User login
Thrombophilia in pregnancy: Whom to screen, when to treat
Why thrombophilia matters
During pregnancy, clotting factors I, VII, VIII, IX, and X rise; protein S and fibrinolytic activity diminish; and resistance to activated protein C develops.1,2 When compounded by thrombophilia—a broad spectrum of coagulation disorders that increase the risk for venous and arterial thrombosis—the hypercoagulable state of pregnancy may increase the risk of thromboembolism during pregnancy or postpartum.3
Pulmonary embolism is the leading cause of maternal death in the United States.1 Concern about this lethal sequela has led to numerous recommendations for screening and subsequent prophylaxis and therapy.
Two types
Thrombophilias are inherited or acquired (TABLE 1). The most common inherited disorders during pregnancy are mutations in factor V Leiden, prothrombin gene, and methylenetetrahydrofolate reductase (MTHFR) (TABLE 2). Caucasians have a higher rate of genetic thrombophilias than other racial groups.
Antiphospholipid antibody (APA) syndrome is the most common acquired thrombophilia of pregnancy. It can be diagnosed when the immunoglobulin G or immunoglobulin M level is 20 g per liter or higher, when lupus anticoagulant is present, or both.4
TABLE 1
Thrombophilias are inherited or acquired
INHERITED
|
ACQUIRED
|
| MTHFR=methylenetetrahydrofolate reductase |
Prevalence of thrombophilias in women with normal pregnancy outcomes
| THROMBOPHILIA | PREVALENCE (%) |
|---|---|
| Factor V Leiden mutation | 2–10 |
| MTHFR mutation | 8–16 |
| Prothrombin gene mutation | 2–6 |
| Protein C and S deficiencies | 0.2–1.0* |
| Anticardiolipin antibodies | 1–7 |
| * Combined rate | |
| MTHFR=methylenetetrahydrofolate reductase | |
Link to adverse pregnancy outcomes
During the past 2 decades, several epidemiologic and case-control studies have explored the association between thrombophilias and adverse pregnancy outcomes,2-6 which include the following maternal effects:
- Venous thromboembolism, including deep vein thrombosis, pulmonary embolism, and cerebral vein thrombosis
- Arterial thrombosis (peripheral, cerebral)
- Severe preeclampsia
- Thrombosis and infarcts
- Abruptio placenta
- Recurrent miscarriage
- Fetal growth restriction
- Death
- Stroke
Preeclampsia and thrombophilia
The association between preeclampsia and thrombophilia remains somewhat unclear because of inconsistent data. Because of this, we do not recommend routine screening for thrombophilia in women with preeclampsia.
An association between inherited thrombophilias and preeclampsia was reported by Dekker et al in 1995.7 Since then, numerous retrospective and case-controlled studies have assessed the incidence of thrombophilia in women with severe preeclampsia.7-25 Their findings range from:
- Factor V Leiden: 3.7% to 26.5%
- Prothrombin gene mutation: 0 to 10.8%
- Protein S deficiency: 0.7% to 24.7%
- MTHFR variant: 6.7% to 24.0%
Other points of contention are the varying levels of severity of preeclampsia and of gestational age at delivery, as well as racial differences. For example, most studies found an association between thrombophilia and severe preeclampsia at less than 34 weeks’ gestation, but not between thrombophilia and mild preeclampsia at term. In addition, a recent prospective observational study at multiple centers involving 5,168 women found a factor V Leiden mutation rate of 6% among white women, 2.3% among Asians, 1.6% in Hispanics, and 0.8% in African Americans.8 This large study found no association between thrombophilia and preeclampsia in these women. Therefore, based on available data, we do not recommend routine screening for factor V Leiden in women with severe preeclampsia.
Preeclampsia and APA syndrome
In 1989, Branch et al26 first reported an association between APA syndrome and severe preeclampsia at less than 34 weeks’ gestation. They recommended that women with severe preeclampsia at this gestational age be screened for APA syndrome and treated when the screen is positive. Several later studies supported or refuted the association between APA syndrome and preeclampsia,26,27 and a recent report concluded that routine testing for APA syndrome in women with early-onset preeclampsia is unwarranted.26 Therefore, we do not recommend routine screening for APA in women with severe preeclampsia.
No need to screen women with abruptio placenta
The placental circulation is comparable to venous circulation, with low pressure and low flow velocity rendering it susceptible to thrombotic complications at the maternal–placental interface and consequent premature separation of the placenta.
It is difficult to confirm an association between thrombophilia and abruptio placenta because of confounding variables such as chronic hypertension, cigarette and cocaine use, and advanced maternal age.3 Studies reviewing this association are scarce, and screening for thrombophilia is discouraged in pregnancies marked by abruptio placenta.
Kupferminc et al28 found that 25%, 20%, and 15% of thrombophilia patients with placental abruption had mutations in factor V Leiden, prothrombin gene, and MTHFR, respectively. In contrast, Prochazka et al29 found 15.7% of their cohort of patients with abruptio placenta to have factor V Leiden mutation.
A large prospective, observational study of more than 5,000 asymptomatic pregnant women at multiple centers found no association between abruptio placenta and factor V Leiden mutation.8 Nor were there cases of abruptio placenta among 134 women who were heterozygous for factor V Leiden.
And no routine screening in cases of IUGR
Routine screening for thrombophilias in women with intrauterine growth restriction (IUGR) is not recommended. One reason: The prevalence of thrombophilias in these women ranges widely, depending on the study cited: from 2.8% to 35% for factor V Leiden and 2.8% to 15.4% for prothrombin gene mutation (TABLE 3). In addition, in contrast to earlier studies, a large case-control trial by Infante-Rivard et al30 found no increased risk of IUGR in women with thrombophilias, except for a subgroup of women with the MTHFR variant who did not take a prenatal multivitamin.
A recent meta-analysis of case-control studies by Howley et al31 found a significant association between factor V Leiden, the prothrombin gene variant, and IUGR, but the investigators cautioned that this strong association may be driven by small, poor-quality studies that yield extreme associations. A multicenter observational study by Dizon-Townson et al8 found no association between thrombophilia and IUGR in asymptomatic gravidas.
TABLE 3
Incidence of thrombophilias in women with intrauterine growth restriction
| STUDY | FACTOR V LEIDEN (%) | PROTHROMBIN GENE MUTATION (%) | ||
|---|---|---|---|---|
| IUGR | CONTROLS | IUGR | CONTROLS | |
| Kupferminc et al50 | 5/44 (11.4) | 7/110 (6.4) | 5/44 (11.4) | 3/110 (2.7) |
| Infante-Rivard et al30 | 22/488 (4.5) | 18/470 (3.8) | 12/488 (2.5) | 11/470 (2.3) |
| Verspyck et al51 | 4/97 (4.1) | 1/97 (1) | 3/97 (3.1) | 1/97 (1) |
| McCowan et al52 | 4/145 (2.8) | 11/290 (3.8) | 4/145 (2.8) | 9/290 (3.1) |
| Dizon-Townson et al*10 | 6/134 (4.5) | 233/4,753 (4.9) | NR | NR |
| Kupferminc**34 | 9/26 (35) | 2/52 (3.8) | 4/26 (15.4) | 2/52 (3.8) |
| * | ||||
| ** Mid-trimester severe intrauterine growth restriction | ||||
| IUGR=intrauterine growth restriction, NR=not recorded | ||||
| SOURCE: Adapted from Clin Obstet Gynecol. 2006;49:850–860 | ||||
Fetal loss is a complication of thrombophilia
One in 10 pregnancies ends in early death of the fetus (before 20 weeks), and 1 in 200 gestations ends in late fetal loss.32 When fetal loss occurs in the second and third trimesters, it is due to excessive thrombosis of the placental vessels, placental infarction, and secondary uteroplacental insufficiency.2,33 Women who are carriers of factor V or prothrombin gene mutations are at higher risk of late fetal loss than noncarriers are (TABLE 4).
Fetal loss is a well-established complication in women with thrombophilia, but not all thrombophilias are associated with fetal loss, according to a meta-analysis of 31 studies.33 In women with thrombophilia, first-trimester loss is generally associated with factor V Leiden, prothrombin gene mutation, and activated protein C resistance. Late, nonrecurrent fetal loss is associated with factor V Leiden, prothrombin gene mutation, and protein S deficiency.33
TABLE 4
Incidence of factor V Leiden mutation in women with recurrent pregnancy loss
| STUDY | PATIENT SELECTION | PATIENTS (%) | CONTROLS (%) | ODDS RATIO | 95% CONFIDENCE INTERVAL |
|---|---|---|---|---|---|
| Grandone et al53 | ≥2 unexplained fetal losses, other causes excluded | 7/43 (16.3) | 5/118 (4.2) | 4.4 | 1.3–14.7 |
| Ridker et al54 | Recurrent, spontaneous abortion, other causes not excluded | 9/113 (8) | 16/437 (3.7) | 2.3 | 1.0–5.2 |
| Sarig et al55 | ≥3 first- or second-trimester losses or ≥1 intrauterine fetal demise, other causes excluded* | 96/145 (66) | 41/145 (28) | 5.0 | 3.0–8.5 |
| * Excluded chromosomal abnormalities, infections, anatomic alterations, and endocrine dysfunction | |||||
History of adverse outcomes? Offer screening
It is well established that women with a history of fetal death, severe preeclampsia, IUGR, abruptio placenta, or recurrent miscarriage have an increased risk of recurrence in subsequent pregnancies.3,30,34-36 The rate of recurrence of any of these outcomes may be as high as 46% with a history of 2 or more adverse outcomes, even before any thrombophilia is taken into account.3 Although there are few studies describing the rate of recurrence of adverse pregnancy outcomes in women with thrombophilia and a previous adverse outcome (TABLE 5), it appears to range from 66% to 83% in untreated women.3,37
Based on these findings, some authors recommend screening for thrombophilia in women who have had adverse pregnancy outcomes3,9,38 and prophylactic therapy in subsequent pregnancies when the test is positive. Therapy includes low-dose aspirin with or without subcutaneous heparin, as well as folic acid and vitamin B6 supplements, according to the type of thrombophilia present as well as the nature of the previous adverse outcome.
TABLE 5
How women with a previous adverse outcome fare on anticoagulation therapy
| STUDY | PATIENTS | PREVIOUS ADVERSE PREGNANCY OUTCOME | ANTICOAGULANT | OUTCOME IN CURRENT PREGNANCY |
|---|---|---|---|---|
| Riyazi et al9 | 26 | Uteroplacental insufficiency | LMWH and low-dose aspirin | Decreased recurrence of preeclampsia (85% to 38%) and IUGR (54% to 15%) |
| Brenner37 | 50 | ≥3 first-trimester recurrent pregnancy losses with thrombophilia | LMWH | Higher live birth rate compared with historical controls (75% vs 20%) |
| Ogueh et al48 | 24 | Previous adverse pregnancy outcome plus history of thromboembolic disease, family history of thrombophilia | UFH | No significant mprovement |
| Kupferminc et al38 | 33 | Thrombophilia with history of preeclampsia or IUGR | LMWH and low-dose aspirin | With treatment, 3% recurrence of preeclampsia |
| Grandone et al53 | 25 | Repeated pregnancy loss, gestational hypertension, HELLP, or IUGR | UFH or LMWH | 90.3% treated with LMWH had good obstetric outcome |
| Paidas et al3 | 158 | Fetal loss, IUGR, placental abruption, or preeclampsia | UFH or LMWH | 80% reduction in risk of adverse pregnancy outcome, compared with historical controls (OR, 0.21; 95% CI, 0.11–0.39) |
| HELLP=hemolysis, elevated liver enzymes, and low platelets; IUGR=intrauterine growth restriction; LMWH=low-molecular-weight heparin; UFH=unfractionated heparin | ||||
| SOURCE: Adapted from Am J Perinatol. 2006;23:499–506 | ||||
No randomized trials on prophylaxis
We lack randomized trials evaluating thromboprophylaxis for prevention of recurrent adverse pregnancy outcomes in women with previous severe preeclampsia, IUGR, or abruptio placenta in association with genetic thrombophilia. Therefore, any recommendation to treat such women with low-molecular-weight heparin with or without low-dose aspirin in subsequent pregnancies should remain empiric and/or prescribed after appropriate counseling of the patients regarding risks and benefits.
TABLE 6 summarizes the risk of thromboembolism in women with thrombophilia—both for asymptomatic patients and for those with a history of thromboembolism. These percentages should be used when counseling women about their risk and determining management and therapy.
TABLE 6
Risk of thromboembolism during pregnancy and postpartum in women with thrombophilia
| THROMBOPHILIA | RISK (%) | |
|---|---|---|
| ASYMPTOMATIC WOMEN | HISTORY OF VENOUS THROMBOEMBOLISM | |
| Factor V Leiden | ||
| Heterozygous | 0.2 | 10 |
| Homozygous | 1–2 | 15–20 |
| Prothrombin gene mutation | ||
| Heterozygous | 0.5 | 10 |
| Homozygous | 2.3 | 20 |
| Factor V Leiden and prothrombin gene mutation | 5 | 20 |
| Antithrombin deficiency | 7 | 40 |
| Protein C deficiency | 0.5 | 5–15 |
| Protein S deficiency | 0.1 | Unknown |
Prophylaxis for APA syndrome and recurrent pregnancy loss
Several randomized trials have described the use of low-dose aspirin and heparin in women with APA syndrome and a history of recurrent pregnancy loss, although the results are inconsistent (TABLE 7).39-45 The inconsistency may be due to varying definitions of APA syndrome and gestational age at the time of randomization, as well as the population studied (previous thromboembolism, presence or absence of lupus anticoagulant, level of titer of anticardiolipin antibodies, presence or absence of previous stillbirth). Nevertheless, we recommend that women with true APA syndrome (presence of lupus anticoagulant, high titers of immunoglobulin G, history of thromboembolism or recurrent stillbirth) receive prophylaxis with low-dose aspirin, with subcutaneous heparin added once fetal cardiac activity is documented.46
TABLE 7
Live births in women with APA and a history of fetal loss
| STUDY | TREATMENT | CONTROL | NO. OF LIVE BIRTHS (%) | |
|---|---|---|---|---|
| TREATED WOMEN | CONTROL GROUP | |||
| Cowchock et al39 | Aspirin/heparin | Aspirin/prednisone | 9/12 (75) | 6/8 (75) |
| Laskin et al40 | Aspirin/prednisone | Placebo | 25/42 (60) | 24/46 (52) |
| Kutteh41 | Aspirin/heparin | Aspirin only | 20/25 (80) | 11/25 (44) |
| Rai et al42 | Aspirin/heparin | Aspirin only | 32/45 (71) | 19/45 (42) |
| Silver et al43 | Aspirin/prednisone | Aspirin only | 12/12 (100) | 22/22 (100) |
| Pattison et al44 | Aspirin | Placebo | 16/20 (80) | 17/20 (85) |
| Farquharson et al45 | Aspirin/LMWH | Aspirin only | 40/51 (78) | 34/47 (72) |
| LMWH=low-molecular-weight heparin | ||||
Genetic thrombophilias
Few published studies describe prophylactic use of low-molecular-weight heparin with or without low-dose aspirin in women with genetic thrombophilia and a history of adverse pregnancy outcomes. All but 1 of these studies are observational, comparing outcome in the treated pregnancy with that of previously untreated gestations in the same woman.3,9,38,44,45,47 These studies included a limited number of women and a heterogeneous group of patients with various thrombophilias; they also involved different therapies (TABLE 7).3,9,38,41,48,49
Gris et al47 performed a randomized trial in 160 women with at least 1 prior fetal loss after 10 weeks’ gestation who were heterozygous for factor V Leiden or prothrombin G20210A mutation, or had protein S deficiency. Beginning at 8 weeks’ gestation, these women were assigned to treatment with 40 mg of enoxaparin (n=80) or 100 mg of low-dose aspirin (n=80) daily. All women also received 5 mg of folic acid daily.
In the women treated with enoxaparin, 69 (86%) had a live birth, compared with 23 (29%) women treated with low-dose aspirin. The women treated with enoxaparin also had significantly higher median neonatal birth weights and a lower rate of IUGR (10% versus 30%). The authors concluded that women with factor V Leiden, prothrombin gene mutation, or protein S deficiency and a history of fetal loss should receive enoxaparin prophylaxis in subsequent pregnancies.
History of severe preeclampsia, IUGR, or abruptio placenta. No randomized trials have evaluated thromboprophylaxis in women with this history who have genetic thrombophilia. For this reason, any recommendation to treat these women with low-molecular-weight heparin with or without low-dose aspirin in subsequent pregnancies remains empiric. Prophylaxis can be prescribed after an appropriate discussion of risks and benefits with the patient.
Unresolved questions keep management experimental
What is the likelihood that a woman carrying a gene mutation that predisposes her to thrombophilia will have a serious complication during pregnancy? And how safe and effective is prophylaxis?
There is a prevailing need for a double-blind placebo-controlled trial to address these questions and evaluate the benefit of heparin in pregnant women with a history of adverse pregnancy outcomes and thrombophilia. Until then, screening and treatment for thrombophilia remain experimental in these women.
The authors report no financial relationships relevant to this article.
1. Thromboembolism in pregnancy. ACOG Practice Bulletin #19. Washington, DC: ACOG; 2000.
2. Kujovich JL. Thrombophilia and pregnancy complications. Am J Obstet Gynecol. 2004;191:412-424.
3. Paidas MJ, De-Hui WK, Arkel YS. Screening and management of inherited thrombophilias in the setting of adverse pregnancy outcome. Clin Perinatol. 2004;31:783-805.
4. Lee RM, Brown MA, Branch DW, Ward K, Silver RM. Anticardiolipin and anti-B2 glycoprotein-I antibodies in preeclampsia. Obstet Gynecol. 2003;102:294-300.
5. Lin L, August P. Genetic thrombophilias and preeclampsia: a meta-analysis. Obstet Gynecol. 2005;105:182-192.
6. Mignini LE, Latthe PM, Villar J, et al. Mapping the theories of preeclampsia: the role of homocysteine. Obstet Gynecol. 2005;105:411-425.
7. Dekker GA, de Vries JI, Doelitzsch PM, et al. Underlying disorders associated with severe early-onset preeclampsia. Am J Obstet Gynecol. 1995;173:1042-1048.
8. Dizon-Townson D, Miller C, Sibai B, et al. The relationship of factor V Leiden mutation and pregnancy outcomes for mother and fetus. Obstet Gynecol. 2005;106:517-524.
9. Riyazi N, Leeda M, de Vries JIP, et al. Low molecular weight heparin combined with aspirin in pregnant women with thrombophilia and a history of preeclampsia or fetal growth restriction: a preliminary study. Eur J Obstet Gynecol Reprod Biol. 1998;80:49-54.
10. Dizon-Townson DS, Nelson LM, Easton K, Ward K. The factor V Leiden mutation may predispose women to severe preeclampsia. Am J Obstet Gynecol. 1996;175:902-905.
11. Nagy B. Detection of factor V Leiden mutation in severe preeclamptic Hungarian women. Clin Genet. 1998;53:478-481.
12. Krauss T. Activated protein C resistance and factor V Leiden in patients with hemolysis, elevated liver enzymes, low platelets syndrome. Obstet Gynecol. 1998;92:457-460.
13. Kupferminc MJ, Eldor A, Steinman N, et al. Increased frequency of genetic thrombophilia in women with complications of pregnancy. N Engl J Med. 1999;341:384.-
14. van Pampus EC. High prevalence of hemostatic abnormalities in women with a history of severe preeclampsia. Am J Obstet Gynecol. 1999;180:1146-1150.
15. DeGroot CJ, Bloemankamp KW, Duvekot EJ, et al. Preeclampsia and genetic factors for thrombosis: a case control study. Am J Obstet Gynecol. 1999;181:975-980.
16. Kupferminc MJ, Fait G, Many A, Girdon D, Eldor A, Lessing JB. Severe preeclampsia: high frequency of genetic thrombophilic mutations. Obstet Gynecol. 2000;96:45-49.
17. Rigo J, Nagy B, Fintor L, et al. Maternal and neonatal outcome of preeclamptic pregnancies: the potential roles of factor V Leiden mutations and 5,10 methylenetetrahydrofolate reductase. Hypertens Pregnancy. 2000;19(2):163-172.
18. von Tempelhoff GF. Incidence of factor V Leiden mutation, coagulation inhibitor deficiency, and elevated antiphospholipid-antibodies in patients with preeclampsia or HELLP syndrome (hemolysis, elevated liver enzymes, low platelets). Thromb Res. 2000;100:363-365.
19. Kupferminc MJ, Peri H, Zwang E, et al. High prevalence of the prothrombin gene mutation in women with intrauterine growth retardation, abruptio placentae and second trimester loss. Acta Obstet Gynecol Scand. 2000;79:963-967.
20. Kim YJ. Genetic susceptibility to preeclampsia: roles of cytosine-to-thymine substitution at nucleotide 677 of the gene for methylenetetrahydrofolate reductase, 68-base pair insertion at nucleotide 844 of the gene for cystathione [beta]-synthase, and factor V Leiden mutation. Am J Obstet Gynecol. 2001;184:1211-1217.
21. Livingston J, Barton JR, Park V, et al. Maternal and fetal inherited thrombophilias are not related to the development of severe preeclampsia. Am J Obstet Gynecol. 2001;185:153-157.
22. Currie L, Peek M, McNiven M, et al. Is there an increased maternal-infant prevalence of factor V Leiden in association with severe pre-eclampsia? BJOG. 2002;109:191-196.
23. Benedetto C, Marozio L, Salton L, et al. Factor V Leiden and factor II G20210A in preeclampsia and HELLP syndrome. Acta Obstet Gynecol. 2002;81:1095-1100.
24. Schlembach D, Beinder E, Zingsem J, et al. Association of maternal and/or fetal factor V Leiden and G20210A prothrombin mutation with HELLP syndrome and intrauterine growth restriction. Clin Sci. 2003;105:279-285.
25. Mello G, Parretti E, Marozio L, et al. Thrombophilia is significantly associated with severe preeclampsia: results of a large-scale, case-controlled study. Hypertension. 2005;46:1270-1274.
26. Branch DW, Andres R, Digre KB, Rote NS, Scott JR. The association of antiphospholipid antibodies with severe preeclampsia. Obstet Gynecol. 1989;73:541-545.
27. Dreyfus M, Hedelin G, Kutnahorsky R, et al. Antiphospholipid antibodies and preeclampsia: a case-control study. Obstet Gynecol. 2001;97:29-34.
28. Kupferminc MJ, Eldor A, Steinman N, et al. Increased frequency of genetic thrombophilia in women with complications of pregnancy. N Engl J Med. 1999;340:9-13.
29. Prochazka M, Happach C, Marsal K, Dahlback B, Lindqvist PG. Factor V Leiden in pregnancies complicated by placental abruption. BJOG. 2003;110:462-466.
30. Infante-Rivard C, Rivard GE, Yotov WV, et al. Absence of association of thrombophilia polymorphisms with intrauterine growth restriction. N Engl J Med. 2002;347:19-25.
31. Howley HE, Walker M, Rodger MA. A systematic review of the association between factor V Leiden or prothrombin gene variant and intrauterine growth restriction. Am J Obstet Gynecol. 2005;192:694-708.
32. Martinelli I, Taioli E, Cetin I, et al. Mutations in coagulation factors in women with unexplained late fetal loss. N Engl J Med. 2000;343:1015-1018.
33. Rey E, Kahn SR, David M, et al. Thrombophilic disorders and fetal loss: a metaanalysis. Lancet. 2003;361:901-908.
34. Kupferminc MJ. Mid-trimester severe intrauterine growth restriction is associated with high prevalence of thrombophilia. BJOG. 2002;109:1373-1376.
35. Sibai BM, el-Nazer A, Gonzalez-Ruiz A. Severe preeclampsia-eclampsia in young primigravid women: subsequent pregnancy outcome and remote prognosis. Am J Obstet Gynecol. 1986;155:1011-1016.
36. Sibai BM, Mercer B, Sarinoglu C. Severe preeclampsia in the second trimester: recurrence risk and long-term prognosis. Am J Obstet Gynecol. 1991;165:1408-1412.
37. Brenner B. Thrombophilia and fetal loss. Semin Thromb Hemost. 2003;29:165-170.
38. Kupferminc MJ, Fait G, Many A, et al. Low molecular weight heparin for the prevention of obstetric complications in women with thrombophilias. Hypertens Pregnancy. 2001;20:35-44.
39. Cowchock FS, Reece EA, Balaban D, et al. Repeated fetal losses associated with antiphospholipid antibodies: a collaborative randomized trial comparing prednisone with low-dose heparin treatment. Am J Obstet Gynecol. 1992;166:1318-1323.
40. Laskin CA, Bombardier C, Hannah ME, et al. Prednisone and aspirin in women with autoantibodies and unexplained recurrent fetal loss. N Engl J Med. 1997;337:148-154.
41. Kutteh WH. Antiphospholipid antibody-associated recurrent pregnancy loss: treatment with heparin and low-dose aspirin is superior to low-dose aspirin alone. Am J Obstet Gynecol. 1996;174:1584-1589.
42. Rai R, Cohen H, Dave M, Regan L. Randomised controlled trial of aspirin and aspirin plus heparin in pregnant women with recurrent miscarriage associated with phospholipid antibodies (or antiphospholipid antibodies). BMJ. 1997;314:253-257.
43. Silver RK, MacGregor SN, Sholl JS, et al. Comparative trial of prednisone versus aspirin alone in the treatment of anticardiolipin antibody-positive obstetric patients. Am J Obstet Gynecol. 1993;169:1411-1417.
44. Pattison NS, Chamley LW, Birdsall M, et al. Does aspirin have a role in improving pregnancy outcome for women with the antiphospholipid syndrome? A randomized controlled trial. Am J Obstet Gynecol. 2000;183:1008-1012.
45. Farquharson RG, Quenby S, Greaves M. Antiphospholipid syndrome in pregnancy: a randomized, controlled trial of treatment. Obstet Gynecol. 2002;100:408-413.
46. Antiphospholipid syndrome. ACOG Practice Bulletin #68. Obstet Gynecol. 2005;106:1113-1121.
47. Gris JC, Mercier E, Quere I, et al. Low-molecular-weight heparin versus low-dose aspirin in women with one fetal loss and a constitutional thrombophilic disorder. Blood. 2004;103:3695-3699.
48. Ogueh O, Chen MF, Spurll G, Benjamin A. Outcome of pregnancy in women with hereditary thrombophilia. Int J Gynecol Obstet. 2001;74:247-253.
49. Brenner B, Hoffman R, Blumenfeld Z, et al. Gestational outcome in thrombophilic women with recurrent pregnancy loss treated with enoxaparin. Thromb Haemost. 2000;83:693-697.
50. Kupferminc MJ, Fait G, Many A, et al. Low molecular weight heparin for the prevention of obstetric complications in women with thrombophilias. Hypertens Pregnancy. 2001;20:35-44.
51. Verspyck E, Borg JY, Le Cam-Duchez V, et al. Thrombophilia and fetal growth restriction. Eur J Obstet Gynecol Reprod Biol. 2004;113:36-40.
52. McCowan LME, Craigie S, Taylor RS, et al. Inherited thrombophilias are not increased in “idiopathic” small-for-gestationalage pregnancies. Am J Obstet Gynecol. 2003;188:981-992.
53. Grandone E, Brancaccio V, Colaizzo D, et al. Preventing adverse obstetric outcomes in women with genetic thrombophilia. Fertil Steril. 2002;78:371-375.
54. Ridker PM, Miletich JP, Buring JE, et al. Factor V Leiden mutation as a risk factor for recurrent pregnancy loss. Ann Intern Med. 1998;128:1000-1003.
55. Sarig G, Younis J, Hoffman R, et al. Thrombophilia is common in women with idiopathic pregnancy loss and is associated with late pregnancy wastage. Fertil Steril. 2002;77:342-347.
Why thrombophilia matters
During pregnancy, clotting factors I, VII, VIII, IX, and X rise; protein S and fibrinolytic activity diminish; and resistance to activated protein C develops.1,2 When compounded by thrombophilia—a broad spectrum of coagulation disorders that increase the risk for venous and arterial thrombosis—the hypercoagulable state of pregnancy may increase the risk of thromboembolism during pregnancy or postpartum.3
Pulmonary embolism is the leading cause of maternal death in the United States.1 Concern about this lethal sequela has led to numerous recommendations for screening and subsequent prophylaxis and therapy.
Two types
Thrombophilias are inherited or acquired (TABLE 1). The most common inherited disorders during pregnancy are mutations in factor V Leiden, prothrombin gene, and methylenetetrahydrofolate reductase (MTHFR) (TABLE 2). Caucasians have a higher rate of genetic thrombophilias than other racial groups.
Antiphospholipid antibody (APA) syndrome is the most common acquired thrombophilia of pregnancy. It can be diagnosed when the immunoglobulin G or immunoglobulin M level is 20 g per liter or higher, when lupus anticoagulant is present, or both.4
TABLE 1
Thrombophilias are inherited or acquired
INHERITED
|
ACQUIRED
|
| MTHFR=methylenetetrahydrofolate reductase |
Prevalence of thrombophilias in women with normal pregnancy outcomes
| THROMBOPHILIA | PREVALENCE (%) |
|---|---|
| Factor V Leiden mutation | 2–10 |
| MTHFR mutation | 8–16 |
| Prothrombin gene mutation | 2–6 |
| Protein C and S deficiencies | 0.2–1.0* |
| Anticardiolipin antibodies | 1–7 |
| * Combined rate | |
| MTHFR=methylenetetrahydrofolate reductase | |
Link to adverse pregnancy outcomes
During the past 2 decades, several epidemiologic and case-control studies have explored the association between thrombophilias and adverse pregnancy outcomes,2-6 which include the following maternal effects:
- Venous thromboembolism, including deep vein thrombosis, pulmonary embolism, and cerebral vein thrombosis
- Arterial thrombosis (peripheral, cerebral)
- Severe preeclampsia
- Thrombosis and infarcts
- Abruptio placenta
- Recurrent miscarriage
- Fetal growth restriction
- Death
- Stroke
Preeclampsia and thrombophilia
The association between preeclampsia and thrombophilia remains somewhat unclear because of inconsistent data. Because of this, we do not recommend routine screening for thrombophilia in women with preeclampsia.
An association between inherited thrombophilias and preeclampsia was reported by Dekker et al in 1995.7 Since then, numerous retrospective and case-controlled studies have assessed the incidence of thrombophilia in women with severe preeclampsia.7-25 Their findings range from:
- Factor V Leiden: 3.7% to 26.5%
- Prothrombin gene mutation: 0 to 10.8%
- Protein S deficiency: 0.7% to 24.7%
- MTHFR variant: 6.7% to 24.0%
Other points of contention are the varying levels of severity of preeclampsia and of gestational age at delivery, as well as racial differences. For example, most studies found an association between thrombophilia and severe preeclampsia at less than 34 weeks’ gestation, but not between thrombophilia and mild preeclampsia at term. In addition, a recent prospective observational study at multiple centers involving 5,168 women found a factor V Leiden mutation rate of 6% among white women, 2.3% among Asians, 1.6% in Hispanics, and 0.8% in African Americans.8 This large study found no association between thrombophilia and preeclampsia in these women. Therefore, based on available data, we do not recommend routine screening for factor V Leiden in women with severe preeclampsia.
Preeclampsia and APA syndrome
In 1989, Branch et al26 first reported an association between APA syndrome and severe preeclampsia at less than 34 weeks’ gestation. They recommended that women with severe preeclampsia at this gestational age be screened for APA syndrome and treated when the screen is positive. Several later studies supported or refuted the association between APA syndrome and preeclampsia,26,27 and a recent report concluded that routine testing for APA syndrome in women with early-onset preeclampsia is unwarranted.26 Therefore, we do not recommend routine screening for APA in women with severe preeclampsia.
No need to screen women with abruptio placenta
The placental circulation is comparable to venous circulation, with low pressure and low flow velocity rendering it susceptible to thrombotic complications at the maternal–placental interface and consequent premature separation of the placenta.
It is difficult to confirm an association between thrombophilia and abruptio placenta because of confounding variables such as chronic hypertension, cigarette and cocaine use, and advanced maternal age.3 Studies reviewing this association are scarce, and screening for thrombophilia is discouraged in pregnancies marked by abruptio placenta.
Kupferminc et al28 found that 25%, 20%, and 15% of thrombophilia patients with placental abruption had mutations in factor V Leiden, prothrombin gene, and MTHFR, respectively. In contrast, Prochazka et al29 found 15.7% of their cohort of patients with abruptio placenta to have factor V Leiden mutation.
A large prospective, observational study of more than 5,000 asymptomatic pregnant women at multiple centers found no association between abruptio placenta and factor V Leiden mutation.8 Nor were there cases of abruptio placenta among 134 women who were heterozygous for factor V Leiden.
And no routine screening in cases of IUGR
Routine screening for thrombophilias in women with intrauterine growth restriction (IUGR) is not recommended. One reason: The prevalence of thrombophilias in these women ranges widely, depending on the study cited: from 2.8% to 35% for factor V Leiden and 2.8% to 15.4% for prothrombin gene mutation (TABLE 3). In addition, in contrast to earlier studies, a large case-control trial by Infante-Rivard et al30 found no increased risk of IUGR in women with thrombophilias, except for a subgroup of women with the MTHFR variant who did not take a prenatal multivitamin.
A recent meta-analysis of case-control studies by Howley et al31 found a significant association between factor V Leiden, the prothrombin gene variant, and IUGR, but the investigators cautioned that this strong association may be driven by small, poor-quality studies that yield extreme associations. A multicenter observational study by Dizon-Townson et al8 found no association between thrombophilia and IUGR in asymptomatic gravidas.
TABLE 3
Incidence of thrombophilias in women with intrauterine growth restriction
| STUDY | FACTOR V LEIDEN (%) | PROTHROMBIN GENE MUTATION (%) | ||
|---|---|---|---|---|
| IUGR | CONTROLS | IUGR | CONTROLS | |
| Kupferminc et al50 | 5/44 (11.4) | 7/110 (6.4) | 5/44 (11.4) | 3/110 (2.7) |
| Infante-Rivard et al30 | 22/488 (4.5) | 18/470 (3.8) | 12/488 (2.5) | 11/470 (2.3) |
| Verspyck et al51 | 4/97 (4.1) | 1/97 (1) | 3/97 (3.1) | 1/97 (1) |
| McCowan et al52 | 4/145 (2.8) | 11/290 (3.8) | 4/145 (2.8) | 9/290 (3.1) |
| Dizon-Townson et al*10 | 6/134 (4.5) | 233/4,753 (4.9) | NR | NR |
| Kupferminc**34 | 9/26 (35) | 2/52 (3.8) | 4/26 (15.4) | 2/52 (3.8) |
| * | ||||
| ** Mid-trimester severe intrauterine growth restriction | ||||
| IUGR=intrauterine growth restriction, NR=not recorded | ||||
| SOURCE: Adapted from Clin Obstet Gynecol. 2006;49:850–860 | ||||
Fetal loss is a complication of thrombophilia
One in 10 pregnancies ends in early death of the fetus (before 20 weeks), and 1 in 200 gestations ends in late fetal loss.32 When fetal loss occurs in the second and third trimesters, it is due to excessive thrombosis of the placental vessels, placental infarction, and secondary uteroplacental insufficiency.2,33 Women who are carriers of factor V or prothrombin gene mutations are at higher risk of late fetal loss than noncarriers are (TABLE 4).
Fetal loss is a well-established complication in women with thrombophilia, but not all thrombophilias are associated with fetal loss, according to a meta-analysis of 31 studies.33 In women with thrombophilia, first-trimester loss is generally associated with factor V Leiden, prothrombin gene mutation, and activated protein C resistance. Late, nonrecurrent fetal loss is associated with factor V Leiden, prothrombin gene mutation, and protein S deficiency.33
TABLE 4
Incidence of factor V Leiden mutation in women with recurrent pregnancy loss
| STUDY | PATIENT SELECTION | PATIENTS (%) | CONTROLS (%) | ODDS RATIO | 95% CONFIDENCE INTERVAL |
|---|---|---|---|---|---|
| Grandone et al53 | ≥2 unexplained fetal losses, other causes excluded | 7/43 (16.3) | 5/118 (4.2) | 4.4 | 1.3–14.7 |
| Ridker et al54 | Recurrent, spontaneous abortion, other causes not excluded | 9/113 (8) | 16/437 (3.7) | 2.3 | 1.0–5.2 |
| Sarig et al55 | ≥3 first- or second-trimester losses or ≥1 intrauterine fetal demise, other causes excluded* | 96/145 (66) | 41/145 (28) | 5.0 | 3.0–8.5 |
| * Excluded chromosomal abnormalities, infections, anatomic alterations, and endocrine dysfunction | |||||
History of adverse outcomes? Offer screening
It is well established that women with a history of fetal death, severe preeclampsia, IUGR, abruptio placenta, or recurrent miscarriage have an increased risk of recurrence in subsequent pregnancies.3,30,34-36 The rate of recurrence of any of these outcomes may be as high as 46% with a history of 2 or more adverse outcomes, even before any thrombophilia is taken into account.3 Although there are few studies describing the rate of recurrence of adverse pregnancy outcomes in women with thrombophilia and a previous adverse outcome (TABLE 5), it appears to range from 66% to 83% in untreated women.3,37
Based on these findings, some authors recommend screening for thrombophilia in women who have had adverse pregnancy outcomes3,9,38 and prophylactic therapy in subsequent pregnancies when the test is positive. Therapy includes low-dose aspirin with or without subcutaneous heparin, as well as folic acid and vitamin B6 supplements, according to the type of thrombophilia present as well as the nature of the previous adverse outcome.
TABLE 5
How women with a previous adverse outcome fare on anticoagulation therapy
| STUDY | PATIENTS | PREVIOUS ADVERSE PREGNANCY OUTCOME | ANTICOAGULANT | OUTCOME IN CURRENT PREGNANCY |
|---|---|---|---|---|
| Riyazi et al9 | 26 | Uteroplacental insufficiency | LMWH and low-dose aspirin | Decreased recurrence of preeclampsia (85% to 38%) and IUGR (54% to 15%) |
| Brenner37 | 50 | ≥3 first-trimester recurrent pregnancy losses with thrombophilia | LMWH | Higher live birth rate compared with historical controls (75% vs 20%) |
| Ogueh et al48 | 24 | Previous adverse pregnancy outcome plus history of thromboembolic disease, family history of thrombophilia | UFH | No significant mprovement |
| Kupferminc et al38 | 33 | Thrombophilia with history of preeclampsia or IUGR | LMWH and low-dose aspirin | With treatment, 3% recurrence of preeclampsia |
| Grandone et al53 | 25 | Repeated pregnancy loss, gestational hypertension, HELLP, or IUGR | UFH or LMWH | 90.3% treated with LMWH had good obstetric outcome |
| Paidas et al3 | 158 | Fetal loss, IUGR, placental abruption, or preeclampsia | UFH or LMWH | 80% reduction in risk of adverse pregnancy outcome, compared with historical controls (OR, 0.21; 95% CI, 0.11–0.39) |
| HELLP=hemolysis, elevated liver enzymes, and low platelets; IUGR=intrauterine growth restriction; LMWH=low-molecular-weight heparin; UFH=unfractionated heparin | ||||
| SOURCE: Adapted from Am J Perinatol. 2006;23:499–506 | ||||
No randomized trials on prophylaxis
We lack randomized trials evaluating thromboprophylaxis for prevention of recurrent adverse pregnancy outcomes in women with previous severe preeclampsia, IUGR, or abruptio placenta in association with genetic thrombophilia. Therefore, any recommendation to treat such women with low-molecular-weight heparin with or without low-dose aspirin in subsequent pregnancies should remain empiric and/or prescribed after appropriate counseling of the patients regarding risks and benefits.
