User login
Encountering the Victim of Sexual Assault
Each year in the United States, between 300,000 and 700,000 adult women are estimated to experience sexual assault, with 40,000 of such victims typically seeking treatment in an emergency department (ED).1 In a survey of hospital EDs published in 2008, only 9.6% of the 117 responding hospitals provided to presenting victims of sexual assault all of the following elements of comprehensive medical care management2:
• Acute medical care
•
History and physical examination
•
Acute and long-term rape crisis counseling
•
Prophylactic and therapeutic management for HIV or other sexually transmitted infection (STI)
•
Provision of emergency contraception, with appropriate counseling.2
Specific data from a similar survey included these findings: appropriate, CDC-recommended prophylaxis against STI prescribed in only 6.7% of cases, HIV serology testing in only 13%, and information about follow-up care given to only 31% of patients. Nearly 80% of sexual assault victims treated in the responding hospital EDs received less than optimal care.3,4
In the ED, where victims of sexual assault are most likely to be evaluated, the responsibilities involved in managing the department may hamper emergency physicians’ ability to provide the detailed, time-consuming, one-on-one care such patients require; often, this care is entrusted to an NP or an RN.1 Clinicians in this setting, as well as those who practice in student health, primary care, and women’s health, must be competent in assessing and treating the injuries assaulted patients have sustained, providing STI prophylaxis and pregnancy prevention, collecting forensic evidence in order to facilitate prosecution of the perpetrator, and providing appropriate referrals to promote physical and emotional recovery through counseling and other follow-up care—in short, meeting these patients’ medical, legal, and psychosocial needs.5,6 (See “Specialized Training, a Team Response.”5-7)
DEFINITIONS: RAPE AND SEXUAL ASSAULT
The definition of rape varies from state to state, but three criteria are typically present:
•
Sexual penetration of the victim’s vagina, mouth, or rectum
•
Absence of consent from the victim
• The use or threat of force.8
Sexual assault is a less restrictive term, referring to the sexual contact of one person with another without appropriate consent. Specified manifestations vary state by state but typically include child sexual assault, incest, marital rape, and other forced sexual acts.7
“Julie,” 18, presents to the ED, accompanied by a female friend, after being sexually assaulted by a male student from the college Julie attends. Earlier that evening, Julie was drinking alcohol at a party in the suspect’s apartment. While everyone else was dancing, he invited Julie to his room. She admits that she was willing to “fool around” with him, but when he asked to have intercourse, she said “no.” The suspect insisted that she “wanted it” and proceeded to engage in unprotected intercourse with her. Julie is distressed because she was a virgin until the encounter and had not been using any form of birth control.
On presentation of a victim of sexual assault, local law enforcement and an advocate from the local rape crisis center should be promptly notified; however, the patient’s permission must be obtained before the police department is contacted. A victim may not want to report a sexual assault to the police for a number of reasons, including:
•
A belief that the police are limited in their ability to intervene effectively
•
A perception that victims of sexual assault are often considered at fault
•
Fear that the assailant may assault the victim again
•
Misplaced feelings of fear and shame.5
The NP or PA who performs the initial examination should make every effort to interview the patient while both law enforcement and the advocate are present so that the victim is not required to describe and relive the traumatic situation repeatedly. The advocate is present to support the victim throughout the ED or office visit and evidence collection process; and to provide referrals for follow-up care.
The clinician must strive to remain objective during the evaluation and evidence collection process. For example, the detection of another person’s DNA on the body of the patient is not proof, in and of itself, of that person’s guilt, but only the presence of his or her DNA.9
HISTORY AND PHYSICAL
A thorough medical history and assessment should always be completed, either before or after the forensic examination, depending on the patient’s condition.
Evidence collection is begun by obtaining consent and interviewing the patient. The patient’s account of the assault will guide the practitioner to specific areas of the body where evidence may be found (for example, the case patient said the suspect had kissed her neck, which was swabbed to corroborate her story). Whatever the patient’s age, the presence of a family member or friend is not recommended during the interview, as this could cause the victim to withhold information, and any emotional reaction may be a distraction for the patient. Additionally, having a family member or friend present during the interview process puts that individual at risk for subpoena and court appearance.7
The interview should be concise, with the patient’s account of the assault recorded in some way so that he or she can later be quoted as closely as possible. The clinician should avoid using medical or legal terms or abbreviations, or altering the patient’s own words.
Before the physical examination is begun, the patient’s clothing must be collected and each piece packaged in a separate paper bag. Women’s underpants are the garment most likely to contain “transfer from the perpetrator.”10
Julie had changed her clothes before coming to the ED but was wearing the same underpants she had on at the time of the assault. This garment was collected in a paper bag.
The physical exam is conducted in a head-to-toe manner. Each marking found on the victim must be charted on a diagram of the body or the genitalia (see Figure 1). Injuries should be described using the mnemonic TEARS: tissue integrity, ecchymoses, abrasions, redness, and swelling.11 The most common descriptors include abrasions that are tangential or patterned, fingernail markings, contusions, and lacerations.

When the clinician examines the patient’s genitalia and anal area, it is important to report a thorough description of any injuries. The most common area of injury in the female sexual assault victim is a small tear to the posterior fourchette. Visualization can be enhanced by use of toluidine blue dye—but this must be applied before use of a speculum,12 and not until after any photographs of the outer genitalia have been taken.
Photographs should be taken of all injuries, then presented to the police. It is suggested that each injury be photographed from a medium distance, and up close with a ruler or other scale.7
Julie stated that she had been a virgin prior to the assault. She was placed in the lithotomy position, and a careful internal inspection was performed. Gentle retraction of the labia with a good light source allowed adequate visualization. Photographs were taken of an acute laceration of the hymen at the 5:00 position.
PHYSICAL EVIDENCE
Next, evidence is collected from the patient’s body. Fingernails are clipped and saved for possible DNA from the suspect, especially if the victim reports having tried to fight back. The fingernail trimmings from each hand should be packaged separately, with labels.7
Debris is combed from the head hair and pubic hair. This can be significant for confirming details from the victim’s story, such as being attacked and thrown into the mud. Next, the patient’s head hair is collected. When plucking the hair, the examiner must ensure that the root is intact, since the patient’s DNA is contained therein. This can be important for distinguishing the patient’s hair from that of the suspect. Hairs should be chosen from a few different areas of the patient’s head.7
Oral, genital, and anal swabs are collected. For collection of evidence from a female patient, a speculum exam is required.12 The vagina is swabbed with at least four different cotton swabs: one for the cervix, and the other three to collect visualized secretions.10 For each area, a clean, sterile swab should be moistened with distilled water and used to swab lightly, rotating downward. A dry sterile swab is then used to re-swab the area lightly and lift the DNA. Collected swabs should be allowed to dry completely before the packaging is sealed to minimize the risk for contamination by bacterial growth.
Use of a Wood’s lamp can help the examiner detect semen and saliva on the patient’s body.10 However, a recent examination of alternate light sources with appropriate wavelengths has demonstrated improved detection of trace DNA evidence.13
Once the steps in evidence collection have been completed, the patient can be permitted to urinate, shower, brush his or her teeth, and make any necessary phone calls.
Storing and Protecting the Evidence
It is imperative for the NP or PA who completes the kit to maintain the chain of custody—that is, never leaving the evidence unattended until the police collect it. This will eliminate the possibility of tampering or any other reason for the legal system to designate the evidence as inadmissible. If it is not feasible for the responsible clinician to guard the evidence, it must be placed under lock and key, with limited availability to others.10
Evidence that cannot be thoroughly dried during the examination (eg, tampon, condom, tissues) should be collected in a sterile specimen cup and sent to the crime lab immediately.7 Otherwise, if such a sample is packaged and left to sit, the risk increases for any DNA to become contaminated by bacterial growth.
To verify that the chain of custody was maintained, several items must be signed or initialed by both the provider and the law enforcement officer who receives the kit:
•
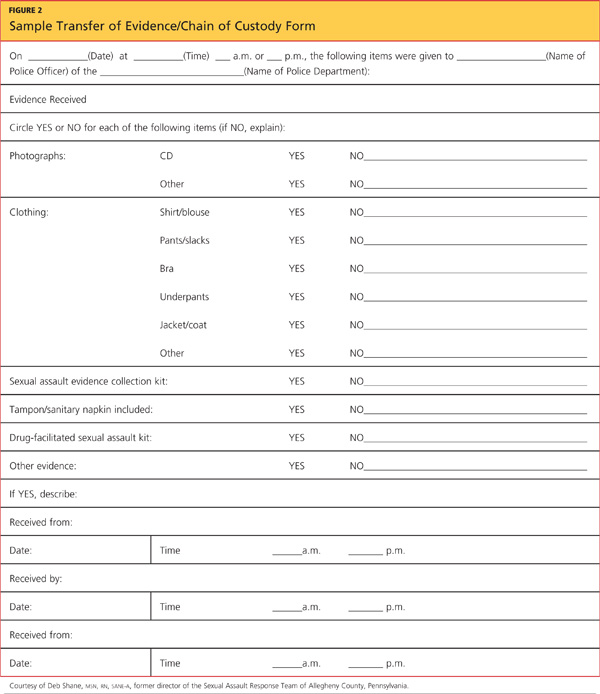
The evidence log sheet. This should be included in the original kit (see Figure 2 for a sample). It should be removed from the kit, completed, and affixed to the outside of the kit before the kit is sealed. A copy of this log should be kept attached to the patient chart.
•
The evidence kit itself. The lid bears a form to be completed by the practitioner.
•
The components of evidence other than the kit (ie, clothing bags, sterile specimen cups containing collected specimens). These bear labels, preprinted with the patient’s name, date of birth, and medical record number, which are signed by the practitioner.
TREATMENT AND
PROPHYLAXIS
The likelihood for a sexual assault victim to have contracted an STI is 26.3%.3 Current recommendations from the CDC,4 including postexposure vaccination against hepatitis B, must be followed for prevention of and treatment for STI. Prophylactic treatment for gonorrhea, chlamydia, and trichomonas should be offered to all victims of sexual assault, as cultures are not taken until patient follow-up at the primary care provider’s office or the county health department.4 Prophylactic treatment for hepatitis B or HIV may be discussed with the patient; he or she must be fully informed about the rigorous follow-up treatment regimens required, as well as the associated adverse effects.
According to the CDC,4 baseline test results for HIV, hepatitis B, and syphilis may be negative, but antibodies can develop over time; thus, reexamination with re-testing should be performed at three months, six months, and 12 months postassault.
Progestin-only emergency contraceptive tablets should be offered through 72 hours postassault to all female sexual assault victims with a negative pregnancy test result in the ED.14
Julie was treated with intramuscular ceftriaxone 250 mg for prevention of gonorrhea, azithromycin 1 g by mouth for prevention of chlamydia, and progestin for pregnancy prevention. She had undergone the hepatitis B vaccination series as a child and had a positive titer drawn before the current school year. Julie declined prophylaxis for HIV because she felt the suspect was at low risk for HIV; however, she was encouraged to undergo HIV testing at her follow-up visit at the local health department.
FOLLOW-UP
Follow-up counseling is a vital component of care for the victim of sexual assault. The police will arrange to ensure the patient’s safety at home before he or she is discharged. A victim of sexual assault should never be discharged if suicidal ideation is evident; in this case, a psychiatry consult must be arranged. For survivors of sexual assault who reside in remote or rural areas, treatment via videoconferencing-based technology has been shown to reduce measures of depression and posttraumatic stress.15
Information regarding rape crisis services should be provided before patients are discharged; the advocate present during the exam should be familiar with services offered in the area. These centers offer emotional support, helpful medical and legal information, and post-rape counseling.7
CONCLUSION
Although the ED is ordinarily the first medical entry point for a sexual assault victim, clinicians in other settings, too, must be prepared to offer medical care to these patients and collect forensic evidence appropriately. Comprehensive care of a sexual assault victim must be completed in a timely and sensitive manner, with documentation that can withstand the exacting requirements of the court system.
REFERENCES
1. Sampsel K, Szobota L, Joyce D, et al. The impact of a sexual assault/domestic violence program on ED care. J Emerg Nurs. 2009;35(4): 282-289.
2. Patel A, Panchal H, Piotrowski ZH, Patel D. Comprehensive medical care for victims of sexual assault: a survey of Illinois hospital emergency departments. Contraception. 2008;77(6):426-430.
3. Straight JD, Heaton PC. Emergency department care for victims of sexual offense. Am J Health Syst Pharm. 2007;64(17):1845-1850.
4. CDC. Sexually transmitted disease treatment guidelines, 2010: sexual assault and STDs (2010). www.cdc.gov/std/treat ment/2010/sexual-assault.htm. Accessed November 26, 2012.
5. Stermac L, Dunlap H, Bainbridge D. Sexual assault services delivered by SANEs. J Forensic Nurs. 2005;1(3):124-128.
6. Plichta SB, Clements PT, Houseman C. Why SANEs matter: models of care for sexual violence victims in the emergency department.
J Forensic Nurs. 2007;3(1):15-23.
7. National Criminal Justice Reference Services. A national protocol for sexual assault medical forensic examinations: adults/adolescents (2004). www.ncjrs.gov/pdffiles1/ovw/206554.pdf. Accessed November 26, 2012.
8. Burgess AW, Hazelwood RR. Victim care services and the Comprehensive Sexual Assault Assessment Tool (CSAAT). In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:47-68.
9. Burg A, Kahn R, Welch K. DNA testing of sexual assault evidence: the laboratory perspective. J Forensic Nurs. 2011;7(3):145-152.
10. Brown K. Forensic examination of sexual assault victims. In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:365-381.
11. Slaughter L, Brown CR, Crowley S, Peck R. Patterns of genital injury in female sexual assault victims. Am J Obstet Gynecol. 1997; 176(3):609-616.
12. Jones JS, Dunnuck C, Rossman L, et al. Significance of toluidine blue positive findings after speculum examination for sexual assault. Am J Emerg Med. 2004;22(3):201-203.
13. Eldredge K, Huggins E, Pugh LC. Alternate light sources in sexual assault examinations: an evidence-based practice project. J Forensic Nurs. 2012;8(1):39-44.
14. Ledray LE. Evidence collection and care of the sexual assault survivor: the SANE/SART response (2001). www.mincava.umn.edu/documents/commissioned/2forensicevidence/2forensicevidence.pdf. Accessed November 26, 2012.
15. Hassija C, Gray MJ. The effectiveness and feasibility of videoconferencing technology to provide evidence-based treatment to rural domestic violence and sexual assault populations. Telemed J E Health. 2011;17(4):30
Each year in the United States, between 300,000 and 700,000 adult women are estimated to experience sexual assault, with 40,000 of such victims typically seeking treatment in an emergency department (ED).1 In a survey of hospital EDs published in 2008, only 9.6% of the 117 responding hospitals provided to presenting victims of sexual assault all of the following elements of comprehensive medical care management2:
• Acute medical care
•
History and physical examination
•
Acute and long-term rape crisis counseling
•
Prophylactic and therapeutic management for HIV or other sexually transmitted infection (STI)
•
Provision of emergency contraception, with appropriate counseling.2
Specific data from a similar survey included these findings: appropriate, CDC-recommended prophylaxis against STI prescribed in only 6.7% of cases, HIV serology testing in only 13%, and information about follow-up care given to only 31% of patients. Nearly 80% of sexual assault victims treated in the responding hospital EDs received less than optimal care.3,4
In the ED, where victims of sexual assault are most likely to be evaluated, the responsibilities involved in managing the department may hamper emergency physicians’ ability to provide the detailed, time-consuming, one-on-one care such patients require; often, this care is entrusted to an NP or an RN.1 Clinicians in this setting, as well as those who practice in student health, primary care, and women’s health, must be competent in assessing and treating the injuries assaulted patients have sustained, providing STI prophylaxis and pregnancy prevention, collecting forensic evidence in order to facilitate prosecution of the perpetrator, and providing appropriate referrals to promote physical and emotional recovery through counseling and other follow-up care—in short, meeting these patients’ medical, legal, and psychosocial needs.5,6 (See “Specialized Training, a Team Response.”5-7)
DEFINITIONS: RAPE AND SEXUAL ASSAULT
The definition of rape varies from state to state, but three criteria are typically present:
•
Sexual penetration of the victim’s vagina, mouth, or rectum
•
Absence of consent from the victim
• The use or threat of force.8
Sexual assault is a less restrictive term, referring to the sexual contact of one person with another without appropriate consent. Specified manifestations vary state by state but typically include child sexual assault, incest, marital rape, and other forced sexual acts.7
“Julie,” 18, presents to the ED, accompanied by a female friend, after being sexually assaulted by a male student from the college Julie attends. Earlier that evening, Julie was drinking alcohol at a party in the suspect’s apartment. While everyone else was dancing, he invited Julie to his room. She admits that she was willing to “fool around” with him, but when he asked to have intercourse, she said “no.” The suspect insisted that she “wanted it” and proceeded to engage in unprotected intercourse with her. Julie is distressed because she was a virgin until the encounter and had not been using any form of birth control.
On presentation of a victim of sexual assault, local law enforcement and an advocate from the local rape crisis center should be promptly notified; however, the patient’s permission must be obtained before the police department is contacted. A victim may not want to report a sexual assault to the police for a number of reasons, including:
•
A belief that the police are limited in their ability to intervene effectively
•
A perception that victims of sexual assault are often considered at fault
•
Fear that the assailant may assault the victim again
•
Misplaced feelings of fear and shame.5
The NP or PA who performs the initial examination should make every effort to interview the patient while both law enforcement and the advocate are present so that the victim is not required to describe and relive the traumatic situation repeatedly. The advocate is present to support the victim throughout the ED or office visit and evidence collection process; and to provide referrals for follow-up care.
The clinician must strive to remain objective during the evaluation and evidence collection process. For example, the detection of another person’s DNA on the body of the patient is not proof, in and of itself, of that person’s guilt, but only the presence of his or her DNA.9
HISTORY AND PHYSICAL
A thorough medical history and assessment should always be completed, either before or after the forensic examination, depending on the patient’s condition.
Evidence collection is begun by obtaining consent and interviewing the patient. The patient’s account of the assault will guide the practitioner to specific areas of the body where evidence may be found (for example, the case patient said the suspect had kissed her neck, which was swabbed to corroborate her story). Whatever the patient’s age, the presence of a family member or friend is not recommended during the interview, as this could cause the victim to withhold information, and any emotional reaction may be a distraction for the patient. Additionally, having a family member or friend present during the interview process puts that individual at risk for subpoena and court appearance.7
The interview should be concise, with the patient’s account of the assault recorded in some way so that he or she can later be quoted as closely as possible. The clinician should avoid using medical or legal terms or abbreviations, or altering the patient’s own words.
Before the physical examination is begun, the patient’s clothing must be collected and each piece packaged in a separate paper bag. Women’s underpants are the garment most likely to contain “transfer from the perpetrator.”10
Julie had changed her clothes before coming to the ED but was wearing the same underpants she had on at the time of the assault. This garment was collected in a paper bag.
The physical exam is conducted in a head-to-toe manner. Each marking found on the victim must be charted on a diagram of the body or the genitalia (see Figure 1). Injuries should be described using the mnemonic TEARS: tissue integrity, ecchymoses, abrasions, redness, and swelling.11 The most common descriptors include abrasions that are tangential or patterned, fingernail markings, contusions, and lacerations.
When the clinician examines the patient’s genitalia and anal area, it is important to report a thorough description of any injuries. The most common area of injury in the female sexual assault victim is a small tear to the posterior fourchette. Visualization can be enhanced by use of toluidine blue dye—but this must be applied before use of a speculum,12 and not until after any photographs of the outer genitalia have been taken.
Photographs should be taken of all injuries, then presented to the police. It is suggested that each injury be photographed from a medium distance, and up close with a ruler or other scale.7
Julie stated that she had been a virgin prior to the assault. She was placed in the lithotomy position, and a careful internal inspection was performed. Gentle retraction of the labia with a good light source allowed adequate visualization. Photographs were taken of an acute laceration of the hymen at the 5:00 position.
