User login
Online reviews
The last time I gave the talk, "Help! I’ve Been Yelped!" to physicians, there was a full house, a sometimes defiant, sometimes incredulous but always engaged full house. Most physicians don’t like Yelp and other online doctor rating sites because of the potential for negative reviews.
In past columns, I’ve written about these sites and how to respond to negative reviews and comments. Now, I’m going to share data on the use of online reviews and why they are important.
We live in a digital world that values reviews. We compare hotels on TripAdvisor.com before booking them and read reviews on Amazon.com before ordering products. We "like" or "dislike" Facebook pages and give thumbs up or thumbs down to videos on YouTube. We even rate physicians’ comments on medical question-and-answer sites such as HealthTap.com.
But how much do all of these online ratings really matter? A 2012 Nielsen report that surveyed more than 28,000 Internet users in 56 countries found that online consumer reviews are the second-most-trusted source of brand information, following only recommendations from family and friends. In other words, we trust online reviews and use them to make our own decisions.
The same is true when it comes to shopping for a doctor. According to an Internet-based survey of 2,137 adults published in the February issue of JAMA, 59% of respondents said that online doctor ratings were either "somewhat important" or "very important" when choosing a physician (2014;11:734-5).
Similarly, the "2013 Industry View Report" by Software Advice found that 62% of respondents said they read online reviews when seeking a new doctor. Although HealthGrades.com was the most commonly used site, Yelp.com was the most trusted. Forty-four percent of those respondents considered Yelp the most trustworthy review site followed by Health Grades (31%), Vitals.com (17%), and ZocDoc.com (7%).
Whether or not we trust Yelp and other online review sites, our patients do. In the JAMA survey, 35% of respondents said that they selected a physician based on good ratings, while 37% said that they avoided a physician with negative reviews. The 2013 Industry View Report also found that 45% of respondents ranked "quality of care" as the most important type of information sought about a doctor. And since many patients equate service with quality, reviews that focus on service matter.
This isn’t an entirely bad thing. If we really listen to what patients are saying, their comments can help us to improve service and communication. And, in some instances, it can lead to stronger doctor-patient relationships. Like many other industries, health care is moving toward transparency, and doctor rating sites are a key component of that.
Dr. Jeffrey Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego and a volunteer clinical assistant professor at the University of California, San Diego. He has published numerous scientific articles and is a member and fellow of the American Academy of Dermatology, and a member of the Telemedicine Association and the American Medical Association, among others. He is board certified in dermatology as well as medicine and surgery in the state of California. Dr. Benabio has a special interest in the uses of social media for education and building dermatology practice. He is the founder of The Derm Blog, an educational website that has had more than 2 million unique visitors. Dr. Benabio is also a founding member and the skin care expert for Livestrong.com, a health and wellness website of Lance Armstrong’s the Livestrong Foundation. Dr. Benabio is @Dermdoc on Twitter.
The last time I gave the talk, "Help! I’ve Been Yelped!" to physicians, there was a full house, a sometimes defiant, sometimes incredulous but always engaged full house. Most physicians don’t like Yelp and other online doctor rating sites because of the potential for negative reviews.
In past columns, I’ve written about these sites and how to respond to negative reviews and comments. Now, I’m going to share data on the use of online reviews and why they are important.
We live in a digital world that values reviews. We compare hotels on TripAdvisor.com before booking them and read reviews on Amazon.com before ordering products. We "like" or "dislike" Facebook pages and give thumbs up or thumbs down to videos on YouTube. We even rate physicians’ comments on medical question-and-answer sites such as HealthTap.com.
But how much do all of these online ratings really matter? A 2012 Nielsen report that surveyed more than 28,000 Internet users in 56 countries found that online consumer reviews are the second-most-trusted source of brand information, following only recommendations from family and friends. In other words, we trust online reviews and use them to make our own decisions.
The same is true when it comes to shopping for a doctor. According to an Internet-based survey of 2,137 adults published in the February issue of JAMA, 59% of respondents said that online doctor ratings were either "somewhat important" or "very important" when choosing a physician (2014;11:734-5).
Similarly, the "2013 Industry View Report" by Software Advice found that 62% of respondents said they read online reviews when seeking a new doctor. Although HealthGrades.com was the most commonly used site, Yelp.com was the most trusted. Forty-four percent of those respondents considered Yelp the most trustworthy review site followed by Health Grades (31%), Vitals.com (17%), and ZocDoc.com (7%).
Whether or not we trust Yelp and other online review sites, our patients do. In the JAMA survey, 35% of respondents said that they selected a physician based on good ratings, while 37% said that they avoided a physician with negative reviews. The 2013 Industry View Report also found that 45% of respondents ranked "quality of care" as the most important type of information sought about a doctor. And since many patients equate service with quality, reviews that focus on service matter.
This isn’t an entirely bad thing. If we really listen to what patients are saying, their comments can help us to improve service and communication. And, in some instances, it can lead to stronger doctor-patient relationships. Like many other industries, health care is moving toward transparency, and doctor rating sites are a key component of that.
Dr. Jeffrey Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego and a volunteer clinical assistant professor at the University of California, San Diego. He has published numerous scientific articles and is a member and fellow of the American Academy of Dermatology, and a member of the Telemedicine Association and the American Medical Association, among others. He is board certified in dermatology as well as medicine and surgery in the state of California. Dr. Benabio has a special interest in the uses of social media for education and building dermatology practice. He is the founder of The Derm Blog, an educational website that has had more than 2 million unique visitors. Dr. Benabio is also a founding member and the skin care expert for Livestrong.com, a health and wellness website of Lance Armstrong’s the Livestrong Foundation. Dr. Benabio is @Dermdoc on Twitter.
The last time I gave the talk, "Help! I’ve Been Yelped!" to physicians, there was a full house, a sometimes defiant, sometimes incredulous but always engaged full house. Most physicians don’t like Yelp and other online doctor rating sites because of the potential for negative reviews.
In past columns, I’ve written about these sites and how to respond to negative reviews and comments. Now, I’m going to share data on the use of online reviews and why they are important.
We live in a digital world that values reviews. We compare hotels on TripAdvisor.com before booking them and read reviews on Amazon.com before ordering products. We "like" or "dislike" Facebook pages and give thumbs up or thumbs down to videos on YouTube. We even rate physicians’ comments on medical question-and-answer sites such as HealthTap.com.
But how much do all of these online ratings really matter? A 2012 Nielsen report that surveyed more than 28,000 Internet users in 56 countries found that online consumer reviews are the second-most-trusted source of brand information, following only recommendations from family and friends. In other words, we trust online reviews and use them to make our own decisions.
The same is true when it comes to shopping for a doctor. According to an Internet-based survey of 2,137 adults published in the February issue of JAMA, 59% of respondents said that online doctor ratings were either "somewhat important" or "very important" when choosing a physician (2014;11:734-5).
Similarly, the "2013 Industry View Report" by Software Advice found that 62% of respondents said they read online reviews when seeking a new doctor. Although HealthGrades.com was the most commonly used site, Yelp.com was the most trusted. Forty-four percent of those respondents considered Yelp the most trustworthy review site followed by Health Grades (31%), Vitals.com (17%), and ZocDoc.com (7%).
Whether or not we trust Yelp and other online review sites, our patients do. In the JAMA survey, 35% of respondents said that they selected a physician based on good ratings, while 37% said that they avoided a physician with negative reviews. The 2013 Industry View Report also found that 45% of respondents ranked "quality of care" as the most important type of information sought about a doctor. And since many patients equate service with quality, reviews that focus on service matter.
This isn’t an entirely bad thing. If we really listen to what patients are saying, their comments can help us to improve service and communication. And, in some instances, it can lead to stronger doctor-patient relationships. Like many other industries, health care is moving toward transparency, and doctor rating sites are a key component of that.
Dr. Jeffrey Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego and a volunteer clinical assistant professor at the University of California, San Diego. He has published numerous scientific articles and is a member and fellow of the American Academy of Dermatology, and a member of the Telemedicine Association and the American Medical Association, among others. He is board certified in dermatology as well as medicine and surgery in the state of California. Dr. Benabio has a special interest in the uses of social media for education and building dermatology practice. He is the founder of The Derm Blog, an educational website that has had more than 2 million unique visitors. Dr. Benabio is also a founding member and the skin care expert for Livestrong.com, a health and wellness website of Lance Armstrong’s the Livestrong Foundation. Dr. Benabio is @Dermdoc on Twitter.

Medical conferences going digital
The medical conferences of the future made a preview appearance at this year’s Transcatheter Cardiovascular Therapeutics annual meeting in San Francisco. Paperless, electronic, interactive, and definitely high tech it was.
Every paid attendee was offered a new Samsung tablet computer, preloaded with pertinent apps and information, to personalize and keep if they wanted or return at the end of the meeting. If attendees preferred to download the apps to their own devices, that was fine too, and many of them did. (I got a loaner through the press room, and found it easy to use.)