TABLE 6 summarizes the risk of thromboembolism in women with thrombophilia—both for asymptomatic patients and for those with a history of thromboembolism. These percentages should be used when counseling women about their risk and determining management and therapy.
TABLE 6
Risk of thromboembolism during pregnancy and postpartum in women with thrombophilia
| THROMBOPHILIA | RISK (%) | |
|---|---|---|
| ASYMPTOMATIC WOMEN | HISTORY OF VENOUS THROMBOEMBOLISM | |
| Factor V Leiden | ||
| Heterozygous | 0.2 | 10 |
| Homozygous | 1–2 | 15–20 |
| Prothrombin gene mutation | ||
| Heterozygous | 0.5 | 10 |
| Homozygous | 2.3 | 20 |
| Factor V Leiden and prothrombin gene mutation | 5 | 20 |
| Antithrombin deficiency | 7 | 40 |
| Protein C deficiency | 0.5 | 5–15 |
| Protein S deficiency | 0.1 | Unknown |
Prophylaxis for APA syndrome and recurrent pregnancy loss
Several randomized trials have described the use of low-dose aspirin and heparin in women with APA syndrome and a history of recurrent pregnancy loss, although the results are inconsistent (TABLE 7).39-45 The inconsistency may be due to varying definitions of APA syndrome and gestational age at the time of randomization, as well as the population studied (previous thromboembolism, presence or absence of lupus anticoagulant, level of titer of anticardiolipin antibodies, presence or absence of previous stillbirth). Nevertheless, we recommend that women with true APA syndrome (presence of lupus anticoagulant, high titers of immunoglobulin G, history of thromboembolism or recurrent stillbirth) receive prophylaxis with low-dose aspirin, with subcutaneous heparin added once fetal cardiac activity is documented.46
TABLE 7
Live births in women with APA and a history of fetal loss
| STUDY | TREATMENT | CONTROL | NO. OF LIVE BIRTHS (%) | |
|---|---|---|---|---|
| TREATED WOMEN | CONTROL GROUP | |||
| Cowchock et al39 | Aspirin/heparin | Aspirin/prednisone | 9/12 (75) | 6/8 (75) |
| Laskin et al40 | Aspirin/prednisone | Placebo | 25/42 (60) | 24/46 (52) |
| Kutteh41 | Aspirin/heparin | Aspirin only | 20/25 (80) | 11/25 (44) |
| Rai et al42 | Aspirin/heparin | Aspirin only | 32/45 (71) | 19/45 (42) |
| Silver et al43 | Aspirin/prednisone | Aspirin only | 12/12 (100) | 22/22 (100) |
| Pattison et al44 | Aspirin | Placebo | 16/20 (80) | 17/20 (85) |
| Farquharson et al45 | Aspirin/LMWH | Aspirin only | 40/51 (78) | 34/47 (72) |
| LMWH=low-molecular-weight heparin | ||||
Genetic thrombophilias
Few published studies describe prophylactic use of low-molecular-weight heparin with or without low-dose aspirin in women with genetic thrombophilia and a history of adverse pregnancy outcomes. All but 1 of these studies are observational, comparing outcome in the treated pregnancy with that of previously untreated gestations in the same woman.3,9,38,44,45,47 These studies included a limited number of women and a heterogeneous group of patients with various thrombophilias; they also involved different therapies (TABLE 7).3,9,38,41,48,49
Gris et al47 performed a randomized trial in 160 women with at least 1 prior fetal loss after 10 weeks’ gestation who were heterozygous for factor V Leiden or prothrombin G20210A mutation, or had protein S deficiency. Beginning at 8 weeks’ gestation, these women were assigned to treatment with 40 mg of enoxaparin (n=80) or 100 mg of low-dose aspirin (n=80) daily. All women also received 5 mg of folic acid daily.
In the women treated with enoxaparin, 69 (86%) had a live birth, compared with 23 (29%) women treated with low-dose aspirin. The women treated with enoxaparin also had significantly higher median neonatal birth weights and a lower rate of IUGR (10% versus 30%). The authors concluded that women with factor V Leiden, prothrombin gene mutation, or protein S deficiency and a history of fetal loss should receive enoxaparin prophylaxis in subsequent pregnancies.
History of severe preeclampsia, IUGR, or abruptio placenta. No randomized trials have evaluated thromboprophylaxis in women with this history who have genetic thrombophilia. For this reason, any recommendation to treat these women with low-molecular-weight heparin with or without low-dose aspirin in subsequent pregnancies remains empiric. Prophylaxis can be prescribed after an appropriate discussion of risks and benefits with the patient.
Unresolved questions keep management experimental
What is the likelihood that a woman carrying a gene mutation that predisposes her to thrombophilia will have a serious complication during pregnancy? And how safe and effective is prophylaxis?
There is a prevailing need for a double-blind placebo-controlled trial to address these questions and evaluate the benefit of heparin in pregnant women with a history of adverse pregnancy outcomes and thrombophilia. Until then, screening and treatment for thrombophilia remain experimental in these women.
The authors report no financial relationships relevant to this article.
Why thrombophilia matters
During pregnancy, clotting factors I, VII, VIII, IX, and X rise; protein S and fibrinolytic activity diminish; and resistance to activated protein C develops.1,2 When compounded by thrombophilia—a broad spectrum of coagulation disorders that increase the risk for venous and arterial thrombosis—the hypercoagulable state of pregnancy may increase the risk of thromboembolism during pregnancy or postpartum.3
Pulmonary embolism is the leading cause of maternal death in the United States.1 Concern about this lethal sequela has led to numerous recommendations for screening and subsequent prophylaxis and therapy.
Two types
Thrombophilias are inherited or acquired (TABLE 1). The most common inherited disorders during pregnancy are mutations in factor V Leiden, prothrombin gene, and methylenetetrahydrofolate reductase (MTHFR) (TABLE 2). Caucasians have a higher rate of genetic thrombophilias than other racial groups.
Antiphospholipid antibody (APA) syndrome is the most common acquired thrombophilia of pregnancy. It can be diagnosed when the immunoglobulin G or immunoglobulin M level is 20 g per liter or higher, when lupus anticoagulant is present, or both.4
TABLE 1
Thrombophilias are inherited or acquired
INHERITED
|
ACQUIRED
|
| MTHFR=methylenetetrahydrofolate reductase |
Prevalence of thrombophilias in women with normal pregnancy outcomes
| THROMBOPHILIA | PREVALENCE (%) |
|---|---|
| Factor V Leiden mutation | 2–10 |
| MTHFR mutation | 8–16 |
| Prothrombin gene mutation | 2–6 |
| Protein C and S deficiencies | 0.2–1.0* |
| Anticardiolipin antibodies | 1–7 |
| * Combined rate | |
| MTHFR=methylenetetrahydrofolate reductase | |
Link to adverse pregnancy outcomes
During the past 2 decades, several epidemiologic and case-control studies have explored the association between thrombophilias and adverse pregnancy outcomes,2-6 which include the following maternal effects:
- Venous thromboembolism, including deep vein thrombosis, pulmonary embolism, and cerebral vein thrombosis
- Arterial thrombosis (peripheral, cerebral)
- Severe preeclampsia
- Thrombosis and infarcts
- Abruptio placenta
- Recurrent miscarriage
- Fetal growth restriction
- Death
- Stroke
Preeclampsia and thrombophilia
The association between preeclampsia and thrombophilia remains somewhat unclear because of inconsistent data. Because of this, we do not recommend routine screening for thrombophilia in women with preeclampsia.
An association between inherited thrombophilias and preeclampsia was reported by Dekker et al in 1995.7 Since then, numerous retrospective and case-controlled studies have assessed the incidence of thrombophilia in women with severe preeclampsia.7-25 Their findings range from:
- Factor V Leiden: 3.7% to 26.5%
- Prothrombin gene mutation: 0 to 10.8%
- Protein S deficiency: 0.7% to 24.7%
- MTHFR variant: 6.7% to 24.0%
Other points of contention are the varying levels of severity of preeclampsia and of gestational age at delivery, as well as racial differences. For example, most studies found an association between thrombophilia and severe preeclampsia at less than 34 weeks’ gestation, but not between thrombophilia and mild preeclampsia at term. In addition, a recent prospective observational study at multiple centers involving 5,168 women found a factor V Leiden mutation rate of 6% among white women, 2.3% among Asians, 1.6% in Hispanics, and 0.8% in African Americans.8 This large study found no association between thrombophilia and preeclampsia in these women. Therefore, based on available data, we do not recommend routine screening for factor V Leiden in women with severe preeclampsia.
Preeclampsia and APA syndrome
In 1989, Branch et al26 first reported an association between APA syndrome and severe preeclampsia at less than 34 weeks’ gestation. They recommended that women with severe preeclampsia at this gestational age be screened for APA syndrome and treated when the screen is positive. Several later studies supported or refuted the association between APA syndrome and preeclampsia,26,27 and a recent report concluded that routine testing for APA syndrome in women with early-onset preeclampsia is unwarranted.26 Therefore, we do not recommend routine screening for APA in women with severe preeclampsia.
No need to screen women with abruptio placenta
The placental circulation is comparable to venous circulation, with low pressure and low flow velocity rendering it susceptible to thrombotic complications at the maternal–placental interface and consequent premature separation of the placenta.
It is difficult to confirm an association between thrombophilia and abruptio placenta because of confounding variables such as chronic hypertension, cigarette and cocaine use, and advanced maternal age.3 Studies reviewing this association are scarce, and screening for thrombophilia is discouraged in pregnancies marked by abruptio placenta.
Kupferminc et al28 found that 25%, 20%, and 15% of thrombophilia patients with placental abruption had mutations in factor V Leiden, prothrombin gene, and MTHFR, respectively. In contrast, Prochazka et al29 found 15.7% of their cohort of patients with abruptio placenta to have factor V Leiden mutation.
A large prospective, observational study of more than 5,000 asymptomatic pregnant women at multiple centers found no association between abruptio placenta and factor V Leiden mutation.8 Nor were there cases of abruptio placenta among 134 women who were heterozygous for factor V Leiden.
And no routine screening in cases of IUGR
Routine screening for thrombophilias in women with intrauterine growth restriction (IUGR) is not recommended. One reason: The prevalence of thrombophilias in these women ranges widely, depending on the study cited: from 2.8% to 35% for factor V Leiden and 2.8% to 15.4% for prothrombin gene mutation (TABLE 3). In addition, in contrast to earlier studies, a large case-control trial by Infante-Rivard et al30 found no increased risk of IUGR in women with thrombophilias, except for a subgroup of women with the MTHFR variant who did not take a prenatal multivitamin.
A recent meta-analysis of case-control studies by Howley et al31 found a significant association between factor V Leiden, the prothrombin gene variant, and IUGR, but the investigators cautioned that this strong association may be driven by small, poor-quality studies that yield extreme associations. A multicenter observational study by Dizon-Townson et al8 found no association between thrombophilia and IUGR in asymptomatic gravidas.
TABLE 3
Incidence of thrombophilias in women with intrauterine growth restriction
| STUDY | FACTOR V LEIDEN (%) | PROTHROMBIN GENE MUTATION (%) | ||
|---|---|---|---|---|
| IUGR | CONTROLS | IUGR | CONTROLS | |
| Kupferminc et al50 | 5/44 (11.4) | 7/110 (6.4) | 5/44 (11.4) | 3/110 (2.7) |
| Infante-Rivard et al30 | 22/488 (4.5) | 18/470 (3.8) | 12/488 (2.5) | 11/470 (2.3) |
| Verspyck et al51 | 4/97 (4.1) | 1/97 (1) | 3/97 (3.1) | 1/97 (1) |
| McCowan et al52 | 4/145 (2.8) | 11/290 (3.8) | 4/145 (2.8) | 9/290 (3.1) |
| Dizon-Townson et al*10 | 6/134 (4.5) | 233/4,753 (4.9) | NR | NR |
| Kupferminc**34 | 9/26 (35) | 2/52 (3.8) | 4/26 (15.4) | 2/52 (3.8) |
| * | ||||
| ** Mid-trimester severe intrauterine growth restriction | ||||
| IUGR=intrauterine growth restriction, NR=not recorded | ||||
| SOURCE: Adapted from Clin Obstet Gynecol. 2006;49:850–860 | ||||
Fetal loss is a complication of thrombophilia
One in 10 pregnancies ends in early death of the fetus (before 20 weeks), and 1 in 200 gestations ends in late fetal loss.32 When fetal loss occurs in the second and third trimesters, it is due to excessive thrombosis of the placental vessels, placental infarction, and secondary uteroplacental insufficiency.2,33 Women who are carriers of factor V or prothrombin gene mutations are at higher risk of late fetal loss than noncarriers are (TABLE 4).
Fetal loss is a well-established complication in women with thrombophilia, but not all thrombophilias are associated with fetal loss, according to a meta-analysis of 31 studies.33 In women with thrombophilia, first-trimester loss is generally associated with factor V Leiden, prothrombin gene mutation, and activated protein C resistance. Late, nonrecurrent fetal loss is associated with factor V Leiden, prothrombin gene mutation, and protein S deficiency.33
TABLE 4
Incidence of factor V Leiden mutation in women with recurrent pregnancy loss
| STUDY | PATIENT SELECTION | PATIENTS (%) | CONTROLS (%) | ODDS RATIO | 95% CONFIDENCE INTERVAL |
|---|---|---|---|---|---|
| Grandone et al53 | ≥2 unexplained fetal losses, other causes excluded | 7/43 (16.3) | 5/118 (4.2) | 4.4 | 1.3–14.7 |
| Ridker et al54 | Recurrent, spontaneous abortion, other causes not excluded | 9/113 (8) | 16/437 (3.7) | 2.3 | 1.0–5.2 |
| Sarig et al55 | ≥3 first- or second-trimester losses or ≥1 intrauterine fetal demise, other causes excluded* | 96/145 (66) | 41/145 (28) | 5.0 | 3.0–8.5 |
| * Excluded chromosomal abnormalities, infections, anatomic alterations, and endocrine dysfunction | |||||
History of adverse outcomes? Offer screening
It is well established that women with a history of fetal death, severe preeclampsia, IUGR, abruptio placenta, or recurrent miscarriage have an increased risk of recurrence in subsequent pregnancies.3,30,34-36 The rate of recurrence of any of these outcomes may be as high as 46% with a history of 2 or more adverse outcomes, even before any thrombophilia is taken into account.3 Although there are few studies describing the rate of recurrence of adverse pregnancy outcomes in women with thrombophilia and a previous adverse outcome (TABLE 5), it appears to range from 66% to 83% in untreated women.3,37
Based on these findings, some authors recommend screening for thrombophilia in women who have had adverse pregnancy outcomes3,9,38 and prophylactic therapy in subsequent pregnancies when the test is positive. Therapy includes low-dose aspirin with or without subcutaneous heparin, as well as folic acid and vitamin B6 supplements, according to the type of thrombophilia present as well as the nature of the previous adverse outcome.
TABLE 5
How women with a previous adverse outcome fare on anticoagulation therapy
| STUDY | PATIENTS | PREVIOUS ADVERSE PREGNANCY OUTCOME | ANTICOAGULANT | OUTCOME IN CURRENT PREGNANCY |
|---|---|---|---|---|
| Riyazi et al9 | 26 | Uteroplacental insufficiency | LMWH and low-dose aspirin | Decreased recurrence of preeclampsia (85% to 38%) and IUGR (54% to 15%) |
| Brenner37 | 50 | ≥3 first-trimester recurrent pregnancy losses with thrombophilia | LMWH | Higher live birth rate compared with historical controls (75% vs 20%) |
| Ogueh et al48 | 24 | Previous adverse pregnancy outcome plus history of thromboembolic disease, family history of thrombophilia | UFH | No significant mprovement |
| Kupferminc et al38 | 33 | Thrombophilia with history of preeclampsia or IUGR | LMWH and low-dose aspirin | With treatment, 3% recurrence of preeclampsia |
| Grandone et al53 | 25 | Repeated pregnancy loss, gestational hypertension, HELLP, or IUGR | UFH or LMWH | 90.3% treated with LMWH had good obstetric outcome |
| Paidas et al3 | 158 | Fetal loss, IUGR, placental abruption, or preeclampsia | UFH or LMWH | 80% reduction in risk of adverse pregnancy outcome, compared with historical controls (OR, 0.21; 95% CI, 0.11–0.39) |
| HELLP=hemolysis, elevated liver enzymes, and low platelets; IUGR=intrauterine growth restriction; LMWH=low-molecular-weight heparin; UFH=unfractionated heparin | ||||
| SOURCE: Adapted from Am J Perinatol. 2006;23:499–506 | ||||
No randomized trials on prophylaxis
We lack randomized trials evaluating thromboprophylaxis for prevention of recurrent adverse pregnancy outcomes in women with previous severe preeclampsia, IUGR, or abruptio placenta in association with genetic thrombophilia. Therefore, any recommendation to treat such women with low-molecular-weight heparin with or without low-dose aspirin in subsequent pregnancies should remain empiric and/or prescribed after appropriate counseling of the patients regarding risks and benefits.
TABLE 6 summarizes the risk of thromboembolism in women with thrombophilia—both for asymptomatic patients and for those with a history of thromboembolism. These percentages should be used when counseling women about their risk and determining management and therapy.
TABLE 6
Risk of thromboembolism during pregnancy and postpartum in women with thrombophilia
| THROMBOPHILIA | RISK (%) | |
|---|---|---|
| ASYMPTOMATIC WOMEN | HISTORY OF VENOUS THROMBOEMBOLISM | |
| Factor V Leiden | ||
| Heterozygous | 0.2 | 10 |
| Homozygous | 1–2 | 15–20 |
| Prothrombin gene mutation | ||
| Heterozygous | 0.5 | 10 |
| Homozygous | 2.3 | 20 |
| Factor V Leiden and prothrombin gene mutation | 5 | 20 |
| Antithrombin deficiency | 7 | 40 |
| Protein C deficiency | 0.5 | 5–15 |
| Protein S deficiency | 0.1 | Unknown |
Prophylaxis for APA syndrome and recurrent pregnancy loss
Several randomized trials have described the use of low-dose aspirin and heparin in women with APA syndrome and a history of recurrent pregnancy loss, although the results are inconsistent (TABLE 7).39-45 The inconsistency may be due to varying definitions of APA syndrome and gestational age at the time of randomization, as well as the population studied (previous thromboembolism, presence or absence of lupus anticoagulant, level of titer of anticardiolipin antibodies, presence or absence of previous stillbirth). Nevertheless, we recommend that women with true APA syndrome (presence of lupus anticoagulant, high titers of immunoglobulin G, history of thromboembolism or recurrent stillbirth) receive prophylaxis with low-dose aspirin, with subcutaneous heparin added once fetal cardiac activity is documented.46
TABLE 7
Live births in women with APA and a history of fetal loss
| STUDY | TREATMENT | CONTROL | NO. OF LIVE BIRTHS (%) | |
|---|---|---|---|---|
| TREATED WOMEN | CONTROL GROUP | |||
| Cowchock et al39 | Aspirin/heparin | Aspirin/prednisone | 9/12 (75) | 6/8 (75) |
| Laskin et al40 | Aspirin/prednisone | Placebo | 25/42 (60) | 24/46 (52) |
| Kutteh41 | Aspirin/heparin | Aspirin only | 20/25 (80) | 11/25 (44) |
| Rai et al42 | Aspirin/heparin | Aspirin only | 32/45 (71) | 19/45 (42) |
| Silver et al43 | Aspirin/prednisone | Aspirin only | 12/12 (100) | 22/22 (100) |
| Pattison et al44 | Aspirin | Placebo | 16/20 (80) | 17/20 (85) |
| Farquharson et al45 | Aspirin/LMWH | Aspirin only | 40/51 (78) | 34/47 (72) |
| LMWH=low-molecular-weight heparin | ||||
Genetic thrombophilias
Few published studies describe prophylactic use of low-molecular-weight heparin with or without low-dose aspirin in women with genetic thrombophilia and a history of adverse pregnancy outcomes. All but 1 of these studies are observational, comparing outcome in the treated pregnancy with that of previously untreated gestations in the same woman.3,9,38,44,45,47 These studies included a limited number of women and a heterogeneous group of patients with various thrombophilias; they also involved different therapies (TABLE 7).3,9,38,41,48,49
Gris et al47 performed a randomized trial in 160 women with at least 1 prior fetal loss after 10 weeks’ gestation who were heterozygous for factor V Leiden or prothrombin G20210A mutation, or had protein S deficiency. Beginning at 8 weeks’ gestation, these women were assigned to treatment with 40 mg of enoxaparin (n=80) or 100 mg of low-dose aspirin (n=80) daily. All women also received 5 mg of folic acid daily.
In the women treated with enoxaparin, 69 (86%) had a live birth, compared with 23 (29%) women treated with low-dose aspirin. The women treated with enoxaparin also had significantly higher median neonatal birth weights and a lower rate of IUGR (10% versus 30%). The authors concluded that women with factor V Leiden, prothrombin gene mutation, or protein S deficiency and a history of fetal loss should receive enoxaparin prophylaxis in subsequent pregnancies.
History of severe preeclampsia, IUGR, or abruptio placenta. No randomized trials have evaluated thromboprophylaxis in women with this history who have genetic thrombophilia. For this reason, any recommendation to treat these women with low-molecular-weight heparin with or without low-dose aspirin in subsequent pregnancies remains empiric. Prophylaxis can be prescribed after an appropriate discussion of risks and benefits with the patient.
Unresolved questions keep management experimental
What is the likelihood that a woman carrying a gene mutation that predisposes her to thrombophilia will have a serious complication during pregnancy? And how safe and effective is prophylaxis?
There is a prevailing need for a double-blind placebo-controlled trial to address these questions and evaluate the benefit of heparin in pregnant women with a history of adverse pregnancy outcomes and thrombophilia. Until then, screening and treatment for thrombophilia remain experimental in these women.
The authors report no financial relationships relevant to this article.
1. Thromboembolism in pregnancy. ACOG Practice Bulletin #19. Washington, DC: ACOG; 2000.
2. Kujovich JL. Thrombophilia and pregnancy complications. Am J Obstet Gynecol. 2004;191:412-424.
3. Paidas MJ, De-Hui WK, Arkel YS. Screening and management of inherited thrombophilias in the setting of adverse pregnancy outcome. Clin Perinatol. 2004;31:783-805.
4. Lee RM, Brown MA, Branch DW, Ward K, Silver RM. Anticardiolipin and anti-B2 glycoprotein-I antibodies in preeclampsia. Obstet Gynecol. 2003;102:294-300.
5. Lin L, August P. Genetic thrombophilias and preeclampsia: a meta-analysis. Obstet Gynecol. 2005;105:182-192.
6. Mignini LE, Latthe PM, Villar J, et al. Mapping the theories of preeclampsia: the role of homocysteine. Obstet Gynecol. 2005;105:411-425.
7. Dekker GA, de Vries JI, Doelitzsch PM, et al. Underlying disorders associated with severe early-onset preeclampsia. Am J Obstet Gynecol. 1995;173:1042-1048.
8. Dizon-Townson D, Miller C, Sibai B, et al. The relationship of factor V Leiden mutation and pregnancy outcomes for mother and fetus. Obstet Gynecol. 2005;106:517-524.
9. Riyazi N, Leeda M, de Vries JIP, et al. Low molecular weight heparin combined with aspirin in pregnant women with thrombophilia and a history of preeclampsia or fetal growth restriction: a preliminary study. Eur J Obstet Gynecol Reprod Biol. 1998;80:49-54.
10. Dizon-Townson DS, Nelson LM, Easton K, Ward K. The factor V Leiden mutation may predispose women to severe preeclampsia. Am J Obstet Gynecol. 1996;175:902-905.
11. Nagy B. Detection of factor V Leiden mutation in severe preeclamptic Hungarian women. Clin Genet. 1998;53:478-481.
12. Krauss T. Activated protein C resistance and factor V Leiden in patients with hemolysis, elevated liver enzymes, low platelets syndrome. Obstet Gynecol. 1998;92:457-460.
13. Kupferminc MJ, Eldor A, Steinman N, et al. Increased frequency of genetic thrombophilia in women with complications of pregnancy. N Engl J Med. 1999;341:384.-
14. van Pampus EC. High prevalence of hemostatic abnormalities in women with a history of severe preeclampsia. Am J Obstet Gynecol. 1999;180:1146-1150.
15. DeGroot CJ, Bloemankamp KW, Duvekot EJ, et al. Preeclampsia and genetic factors for thrombosis: a case control study. Am J Obstet Gynecol. 1999;181:975-980.
16. Kupferminc MJ, Fait G, Many A, Girdon D, Eldor A, Lessing JB. Severe preeclampsia: high frequency of genetic thrombophilic mutations. Obstet Gynecol. 2000;96:45-49.
17. Rigo J, Nagy B, Fintor L, et al. Maternal and neonatal outcome of preeclamptic pregnancies: the potential roles of factor V Leiden mutations and 5,10 methylenetetrahydrofolate reductase. Hypertens Pregnancy. 2000;19(2):163-172.
18. von Tempelhoff GF. Incidence of factor V Leiden mutation, coagulation inhibitor deficiency, and elevated antiphospholipid-antibodies in patients with preeclampsia or HELLP syndrome (hemolysis, elevated liver enzymes, low platelets). Thromb Res. 2000;100:363-365.
19. Kupferminc MJ, Peri H, Zwang E, et al. High prevalence of the prothrombin gene mutation in women with intrauterine growth retardation, abruptio placentae and second trimester loss. Acta Obstet Gynecol Scand. 2000;79:963-967.
20. Kim YJ. Genetic susceptibility to preeclampsia: roles of cytosine-to-thymine substitution at nucleotide 677 of the gene for methylenetetrahydrofolate reductase, 68-base pair insertion at nucleotide 844 of the gene for cystathione [beta]-synthase, and factor V Leiden mutation. Am J Obstet Gynecol. 2001;184:1211-1217.
21. Livingston J, Barton JR, Park V, et al. Maternal and fetal inherited thrombophilias are not related to the development of severe preeclampsia. Am J Obstet Gynecol. 2001;185:153-157.
22. Currie L, Peek M, McNiven M, et al. Is there an increased maternal-infant prevalence of factor V Leiden in association with severe pre-eclampsia? BJOG. 2002;109:191-196.
23. Benedetto C, Marozio L, Salton L, et al. Factor V Leiden and factor II G20210A in preeclampsia and HELLP syndrome. Acta Obstet Gynecol. 2002;81:1095-1100.
24. Schlembach D, Beinder E, Zingsem J, et al. Association of maternal and/or fetal factor V Leiden and G20210A prothrombin mutation with HELLP syndrome and intrauterine growth restriction. Clin Sci. 2003;105:279-285.
25. Mello G, Parretti E, Marozio L, et al. Thrombophilia is significantly associated with severe preeclampsia: results of a large-scale, case-controlled study. Hypertension. 2005;46:1270-1274.
26. Branch DW, Andres R, Digre KB, Rote NS, Scott JR. The association of antiphospholipid antibodies with severe preeclampsia. Obstet Gynecol. 1989;73:541-545.
27. Dreyfus M, Hedelin G, Kutnahorsky R, et al. Antiphospholipid antibodies and preeclampsia: a case-control study. Obstet Gynecol. 2001;97:29-34.
28. Kupferminc MJ, Eldor A, Steinman N, et al. Increased frequency of genetic thrombophilia in women with complications of pregnancy. N Engl J Med. 1999;340:9-13.
29. Prochazka M, Happach C, Marsal K, Dahlback B, Lindqvist PG. Factor V Leiden in pregnancies complicated by placental abruption. BJOG. 2003;110:462-466.
30. Infante-Rivard C, Rivard GE, Yotov WV, et al. Absence of association of thrombophilia polymorphisms with intrauterine growth restriction. N Engl J Med. 2002;347:19-25.
31. Howley HE, Walker M, Rodger MA. A systematic review of the association between factor V Leiden or prothrombin gene variant and intrauterine growth restriction. Am J Obstet Gynecol. 2005;192:694-708.
32. Martinelli I, Taioli E, Cetin I, et al. Mutations in coagulation factors in women with unexplained late fetal loss. N Engl J Med. 2000;343:1015-1018.
33. Rey E, Kahn SR, David M, et al. Thrombophilic disorders and fetal loss: a metaanalysis. Lancet. 2003;361:901-908.
34. Kupferminc MJ. Mid-trimester severe intrauterine growth restriction is associated with high prevalence of thrombophilia. BJOG. 2002;109:1373-1376.
35. Sibai BM, el-Nazer A, Gonzalez-Ruiz A. Severe preeclampsia-eclampsia in young primigravid women: subsequent pregnancy outcome and remote prognosis. Am J Obstet Gynecol. 1986;155:1011-1016.
36. Sibai BM, Mercer B, Sarinoglu C. Severe preeclampsia in the second trimester: recurrence risk and long-term prognosis. Am J Obstet Gynecol. 1991;165:1408-1412.
37. Brenner B. Thrombophilia and fetal loss. Semin Thromb Hemost. 2003;29:165-170.
38. Kupferminc MJ, Fait G, Many A, et al. Low molecular weight heparin for the prevention of obstetric complications in women with thrombophilias. Hypertens Pregnancy. 2001;20:35-44.
39. Cowchock FS, Reece EA, Balaban D, et al. Repeated fetal losses associated with antiphospholipid antibodies: a collaborative randomized trial comparing prednisone with low-dose heparin treatment. Am J Obstet Gynecol. 1992;166:1318-1323.
40. Laskin CA, Bombardier C, Hannah ME, et al. Prednisone and aspirin in women with autoantibodies and unexplained recurrent fetal loss. N Engl J Med. 1997;337:148-154.
41. Kutteh WH. Antiphospholipid antibody-associated recurrent pregnancy loss: treatment with heparin and low-dose aspirin is superior to low-dose aspirin alone. Am J Obstet Gynecol. 1996;174:1584-1589.
42. Rai R, Cohen H, Dave M, Regan L. Randomised controlled trial of aspirin and aspirin plus heparin in pregnant women with recurrent miscarriage associated with phospholipid antibodies (or antiphospholipid antibodies). BMJ. 1997;314:253-257.
43. Silver RK, MacGregor SN, Sholl JS, et al. Comparative trial of prednisone versus aspirin alone in the treatment of anticardiolipin antibody-positive obstetric patients. Am J Obstet Gynecol. 1993;169:1411-1417.
44. Pattison NS, Chamley LW, Birdsall M, et al. Does aspirin have a role in improving pregnancy outcome for women with the antiphospholipid syndrome? A randomized controlled trial. Am J Obstet Gynecol. 2000;183:1008-1012.
45. Farquharson RG, Quenby S, Greaves M. Antiphospholipid syndrome in pregnancy: a randomized, controlled trial of treatment. Obstet Gynecol. 2002;100:408-413.
46. Antiphospholipid syndrome. ACOG Practice Bulletin #68. Obstet Gynecol. 2005;106:1113-1121.
47. Gris JC, Mercier E, Quere I, et al. Low-molecular-weight heparin versus low-dose aspirin in women with one fetal loss and a constitutional thrombophilic disorder. Blood. 2004;103:3695-3699.
48. Ogueh O, Chen MF, Spurll G, Benjamin A. Outcome of pregnancy in women with hereditary thrombophilia. Int J Gynecol Obstet. 2001;74:247-253.
49. Brenner B, Hoffman R, Blumenfeld Z, et al. Gestational outcome in thrombophilic women with recurrent pregnancy loss treated with enoxaparin. Thromb Haemost. 2000;83:693-697.
50. Kupferminc MJ, Fait G, Many A, et al. Low molecular weight heparin for the prevention of obstetric complications in women with thrombophilias. Hypertens Pregnancy. 2001;20:35-44.
51. Verspyck E, Borg JY, Le Cam-Duchez V, et al. Thrombophilia and fetal growth restriction. Eur J Obstet Gynecol Reprod Biol. 2004;113:36-40.
52. McCowan LME, Craigie S, Taylor RS, et al. Inherited thrombophilias are not increased in “idiopathic” small-for-gestationalage pregnancies. Am J Obstet Gynecol. 2003;188:981-992.
53. Grandone E, Brancaccio V, Colaizzo D, et al. Preventing adverse obstetric outcomes in women with genetic thrombophilia. Fertil Steril. 2002;78:371-375.
54. Ridker PM, Miletich JP, Buring JE, et al. Factor V Leiden mutation as a risk factor for recurrent pregnancy loss. Ann Intern Med. 1998;128:1000-1003.
55. Sarig G, Younis J, Hoffman R, et al. Thrombophilia is common in women with idiopathic pregnancy loss and is associated with late pregnancy wastage. Fertil Steril. 2002;77:342-347.
1. Thromboembolism in pregnancy. ACOG Practice Bulletin #19. Washington, DC: ACOG; 2000.
2. Kujovich JL. Thrombophilia and pregnancy complications. Am J Obstet Gynecol. 2004;191:412-424.
3. Paidas MJ, De-Hui WK, Arkel YS. Screening and management of inherited thrombophilias in the setting of adverse pregnancy outcome. Clin Perinatol. 2004;31:783-805.
4. Lee RM, Brown MA, Branch DW, Ward K, Silver RM. Anticardiolipin and anti-B2 glycoprotein-I antibodies in preeclampsia. Obstet Gynecol. 2003;102:294-300.
5. Lin L, August P. Genetic thrombophilias and preeclampsia: a meta-analysis. Obstet Gynecol. 2005;105:182-192.
6. Mignini LE, Latthe PM, Villar J, et al. Mapping the theories of preeclampsia: the role of homocysteine. Obstet Gynecol. 2005;105:411-425.
7. Dekker GA, de Vries JI, Doelitzsch PM, et al. Underlying disorders associated with severe early-onset preeclampsia. Am J Obstet Gynecol. 1995;173:1042-1048.
8. Dizon-Townson D, Miller C, Sibai B, et al. The relationship of factor V Leiden mutation and pregnancy outcomes for mother and fetus. Obstet Gynecol. 2005;106:517-524.
9. Riyazi N, Leeda M, de Vries JIP, et al. Low molecular weight heparin combined with aspirin in pregnant women with thrombophilia and a history of preeclampsia or fetal growth restriction: a preliminary study. Eur J Obstet Gynecol Reprod Biol. 1998;80:49-54.
10. Dizon-Townson DS, Nelson LM, Easton K, Ward K. The factor V Leiden mutation may predispose women to severe preeclampsia. Am J Obstet Gynecol. 1996;175:902-905.
11. Nagy B. Detection of factor V Leiden mutation in severe preeclamptic Hungarian women. Clin Genet. 1998;53:478-481.
12. Krauss T. Activated protein C resistance and factor V Leiden in patients with hemolysis, elevated liver enzymes, low platelets syndrome. Obstet Gynecol. 1998;92:457-460.
13. Kupferminc MJ, Eldor A, Steinman N, et al. Increased frequency of genetic thrombophilia in women with complications of pregnancy. N Engl J Med. 1999;341:384.-
14. van Pampus EC. High prevalence of hemostatic abnormalities in women with a history of severe preeclampsia. Am J Obstet Gynecol. 1999;180:1146-1150.
15. DeGroot CJ, Bloemankamp KW, Duvekot EJ, et al. Preeclampsia and genetic factors for thrombosis: a case control study. Am J Obstet Gynecol. 1999;181:975-980.
16. Kupferminc MJ, Fait G, Many A, Girdon D, Eldor A, Lessing JB. Severe preeclampsia: high frequency of genetic thrombophilic mutations. Obstet Gynecol. 2000;96:45-49.
17. Rigo J, Nagy B, Fintor L, et al. Maternal and neonatal outcome of preeclamptic pregnancies: the potential roles of factor V Leiden mutations and 5,10 methylenetetrahydrofolate reductase. Hypertens Pregnancy. 2000;19(2):163-172.
18. von Tempelhoff GF. Incidence of factor V Leiden mutation, coagulation inhibitor deficiency, and elevated antiphospholipid-antibodies in patients with preeclampsia or HELLP syndrome (hemolysis, elevated liver enzymes, low platelets). Thromb Res. 2000;100:363-365.
19. Kupferminc MJ, Peri H, Zwang E, et al. High prevalence of the prothrombin gene mutation in women with intrauterine growth retardation, abruptio placentae and second trimester loss. Acta Obstet Gynecol Scand. 2000;79:963-967.
20. Kim YJ. Genetic susceptibility to preeclampsia: roles of cytosine-to-thymine substitution at nucleotide 677 of the gene for methylenetetrahydrofolate reductase, 68-base pair insertion at nucleotide 844 of the gene for cystathione [beta]-synthase, and factor V Leiden mutation. Am J Obstet Gynecol. 2001;184:1211-1217.
21. Livingston J, Barton JR, Park V, et al. Maternal and fetal inherited thrombophilias are not related to the development of severe preeclampsia. Am J Obstet Gynecol. 2001;185:153-157.
22. Currie L, Peek M, McNiven M, et al. Is there an increased maternal-infant prevalence of factor V Leiden in association with severe pre-eclampsia? BJOG. 2002;109:191-196.
23. Benedetto C, Marozio L, Salton L, et al. Factor V Leiden and factor II G20210A in preeclampsia and HELLP syndrome. Acta Obstet Gynecol. 2002;81:1095-1100.
24. Schlembach D, Beinder E, Zingsem J, et al. Association of maternal and/or fetal factor V Leiden and G20210A prothrombin mutation with HELLP syndrome and intrauterine growth restriction. Clin Sci. 2003;105:279-285.
25. Mello G, Parretti E, Marozio L, et al. Thrombophilia is significantly associated with severe preeclampsia: results of a large-scale, case-controlled study. Hypertension. 2005;46:1270-1274.
26. Branch DW, Andres R, Digre KB, Rote NS, Scott JR. The association of antiphospholipid antibodies with severe preeclampsia. Obstet Gynecol. 1989;73:541-545.
27. Dreyfus M, Hedelin G, Kutnahorsky R, et al. Antiphospholipid antibodies and preeclampsia: a case-control study. Obstet Gynecol. 2001;97:29-34.
28. Kupferminc MJ, Eldor A, Steinman N, et al. Increased frequency of genetic thrombophilia in women with complications of pregnancy. N Engl J Med. 1999;340:9-13.
29. Prochazka M, Happach C, Marsal K, Dahlback B, Lindqvist PG. Factor V Leiden in pregnancies complicated by placental abruption. BJOG. 2003;110:462-466.