PHYSICAL EVIDENCE
Next, evidence is collected from the patient’s body. Fingernails are clipped and saved for possible DNA from the suspect, especially if the victim reports having tried to fight back. The fingernail trimmings from each hand should be packaged separately, with labels.7
Debris is combed from the head hair and pubic hair. This can be significant for confirming details from the victim’s story, such as being attacked and thrown into the mud. Next, the patient’s head hair is collected. When plucking the hair, the examiner must ensure that the root is intact, since the patient’s DNA is contained therein. This can be important for distinguishing the patient’s hair from that of the suspect. Hairs should be chosen from a few different areas of the patient’s head.7
Oral, genital, and anal swabs are collected. For collection of evidence from a female patient, a speculum exam is required.12 The vagina is swabbed with at least four different cotton swabs: one for the cervix, and the other three to collect visualized secretions.10 For each area, a clean, sterile swab should be moistened with distilled water and used to swab lightly, rotating downward. A dry sterile swab is then used to re-swab the area lightly and lift the DNA. Collected swabs should be allowed to dry completely before the packaging is sealed to minimize the risk for contamination by bacterial growth.
Use of a Wood’s lamp can help the examiner detect semen and saliva on the patient’s body.10 However, a recent examination of alternate light sources with appropriate wavelengths has demonstrated improved detection of trace DNA evidence.13
Once the steps in evidence collection have been completed, the patient can be permitted to urinate, shower, brush his or her teeth, and make any necessary phone calls.
Storing and Protecting the Evidence
It is imperative for the NP or PA who completes the kit to maintain the chain of custody—that is, never leaving the evidence unattended until the police collect it. This will eliminate the possibility of tampering or any other reason for the legal system to designate the evidence as inadmissible. If it is not feasible for the responsible clinician to guard the evidence, it must be placed under lock and key, with limited availability to others.10
Evidence that cannot be thoroughly dried during the examination (eg, tampon, condom, tissues) should be collected in a sterile specimen cup and sent to the crime lab immediately.7 Otherwise, if such a sample is packaged and left to sit, the risk increases for any DNA to become contaminated by bacterial growth.
To verify that the chain of custody was maintained, several items must be signed or initialed by both the provider and the law enforcement officer who receives the kit:
•
The evidence log sheet. This should be included in the original kit (see Figure 2 for a sample). It should be removed from the kit, completed, and affixed to the outside of the kit before the kit is sealed. A copy of this log should be kept attached to the patient chart.
•
The evidence kit itself. The lid bears a form to be completed by the practitioner.
•
The components of evidence other than the kit (ie, clothing bags, sterile specimen cups containing collected specimens). These bear labels, preprinted with the patient’s name, date of birth, and medical record number, which are signed by the practitioner.
TREATMENT AND
PROPHYLAXIS
The likelihood for a sexual assault victim to have contracted an STI is 26.3%.3 Current recommendations from the CDC,4 including postexposure vaccination against hepatitis B, must be followed for prevention of and treatment for STI. Prophylactic treatment for gonorrhea, chlamydia, and trichomonas should be offered to all victims of sexual assault, as cultures are not taken until patient follow-up at the primary care provider’s office or the county health department.4 Prophylactic treatment for hepatitis B or HIV may be discussed with the patient; he or she must be fully informed about the rigorous follow-up treatment regimens required, as well as the associated adverse effects.
According to the CDC,4 baseline test results for HIV, hepatitis B, and syphilis may be negative, but antibodies can develop over time; thus, reexamination with re-testing should be performed at three months, six months, and 12 months postassault.
Progestin-only emergency contraceptive tablets should be offered through 72 hours postassault to all female sexual assault victims with a negative pregnancy test result in the ED.14
Julie was treated with intramuscular ceftriaxone 250 mg for prevention of gonorrhea, azithromycin 1 g by mouth for prevention of chlamydia, and progestin for pregnancy prevention. She had undergone the hepatitis B vaccination series as a child and had a positive titer drawn before the current school year. Julie declined prophylaxis for HIV because she felt the suspect was at low risk for HIV; however, she was encouraged to undergo HIV testing at her follow-up visit at the local health department.
FOLLOW-UP
Follow-up counseling is a vital component of care for the victim of sexual assault. The police will arrange to ensure the patient’s safety at home before he or she is discharged. A victim of sexual assault should never be discharged if suicidal ideation is evident; in this case, a psychiatry consult must be arranged. For survivors of sexual assault who reside in remote or rural areas, treatment via videoconferencing-based technology has been shown to reduce measures of depression and posttraumatic stress.15
Information regarding rape crisis services should be provided before patients are discharged; the advocate present during the exam should be familiar with services offered in the area. These centers offer emotional support, helpful medical and legal information, and post-rape counseling.7
CONCLUSION
Although the ED is ordinarily the first medical entry point for a sexual assault victim, clinicians in other settings, too, must be prepared to offer medical care to these patients and collect forensic evidence appropriately. Comprehensive care of a sexual assault victim must be completed in a timely and sensitive manner, with documentation that can withstand the exacting requirements of the court system.
REFERENCES
1. Sampsel K, Szobota L, Joyce D, et al. The impact of a sexual assault/domestic violence program on ED care. J Emerg Nurs. 2009;35(4): 282-289.
2. Patel A, Panchal H, Piotrowski ZH, Patel D. Comprehensive medical care for victims of sexual assault: a survey of Illinois hospital emergency departments. Contraception. 2008;77(6):426-430.
3. Straight JD, Heaton PC. Emergency department care for victims of sexual offense. Am J Health Syst Pharm. 2007;64(17):1845-1850.
4. CDC. Sexually transmitted disease treatment guidelines, 2010: sexual assault and STDs (2010). www.cdc.gov/std/treat ment/2010/sexual-assault.htm. Accessed November 26, 2012.
5. Stermac L, Dunlap H, Bainbridge D. Sexual assault services delivered by SANEs. J Forensic Nurs. 2005;1(3):124-128.
6. Plichta SB, Clements PT, Houseman C. Why SANEs matter: models of care for sexual violence victims in the emergency department.
J Forensic Nurs. 2007;3(1):15-23.
7. National Criminal Justice Reference Services. A national protocol for sexual assault medical forensic examinations: adults/adolescents (2004). www.ncjrs.gov/pdffiles1/ovw/206554.pdf. Accessed November 26, 2012.
8. Burgess AW, Hazelwood RR. Victim care services and the Comprehensive Sexual Assault Assessment Tool (CSAAT). In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:47-68.
9. Burg A, Kahn R, Welch K. DNA testing of sexual assault evidence: the laboratory perspective. J Forensic Nurs. 2011;7(3):145-152.
10. Brown K. Forensic examination of sexual assault victims. In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:365-381.
11. Slaughter L, Brown CR, Crowley S, Peck R. Patterns of genital injury in female sexual assault victims. Am J Obstet Gynecol. 1997; 176(3):609-616.
12. Jones JS, Dunnuck C, Rossman L, et al. Significance of toluidine blue positive findings after speculum examination for sexual assault. Am J Emerg Med. 2004;22(3):201-203.
13. Eldredge K, Huggins E, Pugh LC. Alternate light sources in sexual assault examinations: an evidence-based practice project. J Forensic Nurs. 2012;8(1):39-44.
14. Ledray LE. Evidence collection and care of the sexual assault survivor: the SANE/SART response (2001). www.mincava.umn.edu/documents/commissioned/2forensicevidence/2forensicevidence.pdf. Accessed November 26, 2012.
15. Hassija C, Gray MJ. The effectiveness and feasibility of videoconferencing technology to provide evidence-based treatment to rural domestic violence and sexual assault populations. Telemed J E Health. 2011;17(4):30
Each year in the United States, between 300,000 and 700,000 adult women are estimated to experience sexual assault, with 40,000 of such victims typically seeking treatment in an emergency department (ED).1 In a survey of hospital EDs published in 2008, only 9.6% of the 117 responding hospitals provided to presenting victims of sexual assault all of the following elements of comprehensive medical care management2:
• Acute medical care
•
History and physical examination
•
Acute and long-term rape crisis counseling
•
Prophylactic and therapeutic management for HIV or other sexually transmitted infection (STI)
•
Provision of emergency contraception, with appropriate counseling.2
Specific data from a similar survey included these findings: appropriate, CDC-recommended prophylaxis against STI prescribed in only 6.7% of cases, HIV serology testing in only 13%, and information about follow-up care given to only 31% of patients. Nearly 80% of sexual assault victims treated in the responding hospital EDs received less than optimal care.3,4
In the ED, where victims of sexual assault are most likely to be evaluated, the responsibilities involved in managing the department may hamper emergency physicians’ ability to provide the detailed, time-consuming, one-on-one care such patients require; often, this care is entrusted to an NP or an RN.1 Clinicians in this setting, as well as those who practice in student health, primary care, and women’s health, must be competent in assessing and treating the injuries assaulted patients have sustained, providing STI prophylaxis and pregnancy prevention, collecting forensic evidence in order to facilitate prosecution of the perpetrator, and providing appropriate referrals to promote physical and emotional recovery through counseling and other follow-up care—in short, meeting these patients’ medical, legal, and psychosocial needs.5,6 (See “Specialized Training, a Team Response.”5-7)
DEFINITIONS: RAPE AND SEXUAL ASSAULT
The definition of rape varies from state to state, but three criteria are typically present:
•
Sexual penetration of the victim’s vagina, mouth, or rectum
•
Absence of consent from the victim
• The use or threat of force.8
Sexual assault is a less restrictive term, referring to the sexual contact of one person with another without appropriate consent. Specified manifestations vary state by state but typically include child sexual assault, incest, marital rape, and other forced sexual acts.7
“Julie,” 18, presents to the ED, accompanied by a female friend, after being sexually assaulted by a male student from the college Julie attends. Earlier that evening, Julie was drinking alcohol at a party in the suspect’s apartment. While everyone else was dancing, he invited Julie to his room. She admits that she was willing to “fool around” with him, but when he asked to have intercourse, she said “no.” The suspect insisted that she “wanted it” and proceeded to engage in unprotected intercourse with her. Julie is distressed because she was a virgin until the encounter and had not been using any form of birth control.
On presentation of a victim of sexual assault, local law enforcement and an advocate from the local rape crisis center should be promptly notified; however, the patient’s permission must be obtained before the police department is contacted. A victim may not want to report a sexual assault to the police for a number of reasons, including:
•
A belief that the police are limited in their ability to intervene effectively
•
A perception that victims of sexual assault are often considered at fault
•
Fear that the assailant may assault the victim again
•
Misplaced feelings of fear and shame.5
The NP or PA who performs the initial examination should make every effort to interview the patient while both law enforcement and the advocate are present so that the victim is not required to describe and relive the traumatic situation repeatedly. The advocate is present to support the victim throughout the ED or office visit and evidence collection process; and to provide referrals for follow-up care.
The clinician must strive to remain objective during the evaluation and evidence collection process. For example, the detection of another person’s DNA on the body of the patient is not proof, in and of itself, of that person’s guilt, but only the presence of his or her DNA.9
HISTORY AND PHYSICAL
A thorough medical history and assessment should always be completed, either before or after the forensic examination, depending on the patient’s condition.
Evidence collection is begun by obtaining consent and interviewing the patient. The patient’s account of the assault will guide the practitioner to specific areas of the body where evidence may be found (for example, the case patient said the suspect had kissed her neck, which was swabbed to corroborate her story). Whatever the patient’s age, the presence of a family member or friend is not recommended during the interview, as this could cause the victim to withhold information, and any emotional reaction may be a distraction for the patient. Additionally, having a family member or friend present during the interview process puts that individual at risk for subpoena and court appearance.7
The interview should be concise, with the patient’s account of the assault recorded in some way so that he or she can later be quoted as closely as possible. The clinician should avoid using medical or legal terms or abbreviations, or altering the patient’s own words.
Before the physical examination is begun, the patient’s clothing must be collected and each piece packaged in a separate paper bag. Women’s underpants are the garment most likely to contain “transfer from the perpetrator.”10
Julie had changed her clothes before coming to the ED but was wearing the same underpants she had on at the time of the assault. This garment was collected in a paper bag.
The physical exam is conducted in a head-to-toe manner. Each marking found on the victim must be charted on a diagram of the body or the genitalia (see Figure 1). Injuries should be described using the mnemonic TEARS: tissue integrity, ecchymoses, abrasions, redness, and swelling.11 The most common descriptors include abrasions that are tangential or patterned, fingernail markings, contusions, and lacerations.
When the clinician examines the patient’s genitalia and anal area, it is important to report a thorough description of any injuries. The most common area of injury in the female sexual assault victim is a small tear to the posterior fourchette. Visualization can be enhanced by use of toluidine blue dye—but this must be applied before use of a speculum,12 and not until after any photographs of the outer genitalia have been taken.
Photographs should be taken of all injuries, then presented to the police. It is suggested that each injury be photographed from a medium distance, and up close with a ruler or other scale.7
Julie stated that she had been a virgin prior to the assault. She was placed in the lithotomy position, and a careful internal inspection was performed. Gentle retraction of the labia with a good light source allowed adequate visualization. Photographs were taken of an acute laceration of the hymen at the 5:00 position.
PHYSICAL EVIDENCE
Next, evidence is collected from the patient’s body. Fingernails are clipped and saved for possible DNA from the suspect, especially if the victim reports having tried to fight back. The fingernail trimmings from each hand should be packaged separately, with labels.7
Debris is combed from the head hair and pubic hair. This can be significant for confirming details from the victim’s story, such as being attacked and thrown into the mud. Next, the patient’s head hair is collected. When plucking the hair, the examiner must ensure that the root is intact, since the patient’s DNA is contained therein. This can be important for distinguishing the patient’s hair from that of the suspect. Hairs should be chosen from a few different areas of the patient’s head.7
Oral, genital, and anal swabs are collected. For collection of evidence from a female patient, a speculum exam is required.12 The vagina is swabbed with at least four different cotton swabs: one for the cervix, and the other three to collect visualized secretions.10 For each area, a clean, sterile swab should be moistened with distilled water and used to swab lightly, rotating downward. A dry sterile swab is then used to re-swab the area lightly and lift the DNA. Collected swabs should be allowed to dry completely before the packaging is sealed to minimize the risk for contamination by bacterial growth.
Use of a Wood’s lamp can help the examiner detect semen and saliva on the patient’s body.10 However, a recent examination of alternate light sources with appropriate wavelengths has demonstrated improved detection of trace DNA evidence.13
Once the steps in evidence collection have been completed, the patient can be permitted to urinate, shower, brush his or her teeth, and make any necessary phone calls.
Storing and Protecting the Evidence
It is imperative for the NP or PA who completes the kit to maintain the chain of custody—that is, never leaving the evidence unattended until the police collect it. This will eliminate the possibility of tampering or any other reason for the legal system to designate the evidence as inadmissible. If it is not feasible for the responsible clinician to guard the evidence, it must be placed under lock and key, with limited availability to others.10
Evidence that cannot be thoroughly dried during the examination (eg, tampon, condom, tissues) should be collected in a sterile specimen cup and sent to the crime lab immediately.7 Otherwise, if such a sample is packaged and left to sit, the risk increases for any DNA to become contaminated by bacterial growth.
To verify that the chain of custody was maintained, several items must be signed or initialed by both the provider and the law enforcement officer who receives the kit:
•
The evidence log sheet. This should be included in the original kit (see Figure 2 for a sample). It should be removed from the kit, completed, and affixed to the outside of the kit before the kit is sealed. A copy of this log should be kept attached to the patient chart.
•
The evidence kit itself. The lid bears a form to be completed by the practitioner.
•
The components of evidence other than the kit (ie, clothing bags, sterile specimen cups containing collected specimens). These bear labels, preprinted with the patient’s name, date of birth, and medical record number, which are signed by the practitioner.
TREATMENT AND
PROPHYLAXIS
The likelihood for a sexual assault victim to have contracted an STI is 26.3%.3 Current recommendations from the CDC,4 including postexposure vaccination against hepatitis B, must be followed for prevention of and treatment for STI. Prophylactic treatment for gonorrhea, chlamydia, and trichomonas should be offered to all victims of sexual assault, as cultures are not taken until patient follow-up at the primary care provider’s office or the county health department.4 Prophylactic treatment for hepatitis B or HIV may be discussed with the patient; he or she must be fully informed about the rigorous follow-up treatment regimens required, as well as the associated adverse effects.
According to the CDC,4 baseline test results for HIV, hepatitis B, and syphilis may be negative, but antibodies can develop over time; thus, reexamination with re-testing should be performed at three months, six months, and 12 months postassault.
Progestin-only emergency contraceptive tablets should be offered through 72 hours postassault to all female sexual assault victims with a negative pregnancy test result in the ED.14
Julie was treated with intramuscular ceftriaxone 250 mg for prevention of gonorrhea, azithromycin 1 g by mouth for prevention of chlamydia, and progestin for pregnancy prevention. She had undergone the hepatitis B vaccination series as a child and had a positive titer drawn before the current school year. Julie declined prophylaxis for HIV because she felt the suspect was at low risk for HIV; however, she was encouraged to undergo HIV testing at her follow-up visit at the local health department.
FOLLOW-UP
Follow-up counseling is a vital component of care for the victim of sexual assault. The police will arrange to ensure the patient’s safety at home before he or she is discharged. A victim of sexual assault should never be discharged if suicidal ideation is evident; in this case, a psychiatry consult must be arranged. For survivors of sexual assault who reside in remote or rural areas, treatment via videoconferencing-based technology has been shown to reduce measures of depression and posttraumatic stress.15
Information regarding rape crisis services should be provided before patients are discharged; the advocate present during the exam should be familiar with services offered in the area. These centers offer emotional support, helpful medical and legal information, and post-rape counseling.7
CONCLUSION
Although the ED is ordinarily the first medical entry point for a sexual assault victim, clinicians in other settings, too, must be prepared to offer medical care to these patients and collect forensic evidence appropriately. Comprehensive care of a sexual assault victim must be completed in a timely and sensitive manner, with documentation that can withstand the exacting requirements of the court system.
REFERENCES
1. Sampsel K, Szobota L, Joyce D, et al. The impact of a sexual assault/domestic violence program on ED care. J Emerg Nurs. 2009;35(4): 282-289.
2. Patel A, Panchal H, Piotrowski ZH, Patel D. Comprehensive medical care for victims of sexual assault: a survey of Illinois hospital emergency departments. Contraception. 2008;77(6):426-430.
3. Straight JD, Heaton PC. Emergency department care for victims of sexual offense. Am J Health Syst Pharm. 2007;64(17):1845-1850.
4. CDC. Sexually transmitted disease treatment guidelines, 2010: sexual assault and STDs (2010). www.cdc.gov/std/treat ment/2010/sexual-assault.htm. Accessed November 26, 2012.
5. Stermac L, Dunlap H, Bainbridge D. Sexual assault services delivered by SANEs. J Forensic Nurs. 2005;1(3):124-128.
6. Plichta SB, Clements PT, Houseman C. Why SANEs matter: models of care for sexual violence victims in the emergency department.
J Forensic Nurs. 2007;3(1):15-23.
7. National Criminal Justice Reference Services. A national protocol for sexual assault medical forensic examinations: adults/adolescents (2004). www.ncjrs.gov/pdffiles1/ovw/206554.pdf. Accessed November 26, 2012.
8. Burgess AW, Hazelwood RR. Victim care services and the Comprehensive Sexual Assault Assessment Tool (CSAAT). In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:47-68.
9. Burg A, Kahn R, Welch K. DNA testing of sexual assault evidence: the laboratory perspective. J Forensic Nurs. 2011;7(3):145-152.
10. Brown K. Forensic examination of sexual assault victims. In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:365-381.
11. Slaughter L, Brown CR, Crowley S, Peck R. Patterns of genital injury in female sexual assault victims. Am J Obstet Gynecol. 1997; 176(3):609-616.
12. Jones JS, Dunnuck C, Rossman L, et al. Significance of toluidine blue positive findings after speculum examination for sexual assault. Am J Emerg Med. 2004;22(3):201-203.
13. Eldredge K, Huggins E, Pugh LC. Alternate light sources in sexual assault examinations: an evidence-based practice project. J Forensic Nurs. 2012;8(1):39-44.
14. Ledray LE. Evidence collection and care of the sexual assault survivor: the SANE/SART response (2001). www.mincava.umn.edu/documents/commissioned/2forensicevidence/2forensicevidence.pdf. Accessed November 26, 2012.
15. Hassija C, Gray MJ. The effectiveness and feasibility of videoconferencing technology to provide evidence-based treatment to rural domestic violence and sexual assault populations. Telemed J E Health. 2011;17(4):30
Grand Rounds: Woman, 38, With Pulseless Electrical Activity
On an autumn day, a 38-year-old woman with a history of asthma presented to the emergency department (ED) with the chief complaint of shortness of breath (SOB). The patient described her SOB as sudden in onset and not relieved by use of her albuterol inhaler; hence the ED visit.