Rather than tack the cost of the tablets onto registration fees, the organizers shifted funds from the no-longer-needed bulky printed programs and other materials to pay for the tablets, according to the Cardiovascular Research Foundation, cosponsor of the TCT meeting with the American College of Cardiology. No funds from industry were solicited for the tablets, no advertising appeared on the home screens, and the tablets were not being used to mine for user data of any kind, but the preloaded apps did contain some advertisements.
Paperless medical conferences are not new – many conferences eschew pulp these days, providing materials on zip drives instead of printed programs that attendees can load onto their computers. And apps for the larger medical conferences now are commonplace, too, for those who have their own smartphones or tablets. But this is the first time I’ve seen a conference give out tablets and include interactive social media features, convenient continuing medical education mechanisms, and more.
Through the apps, attendees could navigate the convention center; view abstracts; download speaker slides and disclosures; watch live cases; take notes; contact some faculty; find shuttle buses, hotels, and restaurants; and access exhibition materials. After attending a session, they could log their hours, write a review, and apply for CME credits through the apps. If they were willing to enable certain settings, they could see who else at the meeting was in their vicinity, and communicate with them.

Each of the major sessions I covered included a "digital moderator" in addition to the regular moderator. Instead of standing in line at microphones to ask questions, members of the audience texted comments and questions that appeared on a screen to the side of the main screen showing the presenter’s slides, so everyone could see them in real time. This feature wasn’t as much used as one might fear – doctors were still paying attention to the speaker, not staring down at their devices, for the most part. From what I could see, the digital moderators provided most of the texted comments and questions, though at one session the live moderator noted that audience texts were asking the speaker to comment about stroke risk, so he raised the question.
Keep in mind, the TCT always has been one of the most high-tech conferences happening in a very high-tech specialty, interventional cardiology. The typical setup in their main forum was similar to that in past meetings, a multitasking-palooza featuring a long dais of speakers and multiple video screens, with individual headsets that let you tune into whichever "channel" interests you most at the moment. Screens with live cases flank either end, with the presenter and his or her slides in the middle and screens promoting upcoming sessions and showing the audience texts in between the other screens.
TCT comes to San Francisco regularly because the city has the infrastructure to support these technologic demands, a spokeswoman in their press room told me. Some other locations haven’t been able to handle their needs.
I wondered if the technology will be so appealing that attendees might prefer virtual attendance rather than having to be there. It’s possible, she said, but unlikely. Like most people, these doctors value their face time.
On Twitter @sherryboschert
The medical conferences of the future made a preview appearance at this year’s Transcatheter Cardiovascular Therapeutics annual meeting in San Francisco. Paperless, electronic, interactive, and definitely high tech it was.
Every paid attendee was offered a new Samsung tablet computer, preloaded with pertinent apps and information, to personalize and keep if they wanted or return at the end of the meeting. If attendees preferred to download the apps to their own devices, that was fine too, and many of them did. (I got a loaner through the press room, and found it easy to use.)
Rather than tack the cost of the tablets onto registration fees, the organizers shifted funds from the no-longer-needed bulky printed programs and other materials to pay for the tablets, according to the Cardiovascular Research Foundation, cosponsor of the TCT meeting with the American College of Cardiology. No funds from industry were solicited for the tablets, no advertising appeared on the home screens, and the tablets were not being used to mine for user data of any kind, but the preloaded apps did contain some advertisements.
Paperless medical conferences are not new – many conferences eschew pulp these days, providing materials on zip drives instead of printed programs that attendees can load onto their computers. And apps for the larger medical conferences now are commonplace, too, for those who have their own smartphones or tablets. But this is the first time I’ve seen a conference give out tablets and include interactive social media features, convenient continuing medical education mechanisms, and more.
Through the apps, attendees could navigate the convention center; view abstracts; download speaker slides and disclosures; watch live cases; take notes; contact some faculty; find shuttle buses, hotels, and restaurants; and access exhibition materials. After attending a session, they could log their hours, write a review, and apply for CME credits through the apps. If they were willing to enable certain settings, they could see who else at the meeting was in their vicinity, and communicate with them.
Each of the major sessions I covered included a "digital moderator" in addition to the regular moderator. Instead of standing in line at microphones to ask questions, members of the audience texted comments and questions that appeared on a screen to the side of the main screen showing the presenter’s slides, so everyone could see them in real time. This feature wasn’t as much used as one might fear – doctors were still paying attention to the speaker, not staring down at their devices, for the most part. From what I could see, the digital moderators provided most of the texted comments and questions, though at one session the live moderator noted that audience texts were asking the speaker to comment about stroke risk, so he raised the question.
Keep in mind, the TCT always has been one of the most high-tech conferences happening in a very high-tech specialty, interventional cardiology. The typical setup in their main forum was similar to that in past meetings, a multitasking-palooza featuring a long dais of speakers and multiple video screens, with individual headsets that let you tune into whichever "channel" interests you most at the moment. Screens with live cases flank either end, with the presenter and his or her slides in the middle and screens promoting upcoming sessions and showing the audience texts in between the other screens.
TCT comes to San Francisco regularly because the city has the infrastructure to support these technologic demands, a spokeswoman in their press room told me. Some other locations haven’t been able to handle their needs.
I wondered if the technology will be so appealing that attendees might prefer virtual attendance rather than having to be there. It’s possible, she said, but unlikely. Like most people, these doctors value their face time.
On Twitter @sherryboschert
The medical conferences of the future made a preview appearance at this year’s Transcatheter Cardiovascular Therapeutics annual meeting in San Francisco. Paperless, electronic, interactive, and definitely high tech it was.
Every paid attendee was offered a new Samsung tablet computer, preloaded with pertinent apps and information, to personalize and keep if they wanted or return at the end of the meeting. If attendees preferred to download the apps to their own devices, that was fine too, and many of them did. (I got a loaner through the press room, and found it easy to use.)
Rather than tack the cost of the tablets onto registration fees, the organizers shifted funds from the no-longer-needed bulky printed programs and other materials to pay for the tablets, according to the Cardiovascular Research Foundation, cosponsor of the TCT meeting with the American College of Cardiology. No funds from industry were solicited for the tablets, no advertising appeared on the home screens, and the tablets were not being used to mine for user data of any kind, but the preloaded apps did contain some advertisements.
Paperless medical conferences are not new – many conferences eschew pulp these days, providing materials on zip drives instead of printed programs that attendees can load onto their computers. And apps for the larger medical conferences now are commonplace, too, for those who have their own smartphones or tablets. But this is the first time I’ve seen a conference give out tablets and include interactive social media features, convenient continuing medical education mechanisms, and more.
Through the apps, attendees could navigate the convention center; view abstracts; download speaker slides and disclosures; watch live cases; take notes; contact some faculty; find shuttle buses, hotels, and restaurants; and access exhibition materials. After attending a session, they could log their hours, write a review, and apply for CME credits through the apps. If they were willing to enable certain settings, they could see who else at the meeting was in their vicinity, and communicate with them.
Each of the major sessions I covered included a "digital moderator" in addition to the regular moderator. Instead of standing in line at microphones to ask questions, members of the audience texted comments and questions that appeared on a screen to the side of the main screen showing the presenter’s slides, so everyone could see them in real time. This feature wasn’t as much used as one might fear – doctors were still paying attention to the speaker, not staring down at their devices, for the most part. From what I could see, the digital moderators provided most of the texted comments and questions, though at one session the live moderator noted that audience texts were asking the speaker to comment about stroke risk, so he raised the question.
Keep in mind, the TCT always has been one of the most high-tech conferences happening in a very high-tech specialty, interventional cardiology. The typical setup in their main forum was similar to that in past meetings, a multitasking-palooza featuring a long dais of speakers and multiple video screens, with individual headsets that let you tune into whichever "channel" interests you most at the moment. Screens with live cases flank either end, with the presenter and his or her slides in the middle and screens promoting upcoming sessions and showing the audience texts in between the other screens.
TCT comes to San Francisco regularly because the city has the infrastructure to support these technologic demands, a spokeswoman in their press room told me. Some other locations haven’t been able to handle their needs.
I wondered if the technology will be so appealing that attendees might prefer virtual attendance rather than having to be there. It’s possible, she said, but unlikely. Like most people, these doctors value their face time.
On Twitter @sherryboschert

Online tool calculates Medicare incentives, penalties
Not sure if you’re going to be getting a bonus or paying a penalty to Medicare this year? You’re not alone.
Between the Medicare e-prescribing program, the "meaningful use" incentives for implementing electronic health records (EHRs), and the Physician Quality Reporting System (PQRS) – all with different incentive and penalty schedules – it’s hard to keep track of whether payments are going up or down and by how much.

