User login
Kidney Failure in the 21st Century
The Initiating Dialysis Early and Late (IDEAL) study in Australia and New Zealand1 examined the optimal time to initiate dialysis. This well-designed, randomized, controlled trial gave the nephrology community guidelines for treating patients as they progress through chronic kidney disease to stage 5 (CKD 5). The IDEAL investigators demonstrated that planned early initiation of dialysis did not enhance survival—and in some cases, it hastened death.1
Although most patients have a nephrology provider by the time they reach CKD 5 (ie, kidney failure), primary care providers can be instrumental in preparing the patient for what lies ahead as kidney failure progresses. Presented here is an overview of diagnosis and management of the patient with CKD 5 in the 21st century.
CASE PRESENTATION
A 70-year-old woman with an extensive history of diabetes and hypertension presents to her primary care clinician complaining of a lack of energy. She has just returned from a trip to Disney World, where she says she was unable to keep up with her grandchildren. She sat in the shade while they enjoyed Space Mountain and other attractions, and because of uncustomary fatigue, she required a nap every afternoon.
Physical examination shows an elderly female in no acute distress. Cardiac exam shows a regular heart rate and rhythm, the patient’s lungs are clear, and she has 1+ pitting leg edema bilaterally. The patient’s blood pressure is slightly elevated at 142/92 mm Hg, and no protein is detected on spot urine testing.
Blood work is ordered, including a complete blood count, a comprehensive metabolic panel, and an A1C. Results include a hemoglobin level of 8.7 g/dL (reference range for women, 12.0 to 16.0 g/dL), a serum creatinine level (SCr) of 3 mg/dL (range, 0.6 to 1.2 mg/dL; estimated glomerular filtration rate [eGFR], 15 mL/min/1.73 m2), and an A1C value of 7.5% (normal, & < 7%).
The patient is told that she is in kidney failure and is referred immediately to a nephrology practice, where she is seen the following day. After her appointment, she returns to the primary care office. When she is asked when she will be starting dialysis, she seems surprised, saying, “They told me I was doing well. I need some shots for my blood, but they didn’t seem worried at all.”
Is this patient being managed correctly by the nephrology practitioner?
EPIDEMIOLOGY
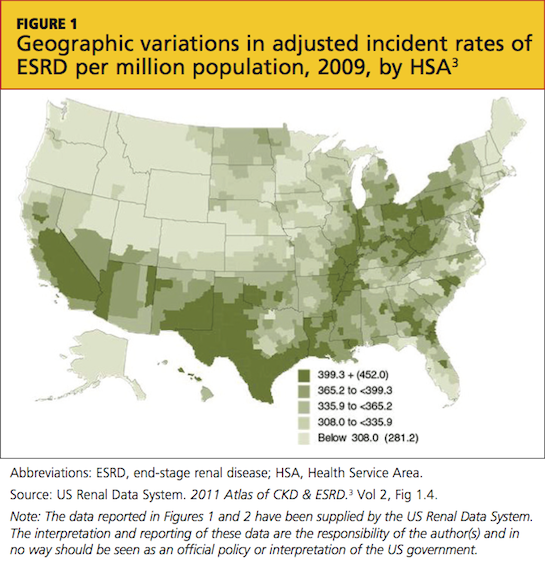
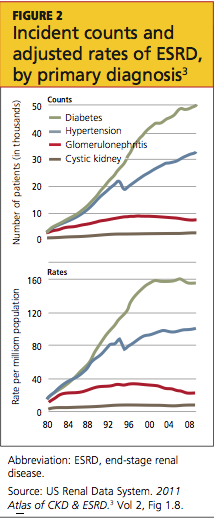
Presently, more than 1 million persons in the United States have CKD 5, and 500,000 are undergoing dialysis. The number of patients with CDK 5 who are on dialysis has doubled since 1994 and is projected to reach 774,000 by 20202,3 (see Figure 13 and Figure 23).
CKD 5 is defined as an eGFR below 15 mL/min/1.73 m2, according to the Modification of Diet in Renal Disease (MDRD) study group formula; or as a creatinine clearance of less than 15 mL/min, using the Cockcroft-Gault formula.4-6 Both formulas have limitations, since they are not fully accurate at extremes of age, with variations in weight, for some racial mixes, or for the very malnourished patient.7,8 However, they do correct for normal age-related loss of kidney function, gender, and SCr, and they are currently the generally accepted formulas.4
A rise in SCr is exponential; for each doubling of the SCr, a reduction in kidney function of approximately 50% occurs. This means that a rise in SCr from 4 to 8 mg/dL is equivalent (in the proportion of loss of kidney function) to a rise of SCr from 0.5 to 1 mg/dL. Commonly, patients are not referred to nephrology until the SCr doubles to 4 or 6 mg/dL—whereas the rise in SCr from 0.5 to 1 mg/dL should be of greatest concern to the primary care provider, prompting a referral.9 Early recognition of reduced renal function allows for identification of potentially reversible etiologies and the slowing of CKD progression.
INDICATIONS FOR RENAL REPLACEMENT THERAPY
Not all patients with an eGFR below 15 mL/min/1.73 m2 are started on dialysis immediately. The decision to initiate dialysis is guided by assessment of a constellation of uremic manifestations—not eGFR alone. Newer data suggest that early initiation of dialysis may be associated with increased mortality.10-15
The IDEAL study,1 a well-designed, randomized, controlled trial of all patients who started dialysis in Australia and New Zealand over a multiyear period, was designed to determine the optimal time to initiate dialysis. Patients were randomized to start dialysis (hemodialysis or peritoneal dialysis) at an eGFR between 10 and 14 mL/min/1.73 m2 or between 5 and 7 mL/min/1.73 m2. While there was some overlap and some patients were started on dialysis outside their randomized eGFR (eg, earlier than the allotted time because symptoms developed), what the IDEAL investigators found surprised the entire nephrology community: Early dialysis starts did not enhance survival and, in some cases, it hastened death.1
The indications for initiation of dialysis often develop long after the patient has progressed within CKD 5, commonly with an eGFR of 10 mL/min/1.73 m2 or less. Medicare has acknowledged this by reimbursing dialysis only in eligible patients whose eGFR is below 10 mL/min/1.73 m2.16 There are also acute indications for initiation of dialysis, such as uremic pericarditis, hyperkalemia, bleeding related to uremic platelet dysfunction, and metabolic encephalopathy related to uremia (and reimbursement for dialysis can be justified), but these are uncommon.
RENAL REPLACEMENT THERAPY CHOICES
The choices of treatment for kidney failure (note: treatment, not cure) are medical management, hemodialysis, peritoneal dialysis, and transplant. Each choice has its advantages and disadvantages, and all patients should receive clear explanations of what they can expect from each modality.
While younger, higher-functioning individuals are likely to benefit from dialysis, patients with extensive comorbid illnesses and/or low functional status tend to respond poorly17; medical management may be the best choice for these patients. In one recent study, the functional status of residents in skilled nursing homes was examined, before and after initiation of dialysis. At one year, 58% of the nursing home residents who underwent dialysis had died, and only 13% had maintained their pre-dialysis functional status.18
Another research team recently compared conservative management of CKD 5 (ie, medical therapy without dialysis) with dialysis in elderly patients. For patients 75 and older with extensive comorbid illness, the researchers found no statistically significant survival benefit to dialysis.19
Dialysis, whether administered as hemodialysis or peritoneal dialysis, is a rigorous, intensive medical therapy. Dialysis does not necessarily prolong life in patients with extensive comorbidities, and it does not always enhance quality of life.18,20-23 The decision to undergo dialysis is personal and individual, and both the patient and family should be actively involved in making it. Primary care providers should be the nephrologist’s ally in the discussion of therapy for renal failure; often, they have cared for the patient for years, and they understand the patient and family dynamics.
An important message the nephrology practitioner must communicate is that choosing medical management without dialysis is not withholding care; sometimes it is a more humane choice.24 Dying of kidney failure can be a peaceful and comfortable death: As the uremic toxins build up (with eGFR ≤ 2 mL/min/1.73 m2, although this can take many years), the patient becomes confused and slowly slips into a sleepiness that leads to death.25 Hospice is usually involved to support the patient and family.
Hemodialysis
Hemodialysis is the most common, best-known treatment modality for CKD in the US, with about 94% of patients choosing it.3 In this process, blood is removed from the body (approximately 500 cc at a time) and filtered through a semipermeable membrane that removes uremic toxins and excess fluid, normalizing the metabolic and electrolyte derangements. The filtered blood is then returned to the patient.
The average dialysis session is four hours long and is conducted three times per week, following recommendations from the 2002 Hemodialysis Study (HEMO).26 Most patients come to a free-standing dialysis center on a Monday/Wednesday/Friday or a Tuesday/Thursday/Saturday schedule.
In theory, there is no such thing as too much dialysis (since the kidneys work 24 hours per day, seven days per week); thus, researchers have recently examined lengthening dialysis in an attempt to extend survival.27-29 According to study results, patients who undergo longer dialysis times generally enjoy better nutrition with a more liberal diet, require fewer medications, have reduced incidence of increased left ventricular mass (a marker for coronary artery disease), and report better quality of life, all in addition to a survival benefit; however, the latter was not considered statistically significant in any of the studies.27-29 Additionally, this survival benefit may not extend to daily hemodialysis; in a recent publication, daily hemodialysis was associated with a 60% higher death rate.30
A number of dialysis units have begun to offer nocturnal dialysis. In this option, patients sleep at the unit for eight hours, three nights per week, for a total of 24 hours of dialysis (vs the typical 12 hours per week). Some patients receive dialysis at home, allowing them to dialyze for six weekly sessions of two to three hours. This strategy attempts to mimic a more “natural” state.
One of the primary challenges associated with hemodialysis is establishing and maintaining a vascular access. An arteriovenous (AV) fistula is the access of choice because its use reduces the likelihood of clotting, improves access survival, and increases clearances during dialysis.31 However, the AV fistula is most effective if it is placed a minimum of six months before use.32
For many patients, an AV fistula is created surgically when the eGFR falls to 15 mL/min/1.73 m2. Fistula placement in preparation for the initiation of hemodialysis is important to reduce the need for hemodialysis catheters, which are associated with higher risk for infection and poorer outcomes.33
Peritoneal Dialysis
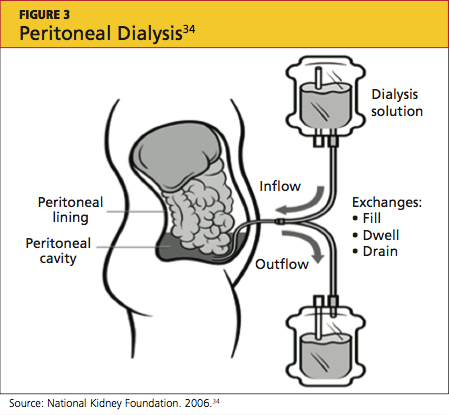
Peritoneal dialysis (PD) filters out uremic toxins and normalizes the metabolic and electrolyte derangements by using the patient’s peritoneal membrane as a filter. Dialysate is instilled through a catheter into the peritoneal cavity where it is allowed to dwell, often for four to six hours (see Figure 334). Exchanges can be performed three to four times per day (allowing six to eight hours of dwell time per exchange for the dialysate), or by way of a cycler at night.35,36
Performing exchanges by way of a cycler requires the patient to be connected via the PD catheter for eight hours; thus the advantage of performing the exchange during sleep. The cycler has a soft, whooshing sound that many patients describe as “white noise” that does not disturb their sleep.
The principal advantage of peritoneal dialysis is extended survival of the patient.37-39 PD also allows the patient a more liberal diet. Although PD must be performed every day, exchanges can be adjusted to the patient’s timing preference. PD reduces cost and time, since the patient need not travel to a dialysis center. PD also preserves residual renal function,39 which is associated with a survival benefit and contributes to the patient’s overall health and well-being. The use of PD requires a committed, competent patient in a clean home environment.
This intervention may not be suitable for patients with a history of abdominal surgeries. However, as a therapy considered gentler than hemodialysis, PD is an excellent choice for the patient with congestive heart failure.40 The PD catheter is not placed until two to four weeks before it will be needed.41
Kidney Transplantation
Last, but certainly not least, is transplant. As entire books have been written on this modality, only the highlights will be addressed here.42 Survival rates following transplantation are reported to exceed those associated with any other treatment modality, even when controlling for comorbidities and patient selection bias.43 A patient can receive a kidney from either a living or a deceased donor. Apart from the perioperative risks associated with transplantation surgery, long-term surgical or medical problems are not common for the living kidney donor.44-46
Since 2002, as a result of a policy change from the United Network for Organ Sharing (UNOS),47 the donor pool has been expanded by including kidneys from what are commonly referred to as extended criteria donors: those who are older than 60, or who are 50 to 59 and have two of the following factors: cerebrovascular accident as the cause of death; preexisting hypertension; or an SCr level exceeding 1.5 mg/dL. These kidneys may be given to any recipients but are primarily used for those age 50 or older.47
Graft survival is statistically shorter in a cadaver kidney than in a living donor kidney.48 However, the larger problem is the long wait time for a cadaver transplant—seven to eight years (or possibly longer) for some centers and some blood types.49 A patient can be referred to a transplant center when the eGFR falls below 25 mL/min/1.73 m2; he or she will then be actively listed for transplant when eGFR reaches 20 mL/min/1.73 m2 or lower.
Early referral for transplant listing buys the patient time before dialysis becomes essential. Patients can receive preemptive transplants (ie, transplantation before dialysis is initiated); these are becoming increasingly popular because they generally extend survival for the recipient.50,51
UNOS (www.unos.org) has set few limits on transplant recipients: patients are required to undergo an extensive medical work-up, but there are no upper age limits (although some centers do set their own) and usually no limits on patients infected with HIV, hepatitis B, or hepatitis C (although there may be separate listing requirements). Patients who are not US citizens are not denied.
Because more than 100,000 patients are currently on the wait list, domino kidney transplants are now being offered at many centers.52-54 These organ exchanges involve altruistic donors who do not match their targeted kidney recipients. Since publication of the first article describing this procedure at Johns Hopkins Medical Center,53 there have been two-way, three-way, and up to 32-way domino transplants. However, patients wishing to engage in this type of trade require a donor; not every patient has access to an altruistic donor.
CKD PATIENT EDUCATION
When Congress passed the Medicare Improvements for Patients and Providers Act of 2008,55 a component little noted outside the nephrology community was the offer of kidney disease education (KDE) classes to Medicare-eligible patients with CKD 4.56-58 Medicare patients with an eGFR of 15 to 30 mL/min/1.73 m2 are eligible to attend KDE classes presented by a physician, an NP, a PA, or a clinical nurse specialist. Medicare will reimburse for six hours of education.
This groundbreaking educational benefit, the first such program paid for by Medicare, was championed by the National Kidney Foundation and other nephrology groups. Many nephrology practices now offer these classes to all their CKD patients, regardless of health insurance status. Instructors educate patients on the choices of renal replacement therapy and help patients select their best option.
KDE classes can be conducted in the office setting or at the patient’s home, and they can be billed on the same day as an evaluation and management (E/M) visit.56,57 This may help explain why, in 2010, gerontologists billed for more home KDE classes than did nephrologists.58
FUTURE TRENDS AND ONGOING TRIALS
The overarching goal of therapy for CKD patients is to diagnose accurately and treat effectively in order to slow or prevent progression to end-stage renal disease (ESRD). Following is a brief review of a selection of new diagnostic tools and therapeutic interventions that may impact the management of CKD in the coming years.
The QxMD Kidney Failure Risk Equation is a newly developed, well-validated predictive model that offers relatively accurate prediction of a patient’s likelihood of progression to ESRD, based on age, sex, eGFR, and levels of albuminuria, SCr, serum phosphorus, serum bicarbonate, and serum albumin59 (see table59). This tool can be accessed online at www.qxmd.com/calculate-online/nephrology/kidney-failure-risk-equation.

Increased awareness of the role that phosphorus plays in the development of vascular calcifications has led to an emphasis on earlier, more aggressive control of dietary phosphorus. Historically, dietary phosphorus control and phosphorus binders were recommended only when the patient’s serum phosphorus exceeded normal limits. Dietary phosphorus control may now be advised as early as CKD 3, based on the understanding that phosphorus is a key component in driving the development of vascular calcifications—which in turn contribute to the high incidence of cardiovascular disease in patients with CKD.60
Bardoxolone is a new medication developed for treatment of diabetic nephropathy.61,62 It works by inhibiting proinflammatory mediators and moderating the effects of oxidative stress, thus interrupting the cascade of inflammation and cellular injury that result in diabetic nephropathy.62 Early clinical trials examining this agent have shown promise in terms of raising eGFR and reducing serum creatinine, but tolerability and toxicity profiles have been an issue.61 Additionally, some reduction in serum creatinine may have been attributable to weight loss as opposed to true improvement of renal function.62
Data have recently been released regarding the use of the herb silymarin for treatment of patients with macroalbuminuria related to diabetic nephropathy. Results from a small (n = 60), randomized, nonblinded clinical trial by Fallahzadeh et al63 indicate that silymarin decreases proteinuria when used in combination with an ACE inhibitor or an angiotensin receptor blocker (ARB). Silymarin, an extract from milk thistle, has been used medicinally for centuries for its antioxidant, anti-inflammatory, and antiviral properties in those with liver “ailments.” In this clinical trial, silymarin was well tolerated and associated with a reduction in pro-inflammatory markers.63
AST-120 is another agent intended to slow progression of CKD. It promotes intestinal adsorption and fecal excretion of the uremic toxin indoxyl sulfate.64 A recently published study demonstrated an association between use of AST-120 and a delay in required initiation of hemodialysis, but no survival benefit.65 This was a nonrandomized trial, and previous research showed no effect of AST-120 on progression of CKD.66 However, patients close to requiring dialysis are likely to welcome a means to delay it.
A growing body of evidence suggests that reversal of CKD-associated acidemia by administering sodium bicarbonate may actually forestall progression of CKD.67 However, treatment with sodium bicarbonate can lead to complications of hypertension and fluid volume overload. In one study, patients at risk for these complications derived equivalent benefit by increasing dietary fruit and vegetable intake to reduce renal acid load.68 However, providers must be mindful of patients’ serum potassium levels, especially patients who are taking an ACE inhibitor or an ARB.
The Provider’s Current Role
Despite the hope offered by new and novel therapies, the mainstay of treatment for CKD continues to be aggressive management of diabetes, hypertension, and the cardiovascular risk profile. As a result of vigorous preventive strategies to address the cardiovascular risks inherent in this patient population, the patient with type 2 diabetes is now more likely to progress to ESRD than to die of a cardiovascular event.69
The well-informed clinician can be instrumental in providing evidence-based medical therapy and excellent patient education from the time of initial CKD diagnosis through CKD 5.
PATIENT OUTCOME
The case patient was started on injections of epoietin alfa for her anemia. She attended KDE classes led by an advanced practitioner in her nephrology group and decided to undergo peritoneal dialysis, since it would allow her to maintain her travel schedule. When last heard from, the patient was preparing for a trip to see the Great Barrier Reef in Australia.
CONCLUSION
The decision to begin renal replacement therapy—whether a form of dialysis, or another management option—depends not on SCr or eGFR alone. Rather, a number of uremic manifestations, comorbidities, lifestyle factors, and other variables must be carefully weighed before the patient, the family, and the clinicians involved can decide on the management plan most likely to enhance the patient’s quality of life and extend survival.
1. Cooper BA, Branley P, Bulfone L, et al; IDEAL Study. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010; 363(7):609-619.
2. Olan G. Policy Update: ASN to CDC: data collection of creatinine levels will advance research. ASN Kidney News. 2012;4(6):16. www.asn-online.org/publications/kidneynews/archives/2012/KN_jun2012.pdf. Accessed August 27, 2012.
3. US Renal Data System, National Institute of Diabetes and Digestive and Kidney Diseases, NIH. 2011 Atlas of CKD & ESRD. Vol 2. Chap 1: Incidence, prevalence, patient characteristics, and modalities. www.usrds.org/2011/pdf/v2_ch01_11.pdf. Accessed September 26, 2012.
4. National Kidney Foundation. Kidney Disease Outcomes Quality Initiative (KDOQI). Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. ?Part 4. Definition and classification of the stages of chronic kidney disease. 2002:43-80. www.kidney.org/professionals/kdoqi/pdf/ckd_evalua tion_classification_stratification.pdf. Accessed August 27, 2012.
5. Levey AS, Bosch JP, Lewis JB, et al; Modification of Diet in Renal Disease Study Group. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Internal Med. 1999;130 (6):461-470.
6. Froissart M, Rossert J, Jacquot C, et al. Predictive performance of the Modification of Diet in Renal Disease and Cockcroft-Gault equations for estimating renal function. J Am Soc Nephrol. 2005;16(3):763-773.
7. Jafar TH, Schmid CH, Levey AS. Serum creatinine as marker of kidney function in South Asians: a study of reduced GFR in adults in Pakistan. J Am Soc Nephrol. 2005;16(5):1413-1419.
8. Zuo L, Ma YC, Zhou YH, et al. Application of GFR-estimating equations in Chinese patients with chronic kidney disease. Am J Kidney Dis. 2005;45(3):463-472.
9. Stevens LA, Stoycheff N, Levey AS. Staging and management of chronic kidney disease. In: Greenberg A, ed. Primer of Kidney Diseases: Expert Consult. 5th ed. Philadelphia, PA: WB Saunders; 2009:436-445.
10. Clark WF, Na Y, Rosansky SJ, et al. Association between estimated glomerular filtration rate at initiation of dialysis and mortality. CMAJ. 2011;183(1):47-53.
11. Beddhu S, Samore MH, Roberts MS, et al. Impact of timing of initiation of dialysis on mortality. J Am Soc Nephrol. 2003;14(9):2305-2312.
12. Kazmi WH, Gilbertson DT, Obrador GT, et al. Effect of comorbidity on the increased mortality associated with early initiation of dialysis. Am J Kidney Dis. 2005;46(5):887-896.
13. Lassalle M, Labeeuw M, Frimat L, et al. Age and comorbidity may explain the paradoxical association of an early dialysis start with poor survival. Kidney Int. 2010;77(8):700-707.
14. Stel VS, Dekker FW, Ansell D, et al. Residual renal function at the start of dialysis and clinical outcomes. Nephrol Dial Transplant. 2009;24 (10):3175-3182.
15. Traynor JP, Simpson K, Geddes CC, et al. Early initiation of dialysis fails to prolong survival in patients with end-stage renal failure. J Am Soc Nephrol. 2002;13(8):2125-2132.
16. US Department of Health and Human Services, Centers for Medicare and Medicaid Services. CMS Form 2728. End-Stage Renal Disease Medical Evidence Report: Medicare Entitlement and/or Patient Registration. www.usrds.org/2008/rg/forms/02_2728_1965.pdf. Accessed September 25, 2012.
17. Renal Physicians Association. Shared Decision-Making in the Appropriate Initiation of and Withdrawal from Dialysis: Clinical Practice Guideline. 2nd ed. Rockville, MD: Renal Physicians Association; Oct 2010:1-12.
18. Kurella Tamura M, Covinsky KE, Chertow GM, et al. Functional status of elderly adults before and after initiation of dialysis. N Engl J Med. 2009;361(16):1539-1547.
19. Chandna SM, Da Silva-Gane M, Marshall C, et al. Survival of elderly patients with stage 5 CKD: comparison of conservative management and renal replacement therapy. Nephrol Dial Transplant. 2011;26(5):1608-1614.
20. Smith C, Da Silva-Gane M, Chandna S, Warwicker P, Greenwood R, Farrington K. Choosing not to dialyse: evaluation of planned non-dialytic management in a cohort of patients with end-stage renal failure. Nephron Clin Pract. 2003;95:c40-c46.
21. Lamping DL, Constantinovici N, Roderick P, et al. Clinical outcomes, quality of life, and costs in the North Thames Dialysis Study of elderly people on dialysis: a prospective cohort study. Lancet. 2000;356:1543-1550.
22. O’Connor NR, Kumar P. Conservative management of end-stage renal disease without dialysis: a systematic review. J Palliat Med. 2012; 15(2):228-235.
23. Jassal SV, Trpeski L, Zhu N, et al. Changes in survival among elderly patients initiating dialysis from 1990 to 1999. CMAJ. 2007;177(9):?1033-1038.
24. Schmidt RJ. Informing our elders about dialysis: is an age-attuned approach warranted? Clin J Am Soc Nephrol. 2012;7(1):185-191.
25. Holley JL. Providing optimal care before and after discontinuation. Semin Dial. 2012;25(1):?33-34.
26. Eknoyan G, Beck GJ, Cheung AK, et al; Hemodialysis (HEMO) Study Group. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med. 2002;347(25):?2010-2019.
27. Lacson E, Lazarus M. Dialysis time: does it matter? A reappraisal of existing literature. Curr Opin Nephrol Hypertens. 2011;20(2):189-194.