She denied any chest pain, palpitations, dizziness, orthopnea, upper respiratory tract infection, cough, wheezing, fever or chills, headache, vision changes, body aches, sick contacts, or pets at home. She said she uses her albuterol inhaler as needed, and that she had used it that day for the first time in “a few months.” She denied any history of intubation or steroid use. Additionally, she had not been seen by a primary care provider in years.
The woman, a native of Ghana, had been living in the United States for many years. She denied any recent travel or exposure to toxic chemicals; any use of tobacco, alcohol, or illicit drugs; or any history of sexually transmitted disease.
The patient was afebrile (temperature, 98.6°F), with a respiratory rate of 20 breaths/min; blood pressure, 144/69 mm Hg; and ventricular rate, 125 beats/min. On physical examination, her extraocular movements were intact; pupils were equal, round, reactive to light and accommodation; and sclera were nonicteric. The patient’s head was normocephalic and atraumatic, and the neck was supple with normal range of motion and no jugular venous distension or lymphadenopathy. Her mucous membranes were moist with no pharyngeal erythema or exudates. Cardiovascular examination, including ECG, revealed tachycardia but no murmurs or gallops.
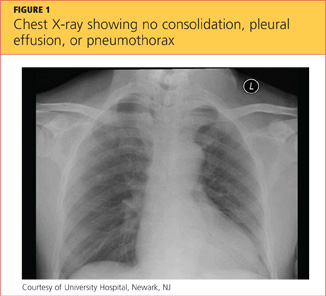
While being evaluated in the ED, the patient became tachypneic and began to experience respiratory distress. She was intubated for airway protection, at which time she developed pulseless electrical activity (PEA), with 30 beats/min. She responded to atropine and epinephrine injections. A repeat ECG showed sinus tachycardia and right atrial enlargement with right-axis deviation. Chest x-ray (see Figure 1) showed no consolidation, pleural effusion, or pneumothorax.
Results from the patient’s lab work are shown in the table, above. Negative results were reported for a urine pregnancy test.

Since there was no clear etiology for the patient’s PEA, she underwent pan-culturing, with the following tests ordered: HIV antibody testing, immunovirology for influenza A and B viruses, and urine toxicology. Doppler ultrasound of the bilateral lower extremities was also ordered, in addition to chest CT and transthoracic and transesophageal echocardiography (TTE and TEE, respectively). The patient was intubated and transferred to the medical ICU for further management.
The differential diagnosis included cardiac tamponade, acute MI, acute pulmonary embolus (PE), tension pneumothorax, hypovolemia, and asthma exacerbated by viral or bacterial infection.1,2 Although the case patient presented with PEA, she did not have the presenting signs of cardiac tamponade known as Beck’s triad: hypotension, jugular venous distension, and muffled heart sounds.3 TTE showed an ejection fraction of 65% and grade 2 diastolic dysfunction but no pericardial effusions (which accumulate rapidly in the patient with cardiac tamponade, resulting from fluid buildup in the pericardial layers),4 and TEE showed no atrial thrombi (which can masquerade as cardiac tamponade5). The patient had no signs of trauma and denied any history of malignancy (both potential causes of cardiac tamponade). Chest x-ray showed normal heart size and no pneumothorax, consolidations, or pleural effusions.4,6-8 Thus, the diagnosis of cardiac tamponade was ruled out.
Common presenting symptoms of acute MI include sudden-onset chest pain, SOB, palpitations, dizziness, nausea, and/or vomiting. Women may experience less dramatic symptoms—often little more than SOB and fatigue.9 According to a 2000 consensus document from a joint European Society of Cardiology/American College of Cardiology committee10 in which MI was redefined, the diagnosis of MI relies on a rise in cardiac troponin levels, typical MI symptoms, and changes in ECG showing pathological Q waves or ST elevation or depression. The case patient’s troponin I level was less than 0.02 ng/mL, and ECG did not reveal Q waves or ST-T wave changes; additionally, since the patient had no chest pain, palpitations, diaphoresis, nausea, or vomiting, acute MI was ruled out.
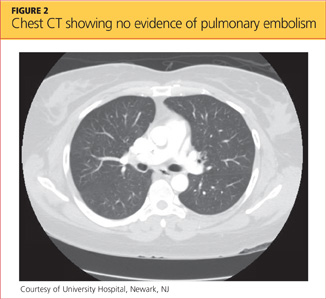
Blood clots capable of blocking the pulmonary artery usually originate in the deep veins of the lower extremities.11 Three main factors, called Virchow’s triad, are known to contribute to these deep vein thromboses (DVTs): venous stasis, endothelial injury, and a hypercoagulability state.12,13 The patient had denied any trauma, recent travel, history of malignancy, or use of tobacco or oral contraceptives, and the result of her urine pregnancy test was negative. Even though the patient presented with tachypnea and acute SOB, with ECG showing right-axis deviation and tachycardia (common presenting signs and symptoms for PE), her chest CT showed no evidence of PE (see Figure 2); additionally, Doppler ultrasound of the bilateral lower extremities revealed no DVTs. Thus, PE was also excluded.
Tension pneumothorax was also ruled out, as chest x-ray showed neither mediastinal shift nor tracheal deviation, and the patient had denied any trauma. Laboratory analyses did not indicate hyponatremia, and the patient’s hemoglobin and hematocrit were satisfactory. She was tachycardic on admission, but her blood pressure was stable. As the patient denied any use of vasodilators or diuretics, hypovolemia was ruled out.
Patients experiencing asthma exacerbation can present with acute SOB, which usually resolves following use of IV steroids, nebulizer therapy, and inhaler treatments. Despite being administered IV methylprednisolone and magnesium sulfate in the ED, the patient experienced PEA and respiratory distress and required intubation for airway protection.
The HIV test was nonreactive, and blood and urine cultures did not show any growth. Results of tests for Legionella urinary antigen and Streptococcus pneumoniae antigen were negative. Sputum culture showed normal flora. Immunovirology testing, however, was positive for both influenza A and B antigens.
Chest X-ray showed no acute pulmonary pathology, nor did chest CT show any central, interlobar, or segmental embolism or mediastinal lymphadenopathy. It was determined that the patient’s acute SOB might represent asthma exacerbation secondary to influenza viral infection. Her PEA was attributed to possible acute pericarditis secondary to concomitant influenza A and B viral infection.
DISCUSSION
Currently, the CDC recognizes three types of influenza virus: A, B, and C.14 Only influenza A viruses are further classified into subtypes, based on the presence of surface proteins called hemagglutinin (HA) or neuraminidase (NA) glycoproteins. Humans can be infected by influenza A subtypes H1N1 and H3N2.14 Influenza B viruses, found mostly in humans, are associated with significant morbidity and mortality.
Influenza A and B viruses are further classified into strains that change with each flu season—thus, the need to update vaccinations against influenza A and B each year. No vaccination exists against influenza C virus, which is known to cause only mild illness in humans.15
In patients with asthma (as in the case patient), chronic bronchitis, or emphysema, infection with the influenza virus can manifest with SOB, in addition to the more common symptoms of fever, sore throat, headache, rhinorrhea, chills, muscle aches, and general discomfort.16 Patients with coronary artery disease, congestive heart failure (CHF), and/or a history of smoking may experience more severe symptoms and increased risk for influenza-associated mortality than do other patients.17,18
Rare cardiac complications of influenza infections are myocarditis and benign acute pericarditis; myocarditis can progress to CHF and death.19,20 A case of acute myopericarditis was reported by Proby et al21 in a patient with acute influenza A infection who developed pericardial effusions, myositis, tamponade, and pleurisy. That patient recovered after pericardiocentesis and administration of inotropic drugs.
In the literature, a few cases of acute pericarditis have been reported in association with administration of the influenza vaccination.22,23
In the case patient, the diagnosis of influenza A and B was made following testing of nasal and nasopharyngeal swabs with an immunochromatographic assay that uses highly sensitive monoclonal antibodies to detect influenza A and B nucleoprotein antigens.24,25
According to reports in the literature, two-thirds of cases of acute pericarditis are caused by infection, most commonly viral infection (including influenza virus, adenovirus, enterovirus, cytomegalovirus, hepatitis B virus, and herpes simplex virus).26,27 Other etiologies for acute pericarditis are autoimmune (accounting for less than 10% of cases) and neoplastic conditions (5% to 7% of cases).26
PATIENT OUTCOME
Consultation with an infectious disease specialist was obtained. The patient was placed under droplet isolation precautions and was started on a nebulizer, IV steroid treatments, and oseltamivir 75 mg by mouth every 12 hours. She was transferred to a medical floor, where she completed a five-day course of oseltamivir.
As a result of timely intervention, the patient was discharged in stable condition on a therapeutic regimen that included albuterol, fluticasone, and salmeterol inhalation, in addition to tapered-dose steroids. She was advised to follow up with her primary care provider and at the pulmonary clinic.
CONCLUSION
To our knowledge, this is the first reported case of acute pericarditis in a patient with concomitant acute infections with influenza A and B. According to conclusions reached in recent literature, further research is needed to explain the pathophysiology of influenza viral infections, associated cardiovascular morbidity and mortality, and the degree to which these can be prevented by influenza vaccination.1,28 Also to be pursued through research is a better understanding of the morbidity and mortality associated with influenza viruses, especially in children and in adults affected by asthma, cardiac disease, and/or obesity.
REFERENCES
1. Finelli L, Chaves SS. Influenza and acute myocardial infarction. J Infect Dis. 2011;203(12):
1701-1704.
2. Steiger HV, Rimbach K, Müller E, Breitkreutz R. Focused emergency echocardiography: lifesaving tool for a 14-year-old girl suffering out-of-hospital pulseless electrical activity arrest because of cardiac tamponade. Eur J Emerg Med. 2009;16(2): 103-105.
3. Goodman A, Perera P, Mailhot T, Mandavia D. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade.
J Emerg Trauma Shock. 2012;5(1):72-75.
4. Restrepo CS, Lemos DF, Lemos JA, et al. Imaging findings in cardiac tamponade with emphasis on CT. Radiographics. 2007;27(6):1595-1610.
5. Papanagnou D, Stone MB. Massive right atrial thrombus masquerading as cardiac tamponade. Acad Emerg Med. 2010;17(2):E11.
6. Saito Y, Donohue A, Attai S, et al. The syndrome of cardiac tamponade with “small” pericardial effusion. Echocardiography. 2008;25(3): 321-327.
7. Lin E, Boire A, Hemmige V, et al. Cardiac tamponade mimicking tuberculous pericarditis as the initial presentation of chronic lymphocytic leukemia in a 58-year-old woman: a case report. J Med Case Rep. 2010;4:246.
8. Meniconi A, Attenhofer Jost CH, Jenni R. How to survive myocardial rupture after myocardial infarction. Heart. 2000;84(5):552.
9. Kosuge M, Kimura K, Ishikawa T, et al. Differences between men and women in terms of clinical features of ST-segment elevation acute myocardial infarction. Circ J. 2006;70(3):222-226.
10. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-969.
11. Goldhaber SZ. Deep venous thrombosis and pulmonary thromboembolism. In: Fauci AS, Braunwald E, Kasper DL, et al. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw-Hill Medical; 2008:1651–1657.
12. Brooks EG, Trotman W, Wadsworth MP, et al. Valves of the deep venous system: an overlooked risk factor. Blood. 2009;114(6):1276-1279.
13. Kyrle PA, Eichinger S. Is Virchow’s triad complete? Blood. 2009;114(6):1138-1139.
14. CDC. Seasonal influenza (flu): types of influenza viruses (2012). www.cdc.gov/flu/about/viruses/types.htm. Accessed October 24, 2012.
15. CDC. Seasonal influenza (flu)(2012). www.cdc .gov/flu. Accessed October 24, 2012.
16. Eccles R. Understanding the symptoms of the common cold and influenza. Lancet Infect Dis. 2005;5(11):718-725.
17. Angelo SJ, Marshall PS, Chrissoheris MP, Chaves AM. Clinical characteristics associated with poor outcome in patients acutely infected with Influenza A. Conn Med. 2004;68(4):199-205.
18. Murin S, Bilello K. Respiratory tract infections: another reason not to smoke. Cleve Clin J Med. 2005;72(10):916-920.
19. Ray CG, Icenogle TB, Minnich LL, et al. The use of intravenous ribavirin to treat influenza virus–associated acute myocarditis. J Infect Dis. 1989; 159(5):829-836.
20. Fairley CK, Ryan M, Wall PG, Weinberg J. The organism reported to cause infective myocarditis and pericarditis in England and Wales. J Infect. 1996;32(3):223-225.
21. Proby CM, Hackett D, Gupta S, Cox TM. Acute myopericarditis in influenza A infection. Q J Med. 1986;60(233):887-892.
22. Streifler JJ, Dux S, Garty M, Rosenfeld JB. Recurrent pericarditis: a rare complication of influenza vaccination. Br Med J (Clin Res Ed). 1981; 283(6290):526-527.
23. Desson JF, Leprévost M, Vabret F, Davy A. Acute benign pericarditis after anti-influenza vaccination [in French]. Presse Med. 1997;26 (9):415.
24. BinaxNOW® Influenza A&B Test Kit (product instructions). www.diagnosticsdirect2u.com/images/PDF/Binax%20Now%20416-022%20PPI .pdf. Accessed October 24, 2012.
25. 510(k) Substantial Equivalence Determination Decision Summary [BinaxNow® Influenza A & B Test] (2009). www.accessdata.fda.gov/cdrh_docs/reviews/K062109.pdf. Accessed October 24, 2012.
26. Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121(7):916-928.
27. Maisch B, Seferovic PM, Ristic AD, et al; Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases: executive summary. Eur Heart J. 2004;25(7):587-610.
28. McCullers JA, Hayden FG. Fatal influenza B infections: time to reexamine influenza research priorities. J Infect Dis. 2012;205(6):870-872.
On an autumn day, a 38-year-old woman with a history of asthma presented to the emergency department (ED) with the chief complaint of shortness of breath (SOB). The patient described her SOB as sudden in onset and not relieved by use of her albuterol inhaler; hence the ED visit.
She denied any chest pain, palpitations, dizziness, orthopnea, upper respiratory tract infection, cough, wheezing, fever or chills, headache, vision changes, body aches, sick contacts, or pets at home. She said she uses her albuterol inhaler as needed, and that she had used it that day for the first time in “a few months.” She denied any history of intubation or steroid use. Additionally, she had not been seen by a primary care provider in years.
The woman, a native of Ghana, had been living in the United States for many years. She denied any recent travel or exposure to toxic chemicals; any use of tobacco, alcohol, or illicit drugs; or any history of sexually transmitted disease.
The patient was afebrile (temperature, 98.6°F), with a respiratory rate of 20 breaths/min; blood pressure, 144/69 mm Hg; and ventricular rate, 125 beats/min. On physical examination, her extraocular movements were intact; pupils were equal, round, reactive to light and accommodation; and sclera were nonicteric. The patient’s head was normocephalic and atraumatic, and the neck was supple with normal range of motion and no jugular venous distension or lymphadenopathy. Her mucous membranes were moist with no pharyngeal erythema or exudates. Cardiovascular examination, including ECG, revealed tachycardia but no murmurs or gallops.
While being evaluated in the ED, the patient became tachypneic and began to experience respiratory distress. She was intubated for airway protection, at which time she developed pulseless electrical activity (PEA), with 30 beats/min. She responded to atropine and epinephrine injections. A repeat ECG showed sinus tachycardia and right atrial enlargement with right-axis deviation. Chest x-ray (see Figure 1) showed no consolidation, pleural effusion, or pneumothorax.
Results from the patient’s lab work are shown in the table, above. Negative results were reported for a urine pregnancy test.
Since there was no clear etiology for the patient’s PEA, she underwent pan-culturing, with the following tests ordered: HIV antibody testing, immunovirology for influenza A and B viruses, and urine toxicology. Doppler ultrasound of the bilateral lower extremities was also ordered, in addition to chest CT and transthoracic and transesophageal echocardiography (TTE and TEE, respectively). The patient was intubated and transferred to the medical ICU for further management.
The differential diagnosis included cardiac tamponade, acute MI, acute pulmonary embolus (PE), tension pneumothorax, hypovolemia, and asthma exacerbated by viral or bacterial infection.1,2 Although the case patient presented with PEA, she did not have the presenting signs of cardiac tamponade known as Beck’s triad: hypotension, jugular venous distension, and muffled heart sounds.3 TTE showed an ejection fraction of 65% and grade 2 diastolic dysfunction but no pericardial effusions (which accumulate rapidly in the patient with cardiac tamponade, resulting from fluid buildup in the pericardial layers),4 and TEE showed no atrial thrombi (which can masquerade as cardiac tamponade5). The patient had no signs of trauma and denied any history of malignancy (both potential causes of cardiac tamponade). Chest x-ray showed normal heart size and no pneumothorax, consolidations, or pleural effusions.4,6-8 Thus, the diagnosis of cardiac tamponade was ruled out.
Common presenting symptoms of acute MI include sudden-onset chest pain, SOB, palpitations, dizziness, nausea, and/or vomiting. Women may experience less dramatic symptoms—often little more than SOB and fatigue.9 According to a 2000 consensus document from a joint European Society of Cardiology/American College of Cardiology committee10 in which MI was redefined, the diagnosis of MI relies on a rise in cardiac troponin levels, typical MI symptoms, and changes in ECG showing pathological Q waves or ST elevation or depression. The case patient’s troponin I level was less than 0.02 ng/mL, and ECG did not reveal Q waves or ST-T wave changes; additionally, since the patient had no chest pain, palpitations, diaphoresis, nausea, or vomiting, acute MI was ruled out.
Blood clots capable of blocking the pulmonary artery usually originate in the deep veins of the lower extremities.11 Three main factors, called Virchow’s triad, are known to contribute to these deep vein thromboses (DVTs): venous stasis, endothelial injury, and a hypercoagulability state.12,13 The patient had denied any trauma, recent travel, history of malignancy, or use of tobacco or oral contraceptives, and the result of her urine pregnancy test was negative. Even though the patient presented with tachypnea and acute SOB, with ECG showing right-axis deviation and tachycardia (common presenting signs and symptoms for PE), her chest CT showed no evidence of PE (see Figure 2); additionally, Doppler ultrasound of the bilateral lower extremities revealed no DVTs. Thus, PE was also excluded.
Tension pneumothorax was also ruled out, as chest x-ray showed neither mediastinal shift nor tracheal deviation, and the patient had denied any trauma. Laboratory analyses did not indicate hyponatremia, and the patient’s hemoglobin and hematocrit were satisfactory. She was tachycardic on admission, but her blood pressure was stable. As the patient denied any use of vasodilators or diuretics, hypovolemia was ruled out.
Patients experiencing asthma exacerbation can present with acute SOB, which usually resolves following use of IV steroids, nebulizer therapy, and inhaler treatments. Despite being administered IV methylprednisolone and magnesium sulfate in the ED, the patient experienced PEA and respiratory distress and required intubation for airway protection.
The HIV test was nonreactive, and blood and urine cultures did not show any growth. Results of tests for Legionella urinary antigen and Streptococcus pneumoniae antigen were negative. Sputum culture showed normal flora. Immunovirology testing, however, was positive for both influenza A and B antigens.
Chest X-ray showed no acute pulmonary pathology, nor did chest CT show any central, interlobar, or segmental embolism or mediastinal lymphadenopathy. It was determined that the patient’s acute SOB might represent asthma exacerbation secondary to influenza viral infection. Her PEA was attributed to possible acute pericarditis secondary to concomitant influenza A and B viral infection.
DISCUSSION
Currently, the CDC recognizes three types of influenza virus: A, B, and C.14 Only influenza A viruses are further classified into subtypes, based on the presence of surface proteins called hemagglutinin (HA) or neuraminidase (NA) glycoproteins. Humans can be infected by influenza A subtypes H1N1 and H3N2.14 Influenza B viruses, found mostly in humans, are associated with significant morbidity and mortality.
Influenza A and B viruses are further classified into strains that change with each flu season—thus, the need to update vaccinations against influenza A and B each year. No vaccination exists against influenza C virus, which is known to cause only mild illness in humans.15
In patients with asthma (as in the case patient), chronic bronchitis, or emphysema, infection with the influenza virus can manifest with SOB, in addition to the more common symptoms of fever, sore throat, headache, rhinorrhea, chills, muscle aches, and general discomfort.16 Patients with coronary artery disease, congestive heart failure (CHF), and/or a history of smoking may experience more severe symptoms and increased risk for influenza-associated mortality than do other patients.17,18
Rare cardiac complications of influenza infections are myocarditis and benign acute pericarditis; myocarditis can progress to CHF and death.19,20 A case of acute myopericarditis was reported by Proby et al21 in a patient with acute influenza A infection who developed pericardial effusions, myositis, tamponade, and pleurisy. That patient recovered after pericardiocentesis and administration of inotropic drugs.