Apparently, officials at the Centers for Medicare and Medicaid Services (CMS) agree. They have launched an online tool that allows physicians to click through a few questions and figure out what their payment adjustments will look like based on 2013 participation in the eRx Incentive Program, the Medicare EHR Incentive Program, and the PQRS.
For instance, if a physician attested to meaningful use of certified EHR technology in 2013 and plans on demonstrating that use, then he will avoid the 2015 payment adjustment and be eligible for incentive payments of between $8,000 and $12,000, depending on the year that he first demonstrated meaningful use.
The tool can also help physicians figure out how the three programs interact. If a physician reported the eRx measure’s numerator code at least 25 times in 2012, he will avoid the 2014 eRx penalty. But if he also successfully attested to meaningful use in 2012, then he can’t "double dip" and pick up the 1% eRx bonus, according to the CMS.
–By Mary Ellen Schneider
Dr. Stuart M. Garay, FCCP, comments:
Meeting CMS requirements for Medicare reimbursement is becoming increasingly complicated. During the past few years e-prescribing, EHR meaningful use, and PQRS have been rolled out to physicians with different incentive and penalty schedules. Physicians have been presented a confusing mess! Finally CMS has provided an online tool to sort this out. Take advantage; don't miss out!
Dr. Stuart M. Garay, FCCP, comments:
Meeting CMS requirements for Medicare reimbursement is becoming increasingly complicated. During the past few years e-prescribing, EHR meaningful use, and PQRS have been rolled out to physicians with different incentive and penalty schedules. Physicians have been presented a confusing mess! Finally CMS has provided an online tool to sort this out. Take advantage; don't miss out!
Dr. Stuart M. Garay, FCCP, comments:
Meeting CMS requirements for Medicare reimbursement is becoming increasingly complicated. During the past few years e-prescribing, EHR meaningful use, and PQRS have been rolled out to physicians with different incentive and penalty schedules. Physicians have been presented a confusing mess! Finally CMS has provided an online tool to sort this out. Take advantage; don't miss out!
Not sure if you’re going to be getting a bonus or paying a penalty to Medicare this year? You’re not alone.
Between the Medicare e-prescribing program, the "meaningful use" incentives for implementing electronic health records (EHRs), and the Physician Quality Reporting System (PQRS) – all with different incentive and penalty schedules – it’s hard to keep track of whether payments are going up or down and by how much.
Apparently, officials at the Centers for Medicare and Medicaid Services (CMS) agree. They have launched an online tool that allows physicians to click through a few questions and figure out what their payment adjustments will look like based on 2013 participation in the eRx Incentive Program, the Medicare EHR Incentive Program, and the PQRS.
For instance, if a physician attested to meaningful use of certified EHR technology in 2013 and plans on demonstrating that use, then he will avoid the 2015 payment adjustment and be eligible for incentive payments of between $8,000 and $12,000, depending on the year that he first demonstrated meaningful use.
The tool can also help physicians figure out how the three programs interact. If a physician reported the eRx measure’s numerator code at least 25 times in 2012, he will avoid the 2014 eRx penalty. But if he also successfully attested to meaningful use in 2012, then he can’t "double dip" and pick up the 1% eRx bonus, according to the CMS.
–By Mary Ellen Schneider
Not sure if you’re going to be getting a bonus or paying a penalty to Medicare this year? You’re not alone.
Between the Medicare e-prescribing program, the "meaningful use" incentives for implementing electronic health records (EHRs), and the Physician Quality Reporting System (PQRS) – all with different incentive and penalty schedules – it’s hard to keep track of whether payments are going up or down and by how much.
Apparently, officials at the Centers for Medicare and Medicaid Services (CMS) agree. They have launched an online tool that allows physicians to click through a few questions and figure out what their payment adjustments will look like based on 2013 participation in the eRx Incentive Program, the Medicare EHR Incentive Program, and the PQRS.
For instance, if a physician attested to meaningful use of certified EHR technology in 2013 and plans on demonstrating that use, then he will avoid the 2015 payment adjustment and be eligible for incentive payments of between $8,000 and $12,000, depending on the year that he first demonstrated meaningful use.
The tool can also help physicians figure out how the three programs interact. If a physician reported the eRx measure’s numerator code at least 25 times in 2012, he will avoid the 2014 eRx penalty. But if he also successfully attested to meaningful use in 2012, then he can’t "double dip" and pick up the 1% eRx bonus, according to the CMS.
–By Mary Ellen Schneider

Apps for physicians
When it comes to health, wellness, and fitness apps, we physicians tend to think of our patients. As in, how can this app help my patient lose weight, exercise more, monitor his diabetes, or help her stay compliant with her medications?
But what about physicians and other health care workers? Can apps help us? Absolutely. According to Dr. Craig Burkhart, a dermatologist and apps expert at the University of North Carolina at Chapel Hill, many physicians aren’t taking advantage of apps that can improve efficiency. "Most physicians I encounter have $1,000-$2,000 smartphones and tablets (when you include the service plans) and only make phone calls, check e-mails, text, and listen to music on them – all things they could do with much less expensive devices."
Dr. Burkhart says that many apps "can turn your devices into tools that help organize your e-mails, organize your schedule, bring clinical information to your fingertips, aid patient-doctor communication, secure important information, speed up and improve note taking, and more."
Apps for physicians are available in categories including patient education, drug reference, medical literature, and general reference.
Check out these handy apps and see what works for you:
• Read by QxMD. Staying up to date on medical journals is a challenge. This app lets you access, organize, and share articles from your favorite medical journals. Its magazinelike interface is popular with users, and makes reading medical journals "as fun as it can be," says Dr. Burkhart.
• PDFpen. Dr. Burkhart says this app is "essential to a paperless workflow." It allows users to sign and send documents without printing actual sheets of paper, making for a greener and more efficient office.
• Visual DX. A reference tool for physicians, this app is a digital medical image library with more than 25,000 images. It allows you to visually confirm a diagnosis and to quickly search on a disease, including symptoms and patient care management. A key feature is its ability to let you create a visual differential of medication-induced diseases for more than 700 different drugs.
• 1Password. We’ve all forgotten passwords from time to time. This app allows you to make and store highly secure and complex passwords. For Dr. Burkhart, it has "replaced memory and random sheets of paper as his password repository."
• Draw MD. We know that visuals often help us to explain complex issues to patients more effectively. This app enables you to draw and modify medical images and surgical procedures in a way that is clear and understandable to patients.
• 3D4Medical. This app can enhance patient education by using 3D technology to allow navigation around the body. You can zoom, rotate, and cut images to create different perspectives.
Dr. Jeffrey Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego and a volunteer clinical assistant professor at the University of California, San Diego. He has published numerous scientific articles and is a member and fellow of the American Academy of Dermatology, and a member of the Telemedicine Association and the American Medical Association, among others. He is board certified in dermatology as well as medicine and surgery in the state of California. Dr. Benabio has a special interest in the uses of social media for education and building a dermatology practice. He is the founder of The Derm Blog, an educational website which has had over 2 million unique visitors. Dr. Benabio is also a founding member and the skin care expert for Livestrong.com, a health and wellness website of Lance Armstrong’s the Livestrong Foundation. Dr. Benabio is @Dermdoc on Twitter.
When it comes to health, wellness, and fitness apps, we physicians tend to think of our patients. As in, how can this app help my patient lose weight, exercise more, monitor his diabetes, or help her stay compliant with her medications?
But what about physicians and other health care workers? Can apps help us? Absolutely. According to Dr. Craig Burkhart, a dermatologist and apps expert at the University of North Carolina at Chapel Hill, many physicians aren’t taking advantage of apps that can improve efficiency. "Most physicians I encounter have $1,000-$2,000 smartphones and tablets (when you include the service plans) and only make phone calls, check e-mails, text, and listen to music on them – all things they could do with much less expensive devices."
Dr. Burkhart says that many apps "can turn your devices into tools that help organize your e-mails, organize your schedule, bring clinical information to your fingertips, aid patient-doctor communication, secure important information, speed up and improve note taking, and more."
Apps for physicians are available in categories including patient education, drug reference, medical literature, and general reference.
Check out these handy apps and see what works for you:
• Read by QxMD. Staying up to date on medical journals is a challenge. This app lets you access, organize, and share articles from your favorite medical journals. Its magazinelike interface is popular with users, and makes reading medical journals "as fun as it can be," says Dr. Burkhart.
• PDFpen. Dr. Burkhart says this app is "essential to a paperless workflow." It allows users to sign and send documents without printing actual sheets of paper, making for a greener and more efficient office.
• Visual DX. A reference tool for physicians, this app is a digital medical image library with more than 25,000 images. It allows you to visually confirm a diagnosis and to quickly search on a disease, including symptoms and patient care management. A key feature is its ability to let you create a visual differential of medication-induced diseases for more than 700 different drugs.
• 1Password. We’ve all forgotten passwords from time to time. This app allows you to make and store highly secure and complex passwords. For Dr. Burkhart, it has "replaced memory and random sheets of paper as his password repository."
• Draw MD. We know that visuals often help us to explain complex issues to patients more effectively. This app enables you to draw and modify medical images and surgical procedures in a way that is clear and understandable to patients.
• 3D4Medical. This app can enhance patient education by using 3D technology to allow navigation around the body. You can zoom, rotate, and cut images to create different perspectives.
Dr. Jeffrey Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego and a volunteer clinical assistant professor at the University of California, San Diego. He has published numerous scientific articles and is a member and fellow of the American Academy of Dermatology, and a member of the Telemedicine Association and the American Medical Association, among others. He is board certified in dermatology as well as medicine and surgery in the state of California. Dr. Benabio has a special interest in the uses of social media for education and building a dermatology practice. He is the founder of The Derm Blog, an educational website which has had over 2 million unique visitors. Dr. Benabio is also a founding member and the skin care expert for Livestrong.com, a health and wellness website of Lance Armstrong’s the Livestrong Foundation. Dr. Benabio is @Dermdoc on Twitter.
When it comes to health, wellness, and fitness apps, we physicians tend to think of our patients. As in, how can this app help my patient lose weight, exercise more, monitor his diabetes, or help her stay compliant with her medications?
But what about physicians and other health care workers? Can apps help us? Absolutely. According to Dr. Craig Burkhart, a dermatologist and apps expert at the University of North Carolina at Chapel Hill, many physicians aren’t taking advantage of apps that can improve efficiency. "Most physicians I encounter have $1,000-$2,000 smartphones and tablets (when you include the service plans) and only make phone calls, check e-mails, text, and listen to music on them – all things they could do with much less expensive devices."
Dr. Burkhart says that many apps "can turn your devices into tools that help organize your e-mails, organize your schedule, bring clinical information to your fingertips, aid patient-doctor communication, secure important information, speed up and improve note taking, and more."
Apps for physicians are available in categories including patient education, drug reference, medical literature, and general reference.
Check out these handy apps and see what works for you:
• Read by QxMD. Staying up to date on medical journals is a challenge. This app lets you access, organize, and share articles from your favorite medical journals. Its magazinelike interface is popular with users, and makes reading medical journals "as fun as it can be," says Dr. Burkhart.
• PDFpen. Dr. Burkhart says this app is "essential to a paperless workflow." It allows users to sign and send documents without printing actual sheets of paper, making for a greener and more efficient office.
• Visual DX. A reference tool for physicians, this app is a digital medical image library with more than 25,000 images. It allows you to visually confirm a diagnosis and to quickly search on a disease, including symptoms and patient care management. A key feature is its ability to let you create a visual differential of medication-induced diseases for more than 700 different drugs.
• 1Password. We’ve all forgotten passwords from time to time. This app allows you to make and store highly secure and complex passwords. For Dr. Burkhart, it has "replaced memory and random sheets of paper as his password repository."
• Draw MD. We know that visuals often help us to explain complex issues to patients more effectively. This app enables you to draw and modify medical images and surgical procedures in a way that is clear and understandable to patients.
• 3D4Medical. This app can enhance patient education by using 3D technology to allow navigation around the body. You can zoom, rotate, and cut images to create different perspectives.
Dr. Jeffrey Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego and a volunteer clinical assistant professor at the University of California, San Diego. He has published numerous scientific articles and is a member and fellow of the American Academy of Dermatology, and a member of the Telemedicine Association and the American Medical Association, among others. He is board certified in dermatology as well as medicine and surgery in the state of California. Dr. Benabio has a special interest in the uses of social media for education and building a dermatology practice. He is the founder of The Derm Blog, an educational website which has had over 2 million unique visitors. Dr. Benabio is also a founding member and the skin care expert for Livestrong.com, a health and wellness website of Lance Armstrong’s the Livestrong Foundation. Dr. Benabio is @Dermdoc on Twitter.