30. Infante-Rivard C, Rivard GE, Yotov WV, et al. Absence of association of thrombophilia polymorphisms with intrauterine growth restriction. N Engl J Med. 2002;347:19-25.
31. Howley HE, Walker M, Rodger MA. A systematic review of the association between factor V Leiden or prothrombin gene variant and intrauterine growth restriction. Am J Obstet Gynecol. 2005;192:694-708.
32. Martinelli I, Taioli E, Cetin I, et al. Mutations in coagulation factors in women with unexplained late fetal loss. N Engl J Med. 2000;343:1015-1018.
33. Rey E, Kahn SR, David M, et al. Thrombophilic disorders and fetal loss: a metaanalysis. Lancet. 2003;361:901-908.
34. Kupferminc MJ. Mid-trimester severe intrauterine growth restriction is associated with high prevalence of thrombophilia. BJOG. 2002;109:1373-1376.
35. Sibai BM, el-Nazer A, Gonzalez-Ruiz A. Severe preeclampsia-eclampsia in young primigravid women: subsequent pregnancy outcome and remote prognosis. Am J Obstet Gynecol. 1986;155:1011-1016.
36. Sibai BM, Mercer B, Sarinoglu C. Severe preeclampsia in the second trimester: recurrence risk and long-term prognosis. Am J Obstet Gynecol. 1991;165:1408-1412.
37. Brenner B. Thrombophilia and fetal loss. Semin Thromb Hemost. 2003;29:165-170.
38. Kupferminc MJ, Fait G, Many A, et al. Low molecular weight heparin for the prevention of obstetric complications in women with thrombophilias. Hypertens Pregnancy. 2001;20:35-44.
39. Cowchock FS, Reece EA, Balaban D, et al. Repeated fetal losses associated with antiphospholipid antibodies: a collaborative randomized trial comparing prednisone with low-dose heparin treatment. Am J Obstet Gynecol. 1992;166:1318-1323.
40. Laskin CA, Bombardier C, Hannah ME, et al. Prednisone and aspirin in women with autoantibodies and unexplained recurrent fetal loss. N Engl J Med. 1997;337:148-154.
41. Kutteh WH. Antiphospholipid antibody-associated recurrent pregnancy loss: treatment with heparin and low-dose aspirin is superior to low-dose aspirin alone. Am J Obstet Gynecol. 1996;174:1584-1589.
42. Rai R, Cohen H, Dave M, Regan L. Randomised controlled trial of aspirin and aspirin plus heparin in pregnant women with recurrent miscarriage associated with phospholipid antibodies (or antiphospholipid antibodies). BMJ. 1997;314:253-257.
43. Silver RK, MacGregor SN, Sholl JS, et al. Comparative trial of prednisone versus aspirin alone in the treatment of anticardiolipin antibody-positive obstetric patients. Am J Obstet Gynecol. 1993;169:1411-1417.
44. Pattison NS, Chamley LW, Birdsall M, et al. Does aspirin have a role in improving pregnancy outcome for women with the antiphospholipid syndrome? A randomized controlled trial. Am J Obstet Gynecol. 2000;183:1008-1012.
45. Farquharson RG, Quenby S, Greaves M. Antiphospholipid syndrome in pregnancy: a randomized, controlled trial of treatment. Obstet Gynecol. 2002;100:408-413.
46. Antiphospholipid syndrome. ACOG Practice Bulletin #68. Obstet Gynecol. 2005;106:1113-1121.
47. Gris JC, Mercier E, Quere I, et al. Low-molecular-weight heparin versus low-dose aspirin in women with one fetal loss and a constitutional thrombophilic disorder. Blood. 2004;103:3695-3699.
48. Ogueh O, Chen MF, Spurll G, Benjamin A. Outcome of pregnancy in women with hereditary thrombophilia. Int J Gynecol Obstet. 2001;74:247-253.
49. Brenner B, Hoffman R, Blumenfeld Z, et al. Gestational outcome in thrombophilic women with recurrent pregnancy loss treated with enoxaparin. Thromb Haemost. 2000;83:693-697.
50. Kupferminc MJ, Fait G, Many A, et al. Low molecular weight heparin for the prevention of obstetric complications in women with thrombophilias. Hypertens Pregnancy. 2001;20:35-44.
51. Verspyck E, Borg JY, Le Cam-Duchez V, et al. Thrombophilia and fetal growth restriction. Eur J Obstet Gynecol Reprod Biol. 2004;113:36-40.
52. McCowan LME, Craigie S, Taylor RS, et al. Inherited thrombophilias are not increased in “idiopathic” small-for-gestationalage pregnancies. Am J Obstet Gynecol. 2003;188:981-992.
53. Grandone E, Brancaccio V, Colaizzo D, et al. Preventing adverse obstetric outcomes in women with genetic thrombophilia. Fertil Steril. 2002;78:371-375.
54. Ridker PM, Miletich JP, Buring JE, et al. Factor V Leiden mutation as a risk factor for recurrent pregnancy loss. Ann Intern Med. 1998;128:1000-1003.
55. Sarig G, Younis J, Hoffman R, et al. Thrombophilia is common in women with idiopathic pregnancy loss and is associated with late pregnancy wastage. Fertil Steril. 2002;77:342-347.
Efficacy of Group Education in Veterans with Hepatitis C
Use of Optical Coherence Tomography to Quantify Macular Edema
URINARY INCONTINENCE
Surgery for stress incontinence
Another year is drawing to a close and, looking back, what have we learned about urinary incontinence? A clear understanding of etiology stubbornly eludes us. How would a clear understanding of etiology affect management? It’s difficult to be specific until we actually do understand it, but generally:
The “multiple-hit” theory probably applies to urinary incontinence, too
The “multiple-hit” theory usually ascribed to cancer probably also fits the development of urinary incontinence, a likewise multifaceted condition. A woman begins life with genetic predisposition at some level that we cannot currently measure, but which is influenced by the environment (eg, nutrition, toxic exposures) and life events (eg, childbirth, aging)—all of which determine her likelihood of developing incontinence.
Until the time when we do have a clear understanding on which to base diagnosis, treatment, and prevention, of course, we must continue to manage incontinence with the tools of today.
A few pieces of the puzzle are slowly coming together.
Surgery for stress incontinence
Even as new surgical techniques or modifications continue to proliferate, evidence to guide clinical practice accumulates belatedly. MEDLINE lists 325 articles since 1996 (combining surgical mesh and urinary incontinence, limited to human females and published in English). Nonetheless, a consensus may be emerging that the safest synthetic material is monofilament polypropylene with pore size larger than 70 μm.
Unfortunately, by the time research reports are published showing higher complications with certain products, countless women have already been treated.
Mesh erosion (or exposure, extrusion), sometimes accompanied by infection, is a common complication when multifilament or small-pore meshes are used. Even worse, companies commonly withdraw products, modify them, and re-introduce them to the market, accompanied by intensive marketing but, as with the original product, without any real evidence of safety and effectiveness.
In an ideal world, clinicians (and patients) would insist on evidence before accepting new products and techniques. Failing that, clinicians (and patients!) should clearly understand that all new products and techniques are experimental until they are proven equal to or better than traditional techniques. As we have learned with the most subtle differences between synthetic materials, “almost the same” or “looks the same” is not the same.
Among the most important evidence on slings this year are reports of investigations that demonstrated what should not be done.
Are monofilament, large-pore mesh products safer?
Abdel-Fattah M, Sivanesan K, Ramsay I, Pringle S, Bjornsson S. How common are tape erosions? A comparison of two versions of the transobturator tension-free vaginal tape procedure. BJU Int. 2006;98:594–598.
Yamada BS, Govier FE, Stefanovic KB, Kobashi KC. High rate of vaginal erosions associated with the Mentor Obtape. J Urol. 2006;176:651–654.
Siegel AL, Kim M, Goldstein M, Levey S, Ilbeigi P. High incidence of vaginal mesh extrusion using the Intravaginal Slingplasty sling. J Urol. 2005;174:1308–1311.
The risk of vaginal erosion is much higher with synthetic meshes used for sling procedures when the mesh is multifilament and/or small-pore (<70 μm). In some cases, companies have replaced products (Mentor Obtape small-pore polypropylene sling product was replaced with macroporous Aris), whereas others continue to market products reported to have unacceptably high rates of vaginal erosion and mesh extrusion (Intravaginal Slingplasty multifilament mesh) (TABLE 1).
TABLE 1
Comparison of selected multifilament and small-pore mesh products
| REFERENCE | SLING PRODUCT | EROSION RATE | MANAGEMENT |
|---|---|---|---|
| Abdel-Fattah et al (2006) | Obtape | 7.3% (14 of 192) | 7: partial excision 7: complete excision with infection |
| TVT-O | 1.8% (2 of 112) | 1: partial excision 1: vaginal closure | |
| Yamada et al (2006) | Obtape | 13.4% (9 of 67) | 9: complete excision (1 with abscess) |
| Monarc | 0 of 56 | — | |
| Siegel et al (2005) | IVS | 17% (6 of 35) | 6: complete excision (1 with pelvic abscess) |
Avoid cadaveric fascia in sling procedures
Howden NS, Zyczynski HM, Moalli PA, Sagan ER, Meyn LA, Weber AM. Comparison of autologous rectus fascia and cadaveric fascia in pubovaginal sling continence outcomes. Am J Obstet Gynecol. 2006;194:1444–1449.
Evidence has accumulated that sling procedures performed with cadaveric fascia have substantially worse continence outcomes, compared with those using autologous fascia. In a retrospective cohort study of 150 women with cadaveric fascial slings and 153 women who had autologous rectus fascial slings, urinary incontinence (16 vs 5 per 100 women-years) and reoperation for stress incontinence (4 vs 1 per 100 women-years) occurred more frequently after cadaveric versus autologous rectus fascial slings.
Should xenograft materials be used in sling procedures?
Giri SK, Hickey JP, Sil D, et al. Long-term results of pubovaginal sling surgery using acellular cross-linked porcine dermis in the treatment of urodynamic stress incontinence. J Urol. 2006; 175:1788–1792.
Several companies market specific products integrated into sling techniques, such as In-First Ultra (porcine dermal matrix secured with bone anchors) and Stratasis (porcine small intestinal submucosa in urethral sling and tension-free versions). Other companies market only the xenograft for application in sling procedures, such as Pelvicol (acellular porcine collagen matrix). However, relatively little information is available to support or discourage use of xenograft materials in sling procedures.
Giri et al found worse outcomes using Pelvicol compared with autologous rectus fascia for pubovaginal slings. With 3-year follow-up, 54% (26 of 48 women) with Pelvicol were considered successfully cured or improved, compared with 80.4% (37 of 46 women) with rectus fascia. Of interest, women continued to report recurrent incontinence with Pelvicol through the 3-year period, whereas women with rectus fascia had recurrence within the first 9 months after surgery.
Midurethral slings: Retropubic or transobturator?
Waltregny D, Reul O, Mathantu B, Gaspar Y, Bonnet P, de Leval J. Inside out transobturator vaginal tape for the treatment of female stress urinary incontinence: interim results of a prospective study after a 1-year minimum followup. J Urol. 2006;175:2191–2195.
Morey AF, Medendorp AR, Noller MW, et al. Transobturator versus transabdominal midurethral slings: a multi-institutional comparison of obstructive voiding complications. J Urol. 2006;175:1014–1017.
Midurethral sling placement was modified from the retropubic to the obturator approach with the objective of reducing the risk of major bladder and urethral injury and vascular complications. Does the obturator approach actually have fewer intraoperative complications compared with the retropubic approach? Unknown. (As noted below, even within retropubic procedures, it is possible—although currently unknown—that vaginal and abdominal approaches have different complication rates.) This is a good news–bad news problem:
Results of the obturator approach are beginning to appear in the literature as case series and uncontrolled comparative studies. Waltregney et al reported cure of stress incontinence in 91% of 99 patients after 1 year of follow-up. Morey et al reported similar continence outcomes: 89% success for 154 patients after the obturator approach compared with 86% success for 350 patients after the abdominal approach, although follow-up in the abdominal group was substantially longer (mean 20 months, range 18–26) than in the obturator group (mean 9 months, range 6–16). Of interest, urethrolysis was performed more frequently in the abdominal group (2.3%) than in the obturator group (0%).
Randomized trials are necessary to obtain unbiased comparisons of techniques. Investigators in the NIH-sponsored Urinary Incontinence Treatment Network are currently performing a randomized trial comparing obturator and abdominal approaches with midurethral slings for women with stress and stress-predominant mixed incontinence. The primary outcome will compare objective and subjective treatment success between the 2 groups at 1 and 2 years after surgery. Enrollment is expected to be complete by early 2008, and 1-year follow-up by early 2009. Stay tuned for the results!
Retropubic midurethral slings: Which brand?
Gandhi S, Abramov Y, Kwon C, et al. TVT versus SPARC: comparison of outcomes for two midurethral tape procedures. Int Urogynecol J Pelvic Floor Dysfunct. 2006;17:125–130.
Lord HE, Taylor JD, Finn JC, et al. A randomized controlled equivalence trial of short-term complications and efficacy of tension-free vaginal tape and suprapubic urethral support sling for treating stress incontinence. BJU Int. 2006;98:367–376.
As the first midurethral sling, the tension-free vaginal tape (Gynecare TVT) has the most evidence and longest follow-up available in the literature. It was originally described using the vaginal approach (“bottom-up”); the company now markets all 3 approaches: vaginal, abdominal (“top-down”), and obturator. Other companies market different products along the same lines, but it cannot be assumed that midurethral slings are interchangeable. Studies are starting to appear that compare different retropubic midurethral slings. In a retrospective case series (Gandhi et al) and a randomized trial (Lord et al), Gynecare TVT had better continence outcomes compared with SPARC (TABLE 2).
TABLE 2
Comparison of 2 retropubic midurethral slings
| OUTCOMES | GYNECARE TVT | SPARC | STATISTICAL SIGNIFICANCE |
|---|---|---|---|
| Subjective continence | |||
| Series by Gandhi et al | 86% (61 of 71) | 60% (28 of 47) | 0.001 |
| RCT by Lord et al | 87% (128 of 147) | 76% (117 of 153) | 0.03 |
| Objective stress continence | |||
| Series by Gandhi et al | 95% (58 of 61) | 70% (32 of 46) | <0.001 |
| RCT by Lord et al | 97.3% (143 of 147) | 97.4% (148 of 152) | NS |
| Follow-up | |||
| Series by Gandhi et al (median, range) | 17 weeks (6–197) | 16 weeks (6–129) | — |
| RCT by Lord et al | 6 weeks | 6 weeks | — |
| Retention requiring reoperation | |||
| Series by Gandhi et al | 2.7% (2 of 73) | 2.0% (1 of 49) | NS |
| RCT by Lord et al | 0 of 147 | 6.5% (10 of 154) | 0.002 |
| Mesh erosions* | |||
| RCT by Lord et al | 4.8% (7 of 147) | 10.5% (16 of 152) | 0.08 |
| *Mesh erosions not reported in Gandhi et al. | |||
Particularly for urge incontinence and associated symptoms falling under the heading of “overactive bladder,” new drugs are always being developed and existing drugs can be found to have a potentially new application. Drugs recently added to those FDA-approved for urge incontinence have relied primarily on their anticholinergic effects. In contrast, tramadol, a drug FDA-approved for pain relief (marketed in the United States as Ultram), was tested for this use. Although the mechanism of action is unknown, the authors proposed a possible change in dopamine receptor activation.
Treated group improved, placebo group did not
Safarinejad MR, Hosseini SY. Safety and efficacy of tramadol in the treatment of idiopathic detrusor overactivity: a double-blind, placebo-controlled, randomized study. Br J Clin Pharmacol. 2006;61:456–463.
This randomized, placebo-controlled trial included 76 men and women with detrusor overactivity. The study population was relatively young, with mean ages of 39 and 37 years in the drug and placebo groups, respectively, and included about 2/3 women. At a sustained-release dose of 100 mg twice a day for 12 weeks of study, tramadol was effective for reducing the number of urge incontinence episodes per 24 hours from a baseline mean of 3.2 ±3.3 episodes to a mean of 1.6 ± 2.8 episodes. In addition, frequency of voiding per 24 hours was reduced (baseline mean 9.3 ± 3.2 episodes, to 5.1 ± 2.1) and the mean volume per void increased substantially (158 ± 32 mL, to 198 ± 76 mL) without an increase in postvoid residual urine volume.
In contrast to the results of many placebo-controlled drug trials and even with the use of 24-hour voiding diaries every 2 weeks for the 12-week study, the placebo group showed essentially no change in clinical and urodynamic outcomes. For example, the number of urge incontinence episodes per 24 hours was unchanged, from a baseline mean of 3.3 ± 3.1 episodes, to a mean of 3.1 ± 3.0 after 12 weeks. Nausea was the most commonly reported side effect (18% vs 5% in the drug and placebo groups, respectively); 2 of 35 participants in the tramadol group dropped out of the study due to nausea.
Confirmation of these results and further study may shed light on the complex control of normal voiding and the true etiology behind the symptoms that we call “detrusor overactivity,” and potentially open a new class of drugs for treatment.
Delivery mode and genetic influences on urinary incontinence
Rohr G, Kragstrup J, Gaist D, Christensen K. Genetic and environmental influences on urinary incontinence: a Danish population-based twin study of middle-aged and elderly women. Acta Obstet Gynecol Scand. 2004;83:978–982.
Goldberg RP, Abramov Y, Botros S, et al. Delivery mode is a major environmental determinant of stress urinary incontinence: results of the Evanston–Northwestern Twin Sisters Study. Am J Obstet Gynecol. 2005;193:2149–2153.
The genetic predisposition for urinary incontinence, seen in clinical practice as clustering in families—mothers, daughters, sisters—has been long suspected, and has been supported in recent studies of nature’s gift to genetic research—twins. In a study of more than 1,000 Danish twins in 2 age groups, Rohr et al were able to quantitatively estimate the heritable component for urinary incontinence, which was categorized by questionnaire into urge, mixed, and stress incontinence. The study included 548 monozygotic twin pairs (who share identical genetic material) and 620 dizygotic twin pairs (who, on average, share 50% of their genes like ordinary sisters).
Urge incontinence, in both age groups, had a similar level of heritability: 42% for ages 46–68 and 49% for ages 70–94.
Mixed incontinence had a lower level of heritability: 27% in middle age and 55% in the older group.
Stress incontinence in the older group had a significant heritable component at 39%, but stress incontinence in the middle-aged group was more strongly associated with environmental factors than with heritability.
Another study focused on stress incontinence in a study of 271 monozygotic twin pairs with a mean age of 47 years. Within the 173 parous twin pairs, environmental factors associated with stress incontinence were identified: age, parity, obesity, and mode of delivery.
Childbirth and genetic factors. These data clarify an important area of (apparently) inconsistent epidemiologic literature on the role of childbirth, and particularly mode of delivery, in lifetime risk of urinary incontinence. The inconsistency resolves once age of the study cohort and type of incontinence are considered. Stress incontinence is influenced most strongly by mode of delivery in middle-aged women. Later in life, genetic factors play a more important role in risk of stress incontinence, and mode of delivery becomes less important. Urge incontinence, perhaps developing along a different etiologic path than stress incontinence, is strongly influenced by heritability in both middle-aged and older women; environmental factors influencing the development of urge incontinence are less important through the lifespan.
Nonetheless, indications of a genetic component do not begin to tell us what exactly is affected that increases the likelihood of urinary incontinence. Speculation is easy enough—perhaps the inherent strength, elasticity, or regeneration potential of critically important tissues in the urethra and pelvis is affected—but the details are not yet fully known.
Again, until we have a clearer understanding, we must continue to manage incontinence with the tools of today.
The author reports no financial relationships.

Anne M. Weber, MD, MS
Program Officer, Female Pelvic
Floor Disorders Program,
Contraception and Reproductive
Health Branch, Center for
Population Research, National
Institute of Child Health
and Human Development,
National Institutes of Health,
Bethesda
Anne M. Weber, MD, MS
Program Officer, Female Pelvic
Floor Disorders Program,
Contraception and Reproductive
Health Branch, Center for
Population Research, National
Institute of Child Health
and Human Development,
National Institutes of Health,
Bethesda
Anne M. Weber, MD, MS
Program Officer, Female Pelvic
Floor Disorders Program,
Contraception and Reproductive
Health Branch, Center for
Population Research, National
Institute of Child Health
and Human Development,
National Institutes of Health,
Bethesda
Surgery for stress incontinence
Another year is drawing to a close and, looking back, what have we learned about urinary incontinence? A clear understanding of etiology stubbornly eludes us. How would a clear understanding of etiology affect management? It’s difficult to be specific until we actually do understand it, but generally:
The “multiple-hit” theory probably applies to urinary incontinence, too
The “multiple-hit” theory usually ascribed to cancer probably also fits the development of urinary incontinence, a likewise multifaceted condition. A woman begins life with genetic predisposition at some level that we cannot currently measure, but which is influenced by the environment (eg, nutrition, toxic exposures) and life events (eg, childbirth, aging)—all of which determine her likelihood of developing incontinence.
Until the time when we do have a clear understanding on which to base diagnosis, treatment, and prevention, of course, we must continue to manage incontinence with the tools of today.
A few pieces of the puzzle are slowly coming together.
Surgery for stress incontinence
Even as new surgical techniques or modifications continue to proliferate, evidence to guide clinical practice accumulates belatedly. MEDLINE lists 325 articles since 1996 (combining surgical mesh and urinary incontinence, limited to human females and published in English). Nonetheless, a consensus may be emerging that the safest synthetic material is monofilament polypropylene with pore size larger than 70 μm.
Unfortunately, by the time research reports are published showing higher complications with certain products, countless women have already been treated.
Mesh erosion (or exposure, extrusion), sometimes accompanied by infection, is a common complication when multifilament or small-pore meshes are used. Even worse, companies commonly withdraw products, modify them, and re-introduce them to the market, accompanied by intensive marketing but, as with the original product, without any real evidence of safety and effectiveness.
In an ideal world, clinicians (and patients) would insist on evidence before accepting new products and techniques. Failing that, clinicians (and patients!) should clearly understand that all new products and techniques are experimental until they are proven equal to or better than traditional techniques. As we have learned with the most subtle differences between synthetic materials, “almost the same” or “looks the same” is not the same.
Among the most important evidence on slings this year are reports of investigations that demonstrated what should not be done.
Are monofilament, large-pore mesh products safer?
Abdel-Fattah M, Sivanesan K, Ramsay I, Pringle S, Bjornsson S. How common are tape erosions? A comparison of two versions of the transobturator tension-free vaginal tape procedure. BJU Int. 2006;98:594–598.
Yamada BS, Govier FE, Stefanovic KB, Kobashi KC. High rate of vaginal erosions associated with the Mentor Obtape. J Urol. 2006;176:651–654.
Siegel AL, Kim M, Goldstein M, Levey S, Ilbeigi P. High incidence of vaginal mesh extrusion using the Intravaginal Slingplasty sling. J Urol. 2005;174:1308–1311.
The risk of vaginal erosion is much higher with synthetic meshes used for sling procedures when the mesh is multifilament and/or small-pore (<70 μm). In some cases, companies have replaced products (Mentor Obtape small-pore polypropylene sling product was replaced with macroporous Aris), whereas others continue to market products reported to have unacceptably high rates of vaginal erosion and mesh extrusion (Intravaginal Slingplasty multifilament mesh) (TABLE 1).
TABLE 1
Comparison of selected multifilament and small-pore mesh products
| REFERENCE | SLING PRODUCT | EROSION RATE | MANAGEMENT |
|---|---|---|---|
| Abdel-Fattah et al (2006) | Obtape | 7.3% (14 of 192) | 7: partial excision 7: complete excision with infection |
| TVT-O | 1.8% (2 of 112) | 1: partial excision 1: vaginal closure | |
| Yamada et al (2006) | Obtape | 13.4% (9 of 67) | 9: complete excision (1 with abscess) |
| Monarc | 0 of 56 | — | |
| Siegel et al (2005) | IVS | 17% (6 of 35) | 6: complete excision (1 with pelvic abscess) |
Avoid cadaveric fascia in sling procedures
Howden NS, Zyczynski HM, Moalli PA, Sagan ER, Meyn LA, Weber AM. Comparison of autologous rectus fascia and cadaveric fascia in pubovaginal sling continence outcomes. Am J Obstet Gynecol. 2006;194:1444–1449.
Evidence has accumulated that sling procedures performed with cadaveric fascia have substantially worse continence outcomes, compared with those using autologous fascia. In a retrospective cohort study of 150 women with cadaveric fascial slings and 153 women who had autologous rectus fascial slings, urinary incontinence (16 vs 5 per 100 women-years) and reoperation for stress incontinence (4 vs 1 per 100 women-years) occurred more frequently after cadaveric versus autologous rectus fascial slings.
Should xenograft materials be used in sling procedures?
Giri SK, Hickey JP, Sil D, et al. Long-term results of pubovaginal sling surgery using acellular cross-linked porcine dermis in the treatment of urodynamic stress incontinence. J Urol. 2006; 175:1788–1792.
Several companies market specific products integrated into sling techniques, such as In-First Ultra (porcine dermal matrix secured with bone anchors) and Stratasis (porcine small intestinal submucosa in urethral sling and tension-free versions). Other companies market only the xenograft for application in sling procedures, such as Pelvicol (acellular porcine collagen matrix). However, relatively little information is available to support or discourage use of xenograft materials in sling procedures.
Giri et al found worse outcomes using Pelvicol compared with autologous rectus fascia for pubovaginal slings. With 3-year follow-up, 54% (26 of 48 women) with Pelvicol were considered successfully cured or improved, compared with 80.4% (37 of 46 women) with rectus fascia. Of interest, women continued to report recurrent incontinence with Pelvicol through the 3-year period, whereas women with rectus fascia had recurrence within the first 9 months after surgery.
Midurethral slings: Retropubic or transobturator?
Waltregny D, Reul O, Mathantu B, Gaspar Y, Bonnet P, de Leval J. Inside out transobturator vaginal tape for the treatment of female stress urinary incontinence: interim results of a prospective study after a 1-year minimum followup. J Urol. 2006;175:2191–2195.
Morey AF, Medendorp AR, Noller MW, et al. Transobturator versus transabdominal midurethral slings: a multi-institutional comparison of obstructive voiding complications. J Urol. 2006;175:1014–1017.
Midurethral sling placement was modified from the retropubic to the obturator approach with the objective of reducing the risk of major bladder and urethral injury and vascular complications. Does the obturator approach actually have fewer intraoperative complications compared with the retropubic approach? Unknown. (As noted below, even within retropubic procedures, it is possible—although currently unknown—that vaginal and abdominal approaches have different complication rates.) This is a good news–bad news problem:
Results of the obturator approach are beginning to appear in the literature as case series and uncontrolled comparative studies. Waltregney et al reported cure of stress incontinence in 91% of 99 patients after 1 year of follow-up. Morey et al reported similar continence outcomes: 89% success for 154 patients after the obturator approach compared with 86% success for 350 patients after the abdominal approach, although follow-up in the abdominal group was substantially longer (mean 20 months, range 18–26) than in the obturator group (mean 9 months, range 6–16). Of interest, urethrolysis was performed more frequently in the abdominal group (2.3%) than in the obturator group (0%).
Randomized trials are necessary to obtain unbiased comparisons of techniques. Investigators in the NIH-sponsored Urinary Incontinence Treatment Network are currently performing a randomized trial comparing obturator and abdominal approaches with midurethral slings for women with stress and stress-predominant mixed incontinence. The primary outcome will compare objective and subjective treatment success between the 2 groups at 1 and 2 years after surgery. Enrollment is expected to be complete by early 2008, and 1-year follow-up by early 2009. Stay tuned for the results!
Retropubic midurethral slings: Which brand?
Gandhi S, Abramov Y, Kwon C, et al. TVT versus SPARC: comparison of outcomes for two midurethral tape procedures. Int Urogynecol J Pelvic Floor Dysfunct. 2006;17:125–130.
Lord HE, Taylor JD, Finn JC, et al. A randomized controlled equivalence trial of short-term complications and efficacy of tension-free vaginal tape and suprapubic urethral support sling for treating stress incontinence. BJU Int. 2006;98:367–376.
As the first midurethral sling, the tension-free vaginal tape (Gynecare TVT) has the most evidence and longest follow-up available in the literature. It was originally described using the vaginal approach (“bottom-up”); the company now markets all 3 approaches: vaginal, abdominal (“top-down”), and obturator. Other companies market different products along the same lines, but it cannot be assumed that midurethral slings are interchangeable. Studies are starting to appear that compare different retropubic midurethral slings. In a retrospective case series (Gandhi et al) and a randomized trial (Lord et al), Gynecare TVT had better continence outcomes compared with SPARC (TABLE 2).
TABLE 2
Comparison of 2 retropubic midurethral slings
| OUTCOMES | GYNECARE TVT | SPARC | STATISTICAL SIGNIFICANCE |
|---|---|---|---|
| Subjective continence | |||
| Series by Gandhi et al | 86% (61 of 71) | 60% (28 of 47) | 0.001 |
| RCT by Lord et al | 87% (128 of 147) | 76% (117 of 153) | 0.03 |
| Objective stress continence | |||
| Series by Gandhi et al | 95% (58 of 61) | 70% (32 of 46) | <0.001 |
| RCT by Lord et al | 97.3% (143 of 147) | 97.4% (148 of 152) | NS |
| Follow-up | |||
| Series by Gandhi et al (median, range) | 17 weeks (6–197) | 16 weeks (6–129) | — |
| RCT by Lord et al | 6 weeks | 6 weeks | — |
| Retention requiring reoperation | |||
| Series by Gandhi et al | 2.7% (2 of 73) | 2.0% (1 of 49) | NS |
| RCT by Lord et al | 0 of 147 | 6.5% (10 of 154) | 0.002 |
| Mesh erosions* | |||
| RCT by Lord et al | 4.8% (7 of 147) | 10.5% (16 of 152) | 0.08 |
| *Mesh erosions not reported in Gandhi et al. | |||
Particularly for urge incontinence and associated symptoms falling under the heading of “overactive bladder,” new drugs are always being developed and existing drugs can be found to have a potentially new application. Drugs recently added to those FDA-approved for urge incontinence have relied primarily on their anticholinergic effects. In contrast, tramadol, a drug FDA-approved for pain relief (marketed in the United States as Ultram), was tested for this use. Although the mechanism of action is unknown, the authors proposed a possible change in dopamine receptor activation.
Treated group improved, placebo group did not
Safarinejad MR, Hosseini SY. Safety and efficacy of tramadol in the treatment of idiopathic detrusor overactivity: a double-blind, placebo-controlled, randomized study. Br J Clin Pharmacol. 2006;61:456–463.
This randomized, placebo-controlled trial included 76 men and women with detrusor overactivity. The study population was relatively young, with mean ages of 39 and 37 years in the drug and placebo groups, respectively, and included about 2/3 women. At a sustained-release dose of 100 mg twice a day for 12 weeks of study, tramadol was effective for reducing the number of urge incontinence episodes per 24 hours from a baseline mean of 3.2 ±3.3 episodes to a mean of 1.6 ± 2.8 episodes. In addition, frequency of voiding per 24 hours was reduced (baseline mean 9.3 ± 3.2 episodes, to 5.1 ± 2.1) and the mean volume per void increased substantially (158 ± 32 mL, to 198 ± 76 mL) without an increase in postvoid residual urine volume.
In contrast to the results of many placebo-controlled drug trials and even with the use of 24-hour voiding diaries every 2 weeks for the 12-week study, the placebo group showed essentially no change in clinical and urodynamic outcomes. For example, the number of urge incontinence episodes per 24 hours was unchanged, from a baseline mean of 3.3 ± 3.1 episodes, to a mean of 3.1 ± 3.0 after 12 weeks. Nausea was the most commonly reported side effect (18% vs 5% in the drug and placebo groups, respectively); 2 of 35 participants in the tramadol group dropped out of the study due to nausea.
Confirmation of these results and further study may shed light on the complex control of normal voiding and the true etiology behind the symptoms that we call “detrusor overactivity,” and potentially open a new class of drugs for treatment.
Delivery mode and genetic influences on urinary incontinence
Rohr G, Kragstrup J, Gaist D, Christensen K. Genetic and environmental influences on urinary incontinence: a Danish population-based twin study of middle-aged and elderly women. Acta Obstet Gynecol Scand. 2004;83:978–982.
Goldberg RP, Abramov Y, Botros S, et al. Delivery mode is a major environmental determinant of stress urinary incontinence: results of the Evanston–Northwestern Twin Sisters Study. Am J Obstet Gynecol. 2005;193:2149–2153.
The genetic predisposition for urinary incontinence, seen in clinical practice as clustering in families—mothers, daughters, sisters—has been long suspected, and has been supported in recent studies of nature’s gift to genetic research—twins. In a study of more than 1,000 Danish twins in 2 age groups, Rohr et al were able to quantitatively estimate the heritable component for urinary incontinence, which was categorized by questionnaire into urge, mixed, and stress incontinence. The study included 548 monozygotic twin pairs (who share identical genetic material) and 620 dizygotic twin pairs (who, on average, share 50% of their genes like ordinary sisters).
Urge incontinence, in both age groups, had a similar level of heritability: 42% for ages 46–68 and 49% for ages 70–94.
Mixed incontinence had a lower level of heritability: 27% in middle age and 55% in the older group.
Stress incontinence in the older group had a significant heritable component at 39%, but stress incontinence in the middle-aged group was more strongly associated with environmental factors than with heritability.
Another study focused on stress incontinence in a study of 271 monozygotic twin pairs with a mean age of 47 years. Within the 173 parous twin pairs, environmental factors associated with stress incontinence were identified: age, parity, obesity, and mode of delivery.
Childbirth and genetic factors. These data clarify an important area of (apparently) inconsistent epidemiologic literature on the role of childbirth, and particularly mode of delivery, in lifetime risk of urinary incontinence. The inconsistency resolves once age of the study cohort and type of incontinence are considered. Stress incontinence is influenced most strongly by mode of delivery in middle-aged women. Later in life, genetic factors play a more important role in risk of stress incontinence, and mode of delivery becomes less important. Urge incontinence, perhaps developing along a different etiologic path than stress incontinence, is strongly influenced by heritability in both middle-aged and older women; environmental factors influencing the development of urge incontinence are less important through the lifespan.
Nonetheless, indications of a genetic component do not begin to tell us what exactly is affected that increases the likelihood of urinary incontinence. Speculation is easy enough—perhaps the inherent strength, elasticity, or regeneration potential of critically important tissues in the urethra and pelvis is affected—but the details are not yet fully known.
Again, until we have a clearer understanding, we must continue to manage incontinence with the tools of today.
Surgery for stress incontinence
Another year is drawing to a close and, looking back, what have we learned about urinary incontinence? A clear understanding of etiology stubbornly eludes us. How would a clear understanding of etiology affect management? It’s difficult to be specific until we actually do understand it, but generally:
The “multiple-hit” theory probably applies to urinary incontinence, too
The “multiple-hit” theory usually ascribed to cancer probably also fits the development of urinary incontinence, a likewise multifaceted condition. A woman begins life with genetic predisposition at some level that we cannot currently measure, but which is influenced by the environment (eg, nutrition, toxic exposures) and life events (eg, childbirth, aging)—all of which determine her likelihood of developing incontinence.
Until the time when we do have a clear understanding on which to base diagnosis, treatment, and prevention, of course, we must continue to manage incontinence with the tools of today.
A few pieces of the puzzle are slowly coming together.
Surgery for stress incontinence
Even as new surgical techniques or modifications continue to proliferate, evidence to guide clinical practice accumulates belatedly. MEDLINE lists 325 articles since 1996 (combining surgical mesh and urinary incontinence, limited to human females and published in English). Nonetheless, a consensus may be emerging that the safest synthetic material is monofilament polypropylene with pore size larger than 70 μm.
Unfortunately, by the time research reports are published showing higher complications with certain products, countless women have already been treated.
Mesh erosion (or exposure, extrusion), sometimes accompanied by infection, is a common complication when multifilament or small-pore meshes are used. Even worse, companies commonly withdraw products, modify them, and re-introduce them to the market, accompanied by intensive marketing but, as with the original product, without any real evidence of safety and effectiveness.
In an ideal world, clinicians (and patients) would insist on evidence before accepting new products and techniques. Failing that, clinicians (and patients!) should clearly understand that all new products and techniques are experimental until they are proven equal to or better than traditional techniques. As we have learned with the most subtle differences between synthetic materials, “almost the same” or “looks the same” is not the same.
Among the most important evidence on slings this year are reports of investigations that demonstrated what should not be done.
Are monofilament, large-pore mesh products safer?
Abdel-Fattah M, Sivanesan K, Ramsay I, Pringle S, Bjornsson S. How common are tape erosions? A comparison of two versions of the transobturator tension-free vaginal tape procedure. BJU Int. 2006;98:594–598.
Yamada BS, Govier FE, Stefanovic KB, Kobashi KC. High rate of vaginal erosions associated with the Mentor Obtape. J Urol. 2006;176:651–654.
Siegel AL, Kim M, Goldstein M, Levey S, Ilbeigi P. High incidence of vaginal mesh extrusion using the Intravaginal Slingplasty sling. J Urol. 2005;174:1308–1311.
The risk of vaginal erosion is much higher with synthetic meshes used for sling procedures when the mesh is multifilament and/or small-pore (<70 μm). In some cases, companies have replaced products (Mentor Obtape small-pore polypropylene sling product was replaced with macroporous Aris), whereas others continue to market products reported to have unacceptably high rates of vaginal erosion and mesh extrusion (Intravaginal Slingplasty multifilament mesh) (TABLE 1).
TABLE 1
Comparison of selected multifilament and small-pore mesh products
| REFERENCE | SLING PRODUCT | EROSION RATE | MANAGEMENT |
|---|---|---|---|
| Abdel-Fattah et al (2006) | Obtape | 7.3% (14 of 192) | 7: partial excision 7: complete excision with infection |
| TVT-O | 1.8% (2 of 112) | 1: partial excision 1: vaginal closure | |
| Yamada et al (2006) | Obtape | 13.4% (9 of 67) | 9: complete excision (1 with abscess) |
| Monarc | 0 of 56 | — | |
| Siegel et al (2005) | IVS | 17% (6 of 35) | 6: complete excision (1 with pelvic abscess) |
Avoid cadaveric fascia in sling procedures
Howden NS, Zyczynski HM, Moalli PA, Sagan ER, Meyn LA, Weber AM. Comparison of autologous rectus fascia and cadaveric fascia in pubovaginal sling continence outcomes. Am J Obstet Gynecol. 2006;194:1444–1449.
Evidence has accumulated that sling procedures performed with cadaveric fascia have substantially worse continence outcomes, compared with those using autologous fascia. In a retrospective cohort study of 150 women with cadaveric fascial slings and 153 women who had autologous rectus fascial slings, urinary incontinence (16 vs 5 per 100 women-years) and reoperation for stress incontinence (4 vs 1 per 100 women-years) occurred more frequently after cadaveric versus autologous rectus fascial slings.