In the literature, a few cases of acute pericarditis have been reported in association with administration of the influenza vaccination.22,23
In the case patient, the diagnosis of influenza A and B was made following testing of nasal and nasopharyngeal swabs with an immunochromatographic assay that uses highly sensitive monoclonal antibodies to detect influenza A and B nucleoprotein antigens.24,25
According to reports in the literature, two-thirds of cases of acute pericarditis are caused by infection, most commonly viral infection (including influenza virus, adenovirus, enterovirus, cytomegalovirus, hepatitis B virus, and herpes simplex virus).26,27 Other etiologies for acute pericarditis are autoimmune (accounting for less than 10% of cases) and neoplastic conditions (5% to 7% of cases).26
PATIENT OUTCOME
Consultation with an infectious disease specialist was obtained. The patient was placed under droplet isolation precautions and was started on a nebulizer, IV steroid treatments, and oseltamivir 75 mg by mouth every 12 hours. She was transferred to a medical floor, where she completed a five-day course of oseltamivir.
As a result of timely intervention, the patient was discharged in stable condition on a therapeutic regimen that included albuterol, fluticasone, and salmeterol inhalation, in addition to tapered-dose steroids. She was advised to follow up with her primary care provider and at the pulmonary clinic.
CONCLUSION
To our knowledge, this is the first reported case of acute pericarditis in a patient with concomitant acute infections with influenza A and B. According to conclusions reached in recent literature, further research is needed to explain the pathophysiology of influenza viral infections, associated cardiovascular morbidity and mortality, and the degree to which these can be prevented by influenza vaccination.1,28 Also to be pursued through research is a better understanding of the morbidity and mortality associated with influenza viruses, especially in children and in adults affected by asthma, cardiac disease, and/or obesity.
REFERENCES
1. Finelli L, Chaves SS. Influenza and acute myocardial infarction. J Infect Dis. 2011;203(12):
1701-1704.
2. Steiger HV, Rimbach K, Müller E, Breitkreutz R. Focused emergency echocardiography: lifesaving tool for a 14-year-old girl suffering out-of-hospital pulseless electrical activity arrest because of cardiac tamponade. Eur J Emerg Med. 2009;16(2): 103-105.
3. Goodman A, Perera P, Mailhot T, Mandavia D. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade.
J Emerg Trauma Shock. 2012;5(1):72-75.
4. Restrepo CS, Lemos DF, Lemos JA, et al. Imaging findings in cardiac tamponade with emphasis on CT. Radiographics. 2007;27(6):1595-1610.
5. Papanagnou D, Stone MB. Massive right atrial thrombus masquerading as cardiac tamponade. Acad Emerg Med. 2010;17(2):E11.
6. Saito Y, Donohue A, Attai S, et al. The syndrome of cardiac tamponade with “small” pericardial effusion. Echocardiography. 2008;25(3): 321-327.
7. Lin E, Boire A, Hemmige V, et al. Cardiac tamponade mimicking tuberculous pericarditis as the initial presentation of chronic lymphocytic leukemia in a 58-year-old woman: a case report. J Med Case Rep. 2010;4:246.
8. Meniconi A, Attenhofer Jost CH, Jenni R. How to survive myocardial rupture after myocardial infarction. Heart. 2000;84(5):552.
9. Kosuge M, Kimura K, Ishikawa T, et al. Differences between men and women in terms of clinical features of ST-segment elevation acute myocardial infarction. Circ J. 2006;70(3):222-226.
10. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-969.
11. Goldhaber SZ. Deep venous thrombosis and pulmonary thromboembolism. In: Fauci AS, Braunwald E, Kasper DL, et al. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw-Hill Medical; 2008:1651–1657.
12. Brooks EG, Trotman W, Wadsworth MP, et al. Valves of the deep venous system: an overlooked risk factor. Blood. 2009;114(6):1276-1279.
13. Kyrle PA, Eichinger S. Is Virchow’s triad complete? Blood. 2009;114(6):1138-1139.
14. CDC. Seasonal influenza (flu): types of influenza viruses (2012). www.cdc.gov/flu/about/viruses/types.htm. Accessed October 24, 2012.
15. CDC. Seasonal influenza (flu)(2012). www.cdc .gov/flu. Accessed October 24, 2012.
16. Eccles R. Understanding the symptoms of the common cold and influenza. Lancet Infect Dis. 2005;5(11):718-725.
17. Angelo SJ, Marshall PS, Chrissoheris MP, Chaves AM. Clinical characteristics associated with poor outcome in patients acutely infected with Influenza A. Conn Med. 2004;68(4):199-205.
18. Murin S, Bilello K. Respiratory tract infections: another reason not to smoke. Cleve Clin J Med. 2005;72(10):916-920.
19. Ray CG, Icenogle TB, Minnich LL, et al. The use of intravenous ribavirin to treat influenza virus–associated acute myocarditis. J Infect Dis. 1989; 159(5):829-836.
20. Fairley CK, Ryan M, Wall PG, Weinberg J. The organism reported to cause infective myocarditis and pericarditis in England and Wales. J Infect. 1996;32(3):223-225.
21. Proby CM, Hackett D, Gupta S, Cox TM. Acute myopericarditis in influenza A infection. Q J Med. 1986;60(233):887-892.
22. Streifler JJ, Dux S, Garty M, Rosenfeld JB. Recurrent pericarditis: a rare complication of influenza vaccination. Br Med J (Clin Res Ed). 1981; 283(6290):526-527.
23. Desson JF, Leprévost M, Vabret F, Davy A. Acute benign pericarditis after anti-influenza vaccination [in French]. Presse Med. 1997;26 (9):415.
24. BinaxNOW® Influenza A&B Test Kit (product instructions). www.diagnosticsdirect2u.com/images/PDF/Binax%20Now%20416-022%20PPI .pdf. Accessed October 24, 2012.
25. 510(k) Substantial Equivalence Determination Decision Summary [BinaxNow® Influenza A & B Test] (2009). www.accessdata.fda.gov/cdrh_docs/reviews/K062109.pdf. Accessed October 24, 2012.
26. Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121(7):916-928.
27. Maisch B, Seferovic PM, Ristic AD, et al; Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases: executive summary. Eur Heart J. 2004;25(7):587-610.
28. McCullers JA, Hayden FG. Fatal influenza B infections: time to reexamine influenza research priorities. J Infect Dis. 2012;205(6):870-872.
On an autumn day, a 38-year-old woman with a history of asthma presented to the emergency department (ED) with the chief complaint of shortness of breath (SOB). The patient described her SOB as sudden in onset and not relieved by use of her albuterol inhaler; hence the ED visit.
She denied any chest pain, palpitations, dizziness, orthopnea, upper respiratory tract infection, cough, wheezing, fever or chills, headache, vision changes, body aches, sick contacts, or pets at home. She said she uses her albuterol inhaler as needed, and that she had used it that day for the first time in “a few months.” She denied any history of intubation or steroid use. Additionally, she had not been seen by a primary care provider in years.
The woman, a native of Ghana, had been living in the United States for many years. She denied any recent travel or exposure to toxic chemicals; any use of tobacco, alcohol, or illicit drugs; or any history of sexually transmitted disease.
The patient was afebrile (temperature, 98.6°F), with a respiratory rate of 20 breaths/min; blood pressure, 144/69 mm Hg; and ventricular rate, 125 beats/min. On physical examination, her extraocular movements were intact; pupils were equal, round, reactive to light and accommodation; and sclera were nonicteric. The patient’s head was normocephalic and atraumatic, and the neck was supple with normal range of motion and no jugular venous distension or lymphadenopathy. Her mucous membranes were moist with no pharyngeal erythema or exudates. Cardiovascular examination, including ECG, revealed tachycardia but no murmurs or gallops.
While being evaluated in the ED, the patient became tachypneic and began to experience respiratory distress. She was intubated for airway protection, at which time she developed pulseless electrical activity (PEA), with 30 beats/min. She responded to atropine and epinephrine injections. A repeat ECG showed sinus tachycardia and right atrial enlargement with right-axis deviation. Chest x-ray (see Figure 1) showed no consolidation, pleural effusion, or pneumothorax.
Results from the patient’s lab work are shown in the table, above. Negative results were reported for a urine pregnancy test.
Since there was no clear etiology for the patient’s PEA, she underwent pan-culturing, with the following tests ordered: HIV antibody testing, immunovirology for influenza A and B viruses, and urine toxicology. Doppler ultrasound of the bilateral lower extremities was also ordered, in addition to chest CT and transthoracic and transesophageal echocardiography (TTE and TEE, respectively). The patient was intubated and transferred to the medical ICU for further management.
The differential diagnosis included cardiac tamponade, acute MI, acute pulmonary embolus (PE), tension pneumothorax, hypovolemia, and asthma exacerbated by viral or bacterial infection.1,2 Although the case patient presented with PEA, she did not have the presenting signs of cardiac tamponade known as Beck’s triad: hypotension, jugular venous distension, and muffled heart sounds.3 TTE showed an ejection fraction of 65% and grade 2 diastolic dysfunction but no pericardial effusions (which accumulate rapidly in the patient with cardiac tamponade, resulting from fluid buildup in the pericardial layers),4 and TEE showed no atrial thrombi (which can masquerade as cardiac tamponade5). The patient had no signs of trauma and denied any history of malignancy (both potential causes of cardiac tamponade). Chest x-ray showed normal heart size and no pneumothorax, consolidations, or pleural effusions.4,6-8 Thus, the diagnosis of cardiac tamponade was ruled out.
Common presenting symptoms of acute MI include sudden-onset chest pain, SOB, palpitations, dizziness, nausea, and/or vomiting. Women may experience less dramatic symptoms—often little more than SOB and fatigue.9 According to a 2000 consensus document from a joint European Society of Cardiology/American College of Cardiology committee10 in which MI was redefined, the diagnosis of MI relies on a rise in cardiac troponin levels, typical MI symptoms, and changes in ECG showing pathological Q waves or ST elevation or depression. The case patient’s troponin I level was less than 0.02 ng/mL, and ECG did not reveal Q waves or ST-T wave changes; additionally, since the patient had no chest pain, palpitations, diaphoresis, nausea, or vomiting, acute MI was ruled out.
Blood clots capable of blocking the pulmonary artery usually originate in the deep veins of the lower extremities.11 Three main factors, called Virchow’s triad, are known to contribute to these deep vein thromboses (DVTs): venous stasis, endothelial injury, and a hypercoagulability state.12,13 The patient had denied any trauma, recent travel, history of malignancy, or use of tobacco or oral contraceptives, and the result of her urine pregnancy test was negative. Even though the patient presented with tachypnea and acute SOB, with ECG showing right-axis deviation and tachycardia (common presenting signs and symptoms for PE), her chest CT showed no evidence of PE (see Figure 2); additionally, Doppler ultrasound of the bilateral lower extremities revealed no DVTs. Thus, PE was also excluded.
Tension pneumothorax was also ruled out, as chest x-ray showed neither mediastinal shift nor tracheal deviation, and the patient had denied any trauma. Laboratory analyses did not indicate hyponatremia, and the patient’s hemoglobin and hematocrit were satisfactory. She was tachycardic on admission, but her blood pressure was stable. As the patient denied any use of vasodilators or diuretics, hypovolemia was ruled out.
Patients experiencing asthma exacerbation can present with acute SOB, which usually resolves following use of IV steroids, nebulizer therapy, and inhaler treatments. Despite being administered IV methylprednisolone and magnesium sulfate in the ED, the patient experienced PEA and respiratory distress and required intubation for airway protection.
The HIV test was nonreactive, and blood and urine cultures did not show any growth. Results of tests for Legionella urinary antigen and Streptococcus pneumoniae antigen were negative. Sputum culture showed normal flora. Immunovirology testing, however, was positive for both influenza A and B antigens.
Chest X-ray showed no acute pulmonary pathology, nor did chest CT show any central, interlobar, or segmental embolism or mediastinal lymphadenopathy. It was determined that the patient’s acute SOB might represent asthma exacerbation secondary to influenza viral infection. Her PEA was attributed to possible acute pericarditis secondary to concomitant influenza A and B viral infection.
DISCUSSION
Currently, the CDC recognizes three types of influenza virus: A, B, and C.14 Only influenza A viruses are further classified into subtypes, based on the presence of surface proteins called hemagglutinin (HA) or neuraminidase (NA) glycoproteins. Humans can be infected by influenza A subtypes H1N1 and H3N2.14 Influenza B viruses, found mostly in humans, are associated with significant morbidity and mortality.
Influenza A and B viruses are further classified into strains that change with each flu season—thus, the need to update vaccinations against influenza A and B each year. No vaccination exists against influenza C virus, which is known to cause only mild illness in humans.15
In patients with asthma (as in the case patient), chronic bronchitis, or emphysema, infection with the influenza virus can manifest with SOB, in addition to the more common symptoms of fever, sore throat, headache, rhinorrhea, chills, muscle aches, and general discomfort.16 Patients with coronary artery disease, congestive heart failure (CHF), and/or a history of smoking may experience more severe symptoms and increased risk for influenza-associated mortality than do other patients.17,18
Rare cardiac complications of influenza infections are myocarditis and benign acute pericarditis; myocarditis can progress to CHF and death.19,20 A case of acute myopericarditis was reported by Proby et al21 in a patient with acute influenza A infection who developed pericardial effusions, myositis, tamponade, and pleurisy. That patient recovered after pericardiocentesis and administration of inotropic drugs.
In the literature, a few cases of acute pericarditis have been reported in association with administration of the influenza vaccination.22,23
In the case patient, the diagnosis of influenza A and B was made following testing of nasal and nasopharyngeal swabs with an immunochromatographic assay that uses highly sensitive monoclonal antibodies to detect influenza A and B nucleoprotein antigens.24,25
According to reports in the literature, two-thirds of cases of acute pericarditis are caused by infection, most commonly viral infection (including influenza virus, adenovirus, enterovirus, cytomegalovirus, hepatitis B virus, and herpes simplex virus).26,27 Other etiologies for acute pericarditis are autoimmune (accounting for less than 10% of cases) and neoplastic conditions (5% to 7% of cases).26
PATIENT OUTCOME
Consultation with an infectious disease specialist was obtained. The patient was placed under droplet isolation precautions and was started on a nebulizer, IV steroid treatments, and oseltamivir 75 mg by mouth every 12 hours. She was transferred to a medical floor, where she completed a five-day course of oseltamivir.
As a result of timely intervention, the patient was discharged in stable condition on a therapeutic regimen that included albuterol, fluticasone, and salmeterol inhalation, in addition to tapered-dose steroids. She was advised to follow up with her primary care provider and at the pulmonary clinic.
CONCLUSION
To our knowledge, this is the first reported case of acute pericarditis in a patient with concomitant acute infections with influenza A and B. According to conclusions reached in recent literature, further research is needed to explain the pathophysiology of influenza viral infections, associated cardiovascular morbidity and mortality, and the degree to which these can be prevented by influenza vaccination.1,28 Also to be pursued through research is a better understanding of the morbidity and mortality associated with influenza viruses, especially in children and in adults affected by asthma, cardiac disease, and/or obesity.
REFERENCES
1. Finelli L, Chaves SS. Influenza and acute myocardial infarction. J Infect Dis. 2011;203(12):
1701-1704.
2. Steiger HV, Rimbach K, Müller E, Breitkreutz R. Focused emergency echocardiography: lifesaving tool for a 14-year-old girl suffering out-of-hospital pulseless electrical activity arrest because of cardiac tamponade. Eur J Emerg Med. 2009;16(2): 103-105.
3. Goodman A, Perera P, Mailhot T, Mandavia D. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade.
J Emerg Trauma Shock. 2012;5(1):72-75.
4. Restrepo CS, Lemos DF, Lemos JA, et al. Imaging findings in cardiac tamponade with emphasis on CT. Radiographics. 2007;27(6):1595-1610.
5. Papanagnou D, Stone MB. Massive right atrial thrombus masquerading as cardiac tamponade. Acad Emerg Med. 2010;17(2):E11.
6. Saito Y, Donohue A, Attai S, et al. The syndrome of cardiac tamponade with “small” pericardial effusion. Echocardiography. 2008;25(3): 321-327.
7. Lin E, Boire A, Hemmige V, et al. Cardiac tamponade mimicking tuberculous pericarditis as the initial presentation of chronic lymphocytic leukemia in a 58-year-old woman: a case report. J Med Case Rep. 2010;4:246.
8. Meniconi A, Attenhofer Jost CH, Jenni R. How to survive myocardial rupture after myocardial infarction. Heart. 2000;84(5):552.
9. Kosuge M, Kimura K, Ishikawa T, et al. Differences between men and women in terms of clinical features of ST-segment elevation acute myocardial infarction. Circ J. 2006;70(3):222-226.
10. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-969.
11. Goldhaber SZ. Deep venous thrombosis and pulmonary thromboembolism. In: Fauci AS, Braunwald E, Kasper DL, et al. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw-Hill Medical; 2008:1651–1657.
12. Brooks EG, Trotman W, Wadsworth MP, et al. Valves of the deep venous system: an overlooked risk factor. Blood. 2009;114(6):1276-1279.
13. Kyrle PA, Eichinger S. Is Virchow’s triad complete? Blood. 2009;114(6):1138-1139.
14. CDC. Seasonal influenza (flu): types of influenza viruses (2012). www.cdc.gov/flu/about/viruses/types.htm. Accessed October 24, 2012.
15. CDC. Seasonal influenza (flu)(2012). www.cdc .gov/flu. Accessed October 24, 2012.
16. Eccles R. Understanding the symptoms of the common cold and influenza. Lancet Infect Dis. 2005;5(11):718-725.
17. Angelo SJ, Marshall PS, Chrissoheris MP, Chaves AM. Clinical characteristics associated with poor outcome in patients acutely infected with Influenza A. Conn Med. 2004;68(4):199-205.
18. Murin S, Bilello K. Respiratory tract infections: another reason not to smoke. Cleve Clin J Med. 2005;72(10):916-920.
19. Ray CG, Icenogle TB, Minnich LL, et al. The use of intravenous ribavirin to treat influenza virus–associated acute myocarditis. J Infect Dis. 1989; 159(5):829-836.
20. Fairley CK, Ryan M, Wall PG, Weinberg J. The organism reported to cause infective myocarditis and pericarditis in England and Wales. J Infect. 1996;32(3):223-225.
21. Proby CM, Hackett D, Gupta S, Cox TM. Acute myopericarditis in influenza A infection. Q J Med. 1986;60(233):887-892.
22. Streifler JJ, Dux S, Garty M, Rosenfeld JB. Recurrent pericarditis: a rare complication of influenza vaccination. Br Med J (Clin Res Ed). 1981; 283(6290):526-527.
23. Desson JF, Leprévost M, Vabret F, Davy A. Acute benign pericarditis after anti-influenza vaccination [in French]. Presse Med. 1997;26 (9):415.
24. BinaxNOW® Influenza A&B Test Kit (product instructions). www.diagnosticsdirect2u.com/images/PDF/Binax%20Now%20416-022%20PPI .pdf. Accessed October 24, 2012.
25. 510(k) Substantial Equivalence Determination Decision Summary [BinaxNow® Influenza A & B Test] (2009). www.accessdata.fda.gov/cdrh_docs/reviews/K062109.pdf. Accessed October 24, 2012.
26. Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121(7):916-928.
27. Maisch B, Seferovic PM, Ristic AD, et al; Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases: executive summary. Eur Heart J. 2004;25(7):587-610.
28. McCullers JA, Hayden FG. Fatal influenza B infections: time to reexamine influenza research priorities. J Infect Dis. 2012;205(6):870-872.
Cover

A Compounded Problem
Preoperative Templating and Its Intraoperative Applications for Hip Resurfacing Arthroplasty
Orthopedic Surgery Is Possible in Hemophilic Patients With Inhibitors
Evolving applications of first-trimester ultrasound
The authors report no financial relationships relevant to this article.
In recent years, prenatal screening and testing have begun to shift from the second trimester to the first. Ultrasonographic evaluation—a large component of fetal testing—is also applied earlier in gestation to provide information to clinicians and patients about the integrity of the pregnancy. The shifting of the classic, “gold standard” anatomy scan to the first trimester was made possible by high-frequency transvaginal transducers and by greater understanding of the early signs of fetal pathology.