28. Chertow GM, Levin NW, Beck GJ, et al; FHN Trial Group. In-center hemodialysis six times per week versus three times per week. N Engl J Med. 2010;363(24):22878-2300.
29. Lacson E Jr, Xu J, Suri RS, et al. Survival with three-times weekly in-center nocturnal versus conventional hemodialysis. J Am Soc Nephrol. 2012;23(4):687-695.
30. Suri RS, Lindsay RM, Bieber BA, et al. A multinational cohort study of in-center daily hemodialysis and patient survival. Kidney Int. 2012 Sep 12. [Epub ahead of print]
31. Sidawy AN, Spergel LM, Besarab A, et al; Society for Vascular Surgery. Clinical practice guidelines for the surgical placement and maintenance of arteriovenous hemodialysis access. ?J Vasc Surg. 2008;48(5 Suppl):2S-25S.
32. Heaf JG. Algorithm for optimal dialysis access timing. Clin Nephrol. 2007;67(2):96-104.
33. Nassar GM, Ayus JC. Infectious complications of the hemodialysis access. Kidney Int. 2001;60(1):1-13.
34. National Kidney Foundation. Peritoneal dialysis: what you need to know (2006;11-50-0215). www.kidney.org/atoz/pdf/PeritonealDialysis.pdf. Accessed September 24, 2012.
35. Davison SN, Ghangri GS, Jindal K, Pannu N. Comparison of volume overload with cycler-assisted versus continuous ambulatory peritoneal dialysis. Clin J Am Soc Nephrol. 2009;4(6):1044-1050.
36. Juergensen P, Eras J, McClure B, et al. The impact of various cycling regimens on phosphorus removal in chronic peritoneal dialysis patients. Int J Artif Organs. 2005;28(12):1219-1223.
37. Vonesh EF, Snyder JJ, Foley RN, Collins AJ. Mortality studies comparing peritoneal dialysis and hemodialysis: what do they tell us? Kidney Int Suppl. 2006 Nov;(103):S3-S11.
38. Heaf J, Løkkegaard H, Madsen M. Initial survival advantage of peritoneal dialysis relative to haemodialysis. Nephrol Dial Transplant. 2002;17(1):112-117.
39. Wang AY, Lai KN. The importance of residual renal function in dialysis patients. Kidney Int. 2006;69(10):1726-1732.
40. Cnossen N, Kooman JP, Konings CJ, et al. Peritoneal dialysis in patients with congestive heart failure. Nephrol Dial Transplant. 2006;21 suppl 2: ii63-ii66.
The Initiating Dialysis Early and Late (IDEAL) study in Australia and New Zealand1 examined the optimal time to initiate dialysis. This well-designed, randomized, controlled trial gave the nephrology community guidelines for treating patients as they progress through chronic kidney disease to stage 5 (CKD 5). The IDEAL investigators demonstrated that planned early initiation of dialysis did not enhance survival—and in some cases, it hastened death.1
Although most patients have a nephrology provider by the time they reach CKD 5 (ie, kidney failure), primary care providers can be instrumental in preparing the patient for what lies ahead as kidney failure progresses. Presented here is an overview of diagnosis and management of the patient with CKD 5 in the 21st century.
CASE PRESENTATION
A 70-year-old woman with an extensive history of diabetes and hypertension presents to her primary care clinician complaining of a lack of energy. She has just returned from a trip to Disney World, where she says she was unable to keep up with her grandchildren. She sat in the shade while they enjoyed Space Mountain and other attractions, and because of uncustomary fatigue, she required a nap every afternoon.
Physical examination shows an elderly female in no acute distress. Cardiac exam shows a regular heart rate and rhythm, the patient’s lungs are clear, and she has 1+ pitting leg edema bilaterally. The patient’s blood pressure is slightly elevated at 142/92 mm Hg, and no protein is detected on spot urine testing.
Blood work is ordered, including a complete blood count, a comprehensive metabolic panel, and an A1C. Results include a hemoglobin level of 8.7 g/dL (reference range for women, 12.0 to 16.0 g/dL), a serum creatinine level (SCr) of 3 mg/dL (range, 0.6 to 1.2 mg/dL; estimated glomerular filtration rate [eGFR], 15 mL/min/1.73 m2), and an A1C value of 7.5% (normal, & < 7%).
The patient is told that she is in kidney failure and is referred immediately to a nephrology practice, where she is seen the following day. After her appointment, she returns to the primary care office. When she is asked when she will be starting dialysis, she seems surprised, saying, “They told me I was doing well. I need some shots for my blood, but they didn’t seem worried at all.”
Is this patient being managed correctly by the nephrology practitioner?
EPIDEMIOLOGY
Presently, more than 1 million persons in the United States have CKD 5, and 500,000 are undergoing dialysis. The number of patients with CDK 5 who are on dialysis has doubled since 1994 and is projected to reach 774,000 by 20202,3 (see Figure 13 and Figure 23).
CKD 5 is defined as an eGFR below 15 mL/min/1.73 m2, according to the Modification of Diet in Renal Disease (MDRD) study group formula; or as a creatinine clearance of less than 15 mL/min, using the Cockcroft-Gault formula.4-6 Both formulas have limitations, since they are not fully accurate at extremes of age, with variations in weight, for some racial mixes, or for the very malnourished patient.7,8 However, they do correct for normal age-related loss of kidney function, gender, and SCr, and they are currently the generally accepted formulas.4
A rise in SCr is exponential; for each doubling of the SCr, a reduction in kidney function of approximately 50% occurs. This means that a rise in SCr from 4 to 8 mg/dL is equivalent (in the proportion of loss of kidney function) to a rise of SCr from 0.5 to 1 mg/dL. Commonly, patients are not referred to nephrology until the SCr doubles to 4 or 6 mg/dL—whereas the rise in SCr from 0.5 to 1 mg/dL should be of greatest concern to the primary care provider, prompting a referral.9 Early recognition of reduced renal function allows for identification of potentially reversible etiologies and the slowing of CKD progression.
INDICATIONS FOR RENAL REPLACEMENT THERAPY
Not all patients with an eGFR below 15 mL/min/1.73 m2 are started on dialysis immediately. The decision to initiate dialysis is guided by assessment of a constellation of uremic manifestations—not eGFR alone. Newer data suggest that early initiation of dialysis may be associated with increased mortality.10-15
The IDEAL study,1 a well-designed, randomized, controlled trial of all patients who started dialysis in Australia and New Zealand over a multiyear period, was designed to determine the optimal time to initiate dialysis. Patients were randomized to start dialysis (hemodialysis or peritoneal dialysis) at an eGFR between 10 and 14 mL/min/1.73 m2 or between 5 and 7 mL/min/1.73 m2. While there was some overlap and some patients were started on dialysis outside their randomized eGFR (eg, earlier than the allotted time because symptoms developed), what the IDEAL investigators found surprised the entire nephrology community: Early dialysis starts did not enhance survival and, in some cases, it hastened death.1
The indications for initiation of dialysis often develop long after the patient has progressed within CKD 5, commonly with an eGFR of 10 mL/min/1.73 m2 or less. Medicare has acknowledged this by reimbursing dialysis only in eligible patients whose eGFR is below 10 mL/min/1.73 m2.16 There are also acute indications for initiation of dialysis, such as uremic pericarditis, hyperkalemia, bleeding related to uremic platelet dysfunction, and metabolic encephalopathy related to uremia (and reimbursement for dialysis can be justified), but these are uncommon.
RENAL REPLACEMENT THERAPY CHOICES
The choices of treatment for kidney failure (note: treatment, not cure) are medical management, hemodialysis, peritoneal dialysis, and transplant. Each choice has its advantages and disadvantages, and all patients should receive clear explanations of what they can expect from each modality.
While younger, higher-functioning individuals are likely to benefit from dialysis, patients with extensive comorbid illnesses and/or low functional status tend to respond poorly17; medical management may be the best choice for these patients. In one recent study, the functional status of residents in skilled nursing homes was examined, before and after initiation of dialysis. At one year, 58% of the nursing home residents who underwent dialysis had died, and only 13% had maintained their pre-dialysis functional status.18
Another research team recently compared conservative management of CKD 5 (ie, medical therapy without dialysis) with dialysis in elderly patients. For patients 75 and older with extensive comorbid illness, the researchers found no statistically significant survival benefit to dialysis.19
Dialysis, whether administered as hemodialysis or peritoneal dialysis, is a rigorous, intensive medical therapy. Dialysis does not necessarily prolong life in patients with extensive comorbidities, and it does not always enhance quality of life.18,20-23 The decision to undergo dialysis is personal and individual, and both the patient and family should be actively involved in making it. Primary care providers should be the nephrologist’s ally in the discussion of therapy for renal failure; often, they have cared for the patient for years, and they understand the patient and family dynamics.
An important message the nephrology practitioner must communicate is that choosing medical management without dialysis is not withholding care; sometimes it is a more humane choice.24 Dying of kidney failure can be a peaceful and comfortable death: As the uremic toxins build up (with eGFR ≤ 2 mL/min/1.73 m2, although this can take many years), the patient becomes confused and slowly slips into a sleepiness that leads to death.25 Hospice is usually involved to support the patient and family.
Hemodialysis
Hemodialysis is the most common, best-known treatment modality for CKD in the US, with about 94% of patients choosing it.3 In this process, blood is removed from the body (approximately 500 cc at a time) and filtered through a semipermeable membrane that removes uremic toxins and excess fluid, normalizing the metabolic and electrolyte derangements. The filtered blood is then returned to the patient.
The average dialysis session is four hours long and is conducted three times per week, following recommendations from the 2002 Hemodialysis Study (HEMO).26 Most patients come to a free-standing dialysis center on a Monday/Wednesday/Friday or a Tuesday/Thursday/Saturday schedule.
In theory, there is no such thing as too much dialysis (since the kidneys work 24 hours per day, seven days per week); thus, researchers have recently examined lengthening dialysis in an attempt to extend survival.27-29 According to study results, patients who undergo longer dialysis times generally enjoy better nutrition with a more liberal diet, require fewer medications, have reduced incidence of increased left ventricular mass (a marker for coronary artery disease), and report better quality of life, all in addition to a survival benefit; however, the latter was not considered statistically significant in any of the studies.27-29 Additionally, this survival benefit may not extend to daily hemodialysis; in a recent publication, daily hemodialysis was associated with a 60% higher death rate.30
A number of dialysis units have begun to offer nocturnal dialysis. In this option, patients sleep at the unit for eight hours, three nights per week, for a total of 24 hours of dialysis (vs the typical 12 hours per week). Some patients receive dialysis at home, allowing them to dialyze for six weekly sessions of two to three hours. This strategy attempts to mimic a more “natural” state.
One of the primary challenges associated with hemodialysis is establishing and maintaining a vascular access. An arteriovenous (AV) fistula is the access of choice because its use reduces the likelihood of clotting, improves access survival, and increases clearances during dialysis.31 However, the AV fistula is most effective if it is placed a minimum of six months before use.32
For many patients, an AV fistula is created surgically when the eGFR falls to 15 mL/min/1.73 m2. Fistula placement in preparation for the initiation of hemodialysis is important to reduce the need for hemodialysis catheters, which are associated with higher risk for infection and poorer outcomes.33
Peritoneal Dialysis
Peritoneal dialysis (PD) filters out uremic toxins and normalizes the metabolic and electrolyte derangements by using the patient’s peritoneal membrane as a filter. Dialysate is instilled through a catheter into the peritoneal cavity where it is allowed to dwell, often for four to six hours (see Figure 334). Exchanges can be performed three to four times per day (allowing six to eight hours of dwell time per exchange for the dialysate), or by way of a cycler at night.35,36
Performing exchanges by way of a cycler requires the patient to be connected via the PD catheter for eight hours; thus the advantage of performing the exchange during sleep. The cycler has a soft, whooshing sound that many patients describe as “white noise” that does not disturb their sleep.
The principal advantage of peritoneal dialysis is extended survival of the patient.37-39 PD also allows the patient a more liberal diet. Although PD must be performed every day, exchanges can be adjusted to the patient’s timing preference. PD reduces cost and time, since the patient need not travel to a dialysis center. PD also preserves residual renal function,39 which is associated with a survival benefit and contributes to the patient’s overall health and well-being. The use of PD requires a committed, competent patient in a clean home environment.
This intervention may not be suitable for patients with a history of abdominal surgeries. However, as a therapy considered gentler than hemodialysis, PD is an excellent choice for the patient with congestive heart failure.40 The PD catheter is not placed until two to four weeks before it will be needed.41
Kidney Transplantation
Last, but certainly not least, is transplant. As entire books have been written on this modality, only the highlights will be addressed here.42 Survival rates following transplantation are reported to exceed those associated with any other treatment modality, even when controlling for comorbidities and patient selection bias.43 A patient can receive a kidney from either a living or a deceased donor. Apart from the perioperative risks associated with transplantation surgery, long-term surgical or medical problems are not common for the living kidney donor.44-46
Since 2002, as a result of a policy change from the United Network for Organ Sharing (UNOS),47 the donor pool has been expanded by including kidneys from what are commonly referred to as extended criteria donors: those who are older than 60, or who are 50 to 59 and have two of the following factors: cerebrovascular accident as the cause of death; preexisting hypertension; or an SCr level exceeding 1.5 mg/dL. These kidneys may be given to any recipients but are primarily used for those age 50 or older.47
Graft survival is statistically shorter in a cadaver kidney than in a living donor kidney.48 However, the larger problem is the long wait time for a cadaver transplant—seven to eight years (or possibly longer) for some centers and some blood types.49 A patient can be referred to a transplant center when the eGFR falls below 25 mL/min/1.73 m2; he or she will then be actively listed for transplant when eGFR reaches 20 mL/min/1.73 m2 or lower.
Early referral for transplant listing buys the patient time before dialysis becomes essential. Patients can receive preemptive transplants (ie, transplantation before dialysis is initiated); these are becoming increasingly popular because they generally extend survival for the recipient.50,51
UNOS (www.unos.org) has set few limits on transplant recipients: patients are required to undergo an extensive medical work-up, but there are no upper age limits (although some centers do set their own) and usually no limits on patients infected with HIV, hepatitis B, or hepatitis C (although there may be separate listing requirements). Patients who are not US citizens are not denied.
Because more than 100,000 patients are currently on the wait list, domino kidney transplants are now being offered at many centers.52-54 These organ exchanges involve altruistic donors who do not match their targeted kidney recipients. Since publication of the first article describing this procedure at Johns Hopkins Medical Center,53 there have been two-way, three-way, and up to 32-way domino transplants. However, patients wishing to engage in this type of trade require a donor; not every patient has access to an altruistic donor.
CKD PATIENT EDUCATION
When Congress passed the Medicare Improvements for Patients and Providers Act of 2008,55 a component little noted outside the nephrology community was the offer of kidney disease education (KDE) classes to Medicare-eligible patients with CKD 4.56-58 Medicare patients with an eGFR of 15 to 30 mL/min/1.73 m2 are eligible to attend KDE classes presented by a physician, an NP, a PA, or a clinical nurse specialist. Medicare will reimburse for six hours of education.
This groundbreaking educational benefit, the first such program paid for by Medicare, was championed by the National Kidney Foundation and other nephrology groups. Many nephrology practices now offer these classes to all their CKD patients, regardless of health insurance status. Instructors educate patients on the choices of renal replacement therapy and help patients select their best option.
KDE classes can be conducted in the office setting or at the patient’s home, and they can be billed on the same day as an evaluation and management (E/M) visit.56,57 This may help explain why, in 2010, gerontologists billed for more home KDE classes than did nephrologists.58
FUTURE TRENDS AND ONGOING TRIALS
The overarching goal of therapy for CKD patients is to diagnose accurately and treat effectively in order to slow or prevent progression to end-stage renal disease (ESRD). Following is a brief review of a selection of new diagnostic tools and therapeutic interventions that may impact the management of CKD in the coming years.
The QxMD Kidney Failure Risk Equation is a newly developed, well-validated predictive model that offers relatively accurate prediction of a patient’s likelihood of progression to ESRD, based on age, sex, eGFR, and levels of albuminuria, SCr, serum phosphorus, serum bicarbonate, and serum albumin59 (see table59). This tool can be accessed online at www.qxmd.com/calculate-online/nephrology/kidney-failure-risk-equation.
Increased awareness of the role that phosphorus plays in the development of vascular calcifications has led to an emphasis on earlier, more aggressive control of dietary phosphorus. Historically, dietary phosphorus control and phosphorus binders were recommended only when the patient’s serum phosphorus exceeded normal limits. Dietary phosphorus control may now be advised as early as CKD 3, based on the understanding that phosphorus is a key component in driving the development of vascular calcifications—which in turn contribute to the high incidence of cardiovascular disease in patients with CKD.60
Bardoxolone is a new medication developed for treatment of diabetic nephropathy.61,62 It works by inhibiting proinflammatory mediators and moderating the effects of oxidative stress, thus interrupting the cascade of inflammation and cellular injury that result in diabetic nephropathy.62 Early clinical trials examining this agent have shown promise in terms of raising eGFR and reducing serum creatinine, but tolerability and toxicity profiles have been an issue.61 Additionally, some reduction in serum creatinine may have been attributable to weight loss as opposed to true improvement of renal function.62
Data have recently been released regarding the use of the herb silymarin for treatment of patients with macroalbuminuria related to diabetic nephropathy. Results from a small (n = 60), randomized, nonblinded clinical trial by Fallahzadeh et al63 indicate that silymarin decreases proteinuria when used in combination with an ACE inhibitor or an angiotensin receptor blocker (ARB). Silymarin, an extract from milk thistle, has been used medicinally for centuries for its antioxidant, anti-inflammatory, and antiviral properties in those with liver “ailments.” In this clinical trial, silymarin was well tolerated and associated with a reduction in pro-inflammatory markers.63
AST-120 is another agent intended to slow progression of CKD. It promotes intestinal adsorption and fecal excretion of the uremic toxin indoxyl sulfate.64 A recently published study demonstrated an association between use of AST-120 and a delay in required initiation of hemodialysis, but no survival benefit.65 This was a nonrandomized trial, and previous research showed no effect of AST-120 on progression of CKD.66 However, patients close to requiring dialysis are likely to welcome a means to delay it.
A growing body of evidence suggests that reversal of CKD-associated acidemia by administering sodium bicarbonate may actually forestall progression of CKD.67 However, treatment with sodium bicarbonate can lead to complications of hypertension and fluid volume overload. In one study, patients at risk for these complications derived equivalent benefit by increasing dietary fruit and vegetable intake to reduce renal acid load.68 However, providers must be mindful of patients’ serum potassium levels, especially patients who are taking an ACE inhibitor or an ARB.
The Provider’s Current Role
Despite the hope offered by new and novel therapies, the mainstay of treatment for CKD continues to be aggressive management of diabetes, hypertension, and the cardiovascular risk profile. As a result of vigorous preventive strategies to address the cardiovascular risks inherent in this patient population, the patient with type 2 diabetes is now more likely to progress to ESRD than to die of a cardiovascular event.69
The well-informed clinician can be instrumental in providing evidence-based medical therapy and excellent patient education from the time of initial CKD diagnosis through CKD 5.
PATIENT OUTCOME
The case patient was started on injections of epoietin alfa for her anemia. She attended KDE classes led by an advanced practitioner in her nephrology group and decided to undergo peritoneal dialysis, since it would allow her to maintain her travel schedule. When last heard from, the patient was preparing for a trip to see the Great Barrier Reef in Australia.
CONCLUSION
The decision to begin renal replacement therapy—whether a form of dialysis, or another management option—depends not on SCr or eGFR alone. Rather, a number of uremic manifestations, comorbidities, lifestyle factors, and other variables must be carefully weighed before the patient, the family, and the clinicians involved can decide on the management plan most likely to enhance the patient’s quality of life and extend survival.
The Initiating Dialysis Early and Late (IDEAL) study in Australia and New Zealand1 examined the optimal time to initiate dialysis. This well-designed, randomized, controlled trial gave the nephrology community guidelines for treating patients as they progress through chronic kidney disease to stage 5 (CKD 5). The IDEAL investigators demonstrated that planned early initiation of dialysis did not enhance survival—and in some cases, it hastened death.1
Although most patients have a nephrology provider by the time they reach CKD 5 (ie, kidney failure), primary care providers can be instrumental in preparing the patient for what lies ahead as kidney failure progresses. Presented here is an overview of diagnosis and management of the patient with CKD 5 in the 21st century.
CASE PRESENTATION
A 70-year-old woman with an extensive history of diabetes and hypertension presents to her primary care clinician complaining of a lack of energy. She has just returned from a trip to Disney World, where she says she was unable to keep up with her grandchildren. She sat in the shade while they enjoyed Space Mountain and other attractions, and because of uncustomary fatigue, she required a nap every afternoon.
Physical examination shows an elderly female in no acute distress. Cardiac exam shows a regular heart rate and rhythm, the patient’s lungs are clear, and she has 1+ pitting leg edema bilaterally. The patient’s blood pressure is slightly elevated at 142/92 mm Hg, and no protein is detected on spot urine testing.
Blood work is ordered, including a complete blood count, a comprehensive metabolic panel, and an A1C. Results include a hemoglobin level of 8.7 g/dL (reference range for women, 12.0 to 16.0 g/dL), a serum creatinine level (SCr) of 3 mg/dL (range, 0.6 to 1.2 mg/dL; estimated glomerular filtration rate [eGFR], 15 mL/min/1.73 m2), and an A1C value of 7.5% (normal, & < 7%).
The patient is told that she is in kidney failure and is referred immediately to a nephrology practice, where she is seen the following day. After her appointment, she returns to the primary care office. When she is asked when she will be starting dialysis, she seems surprised, saying, “They told me I was doing well. I need some shots for my blood, but they didn’t seem worried at all.”
Is this patient being managed correctly by the nephrology practitioner?
EPIDEMIOLOGY
Presently, more than 1 million persons in the United States have CKD 5, and 500,000 are undergoing dialysis. The number of patients with CDK 5 who are on dialysis has doubled since 1994 and is projected to reach 774,000 by 20202,3 (see Figure 13 and Figure 23).
CKD 5 is defined as an eGFR below 15 mL/min/1.73 m2, according to the Modification of Diet in Renal Disease (MDRD) study group formula; or as a creatinine clearance of less than 15 mL/min, using the Cockcroft-Gault formula.4-6 Both formulas have limitations, since they are not fully accurate at extremes of age, with variations in weight, for some racial mixes, or for the very malnourished patient.7,8 However, they do correct for normal age-related loss of kidney function, gender, and SCr, and they are currently the generally accepted formulas.4
A rise in SCr is exponential; for each doubling of the SCr, a reduction in kidney function of approximately 50% occurs. This means that a rise in SCr from 4 to 8 mg/dL is equivalent (in the proportion of loss of kidney function) to a rise of SCr from 0.5 to 1 mg/dL. Commonly, patients are not referred to nephrology until the SCr doubles to 4 or 6 mg/dL—whereas the rise in SCr from 0.5 to 1 mg/dL should be of greatest concern to the primary care provider, prompting a referral.9 Early recognition of reduced renal function allows for identification of potentially reversible etiologies and the slowing of CKD progression.
INDICATIONS FOR RENAL REPLACEMENT THERAPY
Not all patients with an eGFR below 15 mL/min/1.73 m2 are started on dialysis immediately. The decision to initiate dialysis is guided by assessment of a constellation of uremic manifestations—not eGFR alone. Newer data suggest that early initiation of dialysis may be associated with increased mortality.10-15
The IDEAL study,1 a well-designed, randomized, controlled trial of all patients who started dialysis in Australia and New Zealand over a multiyear period, was designed to determine the optimal time to initiate dialysis. Patients were randomized to start dialysis (hemodialysis or peritoneal dialysis) at an eGFR between 10 and 14 mL/min/1.73 m2 or between 5 and 7 mL/min/1.73 m2. While there was some overlap and some patients were started on dialysis outside their randomized eGFR (eg, earlier than the allotted time because symptoms developed), what the IDEAL investigators found surprised the entire nephrology community: Early dialysis starts did not enhance survival and, in some cases, it hastened death.1
The indications for initiation of dialysis often develop long after the patient has progressed within CKD 5, commonly with an eGFR of 10 mL/min/1.73 m2 or less. Medicare has acknowledged this by reimbursing dialysis only in eligible patients whose eGFR is below 10 mL/min/1.73 m2.16 There are also acute indications for initiation of dialysis, such as uremic pericarditis, hyperkalemia, bleeding related to uremic platelet dysfunction, and metabolic encephalopathy related to uremia (and reimbursement for dialysis can be justified), but these are uncommon.
RENAL REPLACEMENT THERAPY CHOICES
The choices of treatment for kidney failure (note: treatment, not cure) are medical management, hemodialysis, peritoneal dialysis, and transplant. Each choice has its advantages and disadvantages, and all patients should receive clear explanations of what they can expect from each modality.