Apps for your smart phone
The number of health apps continues to grow at a rapid pace, and if you’re in search of more apps to download and experiment with, Dr. Craig Burkhart has a list for you.
To give a sense of how fast health apps are arriving in the market, Dr. Burkhart of the University of North Carolina at Chapel Hill, broke down the number of health applications for Apple devices at the times of American Academy of Dermatology’s meetings: At the 2012 AAD annual meeting, there were 5,000 iOS health apps. That number went up to 13,000 during the 2012 Summer AAD, and 40,000 at the 2013 AAD annual meeting.

He listed some of his favorites during the 2013 AAD summer academy meeting:
1password – to remember passwords
Byword – a simple writing app
Drafts – to automate text actions, also good for transcriptions
Dropbox – to store and share documents, large or small
Epocrates – for drug reference
Evernote – for note-taking
Flipboard – popular news reader
Google Drive – for documents and spreadsheets
Launch Center Pro – to get quick shortcuts for specific features buried in apps
Mind Node – for mind mapping
Omnifocus – for task management, based on GDT system
PDF Pen and Good Reader – PDF readers with annotating capabilities
PubMed Mobile – to search PubMed for journal articles
Read by QXMD – to keep up with medical and scientific research
Scanner Pro – to capture documents and receipts as PDF
Text Expander Touch – for those who write
Tweetbot – if you use twitter for news
What health apps would you recommend to your colleagues? Write to [email protected] and let us know, or post your favorites on the Skin & Allergy News Facebook page.
Dr. Burkhart had no disclosures relevant to mobile apps.
[email protected] On Twitter @NaseemSMiller
The number of health apps continues to grow at a rapid pace, and if you’re in search of more apps to download and experiment with, Dr. Craig Burkhart has a list for you.
To give a sense of how fast health apps are arriving in the market, Dr. Burkhart of the University of North Carolina at Chapel Hill, broke down the number of health applications for Apple devices at the times of American Academy of Dermatology’s meetings: At the 2012 AAD annual meeting, there were 5,000 iOS health apps. That number went up to 13,000 during the 2012 Summer AAD, and 40,000 at the 2013 AAD annual meeting.
He listed some of his favorites during the 2013 AAD summer academy meeting:
1password – to remember passwords
Byword – a simple writing app
Drafts – to automate text actions, also good for transcriptions
Dropbox – to store and share documents, large or small
Epocrates – for drug reference
Evernote – for note-taking
Flipboard – popular news reader
Google Drive – for documents and spreadsheets
Launch Center Pro – to get quick shortcuts for specific features buried in apps
Mind Node – for mind mapping
Omnifocus – for task management, based on GDT system
PDF Pen and Good Reader – PDF readers with annotating capabilities
PubMed Mobile – to search PubMed for journal articles
Read by QXMD – to keep up with medical and scientific research
Scanner Pro – to capture documents and receipts as PDF
Text Expander Touch – for those who write
Tweetbot – if you use twitter for news
What health apps would you recommend to your colleagues? Write to [email protected] and let us know, or post your favorites on the Skin & Allergy News Facebook page.
Dr. Burkhart had no disclosures relevant to mobile apps.
[email protected] On Twitter @NaseemSMiller
The number of health apps continues to grow at a rapid pace, and if you’re in search of more apps to download and experiment with, Dr. Craig Burkhart has a list for you.
To give a sense of how fast health apps are arriving in the market, Dr. Burkhart of the University of North Carolina at Chapel Hill, broke down the number of health applications for Apple devices at the times of American Academy of Dermatology’s meetings: At the 2012 AAD annual meeting, there were 5,000 iOS health apps. That number went up to 13,000 during the 2012 Summer AAD, and 40,000 at the 2013 AAD annual meeting.
He listed some of his favorites during the 2013 AAD summer academy meeting:
1password – to remember passwords
Byword – a simple writing app
Drafts – to automate text actions, also good for transcriptions
Dropbox – to store and share documents, large or small
Epocrates – for drug reference
Evernote – for note-taking
Flipboard – popular news reader
Google Drive – for documents and spreadsheets
Launch Center Pro – to get quick shortcuts for specific features buried in apps
Mind Node – for mind mapping
Omnifocus – for task management, based on GDT system
PDF Pen and Good Reader – PDF readers with annotating capabilities
PubMed Mobile – to search PubMed for journal articles
Read by QXMD – to keep up with medical and scientific research
Scanner Pro – to capture documents and receipts as PDF
Text Expander Touch – for those who write
Tweetbot – if you use twitter for news
What health apps would you recommend to your colleagues? Write to [email protected] and let us know, or post your favorites on the Skin & Allergy News Facebook page.
Dr. Burkhart had no disclosures relevant to mobile apps.
[email protected] On Twitter @NaseemSMiller

Health IT coordinator moving on
Upset about the federal government’s meaningful use standards? Don’t take your complaints to Dr. Farzad Mostashari. He’s stepping down from his post as national coordinator for health information technology sometime this fall.
His departure comes as physicians and hospitals are moving toward adoption of Stage 2 of meaningful use, part of the Medicare Electronic Health Record (EHR) incentive program. Dr. Mostashari also has been called to Capitol Hill in recent weeks to field questions from lawmakers on why it is taking so long to make EHR systems talk to one another.