![]()
Real-time video of fetal anatomy ultrasonography at 11 weeks

Ilan E. Timor-Tritsch, MD
Dr. Timor-Tritsch is Professor of Obstetrics and Gynecology at New York University School of Medicine and
Director of the Division of ObGyn Imaging at NYU Langone Medical Center
in New York City.
Simi K. Gupta, MD
Dr. Gupta is a Fellow in Maternal-Fetal Medicine in the Department of Obstetrics and Gynecology at New York University School of Medicine in New York City.
![]()
Real-time video of fetal anatomy ultrasonography at 11 weeks
Ilan E. Timor-Tritsch, MD
Dr. Timor-Tritsch is Professor of Obstetrics and Gynecology at New York University School of Medicine and
Director of the Division of ObGyn Imaging at NYU Langone Medical Center
in New York City.
Simi K. Gupta, MD
Dr. Gupta is a Fellow in Maternal-Fetal Medicine in the Department of Obstetrics and Gynecology at New York University School of Medicine in New York City.
![]()
Real-time video of fetal anatomy ultrasonography at 11 weeks
Ilan E. Timor-Tritsch, MD
Dr. Timor-Tritsch is Professor of Obstetrics and Gynecology at New York University School of Medicine and
Director of the Division of ObGyn Imaging at NYU Langone Medical Center
in New York City.
Simi K. Gupta, MD
Dr. Gupta is a Fellow in Maternal-Fetal Medicine in the Department of Obstetrics and Gynecology at New York University School of Medicine in New York City.
The authors report no financial relationships relevant to this article.
In recent years, prenatal screening and testing have begun to shift from the second trimester to the first. Ultrasonographic evaluation—a large component of fetal testing—is also applied earlier in gestation to provide information to clinicians and patients about the integrity of the pregnancy. The shifting of the classic, “gold standard” anatomy scan to the first trimester was made possible by high-frequency transvaginal transducers and by greater understanding of the early signs of fetal pathology.
The authors report no financial relationships relevant to this article.
In recent years, prenatal screening and testing have begun to shift from the second trimester to the first. Ultrasonographic evaluation—a large component of fetal testing—is also applied earlier in gestation to provide information to clinicians and patients about the integrity of the pregnancy. The shifting of the classic, “gold standard” anatomy scan to the first trimester was made possible by high-frequency transvaginal transducers and by greater understanding of the early signs of fetal pathology.
Vaginal dilation: When it’s indicated and tips on teaching it
Vaginal dilators are used to restore vaginal capacity, to expand the vagina in width and depth, to provide elasticity to the tissues, and to allow for comfortable sexual activity. Vaginal dilators are smooth plastic, rubber, or glass cylinder-shaped objects that come in a variety of graduated sizes and weights.
Several medical conditions may warrant the use of vaginal dilation, including superficial dyspareunia, high-tone pelvic floor dysfunction, vaginismus, provoked vestibulodynia, vaginal atrophy, vulvar dermatoses, vaginal agenesis, and postradiation adhesions. Dilation also can be used as deconditioning therapy for psychogenic dyspareunia.1-4 In addition, Masters and Johnson advocated the use of dilators for patients with female sexual dysfunction in order to interrupt the cycle of pain–fear–muscle spasm–more pain, and to build confidence “in the privacy of the marital bedroom.”5
Vaginal dilators often are sufficient to restore function, with dilator therapy considered successful if a woman is able to resume comfortable sexual intercourse or self-stimulation, as desired.1,6 Vaginal dilation also can be used as an adjunct to pelvic floor muscle physical therapy, psychotherapy, sex therapy, minimally absorbed local vaginal estrogen therapy, intravaginal muscle relaxants, lubricants, moisturizers, and vibrators.
Each patient in these case studies achieved success resuming sexual activity after several months of dilator therapy used in combination with other medical interventions.
CASE 1: Chronic vulvovaginal infection and pain
A 26-year-old G0P0 woman presented with a 2-year history of prohibitive penetrative dyspareunia. She had a history of chronic vulvovaginal candidiasis, treated by another clinician with multiple courses of intravaginal antifungal cream.
After extensive evaluation for sexual pain, a diagnosis of pelvic floor muscle spasm, sexual aversion, fear secondary to pain, and contact irritant dermatitis was reached. After vaginal fungal cultures indicated negative results, a size small dilator was introduced in the office using a hypoallergenic intravaginal moisturizer. After daily use of the vaginal dilator for 4 months, with progressed introduction of graduated sizes (small, medium, medium+, large), she was able to accommodate intravaginal intercourse with her partner.
CASE 2: Interstitial cystitis and fear of pain
A 58-year-old G3P3 postmenopausal woman presented with interstitial cystitis (IC), pelvic floor muscle hypertonus, vulvovaginal atrophy, and provoked vestibulodynia. Although her IC symptoms were well-controlled, she was fearful about reestablishing physical intimacy with her partner after 7 years of abstinence.
A program of intravaginal estrogen (Vagifem) 2 to 3 times per week, introital cutaneous lysate (Neogyn) vulvar soothing cream twice per day, and compounded muscle-relaxing intravaginal diazepam suppositories 2 to 3 times per week was initiated. After 2 months of treatment, she was taught in the office to use a size extra small vaginal dilator. She was delighted that use did not result in pain. Two months later, she was able to use a size small dilator, and 4 months later, a size medium dilator. At this point, the patient is confident that she can have sexual intercourse.
CASE 3: Lichen sclerosus
A 50-year-old G0P0 premenopausal woman had a history of IC and biopsy-proven lichen sclerosus. The white plaques surrounding her introitus had become so severe in the past year that she was no longer able to tolerate penile penetration without tearing. Nightly use of topical clobetasol cream and introital estrogen cream (Estrace) was recommended. After 30 days, the patient began twice-a-week maintenance with the creams and also began to use vaginal dilators. After success inserting a size extra large dilator following 5 months of dilator use, she was able to resume intercourse without tearing.
CASE 4: Vestibulodynia and vaginismus
A 25-year-old G0P0 woman underwent vestibulectomy for primary provoked vestibulodynia followed by pelvic floor muscle physical therapy for primary vaginismus. Her marriage of 6 years was unconsummated. Two weeks postoperatively, she began using a size small dilator daily and progressed to a size medium plus dilator after 6 weeks. She managed her chronic constipation and pelvic floor muscle hypertonus with daily fiber supplements, stool softeners, and self-transvaginal massage of the pelvic floor muscles. Seven weeks after surgery, she accomplished intercourse with her husband for the first time.
How to teach your patient to use vaginal dilation successfully
Before ordering vaginal dilation for your patient, 1) assess the levator ani muscle group for hypertonus or spasm and 2) choose the size dilator to start therapy that does not cause pain with insertion but enters with some resistance.
When beginning to teach your patient to use a vaginal dilator in the office, a mirror demonstration may be helpful. Be sure to instruct your patient regarding the following elements to help her achieve success with dilation therapy.
Relax and allow for privacy. About 10 to 15 minutes of privacy before vaginal dilation can help with the success of each individual therapy session. Relaxation can be facilitated with activities such as deep breathing, soaking in a warm bath, or using prescribed muscle relaxants 30 to 60 minutes prior to dilation.
Use proper positioning. Instruct the patient to lie on the bed with her knees bent and placed apart. Advise her to place the lubricated dilator in the vagina as far as it can go without causing any pain (FIGURE 1). It may be helpful for her to bear down when first inserting the dilator. An in-and-out motion is not necessary.

FIGURE 1 Inserting the dilator
Tell the patient to lie on the bed with her knees bent and to insert the lubricated dilator into her vagina as far as it will go without causing pain.Be sure to inform her to use a water-based lubricant—not lotion, petroleum jelly, or any non-water-based lubricant.
Dilate daily. The dilator should be used daily and left in place for 5 to 15 minutes. She may experience a small amount of spotting initially, but spotting should abate within 2 weeks of initiating dilator use. Each dilator size should be used for 3 to 4 weeks. When your patient is changing sizes, she should transition to the larger size over several days by dilating for the first few minutes with the smaller dilator, then changing to the larger dilator for the remainder of the time. If she experiences pain or heavy bleeding, she should cease dilation and follow-up with you.
Proper cleaning. Instruct her to wash the dilator with antibacterial soap and water and to dry it thoroughly between uses.
Follow-up. When undergoing vaginal dilation therapy, your patient should be following up with you at regular intervals, usually once a month, to facilitate compliance with the program.
You can purchase dilators for your medical practice and resell them in your office. Patients also can be directed to purchase dilators directly from a manufacturer (such as Syracuse Medical Devices or AmeriMed Direct) or through a number of Internet sites, including Middlesexmd.com6 or Vaginismus.com.7 Both of these Web sites also offer educational materials, including videos and books and a private support forum or blog.

FIGURE 2 Vaginal dilators come in 8 different circumferences
Vaginal dilators range in size from Extra Small at 1/2 in (13 mm) to Large Plus at 1 1/2 in (39 mm). Each is 6 in (15 cm) long, has one rounded end, and is constructed of sterilizable, medical-grade plastic.
Printed with permission of Syracuse Medical Devices, Inc., Syracuse, New York.Most dilators used in the United States are 6 in (15 cm) long and are made from sterilizable, medical-grade, latex-free, rigid plastic with a smooth surface. Some dilators are made of softer material such as silicone, and others have a vibrating inner wand.6 They are available to purchase as single dilators or in sets of 5 to 8 graduated sizes (FIGURE 2). Some sets come with a storage bag and universal handles that lock-on for insertion. Graduated circumference sizes are fairly universal in the United States (TABLE).
Average dilator sizes and circumferences*
| Size | Circumference |
|---|---|
| Extra small | 1/2 in; 13 mm |
| Extra small plus | 11/16 in; 18 mm |
| Small | 7/8 in; 22 mm |
| Small plus | 1 in; 25 mm |
| Medium | 1 1/8 in; 29 mm |
| Medium plus | 1 1/4 in; 32 mm |
| Large | 1 3/8 in; 35 mm |
| Large plus | 1 5/8 in; 38 mm |
| *Based on Syracuse Medical Devices, Inc. product information. | |
Restoring her sexual health: Our goal
Sexual health is a vitally important quality-of-life issue; restoring that health should be our priority. We need to educate our patients on nonprescription methods to promote their vaginal and sexual health, as vaginal dilation therapy can result in the reduction or elimination of dyspareunia.
We want to hear from you! Tell us what you think.
Your age-based guide to comprehensive well-woman care
Robert L. Barbieri, MD (October 2012)
Sexual dysfunction
Barbara S. Levy, MD (Update, September 2012)
New study: ObGyns aren’t fully addressing their patients’ sexual function
(Web News, April 2012)
How to prepare your patient for the many nuances of postpartum sexuality
Roya Rezaee, MD, and Sheryl Kingsberg, PhD (January 2012)

Susan Kellogg Spadt, PhD, CRNP
Dr. Kellogg Spadt is Director of Sexual Medicine.

Jennifer Iorio, MSN, CRNP
Ms. Iorio is a Nurse Practitioner, Female Sexual Medicine.

Jennifer Yonaitis Fariello, MSN, CRNP
Ms. Fariello is a Nurse Practitioner, Male and Female Sexual Medicine.

Kristene E. Whitmore, MD
Dr. Whitmore is Medical Director and Chief of Surgery.
All are colleagues at the Pelvic & Sexual Health Institute, Philadelphia, Pennsylvania.
The authors report no financial relationships relevant to this article.
Susan Kellogg Spadt, PhD, CRNP
Dr. Kellogg Spadt is Director of Sexual Medicine.
Jennifer Iorio, MSN, CRNP
Ms. Iorio is a Nurse Practitioner, Female Sexual Medicine.
Jennifer Yonaitis Fariello, MSN, CRNP
Ms. Fariello is a Nurse Practitioner, Male and Female Sexual Medicine.
Kristene E. Whitmore, MD
Dr. Whitmore is Medical Director and Chief of Surgery.
All are colleagues at the Pelvic & Sexual Health Institute, Philadelphia, Pennsylvania.
The authors report no financial relationships relevant to this article.
Susan Kellogg Spadt, PhD, CRNP
Dr. Kellogg Spadt is Director of Sexual Medicine.
Jennifer Iorio, MSN, CRNP
Ms. Iorio is a Nurse Practitioner, Female Sexual Medicine.
Jennifer Yonaitis Fariello, MSN, CRNP
Ms. Fariello is a Nurse Practitioner, Male and Female Sexual Medicine.
Kristene E. Whitmore, MD
Dr. Whitmore is Medical Director and Chief of Surgery.
All are colleagues at the Pelvic & Sexual Health Institute, Philadelphia, Pennsylvania.
The authors report no financial relationships relevant to this article.
Vaginal dilators are used to restore vaginal capacity, to expand the vagina in width and depth, to provide elasticity to the tissues, and to allow for comfortable sexual activity. Vaginal dilators are smooth plastic, rubber, or glass cylinder-shaped objects that come in a variety of graduated sizes and weights.
Several medical conditions may warrant the use of vaginal dilation, including superficial dyspareunia, high-tone pelvic floor dysfunction, vaginismus, provoked vestibulodynia, vaginal atrophy, vulvar dermatoses, vaginal agenesis, and postradiation adhesions. Dilation also can be used as deconditioning therapy for psychogenic dyspareunia.1-4 In addition, Masters and Johnson advocated the use of dilators for patients with female sexual dysfunction in order to interrupt the cycle of pain–fear–muscle spasm–more pain, and to build confidence “in the privacy of the marital bedroom.”5
Vaginal dilators often are sufficient to restore function, with dilator therapy considered successful if a woman is able to resume comfortable sexual intercourse or self-stimulation, as desired.1,6 Vaginal dilation also can be used as an adjunct to pelvic floor muscle physical therapy, psychotherapy, sex therapy, minimally absorbed local vaginal estrogen therapy, intravaginal muscle relaxants, lubricants, moisturizers, and vibrators.
Each patient in these case studies achieved success resuming sexual activity after several months of dilator therapy used in combination with other medical interventions.
CASE 1: Chronic vulvovaginal infection and pain
A 26-year-old G0P0 woman presented with a 2-year history of prohibitive penetrative dyspareunia. She had a history of chronic vulvovaginal candidiasis, treated by another clinician with multiple courses of intravaginal antifungal cream.
After extensive evaluation for sexual pain, a diagnosis of pelvic floor muscle spasm, sexual aversion, fear secondary to pain, and contact irritant dermatitis was reached. After vaginal fungal cultures indicated negative results, a size small dilator was introduced in the office using a hypoallergenic intravaginal moisturizer. After daily use of the vaginal dilator for 4 months, with progressed introduction of graduated sizes (small, medium, medium+, large), she was able to accommodate intravaginal intercourse with her partner.
CASE 2: Interstitial cystitis and fear of pain
A 58-year-old G3P3 postmenopausal woman presented with interstitial cystitis (IC), pelvic floor muscle hypertonus, vulvovaginal atrophy, and provoked vestibulodynia. Although her IC symptoms were well-controlled, she was fearful about reestablishing physical intimacy with her partner after 7 years of abstinence.
A program of intravaginal estrogen (Vagifem) 2 to 3 times per week, introital cutaneous lysate (Neogyn) vulvar soothing cream twice per day, and compounded muscle-relaxing intravaginal diazepam suppositories 2 to 3 times per week was initiated. After 2 months of treatment, she was taught in the office to use a size extra small vaginal dilator. She was delighted that use did not result in pain. Two months later, she was able to use a size small dilator, and 4 months later, a size medium dilator. At this point, the patient is confident that she can have sexual intercourse.
CASE 3: Lichen sclerosus
A 50-year-old G0P0 premenopausal woman had a history of IC and biopsy-proven lichen sclerosus. The white plaques surrounding her introitus had become so severe in the past year that she was no longer able to tolerate penile penetration without tearing. Nightly use of topical clobetasol cream and introital estrogen cream (Estrace) was recommended. After 30 days, the patient began twice-a-week maintenance with the creams and also began to use vaginal dilators. After success inserting a size extra large dilator following 5 months of dilator use, she was able to resume intercourse without tearing.
CASE 4: Vestibulodynia and vaginismus
A 25-year-old G0P0 woman underwent vestibulectomy for primary provoked vestibulodynia followed by pelvic floor muscle physical therapy for primary vaginismus. Her marriage of 6 years was unconsummated. Two weeks postoperatively, she began using a size small dilator daily and progressed to a size medium plus dilator after 6 weeks. She managed her chronic constipation and pelvic floor muscle hypertonus with daily fiber supplements, stool softeners, and self-transvaginal massage of the pelvic floor muscles. Seven weeks after surgery, she accomplished intercourse with her husband for the first time.
How to teach your patient to use vaginal dilation successfully
Before ordering vaginal dilation for your patient, 1) assess the levator ani muscle group for hypertonus or spasm and 2) choose the size dilator to start therapy that does not cause pain with insertion but enters with some resistance.
When beginning to teach your patient to use a vaginal dilator in the office, a mirror demonstration may be helpful. Be sure to instruct your patient regarding the following elements to help her achieve success with dilation therapy.
Relax and allow for privacy. About 10 to 15 minutes of privacy before vaginal dilation can help with the success of each individual therapy session. Relaxation can be facilitated with activities such as deep breathing, soaking in a warm bath, or using prescribed muscle relaxants 30 to 60 minutes prior to dilation.
Use proper positioning. Instruct the patient to lie on the bed with her knees bent and placed apart. Advise her to place the lubricated dilator in the vagina as far as it can go without causing any pain (FIGURE 1). It may be helpful for her to bear down when first inserting the dilator. An in-and-out motion is not necessary.
FIGURE 1 Inserting the dilator
Tell the patient to lie on the bed with her knees bent and to insert the lubricated dilator into her vagina as far as it will go without causing pain.Be sure to inform her to use a water-based lubricant—not lotion, petroleum jelly, or any non-water-based lubricant.
Dilate daily. The dilator should be used daily and left in place for 5 to 15 minutes. She may experience a small amount of spotting initially, but spotting should abate within 2 weeks of initiating dilator use. Each dilator size should be used for 3 to 4 weeks. When your patient is changing sizes, she should transition to the larger size over several days by dilating for the first few minutes with the smaller dilator, then changing to the larger dilator for the remainder of the time. If she experiences pain or heavy bleeding, she should cease dilation and follow-up with you.
Proper cleaning. Instruct her to wash the dilator with antibacterial soap and water and to dry it thoroughly between uses.
Follow-up. When undergoing vaginal dilation therapy, your patient should be following up with you at regular intervals, usually once a month, to facilitate compliance with the program.
You can purchase dilators for your medical practice and resell them in your office. Patients also can be directed to purchase dilators directly from a manufacturer (such as Syracuse Medical Devices or AmeriMed Direct) or through a number of Internet sites, including Middlesexmd.com6 or Vaginismus.com.7 Both of these Web sites also offer educational materials, including videos and books and a private support forum or blog.
FIGURE 2 Vaginal dilators come in 8 different circumferences
Vaginal dilators range in size from Extra Small at 1/2 in (13 mm) to Large Plus at 1 1/2 in (39 mm). Each is 6 in (15 cm) long, has one rounded end, and is constructed of sterilizable, medical-grade plastic.
Printed with permission of Syracuse Medical Devices, Inc., Syracuse, New York.Most dilators used in the United States are 6 in (15 cm) long and are made from sterilizable, medical-grade, latex-free, rigid plastic with a smooth surface. Some dilators are made of softer material such as silicone, and others have a vibrating inner wand.6 They are available to purchase as single dilators or in sets of 5 to 8 graduated sizes (FIGURE 2). Some sets come with a storage bag and universal handles that lock-on for insertion. Graduated circumference sizes are fairly universal in the United States (TABLE).
Average dilator sizes and circumferences*
| Size | Circumference |
|---|---|
| Extra small | 1/2 in; 13 mm |
| Extra small plus | 11/16 in; 18 mm |
| Small | 7/8 in; 22 mm |
| Small plus | 1 in; 25 mm |
| Medium | 1 1/8 in; 29 mm |
| Medium plus | 1 1/4 in; 32 mm |
| Large | 1 3/8 in; 35 mm |
| Large plus | 1 5/8 in; 38 mm |
| *Based on Syracuse Medical Devices, Inc. product information. | |
Restoring her sexual health: Our goal
Sexual health is a vitally important quality-of-life issue; restoring that health should be our priority. We need to educate our patients on nonprescription methods to promote their vaginal and sexual health, as vaginal dilation therapy can result in the reduction or elimination of dyspareunia.
We want to hear from you! Tell us what you think.