Should xenograft materials be used in sling procedures?
Giri SK, Hickey JP, Sil D, et al. Long-term results of pubovaginal sling surgery using acellular cross-linked porcine dermis in the treatment of urodynamic stress incontinence. J Urol. 2006; 175:1788–1792.
Several companies market specific products integrated into sling techniques, such as In-First Ultra (porcine dermal matrix secured with bone anchors) and Stratasis (porcine small intestinal submucosa in urethral sling and tension-free versions). Other companies market only the xenograft for application in sling procedures, such as Pelvicol (acellular porcine collagen matrix). However, relatively little information is available to support or discourage use of xenograft materials in sling procedures.
Giri et al found worse outcomes using Pelvicol compared with autologous rectus fascia for pubovaginal slings. With 3-year follow-up, 54% (26 of 48 women) with Pelvicol were considered successfully cured or improved, compared with 80.4% (37 of 46 women) with rectus fascia. Of interest, women continued to report recurrent incontinence with Pelvicol through the 3-year period, whereas women with rectus fascia had recurrence within the first 9 months after surgery.
Midurethral slings: Retropubic or transobturator?
Waltregny D, Reul O, Mathantu B, Gaspar Y, Bonnet P, de Leval J. Inside out transobturator vaginal tape for the treatment of female stress urinary incontinence: interim results of a prospective study after a 1-year minimum followup. J Urol. 2006;175:2191–2195.
Morey AF, Medendorp AR, Noller MW, et al. Transobturator versus transabdominal midurethral slings: a multi-institutional comparison of obstructive voiding complications. J Urol. 2006;175:1014–1017.
Midurethral sling placement was modified from the retropubic to the obturator approach with the objective of reducing the risk of major bladder and urethral injury and vascular complications. Does the obturator approach actually have fewer intraoperative complications compared with the retropubic approach? Unknown. (As noted below, even within retropubic procedures, it is possible—although currently unknown—that vaginal and abdominal approaches have different complication rates.) This is a good news–bad news problem:
Results of the obturator approach are beginning to appear in the literature as case series and uncontrolled comparative studies. Waltregney et al reported cure of stress incontinence in 91% of 99 patients after 1 year of follow-up. Morey et al reported similar continence outcomes: 89% success for 154 patients after the obturator approach compared with 86% success for 350 patients after the abdominal approach, although follow-up in the abdominal group was substantially longer (mean 20 months, range 18–26) than in the obturator group (mean 9 months, range 6–16). Of interest, urethrolysis was performed more frequently in the abdominal group (2.3%) than in the obturator group (0%).
Randomized trials are necessary to obtain unbiased comparisons of techniques. Investigators in the NIH-sponsored Urinary Incontinence Treatment Network are currently performing a randomized trial comparing obturator and abdominal approaches with midurethral slings for women with stress and stress-predominant mixed incontinence. The primary outcome will compare objective and subjective treatment success between the 2 groups at 1 and 2 years after surgery. Enrollment is expected to be complete by early 2008, and 1-year follow-up by early 2009. Stay tuned for the results!
Retropubic midurethral slings: Which brand?
Gandhi S, Abramov Y, Kwon C, et al. TVT versus SPARC: comparison of outcomes for two midurethral tape procedures. Int Urogynecol J Pelvic Floor Dysfunct. 2006;17:125–130.
Lord HE, Taylor JD, Finn JC, et al. A randomized controlled equivalence trial of short-term complications and efficacy of tension-free vaginal tape and suprapubic urethral support sling for treating stress incontinence. BJU Int. 2006;98:367–376.
As the first midurethral sling, the tension-free vaginal tape (Gynecare TVT) has the most evidence and longest follow-up available in the literature. It was originally described using the vaginal approach (“bottom-up”); the company now markets all 3 approaches: vaginal, abdominal (“top-down”), and obturator. Other companies market different products along the same lines, but it cannot be assumed that midurethral slings are interchangeable. Studies are starting to appear that compare different retropubic midurethral slings. In a retrospective case series (Gandhi et al) and a randomized trial (Lord et al), Gynecare TVT had better continence outcomes compared with SPARC (TABLE 2).
TABLE 2
Comparison of 2 retropubic midurethral slings
| OUTCOMES | GYNECARE TVT | SPARC | STATISTICAL SIGNIFICANCE |
|---|---|---|---|
| Subjective continence | |||
| Series by Gandhi et al | 86% (61 of 71) | 60% (28 of 47) | 0.001 |
| RCT by Lord et al | 87% (128 of 147) | 76% (117 of 153) | 0.03 |
| Objective stress continence | |||
| Series by Gandhi et al | 95% (58 of 61) | 70% (32 of 46) | <0.001 |
| RCT by Lord et al | 97.3% (143 of 147) | 97.4% (148 of 152) | NS |
| Follow-up | |||
| Series by Gandhi et al (median, range) | 17 weeks (6–197) | 16 weeks (6–129) | — |
| RCT by Lord et al | 6 weeks | 6 weeks | — |
| Retention requiring reoperation | |||
| Series by Gandhi et al | 2.7% (2 of 73) | 2.0% (1 of 49) | NS |
| RCT by Lord et al | 0 of 147 | 6.5% (10 of 154) | 0.002 |
| Mesh erosions* | |||
| RCT by Lord et al | 4.8% (7 of 147) | 10.5% (16 of 152) | 0.08 |
| *Mesh erosions not reported in Gandhi et al. | |||
Particularly for urge incontinence and associated symptoms falling under the heading of “overactive bladder,” new drugs are always being developed and existing drugs can be found to have a potentially new application. Drugs recently added to those FDA-approved for urge incontinence have relied primarily on their anticholinergic effects. In contrast, tramadol, a drug FDA-approved for pain relief (marketed in the United States as Ultram), was tested for this use. Although the mechanism of action is unknown, the authors proposed a possible change in dopamine receptor activation.
Treated group improved, placebo group did not
Safarinejad MR, Hosseini SY. Safety and efficacy of tramadol in the treatment of idiopathic detrusor overactivity: a double-blind, placebo-controlled, randomized study. Br J Clin Pharmacol. 2006;61:456–463.
This randomized, placebo-controlled trial included 76 men and women with detrusor overactivity. The study population was relatively young, with mean ages of 39 and 37 years in the drug and placebo groups, respectively, and included about 2/3 women. At a sustained-release dose of 100 mg twice a day for 12 weeks of study, tramadol was effective for reducing the number of urge incontinence episodes per 24 hours from a baseline mean of 3.2 ±3.3 episodes to a mean of 1.6 ± 2.8 episodes. In addition, frequency of voiding per 24 hours was reduced (baseline mean 9.3 ± 3.2 episodes, to 5.1 ± 2.1) and the mean volume per void increased substantially (158 ± 32 mL, to 198 ± 76 mL) without an increase in postvoid residual urine volume.
In contrast to the results of many placebo-controlled drug trials and even with the use of 24-hour voiding diaries every 2 weeks for the 12-week study, the placebo group showed essentially no change in clinical and urodynamic outcomes. For example, the number of urge incontinence episodes per 24 hours was unchanged, from a baseline mean of 3.3 ± 3.1 episodes, to a mean of 3.1 ± 3.0 after 12 weeks. Nausea was the most commonly reported side effect (18% vs 5% in the drug and placebo groups, respectively); 2 of 35 participants in the tramadol group dropped out of the study due to nausea.
Confirmation of these results and further study may shed light on the complex control of normal voiding and the true etiology behind the symptoms that we call “detrusor overactivity,” and potentially open a new class of drugs for treatment.
Delivery mode and genetic influences on urinary incontinence
Rohr G, Kragstrup J, Gaist D, Christensen K. Genetic and environmental influences on urinary incontinence: a Danish population-based twin study of middle-aged and elderly women. Acta Obstet Gynecol Scand. 2004;83:978–982.
Goldberg RP, Abramov Y, Botros S, et al. Delivery mode is a major environmental determinant of stress urinary incontinence: results of the Evanston–Northwestern Twin Sisters Study. Am J Obstet Gynecol. 2005;193:2149–2153.
The genetic predisposition for urinary incontinence, seen in clinical practice as clustering in families—mothers, daughters, sisters—has been long suspected, and has been supported in recent studies of nature’s gift to genetic research—twins. In a study of more than 1,000 Danish twins in 2 age groups, Rohr et al were able to quantitatively estimate the heritable component for urinary incontinence, which was categorized by questionnaire into urge, mixed, and stress incontinence. The study included 548 monozygotic twin pairs (who share identical genetic material) and 620 dizygotic twin pairs (who, on average, share 50% of their genes like ordinary sisters).
Urge incontinence, in both age groups, had a similar level of heritability: 42% for ages 46–68 and 49% for ages 70–94.
Mixed incontinence had a lower level of heritability: 27% in middle age and 55% in the older group.
Stress incontinence in the older group had a significant heritable component at 39%, but stress incontinence in the middle-aged group was more strongly associated with environmental factors than with heritability.
Another study focused on stress incontinence in a study of 271 monozygotic twin pairs with a mean age of 47 years. Within the 173 parous twin pairs, environmental factors associated with stress incontinence were identified: age, parity, obesity, and mode of delivery.
Childbirth and genetic factors. These data clarify an important area of (apparently) inconsistent epidemiologic literature on the role of childbirth, and particularly mode of delivery, in lifetime risk of urinary incontinence. The inconsistency resolves once age of the study cohort and type of incontinence are considered. Stress incontinence is influenced most strongly by mode of delivery in middle-aged women. Later in life, genetic factors play a more important role in risk of stress incontinence, and mode of delivery becomes less important. Urge incontinence, perhaps developing along a different etiologic path than stress incontinence, is strongly influenced by heritability in both middle-aged and older women; environmental factors influencing the development of urge incontinence are less important through the lifespan.
Nonetheless, indications of a genetic component do not begin to tell us what exactly is affected that increases the likelihood of urinary incontinence. Speculation is easy enough—perhaps the inherent strength, elasticity, or regeneration potential of critically important tissues in the urethra and pelvis is affected—but the details are not yet fully known.
Again, until we have a clearer understanding, we must continue to manage incontinence with the tools of today.
The author reports no financial relationships.
The author reports no financial relationships.
Noninvasive vulvar lesions: An illustrated guide to diagnosis and treatment
CASE Postmenopausal dyspareunia
A 60-year-old widow who recently remarried complains of dyspareunia. Examination of the vulva reveals firm but thin white skin over the periclitoral area and labia minora and shrinking of the vulvar skin.
What is the likely diagnosis?
Lichen sclerosus is the probable diagnosis, given her age and the appearance of the vulva, although it is impossible to assure the diagnosis without a biopsy. The preferred treatment is clobetasol, an ultrapotent steroid, applied daily.
True, powerful steroids can cause atrophy if applied regularly to other areas of the skin, but clobetasol does not cause atrophy of vulvar skin. After several weeks of nightly application, the skin should be softer and more pliable, and dyspareunia should be resolved. The patient can then reduce the clobetasol application to twice weekly—but she must continue the treatment indefinitely.
The vulva over the lifespan
The vulva is sensitive to both physiologic and pathologic changes, as well as to the sex hormones that govern the menstrual cycle. The mucosa on the inner aspects of the labia minora is very similar to the skin of the vagina and thus very sensitive to estrogen. The skin of the labia majora and the outer surface of the labia minora is more consistent with hair-bearing skin in the perineal area and more sensitive to androgens, which help thicken the skin. At menopause, the loss of estrogen leads to atrophy, and the vulvar epithelium is reduced to a few layers of mostly intermediate and parabasal cell types. The labia minora and majora as well as the clitoris gradually become less prominent with age.
The skin of the vulva consists of both dermis and epidermis, which interact with each other and respond to different nutritional and hormonal influences. For example, estrogen has little effect on vulvar epidermis, but considerable effect on the dermis, thickening the skin and preventing atrophy.
Postmenopausal atrophic changes can become a clinical problem when a woman resumes sexual intercourse after a long period of abstinence, as in the opening case. If atrophy is the main complaint, estrogen replacement therapy will alleviate symptoms of tightness, irritation, and dyspareunia, but it may take 6 weeks to 6 months to achieve optimal results. In the interim, women need to be reassured that reasonable function can be achieved.
Hygienic considerations
With any vulvar irritation, the patient should discontinue the use of synthetic undergarments in favor of cotton panties, which permit more adequate circulation and do not trap moisture.
Sitz baths often help relieve local discomfort, but should be followed by thorough drying.
The new ACOG Committee Opinion reflects recommendations of the American Society for Colposcopy and Cervical Pathology.17
Vulvodynia. American College of Obstetricians and Gynecologists Committee Opinion No. 345. Obstet Gynecol. October 2006;108:1049–1052.
Vulvar dystrophies: Think “white”
In the past, these diseases have been defined as non-neoplastic epithelial disorders of the vulva. Although there have been many attempts to more accurately define vulvar dystrophies, none have completely described the wide variety of clinical presentations.
In general, dystrophies are disorders of epithelial growth and nutrition that often result in a white surface color change. This definition includes intraepithelial neoplasia and Paget’s disease of the vulva. The International Society for the Study of Vulvovaginal Disease has proposed multiple classifications since 1975. I prefer the clarity of the 1987 classification system.1 I also consider these terms out-of-date: lichen sclerosus et atrophicus, carcinoma simplex, leukoplakic vulvitis, leukoplakia, hyperplastic vulvitis, neurodermatitis, kraurosis vulvae, leukokeratosis, erythroplasia of Queyrat, and Bowen’s disease.
What makes the lesions white?
The white appearance of dystrophic lesions is due to excessive keratin, at times deep pigmentation, and relative avascularity. All 3 of these characteristics are present in the spectrum of vulvar dystrophies. Biopsy of the affected skin is the key to accurate diagnosis and successful therapy.
Lichen sclerosus
Does not raise risk of carcinoma
The most common of the 3 groups of white lesions described in the 1987 classification of dystrophies, lichen sclerosus usually occurs in postmenopausal women, but can appear at any age, including childhood (FIGURE 1). Despite claims to the contrary, there is no good evidence that women with lichen sclerosus face a higher risk for vulvar carcinoma.
FIGURE 1
Lichen sclerosus affects all ages
3-year-old child. Note the inflammation secondary to excoriations.
20-year-old woman. The glans clitoris has begun the hooding process.
70-year-old woman. The introitus has shrunk, making intercourse impossible.
Signs and symptoms
In lichen sclerosus, the skin of the vulva appears very thin, atrophic, and dry, resembling parchment. It is also white, with loss of pigmentation.
Pruritus is the most common symptom and is usually the presenting symptom. Scratching during sleep may create ulcerations and areas of ecchymosis, and there is generalized shrinking of the vulvar skin, with eventual loss of the labia minora.
The edema and shrinking that occur around the clitoris cause a “hooding” of the glans clitoris. If the process continues unchecked, it can involve the labia majora as well as the skin of the inner thigh and anal region.
Prescribe clobetasol ointment
The patient should be instructed to use clobetasol 0.05% ointment on a continuing basis. This drug is so successful it has eclipsed the use of testosterone propionate for this indication. Lorenz and colleagues2 found very high success rates in 81 symptomatic patients with biopsy-proven disease who had failed previous therapy.
For reasons that are unknown, persistent use of this steroid on vulvar skin does not cause the atrophy commonly seen with prolonged use of high-potency steroids on other areas of the skin.
Start with twice-daily application and taper to less frequent use as the symptoms come under control. Most patients in remission can be maintained with twice-weekly application. Pruritus should disappear completely, and the skin itself will become less “leathery.”
Surgical treatment is not advised
Surgery does not appear to have a role because lichen sclerosus often recurs outside excised areas. Several reports have even described the return of disease in skin grafts used to replace large diseased areas.
I do not recommend surgery except in dire circumstances, when symptom relief is essential to the patient’s quality of life and all other therapies have failed.
Squamous cell hyperplasia
This disease is probably the same entity as lichen simplex chronicus. Changes in vulvar skin appear to result from chronic scratching secondary to intense pruritus. This complaint often involves a vicious cycle of scratching, increased pruritus, and more scratching, until excoriations occur. The aim of therapy is to eliminate the pruritus (FIGURE 2).

FIGURE 2
Squamous cell hyperplasia
75-year-old woman. The skin is thickened and may be leathery.
Intense pruritus and aggressive scratching lead to excoriations.
Signs and symptoms
Vulvar skin is typically white or pink. Biopsy will confirm the diagnosis, revealing a markedly thickened keratin layer (hyperkeratosis) and irregular thickening of the Malpighian ridges (acanthosis).
Inflammatory changes are also present, especially when there are areas of excoriation.
Treatment is similar to therapy for lichen sclerosus
Potent topical corticosteroids are the backbone of treatment; clobetasol is the preferred drug. The frequency of application is identical to that described for lichen sclerosus, and response to therapy usually takes 2 months. In the interim, it is advisable to prescribe other medications for the pruritus.
Lichen sclerosus and squamous cell hyperplasia sometimes coincide. Fortunately, the therapies are quite similar and both conditions tend to respond.
Vulvodynia
This disorder consists of chronic vulvar discomfort due to itching, burning, and/or pain that causes physical, sexual, and psychological distress.3,4 Once referred to as essential vulvodynia, it now is defined as generalized vulvar dysesthesia.
Signs and symptoms
Women with this condition tend to have difficulty localizing their pain. They often present with a complaint of recurrent yeast infection or constant irritation at the introitus. Dyspareunia may or may not be a presenting symptom, although intercourse often triggers this condition. Tight pants or rough undergarments also may trigger symptoms.
Common symptoms. In a study by Sadownik,5 women with vulvar dysesthesia reported the following symptoms:
Women with vulvar dysesthesia who appear to have urinary tract symptoms should undergo a urine culture, though it will often be negative and antibiotic therapy will have little effect.
A diagnosis of exclusion
The pain of dysesthesia appears to be neuropathic in origin in that it mimics pain of the sensory nervous system. It may be diffuse or focal, unilateral or bilateral, constant or sporadic. Thus, it is a diagnosis of exclusion.
Recommended therapies
Vulvar dysesthesia should be regarded as a chronic pain syndrome and treated accordingly, with emphasis on generalized improvements in health and attitude rather than single-therapy approaches.
Potent topical corticosteroids are usually of no benefit. Nor does topical estrogen produce long-term relief.
Once all possible causes of symptoms are excluded, refer the patient for education, support, and treatment of depression, if present. Occasionally, topical anesthetics will provide short-term relief.
At least 2 vulvar pain societies—the National Vulvodynia Association and the Vulvar Pain Foundation—have newsletters, outreach programs, and Web sites.
Vulvar vestibulitis
A more readily definable condition in the same category as vulvodynia is so-called vulvar vestibulitis, also known as localized vulvodynia (as classified by the new ACOG Committee Opinion on vulvodynia).
Signs and symptoms
The defining presentation is severe pain on vestibular touch (eg, entry at intercourse), with tenderness to pressure localized within the vulvar vestibule in a horseshoe distribution pattern encompassing 3, 6, and 9 o’clock on the vestibule. Erythema is often present, especially at the 5 and 7 o’clock positions (FIGURE 3).
Patients have no symptoms during normal daily activities, but complain of dyspareunia and an inability to use tampons.
FIGURE 3
Vestibular adenitis
Intense erythema at the 5 o’clock position in the vestibule.
Diagnostic strategies
Vulvar vestibulitis can be diagnosed using a moistened cotton-tip applicator. Pressure applied in the area of the urethral meatus will result in minimal discomfort, but pressure in the horseshoe area of the vestibule will cause exquisite discomfort.
Careful inspection at 5 and 7 o’clock in the vestibule usually uncovers intense erythema over an area of 4 or 5 mm. To distinguish vestibulitis from dysesthesia, see the comparison in TABLE 1.
TABLE 1
Distinguishing vulvar vestibulitis and dysesthesia
| VULVAR VESTIBULITIS | ESSENTIAL VULVAR DYSESTHESIA |
|---|---|
| Pain is usually not constant | Pain is a constant burning sensation |
| Erythema in sensitive areas | No erythema or abnormal appearance |
| Lidocaine quells sensitivity | Lidocaine has no effect |
| Cause is dermal inflammation | Cause is allodynia (heightened nerve sensitivity) |
Recommended therapies
Treatment of vulvar vestibulitis is complex. It is important to see the patient often to ensure that this syndrome is truly present rather than vulvar dysesthesia. Xylocaine jelly should be given in an attempt to relieve symptoms; topical steroid ointments are another option.
Women with persistent symptoms are difficult to treat medically. Earlier theories pointing to infection as the cause of vestibulitis have been discounted.
Some experts believe that foods containing oxalates precipitate these symptoms. It may be advisable to have the patient reduce the content of oxalates in her diet in an effort to address all possible remedies.
For refractory cases, consider surgery
Consider surgical removal of the tender vestibule if all other therapies fail to provide adequate relief. Surgery for this indication has a high success rate (TABLE 2).7
Some surgeons have attempted treatment with laser ablation, but most have found excision more satisfactory, with faster recovery and excellent cosmesis.
Schneider and colleagues8 had 69 women complete a questionnaire 6 months after surgery, 54 (78%) of whom replied. Moderate to excellent improvement was reported by 45 women (83%); 7 had repeat surgery, after which 4 improved.
TABLE 2
Impressive track record for surgical treatment of vestibulitis
| % RESPONSE | |||
|---|---|---|---|
| STUDY | COMPLETE | PARTIAL | NONE |
| Bornstein et al7 | 76 | 24 | 0 |
| Bergeron et al12 | 63 | 37 | 0 |
| Kehoe and Luesley13 | 60 | 29 | 11 |
| Mann et al14 | 66 | 21 | 13 |
| Schover et al15 | 47 | 37 | 16 |
| Marinoff and Turner16 | 82 | 15 | 3 |
| Adapted from Bornstein et al7 | |||
Pigmented lesions
Are they cancer precursors?
Precursors of malignant melanoma of the vulva have yet to be clearly defined. The majority of these melanomas appear to arise de novo; however, some are associated with precursor nevi, especially junctional nevi. The 3 most common types of nevi that appear on the vulva are:
Assessing malignant potential
Only a small number of dysplastic nevi progress to malignant melanoma, but the frequency increases when the dysplastic nevus is familial and not acquired.
In general, the more severe the dysplasia, the greater the likelihood it will progress to malignancy. In dysplastic nevi, the pattern and appearance of the melanocytic cells are atypical. Bridging of melanocytic clusters of atypical cells may occur. Often, the atypical melanocytes are varied in size and shape, increasing in cell and nuclear size as severity increases. In the most severe cases, nucleoli are very prominent.
Many pigmented lesions of the vulva are lentigines, similar to freckles. Distinguishing one pigmented lesion from another is difficult even with magnification, and the clinician often must decide whether or not to biopsy. One set of guidelines recommends excisional biopsy of vulvar nevi when there is a change in:
Note that a reddish lesion may be basal cell hyperplasia, which has been associated with the development of basal cell carcinoma (FIGURE 4).

FIGURE 4
Basal cell carcinoma
An uncommon type of vulvar cancer, this tumor rarely metastasizes.
Premalignant lesions of squamous epithelium
The variable appearance of vulvar intraepithelial neoplasia (VIN) necessitates the liberal use of diagnostic biopsies, particularly when lesions persist or recur. VIN can present as a white lesion, or as pseudopigmented, pink, or raised and eroded.
Cigarette smoking is a risk factor.
Clinical appearance
Macroscopically, VIN lesions are often multiple and appear slightly raised and papular. Hyper- or pseudopigmented lesions are seen in about 30% of cases.
A confluence of VIN can create an appearance of diffuse plaques. In VIN, as for CIN, carcinoma in situ involves a full-thickness abnormality.
Terminology
If the abnormal parabasal layer extends to one half to two thirds of the epithelium, moderate dysplasia is present. A lower degree of involvement is called mild dysplasia, and full-thickness involvement is severe dysplasia or carcinoma in situ.
High rate of persistence, recurrence
Herod and colleagues9 reported on a 15-year follow-up of VIN and found that disease persisted or recurred in 48% of women managed surgically, and 7% of patients progressed to frankly invasive carcinoma. These investigators used the following classification system:
Joura et al10 strongly suggested that the incidence of this condition is increasing, especially in women prior to the 7th decade of life. Whether this increase is due to better recognition or a true rise in prevalence has been debated.
Diagnostic strategies
Application of 5% acetic acid to the vulvar skin will, after 3 to 5 minutes, allow areas of involvement to be readily seen with a handheld magnifying glass. Colposcopy can be used, but is slower and not as efficient as a simple magnifying lens. Most clinicians have abandoned the use of toluidine blue to identify multicentric lesions, since acetic acid appears to be less cumbersome and just as efficient.
White or pseudopigmented lesions (FIGURE 5) can be seen anywhere on the vulva and represent 2 of the 3 presentations of VIN. Pink lesions (FIGURE 5) are usually seen on moist surfaces near mucous membranes, whereas the white or pseudopigmented lesions are usually seen on the drier, hair-bearing areas of the vulva. Biopsy reveals similar histology.
The cause of the pseudopigmented lesions is unclear, but is unrelated to a disturbance of the melanin cells. As with other vulvar lesions, biopsy is essential for a correct diagnosis.

FIGURE 5
VIN III lesions: A trio of presentations
White lesion.
Pseudopigmented lesions.
Pink lesion.
Recommended therapies
VIN is treated by destroying or excising the epithelium involved. When the area is limited in size, simple excision or laser vaporization is preferred. A 2- to 3-mm margin is adequate, because these lesions have sharp borders.
Laser therapy warrants extra care because the epithelium is rarely thicker than 0.5 mm. For this reason, vaporization of the vulva should be limited to the following depths:
These limits will speed healing and prevent the unnecessary destruction of dermis.
Also be aware that the depth of hair-follicle involvement rarely exceeds 1 mm. Vaporization of the full thickness of the dermis will lead to alopecia and vulvar dryness.
When disease is multifocal or confluent, treatment is more challenging. Several decades ago, simple vulvectomy was performed, but the patient was left a sexual cripple.
Since then, laser therapy has been attempted in these cases, and has proved to be effective when the area treated does not exceed 25% of the total area of the vulva. Extensive laser therapy leads to considerable postoperative pain and an unhappy result.
Extensive involvement may necessitate laser treatment by quadrant to achieve the best results. Another option is “skinning vulvectomy” using a skin graft. This procedure, first described by Felix Rutledge,11 requires a 7- or 8-day hospitalization, but allows for complete therapy in 1 session.
Paget’s disease of the vulva
This disease is most frequently seen in the breast nipple (FIGURE 6), where it is usually associated with an underlying infiltrating ductal carcinoma. Extramammary sites include the vulvar, perianal, and axillary regions. The disease has also been seen in the ear canal.
Paget’s disease is an intraepithelial adenocarcinoma of eccrine or apocrine origin.

FIGURE 6
Paget disease: Not just a breast complaint
Paget disease of the nipple with underlying ductal adenocarcinoma.
Vulvar Paget disease: lesion (left) and photomicrograph of the lesion.
Clinical appearance
Paget’s disease of the vulva appears as a superficial, red to pink, velvety, eczematoid lesion (FIGURE 6), which is very pruritic and often associated with exfoliation. Margins are difficult to identify grossly.
On rare occasions, a nodular tumor can be found in the middle of the skin involvement, but in most cases no invasive malignancy is found at extramammary sites on the vulva.
Diagnostic strategies
Microscopic appearance of Paget cells (FIGURE 6) are pathognomonic of the disease.
Older textbooks suggest that 10% to 20% of patients have an associated, underlying, invasive carcinoma of a skin appendage, Bartholin’s gland, urinary tract, or bowel or rectal site, but later experience has not confirmed this. Rather, the likelihood of concomitant invasive disease is much lower than 10%.
Excision is the treatment of choice
Any attempt to achieve negative margins must utilize frozen section. Some studies have suggested that negative margins are not associated with a reduced rate of recurrence, but these findings have been inconsistent.
Recurrence is common
Paget’s disease of the vulva often recurs, especially when the initial lesion is large. Close monitoring will detect these recurrences when they’re quite small and easily removed via local excision. Occasionally, the initial disease is so extensive that skin grafting may be necessary to cover the defect.
The author reports no financial relationships relevant to this article.
1. Voet RL. Classification of vulvar dystrophies and premalignant squamous lesions. J Cutan Pathol. 1994;21:86-90.
2. Lorenz B, Kaufman RH, Kutzner SK. Lichen sclerosus. Therapy with clobetasol propionate. J Reprod Med. 1998;43:790-794.
3. Proceedings of the XVth World Congress. International Society for the Study of Vulvovaginal Disease, Santa Fe, NM; September 26-30, 1999. International Society for the Study of Vulvovaginal Disease Newsletter, Summer 2000.
4. Masheb RM, Nash JM, Brondolo E, Kerns RD. Vulvodynia: an introduction and critical review of a chronic pain condition. Pain. 2000;86-93.
5. Sadownik A. Clinical profile of vulvodynia patients. J Reprod Med. 2000;45:679-684.
6. Edwards A, Wojnarowska F. The vulvar pain syndromes. Int J STD AIDS. 1998;9:74-78.
7. Bornstein J, Zarfati D, Goldik Z, Abramovici H. Vulvar vestibulitis: physical or psychosexual problem? Obstet Gynecol. 1999;93(5 Pt 2):876-880.
8. Schneider D, Yaron M, Bukovsky I, Soffer Y, Halpern R. Outcome of surgical treatment for superficial dyspareunia from vulvar vestibulitis. J Reprod Med. 2001;46:227-231.
9. Herod JJ, Shafi MI, Rollason TP, Jordan JA, Luesley DM. Vulvar intraepithelial neoplasia: long-term follow-up of treated and untreated women. Br J Obstet Gynaecol. 1996;103:446-452.
10. Joura EA, Lösch A, Haider-Angeler M-G, Breitenecker G, Leodolter S. Trends in vulvar neoplasia. J Reprod Med. 2000;45:613-615.
11. Rutledge F, Sinclair M. Treatment of intraepithelial carcinoma of the vulva by skin excision and graft. Am J Obstet Gynecol. 1968;102:807-818.
12. Bergeron S, Bouchard C, Fortier M, Binik YM, Khalife S. The surgical treatment of vulvar vestibulitis syndrome: a follow-up study. J Sex Marital Ther. 1997;23:317-325.
13. Kehoe S, Luesley D. An evaluation of modified vestibulectomy in the treatment of vulvar vestibulitis: preliminary results. Acta Obstet Gynecol Scand. 1996;75:676-677.
14. Mann MS, Kaufman RH, Brown D, Jr, Adam E. Vulvar vestibulitis: significant clinical variables and treatment outcome. Obstet Gynecol. 1992;79:122-125.
15. Schover LR, Youngs DD, Cannata R. Psychosexual aspects of the evaluation and management of vulvar vestibulitis. Am J Obstet Gynecol. 1992;167:630-636.
16. Marinoff SC, Turner ML. Vulvar vestibulitis syndrome: an overview. Am J Obstet Gynecol. 1991;165:1228-1233.
17. Haefner HK, Collins ME, Davis GD, et al. The vulvodynia guideline. J Low Genit Tract Dis. 2005;9:45-51.
CASE Postmenopausal dyspareunia
A 60-year-old widow who recently remarried complains of dyspareunia. Examination of the vulva reveals firm but thin white skin over the periclitoral area and labia minora and shrinking of the vulvar skin.
What is the likely diagnosis?
Lichen sclerosus is the probable diagnosis, given her age and the appearance of the vulva, although it is impossible to assure the diagnosis without a biopsy. The preferred treatment is clobetasol, an ultrapotent steroid, applied daily.
True, powerful steroids can cause atrophy if applied regularly to other areas of the skin, but clobetasol does not cause atrophy of vulvar skin. After several weeks of nightly application, the skin should be softer and more pliable, and dyspareunia should be resolved. The patient can then reduce the clobetasol application to twice weekly—but she must continue the treatment indefinitely.
The vulva over the lifespan
The vulva is sensitive to both physiologic and pathologic changes, as well as to the sex hormones that govern the menstrual cycle. The mucosa on the inner aspects of the labia minora is very similar to the skin of the vagina and thus very sensitive to estrogen. The skin of the labia majora and the outer surface of the labia minora is more consistent with hair-bearing skin in the perineal area and more sensitive to androgens, which help thicken the skin. At menopause, the loss of estrogen leads to atrophy, and the vulvar epithelium is reduced to a few layers of mostly intermediate and parabasal cell types. The labia minora and majora as well as the clitoris gradually become less prominent with age.
The skin of the vulva consists of both dermis and epidermis, which interact with each other and respond to different nutritional and hormonal influences. For example, estrogen has little effect on vulvar epidermis, but considerable effect on the dermis, thickening the skin and preventing atrophy.
Postmenopausal atrophic changes can become a clinical problem when a woman resumes sexual intercourse after a long period of abstinence, as in the opening case. If atrophy is the main complaint, estrogen replacement therapy will alleviate symptoms of tightness, irritation, and dyspareunia, but it may take 6 weeks to 6 months to achieve optimal results. In the interim, women need to be reassured that reasonable function can be achieved.
Hygienic considerations
With any vulvar irritation, the patient should discontinue the use of synthetic undergarments in favor of cotton panties, which permit more adequate circulation and do not trap moisture.
Sitz baths often help relieve local discomfort, but should be followed by thorough drying.
The new ACOG Committee Opinion reflects recommendations of the American Society for Colposcopy and Cervical Pathology.17
Vulvodynia. American College of Obstetricians and Gynecologists Committee Opinion No. 345. Obstet Gynecol. October 2006;108:1049–1052.
Vulvar dystrophies: Think “white”
In the past, these diseases have been defined as non-neoplastic epithelial disorders of the vulva. Although there have been many attempts to more accurately define vulvar dystrophies, none have completely described the wide variety of clinical presentations.
In general, dystrophies are disorders of epithelial growth and nutrition that often result in a white surface color change. This definition includes intraepithelial neoplasia and Paget’s disease of the vulva. The International Society for the Study of Vulvovaginal Disease has proposed multiple classifications since 1975. I prefer the clarity of the 1987 classification system.1 I also consider these terms out-of-date: lichen sclerosus et atrophicus, carcinoma simplex, leukoplakic vulvitis, leukoplakia, hyperplastic vulvitis, neurodermatitis, kraurosis vulvae, leukokeratosis, erythroplasia of Queyrat, and Bowen’s disease.
What makes the lesions white?
The white appearance of dystrophic lesions is due to excessive keratin, at times deep pigmentation, and relative avascularity. All 3 of these characteristics are present in the spectrum of vulvar dystrophies. Biopsy of the affected skin is the key to accurate diagnosis and successful therapy.
Lichen sclerosus
Does not raise risk of carcinoma
The most common of the 3 groups of white lesions described in the 1987 classification of dystrophies, lichen sclerosus usually occurs in postmenopausal women, but can appear at any age, including childhood (FIGURE 1). Despite claims to the contrary, there is no good evidence that women with lichen sclerosus face a higher risk for vulvar carcinoma.
FIGURE 1
Lichen sclerosus affects all ages
3-year-old child. Note the inflammation secondary to excoriations.
20-year-old woman. The glans clitoris has begun the hooding process.
70-year-old woman. The introitus has shrunk, making intercourse impossible.
Signs and symptoms
In lichen sclerosus, the skin of the vulva appears very thin, atrophic, and dry, resembling parchment. It is also white, with loss of pigmentation.
Pruritus is the most common symptom and is usually the presenting symptom. Scratching during sleep may create ulcerations and areas of ecchymosis, and there is generalized shrinking of the vulvar skin, with eventual loss of the labia minora.
The edema and shrinking that occur around the clitoris cause a “hooding” of the glans clitoris. If the process continues unchecked, it can involve the labia majora as well as the skin of the inner thigh and anal region.
Prescribe clobetasol ointment
The patient should be instructed to use clobetasol 0.05% ointment on a continuing basis. This drug is so successful it has eclipsed the use of testosterone propionate for this indication. Lorenz and colleagues2 found very high success rates in 81 symptomatic patients with biopsy-proven disease who had failed previous therapy.
For reasons that are unknown, persistent use of this steroid on vulvar skin does not cause the atrophy commonly seen with prolonged use of high-potency steroids on other areas of the skin.
Start with twice-daily application and taper to less frequent use as the symptoms come under control. Most patients in remission can be maintained with twice-weekly application. Pruritus should disappear completely, and the skin itself will become less “leathery.”
Surgical treatment is not advised
Surgery does not appear to have a role because lichen sclerosus often recurs outside excised areas. Several reports have even described the return of disease in skin grafts used to replace large diseased areas.
I do not recommend surgery except in dire circumstances, when symptom relief is essential to the patient’s quality of life and all other therapies have failed.
Squamous cell hyperplasia
This disease is probably the same entity as lichen simplex chronicus. Changes in vulvar skin appear to result from chronic scratching secondary to intense pruritus. This complaint often involves a vicious cycle of scratching, increased pruritus, and more scratching, until excoriations occur. The aim of therapy is to eliminate the pruritus (FIGURE 2).
FIGURE 2
Squamous cell hyperplasia
75-year-old woman. The skin is thickened and may be leathery.
Intense pruritus and aggressive scratching lead to excoriations.
Signs and symptoms
Vulvar skin is typically white or pink. Biopsy will confirm the diagnosis, revealing a markedly thickened keratin layer (hyperkeratosis) and irregular thickening of the Malpighian ridges (acanthosis).
Inflammatory changes are also present, especially when there are areas of excoriation.
Treatment is similar to therapy for lichen sclerosus
Potent topical corticosteroids are the backbone of treatment; clobetasol is the preferred drug. The frequency of application is identical to that described for lichen sclerosus, and response to therapy usually takes 2 months. In the interim, it is advisable to prescribe other medications for the pruritus.
Lichen sclerosus and squamous cell hyperplasia sometimes coincide. Fortunately, the therapies are quite similar and both conditions tend to respond.
Vulvodynia
This disorder consists of chronic vulvar discomfort due to itching, burning, and/or pain that causes physical, sexual, and psychological distress.3,4 Once referred to as essential vulvodynia, it now is defined as generalized vulvar dysesthesia.
Signs and symptoms
Women with this condition tend to have difficulty localizing their pain. They often present with a complaint of recurrent yeast infection or constant irritation at the introitus. Dyspareunia may or may not be a presenting symptom, although intercourse often triggers this condition. Tight pants or rough undergarments also may trigger symptoms.
Common symptoms. In a study by Sadownik,5 women with vulvar dysesthesia reported the following symptoms:
Women with vulvar dysesthesia who appear to have urinary tract symptoms should undergo a urine culture, though it will often be negative and antibiotic therapy will have little effect.
A diagnosis of exclusion
The pain of dysesthesia appears to be neuropathic in origin in that it mimics pain of the sensory nervous system. It may be diffuse or focal, unilateral or bilateral, constant or sporadic. Thus, it is a diagnosis of exclusion.
Recommended therapies
Vulvar dysesthesia should be regarded as a chronic pain syndrome and treated accordingly, with emphasis on generalized improvements in health and attitude rather than single-therapy approaches.