In an e-mail to agency staff on Aug. 6, Health and Human Services Secretary Kathleen Sebelius praised Dr. Mostashari for his work in linking the meaningful use of EHRs to population health goals and laying a "strong foundation" for increasing the interoperability of health records.
Dr. Mostashari, who became national coordinator in 2011, will stay on in his current post for a little while as HHS officials search for a replacement. As for his plans after leaving HHS, Dr. Mostashari said that he’s not sure.
"It is difficult for me to announce that I am leaving," he wrote in an e-mail to staff at the Office of the National Coordinator of Health Information Technology. "I don’t know what I will be doing after I leave public service, but be assured that I will be by your side as we continue to battle for healthcare transformation, cheering you on."
–By Mary Ellen Schneider
On Twitter @MaryEllenNY
Upset about the federal government’s meaningful use standards? Don’t take your complaints to Dr. Farzad Mostashari. He’s stepping down from his post as national coordinator for health information technology sometime this fall.
His departure comes as physicians and hospitals are moving toward adoption of Stage 2 of meaningful use, part of the Medicare Electronic Health Record (EHR) incentive program. Dr. Mostashari also has been called to Capitol Hill in recent weeks to field questions from lawmakers on why it is taking so long to make EHR systems talk to one another.
In an e-mail to agency staff on Aug. 6, Health and Human Services Secretary Kathleen Sebelius praised Dr. Mostashari for his work in linking the meaningful use of EHRs to population health goals and laying a "strong foundation" for increasing the interoperability of health records.
Dr. Mostashari, who became national coordinator in 2011, will stay on in his current post for a little while as HHS officials search for a replacement. As for his plans after leaving HHS, Dr. Mostashari said that he’s not sure.
"It is difficult for me to announce that I am leaving," he wrote in an e-mail to staff at the Office of the National Coordinator of Health Information Technology. "I don’t know what I will be doing after I leave public service, but be assured that I will be by your side as we continue to battle for healthcare transformation, cheering you on."
–By Mary Ellen Schneider
On Twitter @MaryEllenNY
Upset about the federal government’s meaningful use standards? Don’t take your complaints to Dr. Farzad Mostashari. He’s stepping down from his post as national coordinator for health information technology sometime this fall.
His departure comes as physicians and hospitals are moving toward adoption of Stage 2 of meaningful use, part of the Medicare Electronic Health Record (EHR) incentive program. Dr. Mostashari also has been called to Capitol Hill in recent weeks to field questions from lawmakers on why it is taking so long to make EHR systems talk to one another.
In an e-mail to agency staff on Aug. 6, Health and Human Services Secretary Kathleen Sebelius praised Dr. Mostashari for his work in linking the meaningful use of EHRs to population health goals and laying a "strong foundation" for increasing the interoperability of health records.
Dr. Mostashari, who became national coordinator in 2011, will stay on in his current post for a little while as HHS officials search for a replacement. As for his plans after leaving HHS, Dr. Mostashari said that he’s not sure.
"It is difficult for me to announce that I am leaving," he wrote in an e-mail to staff at the Office of the National Coordinator of Health Information Technology. "I don’t know what I will be doing after I leave public service, but be assured that I will be by your side as we continue to battle for healthcare transformation, cheering you on."
–By Mary Ellen Schneider
On Twitter @MaryEllenNY

Will a novel antibody fix the anticoagulant-bleeding problem?
It seems inescapable: If patients are made less able to form blood clots, they bleed more.
Bleeding is the perennial problem for anticoagulants. Whether it’s the traditional anticoagulants (heparin, warfarin, and the low-molecular-weight heparins) or new drugs (fondaparinux, dabigatran, rivaroxaban, and apixaban), as the anticoagulant’s potency or dosage increases to stop blood clots from forming, the inevitable downside is increased bleeding.
Maybe not.
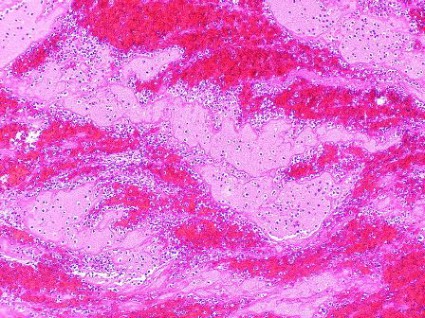
A newly developed, synthetic human IgG antibody appears, in animal and in vitro models, to allow normal clotting to occur and stop bleeding at vessel tears and cuts, while short-circuiting pathologic clotting in intravascular spaces – the sorts of clots that cause venous thromboembolisms, myocardial infarctions, and strokes.

"It seems too good to be true. It’s beyond comprehension," said Dr. Trevor Baglin, the University of Cambridge, England, hematologist who discovered the first identified, naturally occurring example of this antibody, in IgA form, in a patient he initially saw in 2008. "All we can do is go forward and see if it genuinely is as good as it seems," he said while presenting his group’s initial animal findings with the antibody at the Congress of the International Society on Thrombosis and Haemostasis in Amsterdam earlier this month.
The antibody – which has been patented, synthesized, and is in extensive preclinical testing – has been named ichorcumab. In Greek mythology, "ichor" was the blood factor in gods that made them immortal.
The secret behind ichorcumab is that it binds to and inactivates exosite 1, the part of the thrombin molecule that cleaves fibrinogen into fibrin, an effective brake on clotting. Study results suggest that whether the exosite 1 portion of thrombin is exposed or hidden at various body sites accounts for ichorcumab’s varied effects.
"Our hypothesis is that exosite 1 is protected from the antibody [when a thrombin molecule sits] on a cell or clot surface, so hemostasis is unaffected, but thrombosis occurs in the luminal space, where exosite 1 is exposed an available to the antibody," Dr. Baglin explained.
"While before we thought of just one type of clot, [the work with ichorcumab so far] suggests there is not one clotting mechanism but two," he noted, one that leads to clot formation that stops bleeding, and a second mechanism that produces clots that cause thrombosis. Ichorcumab blocks the bad clots but not the good ones, because the clots form at different locations that affect the way that exosite 1 on thrombin is exposed.
It may sound farfetched, but it’s a way for the researchers to explain the curious patient whom Dr. Baglin first met in 2008, a 53-year old woman who spontaneously makes and carries the IgA prototype of ichorcumab in her blood.
Dr. Baglin said that he consulted on her case after a preprocedural clotting screen revealed that her blood was unclottable by standard tests, yet she had no history of any bleeding disorder. In fact, her history showed that she had undergone knee surgery (when no clotting screen had been done) 5 months before Dr. Baglin first saw her without any hint of a bleeding incident. She subsequently cut the tip of a finger while slicing with a mandolin, but her bleeding stopped spontaneously.
The patient goes through life with this antibody in her blood at a level of about 3 g/L with no bleeding problems whatsoever; yet in a mouse model, a substantially lower level of the mimic antibody, ichorcumab, effectively blocked thrombosis. In the mouse model, this effective dose of ichorcumab does not cause bleeding if the mouse’s tail is cut.
Dr. Baglin and his associates started a company in Cambridge, XO1, to fund the preclinical work and eventually commercialize ichorcumab. They believe it will be another 2 years before any person receives a dose of the antibody.
–BY MITCHEL L. ZOLER
On Twitter @mitchelzoler
It seems inescapable: If patients are made less able to form blood clots, they bleed more.
Bleeding is the perennial problem for anticoagulants. Whether it’s the traditional anticoagulants (heparin, warfarin, and the low-molecular-weight heparins) or new drugs (fondaparinux, dabigatran, rivaroxaban, and apixaban), as the anticoagulant’s potency or dosage increases to stop blood clots from forming, the inevitable downside is increased bleeding.
Maybe not.
A newly developed, synthetic human IgG antibody appears, in animal and in vitro models, to allow normal clotting to occur and stop bleeding at vessel tears and cuts, while short-circuiting pathologic clotting in intravascular spaces – the sorts of clots that cause venous thromboembolisms, myocardial infarctions, and strokes.
"It seems too good to be true. It’s beyond comprehension," said Dr. Trevor Baglin, the University of Cambridge, England, hematologist who discovered the first identified, naturally occurring example of this antibody, in IgA form, in a patient he initially saw in 2008. "All we can do is go forward and see if it genuinely is as good as it seems," he said while presenting his group’s initial animal findings with the antibody at the Congress of the International Society on Thrombosis and Haemostasis in Amsterdam earlier this month.
The antibody – which has been patented, synthesized, and is in extensive preclinical testing – has been named ichorcumab. In Greek mythology, "ichor" was the blood factor in gods that made them immortal.
The secret behind ichorcumab is that it binds to and inactivates exosite 1, the part of the thrombin molecule that cleaves fibrinogen into fibrin, an effective brake on clotting. Study results suggest that whether the exosite 1 portion of thrombin is exposed or hidden at various body sites accounts for ichorcumab’s varied effects.
"Our hypothesis is that exosite 1 is protected from the antibody [when a thrombin molecule sits] on a cell or clot surface, so hemostasis is unaffected, but thrombosis occurs in the luminal space, where exosite 1 is exposed an available to the antibody," Dr. Baglin explained.
"While before we thought of just one type of clot, [the work with ichorcumab so far] suggests there is not one clotting mechanism but two," he noted, one that leads to clot formation that stops bleeding, and a second mechanism that produces clots that cause thrombosis. Ichorcumab blocks the bad clots but not the good ones, because the clots form at different locations that affect the way that exosite 1 on thrombin is exposed.
It may sound farfetched, but it’s a way for the researchers to explain the curious patient whom Dr. Baglin first met in 2008, a 53-year old woman who spontaneously makes and carries the IgA prototype of ichorcumab in her blood.
Dr. Baglin said that he consulted on her case after a preprocedural clotting screen revealed that her blood was unclottable by standard tests, yet she had no history of any bleeding disorder. In fact, her history showed that she had undergone knee surgery (when no clotting screen had been done) 5 months before Dr. Baglin first saw her without any hint of a bleeding incident. She subsequently cut the tip of a finger while slicing with a mandolin, but her bleeding stopped spontaneously.
The patient goes through life with this antibody in her blood at a level of about 3 g/L with no bleeding problems whatsoever; yet in a mouse model, a substantially lower level of the mimic antibody, ichorcumab, effectively blocked thrombosis. In the mouse model, this effective dose of ichorcumab does not cause bleeding if the mouse’s tail is cut.
Dr. Baglin and his associates started a company in Cambridge, XO1, to fund the preclinical work and eventually commercialize ichorcumab. They believe it will be another 2 years before any person receives a dose of the antibody.
–BY MITCHEL L. ZOLER
On Twitter @mitchelzoler
It seems inescapable: If patients are made less able to form blood clots, they bleed more.
Bleeding is the perennial problem for anticoagulants. Whether it’s the traditional anticoagulants (heparin, warfarin, and the low-molecular-weight heparins) or new drugs (fondaparinux, dabigatran, rivaroxaban, and apixaban), as the anticoagulant’s potency or dosage increases to stop blood clots from forming, the inevitable downside is increased bleeding.
Maybe not.
A newly developed, synthetic human IgG antibody appears, in animal and in vitro models, to allow normal clotting to occur and stop bleeding at vessel tears and cuts, while short-circuiting pathologic clotting in intravascular spaces – the sorts of clots that cause venous thromboembolisms, myocardial infarctions, and strokes.
"It seems too good to be true. It’s beyond comprehension," said Dr. Trevor Baglin, the University of Cambridge, England, hematologist who discovered the first identified, naturally occurring example of this antibody, in IgA form, in a patient he initially saw in 2008. "All we can do is go forward and see if it genuinely is as good as it seems," he said while presenting his group’s initial animal findings with the antibody at the Congress of the International Society on Thrombosis and Haemostasis in Amsterdam earlier this month.
The antibody – which has been patented, synthesized, and is in extensive preclinical testing – has been named ichorcumab. In Greek mythology, "ichor" was the blood factor in gods that made them immortal.
The secret behind ichorcumab is that it binds to and inactivates exosite 1, the part of the thrombin molecule that cleaves fibrinogen into fibrin, an effective brake on clotting. Study results suggest that whether the exosite 1 portion of thrombin is exposed or hidden at various body sites accounts for ichorcumab’s varied effects.
"Our hypothesis is that exosite 1 is protected from the antibody [when a thrombin molecule sits] on a cell or clot surface, so hemostasis is unaffected, but thrombosis occurs in the luminal space, where exosite 1 is exposed an available to the antibody," Dr. Baglin explained.
"While before we thought of just one type of clot, [the work with ichorcumab so far] suggests there is not one clotting mechanism but two," he noted, one that leads to clot formation that stops bleeding, and a second mechanism that produces clots that cause thrombosis. Ichorcumab blocks the bad clots but not the good ones, because the clots form at different locations that affect the way that exosite 1 on thrombin is exposed.
It may sound farfetched, but it’s a way for the researchers to explain the curious patient whom Dr. Baglin first met in 2008, a 53-year old woman who spontaneously makes and carries the IgA prototype of ichorcumab in her blood.
Dr. Baglin said that he consulted on her case after a preprocedural clotting screen revealed that her blood was unclottable by standard tests, yet she had no history of any bleeding disorder. In fact, her history showed that she had undergone knee surgery (when no clotting screen had been done) 5 months before Dr. Baglin first saw her without any hint of a bleeding incident. She subsequently cut the tip of a finger while slicing with a mandolin, but her bleeding stopped spontaneously.
The patient goes through life with this antibody in her blood at a level of about 3 g/L with no bleeding problems whatsoever; yet in a mouse model, a substantially lower level of the mimic antibody, ichorcumab, effectively blocked thrombosis. In the mouse model, this effective dose of ichorcumab does not cause bleeding if the mouse’s tail is cut.
Dr. Baglin and his associates started a company in Cambridge, XO1, to fund the preclinical work and eventually commercialize ichorcumab. They believe it will be another 2 years before any person receives a dose of the antibody.
–BY MITCHEL L. ZOLER
On Twitter @mitchelzoler
Mammas, don't let your babies grow up to be doctors
When country singer Ed Bruce released "Mammas, Don’t Let Your Babies Grow Up to be Cowboys" in 1975, he suggested that they should consider becoming doctors instead, but if a new national survey of doctors is to be believed, that’s not such a good career move either.
The survey, conducted by the Georgia-based staffing company Jackson Healthcare, found that 59% of physicians would be unlikely to encourage a young person to become a doctor. The findings are based on the responses of 3,456 physicians who completed e-mailed surveys between March 7 and April 1, 2013.