Your age-based guide to comprehensive well-woman care
Robert L. Barbieri, MD (October 2012)
Sexual dysfunction
Barbara S. Levy, MD (Update, September 2012)
New study: ObGyns aren’t fully addressing their patients’ sexual function
(Web News, April 2012)
How to prepare your patient for the many nuances of postpartum sexuality
Roya Rezaee, MD, and Sheryl Kingsberg, PhD (January 2012)
Vaginal dilators are used to restore vaginal capacity, to expand the vagina in width and depth, to provide elasticity to the tissues, and to allow for comfortable sexual activity. Vaginal dilators are smooth plastic, rubber, or glass cylinder-shaped objects that come in a variety of graduated sizes and weights.
Several medical conditions may warrant the use of vaginal dilation, including superficial dyspareunia, high-tone pelvic floor dysfunction, vaginismus, provoked vestibulodynia, vaginal atrophy, vulvar dermatoses, vaginal agenesis, and postradiation adhesions. Dilation also can be used as deconditioning therapy for psychogenic dyspareunia.1-4 In addition, Masters and Johnson advocated the use of dilators for patients with female sexual dysfunction in order to interrupt the cycle of pain–fear–muscle spasm–more pain, and to build confidence “in the privacy of the marital bedroom.”5
Vaginal dilators often are sufficient to restore function, with dilator therapy considered successful if a woman is able to resume comfortable sexual intercourse or self-stimulation, as desired.1,6 Vaginal dilation also can be used as an adjunct to pelvic floor muscle physical therapy, psychotherapy, sex therapy, minimally absorbed local vaginal estrogen therapy, intravaginal muscle relaxants, lubricants, moisturizers, and vibrators.
Each patient in these case studies achieved success resuming sexual activity after several months of dilator therapy used in combination with other medical interventions.
CASE 1: Chronic vulvovaginal infection and pain
A 26-year-old G0P0 woman presented with a 2-year history of prohibitive penetrative dyspareunia. She had a history of chronic vulvovaginal candidiasis, treated by another clinician with multiple courses of intravaginal antifungal cream.
After extensive evaluation for sexual pain, a diagnosis of pelvic floor muscle spasm, sexual aversion, fear secondary to pain, and contact irritant dermatitis was reached. After vaginal fungal cultures indicated negative results, a size small dilator was introduced in the office using a hypoallergenic intravaginal moisturizer. After daily use of the vaginal dilator for 4 months, with progressed introduction of graduated sizes (small, medium, medium+, large), she was able to accommodate intravaginal intercourse with her partner.
CASE 2: Interstitial cystitis and fear of pain
A 58-year-old G3P3 postmenopausal woman presented with interstitial cystitis (IC), pelvic floor muscle hypertonus, vulvovaginal atrophy, and provoked vestibulodynia. Although her IC symptoms were well-controlled, she was fearful about reestablishing physical intimacy with her partner after 7 years of abstinence.
A program of intravaginal estrogen (Vagifem) 2 to 3 times per week, introital cutaneous lysate (Neogyn) vulvar soothing cream twice per day, and compounded muscle-relaxing intravaginal diazepam suppositories 2 to 3 times per week was initiated. After 2 months of treatment, she was taught in the office to use a size extra small vaginal dilator. She was delighted that use did not result in pain. Two months later, she was able to use a size small dilator, and 4 months later, a size medium dilator. At this point, the patient is confident that she can have sexual intercourse.
CASE 3: Lichen sclerosus
A 50-year-old G0P0 premenopausal woman had a history of IC and biopsy-proven lichen sclerosus. The white plaques surrounding her introitus had become so severe in the past year that she was no longer able to tolerate penile penetration without tearing. Nightly use of topical clobetasol cream and introital estrogen cream (Estrace) was recommended. After 30 days, the patient began twice-a-week maintenance with the creams and also began to use vaginal dilators. After success inserting a size extra large dilator following 5 months of dilator use, she was able to resume intercourse without tearing.
CASE 4: Vestibulodynia and vaginismus
A 25-year-old G0P0 woman underwent vestibulectomy for primary provoked vestibulodynia followed by pelvic floor muscle physical therapy for primary vaginismus. Her marriage of 6 years was unconsummated. Two weeks postoperatively, she began using a size small dilator daily and progressed to a size medium plus dilator after 6 weeks. She managed her chronic constipation and pelvic floor muscle hypertonus with daily fiber supplements, stool softeners, and self-transvaginal massage of the pelvic floor muscles. Seven weeks after surgery, she accomplished intercourse with her husband for the first time.
How to teach your patient to use vaginal dilation successfully
Before ordering vaginal dilation for your patient, 1) assess the levator ani muscle group for hypertonus or spasm and 2) choose the size dilator to start therapy that does not cause pain with insertion but enters with some resistance.
When beginning to teach your patient to use a vaginal dilator in the office, a mirror demonstration may be helpful. Be sure to instruct your patient regarding the following elements to help her achieve success with dilation therapy.
Relax and allow for privacy. About 10 to 15 minutes of privacy before vaginal dilation can help with the success of each individual therapy session. Relaxation can be facilitated with activities such as deep breathing, soaking in a warm bath, or using prescribed muscle relaxants 30 to 60 minutes prior to dilation.
Use proper positioning. Instruct the patient to lie on the bed with her knees bent and placed apart. Advise her to place the lubricated dilator in the vagina as far as it can go without causing any pain (FIGURE 1). It may be helpful for her to bear down when first inserting the dilator. An in-and-out motion is not necessary.
FIGURE 1 Inserting the dilator
Tell the patient to lie on the bed with her knees bent and to insert the lubricated dilator into her vagina as far as it will go without causing pain.Be sure to inform her to use a water-based lubricant—not lotion, petroleum jelly, or any non-water-based lubricant.
Dilate daily. The dilator should be used daily and left in place for 5 to 15 minutes. She may experience a small amount of spotting initially, but spotting should abate within 2 weeks of initiating dilator use. Each dilator size should be used for 3 to 4 weeks. When your patient is changing sizes, she should transition to the larger size over several days by dilating for the first few minutes with the smaller dilator, then changing to the larger dilator for the remainder of the time. If she experiences pain or heavy bleeding, she should cease dilation and follow-up with you.
Proper cleaning. Instruct her to wash the dilator with antibacterial soap and water and to dry it thoroughly between uses.
Follow-up. When undergoing vaginal dilation therapy, your patient should be following up with you at regular intervals, usually once a month, to facilitate compliance with the program.
You can purchase dilators for your medical practice and resell them in your office. Patients also can be directed to purchase dilators directly from a manufacturer (such as Syracuse Medical Devices or AmeriMed Direct) or through a number of Internet sites, including Middlesexmd.com6 or Vaginismus.com.7 Both of these Web sites also offer educational materials, including videos and books and a private support forum or blog.
FIGURE 2 Vaginal dilators come in 8 different circumferences
Vaginal dilators range in size from Extra Small at 1/2 in (13 mm) to Large Plus at 1 1/2 in (39 mm). Each is 6 in (15 cm) long, has one rounded end, and is constructed of sterilizable, medical-grade plastic.
Printed with permission of Syracuse Medical Devices, Inc., Syracuse, New York.Most dilators used in the United States are 6 in (15 cm) long and are made from sterilizable, medical-grade, latex-free, rigid plastic with a smooth surface. Some dilators are made of softer material such as silicone, and others have a vibrating inner wand.6 They are available to purchase as single dilators or in sets of 5 to 8 graduated sizes (FIGURE 2). Some sets come with a storage bag and universal handles that lock-on for insertion. Graduated circumference sizes are fairly universal in the United States (TABLE).
Average dilator sizes and circumferences*
| Size | Circumference |
|---|---|
| Extra small | 1/2 in; 13 mm |
| Extra small plus | 11/16 in; 18 mm |
| Small | 7/8 in; 22 mm |
| Small plus | 1 in; 25 mm |
| Medium | 1 1/8 in; 29 mm |
| Medium plus | 1 1/4 in; 32 mm |
| Large | 1 3/8 in; 35 mm |
| Large plus | 1 5/8 in; 38 mm |
| *Based on Syracuse Medical Devices, Inc. product information. | |
Restoring her sexual health: Our goal
Sexual health is a vitally important quality-of-life issue; restoring that health should be our priority. We need to educate our patients on nonprescription methods to promote their vaginal and sexual health, as vaginal dilation therapy can result in the reduction or elimination of dyspareunia.
We want to hear from you! Tell us what you think.
Your age-based guide to comprehensive well-woman care
Robert L. Barbieri, MD (October 2012)
Sexual dysfunction
Barbara S. Levy, MD (Update, September 2012)
New study: ObGyns aren’t fully addressing their patients’ sexual function
(Web News, April 2012)
How to prepare your patient for the many nuances of postpartum sexuality
Roya Rezaee, MD, and Sheryl Kingsberg, PhD (January 2012)
Polycystic ovary syndrome: Cosmetic and dietary approaches
Part 1. Where we stand with diagnosis and treatment—and
where we're going
Although polycystic ovary syndrome (PCOS) is the most common endocrine abnormality in women of reproductive age, affecting at least 1 in 15 women in this population, its precise cause is unknown. As a result, management of PCOS requires a focus on its individual effects, among them anovulation, infertility, hyperandrogenism, and insulin resistance.
So far in this four-part series, we have covered diagnosis and treatment, the role of obesity and insulin resistance, and long-term metabolic risks. In this concluding article, we focus on cosmetic and dietary issues, and describe emerging diagnostic approaches to this common disorder.
![]()
Management of hirsutism and acne should focus on combination therapy that includes androgen suppression and peripheral androgen blockade, with or without mechanical or cosmetic reduction or destruction of unwanted hair. The choice of treatment depends on the side-effect profile. To maximize benefits, treatments should be continued for at least 2 years. All of the therapies described in this article have teratogenic potential (inhibiting normal development of male external genitalia) and should be prescribed only with adequate contraception that is used consistently.
Medical treatment of hirsutism and acne
Oral contraceptives are the most popular treatment for hirsutism. They suppress pituitary production of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which in turn suppress ovarian androgen production. OCs also may reduce adrenal androgen production, although the mechanism of action is unclear.
The estrogen component in OCs increases hepatic production of sex hormone-binding globulin (SHBG), thereby decreasing free testosterone levels. The progestin component antagonizes 5α-reductase and the androgen receptor; it also may increase hepatic metabolism of testosterone and can increase SHBG when the OC has low androgenic activity.
Spironolactone is an aldosterone antagonist and mild diuretic that competes primarily with androgens for the androgen receptor. It also:
- inhibits the 5α-reductase enzyme, preventing the conversion of testosterone to the more potent dihydrotestosterone (DHT)
- increases hepatic production of SHBG, thereby decreasing free testosterone levels
- suppresses enzymes in the biosynthesis of androgens.
A dose of 100 mg twice daily is effective, although higher doses of 200 mg to 300 mg may be required. Start with a dose of 25 mg daily, with a progressive increase over 3 weeks to minimize side effects (TABLE).
Medical treatment of hirsutism in women with PCOS
| Drug | Brand name | Cost | Side effects |
|---|---|---|---|
| Spironolactone | Aldactone, Novo-Spiroton, Aldactazide, Spiractin, Spirotone, Verospiron, Berlactone | $30 for thirty 50-mg tabs | Dyspepsia, nausea, polyuria, nocturia, fatigue, headache, breast tenderness, reduced libido, photosensitivity, hyperkalemia (rare) |
| Flutamide | Eulexin | $170 for one hundred 250-mg tabs | Greenish urine, excessive dryness of skin and scalp, liver enzyme abnormalities, hepatic toxicity |
| Bicalutamide | Casodex, Cosudex, Calutide, Kalumid | $30–$490 for thirty 50-mg tabs | Breast tenderness, gynecomastia, hot flushes, gastrointestinal disorders, diarrhea, nausea, hepatic changes, asthenia, pruritus |
| Cyproterone acetate | Androcur, Cyprostat, Cyproteron, Procur, Cyprone, Cyprohexal, Ciproterona, Cyproteronum, Neoproxil, Siterone | $35–$50 for twenty 50-mg tabs (generic) $90 for sixty 50-mg tabs (Androcur) | Liver toxicity, adrenal insufficiency, loss of libido, and depressive mood changes |
| Finasteride | Proscar, Propecia | $8.75–$17.50 for thirty to sixty 5-mg tabs | Teratogenicity is a major concern |
Flutamide (Eulexin) is approved by the US Food and Drug Administration as an adjuvant treatment for prostate cancer. It is not a steroid but a substituted anilide that competes with testosterone and its powerful metabolite, DHT, for binding to androgen receptors. Flutamide may also be used to treat excess androgen levels and hirsutism in women. It is given at a dose of 500 mg daily. Side effects include greenish urine, excessive dryness of skin and scalp, liver enzyme abnormalities, and hepatic toxicity.
Flutamide is now being replaced by a newer member of this class of drugs, bicalutamide (launched in 1995 and marketed as Casodex, Cosudex, Calutide, Kalumid), due to a better side-effect profile. Bicalutamide acts as a pure antiandrogen by binding to the androgen receptor and preventing its activation and subsequent upregulation of androgen-responsive genes by androgenic hormones. In addition, bicalutamide accelerates the degradation of the androgen receptor. Preliminary studies suggest that a dose of 25 mg daily produces significant improvement in Ferriman-Gallwey scores. Side effects include breast tenderness, gynecomastia, hot flushes, gastrointestinal disorders, diarrhea, nausea, hepatic changes (elevated levels of transaminases; jaundice), asthenia, and pruritus.
Cyproterone acetate is a synthetic derivative of 17-hydroxyprogesterone. It inhibits the steroidogenic enzyme 21-hydroxylase and, to a lesser extent, 3-beta-hydroxysteroid dehydrogenase, both of which are needed to synthesize cortisol and aldosterone.
Gonadotropin production is reduced by the progestational and glucocorticoid effects of cyproterone acetate and may result in lower testosterone levels. However, the blockade of adrenal 21-hydroxylase may lead to the accumulation of androgen precursors, which may be converted to testosterone, reducing the efficacy of antiandrogen treatment. For this reason, cyproterone acetate is sometimes combined with other agents. Studies of hirsutism have demonstrated increased efficacy with combination therapy, compared with cyproterone acetate alone. This drug is approved for use only in the United Kingdom and Canada.
A dose of 50 mg to 100 mg is recommended. The most serious potential side effect is liver toxicity. Patients should be monitored for changes in liver enzymes, especially if they are taking a high dose (200–300 mg/day). Other side effects include adrenal insufficiency, loss of libido, and depressive mood changes.
Finasteride (approved in 1992 and marketed as Proscar, Propecia) is a synthetic antiandrogen that inhibits 5a-reductase, the enzyme that converts testosterone to DHT. It is used as a treatment for benign prostatic hyperplasia in low doses, and for prostate cancer in higher doses. A dose of 2.5 mg to 5 mg daily is typical for women with hirsutism.
In randomized clinical trials, finasteride has produced significant improvements in hirsutism, compared with placebo, but no significant differences compared with other therapies. Although the side-effect profile is less severe than that of other therapies, teratogenicity is a major concern.
![]()
Numerous dietary interventions have been explored in women with PCOS.1 A few studies have involved manipulation of the dietary macronutrient profile, but only two have used a controlled study design to compare different macronutrient compositions. Two different groups tested a high-protein (30%) diet, compared with lower protein (15%), while keeping fat intake (30%) the same.2,3
In a study by Moran and colleagues, women were prescribed a reduced-calorie diet for 12 weeks, followed by a maintenance diet for 4 weeks.2 There were no differences between the high-protein and low-protein groups in terms of weight or fat loss (as assessed by dual-energy x-ray absorptiometry). However, the 38% dropout rate was higher than anticipated, and the authors acknowledge that the inability to detect a difference between groups could be due to insufficient power.2
In the study by Stamets and colleagues, the same macronutrient profile was used, but for only 4 weeks—too short a time to detect much difference in weight loss.3 Not surprisingly, no difference in weight loss was found between groups.
In both studies, dietary compliance and the rate of study retention were confounding and limiting factors.2,3 To date, there is insufficient evidence that a particular dietary approach, such as modified macronutrient composition, will enhance weight loss in women with PCOS. However, general dietary and lifestyle modifications still remain the first line of therapy to address the metabolic consequences of PCOS for overweight and obese women.1 In appropriate clinical situations, consideration should also be given to alternative weight-loss approaches, such as weight-loss medication or bariatric surgery.
![]()
Although the fundamental pathophysiologic mechanism is unclear, both lean and obese women with PCOS have greater LH pulse frequency and amplitude, leading to increased 24-hour mean concentrations of LH. Because androgen production by theca cells is LH-dependent, it would seem to follow that the elevated LH levels seen in women with PCOS are responsible for excess androgen production. The most likely cause of anovulation is an FSH level too low to fully mature the follicles. FSH levels may be suppressed by negative feedback inhibition from midfollicular estradiol levels.
While the defect in PCOS is unknown, it is clear that there are altered gonadotropin dynamics. Nonetheless, current consensus is that elevated LH is not essential for the definition of PCOS, despite this frequent finding and the understanding that high LH levels have adverse effects on oocyte quality, maturity, pregnancy outcomes, and miscarriages.4,5
![]()
In recent years there has been increasing interest in anti-Müllerian hormone (AMH) (also known as Müllerian-inhibiting substance), which is exclusively of ovarian origin in women, as a marker of ovarian reserve and female reproductive function. Several studies on the role of AMH in ovarian physiology indicate that the hormone has two main functions with respect to folliculogenesis, at least according to mice models:
- It plays a negative role in follicular recruitment.
- It reduces preantral and antral follicle responsiveness to FSH.6-8
We know that serum AMH levels decline with age, as there is a decline in female reproductive function due to the reduction in the ovarian follicle pool and the quality of the oocytes. Undetectable AMH levels after premature ovarian failure have been reported, and oophorectomy in regularly cycling women is associated with the disappearance of AMH within 3 to 5 days. In contrast, AMH serum levels are normal in women affected by functional hypothalamic (hypogonadotrophic) amenorrhea.
In the past, FSH, inhibin B, and the antral follicle count have been the most reliable markers for investigating ovarian reserve during assisted reproductive treatment and predicting ovarian response to ovulation induction in intrauterine insemination and in vitro fertilization cycles, and are also useful in monitoring other reproductive disorders. However, AMH seems to better reflect the continuous decline of the oocyte/follicle pool with age and may be the best marker of ovarian aging and the menopausal transition. Moreover, serum levels can be drawn at any time of the menstrual cycle, unlike the measurement of FSH, which must be performed on day 3 of the cycle.8,9
Increased AMH production also has been reported in women with PCOS, compared with controls.10 The increased production may be the result of aberrant activity of the granulosa cells in polycystic ovaries. AMH production may exert a paracrine negative control on follicle growth sufficient to prevent selection of a dominant follicle. Coupled with higher inhibin B levels, this may lead to a relative deficit of FSH in women with PCOS.
AMH measurement offers high specificity and sensitivity as a marker for PCOS. On this basis, it has been proposed that, in situations in which accurate ultrasonographic data are unavailable, AMH could be used instead of the follicle count as a diagnostic criterion for PCOS. Therapeutic interventions, including metformin administration to improve insulin resistance in women affected by PCOS, are associated with a reduction in both serum AMH levels and antral follicles. This suggests that the measurement of AMH could be used to evaluate treatment efficacy, may be a better predictor of ovarian hyperstimulation syndrome (OHSS) than body mass index, and could help direct the application of mild ovulation induction protocols to avoid moderate and severe OHSS.
There seems to be little doubt that research on AMH will continue in years to come. A clearer understanding of its effects on ovarian physiology may help clinicians find a role for AMH measurement in the field of reproductive medicine, thereby simplifying the diagnosis of PCOS and the evaluation of its treatment efficacy.
We want to hear from you! Tell us what you think.
1. Moran LJ, Pasquali R, Teede HJ, Hoeger KM, Norman RJ. Treatment of obesity in polycystic ovary syndrome: a position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertil Steril. 2009;92(6):1966-1982.
2. Moran LJ, Noakes M, Clifton PM, Tomlinson L, Galletly C, Norman RJ. Dietary composition in restoring reproductive and metabolic physiology in overweight women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2003;88(2):812-819.
3. Stamets K, Taylor DS, Kunselman A, Demers LM, Pelkman CL, Legro RS. A randomized trial of the effects of two types of short-term hypocaloric diets on weight loss in women with polycystic ovary syndrome. Fertil Steril. 2004;81(3):630-637.
4. Morales AJ, Laughlin GA, Bützow T, Maheshwari H, Baumann G, Yen SS. Insulin somatotropic, and luteinizing hormone axes in lean and obese women with polycystic ovary syndrome: common and distinct features. J Clin Endocrinol Metab. 1996;81(8):2854-2864.