While younger, higher-functioning individuals are likely to benefit from dialysis, patients with extensive comorbid illnesses and/or low functional status tend to respond poorly17; medical management may be the best choice for these patients. In one recent study, the functional status of residents in skilled nursing homes was examined, before and after initiation of dialysis. At one year, 58% of the nursing home residents who underwent dialysis had died, and only 13% had maintained their pre-dialysis functional status.18
Another research team recently compared conservative management of CKD 5 (ie, medical therapy without dialysis) with dialysis in elderly patients. For patients 75 and older with extensive comorbid illness, the researchers found no statistically significant survival benefit to dialysis.19
Dialysis, whether administered as hemodialysis or peritoneal dialysis, is a rigorous, intensive medical therapy. Dialysis does not necessarily prolong life in patients with extensive comorbidities, and it does not always enhance quality of life.18,20-23 The decision to undergo dialysis is personal and individual, and both the patient and family should be actively involved in making it. Primary care providers should be the nephrologist’s ally in the discussion of therapy for renal failure; often, they have cared for the patient for years, and they understand the patient and family dynamics.
An important message the nephrology practitioner must communicate is that choosing medical management without dialysis is not withholding care; sometimes it is a more humane choice.24 Dying of kidney failure can be a peaceful and comfortable death: As the uremic toxins build up (with eGFR ≤ 2 mL/min/1.73 m2, although this can take many years), the patient becomes confused and slowly slips into a sleepiness that leads to death.25 Hospice is usually involved to support the patient and family.
Hemodialysis
Hemodialysis is the most common, best-known treatment modality for CKD in the US, with about 94% of patients choosing it.3 In this process, blood is removed from the body (approximately 500 cc at a time) and filtered through a semipermeable membrane that removes uremic toxins and excess fluid, normalizing the metabolic and electrolyte derangements. The filtered blood is then returned to the patient.
The average dialysis session is four hours long and is conducted three times per week, following recommendations from the 2002 Hemodialysis Study (HEMO).26 Most patients come to a free-standing dialysis center on a Monday/Wednesday/Friday or a Tuesday/Thursday/Saturday schedule.
In theory, there is no such thing as too much dialysis (since the kidneys work 24 hours per day, seven days per week); thus, researchers have recently examined lengthening dialysis in an attempt to extend survival.27-29 According to study results, patients who undergo longer dialysis times generally enjoy better nutrition with a more liberal diet, require fewer medications, have reduced incidence of increased left ventricular mass (a marker for coronary artery disease), and report better quality of life, all in addition to a survival benefit; however, the latter was not considered statistically significant in any of the studies.27-29 Additionally, this survival benefit may not extend to daily hemodialysis; in a recent publication, daily hemodialysis was associated with a 60% higher death rate.30
A number of dialysis units have begun to offer nocturnal dialysis. In this option, patients sleep at the unit for eight hours, three nights per week, for a total of 24 hours of dialysis (vs the typical 12 hours per week). Some patients receive dialysis at home, allowing them to dialyze for six weekly sessions of two to three hours. This strategy attempts to mimic a more “natural” state.
One of the primary challenges associated with hemodialysis is establishing and maintaining a vascular access. An arteriovenous (AV) fistula is the access of choice because its use reduces the likelihood of clotting, improves access survival, and increases clearances during dialysis.31 However, the AV fistula is most effective if it is placed a minimum of six months before use.32
For many patients, an AV fistula is created surgically when the eGFR falls to 15 mL/min/1.73 m2. Fistula placement in preparation for the initiation of hemodialysis is important to reduce the need for hemodialysis catheters, which are associated with higher risk for infection and poorer outcomes.33
Peritoneal Dialysis
Peritoneal dialysis (PD) filters out uremic toxins and normalizes the metabolic and electrolyte derangements by using the patient’s peritoneal membrane as a filter. Dialysate is instilled through a catheter into the peritoneal cavity where it is allowed to dwell, often for four to six hours (see Figure 334). Exchanges can be performed three to four times per day (allowing six to eight hours of dwell time per exchange for the dialysate), or by way of a cycler at night.35,36
Performing exchanges by way of a cycler requires the patient to be connected via the PD catheter for eight hours; thus the advantage of performing the exchange during sleep. The cycler has a soft, whooshing sound that many patients describe as “white noise” that does not disturb their sleep.
The principal advantage of peritoneal dialysis is extended survival of the patient.37-39 PD also allows the patient a more liberal diet. Although PD must be performed every day, exchanges can be adjusted to the patient’s timing preference. PD reduces cost and time, since the patient need not travel to a dialysis center. PD also preserves residual renal function,39 which is associated with a survival benefit and contributes to the patient’s overall health and well-being. The use of PD requires a committed, competent patient in a clean home environment.
This intervention may not be suitable for patients with a history of abdominal surgeries. However, as a therapy considered gentler than hemodialysis, PD is an excellent choice for the patient with congestive heart failure.40 The PD catheter is not placed until two to four weeks before it will be needed.41
Kidney Transplantation
Last, but certainly not least, is transplant. As entire books have been written on this modality, only the highlights will be addressed here.42 Survival rates following transplantation are reported to exceed those associated with any other treatment modality, even when controlling for comorbidities and patient selection bias.43 A patient can receive a kidney from either a living or a deceased donor. Apart from the perioperative risks associated with transplantation surgery, long-term surgical or medical problems are not common for the living kidney donor.44-46
Since 2002, as a result of a policy change from the United Network for Organ Sharing (UNOS),47 the donor pool has been expanded by including kidneys from what are commonly referred to as extended criteria donors: those who are older than 60, or who are 50 to 59 and have two of the following factors: cerebrovascular accident as the cause of death; preexisting hypertension; or an SCr level exceeding 1.5 mg/dL. These kidneys may be given to any recipients but are primarily used for those age 50 or older.47
Graft survival is statistically shorter in a cadaver kidney than in a living donor kidney.48 However, the larger problem is the long wait time for a cadaver transplant—seven to eight years (or possibly longer) for some centers and some blood types.49 A patient can be referred to a transplant center when the eGFR falls below 25 mL/min/1.73 m2; he or she will then be actively listed for transplant when eGFR reaches 20 mL/min/1.73 m2 or lower.
Early referral for transplant listing buys the patient time before dialysis becomes essential. Patients can receive preemptive transplants (ie, transplantation before dialysis is initiated); these are becoming increasingly popular because they generally extend survival for the recipient.50,51
UNOS (www.unos.org) has set few limits on transplant recipients: patients are required to undergo an extensive medical work-up, but there are no upper age limits (although some centers do set their own) and usually no limits on patients infected with HIV, hepatitis B, or hepatitis C (although there may be separate listing requirements). Patients who are not US citizens are not denied.
Because more than 100,000 patients are currently on the wait list, domino kidney transplants are now being offered at many centers.52-54 These organ exchanges involve altruistic donors who do not match their targeted kidney recipients. Since publication of the first article describing this procedure at Johns Hopkins Medical Center,53 there have been two-way, three-way, and up to 32-way domino transplants. However, patients wishing to engage in this type of trade require a donor; not every patient has access to an altruistic donor.
CKD PATIENT EDUCATION
When Congress passed the Medicare Improvements for Patients and Providers Act of 2008,55 a component little noted outside the nephrology community was the offer of kidney disease education (KDE) classes to Medicare-eligible patients with CKD 4.56-58 Medicare patients with an eGFR of 15 to 30 mL/min/1.73 m2 are eligible to attend KDE classes presented by a physician, an NP, a PA, or a clinical nurse specialist. Medicare will reimburse for six hours of education.
This groundbreaking educational benefit, the first such program paid for by Medicare, was championed by the National Kidney Foundation and other nephrology groups. Many nephrology practices now offer these classes to all their CKD patients, regardless of health insurance status. Instructors educate patients on the choices of renal replacement therapy and help patients select their best option.
KDE classes can be conducted in the office setting or at the patient’s home, and they can be billed on the same day as an evaluation and management (E/M) visit.56,57 This may help explain why, in 2010, gerontologists billed for more home KDE classes than did nephrologists.58
FUTURE TRENDS AND ONGOING TRIALS
The overarching goal of therapy for CKD patients is to diagnose accurately and treat effectively in order to slow or prevent progression to end-stage renal disease (ESRD). Following is a brief review of a selection of new diagnostic tools and therapeutic interventions that may impact the management of CKD in the coming years.
The QxMD Kidney Failure Risk Equation is a newly developed, well-validated predictive model that offers relatively accurate prediction of a patient’s likelihood of progression to ESRD, based on age, sex, eGFR, and levels of albuminuria, SCr, serum phosphorus, serum bicarbonate, and serum albumin59 (see table59). This tool can be accessed online at www.qxmd.com/calculate-online/nephrology/kidney-failure-risk-equation.
Increased awareness of the role that phosphorus plays in the development of vascular calcifications has led to an emphasis on earlier, more aggressive control of dietary phosphorus. Historically, dietary phosphorus control and phosphorus binders were recommended only when the patient’s serum phosphorus exceeded normal limits. Dietary phosphorus control may now be advised as early as CKD 3, based on the understanding that phosphorus is a key component in driving the development of vascular calcifications—which in turn contribute to the high incidence of cardiovascular disease in patients with CKD.60
Bardoxolone is a new medication developed for treatment of diabetic nephropathy.61,62 It works by inhibiting proinflammatory mediators and moderating the effects of oxidative stress, thus interrupting the cascade of inflammation and cellular injury that result in diabetic nephropathy.62 Early clinical trials examining this agent have shown promise in terms of raising eGFR and reducing serum creatinine, but tolerability and toxicity profiles have been an issue.61 Additionally, some reduction in serum creatinine may have been attributable to weight loss as opposed to true improvement of renal function.62
Data have recently been released regarding the use of the herb silymarin for treatment of patients with macroalbuminuria related to diabetic nephropathy. Results from a small (n = 60), randomized, nonblinded clinical trial by Fallahzadeh et al63 indicate that silymarin decreases proteinuria when used in combination with an ACE inhibitor or an angiotensin receptor blocker (ARB). Silymarin, an extract from milk thistle, has been used medicinally for centuries for its antioxidant, anti-inflammatory, and antiviral properties in those with liver “ailments.” In this clinical trial, silymarin was well tolerated and associated with a reduction in pro-inflammatory markers.63
AST-120 is another agent intended to slow progression of CKD. It promotes intestinal adsorption and fecal excretion of the uremic toxin indoxyl sulfate.64 A recently published study demonstrated an association between use of AST-120 and a delay in required initiation of hemodialysis, but no survival benefit.65 This was a nonrandomized trial, and previous research showed no effect of AST-120 on progression of CKD.66 However, patients close to requiring dialysis are likely to welcome a means to delay it.
A growing body of evidence suggests that reversal of CKD-associated acidemia by administering sodium bicarbonate may actually forestall progression of CKD.67 However, treatment with sodium bicarbonate can lead to complications of hypertension and fluid volume overload. In one study, patients at risk for these complications derived equivalent benefit by increasing dietary fruit and vegetable intake to reduce renal acid load.68 However, providers must be mindful of patients’ serum potassium levels, especially patients who are taking an ACE inhibitor or an ARB.
The Provider’s Current Role
Despite the hope offered by new and novel therapies, the mainstay of treatment for CKD continues to be aggressive management of diabetes, hypertension, and the cardiovascular risk profile. As a result of vigorous preventive strategies to address the cardiovascular risks inherent in this patient population, the patient with type 2 diabetes is now more likely to progress to ESRD than to die of a cardiovascular event.69
The well-informed clinician can be instrumental in providing evidence-based medical therapy and excellent patient education from the time of initial CKD diagnosis through CKD 5.
PATIENT OUTCOME
The case patient was started on injections of epoietin alfa for her anemia. She attended KDE classes led by an advanced practitioner in her nephrology group and decided to undergo peritoneal dialysis, since it would allow her to maintain her travel schedule. When last heard from, the patient was preparing for a trip to see the Great Barrier Reef in Australia.
CONCLUSION
The decision to begin renal replacement therapy—whether a form of dialysis, or another management option—depends not on SCr or eGFR alone. Rather, a number of uremic manifestations, comorbidities, lifestyle factors, and other variables must be carefully weighed before the patient, the family, and the clinicians involved can decide on the management plan most likely to enhance the patient’s quality of life and extend survival.
1. Cooper BA, Branley P, Bulfone L, et al; IDEAL Study. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010; 363(7):609-619.
2. Olan G. Policy Update: ASN to CDC: data collection of creatinine levels will advance research. ASN Kidney News. 2012;4(6):16. www.asn-online.org/publications/kidneynews/archives/2012/KN_jun2012.pdf. Accessed August 27, 2012.
3. US Renal Data System, National Institute of Diabetes and Digestive and Kidney Diseases, NIH. 2011 Atlas of CKD & ESRD. Vol 2. Chap 1: Incidence, prevalence, patient characteristics, and modalities. www.usrds.org/2011/pdf/v2_ch01_11.pdf. Accessed September 26, 2012.
4. National Kidney Foundation. Kidney Disease Outcomes Quality Initiative (KDOQI). Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. ?Part 4. Definition and classification of the stages of chronic kidney disease. 2002:43-80. www.kidney.org/professionals/kdoqi/pdf/ckd_evalua tion_classification_stratification.pdf. Accessed August 27, 2012.
5. Levey AS, Bosch JP, Lewis JB, et al; Modification of Diet in Renal Disease Study Group. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Internal Med. 1999;130 (6):461-470.
6. Froissart M, Rossert J, Jacquot C, et al. Predictive performance of the Modification of Diet in Renal Disease and Cockcroft-Gault equations for estimating renal function. J Am Soc Nephrol. 2005;16(3):763-773.
7. Jafar TH, Schmid CH, Levey AS. Serum creatinine as marker of kidney function in South Asians: a study of reduced GFR in adults in Pakistan. J Am Soc Nephrol. 2005;16(5):1413-1419.
8. Zuo L, Ma YC, Zhou YH, et al. Application of GFR-estimating equations in Chinese patients with chronic kidney disease. Am J Kidney Dis. 2005;45(3):463-472.
9. Stevens LA, Stoycheff N, Levey AS. Staging and management of chronic kidney disease. In: Greenberg A, ed. Primer of Kidney Diseases: Expert Consult. 5th ed. Philadelphia, PA: WB Saunders; 2009:436-445.
10. Clark WF, Na Y, Rosansky SJ, et al. Association between estimated glomerular filtration rate at initiation of dialysis and mortality. CMAJ. 2011;183(1):47-53.
11. Beddhu S, Samore MH, Roberts MS, et al. Impact of timing of initiation of dialysis on mortality. J Am Soc Nephrol. 2003;14(9):2305-2312.
12. Kazmi WH, Gilbertson DT, Obrador GT, et al. Effect of comorbidity on the increased mortality associated with early initiation of dialysis. Am J Kidney Dis. 2005;46(5):887-896.
13. Lassalle M, Labeeuw M, Frimat L, et al. Age and comorbidity may explain the paradoxical association of an early dialysis start with poor survival. Kidney Int. 2010;77(8):700-707.
14. Stel VS, Dekker FW, Ansell D, et al. Residual renal function at the start of dialysis and clinical outcomes. Nephrol Dial Transplant. 2009;24 (10):3175-3182.
15. Traynor JP, Simpson K, Geddes CC, et al. Early initiation of dialysis fails to prolong survival in patients with end-stage renal failure. J Am Soc Nephrol. 2002;13(8):2125-2132.
16. US Department of Health and Human Services, Centers for Medicare and Medicaid Services. CMS Form 2728. End-Stage Renal Disease Medical Evidence Report: Medicare Entitlement and/or Patient Registration. www.usrds.org/2008/rg/forms/02_2728_1965.pdf. Accessed September 25, 2012.
17. Renal Physicians Association. Shared Decision-Making in the Appropriate Initiation of and Withdrawal from Dialysis: Clinical Practice Guideline. 2nd ed. Rockville, MD: Renal Physicians Association; Oct 2010:1-12.
18. Kurella Tamura M, Covinsky KE, Chertow GM, et al. Functional status of elderly adults before and after initiation of dialysis. N Engl J Med. 2009;361(16):1539-1547.
19. Chandna SM, Da Silva-Gane M, Marshall C, et al. Survival of elderly patients with stage 5 CKD: comparison of conservative management and renal replacement therapy. Nephrol Dial Transplant. 2011;26(5):1608-1614.
20. Smith C, Da Silva-Gane M, Chandna S, Warwicker P, Greenwood R, Farrington K. Choosing not to dialyse: evaluation of planned non-dialytic management in a cohort of patients with end-stage renal failure. Nephron Clin Pract. 2003;95:c40-c46.
21. Lamping DL, Constantinovici N, Roderick P, et al. Clinical outcomes, quality of life, and costs in the North Thames Dialysis Study of elderly people on dialysis: a prospective cohort study. Lancet. 2000;356:1543-1550.
22. O’Connor NR, Kumar P. Conservative management of end-stage renal disease without dialysis: a systematic review. J Palliat Med. 2012; 15(2):228-235.
23. Jassal SV, Trpeski L, Zhu N, et al. Changes in survival among elderly patients initiating dialysis from 1990 to 1999. CMAJ. 2007;177(9):?1033-1038.
24. Schmidt RJ. Informing our elders about dialysis: is an age-attuned approach warranted? Clin J Am Soc Nephrol. 2012;7(1):185-191.
25. Holley JL. Providing optimal care before and after discontinuation. Semin Dial. 2012;25(1):?33-34.
26. Eknoyan G, Beck GJ, Cheung AK, et al; Hemodialysis (HEMO) Study Group. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med. 2002;347(25):?2010-2019.
27. Lacson E, Lazarus M. Dialysis time: does it matter? A reappraisal of existing literature. Curr Opin Nephrol Hypertens. 2011;20(2):189-194.
28. Chertow GM, Levin NW, Beck GJ, et al; FHN Trial Group. In-center hemodialysis six times per week versus three times per week. N Engl J Med. 2010;363(24):22878-2300.
29. Lacson E Jr, Xu J, Suri RS, et al. Survival with three-times weekly in-center nocturnal versus conventional hemodialysis. J Am Soc Nephrol. 2012;23(4):687-695.
30. Suri RS, Lindsay RM, Bieber BA, et al. A multinational cohort study of in-center daily hemodialysis and patient survival. Kidney Int. 2012 Sep 12. [Epub ahead of print]
31. Sidawy AN, Spergel LM, Besarab A, et al; Society for Vascular Surgery. Clinical practice guidelines for the surgical placement and maintenance of arteriovenous hemodialysis access. ?J Vasc Surg. 2008;48(5 Suppl):2S-25S.
32. Heaf JG. Algorithm for optimal dialysis access timing. Clin Nephrol. 2007;67(2):96-104.
33. Nassar GM, Ayus JC. Infectious complications of the hemodialysis access. Kidney Int. 2001;60(1):1-13.
34. National Kidney Foundation. Peritoneal dialysis: what you need to know (2006;11-50-0215). www.kidney.org/atoz/pdf/PeritonealDialysis.pdf. Accessed September 24, 2012.
35. Davison SN, Ghangri GS, Jindal K, Pannu N. Comparison of volume overload with cycler-assisted versus continuous ambulatory peritoneal dialysis. Clin J Am Soc Nephrol. 2009;4(6):1044-1050.
36. Juergensen P, Eras J, McClure B, et al. The impact of various cycling regimens on phosphorus removal in chronic peritoneal dialysis patients. Int J Artif Organs. 2005;28(12):1219-1223.
37. Vonesh EF, Snyder JJ, Foley RN, Collins AJ. Mortality studies comparing peritoneal dialysis and hemodialysis: what do they tell us? Kidney Int Suppl. 2006 Nov;(103):S3-S11.
38. Heaf J, Løkkegaard H, Madsen M. Initial survival advantage of peritoneal dialysis relative to haemodialysis. Nephrol Dial Transplant. 2002;17(1):112-117.
39. Wang AY, Lai KN. The importance of residual renal function in dialysis patients. Kidney Int. 2006;69(10):1726-1732.
40. Cnossen N, Kooman JP, Konings CJ, et al. Peritoneal dialysis in patients with congestive heart failure. Nephrol Dial Transplant. 2006;21 suppl 2: ii63-ii66.
1. Cooper BA, Branley P, Bulfone L, et al; IDEAL Study. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010; 363(7):609-619.
2. Olan G. Policy Update: ASN to CDC: data collection of creatinine levels will advance research. ASN Kidney News. 2012;4(6):16. www.asn-online.org/publications/kidneynews/archives/2012/KN_jun2012.pdf. Accessed August 27, 2012.
3. US Renal Data System, National Institute of Diabetes and Digestive and Kidney Diseases, NIH. 2011 Atlas of CKD & ESRD. Vol 2. Chap 1: Incidence, prevalence, patient characteristics, and modalities. www.usrds.org/2011/pdf/v2_ch01_11.pdf. Accessed September 26, 2012.
4. National Kidney Foundation. Kidney Disease Outcomes Quality Initiative (KDOQI). Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. ?Part 4. Definition and classification of the stages of chronic kidney disease. 2002:43-80. www.kidney.org/professionals/kdoqi/pdf/ckd_evalua tion_classification_stratification.pdf. Accessed August 27, 2012.
5. Levey AS, Bosch JP, Lewis JB, et al; Modification of Diet in Renal Disease Study Group. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Internal Med. 1999;130 (6):461-470.
6. Froissart M, Rossert J, Jacquot C, et al. Predictive performance of the Modification of Diet in Renal Disease and Cockcroft-Gault equations for estimating renal function. J Am Soc Nephrol. 2005;16(3):763-773.
7. Jafar TH, Schmid CH, Levey AS. Serum creatinine as marker of kidney function in South Asians: a study of reduced GFR in adults in Pakistan. J Am Soc Nephrol. 2005;16(5):1413-1419.
8. Zuo L, Ma YC, Zhou YH, et al. Application of GFR-estimating equations in Chinese patients with chronic kidney disease. Am J Kidney Dis. 2005;45(3):463-472.
9. Stevens LA, Stoycheff N, Levey AS. Staging and management of chronic kidney disease. In: Greenberg A, ed. Primer of Kidney Diseases: Expert Consult. 5th ed. Philadelphia, PA: WB Saunders; 2009:436-445.
10. Clark WF, Na Y, Rosansky SJ, et al. Association between estimated glomerular filtration rate at initiation of dialysis and mortality. CMAJ. 2011;183(1):47-53.
11. Beddhu S, Samore MH, Roberts MS, et al. Impact of timing of initiation of dialysis on mortality. J Am Soc Nephrol. 2003;14(9):2305-2312.
12. Kazmi WH, Gilbertson DT, Obrador GT, et al. Effect of comorbidity on the increased mortality associated with early initiation of dialysis. Am J Kidney Dis. 2005;46(5):887-896.
13. Lassalle M, Labeeuw M, Frimat L, et al. Age and comorbidity may explain the paradoxical association of an early dialysis start with poor survival. Kidney Int. 2010;77(8):700-707.
14. Stel VS, Dekker FW, Ansell D, et al. Residual renal function at the start of dialysis and clinical outcomes. Nephrol Dial Transplant. 2009;24 (10):3175-3182.
15. Traynor JP, Simpson K, Geddes CC, et al. Early initiation of dialysis fails to prolong survival in patients with end-stage renal failure. J Am Soc Nephrol. 2002;13(8):2125-2132.
16. US Department of Health and Human Services, Centers for Medicare and Medicaid Services. CMS Form 2728. End-Stage Renal Disease Medical Evidence Report: Medicare Entitlement and/or Patient Registration. www.usrds.org/2008/rg/forms/02_2728_1965.pdf. Accessed September 25, 2012.
17. Renal Physicians Association. Shared Decision-Making in the Appropriate Initiation of and Withdrawal from Dialysis: Clinical Practice Guideline. 2nd ed. Rockville, MD: Renal Physicians Association; Oct 2010:1-12.
18. Kurella Tamura M, Covinsky KE, Chertow GM, et al. Functional status of elderly adults before and after initiation of dialysis. N Engl J Med. 2009;361(16):1539-1547.
19. Chandna SM, Da Silva-Gane M, Marshall C, et al. Survival of elderly patients with stage 5 CKD: comparison of conservative management and renal replacement therapy. Nephrol Dial Transplant. 2011;26(5):1608-1614.
20. Smith C, Da Silva-Gane M, Chandna S, Warwicker P, Greenwood R, Farrington K. Choosing not to dialyse: evaluation of planned non-dialytic management in a cohort of patients with end-stage renal failure. Nephron Clin Pract. 2003;95:c40-c46.
21. Lamping DL, Constantinovici N, Roderick P, et al. Clinical outcomes, quality of life, and costs in the North Thames Dialysis Study of elderly people on dialysis: a prospective cohort study. Lancet. 2000;356:1543-1550.