Their dissatisfaction with medical practice is reflected in the career satisfaction numbers in the survey. Only 20% of physicians said that they were very satisfied in their work, while 39% were somewhat satisfied and 42% were somewhat or very dissatisfied.
The satisfied ones tended to be those employed by a hospital or working at a physician-owned practice where they had no ownership stake, according to the survey.
Satisfied doctors reported that they worked 11 hours a day or less and were supported by nurse practitioners or physician assistants.
In contrast, dissatisfied doctors tended to own their practices, work as locum tenens physicians, or work for a hospital-owned practice. They also worked longer hours and had few physician extenders.
Maybe the next generation will take Ed Bruce’s other suggested career path and become lawyers.
When country singer Ed Bruce released "Mammas, Don’t Let Your Babies Grow Up to be Cowboys" in 1975, he suggested that they should consider becoming doctors instead, but if a new national survey of doctors is to be believed, that’s not such a good career move either.
The survey, conducted by the Georgia-based staffing company Jackson Healthcare, found that 59% of physicians would be unlikely to encourage a young person to become a doctor. The findings are based on the responses of 3,456 physicians who completed e-mailed surveys between March 7 and April 1, 2013.
Their dissatisfaction with medical practice is reflected in the career satisfaction numbers in the survey. Only 20% of physicians said that they were very satisfied in their work, while 39% were somewhat satisfied and 42% were somewhat or very dissatisfied.
The satisfied ones tended to be those employed by a hospital or working at a physician-owned practice where they had no ownership stake, according to the survey.
Satisfied doctors reported that they worked 11 hours a day or less and were supported by nurse practitioners or physician assistants.
In contrast, dissatisfied doctors tended to own their practices, work as locum tenens physicians, or work for a hospital-owned practice. They also worked longer hours and had few physician extenders.
Maybe the next generation will take Ed Bruce’s other suggested career path and become lawyers.
When country singer Ed Bruce released "Mammas, Don’t Let Your Babies Grow Up to be Cowboys" in 1975, he suggested that they should consider becoming doctors instead, but if a new national survey of doctors is to be believed, that’s not such a good career move either.
The survey, conducted by the Georgia-based staffing company Jackson Healthcare, found that 59% of physicians would be unlikely to encourage a young person to become a doctor. The findings are based on the responses of 3,456 physicians who completed e-mailed surveys between March 7 and April 1, 2013.
Their dissatisfaction with medical practice is reflected in the career satisfaction numbers in the survey. Only 20% of physicians said that they were very satisfied in their work, while 39% were somewhat satisfied and 42% were somewhat or very dissatisfied.
The satisfied ones tended to be those employed by a hospital or working at a physician-owned practice where they had no ownership stake, according to the survey.
Satisfied doctors reported that they worked 11 hours a day or less and were supported by nurse practitioners or physician assistants.
In contrast, dissatisfied doctors tended to own their practices, work as locum tenens physicians, or work for a hospital-owned practice. They also worked longer hours and had few physician extenders.
Maybe the next generation will take Ed Bruce’s other suggested career path and become lawyers.