5. Guzick DS. Polycystic ovary syndrome. Obstet Gynecol. 2004;103(1):181-193.
6. Durlinger AL, Grijters MJ, Kramer P, et al. Anti- Müllerian hormone attenuates the effects of FSH on follicle development in the mouse ovary. Endocrinology. 2001;142(11):4891-4899.
7. Durlinger AL, Kramer P, Karels B, et al. Control of primordial follicle recruitment by anti-Müllerian hormone in the mouse ovary. Endocrinology. 1990;140(12):5789-5796.
8. Cook CL, Siow Y, Taylor S, et al. Serum Müllerian inhibiting substance levels during normal menstrual cycles. Fertil Steril. 2000;73(4):859-861.
9. Muttukrishna S, Suharjono H, McGarrigle H, et al. Inhibin B and anti-Müllerian hormone: markers of ovarian response in IVF/ICSI patients? BJOG. 2004;111(11):1248-1253.
10. Fallat M, Slow Y, Mara M, et al. Müllerian-inhibiting substance in follicular fluid and serum: a comparison of patients with tubal factor infertility, polycystic ovary syndrome, and endometriosis. Fertil Steril. 1997;67(5):962-965.
Part 1. Where we stand with diagnosis and treatment—and
where we're going
Although polycystic ovary syndrome (PCOS) is the most common endocrine abnormality in women of reproductive age, affecting at least 1 in 15 women in this population, its precise cause is unknown. As a result, management of PCOS requires a focus on its individual effects, among them anovulation, infertility, hyperandrogenism, and insulin resistance.
So far in this four-part series, we have covered diagnosis and treatment, the role of obesity and insulin resistance, and long-term metabolic risks. In this concluding article, we focus on cosmetic and dietary issues, and describe emerging diagnostic approaches to this common disorder.
![]()
Management of hirsutism and acne should focus on combination therapy that includes androgen suppression and peripheral androgen blockade, with or without mechanical or cosmetic reduction or destruction of unwanted hair. The choice of treatment depends on the side-effect profile. To maximize benefits, treatments should be continued for at least 2 years. All of the therapies described in this article have teratogenic potential (inhibiting normal development of male external genitalia) and should be prescribed only with adequate contraception that is used consistently.
Medical treatment of hirsutism and acne
Oral contraceptives are the most popular treatment for hirsutism. They suppress pituitary production of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which in turn suppress ovarian androgen production. OCs also may reduce adrenal androgen production, although the mechanism of action is unclear.
The estrogen component in OCs increases hepatic production of sex hormone-binding globulin (SHBG), thereby decreasing free testosterone levels. The progestin component antagonizes 5α-reductase and the androgen receptor; it also may increase hepatic metabolism of testosterone and can increase SHBG when the OC has low androgenic activity.
Spironolactone is an aldosterone antagonist and mild diuretic that competes primarily with androgens for the androgen receptor. It also:
- inhibits the 5α-reductase enzyme, preventing the conversion of testosterone to the more potent dihydrotestosterone (DHT)
- increases hepatic production of SHBG, thereby decreasing free testosterone levels
- suppresses enzymes in the biosynthesis of androgens.
A dose of 100 mg twice daily is effective, although higher doses of 200 mg to 300 mg may be required. Start with a dose of 25 mg daily, with a progressive increase over 3 weeks to minimize side effects (TABLE).
Medical treatment of hirsutism in women with PCOS
| Drug | Brand name | Cost | Side effects |
|---|---|---|---|
| Spironolactone | Aldactone, Novo-Spiroton, Aldactazide, Spiractin, Spirotone, Verospiron, Berlactone | $30 for thirty 50-mg tabs | Dyspepsia, nausea, polyuria, nocturia, fatigue, headache, breast tenderness, reduced libido, photosensitivity, hyperkalemia (rare) |
| Flutamide | Eulexin | $170 for one hundred 250-mg tabs | Greenish urine, excessive dryness of skin and scalp, liver enzyme abnormalities, hepatic toxicity |
| Bicalutamide | Casodex, Cosudex, Calutide, Kalumid | $30–$490 for thirty 50-mg tabs | Breast tenderness, gynecomastia, hot flushes, gastrointestinal disorders, diarrhea, nausea, hepatic changes, asthenia, pruritus |
| Cyproterone acetate | Androcur, Cyprostat, Cyproteron, Procur, Cyprone, Cyprohexal, Ciproterona, Cyproteronum, Neoproxil, Siterone | $35–$50 for twenty 50-mg tabs (generic) $90 for sixty 50-mg tabs (Androcur) | Liver toxicity, adrenal insufficiency, loss of libido, and depressive mood changes |
| Finasteride | Proscar, Propecia | $8.75–$17.50 for thirty to sixty 5-mg tabs | Teratogenicity is a major concern |
Flutamide (Eulexin) is approved by the US Food and Drug Administration as an adjuvant treatment for prostate cancer. It is not a steroid but a substituted anilide that competes with testosterone and its powerful metabolite, DHT, for binding to androgen receptors. Flutamide may also be used to treat excess androgen levels and hirsutism in women. It is given at a dose of 500 mg daily. Side effects include greenish urine, excessive dryness of skin and scalp, liver enzyme abnormalities, and hepatic toxicity.
Flutamide is now being replaced by a newer member of this class of drugs, bicalutamide (launched in 1995 and marketed as Casodex, Cosudex, Calutide, Kalumid), due to a better side-effect profile. Bicalutamide acts as a pure antiandrogen by binding to the androgen receptor and preventing its activation and subsequent upregulation of androgen-responsive genes by androgenic hormones. In addition, bicalutamide accelerates the degradation of the androgen receptor. Preliminary studies suggest that a dose of 25 mg daily produces significant improvement in Ferriman-Gallwey scores. Side effects include breast tenderness, gynecomastia, hot flushes, gastrointestinal disorders, diarrhea, nausea, hepatic changes (elevated levels of transaminases; jaundice), asthenia, and pruritus.
Cyproterone acetate is a synthetic derivative of 17-hydroxyprogesterone. It inhibits the steroidogenic enzyme 21-hydroxylase and, to a lesser extent, 3-beta-hydroxysteroid dehydrogenase, both of which are needed to synthesize cortisol and aldosterone.
Gonadotropin production is reduced by the progestational and glucocorticoid effects of cyproterone acetate and may result in lower testosterone levels. However, the blockade of adrenal 21-hydroxylase may lead to the accumulation of androgen precursors, which may be converted to testosterone, reducing the efficacy of antiandrogen treatment. For this reason, cyproterone acetate is sometimes combined with other agents. Studies of hirsutism have demonstrated increased efficacy with combination therapy, compared with cyproterone acetate alone. This drug is approved for use only in the United Kingdom and Canada.
A dose of 50 mg to 100 mg is recommended. The most serious potential side effect is liver toxicity. Patients should be monitored for changes in liver enzymes, especially if they are taking a high dose (200–300 mg/day). Other side effects include adrenal insufficiency, loss of libido, and depressive mood changes.
Finasteride (approved in 1992 and marketed as Proscar, Propecia) is a synthetic antiandrogen that inhibits 5a-reductase, the enzyme that converts testosterone to DHT. It is used as a treatment for benign prostatic hyperplasia in low doses, and for prostate cancer in higher doses. A dose of 2.5 mg to 5 mg daily is typical for women with hirsutism.
In randomized clinical trials, finasteride has produced significant improvements in hirsutism, compared with placebo, but no significant differences compared with other therapies. Although the side-effect profile is less severe than that of other therapies, teratogenicity is a major concern.
![]()
Numerous dietary interventions have been explored in women with PCOS.1 A few studies have involved manipulation of the dietary macronutrient profile, but only two have used a controlled study design to compare different macronutrient compositions. Two different groups tested a high-protein (30%) diet, compared with lower protein (15%), while keeping fat intake (30%) the same.2,3
In a study by Moran and colleagues, women were prescribed a reduced-calorie diet for 12 weeks, followed by a maintenance diet for 4 weeks.2 There were no differences between the high-protein and low-protein groups in terms of weight or fat loss (as assessed by dual-energy x-ray absorptiometry). However, the 38% dropout rate was higher than anticipated, and the authors acknowledge that the inability to detect a difference between groups could be due to insufficient power.2
In the study by Stamets and colleagues, the same macronutrient profile was used, but for only 4 weeks—too short a time to detect much difference in weight loss.3 Not surprisingly, no difference in weight loss was found between groups.
In both studies, dietary compliance and the rate of study retention were confounding and limiting factors.2,3 To date, there is insufficient evidence that a particular dietary approach, such as modified macronutrient composition, will enhance weight loss in women with PCOS. However, general dietary and lifestyle modifications still remain the first line of therapy to address the metabolic consequences of PCOS for overweight and obese women.1 In appropriate clinical situations, consideration should also be given to alternative weight-loss approaches, such as weight-loss medication or bariatric surgery.
![]()
Although the fundamental pathophysiologic mechanism is unclear, both lean and obese women with PCOS have greater LH pulse frequency and amplitude, leading to increased 24-hour mean concentrations of LH. Because androgen production by theca cells is LH-dependent, it would seem to follow that the elevated LH levels seen in women with PCOS are responsible for excess androgen production. The most likely cause of anovulation is an FSH level too low to fully mature the follicles. FSH levels may be suppressed by negative feedback inhibition from midfollicular estradiol levels.
While the defect in PCOS is unknown, it is clear that there are altered gonadotropin dynamics. Nonetheless, current consensus is that elevated LH is not essential for the definition of PCOS, despite this frequent finding and the understanding that high LH levels have adverse effects on oocyte quality, maturity, pregnancy outcomes, and miscarriages.4,5
![]()
In recent years there has been increasing interest in anti-Müllerian hormone (AMH) (also known as Müllerian-inhibiting substance), which is exclusively of ovarian origin in women, as a marker of ovarian reserve and female reproductive function. Several studies on the role of AMH in ovarian physiology indicate that the hormone has two main functions with respect to folliculogenesis, at least according to mice models:
- It plays a negative role in follicular recruitment.
- It reduces preantral and antral follicle responsiveness to FSH.6-8
We know that serum AMH levels decline with age, as there is a decline in female reproductive function due to the reduction in the ovarian follicle pool and the quality of the oocytes. Undetectable AMH levels after premature ovarian failure have been reported, and oophorectomy in regularly cycling women is associated with the disappearance of AMH within 3 to 5 days. In contrast, AMH serum levels are normal in women affected by functional hypothalamic (hypogonadotrophic) amenorrhea.
In the past, FSH, inhibin B, and the antral follicle count have been the most reliable markers for investigating ovarian reserve during assisted reproductive treatment and predicting ovarian response to ovulation induction in intrauterine insemination and in vitro fertilization cycles, and are also useful in monitoring other reproductive disorders. However, AMH seems to better reflect the continuous decline of the oocyte/follicle pool with age and may be the best marker of ovarian aging and the menopausal transition. Moreover, serum levels can be drawn at any time of the menstrual cycle, unlike the measurement of FSH, which must be performed on day 3 of the cycle.8,9
Increased AMH production also has been reported in women with PCOS, compared with controls.10 The increased production may be the result of aberrant activity of the granulosa cells in polycystic ovaries. AMH production may exert a paracrine negative control on follicle growth sufficient to prevent selection of a dominant follicle. Coupled with higher inhibin B levels, this may lead to a relative deficit of FSH in women with PCOS.
AMH measurement offers high specificity and sensitivity as a marker for PCOS. On this basis, it has been proposed that, in situations in which accurate ultrasonographic data are unavailable, AMH could be used instead of the follicle count as a diagnostic criterion for PCOS. Therapeutic interventions, including metformin administration to improve insulin resistance in women affected by PCOS, are associated with a reduction in both serum AMH levels and antral follicles. This suggests that the measurement of AMH could be used to evaluate treatment efficacy, may be a better predictor of ovarian hyperstimulation syndrome (OHSS) than body mass index, and could help direct the application of mild ovulation induction protocols to avoid moderate and severe OHSS.
There seems to be little doubt that research on AMH will continue in years to come. A clearer understanding of its effects on ovarian physiology may help clinicians find a role for AMH measurement in the field of reproductive medicine, thereby simplifying the diagnosis of PCOS and the evaluation of its treatment efficacy.
We want to hear from you! Tell us what you think.
Part 1. Where we stand with diagnosis and treatment—and
where we're going
Although polycystic ovary syndrome (PCOS) is the most common endocrine abnormality in women of reproductive age, affecting at least 1 in 15 women in this population, its precise cause is unknown. As a result, management of PCOS requires a focus on its individual effects, among them anovulation, infertility, hyperandrogenism, and insulin resistance.
So far in this four-part series, we have covered diagnosis and treatment, the role of obesity and insulin resistance, and long-term metabolic risks. In this concluding article, we focus on cosmetic and dietary issues, and describe emerging diagnostic approaches to this common disorder.
![]()
Management of hirsutism and acne should focus on combination therapy that includes androgen suppression and peripheral androgen blockade, with or without mechanical or cosmetic reduction or destruction of unwanted hair. The choice of treatment depends on the side-effect profile. To maximize benefits, treatments should be continued for at least 2 years. All of the therapies described in this article have teratogenic potential (inhibiting normal development of male external genitalia) and should be prescribed only with adequate contraception that is used consistently.
Medical treatment of hirsutism and acne
Oral contraceptives are the most popular treatment for hirsutism. They suppress pituitary production of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which in turn suppress ovarian androgen production. OCs also may reduce adrenal androgen production, although the mechanism of action is unclear.
The estrogen component in OCs increases hepatic production of sex hormone-binding globulin (SHBG), thereby decreasing free testosterone levels. The progestin component antagonizes 5α-reductase and the androgen receptor; it also may increase hepatic metabolism of testosterone and can increase SHBG when the OC has low androgenic activity.
Spironolactone is an aldosterone antagonist and mild diuretic that competes primarily with androgens for the androgen receptor. It also:
- inhibits the 5α-reductase enzyme, preventing the conversion of testosterone to the more potent dihydrotestosterone (DHT)
- increases hepatic production of SHBG, thereby decreasing free testosterone levels
- suppresses enzymes in the biosynthesis of androgens.
A dose of 100 mg twice daily is effective, although higher doses of 200 mg to 300 mg may be required. Start with a dose of 25 mg daily, with a progressive increase over 3 weeks to minimize side effects (TABLE).
Medical treatment of hirsutism in women with PCOS
| Drug | Brand name | Cost | Side effects |
|---|---|---|---|
| Spironolactone | Aldactone, Novo-Spiroton, Aldactazide, Spiractin, Spirotone, Verospiron, Berlactone | $30 for thirty 50-mg tabs | Dyspepsia, nausea, polyuria, nocturia, fatigue, headache, breast tenderness, reduced libido, photosensitivity, hyperkalemia (rare) |
| Flutamide | Eulexin | $170 for one hundred 250-mg tabs | Greenish urine, excessive dryness of skin and scalp, liver enzyme abnormalities, hepatic toxicity |
| Bicalutamide | Casodex, Cosudex, Calutide, Kalumid | $30–$490 for thirty 50-mg tabs | Breast tenderness, gynecomastia, hot flushes, gastrointestinal disorders, diarrhea, nausea, hepatic changes, asthenia, pruritus |
| Cyproterone acetate | Androcur, Cyprostat, Cyproteron, Procur, Cyprone, Cyprohexal, Ciproterona, Cyproteronum, Neoproxil, Siterone | $35–$50 for twenty 50-mg tabs (generic) $90 for sixty 50-mg tabs (Androcur) | Liver toxicity, adrenal insufficiency, loss of libido, and depressive mood changes |
| Finasteride | Proscar, Propecia | $8.75–$17.50 for thirty to sixty 5-mg tabs | Teratogenicity is a major concern |
Flutamide (Eulexin) is approved by the US Food and Drug Administration as an adjuvant treatment for prostate cancer. It is not a steroid but a substituted anilide that competes with testosterone and its powerful metabolite, DHT, for binding to androgen receptors. Flutamide may also be used to treat excess androgen levels and hirsutism in women. It is given at a dose of 500 mg daily. Side effects include greenish urine, excessive dryness of skin and scalp, liver enzyme abnormalities, and hepatic toxicity.
Flutamide is now being replaced by a newer member of this class of drugs, bicalutamide (launched in 1995 and marketed as Casodex, Cosudex, Calutide, Kalumid), due to a better side-effect profile. Bicalutamide acts as a pure antiandrogen by binding to the androgen receptor and preventing its activation and subsequent upregulation of androgen-responsive genes by androgenic hormones. In addition, bicalutamide accelerates the degradation of the androgen receptor. Preliminary studies suggest that a dose of 25 mg daily produces significant improvement in Ferriman-Gallwey scores. Side effects include breast tenderness, gynecomastia, hot flushes, gastrointestinal disorders, diarrhea, nausea, hepatic changes (elevated levels of transaminases; jaundice), asthenia, and pruritus.
Cyproterone acetate is a synthetic derivative of 17-hydroxyprogesterone. It inhibits the steroidogenic enzyme 21-hydroxylase and, to a lesser extent, 3-beta-hydroxysteroid dehydrogenase, both of which are needed to synthesize cortisol and aldosterone.
Gonadotropin production is reduced by the progestational and glucocorticoid effects of cyproterone acetate and may result in lower testosterone levels. However, the blockade of adrenal 21-hydroxylase may lead to the accumulation of androgen precursors, which may be converted to testosterone, reducing the efficacy of antiandrogen treatment. For this reason, cyproterone acetate is sometimes combined with other agents. Studies of hirsutism have demonstrated increased efficacy with combination therapy, compared with cyproterone acetate alone. This drug is approved for use only in the United Kingdom and Canada.
A dose of 50 mg to 100 mg is recommended. The most serious potential side effect is liver toxicity. Patients should be monitored for changes in liver enzymes, especially if they are taking a high dose (200–300 mg/day). Other side effects include adrenal insufficiency, loss of libido, and depressive mood changes.
Finasteride (approved in 1992 and marketed as Proscar, Propecia) is a synthetic antiandrogen that inhibits 5a-reductase, the enzyme that converts testosterone to DHT. It is used as a treatment for benign prostatic hyperplasia in low doses, and for prostate cancer in higher doses. A dose of 2.5 mg to 5 mg daily is typical for women with hirsutism.
In randomized clinical trials, finasteride has produced significant improvements in hirsutism, compared with placebo, but no significant differences compared with other therapies. Although the side-effect profile is less severe than that of other therapies, teratogenicity is a major concern.
![]()
Numerous dietary interventions have been explored in women with PCOS.1 A few studies have involved manipulation of the dietary macronutrient profile, but only two have used a controlled study design to compare different macronutrient compositions. Two different groups tested a high-protein (30%) diet, compared with lower protein (15%), while keeping fat intake (30%) the same.2,3
In a study by Moran and colleagues, women were prescribed a reduced-calorie diet for 12 weeks, followed by a maintenance diet for 4 weeks.2 There were no differences between the high-protein and low-protein groups in terms of weight or fat loss (as assessed by dual-energy x-ray absorptiometry). However, the 38% dropout rate was higher than anticipated, and the authors acknowledge that the inability to detect a difference between groups could be due to insufficient power.2
In the study by Stamets and colleagues, the same macronutrient profile was used, but for only 4 weeks—too short a time to detect much difference in weight loss.3 Not surprisingly, no difference in weight loss was found between groups.
In both studies, dietary compliance and the rate of study retention were confounding and limiting factors.2,3 To date, there is insufficient evidence that a particular dietary approach, such as modified macronutrient composition, will enhance weight loss in women with PCOS. However, general dietary and lifestyle modifications still remain the first line of therapy to address the metabolic consequences of PCOS for overweight and obese women.1 In appropriate clinical situations, consideration should also be given to alternative weight-loss approaches, such as weight-loss medication or bariatric surgery.
![]()
Although the fundamental pathophysiologic mechanism is unclear, both lean and obese women with PCOS have greater LH pulse frequency and amplitude, leading to increased 24-hour mean concentrations of LH. Because androgen production by theca cells is LH-dependent, it would seem to follow that the elevated LH levels seen in women with PCOS are responsible for excess androgen production. The most likely cause of anovulation is an FSH level too low to fully mature the follicles. FSH levels may be suppressed by negative feedback inhibition from midfollicular estradiol levels.
