbalta
- Haloperidol decanoate • Haloperidol decanoate
- Haloperidol • Haldol
- Naproxen • Naproxyn, Aleve, others
- Zolpidem • Ambien
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rush CR. Behavioral pharmacology of zolpidem relative to benzodiazepines: a review. Pharmacol Biochem Behav. 1998;61(3):253-269.
2. Hajak G, Müller WE, Wittchen HU, et al. Abuse and dependence potential for the non-benzodiazepine hypnotics zolpidem and zopiclone: a review of case reports and epidemiological data. Addiction. 2003;98(10):1371-1378.
3. Madrak LN, Rosenberg M. Zolpidem abuse. Am J Psychiatry. 2001;158(8):1330-1331.
4. Victorri-Vigneau C, Dailly E, Veyrac G, et al. Evidence of zolpidem abuse and dependence: results of the French Centre for Evaluation and Information on Pharmacodepencence (CEIP) network survey. Br J Clin Pharmacol. 2007;64(2):198-209.
5. Markowitz JS, Brewerton TD. Zolpidem-induced psychosis. Ann Clin Psychiatry. 1996;8(2):89-91.
6. Tsai MJ, Huang YB, Wu PC. A novel clinical pattern of visual hallucination after zolpidem use. J Toxicol Clin Toxicol. 2003;41(6):869-872.
1. Rush CR. Behavioral pharmacology of zolpidem relative to benzodiazepines: a review. Pharmacol Biochem Behav. 1998;61(3):253-269.
2. Hajak G, Müller WE, Wittchen HU, et al. Abuse and dependence potential for the non-benzodiazepine hypnotics zolpidem and zopiclone: a review of case reports and epidemiological data. Addiction. 2003;98(10):1371-1378.
3. Madrak LN, Rosenberg M. Zolpidem abuse. Am J Psychiatry. 2001;158(8):1330-1331.
4. Victorri-Vigneau C, Dailly E, Veyrac G, et al. Evidence of zolpidem abuse and dependence: results of the French Centre for Evaluation and Information on Pharmacodepencence (CEIP) network survey. Br J Clin Pharmacol. 2007;64(2):198-209.
5. Markowitz JS, Brewerton TD. Zolpidem-induced psychosis. Ann Clin Psychiatry. 1996;8(2):89-91.
6. Tsai MJ, Huang YB, Wu PC. A novel clinical pattern of visual hallucination after zolpidem use. J Toxicol Clin Toxicol. 2003;41(6):869-872.
A curious case of depression
Discuss this article at www.facebook.com/CurrentPsychiatry
Mr. Z, age 61, is referred by his primary care clinician to the hospital’s medical service with increasing depressive symptoms and non-pruritic rash. He has a history of bipolar I disorder for >30 years. When the primary care physician evaluated Mr. Z, his vitals were normal, but blood work revealed mild anemia and thrombocytopenia of 34 x103/μL, which prompted referral to the hospital. During admission, the psychiatric consultation service is called to evaluate Mr. Z’s depressive symptoms.
Mr. Z reports having chronic sleep problems and feeling cold and tired, shivering at times, but has no pain. He says he’s worried because he feels severely depressed, worthless, and hopeless, but denies suicidal ideation and psychosis. Mr. Z says he started experiencing increasingly depressed mood, anhedonia, insomnia, fatigue, poor appetite, and concentration 2 months ago. At that time his outpatient psychiatrist started Mr. Z on risperidone, 6 mg/d, and divalproex, 1,500 mg at bedtime because of emerging mood symptoms, after he was off medication for 7 months. Mr. Z attributed his worsened mood symptoms to being overwhelmed by several psychosocial stressors, including going through a complicated divorce, financial problems, and homelessness after being evicted from his apartment.
A review of Mr. Z’s psychiatric history reveals several remote hospitalizations—the last was 7 years ago—for escalated manic symptoms after he stopped taking his medication. He denies past suicide attempts. Mr. Z says he is compliant with his current medication regimen—risperidone, 6 mg/d, and divalproex, 1,500 mg at bedtime. He denies illicit drug use and says he drinks “a couple of beers, mostly on weekends.” Family history is positive for depression and bipolar II disorder.
His medical history is significant for hypothyroidism after goiter removal 6 years ago, for which he takes levothyroxine, 150 mcg/d, and a sports injury-related splenectomy in childhood. He reports no allergies. Vital signs at the time of admission are temperature, 99.1°F; pulse, 98 beats per minute; respiration, 16 breaths per minute; blood pressure, 123/73 mm/Hg; and oxygen saturation, 97%.
During the interview, Mr. Z presents with tired facies and exhibits psychomotor retardation. He has to force himself to stay engaged in the evaluation and maintain eye contact. His speech is clear, regular, and soft. Mr. Z says he is “very depressed”; his affect is constricted, almost flat, stable, and consistent with depressed mood. His thought process is linear and somewhat concrete and his thought content is notable for hopelessness, although Mr. Z continues to deny suicidal or homicidal ideations. No hallucinations or apparent delusions are noted. Insight and judgment are fair. Mr. Z understands his current mental state; however, he displays some lack of knowledge regarding his current hospitalization. Cognition is intact.
The authors’ observations
The differential diagnosis in patients presenting with mood changes is extensive (Table 1)1 and in Mr. Z’s case includes several precipitating and perpetuating factors. Mr. Z presents with severe depressive symptoms and meets DSM-IV-TR criteria for a major depressive episode (MDE). This presentation is not typical of his bipolar I disorder because Mr. Z has never experienced an MDE and usually presents with escalating hypomanic/manic symptoms in the context of medication nonadherence. Nevertheless, Mr. Z has several risk factors for severe depression, including a family psychiatric history, multiple enduring social stressors and life crises, and medical conditions.
In the general population, the lifetime risk for developing depression is 8% to 17%.2 The risk of developing a mood disorder increases significantly if a first-degree relative is diagnosed with a mood disorder; the relative risk is 10.3 for bipolar disorder and 3.2 for depression.3 Additionally, Mr. Z is going through a complicated divorce, has financial problems, and is homeless, all of which could trigger an MDE. Furthermore, hypothyroidism shares many symptoms of depression, including fatigue, lethargy, anhedonia, cold intolerance, and low mood; mental status changes frequently are the initial presentation of thyroid problems.4 Physicians started Mr. Z on a new medication regimen (risperidone and divalproex) to control mood instability, which coincided with symptom onset. Atypical antipsychotics have been reported to precipitate depressive symptoms; their side effect profile includes extrapyramidal effects, such as flat affect, which can be mistaken for depression.5 Rapid valproate titration can mimic neurovegetative symptoms of depression and cause dose-dependent thrombocytopenia and rash, which could explain his initial presentation.6 Finally, Mr. Z’s history of traumatic splenectomy, change in mental status, and thrombocytopenia suggest an infectious etiology.
Table 1
Differential diagnosis in patients presenting with mood changes
| Cerebrovascular disease |
| Degenerative disorders (Parkinson’s disease, Huntington’s disease, Wilson’s disease) |
| Demyelinating disorders (multiple sclerosis, amyotrophic lateral sclerosis, lipid storage disease) |
| Endocrine disorders (Addison’s disease, Cushing’s disease, hyperthyroidism, hypothyroidism, hyperparathyroidism, pituitary dysfunction) |
| Epilepsy |
| Infectious diseases |
| Immune diseases |
| Metabolic encephalopathy |
| Neoplasm |
| Nutritional deficits (thiamine, niacin, vitamin B12) |
| Primary psychiatric disorders (mood disorders, dementia, sleep disorders) |
| Substance use |
| Toxins/medications |
| Traumatic brain injury |
| Source: Reference 1 |
Possible infectious causes
The increased prevalence of immune suppression due to human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) or from therapeutic modalities such as cancer therapy or splenectomy has led to an increased number of chronic CNS infections, manifesting with an array of neuropsychiatric symptoms and nonspecific physiological reactions.1,7 Mr. Z complains of a 2-month period of worsening depression that could suggest an infectious process with an insidious onset. Some infectious agents that can cause chronic CNS infection and encephalopathy are presented in Table 2.8 HIV, tuberculosis, syphilis, Lyme disease, and herpes simplex virus are becoming more prevalent and can present with neuropsychiatric symptoms.1 For example, in addition to thrombocytopenia and low-grade fever, patients with HIV may exhibit a broad range of neuropsychiatric symptoms such as cognitive problems, impaired executive and motor functioning, sleep disturbance, and anxiety. These patients frequently present with low mood and neurovegetative symptoms of depression.7 Similarly, the same tick responsible for Lyme disease infection can transmit other infectious agents that can cause thrombocytopenia, including Babesia, Ehrlichia chaffeensis, Anaplasma phagocytophilum, and human Ewingii ehrlichiosis.
The authors’ observations
Diagnosis of a mood change, particularly an MDE, is clinical, based on careful psychiatric evaluation using standardized criteria rather than a specific lab test. However, some laboratory studies (Table 3)1 are useful in differentiating medical illnesses that may present with depression. Mr. Z’s presentation warrants investigating these tests. His history of traumatic splenectomy and night sweats suggests an infection. The team’s initial recommendations include laboratory tests, discontinuing divalproex because it may be causing thrombocytopenia, and decreasing risperidone to 2 mg/d to improve his fatigue and possibly developed extrapyramidal symptoms.
Table 2
Potential infectious causes of chronic encephalopathy
| Type of infection | Organism/disease |
|---|---|
| Mycobacterial | Mycobacterium tuberculosis |
| Spirochetal | Treponema pallidum (syphilis), Borrelia burgdorferi (Lyme disease), Leptospira |
| Bacterial | Brucella, Listeria, Nocardia, Actinomyces israelii, Whipple’s disease |
| Viral | HIV/AIDS, cytomegalovirus, varicella zoster virus, herpes simplex virus, enterovirus |
| Fungal | Histoplasmosis, coccidiosis, sporothrix, Blastomyces, Cryptococcus |
| Parasitic | Toxoplasmosis, taenia solium (cysticercosis), Schistosoma, Acanthamoeba |
| AIDS: acquired immunodeficiency syndrome; HIV: human immunodeficiency virus Source: Reference 8 | |
Table 3
Differentiating medical illnesses that may mimic depression
| Laboratory tests |
|
| Imaging studies |
|
| Other tests |
|
| Procedures |
|
| ABG: arterial blood gases; CBC: complete blood count; EEG: electroencephalogram; ELISA: enzyme-linked immunosorbent assay; HIV: human immunodeficiency virus; VDRL: venereal disease research laboratory Source: Reference 1 |
TREATMENT: Cause revealed
Mr. Z develops a persistent fever of 102°F with continuous profuse sweating and a hypotensive episode. Blood work reveals mild anemia, thrombocytopenia, and increased coagulation parameters with high D-dimer and low fibrinogen, consistent with diagnosis of disseminated intravascular coagulation (DIC) secondary to infectious etiology. Thyroid and HIV tests are negative. After further evaluation, Mr. Z remembers that 4 months earlier he removed several ticks from his legs after hunting; he also remembers experiencing shivering and night sweats several weeks before he was hospitalized. His blood smear is positive for babesiosis and further testing confirms positive Lyme antibodies. Mr. Z is started on aggressive hemodynamic stabilization and a pathogen-tailored course of antibiotics for several weeks. This results in improvement and discharge home in a stable condition. His depression and fatigue improve but do not fully remit by the time he is discharged.
The authors’ observations
Lyme disease is one of the fastest-growing infectious diseases in the United States.9 The prevalence of positive Lyme antibodies is 30% higher in psychiatric populations than the general population.10 Lyme disease is transmitted by deer tick bite, often undetected, that is infected with spirochete Borrelia burgdorferi. To be infectious, ticks need to be attached to the skin for 24 to 48 hours,11,12 although individual cases have reported transmission in <24 hours. The clinical manifestations of Lyme disease can be divided into 3 phases:
- early localized phase, characterized by the distinctive skin lesion erythema migrans with or without constitutional symptoms
- early disseminated phase, characterized by multiple erythema migrans lesions and neurologic and/or cardiac findings
- late or chronic disease associated with intermittent/persistent arthritis and/or neurologic problems.11,13
The clinical features of each stage frequently overlap and some patients in a later stage of Lyme disease do not have prior signs or symptoms of the disease. Because it is a multisystem disease, Lyme disease can attack the CNS in the form of neuroborreliosis, a clinical diagnosis, without involving other systems, and its neuropsychiatric manifestations can resemble neurosyphilis because both organisms are spirochetes.11,13,14 CNS disorders have been found in up to 40% of Lyme disease cases.11 In neuroborreliosis, cognitive problems usually predominate; however, neuroborreliosis can mimic multiple brain diseases presenting with various neurologic and psychiatric symptoms (Table 4)14,15 and can present at any time after the tick bite. Furthermore neuroborreliosis is difficult to diagnose because symptoms may remain dormant and emerge after several years.11,13,14Borrelia burgdorferi is challenging to isolate and grow in the lab, and enzyme-linked immunosorbent assay (ELISA) testing for antibodies is highly specific but not very sensitive,16 frequently giving false negative results. Western blot confirms the diagnosis.
Table 4
Late-stage neuropsychiatric symptoms of Lyme disease
| Cognitive problems, memory problems, forgetfulness, slowing of thought processing, dysfunction in visuospatial orientation, dyslexia |
| Depression |
| Mood swings |
| Psychosis |
| Violent behavior/irritability |
| OCD |
| Anxiety |
| Panic attacks |
| Sleep disorders |
| Seizures |
| ADHD-like symptoms |
| Autism-like behavior |
| Chronic fatigue syndrome |
| Fibromyalgia |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder Source: References 14,15 |
Mr. Z’s presentation also reflects co-infection with babesiosis. Babesia is malaria-like protozoa diagnosed by blood smear that can cause a fatal illness in immuno-compromised patients. The clinical picture varies from mild symptoms such as night sweats, chills, arthralgias, and anorexia with thrombocytopenia to severe and potentially fatal outcomes in immunocompromised patients, including DIC, acute renal failure, sepsis, congestive heart failure, and myocardial infarction.11 Risk factors for the severest forms of babesiosis are age >50, co-infection with Lyme disease, and splenectomy,11 all of which were present in Mr. Z. Co-infected patients experience fatigue, headache, anorexia, and emotional lability more frequently than those with Lyme disease alone.12
Treatment options
Treatment of Lyme disease/neuroborreliosis is complex. The mainstay approach is antibiotics. Despite adequate treatment, many patients experience continued impairment, including chronic pain, fatigue, and cognitive and psychiatric symptoms.11,14 There is some evidence Borrelia burgdorferi can persist and re-emerge after adequate treatment.14,17 The National Institute of Health sponsored several clinical trials of prolonged antibiotic treatment for chronic Lyme disease. Some results suggested improvement in fatigue and cognitive function, although these results were not sustained.18
There is a strong link between mental illness and increased prevalence of positive Lyme disease antibodies.10 Several studies report increased risk of infection during psychological stress that may be related to an altered immune system response.19 Evidence suggests that Borrelia burgdorferi can alter immune system response, making T cells more reactive not only to Borrelia burgdorferi antigens but also to host antigens,20 creating autoimmune inflammatory reactions that could explain chronic neuropsychiatric symptoms. It appears Lyme disease antigens can mimic certain autoantigens (for example, in the thyroid gland).21 Whether there is a role for autoimmune therapy in treating chronic symptoms needs to be investigated.
Once Lyme disease is diagnosed, educating patients and families becomes an important part of treatment because many patients report feeling stigmatized by the diagnosis. Referral to a Lyme disease support group may be beneficial. Patients with neuropsychiatric symptoms that persist after antibiotic treatment should be offered symptom-based treatment, including medications and therapy.
Related Resource
- Centers for Disease Control and Prevention. Lyme disease: Resources for clinicians. www.cdc.gov/lyme/healthcare/clinicians.html.
Drug Brand Names
- Divalproex sodium • Depakote
- Levothyroxine • Levoxyl, Synthroid
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Stern TA, Rosenbaum JF, Fava M, et al. eds. Massachusetts General Hospital comprehensive clinical psychiatry. Philadelphia, PA: Mosby; 2008;257-277.
2. Andrade L, Caraveo-Anduaga JJ, Berglund P, et al. The epidemiology of major depressive episodes: results from the International Consortium of Psychiatric Epidemiology (ICPE) Surveys. Int J Methods Psychiatr Res. 2003;12(1):3-21.