22. O’Connor NR, Kumar P. Conservative management of end-stage renal disease without dialysis: a systematic review. J Palliat Med. 2012; 15(2):228-235.
23. Jassal SV, Trpeski L, Zhu N, et al. Changes in survival among elderly patients initiating dialysis from 1990 to 1999. CMAJ. 2007;177(9):?1033-1038.
24. Schmidt RJ. Informing our elders about dialysis: is an age-attuned approach warranted? Clin J Am Soc Nephrol. 2012;7(1):185-191.
25. Holley JL. Providing optimal care before and after discontinuation. Semin Dial. 2012;25(1):?33-34.
26. Eknoyan G, Beck GJ, Cheung AK, et al; Hemodialysis (HEMO) Study Group. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med. 2002;347(25):?2010-2019.
27. Lacson E, Lazarus M. Dialysis time: does it matter? A reappraisal of existing literature. Curr Opin Nephrol Hypertens. 2011;20(2):189-194.
28. Chertow GM, Levin NW, Beck GJ, et al; FHN Trial Group. In-center hemodialysis six times per week versus three times per week. N Engl J Med. 2010;363(24):22878-2300.
29. Lacson E Jr, Xu J, Suri RS, et al. Survival with three-times weekly in-center nocturnal versus conventional hemodialysis. J Am Soc Nephrol. 2012;23(4):687-695.
30. Suri RS, Lindsay RM, Bieber BA, et al. A multinational cohort study of in-center daily hemodialysis and patient survival. Kidney Int. 2012 Sep 12. [Epub ahead of print]
31. Sidawy AN, Spergel LM, Besarab A, et al; Society for Vascular Surgery. Clinical practice guidelines for the surgical placement and maintenance of arteriovenous hemodialysis access. ?J Vasc Surg. 2008;48(5 Suppl):2S-25S.
32. Heaf JG. Algorithm for optimal dialysis access timing. Clin Nephrol. 2007;67(2):96-104.
33. Nassar GM, Ayus JC. Infectious complications of the hemodialysis access. Kidney Int. 2001;60(1):1-13.
34. National Kidney Foundation. Peritoneal dialysis: what you need to know (2006;11-50-0215). www.kidney.org/atoz/pdf/PeritonealDialysis.pdf. Accessed September 24, 2012.
35. Davison SN, Ghangri GS, Jindal K, Pannu N. Comparison of volume overload with cycler-assisted versus continuous ambulatory peritoneal dialysis. Clin J Am Soc Nephrol. 2009;4(6):1044-1050.
36. Juergensen P, Eras J, McClure B, et al. The impact of various cycling regimens on phosphorus removal in chronic peritoneal dialysis patients. Int J Artif Organs. 2005;28(12):1219-1223.
37. Vonesh EF, Snyder JJ, Foley RN, Collins AJ. Mortality studies comparing peritoneal dialysis and hemodialysis: what do they tell us? Kidney Int Suppl. 2006 Nov;(103):S3-S11.
38. Heaf J, Løkkegaard H, Madsen M. Initial survival advantage of peritoneal dialysis relative to haemodialysis. Nephrol Dial Transplant. 2002;17(1):112-117.
39. Wang AY, Lai KN. The importance of residual renal function in dialysis patients. Kidney Int. 2006;69(10):1726-1732.
40. Cnossen N, Kooman JP, Konings CJ, et al. Peritoneal dialysis in patients with congestive heart failure. Nephrol Dial Transplant. 2006;21 suppl 2: ii63-ii66.
Mentally Healthful Eating
Pulsed Radio Frequency Energy for the Treatment of Phantom Limb Pain
Feasibility of Same-Day Postoperative Evaluation Following Phacoemulsification With Intraocular Lens Implantation at a Veterans Health Administration Teaching Hospital
Don't Quit on a Quitter: Helping Your Patient Stop Smoking
Although smoking prevalence among US adults declined by about 42% between 1965 and 2011, this reduction has slowed in recent years. According to 2010 figures from the CDC, 19.3% of US adults (nearly one in five) remain current smokers,1 despite all the evidence of negative effects that tobacco use and smoke exposure exert on good health.2 Each year, 443,000 premature deaths in the US are attributed to cigarette smoking.3
In the face of these discouraging data, and in ongoing efforts to minimize the deadly effects of cigarette smoking, the US Department of Health and Human Services’ program, Healthy People 2020,4 restated its 10-year goals pertaining to tobacco use as put forth in Healthy People 2010.5 These are to reduce the proportion of Americans who currently smoke to 12%, and to increase the proportion of current smokers who have attempted cessation to 80%.4
Though trained to encourage smoking cessation in their patients, health care providers often lack the knowledge, skills, or resources to support patients through the difficulties of discontinuing tobacco use. Whatever barriers clinicians may face in accessing smoking cessation services, the barriers faced by underserved patients are often greater.6 A heightened awareness of these barriers and improved understanding of common smoking cessation methods will help providers better support their patients who are trying to quit.
ASSESSING READINESS AND MOTIVATING PATIENTS
In 2008, the Public Health Service, US Department of Health and Human Services, updated its clinical practice guidelines for clinicians who manage tobacco-dependent patients.7 According to evidence from randomized controlled trials, even brief interventions on the health care provider’s part (such as raising the issue of smoking cessation at each patient visit to determine whether the patient is ready to quit) can prompt the patient to seriously consider smoking abstinence.3,8 Being asked repeatedly can advance a patient’s readiness, and any attempts patients make to quit must be robustly supported.9
The Public Health Service’s five A’s3,7 outline the recommended conversation with patients:
Ask about tobacco use;
Advise tobacco users to quit in strong, clear terms;
Assess readiness for tobacco cessation;
Assist in developing a plan to stop tobacco use; and
Arrange a follow-up consultation to review the patient’s success or to reassess cessation readiness.
Whenever a patient expresses any interest in smoking cessation, it is essential for the clinician to respond with motivation. To help the patient prepare to stop, the clinician must address the five R’s7:
Relevance—the importance of smoking cessation to the patient;
Risks of continuing to smoke, particularly health concerns;
Rewards of smoking cessation, especially alleviation of health complaints;
Roadblocks that contribute to the threat of relapse—but which can be overcome with sufficient motivation; and
Repetition of support and reinforcement for this healthy lifestyle choice, be it from family, friends, coworkers, or the clinician. To prepare for times when support seems to wane, patients should be encouraged to phone 1-800-QUITNOW, a number that will connect the caller to his or her state’s quit line.
Repetition may also imply repeated cessation attempts if the first (or most recent) was unsuccessful. According to findings from a literature review, the reasons smokers relapse are numerous, including cravings (the most common) and withdrawal symptoms, weight gain, stress, and exposure to other smokers.10,11 Interventions based on patients’ given reasons for relapse have no apparent impact on the rate of return to smoking.12 Nevertheless, clinicians must take responsibility to motivate patients and reinforce their successes at every encounter.
UNAIDED CESSATION
In a culture demanding quick results and in the context of ongoing pharmaceutical advertisements and aisles lined with quit-smoking products, it may be easy to dismiss unaided cessation. Options range from gradual cutting down to the abrupt discontinuation of tobacco—going cold turkey. Although little research has been devoted to these strategies,13 unaided cessation is the method patients most often cite in their attempts to quit—and the method successful quitters report as most effective.14,15 The patients most likely to succeed at quitting are those who do not ask for help.
ASSISTED CESSATION
Patients with a significant dependence on nicotine are likely to request assistance with cessation.15 Identifying those who struggle to quit smoking and offering appropriate support may represent the difference between their success and failure.9
Several available tools to support patients’ “quit smoking” efforts, including pharmacologic options (see table7), are described here.
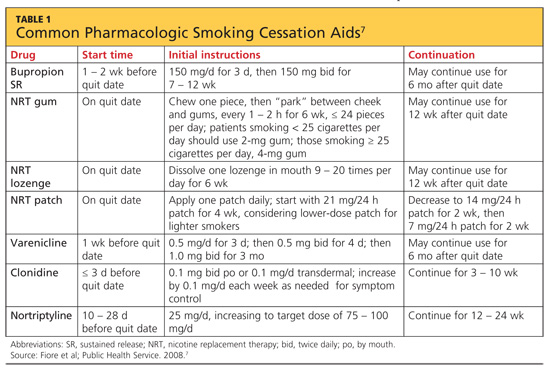
Nicotine Replacement Therapy
Nicotine replacement therapy (NRT) is used to reduce nicotine withdrawal symptoms by replacing smoking-produced nicotine with an alternate source of delivery. NRT is currently available in several forms: a transdermal patch, gum, lozenge, or the electronic cigarette. The chance of successful quitting is increased 50% to 70% when NRT is used, compared with patients using placebo.16 While the various forms of NRT share the same goal, they are not equally effective.17
Nicotine transdermal patches have been used in the US since 1991. The patches are used in a stepwise fashion; each patch delivers nicotine at a consistent quantity per hour, and over time, patches with increasingly lower doses of nicotine are substituted. There is some evidence that the patch is more efficacious for maintenance after smoking cessation than for the initial effort to quit.18
Nicotine gum and lozenges, orally absorbed forms of NRT, are used as needed, depending on patients’ withdrawal symptoms. Japuntich et al18 found that these products alone are not beneficial. However, combining bupropion with gum or lozenge therapy was found more effective for patients attempting to stop smoking than either agent alone.18 Lozenges have also been described as increasingly beneficial when combined with a longer-acting NRT, such as a transdermal patch, when cravings increase and rapid delivery of nicotine is required.16
The electronic cigarette (e-cigarette) is a battery-operated device that aerosolizes liquid nicotine, which is then orally absorbed. In a 2011 study, Siegel et al19 found that more than two-thirds of smokers reduced the number of cigarettes smoked after using an e-cigarette. Six months after subjects first purchased e-cigarettes, 31% remained tobacco-abstinent.
Since e-cigarettes are flameless, their use has been suggested in areas where smoking was previously prohibited. This short-acting NRT may benefit a patient when craving is provoked by forced denial of nicotine.
Current research is under way to examine two newer potential NRT tools: a nicotine mouth spray and a nicotine vaccine.20,21 In a randomized, double-blind, placebo-controlled study, Tønnesen et al20 found that use of a nicotine mouth spray was associated with significantly higher rates of tobacco abstinence at six, 24, and 52 weeks, compared with patients receiving placebo; however, rates of adverse effects were high in both groups (88% and 71%, respectively).
NRT is inexpensive and easily accessible to patients. Since its forms are all available OTC, consultation with health care providers is unnecessary. For patients who have tried to quit smoking unaided and who need short-term or immediate assistance to prevent a smoking relapse, NRT can be a helpful resource.
Bupropion
For smokers who want to quit without using a nicotine-based intervention, the antidepressant bupropion can be a promising smoking cessation aid. It is not clear what mechanism of action helps smokers who take bupropion to stop, although its chemical structure resembles that of diethylpropion, a drug used as an appetite suppressant.22 Bupropion does hinder norepinephrine and dopamine reuptake in the nervous system—opposing an effect of nicotine withdrawal.
Bupropion’s effects as an antidepressant and as a smoking cessation aid do not appear to be related.22 For this reason, even a patient who has not responded to bupropion for treatment of depression may benefit from using it as a smoking cessation aid.
Bupropion may be used alone or with other agents to stop nicotine use. Many study groups report that a combination of medications is more effective than monotherapy, and this is true for combinations that include bupropion.23-26 When used with nicotine lozenges, bupropion has been found effective in preventing a return to tobacco after previous lapses in smoking abstinence. Aside from a nicotine patch, no other monotherapy or combination was effective at achieving this goal.18 Thus, bupropion may be best utilized as a component in combination therapy.
Varenicline
Approved for use in the US in 2006, varenicline is the newest pharmaceutical therapy for smoking cessation. As a partial nicotinic receptor agonist,7 varenicline prevents nicotine from activating the mesolimbic dopamine system, which is associated with pleasure and reward (among other functions). By stimulating the nervous system’s dopamine (though to a lesser extent than nicotine), this agent reduces cravings for tobacco and symptoms of nicotine withdrawal—which are among the greatest barriers to smoking cessation.10 Because of its mechanism of action, varenicline is not often used in combination with NRT.
Varenicline has been shown to be as effective as the combination therapy of bupropion with nicotine lozenges.7,27 UK investigators Hajek et al27 found that using varenicline for four weeks before attempting to stop smoking had minimal effect on smoking urges and withdrawal symptoms, compared with using varenicline for just one week before attempting to quit. However, those who used varenicline for four weeks before stopping smoking were more likely to be smoke-free at 12 weeks than those who had used it for just one week before quitting.27
Other Pharmaceutical Options
Clonidine, long recognized as an effective antihypertensive medication, was determined by Gourlay et al9 in a 2004 review to have potential for use in supporting smoking cessation. Because significant adverse events (including drowsiness, sedation, and postural hypotension) have been associated with clonidine use7,28 and the FDA has not yet approved it for the indication of smoking cessation, its use may be most appropriate as a second-line treatment option, in combination with bupropion or nortriptyline, or for specialists’ use.28 Clonidine should not be discontinued suddenly.
Like bupropion, the tricyclic antidepressant nortriptyline has been investigated for its potential in tobacco cessation therapy. While a significant amount is known about plasma concentrations of nortriptyline needed to treat depression, levels required for effective tobacco cessation are less clear. Mooney et al29 found that therapeutic plasma concentrations of nortriptyline varied among subjects by race and smoking habits; although a lower concentration was usually required to assist smoking cessation than to treat depression, adverse effects were common even at lower concentrations. Thus, it was recommended that nortriptyline be reserved for second-line treatment.
This summer, researchers for the Cochrane Tobacco Addiction Review Group published a review of the literature (including phase II and phase III trials conducted by pharmaceutical companies—making the risk for bias “high or unclear”) pertaining to two nicotine vaccines in development.21 In two studies, the level of development of nicotine antibodies was associated with commensurate cessation rates; in two others, the outcome measure (12 months’ abstinence from smoking) was met in 11% of subjects, whether they received the vaccine or placebo. Thus, no strong evidence yet exists that nicotine vaccination supports smoking cessation in the long term; further research is needed.
NONPHARMACEUTICAL
INTERVENTIONS
Acupuncture
Variations and modifications of the traditional Chinese therapy of acupuncture, including acupressure and electrostimulation, have been examined in a number of clinical trials. Despite the supporting rhetoric, objective research of good quality in this area is limited. However, one systematic literature review showed acupuncture to be only slightly more effective than sham interventions and less effective than NRT.30 Insufficient evidence was reported on acupressure and laser stimulation, and acupressure was no more effective than psychological treatments. Considering questionable study quality and other limitations in the currently available research, practitioners should not consider acupuncture or related interventions as first-line options—nor should their potential be dismissed altogether.
Hypnotherapy
Conclusive research findings regarding hypnotherapy as an effective treatment for tobacco dependence are also limited. In 2010, Barnes at al31 reviewed 11 studies comparing hypnotherapy with various alternate methods and found little difference in effectiveness among hypnotherapy, psychological counseling, and rapid smoking therapy. Despite the limitations in these data, however, hypnotherapy may be appropriate for some patients.
CONCLUSION
Tobacco dependence is not the same for any two patients. Just as health care providers do not use the same treatment option for every patient with hypertension or diabetes, treatment for tobacco-dependent patients must also be individualized.
Our professional goal is to care for the health of patients. We clinicians must recommend cessation to our patients who smoke at every encounter—and offer support often. When we miss an opportunity to counsel a patient on the importance of quitting, the patient may interpret our silence as condoning the behavior. Empowering patients with an understanding of the options can contribute to their success—a significant move toward better health.
The authors of Healthy People 2020 hope that 80% of current smokers will have tried to stop smoking by that year. Have 80% of your patients been counseled and offered assistance to stop?
REFERENCES
1. CDC. Current cigarette smoking prevalence among working adults—United States, 2004-2010. MMWR Morb Mortal Wkly Rep. 2011;60(38):1305-1309.
2. CDC. Vital signs: current cigarette smoking among adults aged ≥ 18 years—United States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59(35):1135-1140.
3. Jamal A, Dube SR, Malarcher AM, et al; CDC. Tobacco use screening and counseling during physician office visits among adults—National Ambulatory Medical Care Survey and National Health Interview Survey, United States, 2005-2009. MMWR Morb Mortal Wkly Rep. 2012;61 suppl: 38-45.
4. US Department of Health and Human Services. Healthy People 2020 summary of objectives: tobacco use. http://healthypeople.gov/2020/topicsobjectives2020/pdfs/TobaccoUse.pdf. Accessed October 18, 2012.
5. US Department of Health and Human Services. Healthy People 2010 archives. www.healthypeople.gov/2010. Accessed October 18, 2012.
6. Blumenthal DS. Barriers to the provision of smoking cessation services reported by clinicians in underserved communities. J Am Board Fam Med. 2007;20(3):272-279.
7. Fiore MC, Jaén CR, Baker TB, et al; Public Health Service, US Department of Health and Human Services. Clinical practice guideline: treating tobacco use and dependence: 2008 update. www.ahrq.gov/clinic/tobacco/treating_tobacco_use08.pdf. Accessed October 18, 2012.
8. Carson KV, Verbiest ME, Crone MR, et al. Training health professionals in smoking cessation. Cochrane Database Syst Rev. 2012 May 16; 5:CD000214.
9. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000058.
10. Guirguis AB, Ray SM, Zingone MM, et al. Smoking cessation: barriers to success and readiness to change. Tenn Med. 2010;103(9):45-49.
11. Nørregaard J, Tønnesen P, Petersen L. Predictors and reasons for relapse in smoking cessation with nicotine and placebo patches. Prev Med. 1993;22(2):261-271.
12. Lancaster T, Hajek P, Stead LF, et al. Prevention of relapse after quitting smoking: a systematic review of trials. Arch Intern Med. 2006;166(8): 828-835.
13. Chapman S, MacKenzie R. The global research neglect of unassisted smoking cessation: causes and consequences. PLoS Med. 2010;7(2):e1000216.
14. Hung WT, Dunlop SM, Perez D, Cotter T. Use and perceived helpfulness of smoking cessation methods: results from a population survey of recent quitters. BMC Public Health. 2011;11:592.
15. Shiffman S, Brockwell SE, Pillitteri JL, Gitchell JG. Use of smoking-cessation treatments in the United States. Am J Prev Med. 2008;34(2):102-111.
16. Stead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008 Jan 23;(1):CD000146.
17. Robles GI, Singh-Franco D, Ghin HL. A review of the efficacy of smoking-cessation pharmacotherapies in nonwhite populations. Clin Ther. 2008;30(5):800-812.
18. Japuntich SJ, Piper ME, Leventhal AM, et al. The effect of five smoking cessation pharmacotherapies on smoking cessation milestones. J Consult Clin Psychol. 2011;79(1):34-42.
19. Siegel MB, Tanwar KL, Wood KS. Electronic cigarettes as a smoking-cessation tool: results from an online survey. Am J Prev Med. 2011;40 (4):472-475.
20. Tønnesen P, Lauri H, Perfekt R, et al. Efficacy of a nicotine mouth spray in smoking cessation: a randomised, double-blind trial. Eur Respir J. 2012;40(3):548-554.
21. Hartmann-Boyce J, Cahill K, Hatsukami D, Cornuz J. Nicotine vaccines for smoking cessation. Cochrane Database Syst Rev. 2012 Aug 15;8:CD007072.
22. Roddy E. Bupropion and other non-nicotine pharmacotherapies. BMJ. 2004;328(7438):
509-511.
23. Loh WY, Piper ME, Schlam TR, et al. Should all smokers use combination smoking cessation pharmacotherapy? Using novel analytic methods to detect differential treatment effects over 8 weeks of pharmacotherapy. Nicotine Tob Res. 2012;14(2):131-141.
24. Bolt DM, Piper ME, Theobald WE, Baker TB. Why two smoking cessation agents work better than one: role of craving suppression. J Consult Clin Psychol. 2012;80(1):44-65.
25. McNeil JJ, Piccenna L, Ioannides-Demos LL. Smoking cessation: recent advances. Cardiovasc Drugs Ther. 2010;24(4):359-367.
26. Ebbert JO, Hays JT, Hurt RD. Combination pharmacotherapy for stopping smoking: what advantages does it offer? Drugs. 2010;70(6):643-650.
27. Hajek P, McRobbie HJ, Myers KE, et al. Use of varenicline for 4 weeks before quitting smoking: decrease in ad lib smoking and increase in smoking cessation rates. Arch Intern Med. 2011;171 (8):770-777.
28. Bentz CJ. Review: clonidine is more effective than placebo for long-term smoking cessation, but has side effects. ACP J Club. 2005;142(1):12.
29. Mooney ME, Reus VI, Gorecki J, et al. Therapeutic drug monitoring of nortriptyline in smoking cessation: a multistudy analysis. Clin Pharmacol Ther. 2008;83(3):436-442.
30. White AR, Rampes H, Liu JP, et al. Acupuncture and related interventions for smoking cessation. Cochrane Database Syst Rev. 2011;(1): CD000009.
31. Barnes J, Dong CY, McRobbie H, et al. Hypnotherapy for smoking cessation. Cochrane Database Syst Rev. 2010;(10):CD001008.
Although smoking prevalence among US adults declined by about 42% between 1965 and 2011, this reduction has slowed in recent years. According to 2010 figures from the CDC, 19.3% of US adults (nearly one in five) remain current smokers,1 despite all the evidence of negative effects that tobacco use and smoke exposure exert on good health.2 Each year, 443,000 premature deaths in the US are attributed to cigarette smoking.3
In the face of these discouraging data, and in ongoing efforts to minimize the deadly effects of cigarette smoking, the US Department of Health and Human Services’ program, Healthy People 2020,4 restated its 10-year goals pertaining to tobacco use as put forth in Healthy People 2010.5 These are to reduce the proportion of Americans who currently smoke to 12%, and to increase the proportion of current smokers who have attempted cessation to 80%.4
Though trained to encourage smoking cessation in their patients, health care providers often lack the knowledge, skills, or resources to support patients through the difficulties of discontinuing tobacco use. Whatever barriers clinicians may face in accessing smoking cessation services, the barriers faced by underserved patients are often greater.6 A heightened awareness of these barriers and improved understanding of common smoking cessation methods will help providers better support their patients who are trying to quit.
ASSESSING READINESS AND MOTIVATING PATIENTS
In 2008, the Public Health Service, US Department of Health and Human Services, updated its clinical practice guidelines for clinicians who manage tobacco-dependent patients.7 According to evidence from randomized controlled trials, even brief interventions on the health care provider’s part (such as raising the issue of smoking cessation at each patient visit to determine whether the patient is ready to quit) can prompt the patient to seriously consider smoking abstinence.3,8 Being asked repeatedly can advance a patient’s readiness, and any attempts patients make to quit must be robustly supported.9
The Public Health Service’s five A’s3,7 outline the recommended conversation with patients:
Ask about tobacco use;
Advise tobacco users to quit in strong, clear terms;
Assess readiness for tobacco cessation;
Assist in developing a plan to stop tobacco use; and
Arrange a follow-up consultation to review the patient’s success or to reassess cessation readiness.
Whenever a patient expresses any interest in smoking cessation, it is essential for the clinician to respond with motivation. To help the patient prepare to stop, the clinician must address the five R’s7:
Relevance—the importance of smoking cessation to the patient;
Risks of continuing to smoke, particularly health concerns;
Rewards of smoking cessation, especially alleviation of health complaints;
Roadblocks that contribute to the threat of relapse—but which can be overcome with sufficient motivation; and
Repetition of support and reinforcement for this healthy lifestyle choice, be it from family, friends, coworkers, or the clinician. To prepare for times when support seems to wane, patients should be encouraged to phone 1-800-QUITNOW, a number that will connect the caller to his or her state’s quit line.
Repetition may also imply repeated cessation attempts if the first (or most recent) was unsuccessful. According to findings from a literature review, the reasons smokers relapse are numerous, including cravings (the most common) and withdrawal symptoms, weight gain, stress, and exposure to other smokers.10,11 Interventions based on patients’ given reasons for relapse have no apparent impact on the rate of return to smoking.12 Nevertheless, clinicians must take responsibility to motivate patients and reinforce their successes at every encounter.
UNAIDED CESSATION
In a culture demanding quick results and in the context of ongoing pharmaceutical advertisements and aisles lined with quit-smoking products, it may be easy to dismiss unaided cessation. Options range from gradual cutting down to the abrupt discontinuation of tobacco—going cold turkey. Although little research has been devoted to these strategies,13 unaided cessation is the method patients most often cite in their attempts to quit—and the method successful quitters report as most effective.14,15 The patients most likely to succeed at quitting are those who do not ask for help.
ASSISTED CESSATION
Patients with a significant dependence on nicotine are likely to request assistance with cessation.15 Identifying those who struggle to quit smoking and offering appropriate support may represent the difference between their success and failure.9
Several available tools to support patients’ “quit smoking” efforts, including pharmacologic options (see table7), are described here.