Potent topical corticosteroids are usually of no benefit. Nor does topical estrogen produce long-term relief.
Once all possible causes of symptoms are excluded, refer the patient for education, support, and treatment of depression, if present. Occasionally, topical anesthetics will provide short-term relief.
At least 2 vulvar pain societies—the National Vulvodynia Association and the Vulvar Pain Foundation—have newsletters, outreach programs, and Web sites.
Vulvar vestibulitis
A more readily definable condition in the same category as vulvodynia is so-called vulvar vestibulitis, also known as localized vulvodynia (as classified by the new ACOG Committee Opinion on vulvodynia).
Signs and symptoms
The defining presentation is severe pain on vestibular touch (eg, entry at intercourse), with tenderness to pressure localized within the vulvar vestibule in a horseshoe distribution pattern encompassing 3, 6, and 9 o’clock on the vestibule. Erythema is often present, especially at the 5 and 7 o’clock positions (FIGURE 3).
Patients have no symptoms during normal daily activities, but complain of dyspareunia and an inability to use tampons.
FIGURE 3
Vestibular adenitis
Intense erythema at the 5 o’clock position in the vestibule.
Diagnostic strategies
Vulvar vestibulitis can be diagnosed using a moistened cotton-tip applicator. Pressure applied in the area of the urethral meatus will result in minimal discomfort, but pressure in the horseshoe area of the vestibule will cause exquisite discomfort.
Careful inspection at 5 and 7 o’clock in the vestibule usually uncovers intense erythema over an area of 4 or 5 mm. To distinguish vestibulitis from dysesthesia, see the comparison in TABLE 1.
TABLE 1
Distinguishing vulvar vestibulitis and dysesthesia
| VULVAR VESTIBULITIS | ESSENTIAL VULVAR DYSESTHESIA |
|---|---|
| Pain is usually not constant | Pain is a constant burning sensation |
| Erythema in sensitive areas | No erythema or abnormal appearance |
| Lidocaine quells sensitivity | Lidocaine has no effect |
| Cause is dermal inflammation | Cause is allodynia (heightened nerve sensitivity) |
Recommended therapies
Treatment of vulvar vestibulitis is complex. It is important to see the patient often to ensure that this syndrome is truly present rather than vulvar dysesthesia. Xylocaine jelly should be given in an attempt to relieve symptoms; topical steroid ointments are another option.
Women with persistent symptoms are difficult to treat medically. Earlier theories pointing to infection as the cause of vestibulitis have been discounted.
Some experts believe that foods containing oxalates precipitate these symptoms. It may be advisable to have the patient reduce the content of oxalates in her diet in an effort to address all possible remedies.
For refractory cases, consider surgery
Consider surgical removal of the tender vestibule if all other therapies fail to provide adequate relief. Surgery for this indication has a high success rate (TABLE 2).7
Some surgeons have attempted treatment with laser ablation, but most have found excision more satisfactory, with faster recovery and excellent cosmesis.
Schneider and colleagues8 had 69 women complete a questionnaire 6 months after surgery, 54 (78%) of whom replied. Moderate to excellent improvement was reported by 45 women (83%); 7 had repeat surgery, after which 4 improved.
TABLE 2
Impressive track record for surgical treatment of vestibulitis
| % RESPONSE | |||
|---|---|---|---|
| STUDY | COMPLETE | PARTIAL | NONE |
| Bornstein et al7 | 76 | 24 | 0 |
| Bergeron et al12 | 63 | 37 | 0 |
| Kehoe and Luesley13 | 60 | 29 | 11 |
| Mann et al14 | 66 | 21 | 13 |
| Schover et al15 | 47 | 37 | 16 |
| Marinoff and Turner16 | 82 | 15 | 3 |
| Adapted from Bornstein et al7 | |||
Pigmented lesions
Are they cancer precursors?
Precursors of malignant melanoma of the vulva have yet to be clearly defined. The majority of these melanomas appear to arise de novo; however, some are associated with precursor nevi, especially junctional nevi. The 3 most common types of nevi that appear on the vulva are:
Assessing malignant potential
Only a small number of dysplastic nevi progress to malignant melanoma, but the frequency increases when the dysplastic nevus is familial and not acquired.
In general, the more severe the dysplasia, the greater the likelihood it will progress to malignancy. In dysplastic nevi, the pattern and appearance of the melanocytic cells are atypical. Bridging of melanocytic clusters of atypical cells may occur. Often, the atypical melanocytes are varied in size and shape, increasing in cell and nuclear size as severity increases. In the most severe cases, nucleoli are very prominent.
Many pigmented lesions of the vulva are lentigines, similar to freckles. Distinguishing one pigmented lesion from another is difficult even with magnification, and the clinician often must decide whether or not to biopsy. One set of guidelines recommends excisional biopsy of vulvar nevi when there is a change in:
Note that a reddish lesion may be basal cell hyperplasia, which has been associated with the development of basal cell carcinoma (FIGURE 4).
FIGURE 4
Basal cell carcinoma
An uncommon type of vulvar cancer, this tumor rarely metastasizes.
Premalignant lesions of squamous epithelium
The variable appearance of vulvar intraepithelial neoplasia (VIN) necessitates the liberal use of diagnostic biopsies, particularly when lesions persist or recur. VIN can present as a white lesion, or as pseudopigmented, pink, or raised and eroded.
Cigarette smoking is a risk factor.
Clinical appearance
Macroscopically, VIN lesions are often multiple and appear slightly raised and papular. Hyper- or pseudopigmented lesions are seen in about 30% of cases.
A confluence of VIN can create an appearance of diffuse plaques. In VIN, as for CIN, carcinoma in situ involves a full-thickness abnormality.
Terminology
If the abnormal parabasal layer extends to one half to two thirds of the epithelium, moderate dysplasia is present. A lower degree of involvement is called mild dysplasia, and full-thickness involvement is severe dysplasia or carcinoma in situ.
High rate of persistence, recurrence
Herod and colleagues9 reported on a 15-year follow-up of VIN and found that disease persisted or recurred in 48% of women managed surgically, and 7% of patients progressed to frankly invasive carcinoma. These investigators used the following classification system:
Joura et al10 strongly suggested that the incidence of this condition is increasing, especially in women prior to the 7th decade of life. Whether this increase is due to better recognition or a true rise in prevalence has been debated.
Diagnostic strategies
Application of 5% acetic acid to the vulvar skin will, after 3 to 5 minutes, allow areas of involvement to be readily seen with a handheld magnifying glass. Colposcopy can be used, but is slower and not as efficient as a simple magnifying lens. Most clinicians have abandoned the use of toluidine blue to identify multicentric lesions, since acetic acid appears to be less cumbersome and just as efficient.
White or pseudopigmented lesions (FIGURE 5) can be seen anywhere on the vulva and represent 2 of the 3 presentations of VIN. Pink lesions (FIGURE 5) are usually seen on moist surfaces near mucous membranes, whereas the white or pseudopigmented lesions are usually seen on the drier, hair-bearing areas of the vulva. Biopsy reveals similar histology.
The cause of the pseudopigmented lesions is unclear, but is unrelated to a disturbance of the melanin cells. As with other vulvar lesions, biopsy is essential for a correct diagnosis.
FIGURE 5
VIN III lesions: A trio of presentations
White lesion.
Pseudopigmented lesions.
Pink lesion.
Recommended therapies
VIN is treated by destroying or excising the epithelium involved. When the area is limited in size, simple excision or laser vaporization is preferred. A 2- to 3-mm margin is adequate, because these lesions have sharp borders.
Laser therapy warrants extra care because the epithelium is rarely thicker than 0.5 mm. For this reason, vaporization of the vulva should be limited to the following depths:
These limits will speed healing and prevent the unnecessary destruction of dermis.
Also be aware that the depth of hair-follicle involvement rarely exceeds 1 mm. Vaporization of the full thickness of the dermis will lead to alopecia and vulvar dryness.
When disease is multifocal or confluent, treatment is more challenging. Several decades ago, simple vulvectomy was performed, but the patient was left a sexual cripple.
Since then, laser therapy has been attempted in these cases, and has proved to be effective when the area treated does not exceed 25% of the total area of the vulva. Extensive laser therapy leads to considerable postoperative pain and an unhappy result.
Extensive involvement may necessitate laser treatment by quadrant to achieve the best results. Another option is “skinning vulvectomy” using a skin graft. This procedure, first described by Felix Rutledge,11 requires a 7- or 8-day hospitalization, but allows for complete therapy in 1 session.
Paget’s disease of the vulva
This disease is most frequently seen in the breast nipple (FIGURE 6), where it is usually associated with an underlying infiltrating ductal carcinoma. Extramammary sites include the vulvar, perianal, and axillary regions. The disease has also been seen in the ear canal.
Paget’s disease is an intraepithelial adenocarcinoma of eccrine or apocrine origin.
FIGURE 6
Paget disease: Not just a breast complaint
Paget disease of the nipple with underlying ductal adenocarcinoma.
Vulvar Paget disease: lesion (left) and photomicrograph of the lesion.
Clinical appearance
Paget’s disease of the vulva appears as a superficial, red to pink, velvety, eczematoid lesion (FIGURE 6), which is very pruritic and often associated with exfoliation. Margins are difficult to identify grossly.
On rare occasions, a nodular tumor can be found in the middle of the skin involvement, but in most cases no invasive malignancy is found at extramammary sites on the vulva.
Diagnostic strategies
Microscopic appearance of Paget cells (FIGURE 6) are pathognomonic of the disease.
Older textbooks suggest that 10% to 20% of patients have an associated, underlying, invasive carcinoma of a skin appendage, Bartholin’s gland, urinary tract, or bowel or rectal site, but later experience has not confirmed this. Rather, the likelihood of concomitant invasive disease is much lower than 10%.
Excision is the treatment of choice
Any attempt to achieve negative margins must utilize frozen section. Some studies have suggested that negative margins are not associated with a reduced rate of recurrence, but these findings have been inconsistent.
Recurrence is common
Paget’s disease of the vulva often recurs, especially when the initial lesion is large. Close monitoring will detect these recurrences when they’re quite small and easily removed via local excision. Occasionally, the initial disease is so extensive that skin grafting may be necessary to cover the defect.
The author reports no financial relationships relevant to this article.
CASE Postmenopausal dyspareunia
A 60-year-old widow who recently remarried complains of dyspareunia. Examination of the vulva reveals firm but thin white skin over the periclitoral area and labia minora and shrinking of the vulvar skin.
What is the likely diagnosis?
Lichen sclerosus is the probable diagnosis, given her age and the appearance of the vulva, although it is impossible to assure the diagnosis without a biopsy. The preferred treatment is clobetasol, an ultrapotent steroid, applied daily.
True, powerful steroids can cause atrophy if applied regularly to other areas of the skin, but clobetasol does not cause atrophy of vulvar skin. After several weeks of nightly application, the skin should be softer and more pliable, and dyspareunia should be resolved. The patient can then reduce the clobetasol application to twice weekly—but she must continue the treatment indefinitely.
The vulva over the lifespan
The vulva is sensitive to both physiologic and pathologic changes, as well as to the sex hormones that govern the menstrual cycle. The mucosa on the inner aspects of the labia minora is very similar to the skin of the vagina and thus very sensitive to estrogen. The skin of the labia majora and the outer surface of the labia minora is more consistent with hair-bearing skin in the perineal area and more sensitive to androgens, which help thicken the skin. At menopause, the loss of estrogen leads to atrophy, and the vulvar epithelium is reduced to a few layers of mostly intermediate and parabasal cell types. The labia minora and majora as well as the clitoris gradually become less prominent with age.
The skin of the vulva consists of both dermis and epidermis, which interact with each other and respond to different nutritional and hormonal influences. For example, estrogen has little effect on vulvar epidermis, but considerable effect on the dermis, thickening the skin and preventing atrophy.
Postmenopausal atrophic changes can become a clinical problem when a woman resumes sexual intercourse after a long period of abstinence, as in the opening case. If atrophy is the main complaint, estrogen replacement therapy will alleviate symptoms of tightness, irritation, and dyspareunia, but it may take 6 weeks to 6 months to achieve optimal results. In the interim, women need to be reassured that reasonable function can be achieved.
Hygienic considerations
With any vulvar irritation, the patient should discontinue the use of synthetic undergarments in favor of cotton panties, which permit more adequate circulation and do not trap moisture.
Sitz baths often help relieve local discomfort, but should be followed by thorough drying.
The new ACOG Committee Opinion reflects recommendations of the American Society for Colposcopy and Cervical Pathology.17
Vulvodynia. American College of Obstetricians and Gynecologists Committee Opinion No. 345. Obstet Gynecol. October 2006;108:1049–1052.
Vulvar dystrophies: Think “white”
In the past, these diseases have been defined as non-neoplastic epithelial disorders of the vulva. Although there have been many attempts to more accurately define vulvar dystrophies, none have completely described the wide variety of clinical presentations.
In general, dystrophies are disorders of epithelial growth and nutrition that often result in a white surface color change. This definition includes intraepithelial neoplasia and Paget’s disease of the vulva. The International Society for the Study of Vulvovaginal Disease has proposed multiple classifications since 1975. I prefer the clarity of the 1987 classification system.1 I also consider these terms out-of-date: lichen sclerosus et atrophicus, carcinoma simplex, leukoplakic vulvitis, leukoplakia, hyperplastic vulvitis, neurodermatitis, kraurosis vulvae, leukokeratosis, erythroplasia of Queyrat, and Bowen’s disease.
What makes the lesions white?
The white appearance of dystrophic lesions is due to excessive keratin, at times deep pigmentation, and relative avascularity. All 3 of these characteristics are present in the spectrum of vulvar dystrophies. Biopsy of the affected skin is the key to accurate diagnosis and successful therapy.
Lichen sclerosus
Does not raise risk of carcinoma
The most common of the 3 groups of white lesions described in the 1987 classification of dystrophies, lichen sclerosus usually occurs in postmenopausal women, but can appear at any age, including childhood (FIGURE 1). Despite claims to the contrary, there is no good evidence that women with lichen sclerosus face a higher risk for vulvar carcinoma.
FIGURE 1
Lichen sclerosus affects all ages
3-year-old child. Note the inflammation secondary to excoriations.
20-year-old woman. The glans clitoris has begun the hooding process.
70-year-old woman. The introitus has shrunk, making intercourse impossible.
Signs and symptoms
In lichen sclerosus, the skin of the vulva appears very thin, atrophic, and dry, resembling parchment. It is also white, with loss of pigmentation.
Pruritus is the most common symptom and is usually the presenting symptom. Scratching during sleep may create ulcerations and areas of ecchymosis, and there is generalized shrinking of the vulvar skin, with eventual loss of the labia minora.
The edema and shrinking that occur around the clitoris cause a “hooding” of the glans clitoris. If the process continues unchecked, it can involve the labia majora as well as the skin of the inner thigh and anal region.
Prescribe clobetasol ointment
The patient should be instructed to use clobetasol 0.05% ointment on a continuing basis. This drug is so successful it has eclipsed the use of testosterone propionate for this indication. Lorenz and colleagues2 found very high success rates in 81 symptomatic patients with biopsy-proven disease who had failed previous therapy.
For reasons that are unknown, persistent use of this steroid on vulvar skin does not cause the atrophy commonly seen with prolonged use of high-potency steroids on other areas of the skin.
Start with twice-daily application and taper to less frequent use as the symptoms come under control. Most patients in remission can be maintained with twice-weekly application. Pruritus should disappear completely, and the skin itself will become less “leathery.”
Surgical treatment is not advised
Surgery does not appear to have a role because lichen sclerosus often recurs outside excised areas. Several reports have even described the return of disease in skin grafts used to replace large diseased areas.
I do not recommend surgery except in dire circumstances, when symptom relief is essential to the patient’s quality of life and all other therapies have failed.
Squamous cell hyperplasia
This disease is probably the same entity as lichen simplex chronicus. Changes in vulvar skin appear to result from chronic scratching secondary to intense pruritus. This complaint often involves a vicious cycle of scratching, increased pruritus, and more scratching, until excoriations occur. The aim of therapy is to eliminate the pruritus (FIGURE 2).
FIGURE 2
Squamous cell hyperplasia
75-year-old woman. The skin is thickened and may be leathery.
Intense pruritus and aggressive scratching lead to excoriations.
Signs and symptoms
Vulvar skin is typically white or pink. Biopsy will confirm the diagnosis, revealing a markedly thickened keratin layer (hyperkeratosis) and irregular thickening of the Malpighian ridges (acanthosis).
Inflammatory changes are also present, especially when there are areas of excoriation.
Treatment is similar to therapy for lichen sclerosus
Potent topical corticosteroids are the backbone of treatment; clobetasol is the preferred drug. The frequency of application is identical to that described for lichen sclerosus, and response to therapy usually takes 2 months. In the interim, it is advisable to prescribe other medications for the pruritus.
Lichen sclerosus and squamous cell hyperplasia sometimes coincide. Fortunately, the therapies are quite similar and both conditions tend to respond.
Vulvodynia
This disorder consists of chronic vulvar discomfort due to itching, burning, and/or pain that causes physical, sexual, and psychological distress.3,4 Once referred to as essential vulvodynia, it now is defined as generalized vulvar dysesthesia.
Signs and symptoms
Women with this condition tend to have difficulty localizing their pain. They often present with a complaint of recurrent yeast infection or constant irritation at the introitus. Dyspareunia may or may not be a presenting symptom, although intercourse often triggers this condition. Tight pants or rough undergarments also may trigger symptoms.
Common symptoms. In a study by Sadownik,5 women with vulvar dysesthesia reported the following symptoms:
Women with vulvar dysesthesia who appear to have urinary tract symptoms should undergo a urine culture, though it will often be negative and antibiotic therapy will have little effect.
A diagnosis of exclusion
The pain of dysesthesia appears to be neuropathic in origin in that it mimics pain of the sensory nervous system. It may be diffuse or focal, unilateral or bilateral, constant or sporadic. Thus, it is a diagnosis of exclusion.
Recommended therapies
Vulvar dysesthesia should be regarded as a chronic pain syndrome and treated accordingly, with emphasis on generalized improvements in health and attitude rather than single-therapy approaches.
Potent topical corticosteroids are usually of no benefit. Nor does topical estrogen produce long-term relief.
Once all possible causes of symptoms are excluded, refer the patient for education, support, and treatment of depression, if present. Occasionally, topical anesthetics will provide short-term relief.
At least 2 vulvar pain societies—the National Vulvodynia Association and the Vulvar Pain Foundation—have newsletters, outreach programs, and Web sites.
Vulvar vestibulitis
A more readily definable condition in the same category as vulvodynia is so-called vulvar vestibulitis, also known as localized vulvodynia (as classified by the new ACOG Committee Opinion on vulvodynia).
Signs and symptoms
The defining presentation is severe pain on vestibular touch (eg, entry at intercourse), with tenderness to pressure localized within the vulvar vestibule in a horseshoe distribution pattern encompassing 3, 6, and 9 o’clock on the vestibule. Erythema is often present, especially at the 5 and 7 o’clock positions (FIGURE 3).
Patients have no symptoms during normal daily activities, but complain of dyspareunia and an inability to use tampons.
FIGURE 3
Vestibular adenitis
Intense erythema at the 5 o’clock position in the vestibule.
Diagnostic strategies
Vulvar vestibulitis can be diagnosed using a moistened cotton-tip applicator. Pressure applied in the area of the urethral meatus will result in minimal discomfort, but pressure in the horseshoe area of the vestibule will cause exquisite discomfort.
Careful inspection at 5 and 7 o’clock in the vestibule usually uncovers intense erythema over an area of 4 or 5 mm. To distinguish vestibulitis from dysesthesia, see the comparison in TABLE 1.
TABLE 1
Distinguishing vulvar vestibulitis and dysesthesia
| VULVAR VESTIBULITIS | ESSENTIAL VULVAR DYSESTHESIA |
|---|---|
| Pain is usually not constant | Pain is a constant burning sensation |
| Erythema in sensitive areas | No erythema or abnormal appearance |
| Lidocaine quells sensitivity | Lidocaine has no effect |
| Cause is dermal inflammation | Cause is allodynia (heightened nerve sensitivity) |
Recommended therapies
Treatment of vulvar vestibulitis is complex. It is important to see the patient often to ensure that this syndrome is truly present rather than vulvar dysesthesia. Xylocaine jelly should be given in an attempt to relieve symptoms; topical steroid ointments are another option.
Women with persistent symptoms are difficult to treat medically. Earlier theories pointing to infection as the cause of vestibulitis have been discounted.
Some experts believe that foods containing oxalates precipitate these symptoms. It may be advisable to have the patient reduce the content of oxalates in her diet in an effort to address all possible remedies.
For refractory cases, consider surgery
Consider surgical removal of the tender vestibule if all other therapies fail to provide adequate relief. Surgery for this indication has a high success rate (TABLE 2).7
Some surgeons have attempted treatment with laser ablation, but most have found excision more satisfactory, with faster recovery and excellent cosmesis.
Schneider and colleagues8 had 69 women complete a questionnaire 6 months after surgery, 54 (78%) of whom replied. Moderate to excellent improvement was reported by 45 women (83%); 7 had repeat surgery, after which 4 improved.
TABLE 2
Impressive track record for surgical treatment of vestibulitis
| % RESPONSE | |||
|---|---|---|---|
| STUDY | COMPLETE | PARTIAL | NONE |
| Bornstein et al7 | 76 | 24 | 0 |
| Bergeron et al12 | 63 | 37 | 0 |
| Kehoe and Luesley13 | 60 | 29 | 11 |
| Mann et al14 | 66 | 21 | 13 |
| Schover et al15 | 47 | 37 | 16 |
| Marinoff and Turner16 | 82 | 15 | 3 |
| Adapted from Bornstein et al7 | |||
Pigmented lesions
Are they cancer precursors?
Precursors of malignant melanoma of the vulva have yet to be clearly defined. The majority of these melanomas appear to arise de novo; however, some are associated with precursor nevi, especially junctional nevi. The 3 most common types of nevi that appear on the vulva are:
Assessing malignant potential
Only a small number of dysplastic nevi progress to malignant melanoma, but the frequency increases when the dysplastic nevus is familial and not acquired.
In general, the more severe the dysplasia, the greater the likelihood it will progress to malignancy. In dysplastic nevi, the pattern and appearance of the melanocytic cells are atypical. Bridging of melanocytic clusters of atypical cells may occur. Often, the atypical melanocytes are varied in size and shape, increasing in cell and nuclear size as severity increases. In the most severe cases, nucleoli are very prominent.
Many pigmented lesions of the vulva are lentigines, similar to freckles. Distinguishing one pigmented lesion from another is difficult even with magnification, and the clinician often must decide whether or not to biopsy. One set of guidelines recommends excisional biopsy of vulvar nevi when there is a change in:
Note that a reddish lesion may be basal cell hyperplasia, which has been associated with the development of basal cell carcinoma (FIGURE 4).
FIGURE 4
Basal cell carcinoma
An uncommon type of vulvar cancer, this tumor rarely metastasizes.
Premalignant lesions of squamous epithelium
The variable appearance of vulvar intraepithelial neoplasia (VIN) necessitates the liberal use of diagnostic biopsies, particularly when lesions persist or recur. VIN can present as a white lesion, or as pseudopigmented, pink, or raised and eroded.
Cigarette smoking is a risk factor.
Clinical appearance
Macroscopically, VIN lesions are often multiple and appear slightly raised and papular. Hyper- or pseudopigmented lesions are seen in about 30% of cases.
A confluence of VIN can create an appearance of diffuse plaques. In VIN, as for CIN, carcinoma in situ involves a full-thickness abnormality.
Terminology
If the abnormal parabasal layer extends to one half to two thirds of the epithelium, moderate dysplasia is present. A lower degree of involvement is called mild dysplasia, and full-thickness involvement is severe dysplasia or carcinoma in situ.
High rate of persistence, recurrence
Herod and colleagues9 reported on a 15-year follow-up of VIN and found that disease persisted or recurred in 48% of women managed surgically, and 7% of patients progressed to frankly invasive carcinoma. These investigators used the following classification system:
Joura et al10 strongly suggested that the incidence of this condition is increasing, especially in women prior to the 7th decade of life. Whether this increase is due to better recognition or a true rise in prevalence has been debated.
Diagnostic strategies
Application of 5% acetic acid to the vulvar skin will, after 3 to 5 minutes, allow areas of involvement to be readily seen with a handheld magnifying glass. Colposcopy can be used, but is slower and not as efficient as a simple magnifying lens. Most clinicians have abandoned the use of toluidine blue to identify multicentric lesions, since acetic acid appears to be less cumbersome and just as efficient.
White or pseudopigmented lesions (FIGURE 5) can be seen anywhere on the vulva and represent 2 of the 3 presentations of VIN. Pink lesions (FIGURE 5) are usually seen on moist surfaces near mucous membranes, whereas the white or pseudopigmented lesions are usually seen on the drier, hair-bearing areas of the vulva. Biopsy reveals similar histology.
The cause of the pseudopigmented lesions is unclear, but is unrelated to a disturbance of the melanin cells. As with other vulvar lesions, biopsy is essential for a correct diagnosis.
FIGURE 5
VIN III lesions: A trio of presentations
White lesion.
Pseudopigmented lesions.
Pink lesion.
Recommended therapies
VIN is treated by destroying or excising the epithelium involved. When the area is limited in size, simple excision or laser vaporization is preferred. A 2- to 3-mm margin is adequate, because these lesions have sharp borders.
Laser therapy warrants extra care because the epithelium is rarely thicker than 0.5 mm. For this reason, vaporization of the vulva should be limited to the following depths:
These limits will speed healing and prevent the unnecessary destruction of dermis.
Also be aware that the depth of hair-follicle involvement rarely exceeds 1 mm. Vaporization of the full thickness of the dermis will lead to alopecia and vulvar dryness.
When disease is multifocal or confluent, treatment is more challenging. Several decades ago, simple vulvectomy was performed, but the patient was left a sexual cripple.
Since then, laser therapy has been attempted in these cases, and has proved to be effective when the area treated does not exceed 25% of the total area of the vulva. Extensive laser therapy leads to considerable postoperative pain and an unhappy result.
Extensive involvement may necessitate laser treatment by quadrant to achieve the best results. Another option is “skinning vulvectomy” using a skin graft. This procedure, first described by Felix Rutledge,11 requires a 7- or 8-day hospitalization, but allows for complete therapy in 1 session.
Paget’s disease of the vulva
This disease is most frequently seen in the breast nipple (FIGURE 6), where it is usually associated with an underlying infiltrating ductal carcinoma. Extramammary sites include the vulvar, perianal, and axillary regions. The disease has also been seen in the ear canal.
Paget’s disease is an intraepithelial adenocarcinoma of eccrine or apocrine origin.
FIGURE 6
Paget disease: Not just a breast complaint
Paget disease of the nipple with underlying ductal adenocarcinoma.
Vulvar Paget disease: lesion (left) and photomicrograph of the lesion.
Clinical appearance
Paget’s disease of the vulva appears as a superficial, red to pink, velvety, eczematoid lesion (FIGURE 6), which is very pruritic and often associated with exfoliation. Margins are difficult to identify grossly.
On rare occasions, a nodular tumor can be found in the middle of the skin involvement, but in most cases no invasive malignancy is found at extramammary sites on the vulva.
Diagnostic strategies
Microscopic appearance of Paget cells (FIGURE 6) are pathognomonic of the disease.
Older textbooks suggest that 10% to 20% of patients have an associated, underlying, invasive carcinoma of a skin appendage, Bartholin’s gland, urinary tract, or bowel or rectal site, but later experience has not confirmed this. Rather, the likelihood of concomitant invasive disease is much lower than 10%.
Excision is the treatment of choice
Any attempt to achieve negative margins must utilize frozen section. Some studies have suggested that negative margins are not associated with a reduced rate of recurrence, but these findings have been inconsistent.
Recurrence is common
Paget’s disease of the vulva often recurs, especially when the initial lesion is large. Close monitoring will detect these recurrences when they’re quite small and easily removed via local excision. Occasionally, the initial disease is so extensive that skin grafting may be necessary to cover the defect.
The author reports no financial relationships relevant to this article.
1. Voet RL. Classification of vulvar dystrophies and premalignant squamous lesions. J Cutan Pathol. 1994;21:86-90.
2. Lorenz B, Kaufman RH, Kutzner SK. Lichen sclerosus. Therapy with clobetasol propionate. J Reprod Med. 1998;43:790-794.
3. Proceedings of the XVth World Congress. International Society for the Study of Vulvovaginal Disease, Santa Fe, NM; September 26-30, 1999. International Society for the Study of Vulvovaginal Disease Newsletter, Summer 2000.
4. Masheb RM, Nash JM, Brondolo E, Kerns RD. Vulvodynia: an introduction and critical review of a chronic pain condition. Pain. 2000;86-93.
5. Sadownik A. Clinical profile of vulvodynia patients. J Reprod Med. 2000;45:679-684.
6. Edwards A, Wojnarowska F. The vulvar pain syndromes. Int J STD AIDS. 1998;9:74-78.
7. Bornstein J, Zarfati D, Goldik Z, Abramovici H. Vulvar vestibulitis: physical or psychosexual problem? Obstet Gynecol. 1999;93(5 Pt 2):876-880.
8. Schneider D, Yaron M, Bukovsky I, Soffer Y, Halpern R. Outcome of surgical treatment for superficial dyspareunia from vulvar vestibulitis. J Reprod Med. 2001;46:227-231.
9. Herod JJ, Shafi MI, Rollason TP, Jordan JA, Luesley DM. Vulvar intraepithelial neoplasia: long-term follow-up of treated and untreated women. Br J Obstet Gynaecol. 1996;103:446-452.
10. Joura EA, Lösch A, Haider-Angeler M-G, Breitenecker G, Leodolter S. Trends in vulvar neoplasia. J Reprod Med. 2000;45:613-615.
11. Rutledge F, Sinclair M. Treatment of intraepithelial carcinoma of the vulva by skin excision and graft. Am J Obstet Gynecol. 1968;102:807-818.
12. Bergeron S, Bouchard C, Fortier M, Binik YM, Khalife S. The surgical treatment of vulvar vestibulitis syndrome: a follow-up study. J Sex Marital Ther. 1997;23:317-325.
13. Kehoe S, Luesley D. An evaluation of modified vestibulectomy in the treatment of vulvar vestibulitis: preliminary results. Acta Obstet Gynecol Scand. 1996;75:676-677.
14. Mann MS, Kaufman RH, Brown D, Jr, Adam E. Vulvar vestibulitis: significant clinical variables and treatment outcome. Obstet Gynecol. 1992;79:122-125.
15. Schover LR, Youngs DD, Cannata R. Psychosexual aspects of the evaluation and management of vulvar vestibulitis. Am J Obstet Gynecol. 1992;167:630-636.
16. Marinoff SC, Turner ML. Vulvar vestibulitis syndrome: an overview. Am J Obstet Gynecol. 1991;165:1228-1233.
17. Haefner HK, Collins ME, Davis GD, et al. The vulvodynia guideline. J Low Genit Tract Dis. 2005;9:45-51.
1. Voet RL. Classification of vulvar dystrophies and premalignant squamous lesions. J Cutan Pathol. 1994;21:86-90.
2. Lorenz B, Kaufman RH, Kutzner SK. Lichen sclerosus. Therapy with clobetasol propionate. J Reprod Med. 1998;43:790-794.
3. Proceedings of the XVth World Congress. International Society for the Study of Vulvovaginal Disease, Santa Fe, NM; September 26-30, 1999. International Society for the Study of Vulvovaginal Disease Newsletter, Summer 2000.
4. Masheb RM, Nash JM, Brondolo E, Kerns RD. Vulvodynia: an introduction and critical review of a chronic pain condition. Pain. 2000;86-93.
5. Sadownik A. Clinical profile of vulvodynia patients. J Reprod Med. 2000;45:679-684.
6. Edwards A, Wojnarowska F. The vulvar pain syndromes. Int J STD AIDS. 1998;9:74-78.
7. Bornstein J, Zarfati D, Goldik Z, Abramovici H. Vulvar vestibulitis: physical or psychosexual problem? Obstet Gynecol. 1999;93(5 Pt 2):876-880.
8. Schneider D, Yaron M, Bukovsky I, Soffer Y, Halpern R. Outcome of surgical treatment for superficial dyspareunia from vulvar vestibulitis. J Reprod Med. 2001;46:227-231.
9. Herod JJ, Shafi MI, Rollason TP, Jordan JA, Luesley DM. Vulvar intraepithelial neoplasia: long-term follow-up of treated and untreated women. Br J Obstet Gynaecol. 1996;103:446-452.
10. Joura EA, Lösch A, Haider-Angeler M-G, Breitenecker G, Leodolter S. Trends in vulvar neoplasia. J Reprod Med. 2000;45:613-615.
11. Rutledge F, Sinclair M. Treatment of intraepithelial carcinoma of the vulva by skin excision and graft. Am J Obstet Gynecol. 1968;102:807-818.
12. Bergeron S, Bouchard C, Fortier M, Binik YM, Khalife S. The surgical treatment of vulvar vestibulitis syndrome: a follow-up study. J Sex Marital Ther. 1997;23:317-325.
13. Kehoe S, Luesley D. An evaluation of modified vestibulectomy in the treatment of vulvar vestibulitis: preliminary results. Acta Obstet Gynecol Scand. 1996;75:676-677.
14. Mann MS, Kaufman RH, Brown D, Jr, Adam E. Vulvar vestibulitis: significant clinical variables and treatment outcome. Obstet Gynecol. 1992;79:122-125.
15. Schover LR, Youngs DD, Cannata R. Psychosexual aspects of the evaluation and management of vulvar vestibulitis. Am J Obstet Gynecol. 1992;167:630-636.
16. Marinoff SC, Turner ML. Vulvar vestibulitis syndrome: an overview. Am J Obstet Gynecol. 1991;165:1228-1233.
17. Haefner HK, Collins ME, Davis GD, et al. The vulvodynia guideline. J Low Genit Tract Dis. 2005;9:45-51.
Measuring Wellness in a Staff Health Promotion Program
Assessing Diagnostic Test Result Management in a VA Health Care Network
Nonestrogen therapies for menopausal symptoms
With more women steering clear of estrogen in the wake of the Women’s Health Initiative and other trials,page 24). Nonetheless, many physicians and patients seek nonestrogen alternatives for this menopause-related symptom.
Over-the-counter lubricants are a mixed lot
Although many lubricants are marketed today, clinical study has been limited because they are regulated by the FDA as cosmetics. Of these products, Replens, a bioadhesive vaginal lubricant, has been studied the most intensively.
A unique formulation. Replens, a polycarbophil-based polymer, attaches to the vaginal wall and can hold 60 times its weight in water. It remains against the vaginal epithelial surface for more than 24 hours before it is sloughed off. This mechanism provides longer relief and requires less frequent application than other lubricants.17
Replens vs estrogen. Thrice-weekly Replens was compared with 12 weeks of daily vaginal estrogen cream18 and with vaginal estrogen cream applied daily for 2 weeks and then 3 times weekly for a total of 3 months.19 The comparison of Replens with conjugated estrogen cream (Premarin) showed significant improvements in vaginal moisture, fluid volume, elasticity, and pH levels in both treatment groups.18 Vaginal atrophy (assessed via Papanicolaou smear) reversed in 100% of estrogen-treated patients and 60% of Replens-treated patients.
When Replens was compared with dienoestrol vaginal cream, both therapies produced significant improvement in the vaginal dryness index (a score based on vaginal moisture, fluid volume, elasticity, and mucosa) within the first week.19 However, dienoestrol-treated patients had greater improvement in mean vaginal dryness (21.78 vs 17.32) at 12 weeks of therapy (P=.0001), compared with baseline values of 13 (dienoestrol) and 13.45 (Replens). Vaginal symptoms and dyspareunia improved at similar rates in the 2 groups. Patient satisfaction also was high in both groups, with 60% of Replens-treated patients and 84% of dienoestrol-treated patients reporting good to excellent effects.
No serious side effects were reported.18,19
Start with Replens for vaginal dryness, as it is a safe and effective alternative. If it is ineffective, vaginal estrogen may be more effective than vaginal lubricants.
The authors report no financial relationships relevant to this article
By Joann V. Pinkerton, MD, OBG Management Board of Editors, Professor of Obstetrics and Gynecology and Director, The Women’s Place Midlife Health Center, University of Virginia Health System, Charlottesville, Va
CASE 1 Perimenopausal, daily hot flashes
THERAPY
Exercise, soy products, vitamin E, and black cohosh
THE PATIENT: “V.S.,” 51, has been a patient for some time. At her latest visit, she reports that her menstrual periods are irregular, occurring every 3 to 12 weeks. She also has as many as 5 hot flashes a day, wakes in the very early morning, and occasionally experiences mild night sweats. Because she underwent bilateral tubal ligation many years ago, there is no need for contraception. She has no family history of breast cancer, but prefers to avoid drugs and asks if there are any herbal remedies and/or lifestyle changes that will ease her transition through menopause. She has a body mass index (BMI) of 31.6, and her breast and pelvic examinations are negative.

INTERVENTION: We discuss several simple options. For example, regular exercise may reduce vasomotor symptoms, although intense exertion with sweating can provoke hot flashes. Soy products and soy extracts have had mixed results, but appear to have some benefit. I suggest adding 1 soy dietary product per day. Vitamin E also may reduce hot flashes very modestly. The most promising product is black cohosh; I advise V.S. to take 20 mg twice a day.
OUTCOME: V.S. begins exercising regularly and sets a weight loss goal of 10%. She also begins taking 400 IU of vitamin E daily, adds soy nuts to her diet, and starts taking black cohosh. Three months later, she reports that her hot flashes have decreased to about 3 per day and are tolerable. She has had 1 menstrual cycle in the interim. If her symptoms worsen, she will consider medical therapy.
CASE 2 Severe symptoms, mood effects
THERAPY
Venlafaxine and vaginal moisturizers
THE PATIENT: “A.B.,” 54, a cancer survivor, is menopausal and has 10 to 20 hot flashes a day and soaking night sweats. She also reports low mood, frequent crying, and irritability. Before her cancer diagnosis, A.B. took hormone therapy for 6 months for severe menopausal symptoms. She recently underwent lumpectomy, axillary node dissection, radiation, and chemotherapy for a 3-cm, grade 3, invasive lobular carcinoma that was estrogen- and progesterone-receptor positive, and she is about to begin an aromatase inhibitor for chemoprevention. She and her husband have attempted intercourse since her chemotherapy ended, but the experience was painful. She would prefer to restart hormone therapy, but is willing to try nonhormonal options first. Her examination is unremarkable except for significant atrophy, with a vaginal pH of 7.0.
INTERVENTION: After a discussion of the data on SSRIs, SNRIs, and gabapentin, A.B. decides to try venlafaxine, 37.5 mg daily. If she has no improvement after 2 weeks, she will increase the dosage to 75 mg daily. For the vulvovaginal atrophy, she will try both vaginal moisturizers and vaginal lubricants, recognizing that this will not rethicken the epithelium. She also will exercise 5 days per week.