3. Merikangas KR, Low NC. The epidemiology of mood disorders. Curr Psychiatry Rep. 2004;6:411-421.
4. Brown GM. Psychiatric and neurologic aspects of endocrine disease. In Krieger DT Hughes JC, eds. Neuroendocrinology. Sunderland, MA: Sinauer Associates; 1980;185-194.
5. Maguire GA. Comprehensive understanding of schizophrenia and its treatment. Am J Health Syst Pharm. 2002;59(17 suppl 5):S4-S11.
6. Dreifuss FE, Langer DH. Side effects of valproate. Am J Med. 1988;84(1A):34-41.
7. Perry S, Jacobsen P. Neuropsychiatric manifestations of AIDS-spectrum disorders. Hosp Community Psychiatry. 1986;37:135-142.
8. Hildebrand J, Aoun M. Chronic meningitis: still a diagnostic challenge. J Neurol. 2003;250(6):653-660.
9. Bacon RM, Kugeler KJ, Mead PS. Centers for Disease Control and Prevention (CDC). Surveillance for Lyme disease—United States 1992-2006. MMWR Surveill Summ. 2008;57(10):1-9.
10. Hájek T, Pasková B, Janovská D, et al. Higher prevalence of antibodies to Borrelia burgdorferi in psychiatric patients than in healthy subjects. Am J Psychiatry. 2002;159:297-301.
11. Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43(9):1089-1134.
12. Krause PJ, Telford SR 3rd, Spielman A, et al. Concurrent Lyme disease and babesiosis. Evidence for increased severity and duration of illness. JAMA. 1996;275(21):1657-1660.
13. Hildenbrand P, Craven DE, Jones R, et al. Lyme neuroborreliosis: manifestations of a rapidly emerging zoonosis. AJNR Am J Neuroradiol. 2009;30:1079-1087.
14. Fallon BA, Nields JA. Lyme disease: a neuropsychiatric illness. Am J Psychiatry. 1994;151:1571-1583.
15. Fallon BA, Nields JA, Burrascano JJ, et al. The neuropsychiatric manifestations of Lyme borreliosis. Psychiatr Q. 1992;63(1):95-117.
16. Stricker RB, Johnson L. Lyme wars: let’s tackle the testing. BMJ. 2007;335:1008.-
17. Hodzic E, Feng S, Holden K, et al. Persistence of Borrelia burgdorferi following antibiotic treatment in mice. Antimicrob Agents Chemother. 2008;52(5):1728-1736.
18. Fallon BA, Keilp JG, Corbera KM, et al. A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy. Neurology. 2008;70(13):992-1003.
19. Sheridan JF, Dobbs C, Brown D, et al. Psychoneuroimmunology: stress effects on pathogenesis and immunity during infection. Clin Microbiol Rev. 1994;7(2):200-212.
20. Yssel H, Shanafelt MC, Soderberg C, et al. Borrelia burgdorferi activates a T helper 1-like T cell subset in Lyme arthritis. J Exp Med. 1991;174:593-601.
21. Benvenga S, Guarneri F, Vaccaro M, et al. Homologies between proteins of Borrelia burgdorferi and thyroid autoantigens. Thyroid. 2004;14(11):964-966.
Discuss this article at www.facebook.com/CurrentPsychiatry
Mr. Z, age 61, is referred by his primary care clinician to the hospital’s medical service with increasing depressive symptoms and non-pruritic rash. He has a history of bipolar I disorder for >30 years. When the primary care physician evaluated Mr. Z, his vitals were normal, but blood work revealed mild anemia and thrombocytopenia of 34 x103/μL, which prompted referral to the hospital. During admission, the psychiatric consultation service is called to evaluate Mr. Z’s depressive symptoms.
Mr. Z reports having chronic sleep problems and feeling cold and tired, shivering at times, but has no pain. He says he’s worried because he feels severely depressed, worthless, and hopeless, but denies suicidal ideation and psychosis. Mr. Z says he started experiencing increasingly depressed mood, anhedonia, insomnia, fatigue, poor appetite, and concentration 2 months ago. At that time his outpatient psychiatrist started Mr. Z on risperidone, 6 mg/d, and divalproex, 1,500 mg at bedtime because of emerging mood symptoms, after he was off medication for 7 months. Mr. Z attributed his worsened mood symptoms to being overwhelmed by several psychosocial stressors, including going through a complicated divorce, financial problems, and homelessness after being evicted from his apartment.
A review of Mr. Z’s psychiatric history reveals several remote hospitalizations—the last was 7 years ago—for escalated manic symptoms after he stopped taking his medication. He denies past suicide attempts. Mr. Z says he is compliant with his current medication regimen—risperidone, 6 mg/d, and divalproex, 1,500 mg at bedtime. He denies illicit drug use and says he drinks “a couple of beers, mostly on weekends.” Family history is positive for depression and bipolar II disorder.
His medical history is significant for hypothyroidism after goiter removal 6 years ago, for which he takes levothyroxine, 150 mcg/d, and a sports injury-related splenectomy in childhood. He reports no allergies. Vital signs at the time of admission are temperature, 99.1°F; pulse, 98 beats per minute; respiration, 16 breaths per minute; blood pressure, 123/73 mm/Hg; and oxygen saturation, 97%.
During the interview, Mr. Z presents with tired facies and exhibits psychomotor retardation. He has to force himself to stay engaged in the evaluation and maintain eye contact. His speech is clear, regular, and soft. Mr. Z says he is “very depressed”; his affect is constricted, almost flat, stable, and consistent with depressed mood. His thought process is linear and somewhat concrete and his thought content is notable for hopelessness, although Mr. Z continues to deny suicidal or homicidal ideations. No hallucinations or apparent delusions are noted. Insight and judgment are fair. Mr. Z understands his current mental state; however, he displays some lack of knowledge regarding his current hospitalization. Cognition is intact.
The authors’ observations
The differential diagnosis in patients presenting with mood changes is extensive (Table 1)1 and in Mr. Z’s case includes several precipitating and perpetuating factors. Mr. Z presents with severe depressive symptoms and meets DSM-IV-TR criteria for a major depressive episode (MDE). This presentation is not typical of his bipolar I disorder because Mr. Z has never experienced an MDE and usually presents with escalating hypomanic/manic symptoms in the context of medication nonadherence. Nevertheless, Mr. Z has several risk factors for severe depression, including a family psychiatric history, multiple enduring social stressors and life crises, and medical conditions.
In the general population, the lifetime risk for developing depression is 8% to 17%.2 The risk of developing a mood disorder increases significantly if a first-degree relative is diagnosed with a mood disorder; the relative risk is 10.3 for bipolar disorder and 3.2 for depression.3 Additionally, Mr. Z is going through a complicated divorce, has financial problems, and is homeless, all of which could trigger an MDE. Furthermore, hypothyroidism shares many symptoms of depression, including fatigue, lethargy, anhedonia, cold intolerance, and low mood; mental status changes frequently are the initial presentation of thyroid problems.4 Physicians started Mr. Z on a new medication regimen (risperidone and divalproex) to control mood instability, which coincided with symptom onset. Atypical antipsychotics have been reported to precipitate depressive symptoms; their side effect profile includes extrapyramidal effects, such as flat affect, which can be mistaken for depression.5 Rapid valproate titration can mimic neurovegetative symptoms of depression and cause dose-dependent thrombocytopenia and rash, which could explain his initial presentation.6 Finally, Mr. Z’s history of traumatic splenectomy, change in mental status, and thrombocytopenia suggest an infectious etiology.
Table 1
Differential diagnosis in patients presenting with mood changes
| Cerebrovascular disease |
| Degenerative disorders (Parkinson’s disease, Huntington’s disease, Wilson’s disease) |
| Demyelinating disorders (multiple sclerosis, amyotrophic lateral sclerosis, lipid storage disease) |
| Endocrine disorders (Addison’s disease, Cushing’s disease, hyperthyroidism, hypothyroidism, hyperparathyroidism, pituitary dysfunction) |
| Epilepsy |
| Infectious diseases |
| Immune diseases |
| Metabolic encephalopathy |
| Neoplasm |
| Nutritional deficits (thiamine, niacin, vitamin B12) |
| Primary psychiatric disorders (mood disorders, dementia, sleep disorders) |
| Substance use |
| Toxins/medications |
| Traumatic brain injury |
| Source: Reference 1 |
Possible infectious causes
The increased prevalence of immune suppression due to human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) or from therapeutic modalities such as cancer therapy or splenectomy has led to an increased number of chronic CNS infections, manifesting with an array of neuropsychiatric symptoms and nonspecific physiological reactions.1,7 Mr. Z complains of a 2-month period of worsening depression that could suggest an infectious process with an insidious onset. Some infectious agents that can cause chronic CNS infection and encephalopathy are presented in Table 2.8 HIV, tuberculosis, syphilis, Lyme disease, and herpes simplex virus are becoming more prevalent and can present with neuropsychiatric symptoms.1 For example, in addition to thrombocytopenia and low-grade fever, patients with HIV may exhibit a broad range of neuropsychiatric symptoms such as cognitive problems, impaired executive and motor functioning, sleep disturbance, and anxiety. These patients frequently present with low mood and neurovegetative symptoms of depression.7 Similarly, the same tick responsible for Lyme disease infection can transmit other infectious agents that can cause thrombocytopenia, including Babesia, Ehrlichia chaffeensis, Anaplasma phagocytophilum, and human Ewingii ehrlichiosis.
The authors’ observations
Diagnosis of a mood change, particularly an MDE, is clinical, based on careful psychiatric evaluation using standardized criteria rather than a specific lab test. However, some laboratory studies (Table 3)1 are useful in differentiating medical illnesses that may present with depression. Mr. Z’s presentation warrants investigating these tests. His history of traumatic splenectomy and night sweats suggests an infection. The team’s initial recommendations include laboratory tests, discontinuing divalproex because it may be causing thrombocytopenia, and decreasing risperidone to 2 mg/d to improve his fatigue and possibly developed extrapyramidal symptoms.
Table 2
Potential infectious causes of chronic encephalopathy
| Type of infection | Organism/disease |
|---|---|
| Mycobacterial | Mycobacterium tuberculosis |
| Spirochetal | Treponema pallidum (syphilis), Borrelia burgdorferi (Lyme disease), Leptospira |
| Bacterial | Brucella, Listeria, Nocardia, Actinomyces israelii, Whipple’s disease |
| Viral | HIV/AIDS, cytomegalovirus, varicella zoster virus, herpes simplex virus, enterovirus |
| Fungal | Histoplasmosis, coccidiosis, sporothrix, Blastomyces, Cryptococcus |
| Parasitic | Toxoplasmosis, taenia solium (cysticercosis), Schistosoma, Acanthamoeba |
| AIDS: acquired immunodeficiency syndrome; HIV: human immunodeficiency virus Source: Reference 8 | |
Table 3
Differentiating medical illnesses that may mimic depression
| Laboratory tests |
|
| Imaging studies |
|
| Other tests |
|
| Procedures |
|
| ABG: arterial blood gases; CBC: complete blood count; EEG: electroencephalogram; ELISA: enzyme-linked immunosorbent assay; HIV: human immunodeficiency virus; VDRL: venereal disease research laboratory Source: Reference 1 |
TREATMENT: Cause revealed
Mr. Z develops a persistent fever of 102°F with continuous profuse sweating and a hypotensive episode. Blood work reveals mild anemia, thrombocytopenia, and increased coagulation parameters with high D-dimer and low fibrinogen, consistent with diagnosis of disseminated intravascular coagulation (DIC) secondary to infectious etiology. Thyroid and HIV tests are negative. After further evaluation, Mr. Z remembers that 4 months earlier he removed several ticks from his legs after hunting; he also remembers experiencing shivering and night sweats several weeks before he was hospitalized. His blood smear is positive for babesiosis and further testing confirms positive Lyme antibodies. Mr. Z is started on aggressive hemodynamic stabilization and a pathogen-tailored course of antibiotics for several weeks. This results in improvement and discharge home in a stable condition. His depression and fatigue improve but do not fully remit by the time he is discharged.
The authors’ observations
Lyme disease is one of the fastest-growing infectious diseases in the United States.9 The prevalence of positive Lyme antibodies is 30% higher in psychiatric populations than the general population.10 Lyme disease is transmitted by deer tick bite, often undetected, that is infected with spirochete Borrelia burgdorferi. To be infectious, ticks need to be attached to the skin for 24 to 48 hours,11,12 although individual cases have reported transmission in <24 hours. The clinical manifestations of Lyme disease can be divided into 3 phases:
- early localized phase, characterized by the distinctive skin lesion erythema migrans with or without constitutional symptoms
- early disseminated phase, characterized by multiple erythema migrans lesions and neurologic and/or cardiac findings
- late or chronic disease associated with intermittent/persistent arthritis and/or neurologic problems.11,13
The clinical features of each stage frequently overlap and some patients in a later stage of Lyme disease do not have prior signs or symptoms of the disease. Because it is a multisystem disease, Lyme disease can attack the CNS in the form of neuroborreliosis, a clinical diagnosis, without involving other systems, and its neuropsychiatric manifestations can resemble neurosyphilis because both organisms are spirochetes.11,13,14 CNS disorders have been found in up to 40% of Lyme disease cases.11 In neuroborreliosis, cognitive problems usually predominate; however, neuroborreliosis can mimic multiple brain diseases presenting with various neurologic and psychiatric symptoms (Table 4)14,15 and can present at any time after the tick bite. Furthermore neuroborreliosis is difficult to diagnose because symptoms may remain dormant and emerge after several years.11,13,14Borrelia burgdorferi is challenging to isolate and grow in the lab, and enzyme-linked immunosorbent assay (ELISA) testing for antibodies is highly specific but not very sensitive,16 frequently giving false negative results. Western blot confirms the diagnosis.
Table 4
Late-stage neuropsychiatric symptoms of Lyme disease
| Cognitive problems, memory problems, forgetfulness, slowing of thought processing, dysfunction in visuospatial orientation, dyslexia |
| Depression |
| Mood swings |
| Psychosis |
| Violent behavior/irritability |
| OCD |
| Anxiety |
| Panic attacks |
| Sleep disorders |
| Seizures |
| ADHD-like symptoms |
| Autism-like behavior |
| Chronic fatigue syndrome |
| Fibromyalgia |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder Source: References 14,15 |
Mr. Z’s presentation also reflects co-infection with babesiosis. Babesia is malaria-like protozoa diagnosed by blood smear that can cause a fatal illness in immuno-compromised patients. The clinical picture varies from mild symptoms such as night sweats, chills, arthralgias, and anorexia with thrombocytopenia to severe and potentially fatal outcomes in immunocompromised patients, including DIC, acute renal failure, sepsis, congestive heart failure, and myocardial infarction.11 Risk factors for the severest forms of babesiosis are age >50, co-infection with Lyme disease, and splenectomy,11 all of which were present in Mr. Z. Co-infected patients experience fatigue, headache, anorexia, and emotional lability more frequently than those with Lyme disease alone.12
Treatment options
Treatment of Lyme disease/neuroborreliosis is complex. The mainstay approach is antibiotics. Despite adequate treatment, many patients experience continued impairment, including chronic pain, fatigue, and cognitive and psychiatric symptoms.11,14 There is some evidence Borrelia burgdorferi can persist and re-emerge after adequate treatment.14,17 The National Institute of Health sponsored several clinical trials of prolonged antibiotic treatment for chronic Lyme disease. Some results suggested improvement in fatigue and cognitive function, although these results were not sustained.18
There is a strong link between mental illness and increased prevalence of positive Lyme disease antibodies.10 Several studies report increased risk of infection during psychological stress that may be related to an altered immune system response.19 Evidence suggests that Borrelia burgdorferi can alter immune system response, making T cells more reactive not only to Borrelia burgdorferi antigens but also to host antigens,20 creating autoimmune inflammatory reactions that could explain chronic neuropsychiatric symptoms. It appears Lyme disease antigens can mimic certain autoantigens (for example, in the thyroid gland).21 Whether there is a role for autoimmune therapy in treating chronic symptoms needs to be investigated.
Once Lyme disease is diagnosed, educating patients and families becomes an important part of treatment because many patients report feeling stigmatized by the diagnosis. Referral to a Lyme disease support group may be beneficial. Patients with neuropsychiatric symptoms that persist after antibiotic treatment should be offered symptom-based treatment, including medications and therapy.
Related Resource
- Centers for Disease Control and Prevention. Lyme disease: Resources for clinicians. www.cdc.gov/lyme/healthcare/clinicians.html.