Nicotine Replacement Therapy
Nicotine replacement therapy (NRT) is used to reduce nicotine withdrawal symptoms by replacing smoking-produced nicotine with an alternate source of delivery. NRT is currently available in several forms: a transdermal patch, gum, lozenge, or the electronic cigarette. The chance of successful quitting is increased 50% to 70% when NRT is used, compared with patients using placebo.16 While the various forms of NRT share the same goal, they are not equally effective.17
Nicotine transdermal patches have been used in the US since 1991. The patches are used in a stepwise fashion; each patch delivers nicotine at a consistent quantity per hour, and over time, patches with increasingly lower doses of nicotine are substituted. There is some evidence that the patch is more efficacious for maintenance after smoking cessation than for the initial effort to quit.18
Nicotine gum and lozenges, orally absorbed forms of NRT, are used as needed, depending on patients’ withdrawal symptoms. Japuntich et al18 found that these products alone are not beneficial. However, combining bupropion with gum or lozenge therapy was found more effective for patients attempting to stop smoking than either agent alone.18 Lozenges have also been described as increasingly beneficial when combined with a longer-acting NRT, such as a transdermal patch, when cravings increase and rapid delivery of nicotine is required.16
The electronic cigarette (e-cigarette) is a battery-operated device that aerosolizes liquid nicotine, which is then orally absorbed. In a 2011 study, Siegel et al19 found that more than two-thirds of smokers reduced the number of cigarettes smoked after using an e-cigarette. Six months after subjects first purchased e-cigarettes, 31% remained tobacco-abstinent.
Since e-cigarettes are flameless, their use has been suggested in areas where smoking was previously prohibited. This short-acting NRT may benefit a patient when craving is provoked by forced denial of nicotine.
Current research is under way to examine two newer potential NRT tools: a nicotine mouth spray and a nicotine vaccine.20,21 In a randomized, double-blind, placebo-controlled study, Tønnesen et al20 found that use of a nicotine mouth spray was associated with significantly higher rates of tobacco abstinence at six, 24, and 52 weeks, compared with patients receiving placebo; however, rates of adverse effects were high in both groups (88% and 71%, respectively).
NRT is inexpensive and easily accessible to patients. Since its forms are all available OTC, consultation with health care providers is unnecessary. For patients who have tried to quit smoking unaided and who need short-term or immediate assistance to prevent a smoking relapse, NRT can be a helpful resource.
Bupropion
For smokers who want to quit without using a nicotine-based intervention, the antidepressant bupropion can be a promising smoking cessation aid. It is not clear what mechanism of action helps smokers who take bupropion to stop, although its chemical structure resembles that of diethylpropion, a drug used as an appetite suppressant.22 Bupropion does hinder norepinephrine and dopamine reuptake in the nervous system—opposing an effect of nicotine withdrawal.
Bupropion’s effects as an antidepressant and as a smoking cessation aid do not appear to be related.22 For this reason, even a patient who has not responded to bupropion for treatment of depression may benefit from using it as a smoking cessation aid.
Bupropion may be used alone or with other agents to stop nicotine use. Many study groups report that a combination of medications is more effective than monotherapy, and this is true for combinations that include bupropion.23-26 When used with nicotine lozenges, bupropion has been found effective in preventing a return to tobacco after previous lapses in smoking abstinence. Aside from a nicotine patch, no other monotherapy or combination was effective at achieving this goal.18 Thus, bupropion may be best utilized as a component in combination therapy.
Varenicline
Approved for use in the US in 2006, varenicline is the newest pharmaceutical therapy for smoking cessation. As a partial nicotinic receptor agonist,7 varenicline prevents nicotine from activating the mesolimbic dopamine system, which is associated with pleasure and reward (among other functions). By stimulating the nervous system’s dopamine (though to a lesser extent than nicotine), this agent reduces cravings for tobacco and symptoms of nicotine withdrawal—which are among the greatest barriers to smoking cessation.10 Because of its mechanism of action, varenicline is not often used in combination with NRT.
Varenicline has been shown to be as effective as the combination therapy of bupropion with nicotine lozenges.7,27 UK investigators Hajek et al27 found that using varenicline for four weeks before attempting to stop smoking had minimal effect on smoking urges and withdrawal symptoms, compared with using varenicline for just one week before attempting to quit. However, those who used varenicline for four weeks before stopping smoking were more likely to be smoke-free at 12 weeks than those who had used it for just one week before quitting.27
Other Pharmaceutical Options
Clonidine, long recognized as an effective antihypertensive medication, was determined by Gourlay et al9 in a 2004 review to have potential for use in supporting smoking cessation. Because significant adverse events (including drowsiness, sedation, and postural hypotension) have been associated with clonidine use7,28 and the FDA has not yet approved it for the indication of smoking cessation, its use may be most appropriate as a second-line treatment option, in combination with bupropion or nortriptyline, or for specialists’ use.28 Clonidine should not be discontinued suddenly.
Like bupropion, the tricyclic antidepressant nortriptyline has been investigated for its potential in tobacco cessation therapy. While a significant amount is known about plasma concentrations of nortriptyline needed to treat depression, levels required for effective tobacco cessation are less clear. Mooney et al29 found that therapeutic plasma concentrations of nortriptyline varied among subjects by race and smoking habits; although a lower concentration was usually required to assist smoking cessation than to treat depression, adverse effects were common even at lower concentrations. Thus, it was recommended that nortriptyline be reserved for second-line treatment.
This summer, researchers for the Cochrane Tobacco Addiction Review Group published a review of the literature (including phase II and phase III trials conducted by pharmaceutical companies—making the risk for bias “high or unclear”) pertaining to two nicotine vaccines in development.21 In two studies, the level of development of nicotine antibodies was associated with commensurate cessation rates; in two others, the outcome measure (12 months’ abstinence from smoking) was met in 11% of subjects, whether they received the vaccine or placebo. Thus, no strong evidence yet exists that nicotine vaccination supports smoking cessation in the long term; further research is needed.
NONPHARMACEUTICAL
INTERVENTIONS
Acupuncture
Variations and modifications of the traditional Chinese therapy of acupuncture, including acupressure and electrostimulation, have been examined in a number of clinical trials. Despite the supporting rhetoric, objective research of good quality in this area is limited. However, one systematic literature review showed acupuncture to be only slightly more effective than sham interventions and less effective than NRT.30 Insufficient evidence was reported on acupressure and laser stimulation, and acupressure was no more effective than psychological treatments. Considering questionable study quality and other limitations in the currently available research, practitioners should not consider acupuncture or related interventions as first-line options—nor should their potential be dismissed altogether.
Hypnotherapy
Conclusive research findings regarding hypnotherapy as an effective treatment for tobacco dependence are also limited. In 2010, Barnes at al31 reviewed 11 studies comparing hypnotherapy with various alternate methods and found little difference in effectiveness among hypnotherapy, psychological counseling, and rapid smoking therapy. Despite the limitations in these data, however, hypnotherapy may be appropriate for some patients.
CONCLUSION
Tobacco dependence is not the same for any two patients. Just as health care providers do not use the same treatment option for every patient with hypertension or diabetes, treatment for tobacco-dependent patients must also be individualized.
Our professional goal is to care for the health of patients. We clinicians must recommend cessation to our patients who smoke at every encounter—and offer support often. When we miss an opportunity to counsel a patient on the importance of quitting, the patient may interpret our silence as condoning the behavior. Empowering patients with an understanding of the options can contribute to their success—a significant move toward better health.
The authors of Healthy People 2020 hope that 80% of current smokers will have tried to stop smoking by that year. Have 80% of your patients been counseled and offered assistance to stop?
REFERENCES
1. CDC. Current cigarette smoking prevalence among working adults—United States, 2004-2010. MMWR Morb Mortal Wkly Rep. 2011;60(38):1305-1309.
2. CDC. Vital signs: current cigarette smoking among adults aged ≥ 18 years—United States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59(35):1135-1140.
3. Jamal A, Dube SR, Malarcher AM, et al; CDC. Tobacco use screening and counseling during physician office visits among adults—National Ambulatory Medical Care Survey and National Health Interview Survey, United States, 2005-2009. MMWR Morb Mortal Wkly Rep. 2012;61 suppl: 38-45.
4. US Department of Health and Human Services. Healthy People 2020 summary of objectives: tobacco use. http://healthypeople.gov/2020/topicsobjectives2020/pdfs/TobaccoUse.pdf. Accessed October 18, 2012.
5. US Department of Health and Human Services. Healthy People 2010 archives. www.healthypeople.gov/2010. Accessed October 18, 2012.
6. Blumenthal DS. Barriers to the provision of smoking cessation services reported by clinicians in underserved communities. J Am Board Fam Med. 2007;20(3):272-279.
7. Fiore MC, Jaén CR, Baker TB, et al; Public Health Service, US Department of Health and Human Services. Clinical practice guideline: treating tobacco use and dependence: 2008 update. www.ahrq.gov/clinic/tobacco/treating_tobacco_use08.pdf. Accessed October 18, 2012.
8. Carson KV, Verbiest ME, Crone MR, et al. Training health professionals in smoking cessation. Cochrane Database Syst Rev. 2012 May 16; 5:CD000214.
9. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000058.
10. Guirguis AB, Ray SM, Zingone MM, et al. Smoking cessation: barriers to success and readiness to change. Tenn Med. 2010;103(9):45-49.
11. Nørregaard J, Tønnesen P, Petersen L. Predictors and reasons for relapse in smoking cessation with nicotine and placebo patches. Prev Med. 1993;22(2):261-271.
12. Lancaster T, Hajek P, Stead LF, et al. Prevention of relapse after quitting smoking: a systematic review of trials. Arch Intern Med. 2006;166(8): 828-835.
13. Chapman S, MacKenzie R. The global research neglect of unassisted smoking cessation: causes and consequences. PLoS Med. 2010;7(2):e1000216.
14. Hung WT, Dunlop SM, Perez D, Cotter T. Use and perceived helpfulness of smoking cessation methods: results from a population survey of recent quitters. BMC Public Health. 2011;11:592.
15. Shiffman S, Brockwell SE, Pillitteri JL, Gitchell JG. Use of smoking-cessation treatments in the United States. Am J Prev Med. 2008;34(2):102-111.
16. Stead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008 Jan 23;(1):CD000146.
17. Robles GI, Singh-Franco D, Ghin HL. A review of the efficacy of smoking-cessation pharmacotherapies in nonwhite populations. Clin Ther. 2008;30(5):800-812.
18. Japuntich SJ, Piper ME, Leventhal AM, et al. The effect of five smoking cessation pharmacotherapies on smoking cessation milestones. J Consult Clin Psychol. 2011;79(1):34-42.
19. Siegel MB, Tanwar KL, Wood KS. Electronic cigarettes as a smoking-cessation tool: results from an online survey. Am J Prev Med. 2011;40 (4):472-475.
20. Tønnesen P, Lauri H, Perfekt R, et al. Efficacy of a nicotine mouth spray in smoking cessation: a randomised, double-blind trial. Eur Respir J. 2012;40(3):548-554.
21. Hartmann-Boyce J, Cahill K, Hatsukami D, Cornuz J. Nicotine vaccines for smoking cessation. Cochrane Database Syst Rev. 2012 Aug 15;8:CD007072.
22. Roddy E. Bupropion and other non-nicotine pharmacotherapies. BMJ. 2004;328(7438):
509-511.
23. Loh WY, Piper ME, Schlam TR, et al. Should all smokers use combination smoking cessation pharmacotherapy? Using novel analytic methods to detect differential treatment effects over 8 weeks of pharmacotherapy. Nicotine Tob Res. 2012;14(2):131-141.
24. Bolt DM, Piper ME, Theobald WE, Baker TB. Why two smoking cessation agents work better than one: role of craving suppression. J Consult Clin Psychol. 2012;80(1):44-65.
25. McNeil JJ, Piccenna L, Ioannides-Demos LL. Smoking cessation: recent advances. Cardiovasc Drugs Ther. 2010;24(4):359-367.
26. Ebbert JO, Hays JT, Hurt RD. Combination pharmacotherapy for stopping smoking: what advantages does it offer? Drugs. 2010;70(6):643-650.
27. Hajek P, McRobbie HJ, Myers KE, et al. Use of varenicline for 4 weeks before quitting smoking: decrease in ad lib smoking and increase in smoking cessation rates. Arch Intern Med. 2011;171 (8):770-777.
28. Bentz CJ. Review: clonidine is more effective than placebo for long-term smoking cessation, but has side effects. ACP J Club. 2005;142(1):12.
29. Mooney ME, Reus VI, Gorecki J, et al. Therapeutic drug monitoring of nortriptyline in smoking cessation: a multistudy analysis. Clin Pharmacol Ther. 2008;83(3):436-442.
30. White AR, Rampes H, Liu JP, et al. Acupuncture and related interventions for smoking cessation. Cochrane Database Syst Rev. 2011;(1): CD000009.
31. Barnes J, Dong CY, McRobbie H, et al. Hypnotherapy for smoking cessation. Cochrane Database Syst Rev. 2010;(10):CD001008.
Although smoking prevalence among US adults declined by about 42% between 1965 and 2011, this reduction has slowed in recent years. According to 2010 figures from the CDC, 19.3% of US adults (nearly one in five) remain current smokers,1 despite all the evidence of negative effects that tobacco use and smoke exposure exert on good health.2 Each year, 443,000 premature deaths in the US are attributed to cigarette smoking.3
In the face of these discouraging data, and in ongoing efforts to minimize the deadly effects of cigarette smoking, the US Department of Health and Human Services’ program, Healthy People 2020,4 restated its 10-year goals pertaining to tobacco use as put forth in Healthy People 2010.5 These are to reduce the proportion of Americans who currently smoke to 12%, and to increase the proportion of current smokers who have attempted cessation to 80%.4
Though trained to encourage smoking cessation in their patients, health care providers often lack the knowledge, skills, or resources to support patients through the difficulties of discontinuing tobacco use. Whatever barriers clinicians may face in accessing smoking cessation services, the barriers faced by underserved patients are often greater.6 A heightened awareness of these barriers and improved understanding of common smoking cessation methods will help providers better support their patients who are trying to quit.
ASSESSING READINESS AND MOTIVATING PATIENTS
In 2008, the Public Health Service, US Department of Health and Human Services, updated its clinical practice guidelines for clinicians who manage tobacco-dependent patients.7 According to evidence from randomized controlled trials, even brief interventions on the health care provider’s part (such as raising the issue of smoking cessation at each patient visit to determine whether the patient is ready to quit) can prompt the patient to seriously consider smoking abstinence.3,8 Being asked repeatedly can advance a patient’s readiness, and any attempts patients make to quit must be robustly supported.9
The Public Health Service’s five A’s3,7 outline the recommended conversation with patients:
Ask about tobacco use;
Advise tobacco users to quit in strong, clear terms;
Assess readiness for tobacco cessation;
Assist in developing a plan to stop tobacco use; and
Arrange a follow-up consultation to review the patient’s success or to reassess cessation readiness.
Whenever a patient expresses any interest in smoking cessation, it is essential for the clinician to respond with motivation. To help the patient prepare to stop, the clinician must address the five R’s7:
Relevance—the importance of smoking cessation to the patient;
Risks of continuing to smoke, particularly health concerns;
Rewards of smoking cessation, especially alleviation of health complaints;
Roadblocks that contribute to the threat of relapse—but which can be overcome with sufficient motivation; and
Repetition of support and reinforcement for this healthy lifestyle choice, be it from family, friends, coworkers, or the clinician. To prepare for times when support seems to wane, patients should be encouraged to phone 1-800-QUITNOW, a number that will connect the caller to his or her state’s quit line.
Repetition may also imply repeated cessation attempts if the first (or most recent) was unsuccessful. According to findings from a literature review, the reasons smokers relapse are numerous, including cravings (the most common) and withdrawal symptoms, weight gain, stress, and exposure to other smokers.10,11 Interventions based on patients’ given reasons for relapse have no apparent impact on the rate of return to smoking.12 Nevertheless, clinicians must take responsibility to motivate patients and reinforce their successes at every encounter.
UNAIDED CESSATION
In a culture demanding quick results and in the context of ongoing pharmaceutical advertisements and aisles lined with quit-smoking products, it may be easy to dismiss unaided cessation. Options range from gradual cutting down to the abrupt discontinuation of tobacco—going cold turkey. Although little research has been devoted to these strategies,13 unaided cessation is the method patients most often cite in their attempts to quit—and the method successful quitters report as most effective.14,15 The patients most likely to succeed at quitting are those who do not ask for help.
ASSISTED CESSATION
Patients with a significant dependence on nicotine are likely to request assistance with cessation.15 Identifying those who struggle to quit smoking and offering appropriate support may represent the difference between their success and failure.9
Several available tools to support patients’ “quit smoking” efforts, including pharmacologic options (see table7), are described here.
Nicotine Replacement Therapy
Nicotine replacement therapy (NRT) is used to reduce nicotine withdrawal symptoms by replacing smoking-produced nicotine with an alternate source of delivery. NRT is currently available in several forms: a transdermal patch, gum, lozenge, or the electronic cigarette. The chance of successful quitting is increased 50% to 70% when NRT is used, compared with patients using placebo.16 While the various forms of NRT share the same goal, they are not equally effective.17
Nicotine transdermal patches have been used in the US since 1991. The patches are used in a stepwise fashion; each patch delivers nicotine at a consistent quantity per hour, and over time, patches with increasingly lower doses of nicotine are substituted. There is some evidence that the patch is more efficacious for maintenance after smoking cessation than for the initial effort to quit.18
Nicotine gum and lozenges, orally absorbed forms of NRT, are used as needed, depending on patients’ withdrawal symptoms. Japuntich et al18 found that these products alone are not beneficial. However, combining bupropion with gum or lozenge therapy was found more effective for patients attempting to stop smoking than either agent alone.18 Lozenges have also been described as increasingly beneficial when combined with a longer-acting NRT, such as a transdermal patch, when cravings increase and rapid delivery of nicotine is required.16
The electronic cigarette (e-cigarette) is a battery-operated device that aerosolizes liquid nicotine, which is then orally absorbed. In a 2011 study, Siegel et al19 found that more than two-thirds of smokers reduced the number of cigarettes smoked after using an e-cigarette. Six months after subjects first purchased e-cigarettes, 31% remained tobacco-abstinent.
Since e-cigarettes are flameless, their use has been suggested in areas where smoking was previously prohibited. This short-acting NRT may benefit a patient when craving is provoked by forced denial of nicotine.
Current research is under way to examine two newer potential NRT tools: a nicotine mouth spray and a nicotine vaccine.20,21 In a randomized, double-blind, placebo-controlled study, Tønnesen et al20 found that use of a nicotine mouth spray was associated with significantly higher rates of tobacco abstinence at six, 24, and 52 weeks, compared with patients receiving placebo; however, rates of adverse effects were high in both groups (88% and 71%, respectively).
NRT is inexpensive and easily accessible to patients. Since its forms are all available OTC, consultation with health care providers is unnecessary. For patients who have tried to quit smoking unaided and who need short-term or immediate assistance to prevent a smoking relapse, NRT can be a helpful resource.
Bupropion
For smokers who want to quit without using a nicotine-based intervention, the antidepressant bupropion can be a promising smoking cessation aid. It is not clear what mechanism of action helps smokers who take bupropion to stop, although its chemical structure resembles that of diethylpropion, a drug used as an appetite suppressant.22 Bupropion does hinder norepinephrine and dopamine reuptake in the nervous system—opposing an effect of nicotine withdrawal.
Bupropion’s effects as an antidepressant and as a smoking cessation aid do not appear to be related.22 For this reason, even a patient who has not responded to bupropion for treatment of depression may benefit from using it as a smoking cessation aid.
Bupropion may be used alone or with other agents to stop nicotine use. Many study groups report that a combination of medications is more effective than monotherapy, and this is true for combinations that include bupropion.23-26 When used with nicotine lozenges, bupropion has been found effective in preventing a return to tobacco after previous lapses in smoking abstinence. Aside from a nicotine patch, no other monotherapy or combination was effective at achieving this goal.18 Thus, bupropion may be best utilized as a component in combination therapy.
Varenicline
Approved for use in the US in 2006, varenicline is the newest pharmaceutical therapy for smoking cessation. As a partial nicotinic receptor agonist,7 varenicline prevents nicotine from activating the mesolimbic dopamine system, which is associated with pleasure and reward (among other functions). By stimulating the nervous system’s dopamine (though to a lesser extent than nicotine), this agent reduces cravings for tobacco and symptoms of nicotine withdrawal—which are among the greatest barriers to smoking cessation.10 Because of its mechanism of action, varenicline is not often used in combination with NRT.
Varenicline has been shown to be as effective as the combination therapy of bupropion with nicotine lozenges.7,27 UK investigators Hajek et al27 found that using varenicline for four weeks before attempting to stop smoking had minimal effect on smoking urges and withdrawal symptoms, compared with using varenicline for just one week before attempting to quit. However, those who used varenicline for four weeks before stopping smoking were more likely to be smoke-free at 12 weeks than those who had used it for just one week before quitting.27
Other Pharmaceutical Options
Clonidine, long recognized as an effective antihypertensive medication, was determined by Gourlay et al9 in a 2004 review to have potential for use in supporting smoking cessation. Because significant adverse events (including drowsiness, sedation, and postural hypotension) have been associated with clonidine use7,28 and the FDA has not yet approved it for the indication of smoking cessation, its use may be most appropriate as a second-line treatment option, in combination with bupropion or nortriptyline, or for specialists’ use.28 Clonidine should not be discontinued suddenly.
Like bupropion, the tricyclic antidepressant nortriptyline has been investigated for its potential in tobacco cessation therapy. While a significant amount is known about plasma concentrations of nortriptyline needed to treat depression, levels required for effective tobacco cessation are less clear. Mooney et al29 found that therapeutic plasma concentrations of nortriptyline varied among subjects by race and smoking habits; although a lower concentration was usually required to assist smoking cessation than to treat depression, adverse effects were common even at lower concentrations. Thus, it was recommended that nortriptyline be reserved for second-line treatment.
This summer, researchers for the Cochrane Tobacco Addiction Review Group published a review of the literature (including phase II and phase III trials conducted by pharmaceutical companies—making the risk for bias “high or unclear”) pertaining to two nicotine vaccines in development.21 In two studies, the level of development of nicotine antibodies was associated with commensurate cessation rates; in two others, the outcome measure (12 months’ abstinence from smoking) was met in 11% of subjects, whether they received the vaccine or placebo. Thus, no strong evidence yet exists that nicotine vaccination supports smoking cessation in the long term; further research is needed.
NONPHARMACEUTICAL
INTERVENTIONS
Acupuncture
Variations and modifications of the traditional Chinese therapy of acupuncture, including acupressure and electrostimulation, have been examined in a number of clinical trials. Despite the supporting rhetoric, objective research of good quality in this area is limited. However, one systematic literature review showed acupuncture to be only slightly more effective than sham interventions and less effective than NRT.30 Insufficient evidence was reported on acupressure and laser stimulation, and acupressure was no more effective than psychological treatments. Considering questionable study quality and other limitations in the currently available research, practitioners should not consider acupuncture or related interventions as first-line options—nor should their potential be dismissed altogether.
Hypnotherapy
Conclusive research findings regarding hypnotherapy as an effective treatment for tobacco dependence are also limited. In 2010, Barnes at al31 reviewed 11 studies comparing hypnotherapy with various alternate methods and found little difference in effectiveness among hypnotherapy, psychological counseling, and rapid smoking therapy. Despite the limitations in these data, however, hypnotherapy may be appropriate for some patients.
CONCLUSION
Tobacco dependence is not the same for any two patients. Just as health care providers do not use the same treatment option for every patient with hypertension or diabetes, treatment for tobacco-dependent patients must also be individualized.
Our professional goal is to care for the health of patients. We clinicians must recommend cessation to our patients who smoke at every encounter—and offer support often. When we miss an opportunity to counsel a patient on the importance of quitting, the patient may interpret our silence as condoning the behavior. Empowering patients with an understanding of the options can contribute to their success—a significant move toward better health.
The authors of Healthy People 2020 hope that 80% of current smokers will have tried to stop smoking by that year. Have 80% of your patients been counseled and offered assistance to stop?
REFERENCES
1. CDC. Current cigarette smoking prevalence among working adults—United States, 2004-2010. MMWR Morb Mortal Wkly Rep. 2011;60(38):1305-1309.
2. CDC. Vital signs: current cigarette smoking among adults aged ≥ 18 years—United States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59(35):1135-1140.
3. Jamal A, Dube SR, Malarcher AM, et al; CDC. Tobacco use screening and counseling during physician office visits among adults—National Ambulatory Medical Care Survey and National Health Interview Survey, United States, 2005-2009. MMWR Morb Mortal Wkly Rep. 2012;61 suppl: 38-45.