OUTCOME: After 3 months and an increase to 75 mg daily venlafaxine, the patient reports a 50% decrease in hot flashes and a more stable mood. The dyspareunia remains a problem. She decides to try a small amount of estradiol cream—somewhere between the size of a pea and the size of a dime—applied externally around the introital opening. She will start by applying it daily for 2 weeks, then reduce to twice a week.
CASE 3 Severe symptoms after TAH/BSO
THERAPY
Unsatisfactory improvement, a return to estrogen
THE PATIENT: “A.G.,” 46, complains of severe vasomotor symptoms. Two months ago she underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy for bilateral complex masses, which turned out to be endometriomas. At that time, endometriosis was observed along the left ureter, with residual peritoneal implants and a small nodule within the rectovaginal septum. A.G. was offered leuprolide acetate (Lupron Depot) postoperatively, but declined. She did well for about 2 months and then began having vasomotor symptoms. Her physician was hesitant to prescribe estrogen because of fear of reactivating endometriosis. A.G. toughed it out for 3 months, but now reports “misery.” She is moody, cries easily, and has not had sex with her husband since her surgery. An examination reveals a small, 8-mm nodule within the rectovaginal septum, decreased vulvar color, vaginal pallor, and levator ani spasm with exam. Vaginal pH is 6.5.
INTERVENTION: Although I suggest systemic progesterone therapy—oral, vaginal, or intramuscular—and explain that it would decrease any residual endometriosis and relieve the hot flashes, the patient does not want to take any hormonal therapy and is concerned about worsening her mood. Despite reassurance that hormone therapy would have less than a 5% chance of reactivating the endometriosis, A.G. decides to try an antidepressant first. Since she had taken paroxetine (Paxil) for postpartum depression, with no major side effects, she decides to try it again, starting with 10 mg daily.
OUTCOME: A.G. continues to have at least 5 bothersome hot flashes per day, which interrupt her work with profuse sweating. She also wakes at night for the same reason. However, she is less irritable. It has been 7 months since her surgery, and both she and her husband want her to try hormone therapy. She elects to begin a low-dose combined estrogen–progesterone product, as well as estradiol vaginal cream twice daily.
Three months later, she reports no pain, a gradual reduction in hot flashes, and significant improvement overall. Her vaginal color has returned, her pH is 5.5, and intercourse is no longer painful. She decides to continue taking oral hormone therapy at a low dose despite occasional vasomotor symptoms, and to keep using vaginal estrogen, but will stop the paroxetine.
How does one hot flash differ from another?
By Joann V. Pinkerton, MD, OBG Management Board of Editors, Professor of Obstetrics and Gynecology and Director of The Women’s Place Midlife Health Center, University of Virginia Health System, Charlottesville, Va

Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. JAMA. 2006;295:2057–2071.
Nedrow A, Miller J, Walker M, Nygren P, Huffman LH, Nelson HD. Complementary and alternative therapies for the management of menopause-related symptoms. Arch Intern Med. 2006;166:1453–1465.
The hot flash, long synonymous with menopause, is the bane of many women facing the midlife transition. Despite the intensity of the sensation, hot flashes appear to be triggered by small elevations in core body temperature within a greatly reduced thermoneutral zone.1-4 If the core temperature crosses the upper threshold, a hot flash with sweating and peripheral vasodilation occurs. If the lower threshold is crossed, shivering results. Core temperature elevations occur in both symptomatic and asymptomatic women.
The difference: In symptomatic women, the thermoneutral zone is narrowed.
2 randomized trials attest to mostly modest efficacy
In their rigorous study of nonhormonal therapies for hot flashes, Nelson et al reviewed MEDLINE, PsycINFO, and the Cochrane Clinical Trials Register Database for randomized, double-blind, placebo-controlled trials of oral nonhormonal treatments for hot flashes, ultimately selecting 43 trials. These included 10 trials of antidepressants, 10 trials of clonidine, 17 trials of isoflavones, and 6 trials of other prescription drugs. They found at least some evidence of efficacy for SSRIs, SNRIs, clonidine, and gabapentin, but all were considerably less effective than estrogen.
Nedrow and colleagues searched the same databases plus MANTIS and AMED, selecting 70 trials for inclusion. Overall, the data were insufficient to support the effectiveness of any complementary or alternative therapy. For example, a good-quality study enrolling breast cancer survivors compared 56 patients ingesting 90 mg daily of isoflavone soy drink with 55 patients who took placebo, with no differences reported between the groups in hot flash frequency or intensity, yet both groups improved over baseline.
The placebo effect and other challenges
Randomized, controlled trials of alternative medicines and nonhormonal prescription therapies have found a placebo effect that ranges from about 1% to as high as 77%.5,6 In estrogen trials, the mean placebo response is 50.8%.7 The study of nonhormonal therapies involves several challenges, such as difficulty locating a proper control or placebo, and double-blinding is often impossible.
A big problem faced in both studies was the lack of consistency in inclusion criteria. Study samples differed in age range, menopausal status, type of menopause, inclusion of breast cancer survivors, or use of antiestrogen therapy such as tamoxifen, raloxifene, or aromatase inhibitors—drugs that are associated with hot flashes.
Studies also varied in the degree of hot-flash severity required for enrollment. Some studies of alternative therapies enrolled women with 1 or 2 hot flashes per day, or 14 per week, whereas the US FDA requires women in hormone-therapy trials to have at least 7 moderate to severe hot flashes daily, or 50 to 60 per week, with specific definitions of severity.
Moreover, botanical products may have milder effects overall or take longer to elicit a response. Most studies are of short duration with small numbers of women, increasing the potential for confounding by the placebo effect.
REFERENCES
1. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. JAMA. 1998;280:605-613.
2. Roussouw JE, Anderson GL, Prentice RL, et al. Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288:321-333.
3. Fugate SE, Church CO. Nonestrogen treatment modalities for vasomotor symptoms associated with menopause. Ann Pharmacother. 2004;38:1482-1499.
4. Guttuso T, Kurlan R, McDermott MP, Kieburtz K. Gabapentin’s effects on hot flashes in postmenopausal women: a randomized controlled trial. Obstet Gynecol. 2003;101:337-345.
5. Marchesoni D, Mozzanega B, Maggino T, Nardelli GB. Postmenopausal hot flushes: endocrine correlations and progestinic treatment. Double blind crossed clinical trials using MPA versus placebo. J Gynaecol Endocrinol. 1985;1:63-69.
6. Bullock JL, Massey FM, Gambrell RD. Use of medroxyprogesterone acetate to prevent menopausal symptoms. Obstet Gynecol. 1975;46:165-168.
7. Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes. JAMA. 2006;295:2057-2071.
8. Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes: a randomized controlled trial. JAMA. 2003;289:2827-2834.
9. Suvanto-Luukkonen E, Koivunen R, Sundstrom H, et al. Citalopram and fluoxetine in the treatment of postmenopausal symptoms: a prospective, randomized, 9-month, placebo-controlled, double-blind study. Menopause. 2005;12:18-26.
10. Evans ML, Pritts E, Vittinghoff E, McClish K, Morgan KS, Jaffe RB. Management of postmenopausal hot flashes with venlafaxine hydrochloride: a randomized, controlled trial. Obstet Gynecol. 2005;105:161-166.
11. Blumenthal M, Busse WR, Goldberg A, et al. German Commision E Monographs: therapeutic monographs on medicinal plants for human use. Austin, Tex: American Botanical Council; 1998.
12. Nappi RE, Malavasi B, Brundu B, Facchinetti F. Efficacy of Cimicifuga racemosa on climacteric complaints: a randomized study versus low-dose transdermal estradiol. Gynecol Endocrinol. 2005;20:30-35.
13. Liske E, Hänggi W, Henneicke-Von Zepelin H-H, Boblitz N, Wüstenberg P, Rahlfs VW. Physiological investigation of a unique extract of black cohosh (Cimicifugae racemosae rhizoma): a 6-month clinical study demonstrates no systemic estrogenic effect. J Womens Health Gender Based Med. 2002;11:163-174.
14. Aiello EJ, Yasui Y, Tworoger SS, et al. Effect of a yearlong, moderate-intensity exercise intervention on the occurrence and severity of menopause symptoms in postmenopausal women. Menopause. 2004;11:382-388.
15. NIH State-of-the-Science Conference Statement on management of menopause-related symptoms National Institute of Health Consensus Development Program, March 21-23, 2005. Available at: http://consensus.nih.gov/2005/2005MenopausalSymptomsSOS025html.htm. Accessed October 9, 2006.
16. Kass-Annese B. Alternative therapies for menopause. Clin Obstet Gynecol. 2000;43:162-183.
17. Willhite LA, O’Connell MB. Urogenital atrophy: prevention and treatment. Pharmacotherapy. 2001;21:464-480.
18. Nachtigall LE. Comparative study: Replens versus local estrogen in menopausal women. Fertil Steril. 1994;61:178-180.
19. Bygdeman M, Swahn ML. Replens versus dienoestrol cream in the symptomatic treatment of vaginal atrophy in postmenopausal women. Maturitas. 1996;23:259-263.
With more women steering clear of estrogen in the wake of the Women’s Health Initiative and other trials,page 24). Nonetheless, many physicians and patients seek nonestrogen alternatives for this menopause-related symptom.
Over-the-counter lubricants are a mixed lot
Although many lubricants are marketed today, clinical study has been limited because they are regulated by the FDA as cosmetics. Of these products, Replens, a bioadhesive vaginal lubricant, has been studied the most intensively.
A unique formulation. Replens, a polycarbophil-based polymer, attaches to the vaginal wall and can hold 60 times its weight in water. It remains against the vaginal epithelial surface for more than 24 hours before it is sloughed off. This mechanism provides longer relief and requires less frequent application than other lubricants.17
Replens vs estrogen. Thrice-weekly Replens was compared with 12 weeks of daily vaginal estrogen cream18 and with vaginal estrogen cream applied daily for 2 weeks and then 3 times weekly for a total of 3 months.19 The comparison of Replens with conjugated estrogen cream (Premarin) showed significant improvements in vaginal moisture, fluid volume, elasticity, and pH levels in both treatment groups.18 Vaginal atrophy (assessed via Papanicolaou smear) reversed in 100% of estrogen-treated patients and 60% of Replens-treated patients.
When Replens was compared with dienoestrol vaginal cream, both therapies produced significant improvement in the vaginal dryness index (a score based on vaginal moisture, fluid volume, elasticity, and mucosa) within the first week.19 However, dienoestrol-treated patients had greater improvement in mean vaginal dryness (21.78 vs 17.32) at 12 weeks of therapy (P=.0001), compared with baseline values of 13 (dienoestrol) and 13.45 (Replens). Vaginal symptoms and dyspareunia improved at similar rates in the 2 groups. Patient satisfaction also was high in both groups, with 60% of Replens-treated patients and 84% of dienoestrol-treated patients reporting good to excellent effects.
No serious side effects were reported.18,19
Start with Replens for vaginal dryness, as it is a safe and effective alternative. If it is ineffective, vaginal estrogen may be more effective than vaginal lubricants.
The authors report no financial relationships relevant to this article
By Joann V. Pinkerton, MD, OBG Management Board of Editors, Professor of Obstetrics and Gynecology and Director, The Women’s Place Midlife Health Center, University of Virginia Health System, Charlottesville, Va
CASE 1 Perimenopausal, daily hot flashes
THERAPY
Exercise, soy products, vitamin E, and black cohosh
THE PATIENT: “V.S.,” 51, has been a patient for some time. At her latest visit, she reports that her menstrual periods are irregular, occurring every 3 to 12 weeks. She also has as many as 5 hot flashes a day, wakes in the very early morning, and occasionally experiences mild night sweats. Because she underwent bilateral tubal ligation many years ago, there is no need for contraception. She has no family history of breast cancer, but prefers to avoid drugs and asks if there are any herbal remedies and/or lifestyle changes that will ease her transition through menopause. She has a body mass index (BMI) of 31.6, and her breast and pelvic examinations are negative.
INTERVENTION: We discuss several simple options. For example, regular exercise may reduce vasomotor symptoms, although intense exertion with sweating can provoke hot flashes. Soy products and soy extracts have had mixed results, but appear to have some benefit. I suggest adding 1 soy dietary product per day. Vitamin E also may reduce hot flashes very modestly. The most promising product is black cohosh; I advise V.S. to take 20 mg twice a day.
OUTCOME: V.S. begins exercising regularly and sets a weight loss goal of 10%. She also begins taking 400 IU of vitamin E daily, adds soy nuts to her diet, and starts taking black cohosh. Three months later, she reports that her hot flashes have decreased to about 3 per day and are tolerable. She has had 1 menstrual cycle in the interim. If her symptoms worsen, she will consider medical therapy.
CASE 2 Severe symptoms, mood effects
THERAPY
Venlafaxine and vaginal moisturizers
THE PATIENT: “A.B.,” 54, a cancer survivor, is menopausal and has 10 to 20 hot flashes a day and soaking night sweats. She also reports low mood, frequent crying, and irritability. Before her cancer diagnosis, A.B. took hormone therapy for 6 months for severe menopausal symptoms. She recently underwent lumpectomy, axillary node dissection, radiation, and chemotherapy for a 3-cm, grade 3, invasive lobular carcinoma that was estrogen- and progesterone-receptor positive, and she is about to begin an aromatase inhibitor for chemoprevention. She and her husband have attempted intercourse since her chemotherapy ended, but the experience was painful. She would prefer to restart hormone therapy, but is willing to try nonhormonal options first. Her examination is unremarkable except for significant atrophy, with a vaginal pH of 7.0.
INTERVENTION: After a discussion of the data on SSRIs, SNRIs, and gabapentin, A.B. decides to try venlafaxine, 37.5 mg daily. If she has no improvement after 2 weeks, she will increase the dosage to 75 mg daily. For the vulvovaginal atrophy, she will try both vaginal moisturizers and vaginal lubricants, recognizing that this will not rethicken the epithelium. She also will exercise 5 days per week.
OUTCOME: After 3 months and an increase to 75 mg daily venlafaxine, the patient reports a 50% decrease in hot flashes and a more stable mood. The dyspareunia remains a problem. She decides to try a small amount of estradiol cream—somewhere between the size of a pea and the size of a dime—applied externally around the introital opening. She will start by applying it daily for 2 weeks, then reduce to twice a week.
CASE 3 Severe symptoms after TAH/BSO
THERAPY
Unsatisfactory improvement, a return to estrogen
THE PATIENT: “A.G.,” 46, complains of severe vasomotor symptoms. Two months ago she underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy for bilateral complex masses, which turned out to be endometriomas. At that time, endometriosis was observed along the left ureter, with residual peritoneal implants and a small nodule within the rectovaginal septum. A.G. was offered leuprolide acetate (Lupron Depot) postoperatively, but declined. She did well for about 2 months and then began having vasomotor symptoms. Her physician was hesitant to prescribe estrogen because of fear of reactivating endometriosis. A.G. toughed it out for 3 months, but now reports “misery.” She is moody, cries easily, and has not had sex with her husband since her surgery. An examination reveals a small, 8-mm nodule within the rectovaginal septum, decreased vulvar color, vaginal pallor, and levator ani spasm with exam. Vaginal pH is 6.5.
INTERVENTION: Although I suggest systemic progesterone therapy—oral, vaginal, or intramuscular—and explain that it would decrease any residual endometriosis and relieve the hot flashes, the patient does not want to take any hormonal therapy and is concerned about worsening her mood. Despite reassurance that hormone therapy would have less than a 5% chance of reactivating the endometriosis, A.G. decides to try an antidepressant first. Since she had taken paroxetine (Paxil) for postpartum depression, with no major side effects, she decides to try it again, starting with 10 mg daily.
OUTCOME: A.G. continues to have at least 5 bothersome hot flashes per day, which interrupt her work with profuse sweating. She also wakes at night for the same reason. However, she is less irritable. It has been 7 months since her surgery, and both she and her husband want her to try hormone therapy. She elects to begin a low-dose combined estrogen–progesterone product, as well as estradiol vaginal cream twice daily.
Three months later, she reports no pain, a gradual reduction in hot flashes, and significant improvement overall. Her vaginal color has returned, her pH is 5.5, and intercourse is no longer painful. She decides to continue taking oral hormone therapy at a low dose despite occasional vasomotor symptoms, and to keep using vaginal estrogen, but will stop the paroxetine.
How does one hot flash differ from another?
By Joann V. Pinkerton, MD, OBG Management Board of Editors, Professor of Obstetrics and Gynecology and Director of The Women’s Place Midlife Health Center, University of Virginia Health System, Charlottesville, Va
Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. JAMA. 2006;295:2057–2071.
Nedrow A, Miller J, Walker M, Nygren P, Huffman LH, Nelson HD. Complementary and alternative therapies for the management of menopause-related symptoms. Arch Intern Med. 2006;166:1453–1465.
The hot flash, long synonymous with menopause, is the bane of many women facing the midlife transition. Despite the intensity of the sensation, hot flashes appear to be triggered by small elevations in core body temperature within a greatly reduced thermoneutral zone.1-4 If the core temperature crosses the upper threshold, a hot flash with sweating and peripheral vasodilation occurs. If the lower threshold is crossed, shivering results. Core temperature elevations occur in both symptomatic and asymptomatic women.
The difference: In symptomatic women, the thermoneutral zone is narrowed.
2 randomized trials attest to mostly modest efficacy
In their rigorous study of nonhormonal therapies for hot flashes, Nelson et al reviewed MEDLINE, PsycINFO, and the Cochrane Clinical Trials Register Database for randomized, double-blind, placebo-controlled trials of oral nonhormonal treatments for hot flashes, ultimately selecting 43 trials. These included 10 trials of antidepressants, 10 trials of clonidine, 17 trials of isoflavones, and 6 trials of other prescription drugs. They found at least some evidence of efficacy for SSRIs, SNRIs, clonidine, and gabapentin, but all were considerably less effective than estrogen.
Nedrow and colleagues searched the same databases plus MANTIS and AMED, selecting 70 trials for inclusion. Overall, the data were insufficient to support the effectiveness of any complementary or alternative therapy. For example, a good-quality study enrolling breast cancer survivors compared 56 patients ingesting 90 mg daily of isoflavone soy drink with 55 patients who took placebo, with no differences reported between the groups in hot flash frequency or intensity, yet both groups improved over baseline.
The placebo effect and other challenges
Randomized, controlled trials of alternative medicines and nonhormonal prescription therapies have found a placebo effect that ranges from about 1% to as high as 77%.5,6 In estrogen trials, the mean placebo response is 50.8%.7 The study of nonhormonal therapies involves several challenges, such as difficulty locating a proper control or placebo, and double-blinding is often impossible.
A big problem faced in both studies was the lack of consistency in inclusion criteria. Study samples differed in age range, menopausal status, type of menopause, inclusion of breast cancer survivors, or use of antiestrogen therapy such as tamoxifen, raloxifene, or aromatase inhibitors—drugs that are associated with hot flashes.
Studies also varied in the degree of hot-flash severity required for enrollment. Some studies of alternative therapies enrolled women with 1 or 2 hot flashes per day, or 14 per week, whereas the US FDA requires women in hormone-therapy trials to have at least 7 moderate to severe hot flashes daily, or 50 to 60 per week, with specific definitions of severity.
Moreover, botanical products may have milder effects overall or take longer to elicit a response. Most studies are of short duration with small numbers of women, increasing the potential for confounding by the placebo effect.
REFERENCES
With more women steering clear of estrogen in the wake of the Women’s Health Initiative and other trials,page 24). Nonetheless, many physicians and patients seek nonestrogen alternatives for this menopause-related symptom.
Over-the-counter lubricants are a mixed lot
Although many lubricants are marketed today, clinical study has been limited because they are regulated by the FDA as cosmetics. Of these products, Replens, a bioadhesive vaginal lubricant, has been studied the most intensively.
A unique formulation. Replens, a polycarbophil-based polymer, attaches to the vaginal wall and can hold 60 times its weight in water. It remains against the vaginal epithelial surface for more than 24 hours before it is sloughed off. This mechanism provides longer relief and requires less frequent application than other lubricants.17
Replens vs estrogen. Thrice-weekly Replens was compared with 12 weeks of daily vaginal estrogen cream18 and with vaginal estrogen cream applied daily for 2 weeks and then 3 times weekly for a total of 3 months.19 The comparison of Replens with conjugated estrogen cream (Premarin) showed significant improvements in vaginal moisture, fluid volume, elasticity, and pH levels in both treatment groups.18 Vaginal atrophy (assessed via Papanicolaou smear) reversed in 100% of estrogen-treated patients and 60% of Replens-treated patients.
When Replens was compared with dienoestrol vaginal cream, both therapies produced significant improvement in the vaginal dryness index (a score based on vaginal moisture, fluid volume, elasticity, and mucosa) within the first week.19 However, dienoestrol-treated patients had greater improvement in mean vaginal dryness (21.78 vs 17.32) at 12 weeks of therapy (P=.0001), compared with baseline values of 13 (dienoestrol) and 13.45 (Replens). Vaginal symptoms and dyspareunia improved at similar rates in the 2 groups. Patient satisfaction also was high in both groups, with 60% of Replens-treated patients and 84% of dienoestrol-treated patients reporting good to excellent effects.
No serious side effects were reported.18,19
Start with Replens for vaginal dryness, as it is a safe and effective alternative. If it is ineffective, vaginal estrogen may be more effective than vaginal lubricants.
The authors report no financial relationships relevant to this article
By Joann V. Pinkerton, MD, OBG Management Board of Editors, Professor of Obstetrics and Gynecology and Director, The Women’s Place Midlife Health Center, University of Virginia Health System, Charlottesville, Va
CASE 1 Perimenopausal, daily hot flashes
THERAPY
Exercise, soy products, vitamin E, and black cohosh
THE PATIENT: “V.S.,” 51, has been a patient for some time. At her latest visit, she reports that her menstrual periods are irregular, occurring every 3 to 12 weeks. She also has as many as 5 hot flashes a day, wakes in the very early morning, and occasionally experiences mild night sweats. Because she underwent bilateral tubal ligation many years ago, there is no need for contraception. She has no family history of breast cancer, but prefers to avoid drugs and asks if there are any herbal remedies and/or lifestyle changes that will ease her transition through menopause. She has a body mass index (BMI) of 31.6, and her breast and pelvic examinations are negative.
INTERVENTION: We discuss several simple options. For example, regular exercise may reduce vasomotor symptoms, although intense exertion with sweating can provoke hot flashes. Soy products and soy extracts have had mixed results, but appear to have some benefit. I suggest adding 1 soy dietary product per day. Vitamin E also may reduce hot flashes very modestly. The most promising product is black cohosh; I advise V.S. to take 20 mg twice a day.
OUTCOME: V.S. begins exercising regularly and sets a weight loss goal of 10%. She also begins taking 400 IU of vitamin E daily, adds soy nuts to her diet, and starts taking black cohosh. Three months later, she reports that her hot flashes have decreased to about 3 per day and are tolerable. She has had 1 menstrual cycle in the interim. If her symptoms worsen, she will consider medical therapy.
CASE 2 Severe symptoms, mood effects
THERAPY
Venlafaxine and vaginal moisturizers
THE PATIENT: “A.B.,” 54, a cancer survivor, is menopausal and has 10 to 20 hot flashes a day and soaking night sweats. She also reports low mood, frequent crying, and irritability. Before her cancer diagnosis, A.B. took hormone therapy for 6 months for severe menopausal symptoms. She recently underwent lumpectomy, axillary node dissection, radiation, and chemotherapy for a 3-cm, grade 3, invasive lobular carcinoma that was estrogen- and progesterone-receptor positive, and she is about to begin an aromatase inhibitor for chemoprevention. She and her husband have attempted intercourse since her chemotherapy ended, but the experience was painful. She would prefer to restart hormone therapy, but is willing to try nonhormonal options first. Her examination is unremarkable except for significant atrophy, with a vaginal pH of 7.0.
INTERVENTION: After a discussion of the data on SSRIs, SNRIs, and gabapentin, A.B. decides to try venlafaxine, 37.5 mg daily. If she has no improvement after 2 weeks, she will increase the dosage to 75 mg daily. For the vulvovaginal atrophy, she will try both vaginal moisturizers and vaginal lubricants, recognizing that this will not rethicken the epithelium. She also will exercise 5 days per week.
OUTCOME: After 3 months and an increase to 75 mg daily venlafaxine, the patient reports a 50% decrease in hot flashes and a more stable mood. The dyspareunia remains a problem. She decides to try a small amount of estradiol cream—somewhere between the size of a pea and the size of a dime—applied externally around the introital opening. She will start by applying it daily for 2 weeks, then reduce to twice a week.
CASE 3 Severe symptoms after TAH/BSO
THERAPY
Unsatisfactory improvement, a return to estrogen
THE PATIENT: “A.G.,” 46, complains of severe vasomotor symptoms. Two months ago she underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy for bilateral complex masses, which turned out to be endometriomas. At that time, endometriosis was observed along the left ureter, with residual peritoneal implants and a small nodule within the rectovaginal septum. A.G. was offered leuprolide acetate (Lupron Depot) postoperatively, but declined. She did well for about 2 months and then began having vasomotor symptoms. Her physician was hesitant to prescribe estrogen because of fear of reactivating endometriosis. A.G. toughed it out for 3 months, but now reports “misery.” She is moody, cries easily, and has not had sex with her husband since her surgery. An examination reveals a small, 8-mm nodule within the rectovaginal septum, decreased vulvar color, vaginal pallor, and levator ani spasm with exam. Vaginal pH is 6.5.
INTERVENTION: Although I suggest systemic progesterone therapy—oral, vaginal, or intramuscular—and explain that it would decrease any residual endometriosis and relieve the hot flashes, the patient does not want to take any hormonal therapy and is concerned about worsening her mood. Despite reassurance that hormone therapy would have less than a 5% chance of reactivating the endometriosis, A.G. decides to try an antidepressant first. Since she had taken paroxetine (Paxil) for postpartum depression, with no major side effects, she decides to try it again, starting with 10 mg daily.
OUTCOME: A.G. continues to have at least 5 bothersome hot flashes per day, which interrupt her work with profuse sweating. She also wakes at night for the same reason. However, she is less irritable. It has been 7 months since her surgery, and both she and her husband want her to try hormone therapy. She elects to begin a low-dose combined estrogen–progesterone product, as well as estradiol vaginal cream twice daily.
Three months later, she reports no pain, a gradual reduction in hot flashes, and significant improvement overall. Her vaginal color has returned, her pH is 5.5, and intercourse is no longer painful. She decides to continue taking oral hormone therapy at a low dose despite occasional vasomotor symptoms, and to keep using vaginal estrogen, but will stop the paroxetine.
How does one hot flash differ from another?
By Joann V. Pinkerton, MD, OBG Management Board of Editors, Professor of Obstetrics and Gynecology and Director of The Women’s Place Midlife Health Center, University of Virginia Health System, Charlottesville, Va
Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. JAMA. 2006;295:2057–2071.
Nedrow A, Miller J, Walker M, Nygren P, Huffman LH, Nelson HD. Complementary and alternative therapies for the management of menopause-related symptoms. Arch Intern Med. 2006;166:1453–1465.
The hot flash, long synonymous with menopause, is the bane of many women facing the midlife transition. Despite the intensity of the sensation, hot flashes appear to be triggered by small elevations in core body temperature within a greatly reduced thermoneutral zone.1-4 If the core temperature crosses the upper threshold, a hot flash with sweating and peripheral vasodilation occurs. If the lower threshold is crossed, shivering results. Core temperature elevations occur in both symptomatic and asymptomatic women.
The difference: In symptomatic women, the thermoneutral zone is narrowed.
2 randomized trials attest to mostly modest efficacy
In their rigorous study of nonhormonal therapies for hot flashes, Nelson et al reviewed MEDLINE, PsycINFO, and the Cochrane Clinical Trials Register Database for randomized, double-blind, placebo-controlled trials of oral nonhormonal treatments for hot flashes, ultimately selecting 43 trials. These included 10 trials of antidepressants, 10 trials of clonidine, 17 trials of isoflavones, and 6 trials of other prescription drugs. They found at least some evidence of efficacy for SSRIs, SNRIs, clonidine, and gabapentin, but all were considerably less effective than estrogen.
Nedrow and colleagues searched the same databases plus MANTIS and AMED, selecting 70 trials for inclusion. Overall, the data were insufficient to support the effectiveness of any complementary or alternative therapy. For example, a good-quality study enrolling breast cancer survivors compared 56 patients ingesting 90 mg daily of isoflavone soy drink with 55 patients who took placebo, with no differences reported between the groups in hot flash frequency or intensity, yet both groups improved over baseline.
The placebo effect and other challenges
Randomized, controlled trials of alternative medicines and nonhormonal prescription therapies have found a placebo effect that ranges from about 1% to as high as 77%.5,6 In estrogen trials, the mean placebo response is 50.8%.7 The study of nonhormonal therapies involves several challenges, such as difficulty locating a proper control or placebo, and double-blinding is often impossible.
A big problem faced in both studies was the lack of consistency in inclusion criteria. Study samples differed in age range, menopausal status, type of menopause, inclusion of breast cancer survivors, or use of antiestrogen therapy such as tamoxifen, raloxifene, or aromatase inhibitors—drugs that are associated with hot flashes.
Studies also varied in the degree of hot-flash severity required for enrollment. Some studies of alternative therapies enrolled women with 1 or 2 hot flashes per day, or 14 per week, whereas the US FDA requires women in hormone-therapy trials to have at least 7 moderate to severe hot flashes daily, or 50 to 60 per week, with specific definitions of severity.
Moreover, botanical products may have milder effects overall or take longer to elicit a response. Most studies are of short duration with small numbers of women, increasing the potential for confounding by the placebo effect.
REFERENCES
1. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. JAMA. 1998;280:605-613.
2. Roussouw JE, Anderson GL, Prentice RL, et al. Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288:321-333.
3. Fugate SE, Church CO. Nonestrogen treatment modalities for vasomotor symptoms associated with menopause. Ann Pharmacother. 2004;38:1482-1499.
4. Guttuso T, Kurlan R, McDermott MP, Kieburtz K. Gabapentin’s effects on hot flashes in postmenopausal women: a randomized controlled trial. Obstet Gynecol. 2003;101:337-345.
5. Marchesoni D, Mozzanega B, Maggino T, Nardelli GB. Postmenopausal hot flushes: endocrine correlations and progestinic treatment. Double blind crossed clinical trials using MPA versus placebo. J Gynaecol Endocrinol. 1985;1:63-69.
6. Bullock JL, Massey FM, Gambrell RD. Use of medroxyprogesterone acetate to prevent menopausal symptoms. Obstet Gynecol. 1975;46:165-168.
7. Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes. JAMA. 2006;295:2057-2071.
8. Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes: a randomized controlled trial. JAMA. 2003;289:2827-2834.
9. Suvanto-Luukkonen E, Koivunen R, Sundstrom H, et al. Citalopram and fluoxetine in the treatment of postmenopausal symptoms: a prospective, randomized, 9-month, placebo-controlled, double-blind study. Menopause. 2005;12:18-26.
10. Evans ML, Pritts E, Vittinghoff E, McClish K, Morgan KS, Jaffe RB. Management of postmenopausal hot flashes with venlafaxine hydrochloride: a randomized, controlled trial. Obstet Gynecol. 2005;105:161-166.
11. Blumenthal M, Busse WR, Goldberg A, et al. German Commision E Monographs: therapeutic monographs on medicinal plants for human use. Austin, Tex: American Botanical Council; 1998.
12. Nappi RE, Malavasi B, Brundu B, Facchinetti F. Efficacy of Cimicifuga racemosa on climacteric complaints: a randomized study versus low-dose transdermal estradiol. Gynecol Endocrinol. 2005;20:30-35.
13. Liske E, Hänggi W, Henneicke-Von Zepelin H-H, Boblitz N, Wüstenberg P, Rahlfs VW. Physiological investigation of a unique extract of black cohosh (Cimicifugae racemosae rhizoma): a 6-month clinical study demonstrates no systemic estrogenic effect. J Womens Health Gender Based Med. 2002;11:163-174.
14. Aiello EJ, Yasui Y, Tworoger SS, et al. Effect of a yearlong, moderate-intensity exercise intervention on the occurrence and severity of menopause symptoms in postmenopausal women. Menopause. 2004;11:382-388.
15. NIH State-of-the-Science Conference Statement on management of menopause-related symptoms National Institute of Health Consensus Development Program, March 21-23, 2005. Available at: http://consensus.nih.gov/2005/2005MenopausalSymptomsSOS025html.htm. Accessed October 9, 2006.
16. Kass-Annese B. Alternative therapies for menopause. Clin Obstet Gynecol. 2000;43:162-183.
17. Willhite LA, O’Connell MB. Urogenital atrophy: prevention and treatment. Pharmacotherapy. 2001;21:464-480.
18. Nachtigall LE. Comparative study: Replens versus local estrogen in menopausal women. Fertil Steril. 1994;61:178-180.
19. Bygdeman M, Swahn ML. Replens versus dienoestrol cream in the symptomatic treatment of vaginal atrophy in postmenopausal women. Maturitas. 1996;23:259-263.
1. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. JAMA. 1998;280:605-613.
2. Roussouw JE, Anderson GL, Prentice RL, et al. Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288:321-333.
3. Fugate SE, Church CO. Nonestrogen treatment modalities for vasomotor symptoms associated with menopause. Ann Pharmacother. 2004;38:1482-1499.
4. Guttuso T, Kurlan R, McDermott MP, Kieburtz K. Gabapentin’s effects on hot flashes in postmenopausal women: a randomized controlled trial. Obstet Gynecol. 2003;101:337-345.
5. Marchesoni D, Mozzanega B, Maggino T, Nardelli GB. Postmenopausal hot flushes: endocrine correlations and progestinic treatment. Double blind crossed clinical trials using MPA versus placebo. J Gynaecol Endocrinol. 1985;1:63-69.
6. Bullock JL, Massey FM, Gambrell RD. Use of medroxyprogesterone acetate to prevent menopausal symptoms. Obstet Gynecol. 1975;46:165-168.
7. Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes. JAMA. 2006;295:2057-2071.
8. Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes: a randomized controlled trial. JAMA. 2003;289:2827-2834.
9. Suvanto-Luukkonen E, Koivunen R, Sundstrom H, et al. Citalopram and fluoxetine in the treatment of postmenopausal symptoms: a prospective, randomized, 9-month, placebo-controlled, double-blind study. Menopause. 2005;12:18-26.
10. Evans ML, Pritts E, Vittinghoff E, McClish K, Morgan KS, Jaffe RB. Management of postmenopausal hot flashes with venlafaxine hydrochloride: a randomized, controlled trial. Obstet Gynecol. 2005;105:161-166.
11. Blumenthal M, Busse WR, Goldberg A, et al. German Commision E Monographs: therapeutic monographs on medicinal plants for human use. Austin, Tex: American Botanical Council; 1998.
12. Nappi RE, Malavasi B, Brundu B, Facchinetti F. Efficacy of Cimicifuga racemosa on climacteric complaints: a randomized study versus low-dose transdermal estradiol. Gynecol Endocrinol. 2005;20:30-35.
13. Liske E, Hänggi W, Henneicke-Von Zepelin H-H, Boblitz N, Wüstenberg P, Rahlfs VW. Physiological investigation of a unique extract of black cohosh (Cimicifugae racemosae rhizoma): a 6-month clinical study demonstrates no systemic estrogenic effect. J Womens Health Gender Based Med. 2002;11:163-174.
14. Aiello EJ, Yasui Y, Tworoger SS, et al. Effect of a yearlong, moderate-intensity exercise intervention on the occurrence and severity of menopause symptoms in postmenopausal women. Menopause. 2004;11:382-388.
15. NIH State-of-the-Science Conference Statement on management of menopause-related symptoms National Institute of Health Consensus Development Program, March 21-23, 2005. Available at: http://consensus.nih.gov/2005/2005MenopausalSymptomsSOS025html.htm. Accessed October 9, 2006.
16. Kass-Annese B. Alternative therapies for menopause. Clin Obstet Gynecol. 2000;43:162-183.
17. Willhite LA, O’Connell MB. Urogenital atrophy: prevention and treatment. Pharmacotherapy. 2001;21:464-480.
18. Nachtigall LE. Comparative study: Replens versus local estrogen in menopausal women. Fertil Steril. 1994;61:178-180.
19. Bygdeman M, Swahn ML. Replens versus dienoestrol cream in the symptomatic treatment of vaginal atrophy in postmenopausal women. Maturitas. 1996;23:259-263.
Real-life risks and benefits of fracture-reducing drugs
It is all too easy to focus on T-scores and lose sight of why we check bone mass: we want to prevent fragility fractures—not osteoporosis per se. Fracture incidence is greater in women with osteoporosis, but the absolute number of fragility fractures is far greater in the women who have not yet reached that threshold. That was my main message last year. It still is, although I had hoped we would by now have in our hands a fracture risk assessment tool due from the World Health Organization. It will use age, DXA score, history, and other factors to project 5- and 10-year risk of fracture. Then we will simply have to decide at what level of risk, for an individual patient, drug therapy is indicated. Watch this space!
1 Osteonecrosis of the jaw: What clinicians need to know
2 Raloxifene: A bone drug that reduces new onset breast cancer
3 Estrogen for bone protection: Time for a comeback?
4 Risedronate: Not just for fracture prevention?
1 Osteonecrosis of the jaw: What clinicians need to know
Woo SB, Hellstein JW, Kalmar JR. Systematic review: bisphosphonates and osteonecrosis of the jaws. Ann Intern Med. 2006;144:753–761.
This was the year of massive media attention on bisphosphonate therapy and osteonecrosis of the jaw. A bone specialist I know said he got even more phone calls after this report was published than after the WHI blitz 4 years ago.
Patients started calling when the lay press limelight focused on a report by Woo et al, who reviewed all of the world’s literature published since 1966, and identified 368 reported cases of bisphosphonate-associated osteonecrosis of the jaw (ONJ).
Main findings
Of the 368 cases, 94% were being treated with intravenous bisphosphonate therapy; 85% of the patients had either multiple myeloma or metastatic cancer of the breast. More than half of all cases (60%) were preceded by tooth extraction or other dentoalveolar surgical procedure to treat infections, and the remaining 40% were related to infection, denture trauma, or other physical trauma.
The latter group of cases occurred spontaneously, although the patients affected often wore dentures. The mandible was more commonly affected than the maxilla by a ratio of 2:1.
Other studies have reported 75% of patients with ONJ were receiving chemotherapy at the time of diagnosis, and 38% were on corticosteroids.
Do these findings affect prescribing?
A small number of cases of ONJ in postmenopausal women taking oral bisphosphonates have occurred, though rarely—well under 1 per 100,000 patients treated. Realize that patients with myeloma or metastatic breast cancer are usually treated with high-dose, high-potency intravenous bisphosphonate.
There were no reports of ONJ in any of the controlled trials on use of bisphosphonates for osteoporosis; this represents more than 60,000 patients who in some cases were treated for more than 8 years.