Drug Brand Names
- Divalproex sodium • Depakote
- Levothyroxine • Levoxyl, Synthroid
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Mr. Z, age 61, is referred by his primary care clinician to the hospital’s medical service with increasing depressive symptoms and non-pruritic rash. He has a history of bipolar I disorder for >30 years. When the primary care physician evaluated Mr. Z, his vitals were normal, but blood work revealed mild anemia and thrombocytopenia of 34 x103/μL, which prompted referral to the hospital. During admission, the psychiatric consultation service is called to evaluate Mr. Z’s depressive symptoms.
Mr. Z reports having chronic sleep problems and feeling cold and tired, shivering at times, but has no pain. He says he’s worried because he feels severely depressed, worthless, and hopeless, but denies suicidal ideation and psychosis. Mr. Z says he started experiencing increasingly depressed mood, anhedonia, insomnia, fatigue, poor appetite, and concentration 2 months ago. At that time his outpatient psychiatrist started Mr. Z on risperidone, 6 mg/d, and divalproex, 1,500 mg at bedtime because of emerging mood symptoms, after he was off medication for 7 months. Mr. Z attributed his worsened mood symptoms to being overwhelmed by several psychosocial stressors, including going through a complicated divorce, financial problems, and homelessness after being evicted from his apartment.
A review of Mr. Z’s psychiatric history reveals several remote hospitalizations—the last was 7 years ago—for escalated manic symptoms after he stopped taking his medication. He denies past suicide attempts. Mr. Z says he is compliant with his current medication regimen—risperidone, 6 mg/d, and divalproex, 1,500 mg at bedtime. He denies illicit drug use and says he drinks “a couple of beers, mostly on weekends.” Family history is positive for depression and bipolar II disorder.
His medical history is significant for hypothyroidism after goiter removal 6 years ago, for which he takes levothyroxine, 150 mcg/d, and a sports injury-related splenectomy in childhood. He reports no allergies. Vital signs at the time of admission are temperature, 99.1°F; pulse, 98 beats per minute; respiration, 16 breaths per minute; blood pressure, 123/73 mm/Hg; and oxygen saturation, 97%.
During the interview, Mr. Z presents with tired facies and exhibits psychomotor retardation. He has to force himself to stay engaged in the evaluation and maintain eye contact. His speech is clear, regular, and soft. Mr. Z says he is “very depressed”; his affect is constricted, almost flat, stable, and consistent with depressed mood. His thought process is linear and somewhat concrete and his thought content is notable for hopelessness, although Mr. Z continues to deny suicidal or homicidal ideations. No hallucinations or apparent delusions are noted. Insight and judgment are fair. Mr. Z understands his current mental state; however, he displays some lack of knowledge regarding his current hospitalization. Cognition is intact.
The authors’ observations
The differential diagnosis in patients presenting with mood changes is extensive (Table 1)1 and in Mr. Z’s case includes several precipitating and perpetuating factors. Mr. Z presents with severe depressive symptoms and meets DSM-IV-TR criteria for a major depressive episode (MDE). This presentation is not typical of his bipolar I disorder because Mr. Z has never experienced an MDE and usually presents with escalating hypomanic/manic symptoms in the context of medication nonadherence. Nevertheless, Mr. Z has several risk factors for severe depression, including a family psychiatric history, multiple enduring social stressors and life crises, and medical conditions.
In the general population, the lifetime risk for developing depression is 8% to 17%.2 The risk of developing a mood disorder increases significantly if a first-degree relative is diagnosed with a mood disorder; the relative risk is 10.3 for bipolar disorder and 3.2 for depression.3 Additionally, Mr. Z is going through a complicated divorce, has financial problems, and is homeless, all of which could trigger an MDE. Furthermore, hypothyroidism shares many symptoms of depression, including fatigue, lethargy, anhedonia, cold intolerance, and low mood; mental status changes frequently are the initial presentation of thyroid problems.4 Physicians started Mr. Z on a new medication regimen (risperidone and divalproex) to control mood instability, which coincided with symptom onset. Atypical antipsychotics have been reported to precipitate depressive symptoms; their side effect profile includes extrapyramidal effects, such as flat affect, which can be mistaken for depression.5 Rapid valproate titration can mimic neurovegetative symptoms of depression and cause dose-dependent thrombocytopenia and rash, which could explain his initial presentation.6 Finally, Mr. Z’s history of traumatic splenectomy, change in mental status, and thrombocytopenia suggest an infectious etiology.
Table 1
Differential diagnosis in patients presenting with mood changes
| Cerebrovascular disease |
| Degenerative disorders (Parkinson’s disease, Huntington’s disease, Wilson’s disease) |
| Demyelinating disorders (multiple sclerosis, amyotrophic lateral sclerosis, lipid storage disease) |
| Endocrine disorders (Addison’s disease, Cushing’s disease, hyperthyroidism, hypothyroidism, hyperparathyroidism, pituitary dysfunction) |
| Epilepsy |
| Infectious diseases |
| Immune diseases |
| Metabolic encephalopathy |
| Neoplasm |
| Nutritional deficits (thiamine, niacin, vitamin B12) |
| Primary psychiatric disorders (mood disorders, dementia, sleep disorders) |
| Substance use |
| Toxins/medications |
| Traumatic brain injury |
| Source: Reference 1 |
Possible infectious causes
The increased prevalence of immune suppression due to human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) or from therapeutic modalities such as cancer therapy or splenectomy has led to an increased number of chronic CNS infections, manifesting with an array of neuropsychiatric symptoms and nonspecific physiological reactions.1,7 Mr. Z complains of a 2-month period of worsening depression that could suggest an infectious process with an insidious onset. Some infectious agents that can cause chronic CNS infection and encephalopathy are presented in Table 2.8 HIV, tuberculosis, syphilis, Lyme disease, and herpes simplex virus are becoming more prevalent and can present with neuropsychiatric symptoms.1 For example, in addition to thrombocytopenia and low-grade fever, patients with HIV may exhibit a broad range of neuropsychiatric symptoms such as cognitive problems, impaired executive and motor functioning, sleep disturbance, and anxiety. These patients frequently present with low mood and neurovegetative symptoms of depression.7 Similarly, the same tick responsible for Lyme disease infection can transmit other infectious agents that can cause thrombocytopenia, including Babesia, Ehrlichia chaffeensis, Anaplasma phagocytophilum, and human Ewingii ehrlichiosis.
The authors’ observations
Diagnosis of a mood change, particularly an MDE, is clinical, based on careful psychiatric evaluation using standardized criteria rather than a specific lab test. However, some laboratory studies (Table 3)1 are useful in differentiating medical illnesses that may present with depression. Mr. Z’s presentation warrants investigating these tests. His history of traumatic splenectomy and night sweats suggests an infection. The team’s initial recommendations include laboratory tests, discontinuing divalproex because it may be causing thrombocytopenia, and decreasing risperidone to 2 mg/d to improve his fatigue and possibly developed extrapyramidal symptoms.
Table 2
Potential infectious causes of chronic encephalopathy
| Type of infection | Organism/disease |
|---|---|
| Mycobacterial | Mycobacterium tuberculosis |
| Spirochetal | Treponema pallidum (syphilis), Borrelia burgdorferi (Lyme disease), Leptospira |
| Bacterial | Brucella, Listeria, Nocardia, Actinomyces israelii, Whipple’s disease |
| Viral | HIV/AIDS, cytomegalovirus, varicella zoster virus, herpes simplex virus, enterovirus |
| Fungal | Histoplasmosis, coccidiosis, sporothrix, Blastomyces, Cryptococcus |
| Parasitic | Toxoplasmosis, taenia solium (cysticercosis), Schistosoma, Acanthamoeba |
| AIDS: acquired immunodeficiency syndrome; HIV: human immunodeficiency virus Source: Reference 8 | |
Table 3
Differentiating medical illnesses that may mimic depression
| Laboratory tests |
|
| Imaging studies |
|
| Other tests |
|
| Procedures |
|
| ABG: arterial blood gases; CBC: complete blood count; EEG: electroencephalogram; ELISA: enzyme-linked immunosorbent assay; HIV: human immunodeficiency virus; VDRL: venereal disease research laboratory Source: Reference 1 |
TREATMENT: Cause revealed
Mr. Z develops a persistent fever of 102°F with continuous profuse sweating and a hypotensive episode. Blood work reveals mild anemia, thrombocytopenia, and increased coagulation parameters with high D-dimer and low fibrinogen, consistent with diagnosis of disseminated intravascular coagulation (DIC) secondary to infectious etiology. Thyroid and HIV tests are negative. After further evaluation, Mr. Z remembers that 4 months earlier he removed several ticks from his legs after hunting; he also remembers experiencing shivering and night sweats several weeks before he was hospitalized. His blood smear is positive for babesiosis and further testing confirms positive Lyme antibodies. Mr. Z is started on aggressive hemodynamic stabilization and a pathogen-tailored course of antibiotics for several weeks. This results in improvement and discharge home in a stable condition. His depression and fatigue improve but do not fully remit by the time he is discharged.
The authors’ observations
Lyme disease is one of the fastest-growing infectious diseases in the United States.9 The prevalence of positive Lyme antibodies is 30% higher in psychiatric populations than the general population.10 Lyme disease is transmitted by deer tick bite, often undetected, that is infected with spirochete Borrelia burgdorferi. To be infectious, ticks need to be attached to the skin for 24 to 48 hours,11,12 although individual cases have reported transmission in <24 hours. The clinical manifestations of Lyme disease can be divided into 3 phases:
- early localized phase, characterized by the distinctive skin lesion erythema migrans with or without constitutional symptoms
- early disseminated phase, characterized by multiple erythema migrans lesions and neurologic and/or cardiac findings
- late or chronic disease associated with intermittent/persistent arthritis and/or neurologic problems.11,13
The clinical features of each stage frequently overlap and some patients in a later stage of Lyme disease do not have prior signs or symptoms of the disease. Because it is a multisystem disease, Lyme disease can attack the CNS in the form of neuroborreliosis, a clinical diagnosis, without involving other systems, and its neuropsychiatric manifestations can resemble neurosyphilis because both organisms are spirochetes.11,13,14 CNS disorders have been found in up to 40% of Lyme disease cases.11 In neuroborreliosis, cognitive problems usually predominate; however, neuroborreliosis can mimic multiple brain diseases presenting with various neurologic and psychiatric symptoms (Table 4)14,15 and can present at any time after the tick bite. Furthermore neuroborreliosis is difficult to diagnose because symptoms may remain dormant and emerge after several years.11,13,14Borrelia burgdorferi is challenging to isolate and grow in the lab, and enzyme-linked immunosorbent assay (ELISA) testing for antibodies is highly specific but not very sensitive,16 frequently giving false negative results. Western blot confirms the diagnosis.
Table 4
Late-stage neuropsychiatric symptoms of Lyme disease
| Cognitive problems, memory problems, forgetfulness, slowing of thought processing, dysfunction in visuospatial orientation, dyslexia |
| Depression |
| Mood swings |
| Psychosis |
| Violent behavior/irritability |
| OCD |
| Anxiety |
| Panic attacks |
| Sleep disorders |
| Seizures |
| ADHD-like symptoms |
| Autism-like behavior |
| Chronic fatigue syndrome |
| Fibromyalgia |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder Source: References 14,15 |
Mr. Z’s presentation also reflects co-infection with babesiosis. Babesia is malaria-like protozoa diagnosed by blood smear that can cause a fatal illness in immuno-compromised patients. The clinical picture varies from mild symptoms such as night sweats, chills, arthralgias, and anorexia with thrombocytopenia to severe and potentially fatal outcomes in immunocompromised patients, including DIC, acute renal failure, sepsis, congestive heart failure, and myocardial infarction.11 Risk factors for the severest forms of babesiosis are age >50, co-infection with Lyme disease, and splenectomy,11 all of which were present in Mr. Z. Co-infected patients experience fatigue, headache, anorexia, and emotional lability more frequently than those with Lyme disease alone.12
Treatment options
Treatment of Lyme disease/neuroborreliosis is complex. The mainstay approach is antibiotics. Despite adequate treatment, many patients experience continued impairment, including chronic pain, fatigue, and cognitive and psychiatric symptoms.11,14 There is some evidence Borrelia burgdorferi can persist and re-emerge after adequate treatment.14,17 The National Institute of Health sponsored several clinical trials of prolonged antibiotic treatment for chronic Lyme disease. Some results suggested improvement in fatigue and cognitive function, although these results were not sustained.18
There is a strong link between mental illness and increased prevalence of positive Lyme disease antibodies.10 Several studies report increased risk of infection during psychological stress that may be related to an altered immune system response.19 Evidence suggests that Borrelia burgdorferi can alter immune system response, making T cells more reactive not only to Borrelia burgdorferi antigens but also to host antigens,20 creating autoimmune inflammatory reactions that could explain chronic neuropsychiatric symptoms. It appears Lyme disease antigens can mimic certain autoantigens (for example, in the thyroid gland).21 Whether there is a role for autoimmune therapy in treating chronic symptoms needs to be investigated.
Once Lyme disease is diagnosed, educating patients and families becomes an important part of treatment because many patients report feeling stigmatized by the diagnosis. Referral to a Lyme disease support group may be beneficial. Patients with neuropsychiatric symptoms that persist after antibiotic treatment should be offered symptom-based treatment, including medications and therapy.
Related Resource
- Centers for Disease Control and Prevention. Lyme disease: Resources for clinicians. www.cdc.gov/lyme/healthcare/clinicians.html.
Drug Brand Names
- Divalproex sodium • Depakote
- Levothyroxine • Levoxyl, Synthroid
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Stern TA, Rosenbaum JF, Fava M, et al. eds. Massachusetts General Hospital comprehensive clinical psychiatry. Philadelphia, PA: Mosby; 2008;257-277.
2. Andrade L, Caraveo-Anduaga JJ, Berglund P, et al. The epidemiology of major depressive episodes: results from the International Consortium of Psychiatric Epidemiology (ICPE) Surveys. Int J Methods Psychiatr Res. 2003;12(1):3-21.
3. Merikangas KR, Low NC. The epidemiology of mood disorders. Curr Psychiatry Rep. 2004;6:411-421.
4. Brown GM. Psychiatric and neurologic aspects of endocrine disease. In Krieger DT Hughes JC, eds. Neuroendocrinology. Sunderland, MA: Sinauer Associates; 1980;185-194.
5. Maguire GA. Comprehensive understanding of schizophrenia and its treatment. Am J Health Syst Pharm. 2002;59(17 suppl 5):S4-S11.
6. Dreifuss FE, Langer DH. Side effects of valproate. Am J Med. 1988;84(1A):34-41.
7. Perry S, Jacobsen P. Neuropsychiatric manifestations of AIDS-spectrum disorders. Hosp Community Psychiatry. 1986;37:135-142.
8. Hildebrand J, Aoun M. Chronic meningitis: still a diagnostic challenge. J Neurol. 2003;250(6):653-660.
9. Bacon RM, Kugeler KJ, Mead PS. Centers for Disease Control and Prevention (CDC). Surveillance for Lyme disease—United States 1992-2006. MMWR Surveill Summ. 2008;57(10):1-9.
10. Hájek T, Pasková B, Janovská D, et al. Higher prevalence of antibodies to Borrelia burgdorferi in psychiatric patients than in healthy subjects. Am J Psychiatry. 2002;159:297-301.
11. Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43(9):1089-1134.
12. Krause PJ, Telford SR 3rd, Spielman A, et al. Concurrent Lyme disease and babesiosis. Evidence for increased severity and duration of illness. JAMA. 1996;275(21):1657-1660.
13. Hildenbrand P, Craven DE, Jones R, et al. Lyme neuroborreliosis: manifestations of a rapidly emerging zoonosis. AJNR Am J Neuroradiol. 2009;30:1079-1087.
14. Fallon BA, Nields JA. Lyme disease: a neuropsychiatric illness. Am J Psychiatry. 1994;151:1571-1583.
15. Fallon BA, Nields JA, Burrascano JJ, et al. The neuropsychiatric manifestations of Lyme borreliosis. Psychiatr Q. 1992;63(1):95-117.
16. Stricker RB, Johnson L. Lyme wars: let’s tackle the testing. BMJ. 2007;335:1008.-
17. Hodzic E, Feng S, Holden K, et al. Persistence of Borrelia burgdorferi following antibiotic treatment in mice. Antimicrob Agents Chemother. 2008;52(5):1728-1736.
18. Fallon BA, Keilp JG, Corbera KM, et al. A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy. Neurology. 2008;70(13):992-1003.
19. Sheridan JF, Dobbs C, Brown D, et al. Psychoneuroimmunology: stress effects on pathogenesis and immunity during infection. Clin Microbiol Rev. 1994;7(2):200-212.