4. US Department of Health and Human Services. Healthy People 2020 summary of objectives: tobacco use. http://healthypeople.gov/2020/topicsobjectives2020/pdfs/TobaccoUse.pdf. Accessed October 18, 2012.
5. US Department of Health and Human Services. Healthy People 2010 archives. www.healthypeople.gov/2010. Accessed October 18, 2012.
6. Blumenthal DS. Barriers to the provision of smoking cessation services reported by clinicians in underserved communities. J Am Board Fam Med. 2007;20(3):272-279.
7. Fiore MC, Jaén CR, Baker TB, et al; Public Health Service, US Department of Health and Human Services. Clinical practice guideline: treating tobacco use and dependence: 2008 update. www.ahrq.gov/clinic/tobacco/treating_tobacco_use08.pdf. Accessed October 18, 2012.
8. Carson KV, Verbiest ME, Crone MR, et al. Training health professionals in smoking cessation. Cochrane Database Syst Rev. 2012 May 16; 5:CD000214.
9. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000058.
10. Guirguis AB, Ray SM, Zingone MM, et al. Smoking cessation: barriers to success and readiness to change. Tenn Med. 2010;103(9):45-49.
11. Nørregaard J, Tønnesen P, Petersen L. Predictors and reasons for relapse in smoking cessation with nicotine and placebo patches. Prev Med. 1993;22(2):261-271.
12. Lancaster T, Hajek P, Stead LF, et al. Prevention of relapse after quitting smoking: a systematic review of trials. Arch Intern Med. 2006;166(8): 828-835.
13. Chapman S, MacKenzie R. The global research neglect of unassisted smoking cessation: causes and consequences. PLoS Med. 2010;7(2):e1000216.
14. Hung WT, Dunlop SM, Perez D, Cotter T. Use and perceived helpfulness of smoking cessation methods: results from a population survey of recent quitters. BMC Public Health. 2011;11:592.
15. Shiffman S, Brockwell SE, Pillitteri JL, Gitchell JG. Use of smoking-cessation treatments in the United States. Am J Prev Med. 2008;34(2):102-111.
16. Stead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008 Jan 23;(1):CD000146.
17. Robles GI, Singh-Franco D, Ghin HL. A review of the efficacy of smoking-cessation pharmacotherapies in nonwhite populations. Clin Ther. 2008;30(5):800-812.
18. Japuntich SJ, Piper ME, Leventhal AM, et al. The effect of five smoking cessation pharmacotherapies on smoking cessation milestones. J Consult Clin Psychol. 2011;79(1):34-42.
19. Siegel MB, Tanwar KL, Wood KS. Electronic cigarettes as a smoking-cessation tool: results from an online survey. Am J Prev Med. 2011;40 (4):472-475.
20. Tønnesen P, Lauri H, Perfekt R, et al. Efficacy of a nicotine mouth spray in smoking cessation: a randomised, double-blind trial. Eur Respir J. 2012;40(3):548-554.
21. Hartmann-Boyce J, Cahill K, Hatsukami D, Cornuz J. Nicotine vaccines for smoking cessation. Cochrane Database Syst Rev. 2012 Aug 15;8:CD007072.
22. Roddy E. Bupropion and other non-nicotine pharmacotherapies. BMJ. 2004;328(7438):
509-511.
23. Loh WY, Piper ME, Schlam TR, et al. Should all smokers use combination smoking cessation pharmacotherapy? Using novel analytic methods to detect differential treatment effects over 8 weeks of pharmacotherapy. Nicotine Tob Res. 2012;14(2):131-141.
24. Bolt DM, Piper ME, Theobald WE, Baker TB. Why two smoking cessation agents work better than one: role of craving suppression. J Consult Clin Psychol. 2012;80(1):44-65.
25. McNeil JJ, Piccenna L, Ioannides-Demos LL. Smoking cessation: recent advances. Cardiovasc Drugs Ther. 2010;24(4):359-367.
26. Ebbert JO, Hays JT, Hurt RD. Combination pharmacotherapy for stopping smoking: what advantages does it offer? Drugs. 2010;70(6):643-650.
27. Hajek P, McRobbie HJ, Myers KE, et al. Use of varenicline for 4 weeks before quitting smoking: decrease in ad lib smoking and increase in smoking cessation rates. Arch Intern Med. 2011;171 (8):770-777.
28. Bentz CJ. Review: clonidine is more effective than placebo for long-term smoking cessation, but has side effects. ACP J Club. 2005;142(1):12.
29. Mooney ME, Reus VI, Gorecki J, et al. Therapeutic drug monitoring of nortriptyline in smoking cessation: a multistudy analysis. Clin Pharmacol Ther. 2008;83(3):436-442.
30. White AR, Rampes H, Liu JP, et al. Acupuncture and related interventions for smoking cessation. Cochrane Database Syst Rev. 2011;(1): CD000009.
31. Barnes J, Dong CY, McRobbie H, et al. Hypnotherapy for smoking cessation. Cochrane Database Syst Rev. 2010;(10):CD001008.
Cover

Opioid-Induced Hearing Loss:
A Trend to Keep Listening For?
When and how to place an autologous rectus fascia pubovaginal sling
Watch 2 intraoperative videos
These videos were selected by Mickey Karram, MD, and are presented courtesy of the International Academy of Pelvic Surgery (IAPS)
The authors report no financial relationships relevant to this article.
Developed in partnership with International Academy of Pelvic Surgery.
CASE 1: Recurrent SUI and mesh erosion
A 50-year-old woman reports urinary incontinence that is associated with activity and exertion—stress urinary incontinence (SUI)—and says it has worsened over the past year. She mentions that she underwent vaginal hysterectomy, with placement of a tension-free vaginal tape (TVT), about 2 years earlier.
During physical examination, the patient becomes incontinent when abdominal pressure is increased, with some urethral mobility (cotton-swab deflection to 25° from the horizontal). She is also noted to have erosion of the TVT tape into the vaginal lumen.
Urodynamic testing reveals easily demonstrable SUI at a volume of 150 mL when she is in the sitting position, with a Valsalva leak-point pressure of 55 cm H2O. Her bladder remains stable to a capacity of 520 mL. Cystoscopy yields unremarkable findings.
When she is offered surgical correction of her SUI, the patient expresses a preference for the use of her own tissues and says she does not want to have synthetic mesh placed.
Is this patient a candidate for a rectus fascia pubovaginal sling?

Mickey Karram, MD
Dr. Karram is Director of the Fellowship Program in Female Pelvic Medicine and Reconstructive Pelvic Surgery, University of Cincinnati/The Christ Hospital, Cincinnati, Ohio; Co-Editor in Chief of the International Academy of Pelvic Surgery (IAPS); and Course Director of the Pelvic Anatomy and Gynecologic Surgery Symposium (PAGS) and the Female Urology and Urogynecology Symposium (FUUS), both co-sponsored by OBG Management.
Dani Zoorob, MD
Dr. Zoorob is a Fellow in Urogynecology at the University of Cincinnati/The Christ Hospital in Cincinnati, Ohio.
Mickey Karram, MD
Dr. Karram is Director of the Fellowship Program in Female Pelvic Medicine and Reconstructive Pelvic Surgery, University of Cincinnati/The Christ Hospital, Cincinnati, Ohio; Co-Editor in Chief of the International Academy of Pelvic Surgery (IAPS); and Course Director of the Pelvic Anatomy and Gynecologic Surgery Symposium (PAGS) and the Female Urology and Urogynecology Symposium (FUUS), both co-sponsored by OBG Management.
Dani Zoorob, MD
Dr. Zoorob is a Fellow in Urogynecology at the University of Cincinnati/The Christ Hospital in Cincinnati, Ohio.
Mickey Karram, MD
Dr. Karram is Director of the Fellowship Program in Female Pelvic Medicine and Reconstructive Pelvic Surgery, University of Cincinnati/The Christ Hospital, Cincinnati, Ohio; Co-Editor in Chief of the International Academy of Pelvic Surgery (IAPS); and Course Director of the Pelvic Anatomy and Gynecologic Surgery Symposium (PAGS) and the Female Urology and Urogynecology Symposium (FUUS), both co-sponsored by OBG Management.
Dani Zoorob, MD
Dr. Zoorob is a Fellow in Urogynecology at the University of Cincinnati/The Christ Hospital in Cincinnati, Ohio.
Watch 2 intraoperative videos
These videos were selected by Mickey Karram, MD, and are presented courtesy of the International Academy of Pelvic Surgery (IAPS)
The authors report no financial relationships relevant to this article.
Developed in partnership with International Academy of Pelvic Surgery.
CASE 1: Recurrent SUI and mesh erosion
A 50-year-old woman reports urinary incontinence that is associated with activity and exertion—stress urinary incontinence (SUI)—and says it has worsened over the past year. She mentions that she underwent vaginal hysterectomy, with placement of a tension-free vaginal tape (TVT), about 2 years earlier.
During physical examination, the patient becomes incontinent when abdominal pressure is increased, with some urethral mobility (cotton-swab deflection to 25° from the horizontal). She is also noted to have erosion of the TVT tape into the vaginal lumen.
Urodynamic testing reveals easily demonstrable SUI at a volume of 150 mL when she is in the sitting position, with a Valsalva leak-point pressure of 55 cm H2O. Her bladder remains stable to a capacity of 520 mL. Cystoscopy yields unremarkable findings.
When she is offered surgical correction of her SUI, the patient expresses a preference for the use of her own tissues and says she does not want to have synthetic mesh placed.
Is this patient a candidate for a rectus fascia pubovaginal sling?
Watch 2 intraoperative videos
These videos were selected by Mickey Karram, MD, and are presented courtesy of the International Academy of Pelvic Surgery (IAPS)
The authors report no financial relationships relevant to this article.
Developed in partnership with International Academy of Pelvic Surgery.
CASE 1: Recurrent SUI and mesh erosion
A 50-year-old woman reports urinary incontinence that is associated with activity and exertion—stress urinary incontinence (SUI)—and says it has worsened over the past year. She mentions that she underwent vaginal hysterectomy, with placement of a tension-free vaginal tape (TVT), about 2 years earlier.
During physical examination, the patient becomes incontinent when abdominal pressure is increased, with some urethral mobility (cotton-swab deflection to 25° from the horizontal). She is also noted to have erosion of the TVT tape into the vaginal lumen.
Urodynamic testing reveals easily demonstrable SUI at a volume of 150 mL when she is in the sitting position, with a Valsalva leak-point pressure of 55 cm H2O. Her bladder remains stable to a capacity of 520 mL. Cystoscopy yields unremarkable findings.
When she is offered surgical correction of her SUI, the patient expresses a preference for the use of her own tissues and says she does not want to have synthetic mesh placed.
Is this patient a candidate for a rectus fascia pubovaginal sling?
UPDATE ON OSTEOPOROSIS
What is the optimal interval for osteoporosis screening in postmenopausal women before fracture occurrence and osteoporosis?
Steven R. Goldstein, MD (Examining the Evidence, August 2012)
Update on Menopause
Andrew M. Kaunitz, MD (May 2012)
Update on Osteoporosis
Steven R. Goldstein, MD (November 2011)
An appeal to the FDA: Remove the black-box warning for depot medroxyprogesterone acetate?
Andrew M. Kaunitz, MD; David A. Grimes, MD (Guest Editorial, August 2011)
Osteoporosis is a significant health issue—and it is likely to remain so as more and more women live longer and longer. In fact, increasing age is the single biggest risk factor for osteoporotic fragility fracture.
Over the past year, important research has improved our understanding in diverse areas of bone health. In this Update, I highlight studies that:
- seek to elucidate the optimal frequency of dual-energy x-ray absorptiometry (DXA) imaging to assess bone mineral density
- review secondary causes of osteoporosis besides menopause-related estrogen deficiency
- explore the use of quantitative ultrasound (QUS) to predict the risk of fracture
- report on a new class of pharmaceutical agents that inhibit the bone-resorption enzyme Cathepsin K.
All of these issues are clinically relevant to the ObGyn specialty because, when it comes to our patients’ bone health, we often function as the primary care physician.
When is DXA indicated—and how often should it be repeated?
Gourlay ML, Fine JP, Preisser JS, et al; Study of Osteoporotic Fractures Research Group. Bone-density testing interval and transition to osteoporosis in older women. N Engl J Med. 2012;366(3):225–233.
Lewiecki EM, Laster AJ, Miller PD, Bilezikian JP. More bone density testing is needed, not less. J Bone Miner Res. 2012;27(4):739–742.
American Society for Bone and Mineral Research response to media coverage of New England Journal of Medicine study: “Bone density testing interval and transition to osteoporosis in older women” [press release]. http://www.asbmr.org/about/pressreleases/detail.aspx?cid=3801baff-0df3-47c0-874f-08a185d67001. Published February 1, 2012. Accessed October 15, 2012.
Recommendations from professional societies, such as the National Osteoporosis Foundation, the International Society of Clinical Densitometry, and the American College of Obstetricians and Gynecologists say virtually the same thing about DXA imaging: Screening is appropriate for women 65 years and older and for postmenopausal women younger than age 65 who have risk factors for fracture. Risk factors include:
- history of a fragility fracture
- body weight less than 127 lb
- medical causes of bone loss, such as medication or disease
- parental history of hip fracture
- current smoker
- alcoholism
- rheumatoid arthritis.
The measurement of bone mineral density (BMD) has been the cornerstone of the diagnosis of osteopenia and osteoporosis since these classifications were introduced by the World Health Organization (WHO) in 1994. Although we are now able to evaluate a woman’s fracture risk using the FRAX tool, which does not require BMD assessment, DXA scanning has become entrenched in routine clinical practice in the United States. In addition, patients who use drugs to reduce their fracture risk often demand periodic testing to see how they are doing. Even women who do not take medications often want periodic assessment to confirm that they are not “losing bone.” Medicare allows for testing every 23 months.
23-month screening interval does not fit all women
Gourlay and colleagues prospectively followed 4,957 women aged 67 years or older who had no history of hip or vertebral fracture and who were not being treated for osteoporosis. After follow-up for as long as 15 years, investigators found that the better a woman’s initial bone density, the longer it took for her to develop osteoporosis. For example, among women over 67 years of age who had a T-score of –1.0 or better, it would take 16.8 years for 10% of this population to develop osteoporosis. In contrast, among women over 67 years of age who had a T-score of –2.0, it would take only 1.1 years for 10% of this population to develop osteoporosis.
This finding certainly calls into question the notion that all patients should be screened every 23 months. It may be better to think of screening as a way of triaging patients for decisions relative to subsequent follow-up.
Media distorted take-home message
This study was the focus of considerable attention from the media, which implied that too much DXA screening is being performed. In reality, only 13% of women over the age of 65 undergo a baseline DXA scan. However, routine follow-up of all patients at 23-month intervals is clearly not appropriate.
Because this study primarily involved white women older than age 67, extrapolation of its findings to other groups may not be appropriate. Nevertheless, the study helps to underscore the fact that reliance on BMD measurement alone should not be used to determine the need for therapeutic intervention. The FRAX tool can be used on an annual basis to assess a woman’s risk of fracture and does not require follow-up DXA imaging at any arbitrary interval.
In healthy older women, an interval of 23 months for repeat BMD assessment makes little sense. For women who have excellent initial T-scores, clinicians can lengthen this interval significantly.
However, strict reliance on the T-score isn’t the best way to predict a woman’s fracture risk or determine when pharmacologic intervention is warranted. Rather, yearly assessment using a tool such as FRAX should become the standard of care.
Some secondary causes of osteoporosis are overlooked or underappreciated
Miller PD. Unrecognized and unappreciated secondary causes of osteoporosis. Endocrinol Metab Clin North Am. 2012;41(3):613–628.
The fractures traditionally associated with osteoporosis involve the hip and vertebrae, although low-trauma fractures of the humerus, forearm, femur shaft, tibia, and fibula are also associated with a high risk of future fracture in untreated women.
Once a clinician is confident that a patient has osteoporosis, the question is whether the diagnosis is postmenopausal osteoporosis—or some other form of the disease. Although estrogen deficiency is the most common cause of osteoporosis in postmenopausal women, many other conditions may accompany estrogen deficiency and contribute to impaired bone strength in this population.
Among the culprits are some conditions that are not often encountered in the average gynecologic practice: monoclonal gammopathy of undetermined significance (MGUS), multiple myeloma, celiac disease, Crohn’s disease, and other inflammatory bowel diseases. In addition, bariatric surgery, eating disorders, primary hyperparathyroidism, and a number of medications have been implicated in BMD loss or increased risk of fracture, or both. Among the problematic drugs of particular interest to us as gynecologists are aromatase inhibitors, depot medroxyprogesterone acetate, proton pump inhibitors, and gonadotropin-releasing hormone (GnRH) agonists.
Other medications that can affect BMD are glucocorticoids, unfractionated heparin, selective serotonin reuptake inhibitors, excessive amounts of thyroid replacement agents, and some antiseizure medications.
If you suspect a secondary cause of osteoporosis, be prepared to perform a basic workup that includes:
- a careful history and physical examination
- complete blood count
- a chemistry profile, including serum calcium, phosphorous, electrolytes, alkaline phosphatase, and creatinine.
In addition, measurement of 25-hydroxy vitamin D and thyroid-stimulating hormone (TSH) may be helpful, as may serum protein electrophoresis.
Patients who have clinical or laboratory abnormalities suggestive of a secondary cause of osteoporosis are usually referred to a metabolic bone specialist (endocrinology or rheumatology).
When a patient has any clinical history that suggests a secondary cause of bone loss other than menopause-related estrogen deficiency, simple laboratory tests are appropriate and may uncover a condition that necessitates referral to a metabolic bone expert.
Quantitative ultrasound assessment of bone can help predict a woman’s risk of fracture
Guglielmi G, Rossini M, Nicolosi MG, Tagno A, Lentini G, de Terlizzi F. Three-year prospective study on fracture risk in postmenopausal women by quantitative ultrasound at the phalanges [published online ahead of print August 15, 2012]. J Clin Densitom. doi:10.1016 /j.jocd.2012.07.006.
Chan MY, Nguyen ND, Center JR, Eisman JA, Nguyen TV. Quantitative ultrasound and fracture risk prediction in non-osteoporotic men and women as defined by WHO criteria [published online ahead of print August 10, 2012]. Osteoporos Int. doi:10.1007/s00198-012 -2001-2.
I became interested in bone health through my longstanding interest in ultrasound, when a manufacturer asked me to evaluate equipment designed to assess bone density of the heel through quantitative ultrasound (QUS). This modality is not the diagnostic imaging we are familiar with in obstetrics and gynecology. In QUS, the homogeneity of healthy bone promotes sound transmission, whereas the voids and discontinuity of osteoporotic bone impede it. Therefore, normal bone has a faster speed of sound than less healthy bone. The other important quantitative measure is broadband ultrasound attenuation (BUA). Healthy bone is dense and absorbs and scatters sound to a greater extent than osteoporotic bone does.
Two trials of QUS
In 2010, Guglielmi and colleagues contacted 2,210 Italian women who had undergone QUS of the phalanges in 2006–2007. These women had an average age of 60.9 years, entered menopause at an average age of 49.3 years, and had a mean body mass index (BMI) of 26.5 kg/m2. By 2010, this group had experienced 108 new major osteoporotic fractures, including 23 hip fractures and 56 vertebral fractures. Investigators found a statistically significant correlation between QUS findings and fracture risk.
Chan and colleagues focused on 312 women 62 to 92 years of age who had femoral neck BMD, as measured by DXA, of –2.5 or better. QUS was measured as BUA at the calcaneus. The incidence of any fragility fracture was ascertained by radiographic reports during the follow-up period from 1994 to 2011. Eighty women (26%) experienced at least one fragility fracture during follow-up. After adjustment for covariates, women were significantly more likely to experience any fracture if BUA was decreased (hazard ratio [HR], 1.50; 95% confidence interval [CI], 1.13–1.99).
When the models that included BUA were compared with those that used femoral neck BMD, they had a greater area under the curve (0.71, 0.85, 0.71 for any fracture, hip fracture, and vertebral fracture, respectively) and yielded a net reclassification improvement of 16.4% (P=.009) when combined with femoral neck BMD. These findings suggest that calcaneal BUA is an independent predictor of fracture risk in women who have nonosteoporotic BMD.
In an era of increasing pressure to reduce costs, QUS assessment of bone is a promising modality that may be useful as a screening tool. Although it measures different variables than DXA imaging (more microarchitecture, less true density), it seems to predict the risk of fracture at less cost without ionizing radiation.
In the pipeline: A drug that curbs bone resorption without diminishing bone formation
Williams SC. Potential first-in-class osteoporosis drug speeds through trials. Nat Med. 2012;18(8):1158.
Ng KW. Potential role of odanacatib in the treatment of osteoporosis. Clin Interv Aging. 2012;7:235–247.
Alendronate was the first of the oral bisphosphonates to be approved by the US Food and Drug Administration (FDA). Once it was approved in 1999, the drug quickly became the most widely used bone agent in clinical practice and was soon joined by other oral and intravenous bisphosphonates. Regrettably, highly publicized adverse effects have caused many patients to shy away from this class of drugs. Two years ago, the FDA approved denosumab, a subcutaneous injectable agent that is a RANK ligand inhibitor.
The bisphosphonates and denosumab increase bone mass by shutting down the osteoclasts responsible for bone resorption, but they also inhibit creation of new bone. A new category of drug that inhibits the bone-resorption enzyme Cathepsin K appears to inhibit bone resorption without diminishing bone formation. Trials of two previous agents in this class were halted because of adverse effects—particularly effects to the skin, where the enzyme is expressed in addition to bone. However, Phase 2 trials in which odanacatib was compared with alendronate found that the new drug increased BMD almost twice as much as alendronate did, with less reduction in serum markers of bone formation.
Phase 3 trials of odanacatib in 16,000 women older than age 65 recently were halted so that the manufacturer could pursue regulatory approval ahead of the previous schedule. Although Phase 3 data have not been published yet, odanacatib may prove to be an exciting alternative to existing therapies.
Odanacatib is not yet available. However, by discussing therapies that may be “around the corner” with our patients, we demonstrate that we are staying ahead of the curve of scientific development.
We want to hear from you! Tell us what you think.
| Dr. Goldstein describes an evidence-based approach to BMD assessment |

Steven R. Goldstein, MD
Dr. Goldstein is Professor of Obstetrics and Gynecology at New York University School of Medicine. He is also Director of Gynecologic Ultrasound and Co-Director of Bone Densitometry at New York University Medical Center in New York City. He serves on the OBG Management Board of Editors.
Dr. Goldstein reports that he is a consultant to Cook ObGyn and Phillips Ultrasound; a speaker for Merck and Warner Chilcott; and is on the Gyn Advisory Boards of Bayer, Depomed, Novo Nordisk, and Shionogi. He serves on the OBG Management Board of Editors.
| Dr. Goldstein describes an evidence-based approach to BMD assessment |
Steven R. Goldstein, MD
Dr. Goldstein is Professor of Obstetrics and Gynecology at New York University School of Medicine. He is also Director of Gynecologic Ultrasound and Co-Director of Bone Densitometry at New York University Medical Center in New York City. He serves on the OBG Management Board of Editors.
Dr. Goldstein reports that he is a consultant to Cook ObGyn and Phillips Ultrasound; a speaker for Merck and Warner Chilcott; and is on the Gyn Advisory Boards of Bayer, Depomed, Novo Nordisk, and Shionogi. He serves on the OBG Management Board of Editors.
| Dr. Goldstein describes an evidence-based approach to BMD assessment |
Steven R. Goldstein, MD
Dr. Goldstein is Professor of Obstetrics and Gynecology at New York University School of Medicine. He is also Director of Gynecologic Ultrasound and Co-Director of Bone Densitometry at New York University Medical Center in New York City. He serves on the OBG Management Board of Editors.
Dr. Goldstein reports that he is a consultant to Cook ObGyn and Phillips Ultrasound; a speaker for Merck and Warner Chilcott; and is on the Gyn Advisory Boards of Bayer, Depomed, Novo Nordisk, and Shionogi. He serves on the OBG Management Board of Editors.
What is the optimal interval for osteoporosis screening in postmenopausal women before fracture occurrence and osteoporosis?
Steven R. Goldstein, MD (Examining the Evidence, August 2012)
Update on Menopause
Andrew M. Kaunitz, MD (May 2012)
Update on Osteoporosis
Steven R. Goldstein, MD (November 2011)
An appeal to the FDA: Remove the black-box warning for depot medroxyprogesterone acetate?
Andrew M. Kaunitz, MD; David A. Grimes, MD (Guest Editorial, August 2011)
Osteoporosis is a significant health issue—and it is likely to remain so as more and more women live longer and longer. In fact, increasing age is the single biggest risk factor for osteoporotic fragility fracture.