How EHRs went wrong
If, like me, you believe that electronic health records will play an important role in future of medicine but can’t figure out why the federal government is spending $19 billion dollars incentivizing the adoption of systems that aren’t ready for prime time, I have found an answer.
An article in the New York Times ("A Digital Shift on Health Data Swells Profits in an Industry," Feb. 19, 2013) provided a glimpse into the backstage story of some questionable associations that led to bad decisions.
Glen E. Tullman, who until recently was the chief executive of Allscripts, one of the three dominant players in the electronic health information business, was health technology advisor to the 2008 Obama campaign. Since President Obama took office in 2009, he has reportedly visited the White House on at least seven occasions. Mr. Tullman, who was quoted as saying, "We really haven’t done any lobbying," characterized his time in Washington as education. According to the New York Times article, Allscripts annual sales have more than doubled since 2009 to an estimated $1.44 billion dollars in 2012.
It appears that the lobbying efforts by Mr. Tullman and other members of the industry were instrumental in creating a timetable of incentives that had physicians and hospitals rushing to jump on the EHR train before it left the station – and before it was road worthy. The result has been huge profits to the largest digital records companies while smaller companies that may have been less ready to compete have withered, the Times said.
One could argue that this is just another example of survival of the fittest in the best tradition of American free market capitalism. The problem is that the subsidies have tilted the playing field, and the resulting products have not met the promises made by those who lobbied for them. The even bigger problem is that the government also failed to secure from the industry any guarantees that EHR systems would meet a set of minimum standards and be compatible with one another.
As physicians, we also must share some of the blame for this EHR debacle.
We have not been thoughtful consumers. Those of us in small physician-owned groups must understand the relationship between our overhead and the bottom line and carefully weigh whether an incentive makes sense for us financially. If we decide to buy an EHR, we must be good shoppers. We must visit several practices that match our demographic and have been using for several years the system we are considering – even if this means flying to other cities to get a broad sampling. We should drive a hard bargain with incentives for support and severe financial penalties for failure to produce. And we mustn’t be afraid to say to the vendors that either we or they aren’t ready.
Most of us, however, no longer practice in physician-owned practices anymore. For a variety of reasons, we have allowed others to make decisions that dictate how we practice medicine in the real world. Most of these "others" aren’t physicians, and if they were once physicians, they certainly aren’t now in the true sense of the word and they don’t have recent practical experience of seeing real patients in real time. These others are often the folks who choose when and from which vendors medical practices buy their EHRs.
By joining larger and larger provider organizations, practicing physicians have lost their ability to provide critical input into the choice of tools with which they will practice. The result has been large investments in EHR systems that neither save money nor provide better care. We can only hope that from the ashes of this first failed attempt will come a system that does what we and our patients want it to do.
Dr. Wilkoff practices general pediatrics in a multispecialty group practice in Brunswick, Maine. E-mail Dr. Wilkoff at [email protected].
If, like me, you believe that electronic health records will play an important role in future of medicine but can’t figure out why the federal government is spending $19 billion dollars incentivizing the adoption of systems that aren’t ready for prime time, I have found an answer.
An article in the New York Times ("A Digital Shift on Health Data Swells Profits in an Industry," Feb. 19, 2013) provided a glimpse into the backstage story of some questionable associations that led to bad decisions.
Glen E. Tullman, who until recently was the chief executive of Allscripts, one of the three dominant players in the electronic health information business, was health technology advisor to the 2008 Obama campaign. Since President Obama took office in 2009, he has reportedly visited the White House on at least seven occasions. Mr. Tullman, who was quoted as saying, "We really haven’t done any lobbying," characterized his time in Washington as education. According to the New York Times article, Allscripts annual sales have more than doubled since 2009 to an estimated $1.44 billion dollars in 2012.
It appears that the lobbying efforts by Mr. Tullman and other members of the industry were instrumental in creating a timetable of incentives that had physicians and hospitals rushing to jump on the EHR train before it left the station – and before it was road worthy. The result has been huge profits to the largest digital records companies while smaller companies that may have been less ready to compete have withered, the Times said.
One could argue that this is just another example of survival of the fittest in the best tradition of American free market capitalism. The problem is that the subsidies have tilted the playing field, and the resulting products have not met the promises made by those who lobbied for them. The even bigger problem is that the government also failed to secure from the industry any guarantees that EHR systems would meet a set of minimum standards and be compatible with one another.
As physicians, we also must share some of the blame for this EHR debacle.
We have not been thoughtful consumers. Those of us in small physician-owned groups must understand the relationship between our overhead and the bottom line and carefully weigh whether an incentive makes sense for us financially. If we decide to buy an EHR, we must be good shoppers. We must visit several practices that match our demographic and have been using for several years the system we are considering – even if this means flying to other cities to get a broad sampling. We should drive a hard bargain with incentives for support and severe financial penalties for failure to produce. And we mustn’t be afraid to say to the vendors that either we or they aren’t ready.
Most of us, however, no longer practice in physician-owned practices anymore. For a variety of reasons, we have allowed others to make decisions that dictate how we practice medicine in the real world. Most of these "others" aren’t physicians, and if they were once physicians, they certainly aren’t now in the true sense of the word and they don’t have recent practical experience of seeing real patients in real time. These others are often the folks who choose when and from which vendors medical practices buy their EHRs.
By joining larger and larger provider organizations, practicing physicians have lost their ability to provide critical input into the choice of tools with which they will practice. The result has been large investments in EHR systems that neither save money nor provide better care. We can only hope that from the ashes of this first failed attempt will come a system that does what we and our patients want it to do.
Dr. Wilkoff practices general pediatrics in a multispecialty group practice in Brunswick, Maine. E-mail Dr. Wilkoff at [email protected].
If, like me, you believe that electronic health records will play an important role in future of medicine but can’t figure out why the federal government is spending $19 billion dollars incentivizing the adoption of systems that aren’t ready for prime time, I have found an answer.
An article in the New York Times ("A Digital Shift on Health Data Swells Profits in an Industry," Feb. 19, 2013) provided a glimpse into the backstage story of some questionable associations that led to bad decisions.
Glen E. Tullman, who until recently was the chief executive of Allscripts, one of the three dominant players in the electronic health information business, was health technology advisor to the 2008 Obama campaign. Since President Obama took office in 2009, he has reportedly visited the White House on at least seven occasions. Mr. Tullman, who was quoted as saying, "We really haven’t done any lobbying," characterized his time in Washington as education. According to the New York Times article, Allscripts annual sales have more than doubled since 2009 to an estimated $1.44 billion dollars in 2012.
It appears that the lobbying efforts by Mr. Tullman and other members of the industry were instrumental in creating a timetable of incentives that had physicians and hospitals rushing to jump on the EHR train before it left the station – and before it was road worthy. The result has been huge profits to the largest digital records companies while smaller companies that may have been less ready to compete have withered, the Times said.
One could argue that this is just another example of survival of the fittest in the best tradition of American free market capitalism. The problem is that the subsidies have tilted the playing field, and the resulting products have not met the promises made by those who lobbied for them. The even bigger problem is that the government also failed to secure from the industry any guarantees that EHR systems would meet a set of minimum standards and be compatible with one another.
As physicians, we also must share some of the blame for this EHR debacle.
We have not been thoughtful consumers. Those of us in small physician-owned groups must understand the relationship between our overhead and the bottom line and carefully weigh whether an incentive makes sense for us financially. If we decide to buy an EHR, we must be good shoppers. We must visit several practices that match our demographic and have been using for several years the system we are considering – even if this means flying to other cities to get a broad sampling. We should drive a hard bargain with incentives for support and severe financial penalties for failure to produce. And we mustn’t be afraid to say to the vendors that either we or they aren’t ready.
Most of us, however, no longer practice in physician-owned practices anymore. For a variety of reasons, we have allowed others to make decisions that dictate how we practice medicine in the real world. Most of these "others" aren’t physicians, and if they were once physicians, they certainly aren’t now in the true sense of the word and they don’t have recent practical experience of seeing real patients in real time. These others are often the folks who choose when and from which vendors medical practices buy their EHRs.
By joining larger and larger provider organizations, practicing physicians have lost their ability to provide critical input into the choice of tools with which they will practice. The result has been large investments in EHR systems that neither save money nor provide better care. We can only hope that from the ashes of this first failed attempt will come a system that does what we and our patients want it to do.
Dr. Wilkoff practices general pediatrics in a multispecialty group practice in Brunswick, Maine. E-mail Dr. Wilkoff at [email protected].
Only doctors can save America
Dr. Ezekiel J. Emanuel, one of the brains behind Obamacare, has a blunt message for his fellow physicians:
Only you can save America.
He's not just talking about medicine. As might befit someone who holds a faculty title at the business-oriented Wharton School at the University of Pennsylvania, Dr. Emanuel spent much of his keynote address here at the American College of Physicians' annual meeting in San Francisco talking about the U.S. economy. The enormous impact of runaway spending on U.S. health care threatens "everything we care about," including access to health care, state funds available for education, corporate wages for the middle class, and the fiscal health of the nation, he said.
"More than any other group in America, doctors have the power to solve our long-term economic challenges to ensure a prosperous future," Dr. Emanuel said.