20. Yssel H, Shanafelt MC, Soderberg C, et al. Borrelia burgdorferi activates a T helper 1-like T cell subset in Lyme arthritis. J Exp Med. 1991;174:593-601.
21. Benvenga S, Guarneri F, Vaccaro M, et al. Homologies between proteins of Borrelia burgdorferi and thyroid autoantigens. Thyroid. 2004;14(11):964-966.
1. Stern TA, Rosenbaum JF, Fava M, et al. eds. Massachusetts General Hospital comprehensive clinical psychiatry. Philadelphia, PA: Mosby; 2008;257-277.
2. Andrade L, Caraveo-Anduaga JJ, Berglund P, et al. The epidemiology of major depressive episodes: results from the International Consortium of Psychiatric Epidemiology (ICPE) Surveys. Int J Methods Psychiatr Res. 2003;12(1):3-21.
3. Merikangas KR, Low NC. The epidemiology of mood disorders. Curr Psychiatry Rep. 2004;6:411-421.
4. Brown GM. Psychiatric and neurologic aspects of endocrine disease. In Krieger DT Hughes JC, eds. Neuroendocrinology. Sunderland, MA: Sinauer Associates; 1980;185-194.
5. Maguire GA. Comprehensive understanding of schizophrenia and its treatment. Am J Health Syst Pharm. 2002;59(17 suppl 5):S4-S11.
6. Dreifuss FE, Langer DH. Side effects of valproate. Am J Med. 1988;84(1A):34-41.
7. Perry S, Jacobsen P. Neuropsychiatric manifestations of AIDS-spectrum disorders. Hosp Community Psychiatry. 1986;37:135-142.
8. Hildebrand J, Aoun M. Chronic meningitis: still a diagnostic challenge. J Neurol. 2003;250(6):653-660.
9. Bacon RM, Kugeler KJ, Mead PS. Centers for Disease Control and Prevention (CDC). Surveillance for Lyme disease—United States 1992-2006. MMWR Surveill Summ. 2008;57(10):1-9.
10. Hájek T, Pasková B, Janovská D, et al. Higher prevalence of antibodies to Borrelia burgdorferi in psychiatric patients than in healthy subjects. Am J Psychiatry. 2002;159:297-301.
11. Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43(9):1089-1134.
12. Krause PJ, Telford SR 3rd, Spielman A, et al. Concurrent Lyme disease and babesiosis. Evidence for increased severity and duration of illness. JAMA. 1996;275(21):1657-1660.
13. Hildenbrand P, Craven DE, Jones R, et al. Lyme neuroborreliosis: manifestations of a rapidly emerging zoonosis. AJNR Am J Neuroradiol. 2009;30:1079-1087.
14. Fallon BA, Nields JA. Lyme disease: a neuropsychiatric illness. Am J Psychiatry. 1994;151:1571-1583.
15. Fallon BA, Nields JA, Burrascano JJ, et al. The neuropsychiatric manifestations of Lyme borreliosis. Psychiatr Q. 1992;63(1):95-117.
16. Stricker RB, Johnson L. Lyme wars: let’s tackle the testing. BMJ. 2007;335:1008.-
17. Hodzic E, Feng S, Holden K, et al. Persistence of Borrelia burgdorferi following antibiotic treatment in mice. Antimicrob Agents Chemother. 2008;52(5):1728-1736.
18. Fallon BA, Keilp JG, Corbera KM, et al. A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy. Neurology. 2008;70(13):992-1003.
19. Sheridan JF, Dobbs C, Brown D, et al. Psychoneuroimmunology: stress effects on pathogenesis and immunity during infection. Clin Microbiol Rev. 1994;7(2):200-212.
20. Yssel H, Shanafelt MC, Soderberg C, et al. Borrelia burgdorferi activates a T helper 1-like T cell subset in Lyme arthritis. J Exp Med. 1991;174:593-601.
21. Benvenga S, Guarneri F, Vaccaro M, et al. Homologies between proteins of Borrelia burgdorferi and thyroid autoantigens. Thyroid. 2004;14(11):964-966.
Is there a link between aripiprazole and treatment-emergent psychosis?
Discuss this article at www.facebook.com/CurrentPsychiatry
• Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonist.
• Clinical predictors of aripiprazole-associated worsening of psychosis include low baseline level of psychopathology and previous treatment with high-dose antipsychotics.
• Rapid transition from a medication with significant anticholinergic properties to 1 without these properties may result in symptoms of activation, including restlessness, insomnia, and anxiety, which can be mistaken for worsening psychosis.
• Akathisia, a common adverse effect of aripiprazole, may masquerade as treatment-emergent worsening of psychotic symptoms.
Mr. N, age 29, presents to the emergency department at the urging of his family because of poor self-care, bizarre behavior, and disturbed sleep. He first experienced psychiatric symptoms 10 years ago after his mother died. He became dysphoric and paranoid, displaying bizarre responses and behaviors with poor self-care and a gradual functional decline. He has been taking sertraline, 100 mg/d, for 10 years.
Upon arrival at the hospital’s inpatient unit, Mr. N is unkempt, oddly related, and paranoid. His affect is constricted. Mr. N displays thought blocking and possibly is responding to internal stimuli. Sertraline is continued and haloperidol, 1 mg/d, is initiated. For the next 2 weeks, Mr. N continues to be oddly related, irritable, and paranoid, and experiences disturbed sleep and thought blocking. After an episode of impulsive aggression, the treatment team initiates aripiprazole, which is titrated to 30 mg/d for 1 week. Mr. N’s clinical status worsens; he is menacing toward other patients and his thinking is more disorganized, with loose associations and ideas of reference. He requires 4 injections of IM haloperidol, 5 mg, and several visits to the seclusion room over the next week. Haloperidol is increased to 30 mg/d over the next 10 days, then aripiprazole is discontinued because of a putative drug interaction with haloperidol. Following the medication changes Mr. N demonstrates better behavioral control, but still is grossly psychotic. While awaiting transfer to a state hospital, Mr. N receives a trial of olanzapine, 20 to 40 mg/d, for 2 weeks without significant benefit.
Several clinical trials demonstrate a significant reduction in intensity of psychotic symptoms with aripiprazole, which has a unique mechanism of action.1 However, since its FDA approval in 2002, several case reports have described treatment-emergent psychotic symptoms associated with aripiprazole initiation. Over the past 40 years, reports of worsening psychosis associated with antipsychotics have been limited to patients with schizophrenia who were taking high dosages or who had high plasma concentrations, when anticholinergic delirium may have explained increased psychotic symptoms.2-4
How can a drug effectively treat psychotic symptoms and occasionally worsen them? In this article, we discuss the relevant pharmacology and clinical literature on aripiprazole and try to make sense of this apparent paradox.
Unique pharmacologic profile
Antipsychotics have been reported to be either neutral antagonists or inverse agonists at the D2 receptor, based on in vitro data.5 Aripiprazole and its main metabolite, dehydroaripiprazole, originally were described as partial agonists at D2 dopamine receptors.6,7 However, it appears aripiprazole’s pharmacologic action is better explained by the concept of functional selectivity. Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonistic.5
Researchers have hypothesized that the pathophysiology of schizophrenia may, in part, be caused by dysfunction of mesocorticolimbic dopaminergic neurons characterized by an enhanced sensitivity of postsynaptic D2 receptors and increased sensitivity to dopaminergic drugs.8,9 In addition, chronic treatment with a D2 receptor antagonist is associated with increases in postsynaptic dopamine receptor density (ie, an increase in receptor reserve).10,11 Upregulation of D2 receptors may explain several features seen in patients chronically treated with antipsychotics, including tardive dyskinesia12 and rapid psychotic relapse after discontinuing an antipsychotic (supersensitivity psychosis).13 Because chronic antipsychotic treatment leads to high postsynaptic receptor reserve, aripiprazole initiation may produce overactivation of D2 receptors, which might worsen a patient’s condition.14 In vitro data15-18 and clinical observations indicate that aripiprazole has intrinsic efficacy at D2 receptors, as do clinical observations, such as:
- its propensity to reduce serum prolactin19
- a decreased likelihood of producing extrapyramidal side effects despite >80% occupancy of D2 receptors6
- case reports documenting aripiprazole-associated mania,20 improvement of risperidone-associated cognitive impairment,21 and pathologic gambling.22
Emergence or worsening of psychotic symptoms or a marginal antipsychotic effect may occur if aripiprazole is indeed a postsynaptic D2 receptor agonist. An individual patient’s outcome likely would depend on his or her sensitivity to psychosis and concurrent or previous exposure to a D2 receptor antagonist. For example, stimulation of postsynaptic D2 receptors may be further augmented if the dosage of the previous antipsychotic was reduced or withdrawn before initiating aripiprazole because additional receptors would be available for interaction with aripiprazole.
Case reports
A literature review revealed 23 reports of treatment-emergent psychosis associated with aripiprazole initiation (Table). The mean age of the patients was 47 (range: 17 to 69) and 57% were men. Most patients (87%) were diagnosed with a schizophrenia-spectrum illness before aripiprazole initiation. Most (57%) had mild, stable, or no psychotic symptoms before aripiprazole initiation. Most were receiving relatively high doses of antipsychotics (average chlorpromazine equivalents [CPZE]: 648 mg/d) before aripiprazole initiation. This medication was either decreased or discontinued in 70% of patients.
Emergence or worsening of psychotic symptoms included agitation, aggressive behavior, and increased psychomotor activity. However, akathisia evaluation was described in only 2 reports: 1 author identified akathisia symptoms, but attributed them to a concomitant antipsychotic (fluphenazine)23 and the other report specifically excluded the possibility of akathisia.24 Two systematic studies have attempted to establish risk factors for aripiprazole-associated worsening psychosis (Box).14,25
In our literature review, the mean final dose of aripiprazole was 21.5 mg/d (range: 2 to 60 mg/d). In the cases describing subsequent treatment, all but 1 patient were switched to another antipsychotic, including 2 whose psychotic symptoms stabilized with continuation of aripiprazole and addition of a second antipsychotic. Interestingly, in the case reported by Adan-Manes et al,26 initial treatment with aripiprazole monotherapy was efficacious, but a subsequent trial of adjunctive aripiprazole resulted in worsening psychosis.
Table
Case reports: Treatment-emergent psychosis associated with aripiprazole
| Study | Age, sex | Diagnosis | Before aripiprazole initiation | Pre-aripiprazole treatment | Aripiprazole dose | Concomitant psychotropic treatment | Subsequent treatment |
|---|---|---|---|---|---|---|---|
| Chiu et al, 2011a | 39, M | Schizophrenia | Psychiatrically stable, tardive dystonia | Clozapine, 300 mg/d | 10 mg/d | Valproic acid, 1,000 mg/d, clonazepam, 2 mg/d, mephenoxalone, 800 mg/d | Clozapine |
| Ekinci et al, 2010b | 17, M | ADHD | Inattention and impulsive aggression | Tapered and discontinued risperidone, 2.5 mg/d | 5 mg/d | Methylphenidate, 54 mg/d | Risperidone, 2 mg/d, methylphenidate, 36 mg/d |
| Selvaraj et al, 2010c | 49, F | Chronic depression | Depressive symptoms, suicidal ideation | None stated | 2 mg/d | Duloxetine, 80 mg/d, clonazepam, 2 mg/d | Duloxetine, 120 mg/d |
| Adan-Manes et al, 2009d | 23, M | Schizophrenia | No psychotic symptoms | Abrupt decrease of amisulpride dose from 800 mg/d to 400 mg/d | 20 mg/d | Biperiden, 4 mg/d | Amisulpride, 800 mg/d |
| Cho et al, 2009e | 45, F | Schizophrenia | Persistent psychotic symptoms, new onset diabetes with acute ketoacidosis | Haloperidol, 20 mg/d, abrupt clozapine discontinuation | 15 mg/d | Valproic acid, nortriptyline | Molindone, 150 mg/d |
| Ahuja et al, 2007f | 35, F | Schizoaffective disorder | Stable before medication change | Tapered amisulpride, 400 mg/d, over 6 weeks | 15 mg/d | None | Amisulpride, 600 mg/d |
| Lea et al, 2007g | 57, M | Schizophrenia | Persistent psychotic symptoms, treatment resistance, recent recovery from NMS | Discontinued ziprasidone, 200 mg/d | 30 mg/d | Lorazepam, 2 mg/d, amantadine, 100 mg, sertraline, 50 mg/d | Clozapine |
| Lea et al, 2007g | 49, M | Schizoaffective disorder | Delusions, verbal aggression, substance abuse, HCV | Decreased quetiapine dose from 800 mg/d to 400 mg/d | 15 mg/d | Divalproex, 1,000 mg/d, fluvoxamine, 200 mg/d, clonazepam, 2 mg/d | Lithium, quetiapine, 500 mg/d, haloperidol, 2 mg/d |
| Lea et al, 2007g | 60, M | Schizophrenia | Delusions, labile mood, aggression | Risperidone, 3 mg/d, interruption of fluphenazine, 75 mg/d | 20 mg/d | Divalproex, 4,500 mg/d, benztropine, 3 mg/d | Not discussed |
| Raja, 2007h | 30, M | Schizoaffective disorder | Negative symptoms, otherwise stable, recent citalopram discontinuation | Discontinued amisulpride, 800 mg/d over 2 weeks | 30 mg/d | Lithium | Amisulpride, 500 mg/d |
| Raja, 2007h | 69, F | Bipolar disorder | History of multiple relapses; presented with tremor, akathisia, weight gain | Discontinued risperidone, 2 mg/d, over 2 weeks | 15 mg/d | Lithium | Risperidone, 4 mg |
| Raja, 2007h | 59, F | Schizophrenia | Negative symptoms, otherwise stable | Reduced risperidone dosage from 5 mg/d to 4 mg/d | 7.5 mg/d | None | Risperidone, 5 mg/d |
| Thone, 2007i | 31, M | Schizophrenia | Confusion, agitation, delusions worsened with aripiprazole dose increase | None | 60 mg/d | None | Aripiprazole dose reduction to 15 mg/d, olanzapine, 10 mg/d |
| Glick et al, 2006j | 55, F | Schizophrenia | Stable before medication change | Tapered and discontinued thioridazine, 600 mg/d, over 3 months | 30 mg/d | None | Chlorpromazine, 200 mg/d, aripiprazole, 30 mg/d |
| Glick et al, 2006j | 52, M | Schizophrenia | Negative symptoms | Decreased olanzapine dose from 30 mg/d to 20 mg/d | 30 mg/d | None | Olanzapine, 30 mg/d |
| Barnas et al, 2005k | 57, F | Schizoaffective disorder | Stable before medication change | Discontinued perphenazine, 8 mg/d | 30 mg/d | None | Quetiapine, 350 mg/d |
| DeQuardo, 2004l | 54, M | Schizophrenia | History of aggression, residual paranoia, severe EPS | Haloperidol, 200 mg/d | 15 mg/d | Benztropine | Haloperidol |
| DeQuardo, 2004l | 51, M | Schizophrenia | History of aggression, persistent psychotic symptoms, treatment resistance | Olanzapine, 60 mg/d | 10 mg/d | None | Olanzapine |
| Ramaswamy et al, 2004m | 43, F | Schizoaffective disorder | Psychiatrically stable, multiple medication changes, including substituting carbamazepine for valproic acid | Discontinued ziprasidone, 160 mg/d, discontinued quetiapine, 400 mg/d, over 2 weeks | 30 mg/d | Propranolol, 30 mg/d, l-thyroxine, .05 mg/d, carbamazepine, 600 mg/d | Not available |
| Ramaswawamy et al, 2004m | 57, F | Schizoaffective disorder | History of multiple hospitalizations, but stable before medication change | Decreased olanzapine dose from 20 mg/d to 15 mg/d | 30 mg/d | Valproic acid, 2,000 mg/d | Ziprasidone |
| Ramaswawamy et al, 2004m | 67, F | Schizophrenia | Remote hospitalizations, recent worsened psychosis | Decreased ziprasidone dose from 200 mg/d to 160 mg/d 2 months previously | 30 mg/d | Carbamazepine, 200 mg/d | Not discussed |
| Ramaswamy et al, 2004m | 46, M | Schizophrenia | Persistent delusions while receiving risperidone, TD | Risperidone, 3 mg/d | 15 mg/d | Valproic acid, 1,500 mg/d | Risperidone, 3 mg/d |
| Reeves et al, 2004n | 50, M | Schizoaffective disorder | Relatively stable with nonthreatening delusions, hallucinations | Quetiapine, 800 mg/d | 30 mg/d | Divalproex, 2,000 mg/d | Olanzapine, 20 mg/d |
| ADHD: attention-deficit/hyperactivity disorder; EPS: extrapyramidal symptoms; HCV: hepatitis C virus; NMS: neuroleptic malignant syndrome; TD: tardive dyskinesia Source: References a. Chiu YH, Chen CH, Lu ML. Worsening psychosis after adding aripiprazole to clozapine. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):291-292. b. Ekinci O, Sabuncuoglu O. Psychosis associated with switching from risperidone to aripiprazole in an adolescent on methylphenidate treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(2):648-649. c. Selvaraj V, Ramaswamy S, Sharma A, et al. New-onset psychosis and emergence of suicidal ideation with aripiprazole. Am J Psychiatry. 2010;167(12):1535-1536. d. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246. e. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143. f. Ahuja N, Lloyd AJ. Aripiprazole and worsening of psychosis: a case report. J Clin Psychiatry. 2007;68(5):805-806. g. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342. h. Raja M. Improvement or worsening of psychotic symptoms after treatment with low doses of aripiprazole. Int J Neuropsychopharmacol. 2007;10(1):107-110. i. Thone J. Worsened agitation and confusion in schizophrenia subsequent to high-dose aripiprazole. J Neuropsychiatry Clin Neurosci. 2007;19(4):481-482. j. Glick ID, Duggal V, Hodulik C. Aripiprazole as a dopamine partial agonist: positive and negative effects. J Clin Psychopharmacol. 2006;26(1):101-103. k. Barnas ME, Hussain N, Petrides G. Treatment-emergent psychosis with aripiprazole. J Clin Psychiatry. 2005;66(10):1339. l. DeQuardo JR. Worsened agitation with aripiprazole: adverse effect of dopamine partial agonism? J Clin Psychiatry. 2004;65(1):132-133. m. Ramaswamy S, Vijay D, William M, et al. Aripiprazole possibly worsens psychosis. Int Clin Psychopharmacol. 2004;19(1):45-48. n. Reeves RR, Mack JE. Worsening schizoaffective disorder with aripiprazole. Am J Psychiatry. 2004;161(7):1308. | |||||||
Takeuchi et al14 aimed to establish predictors of worsening psychosis in a naturalistic setting where patients slowly transitioned to aripiprazole from previous antipsychotic treatment. Patients were required to be on a stable dose of an antipsychotic before participating in the study. Aripiprazole was started at 12 mg/d for 2 weeks with flexible dosing from weeks 2 to 52. Previous antipsychotic therapy was reduced biweekly by 25%. The incidence of worsening psychopathology after aripiprazole initiation was higher in the group of patients who had previously received high-dose antipsychotic therapy (average chlorpromazine equivalents [CPZE]: 727 mg/d) compared with the group on low dosages (average CPZE: 382 mg/d). It is possible that previous high-dose antipsychotic therapy was indicative of more significant baseline psychopathology; however, the worsened group and stabilized group had similar baseline Clinical Global Impressions-Severity scores.