Over the past year, important research has improved our understanding in diverse areas of bone health. In this Update, I highlight studies that:
- seek to elucidate the optimal frequency of dual-energy x-ray absorptiometry (DXA) imaging to assess bone mineral density
- review secondary causes of osteoporosis besides menopause-related estrogen deficiency
- explore the use of quantitative ultrasound (QUS) to predict the risk of fracture
- report on a new class of pharmaceutical agents that inhibit the bone-resorption enzyme Cathepsin K.
All of these issues are clinically relevant to the ObGyn specialty because, when it comes to our patients’ bone health, we often function as the primary care physician.
When is DXA indicated—and how often should it be repeated?
Gourlay ML, Fine JP, Preisser JS, et al; Study of Osteoporotic Fractures Research Group. Bone-density testing interval and transition to osteoporosis in older women. N Engl J Med. 2012;366(3):225–233.
Lewiecki EM, Laster AJ, Miller PD, Bilezikian JP. More bone density testing is needed, not less. J Bone Miner Res. 2012;27(4):739–742.
American Society for Bone and Mineral Research response to media coverage of New England Journal of Medicine study: “Bone density testing interval and transition to osteoporosis in older women” [press release]. http://www.asbmr.org/about/pressreleases/detail.aspx?cid=3801baff-0df3-47c0-874f-08a185d67001. Published February 1, 2012. Accessed October 15, 2012.
Recommendations from professional societies, such as the National Osteoporosis Foundation, the International Society of Clinical Densitometry, and the American College of Obstetricians and Gynecologists say virtually the same thing about DXA imaging: Screening is appropriate for women 65 years and older and for postmenopausal women younger than age 65 who have risk factors for fracture. Risk factors include:
- history of a fragility fracture
- body weight less than 127 lb
- medical causes of bone loss, such as medication or disease
- parental history of hip fracture
- current smoker
- alcoholism
- rheumatoid arthritis.
The measurement of bone mineral density (BMD) has been the cornerstone of the diagnosis of osteopenia and osteoporosis since these classifications were introduced by the World Health Organization (WHO) in 1994. Although we are now able to evaluate a woman’s fracture risk using the FRAX tool, which does not require BMD assessment, DXA scanning has become entrenched in routine clinical practice in the United States. In addition, patients who use drugs to reduce their fracture risk often demand periodic testing to see how they are doing. Even women who do not take medications often want periodic assessment to confirm that they are not “losing bone.” Medicare allows for testing every 23 months.
23-month screening interval does not fit all women
Gourlay and colleagues prospectively followed 4,957 women aged 67 years or older who had no history of hip or vertebral fracture and who were not being treated for osteoporosis. After follow-up for as long as 15 years, investigators found that the better a woman’s initial bone density, the longer it took for her to develop osteoporosis. For example, among women over 67 years of age who had a T-score of –1.0 or better, it would take 16.8 years for 10% of this population to develop osteoporosis. In contrast, among women over 67 years of age who had a T-score of –2.0, it would take only 1.1 years for 10% of this population to develop osteoporosis.
This finding certainly calls into question the notion that all patients should be screened every 23 months. It may be better to think of screening as a way of triaging patients for decisions relative to subsequent follow-up.
Media distorted take-home message
This study was the focus of considerable attention from the media, which implied that too much DXA screening is being performed. In reality, only 13% of women over the age of 65 undergo a baseline DXA scan. However, routine follow-up of all patients at 23-month intervals is clearly not appropriate.
Because this study primarily involved white women older than age 67, extrapolation of its findings to other groups may not be appropriate. Nevertheless, the study helps to underscore the fact that reliance on BMD measurement alone should not be used to determine the need for therapeutic intervention. The FRAX tool can be used on an annual basis to assess a woman’s risk of fracture and does not require follow-up DXA imaging at any arbitrary interval.
In healthy older women, an interval of 23 months for repeat BMD assessment makes little sense. For women who have excellent initial T-scores, clinicians can lengthen this interval significantly.
However, strict reliance on the T-score isn’t the best way to predict a woman’s fracture risk or determine when pharmacologic intervention is warranted. Rather, yearly assessment using a tool such as FRAX should become the standard of care.
Some secondary causes of osteoporosis are overlooked or underappreciated
Miller PD. Unrecognized and unappreciated secondary causes of osteoporosis. Endocrinol Metab Clin North Am. 2012;41(3):613–628.
The fractures traditionally associated with osteoporosis involve the hip and vertebrae, although low-trauma fractures of the humerus, forearm, femur shaft, tibia, and fibula are also associated with a high risk of future fracture in untreated women.
Once a clinician is confident that a patient has osteoporosis, the question is whether the diagnosis is postmenopausal osteoporosis—or some other form of the disease. Although estrogen deficiency is the most common cause of osteoporosis in postmenopausal women, many other conditions may accompany estrogen deficiency and contribute to impaired bone strength in this population.
Among the culprits are some conditions that are not often encountered in the average gynecologic practice: monoclonal gammopathy of undetermined significance (MGUS), multiple myeloma, celiac disease, Crohn’s disease, and other inflammatory bowel diseases. In addition, bariatric surgery, eating disorders, primary hyperparathyroidism, and a number of medications have been implicated in BMD loss or increased risk of fracture, or both. Among the problematic drugs of particular interest to us as gynecologists are aromatase inhibitors, depot medroxyprogesterone acetate, proton pump inhibitors, and gonadotropin-releasing hormone (GnRH) agonists.
Other medications that can affect BMD are glucocorticoids, unfractionated heparin, selective serotonin reuptake inhibitors, excessive amounts of thyroid replacement agents, and some antiseizure medications.
If you suspect a secondary cause of osteoporosis, be prepared to perform a basic workup that includes:
- a careful history and physical examination
- complete blood count
- a chemistry profile, including serum calcium, phosphorous, electrolytes, alkaline phosphatase, and creatinine.
In addition, measurement of 25-hydroxy vitamin D and thyroid-stimulating hormone (TSH) may be helpful, as may serum protein electrophoresis.
Patients who have clinical or laboratory abnormalities suggestive of a secondary cause of osteoporosis are usually referred to a metabolic bone specialist (endocrinology or rheumatology).
When a patient has any clinical history that suggests a secondary cause of bone loss other than menopause-related estrogen deficiency, simple laboratory tests are appropriate and may uncover a condition that necessitates referral to a metabolic bone expert.
Quantitative ultrasound assessment of bone can help predict a woman’s risk of fracture
Guglielmi G, Rossini M, Nicolosi MG, Tagno A, Lentini G, de Terlizzi F. Three-year prospective study on fracture risk in postmenopausal women by quantitative ultrasound at the phalanges [published online ahead of print August 15, 2012]. J Clin Densitom. doi:10.1016 /j.jocd.2012.07.006.
Chan MY, Nguyen ND, Center JR, Eisman JA, Nguyen TV. Quantitative ultrasound and fracture risk prediction in non-osteoporotic men and women as defined by WHO criteria [published online ahead of print August 10, 2012]. Osteoporos Int. doi:10.1007/s00198-012 -2001-2.
I became interested in bone health through my longstanding interest in ultrasound, when a manufacturer asked me to evaluate equipment designed to assess bone density of the heel through quantitative ultrasound (QUS). This modality is not the diagnostic imaging we are familiar with in obstetrics and gynecology. In QUS, the homogeneity of healthy bone promotes sound transmission, whereas the voids and discontinuity of osteoporotic bone impede it. Therefore, normal bone has a faster speed of sound than less healthy bone. The other important quantitative measure is broadband ultrasound attenuation (BUA). Healthy bone is dense and absorbs and scatters sound to a greater extent than osteoporotic bone does.
Two trials of QUS
In 2010, Guglielmi and colleagues contacted 2,210 Italian women who had undergone QUS of the phalanges in 2006–2007. These women had an average age of 60.9 years, entered menopause at an average age of 49.3 years, and had a mean body mass index (BMI) of 26.5 kg/m2. By 2010, this group had experienced 108 new major osteoporotic fractures, including 23 hip fractures and 56 vertebral fractures. Investigators found a statistically significant correlation between QUS findings and fracture risk.
Chan and colleagues focused on 312 women 62 to 92 years of age who had femoral neck BMD, as measured by DXA, of –2.5 or better. QUS was measured as BUA at the calcaneus. The incidence of any fragility fracture was ascertained by radiographic reports during the follow-up period from 1994 to 2011. Eighty women (26%) experienced at least one fragility fracture during follow-up. After adjustment for covariates, women were significantly more likely to experience any fracture if BUA was decreased (hazard ratio [HR], 1.50; 95% confidence interval [CI], 1.13–1.99).
When the models that included BUA were compared with those that used femoral neck BMD, they had a greater area under the curve (0.71, 0.85, 0.71 for any fracture, hip fracture, and vertebral fracture, respectively) and yielded a net reclassification improvement of 16.4% (P=.009) when combined with femoral neck BMD. These findings suggest that calcaneal BUA is an independent predictor of fracture risk in women who have nonosteoporotic BMD.
In an era of increasing pressure to reduce costs, QUS assessment of bone is a promising modality that may be useful as a screening tool. Although it measures different variables than DXA imaging (more microarchitecture, less true density), it seems to predict the risk of fracture at less cost without ionizing radiation.
In the pipeline: A drug that curbs bone resorption without diminishing bone formation
Williams SC. Potential first-in-class osteoporosis drug speeds through trials. Nat Med. 2012;18(8):1158.
Ng KW. Potential role of odanacatib in the treatment of osteoporosis. Clin Interv Aging. 2012;7:235–247.
Alendronate was the first of the oral bisphosphonates to be approved by the US Food and Drug Administration (FDA). Once it was approved in 1999, the drug quickly became the most widely used bone agent in clinical practice and was soon joined by other oral and intravenous bisphosphonates. Regrettably, highly publicized adverse effects have caused many patients to shy away from this class of drugs. Two years ago, the FDA approved denosumab, a subcutaneous injectable agent that is a RANK ligand inhibitor.
The bisphosphonates and denosumab increase bone mass by shutting down the osteoclasts responsible for bone resorption, but they also inhibit creation of new bone. A new category of drug that inhibits the bone-resorption enzyme Cathepsin K appears to inhibit bone resorption without diminishing bone formation. Trials of two previous agents in this class were halted because of adverse effects—particularly effects to the skin, where the enzyme is expressed in addition to bone. However, Phase 2 trials in which odanacatib was compared with alendronate found that the new drug increased BMD almost twice as much as alendronate did, with less reduction in serum markers of bone formation.
Phase 3 trials of odanacatib in 16,000 women older than age 65 recently were halted so that the manufacturer could pursue regulatory approval ahead of the previous schedule. Although Phase 3 data have not been published yet, odanacatib may prove to be an exciting alternative to existing therapies.
Odanacatib is not yet available. However, by discussing therapies that may be “around the corner” with our patients, we demonstrate that we are staying ahead of the curve of scientific development.
We want to hear from you! Tell us what you think.
What is the optimal interval for osteoporosis screening in postmenopausal women before fracture occurrence and osteoporosis?
Steven R. Goldstein, MD (Examining the Evidence, August 2012)
Update on Menopause
Andrew M. Kaunitz, MD (May 2012)
Update on Osteoporosis
Steven R. Goldstein, MD (November 2011)
An appeal to the FDA: Remove the black-box warning for depot medroxyprogesterone acetate?
Andrew M. Kaunitz, MD; David A. Grimes, MD (Guest Editorial, August 2011)
Osteoporosis is a significant health issue—and it is likely to remain so as more and more women live longer and longer. In fact, increasing age is the single biggest risk factor for osteoporotic fragility fracture.
Over the past year, important research has improved our understanding in diverse areas of bone health. In this Update, I highlight studies that:
- seek to elucidate the optimal frequency of dual-energy x-ray absorptiometry (DXA) imaging to assess bone mineral density
- review secondary causes of osteoporosis besides menopause-related estrogen deficiency
- explore the use of quantitative ultrasound (QUS) to predict the risk of fracture
- report on a new class of pharmaceutical agents that inhibit the bone-resorption enzyme Cathepsin K.
All of these issues are clinically relevant to the ObGyn specialty because, when it comes to our patients’ bone health, we often function as the primary care physician.
When is DXA indicated—and how often should it be repeated?
Gourlay ML, Fine JP, Preisser JS, et al; Study of Osteoporotic Fractures Research Group. Bone-density testing interval and transition to osteoporosis in older women. N Engl J Med. 2012;366(3):225–233.
Lewiecki EM, Laster AJ, Miller PD, Bilezikian JP. More bone density testing is needed, not less. J Bone Miner Res. 2012;27(4):739–742.
American Society for Bone and Mineral Research response to media coverage of New England Journal of Medicine study: “Bone density testing interval and transition to osteoporosis in older women” [press release]. http://www.asbmr.org/about/pressreleases/detail.aspx?cid=3801baff-0df3-47c0-874f-08a185d67001. Published February 1, 2012. Accessed October 15, 2012.
Recommendations from professional societies, such as the National Osteoporosis Foundation, the International Society of Clinical Densitometry, and the American College of Obstetricians and Gynecologists say virtually the same thing about DXA imaging: Screening is appropriate for women 65 years and older and for postmenopausal women younger than age 65 who have risk factors for fracture. Risk factors include:
- history of a fragility fracture
- body weight less than 127 lb
- medical causes of bone loss, such as medication or disease
- parental history of hip fracture
- current smoker
- alcoholism
- rheumatoid arthritis.
The measurement of bone mineral density (BMD) has been the cornerstone of the diagnosis of osteopenia and osteoporosis since these classifications were introduced by the World Health Organization (WHO) in 1994. Although we are now able to evaluate a woman’s fracture risk using the FRAX tool, which does not require BMD assessment, DXA scanning has become entrenched in routine clinical practice in the United States. In addition, patients who use drugs to reduce their fracture risk often demand periodic testing to see how they are doing. Even women who do not take medications often want periodic assessment to confirm that they are not “losing bone.” Medicare allows for testing every 23 months.
23-month screening interval does not fit all women
Gourlay and colleagues prospectively followed 4,957 women aged 67 years or older who had no history of hip or vertebral fracture and who were not being treated for osteoporosis. After follow-up for as long as 15 years, investigators found that the better a woman’s initial bone density, the longer it took for her to develop osteoporosis. For example, among women over 67 years of age who had a T-score of –1.0 or better, it would take 16.8 years for 10% of this population to develop osteoporosis. In contrast, among women over 67 years of age who had a T-score of –2.0, it would take only 1.1 years for 10% of this population to develop osteoporosis.
This finding certainly calls into question the notion that all patients should be screened every 23 months. It may be better to think of screening as a way of triaging patients for decisions relative to subsequent follow-up.
Media distorted take-home message
This study was the focus of considerable attention from the media, which implied that too much DXA screening is being performed. In reality, only 13% of women over the age of 65 undergo a baseline DXA scan. However, routine follow-up of all patients at 23-month intervals is clearly not appropriate.
Because this study primarily involved white women older than age 67, extrapolation of its findings to other groups may not be appropriate. Nevertheless, the study helps to underscore the fact that reliance on BMD measurement alone should not be used to determine the need for therapeutic intervention. The FRAX tool can be used on an annual basis to assess a woman’s risk of fracture and does not require follow-up DXA imaging at any arbitrary interval.
In healthy older women, an interval of 23 months for repeat BMD assessment makes little sense. For women who have excellent initial T-scores, clinicians can lengthen this interval significantly.
However, strict reliance on the T-score isn’t the best way to predict a woman’s fracture risk or determine when pharmacologic intervention is warranted. Rather, yearly assessment using a tool such as FRAX should become the standard of care.
Some secondary causes of osteoporosis are overlooked or underappreciated
Miller PD. Unrecognized and unappreciated secondary causes of osteoporosis. Endocrinol Metab Clin North Am. 2012;41(3):613–628.
The fractures traditionally associated with osteoporosis involve the hip and vertebrae, although low-trauma fractures of the humerus, forearm, femur shaft, tibia, and fibula are also associated with a high risk of future fracture in untreated women.
Once a clinician is confident that a patient has osteoporosis, the question is whether the diagnosis is postmenopausal osteoporosis—or some other form of the disease. Although estrogen deficiency is the most common cause of osteoporosis in postmenopausal women, many other conditions may accompany estrogen deficiency and contribute to impaired bone strength in this population.
Among the culprits are some conditions that are not often encountered in the average gynecologic practice: monoclonal gammopathy of undetermined significance (MGUS), multiple myeloma, celiac disease, Crohn’s disease, and other inflammatory bowel diseases. In addition, bariatric surgery, eating disorders, primary hyperparathyroidism, and a number of medications have been implicated in BMD loss or increased risk of fracture, or both. Among the problematic drugs of particular interest to us as gynecologists are aromatase inhibitors, depot medroxyprogesterone acetate, proton pump inhibitors, and gonadotropin-releasing hormone (GnRH) agonists.
Other medications that can affect BMD are glucocorticoids, unfractionated heparin, selective serotonin reuptake inhibitors, excessive amounts of thyroid replacement agents, and some antiseizure medications.
If you suspect a secondary cause of osteoporosis, be prepared to perform a basic workup that includes:
- a careful history and physical examination
- complete blood count
- a chemistry profile, including serum calcium, phosphorous, electrolytes, alkaline phosphatase, and creatinine.
In addition, measurement of 25-hydroxy vitamin D and thyroid-stimulating hormone (TSH) may be helpful, as may serum protein electrophoresis.
Patients who have clinical or laboratory abnormalities suggestive of a secondary cause of osteoporosis are usually referred to a metabolic bone specialist (endocrinology or rheumatology).
When a patient has any clinical history that suggests a secondary cause of bone loss other than menopause-related estrogen deficiency, simple laboratory tests are appropriate and may uncover a condition that necessitates referral to a metabolic bone expert.
Quantitative ultrasound assessment of bone can help predict a woman’s risk of fracture
Guglielmi G, Rossini M, Nicolosi MG, Tagno A, Lentini G, de Terlizzi F. Three-year prospective study on fracture risk in postmenopausal women by quantitative ultrasound at the phalanges [published online ahead of print August 15, 2012]. J Clin Densitom. doi:10.1016 /j.jocd.2012.07.006.
Chan MY, Nguyen ND, Center JR, Eisman JA, Nguyen TV. Quantitative ultrasound and fracture risk prediction in non-osteoporotic men and women as defined by WHO criteria [published online ahead of print August 10, 2012]. Osteoporos Int. doi:10.1007/s00198-012 -2001-2.
I became interested in bone health through my longstanding interest in ultrasound, when a manufacturer asked me to evaluate equipment designed to assess bone density of the heel through quantitative ultrasound (QUS). This modality is not the diagnostic imaging we are familiar with in obstetrics and gynecology. In QUS, the homogeneity of healthy bone promotes sound transmission, whereas the voids and discontinuity of osteoporotic bone impede it. Therefore, normal bone has a faster speed of sound than less healthy bone. The other important quantitative measure is broadband ultrasound attenuation (BUA). Healthy bone is dense and absorbs and scatters sound to a greater extent than osteoporotic bone does.
Two trials of QUS
In 2010, Guglielmi and colleagues contacted 2,210 Italian women who had undergone QUS of the phalanges in 2006–2007. These women had an average age of 60.9 years, entered menopause at an average age of 49.3 years, and had a mean body mass index (BMI) of 26.5 kg/m2. By 2010, this group had experienced 108 new major osteoporotic fractures, including 23 hip fractures and 56 vertebral fractures. Investigators found a statistically significant correlation between QUS findings and fracture risk.
Chan and colleagues focused on 312 women 62 to 92 years of age who had femoral neck BMD, as measured by DXA, of –2.5 or better. QUS was measured as BUA at the calcaneus. The incidence of any fragility fracture was ascertained by radiographic reports during the follow-up period from 1994 to 2011. Eighty women (26%) experienced at least one fragility fracture during follow-up. After adjustment for covariates, women were significantly more likely to experience any fracture if BUA was decreased (hazard ratio [HR], 1.50; 95% confidence interval [CI], 1.13–1.99).
When the models that included BUA were compared with those that used femoral neck BMD, they had a greater area under the curve (0.71, 0.85, 0.71 for any fracture, hip fracture, and vertebral fracture, respectively) and yielded a net reclassification improvement of 16.4% (P=.009) when combined with femoral neck BMD. These findings suggest that calcaneal BUA is an independent predictor of fracture risk in women who have nonosteoporotic BMD.
In an era of increasing pressure to reduce costs, QUS assessment of bone is a promising modality that may be useful as a screening tool. Although it measures different variables than DXA imaging (more microarchitecture, less true density), it seems to predict the risk of fracture at less cost without ionizing radiation.
In the pipeline: A drug that curbs bone resorption without diminishing bone formation
Williams SC. Potential first-in-class osteoporosis drug speeds through trials. Nat Med. 2012;18(8):1158.
Ng KW. Potential role of odanacatib in the treatment of osteoporosis. Clin Interv Aging. 2012;7:235–247.
Alendronate was the first of the oral bisphosphonates to be approved by the US Food and Drug Administration (FDA). Once it was approved in 1999, the drug quickly became the most widely used bone agent in clinical practice and was soon joined by other oral and intravenous bisphosphonates. Regrettably, highly publicized adverse effects have caused many patients to shy away from this class of drugs. Two years ago, the FDA approved denosumab, a subcutaneous injectable agent that is a RANK ligand inhibitor.
The bisphosphonates and denosumab increase bone mass by shutting down the osteoclasts responsible for bone resorption, but they also inhibit creation of new bone. A new category of drug that inhibits the bone-resorption enzyme Cathepsin K appears to inhibit bone resorption without diminishing bone formation. Trials of two previous agents in this class were halted because of adverse effects—particularly effects to the skin, where the enzyme is expressed in addition to bone. However, Phase 2 trials in which odanacatib was compared with alendronate found that the new drug increased BMD almost twice as much as alendronate did, with less reduction in serum markers of bone formation.
Phase 3 trials of odanacatib in 16,000 women older than age 65 recently were halted so that the manufacturer could pursue regulatory approval ahead of the previous schedule. Although Phase 3 data have not been published yet, odanacatib may prove to be an exciting alternative to existing therapies.
Odanacatib is not yet available. However, by discussing therapies that may be “around the corner” with our patients, we demonstrate that we are staying ahead of the curve of scientific development.
We want to hear from you! Tell us what you think.
Polycystic ovary syndrome: The long-term metabolic risks
Part 1. Where we stand with diagnosis and treatment—and
where we're going
Women with polycystic ovary syndrome (PCOS), compared with women without the condition, have a greater chance of developing metabolic syndrome (also known as syndrome X). Recent data have drawn attention to these long-term metabolic risks of PCOS. What is metabolic syndrome, and how can its first-line treatment, metformin, affect my patient’s symptoms of PCOS, including hyperandrogenism, anovulation, infertility, weight loss, and early pregnancy loss?
We address these questions in part 3 of this four-part series, which will continue to be posted on the OBG Management Web site. [Editor’s note: For readers’ ease of access, all installments of this series will, as they are published, be collected on a single Web page of links.]
Metabolic syndrome
![]()
Metabolic syndrome is a cluster of risk factors for cardiovascular disease that, together, increase a woman’s likelihood of a heart attack or stroke (by fourfold compared with those free of the condition) and increase the chance of her developing diabetes mellitus (DM). According to the American Heart Association, between 20% and 25% of the US adult population (between 58 and 73 million men and women) has metabolic syndrome.1
The diagnostic criteria for metabolic syndrome are presence of at least three of the following:
- abdominal obesity (excessive fat tissue in and around the abdomen)
- atherogenic dyslipidemia (blood fat disorders—including elevated triglyceride level, low high-density lipoprotein cholesterol [HDL-C] level, and elevated low-density cholesterol [LDL-C] level—that foster arterial plaque buildup)
- elevated blood pressure
- insulin resistance or glucose intolerance
- prothrombotic state (which is a high level of fibrinogen or plasminogen activator inhibitor–1 in the blood)
- proinflammatory state (which is elevated plasma C-reactive protein level).
Metformin
![]()
Metformin, a biguanide antidiabetic drug, was first described in the scientific literature in 1957.2 It was first marketed in France in 1979, but it did not receive approval by the US Food and Drug Administration (FDA) for DM until 1994. In contrast to sulfonylurea medications, which work rapidly to control elevated blood glucose levels by increasing pancreatic insulin production, metformin is an insulin-sensitizing agent—it improves peripheral insulin sensitivity and suppresses hepatic gluconeogenesis. Metformin is preferred for initial DM treatment because it does not induce hypoglycemia. Although metformin is not FDA-approved to treat PCOS, it is increasingly being used to treat the syndrome in patients with impaired glucose tolerance and those with no impaired glucose tolerance. More recent research has focused on metformin’s effect on other associated maladies of PCOS, including hirsutism, acne, weight loss, anovulation, pregnancy, and pregnancy loss.