If the U.S. health care system were a country, its nearly $3 trillion economy in 2012 would be the fifth largest in the world, behind only the U.S. as a whole, China, Japan, and Germany. "We spend more on health care in this country than the 66 million French spend on everything in their society," he said. "It is an astounding number how much we spend on health care."
Take just the federal portions of Medicare and Medicaid, excluding state spending, and you've still got the 16th largest economy in the world, bigger than the economies of Switzerland, Turkey, or the Netherlands, for example. The impact of any other fiscal variable on the U.S. economy, including Social Security, is swamped by the impact of health care costs, said Dr. Emanuel, who is also chair of medical ethics and health policy at the University of Pennsylvania, Philadelphia.
Per person, the United States far outspends other countries when it comes to health care, and the proportion of the gross domestic product consumed by health care keeps getting larger and larger.
Dr. Emanuel served as a special adviser for health policy to the director of the federal Office of Management and Budget in 2009-2011 - during the design, passage, and first steps to implementation of the Patient Protection and Affordable Care Act (commonly known as Obamacare) - and he seemed to address some critics in absentia who have claimed that health care reform will lead to unwanted rationing of care. There's no need to ration, Dr. Emanuel said. Switzerland doesn't ration care, and it spends far less per capita for what is considered quality health care. "We can do a better job in this country of controlling costs without the need to ration care," he said.
The only way to really control costs is to transform the way U.S. health care is delivered, he said. Ten percent of U.S. patients account for 63% of dollars spent on health care. "You know who they are - people with congestive heart failure, COPD, diabetes, adult asthma, coronary artery disease, cancer. People with chronic multiple chronic illnesses. That's where the money's going. That's where the uneven quality is," and that's where health care delivery needs to improve, he said.
Dr. Emanuel proposed six essential components to transforming the health care system. Among them: The focus needs to be on cost according to value, and getting rid of services with no value. The system must focus on patients' needs, not on physicians' schedules or other concerns. And the system must evolve toward clinicians working as teams including allied health professionals, not as individuals. "We are not going to be, going forward, one-sies and two-sies in practice" anymore, he said.
Greater emphasis on delivering health care via organizations and systems, standardization of processes, and transparency around price and quality will be essential, he added.
Transparency in pricing and quality isn't just something consumers will want. Physicians will want it in order to refer patients to quality care and set prices appropriately, Dr. Emanuel argued. "I think this is inevitable, and I think it's going to happen faster than you think," he said.
Most U.S. physicians are stuck in fee-for-service payment systems, which don't provide the incentives needed for change, he said. Doctors "as a group" should push for changes to the payment system, which will increase physician autonomy but also will assign more financial risk to physicians. "I see no way of getting out of that," Dr. Emanuel said.
In his eyes, if doctors don't push for changes in how health care is delivered, we basically can kiss the U.S. economy and future prosperity good-bye. "Doctors are the only people who can re-engineer the delivery system," he said. "If you don't do it, it ain't gonna happen. It's that simple," he said. All previous reform efforts that did not have physician leadership have failed.
"You have to lead this," he explained.
No one should expect that reforming the fifth-largest economy in the world could be accomplished in just a few years, however. "It's going to take this decade," Dr. Emanuel predicted.
Dr. Emanuel reported having no financial disclosures.
Twitter: @sherryboschert
Dr. Ezekiel J. Emanuel, one of the brains behind Obamacare, has a blunt message for his fellow physicians:
Only you can save America.
He's not just talking about medicine. As might befit someone who holds a faculty title at the business-oriented Wharton School at the University of Pennsylvania, Dr. Emanuel spent much of his keynote address here at the American College of Physicians' annual meeting in San Francisco talking about the U.S. economy. The enormous impact of runaway spending on U.S. health care threatens "everything we care about," including access to health care, state funds available for education, corporate wages for the middle class, and the fiscal health of the nation, he said.
"More than any other group in America, doctors have the power to solve our long-term economic challenges to ensure a prosperous future," Dr. Emanuel said.
If the U.S. health care system were a country, its nearly $3 trillion economy in 2012 would be the fifth largest in the world, behind only the U.S. as a whole, China, Japan, and Germany. "We spend more on health care in this country than the 66 million French spend on everything in their society," he said. "It is an astounding number how much we spend on health care."
Take just the federal portions of Medicare and Medicaid, excluding state spending, and you've still got the 16th largest economy in the world, bigger than the economies of Switzerland, Turkey, or the Netherlands, for example. The impact of any other fiscal variable on the U.S. economy, including Social Security, is swamped by the impact of health care costs, said Dr. Emanuel, who is also chair of medical ethics and health policy at the University of Pennsylvania, Philadelphia.
Per person, the United States far outspends other countries when it comes to health care, and the proportion of the gross domestic product consumed by health care keeps getting larger and larger.
Dr. Emanuel served as a special adviser for health policy to the director of the federal Office of Management and Budget in 2009-2011 - during the design, passage, and first steps to implementation of the Patient Protection and Affordable Care Act (commonly known as Obamacare) - and he seemed to address some critics in absentia who have claimed that health care reform will lead to unwanted rationing of care. There's no need to ration, Dr. Emanuel said. Switzerland doesn't ration care, and it spends far less per capita for what is considered quality health care. "We can do a better job in this country of controlling costs without the need to ration care," he said.
The only way to really control costs is to transform the way U.S. health care is delivered, he said. Ten percent of U.S. patients account for 63% of dollars spent on health care. "You know who they are - people with congestive heart failure, COPD, diabetes, adult asthma, coronary artery disease, cancer. People with chronic multiple chronic illnesses. That's where the money's going. That's where the uneven quality is," and that's where health care delivery needs to improve, he said.
Dr. Emanuel proposed six essential components to transforming the health care system. Among them: The focus needs to be on cost according to value, and getting rid of services with no value. The system must focus on patients' needs, not on physicians' schedules or other concerns. And the system must evolve toward clinicians working as teams including allied health professionals, not as individuals. "We are not going to be, going forward, one-sies and two-sies in practice" anymore, he said.
Greater emphasis on delivering health care via organizations and systems, standardization of processes, and transparency around price and quality will be essential, he added.
Transparency in pricing and quality isn't just something consumers will want. Physicians will want it in order to refer patients to quality care and set prices appropriately, Dr. Emanuel argued. "I think this is inevitable, and I think it's going to happen faster than you think," he said.
Most U.S. physicians are stuck in fee-for-service payment systems, which don't provide the incentives needed for change, he said. Doctors "as a group" should push for changes to the payment system, which will increase physician autonomy but also will assign more financial risk to physicians. "I see no way of getting out of that," Dr. Emanuel said.
In his eyes, if doctors don't push for changes in how health care is delivered, we basically can kiss the U.S. economy and future prosperity good-bye. "Doctors are the only people who can re-engineer the delivery system," he said. "If you don't do it, it ain't gonna happen. It's that simple," he said. All previous reform efforts that did not have physician leadership have failed.
"You have to lead this," he explained.
No one should expect that reforming the fifth-largest economy in the world could be accomplished in just a few years, however. "It's going to take this decade," Dr. Emanuel predicted.
Dr. Emanuel reported having no financial disclosures.
Twitter: @sherryboschert
Dr. Ezekiel J. Emanuel, one of the brains behind Obamacare, has a blunt message for his fellow physicians:
Only you can save America.
He's not just talking about medicine. As might befit someone who holds a faculty title at the business-oriented Wharton School at the University of Pennsylvania, Dr. Emanuel spent much of his keynote address here at the American College of Physicians' annual meeting in San Francisco talking about the U.S. economy. The enormous impact of runaway spending on U.S. health care threatens "everything we care about," including access to health care, state funds available for education, corporate wages for the middle class, and the fiscal health of the nation, he said.
"More than any other group in America, doctors have the power to solve our long-term economic challenges to ensure a prosperous future," Dr. Emanuel said.
If the U.S. health care system were a country, its nearly $3 trillion economy in 2012 would be the fifth largest in the world, behind only the U.S. as a whole, China, Japan, and Germany. "We spend more on health care in this country than the 66 million French spend on everything in their society," he said. "It is an astounding number how much we spend on health care."
Take just the federal portions of Medicare and Medicaid, excluding state spending, and you've still got the 16th largest economy in the world, bigger than the economies of Switzerland, Turkey, or the Netherlands, for example. The impact of any other fiscal variable on the U.S. economy, including Social Security, is swamped by the impact of health care costs, said Dr. Emanuel, who is also chair of medical ethics and health policy at the University of Pennsylvania, Philadelphia.
Per person, the United States far outspends other countries when it comes to health care, and the proportion of the gross domestic product consumed by health care keeps getting larger and larger.
Dr. Emanuel served as a special adviser for health policy to the director of the federal Office of Management and Budget in 2009-2011 - during the design, passage, and first steps to implementation of the Patient Protection and Affordable Care Act (commonly known as Obamacare) - and he seemed to address some critics in absentia who have claimed that health care reform will lead to unwanted rationing of care. There's no need to ration, Dr. Emanuel said. Switzerland doesn't ration care, and it spends far less per capita for what is considered quality health care. "We can do a better job in this country of controlling costs without the need to ration care," he said.
The only way to really control costs is to transform the way U.S. health care is delivered, he said. Ten percent of U.S. patients account for 63% of dollars spent on health care. "You know who they are - people with congestive heart failure, COPD, diabetes, adult asthma, coronary artery disease, cancer. People with chronic multiple chronic illnesses. That's where the money's going. That's where the uneven quality is," and that's where health care delivery needs to improve, he said.
Dr. Emanuel proposed six essential components to transforming the health care system. Among them: The focus needs to be on cost according to value, and getting rid of services with no value. The system must focus on patients' needs, not on physicians' schedules or other concerns. And the system must evolve toward clinicians working as teams including allied health professionals, not as individuals. "We are not going to be, going forward, one-sies and two-sies in practice" anymore, he said.
Greater emphasis on delivering health care via organizations and systems, standardization of processes, and transparency around price and quality will be essential, he added.
Transparency in pricing and quality isn't just something consumers will want. Physicians will want it in order to refer patients to quality care and set prices appropriately, Dr. Emanuel argued. "I think this is inevitable, and I think it's going to happen faster than you think," he said.
Most U.S. physicians are stuck in fee-for-service payment systems, which don't provide the incentives needed for change, he said. Doctors "as a group" should push for changes to the payment system, which will increase physician autonomy but also will assign more financial risk to physicians. "I see no way of getting out of that," Dr. Emanuel said.
In his eyes, if doctors don't push for changes in how health care is delivered, we basically can kiss the U.S. economy and future prosperity good-bye. "Doctors are the only people who can re-engineer the delivery system," he said. "If you don't do it, it ain't gonna happen. It's that simple," he said. All previous reform efforts that did not have physician leadership have failed.
"You have to lead this," he explained.
No one should expect that reforming the fifth-largest economy in the world could be accomplished in just a few years, however. "It's going to take this decade," Dr. Emanuel predicted.
Dr. Emanuel reported having no financial disclosures.
Twitter: @sherryboschert