Pae et al25 aimed to find predictors of worsening psychosis with aripiprazole in patients whose previous antipsychotic therapy was immediately discontinued. They found lower baseline disease severity was associated with significant worsening during the first month of aripiprazole treatment.
Other potential explanations
Aripiprazole’s manufacturer reported the incidence of psychosis-related adverse events in an analysis of 9 randomized schizophrenia trials.27 The rates of psychosis-related adverse events ranged from 0.6% to 18%, but there was no apparent relationship to study design or method of transitioning to aripiprazole. Rates of psychosis-related adverse events were similar between aripiprazole and the control group (placebo in 3 studies, another antipsychotic in 2 studies).
Emergence or worsening of psychotic symptoms temporally associated with aripiprazole initiation does not necessarily imply causation. As in Mr. N’s case, it is not always possible to determine whether worsening psychosis is the natural disease course or a treatment effect. In addition, it is not possible to differentiate lack of efficacy from a true propensity for aripiprazole to worsen psychosis.
It also is conceivable discontinuation or dosage reduction of a previous antipsychotic would worsen psychotic symptoms or cause side effects. When significant changes in psychopathology or side effects develop during the transition from 1 antipsychotic to another, it is difficult to determine etiology. Specifically, rapid transition from a medication with significant anticholinergic and antihistaminic properties—such as quetiapine or olanzapine—to 1 without these properties—such as aripiprazole—may result in symptoms of activation, including restlessness, insomnia, and anxiety. Consequently, these symptoms could be mistaken for worsening psychosis.28 Only 1 patient in this series was reported to abruptly discontinue an antipsychotic with significant anticholinergic properties (clozapine) before initiating aripiprazole.24 Studies by Takeuchi et al14 and Pae et al25 did not report the relative baseline use of antipsychotic medication with anticholinergic properties.
In a pooled analysis of treatment-emergent adverse events in 5 randomized clinical trials of patients receiving aripiprazole for acute relapse of schizophrenia, the incidence of akathisia was 10%, although it is not clear if this is a dose-related adverse effect.29 Because akathisia may be confused for worsening psychosis,30 it is possible akathisia was mistakenly identified as worsening psychotic symptoms in Mr. N’s case, as well as several reports from our literature review.
Covert akathisia is unlikely to explain worsening psychopathology observed in all patients in our literature review because confusion of akathisia and worsening psychosis is not a widespread phenomenon. In a post hoc analysis of pooled safety data from aripiprazole trials, Kane et al31 did not find a correlation between presence of akathisia and aripiprazole efficacy as measured by the Positive and Negative Syndrome Scale (PANSS) total, PANSS positive, PANSS negative, Clinical Global Impressions-Severity, Clinical Global Impressions-Improvement, and percentage of responders. Pae et al25 also noted there was no correlation between scores on the Barnes Akathisia Rating Scale and worsening psychopathology in patients switched to aripiprazole.
An antagonist always is an antagonist and clinicians have appreciated this concept since the days of chlorpromazine. The activity of aripiprazole, however, is on a pharmacologic continuum between a neutral antagonist and full agonist and currently there is no way to precisely determine the level of D2 receptor agonist action in a patient.
Although it is interesting to speculate that aripiprazole’s D2 receptor agonist action may contribute to worsening psychosis,32-34 there are other plausible explanations to consider. Rapid transition from a drug with significant anticholinergic properties and aripiprazole-associated akathisia may contribute to worsening psychopathology in patients starting aripiprazole. Because covert side effects may be incorrectly identified as psychotic agitation, we cannot exclude this as a possible etiologic factor in Mr. N’s case as well as the cases in our literature review.
Related Resource
- Abilify [package insert]. Princeton, NJ: Bristol-Myers Squibb; 2011.
Drug Brand Names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Biperiden • Akineton
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fluphenazine • Permitil, Prolixin
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Nortriptyline • Aventyl, Pamelor
- Methylphenidate • Concerta
- Molindone • Moban
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Mellaril
- Thyroxine • Synthroid
- Valproic acid • Depakene
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Citrome L. A review of aripiprazole in the treatment of patients with schizophrenia or bipolar I disorder. Neuropsychiatr Dis Treat. 2006;2(4):427-443.
2. Chong SA, Tan CH, Lee HS. Worsening of psychosis with clozapine and selective serotonin reuptake inhibitor combination: two case reports. J Clin Psychopharmacol. 1997;17(1):68-69.
3. Bowers MB Jr, Swigar ME. Psychotic patients who become worse on neuroleptics. J Clin Psychopharmacol. 1988;8(6):417-421.
4. Tornatore FL, Lee D, Sramek JJ. Psychotic exacerbation with haloperidol. Drug Intell Clin Pharm. 1981;15(3):209-213.
5. Beaulieu JM, Gainetdinov RR. The physiology signaling, and pharmacology of dopamine receptors. Pharmacol Rev. 2011;63(1):182-217.
6. Grunder G, Carlsson A, Wong DF. Mechanism of new antipsychotic medications: occupancy is not just antagonism. Arch Gen Psychiatry. 2003;60(10):974-977.
7. Wood MD, Scott C, Clarke K, et al. Aripiprazole and its human metabolite are partial agonists at the human dopamine D2 receptor, but the rodent metabolite displays antagonist properties. Eur J Pharmacol. 2006;546(1-3):88-94.
8. Seeman P, Weinshenker D, Quirion R, et al. Dopamine supersensitivity correlates with D2High states, implying many paths to psychosis. Proc Natl Acad Sci U S A. 2005;102(9):3513-3518.
9. Seeman P, Ko F, Jack E, et al. Consistent with dopamine supersensitivity, RGS9 expression is diminished in the amphetamine-treated animal model of schizophrenia and in postmortem schizophrenia brain. Synapse. 2007;61(5):303-309.
10. Burt DR, Creese I, Snyder SH. Antischizophrenic drugs: chronic treatment elevates dopamine receptor binding in brain. Science. 1977;196(4287):326-328.
11. Silvestri S, Seeman MV, Negrete JC, et al. Increased dopamine D2 receptor binding after long-term treatment with antipsychotics in humans: a clinical PET study. Psychopharmacology (Berl). 2000;152(2):174-180.
12. Sayers AC, Bürki HR, Ruch W, et al. Neuroleptic-induced hypersensitivity of striatal dopamine receptors in the rat as a model of tardive dyskinesias. Effects of clozapine, haloperidol, loxapine and chlorpromazine. Psychopharmacologia. 1975;41(2):97-104.
13. Moncrieff J. Does antipsychotic withdrawal provoke psychosis? Review of the literature on rapid onset psychosis (supersensitivity psychosis) and withdrawal-related relapse. Acta Psychiatr Scand. 2006;114(1):3-13.
14. Takeuchi H, Uchida H, Suzuki T, et al. Predictors of clinical worsening after a switch to aripiprazole in patients with schizophrenia: a 1-year naturalistic follow-up study. J Clin Psychopharmacol. 2009;29(4):394-395.
15. Shapiro DA, Renock S, Arrington E, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology. 2003;28(8):1400-1411.
16. Urban JD, Vargas GA, von Zastrow M, et al. Aripiprazole has functionally selective actions at dopamine D2 receptor-mediated signaling pathways. Neuropsychopharmacology. 2007;32(1):67-77.
17. Klewe IV, Nielsen SM, Tarpo L, et al. Recruitment of beta-arrestin2 to the dopamine D2 receptor: Insights into anti-psychotic and anti-parkinsonian drug receptor signaling. Neuropharmacology. 2008;54(8):1215-1222.
18. Masri B, Salahpour A, Didriksen M, et al. Antagonism of dopamine D2 receptor/beta-arrestin 2 interaction is a common property of clinically effective antipsychotics. Proc Natl Acad Sci U S A. 2008;105(36):13656-13661.
19. Shim JC, Shin JG, Kelly DL, et al. Adjunctive treatment with a dopamine partial agonist, aripiprazole, for antipsychotic-induced hyperprolactinemia: a placebo-controlled trial. Am J Psychiatry. 2007;164(9):1404-1410.
20. Padala PR, Wengel SP, Petty F. Manic episode during treatment with aripiprazole. Am J Psychiatry. 2007;164(1):172-173.
21. Hu CH, Pai N, Huang XF, et al. Potential control of risperidone-related cognitive deficits by adjunctive aripiprazole treatment. J Clin Psychopharmacol. 2011;31(1):135-136;author reply 136–137.
22. Cohen J, Magalon D, Boyer L, et al. Aripiprazole-induced pathological gambling: a report of 3 cases. Curr Drug Saf. 2011;6(1):51-53.
23. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342.
24. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143.
25. Pae CU, Chiesa A, Mandelli L, et al. Predictors of early worsening after switch to aripiprazole: a randomized, controlled, open-label study. Clin Drug Investig. 2010;30(3):187-193.
26. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246.
27. Cognata-Smith C, Baker RA, Pikalov A, et al. Analysis of nine aripiprazole trials to evaluate strategies for switching patients with schizophrenia to aripiprazole. Paper presented at: 162nd Annual Meeting American Psychiatric Association; May 16-21, 2009; San Francisco, CA.
28. Lieberman J. Cholinergic rebound in neuroleptic withdrawal syndromes. Psychosomatics. 1981;22(3):253-254.
29. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: Safety and tolerability in short-term, placebo-controlled trials. Schizophr Res. 2003;61(2-3):123-136.
30. Kane JM, Fleischhacker WW, Hansen L, et al. Akathisia: an updated review focusing on second-generation antipsychotics. J Clin Psychiatry. 2009;70(5):627-643.
31. Kane JM, Barnes TR, Correll CU, et al. Evaluation of akathisia in patients with schizophrenia, schizoaffective disorder, or bipolar I disorder: A post hoc analysis of pooled data from short- and long-term aripiprazole trials. J Psychopharmacol. 2010;24(7):1019-1029.
32. Fleischhacker WW, McQuade RD, Marcus RN, et al. A double-blind, randomized comparative study of aripiprazole and olanzapine in patients with schizophrenia. Biol Psychiatry. 2009;65(6):510-517.
33. Kane JM, Osuntokun O, Kryzhanovskaya LA, et al. A 28-week, randomized, double-blind study of olanzapine versus aripiprazole in the treatment of schizophrenia. J Clin Psychiatry. 2009;70(4):572-581.
34. Kane JM, Correll CU, Goff DC, et al. A multicenter, randomized, double-blind, placebo-controlled, 16-week study of adjunctive aripiprazole for schizophrenia or schizoaffective disorder inadequately treated with quetiapine or risperidone monotherapy. J Clin Psychiatry. 2009;70(10):1348-1357.
James J. Gugger, PharmD, BCPP
Dr. Gugger is Assistant Clinical Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Courtney L. Tam, PharmD
Dr. Tam is Pharmacy Practice Resident, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Charles R. Ashby, Jr, PhD
Dr. Ashby is Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
James J. Gugger, PharmD, BCPP
Dr. Gugger is Assistant Clinical Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Courtney L. Tam, PharmD
Dr. Tam is Pharmacy Practice Resident, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Charles R. Ashby, Jr, PhD
Dr. Ashby is Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
James J. Gugger, PharmD, BCPP
Dr. Gugger is Assistant Clinical Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Courtney L. Tam, PharmD
Dr. Tam is Pharmacy Practice Resident, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Charles R. Ashby, Jr, PhD
Dr. Ashby is Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Discuss this article at www.facebook.com/CurrentPsychiatry
• Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonist.
• Clinical predictors of aripiprazole-associated worsening of psychosis include low baseline level of psychopathology and previous treatment with high-dose antipsychotics.
• Rapid transition from a medication with significant anticholinergic properties to 1 without these properties may result in symptoms of activation, including restlessness, insomnia, and anxiety, which can be mistaken for worsening psychosis.
• Akathisia, a common adverse effect of aripiprazole, may masquerade as treatment-emergent worsening of psychotic symptoms.
Mr. N, age 29, presents to the emergency department at the urging of his family because of poor self-care, bizarre behavior, and disturbed sleep. He first experienced psychiatric symptoms 10 years ago after his mother died. He became dysphoric and paranoid, displaying bizarre responses and behaviors with poor self-care and a gradual functional decline. He has been taking sertraline, 100 mg/d, for 10 years.
Upon arrival at the hospital’s inpatient unit, Mr. N is unkempt, oddly related, and paranoid. His affect is constricted. Mr. N displays thought blocking and possibly is responding to internal stimuli. Sertraline is continued and haloperidol, 1 mg/d, is initiated. For the next 2 weeks, Mr. N continues to be oddly related, irritable, and paranoid, and experiences disturbed sleep and thought blocking. After an episode of impulsive aggression, the treatment team initiates aripiprazole, which is titrated to 30 mg/d for 1 week. Mr. N’s clinical status worsens; he is menacing toward other patients and his thinking is more disorganized, with loose associations and ideas of reference. He requires 4 injections of IM haloperidol, 5 mg, and several visits to the seclusion room over the next week. Haloperidol is increased to 30 mg/d over the next 10 days, then aripiprazole is discontinued because of a putative drug interaction with haloperidol. Following the medication changes Mr. N demonstrates better behavioral control, but still is grossly psychotic. While awaiting transfer to a state hospital, Mr. N receives a trial of olanzapine, 20 to 40 mg/d, for 2 weeks without significant benefit.
Several clinical trials demonstrate a significant reduction in intensity of psychotic symptoms with aripiprazole, which has a unique mechanism of action.1 However, since its FDA approval in 2002, several case reports have described treatment-emergent psychotic symptoms associated with aripiprazole initiation. Over the past 40 years, reports of worsening psychosis associated with antipsychotics have been limited to patients with schizophrenia who were taking high dosages or who had high plasma concentrations, when anticholinergic delirium may have explained increased psychotic symptoms.2-4
How can a drug effectively treat psychotic symptoms and occasionally worsen them? In this article, we discuss the relevant pharmacology and clinical literature on aripiprazole and try to make sense of this apparent paradox.