Metformin and hirsutism
![]()
PCOS and its associated hyperinsulinemic state causes excess ovarian androgen production and reduces hepatic sex hormone binding globulin (SHBG) production. As treatment with metformin results in lower circulating insulin, the net affect is reduced ovarian androgen production and less free testosterone. Thus, it is reasonable to think metformin would be effective in the treatment of hirsutism. However, conflicting results have been reported with respect to this issue.
While some study results suggest an improvement in patients’ hirsutism symptoms with metformin treatment, results of a recent meta-analysis of randomized controlled trials involving treatment with metformin for at least 6 months for hirsutism suggest that insulin sensitizers provide limited or no important benefit for women with hirsutism. Of 348 studies, 16 trials (22 comparisons) that were eligible for inclusion in the meta-analysis showed a small decrease in Ferriman-Gallwey scores in women treated with insulin sensitizers compared with women treated with placebo. There was no significant difference in hirsutism between women treated with insulin sensitizers and women treated with oral contraceptives; metformin was inferior to both spironolactone and flutamide. Further study into metformin’s role in treatment for hirsutism is warranted.3
Metformin and acne
![]()
The use of insulin-sensitizing agents, such as metformin, to treat acne also requires more research. The same mechanism of action that infers metformin’s use in hirsutism also applies to its use in acne treatment. In a Cochrane Review4 of randomized controlled trials comparing insulin-sensitizing agents to OCs (alone or in combination) for treating acne, limited data demonstrated no evidence of difference in effect between metformin and the OC. This analysis included six trials, four of which compared metformin with an OC (104 participants) and two of which compared an OC combined with metformin with an OC alone (70 participants).
Metformin and weight loss
![]()
Weight loss leads to greater improvements in overall health, increased fecundity, and improved pregnancy outcome. In spite of the advantages, most patients with PCOS have difficulty losing weight and often regain lost weight over time. Many investigators have raised the question as to whether treatment with insulin-sensitizing drugs contributes to weight loss, compared with diet or a lifestyle modification program.
A systematic search of the literature for randomized controlled trials in women of reproductive age that assessed the effect of insulin-sensitizing drugs on weight loss compared with placebo and diet and/or a lifestyle modification program, revealed 14 trials in the literature, including two in women with PCOS.5 Treatment with metformin showed a statistically significant decrease in body mass index compared with placebo, with some indication of greater effect with high-dose metformin (>1,500 mg/day) and longer duration of therapy (>8 weeks).
Clearly, a structured lifestyle modification program to achieve weight loss should still be the first-line treatment in obese women with or without PCOS. Further adequately powered studies are necessary to confirm such findings.2 As new weight loss drugs become available, they should also be considered for treatment of obesity in women with PCOS.
Metformin and anovulation
![]()
While metformin may offer limited assistance with weight loss, especially when combined with diet and lifestyle therapy, and weight loss generally improves ovulation in overweight women with PCOS, there is no evidence that metformin is a powerful ovulatory drug.6 However, results of a meta-analysis that included 17 studies totaling more than 1,600 women with PCOS, showed that metformin did improve ovulation, especially in non-clomiphene–resistant women.7 Metformin alone did not increase the odds of pregnancy, but in combination with clomiphene, pregnancy was increased. The combination of metformin and clomiphene was especially beneficial in clomiphene-resistant women.
It is important to note that, in women with PCOS, treatment with metformin alone, and in combination with clomiphene, helps to reduce the number of multiple pregnancies, compared with treatment with clomiphine alone.9
Metformin and early pregnancy loss
![]()
While there is mixed evidence as to metformin’s effect on early pregnancy loss, the strongest evidence to date does not indicate a beneficial effect. In a large, randomized, prospective study of 626 infertile women with PCOS, the rate of pregnancy loss was similar between the clomiphene only and clomiphene plus metformin groups, and there was a slight trend for an increase in pregnancy loss in the metformin alone group.9
In a comprehensive review of the literature, Mathur and colleagues concludes that, while some studies have found improvements or no difference in the rates of early pregnancy loss with metformin (alone or in combination with clomiphene), there are “no conclusive data to support a beneficial effect of metformin on pregnancy loss.”6
Metformin and pregnancy outcomes
![]()
In a meta-analysis of eight studies of women with PCOS or DM exposed to metformin during the first trimester of pregnancy with major fetal malformations as the primary outcome, the authors concluded there was no evidence of an increased risk with metformin.8
While it is logical to say that metformin could even be beneficial during pregnancy, given its effect of reducing the risk of developing gestational diabetes, there is inadequate evidence to support the use of metformin during pregnancy at this time.6,8
In the next installment: The authors address several questions about current opinion and future considerations:
|
We want to hear from you! Tell us what you think.
1. Nguyen NT, Magno CP, Lane KT, Hinojosa MW, Lane JS. Association of hypertension diabetes, dyslipidemia, and metabolic syndrome with obesity: findings from the National Health and Nutrition Examination Survey, 1999 to 2004. J Am Coll Surg. 2008;207(6):928-934.
2. Bailey CJ. Biguanides and NIDDM. Diabetes Care. 1992;15(6):755-772.
3. Cosma M, Swiglo BA, Flynn DN, et al. Insulin sensitizers for the treatment of hirsutism: a systematic review and meta-analyses of randomized controlled trials. J Clin Endocrinol Metab. 2008;93(4):1135-1142.
4. Costello M, Shrestha B, Eden J, Sjoblom P, Johnson N. Insulin-sensitising drugs versus the combined oral contraceptive pill for hirsuitism acne, and risk of diabetes, cardiovascular disease, and endometrial cancer in polycystic ovary syndrome. Cochrane Database Syst Rev. 2007;(1):CD005552.-
5. Nieuwenhuis-Ruifrok AE, Kuchenbecker WK, Hoek A, Middleton P, Norman RJ. Insulin sensitizing drugs for weight loss in women of reproductive age who are overweight or obese: systematic review and meta-analysis. Hum Reprod Update. 2009;15(1):57-58.
6. Mathur R, Alexander CJ, Yano J, Trivax B, Azziz R. Use of metformin in polycystic ovary syndrome. Am J Obstet Gynecol. 2008;199(6):596-609.
7. Creanga AA, Bradley HM, McCormick C, Witkop CT. Use of metformin in polycystic ovary syndrome: a meta-analysis. Obstet Gynecol. 2008;111(4):959-968.
8. Gilbert C, Valois M, Koren G. Pregnancy outcome after first-trimester exposure to metformin: a meta-analysis. Fertil Steril. 2006;86(3):658-663.
9. Legro RS, Barnhart HX, Schlaff WD, et al. Cooperative Multicenter Reproductive Medicine Network. Clomiphene metformin, or both for infertility in the polycystic ovary syndrome. N Engl J Med. 2007;356(6):551-566.
Part 1. Where we stand with diagnosis and treatment—and
where we're going
Women with polycystic ovary syndrome (PCOS), compared with women without the condition, have a greater chance of developing metabolic syndrome (also known as syndrome X). Recent data have drawn attention to these long-term metabolic risks of PCOS. What is metabolic syndrome, and how can its first-line treatment, metformin, affect my patient’s symptoms of PCOS, including hyperandrogenism, anovulation, infertility, weight loss, and early pregnancy loss?
We address these questions in part 3 of this four-part series, which will continue to be posted on the OBG Management Web site. [Editor’s note: For readers’ ease of access, all installments of this series will, as they are published, be collected on a single Web page of links.]
Metabolic syndrome
![]()
Metabolic syndrome is a cluster of risk factors for cardiovascular disease that, together, increase a woman’s likelihood of a heart attack or stroke (by fourfold compared with those free of the condition) and increase the chance of her developing diabetes mellitus (DM). According to the American Heart Association, between 20% and 25% of the US adult population (between 58 and 73 million men and women) has metabolic syndrome.1
The diagnostic criteria for metabolic syndrome are presence of at least three of the following:
- abdominal obesity (excessive fat tissue in and around the abdomen)
- atherogenic dyslipidemia (blood fat disorders—including elevated triglyceride level, low high-density lipoprotein cholesterol [HDL-C] level, and elevated low-density cholesterol [LDL-C] level—that foster arterial plaque buildup)
- elevated blood pressure
- insulin resistance or glucose intolerance
- prothrombotic state (which is a high level of fibrinogen or plasminogen activator inhibitor–1 in the blood)
- proinflammatory state (which is elevated plasma C-reactive protein level).
Metformin
![]()
Metformin, a biguanide antidiabetic drug, was first described in the scientific literature in 1957.2 It was first marketed in France in 1979, but it did not receive approval by the US Food and Drug Administration (FDA) for DM until 1994. In contrast to sulfonylurea medications, which work rapidly to control elevated blood glucose levels by increasing pancreatic insulin production, metformin is an insulin-sensitizing agent—it improves peripheral insulin sensitivity and suppresses hepatic gluconeogenesis. Metformin is preferred for initial DM treatment because it does not induce hypoglycemia. Although metformin is not FDA-approved to treat PCOS, it is increasingly being used to treat the syndrome in patients with impaired glucose tolerance and those with no impaired glucose tolerance. More recent research has focused on metformin’s effect on other associated maladies of PCOS, including hirsutism, acne, weight loss, anovulation, pregnancy, and pregnancy loss.
Metformin and hirsutism
![]()
PCOS and its associated hyperinsulinemic state causes excess ovarian androgen production and reduces hepatic sex hormone binding globulin (SHBG) production. As treatment with metformin results in lower circulating insulin, the net affect is reduced ovarian androgen production and less free testosterone. Thus, it is reasonable to think metformin would be effective in the treatment of hirsutism. However, conflicting results have been reported with respect to this issue.
While some study results suggest an improvement in patients’ hirsutism symptoms with metformin treatment, results of a recent meta-analysis of randomized controlled trials involving treatment with metformin for at least 6 months for hirsutism suggest that insulin sensitizers provide limited or no important benefit for women with hirsutism. Of 348 studies, 16 trials (22 comparisons) that were eligible for inclusion in the meta-analysis showed a small decrease in Ferriman-Gallwey scores in women treated with insulin sensitizers compared with women treated with placebo. There was no significant difference in hirsutism between women treated with insulin sensitizers and women treated with oral contraceptives; metformin was inferior to both spironolactone and flutamide. Further study into metformin’s role in treatment for hirsutism is warranted.3
Metformin and acne
![]()
The use of insulin-sensitizing agents, such as metformin, to treat acne also requires more research. The same mechanism of action that infers metformin’s use in hirsutism also applies to its use in acne treatment. In a Cochrane Review4 of randomized controlled trials comparing insulin-sensitizing agents to OCs (alone or in combination) for treating acne, limited data demonstrated no evidence of difference in effect between metformin and the OC. This analysis included six trials, four of which compared metformin with an OC (104 participants) and two of which compared an OC combined with metformin with an OC alone (70 participants).
Metformin and weight loss
![]()
Weight loss leads to greater improvements in overall health, increased fecundity, and improved pregnancy outcome. In spite of the advantages, most patients with PCOS have difficulty losing weight and often regain lost weight over time. Many investigators have raised the question as to whether treatment with insulin-sensitizing drugs contributes to weight loss, compared with diet or a lifestyle modification program.
A systematic search of the literature for randomized controlled trials in women of reproductive age that assessed the effect of insulin-sensitizing drugs on weight loss compared with placebo and diet and/or a lifestyle modification program, revealed 14 trials in the literature, including two in women with PCOS.5 Treatment with metformin showed a statistically significant decrease in body mass index compared with placebo, with some indication of greater effect with high-dose metformin (>1,500 mg/day) and longer duration of therapy (>8 weeks).
Clearly, a structured lifestyle modification program to achieve weight loss should still be the first-line treatment in obese women with or without PCOS. Further adequately powered studies are necessary to confirm such findings.2 As new weight loss drugs become available, they should also be considered for treatment of obesity in women with PCOS.
Metformin and anovulation
![]()
While metformin may offer limited assistance with weight loss, especially when combined with diet and lifestyle therapy, and weight loss generally improves ovulation in overweight women with PCOS, there is no evidence that metformin is a powerful ovulatory drug.6 However, results of a meta-analysis that included 17 studies totaling more than 1,600 women with PCOS, showed that metformin did improve ovulation, especially in non-clomiphene–resistant women.7 Metformin alone did not increase the odds of pregnancy, but in combination with clomiphene, pregnancy was increased. The combination of metformin and clomiphene was especially beneficial in clomiphene-resistant women.
It is important to note that, in women with PCOS, treatment with metformin alone, and in combination with clomiphene, helps to reduce the number of multiple pregnancies, compared with treatment with clomiphine alone.9
Metformin and early pregnancy loss
![]()
While there is mixed evidence as to metformin’s effect on early pregnancy loss, the strongest evidence to date does not indicate a beneficial effect. In a large, randomized, prospective study of 626 infertile women with PCOS, the rate of pregnancy loss was similar between the clomiphene only and clomiphene plus metformin groups, and there was a slight trend for an increase in pregnancy loss in the metformin alone group.9
In a comprehensive review of the literature, Mathur and colleagues concludes that, while some studies have found improvements or no difference in the rates of early pregnancy loss with metformin (alone or in combination with clomiphene), there are “no conclusive data to support a beneficial effect of metformin on pregnancy loss.”6
Metformin and pregnancy outcomes
![]()
In a meta-analysis of eight studies of women with PCOS or DM exposed to metformin during the first trimester of pregnancy with major fetal malformations as the primary outcome, the authors concluded there was no evidence of an increased risk with metformin.8
While it is logical to say that metformin could even be beneficial during pregnancy, given its effect of reducing the risk of developing gestational diabetes, there is inadequate evidence to support the use of metformin during pregnancy at this time.6,8
In the next installment: The authors address several questions about current opinion and future considerations:
|
We want to hear from you! Tell us what you think.
Part 1. Where we stand with diagnosis and treatment—and
where we're going
Women with polycystic ovary syndrome (PCOS), compared with women without the condition, have a greater chance of developing metabolic syndrome (also known as syndrome X). Recent data have drawn attention to these long-term metabolic risks of PCOS. What is metabolic syndrome, and how can its first-line treatment, metformin, affect my patient’s symptoms of PCOS, including hyperandrogenism, anovulation, infertility, weight loss, and early pregnancy loss?
We address these questions in part 3 of this four-part series, which will continue to be posted on the OBG Management Web site. [Editor’s note: For readers’ ease of access, all installments of this series will, as they are published, be collected on a single Web page of links.]
Metabolic syndrome
![]()
Metabolic syndrome is a cluster of risk factors for cardiovascular disease that, together, increase a woman’s likelihood of a heart attack or stroke (by fourfold compared with those free of the condition) and increase the chance of her developing diabetes mellitus (DM). According to the American Heart Association, between 20% and 25% of the US adult population (between 58 and 73 million men and women) has metabolic syndrome.1
The diagnostic criteria for metabolic syndrome are presence of at least three of the following:
- abdominal obesity (excessive fat tissue in and around the abdomen)
- atherogenic dyslipidemia (blood fat disorders—including elevated triglyceride level, low high-density lipoprotein cholesterol [HDL-C] level, and elevated low-density cholesterol [LDL-C] level—that foster arterial plaque buildup)
- elevated blood pressure
- insulin resistance or glucose intolerance
- prothrombotic state (which is a high level of fibrinogen or plasminogen activator inhibitor–1 in the blood)
- proinflammatory state (which is elevated plasma C-reactive protein level).
Metformin
![]()
Metformin, a biguanide antidiabetic drug, was first described in the scientific literature in 1957.2 It was first marketed in France in 1979, but it did not receive approval by the US Food and Drug Administration (FDA) for DM until 1994. In contrast to sulfonylurea medications, which work rapidly to control elevated blood glucose levels by increasing pancreatic insulin production, metformin is an insulin-sensitizing agent—it improves peripheral insulin sensitivity and suppresses hepatic gluconeogenesis. Metformin is preferred for initial DM treatment because it does not induce hypoglycemia. Although metformin is not FDA-approved to treat PCOS, it is increasingly being used to treat the syndrome in patients with impaired glucose tolerance and those with no impaired glucose tolerance. More recent research has focused on metformin’s effect on other associated maladies of PCOS, including hirsutism, acne, weight loss, anovulation, pregnancy, and pregnancy loss.
Metformin and hirsutism
![]()
PCOS and its associated hyperinsulinemic state causes excess ovarian androgen production and reduces hepatic sex hormone binding globulin (SHBG) production. As treatment with metformin results in lower circulating insulin, the net affect is reduced ovarian androgen production and less free testosterone. Thus, it is reasonable to think metformin would be effective in the treatment of hirsutism. However, conflicting results have been reported with respect to this issue.
While some study results suggest an improvement in patients’ hirsutism symptoms with metformin treatment, results of a recent meta-analysis of randomized controlled trials involving treatment with metformin for at least 6 months for hirsutism suggest that insulin sensitizers provide limited or no important benefit for women with hirsutism. Of 348 studies, 16 trials (22 comparisons) that were eligible for inclusion in the meta-analysis showed a small decrease in Ferriman-Gallwey scores in women treated with insulin sensitizers compared with women treated with placebo. There was no significant difference in hirsutism between women treated with insulin sensitizers and women treated with oral contraceptives; metformin was inferior to both spironolactone and flutamide. Further study into metformin’s role in treatment for hirsutism is warranted.3
Metformin and acne
![]()
The use of insulin-sensitizing agents, such as metformin, to treat acne also requires more research. The same mechanism of action that infers metformin’s use in hirsutism also applies to its use in acne treatment. In a Cochrane Review4 of randomized controlled trials comparing insulin-sensitizing agents to OCs (alone or in combination) for treating acne, limited data demonstrated no evidence of difference in effect between metformin and the OC. This analysis included six trials, four of which compared metformin with an OC (104 participants) and two of which compared an OC combined with metformin with an OC alone (70 participants).
Metformin and weight loss
![]()
Weight loss leads to greater improvements in overall health, increased fecundity, and improved pregnancy outcome. In spite of the advantages, most patients with PCOS have difficulty losing weight and often regain lost weight over time. Many investigators have raised the question as to whether treatment with insulin-sensitizing drugs contributes to weight loss, compared with diet or a lifestyle modification program.
A systematic search of the literature for randomized controlled trials in women of reproductive age that assessed the effect of insulin-sensitizing drugs on weight loss compared with placebo and diet and/or a lifestyle modification program, revealed 14 trials in the literature, including two in women with PCOS.5 Treatment with metformin showed a statistically significant decrease in body mass index compared with placebo, with some indication of greater effect with high-dose metformin (>1,500 mg/day) and longer duration of therapy (>8 weeks).
Clearly, a structured lifestyle modification program to achieve weight loss should still be the first-line treatment in obese women with or without PCOS. Further adequately powered studies are necessary to confirm such findings.2 As new weight loss drugs become available, they should also be considered for treatment of obesity in women with PCOS.
Metformin and anovulation
![]()
While metformin may offer limited assistance with weight loss, especially when combined with diet and lifestyle therapy, and weight loss generally improves ovulation in overweight women with PCOS, there is no evidence that metformin is a powerful ovulatory drug.6 However, results of a meta-analysis that included 17 studies totaling more than 1,600 women with PCOS, showed that metformin did improve ovulation, especially in non-clomiphene–resistant women.7 Metformin alone did not increase the odds of pregnancy, but in combination with clomiphene, pregnancy was increased. The combination of metformin and clomiphene was especially beneficial in clomiphene-resistant women.
It is important to note that, in women with PCOS, treatment with metformin alone, and in combination with clomiphene, helps to reduce the number of multiple pregnancies, compared with treatment with clomiphine alone.9
Metformin and early pregnancy loss
![]()
While there is mixed evidence as to metformin’s effect on early pregnancy loss, the strongest evidence to date does not indicate a beneficial effect. In a large, randomized, prospective study of 626 infertile women with PCOS, the rate of pregnancy loss was similar between the clomiphene only and clomiphene plus metformin groups, and there was a slight trend for an increase in pregnancy loss in the metformin alone group.9
In a comprehensive review of the literature, Mathur and colleagues concludes that, while some studies have found improvements or no difference in the rates of early pregnancy loss with metformin (alone or in combination with clomiphene), there are “no conclusive data to support a beneficial effect of metformin on pregnancy loss.”6
Metformin and pregnancy outcomes
![]()
In a meta-analysis of eight studies of women with PCOS or DM exposed to metformin during the first trimester of pregnancy with major fetal malformations as the primary outcome, the authors concluded there was no evidence of an increased risk with metformin.8
While it is logical to say that metformin could even be beneficial during pregnancy, given its effect of reducing the risk of developing gestational diabetes, there is inadequate evidence to support the use of metformin during pregnancy at this time.6,8
In the next installment: The authors address several questions about current opinion and future considerations:
|
We want to hear from you! Tell us what you think.
1. Nguyen NT, Magno CP, Lane KT, Hinojosa MW, Lane JS. Association of hypertension diabetes, dyslipidemia, and metabolic syndrome with obesity: findings from the National Health and Nutrition Examination Survey, 1999 to 2004. J Am Coll Surg. 2008;207(6):928-934.
2. Bailey CJ. Biguanides and NIDDM. Diabetes Care. 1992;15(6):755-772.
3. Cosma M, Swiglo BA, Flynn DN, et al. Insulin sensitizers for the treatment of hirsutism: a systematic review and meta-analyses of randomized controlled trials. J Clin Endocrinol Metab. 2008;93(4):1135-1142.
4. Costello M, Shrestha B, Eden J, Sjoblom P, Johnson N. Insulin-sensitising drugs versus the combined oral contraceptive pill for hirsuitism acne, and risk of diabetes, cardiovascular disease, and endometrial cancer in polycystic ovary syndrome. Cochrane Database Syst Rev. 2007;(1):CD005552.-
5. Nieuwenhuis-Ruifrok AE, Kuchenbecker WK, Hoek A, Middleton P, Norman RJ. Insulin sensitizing drugs for weight loss in women of reproductive age who are overweight or obese: systematic review and meta-analysis. Hum Reprod Update. 2009;15(1):57-58.
6. Mathur R, Alexander CJ, Yano J, Trivax B, Azziz R. Use of metformin in polycystic ovary syndrome. Am J Obstet Gynecol. 2008;199(6):596-609.
7. Creanga AA, Bradley HM, McCormick C, Witkop CT. Use of metformin in polycystic ovary syndrome: a meta-analysis. Obstet Gynecol. 2008;111(4):959-968.
8. Gilbert C, Valois M, Koren G. Pregnancy outcome after first-trimester exposure to metformin: a meta-analysis. Fertil Steril. 2006;86(3):658-663.
9. Legro RS, Barnhart HX, Schlaff WD, et al. Cooperative Multicenter Reproductive Medicine Network. Clomiphene metformin, or both for infertility in the polycystic ovary syndrome. N Engl J Med. 2007;356(6):551-566.
1. Nguyen NT, Magno CP, Lane KT, Hinojosa MW, Lane JS. Association of hypertension diabetes, dyslipidemia, and metabolic syndrome with obesity: findings from the National Health and Nutrition Examination Survey, 1999 to 2004. J Am Coll Surg. 2008;207(6):928-934.
2. Bailey CJ. Biguanides and NIDDM. Diabetes Care. 1992;15(6):755-772.
3. Cosma M, Swiglo BA, Flynn DN, et al. Insulin sensitizers for the treatment of hirsutism: a systematic review and meta-analyses of randomized controlled trials. J Clin Endocrinol Metab. 2008;93(4):1135-1142.
4. Costello M, Shrestha B, Eden J, Sjoblom P, Johnson N. Insulin-sensitising drugs versus the combined oral contraceptive pill for hirsuitism acne, and risk of diabetes, cardiovascular disease, and endometrial cancer in polycystic ovary syndrome. Cochrane Database Syst Rev. 2007;(1):CD005552.-
5. Nieuwenhuis-Ruifrok AE, Kuchenbecker WK, Hoek A, Middleton P, Norman RJ. Insulin sensitizing drugs for weight loss in women of reproductive age who are overweight or obese: systematic review and meta-analysis. Hum Reprod Update. 2009;15(1):57-58.
6. Mathur R, Alexander CJ, Yano J, Trivax B, Azziz R. Use of metformin in polycystic ovary syndrome. Am J Obstet Gynecol. 2008;199(6):596-609.
7. Creanga AA, Bradley HM, McCormick C, Witkop CT. Use of metformin in polycystic ovary syndrome: a meta-analysis. Obstet Gynecol. 2008;111(4):959-968.
8. Gilbert C, Valois M, Koren G. Pregnancy outcome after first-trimester exposure to metformin: a meta-analysis. Fertil Steril. 2006;86(3):658-663.
9. Legro RS, Barnhart HX, Schlaff WD, et al. Cooperative Multicenter Reproductive Medicine Network. Clomiphene metformin, or both for infertility in the polycystic ovary syndrome. N Engl J Med. 2007;356(6):551-566.