Recommendations
The American Society for Bone and Mineral Research advises:
2 Raloxifene: An osteoporosis drug that reduces new onset breast cancer
Vogel VG, Costantino JP, Wickerham DL, et al. Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes. The NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 Trial. JAMA 2006;295:2727–2741.
Barrett-Connor E, Mosca L, Collins P, et al. Effects of raloxifene on cardiovascular events and breast cancer in postmenopausal women. N Engl J Med. 2006;355:125–137.
Two large trials cause me to believe that raloxifene significantly reduces new onset breast cancer in virtually every group of women in which it has been studied.
Why you didn’t hear about this until now
Raloxifene was FDA-approved for prevention of osteoporosis in 1997 and for treatment of osteoporosis in 1999. There was a statistically significant 76% reduction in new onset breast cancer in raloxifene-treated patients versus placebo through 4 years of the MORE (Multiple Outcomes of Raloxifene Evaluation) trial, and this persisted at a 66% reduction through the additional years of the CORE (Continued Observation of Raloxifene Evaluation) trial.
Findings effectively buried. However, because of the wording of the FDA label, and, as a result of a $36 million fine from the Department of Justice, for promotional activities in the early years after its release, these findings were effectively buried and not well promulgated.
STAR and RUTH trials
Study of Tamoxifen and Raloxifene
The STAR trial reported by Vogel et al involved 19,747 postmenopausal women enrolled on the basis of their high risk for breast cancer. The patients were randomized to tamoxifen (already approved for breast cancer prevention) or raloxifene.
Over 5 years of study, the incidence of invasive breast cancer was virtually identical in both groups. However, the raloxifene group had statistically significant lower numbers of thromboembolic events, cataracts, hysterectomies performed, and endometrial hyperplasias. A 38% reduction in endometrial cancer in the raloxifene group had not reached statistical significance but was trending in that direction.
Studies of fracture reduction in populations with existing osteoporosis include the Fracture Intervention Trial, which enrolled women with low bone mass and existing vertebral fractures. Clinical vertebral and other fractures were substantially reduced in the treatment group
Raloxifene Use in The Heart
The RUTH trial reported by Barrett-Connor et al involved 10,101 post-menopausal women selected for multiple risks for coronary heart disease.
Although there was no reduction in coronary heart disease, there was no increase, unlike the estrogen and progesterone arm of the Women’s Health Initiative (WHI). Additionally, however, there was a 44% reduction in invasive breast cancer (95% CI 0.38–0.83). Remember, these women were chosen for their risk of heart disease. The rate of breast cancer in the placebo group was 2.7 cases per 1,000 women per year, and thus the 44% reduction means the rate in the treatment group was 1.5 cases per 1,000 women per year.
Consider the context
For comparison purposes, consider an average-risk group in the WHI, where the incidence of breast cancer was 3.3 cases per 1,000 women per year. Contrast this rate to that of a high-risk group, such as the placebo group in the original breast cancer prevention trial (BCPT), where the incidence was 6.8 cancers per 1,000 women per year.
I believe that such information must be available to clinicians and must be factored into your decision when contemplating a bone drug. A recent anecdote underscores the problem.
4 out of 10 Caucasian women over age 50 will fracture a hip, spine, or wrist sooner or later
1 of every 5 who fracture a hip ends up in a nursing home
DXA T-score of -2.0 in the hip and atypical ductal hyperplasia
An internist called me to discuss a mutual patient whom I had placed on raloxifene 2 years earlier. His comment was that raloxifene does not work in the hip. Our mutual patient had a T-score on DXA in the hip of -2.0 and in the spine of -0.7 (falsely improved by some osteophytes). In addition, she had been diagnosed with atypical ductal hyperplasia of the breast 2 years earlier.
I pointed out to him that studies of hip fracture reduction with bisphosphonate were all performed in women with osteoporosis. Furthermore, after the NHANES III correction, a sizable number of women in the MORE trial were not osteoporotic. In fact, the fracture incidence in the MORE trial placebo group was 0.7%—an extremely low risk—compared with 2.2% in the treatment group in the Fracture Intervention Trial I, and 3.0% in the treatment group in the Hip Intervention Program.
Stated another way, the incidence of hip fracture in the MORE placebo group was less than that in the treated groups in the Fracture Intervention Trial I and the Hip Intervention Program.
But perhaps the most important point in my anecdotal case is that the woman had a diagnosis of atypical ductal hyperplasia of the breast, a lesion that significantly increases her risk of invasive breast cancer. For these reasons, raloxifene was a much better choice for her fracture reduction pharmacotherapy. Her internist was unaware of these breast effects and had not taken this into account.
3 Estrogen for bone protection: Time for a comeback?
Stefanick ML, Anderson GL, Margolis KL, et al. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. JAMA. 2006;295:1647–1657.
Jackson RD, Wactawski-Wende J, LaCroix AZ, et al. Effects of conjugated equine estrogen on risk of fractures and BMD in postmenopausal women with hysterectomy: results from the Women’s Health Initiative randomized trial. J Bone Miner Res. 2006;6:817–828.
It may be time to revisit our initial reaction to the WHI. Although most estrogens are FDA-approved for treatment of osteoporosis, recommendations since the WHI have generally been that we should reserve hormone therapy or estrogen therapy for disruptive transitional symptoms (hot flashes, night sweats, etc.), and prescribe the lowest dose possible for the shortest time possible, consistent with the patient’s treatment goals.
Rethink therapy for 2 types of patients?
Recent reports, however, may cause us to rethink that approach, especially in 2 types of patients:
Stefanick et al reported on the 10,739 women aged 50–79 in the estrogen-only arm of the WHI, who received placebo or0.625 mg of conjugated equine estrogen. After a mean follow-up of 7.1 years, there were 104 cases of invasive breast cancer in this CEE group and 133 cases in the placebo group.
Stated another way, this represents a 20% reduction in breast cancer in women in the CEE group. Although this reduction was not statistically significant, it is in stark contrast with the increase in breast cancer seen in numerous studies of estrogen and progestogen together.

Statistically significant reductions in fracture, compared with placebo, in the WHI E2-only arm were:
wrist 42%
clinical vertebral 36%
hip 35%
total fractures 29%
Women in the WHI had all levels of fracture risk
Jackson et al also analyzed fracture incidence in the WHI E2-only arm, as assessed by semiannual questionnaires and verified by adjudication of radiology reports.
Women on CEE had statistically significant reductions in hip fracture (35%), clinical vertebral fracture (36%), wrist fracture (42%), and total fractures (29%), compared with placebo. This trend held across all levels of fracture, although the reductions were greatest in patients at highest risk.
This is notable, however, because the WHI was primarily studying the effect of CEE on coronary heart disease. Unlike virtually all osteoporosis studies, in which women with increased risk of fracture are studied, the women selected for the Women’s Health Initiative represent all levels of fracture risk—and this placebo-controlled, large, randomized study discovered that all fractures, across all levels of risk, were significantly reduced. And there was no increase in breast cancer.
This may well weigh in on many a clinician’s thought process about indications and real risks of estrogen therapy.
4 Risedronate: Not just for fracture prevention?
Buckland-Wright JC, Messent EA, Bingham CO III, et al. A 2 yr longitudinal radiographic study examining the effect of a bisphosphonate (risedronate) upon subchondral bone loss in osteoarthritic knee patients. Rheumatology (Oxford). 2006 Jul 11; [Epub ahead of print].
Bone formation in osteoarthritic knees reversed disease-related bone loss while maintaining structural integrity within the subchondral cancellous bone in patients treated with risedronate, in this 2-year study. Patients with progressive knee osteoarthritis were enrolled in this double-blinded, multicenter, randomized, placebo-controlled trial.
The treatment groups included placebo, risedronate 5 mg/day, 15 mg/day, and 50 mg/week. Patients receiving risedronate 15 mg/day retained vertical trabecular structure and those receiving 50 mg/week increased vertical trabecular number, thereby preserving the structural integrity of the subchondral bone.
This is important because weakening and loss of vertical trabecular support, when combined with the biomechanical weakening of the bone due to disease-related reduction in mineral content, are believed to contribute to collapse of the tibial compartment in late-stage osteoarthritis. It has been suggested that bisphosphonates are associated with decreased bone formation as an expected consequence of suppressing the coupled bone remodeling process. This did not appear to be the case in this study. In fact, the study tends to agree with experimental work that shows that high doses of bisphosphonates, as well as repeated administration, may enhance bone accretion.
The author serves on the advisory boards for Eli Lilly, Merck, Pfizer, Procter & Gamble, and GlaxoSmithKline.

Steven Goldstein, MD
Professor of Obstetrics and Gynecology, New York University School of Medicine, New York City
Steven Goldstein, MD
Professor of Obstetrics and Gynecology, New York University School of Medicine, New York City
Steven Goldstein, MD
Professor of Obstetrics and Gynecology, New York University School of Medicine, New York City
It is all too easy to focus on T-scores and lose sight of why we check bone mass: we want to prevent fragility fractures—not osteoporosis per se. Fracture incidence is greater in women with osteoporosis, but the absolute number of fragility fractures is far greater in the women who have not yet reached that threshold. That was my main message last year. It still is, although I had hoped we would by now have in our hands a fracture risk assessment tool due from the World Health Organization. It will use age, DXA score, history, and other factors to project 5- and 10-year risk of fracture. Then we will simply have to decide at what level of risk, for an individual patient, drug therapy is indicated. Watch this space!
1 Osteonecrosis of the jaw: What clinicians need to know
2 Raloxifene: A bone drug that reduces new onset breast cancer
3 Estrogen for bone protection: Time for a comeback?
4 Risedronate: Not just for fracture prevention?
1 Osteonecrosis of the jaw: What clinicians need to know
Woo SB, Hellstein JW, Kalmar JR. Systematic review: bisphosphonates and osteonecrosis of the jaws. Ann Intern Med. 2006;144:753–761.
This was the year of massive media attention on bisphosphonate therapy and osteonecrosis of the jaw. A bone specialist I know said he got even more phone calls after this report was published than after the WHI blitz 4 years ago.
Patients started calling when the lay press limelight focused on a report by Woo et al, who reviewed all of the world’s literature published since 1966, and identified 368 reported cases of bisphosphonate-associated osteonecrosis of the jaw (ONJ).
Main findings
Of the 368 cases, 94% were being treated with intravenous bisphosphonate therapy; 85% of the patients had either multiple myeloma or metastatic cancer of the breast. More than half of all cases (60%) were preceded by tooth extraction or other dentoalveolar surgical procedure to treat infections, and the remaining 40% were related to infection, denture trauma, or other physical trauma.
The latter group of cases occurred spontaneously, although the patients affected often wore dentures. The mandible was more commonly affected than the maxilla by a ratio of 2:1.
Other studies have reported 75% of patients with ONJ were receiving chemotherapy at the time of diagnosis, and 38% were on corticosteroids.
Do these findings affect prescribing?
A small number of cases of ONJ in postmenopausal women taking oral bisphosphonates have occurred, though rarely—well under 1 per 100,000 patients treated. Realize that patients with myeloma or metastatic breast cancer are usually treated with high-dose, high-potency intravenous bisphosphonate.
There were no reports of ONJ in any of the controlled trials on use of bisphosphonates for osteoporosis; this represents more than 60,000 patients who in some cases were treated for more than 8 years.
Recommendations
The American Society for Bone and Mineral Research advises:
2 Raloxifene: An osteoporosis drug that reduces new onset breast cancer
Vogel VG, Costantino JP, Wickerham DL, et al. Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes. The NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 Trial. JAMA 2006;295:2727–2741.
Barrett-Connor E, Mosca L, Collins P, et al. Effects of raloxifene on cardiovascular events and breast cancer in postmenopausal women. N Engl J Med. 2006;355:125–137.
Two large trials cause me to believe that raloxifene significantly reduces new onset breast cancer in virtually every group of women in which it has been studied.
Why you didn’t hear about this until now
Raloxifene was FDA-approved for prevention of osteoporosis in 1997 and for treatment of osteoporosis in 1999. There was a statistically significant 76% reduction in new onset breast cancer in raloxifene-treated patients versus placebo through 4 years of the MORE (Multiple Outcomes of Raloxifene Evaluation) trial, and this persisted at a 66% reduction through the additional years of the CORE (Continued Observation of Raloxifene Evaluation) trial.
Findings effectively buried. However, because of the wording of the FDA label, and, as a result of a $36 million fine from the Department of Justice, for promotional activities in the early years after its release, these findings were effectively buried and not well promulgated.
STAR and RUTH trials
Study of Tamoxifen and Raloxifene
The STAR trial reported by Vogel et al involved 19,747 postmenopausal women enrolled on the basis of their high risk for breast cancer. The patients were randomized to tamoxifen (already approved for breast cancer prevention) or raloxifene.
Over 5 years of study, the incidence of invasive breast cancer was virtually identical in both groups. However, the raloxifene group had statistically significant lower numbers of thromboembolic events, cataracts, hysterectomies performed, and endometrial hyperplasias. A 38% reduction in endometrial cancer in the raloxifene group had not reached statistical significance but was trending in that direction.
Studies of fracture reduction in populations with existing osteoporosis include the Fracture Intervention Trial, which enrolled women with low bone mass and existing vertebral fractures. Clinical vertebral and other fractures were substantially reduced in the treatment group
Raloxifene Use in The Heart
The RUTH trial reported by Barrett-Connor et al involved 10,101 post-menopausal women selected for multiple risks for coronary heart disease.
Although there was no reduction in coronary heart disease, there was no increase, unlike the estrogen and progesterone arm of the Women’s Health Initiative (WHI). Additionally, however, there was a 44% reduction in invasive breast cancer (95% CI 0.38–0.83). Remember, these women were chosen for their risk of heart disease. The rate of breast cancer in the placebo group was 2.7 cases per 1,000 women per year, and thus the 44% reduction means the rate in the treatment group was 1.5 cases per 1,000 women per year.
Consider the context
For comparison purposes, consider an average-risk group in the WHI, where the incidence of breast cancer was 3.3 cases per 1,000 women per year. Contrast this rate to that of a high-risk group, such as the placebo group in the original breast cancer prevention trial (BCPT), where the incidence was 6.8 cancers per 1,000 women per year.
I believe that such information must be available to clinicians and must be factored into your decision when contemplating a bone drug. A recent anecdote underscores the problem.
4 out of 10 Caucasian women over age 50 will fracture a hip, spine, or wrist sooner or later
1 of every 5 who fracture a hip ends up in a nursing home
DXA T-score of -2.0 in the hip and atypical ductal hyperplasia
An internist called me to discuss a mutual patient whom I had placed on raloxifene 2 years earlier. His comment was that raloxifene does not work in the hip. Our mutual patient had a T-score on DXA in the hip of -2.0 and in the spine of -0.7 (falsely improved by some osteophytes). In addition, she had been diagnosed with atypical ductal hyperplasia of the breast 2 years earlier.
I pointed out to him that studies of hip fracture reduction with bisphosphonate were all performed in women with osteoporosis. Furthermore, after the NHANES III correction, a sizable number of women in the MORE trial were not osteoporotic. In fact, the fracture incidence in the MORE trial placebo group was 0.7%—an extremely low risk—compared with 2.2% in the treatment group in the Fracture Intervention Trial I, and 3.0% in the treatment group in the Hip Intervention Program.
Stated another way, the incidence of hip fracture in the MORE placebo group was less than that in the treated groups in the Fracture Intervention Trial I and the Hip Intervention Program.
But perhaps the most important point in my anecdotal case is that the woman had a diagnosis of atypical ductal hyperplasia of the breast, a lesion that significantly increases her risk of invasive breast cancer. For these reasons, raloxifene was a much better choice for her fracture reduction pharmacotherapy. Her internist was unaware of these breast effects and had not taken this into account.
3 Estrogen for bone protection: Time for a comeback?
Stefanick ML, Anderson GL, Margolis KL, et al. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. JAMA. 2006;295:1647–1657.
Jackson RD, Wactawski-Wende J, LaCroix AZ, et al. Effects of conjugated equine estrogen on risk of fractures and BMD in postmenopausal women with hysterectomy: results from the Women’s Health Initiative randomized trial. J Bone Miner Res. 2006;6:817–828.
It may be time to revisit our initial reaction to the WHI. Although most estrogens are FDA-approved for treatment of osteoporosis, recommendations since the WHI have generally been that we should reserve hormone therapy or estrogen therapy for disruptive transitional symptoms (hot flashes, night sweats, etc.), and prescribe the lowest dose possible for the shortest time possible, consistent with the patient’s treatment goals.
Rethink therapy for 2 types of patients?
Recent reports, however, may cause us to rethink that approach, especially in 2 types of patients:
Stefanick et al reported on the 10,739 women aged 50–79 in the estrogen-only arm of the WHI, who received placebo or0.625 mg of conjugated equine estrogen. After a mean follow-up of 7.1 years, there were 104 cases of invasive breast cancer in this CEE group and 133 cases in the placebo group.
Stated another way, this represents a 20% reduction in breast cancer in women in the CEE group. Although this reduction was not statistically significant, it is in stark contrast with the increase in breast cancer seen in numerous studies of estrogen and progestogen together.
Statistically significant reductions in fracture, compared with placebo, in the WHI E2-only arm were:
wrist 42%
clinical vertebral 36%
hip 35%
total fractures 29%
Women in the WHI had all levels of fracture risk
Jackson et al also analyzed fracture incidence in the WHI E2-only arm, as assessed by semiannual questionnaires and verified by adjudication of radiology reports.
Women on CEE had statistically significant reductions in hip fracture (35%), clinical vertebral fracture (36%), wrist fracture (42%), and total fractures (29%), compared with placebo. This trend held across all levels of fracture, although the reductions were greatest in patients at highest risk.
This is notable, however, because the WHI was primarily studying the effect of CEE on coronary heart disease. Unlike virtually all osteoporosis studies, in which women with increased risk of fracture are studied, the women selected for the Women’s Health Initiative represent all levels of fracture risk—and this placebo-controlled, large, randomized study discovered that all fractures, across all levels of risk, were significantly reduced. And there was no increase in breast cancer.
This may well weigh in on many a clinician’s thought process about indications and real risks of estrogen therapy.
4 Risedronate: Not just for fracture prevention?
Buckland-Wright JC, Messent EA, Bingham CO III, et al. A 2 yr longitudinal radiographic study examining the effect of a bisphosphonate (risedronate) upon subchondral bone loss in osteoarthritic knee patients. Rheumatology (Oxford). 2006 Jul 11; [Epub ahead of print].
Bone formation in osteoarthritic knees reversed disease-related bone loss while maintaining structural integrity within the subchondral cancellous bone in patients treated with risedronate, in this 2-year study. Patients with progressive knee osteoarthritis were enrolled in this double-blinded, multicenter, randomized, placebo-controlled trial.
The treatment groups included placebo, risedronate 5 mg/day, 15 mg/day, and 50 mg/week. Patients receiving risedronate 15 mg/day retained vertical trabecular structure and those receiving 50 mg/week increased vertical trabecular number, thereby preserving the structural integrity of the subchondral bone.
This is important because weakening and loss of vertical trabecular support, when combined with the biomechanical weakening of the bone due to disease-related reduction in mineral content, are believed to contribute to collapse of the tibial compartment in late-stage osteoarthritis. It has been suggested that bisphosphonates are associated with decreased bone formation as an expected consequence of suppressing the coupled bone remodeling process. This did not appear to be the case in this study. In fact, the study tends to agree with experimental work that shows that high doses of bisphosphonates, as well as repeated administration, may enhance bone accretion.
The author serves on the advisory boards for Eli Lilly, Merck, Pfizer, Procter & Gamble, and GlaxoSmithKline.
It is all too easy to focus on T-scores and lose sight of why we check bone mass: we want to prevent fragility fractures—not osteoporosis per se. Fracture incidence is greater in women with osteoporosis, but the absolute number of fragility fractures is far greater in the women who have not yet reached that threshold. That was my main message last year. It still is, although I had hoped we would by now have in our hands a fracture risk assessment tool due from the World Health Organization. It will use age, DXA score, history, and other factors to project 5- and 10-year risk of fracture. Then we will simply have to decide at what level of risk, for an individual patient, drug therapy is indicated. Watch this space!
1 Osteonecrosis of the jaw: What clinicians need to know
2 Raloxifene: A bone drug that reduces new onset breast cancer
3 Estrogen for bone protection: Time for a comeback?
4 Risedronate: Not just for fracture prevention?
1 Osteonecrosis of the jaw: What clinicians need to know
Woo SB, Hellstein JW, Kalmar JR. Systematic review: bisphosphonates and osteonecrosis of the jaws. Ann Intern Med. 2006;144:753–761.
This was the year of massive media attention on bisphosphonate therapy and osteonecrosis of the jaw. A bone specialist I know said he got even more phone calls after this report was published than after the WHI blitz 4 years ago.
Patients started calling when the lay press limelight focused on a report by Woo et al, who reviewed all of the world’s literature published since 1966, and identified 368 reported cases of bisphosphonate-associated osteonecrosis of the jaw (ONJ).
Main findings
Of the 368 cases, 94% were being treated with intravenous bisphosphonate therapy; 85% of the patients had either multiple myeloma or metastatic cancer of the breast. More than half of all cases (60%) were preceded by tooth extraction or other dentoalveolar surgical procedure to treat infections, and the remaining 40% were related to infection, denture trauma, or other physical trauma.
The latter group of cases occurred spontaneously, although the patients affected often wore dentures. The mandible was more commonly affected than the maxilla by a ratio of 2:1.
Other studies have reported 75% of patients with ONJ were receiving chemotherapy at the time of diagnosis, and 38% were on corticosteroids.
Do these findings affect prescribing?
A small number of cases of ONJ in postmenopausal women taking oral bisphosphonates have occurred, though rarely—well under 1 per 100,000 patients treated. Realize that patients with myeloma or metastatic breast cancer are usually treated with high-dose, high-potency intravenous bisphosphonate.
There were no reports of ONJ in any of the controlled trials on use of bisphosphonates for osteoporosis; this represents more than 60,000 patients who in some cases were treated for more than 8 years.
Recommendations
The American Society for Bone and Mineral Research advises:
2 Raloxifene: An osteoporosis drug that reduces new onset breast cancer
Vogel VG, Costantino JP, Wickerham DL, et al. Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes. The NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 Trial. JAMA 2006;295:2727–2741.
Barrett-Connor E, Mosca L, Collins P, et al. Effects of raloxifene on cardiovascular events and breast cancer in postmenopausal women. N Engl J Med. 2006;355:125–137.
Two large trials cause me to believe that raloxifene significantly reduces new onset breast cancer in virtually every group of women in which it has been studied.
Why you didn’t hear about this until now
Raloxifene was FDA-approved for prevention of osteoporosis in 1997 and for treatment of osteoporosis in 1999. There was a statistically significant 76% reduction in new onset breast cancer in raloxifene-treated patients versus placebo through 4 years of the MORE (Multiple Outcomes of Raloxifene Evaluation) trial, and this persisted at a 66% reduction through the additional years of the CORE (Continued Observation of Raloxifene Evaluation) trial.
Findings effectively buried. However, because of the wording of the FDA label, and, as a result of a $36 million fine from the Department of Justice, for promotional activities in the early years after its release, these findings were effectively buried and not well promulgated.
STAR and RUTH trials
Study of Tamoxifen and Raloxifene
The STAR trial reported by Vogel et al involved 19,747 postmenopausal women enrolled on the basis of their high risk for breast cancer. The patients were randomized to tamoxifen (already approved for breast cancer prevention) or raloxifene.
Over 5 years of study, the incidence of invasive breast cancer was virtually identical in both groups. However, the raloxifene group had statistically significant lower numbers of thromboembolic events, cataracts, hysterectomies performed, and endometrial hyperplasias. A 38% reduction in endometrial cancer in the raloxifene group had not reached statistical significance but was trending in that direction.
Studies of fracture reduction in populations with existing osteoporosis include the Fracture Intervention Trial, which enrolled women with low bone mass and existing vertebral fractures. Clinical vertebral and other fractures were substantially reduced in the treatment group
Raloxifene Use in The Heart
The RUTH trial reported by Barrett-Connor et al involved 10,101 post-menopausal women selected for multiple risks for coronary heart disease.
Although there was no reduction in coronary heart disease, there was no increase, unlike the estrogen and progesterone arm of the Women’s Health Initiative (WHI). Additionally, however, there was a 44% reduction in invasive breast cancer (95% CI 0.38–0.83). Remember, these women were chosen for their risk of heart disease. The rate of breast cancer in the placebo group was 2.7 cases per 1,000 women per year, and thus the 44% reduction means the rate in the treatment group was 1.5 cases per 1,000 women per year.
Consider the context
For comparison purposes, consider an average-risk group in the WHI, where the incidence of breast cancer was 3.3 cases per 1,000 women per year. Contrast this rate to that of a high-risk group, such as the placebo group in the original breast cancer prevention trial (BCPT), where the incidence was 6.8 cancers per 1,000 women per year.
I believe that such information must be available to clinicians and must be factored into your decision when contemplating a bone drug. A recent anecdote underscores the problem.
4 out of 10 Caucasian women over age 50 will fracture a hip, spine, or wrist sooner or later
1 of every 5 who fracture a hip ends up in a nursing home
DXA T-score of -2.0 in the hip and atypical ductal hyperplasia
An internist called me to discuss a mutual patient whom I had placed on raloxifene 2 years earlier. His comment was that raloxifene does not work in the hip. Our mutual patient had a T-score on DXA in the hip of -2.0 and in the spine of -0.7 (falsely improved by some osteophytes). In addition, she had been diagnosed with atypical ductal hyperplasia of the breast 2 years earlier.
I pointed out to him that studies of hip fracture reduction with bisphosphonate were all performed in women with osteoporosis. Furthermore, after the NHANES III correction, a sizable number of women in the MORE trial were not osteoporotic. In fact, the fracture incidence in the MORE trial placebo group was 0.7%—an extremely low risk—compared with 2.2% in the treatment group in the Fracture Intervention Trial I, and 3.0% in the treatment group in the Hip Intervention Program.
Stated another way, the incidence of hip fracture in the MORE placebo group was less than that in the treated groups in the Fracture Intervention Trial I and the Hip Intervention Program.
But perhaps the most important point in my anecdotal case is that the woman had a diagnosis of atypical ductal hyperplasia of the breast, a lesion that significantly increases her risk of invasive breast cancer. For these reasons, raloxifene was a much better choice for her fracture reduction pharmacotherapy. Her internist was unaware of these breast effects and had not taken this into account.
3 Estrogen for bone protection: Time for a comeback?
Stefanick ML, Anderson GL, Margolis KL, et al. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. JAMA. 2006;295:1647–1657.
Jackson RD, Wactawski-Wende J, LaCroix AZ, et al. Effects of conjugated equine estrogen on risk of fractures and BMD in postmenopausal women with hysterectomy: results from the Women’s Health Initiative randomized trial. J Bone Miner Res. 2006;6:817–828.
It may be time to revisit our initial reaction to the WHI. Although most estrogens are FDA-approved for treatment of osteoporosis, recommendations since the WHI have generally been that we should reserve hormone therapy or estrogen therapy for disruptive transitional symptoms (hot flashes, night sweats, etc.), and prescribe the lowest dose possible for the shortest time possible, consistent with the patient’s treatment goals.
Rethink therapy for 2 types of patients?
Recent reports, however, may cause us to rethink that approach, especially in 2 types of patients:
Stefanick et al reported on the 10,739 women aged 50–79 in the estrogen-only arm of the WHI, who received placebo or0.625 mg of conjugated equine estrogen. After a mean follow-up of 7.1 years, there were 104 cases of invasive breast cancer in this CEE group and 133 cases in the placebo group.
Stated another way, this represents a 20% reduction in breast cancer in women in the CEE group. Although this reduction was not statistically significant, it is in stark contrast with the increase in breast cancer seen in numerous studies of estrogen and progestogen together.
Statistically significant reductions in fracture, compared with placebo, in the WHI E2-only arm were:
wrist 42%
clinical vertebral 36%
hip 35%
total fractures 29%
Women in the WHI had all levels of fracture risk
Jackson et al also analyzed fracture incidence in the WHI E2-only arm, as assessed by semiannual questionnaires and verified by adjudication of radiology reports.
Women on CEE had statistically significant reductions in hip fracture (35%), clinical vertebral fracture (36%), wrist fracture (42%), and total fractures (29%), compared with placebo. This trend held across all levels of fracture, although the reductions were greatest in patients at highest risk.
This is notable, however, because the WHI was primarily studying the effect of CEE on coronary heart disease. Unlike virtually all osteoporosis studies, in which women with increased risk of fracture are studied, the women selected for the Women’s Health Initiative represent all levels of fracture risk—and this placebo-controlled, large, randomized study discovered that all fractures, across all levels of risk, were significantly reduced. And there was no increase in breast cancer.
This may well weigh in on many a clinician’s thought process about indications and real risks of estrogen therapy.
4 Risedronate: Not just for fracture prevention?
Buckland-Wright JC, Messent EA, Bingham CO III, et al. A 2 yr longitudinal radiographic study examining the effect of a bisphosphonate (risedronate) upon subchondral bone loss in osteoarthritic knee patients. Rheumatology (Oxford). 2006 Jul 11; [Epub ahead of print].
Bone formation in osteoarthritic knees reversed disease-related bone loss while maintaining structural integrity within the subchondral cancellous bone in patients treated with risedronate, in this 2-year study. Patients with progressive knee osteoarthritis were enrolled in this double-blinded, multicenter, randomized, placebo-controlled trial.
The treatment groups included placebo, risedronate 5 mg/day, 15 mg/day, and 50 mg/week. Patients receiving risedronate 15 mg/day retained vertical trabecular structure and those receiving 50 mg/week increased vertical trabecular number, thereby preserving the structural integrity of the subchondral bone.
This is important because weakening and loss of vertical trabecular support, when combined with the biomechanical weakening of the bone due to disease-related reduction in mineral content, are believed to contribute to collapse of the tibial compartment in late-stage osteoarthritis. It has been suggested that bisphosphonates are associated with decreased bone formation as an expected consequence of suppressing the coupled bone remodeling process. This did not appear to be the case in this study. In fact, the study tends to agree with experimental work that shows that high doses of bisphosphonates, as well as repeated administration, may enhance bone accretion.
The author serves on the advisory boards for Eli Lilly, Merck, Pfizer, Procter & Gamble, and GlaxoSmithKline.
Management of prolonged decelerations
A prolonged deceleration may signal danger—or reflect a perfectly normal fetal response to maternal pelvic examination. Because of the wide range of possibilities, this fetal heart rate pattern justifies close attention. For example, repetitive prolonged decelerations may indicate cord compression from oligohydramnios. Even more troubling, a prolonged deceleration may occur for the first time during the evolution of a profound catastrophe, such as amniotic fluid embolism or uterine rupture during vaginal birth after cesarean delivery (VBAC). In some circumstances, a prolonged deceleration may be the terminus of a progression of nonreassuring fetal heart rate (FHR) changes, and becomes the immediate precursor to fetal death (TABLE 1).1
When FHR patterns exhibit these aberrations, we rightly worry about fetal well-being and the possible need for operative intervention. Unfortunately, the degree of fetal compromise is difficult to predict and depends on preexisting fetal condition, physiologic reserve, degree and duration of the insult, and other variables.
TABLE 1
Some causes of prolonged decelerations and bradycardias
| PROLONGED DECELERATION | BRADYCARDIA |
|---|---|
| Cord compression Oligohydramnios Cord prolapse Uteroplacental insufficiency Anesthesia (paracervical, spinal, epidural) Maternal valsalva Maternal supine hypotension Hypertonic or prolonged contractions Abruptio placentae Uterine rupture Cocaine ingestion Maternal hypoxia Maternal seizures, eclampsia Respiratory depression from medications Cardiopulmonary arrest Amniotic fluid embolism Fetal hemorrhage Vasa previa Traumatic amniocentesis Fetal vagal reaction Rapid descent, impending birth Cervical examination Fetal scalp electrode placement Fetal blood sampling Fetal central nervous system anomalies Idiopathic (cord compression?) | Congenital conduction abnormalities Complete heart block Long QT syndrome Congenital heart defects Tachyarrhythmia (Fetal tachyarrhythmia may produce an EFM tracing that appears to be a bradycardia and can only be distinguished by ultrasound) Medications Beta blockers Hypothermia Infection Chorioamnionitis Endotoxemia |
Ultimately, a judgment call
The 22nd edition of Williams Obstetrics2 summarizes the clinical challenges involved in the management of prolonged decelerations during labor: “Management of isolated prolonged decelerations is based on bedside clinical judgment, which inevitably will sometimes be imperfect given the unpredictability of these decelerations.”
“Fetal bradycardia” and “prolonged deceleration” are distinct entities
In general parlance, we often use the terms “fetal bradycardia” and “prolonged deceleration” loosely. In practice, we must differentiate these entities because underlying pathophysiologic mechanisms and clinical management may differ substantially.
The problem: Since the introduction of electronic fetal monitoring (EFM) in the 1960s, numerous descriptions of FHR patterns have been published, each slightly different from the others. The result: confusing nomenclature, miscommunication among clinicians, and stymied research efforts.
To standardize definitions of intrapartum FHR patterns so that the effectiveness of EFM could be better assessed in observational studies and clinical trials, the National Institute of Child Health and Human Development organized a workshop.3 Its recommendations were subsequently adopted by the American College of Obstetricians and Gynecologists (ACOG).4 Among the definitions:
Differentiation between the 2 entities is critical because, in many cases, bradycardias are chronic patterns that may not be associated with immediate fetal compromise and do not require immediate intervention. For example, a fetal bradycardia due to congenital heart block would not benefit from immediate delivery, especially prior to term.
“Moderate fetal bradycardia,” defined as a baseline of 100 to 119 bpm, was reported in 1.8% of 1,386 continuously monitored patients and is attributed to relative cephalopelvic disproportion, resolving after rotation of the fetal vertex and associated with normal neonatal outcome.5,6
Similar decelerations can reflect different events
The exact depth and duration of a prolonged deceleration leading to fetal compromise and requiring prompt delivery is difficult to define, although some observations warrant consideration. Experiments with fetal lambs show that the deceleration in response to umbilical vein occlusion is associated with a fall in fetal blood pressure, whereas deceleration in response to umbilical artery occlusion is associated with a rise in fetal blood pressure. This reflex can be abolished by vagotomy, but will eventually recur due to anoxia.7
Vital clue: What happened before the prolonged deceleration?
In clinical practice, it is important to appreciate characteristics of the FHR pattern preceding the prolonged deceleration.8 Williams and Galerneau9 correlated baseline FHR variability and duration of prolonged decelerations with neonatal acid–base status in 186 term gestations with an identified prolonged deceleration within 30 minutes of delivery. Patients were divided into 4 groups, based on FHR variability and recovery of the FHR baseline (TABLE 2).
The findings:
TABLE 2
Neonatal outcomes associated with variability and recovery of FHR patterns after prolonged deceleration
| UMBILICAL ARTERY | GROUP 1 V+ R+ (N=128) | GROUP 2 V+ R- (N=40) | GROUP 3 V- R+ (N=9) | GROUP 4 V- R- (N=9) | P VALUE |
|---|---|---|---|---|---|
| pH (mean±SD) | 7.17±0.09 | 7.13±0.15 | 7.11±0.11 | 6.83±0.16 | <.001 |
| Base deficit (mean±SD) | -6.5±3.9 | -7.2±5.1 | -10±4 | -20±6 | <.001 |
| pH <7.0 (%) | 2 | 18 | 44 | 78 | <.001 |
| pH <7.1 (%) | 22 | 33 | 56 | 89 | <.001 |
| Base deficit <16 (%) | 1 | 8 | 11 | 78 | <.001 |
| Base deficit <12 (%) | 5 | 13 | 22 | 89 | <.001 |
| V=variability | |||||
| R=recovery | |||||
| SOURCE: Williams and Galerneau9 | |||||
Acid–base changes likely begin within minutes of cord compression
Zilianti and colleagues10 evaluated 29 fetuses with normal FHR patterns during labor with FHR deceleration during the expulsion phase of delivery. When the FHR deceleration was prolonged (>120 seconds), umbilical artery pH significantly decreased (7.19 vs 7.27), umbilical vein pH remained unchanged (7.32), and the umbilical venous–arterial pH difference was significantly increased (0.13 vs 0.05). Thus, acid–base changes likely begin within minutes of cord compression.
The correlation between acidemia and loss of variability
In their review of 43 vacuum extractions, Gull and colleagues22 found that 27 infants were delivered for “end-stage bradycardia” (abrupt persistent decrease in FHR to less than 100 bpm for more than 2 minutes, or repeated deceleration more than 60 bpm below baseline with poor recovery), and 16 were delivered electively (controls). Umbilical-cord base deficit was greater in the newborns with bradycardia than in controls, and the length of time FHR variability was lost correlated with the degree of base deficit. Acidemic fetuses lost FHR variability during the bradycardia for more than 4 minutes, or started to lose FHR variability less than 3 minutes from the beginning of the bradycardia.
What is optimal interval between deceleration and delivery?
In a series of 106 cases of uterine rupture during VBAC, Leung et al11 found significant neonatal morbidity when 18 minutes or more lapsed between the onset of the prolonged deceleration and delivery.
First, remain calm when decelerations occur
Freeman and colleagues12 advocate staying calm and avoiding overreaction, because many cases will resolve spontaneously. Nonetheless, prolonged decelerations should prompt the physician to:
TABLE 3
6 pearls for managing prolonged decelerations
| GOAL | PEARL | |
|---|---|---|
| 1 | Reduce aorto-caval and/or cord compression | Change patient positioning |
| 2 | Restore intravascular volume | Administer intravenous fluid bolus |
| 3 | Reduce uterine activity | Discontinue oxytocin drip and give tocolytic therapy (terbutaline) |
| 4 | Enhance oxygen delivery to fetus | Give supplemental oxygen |
| 5 | Resolve hypotension | Administer vasopressor therapy (ephedrine) |
| 6 | Resolve oligohydramnios and cord compression | Perform transcervical amnioinfusion |
TABLE 4
Stepwise management of prolonged decelerations
| Examine the cervix Check for umbilical cord prolapse Check progress of dilation and descent Place internal monitors, if indicated |
| Determine probable cause |
| Start therapies |
| Prepare for intervention by operative delivery Intravenous access Blood type and screen Indwelling urinary catheter Obtain consents for operative vaginal delivery and cesarean delivery Notify appropriate personnel (eg, anesthesiology, pediatrics) |
| Deliver If fetal condition is nonreassuring despite therapies If prolonged decelerations recur and spontaneous delivery is remote (cases must be individualized) |
Consider amnioinfusion when cord compression is suspected
Many cases of prolonged decelerations are secondary to cord compression resulting from oligohydramnios. Miyazaki13 showed that saline amnioinfusion helped correct the FHR problem in most cases of repetitive variable decelerations (19 of 28) and prolonged decelerations (12 of 14 cases).
Several randomized clinical trials analyzed in a recent Cochrane Review14 suggest that amnioinfusion for cord compression reduces the occurrence of variable FHR decelerations and the need for cesarean section; this applies to settings in which nonreassuring FHR patterns were not further assessed by fetal blood sampling, which is reflective of practice in most US labor units.