Unique pharmacologic profile
Antipsychotics have been reported to be either neutral antagonists or inverse agonists at the D2 receptor, based on in vitro data.5 Aripiprazole and its main metabolite, dehydroaripiprazole, originally were described as partial agonists at D2 dopamine receptors.6,7 However, it appears aripiprazole’s pharmacologic action is better explained by the concept of functional selectivity. Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonistic.5
Researchers have hypothesized that the pathophysiology of schizophrenia may, in part, be caused by dysfunction of mesocorticolimbic dopaminergic neurons characterized by an enhanced sensitivity of postsynaptic D2 receptors and increased sensitivity to dopaminergic drugs.8,9 In addition, chronic treatment with a D2 receptor antagonist is associated with increases in postsynaptic dopamine receptor density (ie, an increase in receptor reserve).10,11 Upregulation of D2 receptors may explain several features seen in patients chronically treated with antipsychotics, including tardive dyskinesia12 and rapid psychotic relapse after discontinuing an antipsychotic (supersensitivity psychosis).13 Because chronic antipsychotic treatment leads to high postsynaptic receptor reserve, aripiprazole initiation may produce overactivation of D2 receptors, which might worsen a patient’s condition.14 In vitro data15-18 and clinical observations indicate that aripiprazole has intrinsic efficacy at D2 receptors, as do clinical observations, such as:
- its propensity to reduce serum prolactin19
- a decreased likelihood of producing extrapyramidal side effects despite >80% occupancy of D2 receptors6
- case reports documenting aripiprazole-associated mania,20 improvement of risperidone-associated cognitive impairment,21 and pathologic gambling.22
Emergence or worsening of psychotic symptoms or a marginal antipsychotic effect may occur if aripiprazole is indeed a postsynaptic D2 receptor agonist. An individual patient’s outcome likely would depend on his or her sensitivity to psychosis and concurrent or previous exposure to a D2 receptor antagonist. For example, stimulation of postsynaptic D2 receptors may be further augmented if the dosage of the previous antipsychotic was reduced or withdrawn before initiating aripiprazole because additional receptors would be available for interaction with aripiprazole.
Case reports
A literature review revealed 23 reports of treatment-emergent psychosis associated with aripiprazole initiation (Table). The mean age of the patients was 47 (range: 17 to 69) and 57% were men. Most patients (87%) were diagnosed with a schizophrenia-spectrum illness before aripiprazole initiation. Most (57%) had mild, stable, or no psychotic symptoms before aripiprazole initiation. Most were receiving relatively high doses of antipsychotics (average chlorpromazine equivalents [CPZE]: 648 mg/d) before aripiprazole initiation. This medication was either decreased or discontinued in 70% of patients.
Emergence or worsening of psychotic symptoms included agitation, aggressive behavior, and increased psychomotor activity. However, akathisia evaluation was described in only 2 reports: 1 author identified akathisia symptoms, but attributed them to a concomitant antipsychotic (fluphenazine)23 and the other report specifically excluded the possibility of akathisia.24 Two systematic studies have attempted to establish risk factors for aripiprazole-associated worsening psychosis (Box).14,25
In our literature review, the mean final dose of aripiprazole was 21.5 mg/d (range: 2 to 60 mg/d). In the cases describing subsequent treatment, all but 1 patient were switched to another antipsychotic, including 2 whose psychotic symptoms stabilized with continuation of aripiprazole and addition of a second antipsychotic. Interestingly, in the case reported by Adan-Manes et al,26 initial treatment with aripiprazole monotherapy was efficacious, but a subsequent trial of adjunctive aripiprazole resulted in worsening psychosis.
Table
Case reports: Treatment-emergent psychosis associated with aripiprazole
| Study | Age, sex | Diagnosis | Before aripiprazole initiation | Pre-aripiprazole treatment | Aripiprazole dose | Concomitant psychotropic treatment | Subsequent treatment |
|---|---|---|---|---|---|---|---|
| Chiu et al, 2011a | 39, M | Schizophrenia | Psychiatrically stable, tardive dystonia | Clozapine, 300 mg/d | 10 mg/d | Valproic acid, 1,000 mg/d, clonazepam, 2 mg/d, mephenoxalone, 800 mg/d | Clozapine |
| Ekinci et al, 2010b | 17, M | ADHD | Inattention and impulsive aggression | Tapered and discontinued risperidone, 2.5 mg/d | 5 mg/d | Methylphenidate, 54 mg/d | Risperidone, 2 mg/d, methylphenidate, 36 mg/d |
| Selvaraj et al, 2010c | 49, F | Chronic depression | Depressive symptoms, suicidal ideation | None stated | 2 mg/d | Duloxetine, 80 mg/d, clonazepam, 2 mg/d | Duloxetine, 120 mg/d |
| Adan-Manes et al, 2009d | 23, M | Schizophrenia | No psychotic symptoms | Abrupt decrease of amisulpride dose from 800 mg/d to 400 mg/d | 20 mg/d | Biperiden, 4 mg/d | Amisulpride, 800 mg/d |
| Cho et al, 2009e | 45, F | Schizophrenia | Persistent psychotic symptoms, new onset diabetes with acute ketoacidosis | Haloperidol, 20 mg/d, abrupt clozapine discontinuation | 15 mg/d | Valproic acid, nortriptyline | Molindone, 150 mg/d |
| Ahuja et al, 2007f | 35, F | Schizoaffective disorder | Stable before medication change | Tapered amisulpride, 400 mg/d, over 6 weeks | 15 mg/d | None | Amisulpride, 600 mg/d |
| Lea et al, 2007g | 57, M | Schizophrenia | Persistent psychotic symptoms, treatment resistance, recent recovery from NMS | Discontinued ziprasidone, 200 mg/d | 30 mg/d | Lorazepam, 2 mg/d, amantadine, 100 mg, sertraline, 50 mg/d | Clozapine |
| Lea et al, 2007g | 49, M | Schizoaffective disorder | Delusions, verbal aggression, substance abuse, HCV | Decreased quetiapine dose from 800 mg/d to 400 mg/d | 15 mg/d | Divalproex, 1,000 mg/d, fluvoxamine, 200 mg/d, clonazepam, 2 mg/d | Lithium, quetiapine, 500 mg/d, haloperidol, 2 mg/d |
| Lea et al, 2007g | 60, M | Schizophrenia | Delusions, labile mood, aggression | Risperidone, 3 mg/d, interruption of fluphenazine, 75 mg/d | 20 mg/d | Divalproex, 4,500 mg/d, benztropine, 3 mg/d | Not discussed |
| Raja, 2007h | 30, M | Schizoaffective disorder | Negative symptoms, otherwise stable, recent citalopram discontinuation | Discontinued amisulpride, 800 mg/d over 2 weeks | 30 mg/d | Lithium | Amisulpride, 500 mg/d |
| Raja, 2007h | 69, F | Bipolar disorder | History of multiple relapses; presented with tremor, akathisia, weight gain | Discontinued risperidone, 2 mg/d, over 2 weeks | 15 mg/d | Lithium | Risperidone, 4 mg |
| Raja, 2007h | 59, F | Schizophrenia | Negative symptoms, otherwise stable | Reduced risperidone dosage from 5 mg/d to 4 mg/d | 7.5 mg/d | None | Risperidone, 5 mg/d |
| Thone, 2007i | 31, M | Schizophrenia | Confusion, agitation, delusions worsened with aripiprazole dose increase | None | 60 mg/d | None | Aripiprazole dose reduction to 15 mg/d, olanzapine, 10 mg/d |
| Glick et al, 2006j | 55, F | Schizophrenia | Stable before medication change | Tapered and discontinued thioridazine, 600 mg/d, over 3 months | 30 mg/d | None | Chlorpromazine, 200 mg/d, aripiprazole, 30 mg/d |
| Glick et al, 2006j | 52, M | Schizophrenia | Negative symptoms | Decreased olanzapine dose from 30 mg/d to 20 mg/d | 30 mg/d | None | Olanzapine, 30 mg/d |
| Barnas et al, 2005k | 57, F | Schizoaffective disorder | Stable before medication change | Discontinued perphenazine, 8 mg/d | 30 mg/d | None | Quetiapine, 350 mg/d |
| DeQuardo, 2004l | 54, M | Schizophrenia | History of aggression, residual paranoia, severe EPS | Haloperidol, 200 mg/d | 15 mg/d | Benztropine | Haloperidol |
| DeQuardo, 2004l | 51, M | Schizophrenia | History of aggression, persistent psychotic symptoms, treatment resistance | Olanzapine, 60 mg/d | 10 mg/d | None | Olanzapine |
| Ramaswamy et al, 2004m | 43, F | Schizoaffective disorder | Psychiatrically stable, multiple medication changes, including substituting carbamazepine for valproic acid | Discontinued ziprasidone, 160 mg/d, discontinued quetiapine, 400 mg/d, over 2 weeks | 30 mg/d | Propranolol, 30 mg/d, l-thyroxine, .05 mg/d, carbamazepine, 600 mg/d | Not available |
| Ramaswawamy et al, 2004m | 57, F | Schizoaffective disorder | History of multiple hospitalizations, but stable before medication change | Decreased olanzapine dose from 20 mg/d to 15 mg/d | 30 mg/d | Valproic acid, 2,000 mg/d | Ziprasidone |
| Ramaswawamy et al, 2004m | 67, F | Schizophrenia | Remote hospitalizations, recent worsened psychosis | Decreased ziprasidone dose from 200 mg/d to 160 mg/d 2 months previously | 30 mg/d | Carbamazepine, 200 mg/d | Not discussed |
| Ramaswamy et al, 2004m | 46, M | Schizophrenia | Persistent delusions while receiving risperidone, TD | Risperidone, 3 mg/d | 15 mg/d | Valproic acid, 1,500 mg/d | Risperidone, 3 mg/d |
| Reeves et al, 2004n | 50, M | Schizoaffective disorder | Relatively stable with nonthreatening delusions, hallucinations | Quetiapine, 800 mg/d | 30 mg/d | Divalproex, 2,000 mg/d | Olanzapine, 20 mg/d |
| ADHD: attention-deficit/hyperactivity disorder; EPS: extrapyramidal symptoms; HCV: hepatitis C virus; NMS: neuroleptic malignant syndrome; TD: tardive dyskinesia Source: References a. Chiu YH, Chen CH, Lu ML. Worsening psychosis after adding aripiprazole to clozapine. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):291-292. b. Ekinci O, Sabuncuoglu O. Psychosis associated with switching from risperidone to aripiprazole in an adolescent on methylphenidate treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(2):648-649. c. Selvaraj V, Ramaswamy S, Sharma A, et al. New-onset psychosis and emergence of suicidal ideation with aripiprazole. Am J Psychiatry. 2010;167(12):1535-1536. d. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246. e. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143. f. Ahuja N, Lloyd AJ. Aripiprazole and worsening of psychosis: a case report. J Clin Psychiatry. 2007;68(5):805-806. g. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342. h. Raja M. Improvement or worsening of psychotic symptoms after treatment with low doses of aripiprazole. Int J Neuropsychopharmacol. 2007;10(1):107-110. i. Thone J. Worsened agitation and confusion in schizophrenia subsequent to high-dose aripiprazole. J Neuropsychiatry Clin Neurosci. 2007;19(4):481-482. j. Glick ID, Duggal V, Hodulik C. Aripiprazole as a dopamine partial agonist: positive and negative effects. J Clin Psychopharmacol. 2006;26(1):101-103. k. Barnas ME, Hussain N, Petrides G. Treatment-emergent psychosis with aripiprazole. J Clin Psychiatry. 2005;66(10):1339. l. DeQuardo JR. Worsened agitation with aripiprazole: adverse effect of dopamine partial agonism? J Clin Psychiatry. 2004;65(1):132-133. m. Ramaswamy S, Vijay D, William M, et al. Aripiprazole possibly worsens psychosis. Int Clin Psychopharmacol. 2004;19(1):45-48. n. Reeves RR, Mack JE. Worsening schizoaffective disorder with aripiprazole. Am J Psychiatry. 2004;161(7):1308. | |||||||
Takeuchi et al14 aimed to establish predictors of worsening psychosis in a naturalistic setting where patients slowly transitioned to aripiprazole from previous antipsychotic treatment. Patients were required to be on a stable dose of an antipsychotic before participating in the study. Aripiprazole was started at 12 mg/d for 2 weeks with flexible dosing from weeks 2 to 52. Previous antipsychotic therapy was reduced biweekly by 25%. The incidence of worsening psychopathology after aripiprazole initiation was higher in the group of patients who had previously received high-dose antipsychotic therapy (average chlorpromazine equivalents [CPZE]: 727 mg/d) compared with the group on low dosages (average CPZE: 382 mg/d). It is possible that previous high-dose antipsychotic therapy was indicative of more significant baseline psychopathology; however, the worsened group and stabilized group had similar baseline Clinical Global Impressions-Severity scores.
Pae et al25 aimed to find predictors of worsening psychosis with aripiprazole in patients whose previous antipsychotic therapy was immediately discontinued. They found lower baseline disease severity was associated with significant worsening during the first month of aripiprazole treatment.
Other potential explanations
Aripiprazole’s manufacturer reported the incidence of psychosis-related adverse events in an analysis of 9 randomized schizophrenia trials.27 The rates of psychosis-related adverse events ranged from 0.6% to 18%, but there was no apparent relationship to study design or method of transitioning to aripiprazole. Rates of psychosis-related adverse events were similar between aripiprazole and the control group (placebo in 3 studies, another antipsychotic in 2 studies).
Emergence or worsening of psychotic symptoms temporally associated with aripiprazole initiation does not necessarily imply causation. As in Mr. N’s case, it is not always possible to determine whether worsening psychosis is the natural disease course or a treatment effect. In addition, it is not possible to differentiate lack of efficacy from a true propensity for aripiprazole to worsen psychosis.
It also is conceivable discontinuation or dosage reduction of a previous antipsychotic would worsen psychotic symptoms or cause side effects. When significant changes in psychopathology or side effects develop during the transition from 1 antipsychotic to another, it is difficult to determine etiology. Specifically, rapid transition from a medication with significant anticholinergic and antihistaminic properties—such as quetiapine or olanzapine—to 1 without these properties—such as aripiprazole—may result in symptoms of activation, including restlessness, insomnia, and anxiety. Consequently, these symptoms could be mistaken for worsening psychosis.28 Only 1 patient in this series was reported to abruptly discontinue an antipsychotic with significant anticholinergic properties (clozapine) before initiating aripiprazole.24 Studies by Takeuchi et al14 and Pae et al25 did not report the relative baseline use of antipsychotic medication with anticholinergic properties.
In a pooled analysis of treatment-emergent adverse events in 5 randomized clinical trials of patients receiving aripiprazole for acute relapse of schizophrenia, the incidence of akathisia was 10%, although it is not clear if this is a dose-related adverse effect.29 Because akathisia may be confused for worsening psychosis,30 it is possible akathisia was mistakenly identified as worsening psychotic symptoms in Mr. N’s case, as well as several reports from our literature review.
Covert akathisia is unlikely to explain worsening psychopathology observed in all patients in our literature review because confusion of akathisia and worsening psychosis is not a widespread phenomenon. In a post hoc analysis of pooled safety data from aripiprazole trials, Kane et al31 did not find a correlation between presence of akathisia and aripiprazole efficacy as measured by the Positive and Negative Syndrome Scale (PANSS) total, PANSS positive, PANSS negative, Clinical Global Impressions-Severity, Clinical Global Impressions-Improvement, and percentage of responders. Pae et al25 also noted there was no correlation between scores on the Barnes Akathisia Rating Scale and worsening psychopathology in patients switched to aripiprazole.
An antagonist always is an antagonist and clinicians have appreciated this concept since the days of chlorpromazine. The activity of aripiprazole, however, is on a pharmacologic continuum between a neutral antagonist and full agonist and currently there is no way to precisely determine the level of D2 receptor agonist action in a patient.
Although it is interesting to speculate that aripiprazole’s D2 receptor agonist action may contribute to worsening psychosis,32-34 there are other plausible explanations to consider. Rapid transition from a drug with significant anticholinergic properties and aripiprazole-associated akathisia may contribute to worsening psychopathology in patients starting aripiprazole. Because covert side effects may be incorrectly identified as psychotic agitation, we cannot exclude this as a possible etiologic factor in Mr. N’s case as well as the cases in our literature review.