While the defect in PCOS is unknown, it is clear that there are altered gonadotropin dynamics. Nonetheless, current consensus is that elevated LH is not essential for the definition of PCOS, despite this frequent finding and the understanding that high LH levels have adverse effects on oocyte quality, maturity, pregnancy outcomes, and miscarriages.4,5
![]()
In recent years there has been increasing interest in anti-Müllerian hormone (AMH) (also known as Müllerian-inhibiting substance), which is exclusively of ovarian origin in women, as a marker of ovarian reserve and female reproductive function. Several studies on the role of AMH in ovarian physiology indicate that the hormone has two main functions with respect to folliculogenesis, at least according to mice models:
- It plays a negative role in follicular recruitment.
- It reduces preantral and antral follicle responsiveness to FSH.6-8
We know that serum AMH levels decline with age, as there is a decline in female reproductive function due to the reduction in the ovarian follicle pool and the quality of the oocytes. Undetectable AMH levels after premature ovarian failure have been reported, and oophorectomy in regularly cycling women is associated with the disappearance of AMH within 3 to 5 days. In contrast, AMH serum levels are normal in women affected by functional hypothalamic (hypogonadotrophic) amenorrhea.
In the past, FSH, inhibin B, and the antral follicle count have been the most reliable markers for investigating ovarian reserve during assisted reproductive treatment and predicting ovarian response to ovulation induction in intrauterine insemination and in vitro fertilization cycles, and are also useful in monitoring other reproductive disorders. However, AMH seems to better reflect the continuous decline of the oocyte/follicle pool with age and may be the best marker of ovarian aging and the menopausal transition. Moreover, serum levels can be drawn at any time of the menstrual cycle, unlike the measurement of FSH, which must be performed on day 3 of the cycle.8,9
Increased AMH production also has been reported in women with PCOS, compared with controls.10 The increased production may be the result of aberrant activity of the granulosa cells in polycystic ovaries. AMH production may exert a paracrine negative control on follicle growth sufficient to prevent selection of a dominant follicle. Coupled with higher inhibin B levels, this may lead to a relative deficit of FSH in women with PCOS.
AMH measurement offers high specificity and sensitivity as a marker for PCOS. On this basis, it has been proposed that, in situations in which accurate ultrasonographic data are unavailable, AMH could be used instead of the follicle count as a diagnostic criterion for PCOS. Therapeutic interventions, including metformin administration to improve insulin resistance in women affected by PCOS, are associated with a reduction in both serum AMH levels and antral follicles. This suggests that the measurement of AMH could be used to evaluate treatment efficacy, may be a better predictor of ovarian hyperstimulation syndrome (OHSS) than body mass index, and could help direct the application of mild ovulation induction protocols to avoid moderate and severe OHSS.
There seems to be little doubt that research on AMH will continue in years to come. A clearer understanding of its effects on ovarian physiology may help clinicians find a role for AMH measurement in the field of reproductive medicine, thereby simplifying the diagnosis of PCOS and the evaluation of its treatment efficacy.
We want to hear from you! Tell us what you think.
1. Moran LJ, Pasquali R, Teede HJ, Hoeger KM, Norman RJ. Treatment of obesity in polycystic ovary syndrome: a position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertil Steril. 2009;92(6):1966-1982.
2. Moran LJ, Noakes M, Clifton PM, Tomlinson L, Galletly C, Norman RJ. Dietary composition in restoring reproductive and metabolic physiology in overweight women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2003;88(2):812-819.
3. Stamets K, Taylor DS, Kunselman A, Demers LM, Pelkman CL, Legro RS. A randomized trial of the effects of two types of short-term hypocaloric diets on weight loss in women with polycystic ovary syndrome. Fertil Steril. 2004;81(3):630-637.
4. Morales AJ, Laughlin GA, Bützow T, Maheshwari H, Baumann G, Yen SS. Insulin somatotropic, and luteinizing hormone axes in lean and obese women with polycystic ovary syndrome: common and distinct features. J Clin Endocrinol Metab. 1996;81(8):2854-2864.
5. Guzick DS. Polycystic ovary syndrome. Obstet Gynecol. 2004;103(1):181-193.
6. Durlinger AL, Grijters MJ, Kramer P, et al. Anti- Müllerian hormone attenuates the effects of FSH on follicle development in the mouse ovary. Endocrinology. 2001;142(11):4891-4899.
7. Durlinger AL, Kramer P, Karels B, et al. Control of primordial follicle recruitment by anti-Müllerian hormone in the mouse ovary. Endocrinology. 1990;140(12):5789-5796.
8. Cook CL, Siow Y, Taylor S, et al. Serum Müllerian inhibiting substance levels during normal menstrual cycles. Fertil Steril. 2000;73(4):859-861.
9. Muttukrishna S, Suharjono H, McGarrigle H, et al. Inhibin B and anti-Müllerian hormone: markers of ovarian response in IVF/ICSI patients? BJOG. 2004;111(11):1248-1253.
10. Fallat M, Slow Y, Mara M, et al. Müllerian-inhibiting substance in follicular fluid and serum: a comparison of patients with tubal factor infertility, polycystic ovary syndrome, and endometriosis. Fertil Steril. 1997;67(5):962-965.
1. Moran LJ, Pasquali R, Teede HJ, Hoeger KM, Norman RJ. Treatment of obesity in polycystic ovary syndrome: a position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertil Steril. 2009;92(6):1966-1982.
2. Moran LJ, Noakes M, Clifton PM, Tomlinson L, Galletly C, Norman RJ. Dietary composition in restoring reproductive and metabolic physiology in overweight women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2003;88(2):812-819.
3. Stamets K, Taylor DS, Kunselman A, Demers LM, Pelkman CL, Legro RS. A randomized trial of the effects of two types of short-term hypocaloric diets on weight loss in women with polycystic ovary syndrome. Fertil Steril. 2004;81(3):630-637.
4. Morales AJ, Laughlin GA, Bützow T, Maheshwari H, Baumann G, Yen SS. Insulin somatotropic, and luteinizing hormone axes in lean and obese women with polycystic ovary syndrome: common and distinct features. J Clin Endocrinol Metab. 1996;81(8):2854-2864.
5. Guzick DS. Polycystic ovary syndrome. Obstet Gynecol. 2004;103(1):181-193.
6. Durlinger AL, Grijters MJ, Kramer P, et al. Anti- Müllerian hormone attenuates the effects of FSH on follicle development in the mouse ovary. Endocrinology. 2001;142(11):4891-4899.
7. Durlinger AL, Kramer P, Karels B, et al. Control of primordial follicle recruitment by anti-Müllerian hormone in the mouse ovary. Endocrinology. 1990;140(12):5789-5796.
8. Cook CL, Siow Y, Taylor S, et al. Serum Müllerian inhibiting substance levels during normal menstrual cycles. Fertil Steril. 2000;73(4):859-861.
9. Muttukrishna S, Suharjono H, McGarrigle H, et al. Inhibin B and anti-Müllerian hormone: markers of ovarian response in IVF/ICSI patients? BJOG. 2004;111(11):1248-1253.
10. Fallat M, Slow Y, Mara M, et al. Müllerian-inhibiting substance in follicular fluid and serum: a comparison of patients with tubal factor infertility, polycystic ovary syndrome, and endometriosis. Fertil Steril. 1997;67(5):962-965.
WellMed Uses Peer Mentoring to Boost Diabetes Management
PHILADELPHIA – Participants in a peer-mentoring program had lower hemoglobin A1c levels and less severe diabetes over 6-10 months in an initiative that involved more than 550 patients at a single Texas health care organization.
Run at WellMed Medical Management in San Antonio, a primary care–oriented health care organization, the peer-mentoring program "shows what is possible with a well-designed health care system," Dr. Wilson D. Pace said at the annual Congress of Delegates of the American Academy of Family Physicians.
Peer mentoring "is what’s possible with reorganization [of health care delivery] from a strong primary care perspective. WellMed has worked on their model for more than 20 years," said Dr. Pace, a professor of family medicine at the University of Colorado in Denver, and director of the National Research Network of the American Academy of Family Physicians.
Programs like peer mentoring "are much more resource intensive at the primary care level" compared with standard models of care delivery, "but overall costs actually are reduced. Going beyond just health care is how you achieve health," Dr. Pace said in an interview.
"Putting in social systems and thinking about community resources are not usually seen in our health care systems. It takes [a system] willing to take on risk early, because it takes time to see the savings; they don’t happen in the first 6 months," he said.
Dr. Pace and his associates conducted a case study of WellMed to document the effect of management programs that the Accountable Care Organization already had in place. During the course of that evaluation, they suggested to WellMed officials that they also consider starting a peer-mentoring program. To bolster their case, the researchers reviewed reported results from 69 studies on peer mentoring, and found that 60 reported net benefits from this approach.
"We thought that we could put peer mentoring [at WellMed] and show some impact, and when we called they said that they had already been thinking about it; they were very receptive," Dr. Pace recalled.
The WellMed program initially rolled out to 15 of the 23 San Antonio practices in the plan. Over the course of the next 2 years, the peer-mentoring program, which is managed by a nurse practitioner, expanded to all 23 practices and is now overseen by six nurse practitioners. After full implementation, the program involved more than 50 recruited and trained patient mentors, and more than 500 patients with diabetes who were interested in being mentees.
Mentees attended a series of twelve 3-hour, peer-led workshop sessions that dealt with diabetes and self-management. Participants also attended one-on-one and small-group mentoring sessions. In addition, they received personal health records with information that included their blood sugar levels over time, their lab results, and their appointments, to help patients "own" their information.
After 6 months, mentored patients had statistically significant increases in the number of times a week they checked their blood glucose, their knowledge of what hemoglobin A1c means, the quality of their diet, and their activity level. The percent of participants who knew their own A1c level rose from 32% at baseline to 76% after 6 months.
Average hemoglobin A1c levels among the mentored patients fell significantly more after 6 months compared with a control group of patients. Among the patients who received mentorship, average A1c levels dropped from 6.34% at baseline to 6.13% at 6-10 months after the end of the mentoring program. Their average level of disease-related distress fell from a score of 4.08 at baseline to 3.40 6 months after the end of mentoring. The percentage of patients with a disease-related distress score greater than 6 – a marker of clinically significant distress – fell from 24% at baseline to 18% after 6 months. Both changes were statistically significant.
Even before peer mentoring started, WellMed outperformed most other health providers, according to an assessment of their methods and outcomes led by Dr. Robert L. Phillips, Jr., vice president for research and policy at the American Board of Family Medicine in Lexington, Ky.
In a case study led by Dr. Phillips, WellMed members in 2008 had an 18% rate of emergency department visits, a 14% hospitalization rate, a 14% rate of 30-day rehospitalizations, and a rate of 1,002 hospital bed days per 1,000 program members. In contrast, the Texas region’s Medicare program in 2006 had a 28% rate of ED visits, a 22% hospitalization rate, a 20% rate of 30-day rehospitalizations, and 2,559 hospital bed days per 1,000 program members. Those numbers were seen in a study that matched enrollees by age, gender, and number of chronic conditions. Dr. Phillips published a full report of his case study findings last year (J. Ambul. Care Manage. 2001;34:67-77).
"WellMed is really interesting because it does not include a hospital, and it’s primary care driven," Dr. Pace said. "The biggest issue [in creating a health care company like WellMed] is the way the health care dollars flow, and getting rid of the ‘silo-ing’ of dollars. The vision now is that hospitals and specialists are revenue centers that drive everything else; that’s how we think of health care."
WellMed "is an interesting model because it’s different from a hospital-led Accountable Care Organization. That gets you away from hospitals arguing about their bed days. Hospitals need to right-size. We think we can maintain this crazy misdistribution of specialists and hospitals, and it just can’t happen."
Dr. Pace and Dr. Phillips said that they had no disclosures.
PHILADELPHIA – Participants in a peer-mentoring program had lower hemoglobin A1c levels and less severe diabetes over 6-10 months in an initiative that involved more than 550 patients at a single Texas health care organization.
Run at WellMed Medical Management in San Antonio, a primary care–oriented health care organization, the peer-mentoring program "shows what is possible with a well-designed health care system," Dr. Wilson D. Pace said at the annual Congress of Delegates of the American Academy of Family Physicians.
Peer mentoring "is what’s possible with reorganization [of health care delivery] from a strong primary care perspective. WellMed has worked on their model for more than 20 years," said Dr. Pace, a professor of family medicine at the University of Colorado in Denver, and director of the National Research Network of the American Academy of Family Physicians.
Programs like peer mentoring "are much more resource intensive at the primary care level" compared with standard models of care delivery, "but overall costs actually are reduced. Going beyond just health care is how you achieve health," Dr. Pace said in an interview.
"Putting in social systems and thinking about community resources are not usually seen in our health care systems. It takes [a system] willing to take on risk early, because it takes time to see the savings; they don’t happen in the first 6 months," he said.
Dr. Pace and his associates conducted a case study of WellMed to document the effect of management programs that the Accountable Care Organization already had in place. During the course of that evaluation, they suggested to WellMed officials that they also consider starting a peer-mentoring program. To bolster their case, the researchers reviewed reported results from 69 studies on peer mentoring, and found that 60 reported net benefits from this approach.
"We thought that we could put peer mentoring [at WellMed] and show some impact, and when we called they said that they had already been thinking about it; they were very receptive," Dr. Pace recalled.
The WellMed program initially rolled out to 15 of the 23 San Antonio practices in the plan. Over the course of the next 2 years, the peer-mentoring program, which is managed by a nurse practitioner, expanded to all 23 practices and is now overseen by six nurse practitioners. After full implementation, the program involved more than 50 recruited and trained patient mentors, and more than 500 patients with diabetes who were interested in being mentees.
Mentees attended a series of twelve 3-hour, peer-led workshop sessions that dealt with diabetes and self-management. Participants also attended one-on-one and small-group mentoring sessions. In addition, they received personal health records with information that included their blood sugar levels over time, their lab results, and their appointments, to help patients "own" their information.
After 6 months, mentored patients had statistically significant increases in the number of times a week they checked their blood glucose, their knowledge of what hemoglobin A1c means, the quality of their diet, and their activity level. The percent of participants who knew their own A1c level rose from 32% at baseline to 76% after 6 months.
Average hemoglobin A1c levels among the mentored patients fell significantly more after 6 months compared with a control group of patients. Among the patients who received mentorship, average A1c levels dropped from 6.34% at baseline to 6.13% at 6-10 months after the end of the mentoring program. Their average level of disease-related distress fell from a score of 4.08 at baseline to 3.40 6 months after the end of mentoring. The percentage of patients with a disease-related distress score greater than 6 – a marker of clinically significant distress – fell from 24% at baseline to 18% after 6 months. Both changes were statistically significant.
Even before peer mentoring started, WellMed outperformed most other health providers, according to an assessment of their methods and outcomes led by Dr. Robert L. Phillips, Jr., vice president for research and policy at the American Board of Family Medicine in Lexington, Ky.
In a case study led by Dr. Phillips, WellMed members in 2008 had an 18% rate of emergency department visits, a 14% hospitalization rate, a 14% rate of 30-day rehospitalizations, and a rate of 1,002 hospital bed days per 1,000 program members. In contrast, the Texas region’s Medicare program in 2006 had a 28% rate of ED visits, a 22% hospitalization rate, a 20% rate of 30-day rehospitalizations, and 2,559 hospital bed days per 1,000 program members. Those numbers were seen in a study that matched enrollees by age, gender, and number of chronic conditions. Dr. Phillips published a full report of his case study findings last year (J. Ambul. Care Manage. 2001;34:67-77).
"WellMed is really interesting because it does not include a hospital, and it’s primary care driven," Dr. Pace said. "The biggest issue [in creating a health care company like WellMed] is the way the health care dollars flow, and getting rid of the ‘silo-ing’ of dollars. The vision now is that hospitals and specialists are revenue centers that drive everything else; that’s how we think of health care."
WellMed "is an interesting model because it’s different from a hospital-led Accountable Care Organization. That gets you away from hospitals arguing about their bed days. Hospitals need to right-size. We think we can maintain this crazy misdistribution of specialists and hospitals, and it just can’t happen."
Dr. Pace and Dr. Phillips said that they had no disclosures.
PHILADELPHIA – Participants in a peer-mentoring program had lower hemoglobin A1c levels and less severe diabetes over 6-10 months in an initiative that involved more than 550 patients at a single Texas health care organization.
Run at WellMed Medical Management in San Antonio, a primary care–oriented health care organization, the peer-mentoring program "shows what is possible with a well-designed health care system," Dr. Wilson D. Pace said at the annual Congress of Delegates of the American Academy of Family Physicians.
Peer mentoring "is what’s possible with reorganization [of health care delivery] from a strong primary care perspective. WellMed has worked on their model for more than 20 years," said Dr. Pace, a professor of family medicine at the University of Colorado in Denver, and director of the National Research Network of the American Academy of Family Physicians.
Programs like peer mentoring "are much more resource intensive at the primary care level" compared with standard models of care delivery, "but overall costs actually are reduced. Going beyond just health care is how you achieve health," Dr. Pace said in an interview.
"Putting in social systems and thinking about community resources are not usually seen in our health care systems. It takes [a system] willing to take on risk early, because it takes time to see the savings; they don’t happen in the first 6 months," he said.
Dr. Pace and his associates conducted a case study of WellMed to document the effect of management programs that the Accountable Care Organization already had in place. During the course of that evaluation, they suggested to WellMed officials that they also consider starting a peer-mentoring program. To bolster their case, the researchers reviewed reported results from 69 studies on peer mentoring, and found that 60 reported net benefits from this approach.
"We thought that we could put peer mentoring [at WellMed] and show some impact, and when we called they said that they had already been thinking about it; they were very receptive," Dr. Pace recalled.
The WellMed program initially rolled out to 15 of the 23 San Antonio practices in the plan. Over the course of the next 2 years, the peer-mentoring program, which is managed by a nurse practitioner, expanded to all 23 practices and is now overseen by six nurse practitioners. After full implementation, the program involved more than 50 recruited and trained patient mentors, and more than 500 patients with diabetes who were interested in being mentees.
Mentees attended a series of twelve 3-hour, peer-led workshop sessions that dealt with diabetes and self-management. Participants also attended one-on-one and small-group mentoring sessions. In addition, they received personal health records with information that included their blood sugar levels over time, their lab results, and their appointments, to help patients "own" their information.
After 6 months, mentored patients had statistically significant increases in the number of times a week they checked their blood glucose, their knowledge of what hemoglobin A1c means, the quality of their diet, and their activity level. The percent of participants who knew their own A1c level rose from 32% at baseline to 76% after 6 months.
Average hemoglobin A1c levels among the mentored patients fell significantly more after 6 months compared with a control group of patients. Among the patients who received mentorship, average A1c levels dropped from 6.34% at baseline to 6.13% at 6-10 months after the end of the mentoring program. Their average level of disease-related distress fell from a score of 4.08 at baseline to 3.40 6 months after the end of mentoring. The percentage of patients with a disease-related distress score greater than 6 – a marker of clinically significant distress – fell from 24% at baseline to 18% after 6 months. Both changes were statistically significant.
Even before peer mentoring started, WellMed outperformed most other health providers, according to an assessment of their methods and outcomes led by Dr. Robert L. Phillips, Jr., vice president for research and policy at the American Board of Family Medicine in Lexington, Ky.
In a case study led by Dr. Phillips, WellMed members in 2008 had an 18% rate of emergency department visits, a 14% hospitalization rate, a 14% rate of 30-day rehospitalizations, and a rate of 1,002 hospital bed days per 1,000 program members. In contrast, the Texas region’s Medicare program in 2006 had a 28% rate of ED visits, a 22% hospitalization rate, a 20% rate of 30-day rehospitalizations, and 2,559 hospital bed days per 1,000 program members. Those numbers were seen in a study that matched enrollees by age, gender, and number of chronic conditions. Dr. Phillips published a full report of his case study findings last year (J. Ambul. Care Manage. 2001;34:67-77).
"WellMed is really interesting because it does not include a hospital, and it’s primary care driven," Dr. Pace said. "The biggest issue [in creating a health care company like WellMed] is the way the health care dollars flow, and getting rid of the ‘silo-ing’ of dollars. The vision now is that hospitals and specialists are revenue centers that drive everything else; that’s how we think of health care."
WellMed "is an interesting model because it’s different from a hospital-led Accountable Care Organization. That gets you away from hospitals arguing about their bed days. Hospitals need to right-size. We think we can maintain this crazy misdistribution of specialists and hospitals, and it just can’t happen."
Dr. Pace and Dr. Phillips said that they had no disclosures.
AT THE ANNUAL CONGRESS OF DELEGATES OF THE AMERICAN ACADEMY OF FAMILY PHYSICIANS