The recent ACOG practice bulletin on intrapartum monitoring4 advocates amnioinfusion for recurrent variable FHR decelerations, but does not address prolonged decelerations specifically.
Although most data on amnioinfusion address treatment of recurrent variable FHR decelerations, it also seems reasonable to consider this option for prolonged decelerations when oligohydramnios is suspected.12
Other possible causes of prolonged decelerations
Vasa previa. A sudden prolonged deceleration following rupture of membranes with concomitant vaginal bleeding should prompt the physician to consider the possibility of a disrupted velamentous cord insertion (vasa previa), which can lead to rapid fetal exsanguination.15
Acute profound maternal hypoxemia may lead to a first prolonged FHR deceleration, often preceded by increased uterine tone, as described in both eclampsia16 and amniotic fluid embolism.17 With eclampsia, the prolonged deceleration is reversible; treatment and expectant management will allow for fetal recovery after the seizure abates.
When acute amniotic fluid embolism leads to profound cardiovascular collapse, prompt perimortem cesarean delivery may be required within minutes if CPR does not restore normal maternal cardiopulmonary function and recovery of FHR.
When is scalp stimulation helpful?
Stimulation of the fetal scalp is an effective technique for assessing fetal status during periods of nonreassuring FHR patterns.18 However, the technique is intended to be performed during periods of FHR baseline and is sometimes misapplied during prolonged decelerations. Scalp stimulation during a prolonged deceleration would not likely provide valid information or change clinical management and could in theory exacerbate fetal compromise if additional parasympathetic tone were elicited.
Avoid fetal pulse oximetry
Although fetal pulse oximetry is FDA-approved and commercially available in the United States, and may be well suited for monitoring fetal arrhythmias,19,20 a prolonged deceleration is an absolute contraindication to its use.21
Summary
Overall, in managing a delivery marked by prolonged decelerations, we should strive to minimize maternal–fetal complications by carefully assessing the clinical situation, correcting reversible problems, and preparing for expeditious delivery if the fetal condition is of sufficient concern that further expectant management is unlikely to allow for safe spontaneous delivery. Still, “…bedside judgment inevitably will sometimes be imperfect given the unpredictability of these decelerations.”2
The author reports no financial affiliations relevant to this article.
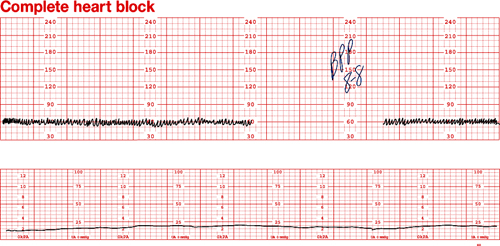
Dilemma: Fetal bradycardia due to congenital complete heart block secondary to anti-SSA/Ro and anti-SS-B/La antibodies. The fetal ventricular rate is fixed at 60 bpm
Management: At 30 weeks’ gestation, with no sonographic evidence of heart failure and a biophysical profile score of 8/8, expectant management is indicated
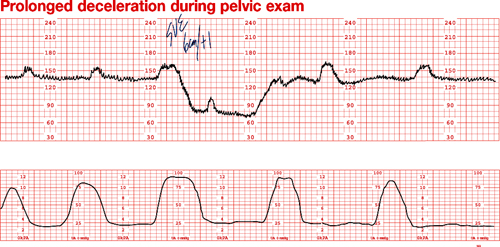
Dilemma: Prolonged deceleration during pelvic examination in an uncomplicated term pregnancy. Note that fetal heart rate (FHR) variability was maintained during recovery of the FHR baseline
Outcome: Uneventful spontaneous vaginal delivery
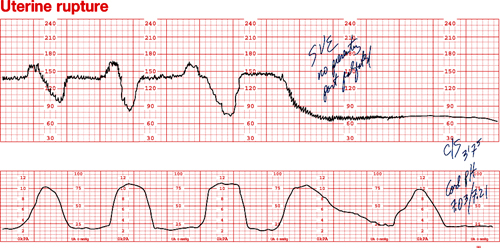
Dilemma: Prolonged deceleration due to uterine rupture during trial of labor after cesarean. Repetitive variable decelerations preceded the prolonged deceleration. FHR variability was lost after several minutes
Management: Emergency cesarean
1. Cetrulo CL, Schifrin BS. Fetal heart rate patterns preceding death in utero. Obstet Gynecol. 1976;48:521-527.
2. Cunningham FG, Leveno KJ, Bloom SL, et al. Williams Obstetrics. 22nd ed. New York: McGraw-Hill; 2005.
3. Electronic fetal heart rate monitoring: research guidelines for interpretation. National Institute of Child Health and Human Development Research Planning Workshop. Am J Obstet Gynecol. 1997;177:1385-1390.
4. Intrapartum fetal heart rate monitoring. ACOG Practice Bulletin #70. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2005;106:1453-1461.
5. Young BK, Weinstein HM. Moderate fetal bradycardia. Am J Obstet Gynecol. 1976;126:271-275.
6. Young BK, Katz M, et al. Fetal blood and tissue pH with moderate bradycardia. Am J Obstet Gynecol. 1979;135:45-47.
7. Reynolds SR. Bradycardia in the lamb fetus in response to circulatory distress. Am J Physiol. 1954;176:169-174.
8. Langer O, Sonnendecker EW. Characteristics and management of intrapartum prolonged fetal bradycardia. Br J Obstet Gynaecol. 1982;89:904-912.
9. Williams KP, Galerneau F. Fetal heart rate parameters predictive of neonatal outcome in the presence of a prolonged deceleration. Obstet Gynecol. 2002;100:951-954.
10. Zilianti M, Segura CL, et al. Studies on fetal bradycardia during birth process. II. Obstet Gynecol. 1973;42:840-843.
11. Leung AS, Leung EK, Paul RH. Uterine rupture after previous cesarean delivery: maternal and fetal consequences. Am J Obstet Gynecol. 1993;169:945-950.
12. Freeman RK, Garite TG, Nageotte MP. Fetal Heart Rate Monitoring. Philadelphia: Lippincott Williams & Wilkins; 2003.
13. Miyazaki FS, Taylor NA. Saline amnioinfusion for relief of variable or prolonged decelerations. A preliminary report. Am J Obstet Gynecol. 1983;146:670-678.
14. Hofmeyr GJ. Amnioinfusion for umbilical cord compression in labour. Cochrane Database Syst Rev. 2000;CD000013.-
15. Gabbe SG, Nelson LM, Paul RH. Fetal heart rate response to acute hemorrhage. Obstet Gynecol. 1977;49:247-251.
16. Paul RH, Koh KS, Bernstein SG. Changes in fetal heart rateuterine contraction patterns associated with eclampsia. Am J Obstet Gynecol. 1978;130:165-169.
17. Clark SL, Hankins GD, Dudley DA, Dildy GA, Porter TF. Amniotic fluid embolism: analysis of the national registry. Am J Obstet Gynecol. 1995;172:1158-1167;discussion 1167-1169.
18. Clark SL, Gimovsky ML, Miller FC. The scalp stimulation test: a clinical alternative to fetal scalp blood sampling. Am J Obstet Gynecol. 1984;148:274-277.
19. Dildy GA, Loucks CA, Clark SL. Intrapartum fetal pulse oximetry in the presence of fetal cardiac arrhythmia. Am J Obstet Gynecol. 1993;169:1609-1611.
20. van den Berg PP, Nijland R, van den Brand SF, Jongsma HW, Nijhuis JG. Intrapartum fetal surveillance of congenital heart block with pulse oximetry. Obstet Gynecol. 1994;84:683-686.
21. Garite TJ, Dildy GA, McNamara H, et al. A multicenter controlled trial of fetal pulse oximetry in the intrapartum management of nonreassuring fetal heart rate patterns. Am J Obstet Gynecol. 2000;183:1049-1058.
22. Gull I, Jaffa AJ, Oren M, Grisaru D, Peyser MR, Lessing JB. Acid accumulation during end-stage bradycardia in term fetuses: how long is too long? Br J Obstet Gynaecol. 1996;103:1096-1101.
A prolonged deceleration may signal danger—or reflect a perfectly normal fetal response to maternal pelvic examination. Because of the wide range of possibilities, this fetal heart rate pattern justifies close attention. For example, repetitive prolonged decelerations may indicate cord compression from oligohydramnios. Even more troubling, a prolonged deceleration may occur for the first time during the evolution of a profound catastrophe, such as amniotic fluid embolism or uterine rupture during vaginal birth after cesarean delivery (VBAC). In some circumstances, a prolonged deceleration may be the terminus of a progression of nonreassuring fetal heart rate (FHR) changes, and becomes the immediate precursor to fetal death (TABLE 1).1
When FHR patterns exhibit these aberrations, we rightly worry about fetal well-being and the possible need for operative intervention. Unfortunately, the degree of fetal compromise is difficult to predict and depends on preexisting fetal condition, physiologic reserve, degree and duration of the insult, and other variables.
TABLE 1
Some causes of prolonged decelerations and bradycardias
| PROLONGED DECELERATION | BRADYCARDIA |
|---|---|
| Cord compression Oligohydramnios Cord prolapse Uteroplacental insufficiency Anesthesia (paracervical, spinal, epidural) Maternal valsalva Maternal supine hypotension Hypertonic or prolonged contractions Abruptio placentae Uterine rupture Cocaine ingestion Maternal hypoxia Maternal seizures, eclampsia Respiratory depression from medications Cardiopulmonary arrest Amniotic fluid embolism Fetal hemorrhage Vasa previa Traumatic amniocentesis Fetal vagal reaction Rapid descent, impending birth Cervical examination Fetal scalp electrode placement Fetal blood sampling Fetal central nervous system anomalies Idiopathic (cord compression?) | Congenital conduction abnormalities Complete heart block Long QT syndrome Congenital heart defects Tachyarrhythmia (Fetal tachyarrhythmia may produce an EFM tracing that appears to be a bradycardia and can only be distinguished by ultrasound) Medications Beta blockers Hypothermia Infection Chorioamnionitis Endotoxemia |
Ultimately, a judgment call
The 22nd edition of Williams Obstetrics2 summarizes the clinical challenges involved in the management of prolonged decelerations during labor: “Management of isolated prolonged decelerations is based on bedside clinical judgment, which inevitably will sometimes be imperfect given the unpredictability of these decelerations.”
“Fetal bradycardia” and “prolonged deceleration” are distinct entities
In general parlance, we often use the terms “fetal bradycardia” and “prolonged deceleration” loosely. In practice, we must differentiate these entities because underlying pathophysiologic mechanisms and clinical management may differ substantially.
The problem: Since the introduction of electronic fetal monitoring (EFM) in the 1960s, numerous descriptions of FHR patterns have been published, each slightly different from the others. The result: confusing nomenclature, miscommunication among clinicians, and stymied research efforts.
To standardize definitions of intrapartum FHR patterns so that the effectiveness of EFM could be better assessed in observational studies and clinical trials, the National Institute of Child Health and Human Development organized a workshop.3 Its recommendations were subsequently adopted by the American College of Obstetricians and Gynecologists (ACOG).4 Among the definitions:
Differentiation between the 2 entities is critical because, in many cases, bradycardias are chronic patterns that may not be associated with immediate fetal compromise and do not require immediate intervention. For example, a fetal bradycardia due to congenital heart block would not benefit from immediate delivery, especially prior to term.
“Moderate fetal bradycardia,” defined as a baseline of 100 to 119 bpm, was reported in 1.8% of 1,386 continuously monitored patients and is attributed to relative cephalopelvic disproportion, resolving after rotation of the fetal vertex and associated with normal neonatal outcome.5,6
Similar decelerations can reflect different events
The exact depth and duration of a prolonged deceleration leading to fetal compromise and requiring prompt delivery is difficult to define, although some observations warrant consideration. Experiments with fetal lambs show that the deceleration in response to umbilical vein occlusion is associated with a fall in fetal blood pressure, whereas deceleration in response to umbilical artery occlusion is associated with a rise in fetal blood pressure. This reflex can be abolished by vagotomy, but will eventually recur due to anoxia.7
Vital clue: What happened before the prolonged deceleration?
In clinical practice, it is important to appreciate characteristics of the FHR pattern preceding the prolonged deceleration.8 Williams and Galerneau9 correlated baseline FHR variability and duration of prolonged decelerations with neonatal acid–base status in 186 term gestations with an identified prolonged deceleration within 30 minutes of delivery. Patients were divided into 4 groups, based on FHR variability and recovery of the FHR baseline (TABLE 2).
The findings:
TABLE 2
Neonatal outcomes associated with variability and recovery of FHR patterns after prolonged deceleration
| UMBILICAL ARTERY | GROUP 1 V+ R+ (N=128) | GROUP 2 V+ R- (N=40) | GROUP 3 V- R+ (N=9) | GROUP 4 V- R- (N=9) | P VALUE |
|---|---|---|---|---|---|
| pH (mean±SD) | 7.17±0.09 | 7.13±0.15 | 7.11±0.11 | 6.83±0.16 | <.001 |
| Base deficit (mean±SD) | -6.5±3.9 | -7.2±5.1 | -10±4 | -20±6 | <.001 |
| pH <7.0 (%) | 2 | 18 | 44 | 78 | <.001 |
| pH <7.1 (%) | 22 | 33 | 56 | 89 | <.001 |
| Base deficit <16 (%) | 1 | 8 | 11 | 78 | <.001 |
| Base deficit <12 (%) | 5 | 13 | 22 | 89 | <.001 |
| V=variability | |||||
| R=recovery | |||||
| SOURCE: Williams and Galerneau9 | |||||
Acid–base changes likely begin within minutes of cord compression
Zilianti and colleagues10 evaluated 29 fetuses with normal FHR patterns during labor with FHR deceleration during the expulsion phase of delivery. When the FHR deceleration was prolonged (>120 seconds), umbilical artery pH significantly decreased (7.19 vs 7.27), umbilical vein pH remained unchanged (7.32), and the umbilical venous–arterial pH difference was significantly increased (0.13 vs 0.05). Thus, acid–base changes likely begin within minutes of cord compression.
The correlation between acidemia and loss of variability
In their review of 43 vacuum extractions, Gull and colleagues22 found that 27 infants were delivered for “end-stage bradycardia” (abrupt persistent decrease in FHR to less than 100 bpm for more than 2 minutes, or repeated deceleration more than 60 bpm below baseline with poor recovery), and 16 were delivered electively (controls). Umbilical-cord base deficit was greater in the newborns with bradycardia than in controls, and the length of time FHR variability was lost correlated with the degree of base deficit. Acidemic fetuses lost FHR variability during the bradycardia for more than 4 minutes, or started to lose FHR variability less than 3 minutes from the beginning of the bradycardia.
What is optimal interval between deceleration and delivery?
In a series of 106 cases of uterine rupture during VBAC, Leung et al11 found significant neonatal morbidity when 18 minutes or more lapsed between the onset of the prolonged deceleration and delivery.
First, remain calm when decelerations occur
Freeman and colleagues12 advocate staying calm and avoiding overreaction, because many cases will resolve spontaneously. Nonetheless, prolonged decelerations should prompt the physician to:
TABLE 3
6 pearls for managing prolonged decelerations
| GOAL | PEARL | |
|---|---|---|
| 1 | Reduce aorto-caval and/or cord compression | Change patient positioning |
| 2 | Restore intravascular volume | Administer intravenous fluid bolus |
| 3 | Reduce uterine activity | Discontinue oxytocin drip and give tocolytic therapy (terbutaline) |
| 4 | Enhance oxygen delivery to fetus | Give supplemental oxygen |
| 5 | Resolve hypotension | Administer vasopressor therapy (ephedrine) |
| 6 | Resolve oligohydramnios and cord compression | Perform transcervical amnioinfusion |
TABLE 4
Stepwise management of prolonged decelerations
| Examine the cervix Check for umbilical cord prolapse Check progress of dilation and descent Place internal monitors, if indicated |
| Determine probable cause |
| Start therapies |
| Prepare for intervention by operative delivery Intravenous access Blood type and screen Indwelling urinary catheter Obtain consents for operative vaginal delivery and cesarean delivery Notify appropriate personnel (eg, anesthesiology, pediatrics) |
| Deliver If fetal condition is nonreassuring despite therapies If prolonged decelerations recur and spontaneous delivery is remote (cases must be individualized) |
Consider amnioinfusion when cord compression is suspected
Many cases of prolonged decelerations are secondary to cord compression resulting from oligohydramnios. Miyazaki13 showed that saline amnioinfusion helped correct the FHR problem in most cases of repetitive variable decelerations (19 of 28) and prolonged decelerations (12 of 14 cases).
Several randomized clinical trials analyzed in a recent Cochrane Review14 suggest that amnioinfusion for cord compression reduces the occurrence of variable FHR decelerations and the need for cesarean section; this applies to settings in which nonreassuring FHR patterns were not further assessed by fetal blood sampling, which is reflective of practice in most US labor units.
The recent ACOG practice bulletin on intrapartum monitoring4 advocates amnioinfusion for recurrent variable FHR decelerations, but does not address prolonged decelerations specifically.
Although most data on amnioinfusion address treatment of recurrent variable FHR decelerations, it also seems reasonable to consider this option for prolonged decelerations when oligohydramnios is suspected.12
Other possible causes of prolonged decelerations
Vasa previa. A sudden prolonged deceleration following rupture of membranes with concomitant vaginal bleeding should prompt the physician to consider the possibility of a disrupted velamentous cord insertion (vasa previa), which can lead to rapid fetal exsanguination.15
Acute profound maternal hypoxemia may lead to a first prolonged FHR deceleration, often preceded by increased uterine tone, as described in both eclampsia16 and amniotic fluid embolism.17 With eclampsia, the prolonged deceleration is reversible; treatment and expectant management will allow for fetal recovery after the seizure abates.
When acute amniotic fluid embolism leads to profound cardiovascular collapse, prompt perimortem cesarean delivery may be required within minutes if CPR does not restore normal maternal cardiopulmonary function and recovery of FHR.
When is scalp stimulation helpful?
Stimulation of the fetal scalp is an effective technique for assessing fetal status during periods of nonreassuring FHR patterns.18 However, the technique is intended to be performed during periods of FHR baseline and is sometimes misapplied during prolonged decelerations. Scalp stimulation during a prolonged deceleration would not likely provide valid information or change clinical management and could in theory exacerbate fetal compromise if additional parasympathetic tone were elicited.
Avoid fetal pulse oximetry
Although fetal pulse oximetry is FDA-approved and commercially available in the United States, and may be well suited for monitoring fetal arrhythmias,19,20 a prolonged deceleration is an absolute contraindication to its use.21
Summary
Overall, in managing a delivery marked by prolonged decelerations, we should strive to minimize maternal–fetal complications by carefully assessing the clinical situation, correcting reversible problems, and preparing for expeditious delivery if the fetal condition is of sufficient concern that further expectant management is unlikely to allow for safe spontaneous delivery. Still, “…bedside judgment inevitably will sometimes be imperfect given the unpredictability of these decelerations.”2
The author reports no financial affiliations relevant to this article.
Dilemma: Fetal bradycardia due to congenital complete heart block secondary to anti-SSA/Ro and anti-SS-B/La antibodies. The fetal ventricular rate is fixed at 60 bpm
Management: At 30 weeks’ gestation, with no sonographic evidence of heart failure and a biophysical profile score of 8/8, expectant management is indicated
Dilemma: Prolonged deceleration during pelvic examination in an uncomplicated term pregnancy. Note that fetal heart rate (FHR) variability was maintained during recovery of the FHR baseline
Outcome: Uneventful spontaneous vaginal delivery
Dilemma: Prolonged deceleration due to uterine rupture during trial of labor after cesarean. Repetitive variable decelerations preceded the prolonged deceleration. FHR variability was lost after several minutes
Management: Emergency cesarean
A prolonged deceleration may signal danger—or reflect a perfectly normal fetal response to maternal pelvic examination. Because of the wide range of possibilities, this fetal heart rate pattern justifies close attention. For example, repetitive prolonged decelerations may indicate cord compression from oligohydramnios. Even more troubling, a prolonged deceleration may occur for the first time during the evolution of a profound catastrophe, such as amniotic fluid embolism or uterine rupture during vaginal birth after cesarean delivery (VBAC). In some circumstances, a prolonged deceleration may be the terminus of a progression of nonreassuring fetal heart rate (FHR) changes, and becomes the immediate precursor to fetal death (TABLE 1).1
When FHR patterns exhibit these aberrations, we rightly worry about fetal well-being and the possible need for operative intervention. Unfortunately, the degree of fetal compromise is difficult to predict and depends on preexisting fetal condition, physiologic reserve, degree and duration of the insult, and other variables.
TABLE 1
Some causes of prolonged decelerations and bradycardias
| PROLONGED DECELERATION | BRADYCARDIA |
|---|---|
| Cord compression Oligohydramnios Cord prolapse Uteroplacental insufficiency Anesthesia (paracervical, spinal, epidural) Maternal valsalva Maternal supine hypotension Hypertonic or prolonged contractions Abruptio placentae Uterine rupture Cocaine ingestion Maternal hypoxia Maternal seizures, eclampsia Respiratory depression from medications Cardiopulmonary arrest Amniotic fluid embolism Fetal hemorrhage Vasa previa Traumatic amniocentesis Fetal vagal reaction Rapid descent, impending birth Cervical examination Fetal scalp electrode placement Fetal blood sampling Fetal central nervous system anomalies Idiopathic (cord compression?) | Congenital conduction abnormalities Complete heart block Long QT syndrome Congenital heart defects Tachyarrhythmia (Fetal tachyarrhythmia may produce an EFM tracing that appears to be a bradycardia and can only be distinguished by ultrasound) Medications Beta blockers Hypothermia Infection Chorioamnionitis Endotoxemia |
Ultimately, a judgment call
The 22nd edition of Williams Obstetrics2 summarizes the clinical challenges involved in the management of prolonged decelerations during labor: “Management of isolated prolonged decelerations is based on bedside clinical judgment, which inevitably will sometimes be imperfect given the unpredictability of these decelerations.”
“Fetal bradycardia” and “prolonged deceleration” are distinct entities
In general parlance, we often use the terms “fetal bradycardia” and “prolonged deceleration” loosely. In practice, we must differentiate these entities because underlying pathophysiologic mechanisms and clinical management may differ substantially.
The problem: Since the introduction of electronic fetal monitoring (EFM) in the 1960s, numerous descriptions of FHR patterns have been published, each slightly different from the others. The result: confusing nomenclature, miscommunication among clinicians, and stymied research efforts.
To standardize definitions of intrapartum FHR patterns so that the effectiveness of EFM could be better assessed in observational studies and clinical trials, the National Institute of Child Health and Human Development organized a workshop.3 Its recommendations were subsequently adopted by the American College of Obstetricians and Gynecologists (ACOG).4 Among the definitions:
Differentiation between the 2 entities is critical because, in many cases, bradycardias are chronic patterns that may not be associated with immediate fetal compromise and do not require immediate intervention. For example, a fetal bradycardia due to congenital heart block would not benefit from immediate delivery, especially prior to term.
“Moderate fetal bradycardia,” defined as a baseline of 100 to 119 bpm, was reported in 1.8% of 1,386 continuously monitored patients and is attributed to relative cephalopelvic disproportion, resolving after rotation of the fetal vertex and associated with normal neonatal outcome.5,6
Similar decelerations can reflect different events
The exact depth and duration of a prolonged deceleration leading to fetal compromise and requiring prompt delivery is difficult to define, although some observations warrant consideration. Experiments with fetal lambs show that the deceleration in response to umbilical vein occlusion is associated with a fall in fetal blood pressure, whereas deceleration in response to umbilical artery occlusion is associated with a rise in fetal blood pressure. This reflex can be abolished by vagotomy, but will eventually recur due to anoxia.7
Vital clue: What happened before the prolonged deceleration?
In clinical practice, it is important to appreciate characteristics of the FHR pattern preceding the prolonged deceleration.8 Williams and Galerneau9 correlated baseline FHR variability and duration of prolonged decelerations with neonatal acid–base status in 186 term gestations with an identified prolonged deceleration within 30 minutes of delivery. Patients were divided into 4 groups, based on FHR variability and recovery of the FHR baseline (TABLE 2).
The findings:
TABLE 2
Neonatal outcomes associated with variability and recovery of FHR patterns after prolonged deceleration
| UMBILICAL ARTERY | GROUP 1 V+ R+ (N=128) | GROUP 2 V+ R- (N=40) | GROUP 3 V- R+ (N=9) | GROUP 4 V- R- (N=9) | P VALUE |
|---|---|---|---|---|---|
| pH (mean±SD) | 7.17±0.09 | 7.13±0.15 | 7.11±0.11 | 6.83±0.16 | <.001 |
| Base deficit (mean±SD) | -6.5±3.9 | -7.2±5.1 | -10±4 | -20±6 | <.001 |
| pH <7.0 (%) | 2 | 18 | 44 | 78 | <.001 |
| pH <7.1 (%) | 22 | 33 | 56 | 89 | <.001 |
| Base deficit <16 (%) | 1 | 8 | 11 | 78 | <.001 |
| Base deficit <12 (%) | 5 | 13 | 22 | 89 | <.001 |
| V=variability | |||||
| R=recovery | |||||
| SOURCE: Williams and Galerneau9 | |||||
Acid–base changes likely begin within minutes of cord compression
Zilianti and colleagues10 evaluated 29 fetuses with normal FHR patterns during labor with FHR deceleration during the expulsion phase of delivery. When the FHR deceleration was prolonged (>120 seconds), umbilical artery pH significantly decreased (7.19 vs 7.27), umbilical vein pH remained unchanged (7.32), and the umbilical venous–arterial pH difference was significantly increased (0.13 vs 0.05). Thus, acid–base changes likely begin within minutes of cord compression.
The correlation between acidemia and loss of variability
In their review of 43 vacuum extractions, Gull and colleagues22 found that 27 infants were delivered for “end-stage bradycardia” (abrupt persistent decrease in FHR to less than 100 bpm for more than 2 minutes, or repeated deceleration more than 60 bpm below baseline with poor recovery), and 16 were delivered electively (controls). Umbilical-cord base deficit was greater in the newborns with bradycardia than in controls, and the length of time FHR variability was lost correlated with the degree of base deficit. Acidemic fetuses lost FHR variability during the bradycardia for more than 4 minutes, or started to lose FHR variability less than 3 minutes from the beginning of the bradycardia.
What is optimal interval between deceleration and delivery?
In a series of 106 cases of uterine rupture during VBAC, Leung et al11 found significant neonatal morbidity when 18 minutes or more lapsed between the onset of the prolonged deceleration and delivery.
First, remain calm when decelerations occur
Freeman and colleagues12 advocate staying calm and avoiding overreaction, because many cases will resolve spontaneously. Nonetheless, prolonged decelerations should prompt the physician to:
TABLE 3
6 pearls for managing prolonged decelerations
| GOAL | PEARL | |
|---|---|---|
| 1 | Reduce aorto-caval and/or cord compression | Change patient positioning |
| 2 | Restore intravascular volume | Administer intravenous fluid bolus |
| 3 | Reduce uterine activity | Discontinue oxytocin drip and give tocolytic therapy (terbutaline) |
| 4 | Enhance oxygen delivery to fetus | Give supplemental oxygen |
| 5 | Resolve hypotension | Administer vasopressor therapy (ephedrine) |
| 6 | Resolve oligohydramnios and cord compression | Perform transcervical amnioinfusion |
TABLE 4
Stepwise management of prolonged decelerations
| Examine the cervix Check for umbilical cord prolapse Check progress of dilation and descent Place internal monitors, if indicated |
| Determine probable cause |
| Start therapies |
| Prepare for intervention by operative delivery Intravenous access Blood type and screen Indwelling urinary catheter Obtain consents for operative vaginal delivery and cesarean delivery Notify appropriate personnel (eg, anesthesiology, pediatrics) |
| Deliver If fetal condition is nonreassuring despite therapies If prolonged decelerations recur and spontaneous delivery is remote (cases must be individualized) |
Consider amnioinfusion when cord compression is suspected
Many cases of prolonged decelerations are secondary to cord compression resulting from oligohydramnios. Miyazaki13 showed that saline amnioinfusion helped correct the FHR problem in most cases of repetitive variable decelerations (19 of 28) and prolonged decelerations (12 of 14 cases).
Several randomized clinical trials analyzed in a recent Cochrane Review14 suggest that amnioinfusion for cord compression reduces the occurrence of variable FHR decelerations and the need for cesarean section; this applies to settings in which nonreassuring FHR patterns were not further assessed by fetal blood sampling, which is reflective of practice in most US labor units.
The recent ACOG practice bulletin on intrapartum monitoring4 advocates amnioinfusion for recurrent variable FHR decelerations, but does not address prolonged decelerations specifically.
Although most data on amnioinfusion address treatment of recurrent variable FHR decelerations, it also seems reasonable to consider this option for prolonged decelerations when oligohydramnios is suspected.12
Other possible causes of prolonged decelerations
Vasa previa. A sudden prolonged deceleration following rupture of membranes with concomitant vaginal bleeding should prompt the physician to consider the possibility of a disrupted velamentous cord insertion (vasa previa), which can lead to rapid fetal exsanguination.15
Acute profound maternal hypoxemia may lead to a first prolonged FHR deceleration, often preceded by increased uterine tone, as described in both eclampsia16 and amniotic fluid embolism.17 With eclampsia, the prolonged deceleration is reversible; treatment and expectant management will allow for fetal recovery after the seizure abates.
When acute amniotic fluid embolism leads to profound cardiovascular collapse, prompt perimortem cesarean delivery may be required within minutes if CPR does not restore normal maternal cardiopulmonary function and recovery of FHR.
When is scalp stimulation helpful?
Stimulation of the fetal scalp is an effective technique for assessing fetal status during periods of nonreassuring FHR patterns.18 However, the technique is intended to be performed during periods of FHR baseline and is sometimes misapplied during prolonged decelerations. Scalp stimulation during a prolonged deceleration would not likely provide valid information or change clinical management and could in theory exacerbate fetal compromise if additional parasympathetic tone were elicited.
Avoid fetal pulse oximetry
Although fetal pulse oximetry is FDA-approved and commercially available in the United States, and may be well suited for monitoring fetal arrhythmias,19,20 a prolonged deceleration is an absolute contraindication to its use.21
Summary
Overall, in managing a delivery marked by prolonged decelerations, we should strive to minimize maternal–fetal complications by carefully assessing the clinical situation, correcting reversible problems, and preparing for expeditious delivery if the fetal condition is of sufficient concern that further expectant management is unlikely to allow for safe spontaneous delivery. Still, “…bedside judgment inevitably will sometimes be imperfect given the unpredictability of these decelerations.”2
The author reports no financial affiliations relevant to this article.
Dilemma: Fetal bradycardia due to congenital complete heart block secondary to anti-SSA/Ro and anti-SS-B/La antibodies. The fetal ventricular rate is fixed at 60 bpm
Management: At 30 weeks’ gestation, with no sonographic evidence of heart failure and a biophysical profile score of 8/8, expectant management is indicated
Dilemma: Prolonged deceleration during pelvic examination in an uncomplicated term pregnancy. Note that fetal heart rate (FHR) variability was maintained during recovery of the FHR baseline
Outcome: Uneventful spontaneous vaginal delivery
Dilemma: Prolonged deceleration due to uterine rupture during trial of labor after cesarean. Repetitive variable decelerations preceded the prolonged deceleration. FHR variability was lost after several minutes
Management: Emergency cesarean
1. Cetrulo CL, Schifrin BS. Fetal heart rate patterns preceding death in utero. Obstet Gynecol. 1976;48:521-527.
2. Cunningham FG, Leveno KJ, Bloom SL, et al. Williams Obstetrics. 22nd ed. New York: McGraw-Hill; 2005.
3. Electronic fetal heart rate monitoring: research guidelines for interpretation. National Institute of Child Health and Human Development Research Planning Workshop. Am J Obstet Gynecol. 1997;177:1385-1390.
4. Intrapartum fetal heart rate monitoring. ACOG Practice Bulletin #70. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2005;106:1453-1461.
5. Young BK, Weinstein HM. Moderate fetal bradycardia. Am J Obstet Gynecol. 1976;126:271-275.
6. Young BK, Katz M, et al. Fetal blood and tissue pH with moderate bradycardia. Am J Obstet Gynecol. 1979;135:45-47.
7. Reynolds SR. Bradycardia in the lamb fetus in response to circulatory distress. Am J Physiol. 1954;176:169-174.
8. Langer O, Sonnendecker EW. Characteristics and management of intrapartum prolonged fetal bradycardia. Br J Obstet Gynaecol. 1982;89:904-912.
9. Williams KP, Galerneau F. Fetal heart rate parameters predictive of neonatal outcome in the presence of a prolonged deceleration. Obstet Gynecol. 2002;100:951-954.
10. Zilianti M, Segura CL, et al. Studies on fetal bradycardia during birth process. II. Obstet Gynecol. 1973;42:840-843.
11. Leung AS, Leung EK, Paul RH. Uterine rupture after previous cesarean delivery: maternal and fetal consequences. Am J Obstet Gynecol. 1993;169:945-950.
12. Freeman RK, Garite TG, Nageotte MP. Fetal Heart Rate Monitoring. Philadelphia: Lippincott Williams & Wilkins; 2003.
13. Miyazaki FS, Taylor NA. Saline amnioinfusion for relief of variable or prolonged decelerations. A preliminary report. Am J Obstet Gynecol. 1983;146:670-678.
14. Hofmeyr GJ. Amnioinfusion for umbilical cord compression in labour. Cochrane Database Syst Rev. 2000;CD000013.-
15. Gabbe SG, Nelson LM, Paul RH. Fetal heart rate response to acute hemorrhage. Obstet Gynecol. 1977;49:247-251.
16. Paul RH, Koh KS, Bernstein SG. Changes in fetal heart rateuterine contraction patterns associated with eclampsia. Am J Obstet Gynecol. 1978;130:165-169.
17. Clark SL, Hankins GD, Dudley DA, Dildy GA, Porter TF. Amniotic fluid embolism: analysis of the national registry. Am J Obstet Gynecol. 1995;172:1158-1167;discussion 1167-1169.
18. Clark SL, Gimovsky ML, Miller FC. The scalp stimulation test: a clinical alternative to fetal scalp blood sampling. Am J Obstet Gynecol. 1984;148:274-277.
19. Dildy GA, Loucks CA, Clark SL. Intrapartum fetal pulse oximetry in the presence of fetal cardiac arrhythmia. Am J Obstet Gynecol. 1993;169:1609-1611.
20. van den Berg PP, Nijland R, van den Brand SF, Jongsma HW, Nijhuis JG. Intrapartum fetal surveillance of congenital heart block with pulse oximetry. Obstet Gynecol. 1994;84:683-686.
21. Garite TJ, Dildy GA, McNamara H, et al. A multicenter controlled trial of fetal pulse oximetry in the intrapartum management of nonreassuring fetal heart rate patterns. Am J Obstet Gynecol. 2000;183:1049-1058.
22. Gull I, Jaffa AJ, Oren M, Grisaru D, Peyser MR, Lessing JB. Acid accumulation during end-stage bradycardia in term fetuses: how long is too long? Br J Obstet Gynaecol. 1996;103:1096-1101.
1. Cetrulo CL, Schifrin BS. Fetal heart rate patterns preceding death in utero. Obstet Gynecol. 1976;48:521-527.
2. Cunningham FG, Leveno KJ, Bloom SL, et al. Williams Obstetrics. 22nd ed. New York: McGraw-Hill; 2005.
3. Electronic fetal heart rate monitoring: research guidelines for interpretation. National Institute of Child Health and Human Development Research Planning Workshop. Am J Obstet Gynecol. 1997;177:1385-1390.
4. Intrapartum fetal heart rate monitoring. ACOG Practice Bulletin #70. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2005;106:1453-1461.
5. Young BK, Weinstein HM. Moderate fetal bradycardia. Am J Obstet Gynecol. 1976;126:271-275.
6. Young BK, Katz M, et al. Fetal blood and tissue pH with moderate bradycardia. Am J Obstet Gynecol. 1979;135:45-47.
7. Reynolds SR. Bradycardia in the lamb fetus in response to circulatory distress. Am J Physiol. 1954;176:169-174.
8. Langer O, Sonnendecker EW. Characteristics and management of intrapartum prolonged fetal bradycardia. Br J Obstet Gynaecol. 1982;89:904-912.
9. Williams KP, Galerneau F. Fetal heart rate parameters predictive of neonatal outcome in the presence of a prolonged deceleration. Obstet Gynecol. 2002;100:951-954.
10. Zilianti M, Segura CL, et al. Studies on fetal bradycardia during birth process. II. Obstet Gynecol. 1973;42:840-843.
11. Leung AS, Leung EK, Paul RH. Uterine rupture after previous cesarean delivery: maternal and fetal consequences. Am J Obstet Gynecol. 1993;169:945-950.
12. Freeman RK, Garite TG, Nageotte MP. Fetal Heart Rate Monitoring. Philadelphia: Lippincott Williams & Wilkins; 2003.
13. Miyazaki FS, Taylor NA. Saline amnioinfusion for relief of variable or prolonged decelerations. A preliminary report. Am J Obstet Gynecol. 1983;146:670-678.
14. Hofmeyr GJ. Amnioinfusion for umbilical cord compression in labour. Cochrane Database Syst Rev. 2000;CD000013.-
15. Gabbe SG, Nelson LM, Paul RH. Fetal heart rate response to acute hemorrhage. Obstet Gynecol. 1977;49:247-251.
16. Paul RH, Koh KS, Bernstein SG. Changes in fetal heart rateuterine contraction patterns associated with eclampsia. Am J Obstet Gynecol. 1978;130:165-169.
17. Clark SL, Hankins GD, Dudley DA, Dildy GA, Porter TF. Amniotic fluid embolism: analysis of the national registry. Am J Obstet Gynecol. 1995;172:1158-1167;discussion 1167-1169.
18. Clark SL, Gimovsky ML, Miller FC. The scalp stimulation test: a clinical alternative to fetal scalp blood sampling. Am J Obstet Gynecol. 1984;148:274-277.
19. Dildy GA, Loucks CA, Clark SL. Intrapartum fetal pulse oximetry in the presence of fetal cardiac arrhythmia. Am J Obstet Gynecol. 1993;169:1609-1611.
20. van den Berg PP, Nijland R, van den Brand SF, Jongsma HW, Nijhuis JG. Intrapartum fetal surveillance of congenital heart block with pulse oximetry. Obstet Gynecol. 1994;84:683-686.
21. Garite TJ, Dildy GA, McNamara H, et al. A multicenter controlled trial of fetal pulse oximetry in the intrapartum management of nonreassuring fetal heart rate patterns. Am J Obstet Gynecol. 2000;183:1049-1058.
22. Gull I, Jaffa AJ, Oren M, Grisaru D, Peyser MR, Lessing JB. Acid accumulation during end-stage bradycardia in term fetuses: how long is too long? Br J Obstet Gynaecol. 1996;103:1096-1101.