Related Resource
- Abilify [package insert]. Princeton, NJ: Bristol-Myers Squibb; 2011.
Drug Brand Names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Biperiden • Akineton
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fluphenazine • Permitil, Prolixin
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Nortriptyline • Aventyl, Pamelor
- Methylphenidate • Concerta
- Molindone • Moban
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Mellaril
- Thyroxine • Synthroid
- Valproic acid • Depakene
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
• Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonist.
• Clinical predictors of aripiprazole-associated worsening of psychosis include low baseline level of psychopathology and previous treatment with high-dose antipsychotics.
• Rapid transition from a medication with significant anticholinergic properties to 1 without these properties may result in symptoms of activation, including restlessness, insomnia, and anxiety, which can be mistaken for worsening psychosis.
• Akathisia, a common adverse effect of aripiprazole, may masquerade as treatment-emergent worsening of psychotic symptoms.
Mr. N, age 29, presents to the emergency department at the urging of his family because of poor self-care, bizarre behavior, and disturbed sleep. He first experienced psychiatric symptoms 10 years ago after his mother died. He became dysphoric and paranoid, displaying bizarre responses and behaviors with poor self-care and a gradual functional decline. He has been taking sertraline, 100 mg/d, for 10 years.
Upon arrival at the hospital’s inpatient unit, Mr. N is unkempt, oddly related, and paranoid. His affect is constricted. Mr. N displays thought blocking and possibly is responding to internal stimuli. Sertraline is continued and haloperidol, 1 mg/d, is initiated. For the next 2 weeks, Mr. N continues to be oddly related, irritable, and paranoid, and experiences disturbed sleep and thought blocking. After an episode of impulsive aggression, the treatment team initiates aripiprazole, which is titrated to 30 mg/d for 1 week. Mr. N’s clinical status worsens; he is menacing toward other patients and his thinking is more disorganized, with loose associations and ideas of reference. He requires 4 injections of IM haloperidol, 5 mg, and several visits to the seclusion room over the next week. Haloperidol is increased to 30 mg/d over the next 10 days, then aripiprazole is discontinued because of a putative drug interaction with haloperidol. Following the medication changes Mr. N demonstrates better behavioral control, but still is grossly psychotic. While awaiting transfer to a state hospital, Mr. N receives a trial of olanzapine, 20 to 40 mg/d, for 2 weeks without significant benefit.
Several clinical trials demonstrate a significant reduction in intensity of psychotic symptoms with aripiprazole, which has a unique mechanism of action.1 However, since its FDA approval in 2002, several case reports have described treatment-emergent psychotic symptoms associated with aripiprazole initiation. Over the past 40 years, reports of worsening psychosis associated with antipsychotics have been limited to patients with schizophrenia who were taking high dosages or who had high plasma concentrations, when anticholinergic delirium may have explained increased psychotic symptoms.2-4
How can a drug effectively treat psychotic symptoms and occasionally worsen them? In this article, we discuss the relevant pharmacology and clinical literature on aripiprazole and try to make sense of this apparent paradox.
Unique pharmacologic profile
Antipsychotics have been reported to be either neutral antagonists or inverse agonists at the D2 receptor, based on in vitro data.5 Aripiprazole and its main metabolite, dehydroaripiprazole, originally were described as partial agonists at D2 dopamine receptors.6,7 However, it appears aripiprazole’s pharmacologic action is better explained by the concept of functional selectivity. Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonistic.5
Researchers have hypothesized that the pathophysiology of schizophrenia may, in part, be caused by dysfunction of mesocorticolimbic dopaminergic neurons characterized by an enhanced sensitivity of postsynaptic D2 receptors and increased sensitivity to dopaminergic drugs.8,9 In addition, chronic treatment with a D2 receptor antagonist is associated with increases in postsynaptic dopamine receptor density (ie, an increase in receptor reserve).10,11 Upregulation of D2 receptors may explain several features seen in patients chronically treated with antipsychotics, including tardive dyskinesia12 and rapid psychotic relapse after discontinuing an antipsychotic (supersensitivity psychosis).13 Because chronic antipsychotic treatment leads to high postsynaptic receptor reserve, aripiprazole initiation may produce overactivation of D2 receptors, which might worsen a patient’s condition.14 In vitro data15-18 and clinical observations indicate that aripiprazole has intrinsic efficacy at D2 receptors, as do clinical observations, such as:
- its propensity to reduce serum prolactin19
- a decreased likelihood of producing extrapyramidal side effects despite >80% occupancy of D2 receptors6
- case reports documenting aripiprazole-associated mania,20 improvement of risperidone-associated cognitive impairment,21 and pathologic gambling.22
Emergence or worsening of psychotic symptoms or a marginal antipsychotic effect may occur if aripiprazole is indeed a postsynaptic D2 receptor agonist. An individual patient’s outcome likely would depend on his or her sensitivity to psychosis and concurrent or previous exposure to a D2 receptor antagonist. For example, stimulation of postsynaptic D2 receptors may be further augmented if the dosage of the previous antipsychotic was reduced or withdrawn before initiating aripiprazole because additional receptors would be available for interaction with aripiprazole.
Case reports
A literature review revealed 23 reports of treatment-emergent psychosis associated with aripiprazole initiation (Table). The mean age of the patients was 47 (range: 17 to 69) and 57% were men. Most patients (87%) were diagnosed with a schizophrenia-spectrum illness before aripiprazole initiation. Most (57%) had mild, stable, or no psychotic symptoms before aripiprazole initiation. Most were receiving relatively high doses of antipsychotics (average chlorpromazine equivalents [CPZE]: 648 mg/d) before aripiprazole initiation. This medication was either decreased or discontinued in 70% of patients.
Emergence or worsening of psychotic symptoms included agitation, aggressive behavior, and increased psychomotor activity. However, akathisia evaluation was described in only 2 reports: 1 author identified akathisia symptoms, but attributed them to a concomitant antipsychotic (fluphenazine)23 and the other report specifically excluded the possibility of akathisia.24 Two systematic studies have attempted to establish risk factors for aripiprazole-associated worsening psychosis (Box).14,25
In our literature review, the mean final dose of aripiprazole was 21.5 mg/d (range: 2 to 60 mg/d). In the cases describing subsequent treatment, all but 1 patient were switched to another antipsychotic, including 2 whose psychotic symptoms stabilized with continuation of aripiprazole and addition of a second antipsychotic. Interestingly, in the case reported by Adan-Manes et al,26 initial treatment with aripiprazole monotherapy was efficacious, but a subsequent trial of adjunctive aripiprazole resulted in worsening psychosis.
Table
Case reports: Treatment-emergent psychosis associated with aripiprazole
| Study | Age, sex | Diagnosis | Before aripiprazole initiation | Pre-aripiprazole treatment | Aripiprazole dose | Concomitant psychotropic treatment | Subsequent treatment |
|---|---|---|---|---|---|---|---|
| Chiu et al, 2011a | 39, M | Schizophrenia | Psychiatrically stable, tardive dystonia | Clozapine, 300 mg/d | 10 mg/d | Valproic acid, 1,000 mg/d, clonazepam, 2 mg/d, mephenoxalone, 800 mg/d | Clozapine |
| Ekinci et al, 2010b | 17, M | ADHD | Inattention and impulsive aggression | Tapered and discontinued risperidone, 2.5 mg/d | 5 mg/d | Methylphenidate, 54 mg/d | Risperidone, 2 mg/d, methylphenidate, 36 mg/d |
| Selvaraj et al, 2010c | 49, F | Chronic depression | Depressive symptoms, suicidal ideation | None stated | 2 mg/d | Duloxetine, 80 mg/d, clonazepam, 2 mg/d | Duloxetine, 120 mg/d |
| Adan-Manes et al, 2009d | 23, M | Schizophrenia | No psychotic symptoms | Abrupt decrease of amisulpride dose from 800 mg/d to 400 mg/d | 20 mg/d | Biperiden, 4 mg/d | Amisulpride, 800 mg/d |
| Cho et al, 2009e | 45, F | Schizophrenia | Persistent psychotic symptoms, new onset diabetes with acute ketoacidosis | Haloperidol, 20 mg/d, abrupt clozapine discontinuation | 15 mg/d | Valproic acid, nortriptyline | Molindone, 150 mg/d |
| Ahuja et al, 2007f | 35, F | Schizoaffective disorder | Stable before medication change | Tapered amisulpride, 400 mg/d, over 6 weeks | 15 mg/d | None | Amisulpride, 600 mg/d |
| Lea et al, 2007g | 57, M | Schizophrenia | Persistent psychotic symptoms, treatment resistance, recent recovery from NMS | Discontinued ziprasidone, 200 mg/d | 30 mg/d | Lorazepam, 2 mg/d, amantadine, 100 mg, sertraline, 50 mg/d | Clozapine |
| Lea et al, 2007g | 49, M | Schizoaffective disorder | Delusions, verbal aggression, substance abuse, HCV | Decreased quetiapine dose from 800 mg/d to 400 mg/d | 15 mg/d | Divalproex, 1,000 mg/d, fluvoxamine, 200 mg/d, clonazepam, 2 mg/d | Lithium, quetiapine, 500 mg/d, haloperidol, 2 mg/d |
| Lea et al, 2007g | 60, M | Schizophrenia | Delusions, labile mood, aggression | Risperidone, 3 mg/d, interruption of fluphenazine, 75 mg/d | 20 mg/d | Divalproex, 4,500 mg/d, benztropine, 3 mg/d | Not discussed |
| Raja, 2007h | 30, M | Schizoaffective disorder | Negative symptoms, otherwise stable, recent citalopram discontinuation | Discontinued amisulpride, 800 mg/d over 2 weeks | 30 mg/d | Lithium | Amisulpride, 500 mg/d |
| Raja, 2007h | 69, F | Bipolar disorder | History of multiple relapses; presented with tremor, akathisia, weight gain | Discontinued risperidone, 2 mg/d, over 2 weeks | 15 mg/d | Lithium | Risperidone, 4 mg |
| Raja, 2007h | 59, F | Schizophrenia | Negative symptoms, otherwise stable | Reduced risperidone dosage from 5 mg/d to 4 mg/d | 7.5 mg/d | None | Risperidone, 5 mg/d |
| Thone, 2007i | 31, M | Schizophrenia | Confusion, agitation, delusions worsened with aripiprazole dose increase | None | 60 mg/d | None | Aripiprazole dose reduction to 15 mg/d, olanzapine, 10 mg/d |
| Glick et al, 2006j | 55, F | Schizophrenia | Stable before medication change | Tapered and discontinued thioridazine, 600 mg/d, over 3 months | 30 mg/d | None | Chlorpromazine, 200 mg/d, aripiprazole, 30 mg/d |
| Glick et al, 2006j | 52, M | Schizophrenia | Negative symptoms | Decreased olanzapine dose from 30 mg/d to 20 mg/d | 30 mg/d | None | Olanzapine, 30 mg/d |
| Barnas et al, 2005k | 57, F | Schizoaffective disorder | Stable before medication change | Discontinued perphenazine, 8 mg/d | 30 mg/d | None | Quetiapine, 350 mg/d |
| DeQuardo, 2004l | 54, M | Schizophrenia | History of aggression, residual paranoia, severe EPS | Haloperidol, 200 mg/d | 15 mg/d | Benztropine | Haloperidol |
| DeQuardo, 2004l | 51, M | Schizophrenia | History of aggression, persistent psychotic symptoms, treatment resistance | Olanzapine, 60 mg/d | 10 mg/d | None | Olanzapine |
| Ramaswamy et al, 2004m | 43, F | Schizoaffective disorder | Psychiatrically stable, multiple medication changes, including substituting carbamazepine for valproic acid | Discontinued ziprasidone, 160 mg/d, discontinued quetiapine, 400 mg/d, over 2 weeks | 30 mg/d | Propranolol, 30 mg/d, l-thyroxine, .05 mg/d, carbamazepine, 600 mg/d | Not available |
| Ramaswawamy et al, 2004m | 57, F | Schizoaffective disorder | History of multiple hospitalizations, but stable before medication change | Decreased olanzapine dose from 20 mg/d to 15 mg/d | 30 mg/d | Valproic acid, 2,000 mg/d | Ziprasidone |
| Ramaswawamy et al, 2004m | 67, F | Schizophrenia | Remote hospitalizations, recent worsened psychosis | Decreased ziprasidone dose from 200 mg/d to 160 mg/d 2 months previously | 30 mg/d | Carbamazepine, 200 mg/d | Not discussed |
| Ramaswamy et al, 2004m | 46, M | Schizophrenia | Persistent delusions while receiving risperidone, TD | Risperidone, 3 mg/d | 15 mg/d | Valproic acid, 1,500 mg/d | Risperidone, 3 mg/d |
| Reeves et al, 2004n | 50, M | Schizoaffective disorder | Relatively stable with nonthreatening delusions, hallucinations | Quetiapine, 800 mg/d | 30 mg/d | Divalproex, 2,000 mg/d | Olanzapine, 20 mg/d |
| ADHD: attention-deficit/hyperactivity disorder; EPS: extrapyramidal symptoms; HCV: hepatitis C virus; NMS: neuroleptic malignant syndrome; TD: tardive dyskinesia Source: References a. Chiu YH, Chen CH, Lu ML. Worsening psychosis after adding aripiprazole to clozapine. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):291-292. b. Ekinci O, Sabuncuoglu O. Psychosis associated with switching from risperidone to aripiprazole in an adolescent on methylphenidate treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(2):648-649. c. Selvaraj V, Ramaswamy S, Sharma A, et al. New-onset psychosis and emergence of suicidal ideation with aripiprazole. Am J Psychiatry. 2010;167(12):1535-1536. d. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246. e. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143. f. Ahuja N, Lloyd AJ. Aripiprazole and worsening of psychosis: a case report. J Clin Psychiatry. 2007;68(5):805-806. g. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342. h. Raja M. Improvement or worsening of psychotic symptoms after treatment with low doses of aripiprazole. Int J Neuropsychopharmacol. 2007;10(1):107-110. i. Thone J. Worsened agitation and confusion in schizophrenia subsequent to high-dose aripiprazole. J Neuropsychiatry Clin Neurosci. 2007;19(4):481-482. j. Glick ID, Duggal V, Hodulik C. Aripiprazole as a dopamine partial agonist: positive and negative effects. J Clin Psychopharmacol. 2006;26(1):101-103. k. Barnas ME, Hussain N, Petrides G. Treatment-emergent psychosis with aripiprazole. J Clin Psychiatry. 2005;66(10):1339. l. DeQuardo JR. Worsened agitation with aripiprazole: adverse effect of dopamine partial agonism? J Clin Psychiatry. 2004;65(1):132-133. m. Ramaswamy S, Vijay D, William M, et al. Aripiprazole possibly worsens psychosis. Int Clin Psychopharmacol. 2004;19(1):45-48. n. Reeves RR, Mack JE. Worsening schizoaffective disorder with aripiprazole. Am J Psychiatry. 2004;161(7):1308. | |||||||
Takeuchi et al14 aimed to establish predictors of worsening psychosis in a naturalistic setting where patients slowly transitioned to aripiprazole from previous antipsychotic treatment. Patients were required to be on a stable dose of an antipsychotic before participating in the study. Aripiprazole was started at 12 mg/d for 2 weeks with flexible dosing from weeks 2 to 52. Previous antipsychotic therapy was reduced biweekly by 25%. The incidence of worsening psychopathology after aripiprazole initiation was higher in the group of patients who had previously received high-dose antipsychotic therapy (average chlorpromazine equivalents [CPZE]: 727 mg/d) compared with the group on low dosages (average CPZE: 382 mg/d). It is possible that previous high-dose antipsychotic therapy was indicative of more significant baseline psychopathology; however, the worsened group and stabilized group had similar baseline Clinical Global Impressions-Severity scores.
Pae et al25 aimed to find predictors of worsening psychosis with aripiprazole in patients whose previous antipsychotic therapy was immediately discontinued. They found lower baseline disease severity was associated with significant worsening during the first month of aripiprazole treatment.
Other potential explanations
Aripiprazole’s manufacturer reported the incidence of psychosis-related adverse events in an analysis of 9 randomized schizophrenia trials.27 The rates of psychosis-related adverse events ranged from 0.6% to 18%, but there was no apparent relationship to study design or method of transitioning to aripiprazole. Rates of psychosis-related adverse events were similar between aripiprazole and the control group (placebo in 3 studies, another antipsychotic in 2 studies).
Emergence or worsening of psychotic symptoms temporally associated with aripiprazole initiation does not necessarily imply causation. As in Mr. N’s case, it is not always possible to determine whether worsening psychosis is the natural disease course or a treatment effect. In addition, it is not possible to differentiate lack of efficacy from a true propensity for aripiprazole to worsen psychosis.
It also is conceivable discontinuation or dosage reduction of a previous antipsychotic would worsen psychotic symptoms or cause side effects. When significant changes in psychopathology or side effects develop during the transition from 1 antipsychotic to another, it is difficult to determine etiology. Specifically, rapid transition from a medication with significant anticholinergic and antihistaminic properties—such as quetiapine or olanzapine—to 1 without these properties—such as aripiprazole—may result in symptoms of activation, including restlessness, insomnia, and anxiety. Consequently, these symptoms could be mistaken for worsening psychosis.28 Only 1 patient in this series was reported to abruptly discontinue an antipsychotic with significant anticholinergic properties (clozapine) before initiating aripiprazole.24 Studies by Takeuchi et al14 and Pae et al25 did not report the relative baseline use of antipsychotic medication with anticholinergic properties.
In a pooled analysis of treatment-emergent adverse events in 5 randomized clinical trials of patients receiving aripiprazole for acute relapse of schizophrenia, the incidence of akathisia was 10%, although it is not clear if this is a dose-related adverse effect.29 Because akathisia may be confused for worsening psychosis,30 it is possible akathisia was mistakenly identified as worsening psychotic symptoms in Mr. N’s case, as well as several reports from our literature review.
Covert akathisia is unlikely to explain worsening psychopathology observed in all patients in our literature review because confusion of akathisia and worsening psychosis is not a widespread phenomenon. In a post hoc analysis of pooled safety data from aripiprazole trials, Kane et al31 did not find a correlation between presence of akathisia and aripiprazole efficacy as measured by the Positive and Negative Syndrome Scale (PANSS) total, PANSS positive, PANSS negative, Clinical Global Impressions-Severity, Clinical Global Impressions-Improvement, and percentage of responders. Pae et al25 also noted there was no correlation between scores on the Barnes Akathisia Rating Scale and worsening psychopathology in patients switched to aripiprazole.
An antagonist always is an antagonist and clinicians have appreciated this concept since the days of chlorpromazine. The activity of aripiprazole, however, is on a pharmacologic continuum between a neutral antagonist and full agonist and currently there is no way to precisely determine the level of D2 receptor agonist action in a patient.
Although it is interesting to speculate that aripiprazole’s D2 receptor agonist action may contribute to worsening psychosis,32-34 there are other plausible explanations to consider. Rapid transition from a drug with significant anticholinergic properties and aripiprazole-associated akathisia may contribute to worsening psychopathology in patients starting aripiprazole. Because covert side effects may be incorrectly identified as psychotic agitation, we cannot exclude this as a possible etiologic factor in Mr. N’s case as well as the cases in our literature review.
Related Resource
- Abilify [package insert]. Princeton, NJ: Bristol-Myers Squibb; 2011.
Drug Brand Names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Biperiden • Akineton
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fluphenazine • Permitil, Prolixin
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Nortriptyline • Aventyl, Pamelor
- Methylphenidate • Concerta
- Molindone • Moban
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Mellaril
- Thyroxine • Synthroid
- Valproic acid • Depakene
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Citrome L. A review of aripiprazole in the treatment of patients with schizophrenia or bipolar I disorder. Neuropsychiatr Dis Treat. 2006;2(4):427-443.
2. Chong SA, Tan CH, Lee HS. Worsening of psychosis with clozapine and selective serotonin reuptake inhibitor combination: two case reports. J Clin Psychopharmacol. 1997;17(1):68-69.
3. Bowers MB Jr, Swigar ME. Psychotic patients who become worse on neuroleptics. J Clin Psychopharmacol. 1988;8(6):417-421.
4. Tornatore FL, Lee D, Sramek JJ. Psychotic exacerbation with haloperidol. Drug Intell Clin Pharm. 1981;15(3):209-213.
5. Beaulieu JM, Gainetdinov RR. The physiology signaling, and pharmacology of dopamine receptors. Pharmacol Rev. 2011;63(1):182-217.
6. Grunder G, Carlsson A, Wong DF. Mechanism of new antipsychotic medications: occupancy is not just antagonism. Arch Gen Psychiatry. 2003;60(10):974-977.
7. Wood MD, Scott C, Clarke K, et al. Aripiprazole and its human metabolite are partial agonists at the human dopamine D2 receptor, but the rodent metabolite displays antagonist properties. Eur J Pharmacol. 2006;546(1-3):88-94.
8. Seeman P, Weinshenker D, Quirion R, et al. Dopamine supersensitivity correlates with D2High states, implying many paths to psychosis. Proc Natl Acad Sci U S A. 2005;102(9):3513-3518.
9. Seeman P, Ko F, Jack E, et al. Consistent with dopamine supersensitivity, RGS9 expression is diminished in the amphetamine-treated animal model of schizophrenia and in postmortem schizophrenia brain. Synapse. 2007;61(5):303-309.
10. Burt DR, Creese I, Snyder SH. Antischizophrenic drugs: chronic treatment elevates dopamine receptor binding in brain. Science. 1977;196(4287):326-328.
11. Silvestri S, Seeman MV, Negrete JC, et al. Increased dopamine D2 receptor binding after long-term treatment with antipsychotics in humans: a clinical PET study. Psychopharmacology (Berl). 2000;152(2):174-180.
12. Sayers AC, Bürki HR, Ruch W, et al. Neuroleptic-induced hypersensitivity of striatal dopamine receptors in the rat as a model of tardive dyskinesias. Effects of clozapine, haloperidol, loxapine and chlorpromazine. Psychopharmacologia. 1975;41(2):97-104.
13. Moncrieff J. Does antipsychotic withdrawal provoke psychosis? Review of the literature on rapid onset psychosis (supersensitivity psychosis) and withdrawal-related relapse. Acta Psychiatr Scand. 2006;114(1):3-13.
14. Takeuchi H, Uchida H, Suzuki T, et al. Predictors of clinical worsening after a switch to aripiprazole in patients with schizophrenia: a 1-year naturalistic follow-up study. J Clin Psychopharmacol. 2009;29(4):394-395.
15. Shapiro DA, Renock S, Arrington E, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology. 2003;28(8):1400-1411.
16. Urban JD, Vargas GA, von Zastrow M, et al. Aripiprazole has functionally selective actions at dopamine D2 receptor-mediated signaling pathways. Neuropsychopharmacology. 2007;32(1):67-77.
17. Klewe IV, Nielsen SM, Tarpo L, et al. Recruitment of beta-arrestin2 to the dopamine D2 receptor: Insights into anti-psychotic and anti-parkinsonian drug receptor signaling. Neuropharmacology. 2008;54(8):1215-1222.
18. Masri B, Salahpour A, Didriksen M, et al. Antagonism of dopamine D2 receptor/beta-arrestin 2 interaction is a common property of clinically effective antipsychotics. Proc Natl Acad Sci U S A. 2008;105(36):13656-13661.
19. Shim JC, Shin JG, Kelly DL, et al. Adjunctive treatment with a dopamine partial agonist, aripiprazole, for antipsychotic-induced hyperprolactinemia: a placebo-controlled trial. Am J Psychiatry. 2007;164(9):1404-1410.
20. Padala PR, Wengel SP, Petty F. Manic episode during treatment with aripiprazole. Am J Psychiatry. 2007;164(1):172-173.
21. Hu CH, Pai N, Huang XF, et al. Potential control of risperidone-related cognitive deficits by adjunctive aripiprazole treatment. J Clin Psychopharmacol. 2011;31(1):135-136;author reply 136–137.
22. Cohen J, Magalon D, Boyer L, et al. Aripiprazole-induced pathological gambling: a report of 3 cases. Curr Drug Saf. 2011;6(1):51-53.
23. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342.
24. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143.
25. Pae CU, Chiesa A, Mandelli L, et al. Predictors of early worsening after switch to aripiprazole: a randomized, controlled, open-label study. Clin Drug Investig. 2010;30(3):187-193.
26. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246.
27. Cognata-Smith C, Baker RA, Pikalov A, et al. Analysis of nine aripiprazole trials to evaluate strategies for switching patients with schizophrenia to aripiprazole. Paper presented at: 162nd Annual Meeting American Psychiatric Association; May 16-21, 2009; San Francisco, CA.
28. Lieberman J. Cholinergic rebound in neuroleptic withdrawal syndromes. Psychosomatics. 1981;22(3):253-254.
29. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: Safety and tolerability in short-term, placebo-controlled trials. Schizophr Res. 2003;61(2-3):123-136.
30. Kane JM, Fleischhacker WW, Hansen L, et al. Akathisia: an updated review focusing on second-generation antipsychotics. J Clin Psychiatry. 2009;70(5):627-643.
31. Kane JM, Barnes TR, Correll CU, et al. Evaluation of akathisia in patients with schizophrenia, schizoaffective disorder, or bipolar I disorder: A post hoc analysis of pooled data from short- and long-term aripiprazole trials. J Psychopharmacol. 2010;24(7):1019-1029.
32. Fleischhacker WW, McQuade RD, Marcus RN, et al. A double-blind, randomized comparative study of aripiprazole and olanzapine in patients with schizophrenia. Biol Psychiatry. 2009;65(6):510-517.
33. Kane JM, Osuntokun O, Kryzhanovskaya LA, et al. A 28-week, randomized, double-blind study of olanzapine versus aripiprazole in the treatment of schizophrenia. J Clin Psychiatry. 2009;70(4):572-581.
34. Kane JM, Correll CU, Goff DC, et al. A multicenter, randomized, double-blind, placebo-controlled, 16-week study of adjunctive aripiprazole for schizophrenia or schizoaffective disorder inadequately treated with quetiapine or risperidone monotherapy. J Clin Psychiatry. 2009;70(10):1348-1357.
1. Citrome L. A review of aripiprazole in the treatment of patients with schizophrenia or bipolar I disorder. Neuropsychiatr Dis Treat. 2006;2(4):427-443.
2. Chong SA, Tan CH, Lee HS. Worsening of psychosis with clozapine and selective serotonin reuptake inhibitor combination: two case reports. J Clin Psychopharmacol. 1997;17(1):68-69.
3. Bowers MB Jr, Swigar ME. Psychotic patients who become worse on neuroleptics. J Clin Psychopharmacol. 1988;8(6):417-421.
4. Tornatore FL, Lee D, Sramek JJ. Psychotic exacerbation with haloperidol. Drug Intell Clin Pharm. 1981;15(3):209-213.
5. Beaulieu JM, Gainetdinov RR. The physiology signaling, and pharmacology of dopamine receptors. Pharmacol Rev. 2011;63(1):182-217.
6. Grunder G, Carlsson A, Wong DF. Mechanism of new antipsychotic medications: occupancy is not just antagonism. Arch Gen Psychiatry. 2003;60(10):974-977.
7. Wood MD, Scott C, Clarke K, et al. Aripiprazole and its human metabolite are partial agonists at the human dopamine D2 receptor, but the rodent metabolite displays antagonist properties. Eur J Pharmacol. 2006;546(1-3):88-94.
8. Seeman P, Weinshenker D, Quirion R, et al. Dopamine supersensitivity correlates with D2High states, implying many paths to psychosis. Proc Natl Acad Sci U S A. 2005;102(9):3513-3518.
9. Seeman P, Ko F, Jack E, et al. Consistent with dopamine supersensitivity, RGS9 expression is diminished in the amphetamine-treated animal model of schizophrenia and in postmortem schizophrenia brain. Synapse. 2007;61(5):303-309.
10. Burt DR, Creese I, Snyder SH. Antischizophrenic drugs: chronic treatment elevates dopamine receptor binding in brain. Science. 1977;196(4287):326-328.
11. Silvestri S, Seeman MV, Negrete JC, et al. Increased dopamine D2 receptor binding after long-term treatment with antipsychotics in humans: a clinical PET study. Psychopharmacology (Berl). 2000;152(2):174-180.
12. Sayers AC, Bürki HR, Ruch W, et al. Neuroleptic-induced hypersensitivity of striatal dopamine receptors in the rat as a model of tardive dyskinesias. Effects of clozapine, haloperidol, loxapine and chlorpromazine. Psychopharmacologia. 1975;41(2):97-104.
13. Moncrieff J. Does antipsychotic withdrawal provoke psychosis? Review of the literature on rapid onset psychosis (supersensitivity psychosis) and withdrawal-related relapse. Acta Psychiatr Scand. 2006;114(1):3-13.
14. Takeuchi H, Uchida H, Suzuki T, et al. Predictors of clinical worsening after a switch to aripiprazole in patients with schizophrenia: a 1-year naturalistic follow-up study. J Clin Psychopharmacol. 2009;29(4):394-395.
15. Shapiro DA, Renock S, Arrington E, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology. 2003;28(8):1400-1411.
16. Urban JD, Vargas GA, von Zastrow M, et al. Aripiprazole has functionally selective actions at dopamine D2 receptor-mediated signaling pathways. Neuropsychopharmacology. 2007;32(1):67-77.
17. Klewe IV, Nielsen SM, Tarpo L, et al. Recruitment of beta-arrestin2 to the dopamine D2 receptor: Insights into anti-psychotic and anti-parkinsonian drug receptor signaling. Neuropharmacology. 2008;54(8):1215-1222.
18. Masri B, Salahpour A, Didriksen M, et al. Antagonism of dopamine D2 receptor/beta-arrestin 2 interaction is a common property of clinically effective antipsychotics. Proc Natl Acad Sci U S A. 2008;105(36):13656-13661.
19. Shim JC, Shin JG, Kelly DL, et al. Adjunctive treatment with a dopamine partial agonist, aripiprazole, for antipsychotic-induced hyperprolactinemia: a placebo-controlled trial. Am J Psychiatry. 2007;164(9):1404-1410.
20. Padala PR, Wengel SP, Petty F. Manic episode during treatment with aripiprazole. Am J Psychiatry. 2007;164(1):172-173.
21. Hu CH, Pai N, Huang XF, et al. Potential control of risperidone-related cognitive deficits by adjunctive aripiprazole treatment. J Clin Psychopharmacol. 2011;31(1):135-136;author reply 136–137.
22. Cohen J, Magalon D, Boyer L, et al. Aripiprazole-induced pathological gambling: a report of 3 cases. Curr Drug Saf. 2011;6(1):51-53.
23. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342.
24. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143.
25. Pae CU, Chiesa A, Mandelli L, et al. Predictors of early worsening after switch to aripiprazole: a randomized, controlled, open-label study. Clin Drug Investig. 2010;30(3):187-193.
26. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246.
27. Cognata-Smith C, Baker RA, Pikalov A, et al. Analysis of nine aripiprazole trials to evaluate strategies for switching patients with schizophrenia to aripiprazole. Paper presented at: 162nd Annual Meeting American Psychiatric Association; May 16-21, 2009; San Francisco, CA.
28. Lieberman J. Cholinergic rebound in neuroleptic withdrawal syndromes. Psychosomatics. 1981;22(3):253-254.
29. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: Safety and tolerability in short-term, placebo-controlled trials. Schizophr Res. 2003;61(2-3):123-136.
30. Kane JM, Fleischhacker WW, Hansen L, et al. Akathisia: an updated review focusing on second-generation antipsychotics. J Clin Psychiatry. 2009;70(5):627-643.
31. Kane JM, Barnes TR, Correll CU, et al. Evaluation of akathisia in patients with schizophrenia, schizoaffective disorder, or bipolar I disorder: A post hoc analysis of pooled data from short- and long-term aripiprazole trials. J Psychopharmacol. 2010;24(7):1019-1029.
32. Fleischhacker WW, McQuade RD, Marcus RN, et al. A double-blind, randomized comparative study of aripiprazole and olanzapine in patients with schizophrenia. Biol Psychiatry. 2009;65(6):510-517.
33. Kane JM, Osuntokun O, Kryzhanovskaya LA, et al. A 28-week, randomized, double-blind study of olanzapine versus aripiprazole in the treatment of schizophrenia. J Clin Psychiatry. 2009;70(4):572-581.
34. Kane JM, Correll CU, Goff DC, et al. A multicenter, randomized, double-blind, placebo-controlled, 16-week study of adjunctive aripiprazole for schizophrenia or schizoaffective disorder inadequately treated with quetiapine or risperidone monotherapy. J Clin Psychiatry. 2009;70(10):1348-1357.